AJR:182, February 2004 283 Pre valence and Patterns of Occult Hip Fractures and Mimics Rev ealed by MRI OBJECTIVE. The diagnosis of hip fractures can be difficult on radiography alone. MRI is frequently used to confirm or deny the presence of a minimally displaced hip fracture. This study evaluates the patterns of injury seen on MRI that ar e difficult to diagnose on radiography. MATERIALS AND METHODS. MRIs of 73 patients who were examined for possible hip fractures and whose radiographic findings were negative or equivocal for hip fracture were reviewed. Seventy-six studies were performed in 73 patients who were between 24 and 102 years old. MRIs were evaluated for the pr esence and location of bone or sof t-tissue injury. Muscle injuries were categorized on the basis of location and type of injury. RESULTS. Forty-six percent (35/76) of the studies showed subtle fractures. Seventeen fractures were in the proximal femur and 18 in the innominate bone. Soft-tissue abnormali- ties were common, found in 65% of the studies. Twenty percent of the MRI findings were considered normal because there was no apparent finding on the images to explain the pa- tients’ symptoms. CONCLUSION. Soft-tissue abnormalities are commonly seen alone or in association with subtle fractures on MRI in the evaluation of patients with a clinical suspicion of hip frac- ture. MRI is recommended for all symptomatic patients whose radiographic findings are neg- ative for hip fracture. ip injury is a growing medical prob- lem, mostly because of an increase in the elderly population and in high-velocity motor vehicle trauma affecting young people [1]. Prompt and early diagnosis is important in minimally displaced fractures of the femoral neck because delayed diagnosis and treatment may result in signi ficant displacement of the fracture fragment [2]. Signi ficant displace- ment will alter the treatment and require more extensive surgery, such as hemiarthroplasty in- stead of stabilization with internal fixation. Diagnosis of minimally displaced hip frac- tures on radiographs can be challenging, es- pecially in elderly patients with osteoporosis [3–7]. In these patients, in the face of reason- able clinical suspicion for fracture, MRI is recommended for further evaluation when conventional radiographic findings are nega- tive or equivocal [7–10]. A subset of patients exist who have clini- cal signs and symptoms of hip fracture but do not show a fracture on MRI. Various soft- tissue injuries have been found on MRI of some of these patients [11, 12]. Evaluating the incidence and type of bone and muscle injuries in cases of clinical suspicion of hip fracture will help clarify injury patterns that clinically mimic femoral neck fractures. Materials and Methods Patients with a clinical suspicion of hip fracture who underwent MRI of the hip because radio- graphic findings were reported to be negative were retrospectively identified from our radiology data- base. Seventy-six studies from 73 patients—28 men and 45 women—satisfied the selection crite- ria and form the population of this study. One pa- tient was evaluated for bilateral hip fractures, and one patient with systemic lupus erythematosus who was undergoing steroid therapy was evaluated on three occasions. The patients were 24–102 years old (average, 67 years). All images were reviewed in conference by both authors, one a fellowship-trained and experienced musculoskeletal radiologist and the other a trainee radiologist. Except for three patients who were evaluated with only frontal radiography of the pel- vis, all patients underwent radiography of the pel- vis in the anteroposterior projection and of the hip in anteroposterior and cross-table lateral projec- Mayumi Oka 1,2 Johnny U. V. Monu 1 Received April 5, 2002; accepted after revision August 19, 2003. Presented at the 2001 annual meeting of the American Roentgen Ray Society, Seattle, WA. 1 Department of Radiology, University of Rochester School of Medicine and Dentistry, University of Rochester Medical Center, 601 Elmwood Ave., Box 648, Rochester, NY 14642. Address correspondence to J. U. V. Monu. 2 Present address: Department of Radiology, Johns Hopkins Hospital, 600 N Wolfe St., Baltimore, MD 21287. AJR 2004;182:283–288 0361–803X/04/1822–283 © American Roentgen Ray Society H

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

8/3/2019 Patterns of Occult Hip Fractures and Mimics Revealed by MRI
http://slidepdf.com/reader/full/patterns-of-occult-hip-fractures-and-mimics-revealed-by-mri 1/6
AJR:182, February 2004 283
Prevalence and Patterns of OccultHip Fractures and Mimics Revealedby MRI
OBJECTIVE.
The diagnosis of hip fractures can be difficult on radiography alone. MRI is
frequently used to confirm or deny the presence of a minimally displaced hip fracture. This
study evaluates the patterns of injury seen on MRI that are difficult to diagnose on radiography.
MATERIALS AND METHODS. MRIs of 73 patients who were examined for possible
hip fractures and whose radiographic findings were negative or equivocal for hip fracture
were reviewed. Seventy-six studies were performed in 73 patients who were between 24 and
102 years old. MRIs were evaluated for the presence and location of bone or soft-tissue injury.Muscle injuries were categorized on the basis of location and type of injury.
RESULTS.
Forty-six percent (35/76) of the studies showed subtle fractures. Seventeen
fractures were in the proximal femur and 18 in the innominate bone. Soft-tissue abnormali-
ties were common, found in 65% of the studies. Twenty percent of the MRI findings were
considered normal because there was no apparent finding on the images to explain the pa-
tients’ symptoms.
CONCLUSION.
Soft-tissue abnormalities are commonly seen alone or in association
with subtle fractures on MRI in the evaluation of patients with a clinical suspicion of hip frac-
ture. MRI is recommended for all symptomatic patients whose radiographic findings are neg-
ative for hip fracture.
ip injury is a growing medical prob-
lem, mostly because of an increasein the elderly population and in
high-velocity motor vehicle trauma affecting
young people [1]. Prompt and early diagnosis is
important in minimally displaced fractures of the
femoral neck because delayed diagnosis and
treatment may result in significant displacement
of the fracture fragment [2]. Significant displace-
ment will alter the treatment and require more
extensive surgery, such as hemiarthroplasty in-
stead of stabilization with internal fixation.
Diagnosis of minimally displaced hip frac-
tures on radiographs can be challenging, es-
pecially in elderly patients with osteoporosis
[3–7]. In these patients, in the face of reason-able clinical suspicion for fracture, MRI is
recommended for further evaluation when
conventional radiographic findings are nega-
tive or equivocal [7–10].
A subset of patients exist who have clini-
cal signs and symptoms of hip fracture but
do not show a fracture on MRI. Various soft-
tissue injuries have been found on MRI of
some of these patients [11, 12].
Evaluating the incidence and type of bone
and muscle injuries in cases of clinical suspicionof hip fracture will help clarify injury patterns
that clinically mimic femoral neck fractures.
Materials and Methods
Patients with a clinical suspicion of hip fracture
who underwent MRI of the hip because radio-
graphic findings were reported to be negative were
retrospectively identified from our radiology data-
base. Seventy-six studies from 73 patients—28
men and 45 women—satisfied the selection crite-
ria and form the population of this study. One pa-
tient was evaluated for bilateral hip fractures, and
one patient with systemic lupus erythematosus
who was undergoing steroid therapy was evaluatedon three occasions. The patients were 24–102
years old (average, 67 years).
All images were reviewed in conference by both
authors, one a fellowship-trained and experienced
musculoskeletal radiologist and the other a trainee
radiologist. Except for three patients who were
evaluated with only frontal radiography of the pel-
vis, all patients underwent radiography of the pel-
vis in the anteroposterior projection and of the hip
in anteroposterior and cross-table lateral projec-
Mayumi Oka
1,2
Johnny U. V. Monu
1
Received April 5, 2002; accepted after revisionAugust 19, 2003.
Presented at the 2001 annual meeting of the American
Roentgen Ray Society, Seattle, WA.
1
Department of Radiology, University of Rochester Schoolof Medicine and Dentistry, University of RochesterMedical Center, 601 Elmwood Ave., Box 648, Rochester, NY14642. Address correspondence to J. U. V. Monu.
2
Present address: Department of Radiology, JohnsHopkins Hospital, 600 N Wolfe St., Baltimore, MD 21287.
AJR
2004;182:283–288
0361–803X/04/1822–283
© American Roentgen Ray Society
H

8/3/2019 Patterns of Occult Hip Fractures and Mimics Revealed by MRI
http://slidepdf.com/reader/full/patterns-of-occult-hip-fractures-and-mimics-revealed-by-mri 2/6
284
AJR:182, February 2004
Oka and Monu
tions. The radiographs were reviewed for adequacy
of the image quality and the presence of fractures.
A study was deemed adequate when the acetabu-
lum, femoral head, and femoral neck were visual-
ized on two images. No patients were excluded
because of inadequate radiographs.
Sixty-four of the 76 MRIs of the hip were ob-
tained within 48 hr after the radiographs. However,the interval between radiographs and MRI studies
ranged from 5 days to 3 weeks in the other 12 cases.
All MRI studies were performed on a 1.5-T unit
(Signa, General Electric Medical Systems, Milwau-
kee, WI) using a commercially available pelvic
phased array surface coil as a receiver. Imaging pro-
tocols varied but generally included T1-weighted
spin-echo images (TR/TE range, 600/14–18; slice
thickness, 5 mm; interslice gap, 0.5–1.0 mm; matrix,
256 ×
192) in the axial and oblique coronal planes;
T2-weighted fast spin-echo images (TR range/TE
range, 3,200–5,000/96–102; slice thickness, 5 mm;
interslice gap, 0.5–1.0 mm; matrix, 256 ×
192) with
fat saturation; and occasional STIR images (TR/TE,
4,800/60; inversion time, 150 msec; slice thickness, 5
mm; interslice gap, 0.5–1.0 mm; matrix, 256 × 192)
in the coronal or axial plane. Images in the sagittal
plane using dual-echo spin-echo pulse sequences
were infrequently obtained. Field of view ranged be-
tween 16 and 22 cm to cover the index hip joint.
The MRIs were evaluated for the presence and
site of bone or soft-tissue injury. The bone injuries
were characterized as bone contusion or fracture.
A fracture was diagnosed when a linear low-
signal focus was surrounded by an intermediate-
signal area on T1-weighted images and the linear
low-signal focus was surrounded by high signal on
T2-weighted images [9, 10, 12]. Ill-defined areas
of altered signal intensity on T1-weighted images
and high signal intensity on T2-weighted images
were interpreted as bone marrow edema.
Soft-tissue injuries were further characterized
as muscle edema, hematoma, partial muscle tear,
or complete muscle tear using criteria that have
been previously defined [13–19].Acute muscle injuries have associated edema and
hemorrhage that cause prolongation of the T1 and T2
relaxation times of the injured tissue [14]. Muscle in-
juries were diagnosed when areas of increased signal
intensity were seen on T2-weighted or STIR images.
Complete tears showed total disruption of the muscle,
muscle retraction, blood, and edema in the tear. A par-
tial tear is seen as a focal interruption of continuity of
the muscle without complete transection of the mus-
cle or tendon. Muscle edema was seen as a nongeo-
graphic area or an infiltrative pattern of low signal on
T1-weighted and high signal on T2-weighted images
that could not be distinguished from early interstitial
hemorrhage. Any confined area of altered signal
within or outside the muscle fibers was identified as a
hematoma, which is a form of muscle injury [13, 14].
In a setting of trauma, it may be difficult to differenti-
ate an isolated hematoma from a hematoma arising
from a muscle injury; a hematoma was therefore con-
sidered to be muscle injury in this study. A hematoma
may show varying signal intensities on both T1- and
T2-weighted images, depending on the evolving state
of hemoglobin [20].
We further analyzed our results in terms of
muscle function and stratified the muscles around
the hip joint into groups as follows: thigh adduc-
tor, thigh abductor, external rotator, internal rota-
tor, flexor, and extensor. This stratification was
based on their primary function or function when
the hip was in a neutral position [21]. The individ-
ual muscles and the functional muscle groups are
shown in Appendix 1.
Results
Our retrospective review showed that no
fractures were missed on radiographs.
Thirty-five (46%) of 76 studies were found
to have fractures on MRI (Table 1). The frac-
tures were four fractures of the greater tro-
chanter (Fig. 1), five intertrochanteric
fractures, and eight femoral neck fractures.
TABLE 1Fractures and Locations(n = 35)
Fracture Location No.
Femoral fractures
Neck 8
Intertrochanteric 5
Greater trochanteric 4
Total 17
Pelvic fractures
Pubic rami alone 13
Acetabulum alone 2
Pubic rami and acetabulum 3
Total 18
Grand total 35
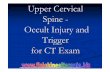
Fig. 1.—77-year-old woman with fracture of greater trochanter after fall. Fracture was difficult to visualize on conventional radiographs.A, Frontal radiograph of left hip appears to show normal findings.B, T1-weighted coronal image of left hip shows linear low-signal focus (arrowheads ), indicating fracture.
BA

8/3/2019 Patterns of Occult Hip Fractures and Mimics Revealed by MRI
http://slidepdf.com/reader/full/patterns-of-occult-hip-fractures-and-mimics-revealed-by-mri 3/6
MRI of Hip Fractures
AJR:182, February 2004
285
In the innominate bones, there were five ace-
tabular fractures and 13 fractures of the obtura-
tor ring. Two patients had bone marrow edema
without focal cortical disruption (Fig. 2).
In the group with fractures on MRI, 24
(69%) had associated muscle injury. The obtu-
rator externus muscle, a major external rotator,
was abnormal in 15 studies (43%). Injury to
the other external rotators of the hip, which in-
clude the gluteus maximus, piriformis, obtura-
torius internus, gemelli, and quadratus
femoris, was seen in 17 studies (49%). Injury
Fig. 2.—67-year-old woman who presented with persistent right hip pain after fall 3 weeks earlier.
A, Frontal radiograph of right hip shows unremarkable findings.B, Coronal T2-weighted image shows abnormally high signal in anterior column of hip and in area of superior pubic ramus, consistent with trabecular fracture. Linear ab-normally high signal is seen in adductors and obturator externus and is compatible with presence of interstitial edema or hemorrhage.
BA
Fig. 3.—73-year-old man who experienced hip pain after fall. He had no fractures, but MRI showed muscle injury.A, T1-weighted coronal image shows abnormal signal of interstitial muscle hemorrhage (arrows ) in obturator externus muscle near its attachment to greater trochanterand in musculotendinous junction.B, T2-weighted coronal image shows abnormal signal in obturator externus muscle near its attachment to greater trochanter and in musculotendinous junction. Thesefindings are compatible with interstitial hemorrhage (arrows ).
BA

8/3/2019 Patterns of Occult Hip Fractures and Mimics Revealed by MRI
http://slidepdf.com/reader/full/patterns-of-occult-hip-fractures-and-mimics-revealed-by-mri 4/6
286
AJR:182, February 2004
Oka and Monu
to the thigh adductor was seen in 22 studies
(63%). In this group of patients with adductor
muscle injuries, five (23%) were associated
with femoral fractures and 17 (77%) were re-
lated to fractures of the innominate bone.
On the basis of MRI findings, 41 patients
(56%) did not have a fracture. Twenty-six
(63%) of the patients in this group had muscle
injuries. The obturator externus muscle was the
most frequently injured muscle, with abnormal-
ity seen in 13 (32%) of the 41 patients (Fig. 3).
Injury to the other external rotators of the hip
was seen in 14 studies (34%). Twelve studies
(29%) showed injuries in the abductor group(Tables 2 and 3 and Appendix 1).
Trauma was the indication for the study in
42 patients (58%), including 27 (77%) of the
35 studies showing fractures and 15 (37%) of
the 41 studies showing no fracture. The re-
maining 31 patients (43%) had pain but no
history of recent trauma, and the study was
requested to consider unexpected fractures.
Among these patients were eight fractures
(26%) and 13 muscle injuries (42%).
Overall, muscle injuries were seen in 50
studies (66%). Muscle edema, hemorrhage,
and partial tear represented most of the muscle
injuries and were seen in 49 studies. One pa-
tient had an iliopsoas muscle abscess (Fig. 4).
Mean patient age was 70 years in the fracture
group and 63 years in the nonfracture group.
The distribution of abnormalities detected in
individual muscles and in various functional
muscle groups is shown in Appendix 1 and Ta-
ble 2. Injury to the gluteus medius and gluteus
minimus, which are strong internal rotators of
the hip and thigh abductors, was seen with
equal frequency in patients with and withoutfractures. Injury to the gluteus maximus was
more frequently seen in patients without frac-
ture. The external rotators are the most com-
monly injured muscles in both groups.
Fifteen patients (21%) (13 women and
two men) had no fractures or muscle injuries
on MRI. The mean age in this group was
57.3 years (range, 33–81 years).
Discussion
The term “hip fracture” implies a proximal
femoral fracture, usually involving the femoral
neck. Proximal femoral fractures involving thefemoral neck or intertrochanteric regions are
devastating injuries to the hip that need to be
promptly diagnosed. However, injuries that in-
volve the innominate bone or adjacent muscles
may present with similar signs and symptoms.
In this series, 24% of the studies showed pel-
vic fractures that were occult on radiography,
with fractures of the obturator ring (21%) be-
ing the most common.
Generally, patients who sustain obturator
ring fractures or muscle injury around the
hip joint do not require surgery; however,
they can still have prolonged immobilization,
difficulty with ambulation as a result of pain,
and subsequent impaired hip function if the
fracture is not properly treated. Physical
therapy and early mobilization are essential
for these patients to recover as much func-
tion as possible.
Muscle injuries were present in 65% (49/
76) of studies regardless of the presence or
absence of fracture. Muscle injury may be
caused by a direct blow (contusion) or an in-
direct injury (strain due to abnormal stretch-
ing) and may result in edema, hemorrhage,
muscle tear, and hematoma. Edema and
hemorrhage present as high signal intensity
interspersed in muscles on T2-weighted im-
ages. In this series, the adductor muscle
group was frequently injured in association
with an obturator ring fracture.
Muscle tears tend to occur at or near the
musculotendinous junction and are seen as
focal high signal intensity on T2-weighted
images. Moderate strain and partial tears are
difficult to distinguish from hemorrhage
when the latter are located near the junction.
MRI may not always differentiate between a
muscle strain or tear that is associated with a
fracture and hemorrhage into the muscles
from a fracture. MRI findings reflect only the
relative presence of edema, deoxyhemoglo-
bin, and methemoglobin (Fig. 5).
The frequency and distribution of muscleinjuries were similar in the group of patients
with fractures (69%) and in the group with
no bone injuries (63%). Some of the ob-
served clinical signs and symptoms are
caused by associated muscle injuries [11].
The 46% occult fracture rate in this study is
similar to a fracture rate of 54% in the study by
Bogost et al. [11]. The differences in our fig-
ures may be partly explained by the fact that
Bogost et al. studied only patients with a clear
history of trauma. Because a clear history of
trauma may not be readily available in elderly
patients, we included in our study population
patients with a clinically suspected hip fracturewith no history of trauma. Our position is sup-
ported by the subsequent observation that
nearly 23% (35 patients) of the fractures were
in our group of patients who did not recall or
give a clear history of trauma.
In addition to obturator ring fractures,
Bogost et al. [11] reported a small number of
sacral fractures. We found no sacral fractures
in our study population. The sacrum was not
TABLE 2 Muscle Injury, by Individual Muscles (n = 76)
Muscle No Fracture (n = 41) Fracture (n = 35) Total (n = 76)
Iliopsoas 5 5 10
Obturator internus 3 7 10
Obturator externus 13 15 28
Pectineus 3 5 8Adductor longus 6 7 13
Adductor brevis 7 10 17
Adductor magnus 7 5 12
Gluteus minimus 7 8 15
Gluteus medius 7 6 13
Gluteus maximus 6 3 9
Tensor fasciae latae 1 1
Rectus femoris 2 2
Vastus lateralis 2 2
Piriformis 2 2
TABLE 3Muscle Injury, by MuscleGroup (n = 76)
Muscle GroupNo Fracture
(n = 41)
Fracture
(n = 35)
Extensors 11 8
Flexors 5 5
Adductors 7 12
Abductors 11 9
Internal rotators 13 14
External rotators 17 19

8/3/2019 Patterns of Occult Hip Fractures and Mimics Revealed by MRI
http://slidepdf.com/reader/full/patterns-of-occult-hip-fractures-and-mimics-revealed-by-mri 5/6
MRI of Hip Fractures
AJR:182, February 2004
287
routinely included in our images because our
imaging protocol called for a smaller field of
view. The incidence of muscle injury in our
study population was similar to that of Bogost
et al., which was 61% (40% in the fracture
group and 21% in the no-fracture group).
The elderly patient is generally fragile and
does not require a major traumatic event to
sustain a fracture or significant muscle in-
jury. A history of trauma may not be readilyavailable or recalled. Furthermore, hip frac-
tures in the elderly may present with atypical
symptoms, such as several weeks of pain or
gait instability. Occasionally in this popula-
tion, some nontraumatic causes of hip pain
such as an iliopsoas abscess (Fig. 4) and
even exacerbation of hip arthritis may
present acutely and mimic a hip fracture.
Frequently, these elderly patients have coex-
isting morbidity that confuses the clinical
picture and confounds accurate diagnosis.
Because morbidity and mortality after hip
injury in the elderly have a significant socio-
economic impact, prompt and accurate diag-nosis is imperative [1].
MRI not only facilitates the diagnosis of
nondisplaced fractures not seen on radio-
graphs [8, 10, 22, 23] but also provides infor-
mation that may be beneficial for the
appropriate treatment of other injuries. Lim-
ited MRI protocols with T1-weighted coro-
nal images were previously reported to be
sufficient to detect proximal femoral frac-
tures [9, 24]. However, we emphasize the
usefulness of T2-weighted sequences in the
diagnosis of injuries other than hip fractures.
T2-weighted images facilitate recognition of
soft-tissue injuries. In addition, areas of bone
marrow edema cannot be distinguished from
sclerosis using T1-weighted images alone.
The main limitation of this study is that it
was retrospective. The study population was too
small for statistical confirmation. The protocols
BA
Fig. 4.—81-year-old woman with abscess in iliopsoas muscle who presented with left hip pain, no history of trauma, and clinical suspicion of occult fracture.A, T1-weighted axial image shows rounded low-signal focus (arrow ) adjacent to left iliacus muscle.B, T2-weighted image shows central area of high signal surrounded by concentric focus of low- and high-signal zones, consistent with abscess (solid arrow ). Abnormallyhigh signal in iliacus muscle (open arrows ) is result of muscle inflammation.
Fig. 5.—74-year-old woman with iliopsoas avulsion injury after fall 2 days before MRI examination. T2-weightedaxial fast spin-echo fat-suppressed image shows abnormally high signal (arrows ) in and surrounding iliopsoasmuscle, which is consistent with partial tear of muscle and surrounding hemorrhage. Note also some abnormalsignal around gluteus minimus muscle (asterisks ).

8/3/2019 Patterns of Occult Hip Fractures and Mimics Revealed by MRI
http://slidepdf.com/reader/full/patterns-of-occult-hip-fractures-and-mimics-revealed-by-mri 6/6
288
AJR:182, February 2004
Oka and Monu
for MRI of the hip varied during the study pe-
riod. However, our entire patient population had
both T1-weighted and T2-weighted sequences
as part of their study. Although multiple radiolo-
gists interpreted the conventional radiographs,
our retrospective review showed that no frac-
tures were missed on radiographs.
In conclusion, soft-tissue injuries com-
monly accompany hip fractures but may exist
in isolation and may mimic fractures in that
they can produce similar symptoms. Soft-tis-
sue injuries alone can be a cause of morbidity
and merit additional attention. MRI is useful in
the diagnosis of soft-tissue injuries, especially
in the setting of clinically suspected hip frac-
tures. MRI is recommended for all symptom-
atic patients whose conventional radiographs
do not reveal a hip fracture.
References
1. Rudman N, McIlmail D. Emergency department
evaluation and treatment of hip and thigh injuries.
Emerg Med Clin North Am
2000;18:29–66
2. Lu-Yao GL, Keller RB, Littenberg B, Wennberg
JE. Outcomes after displaced fractures of the
femoral neck: a meta-analysis of one hundred and
six published reports. J Bone Joint Surg Am
1994;76:15–25
3. Schultz E, Miller TT, Boruchov SD, Schmell EB,
Toledano B. Incomplete intertrochanteric frac-
tures: imaging features and clinical management.
Radiology
1999;211:237–240
4. Ganel A, Engel J, Oster Z, et al. Bone scanning in
assessment of fractures of the scaphoid. J Hand
Surg
1979;4:540–543
5. Matin P. Bone scintigraphy in the diagnosis and
management of traumatic injury. Semin Nucl Med
1983;13:104–122
6. Grainger C, Garcia J, Howart NR, May M, Rosier
P. Role of MRI in the diagnosis of insufficiency
fractures of the sacrum and acetabular roof. Skel-
etal Radiol
1997;26:517–524
7. Haramati N, Staron RB, Barax C, Feldman F. Mag-
netic resonance imaging of occult fractures of the
proximal femur. Skeletal Radiol 1994;23:19–22
8. Rubin SJ, Marquardt JD, Gottlieb RH, Meyers
SP, Totterman SMS, O’Mara RE. Magnetic reso-
nance imaging: a cost-effective alternative to
bone scintigraphy in the evaluation of patients
with suspected hip fractures. Skeletal Radiol
1998;27:199–204
9. Quinn SF, McCarthy JL. Prospective evaluation
of patients with suspected hip fracture and inde-
terminate radiographs: use of T1-weighted MR
images. Radiology
1993;187:469–471
10. Deutsch AL, Mink JH, Waxman AD. Occult frac-
tures of the proximal femur: MR imaging. Radi-
ology
1989;170:113–6
11. Bogost GA, Lizerbram EK, Crues JV III. MR im-
aging in evaluation of suspected hip fracture: fre-
quency of unsuspected bone and soft-tissue
injury. Radiology
1995;197:263–267
12. May DA, Purins JL, Smith DK. MR imaging of
occult traumatic fractures and muscular injuries
of the hip and pelvis in elderly patients. AJR
1996;166:1075–1078
13. Kneeland JB. MR imaging of sports injuries of the hip.
Magn Reson Imaging Clin N Am 1999;7:105–115
14. El-Khoury GY, Brandser EA, Kathol MH, Tearse
DS, Callaghan JJ. Imaging of muscle injuries.
Skeletal Radiol 1996;25:3–11
15. De Smet AA. MR imaging of acute and remote
muscle injuries. In: De Smet AA, ed. Musculoskele-
tal MRI: normal anatomy and key pathology
.
(ARRS categorical course syllabus) Leesburg, VA:
American Roentgen Ray Society, 2001:97–103
16. Deutsch AL, Mink JH. Magnetic resonance imag-
ing of musculoskeletal injuries. Radiol Clin North
Am
1989;27:983–1002
17. Palmer WE, Kuong SJ, Elmadbouh HM. MR imag-
ing of myotendinous strain. AJR
1999;173:703–709
18. De Smet AA. Magnetic resonance findings in skele-
tal muscle tears. Skeletal Radiol
1993;22:479–484
19. Arrington ED, Miller MD. Skeletal muscle inju-
ries. Orthop Clin North Am 1995;26:411–422
20. Bush CH. The magnetic resonance imaging of
musculoskeletal hemorrhage. Skeletal Radiol
2000;29:1–9
21. Warwick R, Williams PL.
Gray’s anatomy
, 35th
ed. Edinburgh, Scotland: Longman Group,
1973:559–571
22. Pandey R, McNally E, Ali A, Bulstrode C. The
role of MRI in the diagnosis of occult hip frac-
tures. Injury
1998;29:61–63
23. Rizzo PF, Gould ES, Lyden JP, Asnis SE. Diagno-
sis of occult fractures about the hip: magnetic res-
onance imaging compared with bone scanning.
J
Bone Joint Surg Am
1994;75:395–401
24. Mlinek EJ, Clark KC, Walker CW. Limited mag-
netic resonance imaging in the diagnosis of occult
hip fractures. Am J Emerg Med 1998;16:390–392
APPENDIX 1. Functional Muscle Groups About the Hip
Extensors
Primary:
Gluteus maximus, adductor magnus
Other:
Gluteus medius, gluteus minimus, biceps femoris, semitendinosus,
semimembranosus
Flexors
Primary:
Iliopsoas, pectineus, sartorius, tensor fasciae latae
Other:
Adductors, rectus femoris
Adductors
Primary:
Adductor longus, adductor brevis, adductor magnus, gracilis
Other:
Obturator externus, pectineus, gluteus maximus
Abductors
Primary:
Gluteus medius, gluteus minimus, tensor fasciae latae, sartorius
Other:
Piriformis, quadratus femoris
Internal Rotators
Primary:
Gluteus medius, gluteus minimus, tensor fasciae latae, pectineus
Other:
Semitendinosus, semimembranosus
External Rotators
Primary:
Gluteus maximus, piriformis, obturator internus, obturator externus,
superior gemellus, inferior gemellus, quadratus femoris
Related Documents