PCC Conference 8-30-06 Marcia Lux, MD

PCC Conference 8-30-06 Marcia Lux, MD. By way of introduction… New to the Division of GIM 7/1/06 Harvard Medical School, 2001 Columbia Presbyterian Internal.
Dec 24, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
PCC Conference8-30-06
PCC Conference8-30-06
Marcia Lux, MD
By way of introduction…By way of introduction…
• New to the Division of GIM 7/1/06
• Harvard Medical School, 2001• Columbia Presbyterian Internal Medicine Residency, 2001-2004
• Hospitalist CPMC, 2004-2006• Case 1: July 2004• Case 2: May 2006
Case 1:Case 1:
• 86F readmitted for diarrhea• PMH:
• mild dementia• HTN• DM• CAD s/p MI 1979• ischemic CM EF 25%
History of present illness:History of present illness:
• Multiple CPMC admissions 2003-04• 1/03 syncope PPM• 12/03 fall UTI, CHF• 2/04 NSTEMI, MSSA bacteremia ?veg on PPM wire s/p Vanco x 6wks, UTI, CHF
• 3/04 CHF, unexplained leukocytosis• 4/04 constipation• 5/04 hypoxia ?PE, CHF, contrast-induced ARF, UTI
HPI Cont.HPI Cont.
• June 27, 2004-Readmitted• 10d diarrhea, abdominal pain, dizziness
• Copious, foul smelling, bed bound
• No f/c/n/v• WBC 14.9• Cdif toxin positive• Rx’d Flagyl 500 po TID x 10d• d/c’d on hospital day #2
HPI Cont.HPI Cont.
• Readmitted 7/7/04, cont abd pain, diarrhea, subjective fevers
• 120/80, HR 75, T98, bibasilar rales o/w benign exam
• WBC 14.6, Cr 1.2, stool Cdif +• CXR mild PVC, AXR normal• Rx’d Flagyl 500 TID, Vanco 750mg PO QOD (CrCl 26) approved by ID on Hosp Day #1
HPI Cont.HPI Cont.
• GI Consulted, HD#1• NPO/Bowel rest, judicious IVF• Clinically deteriorating, ongoing diarrhea, dehydration, lethargy, delerium
• Sigmoidoscopy HD #6, severe pseudomembranes
• Vanco dosing adjusted: 250 PO QID
HPI Cont.HPI Cont.
• Labs: WBC 24.9, HCO3 13-16• DNR• HD #13, more alert, WBC 13.8• HD #14 PICC placed for TPN, tolerating clears
HPI Cont.HPI Cont.
• HD #14, 5:30 pm- RN note: “BP 80/50, beeper 3281 paged, no answer”
• 8pm-RN note: “BP 75/48, lopressor held, beeper 4778 paged, no answer”
• 5:30 am- RN note: “pt.w/ agonal breathing, unresponsive, 4778 aware, will evaluate”
• Pronounced by House MD at 6 AM• Family declined autopsy

Historical BackgroundHistorical Background
• C dif first described 1935 gram-positive anaerobic bacillus
• “difficult clostridium”-difficult to grow in culture
• Found in stool specimens from healthy neonates leading to misclassification as a commensal organism
• 1970s: “clindamycin colitis” pseudomembranous colitis in hospitalized pts
• 1978: C dif recognized as causative organism
Confusing terminologyConfusing terminology
• Antibiotic-associated diarrhea• C. difficile is one of many causes(approx 20-30%)
• Clostridium difficile-associated diarrhea• diarrhea + positive stool test
• Clostridium difficile colitis• underlying pathologic process
• Pseudomembranous colitis• endoscopic demonstration of exudative lesions
• Toxic megacolon• radiologic and surgical diagnosis
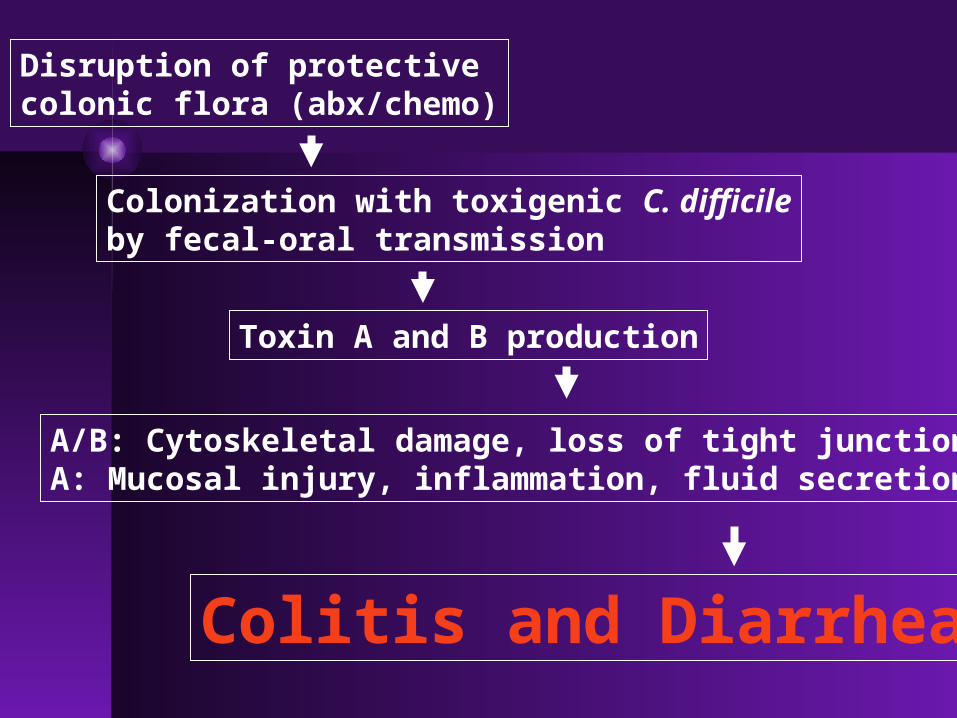
Disruption of protectivecolonic flora (abx/chemo)
Colonization with toxigenic C. difficileby fecal-oral transmission
Toxin A and B production
A/B: Cytoskeletal damage, loss of tight junctions.A: Mucosal injury, inflammation, fluid secretion.
Colitis and Diarrhea
Epidemiology & RFsEpidemiology & RFs
• Leading cause nosocomial enteric infection
• Approx 3 million cases/yr• RISK FACTORS:
• Elderly• debilitated • GI surgery• infected roommate • enteral feeding• prolonged course of abx/multi-agent tx
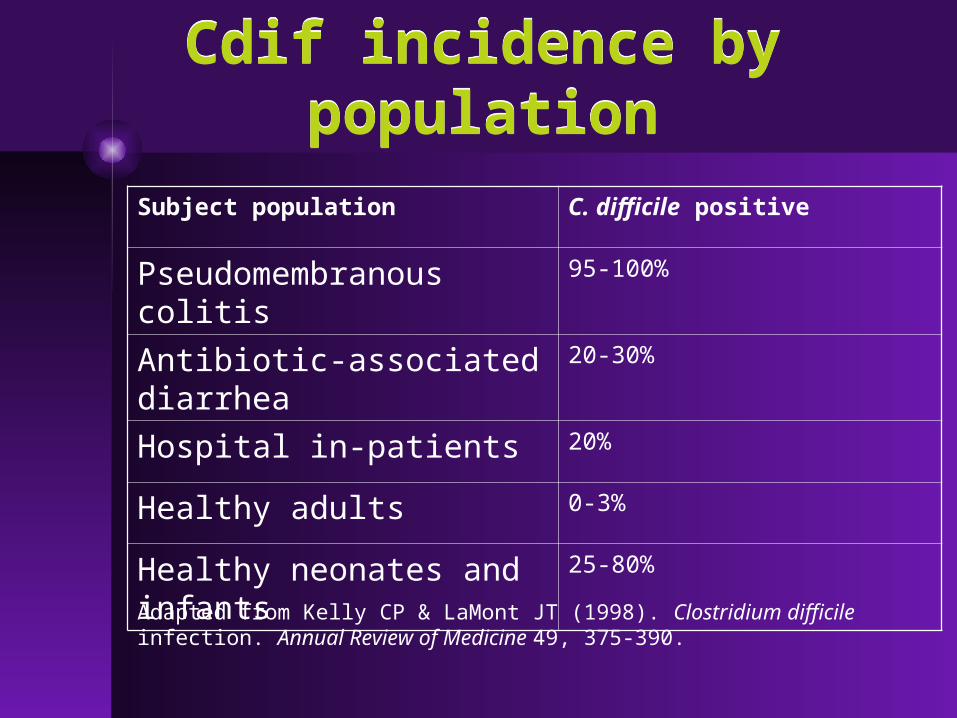
Subject population C. difficile positive
Pseudomembranous colitis 95-100%
Antibiotic-associated diarrhea
20-30%
Hospital in-patients 20%
Healthy adults 0-3%
Healthy neonates and infants
25-80%
Adapted from Kelly CP & LaMont JT (1998). Clostridium difficile infection. Annual Review of Medicine 49, 375-390.
Cdif incidence by populationCdif incidence by population
Clinical ManifestationsClinical Manifestations
• Carrier State: “fecal excretors” asymptomatic-->majority of patients
• Diarrhea without colitis: mild, 3-4 loose BM/d +/- cramps
• Colitis w/o pseudomembranes: more severe systemic c/o, n/v, profuse diarrhea, fever, leukocytosis, abd pain
• Pseudomembranous colitis
Clinical ManifestationsClinical Manifestations
• Fulminant colitis:• Rare, 2-3% of patients, esp elderly• Serious: ileus, perforation, megacolon, death
• High fever, chills, marked leukocytosis (>40K)
• May not have diarrhea if ileus or megacolon• Risk of perforation w/ sigmoid/colonoscopy• Tx surgical
• Unusual presentations:• Long latency period (1-2months)• Absence of antibiotic exposure
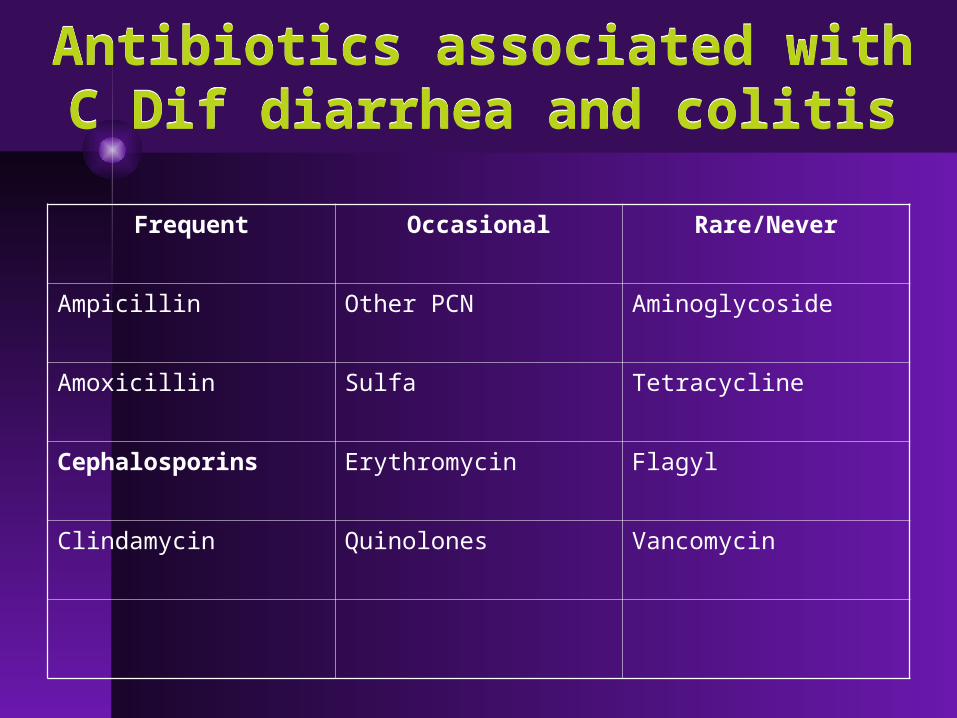
Antibiotics associated with C Dif diarrhea and colitis
Antibiotics associated with C Dif diarrhea and colitis
Frequent Occasional Rare/Never
Ampicillin Other PCN Aminoglycoside
Amoxicillin Sulfa Tetracycline
Cephalosporins Erythromycin Flagyl
Clindamycin Quinolones Vancomycin
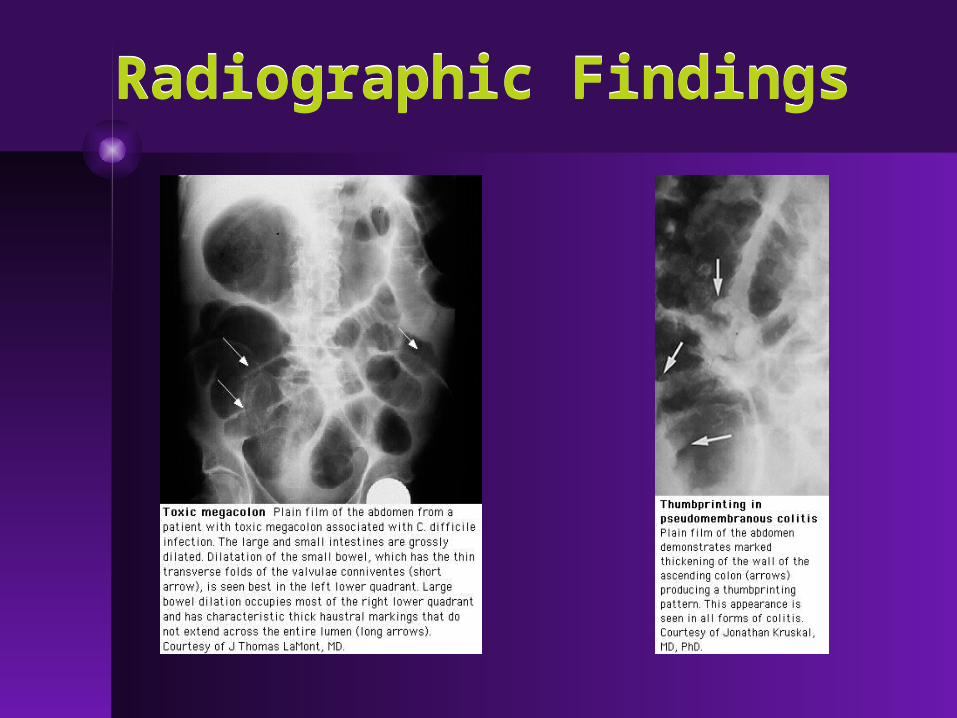
Radiographic FindingsRadiographic Findings
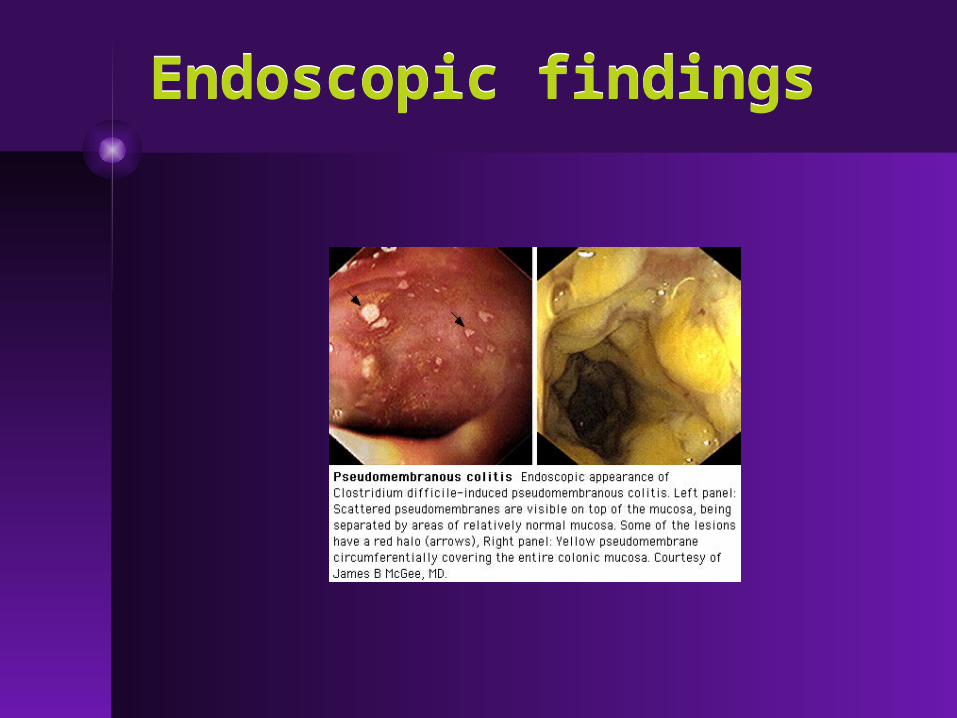
Endoscopic findingsEndoscopic findings
DIAGNOSISDIAGNOSIS
• Endoscopy (pseudomembranous colitis)
• Culture• Cell culture cytotoxin test• ELISA toxin test• PCR toxin gene detection

ELISA toxin testsELISA toxin tests
• Can detect toxin A, toxin B, or both
• Rapid, cheap, and specific• Less sensitive, depends on rapid processing by lab
• Toxin A tests will miss rare C. difficile isolates that produce toxin B only
TREATMENTTREATMENT
1. Discontinue offending agent or modify to less offensive agent (successful in 20% to 25%)
2. Replace fluids and electrolytes3. Avoid antiperistaltic agents: may worsen diarrhea or precipitate toxic megacolon
4. If conservative measures not effective or practical, rx metronidazole 500 mg TID X 10d
[ can also use IV flagyl as good excretion into GI tract via bile and exudation from inflamed colon]
Treatment cont.Treatment cont.
5. Re-treat first-time recurrences with the same regimen used to treat the initial episode
6. Avoid vancomycin if possible: equal efficacy but can lead to VREF. Cannot use IV vanco. Can use vancomycin enemas if NPO
7. Do not treat nosocomial diarrhea empirically without testing, <30% have C. dif infection
Recurrent C. dif InfectionRecurrent C. dif Infection
• 10-25% of patients will relapse• Si/sx similar to initial attack• Most often occurs w/i 1-2 wks but can be up to 2 months later
• Pathogenesis unclear: reinfection vs. failure to mount adequate immune response vs. survival in diverticula
Treatment of RecurrenceTreatment of Recurrence
• First relapse: treat conservatively if mild sx otherwise repeat Flagyl x 10-14d
• Other therapies with some potential efficacy• Pulsed vancomycin taper (4+weeks)• Cholestyramine• Fecal enema (yuck!)
Resistance?Resistance?
• Generally NOT considered a clinically significant problem
• Flagyl resistant strains have been isolated in vitro
• No resistance to vancomycin has been reported

Case 2Case 2
• 54F, no prior hospitalizations• CC: fever, malaise, HA, dry cough x2d
• HPI:denied SOB or pleurisy, +sweats, no chills/rigors, no sick contacts, no prior respiratory illness, no flu shot
• ROS: +4-5/d watery diarrhea and diffuse arthralgias
Case 2, contCase 2, cont
• PMHx:• HTN- well controlled on monotherapy• Morbid obesity
• SHx: telephone operator for Verizon, lived alone, never married, non-smoker
• In ER: T 103.8, 130/80, HR 125, RR 24, O2 94% RA
• PE: mild distress, area of crackles in left lower lung field, benign abdomen

LABS & CXRLABS & CXR
• WBC 18K• 73% PMN, 0 bnd
• Na 134• Cr 1.1• AST 244• ALT 187• CK 2200
QuickTime™ and aTIFF (Uncompressed) decompressor
are needed to see this picture.
ER Dx: CAP; Rx: CTX/Azithro and admit
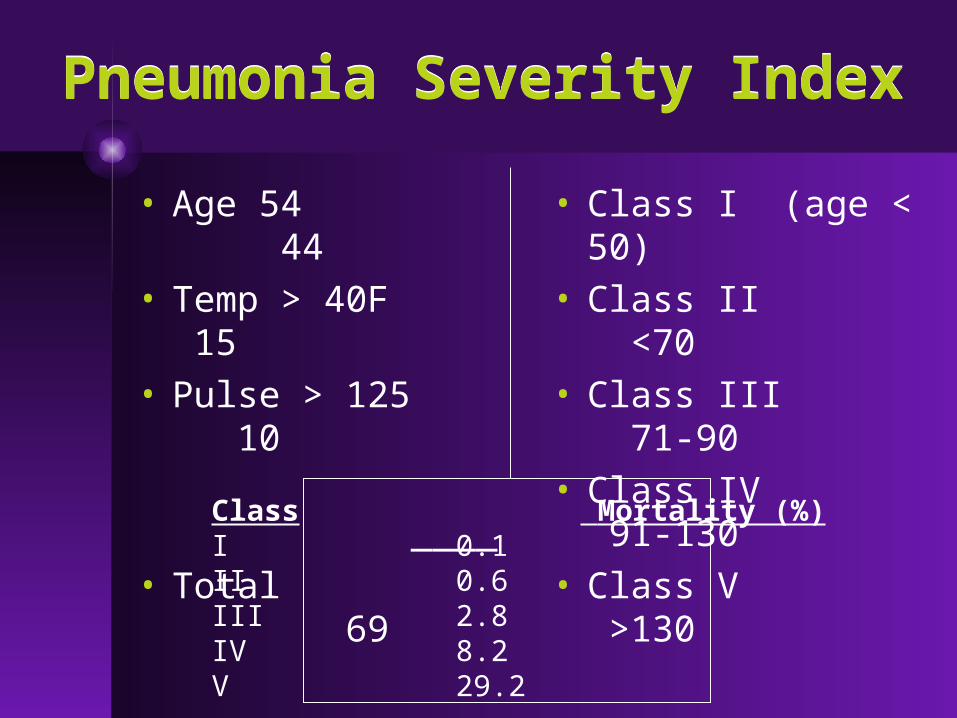
Pneumonia Severity IndexPneumonia Severity Index
• Age 54 44
• Temp > 40F 15
• Pulse > 125 10
____
• Total 69
• Class I (age < 50)
• Class II <70
• Class III 71-90
• Class IV 91-130
• Class V >130
Class Mortality (%)I 0.1II 0.6III 2.8IV 8.2V 29.2
Case 2, contCase 2, cont
• Admit Hospitalist service• Continue CTX/Azithro• Supportive care, IVFs• CK peaked 3400 without renal compromise
• AST/ALT normalized by HD 1
• Pt stable for discharge on Friday but uncomfortable with the plan……….
After 3days of hospitalization without being seen by an
MD……
After 3days of hospitalization without being seen by an
MD……
• Urine Legionella: positive

TerminologyTerminology
• Legionellosis: infectious process caused by Legionella spp..• 1) Legionnaires’ disease: PNA caused
by Legionella species (1976 Philadelphia American Legion Conference)
• 2) Pontiac Fever: acute febrile, self-limited illness linked to Legionella (Pontiac, MI)
• 3) Extrapulmonary Legionella infxn
EpidemiologyEpidemiology
• Incidence linked to degree of water contamination
• Accounts for 2-10% of CAP• Lower incidence for outpatients vs. inpatients
• Nosocomial: 12-70% of hospital water supplies contaminated, also reported outbreaks in NH and LTAC facilities
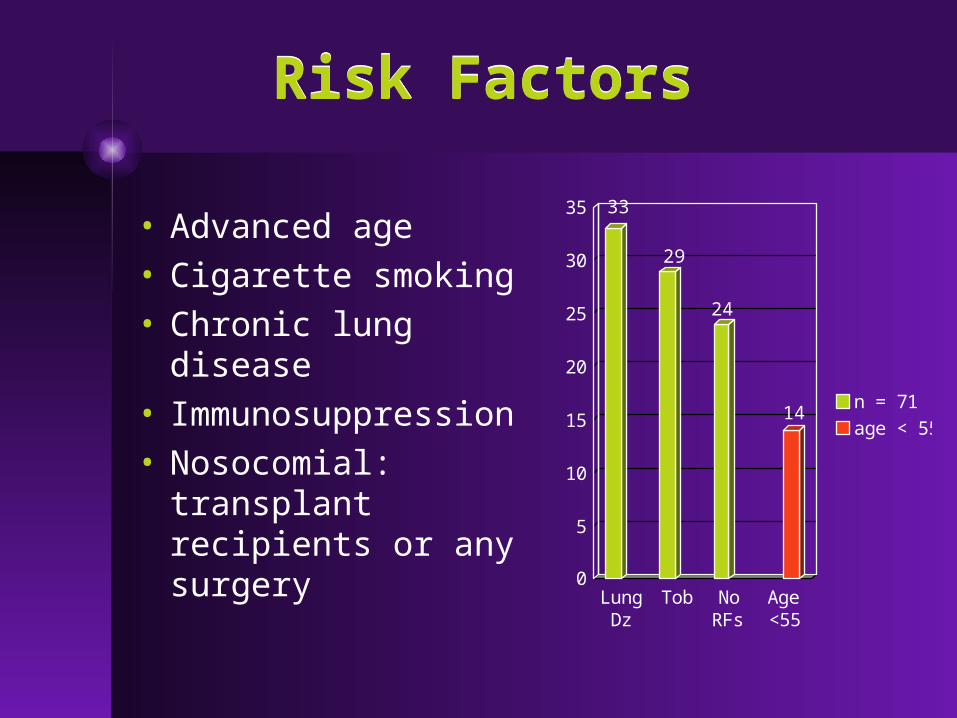
Risk FactorsRisk Factors
• Advanced age• Cigarette smoking
• Chronic lung disease
• Immunosuppression
• Nosocomial: transplant recipients or any surgery
0
5
10
15
20
25
30
35
LungDz
Tob NoRFs
Age<55
n = 71
age < 55
33
29
24
14

CLINICAL MANIFESTIONS:Legionnaires’ Disease
CLINICAL MANIFESTIONS:Legionnaires’ Disease
Sign/Symptom Frequency (%)Cough 41-92
Chills 42-77
Fever > 38 F 88-90
Fever > 40 F 20-62
Dyspnea 25-62
Headache 40-48
Myalgia/Arthralgia 20-40
Diarrhea 21-50
Nausea/Vomiting 8-49
Neurologic Sx 4-53
Chest pain 13-35
Legionella vs. other CAPLegionella vs. other CAP
• GI symptoms, esp. diarrhea• Neurologic findings, esp. confusion
• Fever > 39 F• Sputum w/ many PMNs but no organisms
• Hyponatremia• Hepatic dysfunction• Hematuria• No response to B-Lactam or aminoglycoside abx

PE and Lab findingsPE and Lab findings
• Bradycardia relative to temp elevation
• Rash• Hypophosphatemia• Rhabdomyolysis• Thrombocytopenia• Leukocytosis• DIC

Extrapulmonary LegionellaExtrapulmonary Legionella
• RARE!• Cellulitis• Sinusitis• Septic arthritis• Perirectal abscess
• Pancreatitis• Peritonitis• Pyelonephritis
• Most commonly affects heart:
• Pericarditis• Myocarditis• PV Endocarditis
• Surgical wound infections

Laboratory DiagnosisLaboratory Diagnosis
• Culture:• 3 different media, 3-5 days
• DFA staining:• low Se, high Sp
• Serology:• 4-fold rise in antibody titer
• URINE ANTIGEN
Culture is the Gold Standard
• Culture + antigen testing recommended if legionella is suspected on ddx

Urine AntigenUrine Antigen
• Detects L. pneumonophila serogroup 1(90% of community acq’d Legionella PNA)
• Sensitivity correlates with disease severity, may miss mild cases
• Enzyme immunoassay• Remains positive for days, even after initiation of treatment
• Rapid urinary antigen test: results in 15 min with se/sp 80%/97%
TreatmentTreatment
• Mortality: 16-30% if untreated or treated with wrong antibiotics
• Susceptibility testing not routinely available but significant resistance has not been demonstrated
• Antibiotic choice requires high intracellular penetration• Macrolides, Quinolones, Tetracycline, Rifampin
• ATS recommendations for tx of CAP incorporate either a respiratory quinolone or Azithromycin as standard therapy
TreatmentTreatment
• New macrolides (Azithromycin) or respiratory quinolones (Levaquin) are tx of choice
• No head to head RCT, retrospective studies suggest Levaquin better for severe illness
• Duration of tx: 10-14d • Azithromycin duration 7-10d• Use IV abx if prominent GI symptoms

PrognosisPrognosis
• Mortality <5% if early initiation of appropriate antibiotics
• Defervescence and symptomatic improvement within 3-5d
• Some pts will report prolonged symptoms, usu dyspnea and fatigue for many months following resolution of acute infection
SUMMARYSUMMARY
• Legionella and C. dif are common problems whose disease spectrum bridges primary care and hospital medicine
• C. dif is an extremely common nosocomial infection which can be severe
• Legionella is a frequent cause of CAP that also tends to have a more severe acute presentation
Related Documents











