STROKES IN CHILDREN DR ROBIN THOMAS RESIDENT IN PEDIATRICS JJMMC, DAVANGERE

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

STROKES IN
CHILDREN
DR ROBIN THOMAS
RESIDENT IN PEDIATRICS
JJMMC, DAVANGERE

Stroke-important cause of acquired brain injury in newborns and children.
Relatively rare-children- Arterial or Venous stroke.
Incidence of Arterial ischemic stroke (AIS) and cerebral sinovenous
thrombosis (CSVT)-5/100,000/yr and affects 1 in 2000 newborns.

Blood supply of Brain & Spinal cord

Blood supply of Brain

Circle of Willis
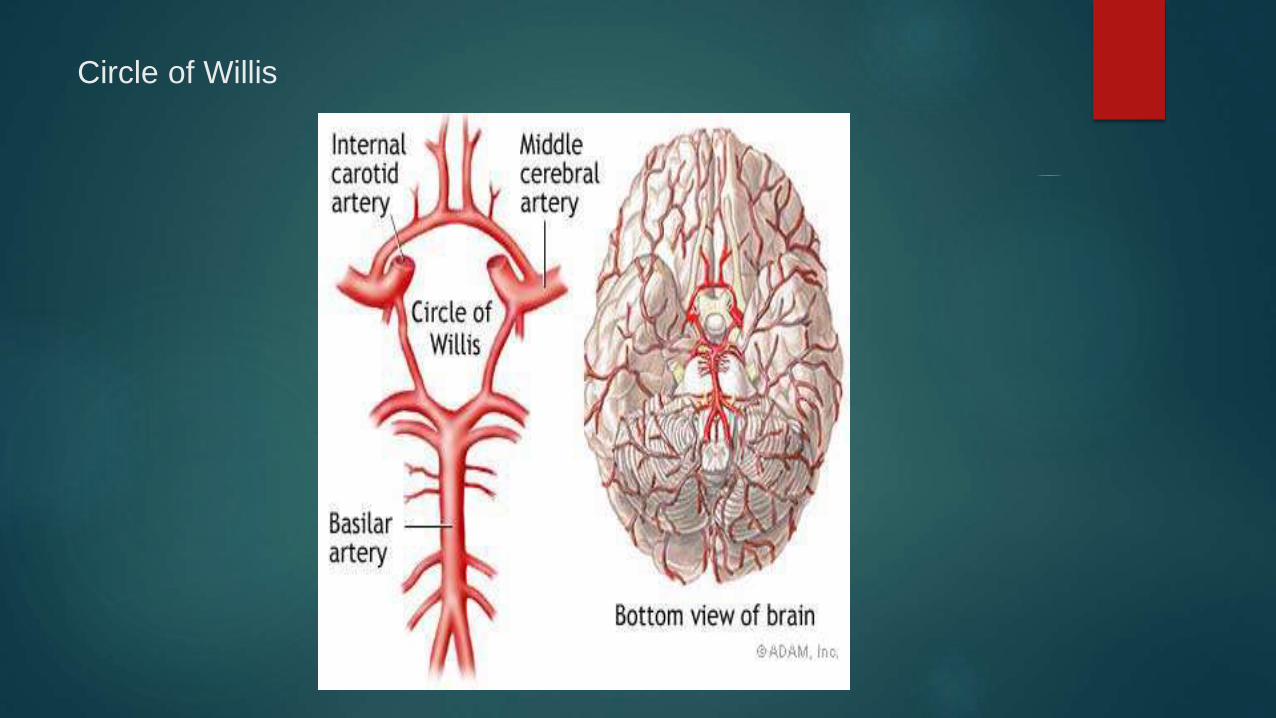
Circle of Willis


Blood supply of Brain
Brain: 700-800 ml blood/min (55ml/100g/min)
< 30 ml/100gm/min: leads to ischemia
80 % blood to gray matter & 20 % to white matter.
Blood supply to brain
Carotid system- 2 Internal Carotid arteries
Vertebro basilar system- 2 Vertebral arteries
Internal carotid artery has 4 portions:
1.Petrous PC3 2.Cervical
3.Cavernous
4.Cerebral

Branches of Cerebral portion of Internal Carotid artery are:
Middle cerebral artery MAAPO Anterior cerebral artery
Anterior choroidal artery
Posterior communicating artery
Ophthalmic artery
Vertebro basilar system
Brain stem, Thalamus, temporal lobe-inferior portion, occipital lobe
1. Vertebral artery
2. Basilar artery
3. Posterior cerebral artery

Circle of Willis
1. Middle cerebral artery (MCA)
2. Anterior cerebral artery (ACA)
3. Posterior cerebral artery (PCA)
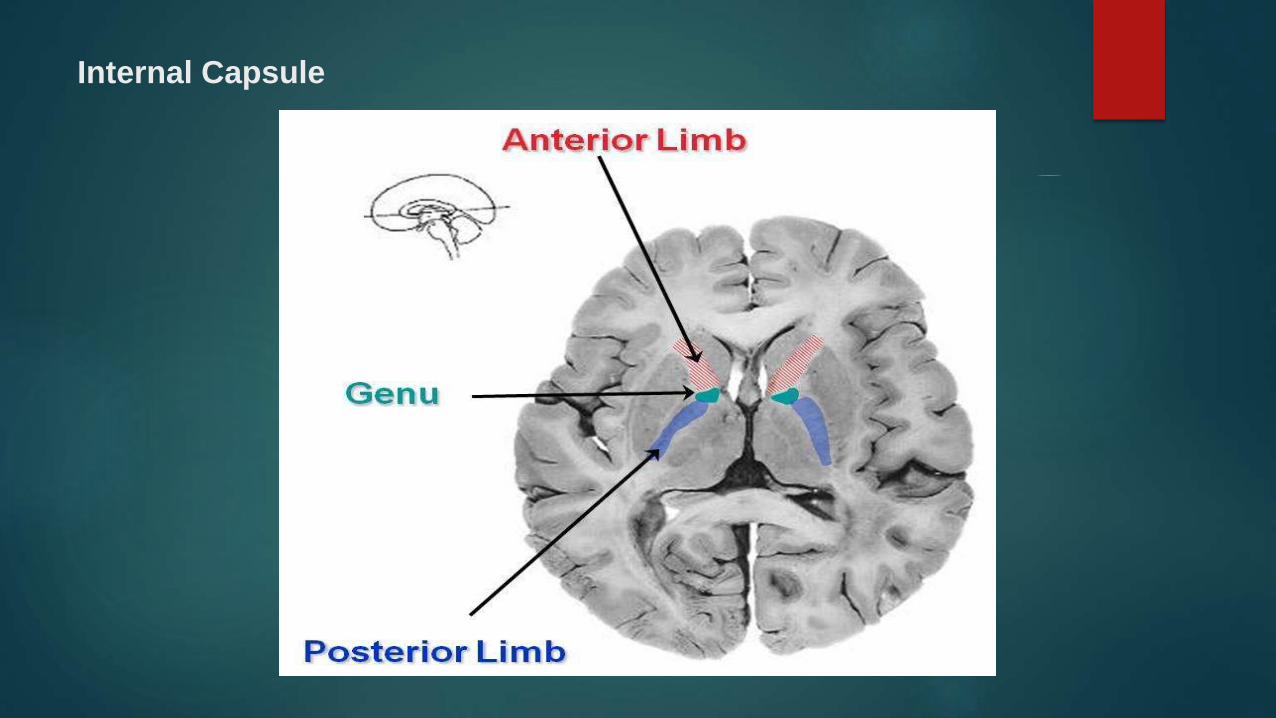
Internal Capsule



Blood Supply of Internal capsule
Anterior limb : Superior half- Lenticulo-striate artery- MCA
Inferior half- ACA- Huebners artery
Genu : Lenticulo-striate artery
Posterior limb : Superior half- Lenticulo-striate artery- MCA
Inferior half- Posterior communicating artery,
Anterior choroidal artery.

Venous drainage of Brain
Sinuses & Veins
Paired Sinuses : Cavernous sinus
Superior & Inferior petrosal sinus
Transverse sinus
Sigmoid sinus
Unpaired Sinuses : Superior & Inferior Sagital sinus
Straight sinus
Anterior & Posterior Intercavernous sinus

Pathophysiology
Interruption of blood flow to the part of the brain
Rupture of blood vessels with bleeding into cerebral parenchyma.
Blood supply of brain- carotid & vertebro-basilar circulations
Numerous anastomosis at the level of circle of willis & through smaller
vessels in leptomeninges.
Diencephalon- supplied by end arteries- anastomosis not adequate-arterial
occlusions have devastating effect.
Water shed zones- portion of cerebral cortex b/w 2 major arteries- less
affected by arterial occlusions –damage when cerebral perfusion pressure
is reduced.
Pathophysiology
Interruption of blood flow of arterial or thrombotic d/s- Ischemic stroke.
Rupture of blood vessels with bleeding into cerebral parenchyma-Hemorrhagic stroke.
Trauma or intimal tears- ICA injury.
Interruption of function – infections, inflammation of intima- severe meningitis, post varicella angiopathy, mycoplasma pneumonia, borrelia, chlamydia, HIV, Helicobactor, Hemolysing streptococci.
Embolisation- Cardioembolism- CCHD, RHD, Prosthetic or Prolapsed cardiac valves, Cardiomyopathy, Arrhythmias.
Decreased cerebral blood flow- high cerebral metabolic rate & paucity of
energy stores in CNS.
Cerebral metabolic rate for oxygen- 3.5 ml/100mg brain/min.
Cerebral hypoxia- oxygen partial pressure < 40 torr.
Glucose storage in brain- survival of cerebral tissue for 90 min.

Preterm infants
Sub ependymal germinal matrix- highly cellular well vascularized area
beneath the ependyma of lateral ventricles- major site of neurogenesis.
Sub ependymal hemorrhage & Intraventricular hemorrhage- common form
of CVD in preterm infants.
Bleeding in highly vascular sub ependymal germinal matrix & then rupture
into lateral ventricle.
Hemorrhagic infarction of periventricular white matter-15% of infants with
intraventricular hemorrhage.

Several factors- fluctuating cerebral blood flow, increase in cerebral
venous pressure, immature capillaries in germinal matrix, abnormal
platelet & coagulation function, low Apgar scores, low birth weight,
prolonged labour, apnea, bradycardia, large PDA, pneumothorax, group B
streptococcal sepsis, hypoxia, hypercapnia, acidosis.
Bed side Ultrasonography- better understanding of subependymal
hemorrhage & intraventricular hemorrhage.

Term infants
Intra cranial hemorrhage- birth trauma- forceps & breech deliveries.
Tears of falx cerebri & tentorium cerebelli.
C/F- apathy, seizures, high pitched cry, irregular respirations.
Tense fontanel, moro reflex abnormalities.
Focal ischemic lesions can occur- DIC, placental infarcts, embolism,
trauma to blood vessels.
Ultrasonography & CT scans- diagnosis.

Neuronal injury & death in hypoxic states- release of excitatory
neurotransmitters: L-glutamate & L-aspartate.
Increased post synaptic stimulation of N-methyl-D-aspartate receptors-
entry of sodium & calcium into neurons & cell death.
Delayed cell death- calcium influx- mitochondrial dysfunction with
breakdown of cell components & free radical formation.
Major factor controlling cerebral metabolic rate-degree of neuronal activity.
Seizures- cerebral metabolic rate increases & reduced to low levels in
coma.

Cerebral blood flow maintained at high levels- substrate for brain
metabolic activity.
< 3 yrs- 30-60 ml/100 mg brain/min.
3-10 yrs- 105 ml/100 mg brain/min.
Adults- 50 ml/100 mg brain/min.
Mature brain- phenomenon of Auto regulation.
Blood flow increases with increased neuronal activity.
Perfusion pressure, intracranial pressure & vascular resistance.
Increasing conc. of CO2- increase of blood flow- dilatation of intracranial
blood vessels.
High conc. of O2- reducing blood flow- causing vasoconstriction.
Most cerebral vascular accidents in children- impairment of arterial blood
flow- result of thrombosis or embolism.
Localized region of metabolic acidosis- dilatation of surrounding blood
vessels- increased vascularity- luxury perfusion.
Damage to neurons & glia- destruction of blood brain barrier- localized
cerebral edema- compress capillaries.
Occlusion of venous structures- increased venous pressure- tendency for
blood vessel to rupture- bleeding & raised intra cranial pressure.
Hemorrhage- intra parenchymal or extra cerebral- acts as mass lesion-
rise in intra cranial pressure.
Damage to blood-brain barrier- promotes cerebral edema.
Blood & blood products of erythrocytes- produce vascular spasm-add to
preexisting damage- cause meningeal irritation- can cause hydrocephalus.

Cerebral infarction pathologic changes- neuronal death & perivascular
hemorrhage- influx of polymorpho-nuclear leukocytes- mononuclear cells
& macrophages.
Astrocytosis results in formation of glial scar.
Preterm infant with sub ependymal germinal matrix hemorrhage-
destruction of white matter- periventricular leukomalacia.
Ventricular dilatation – destruction & disappearance of periventricular white
matter, post hemorrhagic hydrocephalus.







Etiology of Ischemic stroke
Cardio embolism
Congenital cardiac malformations
Acquired
Rheumatic heart disease/endocarditis
Cardiomyopathies, arrhythmias
Prosthetic , Prolapsed valves
Cardiac interventions

Vasculitis & Vasculopathies
Infectious/ Immune/ Iatrogenic vasculitis
Migraine
Hypertensive encephalopathy
Moya moya disease
Hematologic & Hypercoagulable states
Hemoglobinopathies- Sickle cell anemia
Polycythemia
Thrombocytosis

Leukemia, Lympho-reticular malignancy
Protein C, S deficiency
Antithrombin III deficiency
Nephrotic syndrome
Metabolic & related disorders
Homocystinuria
Organic acidemia
Leighs disease
MELAS
Neuroectodermatoses

Trauma
Blunt trauma- ICA.
MELAS- Mitochondrial myopathy, encephalopathy, lactic acidosis, stroke
like episodes.

Etiology of Hemorrhagic stroke
Vascular malformations- AVM/ Aneurysm
Arterial Hypertension
Iatrogenic
Arteritis / Arteriopathies
Cerebral venous occlusive disease
Intracranial tumours
Hematological- Leukemia, Thrombocytopenia,
Vascular disease in older children & infants
Primary vascular diseases
1. Acute infantile hemiplegia
2. Moyamoya disease
3. Takayasu arteritis
4. Fibromuscular dysplasia
5. Hemiplegic migraine

Acute infantile hemiplegia
Sudden onset of pediatric stroke-no specific cause delineated.
Thrombotic occlusions of carotid artery or branches of middle cerebral
artery- frequently documented causes of strokes in children.
3 dimensional MRA- demonstrate significant vascular abnormalities in 75%
of children with strokes. (Wiznitzer & Masaryk, 1991)
Infants- seizures, motor signs few, abnormal hand preference.
Older children- sudden onset of hemiparesis, seizures.

CT or MRI scan- mass lesion, intracranial hemorrhage or arteriovenous
malformation.
Angiography or MRA- moyamoya disease & fibro-muscular dysplasia-
visualization of major blood vessels.
Lumbar puncture- infectious etiological condn.
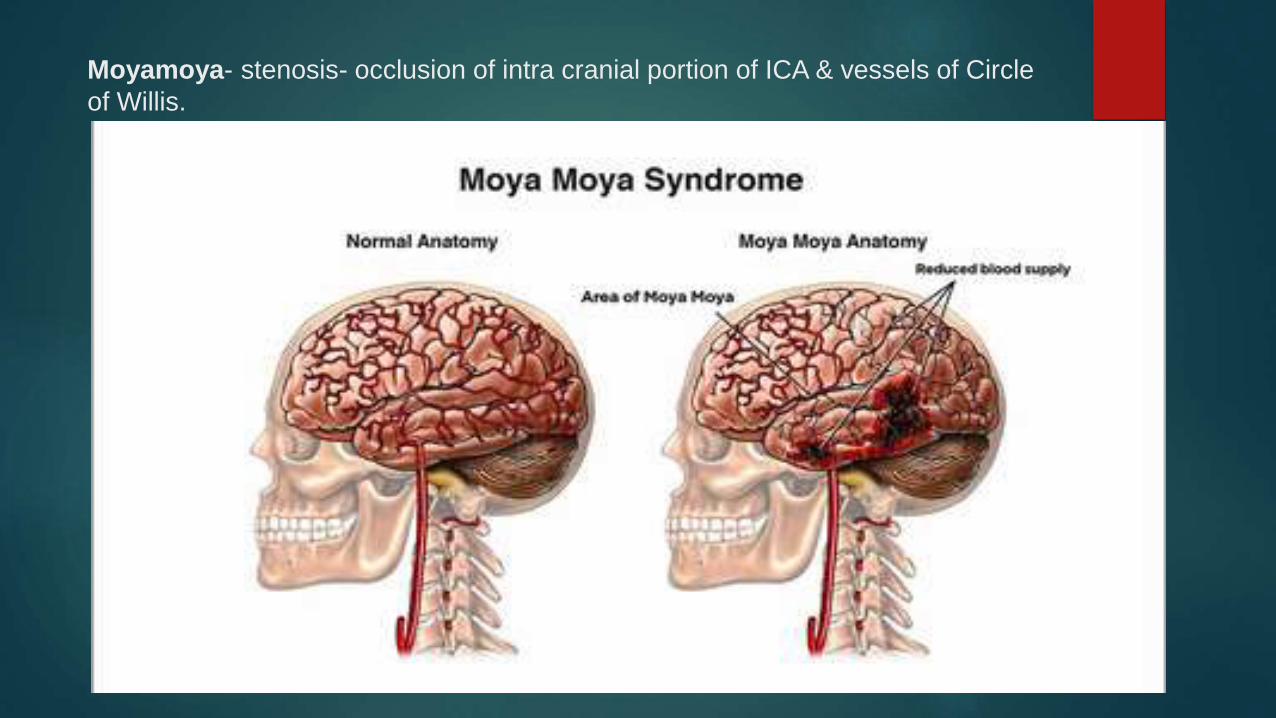
Moyamoya- stenosis- occlusion of intra cranial portion of ICA & vessels of Circle
of Willis.

Stages of Moyamoya disease

Moyamoya- opening of collaterals- smoke like appearance.
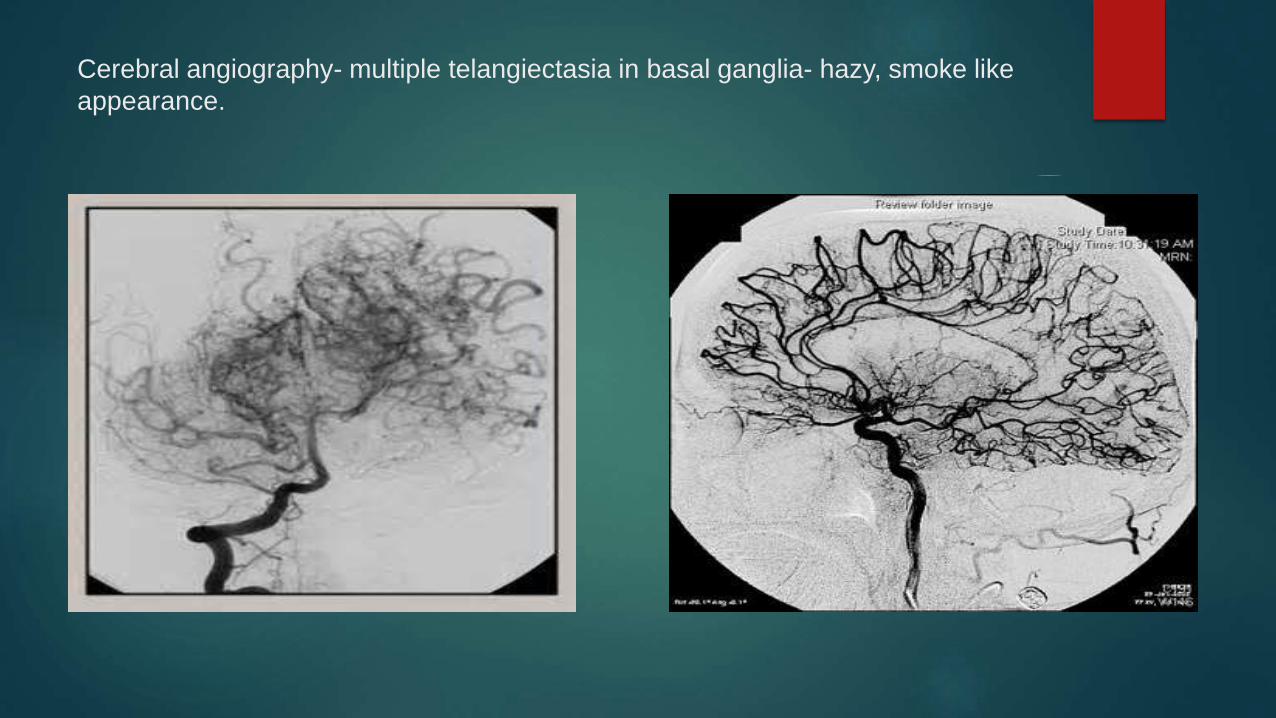
Cerebral angiography- multiple telangiectasia in basal ganglia- hazy, smoke like
appearance.

Contracted internal elastic lamina & focal intimal thickening of vessel wall

Moya moya pattern- opening up of collaterals

Moyamoya disease
Primary vascular disease- stenosis- occlusion of intracranial portion of
Internal carotid artery & other vessels of circle of Willis.
Abnormalities of elastica & focal intimal thickening.
Changes in pulmonary, renal, pancreatic arteries.
Multiple telangiectasias in basal ganglia- hazy, smoke like appearance-
Japanese word moyamoya applied.
Pattern represents opening of collateral channels.
Symptoms in childhood- females frequent.

Chronic inflammatory, occlusive intracranial vasculopathy affecting ACA,
MCA, PCA associated with extensive network of collaterals.
Multiple transient ischemic attacks with permanent residua.
Sudden hemiparesis & multiple transient ishemic attacks without
neurological signs.
Seizures- 33 %- children <6yrs.
Disease is progressive
Poor prognostic factors- early age of onset, typical clinical pattern,
involvement of dominant hemisphere or both hemisphere, complete
occlusion of cerebral blood vessels.
Differentiation from Simple arterial occlusion- recurrent transient
ischemic attacks, progressive mental deterioration, widespread areas of
infarction.
Cerebral angiography- definitive diagnosis.
Progressive vascular changes- occlusion of supra clinoid portion of
internal carotid artery, middle & anterior cerebral arteries & finally
posterior communicating & posterior cerebral arteries.
Cortical atrophy, multiple areas of lucency in cortex & white matter,
ventricular dilatation.
Moyamoya pattern- follow radiation of optic gliomas.

Extra cranial to intra cranial arterial anastomosis

Superficial temporal artery to MCA shunt- enhance cerebral blood flow

Laying STA on arachnoid membrane- STA to MCA shunt
Surgical placement of extracranial to intracranial arterial anastomoses.
Superficial artery to MCA shunt & laying Superficial temporal artery on
arachnoid membrane- enhance cerebral blood flow.
No firm conclusions regarding usefulness of procedure.

Takayasu arteritis
Pulseless disease
Chronic large vessel vasculitis of unknown etiology
Predom. Involves aorta & branches.
Females common-15-20 yrs.
Arteritis involving aorta & its branches.
Inflammation of vessel wall- infiltration of T cells, NK cells, plasma cells, macrophages- giant cells & granulomatous inflammation in media- blood vessel dilatation & aneurysm formation.
Hypertension, absent pulses, vascular bruits.
Strokes in 5-10 % of patients.
Corticosteroids & immunosuppresants.

C/F- Pre pulseless phase of disease- fever, malaise, headache, hypertension, abdominal pain, arthralgia.
Later- diminished pulses, asymmetric blood pressures, claudication, Raynauds phenomenon, renal failure, symptoms of pulmonary & cardiac ischemia.
Classification criteria for TA
Angiographic abnormalities
Decreased peripheral artery pulse or claudication
BP difference b/w arm & legs >10 mmHg
Bruits over aorta
Hypertension
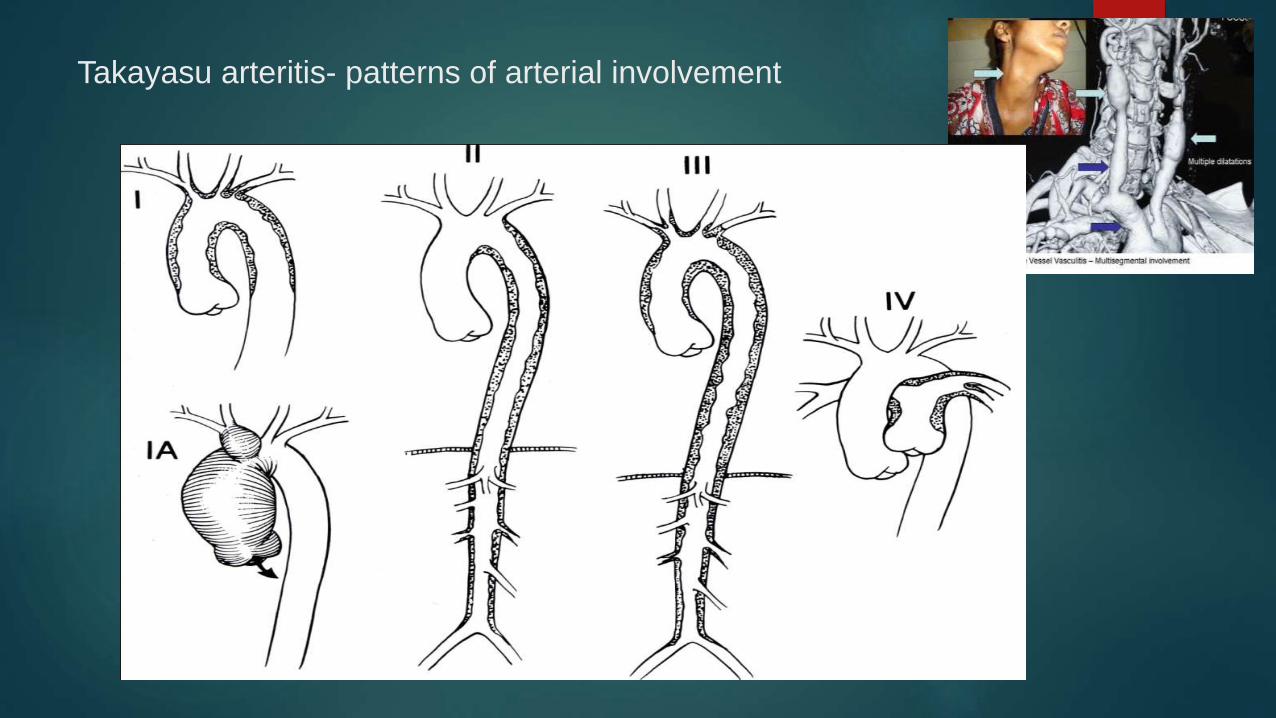
Takayasu arteritis- patterns of arterial involvement
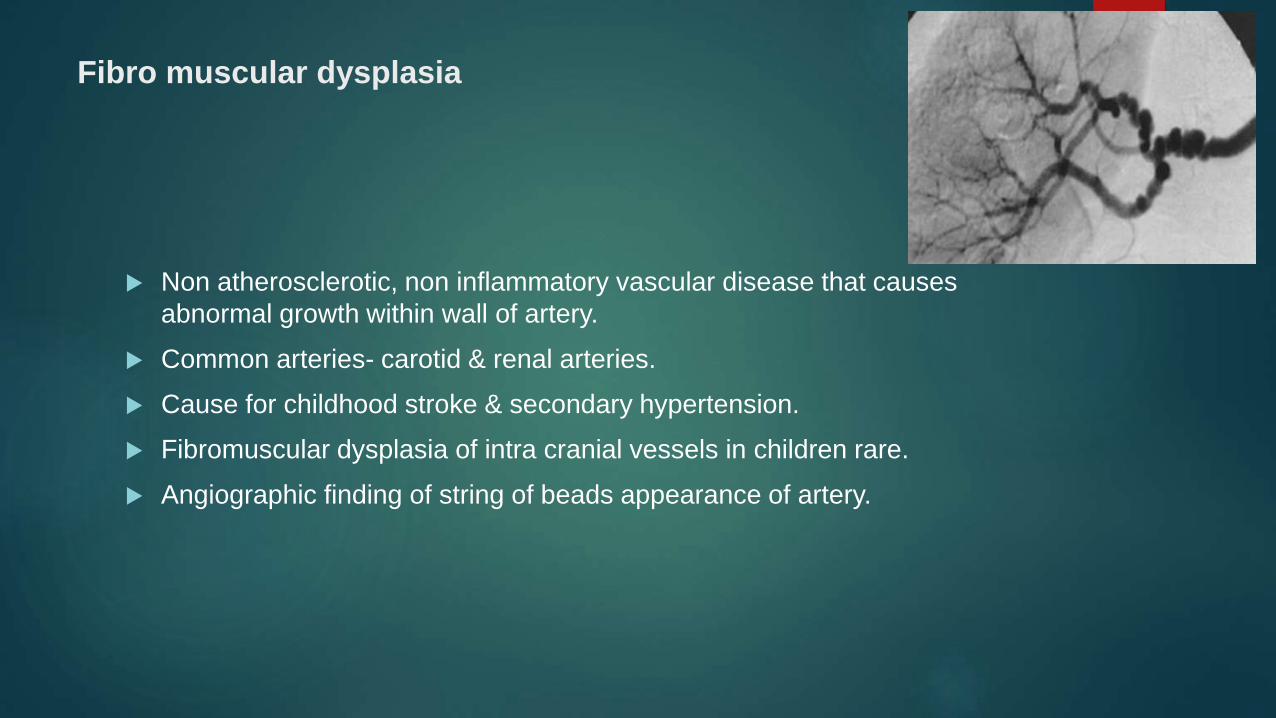
Fibro muscular dysplasia
Non atherosclerotic, non inflammatory vascular disease that causes
abnormal growth within wall of artery.
Common arteries- carotid & renal arteries.
Cause for childhood stroke & secondary hypertension.
Fibromuscular dysplasia of intra cranial vessels in children rare.
Angiographic finding of string of beads appearance of artery.


Migraine
Hemiplegic migraine- transient hemiparesis with severe headache.
Familial forms & sporadic forms.
Transient loss of vision in one eye- amaurosis fugax- adolescent
migraineurs.

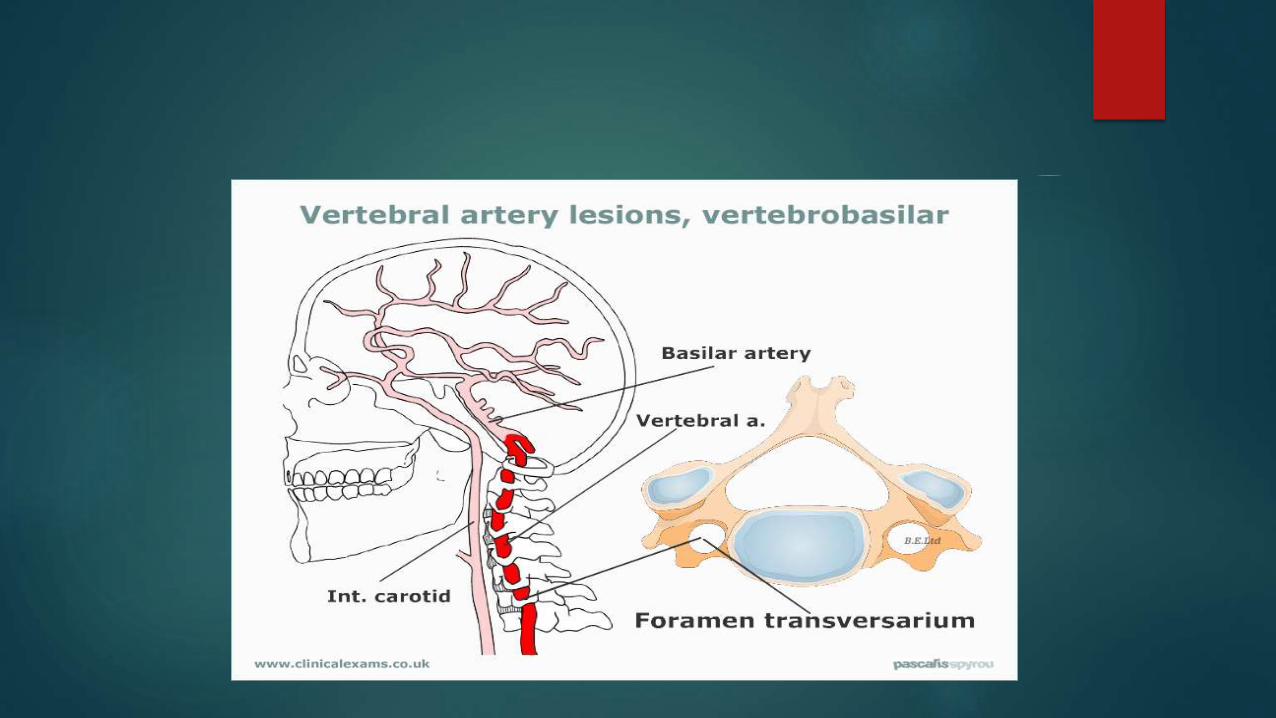
Vertebro basilar occlusion
Decreased blood supply to posterior circulation of brain.
Vertebral artery
Basilar artery
Posterior cerebral artery
Blood supply: brain stem, thalamus, inferior portion of temporal lobe &
occipital lobe.

Vertebro basilar occlusion
Sudden onset or stuttering progression
Brain stem localization- corticospinal & cerebellar signs with oculomotor abnormalities.
Locked in syndrome- infarction at the level of Basilar artery. (Golden etal1987)
Child alert, quadriplegia, facial diplegia, absent horizontal eye movements.
Child cannot speak, preserved vertical eye movements.
Diagnosis considered in a child in coma after a vascular accident but has spontaneous eye opening.

Subclavian steal syndrome
Retrograde flow of blood in vertebral artery, due to proximal stenosis of
subclavian artery.
Follows correction of coarctation of aorta
Headache, dizziness, visual field defects after exercise, seizures.
Angiographic findings characteristic.
Treatment- ligating left vertebral artery or placing a subclavian artery graft.


Cerebrovascular disease secondary to medical conditions
Cardiac disease
Clinical scenario
9/12 old infant k/c/o TOF came with h/o Left sided hemiparesis, seizures,
depressed state of consciousness.
MRI brain showed Right MCA infarct with cerebral edema.

CVA- complication of cyanotic congenital heart disease.
TOF, TGA- common.
Mech : Arterial thrombosis, venous sinus thrombosis, or embolism.
“Any child < 2 yrs with CHD , who has acute onset of neurological
signs- CVA should be considered as primary diagnosis ‘’
After 2 yrs , Brain abscess most common.
Embolic strokes- children with cyanotic congenital heart disease- R-L
shunt bypasses lungs, which normally filter small emboli.

Bacterial endocarditis- congenital heart disease & Rheumatic heart
disease- potential sources of emboli.
Thrombi can form on prosthetic cardiac valves- imp. cause of cerebral
emboli.
Hematologic & Neoplastic diseases
Sickle cell anemia (SCA)
most common Hemoglobinopathy assoc. with CVA.
Stroke in children <19 yrs of age with SCA- 8 %.
Incidence- 700 per 1 lakh children with SCA.
Stroke in SCA- large vessel disease, venous occlusion, subarachnoid or
intracerebral hemorrhage.
Neuroimaging- occlusion of large cerebral vessels or watershed infarction
secondary to disease of large vessels.
Fewer shows isolated subcortical or small cortical branch occlusion.

Neuro pathological examn. confirm infarctions in area supplied by anterior-
middle cerebral artery & thrombi in distal cervical & proximal intracranial
carotid arteries.
Strokes in children with SCA- highest incidence in 5-10 yrs.
Hemiparesis- most common symptom.
Aphasia- 20 %, Seizures- 15 %, TIA- 10 %
Persistent neurologic deficits & neuro psychologic abnorm.
Children with HBSS or SB thalassemia- highest incidence of stroke-
monitor with trans cranial USG.
Blood transfusion & exchange transfusion- standard mode of treatment of
acute stroke in SCA.
Periodic blood transfusions- decrease productions of sickle cells- reduce
recurrence of strokes by 90 %.
Intracranial hemorrhage- serious complication of any bleeding disorder.
Intracerebral, subarachnoid, subdural, intra spinal hemorrhage.
Symptoms- headache, seizures, depressed state of consciousness.
Intra spinal hemorrhages- weakness, back pain.

Hemophilia
Bleeding occurs in 25 %.
Bleeding more common in factor IX deficiency.
Intra cranial Hemorrhage common in children <18 yrs, esp. <3yrs.
Serious permanent deficit- 50 %, mortality- 35 %.
Complications of labour or delivery produce intracranial hemorrhage in
newborns with hemophilia.
Treatment- replace deficient clotting factors- performed prophylactically
after h/o head trauma.

Homozygous deficiency of Protein C in newborns- purpura fulminans & venous thrombosis- thrombosis of cerebral veins.
Strokes –significantly reduced levels of protein C.
ITP- major intracranial hemorrhage can occur.
Subdural, intra parenchymal, intra ventricular hemorrhage- infants b/w 2 weeks & 6/12- Vitamin K deficiency.
Hemolytic uremic syndrome- seizures, depressed consciousness, subarachnoid hemorrhage, hemiparesis, thrombotic strokes.

Leukemia
Intracranial hemorrhage- 20%.
Intracranial bleeding occurs in acute stage of leukemia with extremely
elevated high leukocyte count.
Intracerebral or extra cerebral hemorrhage- results from increased blood
viscosity.
Multiple small thrombi, damage to blood vessels.
Children with high leukocyte count- develop dural sinus occlusion with
increased intracranial pressure & headache.
CVA also occur after bone marrow transplantation.

Infectious diseases
Acute bacterial meningitis- treatment delayed- infectious arteritis-
multiple areas of arterial narrowing & occlusion.
Occlusion of veins or dural sinuses- complication of meningitis & follow
otitis media, mastoiditis, sinusitis & infection of scalp & face.
Clinical picture- convulsions, coma, changing neurologic signs, nuchal
rigidity, signs of infection.
Otitis media & mastoiditis- cause lateral sinus thrombosis associated
with abducens palsy & increased intracranial pressure.
Facial skin & para nasal sinus infections- produce cavernous sinus
thrombosis with proptosis, conjunctival reddening, retinal hemorrhages &
extra ocular palsies.
Retropharyngeal abscess- produces compression or thrombosis of
carotid artery.
Post varicella angiopathy, mycoplasma pneumonia, borrelia-burgdorferi,
chlamydia pneumonia, HIV, helicobactor pylori, hemolysing streptococci-
predisposition for stroke.
Cranial infections
Stroke common sequel of Severe meningitis- H. Influenza, Pneumococcal,
Tuberculous meningitis.
Purulent material around basal cisterns & orbito frontal area, circle of
Willis- envelops small arteries & veins- vasculitis & thrombus.
Collagen vascular disease & Vasculitis
SLE- 40% of patients have neurologic abnormalities- psychiatric,
behavioral abnormalities & focal neurologic signs.
HSP- headaches, mental status changes, seizures, focal neurologic
deficits, involvement of peripheral nerves.
Kawasaki disease- aseptic meningitis, hemiparesis.

Metabolic disorders
Infants with fever & dehydration- primary venous or sinus thrombosis.
C/F- multiple seizures, changing neurological signs, convulsions, coma,
increased intracranial pressure.
Hypernatremic dehydration- seizures, depressed state of
consciousness.
Pathology- multiple hemorrhagic lesion in white matter.
Juvenile onset Insulin dependent Diabetes mellitus- acute
hemiparesis.

MELAS SYNDROME- epilepsia partialis continua or status epilepticus,
repeated strokes.
MRI- multiple areas of hyper intense signal in cortex & subcortical white
matter, sparing deep white matter.

Trauma & physical agents
Trauma to carotid artery- delayed onset of neurological signs-
thrombosis in vessel & extension into cerebral vessels.
Severe cerebral edema- death.
Permanent neurological residua- seizures & neuropsychological deficits.
Children- falling on stick held in mouth, lolli pop injury .

External trauma to carotid artery- hematoma on lateral portion of neck,
Horners syndrome, TIA followed by lucid interval –then sudden onset of
hemiplegia or hemiparesis.
Bone abnormalities of upper cervical spine & odontoid, trauma to cervical
spine- sudden twisting or jerking of head- injure carotid or vertebral
arteries.
Basilar skull fracture can cause laceration of carotid artery at foramen
magnum- severe bleeding from mouth & ipsilateral ear.
Radiation & chemotherapy.

Vascular malformations
Arteriovenous malformations
4 types of vascular malformations- Arteriovenous malformations, venous
angioma, capillary telangiectasias, cavernous angioma.
Admixture of normal & abnormal blood vessels.
Surrounding brain contains areas of fibrosis, inflammation, glotic changes,
calcification.
Seizures- common clinical abnormality than hemorrhage.
Subarachnoid, intraparenchymal, or combined can occur.
Intracerebral hematoma- focal neurological signs & increased intracranial
pressure.
Subarachnoid hemorrhage- sudden onset of headache, meningeal signs.
Vascular malformations may be located in cerebellum & brainstem.
50 % of children with intracranial arteriovenous malformations have bruits
heard over head.
“A cranial bruit heard in an infant younger than 4 months of age ,
even in the presence of loud cardiac murmur , is always assoc. with
intracranial arteriovenous malformation” (Cohen and Levin 1978)

CT with contrast, MRI, Arteriography.
RX- surgical accessibility of lesion.
Total surgical excision is curative, but best approach to treatment ??
Embolization of lesion may be effective.
Stereotactic radiosurgery with linear accelerator – effective modality for
some patients.
Vein of Galen malformations
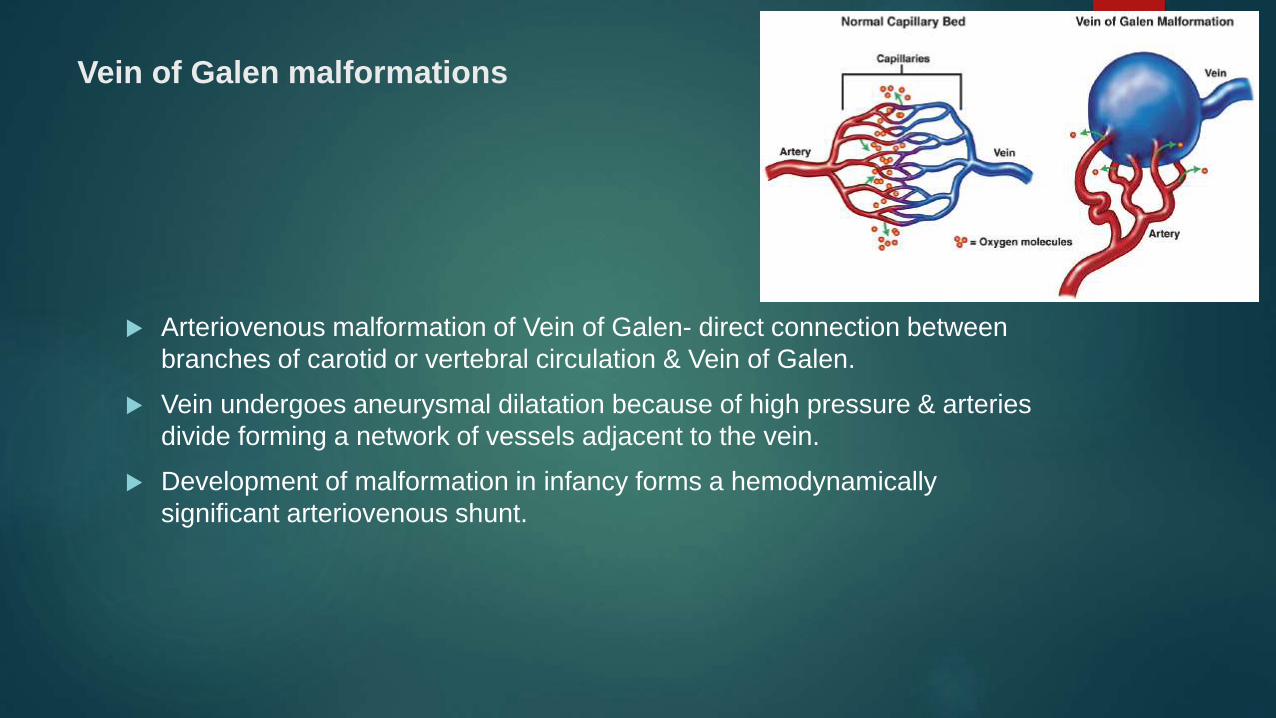
Arteriovenous malformation of Vein of Galen- direct connection between
branches of carotid or vertebral circulation & Vein of Galen.
Vein undergoes aneurysmal dilatation because of high pressure & arteries
divide forming a network of vessels adjacent to the vein.
Development of malformation in infancy forms a hemodynamically
significant arteriovenous shunt.

Neonatal period- signs & symptoms of high output congestive heart failure.
Children- systolic heart murmur, cranial bruit, cardiomegaly, hepatomegaly, tachycardia, respiratory distress, & pulmonary edema.
Death – cardiac failure.
Presentation in later infancy- Hydrocephalus, Subarachnoid hemorrhage.
Dilated veins over scalp, intracranial bruits.
Poor prognosis- death from hemorrhage, increased intracranial pressure or cardiac failure.
Presentation in later life- Headache, signs of intracranial hemorrhage-
convulsions & focal neurological signs.
Signs of brain stem dysfunction & raised intracranial pressure.
Calcification within malformation on CT scan.
Arteriography- diagnostic.
RX- difficult- location, surrounding network of blood vessels, poor
cardiovascular status of pt.
Microsurgical techniques & staged surgical procedures.
Embolization effective in some.
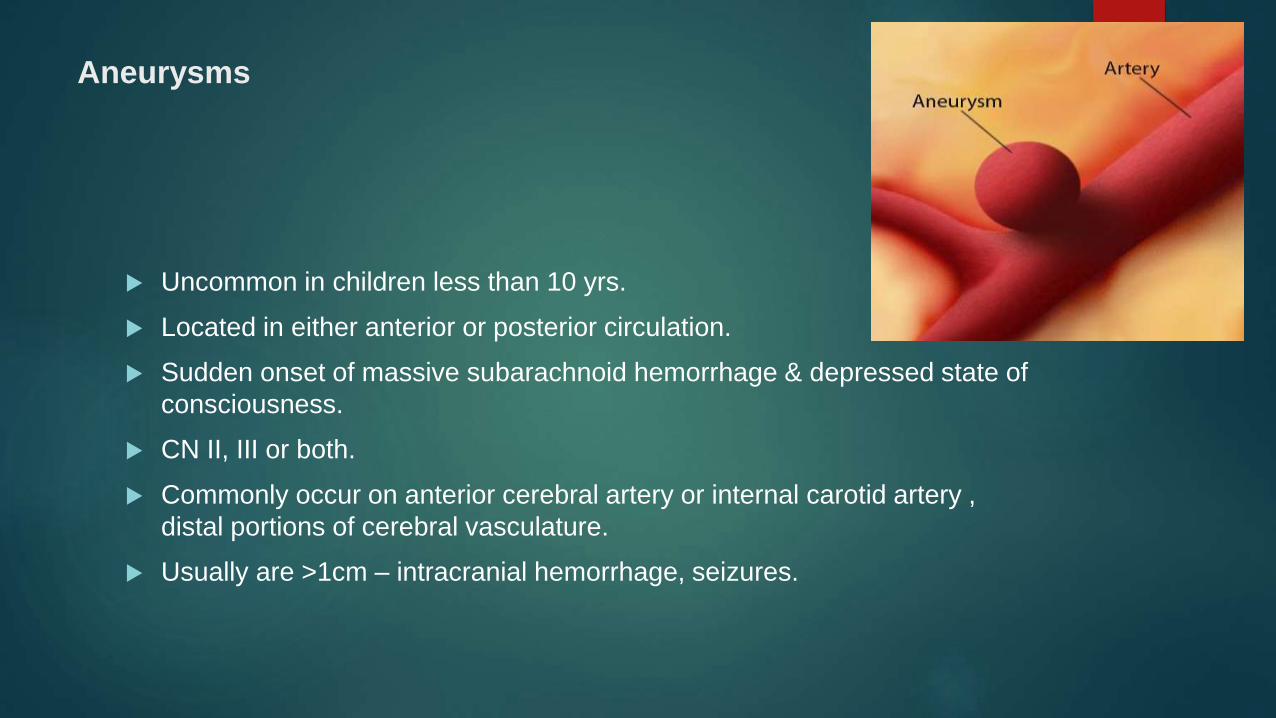
Aneurysms
Uncommon in children less than 10 yrs.
Located in either anterior or posterior circulation.
Sudden onset of massive subarachnoid hemorrhage & depressed state of
consciousness.
CN II, III or both.
Commonly occur on anterior cerebral artery or internal carotid artery ,
distal portions of cerebral vasculature.
Usually are >1cm – intracranial hemorrhage, seizures.

Ruptured Berry Aneurysm- saccular aneurysm, common form of
cerebral aneurysm.

Surgery, microsurgical techniques- definitive RX for aneurysms.
Aneurysm not removed- 50 % will bleed- serious neurological deficits.
Mycotic aneurysms- bleeding.
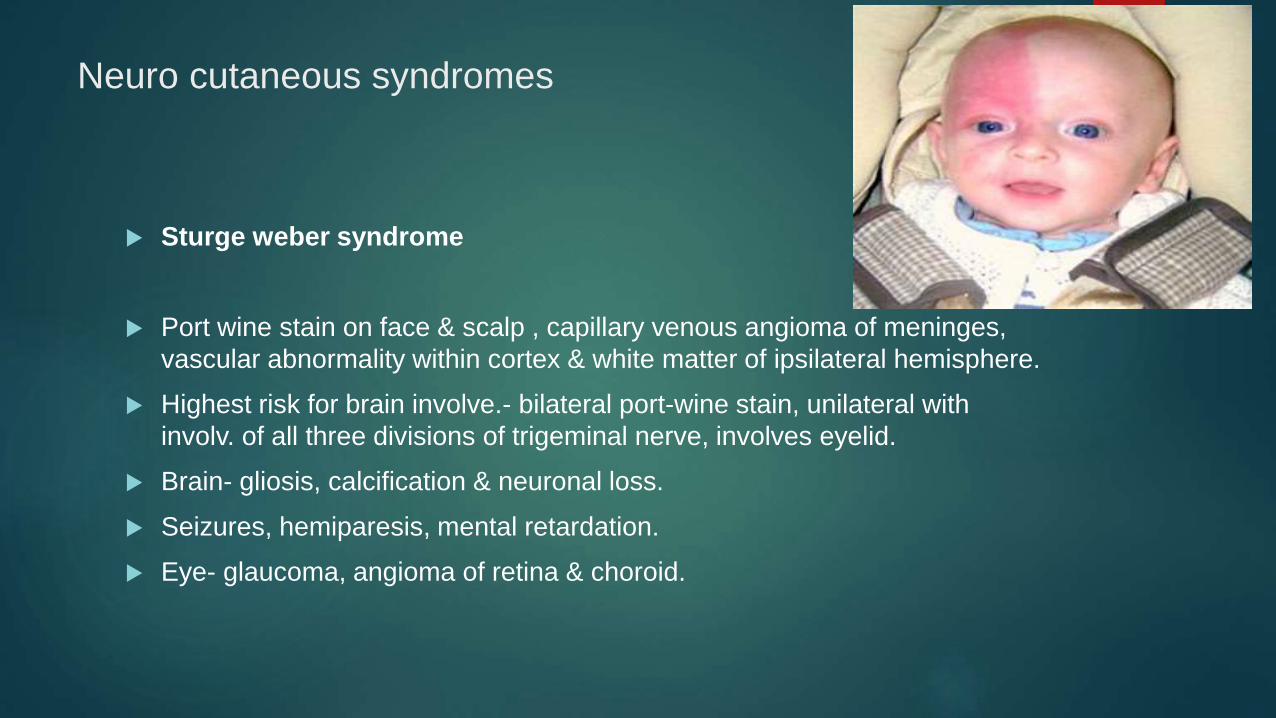
Neuro cutaneous syndromes
Sturge weber syndrome
Port wine stain on face & scalp , capillary venous angioma of meninges,
vascular abnormality within cortex & white matter of ipsilateral hemisphere.
Highest risk for brain involve.- bilateral port-wine stain, unilateral with
involv. of all three divisions of trigeminal nerve, involves eyelid.
Brain- gliosis, calcification & neuronal loss.
Seizures, hemiparesis, mental retardation.
Eye- glaucoma, angioma of retina & choroid.

Progressive abnormalities with areas of calcification, intractable seizures,
intellectual & behavioural deterioration.
Abnormalities of regional cerebral blood flow & progressive cerebral
atrophy.
Early excision of abnormal areas of cortex.
Affected area is large- hemispherectomy.
Lasers- reduce or eliminate port-wine stain.
Dural venous sinus thrombosis
Venous sinuses- major pathway for drainage of intracranial circulation.
Significant proportion of CSF drains into sagittal sinus through pacchionian
granulations.
Thrombosis of major venous sinuses causes increased intracranial
pressure by impeding venous outflow & interfering with resorption of CSF.

Sagital sinus thrombosis
Sagital sinus drains vast majority of cortical veins over brain convexity.
Partial or complete.
Occlusion of sagittal sinus causes stasis & thrombosis in connecting
cortical veins- assoc. hemorrhage over brain surface.
Common in children under 3 yrs, often during first year of life.
Thrombosis extends into cortical veins- rapidly increasing intracranial
pressure, changes in level of consciousness, seizures, focal motor
impairment.
Septic venous sinus thrombosis- most common in neonates.
Spinal fluid resorption impaired-compromise of spinal flow between
arachnoidal granulations & blood in sinus-communicating hydrocephalus.
Venous stasis promotes vascular congestion of brain parenchyma-
increase in intracranial pressure.
Sagital sinus thrombosis-distension of veins over scalp & superior
forehead.

Occlusion of sagittal sinus in older children- syndrome of pseudo tumor
cerebri , headache, CN 6 palsy- false localizing sign, papilledema, visual
loss.
Good prognosis.
Predisposing factors leading to sagittal sinus thrombosis- dehydration,
malnutrition, debilitating d/s, febrile illness, congenital heart disease,
hypercoagulable states.
Spinal fluid studies-normal in early course, later xanthochromic or flankly
blood with increased protein concn.

CT scan- increased density within sinuses-diagnosis of venous sinus
thrombosis. Superficial hemorrhage & cerebral edema.
Delta sign- CT scan with contrast shows enhancement around thrombotic
sinus.
MRA- flow void- thrombosis in the area of sinus.
Conventional angiogram- venous phase of study well documented.
No role for anticoagulant therapy.
Interventional thrombolytic therapy- useful in some.
RX for raised intracranial tension.

Lateral sinus thrombosis
Clinical- seizures, increased intracranial tension, decreased level of
consciousness.
Predisposing factors- otitis media, mastoiditis.
Otitic hydrocephalus- when otitis media & mastoiditis led to lateral sinus
thrombosis & increased intracranial pressure.
Vigorus RX for otitis media & mastoiditis, surgical intervention?

Cavernous sinus thrombosis
Cavernous sinus- CN 3, 4, 6, ophthalmic division of CN5, internal carotid
artery.
Rupture of artery- massive arteriovenous shunt with proptosis, bruit,
involve. of CNs.
Internal carotid artery becomes thrombosed in segment- cavernous sinus-
massive hemispherical infarction.
Predisposing factors- infection of orbit, paranasal sinus, skin of periorbital
& malar areas.

Clinical- conjunctival suffusion- peripheral conjunctival capillaries,
conjunctival edema, retinal edema.
Ptosis- CN 3.
External opthalmoplegia- CN3, 4, 6.
Septic cavernous sinus thrombosis- medical emergency- vigorous
antibiotic therapy.
No role for anticoagulant therapy.

Spinal cord vascular abnormalities
Thrombotic & embolic d/s of spinal cord- rare.
Arteriovenous malformation- back pain, gait abnormalities, bladder &
bowel dysfunction.
Neurological examn.- long tract signs, asymmetric tendon reflexes.
Angioma of skin of back- 20 % accentuated by Valsalva maneuver.
Bruits over spine- rare.
Subarachnoid hemorrhage, no localizing neurological abnorm.
Spinal cord arteriovenous malformation- multiple episodes of subarachnoid
hemorrhage?
High resolution CT or MRI scans- diagnosis.
Selective spinal angiography- outline feeding vessels & extend of
malformation.
Surgical excision possible in many.

History, Physical examination, Clinical presentation

Clinical presentation
Older children : Hemiplegia, Hemi sensory loss, Aphasia &
other neurological deficits.
Younger children : subtle, variable findings, seizure,
early hand preference, limp during walking.

Conditions which mimic stroke
Todds paralysis ( Transient post ictal hemiparesis )
Hemiplegic migraine
Syndrome of alternating hemiplegia
ICSOL ( Intracranial space occupying lesion )
Acute disseminated encephalomyelitis
History & Physical examination
H/O ear, throat, mastoid infection.
H/O intra oral or neck trauma.
H/O cardiac d/s.
H/O Hematological disorders.
H/O multifocal seizures, raised intracranial pressure, vomiting- ? Superior
sagittal sinus thrombosis.
H/O Hemiparesis & seizures in first two years of life- ?
Arterial occlusions.

Localization of Hemiplegia
1. Hemispheric lesion
a. Cortex - cortical features like seizures, dysplasia.
motor deficits are minimum.
Cortical type of sensory loss - Parietal lobe function-
( loss of tactile localization, 2 point discrimination,
stereognosis, graphaesthesia, sensory inattention ).
b. Corona radiata - absence of cortical features
motor deficits- unequal weakness of limbs on
C/L side. Either UL>LL or LL>UL.
Dulling of Primary modalities of sensation- touch,
superficial pain, temperature.

c. Internal capsule : C/L hemiplegia, uniform weakness of limbs on
C/L side, dulling of primary modalities of
sensation-touch, superficial pain, temperature.
Homonymous hemianopia
2. Brain stem : Crossed hemiplegia
I/L LMN cranial nerve palsy
C/L hemiplegia
Brain stem
a. Midbrain : Weber syndrome : I/L 3rd CN & 4th CN palsy,
C/L hemiplegia.
b. Pons : Millard Gubler syndrome : I/L 6th CN & 7th CN palsy,
C/L hemiplegia.
c. Medulla : C/L hemiplegia , I/L CN involv.

Diagnostic Approach
Confirmation of presence of Cerebrovascular lesion.
Exclude other causes of neurological dysfunction.
Etiology of stroke

Evaluation of child with Stroke
Standard Evaluation
CT scan (plain)
If CT scan is normal , MRI scan (plain)
Ischemic Stroke-Investg.
ECG, CXR, Echocardiography
Carotid Doppler studies
Hematological studies
CBC, Platelet count, ESR.
Liver & Renal function test.
Lumbar puncture.
Imaging studies
Magnetic resonance angiography (MRA).
Digital subtraction angiography (DSA).
Collagen vascular screen
PT, APTT.
Protein C, Protein S, Antithrombin 111.
Others- VDRL, HIV, Urinalysis, Lactate/Pyruvate levels, Homocysteine
Urinary & blood aminoacids/ organic acids

Hemorrhagic stroke
CBC, Platelet count, clotting factors.
LFT.
Imaging studies.

Treatment
Arterial Ischemic Stroke
No randomized control trial on children with AIS.
Treatment primary directed towards stabilizing systemic factors &
management of underlying causes.
Supportive care
Manage raised intracranial pressure, blood pressure & fluid balance.
Blood glucose carefully monitored-Hyperglycemia exacerbate infarct size.
Maintain normal body temperature.
Aggressive antiepileptic treatment.
Antithrombotic therapies
Use of anticoagulant therapy increasing in pediatric AIS.
Avoid anticoagulation in hemorrhage, hypertension, or bleeding diathesis.
Heparin
Use anticoagulation in children at high risk of recurrence/extension of
thromboembolic stroke & who are at minimum risk of secondary
hemorrhage.

Loading dose of Heparin 75-100 U/kg iv over 10 min followed by initial
maintenance dose of 28 U/kg/hr in children>1yr & 18 U/kg/hr in
older children.
Adjust Heparin dose to maintain APTT in range of 60-85 sec.
Low molecular weight Heparin
Greater safety & efficacy.
Monitoring done-Antifactor Xa assay once weekly or monthly.
SVT in infants- LMW Heparin for 7-14 days followed by Coumadin for 3/12.

Antiplatelet agents
Traditional role of aspirin in prevention of recurrence after TIA or ischemic
stroke.
Adults-Aspirin reduces stroke by 25 %.
Clopidogrel-no control trials, but may be good choice.
Dose-3-5 mg/kg/day.

Oral anticoagulation
Warfarin used for secondary prevention of stroke if aspirin fails.
Congenital or acquired heart disease
Severe hypercoagulable states
Arterial dissection
Recurrent AIS or TIA while on aspirin.

Thrombolytic agents
Tissue plasminogen activator
Urokinase
Streptokinase
Dissolve the existing thrombus & recanalise the occluded vessel.
Non thrombotic therapies
Transfusion therapy
Neuroprotective agents
Immunosuppressants

Surgical evacuation of hematomas, insertion of ventricular or
lumboperitoneal shunts & rarely revascularization procedures.
Revascularization procedures like Encephalo duroarterio synangiosis
(EDAS) or Pirl Synangiosis- important in treatment of moya moya
disease.
Rehabilitation therapy
Speech therapy
Occupational therapy
Physical & psychological therapy

Summary
Stroke in children relatively rare.
There are fundamental, etiologic & developmental differences in children
compared with adults .
Multiple causes for stroke in children & many risk factors.
Ischemic stroke-interruption of blood flow of arterial or thrombotic d/s.
Hemorrhagic stroke-rupture of blood vessels with bleeding into cerebral
parenchyma.
Hemorrhagic stroke higher mortality than ischemic stroke.
Bibliography
1. Adam K, Gabrielle D. Pediatric stroke syndromes. Nelson textbook of Pediatrics.19th edition;2080-2086.
2. Gerald SG, Keeneth FS. Pediatric Neurology. Edition; 787-803.
3. Veena K. Stroke in the children. 2nd edition;239-246.
4. Gerald MF. Clinical Pediatric Neurology.6th edition; 249-265.
5. Vishram S. Textbook of Clinical Neuro anatomy.3rd edition; 230-249.
6. Amlie LC, Sebire G, Fullerton HJ. Recent developments in childhood arterial ischemic stroke. Lancet Neurol 2010;7:425-435.
7. Benseler SM, Silverman E, Aviv RI etal. Primary central nervous system vasculitis in children. Arthritis Rheum 2011; 54:1291-1297.

8. Birnbaum J, Hellmann DB. Primary angitis of the central nervous
system. Arch Neurol.2008;66:704-709.
9. Danchaivijitr CT, Saunders DE etal. Evolution of cerebral arteriopathies
in childhood arterial ischemic stroke.2006;59:620-626.
10. Chollet F, Tardy J etal. Fluoxitine for motor recovery after acute
ischemic stroke (FLAME): a randomized placebo controlled trial. Lancet
Neurol.2011;10:123-130.

Related Documents











