PCI for STEMI: Fix the Culprit Lesion, or Fix All of James James Hermiller Hermiller, MD, FACC, FSCAI , MD, FACC, FSCAI St Vincent Medical Group St Vincent Medical Group St Vincent Heart Center of Indiana St Vincent Heart Center of Indiana Indianapolis, IN Indianapolis, IN Culprit Lesion, or Fix All of the Lesions

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
PCI for STEMI: Fix theCulprit Lesion, or Fix All of
JamesJames HermillerHermiller, MD, FACC, FSCAI, MD, FACC, FSCAISt Vincent Medical GroupSt Vincent Medical Group
St Vincent Heart Center of IndianaSt Vincent Heart Center of IndianaIndianapolis, INIndianapolis, IN
Culprit Lesion, or Fix All ofthe Lesions
Disclosure Statement of Financial Interest
• Grant/Research Support
• Consulting Fees/Honoraria
• Edwards, Medtronic, Abbott, StJude, BSC
• Edwards, Medtronic, Abbott, StJude, BSC
Within the past 12 months, I or my spouse/partner have had a financialWithin the past 12 months, I or my spouse/partner have had a financialinterest/arrangement or affiliation with the organization(s) listed below.interest/arrangement or affiliation with the organization(s) listed below.
Affiliation/Financial Relationship Company
• Consulting Fees/Honoraria • Edwards, Medtronic, Abbott, StJude, BSC
Outline
• Introduction
• The DATA
• Randomized Trials• Randomized Trials
• Guidelines
• Future Studies
• Summary
Introduction
• 64 year old man presentswith an acute inferior MI
• Prior history of HTN,• Prior history of HTN,hyperlipidemia andsmoking
• Hemodynamically stable
Introduction
Decisions
IntroductionTreat the IRA/RCA and then:
1. PCI LAD during admission only ifrecurrent symptoms or high risk stresstest?
2. PCI LAD during admission or planned2. PCI LAD during admission or plannedstaged intervention?
3. Fix both RCA and LAD at same sitting?
4. FFR LAD at time of primary RCA PCIand treat LAD during hospitalization ifFFR abnormal?
The DataThe Data
PRAMI Trial
NEJM 2013;369:1115
465 STEMI patients
Randomized following infarct-related artery (IRA)-PCI:
Complete revascularization (n=234) – preventative PCI
Culprit-only PCI (n=231) – no preventative PCI
Complete revascularization performed during indexPCI
PRAMI Trial
PCI
1o endpoint: Cardiac death, non-fatal MI or refractoryangina
2o endpoints: repeat PCI, non-cardiac death andindividual components of 1o endpoint
Trial stopped early, mean follow-up 23 months (465 ofthe anticipated 600 patient enrollment)
NEJM 2013;369:1115
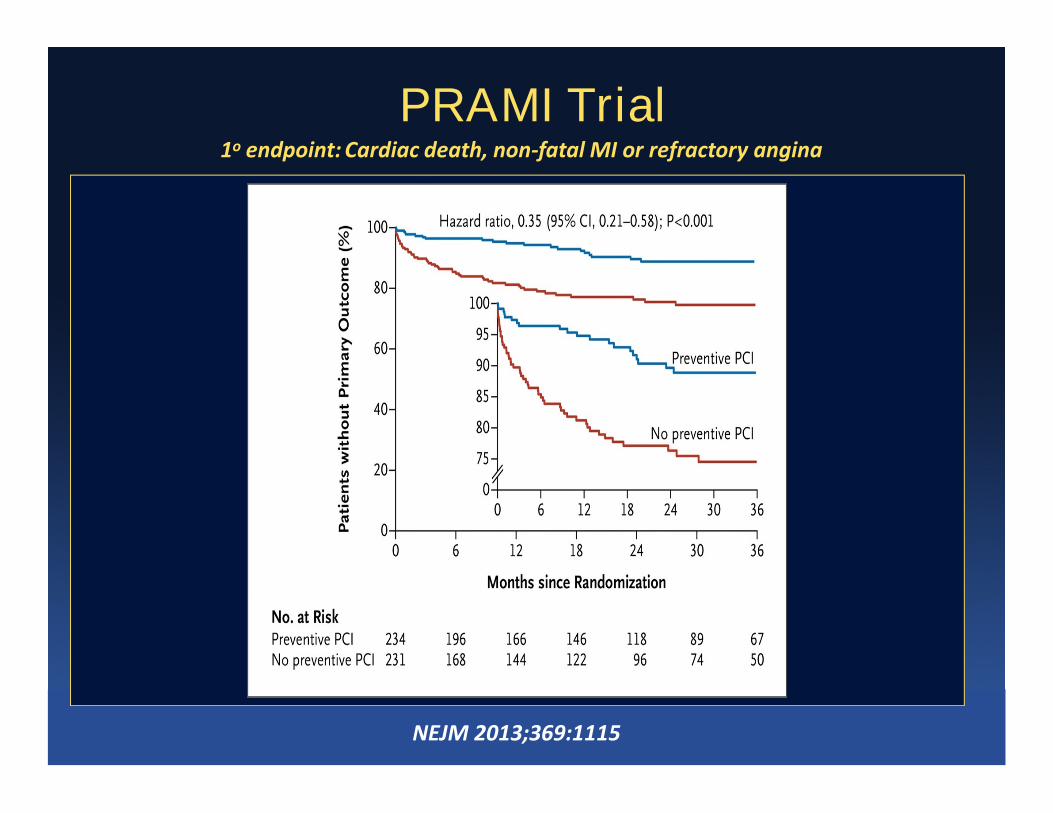
1o endpoint: Cardiac death, non-fatal MI or refractory angina
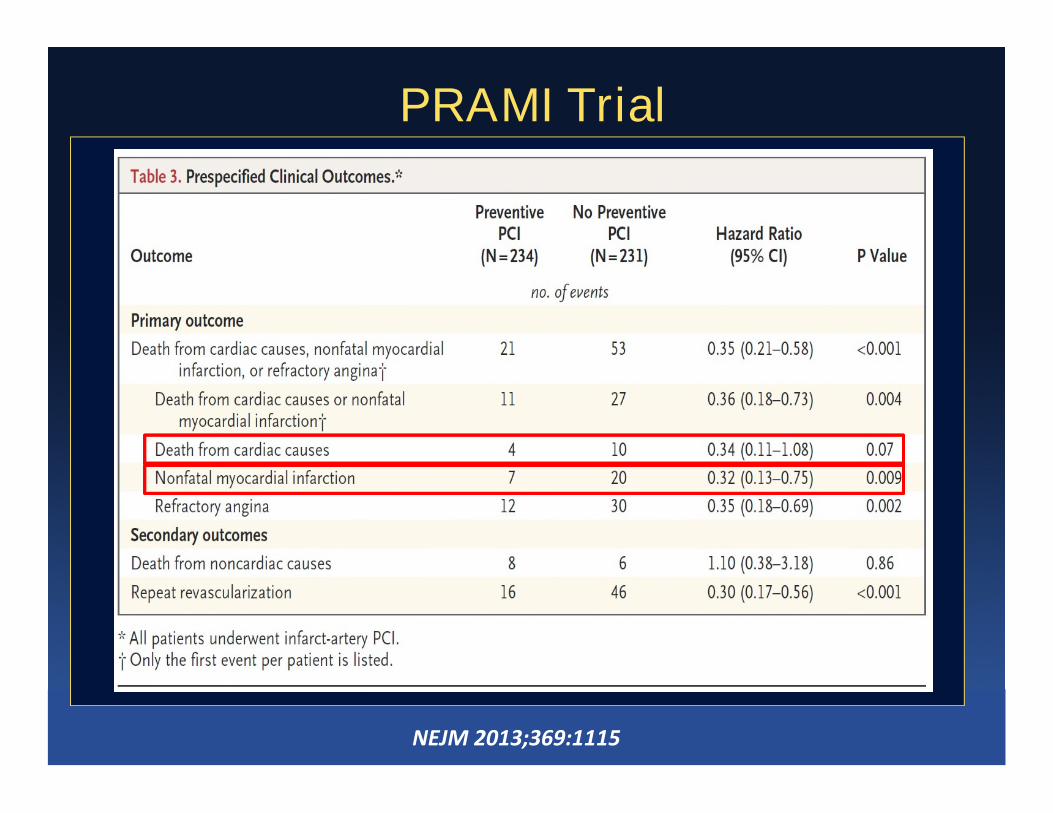
PRAMI Trial
NEJM 2013;369:1115
PRAMI Trial
NEJM 2013;369:1115
PRAMI – Questions?• Five high volume centers in UK (each has > 300
PCIs per year) to enroll 465 patients (2428patients screened) between 2008 and 2003
• Highly selected/selection bias?
• How representative are these patients of those• How representative are these patients of thosewe treat? Generalizibility?
• If there had between 10 rather than 7 events inthe treatment arm, the MI difference would havebeen insignificant
• All 50% lesions or more were stented – whenelse is that done today?
CVLRPIT Trial
JACC 2015;65:963
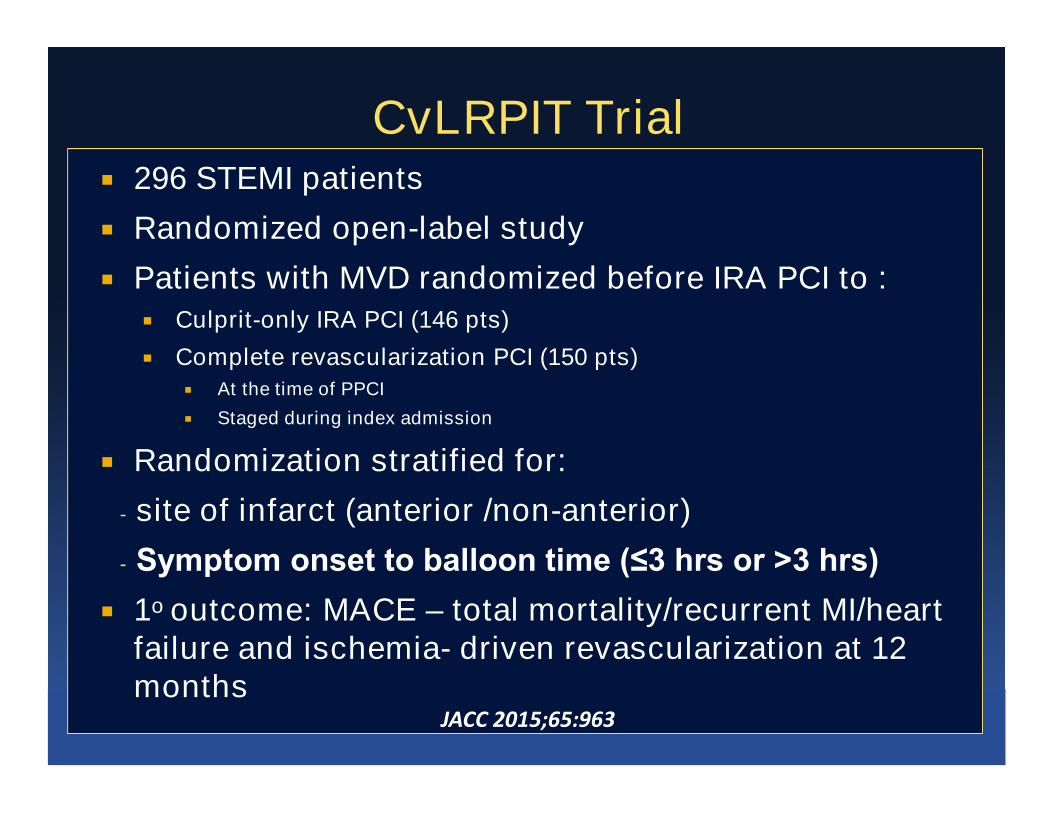
CvLRPIT Trial 296 STEMI patients
Randomized open-label study
Patients with MVD randomized before IRA PCI to : Culprit-only IRA PCI (146 pts)
Complete revascularization PCI (150 pts)
At the time of PPCI
Staged during index admission
Randomization stratified for:
- site of infarct (anterior /non-anterior)
- Symptom onset to balloon time (≤3 hrs or >3 hrs)
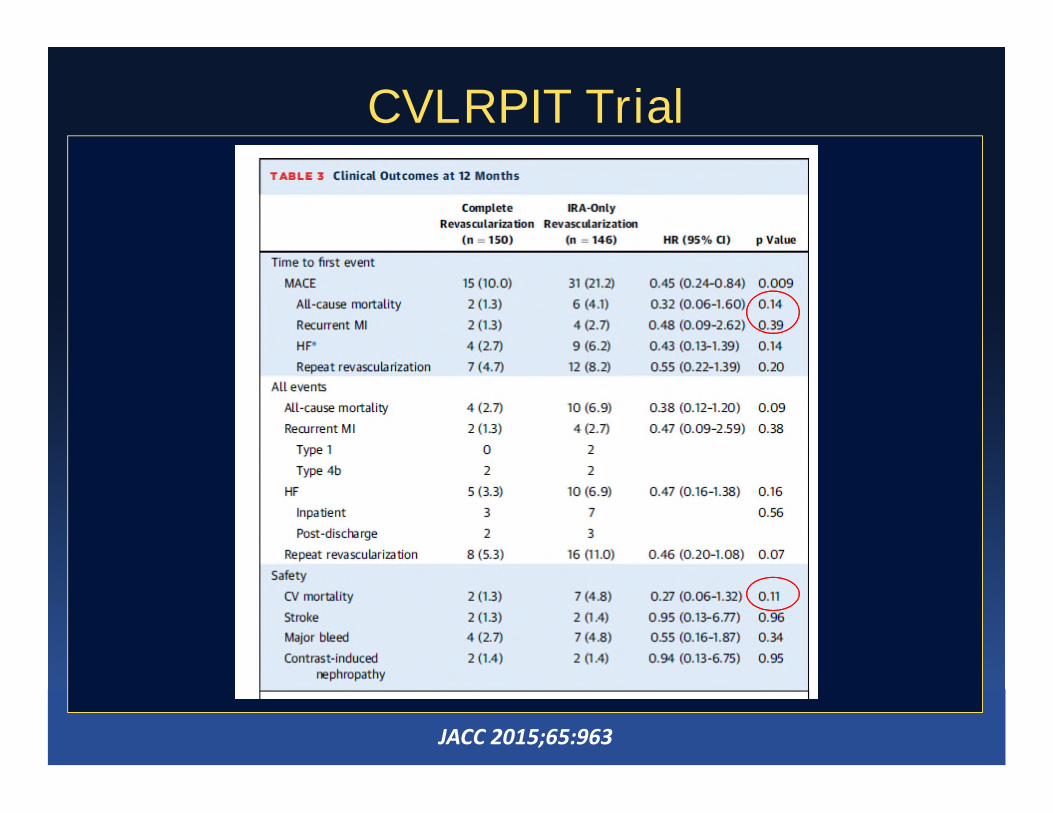
1o outcome: MACE – total mortality/recurrent MI/heartfailure and ischemia- driven revascularization at 12months
JACC 2015;65:963
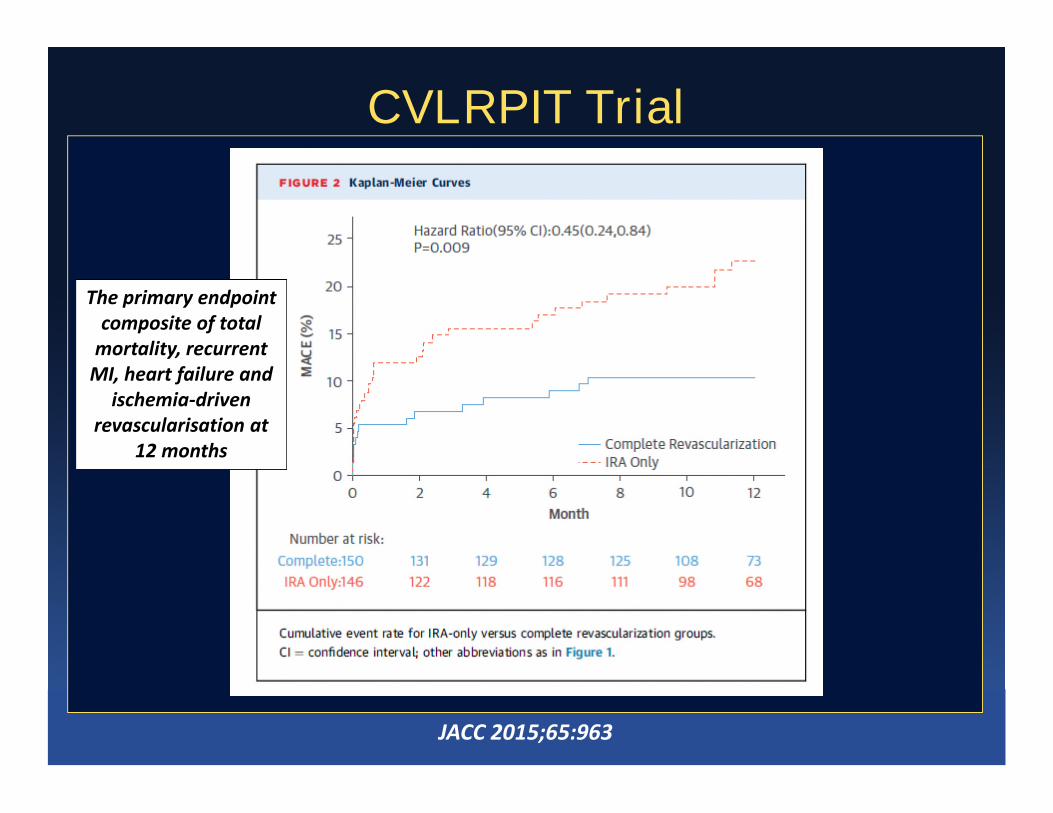
The primary endpointcomposite of total
mortality, recurrentMI, heart failure and
ischemia-driven
CVLRPIT Trial
ischemia-drivenrevascularisation at
12 months
JACC 2015;65:963
CVLRPIT Trial
JACC 2015;65:963
CvLPRIT – Questions?• Small study – sceened 850 patients over 48
months to enroll 296
• Mixed primary endpoint
• Cross-over
Patients with mutli-vessel disease and STEMI at• Patients with mutli-vessel disease and STEMI attime of cath were randomized during IRA PCI
• Of the 146 in the IRA only arm, 7 had completerevascularization
• Of the 150 in the complete revasc arm, 139 hadcomplete revasc, 7 had target IRA PCI only and 3had CABG
DANAMI-3 PRIMULTI Trial
Lancet 2015;386:665
627 STEMI patients
Randomized following infarct-related artery (IRA)-PCI:
Complete FFR-guided revascularization (n=314)
IRA -only PCI (n=313)
Complete revascularization performed as a stagedprocedure in hospital
DANAMI-3 PRIMULTI Trial
procedure in hospital
1o endpoint: All-cause mortality, nonfatal MI, ischemiadriven revascularization of non IRA lesions
2o endpoints: cardiac death, cardiac death/nonfatalMI, urgent PCI, non-urgent PCI and individualcomponents of 1o endpoint
Lancet 2015;386:665
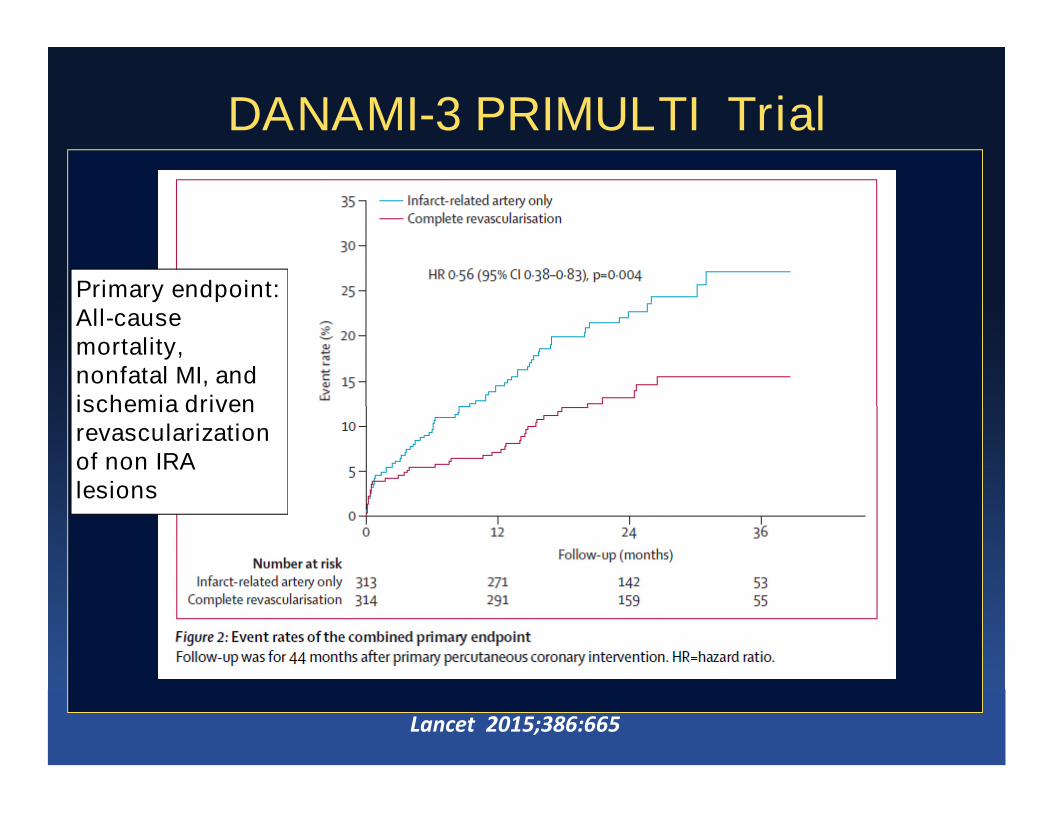
DANAMI-3 PRIMULTI Trial
Primary endpoint:All-causemortality,nonfatal MI, andischemia driven
Lancet 2015;386:665
ischemia drivenrevascularizationof non IRAlesions

Individual components of primary endpoint
Composite Revascularisation
DANAMI-3 PRIMULTI Trial
Non fatal MI All cause death
Lancet 2015;386:665
Multivessel coronary disease diagnosed at the timeof primary PCI for STEMI: complete
revascularization versus conservative strategy.PRAGUE 13 trial
O. HlinomazO. HlinomazICRC, St. Anne University Hospital, Brno, Czech Republic
On behalf of the PRAGUE-13 Investigators
L. Groch, K. Polokova, F. Lehar, T. Vekov, R. Petkov, M. Stoynev, M. Griva, J. Sitar, M. Rezek,M. Novak, J. Semenka, N. Penkov, B. Gersh, D. Holmes, G. Sandhu, P. Widimsky
Grant IGA Czech Republic NT11412-5/2010, VAVPI EU ProjectNCT01332591
EuroPCR 2015
214 STEMI patients
Randomized following infarct-related artery (IRA)-PCI:
Complete revascularization (n=106)
IRA -only PCI (n=108)
Complete revascularization performed as a staged
PRAGUE-13 Trial
Complete revascularization performed as a stagedprocedure
Enrollment ≥48 hrs following onset of symptoms
1o endpoint: All-cause mortality, nonfatal MI, stroke
2o endpoints: cardiac death, all-cause death/nonfatalMI, hospitalization for angina, hospitalization for heartfailure
EuroPCR 2015
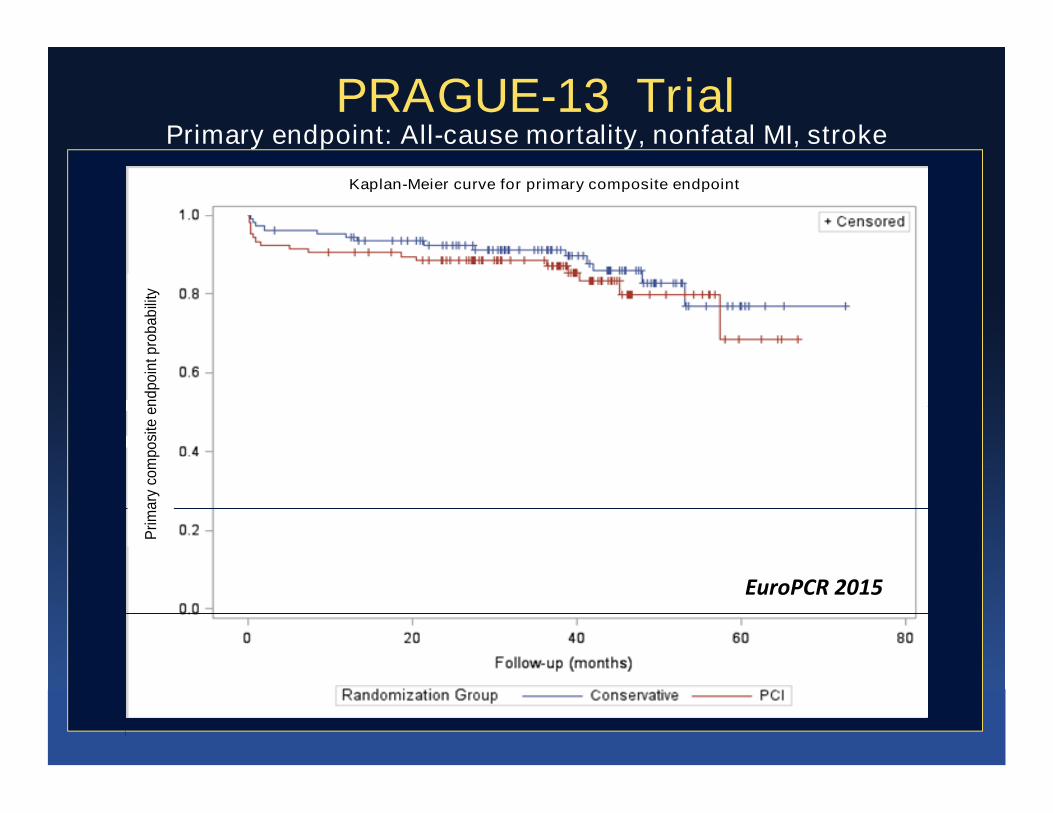
PRAGUE-13 TrialPrimary endpoint: All-cause mortality, nonfatal MI, stroke
Kaplan-Meier curve for primary composite endpoint
Pri
ma
ryco
mpo
site
en
dpo
intp
rob
ab
ility
p=0.407
Pri
ma
ryco
mpo
site
en
dpo
intp
rob
ab
ility
p=0.407
EuroPCR 2015
Conclusions: Complete revascularization of all significantcoronary lesions at the time of primary PCI was associatedwith a reduction in the risk of MACE due to reduction in therisk of urgent re- vascularization. This approach appears to besafe, with no excess major bleeding, or contrast-inducednephropathy.
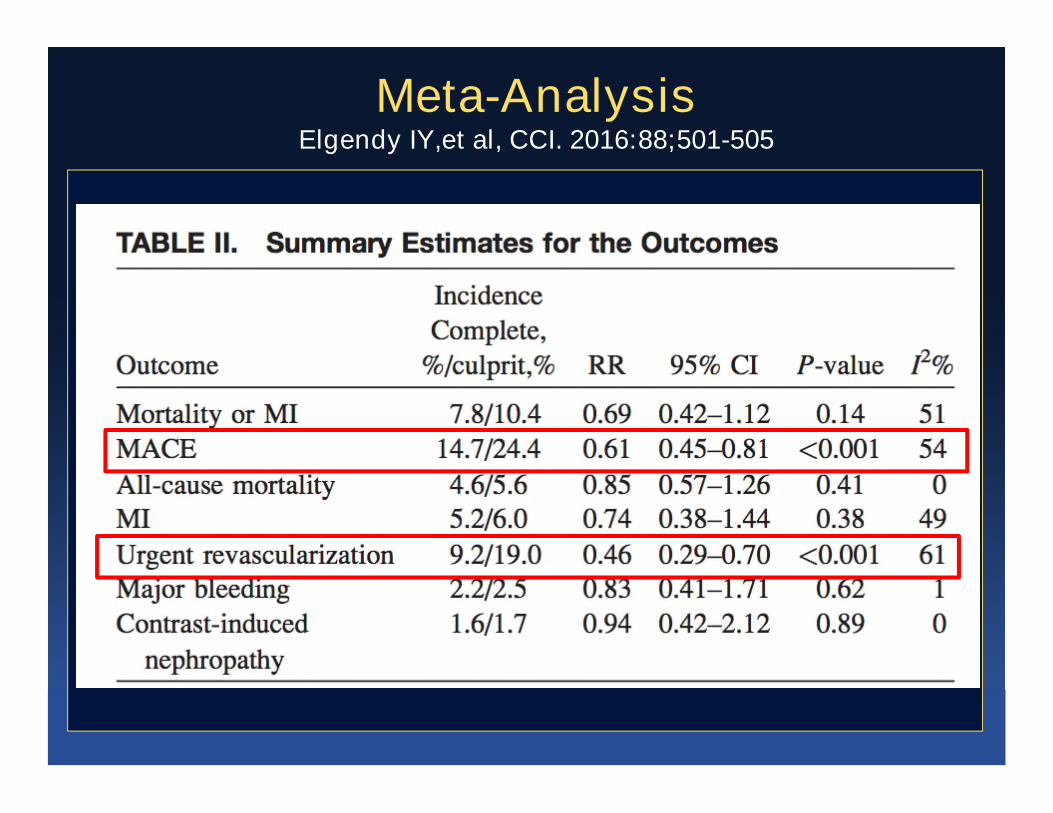
Meta-AnalysisElgendy IY,et al, CCI. 2016:88;501-505
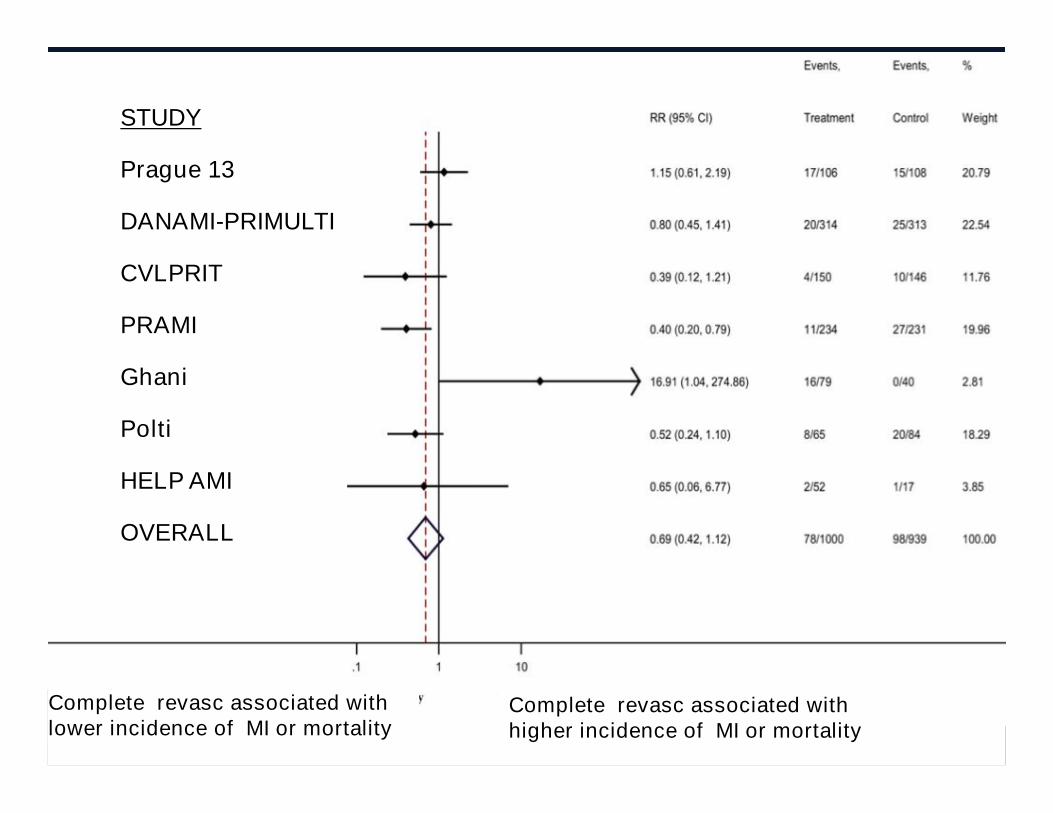
STUDY
Prague 13
DANAMI-PRIMULTI
CVLPRIT
PRAMI
Ghani
Polti
HELP AMI
OVERALL
Complete revasc associated withlower incidence of MI or mortality
Complete revasc associated withhigher incidence of MI or mortality
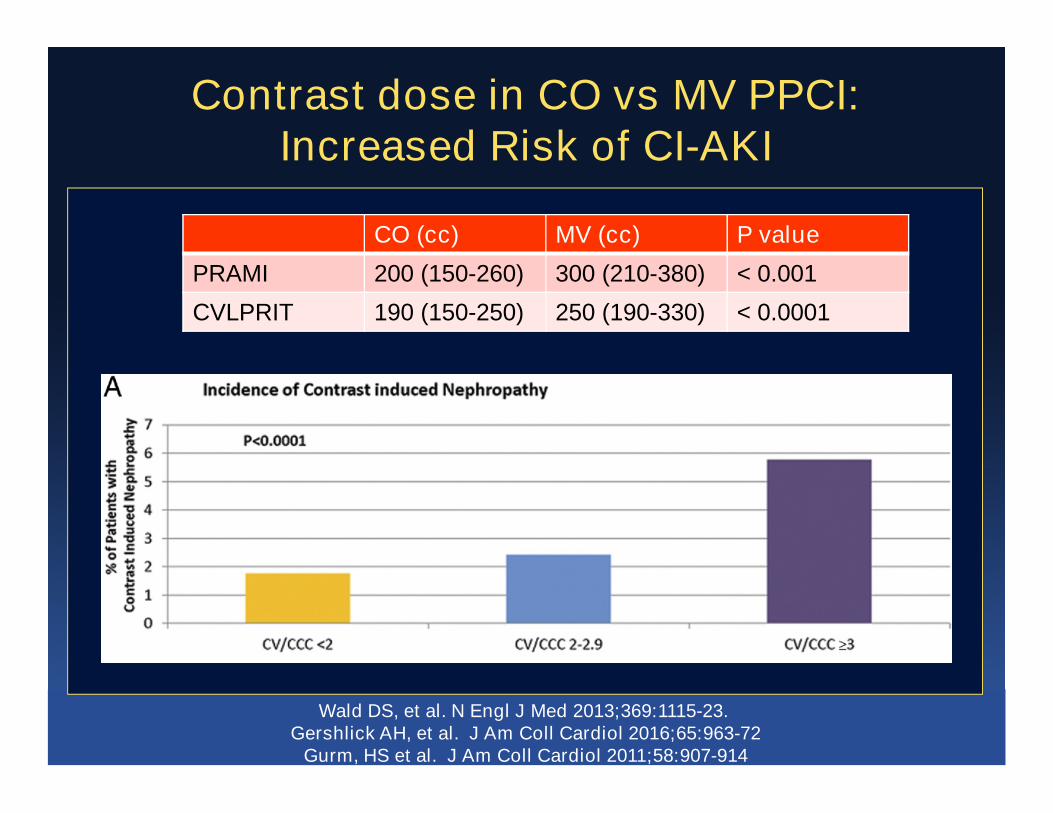
Contrast dose in CO vs MV PPCI:Increased Risk of CI-AKI
CO (cc) MV (cc) P value
PRAMI 200 (150-260) 300 (210-380) < 0.001
CVLPRIT 190 (150-250) 250 (190-330) < 0.0001
Wald DS, et al. N Engl J Med 2013;369:1115-23.Gershlick AH, et al. J Am Coll Cardiol 2016;65:963-72
Gurm, HS et al. J Am Coll Cardiol 2011;58:907-914
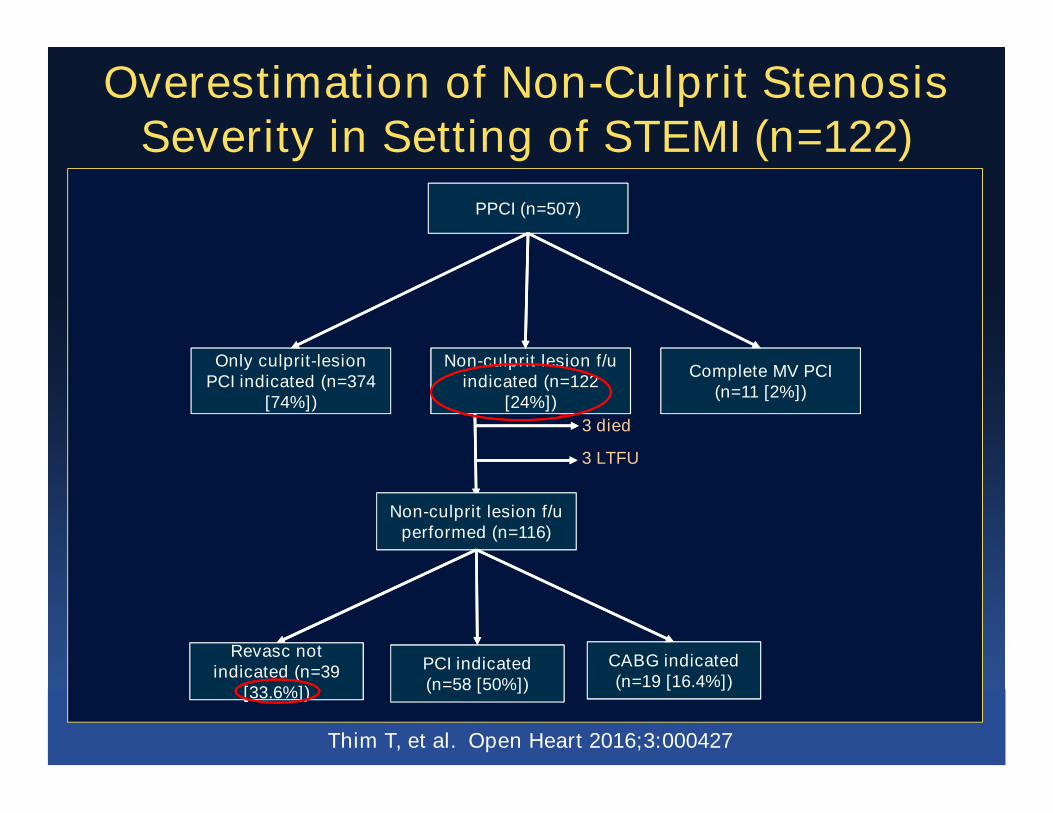
Overestimation of Non-Culprit StenosisSeverity in Setting of STEMI (n=122)
PPCI (n=507)
Only culprit-lesionPCI indicated (n=374
[74%])
Non-culprit lesion f/uindicated (n=122
[24%])
Complete MV PCI(n=11 [2%])
Thim T, et al. Open Heart 2016;3:000427
[74%]) [24%])
3 died
3 LTFU
Non-culprit lesion f/uperformed (n=116)
Revasc not
[33.6%])
Revasc notindicated (n=39
[33.6%])
PCI indicated(n=58 [50%])
CABG indicated(n=19 [16.4%])
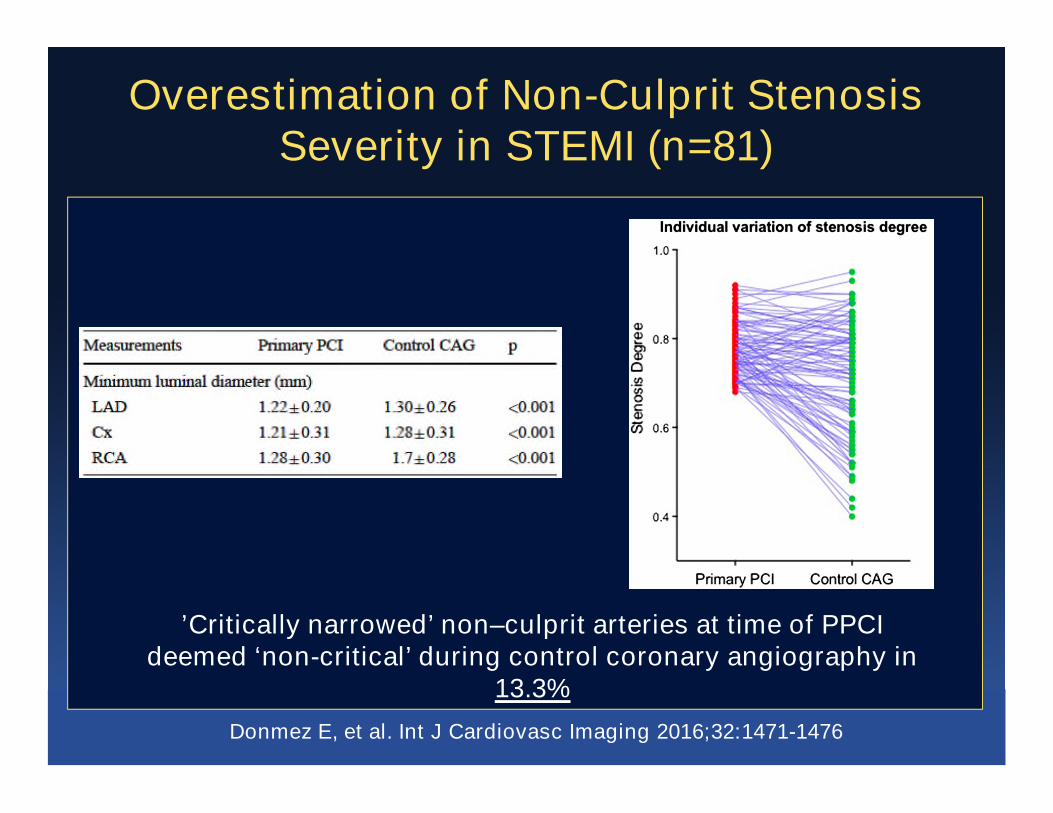
Overestimation of Non-Culprit StenosisSeverity in STEMI (n=81)
Donmez E, et al. Int J Cardiovasc Imaging 2016;32:1471-1476
’Critically narrowed’ non–culprit arteries at time of PPCIdeemed ‘non-critical’ during control coronary angiography in
13.3%
Outline
• Introduction
• The DATA
• Randomized Trials• Randomized Trials
• Guidelines
• Future Studies
• Summary
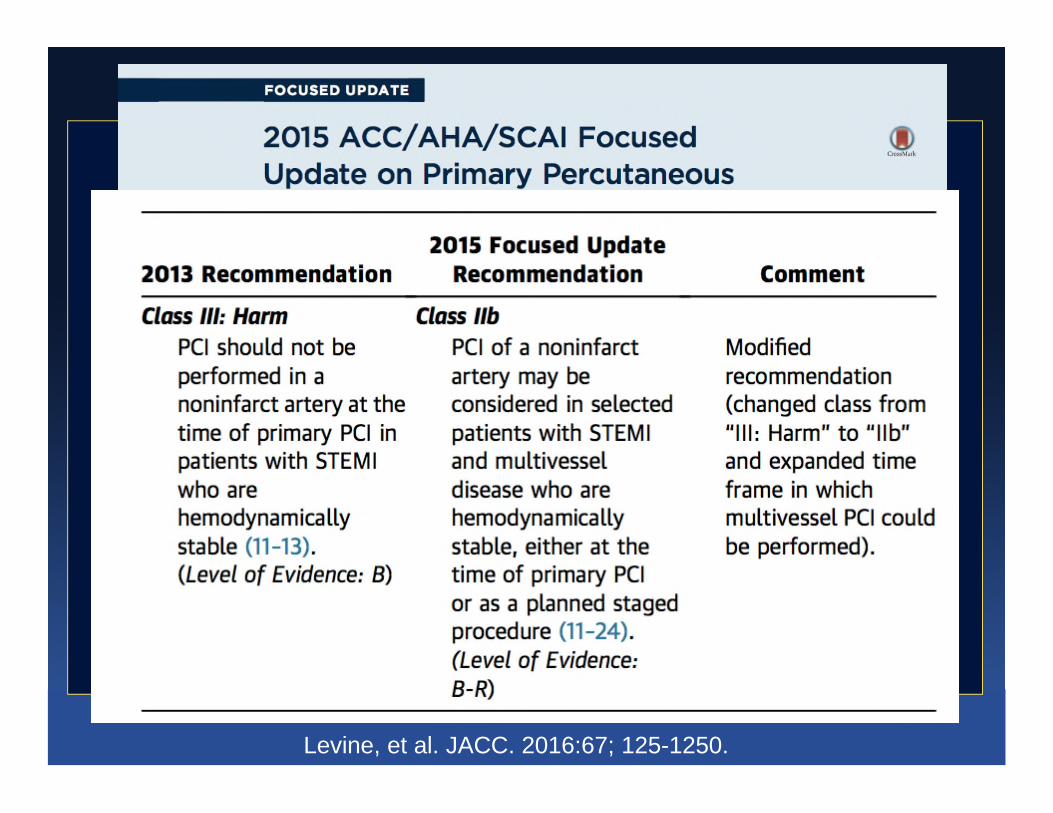
Levine, et al. JACC. 2016:67; 125-1250.
Outline
• Introduction
• The DATA
• Randomized Trials• Randomized Trials
• Guidelines
• Future Studies
• Summary
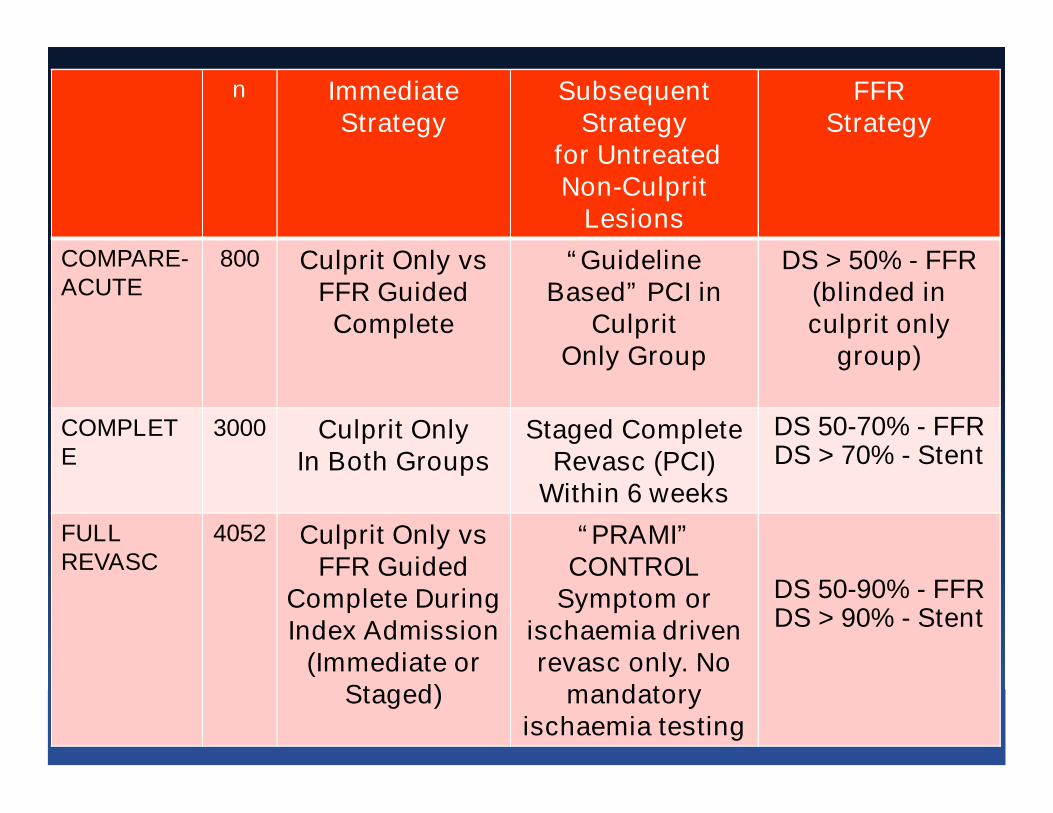
The Ongoing Trialsn ImmediateStrategy
SubsequentStrategy
for UntreatedNon-Culprit
Lesions
FFRStrategy
COMPARE-ACUTE
800 Culprit Only vsFFR GuidedComplete
“GuidelineBased” PCI in
CulpritOnly Group
DS > 50% - FFR(blinded inculprit only
group)
COMPLETE
3000 Culprit OnlyIn Both Groups
Staged CompleteRevasc (PCI)
Within 6 weeks
DS 50-70% - FFRDS > 70% - Stent
FULLREVASC
4052 Culprit Only vsFFR Guided
Complete DuringIndex Admission
(Immediate orStaged)
“PRAMI”CONTROL
Symptom orischaemia drivenrevasc only. No
mandatoryischaemia testing
DS 50-90% - FFRDS > 90% - Stent
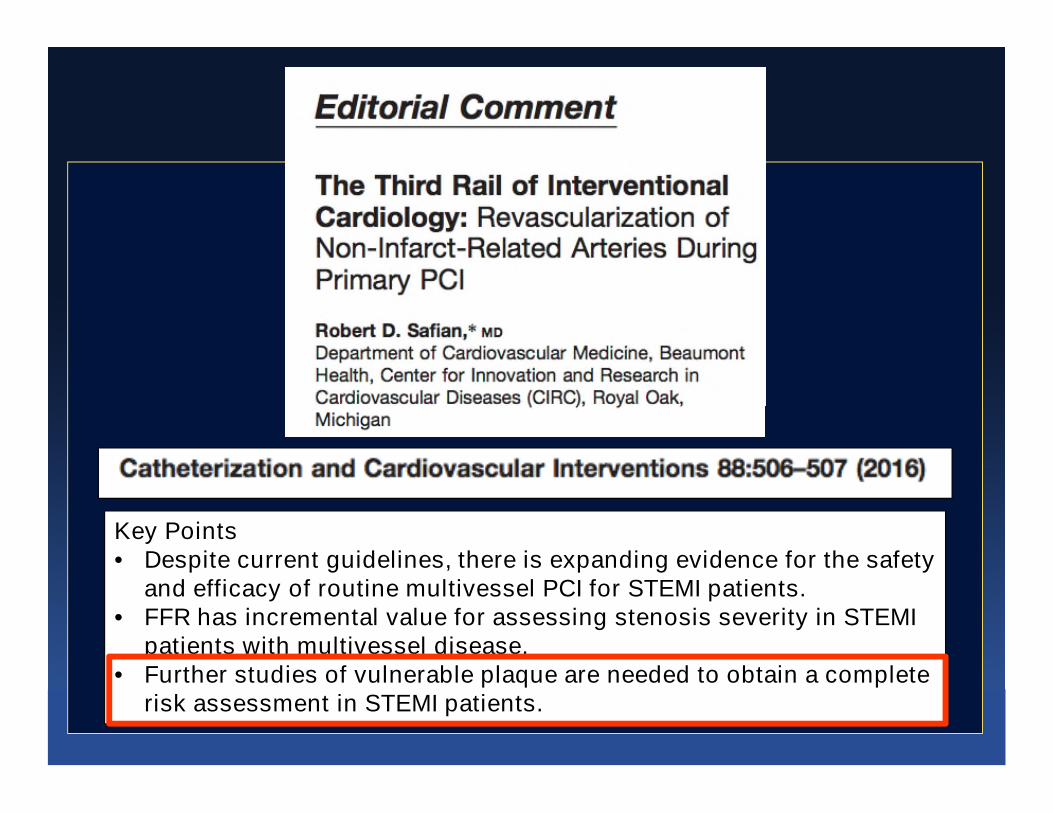
Key Points• Despite current guidelines, there is expanding evidence for the safety
and efficacy of routine multivessel PCI for STEMI patients.• FFR has incremental value for assessing stenosis severity in STEMI
patients with multivessel disease.• Further studies of vulnerable plaque are needed to obtain a complete
risk assessment in STEMI patients.

Outline
• Introduction
• The DATA
• Randomized Trials• Randomized Trials
• Guidelines
• Future Studies
• Summary
Summary
•• The optimal time for completeThe optimal time for complete revascrevasc….….
•• Immediate?Immediate? Staged duringStaged during index?index? Staged a fewStaged a fewdays/weeksdays/weeks later?later?
•• ShouldShould we targetwe target ischemicischemic lesions only using FFR?lesions only using FFR?
•• InIn other situations FFRother situations FFR--guidedguided revascrevasc isisassociated with a better outcomeassociated with a better outcome andandassociated with a better outcomeassociated with a better outcome andand
•• PCIPCI on nonon non--ischaemic lesions has an adverseischaemic lesions has an adverseoutcomeoutcome……
•• Is the real world population so different from theIs the real world population so different from thecarefully selectedcarefully selected groups ingroups in the RCTs that it isthe RCTs that it isimpossible to extrapolateimpossible to extrapolate to real practice?to real practice?
Conclusion
• In patients with STEMI and MVD, there isinsufficient evidence to support areduction in death/MI long-term with multi-vessel PCI
• Await the results of larger RCTs before• Await the results of larger RCTs beforemaking any definitive conclusionsregarding optimal revascularizationstrategy
• For now, PCI is acceptable in selectedpatients (FFR directed at time of staged?)– IIb indication
Case Review
Stented RCA

It’s 2AM --It’s 2AM -- FFR LADFFR LAD
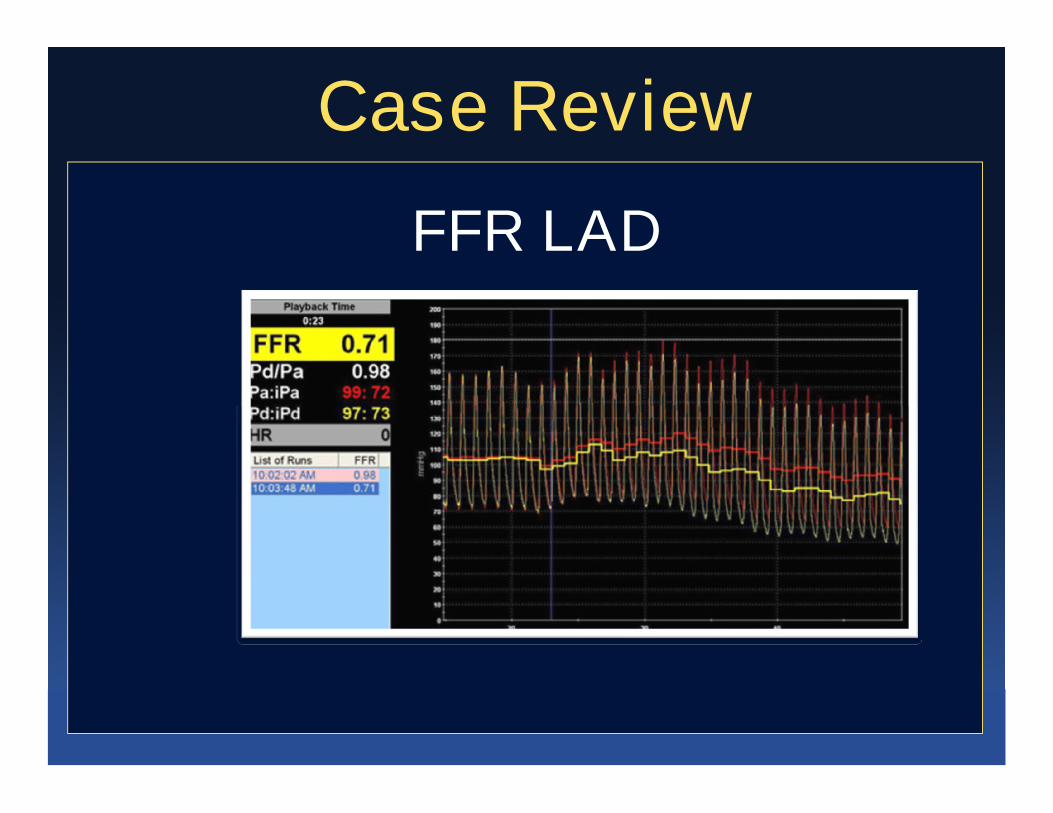
Case Review
FFR LAD

Case ReviewLAD Undilatable – Rota/Stent Prior to
Discharge
Thanks for your attention!Thanks for your attention!
Related Documents



![Journal of Clinical & Experimental Cardiology€¦ · before, we went unable to predict the culprit lesion [1,2]. Although a mild lesion was identified in the middle segment of the](https://static.cupdf.com/doc/110x72/604e57a541576841dc14a7c7/journal-of-clinical-experimental-cardiology-before-we-went-unable-to-predict.jpg)







