Patient tailored ovarian stimulation for IVF Prof.Dr. Bart CJM Fauser

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Patient tailored ovarian
stimulation for IVF
Prof.Dr. Bart CJM Fauser
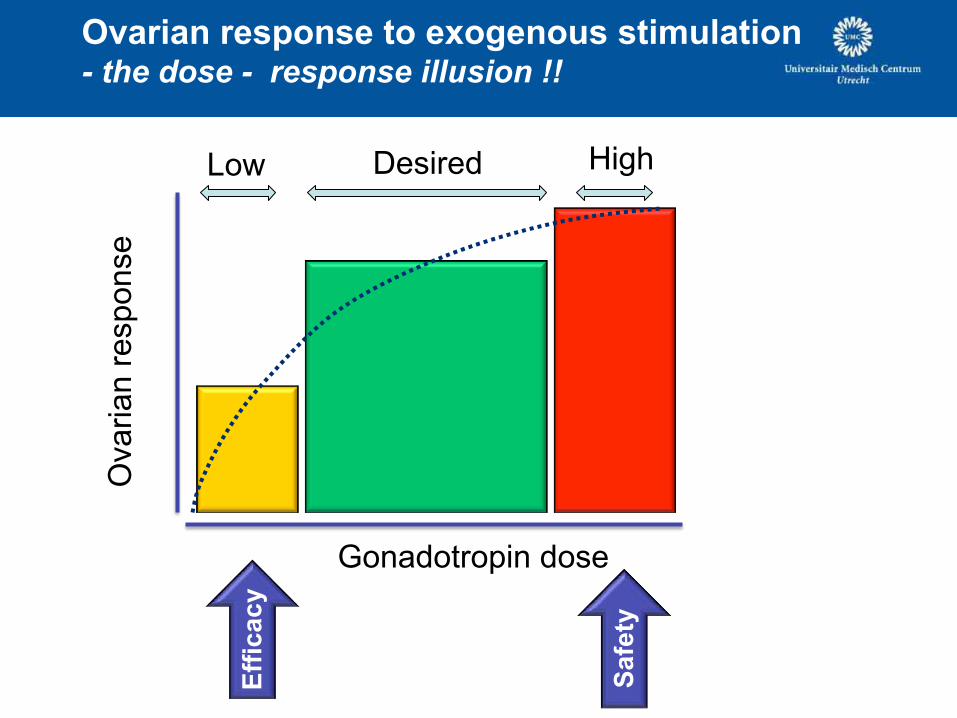
Ovarian response to exogenous stimulation - the dose - response illusion !!
Ovarian
response
Gonadotropin dose
Low Desired High
Eff
ica
cy
Safe
ty
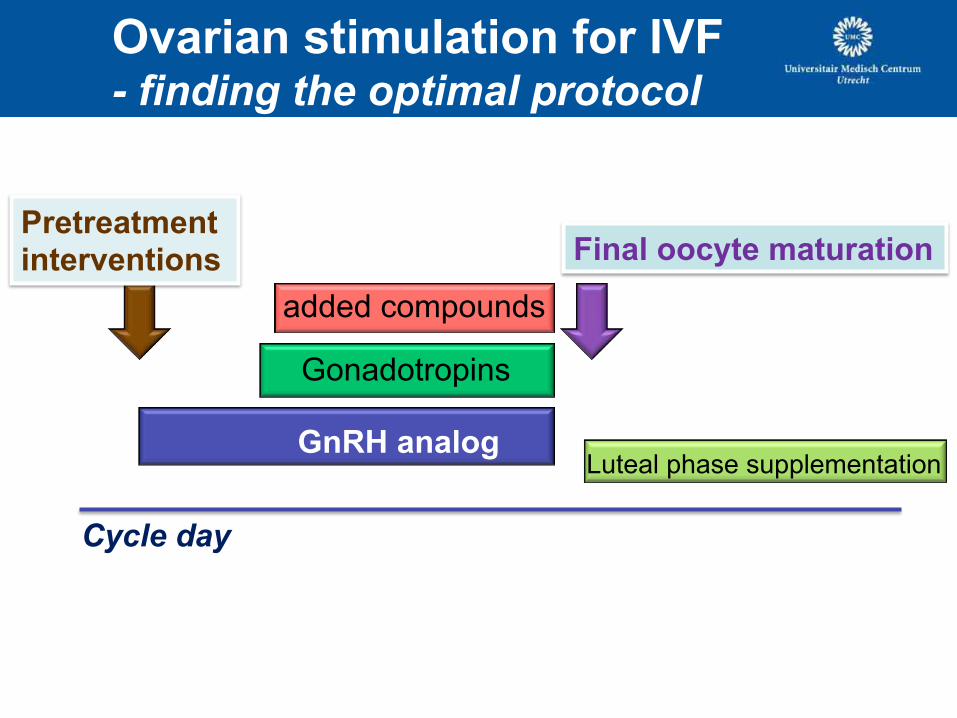
Ovarian stimulation for IVF
- finding the optimal protocol
GnRH analog
Gonadotropins
added compounds
Final oocyte maturation
Luteal phase supplementation
Pretreatment interventions
Cycle day
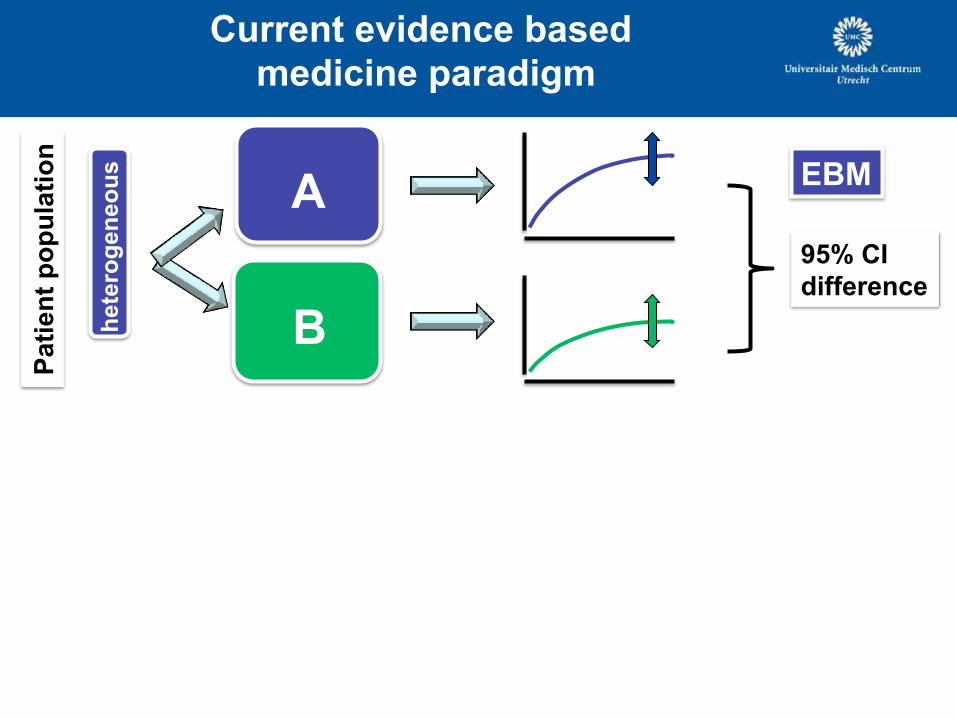
Current evidence based
medicine paradigm P
ati
en
t p
op
ula
tio
n
A
B
EBM
hete
rog
en
eo
us
95% CI
difference
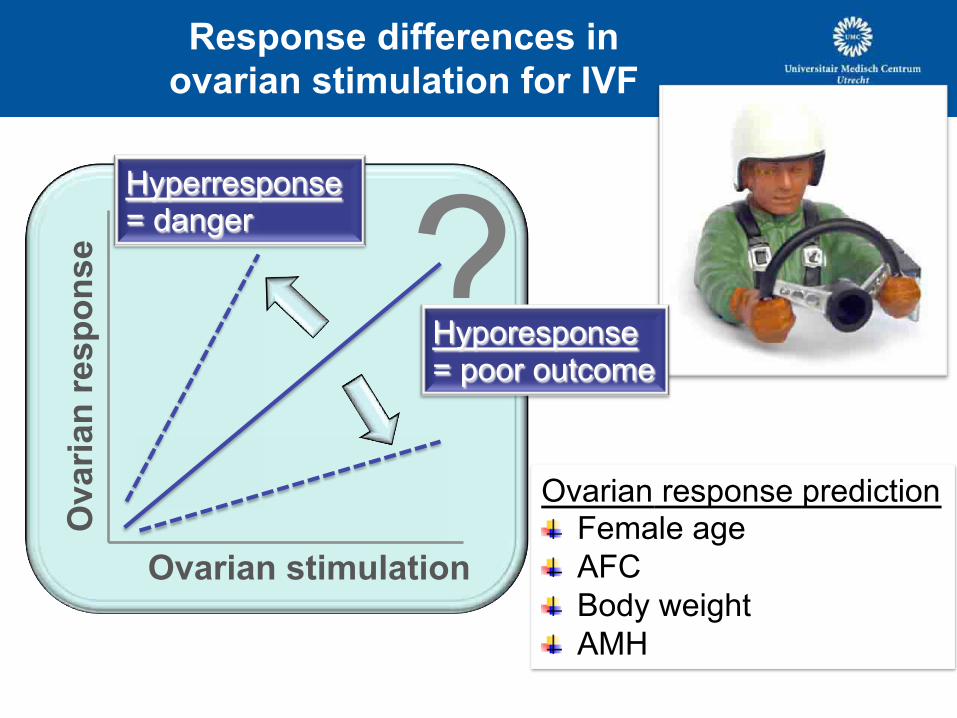
Response differences in
ovarian stimulation for IVF O
vari
an
resp
on
se
Ovarian stimulation
? Hyporesponse = poor outcome
Hyperresponse = danger
Ovarian response prediction ! Female age
! AFC
! Body weight
! AMH
The paradigm shift in medicine
One size fits all
Patient tailored
treatment algorithms
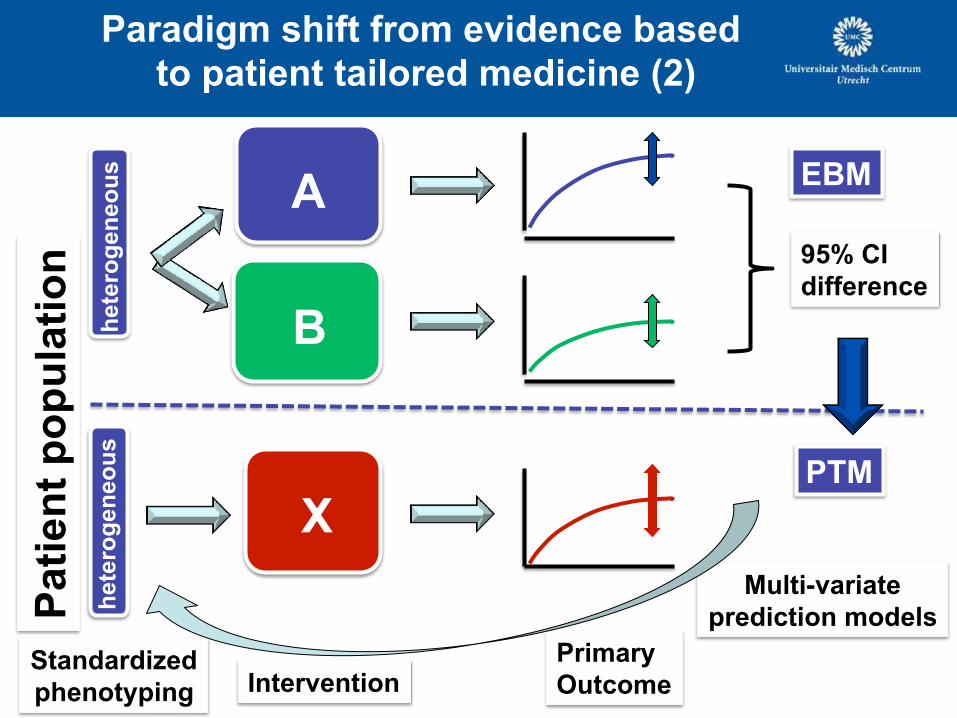
Paradigm shift from evidence based
to patient tailored medicine (2) P
ati
en
t p
op
ula
tio
n
Intervention
A
B
X
Primary
Outcome Standardized
phenotyping
EBM
PTM
Multi-variate
prediction models
hete
rog
en
eo
us
hete
rog
en
eo
us
95% CI
difference
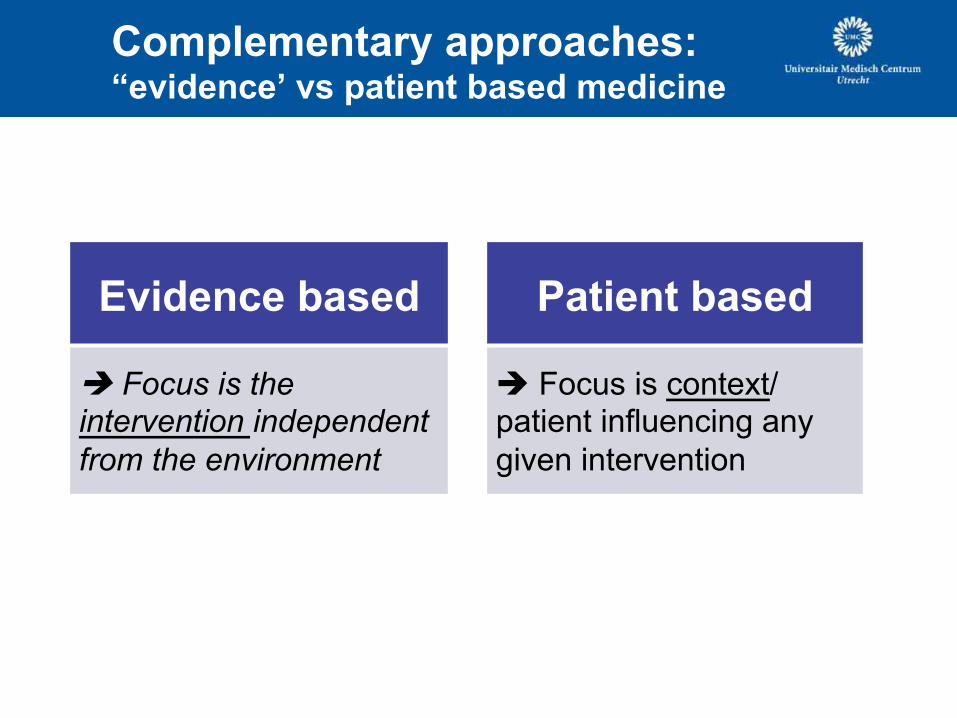
Complementary approaches: “evidence’ vs patient based medicine
Evidence based
è Focus is the intervention independent
from the environment
Patient based
è Focus is context/ patient influencing any
given intervention
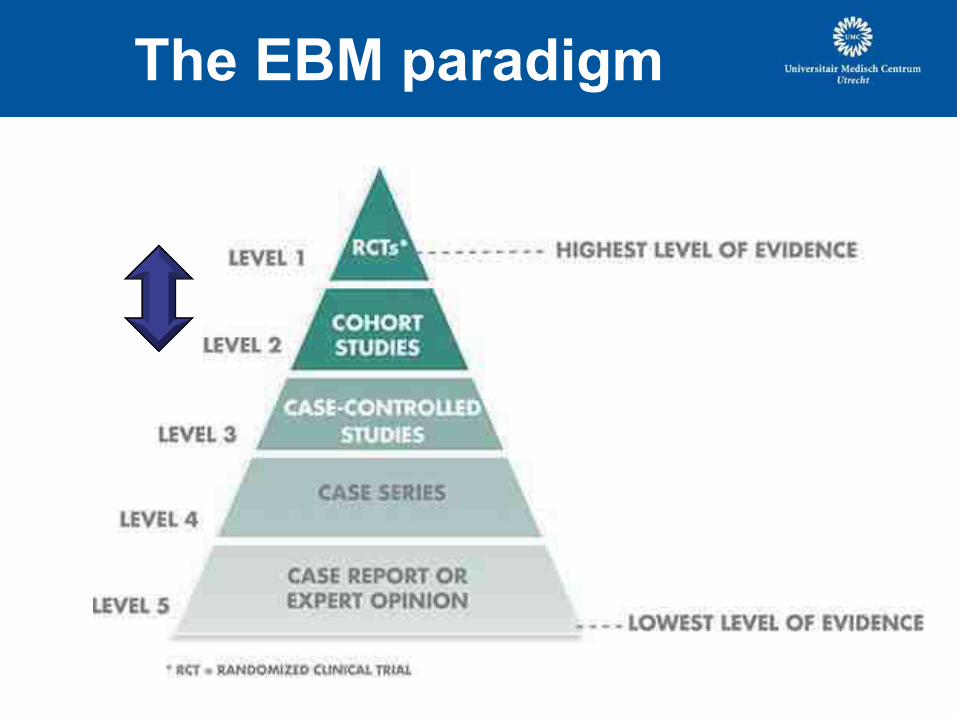
The EBM paradigm
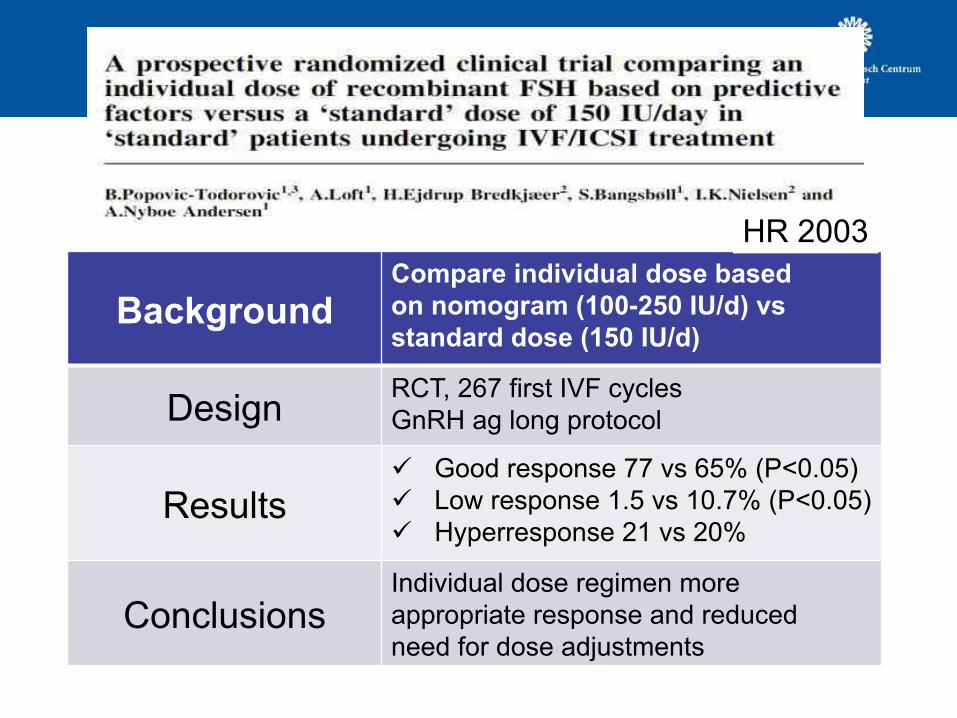
Background Compare individual dose based
on nomogram (100-250 IU/d) vs
standard dose (150 IU/d)
Design RCT, 267 first IVF cycles
GnRH ag long protocol
Results ü Good response 77 vs 65% (P<0.05)
ü Low response 1.5 vs 10.7% (P<0.05)
ü Hyperresponse 21 vs 20%
Conclusions Individual dose regimen more
appropriate response and reduced
need for dose adjustments
HR 2003
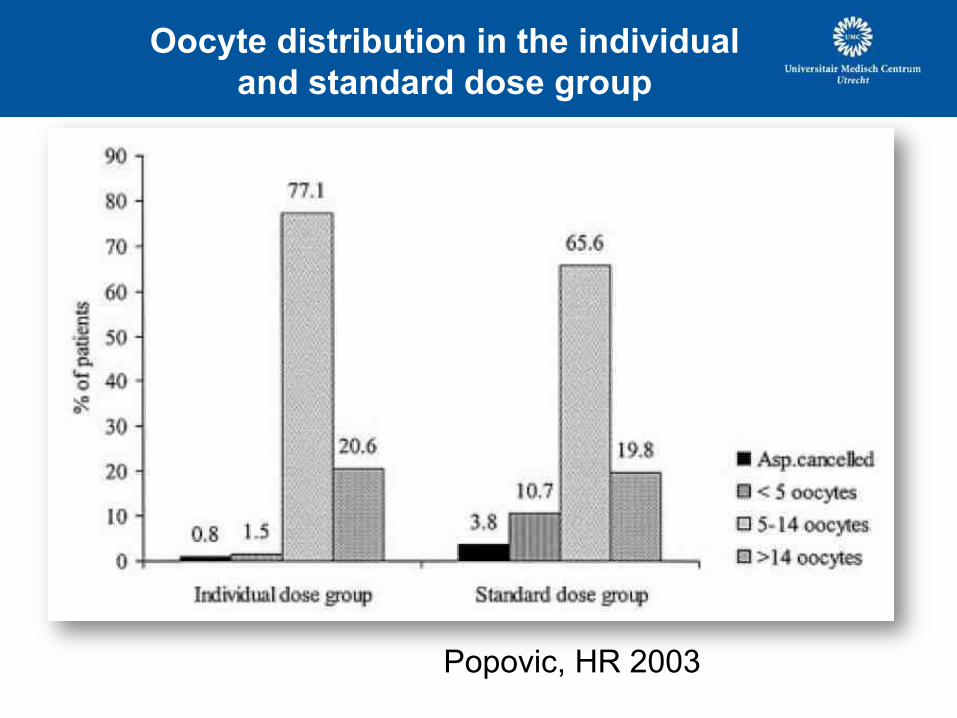
Oocyte distribution in the individual
and standard dose group
Popovic, HR 2003
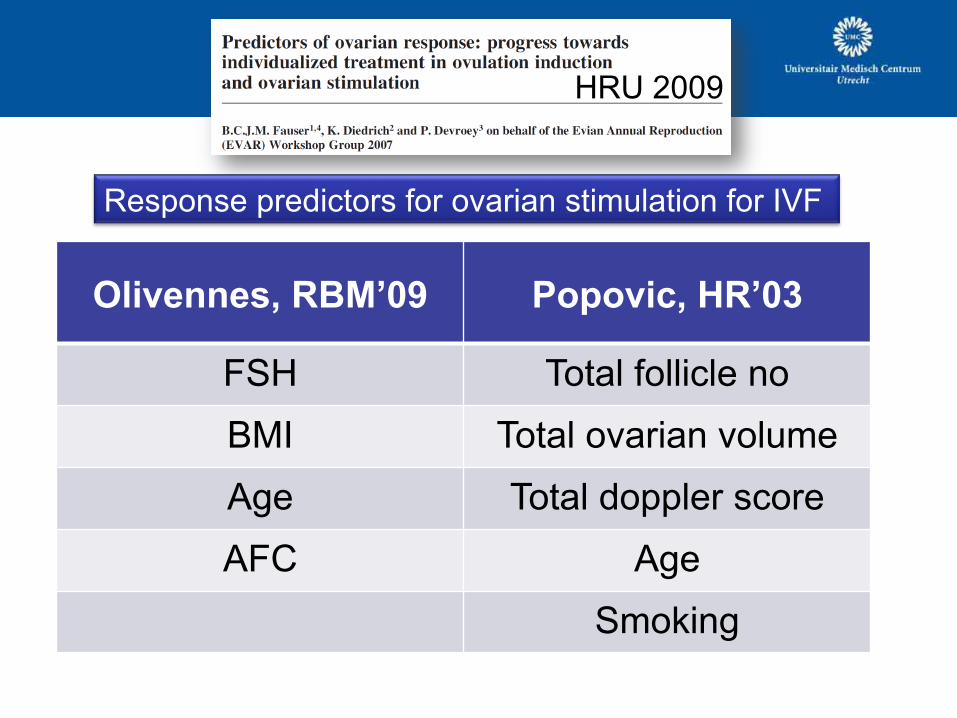
HRU 2009
Olivennes, RBM’09 Popovic, HR’03
FSH Total follicle no
BMI Total ovarian volume
Age Total doppler score
AFC Age
Smoking
Response predictors for ovarian stimulation for IVF
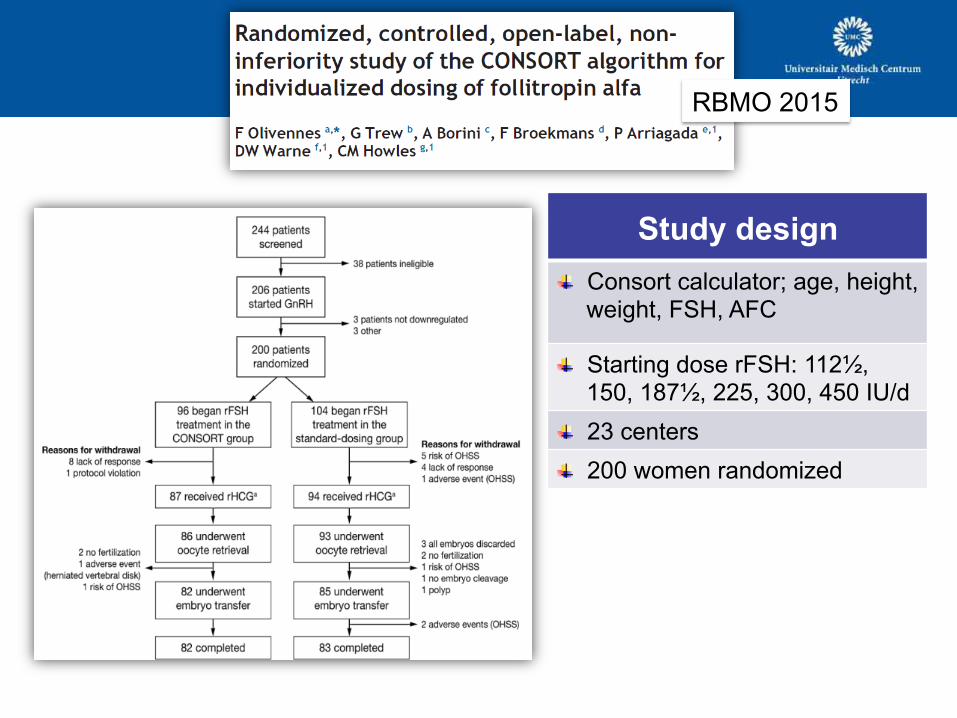
RBMO 2015
Study design
! Consort calculator; age, height, weight, FSH, AFC
! Starting dose rFSH: 112½, 150, 187½, 225, 300, 450 IU/d
! 23 centers
! 200 women randomized
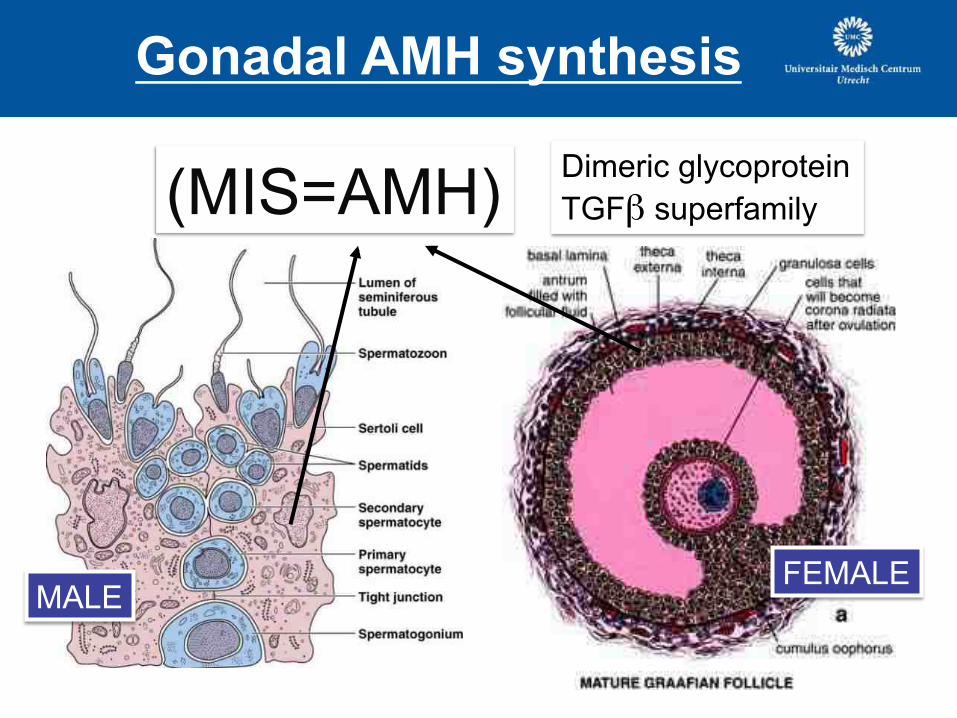
(MIS=AMH)
Gonadal AMH synthesis
Dimeric glycoprotein
TGFβ superfamily
MALE FEMALE
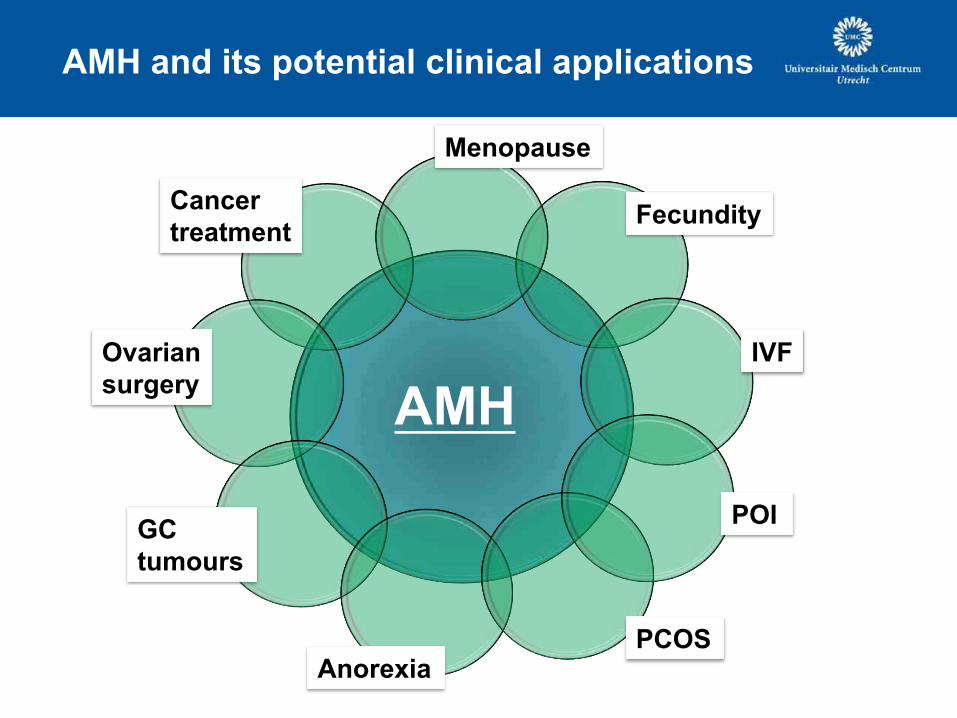
AMH and its potential clinical applications
AMH
Fecundity
IVF
PCOS
POI
Menopause
Cancer
treatment
Ovarian
surgery
GC
tumours
Anorexia
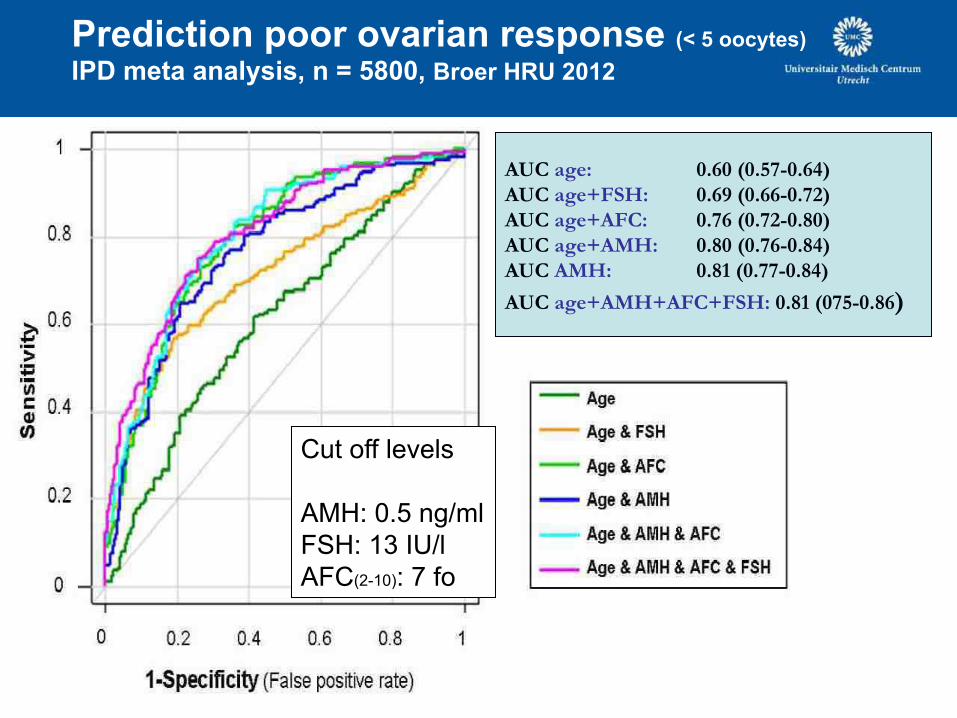
AUC age: 0.60 (0.57-0.64)
AUC age+FSH: 0.69 (0.66-0.72)
AUC age+AFC: 0.76 (0.72-0.80)
AUC age+AMH: 0.80 (0.76-0.84)
AUC AMH: 0.81 (0.77-0.84)
AUC age+AMH+AFC+FSH: 0.81 (075-0.86)
Prediction poor ovarian response (< 5 oocytes)
IPD meta analysis, n = 5800, Broer HRU 2012
Cut off levels
AMH: 0.5 ng/ml
FSH: 13 IU/l
AFC(2-10): 7 fo
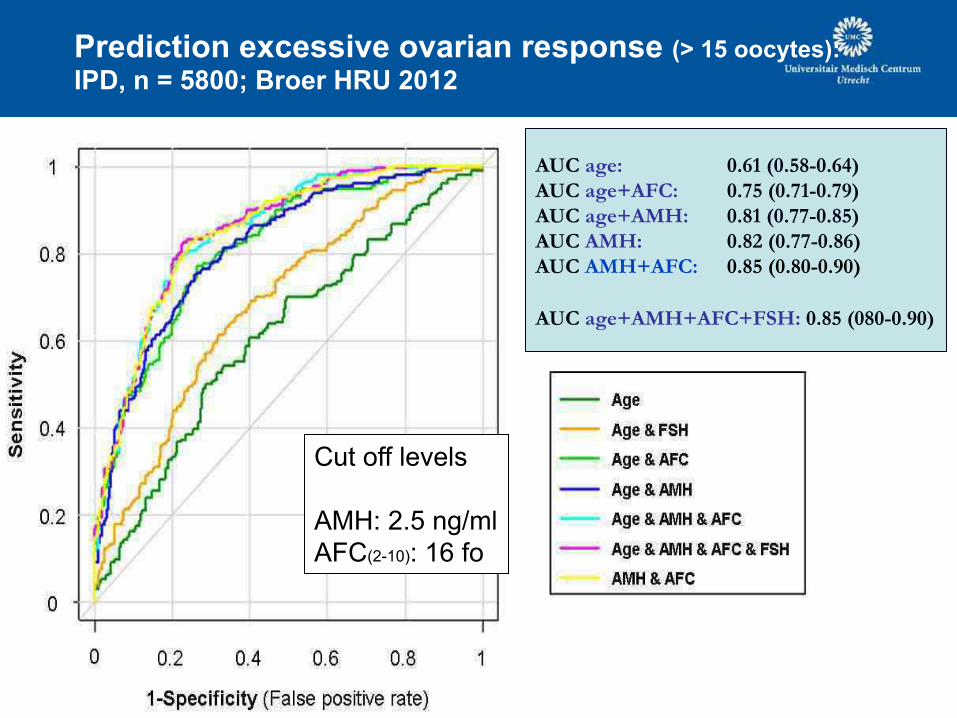
Prediction excessive ovarian response (> 15 oocytes):
IPD, n = 5800; Broer HRU 2012
AUC age: 0.61 (0.58-0.64)
AUC age+AFC: 0.75 (0.71-0.79)
AUC age+AMH: 0.81 (0.77-0.85)
AUC AMH: 0.82 (0.77-0.86)
AUC AMH+AFC: 0.85 (0.80-0.90)
AUC age+AMH+AFC+FSH: 0.85 (080-0.90)
Cut off levels
AMH: 2.5 ng/ml
AFC(2-10): 16 fo
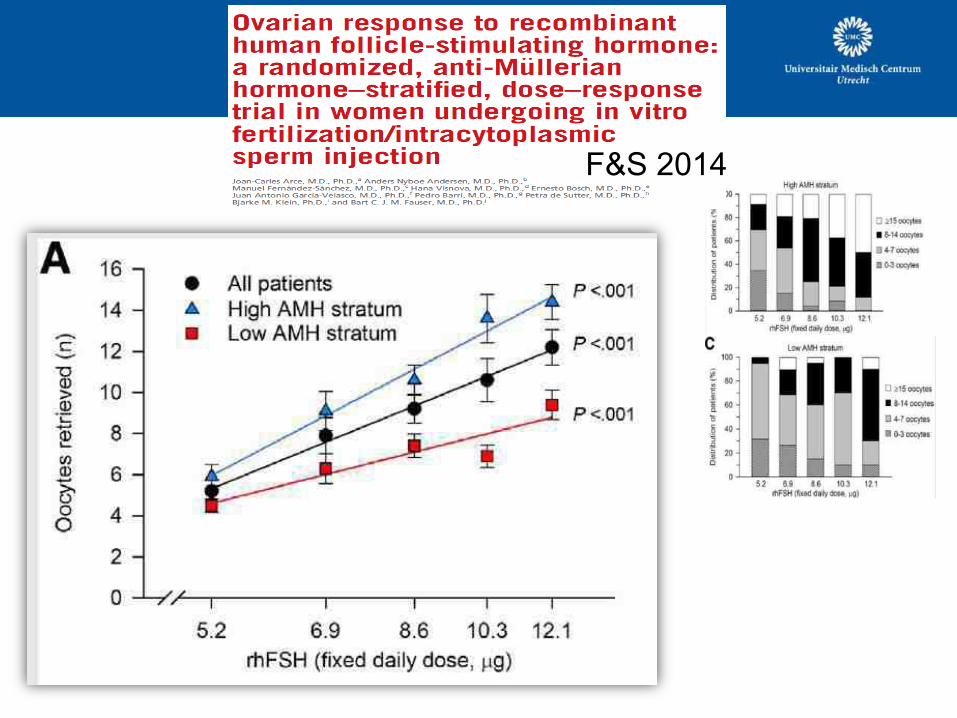
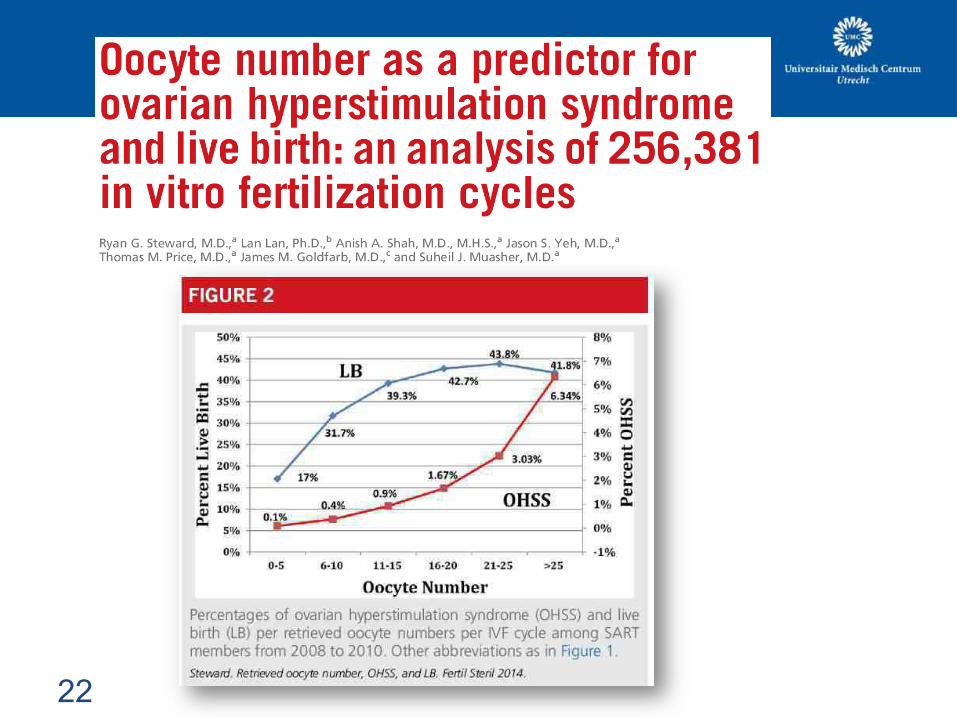
F&S 2014
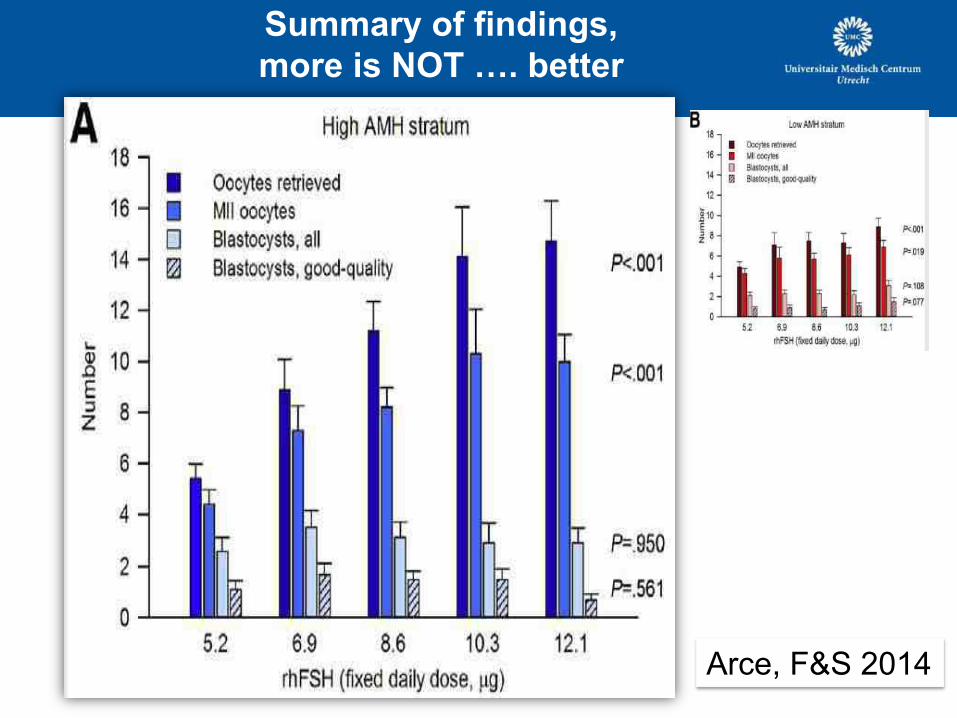
Summary of findings,
more is NOT …. better
Arce, F&S 2014
Optimal number of oocytes for IVF
- the more the better ??
Patient perspective
So
cie
ty
pers
pec
tive
Ch
ild
pers
pectiv
e
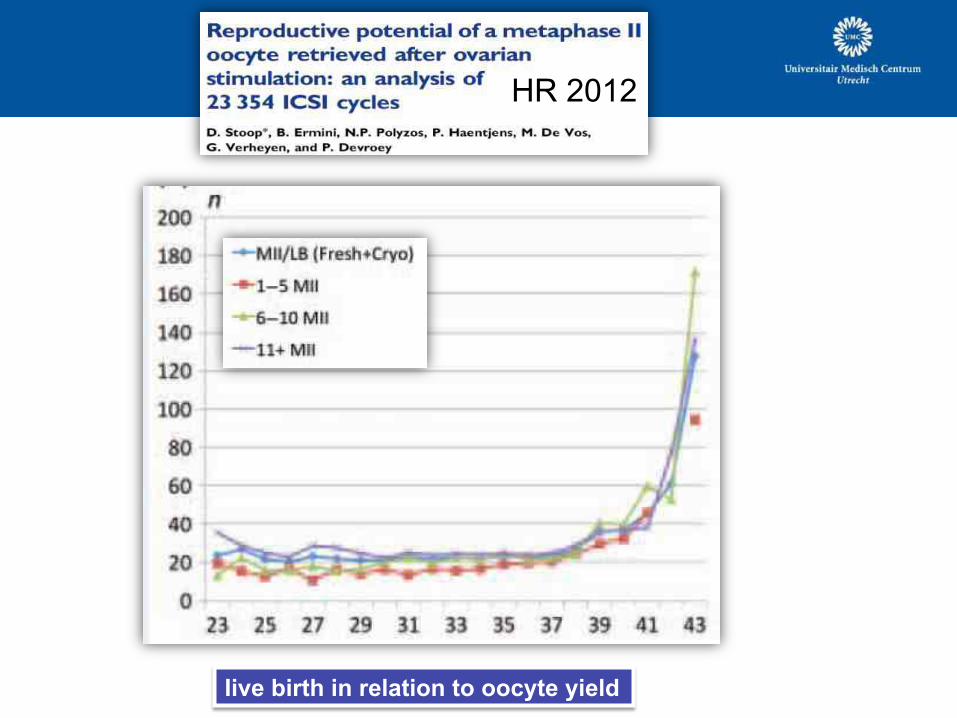
HR 2012
Iive birth in relation to oocyte yield
22
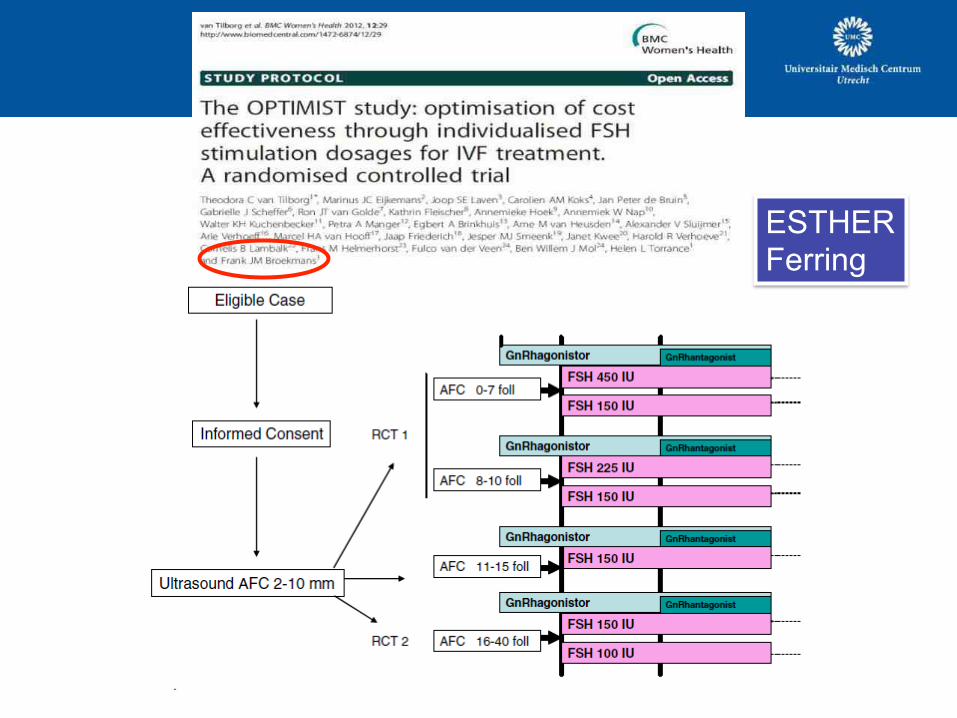
ESTHER Ferring
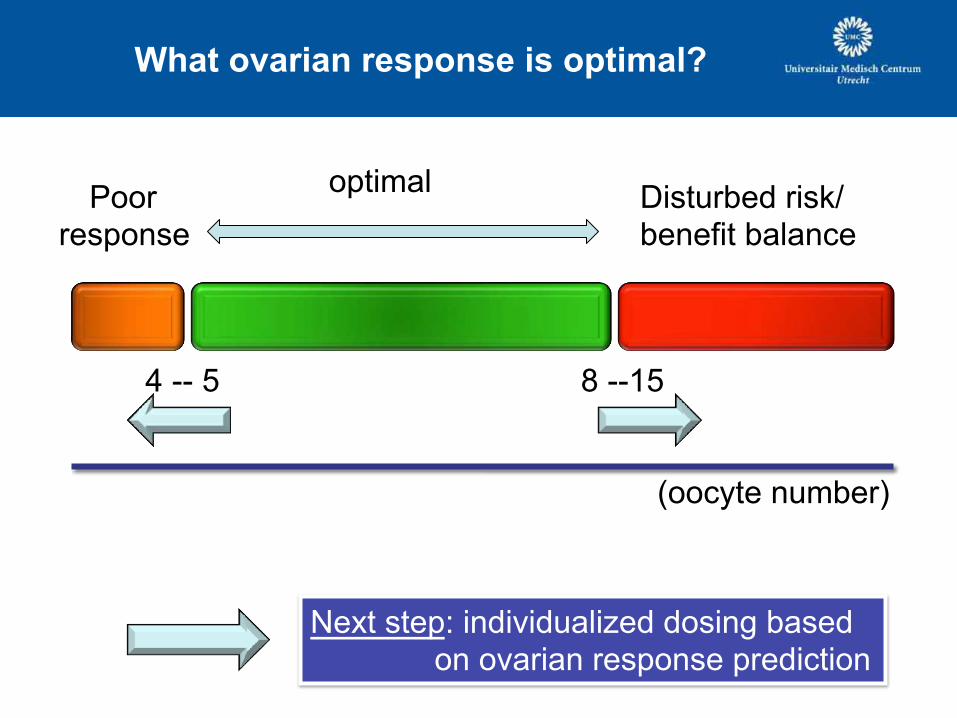
What ovarian response is optimal?
4 -- 5 8 --15
Poor response
optimal Disturbed risk/ benefit balance
(oocyte number)
Next step: individualized dosing based on ovarian response prediction
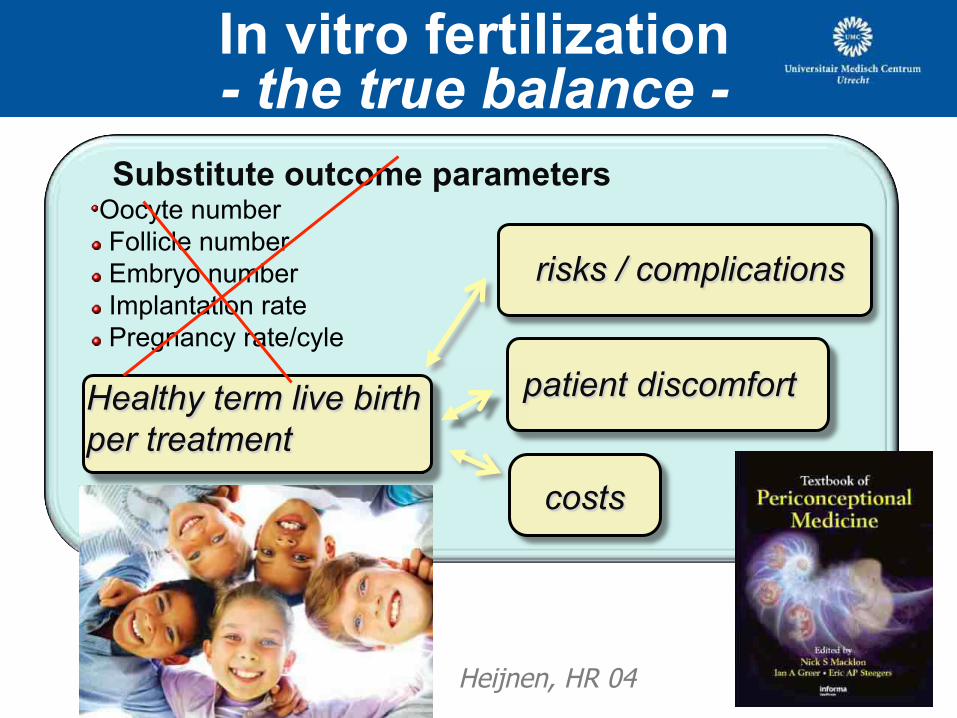
In vitro fertilization - the true balance -
Substitute outcome parameters ! Oocyte number
! Follicle number
! Embryo number
! Implantation rate
! Pregnancy rate/cyle
risks / complications
patient discomfort
costs
Healthy term live birth
per treatment
Heijnen, HR 04
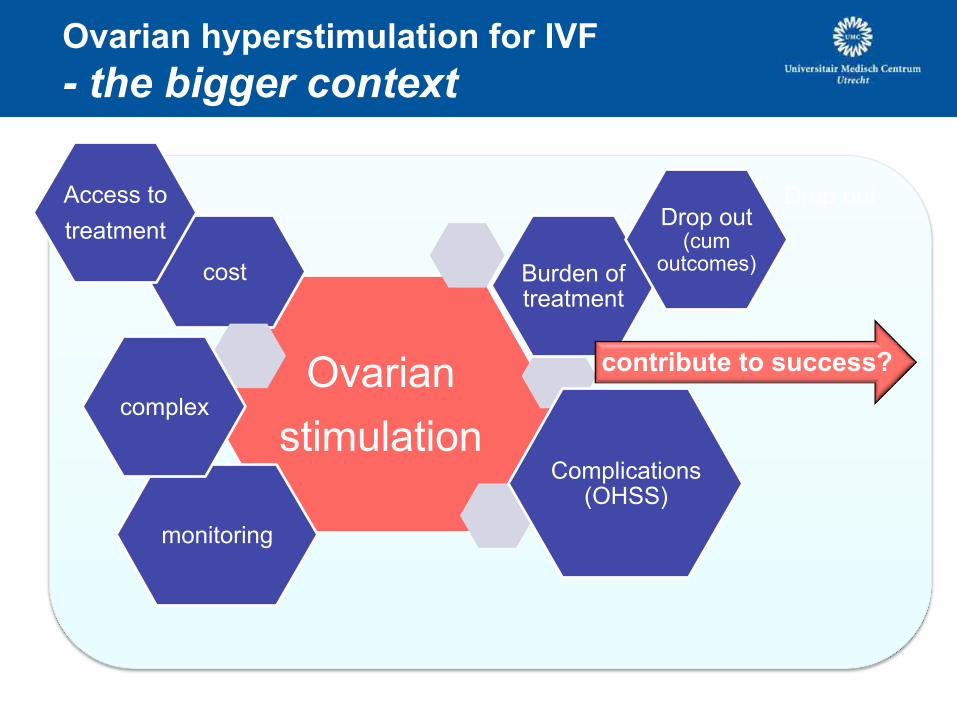
Ovarian hyperstimulation for IVF
- the bigger context
Ovarian
stimulation
cost Burden of treatment
Drop out (cum
outcomes)
monitoring
complex
Complications (OHSS)
contribute to success?
Drop out Access to
treatment
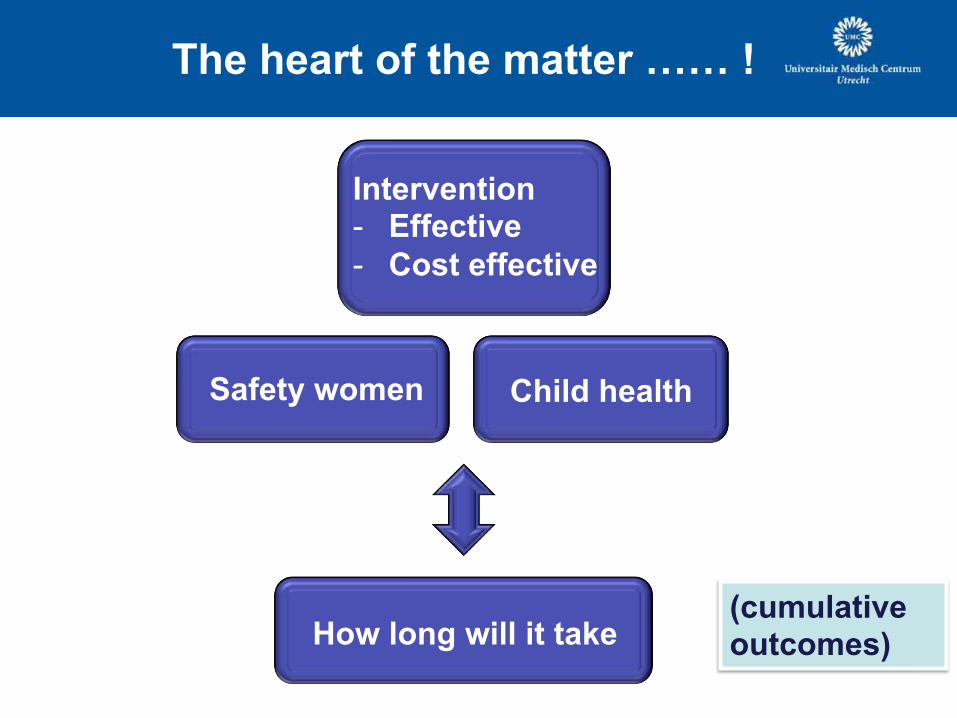
The heart of the matter …… !
Safety women
How long will it take
Child health
Intervention - Effective
- Cost effective
(cumulative outcomes)
Related Documents











