-
7/30/2019 Paulsen 2010
1/13
A COX-2 inhibitor reduces muscle soreness, but does not influencerecovery and adaptation after eccentric exercise
G. Paulsen1, I. M. Egner1, M. Drange1, H. Langberg2, H. B. Benestad3, J. G. Fjeld4, J. Halle n1, T. Raastad1
1Norwegian School of Sport Sciences, Oslo, Norway,
2Institute of Sports Medicine, Bispebjerg Hospital, Copenhagen, Denmark,
3Department of Physiology, Institute of Basic Medical Sciences, University of Oslo, Oslo, Norway, 4Department of Nuclear Medicine,Rikshospitalet University Hospital, Oslo, NorwayCorresponding author: Gran Paulsen, Norwegian School of Sport Sciences, PO Box 4014 U.S., N- 0806 Oslo, Norway. Fax:147 23 26 24 51, E-mail: [email protected]
Accepted for publication 16 February 2009
The aim of this study was to investigate the effect of acyclooxygenase (COX)-2 inhibitor on the recovery of mus-cle function, inflammation, regeneration after, and adapta-tion to, unaccustomed eccentric exercise. Thirty-threeyoung males and females participated in a double-blind,placebo-controlled experiment. Seventy unilateral, volun-tary, maximal eccentric actions with the elbow flexors wereperformed twice(bouts 1 and 2) with the same arm, separatedby 3 weeks. The test group participants were administered400 mg/day of celecoxib for 9 days after bout 1. After bothbouts 1 and 2, concentric and isometric force-generatingcapacity was immediately reduced ($ 4050%), followed bythe later appearance of muscle soreness and increased serum
creatine kinase levels. Radiolabelled autologous leukocytes(detected by scintigraphy) and monocytes/macrophages (his-tology) accumulated in the exercised muscles, simultaneouslywith increased satellite cell activity. These responses werereduced and recovery was faster after bout 2 than 1,demonstrating a repeated-bout effect. No differences betweenthe celecoxib and placebo groups were detected, except formuscle soreness, which was attenuated by celecoxib. Insummary, celecoxib, a COX-2 inhibitor, did not detectablyaffect recovery of muscle function or markers of inflamma-tion and regeneration after unaccustomed eccentric exercise,nor did the drug influence the repeated-bout effect. However,it alleviated muscle soreness.
According to some reports, non-steroidal anti-inflam-matory drugs (NSAIDs) may have detrimental effects
on regeneration and healing processes after injuries tothe different components of the muscleskeletal system(Almekinders, 1999). Therefore, warnings have beenvoiced against the wide use of NSAIDs in exerciseand sports medicine (Almekinders, 1999; Paoloni &Orchard, 2005; Warden, 2005; Mehallo et al., 2006).
The original NSAIDs (e.g. ibuprofen) inhibit boththe constitutive cyclooxygenase (COX)-1 and themore inducible COX-2 enzyme, which both catalyzethe generation of prostanoids [prostaglandins (PGE2and PGF2a), prostacyclins and thromboxanes] thatare involved in numerous physiological processes(Miller, 2006). The more recently developed selectiveCOX-2 inhibitors are in theory more appropriate andspecific to dampen excessive inflammatory reactionsthan the non-selective (COX-1 and COX-2) inhibi-tors (Warden, 2005). However, it has been demon-strated that these new drugs can also have negativelong-term effects on regeneration and healing inanimals (Warden, 2005; Buvanendran & Reuben,2006) especially through inhibition of satellite cell
activity in skeletal muscle (Bondesen et al., 2004; Shenet al., 2006). But there is presently no clear evidence for
detrimental effects of COX-2 inhibitors on regenerationand healing of injuries in humans (Reuben & Ekman,2005, 2007; Warden, 2005; Mehallo et al., 2006;Vuolteenaho et al., 2008). Furthermore, neither clinicalnor experimental exercise-induced muscle damage stu-dies have to our knowledge been conducted in order toevaluate the effect of selective COX-2 inhibitors onrecovery from skeletal muscle injuries in humans.
In humans, some reports have demonstrated thatNSAIDs, such as naproxen and ibuprofen, can reduceeccentric exercise-induced muscle damage and hastenthe recovery process (Baldwin, 2003; Cheung et al.,2003; Connolly et al., 2003). The improved recoverymight stem from the anti-inflammatory effect of thesedrugs (Sayers et al., 2001), but this assumption hasnever been properly documented. Howell et al.(1998a,b) detected no effect of ibuprofen, but a slightlyretarded recovery of maximal isometric torque afterhigh-force eccentric exercise was observed in subjectsadministered flurbiprofen. Other negative effects ofNSAIDs, such as blunted increase in the rate of proteinsynthesis after high-force eccentric exercise (Trappeet al., 2001, 2002), and reduced satellite cell responseto long distance running (Mackey et al., 2007), have
[This article was published online on 10th June 2009. Error were sub-sequently identified. This notice is included in the print and onlineversions to indicate that both have been corrected as at 18th January 2010]
Scand J Med Sci Sports 2010: 20: e195e207 & 2009 John Wiley & Sons A/Sdoi: 10.1111/j.1600-0838.2009.00947.x
e195
mailto:[email protected]:[email protected] -
7/30/2019 Paulsen 2010
2/13
been reported as well. In contrast to these studies,ibuprofen and acetaminophen may actually enhancemuscle growth in response to resistance training inelderly subjects (Carroll et al., 2008), and celecoxib (aCOX-2 inhibitor) can allegedly boost the increased rateof protein synthesis after a bout of high-force resistanceexercise (Burd et al., 2008). Thus, it seems fair toconclude that the jury is still out concerning the effects
of NSAIDs on human skeletal muscle especiallyregarding the COX-2 inhibitors (Warden, 2005).
The repeated-bout effect comprises the physio-logical adaptation that takes place after a single boutof unaccustomed high-force exercise (Clarkson et al.,1987). Basically, the exercised muscles become sig-nificantly more resistant toward damage from arepeated bout, preformed days or weeks after thefirst one. However, the mechanism behind this adap-tation is still not clear (McHugh, 2003). A localinflammatory reaction in the exercised muscle maybe involved in the strengthening of the tissue afterunaccustomed exercise, because when perturbed, areduced repeated-bout effect has been reported (La-pointe et al., 2002a). In the study by Lapointe et al.(2002a), rats were exposed two times to a muscle-damaging exercise protocol. An NSAID was given toone group after the first exercise bout to reduce thepost-exercise inflammation. These rats showedclearly a smaller repeated-bout effect than the con-trols, with larger force deficits and larger accumula-tion of leukocytes in the muscle tissue after thesecond bout. This study design has previously notbeen tested with human subjects, and it is suited toclarify both early and late effects of NSAIDs, includ-
ing the mechanisms behind the repeated-bout effect.Therefore, the aim of the present study was to
investigate whether administration of a COX-2 inhibi-tor would (1) enhance the recovery after maximaleccentric exercise, by reducing the inflammatory reac-tion during the first days after exercise, (2) slow downthe recovery in the final stage (13 weeks after exercise)and (3) reduce the repeated-bout effect.
Materials and methodSubjects
Thirty-three healthy students and employees at the Norwegian
School of Sport Sciences gave written, informed consent to
participate in the study (Table 1). The subjects were physicallyactive and involved in different activities, such as running andcycling, and team sports, such as basketball and soccer. Noneof the subjects were familiar with maximal eccentric exercisewith the elbow flexors. No exercise was performed for 3 daysbefore the experiment. Subjects had a light breakfast at homeand were offered a mixed meal shortly after exercise. Waterwas available ad libitum during exercise. The subjects wereasked to continue their habitual diet and not to take any formof medications or prescription-free supplements (such as
antioxidants) and avoid exercise, stretching and massagetherapy (etc.) during the experimental periods. The studycomplied with the standards set by the Declaration of Helsinkiand was approved by the Regional Ethics Committee ofSouthern Norway.
Study design
This investigation was carried out with a double-blindeddesign. The subjects were randomized to a celecoxib groupand a placebo group. There were no group differences inanthropometric values (Table 1). The celecoxib group wasadministrated 400mg [Celebra (Pfizer, Oslo, Norway); 200 mg
morning and evening] for 9 days, with the first dose approxi-mately 45 min before the exercise (bout 1; Fig. 1). This dosageis the highest recommended dosage in the Norwegian Phar-maceutical Product Compendium (NPPC). Maximal bloodconcentration of the drug is reached after 23 h and the half-life of the drug is 812 h (NPPC). The placebo-group receivedsimilar looking lactose pills. The subjects were contacted everymorning and evening to ascertain that the pills were taken.Three weeks after bout 1, the exercise was repeated (bout 2),but without drug administration (Fig. 1).
The exercise was performed with the same arm, randomlychosen, on both occasions (bouts 1 and 2). The other armserved as a non-exercised control. Before and for 9 days afterthe exercise bouts, tests of muscle function (force-generationcapacity), muscle soreness (pain) and swelling, as well as resting
elbow angle were performed and blood was drawn, daily (Fig.1). Assessments of muscle function were always performed afterblood sampling and the other measurements, except immedi-ately after exercise when muscle function was tested first.
Radionuclide imaging was used to monitor the muscleaccumulation of leukocytes 6 and 20 h after bouts 1 and 2.Microdialysis was performed 2, 24 and 48 h after bout 1 formeasurement of prostaglandins (PGE2). Biopsies from m.biceps brachii were collected from both exercised and controlmuscles 1, 48, 96 and 168 h after bout 1, and 1 and 48 h afterbout 2. The different time points after bout 1 were chosen inorder to evaluate early (1 and 48 h) and late (96 and 168h)inflammatory reactions and regenerating processes.
No subjects withdrew during the study. However, foursubjects did not provide all the scheduled biopsies due to
technical problems or the discomfort experienced. Six subjects
Table 1. Descriptive characteristics of the subjects
Group N Age (years) Height (m) Weight (kg) Celecoxib mg/kg
Males Celecoxib 8 28 5 1.81 0.03 78 7 5.1 0.5Placebo 14 26 4 1.82 0.06 77 6
Females Celecoxib 7 28 5 1.65 0.03 59 6 6.9 0.7Placebo 4 23 5 1.67 0.03 62 3
,1< Celecoxib 15 28 5 1.73 0.08 69 12 6.0 1.1Placebo 18 25 4 1.79 0.08 74 8
Values are means SD.
Paulsen et al.
e196
-
7/30/2019 Paulsen 2010
3/13
(three in the placebo and three in the celecoxib group)performed only the first of the two bouts of exercise, becausethey were specially recruited for the microdialysis experiment.
The double-blind experimental design implied that thesubjects were unaware of which group test or control they belonged to, and during all analyses the subjects groupaffiliation was concealed for the recorders.
Medication side-effect registrationThe subjects were asked to inform the test leader and writedown on a form any symptom they thought could be related tothe pills.
Unilateral arm exercise
For the eccentric exercise the subjects were positioned in achair (Technogym, REV 9000, Gambettola, Italy) and fas-tened with belts over the hip, chest and shoulder, and theupper arm was supported by a cushion. Thus, the shoulderjoint was kept in a slightly flexed position (30351 from thevertical axis) and prevented from moving during the elbow
exercise. The subjects gripped a handle connected to the leverarm of the dynamometer. Because the handle could be rotatedabout the longitudinal axis, the subjects were instructed tosupinate their forearm (elbow joint) for maximal activation ofm. biceps brachii. The exercise protocol consisted of 14 5repetitions of maximal voluntary, eccentric actions using theelbow flexors, with 3035s rest in-between sets. The lever armof the dynamometer was automatically returned to the start-ing point; no muscle force being necessary for the elbowflexion phase. The range of motion (ROM) in the elbow jointwas 401751 (18015 full extension) and the velocity was 301/s.The subjects were verbally motivated to resist maximallythrough the whole ROM and they received real time visualfeedback on their performance on a computer screen.
The total work of each eccentric action was registered andwork per set and total work per exercise were calculated. Allvalues registered during exercise and tests were corrected forgravity and passive tension during the full ROM.
Muscle function
In the same position as during the exercise, maximal force-generating capacity was measured as peak torque during twoconsecutive maximal, isokinetic, concentric elbow flexions at601/s (ROM: 175401) and as peak torque during isometricactions at 901 in the elbow joint (5 s actions; two attempts;Technogym, REV 9000). All subjects participated in one ortwo familiarization tests on separate days within 1 week beforethey entered the study. Two pre-tests were performed on day 1of the experiment (with 3060 min rest in-between) and themean of these tests were used for further analysis. Subjects didalways warm up by 3 min arm cranking (3050 W) and foursubmaximal, concentric, isokinetic actions in the dynam-ometer. The intra-individual coefficient of variation (CV) forthe force-generating capacity measurements were o5%.
Scintigraphic monitoring of leukocyte accumulation
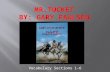
The method has been described by Raastad et al. (2003). Inbrief, 50 mL blood was drawn, and leukocytes (mainly neu-trophilic granulocytes) were isolated and labelled with99mTechnetium (99mTc), before being re-infused. Accumula-tion of 99mTc-leukocytes (radiolabelled leukocytes) in thesubjects arms was quantified scintigraphically (with a gammacamera) on anterior view images (Fig. 4). The radioactivity inthe upper arm elbow flexors was calculated with a custom-made software (from GE Healthcare, Oslo, Norway). Theaccumulation of radioactivity within a region of interest (ROI)in the exercised arm was related to radioactivity in the sameROI in the control arm, corrected for background radiation.
Fig. 1. Overview of the study. The dots, xs and # show the time points for tests and measurements. Note the drugadministration after bout 1 only.
COX-2 inhibition after eccentric exercise
e197
-
7/30/2019 Paulsen 2010
4/13
This procedure was performed on 22 subjects (celecoxib: n5 9,placebo: n513).
Muscle biopsies
A 5 or 6 mm Pelomi-needle (Albertslund, Denmark) withmanual suction was used to obtain tissue samples (23 30100 mg) from the mid-section of m. biceps brachii. Subjects werein supine position, and the procedure was performed under local
anesthesia (10 mg/mL1
5mg/mL, Xylocain
s
adrenaline, Astra-Zeneca, So derta lje, Sweden). Each needle incision was placedapproximately 12 cm medially and laterally to the first incisionand care was taken to avoid tissue affected by earlier biopsies.The muscle samples were rinsed in physiological saline beforevisible fat and connective tissue were removed, and subsequentlyfrozen in isopentane on dry ice and stored at 80 1C untilanalysis.
Twenty-four subjects delivered biopsies from the m. bicepsbrachii of both the exercised arm and the control arm. Toreduce stress on the subjects and to reduce risk of contamina-tion from previous biopsies, each subject was scheduled forbiopsy at three out of the six biopsy time points: 1 h, and 2, 4and 7 days after bout 1, and 1 h and 2 days after bout 2 (Fig. 1).
Immunohistochemistry
Serial cross-sections (7mm) were incubated with antibodies (ab)against leukocytes: CD66b (neutrophilic granulocytes, monoclo-nal ab, M1546, PeliCluster, Sanquin, Amsterdam, the Nether-lands; 1:500), and CD68 (monocytes/macrophages; monoclonalab, M0718, DAKO, Copenhagen, Denmark; 1:300), togetherwith antibodies against laminin (polyclonal ab, Z0097, DAKO;1:1000) or dystrophin (polyclonal ab, ab15277, Abcam, Cam-bridge, UK; 1:2000). The two latter antibodies were used tovisualize the sarcolemma. In order to visualize satellite cells/myoblasts, sections were analyzed for immunoreactivity againstCD56/NCAM (monoclonal ab, ab9018, Abcam; 1:200). Sectionswith overt satellite cell/myoblast activity were double stainedwith CD56 and Ki67 (a marker of proliferation; polyclonal ab,
CP249A, Biocare Medical, Concord, California, USA; 1:200).Alexa-488 (FITC) and -594 (goat anti-rabbit or goat anti-mouse;Invitrogen-Molecular Probes, Eugene, Oregon, USA) were usedas secondary antibodies. The sections were finally counterstainedwith DAPI (for nuclear staining) and mounted under coverslips(ProLong Gold Antifade Reagent with DAPI, P36935, Invitro-gen-Molecular Probes).
Images of the stained cross-sections were captured using anAxiocam camera (Zeiss, Oberkochen, Germany) mounted on aAxioskop-2 light microscope (Zeiss). Multiple images ( 20, 40 and 100 objectives) were taken so that the whole musclebiopsy cross-section was captured. To quantify the number ofcells positive for a leukocyte associated antigen, a cell thatcontained both DAPI and antibody staining was considered aspositive, independent of the staining intensity. Data are pre-
sented as number of positive cells per 100 myofibers.
Microdialysis and prostagandin E2
Tissue fluid (dialysate) from both the exercised arm and thecontrol arm of 12 subjects (six administrated the COX-2inhibitor and six placebo) were collected at three time pointsafter bout 1. All twelve subjects underwent the microdialysisprocedure 26 h after exercise and then again starting at either24 (n55) or 48h (n55) after exercise. A CMA-60 microdialysisprobe (20 kDa molecular cut-off; length 30 mm; CMA/Micro-dialysis AB, Solna, Sweden) was used for collection of tissuefluid for later measurements of PGE2. Before the insertion of the
CMA-60 catheter, positioned 2 cm medial to the centerline ofthe m. biceps brachii muscle, the skin was locally anesthetizedwith 0.3 mL of Lidocain (10 mg/mL; SAD, Copenhagen, Den-mark). The CMA-60 catheters were perfused with a Ringeracetate solution containing 5 nM 3H-PGE2 (specific activity,3.7 GBq/mmol; NEN, Boston, Massachusetts, USA) to deter-mine the recovery of PGE2. The subjects rested for at least90 min before starting the experiment to ensure that any reactionfrom the insertion trauma had minimized. Dialysate sampleswere collected every 30 min. The samples were immediately
frozen ( 80 1C) until analysis.The PGE2 concentration in the dialysate was analyzed by a
commercial competitive enzyme immunoassay (ACEt, catalogno. 514010, Cayman Chemicals Inc., Ann Arbor, Michigan,USA). Standards and samples were analyzed in accordance withthe protocol of the kit. Samples were analyzed in duplicates.Optical density (OD) was measured in a plate-reader (ASYSHitech, Eugendorf, Austria) at 405 nm.
Muscle soreness
Muscle soreness was rated on a visual analogue scale where 0represented not sore at all and 100 mm extremely sore. Thesubjects stretched and contracted their elbow flexors (both arms)
to assess soreness in m. biceps brachii and m. brachialis. In orderto assess soreness/tenderness at the lower (distal) and upper(proximal) part of the upper arm elbow flexors, the subjects satwith their arms extended, but resting, on a bench (901 flexed andlateral-rotated shoulder joints). The upper arm elbow flexormuscles were then palpated manually by the test leader. Inaddition, a probe (3cm2 cross-sectional area), giving 10 N/cm2 ofpressure, was applied perpendicularly to the upper arm elbowflexor muscles at predetermined locations, i.e., a distal and aproximal spot (marked by a water-proof pen). The middle partof the upper arm elbow flexors was discarded because of thelocation of the biopsy incisions.
Muscle swelling and resting arm angle
Swelling was assessed by measuring the arm circumferencewith a tape measuring device, utilizing a spring mechanism toapply constant force (Roche, Oslo, Norway). The circumfer-ence was measured at the persons thickest part of the lowerhalf of the m. biceps brachii (and the m. brachialis under-neath), below the biopsy incisions. A waterproof pen was usedto mark the site for repeated measurements. Resting arm anglewas measured with a goniometer. The intra-individual CV ofthese measurements was o1.8%.
Blood sampling and CK
Blood was drawn from an antecubital vein into a 10 mL serumvacutainer tube. After coagulating for 3045 min at room
temperature ($ 20 1C), the blood was centrifuged at 2700gfor 10min at 4 1C. Serum was immediately pipetted intoEppendorf tubes and stored at 80 1C until analysis. CKwas analyzed with an automated chemistry analyzer (ModularP, Hitachi High- Technologies Corporation, Tokyo, Japan);analytic CV being o5%.
Statistics
All parameters were measured repeatedly after exercise andfor each variable the area under the curve (AUC) wascalculated for each subject. The AUC values, in addition topeak/nadir values, for the celecoxib and placebo group were
Paulsen et al.
e198
-
7/30/2019 Paulsen 2010
5/13
compared with the unpaired Student t-test or the MannWhitney test. A multivariate analysis of variance (MANOVA)with repeated measures and a two-way ANOVA (timegroup and time arm) with Bonferroni post hoc test werealso applied. For the different variables, changes over timewithin each group were followed with a one-way ANOVA orFriedmans test with repeated measures and Dunnetts andTukeys or Dunns post hoc tests. We evaluated the differencesfrom baseline and between selected time points for theexercised arm and the non-exercised (control) arm separately,
as well as the difference between arms. Because of the fact thatdifferent subjects were biopsied at each sampling time point,the unpaired Student t-test and the MannWhitney test wereused to analyze group differences in histological data. Thepaired Student t-test or the Wilcoxon signed rank test wasapplied to evaluate differences between the exercised arm andthe control arm. Data are presented as means with standarderror of the mean (SEM), if not otherwise stated in the text.P 0.05 was considered statistically significant. Cohenseffect size (difference between group means divided by thepooled SD) was calculated with bias correction for unequalnumbers of subjects in the two groups (Hedges). Tests fornormality (Gaussian distribution) dictated the choice of para-metric or non-parametric tests. The statistics were performedwith Microsoft
s
Excel 2003 (including statistiXL 1.8) InStats
3.06, Prisms 5.01 and Statematet 2.0 (GraphPad SoftwareInc., San Diego, California, USA) and SPSS 15.0 (SPSS Inc.,Chicago, Illinois, USA).
ResultsExercise and muscle fatigue
The total work (sum of 14 5 repetitions) performedby each experimental subject during bouts 1 and 2was similar within and between groups: celecoxib:$ 4500 500J (bouts 1 and 2) and placebo:$ 4800 300J (bouts 1 and 2). Total work during
the last (14th) set was reduced by 45 4% and47 4% of the first set values for the celecoxib andplacebo group, respectively, during bout 1 (Po0.01).This reduction was smaller in bout 2 than bout 1 forboth groups (celecoxib: 34 3% and placebo:35 3%; Po0.01). [Correction made to above para-graph after initial online publication.]
Muscle function
The force-generating capacity measured as isometricand isokinetic concentric torque was markedly re-duced ($ 4050%) after both exercise bouts, butthere were no significant differences between groupsat any time point (Fig. 2). The force-generatingcapacity was not recovered 9 days after bout 1, butwas in both groups not detectably different frombaseline values before bout 2, 3 weeks after bout 1.Of note, about half of the subjects in each group were45% (CV for the test) below their baseline values 3weeks after bout 1. After bout 2 the acute reductionin force-generating capacity was only slightly atte-nuated compared with after bout 1 (calculating withthe pre-values of bout 1; Po0.05; Fig. 2). However,
the recovery of both isometric and concentric force-generating capacity was faster after bout 2 than bout1 (comparing AUC values; Po0.01). The force-generating capacity of the non-exercised, controlarm did not change from baseline in either groupduring the experimental periods (Fig. 2).
Muscle soreness
Muscle soreness of the upper arm, as assessed duringcontractions and stretching, was less in the celecoxibgroup than in the placebo group, after both bouts(Fig. 3, AUC: bout 1: P5 0.04, and bout 2: P5 0.06;effect size: 0.75 and 0.86 for bouts 1 and 2, respec-tively). For both groups, less soreness was reportedafter bout 2 than after bout 1 (Po0.01). The peaksoreness values after bout 1 tended to be higher in theplacebo group (6.7 0.6 mm) than in the celecoxibgroup (5.1 0.7 mm; P5 0.08). This was less evidentafter bout 2 [peak values: 2.5 0.4 mm (celecoxib) vs
60
50
40
30
20
10
0
10
CelecoxibPlaceboCelecoxib control
Placebo control
Pre 0 5 24 48 72 9616
821
6P
re 0 5 24 48 72 96168
216
3 weeks#
## #
# #
#
# #
##
##
##
#
##
##
# ##
##
#
#
#
Time (hours after exercise)
Chang
esinisometrictorque(%)
AUC bout 1 > bout 2
60
50
40
30
20
10
0
10
Celecoxib
Placebo
Celecoxib control
Placebo control
Pre 0 5 24 48 72 9616
821
6P
re 0 5 24 48 72 96168
216
3 weeks
#
## #
# #
#
# #
###
###
#
#
#
#
#
##
#
##
#
#
#
Time (hours after exercise)
Changesinconcentrictorque(%)
AUC bout 1 > bout 2
(a)
(b)
Fig. 2. Changes in force-generating capacity of the elbowflexors exposed to two bouts of maximal eccentric exercise(same arm) and no exercise (control). (a) Changes in max-imal voluntary isometric torque (901) and (b) changes inmaximal voluntary isokinetic concentric torque (601/s).N-celecoxib512; n-placebo515. Error bars are SEM.#
Difference from baseline values (before bout 1). The areaunder the curve (AUC) was larger for bout 1 than 2 for bothgroups (Po0.01).
COX-2 inhibition after eccentric exercise
e199
-
7/30/2019 Paulsen 2010
6/13
3.6 0.6 mm (placebo), P5 0.14]. The placebogroup tended to report more soreness in the controlarm than the celecoxib group after bout 1 (AUC;P5 0.1). This soreness/pain seemed to be due to thebiopsy procedure.
For soreness as assessed with palpation, lowerpeak values were reported by the celecoxib groupthan the placebo group, but only in the proximal part
of elbow flexors (3.4 0.8 vs 6.5 0.7; Po0.05).After bout 2, peak soreness values during palpationwere reduced in both groups (Po0.01).
Scintigraphy
The radioactivity, reflecting autologous radiolabelledleukocytes, was in both groups higher in the exer-cised arm than in the control arm 6 and 20 h afterbout 1, and the difference between arms was larger at20 than 6 h after exercise (Po0.05; Fig. 4). Afterbout 2 the radioactivity at 6 h was similar to that
found in bout 1; however, no further increase at 20 hwas detected after bout 2 (Fig. 4). There were nosignificant differences between groups.
The scintigrams confirmed that m. biceps brachiiwas affected by the exercise protocol. We could notprecisely differentiate between the elbow flexors (dueto low image resolution), but, in addition to m.biceps brachii, both m. brachialis and m. brachior-adialis appeared to be affected. There was a trendtoward higher radioactivity in the lower and middlepart than the proximal part of the upper arm (Fig. 4).To exemplify, three subjects demonstrated $ 1000%difference between middle part of the exercised
muscles and control muscles 20 h after exercise. In
five subjects, high radioactivity (4100% higher inthe exercised muscles compared with control) wasfound over a localized area that appeared to corre-spond to the proximal muscletendon junction.
Microdialysis (PGE2)
The PGE2
concentration in the interstitial fluid (dia-lysate) of the exercised muscle was not detectablydifferent from the control muscle at any time point(2, 24 and 48 h after bout 1), and there were no groupdifferences. The mean values (combined over groupsand time points) were 880 134 and 900 135 pg/mLfor the exercised and control muscle, respectively.However, the PGE2 concentration tended to decreasein both the exercised muscle and the control muscleduring the first days after exercise in the celecoxibgroup (mean of both arms: 1000 167 vs 635 187;P5 0.16), but not in the placebo group (mean of botharms: 988 412 vs 1151 296). This suggests that
celecoxib generally lowered the PGE2 levels in theinterstitial fluid over time.
Immunohistochemistry
Leukocytes
CD681 cells, primarily monocytes/macrophages,were observed in the samples from both exercisedand control muscles, but higher numbers werecounted in the exercised muscle after both bouts(74 21 vs 22 3 CD681 cells per 100 myofiber;
data combined over groups and time; Po0.01). Inthe exercised muscles the number of CD681 cellsincreased from 1 to 48 h after exercise and from early(1 and 48 h) to later time points (4 and 7 days) afterexercise (Po0.05). No differences between groupswere observed (Table 2), however, at later timepoints the five highest values registered were allfound in samples from subjects in the placebo group.CD681 cells seemed preferentially related to necroticand regenerated myofibers (Fig. 5). Necrotic myofi-bers (probably segments) were identified as dystro-phin negative fibers (no staining); eight of 23 subjectsdisplayed ! 2% dystrophin negative myofibers onsamples from the exercised muscle: 15% 19 [stan-dard deviation (SD)] of the analyzed fibers. This wasonly observed in samples obtained 4 and 7 days afterexercise. Dystrophin negative fibers were only seen infour of all samples from control. Staining for lamininindicated that the basal membrane (with few excep-tions) stayed intact despite loss of dystrophinstaining, and signs of the regeneration processoccurred within the basal lamina sheath.
CD66b1 cells (neutrophils) were found in very lownumbers and no significant differences between ex-
AUC bout 1 > bout 2AUC placebo > celecoxib (bout 1 and 2)
Pre 0 5 24 48 72 9616
821
6
0
10
20
30
40
50
60
708090
100 Celecoxib
Placebo
Celecoxib control
Placebo control
3 weeks
#
#
#
#
#
#
#
#
## #
##
#
Pre 0 5 24 48 72 9616
821
6
Time (hours after exercise)
Musclesoreness(mm)
Fig. 3. Muscle soreness after two bouts of eccentric exercise,evaluated by visual analogue scale; 0100 mm. N-cele-coxib512; n-placebo515. Error bars are SEM. #Differencefrom baseline. The area under the curve (AUC) was largerfor bout 1 than 2 for both groups (Po0.01). The AUC wassmaller for the celecoxib group than for the placebo groupfor both bouts (bout 1: P50.04; bout 2: P50.06).
Paulsen et al.
e200
-
7/30/2019 Paulsen 2010
7/13
ercised and control muscles, or between groups,could be detected (Table 2).
Satellite cells
No differences between the groups were detected in thenumber of CD561 cells, i.e., satellite cells (locatedunderneath basal lamina, but outside the plasmamembrane) and myoblasts (CD561 cells primarilyinside necrotic myofibres; Table 2). Myoblasts wereobserved only in some subjects and preferentiallyclustered together (see next paragraph). For the groupscombined, the number of satellite cells/myoblasts washigher in exercised than in control muscles at bothearly (1 and 48 h) and late time points (4 and 7 days
after exercise; Po0.05), but there was an increase fromearly to late time points after bout 1 (P50.01). Thenumber of satellite cells/myoblasts per myofiber was0.11 0.04 (SD) in samples from the non-exercised,control arm and 0.19 0.18 (SD) in the exercisesamples (all combined). Expressed as the proportionof the nuclei underneath basal lamina, 4.8% 1.5(SD) were defined as satellite cells in control samplesand 5.7% 1.5 (SD) in the exercise samples. Hence,these latter numbers do not include myoblasts.
Intense satellite cell activity, including increasednumber and cell volume, long cytoplasmatic exten-sions, cell division activity (Ki67 positive nuclei) andfusion of myoblasts were seen in five subjects 1 weekafter exercise (Fig. 6). CD681 cells occasionally were
Table 2. Quantitative immunohistochemical staining: number of neutrophilic granulocytes (CD66b), monocytes/macrophages (CD68) and satellite cells/
myoblasts (CD56) in muscle cross-sections from the exercised muscle
Positive cells per100 myofiber
Bout # Time point Celecoxib Placebo P-value celecoxibvs placebo
CD66b Bout 1 Early 0 (03) 0 (029) P5 0.8Late 0 (02) 0 (03) P5 0.9
Bout 2 Early 0 (02) 0 (03) P5 0.6CD68 Bout 1 Early 21 (681) 25 (10133) P5 0.9
Late 35 (14150) 45 (7968) P5 0.7Bout 2 Early 27 (294) 47 (15104) P5 0.2
CD56 Bout 1 Early 11 (718) 12 (823) P5 0.6Late 16 (1050) 20 (7103) P5 0.7
Bout 2 Early 13 (1125) 14 (1049) P5 0.5
Values are medians and full ranges. N5 814 in each group per time point. The P-values stem from group comparisons.
Infusion of99mTc-leukocytes
Elbow joint;radioactive marker
Shoulder joint
M. biceps brachii/brachialis
Exercised arm Control armBlood sampling
6 hours 20 hours0
25
50
75
100
125
150Celecoxib; bout 1
Placebo; bout 1
Celecoxib; bout 2
Placebo; bout 2*
*
Time
Radioactivity
(%
differencefrom
control)
Fig. 4. Scintigram illustrated. Theimage shows accumulation of radi-olabelled autologous leukocytes inthe exercised arm muscles, mostprominent in the lower/middle partof the upper arm elbow flexors (darkareas reflect high radioactivity). Thefigure shows the relative differencesin radioactivity between the exer-cised arm and the non-exercised,
control arm 6 and 20h after exer-cise. N-celecoxib59; n-placebo513. Error bars are SEM. *denotesdifference between the 6 and 20 hvalues. [Figure has been revised afterinitial online publication]
COX-2 inhibition after eccentric exercise
e201
-
7/30/2019 Paulsen 2010
8/13
(a) (b)
Control
1 week 3 weeks
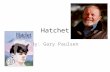
Fig. 5. Immunohistochemical experiments illustrated. The images are from a subject in the placebo group (but similar pictureswere obtained from those in the celecoxib group). Left image (a): CD68 staining of a sample obtained 168 h (1 week) after bout1 (CD685 red, laminin5green, nuclei5blue). The arrow points to a myofiber that is heavily infiltrated by CD68
1 cells(primarily monocytes/macrophages). Note that this myofiber was negative for dystrophin (not shown) and probably in a stageof necrosis. The presence of rounded and apparently swollen myofibers suggests that the myofibers were highly stressed in thissample. Right image (b): CD68 staining on a sample obtained 3 weeks after bout 1 (and 1h after bout 2). Note the smallmyofibers with centrally located nuclei (arrow), indicating regenerated myofibers, surrounded by CD681 macrophages. Thesemyofibers were also positive for CD56 (see Fig. 6). Note that the CD681 cells were most likely remnants from the damagereaction to bout 1 (not bout 2). Thus, the present CD681 cells are probably macrophages/histiocytes that served regenerating
myofibers. There was little or no specific staining in the control samples (lower right corner). Scale bars550 mm.
Fig. 6. Immunohistochemical experiments illustrated (CD565green, Ki675 red, nuclei5blue). Left column of images (a, c):tissue samples from a subject in the celecoxib group. Right column of images (b, d): tissue samples from a subject in the placebogroup. The top row of images (a, b) shows high satellite cell/myoblast activity and Ki671 cells 1 week after bout 1. The insetimage on image a shows accumulation and apparent fusion of myoblasts (CD561), as well as cells that seem to go through celldivision (pink stain5Ki67 [red]1dapi [blue]). The inset images on image b show (i) a normal looking satellite cell, i.e. withCD56 staining around the nucleus, which could be found in samples from both control and exercised muscles, and (ii) a satellitecell positive for Ki67 (sample from a exercised muscle). The second row of images (c, d) shows tissue samples obtained 48 hafter bout 2, i.e., 3 weeks after bout 1. Note the CD56 positive myofibers with relatively small diameter and centrally locatednuclei (arrows), which indicate that these are regenerated myofibers. On image c there is a Ki671 nucleus apparently inside themyofiber (arrowhead). Hence, this seems to be part of the regenerating process after bout 1 (not bout 2). Scale bars 550 mm.
Paulsen et al.
e202
-
7/30/2019 Paulsen 2010
9/13
positive for Ki67 as well. Thus, in areas with largenumber of cells (nuclei), differentiation of the cellscould be very difficult. No detectable differencesbetween the celecoxib and placebo subjects couldbe found.
In biopsies obtained after bout 2, relatively highnumbers of CD561 myofibers with centrally locatednuclei and often small diameters were observed
(! 10% of the myofibers in six subjects; three fromeach group; Fig. 6). A great majority of these CD561
myofibers were also verified to contain embryonicmyosin heavy chain (F1.652, Hybridoma Bank; datanot shown). Although this was observed after bout 2,the regeneration processes were very likely to berelated to bout 1. This implies that complete regen-eration after severe exercise-induced muscle damagetakes more than 3 weeks. There were no signs of failedregeneration in biopsies after bout 2, in either group.
Muscle swelling and resting arm angle
The upper arm circumference increased equally be-tween groups and peaked 4 days after bout 1,4.2 0.9% vs 4.6 1.0% for the celecoxib and pla-cebo group, respectively (Po0.01 from baseline). Theresting arm angle decreased (18015 extended arm)equally between groups by 10 21 and 11 21 24 hafter bout 1 for the celecoxib and placebo group,respectively (Po0.01). Both the circumference and theresting arm angle changed less after bout 2 than bout1 (Po0.01), and no group difference were detected.
CKThe serum CK levels were markedly elevated afterbout 1, but not after bout 2 (AUC; Po0.01; Fig. 7).There were no differences between groups.
Of note, for about half of the subjects the increasein serum CK levels followed a biphasic time course.Thus, there was an early increase during the first 8 h,followed by a more or less steady phase from 8 to24 h, before the values increased markedly until peakvalues were reached typically at 96 h (4 days) afterexercise (Fig. 7).
Gender
There were no gender differences in relative changes ofmuscle function, in muscle soreness or in the histolo-gical data, neither within groups nor across groups.However, the serum CK pre-values (before bout 1)were lower in the females than in the males (P5 0.05),and the females had a lower exercise-response to bout1 (AUC; Po0.05). The three highest values foraccumulation of radiolabelled leukocytes (scintigra-phy data) were observed in female subjects, but wefound no significant differences between the sexes.
Exclusion of the females from these analyses did notchange the group comparisons appreciably.
Adverse effect of the pill administration
Three subjects mentioned slight nausea, but one ofthese subjects was in the placebo group. One subjectfrom the celecoxib group experienced an unexpectedswelling of the forearm of the exercised arm; the excessfluid appeared to be in the subcutaneous tissue.
Discussion
The main finding in this study was that celecoxib, aselective COX-2 inhibitor, did not affect recovery ofmuscle function after a bout of unaccustomed, mus-cle-damaging, eccentric exercise in human subjects.The COX-2 inhibitor did, however, reduce the de-layed onset muscle soreness (DOMS).
A repeated-bout effect was clearly demonstratedby the faster recovery of muscle function and mark-edly blunted DOMS and serum CK response afterthe second bout of exercise. Nine days of celecoxibadministration during the recovery period after bout1 did not have any detectably adverse effect on theadaptation processes and recovery after the secondbout, 3 weeks after the first. The exercise protocolclearly initiated an inflammatory reaction with accu-mulation of leukocytes in the exercised muscles(markedly in some high-responder subjects), andstimulated increased satellite cell activity as well.There were no statistically significant differencesbetween the celecoxib and placebo group concerningindicators of inflammation. Nevertheless, the highestnumbers of accumulated leukocytes at late timepoints (4 and 7 days after bout 1) were found inthe placebo group.
Pre 1 82024 48729616
8
64
128
256
512
1024
2048
4096
8192 Celecoxib
Placebo
Pre 1 8 20 24 48 72 9616
8
3 weeks
# ##
#
##
#
#
# ##
##
Time (hours after exercise)
CK
(IU
L1[log2])
AUC bout 1 > bout 2
Fig. 7. Creatine kinase in serum. N-celecoxib512; n-placebo515. Error bars are SEM. #Difference from baselinevalues. The area under the curve (AUC) was larger for bout1 than 2 for both groups (Po0.01).
COX-2 inhibition after eccentric exercise
e203
-
7/30/2019 Paulsen 2010
10/13
This study is to our knowledge, the first to in-vestigate the effect of a COX-2 inhibitor on recoveryafter exercise-induced muscle damage in humans.Furthermore, the necrosis and regeneration pro-cesses observed in this study are rarely reported forhumans; especially in combination with measure-ments of muscle function.
NSAIDs, changes in muscle function and inflammation
Administration of non-selective NSAIDs in the re-covery phase after high-force, muscle-damaging ex-ercise in human studies has resulted in equivocalfindings (Baldwin, 2003; Cheung et al., 2003; Con-nolly et al., 2003). Some researchers have observedenhanced recovery of muscle function during the firstdays after exercise [e.g. (Dudley et al., 1997)], whileothers observed no such effect in comparison withplacebo-medication [e.g. (Howell et al., 1998a)]. Themost obvious mechanism behind any effect ofNSAIDs on muscle restitution, on which our work-ing hypothesis was founded, is reduced inflammation(Lapointe et al., 2002a, b; Shen et al., 2005).
Accumulation of radiolabelled leukocytes in theexercised muscles 6 and 20 h after exercise indicatesan early inflammatory reaction, but no effect ofcelecoxib was detected. The blood-borne leukocytes(primarily neutrophils) detected by scintigraphy wereprobably either infiltrating the interstitial space ofthe muscle tissue or merely adhering to the luminalside of the local micro-vessels. Neutrophils were,however, histologically not found to have accumu-lated in the muscle tissue 2 days after exercise.
Conversely, the numbers of monocytes and/ormacrophages increased in the muscle tissue, and thehighest values were found 4 and 7 days after exercise,in both the celecoxib and placebo group. Again, therewere no significant differences between groups, butthere was a tendency toward higher leukocyte numbersin high-responder subjects from the placebo group.This could mean that celecoxib had some dampeningeffect when the inflammatory reaction exceeded acertain intensity. The effect size between groups was0.6, but our statistical power to detect such a differencewas very low (26%).
Experimental evidence indicates that high-force,eccentric exercise protocols can cause significantmuscle damage and inflammation in humans (Joneset al., 1986; Newham et al., 1987; Jones et al., 1989;Hellsten et al., 1997; Child et al., 1999). However,scant evidence of a classical local inflammatoryreaction after exercise-induced muscle damage exists[in contrast to findings in rats and mice; (Schneider &Tiidus 2007)]. We found that the most severe muscleweakness occurred well before the cell damage andinflammation had been fully manifested. In linewith this, other workers have also found that peak
accumulation of leukocytes (primarily macrophages)among the myofibers seemed to occur several daysafter exercise (Jones et al., 1986; Hellsten et al., 1997;Child et al., 1999). Bourgeois et al., (1999) reportedenhanced recovery of muscle function after the use ofan NSAID (naproxen), but no inflammatory cellswere seen histologically in muscle samples ob-tained 24 h after resistance exercise. Peterson et al.,
(2003) found accumulation of monocytes/macro-phages (CD68), but not neutrophils (CD15), 24 hafter eccentric exercise, and no effect of acetamino-phen and ibuprofen was reported. The NSAIDs(acetaminophen and ibuprofen) blunted the exer-cise-induced increase of PGF2a, but there were noincrease of the PGE2 levels (Trappe et al., 2001). Wecould not detect any increase of PGE2 in the ex-ercised muscles. Therefore, the lack of an NSAIDeffect as in the present study could be due to theabsence of a sufficiently strong and early inflamma-tory reaction, as reflected by the histological findings,and the lack of a significant prostaglandin response.
NSAIDs and DOMS
The celecoxib group reported less muscle sorenessand pain than the control group after both bouts ofexercise. The DOMS reducing effect of celecoxibafter bout 1 may be due to the drugs knownanalgesic effect (Ekman et al., 2002; Reuben & Ek-man, 2005), in the muscle tissue, in the centralnervous system or both (Veiga et al., 2004).
We obtained circumstantial evidence for a drugeffect on the PGE2 generation in the muscle, but no
evidence for an exercise effect on PGE2. The role oflocal PGE2 in DOMS has been questioned by others,who like us analyzed microdialysis fluid (Tegeder etal., 2002), and by investigators who found noNSAID effect on DOMS [e.g. (Kuipers et al.,1985)]. Our findings are also supported by previousreports (Paulsen et al., 2009), indicating that accu-mulation of leukocytes (as assessed by use of radi-olabelled leukocytes and immunohistochemistry) isboth spatially and temporally out of phase withdevelopment of muscle soreness. To exemplify, sub-
jects with the largest accumulation of radiolabelledleukocytes did not report more intense soreness thanothers. Furthermore, large accumulations of leuko-cytes among the myofibers were seen 1 week afterexercise, but at that time the soreness was almostgone. Thus, our data (PGE2 and accumulation ofleukocytes) indicate that inflammation, in the classi-cal sense, is not a main mechanism behind DOMS.
NSAIDs and satellite cells
A remarkable finding was myofiber necrosis (degra-dation) and regeneration observed in as much as
Paulsen et al.
e204
-
7/30/2019 Paulsen 2010
11/13
$ 1/3 of our subjects. The regeneration process washeralded by cell proliferation leading to increasednumbers of satellite cells/myoblasts (CD56-positivecells), as well as their migration, fusion and develop-ment of new myotubes to replace degraded segmentsof damaged myofibers. This has rarely been reportedin otherwise healthy human muscles after exercise.Indeed, degenerative and regenerative processes have
been captured by histological examination afterstrenuous exercise (Hikida et al., 1983; Jones et al.,1986; Round et al., 1987; Child et al., 1999), butsatellite cell activity in highly damage muscletissue assessed by immunohistochemistry has beenpoorly documented. Crameri et al. (2004) appliedsimilar methodology as us, but found necrosis andmyoblast fusion in only one out of eight subjectsexamined.
Possible retardation of regeneration processes inskeletal muscle tissue by NSAIDs, and especiallyCOX-2 inhibitors (Bondesen et al., 2004; Warden,2005; Shen et al., 2006), has not been thoroughlyinvestigated in humans. However, administration ofindomethacin reduced satellite cell response after longdistance running in endurance-trained subjects(Mackey et al., 2007). The discrepancy between ourstudy, where the satellite cell response in the affectedmuscles was not detectably reduced by celecoxib, andthat of Mackey et al. (2007) is not easily explained.However, the contradictory findings could be due tothe large differences in the exercise protocols andsubject populations, as well as the fact that differentdrugs were administered a non-selective COX-inhibitor vs our selective COX-2 inhibitor. Hence,
any effect on satellite cell proliferation could be due toinhibition of both COX-1 and COX-2, which, interalia, might markedly lower the tissue PGE2 levels (incontrast to our findings).
Our data suggest that the COX-2 inhibitor cele-coxib (at high dosage: $ 6 mg/kg for 9 days) leavesregeneration and adaptation processes unaffectedafter exercise-induced muscle damage. However, thelarge inter-individual differences and the few subjectswith considerable necrosis in the obtained biopsies,made any celecoxib effects of a more subtle natureelusive. Thus, further investigations are warranted,and it should be kept in mind that celecoxib may alsohave diverse COX-2 independent effects on a cell [e.g.(Glebov et al., 2006)].
NSAIDs, inflammation and the repeated-bout effect
The repeated-bout effect is well documented, and asexpected, faster recovery of muscle function, as wellas blunted muscle soreness and serum CK increases,were observed after the repeated exercise bout. Themechanisms behind the repeated-bout effect are,however, still ambiguous (McHugh, 2003), but the
inflammatory reaction might be causative. In anexperiment with rats, Lapointe et al. (2002a) demon-strated that the repeated-bout effect was reducedwhen the accumulation of leukocytes had beenblunted by the NSAID diclofenac in the recoveryphase after the initial bout (Lapointe et al., 2002a).The study design of the present investigation re-sembled Lapointe et al.s (2002a). However, we could
not detect any clear anti-inflammatory effect of ourCOX-2 inhibitor (celecoxib). Moreover, the re-peated-bout effect was seen both in subjects withlarge and low accumulation of leukocytes. Conse-quently, we question the importance of inflammationto the adaptation process after eccentric exercise inhumans. In that sense, our findings are in agreementwith other human studies where signs of myofibrillarremodelling have been observed, without leukocytesdetectably present during the first days after eccentricexercise (Feasson et al., 2002; Yu et al., 2002).
Conclusion
This is the first study to investigate the effect of aCOX-2 inhibitor on inflammation, recovery, regen-eration and adaptation after exercised-induced mus-cle damage in humans. We found no effect of theCOX-2 inhibitor on recovery of muscle function afterdamaging elbow flexor eccentric exercise. However,the drug reduced DOMS. High doses of celecoxibduring 9 days after a bout of eccentric exercise hadno detectable influence on the repeated-bout effectobserved 3 weeks after the first bout. An extensiveinflammatory response to unaccustomed eccentricexercise occurred in some subjects, several days afterthe exercise. The accumulation of leukocytes wasapparently unaffected by celecoxib administrationand seemed to be related to segments of necroticand later regenerating myofibers in the exercisedmuscle. Thereby, our study provided insight intothe basal regeneration processes in healthy humanskeletal muscles.
Perspectives
Celecoxib intake (400 mg/day) over 9 days neitherenhanced nor inhibited recovery, regeneration andadaptation processes after exercise-induced damagein skeletal muscles. The drug alleviated muscle sore-ness, but today it is unclear whether the drug worksprimarily on peripheral factors or in the centralnervous system.
Of clinical relevance, short term use of celecoxib toreduce exercise-induced muscle damage cannot beadvocated. However, celecoxib might be a goodchoice when the intention is to reduce pain andpromote rehabilitation and recovery after injuries
COX-2 inhibition after eccentric exercise
e205
-
7/30/2019 Paulsen 2010
12/13
such as ankle sprains (Ekman et al., 2002; Nadarajahet al., 2006), without detectable adverse effects onthe musculature. The degree of damage from theexercise protocol applied in this study is not asextensive as after strain injuries (including myofiberrupture and intramuscular bleeding). Consequently,our conclusions should not without caution be ex-trapolated to other kinds of muscle injuries. It should
also be noted that celecoxib, and other first genera-tion COX-2 inhibitors, have been associated withincreased risk of cardiovascular events, such as heartattacks (Dajani & Islam, 2008). However, equivocalfindings have been made, and the short term use (fewweeks) of 400 mg/day for healthy people, notsuffering from cardiovascular disease, seems to be
reasonably safe (Kearney et al., 2006; Solomon et al.,2008).
Key words: muscle damage, non-steroidal anti-inflam-
matory drugs, leukocytes, satellite cells.
Acknowledgement
The authors would like to thank Prof. Lars Morkrid and theDepartment of Medical Biochemistry at RikshospitaletUniversity Hospital (Oslo, Norway) for performing the serumCK analyses. This study was partly financed by Pfizer Inc.(Norway). However, the authors have no economical interestsin Pfizer, nor are there any contract-bond restrictions orclauses that potentially could have influenced the study.
References
Almekinders LC. Anti-inflammatory
treatment of muscular injuries in sport.
An update of recent studies. Sports
Med 1999: 28: 383388.
Baldwin LA. Use of nonsteroidal anti-
inflammatory drugs following exercise-
induced muscle injury. Sports Med
2003: 33: 177185.
Bondesen BA, Mills ST, Kegley KM,
Pavlath GK. The COX-2 pathway is
essential during early stages of skeletal
muscle regeneration. Am J Physiol Cell
Physiol 2004: 287: C475C483.
Bourgeois J, MacDougall D, MacDonald J,
Tarnopolsky M. Naproxen does not alter
indices of muscle damage in resistance-
exercise trained men. Med Sci Sports
Exerc 1999: 31: 49.Burd NA, Dickinson JM, LeMoine JK,
Carroll CC, Haus JM, Hughes G,
Sanders C Jr., Trappe TA.
Consumption of a COX-2 inhibitor
stimulates muscle protein synthesis
after resistance exercise in humans. The
FASEB J 2008: 22: 958.
Buvanendran A, Reuben SS. COX-2
inhibitors in sports medicine: utility
and controversy. Br J Sports Med 2006:
40: 895896.
Carroll CC, Dickinson JM, LeMoine JK,
Haus JM, Weinheimer EM, Hollon CJ,
Trappe TA. Ibuprofen and
acetaminophen promote musclehypertrophy and strength gains during
resistance exercise in the elderly. The
FASEB J 2008: 22: 753.
Cheung K, Hume P, Maxwell L. Delayed
onset muscle soreness: treatment
strategies and performance
factors. Sports Med 2003: 33:
145164.
Child R, Brown S, Day S, Donnelly A,
Roper H, Saxton J. Changes in indices
of antioxidant status, lipid
peroxidation and inflammation in
human skeletal muscle after eccentric
muscle actions. Clin Sci (London)
1999: 96: 105115.
Clarkson PM, Byrnes WC, Gillisson E,
Harper E. Adaptation to exercise-
induced muscle damage. Clin Sci
(London) 1987: 73: 383386.
Connolly DA, Sayers SP, McHugh MP.
Treatment and prevention of delayed
onset muscle soreness. J Strength Cond
Res 2003: 17: 197208.
Crameri RM, Langberg H, Magnusson P,
Jensen CH, Schroder HD, Olesen JL,
Suetta C, Teisner B, Kjaer M. Changes
in satellite cells in human skeletal
muscle after a single bout of high
intensity exercise. J Physiol 2004: 558:
333340.
Dajani EZ, Islam K. Cardiovascular andgastrointestinal toxicity of selective
cyclo-oxygenase-2 inhibitors in man. J
Physiol Pharmacol 2008: 59(Suppl. 2):
117133.
Dudley GA, Czerkawski J, Meinrod A,
Gillis G, Baldwin A, Scarpone M.
Efficacy of naproxen sodium for
exercise-induced dysfunction muscle
injury and soreness. Clin J Sport Med
1997: 7: 310.
Ekman EF, Fiechtner JJ, Levy S, Fort
JG. Efficacy of celecoxib versus
ibuprofen in the treatment of acute
pain: a multicenter, double-blind,
randomized controlled trial in acuteankle sprain. Am J Orthop 2002: 31:
445451.
Feasson L, Stockholm D, Freyssenet D,
Richard I, Duguez S, Beckmann JS,
Denis C. Molecular adaptations of
neuromuscular disease-associated
proteins in response to eccentric
exercise in human skeletal muscle. J
Physiol 2002: 543: 297306.
Glebov OK, Rodriguez LM, Lynch P,
Patterson S, Lynch H, Nakahara K,
Jenkins J, Cliatt J, Humbyrd CJ,
Denobile J, Soballe P, Gallinger S,
Buchbinder A, Gordon G, Hawk E,
Kirsch IR. Celecoxib treatment alters
the gene expression profile of normal
colonic mucosa. Cancer Epidemiol
Biomarkers Prev 2006: 15: 13821391.
Hellsten Y, Frandsen U, Orthenblad N,
Sjodin B, Richter EA. Xanthine
oxidase in human skeletal muscle
following eccentric exercise: a role in
inflammation. J Physiol 1997: 498(Part
1): 239248.
Hikida RS, Staron RS, Hagerman FC,
Sherman WM, Costill DL. Muscle fiber
necrosis associated with human
marathon runners. J Neurol Sci 1983:
59: 185203.
Howell JN, Conatser RR, Chleboun GS,
Karapondo DL, Chila AG. The effectof nonsteroidal anti-inflammatory
drugs on recovery from exercise-
induced muscle injury 1. Flurbiprofen.
J Muscoskel Pain 1998a: 6: 5968.
Howell JN, Conatser RR, Chleboun GS,
Karapondo DL, Chila AG. The effect
of nonsteroidal anti-inflammatory
drugs on recovery from exercise-
induced muscle injury 2. Ibuprofen. J
Muscoskel Pain 1998b: 6: 6983.
Jones DA, Newham DJ, Round JM,
Tolfree SE. Experimental human
muscle damage: morphological
changes in relation to other indices of
damage. J Physiol 1986: 375: 435448.Jones DA, Newham DJ, Torgan C.
Mechanical influences on long-lasting
human muscle fatigue and delayed-
onset pain. J Physiol 1989: 412:
415427.
Kearney PM, Baigent C, Godwin J, Halls
H, Emberson JR, Patrono C. Do
selective cyclo-oxygenase-2 inhibitors
and traditional non-steroidal anti-
inflammatory drugs increase the risk of
atherothrombosis? Meta-analysis of
randomised trials. BMJ 2006: 332:
13021308.
Paulsen et al.
e206
-
7/30/2019 Paulsen 2010
13/13
Kuipers H, Keizer HA, Verstappen FT,
Costill DL. Influence of a
prostaglandin-inhibiting drug on
muscle soreness after eccentric
work. Int J Sports Med 1985: 6:
336339.
Lapointe BM, Fremont P, Cote CH.
Adaptation to lengthening contractions
is independent of voluntary muscle
recruitment but relies on inflammation.
Am J Physiol Regul Integr CompPhysiol 2002a: 282: R323R329.
Lapointe BM, Frenette J, Cote CH.
Lengthening contraction-induced
inflammation is linked to secondary
damage but devoid of neutrophil
invasion. J Appl Physiol 2002b: 92:
19952004.
Mackey AL, Kjaer M, Dandanell S,
Mikkelsen KH, Holm L, Dossing S,
Kadi F, Koskinen SO, Jensen CH,
Schroder HD, Langberg H. The
influence of anti-inflammatory
medication on exercise-induced
myogenic precursor cell responses in
humans. J Appl Physiol 2007: 103:425431.
McHugh MP. Recent advances in the
understanding of the repeated bout
effect: the protective effect against
muscle damage from a single bout of
eccentric exercise. Scand J Med Sci
Sports 2003: 13: 8897.
Mehallo CJ, Drezner JA, Bytomski JR.
Practical management: nonsteroidal
antiinflammatory drug (NSAID) use in
athletic injuries. Clin J Sport Med
2006: 16: 170174.
Miller SB. Prostaglandins in health and
disease: an overview. Semin Arthritis
Rheum 2006: 36: 3749.
Nadarajah A, Abrahan L, Lau FL,
Hwang LJ, Fakir-Bolte C. Efficacy and
tolerability of celecoxib compared with
diclofenac slow release in the treatment
of acute ankle sprain in an Asian
population. Singapore Med J 2006: 47:
534542.
Newham DJ, Jones DA, Clarkson PM.
Repeated high-force eccentric
exercise: effects on muscle pain and
damage. J Appl Physiol 1987: 63:
13811386.
Paoloni JA, Orchard JW. The use of
therapeutic medications for soft-tissue
injuries in sports medicine. Med J Aust
2005: 183: 384388.
Paulsen G, Crameri R, Benestad HB,
Fjeld JG, Mrkrid L, Halle n J,
Raastad T. Time course of leukocyte
accumulation in human muscle after
eccentric exercise. Med Sci Sports
Exerc 2009 (in press).
Peterson JM, Trappe TA, Mylona E,White F, Lambert CP, Evans WJ, Pizza
FX. Ibuprofen and acetaminophen:
effect on muscle inflammation after
eccentric exercise. Med Sci Sports
Exerc 2003: 35: 892896.
Raastad T, Risoy BA, Benestad HB,
Fjeld JG, Hallen J. Temporal relation
between leukocyte accumulation in
muscles and halted recovery 1020 h
after strength exercise. J Appl Physiol
2003: 95: 25032509.
Reuben SS, Ekman EF. The effect of
cyclooxygenase-2 inhibition on
analgesia and spinal fusion. J Bone
Joint Surg Am 2005: 87: 536542.Reuben SS, Ekman EF. The effect of
initiating a preventive multimodal
analgesic regimen on long-term patient
outcomes for outpatient anterior
cruciate ligament reconstruction
surgery. Anesth Analg 2007: 105:
228232.
Round JM, Jones DA, Cambridge G.
Cellular infiltrates in human skeletal
muscle: exercise induced damage as a
model for inflammatory muscle
disease? J Neurol Sci 1987: 82: 111.
Sayers SP, Knight CA, Clarkson PM,
Van Wegen EH, Kamen G. Effect of
ketoprofen on muscle function and
sEMG activity after eccentric exercise.
Med Sci Sports Exerc 2001: 33:
702710.
Schneider BS, Tiidus PM. Neutrophil
infiltration in exercise-injured skeletal
muscle: how do we resolve the
controversy? Sports Med 2007: 37:
837856.
Shen W, Li Y, Tang Y, Cummins J,
Huard J. NS-398, a cyclooxygenase-
2-specific inhibitor, delays skeletal
muscle healing by decreasing
regeneration and promoting fibrosis.
Am J Pathol 2005: 167: 11051117.
Shen W, Prisk V, Li Y, Foster W, Huard
J. Inhibited skeletal muscle healing in
cyclooxygenase-2 gene-deficient mice:
the role of PGE2 and PGF2alpha. J
Appl Physiol 2006: 101: 12151221.
Solomon SD, Wittes J, Finn PV, Fowler
R, Viner J, Bertagnolli MM, Arber N,
Levin B, Meinert CL, Martin B, Pater
JL, Goss PE, Lance P, Obara S, ChewEY, Kim J, Arndt G, Hawk E.
Cardiovascular risk of celecoxib in 6
randomized placebo-controlled trials:
the cross trial safety analysis.
Circulation 2008: 117: 21042113.
Tegeder L, Zimmermann J, Meller ST,
Geisslinger G. Release of algesic
substances in human experimental
muscle pain. Inflamm Res 2002: 51:
393402.
Trappe TA, Fluckey JD, White F,
Lambert CP, Evans WJ. Skeletal
muscle PGF(2)(alpha) and PGE(2) in
response to eccentric resistance
exercise: influence of ibuprofenacetaminophen. J Clin Endocrinol
Metab 2001: 86: 50675070.
Trappe TA, White F, Lambert CP, Cesar
D, Hellerstein M, Evans WJ. Effect of
ibuprofen and acetaminophen on
postexercise muscle protein synthesis.
Am J Physiol Endocrinol Metab 2002:
282: E551E556.
Veiga AP, Duarte ID, Avila MN, da
Motta PG, Tatsuo MA, Francischi JN.
Prevention by celecoxib of secondary
hyperalgesia induced by formalin in
rats. Life Sci 2004: 75: 28072817.
Vuolteenaho K, Moilanen T, Moilanen E.
Non-steroidal anti-inflammatory
drugs, cyclooxygenase-2 and the bone
healing process. Basic Clin Pharmacol
Toxicol 2008: 102: 1014.
Warden SJ. Cyclo-oxygenase-2 inhibitors:
beneficial or detrimental for athletes
with acute musculoskeletal injuries?
Sports Med 2005: 35: 271283.
Yu JG, Malm C, Thornell LE. Eccentric
contractions leading to DOMS do not
cause loss of desmin nor fibre necrosis
in human muscle. Histochem Cell Biol
2002: 118: 2934.
COX-2 inhibition after eccentric exercise
e207