MOI UNIVERSITY SCHOOL OF MEDICINE COMMUNITY BASED EDUCATION AND SERVICE (COBES V) PEDIATRIC EMERGENCY PREPAREDNESS IN SIAYA DISTRICT HOSPITAL Khadolwa Angira S. Med /17/03 A report submitted to Moi University School of Medicine in partial fulfillment of COBES V. ©2010

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

8/8/2019 Pediatric Emergency Preparedness 2010
http://slidepdf.com/reader/full/pediatric-emergency-preparedness-2010 1/31
MOI UNIVERSITY
SCHOOL OF MEDICINECOMMUNITY BASED EDUCATION AND SERVICE
(COBES V)
PEDIATRIC EMERGENCY
PREPAREDNESS IN SIAYADISTRICT HOSPITAL
Khadolwa Angira S.Med
/17/03
A report submitted to Moi University School of Medicine in partial fulfillment of COBES V.
©2010

8/8/2019 Pediatric Emergency Preparedness 2010
http://slidepdf.com/reader/full/pediatric-emergency-preparedness-2010 2/31
[1]
DeclarationI hereby declare that this is my original work done during my district health service attachment at
Siaya District Hospital in fulfillment of COBES 5 requirements.
Name Designation Signature date
Researcher
Khadolwa Angira S.
Supervisors
Dr. Nyabera
Ms.wambui

8/8/2019 Pediatric Emergency Preparedness 2010
http://slidepdf.com/reader/full/pediatric-emergency-preparedness-2010 3/31
[2]
Abstract Study title: Pediatric Emergency preparedness in Siaya district hospital
Introduction: The United Nations Millennium Development Goal (MDG4) number four is to
reduce the global under-five mortality rate by two-thirds between the baseline in 1990 and
2015.The under-five mortality is not declining fast enough in third world countries, the rate in
Kenya has been stagnant at128/1000 for the past 10 years.
Justification: Emergency and critical care services are often cited as one of the weakest parts of
health systems and improving such care has the potential to significantly reduce mortality.
Prevention through preparedness is probably the most important phase of response in emergency
and disaster management.
Objective: Asses’ pediatric emergency preparedness in Siaya district hospital.
Methodology: Prospective, cross-sectional study
Findings: The frequent causes of pediatric emergencies were Malaria27%, respiratory
emergencies 24%sand anemia14%. There was a shortage of essential emergency antibiotics.
Of a possible 59, 42 questionnaires were returned (Response rate 71.2%) Almost allrespondents acknowledged that they were inadequately prepared (90%). As many as 92.9%
believed that there was a protocol in their workplace for dealing with pediatric emergencies, but
only 73.9% had read these protocols. The other 7.1% did not know if there was such a protocol
or did not think there was one. If an emergency was to occur while they were at work, about two-
third (71.4%) of respondents reported that they would follow the available hospital protocol,
while another less than one-third (21.5%) would wait for instructions or direction from their
supervisors. Others would Initiate own ideas (from experience) to deal with the emergency
before the definitive action is settled upon. The majority of respondents considered that specific
course materials and activities related to pediatric emergency management should also be
developed to enable health workers to prepare for pediatric emergencies courses: First Aid
(90.4%), Basic Life Support (85.7%), and Infection Control (78.6%), Triage (66.7%). A protocol
8/8/2019 Pediatric Emergency Preparedness 2010
http://slidepdf.com/reader/full/pediatric-emergency-preparedness-2010 4/31
[3]
for pediatric emergency management was deemed necessary by 85.7%, courses in pediatric
emergencies by 80.9%, and drills were cited by 69% also helpful.
Discussion: Malaria is the frequent pediatric emergency encountered followed closely by
respiratory emergencies this contradicts the findings in Ethiopia were respiratory emergencies
lead followed by meningitis. Anemia is a concern which needs to be addressed in Siaya as well
as dehydration and sepsis. There were high rates of unpreparedness and learning needs for
emergency preparedness among Siaya and Hong Kong respondents.
Conclusion: Major causes of pediatric emergencies are preventable and treatable with available
medical treatment; there is room to reduce childhood deaths and illnesses by improving case
detection and management through preparedness. There is a shortage of essential antibiotics,
Health workers are not adequately prepared for pediatric emergencies, but are aware of the need
for such preparation. Pediatric emergency training should be Included in the basic education of
all health workers’. Therefore the hypothesis holds true that Siaya district hospital is not
adequately prepared for pediatric emergencies
Recommendations: Prioritization and Timely procurement of antibiotics, ensure adequate and
constant supply of blood, emergency management in continuing medical education for all staff.
Partner with NGOs emergency providers to ensure optimal emergency care and training
emergency/disaster readiness for children
8/8/2019 Pediatric Emergency Preparedness 2010
http://slidepdf.com/reader/full/pediatric-emergency-preparedness-2010 5/31
[4]
AcknowledgementsThe accomplishment of this study would not have been possible had it not been for the assistance
of the following individuals:
My first gratitude goes to the Hospital Management Team (HMT) – Siaya District Hospital,
headed by the then acting Medical Superintendent, Dr. Mwai. They granted me the permission to
carry out this study in their facility. The District public health nurse Mrs.Okwach for her
invaluable suggestions on the questionnaire. The staff in maternal and child health clinic,
paediatric ward and the entire hospital staff for the support during the period of my study.
I wish to also acknowledge the efforts of my supervisors aforementioned for guiding me in this
study. They gave me positive criticism and guidance in shaping this study and report. The
assessment team during the oral presentation, Dr.Omolo of the Department of psychiatry
Dr.Buziba of Department of haematology and Ms.Wambui of the Department of Nursing also
offered corrective guidance in my presentation.
The COBES committee facilitated our attachment at Siaya District Hospital and by being the
overall managers ensured that everything went according to schedule and as planned.
My family ensured I had the finances to be able to stay at the District and carry out my
attachment. All those who in one way or another played a role in the success of this work are
highly appreciated
Last but not least to God Almighty for his love, care and for giving me supportive people around
me.

8/8/2019 Pediatric Emergency Preparedness 2010
http://slidepdf.com/reader/full/pediatric-emergency-preparedness-2010 6/31
[5]
Tableof ContentsTable of Contents .......................................................................................................................................... 5
List of tables .................................................................................................................................................. 6
List of
abbreviations
......................................................................................................................................
7
CHAPTER 1: INTRODUCTION ......................................................................................................................... 8
CHAPTER 2: Literature review ..................................................................................................................... 10
Justification ................................................................................................................................................. 11
Aim of the study .......................................................................................................................................... 12
Specific objectives ................................................................................................................................... 12
Research question
...............................................................................................................................
12
Hypothesis .................................................................................................................................................. 12
CHAPTER 3: Methodology ........................................................................................................................... 13
CHAPTER 5: Results/Findings ...................................................................................................................... 15
CHAPTER 4: Discussion ................................................................................................................................ 20
CHAPTER 5: Conclusion ............................................................................................................................... 22
CHAPTER 6:
Recommendations
..................................................................................................................
23
CHAPTER 7: References .............................................................................................................................. 24
CHAPTER 8: Appendix ................................................................................................................................. 25
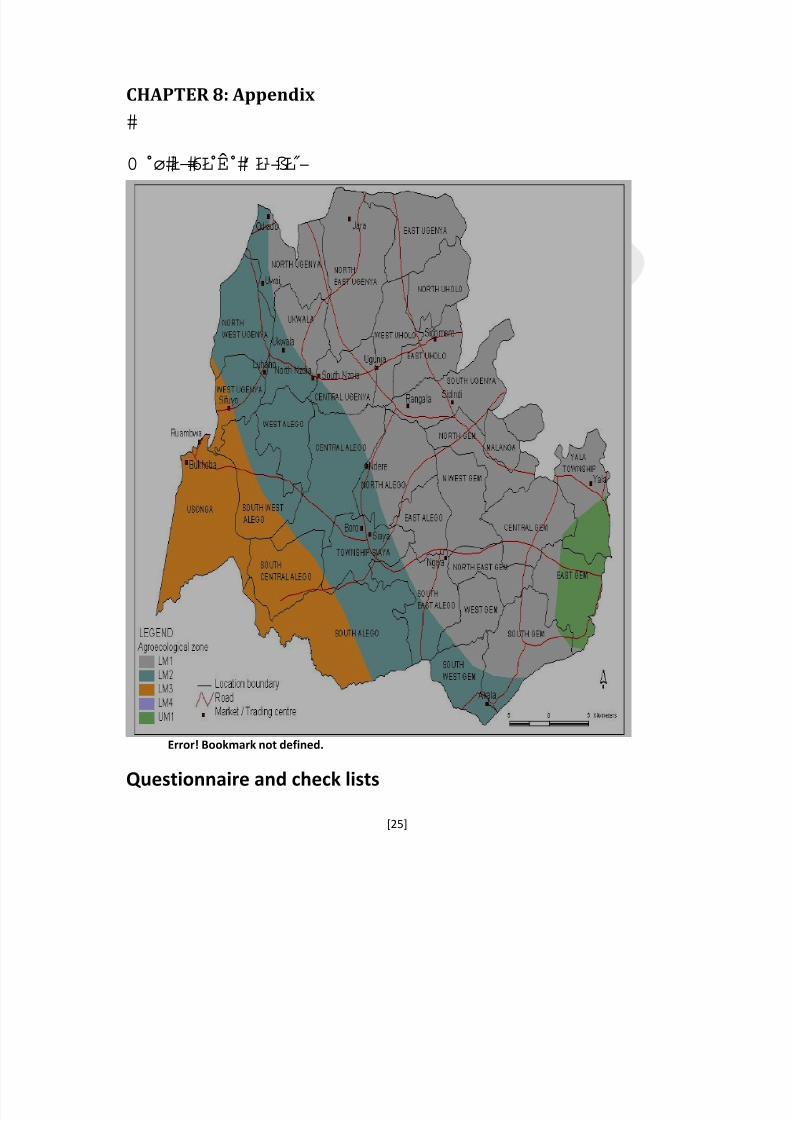
Map of Siaya District ................................................................................................................................... 25

8/8/2019 Pediatric Emergency Preparedness 2010
http://slidepdf.com/reader/full/pediatric-emergency-preparedness-2010 7/31
[6]
List of tablesTable 1: Frequency of pediatric emergency cases for period mid-July to mid-August, 2010…...11
Table 2: Respondents’ demographics…………………………………………………………....13
Table 3: Preparedness for emergencies…………………………………………………………..14
Table 4: Learning needs in relation to preparedness…………………………………………….15
8/8/2019 Pediatric Emergency Preparedness 2010
http://slidepdf.com/reader/full/pediatric-emergency-preparedness-2010 8/31
[7]
List of abbreviationsCOBES……....................................................................Community Based Education and Service
SDH…………………………………………………….Siaya district hospital
DHMT…………………………………………………..District health management team
HMT…………………………………………………… Hospital management team
GoK……………………………………………………..Government of Kenya
KMTC……………………………………………….…. Kenya medical training college
ABCs ……………………………………………………Airway breathing and circulation
KPA……………………………………………………... Kenya pediatric association
MDG………………………………………………….… Millennium Development Goals
8/8/2019 Pediatric Emergency Preparedness 2010
http://slidepdf.com/reader/full/pediatric-emergency-preparedness-2010 9/31
[8]
CHAPTER1:INTRODUCTION
In the fifth year of study, Medical students are attached to various District hospitals to
participate in health administrative work, community outreach as well as to rotate in the clinical
areas they are expected to learn teamwork, to acquire administrative skills, take part in
promotive, preventive, curative and rehabilitative services and conduct a research with view to
provide interventional recommendations.
Siaya district is one of the 21 districts that comprise Nyanza Province. It is bordered by Bunyala
District to the north, Emuhaya and Butere District to the north-east, Bondo District to the south
and Kisumu West District to the south-east. The total area of the district is approximately
1520km2. The district lies between latitude 0 26’ to 0 18’ north and longitude 33 58’ east and
34 33’ west.
Siaya District is divided into seven administrative divisions namely; Yala, Wagai, Karemo,
Ugunja, Uranga, Boro and Ukwala. The divisions are further divided into 30 locations and 130
sub-locations. Ukwala Division is the largest division covering an area of 319.5 km2 and also
has the most locations and sub-locations while Boro division is the smallest covering an area of
180.1 km2, with 3 locations and 12 sub-locations. Politically, the district has 3 political
constituencies and 5 local authorities with a total of 39 electoral wards distributed as follows;
Siaya County Council (22 wards), Siaya Municipal Council (5 wards), Ugunja Town Council (4
wards), Ukwala Town Council (4 wards) and Yala Town Council (4 wards).
The projected district population as at end of year 2010 would be 539,961. (According to the
district’s annual operational plan), with 46%males and 54%females.children under one year 3.6
%, the under-five comprise 18% of the total population. The districts Infant Mortality rate
135.6/1000, under 5 mortality rate 234/1000 estimated growth rate is 0.9%. There are 56

8/8/2019 Pediatric Emergency Preparedness 2010
http://slidepdf.com/reader/full/pediatric-emergency-preparedness-2010 10/31
[9]
Government of Kenya (GoK) health facilities comprising of one district hospital 2 sub-district
hospital 20 health centers 33 dispensaries.
Siaya district hospital (SDH) is one of the level 4 health institutions in Kenya; it has a catchment
population of 44,923 and is categorized as a low volume load district hospital. It acts as a referral
to the surrounding sub district hospitals health centers and dispensaries: It has a bed capacity of
240.Two operating rooms in the theatres. Bed occupancy ranges between 4 and 6 days. It records
an average of 16 deliveries monthly. It is a teaching hospital receiving students from Kenya
medical training college KMTC. It was recently gazzeted as an internship Centre for doctors,
clinical officers, pharmacists and nurses. The top ten causes of admission at the hospital are
Malaria, respiratory infections, skin infections, diarrheal diseases, anemia and accidents.
Pediatric emergency is an injury or illness that is acute and poses an immediate risk to a child's
life or long term health. In Siaya district hospital common causes of pediatric morbidity include:
malaria, respiratory emergencies, febrile infections, anemia and severe dehydration.
Preparedness refers to the state of being prepared for specific or unpredictable events or
situations. Preparedness is an important quality in achieving goals and in avoiding and mitigating
negative outcomes. It is a major phase of emergency management. During preparedness,
governments, organizations, and individuals develop plans to save lives, minimize delays, and
enhance emergency response. Preparedness efforts include preparedness; emergency exercises
and training; warning systems; emergency communication systems; public information and
education; and development of resource inventories; these comprise the basic emergency
equipment, drugs, fluids for resuscitation, personnel contact lists, and mutual aid agreements.
Physicians participate in preparedness and prevention in many different ways, including:
immunization programs, dietary advice, health education, and safety precautions and planning
(Esamai etal). As participants in an emergency action plan, physicians need to help formulate
ways of preventing incidents from occurring or limiting the consequences from an incident thathas already occurred. Physicians need to know what will be expected of their hospital in the case
of a potential infectious disease outbreak. They should also be prepared with the knowledge and
resources needed to help identify the etiology of a problem and to provide timely treatment.
8/8/2019 Pediatric Emergency Preparedness 2010
http://slidepdf.com/reader/full/pediatric-emergency-preparedness-2010 11/31
[10]
CHAPTER2:LiteraturereviewEmergency and critical care services are often cited as one of the weakest parts of health systems
and improving such care has the potential to significantly reduce mortality, Introducing effective
triage and emergency treatments and establishing health care systems that prioritize the critically
ill and ensuring a reliable emergency treatment scheme need not be resource intensive (Tim
Baker 2008) Improving emergency care units, training health staff in fundamentals of critical
care concentrating on airway, breathing and circulation (ABCs) and developing guidelines of
common medical emergencies could all improve the quality of pediatric care. According to the
Kenya pediatric association (KPA) and the ministry of health: respiratory emergencies, severe
Malaria, febrile infections, severe dehydration and Anemia are some of the most common
pediatric emergencies in Kenya. Integration with obstetrics, adult medicine and surgery in a
combined emergency and critical care service would concentrate resources and expertise (Baker
2008)
In a study in Tikur Anbessa Hospital in Addis Ababa, Ethiopia pediatric emergencies accounted
for 40% of pediatric admissions with 14.3% death in the emergency ward (Daniel benti etal
2006). The most common pediatric emergencies included: Severe pneumonia 44% , Meningitis
8.3% ,Sepsis 7.1%,Severe Dehydration 7.9%,Trauma 4.2%,Bronchial asthma 1.7%,Severe
malaria 1.4%,Burns 1.1%,DKA 1.0%,Anemia 0.9%,Seizure disorder 0.6%Others 12.4%.
Although we usually cannot predict emergencies, we can control them through prevention and
planning efforts. Prevention through preparedness is probably the most important phase of
response in emergency and disaster management. In an emergency preparedness study done in
Hong Kong among nurses; almost all respondents acknowledged that they were inadequately
prepared (97%). As many as 84% believed that there was a protocol in their workplace for
dealing with emergencies and disastrous events, but only 61% had read these protocols. All
participants agreed that there are courses which they should take to be prepared for these
situations. Some of these courses, in order of importance, were: First Aid (72%), Basic LifeSupport (75%), Infection Control (63%), Field Triage (58%) and others .The majority of
respondents considered that specific materials and activities related to emergency and disaster
management should also be developed to enable them to prepare for emergencies and disasters.
A protocol for emergency and disaster management was deemed necessary by 85%, pamphlets

8/8/2019 Pediatric Emergency Preparedness 2010
http://slidepdf.com/reader/full/pediatric-emergency-preparedness-2010 12/31
[11]
by 84%, and drills for disaster were cited by 84% as helpful to prepare them for emergencies and
disasters.
JustificationPediatric emergencies are common occurrences’ in many health care facilities. In 2000, the
United Nations adopted the eight Millennium Development Goals (MDGs) as a focus for
international development. Goal number four is to reduce the global under-five mortality rate bytwo-thirds between the baseline in 1990 and 2015. Achieving the goal would save over six
million lives each year. There has been some progress but in 62 countries, under-five mortality is
not declining fast enough and in 27 countries the rate is stagnant (Kenya; 128/1000 over the past
10 years) or getting worse. The majority of deaths are occurring in low-income countries. Over
150 out of every 1000 children born in sub-Saharan Africa today will die before the age of five
whereas in developed countries the rate is only six per 1000. Emergency and critical care
services are often cited as one of the weakest parts of health systems and improving such care
has the potential to significantly reduce mortality(Baker2008) Introducing effective triage and
emergency treatments and establishing health care systems that prioritize the critically ill and
ensuring a reliable emergency treatment, Prevention through preparedness is probably the most
important phase of response in emergency and disaster management. Improving emergency care
units, training health staff in fundamentals of critical care concentrating on ABCs and developing
guidelines of common medical emergencies could all improve the quality of pediatric care.
Without a radical improvement in child health in low-income countries, MDG4 will not be
achieved.
8/8/2019 Pediatric Emergency Preparedness 2010
http://slidepdf.com/reader/full/pediatric-emergency-preparedness-2010 13/31
[12]
Aimof thestudyAsses’ pediatric emergency preparedness in Siaya district hospital
Specific objectives1. Identify common pediatric emergencies and their prevalence
2. Evaluate the health facility preparedness for pediatric emergencies, the emergency
equipment, medication and documentation.
3. Evaluate Health care provider preparedness for pediatric emergencies
ResearchquestionIs Siaya district hospital well prepared for pediatric emergencies?
Hypothesis
Siaya district is not well prepared for pediatric emergencies.

8/8/2019 Pediatric Emergency Preparedness 2010
http://slidepdf.com/reader/full/pediatric-emergency-preparedness-2010 14/31
[13]
CHAPTER3:Methodology
3.1 STUDY AREA Siaya district hospital in Karemo division Siaya district 3.2 STUDY DESIGNS Prospective, cross‐sectional study
3.2 STUDY POPULATION The study population included all health workers in the hospital clinical officers, medical
officers, nurses, counselors, and medical technicians. The total number of health workers was
118 at the time of the study, 6 doctors, 14 clinical officers, 47 nurses, 30 other health
workers. Due to limited resources and time the target was conveniently set at 59(50%) of the
population 3.4. SAMPLE SIZE ESTIMATION:
Proportional ratios according to the number of staff in a given profession. 3.5 SAMPLING METHODS AND TECHNIQUES Convenience sampling method was utilized
INCLUSION CRITERIA Health workers in Siaya district hospital working under the hospitals management.
EXCLUSION CRITERIA Health workers affiliated to non-govern mental organizations working in the hospital.
3.6 METHODS OF DATA COLLECTION Direct observation
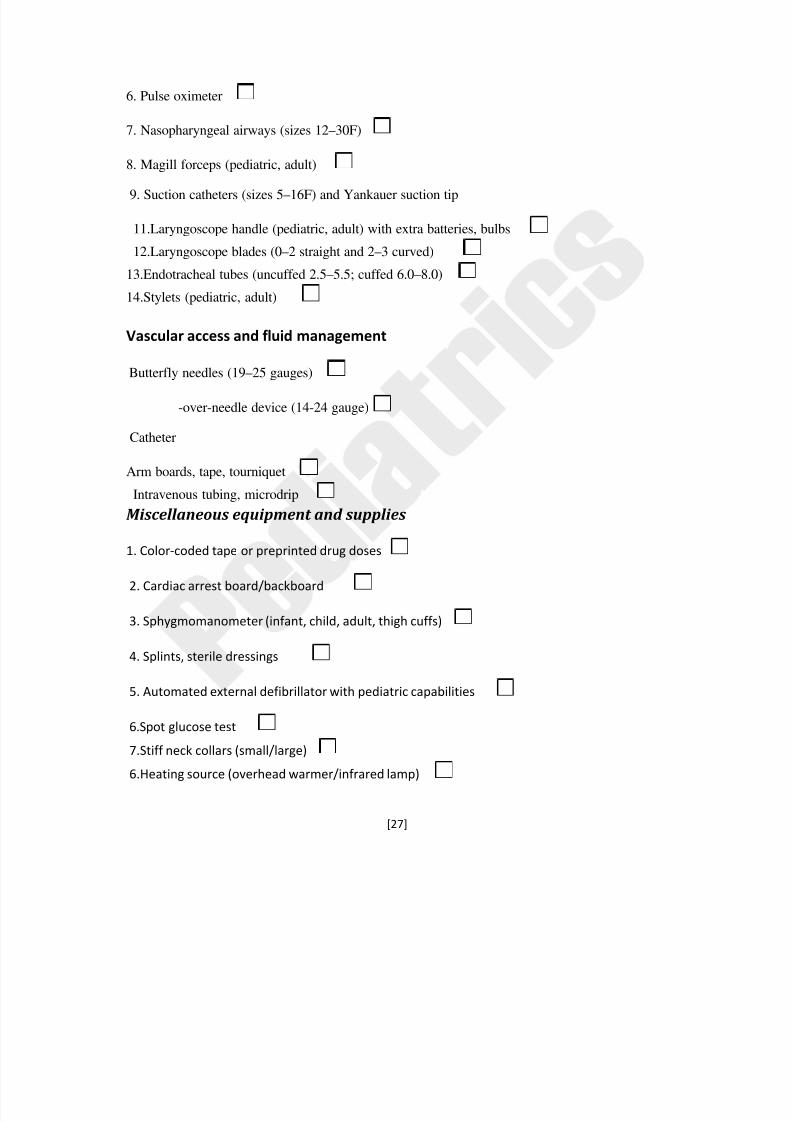
Use of check lists: (which were adopted from the Association of American pediatricians and the
ministry of health GoK emergency tray requisites) listing basic pediatric emergency equipment
and drugs contained in the emergency tray was filled during the research period
8/8/2019 Pediatric Emergency Preparedness 2010
http://slidepdf.com/reader/full/pediatric-emergency-preparedness-2010 15/31
[14]
Questionnaire: a specially designed questionnaire that was validated by my supervisors was
administered to the health workers who obliged to participate in the study it comprised two
sections; health worker preparedness and learning needs pertaining to pediatric emergency
preparedness
3.7 DATA MANAGEMENT AND PRESENTATION Data was analyzed by the following:
1. Tallying
2. Microsoft excel spreadsheet
Data presentation Continuous prose and tables
3.8 BIAS MINIMIZATION The sampling technique adopted minimized most forms of biases.
Proportional ratios were used to allocate questionnaires’
Information bias: Familiarization of the researcher on the information to be collected prior to
implementation of the study
Questionnaire developed and handed to respondents
3.9 ETHICAL CONSIDERATIONS Consent: consent from medical superintendent and health workers involved in the research.
Team clearly explained the purpose of research and anticipated benefits.
Benefits: There will be no direct benefit from participating in the study. However, the findings
and recommendations of the study will benefit the hospital and other stakeholders in policy
formulation and planning.
Confidentiality: All information will be treated with total confidentiality
Right to refuse or withdraw: The subject’s participation in the study is entirely voluntary and
one is free to refuse to take part or withdraw at any stage of study without any consequences.
Purpose: This study is purely meant for academic purposes. However findings will be
disseminated to relevant authorities and other stakeholders with specific interest.
8/8/2019 Pediatric Emergency Preparedness 2010
http://slidepdf.com/reader/full/pediatric-emergency-preparedness-2010 16/31
[15]
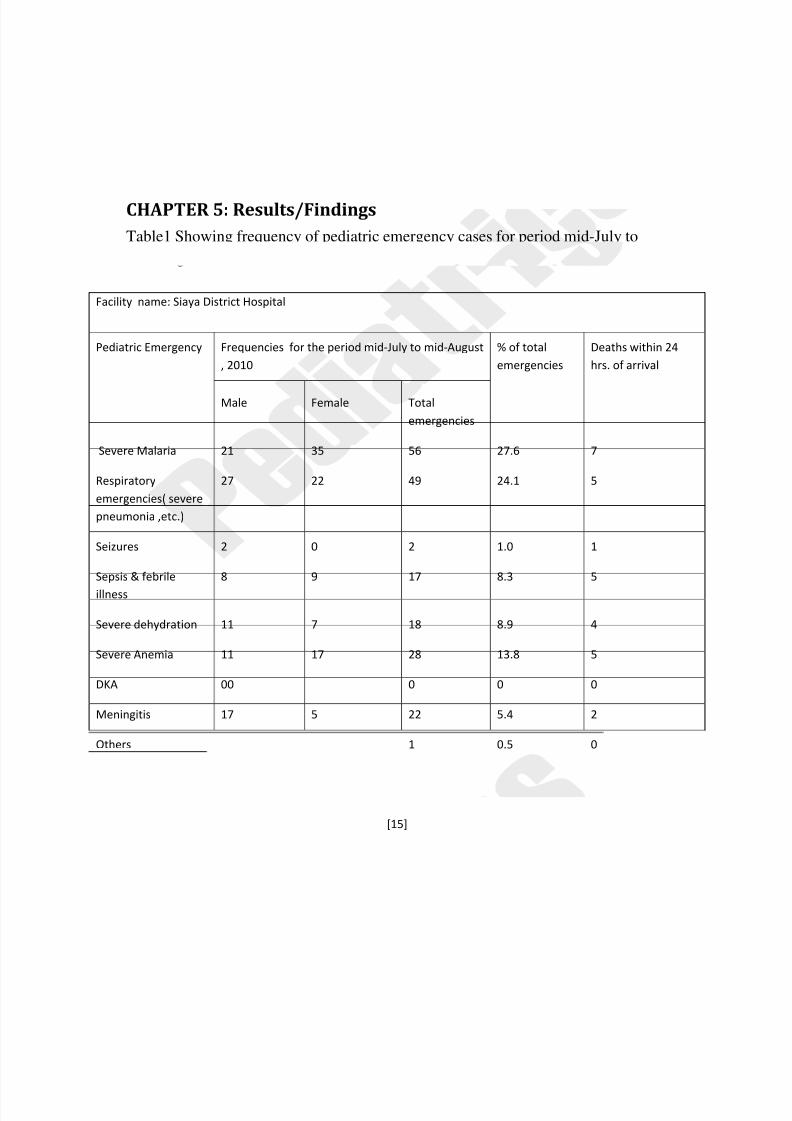
CHAPTER5:Results/FindingsTable1 Showing frequency of pediatric emergency cases for period mid-July to
mid-August, 2010
Facility name: Siaya District Hospital
Pediatric Emergency Frequencies for the period mid‐July to mid‐August
, 2010
% of total
emergencies
Deaths within 24
hrs. of arrival
Male Female Total
emergencies
Severe Malaria 21 35 56 27.6 7
Respiratory
emergencies( severe
pneumonia ,etc.)
27 22 49 24.1 5
Seizures 2 0 2 1.0 1
Sepsis & febrile
illness
8 9 17 8.3 5
Severe dehydration 11 7 18 8.9 4
Severe Anemia 11 17 28 13.8 5
DKA 00 0 0 0
Meningitis 17 5 22 5.4 2
Others 1 0.5 0
Grand Totals 97 106 203 100 27
8/8/2019 Pediatric Emergency Preparedness 2010
http://slidepdf.com/reader/full/pediatric-emergency-preparedness-2010 17/31
[16]
Table 1 shows that there were a total of 203 emergency cases of these 47% were male and 53%
were female, it also shows that severe malaria 27.6% and severe respiratory emergencies 24.1%
were the most common causes of pediatric emergencies at Siaya. Severe anemia accounted for
13.8%, meningitis 5.4%, sepsis 8.3%, severe dehydration 8.9% and others 0.5%. There were 27
deaths recorded during the study period. Table 1 reveals that severe malaria was responsible for
7 (25%) of the total deaths. Total emergency related deaths accounted for 13.3% of encountered
emergencies (not shown on the table).
Facility, equipment and medication
The emergency department was the part of first building you encounter as you enter the
hospital was well labeled with a luminous white signboard facing the main gate. The department
is composed of four rooms with adequate spacing, they were in good condition; two rooms had
an emergency tray each which was constantly at work. Pediatric emergency cases are mostly
handled by the maternal and child health clinic (MCH) and the acute room in the pediatric ward
during the day, while at night all emergency cases are handled by the emergency department.
The highest staffing point in the emergency department during the day on working days is eight
while at night and on weekends is four. There is no anticipatory guidance and education given toparents regarding injury prevention and first aid, though recognition and response to febrile
illnesses is given. The waiting bay is always under direct observation and is screened frequently
by a clinical officer about four times a day. The facility hasn’t yet developed a written pediatric
emergency protocol; the facility has two ambulance and emergency hotline which are used for
response to obstetric and other emergency cases. Siaya district hospital is currently developing a
mass disaster emergency protocol. As regarding pediatric emergency and equipment, majority
are available as per the check list, there is a reliable supply of oxygen in the facility. All the
equipment is operational and well maintained. Majority of the pediatric emergency drugs were
available except for antibiotics; ceftriaxone and naloxone. There was no documentation of
emergency cases but only morbidity cases for which were entered in a specially designed

8/8/2019 Pediatric Emergency Preparedness 2010
http://slidepdf.com/reader/full/pediatric-emergency-preparedness-2010 18/31
[17]
template by the ministry of health. Therefore the hypothesis holds true that Siaya district hospital
is not adequately prepared for pediatric emergencies.
Health professional preparedness
Table 2 Respondent demographics (n = 42)
n %
1.Proffesion
Doctors 3 7.1
Nurses 25 59.5
Clinical officers 5 11.9
Others 9 21.5
2.Sex
Female 31 73.8
Male 11 26.2
4.Age
18-25 years 3 7.1
26-35 years 25 59.5
36 or above 14 43.4
5.Years of experience
Less than 1 year 5 11.9
1 to 5 years 19 45.2
More than 5 years 18 42.9
Demographics
Table 2 shows the participant demographics. Of a possible 59, 42 questionnaires were returned
(Response rate 71.2%). The majority were nurses 59.5% while the minority was doctors7.1%.

8/8/2019 Pediatric Emergency Preparedness 2010
http://slidepdf.com/reader/full/pediatric-emergency-preparedness-2010 19/31
[18]
Female 73.8% were the majority of the respondents and the modal aged 26–35 years (59.5%).
Nearly one-half (45.2%) had 1-5 years of his/her current work experience.
Table 3; Preparedness for emergencies n=42
n %
Health worker perceptions of their own preparedness for pediatric emergencies
Prepared in some ways 30 71.5
Not prepared at all 8 19
Confident of own preparation 4 9.5
Awareness of available protocol for pediatric emergencies in the work place
Available and has read 31 73.9
Available but has not read 8 19
Doesn’t know if there is any/doesn’t think there is any 3 7.1
Immediate action in pediatric emergency situation
Initiate own ideas (from experience) 3 7.1
Follow available hospital protocol 30 71.4
Follow instruction from immediate supervisor 9 21.5
Almost all respondents acknowledged that they were inadequately prepared (90%). As many as
92.9% believe that there was a protocol in their workplace for dealing with pediatric
emergencies, but only 73.9% had read these protocols. The other 7.1% did not know if there was
such a protocol or did not think there was one. If an emergency was to occur while they were at
work, about two-third (71.4%) of respondents reported that they would follow the available
hospital protocol, while another less than one-third (21.5%) would wait for instructions or
direction from their supervisors. Others would Initiate own ideas (from experience) to deal with
the emergency before the definitive action is settled upon.
8/8/2019 Pediatric Emergency Preparedness 2010
http://slidepdf.com/reader/full/pediatric-emergency-preparedness-2010 20/31
[19]
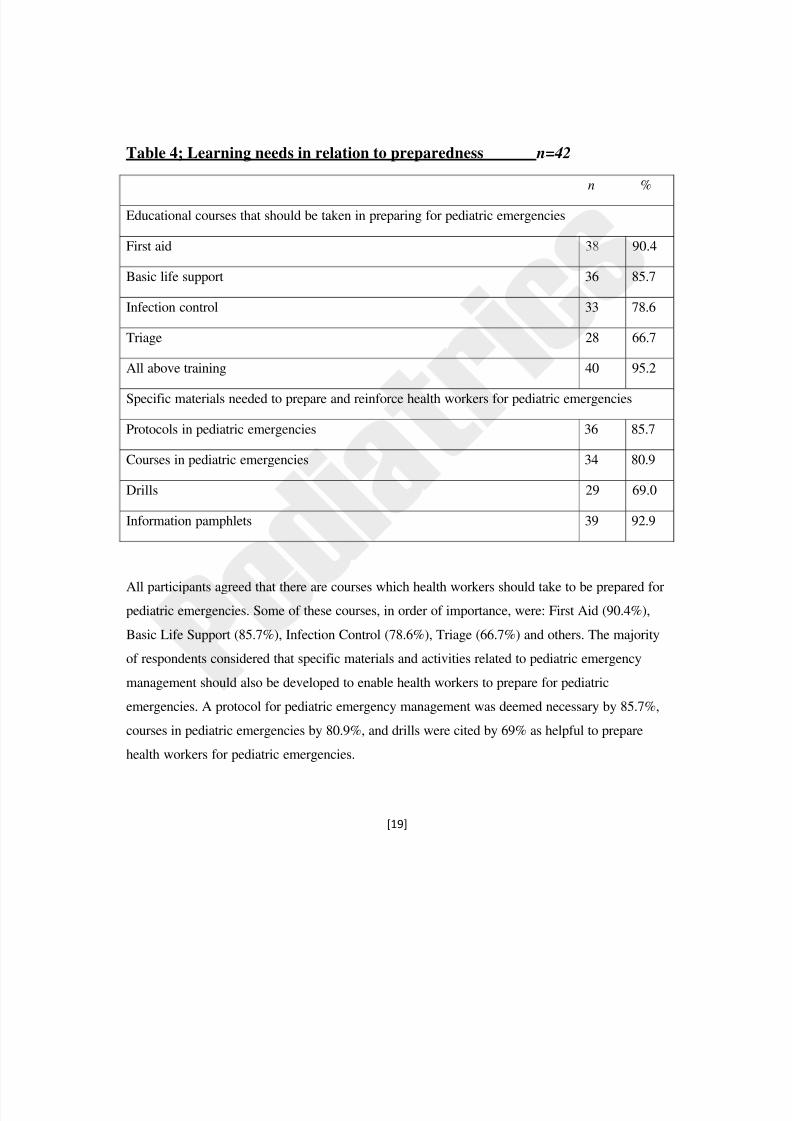
Table 4; Learning needs in relation to preparedness n= 42
n %
Educational courses that should be taken in preparing for pediatric emergencies
First aid 38 90.4
Basic life support 36 85.7
Infection control 33 78.6
Triage 28 66.7
All above training 40 95.2
Specific materials needed to prepare and reinforce health workers for pediatric emergencies
Protocols in pediatric emergencies 36 85.7
Courses in pediatric emergencies 34 80.9
Drills 29 69.0
Information pamphlets 39 92.9
All participants agreed that there are courses which health workers should take to be prepared for
pediatric emergencies. Some of these courses, in order of importance, were: First Aid (90.4%),
Basic Life Support (85.7%), Infection Control (78.6%), Triage (66.7%) and others. The majority
of respondents considered that specific materials and activities related to pediatric emergency
management should also be developed to enable health workers to prepare for pediatric
emergencies. A protocol for pediatric emergency management was deemed necessary by 85.7%,
courses in pediatric emergencies by 80.9%, and drills were cited by 69% as helpful to prepare
health workers for pediatric emergencies.

8/8/2019 Pediatric Emergency Preparedness 2010
http://slidepdf.com/reader/full/pediatric-emergency-preparedness-2010 21/31
[20]
CHAPTER4:Discussion
The study was carried out at the Siaya district hospital (SDH).It was explorative.
There were 203 pediatric emergency cases recorded during the study period, of these 47 %were
males and 53% were female. There were 27 deaths due to emergency related cases representing
13.3% of the encountered emergency cases. This is closely similar to the finding at the pediatric
emergency ward of Tikur Anbessa Hospital in Addis Ababa, Ethiopia which was 14.3%.The
most frequent pediatric emergency was severe malaria27.6%followed closely by respiratory
emergencies 24.1% while at Tikur Anbessa severe pneumonia was leading (44%), followed by
meningitis (8.3%) malaria was not a cause major of emergency in Ethiopia. The frequency of
severe dehydration 8.9% and sepsis 8.3% are almost similar in Ethiopia 7.9% and 7.1%
respectively. Anemia (13.8%) present as a major challenge for SDH.
There were adequate functional emergency trays with basic emergency equipment and
medication except for antibiotics which were in short supply. This was attributed to delays in
procurement procedures and high consumption of the medications in the facility.
There was a high level of unpreparedness almost all the health workers in SDH acknowledgedthat they were not prepared 90% similar to the study done in Hong Kong where 97% agreed to
not being prepared.In both studies a large number of health workers As many as 92.9% in SDH
and Hong Kong 84% believed that there was a protocol in their workplace for dealing with
pediatric emergencies, but only 73.9% had read these protocols. The other 7.1% did not know if
there was such a protocol or did not think there was one. There is statically significant difference
found .If an emergency was to occur while they were at work, about two-third (71.4%) of
respondents reported that they would follow the available hospital protocol, while another less
than one-third (21.5%) would just wait for instructions or direction from their supervisors while
in Hong Kong about a third 38.4 would use the protocol and another third 31.4% would Initiate
own ideas (from experience).
8/8/2019 Pediatric Emergency Preparedness 2010
http://slidepdf.com/reader/full/pediatric-emergency-preparedness-2010 22/31
[21]
On learning needs the findings in this study at SDH augments’ the Hong Kong
study in that All participants agreed that there are courses which health workers should take to
be prepared for pediatric emergencies. These courses, in order of importance remained the same,
were: First Aid, Basic Life Support, Infection Control and Triage. The majority of respondents in
both studies considered that specific materials and activities related to pediatric emergency
management should also be developed to enable health workers to prepare for pediatric
emergencies. A protocol for emergency management was deemed necessary by 85.7% of SDH
respondents as well as 85% of Hong Kong respondents while the figure remained the same
courses in pediatric emergencies by 80.9%, and drills were cited by 69% as helpful to prepare
health workers for pediatric emergencies.

8/8/2019 Pediatric Emergency Preparedness 2010
http://slidepdf.com/reader/full/pediatric-emergency-preparedness-2010 23/31
[22]
CHAPTER5:ConclusionAs major causes of pediatric emergencies and deaths are severe malaria, severe pneumonia,
anemia, sepsis and severe dehydration which are preventable and treatable with available
medical treatment, there is a room to reduce childhood deaths and illnesses by improving case
detection and management through preparedness. Preventable infectious diseases are still
persisting as important causes for childhood illness and deaths across several decades in this
country. Considering the impact of large scale intensified Malaria and water treatment in the
country, surveillance of etiologic agents of these diseases and identifying and introducing
available effective technologies that could result in reducing childhood morbidity and mortality
is of paramount importance. Prioritization and Timely procurement of antibiotics though the
Facility improvement fund would ensure adequate stocking of these drugs.
Health workers in Siaya District hospital are not adequately prepared for pediatric
emergencies, but are aware of the need for such preparation. Pediatric emergency management
training should be Included in the basic education and continuous medical education of all health
workers’. Therefore the hypothesis holds true that Siaya district hospital is not adequately
prepared for pediatric emergencies.
8/8/2019 Pediatric Emergency Preparedness 2010
http://slidepdf.com/reader/full/pediatric-emergency-preparedness-2010 24/31
[23]
CHAPTER6:Recommendations . Prioritization and Timely procurement of antibiotics through the Facility improvement fund
would ensure adequate stocking of these drugs.
Develop an organizational plan for emergency responses in the hospital, which includes:
recognition of an emergency; staff communication, roles, and responsibilities at the time of an
emergency during times of high and low staffing; and maintaining readiness through practice
(mock codes).
Maintain recommended emergency equipment. Organize emergency equipment in a way that
facilitates access to appropriate type and size at the time of an emergency. Develop a system
to check equipment on a regular basis to make sure that it is immediately available and
functioning properly.
Maintain recommended emergency medications and use a resuscitation aid or tool that
provides suggested protocols with precalculated medication doses (broslows tape).
Develop a system to check medications on a regular basis to make sure that stock is always
present and liaise with the obstetric emergency team to ensure adequate and constant supply
of blood.
Include emergency management in continuing medical education for all staff.
Practice mock codes in the hospital on a regular basis (quarterly or biannually). Involve as
many staff members as possible.
Include disaster-preparedness scenarios in mock drills.
Educate families about symptoms and situations for which they should access hospital advice,
Emergency medical services and Educate families about what to do in an emergency.
Encourage first aid and CPR training for parents and caregivers.
Partner with NGOs emergency providers to ensure optimal emergency care and training
emergency/disaster readiness for children.
8/8/2019 Pediatric Emergency Preparedness 2010
http://slidepdf.com/reader/full/pediatric-emergency-preparedness-2010 25/31
[24]
CHAPTER7:References1. Anabwani G. Menge I, Esamai F, Van Reken D, Pediatric morbidity and mortality at the
Eldoret District Hospital, Kenya. East Africa Medical journal 1995; 72(3)165-169
2. Baker Tim (2008) Pediatric emergency and critical care in low-income countries
Pediatric Anesthesia Volume 19, Issue 1, Article first published online: 27 NOV 2008
3. Daniel Benti Dagnew Muluneh and Damte Shimelis (2003) Analysis of admissions to the
pediatric emergency ward of Tikur Anbessa Hospital in Addis Ababa, Ethiopia
September 2002-August 2003)
4. Gebbie K.M. & Qureshi K. (2002) Emergency and disaster preparedness: core
competencies for nurses. What every nurse should know but may not know . American
Journal of Nursing 102(91),5. International Nursing Coalition for Mass Casualty (2003). Educational Competencies for
Registered Nurses Responding to Mass Casualty Incidents. Available at
http://www.nursing.vanderbilt.edu/incmce/competencies.html on January 2008. Accessed
on February 2010.46–51.
6. Siaya district health records office of the prime minister
7. Veenema T.G. (2006) Expanding education opportunities in disaster response and
emergency preparedness for nurses. Nursing Education Perspectives 27(2), 93–98.World Health Organization, Expert Consultation Report (2006) Emergency preparedness
for the health sector and communities – Challenges and the way forward. Pre-hospital
and Disaster Medicine 21(Suppl. 4), s97–s109.
8/8/2019 Pediatric Emergency Preparedness 2010
http://slidepdf.com/reader/full/pediatric-emergency-preparedness-2010 26/31
[25]
CHAPTER8: Appendix
Error! Bookmark not defined. Questionnaire and check lists

8/8/2019 Pediatric Emergency Preparedness 2010
http://slidepdf.com/reader/full/pediatric-emergency-preparedness-2010 27/31
[26]
Evaluation of health facility preparedness check list Name of facility:
Level of
facility:
1. Is there an emergency room?
2. Where is it located and is it easily identifiable
3. What is its capacity?
4. What are the high and low staffing points in the emergency department during the time when
the hospital is operational?(including nights and weekends)
5. Is there any anticipatory guidance and education given to parents regarding injury prevention,
first aid, and basic life support, recognition and response to emergency?
6. Is the waiting bay under direct observation or screened frequently by a clinical staff member, no
of times in a day?
7. Does the facility have a written protocol for pediatric emergencies/emergencies? If yes does it
cater for low staffing hours?
8. Does your staff know the pediatric referral requisites i.e. TWO SIDES(Tubes, Warmth ,Oxygen,
Samples ,IV fluids, Documentation ,Escort)
9. Does the facility have an emergency hotline?
10. Is there a mass emergency protocol to cover for disasters for either pediatric or adults
Emergency Equipment
and
Supplies
check
list
Airway management 1. Oxygen-delivery system
2. Bag-valve-mask (450 and 1000 mL)
3. Clear oxygen masks, breather and nonrebreather, with reservoirs (infant, child, adult)
4.Suction device, tonsil tip, and bulb syringe
5. Nebulizer (or metered-dose inhaler with spacer/mask)
5. Oropharyngeal airways (sizes 00–5)
8/8/2019 Pediatric Emergency Preparedness 2010
http://slidepdf.com/reader/full/pediatric-emergency-preparedness-2010 28/31
[27]
6. Pulse oximeter
7. Nasopharyngeal airways (sizes 12–30F)
8. Magill forceps (pediatric, adult)
9. Suction catheters (sizes 5–16F) and Yankauer suction tip
11.Laryngoscope handle (pediatric, adult) with extra batteries, bulbs
12.Laryngoscope blades (0–2 straight and 2–3 curved)
13.Endotracheal tubes (uncuffed 2.5–5.5; cuffed 6.0–8.0)
14.Stylets (pediatric, adult)
Vascular access and fluid management
Butterfly needles (19–25 gauges)
-over-needle device (14-24 gauge)
Catheter
Arm boards, tape, tourniquet
Intravenous tubing, microdrip
Miscellaneousequipment and supplies 1. Color‐coded tape or preprinted drug doses
2. Cardiac arrest board/backboard
3. Sphygmomanometer (infant, child, adult, thigh cuffs)
4. Splints, sterile dressings
5. Automated external defibrillator with pediatric capabilities
6.Spot glucose test
7.Stiff neck collars (small/large)
6.Heating source (overhead warmer/infrared lamp)
8/8/2019 Pediatric Emergency Preparedness 2010
http://slidepdf.com/reader/full/pediatric-emergency-preparedness-2010 29/31
[28]
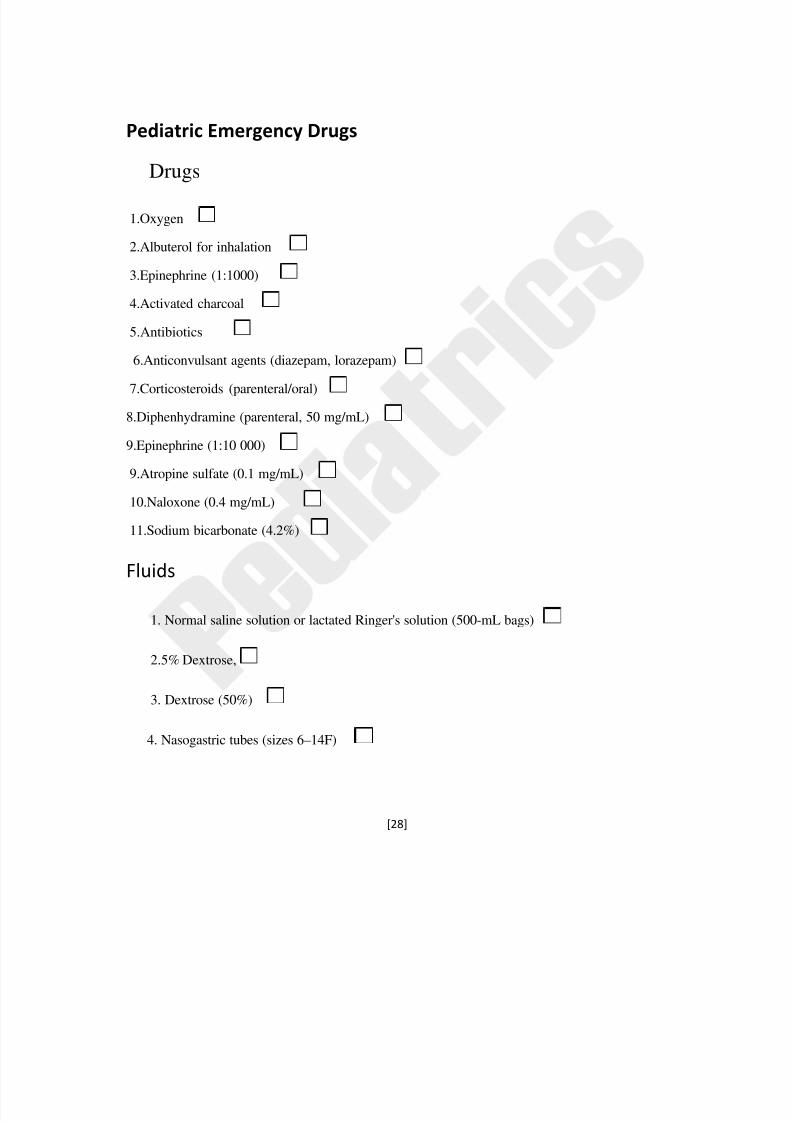
Pediatric Emergency Drugs Drugs
1.Oxygen
2.Albuterol for inhalation
3.Epinephrine (1:1000)
4.Activated charcoal
5.Antibiotics
6.Anticonvulsant agents (diazepam, lorazepam)
7.Corticosteroids (parenteral/oral)
8.Diphenhydramine (parenteral, 50 mg/mL)
9.Epinephrine (1:10 000)
9.Atropine sulfate (0.1 mg/mL)
10.Naloxone (0.4 mg/mL)
11.Sodium bicarbonate (4.2%)
Fluids
1. Normal saline solution or lactated Ringer's solution (500-mL bags)
2.5% Dextrose,
3. Dextrose (50%)
4. Nasogastric tubes (sizes 6–14F)
8/8/2019 Pediatric Emergency Preparedness 2010
http://slidepdf.com/reader/full/pediatric-emergency-preparedness-2010 30/31
[29]
Adapted from: American Academy of Pediatrics: Committee on Pediatric Emergency Medicine.
Emergency Medical Services for Children: The Role of the Primary Care Provider. Singer J,
Ludwig S, eds. Elk Grove
Village, IL: American Academy of Pediatrics; 1992.
Health professional preparedness for pediatric emergencies
Title: Doctor Nurse Clinical officer other
Sex Male Female
Age
Years of
work
experience
:(
tick
appropriately)
<1
yrs.
1‐5 yrs.
6>yrs.
1. Perception of self ‐preparedness:
Prepared in some way
Not prepared at all
Confident of self ‐preparedness
2. Awareness of available protocols for pediatric emergencies in the hospital?
Yes no if yes
Available and has read
Available and has not read
Doesn’t know if there is any and don’t think there is any
3. Immediate action in pediatric emergency situation
Initiate own ideas
Follow hospital protocol
Follow instruction from immediate supervisor
8/8/2019 Pediatric Emergency Preparedness 2010
http://slidepdf.com/reader/full/pediatric-emergency-preparedness-2010 31/31
[30]
4.Learning needs to add on current qualification to enhance management of p emergencies
First aid
Basic life support
Infection control
Triage
5. Specific materials /activities needing to be developed to prepare for pediatric emergencies
Protocol in pediatric emergency yes no
Courses in pediatric emergencies yes no
Drills yes no
Information pamphlets yes no
Related Documents











