Pediatric CRRT: Terminology and Physiology Jordan M. Symons, MD University of Washington School of Medicine Seattle Children’s Hospital

Pediatric CRRT: Terminology and Physiology Jordan M. Symons, MD University of Washington School of Medicine Seattle Childrens Hospital.
Mar 31, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Pediatric CRRT: Terminology and Physiology
Jordan M. Symons, MD
University of Washington School of Medicine
Seattle Children’s Hospital

CRRT: What is it?
Continuous
Renal
Replacement
Therapy
•Strict definition: any form of kidney dialysis therapy that operates continuously, rather than intermittently
•More common definition: continuous hemofiltration technique, often used for hemodynamically unstable patients

Current Nomenclature for CRRT
SCUF: Slow Continuous Ultrafiltration
CVVH: Continuous Veno-Venous Hemofiltration
CVVHD: Continuous Veno-Venous Hemodialysis
CVVHDF: Continuous Veno-Venous Hemodiafiltration

C VV H
Basis for CRRT Nomenclature
Rate/Interval for Therapy
Blood Access
Method for Solute Removal

Solute Removal Mechanisms in RRT• Diffusion
– transmembrane solute movement in response to a concentration gradient
– importance inversely proportional to solute size
• Convection– transmembrane solute movement in association
with ultrafiltered plasma water (“solvent drag”)– mass transfer determined by UF rate (pressure
gradient) and membrane sieving properties– importance directly proportional to solute size

Diffusion

Convection

Clearance: Convection vs. Diffusion

• SCUF
• CVVH
• CVVHD
• CVVHDF
UF
D
R
CRRT Schematic

Rate Limitations of Volume Removal
Vascular Compartment
Extra-Vascular Compartment
BP

Improved Volume Removal with Slower Ultrafiltration Rates
Vascular Compartment
Extra-Vascular Compartment
BP Stable

CRRT for Metabolic Control
0
20
40
60
80
100
120
Time
BU
N (
mg
/dL
)
IHD CRRT

Hollow Fiber Hemofilter

Hemofiltration Membranes
Capillary Cross Section Blood Side

Hemofilter Characteristics
• Pore size– “High Flux” vs. “High cut-off”
• Surface area; porosity– Effects on maximum ultrafiltration capacity
• Membrane material– polysulfone, PAN, etc.; modifications
• Adsorption• Prime volume

Effect of Pore Size on Membrane Selectivity
Creatinine 113 D
Urea 60 D
Glucose 180 D
Vancomycin~1,500 D
IL-6~25,000 D
Albumin~66,000 D

Effect of Pore Size on Membrane Selectivity
Creatinine 113 D
Urea 60 D
Glucose 180 D
Vancomycin~1,500 D
Albumin~66,000 D
IL-6~25,000 D
These effects are maximized in convection

--
--
--
--
--
-
-
-
-
-
-
-
-
Other Membrane Characteristics: e.g., Charge Negative charge
on membrane:• Negatively charged
particles may be repelled, limiting filtration

--
--
--
--
--
+
+
+
+
+
+
+
+
Other Membrane Characteristics: e.g., Charge Negative charge
on membrane:• Negatively charged
particles may be repelled, limiting filtration
• Positively charged particles may have increased sieving

--
--
--
--
--
Other Membrane Characteristics: e.g., Charge Negative charge
on membrane:• Negatively charged
particles may be repelled, limiting filtration
• Positively charged particles may have increased sieving
• Charge may change adsorption

Blood Flow and Dialyzer Have Major Impact on Intermittent HD Clearance
Dialyzer 2: Higher K0A
Dialyzer 1: Lower K0A
Dialysate flow rate (QD) always exceeds QB

Solution/Effluent Flow Rate is Limiting Factor in CRRT
QB 150ml/min
QD 600ml/hr
QR 600ml/hr
Effluent 1200ml/hr +

Solution/Effluent Flow Rate is Limiting Factor in CRRT
QB 150ml/min
QD 1000ml/hr
QR 1000ml/hr
Effluent 2000ml/hr +

Patient’s Chemical Balance on CRRT Approximates Delivered Fluids
• Diffusion: blood equilibrates to dialysate
• Convection: loss is isotonic; volume is “replaced”
• Consider large volumes for other fluids (IVF, feeds, meds, etc.)
• Watch for deficits of solutes not in fluids

Diffusion• Small molecules
diffuse easily• Larger molecules
diffuse slowly• Dialysate required
– Concentration gradient– Faster dialysate flow
increases mass transfer

Convection• Small/large molecules
move equally• Limit is cut-off size of
membrane• Higher UF rate yields
higher convection but risk of hypotension
• May need to Replace excess UF volume
H2O
H2O
H2O
H2O
Net Pressure

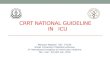
Kramer, P, et al. Arteriovenous haemofiltration: A new and simple method for treatment of over-hydrated patients resistant to diuretics. Klin Wochenschr 55:1121-2, 1977.
First CAVH Circuit


CRRT Machines

Pediatric CRRT Terminology and Physiology: Summary
• CRRT comes in several flavors– SCUF, CVVH, CVVHD, CVVHDF
• Solute transport: diffusion/convection• UF approximates 1-compartment model• Membrane characteristics affect therapy• Fluid composition, rates drive clearance• Advancing technology provides more
options

One of the first infants to receive CRRTVicenza, 1984
Related Documents