Pediatric Sedation Pediatric Sedation Cindy Sanders, RN, MSN Cindy Sanders, RN, MSN November 1, 2008 November 1, 2008

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Pediatric SedationPediatric SedationPediatric SedationPediatric Sedation
Cindy Sanders, RN, MSNCindy Sanders, RN, MSNNovember 1, 2008November 1, 2008
Kids are different• Goals for sedation to control behavior to allow
procedure to be completed successfully• Kids under age 5 or 6 (chronologically or
developmentally) may require deep sedation• Anatomical and physiological differences must
be considered• May be more vulnerable to respiratory
depression and may pass into deeper sedation state than was intended
“Rules” are the same• American Academy of Pediatrics,
(AAP) American Society of Anesthesiologists, (ASA) American Academy of Pediatric Dentists (AAPD) and Joint commission on Accrediation of Healthcare Organizations (JCAHO) issued guidelines for pediatric sedation
Safe sedation requirements
– Systematic approach – No administration of sedation with safety
net– Careful focused pre-sedation assessment– Appropriate NPO– Focused airway exam– Clear understanding of meds, interactions,
etc.
Goals of Pediatric Sedation
• Guard Patient safety• Minimize discomfort and pain• Control anxiety, minimize psychological
trauma, maximize amnesia• Control behavior to allow successful
completion of exam• Return patient to a state in which safe
discharge is possible
Who is an infant/ child?• AAP: birth to 21 years• PALS: infant to age 1, child 1yr to
puberty• Some institutions: to age 18
• Chronologic vs. developmental age
The Sedation Continuum
Moderate/conscious
Deep
Mild/conscious/anxiolysis
The sedation continuum
• Must be able to “rescue” patient from next level
• Failure to rescue may be more common in non hospital setting
• Conscious sedation may be an oxymoron for the young peds patient
Regardless of the medication given, the route of administration or the intended level of sedation, the sedation of a pediatric patient may result in respiratory depression and loss of airway protective reflexes
Candidates for pediatric sedation
• ASA class I and II generally good candidates
• ASA II and IV-require consideration, consultation with anesthesia, etc
• Pediatric specific considerations must be evaluated
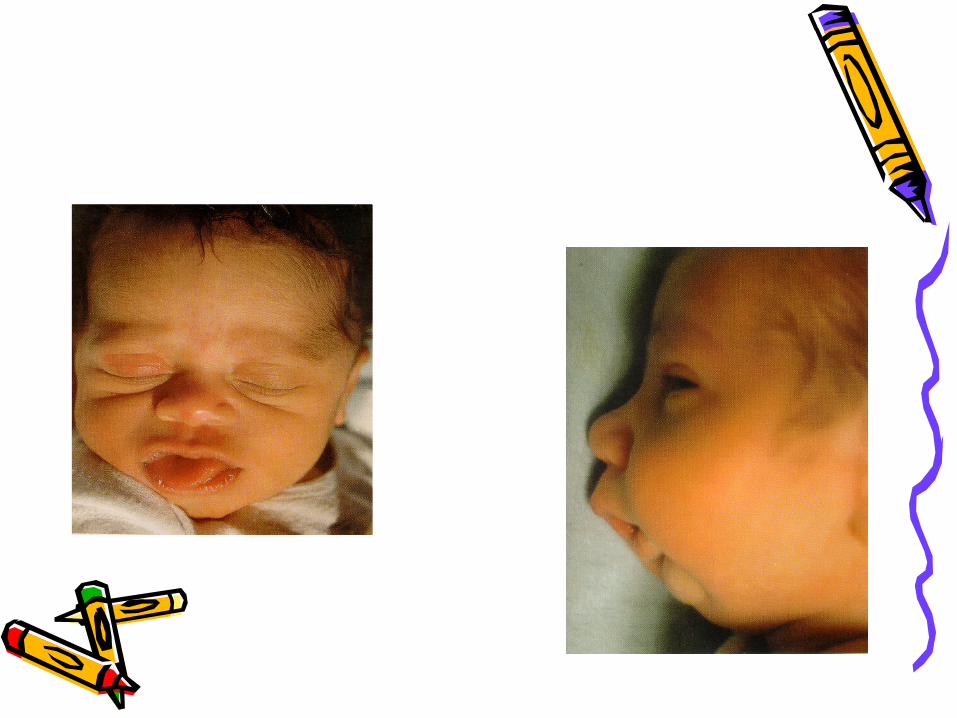
Peds specific risks• Untreated severe GERD (Gastro-
esophageal reflux disease)• Recent apnea monitor/history• Congenital airway anomalies such
as macroglossia, micronathia, etc.• Extreme Tonsillar hypertrophy• Mitochondrial or metabolic disease
Sedation history• Prior sedation history• Medication history/allergies• Significant medical history• Does patient snore• Recent cold, asthma, etc.• NPO status• NPO status• Parent/guardian accompanying child
NPO guidelines• Elective procedures require fasting
guidelines• Risk of aspiration less than with general
anesthesia but absolute risk not known• Generally same guidelines as for general
anesthesia are followed• Solids 6-8 hours, breast milk (considered
semi-solid by some and clear by others-2-4 hours, clears 2 hours
Fluid status• Some patients will have been NPO for 12
or more hours.• May give pre-sedation bolus of 20cc/kg
of isotonic solution like Normal saline• This may decrease the risk of
hypotension and hemodynamic compromise
• May want to leave IV in at procedure end till patient awakens and drinks.
Pre sedation assessment
• Vital signs including heart rate, respirations, b/p, temperature
• Pulse oximetry reading• If using ETCO2 monitoring,
baseline reading• Accurate weight
Pre sedation assessment
• Focused physical exam including respiratory and cardiac rate rhythm and quality
• Renal or hepatic function ok?
• Ability of child to cooperate-is non sedation an option?
• Any contraindications to procedure (MRI, etc)
Pre sedation• Informed consent• Time out
procedure
IV access• Use of topical analgesia if possible
– EMLA, LMX, Synera (>3 years)-use care to follow age and duration guidelines
– New product on market called Zingo (>3 as well) being trialed at several pediatric institutions
• Take time to find best site• Secure well!• Consider contrast requirements if CT
Personnel and equipment
• Must have pediatric specific emergency equipment immediately available
• Sedation providers must be trained in he administration of sedation medications and the management of complications associated with these medications
• Must have skills necessary to rescue patient from next level of sedation
RN requirements• Institution specific but minimal
requirements include• BLS and PALS certifications• “Additional” competency based
training in sedation medications, procedural requirements and rescue skills that is ongoing
AZ State board of Nursing
• Employers must identify medication allowed for conscious sedation
• Licensed provider must be present in the dept from the time the medication is initiated to the completion of the procedure and must be readily available in the facility to assume care of the patient during the post-procedure period
AZ Board of Nursing• Registered nurse responsible must not
“leave patient unattended or engage in other tasks that compromise continuous monitoring”
• Specific list of educational requirements for RNs who administer sedation.
• Advisory opinion Conscious sedation for Diagnostic and Therapeutic Proceduresrevised 5/08.
Monitoring Intraprocedure
• Continuous monitoring of heart rate and pulse oximetry and intermittent recording of respiratory rate and blood pressure
• Standard is within 5 minutes prior to sedation and every 5 minutes till procedure is complete
• Post procedure-vital signs at regular intervals (most often q 15 minutes)
End Tidal CO2• Anesthesia literature validate rapid
response in respiratory depression/hypoventilation
• Most guidelines recommend or state should be immediately available for moderate and esp. deep sedation
• In areas where can’t see patient (MRI) has become more of a standard of care
General pediatric medication
considerations• Dose must be individualized and double
checked• Give small increments and wait for effect• Expect variations in responses• Be prepared to assist respirations, etc.• Remember to consider other
medications and combinations
Pediatric sedatives• Standard pre-printed orders may
decrease potential for error in dosages
• Special care with route
Sedation medications• Goal:• Use the lowest dose of the medication
with the highest therapeutic index for the procedure
• Perfect drug: Causes no respiratory or cardiovascular compromise, effects last the exact length of the procedure and has no contraindications
Real medication choices
• Chloral hydrate• Benzodiazepines• Opiates • Barbiturates• Anesthetic agents• Dexmedetomidine
Chloral hydrate• Has been used for more than 100 years• Classified as a sedative/hypnotic• No analgesic properties• May be given orally or rectally• Sometimes referred to as “not really a
sedative” and therefore outside of the guidelines in any given institution
Chloral Hydrate• Doses range from 25-125mg/kg-most
common is 50mg/kg• Single dose max of 1000mg reported• Onset of action is very variable
ranging from 10-60 minutes• Long sedation has been reported• Premature discharge has led to death
Chloral Hydrate• Hepatic accumulation of metabolites
reported in premature infants• Unpleasant taste, nausea and vomiting
common• Many studies citing other drugs as
more efficient• Some data supporting increased
success if patient under 2 years.• No reversal agent
Benzodiazepines• Has sedative, anti -anxiety and
amnesic properties• No analgesic properties• Commonly used as pre-med• Often not able to provide adequate
sedation for procedures that require immobility as a single agent
• Versed most commonly used agent
Versed (Midazolam)• May be given in a variety of ways• Doses:
– IV 0.05-0.1mg/kg– Oral 0.5-0.7 mg/kg– Rectal 0.5-1.0 mg/kg– Nasal 0.2-0.4 mg/kg– Sublingual 0.2mg/kg
Midazolam• Concomitant use of opiate will increase
effects• Onset of action depends upon route-1-5
minutes IV up to 20-60 minutes orally• Can cause hypotension, respiratory
depression• Reversal agent is Flumazenil
(Romazicon)
Opiates• Used for painful procedures• Often combined with benzodiazepines• Fentanyl most common opiate used in
pediatric procedures due to relatively short half life
• Reversal agent is Naloxone (Narcan)• May need to repeat Narcan dose due to
short ½ life.
Fentanyl• IV form used for sedation (lollipop
and patch extended release)• Dose is usually 1 mcg/kg• Duration of action generally ½-1
hour• Can cause chest wall rigidity if
given as rapid bolus
Barbiturates• Pentobarbital historically used Radiology
sedative-is not an analgesic• Given IV up to 6mg/kg• Long half life a concern as related to
increased recovery times• Attempts to awaken early may
contribute to emergence reaction or pentobarb rage
• No reversal agent
Anesthetic agents• Ketamine• Propofal
Ketamine• Has dissociative properties and is
therefore somewhat unique• Used in human and vet medicine• Provides sedation and analgesia• At high doses is a general
anesthetic agent• May be given IV or IM
Ketamine• To be used only “under direct
supervision of a LIP with experience with anesthetic agents”
• Causes discongigant eye movements • Can cause hallucinations (visual and
auditory) usually at emergence-versed given in combination to reduce
Ketamine
• Dose-– IV 0.5-2mg/kg-usually use 0.5-1 for
procedural sedation– IM 3-7mg/kg
• Onset of action 30 secs. IV. 3-4 minutes IM
• Duration 12-25 minutes IM, 5-10 minutes IV
Propofal• No analgesic properties• General anesthetic agent with very rapid
onset and potential for apnea• State and institution guidelines vary as to RNs
ability to manage infusions• Bolus dosing by LIP• Study in 2005 showed that 42% of 54
pediatric hospitals were using propofal outside of the OR given by non anesthesiologists

Propofal
• Bolus then drip essential as drug is degradated in single pass through the liver
• Bolus is usually 1-2mg/kg• Infusion rates of 50-250mcg/kg/min for
short term procedural sedation• Pediatric specific mortality reported from
irreversible metabolic acidosis in 1999 from long term high dose infusions
Dexmedetomidine (Precedex)
• Highly selective alpha2 adrenoceptor agonist with both analgesic and sedative effects
• Classified as anesthetic agent• Mechanism of action is induction of
stage 2 (non REM sleep)• Bolus then infusion delivery• Short ½ life and lack of respiratory
depression reported
Precedex• Advantages
– Less interference with EEG waves so therefore more diagnostic quality
– Promising results for consistency in achieving adequate sedation for imaging studies
– Large on-going study at Boston Children’s Hospital demonstrating positive safety profile
Precedex• Hemodynamic changes can occur but
are not usually clinically significant• Specifically, bradycardia is common but
without hemodynamic compromise• Contraindications include patients on
Digoxin (cardiac arrest reported in adults) and other cardiac conditions
Post Sedation Considerations
• Patients may still be at significant risk for complications
• Removal of stimulation (pain, MRI noise) may cause deeper sedation level especially if multiple doses have been given
• Delayed drug absorption (oral, rectal, IM) and slow drug elimination also may contribute
Post Sedation Considerations
• Continued monitoring and observation necessary
• Pre-determined discharged criteria – Aldrete most common– Score of 9 or back to baseline usual criteria
• With kids, ability to drink also important to avoid dehydration and hypoglycemia (infants)
Post Sedation Considerations
• Written discharge instructions that are age specific desirable
• Toddlers especially at risk for falls, etc
• Positioning in car seats, etc with infants also very important due to pediatric airway anatomy
QA/QI outcome data• Guidelines state there should be
an analysis of any adverse events• Collecting data regarding success
rates, etc helps drive practice change
• One Benchmark: Pediatric Sedation Research Consortium

Take home points
Take home points• Kids are not little adults• Know age specific vital sign norms• Know where your pediatric airway
equipment is and how to use it• Remember airway position• Double check your meds
Remember if your intent is to Remember if your intent is to sedate a patient, irregardless sedate a patient, irregardless of the medication or dose you of the medication or dose you use, sedation guidelines applyuse, sedation guidelines apply
Remember if your intent is to Remember if your intent is to sedate a patient, irregardless sedate a patient, irregardless of the medication or dose you of the medication or dose you use, sedation guidelines applyuse, sedation guidelines apply
Any Questions?????
Pediatric Sedation References
Guidelines for Monitoring and Management of Pediatric Patients During and After Sedation for Therapeutic and Diagnostic Procedures: An Update. American Academy of Pediatrics, American Academy of Pediatric Dentists, Cote, C.J, MD, Wilson, S/ DMD, MA, PhD the WorkGroup on Sedation. Pediatrics Vol 118 No.6 December 2006 pp 2587-2602. Practice Guidelines for Sedation and Analgesia by Non-Anesthesiologists: an updates report by the American Society of Anesthesiologists Task Force on Sedation and Analgesia by Non-Anesthesiologists. Anesthesiology. V 96 No. 4, April 2002 Incidence and Nature of Adverse Events During Pediatric Sedation /Anesthesia for Procedures Outside the Operating Room: Report from the pediatric Research Consortium. Cravero, J.P. MD, Blike, G.T. MD, Beach, M. MD, Gallagher, S. M. BS, Hertzog, J.H. MD, Havidich, J.E. MD, Gelman, B.MD, and the Pediatric Sedation Consortium. Pediatrics Vol. 118, No 3. September 2006, PP 1087-1096. Advisory Opinion Conscious sedation for Diagnostic and Therapeutic procedures. Arizona State Board of Nursing.
Related Documents











