1 Patient Safety: The Reuse of Single Use Devices Institute for Science and Society University of Nottingham University Park Nottingham NG7 2RD Tel: +44 (0)115 846 8144 Fax: +44 (0)115 846 6349 Web: www.nottingham.ac.uk/igbis/singleuse Email: [email protected] [email protected] Competing interests: none Word count: 33,319 February 2007

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

1
Patient Safety: The Reuse of Single Use Devices
Institute for Science and Society
University of Nottingham
University Park
Nottingham
NG7 2RD
Tel: +44 (0)115 846 8144
Fax: +44 (0)115 846 6349
Web: www.nottingham.ac.uk/igbis/singleuse
Email: [email protected]
Competing interests: none
Word count: 33,319
February 2007

2
Abbreviations
AAGBI Association of Anaesthetists of Great Britain and Ireland
AfPP Association for Perioperative Practice (previously NATN)
AODP Association of Operating Department Practitioners
ASGBI Association of Surgeons of Great Britain and Ireland
BAREMA Trade Association for Anaesthetic and Respiratory Equipment
CDA Clinical Director of Anaesthesia
CJD Creutzfeld Jakob Disease
COREC Central Office for Research Ethics Committee
CRB Criminal Records Bureau
CSD Central Sterilisation Department
DNA Do Not Attend
DVT Deep Vein Thrombosis
EGBAT Expert Group on Blocked Anaesthetic Tubng
EU CEN European Union’s European Standardisation Committee
FT Full Time
HIV Human Immunodeficiency Virus
HR Human Resources
IV Intra Venous
LMA Laryngeal Mask Airway
LOS Length of Stay
LREC Local Research Ethics Committee
MCA Medicines Control Agency
MDA Medical Device Agency
MDD Medical Devices Directive
MHRA Medicine and Healthcare products Regulatory Agency
MHRA CSD MHRA’s Committee for the Safety of Medical Devices
MREC Multi-centre Research Ethics Committee
NATN National Association of Theatre Nurses (now AfPP)
NHS National Health Service
NHS PASA National Health Service Logistics, Purchasing and Supply Agency
NICE National Institute for Clinical Effectiveness
NPSA National Patient Safety Agency
NSF National Service Framework
ODP Operating Department Practitioner

3
OEM Original Equipment Manufacturer
OTJ Operating Theatre Journal
PCA Patient Controlled Analgesia
R&D Research and Development
RCOA Royal College of Anaesthetists
RGF Research Governance Framework
SABS Safety Alert Broadcast System
SEAC Spongiform Encephalopathy Advisory Committee
SHA Strategic Health Authority
SM Sterilisation Manager
SPSS Statistical Package for the Social Sciences
SUD Single Use Devices
TM Theatre Manager
TSEs Transmissible Spongiform Encephalopathies
vCJD Variant Creutzfeld Jakob Disease

4
Glossary
Ablation catheter Long, thin tube (catheter) is threaded into the heart to
destroy (ablate) an area of heart tissue that is causing
abnormal heart rhythms. Given the thin nature of tube,
decontamination is considered ineffective, due to
difficulties in establishing that all parts of the device are
‘clean’ and contaminant free.
Adenoidectomy Operation to remove swollen adenoids, tissue lying
between the throat and the noise.
‘Ambu’ bag Manual resuscitation bag; Ambu (manufacturer). Other
products are available.
Anaesthetic breathing
system
(also referred to as
circuit / ventilator)
Forms part of the anaesthetic system. Device delivers
gases to ventilate the anaesthetised patient. Made of
corrugated plastic tubing.
Anglepieces Part of the anaesthetic breathing system.
Biopsy forcep Instrument with metal jaw which can be used to remove
biopsies (samples) from tissue.
Breathing filter Used in conjunction with an anaesthetic breathing system.
The filter precludes any infective or hazardous particles
entering the patient’s respiratory tract from the anaesthetic
gases. A new breathing filter must be used with each
patient.
Burr Surgical instrument used to drill holes in bones.
Capnograph lines Used to measure CO2 levels during anaesthesia.
Cardiac catheter Similar to ablation catheter; long thin tube (catheter) is

5
threaded though body (usually from an incision in the
groin) to the heart, and is used to obtain diagnostic
information regarding heart disease.
Catheter mounts Transparent tubing, connecting the patient to the breathing
circuit.
CJD / vCJD Creutzfeld-Jakob Disease / variant Creutzfeld-Jakob
Disease – a rare and fatal neurodegenerative disease;
linked to presence of prion protein, which is found
principally in the brain, spinal cord and lympatic tissue
such as the spleen, appendix and tonsils.
CO2 adaptors Component of the breathing system.
Compression
(anti DVT) garment
Non-invasive, intermittent pneumatic compression devices.
Used to boost circulation and thus prevent episodes of
deep vein thrombosis following immobility. Examples
include ‘Flowtron boots’.
Cornea The front of the eye; transparent.
Decontamination
process
Eliminates or reduces the level of microbes and other
unwanted material from devices, which may otherwise
cause infection or colonisation. Achieved through a
combination of cleaning, disinfecting and sterilising, using
chemical agents and steam autoclaves.
Diphtheroids Type of bacteria.
Doppler probe Used to monitor venous flow.
Electrophysiological
catheter
Used to examine cardiac output and gather electrical
tracings and measurement of the heart.
Elephant tubing Part of the anaesthetic breathing system, connecting

6
patient to the anaesthetic machine. Made from plastic.
Endoscopic Type of surgical procedure, in which the surgeon operates
in the body cavity through small incisions. Also see
laparoscopic.
Endoscopic
biopsy forceps
Device used to remove tissue samples. Used in
conjunction with an endoscope (an instrument which is
used to examine the internal body via a small incision).
Endotoxins Toxins linked to bacteria, which result in fevers and altered
resistance to bacterial infections.
Endotrachael tube Tube placed in the patient’s mouth or nose, which assists
with breathing when ventilated.
Enteral system Method of delivering a substance to gastrointestinal
system.
Facemask Used to administer anaesthetic gases and/or oxygen to
patients.
‘Flowtron’ boots Anti DVT garments.
Gas sampling line Thin plastic tube attached to anaesthetic breathing system.
Allows anaesthetist to monitor gases given to and used by
patient.
Green bubble tubing Tubing used to deliver oxygen therapy. Made from plastic.
Gum elastic bougies
(Bougies / Intubating
stylets)
Rubber or plastic device, shaped like a thin cylinder and
malleable; inserted into oesophagus to guide another
instrument (such as LMA or other breathing assistance
device) into place.
Hepatitis B A virus that attacks the liver and causes it to become

7
inflamed; long term infection can lead to liver disease,
death from liver cancer or cirrhosis.
Hepatitis C A virus resulting in serious damage of the liver and affects
its ability to function correctly. Also found in digestive
system, the lymphatic system, the immune system and the
brain. It is mainly spread through contact with the blood of
a person who is infected.
Hypoxia Deficiency of oxygen.
Iatrogenic Medically induced harm.
Invasive / Non invasive
devices
Classification of medical devices, as defined by MHRA and
Medical Device Directive. Generally speaking, devices are
classified according to whether they enter bodily orifices or
the surgical site (invasive), or whether they come into
contact with injured skin or are used to collect blood and
other liquids (non-invasive).
Laparoscopic Refers to surgery carried out through small incisions in
body, during which instruments are passed down a small
tube.
Laryngoscope Device used by anaesthetist to obtain a view of the glottis
(narrow opening in the trachea airway) whilst performing
intubation. It consists of a metal handle and blade, which
can be either plastic or metal. Available as both single use
and reprocessable. Concern lies with 1) impatternation of
handle and potential for blood/tissue to become ingrained
in the markings, and subsequently come into contact with
the blade, and 2) likely presence of blood/tissue on the
blade.
Larynx Area of the throat containing vocal chords.

8
Laryngeal Mask Airway
(LMA)
Airway device used to ventilate patient during anaesthesia.
Inserted into patient’s larynx.
Lumen A hollow area within a tube / device.
Lymphatic tissue Refers to cells containing and carrying blood throughout
the body.
Macintosh
laryngoscope
Type of laryngoscope blade.
Magill forceps
Metal forceps used to assist with the removal of
objects/foreign bodies.
Mapleson C Circuit Type of anaesthetic breathing system.
McCoy laryngoscope Type of laryngoscope blade.
Mucous membranes Moist tissue lining the interior bodily cavity.
Nephrectomy Removal of the kidney.
Nosocomial Infection originating in a hospital.
Oesophagus
/ Oesophagectomy
Piece of the gullet running from the throat to the intestines;
operation to remove oesophagus.
Oxygen bags Rubber inflatable bags used to deliver oxygen to patient.
Pacing electrode Used to observe cardiac output.
Pressure (infuser) bag Inflatable bag (bladder) used to assist with the
administration of intra-venous fluids to patient.
Prion / Prion disease Infectious agent derived from protein. Linked to
transmissible spongiform encephalopathy, such as CJD.

9
Probes Device used to explore body cavity such as brain.
Proteinaceous Describes presence of protein, prions or other material
linked to disease causation.
Recovery T pieces
Part of the anaesthetic breathing system, connecting
patient to oxygen delivery system.
Saw blades Orthopaedic surgical tool.
Sclerosing needle Instrument used to deliver solution; used to treat varicose
veins.
Snare Instrument with a closable wire loop. Often used to take
samples.
Spirometry tubing Used to monitor patient’s breathing whilst under
anaesthesia.
Splencectomy Removal of the spleen.
Subcutaneous Under the skin.
Trocar Instrument placed into the body, through which other,
endoscopic and laparoscopic instruments can be placed.
TSE Transmissible Spongiform Encephalopathy; linked to
prions.
Vascular Relating to the blood vessels.
Ventilator tubing Used with anaesthetic breathing system. Made from
plastic.
.
10
Contents
Abbreviations 2-3
Glossary 4-9
Contents 10
List of tables and figures 11-12
Executive summary 13-17
Introduction 18
Part 1: The Inventory 19-21
Part 2: The Survey 22-55
Part 3: The Interviews 56-111
Conclusion and Recommendations 112-117
Acknowledgements 118-119
References 120-130
Appendix 1: Inventory of reused single use devices 131-192
Appendix 2: Survey Methodology
Appendix 3: Ineligible survey data
Appendix 4: Interview Methodological Details
Appendix 5: R&D log
193-197
198-201
202-206
207-210
Appendix 6: Ergonomics of single use devices, incl. recommendations 211-225
11
List of figures and tables
Table 1 The most frequently reported single use devices reused
(Inventory)
20
Table 2 Occupational characteristics of sample (Survey) 25
Table 3 Single use definitions (Survey) 27
Table 4 Reused single use devices (Survey) 30
Table 5 Reuse of facemasks (Survey) 36
Table 6 Rationales for reuse of single use devices (Survey) 41
Table 7 Number of operations performed per annum / cost (Survey) 43
Table 8 Proposed cost savings linked to reuse of single use devices 43
Table 9 Number of operations performed per annum / waste
(Survey)
45
Table 10 Number of operations performed per annum / number of
beds / reuse (Survey)
47
Table 11 Reuse of single use devices in other hospitals (Survey) 48
Table 12 Comparing reuse of single use devices in own and other
hospitals (Survey)
48
Table 13 Perceived dangers and risks associated with the reuse of
single use devices (Survey)
49
Table 14 Awareness and understanding of guidance relating to the
use of single use devices (Survey)
53
Table 15 Awareness of Trust policy on the use of single use devices
(Survey)
54
Table 16 Trusts participating in the survey recruited for interview
phase (Interview)
56
Table 17 Reuse of single use devices reported by survey participants
recruited for interview phase (Interview)
56
Table 18 Overview of additional Trusts recruited for interview phase
(Interview)
57
Table 19 Sample composition (Interviews) 58
Table 20 Popular definitions of single use (Interview) 72
Table 21 Reused single use reported by participants (Interview) 81
Table 22 Benefits / impact of service change model (Interview) 84
Table 23 Ineligible data: sample characteristics (Appendix 1) 198
Table 24 Ineligible data: definitions of single use (Appendix 1) 199
12
Table 25 Ineligible data: reported reuse (Appendix 1) 200
Table 26 Ergonomic report: detailed description of labelling
(Appendix 6)
216-
219
Figure 1 Geographical characteristics of sample (Survey) 26
Figure 2 Positioning of the laryngoscope 38
Figure 3 Location of the tonsils 39
Figure 4 Positioning of the laryngeal mask 66
Figure 5 Inconsistent labelling (Interview) 68
Figure 6 Single use logo (Interview) 72
Figure 7 Contaminated, reused single use laryngoscope blade
(Interview)
74
Figure 8 Intavent Orthofix LMA colour coding scheme (Interview) 75
Figure 9 Eschmann bougie: Instructions for cleaning, disinfection and
storage (Interview)
76
Figure 10 Eschmann and Portex bougies (Interview) 77
Figure 11 Sample breathing circuits (Interview) 79
Figure 12 ET connector and IV giving set (Interview) 80
Figure 13 Time-motion image of bougie and its ability to retain its
shape
92
Figure 14 Single use laryngoscope blade (Interview) 96
Figure 15 Reusable laryngoscope handle (Interview) 96
Figure 16 Europa laryngoscope pouch (Appendix 6) 213
Figure 17 Example of multiple use symbol (Appendix 6) 215
Figure 18 Example of single use label using text (Appendix 6) 215
Figure 19 Examples of inconsistency in font style and size in labelling
(Appendix 6)
219
Figure 20 Labelling observed on devices (Appendix 6) 220
Figure 21 Examples of the similarities between the single use icon
and other item labelling (Appendix 6)
220

13
Executive Summary
Patient safety has become an increasing concern for the National Health Service
since the publication of An Organisation with a Memory. The National Patient Safety
Agency was created with the express aim of learning from critical incidents (patient
safety incidents), identifying safety risks, and developing methods to prevent such
risks and incidents from re-occurring.
This report examines one identified risk to patient safety: the reuse of ‘single use’
devices. Reuse poses a threat to patient safety in terms of cross infection, including
blood borne diseases such as HIV and Hepatitis B and C, and prion diseases such
as CJD. Patient safety is also threatened by device malfunction and breakage linked
to reuse, for which the devices are not designed.
This report provides an account of a programme of research undertaken over 24
months. This examines data collected via an inventory of published accounts of
reuse, a web-based survey and in-depth interviews with clinical staff working in
theatre and anaesthetic departments in NHS acute hospitals in England.
The inventory of published accounts of reused single use devices revealed a varied
pattern of practice across North America, Europe and Australasia. A total of 477
accounts were found, detailing the reuse of 291 different anaesthetic and surgical
devices. These included: catheters, needles, laparoscopic and endoscopic
instruments, biopsy forceps, breathing filters, airway devices, endotracheal tubes and
laryngeal masks. As expected, reuse was most prevalent in the USA, where
reprocessing of single use devices is regulated by the FDA. However, reuse was also
reported in countries where the practice has been outlawed. For example, single use
anaesthetic devices including breathing filters, laryngoscope blades and laryngeal
masks were reported as being reused in the UK, despite official guidance to the
contrary.
The web-based survey of theatre personnel extended our focus on the reuse of
single use devices in the English NHS. We had intended that the survey data could
be used to estimate the prevalence and incidence of reuse, as well as the categories
of device involved. However, bureaucratic obstacles introduced by the Research
Governance Framework for Health and Social Care and European Clinical Trials
Directive, resulted in a much smaller sample of informants with an unknown
14
relationship to the population of hospitals and possible response biases.
Unfortunately, this means that the survey data cannot be extrapolated to calculate
the extent of reuse in the NHS.
Despite its methodological shortcomings, the survey data provides a revealing insight
into the use and reuse of single use devices in a small number of hospitals. The data
demonstrates that clinicians find the definition of ‘single use’ to be confusing, and that
‘single use’ and ‘single patient use’ are understood differently, despite both falling
under the same guidance offered by the Medicines and Healthcare products
Regulatory Agency.
Examples of reuse reported by survey participants included breathing circuits,
facemasks, monitoring and sampling lines, intubating equipment, anti DVT garments
and diathermy equipment. Reuse was rationalised in relation to the prohibitive cost of
replacing each device after just one use, the environmental impact of disposing of the
clinical waste, a perceived lack of risk associated with reuse, and problems with the
supply chain resulting in a lack of other equipment.
The third phase of the research built on the survey findings to gain further
understanding of the context in which decisions relating to the use and reuse of
single use devices are made. 23 in-depth interviews with frontline theatre staff were
carried out in 10 acute NHS hospitals across England. Participants included theatre
managers, operating department practitioners, sterilisation managers and clinical
directors of anaesthesia.
While reuse was only reported by a small proportion of the respondents, the data
allows an understanding of the clinical and financial context in which reuse occurs to
be gained. The factors that lead a clinician to reuse a single use device include the
design and labelling of devices, awareness and understanding of the single use logo,
issues relating to the quality and effectiveness of equipment, contradictory guidance,
and human failings linked to knowledge and situational awareness.
Our survey and interview participants rationalised the reuse of single use devices in
terms of the financial implications of discarding the devices after just one use. Yet
economic analysis of cost data supplied by one participant and the NHS Purchasing
and Supply Agency, demonstrates that, when all associated costs are linked to
reuse, including original purchase price, decontamination, packaging and costs

15
incurred as a result of a critical incident, this is unlikely to yield any significant cost
savings. Lastly, we performed an ergonomic analysis of the single use devices which
were most frequently reported as being reused, both by survey and interview
participants. This analysis concluded that reuse may be influenced by the labelling,
packaging and material properties of the devices. In particular, the ergonomic
analysis reiterates our concerns about the single use logo and its familiarity, and
ambiguities regarding whether a device should be used on a single occasion or in the
treatment of a single patient.
The results from this study appear to show that, although not widespread, reuse of
single use devices is still an important issue and of considerable concern. Clinicians
were insistent that the use of single use devices is in the patient’s best interest, and
is best clinical practice. Although some participants voiced concerns about the
effectiveness of some single use devices and the negative environmental impact of
disposing of the devices, tellingly, most would want single use devices used on
themselves or family members if they were ever patients.
We found that there are several physical reasons why single use devices might be
misused, including:
• Misunderstanding of the definition
• Design characteristics
• Suitability and safety of other devices.
• Discrepancies in labelling
The safe delivery of healthcare is also threatened by organisational factors,
including:
• Lack of awareness about single use devices
• Perception that reuse of single use devices is cheaper
• Fragmented hospital budgets which have resulted in the true costs of single
use and reprocessable devices being obscured from clinicians
• Perception that cost is a more important driver than quality when making
purchasing devices
16
Clinicians felt that by cutting costs, patients were put at risk. Cheaper single use
devices were perceived to be placing the patient at greater risk of harm than using a
reprocessable device. We recommend that these perceptions are addressed, both
substantively through the design and cost of devices, and educationally, via an
awareness programme aimed at clinicians.
A fundamental question that has arisen from this research is how to deliver the best,
safest care to patients and at the same time protect the NHS from the higher costs
associated with such practice. Is it appropriate, for example, to continue to
repeatedly purchase and discard certain, non-invasive single use devices (which are
likely to pose very little iatrogenic risk) when the NHS is in financial difficulties? Is it
possible to balance known financial risks against unknown risks of contracting an
iatrogenic infection linked to the use of a medical device? Which is more of a threat:
financial disaster or the potential for patient harm?
Single use devices are beneficial in that they protect against iatrogenic cross
infection and contamination, and ensure that each patient has clean instruments
used on them. This research clearly demonstrates that clinicians feel that the use of
single use devices is in the patient’s best interest. The use of single use devices is
seen to be a sign of clinicians’ professionalism and adherence to good clinical
practice standards. However, as our data demonstrates, single use devices do not
always function as well as clinicians would want them to. Some are unfit for use and
can endanger the patient.
It is not our aim in this report to blame or identify individuals who have admitted to
reusing single use devices. The opportunity for shared learning and improvement in
the design and use of medical devices is a greater good. This report and its
Appendices outline the processes leading to the misuse of devices, as well as
providing a forum for clinicians to voice their concerns. It is now for the regulators
(including the Department of Health, Medicines and Healthcare products Regulatory
Agency and the National Patient Safety Agency), manufacturing community, Royal
Colleges and Royal Associations, front line clinical staff and NHS managers to work
together to address the problems and weaknesses identified in this report. However,
we offer the following nine suggestions:
1. Professional associations and Royal Colleges should work together to address
inconsistencies in infection control guidelines. In particular:

17
a. Use of single use laryngoscope blades
b. Contrasting guidance for different invasive intubating equipment
(laryngoscope, laryngeal mask, bougie)
2. Clearer microbiology guidance is required on the actual threat of vCJD and other
iatrogenic infections from reused devices
3. The definition of single use should be re-examined. Do the terms ‘single use’
and ‘single patient use’ describe the same expected usage pattern? If so, we
recommend that the term single patient use is removed from all devices.
Additionally, regardless of the resulting definition, a high profile educational
campaign targeting all stakeholders should be designed and implemented
4. Labelling inconsistencies need to be addressed:
a. Labelling on each device should be consistent. For example, a device
should not be labelled as both single use and single patient use
b. Labelling on the device, packaging and paper insert (instructions) should
be consistent
c. Size of single use logo, font and position of the logo should be examined
d. Use of wording to replace single use logo should be examined
5. Colour coding of devices, thus differentiating between single use and
reprocessable should be investigated. Views of users, purchasers and
manufacturers will need to be sought
6. Robust system for the replacement of breathing circuits after seven days to be
designed and implemented throughout the health care system
7. All clinical stakeholders should revisit EGBAT’s fifth recommendation, regarding
removing devices from their packaging prior to use. Practice should be amended
where at odds with proposal
8. MHRA and device manufacturers to seek independent scientific expertise on the
contamination risks of certain single use devices (such as blood pressure cuffs
and pressure infuser bags) and remove the single use logo if evidence suggests
that this is feasible
9. All parties should look for ways to remedy the perceived quality/cost conflict.
Equipment must be fit for purpose in order to be both cost effective and protect
staff and patients against infection / cross contamination

18
Introduction
Patient safety has become a matter of increasing concern to the National Health
Service (NHS), both to reduce litigation risks and costs and to demonstrate the
delivery of a high quality service to users. Following the Chief Medical Officer’s
report, An Organisation with a Memory1, the government created the National Patient
Safety Agency to champion learning from critical incidents and to encourage
systematic institutional attention to the identification of safety risks and the
development of methods for their prevention.
This report focuses on one identified source of risk: the reuse of medical devices
intended to be used on a single occasion. Reuse of these devices is believed to
increase the chances of cross infection and device failure.
This research, commissioned by the Department of Health’s Patient Safety Research
Portfolio, has three objectives:
1. An inventory of single use devices reported as being reused
2. A survey to investigate current practice
3. An in-depth qualitative study of reusers’ and non-reusers’ rationales for reuse
of single use devices.
19
Part One: The Inventory
An inventory of published accounts of the reuse of single use devices (SUDs) was
compiled through a search of the scientific literature (June - September 2004;
updated June 2006). It was necessary to restrict the cases to those reported in
Western societies, as reuse may be considered a more acceptable practice in less
developed countries due to a lack of financial and material resources. The inventory
data derives from reported cases of SUD reuse in the UK, the European Union, North
America and Australasia.
Using a popular citation index (PubMed), the following search terms were
investigated:
• Reuse of single use (medical) devices
• Reprocessed single use (medical) devices
• Recycled single use (medical) devices
Reports were only included in the inventory if they were published in the English
language and had online full-text availability. These criteria were selected to specify
the task in the most replicable and accessible manner. While it is possible that a
different strategy would have resulted in a different outcome, the inventory included
the main high-ranking journals from the ISI Web of Science. The use of PubMed
citations, in conjunction with International reports and documents, allows us to be
confident that we have an accurate picture of the data available at the time.
477 reports of reuse were found, although this figure contains many repeated
devices. In total, 291 single use devices were reported as being reused. A full version
of the inventory (listed both by device and country) can be found in Appendix one;
this is also supplemented by a full reference list. An overview of the inventory data is
presented in Table 1.

20
Table 1: The most frequently reported devices
Surgical Devices:
• Catheters (N=95)
• Needles (N=41)
• Laparoscopic instruments (N=34)
• Biopsy forceps (N=27)
• Endoscopic instruments (N=17)
• Trocars (N=12)
• Syringes (N=10)
• Diathermy instruments (N=10)
• Burrs (N=9)
Anaesthetic Devices:
• Breathing filters and associated
devices (N=22)
• Breathing circuits (N=7)
• Endotracheal tubes (N=6)
• Oxygen masks (N=5)
• Laryngeal masks (N=2)
The majority of cases of reused SUDs derived from the USA (N=207) and Canada
(N=60). However, reprocessing of (re)used single use devices is permitted in both
countries. In the USA, prior to 2000, hospitals were able to reprocess SUDs ‘in-
house’ through the use of bench-top sterilisation units and central sterilisation
departments (CSDs). However, concerns regarding insufficient safety data led to
such activity being regulated. Post 2000, the USA Food and Drug Administration
(FDA) have issued regulations to which all third party reprocessors and reprocessing
hospitals are required to conform2. Reprocessors (both in-house and third parties)
take on the responsibilities once held by the original equipment manufacturers
(OEMs), and thus become liable should an adverse event arise because of the use of
a reused SUD. Canada does not regulate the reuse of SUDs3. Whilst the
governments of Australia and New Zealand recommend that reuse should not occur,
evidence suggests that reuse is taking place (Australia: N=31; New Zealand: N=15).
Despite the Medical Devices Directive (MDD) 93/42/EEC4, reports suggest that reuse
is still occurring throughout Europe. Reports of reuse originated from Germany
(N=37), the UK (N=20), European Union umbrella organisations (N=19), Denmark
(N=14), Sweden (N=2) and Italy (N=1), despite the implementation of the MDD in
national regulations throughout the EU. However, the onus of the MDD regulations is
placed on the device manufacturers, who are required to prove that the device is safe
and fit for its intended purpose. There is little in the MDD about reuse by clinical staff,
although individual EU member states have made provision for reuse in their own
regulatory systems. Denmark went further than merely advising against reuse, and

21
described reuse as ‘substandard practice’5 whilst the UK’s Medicines and Healthcare
products Regulatory Agency (MHRA) states that reuse must not occur under any
circumstances6. Germany allows SUD reprocessing but demands that evidence of
the device’s safety is obtained before reuse3. In Sweden, the physician reusing the
device is held liable for any adverse event, and the patient must consent to the use of
a reused SUD.
The inventory has demonstrated that, despite guidance to the contrary, SUDs have
been reused in countries where such practice had been outlawed. However, a
secondary outcome of the inventory is the finding that regulators and clinicians in
some countries appear to consider that there is little risk involved in reuse.
22
Part Two: The Survey
The second phase of the research aimed to explore the reuse of SUDs within the
context of the English NHS, and in particular, operating and anaesthetic departments
within the acute sector. In order to accomplish this, a survey tool was utilised.
The commissioners requested that a sufficiently large survey be carried out to
establish the incidence and prevalence of the reuse of single use medical devices in
theatre and anaesthetic departments, and that the survey should target ‘relevant
frontline staff’. Preliminary investigation identified approximately 350 NHS hospitals in
England with surgical theatres and anaesthetic departments. Given the size of the
population, it was considered practicable to invite all of them to participate in the
initial survey.
The aim of this survey, then, was to establish:
1. The incidence and prevalence of the reuse of single use medical devices in
theatre and anaesthetic departments.
2. The categories of devices involved.
The survey would collect documentary, attitudinal and explanatory data about the
reuse of SUDs in English operating theatres and anaesthetic departments. Jupp et
al7 describe how self-report surveys are an option for uncovering hidden crime
figures and our approach drew extensively on the experience of criminological
research in inviting respondents to disclose deviant behaviour.
We originally planned to use telephone contacts with theatre managers and clinical
directors of anaesthesia to identify appropriate informants for each hospital (i.e. staff
who were likely to know about the extent of reuse). This would yield a sampling
frame of approximately seven hundred health professionals, who would be asked to
participate in the survey. We hoped to achieve a response rate of 30-40 per cent.
The inclusion of two informants per hospital would allow us to achieve a higher
proportion of hospitals, with the possibility of internal error checking where both
responded from the same site. The respondent hospitals could be compared with
published statistics on the population of hospitals to determine whether they could be
considered to be a representative sample or in what ways they might be skewed by
size, type or location.

23
Three survey methods were considered for this study:
• Postal surveys
• Telephone surveys
• Web-based surveys
Postal surveys can achieve wide population coverage at a relatively low cost8.
However, the method often leads to low response rates and questionnaires may be
returned with illegible writing9. Previous research investigating the reuse of SUDs via
postal surveys has reported response rates of 57%10, 43%11, and 40%12. However,
McAvoy and Kaner13 caution that response rates for postal questionnaires involving
doctors have been falling. They suggest that reasons for this include: being swamped
by the volume of questionnaires arriving on their desks; doctors resenting
interference in their activities by outside researchers; the length of questionnaires;
and the time taken to participate in research.
Given this obstacle, a telephone survey was considered, but rejected given the
sensitive nature of the survey questions, and the concern that participants might find
the method unduly intrusive. This approach is also less conducive to anonymisation.
Finally, we considered a web-based survey. This method has recently been favoured
when researching health professionals14. Whilst more expensive to set-up than paper
questionnaires, web-based surveys offer many advantages: they are highly cost
efficient because of the elimination of paper and postage, whilst providing the
opportunity for rapid coding and analysis15,16,17,18,19. Moreover, Joinson20 has argued
that respondents are more likely to be “disinhibited” when responding to web-based
surveys, and more willing to share sensitive information. Umbach17 reinforces this
line of argument, suggesting that respondents are more likely to respond to socially
threatening questions because of the perceived distance between researcher and
respondent. While Flatley21 cautioned about difficulties that respondents may face
regarding their ability to use the internet, we reasoned that, since our sample would
need to be computer literate in order to perform their jobs successfully, such a
problem would not arise.
The survey was designed in collaboration with the University of Nottingham Survey
Unit, acting as sub-contractors. It aimed to produce estimates of the prevalence of
reuse and identify possible variations in incidence associated with hospital types.

24
Questions addressed the types of devices that may be reused and the specific
contexts within which this might occur. Given the perceived sensitivity in reporting
reuse of SUDs, it was likely that some under-reporting would occur, as respondents
sought to protect both themselves and their colleagues. Consequently, the question
wording was designed to normalise reuse, reducing any threat or negative
association with reporting. ‘Census-type’ questions would also be asked about the
mix of specialties, volume of operations, hospital location (urban, suburban, rural)
and involvement in teaching.
The questionnaire was piloted by members of the Association of Anaesthetists of
Great Britain and Ireland (AAGBI) council, and the anaesthetic teams at York District
Hospital and Nottingham University Hospitals. Recommendations following piloting
included reducing the length of the questionnaire and clarifying the wording of some
questions, so that participants were more likely to feel able to admit to ‘deviant’ acts
based on their own experience or knowledge of colleagues’ experiences.
The final version of the questionnaire comprised 16 questions about: the participant
(job title, level of experience); the hospital they were employed in (geographical
region, number of beds, theatres, and operations performed each year); the reuse of
SUDs (definitions, experience of reuse, rationales for reuse, awareness of policies
and guidance against reuse; and the possible dangers of reuse). The majority of
questions were closed-ended, with participants responding using check boxes and
Likert scales. A minority of questions were open-ended and required participants to
enter textual answers.
The survey went ‘live’ on 29th September 2004. Despite the web pages being tested
by the Survey Unit, respondents reported a few minor technical hitches, which were
immediately rectified.
Our commissioned design for a nation-wide survey of hospitals proved unworkable,
due to NHS research governance regulations. The need for individual Trust approval
made it impossible to carry out the planned survey within the funded time and
resources. This imposed a change in research design. Rather than recruiting our
sample through NHS routes, we used the membership lists of the professional
associations for relevant healthcare staff working within theatres and anaesthetic
departments.

25
This change introduced two important limitations. First, it was impossible to relate
respondents to their workplaces so that the relationship between the sample and the
population was unknowable, preventing the realisation of the commissioners’ original
goal of estimating incidence and prevalence. Second, there is a greater risk of bias
because those responding were likely to have done so because they were interested
in single use devices, or felt that they had a particular story to tell, rather than
participating solely in their official capacity as NHS employees. We sought to mitigate
the impact of these factors by adopting a more formal case-control design for the
interview phase. An account of the original plans and a detailed explanation of the
new sample design and recruitment strategy can be found in Appendix two.
Survey data were collected over a period of 76 days (29.09.04 – 15.12.04). We
received 113 responses in total, which represents a response rate of just over 1%
(total invitations sent was 10,119, plus an unknown number of responses to an
advertisement placed in The Operating Theatre Journal). 22 of these responses were
considered ineligible because the respondents were not working in the English NHS.1
The following discussion focuses solely on the 91 eligible responses. Respondents
identified themselves in the following manner:
Table 2: Occupational Characteristics of Survey Sample
N %
Nurse 41 45
Anaesthetist 33 36
ODP 11 12
Theatre Manager 6 7
Surgeon 0 0
Total 91 100
The failure to recruit any surgeons is disappointing, and has undoubtedly influenced
the results. However, as Appendix two makes clear, this lack of engagement was not 1 Whilst interesting, these 22 cases have been removed from the main dataset, in
order that the remaining data not be ‘contaminated’ by cases that did not meet the
sampling criteria. A brief discussion of the ineligible data can be found in Appendix
three at the end of this report.

26
planned, but resulted from a logistical breakdown, or apparent indifference towards
the topic among the target population.
The majority of the participants had been working in their role for over one year
(97%), with just under 95% at their current place of employment for over a year.
Explanations for reuse have noted the different guidelines that exist in different
hospitals, despite the general regulatory advice from the MDA2 6. However, it is
reasonable to assume that experienced staff will be aware of the MDA guidelines.
Additionally, 69% of respondents had worked in their post for more than five years,
and so would have experienced the change in procedures involving SUDs/reusable
devices for Tonsillectomy and Adenoidectomy in 200122, and would therefore be
aware of the debate regarding the usage of single use devices and patient safety.
Responses were received from all eight geographical regions in England:
Figure 1: Geographical Characteristics of Survey Sample
2 The current guidance on the use of single use medical devices was published in
2000 by the Medical Devices Agency6. Subsequently, the Medical Devices Agency
(MDA) has been merged with the Medicines Control Agency (MCA), forming the
Medicines and Healthcare products Regulatory Agency (MHRA).
16%
10%
10%
9% 11%
13%
12% 19%
27
57% of respondents defined their place of employment as falling within an urban
area, followed by 33% falling within a suburban area, and 10% in a rural location.
Participants were more likely to be employed in hospitals with over 300 in-patient
beds (70%) and over ten operating theatres (52%). 23% of respondents worked in
hospitals which performed less than 5,000 operations per year, and 25% of
respondents in hospitals performing over 20,000 operations per year.
The quantitative data resulting from the questionnaire has been analysed using
SPSS 3, whilst the textual, qualitative data has been thematically analysed.
Results
The survey data reinforce our finding from the scientific literature that there is little
consistent understanding about what ‘single use’ or the single use logo means in
practice.
Respondents were given five different definitions of SUD, all taken from the literature
(‘single patient’, ‘single episode’, ‘used on a single occasion within a single episode’,
‘non-reprocessable’ and ‘disposable’), and asked to tick all that they considered
relevant to the term ‘single use device’ (Table 3). They were also able to elaborate
upon their response if they wished.
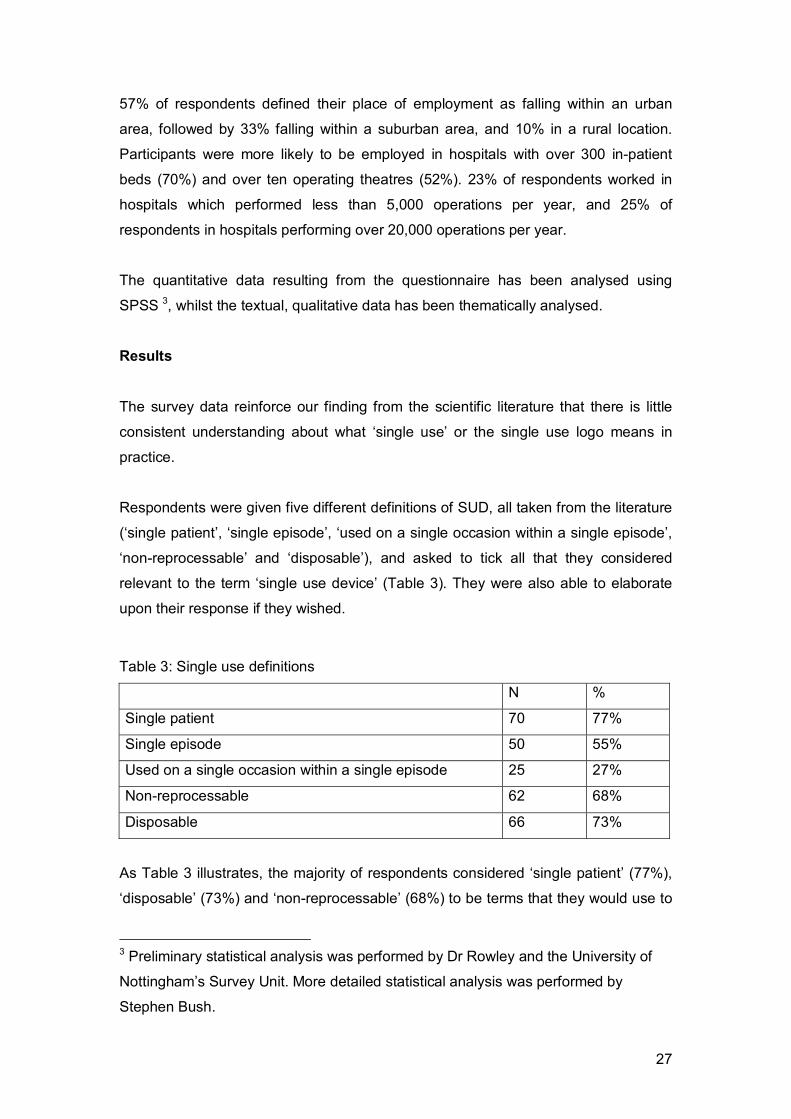
Table 3: Single use definitions
N %
Single patient 70 77%
Single episode 50 55%
Used on a single occasion within a single episode 25 27%
Non-reprocessable 62 68%
Disposable 66 73%
As Table 3 illustrates, the majority of respondents considered ‘single patient’ (77%),
‘disposable’ (73%) and ‘non-reprocessable’ (68%) to be terms that they would use to
3 Preliminary statistical analysis was performed by Dr Rowley and the University of
Nottingham’s Survey Unit. More detailed statistical analysis was performed by
Stephen Bush.

28
describe a SUD. There was less support for definitions that referred to a single
episode of use (54%), and even less for the definition that fits the manufacturing
industry’s recommendation of ‘to be used once and then discarded’, that of ‘to be
used on a single occasion within a single episode’ (27%).
Few participants offered any elaboration upon their understanding of the term ‘single
use device’ (N=5). The explanations that we received were all similar, which is
surprisingly given the inconsistency in the definitions offered in the scientific
literature. However, none offered a definitive explanation of the term ‘SUD’.
According to our survey respondents, the meaning of the term ‘single use device’ is
dependent upon the specific device in question. For example, “a device may or may
not be a single use within an episode - depends on device. e.g. an IV cannula is
single use within episode, a disposable PCA pump is single patient but often refillable
for that patient” (ID 80 / Anaesthetist). Moreover, given the similar level of support
that single patient, non-reprocessable and disposable received, it is likely that “all
[terms] may apply dependant on the item, its use, whether sterility is required and the
likelihood of damage occurring during use” (ID 89 / Anaesthetist).
The data demonstrates that there is no agreed definition of a SUD, and strengthens
our argument that there is little objective understanding regarding what ‘single use’
should be recognised as meaning. Moreover, in light of the gulf in levels of support
for ‘single patient use’ (77%) and ‘single use’ (27%), it is apparent that in clinical
practice, ‘single use’ and ‘single patient use’ are considered to be different
phenomena.
Although the MHRA6 acknowledge that manufacturers intend that SUDs should “be
used once and then discarded [and] consider the device is not suitable for use on
more than one occasion”, their own definition is inconsistent with this, as the
following definition of ‘single use’ illustrates:
Single use – The medical device is intended to be used on an individual
patient during a single procedure and then discarded. It is not intended to be
reprocessed and used on another patient. The labelling identifies the device
as disposable and not intended to be reprocessed and used again (p.14)
The MHRA’s own definition of ‘single use’ makes a distinction between use on a
single procedure and the intention that the device should not be reprocessed and

29
used on another patient4. However, this definition differs from the manufacturers’
approach, in the first definition quoted by the MHRA. In highlighting this subtle
difference, we draw attention to the possibility for confusion. The manufacturers’
definition is clear: the device is designed to be used on a single occasion. However,
the MHRA’s definition implies that single use can be taken as meaning single patient
use during one procedure. Their definition is supported by further explanations of
‘reuse’ and ‘single patient use’, which both describe the second and subsequent use
of a SUD that either has, or may have, been reprocessed (cleaned / sterilised)
between usages. There is also an issue with how to define a ‘single procedure’. For
some procedures the length of usage may be quite short, while for others it may be
lengthy and periodic. For example, a single use facemask will be transferred with the
patient back to the ward following surgery. The facemask will be used solely by that
patient, but the period of usage may span several hours. Moreover, there is a risk of
infection from the facemask being transferred from the theatre and recovery suite to
the ward environment, where greater numbers of patients could become exposed to
the risk that the reused facemask might present.
Whilst only a small difference, the lack of consistency between the two definitions
may result in patient harm. Anecdotal reports suggest that there have been cases of
scalpel blades snapping and needles becoming blunt through extended use, but with
the usage pattern falling within the MHRA definition – used on a single patient and
not reprocessed (Personal communication with manufacturing representative). We
suggest that this definitional inconsistency requires attention. Such variation can
have an impact upon patient safety, as SUDs are not designed or manufactured to
be used on more than one patient or undergo any form of reprocessing.
4 The MHRA have subsequently altered their definition of 'single use' (see DB
2006(04) Single-use Medical Devices: Implications and Consequences of Reuse).
The definition now reads: “a device designated for single use must not be re-used. It
should only be used on a single patient during a single procedure and then
discarded. It is not intended to be reprocessed and used again, even on the same
patient”. This has clarified the difference between single use and single patient use.
However, we have not altered our argument in the text, as this definition was not
operational when the data discussed in this section was collected. Rather, the
definition seen in MDA DB 2000(04) was still utilised.

30
Respondents were asked to list SUDs that, to their knowledge, had been reused at
their hospital either by themselves or by colleagues. They were also asked how
frequently they thought the devices were being reused 5. 62% of respondents were
able to report reuse. The SUDs reported as being reused, and the frequency of such
reuse occurring is shown in the following chart:
Table 4: Reused SUDs
Total
(N)
Every
operation
More
than
once a
week
More
than
once a
month
More
than
once a
year
Unknown
Anaesthetic breathing
systems 37 22 13 2 0
0
Facemasks 17 5 9 1 0 2
Circulation /
Compression garments 13 5 7 1 0
0
Monitoring / Sampling
lines 12 10 2 0 0
0
Intubating bougies 11 2 4 4 1 0
Laryngoscope blades 6 3 1 1 1 0
Pressure infusion bags 4 0 3 0 1 0
Syringes 4 3 0 0 0 1
Probes 4 1 1 1 1 0
Diathermy equipment 2 0 2 0 0 0
An outcome of the recruitment strategy, and the lack of participation from surgeons,
is that the SUDs reported as being reused are predominantly found in anaesthesia.
127 reports of reused SUDs were received. These described the reuse of 13
anaesthetic devices, ten surgical devices, and seven devices that are neither solely
used in surgery nor in anaesthesia. The ratio of reuse reported for SUD anaesthetic
and surgical devices is 89:11.
5 The question was worded to gain data on the patterns of reuse, rather than the
number of times a particular instrument might be reused. At present, it is impossible
to collect data on the frequency of reuse for individual SUDs, as records are not kept.

31
A further limitation of the recruitment method has been the inability to draw any
statistical inference from all but a few of the relationships expected between reused
SUDs and the rationales given to explain such practice. For example, it is impossible
to demonstrate that there is an association between the reuse of a SUD, the number
of procedures carried out in which the SUD is used and the rationale that reuse
occurs due to the prohibitive cost of replacing the SUD each time.
The most frequent device reported as being reused
was the anaesthetic breathing system (N=37). 22
individuals reporting reuse considered that anaesthetic
breathing systems were likely to be reused in every
operation. It is known that anaesthetic equipment
shared between patients poses a risk of cross-
contamination23,24,25,26. For example, in 1993 an Australian hospital reported the
nosocomial infection Hepatitis C in five patients whose anaesthetic therapy was
provided using a reused breathing circuit27. Consequently, breathing circuits became
labelled as ‘single use’.
However, while the extent of reported reuse may seem surprising, the reuse of
breathing circuits has now been sanctioned in the UK. The AAGBI28 has endorsed
the reuse of single use breathing circuits on than one patient and for more than one
operating session, if the circuit is protected by a new breathing (bacteria/viral) filter
for every patient. To this extent, manufacturers now market their breathing circuits as
being able to withstand limited reuse. For example, Flexicare Medical sell their
breathing circuits without a symbol or wording restricting them to single use, and
suggest that circuits then require the use of a suitable Breathing Filter between the
patient and breathing circuit, with the Breathing Filter being discarded after each
patient29. Intersurgical describe the “limited repeated use” of single use breathing
circuits, on condition that all reference to ‘single use’ is removed from the packaging
and instructions, and a single use breathing filter is used30. It is assumed that it is this
kind of reuse that respondents have reported.
32
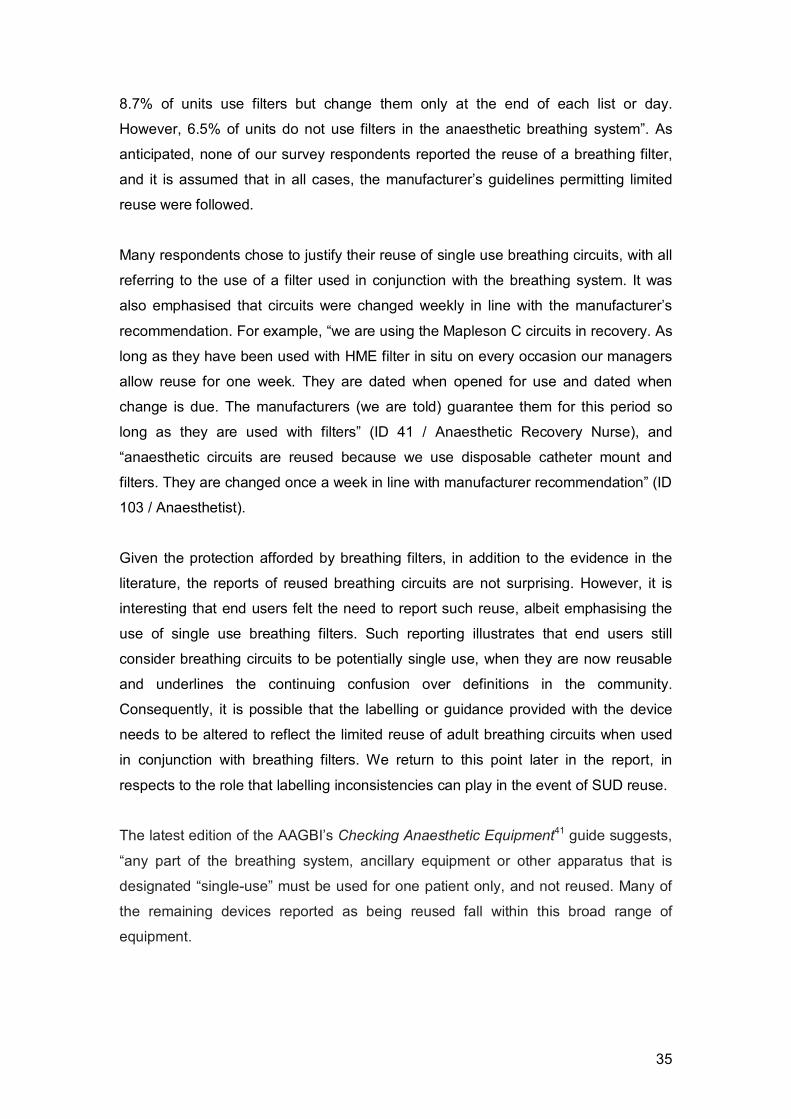
Breathing filters are placed at the Y-piece
of the breathing system, and prevent the
patient from inhaling hazardous or
infectious particles whilst the upper
airways are bypassed33.
Manufacturers now advise that anaesthetic breathing systems can be reused for up
to a one week, subject to a new single use breathing filter being used for each
patient29,31. NHS Purchasing and Supply Agency35 endorsed this reclassification, and
provided the following statement:
Following lengthy consultation between the Medical Devices Agency, the
Royal College of Anaesthetists, the Association of Anaesthetists, product
manufacturers, BAREMA, and the NHS Purchasing and Supply Agency,
agreement has now been reached on the principle of limited repeated use of
breathing systems.
It is understood that this change in reclassification was brought about following a
meeting between the MDA, AAGBI, Royal College of Anaesthetists (RCOA), NHS
PASA and BAREMA in Summer 2001, in response to the publication of the MDA’s
Device Bulletin DB2000(04)6,36. It seems that limited reuse of breathing circuits
labelled as single use, providing they were protected by a new, single use breathing
filter for each patient, had been a long-standing practice. Smith and Birks37 described
how:
In most anaesthetic departments, in conjunction with a single use disposable
bacterial/viral filter, an anaesthetic breathing system designated single use is
often used for one list, one day or even for one week. The perceived risk of a
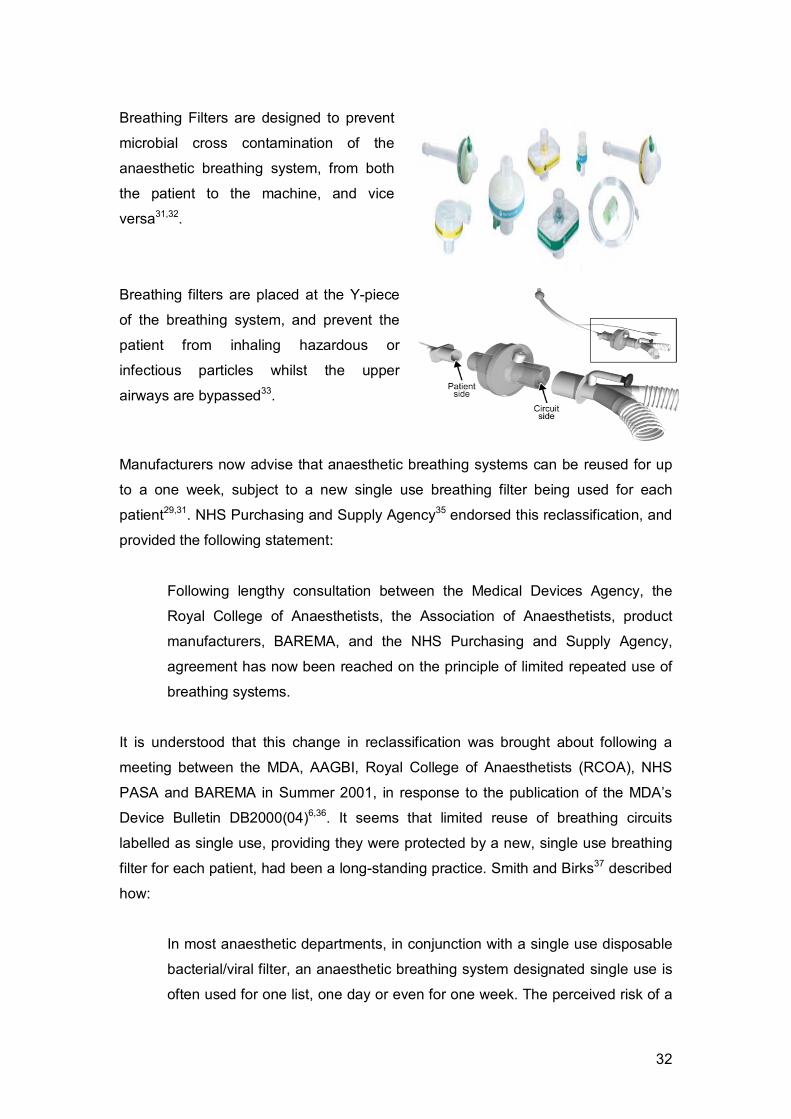
Breathing Filters are designed to prevent
microbial cross contamination of the
anaesthetic breathing system, from both
the patient to the machine, and vice
versa31,32.

33
patient contracting a disease such as a prion disease from anaesthetic
breathing systems is exceptionally small, whilst the cost of replacing all the
tubing and other parts of the anaesthetic breathing system for each individual
patient is high.
Although no official statement on the ‘limited reuse’ of breathing circuits has ever
been made by MHRA, all parties agreed to the limited reuse of breathing circuits on
condition that such reuse was sanctioned by the notified bodies. BAREMA made the
following statement38:
This statement is intended to clarify the current position regarding the supply
and use of anaesthetic breathing circuits. Up until August 2000, it was the
common practice in most UK hospitals for anaesthetic breathing circuits to be
used for more than a single case – e.g. anything from a list to several days,
even if the circuits were originally supplied for ‘single use only’. In August
2000, the Medical Devices Agency publication DB 200 (04) reiterated that any
product sold by a manufacturer for ‘Single Use’ should not be used for more
than one patient. Since August 2000, there has been considerable debate
between users, MDA and suppliers on the practice to be adopted in hospitals.
Under the requirements of the Medical Devices Directive, it is the
responsibility of the manufacturer to specify how products are to be used and
be able to demonstrate to independent authorities (namely Notified Bodies)
that the appropriate validation for that use has been done. During the recent
past a number of suppliers in the UK have been able to show that anaesthetic
breathing circuits can be safely reused and are now selling these products
with appropriate instructions to be followed in hospitals. It is expected all
suppliers of circuits will be selling for reuse in the next few weeks.
The notified bodies were satisfied with the reclassification proposed, on proviso that
all reference to single use would be removed from breathing circuits36.
One respondent reported the reuse of paediatric breathing circuits, providing the
circuit was protected by a ‘Pall’ BB25 filter (ID 104 / Anaesthetist). Reuse was
reported to occur more than once a week. Currently, paediatric breathing circuits, like
their adult counterparts, can be reused if a single use breathing filter is utilised.

34
The respondent referred to the use of a BB25 filter manufactured by Pall Medical,
who describe their filter as offering effective barrier with bacterial/viral removal
efficiency of 99.999%. However, the scientific literature has reported that paediatric
breathing filters are not as effective as their adult equivalent in reducing risk of cross-
infection32,33,34. In the light of this, debate between the manufacturers and paediatric
anaesthetists is ongoing38, and it is likely that paediatric breathing circuits will
become single use.
Referring to the ‘reuse’ of breathing systems with the use of a new breathing filter for
each patient, Bennett and Bingham39 advise that, until new guidelines can be issued,
clinical end users must be aware that “in the absence of a written local policy to the
contrary, reuse of single use equipment, even with a filter, remains the responsibility
of individual practitioners”. A risk assessment carried out by North Lincolnshire and
Goole Hospitals NHS Trust, has led to the sanctioned reuse of breathing systems if
the devices are used in conjunction with breathing filters40. If this guidance is
followed, then the Trust will accept liability for reuse.
Wilkes33 reported that, in a 1993 outbreak of nosocomial Hepatitis C in Australia, “it
was hypothesized that an infected patient had coughed secretions into the breathing
system which then acted as a reservoir of infection for subsequent patients”.
Breathing filters were not used during the operating list that led to this incident.
Wilkes conjectured that “if filters had been used, cross-infection might have been
prevented by intercepting either air-borne particles or contaminated liquid”.
Given the risk of transmission of bacteria and viral infectious particles, a new, single
use breathing filter should be connected to the anaesthetic breathing circuit, at the
patient end of the circuit for each new patient. The breathing filter acts to protect the
patient “from any microbes that may be present in the breathing system delivering
gases to their lungs. A filter can also reduce the likelihood of microbes passing from
the patient’s respiratory tract to the breathing system”32. Given that the filter acts as a
barrier that prevents infectious particles reaching the patient, and or the breathing
circuit, it is recommended that “anything between the filter and the patient should be
disposed of or sterilised appropriately after use” 29,34.
Atkinson et al23 carried out a survey of UK anaesthetists to discover the extent to
which breathing filters were used. They found that “seventy-seven per cent of
respondents use a new filter in the anaesthetic circuit for each patient. Filters are
used by 6.5% of respondents for selected cases only (e.g. ‘high-risk patients’), whilst
35
8.7% of units use filters but change them only at the end of each list or day.
However, 6.5% of units do not use filters in the anaesthetic breathing system”. As
anticipated, none of our survey respondents reported the reuse of a breathing filter,
and it is assumed that in all cases, the manufacturer’s guidelines permitting limited
reuse were followed.
Many respondents chose to justify their reuse of single use breathing circuits, with all
referring to the use of a filter used in conjunction with the breathing system. It was
also emphasised that circuits were changed weekly in line with the manufacturer’s
recommendation. For example, “we are using the Mapleson C circuits in recovery. As
long as they have been used with HME filter in situ on every occasion our managers
allow reuse for one week. They are dated when opened for use and dated when
change is due. The manufacturers (we are told) guarantee them for this period so
long as they are used with filters” (ID 41 / Anaesthetic Recovery Nurse), and
“anaesthetic circuits are reused because we use disposable catheter mount and
filters. They are changed once a week in line with manufacturer recommendation” (ID
103 / Anaesthetist).
Given the protection afforded by breathing filters, in addition to the evidence in the
literature, the reports of reused breathing circuits are not surprising. However, it is
interesting that end users felt the need to report such reuse, albeit emphasising the
use of single use breathing filters. Such reporting illustrates that end users still
consider breathing circuits to be potentially single use, when they are now reusable
and underlines the continuing confusion over definitions in the community.
Consequently, it is possible that the labelling or guidance provided with the device
needs to be altered to reflect the limited reuse of adult breathing circuits when used
in conjunction with breathing filters. We return to this point later in the report, in
respects to the role that labelling inconsistencies can play in the event of SUD reuse.
The latest edition of the AAGBI’s Checking Anaesthetic Equipment41 guide suggests,
“any part of the breathing system, ancillary equipment or other apparatus that is
designated “single-use” must be used for one patient only, and not reused. Many of
the remaining devices reported as being reused fall within this broad range of
equipment.

36
The second most frequently
reported devices being
reused were facemasks
(N=17).
Of these 17 reports, 12 referred to facemasks used for oxygen therapy, and 5
mentioned anaesthetic facemasks. Respondents were most likely to report that
facemasks were reused in every operation (N=5) or more than one a week (N=9).
When separated into each type of facemask, the reported reuse had similar patterns
(Table 5):
Table 5: Reuse of Facemasks
Total
(N)
Every
operation
More
than
once a
week
More
than
once a
month
More
than
once a
year
Unknown
Anaesthetic Facemask 5 2 3 0 0 0
Oxygen Facemask 12 3 6 1 0 2
Both types of mask are intended to be single use, yet, in practice, an oxygen mask is
likely to be classified as single patient use. Although one respondent considered
there were “no perceived risks” to the reuse of facemasks, and that they could be
“socially cleaned” (ID 90 / Anaesthetist), they are known to pose a threat of cross
infection due to contamination by patient secretions26,29. During the pilot phase of the
project, anaesthetists were observed re-using single use anaesthetic masks that had
been ‘cleaned’ by the ODP using an alcohol wipe. Following ‘cleaning’, the mask was
placed unwrapped on the anaesthetic machine for reuse on the next patient.
Given the large volume of anaesthetic inductions performed, is it realistic to expect
SUD anaesthetic masks to be discarded after one use? Does this device require
reclassifying, or is there a real threat of cross infection? If the risk of cross infection is
so great, then why are anaesthetic facemasks reused at all? The answers to these
questions are outside the remit of this report, but we suggest that a microbiological
study of the risks relating to the reuse of masks may be desirable.

37
Monitoring and Sampling lines are used to examine
the gases that are delivered and exhaled during
anaesthesia. Monitoring provides essential
information to the anaesthetist about the patient’s
pulmonary function whilst they are ventilated.
Sampling lines are labelled ‘single use’ as it is possible for patient secretions to
collect in the tubing. Despite such concerns, sampling and monitoring lines were
reported as being reused. Ten respondents reporting such reuse considered that this
was likely to occur in every operation.
A range of intubation devices, including bougies, laryngeal mask airways (LMAs) and
laryngoscope blades were reported as being reused, despite their ‘single use’
labelling.
11 respondents reported the reuse of single use elastic gum bougies. These devices
are also referred to as Endotracheal Tube Introducers, Endotracheal Stylets and
Bougies. They are used to enable the anaesthetist to gain directional control when
experiencing a difficult intubation. Bougies carry a risk of cross infection, as the
device “has the potential to introduce pathogens into the respiratory tract”42. In his
examination of used bougies, Cupitt46 reported incidences of Coagulase -ve
Staphylococcus, unknown species of Staphylococcus, Diphtheroids, Bacillus species,
Micrococcus, Coliform, and Fungus growing on bougies. Shah et al43 have found
similar levels of bacterial contamination, and report concerns that such contamination
may lead to greater incidences of iatrogenic pneumonia6.
There is also a risk of viral transmission of disease via cross contamination from
blood residue on the outer structure of the bougie. Philips and Monaghan44 found
residual blood contamination on 40% of ‘clean’ laryngoscope blades awaiting reuse,
and Smith45 described blood contamination of the handle. Given that the bougie is
often used in collaboration with a laryngoscope, it is reasonable to expect a similar
extent of residual blood from the patient’s respiratory tract to remain on the bougie.
6 It is recognised that iatrogenic pneumonia can be caused by ventilation and airway
manipulation46. Shah et al43 consider that the presence of contaminated bougies
creates a further risk of infection.

38
Despite the risk of bacterial and blood borne cross contamination, two respondents
reporting the reuse of bougies considered that reuse was likely to occur in every
operation, while another four thought that reuse was likely to take place at least once
a week or more. One respondent provided a rationale to explain their reuse of a
single use bougie, describing how there is “no suitable alternative of sufficient quality”
(ID 103 / Anaesthetist).
Bougies are manufactured in both reusable and single use forms. Reusable bougies
can be used up to five times if disinfected between patients28. However, as Cupitt42
notes, “no formal record is kept of their use, therefore each bougie is probably used
many times. [Moreover] since they function perfectly well after five uses, is the
indication for discarding them an infection issue or does it relate to actual physical
deterioration? With repeated use, localised areas of weakness can develop in the
outer layer of the bougie. In many hospitals they are only replaced when actual
damage becomes visible”. The reuse of bougies beyond their intended lifespan is
clearly a threat to patient safety. Given that Cupitt describes the deterioration of
reusable bougies, and our respondent rationalised reuse in terms of the lack of
another device of suitable quality, it seems as if the manufacturing and design of
bougies could be examined in order that reuse cannot be justified in relation to
quality issues.
Six respondents reported the reuse of a single use laryngoscope, with three of them
considering reuse to occur in every operation. Laryngoscopy is an invasive
procedure by which a blade is placed into the patient’s mouth and throat, enabling
the anaesthetist to visualise trachea when attempting to ventilate the patient, as
figure 2 illustrates.
Figure 2: Position of the laryngoscope.
Source: http://health.allrefer.com/pictures-images/laryngoscope.html

39
Following concerns regarding the possible spread of TSEs and prions (including
vCJD) from the tonsils47,48,49 (see figure 3), single use laryngoscopes were
introduced. Given the proximity of the tonsils and the laryngoscope (
Figure 3), it was suggested that anaesthetists should only single use laryngoscopes
in an attempt to minimise the risk of cross infection28.
Figure 3: Location of the tonsils.
Source: http://health.allrefer.com/health/epiglottitis-throat-anatomy.html
Esler et al50 describe how “mixed cultures have been grown from laryngoscopes
following routine use, including a wide range of potentially harmful micro-organisms.
Laryngoscope blades come into contact with mucous membranes, saliva and blood.
Consequently, cross-infection has been reported28,50. For example, Esler et al
discussed cross-infections deriving from delivery suites and in neonatal intensive
care units involving infection with Listeria monocytogenes and Pseudomonas
aeruginosa. Later in this report, we provide visual evidence of the inability of
reprocessing methods to remove tissue and blood contamination on a single use
laryngoscope blade.
Laryngoscopes are manufactured as both reusable and single use devices, and we
return to this issue later in the report. Reusable examples can be used in conjunction
with either a single use or a reusable blade. Practitioners also have the option to use
disposable sheaths that fit over the blade and the handle. However, even if a new
single use blade is used, patient safety may still be compromised. Esler et al50
describe how, “although the laryngoscope handle does not contact the patient
directly, it may be contaminated by the tip of the blade, which often touches the
handle when in the folded closed position, and hence the handle must also be

40
considered a potential source of cross-infection”. Consequently, any risk analysis of
laryngoscopes must take into account the threat posed by reused handles.
Reuse of laryngeal mask airways (LMAs) were reported by a minority of respondents
(N=4). The LMA allows the anaesthetist to manage the patient’s airway when the
more traditional technique of an endotracheal tube attached to a breathing system,
would interfere with the surgical field. LMAs, in both their single use and reusable
guises, are expensive devices, and are not used in every operation.
Like laryngoscopes, LMAs are placed down the patient’s trachea and thus “have the
potential to act as a vector for the transmission of prion diseases”51. LMAs come into
contact with the patient’s tonsils, which are known to carry a risk of prion
transmission. Parker and Day52 examined 50 LMAs and found blood contamination
on 76% of the devices. However, contamination visible to the human eye was only
found on 12% of devices, demonstrating that instruments which appear to be ‘clean’,
may not be as sterile as anticipated.
Other anaesthetic devices reported as being reused included: capnographs lines,
spirometry tubing, ventilator tubing, green bubble tubing and elephant tubing,
breathing system bags, oxygen bags, pressure infusion bags, anglepieces, C02
adaptors, recovery T-pieces and catheter mounts.
Respondents listed 26 SUDs that although used within the operating theatre, cannot
be clearly categorised as an anaesthetic or surgical device. These include syringes
(n=3), drapes (n=1), circulation / compression garments (n=13), gloves (n=1),
warming blankets (n=1), spinal needles (n=1) and bottles of prep solution and saline
(n=2). Given that the data on the above devices is sparse, any in-depth discussion
about reuse patterns can only be made in regards to circulation and compression
garments.

41
The third most frequently reported category of
device to be reused were circulation and
compression garments (N=13). Although a range of
terms were given to describe the devices, including
‘Flowtron Boots’, ‘gaiter inflation DVT prohylaxis’
and ‘compression garments’, they have been
grouped together in the analysis.
Compression garments are used perioperatively to
aid the patient’s circulation and prevent pooling of
blood at lower extremities of the body. Used post-
operatively, they can aid with DVT prophylaxis.
Five individuals reporting reuse considered it was likely to occur in each operation,
with another seven reporters estimating reuse at least once a week. Compression
garments are likely to be in direct contact with the patient’s skin, but some
respondents considered that the device could be reclassified as reprocessable. For
example, “many ‘single use items’ could actually be simply washed and reused, such
things that are non-invasive and are in contact with unbroken skin. The
manufacturers should alter the design to that can be done safely; for example, with
‘Flowtron leggings’” (ID 77 / Theatre Nurse). Considering that compression garments
are unlikely to come into contact with the clinical site, it is possible that they might be
an appropriate device for reclassification. We suggest that there should be further
examination of this issue.
As already discussed, the lack of participating surgeons in the survey has had an
impact on the types of devices that are reported as reused. Respondents reported
the reuse of just 11 surgical devices, and it is impossible to provide any in-depth
analysis. The devices reported as reused can be categorised as: diathermy
instruments (n=2), laparoscopic instruments (n=1), probes (n=4), saw blades (n=1),
jugs (n=1), buckets (n=1) and “most surgical instruments” (ID 81 / Anaesthetist).
Respondents were asked why they thought SUDs were reused in their hospital, and
could check as many of the factors listed as they wished (Table 6).
Table 6: Rationales for reuse

42
N %
Cost 46 50
No risks involved in reuse 25 27
Don't know / am not aware SUDs are reused 19 21
Waste/environmental issues 18 20
Other 17 19
Only available equipment 10 11
Reuse of SUDs is frequently rationalised in terms of the financial and environmental
impact that results from repeated purchasing and disposal of medical
devices53,54,55,56. The survey showed that 50% of respondents considered that SUDs
were reused at their hospital due to the prohibitive cost of replacing the device after
each procedure. Statistical tests demonstrated that cost was a significant factor in the
decision to reuse breathing circuits (χ2 = 8.26, p < 0.004), facemasks (χ2 = 5.94, p <
0.05) and compression garments (χ2 = 7.04, p < 0.01).
One anaesthetist rationalised the reuse of a single use syringe in terms of the cost: “I
personally reuse syringes on same patient because of cost” (ID 103), whilst another
justified the reuse of a pressure infusor bag because of the financial implications (ID
101).
The average cost of a syringe, according to the NHS PASA catalogue57, is 15 pence.
Although the large volume of use multiplies this cost many thousands of times over,
there are real dangers from reusing syringes. For example, if a syringe is used to
draw medication, and subsequently reused to draw a different medication, the two
substances may react with each other. It is likely that, following its first use, the
syringe is no longer sterile. Whilst undertaking piloting, the reuse of a syringe was
witnessed. A non-sterile syringe was picked up from a tray on the anaesthetic
machine and used to test the inflation of the cuff to a tracheal tube. Once this had
been checked, the syringe was disconnected and returned to the tray for further use.
The cost of LMAs provides a further example of the financial justifications for SUD
reuse. All respondents reporting reuse of a SUD LMA justified the practice on
grounds of cost. Smith45 compared the cost of a single use LMA with its reusable
equivalent. The SUD LMA was reported to cost approximately £27. The reusable
LMA, which, according to the manufacturer, can be sterilised up to 39 times (i.e.

43
disposed of after 40 uses), costs over £80. As discussed earlier, the use of a SUD
LMA is favoured because of the certainty of sterility. However, as Smith states, for
some hospitals, SUD LMAs are “not an attractive financial option”. We shall further
examine the costs differences between single use and reprocessable devices later.
Respondents employed in hospitals carrying out more than 15,000 procedures per
annum were more likely to rationalise reuse of SUDs in terms of the negative
financial impact of the purchase and use of new single use devices for each patient.

44
Table 7: Reuse rationalised according to prohibitive cost of replacing SUDs,
measured against the number of operations performed per annum
N %
999 or less 1 2
1,000 - 4,999 7 15
5,000 - 9,999 5 11
10,000 - 14,999 5 11
15,000 - 19,999 7 15
20,000 or more 12 26
Unknown 9 20
Total 46 100
However, the small sample makes it impossible to test this apparent association.
Haley58a described how, in the USA, a SUD reprocessing programme in a 600 bed
hospital could halve expenditure on devices (Table 8). Although the exact products to
be reused are not identified, Haley works for Vanguard Medical Concepts, a US third
party reprocessor handling arthroscopic instruments, biopsy forceps, EP catheters,
anti DVT garments and laparoscopic equipment58b.
Table 8: Proposed cost savings linked to reuse58a
Number of beds Average savings in US $
100-150 71,910
151-200 137,700
201-300 313,650
301-450 465,120
451-600 639,540
600-1000 755,820
The reuse of SUDs as a financial solution, places a burden on both staff and patient
safety, and on the professional obligations of clinicians. In a recent editorial in
‘Anaesthesia’, Woods59, formerly anaesthetic clinical speciality advisor for the NPSA,
argued that it is up to “practitioners to stand up for themselves and demand that the
safest rather than the cheapest options are considered when purchasing the
materials we use in our daily work”. When questioned, very few clinical practitioners

45
would be happy to have a reused SUD used on themselves or their family60. 82% of
nurses and 71% of surgeons surveyed say they would be uncomfortable if a
reprocessed single use device were used in this context.
However, while some of our survey respondents were resolute that they would
“refuse to accept a reprocessed single use item onto my trolley” (ID 12 / Nurse),
patient safety is compromised by SUD reuse. By placing the patient at risk of cross
contamination or iatrogenic injury and disease, a practitioner is not meeting the
professional obligation ‘to do no harm’. Moreover, placing a patient at risk from a
contaminated instrument is costly. Medico-legal costs associated with unclean,
unsterilised or contaminated surgical devices (whether SUD or reusable), are
estimated to exceed £1.5 million since 1995 (personal communication with NHSLA).
Surprisingly, given its emphasis within the literature12,61 only 18 respondents
considered that waste or environmental issues could justify SUD reuse. One
anaesthetist commented, “I personally reuse syringes on same patient because of
environment issues (ID 103). However, another expressed doubts about the validity
of the environmental argument when rationalizing SUD reuse: “I feel environmental
issues ought to be a reason for reuse but am sure this is not the case” (ID 97).
As with the justification of reuse in terms of the cost of replacing every device,
respondents who justified reuse of SUDs in terms of wastage and environmental
issues were more likely to work in hospitals that performed over 15,000 operations
per year (50%) and would consequently generate greater levels of waste (table 9).

46
Table 9: Reused rationalised in terms of excessive waste, measured against number
of operations performed per annum
N %
999 or less 0 0
1,000 - 4,999 2 11
5,000 - 9,999 1 6
10,000 - 14,999 2 11
15,000 - 19,999 3 17
20,000 or more 6 33
Unknown 4 22
Total 18 100
However, whilst SUDs and their packaging “contribute to the solid waste stream”62,
the reprocessing of reusable devices also has an environmental impact from the
waste generated during sterilisation55. At the end of its lifecycle, the reprocessable
device will still contribute to the solid waste stream, as Schultz62 describes. Repeated
re-packaging following sterilisation also places increased waste into the environment.
25 respondents considered that the rationale for reuse of SUDs was the lack of risk
involved in the practice. For example, one ODP declared that there were “very few
risks from routine patients so some items have always been classed as multi-use
even though they are classed as single use” (ID 92). This respondent reported the
reuse of laryngoscope blades, bougies and facemasks. All these devices have the
potential to come into contact with infectious agents.
It is interesting that staff perceived that reuse of many SUDs does not involve any
real risks. Woollard63 argued that, in the absence of demonstrated adverse effects,
Australian hospitals were not prepared to divert resources from other areas of
medical care to replace equipment. However, research has found evidence of
contamination on surgical instruments56,61,64,65 and it is acknowledged that the long-
term safety and efficacy of reused SUDs has “never been properly proven”66. It is
therefore proposed that it is not solely that there has been an absence of adverse
events linked to surgical devices, but that “patient adverse events directly related to
the reuse of SUDs are often under-reported due to the difficulties in determining the
actual causes of such events, the potential liability issues of such events and the

47
inadequacy of the reporting systems”67. However, many items listed in the inventory
of reuse and reported by respondents, are non-critical, non-invasive devices (e.g.
anti DVT garments such as ‘flowtron boots’). It is likely that the risk of iatrogenic
transmission of disease, bacteria or prions via such devices is indeed extremely low.
Lastly, ten respondents blamed a lack of equipment or the lack of “suitable
alternative[s] of sufficient quality” (ID 101 / Anaesthetist) for SUDs reuse. When we
raised the supply chain issue with manufacturers, they argued strongly that they did
all they could to meet orders and not place patients in danger or risk their company’s
reputation. They claimed that supply problems often occurred in the hospital, either
before they received an order, because of a problem in the hospital’s administration
system, or after the order was despatched and before it was delivered to theatre. The
interview phase of the study investigated these claims further, whilst our ergonomic
analysis reviewed the quality issues.
Collignon et al12 examined the reuse of SUDs in Australia, and found that large
metropolitan hospitals were more likely to reuse (or report the reuse of) SUDs. The
survey data suggests that a similar conclusion could be reached about the reuse of
SUDs in the English NHS. Most SUD reuse was reported from staff who work in
hospitals with over 300 inpatient beds (N=34), and performing over 20,000 surgical
procedures are performed per annum (N=18). Table 10 outlines the relationship
between number of operations performed, hospital bed numbers and SUD reuse.

48
Tabl
e 10
: App
roxi
mat
e nu
mbe
r of o
pera
tions
per
form
ed /
Num
ber o
f inp
atie
nt b
eds
/ Reu
se o
f SU
Ds
N
umbe
r of i
npat
ient
bed
s To
tal
50
or l
ess
51-1
00
101-
150
151-
200
201-
300
Mor
e th
an
300
No
reus
e A
ppro
xim
ate
num
ber
of
oper
atio
ns
perfo
rmed
1,00
0 - 4
,999
3
1 3
1 4
12
5,00
0 - 9
,999
0 0
0 0
2 2
10,0
00 -
14,9
99
0
0 0
1 1
2
15,0
00 –
19,
999
0
0 0
0 2
2
20,0
00 o
r mor
e
0 0
0 0
5 5
To
tal
3
1 3
2 14
23
Reu
se
App
roxi
mat
e
num
ber
of
oper
atio
ns
perfo
rmed
999
or le
ss
0 0
1 0
0 0
1
1,00
0 - 4
,999
0
2 0
1 1
4 8
5,00
0 - 9
,999
2
0 1
0 2
1 6
10,0
00 -
14,9
99
0 0
0 1
0 5
6
15,0
00 -
19,9
99
0 0
0 0
1 6
7
20,0
00 o
r mor
e 0
0 0
0 0
18
18
To
tal
2 2
2 2
4 34
46

49
Respondents were asked whether they thought reuse of SUDs occurred in other
hospitals (Table 11). 25 individuals reporting such a practice thought it was likely to
be occurring in more than 75% of other English NHS hospitals. However, 27 of those
responding to the question thought that reuse of SUDs was only likely to happen in
less than a quarter of all English NHS hospitals.
Table 11: Reuse in other hospitals
N %
75% or more 25 29
50-74% 18 21
25 –49% 15 18
Less than 25% 27 32
Total 85 100
When comparing these responses to their own reported pattern of use or reuse,
respondents whom themselves reported SUDs reuse were more likely to consider
that other hospitals were practising SUDs reuse (χ2 = 25.42, p < 0.001) (Table 12).
Similarly, respondents who did not reuse SUDs thought that other NHS hospitals
were also unlikely to reuse SUDs.
Table 12: Comparing reuse in own and other hospitals
Reuse in other hospitals Total
75% or
more 50-74% 25-49%
24% or
less
Reuse No items
listed as
reused
1 4 8 18 31
Items listed as
reused 24 14 7 9 54
Total 25 18 15 27 85

50
Respondents were asked to respond to the question “what do you think the risks and
dangers of re-using single use devices might be?”. Responses fell into five
categories, which are shown in Table 13:
Table 13: Perceived danger / risk of reuse
N %
Cross contamination and infection 59 65
Device failure 57 63
Inability to adequately clean 23 21
Ethics of care and safety 14 15
Compromising manufacturers guarantee 11 12
Risk of litigation 11 12
59 respondents perceived cross contamination and infection to be a danger or risk
associated with the reuse of SUDs. Of these, 24 were nurses, 21 were anaesthetists,
nine were ODPs and five were theatre managers. However, when compared to the
total number of each occupation within the sample, a different pattern is seen. 83% of
all theatre managers and 82% of all ODPs in the sample were concerned about the
risk of cross contamination and infection from SUD reuse, with anaesthetists (64%)
and nurses (59%) least likely to consider that reuse posed an infection risk.
Statements described “bacterial / viral cross contamination between patients” (ID 1 /
ODP), the “increase risk of cross infection which therefore ignores [the] principals of
universal precautions” (ID 7/ Nurse), “cross infection, CJD etc” (ID 54 / Nurse) and
“infective risk / prion risk” (ID 81 / Anaesthetist).
The argument that reuse could be justified on grounds of the lack of risk was
discussed earlier in this report. However, Collignon et al61 point to the lengthy
incubation period associated with TSE diseases, and argue that linking a subsequent
surgical infection to the reuse of a SUD “will be very difficult”. Our data do show that
clinical end users have real concerns about the possibility of cross contamination and
infection. Moreover, “even a small risk is unacceptable to the patient who acquires an
infection”55, and reuse of SUDs does generate a credible threat to patient safety.
Despite Woollard’s 63 complaint about the lack of scientific evidence of risk from SUD
reuse, cases are beginning to be reported. Bacteria have been found on ablation

51
catheters665, gum elastic bougies42, endoscopic biopsy forceps64,68 and anaesthetic
ventilators25.
In recent years, two cases of reuse of contaminated surgical devices have occurred
in England, and received high profile media coverage. Whilst it is unclear whether the
devices in either case were SUDs, they demonstrate how even instruments that are
designed to be decontaminated can lead to cross-contamination and infection
transmission between patients. The risk of contamination to instruments that are not
designed to be cleaned and sterilised, may, then, be very real.
In 2001, Alan Brant underwent a procedure to dilate his oesophagus at St Peters
Hospital, Chertsey. During the procedure, a biopsy was taken and found to show
signs of a malignancy. Mr Brant underwent an oesophagectomy and splenectomy to
remove the malignancy. However when this was later examined, no evidence of a
carcinoma could be found. Investigation attributed the error to a contaminated biopsy
forcep that had been used on a previous patient, and upon which a malignant
“fragment” remained (personal communication).
In 2002, staff at Middlesbrough General Hospital unknowingly reused surgical
instruments that had been previously used on a patient diagnosed with CJD69,70.
Instruments used on patients thought to be at-risk of CJD should be quarantined until
the diagnosis is confirmed but this did not happen. Investigation determined that 34
patients might be at risk of cross contamination, having had a similar procedure to
the original patient7. This figure was subsequently reduced to 24, but was expected
to fall further: “it appears that the number of patients who may be at any real risk of
exposure – albeit a very small risk – is likely to be less than the 24 identified”70.
57 respondents considered that there was a risk of device failure if SUDs were
reused. Of these, 30 were nurses, 15 were anaesthetists, seven were ODPs and four
were theatre managers. When assessed against the total number within each
occupation group, anaesthetists (45%) were least likely to foresee device failure as a
risk or danger associated with SUD reuse. Nurses and ODPs (both 73%) were most
concerned, followed by theatre managers (67%). Explanations ranged from complex
7 At the time of the incident, Middlesbrough General Hospital did not have a
procedure for tracking surgical instruments, or linking their usage to individual
patients70.
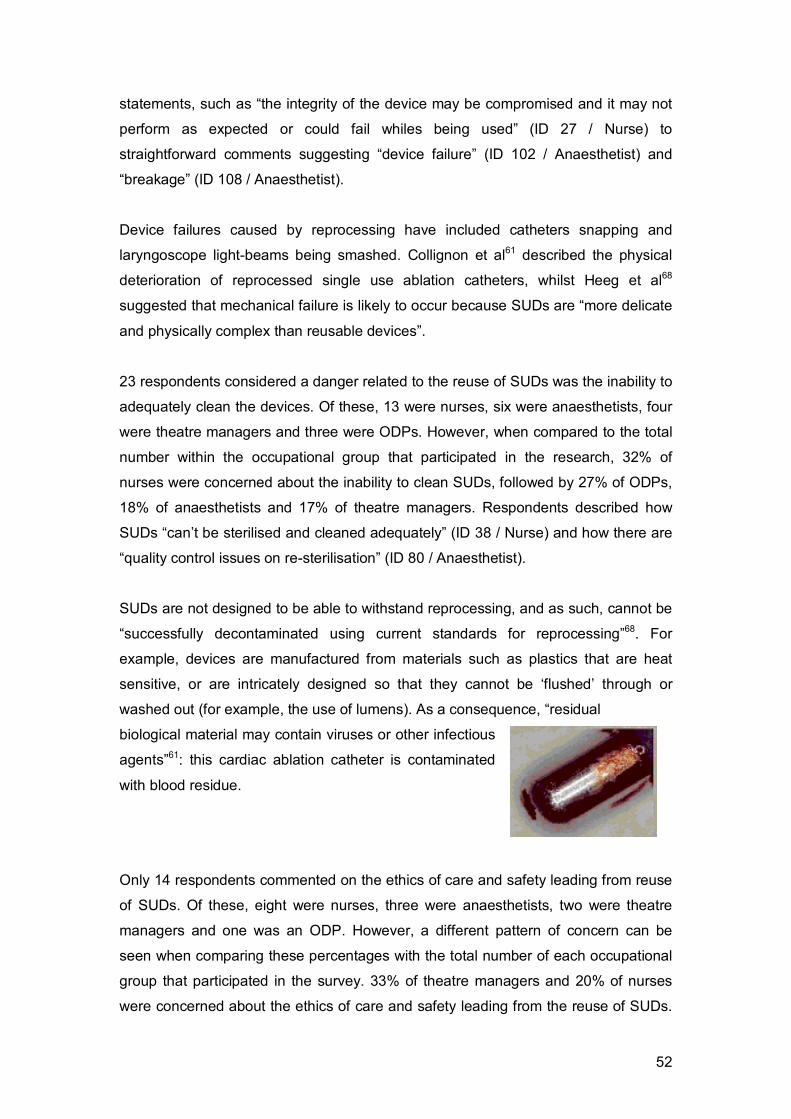
52
statements, such as “the integrity of the device may be compromised and it may not
perform as expected or could fail whiles being used” (ID 27 / Nurse) to
straightforward comments suggesting “device failure” (ID 102 / Anaesthetist) and
“breakage” (ID 108 / Anaesthetist).
Device failures caused by reprocessing have included catheters snapping and
laryngoscope light-beams being smashed. Collignon et al61 described the physical
deterioration of reprocessed single use ablation catheters, whilst Heeg et al68
suggested that mechanical failure is likely to occur because SUDs are “more delicate
and physically complex than reusable devices”.
23 respondents considered a danger related to the reuse of SUDs was the inability to
adequately clean the devices. Of these, 13 were nurses, six were anaesthetists, four
were theatre managers and three were ODPs. However, when compared to the total
number within the occupational group that participated in the research, 32% of
nurses were concerned about the inability to clean SUDs, followed by 27% of ODPs,
18% of anaesthetists and 17% of theatre managers. Respondents described how
SUDs “can’t be sterilised and cleaned adequately” (ID 38 / Nurse) and how there are
“quality control issues on re-sterilisation” (ID 80 / Anaesthetist).
SUDs are not designed to be able to withstand reprocessing, and as such, cannot be
“successfully decontaminated using current standards for reprocessing”68. For
example, devices are manufactured from materials such as plastics that are heat
sensitive, or are intricately designed so that they cannot be ‘flushed’ through or
washed out (for example, the use of lumens). As a consequence, “residual
biological material may contain viruses or other infectious
agents”61: this cardiac ablation catheter is contaminated
with blood residue.
Only 14 respondents commented on the ethics of care and safety leading from reuse
of SUDs. Of these, eight were nurses, three were anaesthetists, two were theatre
managers and one was an ODP. However, a different pattern of concern can be
seen when comparing these percentages with the total number of each occupational
group that participated in the survey. 33% of theatre managers and 20% of nurses
were concerned about the ethics of care and safety leading from the reuse of SUDs.

53
Just 9% of anaesthetists and ODPs mentioned how reuse of SUDs might
compromise safety and ethics. Respondents described how SUD reuse
“compromise[s the] safety of patient[s] and staff” (ID 37 / Nurse), and “giv[es] a less
than quality service to the second and subsequent patients who did not have the
instrument first” (ID 48 / Theatre Manager).
The reuse of SUDs places both patients and staff at risk, and is also ethically
contentious in that it compromises the quality of care received by the patient55,71.
Consequently, the practice has been described as “medical experimentation without
benefit, written consent – or even patient knowledge”71. What makes SUD reuse
even more ethically controversial, is that most patients will be unaware of the
practice, and will give their consent to medical treatment without knowing all the facts
about the care that they will receive.
SUDs are designed to be used once and be discarded. Reuse of a SUD therefore
invalidates the manufacturer’s warranty. Only 11 respondents recognized that reuse
rendered the guarantee void. Of these, eight were nurses, and three were
anaesthetists. However, they represented just 20% and 9% of all nurses and
anaesthetists participating in the survey.
Reuse of SUDs can place both patients and staff in danger of iatrogenic transmission
of disease, and for the patient, can result in harm caused by breakage or failure of
the device in use. Since reuse invalidates the manufacturer’s warranty, any litigation
costs arising from device failure will be met by the hospital and the staff members
concerned.
11 respondents referred to the risk of litigation as a consequence of reusing SUDs.
Of these, six were nurses, three were anaesthetists and two were ODPs. They
represented 15%, 9% and 18% of all nurses, anaesthetists and ODPs participating in
the survey.
Respondents were asked if they were aware of any Hospital or Trust guidelines or
policies relating to the reuse of SUDs (table 14).
74% of respondents reported that they were aware of hospital guidelines detailing the
use of SUDs. These guidelines could be broken down into 3 main categories which
accounted for 92% of responses: reuse of any kind must not occur, specific low risk

54
items can be reused, and manufacturers’ guidelines are followed. Two further
categories – lack of awareness and other - accounted for the remaining 8% of
responses.
Table 14: Awareness and understanding of SUDs guidance
N %
Reuse of any kind must not occur 30 57
Follow manufacturers guidance on reuse 13 25
Specific low risk items reused 5 10
Unaware of policy 2 4
Other 2 4
Total 52 100
Surprisingly, a few respondents who earlier in the survey had reported the reuse of
certain SUDs, now claimed that SUDs were not reused at their hospital. One
anaesthetist commented, “the risk management group have stated that all devices
labelled single use should be single use and that we should move to a position where
most items in contact with the patient are single use” (ID 81). However, despite this
statement, the respondent had earlier reported the current reuse of bougies,
laryngoscope blades, LMAs, breathing circuits, recovery T pieces, doppler probes,
facemasks and most surgical instruments. Devices reported as being reused by other
respondents included laser probes used in glaucoma surgery, compression
garments, sampling lines and angle pieces.
Nevertheless, the majority of respondents were clear that “no SUD is to be reused
under any circumstance” (ID 13 / Nurse). Despite respondents explaining that no
reuse of SUDs should occur, and paraphrasing the guidance issued by the MDA6,
only one respondent referred to the “national guidelines” (ID 106 / Anaesthetist). This
may suggest that greater awareness of the MDA’s6 guidelines is required. This lack
of awareness was emphasised by the comments made by three nurse respondents.
They described how they were either not aware of the written policy, or had not read
it recently, but simply followed the practice of others and did not reuse SUDs.
Certain devices were perceived as only having a low risk of cross contamination,
infection or failure if reused. These were breathing circuits (if protected by the

55
appropriate breathing filter) and compression garments. For example, one nurse
described how compression garments “are disposed of if they come into contact with
the patient’s skin” (ID 21), whilst an anaesthetist commented that “gas sampling lines
[are] changed only when damaged or contaminate[d] but are always used behind a
breathing filter” (ID 107). However, in both of these cases, the contaminant may be
invisible to the human eye.
55% of respondents were aware of Trust guidelines. The majority of these
respondents described how Trust guidelines stated that reuse of SUDs must not
occur (Table 15).
Table 15: Awareness of Trust policies on SUDs
Trust policy consistently matches the policies of individual hospitals, as described
above. However, in many cases, the hospitals and the Trust are one organisation.
Conclusion
Despite the guidelines issued by the MDA6 in 2000, which effectively ‘banned’ the
reuse of SUDs, this survey has demonstrated that the practice of reusing SUDs still
exists. Whilst we are unable to determine the extent of reuse, due to our sampling
difficulties, our data demonstrates that the practice continues.
There is already substantial concern about the risk of hospital - or healthcare -
acquired infections, affecting 95,000 people a year, and leading to approximately
5,000 fatalities72. The reuse of SUDs poses an additional threat to patient safety
through cross infection, contamination or device malfunction.
N %
Reuse of any kind must not occur 29 59
Follow manufacturers guidance on reuse 13 27
Specific low risk items reused 3 6
Unaware of policy/policy in development 2 4
Follow other guidelines for reuse 2 4
Total 49 100

56
This survey has shown that reuse of SUDs is likely to occur because of:
Confusion about what single use means.
A perceived lack of risk associated with reuse.
The lack of other available equipment.
The cost of replacing each SUD with a new SUD.
Unrealistic expectations about disposal of certain devices after just one
use.
While there are strong suggestions in the data that reuse is most likely to occur in
large, high-throughput hospitals, the sampling problems mean that this cannot be
stated as a firm conclusion. This is a particularly unfortunate consequence of the
abandonment of the original design. Similarly, there are insufficient data to explore
the possibility of other associations and, in particular, of regional variations in the
practice. We suggest that this continues to be an area that warrants detailed
examination.
Further educational and regulatory efforts to discourage reuse are clearly desirable,
but it is questionable how effective these can be without more fundamental
agreement on what actually constitutes reuse and to what devices this classification
should be applied. An enhanced communication programme needs to rest on
greater clarity about what is to be communicated.

57
Part Three: The Interviews
All fieldwork for the interview phase was conducted by Dr Rowley, under the
supervision of Professor Dingwall. Professor Currie assisted with a small number of
interviews. Dr Sharples and Dr Norris carried out an ergonomic analysis of
anaesthetic devices kindly supplied by leading manufacturers (see Appendix six),
and Professor Whynes performed a formal cost-benefit analysis of the available
financial data, which can be found towards the end of the main body of the report.
A purposive sample of hospitals was constructed for the interview phase,
incorporating some where individual staff members had responded to the survey and
a parallel, but not strictly matched, group where staff did not. The purposive sample
covered a range of hospital characteristics (location (urban/rural), geography
(Strategic Health Authorities), hospital size (bed numbers) and Healthcare
Commission star rating). Staff from 55 hospitals reported reuse of SUDs during the
earlier survey: 5 of these were included in the sample (table 16).
Table 16: Trusts responding to the survey and included in the interview sample
Hospital ID Trust SHA Star Rating
2003-4
Star Rating
2004-05
No. Beds
1 A A 1 3 ↑ 503
2 B A 3 3 ↔ 1300
3 C B 0 0 ↔ 1140
4 D B 2 2 ↔ 660
5 F A 3 3 ↔ 1000
Table 17 lists the devices that staff reported as being reused:
Table 17: Reuse reported by survey respondents
Hospital ID Reused SUDs
1 Facemasks, Anaesthetic Circuits, Compression Garments
2 Facemasks, Anaesthetic Circuits, Compression Garments, Gas
Sampling Lines
3 Pressure Infusor Bags, Intubating Bougies
4 Anaesthetic Circuits, Intubating Bougies, Non-Sterile Gloves
5 Facemasks, Anaesthetic Circuits

58
An additional eight hospitals, whose staff had not responded to the survey, were
included in the sample (Table 18). Five of these were located in the same Strategic
Health Authorities (SHA), whilst the remaining three were from a third SHA selected
for comparative purposes (socio-economic differences and influence of industrial
workers in urban/rural region).
Table 18: Additional Trusts selected for interview sample
Hospital ID Trust SHA Star Rating
2003-4
Star Rating
2004-05
No. Beds
6 E B 2 2 ↔ 450
7 G A 3 3 ↔ 635
8 A A 1 3 ↑ 108
9 A A 1 3 ↑ 690
10 A A 1 3 ↑ 212
11 H C 2 2 ↔ 535
12 H C 2 2 ↔ 530
13 H C 2 2 ↔ 67
In total, 13 hospitals spread across 8 NHS Trusts and 3 SHAs were invited to
participate in the interview phase of the study. As with the survey, NHS research
governance presented serious obstacles to the efficient, effective and timely conduct
of the research. These are detailed in Appendix five. However, MREC and R&D
approvals were eventually gained for all participating Trusts.
In each hospital, the Theatre Manager and Clinical Director of Anaesthesia were
invited to participate in an interview. Each was asked to recruit one ODP, who would
also be invited to participate. These individuals were selected as they are likely to be
involved in the practice of using single use devices, or are directly responsible for the
management of the theatre/anaesthetic room environment and for stocks of
equipment. Given the lack of success at recruiting surgeons to participate in the
earlier survey, we considered it more cost-effective to pursue the recruitment of
anaesthetists, theatre managers and ODPs. However, this has resulted in the study
being more focused on anaesthetic devices than had been planned.

59
In total, 60 invitation letters and emails were sent to 37 individuals, resulting in 23
interviews 8. The final sample (23/37) therefore reflected a response rate of 62%.
The sample comprised one sterilisation manager (SM), eight ODPs, nine theatre
managers (TM) and five clinical directors of anaesthesia (CDA) (
Table 19). The lower number of CDAs recruited was due to a number of job
vacancies and the nature of the role, where a clinical director may work across
multiple sites within a Trust. Where ODPs were recruited via theatre managers or
clinical directors of anaesthesia, only one was ever available for interview.
Table 19: Sample Composition
Hospital ID Theatre
Manager
Clinical
Director of
Anaesthesia
ODP Sterilisation
Manager
1 No No No N/A
2 Yes Yes Yes N/A
3 Yes No Yes N/A
4 Yes Yes Yes N/A
5 Yes Yes No N/A
6 Yes Yes Yes Yes
7 Yes Yes Yes N/A
8 Yes No No N/A
9 Yes No Yes N/A
10 N/A N/A N/A N/A
11 Yes No Yes N/A
12 No No No N/A
13 No No Yes N/A
At no stage is any individual or Trust identified by name. Direct quotations are identified by hospital number (as in Table 19) and the individual’s occupational role: for example, ‘1CDA’ would be the
clinical director of anaesthesia from hospital 1.
8 The final sample contained 12 hospitals. Hospital 10 was omitted as the Surgical
Services Manager failed to sign the R&D form, despite repeated requests. After the
fourth attempt, it was considered uneconomic to pursue the signature further.

60
Interviews built on the scientific background and survey findings and were designed
to collect data on:
1. Rationales for the reuse of specific medical devices in specific settings, where
this is occurring, or for avoiding reuse, where this is not;
2. Cost differences between single use and equivalent re-usable devices; and
3. Procedures employed for decontamination and their associated costs (where
reuse was reported).
Respondents were sent the following list of questions and advised that, whilst the
interviews would cover the topics outlined, they could also include issues that
respondents wanted to raise and discuss with the research team.
1. What is the department’s / hospital’s policy relating to the use and reuse of single
use devices?
2. How many single use devices are used in the department each year?
3. How many single use devices are purchased by your department each year?
4. What are the cost differences between similar single use and reprocessable
devices? (For example, a laryngeal mask is available in both a single use and
reusable form.) Please provide examples of devices and their costs.
5. What are the cost differences between re-using single use devices and
purchasing new equipment? Please provide some examples, and include all
costs associated with the device lifecycle, as detailed in the chart below.

61
6. What procedures are undertaken to return a single use device to a state where it
can be reused?
a. What are the costs involved in these procedures?
b. What is the time delay involved in these procedures?
7. What are the indemnity costs involved regarding the use and reuse of single use
devices?
8. Are the lifecycle and indemnity costs associated with re-using single use devices
included within your department’s calculations/budgeting decisions? For
example, are these lifecycle costs factored into the decision to use single use
devices verses reprocessable devices or to purchase new single use devices
verses re-using single use devices? If they are not, which department picks up
the cost of the reprocessing?
9. How is the balance of likely adverse effect against cost & performance pressures
assessed and what is the response?
We anticipated that two interviewing formats would be followed:
• Task-based interviews with Theatre Managers and Clinical Directors of
Anaesthesia, where they would be asked to explain their rationales for the
local practice of using (and/or re-using) single use devices and to relate
these to current national and local policies and guidelines. Theatre Managers
would also be asked about the number of single use devices purchased and
the number of single use devices used.
• Situational interviews, a process that incorporates both observation and
interview, would be carried out with ODPs. This format built on the
experience of Dingwall and colleagues73 when interviewing child protection
workers about their work as documented by their own selected case files.
This allowed the interview responses to be disciplined by reference to
decisions actually made rather than being coloured by knowledge of official
policies or socially desirable responses. As such, it represented a better
proxy for observational data than traditional interviewing techniques. ODPs
would be interviewed in their own workspaces and asked to talk through the
local stocks of devices and the circumstances in which they are used.
However, in practice, all the interviews tended to combine these formats. Formal
question and answer exchanges were used in combination with more informal,
situational accounts and demonstrations of devices, cost data and decision-making
models. Moreover, whilst interviews in the workplace were possible in a minority of

62
cases, the majority of the interviews took place in offices or meeting rooms within the
theatre department but away from the clinical (sterile) areas. On two occasions
however, Dr Rowley was required to ‘gown up’ in order to enter the clinical area
where the interview took place.
All interviews were semi-structured and presented comparable questions to all
participants. This format allowed the research team space to adapt the interview and
elicit further responses from participants in the light of local circumstances7. All
interviews bar one were audio recorded, with the informants’ consent, using digital
recording equipment. Once transcriptions were completed, data analysis began.
Bryman and Burgess74 describe how, “data are collected and after a general
reflection on ‘issues of concern’ categories which fit the data are generated”.
Similarly, ten Have75 suggested, “analytic induction is a technique used primarily by
qualitative researchers to access commonalities across a number of cases and
thereby clarify empirical categories and the concepts that are exemplified by the
cases included in a category”. Consequently, data analysis was driven and
“developed from phenomena which are in various ways evidenced in the data”76.
Results
The widespread introduction of single use devices followed awareness that
sterilisation and decontamination processes were ineffective at removing all microbial
and proteinaceous materials from surgical and anaesthetic instruments41,79. Evidence
of iatrogenic transmission of Creuztfeld Jacob Disease (CJD) first emerged in the
1950s, when concerns were mooted about the possibility that contaminated surgical
instruments could infect patients78. These were reiterated in the 1970s following
iatrogenic cross infection stemming from the use of cadaveric corneas during
transplantation79. However, it was not until the iatrogenic transmission of variant CJD
(vCJD) from one neurosurgery patient to another that alarm was raised about the
medically induced transmission of vCJD. Then, in 1998, prion protein was discovered
in the lymphatic tissue (appendix) of a patient who subsequently developed vCJD80.
When asked to account for the introduction of single use devices into anaesthesia 9,
respondents were clear about the role of the threat of vCJD transmission, and their
9 As noted earlier, the absence of any surgeons from the sample means we can only
examine the use of single use devices in anaesthesia. This does not imply that there
are no problems with the use of SUDs by surgeons.

63
increased awareness that prions remained on stainless steel surgical instruments
despite the decontamination process:
Well I think what prompted all this to happen was when they brought in single
use tonsillectomy instruments and things. And there was this big like ‘oh my
goodness’ you know and then we’re thinking, ‘well we’re working in exactly
the same area, why aren’t we doing anything, we’re just washing ours under
the tap and they’re having to spend millions on single use instruments’
(3ODP)
With new variant CJD coming to the fore and the risk of transmission through
tonsil tissue and any tube that’s going to pass them, hence that was mainly
the main spur for us moving to single use bougies, laryngoscope blades
(3TM)
Disposable laryngoscope blades are used in ENT cases due to risk of vCJD
and the presence of prions in tonsil region (4CDA)
Given the emphasis that has been placed on the threat of iatrogenic transmission of
vCJD, and other transmissible spongiform encephalopathies (TSEs), it is generally
agreed amongst clinicians that their “awareness of risk has become much higher
than it used to be” (2TM). They disagreed, however, about how ‘real’ or significant
the threat of iatrogenic vCJD, or any other disease, may actually be. Whilst one
anaesthetist considered that “clearly there’s a risk of transmission of diseases we
know about and I’m sure some we don’t yet know about, so single use would appear
to be the way to go” (2CDA), others questioned whether the extent of the actual risk
had been exaggerated:
I mean, we don’t know what size the risk was, but presumably there was a
small measurable risk there that is no longer there (6CDA)
Well before they went to single use was there ever a cross infection risk? And
the answer is no, because I don’t think there’s ever been a case of it, not
even for something like herpes or something like that. I don’t think that’s ever
been reported from one patient to another because they used to go and get
sterilised, sent back and that was it. So it wasn’t that they weren’t clean, we
used to clean them thoroughly after use, dry them and put them back….it’s

64
just creating more money for these companies that are jumping onto the band
wagon saying that something should be single use (4TM)
A number of authors have argued that there is “no firm evidence to indicate that the
reuse of SUDs ha[s] caused a health hazard”81,82. However, others have disagreed,
pointing to the long incubation period of prion related diseases61, and arguing that the
long term safety and efficacy of reuse is still unknown66. More recently, Walsh83 has
suggested that, if the risk from airway devices such as breathing circuits and
laryngeal masks had been significant, the consequences would have been visible by
now. Respondents frequently compared the ‘actual’ threat of cross contamination
linked with medical devices and everyday items, like china or cutlery:
If you’re eating with knives and forks in public restaurants that aren’t sort of
autoclaved in any way but washed as they are, you don’t see them, you’re
probably just at risk of getting anything as if you put a laryngoscope blade into
somebody’s mouth (5CDA)
It’s like you eat off a plate that somebody else has eaten off, it’s been washed
you don’t think “I need a new plate…” (7CDA)
Whilst discussing the influence that being risk aware had on their practice and use of
disposable and reusable equipment, respondents drew distinctions between the
know and unknown risk status of patients. For example:
Disposable laryngoscope blades are used in resuscitation, as the patient’s
disease status and risk level is unknown (4CDA)
Patients that generally aren’t screened come ‘off the road’, shall we say, like
our emergency theatre and our trauma theatre, and we change the
anaesthetic circuits at the end of each list. But those that are in a controlled
environment where we know their pathology or whatever else you’d like to
call it, we change at the end of each week (4TM)
Whilst respondents felt able to balance the risk of the known against the unknown,
there are dangers in relying too heavily on apparent evidence of a patient’s risk
status, as in the Middlesbrough case, where a CJD diagnosis was apparently
unanticipated. Instead, the instruments underwent a routine sterilisation cycle (known
65
to be ineffective in the decontamination of TSE proteins) and were used on a further
24 patients. Clinicians considered the risk status of patient A (diagnosed post-
operatively with CJD) to be known (initial diagnosis of dementia) but, with hindsight,
the patient’s risk status was unknown. During an interview for this study, an ODP
noted how a system relying on known and unknown risk status was inherently
flawed:
We do have disposables, we tend to keep those for infected cases where a
patient is known to be Hep B or you know. You never know, everybody that
walks into theatre should be treated the same because you don’t know who’s
got Hep B and who hasn’t (11ODP)
A further distinction between safety and exposure to prions was made by an ODP
who argued that exposure to possible cross contamination from a reusable device
was less of a consideration in an emergency situation:
If you’ve got someone that’s about to die, then sod the prions, you just use
the reusable (3ODP)
This ODP considered that when the small risk of keeping a patient alive by using a
reusable device, which might have been exposed to prions, was compared to the
probable fatality if the equipment were not used, the exposure was acceptable. This
example, as well as a similar case discussed later, was informally discussed with a
contact at the MHRA, who considered that the account provided by the ODP
demonstrated that an adequate risk analysis had been performed.
As these quotes illustrate, clinicians are concerned about the threats of exposure to
cross contamination, but, at the same time, are also aware that the risks might have
been overestimated. Those questioning whether the risk of cross contamination has
been exaggerated pointed to the discrepancy between the guidance issued about
the risk of cross infection with anaesthetic devices and that issued about surgical
instruments, and also to the inconsistency between different anaesthetic devices.
In 2001, the Department of Health published a circular directing that all
instrumentation used in tonsillectomy (lymphatic tissue) surgery must be single use,
following advice from the Spongiform Encephalopathy Advisory Committee (SEAC)
that there was a theoretical risk of transmission of vCJD22,84. Almost simultaneously,

66
the AAGBI issued guidance28, which suggested that anaesthetists should use single
use laryngoscope blades due to the proximity of the tonsils. While the Department of
Health guidance about the utilisation of single use diathermy equipment during
tonsillectomy was later withdrawn, following an increase in adverse incidents (post-
operative bleeding) and at least one patient fatality, the guidance to anaesthetists
remains in force. There is however some confusion about this. Whilst the AAGBI’s
Infection Control guidelines are still in place, advising the use of single use
laryngoscopes, documents from the Royal College of Anaesthetists imply that this
guidance has been withdrawn and encourage anaesthetists to use single use
devices only if they consider them to offer optimum practice85.
In contrasting the infection risks from facemasks and intubating devices, the
suggestion that the risks of medical devices and cutlery are similar, was repeated.
However, one ODP cautioned about devices inserted into the larynx:
I think things like anaesthetic facemasks I don’t, you know I’d be quite happy
to have one that had been washed thoroughly under a tap. You know, you go
into a restaurant and you have cutlery that hasn’t been through an autoclave
don’t you? But I wouldn’t want to use a knife that someone had shoved right
down into their larynx (3ODP)
The AAGBI28 recommends that anaesthetists use single use laryngoscope blades
because of the potential for cross infection, but similar guidance has not been issued
about single use laryngeal masks and bougies. As figure 4 demonstrates, both are
inserted into the same area as the laryngoscope (the larynx) and will carry ‘risky’
protein and biofilm past the tonsils83.

67
Figure 4: Positioning of laryngeal mask.
Source:
http://health.allrefer.com/health/epiglottitis-throat-anatomy.html
Source: www.brandianestesia.it/Images/LMA-ins.jpg
The inconsistency in advice was noted by an anaesthetist:
My personal opinion doesn’t matter because there is national guidance on
this, but my own personal opinion is that if you only had money for one thing,
continue to wash laryngoscope blades or you have the money to have
disposable laryngeal masks, I would go disposable rather than to
autoclavable laryngeal masks. And yet the dictates of contamination are that
that fits the bill but that is against national guidelines therefore it’s the other
way round ...If I had a choice between having a laryngeal mask that had been
shoved down forty other people or a brand new one I’d want a brand new one
put down me and then have it thrown away, because if you are talking
seriously about infection risks and protein contamination and you know,
variant CJD, then laryngeal masks are going to be prime bits of kit that could
potentially transmit it. And they are autoclaved, but as you well know,
autoclaving does not get rid of this specific problem (5CDA)
The discrepancy between guidance to anaesthetists and to surgeons was
emphasised by one ODP, who compared their inability to use a reusable set of
stainless steel Magill forceps, which, although used to assist intubation, are unlikely
to come into direct contact with any lymphatic tissue, with a surgeon’s ability to
undertake appendectomy and neurosurgery without using single use equipment,
despite the greater likelihood of exposure to prions:

68
Magill’s forceps: you could use reusable and
sterilise them like you do surgical instruments
but it’s the prion thing. But they’re still cutting
out appendix and you know that’s a prion risk of
doing neurosurgery without single use
instruments (3ODP)
The ODP’s reaction is understandable; Magill forceps are non-invasive devices, yet
are single use. In comparison, surgeons are able to reuse instruments which come
into close contact with areas of the body where prions are likely to occur.
It would seem desirable that more consistent and principled guidance should be
developed both within and between specialties working in operating areas.
The survey findings, of considerable confusion about the definition of the term ‘single
use’, were replicated in the qualitative interviews.
As noted previously, the official UK definition is set out by the MHRA6:
Single use - the medical device is intended to be used on an individual patient
during a single procedure and then discarded. It is not intended to be
reprocessed and used on another patient. The labelling identifies the device
as disposable and not intended to be reprocessed and used again.
We have argued that this definition is confusing and does not effectively distinguish
between a single episode of use and single patient use10.
• Some single use devices, such as stapling guns used in a bowel anastomosis
procedure, can only be used on a single episode. They are pre-loaded with a
number of staples, but once removed from the rectum cannot be re-loaded
and reinserted (single episode of use)
• Some single use devices, such as laryngoscopes are used to assist the
intubation and extubation of the patient, and may be used on more than one 10 The MHRA definition of ‘single use’ was altered in DB2006(04). We discuss this
alteration and what consequences it has for our argument in footnote 4 (page 29).

69
occasion in each of these episodes. Flowtron boots are anti DVT devices
which the patient wears for an extended period of time throughout their
hospital stay (single patient use).
Both types of event are covered by the same MHRA definition, which considers
reuse to have occurred only if the device has undergone some form of reprocessing
between each episode of use.
Our interviews confirmed the confusion about the difference between single use and
single patient use devices. In one Trust, for example, different interpretations were
held by the sterilisation manager and the theatre manager:
It’s a classic: the differences between single use and single patient use.
Really, it’s all single use in my view (6SM)
It depends on how the packaging is labelled; if it’s for single patient use or
single sort of anaesthetic gear could be used for a session, for a day and the
disposed of. As I say, it depends on what the items are (6TM)
However, as we show later when discussing device labelling, current provision is
inconsistent, notwithstanding EU CEN directives86. Moreover, our ergonomic analysis
(Appendix six) found at least one device where the packaging was labelled single
use, but the device itself was labelled single patient use (Figure 5).
Figure 5: Inconsistent labelling
Unlike the sterilisation manager quoted above, participants who were working in
theatres tended to prefer the definition that referred to single patient use:
SINGLE PATIENT USE
70
If it’s single use …..well to me, a single use means single patient use so they
would just dispose of it after the single patient use (8TM)
Respondents were suspicious of the basis on which devices were labelled as single
use. This was thought to be more a question of quality – that the manufacturer could
not guarantee that they would be fit for use on a second occasion or would withstand
reprocessing - than of the assessed risk of cross infection or contamination:
I think with the Flowtron boots that’s, it’s not always necessarily easy to see
what the issue is because that’s, it’s single patient use rather than single use,
and it’s that confusion isn’t it? There’s a single patient use and a single use
so you usually when you say single use it means that the company won’t,
obviously the company won’t guarantee that to be used again. Whereas the
single patient use what they’re saying is it’s the infection control or cross
contamination or whatever that’s the issue (5TM)
Our survey data demonstrated confusion over the lifespan of breathing circuits, and
we have previously discussed the history of this issue. The same confusion emerged
in the interviews about whether single use status was mainly intended to address
risks of cross contamination or infection or device malfunction.
Whilst some breathing circuits are labelled as single use, the instructions provided
with others state that the device can be used for seven days (see figure 10). We
outlined earlier in the report how manufacturers will guarantee the use of breathing
circuits for seven days if they are protected with a single use breathing filter, which
must be changed for each patient. However, one participant, who was generally
against the use of single use devices, considered this practice to be misleading and
diverged from the true meaning of single use:
We’ve got round the breathing circuit, single use, put it on, have a clean filter,
but we don’t actually change the breathing circuit except every week or every
X days when we decide. We sort of cheat, that isn’t single use. Yes it is
because we only put it on once (7CDA)
At the centre of this definition is a rationale that concentrates upon relative risk. By
using a filter with each patient, the risk of cross contamination is perceived to be
miniscule32 and so the apparent reuse of breathing circuits is justified. The filter

71
precludes any infective or hazardous particles entering the patient’s respiratory tract
from the anaesthetic gases32,33. However, when patients’ risk status is unknown, the
manner in which breathing circuits are used and replaced appears to change:
The manufacturer recommends that the circuits are changed weekly.
However, when used in our emergency or resus’ theatres, they suggest that
we should change them at the end of each day, due to the high-risk status of
patients (4CDA)
As might be expected in the current climate, the rationale for the use and limited
reuse of breathing circuits was governed by cost, and the need to balance
expenditure and risk:
I’ve not worked anywhere where a single use breathing circuit is used once
and thrown away, it just couldn’t be done, the Health Service would’ve gone
out of business years ago (4TM)
An average cost of a single use breathing circuit is approximately £8.00. By using it
in a manner meeting the definition of ‘limited reuse’, considerable financial savings
can be made. For example, one circuit used in a limited reuse fashion (i.e. over
seven days), with an average of five operations per day, 35 operations per week,
would save in excess of £280 in each theatre per week. Over a year this equates to
approximately £14,500 per theatre 11.
The management of the seven-day time limit for the use of breathing circuits
highlighted a potential system weakness. The following quotation illustrates how a
badly designed system could harm patient safety:
11 All pricing figures are taken from the NHS Purchasing and Supply Agency’s October 2004 catalogue.

72
Respondent: All the circuits we have are all date stamped as they’re put onto the
machines so in seven days’ time they’ll be changed and thrown away.
Interviewer: Is there a person whose sole responsibility it is to change them or is it
whoever sees it changes it?
Respondent: It’s the anaesthetic staff who change it. Sometimes it’s the night staff,
sometimes it’s the weekend staff.
Interviewer: Is there ever an opportunity where somebody might forget and it gets
left?
Respondent: It’s always possible. That wouldn’t be intentionally though (3TM)
Without an explicit procedure for changing the circuits, patient safety may be placed
in jeopardy. In the absence of a procedure, it is not clear whose responsibility it
would be to change the circuit. The circuit may not be replaced if an individual is on
leave, if someone forgets or if no one notices that the stamp is out of date.
If microbiological evidence suggests that breathing circuits can withstand limited
reuse, then any wording or labelling implying that they are single use devices should
be removed. Clinicians seem to need better education about the status of ‘limited
reuse’ and to develop appropriate Standard Operating Procedures to ensure that this
is monitored and enforced. However, we are also concerned that, in their present
form, the labelling and instructions concerning limited reuse are problematic.
We are not alone in voicing our concerns about the confusing nature of single use
device labelling or the use of the single use logo. The following table documents 14
definitions of ‘single use’ found during the study.
73
Table 20: Popular definitions of 'single use'
Named patient87
Single patient (X number of days) 87
Single patient (X number of separate episodes) 87
Single episode87
Single patient87
Single use87,88,6SM
Disposable89,90,91
Single patient, single procedure89
Suitable for one episode of use only92
A single use medical device is intended to be used on an individual patient
during a single procedure and then discarded65
Single use disposable93, 6ODP
Throw-away kit90
Designed to be used only once60
Reusable disposable www.ce-mark.com
Single use devices should be identified by the following symbol, which can replace
any wording to the same effect86,95.
Figure 6: Single Use Symbol.
The symbol, mandated in European Union guidelines86 and harmonised in the
Medical Device Directive4 and by ISO96, is considered to be reasonably intuitive (see
Appendix six for further discussion). However, the symbol in figure 6 can be
supplemented by the following three descriptive statements:
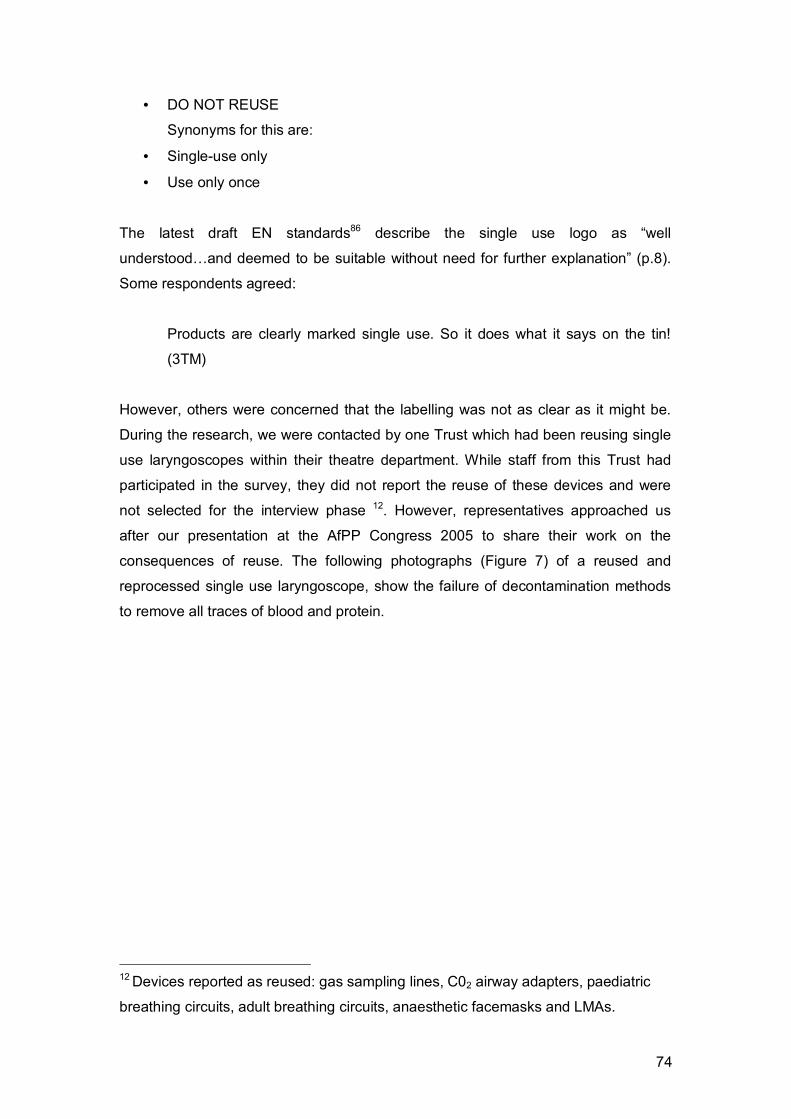
74
• DO NOT REUSE
Synonyms for this are:
• Single-use only
• Use only once
The latest draft EN standards86 describe the single use logo as “well
understood…and deemed to be suitable without need for further explanation” (p.8).
Some respondents agreed:
Products are clearly marked single use. So it does what it says on the tin!
(3TM)
However, others were concerned that the labelling was not as clear as it might be.
During the research, we were contacted by one Trust which had been reusing single
use laryngoscopes within their theatre department. While staff from this Trust had
participated in the survey, they did not report the reuse of these devices and were
not selected for the interview phase 12. However, representatives approached us
after our presentation at the AfPP Congress 2005 to share their work on the
consequences of reuse. The following photographs (Figure 7) of a reused and
reprocessed single use laryngoscope, show the failure of decontamination methods
to remove all traces of blood and protein.
12 Devices reported as reused: gas sampling lines, C02 airway adapters, paediatric
breathing circuits, adult breathing circuits, anaesthetic facemasks and LMAs.
75
Figure 7: Contaminated single use laryngoscope blade
Source: Rowley, personal communication 2006
It is not known how many times this blade had been reused and how many patients
may have been put at risk. However, as the images demonstrate, residual debris
(most likely to be blood and lymphatic tissue) can be seen on the blade. The reuse of
laryngoscope blades reported by this Trust was explained in the following terms:
We are using both reusable and single use versions and there is staff
confusion and lack of knowledge of the single use symbol and its implications.
This reported confusion and lack of knowledge of the SUDs logo endorses the recent
views of the MHRA’s committee for the safety of devices93, who described the
symbol as “misunderstood and confusing”. One anaesthetist explained:
Single use labelling is not obvious enough – for example, single use
laryngoscope blades look like reusable blades to the untrained eye. The
result of this is that reusable blades get thrown away, as they are mistaken
for single use devices. The solution is to colour code devices, as the single
use status needs to be visual and noticeable (4CDA)
SINGLE PATIENT USE

76
Colour coding single use devices to distinguish them from reusable equivalents was
suggested by other participants. If established, this would follow the precedent set by
the national colour coding of syringes and drug ampoules59,97,98. Indeed, some
hospitals had begun to source colour coded devices in a bid to differentiate single
use and reusable equipment:
The laryngoscope blades and things like that, if you held a reusable and
single use one up, you can hardly tell. What I’ve done with ours…is get a
yellow marking on it (3ODP)
Recently, Intavent Orthofix have offered colour coded laryngeal masks, to mark the
departments in which the device is used (Figure 8). Blue caps signify that the mask
should be used only in theatre, for example, and clear caps that it is single use
Figure 8: Intavent Orthofix Laryngeal Mask Colour Coding
Source: Intavent Orthofix.
However, respondents feared that design alterations would lead to price increases.
If you made people change things and make them a different colour all they
would do is they’d make them one or two pence more expensive, it would just
cost us more money (9ODP)
Yet, it was also appreciated that better identification of reusable devices would be
useful:
BLUE
LILAC
GREEN
YELLOW
CLEAR

77
Some quite expensive things have been disposed of by accident, because it
works the other way, because the piece looks single use, they chuck it (6TM)
Des-Côteaux et al99 had to abort their study comparing the costs of reusable and
limited-reuse laparoscopic instruments, as the reprocessable devices were mistaken
for single use and thrown away. Any initial outlay in developing colour coding could
be offset by savings from reducing mistaken disposal. However, manufacturers were
reluctant to ‘spoon feed’ customers (personal communication, Barema meeting,
February 2006). Colour coding was considered likely to offend some customers and
consequently damage sales.
Labels also contained contradictory advice. As one anaesthetist (4CDA) pointed out,
cleaning and disinfecting instructions are provided for the, single use, Eschmann
bougie (Figure 9).
Figure 9: Eschmann bougie: Instructions for Cleaning, Disinfection and Storage
1. Prior to disinfection, thoroughly
wash the introducer in an aqueous
solution of neutral soap, removing
all visible soiling. Abrasion should
be avoided. Rinse with clean water
and dry.
2. Immerse the product in a liquid
disinfectant prior to use according
to the manufacturer’s
recommendations.
3. Devices should be rinsed in sterile
water after treatment with
disinfectant solutions to remove any
residues before use
4. Between uses, the introducer should
be stored in its original container.

78
The technical data sheet also described how the bougie could be reused up to five
times following cleaning and disinfection, despite the presence of the SUD logo.
However, as figure 9 demonstrates, the Eschmann bougie itself (top image) does not
have any single use labelling, unlike the Portex single use version (bottom image).
Figure 10: Eschmann (Portex) and Portex bougies
Inconsistencies in labelling also arose from devices changing from reusable to single
use. One theatre manager recalled:
We had a problem in the past, and the problems that we have had is that
when companies have changed from reusables to single use, unless people
are very vigilant. Companies wouldn’t always let us know that it had changed,
and the people in stores weren’t educated enough in their use to know that
the two on the side were single use, and we had a problem with that (9TM)
As this quote suggests, the lack of recognition that the device had changed status
from a reusable to a disposable (or vice versa) was not seen to be a current problem.
However, the incidence of this type of situation points to the need for manufacturers
to keep purchasers and users informed and educated about any alterations. Whilst
Portex 15ch SIZES 6.0-11.0mm SINGLE USE
Eschmann UK 15ch sizes 6.0-11.0mm

79
the Chief Medical Officer’s Safety Alert Broadcast System (SABS) and the MHRA
Medical Device Alerts are suitable forums to publish such modifications, the
information does not appear to reach all members of staff who use the devices.
The communication of the idea of ‘limited reuse’ on breathing circuits clearly
presented particular problems, despite the efforts of manufacturers and the PaSA:
I think the only outstanding issue in anaesthetics is possibly the tubing, the,
and the tubing that’s used on the anaesthetic machines is a little bit
complicated because the company sell them on the basis, and they were
marking them single use but they were also putting in the advice on a card
saying that they could be used over so many days providing they were used
with an in-line filter…it’s a little bit ambiguous that because what is limited
reuse, what securities have you got that you change them? (2TM)
Anaesthetic circuits was the big grey area, and we follow the manufacturer
instructions now (7ODP)
Our circuits…have a seven-day life and that’s what the manufacturers say. If
anything comes up with a two and a line through it, then it’s used in that way.
All the circuits we have are all date stamped as they’re put onto the
machines, so in 7 days time, they’ll be changed and thrown away (3TM)
Analysis of two circuits from the manufacturer supplying hospital 3 illustrate the
problems with current labelling practice (figure 11).

80
Figure 11: Sample Breathing Circuits (Hospital 3).
These two samples, both manufactured by the same company, contain contradictory
labelling. The instructions for the circuit on the left describe how “the maximum
period of use is 7 days”, whilst the instructions provided with the circuit on the right
contain the single use symbol. Such inconsistencies continue to confuse clinicians
and may jeopardise patient safety.
Respondents were concerned about the potential risk from device packaging. This
included the difficulty of opening some plastic bags quickly in an emergency, and the
threat that pieces of plastic could occlude devices and cause an obstruction:
One thing that we have noticed is that these things come in plastic bags now,
and what can happen is that ODPs can connect up the tube with the
connector, pushing the plastic bag, and as they rip the plastic bag off, a bit of
it gets caught in it, and that can cause obstruction, and there have been
instances of those occurring, probably two or three, and now we have clear
tubes and you would think that you would see it, see the items and that would
maybe improve things, but nevertheless, it’s an additional connection and so
THE MAXIMUM PERIOD OF USE IS 7 DAYS

81
is an additional point where things might get into the system and can cause a
problem (6CDA)
The report of the Expert Group on Blocked Anaesthetic Tubing (EGBAT)100, set up
following the death of Tony Clowes, which was linked to an occluded component
within the anaesthetic circuit, identified the storage and wrapping of devices to be an
issue warranting further investigation. EGBAT recommended that devices should not
be opened prior to use and then stored away, where obstruction could occur (as is
believed to have happened in the Clowes case). Nevertheless, as the above
quotation illustrates, our data suggests that potential for occlusion exists even when
devices are opened at the point of use. The recent example of a blocked airway at
Hope Hospital in Salford again demonstrates the dangers associated with
anaesthetic equipment. In a case similar to that of Tony Clowes, a connector used
within the breathing system was occluded by the cap from an IV giving set (Figure
12) (Anon; personal communication, April 2006). Our argument here is not
specifically related to single use devices, but devices in general. Our data suggests
that simple patient safety lessons seem not to have been learnt.
Figure 12: ET connector and IV giving set
Our survey showed that SUDs are reused despite the MDA6 guidelines prohibiting
such practice. Such practice is neither unusual nor contained to the UK. Reuse has
been reported worldwide - a detailed inventory of published reports can be found in
Appendix one. Reused SUDs have included: diathermy pencils, laparoscopic
scissors and forceps, electrophysiological (EP) and cardiac catheters, snares,
sclerosing needles, pacing electrodes, biopsy needles and patient breathing circuits.

82
Reuse is considered to be ‘risky’ and to present dangers to the health and safety of
staff and patients. It may result in both physical and physiological harm68. Reports of
such harm include: a reused cardiac catheter that snapped and become lodged in a
patient’s heart, bacterial cross contamination of a reused cardiac catheter which led
to a patient’s death, and a case of iatrogenic Hepatitis B due to the reuse of a
contaminated blood sampling stick71. Many SUDs are delicate and intricate pieces of
equipment68. They have complex design features, such as small lumens or oblique
corners12,101. They are not designed to withstand decontamination and reprocessing
cycles and so may become impaired, damaged or weakened, and thus not function
efficiently, or as designed, on second and subsequent uses.
In addition to the 127 cases of reuse reported in the survey, we received an
additional 15 reports of SUD reuse during our interviews. Three of these
(laryngoscope, bougie and nasal probe) were based on experiences in the
respondents’ previous job. Devices reported as being reused are shown in Table 21.
Table 21: Reused single use devices
Specialist laryngoscope blades (1) Ambu bags (1)
Anaesthetic facemasks (1) Anaesthetic breathing circuits (2)
Blood pressure cuffs (1) Pressure infuser bags (1)
ECG leads (1) Magill forceps (1)
Anti DVT garments (3) Laryngoscope blades (1)
Bougies (1) Nasal probes (1)
The accounts provided by respondents in justifying reuse matched those identified
from our survey data and from other investigations55,64,102,103.
Reuse was overwhelmingly rationalised in terms of perceived costs and lack of risk.
If there were a bottomless pit of money in the NHS then I would be delighted
to use single use devices for everything and throw them away and get a new
one out each time (5CDA)
The perceived costs of SUDs largely reflect the purchasing price of the devices,
which is seen as prohibitive in the current state of NHS finances. Reuse was a cost
saving initiative:
83
The previous manager wanted us to reuse anaesthetic theatre masks and it
does say on them single use only. I think his main reason was just cost but if
it says single use it’s single use isn’t it? (13ODP)
What stands out from many of the examples of reuse
reported, both during the interview and survey phases of this
research, is how several of the items that are reused are non
critical, non invasive devices. Moreover, such devices may
previously have been reusable. Anaesthetic theatre masks
would have been run under a tap and/or wiped down by the
ODP and reused on subsequent patients.
Anti DVT garments are another example of SUDs whose labelling has altered.
However, as the following data extracts demonstrate, following their re-labelling,
many hospitals have not had the infrastructure to use the devices effectively outside
of the operating theatre.
We did used to reuse them unless they were contaminated obviously and
now we just leave them on the patient, they go back to the ward, we’ve got
much better systems so they do go back to the orthopaedic ward with them
on. Because initially when we went over to using them as single use, we’d
put them on the patient and they didn’t have pumps up on the ward, so then
we’d be throwing them in the bin and at £19 a pair, when you’ve got a
throughput of 10,000 patients, it’s an awful lot of money (3ODP)
The only things we currently reuse that was designed for single patient use
are anti-embolism devices, DVT prevention stuff. However saying that,
recently recovery have now bought a load of DVT pumps so the, once the
patient is on the table we put the DVT stockings on they then can now go to
recovery and keep them on. So they’re at least not thrown away at the end of
an operation, they can still be used throughout the entire patient’s visit so it’s
not a waste of money (2ODP).
The reuse of such devices is apparently based on an assessment of the cost of
continually replacing the equipment. However, these accounts also imply that there is
little risk involved. These garments are unlikely to come into direct contact with the

84
clinical site. They are made of nylon and can be washed/wiped if required. Moreover,
as the quotations show, staff will discard these devices if they are visibly
contaminated.
One Trust had formally risk assessed the contamination/infection threat provided by
anti DVT garments (Flowtron boots), and decided that, if patients wore anti-embolism
(TED) stockings, then reuse could be sanctioned:
The main one for us is the Flowtron boots, it was decided with Infection
Control that we if we put an inner lining to those, to those Flowtron boots that
you know it would still be okay to use them in-between patients and to throw
them away at the end of the week, or at the end of the day (5TM)
This Trust reported that any decisions related to service delivery and medical devices
were based on an assessment of five criteria shown in table 22:

85
Table 22: Benefits / Impact of Service Change
Service Delivery/ Business Impact
More patients being treated more quickly
More patients treated
Faster turnaround
LOS (length of stay) reduced
Waiting times reduced
Follow ups reduced
Reduction in unnecessary admissions or
appointments
Reduces DNAs
Innovation in Deployment of Staff
Extending roles
Sharing tasks between
team members
Extending availability of
services
Financial Impact
Contribution to improved financial position
Meets recurrent balance
Meets CIP
Cost avoidance
Increased productivity / reduced costs
Clinical Outcomes
Higher Quality Care
Access to appropriate
care at right time and
place
Intervention – timely
Increase clinical care time
Eliminate unnecessary admissions
Reduce:
1. complaints
2. adverse incidents
3. drug errors
4. infection rates
5. morbidity / mortality
Compliance with national targets (NICE,
NSFs etc)
Staff Experience
Knowledge and skills
framework
Aspirations – opportunity for
professional development
Enhanced roles
Better Morale
‘Managed’ activity
Reduce fire fighting
Recruitment and retention
Implementation Consistent with IWL
Staff involvement (FT+)
Partnerships, teams
Making better use of skills
Contribute working time directive
Patient Experience Better Team work (breaking down barriers) Access (waiting times) Shorter LOS Fewer handoffs Reductions (unnecessary visits, admissions, cancellations) Information and communication Choice Soft issues
86
The balance between cost and lack of risk is central to the reuse debate:
We reuse blood pressure cuffs all the time but we do
clean them here in between patients. We have a box
full of ones that have come off and a box of clean ones
so I think that’s good that we do that. Same with ECG
leads, we clean it all before we reuse them. But again
then that has impact, I know it sounds silly but it has a
time impact because it takes time to clean all these
things (13ODP)
Whilst this respondent rationalised the reuse of blood pressure cuffs in terms of
financial savings (Single use approximate cost: £18.00; reusable approximate cost:
£77.0057), the cost of the time taken to ‘clean’ them, diverting staff from other tasks,
must be taken into account. The second respondent’s attempt at balancing the cost
and perceived risk against reuse, involved rejecting the single use nature of the
device:
Blood pressure cuffs they’re supposed to be single use but we don’t count
them as, you know they’re only on the skin. You know, if we reused
everything it would cost a fortune and we’d never have it, because we’d never
be able to replace them (2ODP)
As the last quotation suggests, respondents perceived that, if the device was only
touching the patient’s skin (as with a blood pressure cuff or anti DVT garment), then
there was no reason to use the device on a single occasion only. Other cases of
reuse were defended in similar terms, although these devices did not come into
contact with the patients’ skin:
Items like pressure infusor bags are meant to
be single use but we reuse them. Obviously if
they are contaminated in any way they get
thrown, but we do reuse them…because they
just hold a bag of fluid; they don’t go near the
patient, so we assume we can reuse them
(11ODP)

87
As the above illustration shows, pressure infuser bags have a plastic bladder that
acts as an external sleeve, which can be inflated to increase the pressure with which
intravenous fluid is administered to the patient. The device does not need to be
sterile and is unlikely to come into physical contact with the patient. At a
commonsense level, it is easy to understand respondents’ claims that reuse poses
little or no risk. We cannot comment on the validity of this claim but, if it is correct,
there may be an argument for reviewing the classification of such devices.
Taking single use devices straight from their packaging means that clinicians have a
consistent expectation about the device that they are handling. Unlike reusable
devices, which can experience fatigue, general wear and tear, and can become
damaged during use and the reprocessing cycle, single use devices should be fit for
use 100% of the time. Three participants confirmed this, and explained:
You know if you’re going to open a disposable one it’s going to be pukka (4ODP)
Generally speaking, a disposable single use is better than a non-disposable
500 use (11TM)
Well we have diathermy, finger switching diathermy, they cost quite a lot of
money to buy originally, we have to reprocess them and all of the
manufacturers say it will last this long and invariably they don’t…. you know,
you can only lean on people and sort of encourage them towards using these
things single use but it’s their decision. I mean it’s, I’d say diathermy as an
example, a finger switching diathermy you can buy for £1.50. We will buy one
for £100 and if we use it forty times that’s £2.50 a go isn’t it so that’s already
more expensive. Then you add on the cost of cleaning it, the cost of a tip
each time, the cost of reprocessing it, unpacking it and it’s just ridiculous. And
the other thing is because they break down we end up with a situation
whereby the surgeon will plug in a machine and say “it’s not working, it’s not
working, the machine is not working”, and we’ll be like “no, no the machine
was working fine, it’s probably the finger switch.” Well you know they cost
100 quid but chop it in half and throw it in the bin, get another one because
the patient is bleeding. You can’t stand there having a debate….get another
sterile one and have a go. If you have a single use one and you plug it in and
it don’t work you can then go back to the people who make it and you can say

88
“right, you know you’re selling pants,” but that’s, that’s how I would do it
personally (9ODP)
However, it should not be assumed that workable equipment was necessarily
perceived as high-quality equipment:
Sometimes they may say that this is a single use device and it’s comparable
to a reusable one but obviously a lot cheaper and it’ll, the actual quality of the
device is not always exactly the same and straight away on usability and
appropriateness it’s sort of you know not used (5TM)
While this should not be read as condemning the quality of all single use devices,
there is a potential problem, for both the health service and the device industry, from
the perception that devices have been designed to minimise NHS costs at the
expense of quality and efficacy. For example:
Sometimes I think you might worry about the strength of things, as things are
often cheaper (6ODP)
Some of the single use items obviously because they’re single use, they’re
cheap and they’re not quite as good a quality as other things (13ODP)
There is pressure on the stores manager to get things as cheap as he can.
We’ve had one or two instances where he’s brought something in and then
everybody just turns round and says “Its pants, I’m not going to use it, its
rubbish, get the old ones back,” and he doesn’t have a choice (9ODP)
A particular concern was the perceived ‘under engineering’ of plastic laryngoscope
blades. Traditionally, metal (stainless-steel) laryngoscope blades have been used by
anaesthetists to assist with the induction of anaesthesia. The patient’s mouth is kept
open whilst an intubating device (such as an endotrachael tube or laryngeal mask) is
inserted. However, whilst satisfying the objective to minimise the risk of cross
infection of TSEs from one patient to another, the quality and suitability for purpose
of the disposable blades has been criticised48,49,105,106. In this study, one anaesthetist
commented:

89
Plastic [laryngoscopes]…are in fact under engineered, they’re actually not
up to the job (2CDA)
Others also picked up the notion of unsuitability. Respondents spoke of their
dissatisfaction with the quality of the blades. One anaesthetist recalled how:
The original laryngoscope blades that came out, they were quite cheap…and
the plastic blades were just bloody dangerous, because they just contorted. If
you got a difficult airway and you lifted it, it just bent across (6CDA)
However, it was not only the plastic blades that were criticised for their unsuitability:
similar criticisms were also made of disposable metal blades. One theatre manager
described how their discontent with single use blades had led to them to return to
using non-disposable metal blades. This was despite recognition that reusable
blades present a risk of cross infection due to the inability to remove proteinaceous
material from stainless steel:
Laryngoscope blades, because of the scare with CJD, we were told we had to
use disposable single use laryngoscope blades. So we ordered a load of
them, even though they were made of metal they were rubbish because they
were flexible….so in that instance, the single use wasn’t as good as the
autoclavable version, so we’ve stuck with the autoclavable (11TM)
For these clinicians, disposable laryngoscope blades were perceived as providing a
greater threat to patient safety from iatrogenic injury than from cross infection. If the
blades were to slip, contort or flex unexpectedly, the patient’s larynx could be
damaged. Concerns regarding perceived differences in the efficacy of single use
laryngoscopes compared to reusable devices were also voiced by another
anaesthetist:
It’s okay if it’s an easy intubation but then you know that’s not really the issue
it’s, the problem is the one whatever it is that’s actually a bit more tricky,
requires a bit more force and sometimes, but not always, but sometimes it’s a
life, you’re in a life critical situation and you can’t have your equipment not
being up to the job, you don’t know which of the patients that will happen in
so you have to have an instrument that’s going to be able to do it for every

90
patient unfortunately. And I’m saying unfortunately because that means
slightly more cost implications (2CDA)
There seems to be a distinction between equipment that is acceptable for use with a
routine patient, and equipment that is incompatible with difficult cases. However,
when treating difficult cases, participants felt that they did not have time to source
alternative equipment, but wanted to be able to rely on the devices to hand, and so
often turned to reusable kit:
It’s nice to know that you’ve got the back up of the emergency reusables,
handy for safety reasons. Because every individual can do very strange
things suddenly in an anaesthetic, so I think it would be very foolish to go
over. It would be very foolish to get rid of all the reusable laryngeal masks
(3ODP)
These comments reinforce Twigg et al’s107 warning about the need for equipment to
be fit for purpose. One anaesthetist commented:
Sometimes I think ‘I’m using this single use laryngoscope blade and I don’t
think it’s as good as the one I would like or it isn’t shaped in exactly the way
that I’m used to’ and therefore my practice is probably inferior to what it would
be if I’d got a re-sterilised laryngoscope (7CDA)
Whilst the use of single use laryngoscope blades was mandated because of the
theoretical risk of cross contamination from prions, the unsatisfactory quality of some
laryngoscope blades has resulted in actual risks to patients’ health and safety.
Hutton108 described how:
New, inferior equipment has now claimed its first victims and the real danger
of responding to theoretical risks in the face of practical experience has been
exposed. The message is clear: hypoxia threatens life in minutes,
haemorrhage in hours and tonsilla prions (maybe) in decades.
Disposable laryngoscope blades were also criticised for their inadequate light source.
Two anaesthetists explained:

91
There have been some queries about the quality of some single use
equipment. The [laryngoscope] blades aren’t quite good enough to offer you
as excellent a view as you might wish in difficult patients, but I know the
quality of them has improved quite a lot (5CDA)
Single use laryngoscope blades led to a higher risk of failed intubation, as
plastic blade was more flexible and had a poorer light source, but disposable
blade is in the patient’s best interest in terms of risk transmission (4CDA)
Rassam’s et al’s109 evaluation of 20 Macintosh type laryngoscope blades included 19
single use blades sourced from different manufacturers. Anaesthetists were asked
about the quality of illumination given by each blade, their satisfaction with the
resultant view, and their perception of clinical appropriateness. Two plastic single use
blades were found to have a poorer illumination score than the others, and one of
these blades was also found to result in an inferior view that was perceived as being
a disadvantage in clinical use. The illumination quality of laryngoscopes is clearly
important, as a difficult view of the larynx is associated with increased morbidity 108,110.
Many of the respondents criticised single use devices in terms of the potentially fatal
outcomes from the use of ineffective equipment. The strongest criticism related to
single use bougies:
With regards to the bougies, I know there are new bougies which cost a fiver
compared to the £85 gum elastic ones, which look similar, but I have to say,
they don’t function similarly at all. And one of the areas that we are unhappy
about is that the gum elastic bougie has been replaced by a plastic thing, and
I am slightly concerned that they get put back and somebody thinks of
washing those out and using them again. We do say that they are disposable,
but they certainly don’t function as well: they’ve got flat ends as opposed to
the parabolic ends, and they don’t have the nice characteristics of bendy and
then gradually take the shapes of things, so if you bend it, it manages to get
into position and smoothly glides in, but this one flatly doesn’t want to go in,
and in slightly straightens as you put the [endotrachael] tube over it, so the
older one did function significantly better. The new ones could potentially
present at problem (6CDA)

92
The altered design of bougies led participants to describe them as ‘substandard’,
‘dangerous’ and ‘awful’. The main area of concern, as implied in the quote above,
was the single use bougie’s failure to retain its memory of shape. One ODP
compared the efficacy of the original, reusable gum elastic bougie (Eschmann) and a
single use bougie:
They’ve got memory on them…. the gum elastic Eschmann [now Portex
Venn] one, and Cooke have got one as well, they’re blue, and basically when
you bend them up if you’ve got a very anterior larynx, when you bend the tip
up by the time you put the laryngoscope in you want that bit to stay in the
position and with the Portex [single use] one, they’re just urgh. A lot of the
anaesthetists still keep them in their briefcase, their gum elastics, you know
it’s just their little security blanket (3ODP)
The inability of the single use bougie to retain its memory has been acknowledged,
and the Portex device deemed inappropriate for use as an intubation aid111. Wilkes et
al112 found that single use bougies tended to be stiffer than their reusable
equivalents. Annamaneni et al113 compared the ability of single use and multiple use
bougies to retain their shape, and found that multiple use bougies were superior
(figure 13). The authors demonstrated the bougies’ ability to retain their shape via a
time-motion image captured over four seconds:

93
Figure 13: Time motion capture of memory retention of single use and multiple use
bougies113.
The manufacturers recognise that the performance of the reusable bougie has been
difficult to replicate in the single use equivalent114.
Concern was also expressed about the quality of anaesthetic breathing circuits. One
anaesthetist compared the ‘sturdy’ quality of old-fashioned circuits with the ‘flimsy’
tubing that is now used:
I think things like anaesthetic circuits, there clearly has been a change from a
very sturdy horrible black rubber stuff that was sort of just going out when I
first started anaesthetics but now has completely gone, to what we have now
which are very flimsy circuits and in fact actually are kept on machines for a
week. I don’t know if they’re supposed to be single use or not but they are
kept on for a week here (2CDA)
The fragility of breathing circuits has recently been noted by the MHRA115 in
MDA/2005/062, which warns against the entrapment of breathing circuits between
the operating table and patient transfer trolley, following one patient fatality and
hypoxic brain damage to another.
Similar comparisons were made between the robustness of other disposable and
non-disposable devices. For example, the original LMA developed by Intavent

94
Orthofix, was considered to be the gold standard, with respondents describing how
“nothing is as good as the reusable to be quite honest” (3ODP). Compared to the
original LMA, which has a “plastic balloon on the end of a tube [compared] to a nice
soft latex one” (4ODP), laryngeal masks developed by other companies were
reported to vary in design details and to be made of different materials. These
differences have resulted in clinicians perceiving the masks to be bulkier, which
resulting in tissue trauma and damaged teeth, as well as not producing as good a
seal as the original LMA. One anaesthetist explained:
Certainly some of the laryngeal masks that we are using now, compared to
the original design which looked like it was latex, but in fact wasn’t, it was
made of slightly softer material, the plastic ones that we are using now are
much cheaper, but also they do appear to be much cheaper and there is a
small risk of not getting as good a seal, of causing direct trauma, especially if
people are worried about knocking teeth out with them, as they are bulkier to
put in (6CDA)
Anaesthetists were not solely concerned with the threat of tissue trauma or damage
to the teeth. One anaesthetist was vehement in his assessment of single use
laryngeal masks:
Disposable laryngeal masks can be dangerous and can deform if the patient
has a difficult airway (4CDA)
The materials used in devices also influenced clinicians’ views of a lack of risk in
reuse:
Things like metal Magill forceps that are single use and I know that you could
use probably them more than five times….It can be autoclaved because it’s
metal firstly, it can be cleaned because it’s a smooth surface and they’re not
used in a way that could, if they were damaged it wouldn’t harm the patient.
So I’d be quite comfortable with doing that. Because it’s metal and it’s robust
and there’s nothing electrical on it that can go wrong, there’s nothing on it that
can harm the patient, it’s two pieces of metal with a bolt in the middle of it so
it’s not going to go wrong (11TM)

95
However, whilst devices such as Magill forceps are made
from a metal composite, they are not designed to be reused.
Lower grade composites are used due to the single use
nature of the devices, and consequently, it is possible that
they might fail as a result of being autoclaved. Moreover,
there are small areas on the device that may retain tissue or
blood debris if the device came into contact with the clinical
site or other used instruments.
Despite these specific criticisms, there was a general satisfaction with the quality of
single use devices. Although clinicians might have reservations about device
efficacy, most respondents insisted that, in terms of infection control, the use of
single use devices was in patients’ best interests. This contrasts with findings from
previous research that found anaesthetists reluctant to change from reusable to
single use devices because of concerns about possibly sub-optimal quality116.
In some cases, reuse was sanctioned because of the need for emergency treatment:
There is urgency when a patient needs
an Ambu bag; it is therefore kept
unwrapped. However, as recovery is
unlikely, potential germs and dirt from
unwrapped kit are less of a concern
(9ODP)
This respondent reported throwing away SUDs which had been unused in theatres
but left unwrapped, claiming “a lot of things we end up wasting because if something
is opened, personally, that’s used. I don’t know where it’s been, if I can’t, if I didn’t
open it and I don’t know it’s safe then I chuck it in the bin”. Yet in an emergency
situation, this policy was overridden: the patient needed to be ventilated, and the risk
of hypoxia outweighed the risk of cross infection, echoing Hutton’s120 comments.
However, our respondent also pointed out that the patient was unlikely to survive, so
action with a risk of iatrogenic cross infection was acceptable, if their life could be
saved. Nonetheless, it is not only the risk of cross infection and contamination that is
an issue. We have already referred to the blocked anaesthetic tubing incident at

96
Chelmsford and the potential hazard of foreign bodies becoming lodged in devices
left unwrapped prior to use.
In other cases, reuse was blamed upon a lack of clean equipment and delays in the
sterilisation process. This was especially likely when the supply of certain devices
was limited:
We still have in the Trust laryngoscopes that are specific to situations so
you’ve got different types of laryngoscopes, like McCoy laryngoscopes,
you’ve got polio blade laryngoscopes all of which are, can’t be thrown away,
they’re too expensive so we still have to wash them. I mean in an emergency
situation we would have to wash then put them straight back into use,
otherwise we send them to CSD and they get washed and sterilised and then
brought back to us. We have to gauge every situation on its merits, if you
know you’ve only got one of them it’s not safe to let them go out of sight for
basically six hours until we get it back (2ODP)
Problems and delays linked to the turn-around time for sterilisation departments were
present in many of the accounts received from staff employed in hospitals that still
used reusable laryngoscopes:
We have had problems with the CSD turn around time so we’ve been running
out of laryngoscope blades…they’re sent to the CSD after each patient, so of
course then we’ve got to wait for them to be turned round to get them back
into the department (11ODP)
The CSD turn around time varied according to whether the sterilisation department
was onsite (3-4 hours) or off site (24-48 hours). Given this delay, in addition to the
possibility that devices may be damaged during the sterilisation process, and the
likelihood of general ‘wear and tear’ of devices, extra equipment would be needed to
manage the gaps that would arise117. In turn, this will have cost implications.
The use of single use devices is frequently criticised in terms of the perceived waste
and environmental impact from disposing of equipment after just one use. Collignon
et al’s12 study of Australian healthcare facilities found that reuse of single use devices
was justified by respondents in relation to the minimisation of waste and
environmental concerns, whilst Smith and Berlin118 argued that reuse of single use

97
devices has been driven by the financial cost of disposing of increased volumes of
medical waste.
One issue may be whether certain devices are unnecessarily labelled as single use.
For example, single use laryngoscopy equipment is available in two formats: a single
use blade (Figure 14), which is connected to a reusable autoclavable handle (ade Figure 15), or a single use laryngoscope, in which both the handle and the blade are
disposable.
Figure 14: Single use laryngoscope blade Figure 15: Reusable laryngoscope handle
Respondents questioned whether all parts of the laryngoscope needed to be
disposable:
We have the whole thing, handle and everything. And I think they’re very
wasteful personally, and I think it’s something that we will review in the future
(2TM)
Well laryngoscopes certainly, a very important piece of our equipment, it’s not
only the blades now the whole damn thing is thrown away (7CDA)
The language of waste was also used in relation to devices like infuser bags and
blood pressure cuffs which, as discussed earlier, are unlikely to be in contact with the
clinical site or contaminated with blood or other infective agents:

98
It’s such a waste of money. If you have one of these [pressure infuser] bags
per patient, sometimes you can be using two or three bags per patient, if
they’ve got you know, a number of IVs up, you can be using them, but it’s
such a waste, it really is (11ODP)
Unlike laryngoscopes, pressure infuser bags could simply be wiped down by an
ODP. The single use nature of the device was therefore treated with scepticism, in
accord with Stewart’s119 analysis in the course of a discussion of the ‘spurious
labelling’ of some single use devices:
Disposable pressure infuser: This consists of a bladder with an external
sleeve and an inflating bulb. A plastic bag of sterile fluid for flushing an
artery or other vessel is placed inside the infuser sleeve and the bladder is
inflated. This insider of the sealed bag is sterile; the external surface which
is in contact with the infuser sleeve does not need to be sterile. The
potential for nosocomial infection from this device is probably less than that
of a blood pressure cuff.
The rise of single use devices was certainly seen by some respondents as an
extension of a negative feature associated by them with modern consumer societies:
It’s just a throwaway society isn’t it, I mean, that’s what everyone wants, its
convenience (4TM)
It’s so wasteful, largely unnecessary. I don’t know what the next generation
are going to think of us wasting all these valuable resources and throwing
them away….the earth will run out of resources and the next generation will
be appalled (7CDA)
A secondary outcome from the use of single use devices is the environmental
pollution caused by their destruction109,119,120. The majority of single use devices are
made from plastics or lower-grade metal, and must be disposed of via landfill or
incineration:
I do worry about the environment as well you know which is a negative, you
know the amount of rubbish we throw out is just incredible. It is all plastics
and not biodegradable….it’s not very eco-friendly (3ODP)

99
Well it’s all incinerated and clearly that adds to our environmental pollution
(2CDA)
Cook120 asks whether such a disposal strategy is environmentally responsible, while
the World Health Organisation121 has called for the impact of environmental exposure
to healthcare waste to be minimised. However, the environmental risks or hazards of
disposing of single use devices were contrasted with the threat to patient safety if
such devices were not used:
I know it’s not good for the environment particularly….[but] because of the
CJD most anaesthetic invasive things are around that dangerous area that I
think it would be going backwards to look at reusable (3ODP)
It does seem a shame that this metal is then, goes to the furnace and can’t be
recycled but that’s the way that it is at the minute. It can’t even be melted
down and you know re-extruded or something else but the fear is over you
know disease transmission that we don’t know about I guess, though what
could survive flames I don’t know (2CDA)
The environmental impacts of using single use devices, whilst unfavourable, were
considered by the majority of participants to be tolerable compared to the risk of
iatrogenic infection and the threat to patient safety.
Whilst we have no evidence to suggest that reuse of invasive single use devices is
occurring in the NHS because of the current financial situation, such a practice has
been reported from the USA122,123,124. Cost was however, an influencing factor in
purchasing decisions. Many respondents felt that the cost of the item held more sway
in Trust decision-making than its quality or clinical effectiveness. One theatre
manager described the decision-making and procurement process for purchasing
new devices:
The first driver to what we do is cost, that’s the first thing we look at. Then we
look at how effective the product is second after that (11TM)
Such a scenario however, is not unique to our data or the present period of financial
difficulty for the NHS. Discussing data collected between 2003 and 2004, McDonald
et al125 highlight the discrepancy between cost and quality of goods. They cite a

100
hospital manager, who explained that staff knew they were “working with sub-
standard equipment….we are all under pressure to keep our budget in line” (p.190-
191). We received similar accounts from clinicians in this study, all of whom were
critical of the need to contain costs, regardless of whether the device in question
represented good value. To reinforce the argument, one ODP even compared the
Trust’s purchasing patterns with a particular supermarket brand that is known to offer
cut-price bargains as well as generally lower priced goods:
We have to go with the cheapest option…I call us the ‘Netto’ of the NHS
(11ODP)
We just go for the cheapest all the time, the cheapest, the cheapest but it’s
not always the right way to look at it you know. Something might be cheaper
but it might only last half as long (13ODP)
This last quotation reinforces one of the most important findings of this phase of the
study: the relationship between cost and value or quality.
Participants perceived that single use devices were more expensive pro rata than
reusable devices. For example, a single use laryngeal mask costs approximately
£6.50 and a reusable one, which might be expected to be used up to 40 times, costs
£62 13. Such a price differential influenced the hospital’s decision regarding what
equipment was available for use:
We would prefer single use things, but there are problem with the cost of it
(7TM)
We thought long and hard about reusables verses disposables and we
moved down the route of trying to use disposables for everything. The thing
we found with laryngoscopes is the cost implications of that are phenomenal
really. Disposable blades really are prohibitively expensive (4CDA)
We’re still on reusable laryngeal masks because you know it’s the cash, yeah
you get probably triple the value out of a laryngeal mask, a reusable one
13 All pricing figures are taken from the October 2004 edition of the NHS Purchasing
and Supply Agency’s catalogue57.

101
about £90 and a single use one £4, £5 and you can understand why we do
that at the moment (6TM)
The perception that reusable devices offered greater financial value is based on the
logistics of repeatedly purchasing and disposing of single use devices. However, this
perception is frequently misinformed. When the full lifetime and organisational costs
of each device are factored into the financial equation, single use devices are
unlikely to be any more expensive than reusable devices, and in some cases may
actually be a cheaper option. Given the compartmentalisation of hospital budgets,
few units actually ‘see’ the real costs of reusable devices, as, once they leave the
operating theatre, they are ‘out of sight’ until returned clean and ready for use.
Device users will not experience the costs incurred in decontaminating a reusable
device (including transport of equipment, decontamination, cleaning, sterilisation and
repackaging and return to local storage) or shuffling operating lists so that the
required equipment is available. Many respondents only considered the immediate
purchase price of single use devices rather than the total lifetime or organisational
costs of reusables. For example, if a laryngeal mask could be bought for £5 and
reused on a second occasion, then £5 would have been saved. However, even a
relatively crude analysis demonstrates that single use devices may actually present a
cheaper option, as money is not spent on reprocessing:
There is an increasing trend to get more and more single use. There’s often a
financial implication behind it (7ODP)
More and more has been single use just by the mere fact of all
decontamination issues are reprocessing issues that items would create and
so that you know it’s almost becoming cost neutral when you actually weigh
both up (3TM)
£5 a use [for a single use laryngeal mask] is actually very good, it compares
very well with the reusable mask that costs I think over £100 because they’re
never actually used the forty times they could’ve been used because for
some reason it would been lost to the system and then on top of that you
have to add the cost of autoclaving, packing and what have you so clearly £5
for a single use is great (2CDA)

102
Additional expenses incurred with reusable devices may also include the disruption
caused by the return of damaged or broken equipment from the CSD, which is unfit
for use. This may cause delays and cancellations, which result in unused theatre
time and staff and, possibly, extend the length of in-patient stays, with additional
costs and risks. Lastly, reusable equipment rarely seems to last as long as its
designated lifespan, which appears to be calculated for optimal handling and
reprocessing conditions rather than average experience. Reusables either get lost or
sustain general wear and tear that compromises their usability:
One of the problems we had with laryngeal masks was that they never seem
to get to 40 usages by the mere fact they get slung in bins, they get
damaged, the cuffs get split or they just disappear into the ether and that’s
one of the reasons we look for, to move into single use masks because like if
you’re not getting the full life out of the whatever product either you’re using it
incorrectly or clearly if stuff is getting damaged and disappearing we never
knew where they disappear to (3TM)
Things like laryngeal masks, they don’t go in a black hole – they get taken out
of the Trust. In this Trust alone, an event happens and all the laryngeal
masks disappear, as the consultants go off to the VIP tents with them. At the
same time, you can’t really use them for 40 times. You can’t really clean them
the first time, let alone the second, third or fourth (6SM)
This last quotation re-emphasises concerns about the degree to which reusables can
be adequately cleaned and decontaminated. However, until clinicians have a more
accurate perception of the lifetime and organisational costs of reusable and single
use devices, the balance between cost and benefit is likely to be set at an
inappropriate point.
Variations in the perception of risk also affected the trade-off between costs and
benefits. Where participants thought that the risks had been exaggerated, as
discussed earlier, they were more reluctant to incur the perceived costs of single use
devices. SUDs were not seen as the most cost-effective investment for protecting
patients against iatrogenic infection:
I mean the amount of money we spend on disposal anaesthetic equipment
could be better used on patient care in other areas that’s for sure. I mean I

103
think in the history of anaesthesia there’s never been any major
recontamination of a patient from the breathing circuit (4TM)
Another anaesthetist spoke about the exaggeration of risk and compared the
risk/benefit ratio of infection prevention and single use devices to the policy of placing
cardiac defibrillation equipment at rail stations:
We do risk analysis and try to relate it to reasonable risks and reasonable
costs of procedures, and certainly we use various constraints to what are
reasonable risks and you can use things like ‘numbers needed to treat’, or
you can do it as ‘costs per patient per beneficial life afterwards’, or ‘quality of
life adjusted indicators’. So there are ways of doing these things. I mean, this
is a demonstration of the fact that this current Government has decided to put
defibrillation things at all railway stations in case anyone has a cardiac arrest.
It gets good press, but actually you need to spend about £300 million to save
a person (6CDA)
These respondents thought that a disproportionately large financial outlay was being
made for the health gain achieved, rejecting Webster’s126 argument that “the cost of
a single case of significant iatrogenic harm that would pay for a great deal of patient
safety”. Other respondents were more risk averse, and echoing Webster, considered
that the cost of safety outweighed all other costs:
If safety means you need single use, then you must use single use regardless
of cost issues (4CDA)
I think the biggest thing, ignoring the cost, is that if it is going to benefit the
patient, then you must use single use (7TM)
The patients have to be a priority in everything, from my point of view,
regardless of the costs, because that’s what we’re here for. If we need to
change anything, then it has to be right for the patients. That may then lead to
funding issues (9TM)
Despite the financial implications, one Trust even went as far as using a reusable
orthopaedic cannulated screwdriver as a single use device as the sterilisation

104
department could not guarantee that it would be contaminant free due to its small
bore:
A lot of the instrumentation we use, say for putting screws into feet, they
should be more than one use but we have found with our CSD, who sterilises
our equipment, that because the equipment was so fine bore that they
couldn’t guarantee the cleanliness, so we’re now using those instruments,
that should be used time after time, as single use instrumentation now. It
might bump costs up a bit, but at least we are sure that there is no
contamination going into patients (6ODP)
The device in question was reported to cost in the region of £200, but was being
discarded after just one procedure.
These quotations reflect the typical perception that single use devices are indeed
safer than reusable equipment, although they also demonstrate the common
reluctance of practitioners to recognise the need for cost/safety trade-offs. Whatever
qualifications they introduced, most respondents were quite clear that the use of
disposable devices was in the patient’s best interest, and typically referred to this as
‘best practice’:
For patient safety, it is probably the only alternative (2CDA)
We prefer to stick to single use, I think that’s best practice really (3ODP)
I think we have an obligation to do the best for the patient (9TM)
As a result, respondents looked to use single use devices wherever possible:
I think the more we’ve got, the safer it is for patients (6ODP)
Respondents rationalised that if they, or anyone close to them, were the patient, they
would want single use devices to be employed in their treatment, and they felt that
other patients should not be offered a lower standard of provision
I think the most important thing is that we, as professionals need to make
sure that what we use on the patient, we would be happy to accept for use on

105
ourselves or any member of our own family, and looking at the guidance and
using that guidance thinking, ‘is this the best practice that we can give the
patients’? (9TM)
I think if I was ever in that position, and was the patient having an operation, I
would really prefer that single use was used on me (6ODP)
I want platinum standard – if I could go higher I would. But it costs money to
have platinum standards. I don’t care what the costs are. That’s the standards
that we have to have for our patients. I work on the principal that I’m the
patient. You know, if this is being used on you, then I would want it to be used
on me. I’ve had surgery here, as have my family, and I’m very happy with the
standards here (6SM)
These findings echo the results of a US survey, where 82% of all nurses and 71% of
all surgeons questioned reported that they would feel wary if a reprocessed device
was used on them60. Similarly, Walsh83 carried out his own ‘straw-poll’ of UK theatre
staff, and found that “almost all would prefer an unused laryngeal mask airway for
their anaesthetic, because they see them contaminated with blood and secretions”.
However, as we have already discussed, the perceived safety of single use devices
is to some extent at odds with perceptions of their quality and efficacy. One ODP
acknowledged:
Lots of things aren’t as good you know, you buy cheap and it looks cheap and
it doesn’t work properly, so you know, you have to weigh up the pros and
cons: is it going to be safe for the patient or not? You know certain things are
good, some, and you just, you have got an alternative but it might be
expensive (4ODP)
The appearance of the device, the cost of the device and the functionality of the
device all combine to create the clinician’s perception that buying cheaper devices
does not always save costs in the long-term:
We go for value, we will always consider cost, but we’ll also consider how it
does its job. It’s not good buying a thre’penny laryngoscope blade that
106
doesn’t work, you know it’s cheap as chips but if it doesn’t work then you
know you’re endangering people (9ODP)
As Webster98 suggests, in the long-term, it may be cheaper to follow good clinical
practice in relation to patient safety (and single use devices) than face the financial
implications of an episode of iatrogenic harm. It is not, however, just the financial
threat of iatrogenic harm that should influence the purchasing decisions in relation to
single use devices. These devices can also accelerate workflow and produce quality
and efficiency gains. For example, the adoption of single use devices in the context
of new surgical technologies can reduce the time the patient spends both under
anaesthesia and as an inpatient:
The staple guns and things like that we use are a one off item that tend to
actually save time and will knock half an hour or more off an operation (4TM)
A couple of weeks ago we did a laparoscopic nephrectomy…the patient was
walking around the shops within four days. You know, do a loin incision like
that, and the patient will still be in bed in ten days’ time because he can’t
move, you know it’s, there’s a benefit for all these things to be done. But
we’re just paying maybe a little bit more cost. You know, if you open a patient
the patient is going to be in hospital for a fortnight, you have to pay that, but
what we’ve saved on bed days’ cost, the disposables have cost nothing
really. And I think that’s the way you’ve got to look at it, if it’s going to save a
patient being in hospital, they don’t like being in hospital for ten days or a
week when they can be out in two, you know for a gall bladder, out in two
days, probably less you know (4ODP)
The latter quotation demonstrates a problem with the organisation of the NHS
hospital accounting. As our data show, theatres are under pressure to use the
cheapest possible equipment, yet by performing a slightly more expensive procedure
(for example, laparoscopic rather than open surgery), the extra money spent may be
more than recouped by a reduction in the number of bed days needed and
anaesthetic gases required. As laparoscopic surgery is less invasive and often
quicker, the patient’s recovery time is shortened. Yet, the compartmentalisation of
Trusts’ internal budgets can mean that these savings are not recognised by the
purchasing decision making process. Such a scenario was recalled by an ODP:

107
A lot of the single use disposables that we use save a lot of time, because
like, I can remember for years, we’d take out pieces of a patient’s bowel and
then you’d have to sew them up, it’s much more time consuming than having
a stapler or putting clips in. It’s beneficial to the patient in as much as it’s a
new instrument and it saves time, so there’s less anaesthetic. So then, its
cost effective I guess in a way. The financial part of the hospital don’t really
understand dare I say….If they looked at the whole picture, like laparoscopic
bowel surgery, once you’ve got all the kit, the patient is on the table for less
time and is only in hospital for a few days rather than two weeks (6ODP)
Our data suggests that whilst a variety of constraints affect the decision whether or
not to use single use devices, the primary influences are cost, quality and the
perceived benefit, or otherwise of using disposable equipment.
Specific data on lifetime and organisational costs was hard to obtain from Trusts.
However, we can demonstrate the principles discussed in the last two sections
through a fairly crude analysis of the choice between reusable and single use
laryngoscope blades. Whilst a single use laryngoscope blade is known to withstand
less force and produce a poorer light source than a reusable blade106,127, the risk of
infection or cross contamination from reusable devices is well documented 79,109,128.
Estimates, based on figures in the NHS Logistics catalogue57 and data supplied from
Hospital 3, suggest the following costs:
• Purchase price of a single use laryngoscope handle and blade: £10.70
(average)
• Purchase price of a reusable laryngoscope handle and blade: £120.00
(average)
• However, the reusable device will be used repeatedly, and will undergo a
sterilisation cycle after each use. Using data supplied from Hospital 3, the
sterilisation cost is calculated at £2.50 per item. Hospital 3 estimated that
their laryngoscopes were each used approximately 330 times per annum 14
• Estimated cost of each use of a reusable laryngoscope is therefore: £120.00 /
330 + £5.00 = £5.36
14 It is appreciated that the period of use for a laryngoscope blade could be far less
or far more than a year.

108
However, it is important that other handling and related costs are also included in this
financial calculation. While reusable devices appear to present the cheapest option,
the figures do not take account of the relative risks of infection, generating additional
costs in compensation, additional treatment and extended in-patient stays, the need
for additional reusable stock to buffer the time lag between sending equipment to the
CSD and receiving it, and the impact of missing or broken equipment on the
continuity of theatre working. While these figures are not conclusive, there is every
reason to suppose that the actual cost per use is much closer than the calculation
suggests.
Prior to the inauguration of this study, we had envisaged conducting a formal
economic evaluation, entailing the measurement of costs and benefits. Our
presumption had been that the reuse of SUDs would be both explicit and pervasive,
and that cost and consequence data would be readily collectable. However, during
the course of the study, it became increasingly apparent that, if widespread reuse
was indeed occurring, it was not a matter which individuals within organisations were
prepared to discuss in detail openly. Trusts were unwilling or unable to provide
financial data pertaining to the reuse of SUDs. In only one case was any relevant
economic material made available. This took the form of an uncontroversial
assessment of whether or not to initiate a move from reusable to single use
equipment in a specific context. Understandably, suppliers and manufacturers of
devices were unwilling to release details of actual prices charged or the volume of
sales, owing to concerns over information being made available to competitors. The
unavailability of data has made a formal quantitative evaluation impossible.
This having been said, the data obtained at interview have enabled us to explore the
series of behavioural propositions and hypotheses which we had established initially.
These were essentially economic constructs, potentially explaining micro-behaviour
with respect to single use devices in terms of expected costs and consequences. The
evidence necessary to explore these hypotheses has already been presented
throughout the report. Here, we state six hypotheses and summarise the evidence
available in support or otherwise, before reaching an economic model of the need to
balance cost and benefit in the decision to reuse SUDs. The behavioural propositions
pertain to choices made by individual agents at the appropriate stage of a decision
process, the choice being between:

109
• Should I employ a new single use device?
• Should I re-employ a previously-used single use device?
• Should I employ a reusable device?
Hypothesis 1
Interpreting behaviour as a result of the above three-way choice presupposes
that the decision maker is aware that the device is intended for single use.
There is some evidence that unfamiliarity with the device per se or lack of clarity in
the manufacturer’s instructions can lead to errors in usage, of the form of either (i)
reusables being discarded unnecessarily or, (ii) single use devices being reused
inappropriately. Whilst that inappropriate usage may be unintended, there are still
cost and outcome consequences. Given that the price of reusables tends to exceed
that of single use devices by a wide margin, the former error represents waste for no
health gain, whereas the latter represents cost saving accompanied by a potential
health risk.
Hypothesis 2
Reuse of single use devices can save money. Having been purchased for
the first procedure, the cost of reusing the device is (i) zero for the device
itself, although possibly (ii) positive, if maintenance or reprocessing (e.g.
cleaning) is required. In general, therefore, reuse will be cost-saving if
reprocessing costs are less than replacement costs.
The US General Accounting Office122 study identified cost economies as a principal
explanation for reuse:
Substantial cost savings can be achieved by reprocessing SUDs.
Independent reprocessing firms charge hospitals approximately one-half the
price of a new device, while the in-house cost of reprocessing some devices
can be less than 10 percent of the price of a new device. The competition
created by SUD reprocessing appears to have caused some original device
manufacturers to reduce their prices to certain purchasers (p.5)
However, unlike the USA, in the UK reprocessing of devices by 3rd parties does not
occur. Accordingly, cost advantages following reprocessing may not be so apparent.

110
There were no reported cases of single use devices being reprocessed officially, yet
reuse was obviously occurring. Although cost saving was the most commonly cited
justification, it was not at all clear that the respondents were accurately informed
about the financial implications. Their intuition, in other words, may have been
leading them to believe that reuse “must” be cheaper.
Hypothesis 3
Reuse increases security in supply. If an SUD is necessary for a procedure
then the availability, or otherwise, of the SUD will act as a potential constraint
on that procedure being undertaken. For any given level of stock of the SUD,
reuse increases the likelihood that the procedure will be feasible. Given the
variability of demand for procedures and the possibility that many demands
could be emergencies, non-reuse will require more SUDs to be held in stock
at any one time (with implications for storage costs and tied-up capital).
Our data tend to contradict this hypothesis. SUDs are generally considered superior
to reusable equivalents in terms of security of supply, for three reasons: (i) automatic
stock replenishment systems mean that SUDs are replaced following use as a matter
of routine. Reusable devices have a longer life and therefore require more conscious
ordering, which is vulnerable to mismanagement. (ii) Reliance on a limited number of
reusable devices entails supply insecurity if one or more devices are mislaid,
damaged or are undergoing cleaning. (iii) If the supply of reusables is limited,
individuals face the incentive to reserve devices for their own usage, e.g. by means
of concealment, thereby disrupting supplies for other users. The only exceptional
circumstances would appear to be emergencies, when SUD reuse may be justified
on the basis of needing to use the nearest device available.
Hypothesis 4
Reuse eases the management of patient care. Depending on the practices
of the institution concerned, it might be the case that new SUDs are more
difficult to access than used ones, owing to, for example, physical distance,
need for authorisation and "red tape". Where a maximum level of use of
SUDs is an efficiency criterion for a unit, reuse would enable the unit to reach
its target more easily (or make the unit appear more efficient).
Little information was forthcoming in this area, suggesting that accessing SUDs was
not a particular cause of concern. We infer that individuals who cite the need to save

111
resources as a justification for reuse must be faced with either budget constraints or
performance targets because, without these, cost saving behaviour would be
unnecessary.
Hypothesis 5
The user believes the old SUD to be superior to the new, despite the
intentions of the manufacturer, e.g. the old SUDs were "better made" than the
new ones, the old ones work better as they are "worn in".
Support for this hypothesis was reflected in the data, but in relation to the debate
regarding reusable vs. SUDs (e.g. bougies, laryngoscope blades). Certain SUDs
were indeed perceived to be of poorer quality than reusables. Despite being new,
often lower cost, carrying no risk of cross infection or contamination, SUDs were
rejected on the grounds of offering sub-standard care.
Hypothesis 6
Reuse of SUDs risks contamination. Therefore, the decision to reuse
requires either that the user feels that reuse poses no threat to the welfare of
the patient, or that any increased risk to the patient is more-than-offset by the
advantages of reuse.
There was no evidence that individuals were unaware that, in general terms, reusing
devices posed some degree of iatrogenic risk. Individuals disputed, however, the
magnitude of this risk and the extent to which risk minimisation was consistent with
efficiency and effectiveness. A minority of participants admitted to covert attempts at
reprocessing SUDs. They perceived that objects such as stainless steel forceps were
able to withstand the sterilisation process and reuse would therefore entail no
significant risk. Others who admitted reusing items such as Flowtron boots, pressure
infuser bags and blood pressure cuffs, justified reuse on the basis that such items
were used away from the operative site and were therefore insignificant threats to
health. Both the USA122 and the Australian12,61 studies of SUDs concluded that risks
of adverse consequences following reuse were, in many cases, low. In the
Australian case, terminating reuse on the grounds of risk reduction alone was held to
be cost-ineffective.
These behavioural propositions may be integrated into a simple model of the choice
problem, as follows:

112
• Using the SUD appropriately costs [C + CD], where C = the unit cost of the
SUD and CD = the expected cost of its disposal
• Reusing the SUD costs [CR + RP], where CR = the cost of reprocessing
the SUD for reuse, R = the expected risk of an adverse consequence as a
result of reuse, e.g. infection, and P = the expected penalty incurred as a
result of an adverse consequence, e.g. cost of additional treatment,
litigation, compensation, etc
• Therefore, an SUD will be reused if the user believes [C + CD] > [CR + RP]
Different SUDs exhibit different characteristics, which explains why reuse is more
frequent for some devices than for others. On the basis of the model, the reuse of
any particular SUD is more probable when the individual contemplating its reuse
believes:
• The unit cost of the SUD is high
• The cost of its disposal is high
• The cost of reprocessing the SUD is low
• The risk of an adverse event following re-use is low
• The penalty resulting from an adverse event is low

113
Conclusion and Recommendations:
This study has found that, despite guidance to the contrary, single use devices
continue to be reused. Reuse appears not to be widespread, but sufficient to remain
a matter of concern 15. Whilst some Trusts reported that they risk assessed reuse, in
most cases, device misuse was informed by common sense assumptions and the
clinical experience of participants.
The reuse of SUDs has been described as medical experimentation101, yet, when
reuse occurs, it seldom seems to be a deliberate decision, other than when the reuse
of the device is considered to present little risk. Rather reuse is most likely to be as a
result of underlying (latent) factors, including the physical design of the devices,
organisational breaches and human failings. Risks to patient safety in terms of the
reuse of SUDs therefore go beyond the active errors of individuals who we might
think of as ‘deviant’ or ‘careless’. Rather, as this report has demonstrated, several
different factors influence breaches in patient safety. These latent threats can lead
even the best clinician to be involved in an error that has the potential to harm a
patient.
Single use devices were introduced following awareness that protein and bacteria
remained on instruments following decontamination and sterilisation processes. This
led to fears that patients may contract iatrogenic infections and diseases such as
vCJD, HIV and Hepatitis B&C. The use of single use devices, which by definition
should be used once and then discarded, removed this threat to the delivery of safe
care for patients: new single use devices are guaranteed to be clean and
contaminant free. Moreover, unlike reprocessable equipment, single use devices are
neither fatigued nor suffering from wear and tear. For the most part, the use of single
use devices is in the patient’s best interests.
15 It is appreciated that due to the shortcomings of the survey phase of the research,
these statements cannot be generalised or applied to Trusts across the NHS.
However, given the recurring patterns of practice that we found across three different
SHAs, we consider that our conclusions offer a representative summary of current
usage and reuse.

114
Despite MHRA6 guidance specifying that single use devices should be used once
and then discarded, we have found that reuse continues. In 2004 we undertook a
survey of frontline staff working in Acute English NHS Trusts. 62% of respondents
reported that single use devices had been reused in their hospital. Examples
frequently cited included: breathing circuits, laryngoscope blades, laryngeal masks,
gum elastic bougies, facemasks and compression garments. All (with the exception
of breathing circuits which is a ‘grey’ area in the regulations) are labelled as single
use, and most are used invasively when intubating the patient. Our interview study of
theatre staff, conducted a year later, found a lesser extent of reuse reported,
although this difference may simply reflect the limitations of both samples.
Current thinking is encouraging the health service to move away from a culture of
blame towards a culture of learning129. Consequently, whilst reuse might occasionally
be explained by actions of a rogue or deviant clinician, our interview data points to a
number of organisational and physical reasons why single use devices are misused.
Moreover, many of these findings present an opportunity for learning and
development, both for clinicians and the manufacturing industry.
Misuse of single use devices is most likely the result of latent factors, including the
physical design of the devices and organisational breaches, as well as active failures
linked to human fallibility. During interviews with clinicians, we became aware of
several physical reasons why single use devices might be misused, including:
• Misunderstanding of the definition
• Design characteristics
• Suitability and safety of other devices.
• Discrepancies in labelling
The safe delivery of healthcare is also threatened by organisational factors,
including:
• Lack of awareness about single use devices
• Perception that reuse of single use devices is cheaper
• Fragmented hospital budgets which have resulted in the true costs of single
use and reprocessable devices being obscured from clinicians

115
• Perception that cost is a more important driver than quality when making
purchasing devices
Reuse was also rationalised in terms of the financial implications of continually
purchasing devices after one use, and environmental concerns about their disposal.
Lastly, clinicians questioned the extent of the risk linked to reprocessable devices.
In our survey we asked participants if they were aware of any guidance relating to
the use of single use devices. Only one person explicitly mentioned the MDA6 device
bulletin. This finding has influenced the MHRA’s decision to re-release the document
in October 200693. Recent communication with an orthopaedic surgeon also
reinforces our argument that problems exist with the current communication
strategies employed by the relevant stakeholders. This surgeon reported that they
were unaware of the MHRA guidance regarding single use devices, and asked
whose responsibility it was to communicate this to practitioners. Medical Device
Alerts and Bulletins from the MHRA are automatically sent to Trust SABS (safety
alert broadcast system) liaison officers for onward distribution to all relevant staff.
Evidence shows that this method of communication is not working efficiently: staff
are either not getting the information or are ignoring it. Consequently, this means that
care has been or potentially could be compromised. We recommend that the
SABs/Trust networks are evaluated in terms of the uptake and distribution of advice
transferred via the SABs provision.
Given the current financial crisis in the NHS, we found two important links between
the use and misuse of devices and perceived cost savings:
• Reuse of devices is perceived to present a cheaper alternative to
repeated purchasing
• Cost is a more important driver than quality (and hence effectiveness and
safety) when making purchasing decisions.
Clinicians felt that by cutting costs, patients were put at risk. Cheaper single use
devices were perceived to be placing the patient at greater risk of harm than that
linked to the use of a reprocessable device. We recommend that these perceptions
are addressed, both substantively through the design and cost of devices, and

116
educationally, via an awareness programme aimed at clinicians. However, it is also
important that Webster’s124 stark warning be noted:
The cost of a single case of significant iatrogenic harm would pay for a great
deal of patient safety.
A fundamental question that has arisen from this research is how to deliver the best,
safest care to patients and at the same time protect the NHS from the higher costs
associated with such practice. Is it appropriate, for example, to continue to
repeatedly purchase and discard certain, non-invasive single use devices (which
most likely pose very little iatrogenic risk) when the NHS is in financial difficulties? Is
it possible to balance known financial risks against unknown risks of contracting an
iatrogenic infection linked to the use of a medical device? Which is more of a threat:
financial disaster or the potential for patient harm?
In contrast to clinicians concerns relating to the patient safety risks associated with
inferior quality single use devices, when the quality of the devices was not called into
question, a different stance was taken. Single use devices were considered
beneficial in that they protect against iatrogenic cross infection and contamination,
and ensure that each patient has clean instruments used on them. This research
clearly demonstrates that clinicians feel that the use of single use devices is in the
patient’s best interest. Moreover, the use of single use devices is seen to be a sign of
clinicians’ professionalism and adherence to good clinical practice standards.
However, as our data demonstrates, single use devices do not always function as
well as clinicians would want them to. Some are unfit for use and their use can
endanger the patient.
It is not our aim in this report to blame or identify individuals who have admitted to
reusing single use devices. Rather, the opportunity for shared learning and
improvement in the design and use of medical devices is considered to be a greater
good. This report and its Appendices outline the obstacles leading to the misuse of
devices, as well as providing a forum for clinicians to voice their concerns. It is now
for the regulators (including the Department of Health, Medicines and Healthcare
products Regulatory Agency and the National Patient Safety Agency), manufacturing
community, Royal Colleges and Royal Associations, front line clinical staff and NHS
managers to work together to address the problems and weaknesses identified in
this report. However, we offer the following nine suggestions:

117
1. Professional associations and Royal Colleges should work together to
address inconsistencies in infection control guidelines. In particular:
a. Use of single use laryngoscope blades
b. Contrasting guidance for different invasive intubating equipment
(laryngoscope, laryngeal mask, bougie)
2. Clearer microbiology guidance is required on the actual threat of vCJD and
other iatrogenic infections from reused devices
3. The definition of single use should be re-examined. Do the terms ‘single use’
and ‘single patient use’ describe the same expected usage pattern? If so, we
recommend that the term single patient use is removed from all devices.
Additionally, regardless of the resulting definition, a high profile educational
campaign targeting all stakeholders should be designed and implemented
4. Labelling inconsistencies need to be addressed:
a. Labelling on each device should be consistent. For example, a device
should not be labelled as both single use and single patient use
b. Labelling on the device, packaging and paper insert (instructions)
should be consistent
c. Size of single use logo, font and position of the logo should be
examined
d. Use of wording to replace single use logo should be examined
5. Colour coding of devices, thus differentiating between single use and
reprocessable should be investigated. Views of users, purchasers and
manufacturers will need to be sought
6. Robust system for the replacement of breathing circuits after seven days to
be designed and implemented throughout the health care system
118
7. All clinical stakeholders should revisit EGBAT’s100 fifth recommendation,
regarding removing devices from their packaging prior to use. Practice should
be amended where at odds with proposal
8. MHRA and device manufacturers to seek independent scientific expertise on
the contamination risks of certain single use devices (such as blood pressure
cuffs and pressure infuser bags) and remove the single use logo if evidence
suggests that this is feasible
9. All parties should look for ways to remedy the perceived quality/cost conflict.
Equipment must be fit for purpose in order to be both cost effective and
protect staff and patients against infection / cross contamination

119
Acknowledgments
We would like to acknowledge the support of colleagues in the Institute for Science
and Society and elsewhere in the University of Nottingham. Thanks are also
extended to those individuals who participated in the study, to BAREMA and in
particular to Harrie Cooke, for his helpful advice and guidance, to members of the
anaesthetic manufacturing community, and to all those individuals who have assisted
us in the completion of this study and shown an interest in our research.
Contribution of team members:
Professor Alan Aitkenhead: Advisor
Professor of Anaesthesia
Anaesthetic Safety
Professor Graeme Currie: Advisor and Interviewer
Professor of Public Sector Management
NHS Organisational Management
Professor Robert Dingwall: Chief Investigator; Co-author of report
Professor of Sociology
Organisational Deviancy, Patient Safety
Professor David Whynes: Author of cost-benefit analysis
Professor of Economics
Health Economics
Professor John Wilson: Advisor
Professor of Ergonomics
Human Factors; Design Safety
Dr Beverley Norris: Co-author of ergonomics report
Senior Research Fellow (Ergonomics).
Human Factors; Design Safety
Dr Sarah Sharples: Co-author of ergonomics report
Lecturer in Ergonomics

120
Human Factors; Design Safety
Dr Emma Rowley: Fieldworker; Co-author of report
Research Fellow (Medical Sociology)
Patient Safety, Medical Devices, Research
Governance

121
References
1. Chief Medical Officer. An Organisation with a Memory London: The Stationery
Office 2000.
2. Federal Drug Administration (Center for Devices and Radiological Health).
Reuse of Single Use Devices: FDA Policy 2002
http://www.fda.gov/cdrh/Reuse/index.html
3. MEDEC. Cause For Concern: The Reuse Of Single Use Medical Devices. A
Position Paper Toronto: MEDEC 2004
4. OOPEC. Council Directive 93/42/EEC of June 1993 concerning medical
devices (Amended 2003) CONSELG:1993L0042 - EN - 20.11.2003 –
004.001-1. European Union 2003.
5. Jepsen OB. Infection Control: Preventing Iatrogenic Transmission Of
Spongiform Encephalopathy In Danish Hospitals APMIS 2002;110(1):104-
112.
6. Medical Devices Agency. Device Bulletin: Single-use Medical Devices:
Implications and Consequences of Reuse. MDA DB2000 (04) London:
Medicines and Healthcare products Regulatory Agency 2000.
7. Jupp V, Davies P, Francis P. (eds.) Doing Criminological Research London:
Sage 2000.
8. de Vaus DA. Surveys In Social Research (Third Edition) London: UCL Press
1994.
9. Newell R. Questionnaires in Gilbert, N. (eds.) Researching Social Life
London: Sage 1993.
10. Canadian Nosocomial Infection Surveillance Program Surveillance Project for
the Reuse of Single-Use Medical Devices in Canadian Health Care Facilities.
2001 http:// www.hc-sc.gc.ca/pphb-dgspsp/publicat/cnsip-pcsinin1001/
11. Patients Association (2002) Infection Control and Medical Device
Decontamination: A Survey of Strategic Health Authorities. www.patients-
association.com
12. Collignon PJ, Graham E, Dreimanis DE. Reuse In Sterile Sites Of Single-Use
Medical Devices: How Common Is This In Australia? Med J Aust.
1996;164(9):533-6.
122
13. McAvoy BR, Kaner EF. General Practice Postal Surveys: A Questionnaire
Too Far? Br Med J 1996;313732-733.
14. Braithwaite D, Emery J, De Lusignan S, Sutton S. Using the Internet to
Conduct Surveys of Health Professionals: A Valid Alternative? Fam Pract
2003; 20:545-551.
15. Dillman DA. Mail and Internet Surveys: The Tailored Design Methods
(Second edition) New York: Wiley 2000.
16. Porter SR. Raising response rates: What works? New Directions for
Institutional Research 2004;2004(121):5-21
17. Umbach PD. Web surveys: Best practices New Directions in Institutional
Research 2004; 2004(121):23-38
18. Dillman, D.A. and Bowker, D.K. (2001) The Web Questionnaire Challenge to
Survey Methodologists
http://survey.sesrc.wsu.edu/dillman/zuma_paper_dillman_bowker.pdf
19. Zanutto E. Web & E-mail Surveys 2001 http://www.stat-
wharton.upenn.edu/~zanutto/Annenberg2001/docs/websurveys01.pdf
20. Joinson AN. Causes and Implications of Disinhibited Behaviour On The Net in
Gackenbach, J. (eds.) Psychology of the Internet New York: Academic Press
1998
21. Flatley J. The internet as a mode of data collection in government social
surveys: issues and investigations Social Survey Methodology Bulletin,
2001;2001:1-10
22. Department of Health. Press Release: Re-introduction Of Reusable
Instruments for Tonsil Surgery 2001/0623 2001 London: Department of
Health
23. Atkinson MC, Girgis Y, Broome IJ. Extent and practicalities of filter use in
anaesthetic breathing circuits and attitudes towards their use: a postal survey
of UK hospitals.Anaesthesia 1999; 54(1):37-41
24. AAGBI. A Report Received By Council of the Association of Anaesthetists on
Blood Borne Viruses and Anaesthesia: An Update (January 1996). 1996
London: Association of Anaesthetists of Great Britain and Ireland.

123
25. Nielson E, Jacobsen JB, Stokke DB, Brinklov MM, Christenson KN Cross-
Infection From Contaminated Anaesthetic Equipment Anaesthesia
1980;35:703–8.
26. MacCallum FO, Noble WC. Disinfection of Anaesthetic Face Masks
Anaesthesia 1960;15:307–10.
27. Hogarth I. Anaesthetic Machine And Breathing System Contamination And
The Efficacy Of Bacterial/Viral Filters Anaesth Intensive Care 1996;24 (2)
28. AAGBI. Infection Control in Anaesthesia 2002 London: Association of
Anaesthetists of Great Britain and Ireland.
29. Flexicare Medical. Communication (Fax) Between Flexicare Medical and NHS
Purchasing and Supply December 2001.
30. Intersurgical. Anaesthetic Breathing Systems Validation for Safe Reuse
Personal Communication from Intersurgical to NHS Purchasing and Supply,
October 2001.
31. Wilkes T. An Assessment Of The Performance Of Breathing System Filters
Business Briefing: Medical Device Manufacturing and Technology
2004;2004:1-4.
32. Wilkes AR. The Ability Of Breathing System Filters To Prevent Liquid
Contamination Of Breathing Systems: A Laboratory Study.
Anaesthesia 2002;57 (1):33-39.
33. National Health Service Purchasing and Supply Agency. Breathing Circuits
and Accessories. 2005
http://www.pasa.nhs.uk/medicalconsumables/anaesthesia_examgloves/respir
ation/breathing_circuits/
34. Medicines and Healthcare products Regulatory Agency. MHRA Evaluation
04005: Breathing System Filters London: MHRA 2004.
35. Cooke, H. Personal Communication with Secretary of BAREMA 2005.
36. Smith G, Birks R. Single Use Medical Devices Anaesthesia News 2001a;
170:1.
37. Smith G. and Birks R. Anaesthetic Breathing Circuits and Single Use
Anaesthesia News 2001b;172:1.

124
39. Bennett N, Bingham R. Statement on Paediatric Filters and Breathing
Systems Association of Paediatric Anaesthetists of Great Britain and Ireland
2005 http://www.apagbi.org.uk/docs/APA_Filters.pdf
40. Preston D. Strategy for the Decontamination of Reusable Surgical
Instruments NLG (03)023 North Lincolnshire and Goole Hospitals NHS Trust
2003.
41. AAGBI. Checking Anaesthetic Equipment London: Association of
Anaesthetists of Great Britain and Ireland 2004
42. Cupitt JM. Microbial Contamination of Gum Elastic Bougies Anaesthesia
2000;55:466 – 468.
43. Shah N, Greig JR, Stephenson JR, Jankowski S. Microbial Contamination of
Gum-Elastic Bougies Anaesthesia 2000;55:1225.
44. Phillips RA, Monaghan WP. Incidence Of Visible And Occult Blood On
Laryngoscope Blades And Handles. Journal of the American Association of
Nurse Anaesthetists 1997;65: 241-7.
45. Smith G. Variant CJD: What You Need To Know At Present Royal College of
Anaesthetists Bulletin 2001;May:302 – 304.
46. Strausbergh LJ. Nosocomial Respiratory Infections in Mandell GL. (eds.)
Principles and Practices Of Infectious Diseases Philadelphia: Churchill
Livingstone 1999.
47. Hill AF, Butterworth RJ, Joiner S, McGregor G, Rosser MN, Thomas DJ.
Investigations of variant Creutzfeldt-Jakob Disease and Other Human Prion
Diseases with Tonsil Biopsy Samples Lancet;353:183-189.
48. Laurenson IF, Whyte AS, Fox C, Babb JR. Contaminated Surgical
Instruments And Variant Creutzfeldt-Jakob Disease Lancet 1999;354:1823.
49. Hirsch N, Becette A, Collinge J, Scaravilli F, Tabrizi S, Berry S. Lymphocyte
Contamination Of Laryngoscope Blades – A Possible Vector For
Transmission Of Variant Creutzfeldt-Jacob Disease Anaesthesia 2005;60:
664-667.
50. Esler MD, Wilkinson DJ, Langford RM. Degradation of Laryngoscopes
Anaesthesia 2000;55:300-301.
51. Coetzee GJ. Eliminating Protein From Reusable Laryngeal Mask Airways
Anaesthesia 2003;58:346-352.

125
52. Parker MRJ, Day CJE. Visible and Occult Blood Contamination of Laryngeal
Mask Airways and Trachael Tubes Used in Adult Anaesthesia Anaesthesia
2000;55:367-390.
53. Ontario Hospital Association Report Of Ontario Hospital Associations’ Reuse
Of Single Use Medical Devices Ad-Hoc Working Group January 2004.
54. Lichtman B. Going Once, Going Twice: What Price For A Reprocessed
Device? UCLA Journal of Law and Technology Notes 2003;16.
55. Castille K. To Reuse Or Not To Reuse – That Is The Question Nurs Stand
1999;13 (34):48-52.
56. Brook CW. Reuse of single use medical devices: NHMRC deliberations Med
JAust 1996;164:537
57. National Health Service Purchasing and Supply Agency. Logistics Authority:
Catalogue NHS Logistics: Alfreton 2004.
58a. Haley D. A Case for Outsourcing Medical Device Reprocessing
(Management) The Association of Perioperative Registered Nurses 2004; 79
(4) p806-808.
58b. Haley D. (2004) Reprocessing: 25Million Medical Devices and Counting.
What Does The Future Hold? Today’s Surgicenter: Materials Management,
9/1/2004
http://www.surgicenteronline.com/articles/materials_management/563_491fea
t2.html
59. Woods I. Making Errors: Admitting Them and Learning From Them
Anaesthesia 2005;60:215-217.
60. Brune A. What Knee Patients Need To Know About Single Use Instrument
Reprocessing 2003 http://www.Knee1.com
61. Collignon PJ, Dreimanis DE, Beckingham WD. Reuse of Single-Use Medical
Devices in Sterile Sites: How Often Does This Still Occur in Australia? Med J
Aust 2003;179(2):115-6; discussion 116
62. Schultz J. Reprocessing Single-Use Medical Devices Jan Schultz &
Associates: Roswell GA. 2004
http://www.noharm.org/details.cfm?type=document&ID=490

126
63. Woollard K. Reuse of single-use medical devices: who makes the decision?
The controversy can be resolved by identifying the real risks of cross-infection
Med J Aust 1996;164 (9):538
64. Cohoon BD. Reprocessing single-use medical devices AORN J
2002;75(3):557-62, 565-7
65. Eucomed. Safety Issues: Reuse 2004
http://www.eucomed.be/?x=4&y=46&z=125&id=442
66. Ryden L. Reuse Of Devices in Cardiology Eur Heart J 1998;19:1628-1631.
67. Day P. What Is The Evidence On The Safety And Effectiveness Of the reuse
Of Medical Devices Labelled As Single-Use Only? New Zealand Health
Technology Assessment 2004;3(2).
68. Heeg P, Roth K, Reichl R, Cogdill CP, Bond WW. Decontaminated Single-
Use Devices: An Oxymoron That May Be Placing Patients At Risk For Cross-
Contamination Infect Control Hosp Epidemiol 2001; 22 (9): 542-549.
69. Dean M. UK Concern Over Reuse Of Neurosurgical Tools Lancet
2002;360(9): 1485.
70. Kirkup B. Incident Arising in October 2002 from a Patient with Creutzfeldt-
Jakob Disease in Middlesbrough: Report of Incident Review London:
Department of Health 2003.
71. Carrey D. Reprocessing and Reusing Single Use Only Medical Devices: safe
Medical Practice or Risky Business? J Contemp Health Law Policy 2000
17:657-685.
72. National Audit Office. The Management And Control Of Hospital Acquired
Infection In Acute NHS Trusts In England London Stationary Office 2000.
73. Dingwall R. The Jasmine Beckford Affair Mod Law Rev 1986; 49(4): 489-507.
74. Bryman A, Burgess RG. (eds.) Analysing Qualitative Data London: Routledge
1994.
75. Have PT. Doing Conversation Analysis: A Practical Guide London: Sage
1999.
76. Heritage J. Garfinkel And Ethnomethodology Cambridge: Polity Press 1984.
127
77. Miller DM, Youkhana I, Karunaratne WU, Pearce A. Presence Of Protein
Deposits On ‘Cleaned’ Reusable Anaesthetic Equipment Anaesthesia
2001;56:1069-1072.
78. Nevin S, McMenemey WH, Behrman S, Jones DP. Subacute Spongiform
Encephalopathy – A Subacute Form Of Encephalopathy Attributable To
Vascular Dysfunction (Spongiform Cerebral Atrophy) Brain 1960;83:519-563.
79. Will RG. Acquired Prion Disease: Iatrogenic CJD, Variant CJD, Kuru Br Med
Bull 2003;66:255-265.
80. Chief Medical Officer Protecting The Public: Creutzfeldt-Jakob Disease 2006
www.dh.gov.uk/AboutUs/MinistersandDepartmentLeaders/ChiefMedicalOffice
r
81. Qian Z, Casteńeda WR. Can Labeled Single-Use Devices Be Reused? An
Old Question in the New Era Vasc Interv Radiol 2002;13:1183–1186
82. Furman, PJ. The Reprocessing Of Medical Devices Labelled For “Single Use”
In The US – An Historical Overview, Business Briefings and Technology
Assessment 2002; June:1-5.
83. Walsh EM. Reducing The Risk Of Prion Transmission In Anaesthesia
Anaesthesia 2006; 61: 64-65.
84. Medical Device Agency. DA 2001(08) - Use of Electro-surgery (diathermy) in
Tonsil and Adenoid Surgery London: Medical Devices Agency 2001
85. Smith G. vCJD and Disposable Laryngoscopes: A Reply Royal College of
Anaesthetists Bulletin 2002;March(12): 599.
86. EU / CEN. Draft prEN 980: Symbols for use in the labelling of medical devices
CEN/TC 257 N154 Brussels: European Union 2005
87. National Network of Clinical Procurement Specialists – personal
communication, July 2004
88. Carter JA. Checking anaesthetic equipment and the Expert Group on Blocked
Anaesthetic Tubing (EGBAT). Anaesthesia. 2004;59(2):105-7.
89. Federal Drug Administration. Reusing Medical Devices: Ensuring Safety the
Second Time Around FDA Consumer Magazine 2000:9-10.
http://www.fda.gov/fdac/features/2000/500_reuse.html
90. Milmo C. Mix Up Will Reignite Row Over Surgical Instruments The
Independent 2004: 30.10.04

128
91. Webster P. Canadian hospitals call for restrictions on single-use devices
Lancet 2004;363(9408):542
92. National Health Service Estates. Decontamination Review: Report on a
survey of current decontamination practices in healthcare premises in
England London: Department of Health 2003.
93. Royal College of Anaesthetists. What is the latest college position with regard
to the use of non-disposable equipment (including LMAs) for tonsillectomy?
2003 http://www.rcoa.ac.uk/index.asp?PageID=146
94. Medicines and Healthcare products Regulatory. Minutes Of The Committee
On The Safety Of Devices Meeting: 23 March 2006 2006
http://www.mhra.gov.uk/home/idcplg?IdcService=GET_FILE&dID=21086&no
SaveAs=1&Rendition=WEB
95. Liu L, Hoelscher U, Gruchmann T. Symbol Comprehension in different
countries: experience gained from medical device area, from Auinger A
(Hrsg.) Workshops: Proceedings der 5. fachűbergreifender Konferenz
Mensch und Computer Wien: Oesterreichsche Computer Gesellschaft, 2005,
S81-S87.
96. ISO. ISO/TR 15223:1998 Medical devices: Symbols to be used with medical
device labels, labelling and information to be supplied (Withdrawn – replaced
by BS EN980) 1998 ISO: Geneva
97. Keay S, Callander C. The Safe Use Of Infusion Devices Continuing Education
in Anaesthesia, Critical Care and Pain 2004;4 (3): 81-85.
98. Webster CS. The nuclear power industry as an alternative analogy for safety
in anaesthesia and a novel approach for the conceptualisation of safety goals
Anaesthesia 2005b;60:1115–22
99. Des-Côteaux JG, Blackmore K, Parsons L. A Prospective Comparison of The
Costs of Reusable and Limited-reuse Laparoscopic Instruments Can J Surg
1998;41:136-141.
100. Department of Health. Protecting the Breathing Circuit in Anaesthesia: Report
to the Chief Medical Officer of an Expert Group on Blocked Anaesthetic
Tubing 2004 London: Department of Health.
101. Hawkins D. Risky Recycling: That ‘Disposable’ Catheter May Have Been
Used Before US News.com 1999 (20.09.99)

129
102. Favero MS. Requiem for reuse of single-use devices in US hospitals. Infect
Control Hosp Epidemiol 2001; 22:539-541.
103. Abreu EL, Haire DM, Malchesky PS, Wolf-Bloom DF, Cornhill JF.
Development of a program model to evaluate the potential for reuse of single-
use medical devices: results of a pilot test study Biomed Instrum Technol
2002;36(6):389-404
104. Babb S, Mann S. Disposable Laryngoscope Blades Anaesthesia 2002
57:286-288
105. Cook TM, McCormick B, Twigg S. Reusable and Sheathed Laryngoscope
Blades Anaesthesia 2002;57:823
106. Evans A, Vaughan RS, Hall JE, Mecklenburgh J, Wilkes AR. A Comparison
Of The Forces Exerted During Laryngoscopy Using Disposable And Non-
Disposable Laryngoscope Blades Anaesthesia 2003;58:869-873
107. Twigg SJ, McCormick B, Cook TM. Randomised Evaluation Of The
Performance Of Single-Use Laryngoscopes In Simulated Easy And Difficult
Intubation Br J Anaesth 2003;90(1):8-13.
108. Hutton P. President’s Statement Royal College of Anaesthetists Bulletin
2002;12(March 2002): 555-557.
109. Rassam S, Wilkes A, Hall JE, Mecklenburgh JS. A Comparison Of 20
Laryngoscope Blades Using Intubating Manikin: Visual Analogue Scores And
Forces Exerted During Laryngoscopy Anaesthesia 2005;60:384-394.
110. Rose K, Cohen MM. The Airway: Problems And Predictions In 18,500
Patients Can J Anaesth 1994;41:372-383.
111. Hodzovic I, Latto IP, Wilkes AR, Hall JE, Mapleson, WW. Evaluation Of
Frova, Single Use Intubation Introducer, In A Manikin. Comparison With
Eschmann Multi-Use Introducer And Portex Single-Use Introducer
Anaesthesia 2004;59: 811-816.
112. Wilkes AR, Hodzovic I, Latto IP. Comparison Of The Peak Forces That Can
Be Exerted By Multiple Use And Single Use Bougies In Vitro Br J Anaesth
2002;89: 671
130
113. Annamaneri R, Hodzovic I, Wilkes AR, Latto IP. A Comparison Of Simulated
Difficult Intubation With Multiple-Use And Single-Use Bougies In A Manikin
Anaesthesia 2003;58:45-49.
114. Reay J. A Comparison Of Multiple-Use And Single-Use Bougies Anaesthesia
2005;60:417.
115. Medicines and Healthcare products Regulatory Agency. Medical Device Alert:
MDA/2005/062 All Anaesthetic Breathing Systems London: Medicines and
Healthcare products Regulatory Agency 2005.
116. Scott SH. Put Your Money Where Your Prion Is Royal College of
Anaesthetists Bulletin 2002;March(12):598-99.
117. Esler MD, Baines LC, Wilkinson DJ, Langford RM.
Decontamination of laryngoscopes: a survey of national practice.
Anaesthesia 1999; 54(6): 587-592.
118. Smith JJ, Berlin L. Reusing Catheters and Other Medical Devices AJR Am J
Roentgenol 2001;177:773-776.
119. Stewart I. ‘Single Use Only’ Labelling Of Medical Devices: Always Essential
Or Sometimes Spurious? Med J Aust 1997;167:538-539.
120. Cook TM. The Classic Laryngeal Mask Airway: A Tried And Tested Airway,
What Now? Br J Anaesth 2006;96(2):149-152.
121. World Health Organisation Risks Associated with Healthcare Waste Health
Care Waste Management 2005
www.healthcarewaste.org/en/115_overview.html
122. General Accounting Office. Single Use Medical Devices: Little Available
Evidence of Harm from Reuse But Oversight Warranted 2002 GAO:
Washington DC.
123. Lewis C. Reusing Medical Devices: Ensuring Safety The Second Time
Around FDA Consumer Magazine September/October 2000.
124. Klein A. Good as New? The Reuse of Medical Devices Hospitals Save
Money, But Safety Is Questioned Washington Post 11.12.2005: p.A05
125. McDonald R, Waring J, Harrison S. Rules, Safety and the Narrativisation of
Identity: A Hospital Operating Theatre Case Study Sociol Health Illn
2006;28(2):178-202.

131
126. Webster CS. The Iatrogenic-Harm Cost Equation and New Technology
Anaesthesia 2005;60:843-846.
127. Evans A, Wilkes AR, Hall JE. Strength Requirements Of Laryngoscope
Blades Anaesthesia 2005; 60:289-290.
128. Shafik MT, Bahlman BU, Hall JE, Ali MS. A Comparison Of The Soft SealTM
Disposable And The Classic Re-Usable Laryngeal Mask Airway Anaesthesia
2006;61:178-181.
129. National Patient Safety Agency. Seven Steps to Patient Safety: The Full
Reference Guide London: NPSA 2003.

132
Appendices
1. Inventory of Reuse
i. by device
ii. by country
2. Survey sampling strategy details
3. Ineligible survey data
4. Interview methodology details
5. R&D log (Interview phase)
6. Ergonomics report

13
3
App
endi
x 1.
Inve
ntor
y of
reus
ed S
UD
s
i. R
euse
by
devi
ce
R
euse
d S
ingl
e U
se D
evic
e R
efer
ence
D
ate
C
ount
ry o
f Orig
in
1 A
graf
Equ
ipm
ent
1 19
99
DE
NM
AR
K
2 A
mbu
bag
(Neo
nata
l)
2 20
01
CA
NA
DA
3 A
naes
thes
ia: A
irway
Con
nect
or
3 20
03
US
A
4 A
naes
thes
ia: A
irway
Dev
ice
4 20
04
NEW
ZE
ALA
ND
A
naes
thes
ia: A
irway
Dev
ice
5
2000
G
ER
MA
NY
5 A
naes
thes
ia: A
ngle
pie
ce c
onne
ctor
in P
CB
6
2004
U
K
6 A
naes
thes
ia: B
ite B
lock
2
2001
C
AN
AD
A
7 A
naes
thes
ia: B
reat
hing
Circ
uits
7
2000
U
SA
A
naes
thes
ia: B
reat
hing
Circ
uits
8
2000
U
SA
A
naes
thes
ia: B
reat
hing
Circ
uits
3
2003
U
SA
A
naes
thes
ia: B
reat
hing
Circ
uits
9
20
04
CA
NA
DA
A
naes
thes
ia: B
reat
hing
Circ
uits
10
20
01
CA
NA
DA
A
naes
thes
ia: B
reat
hing
Circ
uits
11
20
04
US
A
A
naes
thes
ia: B
reat
hing
Circ
uits
2
2001
U
SA
8 A
naes
thes
ia: B
ronc
hosc
ope
4 20
04
NEW
ZE
ALA
ND
A
naes
thes
ia: B
ronc
hosc
ope
3 20
03
US
A
A
naes
thes
ia: B
ronc
hosc
ope
3 20
03
US
A
13
4
9 A
naes
thes
ia: C
athe
ter m
ount
on
PC
B
12
2004
U
K
A
naes
thes
ia: C
athe
ter m
ount
on
PC
B
13
2002
U
K
10
Ana
esth
esia
: End
otra
chea
l Tub
e 3
2003
U
SA
A
naes
thes
ia: E
ndot
rach
eal T
ube
3 20
03
NEW
ZE
ALA
ND
A
naes
thes
ia: E
ndot
rach
eal T
ube
10
2001
C
AN
AD
A
A
naes
thes
ia: E
ndot
rach
eal T
ube
2 20
01
CA
NA
DA
A
naes
thes
ia: E
ndot
rach
eal T
ube
8 20
00
US
A
A
naes
thes
ia: E
ndot
rach
eal T
ube
7 20
00
US
A
11
Ana
esth
esia
: Filt
er
4 20
04
NEW
ZE
ALA
ND
A
naes
thes
ia: F
ilter
14
20
04
UK
A
naes
thes
ia: F
ilter
15
20
01
UK
A
naes
thes
ia: F
ilter
21
20
00
US
A
12
Ana
esth
esia
: Int
ubat
ing
styl
ette
s (b
ougi
es)
2 20
01
CA
NA
DA
13
Ana
esth
esia
: Int
ubat
ion
Equ
ipm
ent
1 19
99
DE
NM
AR
K
A
naes
thes
ia: L
aryn
gosc
ope
blad
es
16
2002
U
K
14
Ana
esth
esia
: LM
As
17
20
00
UK
15
Ana
esth
esia
: LM
As
18
19
99
EU
RO
PEA
N U
NIO
N
16
Ana
esth
esia
: Mas
ks
7 20
00
US
A
naes
thes
ia: M
asks
1
1999
D
EN
MA
RK
A
naes
thes
ia: M
asks
19
20
00
UK
A
naes
thes
ia: M
asks
3
2003
U
S

13
5
A
naes
thes
ia: M
asks
2
2001
U
S
17
Ana
esth
esia
: Mou
thpi
eces
3
2003
U
S
A
naes
thes
ia: M
outh
piec
es
7 20
00
US
18
Ana
esth
esia
: Neb
ulis
ers
14
2004
U
K
A
naes
thes
ia: N
ebul
iser
s 10
20
01
CA
NA
DA
19
Ana
esth
esia
: Ora
l airw
ays
2 20
01
CA
NA
DA
20
Ana
esth
esia
: Res
pira
tory
The
rapy
7
2000
U
S
21
Ana
esth
esia
: Spi
rom
etry
Tub
ing
20
2004
U
K
22
Ana
esth
esia
: T-p
iece
(PC
B)
12
2004
U
K
A
naes
thes
ia: T
-pie
ce (P
CB
) 13
20
04
UK
A
naes
thes
ia: T
-pie
ce (P
CB
) 2
2001
C
AN
AD
A
23
Ana
esth
esia
: Tub
ing
17
2000
U
K
A
naes
thes
ia: T
ubin
g 18
19
99
EU
RO
PEA
N U
NIO
N
24
Ana
esth
esia
:: O
xyge
nato
rs
22
2002
U
SA
25
Ang
iosc
ope
4 20
04
NEW
ZE
ALA
ND
26
Car
diac
: Aor
tic p
unch
es
23
2003
U
SA
27
Car
diac
: Bio
psy
Nee
dle
3 20
03
US
A
28
Car
diac
: Bur
r 3
2003
U
SA
29
Car
diac
: Cat
hete
r 24
20
04
GE
RM
AN
Y
C
ardi
ac: C
athe
ter
10
2001
C
AN
AD
A
C
ardi
ac: C
athe
ter
25
1999
U
SA

13
6
C
ardi
ac: C
athe
ter
26
2003
U
SA
C
ardi
ac: C
athe
ter
27
1997
A
US
TRAL
IA
C
ardi
ac: C
athe
ter
9
2004
C
AN
AD
A
C
ardi
ac: C
athe
ter
28
2000
U
SA
C
ardi
ac: C
athe
ter
4 20
04
NEW
ZE
ALA
ND
30
Car
diac
: Cat
hete
r (Ab
latio
n)
29
2001
U
SA
C
ardi
ac: C
athe
ter (
Abla
tion)
4
2004
N
EW Z
EAL
AN
D
C
ardi
ac: C
athe
ter (
Abla
tion)
7
2000
U
SA
C
ardi
ac: C
athe
ter (
Abla
tion)
30
20
04
AU
STR
ALIA
C
ardi
ac: C
athe
ter (
Abla
tion)
31
20
00
US
A
C
ardi
ac: C
athe
ter (
Abla
tion)
32
20
03
AU
STR
ALIA
31
Car
diac
: Cat
hete
r (A
chal
asia
bal
loon
) 24
20
04
GE
RM
AN
Y
32
Car
diac
: Cat
hete
r (An
giog
raph
y)
7 20
00
US
A
C
ardi
ac: C
athe
ter (
Angi
ogra
phy)
9
20
04
CA
NA
DA
C
ardi
ac: C
athe
ter (
Angi
ogra
phy)
3
2003
U
SA
C
ardi
ac: C
athe
ter (
Angi
ogra
phy)
29
20
01
US
A
C
ardi
ac: C
athe
ter (
Angi
ogra
phy)
2
2001
C
AN
AD
A
33
Car
diac
: Cat
hete
r (An
giop
last
y B
allo
ons)
33
19
96
AU
STR
ALIA
C
ardi
ac: C
athe
ter (
Angi
opla
sty
Bal
loon
s)
7 20
00
US
A
C
ardi
ac: C
athe
ter (
Angi
opla
sty
Bal
loon
s)
21
2000
U
SA
C
ardi
ac: C
athe
ter (
Angi
opla
sty
Bal
loon
s)
27
1997
A
US
TRAL
IA
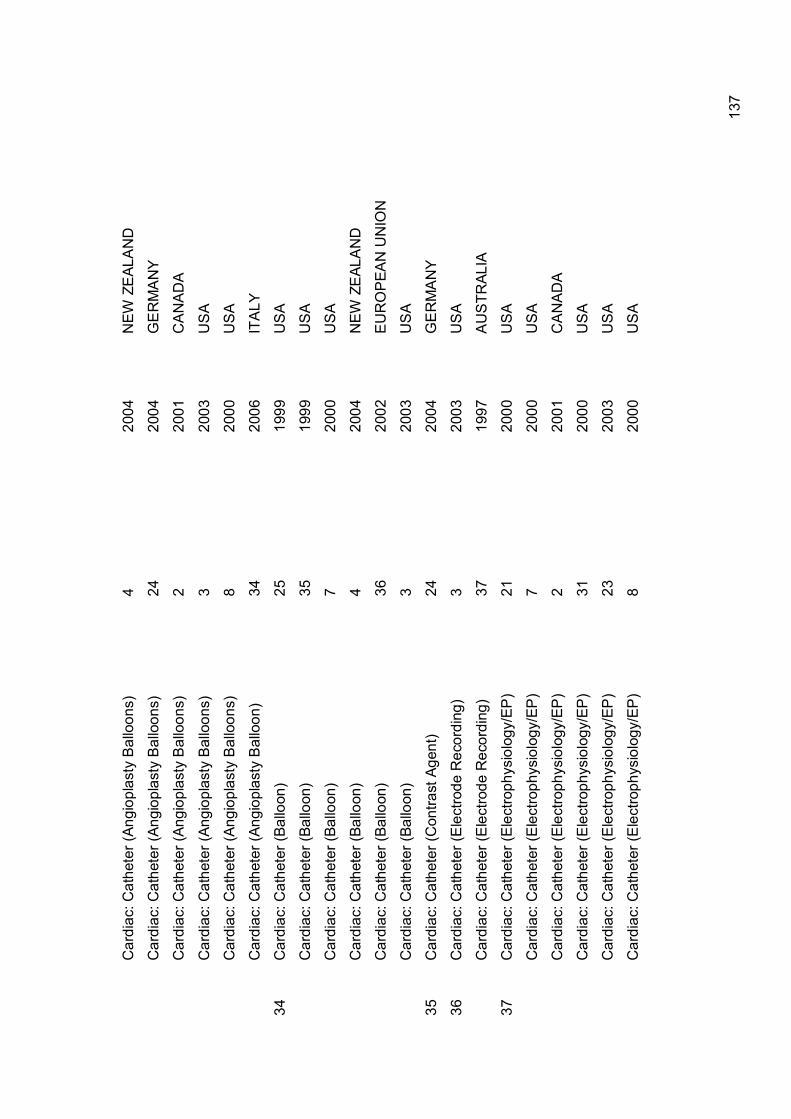
13
7
C
ardi
ac: C
athe
ter (
Angi
opla
sty
Bal
loon
s)
4 20
04
NEW
ZE
ALA
ND
C
ardi
ac: C
athe
ter (
Angi
opla
sty
Bal
loon
s)
24
2004
G
ER
MA
NY
C
ardi
ac: C
athe
ter (
Angi
opla
sty
Bal
loon
s)
2 20
01
CA
NA
DA
C
ardi
ac: C
athe
ter (
Angi
opla
sty
Bal
loon
s)
3 20
03
US
A
C
ardi
ac: C
athe
ter (
Angi
opla
sty
Bal
loon
s)
8 20
00
US
A
C
ardi
ac: C
athe
ter (
Angi
opla
sty
Bal
loon
) 34
20
06
ITA
LY
34
Car
diac
: Cat
hete
r (Ba
lloon
) 25
19
99
US
A
C
ardi
ac: C
athe
ter (
Ballo
on)
35
1999
U
SA
C
ardi
ac: C
athe
ter (
Ballo
on)
7 20
00
US
A
C
ardi
ac: C
athe
ter (
Ballo
on)
4 20
04
NEW
ZE
ALA
ND
C
ardi
ac: C
athe
ter (
Ballo
on)
36
2002
E
UR
OP
EAN
UN
ION
C
ardi
ac: C
athe
ter (
Ballo
on)
3 20
03
US
A
35
Car
diac
: Cat
hete
r (C
ontra
st A
gent
) 24
20
04
GE
RM
AN
Y
36
Car
diac
: Cat
hete
r (E
lect
rode
Rec
ordi
ng)
3 20
03
US
A
C
ardi
ac: C
athe
ter (
Ele
ctro
de R
ecor
ding
) 37
19
97
AU
STR
ALIA
37
Car
diac
: Cat
hete
r (E
lect
roph
ysio
logy
/EP
) 21
20
00
US
A
C
ardi
ac: C
athe
ter (
Ele
ctro
phys
iolo
gy/E
P)
7 20
00
US
A
C
ardi
ac: C
athe
ter (
Ele
ctro
phys
iolo
gy/E
P)
2 20
01
CA
NA
DA
C
ardi
ac: C
athe
ter (
Ele
ctro
phys
iolo
gy/E
P)
31
2000
U
SA
C
ardi
ac: C
athe
ter (
Ele
ctro
phys
iolo
gy/E
P)
23
2003
U
SA
C
ardi
ac: C
athe
ter (
Ele
ctro
phys
iolo
gy/E
P)
8 20
00
US
A

13
8
C
ardi
ac: C
athe
ter (
Ele
ctro
phys
iolo
gy/E
P)
38
2003
U
SA
C
ardi
ac: C
athe
ter (
Ele
ctro
phys
iolo
gy/E
P)
39
2004
U
SA
C
ardi
ac: C
athe
ter (
Ele
ctro
phys
iolo
gy/E
P)
28
2000
U
SA
C
ardi
ac: C
athe
ter (
Ele
ctro
phys
iolo
gy/E
P)
32
2003
A
US
TRAL
IA
C
ardi
ac: C
athe
ter (
Ele
ctro
phys
iolo
gy/E
P)
29
2001
U
SA
C
ardi
ac: C
athe
ter (
Ele
ctro
phys
iolo
gy/E
P)
36
2002
E
UR
OP
EAN
UN
ION
C
ardi
ac: C
athe
ter (
Ele
ctro
phys
iolo
gy/E
P)
4 20
04
NEW
ZE
ALA
ND
C
ardi
ac: E
lect
roph
ysio
logi
cal C
athe
ter
40
2001
U
SA
38
Car
diac
: Cat
hete
r (Fi
ber-o
ptic
Oxi
met
er)
3 20
03
US
A
39
Car
diac
: Cat
hete
r (G
uide
wire
) 3
2003
U
SA
C
ardi
ac: C
athe
ter (
Gui
dew
ire)
1 19
99
DE
NM
AR
K
C
ardi
ac: C
athe
ter (
Gui
dew
ire)
7 20
00
US
A
C
ardi
ac: C
athe
ter (
Gui
dew
ire)
41
2003
E
UR
OP
EAN
UN
ION
C
ardi
ac: C
athe
ter (
Gui
dew
ire)
35
1999
U
SA
C
ardi
ac: C
athe
ter (
Gui
dew
ire)
10
2001
C
AN
AD
A
C
ardi
ac: C
athe
ter (
Gui
dew
ire)
18
1999
E
UR
OP
EAN
UN
ION
C
ardi
ac: C
athe
ter (
Gui
dew
ire)
2 20
01
CA
NA
DA
40
Car
diac
: Cat
hete
r (H
aem
o-di
alys
is)
29
2001
U
SA
41
Car
diac
: Cat
hete
r (H
igh
Den
sity
Arra
y)
3 20
03
US
A
42
Car
diac
: Cat
hete
r 18
19
99
EU
RO
PEA
N U
NIO
N
43
Car
diac
: Cat
hete
r (Ke
rato
me)
3
2003
U
SA

13
9
44
Car
diac
: Cat
hete
r (St
eera
ble)
3
2003
U
SA
45
Car
diac
: Con
cent
ric N
eedl
es (E
P)
2 20
01
CA
NA
DA
46
Car
diac
: Def
ibril
lato
rs (I
mpl
anta
ble)
42
19
99
EU
RO
PEA
N U
NIO
N
C
ardi
ac: D
efib
rilla
tors
(Im
plan
tabl
e)
24
2004
G
ER
MA
NY
47
Car
diac
: Ext
erna
l Vei
n S
tripp
er
3 20
03
US
A
48
Car
diac
: Pac
emak
er
10
2001
C
AN
AD
A
C
ardi
ac: P
acem
aker
24
20
04
GE
RM
AN
Y
C
ardi
ac: P
acem
aker
2
2001
C
AN
AD
A
C
ardi
ac: P
acem
aker
43
19
98
EU
RO
PEA
N U
NIO
N
C
ardi
ac: P
acem
aker
29
20
01
US
A
C
ardi
ac: P
acem
aker
44
19
96
AU
STR
ALIA
C
ardi
ac: P
acem
aker
45
19
92
CA
NA
DA
C
ardi
ac: P
acem
aker
46
19
85
CA
NA
DA
C
ardi
ac: P
acem
aker
47
19
86
US
A
C
ardi
ac: P
acem
aker
46
19
89
CA
NA
DA
C
ardi
ac: P
acem
aker
48
19
98
SWED
EN
C
ardi
ac: P
acem
aker
49
19
99
CA
NA
DA
C
ardi
ac: P
acem
aker
50
19
78
SWED
EN
49
Car
diac
: Sta
biliz
er D
evic
e 3
2003
U
SA
50
Car
diac
: Syr
inge
3
2003
U
SA
C
ardi
ac: S
yrin
ge
7 20
00
US
A

14
0
51
Car
diac
: Syr
inge
(In
ject
or T
ype
Act
uato
r) 3
2003
U
SA
52
Car
diac
: Syr
inge
(Ang
iogr
aphe
r Inj
ecto
r) 3
2000
U
SA
53
Car
diac
: Tra
cers
39
20
04
US
A
54
Car
diac
: Tra
nsdu
cer
10
2001
C
AN
AD
A
C
ardi
ac: T
rans
duce
r 2
2001
C
AN
AD
A
55
Car
diac
: Tro
car
3 20
03
US
A
C
ardi
ac: T
roca
r 7
2000
U
SA
56
Car
diac
: Vei
n S
tripp
er
3 20
03
US
A
57
Car
diac
: Wire
s 25
19
99
US
A
C
ardi
ac: W
ires
35
1999
U
SA
58
Col
orec
tal:
Man
omet
ry T
ubin
g
2 20
01
CA
NA
DA
59
Col
orec
tal:
Sna
res
51
1996
A
US
TRAL
IA
C
olor
ecta
l: S
nare
s 33
19
96
AU
STR
ALIA
60
Der
mat
olog
y: E
lect
roca
uter
y tip
(hyf
reca
tor)
2 20
01
CA
NA
DA
61
Dia
ther
my:
Ele
ctro
des
21
2000
U
SA
D
iath
erm
y: E
lect
rode
s 8
2000
U
SA
D
iath
erm
y: E
lect
rode
s 7
2000
U
SA
62
Dia
ther
my:
Pen
cils
7
2000
U
SA
D
iath
erm
y: P
enci
ls
33
1996
A
US
TRAL
IA
D
iath
erm
y: P
enci
ls
8 20
00
US
A
D
iath
erm
y: P
enci
ls
3 20
03
US
A

14
1
D
iath
erm
y: P
enci
ls
32
2003
A
US
TRAL
IA
D
iath
erm
y: P
enci
ls
3 20
03
US
A
D
iath
erm
y: P
enci
ls
3 20
03
US
A
63
Ele
ctro
de C
able
3
2003
U
SA
64
Ele
ctro
de: P
ercu
tane
ous
Abl
atio
n 3
2003
U
SA
65
Ele
ctro
des
1 19
99
DE
NM
AR
K
66
Ele
ctro
des
and
need
les:
EEG
10
20
01
CA
NA
DA
E
lect
rode
s an
d ne
edle
s: E
EG
33
1996
A
US
TRAL
IA
E
lect
rode
s an
d ne
edle
s: E
EG
18
1999
E
UR
OP
EAN
UN
ION
67
Ele
ctro
des:
Car
diac
pac
ing
33
19
96
AU
STR
ALIA
E
lect
rode
s: C
ardi
ac p
acin
g
32
2003
A
US
TRAL
IA
E
lect
rode
s: C
ardi
ac p
acin
g
51
1996
A
US
TRAL
IA
68
Ele
ctro
des:
Res
ecto
scop
e
24
2004
G
ER
MA
NY
69
Ele
ctro
des:
Silv
er
52
2002
E
UR
OP
EAN
UN
ION
70
Ele
ctro
phys
iolo
gica
l stim
ulat
ion
30
20
04
AU
STR
ALIA
71
Ele
ctro
phys
iolo
gy: E
EG N
eedl
e-B
onne
t 2
2001
C
AN
AD
A
72
End
osco
pe
3 20
03
US
A
E
ndos
cope
7
2000
U
SA
E
ndos
cope
53
20
04
US
A
E
ndos
cope
1
1999
D
EN
MA
RK
E
ndos
cope
54
20
01
US
A
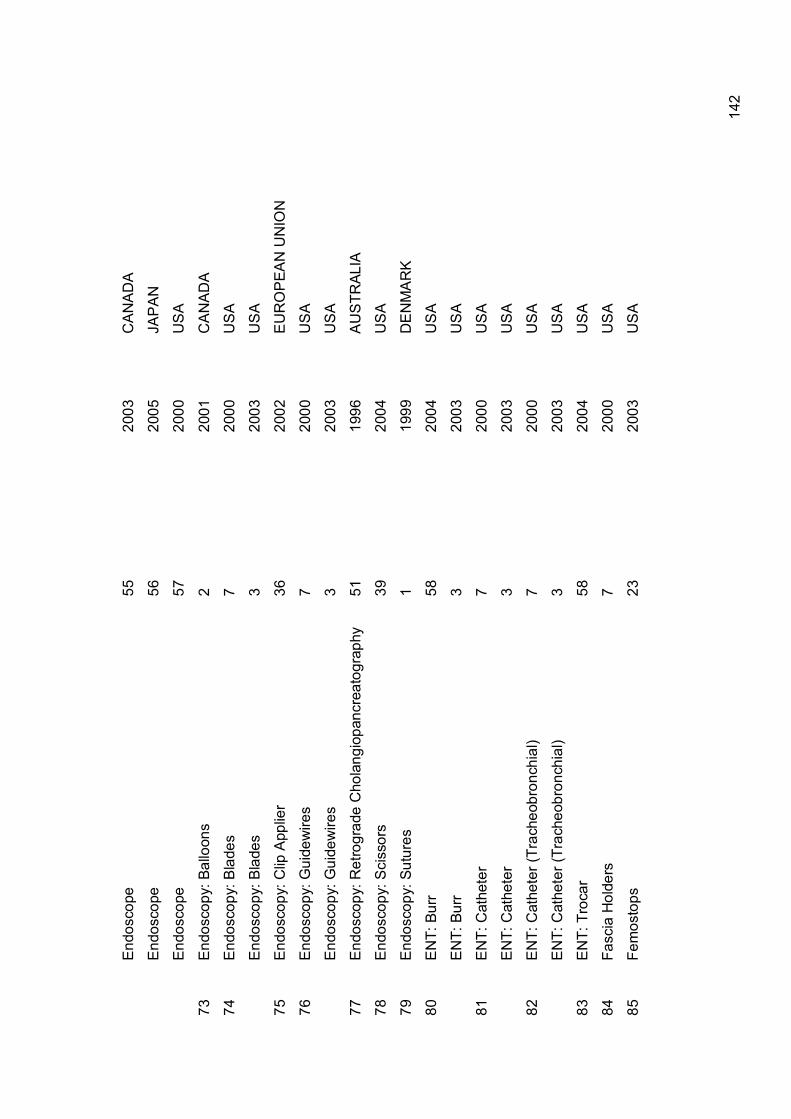
14
2
E
ndos
cope
55
20
03
CA
NA
DA
E
ndos
cope
56
20
05
JAP
AN
E
ndos
cope
57
20
00
US
A
73
End
osco
py: B
allo
ons
2
2001
C
AN
AD
A
74
End
osco
py: B
lade
s 7
2000
U
SA
E
ndos
copy
: Bla
des
3 20
03
US
A
75
End
osco
py: C
lip A
pplie
r 36
20
02
EU
RO
PEA
N U
NIO
N
76
End
osco
py: G
uide
wire
s 7
2000
U
SA
E
ndos
copy
: Gui
dew
ires
3 20
03
US
A
77
End
osco
py: R
etro
grad
e C
hola
ngio
panc
reat
ogra
phy
51
19
96
AU
STR
ALIA
78
End
osco
py: S
ciss
ors
39
2004
U
SA
79
End
osco
py: S
utur
es
1 19
99
DE
NM
AR
K
80
EN
T: B
urr
58
2004
U
SA
E
NT:
Bur
r 3
2003
U
SA
81
EN
T: C
athe
ter
7 20
00
US
A
E
NT:
Cat
hete
r 3
2003
U
SA
82
EN
T: C
athe
ter (
Trac
heob
ronc
hial
) 7
2000
U
SA
E
NT:
Cat
hete
r (Tr
ache
obro
nchi
al)
3 20
03
US
A
83
EN
T: T
roca
r 58
20
04
US
A
84
Fasc
ia H
olde
rs
7 20
00
US
A
85
Fem
osto
ps
23
2003
U
SA

14
3
86
Fibr
eopt
ic L
aser
Cab
le
3 20
03
US
A
87
Gas
troen
tero
logy
/ U
rolo
gy: B
iops
y Fo
rcep
s
3 20
03
US
A
G
astro
ente
rolo
gy /
Uro
logy
: Bio
psy
Forc
eps
28
20
00
US
A
88
Gas
troen
tero
logy
/ U
rolo
gy: B
iops
y Fo
rcep
s (E
lect
ric)
3 20
03
US
A
89
Gas
troen
tero
logy
/ U
rolo
gy: B
iops
y In
stru
men
t 3
2003
U
SA
90
Gas
troen
tero
logy
/ U
rolo
gy: B
iops
y Pu
nch:
3
2003
U
SA
91
Gas
troen
tero
logy
: Bal
loon
Dila
tors
: EC
RP
32
20
03
AU
STR
ALIA
92
Gas
troen
tero
logy
: Bal
loon
Dila
tors
: Upp
er E
ndos
copy
32
20
03
AU
STR
ALIA
93
Gas
troen
tero
logy
: Bal
loon
Ext
ract
or
2 20
01
CA
NA
DA
94
Gas
troen
tero
logy
: Bal
loon
sys
tem
for u
teru
s ab
latio
n 24
20
04
GE
RM
AN
Y
95
Gas
troen
tero
logy
: Bio
psy
Forc
eps
(Mic
roev
asiv
e)
2 20
01
CA
NA
DA
96
Gas
troen
tero
logy
: Bio
psy
Forc
eps
(Non
-ele
ctric
al)
58
2004
U
SA
G
astro
ente
rolo
gy: B
iops
y Fo
rcep
s (N
on-e
lect
rical
) 7
2000
U
SA
G
astro
ente
rolo
gy: B
iops
y Fo
rcep
s (N
on-e
lect
rical
) 3
2003
U
SA
97
Gas
troen
tero
logy
: Can
nula
32
20
03
AU
STR
ALIA
98
Gas
troen
tero
logy
: C
athe
ter
(Coa
gula
tion
Ele
ctro
-
hem
osta
tis)
2 20
01
CA
NA
DA
99
Gas
troen
tero
logy
: Cyt
olog
y br
ushe
s
2 20
01
CA
NA
DA
G
astro
ente
rolo
gy: C
ytol
ogy
brus
hes
3
2003
U
SA
G
astro
ente
rolo
gy: C
ytol
ogy
brus
hes
32
20
03
AU
STR
ALIA
100
Gas
troen
tero
logy
: Dila
tion
Bal
loon
s 1
1999
D
EN
MA
RK

14
4
G
astro
ente
rolo
gy: D
ilatio
n B
allo
ons
10
2001
C
AN
AD
A
101
Gas
troen
tero
logy
: Ele
ctro
de (A
ctiv
e EP
) 3
2003
U
SA
102
Gas
troen
tero
logy
: E
lect
rode
(F
lexi
ble
Suct
ion
Coa
gula
tor)
3
2003
US
A
103
Gas
troen
tero
logy
: Ele
ctro
de (L
oop)
2
2001
C
AN
AD
A
104
Gas
troen
tero
logy
: Eso
phag
eal S
tent
2
2001
C
AN
AD
A
105
Gas
troen
tero
logy
: Pol
yp fo
rcep
s 9
20
04
CA
NA
DA
106
Gas
troen
tero
logy
: Sto
ne D
islo
dger
3
2003
U
SA
107
Gas
troen
tero
logy
: Sto
ne R
emov
ing
Bas
kets
32
20
03
AU
STR
ALIA
108
Gen
eral
Sur
gery
: Bio
psy
Bru
sh
3 20
03
US
A
109
Gen
eral
Sur
gery
: Bio
psy
Dev
ice
53
2004
U
SA
G
ener
al S
urge
ry: B
iops
y D
evic
e
3 20
03
US
A
110
Gen
eral
Sur
gery
: Bio
psy
Forc
eps
39
2004
U
SA
G
ener
al S
urge
ry: B
iops
y Fo
rcep
s 4
2004
N
EW Z
EAL
AN
D
G
ener
al S
urge
ry: B
iops
y Fo
rcep
s 7
2000
U
SA
G
ener
al S
urge
ry: B
iops
y Fo
rcep
s 59
20
03
US
A
G
ener
al S
urge
ry: B
iops
y Fo
rcep
s 26
20
03
US
A
G
ener
al S
urge
ry: B
iops
y Fo
rcep
s 3
2003
U
SA
G
ener
al S
urge
ry: B
iops
y Fo
rcep
s 22
20
02
US
A
G
ener
al S
urge
ry: B
iops
y Fo
rcep
s 11
20
04
CA
NA
DA
G
ener
al S
urge
ry: B
iops
y Fo
rcep
s 41
20
03
EU
RO
PEA
N U
NIO
N

14
5
G
ener
al S
urge
ry: B
iops
y Fo
rcep
s 38
20
03
US
A
G
ener
al S
urge
ry: B
iops
y Fo
rcep
s 35
19
99
US
A
G
ener
al S
urge
ry: B
iops
y Fo
rcep
s 10
20
01
CA
NA
DA
G
ener
al S
urge
ry: B
iops
y Fo
rcep
s 24
.
2004
G
ER
MA
NY
G
ener
al S
urge
ry: B
iops
y Fo
rcep
s 60
20
00
GE
RM
AN
Y
G
ener
al S
urge
ry: B
iops
y Fo
rcep
s 8
2000
U
SA
G
ener
al S
urge
ry: B
iops
y Fo
rcep
s 23
20
03
US
A
G
ener
al S
urge
ry: B
iops
y Fo
rcep
s 2
2001
C
AN
AD
A
111
Gen
eral
Sur
gery
: Bio
psy
Forc
eps
(Arte
rial)
30
2004
A
US
TRAL
IA
112
Gen
eral
Sur
gery
: Bio
psy
Nee
dle
7 20
00
US
A
G
ener
al S
urge
ry: B
iops
y N
eedl
e 61
20
04
US
A
113
Gen
eral
Sur
gery
: Bla
des
39
2004
U
SA
114
Gen
eral
Sur
gery
: Chi
sel
3 20
03
US
A
115
Gen
eral
Sur
gery
: Cla
mp
(Vas
cula
r) 3
2003
U
SA
G
ener
al S
urge
ry: C
lam
p (V
ascu
lar)
24
2004
G
ER
MA
NY
116
Gen
eral
Sur
gery
: Cla
mp
hold
er
24
2004
G
ER
MA
NY
117
Gen
eral
Sur
gery
: Clip
58
20
04
US
A
G
ener
al S
urge
ry: C
lip
24
2004
G
ER
MA
NY
118
Gen
eral
Sur
gery
: Clip
(Im
plan
tabl
e)
3 20
03
US
A
119
Gen
eral
Sur
gery
: Clip
App
lier
52
2002
E
UR
OP
EAN
UN
ION
120
Gen
eral
Sur
gery
: Clip
Rem
over
s 62
20
04
UK
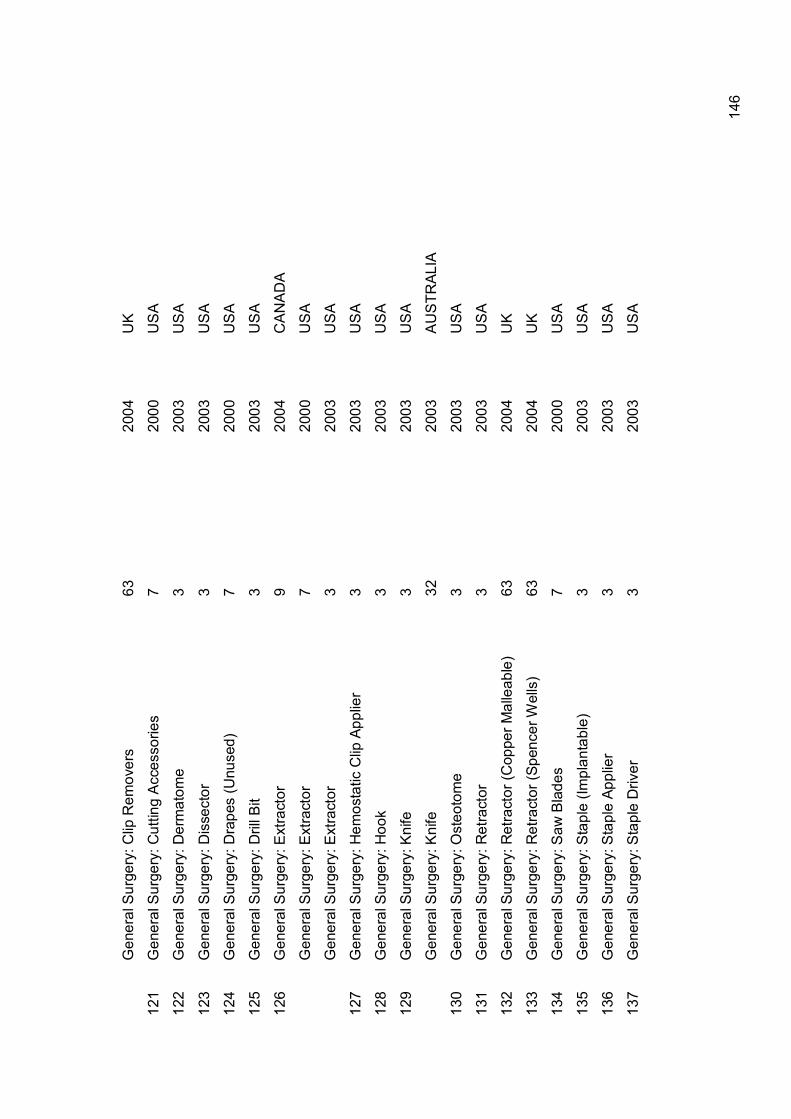
14
6
G
ener
al S
urge
ry: C
lip R
emov
ers
63
2004
U
K
121
Gen
eral
Sur
gery
: Cut
ting
Acc
esso
ries
7 20
00
US
A
122
Gen
eral
Sur
gery
: Der
mat
ome
3
2003
U
SA
123
Gen
eral
Sur
gery
: Dis
sect
or
3 20
03
US
A
124
Gen
eral
Sur
gery
: Dra
pes
(Unu
sed)
7
2000
U
SA
125
Gen
eral
Sur
gery
: Dril
l Bit
3
2003
U
SA
126
Gen
eral
Sur
gery
: Ext
ract
or
9
2004
C
AN
AD
A
G
ener
al S
urge
ry: E
xtra
ctor
7
2000
U
SA
G
ener
al S
urge
ry: E
xtra
ctor
3
2003
U
SA
127
Gen
eral
Sur
gery
: Hem
osta
tic C
lip A
pplie
r 3
2003
U
SA
128
Gen
eral
Sur
gery
: Hoo
k
3 20
03
US
A
129
Gen
eral
Sur
gery
: Kni
fe
3 20
03
US
A
G
ener
al S
urge
ry: K
nife
32
20
03
AU
STR
ALIA
130
Gen
eral
Sur
gery
: Ost
eoto
me
3
2003
U
SA
131
Gen
eral
Sur
gery
: Ret
ract
or
3 20
03
US
A
132
Gen
eral
Sur
gery
: Ret
ract
or (C
oppe
r Mal
leab
le)
63
2004
U
K
133
Gen
eral
Sur
gery
: Ret
ract
or (S
penc
er W
ells
) 63
20
04
UK
134
Gen
eral
Sur
gery
: Saw
Bla
des
7 20
00
US
A
135
Gen
eral
Sur
gery
: Sta
ple
(Impl
anta
ble)
3
2003
U
SA
136
Gen
eral
Sur
gery
: Sta
ple
Appl
ier
3 20
03
US
A
137
Gen
eral
Sur
gery
: Sta
ple
Driv
er
3 20
03
US
A

14
7
138
Gen
eral
Sur
gery
: Sta
pler
3
2003
U
SA
G
ener
al S
urge
ry: S
tapl
er
7 20
00
US
A
G
ener
al S
urge
ry: S
tapl
er
39
2004
U
SA
G
ener
al S
urge
ry: S
tapl
er
3 20
03
US
A
139
Gen
eral
Sur
gery
: Sta
pler
(End
osco
pic)
7
2000
U
SA
140
Gen
eral
Sur
gery
: Sta
pler
(Pla
stic
Sur
gery
) 7
2000
U
SA
G
ener
al S
urge
ry: S
tapl
er (P
last
ic S
urge
ry)
3 20
03
US
A
141
Gen
eral
Sur
gery
: Suc
tion
Tubi
ng
7 20
00
US
A
142
Gen
eral
Sur
gery
: Sut
ures
(non
-ste
rile)
7
2000
U
SA
G
ener
al S
urge
ry: S
utur
es (n
on-s
teril
e)
22
2002
U
SA
143
Gen
eral
Sur
gery
: Sut
ures
(Sto
mac
h / I
ntes
tinal
) 3
2003
U
SA
144
Gen
eral
Sur
gery
: Tro
car
3 20
03
US
A
G
ener
al S
urge
ry: T
roca
r 4
2004
N
EW Z
EAL
AN
D
G
ener
al S
urge
ry: T
roca
r 38
20
03
US
A
G
ener
al S
urge
ry: T
roca
r 18
19
99
EU
RO
PEA
N U
NIO
N
G
ener
al S
urge
ry: T
roca
r 23
20
03
US
A
G
ener
al S
urge
ry: T
roca
r 24
20
04
GE
RM
AN
Y
G
ener
al S
urge
ry: T
roca
r 39
20
04
US
A
G
ener
al S
urge
ry: T
roca
r 7
2000
U
SA
145
Gen
eral
: Ant
i DV
T ga
rmen
ts
7 20
00
US
A
G
ener
al: A
nti D
VT
garm
ents
28
20
01
US
A

14
8
G
ener
al: A
nti D
VT
garm
ents
39
20
04
US
A
G
ener
al: A
nti D
VT
garm
ents
3
2003
U
SA
G
ener
al: A
nti D
VT
garm
ents
53
20
04
US
A
146
Gen
eral
: Blo
od la
ncet
3
2003
U
SA
147
Gen
eral
: Blo
od P
ress
ure
Cuf
fs
53
2004
U
SA
G
ener
al: B
lood
Pre
ssur
e C
uffs
7
2000
U
SA
G
ener
al: B
lood
Pre
ssur
e C
uffs
3
2003
U
SA
G
ener
al: B
lood
Pre
ssur
e C
uffs
39
20
04
US
A
148
Gen
eral
: Bow
ls
63
2004
U
K
149
Gen
eral
: Bru
shes
1
1999
D
EN
MA
RK
150
Gen
eral
: Cab
les
1
1999
D
EN
MA
RK
151
Gen
eral
: Cat
hete
r 22
20
02
US
A
G
ener
al: C
athe
ter
59
2003
U
SA
G
ener
al: C
athe
ter
52
2002
E
UR
OP
EAN
UN
ION
G
ener
al: C
athe
ter
10
2001
U
SA
G
ener
al: C
athe
ter
24
2004
G
ER
MA
NY
G
ener
al: C
athe
ter
18
1999
E
UR
OP
EAN
UN
ION
G
ener
al: C
athe
ter
51
1996
A
US
TRAL
IA
G
ener
al: C
athe
ter
61
2004
U
SA
152
Gen
eral
: Cat
hete
r (D
iagn
ostic
) 24
20
04
GE
RM
AN
Y
G
ener
al: C
athe
ter (
Dia
gnos
tic)
3 20
03
US
A

14
9
153
Gen
eral
: Cat
hete
r (D
rain
age)
3
2003
U
SA
G
ener
al: C
athe
ter (
Dra
inag
e)
24
2004
G
ER
MA
NY
154
Gen
eral
: Cur
ette
(Sur
gery
) 3
2003
U
SA
155
Gen
eral
: Cut
ting
Equi
pmen
t 1
1999
D
EN
MA
RK
156
Gen
eral
: Syr
inge
64
20
03
UK
G
ener
al: S
yrin
ge
18
1999
E
UR
OP
EAN
UN
ION
G
ener
al: S
yrin
ge
61
2004
U
SA
157
Gen
eral
: Syr
inge
(Irri
gatin
g)
3 20
03
US
A
G
ener
al: S
yrin
ge (I
rriga
ting)
7
2000
U
SA
158
Gen
eral
: Syr
inge
(Pis
ton)
3
2003
U
SA
159
Gen
eral
: Tis
sue
Forc
eps
30
2004
A
US
TRAL
IA
160
Gen
eral
: Tou
rniq
uet
3 20
03
US
A
161
Gen
eral
: Tub
es
1 19
99
DE
NM
AR
K
G
ener
al: T
ubes
19
20
00
UK
162
Glo
ves
64
2003
U
K
163
Gou
ge (S
urge
ry)
3 20
03
US
A
164
Gow
ns
7 20
00
US
A
G
owns
3
2003
U
SA
165
Hem
odia
lysi
s B
lood
Circ
uit
3 20
03
US
A
H
emod
ialy
sis
Blo
od C
ircui
t 7
2000
U
SA
H
emod
ialy
sis
Blo
od C
ircui
t 65
20
05
US
A

15
0
H
emod
ialy
sis
Blo
od C
ircui
t 66
19
97
US
A
H
emod
ialy
sis
Blo
od C
ircui
t 67
19
96
US
A
166
Hem
orrh
oida
l Lig
ator
3
2003
U
SA
167
Hos
es
24
2004
G
ER
MA
NY
168
IAB
dev
ice
4 20
04
NEW
ZE
ALA
ND
169
Impl
ants
1
1999
D
EN
MA
RK
170
Infla
tion
Dev
ices
23
20
03
US
A
171
Infu
sion
Pum
p 3
2003
U
SA
172
Lapa
rosc
opes
7
2000
U
SA
La
paro
scop
es
2 20
01
CA
NA
DA
La
paro
scop
es
3 20
03
US
A
La
paro
scop
es
38
2003
U
SA
La
paro
scop
es
10
2001
C
AN
AD
A
La
paro
scop
es
51
1996
A
US
TRAL
IA
La
paro
scop
es
7 20
00
US
A
La
paro
scop
es
58
2004
U
SA
La
paro
scop
es
53
2004
U
SA
173
Lapa
rosc
opes
: Bab
cock
2
2001
C
AN
AD
A
174
Lapa
rosc
opes
: Cav
itron
Mic
ro N
eedl
e Ti
p 2
2001
C
AN
AD
A
175
Lapa
rosc
opes
: Cla
mps
39
20
04
US
A
176
Lapa
rosc
opes
: Dis
sect
ing
Hoo
k 2
2001
C
AN
AD
A

15
1
177
Lapa
rosc
opes
: Dis
sect
ors
7 20
00
US
A
La
paro
scop
es: D
isse
ctor
s 39
20
04
US
A
La
paro
scop
es: D
isse
ctor
s 3
2003
U
SA
La
paro
scop
es: D
isse
ctor
s
7 20
00
US
A
La
paro
scop
ic d
isse
ctio
n 68
20
02
GE
RM
AN
Y
178
Lapa
rosc
opes
: For
ceps
39
20
04
US
A
La
paro
scop
es: F
orce
ps
32
2003
A
US
TRAL
IA
179
Lapa
rosc
opes
: Gra
sper
s 7
2000
U
SA
La
paro
scop
es: G
rasp
ers
39
2004
U
SA
La
paro
scop
es: G
rasp
ers
3
2003
U
SA
180
Lapa
rosc
opes
: Sci
ssor
s 7
2000
U
SA
La
paro
scop
es: S
ciss
ors
21
2000
U
SA
La
paro
scop
es: S
ciss
ors
38
2003
U
SA
La
paro
scop
es: S
ciss
ors
2 20
01
CA
NA
DA
La
paro
scop
es: S
ciss
ors
51
1996
A
US
TRAL
IA
La
paro
scop
es: S
ciss
ors
8 20
00
US
A
La
paro
scop
es: S
ciss
ors
9
2004
C
AN
AD
A
La
paro
scop
es: S
ciss
ors
39
2004
U
SA
La
paro
scop
es: S
ciss
ors
32
2003
A
US
TRAL
IA
La
paro
scop
es: S
ciss
ors
3 20
03
US
A
181
Lapa
rosc
opes
: Tro
car
2 20
01
CA
NA
DA
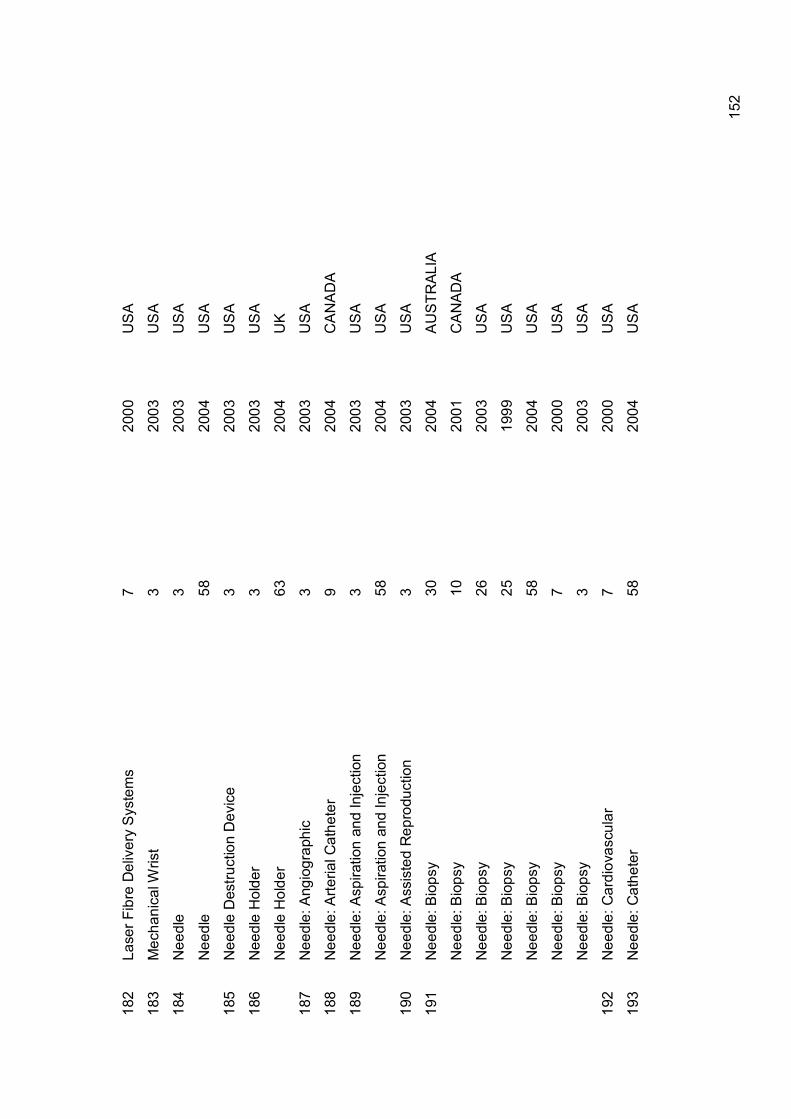
15
2
182
Lase
r Fib
re D
eliv
ery
Sys
tem
s 7
2000
U
SA
183
Mec
hani
cal W
rist
3 20
03
US
A
184
Nee
dle
3 20
03
US
A
N
eedl
e 58
20
04
US
A
185
Nee
dle
Des
truct
ion
Dev
ice
3
2003
U
SA
186
Nee
dle
Hol
der
3
2003
U
SA
N
eedl
e H
olde
r 63
20
04
UK
187
Nee
dle:
Ang
iogr
aphi
c 3
2003
U
SA
188
Nee
dle:
Arte
rial C
athe
ter
9
2004
C
AN
AD
A
189
Nee
dle:
Asp
iratio
n an
d In
ject
ion
3
2003
U
SA
N
eedl
e: A
spira
tion
and
Inje
ctio
n 58
20
04
US
A
190
Nee
dle:
Ass
iste
d R
epro
duct
ion
3 20
03
US
A
191
Nee
dle:
Bio
psy
30
20
04
AU
STR
ALIA
N
eedl
e: B
iops
y
10
2001
C
AN
AD
A
N
eedl
e: B
iops
y
26
2003
U
SA
N
eedl
e: B
iops
y
25
1999
U
SA
N
eedl
e: B
iops
y
58
2004
U
SA
N
eedl
e: B
iops
y
7 20
00
US
A
N
eedl
e: B
iops
y
3 20
03
US
A
192
Nee
dle:
Car
diov
ascu
lar
7 20
00
US
A
193
Nee
dle:
Cat
hete
r 58
20
04
US
A

15
3
194
Nee
dle:
Con
duct
ion
3 20
03
US
A
195
Nee
dle:
Ele
ctro
phys
iolo
gica
l (E
P)
10
2001
C
AN
AD
A
N
eedl
e: E
lect
roph
ysio
logi
cal (
EP
) 33
19
96
AU
STR
ALIA
N
eedl
e: E
lect
roph
ysio
logi
cal (
EP
) 18
19
99
EU
RO
PEA
N U
NIO
N
196
Nee
dle:
Hyp
oder
mic
Sin
gle
Lum
en
3 20
03
US
A
197
Nee
dle:
Isot
ope
3
2003
U
SA
198
Nee
dle:
Liv
er b
iops
y
10
2001
C
AN
AD
A
N
eedl
e: L
iver
bio
psy
2
2001
C
AN
AD
A
199
Nee
dle:
Par
acen
tesi
s
2 20
01
CA
NA
DA
200
Nee
dle:
Pha
ecom
ulsi
ficat
ion
7 20
00
US
A
N
eedl
e: P
haec
omul
sific
atio
n
3 20
03
US
A
201
Nee
dle:
Pne
umpe
riton
eum
3
2003
U
SA
202
Nee
dle:
Scl
erot
hera
py
10
2001
C
AN
AD
A
N
eedl
e: S
cler
othe
rapy
2
2001
C
AN
AD
A
N
eedl
e: S
cler
othe
rapy
32
20
03
AU
STR
ALIA
203
Nee
dle:
Sho
rt-te
rm S
pina
l 3
2003
U
SA
204
Nee
dle:
Sin
gle
Lum
en
3 20
03
US
A
205
Nee
dle:
Ste
reot
actic
2
2001
C
AN
AD
A
206
Ner
ve H
ooks
63
20
04
UK
207
Neu
rosu
rger
y: B
iops
y N
eedl
e 32
20
03
AU
STR
ALIA
208
Neu
rosu
rger
y: B
iops
y To
ol
10
2001
C
AN
AD
A
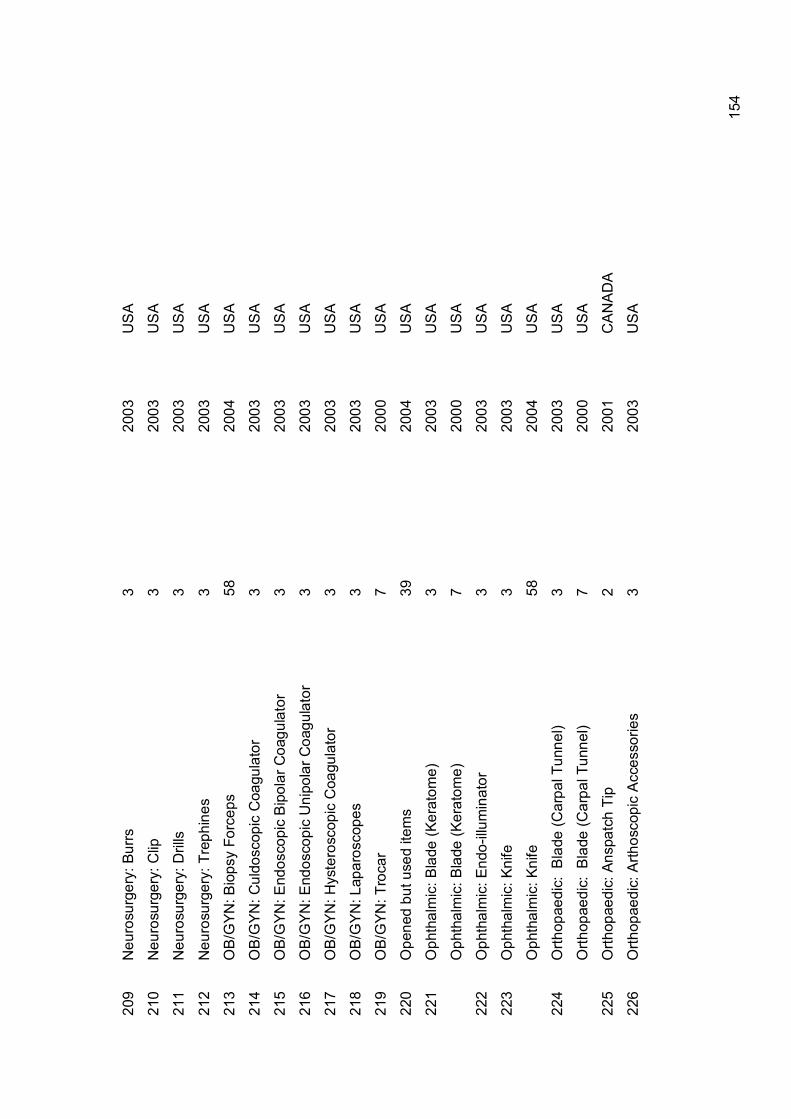
15
4
209
Neu
rosu
rger
y: B
urrs
3
2003
U
SA
210
Neu
rosu
rger
y: C
lip
3 20
03
US
A
211
Neu
rosu
rger
y: D
rills
3
2003
U
SA
212
Neu
rosu
rger
y: T
reph
ines
3
2003
U
SA
213
OB
/GYN
: Bio
psy
Forc
eps
58
2004
U
SA
214
OB
/GYN
: Cul
dosc
opic
Coa
gula
tor
3 20
03
US
A
215
OB
/GYN
: End
osco
pic
Bip
olar
Coa
gula
tor
3 20
03
US
A
216
OB
/GYN
: End
osco
pic
Uni
pola
r Coa
gula
tor
3 20
03
US
A
217
OB
/GYN
: Hys
tero
scop
ic C
oagu
lato
r 3
2003
U
SA
218
OB
/GYN
: Lap
aros
cope
s
3 20
03
US
A
219
OB
/GYN
: Tro
car
7 20
00
US
A
220
Ope
ned
but u
sed
item
s 39
20
04
US
A
221
Oph
thal
mic
: Bla
de (K
erat
ome)
3
2003
U
SA
O
phth
alm
ic: B
lade
(Ker
atom
e)
7 20
00
US
A
222
Oph
thal
mic
: End
o-illu
min
ator
3
2003
U
SA
223
Oph
thal
mic
: Kni
fe
3 20
03
US
A
O
phth
alm
ic: K
nife
58
20
04
US
A
224
Orth
opae
dic:
Bla
de (C
arpa
l Tun
nel)
3
2003
U
SA
O
rthop
aedi
c: B
lade
(Car
pal T
unne
l)
7 20
00
US
A
225
Orth
opae
dic:
Ans
patc
h Ti
p
2 20
01
CA
NA
DA
226
Orth
opae
dic:
Arth
osco
pic
Acc
esso
ries
3
2003
U
SA

15
5
227
Orth
opae
dic:
Arth
osco
pic
shav
ers
& w
ands
38
20
03
US
A
O
rthop
aedi
c: A
rthos
copi
c w
ands
23
20
03
US
A
228
Orth
opae
dic:
Arth
rosc
opic
Inst
rum
ents
24
20
04
GE
RM
AN
Y
O
rthop
aedi
c: A
rthro
scop
ic in
stru
men
ts
7 20
00
US
A
229
Orth
opae
dic:
Arth
rosc
opic
sha
ver b
lade
s 24
20
04
GE
RM
AN
Y
230
Orth
opae
dic:
Arth
rosc
opic
Sha
vers
39
20
04
US
A
231
Orth
opae
dic:
Bla
des
23
20
03
US
A
232
Orth
opae
dic:
Bon
e H
ook
(Sur
gery
) 3
2003
U
SA
233
Orth
opae
dic:
Bon
e Ta
p
3 20
03
US
A
234
Orth
opae
dic:
Bon
e-m
arro
w tr
ephi
ne s
ets
51
1996
A
US
TRAL
IA
235
Orth
opae
dic:
Bur
r
3 20
03
US
A
O
rthop
aedi
c: B
urr
23
20
03
US
A
O
rthop
aedi
c: B
urr
7
2000
U
SA
O
rthop
aedi
c: B
urr
39
20
04
US
A
O
rthop
aedi
c: B
urr
53
20
04
US
A
236
Orth
opae
dic:
Cou
nter
sink
3
2003
U
SA
237
Orth
opae
dic:
Dril
l Bit
3 20
03
US
A
O
rthop
aedi
c: D
rill B
it
7 20
00
US
A
O
rthop
aedi
c: D
rill B
it
39
2004
U
SA
O
rthop
aedi
c: D
rill B
it
61
2004
U
SA
O
rthop
aedi
c: D
rill B
it
7 20
00
US
A
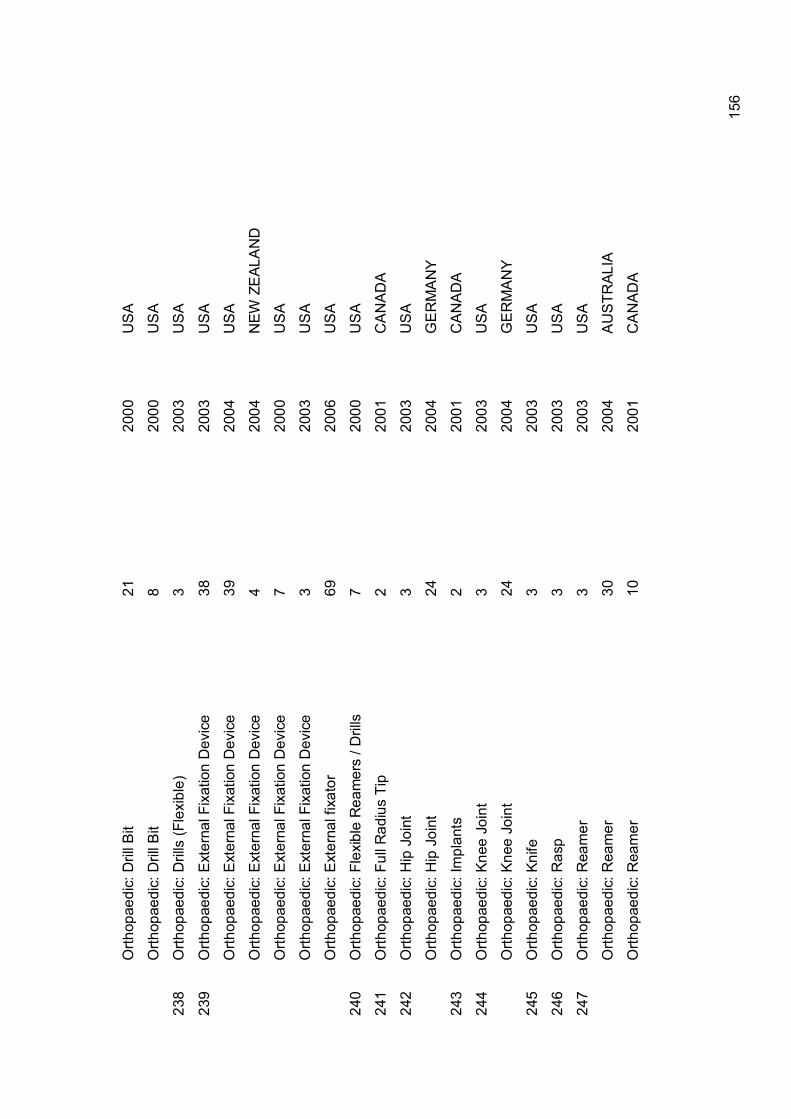
15
6
O
rthop
aedi
c: D
rill B
it
21
2000
U
SA
O
rthop
aedi
c: D
rill B
it
8 20
00
US
A
238
Orth
opae
dic:
Dril
ls (F
lexi
ble)
3
2003
U
SA
239
Orth
opae
dic:
Ext
erna
l Fix
atio
n D
evic
e 38
20
03
US
A
O
rthop
aedi
c: E
xter
nal F
ixat
ion
Dev
ice
39
2004
U
SA
O
rthop
aedi
c: E
xter
nal F
ixat
ion
Dev
ice
4 20
04
NEW
ZE
ALA
ND
O
rthop
aedi
c: E
xter
nal F
ixat
ion
Dev
ice
7 20
00
US
A
O
rthop
aedi
c: E
xter
nal F
ixat
ion
Dev
ice
3 20
03
US
A
O
rthop
aedi
c: E
xter
nal f
ixat
or
69
2006
U
SA
240
Orth
opae
dic:
Fle
xibl
e R
eam
ers
/ Dril
ls
7 20
00
US
A
241
Orth
opae
dic:
Ful
l Rad
ius
Tip
2 20
01
CA
NA
DA
242
Orth
opae
dic:
Hip
Joi
nt
3 20
03
US
A
O
rthop
aedi
c: H
ip J
oint
24
20
04
GE
RM
AN
Y
243
Orth
opae
dic:
Impl
ants
2
2001
C
AN
AD
A
244
Orth
opae
dic:
Kne
e Jo
int
3 20
03
US
A
O
rthop
aedi
c: K
nee
Join
t 24
20
04
GE
RM
AN
Y
245
Orth
opae
dic:
Kni
fe
3 20
03
US
A
246
Orth
opae
dic:
Ras
p
3 20
03
US
A
247
Orth
opae
dic:
Rea
mer
3
2003
U
SA
O
rthop
aedi
c: R
eam
er
30
2004
A
US
TRAL
IA
O
rthop
aedi
c: R
eam
er
10
2001
C
AN
AD
A

15
7
248
Orth
opae
dic:
Sho
ulde
r Joi
nt
3 20
03
US
A
249
Orth
opae
dic:
Tre
phin
e
3 20
03
US
A
250
Orth
opae
dics
: Ron
geur
3
2003
U
SA
251
Pel
visc
ope
24
2004
G
ER
MA
NY
252
Pha
co T
ips
39
2004
U
SA
253
Pha
cofra
gmen
tatio
n sy
stem
3
2003
U
SA
254
PH
-met
ric e
lect
rode
s 24
20
04
GE
RM
AN
Y
255
Pne
umat
ic T
ourn
ique
t Cuf
fs
39
2004
U
SA
256
Pol
ypec
tom
y sl
ing
24
2004
G
ER
MA
NY
257
Pro
be: A
rgon
pla
sma
coag
ulat
ion
25
19
99
US
A
P
robe
: Arg
on p
lasm
a co
agul
atio
n 4
2004
N
EW Z
EAL
AN
D
258
Pro
bes
/ las
er p
robe
s 24
20
04
GE
RM
AN
Y
259
Pro
bes:
Pac
emak
er
24
2004
G
ER
MA
NY
260
Pro
lene
mes
h 7
2000
U
SA
261
Pro
sthe
sis
1 19
99
DE
NM
AR
K
P
rost
hesi
s 24
20
04
GE
RM
AN
Y
P
rost
hesi
s 38
20
03
US
A
262
PTC
A
53
2004
U
SA
263
Pul
se O
xim
eter
3
2003
U
SA
P
ulse
Oxi
met
er
53
2004
U
SA
264
Pul
se O
xim
eter
Sen
sors
39
20
04
US
A

15
8
P
ulse
Oxi
met
er S
enso
rs
28
2002
U
SA
265
Pum
p ho
ses
24
2004
G
ER
MA
NY
266
PV
B pr
essu
re c
onve
rter
24
2004
G
ER
MA
NY
267
Rad
iolo
gy: B
ile D
uct S
tone
Ext
ract
or
2 20
01
CA
NA
DA
268
Rad
iolo
gy: C
athe
ter
29
2001
U
SA
269
Res
pira
tory
/ P
ulm
onar
y: N
asal
Pro
ngs
2 20
01
CA
NA
DA
270
Res
pira
tory
/ P
ulm
onar
y: T
rach
eost
omy
tubi
ng
2 20
01
CA
NA
DA
271
Saw
53
20
04
US
A
S
aw
3 20
03
US
A
S
aw
39
2004
U
SA
272
Saw
Bla
de
3 20
03
US
A
S
aw B
lade
24
20
04
GE
RM
AN
Y
S
aw B
lade
7
2000
U
SA
S
aw B
lade
61
20
04
US
A
S
aw B
lade
21
20
00
US
A
S
aw B
lade
59
20
03
US
A
S
aw B
lade
8
2000
U
SA
273
Sca
lpel
bla
de
3 20
03
US
A
274
Sci
ssor
Tip
s
7 20
00
US
A
275
Sci
ssor
s 39
20
04
US
A
S
ciss
ors
3
2003
U
SA
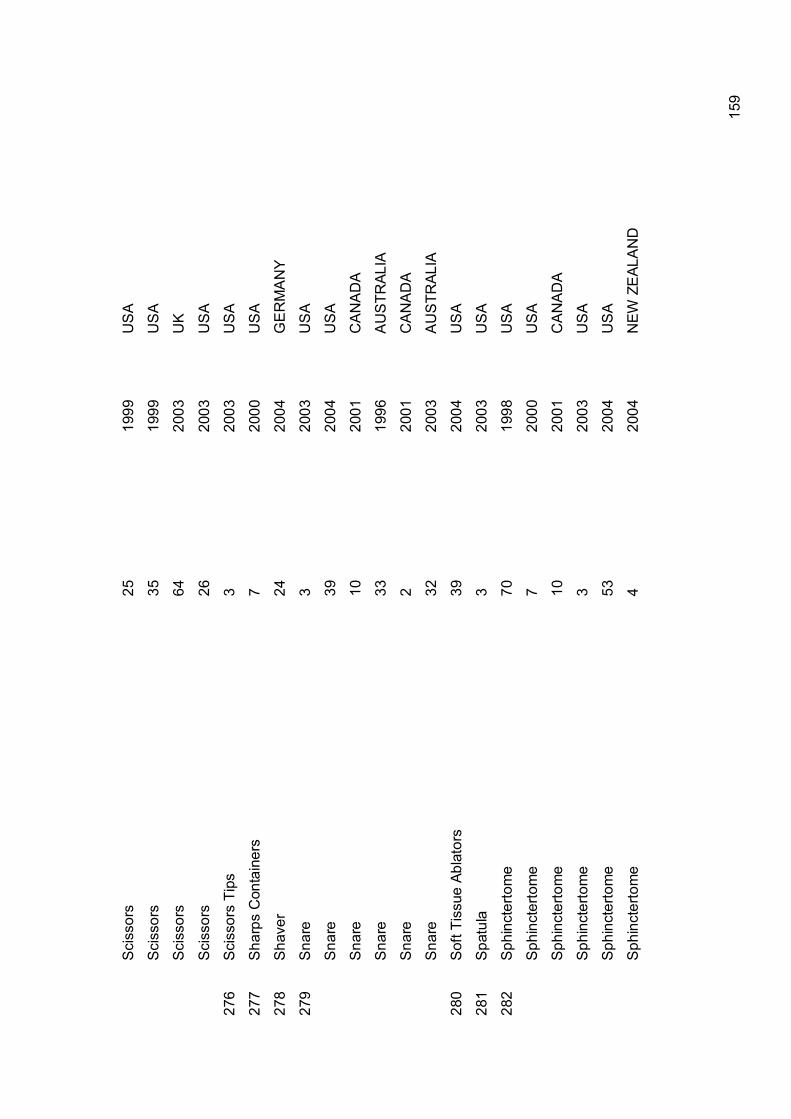
15
9
S
ciss
ors
25
19
99
US
A
S
ciss
ors
35
19
99
US
A
S
ciss
ors
64
20
03
UK
S
ciss
ors
26
20
03
US
A
276
Sci
ssor
s Ti
ps
3 20
03
US
A
277
Sha
rps
Con
tain
ers
7 20
00
US
A
278
Sha
ver
24
2004
G
ER
MA
NY
279
Sna
re
3 20
03
US
A
S
nare
39
20
04
US
A
S
nare
10
20
01
CA
NA
DA
S
nare
33
19
96
AU
STR
ALIA
S
nare
2
2001
C
AN
AD
A
S
nare
32
20
03
AU
STR
ALIA
280
Sof
t Tis
sue
Abla
tors
39
20
04
US
A
281
Spa
tula
3
2003
U
SA
282
Sph
inct
erto
me
70
1998
U
SA
S
phin
cter
tom
e 7
2000
U
SA
S
phin
cter
tom
e 10
20
01
CA
NA
DA
S
phin
cter
tom
e 3
2003
U
SA
S
phin
cter
tom
e 53
20
04
US
A
S
phin
cter
tom
e 4
2004
N
EW Z
EAL
AN
D

16
0
S
phin
cter
otom
e 9
20
04
CA
NA
DA
S
phin
cter
tom
es
71
2003
U
SA
S
phin
cter
tom
es
72
1997
U
SA
283
Suc
tion
Scr
ews
24
2004
G
ER
MA
NY
284
Sur
gery
: Cat
hete
r Nee
dle
3
2003
U
SA
285
Syr
inge
Pis
ton
& In
fusi
on Im
plan
ted
Pum
ps
7 20
00
US
A
286
Uro
logy
: D
ialy
sis
Set
3
2003
U
SA
287
Uro
logy
: Cat
hete
r (B
iliary
) 3
2003
U
SA
U
rolo
gy: C
athe
ter (
Bilia
ry)
24
2004
G
ER
MA
NY
288
Uro
logy
: Cat
hete
r (B
ladd
er &
rect
al c
athe
ters
) 24
20
04
GE
RM
AN
Y
289
Uro
logy
: Cat
hete
r (U
reth
ral)
7 20
00
US
A
U
rolo
gy: C
athe
ter (
Ure
thra
l) 2
2001
C
AN
AD
A
U
rolo
gy: C
athe
ter (
Ure
thra
l) 3
2003
U
SA
290
Uro
logy
: Pap
illoto
me
24
20
04
GE
RM
AN
Y
291
Uro
logy
: Pen
ile R
ing
2
2001
C
AN
AD
A
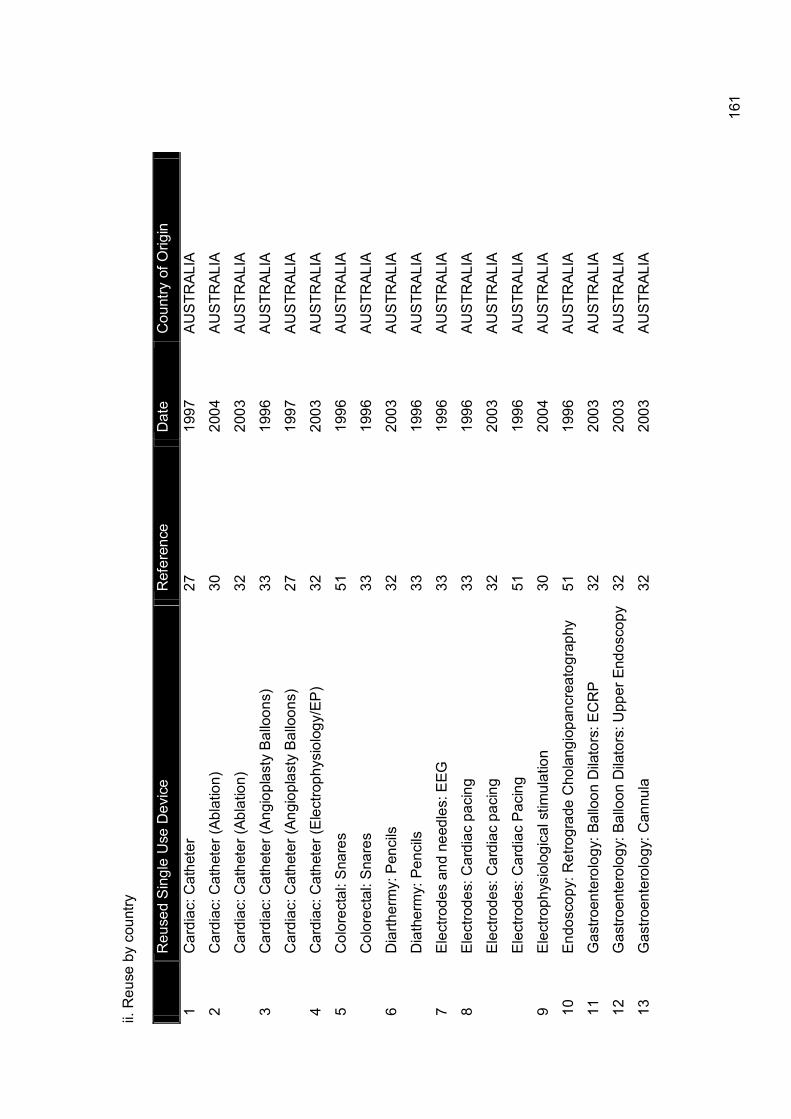
16
1
ii. R
euse
by
coun
try
R
euse
d S
ingl
e U
se D
evic
e R
efer
ence
D
ate
C
ount
ry o
f Orig
in
1 C
ardi
ac: C
athe
ter
27
1997
A
US
TRAL
IA
2 C
ardi
ac: C
athe
ter (
Abla
tion)
30
20
04
AU
STR
ALIA
C
ardi
ac: C
athe
ter (
Abla
tion)
32
20
03
AU
STR
ALIA
3 C
ardi
ac: C
athe
ter (
Angi
opla
sty
Bal
loon
s)
33
1996
A
US
TRAL
IA
C
ardi
ac: C
athe
ter (
Angi
opla
sty
Bal
loon
s)
27
1997
A
US
TRAL
IA
4 C
ardi
ac: C
athe
ter (
Ele
ctro
phys
iolo
gy/E
P)
32
2003
A
US
TRAL
IA
5 C
olor
ecta
l: S
nare
s 51
19
96
AU
STR
ALIA
C
olor
ecta
l: S
nare
s 33
19
96
AU
STR
ALIA
6 D
iarth
erm
y: P
enci
ls
32
2003
A
US
TRAL
IA
D
iath
erm
y: P
enci
ls
33
1996
A
US
TRAL
IA
7 E
lect
rode
s an
d ne
edle
s: E
EG
33
1996
A
US
TRAL
IA
8 E
lect
rode
s: C
ardi
ac p
acin
g
33
1996
A
US
TRAL
IA
E
lect
rode
s: C
ardi
ac p
acin
g
32
2003
A
US
TRAL
IA
E
lect
rode
s: C
ardi
ac P
acin
g
51
1996
A
US
TRAL
IA
9 E
lect
roph
ysio
logi
cal s
timul
atio
n
30
2004
A
US
TRAL
IA
10
End
osco
py: R
etro
grad
e C
hola
ngio
panc
reat
ogra
phy
51
19
96
AU
STR
ALIA
11
Gas
troen
tero
logy
: Bal
loon
Dila
tors
: EC
RP
32
20
03
AU
STR
ALIA
12
Gas
troen
tero
logy
: Bal
loon
Dila
tors
: Upp
er E
ndos
copy
32
20
03
AU
STR
ALIA
13
Gas
troen
tero
logy
: Can
nula
32
20
03
AU
STR
ALIA

16
2
14
Gas
troen
tero
logy
: Cyt
olog
y br
ushe
s
32
2003
A
US
TRAL
IA
15
Gas
troen
tero
logy
: Sto
ne R
emov
ing
Bas
kets
32
20
03
AU
STR
ALIA
16
Gen
eral
Sur
gica
l: B
iops
y Fo
rcep
s (A
rteria
l) 30
20
04
AU
STR
ALIA
17
Gen
eral
Sur
gica
l: K
nife
32
20
03
AU
STR
ALIA
18
Gen
eral
: Cat
hete
r 51
19
96
AU
STR
ALIA
19
Gen
eral
: Tis
sue
Forc
eps
30
2004
A
US
TRAL
IA
20
Lapa
rosc
opes
51
19
96
AU
STR
ALIA
21
Lapa
rosc
opes
: For
ceps
32
20
03
AU
STR
ALIA
22
Lapa
rosc
opes
: Sci
ssor
s 51
19
96
AU
STR
ALIA
La
paro
scop
es: S
ciss
ors
32
2003
A
US
TRAL
IA
23
Nee
dle:
Bio
psy
30
20
04
AU
STR
ALIA
24
Nee
dle:
Ele
ctro
phys
iolo
gica
l (E
P)
33
1996
A
US
TRAL
IA
25
Nee
dle:
Scl
erot
hera
py
32
2003
A
US
TRAL
IA
26
Neu
rosu
rger
y: B
iops
y N
eedl
e 32
20
03
AU
STR
ALIA
27
Orth
opae
dic:
Bon
e-m
arro
w tr
ephi
ne s
ets
51
1996
A
US
TRAL
IA
28
Orth
opae
dic:
Rea
mer
30
20
04
AU
STR
ALIA
29
Sna
re
33
1996
A
US
TRAL
IA
S
nare
32
20
03
AU
STR
ALIA

16
3
1 A
mbu
bag
(Neo
nata
l)
2 20
01
CA
NA
DA
2 A
naes
thes
ia: B
ite B
lock
2
2001
C
AN
AD
A
3 A
naes
thes
ia: B
reat
hing
Circ
uits
9
20
04
CA
NA
DA
A
naes
thes
ia: B
reat
hing
Circ
uits
10
20
01
CA
NA
DA
4 A
naes
thes
ia: E
ndot
rach
eal T
ube
10
2001
C
AN
AD
A
A
naes
thes
ia: E
ndot
rach
eal T
ube
2 20
01
CA
NA
DA
5 A
naes
thes
ia: I
ntub
atin
g st
ylet
tes
(bou
gies
) 2
2001
C
AN
AD
A
6 A
naes
thes
ia: N
ebul
iser
s 10
20
01
CA
NA
DA
7 A
naes
thes
ia: O
ral a
irway
s 2
2001
C
AN
AD
A
8 A
naes
thes
ia: T
-pie
ce
2 20
01
CA
NA
DA
9 C
ardi
ac: C
athe
ter
10
2001
C
AN
AD
A
C
ardi
ac: C
athe
ter
9
2004
C
AN
AD
A
10
Car
diac
: Cat
hete
r (An
giog
raph
y)
9
2004
C
AN
AD
A
C
ardi
ac: C
athe
ter (
Angi
ogra
phy)
2
2001
C
AN
AD
A
11
Car
diac
: Cat
hete
r (An
giop
last
y B
allo
ons)
2
2001
C
AN
AD
A
12
Car
diac
: Cat
hete
r (E
lect
roph
ysio
logy
/EP
) 2
2001
C
AN
AD
A
13
Car
diac
: Cat
hete
r (G
uide
wire
) 10
20
01
CA
NA
DA
C
ardi
ac: C
athe
ter (
Gui
dew
ire)
2 20
01
CA
NA
DA
14
Car
diac
: Con
cent
ric N
eedl
es (E
lect
roph
ysio
logy
) 2
2001
C
AN
AD
A
15
Car
diac
: Pac
emak
er
10
2001
C
AN
AD
A
C
ardi
ac: P
acem
aker
2
2001
C
AN
AD
A

16
4
16
Car
diac
: Tra
nsdu
cer
10
2001
C
AN
AD
A
C
ardi
ac: T
rans
duce
r 2
2001
C
AN
AD
A
17
Col
orec
tal:
Man
omet
ry T
ubin
g
2 20
01
CA
NA
DA
18
Der
mat
olog
y: E
lect
roca
uter
y tip
(hyf
reca
tor)
2 20
01
CA
NA
DA
19
Ele
ctro
des
and
need
les:
EEG
10
20
01
CA
NA
DA
E
lect
roph
ysio
logy
: EEG
Nee
dle-
Bon
net
2 20
01
CA
NA
DA
20
End
osco
py: B
allo
ons
2
2001
C
AN
AD
A
21
Gas
troen
tero
logy
: Bal
loon
Ext
ract
or
2 20
01
CA
NA
DA
22
Gas
troen
tero
logy
: Bio
psy
Forc
eps
(Mic
roev
asiv
e)
2 20
01
CA
NA
DA
23
Gas
troen
tero
logy
: C
athe
ter
(Coa
gula
tion
Ele
ctro
-
hem
osta
tis)
2 20
01
CA
NA
DA
24
Gas
troen
tero
logy
: Cyt
olog
y br
ushe
s
2 20
01
CA
NA
DA
25
Gas
troen
tero
logy
: Dila
tion
Bal
loon
s 10
20
01
CA
NA
DA
26
Gas
troen
tero
logy
: Ele
ctro
de (L
oop)
2
2001
C
AN
AD
A
27
Gas
troen
tero
logy
: Eso
phag
eal S
tent
2
2001
C
AN
AD
A
28
Gas
troen
tero
logy
: Pol
yp fo
rcep
s 9
20
04
CA
NA
DA
29
Gen
eral
Sur
gery
: Ext
ract
or
9
2004
C
AN
AD
A
30
Gen
eral
Sur
gica
l: B
iops
y Fo
rcep
s 11
20
04
CA
NA
DA
G
ener
al S
urgi
cal:
Bio
psy
Forc
eps
10
2001
C
AN
AD
A
G
ener
al S
urgi
cal:
Bio
psy
Forc
eps
2 20
01
CA
NA
DA
31
Lapa
rosc
opes
2
2001
C
AN
AD
A

16
5
La
paro
scop
es
10
2001
C
AN
AD
A
32
Lapa
rosc
opes
: Bab
cock
2
2001
C
AN
AD
A
33
Lapa
rosc
opes
: Cav
itron
Mic
ro N
eedl
e Ti
p 2
2001
C
AN
AD
A
34
Lapa
rosc
opes
: Dis
sect
ing
Hoo
k 2
2001
C
AN
AD
A
35
Lapa
rosc
opes
: Sci
ssor
s 2
2001
C
AN
AD
A
La
paro
scop
es: S
ciss
ors
9
2004
C
AN
AD
A
36
Lapa
rosc
opes
: Tro
car
2 20
01
CA
NA
DA
37
Nee
dle:
Arte
rial C
athe
ter
9
2004
C
AN
AD
A
38
Nee
dle:
Bio
psy
10
20
01
CA
NA
DA
39
Nee
dle:
Ele
ctro
phys
iolo
gica
l (E
P)
10
2001
C
AN
AD
A
40
Nee
dle:
Liv
er b
iops
y
10
2001
C
AN
AD
A
N
eedl
e: L
iver
bio
psy
2
2001
C
AN
AD
A
41
Nee
dle:
Par
acen
tesi
s
2 20
01
CA
NA
DA
42
Nee
dle:
Scl
erot
hera
py
10
2001
C
AN
AD
A
N
eedl
e: S
cler
othe
rapy
2
2001
C
AN
AD
A
43
Nee
dle:
Ste
reot
actic
2
2001
C
AN
AD
A
44
Neu
rosu
rger
y: B
iops
y To
ol
10
2001
C
AN
AD
A
45
Orth
opae
dic:
Ans
patc
h Ti
p
2 20
01
CA
NA
DA
46
Orth
opae
dic:
Ful
l Rad
ius
Tip
2 20
01
CA
NA
DA
47
Orth
opae
dic:
Impl
ants
2
2001
C
AN
AD
A
48
Orth
opae
dic:
Rea
mer
10
20
01
CA
NA
DA

16
6
49
Rad
iolo
gy: B
ile D
uct S
tone
Ext
ract
or
2 20
01
CA
NA
DA
50
Res
pira
tory
/ P
ulm
onar
y: N
asal
Pro
ngs
2 20
01
CA
NA
DA
51
Res
pira
tory
/ P
ulm
onar
y: T
rach
eost
omy
tubi
ng
2 20
01
CA
NA
DA
52
Sna
re
10
2001
C
AN
AD
A
S
nare
2
2001
C
AN
AD
A
53
Sph
inct
erto
me
10
2001
C
AN
AD
A
S
phnc
tero
tom
e 9
20
04
CA
NA
DA
54
Uro
logy
: Cat
hete
r (U
reth
ral)
2 20
01
CA
NA
DA
55
Uro
logy
: Pen
ile R
ing
2
2001
C
AN
AD
A
1 A
graf
Equ
ipm
ent
1 19
99
DE
NM
AR
K
2 A
naes
thes
ia: I
ntub
atio
n E
quip
men
t 1
1999
D
EN
MA
RK
3 A
naes
thes
ia: M
asks
1
1999
D
EN
MA
RK
4 C
ardi
ac: C
athe
ter (
Gui
dew
ire)
1 19
99
DE
NM
AR
K
5 E
lect
rode
s 1
1999
D
EN
MA
RK
6 E
ndos
cope
1
1999
D
EN
MA
RK
7 E
ndos
copy
: Sut
ures
1
1999
D
EN
MA
RK
8 G
astro
ente
rolo
gy: D
ilatio
n B
allo
ons
1 19
99
DE
NM
AR
K
9 G
ener
al: B
rush
es
1 19
99
DE
NM
AR
K
10
Gen
eral
: Cab
les
1
1999
D
EN
MA
RK
11
Gen
eral
: Cut
ting
Equi
pmen
t 1
1999
D
EN
MA
RK

16
7
12
Gen
eral
: Tub
es
1 19
99
DE
NM
AR
K
13
Impl
ants
1
1999
D
EN
MA
RK
14
Pro
sthe
sis
1 19
99
DE
NM
AR
K
1 A
naes
thes
ia: L
MA
s
18
1999
E
UR
OP
EAN
UN
ION
2 A
naes
thes
ia: T
ubin
g 18
19
99
EU
RO
PEA
N U
NIO
N
3 C
ardi
ac: C
athe
ter (
Abla
tion)
29
20
02
EU
RO
PEA
N U
NIO
N
4 C
ardi
ac: C
athe
ter (
Ballo
on)
36
2002
E
UR
OP
EAN
UN
ION
5 C
ardi
ac: C
athe
ter (
Ele
ctro
phys
iolo
gy/E
P)
41
2000
E
UR
OP
EAN
UN
ION
C
ardi
ac: C
athe
ter (
Ele
ctro
phys
iolo
gy/E
P)
36
2002
E
UR
OP
EAN
UN
ION
6 C
ardi
ac: C
athe
ter (
Gui
dew
ire)
41
2003
E
UR
OP
EAN
UN
ION
7 C
ardi
ac: C
athe
ter
18
1999
E
UR
OP
EAN
UN
ION
8 C
ardi
ac: D
efib
rilla
tors
42
19
99
EU
RO
PEA
N U
NIO
N
9 C
ardi
ac: P
acem
aker
43
19
98
EU
RO
PEA
N U
NIO
N
10
Ele
ctro
des
and
need
les:
EEG
18
19
99
EU
RO
PEA
N U
NIO
N
11
Ele
ctro
des:
Silv
er
52
2002
E
UR
OP
EAN
UN
ION
12
End
osco
py: C
lip A
pplie
r 36
20
02
EU
RO
PEA
N U
NIO
N
13
Gen
eral
Sur
gica
l: B
iops
y Fo
rcep
s 41
20
03
EU
RO
PEA
N U
NIO
N
14
Gen
eral
Sur
gica
l: C
lip A
pplie
r 52
20
02
EU
RO
PEA
N U
NIO
N
15
Gen
eral
Sur
gica
l: Tr
ocar
18
19
99
EU
RO
PEA
N U
NIO
N
16
Gen
eral
: Cat
hete
r 52
20
02
EU
RO
PEA
N U
NIO
N

16
8
17
Gen
eral
: Cat
hete
r (D
iagn
ostic
) 18
19
99
EU
RO
PEA
N U
NIO
N
18
Gen
eral
: Syr
inge
18
19
99
EU
RO
PEA
N U
NIO
N
19
Nee
dle:
Ele
ctro
phys
iolo
gica
l (E
P)
18
1999
E
UR
OP
EAN
UN
ION
1 C
ardi
ac: C
athe
ter
24
2004
G
ER
MA
NY
2 C
ardi
ac: C
athe
ter (
Ach
alas
ia b
allo
on)
24
2004
G
ER
MA
NY
3 C
ardi
ac: C
athe
ter (
Angi
opla
sty
Bal
loon
s)
24
2004
G
ER
MA
NY
4 C
ardi
ac: C
athe
ter (
Con
trast
Age
nt)
24
2004
G
ER
MA
NY
5 C
ardi
ac: D
efib
rilla
tors
(Im
plan
tabl
e)
24
2004
G
ER
MA
NY
6 C
ardi
ac: P
acem
aker
24
20
04
GE
RM
AN
Y
7 E
lect
rode
s: R
esec
tosc
ope
24
20
04
GE
RM
AN
Y
8 G
astro
ente
rolo
gy: B
allo
on s
yste
m fo
r ute
rus
abla
tion
24
2004
G
ER
MA
NY
9 G
ener
al S
urgi
cal C
lam
p (V
ascu
lar)
24
2004
G
ER
MA
NY
10
Gen
eral
Sur
gica
l: B
iops
y Fo
rcep
s 24
20
04
GE
RM
AN
Y
G
ener
al S
urgi
cal:
Bio
psy
Forc
eps
60
2000
G
ER
MA
NY
11
Gen
eral
Sur
gica
l: C
lam
p ho
lder
24
20
04
GE
RM
AN
Y
12
Gen
eral
Sur
gica
l: C
lips
24
2004
G
ER
MA
NY
13
Gen
eral
Sur
gica
l: Tr
ocar
24
20
04
GE
RM
AN
Y
14
Gen
eral
: Cat
hete
r 24
20
04
GE
RM
AN
Y
15
Gen
eral
: Cat
hete
r (D
iagn
ostic
) 24
20
04
GE
RM
AN
Y
16
Gen
eral
: Cat
hete
r (D
rain
age)
24
20
04
GE
RM
AN
Y

16
9
17
Hos
es
24
2004
G
ER
MA
NY
18
Orth
opae
dic:
Arth
rosc
opic
Inst
rum
ents
24
20
04
GE
RM
AN
Y
19
Orth
opae
dic:
Arth
rosc
opic
sha
ver b
lade
s 24
20
04
GE
RM
AN
Y
20
Orth
opae
dic:
Hip
Joi
nt
24
2004
G
ER
MA
NY
21
Orth
opae
dic:
Kne
e Jo
int
24
2004
G
ER
MA
NY
22
Pel
visc
ope
24
2004
G
ER
MA
NY
23
PH
-met
ric e
lect
rode
s 24
20
04
GE
RM
AN
Y
24
Pol
ypec
tom
y sl
ing
24
2004
G
ER
MA
NY
25
Pro
bes
/ las
er p
robe
s 24
20
04
GE
RM
AN
Y
26
Pro
bes:
Pac
emak
er
24
2004
G
ER
MA
NY
27
Pro
sthe
sis
24
2004
G
ER
MA
NY
28
Pum
p ho
ses
24
2004
G
ER
MA
NY
29
PV
B pr
essu
re c
onve
rter
24
2004
G
ER
MA
NY
30
Saw
Bla
de
24
2004
G
ER
MA
NY
31
Sha
ver
24
2004
G
ER
MA
NY
32
Suc
tion
Scr
ews
24
2004
G
ER
MA
NY
33
Uro
logy
: Cat
hete
r (B
iliary
) 24
20
04
GE
RM
AN
Y
34
Uro
logy
: Cat
hete
r (B
ladd
er &
rect
al c
athe
ters
) 24
20
04
GE
RM
AN
Y
35
Uro
logy
: Pap
illoto
me
24
20
04
GE
RM
AN
Y

17
0
1 A
naes
thes
ia: A
irway
Dev
ice
4 20
04
NEW
ZE
ALA
ND
2 A
naes
thes
ia: B
ronc
hosc
ope
4 20
04
NEW
ZE
ALA
ND
3 A
naes
thes
ia: F
ilter
4
2004
N
EW Z
EAL
AN
D
4 A
ngio
scop
e 4
2004
N
EW Z
EAL
AN
D
5 C
ardi
ac: C
athe
ter
4 20
04
NEW
ZE
ALA
ND
6 C
ardi
ac: C
athe
ter (
Abla
tion)
4
2004
N
EW Z
EAL
AN
D
7 C
ardi
ac: C
athe
ter (
Angi
opla
sty
Bal
loon
s)
4 20
04
NEW
ZE
ALA
ND
8 C
ardi
ac: C
athe
ter (
Ballo
on)
4 20
04
NEW
ZE
ALA
ND
9 C
ardi
ac: C
athe
ter (
Ele
ctro
phys
iolo
gy/E
P)
4 20
04
NEW
ZE
ALA
ND
10
Gen
eral
Sur
gica
l: B
iops
y Fo
rcep
s 4
2004
N
EW Z
EAL
AN
D
11
Gen
eral
Sur
gica
l: Tr
ocar
4
2004
N
EW Z
EAL
AN
D
12
IAB
dev
ice
4 20
04
NEW
ZE
ALA
ND
13
Orth
opae
dic:
Ext
erna
l Fix
atio
n D
evic
e 4
2004
N
EW Z
EAL
AN
D
14
Pro
be: A
rgon
Pla
sma
Coa
gula
tion
4 20
04
NEW
ZE
ALA
ND
15
Sph
inct
erto
me
4 20
04
NEW
ZE
ALA
ND
1 A
naes
thes
ia: A
ngle
pie
ce c
onne
ctor
in P
CB
6
2004
U
K
2 A
naes
thes
ia: C
athe
ter m
ount
on
PC
B
12
2004
U
K
A
naes
thes
ia: C
athe
ter m
ount
on
PC
B
13
2002
U
K
3 A
naes
thes
ia: F
ilter
14
20
04
UK
A
naes
thes
ia: F
ilter
15
20
01
UK
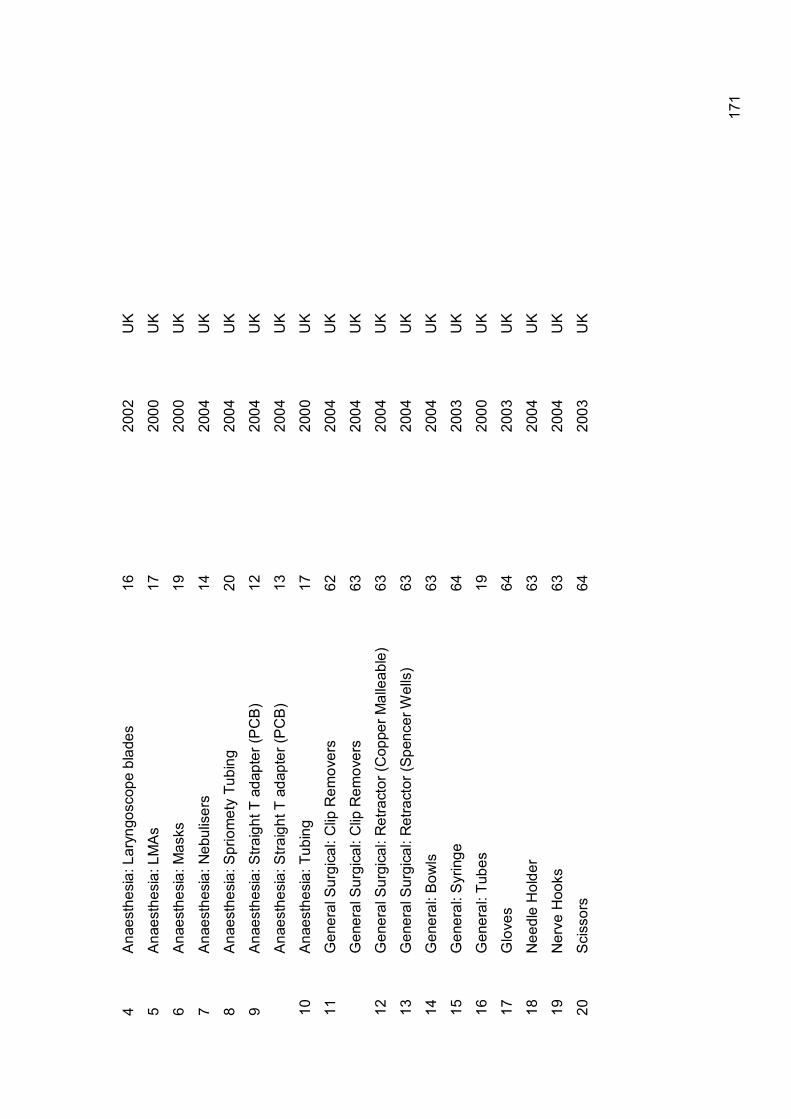
17
1
4 A
naes
thes
ia: L
aryn
gosc
ope
blad
es
16
2002
U
K
5 A
naes
thes
ia: L
MA
s
17
2000
U
K
6 A
naes
thes
ia: M
asks
19
20
00
UK
7 A
naes
thes
ia: N
ebul
iser
s 14
20
04
UK
8 A
naes
thes
ia: S
prio
met
y Tu
bing
20
20
04
UK
9 A
naes
thes
ia: S
traig
ht T
ada
pter
(PC
B)
12
2004
U
K
A
naes
thes
ia: S
traig
ht T
ada
pter
(PC
B)
13
2004
U
K
10
Ana
esth
esia
: Tub
ing
17
2000
U
K
11
Gen
eral
Sur
gica
l: C
lip R
emov
ers
62
2004
U
K
G
ener
al S
urgi
cal:
Clip
Rem
over
s 63
20
04
UK
12
Gen
eral
Sur
gica
l: R
etra
ctor
(Cop
per M
alle
able
) 63
20
04
UK
13
Gen
eral
Sur
gica
l: R
etra
ctor
(Spe
ncer
Wel
ls)
63
2004
U
K
14
Gen
eral
: Bow
ls
63
2004
U
K
15
Gen
eral
: Syr
inge
64
20
03
UK
16
Gen
eral
: Tub
es
19
2000
U
K
17
Glo
ves
64
2003
U
K
18
Nee
dle
Hol
der
63
2004
U
K
19
Ner
ve H
ooks
63
20
04
UK
20
Sci
ssor
s
64
2003
U
K

17
2
1 A
naes
thes
ia: M
asks
7
2000
U
SA
A
naes
thes
ia: M
asks
3
2003
U
SA
A
naes
thes
ia: M
asks
2
2001
U
SA
2 A
naes
thes
ia: M
outh
piec
es
3 20
03
US
A
A
naes
thes
ia: M
outh
piec
es
7 20
00
US
A
3 A
naes
thes
ia: R
espi
rato
ry T
hera
py
7 20
00
US
A
4 A
naes
thes
ia: A
irway
Con
nect
or
3 20
03
US
A
5 A
naes
thes
ia: B
reat
hing
Circ
uits
7
2000
U
SA
A
naes
thes
ia: B
reat
hing
Circ
uits
8
2000
U
SA
A
naes
thes
ia: B
reat
hing
Circ
uits
3
2003
U
SA
A
naes
thes
ia: B
reat
hing
Circ
uits
11
20
04
US
A
A
naes
thes
ia: B
reat
hing
Circ
uits
2
2001
U
SA
6 A
naes
thes
ia: B
ronc
hosc
ope
3 20
03
US
A
A
naes
thes
ia: B
ronc
hosc
ope
3 20
03
US
A
7 A
naes
thes
ia: E
ndot
rach
eal T
ube
3 20
03
US
A
A
naes
thes
ia: E
ndot
rach
eal T
ube
8 20
00
US
A
A
naes
thes
ia: E
ndot
rach
eal T
ube
7 20
00
US
A
8 A
naes
thes
ia: F
ilter
21
20
00
US
A
9 A
naes
thes
ia::
Oxy
gena
tors
22
20
02
US
A
10
Ant
i DV
T ga
rmen
ts
28
2001
U
SA
A
nti D
VT
garm
ents
39
20
04
US
A

17
3
11
Bio
psy
need
le
61
2004
U
SA
12
Car
diac
: Aor
tic p
unch
es
23
2003
U
SA
13
Car
diac
: Bal
loon
s 25
19
99
US
A
C
ardi
ac: B
allo
ons
35
19
99
US
A
14
Car
diac
: Bio
psy
Nee
dle
3 20
03
US
A
15
Car
diac
: Bur
r 3
2003
U
SA
16
Car
diac
: Cat
hete
r 25
19
99
US
A
C
ardi
ac: C
athe
ter
26
2003
U
SA
C
ardi
ac: C
athe
ter
28
2000
U
SA
17
Car
diac
: Cat
hete
r (Ab
latio
n)
29
2001
U
SA
C
ardi
ac: C
athe
ter (
Abla
tion)
7
2000
U
SA
C
ardi
ac: C
athe
ter (
Abla
tion)
31
20
00
US
A
C
ardi
ac: C
athe
ter (
Angi
ogra
phy)
7
2000
U
SA
C
ardi
ac: C
athe
ter (
Angi
ogra
phy)
3
2003
U
SA
C
ardi
ac: C
athe
ter (
Angi
ogra
phy)
29
20
01
US
A
18
Car
diac
: Cat
hete
r (An
giop
last
y B
allo
ons)
7
2000
U
SA
C
ardi
ac: C
athe
ter (
Angi
opla
sty
Bal
loon
s)
21
2000
U
SA
C
ardi
ac: C
athe
ter (
Angi
opla
sty
Bal
loon
s)
3 20
03
US
A
C
ardi
ac: C
athe
ter (
Angi
opla
sty
Bal
loon
s)
8 20
00
US
A
C
ardi
ac: C
athe
ter (
Angi
opla
sty
Bal
loon
s)
21
2003
U
SA
C
ardi
ac: C
athe
ter (
Ballo
on)
7 20
00
US
A

17
4
C
ardi
ac: C
athe
ter (
Ballo
on)
3 20
03
US
A
C
ardi
ac: C
athe
ter (
Ballo
on)
3 20
03
US
A
19
Car
diac
: Cat
hete
r (E
lect
rode
Rec
ordi
ng)
3 20
03
US
A
20
Car
diac
: Cat
hete
r (E
lect
roph
ysio
logy
/EP
) 21
20
00
US
A
C
ardi
ac: C
athe
ter (
Ele
ctro
phys
iolo
gy/E
P)
7 20
00
US
A
C
ardi
ac: C
athe
ter (
Ele
ctro
phys
iolo
gy/E
P)
31
2000
U
SA
C
ardi
ac: C
athe
ter (
Ele
ctro
phys
iolo
gy/E
P)
23
2003
U
SA
C
ardi
ac: C
athe
ter (
Ele
ctro
phys
iolo
gy/E
P)
8 20
00
US
A
C
ardi
ac: C
athe
ter (
Ele
ctro
phys
iolo
gy/E
P)
38
2003
U
SA
C
ardi
ac: C
athe
ter (
Ele
ctro
phys
iolo
gy/E
P)
39
2004
U
SA
C
ardi
ac: C
athe
ter (
Ele
ctro
phys
iolo
gy/E
P)
28
2000
U
SA
C
ardi
ac: C
athe
ter (
Ele
ctro
phys
iolo
gy/E
P)
29
2001
U
SA
21
Car
diac
: Cat
hete
r (Fi
ber-o
ptic
Oxi
met
er)
3 20
03
US
A
22
Car
diac
: Cat
hete
r (G
uide
wire
) 3
2003
U
SA
C
ardi
ac: C
athe
ter (
Gui
dew
ire)
7 20
00
US
A
C
ardi
ac: C
athe
ter (
Gui
dew
ire)
35
1999
U
SA
23
Car
diac
: Cat
hete
r (H
aem
o-di
alys
is)
29
2001
U
SA
24
Car
diac
: Cat
hete
r (H
igh
Den
sity
Arra
y)
3 20
03
US
A
25
Car
diac
: Cat
hete
r (Ke
rato
me)
3
2003
U
SA
26
Car
diac
: Cat
hete
r (St
eera
ble)
3
2003
U
SA
27
Car
diac
: Ext
erna
l Vei
n S
tripp
er
3 20
03
US
A

17
5
28
Car
diac
: Pac
emak
er
29
2001
U
SA
29
Car
diac
: Sta
biliz
er D
evic
e 3
2003
U
SA
30
Car
diac
: Syr
inge
3
2003
U
SA
C
ardi
ac: S
yrin
ge
7 20
00
US
A
31
Car
diac
: Syr
inge
(In
ject
or T
ype
Act
uato
r) 3
2003
U
SA
32
Car
diac
: Syr
inge
(Ang
iogr
aphe
r Inj
ecto
r) 21
20
00
US
A
33
Car
diac
: Tra
cers
39
20
04
US
A
34
Car
diac
: Tro
car
3 20
03
US
A
C
ardi
ac: T
roca
r 7
2000
U
SA
35
Car
diac
: Vei
n S
tripp
er
3 20
03
US
A
36
Car
diac
: Wire
s 25
19
99
US
A
C
ardi
ac: W
ires
35
1999
U
SA
37
Dia
rther
my
3 20
03
US
A
38
Dia
ther
my:
App
arat
us
3 20
03
US
A
D
iath
erm
y: C
uttin
g an
d C
oagu
latio
n D
evic
es
3 20
03
US
A
39
Dia
ther
my:
Ele
ctro
des
21
2000
U
SA
D
iath
erm
y: E
lect
rode
s 8
2000
U
SA
D
iath
erm
y: E
lect
rode
s 7
2000
U
SA
40
Dia
ther
my:
Pen
cils
7
2000
U
SA
D
iath
erm
y: P
enci
ls
8 20
00
US
A
41
Ele
ctro
de C
able
3
2003
U
SA

17
6
42
Ele
ctro
de: P
ercu
tane
ous
Abl
atio
n 3
2003
U
SA
43
End
osco
pe
3 20
03
US
A
E
ndos
cope
7
2000
U
SA
E
ndos
cope
53
20
04
US
A
44
End
osco
py: B
lade
s 7
2000
U
SA
E
ndos
copy
: Bla
des
3 20
03
US
A
45
End
osco
py: G
uide
wire
s 7
2000
U
SA
E
ndos
copy
: Gui
dew
ires
3 20
03
US
A
46
End
osco
py: S
ciss
ors
39
2004
U
SA
47
EN
T: B
urr
58
2004
U
SA
E
NT:
Bur
r 3
2003
U
SA
48
EN
T: C
athe
ter
7 20
00
US
A
49
EN
T: C
athe
ter (
Trac
heob
ronc
hial
) 7
2000
U
SA
E
NT:
Cat
hete
r (Tr
ache
obro
nchi
al)
3 20
03
US
A
E
NT:
Cat
hete
rs
3 20
03
US
A
50
EN
T: T
roca
r 58
20
04
US
A
51
Fasc
ia H
olde
rs
7 20
00
US
A
52
Fem
osto
ps
23
2003
U
SA
53
Fibr
eopt
ic L
aser
Cab
le
3 20
03
US
A
54
Gas
troen
tero
logy
/ U
rolo
gy: B
iops
y Fo
rcep
s
3 20
03
US
A
G
astro
ente
rolo
gy /
Uro
logy
: Bio
psy
Forc
eps
28
20
00
US
A
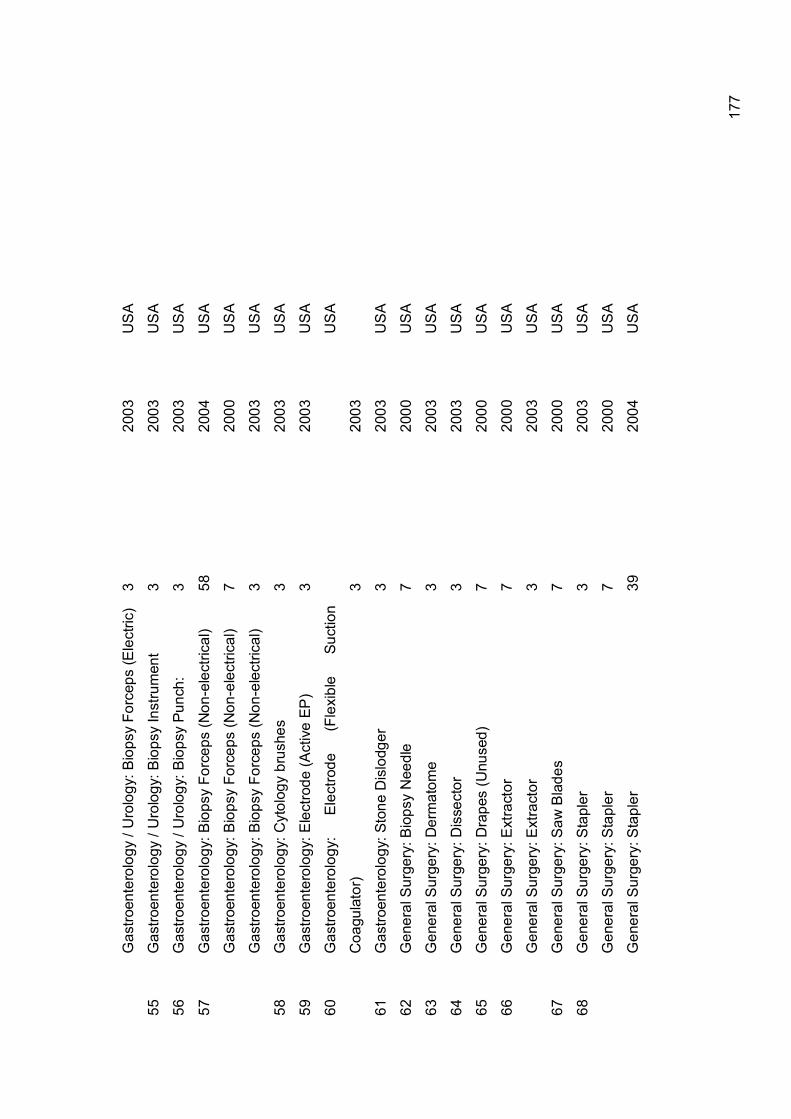
17
7
G
astro
ente
rolo
gy /
Uro
logy
: Bio
psy
Forc
eps
(Ele
ctric
) 3
2003
U
SA
55
Gas
troen
tero
logy
/ U
rolo
gy: B
iops
y In
stru
men
t 3
2003
U
SA
56
Gas
troen
tero
logy
/ U
rolo
gy: B
iops
y Pu
nch:
3
2003
U
SA
57
Gas
troen
tero
logy
: Bio
psy
Forc
eps
(Non
-ele
ctric
al)
58
2004
U
SA
G
astro
ente
rolo
gy: B
iops
y Fo
rcep
s (N
on-e
lect
rical
) 7
2000
U
SA
G
astro
ente
rolo
gy: B
iops
y Fo
rcep
s (N
on-e
lect
rical
) 3
2003
U
SA
58
Gas
troen
tero
logy
: Cyt
olog
y br
ushe
s
3 20
03
US
A
59
Gas
troen
tero
logy
: Ele
ctro
de (A
ctiv
e EP
) 3
2003
U
SA
60
Gas
troen
tero
logy
: E
lect
rode
(F
lexi
ble
Suct
ion
Coa
gula
tor)
3
2003
US
A
61
Gas
troen
tero
logy
: Sto
ne D
islo
dger
3
2003
U
SA
62
Gen
eral
Sur
gery
: Bio
psy
Nee
dle
7 20
00
US
A
63
Gen
eral
Sur
gery
: Der
mat
ome
3
2003
U
SA
64
Gen
eral
Sur
gery
: Dis
sect
or
3 20
03
US
A
65
Gen
eral
Sur
gery
: Dra
pes
(Unu
sed)
7
2000
U
SA
66
Gen
eral
Sur
gery
: Ext
ract
or
7 20
00
US
A
G
ener
al S
urge
ry: E
xtra
ctor
3
2003
U
SA
67
Gen
eral
Sur
gery
: Saw
Bla
des
7 20
00
US
A
68
Gen
eral
Sur
gery
: Sta
pler
3
2003
U
SA
G
ener
al S
urge
ry: S
tapl
er
7 20
00
US
A
G
ener
al S
urge
ry: S
tapl
er
39
2004
U
SA

17
8
G
ener
al S
urge
ry: S
tapl
er
3 20
03
US
A
69
Gen
eral
Sur
gery
: Sta
pler
(End
osco
pic)
7
2000
U
SA
70
Gen
eral
Sur
gery
: Sta
pler
(Pla
stic
Sur
gery
) 7
2000
U
SA
70
Gen
eral
Sur
gica
l Cla
mp
(Vas
cula
r) 3
2003
U
SA
71
Gen
eral
Sur
gica
l: B
iops
y 53
20
04
US
A
G
ener
al S
urgi
cal:
Bio
psy
Bru
sh
3 20
03
US
A
72
Gen
eral
Sur
gica
l: B
iops
y D
evic
e (P
ercu
tane
ous)
3
2003
U
SA
73
Gen
eral
Sur
gica
l: B
iops
y Fo
rcep
s 39
20
04
US
A
G
ener
al S
urgi
cal:
Bio
psy
Forc
eps
7 20
00
US
A
G
ener
al S
urgi
cal:
Bio
psy
Forc
eps
59
2003
U
SA
G
ener
al S
urgi
cal:
Bio
psy
Forc
eps
26
2003
U
SA
G
ener
al S
urgi
cal:
Bio
psy
Forc
eps
3 20
03
US
A
G
ener
al S
urgi
cal:
Bio
psy
Forc
eps
22
2002
U
SA
G
ener
al S
urgi
cal:
Bio
psy
Forc
eps
38
2003
U
SA
G
ener
al S
urgi
cal:
Bio
psy
Forc
eps
35
1999
U
SA
G
ener
al S
urgi
cal:
Bio
psy
Forc
eps
8 20
00
US
A
G
ener
al S
urgi
cal:
Bio
psy
Forc
eps
23
2003
U
SA
74
Gen
eral
Sur
gica
l: B
lade
s 39
20
04
US
A
75
Gen
eral
Sur
gica
l: C
hise
l 3
2003
U
SA
76
Gen
eral
Sur
gica
l: C
lam
p
3 20
03
US
A
77
Gen
eral
Sur
gica
l: C
lip
58
2004
U
SA
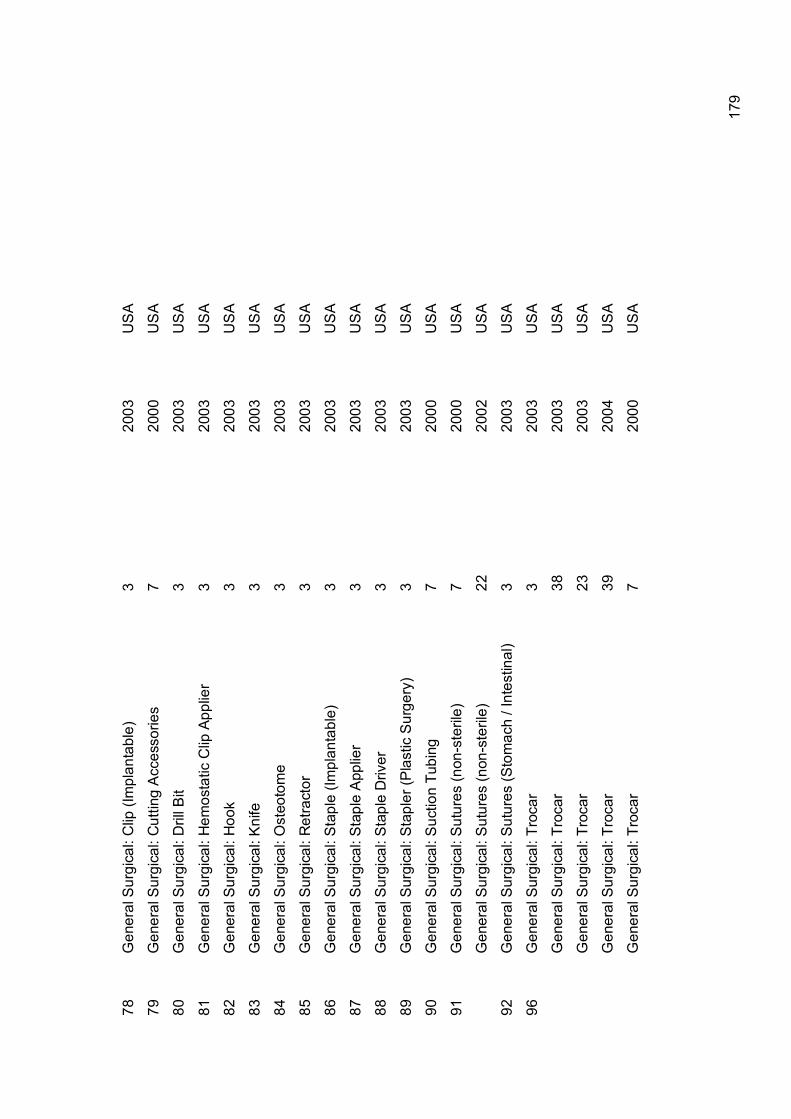
17
9
78
Gen
eral
Sur
gica
l: C
lip (I
mpl
anta
ble)
3
2003
U
SA
79
Gen
eral
Sur
gica
l: C
uttin
g A
cces
sorie
s 7
2000
U
SA
80
Gen
eral
Sur
gica
l: D
rill B
it
3 20
03
US
A
81
Gen
eral
Sur
gica
l: H
emos
tatic
Clip
App
lier
3 20
03
US
A
82
Gen
eral
Sur
gica
l: H
ook
3
2003
U
SA
83
Gen
eral
Sur
gica
l: K
nife
3
2003
U
SA
84
Gen
eral
Sur
gica
l: O
steo
tom
e
3 20
03
US
A
85
Gen
eral
Sur
gica
l: R
etra
ctor
3
2003
U
SA
86
Gen
eral
Sur
gica
l: S
tapl
e (Im
plan
tabl
e)
3 20
03
US
A
87
Gen
eral
Sur
gica
l: S
tapl
e A
pplie
r 3
2003
U
SA
88
Gen
eral
Sur
gica
l: S
tapl
e D
river
3
2003
U
SA
89
Gen
eral
Sur
gica
l: S
tapl
er (P
last
ic S
urge
ry)
3 20
03
US
A
90
Gen
eral
Sur
gica
l: S
uctio
n Tu
bing
7
2000
U
SA
91
Gen
eral
Sur
gica
l: S
utur
es (n
on-s
teril
e)
7 20
00
US
A
G
ener
al S
urgi
cal:
Sut
ures
(non
-ste
rile)
22
20
02
US
A
92
Gen
eral
Sur
gica
l: S
utur
es (S
tom
ach
/ Int
estin
al)
3 20
03
US
A
96
Gen
eral
Sur
gica
l: Tr
ocar
3
2003
U
SA
G
ener
al S
urgi
cal:
Troc
ar
38
2003
U
SA
G
ener
al S
urgi
cal:
Troc
ar
23
2003
U
SA
G
ener
al S
urgi
cal:
Troc
ar
39
2004
U
SA
G
ener
al S
urgi
cal:
Troc
ar
7 20
00
US
A

18
0
G
ener
al: A
nti D
VT
garm
ents
7
2000
U
SA
G
ener
al: A
nti D
VT
garm
ents
3
2003
U
SA
G
ener
al: A
nti D
VT
garm
ents
53
20
04
US
A
97
Gen
eral
: Blo
od a
cces
s de
vice
3
2003
U
SA
G
ener
al: B
lood
Lan
cet
3 20
03
US
A
98
Gen
eral
: Blo
od P
ress
ure
53
2004
U
SA
G
ener
al: B
lood
Pre
ssur
e C
uffs
7
2000
U
SA
G
ener
al: B
lood
Pre
ssur
e C
uffs
3
2003
U
SA
G
ener
al: B
lood
Pre
ssur
e C
uffs
39
20
04
US
A
99
Gen
eral
: Cat
hete
r 22
20
02
US
A
G
ener
al: C
athe
ter
59
2003
U
SA
G
ener
al: C
athe
ter
10
2001
U
SA
G
ener
al: C
athe
ter
61
2004
U
SA
100
Gen
eral
: Cat
hete
r (D
iagn
ostic
) 3
2003
U
SA
101
Gen
eral
: Cat
hete
r (D
rain
age)
3
2003
U
SA
102
Gen
eral
: Cur
ette
(sur
gica
l) 3
2003
U
SA
103
Gen
eral
: Syr
inge
61
20
04
US
A
104
Gen
eral
: Syr
inge
(Irri
gatin
g)
3 20
03
US
A
G
ener
al: S
yrin
ge (I
rriga
ting)
7
2000
U
SA
105
Gen
eral
: Syr
inge
(Pis
ton)
3
2003
U
SA
106
Gen
eral
: Tou
rniq
uet
3 20
03
US
A

18
1
107
Gou
ge (S
urgi
cal)
3 20
03
US
A
108
Gow
ns
7 20
00
US
A
G
owns
3
2003
U
SA
109
Hem
odia
lysi
s B
lood
Circ
uit
3 20
03
US
A
H
emod
ialy
sis
Blo
od C
ircui
t 7
2000
U
SA
110
Hem
orrh
oida
l Lig
ator
3
2003
U
SA
111
Infla
tion
Dev
ices
23
20
03
US
A
112
Infu
sion
Pum
p 3
2003
U
SA
113
Lapa
rosc
opes
7
2000
U
SA
La
paro
scop
es
3 20
03
US
A
La
paro
scop
es
38
2003
U
SA
La
paro
scop
es
7 20
00
US
A
La
paro
scop
es
58
2004
U
SA
La
paro
scop
es
53
2004
U
SA
114
Lapa
rosc
opes
: Cla
mps
39
20
04
US
A
115
Lapa
rosc
opes
: Dis
sect
ors
7 20
00
US
A
La
paro
scop
es: D
isse
ctor
s 39
20
04
US
A
La
paro
scop
es: D
isse
ctor
s 3
2003
U
SA
La
paro
scop
es: D
isse
ctor
s
7 20
00
US
A
116
Lapa
rosc
opes
: For
ceps
39
20
04
US
A
117
Lapa
rosc
opes
: Gra
sper
s 7
2000
U
SA

18
2
La
paro
scop
es: G
rasp
ers
39
2004
U
SA
La
paro
scop
es: G
rasp
ers
3
2003
U
SA
118
Lapa
rosc
opes
: Sci
ssor
s 7
2000
U
SA
La
paro
scop
es: S
ciss
ors
21
2000
U
SA
La
paro
scop
es: S
ciss
ors
38
2003
U
SA
La
paro
scop
es: S
ciss
ors
8 20
00
US
A
La
paro
scop
es: S
ciss
ors
39
2004
U
SA
La
paro
scop
es: S
ciss
ors
3 20
03
US
A
119
Lase
r Fib
re D
eliv
ery
Sys
tem
s 7
2000
U
SA
120
Mec
hani
cal W
rist
3 20
03
US
A
121
Nee
dle
3 20
03
US
A
N
eedl
e 58
20
04
US
A
122
Nee
dle
Des
truct
ion
Dev
ice
3
2003
U
SA
123
Nee
dle
Hol
der
3
2003
U
SA
124
Nee
dle:
Ang
iogr
aphi
c 3
2003
U
SA
125
Nee
dle:
Asp
iratio
n an
d In
ject
ion
3
2003
U
SA
N
eedl
e: A
spira
tion
and
Inje
ctio
n 58
20
04
US
A
126
Nee
dle:
Ass
iste
d R
epro
duct
ion
3 20
03
US
A
127
Nee
dle:
Bio
psy
26
20
03
US
A
N
eedl
e: B
iops
y
25
1999
U
SA
N
eedl
e: B
iops
y
58
2004
U
SA

18
3
N
eedl
e: B
iops
y
7 20
00
US
A
N
eedl
e: B
iops
y
3 20
03
US
A
128
Nee
dle:
Car
diov
ascu
lar
7 20
00
US
A
129
Nee
dle:
Cat
hete
r 58
20
04
US
A
130
Nee
dle:
Con
duct
ion
3 20
03
US
A
131
Nee
dle:
Hyp
oder
mic
Sin
gle
Lum
en
3 20
03
US
A
132
Nee
dle:
Isot
ope
3
2003
U
SA
133
Nee
dle:
Pha
ecom
ulsi
ficat
ion
7 20
00
US
A
N
eedl
e: P
haec
omul
sific
atio
n
3 20
03
US
A
134
Nee
dle:
Pne
umpe
riton
eum
3
2003
U
SA
135
Nee
dle:
Sho
rt-te
rm S
pina
l 3
2003
U
SA
136
Nee
dle:
Sin
gle
Lum
en
3 20
03
US
A
137
Neu
rosu
rger
y: B
urrs
3
2003
U
SA
138
Neu
rosu
rger
y: C
lip
3 20
03
US
A
139
Neu
rosu
rger
y: D
rills
3
2003
U
SA
140
Neu
rosu
rger
y: T
reph
ines
3
2003
U
SA
141
OB
/GYN
: Bio
psy
Forc
eps
58
2004
U
SA
142
OB
/GYN
: Cul
dosc
opic
Coa
gula
tor
3 20
03
US
A
143
OB
/GYN
: End
osco
pic
Bip
olar
Coa
gula
tor
3 20
03
US
A
144
OB
/GYN
: End
osco
pic
Uni
pola
r Coa
gula
tor
3 20
03
US
A
145
OB
/GYN
: Hys
tero
scop
ic C
oagu
lato
r 3
2003
U
SA

18
4
146
OB
/GYN
: Lap
aros
cope
s
3 20
03
US
A
147
OB
/GYN
: Tro
car
7 20
00
US
A
148
Ope
ned
but u
sed
item
s 39
20
04
US
A
149
Oph
thal
mic
: Bla
de (K
erat
ome)
3
2003
U
SA
O
phth
alm
ic: B
lade
(Ker
atom
e)
7 20
00
US
A
150
Oph
thal
mic
: End
o-illu
min
ator
3
2003
U
SA
151
Oph
thal
mic
: Kni
fe
3 20
03
US
A
O
phth
alm
ic: K
nife
58
20
04
US
A
152
Orth
opae
dic:
Bla
de (C
arpa
l Tun
nel)
3
2003
U
SA
O
rthop
aedi
c: B
lade
(Car
pal T
unne
l)
7 20
00
US
A
153
Orth
opae
dic:
Arth
osco
pic
Acc
esso
ries
3
2003
U
SA
154
Orth
opae
dic:
Arth
osco
pic
shav
ers
& w
ands
38
20
03
US
A
O
rthop
aedi
c: A
rthos
copi
c w
ands
23
20
03
US
A
155
Orth
opae
dic:
Arth
rosc
opic
inst
rum
ents
7
2000
U
SA
O
rthop
aedi
c: A
rthro
scop
ic S
have
rs
39
2004
U
SA
156
Orth
opae
dic:
Bla
des
23
20
03
US
A
157
Orth
opae
dic:
Bon
e H
ook
(Sur
gica
l) 3
2003
U
SA
158
Orth
opae
dic:
Bon
e Ta
p
3 20
03
US
A
159
Orth
opae
dic:
Bur
r
3 20
03
US
A
O
rthop
aedi
c: B
urr
23
20
03
US
A
O
rthop
aedi
c: B
urr
7
2000
U
SA
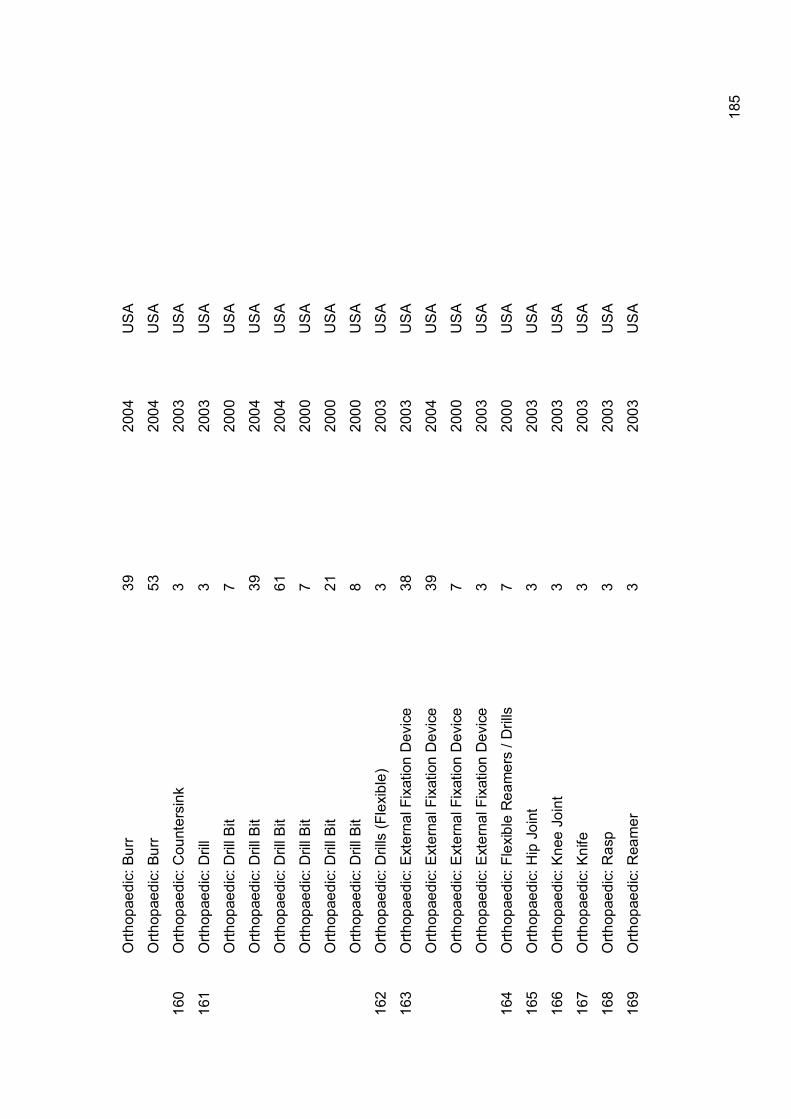
18
5
O
rthop
aedi
c: B
urr
39
20
04
US
A
O
rthop
aedi
c: B
urr
53
20
04
US
A
160
Orth
opae
dic:
Cou
nter
sink
3
2003
U
SA
161
Orth
opae
dic:
Dril
l
3 20
03
US
A
O
rthop
aedi
c: D
rill B
it
7 20
00
US
A
O
rthop
aedi
c: D
rill B
it
39
2004
U
SA
O
rthop
aedi
c: D
rill B
it
61
2004
U
SA
O
rthop
aedi
c: D
rill B
it
7 20
00
US
A
O
rthop
aedi
c: D
rill B
it
21
2000
U
SA
O
rthop
aedi
c: D
rill B
it
8 20
00
US
A
162
Orth
opae
dic:
Dril
ls (F
lexi
ble)
3
2003
U
SA
163
Orth
opae
dic:
Ext
erna
l Fix
atio
n D
evic
e 38
20
03
US
A
O
rthop
aedi
c: E
xter
nal F
ixat
ion
Dev
ice
39
2004
U
SA
O
rthop
aedi
c: E
xter
nal F
ixat
ion
Dev
ice
7 20
00
US
A
O
rthop
aedi
c: E
xter
nal F
ixat
ion
Dev
ice
3 20
03
US
A
164
Orth
opae
dic:
Fle
xibl
e R
eam
ers
/ Dril
ls
7 20
00
US
A
165
Orth
opae
dic:
Hip
Joi
nt
3 20
03
US
A
166
Orth
opae
dic:
Kne
e Jo
int
3 20
03
US
A
167
Orth
opae
dic:
Kni
fe
3 20
03
US
A
168
Orth
opae
dic:
Ras
p
3 20
03
US
A
169
Orth
opae
dic:
Rea
mer
3
2003
U
SA

18
6
170
Orth
opae
dic:
Sho
ulde
r Joi
nt
3 20
03
US
A
171
Orth
opae
dic:
Tre
phin
e
3 20
03
US
A
172
Orth
opae
dics
: Ron
geur
3
2003
U
SA
173
Pha
co T
ips
39
2004
U
SA
174
Pha
cofra
gmen
tatio
n sy
stem
3
2003
U
SA
175
Pne
umat
ic T
ourn
ique
t Cuf
fs
39
2004
U
SA
176
Pro
be: A
rgon
bea
m p
lasm
a co
agul
atio
n
25
1999
U
SA
177
Pro
lene
mes
h 7
2000
U
SA
178
Pro
sthe
sis
38
2003
U
SA
179
PTC
A
53
2004
U
SA
180
Pul
se O
xim
eter
3
2003
U
SA
P
ulse
Oxi
met
er
53
2004
U
SA
181
Pul
se O
xim
eter
Sen
sors
39
20
04
US
A
P
ulse
Oxi
met
er S
enso
rs
28
2002
U
SA
182
Rad
iolo
gy: C
athe
ter
29
2001
U
SA
183
Saw
53
20
04
US
A
S
aw
3 20
03
US
A
S
aw
39
2004
U
SA
184
Saw
Bla
de
3 20
03
US
A
S
aw B
lade
7
2000
U
SA
S
aw B
lade
61
20
04
US
A

18
7
S
aw B
lade
21
20
00
US
A
S
aw B
lade
59
20
03
US
A
S
aw B
lade
8
2000
U
SA
185
Sca
lpel
bla
de
3 20
03
US
A
186
Sci
ssor
Tip
s
7 20
00
US
A
187
Sci
ssor
s 39
20
04
US
A
S
ciss
ors
3
2003
U
SA
S
ciss
ors
25
19
99
US
A
S
ciss
ors
35
19
99
US
A
S
ciss
ors
26
20
03
US
A
S
ciss
ors
Tips
3
2003
U
SA
188
Sha
rps
Con
tain
ers
7 20
00
US
A
189
Sna
re
3 20
03
US
A
S
nare
39
20
04
US
A
190
Sof
t Tis
sue
Abla
tors
39
20
04
US
A
191
Spa
tula
3
2003
U
SA
192
Sph
inct
erto
me
70
1998
U
SA
S
phin
cter
tom
e 7
2000
U
SA
S
phin
cter
tom
e 3
2003
U
SA
S
phin
cter
tom
e 53
20
04
US
A
193
Sur
gica
l: C
athe
ter N
eedl
e
3 20
03
US
A

18
8
194
Syr
inge
Pis
ton
& In
fusi
on Im
plan
ted
Pum
ps
7 20
00
US
A
195
Uro
logy
: D
ialy
sis
Set
3
2003
U
SA
196
Uro
logy
: Cat
hete
r (B
iliary
) 3
2003
U
SA
197
Uro
logy
: Cat
hete
r (U
reth
ral)
7 20
00
US
A
U
rolo
gy: C
athe
ter (
Ure
thra
l) 3
2003
U
SA

189
References
1. Christensen M, Meyer M, Jepsen OB. Reuse of single use sterile medical
devices in Danish hospitals decreases after report discouraging it
Eurosurveillance 1999;4(10):101-102
2. Canadian Nosocomial Infection Surveillance Program Surveillance Project for
the Reuse of Single-Use Medical Devices in Canadian Health Care Facilities.
2001 http:// www.hc-sc.gc.ca/pphb-dgspsp/publicat/cnsip-pcsinin1001
3. Federal Drug Administration. Reuse 2003 www.fda.gov.reuse
4. Day P. What Is The Evidence On The Safety And Effectiveness Of the reuse
Of Medical Devices Labelled As Single-Use Only? New Zealand Health
Technology Assessment 2004;3(2).
5. Lipp MD, Jaehnichen G, Golecki N, Fecht G, Reichl R, Heeg P.
Microbiological, microstructure, and material science examinations of
processed Combitubes after multiple use Anaesth Analg 2000;91(3):693-697.
6. Carter JA. Checking anaesthetic equipment and the Expert Group on Blocked
Anaesthetic Tubing (EGBAT). Anaesthesia. 2004;59(2):105-7.
7. Healthcare Purchasing News. Reuse of single use medical devices 2002;April
2002. www.findarticles.com
8. Feigal DW. Testimony on reuse of medical devices to US Senate 27.06.00
9. Ontario Hospital Association Report Of Ontario Hospital Associations’ Reuse
Of Single Use Medical Devices Ad-Hoc Working Group January 2004.
10. Spurgeon D. Single use equipment is used up to 20 times say report Br Med
J 2001;323:553
11. Webster P. Canadian hospitals call for restrictions on single-use devices
Lancet 2004;363(9408):542
12. Department of Health. Protecting the Breathing Circuit in Anaesthesia: Report
to the Chief Medical Officer of an Expert Group on Blocked Anaesthetic
Tubing 2004 London: Department of Health.
13. Operation Orcadian. Essex police inquiry into blocked anaesthetic tubing at
Broomfield Hospital, Chelmsford. 2001
14. National Network of Clinical Proceurement Specialists, personal
communication, 2004
190
15. AAGBI. Infection Control in Anaesthesia 2002 London: Association of
Anaesthetists of Great Britain and Ireland.
16. Pidduck D. Cross infection and the laryngoscope Br J Peroperative Nurs
2002;12:170-175
17. National Health Service Estates. Decontamination Review: Report on a
survey of current decontamination practices in healthcare premises in
England London: Department of Health 2003.
18. http://www.eurosurveillance.com
19. NHS Estates. A review of the decontamination of surgical instruments in the
NHS in England London: Departmetn of Health, 2001
20. Operating Department Practitioners – personal communication, 2004
21. Federal Drug Administration. Enforced priorities for single use devices
reprocessing by third parties and hospitals www.fda.gov/reuse
22. Cohoon BD. Reprocessing single-use medical devices AORN J
2002;75(3):557-62, 565-7
23. Solomon M. Saving money the safe way: hospitals turn to medical device
reprocessors – business focus Healthcare Review 27.05.03
www.findarticles.com
24. GfK Healthcare. Reuse of single use medical devices
http://www.bvmed.de/themen/reuse/?language=2
25. Kolata G. Single use medical devices are often used several times New York
Times 10.11.99
26. Lichtman B. Going Once, Going Twice: What Price For A Reprocessed
Device? UCLA Journal of Law and Technology Notes 2003;16.
27. Stewart I. Single use only labelling of medical devices: always essential or
sometimes spurious? Med J Aust 1997;167:538-839.
28. General Accounting Office. Single Use Medical Devices: Little Available
Evidence of Harm from Reuse But Oversight Warranted 2002 GAO:
Washington DC.
29. Mickelsen S, Mickelsen C, MacIndoe C, Jaramillo J, Bass S, West G et al.
Trends and patterns in electrophysiologic and Ablation catheter reuse in the
United States Am J of Cardio 2001;87:351-353

191
30. Berenger Sj, Ferguson JK. Reuse of single use medical devices: how often
does this still occur in Australia? Med J Aust 2004;180(1):46
31. Clough J. Testimony to Congressional committees and Federal agencies on
reuse of medical devices. US Senate 27.06.00
32. Collignon PJ, Dreimanis DE, Beckingham WD. Reuse of Single-Use Medical
Devices in Sterile Sites: How Often Does This Still Occur in Australia? Med J
Aust 2003;179(2):115-6; discussion 116
33. Woollard K. Reuse of single-use medical devices: who makes the decision?
The controversy can be resolved by identifying the real risks of cross-infection
Med J Aust 1996;164 (9):538
34. Fedel M. Tessarolo F, Ferrari P, Losche C, Ghassemieh N, Guarrera GM et
al. Functional properties and performance of new and repocesed coronary
angioplasty balloon catheters J Biomed Mater Res B Appl Biomater
2006;Feb27 (e-print)
35. Charatan F. Controvery erupts over reuse of single use medical devices Br
Med J 1999;319:1320
36. Health Policy Forum 2002 www.forum.europa.eu.int
37. Brook CW. Reuse of single use medical devices: NHMRC deliberations Med
JAust 1996;164:537
38. Premierinc. Reuse of single use devices in USA 2003 www.premierinc.com
39. AHRMM. Reprocessing advances 2004 www.premierinc.com
40. Lindsay BD, Kutalek SP, Cannom DS, Hammill SC, Naccarelli GV. NASPE
task force on reprocessing of electrophysiological catheters. North American
society of Pacing and Electrophysiology Pacing Clin Electrophysiol
2001;24(8.1):1297-1305.
41. Eucomed. Reprocessing single use medical technology – a threat to patient
safety 2003 www.eucomed.be
42. Ryden L, Fox KM. Reuse of devices in cardiology Eur Heart J
1999;20(10):709-710
43. Ryden L. Reuse Of Devices in Cardiology Eur Heart J 1998;19:1628-1631.
44. Jackson M. Issues affecting refurbishment and reuse of pacemakers Aust
Health Rev 1996;19(1):68-80.

192
45. McGregor M. The reuse of cardiac pacemakers Can J Cardio 1992;8(7):697-
701.
46. Rosengarten MD, Portnoy, D, Chiu RC, Paterson AK. Reuse of permanent
cardiac pacemakers Can Med Assoc J 1985;133(4):279-283.
47. Myers GH. Is reuse financially worthwhile? Pacing Clin Electrophysiol
1986;9(6.2):1288-1294.
48. LInde CL, Bocray A, Jonasson H, Rosenqvist M, Radegran K, Ryden L.
reused pacemakers – as safe as new? A retrospective case control study Eur
Heart J 1998;19(1):154-157.
49. Braun TC, Hagen NC, Hatfield RE, Wyse DG. Cardiac pacemakers and
implantable defibrillators in terminal care J Pain Symptom Manage
1999;18(2):126-131.
50. Havia T, Schuller H. The reuse of previously implanted pacemakers Scan J
Thorac Cardiocasc Surg Suppl 1978;(22):33-34.
51. Collignon PJ, Graham E, Dreimanis DE. Reuse In Sterile Sites Of Single-Use
Medical Devices: How Common Is This In Australia? Med J Aust.
1996;164(9):533-6.
52. Eucomed. Reuse 2002 www.eucomed.be
53. Alfa MJ, Castillo J. Impact of FDA policy change on the reuse of single use
medical devices in Michigan hospitals Am J Infect Control 2004;32(6):337-
341.
54. Hambrick D 3rd. Reprocessing of single use endoscopic biopsy forceps and
snares. One hospital’s study Gastroenterol Nurs 2001;24(3):112-115
55. Tapp A. Reuse of single use medical devices Can Oper Room Nurs J
2003;21(1):18-19
56. Koh A, Kawahara K. Current practices and problems in the reuse of single
use devices in Japan J Med Dent Sci 2005;52(1):81-89.
57. Furman, PJ. The Reprocessing Of Medical Devices Labelled For “Single Use”
In The US – An Historical Overview, Business Briefings and Technology
Assessment 2002; June:1-5.
58. Federal Drug Administration. Critical Reprocessed single use devices
previously exempt from pre-market notification regulations 2004
www.fda.gov.reuse

193
59. Brune A. What Knee Patients Need To Know About Single Use Instrument
Reprocessing 2003 http://www.Knee1.com
60. Schroder P. Reuse of singe use devices Med Dev Technol
2000;11(10):44,48-53.
61. http://singleusedevices.com
62. Kings Lynn and Wisbech Hospitals NHS Trust Winning Ways 2004
63. Infection Control Nurses Forum. Message board ‘single use surgical
instruments’ 2004 www.icna.co.uk
64. Nursing Times. NT survey reveals NHS equipment crisis Nursing Times
online 01.09.03
65. Fan Q, Liu J, Ebben JP, Collincs AJ. Reuse associated mortality in incident
hemodialysis patients in the United States, 2000 to 2001 Am J Kidney Dis
46(4):661-668
66. National Kidney Foundation. Task force on reuse of dialyzers, council on
dialysis, National Kidney Foundation Am J Kidney Dis 1997;30(6):859-871
67. Dos Santos JP, Loureiro A, Cendoroglo NM, Pereira BJ. Impact of dialysis
room and reuse strategies on the incidence of hepatitis C visus infection in
haemodialysis units Nephrol Dial Transplant 1996;11(10):2017-2022
68. Roth K, Heeg P, Reichl R. Specific hygiene issues relating to reprocessing
and reuse of single use devices for laparoscopic surgery Surg Endosc
2002;16(7):1091-1097.
69. Beck DJ, Seligson D. External fixator parts should not be reused J Orthop
Trauma 2006;20(1):39-42
70. Wilcox CM, Geel SW, Baron TH. How many times can you reuse a single use
sphinctertome: prospective evaluation Gastrointest Endosc 1999;48(1):58-60.
71. Alfa MJ, Nemes R. Inadequacy of manual cleaning for reprocessing single
use, triple lumen spinctertomes: simulated use testing comparing manual with
automated cleaning methods Am J Infect Control 31(4):193-207.
72. Kozarek RA, Sumida SE, Raltz SL, Merriam LD, Irizarry DC. In vitro
evaluation of wire integrity and ability to reprocess single use sphinctertomes
Gastrointest Endosc 1997;45(2):117-121.

194
Appendix 2: Sampling strategy for survey.
We had envisaged that our web-based survey would sample 350 acute NHS
hospitals in England. We had planned to contact the Clinical Directors of Anaesthesia
(CDA) and Theatre Managers (TM) with the aim that they would be able to recruit
one anaesthetist and one surgeon who would be prepared to complete the
questionnaire. However, we discovered that this research design could not be
operationalised without serious delay, which would compromise even a partial
achievement of its goals within the available time and budget. The cause of this was
the introduction of the Research Governance Framework for Health and Social Care1
(RGF) and the European Clinical Trials Directive2 in May 2004, and its impact on
research involving members of NHS staff.
We had intended to recruit participant surgeons and anaesthetists via subscription to
an online database of NHS staff (www.specialistinfo.com) and had also hoped that
the Department of Health might be able to supply a list of contacts. However, having
taken advice from the Research and Development (R&D) department at Nottingham
University Hospitals NHS Trust about the consequences of the RGF, it became clear
that we could not approach NHS staff directly, or be given their personal data (i.e.
name and contact details) by third parties such as Trust Human Resources (HR)
departments. Any approach to NHS staff regarding their participation in the research
would need to come from their employer. Consequently the options available to us
were to recruit via HR departments, or Chief Executives and Clinical Directors if their
contact details were publicly accessible. These parties would then need to ask staff if
they would like to participate in the research and to contact us if they were happy to
take part.
Such a recruitment strategy was considered problematic. Firstly, it was dependent
upon the initial contact’s agreement to follow the strategy, and would then also be
reliant upon staff contacting us. Secondly, such a strategy would be extremely time
consuming.
Moreover, in order to follow this approach, we would need R&D organisational
approval for every NHS Trust invited to participate in the survey. Our original search
had shown that approximately 350 hospitals in England fitted the sampling criteria
(acute NHS hospitals). Although several of these hospitals will have fallen into the

195
same NHS Trust, up to 1400 signatures from R&D and clinical staff would have been
required, even before the sample was recruited or any survey data was collected.
Gaining R&D organisational approval is not a straightforward task. Prior to May 2005,
R&D departments could use either part D of the form issued by the Central Office for
Research Ethics Committees (COREC) or their own version. Using the form from
Nottingham City Hospital as an example, R&D approval to for sample recruitment at
just one site involves:
1. A completed R&D application form (4 pages in length and requiring
signatures from 4 members of hospital staff)
2. Copy of research protocol
3. Copy of completed COREC parts A, B and C
4. A completed copy of the hospital’s own R&D costings form
5. All correspondence between the ethics committee and the research team
6. An independent, external peer review of the research
7. A copy of the invitation letter on hospital letter-headed paper
8. A copy of the consent form on hospital letter-headed paper
9. A copy of the questionnaire on hospital letter-headed paper
10. Researcher’s CV
11. Evidence of sponsorship
In addition to the 1400 signatures, the need for items 7-9 to be on individual hospital
letter-headed paper would create extensive delays. It also emerged that most sites
would require individual honorary contracts involving police record checks and
occupational health examinations for the research fellow. Based on the experience of
undergoing repeated health examinations and renewing CRB checks gained when
completing the last phase of the study, the potential for both delay and facing
repeated testing when hospitals are unwilling to accept others’ data, would have only
further added to be bureaucratic administration involved in gaining R&D approval for
a national survey. Given these obstacles, it was considered that the administrative
burden of gaining R&D approval from 350 sites was prohibitive. Compliance would
have required the team to do nothing else for most of the contracted period of the
project at the expense of the funded objectives.
Finally, we became aware that any data collection request made to the Department
of Health would also involve approval from the Gateway department based in Leeds.

196
The Gateway department would, having assessed the questionnaire, determine if the
request would place a disproportionate burden on the NHS. During this process,
Gateway could have altered the questionnaire against our wishes, and those of the
commissioners, or even prevented the survey from taking place, despite the fact that
it had been commissioned by an NHS body.
Given the obstacles in recruiting survey participants under this regime, an alternative
strategy was developed. The criteria for our sample would be that participants would
be members of professional associations for surgeons, anaesthetists, theatre nurses
and operating department practitioners. The professional backgrounds of these
participants would be similar to those participants whom we had originally hoped to
recruit. However, in this instance they would be recruited because of their
membership of a professional organisation rather than by virtue of their employment
in the NHS. Although this would not enable us to achieve the original goal of mapping
the prevalence of SUD reuse, this approach would give us some information about
incidence that would still enable us to adopt a case-control design for the qualitative
phase of the study: we would be able to use the information collected on the
characteristics of hospitals and test this to see if there was any associated with
reports of SUD reuse. If such associations were found, we could then select our
sample accordingly.
We were advised by contacts in the research ethics and R&D communities that our
change in recruitment strategy would allow us legitimately to circumvent the ethics
and governance system. However, prior agreement to this change in strategy was
also sought from Professor Lilford, in his capacity of director of the Patient Safety
Research Portfolio. With this approval, the Chairs of the relevant professional
organisations (Association of Surgeons of Great Britain and Ireland (ASGBI),
Association of Anaesthetists of Great Britain and Ireland (AAGBI), National
Association of Theatre Nurses (NATN) and Association of Operating Department
Practitioners (AODP)) were contacted and asked if they would agree to allow the
research team to invite their members to participate in the research.
Discussions between the research team and both the NATN and ASGBI led to
agreement over the sampling strategy and the involvement of these organisations
being reached quickly. The research team were not provided with any contact details
for members of either association. Rather, the NATN and ASGBI were sent flyers
which were then forwarded onto their members in their routine mailings. This activity

197
incurred costs that were not budgeted for in the original research proposal, but which
were covered by virement. 8500 flyers were sent to members of the NATN with their
October 2004 edition of the British Journal of Perioperative Nursing. 1,500 flyers
were sent to members of the ASGBI who work in general, breast, coloproctology,
endoscopy, gastroenterology, transplant and vascular surgeries with their
September/October 2004 Executive Newsletter.
Negotiations with the AAGBI were prolonged. Initially, Dr Rowley made contact with
Professor John Carter, then Chairman of the AAGBI Safety Committee. However,
this approach appeared to be unsuccessful and Professor Aitkenhead wrote to
Professor Mike Harmer, President of the AAGBI, repeating our request. A list of
Equipment Officers, anaesthetists with a designated responsibility for equipment
issues, was finally received from the AAGBI Safety Committee in November 2004,
following the Council meeting. The list contained 145 names and addresses, and
after cleaning to remove ineligible cases (non-English places of employment, private
hospital, repeated entries), 119 Equipment Officers were sent a letter inviting their
participation in the research. Two invitations were subsequently returned due to the
addressee being unknown at the address provided.
Recruitment of AODP members was problematic, and remained unresolved by the
deadline for completion of the survey. We had initially contacted the Chair of the
AODP in the same manner as the other professional associations, but did not receive
a response. After much delay, we contacted the President of the AODP, who
explained that the AODP had taken the stance that we were evading the research
governance and ethics frameworks. They consequently requested confirmation from
the commissioning panel that our recruitment strategy was supported. We forwarded
this request to Professor Lilford, Director of the Patient Safety Research Portfolio, but
did not receive the information required by the AODP until after the survey had
closed. As a sign of goodwill, we nonetheless forwarded the paperwork to the AODP.
To counter the lack of involvement of the AODP, a small number of ODPs belonging
to an online message group were invited to participate in the survey. An invitation
was posted on their on-line message board after approval was given from the board’s
administrator.
Lastly, a half page advert was placed in the September/October 2004 edition of The
Operating Theatre Journal (OTJ). As with the flyers sent to the NATN and ASGBI,
the advert in the OTJ also incurred expenses outside the original budget. This

198
monthly journal is sent free of charge to every UK hospital with an operating theatre.
The September/October edition of the OJT had an extended print run, as delegates
at the NATN congress were given a copy in their conference pack.
None of the professional organisations held electronic mailing lists, and as such,
sample recruitment was performed using printed flyers, letters and advertisements.
Consequently, the security features required for the website were reduced.
Participants were only able to gain entrance to the survey site once they had
completed a consent form that was found at the gateway to the survey pages.
Moreover, the inputted data was only saved if the respondent provided details of their
place of employment. This data was destroyed following recruitment of the sample
for the interview phase of the study.
It is likely that the chosen recruitment strategy will have influenced the response rate
that the survey achieved. The lack of electronic contact details meant that we were
unable to track respondents or issue reminder emails. Moreover, the flyers and
letters were sent cold. Respondents neither knew that they would be invited to
participate in a survey, or who the research team were in advance of being sent the
flyer/letter or reading the advertisement. To lessen the impact of this cold contact
strategy, and as an incentive to participate in the survey, we offered the prize of a
case of champagne for one lucky participant. The prize was drawn randomly on 15th
December 2004, after the survey deadline had passed and the recipient was
contacted to arrange delivery.
References
1. Department of Health. Research Governance Framework for Health and
Social Care London: Department of Health 2001
2. European Union. Directive 2001/20/EC of the European parliament and of the
council 4th April 2001 Official Journal of the European Communities
2001;L121:34-44

199
Appendix 3. Ineligible Survey Data
As reported in our discussion of the survey data, of the 113 responses received, 22
of these were ineligible. Respondents were recorded as not working in the English
NHS sector, and therefore did not fit our sampling criteria. However, the results offer
some interesting comparison, and highlight the need for further research into reuse of
single use devices in the private sector.
Data Characteristics
Despite the participation invitation clearly stating that the research was only asking
about reuse of SUDs in English NHS operating theatres, 54% of ineligible cases
were made by staff working in private hospitals in England. The remaining ineligible
cases came from clinical staff working in Wales (9%), Ireland (5%), Scotland (27%),
and unexpectedly, Australia (5%).
Table 23: Data characteristics
Total
Theatre
Nurse
Clinical
Procurement
Theatre
Manager
Location Wales 2 0 0 2
Scotland 4 1 1 6
Ireland 0 0 1 1
Australia 1 0 0 1
Private 11 0 1 12
Total 18 1 3 22
The cases from elsewhere in the British Isles have been excluded as the NHS is
devolved to each country: for example, the policy on SUD usage for tonsillectomy
differs between England and Wales.
Of the 12 private cases excluded from the main analysis, 11 responses were from
nurses, whilst the remaining respondent was a theatre manager. 42% of these
respondents had been in post for up to five years, with 58% working at the hospital
for five years or more.

200
In a similar manner to the main body of data, ineligible cases were geographically
spread.
Single Use Devices and Their Reuse
In the similar manner to the main body of data, respondents working in private
hospitals also demonstrated that there is no consistent understanding of ‘single use’.
Table 24: Definitions of single use
N %
Single patient 10 83
Single episode 8 67
Used on a single occasion within a single episode 2 17
Non-reprocessable 11 92
Disposable 11 92
As with the main body of data, respondents were less likely to support definitions of
‘single use’ that described the single episode of use. Respondents considered that
SUDs should be disposable (92%) and non-reprocessable (92%), and that they
should only be used on one patient (83%). Such support reiterates our earlier
argument that there is little objective understanding about what ‘single use’
constitutes amongst clinical endusers. Respondents working in the private sector
17%
25% 8%
8%
8%
17%
17%

201
were more likely to consider a SUD to be something that cannot be reprocessed and
must be disposed of, rather than a device that should be used once and then
discarded.
Seven respondents reported the reuse of SUDs:
Table 25: Single use devices reported as being reused
Total
(N)
Every
operation
More
than
once a
week
More
than
once a
month
More than
once a
year
Laryngoscope blades 3 2 0 1 0
Drill bits 2 1 1 0 0
Compression garments 2 2 0 0 0
Saw blades 1 0 0 0 1
Disposable suction bottle
liners 1 1 0 0 0
LMAs 1 0 1 0 0
Guidewires 1 0 0 1 0
Anaesthetic tubing 1 0 1 0 0
Dental burrs 1 1 0 0 0
GU irrigation tubing 1 1 0 0 0
Puddle floor vacs 1 1 0 0 0
Pins that hold cutting jigs 1 1 0 0 0
Many of the items listed will not come into direct contact with either the patient’s skin
or the surgical site. Consequently, items such as puddle floor vacs, suction bottle
liners, compression garments and pins that hold cutting jigs may not need to be
labelled as ‘for single use only’.
However, some of the other devices that were reported as being reused do come into
contact with the patient. In addition to devices such as laryngoscope blades, LMAs
and anaesthetic tubing, which were discussed earlier in this report, the reuse of drill
bits, burrs and guidewires might be considered alarming. These devices become

202
fatigued with use, which if reused, can lead to a patient safety incident through
device failure or breakage. Despite this threat, one respondent claimed that a
“Medical rep [had] indicate[d] that guidewires are strong and can be reused even
though the packaging suggest single-use” (ID 42 / Nurse). Further rationales for
reuse included the prohibitive cost of replacing each SUD (25%), the lack of risk
associated with reuse (17%) and the lack of other equipment (17%).
Respondents working in the private sector considered that the dangers of reusing
SUDs included a risk of cross contamination and infection (N=6), the possibility that
the device could be faulty on the second and subsequent use (N= 5), the inability to
adequately clean the devices (N=3) and that reuse breaches the manufacturer’s
guidelines (N=1).
92% of respondents working in the private sector stated that they were aware of their
hospital’s guidelines on the use of SUDs. All described how the guidelines reiterated
that single use means single use. However, as discussed throughout this report,
endusers appear confused about what ‘single use’ actually means in practice.
Similar patterns of reuse have been reported by the 12 respondents working in the
private sector, to those reported by respondents working in the NHS. It is proposed
therefore, that the constraints, which lead to SUDs reuse, are not unique to the NHS.
203
Appendix 4: Interview methodological details
All research involving NHS staff, patients, facilities, records or tissue samples must
be considered by an appropriate ethics committee16. Research falling across more
than one domain (SHA) must be considered by a multi-site research ethics
committee (MREC). Ethical approval was sought from the Trent MREC, and gained
in July 2005.
The initial ethical application and associated documents amounted to 116 A4 pages.
Subsequent amendments created a further 60 pages of paperwork, amounting to a
total of 176 pages. From date of submission to receiving ethical approval, the MREC
process took 63 working days (03.05.05 – 28.07.05). However, COREC operate a
60-day limit on applications, which begins from the final date in which applications
can be submitted for the forthcoming meeting, and contains a start-stop element, in
which the ‘clock’ is stopped between each correspondence being sent and a reply
received. Consequently, the 60-day limit began nine working days following our
submission (16.05.05), and was stopped and started twice (15.06.05 - 23.06.05,
14.07.05 - 26.07.05). The ‘official’ length of the MREC process was therefore 41
working days.
NHS Trust R&D approval was sought concurrently with ethical approval. R&D
approval has been described as a “cumbersome” practice1 and implemented in
different ways and with varying application processes2. The introduction of the
‘standardised’ R&D form in May 2005 was intended to address the problem of
inconsistent processes. Nevertheless, the system continues to be in a state of
confusion.
Locating R&D departments was a problematic and time-consuming process.
Morecroft et al3 described their difficulty in dealing with switchboard personnel, which
we shared: when asking to be put through to the R&D department, we were
transferred, in one instance, to the social care department, and, in another, to the
palliative nursing team. Other hospital switchboards denied the existence of an R&D
16 Following the 2005 Warner review4, it is likely that research involving NHS staff will
not be required to undergo ethical consideration at committee level, unless ‘material
ethical issues’ arise. However, applications will still need approval by COREC
National Research Ethics Advisors.

204
department. Finally, we gained access to an online resource hosted by the NHS
R&D forum. Using this, R&D co-ordinators for each of the Trusts were easily
identified and contacted, to establish their preferred formats for applications.
Despite the standardised form, significant variation in the application process
remains. Five of the eight Trusts accepted the new standardised form. One of these
decided to accept the new form (and only the new form) one week before the
application was due to be submitted. Previously, they had only accepted applications
on their own form, which meant that the paperwork had to be amended at short
notice. All Trusts required authorisation signatures but the job titles of the signatories
varied, introducing further delays and difficulties in making contact.
Applications to the eight Trusts were submitted between May and June 2005. These
averaged 90 pages in length. In addition to the completed R&D application form,
which was an average of nine pages in length and required signatures from up to
four members of hospital staff, each application pack required:
1. A copy of research protocol, in both scientific and lay language
2. A diagram of the research design
3. A copy of the completed ethics (COREC) form
4. A copy of the research budget, in some cases on the hospital’s own financial
proforma
5. A copy of all correspondence between MREC and the research team
6. A copy of an independent, external peer review of the research
7. A copy of the invitation letter
8. A copy of the consent form
9. A copy of the questionnaire
10. The researchers CVs (both Professor Dingwall’s and Dr Rowley’s CVs were
required)
11. Evidence of sponsorship
Following receipt of the applications, the R&D committees considered the study. In
some cases this was carried out quickly (for example, two hospitals considered the
application just a few days after it was received). However, in others, the study had
not been considered for approval four months after the application was made. (A full
log of the application process in each Trust can be found in the Appendix five).

205
Several Trusts questioned some aspect of the application, but there was no
consistency in the queries, despite identical submissions. One hospital queried
whether Professor Dingwall or Dr Rowley should be recognised as the principal
researcher, although COREC guidelines clearly state that the principal researcher is
the field-researcher (Dr Rowley). At a second hospital, the research’s sponsorship
was challenged. Originally, the University of Nottingham had agreed to act as
sponsor, after being told that the Department of Health would not, but Department
policy later changed. A revision of arrangements to reflect this would have introduced
further delays but fortunately the commissioners and the university were able to
resolve the question.
Most sites required individual honorary contracts for the principal researcher. The
RGF requires that “researchers who do not have a paid contract with a NHS body
but whose research involves NHS staff or patients, their organs, tissue or data must
have an honorary contract with a NHS body”5. An honorary contract to cover the
whole of the NHS is unavailable, yet it is intended that once one honorary contract is
gained, subsequent Trusts should accept that. In practice this is not the case, with
Trusts refusing to accept honorary contracts other than their own6.
The process of applying for an honorary contract is inconsistent3,7. In some Trusts,
an honorary contract was received by return of post following an email request. In
others, a formal letter, application form and CV needed to be sent to the R&D
director. This was then passed onto the Human Resources department, and after a
number of conversations to clarify the contract’s purpose, the paperwork was sent.
In others, in addition to the application form, Dr Rowley was required to undergo
occupational health screening (height, weight and blood pressure checks, and urine,
blood and eye sight tests) and criminal records bureau (CRB) investigation. The CRB
process led to prolonged delay. The original application to the CRB was made in
May 2005 (20.05.05) when Dr Rowley travelled to the relevant hospital Human
Resources department to deliver proof of her identity (birth certificate, driving licence
and passport). However, the application was mislaid and once found, was subjected
to repeated requests after the supplementary information that was originally supplied
was lost once more! Clearance was finally received some 83 workdays after the
application was submitted. This delay severely affected the application for an
honorary contract at another Trust, which also required CRB approval. Thus, data
collection at two Trusts (four sites) was delayed.
206
The introduction of the requirement for Trust R&D approval created an unforeseen
increase in workload and expenditure. As Watson and Manthorpe7 note, protocols
written, like ours, prior to Spring 2004 would not have incorporated the additional
time needed to prepare the paperwork, arrange for designated Trust officers to sign
the forms, and await the R&D board’s decision. Wald8 described how an R&D
application at just one Trust created an extra 44 hours of work, and an additional
£850 expenses covering staff time, travelling, telephone calls, fax messages, internet
research and consumables. Brindle9 reported how, in one study requiring 62 R&D
applications, 58 of the Trusts had their own form. These 62 applications produced
5929 pages of paperwork. Eight months after submission, just 20 Trusts had granted
approval. We estimate that this phase of the present study consumed 120 workdays
(27.04.05 – 13.10.05) and incurred additional unbudgeted costs resulting from
telephone calls, paperwork, postage and mileage.
The Theatre Manager and Clinical Director of Anaesthesia were each sent a letter
inviting them to participate in the research. Following the governance regulations,
which prevent research teams having access to any personal data about a third party
without their express agreement, letters were addressed to ‘The Theatre Manager’
and ‘The Clinical Director of Anaesthesia’, unless the individual’s name was already
known. Each respondent was asked to reply to Dr Rowley if they agreed to
participate in the research. If such an agreement was reached, an interview was
arranged and an information sheet, consent form and list of questions sent to the
participant. If a response was not received after four weeks, a follow-up telephone
call was made. Dr Rowley called the hospital's switchboard and asked to speak to
the Theatre Manager or Clinical Director of Anaesthesia (as applicable). If the
individual was unavailable, a message was left asking them to make contact, or an
email was sent if colleagues suggested that this was a more appropriate form of
communication and were able to furnish Dr Rowley with the email address.
The Theatre Manager and Clinical Director of Anaesthesia were each asked to
nominate an ODP who had responsibility for equipment, and to forward a second
letter (enclosed with the first) to them. This letter invited the ODP to participate in the
research, and asked them to contact Dr Rowley if they were happy to be recruited.
Upon such contact, an interview was arranged, and an information sheet, consent
form and list of questions were sent.
207
References
1. Meerabeau E, Ruston A, Clayton J. The Research Governance Framework
For Health And Social Care: Implications For Developing Research In
Primary Care J Res Nurs 2004;9(6):421-429
2. Dumville JC, Watson J, Raynor P, Togerson DJ. Research Governance: A
Barrier To Ethical Research? QJM 2004; 97:113-114.
3. Morecroft C, Ashcroft D, Noyce P. Research Governance And Pharmacy
Practice Research: A Case-Study The Pharmaceutical Journal 2005;274:650-
651
4. Department of Health. Report Of The Ad Hoc Advisory Group On The
Operation Of NHS Research Ethics Committees London: Department of
Health 2005.
5. Department of Health. Guidance Note on Research Governance and
Honorary Contracts London: Department of Health 2003.
6. Hill AF, Butterworth RJ, Joiner S, McGregor G, Rosser MN, Thomas DJ.
Investigation Of Variant Creutzfeldt-Jakob Disease And Other Human Prion
Diseases With Tonsil Biopsy Samples Lancet 1999;353:183-189.
7. Watson R, Manthorpe J. Research Governance: For Whose Benefit? J Adv
Nurs 2002;39(6):515-516
8. Wald D. Bureaucracy Of Research Ethics Br Med J 2004;329:282-284
9. Brindle D. (2005) Scaling Back The Paper Mountain Guardian 5th January
2005

208
Appendix 5. R&D log
Hospitals 1, 8, 9 & 10
24.05.05 Honorary contract requested (letter and CV sent)
05.07.05 Following confusion at Trust level on who should sign forms, 1st
form (H1) signed and returned.
11.07.05 2nd (H8) and 3rd (H9) forms received. Sent to Trust 12.07.05
26.07.05 Still awaiting 4th form, despite 3 follow up calls.
26.07.05 Honorary contract received.
26.07.05 Waiting for 4th form and approval (hospital 10)
18.08.05 MREC approval and documentation sent.
25.08.05 Requested that application proceed without H10
15.09.05 R&D approval received
15.09.05 Invitation letters sent
03.10.05 Arranged interview with 9ODP
05.10.05 Interview with 9ODP
09.10.05 Arranged interview with 8TM
12.10.05 Arranged interview with 9TM
12.10.05 Follow up call to 9CDA: new to post, so refused to participate
13.10.05 Follow up call to 1CDA and 1TM: refused to participate
18.10.05 Interview with 8TM
18.10.05 Interview with 9TM
Hospital 2
27.04.05 R&D finance forms completed and sent to finance director
27.05.05 Clinical Director signs form
31.05.05 Forms delivered to Assistant Medical Director
02.06.05 Honorary contract requested
09.06.05 Honorary contract sent to Assistant Medical Director
24.06.05 Change of guidance: Assistant Medical Director not required to
sign form.
24.06.05 Forms and e-versions submitted
05.07.05 Preliminary R&D approval sought, subject to honorary contract
(awaiting CRB) and REC.
18.08.05 MREC approval and documentation sent.
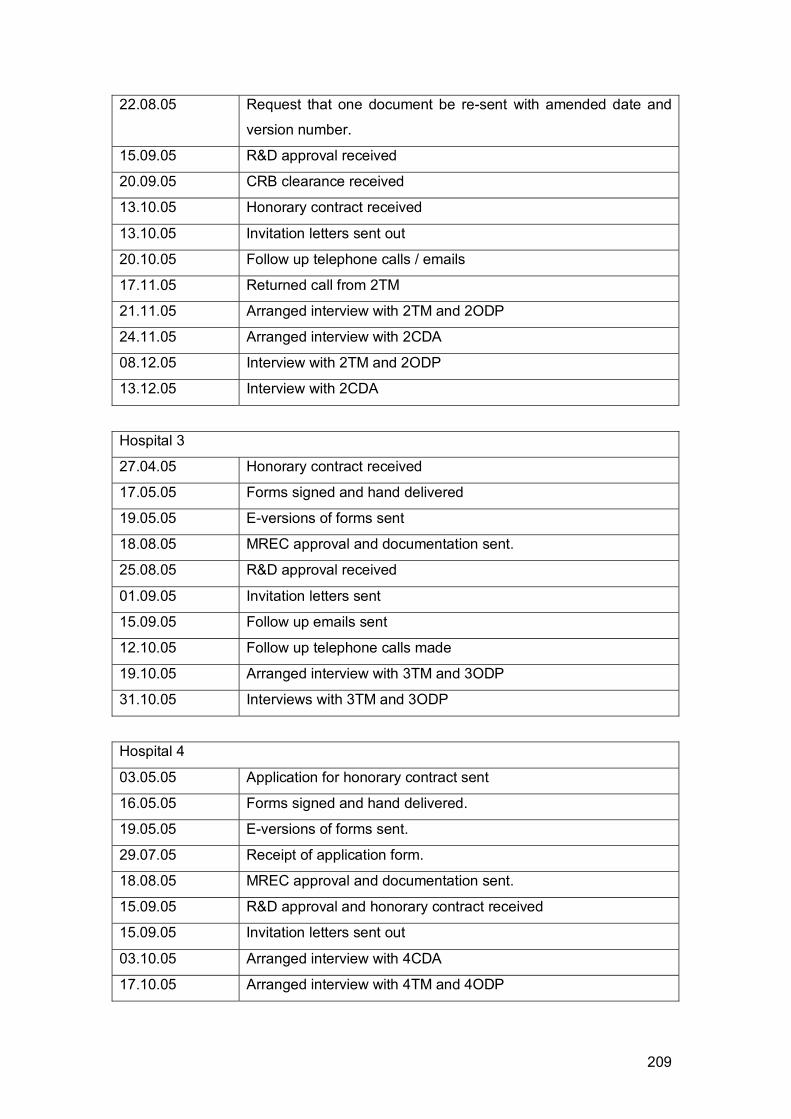
209
22.08.05 Request that one document be re-sent with amended date and
version number.
15.09.05 R&D approval received
20.09.05 CRB clearance received
13.10.05 Honorary contract received
13.10.05 Invitation letters sent out
20.10.05 Follow up telephone calls / emails
17.11.05 Returned call from 2TM
21.11.05 Arranged interview with 2TM and 2ODP
24.11.05 Arranged interview with 2CDA
08.12.05 Interview with 2TM and 2ODP
13.12.05 Interview with 2CDA
Hospital 3
27.04.05 Honorary contract received
17.05.05 Forms signed and hand delivered
19.05.05 E-versions of forms sent
18.08.05 MREC approval and documentation sent.
25.08.05 R&D approval received
01.09.05 Invitation letters sent
15.09.05 Follow up emails sent
12.10.05 Follow up telephone calls made
19.10.05 Arranged interview with 3TM and 3ODP
31.10.05 Interviews with 3TM and 3ODP
Hospital 4
03.05.05 Application for honorary contract sent
16.05.05 Forms signed and hand delivered.
19.05.05 E-versions of forms sent.
29.07.05 Receipt of application form.
18.08.05 MREC approval and documentation sent.
15.09.05 R&D approval and honorary contract received
15.09.05 Invitation letters sent out
03.10.05 Arranged interview with 4CDA
17.10.05 Arranged interview with 4TM and 4ODP

210
31.10.05 Interviews with 4TM, 4CDA and 4ODP
Hospital 5
19.05.05 Forms signed by Clinical Director, and collected
24.05.05 R&D forms and e-versions submitted
24.05.05 Honorary contract application submitted, with CV
21.06.05 Honorary contract received
21.06.05 Occupational health screening
24.06.05 Preliminary R&D approval subject to REC
18.08.05 R&D registration form sent with final REC approval
18.08.05 MREC approval and documentation sent.
22.08.05 R&D re-submission in light of amended MREC documents
20.09.05 R&D approval received
20.09.05 Invitation letters sent
09.10.05 Follow up calls
17.10.05 Follow up calls
20.10.05 Follow up emails
20.10.05 Arrange interview with 5CDA
24.11.05 Follow up email to 5TM
29.11.05 Arrange interview with 5TM
06.12.05 Interview with 5TM
14.12.05 Interview with 5CDA
Hospital 6
16.05.05 Forms signed and delivered by hand.
19.05.05 E-versions of forms sent.
25.05.05 R&D approval subject to REC approval.
27.06.05 Another Trust Honorary Contract accepted.
18.08.05 MREC approval and documentation sent.
30.09.05 Interview with 6TM, 6CDA and 6ODP
06.10.05 Interview with 6SM
Hospital 7
02.06.05 Meet with Surgical Services Manager; Forms signed
03.06.05 Application forms submitted

211
03.06.05 Application for honorary contract sent.
10.06.05 Preliminary approval, subject to REC and honorary contract.
18.08.05 MREC approval and documentation sent.
27.09.05 R&D approval received
10.10.05 Honorary contract received
10.10.05 Invitation letters sent out
20.10.05 Arranged interview with 7CDA
25.10.05 Arranged interview with 7ODP
25.10.05 Arranged interview with 7TM
27.10.05 Interviews with 7CDA, 7TM and 7ODP
Hospitals 11, 12 & 13
05.05.05 R&D form submitted (paper hard copy and e-version).
11.05.05 Offer of honorary contract received, on condition of Criminal
Record Bureau checks and occupational health screening.
20.05.05 Returned forms to HR (in person) along with proof of identity
requested (passport, driving license, bank statement).
08.06.05 Occupational Health Screening (eyesight, weight, height, BMI,
blood pressure, urine sample, rubella (tested previously), general
health questions).
27.07.05 Still waiting for CRB approval
18.08.05 MREC approval and documentation sent.
20.09.05 CRB clearance received
06.10.05 Honorary contract received
13.10.05 R&D approval received
13.10.05 Interview invitation letters sent
24.11.05 Follow up telephone calls/emails
29.11.05 Arranged interview with 11TM and 11ODP
05.12.06 Arrange interview with 13ODP
07.12.05 Interview with 13ODP
12.12.05 Arrange interview with 11CDA
05.01.06 Interview with 11TM and 11ODP
05.01.06 11CDA cancels interview; unable to reschedule

212
Appendix 6. Ergonomics of Single Use Devices
This report describes the design features of a set of nine different types of medical
devices in an attempt to identify how their design properties might influence the
likelihood of the reuse of single use devices. The aim of this is to identify appropriate
design recommendations for single use devices.
It is important to note that whilst the types of devices examined were selected on the
bases of accounts of clinicians in the survey and interviews conducted, the specific
manufacturers whose devices are considered here were not in any way linked to
instances of reuse. The samples used were obtained from those manufacturers
willing to kindly support our study, and this report and any illustrations within it do not
intend to make any specific recommendations regarding particular manufacturers or
companies. A full inventory of the devices considered is available at the end of this
appendix.
Two ergonomics consultants (Dr. Sarah Sharples & Dr. Beverley Norris, Institute for
Occupational Ergonomics, University of Nottingham) evaluated the devices over two
separate meetings. During these meetings, feature of the devices that might
influence reuse were noted, and single and reusable devices compared.
The features identified were classified as relating to:
• Packaging e.g. ease of opening, expense or quality
• Labelling e.g. text and symbols on device itself, card inserts for recording
sterilisation, text and symbols on package
• Material properties and design e.g. apparent quality or durability of material,
potential for sterilisation, durability of fittings etc
The following examples of devices were examined:
• Anaesthesia masks
• Oxygen mask
• Laryngeal mask
• Endotracheal tube
• Breathing system
• Bougies

213
• Electrodes and wires (diathermy)
• Pen (diathermy)
• Laryngoscope handle and blade
These devices included both single use and reusable items. It is noted that a number
of standards for the design of these items and their packaging exist1,2 and that all of
these items conform to these standards. Therefore issues raised in this report reflect
the need for consideration of the way in which these standards and design practice
could potentially change the likelihood of inappropriate reuse of the single use
versions of these devices.
Three main types of design feature were identified as influencing factors on single or
multiple device use. These were labelling, packaging and material properties and
design.
Labelling was felt to be an important influential factor as it was the main (usually only)
explicit way in which the manufacturers informed the purchaser about the appropriate
use of the device. Labelling will be particularly important for new or untrained users,
or for experienced users who are using new or unfamiliar products. However, it is
vital that this labelling is prominent, unambiguous, clear and consistent. There has
been extensive research on the effectiveness of labelling, both on-product and on
packaging3,4,5,6,7,8,9,10,11. Research has shown that effectiveness is difficult to
measure, and a variety of measurement methods have been developed4:
• Comprehension - the level of understanding of a conveyed message
• Warning detection - the time to notice a warning message in-situ on
packaging
• Reading time/rate - the time to understand, or the rate of processing, of a
warning message
• Recall - the retained learning of a warning message over time
• Hazard perception - the awareness of a hazard and the likelihood to comply
with a warning
• Behavioural compliance - a measure of changed behaviour as a result of a
warning.
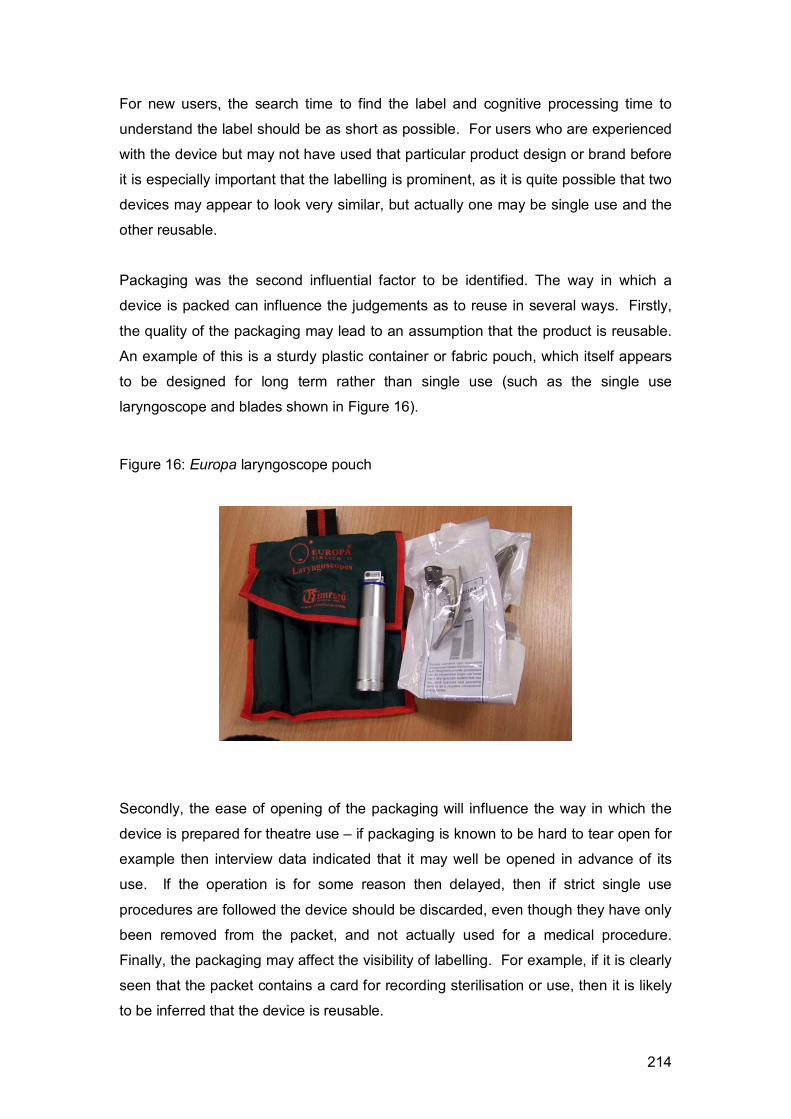
214
For new users, the search time to find the label and cognitive processing time to
understand the label should be as short as possible. For users who are experienced
with the device but may not have used that particular product design or brand before
it is especially important that the labelling is prominent, as it is quite possible that two
devices may appear to look very similar, but actually one may be single use and the
other reusable.
Packaging was the second influential factor to be identified. The way in which a
device is packed can influence the judgements as to reuse in several ways. Firstly,
the quality of the packaging may lead to an assumption that the product is reusable.
An example of this is a sturdy plastic container or fabric pouch, which itself appears
to be designed for long term rather than single use (such as the single use
laryngoscope and blades shown in Figure 16).
Figure 16: Europa laryngoscope pouch
Secondly, the ease of opening of the packaging will influence the way in which the
device is prepared for theatre use – if packaging is known to be hard to tear open for
example then interview data indicated that it may well be opened in advance of its
use. If the operation is for some reason then delayed, then if strict single use
procedures are followed the device should be discarded, even though they have only
been removed from the packet, and not actually used for a medical procedure.
Finally, the packaging may affect the visibility of labelling. For example, if it is clearly
seen that the packet contains a card for recording sterilisation or use, then it is likely
to be inferred that the device is reusable.

215
Materials and design are the final influential factor. The first implication of materials
is the perceived quality (and thus cost) of the device. If a device appears to be
cheaply manufactured then it may be more likely to be considered to be single use.
Secondly, users may make judgements about the ease of sterilising a device – for
example, if a device appears to be made predominately from metal, it may be
assumed that it can withstand high temperatures and thus be sterilised and reused.
Finally, the materials used may affect the user’s perception of the ease of use and
efficacy of the device, and thus their preference for use – for example, if a reusable
device is known to be easier to use or produce a better clinical result than a single
use one then this may be selected in preference to the single use item. An example
of this given from the interviews is that the single-use bougies may not retain their
profile as well as the reusable ones.
The following sections give examples of the labelling, packaging and materials on the
sample products.
As mentioned earlier, it is important that labelling is prominent, unambiguous, clear
and consistent. A wide variety of labelling methods were used in the devices
examined.
The first point of note was how a device’s reusability was indicated. A symbol is
used by some of the manufacturers to indicate reuse. The use of the number “2”
crossed out can be considered to be reasonably intuitive to imply that the device
should not be used two (or more) times, and is indeed used in other forms in
reusable devices where there is a maximum number of uses (e.g. in the re-usable
laryngeal masks the maximum number of use is 40 and this is indicated by a crossed
out ‘41’ symbol see Figure 17).

216
Figure 17. Example of multiple use symbol
However, this symbol does not appear to have a consistent size or font style and is
not consistently used. In some cases, the label simply states in text that the device is
“single use” (see Figure 18).
Figure 18. Example of single use label that uses text only
Whilst the use of a symbol is recommended in preference to text as it is not language
dependent, where there is sufficient space the use of text to supplement a symbol is
often recommended in order to help establish the comprehension of new symbols
such as the single use symbol.
The single use symbol is performing a number of functions:
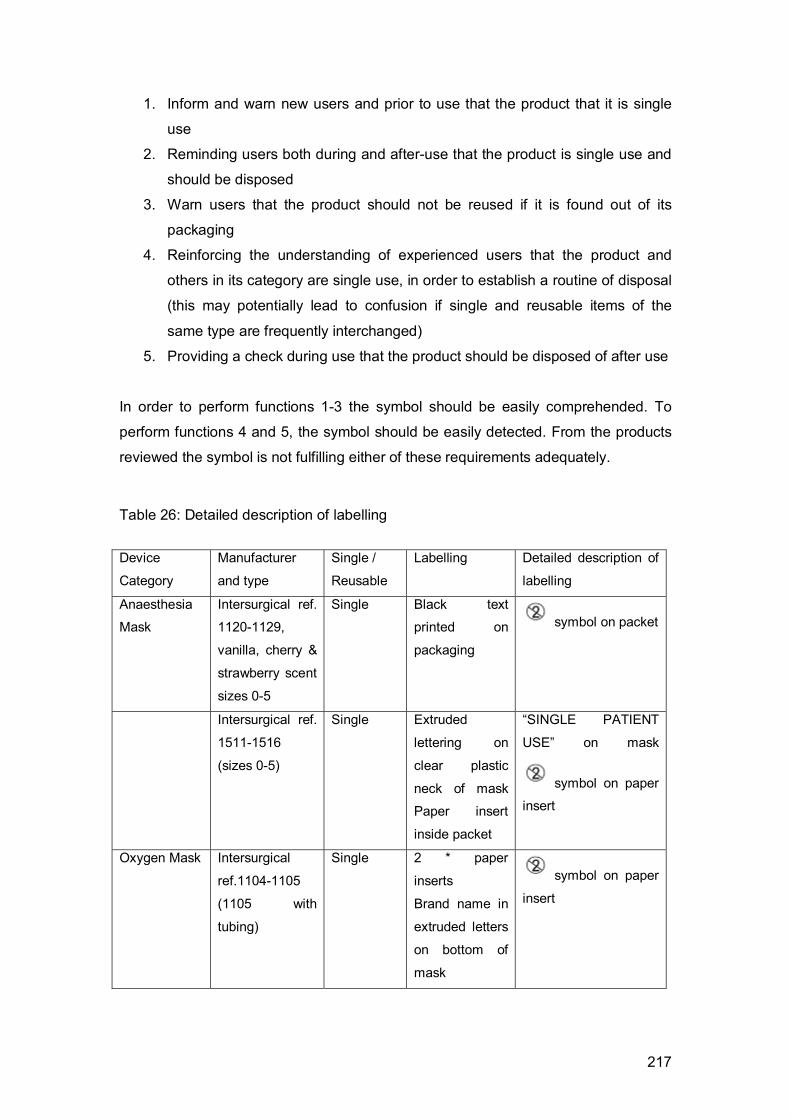
217
1. Inform and warn new users and prior to use that the product that it is single
use
2. Reminding users both during and after-use that the product is single use and
should be disposed
3. Warn users that the product should not be reused if it is found out of its
packaging
4. Reinforcing the understanding of experienced users that the product and
others in its category are single use, in order to establish a routine of disposal
(this may potentially lead to confusion if single and reusable items of the
same type are frequently interchanged)
5. Providing a check during use that the product should be disposed of after use
In order to perform functions 1-3 the symbol should be easily comprehended. To
perform functions 4 and 5, the symbol should be easily detected. From the products
reviewed the symbol is not fulfilling either of these requirements adequately.
Table 26: Detailed description of labelling
Device
Category
Manufacturer
and type
Single /
Reusable
Labelling Detailed description of
labelling
Anaesthesia
Mask
Intersurgical ref.
1120-1129,
vanilla, cherry &
strawberry scent
sizes 0-5
Single Black text
printed on
packaging
symbol on packet
Intersurgical ref.
1511-1516
(sizes 0-5)
Single Extruded
lettering on
clear plastic
neck of mask
Paper insert
inside packet
“SINGLE PATIENT
USE” on mask
symbol on paper
insert
Oxygen Mask Intersurgical
ref.1104-1105
(1105 with
tubing)
Single 2 * paper
inserts
Brand name in
extruded letters
on bottom of
mask
symbol on paper
insert
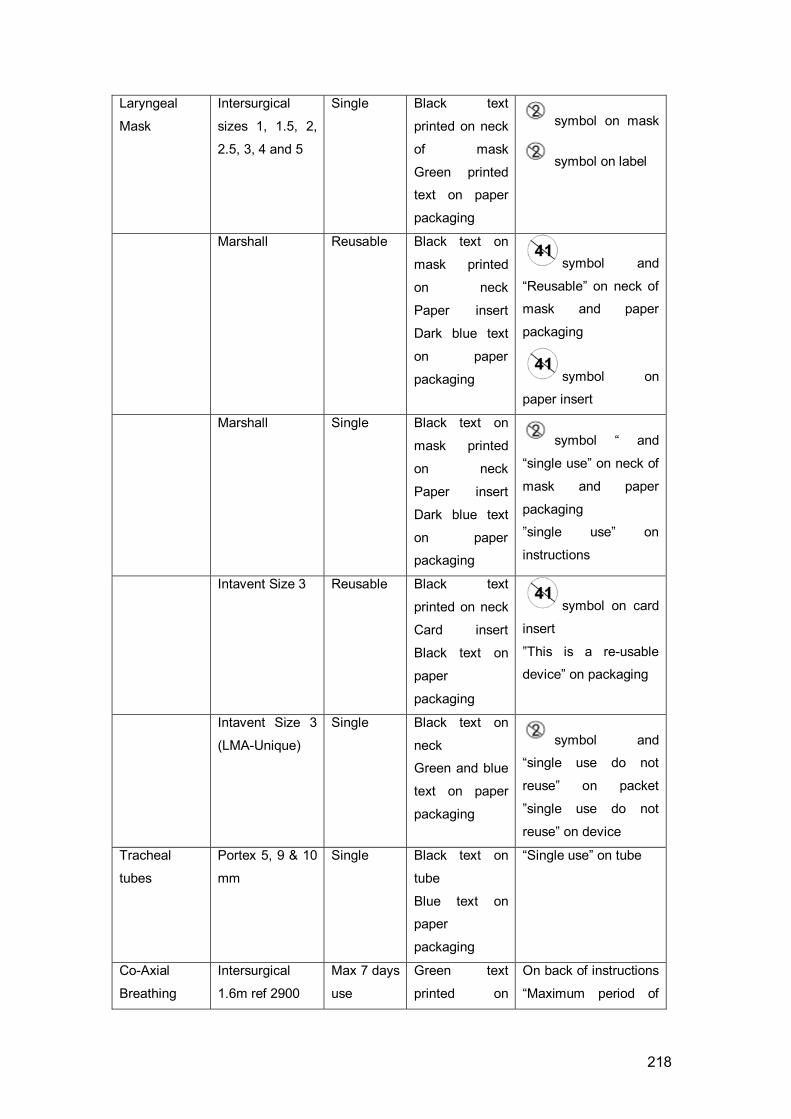
218
Laryngeal
Mask
Intersurgical
sizes 1, 1.5, 2,
2.5, 3, 4 and 5
Single Black text
printed on neck
of mask
Green printed
text on paper
packaging
symbol on mask
symbol on label
Marshall Reusable Black text on
mask printed
on neck
Paper insert
Dark blue text
on paper
packaging
symbol and
“Reusable” on neck of
mask and paper
packaging
symbol on
paper insert
Marshall Single Black text on
mask printed
on neck
Paper insert
Dark blue text
on paper
packaging
symbol “ and
“single use” on neck of
mask and paper
packaging
”single use” on
instructions
Intavent Size 3 Reusable Black text
printed on neck
Card insert
Black text on
paper
packaging
symbol on card
insert
”This is a re-usable
device” on packaging
Intavent Size 3
(LMA-Unique)
Single Black text on
neck
Green and blue
text on paper
packaging
symbol and
“single use do not
reuse” on packet
”single use do not
reuse” on device
Tracheal
tubes
Portex 5, 9 & 10
mm
Single Black text on
tube
Blue text on
paper
packaging
“Single use” on tube
Co-Axial
Breathing
Intersurgical
1.6m ref 2900
Max 7 days
use
Green text
printed on
On back of instructions
“Maximum period of
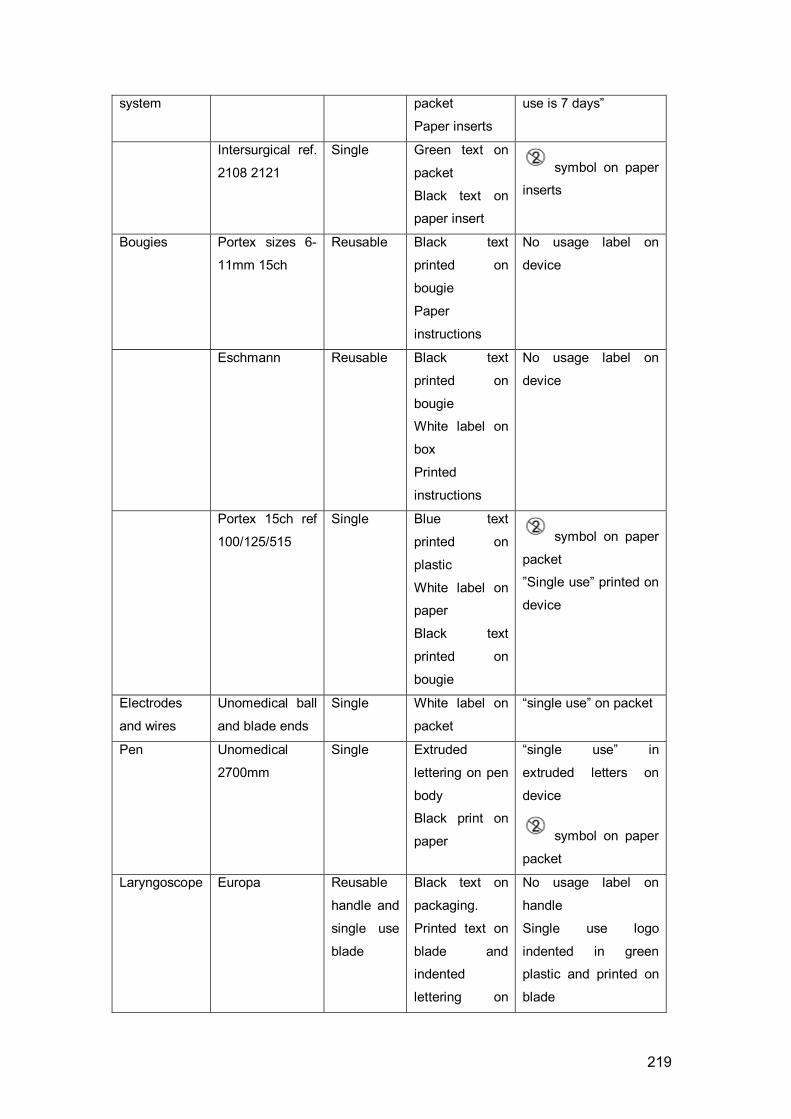
219
system packet
Paper inserts
use is 7 days”
Intersurgical ref.
2108 2121
Single Green text on
packet
Black text on
paper insert
symbol on paper
inserts
Bougies Portex sizes 6-
11mm 15ch
Reusable Black text
printed on
bougie
Paper
instructions
No usage label on
device
Eschmann Reusable Black text
printed on
bougie
White label on
box
Printed
instructions
No usage label on
device
Portex 15ch ref
100/125/515
Single Blue text
printed on
plastic
White label on
paper
Black text
printed on
bougie
symbol on paper
packet
”Single use” printed on
device
Electrodes
and wires
Unomedical ball
and blade ends
Single White label on
packet
“single use” on packet
Pen Unomedical
2700mm
Single Extruded
lettering on pen
body
Black print on
paper
“single use” in
extruded letters on
device
symbol on paper
packet
Laryngoscope Europa Reusable
handle and
single use
blade
Black text on
packaging.
Printed text on
blade and
indented
lettering on
No usage label on
handle
Single use logo
indented in green
plastic and printed on
blade

220
plastic
Penlon Reusable
handle and
single use
blade
Indented label
in clear plastic on packaging
and “single use only”.
Single use logo
indented in plastic
The positioning of the label was not at all consistent. In some cases the labelling
was on the device itself, and in others it was on the packaging. It is preferable for the
usage instructions to be on the device where possible, as the packaging is likely to
become separated from the device at some point.
Figure 19. Examples of inconsistency in font style and size in labelling
SINGLE PATIENT USE
SINGLE PATIENT USE
SINGLE USE
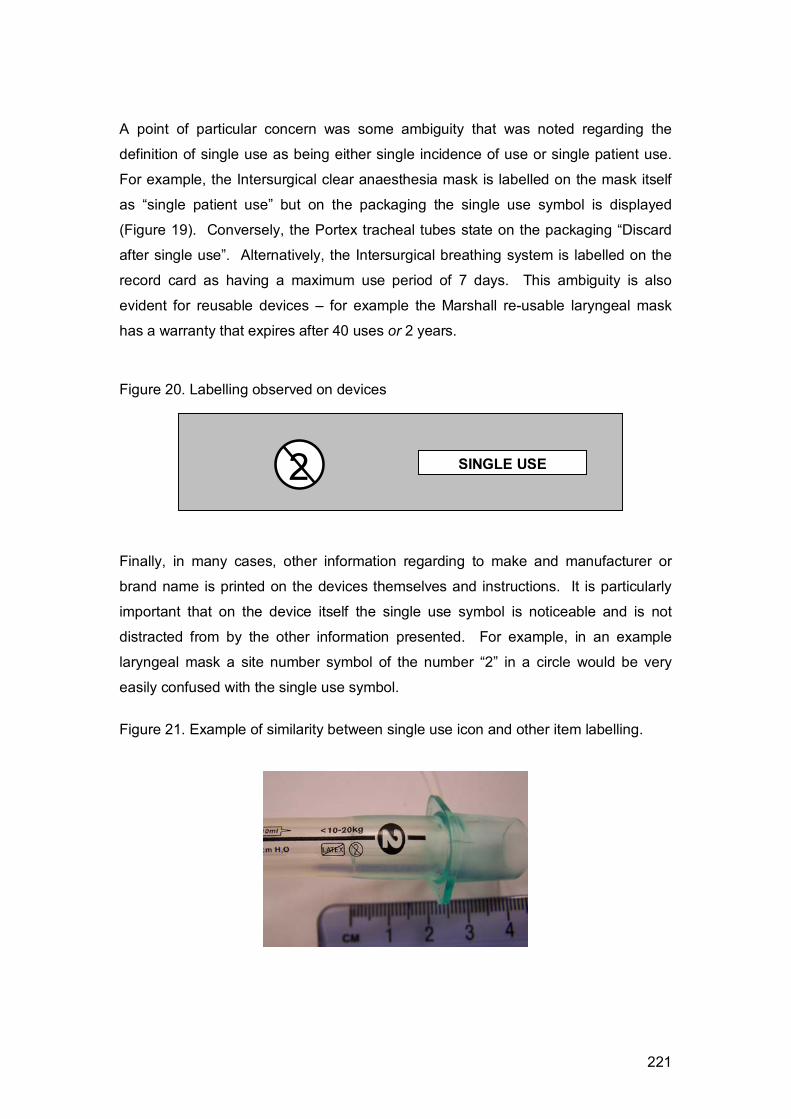
221
A point of particular concern was some ambiguity that was noted regarding the
definition of single use as being either single incidence of use or single patient use.
For example, the Intersurgical clear anaesthesia mask is labelled on the mask itself
as “single patient use” but on the packaging the single use symbol is displayed
(Figure 19). Conversely, the Portex tracheal tubes state on the packaging “Discard
after single use”. Alternatively, the Intersurgical breathing system is labelled on the
record card as having a maximum use period of 7 days. This ambiguity is also
evident for reusable devices – for example the Marshall re-usable laryngeal mask
has a warranty that expires after 40 uses or 2 years.
Figure 20. Labelling observed on devices
Finally, in many cases, other information regarding to make and manufacturer or
brand name is printed on the devices themselves and instructions. It is particularly
important that on the device itself the single use symbol is noticeable and is not
distracted from by the other information presented. For example, in an example
laryngeal mask a site number symbol of the number “2” in a circle would be very
easily confused with the single use symbol.
Figure 21. Example of similarity between single use icon and other item labelling.
2 SINGLE USE

222
The packaging for the devices varied considerably. In most cases the packets were
sealed plastic of some type, but in some cases these plastic packets were partly
made of paper to enable labelling to be printed on them directly. The ease of
opening of the plastic packets varied. For the oxygen mask and breathing system
the plastic packaging was easy to tear or rip, which is likely to make the packets
much easier to open and less likely to be opened in advance of use . However, this
packaging does have the disadvantage of apparently being harder to print on, as in
all cases these packets included loose paper inserts rather than labelling directly on
the packet or device.
Reusable devices tended to come in sturdier packaging, although again this was by
no means a consistent pattern. The reusable laryngoscope and bougies were notable
in that they had packaging that was rigid or apparently long lasting. The advantage
of such containers is that they also provide the opportunity for co-storage of the
sterilisation and use recording cards.
In some cases (e.g. bougies) the single and reusable devices appear to look different
(reusables have weaving visible on inside) but in others the difference is less obvious
(e.g. laryngeal masks). If devices that are reusable and single use look similar then
there is inevitably more likelihood of accidental confusion. In addition, some
materials allow labelling to be printed more visibly than others (e.g. black printing
more noticeable than extruded text).
Conclusions and Recommendations
The primary aim of this report is to identify possible influencing factors on device
single or reuse. On the basis of the short analysis conducted within this report, the
following recommendations can be made.
Recommendations for labelling:
• A consistent size and font style for single use symbol to be adopted
• A similar symbol to indicate reusability to be adopted
• Use of symbol to become industry standard
• Clarification of difference between single use and single patient use
• Symbols to be printed on devices themselves where at all possible

223
• Make size of single use labelling at least the same size as other labelling (e.g.
manufacture information) printed on device
Recommendations for packaging:
• Packaging to be easy and quick to open to prevent advance opening
• Reusable devices to clearly indicate that recording card accompanies item
• Storage for recording card to be provided in packaging for reusable item
• Packaging to be clearly labelled with single or reuse symbol
Recommendations for materials and design:
• Labelling to be printed or inscribed on all parts of device
• Materials to allow visible black printing where possible
• The design of the single use symbol may need to be reviewed to ensure
legibility and noticeability. The current symbol is not easily detected and can
be confused with product numbering systems. In particular the symbol font,
size, contrast and positioning must be standardised across the industry.
In order to establish the symbol throughout the healthcare professions the symbol
should be supplemented by an education campaign. This could take the form of
leaflets supplied with medical devices, or high noticeability information on product
packaging that introduces the symbol and instructs users to look for it on single use
devices.
References
[1] BS EN980:2003 Graphical symbols for use in the labelling of medical devices
2003 BSI: London ISBN: 058042460X
[2] ISO/TR 15223:1998 Medical devices: Symbols to be used with medical device
labels, labelling and information to be supplied. (Withdrawn – replaced by BS EN980)
1998 ISO: Geneva
[3] Cairney P & Sless D. Communication effectiveness of symbolic safety signs with
different user groups. Applied Ergonomics, 1982;13(2):91-97.

224
[4] DeJoy DM. Consumer Product Warnings: Review and analysis of effectiveness
research. Proceedings of Human Factors Society 33rd Annual Meeting, 1989;936-
940.
[5] Easterby RS & Hakiel SR. Field testing of consumer safety signs: The
comprehension of pictorially presented messages. Applied Ergonomics, 1981;12(3):
143-152.
[6] Godfrey SS, Allender L, Laughery KR & Smith VL. Warning messages: Will the
consumer bother to look? Proceedings of Human Factors Society Annual Meeting,
1983;950-954.
[7] Jaynes LS & Boles DB. The effect of symbols on warning compliance.
Proceedings of Human Factors Society 34th Annual Meeting, 1990;984-987.
[8] Kalsher MJ, Pucci S, Wogalter MS & Racicot BM. Enhancing the perceived
readability of pharmaceutical container labels and warnings: the use of alternative
designs and pictorials. Proceedings of the Human Factors and Ergonomics Society
38th Annual Meeting, 1994;384-388.
[9] Mayer DL and Laux LF. Recognisability and effectiveness of warning symbols and
pictorials. Proceedings of the Human Factors 33rd Annual Meeting, 1989; 984-988.
[10] Wogalter MS, Godfrey SS, Fontenelle GA, Desaulniers DR, Rothstein PR and
Laughery KR. Effectiveness of Warnings, Human Factors, 1987;29(5):599-612.
[11] Young SL. Increasing the noticeability of warnings: Effects of pictorial, colour,
signal icon, and border. Proceedings of Human Factors Society 35th Annual Meeting,
1991:580-584.

22
5
Dev
ice
Cat
egor
y M
anuf
actu
rer
and
type
S
ingl
e / R
eusa
ble
Mat
eria
ls
Pac
kagi
ng
Labe
lling
Ana
esth
esia
M
ask
Inte
rsur
gica
l no
s 11
20-1
129,
van
illa,
ch
erry
& s
traw
berr
y sc
ent s
izes
0-5
Sin
gle
Gre
en
trans
luce
nt
plas
tic
and
gree
n ru
bber
C
lear
pla
stic
sea
led
pack
et
Bla
ck te
xt p
rinte
d on
pac
kagi
ng
In
ters
urgi
cal
ref.
1511
-151
6 (s
izes
0-
5)
Sin
gle
Cle
ar
plas
tic
and
clea
r ru
bber
w
ith
whi
te
plas
tic
cuff
Cle
ar p
last
ic s
eale
d pa
cket
E
xtru
ded
lette
ring
on
clea
r pl
astic
ne
ck
of
mas
k P
aper
inse
rt in
side
pac
ket
Oxy
gen
Mas
k In
ters
urgi
cal
1104
-11
05
(110
5 w
ith
tubi
ng)
Sin
gle
Cle
ar p
liabl
e pl
astic
, w
hite
pl
astic
nec
k, g
reen
ela
stic
fix
ing
stra
p
Cle
ar
plas
tic
(‘rip
able
’) pa
cket
2
* pa
per i
nser
ts
Bra
nd n
ame
in e
xtru
ded
lette
rs
on b
otto
m o
f mas
k La
ryng
eal M
ask
Inte
rsur
gica
l si
zes
1, 1
.5,
2, 2
.5,
3, 4
an
d 5
Sin
gle
Cle
ar
and
gree
n tra
nslu
cent
pl
astic
an
d ru
bber
with
red
cap
Pap
er b
acke
d rig
id p
last
ic
Bla
ck t
ext
prin
ted
on n
eck
of
mas
k G
reen
pr
inte
d te
xt
on
pape
r pa
ckag
ing
M
arsh
all
Reu
sabl
e C
lear
pl
astic
ne
ck
with
fle
sh c
olou
red
rubb
er c
uff
and
pum
p
Cle
ar
plas
tic
with
pa
per
back
ing
Bla
ck t
ext
on m
ask
prin
ted
on
neck
P
aper
inse
rt D
ark
blue
te
xt
on
pape
r pa
ckag
ing
M
arsh
all
Sin
gle
use
Cle
ar
plas
tic
neck
w
ith
clea
r rub
ber c
uff a
nd p
ump
Cle
ar
plas
tic
with
pa
per
back
ing
Bla
ck t
ext
on m
ask
prin
ted
on
neck
P
aper
inse
rt D
ark
blue
text
on
pape
r pa
ckag
ing
In
tave
nt S
ize
3 R
eusa
ble
Cle
ar
plas
tic
neck
w
ith
flesh
col
oure
d ru
bber
cuf
f an
d bl
ue p
ump
Pap
er b
acke
d pl
astic
B
lack
te
xt
prin
ted
on
neck
C
ard
inse
rt B
lack
text
on
pape
r pa
ckag
ing
In
tave
nt
Size
3
(LM
A-U
niqu
e)
Sin
gle
Cle
ar
rigid
pl
astic
ne
ck
clea
r cuf
f P
aper
bac
ked
plas
tic
Bla
ck
text
on
ne
ck
Gre
en a
nd b
lue
text
on
pape
r pa
ckag
ing
Trac
heal
tube
s P
orte
x 5,
9
&
10
mm
S
ingl
e C
lear
pl
iabl
e pl
astic
w
ith
blue
tra
nslu
cent
an
d op
aque
end
s an
d pu
mp
Pap
er b
acke
d pl
astic
B
lack
te
xt
on
tube
B
lue
text
on
pape
r pac
kagi
ng
C
o-A
xial
In
ters
urgi
cal
1.6m
M
ax
7 da
ys
Cle
ar/tr
ansl
ucen
t gr
een
Cle
ar p
last
ic b
ag (r
ippa
ble)
G
reen
te
xt
prin
ted
on
pack
et

22
6
Bre
athi
ng
syst
em
ref 2
900
use
plas
tic fl
exib
le tu
bing
P
aper
inse
rts
In
ters
urgi
cal
refs
21
08 2
121
Sin
gle
Gre
en
trans
luce
nt
plas
tic
flexi
ble
tubi
ng
Cle
ar p
last
ic b
ag (r
ippa
ble)
G
reen
te
xt
on
pack
et
Bla
ck te
xt o
n pa
per i
nser
t B
ougi
es
Por
tex
size
s 6-
11m
m 1
5ch
Reu
sabl
e Tr
ansl
ucen
t or
ange
pla
stic
w
eavi
ng v
isib
le in
side
C
ardb
oard
B
lack
te
xt
prin
ted
on
boug
ie
Pap
er
inst
ruct
ions
(a
lthou
gh
say
sing
le u
se)
E
schm
ann
Reu
sabl
e Tr
ansl
ucen
t or
ange
pla
stic
w
eavi
ng v
isib
le in
side
R
igid
pla
stic
box
B
lack
te
xt
prin
ted
on
boug
ie
Whi
te
labe
l on
bo
x P
rinte
d in
stru
ctio
ns
P
orte
x 15
ch
ref
100/
125/
515
Sin
gle
Opa
que
plas
tic
yello
w/o
rang
e P
last
ic w
ith p
aper
bac
king
B
lue
text
pr
inte
d on
pl
astic
W
hite
labe
l on
pape
r B
lack
text
prin
ted
on b
ougi
e E
lect
rode
s an
d w
ires
Uno
med
ical
ba
ll an
d bl
ade
ends
S
ingl
e M
etal
inse
rt in
blu
e op
aque
rig
id p
last
ic
Pla
stic
with
pap
er b
acki
ng
Whi
te la
bel o
n pa
cket
Pen
U
nom
edic
al
2700
mm
S
ingl
e R
igid
opa
que
gree
n pl
astic
w
ith g
reen
pla
stic
cov
ered
le
ad
Pla
stic
with
pap
er b
acki
ng
Ext
rude
d le
tterin
g on
pen
bod
y B
lack
prin
t on
pape
r
Lary
ngos
cope
E
urop
a E
MS
R
eusa
ble
hand
le
Sin
gle
use
blad
e
Sta
inle
ss
stee
l m
etal
ha
ndle
and
sta
inle
ss s
teel
bl
ades
Pla
stic
with
pap
er b
acki
ng
Fabr
ic c
ase
for
hand
le a
nd
blad
es
Bla
ck
text
pr
inte
d on
bl
ade.
In
dent
ed te
xt o
n bl
ack
plas
tic
P
enlo
n R
eusa
ble
hand
le
Sin
gle
use
blad
es
Sta
inle
ss
stee
l m
etal
ha
ndle
an
d cl
ear
plas
tic
blad
es
P
rinte
d on
bla
de
Text
inde
nted
on
plas
tic
Related Documents











