P AY F LEX C LIENT W ELCOME K IT

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

PAYFLEX CLIENT WELCOME KIT
- 2 -
PayFlex Program Highlights
Pages 5-20 Pages 21-43 Pages 44-67
- 3 -
Introduction p. 4
World Class Customer Service Center p. 5 How to Contact PayFlex How to Use the IVR System Online Customer Center
State of the Art Web Portal p. 9
Employer Portal Communications Center Wellness Center Market Watch Participant Center
Participant Center p. 15 Employee Coverage Confirmation Claims-Express Claims & Manual Integrated Voice Response System (IVR) Internet Access
The PayFlex Card
Employee Communications p. 19 Education Materials Participant-Ready Communications e-Notify Explanation of Benefits Correspondence to Participants
PayFlex Plan Highlights
TABLE OF CONTENTS

- 4 -
Introduction Welcome to PayFlex! We are pleased to provide you and your participants the latest in reimbursement account technology and prompt, courteous customer service. Our Client Welcome Kit highlights our programs and services, providing a glimpse of PayFlex products and service offerings. We have developed several tools to help you and your participants make the most of your benefit program. Take a moment to get familiar with the new and innovative Customer Center via www.payflex.com > EMPLOYERS > Employer Portal. In addition to our program highlights, we have included various procedures and forms in the Plan Administration section designed to help you with the administration of your reimbursement accounts. You may or may not use all of the enclosed forms. For example, you may use a customized form or web based process rather than the enrollment form provided on our web site. The purpose of the section is to let you know what's available from PayFlex and what's required to keep your plan in compliance with IRS regulations. We hope our Client Welcome Kit proves to be helpful. If you have any questions, please contact your Client Services Manager. For additional information, visit our website at www.payflex.com. The following is available for you to help your business fully educate your participants:
• Participant Ready-Communications
• Wellness Center
• Legislative Updates
• PayFlex News
• Generic Enrollment Materials
• Customizable Enrollment Materials
• Educational tools: Employer Value Table, Savings calculator, FSA tutorials, etc.
• Healthcare & Dependent Care Expense Planning Worksheets
• FSA Enrollment Slide Show
• Dependent Care Tax Credit Wizard
• Frequently Asked Questions
PayFlex invites you to go green wherever you see this symbol.
- 5 -

- 6 -
How to Contact PayFlex
PayFlex Contact Information For Employers
Client Services Manager Call 1-800-284-4885, press 5, then press 1, then type extension number
Access Employer Portal: Customer Center
Go to www.payflex.com, select “EMPLOYERS” located on left-hand tool bar, then select “Employer Portal”
(If you need a username & password, contact your CSM)
For participant changes regarding: Eligibility, Address, Status and/or
Election changes Fax to 402-231-4283 or Email [email protected]
For Participants PayFlex Website www.mypayflex.com
PayFlex FSA Info Line (IVR 24/7) Toll Free: 800-284-4885 (Select Option 1, then press 1)
Personal Assistance Monday - Friday, 7:00am-7:00pm CST
Toll Free: 800-284-4885 (Select Option 1, then press 3)
Account Information www.mypayflex.com or call 800-284-4885
Claims Filing for Participants Online Process Express Claims at www.mypayflex.com
Fax Claims 402-231-4310
Mailing Address for Claims PayFlex Systems USA, Inc.
P.O. Box 3039 Omaha, NE 68103-3039
Debit Card Letter Response Fax 402-231-4303

- 7 -
How to use: The IVR system
• Dial the toll-free number 1.800.284.4885 • After the introduction, you will have the following choices: Option 1: For account balance information, press 1:
• Enter your member number, followed by the # sign. The number will be repeated to you for verification. If correct, press 1. If the number is not correct, press 2 to try again.
• Then, enter your home zip, followed by the # sign. The number will be repeated to you for verification. If correct, press 1. If the number is not correct, press 2 to try again.
• After successfully entering your member number and your zip, you can press 2 for information on your remaining balance in your health care and/or day care account.
Option 2: If you have questions on why your card has been denied, press 1. Possible Reasons why card has been denied:
• The amount you charged on your debit card exceeded the remaining balance in your health care and/or day care account
• Your card is inactive because requested documentation has not been received for a health care expense charged on your debit card.
Option 3: If you wish to speak to a Customer Service Representative about your account, press 3.
Voice Services

- 8 -
Customer Center
Employers can now manage their PayFlex benefit programs, plan their open enrollment, communicate PayFlex information and keep up-to-date on industry news and PayFlex service offerings all in one place!

- 9 -

- 10 -
Employer Portal: Enhanced Functionality
- 11 -
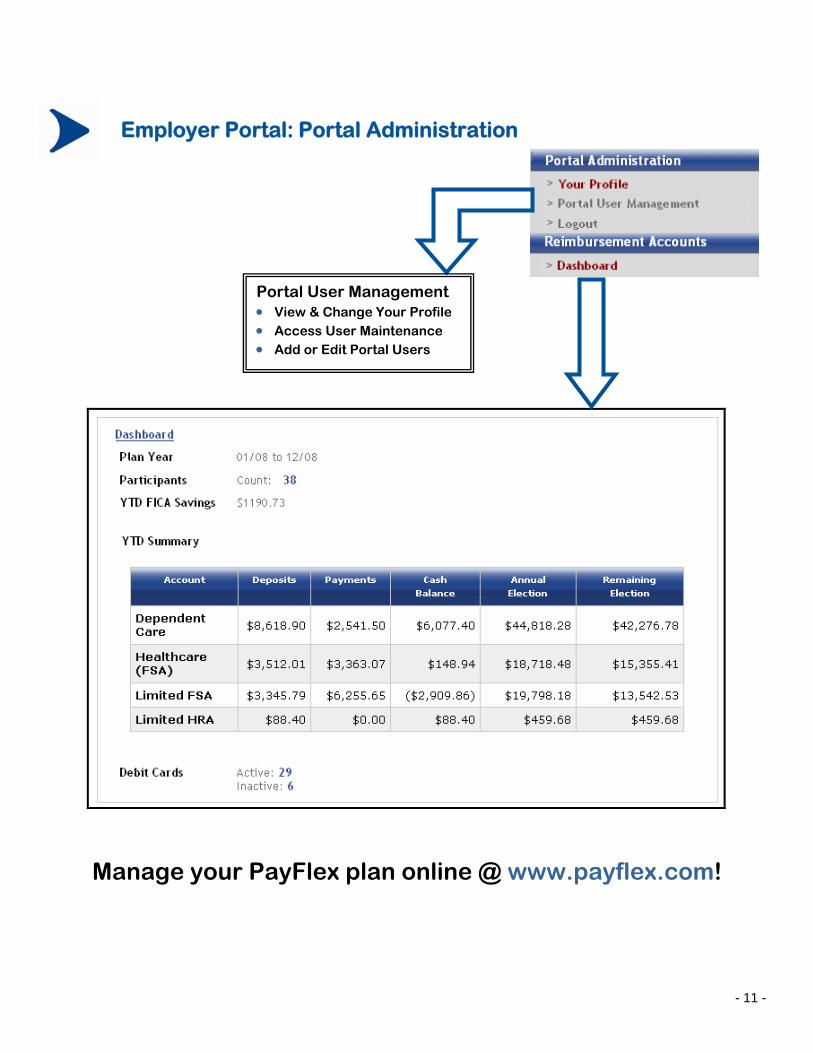
Employer Portal: Portal Administration
Manage your PayFlex plan online @ www.payflex.com!
Portal User Management • View & Change Your Profile • Access User Maintenance • Add or Edit Portal Users
- 12 -
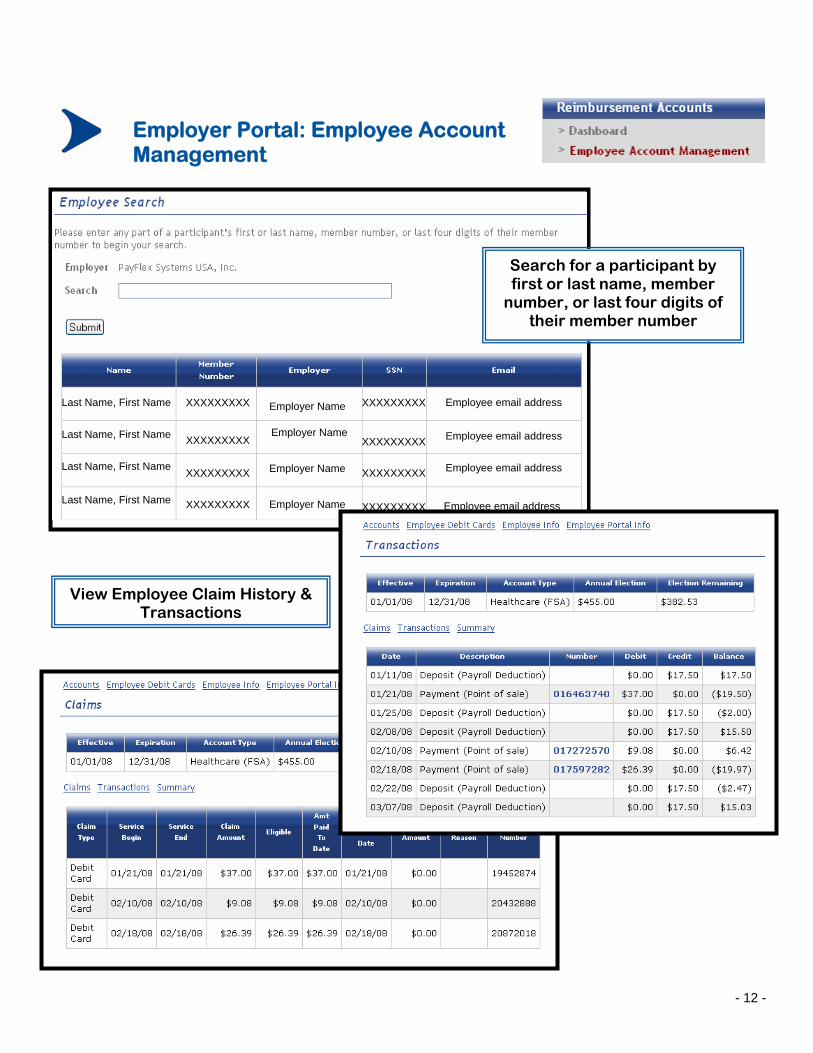
Employer Portal: Employee Account Management
Last Name, First Name XXXXXXXXX
XXXXXXXXX
XXXXXXXXX
XXXXXXXXX
XXXXXXXXX
XXXXXXXXX
XXXXXXXXX
XXXXXXXXX
Last Name, First Name
Last Name, First Name
Last Name, First Name
Employer Name
Employer Name
Employer Name
Employee email address
Employee email address
Employee email address
Employee email address
Employer Name
Search for a participant by first or last name, member
number, or last four digits of their member number
View Employee Claim History & Transactions

- 13 -
Employer Portal: View Employee Debit Card Status
Employer Portal: View & Download Your Reports
LAST NAME, FIRST NAME XXXXXXXXX
XXXXXXXXX
XXXXXXXXX
XXXXXXXXX
Employer Name
####
Search by Active, Inactive (TI) or All
####
####
####
Name of Employer
Employer Name
Employer Name
Employer Name
LAST NAME, FIRST NAME
LAST NAME, FIRST NAME
LAST NAME, FIRST NAME

Communications Center Plan Your Open Enrollment Interested in having an Open Enrollment Meeting? Request a Meeting and Order Your Materials online today via the Communications Center!
Education Materials View, download and print a wide variety of materials and tools via the “Education Materials” link.
Wellness Center
Motivate your employees to get healthy and stay healthy!
Contact your CSM to learn more about our Wellness Partners!
Market Watch
Keep up-to-date on industry news and PayFlex service offerings!
Participant-Ready Communications A library of communications designed to be posted on your intranet or emailed directly to employees!
Legislative Updates PayFlex News IIAS Updates
Asset Health – interactive online healthcare management system
HealthiNation- educational and engaging digital health & wellness videos ⇒ Check out HealthiNation’s
monthly video special via the Customer Center!

- 15 -
Participant Center: www.mypayflex.com
The Participant Center is easy-to-use and always available. Your employees are able to manage their account(s) and spend their FSA dollars 24/7 via www.mypayflex.com.
Reduce Paper – Submit Claims Online

- 16 -
Participant Access Employee Coverage Confirmation Employers should instruct participants to confirm their election online at www.mypayflex.com or by calling the PayFlex Info Line at 1-800-284-4885 (select option 1, then press1). Any changes in election must be made by the employee prior to the effective date, and must be requested through the employer. The employer is responsible for reporting changes by email or fax to PayFlex prior to the effective date. EXPRESS Claims and Manual-Paper Claims To submit claims to PayFlex, participants may use the EXPRESS Claims service available at www.mypayflex.com. This feature allows the participant to submit a claim form online. Participants now have the option to FAX or UPLOAD their documentation. If the participant chooses to FAX, they must print the form, sign and fax the completed claim form with supporting documentation to PayFlex. If UPLOAD is selected, a participant will need to upload supporting documentation in PDF format. By uploading their documentation, this will prevent the participant from having to fax documentation or claim forms to PayFlex. Reimbursements for eligible expenses will be issued on the employer's next reimbursement cycle. Participants will be notified via e-mail from [email protected] when the claim has been processed. The Manual-Paper Claim Form, available at www.mypayflex.com, can also be utilized by the participant to submit a claim to PayFlex for reimbursement. The Claim Form must be fully completed and submitted with proper documentation as described on the form. Detailed information regarding eligible/ineligible expenses, as well as, detailed claim filing instructions are available at www.mypayflex.com. Integrated Voice Response System (IVR) Toll free IVR services are available 24 hours a day at 1-800-284-4885. Employees can check account balances, claims, payment or general information with a touch tone phone. Employees can also speak with a personal service representative, if needed, Monday through Friday from 8:00 a.m. - 8:00 p.m. Eastern Time and 7:00 a.m. - 7:00 p.m. Central Time. Internet Access Employees may also access their account information via the Internet at www.mypayflex.com. Account status is updated on a daily basis. Participants can enroll in direct deposit, order additional debit cards, submit claims via EXPRESS Claims and sign up for e-Notify. There are also additional educational tools to help the participants with their healthcare and/or dependent care account including expense planning worksheets, tutorials, frequently asked questions, savings calculator, and listings of eligible and ineligible expense items.

- 17 -
Participant Access (continued) Internet Access (cont’d) Employees may access detailed account information 24 hours a day, seven days a week at www.mypayflex.com. Available information includes account balance, detail claim information, payment information, as well as educational information regarding flexible spending accounts. First-time users must register their account by entering their member number, home zip code and completing the requested information. Forms available for participants @ www.mypayflex.com:
• Enrollment Form • Direct Deposit Authorization Form • Claim Forms and Filing Instructions • Letter of Medical Necessity • IRS Forms & Publications

- 18 -
The PayFlex Card Offer your employees a convenient way to pay for their healthcare expenses by choosing the PayFlex Card! The card will automatically deduct funds from their healthcare account to pay for eligible expenses. PayFlex Card Pointers
• The PayFlex Card has approximately an 80% auto-substantiation rate for healthcare related expenses
• All healthcare items purchased at a merchant with an inventory information approval system will be approved or denied at the point-of-sale.
• Accepted ONLY at healthcare related merchants AND merchants who have implemented an inventory information approval system
• Merchants must be able to accept MasterCard®
• Over-the-counter items can be purchased with your PayFlex Card
• FSA participants can use the card to pay for items or services up to the annual election amount regardless of how much has been contributed
• Card is valid for three years after the date of issue and PayFlex reloads the card each plan year with the participant’s election amount.
PayFlex invites you to go green… Offer your employees the PayFlex Card!

- 19 -
Employee Communications
Education Materials Employers can access education tools and materials via the Communications Center. The materials are available to view, download and print at your convenience. Our enrollment materials can also be ordered via the Communications Center. Please allow a 10-day lead time when ordering materials. If your organization is interested in customized materials please contact your Client Services Manager.
Participant-Ready Communications Participant-Ready Communications are accessible via the Communications Center in the Customer Center. The communications are designed to be placed on your intranet, emailed as an attachment or copied into an email message for quick and easy communication to your employees. Feel free to use as you see fit for pre-enrollment, during enrollment, throughout the plan year or for year-end reminders.
Participants may take advantage of our e-Notify service. Participants who select this option, automatically receive e-mail indicating that we processed their claim and the dollar amount processed for the claim. The e-mail will be sent within 24 hours of the claim being processed. Participants may also select to receive an electronic explanation of benefits and receipt request letters via e-mail.

- 20 -
Employee Communications
Explanations of Benefits (EOB) All participant reimbursement requests that are processed, paid or denied will be accompanied by an explanation of benefits (EOB) statement. This explanation itemizes the claims being considered with the payment. Reimbursements or notice of direct deposit of reimbursement also include a current statement of account that show the plan year election, year-to-date deposits, year-to-date paid amounts, and current account balance. Correspondence to Participants-Card Transactions Certain transactions that are made with the PayFlex Card also require substantiation. Participants could receive notices for transactions requiring substantiation entitled "Request for Documentation for Purchases Made Using your Flex Card" via e-mail from [email protected] or via postal service depending on the participant's election. If there is no response from the participant within 21 days, a second letter will be sent. If there is no response to the second letter within 21 days, the PayFlex Card is inactivated. A participant can still participate in the plan, however, he/she will not be able to use the PayFlex Card to access their funds. The participant will need to pay for eligible expenses with out of pocket dollars and then submit a claim online via Express Claims, fax or mail.

- 21 -
Employer Services Portal Guide
Confidential and Proprietary This document and the information contained herein are the proprietary and confidential information of PayFlex Systems USA, Inc. No such information may be used, disclosed, reproduced, or modified without the written permission of PayFlex Systems USA, Inc.
- 22 -
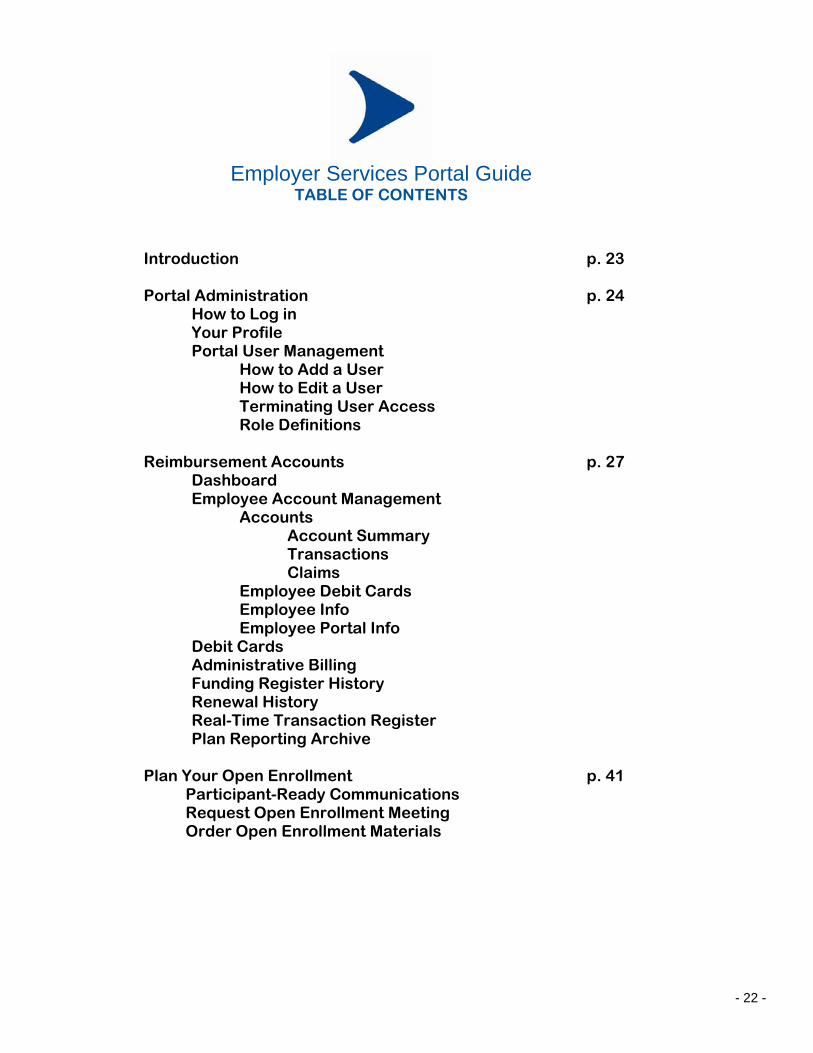
Introduction p. 23 Portal Administration p. 24
How to Log in Your Profile Portal User Management
How to Add a User How to Edit a User Terminating User Access Role Definitions
Reimbursement Accounts p. 27
Dashboard Employee Account Management
Accounts Account Summary Transactions Claims
Employee Debit Cards Employee Info Employee Portal Info Debit Cards Administrative Billing Funding Register History Renewal History Real-Time Transaction Register Plan Reporting Archive
Plan Your Open Enrollment p. 41 Participant-Ready Communications Request Open Enrollment Meeting Order Open Enrollment Materials
Employer Services Portal Guide
TABLE OF CONTENTS

- 23 -
Introduction The newly designed Employer Services Portal was developed to give you convenient access to information regarding your plan, participants, funding and reporting. Through the portal you will be able to setup multiple users and give them access to the various features of the portal by assigning roles. To access the Employer Services Portal, point your web browser to www.payflex.com/employer.
Take note of the left navigation bar in the screenshot above. This is referenced throughout this guide and used to access many of the Employer Services Portal features. Please designate at least one person at your company to be the Website Administrator. This person will initially be set up by your Client Services Manager as the Website Administrator and given a password. Once the Website Administrator logs into the site, they will then be able to add, change, and delete additional users for your company to the Employer Services Portal.

- 24 -
Portal Administration
How to Log in To access the content on the Employer Services Portal, log in using your email and password provided by your Client Services Manager or Website Administrator.
Your Profile (All Users) By selecting Your Profile from the left navigation bar you will be able to edit your personal information such as:
• Email address for communication and login • First and Last Name • Password for login
Client Roles: Any roles granted to you by your Website Administrator will be displayed at the bottom of the page. Throughout this guide, each feature of the Portal will be defined by role in red. It is recommended you change your password periodically, especially after the first time you log in using the password given to you by your Client Services Manager or Website Administrator. Also, make sure to click the Submit button each time you change your information. A confirmation message will appear when you have successfully made your changes. You will not be prompted to change your password.

- 25 -
Portal User Management (Website Administrator) Selecting Portal User Management from the left navigation bar will display a list of Employer Services Portal users and their email addresses. From this screen you can add and edit users. How to Add a User To add a new user to the Employer Services Portal, click Add User at the bottom of the User Maintenance screen. Proceed by filling in the requested information and clicking Submit:
• First and Last Name • Valid Email Address • Password (entered twice for confirmation)
Be sure to keep track of the password assigned to the user, as you will need to communicate it to them. It is recommended you have a standard temporary password for new users and instruct users to change their password after the first time they log in. Users will not be prompted to change their password. A user cannot do anything in the Employer Services Portal until they have been granted roles. See How to Edit a User to see how to grant roles a user. How to Edit a User As a Website Administrator you can also edit a user. You can change their name, password, email or roles. Once a user is added to the Portal, they may not be removed. However, access can be restricted by deleting granted roles and changing the user’s password by selecting Edit User. To edit a user, begin on the User Profile and click on either the Edit User link or Edit/Delete links next to one of the user’s roles. To grant a role to an existing user click Add Role. Select the role you want to add for the user. You will then need to select all employers to which this role applies to:
After you click Submit a confirmation message will appear in blue at the top of the User Profile Screen.

- 26 -
If you need to delete a role granted to a user, find the role you would like to delete and click on Delete. A confirmation message will appear in blue at the top of the screen:
Terminating User Access In the event you need to terminate complete access for a user, PayFlex recommends the following actions be taken:
• Change the user’s password under Edit User. • Delete all of the user’s roles under User Profile.
Role Definitions Below is a listing of the role which applies to each feature:
Feature Role
Your Profile All users
Portal User Management Website Administrator
Dashboard All users
Employee Account Management Benefits Administrator
Debit Cards Benefits Administrator
Administrative Billing Billing Administrator
Funding Register History Funding Administrator
Renewal History Benefits Administrator
Real-Time Transaction Register Funding Administrator
Plan Reporting Archive Funding Administrator
Reimbursement Accounts
- 27 -
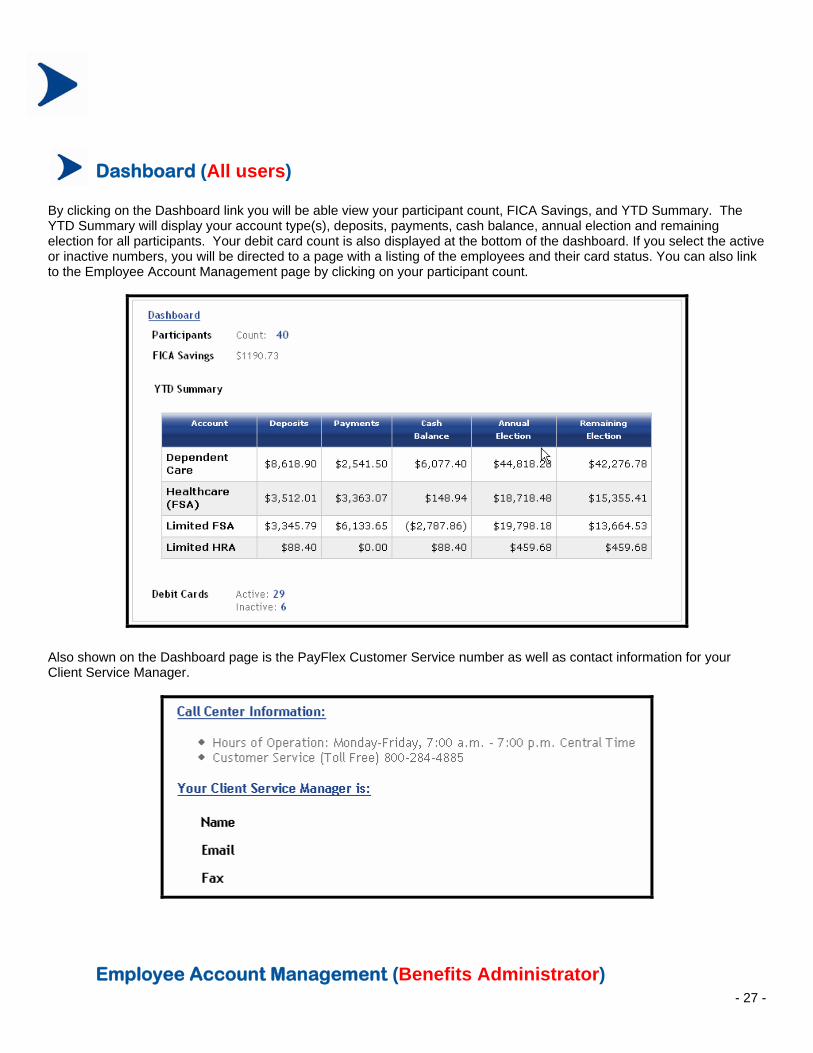
Dashboard (All users) By clicking on the Dashboard link you will be able view your participant count, FICA Savings, and YTD Summary. The YTD Summary will display your account type(s), deposits, payments, cash balance, annual election and remaining election for all participants. Your debit card count is also displayed at the bottom of the dashboard. If you select the active or inactive numbers, you will be directed to a page with a listing of the employees and their card status. You can also link to the Employee Account Management page by clicking on your participant count.
Also shown on the Dashboard page is the PayFlex Customer Service number as well as contact information for your Client Service Manager.
Employee Account Management (Benefits Administrator)
- 28 -
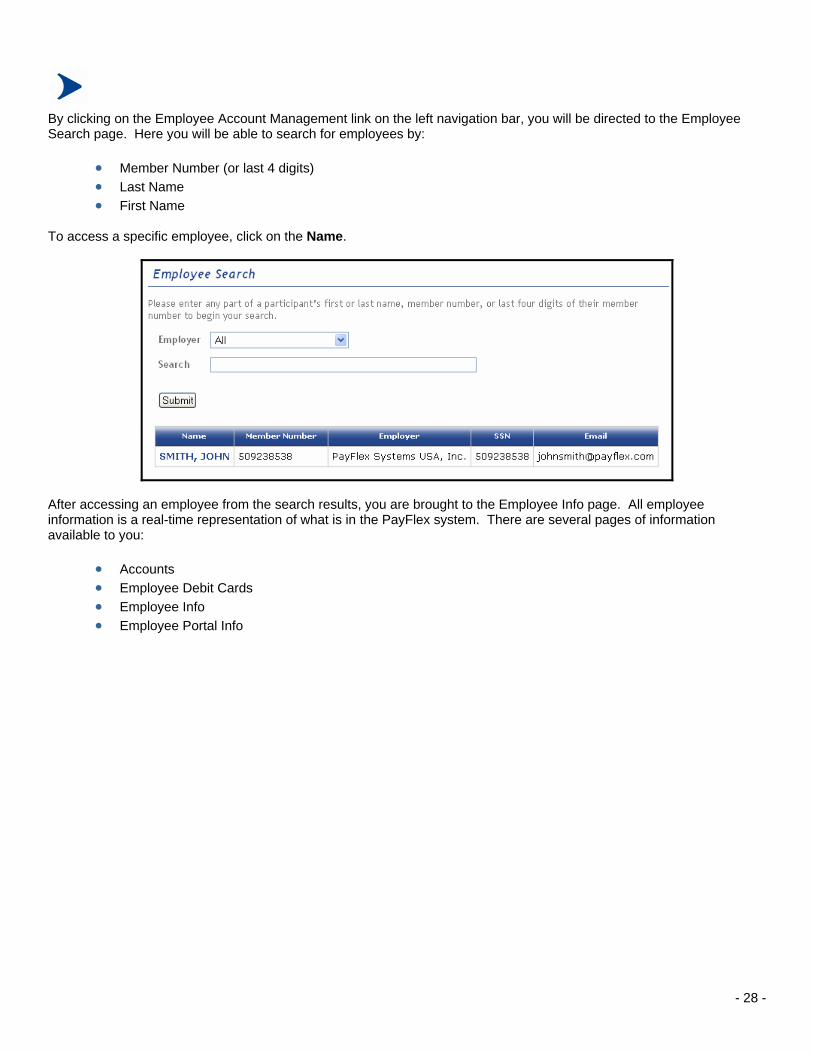
By clicking on the Employee Account Management link on the left navigation bar, you will be directed to the Employee Search page. Here you will be able to search for employees by:
• Member Number (or last 4 digits) • Last Name • First Name
To access a specific employee, click on the Name.
After accessing an employee from the search results, you are brought to the Employee Info page. All employee information is a real-time representation of what is in the PayFlex system. There are several pages of information available to you:
• Accounts • Employee Debit Cards • Employee Info • Employee Portal Info

- 29 -
Accounts Click on Accounts to view a listing of the employee’s accounts. You will be able to review account data from the current and prior plan years. To access an account, click Select and you will be directed to the Account Summary screen for the account you have selected. You can drill down further from this screen to Transactions or Claims.
Account Summary The Account Summary page displays the effective and balance information related to the account you have selected. A few key definitions of the fields are as follows:
• Effective and Expiration: dates between which the employee can incur expenses and be reimbursed from this account.
• Available Balance: the amount of money available to the employee today. For a “pay to election” account such as a Healthcare (FSA), this equals the Annual Election minus Payments. For a “pay to balance” account such as a Dependent Care account, this equals Deposits minus Payments.
• Eligible Claims: the amount of claims which have been submitted and not denied. This represents both claims which have been paid as well as claims pending payment.

- 30 -
Transactions
The Transactions page lists all Deposit or Payment transactions impacting the cash balance of the participant’s account. The running cash balance (Balance) is also displayed in the right-most column.
You can drill-down further on the Payment transactions for a listing of the claims which make up the payment by selecting the Payment Number. Claims
The claims page lists all of the claims the participant has submitted for their account. For convenience you can click on any of the column headers to sort ascending or descending. A few key definitions of the fields are as follows:
• Claim Type: the source of the claim (ie. Debit Card, Web or Manual) • Claim Amount: total amount requested by the participant • Eligible: total amount not denied by the PayFlex examiners • Last Paid Date: the last date a payment was issued for this claim as some claims are paid over multiple payments
(ie. Dependent Care claims) • Denied Reason: the reason the claim was denied

- 31 -
Employee Debit Cards The Debit Cards screen displays all debit cards issued to the employee and their dependent(s). If the Card Status is Temporarily Inactive, PayFlex has requested documentation to substantiate debit card claims and not received proper documentation within the allowed time frame. An employee can have their debit card reactivated by doing one of the following:
• Submit the required documentation • Submit eligible claims to offset the ineligible debit card claim(s) • Reimburse the Plan by writing a check to PayFlex Systems USA, Inc.
Note: A complete listing of employees with Active and Temporarily Inactive debit cards is available by clicking on Debit Cards link. Currently, you are unable to edit an employee’s card status online. Please contact your Client Services Manager with any questions. Employee Info
This screen shows basic demographic information about the employee.

- 32 -
All employee information on the Employer Services Portal is read-only. Should you notice a change is necessary, please pass the appropriate information to PayFlex for updating.
• If you maintain information via an electronic file feed process, please pass changes on the file feed. • If you maintain information manually with PayFlex, please send the changes to our Eligibility Department:
o Email: [email protected] o Fax: (402) 231-4283
Employee Portal Info The Employee Portal Info page displays information if the employee has registered their account on www.mypayflex.com. Employees can choose a Username other than their Member Number to login to the website. You can also see whether or not the employee has registered for one of our three eNotify services and the security question the employee answers when they forget their password. Although you are unable to see, access or change the participant's password, the security question will help you assist your participant if they have forgotten their password.

- 33 -
Debit Cards (Benefits Administrator)
To view a listing of the employees with Active and Temporarily Inactive debit cards, click on Debit Cards on the left navigation bar. You can sort the employee list by Active debit cards, Inactive debit cards or view all. The list will include the cardholder name, member number, last four digits of the card number, card status and status date. The status date represents the date the employee’s debit card was inactivated. PayFlex has requested documentation to substantiate debit card claims and not received proper documentation within the allowed time frame. Therefore, the employee’s debit card has been inactivated. An employee can have their debit card reactivated by doing one of the following:
• Submit the required documentation • Submit eligible claims to offset the ineligible debit card claim(s) • Reimburse the Plan by writing a check to PayFlex Systems USA, Inc.
LAST NAME, FIRST NAME XXXXXXXXX
XXXXXXXXX
XXXXXXXXX
####
####
####
LAST NAME, FIRST NAME
LAST NAME, FIRST NAME

- 34 -
Administrative Billing (Billing Administrator) To view the invoices sent to you, click on Administrative Billing on the left navigation bar. Invoices will be displayed for the previous 18 months. New invoices will appear around the 15th of each month. Your Billing contact will still be sent a copy of the invoice when it is created. By clicking on the Period Start date you can drill-down to the invoice detail. At the bottom of this page you can also download additional copies of your invoice reports:

- 35 -
Funding Register History (Funding Administrator) The Funding Register History page is an archive of funding reports previously sent to your Funding contacts. A Funding Register is created each time PayFlex pays claims for participants and requests custodial funds. The reports available here are:
• Funding Notification Report • Settlement Payment Register Report (Debit Cards) • Production Payment Register Report (Claims) • Commuter Payment Register Report (Transit Passes) • Production Deposit Register Report
The reports can be filtered by using the drop-down Document Type box or sorted by clicking on one of the column headers. You can also provide a start and end date to locate a specific report during that time period.

- 36 -
Renewal History (Benefits Administrator)
The Renewal History screen allows you to see prior renewal packets sent to you by PayFlex. You may search for a specific renewal packet by entering a start and end date or scroll down to select the renewal packet you wish download. A new renewal packet is created for you approximately 90 days prior to the end of each plan year. Your Client Services Manager will mail a copy to you; however you can also retrieve a copy from here as well.

- 37 -
Real-Time Transaction Register (Funding Administrator) The Real-Time Transaction Register page shows all cash transactions impacting your custodial cash balance with PayFlex. The types of transactions you will see on this screen are:
• Money received from you by PayFlex (Employer Funds Received) • Voided Participant Payments and Participant Refunds (Participant Adjustment) • Payments to Participants (Participant Reimbursement)
The source of the transaction is also identified:
• Production (manual/Express claim production) • Settlement (debit card claim settlement) • Manual (receipt posted manually by PayFlex’s accounting department) • Commuter (commuter transit/parking pass orders)
You may select the source as well as enter a beginning and ending date to filter the transaction data. To view your production, settlement and manual transactions by month click on the Calendar View link. Below is a sample calendar view.

- 38 -
Real-Time Transaction Register: Sample Calendar View
To view, download and print a specific register report, click on the dollar amounts shown on your calendar. You may also view the previous and following months by clicking on Previous Month OR Next Month. To go back to the original listing of reports click on Normal View.
- 39 -
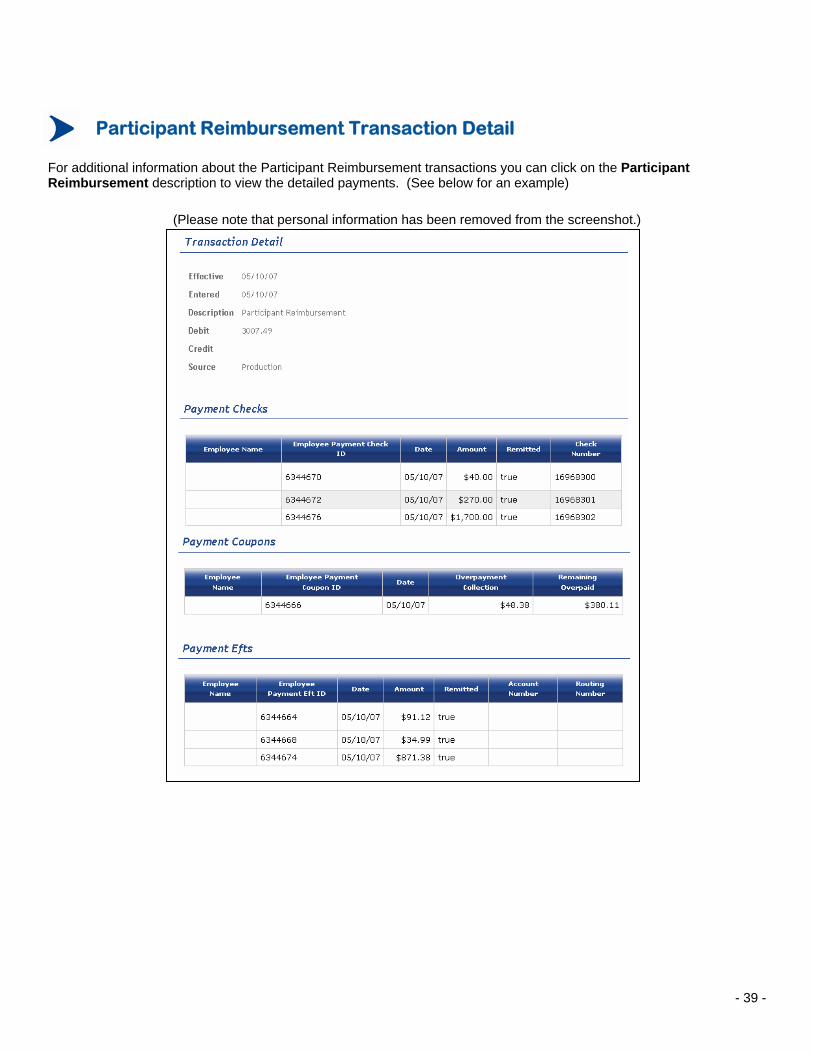
Participant Reimbursement Transaction Detail
For additional information about the Participant Reimbursement transactions you can click on the Participant Reimbursement description to view the detailed payments. (See below for an example)
(Please note that personal information has been removed from the screenshot.)

- 40 -
Plan Reporting Archive (Funding Administrator)
The Plan Reporting Archive page is an archive of reports created by PayFlex. You can download the report to your computer and open it in an appropriate application. The reports available here are:
• Deposit Summary Report • Election Report • Ledger Summary Report • Payment Summary Report • Payroll Report
The reports can be filtered by using the drop-down Document Type box or sorted by clicking on one of the column headers. You can also view a specific time period for your reports, by entering a start and end date and clicking on Apply Filter.

- 41 -
Plan Your Open Enrollment
The Communications Center now available can help you to communicate PayFlex information to your employees with our 22 Participant-Ready Communications. You can also request an open enrollment meeting as well as order your open enrollment materials.
Participant-Ready Communications Our Participant-Ready Communications are designed to be placed on your intranet, emailed as an attachment or copied into an email message for quick and easy communications to your employees. Each category shown below consists of several communications. Click on a category to view, download, copy and/or print the information.

- 42 -
Request Open Enrollment Meeting
If you are interested in having a PayFlex representative at your annual open enrollment meeting, simply go to www.payflex.com > EMPLOYERS > Employer Portal, click on the Communications Center link on the top navigation bar and select Plan Your Open Enrollment. Then select Request Open Enrollment Meeting and fill in the online form to request a meeting. Your information will be submitted to an Enrollment Specialist and you will receive a confirmation within 48 hours letting you know how we can accommodate your request.
Please note that there may be a charge associated with your meeting request. Please review your terms and conditions of your PayFlex contract or contact your Client Services Manager with any questions. We look forward to helping you grow your participation!

- 43 -
Order Open Enrollment Materials If you would like to order standard PayFlex materials for your open enrollment, go to www.payflex.com > EMPLOYERS > Employer Portal, click on the Communications Center and select Plan Your Open Enrollment. Then select Order Open Enrollment Materials and fill in the online form. Please note that we require a 10-day lead time from the date you place your order to the date you receive your materials. You are able to request FSA Brochures, Debit Card Inserts, HSA Flyers, Commuter Brochures, Forms, etc. If you have any questions about our materials, please contact your Client Services Manager or click on Education Materials in the Communications Center to view the materials online.
- 44 -

- 45 -
Enrollment/Change Information p. 46 Enrollment Form Member Number Electronic Reporting of Elections New Participants
Status Changes/Terminations Waivers Electronic Files Address Changes
Discrimination Testing p. 49
Governmental Compliance p. 50
Employer Funding Reports p. 51 Production Payment Register Report
Settlement Payment Register Report Production Deposit Register Report
Employer Plan Reports p. 52 Ledger Summary Report Payment Summary Report Deposit Summary Report Election Report Payroll Schedule Report
Administrative Service Fees
Sample Funding Reports p. 54 Production Payment Register Report
Settlement Payment Register Report Production Deposit Register Report
Sample Plan Reports p. 56 Ledger Summary Report Payment Summary Report Deposit Summary Report Election Report Payroll Schedule Report Administrative Services Fees Invoice
Sample Participant Correspondence p. 60 Request for Documentation for Purchases Explanation of Benefits (EOB)
Sample Forms p. 62 Change in Status Change in Cost or Coverage Election Change Notice Coverage Termination Notice Form Designation of Beneficiary Form Waiver Form
PayFlex Plan Administration
TABLE OF CONTENTS
- 46 -
Enrollment/Change Information
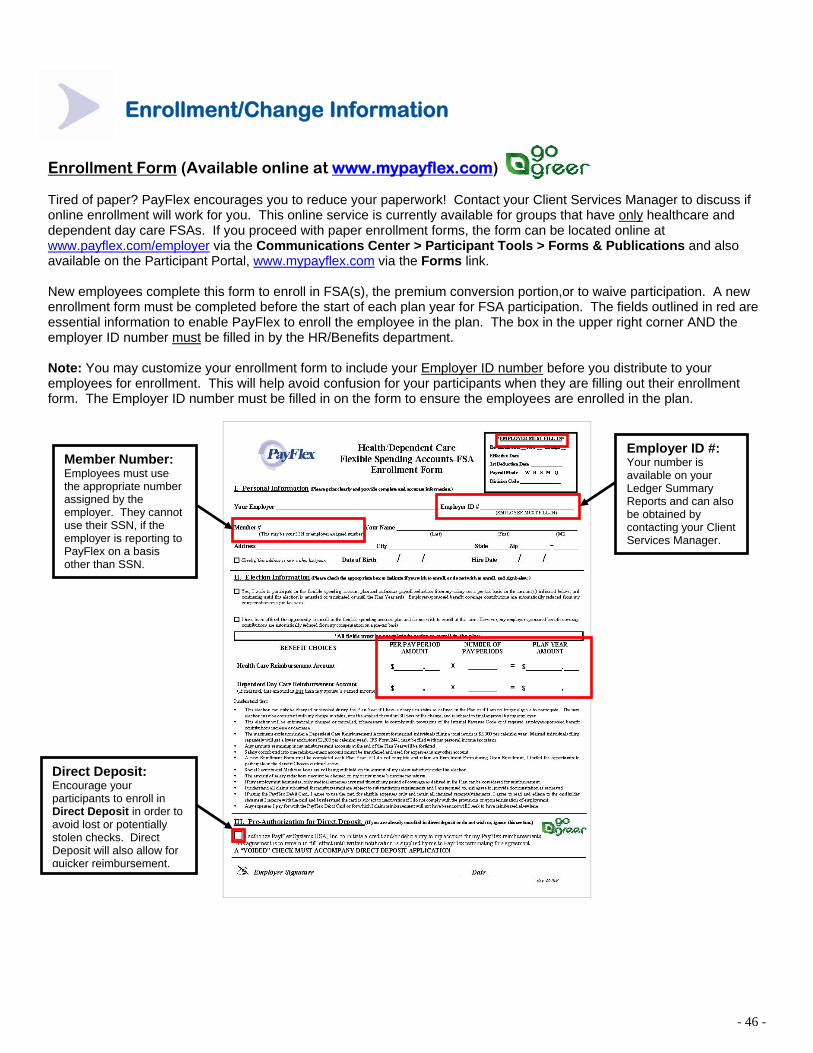
Enrollment Form (Available online at www.mypayflex.com) Tired of paper? PayFlex encourages you to reduce your paperwork! Contact your Client Services Manager to discuss if online enrollment will work for you. This online service is currently available for groups that have only healthcare and dependent day care FSAs. If you proceed with paper enrollment forms, the form can be located online at www.payflex.com/employer via the Communications Center > Participant Tools > Forms & Publications and also available on the Participant Portal, www.mypayflex.com via the Forms link. New employees complete this form to enroll in FSA(s), the premium conversion portion,or to waive participation. A new enrollment form must be completed before the start of each plan year for FSA participation. The fields outlined in red are essential information to enable PayFlex to enroll the employee in the plan. The box in the upper right corner AND the employer ID number must be filled in by the HR/Benefits department. Note: You may customize your enrollment form to include your Employer ID number before you distribute to your employees for enrollment. This will help avoid confusion for your participants when they are filling out their enrollment form. The Employer ID number must be filled in on the form to ensure the employees are enrolled in the plan.
Member Number: Employees must use the appropriate number assigned by the employer. They cannot use their SSN, if the employer is reporting to PayFlex on a basis other than SSN.
Employer ID #: Your number is available on your Ledger Summary Reports and can also be obtained by contacting your Client Services Manager.
Direct Deposit: Encourage your participants to enroll in Direct Deposit in order to avoid lost or potentially stolen checks. Direct Deposit will also allow for quicker reimbursement.

- 47 -
Enrollment/Change Information
IMPORTANT: Member Number (Employee Assigned Number or SSN) Although PayFlex can accommodate an identifying employer assigned number other than the participant’s SSN, the employer must notify participants to use that number to register their account at www.mypayflex.com, and when submitting a paper claim form to PayFlex. Participants will also need the number when utilizing our Integrated Voice Response (IVR) System and when speaking with a PayFlex customer service representative about their account. In addition, if the employer works with a third party such as their insurance carrier to send PayFlex eligibility files or claim information, the correct member number for the participants must be used. If the employer utilizes PayFlex reports or data, participant information will be reported using the member number reported to establish the account. Electronic Reporting of Elections: Using File Feeds If you have more than 50 participants, contact your Client Services Manager to learn more about electronically sending your enrollment information to PayFlex. The process is easy and secure. This information is sent directly from your payroll and/or HR records ensuring that the name, employee member number and election amounts agree with your records. New Participants New participants are to complete the Enrollment Form at the time of enrollment into the plan. If the information is not sent to PayFlex via electronic format, the employer must complete the box in the upper right hand corner of the form and send to PayFlex. A copy of the completed Enrollment Form should be sent to PayFlex for only those employees who enroll in the FSA(s). New PayFlex Debit Cards will be received within 15-20 business days following PayFlex's receipt of the enrollment information. If the participant is re-enrolling, the prior debit card will automatically renew for up to three (3) years. The Designation of Beneficiary Form may be completed only if the employee wishes to name a beneficiary other than what is specified in the Plan Document. A sample form is available in the Sample Forms section. Status Changes/Terminations Mid-year election changes, additions and terminations must be reported to PayFlex in a timely manner in order to avoid the overpayment of claims and to ensure accurate processing. Send to [email protected] or fax to 401-231-4283 attention Eligibility Department. A participant requesting to change or revoke prior elections due to a change in status should complete a Request for Change in Election Form and a new Enrollment Form which should be retained by the employer. The employer must approve or deny the change. If approved, employer must complete the Election Change Notice Form and send to PayFlex for processing. A participant who is terminating coverage must be listed on the Coverage Termination Notice Form, which is then sent to PayFlex for processing. The employer should inform those participants who have a PayFlex Debit Card that the card is inactivated upon termination of employment. Terminated participants who were in the health FSA or those who lose coverage may be eligible for COBRA continuation. If your health FSA is subject to HIPAA, terminated participants or participants who do not renew their election each year should be provided a HIPAA certificate.

- 48 -
Enrollment/Change Information
Waivers If an employee chooses not to participate in the premium conversion portion of the plan for their insurance/benefit coverage premium contribution, depending on the plan document he or she must complete a Participation Waiver Form. This Form is for the employer’s records only. Do not submit it to PayFlex.
Electronic Files If you are transmitting or wish to transmit enrollment and/or payroll deduction information via electronic file, please contact us for file specifications. All electronic files need to be sent to [email protected] or transmitted through FTP. Address Changes For security reasons, the employer is responsible for reporting all employee address changes to PayFlex. This may be done by completing Section I of the Enrollment Form and marking it as “address change only”, or the employer may email the information to [email protected] or fax the change to 402-231-4283, attention Eligibility Department.

- 49 -
Discrimination Testing
PayFlex offers discrimination testing for the health care and dependent care reimbursement accounts for which we provide administration services. However, it remains the Plan Administrator's (employer's) responsibility to provide PayFlex highly compensated and key employee information, review the tests and complete the remaining tests for the entire cafeteria plan by adding Section 125 premium dollars and perform other tests as may be needed. General Information Regarding Testing: The nondiscrimination rules for IRC Section 125 plans examine the following:
• Eligibility - Who is eligible to participate? • Contributions and Benefits - What can participants elect? • Concentrations of Benefits - How much do key employees receive?
Benefits offered under an IRC Section 125 plan must also meet the nondiscrimination rules that apply to those specific benefits:
• Section 105(h) - Self-insured medical reimbursement plans, includes health care flexible spending accounts (FSAs) and health reimbursement arrangements (HRAs)
• Section 129 - Dependent care assistance plans • Section 79 - Group term life plans (if offered) • Section 137 – Adoption assistance plans (if offered)
The prohibited group (those in whose favor the plan cannot discriminate) is different depending on the particular test being applied. In some cases the prohibited group is defined as highly compensated individuals, and in other cases it is defined as key employees. Generally, employees of controlled or affiliated employers are treated as being employed by one employer. In addition, certain leased employees may be counted as employees. It is prudent to monitor the plan and test throughout the plan year if there have been changes that might affect the initial testing results. If the plan is found to be discriminatory during the plan year, corrective action should be taken to bring the plan into compliance. This corrective action must be taken before the end of the plan year.

- 50 -
Governmental Compliance
W-2 Reporting
Wages, tips, and other compensation should exclude any salary reduction amounts. Salary reduction amounts are pretax premium contributions for payment of insurance benefits and Medical or Dependent Care spending account election amounts. Employers are required to report the total amount of Dependent Care benefits for the participant for the calendar year on Form W-2. The amount reported should be the total Dependent Care salary reductions plus any employer credits, regardless of the amount of actual paid claims. Medical Care benefits are not reported as a separate item. Individual employees who have Dependent Care Expenses must file Form 2441 – Child and Dependent Care Expenses along with Form 1040. Form 2441 is available online at www.mypayflex.com. Form 5500 Reporting Employers are required to file Annual Report Form 5500 for welfare benefit plans subject to ERISA. Health flexible spending accounts are considered a welfare plan and are required to file if there are 100 or more participants. However, some government or church groups are exempt from this filing. Please refer to Instructions for Form 5500 for more details. PayFlex can assist employers with this filing requirement if needed. Plan Document/Summary Plan Description PayFlex drafts one copy of the Plan Document and Summary Plan Description to help you initially establish or amend a plan. It is not our intent to act as attorney or accountant regarding these documents. Therefore, you may wish to have your legal counsel review the documents and address any questions you may have. As the IRS code is further clarified and amended, we will keep you informed of these changes, draft amendments and provide notices to keep your plan up to date. Privacy Policy We value your relationship with us, and we know that respect for your privacy is a foundation of that relationship. As a commitment to this foundation, it is our policy not to disclose the information you share with us. Furthermore, we strive to safeguard this information in order to protect your right to privacy and we will continue to review our policies and practices aimed at maintaining the security and confidentiality of our clients’ personal information. PayFlex is required by law to inform its clients of its policies regarding the privacy of client information. Our privacy policy derives from basic principles of trust, ethics and integrity. We use information to provide quality customer service and value. Please refer to www.mypayflex.com for our complete Privacy Notice.

- 51 -
Employer Funding Reports
Funding Reports Funding Reports are sent to the employer’s Funding contacts every time participant payments are generated. Every set of reports includes a Funding Notification Report. This is a voucher-style report which lists the total amount disbursed to participants and provides funding instructions. All Funding Reports are available on the Employer Services Portal under Funding Register History. The Funding Notification Report is also accompanied by one of the following register reports in both PDF and CSV formats. Each register report is broken down by account and plan year. Division/department breakdown is listed if provided. Generally reports are available by 12:00PM CT. If the reports have not arrived by this time but there are still remittances to be funded, funding will be postponed by 1 business day.
Production Payment Register Report
A detailed list of all payments issued to participants for claims adjudicated by PayFlex’s claim examiners. This includes claims submitted by fax, mail and via www.mypayflex.com using Express Claims. Payment adjustments such as Grace Period Adjustments, Refunds (for ineligible debt card transactions) and Voided Checks are also included on this report. These reports are sent each day remittances are created.
Settlement Payment Register Report
A detailed listing of all debit card sale and return transactions settled for participants. These reports are sent each day of the week debit card transactions are settled, including Saturday.
Production Deposit Register Report
A detailed listing of all deposits posted to participant accounts which require funding. These reports are sent each time deposits are posted for a payroll period.

- 52 -
Employer Plan Reports
Plan Reports Plan reports are sent to the employer’s Reporting contacts periodically (ie. Weekly, Monthly, Quarterly). Delivery of scheduled reports is the first day following the close of the calendar reporting period. For example, the August monthly reports arrive on September 1st. Reports can be sent via email, fax or retrieved from the Employer Services Portal, Division/department breakdown is listed if provided.
Ledger Summary Report
Available periodically, this report summarizes the participants’ deposits, payments and balances by account for the reporting period and YTD. It is the employer’s responsibility to review this report and notify us of any discrepancies immediately. Special attention should be given to “Termed” column in addition to the “YTD Deposits” column, as this should agree with payroll deductions. The employer is responsible for reconciling any discrepancies. Formats: CSV and PDF
Payment Summary Report
Available periodically, this report details all payment and payment adjustment transactions posted to participant accounts with an effective date within the reporting period. Transactions are broken down by source (ie. Production and Settlement). Adjustments such as refunds and grace period adjustments are also included. This report will tie to the Payments field on the Ledger Summary Report for the same period. Formats: CSV and PDF Deposit Summary Report
Available periodically, this report details all deposit and deposit adjustment transactions posted to participant accounts with an effective date within the reporting period. This report will tie to the Deposits field on the Ledger Summary Report for the same period. Formats: CSV and PDF Election Report
This report is provided at renewal time, detailing participant elections, scheduled payroll deductions and any employer contributions by account for the plan year. Formats: CSV and PDF Payroll Schedule Report
This report is provided at renewal time, detailing all of the payroll dates for the upcoming plan year for each payroll schedule. Format: PDF

- 53 -
Employer Plan Reports (continued)
Administrative Service Fees An Invoice for the Administrative Service Fees are processed and mailed by the 15th of each month. Changes, additions, or terminations must be submitted to PayFlex by the 5th of each month to be effective for that billing cycle. Any notifications received after the 6th of the month will appear on the next billing invoice. Participants billed for are those in an active status and for those participating who have termed within the past three billing cycles who have an available balance of $10 or more. Debit card fees are applied to those participants in an active status. Initial set-up fees and renewal fees are billed the first month of each new plan year. It is important that the employer pay as billed. Do not make adjustments. Please pay as billed. If adjustments are necessary, be sure to submit all appropriate documentation to your Client Services Manager. Appropriate documentation consists of one or more of the following forms: Coverage Termination Notice Form, Change in Election Form, New Enrollment Form. Adjustments will then be made on a subsequent billing invoice. **Make checks payable to PayFlex Systems USA, Inc. and send to: PayFlex Systems USA, Inc. Accounting Department P.O. Box 3039 Omaha, NE 68103-3039

- 54 -
Sample Funding Reports
Production Payment Register Report (PDF FORMAT)
Plan Year: 01/01/06 MEMBER # LAST NAME FIRST NAME MI PMT # PMT DATE PMT AMT TOTALS Dependent Care
Employee Account Payment XXX-XX-XXXX LAST NAME FIRST NAME MI 2082236 01/12/07 $223.92 XXX-XX-XXXX LAST NAME FIRST NAME MI 2082228 01/12/07 $90.00 EAP Total: $313.92Healthcare (FSA) Dependent Care Total: $313.92
Employee Account Payment XXX-XX-XXXX LAST NAME FIRST NAME MI 2082234 01/12/07 $143.80 XXX-XX-XXXX LAST NAME FIRST NAME MI 16799701 01/12/07 $128.39 XXX-XX-XXXX LAST NAME FIRST NAME MI 16799700 01/12/07 $210.07 EAP Total: $481.86 Healthcare (FSA) Total: $481.86 Plan Year Total: $795.78Plan Year: 01/01/07 Healthcare (FSA) Employee Account Payment XXX-XX-XXXX LAST NAME FIRST NAME MI 16888733 3/15/2007 $116.02
XXX-XX-XXXX LAST NAME FIRST NAME MI 16828268 2/7/2007 $126.00
XXX-XX-XXXX LAST NAME FIRST NAME MI 16836903 2/13/2007 $84.00
XXX-XX-XXXX LAST NAME FIRST NAME MI 16856836 2/23/2007 $214.00
XXX-XX-XXXX LAST NAME FIRST NAME MI 16856836 4/25/2007 $90.00
XXX-XX-XXXX LAST NAME FIRST NAME MI 16888732 3/15/2007 $30.00 EAP Total: $660.02 Healthcare (FSA) Total: $660.02 Plan Year Total: $660.02
NET AMOUNT FOR <Company Name>: $1455.80
EMPLOYER SUMMARY
Plan Year: 01/01/06 Checks Direct Deps Payments Voids Adjustments Net Amount Dependent Care $0.00 313.92 313.92 0.00 0.00 313.92 Healthcare (FSA) $338.46 143.40 481.86 0.00 0.00 481.86 338.46 457.32 795.78 0.00 0.00 795.78 Plan Year: 01/01/07 Healthcare (FSA) 501.62 158.40 660.02 0.00 0.00 660.02 501.62 158.40 660.02 0.00 0.00 660.02 Plan Year: ALL Dependent Care $0.00 313.92 313.92 0.00 0.00 313.92 Healthcare (FSA) 840.08 301.80 1141.88 0.00 0.00 1141.88 840.08 615.72 1455.80 0.00 0.00 1455.80

- 55 -
Sample Funding Reports (continued)
Settlement Payment Register Report (PDF FORMAT)
Plan Year: 01/01/07 MEMBER # LAST NAME FIRST NAME MI PMT # PMT DATE PMT AMT TOTALS Healthcare (FSA) Employee Account Payment XXX-XX-XXXX LAST NAME FIRST NAME MI 13919196 10/25/07 $3.67 XXX-XX-XXXX LAST NAME FIRST NAME MI 13919186 10/25/07 $5.00 XXX-XX-XXXX LAST NAME FIRST NAME MI 13919188 10/25/07 $10.00 XXX-XX-XXXX LAST NAME FIRST NAME MI 13919190 10/25/07 $74.84
XXX-XX-XXXX LAST NAME FIRST NAME MI 13919192 10/25/07 $57.86 XXX-XX-XXXX LAST NAME FIRST NAME MI 13919194 10/25/07 $40.00 EAP Total: $191.37 Healthcare (FSA) Total: $191.37 Plan Year Total: $191.37
NET AMOUNT for <Company Name>: $191.37
Production Deposit Register Report (PDF FORMAT)
Plan Year: 01/01/07 MEMBER # LAST NAME FIRST NAME MI DEP DATE DEP AMT TOTALS Dependent Care Employee Account Deposit XXX-XX-XXXX LAST NAME FIRST NAME MI 6/29/2007 $76.93 XXX-XX-XXXX LAST NAME FIRST NAME MI 6/29/2007 $145.46 XXX-XX-XXXX LAST NAME FIRST NAME MI 6/29/2007 $192.31 XXX-XX-XXXX LAST NAME FIRST NAME MI 6/29/2007 $115.39
XXX-XX-XXXX LAST NAME FIRST NAME MI 6/29/2007 $192.31 XXX-XX-XXXX LAST NAME FIRST NAME MI 6/29/2007 $69.24 EAD Total: 791.64 Dependent Care Total: 791.64 Plan Year Total: 791.64

- 56 -
Sample Plan Reports
Ledger Summary Report (PDF FORMAT) EMPLOYER: XXXXX - <Company Name> PLAN YEAR: 01/01/07 REPORT CREATED: 11/01/07 REPORTING PERIOD: 01/01/07- 10/31/07
MEMBER NUMBER EMPLOYEE ACCOUNT TYPE STATUS STATUS
DATE DEPOSITS (PERIOD)
PAYMENTS(PERIOD)
CHANGE IN CASH
BALANCEDEPOSITS
(YTD) PAYMENTS
(YTD) CASH
BALANCEANNUAL
ELECTIONREMAININGELECTION
XXX-XX-XXXX LAST NAME, FIRST Healthcare (FSA) $400.00 $116.02 $283.98 $400.00 $116.02 $283.98 $480.00 $363.98
XXX-XX-XXXX LAST NAME, FIRST Healthcare (FSA) $700.00 $544.00 $156.00 $700.00 $544.00 $156.00 $840.00 $296.00
XXX-XX-XXXX LAST NAME, FIRST Healthcare (FSA) $1600.00 $1642.68 ($42.68) $1600.00 $1642.68 ($42.68) $1920.00 $277.32
XXX-XX-XXXX LAST NAME, FIRST Healthcare (FSA) $1500.00 $0.00 $1500.00 $1500.00 $0.00 $1500.00 $1800.00 $1800.00
(PAGE 1)
PLAN YEAR 01/01/07 SUMMARY
PLAN TOTAL PARTICIPANTS TOTAL DEPOSITS
(PERIOD)
TOTAL PAYMENTS
PERIOD
TOTAL CHANGE IN
CASH BALANCES
TOTAL DEPOSITS
(YTD)
TOTAL PAYMENTS (PERIOD)
TOTAL CASH
BALANCES
TOTAL ANNUAL
ELECTIONS
TOTAL REMAINING ELECTIONS
Healthcare (FSA) 4 $4200.00 $2302.70 $1897.30 $4200.00 $2302.70 $1897.30 $5040.00 $2737.30
PLAN YEAR TOTALS: 4 $4200.00 $2302.70 $1897.30 $4200.00 $2302.70 $20.00 $100.00 $100.00
(PAGE 2)
Payment Summary Report (CSV FORMAT)
Report Created
Reporting Period Employer ID Employer
Division Code
Member Number Last Name First Name MI Amount Account Type Source Date Amount
Adjustment Reason
11/2/2007 [01/01/07-10/31/07 XXXXX
Company Name
XXX-XX-XXXX LAST NAME FIRST NAME MI $149.40 Healthcare (FSA) Production 8/15/07 $45.00
11/2/2007 [01/01/07-10/31/07 XXXXX
Company Name
XXX-XX-XXXX LAST NAME FIRST NAME MI $10.00 Healthcare (FSA) Production 8/15/07 $7.91
11/2/2007 [01/01/07-10/31/07 XXXXX
Company Name
XXX-XX-XXXX LAST NAME FIRST NAME MI $30.00 Healthcare (FSA) Production 8/15/07 $56.00
11/2/2007 [01/01/07-10/31/07 XXXXX
Company Name
XXX-XX-XXXX LAST NAME FIRST NAME MI $15.00 Healthcare (FSA) Production 8/15/07 $9.92
11/2/2007 [01/01/07-10/31/07 XXXXX
Company Name
XXX-XX-XXXX LAST NAME FIRST NAME MI $20.00 Healthcare (FSA) Production 8/15/07 $5.40
Deposit Summary Report (CSV FORMAT)
Report
Created Reporting
Period Employer ID Employer Division Code
Member Number Last Name First Name MI
Plan Year Account Type Type Date Amount
11/2/2007 [01/01/07-10/31/07 XXXXX
Company Name
XXX-XX-XXXX LAST NAME FIRST NAME MI 1/1/07 Healthcare (FSA)
Payroll Deduction 10/31/07 $20.00
11/2/2007 [01/01/07-10/31/07 XXXXX
Company Name
XXX-XX-XXXX LAST NAME FIRST NAME MI 1/1/07 Healthcare (FSA)
Payroll Deduction 1/31/07 $20.00
11/2/2007 [01/01/07-10/31/07 XXXXX
Company Name
XXX-XX-XXXX LAST NAME FIRST NAME MI 1/1/07 Healthcare (FSA)
Payroll Deduction 2/15/07 $20.00
11/2/2007 [01/01/07-10/31/07 XXXXX
Company Name
XXX-XX-XXXX LAST NAME FIRST NAME MI 1/1/07 Healthcare (FSA)
Payroll Deduction 2/28/07 $20.00
11/2/2007 [01/01/07-10/31/07 XXXXX
Company Name
XXX-XX-XXXX LAST NAME FIRST NAME MI 1/1/07 Healthcare (FSA)
Payroll Deduction 3/7/07 $20.00
- 57 -
Sample Plan Reports (continued)
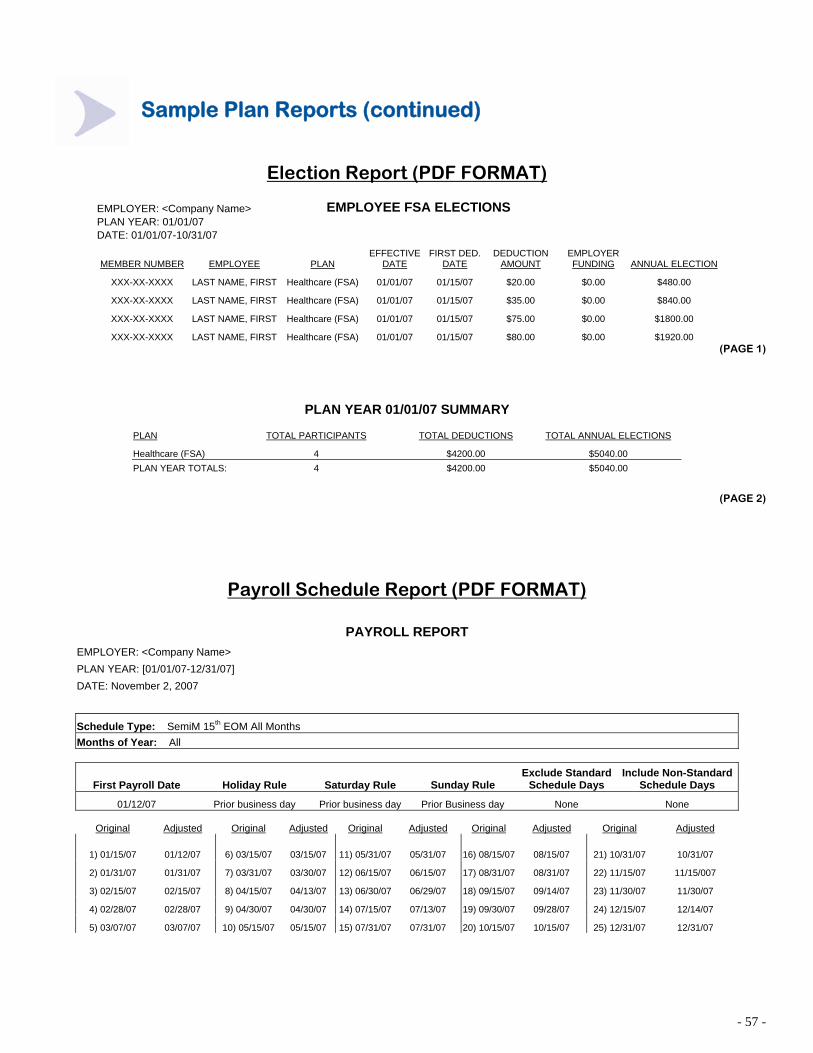
Election Report (PDF FORMAT)
EMPLOYER: <Company Name> EMPLOYEE FSA ELECTIONS PLAN YEAR: 01/01/07 DATE: 01/01/07-10/31/07
MEMBER NUMBER EMPLOYEE PLAN EFFECTIVE
DATE FIRST DED.
DATE DEDUCTION
AMOUNT EMPLOYER FUNDING ANNUAL ELECTION
XXX-XX-XXXX LAST NAME, FIRST Healthcare (FSA) 01/01/07 01/15/07 $20.00 $0.00 $480.00
XXX-XX-XXXX LAST NAME, FIRST Healthcare (FSA) 01/01/07 01/15/07 $35.00 $0.00 $840.00
XXX-XX-XXXX LAST NAME, FIRST Healthcare (FSA) 01/01/07 01/15/07 $75.00 $0.00 $1800.00
XXX-XX-XXXX LAST NAME, FIRST Healthcare (FSA) 01/01/07 01/15/07 $80.00 $0.00 $1920.00 (PAGE 1)
PLAN YEAR 01/01/07 SUMMARY
PLAN TOTAL PARTICIPANTS TOTAL DEDUCTIONS TOTAL ANNUAL ELECTIONS
Healthcare (FSA) 4 $4200.00 $5040.00 PLAN YEAR TOTALS: 4 $4200.00 $5040.00
(PAGE 2)
Payroll Schedule Report (PDF FORMAT)
PAYROLL REPORT EMPLOYER: <Company Name> PLAN YEAR: [01/01/07-12/31/07] DATE: November 2, 2007
Schedule Type: SemiM 15th EOM All Months Months of Year: All
First Payroll Date Holiday Rule Saturday Rule Sunday Rule Exclude Standard
Schedule Days Include Non-Standard
Schedule Days
01/12/07 Prior business day Prior business day Prior Business day None None
Original Adjusted Original Adjusted Original Adjusted Original Adjusted Original Adjusted
1) 01/15/07 01/12/07 6) 03/15/07 03/15/07 11) 05/31/07 05/31/07 16) 08/15/07 08/15/07 21) 10/31/07 10/31/07
2) 01/31/07 01/31/07 7) 03/31/07 03/30/07 12) 06/15/07 06/15/07 17) 08/31/07 08/31/07 22) 11/15/07 11/15/007
3) 02/15/07 02/15/07 8) 04/15/07 04/13/07 13) 06/30/07 06/29/07 18) 09/15/07 09/14/07 23) 11/30/07 11/30/07
4) 02/28/07 02/28/07 9) 04/30/07 04/30/07 14) 07/15/07 07/13/07 19) 09/30/07 09/28/07 24) 12/15/07 12/14/07
5) 03/07/07 03/07/07 10) 05/15/07 05/15/07 15) 07/31/07 07/31/07 20) 10/15/07 10/15/07 25) 12/31/07 12/31/07

- 58 -
FACSIMILE TRANSMISSION TO: ABC COMPANY John Smith FAX #: (123) 456-7890 FROM: PAYFLEX SYSTEMS USA, INC. FAX #: 1-402-231-4310 RE: ADMINISTRATIVE SERVICE FEES INVOICE NUMBER: PAYFLEX0311 INVOICE REFLECTS CHARGES FOR THE PERIOD: 11/01/03 -- 11/30/2003
Total Admin Fee: (22 Participating @ $4.95) $108.90 Total Debit Card Fee: (21 Participating @ $1.50) $31.50 TOTAL AMOUNT DUE: $140.40 Total Adds/Terms: (1 Add(s), 1 Term(s)) $4.95 Adjustments: $560.00 ADJUSTED AMOUNT DUE: $705.35 NOTE: Renewal Fees: $500 + $2 x 30 eligibles. The information contained in this facsimile message and the documents accompanying this facsimile message may contain information that is privileged and confidential intended for the use of the individual or entity named above. If the reader of this message is not the intended recipients or the employee or agent responsible to deliver it to the intended recipient, you are hereby notified that any dissemination, distribution or copying or this communication is strictly prohibited. If you have received this facsimile in error, please immediately notify us by telephone and return the original transmission to us at the above address via the US Postal Service.
Sample Report: Admin Fees Invoice

- 59 -
ABC COMPANY PAYMENT FOR BILLING PERIOD:11/01/03 -- 11/30/2003 TOTAL AMOUNT DUE: $705.35 (see note above) TOTAL AMOUNT PAID:
PAYMENT TERMS: NET 10 DAYS
PLEASE DETACH AND RETURN TOP PORTION WITH PAYMENT ABC COMPANY ROSTER
XXX-XX-XXXX LAST NAME FIRST NAME XXX-XX-XXXX LAST NAME FIRST NAME XXX-XX-XXXX LAST NAME FIRST NAME XXX-XX-XXXX LAST NAME FIRST NAME XXX-XX-XXXX LAST NAME FIRST NAME XXX-XX-XXXX LAST NAME FIRST NAME XXX-XX-XXXX LAST NAME FIRST NAME XXX-XX-XXXX LAST NAME FIRST NAME XXX-XX-XXXX LAST NAME FIRST NAME XXX-XX-XXXX LAST NAME FIRST NAME XXX-XX-XXXX LAST NAME FIRST NAME XXX-XX-XXXX LAST NAME FIRST NAME XXX-XX-XXXX LAST NAME FIRST NAME XXX-XX-XXXX LAST NAME FIRST NAME XXX-XX-XXXX LAST NAME FIRST NAME XXX-XX-XXXX LAST NAME FIRST NAME XXX-XX-XXXX LAST NAME FIRST NAME XXX-XX-XXXX LAST NAME FIRST NAME XXX-XX-XXXX LAST NAME FIRST NAME XXX-XX-XXXX LAST NAME FIRST NAME XXX-XX-XXXX LAST NAME FIRST NAME # Participating: 21 Adds XXX-XX-XXXX LAST NAME FIRST NAME Add @ 1 Month(s): $4.95 # Add: 1 $4.95 Terms XXX-XX-XXXX LAST NAME FIRST NAME Term @ 0 Month(s): $0.00 # Term: 1 $0.00
# Active Employees: 22 Adds/Terms Adjustment: # Termed Employees: 1 $0.00
Sample Report: Admin Service Fees

- 60 -
Request for Documentation for Purchases Made Using Your Flex Card- First Notice
Your Immediate Action Will Ensure Your Card Remains Active
PayFlex Systems USA, Inc. Flex Dept. P.O. Box 3039 Omaha, NE 68103-3039
Date: mm/dd/yy
NAME Document ID: XXXXXXX ADDRESS Employee ID: XXXXXX CITY, STATE, ZIP Employer Name: COMPANY NAME
Dear NAME:
In order to determine the eligibility of each transaction listed below in accordance with IRS guidelines, we are requesting that you please respond to the following:
1. Send an itemized statement for each listed transaction. An itemized statement includes the provider name, service date, service or product description and amount. This may be an Explanation of Benefits (EOB) statement from your insurance company or a detailed cash register receipt. If the expenses on the itemized receipt are not covered by insurance, please note this on the receipt. Credit card statements or non-itemized receipts are not acceptable documentation. The only information we have is the summary listed below, which does not provide the date that the service was performed and the description (type) of service or items purchased with your Flex Card.
2. Include a copy of this letter. 3. Return the requested documentation within 21 days of the date of this letter to ensure that your Flex Card remains active.
Purchases that require documentation: Date Merchant Amount Account
If you discover that an item was not eligible or you are unable to obtain an itemized statement, you must do one of the following within 21 days of the date of this letter to ensure your PayFlex Debit Card remains active:
1. Submit itemized documentation for any other eligible expenses along with a copy of this letter. We will apply those expenses to the ineligible amount and process any remaining expenses as a reimbursement to you. Your submission certifies that: a) you have not yet been reimbursed, b) you will not seek reimbursement elsewhere, and c) the eligible expenses were incurred by you, your spouse or eligible dependent for medical not cosmetic conditions; or
2. Send a personal check or money order payable to PayFlex along with a copy of this letter in the amount of the ineligible expense. DO NOT SEND CASH.
If you have any questions regarding this notice, call PayFlex at (402) 345-0666 or go to our website at www.mypayflex.com. From our website, please follow the “Frequent Questions” and “Eligible Expenses” links for detailed information.
Thank you for participating in your employer’s flexible spending account benefit plan.
mm/dd/yy MERCHANT NAME $91.40 Healthcare (FSA)
If not currently receiving notice via e-mail but would like to, click on the My Info link on the left hand side, and make your selection.
Sample Correspondence: Request for Documentation for Purchases
FAX this letter as your cover sheet MAIL a copy of this letter and the requested
and the requested documentation to: OR documentation to:
FAX: (402) 231-4303 Page 1 of ____ Mail: PayFlex Systems USA, Inc., Flex Dept.,
P.O. Box 3039, Omaha, NE 68103-3039

- 61 -
Sample Correspondence: Explanation of Benefits from PayFlex

- 62 -
REQUEST FOR CHANGE IN ELECTION FORM CHANGE IN STATUS You may request a change in your election to revoke the existing plan election and make a new election for the remainder of the current plan year . Complete Sections 1, 2 and 3 and submit to the HR Department within 30 days of the change in your status. The HR department will review your request and make a determination as to whether the request is appropriate. SECTION 1 Check one of the following change-in-status events that you have experienced:
ο Change in legal marital status (marriage, divorce, annulment, legal separation, death of spouse) ο Change in number of tax dependents (birth, adoption, placement for adoption, death) ο Change in employment status that affects eligibility (termination or commencement of employment; reduction or increase in hours worked
by you, your spouse or your dependent; changing from part-time to full-time or vice versa; strike or lockout; taking of or returning from unpaid leave of absence; change in worksite)
ο Change in dependent eligibility requirements (reaches limiting age, loses or gains student status, marriage) ο Change in residence of you, your spouse or your dependent that affects eligibility (moving in or out of HMO area) Other Changes
ο HIPAA Special Enrollment ο Judgment, Decree, Order ο Medicare/Medicaid Eligibility Change ο COBRA Event Date of the Change in Status event checked above: Note: You may be required to submit appropriate documentation to verify the event. SECTION 2 Please explain below the election change you wish to make. Also explain why your requested change is consistent with your status change. An election change is consistent only if there has been a change affecting eligibility and if the election change is necessary or appropriate as a result of the status change event. ________________________________________________________________________________________________________________________
SECTION 3 I have read and fully understand the regulations to change my election. I understand that my new Agreement Form and this Change in Status Form must be completed within 30 days of the change in status event, and the election change I have requested must be consistent with the change in status event. I understand any election change will be effective on the later of the date of the change in status, or on the date I request the election change. I certify that the above information is true and correct, and agree to provide any necessary third-party documentation to verify the change in status event. __________________________________________________ Employee Signature ________________________________________________ Date Employee Social Security Number Employer
Employer Use Only
Eff. Date Eff. Deduction Date Employer Employer Representative Date

- 63 -
REQUEST FOR CHANGE IN ELECTION FORM CHANGE IN COST OR COVERAGE You may request a change in your election to revoke the existing plan election and make a new election for the remainder of the current plan year. Changes in cost or coverage do not allow changes to a health flexible spending account. Complete Sections 1, 2 and 3 and submit to the HR Department within 30 days of the change in your status. The HR department will review your request and make a determination as to whether the request is appropriate. SECTION 1 Check one of the following changes in cost/coverage events that you have experienced: ο Significant cost increase in your or your dependent’s coverage ο Significant curtailment of your or your dependent’s coverage ο Addition or elimination of benefit package option under your or your dependent’s Employer’s plan ο Change in coverage or open enrollment of spouse or dependent under other Employer’s plan ο Change in cost of daycare by provider who is not a relative by blood or marriage ο Change in daycare provider Date of the Change in cost/coverage event checked above: ____________________________________________________ Note: You may be required to submit appropriate documentation to verify the event. SECTION 2 Please explain below the election change that you wish to make. Also explain why your requested change is consistent with your status change. An election change is consistent only if the election change is necessary or appropriate as a result of the event. ________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________ SECTION 3 I have read and fully understand the regulations to change my election. I understand that my new Agreement Form and this Change in Status Form must be completed within 30 days of the change in cost/coverage event, and the election change I have requested must be consistent with the change in cost/coverage event. I understand any election change will be effective on the later of the date of the change in cost/coverage or on the date I request the election change. I certify that the above information is true and correct, and agree to provide any necessary third-party documentation to verify the change in cost/coverage event. __________________________________________________ Employee Signature __________________________________________________ Date Employee Social Security Number Employer
Employer Use Only
Eff. Date Eff. Deduction Date Employer Employer Representative Date

- 64 -
PAYFLEX REIMBURSMENT ACCOUNT ELECTION CHANGE NOTICE
Participant Name: ___________________________________________________ (FIRST) (MI) (LAST) Member Number: _________________________
Changes made to PayFlex Account Health Care FSA
Dependent Care FSA
Parking/Transit Account
YTD Payroll Contributions prior to change
Total contributions from change effective date through end of plan year
New Annual Election
# of Payrolls Remaining
New Per Payroll Deduction Amount
First Payroll Date of New Election
Company Name: _______________________________________________ Date: ___________ Employer Representative: ________________________________________ Representative Signature: ________________________________________ Employer Phone Number: ________________________________________
Send to: PayFlex Eligibility Dept. P.O. Box 3039 Omaha, NE 68103-3039
Fax to: (402) 231-4283 Email to: [email protected] Page 1 of ______

- 65 -
PAYFLEX FSA ACCOUNT
COVERAGE TERMINATION NOTICE FORM
(If applicable, the PayFlex Debit Card is inactivated upon termination of employment)
Name Member Number
Employment Termination
Date
Coverage Termination
Date
Last Date of Payroll
Contribution
Final YTD Payroll
Contributions Employer: _________________________________Date_________________ Employer Signature: _______________________________________________ Telephone: ______________________________________________________
Fax to: (402) 231-4283 Email to: [email protected] Page 1 of ________
Send to: PayFlex Eligibility Dept. P.O. Box 3039 Omaha, NE 68103-3039

- 66 -
Employer ___________________________________ FSA Plan
DESIGNATION OF BENEFICIARY FORM
(To be completed for reimbursement accounts only)
Name (Please Print): ______________________________________________ ______/______/______ First, M.I., Last Social Security Number
In the event of my death, I hereby designate the following to continue receiving any remaining elected benefits in my reimbursement accounts for any of my remaining eligible expenses or the eligible expenses of my tax dependents that are incurred during my period of coverage as stated in the plan documentation.
Beneficiary Designation
___________________________________________________________________________________________________
(Name) (Relationship) ___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
Information Concerning Primary Beneficiary
_________________________________________________ ______________________________________________
(Street Address) (Social Security Number)
_________________________________________________ ______________________________________________ (City, State, Zip Code) (Date of Birth) Unless I have a Designation of Beneficiary in effect at the time an amount becomes payable to my Beneficiary, that amount will be paid to my spouse. If I do not have a surviving spouse, my children shall share equally as Beneficiaries.
This Designation is intended to replace all prior designations made by me for such amounts. I reserve the right to change any Beneficiary named herein without the consent of such Beneficiary by properly completing and delivering to the Plan’s Administrator a new Designation of Beneficiary. I will promptly notify the Plan Administrator of any change in the name or address of a Beneficiary. Employee’s Signature: ______________________________________ Date:

. 67
Employer: ________________________________________ Flexible Benefit Plan
PARTICIPATION WAIVER FOR PRETAX PREMIUM CONVERSION OPTION
(Used for Employees who do not wish to pay their share of employer-sponsored benefit coverages on a pretax
basis)
Name (Please Print): _________________________________________________________ First, M.I., Last _______/_______/_______ ______________________________________ Social Security Number Effective Payroll Date I have been given an opportunity to participate in this Plan as of ____________________. I decline to participate at this time for the reason(s) stated below. I understand I cannot elect to participate in this Plan until the beginning of the next Plan Year unless I experience a change in status. Reason for declining:
___________________________________________________________________________ ___________________________________________________________________________ ___________________________________________________________________________ ___________________________________________________________________________ ________________________________________________________________ Employee's Signature: ____________________________________ Date: _______________ Company Representative: _________________________________ Date: _______________
Related Documents











