10/7/12 1 Pediatric AirwayYou Swallowed What? Staci Kothbauer, CRNA, MS, APNP University of Wisconsin Hospital American Family Children’s Hospital Madison, WI

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
10/7/12
1
Pediatric Airway-‐You Swallowed What?
Staci Kothbauer, CRNA, MS, APNP
University of Wisconsin Hospital American Family Children’s Hospital
Madison, WI
10/7/12
2
* Understand basic pediatric airway anatomy and how it differs from adults * Identify common syndromes associated with a pediatric difficult airway * Describe techniques to manage a difficult airway * Identify risk factors for airway complications during a general anesthetic in the pediatric patient * Identify common airway emergencies that may present management challenges
Objectives
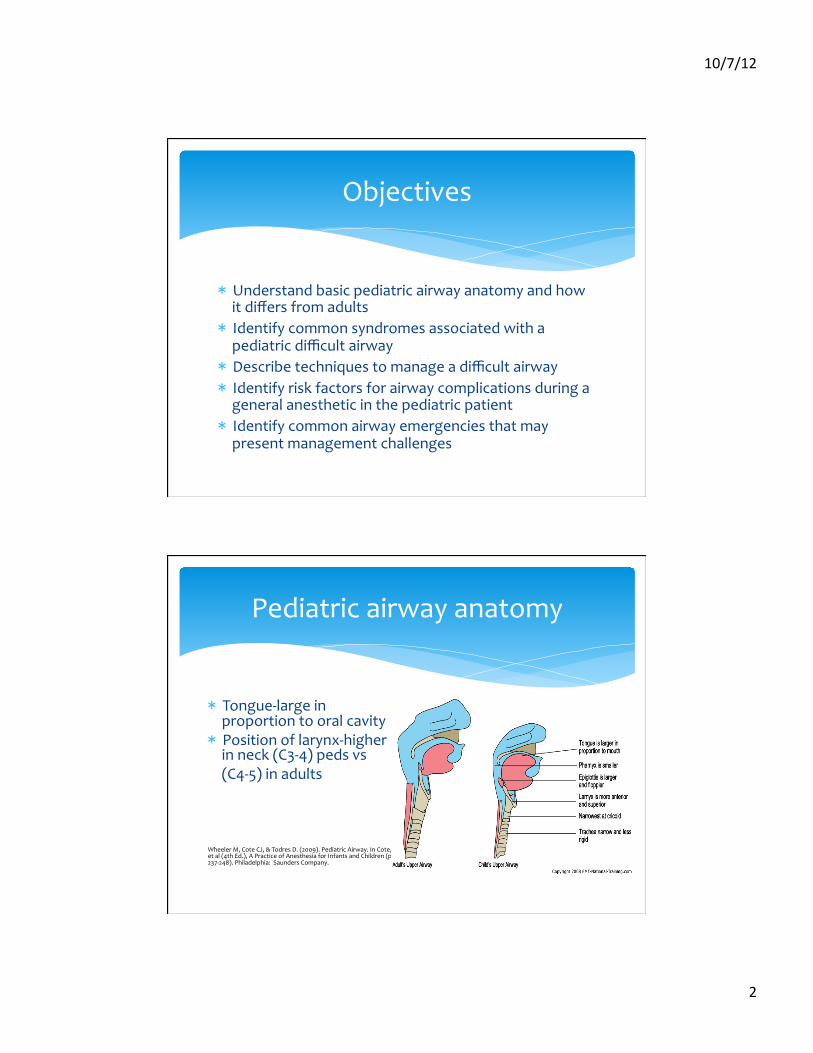
Pediatric airway anatomy
* Tongue-‐large in proportion to oral cavity * Position of larynx-‐higher in neck (C3-‐4) peds vs
(C4-‐5) in adults
Wheeler M, Cote CJ, & Todres D. (2009). Pediatric Airway. In Cote, et al (4th Ed.), A Practice of Anesthesia for Infants and Children (pp.237-‐248). Philadelphia: Saunders Company.
10/7/12
3
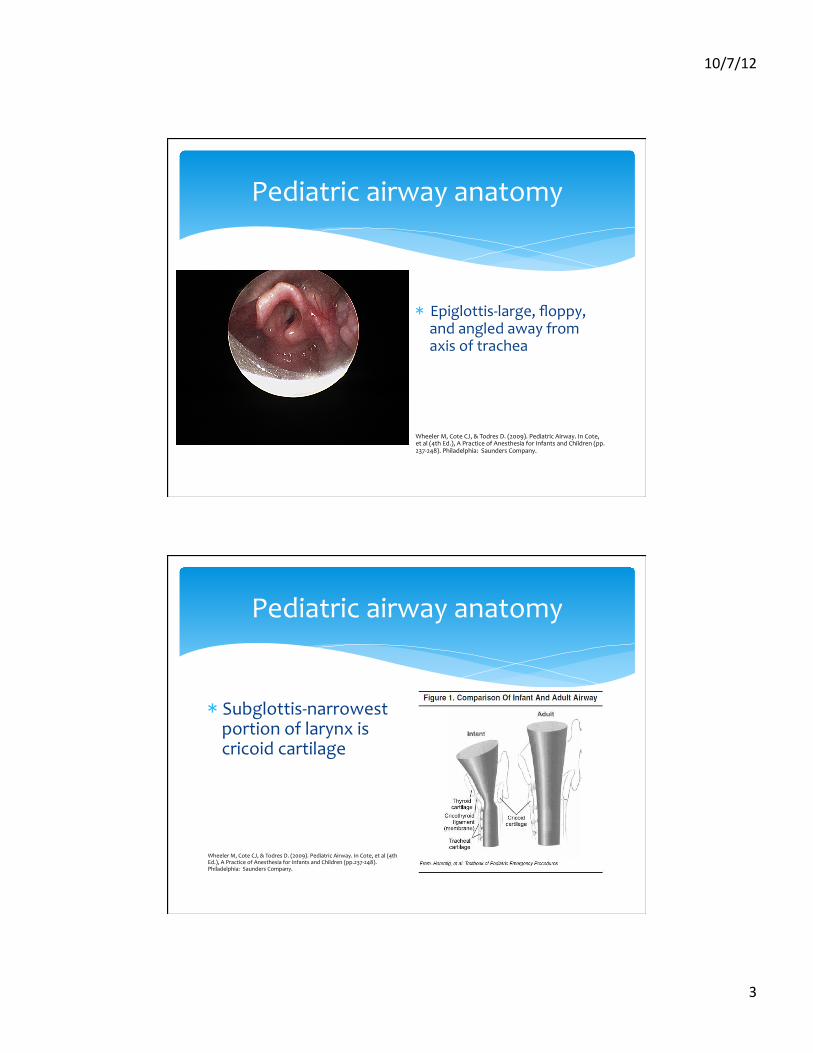
Pediatric airway anatomy
* Epiglottis-‐large, floppy, and angled away from axis of trachea
Wheeler M, Cote CJ, & Todres D. (2009). Pediatric Airway. In Cote, et al (4th Ed.), A Practice of Anesthesia for Infants and Children (pp.237-‐248). Philadelphia: Saunders Company.
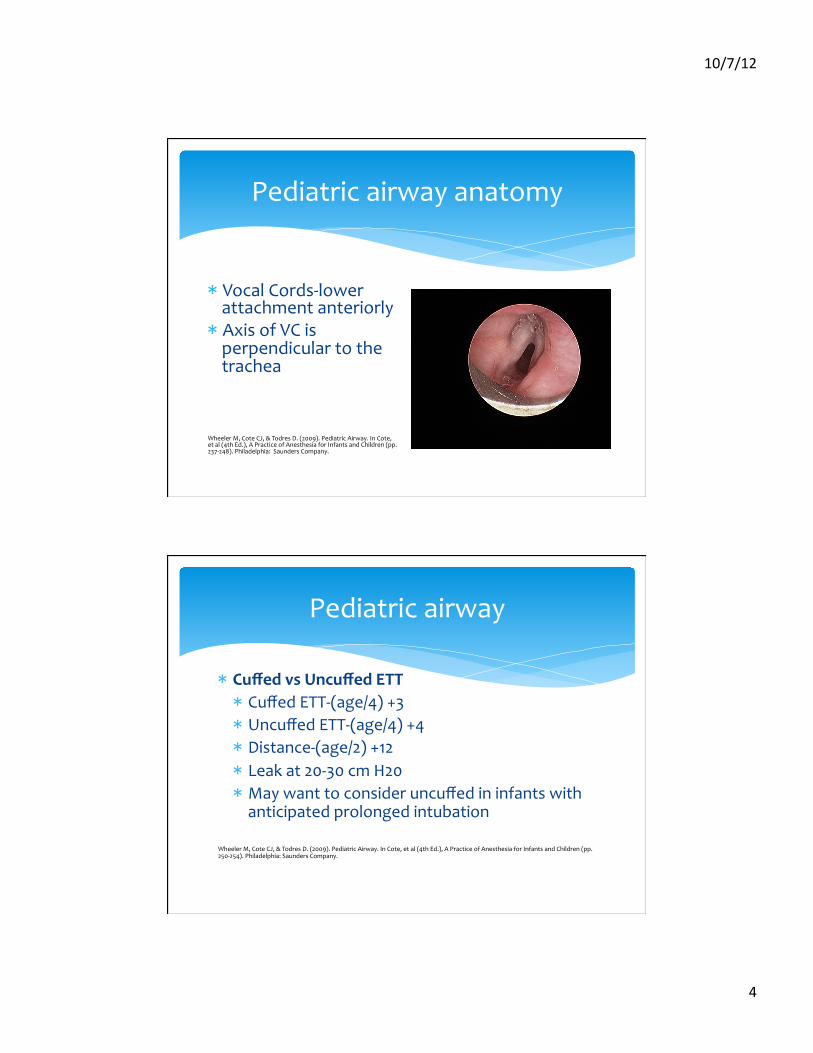
Pediatric airway anatomy
* Subglottis-‐narrowest portion of larynx is cricoid cartilage
Wheeler M, Cote CJ, & Todres D. (2009). Pediatric Airway. In Cote, et al (4th Ed.), A Practice of Anesthesia for Infants and Children (pp.237-‐248). Philadelphia: Saunders Company.
10/7/12
4
Pediatric airway anatomy
* Vocal Cords-‐lower attachment anteriorly * Axis of VC is perpendicular to the trachea
Wheeler M, Cote CJ, & Todres D. (2009). Pediatric Airway. In Cote, et al (4th Ed.), A Practice of Anesthesia for Infants and Children (pp.237-‐248). Philadelphia: Saunders Company.
* Cuffed vs Uncuffed ETT * Cuffed ETT-‐(age/4) +3 * Uncuffed ETT-‐(age/4) +4 * Distance-‐(age/2) +12 * Leak at 20-‐30 cm H20 * May want to consider uncuffed in infants with anticipated prolonged intubation
Wheeler M, Cote CJ, & Todres D. (2009). Pediatric Airway. In Cote, et al (4th Ed.), A Practice of Anesthesia for Infants and Children (pp.250-‐254). Philadelphia: Saunders Company.
Pediatric airway
10/7/12
5
Microcuff ETT
Pediatric airway
* Complications of intubation * Post-‐intubation croup * ETT to large * Surgery > 1 hour * Repeated attempts * Traumatic intubation * Age 1-‐4
Wheeler, M, Cote, C, J, & Todres, D. (2009). Pediatric Airway. In Cote, et al (4th Ed.), A Practice of Anesthesia for Infants and Children (pp.253-‐254). Philadelphia: Saunders Company.
* Position other than supine * Change in position during procedure * Coughing on ETT * Previous history of croup
10/7/12
6
Pediatric syndromes
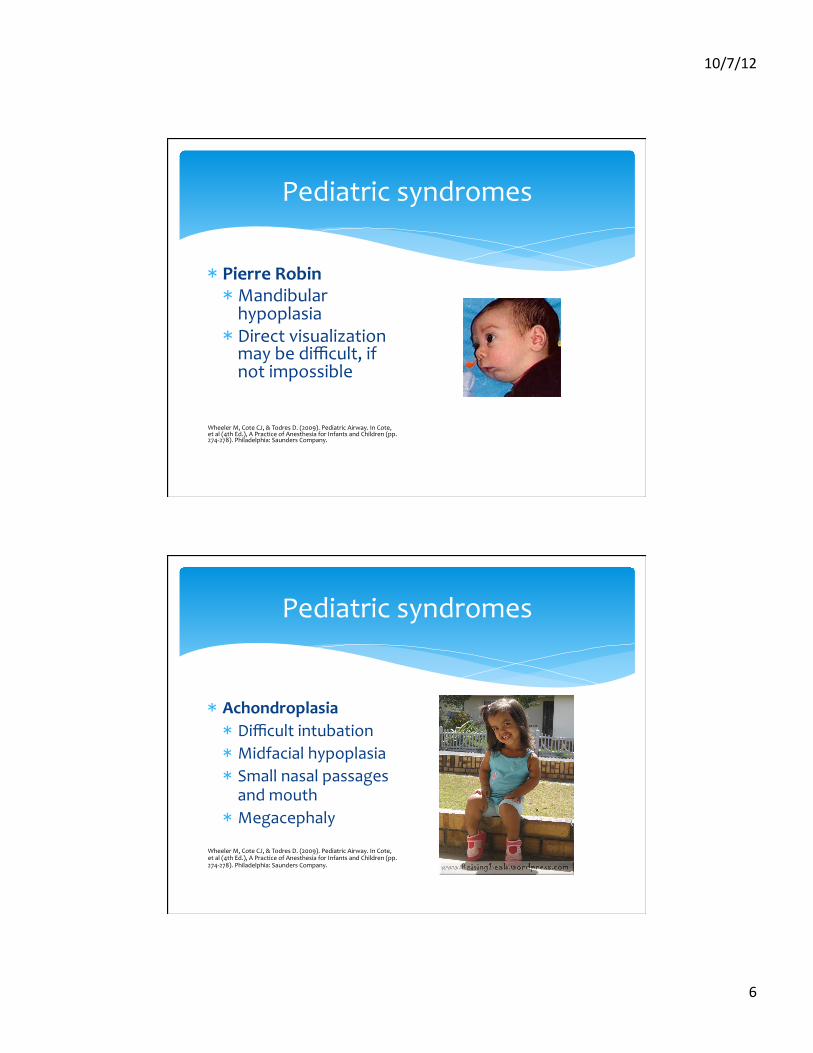
* Pierre Robin * Mandibular hypoplasia * Direct visualization may be difficult, if not impossible
Wheeler M, Cote CJ, & Todres D. (2009). Pediatric Airway. In Cote, et al (4th Ed.), A Practice of Anesthesia for Infants and Children (pp.274-‐278). Philadelphia: Saunders Company.
Pediatric syndromes
* Achondroplasia * Difficult intubation * Midfacial hypoplasia * Small nasal passages and mouth * Megacephaly
Wheeler M, Cote CJ, & Todres D. (2009). Pediatric Airway. In Cote, et al (4th Ed.), A Practice of Anesthesia for Infants and Children (pp.274-‐278). Philadelphia: Saunders Company.

10/7/12
7
Pediatric syndromes
* Marfan syndrome * Difficult intubation * Narrow palate or high arched palate * Scoliosis or kyphosis * Cardiac and pulmonary disease * Dissecting aortic aneurysm
Wheeler M, Cote CJ, & Todres D. (2009). Pediatric Airway. In Cote, et al (4th Ed.), A Practice of Anesthesia for Infants and Children (pp.274-‐278). Philadelphia: Saunders Company.
* Rheumatoid Arthritis * Limited TMJ mobility * Hypoplasic mandible * Cricoarytenoid arthritis with narrow larynx * Cervical spine subluxation, rigid cervical spine
Wheeler M, Cote CJ, & Todres D. (2009). Pediatric Airway. In Cote, et al (4th Ed.), A Practice of Anesthesia for Infants and Children (pp.274-‐278). Philadelphia: Saunders Company.
Pediatric Syndromes
10/7/12
8
Pediatric syndromes
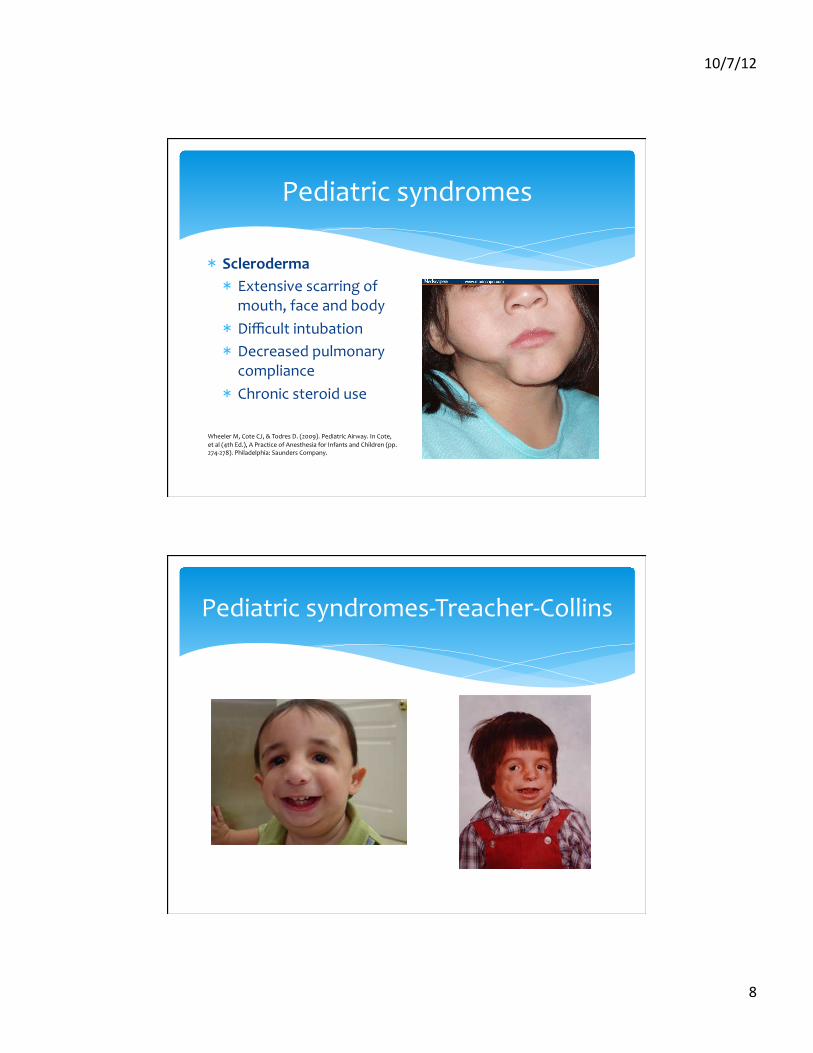
* Scleroderma * Extensive scarring of
mouth, face and body * Difficult intubation * Decreased pulmonary
compliance * Chronic steroid use
Wheeler M, Cote CJ, & Todres D. (2009). Pediatric Airway. In Cote, et al (4th Ed.), A Practice of Anesthesia for Infants and Children (pp.274-‐278). Philadelphia: Saunders Company.
Pediatric syndromes-‐Treacher-‐Collins
10/7/12
9
Pediatric syndromes
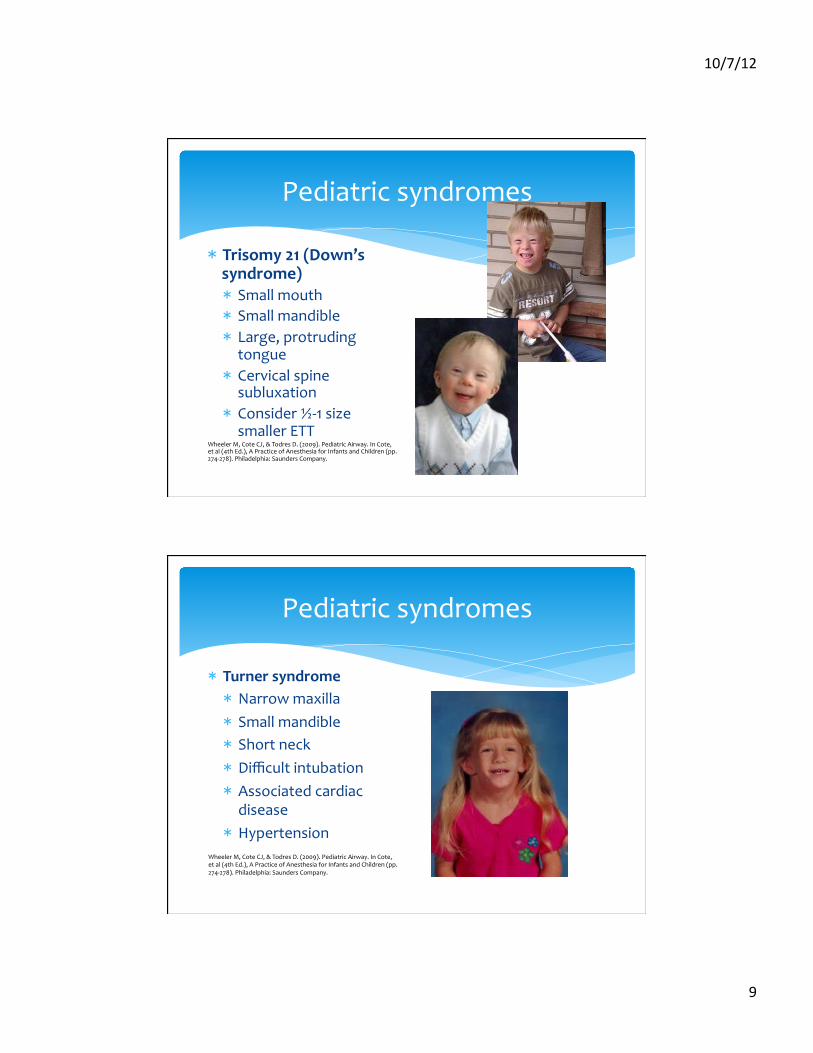
* Trisomy 21 (Down’s syndrome) * Small mouth * Small mandible * Large, protruding
tongue * Cervical spine
subluxation * Consider ½-‐1 size
smaller ETT Wheeler M, Cote CJ, & Todres D. (2009). Pediatric Airway. In Cote, et al (4th Ed.), A Practice of Anesthesia for Infants and Children (pp.274-‐278). Philadelphia: Saunders Company.
Pediatric syndromes
* Turner syndrome * Narrow maxilla * Small mandible * Short neck * Difficult intubation * Associated cardiac
disease * Hypertension
Wheeler M, Cote CJ, & Todres D. (2009). Pediatric Airway. In Cote, et al (4th Ed.), A Practice of Anesthesia for Infants and Children (pp.274-‐278). Philadelphia: Saunders Company.
10/7/12
10
* Awake vs Asleep * Asleep * Spontaneously breathing * Helpful in locating glottis * Avoid neuromuscular blockade
* Sedation-‐if tolerated * Midazolam (0.05 mg/kg IV) and fentanyl (0.5-‐1 mcg/kg IV)
* Ketamine (0.25-‐0.5 mg/kg IV) every 2 minutes * Psychomimetic emergence reactions less in children
Wheeler M, Cote CJ, & Todres D. (2009). Pediatric Airway. In Cote, et al (4th Ed.), A Practice of Anesthesia for Infants and Children (pp.259-‐263). Philadelphia: Saunders Company.
Management of the Pediatric Difficult Airway
* Nebulized lidocaine * Topical spray or jellies * Translaryngeal lidocaine * “spray as you go” with lidocaine * Superior laryngeal nerve block * Use caution not to deliver toxic lidocaine doses * 5 mg/kg or 7 mg/kg with epinephrine
Wheeler M, Cote CJ, & Todres D. (2009). Pediatric Airway. In Cote, et al (4th Ed.), A Practice of Anesthesia for Infants and Children (pp.259-‐263). Philadelphia: Saunders Company.
Anesthetizing the airway
10/7/12
11
* Biggest difference from adult * metabolic rate * FRC * Time from zero 02sat from inspired concentration of 90% to neurological injury * Adults-‐10 minutes * Children-‐4 minutes!!!!
Wheeler M, Cote CJ, & Todres D. (2009). Pediatric Airway. In Cote, et al (4th Ed.), A Practice of Anesthesia for Infants and Children (pp.263). Philadelphia: Saunders Company.
Unexpected Difficult Airway
* Laryngospasm * 14% in <6 year olds to 3.6% in >6 year olds (1)
* Higher ASA score * Type of airway device used (1-‐4) * Upper respiratory infection (URI) (5)
(1) Murat I, Constant I, Maudhuy H. Perioperative anesthetic morbidity in children: a database of 24, 165 anesthetics over a 30-‐month period. Pediatric Anesthesia 2004; 14: 158-‐166.
(2) Parnis SJ, Barker DS, Van Der Walt JH. Clinical predictors of anesthetic complications in children with respiratory tract infections. Pediatric Anesthesia 2001; 11 29-‐40.
(3) Tait AR, Malviya S, Voepel-‐Lewis T et al. Risk factors for perioperative adverse respiratory events in children with upper respiratory tract infections. Anesthesiology 2001; 95: 299-‐306.
(4) Rachel Homer J, Elwood T, Peterson D, Rampersad S et al. Risk factors for adverse events in children with colds emerging from anesthesia: a logistic regression. Pediatric Anesthesia 2007; 17: 154-‐161..
(5) Flick R, Wilder R, Pieper S et al. Risk factors for laryngospasm in children during general anesthesia. Pediatric Anesthesia 2008; 18: 289-‐296.
Who is at risk for respiratory adverse events?
10/7/12
12
* Bordet et al. in Pediatric Anesthesia (2002) (1) * <6 years * Recent RI * Use of LMA * Flick et al. in Pediatric Anesthesia (2008) (2) * 130 children with laryngospasm under GA * Significant association between laryngospasm and
current URI or airway anomaly * LMA + URI=strong association
(1) Bordet F, Allaouchiche B, Lansiaux S et al. Risk factors for airway complications during general anesthesia in pediatric patients. Pediatric Anesthesia 2002; 12: 762-‐769.
(2) Flick R, Wilder R, Pieper S et al. Risk factors for laryngospasm in children during general anesthesia. Pediatric Anesthesia 2008; 18: 289-‐296.
Upper Respiratory Infections
* Croup, bronchitis, bronchiolitis, or pneumonia * Within 4-‐6 weeks * Current or new URI * Dependent on procedure * Fever * Wheezing * “Wet” cough * Patient history-‐asthma
Ghazal EA, Mason LJ, & Cote CJ. (2009). Preoperative Evaluation, Premedication, and Induction of Anesthesia. In Cote, et al (4th Ed.), A Practice of Anesthesia for Infants and Children (pp.60-‐62). Philadelphia: Saunders Company.
When to Cancel?
10/7/12
13
* How long to postpone? * Ideally 7 weeks….not practical * Postpone 2 weeks
* Bottom line-‐proceed with caution if asymptomatic
Ghazal EA. Mason LJ, & Cote CJ. (2009). Preoperative Evaluation Premedication, and Induction of Anesthesia. In Cote, et al (4th Ed.), A Practice of Anesthesia for Infants and Children (pp.60-‐62). Philadelphia: Saunders Company. Orliaguet GA, Olivier G, Savoidelli GL, et al. Case Scenario: Perianesthetic Management of Laryngospasm in Children. Anesthesiology 2012; 116: 458-‐471.
When to Cancel?
* Chin lift * Jaw thrust * Positive pressure * Propofol * Succinylcholine (0.5 mg/kg IV) or (3-‐4 mg/kg IM) (1) * Rocuronium (4-‐5 mg/kg IM) (2) * Treatment depends on severity of laryngospasm (1) Orliaguet GA, Olivier G, Savoidelli GL, et al. Case Scenario: Perianesthetic Management of Laryngospasm in Children. Anesthesiology
2012; 116: 458-‐471. (2) American Academy of Pediatrics, Committee on Drugs. Drugs for Pediatric Emergencies. Pediatrics 1998; 101: e13.
Laryngospasm

10/7/12
14
* Epiglottitis, foreign body, bleeding tonsil * AIRWAY TAKES PRIORITY OVER “FULL STOMACH” * Keep spontaneously breathing * Laryngoscopy under deep volatile agent * ***KEEP CHILD CALM***
* Clear communication with ENT surgeon and OR staff PRIOR to induction
Everett LL, Fuzaylov G, & Todres D. (2009). Pediatric Emergencies. In Cote, et al (4th Ed.), A Practice of Anesthesia for Infants and Children (pp.767-‐772). Philadelphia: Saunders Company.
Airway Emergencies
* IV after induction * Parents into OR ???? * Induce in sitting position * IV-‐ 10-‐30 mL/kg of LR rapidly * Early administration of atropine (10 mcg/kg IV) or glycopyrrolate (10 mcg/kg IV)
Everett LL, Fuzaylov G, & Todres D. (2009). Pediatric Emergencies. In Cote, et al (4th Ed.), A Practice of Anesthesia for Infants and Children (pp.767-‐772). Philadelphia: Saunders Company.
Airway Emergencies
10/7/12
15
* Epiglottitis * Keep child calm * Inhalation induction in sitting position * IV, rapid rehydration, atropine (10 mcg/kg) * Deep intubation * ETT ½ size smaller * Unable to intubate trach * Post-‐op-‐PICU, 24-‐48 hrs.
Everett LL, Fuzaylov G, & Todres D. (2009). Pediatric Emergencies. In Cote, et al (4th Ed.), A Practice of Anesthesia for Infants and Children (pp.772-‐773). Philadelphia: Saunders Company.
Upper Airway Obstruction-‐inspiratory stridor, retractions, tachypnea
Foreign Body Aspiration
* 5th leading cause of death in <1 year olds * May present with wheezing,
cough, and unilateral breath sounds * Emergency treatment if
symptomatic…OR * If stable, radiographic exam * DO NOT INDUCE WITHOUT
ENT SURGEON! Everett LL, Fuzaylov G, & Todres D. (2009). Pediatric Emergencies. In Cote, et al (4th Ed.), A Practice of Anesthesia for Infants and Children (pp.774-‐775). Philadelphia: Saunders Company.
10/7/12
16
What is the foreign body?
LEGO!
10/7/12
17
* Occurs within 6 hours, or 5 to 10 days post-‐op * Considered full stomach * Potential loss of airway * Hemodynamic compromise * ***Replace fluid, if possible, and draw Hgb/Hct
Hannallah RS, Brown KA, & Verghese ST. (2009). Otorhinolaryngologic Procedures. In Cote, et al (4th Ed.), A Practice of Anesthesia for Infants and Children (pp.670-‐671). Philadelphia: Saunders Company.
Tonsil Bleed
* IV access prior to induction * Pretreat with atropine (10 mcg/kg IV) or glycopyrrolate (10 mcg/kg IV) * Induce with ketamine (1-‐2 mg/kg IV) or etomidate (0.3
mg/kg IV), and succinylcholine (1.5-‐2 mg/kg IV)
* RSI * Difficulty visualizing VC-‐press on stomach * Limit opioids * OG tube prior to extubation Campo S, Denman W, & Todres D. (2001). Pediatric Emergencies. In Cote, et al (3rd Ed.), A Practice of Anesthesia for Infants and Children (pp.315-‐330). Philadelphia: Saunders Company.
Tonsil Bleed
10/7/12
18
* Goals: oxygenation, reduce airway obstruction, prevent complications * RSI if full stomach-‐avoid “light” intubation * Premed prior to induction * Opioids, IV lidocaine * Glycopyrrolate or atropine * Increase expiratory time to prevent air trapping * Accept somewhat elevated PaC02 * Limit peak inspiratory pressure to 40-‐45 cm H2o Everett LL, Fuzaylov G, & Todres D. (2009). Pediatric Emergencies. In Cote, et al (4th Ed.), A Practice of Anesthesia for Infants and Children (pp.775-‐). Philadelphia: Saunders Company.
Asthma in Emergency cases
* Treatment * Bronchodilator-‐nebulized or metered-‐dose inhaler * Albuterol
* Beta-‐adrenergic agents * Epinephrine 1:1000 (0.01 mg/kg) SQ every 15 min x3 (max 0.3 mL) * Terbutaline-‐0.01 mL/kg (max 0.25 mL) SQ every 30 min x2 or 0.1 mcg/kg/min, titrate to effect
Campo S, Denman W, & Todres D. (2001). Pediatric Emergencies. In Cote, et al (3rd Ed.), A Practice of Anesthesia for Infants and Children (pp.315-‐330). Philadelphia: Saunders Company.
Bronchospasm
10/7/12
19
* Corticosteroids * Hydrocortisone 7 mg/kg IV immediately and 7 mg/kg/24hr, divided in 6 doses * Methylprednisolone 2 mg/kg IV immediately and 2 mg/kg/24hr, divided in 6 doses * Dexamethasone 0.3 mg/kg IV immediately and 0.3 mg/kg/24hr, divided in 6 doses
Campo S, Denman W, & Todres D. (2001). Pediatric Emergencies. In Cote, et al (3rd Ed.), A Practice of Anesthesia for Infants and Children (pp.315-‐330). Philadelphia: Saunders Company.
Asthma
* Pediatric airway anatomy is different from that of an adult airway * Be alert to children with syndromes and the potential for a difficult airway * Keep the child spontaneously breathing when a difficult airway is suspected * Proceed with caution with recent URI * Keep child calm during emergency airway situations * Avoid “light” anesthesia with asthmatics
Conclusions
Related Documents











