1 23 Intensive Care Medicine ISSN 0342-4642 Intensive Care Med DOI 10.1007/s00134-012-2500-9 Pattern of end-of-life decisions in two Tunisian intensive care units: the role of culture and intensivists’ training Islem Ouanes, Néji Stambouli, Fahmi Dachraoui, Lamia Ouanes-Besbes, Samir Toumi, Faouzi Ben Salem, Mourad Gahbiche & Fekri Abroug

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

1 23
Intensive Care Medicine ISSN 0342-4642 Intensive Care MedDOI 10.1007/s00134-012-2500-9
Pattern of end-of-life decisions in twoTunisian intensive care units: the role ofculture and intensivists’ training
Islem Ouanes, Néji Stambouli, FahmiDachraoui, Lamia Ouanes-Besbes, SamirToumi, Faouzi Ben Salem, MouradGahbiche & Fekri Abroug

1 23
Your article is protected by copyright and all
rights are held exclusively by Copyright jointly
held by Springer and ESICM. This e-offprint
is for personal use only and shall not be self-
archived in electronic repositories. If you
wish to self-archive your work, please use the
accepted author’s version for posting to your
own website or your institution’s repository.
You may further deposit the accepted author’s
version on a funder’s repository at a funder’s
request, provided it is not made publicly
available until 12 months after publication.

Islem OuanesNeji StambouliFahmi DachraouiLamia Ouanes-BesbesSamir ToumiFaouzi Ben SalemMourad GahbicheFekri Abroug
Pattern of end-of-life decisions in two Tunisianintensive care units: the role of cultureand intensivists’ training
Received: 24 June 2011Accepted: 20 November 2011
� Copyright jointly held by Springer andESICM 2012
I. Ouanes � F. Dachraoui �L. Ouanes-Besbes � F. Abroug ())Medical Intensive Care Unit, FattoumaBourguiba University Hospital, Universityof Monastir, 5000 Monastir, Tunisiae-mail: [email protected].: ?216-73-460672Fax: ?216-73-460678
N. Stambouli � S. Toumi �F. Ben Salem � M. GahbicheSurgical Intensive Care Unit,Fattouma Bourguiba University Hospital,University of Monastir, Monastir, Tunisia
Abstract Purpose: End-of-life(EOL) decisions are not well studiedin developing countries. We reportEOL decision patterns in two Tuni-sian intensive care units [ICUs,medical (MICU) and surgical(SICU)] belonging to the sameteaching hospital. Methods: Con-secutive deaths that occurred inparticipating ICUs over 2 years wereanalysed. End-of-life decisions wereprospectively recorded by the seniorattending physicians, while subject’scharacteristics were retrospectivelycollected. Results: Deaths occurredin 326 of 1,733 ICU-admitted patients(median age: 64 years; median SAPSII at admission = 36). Overall, adecision for full support was taken in69%, while decisions to withhold orwithdraw life support were held in22.1 and 8.9% of deaths, respectively.The rate of end-of-life decisions wassimilar in the MICU and the SICU. Inno instance was there MV withdrawalduring ICU stay. Discharging patients
to die at home was observed only inthe MICU (10 out of the 20 patientswith a withdrawal decision). Twofactors were independently associatedwith WH or WD decisions: a severeand ultimately fatal underlying dis-ease was positively associated withsuch decisions (OR = 2.4, 95% CI:1.3–4.36; p = 0.003), while havingan independent functional statusbefore the ICU was associated with adecreased rate of physician decisionsof WH or WD (OR = 0.32, 95% CI:0.15–0.67; p = 0.002). Conclu-sion: Withholding and withdrawinglife support are common in medicaland surgical ICUs of a Tunisian hos-pital. Withholding is more frequentthan withdrawing life support. Thesedecisions appear to be effected byfunctional status and underlyingconditions.
Keywords End of life � Culture �Ethics � Muslim countries � Tunisia
Introduction
Demands on intensive care services are increasingworldwide as the population ages, while intensivistspracticing in developing countries face the additionalchallenge of bed shortages [1, 2]. Recent reports fromdeveloped countries have warned against increasing ICUuse in terminal hospitalisation and the associated increasein end-of-life (EOL) decisions [3]. Meanwhile, the incli-nation to limit treatments with EOL decisions has become
an established indicator of ICU quality of care [4]. End-of-life practice is impacted by religious and culturaldiversities, and by organisational differences [5–9].Reports from 282 ICUs located in seven different geo-graphic regions show that decisions to withhold orwithdraw life support vary from 26% in Latin America to48% in central and Western Europe [10]. Wide variationis also present among occidental countries, as such deci-sions are more common in Northern European countriescompared to Southern European countries [6].
Intensive Care MedDOI 10.1007/s00134-012-2500-9 END OF LIFE: NATIONAL LEGISLATIONS
Author's personal copy

Tunisia is a North African country where most of thepopulation adheres to the Islamic faith. When it comes tocritical and sensitive issues, such as death and organdonation, Islam plays a pivotal role, shaping the behav-iour of the local population. However, in Muslimcountries traditions and precedents regarding withholdingand withdrawing life support decisions for ICU patientsare lacking, and data regarding physicians’ and families’behaviours concerning EOL decisions are scarce [11].However, Islam accepts the principle of putting an end tofutile treatments, allowing death to take its natural course,while overzealous treatment is reprehensible if the phy-sicians are certain about the inevitability of death [11, 12].However, only inferences about Muslim physicians’practice regarding EOL decisions can be made so far[13–15].
Tunisian ICUs face an increasing demand from elderlypatients suffering from acute critical illnesses that mightbe nonreversible, corresponding to the end-of-life process[16]. Religious, cultural, and organisational factors suchas the lack of palliative care facilities, and the risk ofadministrative and legal misunderstandings could alsointerfere with EOL decisions. The fact that our hospitalhas two ICUs (medical and surgical) offers the opportu-nity to explore some additional dimensions other thanthose of religion and culture. Indeed, both ICUs admitdifferent types of patients (older patients with chronicdiseases in the MICU, and younger patients with traumaand other surgical illnesses in the SICU). The medicalstaff training is also different because Tunisian medicalICUs are closed ICUs staffed by medical intensivists,while surgical ICUs are also closed ICUs but are staffedby anaesthesiologists and have a lower physician/ICU bedratio.
The aim of our study was to report the frequency andthe types of EOL decisions in dying patients in twoTunisian ICUs, to compare medical and surgical EOLpractices, and to identify factors associated with EOLdecisions.
Patients and methods
This was a retrospective study conducted in both medicaland surgical ICUs located in an 802-bed teaching hospitalin Monastir, Tunisia.
ICU characteristics
The medical ICU is a 10-bed closed ICU with a dedicatedmedical staff represented by four senior medical intensi-vists. Usually four to five residents in intensive careand internal medicine work with these post-graduate
physicians. The nurse-to-bed ratio is approximately 1/2.The surgical ICU is a 12-bed closed ICU admittingpatients with acute surgical diseases (either pre- or post-operative patients) and victims of trauma. The medicalstaff is represented by anaesthesiologists (two seniors,two residents in anaesthesiology). The bed-to-nurse ratiois also 1/2.
The cohort analysed in this study consisted of 326consecutive patients who died in the two ICUs over aperiod of 2 years from 1 September 2007 to 31 August2009. Given the observational design of the study, theinstitutional review board of our hospital waived the needof a formal study approval.
Data collection
In each deceased patient, demographic data and thoserelated to the current hospitalisation were recorded. TheEOL decision was prospectively recorded by the seniorattending physician in an independent document. Col-lected data on the index admission were the main reasonfor ICU admission, comorbidities, and the severity of thepatient’s condition at admission evaluated by the simpli-fied acute physiological score (SAPS) II and the McCabescore [17]. Both scores are usually calculated in the 24 hfollowing admission by physicians who are usually notinvolved in the definitive EOL decision-making. Thepatient’s functional status before ICU admission was alsorecorded, allowing identification of two groups: inde-pendent patients who needed no help for activities ofdaily living (ADL), and dependent patients who neededhelp for ADL or patients who were bed- or wheelchair-bound. The primary diagnosis, modalities and duration ofventilation, ICU length of stay, and cause of death werealso noted.
In both ICUs, the decision for active care limitationwas usually taken by the medical team, with discussionand input from the nurses in charge. It was usually dis-cussed with families, with special inquiries being madeabout the patient’s preferred location for death (home orhospital).
End-of-life decisions considered in the study includedthe following:
Full support (FS) denotes provision of all measuresneeded for hemodynamic, metabolic, and ventilationsupport.
Withholding of life support (WH) corresponds to adecision to avoid initiating a new treatment or escalateexisting life support should the clinical status worsen.
Withdrawal of life support (WD) corresponds to thecessation of current treatment and removal of an ongoinglife-supporting treatment. In our practice, nutrition isnever removed.
Discharge to die at home (DDH) is a specific modalityof WD corresponding to the decision to discharge a dying
Author's personal copy

patient to let them die at home. This decision is alwaysmade in response to the demand of family members basedon the expressed desire of the patient. In practice amember of the ICU team accompanies the intubatedpatients to their homes where bedside extubations aredone. Sedation and effective analgesia introduced on theICU are routinely maintained thereafter.
Statistical analysis
Continuous variables are expressed as median (inter-quartile range, IQR) and compared with the Mann-Whitney U test; dichotomous variables are expressed inpercentage and compared by chi-square test. A multi-variate logistic regression analysis was performed, withthe EOL decision as the dependent factor. Variables wereintroduced into this multivariate analysis when they weresignificantly associated with a higher risk of end-of-lifedecisions on univariate analysis at p \ 0.2. Goodness offit was assessed by the Hosmer-Lemeshow test; higherp values ([0.05) indicate better fit. All statistics weretwo-tailed, and a p \ 0.05 was considered statisticallysignificant.
Results
Patient’s characteristics
During the study period a total of 1,733 patients wereadmitted to both ICUs (711 to the MICU and 1,022 to the
SICU). A total of 326 patients died (19%), with signifi-cantly more deaths in the MICU (202 out of 711; 28.4%)than in the SICU (124 out of 1,022; 12%) (Fig. 1).
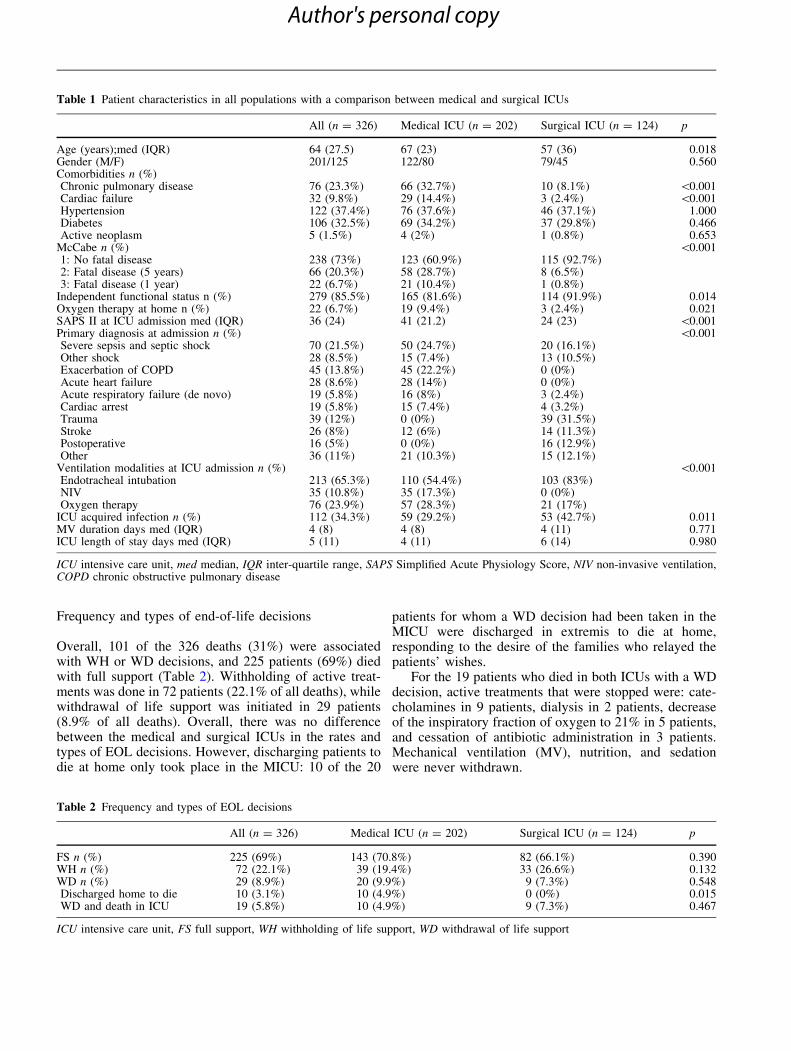
Table 1 summarizes the patient characteristics. Therewere striking differences in the type of diseases cared forat both ICUs, with more decompensation of chronic dis-eases (mainly respiratory and cardiovascular) in theMICU, and a higher rate of postoperative and traumapatients in the SICU. A higher rate of patients wasadmitted for de novo septic shock and acute respiratoryfailure in the MICU.
MICU patients were older and had higher rates ofcomorbidities and functional disabilities (dependency andhome oxygen). They had a poorer short-term prognosiswith significantly more patients in McCabe stages twoand three.
MICU patients had more severe acute disease asreflected by higher SAPS II scores (41 vs. 24 in medicaland surgical patients, respectively; p \ 0.001). Ventila-tion modalities at admission were different principallybecause of the lack of noninvasive ventilation (NIV) inthe SICU, while it was used in 17.3% in MICU patients.ICU-acquired infection was less frequent in the MICUcompared to SICU (29.2 vs. 42.7%; p = 0.011).Mechanical ventilation duration and ICU length of staywere similar.
Death causes
The main causes of death were refractory shock, whichoccurred in 69.3%, and refractory hypoxemia in 12.3%.
326 Dead patients
225/326 (69%) died in ICU witha Full support
101/326 (31%) died with a Withholding or withdrawing of life support decision
72/101 patients: Withholding of life support29/101 patients : withdrawal of life support
19/29: Withdrawing of life support and dead in ICU
10/29 patients were discharged to die at home « in extremis »
202 patients, died in the medical ICU. 124 patients, died in the surgical ICU.Fig. 1 Patient flowchart andmain end-of-life decisions
Author's personal copy
Frequency and types of end-of-life decisions
Overall, 101 of the 326 deaths (31%) were associatedwith WH or WD decisions, and 225 patients (69%) diedwith full support (Table 2). Withholding of active treat-ments was done in 72 patients (22.1% of all deaths), whilewithdrawal of life support was initiated in 29 patients(8.9% of all deaths). Overall, there was no differencebetween the medical and surgical ICUs in the rates andtypes of EOL decisions. However, discharging patients todie at home only took place in the MICU: 10 of the 20
patients for whom a WD decision had been taken in theMICU were discharged in extremis to die at home,responding to the desire of the families who relayed thepatients’ wishes.
For the 19 patients who died in both ICUs with a WDdecision, active treatments that were stopped were: cate-cholamines in 9 patients, dialysis in 2 patients, decreaseof the inspiratory fraction of oxygen to 21% in 5 patients,and cessation of antibiotic administration in 3 patients.Mechanical ventilation (MV), nutrition, and sedationwere never withdrawn.
Table 1 Patient characteristics in all populations with a comparison between medical and surgical ICUs
All (n = 326) Medical ICU (n = 202) Surgical ICU (n = 124) p
Age (years);med (IQR) 64 (27.5) 67 (23) 57 (36) 0.018Gender (M/F) 201/125 122/80 79/45 0.560Comorbidities n (%)Chronic pulmonary disease 76 (23.3%) 66 (32.7%) 10 (8.1%) \0.001Cardiac failure 32 (9.8%) 29 (14.4%) 3 (2.4%) \0.001Hypertension 122 (37.4%) 76 (37.6%) 46 (37.1%) 1.000Diabetes 106 (32.5%) 69 (34.2%) 37 (29.8%) 0.466Active neoplasm 5 (1.5%) 4 (2%) 1 (0.8%) 0.653
McCabe n (%) \0.0011: No fatal disease 238 (73%) 123 (60.9%) 115 (92.7%)2: Fatal disease (5 years) 66 (20.3%) 58 (28.7%) 8 (6.5%)3: Fatal disease (1 year) 22 (6.7%) 21 (10.4%) 1 (0.8%)
Independent functional status n (%) 279 (85.5%) 165 (81.6%) 114 (91.9%) 0.014Oxygen therapy at home n (%) 22 (6.7%) 19 (9.4%) 3 (2.4%) 0.021SAPS II at ICU admission med (IQR) 36 (24) 41 (21.2) 24 (23) \0.001Primary diagnosis at admission n (%) \0.001Severe sepsis and septic shock 70 (21.5%) 50 (24.7%) 20 (16.1%)Other shock 28 (8.5%) 15 (7.4%) 13 (10.5%)Exacerbation of COPD 45 (13.8%) 45 (22.2%) 0 (0%)Acute heart failure 28 (8.6%) 28 (14%) 0 (0%)Acute respiratory failure (de novo) 19 (5.8%) 16 (8%) 3 (2.4%)Cardiac arrest 19 (5.8%) 15 (7.4%) 4 (3.2%)Trauma 39 (12%) 0 (0%) 39 (31.5%)Stroke 26 (8%) 12 (6%) 14 (11.3%)Postoperative 16 (5%) 0 (0%) 16 (12.9%)Other 36 (11%) 21 (10.3%) 15 (12.1%)
Ventilation modalities at ICU admission n (%) \0.001Endotracheal intubation 213 (65.3%) 110 (54.4%) 103 (83%)NIV 35 (10.8%) 35 (17.3%) 0 (0%)Oxygen therapy 76 (23.9%) 57 (28.3%) 21 (17%)
ICU acquired infection n (%) 112 (34.3%) 59 (29.2%) 53 (42.7%) 0.011MV duration days med (IQR) 4 (8) 4 (8) 4 (11) 0.771ICU length of stay days med (IQR) 5 (11) 4 (11) 6 (14) 0.980
ICU intensive care unit, med median, IQR inter-quartile range, SAPS Simplified Acute Physiology Score, NIV non-invasive ventilation,COPD chronic obstructive pulmonary disease
Table 2 Frequency and types of EOL decisions
All (n = 326) Medical ICU (n = 202) Surgical ICU (n = 124) p
FS n (%) 225 (69%) 143 (70.8%) 82 (66.1%) 0.390WH n (%) 72 (22.1%) 39 (19.4%) 33 (26.6%) 0.132WD n (%) 29 (8.9%) 20 (9.9%) 9 (7.3%) 0.548Discharged home to die 10 (3.1%) 10 (4.9%) 0 (0%) 0.015WD and death in ICU 19 (5.8%) 10 (4.9%) 9 (7.3%) 0.467
ICU intensive care unit, FS full support, WH withholding of life support, WD withdrawal of life support
Author's personal copy

Factors associated with the WH or WD decisions areshown in Table 3, which depicts univariate comparison ofpatients who died with full support therapy (n = 225)with those who died with WH or WD decisions. A McC-abe score [ 1 (fatal chronic disease in 1 or 5 years) andthe percentage of patients with an independent functionalstatus prior to ICU admission were significantly differentbetween these groups. Both groups were also differentregarding MV duration and ICU length of stay. Themultivariate logistic regression analysis disclosed onlytwo factors that were independently associated with a WHor WD decision: a McCabe score [ 1 was positivelyassociated with this type of decision [odds ratio(OR) = 2.41; 95% CI: 1.34–4.36; p = 0.003], while anindependent functional status before ICU admission wasassociated with a lack of such decisions [OR = 0.32, 95%CI: 0.15–0.66; p = 0.002]. The Hosmer-Lemeshow testshowed a good fit with a p value equal to 0.786.
Discussion
In this cohort study conducted in two Tunisian ICUsbelonging to the same tertiary teaching hospital, werecorded a 31% frequency of WH or WD decisions inpatients who died. Decisions to withhold life support weretaken more frequently (22.1%) than WD decisions(8.9%). Intensivists from the MICU and SICU had similarbehaviours regarding the rate and pattern of these deci-sions. The only recorded difference concerned thepractice of discharging dying patients in extremis to die athome, which occurred only in the MICU. Two factorswere independently associated with a WH or WD deci-sion: a poor life expectancy (as assessed by the McCabescore), which was positively associated with such
decisions, while an independent functional status beforeICU admission made physicians more reluctant to makesuch decisions.
Our study has some limitations. First, the retrospectiveand observational nature of our study could have ham-pered the strength of some conclusions, especiallyregarding cause-effect associations. Second, the single-hospital design may limit extrapolation of our results.This study was actually performed in two relatively smallICUs belonging to the same hospital with a small numberof admissions per year. Accordingly, we cannot excludesome variations in EOL practices in other Tunisian ICUsor other Muslim countries. A prospective multicenterstudy would be more informative in this regard. Never-theless, our data, which relied on observation rather thanon a survey, provide important insights into the fre-quency, types, and factors associated with WH or WDdecisions in a population of dying patients in two Tuni-sian ICUs where this specific information has not beenpreviously reported.
Previous studies on EOL decisions show considerablevariability in frequency, patterns, and factors associatedwith WH or WD decisions in patients dying in the ICU.Reported frequencies, mostly originating from medical ormixed ICUs, range from 11 to 60% [5, 6, 15, 18–24]. Thiswide variation is usually explained by differences infactors pertaining to patients’ preferences and prognoses,and in others related to physicians’ judgements andmedical training [25] or religious and cultural beliefs [6,26]. The design of our study allowed for controlling forthe cultural aspects of EOL decisions, by comparing therate and pattern of EOL decisions made by two groups ofphysicians sharing the same cultural background, buthaving had two separate medical trainings as intensivists,and dealing with different types of patients carryingvariable prognoses. Despite different trainings, we
Table 3 Univariate analysis
WH or WD decision (n = 101) Full support (n = 225) p
Age med (IQR) 62 (26) 65 (27) 0.440Gender (M/F) 64/37 137/88 0.713ICU type n (%)Medical ICU 59 (58.4%) 143 (63.6%)Surgical ICU 42 (41.6%) 82 (36.4%) 0.390
SAPS II med (IQR) 35 (22.2) 37 (25) 0.383SOFA med (IQR) 6 (4) 6 (4) 0.382APACHE II med (IQR) 17 (10.2) 17.5 (10.2) 0.915McCabe [ 1 (fatal disease at 1 or 5 years) n (%) 47 (46.5%) 41 (18.2%) \0.001Oxygen therapy at home n (%) 9 (8.9%) 13 (5.8%) 0.342Independent functional status n (%) 70 (69.3%) 209 (92.9%) \0.001Hospital-acquired infection n (%) 41 (40.6%) 71 (31.8%) 0.132Current sepsis on the death day n (%) 39 (38.6%) 106 (47.1%) 0.275MV duration med (IQR) 7 (14) 3 (7) 0.002ICU length of stay med (IQR) 7 (14) 4 (10) 0.003
WH Withholding of life support, WD withdrawal of life support,ICU intensive care unit, med median, IQR inter-quartile range,SAPS Simplified Acute Physiology Score, SOFA Sepsis-related
Organ Failure Assessment, APACHE Acute Physiologic andChronic Health Evaluation, MV mechanical ventilation
Author's personal copy

observed similar behaviours regarding both the rate andpattern of EOL decisions in both ICUs belonging to thesame hospital. Obviously, the limitations outlined abovemay mitigate some of our conclusions, but these obser-vations might also suggest that cultural considerationshave more impact on EOL practice than physician’straining or even differences in the diseases treated.
Little is known about EOL decisions in Muslimcountries. A survey reported that among 439 Turkishanaesthesiologists (who were Muslims in 90% of thecases), 66% had initiated a written or oral DNR order atleast once [14]. In one Lebanese ICU, 46% of all deathswere associated with one kind of EOL decision, mainlywithholding life-sustaining treatments (86%) [15]. In theETHICUS study, Muslim physicians were more prone towithhold rather than withdraw active treatments [27].This pattern, which is similar to that observed in ourstudy, was also similar to that observed for Jewish orOrthodox physicians, but contrasted with that recordedwith Catholic or Protestant physicians. The mean per-centage of discussion of EOL decisions with patient’sfamilies, which was 68% in the whole study, was thelowest for Muslim physicians, reflecting their paternalisticattitudes.
Low rates of WH or WD life support decisions likethose reported here may reflect conservative physician’sattitudes or societal and legal barriers to EOL decision-making. The pattern of EOL decisions may also be dif-ferent between countries. Schematically, there is an equaldivision between withholding and withdrawing life sup-port decisions in countries considering these two practicesas ethically equivalent [4, 6, 10, 28, 29], whereas incountries with cultural, religious, or legal barriers con-sidering that withdrawal of life support is morepsychologically demanding than withholding it, physi-cians are more prone to withhold therapy decisions [15,20, 30].
In the current study we did not notice significant dif-ferences in the frequency and modalities of EOLdecisions between the MICU and SICU despite the sharpdifferences between surgical and medical ICU patients interms of severity (higher SAPS II in MICU patients) andprognosis (mortality: 28.4 vs. 12% in the MICU andSICU, respectively). The major difference observedbetween the two ICUs was the practice of discharge to dieat home in the medical ICU and not in the surgical one.The decision to discharge patients to home for a ‘‘better’’end of life (good death) [31] has been previously reportedfrom Tunisian ICUs [32, 33]. Our study provides anappreciation of its frequency and shows that it is anexclusive practice of the medical ICU. Going home to dieis sometimes the last request of a dying person and ispreferred by families. Provided that their dying lovedones do not experience more suffering (which is actuallyensured by the maintainance of analgo-sedation), mostpeople in our culture prefer privacy in these last moments,
and the ICU is probably not the best place for privacy tobe guaranteed. This procedure also has many spiritual andeven administrative advantages. It allows close contactbetween families and their loved ones when death occurs,and avoids all administrative procedures related to intra-hospital death, especially for families living far from theinstitution. It also allows the funeral to take place rapidlyafter death, which is recommended in the Islamic religion[33]. Why this practice is done only in the MICU remainsa matter of speculation, since it could be neither explainedby a particular training of intensivists in comparison toanaesthesiologists nor by cultural differences in our study.A plausible explanation is that surgical and medicalphysicians deal with different types of patients. Elderlypatients who are more frequently admitted in the MICUhave more comorbidities, prompting them to have priordiscussions with their relatives about their wishesregarding death modalities and settings. It is also knownthat the surgical culture makes surgeons very committedto aggressive therapy during the postoperative period,regardless of how severe the condition is, and thus sur-geons may be more reluctant to support WH and WDdecisions than other physicians [4, 34]. Furthermore,trauma is an ‘‘unexpected’’ event for patients and theirfamilies. It can cloud their decision-making and renderthe EOL decision much more challenging. However,Huang et al. [35] recently reported that almost 25% ofpatients dying in their surgical ICU in Taiwan returnedhome to die, underscoring the fact that such a practice isneither exclusively Muslim nor exclusively related tomedical ICUs. In the Chinese culture, dying at home has aspecial meaning and is associated with a sort of ‘‘peacefuldeath’’, which is considered the most fortunate and glo-rious death.
In the current study, factors independently associatedwith WH or WD decisions were the chronic illness andlife expectancy expressed by the McCabe score and thefunctional status before ICU admission, variables thatwere also identified by other studies [4, 6, 20]. Some otherfactors are also reported in the literature, such as demo-graphic characteristics, acute conditions with poorprognosis, environmental factors, sepsis, and multipleorgan failure [4, 6, 22, 34, 36–40]. Although nosocomialinfections were more frequent in patients with WH or WDdecisions compared to those who died with full support,the difference did not achieve the level of statistical sig-nificance in our study.
In conclusion, WH and WD decisions are common,with similar rates in medical and surgical ICUs located inthe same Tunisian hospital. Withholding is more frequentthan withdrawing life support. These decisions areimpacted by prior functional status and the severity of theunderlying condition.
Acknowledgments We thank Dr Abdelkarim Waness for hishelpful comments and critical review of the article.
Author's personal copy

References
1. Angus DC, Kelley MA, Schmitz RJ,White A, Popovich J Jr (2000) Caringfor the critically ill patient. Current andprojected workforce requirements forcare of the critically ill and patientswith pulmonary disease: can we meetthe requirements of an agingpopulation? JAMA 284:2762–2770
2. Adhikari NK, Fowler RA, BhagwanjeeS, Rubenfeld GD (2010) Critical careand the global burden of critical illnessin adults. Lancet 376:1339–1346
3. Wunsch H, Linde-Zwirble WT,Harrison DA, Barnato AE, Rowan KM,Angus DC (2009) Use of intensive careservices during terminalhospitalizations in England and theUnited States. Am J Respir Crit CareMed 180:875–880
4. Bertolini G, Boffelli S, Malacarne P,Peta M, Marchesi M, Barbisan C,Tomelleri S, Spada S, Satolli R, GridelliB, Lizzola I, Mazzon D (2010) End-of-life decision-making and quality of ICUperformance: an observational study in84 Italian units. Intensive Care Med36(9):1495–1504
5. Prendergast TJ, Claessens MT, LuceJM (1998) A national survey of end-of-life care for critically ill patients. Am JRespir Crit Care Med 158:1163–1167
6. Sprung CL, Cohen SL, Sjokvist P,Baras M, Bulow HH, Hovilehto S,Ledoux D, Lippert A, Maia P, PhelanD, Schobersberger W, Wennberg E,Woodcock T (2003) End-of-lifepractices in European intensive careunits: the ethicus study. JAMA290:790–797
7. Sprung CL, Woodcock T, Sjokvist P,Ricou B, Bulow HH, Lippert A, Maia P,Cohen S, Baras M, Hovilehto S, LedouxD, Phelan D, Wennberg E,Schobersberger W (2008) Reasons,considerations, difficulties anddocumentation of end-of-life decisionsin European intensive care units: theETHICUS Study. Intensive Care Med34:271–277
8. Weng L, Joynt GM, Lee A, Du B,Leung P, Peng J, Gomersall CD, Hu X,Yap HY (2011) Attitudes towardsethical problems in critical caremedicine: the Chinese perspective.Intensive Care Med 37:655–664
9. Pochard F, Abroug F (2005) End-of-lifedecisions in ICU and culturalspecificities. Intensive Care Med31:506–507
10. Azoulay E, Metnitz B, Sprung CL,Timsit JF, Lemaire F, Bauer P,Schlemmer B, Moreno R, Metnitz P(2009) End-of-life practices in 282intensive care units: data from theSAPS 3 database. Intensive Care Med35:623–630
11. Bulow HH, Sprung CL, Reinhart K,Prayag S, Du B, Armaganidis A,Abroug F, Levy MM (2008) Theworld’s major religions’ points of viewon end-of-life decisions in the intensivecare unit. Intensive Care Med34:423–430
12. Sachedina A (2005) End-of-life: theIslamic view. Lancet 366:774–779
13. Gouda A, Al-Jabbary A, Fong L (2010)Compliance with DNR policy in atertiary care center in Saudi Arabia.Intensive Care Med 36:2149–2153
14. Iyilikci L, Erbayraktar S, Gokmen N,Ellidokuz H, Kara HC, Gunerli A(2004) Practices of anaesthesiologistswith regard to withholding andwithdrawal of life support from thecritically ill in Turkey. ActaAnaesthesiol Scand 48:457–462
15. Yazigi A, Riachi M, Dabbar G (2005)Withholding and withdrawal of life-sustaining treatment in a Lebaneseintensive care unit: a prospectiveobservational study. Intensive CareMed 31:562–567
16. Chelli H, Besbes L, BenKhelil J, ThabetH, Bouhaja B, Ghedira S, BenLakhal S,Bchir A, Gahbiche M, Bouaziz M,elAtrous S, Besbes M, Amamou M,BenAmmar, Daoud A, Bouchoucha S,Abroug F (2004) [Mechanicalventilation in intensive care units:indications, modalities andcomplications. Results of a prospectivemulticenter survey in Tunisia]. TunisMed 82:12–18
17. McCabe WR, Jackson GG (1962) Gramnegative bacteremia: etiology andecology. Arch Intern Med 110:847–855
18. Soares M, Terzi RG, Piva JP (2007)End-of-life care in Brazil. IntensiveCare Med 33:1014–1017
19. Esteban A, Gordo F, Solsona JF, Alia I,Caballero J, Bouza C, Alcala-Zamora J,Cook DJ, Sanchez JM, Abizanda R,Miro G, FernandezDelCabo MJ, deMiguel E, Santos JA, Balerdi B (2001)Withdrawing and withholding lifesupport in the intensive care unit: aSpanish prospective multi-centreobservational study. Intensive CareMed 27:1744–1749
20. Mani RK, Mandal AK, Bal S, Javeri Y,Kumar R, Nama DK, Pandey P, RawatT, Singh N, Tewari H, Uttam R (2009)End-of-life decisions in an Indianintensive care unit. Intensive Care Med35(10):1713–1719
21. Buckley TA, Joynt GM, Tan PY, ChengCA, Yap FH (2004) Limitation of lifesupport: frequency and practice in aHong Kong intensive care unit. CritCare Med 32:415–420
22. Wood GG, Martin E (1995)Withholding and withdrawing life-sustaining therapy in a Canadianintensive care unit. Can J Anaesth42:186–191
23. Wunsch H, Harrison DA, Harvey S,Rowan K (2005) End-of-life decisions:a cohort study of the withdrawal of allactive treatment in intensive care unitsin the United Kingdom. Intensive CareMed 31:823–831
24. Turner JS, Michell WL, Morgan CJ,Benatar SR (1996) Limitation of lifesupport: frequency and practice in aLondon and a Cape Town intensive careunit. Intensive Care Med 22:1020–1025
25. Hakim RB, Teno JM, Harrell FE Jr,Knaus WA, Wenger N, Phillips RS,Layde P, Califf R, Connors AF Jr, LynnJ (1996) Factors associated with do-not-resuscitate orders: patient’s preferences,prognoses, and physician’s judgments.Support investigators. Study tounderstand prognoses and preferencesfor outcomes and risks of treatment.Ann Intern Med 125:284–293
26. Cohen J, van Delden J, Mortier F,Lofmark R, Norup M, Cartwright C,Faisst K, Canova C, Onwuteaka-Philipsen B, Bilsen J (2008) Influenceof physician’s life stances on attitudesto end-of-life decisions and actual end-of-life decision-making in six countries.J Med Ethics 34:247–253
27. Sprung CL, Maia P, Bulow HH, RicouB, Armaganidis A, Baras M, WennbergE, Reinhart K, Cohen SL, Fries DR,Nakos G, Thijs LG (2007) Theimportance of religious affiliation andculture on end-of-life decisions inEuropean intensive care units. IntensiveCare Med 33:1732–1739
28. Luce JM (1997) Withholding andwithdrawal of life support: ethical,legal, and clinical aspects. New Horiz5:30–37
Author's personal copy

29. (1991) Withholding and withdrawinglife-sustaining therapy. This OfficialStatement of the American ThoracicSociety was adopted by the ATS Boardof Directors, March 1991. Am RevRespir Dis 144:726–731
30. Ganz FD, Benbenishty J, Hersch M,Fischer A, Gurman G, Sprung CL(2006) The impact of regional cultureon intensive care end of life decisionmaking: an Israeli perspective from theETHICUS study. J Med Ethics32:196–199
31. Beuks BC, Nijhof AC, Meertens JH,Ligtenberg JJ, Tulleken JE, Zijlstra JG(2006) A good death. Intensive CareMed 32:752–753
32. Kallel H, Dammak H, Bahloul M,BenHamida C, Chelly H, Rekik N,Bouaziz M (2006) A good death:another break in the wall. IntensiveCare Med 32:1915–1916
33. Boussarsar M, Bouchoucha S (2006)Dying at home: cultural and religiouspreferences. Intensive Care Med32:1917–1918
34. Meissner A, Genga KR, Studart FS,Settmacher U, Hofmann G, Reinhart K,Sakr Y (2010) Epidemiology of andfactors associated with end-of-lifedecisions in a surgical intensive careunit. Crit Care Med 38:1060–1068
35. Huang YC, Huang SJ, Ko WJ (2009)Going home to die from surgicalintensive care units. Intensive Care Med35:810–815
36. Nathens AB, Rivara FP, Wang J,Mackenzie EJ, Jurkovich GJ (2008)Variation in the rates of do notresuscitate orders after major traumaand the impact of intensive care unitenvironment. J Trauma 64:81–88(discussion 88–91)
37. Azoulay E, Pochard F, Garrouste-Orgeas M, Moreau D, Montesino L,Adrie C, de Lassence A, Cohen Y,Timsit JF (2003) Decisions to forgolife-sustaining therapy in ICU patientsindependently predict hospital death.Intensive Care Med 29:1895–1901
38. Keenan SP, Busche KD, Chen LM,McCarthy L, Inman KJ, Sibbald WJ(1997) A retrospective review of a largecohort of patients undergoing theprocess of withholding or withdrawal oflife support. Crit Care Med25:1324–1331
39. Ferrand E, Robert R, Ingrand P,Lemaire F (2001) Withholding andwithdrawal of life support in intensive-care units in France: a prospectivesurvey. French LATAREA Group.Lancet 357:9–14
40. Reignier J, Dumont R, Katsahian S,Martin-Lefevre L, Renard B, FiancetteM, Lebert C, Clementi E, Bontemps F(2008) Patient-related factors andcircumstances surrounding decisionstoforego life-sustaining treatment,including intensive care unit admissionrefusal. Crit Care Med 36:2076–2083
Author's personal copy
Related Documents











