Pediatric Spinal trauma Prof. Pia C Sundgren MD, PhD Diagnostic Centre for Imaging and Functional Medicine, University of Lund, UMAS, Malmoe, Sweden Department of Radiology, University of Michigan Health Systems, Ann Arbor, USA

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Pediatric Spinal trauma
Prof. Pia C Sundgren MD, PhDDiagnostic Centre for Imaging and Functional Medicine, University of Lund, UMAS, Malmoe, Sweden
Department of Radiology, University of Michigan Health Systems, Ann Arbor, USA

injury to the spinal column and spinal cord is a major cause of disability affecting predominatelyyoung healthy individuals
costs of life time care and rehabilitation are extremely high, often over $1,000,000 per individual
spinal cord injuries are rare in infants and children (1-2% of pediatric trauma victims)
Introduction
PC Sundgren Pediatric Spine Trauma Spineradiology´09
Relatore�
Note di presentazione�
läs text slide With the frame of one 30 minutes lecutre it is impossible to present the complete panorama of spinal injury. Insteed I will focus on the three following aspects the technical aspects of imaging and the importance of preset protocols, the possibility of multi-level and complex or combined injuries and finally. I will emphasize to actively search for ligamentous injuries and the possiblity of instability.that might not be obvious at first glance.�

Cause < 3 years2 1-20 years1 overall
Motor vehicle 66% 44% 47.7%
Fall 15% 14% 20.8%
Pedestrian 11%
Bicycle 6%
Violence 14.6%
Sports 16% 14.2%
Spinal trauma and spinal cord injury
1Kokoska E et al. Characteristics of pediatric… J. Ped. Surg. 2001:36;100-105 (408 cases (+))2Polk-Williams A et al. Cervical spine injury…. J. Ped. Surg. 2008:43;1718-1721 (1523 cases (+))
PC Sundgren Pediatric Spine Trauma Spineradiology´09
Relatore�
Note di presentazione�
The majority of injuries are caused by MVA followed by fall as violence and different sport activities may result in trauma to the spinal colum and cord injury�
Spinal trauma and spinal cord injury
<10 years of age 50% in C1-C2 (-C4) region
incidence of dislocations
incidence of cord injuries
> 10 years of age shift towards C5 and below
C-spine fractures
Mortality rates 17% (overall) higher in small children
1Kokoska E et al. Characteristics of pediatric… J. Ped. Surg. 2001:36;100-105 (408 cases (+))PC Sundgren Pediatric Spine Trauma Spineradiology´09
Spinal trauma and spinal cord injury
2Polk-Williams A et al. Cervical spine injury…. J. Ped. Surg. 2008:43;1718-1721 (1523 cases (+))
Children < 3years of age
• injury to upper cervical spine C1-C4
47% cord injuries and 53.4% spine fractures
• injury to lower cervical spine C5-C7
53% cord injuries and 46.6% fractures
• most common sites:C2 (26.5%) followed by C7 (18.5%)
PC Sundgren Pediatric Spine Trauma Spineradiology´09
Misdiagnosis of acute cervical spine injuries
< 8 years of age 24%> 9 years of age 15%
Most common site of diagnostic errorocciput to C2 region
Predisposing factors for misdiagnosis:• unfamiliarity with pediatric cervical spine anatomy• not recognizing normal variants• suboptimal technique
Avellino AM et al The misdiagnosis of acute cervical spine injuries.. Childs Nerv system2005;21;122-127. (37 cases) PC Sundgren Pediatric Spine Trauma Spineradiology´09

Fracture?
PC Sundgren Pediatric Spine Trauma Spineradiology´09

Pitfall
Motion artefacts
PC Sundgren Pediatric Spine Trauma Spineradiology´09
Relatore�
Note di presentazione�
Fallgrop Översta rörelseartefakter, fraktur?? Nedre: Omkörd CT: Ingen fraktur�
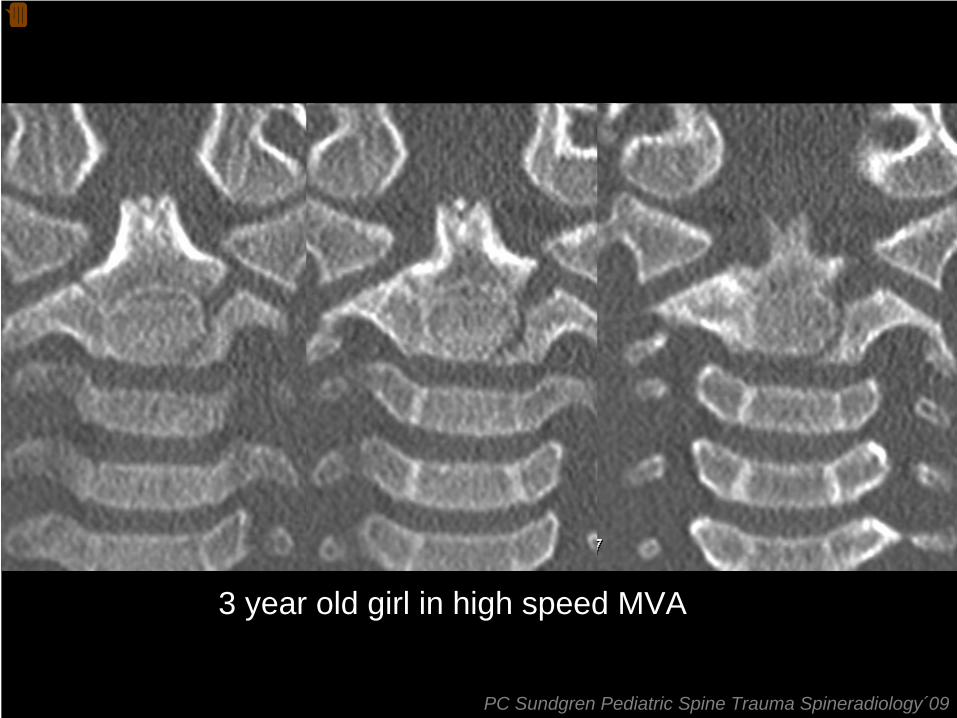
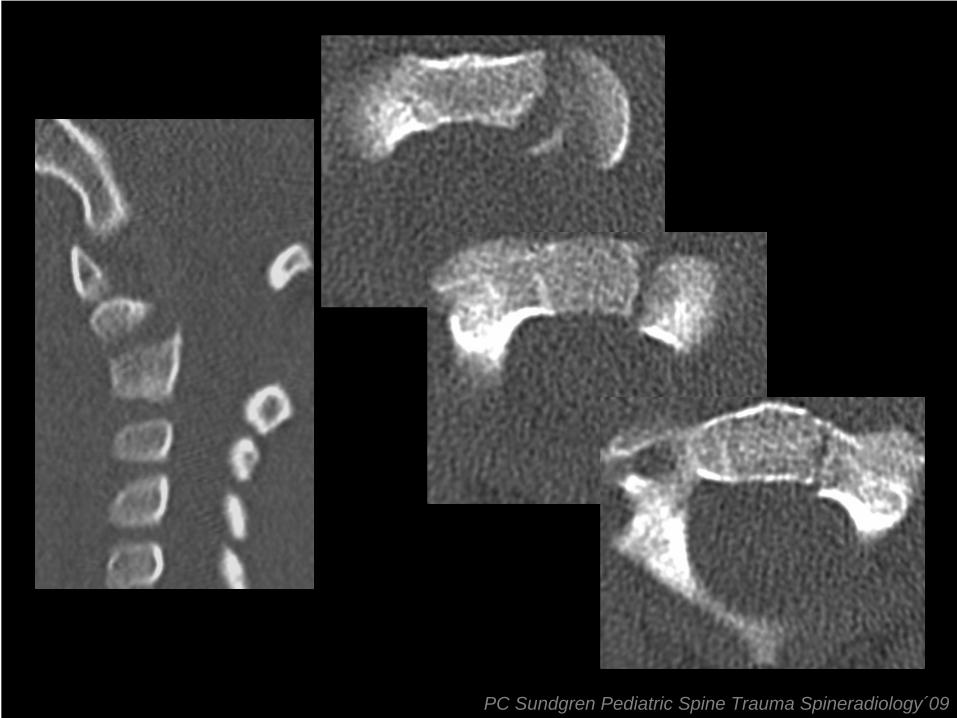
3 year old girl in high speed MVA
PC Sundgren Pediatric Spine Trauma Spineradiology´09
Relatore�
Note di presentazione�
Flicka som varit passagerare i en bil som voltat i känd hastighet. Smärtor i buken som ömmar diffust samt fluktuerande medvetande fraktur på vänster sida med isärsprängning av fysen upp till leden mellan massa lateralis till C1 resp C2. �
PC Sundgren Pediatric Spine Trauma Spineradiology´09

6 month FU the fracture has healed
PC Sundgren Pediatric Spine Trauma Spineradiology´09
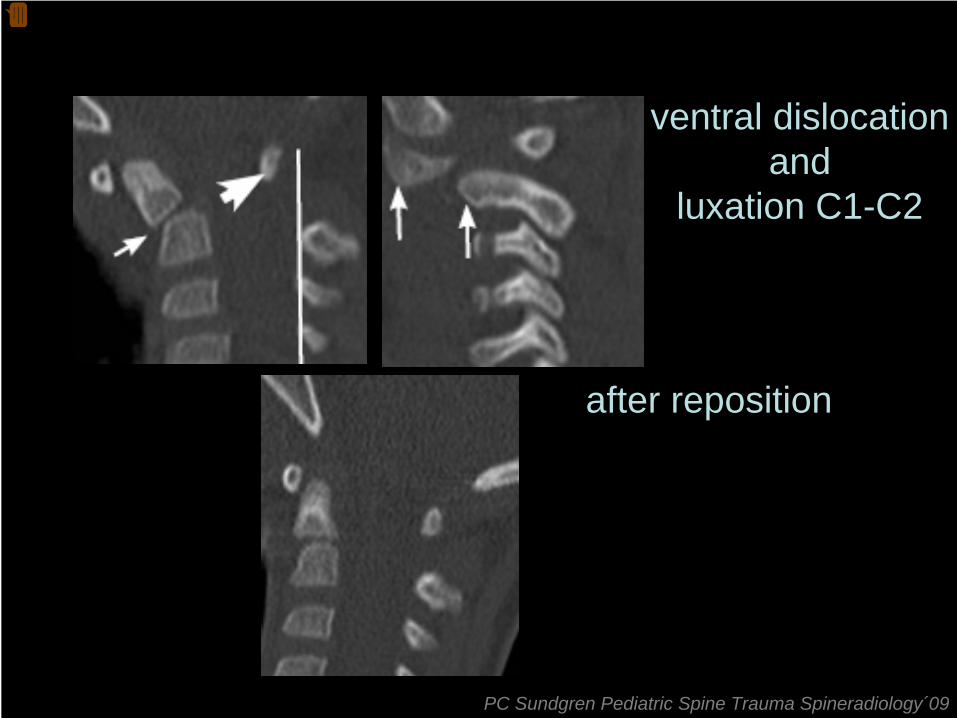
ventral dislocationand
luxation C1-C2
after reposition
PC Sundgren Pediatric Spine Trauma Spineradiology´09
Relatore�
Note di presentazione�
Falltrauma 2 år gammalt barn Fraktur genom synkondrosen av C2 med volar bockning.Luxation mellan C1 och C2 på bild 2. Bild 3 efter reposition i narkos.�

Burst fracture
C7
PC Sundgren Pediatric Spine Trauma Spineradiology´09
Relatore�
Note di presentazione�
CT 17 årig man efter trafikolycka visar två pelarfraktur av burst typ genom C7 MR ung tjej som i berusat tillstånd dykt i en bassäng med grunt vatten Frakturer C4,5,6.�

CT parametersyour choice depends on
• technical specification of the scannersingle slice, helical, multislice
• anatomic regionC1-C2 1-2 mm*C-spine 2-3 mm*T+L-spine <4 mm*
• required detail information• 2D multiplanar reformatting (3D)
* Reconstructed slices, acquisition with sub-millimeter slices (0.6, 0.75…)
PC Sundgren Pediatric Spine Trauma Spineradiology´09
Relatore�
Note di presentazione�
The choice of CT parameters depends on the technial specification of the scanner The anatomic region and and the required detail information The multislice CT (spiral) in high resolution mode with aquiered with submillimeter slices and reconstructed 1.25-2mm thin slices in the C1-C2 region, 3mm thin slices in the rest of the cervical spine and 4mm thin slices in the thoracolumbar spine with 1.5 mm reconstruction interval, for sagittal and coronal reconstructions with bone and soft tissue algorithm is suggested I would like to emphizie the need to have these protocol already preset in the scanner to save time at the ime of examination of these often multitrauma patients �
MR parameters
• sagittal T2 STIR, T2-w, T1-w
• axial T1SE, T2 fast SE,
• axial fat sat T2-w (soft tissue injury)
• axial and sagittal T2* GRE (hemorrhage)
• 3D – ( eg. T2 space (Siemens)
PC Sundgren Pediatric Spine Trauma Spineradiology´09
Relatore�
Note di presentazione�
several of the following imaging fat saturated images are suggested for the MRI trauma proticol again I would like to emphisize the importance of having preset trauma protocol programmed in the scanner. sagittal T2 STIR, T2-w and T1 w images pre and post contrast, axial T1SE, axial T2 fast SE, fat-saturated T2W images for ligamentous and soft tissue injuries, and T2* GRE to evaluate for small hemorrhage or blood products in the spinal cord. 3D faster STIR to see signal abnormaliies in the spine�
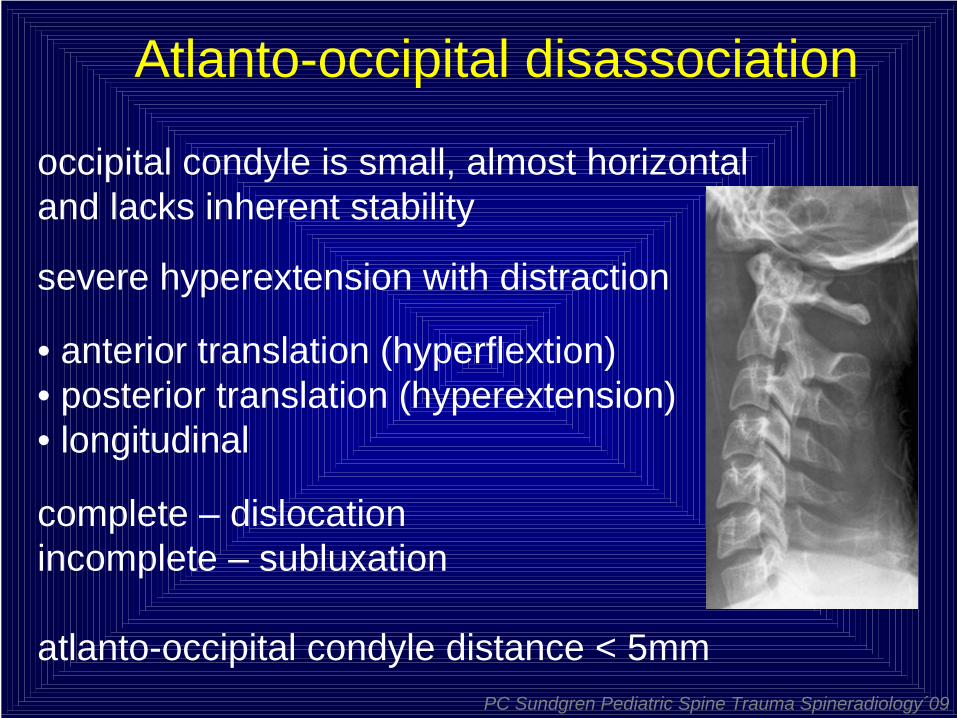
Atlanto-occipital disassociation
occipital condyle is small, almost horizontal and lacks inherent stability
severe hyperextension with distraction
• anterior translation (hyperflextion)• posterior translation (hyperextension)• longitudinal
complete – dislocationincomplete – subluxation
atlanto-occipital condyle distance < 5mmPC Sundgren Pediatric Spine Trauma Spineradiology´09
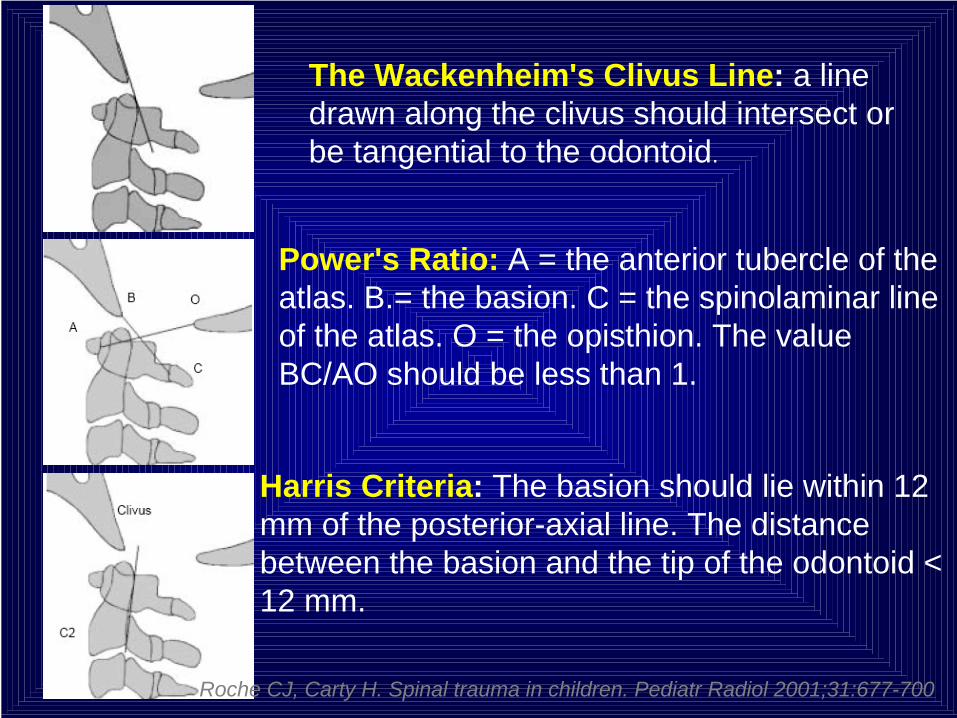
Harris Criteria: The basion should lie within 12 mm of the posterior-axial line. The distance between the basion and the tip of the odontoid < 12 mm.
Power's Ratio: A = the anterior tubercle of the atlas. B.= the basion. C = the spinolaminar line of the atlas. O = the opisthion. The value BC/AO should be less than 1.
The Wackenheim's Clivus Line: a line drawn along the clivus should intersect or be tangential to the odontoid.
Roche CJ, Carty H. Spinal trauma in children. Pediatr Radiol 2001;31:677-700.

2 ½ year-old girl, strapped into a car seat withshoulder harness, facing forward after MVA.
Clinical neurological examination upon admission: child is wide awake,with flaccid tetraparesis
The next day ventilatory assistance is needed
Courtesy Dr P Parizel et al, Antwerp, Belgium PC Sundgren Pediatric Spine Trauma Spineradiology´09
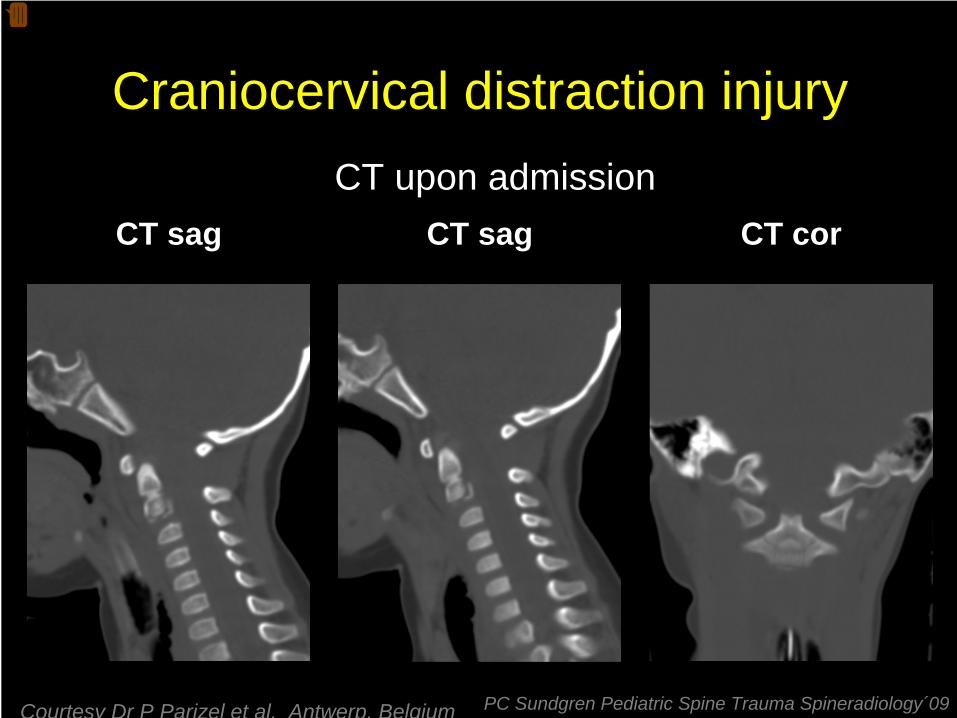
Craniocervical distraction injury
CT sag CT sag CT corCT upon admission
Courtesy Dr P Parizel et al, Antwerp, Belgium PC Sundgren Pediatric Spine Trauma Spineradiology´09
Relatore�
Note di presentazione�
C1-C2 distraction trauma with spinal cord disruption and intramedullary hematoma Motorvehicle accident (frontal collision with another car) The patient is a 2 ½ year-old girl, strapped into a car seat with shoulder harness, facing forward Clinical neurological examination upon admission: child is wide awake, with flaccid tetraparesis The next day ventilatory assistance is needed The child is kept in an artificial coma, on a ventilator �

Craniocervical distraction injuryMRI upon admission
T1 sag T2 corT2 sag
Courtesy Dr P Parizel et al, Antwerp, Belgium PC Sundgren Pediatric Spine Trauma Spineradiology´09
Relatore�
Note di presentazione�
Mechanism of injury and findings: Upon impact the head was accelerated anteriorly CT scan upon admission: distraction injury of C1-2, fracture of the ring apophysis of C2, prevertebral hematoma, intra-and perimedullary hemorrhage, rupture of the interspinous ligament posterior to the spinal canal MRI day of admission: cord edema and rupture, …. etc. etc. MRI 1 week later shows an additional distraction injury through the upper endplate of Th1 DTI with fiber trcking: complete cord transsection Supposedly due to this deceleration injury, the craniocervical junction was distracted at C1_C2, with a second axis of rotation through the cervico-thoracic junction, causing a second distraction injury involving the ring apophysis Th1 �

Craniocervical distraction injuryMRI 6 days later
T1 sag T2 corT2 sag
Courtesy Dr P Parizel et al, Antwerp, Belgium PC Sundgren Pediatric Spine Trauma Spineradiology´09
Relatore�
Note di presentazione�
Mechanism of injury and findings: Upon impact the head was accelerated anteriorly CT scan upon admission: distraction injury of C1-2, fracture of the ring apophysis of C2, prevertebral hematoma, intra-and perimedullary hemorrhage, rupture of the interspinous ligament posterior to the spinal canal MRI day of admission: cord edema and rupture, …. etc. etc. MRI 1 week later shows an additional distraction injury through the upper endplate of Th1 DTI with fiber trcking: complete cord transsection Supposedly due to this deceleration injury, the craniocervical junction was distracted at C1_C2, with a second axis of rotation through the cervico-thoracic junction, causing a second distraction injury involving the ring apophysis Th1 �
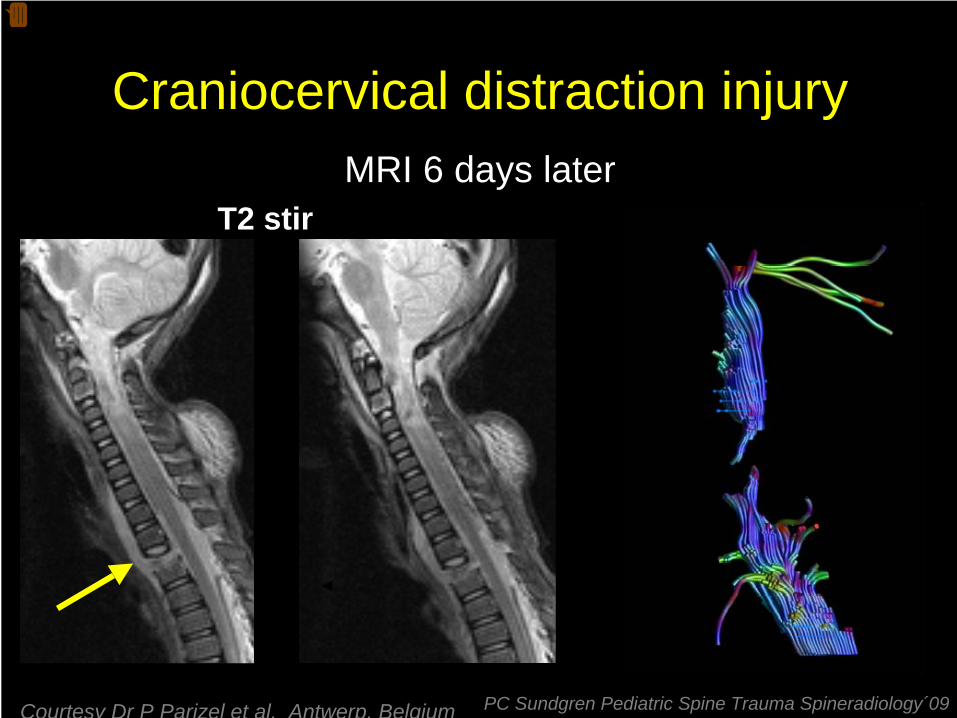
Craniocervical distraction injury
T2 stirMRI 6 days later
Courtesy Dr P Parizel et al, Antwerp, Belgium PC Sundgren Pediatric Spine Trauma Spineradiology´09
Relatore�
Note di presentazione�
Mechanism of injury and findings: Upon impact the head was accelerated anteriorly CT scan upon admission: distraction injury of C1-2, fracture of the ring apophysis of C2, prevertebral hematoma, intra-and perimedullary hemorrhage, rupture of the interspinous ligament posterior to the spinal canal MRI day of admission: cord edema and rupture, …. etc. etc. MRI 1 week later shows an additional distraction injury through the upper endplate of Th1 DTI with fiber trcking: complete cord transsection Supposedly due to this deceleration injury, the craniocervical junction was distracted at C1_C2, with a second axis of rotation through the cervico-thoracic junction, causing a second distraction injury involving the ring apophysis Th1 References: Chang W, Alexander MT, Mirvis SE. AJR Am J Roentgenol. 2009; 192(1): 52-58 Deliganis AV, Baxter AB, Hanson JA, Fisher DJ, Cohen WA, Wilson AJ, Mann FA. Radiographics. 2000; 20 Spec No: S237-250. �
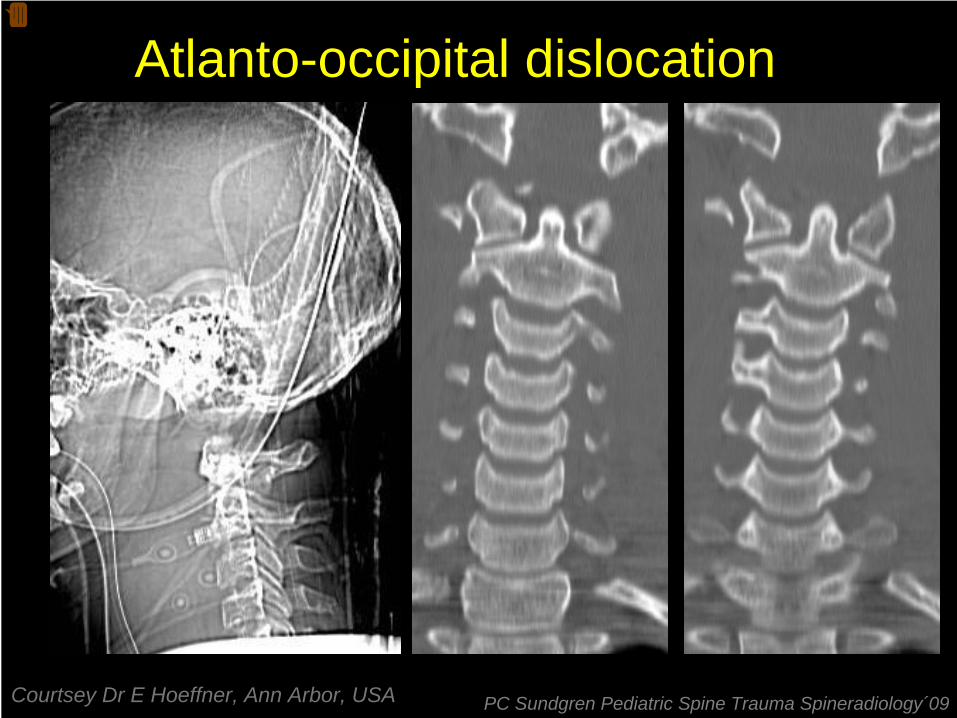
Atlanto-occipital dislocation
Courtsey Dr E Hoeffner, Ann Arbor, USA PC Sundgren Pediatric Spine Trauma Spineradiology´09
Relatore�
Note di presentazione�
Atlanto-occiptal dislocation�

Courtsey Dr E Hoeffner, Ann Arbor, USA
Atlanto-occipital dislocation
PC Sundgren Pediatric Spine Trauma Spineradiology´09
PC Sundgren Pediatric Spine Trauma Spineradiology´09
Relatore�
Note di presentazione�
End ellen hoeffner�

Spinal cord injury without radiographic abnormality- SCIWORA -
Incidence: 19-34% of all spinal cord injuries in children
More common in younger children < 8 years of age
Specific to children and extremely rare in adults
PC Sundgren Pediatric Spine Trauma Spineradiology´09
Spinal cord injury without radiographic abnormality- SCIWORA -
• immature and elastic pediatric spine• vulnerable to external forces• allows for significant inter-segmental movement• transient disc protrusion
compression and stretching of the spinal cord
cord injuryPC Sundgren Pediatric Spine Trauma Spineradiology´09

Normal spine in infants and children
Courtesy Dr M Galluchi, Italy PC Sundgren Pediatric Spine Trauma Spineradiology´09
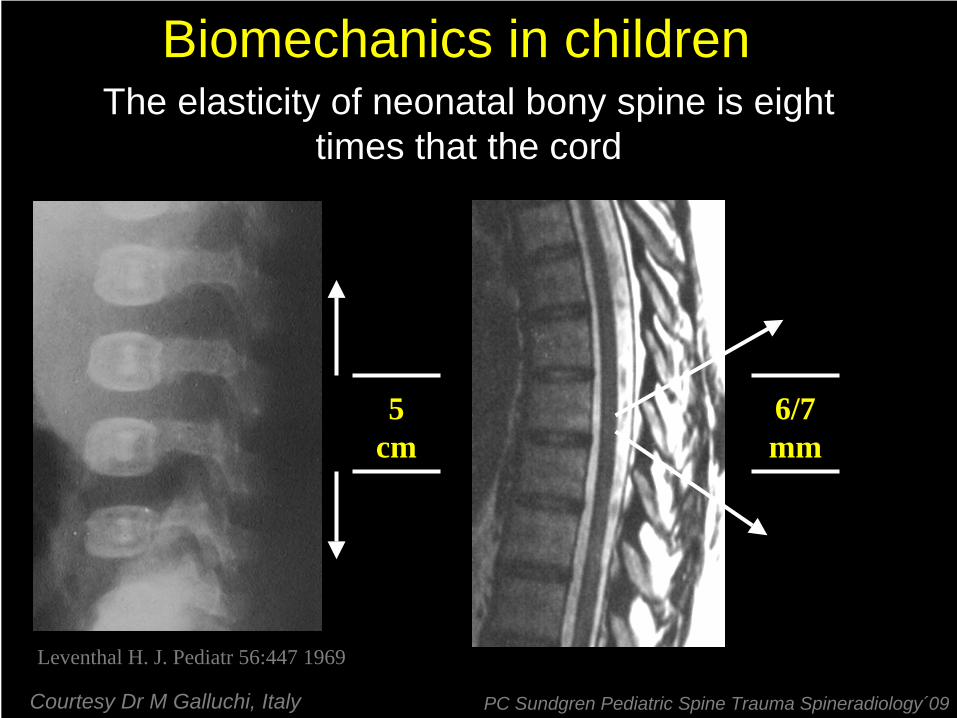
The elasticity of neonatal bony spine is eight times that the cord
Biomechanics in children
5 cm
6/7 mm
Leventhal H. J. Pediatr 56:447 1969
Courtesy Dr M Galluchi, Italy PC Sundgren Pediatric Spine Trauma Spineradiology´09
8 year old boy bound with seat belt, therefore had aflexion trauma in the upper thoracic spine while thelower was immobilized. He became paraplegic
PC Sundgren Pediatric Spine Trauma Spineradiology´09

SCIWORA
Courtesy Dr M Galluchi, Italy PC Sundgren Pediatric Spine Trauma Spineradiology´09
Relatore�
Note di presentazione�
Car accident. 8 yrs old boy, bound with seat belt, therefore had a flexion trauma in the upper thoracic spine while the lower was immobilized. He became paraplegic�

SCIWORA
Courtesy Dr M Galluchi, Italy
Same case 4 month laterPC Sundgren Pediatric Spine Trauma Spineradiology´09
Relatore�
Note di presentazione�
Same case after 4 months. I’m sorry for the quality but it is a quite old case.�

2 year old boy in high speedMVA
Courtsey Dr M Castillo, Chapel Hill,USA
SCIWORA
PC Sundgren Pediatric Spine Trauma Spineradiology´09

14 year old female fell on her head while performing a backward flip at cheer leading
try-out.
Unable to move or breath herself at time of the accident
PC Sundgren Pediatric Spine Trauma Spineradiology´09

CT reformatted images, bone windowscoronal sagittal axial
PC Sundgren Pediatric Spine Trauma Spineradiology´09
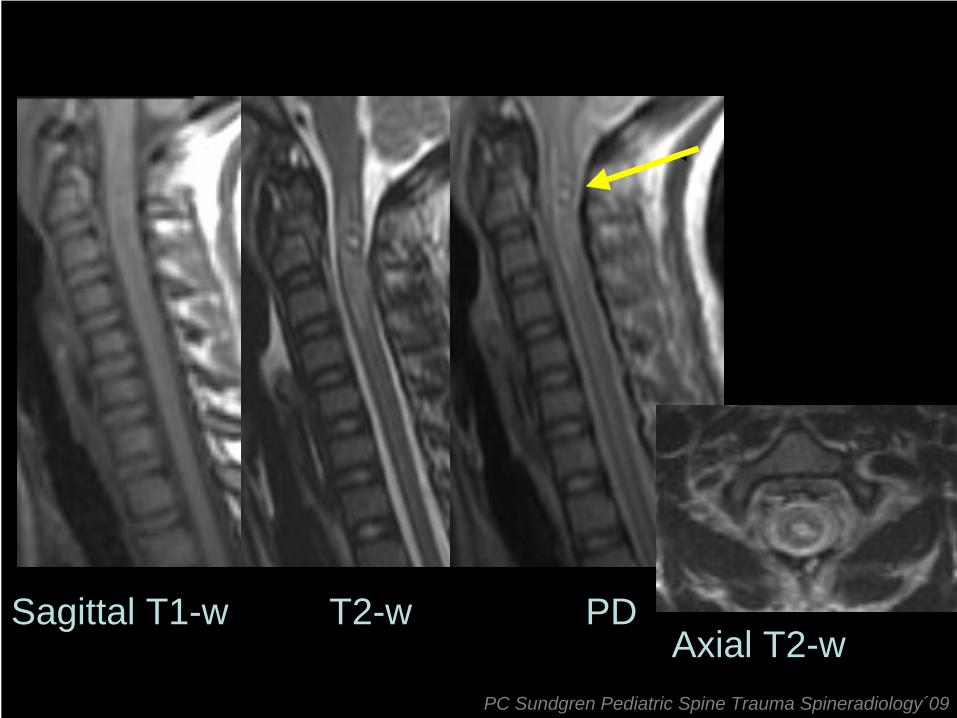
Sagittal T1-w T2-w PDAxial T2-w
PC Sundgren Pediatric Spine Trauma Spineradiology´09

Ligamentous injurytransverse lig.
PC Sundgren Pediatric Spine Trauma Spineradiology´09
Relatore�
Note di presentazione�
Finaly I would like to emphize the nessecitty of actively looking for ligamentous injury that is easy to overlook. The signs are meny ranging from displacement to tears of ligamneous attachments. In particular MRI is very good to both discover and to confirm the supicion made from plain films and CT�
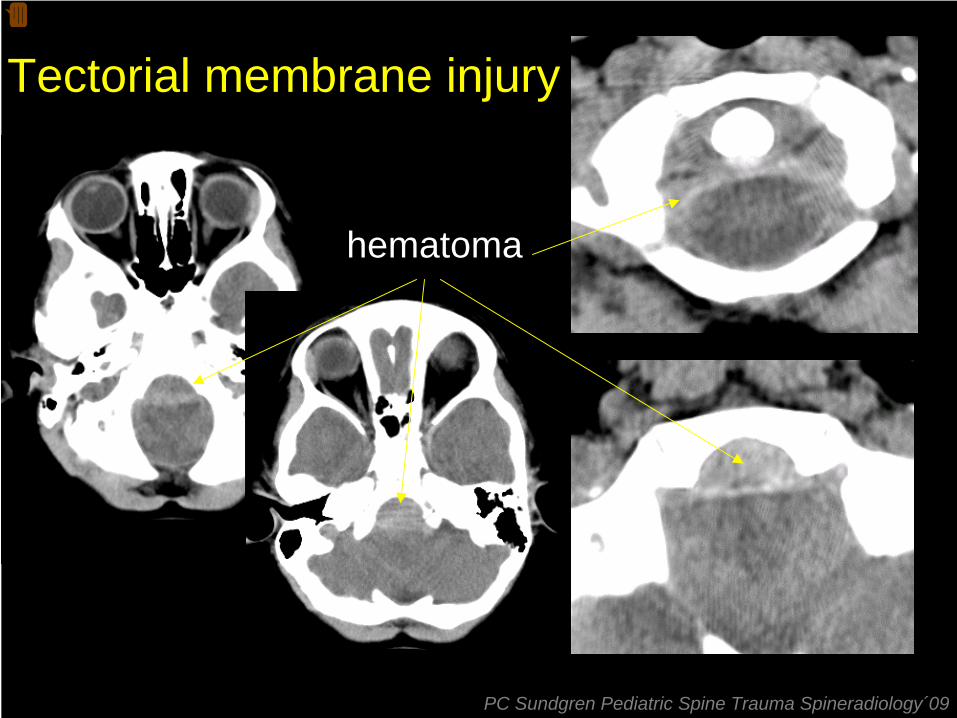
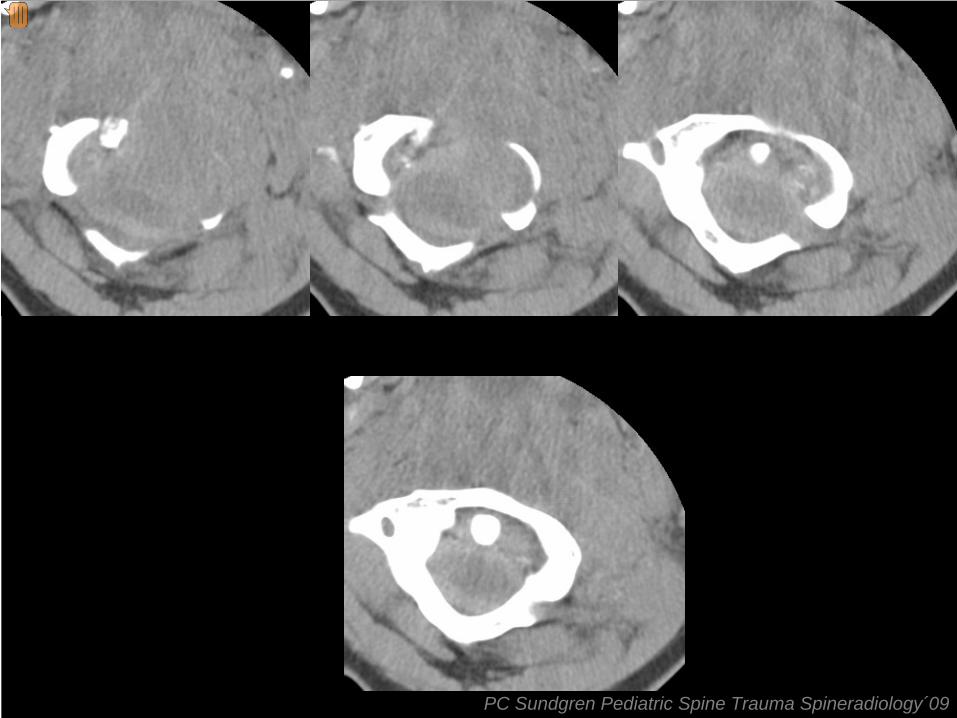
Tectorial membrane injury
hematoma
PC Sundgren Pediatric Spine Trauma Spineradiology´09
Relatore�
Note di presentazione�
I would like to demonstrate this infrequent entity the tectorial membrane injury most commonly seen in children. It can be suspected from careful reading of the CT where we see a unusal hematoma in the low clivus reagion extending to C2 in a 3 year old boy after MVA�

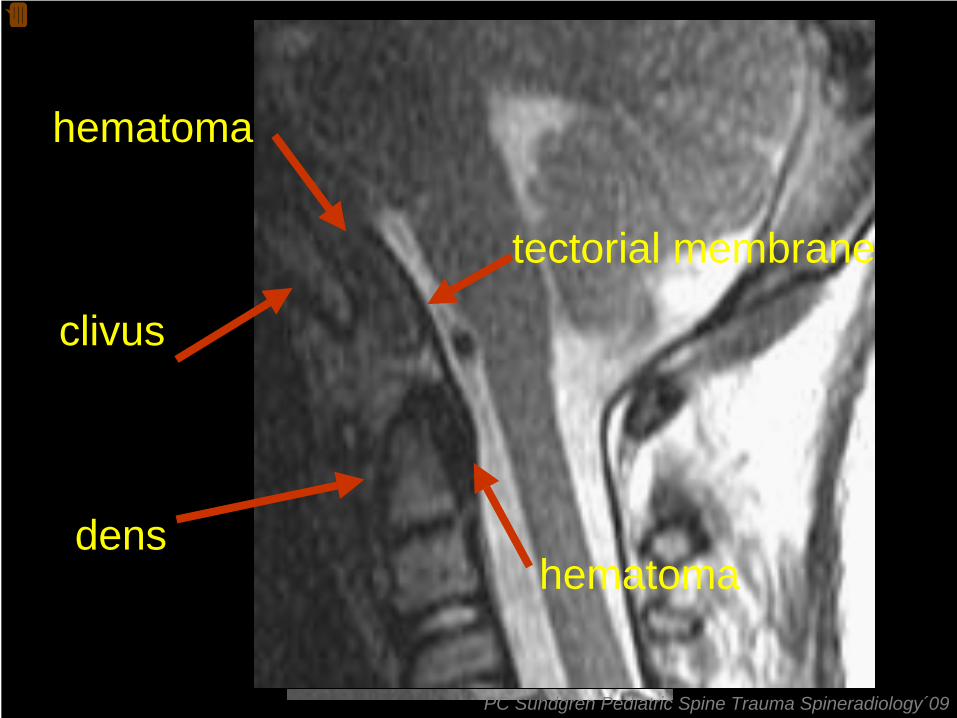
clivus
dens
tectorial membrane
hematoma
hematoma
PC Sundgren Pediatric Spine Trauma Spineradiology´09
Relatore�
Note di presentazione�
Reformatting of these images shows the detached tectorial memebrane and underlying hematoma.�
T2T2
clivus
dens
tectorial membrane
hematoma
hematoma
PC Sundgren Pediatric Spine Trauma Spineradiology´09
Relatore�
Note di presentazione�
MR confirms the diagnosis and shows even better the hemorrhage. CPI #: 32637531 Name: HEANEY, LIAM 3-year-old male, motor vehicle accident, with multiple injuries. Oral and maxillofacial surgery is called to evaluate an intraoral laceration of the upper lip. 3-year-old male, a restrained passenger in the back seat of a van versus other motor vehicle that was hit head-on at approximately 60 miles per hour. The patient was extricated by EMS in full backboard and C spine precautions, and per EMS had decreased level of consciousness en route to this facility. See: Brther Conor with similar AO injury and sister L with normal C-spineThis patient had two new problems which developed today. The first is a very complicated cervical spinal lesion in the C1 region, which may be due to some type of distractive process ligamentous disruption with a hematoma around his spinal cord. Neurosurgery and orthopaedics are carefully involved with this and are following and treating this. A halo device has been placed today for cervical spine stabilization. In addition, a repeat CT scan was done today, which showed free air in the peritoneal cavity and the patient was urgently taken to surgery after the halo was placed, before the patient was extubated, and an exploration of the abdomen was done with sewing of a perforation of his midsmall bowel. The patient was placed on a ventilator postoperatively with excellent saturation and ventilation findings being shown.�

Thank you very much for your attention
PC Sundgren Pediatric Spine Trauma Spineradiology´09
Relatore�
Note di presentazione�
What has this nice image from the backyard of our family summerhouse to do with the severe traumas that I have presented?�

Plexus injury
methemoglobin
Day 4
Day 14
pseudomeningocele
PC Sundgren Pediatric Spine Trauma Spineradiology´09
Relatore�
Note di presentazione�
15 årig pojke efter skidolycka sökt med tecken på plexusskada med engagemang av flera dermatom höger arm. Första raden 4 dagar efter olyckan methemoglobin 10 dagar senare pseudomeningocele�
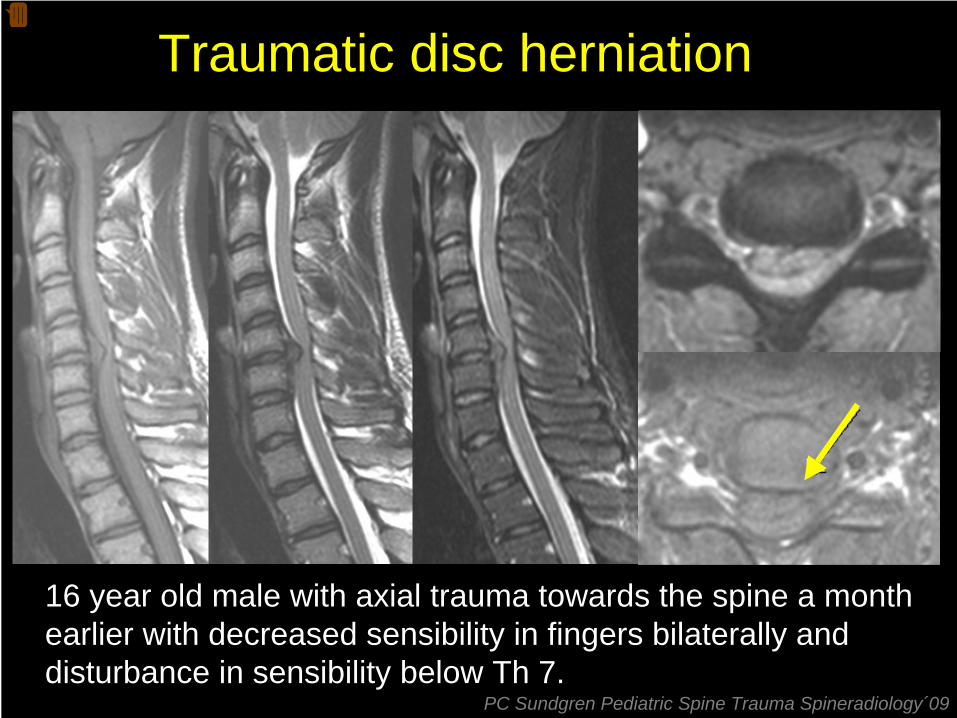
16 year old male with axial trauma towards the spine a monthearlier with decreased sensibility in fingers bilaterally and disturbance in sensibility below Th 7.
Traumatic disc herniation
PC Sundgren Pediatric Spine Trauma Spineradiology´09
Relatore�
Note di presentazione�
våld mot kotpelaren, därefter torticoliis. Rtg �
Related Documents