
Pediatric dentistry update.final
Aug 03, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

PEDIATRIC DENTISTRY UPDATE
By DR/Ali Abdel Fattah pedodontist

THE DENTAL HOME
THE DENTAL HOME WAS
ESTABLISHED AS “AAPD POLICY
IN 2003, AND IS BASED ON
THE SAME CONCEPT AS THE
AMERICAN ACADEMY OF
PEDIATRICS POLICY STATEMENT
DEFINING THE MEDICAL HOME IN
1992.
THE DENTAL HOME The dental home is the ‘ongoing
relationship between the dentist and
the patient, inclusive of all aspects of
oral health care delivered in a
comprehensive, continuously
accessible, coordinated, and family-
centered way. Establishment of a
dental home begins no later than 12
months of age and includes referral to
dental specialists when appropriate
(AAPD def,)
Early Childhood Caries_4.mp4
The Dental Home Provides…
a. Comprehensive oral health care including
“acute care” and preventive services
in accordance with AAPD periodicity
schedules.
b. Comprehensive assessment for oral diseases and conditions.
The Dental Home Provides…
c. “Individualized “ preventive dental health program based upon a caries-risk assessment and a periodontal disease risk assessment.
d. Anticipatory guidance about growth
and development issues,
(ie, teething, digit or pacifier
habits).
The Dental Home Provides…
e. Plan for acute dental trauma.
f. Information about proper care of the child’s teeth and gingivae. This would include prevention, diagnosis, and treatment of disease of the supporting and surrounding tissues and the
“maintenance of health, function, and esthetics of those structures and tissues.”

Why Brush Teeth in”{ Day Care Centers}” ?
• Develop good habits
• Children may not brush at home
• Children learn basic hygiene principals



H2O X X
Tips for Preventing Decay It’s not the bottle, it’s the beverage

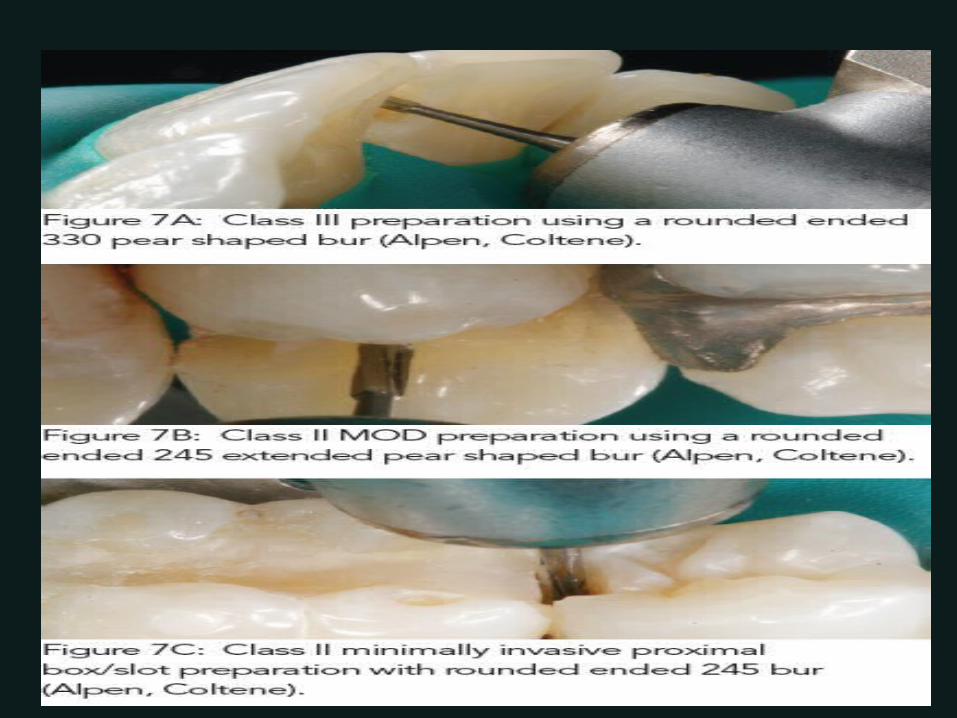
MINIMALLY INVASIVE TECHNIQUES
Minimally invasive techniques today utilize microscope , imaging systems , lasers, air abrasion Prevention protocols can keep the patient disease free indefinitely
Historical Development of Dentistry
- Extraction;
- Surgical approach (“drilling and filling”):
after G.V. Black;- Medical approach – Minimal Intervention.
Minimal Intervention Dentistry
- Modern approach to the treatment
of tooth decay- Based on “Medical Model” of caries management
The Intervention approach Minimal
A medical model; Caries treated as a biological
infection Surgical techniques are {minor}
and stress retention of tooth tissue.
Details of the MI approach
- (1) Reduces cariogenic bacteria; - (2) Uses preventive measures;- (3) Early lesions remineralised;- (4) Minimal surgery on cavities; - (5) Repair of defective restorations.

(1) Cariogenic bacteria
Caries is a bacterial disease;
Depends on dietary sucrose; Driven by frequency of eating; { Modified by saliva }
(2) Preventive measures
• Topical fluoride
• Fissure sealants• Patient education on oral hygiene
(3) Remineralisation
• Requires management by non-intervention {medical model}
• Enhanced by fluoride ion in saliva.
(4) Minimal surgery
Requires adhesive materials (glass-ionomers, adhesive composite systems);
Possibly without drilling (ART technique).
(5) Repair of materials
• To prevent cavity extension;
• Not “botch job”, but appropriate.
The challenge for materials
Adhesion– Occurs naturally for glass-ionomers; problematic for
composites.
Fluoride-release;• Release of other mineralising ions
( PO4, Ca2+ ) Repairable.
Conclusions
• Minimal Intervention dentistry is the future:–Advocated by FDI;
– Cost effective;– Less trauma for the patient.
• A biological approach, not a mechanical one.
• Makes significant demands on materials.

Caries Stabilization Interim therapeutic restorations (ITRs) Resin and glass ionomer sealants Regular recharging of ITRs and sealants
with fluoride Fluoride varnish applications Twice daily brushing with fluoride toothpaste
Why Caries Stabilization?
Poor Dental Access for 0-5 year olds
Only 10% of 0-2 year olds are seen
yearly in the dental clinic. Only 25% of 3-5 year olds are seen
yearly in the dental clinic.
Policy Statement The AAPD recognizes ITR
as a beneficial provisional technique in contemporary pediatric restorative dentistry.
ITR may be used to restore and prevent caries in young patients, uncooperative patients, patients with special needs and situations in which traditional cavity preparation and restorations are not feasible.
Download AAPD policy on ITRs.
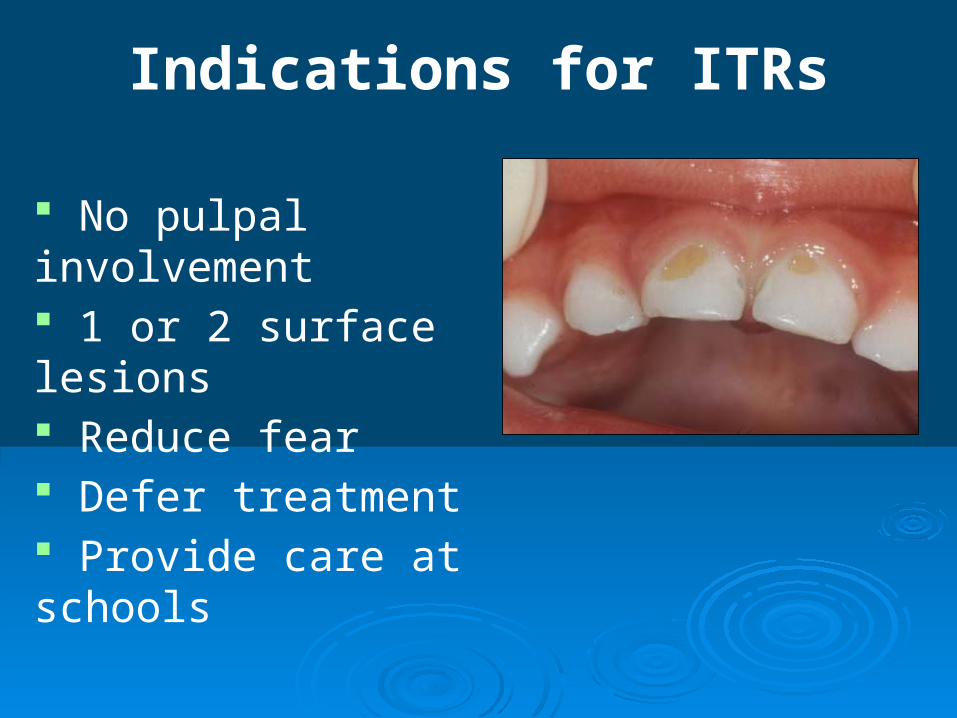
Indications for ITRs
No pulpal involvement 1 or 2 surface lesions Reduce fear Defer treatment Provide care at schools
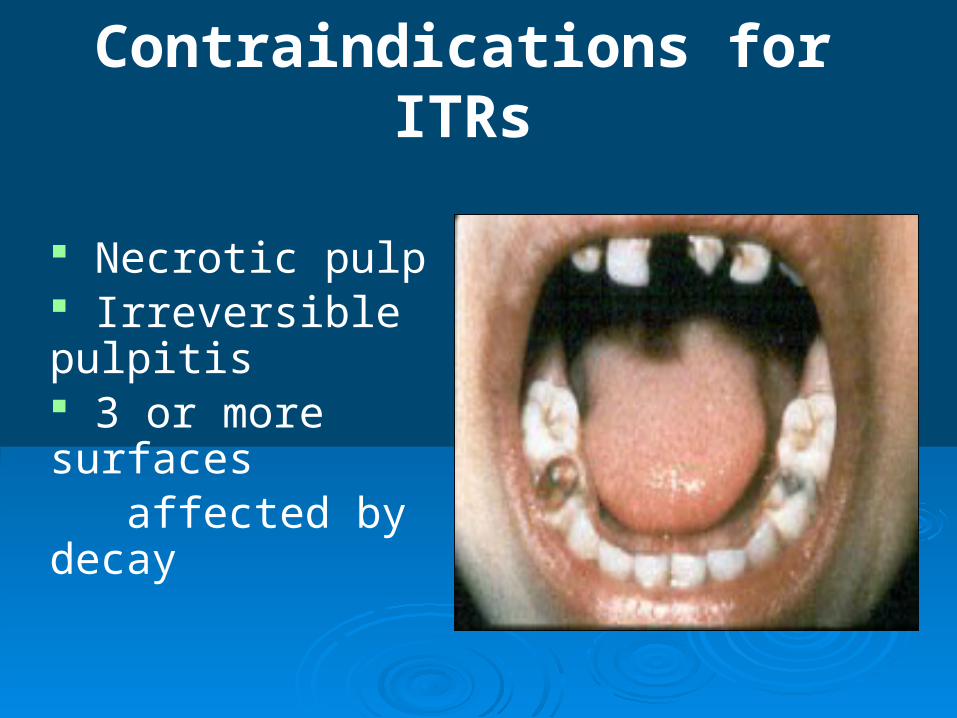
Contraindications for ITRs
Necrotic pulp Irreversible pulpitis 3 or more surfaces affected by decay

Fluoride Varnish “every- every”

Factors for Success
1. Proper diagnosis2. Adequate restoration3. Appropriate excavation4. Margin quality
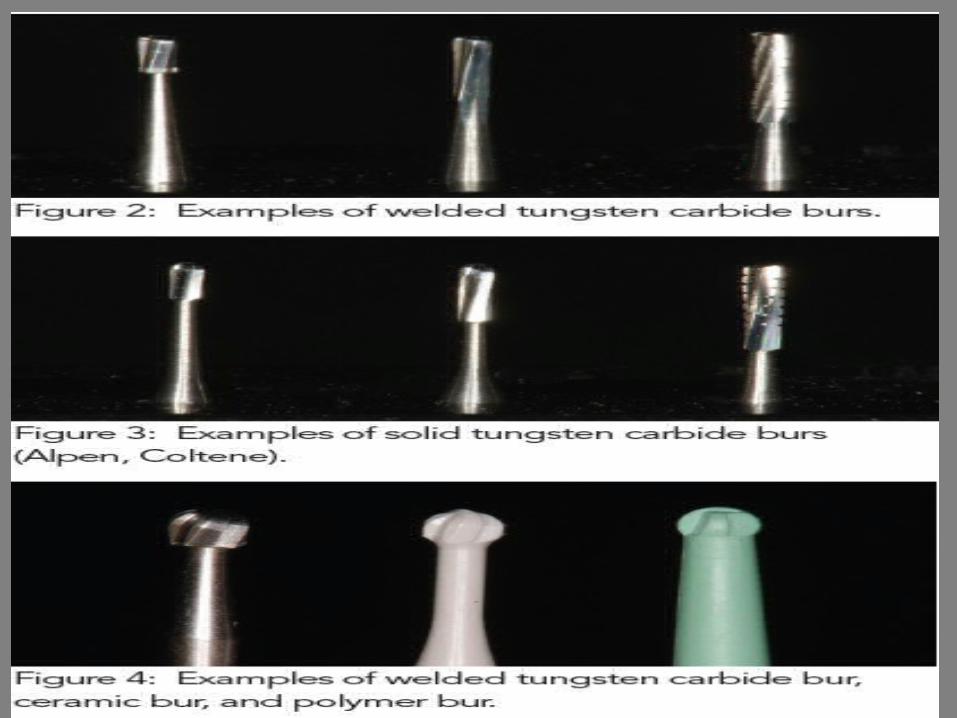

POLYMER BURSmart bur 2 is self – limiting caries removal bur for use in a slow –speed hand piece operating at up to 4000 rpm Research demonstrates that the polymer bur is truly dentin safe & will not cut sound healthy dentine
NuSmile Pediatric Crowns.mp4

NU SIMLE SIGNATURE ARE ST ST CROWNS
WITH TOOTH COLORED COATING
NU SMILE ZR OFFERS SUPERIOR DURABILITY
AND EASY PLACEMENT COMPERED TO
COMPOSITE RESTORATIONS & STRIP CROWNS
NU SMILE & NU SMILE ZR
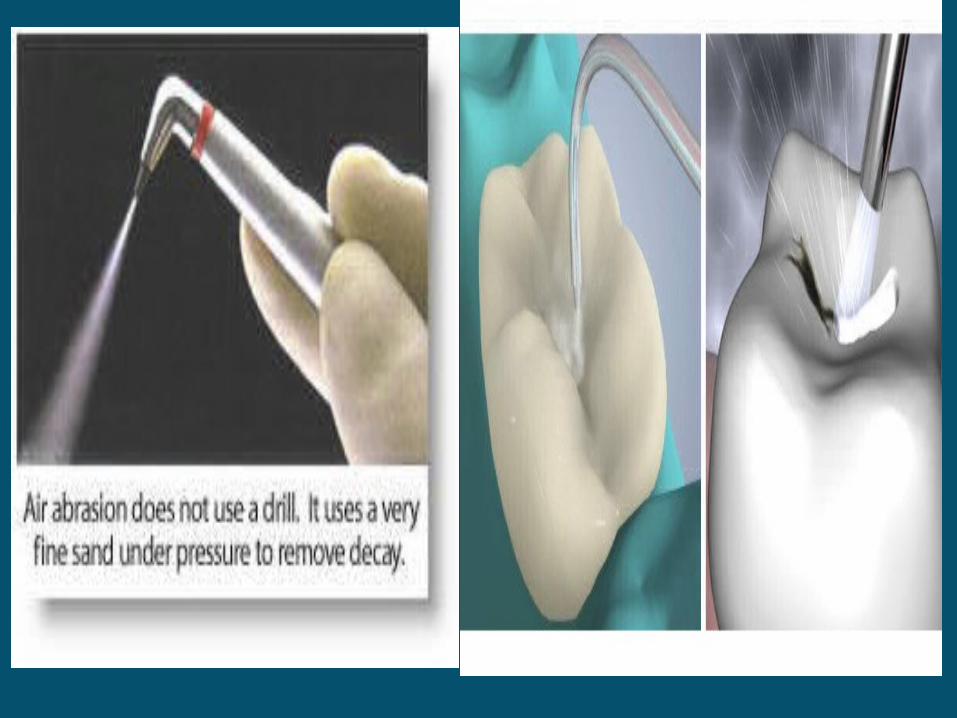
AIR ABRASION
This technique uses a stream of
purified aluminium oxide particles
that are forced under pressure
through a fine –focused nozzle onto
the tooth surface
Quiet Comfort, also called Air Abrasion. - YouTube.mp4
AIR ABRASION
This technique uses a stream of
purified aluminium oxide particles
that are forced under pressure
through a fine –focused nozzle onto
the tooth surface
Pediatrics Air Abrasion.mp4


54
Related Documents











