3D PRINTING IN CHEST WALL PATHOLOGIES Marcelo C. DaSilva, MD, FACS Division of Thoracic Surgery - Brigham and Women’s Hospital. Boston, MA Harvard Medical School

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
3D PRINTING IN CHEST WALL PATHOLOGIES
Marcelo C. DaSilva, MD, FACS Division of Thoracic Surgery - Brigham and Women’s Hospital. Boston, MA
Harvard Medical School

Pectus Excavatum
Marcelo C. DaSilva, MD, FACS
Pectus Excavatum
• Most common congenital sternal deformity
– 1 in 400 children
• Excessive growth of lower costal cartilage resulting in sternal depression
• Deeper depression on the right, pushing heart to the left
• Congenital with progressive worsening over time
• Rarely familial
Marcelo C. DaSilva, MD, FACS
Physiologic Manifestations
• Usually asymptomatic
• “Subjective” decrease in respiratory reserve with exercise
• Scoliosis and mitral valve prolapse have been associated with pectus excavatum
• Mild restrictive pattern on PFTs has been documented in some studies
• Decreased stroke volume and CO during upright exercise has also been demonstrated
Marcelo C. DaSilva, MD, FACS
Operative Indications
• Cosmetic correction is the most common reason
• Psycho-social factors, however, may be quite limiting, particularly in older children and teenagers
• Respiratory insufficiency and recurrent pulmonary infections
• Best results are obtained in patients between the ages of 3 and 5
Marcelo C. DaSilva, MD, FACS
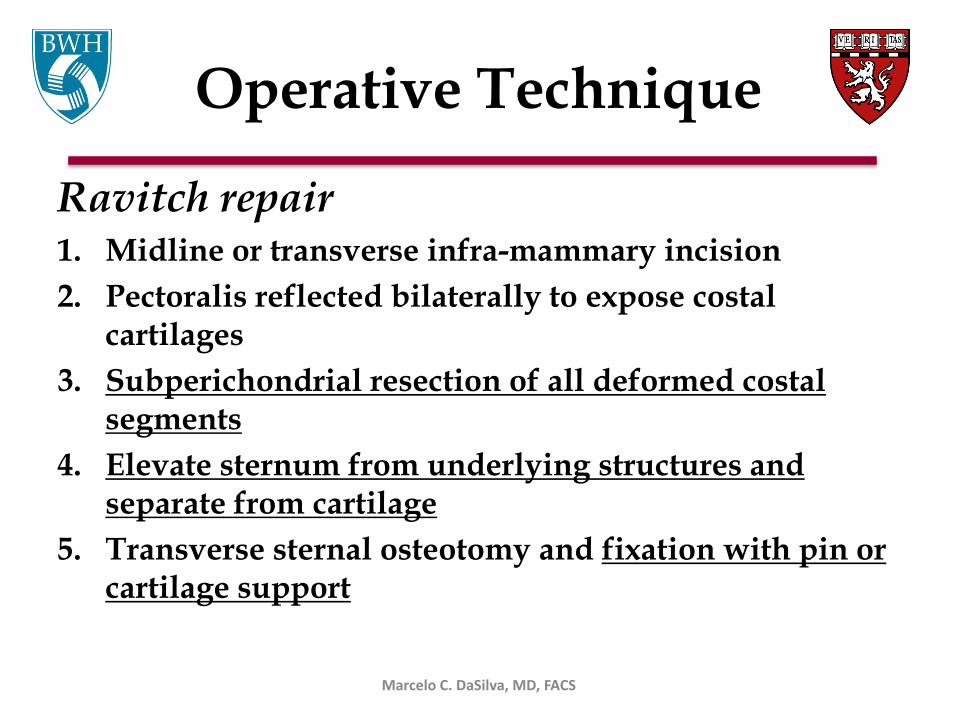
Operative Technique
Ravitch repair 1. Midline or transverse infra-mammary incision
2. Pectoralis reflected bilaterally to expose costal cartilages
3. Subperichondrial resection of all deformed costal segments
4. Elevate sternum from underlying structures and separate from cartilage
5. Transverse sternal osteotomy and fixation with pin or cartilage support
Marcelo C. DaSilva, MD, FACS

Results
• Cosmetic results are good in 80-90%
• Recurrence occurs in about 10-20% of patients
• Return of normal respiratory function and improvement in exercise capacity is possible
Marcelo C. DaSilva, MD, FACS

3D & New Technique for Repair of Pectus Excavatum in Adults
• 43-yo referred for a 2nd opinion for pectus
excavatum
• SOB, DOE progressive worse past 2 years
• CT scan: severe excavatum with AP diameter of 4.5 cm at the xyphoid
– displacement of the heart.
• FVC 3.18 (88%) FEV1 1.33 (45%) DLCO: 18.74
Marcelo C. DaSilva, MD, FACS

Stress Echo
• Left Ventricle: segmental left ventricular wall motion abnormalities present
– Wall motion abnormality involves the septal location
• Tricuspid Valve – Resting
– There is color and spectral Doppler evidence of severe tricuspid regurgitation
Marcelo C. DaSilva, MD, FACS
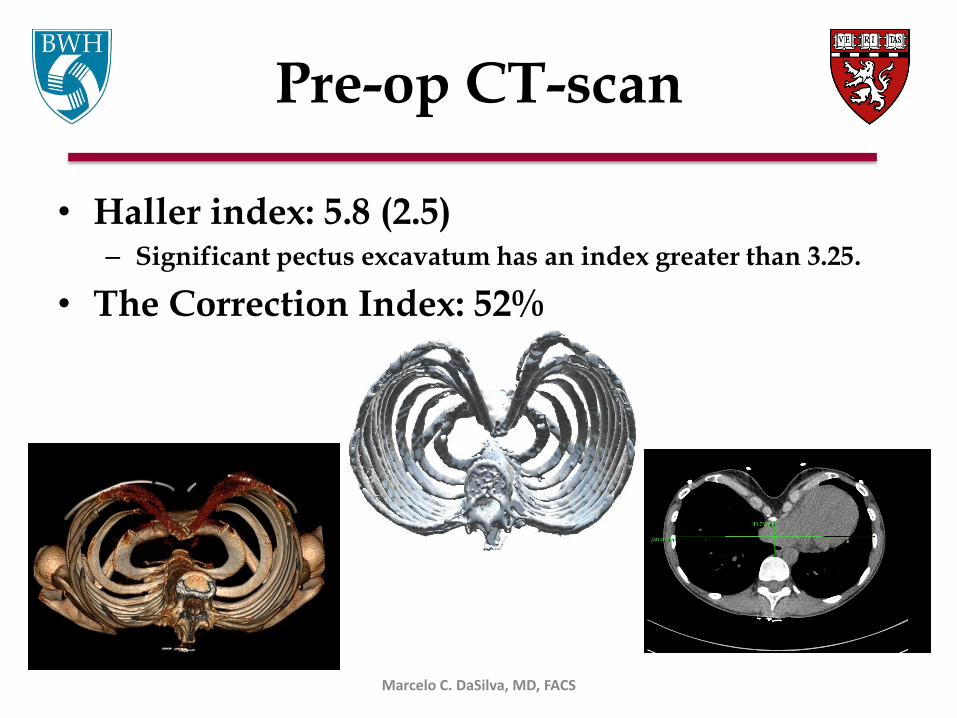
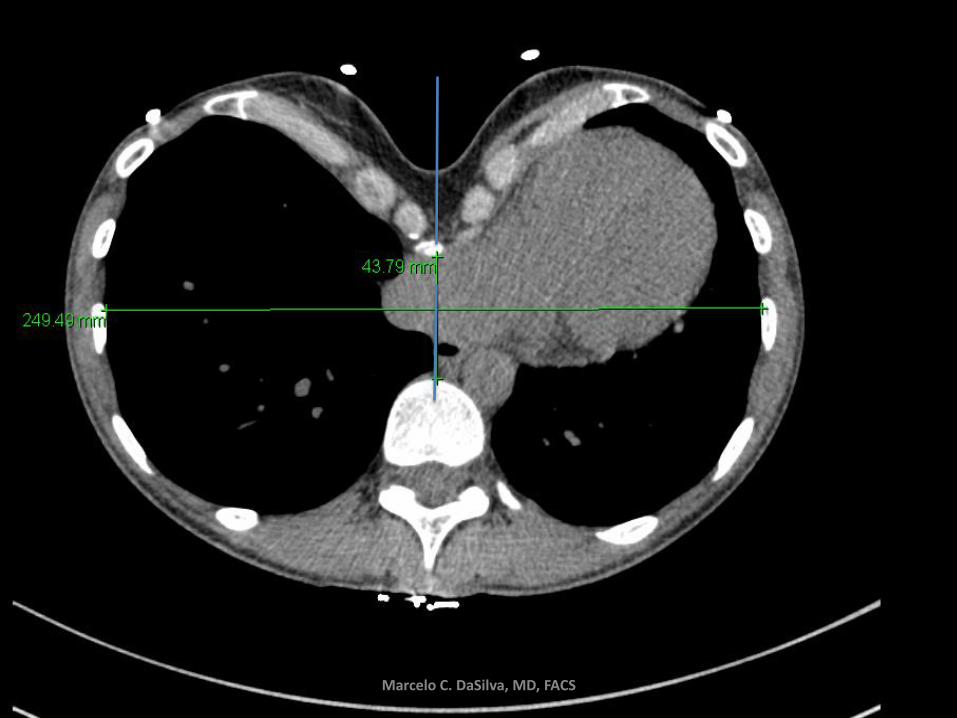
Pre-op CT-scan
• Haller index: 5.8 (2.5) – Significant pectus excavatum has an index greater than 3.25.
• The Correction Index: 52%
Marcelo C. DaSilva, MD, FACS
Marcelo C. DaSilva, MD, FACS
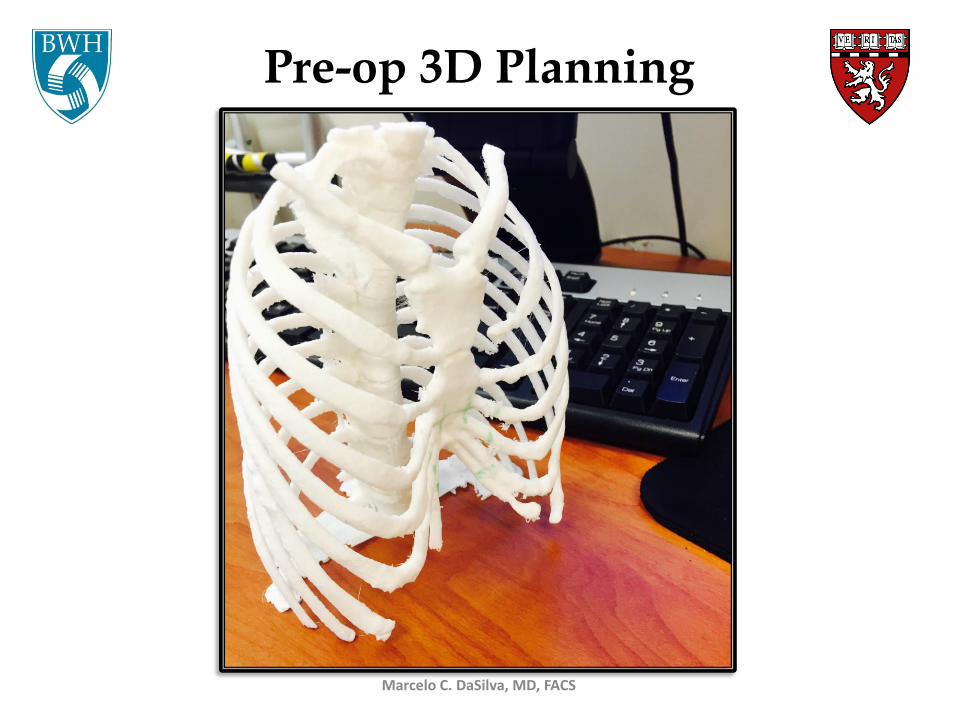
Pre-op 3D Planning
Marcelo C. DaSilva, MD, FACS

Surgery
Marcelo C. DaSilva, MD, FACS
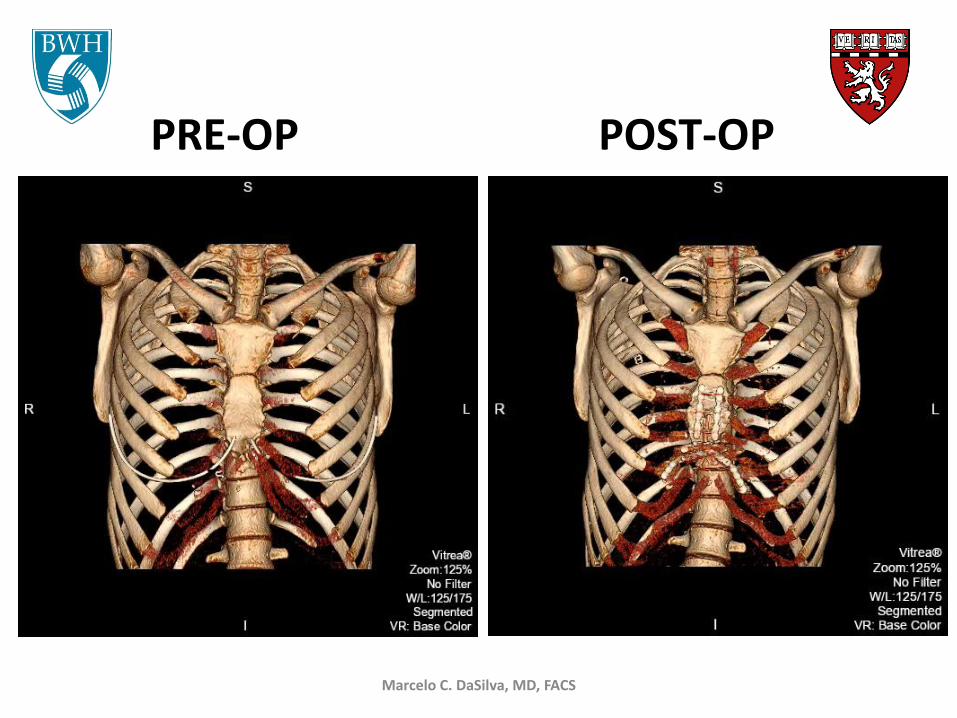
PRE-OP POST-OP
Marcelo C. DaSilva, MD, FACS

Marcelo C. DaSilva, MD, FACS
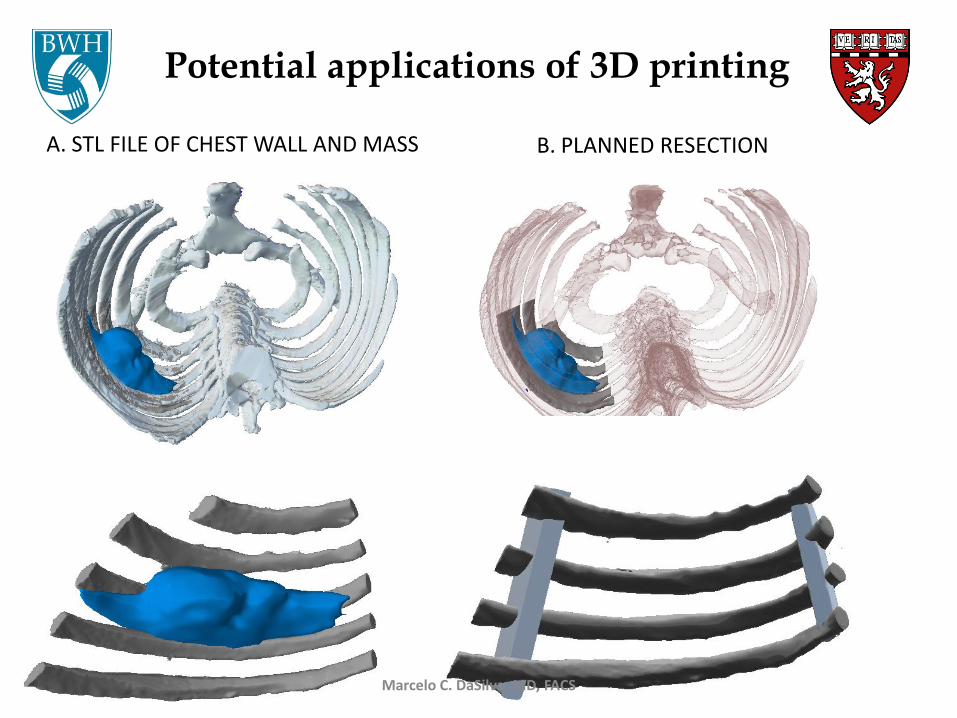
A. STL FILE OF CHEST WALL AND MASS B. PLANNED RESECTION
Potential applications of 3D printing
Marcelo C. DaSilva, MD, FACS

The world is in perpetual motion, and we must invent the things of tomorrow… Act with audacity.” Madame Clicquot
Marcelo C. DaSilva, MD, FACS
Related Documents











