Chapter 1 / Emergency Management: Evaluation of the Critically Ill or Injured Child • 16 Chapter EVALUATION OF THE CYANOTIC NEONATE Cyanosis is a physical sign characterized by blue mucous membranes, nail beds, and skin. Cyanosis results from an absolute concentration of deoxy- genated hemoglobin of at least 3.0 g/dL. Factors that influence whether cyanosis will appear include the hematocrit, which reflects the absolute concentration of hemoglobin, and the factors that affect the O 2 dissociation curve (pH, PCO 2 , temperature, level of 2,3-diphosphoglycerate, and ratio of adult to fetal hemoglobin). Cyanosis should not be confused with acrocyanosis, which is blueness of the extremities due to peripheral vasoconstriction noted in the first 24 to 48 hours of life. Neonates with acrocyanosis have pink mucosal membranes. Differential Diagnosis The causes of cyanosis in the newborn are of cardiac, pulmonary, neurologic, or hematologic origin. The incidence of structural heart disease is about 8 in 1000 live births, and severe congenital heart disease occurs in approximately 1 in 400 live births. Pul- monary disorders may lead to cyanosis as a result of primary lung disease, airway obstruction, or extrinsic compression of the lung. Neurologic causes of cyanosis include central nervous system dysfunction and respiratory neuromuscular dysfunction. Table 3- 1 delineates the causes of cyanosis in the neonate. Clinical Manifestations History and Physical Examination A complete birth history that includes maternal history; prenatal, perinatal, and postnatal complica- tions; history of labor and delivery; and neonatal course should be obtained. Exactly when the child developed cyanosis is critical, because certain con- genital heart defects present at birth, while others may take as long as one month to present themselves. The initial physical examination should focus on the vital signs and cardiac and respiratory examina- tions, looking for evidence of right, left, or biventric- ular congestive heart failure and respiratory distress. Blue or dusky mucous membranes are consistent with cyanosis. Evaluate for rales, stridor, grunting, flaring, retractions, and evidence of consolidation or effusion on pulmonary examination. On cardiovas- cular examination, the precordial impulse is pal- pated, and the clinician should evaluate for systolic or diastolic murmurs, the intensity of S 1 ,S 2 splitting abnormalities, and the presence of an S 3 or S 4 gallop, ejection click, opening snap, or rub. Examination of the extremities should focus on the strength and symmetry of the pulses in the upper and lower extremities, evidence of edema, and cyanosis of the nail beds. Hepatosplenomegaly may be consistent with right ventricular or biventricular heart failure. Diagnostic Evaluation The goal of the initial evaluation of the cyanotic neonate is to determine whether the cyanosis is cardiac or noncardiac in origin. An electrocardiogram (ECG), chest radiograph, and hyperoxia test should be performed. In addition, preductal and postductal oxygen saturation, and four extremity blood pres- sures should be documented. A hyperoxia test should be carried out in neonates with a resting pulse oximetry reading less than 95%, visible cyanosis, or circulatory collapse. The hyperoxia test consists of obtaining a baseline right radial 3 Cardiology

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Chapter 1 / Emergency Management: Evaluation of the Critically Ill or Injured Child • 16Chapter
� EVALUATION OF THE CYANOTIC NEONATE
Cyanosis is a physical sign characterized by bluemucous membranes, nail beds, and skin. Cyanosisresults from an absolute concentration of deoxy-genated hemoglobin of at least 3.0g/dL. Factors thatinfluence whether cyanosis will appear include thehematocrit, which reflects the absolute concentrationof hemoglobin, and the factors that affect the O2
dissociation curve (pH, PCO2, temperature, level of2,3-diphosphoglycerate, and ratio of adult to fetalhemoglobin). Cyanosis should not be confused withacrocyanosis, which is blueness of the extremitiesdue to peripheral vasoconstriction noted in the first24 to 48 hours of life. Neonates with acrocyanosishave pink mucosal membranes.
Differential Diagnosis
The causes of cyanosis in the newborn are of cardiac,pulmonary, neurologic, or hematologic origin. Theincidence of structural heart disease is about 8 in1000 live births, and severe congenital heart diseaseoccurs in approximately 1 in 400 live births. Pul-monary disorders may lead to cyanosis as a result ofprimary lung disease, airway obstruction, or extrinsiccompression of the lung. Neurologic causes ofcyanosis include central nervous system dysfunctionand respiratory neuromuscular dysfunction. Table 3-1 delineates the causes of cyanosis in the neonate.
Clinical Manifestations
History and Physical ExaminationA complete birth history that includes maternalhistory; prenatal, perinatal, and postnatal complica-
tions; history of labor and delivery; and neonatalcourse should be obtained. Exactly when the childdeveloped cyanosis is critical, because certain con-genital heart defects present at birth, while othersmay take as long as one month to present themselves.
The initial physical examination should focus onthe vital signs and cardiac and respiratory examina-tions, looking for evidence of right, left, or biventric-ular congestive heart failure and respiratory distress.Blue or dusky mucous membranes are consistentwith cyanosis. Evaluate for rales, stridor, grunting,flaring, retractions, and evidence of consolidation oreffusion on pulmonary examination. On cardiovas-cular examination, the precordial impulse is pal-pated, and the clinician should evaluate for systolicor diastolic murmurs, the intensity of S1, S2 splittingabnormalities, and the presence of an S3 or S4 gallop,ejection click, opening snap, or rub. Examination ofthe extremities should focus on the strength andsymmetry of the pulses in the upper and lowerextremities, evidence of edema, and cyanosis of thenail beds. Hepatosplenomegaly may be consistentwith right ventricular or biventricular heart failure.
Diagnostic Evaluation
The goal of the initial evaluation of the cyanoticneonate is to determine whether the cyanosis iscardiac or noncardiac in origin. An electrocardiogram(ECG), chest radiograph, and hyperoxia test shouldbe performed. In addition, preductal and postductaloxygen saturation, and four extremity blood pres-sures should be documented.
A hyperoxia test should be carried out in neonateswith a resting pulse oximetry reading less than 95%,visible cyanosis, or circulatory collapse. The hyperoxiatest consists of obtaining a baseline right radial
3 Cardiology

Chapter 3 / Cardiology • 17
(preductal) arterial blood gas measurement with thechild breathing room air, Fio2 = 0.21, and then repeat-ing the measurement with the child inspiring 100%oxygen,Fio2 = 1.00.Interpretation of the hyperoxia testis delineated in Table 3-2.A PaO2 greater than 200mmHg on 100% oxygen makes congenital heart disease
very unlikely. A PaO2 less than 150mmHg on 100%oxygen suggests a cardiac lesion characterized by com-plete mixing without restricted pulmonary blood flow.A PaO2 less than 50 mm Hg on 100% oxygen indicatesa cardiac lesion with parallel circulation, or a mixinglesion with restricted pulmonary blood flow.
Cardiac
Ductal-independent mixing lesionsTruncus arteriosusTotal anomalous pulmonary venous return without obstructionD-transposition of the great arteriesa
Lesions with ductal-dependent PBFTetralogy of Fallot with pulmonary atresiab
Ebstein’s anomalyb
Critical pulmonic stenosisTricuspid valve atresiab with normally related great arteriesb
Pulmonic valve atresia with intact ventricular septumHeterotaxyb
Lesions with ductal-dependent SBFHypoplastic left heart syndromeInterrupted aortic archCritical coarctation of the aortaCritical aortic stenosisTricuspid valve atresia with transposition of the great arteriesb
Differential Diagnosis of Cyanosis in the Neonate
� TABLE 3-1
Pulmonary
Primary lung disease such as respiratory distresssyndrome, meconium aspiration, pneumonia,or persistent pulmonary hypertension of thenewborn
Airway obstruction such as choanal atresia, vocalcord paralysis, or laryngotracheomalacia
Extrinsic compression of the lungs such aspneumothorax, chylothorax, or hemothorax
NeurologicCNS dysfunction such as drug-induced depression
of respiratory drive, postasphyxial cerebraldysfunction, or central apnea
Respiratory neuromuscular dysfunction such asspinal muscular atrophy, infant botulism, orneonatal myasthenia gravis
HematologicMethemoglobinemia or polycythemia
a A patent ductus arteriosus may improve mixing, especially with an intact ventricular septum.b Most forms.PBF, pulmonary blood flow; SBF, systemic blood flow.
PaO2 (mm Hg) at FiO2 = 0.21 PaO2 (mm Hg) at FiO2 = 1.00 PaCO2
(% Saturation) (% Saturation) (mm Hg)
Normal 70 (95) >300 (100) 35
Pulmonary disease 50 (85) >150 (100) 50
Neurologic disease 50 (85) >150 (100) 50
Methemoglobinemia 70 (95) >200 (100) 35
Cardiac diseaseParallel circulationa <40 (<75) <50 (<85) 35Mixing with restricted PBFb <40 (<75) <50 (<85) 35Mixing without restricted PBFc 40–60 (75–93) <150 (<100) 35
a D-Transposition of the great arteries with intact ventricular septum, D-transposition of the great arteries with ventricular septal defect.b Tricuspid atresia with pulmonary stenosis or atresia, pulmonary atresia or critical pulmonary stenosis with intact ventricular septum, tetralogy of Fallot,or Ebstein’s anomaly.c Truncus arteriosus; total anomalous pulmonary venous return; single ventricle, hypoplastic left heart syndrome.PBF, pulmonary blood flow.
Interpretation of the Hyperoxia Test
� TABLE 3-2

The PaO2 should be measured directly via arterialpuncture, though properly acquired transcutaneousoxygen monitor (TCOM) values for PaO2 are alsoacceptable. Pulse oximetry should not be used forinterpretation of the hyperoxia test, because aneonate given 100% inspired oxygen may have aPaO2 of 80mmHg with a pulse oximeter reading of100% (abnormal), or a PaO2 greater than 300mmHgwith a pulse oximeter reading of 100% (normal). Ifa cardiac cause is deemed likely, obtain an echocar-diogram and a cardiology consultation.
Pulse oximetry should be documented at pre-ductal and postductal sites to assess for differentialor reverse differential cyanosis. If the preductal saturation is higher than the postductal satura-tion, differential cyanosis exists, which results when there are normally related great arteries and deoxygenated blood from the pulmonary circula-tion enters the descending aorta through a patent ductus arteriosus. Differential cyanosis is seen in persistent pulmonary hypertension of the newborn(PPHN) and in lesions with left ventricular outflowtract obstruction such as interrupted aortic arch,critical coarctation of the aorta, and critical aorticstenosis.
In rare cases of reverse differential cyanosis, thepostductal saturation is higher than the preductal sat-uration. This occurs only in children with transposi-tion of the great arteries with left ventricular outflowobstruction (i.e., critical coarctation of the aorta,interrupted aortic arch, critical aortic stenosis) orPPHN. Oxygenated blood from the pulmonary cir-culation enters the descending aorta through a patentductus arteriosus.
When either the hyperoxia test or the preductal/postductal oxygen saturation measurement, or both,indicate cardiac disease, the chest radiograph andECG may be used to delineate which cardiac struc-tural defect is the most likely. The chest radiographis obtained to determine the size of the heart andwhether the pulmonary vascularity is increased ordecreased. The ECG evaluates the heart rate,rhythm, axis, intervals, R-wave progression, and P-wave and ST/T wave morphology and helps deter-mine if ischemia, atrial dilatation, or ventricularhypertrophy is present.
To differentiate among cyanotic congenital heartdefects that present with a PaO2 less than 50mmHgon the hyperoxia test, the clinician should firstexamine the chest radiograph. If massive cardiacenlargement is noted, Ebstein’s anomaly is the mostlikely diagnosis. Once massive cardiac enlargement
has been ruled out, the pulmonary vascularitybecomes the focus. Increased pulmonary blood flowsuggests the presence of D-transposition of the greatarteries (D-TGA) with intact ventricular septum,whereas pulmonary edema is a manifestation of total anomalous pulmonary venous return withobstruction.
The remaining diagnoses (tricuspid atresia withnormally related great arteries, pulmonic atresia withintact ventricular septum, critical pulmonic stenosis,and tetralogy of Fallot with or without pulmonaryatresia) all produce decreased pulmonary vascularityand normal or only slightly enlarged heart size. Thesedefects are differentiated by their axis on ECG and the presence or absence of a murmur. Tricuspidatresia with pulmonary stenosis or pulmonary atresiais noted for its superior axis, lying in the 270- to 0-degree quadrant. Critical pulmonic stenosis andpulmonary atresia with intact ventricular septumboth have axes in the 0- to 90-degree quadrant. Theyare differentiated by the presence of the loud systolicejection murmur heard from critical pulmonic steno-sis. Similarly, tetralogy of Fallot and tetralogy of Fallotwith pulmonary atresia both have axes in the 90- to180-degree quadrant; they are distinguished fromeach other by the pulmonic stenosis murmur notedin tetralogy of Fallot.
Treatment
Newborns with mixing lesions without adequatemixing (D-TGA with intact ventricular septum andrestrictive patent foramen ovale) or defects that have ductal-dependent pulmonary blood flow or ductal-dependent systemic blood flow may require prostaglandin E1 (PGE1) infusion to maintainpatency of the ductus arteriosus until definitive surgical treatment can be accomplished. Rarely, thepatient with congenital heart disease may becomeprogressively more unstable after the institution ofPGE1 therapy. This clinical deterioration after insti-tution of PGE1 is an important diagnostic finding thatidentifies the congenital heart defect as one that hasobstructed blood flow out of the pulmonary veins orleft atrium. Lesions that have impaired blood flowfrom the left atrium include hypoplastic left heartsyndrome with restrictive or intact foramen ovale,other variants of mitral atresia with restrictiveforamen ovale, transposition of the great arteries withan intact ventricular septum and restrictive foramenovale, and total anomalous pulmonary venous returnwith obstruction.
18 • Blueprints Pediatrics

Chapter 3 / Cardiology • 19
� CYANOTIC CONGENITAL HEARTDISEASE: DUCTAL-INDEPENDENTMIXING LESIONS
Truncus Arteriosus
Truncus arteriosus (Figure 3-1) is a rare form of cyan-otic congenital heart disease that consists of a singlearterial vessel arising from the base of the heart fromwhich arise the coronary, systemic, and pulmonaryarteries. In this disorder, there is complete mixing ofsystemic and pulmonary venous blood in the truncus.This lesion, along with other conotruncal anomalies(tetralogy of Fallot, interrupted aortic arch, VSD,isolated arch anomalies, and vascular ring), is associ-ated with microdeletion of chromosome 22 (22q11deletion).
Clinical ManifestationsModerate cyanosis is present at birth, and congestiveheart failure develops in a matter of weeks as the pul-monary vascular resistance falls and shunting acrossthe ventricular septal defect begins. On examination,a systolic ejection murmur is heard at the left sternalborder, a widened pulse pressure is present, andbounding arterial pulses are palpated. There is asingle loud second heart sound on cardiovascularexam. Seventy percent of children with truncus arte-
riosus have biventricular hypertrophy on ECG. Onchest radiograph, marked cardiomegaly, increasedpulmonary vascularity, and right aortic arch may beseen. DiGeorge’s syndrome related to the 22q11microdeletion may result in hypocalcemia.
TreatmentAt most centers neonatal surgical repair is per-formed. Surgical repair involves closing the ventric-ular septal defect so the oxygenated blood in the leftventricle is baffled through the VSD to the truncalvalve and a conduit is interposed between the rightventricle and pulmonary arteries, which are discon-nected from the truncal vessel.
1. The absolute concentration of deoxygenatedhemoglobin, and not the ratio of oxygenated todeoxygenated hemoglobin, determines the pres-ence of cyanosis.
2. Once cyanosis has been identified, stabilize theinfant, quickly initiate the preliminary workup(chest radiograph, electrocardiogram, and hyper-oxia test) and define whether the lesion is cardiacor noncardiac in origin.
3. If a cardiac lesion is suspected, determine whetherthe defect is ductal dependent for systemic orpulmonary circulation or a ductal-independentmixing lesion.
4. Once the infant is stabilized, obtain an emergentcardiology consultation, an echocardiogram, and,if indicated, begin PGE1 therapy in preparation forsurgical palliation or correction.
KEY POINTS
Figure 3-1 • Truncus arteriosus (with right aortic arch). Typicalanatomic and hemodynamic findings include: (a) a singleartery arises from the conotruncus giving rise to coronary arter-ies (not shown), pulmonary arteries, and aortic vessels; (b)abnormal truncal valve (quadricuspid shown) with stenosisand/or regurgitation is common; (c) right-sided aortic arch(occurs in approximately 30% of cases); (d) large con-oventricular ventricular septal defect; (e) pulmonary arteryhypertension with a large left-to-right shunt (note superiorvena caval oxygen saturation of 60% and pulmonary arteryoxygen saturation of 85%); (f ) complete mixing (of the systemic and pulmonary venous return) occurs at the greatvessel level.Cloherty JP, Stark AR. Manual of Neonatal Care, 4th ed. Philadelphia:Lippincott-Raven, 1998: 426.

D-Transposition of the Great Arteries
D-Transposition of the great arteries (Figure 3-2)accounts for 5% of congenital heart defects and is themost common form of cyanotic congenital heartdisease presenting in the neonatal period. In thisdefect, the aorta arises anteriorly from the right ven-tricle, and the pulmonary artery rises posteriorlyfrom the left ventricle. There are three basic variants:D-TGA with intact ventricular septum (60%), D-TGA with ventricular septal defect (20%), and D-TGA with ventricular septal defect and pulmonicstenosis (20%).
In this defect, the pulmonary and systemic circuitsare parallel rather than in series. The systemic circuit(deoxygenated blood) is recirculated through thebody, whereas the pulmonary circuit (oxygenatedblood) recirculates through the lungs. A mixinglesion such as an atrial septal defect, ventricularseptal defect, and/or patent ductus arteriosus thatallows mixing of the systemic and pulmonary circu-lations is necessary for survival.
Clinical ManifestationsCyanosis is present from birth, the degree varyingwith the associated mixing lesions. In the absence ofmixing lesions, there is pronounced cyanosis, rightventricular heave, and a single loud S2 on examina-tion. The presence of a systolic murmur indicates thepresence of a VSD or pulmonic stenosis. The ECG isnormal in the newborn; however, right-axis deviationand right ventricular hypertrophy are eventuallyseen. The chest radiograph reveals increased pul-monary vascular markings in D-transposition with orwithout ventricular septal defect, but if pulmonicstenosis is critical, decreased pulmonary vascularmarkings may be present. Cardiomegaly with “egg-shaped silhouette” is often seen on chest radiograph.
TreatmentInitial management may include PGE1 to keep thepatent ductus arteriosus open and increase aorta(deoxygenated) to pulmonary artery (oxygenated)shunting. If needed, the Rashkind balloon atrial sep-tostomy can be utilized to improve atrial mixing andrelieve severe hypoxia. Surgical repair, utilizing thearterial switch procedure, is generally performedduring the first week of life.
Total Anomalous Pulmonary Venous Connection
Total anomalous pulmonary venous connection(TAPVC) (Figure 3-3) is a rare lesion in which thepulmonary venous return is directed to the rightatrium either directly or indirectly through venouschannels. There are four variants:
• Supracardiac (50% of cases): Blood drains via avertical vein into the innominate vein or into thesuperior vena cava
• Cardiac (20% of cases): Blood drains into the coro-nary sinus or directly into the right atrium
20 • Blueprints Pediatrics
Figure 3-2 • Transposition of the great arteries with an intactventricular septum, a large patent ductus arteriosus (on PGE1)and atrial septal defect (status post balloon atrial septostomy).Note the following: (a) The aorta arises from the anatomic rightventricle, and the pulmonary artery from the anatomic left ven-tricle; (b) “transposition physiology,” with a higher oxygen sat-uration in the pulmonary artery than in the aorta; (c) “mixing”between the parallel circulations (see text) at the atrial (after balloon atrial septostomy) and ductal levels; (d) shuntingfrom the left atrium to the right atrium via the atrial septaldefect (not shown) with equalization of atrial pressures; (e)shunting from the aorta to the pulmonary artery via the ductusarteriosus; (f ) pulmonary hypertension due to a large ductusarteriosus.Cloherty JP, Stark AR. Manual of Neonatal Care, 4th ed. Philadelphia:Lippincott-Raven, 1998: 426.

Chapter 3 / Cardiology • 21
• Infradiaphragmatic (20% of cases): Blood drainsvia a vertical vein into the portal or hepatic veins
• Mixed (10% of cases): Blood returns to the heartvia a combination of the above routes
TAPVC can occur with or without obstruction.Obstruction occurs when the anomalous vein enters a vessel at an acute angle. The presence orabsence of obstruction determines whether there is pulmonary venous hypertension and severe
cyanosis or increased pulmonary blood flow and mildcyanosis.
Clinical ManifestationsWithout obstruction, clinical findings are similar tothose of an atrial septal defect. There is an active pre-cordium with a right ventricular heave, a wide andfixed split S2 with a loud pulmonary component, anda systolic ejection murmur at the left upper sternalborder. On chest radiograph, cardiomegaly is notedwith increased pulmonary vascularity. On ECG,right-axis deviation and right ventricular hypertro-phy are seen. A neonate with TAPVC with obstruc-tion presents extremely cyanotic, tachypneic, anddyspneic. Examination reveals a right ventricularheave, a narrowly split S2, and a ventricular gallop(S3).
TreatmentIn TAPVC without obstruction, treatment of con-gestive heart failure is needed initially, and surgicalredirection of aberrant vessels into the left atrium isnecessary in the first month of life. In TAPVC withobstruction, the neonate should be taken to surgeryemergently for correction. PGE1 should not be givenbecause the patent ductus arteriosus adds moreblood volume to an already flooded pulmonarycircuit.
� CYANOTIC CONGENITAL HEART DISEASE: LESIONS WITHDUCTAL-DEPENDENT PULMONARYBLOOD FLOW
Tricuspid Atresia
Tricuspid atresia with normally related great arteries(Figure 3-4) is a rare defect that consists of completeabsence of right atrioventricular connection, whichleads to severe hypoplasia or absence of the rightventricle. Ninety percent of cases of tricuspid atresiahave an associated ventricular septal defect. In chil-dren with tricuspid atresia with normally relatedgreat arteries, the ventricular septal defect allowsblood to pass from the left ventricle to the right ven-tricular outflow and pulmonary arteries. The vastmajority of patients with tricuspid atresia with nor-mally related great arteries also have pulmonarystenosis. In tricuspid atresia the systemic venous
Figure 3-3 • Infradiaphragmatic total anomalous pulmonaryvenous connection. Note the following: (a) pulmonary venousconfluence does not connect with the left atrium, but descendsto connect with the portal circulation below the diaphragm.This connection is frequently severely obstructed as shown; (b)obstruction to pulmonary venous return results in significantlyelevated pulmonary venous pressures, decreased pulmonaryblood flow, pulmonary edema and pulmonary venous desatu-ration (92%); (c) systemic to suprasystemic pressure in the pul-monary artery (in the absence of a patent ductus arteriosus,pulmonary artery pressures may exceed systemic pressureswhen severe pulmonary venous obstruction is present); (d) allsystemic blood flow must be derived via a right-to-left shunt atthe foramen ovale; (e) nearly equal oxygen saturations in allchambers of the heart (i.e., complete mixing at right atrial level),with severe hypoxemia (systemic oxygen saturation 60%) andlow cardiac output (mixed venous oxygen saturation 25%).Cloherty JP, Stark AR. Manual of Neonatal Care, 4th ed. Philadelphia:Lippincott-Raven, 1998: 426.

22 • Blueprints Pediatrics
return is shunted from the right atrium to the leftatrium through the patent foramen ovale or an atrialseptal defect, and the left atrium and left ventriclehandle both systemic and pulmonary venous return.Oxygenated and deoxygenated blood is mixed in theleft atrium. Cyanosis is severe in the neonatal periodand is proportionally related to the amount of pul-monary blood flow. In 30% of cases, there is trans-position of the great arteries, which results in bloodpassing from the left ventricle through the ventricu-lar septal defect to the right ventricular outflow andthe ascending aorta. Tricuspid atresia with transposi-tion of the great arteries is often associated withcoarctation of the aorta or aortic arch hypoplasia.Unlike tricuspid atresia with normally related greatarteries it is a cyanotic lesion with ductal dependentsystemic blood flow.
Clinical ManifestationsNeonates with tricuspid atresia with normally relatedgreat arteries present with progressive cyanosis, poorfeeding, and tachypnea over the first 2 weeks of life.On cardiac examination, the harsh holosystolicmurmur of a ventricular septal defect at the leftlower sternal border and the continuous murmur of a patent ductus arteriosus may be heard. On ECG, there is a superior axis and left ventricular hypertrophy. Findings on chest radiograph include normal heart size and decreased pulmonary vascularmarkings.
TreatmentA child with tricuspid atresia with normally relatedgreat arteries should have PGE1 started to maintainpulmonary flow, and a balloon atrial septostomyshould be performed if the atrial defect is not ade-quate. Surgical management for tricuspid atresiainvolves placing a modified Blalock-Taussig shunt tomaintain pulmonary blood flow. The modifiedBlalock-Taussig shunt is a Gortex conduit placedbetween the subclavian artery and the pulmonaryartery. Ultimately, a cavopulmonary anastomosis(hemi-Fontan or bidirectional Glenn) is performedto provide stable pulmonary blood flow. In mostcenters, a modified Fontan procedure is performed toredirect the inferior vena cava and hepatic vein flowinto the pulmonary circulation.
Pulmonic Atresia with Intact Ventricular Septum
Pulmonic atresia with intact ventricular septum(Figure 3-5) is a rare defect consisting of pulmonaryvalvular and infundibular atresia and varying degreesof right ventricular and tricuspid valve hypoplasia. Inthis disorder, there is an obligate atrial shunt fromright to left, and pulmonary blood flow is dependenton a patent ductus arteriosus. Since there is no pul-monary outflow, the right ventricle is hypertensiveand there is often moderate to severe tricuspid regur-gitation. Pulmonary atresia with intact ventricularseptum may also be associated with coronaryartery–myocardial sinusoid communication. Thecoronary arteries may be quite abnormal, with areasof stenosis or complete atresia. In some cases, coro-nary perfusion may be dependent on the hyperten-sive right ventricle. If the coronaries are rightventricle (RV) dependent, any palliative procedurethat decompresses the right ventricle may lead tomyocardial infarction and death.
Figure 3-4 • Tricuspid atresia with normally related great arter-ies and a small patent ductus arteriosus. Typical anatomic andhemodynamic findings include: (a) atresia of the tricuspid valve;(b) hypoplasia of the right ventricle; (c) restriction to pulmonaryblood flow at two levels: a (usually) small ventricular septaldefect and a stenotic pulmonary valve; (d) all systemic venousreturn must pass through the patent foramen ovale to reachthe left ventricle; (e) complete mixing at the left atrial level, withsystemic oxygen saturation of 78% (in FiO2 of 0:21), suggestingbalanced systemic and pulmonary blood flow.Cloherty JP, Stark AR. Manual of Neonatal Care, 4th ed. Philadelphia:Lippincott-Raven, 1998: 426.

Chapter 3 / Cardiology • 23
Clinical ManifestationsNeonates present at birth extremely cyanotic andtachypneic. Cardiac examination reveals a tricuspidregurgitation murmur in the left lower sternal borderand the continuous murmur of a patent ductus arteriosus. On ECG, left ventricular hypertrophy anda leftward axis are seen. On chest radiograph,decreased pulmonary markings and left ventricularhypertrophy are seen.
TreatmentPGE1 should be started to ensure pulmonary bloodflow initially. Prior to any surgery to provide morestable pulmonary flow, a cardiac catheterization must
be performed to assess the coronary arteries. If thecoronary circulation is not RV dependent, then aright ventricle to pulmonary artery conduit or pul-monary valvotomy is performed to provide antegradepulmonary blood flow. A modified Blalock-Taussigshunt is also typically performed to augment pul-monary blood flow further. Depending on the growthof the right ventricle and tricuspid valve, a single ven-tricle, one and a half ventricle, or two ventricle repairmay be possible. If the coronary circulation is RVdependent, the RV is not decompressed and a mod-ified Blalock-Taussig shunt is performed. After mod-ified Blalock-Taussig shunt placement, patients witha right ventricle dependent coronary circulation areeither listed for heart transplantation or staged to aFontan palliation.
Tetralogy of Fallot
Tetralogy of Fallot (Figure 3-6) is the third mostprevalent cyanotic congenital heart lesion during theneonatal period and after the third week of lifebecomes the leading cause of cyanosis due to con-genital heart disease in childhood. The four defectsFallot noted include an anterior malalignment ven-tricular septal defect, right ventricular outflow tractobstruction (50% infundibular stenosis, 20% pul-monary valve stenosis, and 30% infundibular steno-sis and pulmonary valve stenosis), right ventricularhypertrophy, and an “overriding” large ascendingaorta.
Clinical ManifestationsNeonates with tetralogy of Fallot are cyanoticbecause of right-to-left shunting across the ventricu-lar septal defect and decreased pulmonary flow.Shunting occurs when the combination of the pul-monary vascular resistance and the resistance createdby the right ventricular outflow tract obstructionexceed the peripheral vascular resistance. The degreeof cyanosis is proportional to the severity of the rightventricular outflow tract obstruction. Blood shuntedfrom the aorta to the pulmonary artery through thepatent ductus arteriosus provides additional pul-monary blood flow. Neonates present with cyanosisof varying severity and may have characteristic peri-odic episodic cyanosis and agitation. These episodesof cyanosis are known as “tet spells.” Tet spells arecaused by an increase in right ventricular outflowtract resistance, leading to an increase in the right-left shunt. Such spells may last minutes to hours, may
Figure 3-5 • Pulmonary atresia with intact ventricular septum(PA/IVS) in a neonate with a nonrestrictive patent ductus arte-riosus while receiving PGE1. Typical anatomic and hemody-namic findings include: (a) hypertrophied, hypoplastic rightventricle; (b) hypoplastic tricuspid valve and pulmonaryannulus; (c) atresia of the pulmonary valve with no antegradeflow; (d) suprasystemic right ventricular pressure; (e) pul-monary blood flow via the patent ductus; (f ) right-to-left shuntat the atrial level with systemic desaturation. Many patientshave significant coronary abnormalities with sinusoidal or fis-tulous connections to the hypertensive right ventricle or sig-nificant coronary stenosis (not shown).Cloherty JP, Stark AR. Manual of Neonatal Care, 4th ed. Philadelphia:Lippincott-Raven, 1998: 426.

24 • Blueprints Pediatrics
resolve spontaneously, or may lead to progressivehypoxia, acidosis, and death. On cardiac examina-tion, a right ventricular heave is often felt and a loudsystolic ejection murmur is heard in the left uppersternal border due to right ventricular outflow tractobstruction.The ECG reveals right atrial dilation andright ventricular hypertrophy, whereas the chest radiograph shows normal heart size with decreasedpulmonary vascular markings. Twenty-five percent ofchildren with tetralogy of Fallot have a right-sidedaortic arch.
TreatmentThe treatment of tet spells is aimed at diminishingright-to-left shunting by increasing systemic vascularresistance and decreasing pulmonary vascular resis-tance. Tet spells may be treated with supplementaloxygen, vagal maneuvers, morphine sulfate, vasocon-
strictors, beta-blockers, and volume administration.Holding the infant over the shoulder and placing the child in a knee-chest position decreases preloadand increases systemic vascular resistance. Morphinesulfate suppresses the respiratory center, stops hyperpnea, and dilates the pulmonary arteries. Vaso-constrictors raise the systemic vascular resistance,whereas beta-blockers are thought to minimizeinfundibular spasm. Volume is added to increase thesystemic blood pressure, which minimizes right-to-left shunting. Metabolic acidosis must be corrected,because it increases pulmonary vascular resistanceand thereby promotes right-to-left shunting acrossthe ventricular septal defect. In most institutions,surgical repair is performed during the first 3 to 6months of life, or after the first hypercyanotic episode(tet spell).
Ebstein’s Anomaly
Ebstein’s anomaly (Figure 3-7) is an extremely rareanomaly in which the septal leaflet of the tricuspidvalve is displaced into the right ventricular cavity andthe anterior leaflet of the tricuspid valve is sail-likeand redundant. This results in a portion of the rightventricle being incorporated into the right atrium.Functional hypoplasia of the right ventricle results,as well as tricuspid regurgitation or stenosis or both.A patent foramen ovale is present in 80% of neonateswith the anomaly, and there is a right-to-left shuntat the atrial level. The right atrium is massivelydilated, which may result in supraventricular tachy-cardia. Wolff-Parkinson-White (WPW) syndrome isassociated with Ebstein’s anomaly. In severe cases ofEbstein’s anomaly, the majority of the pulmonaryblood flow comes from the patent ductus arteriosusand not the right ventricle.
Clinical ManifestationsNeonates with the severe form of the disease presentwith cyanosis and congestive heart failure in the first few days of life. The cardiac examination revealsa widely fixed split S2, and a tricuspid regurgitantmurmur is heard at the left lower sternal border. TheECG reveals a right bundle branch block with rightatrial enlargement. Delta waves due to WPW syn-drome and supraventricular tachycardia may mani-fest themselves. Chest radiograph reveals extremecardiomegaly with notable right atrial enlargementand decreased pulmonary vascular markings.
Figure 3-6 • Tetralogy of Fallot. Typical anatomic and hemody-namic findings include: (a) an anteriorly displaced infundibularseptum, resulting in subpulmonary stenosis, a large ventricularseptal defect and overriding of the aorta over the muscularseptum; (b) hypoplasia of the pulmonary valve, main and branch pulmonary arteries; (c) equal right and left ventricularpressures; (d) a right-to-left shunt at ventricular level, with a sys-temic oxygen saturation of 82%.Cloherty JP, Stark AR. Manual of Neonatal Care, 4th ed. Philadelphia:Lippincott-Raven, 1998: 426.
Chapter 3 / Cardiology • 25
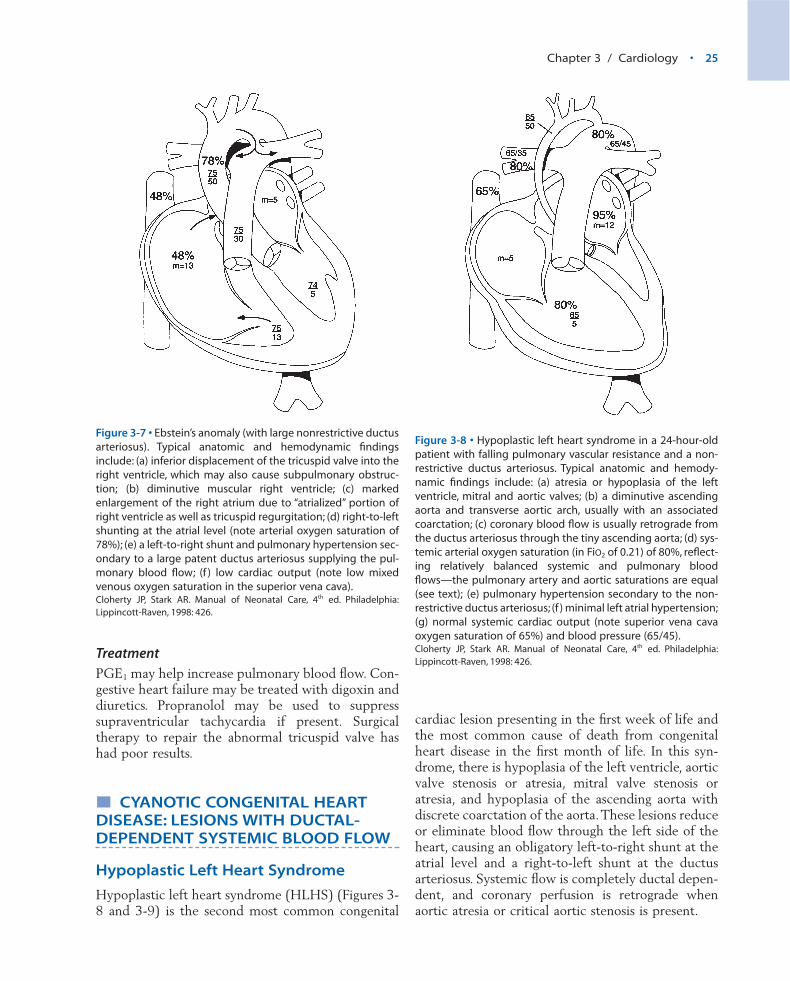
TreatmentPGE1 may help increase pulmonary blood flow. Con-gestive heart failure may be treated with digoxin anddiuretics. Propranolol may be used to suppresssupraventricular tachycardia if present. Surgicaltherapy to repair the abnormal tricuspid valve hashad poor results.
� CYANOTIC CONGENITAL HEARTDISEASE: LESIONS WITH DUCTAL-DEPENDENT SYSTEMIC BLOOD FLOW
Hypoplastic Left Heart Syndrome
Hypoplastic left heart syndrome (HLHS) (Figures 3-8 and 3-9) is the second most common congenital
cardiac lesion presenting in the first week of life andthe most common cause of death from congenitalheart disease in the first month of life. In this syn-drome, there is hypoplasia of the left ventricle, aorticvalve stenosis or atresia, mitral valve stenosis oratresia, and hypoplasia of the ascending aorta withdiscrete coarctation of the aorta.These lesions reduceor eliminate blood flow through the left side of theheart, causing an obligatory left-to-right shunt at theatrial level and a right-to-left shunt at the ductusarteriosus. Systemic flow is completely ductal depen-dent, and coronary perfusion is retrograde whenaortic atresia or critical aortic stenosis is present.
Figure 3-7 • Ebstein’s anomaly (with large nonrestrictive ductusarteriosus). Typical anatomic and hemodynamic findingsinclude: (a) inferior displacement of the tricuspid valve into theright ventricle, which may also cause subpulmonary obstruc-tion; (b) diminutive muscular right ventricle; (c) markedenlargement of the right atrium due to “atrialized” portion ofright ventricle as well as tricuspid regurgitation; (d) right-to-leftshunting at the atrial level (note arterial oxygen saturation of78%); (e) a left-to-right shunt and pulmonary hypertension sec-ondary to a large patent ductus arteriosus supplying the pul-monary blood flow; (f ) low cardiac output (note low mixedvenous oxygen saturation in the superior vena cava).Cloherty JP, Stark AR. Manual of Neonatal Care, 4th ed. Philadelphia:Lippincott-Raven, 1998: 426.
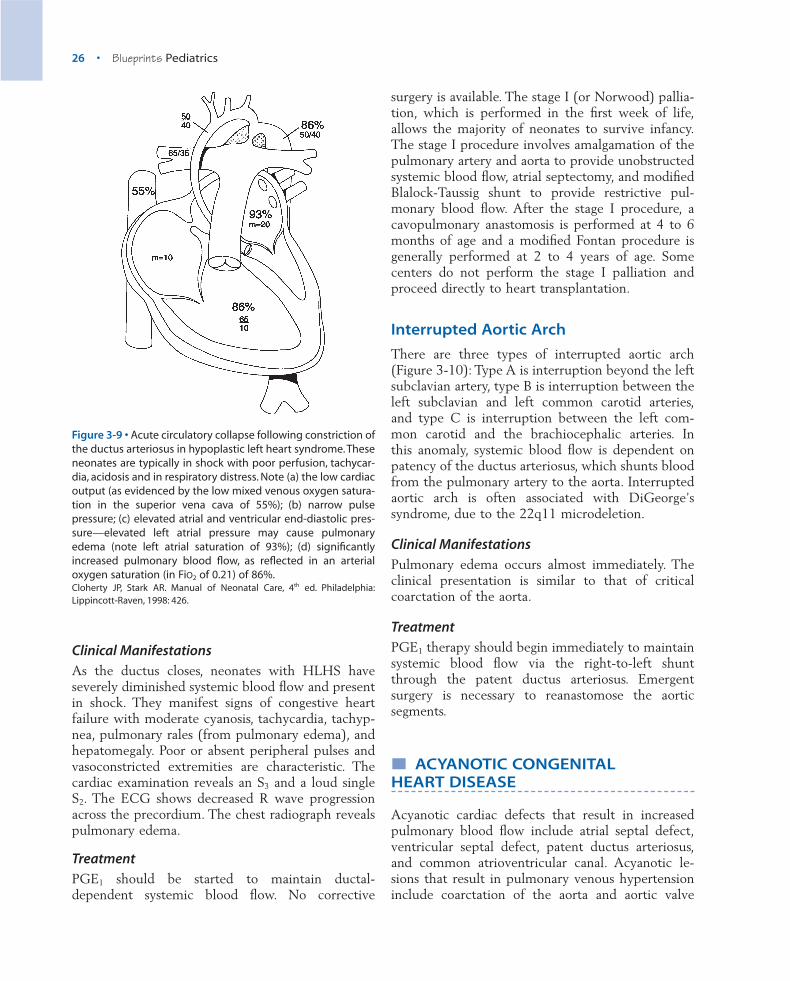
Figure 3-8 • Hypoplastic left heart syndrome in a 24-hour-oldpatient with falling pulmonary vascular resistance and a non-restrictive ductus arteriosus. Typical anatomic and hemody-namic findings include: (a) atresia or hypoplasia of the leftventricle, mitral and aortic valves; (b) a diminutive ascendingaorta and transverse aortic arch, usually with an associatedcoarctation; (c) coronary blood flow is usually retrograde fromthe ductus arteriosus through the tiny ascending aorta; (d) sys-temic arterial oxygen saturation (in FiO2 of 0.21) of 80%, reflect-ing relatively balanced systemic and pulmonary bloodflows—the pulmonary artery and aortic saturations are equal(see text); (e) pulmonary hypertension secondary to the non-restrictive ductus arteriosus; (f ) minimal left atrial hypertension;(g) normal systemic cardiac output (note superior vena cavaoxygen saturation of 65%) and blood pressure (65/45).Cloherty JP, Stark AR. Manual of Neonatal Care, 4th ed. Philadelphia:Lippincott-Raven, 1998: 426.
26 • Blueprints Pediatrics
Clinical ManifestationsAs the ductus closes, neonates with HLHS haveseverely diminished systemic blood flow and presentin shock. They manifest signs of congestive heartfailure with moderate cyanosis, tachycardia, tachyp-nea, pulmonary rales (from pulmonary edema), andhepatomegaly. Poor or absent peripheral pulses andvasoconstricted extremities are characteristic. Thecardiac examination reveals an S3 and a loud singleS2. The ECG shows decreased R wave progressionacross the precordium. The chest radiograph revealspulmonary edema.
TreatmentPGE1 should be started to maintain ductal-dependent systemic blood flow. No corrective
surgery is available. The stage I (or Norwood) pallia-tion, which is performed in the first week of life,allows the majority of neonates to survive infancy.The stage I procedure involves amalgamation of thepulmonary artery and aorta to provide unobstructedsystemic blood flow, atrial septectomy, and modifiedBlalock-Taussig shunt to provide restrictive pul-monary blood flow. After the stage I procedure, acavopulmonary anastomosis is performed at 4 to 6months of age and a modified Fontan procedure isgenerally performed at 2 to 4 years of age. Somecenters do not perform the stage I palliation andproceed directly to heart transplantation.
Interrupted Aortic Arch
There are three types of interrupted aortic arch(Figure 3-10): Type A is interruption beyond the leftsubclavian artery, type B is interruption between theleft subclavian and left common carotid arteries,and type C is interruption between the left com-mon carotid and the brachiocephalic arteries. In this anomaly, systemic blood flow is dependent onpatency of the ductus arteriosus, which shunts bloodfrom the pulmonary artery to the aorta. Interruptedaortic arch is often associated with DiGeorge’s syndrome, due to the 22q11 microdeletion.
Clinical ManifestationsPulmonary edema occurs almost immediately. Theclinical presentation is similar to that of criticalcoarctation of the aorta.
TreatmentPGE1 therapy should begin immediately to maintainsystemic blood flow via the right-to-left shuntthrough the patent ductus arteriosus. Emergentsurgery is necessary to reanastomose the aortic segments.
� ACYANOTIC CONGENITAL HEART DISEASE
Acyanotic cardiac defects that result in increasedpulmonary blood flow include atrial septal defect,ventricular septal defect, patent ductus arteriosus,and common atrioventricular canal. Acyanotic le-sions that result in pulmonary venous hypertensioninclude coarctation of the aorta and aortic valve
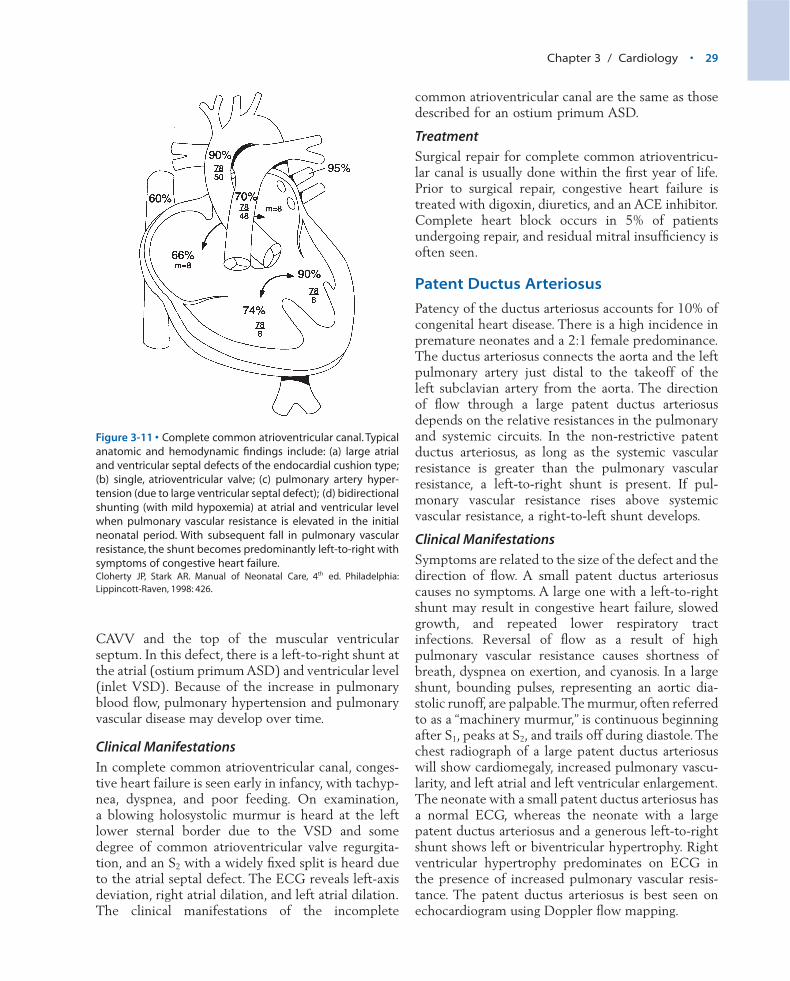
Figure 3-9 • Acute circulatory collapse following constriction ofthe ductus arteriosus in hypoplastic left heart syndrome. Theseneonates are typically in shock with poor perfusion, tachycar-dia, acidosis and in respiratory distress. Note (a) the low cardiacoutput (as evidenced by the low mixed venous oxygen satura-tion in the superior vena cava of 55%); (b) narrow pulse pressure; (c) elevated atrial and ventricular end-diastolic pres-sure—elevated left atrial pressure may cause pulmonaryedema (note left atrial saturation of 93%); (d) significantlyincreased pulmonary blood flow, as reflected in an arterialoxygen saturation (in FiO2 of 0.21) of 86%.Cloherty JP, Stark AR. Manual of Neonatal Care, 4th ed. Philadelphia:Lippincott-Raven, 1998: 426.

Chapter 3 / Cardiology • 27
stenosis. The acyanotic structural anomaly thatresults in relatively normal pulmonary blood flow ispulmonary valve stenosis.
Atrial Septal Defects
Atrial septal defects account for 8% of congenitalheart disease. There are three types of atrial septaldefects:
• Ostium secundum defect, seen in the midportionof the atrial septum
• Ostium primum defect, located in the low atrialseptum
• Sinus venosus defect, found at the junction of theright atrium and the superior or inferior vena cava
The degree of atrial shunting is dependent on thesize of the ASD and the relative compliance of theventricles in diastole. Since right ventricular diastoliccompliance is usually greater than left ventriculardiastolic compliance, left-to-right shunting occurs at the atrial level, thus increasing flow across the tricuspid and pulmonary valves and increasing pulmonary blood flow.
Clinical ManifestationsAtrial septal defects are usually not associated withsymptoms, although there may be a history of slowweight gain and frequent lower respiratory infec-tions. On physical examination, the precordium ishyperdynamic, and a right ventricular heave is oftenpresent. A systolic ejection murmur in the pulmonicarea and a mid-diastolic rumble in the lower rightsternal border reflect the increased flow across thepulmonary and tricuspid valves. S2 is widely and con-stantly split. On chest radiograph, the heart and mainpulmonary artery are enlarged and pulmonary vas-cularity is increased.The ECG often shows right ven-tricular hypertrophy or right ventricular conductiondelay. Right-axis deviation is often seen in secundumdefects, whereas primum defects have characteristicextreme left-axis deviation. The amount of right ventricle and left atrium enlargement is directlypoportional to the size of the left-to-right shunt.On echocardiogram, the defect can be visualized, andDoppler flow mapping demonstrates the direction offlow.
TreatmentSpontaneous closure of small secundum ASDs islikely to occur in the majority of cases in the first yearof life. Ostium primum and sinus venosus ASDs donot close spontaneously and must be addressed sur-gically. The symptomatic child with an ASD shouldhave the defect closed as soon as possible. The timingof ASD repair in the asymptomatic infant or child ismore controversial. In general, the defect should berepaired when circulatory arrest is not needed andwhen the likelihood of needing a blood transfusion
Figure 3-10 • Interrupted aortic arch with restrictive patentductus arteriosus.Typical anatomic and hemodynamic findingsinclude: (a) atresia of a segment of the aortic arch between theleft subclavian artery and the left common carotid (the mostcommon type of interrupted aortic arch—“type B”); (b) a pos-terior malalignment of the conal septum resulting in a largeventricular septal defect and a narrow subaortic area; (c) abicuspid aortic valve occurs in 60% of patients; (d) systemicpressure in the right ventricle and pulmonary artery (due to thelarge, nonrestrictive ventricular septal defect); (e) increasedoxygen saturation in the pulmonary artery due to left-to-rightshunting at the ventricular level; (f ) “differential cyanosis” witha lower oxygen saturation in the descending aorta due to aright-to-left shunt at the patent ductus. Note the lower bloodpressure in the descending aorta due to constriction of theductus; opening the ductus with PGE1 results in equal upperand lower extremity blood pressures, but continued “differen-tial cyanosis.”Cloherty JP, Stark AR. Manual of Neonatal Care, 4th ed. Philadelphia:Lippincott-Raven, 1998: 426.

28 • Blueprints Pediatrics
is low. After 6 months of age, both of these criteriaare generally met. Subacute bacterial endocarditisprophylaxis is not recommended for secundum atrialseptal defects but is indicated in primum and sinusvenosus atrial septal defects.
Ventricular Septal Defects
The ventricular septal defects are the most commoncongenital heart defect, accounting for 25% of allcongenital cardiac lesions. The five types of ventri-cular septal defects are as follows:
• Muscular• Inlet• Conoseptal hypoplasia• Conoventricular• Malalignment
Muscular ventricular septal defects occur in themuscular portion of the septum and may be single ormultiple and located in the posterior, apical, or ante-rior portion of the septum. The inlet VSD is an endo-cardial cushion defect and occurs in the inlet portionof the septum beneath the septal leaflet of the tricuspid valve. Conoseptal hypoplasia VSDs arepositioned in the outflow tract of the right ventriclebeneath the pulmonary valve. The conoventricularVSD occurs in the membranous portion of the ventricular septum. Malalignment VSDs result frommalalignment of the infundibular septum.
When the VSD is non-restrictive, pulmonary vas-cular resistance (PVR) and systemic vascular resis-tance (SVR) determine shunt flow. When the PVR isless than the SVR the shunt flow is left to right. Largedefects eventually result in pulmonary hypertension,whereas small defects do not change PVR. Theamount of left ventricular and left atrial dilatation isdirectly proportional to the size of the left-to-rightshunt. Right ventricular hypertrophy occurs whenpulmonary vascular resistance increases. If leftuntreated, the large VSD may result in elevated pul-monary arterial pressures and may lead to pulmonaryvascular obstructive disease, and Eisenmenger’s syn-drome. In some cases of Eisenmenger’s syndrome, theVSD shunt may reverse right to left. When the VSDis restrictive, shunt flow is left to right from the highpressure LV to the lower pressure RV.
Clinical ManifestationsClinical symptoms are related to the size of theshunt.A small shunt produces no symptoms, whereas
a large shunt without elevated pulmonary arterialpressures gives rise to congestive heart failure andgrowth failure. The patient with a large VSD withEisenmenger physiology presents with shortness ofbreath, dyspnea on exertion, chest pain, and cyanosis.The smaller the defect, the louder the holosystolicmurmur. As pulmonary vascular resistance increases,the holosystolic murmur shortens and the pulmonarycomponent of S2 increases in intensity. In the pres-ence of pulmonary vascular obstructive disease, aright ventricular heave, ejection click, short systolicejection murmur, diastolic murmur of pulmonaryvalve insufficiency, and loud, single S2 are heard.Chest radiograph for small defects may be normal orshow mild cardiomegaly and a slight increase in pul-monary vascularity, whereas in large left-to-rightshunts cardiomegaly, increased pulmonary vascular-ity, and enlargement of the left atrium and left ven-tricle are seen. In small defects the ECG is normal,whereas with a large VSD, left atrial, left ventricular,or biventricular hypertrophy is seen. Right ventricu-lar hypertrophy predominates when pulmonary vas-cular resistance is high. On echocardiogram, thedefect can be visualized, and Doppler flow mappingdemonstrates the direction of flow.
TreatmentMost small VSDs close without intervention (40% by3 years, 75% by 10 years), whereas the treatment forlarge VSDs is surgical closure before pulmonary vas-cular changes become irreversible. Congestive heartfailure is treated with digoxin, diuretics, and anangiotensin-converting enzyme (ACE) inhibitor.
Common Atrioventricular Canal
The common atrioventricular canal defect (Figure 3-11), results from deficiency of the endocardial cush-ions and results in an ostium primum ASD and inletVSD with lack of septation of the mitral and tricus-pid valves (common atrioventricular valve [CAVV]).In an incomplete atrioventricular canal defect, theCAVV leaflets attaches directly to the top of the mus-cular portion of the ventricular septum. As a result,there is no communication beneath the atrioventric-ular valves between the right and left ventricles. Thecommunication at the atrial level is an ostium primumASD.The mitral valve is cleft, and there may be somedegree of mitral regurgitation. In complete commonatrioventricular canal, there is a CAVV that is notattached to the muscular ventricular septum. As aresult, there is a large inlet VSD located between the
Chapter 3 / Cardiology • 29
CAVV and the top of the muscular ventricularseptum. In this defect, there is a left-to-right shunt atthe atrial (ostium primum ASD) and ventricular level(inlet VSD). Because of the increase in pulmonaryblood flow, pulmonary hypertension and pulmonaryvascular disease may develop over time.
Clinical ManifestationsIn complete common atrioventricular canal, conges-tive heart failure is seen early in infancy, with tachyp-nea, dyspnea, and poor feeding. On examination,a blowing holosystolic murmur is heard at the leftlower sternal border due to the VSD and somedegree of common atrioventricular valve regurgita-tion, and an S2 with a widely fixed split is heard dueto the atrial septal defect. The ECG reveals left-axisdeviation, right atrial dilation, and left atrial dilation.The clinical manifestations of the incomplete
common atrioventricular canal are the same as thosedescribed for an ostium primum ASD.
TreatmentSurgical repair for complete common atrioventricu-lar canal is usually done within the first year of life.Prior to surgical repair, congestive heart failure istreated with digoxin, diuretics, and an ACE inhibitor.Complete heart block occurs in 5% of patientsundergoing repair, and residual mitral insufficiency isoften seen.
Patent Ductus Arteriosus
Patency of the ductus arteriosus accounts for 10% ofcongenital heart disease. There is a high incidence inpremature neonates and a 2:1 female predominance.The ductus arteriosus connects the aorta and the leftpulmonary artery just distal to the takeoff of the left subclavian artery from the aorta. The directionof flow through a large patent ductus arteriosusdepends on the relative resistances in the pulmonaryand systemic circuits. In the non-restrictive patentductus arteriosus, as long as the systemic vascularresistance is greater than the pulmonary vascularresistance, a left-to-right shunt is present. If pul-monary vascular resistance rises above systemic vascular resistance, a right-to-left shunt develops.
Clinical ManifestationsSymptoms are related to the size of the defect and thedirection of flow. A small patent ductus arteriosuscauses no symptoms. A large one with a left-to-rightshunt may result in congestive heart failure, slowedgrowth, and repeated lower respiratory tract infections. Reversal of flow as a result of high pulmonary vascular resistance causes shortness ofbreath, dyspnea on exertion, and cyanosis. In a largeshunt, bounding pulses, representing an aortic dia-stolic runoff, are palpable.The murmur, often referredto as a “machinery murmur,” is continuous beginningafter S1, peaks at S2, and trails off during diastole. Thechest radiograph of a large patent ductus arteriosuswill show cardiomegaly, increased pulmonary vascu-larity, and left atrial and left ventricular enlargement.The neonate with a small patent ductus arteriosus hasa normal ECG, whereas the neonate with a largepatent ductus arteriosus and a generous left-to-rightshunt shows left or biventricular hypertrophy. Rightventricular hypertrophy predominates on ECG in the presence of increased pulmonary vascular resis-tance. The patent ductus arteriosus is best seen onechocardiogram using Doppler flow mapping.
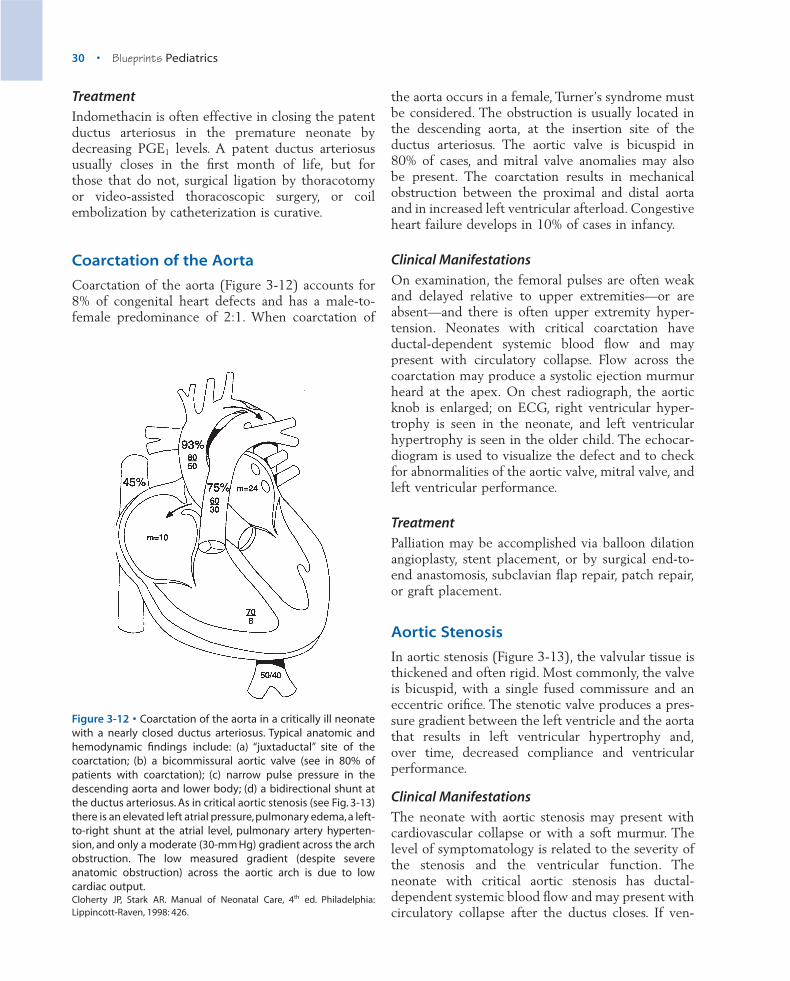
Figure 3-11 • Complete common atrioventricular canal. Typicalanatomic and hemodynamic findings include: (a) large atrialand ventricular septal defects of the endocardial cushion type;(b) single, atrioventricular valve; (c) pulmonary artery hyper-tension (due to large ventricular septal defect); (d) bidirectionalshunting (with mild hypoxemia) at atrial and ventricular levelwhen pulmonary vascular resistance is elevated in the initialneonatal period. With subsequent fall in pulmonary vascularresistance, the shunt becomes predominantly left-to-right withsymptoms of congestive heart failure.Cloherty JP, Stark AR. Manual of Neonatal Care, 4th ed. Philadelphia:Lippincott-Raven, 1998: 426.
30 • Blueprints Pediatrics
TreatmentIndomethacin is often effective in closing the patentductus arteriosus in the premature neonate bydecreasing PGE1 levels. A patent ductus arteriosususually closes in the first month of life, but for those that do not, surgical ligation by thoracotomyor video-assisted thoracoscopic surgery, or coilembolization by catheterization is curative.
Coarctation of the Aorta
Coarctation of the aorta (Figure 3-12) accounts for8% of congenital heart defects and has a male-to-female predominance of 2:1. When coarctation of
the aorta occurs in a female, Turner’s syndrome mustbe considered. The obstruction is usually located inthe descending aorta, at the insertion site of theductus arteriosus. The aortic valve is bicuspid in 80% of cases, and mitral valve anomalies may also be present. The coarctation results in mechanicalobstruction between the proximal and distal aortaand in increased left ventricular afterload. Congestiveheart failure develops in 10% of cases in infancy.
Clinical ManifestationsOn examination, the femoral pulses are often weakand delayed relative to upper extremities—or areabsent—and there is often upper extremity hyper-tension. Neonates with critical coarctation haveductal-dependent systemic blood flow and maypresent with circulatory collapse. Flow across thecoarctation may produce a systolic ejection murmurheard at the apex. On chest radiograph, the aorticknob is enlarged; on ECG, right ventricular hyper-trophy is seen in the neonate, and left ventricularhypertrophy is seen in the older child. The echocar-diogram is used to visualize the defect and to checkfor abnormalities of the aortic valve, mitral valve, andleft ventricular performance.
TreatmentPalliation may be accomplished via balloon dilationangioplasty, stent placement, or by surgical end-to-end anastomosis, subclavian flap repair, patch repair,or graft placement.
Aortic Stenosis
In aortic stenosis (Figure 3-13), the valvular tissue isthickened and often rigid. Most commonly, the valveis bicuspid, with a single fused commissure and aneccentric orifice. The stenotic valve produces a pres-sure gradient between the left ventricle and the aortathat results in left ventricular hypertrophy and,over time, decreased compliance and ventricular performance.
Clinical ManifestationsThe neonate with aortic stenosis may present withcardiovascular collapse or with a soft murmur. Thelevel of symptomatology is related to the severity ofthe stenosis and the ventricular function. Theneonate with critical aortic stenosis has ductal-dependent systemic blood flow and may present withcirculatory collapse after the ductus closes. If ven-
Figure 3-12 • Coarctation of the aorta in a critically ill neonatewith a nearly closed ductus arteriosus. Typical anatomic andhemodynamic findings include: (a) “juxtaductal” site of thecoarctation; (b) a bicommissural aortic valve (see in 80% ofpatients with coarctation); (c) narrow pulse pressure in thedescending aorta and lower body; (d) a bidirectional shunt atthe ductus arteriosus. As in critical aortic stenosis (see Fig. 3-13)there is an elevated left atrial pressure,pulmonary edema,a left-to-right shunt at the atrial level, pulmonary artery hyperten-sion, and only a moderate (30-mm Hg) gradient across the archobstruction. The low measured gradient (despite severeanatomic obstruction) across the aortic arch is due to lowcardiac output.Cloherty JP, Stark AR. Manual of Neonatal Care, 4th ed. Philadelphia:Lippincott-Raven, 1998: 426.

Chapter 3 / Cardiology • 31
tricular function is maintained, a harsh systolic ejec-tion murmur is heard at the right upper sternalborder and is preceded by an ejection click heard bestat the left lower sternal border. If ventricular func-tion is compromised, there may be significant steno-sis with only a soft murmur appreciated. On chestradiograph, poststenotic dilatation of the ascendingaorta is present, and in severe cases, pulmonaryedema can be seen. The ECG may show left ven-tricular hypertrophy, and a strain pattern of STdepressions and inverted T waves may be seen. Thevalvular lesion, the degree of stenosis, and left ven-tricular function are all seen on echocardiogram.
TreatmentIf intervention is required, relief of the aortic valvegradient may be accomplished by open surgicalvalvotomy or by balloon valvuloplasty. Both surgicalvalvotomy and balloon valvuloplasty may result inprogressive aortic regurgitation that may requireaortic valve replacement with a mechanical, homo-graft, or autograft valve (Ross procedure).
Pulmonic Stenosis
Pulmonic valve stenosis accounts for 5% to 8% ofcongenital heart defects. The pulmonary commis-sures are fused, the valve is domed and has a smallcentral opening, and there is poststenotic dilatationof the main pulmonary artery. The valve is bicuspidor dysplastic in 10% of cases. Right ventricular hyper-trophy occurs over time as the ventricle attempts tomaintain cardiac output. In critical pulmonic steno-sis, a decrease in the compliance of the right ventri-cle will increase right atrial pressure and may openthe foramen ovale, producing a small right-to-leftshunt.
Clinical ManifestationsMost patients are asymptomatic. Severe to criticalpulmonary stenosis may cause dyspnea on exertionand angina. Right-sided congestive heart failure israre, except in infants with critical pulmonic steno-sis who may have ductal-dependent pulmonaryblood flow. Characteristically, the ejection click ofpulmonic stenosis varies with inspiration, and a harshsystolic ejection murmur is heard at the left uppersternal border. In severe stenosis, a thrill and rightventricular heave are palpable. On chest radiograph,heart size and pulmonary vascularity are normal,but the pulmonary artery segment is enlarged. OnECG, the degree of right ventricular hypertrophy andright-axis deviation correlates with the degree ofstenosis. The transvalvular gradient and the degree ofright ventricular hypertrophy can be measured byechocardiogram.
TreatmentDefinitive treatment is accomplished by balloonvalvuloplasty of the stenotic valve. Indications forpulmonary valvotomy include a right ventricularpressure greater than 50mm Hg or symptoms ofright-sided congestive heart failure.
Thus far, this chapter has focused on the evalua-tion of the cyanotic neonate and the most common
Figure 3-13 • Critical valvular aortic stenosis with a closedductus arteriosus.Typical anatomic and hemodynamic findingsinclude: (a) a morphologically abnormal,stenotic valve; (b) post-stenotic dilatation of the ascending aorta; (c) elevated left ventricular end diastolic pressure and left atrial pressures con-tributing to pulmonary edema (mild pulmonary venous andarterial desaturation); (d) a left-to-right shunt at the atrial level(note increase in oxygen saturation from superior vena cava toright atrium); (e) pulmonary artery hypertension (also sec-ondary to the elevated left atrial pressure); (f ) only a modest(25-mm Hg) gradient across valve. The low measured gradient(despite severe anatomic obstruction) across the aortic valve isdue to a severely limited cardiac output, as evidenced by thelow mixed venous oxygen saturation (45%) in the superior venacava.Cloherty JP, Stark AR. Manual of Neonatal Care, 4th ed. Philadelphia:Lippincott-Raven, 1998: 426.

32 • Blueprints Pediatrics
cyanotic and acyanotic congenital heart defects.Before moving to acquired structural heart disease,functional heart disease, and arrhythmias, see Table3-3, which lists the classic findings for the 10 mostcommon congenital heart lesions.
� ACQUIRED STRUCTURAL HEART DISEASE
Rheumatic Heart Disease
Rheumatic heart disease results from single or mul-tiple episodes of acute rheumatic fever. Mitral regur-gitation is the most common lesion found. Aorticinsufficiency is also commonly found with or withoutmitral regurgitation. Mitral stenosis is less commonand usually is the end result of multiple attacks ofacute rheumatic fever. Least common is aortic steno-sis. The tricuspid and pulmonary valves are almostnever affected. Symptoms are proportional to thedegree of valvular damage. Rheumatic fever is dis-cussed in Chapter 12.
Kawasaki’s Disease
Cardiac effects may include pericarditis, myocarditis,and transient rhythm disturbances. However, it is
the development of coronary artery aneurysms,with their potential for occlusion or rupture, thatmakes the disease life-threatening. Coronary arteryaneurysms develop during the subacute phase (11thto 25th day) in about 30% of cases but regress in most patients. Early therapy with intravenousimmunoglobulin decreases the incidence of coronaryartery aneurysms to less than 10%. High-dose aspirintherapy lessens the likelihood of late aneurysms. Theechocardiogram is used to assess ventricular functionand visualize pericardial fluid and coronary arteryaneurysms. A thorough discussion of Kawasaki’sdisease is found in Chapter 11.
Endocarditis
PathogenesisBacterial endocarditis is a microbial infection of theendocardium. Although it may occur on normalvalves, bacterial endocarditis is much more likely to occur on congenitally abnormal valves, valvesdamaged by rheumatic fever, acquired valvularlesions (mitral valve prolapse), and prostheticreplacement valves as a consequence of turbulentblood flow. Factors that may precipitate bacterialendocarditis include a previous episode of endo-carditis, dental manipulation or infection, instru-
Lesion Presentation Physical ECG X-rayExamination
Atrial septal defect Murmur Fixed split S2 Mild RVH ±CE, ≠ PBF
Ventricular septal defect Murmur, CHF Holosystolic murmur LVH, RVH +CE, ≠ PBF
Patent ductus Murmur, ±CHF Continuous murmur LVH, ±RVH ±CE, ≠ PBF
AV canal defect Murmur, ±CHF Holosystolic murmur “Superior” axis ± CE, ≠ PBF
Pulmonic stenosis Murmur, ±cyanosis Click, SEM RVH ±CE, NL, or Ø PBF
Tetralogy of Fallot Murmur, cyanosis SEM RVH ±CE, Ø PBF
Aortic stenosis Murmur, ±CHF Click, SEM LVH ±CE, NL, PBF
Coarctation of aorta Hypertension ØFemoral pulses LVH ±CE, NL, PBF
Transposition of the Cyanosis Marked cyanosis RVH ±CE, NL, or ≠ PBFgreat arteries
Single ventricle (Variable) (Variable) (Variable) (Variable)
CE, cardiac enlargement; CHF, congestive heart failure; LVH, left ventricular hypertrophy; NL, normal; PBF, pulmonary blood flow; RVH, right ventricularhypertrophy; SEM, systolic ejection murmur.
Classic Findings for the 10 Most Common Congenital Heart Lesions
� TABLE 3-3

Chapter 3 / Cardiology • 33
mentation of the gastrointestinal or genitourinarytract, intravenous drug abuse, an indwelling centralvenous catheter, and prior cardiac surgery.
In children, alpha hemolytic streptococci (Strepto-coccus viridans) and Staphylococcus aureus are themost common etiologic agents. S. viridans accountsfor approximately 67% of the cases, whereas S.aureus is present in about 20% of cases. When infec-tion complicates cardiac surgery, Staphylococcus epi-dermidis, gram-negative bacilli, and fungi should beconsidered. Gram-negative organisms cause about5% of cases of endocarditis in children and are morelikely in neonates, immunocompromised patients,and intravenous drug abusers. Among the HACEK(Haemophilus, Actinobacillus, Cardiobacterium, Eike-nella, Kingella) organisms, which are a rare cause ofendocarditis, Haemophilus influenzae is the mostcommon, frequently affecting previously damagedvalves.
Clinical ManifestationsFever is the most common finding in children withbacterial endocarditis. Often, a new or changingmurmur is auscultated. Children with endocarditisusually display nonspecific symptoms such as chestpain, dyspnea, arthralgia, myalgia, headache, andmalaise. Embolic phenomena such as hematuria withred cell casts and transient ischemic attack or strokemay be present. Other embolic phenomena, such asRoth spots, splinter hemorrhages, petechiae, Oslernodes, and Janeway lesions, are relatively rare in children with bacterial endocarditis.
Diagnostic EvaluationLaboratory studies include a complete blood count,erythrocyte sedimentation rate (ESR), c-reactiveprotein (CRP), and urinalysis. Multiple blood cul-tures increase the probability of discovering thepathogen. Positive blood cultures, an elevated ESR,elevated CRP, hematuria, and anemia are most oftenfound. The echocardiogram is used to define vegeta-tions or thrombi in the heart.
TreatmentMedical management consists of 6 weeks of intra-venous antibiotics directed against the isolatedpathogen. Surgery is indicated for endocarditis whenmedical treatment is unsuccessful, refractory con-gestive heart failure exists, or there are serious
embolic complications, myocardial abscess forma-tion, or refractory prosthetic valve disease.
Prevention of endocarditis is necessary for high-risk patients. Antibiotic regimens to prevent endo-carditis during dental, respiratory, gastrointestinal, orgenitourinary procedures include oral amoxicillin orparenteral ampicillin and gentamicin prior to theprocedure.
1. Patients with congenitally abnormal valves, valvesdamaged by rheumatic fever, acquired valvularlesions (mitral valve prolapse), or prostheticreplacement valves are at increased risk for endocarditis.
2. Alpha hemolytic streptococci (S. viridans) and S. aureus are the most common etiologic agentsin endocarditis.
KEY POINTS
Coronary Artery Disease
Coronary artery disease is rare in childhood, but theatherosclerotic process appears to begin early in life.There is evidence that progression of atheroscleroticlesions is influenced by genetic factors (familialhypercholesterolemia) and lifestyle (cigarette smok-ing; high-cholesterol diet, high-saturated-fat diet).Because many lifetime habits are formed duringchildhood, the opportunity exists for prevention ofcoronary artery disease.
� FUNCTIONAL HEART DISEASE
Myocarditis
Most cases of myocarditis in North America re-sult from viral infection of the myocardium, pre-dominantly enteroviruses (coxsackie B virus andechovirus). It is unclear whether myocardial damagefrom viral myocarditis results from direct viral inva-sion or an autoimmune antibody response.
Clinical ManifestationsDepending on the degree of damage to themyocardium, patients may be asymptomatic and thediagnosis may be made only by finding ST- and T-
34 • Blueprints Pediatrics
wave changes on an ECG done for an unrelatedreason, whereas others may present with fulminantcongestive heart failure. Common symptoms includefever, dyspnea, fatigue, and chest pain (usually due toa secondary pericarditis). Signs include tachycardia,evidence of congestive heart failure, and S3 ventricular gallop. The ECG often reveals ST-segment depression and T-wave inversion, as well asarrhythmias and conduction defects. The chest radi-ograph varies from mild to marked cardiomegaly.Echocardiogram denotes dilated or hypocontractileventricles, or both. Pericardial effusion may bepresent. Endomyocardial biopsy may be indicated inselect cases to confirm diagnosis. Viral etiologyshould be evaluated by viral culture and PCR fromthe throat, stool, blood, and pericardial fluid, ifpresent.
TreatmentTherapy for patients with viral myocarditis is sup-portive to maintain perfusion and oxygenation. Treatventricular arrhythmias, conduction abnormalities,and congestive heart failure as indicated. Intravenousimmunoglobulin is given to minimize furtherdamage to the myocardium. The prognosis forpatients with myocarditis depends on the extent ofmyocardial damage.
Dilated Cardiomyopathy
Dilated or congestive cardiomyopathy is character-ized by myocardial dysfunction and ventriculardilatation. Although usually an idiopathic disorder, itcan be caused by neuromuscular disease (Duchennemuscular dystrophy) or drug toxicity (anthracy-clines). Dilation of the left ventricle results in congestive heart failure. An increase in left atrialpressure, pulmonary venous pressure, and pulmonarycapillary wedge pressure results in pulmonaryedema.
Clinical ManifestationsSymptoms include dyspnea, orthopnea, and parox-ysmal nocturnal dyspnea. Eventually, right heartfailure with dependent edema occurs, and a pulsusalternans may be noted. On cardiac examination, aright ventricular heave and an S3 gallop are found.The ECG reveals rhythm disturbances, left ventricu-lar hypertrophy, and nonspecific ST- and T-waveischemic changes. Ventricular function is evaluatedby echocardiogram.
TreatmentMedical therapy includes inotropic agents andvasodilators to improve myocardial contractility andto decrease the afterload on the weakened ventricle.Diuretics decrease preload and hopefully improvecardiac output by moving the dilated ventricle to amore favorable position on the Frank-Starling curve,and antiarrhythmic medications are used to controlpotentially fatal ventricular arrhythmias. If medicaltherapy fails, heart transplantation may be necessary.
Hypertrophic Cardiomyopathy
Also known as idiopathic hypertrophic subaorticstenosis, hypertrophic cardiomyopathy is an autoso-mal dominant genetic disorder in which the ventric-ular septum is thickened, resulting in left ventricularoutflow tract obstruction. In the thickened stiff leftventricle, diastolic function is well preserved, but sys-tolic function is compromised. Abnormal motion ofthe mitral valve results in mitral insufficiency.
Clinical ManifestationsSymptoms include dyspnea on exertion, chest pain,and syncope.There is often a bisferious pulse (doublepeaked) because ejection is hindered by septalobstruction, a ventricular gallop (S3), and murmursindicative of mitral regurgitation and left ventricularoutflow tract obstruction. ECG illustrates left-axisdeviation, left ventricular hypertrophy, and possibleST- and T-wave changes consistent with ischemia orstrain. The echocardiogram is diagnostic.
TreatmentTherapy is centered around preventing fatal ventric-ular arrhythmias and decreasing the stiffness of the left ventricle with negative inotropic medi-cations, such as calcium channel blockers, and beta-adrenergic blocking agents. The avoidance ofcompetitive sports is essential because sudden deathduring exertion is a significant risk.
� ARRHYTHMIAS
Arrhythmias in children are much less common thanin adults but can be just as life threatening. Arrhyth-mias result from disorders of impulse formation,impulse conduction, or both and are generally classi-fied as follows.

Chapter 3 / Cardiology • 35
Bradyarrhythmias• Sinus node dysfunction• Conduction block
Tachyarrhythmias• Narrow QRS• Wide QRS
Premature Beats• Atrial• Ventricular
Bradyarrhythmias are the result of either depres-sed automaticity or block of an impulse, whereastachyarrhythmias or premature beats arise fromabnormal impulse formation caused by enhancedautomaticity, a reentrant circuit, or triggered activity.Arrhythmias may result from congenital, functional,or acquired structural heart disease; electrolyte disturbances (potassium, calcium, and magnesium);drug toxicity; poisoning; or an acquired systemic disorder. Table 3-4 lists etiologies predisposing children to arrhythmias.
Bradyarrhythmias
As already stated, bradyarrhythmias result from sinusnode dysfunction or conduction block. Bradycar-dias due to sinus node dysfunction include sinusbradycardia, junctional bradycardia, ectopic atrial
bradycardia, and sinus pauses. Bradycardias due to conduction block include first-degree heart block, second-degree heart block, and third-degree (complete) heart block. Second-degree heart block is further divided into Mobitz type I block (Wenckebach), Mobitz type II block, and fixed-ratioatrioventricular (AV) block.
Differential DiagnosisFigure 3-14 shows the rhythm strips of variousbradycardias. Sinus bradycardia is associated withincreased vagal tone, hypoxia, central nervous systemdisorders with increased intracranial pressure,hypothyroidism, hyperkalemia, hypothermia, drugintoxication (digoxin, beta-blockers, calcium channelblockers), and prior atrial surgery. It is also a normalfinding in healthy athletic teenagers. The ECGreveals a normal P wave with normal AV conductionat rates less than 100bpm in the neonate and 60bpmin the older child. When sinus bradycardia becomestoo slow, sinus pauses or escape rhythms may occur.The escape rhythms most often seen include ectopicatrial bradycardia or ectopic atrial rhythm, junctionalbradycardia or junctional rhythm, or a slow idioven-tricular ventricular rhythm.
First-degree heart block usually results fromslowing of atrioventricular conduction at the level ofthe AV node. It is associated with increased vagal tone,digoxin and beta-blocker administration, infectiousetiologies (viral myocarditis,Lyme disease),hypother-mia, electrolyte abnormalities (hypo/hyperkalemia,hypo/hypercalcemia, hypomagnesemia), congenitalheart disease (ASD, atrioventricular canal defect,Ebstein’s anomaly, TAPVC, and L-transposition of the great arteries or “corrected transposition”),rheumatic fever, and cardiomyopathy. First-degree AV block is characterized on ECG by PR interval prolongation for age and rate. The rhythm is regular,originates in the sinus node, and has a normal QRSmorphology.
Second-degree heart block refers to episodic inter-ruption of AV nodal conduction:
• Mobitz type I (Wenckebach) denotes progressiveprolongation of the PR interval over several beatsuntil a QRS is dropped. This cycle repeats itselfoften, although the number of beats in a cycle maynot be constant. The QRS configuration is normal.Etiologies for this rhythm are the same as those forfirst-degree heart block.
• Mobitz type II is caused by abrupt failure of atri-oventricular conduction below the AV node in the
1. Most cases of myocarditis in North America resultfrom viral infection of the myocardium.
2. Dilated or congestive cardiomyopathy is charac-terized by myocardial dysfunction and ventriculardilatation; it is usually idiopathic.
3. Therapy for dilated cardiomyopathy includesinotropic agents to improve left ventricular con-tractility and vasodilators to decrease afterload.Diuretics decrease preload, and antiarrhythmicmedications are used to control potentially fatalventricular arrhythmias.
4. In hypertrophic cardiomyopathy, the ventricularseptum is thickened, resulting in left ventricularoutflow tract obstruction.
5. Therapy for hypertrophic cardiomyopathy is cen-tered around preventing fatal ventricular arrhyth-mias and decreasing the stiffness of the leftventricle with negative inotropic medications.
KEY POINTS

36 • Blueprints Pediatrics
bundle of His-Purkinje fiber system. It is a moreserious bradycardia than first-degree heart block orWenckebach because it can progress to completeheart block. On ECG, there is sudden AV conduc-tion failure with a dropped QRS after a normal Pwave. No preceding PR interval prolongation isseen in normal conducted impulses.
• Fixed-ratio AV block is an arrhythmia in which theQRS complex follows only after every second(third or fourth) P wave, causing 2:1 (3:1 or 4:1)AV block. There is a normal PR interval in con-ducted beats. There is usually a normal or slightlyprolonged QRS. Fixed-ratio block results fromeither AV node or His bundle injury, and intracar-
diac recordings are required to distinguish the siteof injury. Patients may progress to complete heartblock.
Third-degree heart block occurs when no atrialimpulses are conducted to the ventricles. The atrialrhythm and rate are normal for the patient’s age, andthe ventricular rate is slowed markedly (40–55bpm).If an escape rhythm arises from the AV node (junc-tional rhythm), the QRS interval is of normal dura-tion, but if an escape rhythm arises from the distalHis bundle or Purkinje fibers, the QRS interval is pro-longed (idioventricular rhythm). Congenital com-plete AV block can be an isolated abnormality or can
Congenital heart diseaseSupraventricular dysrhythmias: Ebstein’s anomaly (may also present with WPW syndrome), atrial septal defects, atrial
surgery, L-transposition of the great arteries, after Fontan operationVentricular dysrhythmias: aortic valve disease, pulmonary valve disease, after tetralogy of Fallot repair, anomalous left
coronary artery, RV dysplasiaHeart block (varying degrees): after open-heart surgery (Ebstein’s anomaly, L-transposition of the great arteries,
common atrioventricular canal, VSD repair); congenital complete heart block (idiopathic, associated with maternal systemic lupus erythematosus, L-transposition of the great arteries)
Isolated conduction system disordersWPW syndromeProlonged QT interval syndromes
Associated with systemic illnessInfectious myocarditisKawasaki’s diseaseIdiopathic dilated or hypertrophic cardiomyopathyFriedreich’s ataxia (atrial tachycardia or fibrillation)Muscular dystrophies (Duchenne, periodic paralysis)Glycogen storage diseases (Pompe’s disease)Collagen vascular diseases (rheumatic carditis, systemic lupus erythematosus, periarteritis nodosa, dermatomyositis)Endocrine disorders (hyperthyroidism, adrenal dysfunction)Metabolic and electrolyte disturbances (hypomagnesemia, hyperkalemia, hypocalcemia, hypoxia)Lyme disease
Drug toxicityChemotherapeutic agents (anthracyclines)Tricyclic antidepressantsCocaineDigitalis, beta-adrenergic blockers, calcium channel blockersAsthma medications (sympathomimetics)
Other causesBlunt chest trauma (myocardial contusion)Increased intracranial pressure
Factors Predisposing to Dysrhythmias
� TABLE 3-4

Chapter 3 / Cardiology • 37
be associated with L-transposition of the great arter-ies, atrioventricular canal defect, or maternal lupuserythematosus. Other causes include open-heartsurgery (especially after large ventricular septaldefect closure), cardiomyopathy, or Lyme disease.Newborns with congenital complete heart block maypresent with hydrops fetalis.
TreatmentNo intervention is necessary for sinus bradycardia ifcardiac output is maintained. A management algo-rithm for sinus bradycardia is shown in Figure 3-15.
No treatment is necessary for first- or second-degree heart block (Mobitz type I). Mobitz type II,fixed-ratio AV block, and third-degree heart block allrequire pacemaker placement. In Mobitz type II andfixed-ratio AV block, prophylactic pacemaker inser-tion is essential to protect the patient should he orshe progress to complete heart block with inadequatecardiac output away from medical care.
If the child with complete heart block is hemo-dynamically unstable, transcutaneous or transvenouspacing can be performed acutely, and permanenttransvenous or epicardial pacemaker placement canbe performed later. Third-degree heart block ismanaged with either ventricular demand pacing orAV sequential pacing. Figure 3-16 is a managementalgorithm for AV block.
Tachyarrhythmias
Narrow-complex tachycardias have a QRS morphol-ogy similar or identical to that of normal sinusrhythm. They include most, but not all, SVTs (someSVTs have a widened QRS). Narrow-complex tachy-cardias may be due to increased automaticity or froma reentrant circuit. Narrow-complex tachycardiasdue to increased automaticity include sinus tachy-cardia, ectopic atrial tachycardia, junctional ectopictachycardia, and atrial fibrillation. Narrow-complextachycardias caused by reentrant mechanisms arecategorized as orthodromic reentrant tachycardia(ORT) or antidromic reentrant tachycardia (ART). InORT the SVT propagates down the AV node and upthe bypass tract. Since the ventricles are depolarizedin the normal fashion, down the AV node, the QRScomplex is narrow. In ART the SVT propagates downthe bypass tract and up the AV node. Since the ven-tricles are depolarized down the bypass tract, theQRS is widened. Narrow-complex AV reciprocatingtachycardias include AV node reentrant tachycardia,WPW syndrome orthodromic tachycardia (accessorypathway not concealed on ECG—delta wave), ortho-dromic atrioventricular reciprocating tachycardia(accessory pathway concealed on ECG—no deltawave), sinoatrial reentrant tachycardia, and atrialflutter. Narrow-complex tachycardias are relativelywell tolerated acutely.
Conversely, wide-complex tachycardias, defined astachycardias with a QRS more than 0.12 seconds, area medical emergency. Wide-complex tachycardiasinclude ventricular tachycardia, ventricular fibrilla-tion, WPW syndrome antidromic reentrant tachycar-dia, and orthodromic SVT with aberrancy.
Differential DiagnosisFigure 3-17 shows the rhythm strips of the varioustachycardias. The causes of tachyarrhythmia are asfollows.
Narrow-Complex Tachycardias• Sinus tachycardia: Fever, stress, dehydration, and
anemia• ORT (most common non-sinus tachycardia SVT):
Most cases result from a concealed bypass tractcausing ORT, AV node reentrant tachycardia,WPW syndrome ORT, Ebstein’s anomaly (associ-ated with WPW syndrome), L-transposition of thegreat arteries
• Atrial flutter: Atrial surgery (D-TGA s/p Mustard/Senning procedure, ASD s/p repair Hemi-Fontan,Fontan), myocarditis, structural heart disease with
Sinus bradycardia
First-degree AV block
Mobitz type I(Wenckebach phenomenon)
Complete (third-degree)AV block
Mobitz type II
2:1 AV block
P P P P
P PP P
P P P P P P
P P P P P P
P P PP P P P P P
P P P P P P P P PRRRR
P
RRRR
Figure 3-14 • Bradyarrhythmias.

38 • Blueprints Pediatrics
Isoproterenolinfusion begin at
0.05–0.1 mg/kg/min
< 2 yr HR < 90 2 yr–11 yr HR < 80 > 11 yr HR < 60 P wave upright inleads I, II, aVF normal QRS patternOxygen
Normotension
Determinecause
Observation
Hypotension
Atropine0.02 mg/kg
Epinephrine1 mg/kg
Hypertension
Increasedintracranial pressure?
Yes No
Pacing(transvenous ortranscutaneous)
Determine cause
Treat ICPHyperventilation,
MannitolSee Chapter 8
Treathypertensive crisis,
HydralazineLabetolol
Nitroprusside
Sinus bradycardia
Diagnosis
Figure 3-15 • Management algorithm for sinus bradycardia.
dilated atria (Ebstein’s anomaly, tricuspid atresia,rheumatic heart disease of the mitral valve), severetricuspid regurgitation
• Atrial fibrillation: Most often seen with left atrialenlargement (rheumatic heart disease of the mitralvalve,VSD, systemic to pulmonary artery palliativeshunt placement); other causes that result in rightatrial or biatrial enlargement include Ebstein’sanomaly, WPW syndrome, and myocarditis
Wide-Complex Tachycardia• Ventricular tachycardia: Congenital or acquired
heart disease resulting in ventricular dilation orhypertrophy or ventricular suture line, drug inges-tion, or WPW syndrome ART
• Ventricular fibrillation: Terminal rhythm that devel-ops after hypoxia, ischemia, or high-voltage elec-trical injury; predisposing factors include WPWsyndrome and long QT syndrome
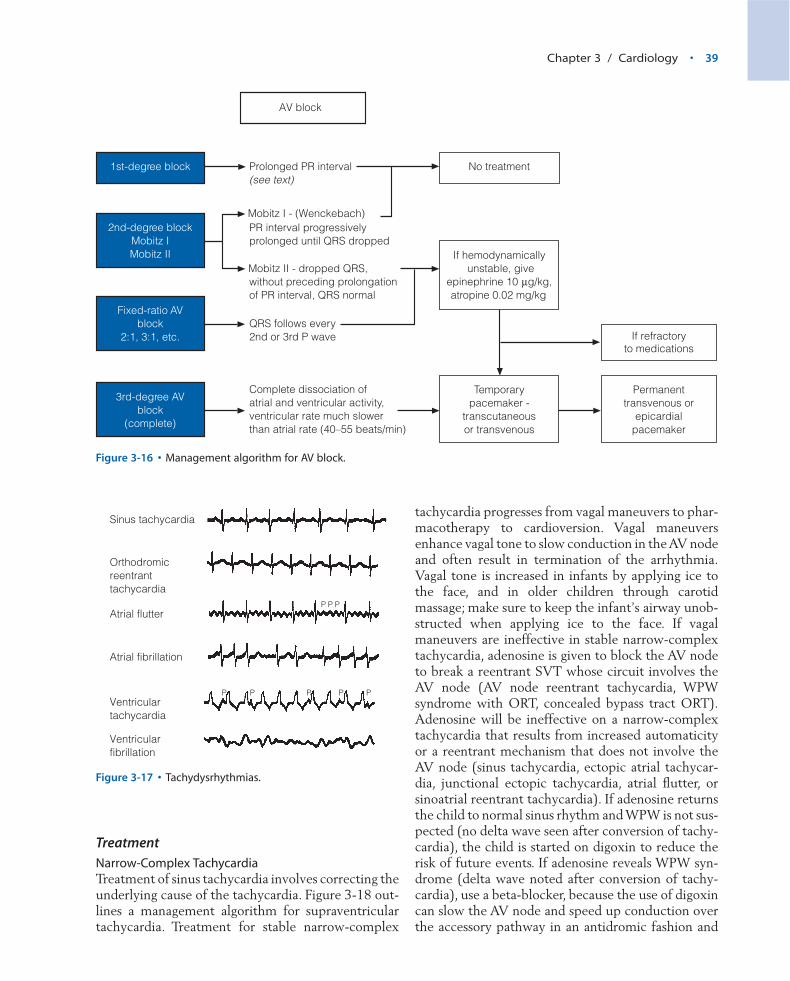
Chapter 3 / Cardiology • 39
TreatmentNarrow-Complex TachycardiaTreatment of sinus tachycardia involves correcting theunderlying cause of the tachycardia. Figure 3-18 out-lines a management algorithm for supraventriculartachycardia. Treatment for stable narrow-complex
tachycardia progresses from vagal maneuvers to phar-macotherapy to cardioversion. Vagal maneuversenhance vagal tone to slow conduction in the AV nodeand often result in termination of the arrhythmia.Vagal tone is increased in infants by applying ice tothe face, and in older children through carotidmassage; make sure to keep the infant’s airway unob-structed when applying ice to the face. If vagalmaneuvers are ineffective in stable narrow-complextachycardia, adenosine is given to block the AV nodeto break a reentrant SVT whose circuit involves theAV node (AV node reentrant tachycardia, WPW syndrome with ORT, concealed bypass tract ORT).Adenosine will be ineffective on a narrow-complextachycardia that results from increased automaticityor a reentrant mechanism that does not involve theAV node (sinus tachycardia, ectopic atrial tachycar-dia, junctional ectopic tachycardia, atrial flutter, orsinoatrial reentrant tachycardia). If adenosine returnsthe child to normal sinus rhythm and WPW is not sus-pected (no delta wave seen after conversion of tachy-cardia), the child is started on digoxin to reduce therisk of future events. If adenosine reveals WPW syn-drome (delta wave noted after conversion of tachy-cardia), use a beta-blocker, because the use of digoxincan slow the AV node and speed up conduction overthe accessory pathway in an antidromic fashion and
If refractoryto medications
1st-degree block Prolonged PR interval(see text)
2nd-degree blockMobitz IMobitz II
PR interval progressivelyprolonged until QRS dropped
Mobitz II - dropped QRS,without preceding prolongationof PR interval, QRS normal
Fixed-ratio AVblock
2:1, 3:1, etc.QRS follows every2nd or 3rd P wave
If hemodynamicallyunstable, give
epinephrine 10 mg/kg,atropine 0.02 mg/kg
3rd-degree AVblock
(complete)
Complete dissociation ofatrial and ventricular activity,ventricular rate much slowerthan atrial rate (40–55 beats/min)
Temporarypacemaker -
transcutaneousor transvenous
No treatment
Permanenttransvenous or
epicardialpacemaker
AV block
Mobitz I - (Wenckebach)
Figure 3-16 • Management algorithm for AV block.
Sinus tachycardia
Atrial flutter
Atrial fibrillation
Ventriculartachycardia
P
Orthodromicreentranttachycardia
Ventricularfibrillation
P P P P
P PP
Figure 3-17 • Tachydysrhythmias.
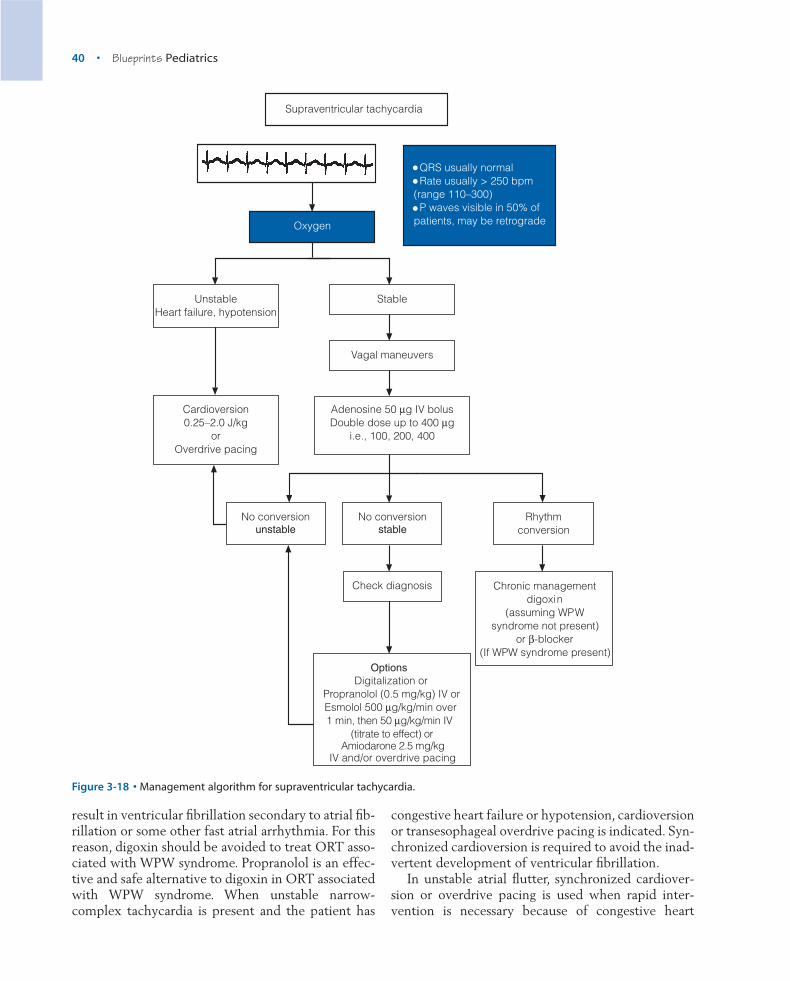
40 • Blueprints Pediatrics
result in ventricular fibrillation secondary to atrial fib-rillation or some other fast atrial arrhythmia. For thisreason, digoxin should be avoided to treat ORT asso-ciated with WPW syndrome. Propranolol is an effec-tive and safe alternative to digoxin in ORT associatedwith WPW syndrome. When unstable narrow-complex tachycardia is present and the patient has
congestive heart failure or hypotension, cardioversionor transesophageal overdrive pacing is indicated. Syn-chronized cardioversion is required to avoid the inad-vertent development of ventricular fibrillation.
In unstable atrial flutter, synchronized cardiover-sion or overdrive pacing is used when rapid inter-vention is necessary because of congestive heart
Cardioversion0.25–2.0 J/kg
orOverdrive pacing
QRS usually normal Rate usually > 250 bpm(range 110–300) P waves visible in 50% ofpatients, may be retrogradeOxygen
UnstableHeart failure, hypotension
Stable
No conversionunstable
Adenosine 50 mg IV bolusDouble dose up to 400 mg
i.e., 100, 200, 400
No conversionstable
Rhythmconversion
Digitalization orPropranolol (0.5 mg/kg) IV or Esmolol 500 mg/kg/min over 1 min, then 50 mg/kg/min IV
(titrate to effect) or Amiodarone 2.5 mg/kg
IV and/or overdrive pacing
Vagal maneuvers
Chronic managementdigoxin
(assuming WPWsyndrome not present)
or b-blocker(If WPW syndrome present)
Check diagnosis
Supraventricular tachycardia
Options
Figure 3-18 • Management algorithm for supraventricular tachycardia.

Chapter 3 / Cardiology • 41
failure. Once cardioversion has occurred, digoxin,beta-blockers, procainamide, amiodarone, sotalol, ora quinidine/digoxin combination may be given tohelp prevent recurrences. If the child is hemody-namically stable, he or she should be loaded withdigoxin and then given procainamide in an attemptto convert the arrhythmia. It is critical to load with digoxin before giving procainamide, becauseprocainamide has vagolytic activity that could inadvertently increase the ventricular rate and causeacute hemodynamic deterioration.
If atrial fibrillation has been present for more than
a few days, anticoagulation is needed before convert-ing the rhythm to decrease the risk of embolization ofpossible intra-atrial clots.An alternative to anticoagu-lation is transesophageal echocardiography to assessfor clots. If no clots are seen, cardioversion mayproceed, although with a slightly increased risk ofthromboembolism relative to anticoagulation. Quini-dine, procainamide, or amiodarone can be effective inpharmacologic conversion of atrial fibrillation, andquinidine and procainamide are good long-term main-tenance drugs. Synchronized cardioversion convertsmost cases to sinus rhythm.
Ventricular tachycardia
Specific Rx for drug-induced VT:Digibind for digitalis
NaHCO3 for tricyclic antidepressantsPhenytoin for cocaine, digoxin, or bupivacaineb-blockers or magnesium sulfate (50 mg/kg IV)
for torsade de pointes
1. ABCs2. Synchronized cardioversion(0.25–2.0 J/kg)(repeat)
Hypotensive orsustained > 30 secs
When stable
P P PP3 or more beatsQRS usually widenedAV dissociationRate: 150–300/minuteFusion beats
Lidocaine 1 mg/kg IV ¥ 2followed by
Lidocaine 20–50 mg/kg/min
Lidocaine 1 mg/kg ¥ 2 IV load10–50 mg/kg/min
procainamide 10 mg/kg IV loadover 30–60 minutes
amiodarone 2.5 mg/kg IV [Do not use amiodarone
and procainamide together –both prolong the QT interval
and both may cause hypotension]
Normotensive
Figure 3-19 • Management algorithm forventricular tachycardia.
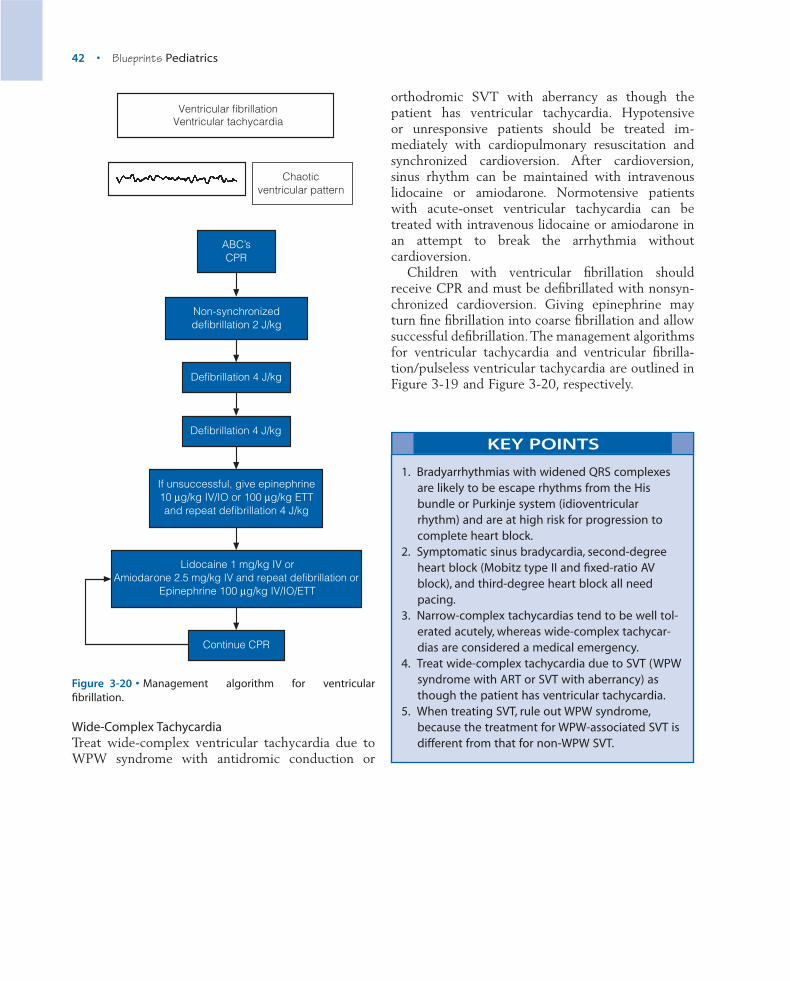
42 • Blueprints Pediatrics
orthodromic SVT with aberrancy as though thepatient has ventricular tachycardia. Hypotensive or unresponsive patients should be treated im-mediately with cardiopulmonary resuscitation andsynchronized cardioversion. After cardioversion,sinus rhythm can be maintained with intravenouslidocaine or amiodarone. Normotensive patients with acute-onset ventricular tachycardia can betreated with intravenous lidocaine or amiodarone inan attempt to break the arrhythmia without cardioversion.
Children with ventricular fibrillation shouldreceive CPR and must be defibrillated with nonsyn-chronized cardioversion. Giving epinephrine mayturn fine fibrillation into coarse fibrillation and allowsuccessful defibrillation.The management algorithmsfor ventricular tachycardia and ventricular fibrilla-tion/pulseless ventricular tachycardia are outlined inFigure 3-19 and Figure 3-20, respectively.
Continue CPR
Chaoticventricular pattern
ABC’sCPR
Non-synchronizeddefibrillation 2 J/kg
Defibrillation 4 J/kg
Defibrillation 4 J/kg
If unsuccessful, give epinephrine10 mg/kg IV/IO or 100 mg/kg ETTand repeat defibrillation 4 J/kg
Lidocaine 1 mg/kg IV orAmiodarone 2.5 mg/kg IV and repeat defibrillation or
Epinephrine 100 mg/kg IV/IO/ETT
Ventricular fibrillationVentricular tachycardia
Figure 3-20 • Management algorithm for ventricular fibrillation.
1. Bradyarrhythmias with widened QRS complexesare likely to be escape rhythms from the Hisbundle or Purkinje system (idioventricularrhythm) and are at high risk for progression tocomplete heart block.
2. Symptomatic sinus bradycardia, second-degreeheart block (Mobitz type II and fixed-ratio AVblock), and third-degree heart block all needpacing.
3. Narrow-complex tachycardias tend to be well tol-erated acutely, whereas wide-complex tachycar-dias are considered a medical emergency.
4. Treat wide-complex tachycardia due to SVT (WPWsyndrome with ART or SVT with aberrancy) asthough the patient has ventricular tachycardia.
5. When treating SVT, rule out WPW syndrome,because the treatment for WPW-associated SVT isdifferent from that for non-WPW SVT.
KEY POINTS
Wide-Complex TachycardiaTreat wide-complex ventricular tachycardia due toWPW syndrome with antidromic conduction or
Related Documents











