
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript


Outcomes in the Patient-Centered Medical HomePaul Grundy MD, MPHFounding President of the PCPCCIBM Director, Healthcare Transformation
@Paul_PCPCChttps://twitter.com/Paul_PCPCC
40% of commercial in-network payments are value-based … up from 11% 2012.
Half of these payments are “at
risk” and half are upside only
Paying for Value

Transformation is Here • HHS to spend $840 million on readying practices for value-based pay,
(part of the $10 Billion) • The Transforming Clinical Practice Initiative will invest $840 million over four
years to support 150,000 clinicians, group practices health systems and medical societies
• It will provide a combination of incentives, tools and information to encourage doctors to team with peers and others to transition to value-based services.
• Momentum is building toward value-based payment methods, this initiative hopes to leverage the success of leading practices, health systems and professional organizations to coach others in how to best move to value-based reimbursement. It fits well into the broader federal strategy.
ARE YOU READY!!!!??
Medicare's Chronic Care Management Payment Part of Payment Reform for Primary Care
A practice that already sees 200 Medicare patients who meet the criteria could gain $100,000 in revenue a year.
But to bill for the fee, there are requirements:•the practice must use a certified electronic health record (EHR)•the practice must offer 24-hour access to staff, who must have EHR access•each patient must have an assigned practitioner•care must be coordinated during transitions to and from hospitals and specialists•practices must create a comprehensive care plan that features medication management and outside
social services, as needed. A staff person must spend 20 minutes on this each month.•Practice must have patient engagements tools to remind, follow up and manage medication.
Section 3021 .
– BUT where the delivery system works, a patient is in a trusting relationship with a healer who is a comprehensivist with DATA in charge.
In much of the world, no one is in charge…and the result is the most wasteful and unsustainable.
Empowered by Data
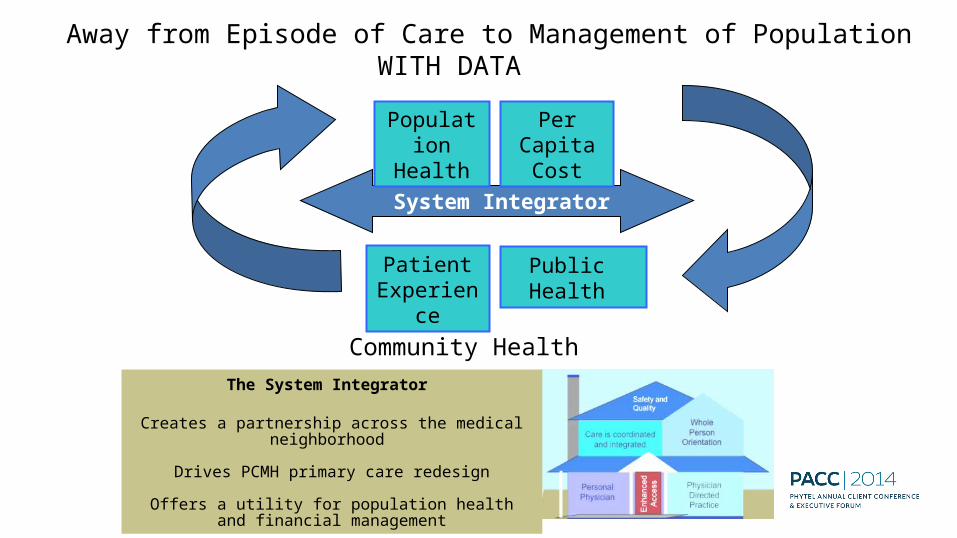
The System Integrator
Creates a partnership across the medical neighborhood
Drives PCMH primary care redesign
Offers a utility for population health and financial management
Away from Episode of Care to Management of PopulationWITH DATA
Community Health
Population
HealthSystem Integrator
PatientExperien
ce
Per Capita Cost
Public Health

36.3% Drop in hospital days32.2% Drop in ER use12.8% Increase Chronic Medication use -15.6% Total cost 10.5% Drop Inpatient specialty care costs 18.9% Ancillary costs down 15.0% Outpatient specialty downSource: Outcomes of Implementing Patient-Centered Medical Home Interventions: A Review of the Evidence from Prospective Evaluation Studies in the US - PCPCC Oct 2012
Smarter Healthcare
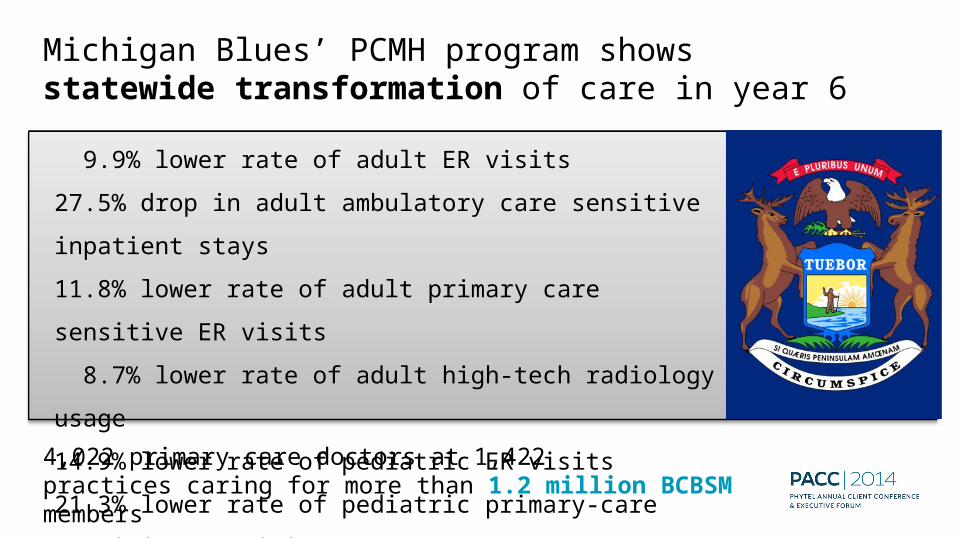
9.9% lower rate of adult ER visits27.5% drop in adult ambulatory care sensitive inpatient stays11.8% lower rate of adult primary care sensitive ER visits 8.7% lower rate of adult high-tech radiology usage14.9% lower rate of pediatric ER visits21.3% lower rate of pediatric primary-care sensitive ER visits
Michigan Blues’ PCMH program shows statewide transformation of care in year 6
4,022 primary care doctors at 1,422 practices caring for more than 1.2 million BCBSM members

USA 2012
Ogden UT


“Mobile First” Patient Consumer

…moving beyond Flexner --- Driven by Actionable, Personalized Data
“The value of experience is not in seeing much, but in seeing wisely.”
-William Osler
Dr. Abraham Flexner

PreventiveMedicine
MedicationRefills Acute Care
Nursing
Test Results
Master Builder
DOCTOR
Source: South-central Foundation, Anchorage AK
BehavioralHealth
CaseManager
MedicalAssistants
Chronic Disease
Monitoring
Practice Transformation Away from an Episode of Care

Source: South-central Foundation, Anchorage AK
PCMH Parallel Team Flow Design*
MedicationRefills
ChronicDisease
MonitoringTest
Results
AcuteCare
PreventiveMedicine
Point of Care Testing
Acute Mental Health
Complaint
ChronicDisease
ComplianceBarriers
HealthcareSupportTeam
Behavioral Health
MedicalAssistants
CaseManager Clinician
* the glue is real data, not a
doctor’s brain
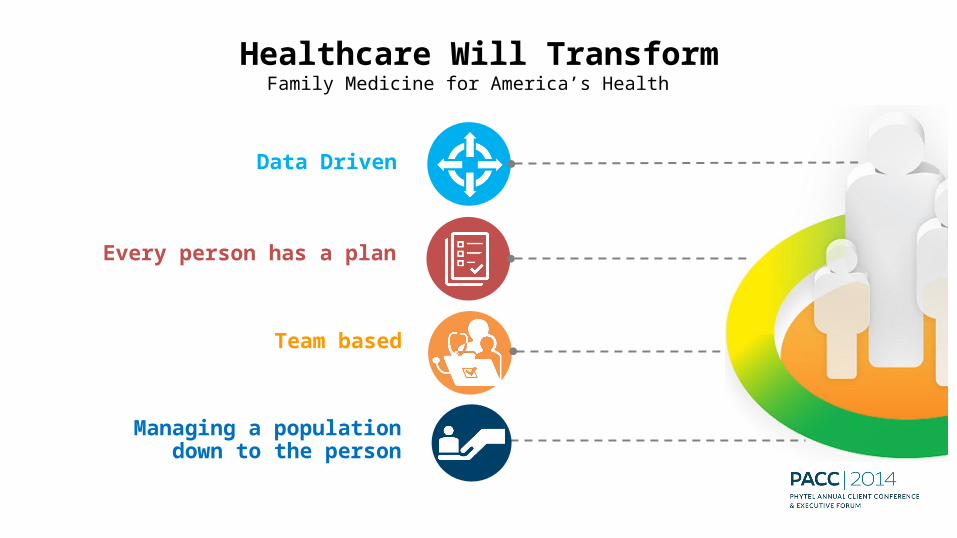
Healthcare Will TransformFamily Medicine for America’s Health
Data Driven
Every person has a plan
Team based
Managing a population down to the person
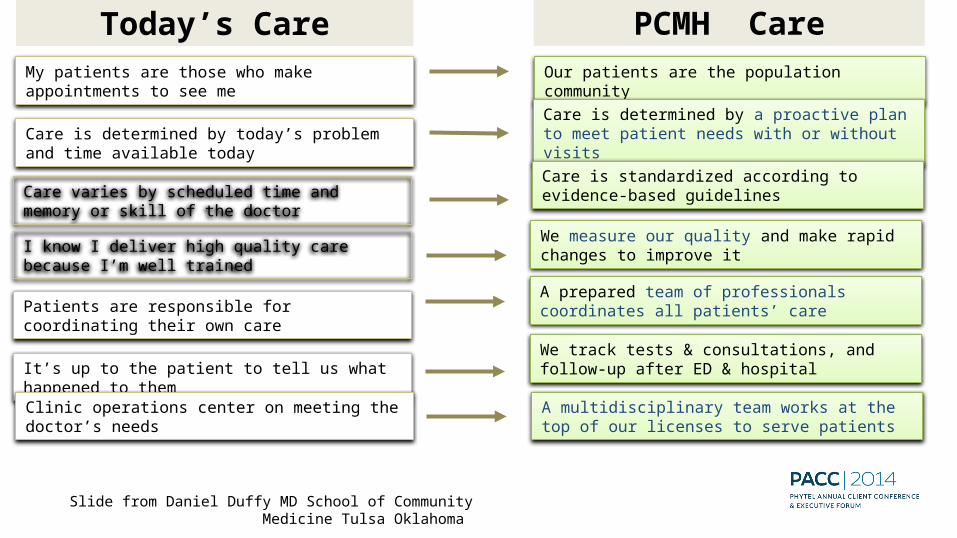
Today’s Care PCMH CareMy patients are those who make appointments to see me
Our patients are the population community
Care is determined by today’s problem and time available today
Care is determined by a proactive plan to meet patient needs with or without visits
Care varies by scheduled time and memory or skill of the doctor
Care is standardized according to evidence-based guidelines
Patients are responsible for coordinating their own care
A prepared team of professionals coordinates all patients’ care
I know I deliver high quality care because I’m well trained
We measure our quality and make rapid changes to improve it
It’s up to the patient to tell us what happened to them
We track tests & consultations, and follow-up after ED & hospital
Clinic operations center on meeting the doctor’s needs
A multidisciplinary team works at the top of our licenses to serve patients
Slide from Daniel Duffy MD School of Community Medicine Tulsa Oklahoma
Superb Access to Care
Patient Engagement in CareClinical Information Systems, Registry Care Coordination
Team Care
Communication Patient Feedback
Mobile easy to use and Available Information
Defining the Care Centered on Patient
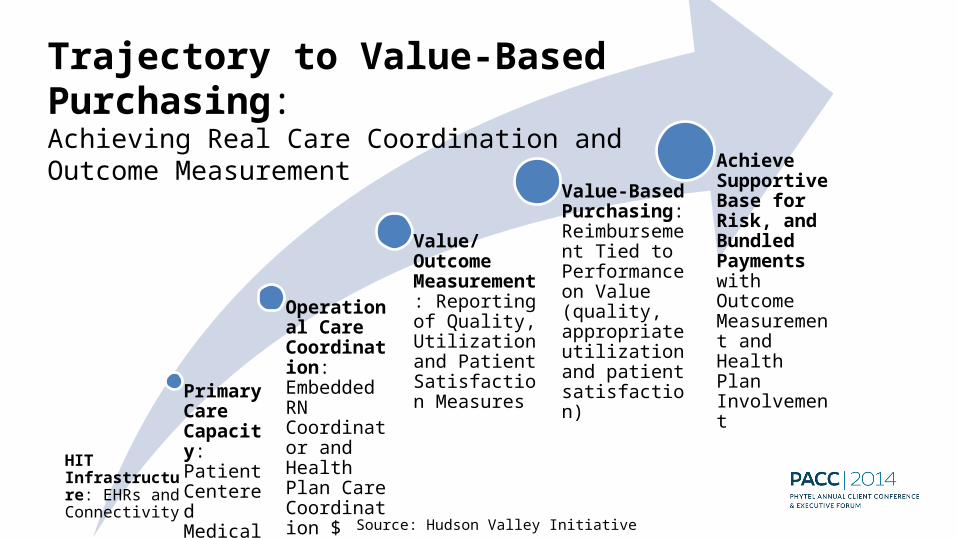
Primary Care Capacity: Patient Centered Medical Home
Operational Care Coordination: Embedded RN Coordinator and Health Plan Care Coordination $
Value/ Outcome Measurement: Reporting of Quality, Utilization and Patient Satisfaction Measures
Value-Based Purchasing: Reimbursement Tied to Performance on Value (quality, appropriate utilization and patient satisfaction)
Achieve Supportive Base for Risk, and Bundled Payments with Outcome Measurement and Health Plan Involvement
Trajectory to Value-Based Purchasing: Achieving Real Care Coordination and Outcome Measurement
Source: Hudson Valley Initiative
HIT Infrastructure: EHRs and Connectivity
Payment reform requires more than one method, you have dials… adjust them!!!
“fee for health”“fee for value” “fee for outcome”“fee for process” “fee for belonging“fee for service” “fee for satisfaction”
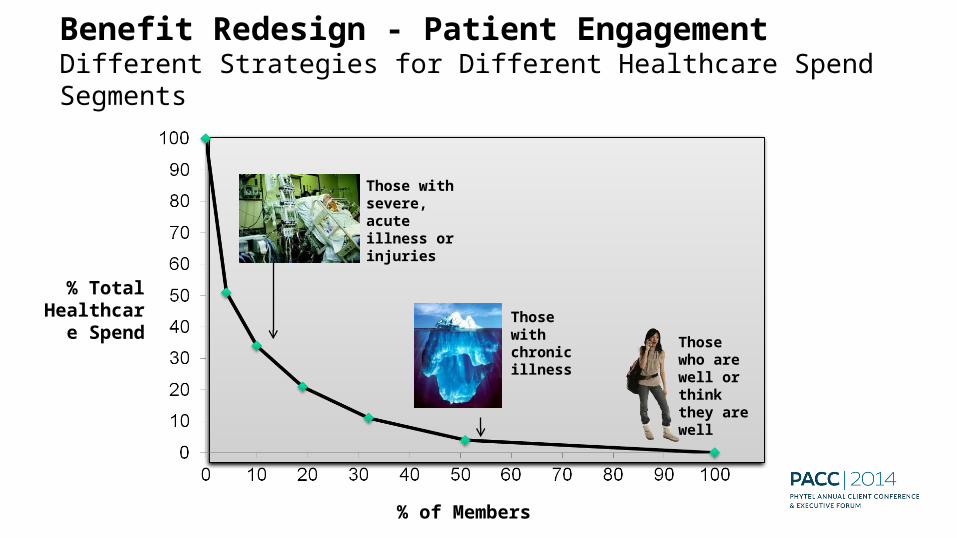
Benefit Redesign - Patient Engagement Different Strategies for Different Healthcare Spend Segments
% Total Healthcar
e Spend
% of Members
Those who are well or think they are well
Those with chronic illness
Those with severe, acute illness or injuries

Public Health
Prevention
Specialists
PCMH 2.0 in Action
Community Care TeamNurse CoordinatorSocial Workers
DieticiansCommunity Health Workers
Care Coordinators
Public Health Prevention HEALTH WELLNESS
Hospitals
PCMH
PCMH
Health IT Framework
Global Information Framework
Evaluation Framework
Operations
A Coordinated Health System

How many patients can you see?How many patients’ problems can you solve?
How can we encourage and convince patients to get required prevention?How can we create systems that significantly increase that patients get required prevention?
How often should a physician see a patient to optimally monitor a condition?What is the best way to optimally monitor a condition?
Asking New QuestionsFromTo
FromTo
FromTo
*Source: 2014 Kaiser Permanente Jack Cochran
Need to move from traditional care provider to health partnerIf you do not choose innovation (play a better game) you will be forced into disruption (game changed for you). An honest assessment is to see it coming and recognize that in some places, it is already there
Millennials are already finding the convenience, economics and technology in virtual health compelling -- so you can chose innovation or disruption
Virtual access will become a required defensive strategy. The primary care team can be engaged in virtual augmented relationship to avoid the loss of the relationship
A Choice for the Future
Thank you


Apply new insights from interactions
and outcomes to enable continuous
transformation
LEARNING
Identify and influence individuals and
populations, and recognize intervention
opportunities
INTERVENTION
COORDINATIONDeliver care and monitor
progress across clinical and social requirements
COLLABORATIONAssess and engage individuals and stakeholders to drive individualized care plans
Drive evidence-based andstandardized care planning
KNOWLEDGE
WELLNESS
A comprehensive approach helps reduce costs while improving care
Related Documents











