Intensive and Critical Care Nursing (2006) 22, 264—273 ORIGINAL ARTICLE Patients’ dreams in ICU: Recall at two years post discharge and comparison to delirium status during ICU admission A multicentre cohort study Brigit L. Roberts a,∗ , Claire M. Rickard b , Dorrilyn Rajbhandari c , Pamela Reynolds d a Sir Charles Gairdner Hospital, Perth, Australia b University of Tasmania, School of Nursing & Midwifery, Clifford Craig Research Trust, Launceston General Hospital, Launceston, Australia c Royal Prince Alfred Hospital, Sydney, Australia d Monash University School of Rural Health and Latrobe Regional Hospital, Traralgon, Australia Accepted 7 February 2006 KEYWORDS Dreams; Memories; ICU; Delirium screening; Interviews Summary Discharged intensive care unit (ICU) patients often recall experience vivid dreams, hallucinations or delusions. These may be persecutory in nature and are sometimes very frightening. It is possible that these memories stem from times when the patient was experiencing delirium, a common syndrome in the critically ill. Routine screening for delirium in ICU is becoming more prevalent, however, lit- tle has been published comparing the objective development of delirium (patient observations using screening tools) and patients’ subjective recollection of dreams and unreal experiences in the ICU. This study describes the relationship between observed behaviour during ICU admission and the subjective memories of ICU experiences amongst 41 partici- pants in three ICUs up to 24 months post discharge. Overall, 44% of patients (n = 18) recalled dreams during their ICU admission. There was a trend to increased preva- lence of dreaming (50% versus 39%) amongst the 18 patients who were delirious during their ICU admission than in the 23 non-delirious patients. Dreaming was sig- nificantly associated on logistic regression with increased length of stay (OR 1.39, 95% CI 1.08—1.79, p = 0.01), but not delirium status (OR 1.56, 95% CI 0.45—5.41, p = 0.49). ∗ Correspondence to: Department of Intensive Care, 4th Floor, G Block, Sir Charles Gairdner Hospital, Nedlands, WA 6009, Australia. Tel +61 8 9346 3333x1010; fax: +61 8 9346 4431. E-mail address: [email protected] (B.L. Roberts). 0964-3397/$ — see front matter © 2006 Elsevier Ltd. All rights reserved. doi:10.1016/j.iccn.2006.02.002

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Intensive and Critical Care Nursing (2006) 22, 264—273
ORIGINAL ARTICLE
Patients’ dreams in ICU: Recall at two years postdischarge and comparison to delirium statusduring ICU admissionA multicentre cohort study
Brigit L. Robertsa,∗, Claire M. Rickardb,Dorrilyn Rajbhandari c, Pamela Reynoldsd
a Sir Charles Gairdner Hospital, Perth, Australiab University of Tasmania, School of Nursing & Midwifery, Clifford Craig Research Trust, LauncestonGeneral Hospital, Launceston, Australiac Royal Prince Alfred Hospital, Sydney, Australiad Monash University School of Rural Health and Latrobe Regional Hospital, Traralgon, Australia
Accepted 7 February 2006
KEYWORDSDreams;Memories;ICU;Delirium screening;Interviews
Summary Discharged intensive care unit (ICU) patients often recall experiencevivid dreams, hallucinations or delusions. These may be persecutory in nature andare sometimes very frightening. It is possible that these memories stem from timeswhen the patient was experiencing delirium, a common syndrome in the criticallyill. Routine screening for delirium in ICU is becoming more prevalent, however, lit-tle has been published comparing the objective development of delirium (patientobservations using screening tools) and patients’ subjective recollection of dreamsand unreal experiences in the ICU.
This study describes the relationship between observed behaviour during ICUadmission and the subjective memories of ICU experiences amongst 41 partici-pants in three ICUs up to 24 months post discharge. Overall, 44% of patients (n = 18)recalled dreams during their ICU admission. There was a trend to increased preva-lence of dreaming (50% versus 39%) amongst the 18 patients who were deliriousduring their ICU admission than in the 23 non-delirious patients. Dreaming was sig-
nificantly associated on logistic regression with increased length of stay (OR 1.39,95% CI 1.08—1.79, p = 0.01), but not delirium status (OR 1.56, 95% CI 0.45—5.41,p = 0.49).∗ Correspondence to: Department of Intensive Care, 4th Floor, G Block, Sir Charles Gairdner Hospital, Nedlands, WA 6009,Australia. Tel +61 8 9346 3333x1010; fax: +61 8 9346 4431.
E-mail address: [email protected] (B.L. Roberts).
0964-3397/$ — see front matter © 2006 Elsevier Ltd. All rights reserved.doi:10.1016/j.iccn.2006.02.002

A longer ICU stay was significantly associated with the experience of ICU dreaming. Asmany dreams are disturbing, we suggest providing information and counselling about
remain in ICU for longer periods.rights reserved.
I
D
DdoeptthatoHou(ptactsal2
D
Pbay2lnipc(feaeb1
delirium to patients who© 2006 Elsevier Ltd. All
ntroduction
elirium
elirium in the intensive care unit (ICU) is now wellocumented in the literature to occur in 20—85%f patients (Ely et al., 2004a). Incidence may riseven further in the future as increasingly oldereople with more complex morbidity are admittedo ICU. Many ICU patients display signs of agita-ion, bizarre or out of character behaviour. Mostealth care workers in ICU are able to identifyn agitated and restless patient as delirious, buto recognise the patient with the lethargic variantf delirium is extremely difficult (Roberts, 2001).ence, symptoms in this group of patients are oftenverlooked, and indeed delirium is reported to bender-diagnosed or unrecognised in 70% of casesEly et al., 2004b). Delirious and agitated patientsose a particular problem in the ICU setting becausehey are often attached to life-saving devices suchs endo-tracheal tubes, inter-costal catheters andentral venous lines where accidental removal ofhese devices may have detrimental effects to theirafety. Delirious patients have increased morbiditynd mortality, and are often linked to an increasedength of both ICU and hospital stay (Ely et al.,001a).
reams and hallucinations
hysical outcomes from ICU are well documentedut the psychological effect of an ICU stay hasttracted interest in the literature only in recentears (Cuthbertson et al., 2004; Schragg et al.,001). Delirious ICU patients (whether agitated orethargic) may experience vivid dreams, halluci-ations or delusions, which can be persecutoryn nature and are sometimes very frightening foratients, who may believe that they are ‘‘goingrazy’’ (Griffith and Jones, 2001). Granberg et al.1998) likens the experience to a state of chaos andurther in 1999 described it as an ‘‘unreal experi-nce’’. The authors defined this as ‘‘visual and/or
uditory phenomena which appear in a conditionxperienced as totally wakeful or in a conditionetween wakefulness and sleep’’ (Granberg et al.,999, p. 29). Some patients may choose ‘‘not toremember anything’’, because they feel ashamedof not remembering properly, or scared of beinglabelled ‘‘mentally unstable’’ (Griffith and Jones,1999).
Jones et al. (2001) divide memories into fourdifferent categories (1) no factual, with some delu-sional recall; (2) factual and delusional recall; (3)factual, with no delusional recall and (4) no fac-tual and no delusional recall. Delusional memo-ries are the commonest in ICU patients and oftenassociated with lack of factual memories of ICU(Capuzzo et al., 2004). Roberts and Chaboyer(2004) reported mixed experiences from a follow-up study of 31 patients with 14 patients recall-ing nightmares whilst in ICU and nine classify-ing the dreams as either good or indifferent.Papathanassoglou and Patiraki (2003) interviewedeight survivors of ICU, who described themes asso-ciated with ICU dreams such as transformation ofperception, distortion of body and bodily sensationswith an emphasised feeling of heightened spiritu-ality, personal rebirth and awe at the wonders oflife.
Delirium assessment in ICU
The incidence and circumstances of the develop-ment of delirium are rapidly gaining interest in theprofessional literature (Dubois et al., 2001; Skrobik,2003; Truman and Ely, 2003). Delirium screeningtools have been developed specifically for criticallyill patients considering their inability to verbalisewhilst intubated (Bergeron et al., 2001; Ely et al.,2001b,c). Similarly, a growing body of literatureexamining the neuropsychological outcome fromICU has emerged. These studies describe patients’memories and experiences as well as the extent oftheir psychological recovery (Cuthbertson et al.,2004; Jackson et al., 2003; Jones et al., 2003;Kapfhammer et al., 2004).
Nevertheless, little has been published on therelationship between the objective developmentof delirium (patient observations using screeningtools) and the patients subjective recollections of
Patients’ dreams in ICU 265
memories, dreams and unreal experiences. Search-ing MEDLINE and CINAHL using MeSH-terms includ-ing delirium, screening, follow-up, memories anddreams revealed only two previous studies, one

ETRmtfmtitaIwmr
oda
S
Ustpsavmb(
iqwsIstSthto
afqc
Definitions
266
by the author BR (Roberts and Chaboyer, 2004).As that study predated the development of vali-dated screening tools for objective patient obser-vation, the ability to interpret the relationshipbetween objective and subjective observations wasimpeded. From the other reported study, Jacksonet al. (2003) suggest that ‘‘future studies shouldexamine the association of severe or prolongeddelirium and negative long-term cognitive out-comes’’ (p. 1232).
This current study describes the relation-ship between patients’ observed behaviour dur-ing their ICU admission using a validated screen-ing tool and their subjective memories of the ICUexperience.
Method
The design was a prospective cohort study.
Setting
Three Australian ICUs, two tertiary referral cen-tres (Level 3) facilities (Sir Charles Gairdner Hos-pital, WA; Royal Prince Alfred Hospital, NSW) andone provider of high standard ICU care (Level 2)(Latrobe Regional Hospital).
Sample
The patient cohort for this study was assembledfrom 152 patients from three of six centres whoparticipated in a previously conducted multi-centreobservational study to determine the incidence ofdelirium in the six Australian and New Zealand ICUs.The inclusion criteria for that study were: informedconsent, admitted to ICU for longer than 36 hours,had been in hospital no longer than 96 hours prior toICU admission and not suffered any cerebral insult,or any past medical history of dementia or delirium.In total 185 patients were screened in the six ICUsacross Australia and New Zealand for delirium inthe second half of 2002, using the ‘‘Intensive CareDelirium Screening Checklist (ICDSC)’’ (Bergeron etal., 2001) for the duration of their ICU admission.Some 84 patients (45%) developed delirium, whichwas associated with higher admission APACHE II andsequential SOFA scores, increased ICU length ofstay, and the use of psychoactive drugs (Roberts etal., 2005).
Review of hospital databases identified that 103
of the 152 patients who participated in the for-mer study at the three centres had been dischargedalive, and these people were invited via mail to par-ticipate.DAa
B.L. Roberts et al.
thics and consenthe study received approval from the local Humanesearch Ethics Committee at each site. An infor-ation sheet outlining the study including its objec-
ives, a consent form, a decline to participateorm and a self-addressed stamped envelope wereailed to each potential participant. The informa-
ion sheet asked permission to contact the partic-pant by telephone to collect follow-up informa-ion and stated that participant’s comments andnswers during the interview would be recorded.f neither consent nor decline to participate formas received, a once off telephone contact wasade to ascertain whether the mail-out had been
eceived.The data for the ‘‘Reference Group’’ were
btained from participants in the previous con-ucted and ethically approved study as describedbove (Roberts et al., 2005).
tudy processes
pon the investigator’s receipt of a signed con-ent form, patients were contacted by telephoneo arrange a suitable time to undertake a tele-hone interview. The same researcher at eachite undertook the interviews, after joint trainingnd discussion to standardise technique. The inter-iewer at each site accessed demographic infor-ation about the cohort prior to the interviewut was blinded to patients’ observed behaviourdelirious/non-delirious) whilst in ICU.
Interviews took approximately 30 minutes andnvolved a mixture of closed-ended and open-endeduestions (Appendix A). The first six questionsere a combination of descriptions and the use of
emantic differential techniques and related to theCU admission by targeting both factual and delu-ional memories/dreams. The closed-ended ques-ions were adapted from Jones et al. (2001) andtoll et al. (1999). One question elicited informa-ion about whether and with whom the participantad discussed the ICU experience and another ques-ion asked if the patients would normally dreamutside the ICU setting.
The interviewer took notes during the interviewnd these notes were read back to the participantsor verification. A copy of these notes was subse-uently mailed to the participants for any furtheromments or changes.
eliriumscore of four or greater at any stage of the ICU
dmission on the Intensive Care Delirium Screening

P
Cc
DDrToaea‘
D
QQwClgwSisadtc
tp
QQsDdawestad
r≥FdvvPapp
amowbnrs
R
S
Iptpstoprtiertitg
F
Rt4sbro(
T
Arivvs
atients’ dreams in ICU
hecklist (Bergeron et al., 2001). These scores werealculated twice daily by ICU nurses.
reamsreams experienced during the ICU admission asecalled by patients 18—24 months post-discharge.hese dreams would either be associated with sleepr wakeful states (hallucinations), or described asn ‘‘unreal’’ feeling or sensation. Clearly delusionalvents were also classed in this category, althoughminority of patients actually perceived them as
‘factual memories’’.
ata analysis
ualitative dataualitative responses regarding recalled dreamsere analysed using thematic analysis as perolaizzi’s method (Colaizzi, 1978). That is, simi-
ar statements were grouped together into cate-ories and the categories given a label. Categoriesere examined for similarities and differences.ignificant statements were extracted and mean-ngs were formulated into themes and fundamentaltatements were developed. This was a two-stagepproach: Firstly, each investigator reviewed theata from each site separately. Secondly, the inves-igators jointly reviewed the data and finalised theategories, statements and themes.
Four case studies were chosen to demonstratehe variability in responses and to provide exem-lars of responses to questions asked.
uantitative datauantitative analysis was undertaken using SPPSoftware (version 11.0, SPSS Inc., Chicago, IL).emographic data were aggregated to allowescription of the sample. The demographic datand delirium status of participants was comparedith a reference group of non-participants. The ref-rence group was also ICU survivors from the priortudy. This provided a means of assessing whetherhere was a likelihood for bias whereby those whogreed to participate might have different recall ofreams than those who did not.
Univariate analysis compared the outcome ofecalled dreams between delirious (ICDSC score of4) and non-delirious patients (ICDSC score <4).urther univariate analysis also compared bothelirious and non-delirious patients, and dreamersersus non-dreamers for demographic and clinicalariables. Categorical data were compared using
earson’s Chi-square, and continuous data weressessed for normality of distribution then com-ared using the t-test or Mann—Whitney U as appro-riate. Univariate logistic regression was used todfCb
267
ssess for a predictive relationship between the pri-ary item of interest (delirium status) and recall
f dreams. Forward step-wise logistic regressionas performed to test for predictive relationshipsetween variables that were significant (p < 0.05) orear significant (p < 0.075) on univariate testing andecall of dreams. A p-value of <0.05 was consideredignificant for all analyses.
esults
ample
nvitations were mailed out to the remaining 103atients of whom 41 patients (40%) consented toake part in the present study. The reason for non-articipation included refusal, lost-to-follow up,erious illness and deaths not captured on hospi-al record databases. Demographic and other databtained during the previous survey from the non-articipants (n = 62) were collected. They formed aeference group to ensure our sample was represen-ative of ICU survivors. Only previously publishednformation was used for non-participants (Robertst al., 2005). When comparing the participant andeference groups for age, gender, ventilation sta-us, admission categories (medical, surgical), delir-um (dichotomous), APACHE II score, and ICU LOS,here were no significant differences between theroups.
actual memories and dreams
esults from the interviewed patients showed thathe highest proportion of participants (n = 20/41,9%) had only factual memories of the ICU. Anotherignificant proportion (n = 14/41, 34%) recalledoth ICU dreams and memories, and the minorityecalled dreams only (n = 4/41, 10%), or had no rec-llection of dreams or indeed the admission at alln = 3/41, 7%).
hematic analysis of dreams
total of 18 patients recalled dreams. Mosteported more than one dream with different top-cs. From this data, seven themes emerged. Thesearied from (1) bodily sensations (n = 9) (e.g. aoid, reminiscing or walking to a light); to (2) per-ecutory experiences (n = 10) (e.g. of impending
eath/buried alive or harm); to (3) metaphysicaleelings (n = 3) such as seeing the face of Jesushrist, different colours for different religions oreing in a temple. Some dreams related to a range
and scary dreams, with laces and frills turning intodirt and filth or beautiful bright light and then beingimprisoned.
Table 1 Thematic analysis with examples of dreamsexperienced in ICU
1 Misperception of places• Waiting in a queue to go to a burial site• On a cloud walking a dog
2 Auditory• Clicking noises like horses• Rock breaking
3 Visual• Glass windows all around• Frills and laces
4 Frightening/persecutory• Buried alive in a glass sided coffin• Nurse trying to steal tablets
5 Divine• The face of Jesus Christ in the wall and ceiling• Being in a temple
6 Bodily experiences• Like in a different world• Feeling a void
7 Indifferent• Two men with a plastic bag and a name tag you
put on a toe• Car/horse racing
E
Iv
CMttciwwstirnsa
CMafwo
owmtIft.
i‘sroihtdd
CMpichpTa
B.L. Roberts et al.
xemplars
nitials have been changed to protect patients’ pri-acy.
ase 1rs. AA was admitted to the ICU following liver
ransplant surgery. She remained in the ICU for aotal of 3 days. Her maximum ICDSC was 0, indi-ating she did not experience delirium. During thenterview AA related a dream where she ‘‘. . . wasalking in clouds—–big fluffy cotton wool clouds,ith a dog and a rabbit, no noise, just quiet.’’ She
tated that she ‘‘did not have a dog or a rabbit buthey were friendly and were just peacefully walk-ng with her.’’ This made her feel very peaceful andelaxed but she often wonders ‘‘why the dog didot chase the rabbit?’’ She has not had this dreamince, but wishes at times she could have the dreamgain to feel the amazing peacefulness.
ase 2r. BB was admitted to ICU with severe communitycquired pneumonia, septic shock and acute renalailure. He remained in ICU for a period of 33 daysith a maximum ICDSC score during his admissionf four, indicating he experienced delirium.
During the interview, BB recalled distinct mem-ries initially of persecutory nature: ‘‘I thought Ias in a prison hospital . . . I thought I’d killed myother and father-in-law’’ This dream was inter-
wined with descriptions of bodily sensations ‘‘. . .
remember having a fan because I was hot . . . butelt like I was still in a prison hospital’’ and descrip-ions of hearing distinct sounds ‘‘. . . clicking doors. . all noises like trucks and earth works happen-ng around me’’. BB described the perception of‘flashing in & out of’’ the dreams. ‘‘I remembereeing an Indian restaurant, sold Indian stuff. Iemembered a woman and man arguing with eachther. I remember coming to, seeing a special-st, would you believe it, he was Indian. He hadis hands around my throat; he was playing withhe lifesaver in my throat’’. BB remembered thesereams as varying between ‘‘scary’’ and ‘‘goodreams’’.
ase 3r. CC was admitted to ICU following electiveeripheral artery bypass graft surgery. He remainedn ICU for 28 days and his ICDSC score was six, indi-ating delirium. During the interview he described
268
of bizarre; (4) auditory (n = 6) and (5) visual phe-nomena (n = 12) (e.g. gruesome rock faces and rockbreaking, a huge pot hanging from the ceiling andcars racing or seeing people fighting). These dreamssometimes led the person to believe they were in(6) places such as a prison hospital, a temple or acafe (n = 13). Some dreams described as (7) indif-ferent (n = 5) included horse/car racing, men usinga plastic bag to tag on a toe, or the ‘‘presence’’ offriends or ‘‘hippies’’ (see Table 1).
Most patients who recalled having dreams inICU had at least one dream that they rememberedas scary or negative. These dreams involved realor impending harm/ death to themselves or oth-ers. It was predominantly delirious patients whoreported scary dreams. The non-delirious tended toclassify their dreams as not unpleasant, althoughoften bizarre. Four participants reported similarphenomenon involving very bright light associatedwith either the inability to move, or resistanceagainst a demand to walk toward the light. A cou-ple of participants recalled their dreams as goodwith beautiful people or being surrounded by glasswindows. Some people reported a mixture of good
ow ‘‘the staff was trying to kill me first in the hos-ital and ultimately moved me to a basement . . ..hey were extracting my blood by force to sell itnd they were doing the same to a friend’s daugh-
P
tlr
CMddshwtab
u
Cp
EatpiaTipc5h
ipnp
(Iqc
C
PtatTntbcduCrafpd
D
Mawdw
atients’ dreams in ICU
er. I was in fear of dying. . . .. I pleaded for myife.’’ These dreams were very scary and have nevere-occurred since ICU discharge.
ase 4s. DD was admitted to ICU due to congestive car-iac failure and transferred to the ward after 11ays. Her maximum ICDCS was four and therefore,he experienced delirium during the ICU stay. Shead a feeling of going back in time ‘‘I was left by aindow with an older guy, it was weird, not upset-
ing . . .. How ICU would have been in olden days?’’nd wondering ‘‘. . . what procedures would haveeen performed to inflate the lungs.’’
These dreams or hallucinations never returnedpon discharge from ICU.
omparison of delirious and non-deliriousatients
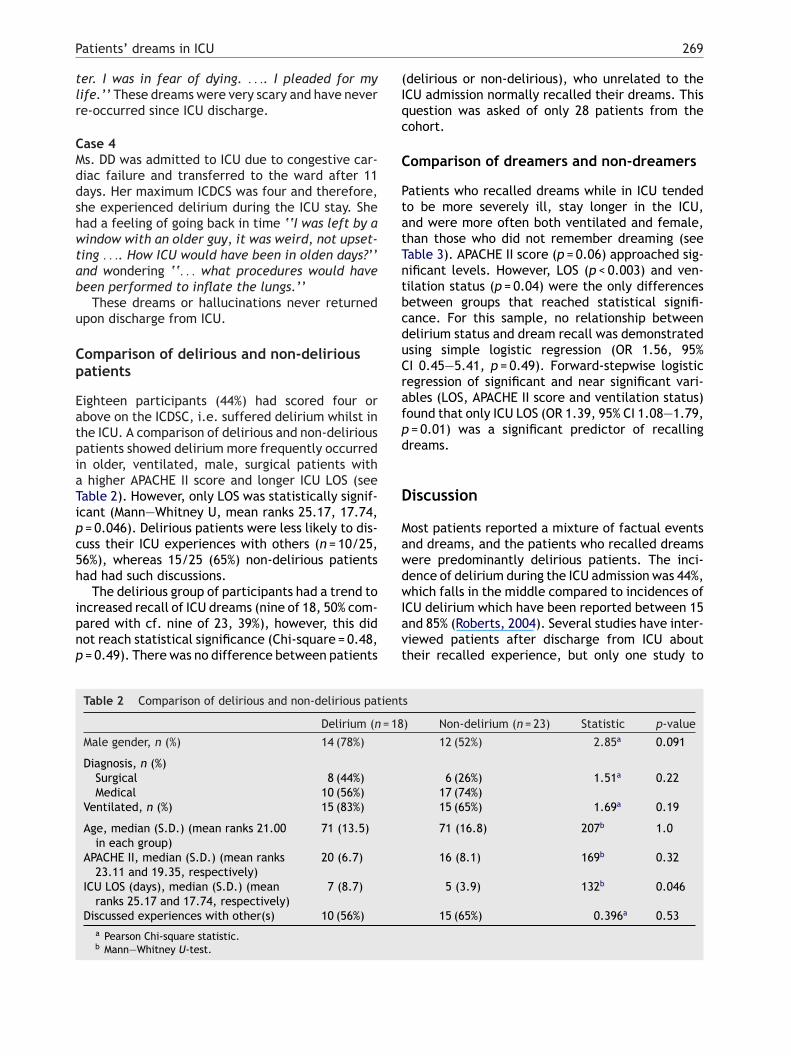
ighteen participants (44%) had scored four orbove on the ICDSC, i.e. suffered delirium whilst inhe ICU. A comparison of delirious and non-deliriousatients showed delirium more frequently occurredn older, ventilated, male, surgical patients with
higher APACHE II score and longer ICU LOS (seeable 2). However, only LOS was statistically signif-cant (Mann—Whitney U, mean ranks 25.17, 17.74,= 0.046). Delirious patients were less likely to dis-uss their ICU experiences with others (n = 10/25,6%), whereas 15/25 (65%) non-delirious patientsad had such discussions.
The delirious group of participants had a trend to
ncreased recall of ICU dreams (nine of 18, 50% com-ared with cf. nine of 23, 39%), however, this didot reach statistical significance (Chi-square = 0.48,= 0.49). There was no difference between patientsIavt
Table 2 Comparison of delirious and non-delirious patient
Delirium (n = 18
Male gender, n (%) 14 (78%)
Diagnosis, n (%)Surgical 8 (44%)Medical 10 (56%)
Ventilated, n (%) 15 (83%)
Age, median (S.D.) (mean ranks 21.00in each group)
71 (13.5)
APACHE II, median (S.D.) (mean ranks23.11 and 19.35, respectively)
20 (6.7)
ICU LOS (days), median (S.D.) (meanranks 25.17 and 17.74, respectively)
7 (8.7)
Discussed experiences with other(s) 10 (56%)a Pearson Chi-square statistic.b Mann—Whitney U-test.
269
delirious or non-delirious), who unrelated to theCU admission normally recalled their dreams. Thisuestion was asked of only 28 patients from theohort.
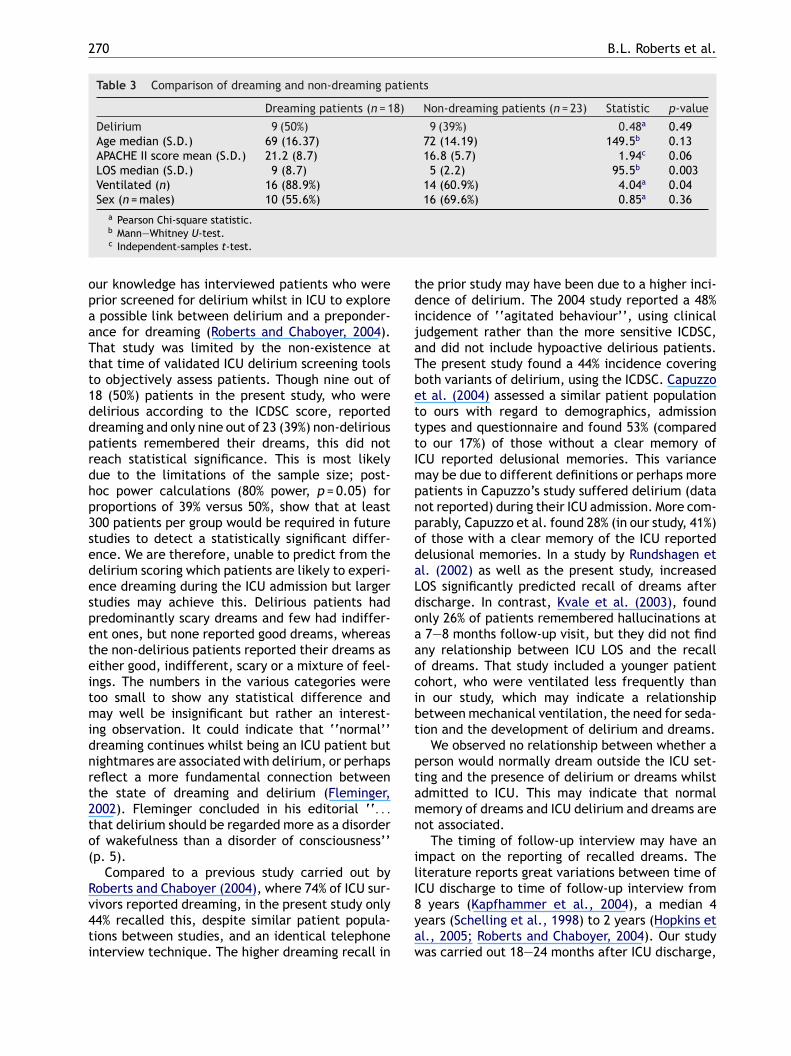
omparison of dreamers and non-dreamers
atients who recalled dreams while in ICU tendedo be more severely ill, stay longer in the ICU,nd were more often both ventilated and female,han those who did not remember dreaming (seeable 3). APACHE II score (p = 0.06) approached sig-ificant levels. However, LOS (p < 0.003) and ven-ilation status (p = 0.04) were the only differencesetween groups that reached statistical signifi-ance. For this sample, no relationship betweenelirium status and dream recall was demonstratedsing simple logistic regression (OR 1.56, 95%I 0.45—5.41, p = 0.49). Forward-stepwise logisticegression of significant and near significant vari-bles (LOS, APACHE II score and ventilation status)ound that only ICU LOS (OR 1.39, 95% CI 1.08—1.79,= 0.01) was a significant predictor of recallingreams.
iscussion
ost patients reported a mixture of factual eventsnd dreams, and the patients who recalled dreamsere predominantly delirious patients. The inci-ence of delirium during the ICU admission was 44%,hich falls in the middle compared to incidences of
CU delirium which have been reported between 15nd 85% (Roberts, 2004). Several studies have inter-iewed patients after discharge from ICU aboutheir recalled experience, but only one study to
s
) Non-delirium (n = 23) Statistic p-value
12 (52%) 2.85a 0.091
6 (26%) 1.51a 0.2217 (74%)15 (65%) 1.69a 0.19
71 (16.8) 207b 1.0
16 (8.1) 169b 0.32
5 (3.9) 132b 0.046
15 (65%) 0.396a 0.53
270 B.L. Roberts et al.
Table 3 Comparison of dreaming and non-dreaming patients
Dreaming patients (n = 18) Non-dreaming patients (n = 23) Statistic p-value
Delirium 9 (50%) 9 (39%) 0.48a 0.49Age median (S.D.) 69 (16.37) 72 (14.19) 149.5b 0.13APACHE II score mean (S.D.) 21.2 (8.7) 16.8 (5.7) 1.94c 0.06LOS median (S.D.) 9 (8.7) 5 (2.2) 95.5b 0.003Ventilated (n) 16 (88.9%) 14 (60.9%) 4.04a 0.04Sex (n = males) 10 (55.6%) 16 (69.6%) 0.85a 0.36
tdijaTbetttImpnpodaLdoaaocibt
ptamn
ilI
a Pearson Chi-square statistic.b Mann—Whitney U-test.c Independent-samples t-test.
our knowledge has interviewed patients who wereprior screened for delirium whilst in ICU to explorea possible link between delirium and a preponder-ance for dreaming (Roberts and Chaboyer, 2004).That study was limited by the non-existence atthat time of validated ICU delirium screening toolsto objectively assess patients. Though nine out of18 (50%) patients in the present study, who weredelirious according to the ICDSC score, reporteddreaming and only nine out of 23 (39%) non-deliriouspatients remembered their dreams, this did notreach statistical significance. This is most likelydue to the limitations of the sample size; post-hoc power calculations (80% power, p = 0.05) forproportions of 39% versus 50%, show that at least300 patients per group would be required in futurestudies to detect a statistically significant differ-ence. We are therefore, unable to predict from thedelirium scoring which patients are likely to experi-ence dreaming during the ICU admission but largerstudies may achieve this. Delirious patients hadpredominantly scary dreams and few had indiffer-ent ones, but none reported good dreams, whereasthe non-delirious patients reported their dreams aseither good, indifferent, scary or a mixture of feel-ings. The numbers in the various categories weretoo small to show any statistical difference andmay well be insignificant but rather an interest-ing observation. It could indicate that ‘‘normal’’dreaming continues whilst being an ICU patient butnightmares are associated with delirium, or perhapsreflect a more fundamental connection betweenthe state of dreaming and delirium (Fleminger,2002). Fleminger concluded in his editorial ‘‘. . .
that delirium should be regarded more as a disorderof wakefulness than a disorder of consciousness’’(p. 5).
Compared to a previous study carried out byRoberts and Chaboyer (2004), where 74% of ICU sur-
vivors reported dreaming, in the present study only44% recalled this, despite similar patient popula-tions between studies, and an identical telephoneinterview technique. The higher dreaming recall in8yaw
he prior study may have been due to a higher inci-ence of delirium. The 2004 study reported a 48%ncidence of ‘‘agitated behaviour’’, using clinicaludgement rather than the more sensitive ICDSC,nd did not include hypoactive delirious patients.he present study found a 44% incidence coveringoth variants of delirium, using the ICDSC. Capuzzot al. (2004) assessed a similar patient populationo ours with regard to demographics, admissionypes and questionnaire and found 53% (comparedo our 17%) of those without a clear memory ofCU reported delusional memories. This varianceay be due to different definitions or perhaps moreatients in Capuzzo’s study suffered delirium (dataot reported) during their ICU admission. More com-arably, Capuzzo et al. found 28% (in our study, 41%)f those with a clear memory of the ICU reportedelusional memories. In a study by Rundshagen etl. (2002) as well as the present study, increasedOS significantly predicted recall of dreams afterischarge. In contrast, Kvale et al. (2003), foundnly 26% of patients remembered hallucinations at7—8 months follow-up visit, but they did not find
ny relationship between ICU LOS and the recallf dreams. That study included a younger patientohort, who were ventilated less frequently thann our study, which may indicate a relationshipetween mechanical ventilation, the need for seda-ion and the development of delirium and dreams.
We observed no relationship between whether aerson would normally dream outside the ICU set-ing and the presence of delirium or dreams whilstdmitted to ICU. This may indicate that normalemory of dreams and ICU delirium and dreams are
ot associated.The timing of follow-up interview may have an
mpact on the reporting of recalled dreams. Theiterature reports great variations between time ofCU discharge to time of follow-up interview from
years (Kapfhammer et al., 2004), a median 4ears (Schelling et al., 1998) to 2 years (Hopkins etl., 2005; Roberts and Chaboyer, 2004). Our studyas carried out 18—24 months after ICU discharge,

P
fWapaoHiuidfa22itr
tascsrsr‘nprw
ddfTmfpseuipcmdbcrmdaeI
fimlh
aaiwo(doPsctcde
tstacm
thvshparIfaTsfiedmh
C
T
atients’ dreams in ICU
alling within the previously reported time-frames.hen Schelling et al. (1998) interviewed patients
t (a median of) 4 years they found 64% to com-lain of nightmares. This was similar to Robertsnd Chaboyer (2004), who found the incidencef dreaming to be 74% at 18 months follow-up.opkins et al. (2005) noted neurocognitive sequelae
n 47% of the patients evaluated at 2-year follow-p, which is similar to the 44%, who recalled dreamsn our study. Many other interviews have been con-ucted immediately after ICU discharge or only aew months after hospital discharge (Capuzzo etl., 2004; Granberg et al., 1999; Rotondi et al.,002; Rundshagen et al., 2002; Swaiss and Badran,004). In these studies recollections of dreams var-ed between 9 and 81%. We might therefore, assumehat delusional memories of ICU will be retainedather than fade with time.
Misperception of place was the most commonheme of dreams, which may indicate the patientsre sub-consciously aware of being in unfamiliarurroundings. Other themes involved bold, brightolours, being surrounded by glass windows andtrange noises may reflect the harsh physical envi-onment of ICU. It is important that health profes-ionals are aware of the influences the ICU envi-onment have on patients and make attempts to‘soften’’ surroundings (dimmed lighting, reduceoise) wherever possible. Divine experiences wereresent, though not common in this study, and mayeflect the near-death-experience often associatedith an ICU admission.Overall, 10 of the 18 patients with dreams
escribed them as scary with a predominance inelirious dreaming patients (six of nine) and onlyour out of nine non-delirious dreaming patients.hese scary dreams such as ‘‘staff trying to kille’’, ‘‘blood being extracted from the body by
orce’’ and ‘‘buried alive’’ must be horrendous foratients. It has been postulated that patients whouffer from delusions may avoid discussing theirxperiences in fear of being labelled ‘‘mentallynstable’’ (Griffith and Jones, 1999). Similar fearn our study population may account for feweratients (n = 10) in the delirious group had dis-ussed their dreams with others, whereas slightlyore (n = 15) non-delirious patients had had thisiscussion, primarily with another family mem-er. Although our results did not reach statisti-al significance, there was a higher incidence ofecalled dreaming in delirious patients, and theyay be most at risk of developing persecutory
elusions regarding their admission. Even if onlysmall number of ICU patients may benefit fromarly identification and intervention; assessing allCU patients for delirium could improve outcome
dfips
271
or those patients, who are suffering from delir-um and dreams. The delirious patient populationay require more intensive and immediate psycho-
ogical follow-up care from appropriately trainedealthcare workers.
Though scary and persecutory hallucinationsppear to attract the most attention in the liter-ture (Fleminger, 2002; Schnyder et al., 2001), thencidence in the present study for scary dreamsere below the number of people reporting goodr indifferent dreams. Allenby-Smith and Pierce2001) interviewed 161 patients and noted thatreams were recounted in 48% of patients, withnly 19% describing severe persecutory beliefs.atients do recall dreams they describe as good,uch as ‘‘beautiful colours’’ or ‘‘walking on aloud’’. It may be assumed that such dreams coun-eract or protect against the stress of ICU, andertainly the patients are happy to recount thesereams, and they may be perceived as positivexperiences.
Dreaming patients tended to be sicker and ven-ilated, and they had a significantly longer ICUtay. These are the patients expected to dominatehe ICU population in the future, and therefore,ttempts must be made to focus our attention onoping strategies through information to and com-unication with patients and their relatives.It is important to provide care for ICU patients
o restore not only physical but also psychologicalealth and well-being. The benefit of adapting pre-entative measures for delirium, the use of deliriumcreening tools for early detection and compre-ensive follow-up care of ICU patients may assistatients in regaining a fulfilling and holistic lifefter discharge from ICU. It is studies like the cur-ent one that focus on the different scenarios ofCU experiences that can be discussed with first theamily, during the acute stage of the patients illnessnd subsequently with the patient him/her self.hough the number of participants in the presenttudy precluded drawing any firm conclusions, ourndings may add to increased awareness and knowl-dge of the plight of ICU patients with regards toelirium and both good and bad dreams. Nursingust play a proactive role by providing the optimal
olistic approach to patient care.
onclusion
he prevalence of 44% of ICU patients reporting
reams from their ICU admission was a significantnding. Dreaming was more widespread amongstatients who were delirious during their ICU admis-ion (nine out of 18) than the non-delirious (nine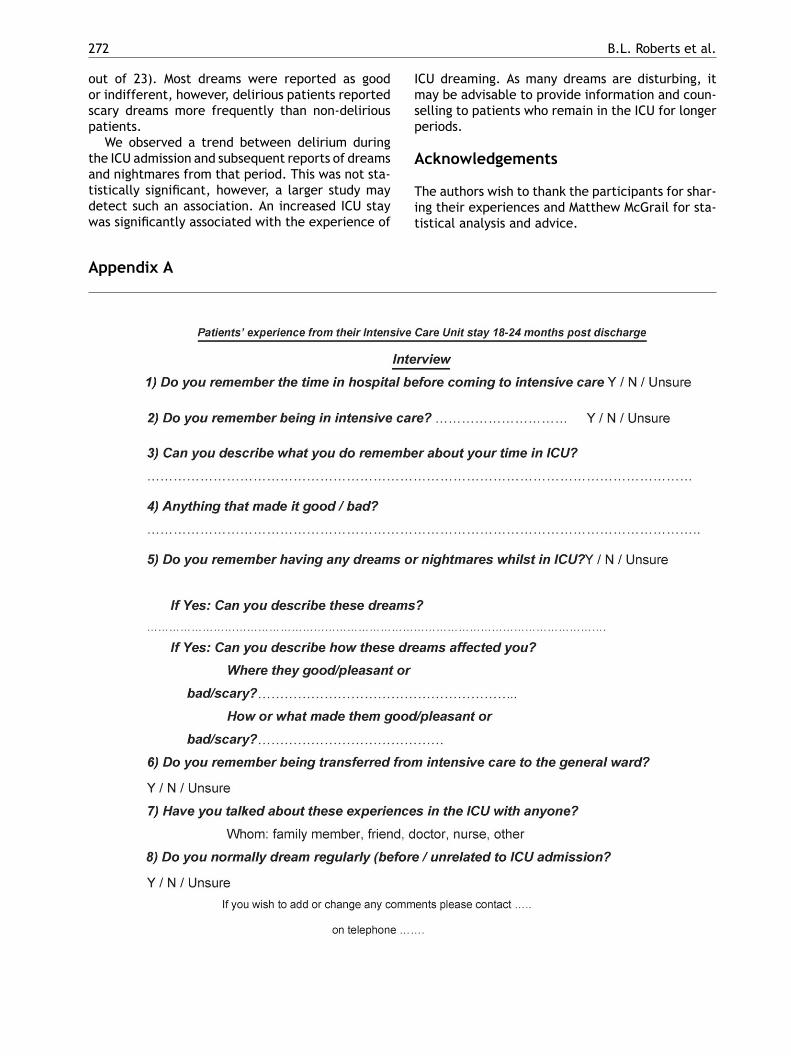
272
out of 23). Most dreams were reported as goodor indifferent, however, delirious patients reportedscary dreams more frequently than non-deliriouspatients.
We observed a trend between delirium duringthe ICU admission and subsequent reports of dreams
and nightmares from that period. This was not sta-tistically significant, however, a larger study maydetect such an association. An increased ICU staywas significantly associated with the experience ofAppendix A
B.L. Roberts et al.
ICU dreaming. As many dreams are disturbing, itmay be advisable to provide information and coun-selling to patients who remain in the ICU for longerperiods.
Acknowledgements
The authors wish to thank the participants for shar-ing their experiences and Matthew McGrail for sta-tistical analysis and advice.
P
R
A
B
C
C
C
D
E
E
E
E
E
F
G
G
G
G
H
atients’ dreams in ICU
eferences
llenby-Smith O, Pierce JMT. Illusions and ‘delusions’ in cardiacsurgical patients after prolonged intensive care unit stay. CritCare 2001;5:46—51.
ergeron N, Dubois M, Dumont M, Dial S, Skrobik Y. Intensive caredelirium screening checklist: evaluation of a new screeningtool. Intensive Care Med 2001;27:859—64.
apuzzo M, Valpondi V, Cingolani E, De Luca S, et al. Applicationof the Italian version of the intensive care unit memory toolin the clinical setting. Crit Care 2004;8(1):R48—56.
olaizzi PF. Psychological research as the phenomenologist viewsit. In: Valle RS, King M, editors. Existential phenomenologi-cal alternatives for psychology. New York: Oxford UniversityPress; 1978. p. 48—71.
uthbertson BH, Hull A, Strachan M, Scott J. Post-traumaticstress disorder after critical illness requiring general inten-sive care. Intensive Care Med 2004;30:450—5.
ubois M, Bergeron N, Dumont M, Dial S, Skrobik Y. Delirium inan intensive care unit: a study of risk factors. Intensive CareMed 2001;27:1297—304.
ly EW, Gautam S, Margolin R, Francis J, et al. The impact ofdelirium in the intensive care unit on hospital length of stay.Intensive Care Med 2001a;27:1892—900.
ly EW, Margolin R, Francis J, May L, et al. Evaluation of deliriumin critically ill patients: validation of the confusion assess-ment method for the intensive care unit (CAM-ICU). Crit CareMed 2001b;29(7):1370—9.
ly EW, Inouye SK, Bernard GR, Gordon S, et al. Delirium inmechanically ventilated patients: validity and reliability ofthe confusion assessment method for the intensive care unit(CAM-ICU). J Am Med Assoc 2001c;286(21):2703—10.
ly EW, Shintani A, Truman B, Speroff T, et al. Delirium as apredictor of mortality in mechanically ventilated patients inthe intensive care unit. J Am Med Assoc 2004a;291:1753—62.
ly EW, Stephens RK, Jackson JC, Thomason JW, et al. Currentopinions regarding the importance, diagnosis, and manage-ment of delirium in the intensive care unit: A survey of 912healthcare professionals. Crit Care Med 2004b;32(1):106—16.
leminger S. Remembering delirium. Br J Psychiatry 2002;180:4—5.
ranberg A, Bergbom Engberg I, Lundberg D. Patients’ experi-ence of being critical ill or severely injured and cared for inan intensive care unit in relation to the ICU syndrome. Part1. Intensive Crit Care Nurs 1998;14:294—307.
ranberg A, Bergbom Engberg I, Lundberg D. Acute confusionand unreal experiences in intensive care patients in rela-tion to the ICU syndrome. Part 2. Intensive Crit Care Nurs1999;15:19—33.
riffith RD, Jones C. Recovery from intensive care. Br Med J1999;319:427—9.
riffith RD, Jones C. Filling the intensive care memory gap?
Intensive Care Med 2001;27:344—6.opkins RO, Weaver LK, Collingridge D, Parkinson RB, et al. Two-year cognitive, emotional, and quality-of-life outcomes inacute respiratory distress syndrome. Am J Respir Crit CareMed 2005;171(4):340—7.
273
Jackson JC, Hart RP, Gordon SM, Shintani A, et al. Six-monthneuropsychological outcome of medical intensive care unitpatients. Crit Care Med 2003;31(4):1226—34.
Jones C, Griffith RD, Humphris G, Skirrow PM. Memory, delu-sion, and the development of acute posttraumatic stressdisorder-related symptoms after intensive care. Crit CareMed 2001;29(3):573—80.
Jones C, Skirrow P, Griffith RD, Humphris GH, et al. Rehabilita-tion after critical illness: a randomized, controlled trial. CritCare Med 2003;31(10):2456—61.
Kapfhammer HP, Rothenhausler HB, Krauseneck T, Stoll C,Schelling G. Posttraumatic stress disorder and health-relatedquality of life in long-term survivors of acute respiratory dis-tress syndrome. Am J Psychiatry 2004;161(1):45—52.
Kvale R, Ulvik A, Flaatten H. Follow-up after intensive care: asingle center study. Intensive Care Med 2003;29:2149—56.
Papathanassoglou EDE, Patiraki EI. Transformations of self: aphenomenological investigation into the lived experience ofsurvivors of critical illness. Nurs Crit Care 2003;8(1):13—21.
Roberts BL. Managing delirium in adult intensive care patients.Crit Care Nurs 2001;21(1):48—55.
Roberts B, Chaboyer W. Patients’ dreams and unreal experi-ences following intensive care unit admission. Nurs Crit Care2004;9(4):173—80.
Roberts B. Screening for delirium in an adult intensive care unit.Intensive Crit Care Nurs 2004;20:206—13.
Roberts BL, Rickard CM, Rajbhandari D, Turner G, et al. Multicen-tre study of delirium in ICU patients using a simple screeningtool. Aust Crit Care 2005;18(1):6—16.
Rotondi AJ, Lakshmipathi C, Sirio C, Mendelsohn A, et al.Patients’ recollections of stressful experiences while receiv-ing prolonged mechanical ventilation in an intensive careunit. Crit Care Med 2002;30(4):746—52.
Rundshagen I, Schnabel K, Wegner C, Schulte am Esch. Incidenceand recall, nightmares, and hallucinations during analgose-dation in intensive care. Intensive Care Med 2002;28:38—43.
Schelling G, Stoll C, Haller M, Briegel J, et al. Health-relatedquality of life and posttraumatic stress disorder in survivorsof the acute respiratory distress syndrome. Crit Care Med1998;26(4):651—9.
Schnyder U, Moergeli H, Trentz O, Klaghofer R, Buddeberg C.Prediction of psychiatric morbidity in severely injured acci-dent victims at one-year follow-up. Am J Respir Crit Care Med2001;164:653—6.
Schragg P, Jones A, Fauvel N. Psychological problems followingICU treatment. Anaesthesia 2001;56(1):9—14.
Skrobik Y. An overview of delirium in the critical care setting.Geriatr Aging 2003;6(10):30—5.
Stoll C, Kapfhammer HP, Rothenhausler HB, Haller M, et al.Sensitivity and specificity of a screening test to documenttraumatic experiences and to diagnose post-traumatic stressdisorder in ARDS patients after intensive care treatment.Intensive Care Med 1999;25:697—704.
Swaiss IG, Badran I. Discomfort, awareness and recall in theintensive care—–still a problem. Middle East J Anesthesiol
2004;17(5):951—8.Truman B, Ely EW. Monitoring delirium in critical ill patients.Using the confusion assessment method for the intensive careunit. Crit Care Nurs 2003;23(2):25—36.
Related Documents