ORLANDO TECH PRACTICAL NURSING PROGRAM PATIENT PROFILE Diana Ariza Olukayode Saseyi

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

8/8/2019 Peds Patient Profile
http://slidepdf.com/reader/full/peds-patient-profile 1/14
ORLANDO TECH
PRACTICAL NURSING PROGRAM
PATIENT PROFILE
Diana Ariza
Olukayode Saseyi
8/8/2019 Peds Patient Profile
http://slidepdf.com/reader/full/peds-patient-profile 2/14
Patient Initials: AV DOB: 01/16/2002 Sex: Female
Age: 8 Yrs Hgt: 41.8 in/106 cm Wgt: 40.5 lbs
Diagnoses:
Cerebral Palsy- Spatic Squad
Patient acquired the cerebral trauma due to misdiagnosis and wrong drug treatment used. Cerebral palsy is
the name given to those cerebral traumas that result in a specific family of symptoms. The spastic form of
Cerebral Palsy is characterized by abnormal control of voluntary limb muscles and by exaggerated reflexes,
sometimes in association with a reduction in muscle tone in the trunk of the body. The muscles are stiffly and
permanently contracted. Making movement awkward and difficult to varying degrees depending upon
severity.
With Full Body Involvement, there are additional complications having to do with eating and breathing due to
the lack of muscle control or the inability of muscles to work together in the normal patterns or rhythms of
contraction.In the pts case, she is not able to be fed due to the lack of muscle tone, therefore she has to be fed
by the feeding pump. Also due to the spasm of muscles, she has breathing problems, which usually leads to an
increase amount of secretions.
The symptoms associated with the spastic form of Cerebral Palsy lessen during sleep and are exacerbated by
stress or voluntary movement .
Developmental Delay
Child development refers to the process in which children go through changes in skill development during
predictable time periods, called developmental milestones. Developmental delay occurs when children have
not reached these milestones by the expected time period. For example, if the normal range for learning to
walk is between 9 and 15 months, and a 20-month-old child has still not begun walking, this would beconsidered a developmental delay.
Developmental delays can occur in all five areas of development or may just happen in one or more of those
areas (to read about the five areas of development). Additionally, growth in each area of development is
related to growth in the other areas. So if there is a difficulty in one area (e.g., speech and language), it is likely
to influence development in other areas (e.g., social and emotional).
Seizure Disorder
brain disorder involving repeated, spontaneous seizures of any type. Seizures ("fits," convulsions) are
episodes of disturbed brain function that cause changes in attention or behavior. They are caused by
abnormally excited electrical signals in the brain.
Seizures ("fits," convulsions) are episodes of disturbed brain function that cause changes in attention or
behavior. They are caused by abnormally excited electrical signals in the brain.
Sometimes a seizure is related to a temporary condition, such as exposure to drugs, withdrawal from certain
drugs, a high fever, or abnormal levels of sodium or glucose in the blood. If the seizure or seizures do not
happen again once the underlying problem is corrected, the person does NOT have epilepsy.
8/8/2019 Peds Patient Profile
http://slidepdf.com/reader/full/peds-patient-profile 3/14
In other cases, permanent injury to or changes in brain tissue cause the brain to be abnormally excitable. In
these cases, the seizures happen without an immediate cause. This is epilepsy. Epilepsy can affect people of
any age.
Epilepsy may be idiopathic, which means the cause cannot be identified. These seizures usually begin
between ages 5 and 20, but they can happen at any age. People with this condition have no other neurological
problems, but sometimes have a family history of seizures or epilepsy.
Almost all seizures are relatively brief, lasting from a few seconds to a few minutes. Most seizures last 1 to 2
minutes. When a seizure stops, people may have a headache, sore muscles, unusual sensations, confusion, and
profound fatigue. These after-effects are called the postictal state. In some people, one side of the body is
weak, and the weakness lasts longer than the seizure (a disorder called Todd's paralysis). Most people who
have a seizure disorder look and behave normally between seizures.
PHYSICAL ASSESSMENT
V/ST:95.0 Axillary
P: 70
R: 22
spO2: 93
Weight: 40.5 lbs
NEURO
Orientation: Alerted, active, hypertonic per norm
Reflexes: no deficits in reflexesPosturing: Chair fast Pupils :PERRL
GENITAL
Female: No signs of menarche
RESPIRATORY Symmetrical
Rate: 22 breaths per min
Retractions: none
Sounds: Labored breathing, Rhonchi and rales
Cough: Active & productive
Secretions: Active- 5 mL
SKINTemperature: Warm
Hydration: Well hydrated & well nourished
Intact: Yes
Jaundiced,Puritis: No
Pain: Pt cant verbally express pain, she shows
uncomfortable facial expressionsWell perfused
CARDIACNo edema present
Rate and quality: Regular HR
Radial p :3+Femoral p: 3+
Color: Pink
Capillary Refill: < 2 sec
Skeletal/MuscleReflexes: No deficits
Range of motion: Limited
Contractures or posturing : present in hands and feet Scoliosis: no present
No acute changes in spasticity
GIAbdomen: Flat
Bowel Sounds: Hypoactive
Feeding Tube: Mic 16 Fr/ 2.5
G/UIncontinent
Color: Amber
Odor: Normal
8/8/2019 Peds Patient Profile
http://slidepdf.com/reader/full/peds-patient-profile 4/14
Eyes, Ears, Nose, Throat:
Cornea clear
Color of sclera: White
Evidence gingival hyperplasia: No
Face: symmetrical
Ears lowest? No
ENDOCRINE
Hx of DM, DI, hypothyroid, adrenal insufficiency?
No
PAST MEDICAL HISTORY
Aspiration Pneumonia Aspiration pneumonia is inflammation of the lungs and airways to the
lungs (bronchial tubes) from breathing in foreign material.
Aspiration pneumonia is caused by breathing foreign materials (usually
food, liquids, vomit, or fluids from the mouth) into the lungs. This may
lead to:
y A collection of pus in the lungs (lung abscess)y An inflammatory reaction
y A lung infection
Aspiration pneumonitis represents chemical damage to the
tracheobronchial tree caused by acute, often witnessed, inhalation of
regurgitated gastric contents in patients with an acute change in mental
status. Aspiration pneumonia results from chronic, usually unwitnessed,
inhalation of small amounts of oropharyngeal contents leading to an
infectious process.
Small Bowel Obstruction A small-bowel obstruction (SBO) is caused by a variety of pathologicprocesses. The leading cause of SBO in developed countries ispostoperative adhesions (60%) followed by malignancy, Crohn'sdisease, and hernias.SBOs can be partial or complete, simple (ie, nonstrangulated) or strangulated. Strangulated obstructions are surgical emergencies. If notdiagnosed and properly treated, vascular compromise leads to bowelischemia and further morbidity and mortality. Because as many as 40%of patients have strangulated obstructions, differentiating thecharacteristics and etiologies of obstruction is critical to proper patienttreatment.
Obstruction of the small bowel leads to proximal dilatation of the
intestine due to accumulation of GI secretions and swallowed air. This
bowel dilatation stimulates cell secretory activity resulting in more fluid
accumulation. This leads to increased peristalsis both above and below
the obstruction with frequent loose stools and flatus early in its course.
Hiatal Hernia condition in which a portion of the stomach protrudes upward into the
chest, through an opening in the diaphragm. The diaphragm is the sheet
of muscle that separates the chest from the abdomen. It is used in
breathing.
8/8/2019 Peds Patient Profile
http://slidepdf.com/reader/full/peds-patient-profile 5/14
The goals of treatment are to relieve symptoms and prevent
complications.
Reducing the backflow of stomach contents into the esophagus
(gastroesophageal reflux) will relieve pain. Medications that neutralize
stomach acidity, decrease acid production, or strengthen the lower
esophageal sphincter (the muscle that prevents acid from backing upinto the esphagus) may be prescribed.
Bowel/ Bladder Incontinence Fecal incontinence is the inability to control your bowels. When
you feel the urge to have a bowel movement, you may not be ableto hold it until you get to a toilet. Or stool may leak from the
rectum unexpectedly, sometimes while passing gas.
Fecal incontinence can be caused by injury to one or both of the
ring-like muscles at the end of the rectum called the anal internaland external sphincters. The sphincters keep stool inside. When
damaged, the muscles aren¶t strong enough to do their job andstool can leak out. In women, the damage often happens when
giving birth. The risk of injury is greatest if the doctor uses forcepsto help deliver the baby or performs an episiotomy, which is a cut
in the vaginal area to prevent it from tearing during birth.Hemorrhoid surgery can also damage the sphincters.
Myringotomy tubessurgical procedure in which a small incision is made in the eardrum (the
tympanic membrane), usually in both ears. The English word is derived from
myringa, modern Latin for drum membrane, and tome, Greek for cutting. It is
also called myringocentesis, tympanotomy, tympanostomy, or paracentesis of
the tympanic membrane. Fluid in the middle ear can be drawn out through the
incision.
Ear tubes, or tympanostomy tubes, are small tubes open at both ends that are
inserted into the incisions in the eardrums during myringotomy. They come in
various shapes and sizes and are made of plastic, metal, or both.
y GT care with soap and water once per day and PRN
y Nasopharyngeal suction PRN with red rubber cathetery Utilize AFOs & splints as directed by Doctor and therapist
Upper Gastrointestinal Bleed
6/16/2009
The underlying mechanisms of nonvariceal bleeding involve either arterial
hemorrhage, such as in ulcer disease and mucosal deep tears, or low-pressure venous hemorrhage, as in telangiectasias and angioectasias. In
variceal hemorrhage, the underlying pathophysiology is due to elevatedportal pressure transmitted to esophageal and gastric varices and resulting
in portal gastropathy.
8/8/2019 Peds Patient Profile
http://slidepdf.com/reader/full/peds-patient-profile 6/14
Duodenal ulcer disease is strongly associated with Helicobacter pylori
infection. The organism causes disruption of the mucous barrier and has a
direct inflammatory effect on gastric and duodenal mucosa. Eradication of
H pylori has been demonstrated to reduce the risk of recurrent ulcers and,
thus, recurrent ulcer hemorrhage.
Allergies: Not Known Drug Allergies
What Immunizations should have at this age?
y rotavirus vaccine- 2 or 3 doses 2 months, 4 months, 6 months.
y Influenza vaccination
y Haemophilus influenzae type b (Hib) conjugate vaccine- Vaccine: 3 or 4 doses 2
months, 4 months, 6 months, 12-15 months
y Hepatitis B - 3 doses Birth, 1-2 months, 6-18 months
y DTaP-Diphtheria, Tetanus & Pertussis- 5 doses 2 months, 4 months, 6 months, 15-
18 months, 4-6 years
y Pneumococcus - 4 doses 2 months, 4 months, 6 months, 12-15 months
y Polio- 4 doses 2 months, 4 months, 6-18 months, 4-6 years
y Meningococcal
y Hepatitis A- 12-23 months of age
y Measles, mumps, and rubella- 12-15 months of age
y Chicken Pox
y Varicella
GROWTH AND DEVELOPMENT
How the disease affects the normal G&D
Stage according to Ericksons stages of development
Where she should be?
Long term effect on the future of this child
SURGICAL AND DIAGNOSTIC PROCEDURES
Name of Procedure Description of Procedure Procedure Results Nursing Interventions & Pt
education (2)
X-RAY Sound waves are sent toward the
organ through a handheld device
that a technician glides over the
Shows a mass and
surgical clips noted
Education about the procedure isgiven to the patient. It is a non-invasive procedure with sound
8/8/2019 Peds Patient Profile
http://slidepdf.com/reader/full/peds-patient-profile 7/14
Why was this ordered? abdomen. The sound waves
bounce off the organs, and their
echoes make electrical impulses
that create a picture - called a
sonogram - on a video monitor. If
there is any hernias or bowel
obstructions, it will bounce off theimage.
behind the heart.
Related to Hiatal
Hernia
Small bowel
obstruction
waves imaging to scan the pancreassize.It is a painless test where a machinewill move while taking the imagesnecessary.
Patient has to remove jewelry,
glasses, and any metal objects.
FUNDOPLICATION
Why was this ordered?
Decompression done
but SBO persisted,
Laparotomy
16 french for Nissan-
type fundoplication
Pre-procedure
Post Procedure
ABNORMAL LAB WORK
Lab Test 1st
Abnormal Most Recent Values Normal ValuesHemoglobin 12.7 15.7 34-40
Hematocrit 39.5 45.9 9.4-14.3
Platelet 313CRP 16.3
Serum Creatinine 0.34 mg/dLNa 131 135-145 mmol/L
K 4.2 3.5-5.0
Ca 9.2 8.5-10.5
Cl 102 98-110
Glucose 148 70-100
BUN 11 5-25
Creatinine 0.37 0.2-0.7
Albumin 3.6 3.2-5.5 WBC 10.7 5.5-15.5
RBC 5.38 4.11-5.59
TREATMENTS AND RATIONALE
Treatments RationaleDIET:Pediasure 5 cans per dayBolus over 1& ½ -2 hrsFlush 180 cc with H2O
Main goal is to give nutritional supplements since patient is not able to eatregular meals.
Also due
Vital Signs: q 4 Hrs Assess any symptoms of Hypertension, any signs or symptoms of distress. Assess for any symptoms of hypoxia by checking the O2 sat and make suresuctioning is done PRN. CPT and postural drainage ABI Vest used to drainsecretions and prevent O2 <90%
I&O Intake and output are important measures to take, to prevent any edema or pulmonary edema due to the inactivity. Also to prevent any dehydration due tothe lack of Liquid intake.
Activity Level Patient is wheelchair bound but any increase of activity level will help with thedecrease of edema or prevent any pulmonary problems due to secretions. It

8/8/2019 Peds Patient Profile
http://slidepdf.com/reader/full/peds-patient-profile 8/14
will help move secretions and let her breath better. It helps with the cognitivelevel as well as her psychological well-being.
PositioningEvery 2 hrsrepositioning
Helps patient to move secretions to prevent a relapse of aspiration pneumonia.Prevents any edema since pt is chair fast. Helps with Range of motionexercises needed to prevent contraction and further level of spasticity.
Catheters N/A
Blood Glucose/Accuchecks everyphysical
Blood glucose level determines the need for insulin and how the Pediasureand medicine might affect her glucose levels.
Special mattresses N/A for Children¶s carePt sleeps for 1 hr in an elevated mattress, restrained to not fall, and positionedon left side, to help move secretions.
Rehab P.T.- activities and education to improve flexibility, strength, mobility, and function. Cognitive skills and fine motor coordination therapy implemented to increaseher level of control. Standing frame, ROM and gait trainer has been used.O.T.- helps to learn physical skills she needs to function and become as independent as possible. Occupational therapy uses people's strengths to help them cope with their disabilities. Pt. is developing head and neck control when she wants. She
responds to verbal directions to reposition herself. Exercises to help her control her extremities without any help and with self-determination has beenimplemented.Botox injection applied to help with the muscle spasticity; pt showedimprovement so further therapy will be used.Speech Therapy- enable pt to make maximum use of their communication skills inexpressing their ideas and understanding those expressed by others Pt has class witha teacher to increase her cognitive level. Pt has not been able to say any word.Her way to communicate is by pressing buttons or choose cards that say ³Yes´or ³No´Resp. Therapy- Pt is evaluated for medicine prescribed for removal of secretions. Chest therapy and ABI Vest used to help move secretions andprevent any pneumonia. Suctioning is scheduled every 2 hours or PRN with
nebulizer medicine to improve asthma symptoms as well as bronchodilator.Play Therapy Improves emotional and social development; reduce aggression; improvecooperation with others. Helps pt to improve cognitive level as well as tointeract with the outside environment. Pt responds well to play therapy andenjoys listening to music. Most of the treatment is to influence the music in her therapy in order to see improvement. Play also induces laughter, which we allknow is the best medicine. Playing also increases hand-eye coordination, canaid in developing fine motor skills, and as they get older, can aid in developingtheir gross motor skills
School Patient goes to class at 9:30 a.m. for 1 hour with a one-to-one contact toincrease cognitive level. Pt responds well to the teacher and the learningmaterials offered, such as colors, figures and music to implement newvocabulary words. Although patient doesn¶t speak, pt is able to show with armsand with facial expressions the likes and dislikes of material. She is able tofollow commands and follow objects and persons when hiding. Teacher implements a lot of exercises for her to recognize when something is in front of her or not. Pt has been showing improvement.
AGE & DIAGNOSIS APPROPRIATE PLAY ACTIVITY & EDUCATIONAL ACTIVITIES
Play activities-

8/8/2019 Peds Patient Profile
http://slidepdf.com/reader/full/peds-patient-profile 9/14
Voice Instructional Equipment with buttons:
Pt likes to hear the voice of a person with the instructions of what she has to do. Pt seems to be able to
press buttons and loves to be able to be independent to do so. Therefore we think it is important to
improve her independency level during class. We can record certain activities explaining what she has
to do, and she is able to pick and choose what she is able to do next, by having different color and
figures in each figure that has the recording. For example, we can use a 4 color table that has 4 different
recording with instructions to choose the color she would like to learn that day. In the color she chooses,
we can describe certain objects and places she can find those colors.While she listens to it, we can give
her the objects so she is able to touch them and play with her hands. This will introduce the touching
and listening activities to improve her vocabulary as well as to learn how to follow instructions.
Since she is choosing the buttons, she will feel a sense of independence and will motivate her to keep
learning and playing. By choosing the different instructions and colors, it also helps with the
neurological development.
Music-
Pt loves and recognize music as an enjoyment time. Not only she is able to recognize the sounds and
follow them but she also move her extremities in order to show enjoyment. This can help her with her
motor development as well as cognitive. It will be great to implement new words and rhythms into her
play therapy so she can increase her cognitive level. "Play permits the child to resolve in symbolic form
unsolved problems of the past and to cope directly or symbolically with present concerns. It is also his
most significant tool for preparing himself for the future and its tasks." Bruno Bettelheim . Therefore it is
important to implement music that helps her interact with other classmates and learn their ways tomove. She tries to imitate their moves, which are important to her physical development and
improvement. Although the pt is not able to move like she would like to, she feels secure trying to move
her extremities and following the example that kids or any person who is playing with her is doing. This
help with her self-expression, adjustability, and potential for interaction.
Music helps the patient to feel secure around sounds and different voices. It will help her to get used to
different directions by different voices, rather than to focus on the everyday people she interacts with.
Also it will help with her motor skills, balance and coordination, by following the rhythm and anyone
around her.
School- Pt receives classes in the morning in the Children¶s care Campus. She is currently ingrade _____. The main activities during her class days are the implementation of new words
into her vocabulary. They used figures that are used everyday (such as fruits, paper and
geometrical figures) to relate it to the colors as well as toys that she can touch. Pt seems to be
able to recognize the colors, once she is able to feel them or associate them in any way with
touch.

8/8/2019 Peds Patient Profile
http://slidepdf.com/reader/full/peds-patient-profile 10/14
Pt reacts positively to music, therefore teacher implements music into the learning activities
such as learning the colors and the rules of behavior while in class. Pt is able to move her head
and hands (even though is not completely in control) following the songs. She follows the
teacher around and gets excited when she hears the music she likes. She enjoys the music
where she sees her classmates dance and the ones that she is able to move her arms to follow
their movements.
Equipment or assistive devices
Patient has to be wheelchair bound in order to move around. In her wheelchair she has to carry
a portable suctioning machine to clear up secretions. She carries her Feeding tube pump in
order to have her feeding every 2 hours at least.
The personnel that go with the child should be somebody who knows the scheduled feeding,
medicines and suctioning. Also somebody who knows to look for Oxygen needs and who knows
that any accumulation of secretions should be avoided as much as possible. They should be
instructed in how to use the suctioning machine as well as the feeding pump.
MEDICATIONS
Medication and doseordered
Safe range ascalculated from
drug guide
Is the Dose safe? If it is outside the
therapeutic rangewhy is it still given?
Why was it ordered?
Albuterol 2.5mgnebulizer tid by
updraft
By dilating the bronchii itwill help patient open theairways and allowsecretions to be coughedout easily
Pulmicort 0.5mgnebulizer bid by
updraft
This is a locally actingsteroid for inhalation, itwill reduce the associatedinflammatory reactiongoing on in the lungs,reduce the amount of secretions and edemathereby improving air entry.
Foradil I caps for inhalation bid byupdraft
Causes bronchodilation inthe patient improvingbreathing
Keppra 500mg bid viang tube
This is an anticovulsantused to reduce frequencyand severity of seizuresthereby helping the childto be quiet and relaxed.
Robinul 1mg qid viang tube
It is used to reducesecretions in therespiratory tract and theGI tract, reducedsecretions promotes air
8/8/2019 Peds Patient Profile
http://slidepdf.com/reader/full/peds-patient-profile 11/14
way patency.
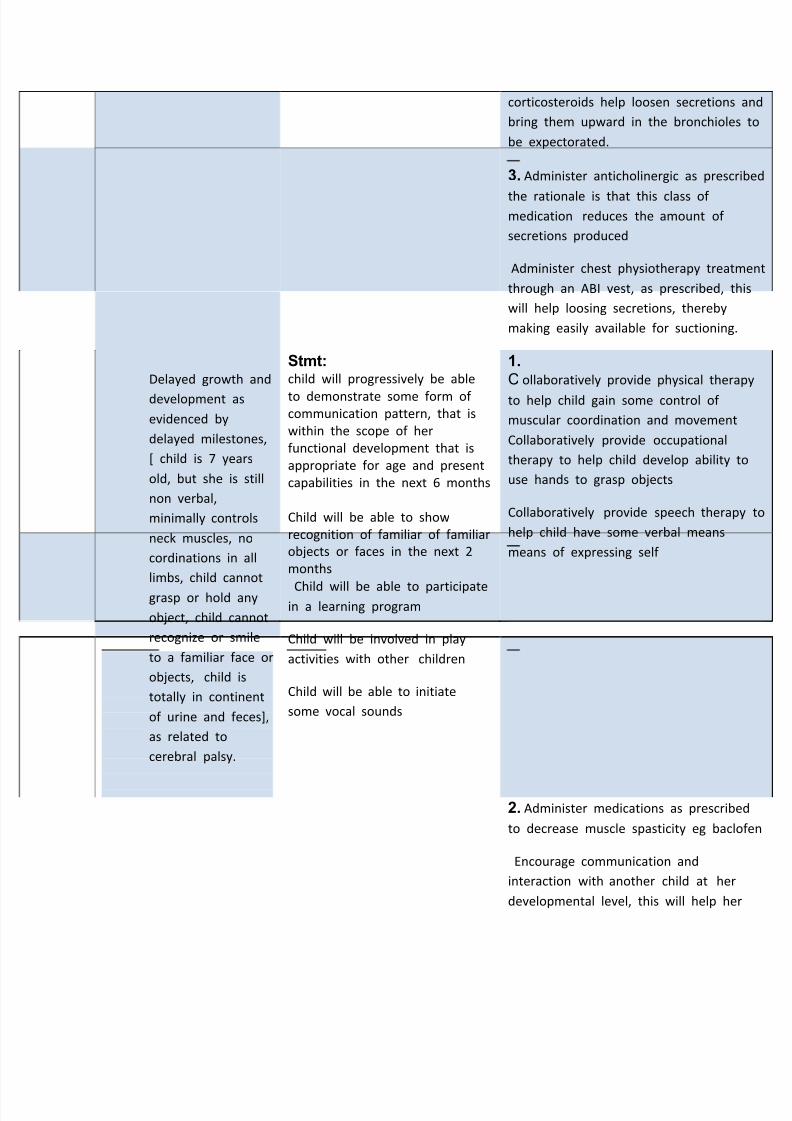
Zantac 200mg at bedtime via ng tube
An anti ulcer drug thatworks by inhibiting protonpumps in the stomachthereby reducing acidity,patient is post
fundiplication, medicationwill help reduce impact of acid on the esophagus
Miralax 8.5mg via ngtube prn
This is used to evacuatethe GI, because mosttimes children withcerebral have problemswith elimination due to uncoordinated and in -effective peristalsis
CARE PLAN
DATE ASSESSMENT/NURSINGDIAGNOSIS
GOAL INTERVENTIONS/NURSING MEASURES &RATIONAL
10/25 /10 Nsg. Dx : : Ineffective air
way clearance, as
evidenced by noisy
breathing, ineffective cough,
decreased air entry in both
lung fields, presence of
crackles, rhonchi and rales
sounds , SPO2<92%
Related to abnormal
voluntary and involuntary
motor performances due to
cerebral palsy
Stmt:Child will have a patent airway
in the next 30 mins
She will have good air entry in
both lung fields in the next 3
mins
Her lung sounds will be
vesicular in the next 3 mins
She will produce less secretions
in the next 2 days
All secretions produced will be
expelled or removed promptly
SPO2 will remain at 96% or
above at all times.
1. Position child in an upright or head
position, or on the side when lying do
at all times, the rationale is that thes
position help prevent blockage of airw
by accumulated secretions.
Suction nasopharynx and oropharynx
necessary as prescribed this will remo
accumulated secretions and eventually
clear the airway.
AEBO2 sat check every 4 hrs suctioning PRN
2. Administer bronchodilator, inhalatio
corticosteroids, prescribed by doctor in
updraft breathing mask, the rationale
that updraft breathing treatment
containing bronchodilators and
8/8/2019 Peds Patient Profile
http://slidepdf.com/reader/full/peds-patient-profile 12/14
corticosteroids help loosen secretions
bring them upward in the bronchioles
be expectorated.
3. Administer anticholinergic as prescr
the rationale is that this class of medication reduces the amount of
secretions produced
Administer chest physiotherapy treatm
through an ABI vest, as prescribed, th
will help loosing secretions, thereby
making easily available for suctioning.
Nsg. DxDelayed growth and
development as
evidenced by
delayed milestones,
[ child is 7 years
old, but she is still
non verbal,
minimally controls
neck muscles, no
cordinations in all
limbs, child cannot
grasp or hold any
object, child cannot
recognize or smile
to a familiar face or
objects, child is
totally in continent
of urine and feces],
as related to
cerebral palsy.
Stmt:child will progressively be able
to demonstrate some form of communication pattern, that is
within the scope of her
functional development that is
appropriate for age and present
capabilities in the next 6 months
Child will be able to show
recognition of familiar of familiar
objects or faces in the next 2
months
Child will be able to participatein a learning program
Child will be involved in play
activities with other children
Child will be able to initiate
some vocal sounds
1.
C ollaboratively provide physical thera
to help child gain some control of
muscular coordination and movement
Collaboratively provide occupational
therapy to help child develop ability t
use hands to grasp objects
Collaboratively provide speech therap
help child have some verbal means
means of expressing self
2. Administer medications as prescribe
to decrease muscle spasticity eg baclo
Encourage communication and
interaction with another child at her
developmental level, this will help her
8/8/2019 Peds Patient Profile
http://slidepdf.com/reader/full/peds-patient-profile 13/14
learn from the other child and help in
setting limits and internal guidance
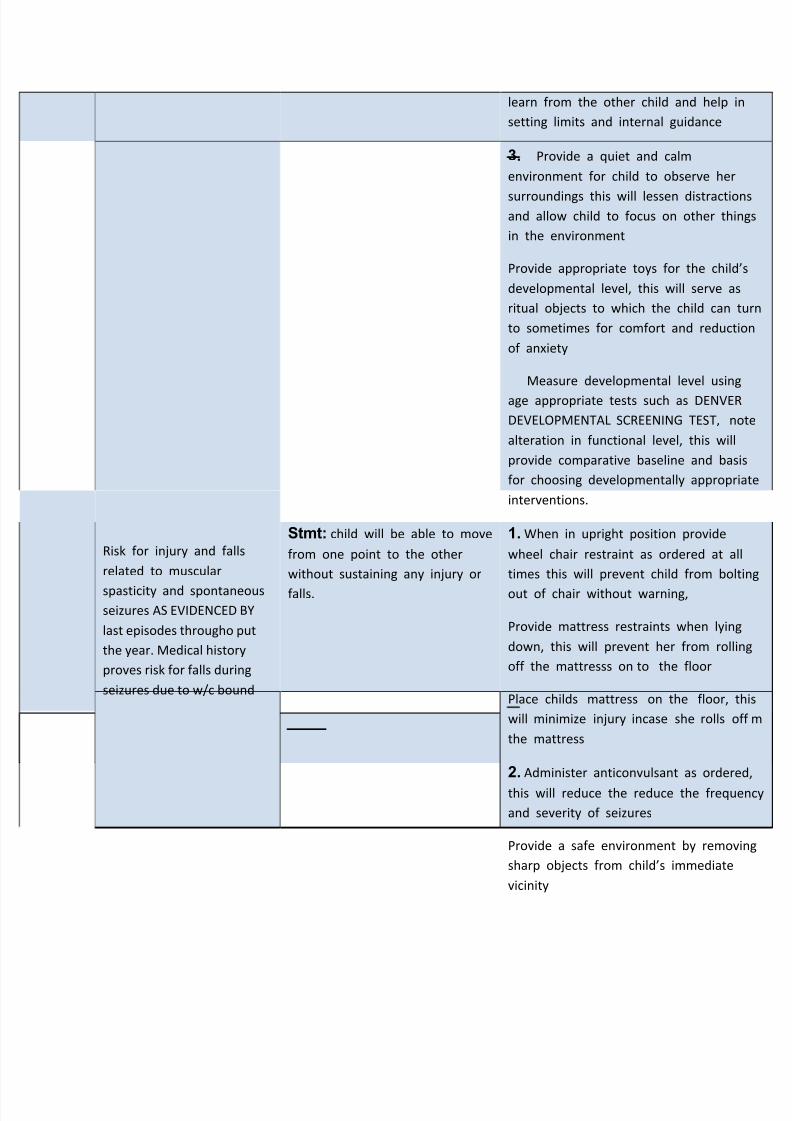
3. Provide a quiet and calm
environment for child to observe her
surroundings this will lessen distractioand allow child to focus on other thin
in the environment
Provide appropriate toys for the child
developmental level, this will serve as
ritual objects to which the child can t
to sometimes for comfort and reducti
of anxiety
Measure developmental level using
age appropriate tests such as DENVER
DEVELOPMENTAL SCREENING TEST, no
alteration in functional level, this will
provide comparative baseline and bas
for choosing developmentally appropri
interventions.
Nsg. DxRisk for injury and falls
related to muscular
spasticity and spontaneousseizures AS EVIDENCED BY
last episodes througho put
the year. Medical history
proves risk for falls during
seizures due to w/c bound
Stmt: child will be able to move
from one point to the other
without sustaining any injury or
falls.
1. When in upright position provide
wheel chair restraint as ordered at al
times this will prevent child from bolt
out of chair without warning,
Provide mattress restraints when lying
down, this will prevent her from rollin
off the mattresss on to the floor
Place childs mattress on the floor, t
will minimize injury incase she rolls of
the mattress
2. Administer anticonvulsant as ordere
this will reduce the reduce the freque
and severity of seizures
Provide a safe environment by remov
sharp objects from childs immediate
vicinity
8/8/2019 Peds Patient Profile
http://slidepdf.com/reader/full/peds-patient-profile 14/14
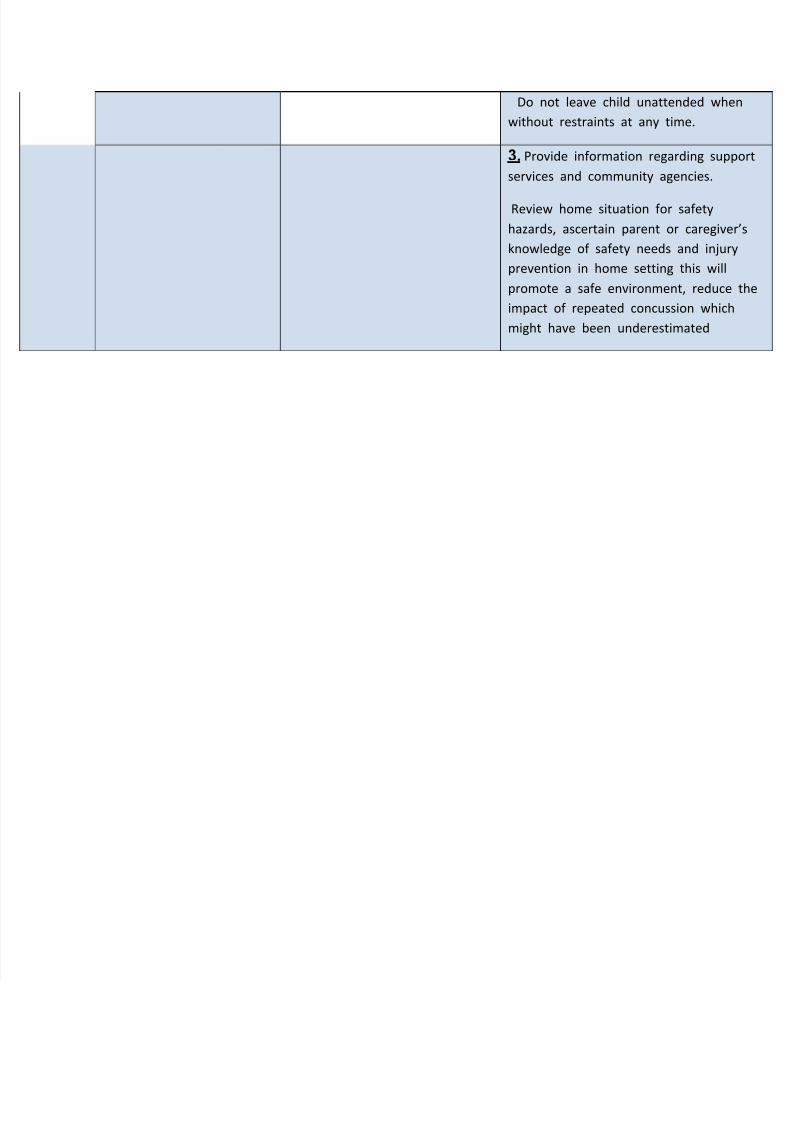
Do not leave child unattended when
without restraints at any time.
3. Provide information regarding suppo
services and community agencies.
Review home situation for safety
hazards, ascertain parent or caregiver
knowledge of safety needs and injury
prevention in home setting this will
promote a safe environment, reduce t
impact of repeated concussion which
might have been underestimated
Related Documents











