782 PEDIATRICS Vol. 63 No. 5 May 1979 The Heart in Acute Glomerulonephritis: An Echocardiographic Study Pnina Vardi, M.D., Walter Markiewicz, M.D., Joseph Levy, M.D., Olga Adler, M.D., Egon Riss, M.D., and Abraham Benderley, M.D. Front the’ !)epartment.s- of Pediatrics, Cardiology, and Diagnostic Radiology, Ra7nbanl .Iedieal Center, Aba Kbiousbiy School of .%h’dicine, Haifa, Israel ABSTRACT. Patients with acute glomerulonephritis often are seen with signs suggesting heart failure. Whether these signs are due to fluid overload secondary to kidney damage only, or whether there is associated inyocardial damage has not been elucidated. Fourteen children with acute glomeru- lonephritis were studied by echocardiography during the edematous phase of the disease and five months later to evaluate cardiac function in this disease. Left ventricular size and function remained normal in all children throughout the study. The most consistent finding was enlargement of the left atrium during the edematous phase with a return toward normal values five nionths later. There was no correlation between blood pressure and the echocardiographic findings. This study suggests that signs of heart failure in acute glomentlonephritis are not due to myocardial damage but probably reflect fluid overload. Pediatrics 63:782-787, 1979, echocardiography, acute glornerulonephritis, heart failure, left atrial enlargement. In many patients with acute glomenilonephri- tis (AGN), signs and symptoms suggesting conges- tive heart failure develop. Despite numerous investigations, it is not clear whether myocardial function is depressed in this disease, or whether the signs suggesting heart failure are due to fluid overload, or to other factors such as hyperten- sion.i In this study, we evaluated a group of children with AGN by echocardiography to gain further insight into the cardiac status of these patients. PATIENTS AND METHODS Fourteen children were studied during an epidemic of poststreptococcal AGN. All had the classic signs of AGN including hematuria, proteinuria, edema, elevated sedimentation rate, and antistreptolysin 0 titer and depressed concen- tration of the third component of the complement (G3). None had a previous history of kidney disease, and all had previously been healthy, except for one child who had chronic hemolytic anemia due to thalassemia (subject no. 4). On admission to the hospital, all children underwent a full clinical examination including a 12-lead electrocardiogram and roentgenogram of the chest. Echocardiographic studies were performed within two days of admission in all subjects, on discharge from the hospital in eight subjects, and five months thereafter in all 14 subjects. The ultrasonic studies were performed on an ultrasonoscope, using a 2.25 MHz transducer focused at 7.5 cm, and a recorder. All the children were examined in the semi-left lateral decubitus position with the head elevated by a wedge. Routine techniques were used for evaluation of the aorta, left atrium, left ventricle, interventricu- lar septum, right ventricle, and pericardiuni. Left ventricular contractile state was evaluated by calculating the ejection fractiont and the percentage of fractional shortening’ from the left ‘ ventricular dimensions (Fig 1). Left atrial and aortic dimensions were obtained at the level of the aortic leaflets. Left atrial dimension was measured at end systole from the anterior border of the posterior aortic wall to the strong anterior edge of the posterior atrial wall echo (Fig 2). Aortic dimension was measured at end diastole. The upper limit for normal values of left atrium, aorta, and left ventricle used in the study are those reported by Feigenbaunr and varied de- pending on the l)ody surface area. The upper Received April 7; revision accepted for publication August 8, 1978. ADDRESS FOR REPRINTS: (P.V.) Department of Pediat- rics “A,” Rambam Medical Center, Haifa, Israel. at Indonesia:AAP Sponsored on January 16, 2015 pediatrics.aappublications.org Downloaded from

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

782 PEDIATRICS Vol. 63 No. 5 May 1979
The Heart in Acute Glomerulonephritis: AnEchocardiographic Study
Pnina Vardi, M.D., Walter Markiewicz, M.D., Joseph Levy, M.D., Olga Adler, M.D.,
Egon Riss, M.D., and Abraham Benderley, M.D.
Front the’ !)epartment.s- of Pediatrics, Cardiology, and Diagnostic Radiology, Ra7nbanl .�Iedieal Center, Aba
Kbiousbiy School of .%h’dicine, Haifa, Israel
ABSTRACT. Patients with acute glomerulonephritis often
are seen with signs suggesting heart failure. Whether thesesigns are due to fluid overload secondary to kidney damageonly, or whether there is associated inyocardial damage hasnot been elucidated. Fourteen children with acute glomeru-
lonephritis were studied by echocardiography during the
edematous phase of the disease and five months later toevaluate cardiac function in this disease. Left ventricular sizeand function remained normal in all children throughout thestudy. The most consistent finding was enlargement of theleft atrium during the edematous phase with a return towardnormal values five nionths later. There was no correlation
between blood pressure and the echocardiographic findings.This study suggests that signs of heart failure in acuteglomentlonephritis are not due to myocardial damage but
probably reflect fluid overload. Pediatrics 63:782-787, 1979,echocardiography, acute glornerulonephritis, heart failure,
left atrial enlargement.
In many patients with acute glomenilonephri-tis (AGN), signs and symptoms suggesting conges-
tive heart failure develop. Despite numerous
investigations, it is not clear whether myocardial
function is depressed in this disease, or whether
the signs suggesting heart failure are due to fluid
overload, or to other factors such as hyperten-sion.i In this study, we evaluated a group of
children with AGN by echocardiography to gain
further insight into the cardiac status of these
patients.
PATIENTS AND METHODS
Fourteen children were studied during an
epidemic of poststreptococcal AGN. All had the
classic signs of AGN including hematuria,
proteinuria, edema, elevated sedimentation rate,
and antistreptolysin 0 titer and depressed concen-
tration of the third component of the complement
(G3). None had a previous history of kidney
disease, and all had previously been healthy,except for one child who had chronic hemolyticanemia due to thalassemia (subject no. 4). On
admission to the hospital, all children underwent
a full clinical examination including a 12-lead
electrocardiogram and roentgenogram of thechest. Echocardiographic studies were performedwithin two days of admission in all subjects, on
discharge from the hospital in eight subjects, andfive months thereafter in all 14 subjects.
The ultrasonic studies were performed on anultrasonoscope, using a 2.25 MHz transducer
focused at 7.5 cm, and a recorder. All the childrenwere examined in the semi-left lateral decubitus
position with the head elevated by a wedge.Routine techniques were used for evaluation of
the aorta, left atrium, left ventricle, interventricu-lar septum, right ventricle, and pericardiuni.�
Left ventricular contractile state was evaluated
by calculating the ejection fractiont and the
percentage of fractional shortening’ from the left‘ventricular dimensions (Fig 1). Left atrial and
aortic dimensions were obtained at the level ofthe aortic leaflets. Left atrial dimension was
measured at end systole from the anterior border
of the posterior aortic wall to the strong anterior
edge of the posterior atrial wall echo (Fig 2).
Aortic dimension was measured at end diastole.
The upper limit for normal values of left atrium,aorta, and left ventricle used in the study are
those reported by Feigenbaunr and varied de-
pending on the l)ody surface area. The upper
Received April 7; revision accepted for publication August 8,
1978.ADDRESS FOR REPRINTS: (P.V.) Department of Pediat-rics “A,” Rambam Medical Center, Haifa, Israel.
at Indonesia:AAP Sponsored on January 16, 2015pediatrics.aappublications.orgDownloaded from

ARTICLES 783
#{149}cg i
� - �T*� � � � �
1� � � � � � I � � � � � � II �
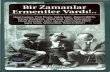
Fig 1. Representative (subject 6) echocardiographic examination of the ventricles taken on
admission (left) and five months later (right). Left ventricular end diastolic dimension remainsunchanged. (ACW = anterior chest wall; RV right ventricle; IVS interventrictilar
se1)ttllll; LV = left ventricle; En = endocardium; P pericardium.)
limit for a noinial left atrial-aorta ratio in our
laboratory is 1.26, whereas the lower limit for
normal ejection fraction and percent of fractional
shortening in children is 55% and 25%, respective-
ly.
For the pllI’pose of this studs’, hypertension was
diagnosed when blood pressure was higher than
1:30/90 flilli Hg. Left ventricular hvpertrophy
was diagnosed by EGG using criteria suggested by
Liebm an . ‘ Chest roentgenograms were reviewed
by an exl)erienced radiologist for evidence of
cardiotnegalv and heart failure. Statistical analy-
sis was performed using two-tailed paired Student
t-tests for analysis of changes in cardiac dimen-
sions, and using the Fisher exact test for the
correlation l)etWeen the presence of hypertension
and increased size or thickness of heart cham-
bers.
RESULTS
There were eight boys and six girls with an age
of 6.7 ± 0.9 years (mean ± SEM) (range 3 to 12
years). Mean body surface area was 0.8 1 ± 0.06
sq m with a range of 0.5 to 1.2 sq m. The clinical
findings on admission and at discharge are given
in Table I. All children were treated by bed rest,low-potassium diet, and penicillin. Patients with
hypertension were treated with water restriction
and intramuscular injections of reserpine. Nonehad evidence of residual kidney damage, andnone was receiving any treatment at the time the
third echocardiogram was performed. All chil-dren had normal sodium, potassium, chloride,bicarbonate, and calcium values throughout thestudy. Mean body weight was 22.4 ± 2.3 kg on
admission and 21.0 ± 2.3 kg on discharge
(P < .01). Mean heart rate increased from
80.6 ± 5.1 to 92.3 ± 3.9 beats per minute duringthe same period (P < .05).
The echocardiographic findings are given in
Table II, and the correlation of selected echocar-
diographic data with roentgenographic and clini-cal findings is given in Table III. Eleven childrenhad an enlarged left atrium on admission. Left
at Indonesia:AAP Sponsored on January 16, 2015pediatrics.aappublications.orgDownloaded from

784 HEART IN GLOMERULONEPHRITIS
Fig 2. Representative echocardiographic study of the aorta and left atrium of the same patient,showing reduction of left atrial size from 3.4 cm on admission (left) to 2.8 cm five months later(right). (RVOT = right ventricular outflow tract; AAo = anterior aortic wall; PAO = posterior
aortic wall; Ao = aorta; LA left atrium.)
TABLE I
CLINICAL FINDINGs IN 14 CHILDREN WITH ACUTE
CLOMERULONEPHHITIS
Clinical bindings’ Number of Patients
On On
Adm iss’ion is5
Hypertension 7 0
Clinical edema 14 0
Proteinuria, cylindruria 14 0
BUN <20 rng/dl 10 0
LVH on ECGt 0 0
Cardiolnegaly on roentgeno- 7 ...
grainl
Congestive heart failure on 7 ...
roentgenogram�
#{176}Nlean of two weeks later.
tLVH = Left ventricular hypertrophy.:1:(;ht’st roentgenograln was not available for review in one
patient.
atrial size returned to normal values in all but onesubject when measured five nionths later. Mean
left atrial size was 3. 1 1 ± 0. 14 cm on admissionvs 2.52 ± 0.10 cm five months later (P < .01).The mean left atriumaorta ratio was similarly
significantly reduced from 1.61 ± 0.07 to
1.33 ± 0.05 (P < .01) during the same period.Seven of eight children already demonstrated areduction in the left atrial size when studied at
the end of hospitalization, a mean of 14 days afterthe first study had been done. Five of these seven
children demonstrated a further reduction in leftatrial size when studied five months later. Leftventricular internal dimension, percentage offractional shortening, and ejection fraction werenormal in all children throughout the study.There was a small but significant decrease in thethickness of the interventricular septum (P < .05)and of the left ventricular posterior wall (P < .05)
at Indonesia:AAP Sponsored on January 16, 2015pediatrics.aappublications.orgDownloaded from

TABLE II
ARTICLES 785
ECHOCARDIOGRAPHIC FINDINGS
hnthng Mean ± SEM P N#{176}
On Admission 5 Months Later
Left atrium (cm) (ES)t 3.11 ± 0.14 2.52 ± 0.10 <.01 14Left atrium/aorta 1.61 ± 0.07 1.33 ± 0.05 <.01 14Aorta (cm) (ED)� 1.96 ± 0.10 1.91 ± 0.07 NS 14Left ventricular internal dimension (cm) 3.65 ± 0.15 3.68 ± 0.13 NS 12
(ED)Interventricular septum (cm) (ED) 0.61 ± 0.05 0.50 ± 0.04 <.05 12Left ventricular posterior wall (cm) (ED) 0.58 ± 0.06 0.48 ± 0.04 < .05 12Right ventricle (cm) (ED) 1.16 ± 0.15 0.85 ± 0.08 NS 12Ejection fraction (%) 79 ± 1.7 78 ± 2.5 NS 12Percentage of fractional shortening 41 ± 1.7 41 ± 2.3 NS 12
5N = Number of patients with adequate echocardiographic measurements.
tES = End systole.
IED = End diastole.
during the study period, whereas no significant
change was observed in the size of the aorta and
right ventricle. No significant relationship was
noted between the presence of hypertension, left
atrial enlargement, and increased thickness of the
left ventricular posterior wall or interventricular
septuni.
DISCUSSION
In many patients with acute glomerulonephri-tis, signs and symptoms suggesting congestive
heart failure . � Various etiologic factors
have been put forth to explain the appearance of
heart failure. In recent years, the attention hasfocused on three possible causative factors:
TABLE III
ConsE�TIoN BETWEEN SELECTED ECHOCARDIOGRAPHIC AND CLINICAL FINDINGs
Subject
No.
Echocardio graphic Findings0 X -Ray an d Clinical Findingst
-�
LA (cm)
-5----,
LVED (cm)
-.-.----‘
%FS
.-‘
Heart
Siz4
CHFI BP
(mm Hg)
BSA
(sq m)
-
Age
(Years)
I III I 111 1 lii
1 2.9(E) 2.4 3.2 2.9 41 45 CDM + 180/120 0.6 32 3.1(E) 1.8 3.4 3.3 35 45 CDM + 120/ 70 0.6 4
3 2.9(E) 1.9 2.9 2.8 34 35 N 0 130/100 0.6 3
4 4.0(E) 3.2(E) 3.8 4.2 39 33 CDM + 150/100 0.7 55 2.9(E) 2.5 4.2 3.8 45 47 N 0 120/ 80 0.8 7
6 3.4(E) 2.8 4.1 4.1 34 44 N + 150/110 0.9 87 3.3(E) 2.8 4.3 4.0 35 35 CDM + 180/120 1.1 10
8 2.6 2.8 3.8 3.5 47 25 N 0 120/ 80 0.9 7
9 3.1(E) 2.8 4.0 3.8 42 53 CDM + 140/100 1.1 1110 2.3 2.2 2.9 3.7 48 41 CDM 0 120/ 80 0.6 3
11 2.8(E) 2.3 NA 3.0 NA 46 N 0 120/ 80 0.5 4
12 2.8 2.7 NA 3.2 NA 37 NA NA 130/ 80 0.7 5
13 4.2(E) 2.6 3.2 4.0 50 40 CDM + 130/ 90 1.0 12
14 3.3(E) 2.5 4.0 4.0 45 50 N 0 170/120 1.2 12
#{176}LA= left atrium; LVED left ventricular dimension at end diastole; %FS percentage of
fractional shortening; I and III refer to echocardiographic measurements on admission and fivemonths later, respectively; E = enlarged; NA not available or inadequate.
tCHF = Congestive heart failure; BP blood press’ure; BSA = body surface area;CDM = cardiomegaly; NA = not available or inadequate.:1:Found on chest roentgenogram.
at Indonesia:AAP Sponsored on January 16, 2015pediatrics.aappublications.orgDownloaded from

786 HEART IN GLOMERULONEPHRITIS
myocardial damage, hypertension, and hyper-
volemia secondary to the renal disease.
Gore and Saphir’ found myocarditis at post-mortem examination in 16 of 160 patients who
died of acute and subacute glomerulonephritis.
The histologic findings consisted of interstitial
edema with few inflaiiiiiiatory cells and little or
no myocardial cell destruction. The role of such
serious myocarditis in causing heart failure has
been questioned. Thus Davies found a normal
cardiac output in five patients with AGN. De
Fazio and associates’ studied seven patients withAGN by cardiac catheterization and found an
increased cardiac output and stroke volume, an
elevation of the pulnionarv capillary wedge and
pulmonary artery pressure, and normal peripher-al and pulmonary arteriolar vascular resistance.
De Fazio et at interpreted these findings asindicating normal nivocardial function and
suggested that the hemodynamic changes ob-
served might be due to hypervolemia.
The suggestion that overload of the vascular
tree may play a critical role in the causation of
circulatory congestion has been advanced by
others.�� Thus Eisenberg,’2 in studying the
blood volunie of ten patients with AGN, found
that the plasma volume was significantly
increased during the edematous phase, without
alteration in circulatory red cell mass. Some
investigators’ have suggested that hypertension is
a causative factor in the development of heart
failure. However, other authors noted that there
was a poor correlation between the presence and
severity of hypertension and the development of
congestion.
In this study, we present data on the heart sizeand function in a group of children examined
during and after an episode of AGN. The percent-
age of fractional shortening and the ejection
fraction remained normal throughout the study.
These measurements are useful indices of myocar-
dial contractilityli although they may be
faulted by variations in other hemodynamic van-
ables. Thus, consideration must be given to the
possibility that the myocardial contractility was
truly reduced during the acute phase of the
disease, but that the measured indices rose in
response to changes in afterload,’4 or in response
to increased sympathetic tone.� This hypothesis
seems unlikely in our patients. First, many
subjects were hypertensive at the time of the first
ultrasonic exam ination ; increased afterload would
tend to depress and not to increase ejection phase
indices. � � Second, five months later, mean heart
rate nieasured during the acute phase of AGN was
significantly lower than during the recovery pen-
od, suggesting that sympathetic tone was notunduly increased at the time of admission to the
hospital. Bradycardia is not uncommon during
the edematous and hypertensive phase of AGN
and has been attributed to increased vagal
tone. �
We think that our findings indicate that left
ventricular function was normal in all the patients
and, therefore, that signs suggesting congestiveheart failure cannot be explained on the basis ofmyocardial dysfunction. Likewise, left ventricularinternal dimension was normal in all subjects
during the edematous phase of the disease andremained unchanged throughout the study. The
mean value for thickness of both the interventnic-
ulan septum and the left ventricular posterior walldecreased slightly but significantly during thestudy, suggesting that the thickness of these walls
might have been slightly increased during the
edematous phase. Diastolic overload of the left
ventricle causing left ventricular hypentrophy orinterstitial infiltration of the myocardmm by fluid
could be responsible for this phenomenon. Since
no significant relationship was noted between
increased thickness of the left ventricular posteni-or wall or of the interventnicular septum and thepresence of hypertension, we are of the opinion
that hypertension was not a causative factor. The
echocardiogram on admission demonstrated in-
creased thickness of the interventricular septumin three children and of the left ventricular
posterior wall in two children, but none of the
children had electrocardiographic evidence ofleft ventricular hypertrophy. In contrast to
patients with chronic glomerulonephritis, chil-
dren with AGN rarely have voltage criteria forleft ventricular hypertrophy and tend to have a
decreased amplitude of the R waves in tracingstaken early in the course of the illness.’ Thisdifference may be related to the transient natureof the hemodynamic and pathologic alterations inmost cases of AGN.
The most consistent echocardiographic finding
in our study was the abnormality noted in the size
of the left atrium. Thus left atnial size wasincreased in all but three children during theedematous phase and returned to normal in all
but one child when measured five months later.
The left atrium-aorta ratio, which is less depen-
dent on body surface area and which has beenproposed as a better indicator of left atrial size,’7
similarly decreased significantly during the study
period. The reason for left atrial enlargement hasnot been directly investigated in this study.However, it has been well documented that leftatnial size can markedly and rapidly change in
at Indonesia:AAP Sponsored on January 16, 2015pediatrics.aappublications.orgDownloaded from

ARTICLES 787
response to variations in pulmonary flow’7 or in
response to fluid infusion,” and we think that it is
reasonable to suggest that the enlargement of the
left atriuni noted on admission was secondary to
the increase in blood volume noted during the
edematous phase of acute glomerulonephritis.
The ratio of the right ventricular preejectionperiod to the right ventricular ejection time
(RPEP/RVET) has been used to evaluate seriallythe pulmonary vascular bedl and might haveprovided information on the pulmonary circula-
tioli of our patients. Since pulmonic valve echo-
grams were not routinely obtained, right ventnic-
ular systolic time intervals could not be measured
in this study.
CONCLUSION
This study demonstrates that signs suggesting
heart failure in patients with acute poststrepto-
coccal glomerulonephnitis are not due to myocar-
dial damage but probably reflect fluid overload.
Treatment should aini at reducing the increased
circulating blood volume rather than trying to
1111 prove myocardial function.
REFERENCES1. Murphy TR, Murphy FD: The heart in acute glomeru-
lonephritis. Ann Intern Med 41:510, 1954.
2. Feigenbaum H: Echocardiography, ed 2. Philadelphia,Lea & Febiger, 1976, pp 87-340.
3. Pombo JF, Troy BL, Russel RO: Left ventricularvolumes and ejection fraction by echocardiography.
Circulation 43:14, 1971.4. McDonald IC, Feigenbaum H, Chang S: Analysis of left
ventricular wall motion by reflected ultra sound.
Application to assessment of myocardial function.
Circulation 46:14, 1972.5. Lowe KG: Systemic hypertension in children, in Watson
H (ed): Pediatric Cardiology. London, Lloyd-Luke
Ltd. 1968, pp 844-845.
6. Liebman J: Electrocardiography, in Moss AJ, Adams FH(eds): heart Disease in infants, Children andAdolescents. Baltimore, Williams & Wilkins Co.
1968, pp 183-231.
7. Rubin MI, Rapoport M: Cardiac complication of acutehemorrhagic nephritis. Am I Dis Child 55:244,
1938.8. Gore I, Saphir 0: Myocarditis associated with acute and
subacute glomerulonephritis. Am Heart I 36:300,
1948.
9. Davies CE: Heart failure in acute glomerulonephritis. QI Med 20:163, 1951.
10. De Fazio V, Chrisensen RC, Regan TJ, et al: Circula-
tory changes in acute glomerulonephritis. Circula-‘tion 20:190, 1959.11. Cardozo EL: Hydremia in acute nephritis. Acta �tIed
Scand 125:333, 1946.12. Eisenberg 5: Blood volume in patients with acute
glomerulonephritis as determined by radioactive
chromium tagged red cells. Am I Med 27:241,1959.
13. Ross J Jr. Sobel BE: Regulation of cardiac contraction.Annii Ree Physiol 34:47, 1972.
14. Hirshleifer J, Crawford M, O’Rourke RA, Karliner JS:
Influence of acute alterations in heart rate and
system arterial pressures on echocardiographicmeasures of left ventricular performance in normalhuman subjects. Circulation 54:835, 1975.
15. Anzola J, Rushmer RF: Cardiac responses to sympathet-ic stimulation. Circulation Res 4:312, 1956.
16. Ash R, Mitchell I, Rapaport M: Electrocardiographicvariations in acute glomerulonephritis. Am I Di.s’
Child 67:106, 1944.17. Silverman NH, Lewis AB, Heyman MA, Rudolph AM:
Echocardiographic assessment of ductus arteriosus
shunt in premature infants. Circulation 50:821,
1974.18. Orlando J, Del Vicario M, Aronow \‘iS, Cassidy J:
Correlation of mean pulmonary artery wedge pres-
sure, left atrial dimension and PTF-V in patientswith acute myocardial infarction. Circulation
55:750, 1977.
at Indonesia:AAP Sponsored on January 16, 2015pediatrics.aappublications.orgDownloaded from

1979;63;782PediatricsBenderley
Pnina Vardi, Walter Markiewicz, Joseph Levy, Olga Adler, Egon Riss and AbrahamThe Heart in Acute Glomerulonephritis: An Echocardiographic Study
ServicesUpdated Information &
http://pediatrics.aappublications.org/content/63/5/782including high resolution figures, can be found at:
Permissions & Licensing
http://pediatrics.aappublications.org/site/misc/Permissions.xhtmlor in its entirety can be found online at: Information about reproducing this article in parts (figures, tables)
Reprints http://pediatrics.aappublications.org/site/misc/reprints.xhtml
Information about ordering reprints can be found online:
Online ISSN: 1098-4275.Copyright © 1979 by the American Academy of Pediatrics. All rights reserved. Print ISSN: 0031-4005. American Academy of Pediatrics, 141 Northwest Point Boulevard, Elk Grove Village, Illinois, 60007.has been published continuously since 1948. PEDIATRICS is owned, published, and trademarked by the PEDIATRICS is the official journal of the American Academy of Pediatrics. A monthly publication, it
at Indonesia:AAP Sponsored on January 16, 2015pediatrics.aappublications.orgDownloaded from

1979;63;782PediatricsBenderley
Pnina Vardi, Walter Markiewicz, Joseph Levy, Olga Adler, Egon Riss and AbrahamThe Heart in Acute Glomerulonephritis: An Echocardiographic Study
http://pediatrics.aappublications.org/content/63/5/782
the World Wide Web at: The online version of this article, along with updated information and services, is located on
ISSN: 0031-4005. Online ISSN: 1098-4275.PrintIllinois, 60007. Copyright © 1979 by the American Academy of Pediatrics. All rights reserved.
by the American Academy of Pediatrics, 141 Northwest Point Boulevard, Elk Grove Village,it has been published continuously since 1948. PEDIATRICS is owned, published, and trademarked PEDIATRICS is the official journal of the American Academy of Pediatrics. A monthly publication,
at Indonesia:AAP Sponsored on January 16, 2015pediatrics.aappublications.orgDownloaded from
Related Documents