STUDENT ARTICLE – DOCTORAL RAHI–SATHI Indo-U.S. Collaboration: The Evolution of a Trainee-Led Twinning Model in Global Health Into a Multidisciplinary Collaborative Program Apurv Soni, a * Nisha Fahey, a,b * Abraham Jaffe, a Shyamsundar Raithatha, c Nitin Raithatha, c Anusha Prabhakaran, c Tiffany A Moore Simas, a Nancy Byatt, a Jagdish Vankar, c Michael Chin, a Ajay G Phatak, c Shirish Srivastava, c David D McManus, a Eileen O’Keefe, d Harshil Patel, c Niket Patel, c Dharti Patel, c Michaela Tracey, a Jasmine A Khubchandani, a Haley Newman, a Allison Earon, a Hannah Rosenfield, a Anna Handorf, a Brittany Novak, a John Bostrom, a Anindita Deb, a Soaham Desai, c Dipen Patel, c Archana Nimbalkar, c Kandarp Talati, c Milagros Rosal, a Patricia McQuilkin, a Himanshu Pandya, c Heena P Santry, a Sunil Thanvi, c Utpala Kharod, c Melissa Fischer, a Jeroan Allison, a Somashekhar M Nimbalkar c RAHI–SATHI presents an innovative twinning model of global health academic partnership, resulting in a number of successful research activities, that features trainees or students as the driving force, complemented by strategic institutional support from both sides of the partnership. Others can promote similar student-led initiatives by: (1) accepting an expanded role for trainees in global health programs, (2) creating structured research and program opportunities for trainees, (3) developing a network of faculty and trainees interested in global health, (4) sharing extramural global health funding opportunities with faculty and trainees, and (5) offering seed funding. ABSTRACT Background: In recent years there has been a surge in the number of global health programs operated by academic insti- tutions. However, most of the existing programs describe partnerships that are primarily faculty-driven and supported by extramural funding. Program Description: Research and Advocacy for Health in India (RAHI, or “pathfinder” in Hindi) and Support and Action Towards Health-Equity in India (SATHI, or “partnership” in Hindi) are 2 interconnected, collaborative efforts between the University of Massachusetts Medical School (UMMS) and Charutar Arogya Mandal (CAM), a medical col- lege and a tertiary care center in rural western India. The RAHI–SATHI program is the culmination of a series of student/ trainee-led research and capacity strengthening initiatives that received institutional support in the form of faculty mentor- ship and seed funding. RAHI–SATHI’s trainee-led twinning approach overcomes traditional barriers faced by global health programs. Trainees help mitigate geographical barriers by acting as a bridge between members from different institutions, garner cultural insight through their ability to immerse themselves in a community, and overcome expertise limitations through pre-planned structured mentorship from faculty of both institutions. Trainees play a central role in cul- tivating trust among the team members and, in the process, they acquire personal leadership skills that may benefit them in their future careers. Conclusion: This paradigm of trainee-led twinning partnership promotes sustainability in an uncertain funding climate and provides a roadmap for conducting foundational work that is essential for the development of a broad, university- wide global health program. BACKGROUND G lobal health, described as a product of international and public health, has gained prominence over the a University of Massachusetts Medical School, Worcester, MA, USA. b Des Moines University, Des Moines, IA, USA. c Pramukhswami Medical College, Karamsad, India. d Boston University, Boston, MA, USA. * Co-first authors. Correspondence to Apurv Soni ([email protected]). Global Health: Science and Practice 2017 | Volume 5 | Number 1 152

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
STUDENT ARTICLE – DOCTORAL
RAHI–SATHI Indo-U.S. Collaboration: The Evolution of aTrainee-Led Twinning Model in Global Health Into aMultidisciplinary Collaborative ProgramApurv Soni,a* Nisha Fahey,a,b* Abraham Jaffe,a Shyamsundar Raithatha,c Nitin Raithatha,c
Anusha Prabhakaran,c Tiffany AMoore Simas,a Nancy Byatt,a Jagdish Vankar,c Michael Chin,a
Ajay G Phatak,c Shirish Srivastava,c David DMcManus,a Eileen O’Keefe,d Harshil Patel,c Niket Patel,c
Dharti Patel,c Michaela Tracey,a Jasmine A Khubchandani,a Haley Newman,a Allison Earon,a
Hannah Rosenfield,a Anna Handorf,a Brittany Novak,a John Bostrom,a Anindita Deb,a Soaham Desai,c
Dipen Patel,c Archana Nimbalkar,c Kandarp Talati,c Milagros Rosal,a Patricia McQuilkin,a
Himanshu Pandya,c Heena P Santry,a Sunil Thanvi,c Utpala Kharod,c Melissa Fischer,a Jeroan Allison,a
Somashekhar M Nimbalkarc
RAHI–SATHI presents an innovative twinning model of global health academic partnership, resulting in anumber of successful research activities, that features trainees or students as the driving force,complemented by strategic institutional support from both sides of the partnership. Others can promotesimilar student-led initiatives by: (1) accepting an expanded role for trainees in global health programs,(2) creating structured research and program opportunities for trainees, (3) developing a network of facultyand trainees interested in global health, (4) sharing extramural global health funding opportunities withfaculty and trainees, and (5) offering seed funding.
ABSTRACTBackground: In recent years there has been a surge in the number of global health programs operated by academic insti-tutions. However, most of the existing programs describe partnerships that are primarily faculty-driven and supported byextramural funding.Program Description: Research and Advocacy for Health in India (RAHI, or “pathfinder” in Hindi) and Support andAction Towards Health-Equity in India (SATHI, or “partnership” in Hindi) are 2 interconnected, collaborative effortsbetween the University of Massachusetts Medical School (UMMS) and Charutar Arogya Mandal (CAM), a medical col-lege and a tertiary care center in rural western India. The RAHI–SATHI program is the culmination of a series of student/trainee-led research and capacity strengthening initiatives that received institutional support in the form of faculty mentor-ship and seed funding. RAHI–SATHI’s trainee-led twinning approach overcomes traditional barriers faced by globalhealth programs. Trainees help mitigate geographical barriers by acting as a bridge between members from differentinstitutions, garner cultural insight through their ability to immerse themselves in a community, and overcome expertiselimitations through pre-planned structured mentorship from faculty of both institutions. Trainees play a central role in cul-tivating trust among the team members and, in the process, they acquire personal leadership skills that may benefit themin their future careers.Conclusion: This paradigm of trainee-led twinning partnership promotes sustainability in an uncertain funding climateand provides a roadmap for conducting foundational work that is essential for the development of a broad, university-wide global health program.
BACKGROUND
Global health, described as a product of internationaland public health, has gained prominence over the
aUniversity of Massachusetts Medical School, Worcester, MA, USA.bDes Moines University, Des Moines, IA, USA.cPramukhswami Medical College, Karamsad, India.dBoston University, Boston, MA, USA.* Co-first authors.Correspondence to Apurv Soni ([email protected]).
Global Health: Science and Practice 2017 | Volume 5 | Number 1 152

past decade or so, specifically in academic centers.1
In the United States alone, there has been a ten-fold increase in the number of global health pro-grams from 2000 to 2012.2
Multiple factors underlie the surge in the num-ber of global health programs in academic institu-tions, includinganincreasedrecognitionofgloballyconnected communities, a strong commitment toservice and philanthropy, and growing studentdemand.3 These collaborative efforts have ledto significant advances in understanding globalhealth disparities as well as curbing epidemicsof HIV/AIDS, malaria, tuberculosis, and, mostrecently, Ebola.4 Emerging evidence suggests thatfaculty and trainees worldwide also benefit fromparticipating in these collaborations that tran-scend national borders5 by heightening theirawareness of social determinants of health,increasing self-awareness, and broadening theirperspectives.6
The current global health landscape representsa paradigm shift from the historical activities ofinternational health.7 Specifically, the conven-tional model of professionals from high-incomecountries providing resources, services, and skillsto “fix” problems ailing low- and middle-incomecountries are being replaced by a more bilateral,twinning approach whereby global and local enti-ties share collective knowledge and resources toachieve a common goal.8,9 Twinning for globalhealth, which has been used in the fields of emer-gency medicine, pediatric oncology, and medicaleducation, emphasizes the role and value of thepartner in the host setting where the majority ofactivities occur.8–12 However, most of the existingprograms in peer-reviewed literature describepartnerships that are faculty-driven and supportedby extramural sources of funding.8–14 Faculty-driven global health programs are often limited tothe interests and expertise of the faculty, and thusa multidisciplinary approach becomes difficult.7
By contrast, we present a student/trainee-ledIndo-U.S. initiative that organically followed thetwinning model and gradually evolved into amultidisciplinary program. The program over-came resource limitations by positioning the train-ees as the driving forces behind the collaboration,complemented by strategic institutional supportand stewardship. To the best of our knowledge,our collaboration represents the first account of atrainee-led twinning program for global health.We believe this account can serve as a roadmapfor other trainee-led initiatives to expand intolarger institution-based global health programswith the help of faculty and institutional support.
THE RAHI–SATHI COLLABORATIONResearch and Advocacy for Health in India (RAHI,which is the Hindi word for pathfinder) andSupport and Action Towards Health-Equity inIndia (SATHI, the Hindi word for partnership) are2 sister collaborations between the Universityof Massachusetts Medical School (UMMS) andCharutar Arogya Mandal (CAM), a charitabletrust that operates a tertiary care center andmedical school in rural western India. RAHI wasformed in 2013 through a formalMemorandumofUnderstanding between UMMS and CAM to sup-port research activities between the 2 institutions.RAHI currently focuses on maternal and childhealth and noncommunicable disease and injurythrough a number of research studies and pro-grams. SATHI was formed in 2015 based on theexperience and feedback from personnel involvedin RAHI to support bilateral capacity strengthen-ing activities, including trainee-exchange, struc-tured mentorship, and biannual seminars onresearch and teaching methodology. The impe-tus behind SATHI was to train learners fromdiverse backgrounds to grow the collaboration.Educational leadership from UMMS and CAMformed a coalition to support this endeavor.
As the only publicly funded medical univer-sity in Massachusetts, UMMS strives to addresshealth disparities locally in central Massachusettsand globally through its legacy partnerships withinstitutions from low- and middle-income coun-tries. Similarly, CAM’s mission is to care for theunderserved of the community and train the nextgeneration of health care providers for ruralIndia. The Central Research Services and Com-munity Extension Department are 2 specificexamples of CAM’s dedication for improvinghealth of local Indian communities throughcommunity-centered research and service, respec-tively. Central Research Services was formed byCAM in 2009 in an effort to support investigator-initiated, community-based research studies andfoster a research culture within the institution.The Community Extension Department is dedi-cated to delivering health programs to the localcommunity. Through this department, CAM hasestablished a network of Village Health Workerswho receive training to perform disease screeningsand deliver health education. Additionally, CAMoperates 7 primary and secondary health centerswithin the region, which increases access to pri-mary and specialist care among rural commun-ities. The shared institutional commitment ofUMMS and CAM to provide equitable health care
The conventionalmodel ofprofessionals fromhigh-incomecountries “fixing”problems in low-income countrieshas been replacedby a twinningapproachwhereby globaland local entitiesshare collectiveknowledge andresources toachievea commongoal.
We present atrainee-ledIndo-U.S. twinningmodel thatgradually evolvedinto amultidisci-plinary program.
Student-Led Twinning Model in Global Health www.ghspjournal.org
Global Health: Science and Practice 2017 | Volume 5 | Number 1 153

to the community formed the bedrock of theRAHI–SATHI collaboration.
The RAHI–SATHI collaboration has beenchampioned thus far by 2 trainee-leaders [A.S.and N.F.] who have led the overall RAHI–SATHIcollaboration with a vision of trainee-centeredresearch and outreach initiatives. These trainee-leaders began as undergraduate students atBoston University and transitioned to medicalschool at UMMS. The RAHI–SATHI collaborationalso receives support from both predoctoral andpostdoctoral trainees from UMMS and CAM whosupport specific ongoing projects or lead develop-ment of new research efforts.
The trainee-leaders recruited predoctoral andpostdoctoral trainees by leveraging existing struc-tured opportunities at UMMS and CAM. Forexample, UMMS medical students are required toparticipate in a scholarly endeavor as part of thelongitudinal 4-year Capstone Scholarship andDiscovery course. In addition, selected UMMSmedical students in the Global Health Pathwayare required to participate in a global health activ-ity in the summer after their first year of medicalschool. Furthermore, UMMS surgical researchscholars are required to dedicate 2 years of theirresidency program to conduct research in a full-time capacity. Finally, CAM residents are requiredto produce a scholarly dissertation at the end oftheir training. Through their participation, train-ees contribute to research and public health activ-ities that directly address the needs of the ruralIndian communities while also meeting theirown educational requirements and developingtheir personal research portfolio.
The trainees are supported by faculty atboth UMMS and CAM (and initially at BostonUniversity). The involvement of faculties fromboth institutions range from high-level advisingon a specific project or scientific product toworking closely in one-on-one mentorship ca-pacity. Typically, faculty who assume a less-involved role, meet with the trainees once asemester to discuss overall progress and respondto questions and solicitations via email or tele-conference. Meanwhile, faculty mentors meetwith the students once a week or once every2 weeks.
TRAINEE-LED TWINNING MODEL FORGLOBAL HEALTHAn international collaboration for strengtheningemergency medicine in Ethiopia described 6 im-portant phases of twinning9:
1. Initiate the partnership
2. Develop a shared work plan
3. Implement the program
4. Monitor outcomes
5. Evaluate results
6. Disseminate information
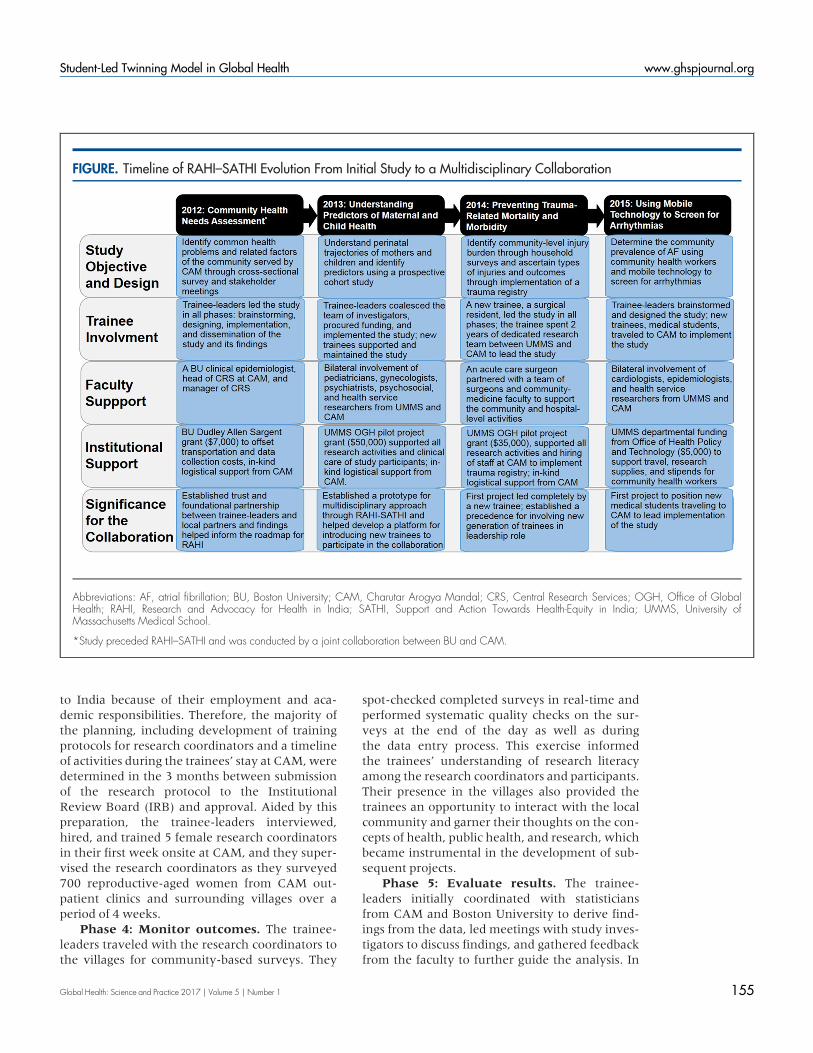
In this article, we describe the role of traineesas the driving force behind all 6 of these phasesin the RAHI–SATHI twinning model for 4 differ-ent activities, selected specifically to illustrate thegradual evolution of the RAHI–SATHI collabora-tion and the transition of the workforce from theinitial trainees to a new generation of trainees(Figure).
Activity 1: Community Health NeedsAssessment in Rural Western India:Cross-Sectional Survey of WomenPhase 1: Initiate a partnership. The officialRAHI–SATHI collaboration was preceded by thefoundational work of the 2 U.S. trainee-leaders[A.S. and N.F.], supported by their clinical epide-miology professor [E.O.] from Boston University,and 2 local leaders from the Central ResearchServices at CAM in India (the head [S.M.N.] andthe manager [A.G.P.]). The 2 U.S. trainee-leaderswere introduced to the Central Research Servicesleaders through a mutual acquaintance who wasa faculty member at CAM. After discussions andidentification of shared interests and local needs,the group decided to conduct an assessment ofwomen’s health status and determinants to pro-duce a snapshot of the community health needs,which would also act as a roadmap for future col-laborative activities.
Phase 2: Develop a shared work plan. Thetrainee-leaders developed a first draft of studymaterials based on feedback from U.S. and Indianinvestigators. The trainee-leaders’ active role inconsolidating feedback from Boston Universityand CAM faculty during this iterative processbecame a crucial learning experience in buildingconsensus, anticipating real-world complications,and understanding the practical limitations ofresearch. This approach also lessened the burdenon the faculty, who were providing in-kind sup-port to this study. The trainee-leaders also gainedexperience in grant writing while successfullyapplying for an institutional grant identified bytheir Boston University mentor.
Phase 3: Implement the program. Thetrainee-leaders were limited to 5 weeks of travel
The RAHI-SATHIcollaboration issupported by bothpre- andpostdoctoralstudents from theUnited States andIndia.
Student-Led Twinning Model in Global Health www.ghspjournal.org
Global Health: Science and Practice 2017 | Volume 5 | Number 1 154
to India because of their employment and aca-demic responsibilities. Therefore, the majority ofthe planning, including development of trainingprotocols for research coordinators and a timelineof activities during the trainees’ stay at CAM,weredetermined in the 3 months between submissionof the research protocol to the InstitutionalReview Board (IRB) and approval. Aided by thispreparation, the trainee-leaders interviewed,hired, and trained 5 female research coordinatorsin their first week onsite at CAM, and they super-vised the research coordinators as they surveyed700 reproductive-aged women from CAM out-patient clinics and surrounding villages over aperiod of 4 weeks.
Phase 4: Monitor outcomes. The trainee-leaders traveled with the research coordinators tothe villages for community-based surveys. They
spot-checked completed surveys in real-time andperformed systematic quality checks on the sur-veys at the end of the day as well as duringthe data entry process. This exercise informedthe trainees’ understanding of research literacyamong the research coordinators and participants.Their presence in the villages also provided thetrainees an opportunity to interact with the localcommunity and garner their thoughts on the con-cepts of health, public health, and research, whichbecame instrumental in the development of sub-sequent projects.
Phase 5: Evaluate results. The trainee-leaders initially coordinated with statisticiansfrom CAM and Boston University to derive find-ings from the data, led meetings with study inves-tigators to discuss findings, and gathered feedbackfrom the faculty to further guide the analysis. In
FIGURE. Timeline of RAHI–SATHI Evolution From Initial Study to a Multidisciplinary Collaboration
Abbreviations: AF, atrial fibrillation; BU, Boston University; CAM, Charutar Arogya Mandal; CRS, Central Research Services; OGH, Office of GlobalHealth; RAHI, Research and Advocacy for Health in India; SATHI, Support and Action Towards Health-Equity in India; UMMS, University ofMassachusetts Medical School.
*Study preceded RAHI–SATHI and was conducted by a joint collaboration between BU and CAM.
Student-Led Twinning Model in Global Health www.ghspjournal.org
Global Health: Science and Practice 2017 | Volume 5 | Number 1 155

the later stages, after cultivating analytic skills, thetrainee-leaders assumed the role of performinganalysis with the support of faculty-level analysts.
The cross-sectional survey identified a highburden of anemia, common mental disorders,chronic pain, and exposure to traumatic events.The factors participants identified as importantfor seeking health care were discordant with thefocus of the Indian National Rural HealthMission. For instance, we found that mothers pri-oritized quality of care over other factors whenconsidering care for their children, and they pri-oritized cost over other factors when seekinghealth care for themselves. By contrast, the gov-ernment’s policies for maternal and child healthlargely focus on reducing costs with limited strat-egies for improving the quality of care provided.15
This preliminary work identified 4 majorneeds, which serves as a roadmap for RAHI:
1. Understanding nutritional, psychosocial, andhealth care influences on mothers and chil-drenduring theperinatal period in rural India.
2. Addressing mortality and long-term disabilitydue to road-traffic accidents and other trau-matic events.
3. Exploring the unique life-course and progres-sion of cardiovascular and other noncommu-nicable diseases.
4. Identifying multidisciplinary approaches tocombat chewable tobacco addiction amongadolescents.
Phase 6: Disseminate information. Find-ings were disseminated using 2 mechanisms tosupport broad communication and further de-velop the partnership:
1. Peer-reviewed publication of manuscriptsand conference abstracts: The trainee-leadersdeveloped first drafts of conference abstractsand manuscripts based on findings from theanalysis and sought specific feedback fromBoston University and CAM investigatorsand, at later stages, the UMMS facultymentors.15,16
2. Discussion of findings with local stakeholdersin rural India: The trainee-leaders returned torural India for a period of 8 weeks to help dis-seminate the findings from the study to localstakeholders. Engaging officials in the publicsector, including health care providers andgovernment health officers, through emailand telephone proved difficult and thusrequired in-person visits by the trainee-
leaders and the head of Central ResearchServices who had a longstanding presence asa clinician in the community. Discussiontopics were tailored to match the purviewof the Chief District Health Officer, theReproductive and Child Health Officer, andthe District Development Officer. A semi-structured interview format was abandonedin favor of a free-flowing conversation abouttheir perception of community needs. Theteam presented findings from the cross-sectional survey in a large-group discussionformat at CAM. The trainee-leaders met withclinicians from various clinical departments atCAMand local government primary care cen-ters to ascertain their impressions about theclinical needs of their patient population andpossible social determinants for health.
Activity 2: Understanding Predictors ofMaternal and Child Health in Rural WesternIndia: Cohort Study of Pregnant WomenPhase 1: Initiate a partnership. In 2012, one ofthe trainee-leaders [A.S.] matriculated to UMMS,where he connected with the institutional Officeof Global Health to identify resources and oppor-tunities for collaboration. Together, both trainee-leaders [A.S. and N.F.] prepared a proposal tostudy predictors of maternal and child healthin rural western India, the first need identifiedthrough their previous community assessment.
India bears the greatest burden worldwide ofchild malnourishment (about 52 million childrenhave stunting) and mortality (in 2008, 1.8 millionchildren under the age of 5 years died).17 Existingeffortsmade by the Indian government to improvehealth outcomes lack the support of evidence-based research.18 The underlying causes of poormaternal and child health and undernutritionmay be multifactorial in nature, and an under-standing of the experiences of Indian womenthroughout the perinatal period is necessaryto help identify entry points for multifacetedinterventions.18,19
In developing their proposal, the trainee-leaders worked with a faculty mentor [J.A.], whocodirects the UMMS Center for Health EquityIntervention Research, and the head of CentralResearch Services at CAM [S.M.N]. Lead investi-gators of the study sought UMMS faculty supportbased on their expertise in peripartum health[T.M.S.], pediatrics [P.M.], women’s mentalhealth [N.B.], and psychosocial determinants ofhealth [M.R.]. Based on their previous ex-
The preliminarywork of thecommunity healthneeds assessmentidentified 4majorneeds, whichserves as aroadmap for theRAHIcollaboration.
Student-Led Twinning Model in Global Health www.ghspjournal.org
Global Health: Science and Practice 2017 | Volume 5 | Number 1 156

perience, the trainee-leaders and the head ofCentral Research Services at CAM activelyrecruited counterpart faculty from CAM [N.R.,A.P., J.V.] to match UMMS faculty in content ex-pertise, thereby facilitating an exchange of clinicaland cultural knowledge. The research team suc-cessfully applied for seed funding through theUMMS Office of Global Health Pilot Project Grantto conduct a prospective cohort study of pregnantwomen in rural India.
Phase 2: Develop a sharedwork plan. Dueto the broad scope of the study, the trainee-leadersmet separately with faculty from each disciplineto identify specific questionnaires, biomarkers,and measurements to be collected during thestudy. Trainee-leaders consolidated the feedbackfrom the investigators and identified critical andoptional components of the study. The trainee-leaders moderated group meetings among UMMSinvestigators and communicatedwith CAM inves-tigators before and after group meetings to buildconsensus and finalize the type of information tobe collected through the study. Thus, the trainee-leaders acted as a bridge between UMMS andCAM investigators as well as principal investiga-tors and co-investigators. The success of trainee-leaders as mediators while developing a sharedwork plan among this multidisciplinary team col-laborating on a project in rural India for the firsttime was predicated on 3 important factors:(1) building on preexisting relationships betweenthe investigators at their respective institutions,(2) engaging faculty early in the process, and(3) demonstrating consistent progress on researchdesign by the trainees at each meeting withfaculty. Ultimately, we designed a prospectivecohort study that recruited and followed pregnantwomen from the first trimester to 2 years post-partumwithmultiple data collection time points.
Phase 3: Implement the program. Thetrainee-leaders traveled to CAM during thesummer after their first year of medical school toimplement the study. The prospective cohortstudy required establishment of standard operat-ing procedures, research space, and sustainedadministrative effort in India. The trainee-leadersand the CAM principal investigator held meetingswith CAM leaders, administration, and facultyfrom relevant departments to describe the studyand outline their roles for supporting the study.To assist with recruitment of pregnant womenfrom the community, the research team, includ-ing trainee-leaders, coordinators, and the CAMprincipal investigator, organized a town hallmeet-ing for community health workers of nearby
villages to describe the study to them, their role ofreferring pregnant women to participate in thestudy, and the honorarium for supporting thestudy.
Phase 4: Monitor outcomes. The trainee-leaders developed standardized forms to track par-ticipant enrollment, follow-up visits, and clinicaldata, which were completed by research assistantson a weekly basis. However, long-term oversightby the trainee-leaders was difficult due to growingcommitments from medical school as they transi-tioned from preclinical to clinical years. Therefore,they recruited a new generation of SATHI traineesto overtakemonitoring of the study. Two graduatestudents from CAM [N.P. and H.P.] performedperiodic data-entry checks and reviewed medicalrecords of the participants. In addition, 4 UMMSmedical students [M.T., H.N., J.K. and H.R.] trav-eled to CAM after their first year of medical schoolto support the research staff with data-entry andquality checks. In addition to monitoring out-comes of the study, the UMMS trainees alsogained cultural and clinical insight into theresearch questions being investigated through thestudy. They used the experience to develop theirresearch interests, which they will pursue for theremainder of their training at UMMS throughtheir capstone course requirement.
Phase 5: Evaluate results. One of thetrainee-leaders [A.S.] led the analysis of theemerging data by leveraging skills acquiredthrough the doctoral program at UMMS Quan-titative Health Sciences and with support fromfaculty-levelstatisticians.Additionally,thetrainee-leader and his mentor [J.A.] conducted biannualworkshops in statistical analysis at CAM to trainlocal statisticians in intermediate and advancedanalyses. The analytical team produced findingsthat were shared by the trainee-leaders withUMMS and CAM investigators, faculty, and stu-dents and continue to be disseminated throughpeer-reviewmechanisms.
Phase 6: Disseminate information. Earlyfindings from the study have identified a high bur-den of low birth weight as well as low maternalhemoglobin and deficiency of essential vitaminsduring pregnancy despite the provision of prenatalcare.20–22 Scholarly products, all first-authored bythe trainee-leaders and second-generation train-ees, were presented at scientific conferences, and2 manuscripts are in development, which discussthe experiences of the pregnant women in ruralwestern India.20–22 Trainees responsible for thefirst draft of the scholarly products solicited feed-back from faculty at both institutions and
The trainee-leaders acted as abridge betweenthe 2 partneruniversities.
Student-Led Twinning Model in Global Health www.ghspjournal.org
Global Health: Science and Practice 2017 | Volume 5 | Number 1 157

incorporated their insights into the work.Additionally, preliminary data from this studyplayed a vital role in successful applications bythe CAM investigators [S.M.N., A.G.P, N.R., andA.P.] for research funding from the IndianCouncil of Medical Research to further study peri-natal health.
Activity 3: Reducing Injury-RelatedMorbidityand Mortality in Rural Western India:Community-Based Survey and TraumaRegistryPhase 1: Initiate a partnership. Prior to imple-mentation of the maternal and child health study(activity 2), the trainee-leaders and the UMMSprincipal investigator hosted the CAM principalinvestigator for a seminar at the UMMS campus.The group presented findings of their communityhealth needs assessment and outlined the scopeof the new maternal and child health study.The seminar was attended by an acute care sur-geon and health services researcher with roots inthe CAM catchment area [H.P.S]. The surgeonexpressed interest in supporting the collaboration.As director of Surgical Research Scholars, the sur-geon recruited a surgical resident [A.J.] entering a2-year period of dedicated research to lead a pro-gram addressing the trauma care needs in ruralwestern India. This undertaking represents thefirst example of a new-generation trainee at thepostdoctoral level leading the design and imple-mentation of a project. The postdoctoral traineetraveled to CAM to gather local feedback aboutthe knowledge gaps that could be addressedthrough the research study and identified facultyfrom the Department for Surgery [S.S.] andCommunity Extension Department [S.R.] to col-laborate on the study.
Phase 2: Develop a shared work plan.During the postdoctoral trainee’s visit to CAM,2 major needs were identified: understandinginjury burden at a community level and develop-ing a mechanism to track and assess outcomes oftrauma patients at CAM.
Road traffic accidents are a leading cause ofmortality in India.23 One out of every 4 road trafficaccidents in India results in a death, and nearlyhalf of the fatal cases never receive any medicalattention.24 CAM’s hospital is situated at the inter-section of 2 major roadways in rural westernIndia. The hospital has more than 20,000 admis-sions per year, and an estimated 70% of these areattributed to road traffic accidents. However, thespecific burden of trauma-related injuries and
outcomes at the hospital and community levelremain unknown. Trauma registries are an inte-gral part of emergency care systems in high-income countries but not in low- and middle-income countries.25 They are important for qual-ity improvement within an institution and sur-veillanceof trauma-relatedoutcomes.26Therefore,the UMMS and CAM team decided to conduct acommunity-based survey and develop a hospital-based trauma registry, which was financially sup-ported by RAHI–SATHI’s second UMMS Office ofGlobalHealthPilotProjectGrant.
Phase 3: Implement the program. UMMSand CAM investigators leveraged a preexistingsampling frame created by CAM as part of theircommunity outreach efforts to carry out bur-den of injury surveys among 5,000 householdfrom 36 villages in the surrounding region. Thepostdoctoral trainee and CAM’s CommunityExtension Department supervised this implemen-tation. Diffusion of trauma registry, a new initia-tive within the busy setting of emergency carein a resource-limited setting, required buy-in atmultiple levels, including the registrar, casualtymedical officers, trauma specialists, and hospitalleaders. TheUMMSpostdoctoral trainee dedicated2 research years to systematically build buy-infor the trauma registry at CAM through a pilotimplementation phase, discussions with physicianchampions, and stakeholder round-table forums.The principal investigator of the study [H.P.S], asdirector of the Surgical Research Scholars pro-gram, modified program requirements and soughtsupport from UMMS leadership to accommodatethe trainee’s time at CAM. A first-year UMMSmedical student [B.N], a member of the third-generation of predoctoral trainees, spent 4 weeksin India working with the postdoctoral traineeduring the implementation phase. Ultimately,the trauma registry was implemented as standardoperating procedures, replacing the existingintake form in the emergency department for alltrauma-related injuries, thereby reducing theadditional burden imposed on care providers andassuring maintenance by existing health care staffat CAM.
Phases 4, 5, and 6: Monitor outcomes,evaluate results, and disseminate informa-tion. The community health workers conduct-ing surveys provided daily tallies of householdssurveyed, and weekly meetings were held to sum-marize the number of injuries and disabilities cap-tured. Data are emerging from this study and havenot yet been analyzed. However, the postdoctoraltrainee and Department of Surgery at UMMS and
Student-Led Twinning Model in Global Health www.ghspjournal.org
Global Health: Science and Practice 2017 | Volume 5 | Number 1 158

CAM have shared their experience of studyingtrauma-related injuries in rural western Indiathrough departmental, institutional, and profes-sional seminars. The understanding of barriers totrauma registry implementation identified in thepilot phase was shared at CAM as well as at meet-ings of the Massachusetts Committee on Traumaand the Association of Academic Surgery confer-ence. Through this outreach, the UMMS teamhas identified the next surgical resident to assumeresponsibilities as the current postdoctoral traineetransitions back to clinical training.
Activity 4: Detecting Unrecognized AtrialFibrillation in Rural Western India UsingMobile-Based Technology: Community-Based ScreeningPhase 1: Initiate a partnership. The trainee-leaders approached the chief of ConnectedCardiovascular Healthcare section at UMMS[D.D.M.] to leverage his research team’s expertisein mobile technology to collaborate with CAM fora joint Indo-U.S. call for proposals. Together, thegroup decided to focus on mobile-based screeningof atrial fibrillation due to recent innovations atUMMS for this technology and its apparent needin India.
Atrial fibrillation is understudied amongIndians but may be an underlying contributorto the ongoing stroke epidemic in India.27,28
Untreated atrial fibrillation can increase the riskof stroke, and in the context of India, where rapidstroke management is suboptimal, prevention ofstroke through early diagnosis of atrial fibrillationbecomes crucial.29 The technology developed bythe UMMS atrial fibrillation research group in col-laboration with local biomedical engineers uses amobile phone to screen for atrial fibrillation.30
The trainee-leaders introduced the group to amember of the Office of Health and Technologyat UMMS [M.C.] who codirects the Global HealthPathway at UMMS and thus oversees the SATHIcomponent of the collaboration. The RAHI leader-ship team at CAM [S.M.N. and A.G.P.] recruited acardiologist from CAM [S.T.] to collaborate on thestudy and provide clinical insight for conducting afeasibility study.
Phase 2: Develop a shared work plan.Conventionally, a 12-lead electrocardiogram(EKG) is required to obtain an electric signal ofcardiac activity, which is interpreted by medicallytrained personnel to diagnose atrial fibrillation orother arrhythmias. However, a single screen foratrial fibrillation may miss cases of paroxysmal
atrial fibrillation. Therefore, the research teamdecided to conduct a feasibility study that usedalgorithm-driven pulse waveform and single-leadEKG technology to screen participants for atrial fi-brillation on 5 consecutive days. Partnership withCAM’s Community Extension Department [S.R.]helped identify villages for community-basedatrial fibrillation screening. CAM investigatorssuggested using community health workers toalign the screening approach with the Indian gov-ernment’s model and develop a proof of conceptthat may be scalable across India.
Phase 3: Implement the program. Twofirst-year UMMS medical students [A.E. andA.H.], representing the third generation of SATHItrainees, were identified to implement the study.The trainees received training at UMMS by thestudy principal investigator, the trainee-leaders,and the atrial fibrillation research staff in usingthe mobile technology. They traveled to CAMwith research equipment and materials with fi-nancial support from the UMMS Office of Healthand Technology. They then trained research coor-dinators in the screening procedures. Ultimately,through a train-the-trainer model and medicalstudents, local community health workers wereable to recruit and screen more than 350 partici-pants in their homes for 5 consecutive days.Although research design was formulated by thefaculty principal investigator and the trainee-leaders, this pilot study represented the firstaccount of a new generation of UMMS predoc-toral trainees [A.E. and A.H.] leading the imple-mentation of a study. It is noteworthy thatneither of the trainees spoke the local Indian lan-guage. Partnering of UMMS and CAM trainees[D.P. and H.P.] helped overcome the linguisticand cultural implementation barriers.
Phase 4, 5, and 6:Monitor outcomes, eval-uate results, and disseminate information.Data from this feasibility study was evaluatedby a team of trainees with statistical [A.S.] andcardiovascular [N.F. and J.B.] training back-grounds. Early findings revealed a prevalence ofatrial fibrillation substantially greater than previ-ously reported in India and comparable with thatfound in the United States and other high-incomecountries. Although large-scale and more repre-sentative screening efforts are currently under-way, noteworthy findings from the feasibilitystudy were presented by a trainee-leader [A.S.] atthe National Institutes of Health Special TopicsConference on Healthcare Innovations and Point-of-Care Technologies and were published ina leading mobile health journal.31 A grant
Student-Led Twinning Model in Global Health www.ghspjournal.org
Global Health: Science and Practice 2017 | Volume 5 | Number 1 159
proposal, coauthored by the trainee-leaders, to le-verage public health infrastructure to establish asystematic screening program for atrial fibrillationwas selected among the finalists for joint consider-ation by the National Institutes of Health andIndian Department of Biotechnology, but ulti-mately was not funded. The group is preparinga similar application in response to a call for pro-posals from the Fogarty International Center.Meanwhile, the UMMS Office of Global Healthhas awarded RAHI–SATHI its third Pilot ProjectGrant, which supports continued screening foratrial fibrillation using mobile technology basedon the promising results from the feasibility study.
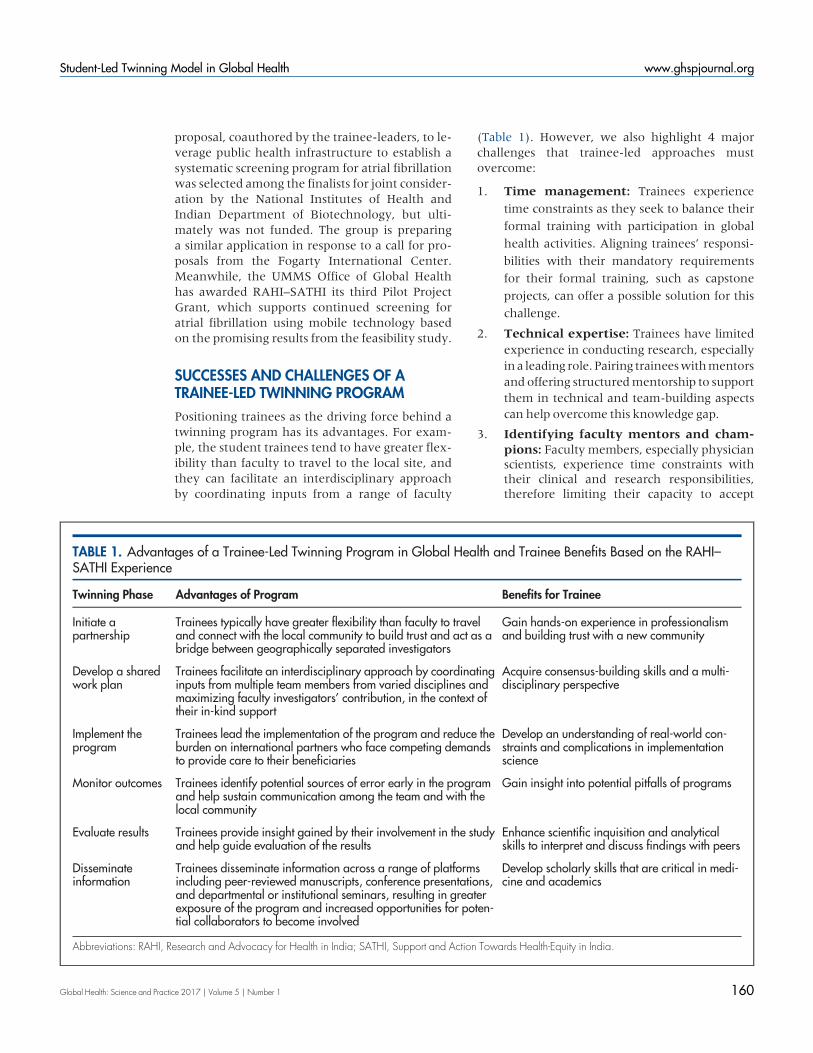
SUCCESSES AND CHALLENGES OF ATRAINEE-LED TWINNING PROGRAMPositioning trainees as the driving force behind atwinning program has its advantages. For exam-ple, the student trainees tend to have greater flex-ibility than faculty to travel to the local site, andthey can facilitate an interdisciplinary approachby coordinating inputs from a range of faculty
(Table 1). However, we also highlight 4 majorchallenges that trainee-led approaches mustovercome:
1. Time management: Trainees experience
time constraints as they seek to balance their
formal training with participation in global
health activities. Aligning trainees’ responsi-
bilities with their mandatory requirements
for their formal training, such as capstone
projects, can offer a possible solution for this
challenge.
2. Technical expertise: Trainees have limitedexperience in conducting research, especiallyina leading role. Pairing traineeswithmentorsand offering structuredmentorship to supportthem in technical and team-building aspectscan help overcome this knowledge gap.
3. Identifying faculty mentors and cham-pions: Faculty members, especially physicianscientists, experience time constraints withtheir clinical and research responsibilities,therefore limiting their capacity to accept
TABLE 1. Advantages of a Trainee-Led Twinning Program in Global Health and Trainee Benefits Based on the RAHI–SATHI Experience
Twinning Phase Advantages of Program Benefits for Trainee
Initiate apartnership
Trainees typically have greater flexibility than faculty to traveland connect with the local community to build trust and act as abridge between geographically separated investigators
Gain hands-on experience in professionalismand building trust with a new community
Develop a sharedwork plan
Trainees facilitate an interdisciplinary approach by coordinatinginputs from multiple team members from varied disciplines andmaximizing faculty investigators’ contribution, in the context oftheir in-kind support
Acquire consensus-building skills and a multi-disciplinary perspective
Implement theprogram
Trainees lead the implementation of the program and reduce theburden on international partners who face competing demandsto provide care to their beneficiaries
Develop an understanding of real-world con-straints and complications in implementationscience
Monitor outcomes Trainees identify potential sources of error early in the programand help sustain communication among the team and with thelocal community
Gain insight into potential pitfalls of programs
Evaluate results Trainees provide insight gained by their involvement in the studyand help guide evaluation of the results
Enhance scientific inquisition and analyticalskills to interpret and discuss findings with peers
Disseminateinformation
Trainees disseminate information across a range of platformsincluding peer-reviewed manuscripts, conference presentations,and departmental or institutional seminars, resulting in greaterexposure of the program and increased opportunities for poten-tial collaborators to become involved
Develop scholarly skills that are critical in medi-cine and academics
Abbreviations: RAHI, Research and Advocacy for Health in India; SATHI, Support and Action Towards Health-Equity in India.
Student-Led Twinning Model in Global Health www.ghspjournal.org
Global Health: Science and Practice 2017 | Volume 5 | Number 1 160

mentees. Identifying grant and manuscriptopportunities can propel faculty to beinvolved.
4. Continuity: Trainees’ involvement in theproject is confined to their time in the aca-demic program. Presence of a faculty cham-pion and explicit transition plans includingsupporting recruitmentof subsequent genera-tion of trainees can helpmaintain continuity.
In addition to these 4 challenges, which areuniversal in nature, Indian trainees experiencedunique challenges that limited their involvement.Medical education in India is intensely regulatedby a national body, the Medical Council of India.Trainees’ academic performance is heavily de-pendent on attendance and curricular-relatedactivities, thereby limiting their elective time andparticipation in extracurricular scholarship.Despite our efforts to promote bilateral involve-ment, these constraints have limited more activeparticipation of Indian trainees. However, inrecent years there has been increased participa-tion due to the combination of continued supportfrom CAM’s leadership and word-of-mouth pro-motion by CAM trainees who have participatedin the RAHI–SATHI collaboration and accom-plished peer-reviewed achievements in the formof publishedmanuscripts and scientific conferencepresentations.
Unsuccessful ProposalsOur collaboration prepared and submitted 4 un-successful proposals for extramural funding.
1. The “Biological Determinants of Type 2 Dia-betes Risk in IndianPopulations”proposalwasdevelopedinresponse toa joint Indo-U.S. call from the National Institutesof Health and the Indian Council ofMedical Research. The proposalaimed to investigate differences inadipose tissue biology among non-Hispanic whites and South AsianIndians as a potential mechanism forhigh risk of diabetes among Indianswithlowbodymassindex(BMI).
2. The “Support and Action TowardsHealth-equity in India” proposalwas developed in response to theObama-Singh Initiative funding op-portunity for higher-education pro-grams. The capacity strengtheningproposal preceded SATHI formation
and included exchange and development pro-gram for trainees.
3. The “Strengthening Kangaroo Mother CareImplementation in Gujarat” proposal wasdeveloped in response to a solicited oppor-tunity from the Bill & Melinda GatesFoundation. The proposal aimed to enhancehospital and community-based KangarooMother Care.
4. The “SmartphoneMonitoring for Atrial fibril-lation inReal-Time–India (SMART–India)”proposal was developed in response to ajoint Indo-U.S. funding opportunity fromthe Indian Department of Biotechnology andthe National Institutes of Health. This pro-posal sought to expand community-basedscreening of atrial fibrillation using mobiletechnology.
Despite these disappointing outcomes, thegrant writing and submission process mobilizedtrainees and faculty members and ultimately pro-vided an opportunity to overcome lack of fundingby seeking alternate resources. The formation ofSATHI despite the unsuccessful application pro-vides a salient example of this approach. In addi-tion to SATHI activities described above, a virtualdevelopment program in global health for traineesand faculty in neurology is underway through abilateral partnership between junior faculty fromUMMS and CAM [A.D. and S.D.]. Such contin-gency plans can help gather preliminary data andfeasibility results, which is becoming increasinglyimportant for extramural funding. Additionally,experience fromotherprogramshas suggested thatcontinuous interaction and activities, independent
BOX. Recommendations for Institutional Leadership and Faculty toPromote Establishment of Trainee-Led Twinning Programs for GlobalHealth
� Accept an expanded role for trainees in global health programs� Create structured opportunities for trainees to engage in research and global
health activities� Develop a network of faculty and trainees interested in global health� Share extramural global health funding opportunities with faculty and trainees� Offer application-based opportunities to seed funding for global health activ-
ities and promote perseverance among partnerships that lack extramuralsupport
Presence of afaculty championand explicittransition planscan helpmaintaincontinuity oftrainee-ledtwinningmodels.
Student-Led Twinning Model in Global Health www.ghspjournal.org
Global Health: Science and Practice 2017 | Volume 5 | Number 1 161

ofextramuralsupport,buildsandfortifiestrustinanacademicpartnership.32
Strategic Institutional SupportUMMS and CAM play a vital role in the growthand success of RAHI–SATHI by providing strategicsupport and fostering a collaborative environmentthat promotes faculty teamwork and encouragesthem to work with trainees. The Box outlinesrecommendations for the parent institutions andfaculty mentors based on our experience withRAHI–SATHI.
Institutional leadership at both sites formal-ized the collaboration in its early stages through amemorandum of understanding, making it possi-ble for the collaboration to harness existing insti-tutional resources. Centers for Health-EquityIntervention Research (CHEIR) and Clinical andTranslational Science (CCTS) have structuredopportunities, which supported the trainees andfaculty working with RAHI–SATHI. Additionally,the Office of Global Health at UMMS providedcrucial seed funding to support the research stud-ies. The International Medical Education Programpartially supported trainees’ travel to CAM.Similarly, CAM’s leadership support of RAHI–SATHI positioned their faculty and trainees toassume an active and leading role in the collabora-tion. The establishment of Central ResearchServices in 2009 as part of the focus of the institu-tion on development of research skills and projectsamong the faculty was germane to the supportreceived by the research activities of RAHI–SATHI. CAM began funding internal researchprojects, capacity building in research and scien-tific writing, and also international travel to dis-seminate the work being done. The annualpublication output by CAM in the last 3 years hasmore than quadrupled that in the past decade. Thehead of Central Research Services [S.M.N.] andhis research team, including trainees, receivedcomplete financial support from CAM to travelto the United States for dissemination of theirwork at professional conferences such as thePediatric Academic Societies and Consortium ofUniversities for Global Health. This travel fortifiedthe interpersonal relationships between UMMSand CAM investigators and helped engage morefaculty and trainees.
CONCLUSIONThis paradigm of trainee-led twinning partnershippresents unique challenges and successes in addi-tion to the ones experienced by traditional,
faculty-led collaborative models. Trainees canhelp mitigate geographical barriers by acting as abridge between members from different institu-tions, garner cultural insight through their abilityto immerse themselves in a community, and over-come expertise limitations through pre-plannedstructured mentorship from faculty of both insti-tutions. In the process, trainees can play a centralrole in cultivating trust among the team membersand acquire personal leadership skills that maybenefit them in their future careers. Our experi-ence shows strategic institutional support totrainee-led initiatives in global health promotessustainability in an uncertain funding climate andprovides a roadmap for conducting foundationalwork that is essential for the development of abroad, university-wide global health program.
Acknowledgments: The research studies described in this manuscriptwere supported by institutional funding. Contribution by coauthors waspartially supported by TL1-TR001454 (to A.S.), KL2TR000160 (to N.B.),8KL2TR000160-03 (to H.P.S.), and UL1-TR001453-01 from theNational Center for Advancing Translational Sciences, 1R15HL121761-01A1, and 1UH2TR000921-02 (to D.D.M.) from the National Heart,Lung, and Blood Institute, P60-MD006912-05 (to J.A. andM.R.) from theNational Institute on Minority Health and Disparities, and Joy McCannEndowment (to T.M.S.). The content is solely the responsibility of theauthors and does not necessarily represent the official views of theNational Institutes of Health.
Competing Interests:None declared.
REFERENCES1. Koplan JP, Bond TC,MersonMH, et al; Consortium of Universities for
Global Health Executive Board. Towards a common definition ofglobal health. Lancet. 2009;373(9679):1993–1995. CrossRef.Medline
2. Matheson AI, Walson JL, Pfeiffer J, Holmes K. Sustainability andgrowth of university global health programs. Washington, DC:Center for Strategic and International Studies; 2014. http://csis.org/publication/sustainability-and-growth-university-global-health-programs. Accessed February 24, 2017.
3. Merson MH, Page KC. The dramatic expansion of universityengagement in global health: implications for U.S. policy.Washington, DC: Center for Strategic and International Studies;2009. http://csis.org/publication/dramatic-expansion-university-engagement-global-health. Accessed February 24, 2017.
4. University of Massachusetts Medical School, Boston Children’sHospital, MIT Humanitarian Response Lab, Avenir Analytics, IcahnSchool of Medicine at Mount Sinai. accel: Academic ConsortiumCombating Ebola in Liberia. https://accel.mit.edu/. AccessedFebruary 24, 2017.
5. Manabe YC, Jacob ST, Thomas D, et al. Resurrecting the triple threat:academic social responsibility in the context of global healthresearch. Clin Infect Dis. 2009;48(10):1420–1422. CrossRef.Medline
6. Smith JK, Weaver DB. Capturing medical students’ idealism. AnnFamMed. 2006;4 (suppl 1):S32–S37, discussion S58-S60.CrossRef. Medline
7. Whitcomb ME. Promoting global health: what role should academichealth centers play? Acad Med. 2007;82(3):217–218. CrossRef.Medline
Student-Led Twinning Model in Global Health www.ghspjournal.org
Global Health: Science and Practice 2017 | Volume 5 | Number 1 162
8. Spicer N, Aleshkina J, Biesma R, et al. National and subnationalHIV/AIDS coordination: are global health initiatives closing the gapbetween intent and practice?Global Health. 2010;6:3. CrossRef.Medline
9. Busse H, Azazh A, Teklu S, et al. Creating change through collabo-ration: a twinning partnership to strengthen emergency medicine atAddis Ababa University/Tikur Anbessa Specialized Hospital–amodel for international medical education partnerships.Acad EmergMed. 2013;20(12):1310–1318. CrossRef. Medline
10. Einterz RM, Kimaiyo S, Mengech HNK, et al. Responding to the HIVpandemic: the power of an academic medical partnership. AcadMed. 2007;82(8):812–818. CrossRef. Medline
11. Hopkins J, Burns E, Eden T. International twinning partnerships: aneffective method of improving diagnosis, treatment and care for chil-dren with cancer in low-middle income countries. J Cancer Policy.2013;1(1-2):e8–e19. CrossRef
12. Monroe-Wise A, Kibore M, Kiarie J, et al. The Clinical EducationPartnership Initiative: an innovative approach to global health edu-cation. BMCMed Educ. 2014;14(1):1043. CrossRef. Medline
13. Macfarlane SB, Agabian N, Novotny TE, Rutherford GW, StewartCC, Debas HT. Think globally, act locally, and collaborate interna-tionally: global health sciences at the University of California, SanFrancisco. Acad Med. 2008;83(2):173–179. CrossRef. Medline
14. Vermund SH, Sahasrabuddhe VV, Khedkar S, Jia Y, Etherington C,Vergara A. Building global health through a center-without-walls:the Vanderbilt Institute for Global Health. Acad Med. 2008;83(2):154–164. CrossRef. Medline
15. Soni A, Fahey N, Phatak AG, et al. Differential in healthcare seekingbehavior of mothers for themselves versus their children in ruralIndia: results of a cross sectional survey. Int Public Heal J. 2014;6(1):57–66. https://www.novapublishers.com/catalog/product_info.php?products_id=50101. Accessed February 24, 2017.
16. Fahey N, Soni A, Allison J, et al. Education mitigates the relationshipof stress and mental disorders among rural Indian women.Ann GlobHeal. 2016;82(5):779–787. CrossRef
17. Paul VK, Sachdev HS, Mavalankar D, et al. Reproductive health, andchild health and nutrition in India: meeting the challenge. Lancet.2011;377(9762):332–349. CrossRef. Medline
18. Liu L, Johnson HL, Cousens S, et al; Child Health EpidemiologyReference Group of WHO and UNICEF. Global, regional, andnational causes of child mortality: an updated systematic analysis for2010 with time trends since 2000. Lancet. 2012;379(9832):2151–2161. CrossRef. Medline
19. Siddalingappa H, Murthy MRN, Kulkarni P, NCA. Prevalence andfactors influencing perinatal mortality in rural mysore, India. J ClinDiagn Res. 2013;7(12):2796–2799. CrossRef. Medline
20. Soni A, Fahey N, Raithatha N, et al. Understanding predictors ofmaternal and child health in rural western India: an internationalprospective study. Presented at: 142nd Annual Meeting of theAmerican Public Health Association; November 15–19, 2014; NewOrleans, LA. https://apha.confex.com/apha/142am/ih/papers/index.cgi?username=312292&password=990045. AccessedFebruary 24, 2017.
21. Fahey N, Soni A, McQuilkin P, Allison J, Nimbalkar SM. Trends inmaternal hemoglobin levels over the course of pregnancy amongwomen from rural western India. Presented at: Pediatrics AcademicSocieties Meeting; April 30–May 3, 2016; Baltimore, MD.
22. Newman H, Fahey N, Soni A, et al. Vitamin D deficiency over thecourse of pregnancy among rural IndianWomen. Presented at:Pediatrics Academic Societies Meeting; April 30–May 3, 2016;Baltimore, MD.
23. Oestern HJ, Garg B, Kotwal P. Trauma care in India and Germany.Clin Orthop Relat Res. 2013;471(9):2869–2877. CrossRef. Medline
24. Fitzharris M, Dandona R, Kumar GA, Dandona L. Crash character-istics and patterns of injury among hospitalized motorised two-wheeled vehicle users in urban India. BMC Public Health. 2009;9(1):11. CrossRef. Medline
25. OReilly GM, Joshipura M, Cameron PA, Gruen R. Trauma registriesin developing countries: a review of the published experience. Injury.2013;44(6):713–721. CrossRef. Medline
26. Moore L, Clark DE. The value of trauma registries. Injury. 2008;39(6):686–695. CrossRef. Medline
27. Sethi NK, Singh MB. Neurologic disability: a hidden epidemic forIndia.Neurology. 2013;81(1):97. CrossRef. Medline
28. Lip GYH, Brechin CM, Lane DA. The global burden of atrial fibrilla-tion and stroke: a systematic review of the epidemiology of atrial fi-brillation in regions outside North America and Europe. Chest.2012;142(6):1489–1498. CrossRef. Medline
29. Pandian JD, Singh G, Kaur P, et al. Incidence, short-term outcome,and spatial distribution of stroke patients in Ludhiana, India.Neurology. 2016;86(5):425–433. CrossRef. Medline
30. McManus DD, Chong JW, Soni A, et al. PULSE-SMART: Pulse-BasedArrhythmia Discrimination Using a Novel Smartphone Application. JCardiovasc Electrophysiol. 2016;27(1):51–57. CrossRef. Medline
31. Soni A, Earon A, Handorf A, et al. High burden of unrecognizedatrial fibrillation in rural India: an innovative community-basedcross-sectional screening program. JMIR Public Health Surveill.2016;2(2):e159. CrossRef. Medline
32. Kolars JC. Should U.S. academic health centers play a leadershiprole in global health initiatives? Observations from three years inChina. Acad Med. 2000;75(4):337–345. CrossRef. Medline
Peer Reviewed
Received: 2016 Jun 14; Accepted: 2017 Jan 25
Cite this article as: Soni A, Fahey N, Jaffe A, et al. RAHI–SATHI Indo-U.S. collaboration: the evolution of a trainee-led twinning model in global healthinto a multidisciplinary collaborative program. Glob Health Sci Pract. 2017;5(1):152-163. https://doi.org/10.9745/GHSP-D-16-00190
© Soni et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use,distribution, and reproduction in any medium, provided the original author and source are properly cited. To view a copy of the license, visit http://creativecommons.org/licenses/by/3.0/. When linking to this article, please use the following permanent link: https://doi.org/10.9745/GHSP-D-16-00190
Student-Led Twinning Model in Global Health www.ghspjournal.org
Global Health: Science and Practice 2017 | Volume 5 | Number 1 163
Related Documents











