University of Nebraska - Lincoln DigitalCommons@University of Nebraska - Lincoln eses, Dissertations, and Student Research: Department of Psychology Psychology, Department of Spring 4-30-2013 Pathways to Social Functioning via Emotion Regulation in People with Serious Mental Illness Hayden C. Booms University of Nebraska-Lincoln, [email protected] Follow this and additional works at: hp://digitalcommons.unl.edu/psychdiss Part of the Clinical Psychology Commons is Article is brought to you for free and open access by the Psychology, Department of at DigitalCommons@University of Nebraska - Lincoln. It has been accepted for inclusion in eses, Dissertations, and Student Research: Department of Psychology by an authorized administrator of DigitalCommons@University of Nebraska - Lincoln. Booms, Hayden C., "Pathways to Social Functioning via Emotion Regulation in People with Serious Mental Illness" (2013). eses, Dissertations, and Student Research: Department of Psychology. 53. hp://digitalcommons.unl.edu/psychdiss/53

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

University of Nebraska - LincolnDigitalCommons@University of Nebraska - LincolnTheses, Dissertations, and Student Research:Department of Psychology Psychology, Department of
Spring 4-30-2013
Pathways to Social Functioning via EmotionRegulation in People with Serious Mental IllnessHayden C. BottomsUniversity of Nebraska-Lincoln, [email protected]
Follow this and additional works at: http://digitalcommons.unl.edu/psychdiss
Part of the Clinical Psychology Commons
This Article is brought to you for free and open access by the Psychology, Department of at DigitalCommons@University of Nebraska - Lincoln. It hasbeen accepted for inclusion in Theses, Dissertations, and Student Research: Department of Psychology by an authorized administrator ofDigitalCommons@University of Nebraska - Lincoln.
Bottoms, Hayden C., "Pathways to Social Functioning via Emotion Regulation in People with Serious Mental Illness" (2013). Theses,Dissertations, and Student Research: Department of Psychology. 53.http://digitalcommons.unl.edu/psychdiss/53

PATHWAYS TO SOCIAL FUNCTIONING VIA EMOTION REGULATION
IN PEOPLE WITH SERIOUS MENTAL ILLNESS
by
Hayden C. Bottoms
A DISSERTATION
Presented to the Faculty of
The Graduate College at the University of Nebraska
In Partial Fulfillment of Requirements
For the Degree of Doctor of Philosophy
Major: Psychology
Under the Supervision of Professor William D. Spaulding
Lincoln, Nebraska
April, 2013

PATHWAYS TO SOCIAL FUNCTIONING VIA EMOTION REGULATION
IN PEOPLE WITH SERIOUS MENTAL ILLNESS
Hayden C. Bottoms, Ph.D.
University of Nebraska, 2014
Adviser: William D. Spaulding
Recent research on social cognitive deficits associated with serious mental illness
(SMI) has demonstrated a range of emotion processing difficulties, from emotion
perception to emotion regulation. Whereas emotion perception deficits are well
documented in this population, little is understood about emotion regulation and the
relationship of emotion regulation to other abilities and impairments.
Method. Participants included 41 individuals with SMI recruited from a day
rehabilitation program. Assessments included a range of functional domains, including
symptom severity, neurocognition, social cognition, emotion regulation, and social
functioning.
Results. Emotion dysregulation was hypothesized to be associated with more
severe positive symptoms, poorer neurocognitive functioning, and poorer social and
community functioning. Results were mixed across the various assessments. There was
some evidence of a relationship between psychiatric symptom severity and emotion
dysregulation. However, global neurocognition explained very little of the variance in
emotion regulation. Individuals with poorer emotion regulation tended to have poorer
self-reported social functioning, and positive symptom severity accounted for some of the
variance in this relationship. Path analysis modeling summarized these relationships.

Conclusions. This study demonstrates that emotion regulation explains variance in
social functioning, but much remains to be understood about how emotion regulation
relates to other biosystemic domains in this population. Limitations in valid assessment in
the SMI population hinder ongoing progress, and this should be a key focus of future
research, as orthogonal functional domains require individual attention in clinical
assessment and research. Assessing segregated processes and investigating interactions
among those processes reveal important relationships among subgroups of this population
that would otherwise be missed. Though symptom severity and neurocognitive
impairments have historically been the focus of treatment development for SMI, this
work clearly demonstrates that individuals with SMI also have impaired emotion
regulation abilities. Furthermore, that these abilities share an interactive relationship with
social functioning and symptom severity reinforces their importance as potential
treatment targets. Integrating emotion regulation skills training into the psychiatric
rehabilitation toolkit is therefore a worthwhile future endeavor.

iv
DEDICATION
To my family,
whose unconditional support
was the foundation of this entire endeavor.

v
ACKNOWLEDGEMENTS
This research is a product of the effort of many individuals. Foremost are the
present and past members of the Serious Mental Illness Research Group at the University
of Nebraska, whose intellectual contributions were instrumental to the conceptualization
of this research project.
I also acknowledge and thank the administrators, staff, and clients of the
Community Mental Health Center. In addition to supporting this particular research
project, they fostered my clinical training and encouraged the integration of research into
the clinical setting.
Finally, I am unspeakably grateful to Will Spaulding, who not only supervised
this project but also gave me the opportunity to fulfill my aspirations of earning a
doctorate in psychology. He’s an inspirational role model, as a researcher, supervisor,
clinician, and advocate. There has been no more rewarding educational experience in my
life than the years I have spent as his student.

vi
FUNDING INFORMATION
This project was funded by a grant from the RAC/Warden Committee of the Department
of Psychology at the University of Nebraska.

vii
TABLE OF CONTENTS
CHAPTER 1: INTRODUCTION ....................................................................................1
CHAPTER 2: CONCEPTUAL FOUNDATIONS ............................................................4
Definitions ...................................................................................................................4
Emotion Regulation Strategies .....................................................................................8
Neural Correlates of Emotion Processing ................................................................... 12
CHAPTER 3: EMOTIONAL ABNORMALITIES IN SMI ........................................... 15
Emotion Perception .................................................................................................... 15
Emotion Paradox........................................................................................................ 18
Emotion Regulation ................................................................................................... 24
CHAPTER 4: INTERVENTIONS TARGETING SOCIAL COGNITIVE DEFICITS ... 27
Interventions Based on the Generalized Deficit Hypothesis ........................................ 27
Interventions Based on the Specific Deficit Hypothesis .............................................. 29
CHAPTER 5: PRESENT STUDY ................................................................................. 32
CHAPTER 6: METHOD ............................................................................................... 39
Participants ................................................................................................................ 39
Measures .................................................................................................................... 41
Procedure ................................................................................................................... 47
CHAPTER 7: RESULTS ............................................................................................... 50
Preliminary Analyses ................................................................................................. 50
Hypothesis 1: Symptom Severity and Emotion Regulation ......................................... 59
Hypothesis 2: Neurocognition and Emotion Regulation ............................................. 61
Hypothesis 3: Social and Community Functioning and Emotion Regulation ............... 68
Hypothesis 4: Group Treatment Participation and Emotion Regulation ...................... 80
Hypothesis 5: Emotion Regulation Pathways to Clinical Outcome ............................. 82
CHAPTER 8: DISCUSSION ......................................................................................... 95
Results Summary ....................................................................................................... 95
Limitations ............................................................................................................... 101
Conclusions ............................................................................................................. 102
REFERENCES ............................................................................................................ 105
FOOTNOTES ............................................................................................................. 130
APPENDIX ................................................................................................................. 131

viii
LIST OF TABLES AND FIGURES
Figure 5.1 Pathway from Neurocognition to Global Functional Outcome from Brekke
et al., 2005
36
Figure 5.2 Pathway from Neurocognition to Occupational Functioning from Lipkovich
et al., 2009
37
Figure 5.3 Hypothesized Path Model 38
Table 6.1 Sample Demographic and Clinical Characteristics 40
Table 7.1 Assessment Descriptive Statistics 50
Table 7.2 Correlation Matrix for Measures of Emotion Regulation and Symptom
Severity
60
Table 7.3 Correlation Matrix for Measures of Emotion Regulation and
Neurocognition
63
Table 7.4 Multiple Regression Models Predicting Emotion Regulation from
Neurocognition
67
Table 7.5 Correlation Matrix for Measures of Emotion Regulation and Social and Community Functioning
70
Table 7.6 Correlation Matrix for Psychiatric Symptom Severity and Measures of
and Social and Community Functioning
71
Table 7.7 Hierarchical Multiple Regression Analyses Predicting Emotion Regulation
from Social Functioning, Positive Symptom Severity, and the Interaction
between Social Functioning and Positive Symptom Severity
72
Figure 7.1 Positive Symptoms Moderate Relationship between SFS and RACERS 74
Figure 7.2 Positive Symptoms Moderate Relationship between SFS and DERS 76
Figure 7.3 Positive Symptoms Moderate Relationship between MCAS and BVAQ 79
Table 7.8 Group Means for Emotion Regulation by Completion of Group Skills Training Modalities
81
Figure 7.4 Hypothesized Path Model with Representative Measures 84
Table 7.9 Parameters of the Hypothesized Path Model 86
Figure 7.5 Final Path Model 88
Table 7.10 Parameters of the Revised Path Model 89

1
PATHWAYS TO SOCIAL FUNCTIONING VIA EMOTION REGULATION
IN PEOPLE WITH SERIOUS MENTAL ILLNESS
CHAPTER 1
INTRODUCTION
The biosystemic paradigm of psychopathology conceptualizes human functioning
as a complex network of interrelated processes and mechanisms (Spaulding, Sullivan, &
Poland, 2003). Those processes and mechanisms can usefully and heuristically be
organized into five categorical levels of analysis (in order of most molecular to most
molar): neurophysiological, neurocognitive, social cognitive, sociobehavioral, and
socioenvironmental. Psychopathology is conceptualized as the result of abnormal or
deficient operation of those processes and mechanisms across all levels as they interact to
maintain stable functioning. Although the processes are causally linked throughout the
biosystem, for the purposes of treatment and rehabilitation, they are independent enough
to require separate, specific targeting. Biosystemic approaches to psychiatric
rehabilitation therefore encourage research that addresses functioning at all the respective
levels.
The last decade of research on schizophrenia has seen an expansion of focus from
the neuropsychological level of analysis to the social cognitive level, in part because it
complements biosystemic psychopathology and also because measures of social
cognitive impairments appear to be more proximal than measures of neurocognitive
impairments to real world behavior and to psychosocial treatment effects. A broad range
of deficits in social cognition are well-documented in the serious mental illness (SMI)
literature (Corrigan & Penn, 2001b; Penn, Sanna, & Roberts, 2008). Furthermore,

2
difficulty processing social information has wide-ranging functional implications, as
normal processing is fundamental for social and occupational relationships, as well as
general community functioning. The development of social cognitive paradigms for
schizophrenia has primarily been guided by the analysis of cognitive processes thought to
be essential to basic social functioning and found to be impaired in SMI. These include
paradigms that range from molecular perceptual processes to more molar processes that
neuropsychologists would consider to be in the executive domain.
On the more molecular end of the biosystemic spectrum, most research on the
social cognitive deficits associated with SMI has focused on emotion processing. This
research has shown that individuals with schizophrenia have a range of difficulties in
processing emotions, from difficulties in perception of others’ emotions to difficulties in
expression and regulation of one’s own emotions. The clinical significance of these
deficits in emotion processing is demonstrated by their association with dimensions of
adaptive social functioning (Couture, Penn, & Roberts, 2006).
The difficulties in emotion processing observed in SMI, particularly emotion
regulation, and their relationship to other biosystemic and functional domains, are the
focus of this dissertation. The following sections address, in turn, (1) the basic concepts
of emotion perception and emotion regulation as they are used in contemporary research
on schizophrenia; (2) the nature of impairment in emotional functioning in schizophrenia
and other serious mental illness; and (3) treatment approaches that target emotional
impairments. Analysis of previous findings and other background information indicates
that further progress in assessment and treatment will require a better understanding of
the relationships between emotion impairments and other aspects of serious mental

3
illness. The subsequent sections describe an empirical, quantitative analysis of those
relationships.

4
CHAPTER 2
CONCEPTUAL FOUNDATIONS
Definitions
Social cognition. Social cognition is defined as “the processes and functions that
allow a person to understand, act on, and benefit from the interpersonal world” (Corrigan
& Penn, 2001a, p. 3). There are generally considered to be four domains of social
cognition: (1) attributional style, or judging the causes of events; (2) theory of mind, or
understanding the contents of others’ minds; (3) social perception, or perceiving social
cues in social situations; and (4) emotion perception, or recognizing emotional
expressions from facial, vocal, and postural cues. Individuals with SMI have been shown
to have deficits in each of these areas (Corrigan & Penn, 2001b; Feinberg, Rifkin,
Schaffer, & Walker, 1986), pointing to a pervasive deficit in the social cognitive domain.
These deficits have functional implications, as each of these domains of social
cognition is associated with functional dimensions such as social skills, social problem
solving, and broad community functioning (Addington, Saeedi, & Addington, 2006;
Brekke, Kay, Lee, & Green, 2005; Corrigan & Toomey, 1995; Ihnen, Penn, Corrigan, &
Martin, 1998; Kee, Green, Mintz, & Brekke, 2003; Kim, Doop, Blake, & Park, 2005;
Mathews & Barch, 2010; Mueser et al., 1996; Pinkham & Penn, 2006; Poole, Tobias, &
Vinogradov, 2000). Thus, deficits in social cognition have both proximal and far-
reaching consequences for daily functioning.
Emotion. Much of the research on social cognitive deficits in schizophrenia has
focused on emotion processing. Indeed, emotional abnormalities have long been observed
as one of the hallmark features of schizophrenia (American Psychiatric Association

5
[APA], 2000; Bleuler, 1950; Kraepelin, 1919). A discussion of these abnormalities must
begin with a conceptualization of what emotions are and how they are normally
processed.
Many researchers have theorized about what emotions are and how they are
generated. The result has been many similar theories and considerable historical debate
regarding a consensual definition of emotion (Bloch, Moran, & Kring, 2010; Kleinginna
& Kleinginna, 1981; Solomon, 2010). Among these are such classic theories as the
James-Lange, Cannon-Bard, and Schachter-Singer theories. William James (1884, 1890),
one of the first psychologists, theorized about emotion. The James-Lange theory posits
that an emotional event is perceived and causes physiological arousal; that physiological
arousal is interpreted, and emotions occur as a result of that interpretation. This theory
was later supplanted by the Cannon-Bard theory, which posits the opposite: an emotional
event is perceived and simultaneously causes physiological arousal and emotion
(Cannon, 1932). Still later, Schachter and Singer’s (1962) two-factor theory was similar
to the James-Lange theory but emphasized the role of cognition in the generation of
emotion. This theory posits that an emotional event is perceived and causes physiological
arousal; that arousal is given a cognitive label which accounts for the situational context.
Each of these classic theories emphasizes (1) the importance of the occurrence of
an event, (2) perception of that event, (3) physiological arousal, and (4) emotional
responses. Gross and Thompson (2009) have combined the salient factors of these and
the many other theories of emotions into the modal model of emotion. The modal model
reflects the core features of emotion emphasized across theories and represents a
consensual understanding of how emotions are generated. Gross and Thompson (2009)

6
establish three core features of emotions. The first feature regards appraisal: Emotions
arise when an individual attends to an event, perceives it, and appraises it for its meaning
(including its personal relevance, familiarity, and valence). Thus, an emotion requires
both attention to a stimulus and an appraisal of that stimulus as pertinent to one’s goals.
The second feature regards the changes that occur as a result of the first feature:
Emotions are multi-faceted phenomena that involve systemic changes – in thoughts
(subjective experience), behavior, and physiology. The final feature regards the flexibility
of emotional responses: The systemic changes associated with emotions are rarely
obligatory. It is this final feature which makes emotion regulation possible, as it is the
flexibility of emotional responses that is regulated.
For the purposes of the present analysis, the modal model’s emphasis on the
typical features of emotions seems most pertinent to understanding what emotions are
and how they can disrupt biosystemic processing when their regulation is dysfunctional,
as in SMI. Such an understanding of how emotions are generated is foundational for the
following discussion of how emotions can be regulated.
Emotion regulation. Gross and Thompson’s (2009) definition of emotion thus
stimulates a definition of emotion regulation: Emotion regulation is a heterogeneous set
of processes that are automatic or controlled and influence emotions in oneself, others, or
both. Thus, emotion regulation strategies influence how emotion is experienced – the
quality, intensity, timing, and dynamic features of thoughts, behaviors, and physiology.
This definition conceptualizes emotion regulation as the regulation of emotions, versus an
alternative conceptualization of regulation by emotions. This second conceptualization
refers to how emotions regulate thoughts, behaviors, physiology, or even other people.

7
The focus of the present analysis is to evaluate how systemic processes are themselves
regulated, thus motivating the choice of a definition consistent with the former
conceptualization.
This definition prompts discussion of the core features of emotion regulation.
First, both positive and negative emotions can be regulated, and they can either be
increased or decreased (Gross & Thompson, 2009). The focus of the majority of the
research on emotion regulation has been on how individuals decrease negative emotions
or increase positive emotions. However, such a focus ignores strategies that increase
negative emotions or decrease positive emotions – strategies that might be associated
with psychopathology. The question arises: Does a pathological excess of negative
emotion arise from underutilization of strategies associated with positive emotion
changes (i.e., decreasing negative emotions, increasing positive emotions), for example,
or alternatively, from overuse of strategies associated with negative emotion changes
(i.e., increasing negative emotions, decreasing positive emotions)? This question is as yet
unanswered.
A second feature of emotion regulation is that regulation can occur either
consciously or unconsciously (Gross & Thompson, 2009). Thus, emotions can be
deliberately changed, or they can be regulated automatically, via habitual processes. For
example, a reaction of disappointment to the receipt of an unsatisfactory gift might be
deliberately hidden (or suppressed) initially; but this reaction may become automatic if
repeated over time. Importantly, it is unclear whether the distinction between conscious
and unconscious regulation is dimensional (i.e., continuous) or categorical (Gross &
Thompson, 2009). That is, it is possible that emotion regulation may have some

8
characteristics of both. Moreover, it is possible that emotion regulation may be a
multidimensional phenomenon with categorical characteristics.
Third, no strategy of regulating emotions is inherently adaptive or maladaptive
(Gross & Thompson, 2009). Consideration of the context in which the emotion is to be
regulated is always key in an evaluation of the adaptive nature of a strategy (Gross, 1998;
Thompson & Calkins, 1996). For example, whereas habitual suppression of emotional
reactions is generally associated with poor functional outcomes (reviewed below),
adopting this strategy in a situation such as receiving an unsatisfactory gift may be the
most adaptive response for social functioning.
Finally, emotion regulation involves changes in how emotional responses are
coordinated (Gross & John, 2003; John & Gross, 2004). As discussed above, emotional
responses entail systemic changes – coordinated and interrelated changes in thoughts
(subjective experience), behavior, and physiology. Various strategies of regulating
emotions are associated with differences in how and when these components of
emotional responses are changed.
Emotion Regulation Strategies
Once an emotional stimulus is perceived and appraised, many strategies exist for
changing the type, timing, experience, or expression of emotions (Gross, 1998). These
strategies can be organized along several dimensions. One dimension separates strategies
into those that are internal (e.g., suppressing disappointment) versus external (e.g., taking
a walk to defuse anger; Thompson, 1994). Another dimension focuses on the resources
used to regulate emotions by separating strategies into those that focus on modifying
cognitions (e.g., reinterpreting a loved one’s death as the end of suffering) versus

9
behaviors (e.g., seeking social support) versus situations (e.g., hiding controversial
artwork from conservative visitors; Eisenberg et al., 1995). A final dimension focuses on
when various strategies impact the emotion generative process by separating strategies
into those that attempt to change the cause of the emotion (antecedent-focused strategies;
e.g., avoiding offensive acquaintances) versus the response to the emotion (response-
focused strategies; e.g., engaging in aerobic exercise to decrease physiological and
experiential components of emotion; Gross & Muñoz, 1995). This dissertation will focus
on the antecedent- versus response-focused dimension, as it appears to be the most
influential in the literature and the most useful for understanding the abnormalities in the
use of these particular strategies in SMI.1
The modal model of emotion implicates areas in the emotion generative process
where regulation might occur: changing the situation, attention, appraisal, or response.
Antecedent- and response-focused strategies vary in the time at which they occur in the
emotion generative process (Gross, 2001; Gross & Muñoz, 1995). In the modal model of
emotion, antecedent-focused strategies occur before appraisals and can affect the
situation, attention, or appraisal. These changes thereby alter the emotional response
(Gross, 2002). In contrast, response-focused strategies occur after appraisals and attempt
to change an emotional response that has already begun to occur (Gross, 2002).
Antecedent-focused strategies. Antecedent-focused strategies are grouped into
four families: situation selection, situation modification, attentional deployment, and
cognitive change (Gross, 2002).
Situation selection and situation modification make it more or less likely that an
emotional situation will occur that leads to desirable or undesirable emotions. They serve

10
to alter an emotional situation that has already occurred to modify the emotional impact.
The “situations” targeted by situation selection and situation modification strategies can
be either internal (e.g., thoughts) or external to the individual.
Attentional deployment strategies are used to select which aspect of a situation is
attended to, and they are typically used when it is impossible to use situation selection or
situation modification strategies. Common examples of attentional deployment are
distraction and concentration. With distraction, attention is deployed to a less
emotionally-arousing aspect of the situation or away from the situation; with
concentration, attention is deployed to the situation. Rumination, common to many forms
of psychopathology, is an example of concentration (Gross & Thompson, 2009).
Finally, cognitive change strategies alter the meaning attached to an emotional
event. An extensively-researched example of cognitive change is reappraisal (Gross,
2002; John & Gross, 2009; Ochsner & Gross, 2009), a strategy in which the meaning of a
situation is interpreted in such a way as to alter the emotional response.
Response-focused strategies. There is only one family of response-focused
strategies, called response modulation (Gross, 2002).
Response modulation strategies attempt to change emotional responses once they
have already been elicited. Common examples include the use of drugs and alcohol
(Morris & Reilly, 1987), exercise (Thayer, Newman, & McClain, 1994), relaxation
(Borkovec & Costello, 1993), and suppression. Suppression refers to the hiding or
avoidance of an emotional expression and has been widely researched as an emotion
regulation strategy (Beevers, Wenzlaff, Hayes, & Scott, 1999; Purdon, 1999; Richards &
Gross, 2006; Salters-Pedneault, Steenkamp, & Litz, 2010).

11
Reappraisal and suppression. Reappraisal, an antecedent-focused strategy that
can alter an emotional response before it has been initiated, and suppression, a response-
focused strategy that alters an emotional response that has already begun, have different
affective, cognitive, and social consequences.
Affective consequences. Individuals who tend to use reappraisal as an emotion
regulation strategy report fewer symptoms of depression, more satisfaction with their
lives, higher self-esteem, higher levels of optimism, and higher levels of general well-
being, versus individuals who tend to use suppression (Gross & John, 2002, 2003).
Moreover, individuals who use reappraisal are better able to regulate negative moods
than are individuals who use suppression.
This may be, in part, because reappraisal tends to be effective at decreasing the
experience of negative emotions, whereas suppression tends to have no effect (Gross,
1998, 2002; Gross & John, 2002, 2003). Both strategies are effective at decreasing
behavioral expressions of disgust (Gross, 1998, 2002); however, suppression increases
sympathetic nervous system activation, whereas reappraisal does not (Gross, 2002). That
is, individuals who habitually suppress negative emotions continue to experience the
negative emotions at at least a physiological level; in contrast, individuals who use
reappraisal may actually experience less negative emotion.
Cognitive consequences. Suppression appears to require more cognitive
resources, thus using resources typically allocated towards other processing. The result is
impaired verbal memory, including memory for social information such as peoples’
names (Gross & John, 2002; Richards & Gross, 2000). No memory impairment is
observed when individuals use reappraisal to manage emotions (Gross & John, 2002;

12
Richards & Gross, 2000). Given the pervasive cognitive deficits associated with SMI, the
effect of emotion regulation strategies on cognitive resources is especially relevant.
Social consequences. Consistent with these differences in affective and cognitive
consequences are differences between reappraisal and suppression in social
consequences. Individuals who reappraise have more social support, both emotionally
and instrumentally; and they are more likely to seek out social support than individuals
who use suppression (Gross & John, 2002). Individuals who reappraise are more likely to
share their emotions with others (Gross & John, 2002, 2003). Consequently, they are
better liked by their peers (Gross & John, 2002, 2003). Individuals who suppress tend to
avoid the attachment and intimacy associated with close relationships (Gross & John,
2003). Suppression even appears to have negative consequences on a conversational
partner – interacting with a person who suppresses is associated with increases in blood
pressure, whereas there appears to be no impact on blood pressure when interacting with
a person who reappraises (Butler et al., 2003). The result of these social consequences is
that individuals who habitually reappraise tend to have improved interpersonal
functioning relative to individuals who suppress (John & Gross, 2004).
Neural Correlates of Emotion Processing
The previous discussion has focused on the social cognitive domain and its
relationship to the neuropsychological and sociobehavioral domains. But in a biosystemic
paradigm, abnormalities potentially extend to more molecular levels of organismic
functioning, including neurophysiology. The human brain is designed for processing
social and emotional information and contains neural circuits specifically designed for
those purposes.

13
Emotional appraisal system. Across electrophysiological, neuropsychological,
and functional neuroimaging studies, the amygdala, insula, striatum, and medial
orbitofrontal cortex are consistently implicated in emotion processing (Bush, Luu, &
Posner, 2000; Davidson & Irwin, 1999; Davidson, Jackson, & Kalin, 2000; Denny,
Silvers, & Ochsner, 2010), with activations during rises in emotion and attenuations
during reductions in emotion. Although individual experiments have implicated
additional areas, the contribution of the above regions has been repeatedly documented
(Brunet-Gouet & Decety, 2006).
The amygdala is broadly implicated in detecting the emotional salience of a
stimulus and generating physiological reactions to emotional events (Adolphs, 2002,
2003; Aleman & Kahn, 2005; Denny et al., 2010; LeDoux, 2000; McDonald, 1998; van
Rijn, Aleman, & Kahn, 2005). Moreover, it appears to have particular importance in the
perception of others’ emotional states, especially perceptions of basic fear and sadness
(Adolphs, 2002, 2003; Calder, Lawrence, & Young, 2001). Although each of the areas in
this emotion processing network is activated for all types of emotions, the insula and
striatum (and, in general, the basal ganglia structures) are specifically implicated in the
evaluation of potentially distressing and aversive stimuli (Scott, Heltzeg, Koeppe,
Stohler, & Zubetla, 2006; Straube & Miltner, 2011). Finally, the medial orbitofrontal
cortex is implicated in evaluating the affective valence of a stimulus and its contextual
meaning (Davidson & Irwin, 1999).
Emotion regulation system. Attempts to regulate emotions require modulation
of the emotional appraisal system. Specifically, across studies, reappraisal consistently
invokes a network including the lateral prefrontal cortex, medial prefrontal cortex, dorsal

14
anterior cingulate cortex, and lateral orbitofrontal cortex (Denny et al., 2010). The
prefrontal regions are the areas most tied to reappraisal and suppression, as they are
associated with developing alternative ways of conceptualizing an emotional situation
(Ochsner & Gross, 2005, 2009; Ochsner et al., 2004). Moreover, these areas are
implicated in general cognitive control of emotion (Allman, Hakeem, Erwin,
Nimchinsky, & Hof, 2001; Banich et al., 2009; Green & Malhi, 2006; Ochsner & Gross,
2005) and development of adaptive responses to shifting social situations. The prefrontal
cortex and anterior cingulate cortex appear to serve an inhibitory role in modulating
activity in the emotional appraisal systems reviewed above. Increased activity in these
areas is correlated with decreased activity in subcortical structures such as the amygdala.
As no direct connections exist between the lateral and dorsal regions of the prefrontal
cortex and the amygdala, the medial prefrontal cortex may serve as the link between
cognitive control of emotion and emotional processing (Green & Malhi, 2006). In
general, these structures serve a top-down interpretive function for emotional stimuli
being processed in subcortical structures in a reciprocal, interactive manner (Denny et al.,
2010; Ochsner & Gross, 2005).

15
CHAPTER 3
EMOTIONAL ABNORMALITIES IN SMI
The foregoing discussion summarized the basic concepts pertinent to researching
emotion processing in SMI and serves as a foundation for discussing the nature of the
impairment in emotion functioning in SMI. Individuals with SMI demonstrate
abnormalities in all aspects of emotion processing – from perception of others’ emotions
to experience and regulation of their own emotions.
Emotion Perception
Individuals with schizophrenia have a general deficit identifying the correct
emotions associated with facial expressions (Feinberg et al., 1986; Novic, Daniel, &
Perline, 1984; Salem, Kring, & Kerr, 1996; Schneider, Gur, Gur, & Shtasel, 1995;
Walker, McGuire, & Bettes, 1984). Whereas psychiatrically healthy individuals
identify an average of 71% of emotional facial expressions correctly, individuals with
schizophrenia accurately identify just 64% (Kohler et al., 2003).
Several studies have attempted to determine the specific features associated with
this emotion perception deficit. Individuals with schizophrenia commit more errors
when identifying negative facial expressions than when identifying positive facial
expressions (Borod, Martin, Alpert, Brozgold, & Welkowitz, 1993; Muzekari & Bates,
1977; Van’t Wout et al., 2007; Zuroff & Colussy, 1986). Specifically, individuals with
schizophrenia appear to be impaired in the recognition of negative emotions such as
fear, anger, shame, and disgust (Dougherty, Bartlett, & Izard, 1974; Kohler et al., 2003;
Mandal & Palchoudhury, 1985) but not positive emotions such as joy and happiness
(Dougherty et al., 1974; Kohler et al., 2003).

16
Accompanying this better recognition of positive versus negative emotions is
increased efficiency in processing positive emotions in schizophrenia (Silver, Bilker, &
Goodman, 2009). Happy facial expressions are not only processed more accurately in
schizophrenia, but they are also processed more rapidly and efficiently than sad facial
expressions. Nevertheless, individuals with schizophrenia process emotional
expressions more slowly and less efficiently than healthy controls. Therefore, it appears
that recognizing emotional facial expressions takes longer and is less productive in
schizophrenia than in comparison participants.
Of note, individuals with schizophrenia also appear to be impaired at
recognizing neutral facial expressions. One study found that they accurately identified
70% of neutral facial expressions, compared to 86% correctly identified by comparison
participants (Kohler et al., 2003). Both groups most often misidentified neutral
expressions as happy or sad. However, of the neutral expressions misidentified by
individuals with schizophrenia, 23% were mislabeled as disgust, versus 5% in the
comparison group. Thus, individuals with schizophrenia appear to have a negative bias
in their emotion perception. Not only are individuals with schizophrenia impaired when
asked to identify neutral facial expressions, they are also impaired when asked to
identify neutral faces (i.e., indicate whether they have seen the face before; Silver et al.,
2009). Thus, individuals with schizophrenia are impaired in processing neutral faces,
regardless of whether they are evaluating its emotional content or its identity; but they
are more impaired when their task involves emotional processing.
Furthermore, whereas increasing the intensity of a facial expression aids control
participants’ identification of the emotion, individuals with schizophrenia benefit

17
significantly less from this compensation (Kohler et al., 2003). That is, they are
impaired at recognizing mild emotional expressions (correctly identifying 5% fewer
expressions than controls) but even more impaired at recognizing extreme emotional
expressions (correctly identifying 7% fewer expressions than controls). Interestingly,
this suggests that increasing the intensity of emotions is unlikely to aid emotion
perception in schizophrenia.
Consistent with these reported difficulties in facial emotion perception,
individuals with schizophrenia also experience difficulty identifying emotions
expressed in voices (Hooker & Park, 2002; Vaskinn et al., 2007). In affective prosody
tasks, they have more difficulty identifying negative emotions, with a particular
impairment for identifying sadness (Bozikas et al., 2006) and fear (Edwards, Pattison,
Jackson, & Wales, 2001). This is the same pattern observed in visual emotion tasks.
However, this is in contrast to what is observed in healthy controls, wherein negative
emotions are easier to perceive in voices than positive emotions (see Edwards, Jackson,
& Pattison, 2002, for review). Interestingly, this impairment is also present in
individuals with schizotypic personality traits (Phillips & Seidman, 2008). Schizotypal
Personality Disorder is considered an attenuated form of schizophrenia, representing a
premorbid stage of the disorder (Raine, 2006). Therefore, that impairment recognizing
emotions in vocal prosody is identifiable in schizotypy suggests that this difficulty may
be fundamental to schizophrenia.
Integrated emotion perception tasks allow participants to benefit from both
visual and vocal affective cues. These more ecologically valid tasks more closely
approximate actual stimuli encountered in daily life. In a videotaped emotion

18
perception task with just video (i.e., no audio), individuals with schizophrenia have
more difficulty identifying happy emotions than controls; however, they perform as
well as controls when identifying sad or angry emotions (Bellack, Blanchard, &
Mueser, 1996). This more accurate perception of positive versus negative emotions
parallels the results reported above with static visual stimuli. When audio is added to
the video, individuals with schizophrenia have more difficulty identifying sad emotions
than controls; however, they perform as well as controls when identifying happy or
angry emotions. This suggests that the vocal cues help individuals with schizophrenia
identify happy and angry emotions. However, integrated cues do not appear to help
their perception of sad emotions.
Emotion Paradox
As discussed previously, similar neural systems are implicated in emotional
expression and emotion perception (Brunet-Gouet & Decety, 2006). As emotion
perception is abnormal in this population, it follows, then, that emotional expression, and
possibly emotional experience, may also show abnormalities.
Schizophrenia has been characterized by flat affect since its very
conceptualization (Bleuler, 1950; Kraepelin, 1919), and indeed flat and inappropriate
affect continue to be considered hallmark characteristics of the disorder (APA, 2000).
However, individuals with schizophrenia report emotional experiences consistent with
the levels reported by psychiatrically healthy individuals. This discrepancy between the
reduced expression but self-reported normal experience of emotion in schizophrenia has
been termed the “emotion paradox” (Aleman & Khan, 2005).

19
Emotional experience. Some research reports that individuals with
schizophrenia demonstrate reduced experience of positive affect (Livingstone, Harper, &
Gillanders, 2009; Reske et al., 2007; Schneider et al., 1995; Suslow, Roestel, Ohrmann,
& Arolt, 2003) and increased experience of negative affect (Livingstone et al., 2009;
Suslow et al., 2003). However, other studies have found that these individuals self-report
similar levels of emotional experience as psychiatrically healthy controls in the
laboratory (Gur, et al., 2006; Kring, Kerr, & Earnst, 1999; Kring & Neale, 1996). This
seems at odds with the increased reporting of anhedonia, defined as the diminished
capacity to experience pleasure, in this population (Horan, Kring, & Blanchard, 2006;
Kirkpatrick, Fenton, Carpenter, & Marder, 2006; Phillips & Seidman, 2008).
The resolution of the discrepancy between normal self-reports of emotional
experience and increased self-reports of anhedonia may lie in the affective valence
being assessed. Individuals with schizophrenia report experiencing significantly more
negative affect and significantly less positive affect in their daily lives than healthy
controls (Myin-Germeys, Delespaul, & Van Os, 2005). This diminished daily
experience of positive affect supports their increased reporting of anhedonia but may in
part be related to biased expectations, whereby they avoid engaging in rewarding
activities because they do not expect to derive pleasure from them (Watson & Naragon-
Gainey, 2010). Nevertheless, it appears that, compared to controls, individuals with
schizophrenia spend a significantly greater proportion of their days experiencing
negative emotions and a significantly lesser proportion of their days experiencing
positive emotions. Overall, the research indicates that, on average, individuals with
schizophrenia are able to experience emotions to a similar degree as normal controls,

20
but their individual experience clearly differs from that of psychiatrically healthy
controls.
These experience sampling findings are supported by findings from a mood
induction task, in which individuals with schizophrenia became less happy in response
to happy induction and less sad in response to sad induction than controls (Schneider et
al., 1995). This suggests that they have an attenuated emotional experience.
Interestingly, they are also sadder during happy induction and happier during sad
induction than controls, indicating some degree of inappropriate emotion induction in
schizophrenia.
In addition to these behavioral findings are physiological findings of abnormal
emotional experience. Individuals with schizophrenia demonstrate greater skin
conductance than normal controls in response to affective stimuli (Kring & Neale,
1996). This suggests that these individuals are experiencing heightened physiological
arousal and is in contrast with the idea that they have a diminished capacity to
experience emotions. Neurologically, individuals with schizophrenia exhibit reduced
activation in emotion processing circuitry (right amygdala, left orbitofrontal cortex,
fusiform gyrus, cuneus) in response to non-aversive (though still affectively arousing)
stimuli and near normal to above normal activation in emotion processing circuitry
(medial prefrontal cortex) in response to aversive stimuli (Taylor, Liberzon, Decker, &
Koeppe, 2002). These physiological and neurological data indicate that emotion
processing may be somewhat disrupted in schizophrenia, which may affect the
experience of emotion.

21
Emotional expression. The crux of the emotion paradox is that although
emotional experience appears to be within normal limits, emotional expression appears to
be abnormal in schizophrenia. Affective flattening, the restriction in the range of
emotional expression in response to emotional stimuli, is a characteristic symptom of
schizophrenia (APA, 2000; Kring & Neale, 1996). Thus, individuals with schizophrenia
appear to have a disjunction between their near-normal emotional experience and their
flattened expression of this experience.
In daily life, individuals with schizophrenia are overall less facially expressive
than psychiatrically healthy controls (Berenbaum & Oltmanns, 1992; Kring & Neale,
1996; Mandal, Pandey, & Prasad, 1998; Martin, Borod, Alpert, Brozgold, &
Welkowitz, 1990; Schneider et al., 1995; Tremeau et al., 2005). Specifically, they
spontaneously smile less often and for a shorter period of time. They also use fewer
facial coverbal gestures (facial or head movements intended to illustrate or replace
speech) and use fewer words in emotional conversation (Gottheil, Paredes, Exline, &
Winkelmayer, 1970; Tremeau et al., 2005). Further, of universally recognized
emotions, they appear to have the greatest impairment expressing happiness verbally
(Gottheil et al., 1970). Interestingly, overall facial expressiveness and the number of
facial coverbal gestures have been found to depend on the number of words used in this
population (Tremeau et al., 2005). This again highlights the interaction between
neurocognition [here, specifically alogia, another common symptom of schizophrenia
(APA, 2000)] and social cognition (here, specifically emotional expression).
Individuals with schizophrenia demonstrate reduced spontaneous, involuntary
facial activity in response to a variety of affective stimuli in the laboratory (Gaebel &

22
Wölwer, 1992; Martin et al., 1990). Research indicates that, like healthy controls,
individuals with schizophrenia make more positive facial expressions in response to
positive film clips than negative facial expressions in response to negative film clips
(Kring & Neale, 1996). However, individuals with schizophrenia make fewer positive
facial expressions in response to positive film clips than normal controls; moreover,
they make fewer negative facial expressions in response to negative film clips than
controls (Kring & Neale, 1996). Further, they appear to have the greatest impairment
expressing anger (Gottheil et al., 1970). Thus, individuals with schizophrenia appear to
make expressions in response to affective stimuli but to an attenuated degree.
Although they make fewer facial expressions, individuals with schizophrenia do
appear to exhibit activity in the facial muscles associated with appropriate facial
reactions to affective stimuli (Earnst et al., 1996; Kring et al., 1999). That is, like
control participants, individuals with schizophrenia show greater activity in the muscles
associated with frowning in response to negative pictures than in response to positive
pictures (Kring et al., 1999). Moreover, individuals with schizophrenia tend to show the
same pattern of facial responsivity in the muscles associated with frowning and smiling
in response to happy, sad, fearful, and angry stimuli (Kring et al., 1999). Thus, it
appears that individuals with schizophrenia are expressing appropriate facial
expressions but to such an attenuated degree that they are not perceived.
As mentioned, individuals with schizophrenia tend to have reduced involuntary
emotional expressiveness, especially for positive emotions (Martin et al., 1990).
Additionally, individuals with schizophrenia demonstrate reduced facial activity when
voluntarily attempting to mimic a facial expression (Gaebel & Wölwer, 1992; Tremeau

23
et al., 2005). Moreover, they are less accurate at generating facial expressions (Gottheil,
Thornton, & Exline, 1976), both by verbal instruction and imitation (Borod et al., 1990;
Schwartz, Mastropaolo, Rosse, Mathis, & Deutsch, 2006). When asked to imitate an
emotional facial expression, individuals with schizophrenia show significantly worse
performance than controls (Gaebel & Wölwer, 1992). They have the most pronounced
deficit when attempting to imitate fearful, sad, and angry expressions (Gaebel &
Wölwer, 1992; Tremeau et al., 2005); they have the least pronounced deficit when
attempting to imitate happy and surprised expressions (Tremeau et al., 2005). Not only
are individuals with schizophrenia less accurate at imitating facial expressions, they
also give fewer emotional expressions on command and spend less time expressing
those emotions (Tremeau et al., 2005). Similarly, they also demonstrate reduced facial
activity when attempting to simulate emotions when the stimulus is an emotional word
(e.g., fear) rather than an emotional facial expression (Gaebel & Wölwer, 1992;
Tremeau et al., 2005). Therefore, it appears that they not only experience difficulty
expressing emotions spontaneously, but they also experience difficulty expressing
emotions voluntarily.
These abnormalities of emotion expression in schizophrenia may be influenced
by emotion perception deficits (Sachs, Steger-Wuchse, Kryspin-Exner, Gur, &
Katschnig, 2004). Individuals with poorer performance on emotion perception measures
tend to have greater affective flattening (Kohler et al., 2003). However, other research
indicates that these processes are independent (Kring & Neale, 1996; Silver & Shlomo,
2001). For example, emotion perception performance was significantly positively
correlated with negative symptoms such as affective flattening in one study, but this

24
correlation was no longer significant when age, length of illness, accumulated time in
the hospital, or education were added as a covariate (Silver, Shlomo, Turner, & Gur,
2002). This suggests that the relationship between emotion perception and emotional
expression may be complicated and deserving of further empirical attention.
Emotion Regulation
This emotion paradox, the disjunction between the experience and the
expression of emotion in schizophrenia, may reflect difficulties in emotion regulation.
That is, the impaired emotion perception, irregular emotional experience, and abnormal
emotional expression observed in this population may be a result of poor skills with
emotion regulation strategies such as reappraisal or suppression.
Indeed, individuals with schizophrenia demonstrate maladaptive coping with
stress (Livingstone et al., 2009), and their chosen methods to regulate distress tend to be
avoidant (e.g., suppression; van den Bosch, van Asma, Rombouts, & Louwerens, 1992).
This preference for avoidant strategies like suppression is in contrast to the preference
for reappraisal made by psychiatrically healthy individuals (Livingstone et al., 2009;
van der Meer, van't Wout, & Aleman, 2009). Frequent use of suppression may help
explain the emotion paradox, wherein suppression leads to an expression of flat affect
that is incongruent with the emotional experience. Suppression may also help explain
the finding of increased skin conductance in this population (van der Meer et al., 2009),
as suppression leads to greater physiological reactivity than reappraisal. Thus, the
choice of regulatory strategy may mediate the relationship between emotional
experience and emotional expression.

25
Some research indicates that individuals with schizophrenia are able to suppress
their feelings in response to emotional film clips but have difficulty amplifying their
feelings (Henry et al., 2007). This suggests that it is easier for them to try to down-
regulate than to up-regulate their emotional experience. Moreover, it suggests that
individuals with schizophrenia not only have a skill deficit (i.e., they do not have the
skills to increase positive experiences) but also maladaptive use of intact skills (i.e.,
overreliance on suppression to decrease negative experiences; Kring & Werner, 2004).
Interestingly, the film clips in this cited study were intended to elicit amusement. The
relative ease with which individuals with schizophrenia were able to adopt the emotion
regulation strategy of suppression to down-regulate positive feelings may relate to their
increased reporting of anhedonia whereby they report diminished levels of pleasure in
their emotional experience.
Further, research indicates that affective flattening, an abnormality in emotional
expression, may be a result of poor use of emotional suppression (Ellgring & Smith,
1998). In other words, it has been argued that individuals presenting with flat affect
may overuse emotional suppression as a regulatory strategy such that they do not
appropriately connect their emotional expression with their emotional experience. The
clinical significance of this poor emotion regulation is shown via the variety of negative
consequences associated with persistent emotional suppression, including impairing
memory, disrupting communication, inhibiting relationship formation, and reducing
rapport (Butler et al., 2003; John & Gross, 2004). Thus, the tendency to overuse the
regulatory strategy of emotional suppression can not only lead to affective flattening
but can also have negative social consequences for individuals with schizophrenia.

26
The neural circuitry associated with emotion processing also shows abnormalities
in schizophrenia (Aleman & Khan, 2005; Brunet-Gouet & Decety, 2006). Generally,
reduced activity in the appraisal regions (amygdala, insula, striatum, and medial
orbitofrontal cortex) is associated with impairments in perception of and response to
emotional stimuli in this population (Brunet-Gouet & Decety, 2006; Denny et al., 2010).
However, the evidence supporting hypoactivations in these areas is equivocal (Brunet-
Gouet & Decety, 2006), as some studies report hyperactivations in these regions,
particularly the amygdala (Holt et al., 2006; Kosaka et al., 2002). The interpretation of
these data that is perhaps most consistent with all current reports is that serious mental
illness involves impairments in emotion appraisal at multiple levels of biosystemic
functioning, including the neurophysiological and neuropsychological levels.
This dysregulation may be due, at least in part, to disrupted connections between
the appraisal regions and the cognitive control (i.e., regulation) regions (Das et al., 2007).
This is apparent even in individuals who are at risk for developing psychosis (Modinos,
Ormel, & Aleman, 2010), indicating that it may be a marker of vulnerability for the
disorder.

27
CHAPTER 4
INTERVENTIONS TARGETING SOCIAL COGNITIVE DEFICITS
The neuropathology associated with schizophrenia and the severity of the
associated social cognitive deficits brings into question whether the emotion processing
deficits associated with that pathology can be remediated. Several interventions have
been developed to target the various systemic deficits associated with SMI. Although
these treatments are far from returning individuals with SMI to “normal” functioning,
preliminary data do indicate that these deficits are responsive to therapeutic remediation.
Interventions Based on the Generalized Deficit Hypothesis
To the degree that functional neurocognition is a prerequisite for success at any
more molar level of processing (e.g., social cognition), strengthening basic
neurocognition may lead to improvements in social cognition (Spaulding & Poland,
2001).2 This is reflected in the generalized deficit hypothesis, that social cognitive deficits
such as the poor emotion processing observed in schizophrenia are due primarily to
cognitive impairment in general, not the failure of some specific cognitive or
neurocognitive subsystem (Archer, Hay, & Young, 1992; Huang, Xu, & Chan, 2011;
Johnston, Katsikitis, & Carr, 2001; Kerr & Neale, 1993; Mueser et al., 1996; Pomarol-
Clotet et al., 2010; Salem et al., 1996). This hypothesis also presumes that remediating
cognitive impairment should likewise remediate emotion processing deficits (van der
Gaag, Kern, van den Bosch, & Liberman, 2002).
Indeed, cognitive remediation, a treatment program aimed at improving executive
functioning deficits, is associated with improvements in social cognition. Cognitive
remediation consists of exercises of varying cognitive complexity, from basic perception

28
to social perception. Although the goal of the program is to target social perception,
neurocognitive skills such as attention, memory, and executive functioning are also
targeted, as these skills are considered fundamental for improved social perception (van
der Gaag et al., 2002). These areas are targeted with training in such strategies as self-
instruction, memory enhancement, inductive reasoning, and compensatory training
procedures, strategies which have proven successful in remediating other types of deficits
in schizophrenia (Kern, Wallace, Hellman, Womack, & Green, 1996).
Consistent with its goal of remediating neurocognitive deficits, cognitive
remediation is associated with improvements in verbal and visual memory, sustained
attention, and executive functioning in schizophrenia (Hodge et al., 2010; Reeder,
Newton, Frangou, & Wykes, 2004). Furthermore, it is associated with improvements in
emotion perception in this population. Although individuals with schizophrenia commit
35-55% more errors in emotion tasks than healthy controls before treatment, their
performance approaches that of untreated healthy controls following treatment (van der
Gaag et al., 2002).
Finally, cognitive remediation is associated with improvements in social and
occupational outcomes, which appear to persist in at least the short-term beyond the
conclusion of treatment (Hodge et al., 2010). Importantly, it has been hypothesized that
cognitive remediation serves as a mediator between changes in neurocognition and social
functioning; without cognitive remediation, changes in neurocognition do not appear to
affect social functioning (Reeder et al., 2004).
A more comprehensive cognitive treatment modality is Integrated Psychological
Therapy (IPT; Brenner, Hodel, Roder, & Corrigan, 1992; Roder, Mueller, Brenner, &

29
Spaulding, 2010). Like cognitive remediation, IPT is founded upon the assumption that
both neurocognitive and social cognitive deficits need to be addressed therapeutically to
effect change in social cognition (Brenner et al., 1992; Wallace et al., 1980). Also like
cognitive remediation, IPT consists of exercises of varying cognitive complexity, from
basic perception to social perception. These exercises are arranged in five hierarchical
subprograms: cognitive differentiation, social perception, verbal communication, social
skills, and interpersonal problem solving. With respect to neurocognitive deficits, IPT is
associated with improvements in attention, concept formation, and abstract thinking, as
well as in spatiotemporal orientation and memory (see Roder, Mueller, Mueser, &
Brenner, 2006, for a review). IPT is also associated with improvements in social
functioning and social competence (Brenner et al., 1992; Roder et al., 2006; Spaulding,
Reed, Sullivan, Richardson, & Weiler, 1999; Zimmer, Duncan, Laitano, Ferreira, &
Belmonte-de-Abreu, 2007).
Interventions Based on the Specific Deficit Hypothesis
Although the generalized deficit hypothesis proposes that deficits in emotion
processing in schizophrenia may be due to general cognitive impairment, its competitor,
the specific deficit hypothesis, proposes that these deficits may be due to a specific deficit
in emotion processing that is independent of general cognitive impairment (Borod et al.,
1993; Edwards et al., 2001; Gaebel & Wölwer, 1992; Heimberg, Gur, Erwin, Shtasel, &
Gur, 1992; Kosmidis et al., 2007; Poole et al., 2000; Shaw et al., 1999). Thus, the
specific deficit hypothesis presumes that remediating emotion processing deficits will
require a targeted intervention, as cognitive remediation may only result in slight

30
improvements in emotion processing (Bryson, Bell, & Lysaker, 1997; Wölwer et al.,
2005).
Several treatments have been developed aimed specifically at remediating
emotion processing deficits. Penn and Combs (2000) randomly assigned inpatients with
schizophrenia to one of four interventions to compare effects on ability to identify facial
affect: repeated practice with facial emotion identification, monetary reinforcement for
correct identifications, imitation of facial emotions (facial feedback), and a combination
of monetary reinforcement and facial feedback. The latter three groups resulted in
improvements in facial affect identification to a degree that was comparable to
performance of untreated healthy controls (Penn & Combs, 2000). Consistent with these
results, two other imitation-based modalities have benefits for improving emotion
recognition, the accuracy of facial expressions, and social and behavioral functioning in
schizophrenia (Mazza et al., 2010; Schwartz et al., 2006).
The Micro-Expression Training Tool (METT; Russell, Chu, & Phillips, 2006) is a
single-session computer-based intervention that attempts to improve emotion recognition.
The program retrains where participants visually attend to faces, and pilot data indicate
that it improves emotion recognition in outpatients with schizophrenia to a level
comparable to untreated healthy controls.
Training of Affect Recognition (TAR; Frommann, Streit, & Wölwer, 2003) is a
modality similar to cognitive remediation and IPT in its emphasis on errorless learning
strategies such as compensation and positive reinforcement. Results indicate that this
program is associated with significant improvements in facial affect recognition and

31
discrimination, to a degree comparable to that of untreated healthy controls (Frommann
et al., 2003; Habel et al., 2010; Wölwer et al., 2005).
Emotion-Focused Therapy (Greenberg, 2004; Greenberg & Bolger, 2001),
Dialectical Behavior Therapy (DBT; Linehan, 1993), and Emotional Management
Training (Hodel & Brenner, 2002) are perhaps the treatments most aimed at developing
emotion regulation skills. These modalities are designed to develop an understanding of
adaptive and maladaptive emotions and their sources and then acquire emotion regulation
skills. Emotion-Focused Therapy and DBT were not developed for schizophrenia, but the
therapeutic goals and skills of both modalities are consistent with deficits observed in
schizophrenia. Thus, these modalities may be useful for helping individuals with
schizophrenia develop more adaptive emotion regulation skills (van der Meer et al.,
2009). In contrast, Emotional Management Training, a subprogram of IPT, was designed
specifically for emotion processing deficits observed in schizophrenia (Hodel & Brenner,
1997). This modality leads to improvements in emotional information processing and
cognitive processing in this population, beyond what is observed for other common
treatments (Hodel & Brenner, 2002).
Finally, Social Cognition and Interaction Training (SCIT; Penn, Roberts, Combs,
& Sterne, 2007) is a group-based treatment modality aimed specifically at remediating
social cognitive deficits in schizophrenia. It targets the three key social cognitive deficits
in this population: emotion perception, attributional style, and theory of mind. It appears
to be effective in inpatients (Combs et al., 2007; Penn et al., 2007) and outpatients
(Roberts & Penn, 2009; Kleinlein, 2010) at remediating deficits in emotion processing
and improving social functioning.

32
CHAPTER 5
PRESENT STUDY
This review has evaluated the abnormalities in emotion processing observed in
schizophrenia. The research on emotion perception clearly demonstrates a deficit in that
domain: Individuals with schizophrenia are impaired at recognizing the emotional
expressions in faces, voices, and integrated tasks. However, the research for emotional
experience and expression are substantially less clear. Although individuals with
schizophrenia self-report similar emotional experiences to controls, physiological and
experience sampling data indicate their actual experiences may conflict with these
reports. This discrepancy points to the possibility that individuals with schizophrenia
may be using emotion regulation strategies to alter their perception of their emotional
experiences, thereby perceiving their abnormal experience as near normal. Finally,
although individuals with schizophrenia frequently present with flattened affect, data
indicate subtle movement in facial regions associated with appropriate emotional
expressions. This again raises the possibility that emotion regulation strategies, such as
suppression, may help explain this observation.
This study further elucidates the relationships between emotion regulation,
biosystemic domains, and treatment modalities in SMI. The importance of understanding
social cognitive functioning, and particularly emotion regulation, in SMI lies in its
relationship to other biosystemic domains, including social and community functioning.
Furthermore, contradictory findings and methodological differences across studies have
limited conclusions that can be drawn about these relationships.

33
The first aim of this study is to evaluate the interrelationships between emotion
processing and psychiatric symptoms. It is hypothesized that more severe positive
symptoms of psychosis will be associated with greater use of suppression as a
regulatory strategy (Hypothesis 1). As discussed, suppression is generally associated
with the experience of more psychiatric symptoms and reappraisal with fewer (Gross &
John, 2003); and this has been replicated in schizophrenia (Henry, Rendell, Green,
McDonald, & O'Donnell, 2008). Positive symptoms of schizophrenia, such as auditory
hallucinations and paranoid delusions, are associated with increases in the emotional
experience of anxiety and depression (Freeman, 2007; Lysaker & Salyers, 2007).
Emotional experiences such as these are typically down-regulated (John & Gross, 2009)
with regulatory strategies such as suppression or reappraisal. This has been replicated in
schizophrenia, whereby the severity of auditory hallucinations has been demonstrated
to be associated with greater use of suppression (Badcock, Paulik, & Maybery, 2011).
The second aim of this study is to evaluate the interrelationships between
emotion processing and neurocognition. It is hypothesized that individuals with better
emotion regulation will have higher scores on neurocognitive assessments of attention,
memory, and executive functioning (Hypothesis 2). Just as any other type of cognitive
processing, emotion processing requires neural resources. At the most basic level,
appraisal of perceived emotional stimuli requires attention to those stimuli. Moreover,
online interpretations of emotional stimuli require intact working memory (Green &
Malhi, 2006). Finally, reinterpretations of these stimuli and self-regulation require
higher order cognitive abilities, such as long-term memory and especially executive
functioning (Declerck, Boone, & De Brabander, 2006; Gyurak et al., 2009). Executive

34
functioning appears to be particularly important for regulating emotions during times of
distress. However, there are discrepant results regarding whether this is also the case in
schizophrenia (Bak et al., 2008; Penn et al., 1993). Limitations in neurocognitive
resources would likely have a greater negative effect on individuals who habitually
suppress (such as the schizophrenia population) than those who reappraise because
suppression requires more cognitive resources (Badcock et al., 2011).
The third aim of this study is to evaluate the interrelationships between emotion
processing and social functioning. It is hypothesized that individuals with better
emotion regulation will have higher scores on assessments of social and community
functioning (Hypothesis 3a). Habitual use of suppression is associated with greater
social functioning difficulties in schizophrenia as compared to habitual use of
reappraisal (Badcock et al., 2011; Henry et al., 2008). It is further hypothesized that the
relationship between emotion regulation and social and community functioning will
interact with severity of positive psychotic symptoms (Hypothesis 3b). Cognitive
deficits limit the neural resources available for allocation toward self-regulation, social
perception, and attention to external stimuli (Ellgring & Smith, 1998), and this may
have negative social consequences. Greater focus on internal stimuli, such as positive
psychotic symptoms, may further limit the resources available for attention to external
stimuli and thereby compromise social functioning.
The fourth aim of this study is to evaluate the interrelationships between
emotion processing and treatment history. It is hypothesized that individuals who have
completed group treatment modalities will have better emotion regulation (Hypothesis
4a). More specifically, it is hypothesized that individuals who have completed a group

35
treatment modality based on the specific deficit hypothesis (e.g., SCIT) will have better
emotion regulation than individuals who have completed a group treatment modality
based on the generalized deficit hypothesis (e.g., IPT) (Hypothesis 4b). As discussed,
treatment modalities have been developed for the purpose of remediating social
cognitive and emotion processing deficits in SMI. Of particular interest is the effect of
“jumping to conclusions” on emotion processing. Individuals who have experienced
psychosis are more likely to jump to conclusions, basing conclusions on limited
evidence (Dudley, John, Young, & Over, 1997a, 1997b). Moreover, jumping to
conclusions is associated with feelings of anxiety, and anxiety with an increase in
paranoia (Lincoln, Lange, Burau, Exner, & Moritz, 2010). However, when given more
information on which to base conclusions, individuals who have experienced psychosis
can change their conclusions (Dudley et al., 1997a, 1997b). The finding that jumping to
conclusions may be related to emotion regulation strategies (Livingstone et al., 2009),
suggests that modalities aimed at teaching individuals how to evaluate evidence and
avoid jumping to conclusions may impact which strategies these individuals use to
regulate emotions.
Finally, this study aims to summarize the hypothesized relationships with a path
model. It is hypothesized that emotion regulation can be incorporated in pathways to
clinical outcome, consistent with pathways previously observed in the SMI population
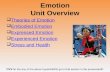
(Hypothesis 5). Previous research has identified pathways to functional outcome in
schizophrenia, but none have incorporated emotion regulation. For example, Brekke et
al. (2005) established the pathway from neurocognition to global functional outcome
via emotion perception. Their results are presented graphically in Figure 5.1.

36
NeurocognitionEmotion
Perception
Social Competence
Global Functional Outcome
0.56 0.30
0.790.74
0.97
Social Support
0.97
Figure 5.1.
Pathway from Neurocognition to Global Functional Outcome from Brekke et al., 2005 Neurocognition was measured by a composite composed of performance on the Controlled Oral Word
Association Test, the Digit Span Distractibility Test, the Degraded-Stimulus Continuous Performance
Test, and perseverative errors from the Wisconsin Card Sorting Test.
Emotion perception was measured by a composite composed of performance on the Facial Emotion
Identification Test, the Videotape Affect Perception Test, and the Voice Emotion Identification Test. Social competence was measured by a subscale of the Community Adjustment Form.
Social support was measured by a self-report social support scale adapted from the Medical Outcomes
Study Social Support Survey.
Global Functional Outcome was measured from the Role Functioning Scale and included ratings of work,
social functioning, and independent living.
In addition, Lipkovich et al. (2009) established the pathway from
neurocognition to occupational functioning via symptom severity. Their results are
presented graphically in Figure 5.2.
Direct effect (β), p < .05
Direct effect (β), p > .05
Residual (Endogenous) Variance ( )

37
Working Memory
Positive Symptoms
Occupational Functioning
error
error
Negative Symptoms
error
Processing Speed
Verbal Memory
Figure 5.2.
Pathway from Neurocognition to Occupational Functioning from Lipkovich et al., 2009 Working memory was measured by the Letter-Number Sequencing verbal subtest of the Wechsler Adult
Intelligence Scale Third Edition.
Processing speed was measured by the average of the WAIS-R Digit-Symbol Coding performance subtest
and the Category Instances, and Controlled Oral Word Association Test.
Verbal memory was measured by the Rey Auditory-Verbal Learning Test with Crawford Alternative.
Positive and negative symptoms were measured with the Positive and Negative Syndrome Scale.
Occupational functioning was measured with the Quality of Life Scale Instrumental Role Functioning
subdomain.
Inclusion of emotional regulation considerations with these known pathways,
and the hypotheses proposed in this study, produces the hypothesized path model
described in Figure 5.3. The hypothesized model adapts the results from Brekke et al.
(2005) and Lipkovich et al. (2009) to pathways from neurocognition to social
functioning via emotion perception and symptom severity. Neurocognition is also
expected to predict emotion regulation, following from Hypothesis 2. The path from
emotion regulation to social functioning follows from Hypothesis 3, and the path from
self-harm to emotion regulation is based on the theory that self-harm is a behavioral
Direct effect (β), p < .05
Direct effect (β), p > .05
Residual (Endogenous) Variance ( )

38
proxy of emotion dysregulation. Finally, the pathways from group skills training
participation to emotion perception and social functioning follow from Hypothesis 4
and the hypothesized effects of modalities such as SCIT and IPT on these constructs.
Figure 5.3. Hypothesized Path Model
Neurocognition
Emotion Perception
Symptom
Severity
Emotion Regulation
Social
Functioning
Group Skills Training
Participation
Self-Harm

39
CHAPTER 6
METHOD
Participants
Participants were recruited from the clients of a local day rehabilitation center
serving adults with SMI. Clients of this day rehabilitation center regularly participate in
rehabilitative group treatment modalities, including IPT and SCIT. The sample included
42 individuals who collectively are fairly representative of the larger SMI population
with respect to psychiatric diagnoses, gender and age distribution, and other demographic
and clinical characteristics. One participant was excluded from the analyses, as detailed
below. Diagnoses were determined by reviewing participants’ clinical records, and all
diagnoses were made by a psychiatrist or clinical psychologist. All participants had
primary Axis I diagnoses of schizophrenia spectrum disorders (78.1%), Bipolar I
Disorder (12.2%), or Major Depressive Disorder (7.3%), and many had secondary Axis I
and Axis II disorders. One exclusion criterion was a primary diagnosis of Borderline
Personality Disorder. This is primarily a disorder of maladaptive emotion regulation, and
the difficulties of individuals with this diagnosis may not be reflective of the difficulties
and experiences of the larger SMI population. Participants in the final sample of 41
individuals (32 males, 9 females) included 37 Caucasians, 2 African Americans, and 2 of
another race or ethnicity, with an age range of 21 to 70 years (M = 43.6 years; SD = 13.7
years) and education of 10 to 16 years (M = 12.2 years; SD = 1.5 years). Most
participants were prescribed antipsychotic medications (85.4%) in addition to other
psychotropic medications. Additional demographic and clinical characteristics of the
sample are included in Table 6.1.

40
Table 6.1. Sample Demographic and Clinical Characteristics
Variable n %
Sex
Male 32 78.0
Female 9 22.0
Ethnicity
Caucasian 37 90.2
African American 2 4.9
Other 2 4.8
Marital Status
Single 33 80.5
Divorced 6 14.6
Legal Status at Admission
Voluntary 18 43.9
Voluntary by Guardian 1 2.4
Mental Health Board Commitment 5 12.2
Court Order 1 2.4
Not Responsible by Reason of Insanity 3 7.3
Axis I Diagnosis
Schizophrenia, Paranoid Type 12 29.3
Schizophrenia, Disorganized or Undifferentiated Type 5 12.2
Schizoaffective Disorder 15 36.6
Bipolar I Disorder 5 12.2
Major Depressive Disorder 3 7.3
Missing 1 2.4
Second Axis I Diagnosis
Paraphilia Disorder 2 4.9
Substance Abuse/Dependence (In Remission) 5 12.2
Anxiety Disorder, Not Otherwise Specified 4 9.8
Posttraumatic Stress Disorder 2 4.9
Other (Cognitive Disorder due to Head Injury; Attention
Deficit/Hyperactivity Disorder; Asperger’s Disorder;
Obsessive Compulsive Disorder) 4 9.8
No Diagnosis/Missing 24 58.5
Third Axis I Diagnosis
Depressive Disorder, Not Otherwise Specified 2 4.9
Other (Substance Abuse/Dependence; Cognitive Disorder,
Not Otherwise Specified; Post-Traumatic Stress Disorder; Intermittent Explosive Disorder; Obsessive Compulsive
Disorder) 5 12.2
No Diagnosis/Missing 34 82.9
Axis II Diagnosis
Personality Disorder, NOS 3 7.3
Borderline Intellectual Functioning 2 4.9
No Diagnosis/Deferred/Missing 36 87.8

41
Variable n %
Medications
Antipsychotic 35 85.4
Anticonvulsant/Mood Stabilizer/Lithium 21 50.4
Antidepressant 18 43.9
Anxiolytic 12 29.3
Addiction 2 4.9
Levothyroxine 2 4.9
Stimulant 1 2.4
Measures
The following measures comprise the battery of instruments included in the study.
Clinical instruments.
Brief Psychiatric Rating Scale (BPRS; Ventura et al., 1993). The Brief
Psychiatric Rating Scale (BPRS) is a semi-structured interview that rates the presence of
24 psychiatric symptoms over the previous two weeks. The severity of each symptom is
rated on a scale from (1) not present to (7) extremely severe. Previous factor analyses
have demonstrated that a four factor solution consisting of Thought Disorder (e.g.,
grandiosity, suspiciousness, hallucinations, unusual thought content), Anergia (motor
retardation, uncooperativeness, blunted affect), Affect (somatic concern, anxiety, guilt,
depression, hostility), and Disorganization (conceptual disorganization, tension, odd
mannerisms and posturing) fits BPRS data well (Mueser, Curran, & McHugo, 1997;
Long & Brekke, 1999). Total scores range from 24 to 168, with higher scores reflecting
greater symptom severity.
Deliberate Self-Harm Inventory (DSHI; Gratz, 2001). The Deliberate Self-Harm
Inventory (DSHI) is a 17-item self-report questionnaire to assess deliberate self-harm.
Each item asks participants to indicate whether they have engaged in a particular type of

42
self-harm and follows affirmative responses with questions about frequency, severity, and
duration of harm. This measure will serve as a functional indicator of difficulties with
emotion regulation.
In undergraduates, the overall internal consistency (α) is .82. Item-total
correlations (r) range from .12 to .65. Test-retest reliability is adequate (ϕ = .68, p
<.001). Scores correlate with other measures of self-harm, history of suicide attempts,
social desirability, and history of psychotherapy.
Researcher and Consumer Emotion Regulation Scale (RACERS; Bottoms,
2011). The Researcher and Consumer Emotion Regulation Scale (RACERS) is a 30-item
self-report measure of emotion regulation developed collaboratively with participants at a
day rehabilitation center. This new instrument was designed to measure aspects of
emotion regulation maximally pertinent to the particular difficulties in this domain
associated with SMI. Preliminary psychometric analyses indicate that RACERS has
adequate construct validity and internal consistency (α = .77). Scores range from 30 to
180, with higher scores reflecting better emotion regulation.
Difficulties in Emotion Regulation Scale (DERS; Gratz & Roemer, 2004). The
Difficulties in Emotion Regulation Scale (DERS) is a 36-item self-report measure of
difficulties with emotion regulation. Participants rate how often the items describe their
emotional and behavioral responses to being upset. Each item is rated on a Likert-type
scale ranging from (1) almost never to (5) almost always. Items are arranged into 6
subscales: Nonacceptance of Emotional Responses; Difficulties Engaging in Goal-
Directed Behavior; Impulse Control Difficulties; Lack of Emotional Awareness; Limited

43
Access to Emotion Regulation Strategies; and Lack of Emotional Clarity. Scores range
from 36 to 180, with higher scores reflecting greater emotion dysregulation.
In undergraduates, the overall internal consistency (α) is .93, ranging from .80 to
.89 on subscales. Item-total correlations (r) range from .16 to .69.
Emotion Regulation Questionnaire (ERQ; Gross & John, 2003). The Emotion
Regulation Questionnaire (ERQ) is a 10-item self-report questionnaire designed to
measure the habitual use of suppression and reappraisal. Each item describes a way of
controlling particular emotions and is rated on a 7-point Likert scale from (1) strongly
agree to (7) strongly agree. Reappraisal scores range from 6 to 42, and suppression scores
range from 4 to 28, with higher scores representing greater use of that regulatory strategy.
No total score is obtained, as the reappraisal and suppression factors are considered
independent.
In undergraduates, the internal consistency (α) for Reappraisal is .79 and for
Suppression is .73. Test-retest reliability is .69 for both scales.
Bermond-Vorst Alexithymia Questionnaire (BVAQ; Vorst & Bermond, 2001).
The Bermond-Vorst Alexithymia Questionnaire (BVAQ) is a 40-item self-report
questionnaire that assesses alexithymia, or a deficiency in the ability to recognize,
identify, and distinguish between emotional states. Each item is rated on a 5-point Likert
scale from (1) strongly agree to (5) strongly disagree. The items are divided into five
subscales in two domains. In the Cognitive domain are the following subscales:
Identifying (degree of ability to describe the nature of one’s own emotions); Analyzing
(degree to which one tries to explain personal emotional states); and Verbalizing (degree
to which one is able to verbally communicate about emotional states). In the Affective

44
domain are the following subscales: Emotionalizing (degree of arousal from emotional
stimuli); and Fantasizing (degree of likelihood to fantasize about virtual matters). Scores
range from 40 to 200, with higher scores reflecting greater alexithymia. The overall
internal consistency (α) is .81 in undergraduates, ranging from .67 to .85 on subscales.
Neurocognition.
The Neuropsychological Assessment Battery – Screening Module (Stern &
White, 2003). The Neuropsychological Assessment Battery – Screening Module (NAB-
S) is designed to evaluate the neuropsychological functioning of adults aged 18 to 97 who
have disorders affecting the central nervous system. As such, it is particularly useful for
individuals with SMI, who demonstrate aberrant neurological functioning as reviewed
above. The Screening Module briefly screens for impairment in each of five
neuropsychological domains: Attention, Language, Memory, Spatial Ability, and
Executive Functions. The internal consistency (α) of the NAB-S ranges from .24 to .79.
The reliability (G) of the NAB-S ranges from .55 to .91, with an overall reliability of .80.
Trail Making Test - Trails A and B (Reitan & Davidson, 1974). The Trail
Making Test (TMT) is a visual search test to assess brain dysfunction and rehabilitative
progress in individuals between the ages of 15 and 89 (Strauss, Sherman, & Spreen,
2006). The test is given in two parts, Trails A and Trails B. On Trails A, participants are
asked to connect a series of 25 numbered circles in numerical order as quickly as
possible; on Trails B, they are asked to connect a series of 25 numbered and lettered
circles by alternating the numerical and alphabetical sequences (e.g., connect 1 to A to 2
to B, etc.) as quickly as possible. Generally, the test measures attention, psychomotor

45
processing speed, and mental flexibility. Scores reflect the time required to complete each
part; higher scores reflect slower time to completion.
Reliability of the TMT in individuals with schizophrenia is quite low (α = .36 for
Trails A and α = .63 for Trails B). Nevertheless, performance on the TMT is associated
with vocational outcome, psychosocial outcome, performance of independent living skills
and thus demonstrates substantial utility in this population.
Social cognition.
Face Emotion Identification Task ( Kerr and Neale, 1993). The Face Emotion
Identification Task (FEIT) is a computer-based task developed to measure emotion
recognition in schizophrenia. Participants are shown 19 photographs from Izard (1971)
and Ekman (1976), representing happiness, sadness, anger, fear, surprise, and shame.
After each photograph, they are asked to identify the present emotion from six choices
corresponding to the emotions included in the pictures. The task has an internal
consistency (α) of .71 in schizophrenia.
Benton Facial Recognition Test (Benton, Hamsher, Varney, & Spreen, 1983).
The Benton Facial Recognition Test (BFRT) measures the ability to recognize unfamiliar
faces and is an assessment of perceptual discrimination. Participants are shown a target
face and are asked to match that face to other photographs. The first 6 trials consist of
straightforward matching of the target to one of six other faces; and the final 16 trials
consist of matching the target to three of six faces with altered lighting or orientation.
Scores range from 0 to 54, with higher scores reflecting greater perceptual discrimination.

46
Social functioning.
Social Functioning Scale (Birchwood, Smith, Cochrane, Wetton, & Copestacke,
1990). The Social Functioning Scale (SFS) is a measure of social functioning to assess
the efficacy of treatment for schizophrenia. The scale measures skills and behaviors
relevant to the impairments of this population. Items are grouped into 7 subscales: Social
engagement, Interpersonal behavior, Prosocial activities, Recreation, Independence-
Competence (ability to perform independent living skills), Independence-Performance
(performance of independent living skills), and Employment/Occupation. Scores range
from 0 to 223, with higher scores reflecting better social functioning.
The SFS has good reliability and validity in a sample of individuals with
schizophrenia. The overall inter-rater reliability is .94, ranging from .69 to .96 on
subscales. The overall scale has an internal consistency (α) of .80, ranging from .69 to .87
on subscales. SFS scores are related to symptom presentation, prosocial behaviors,
employment, and performance independent living skills.
Multnomah Community Ability Scale (Barker, Barron, McFarland, & Bigelow,
1994). The Multnomah Community Ability Scale (MCAS) is a functional assessment
instrument designed specifically for measuring community functioning in individuals
with severe and persistent mental illness living in the community. The original version is
intended for clinician completion (most often, case managers) regarding their clients’
functioning over the past 30 days; the self-report version (MCAS-SR; Barker,
McFarland, & O’Malia, 2004) is intended for consumer completion. The scale includes
17 items covering a range of community abilities in 4 domains: Health, Adaptation,
Social Skills, and Behavior. Each item is rated on a 5-point Likert scale; descriptive

47
anchors vary for each item, but higher ratings reflect greater community functioning.
Scores range from 17 to 85, with higher scores reflecting greater community functioning.
The MCAS has good reliability and validity in large community-based SMI
populations (Barker et al., 1994; Hendryx, Dyck, McBride, & Whitbeck, 2001; Trauer,
2001; Zani, McFarland, Wachal, Barker, & Barron, 1999). The overall inter-rater
reliability is .85, ranging from .32 to .75 on individual items and from .70 to .78 on
subscales. The overall test-retest reliability is .83, ranging from .31 to .90 on individual
items and from .70 to .82 on subscales. The items appear to be measuring the same
construct, as the internal consistency is high (α = .90).
Treatment. Participants’ completion of IPT and SCIT at the day rehabilitation
center will be obtained from their clinical records.
Procedure
Participants were recruited at regular community meetings at a local day
rehabilitation center. After a participant expressed interest in the study, the experimental
purpose, procedures, risks and benefits were fully explained, and written informed
consent was obtained. For participants with legal guardians, guardian consent was
obtained before participant assent was obtained.
Participants were asked to complete a battery of measures administered by the
author. In total, the battery of self-report and researcher-administered instruments took
approximately 3 hours to complete. Most participants completed the battery in one to
three sessions over two weeks, depending on individual preferences and fatigue. Two
participants did not complete the entire battery, as one was hospitalized before
completion of the study and one chose to withdraw from the study. These participants are

48
included in the analyses for the completed portions of the battery. Participants were
compensated $20 for completing the study.
Demographic, clinical, and treatment information was retrieved from treatment
records. All data was compiled into a de-identified database for analysis.
Statistical Analyses
Path analyses were conducted in Mplus. Mplus allows for specification of
simultaneous regression equations and therefore implies a very specific covariance matrix
that better approximates the data than sequential regression equations. Beginning with the
hypothesized model, each model specified endogenous (dependent) and exogenous
(independent) variables and the covariance between them. Estimated models were
evaluated by ensuring that the algorithm converged. Converged models were modified
according to theoretical guidance, beginning by examining the normalized residual
covariance matrix and individually removing parameters with abnormally large standard
errors. Next, parameters with abnormally large modification indices were removed
individually, again according to theoretical guidance. Then, model fit statistics were used
to evaluate the overall model fit. These included the log-likelihood from the tested model;
the log-likelihood of the saturated (unstructured) model in which all variances,
covariances, and means are estimated; the Akaike Information Criterion; the Bayesian
Information Criterion; the Chi-Square Test of Model Fit; the Root Mean Square Error of
Approximation; the Comparative Fit Index; the Tucker Lewis Index; and the
Standardized Root Mean Squared Residual. If the estimated model did not have adequate
fit, the model parameters were evaluated, and those with non-significant p-values were
removed individually. Effect on the model fit was assessed, and those non-significant

49
parameters that improved model fit when removed were excluded from the model. The
model was considered complete when it contained a converged algorithm, stable standard
errors, and adequate model fit.

50
CHAPTER 7
RESULTS
Preliminary Analyses
Mean scores for each of the instruments included in the battery are included in
Table 7.1, and the correlation matrices are included in Appendices A – C. Total scores for
the Deliberate Self-Harm Inventory were not obtained because many participants with a
history of chronic self-harm could not estimate the frequency of this behavior. Therefore,
this instrument was used to categorize participants into two groups: Those with a history
of self-harm and those with no history of self-harm. Results indicated that 21 participants
reported no history of self-harm. Of the 18 participants who indicated a history of self-
harm, 8 reported having injured themselves fewer than 6 times, and the remaining 10
individuals had more chronic histories of self-harm.
Table 7.1. Assessment Descriptive Statistics
Instrument n Scale Range M SE SD Brief Psychiatric Rating Scale 40 24-168 43.20 1.47 9.31
Thought Disorder Factor 39 3.23-16.32 5.73 0.39 2.41
Anergia Factor 40 2.33-16.32 5.58 0.29 1.80
Affect Factor 40 2.28-15.97 5.87 0.47 2.96
Disorganization Factor 40 1.27-8.88 1.94 0.15 0.92 Researcher & Consumer Emotion Regulation Scale 39 30-180 108.35 2.55 15.95
Difficulties in Emotion Regulation Scale
Nonacceptance 38 6-30 14.92 1.05 6.47
Goals 38 5-25 13.24 0.72 4.44 Awareness 38 6-30 15.47 0.77 4.75
Strategies 38 8-40 18.08 1.25 7.69 Clarity 38 5-25 11.55 0.66 4.04
Impulse 38 6-30 12.21 0.79 4.88 Total 38 36-180 85.47 3.89 23.95
Emotion Regulation Questionnaire
Reappraisal 38 6-42 28.97 1.12 6.88
Suppression 38 4-28 16.45 0.74 4.58

51
Instrument n Scale Range M SE SD
Bermond-Vorst Alexithymia Questionnaire
Cognitive Domain 41 24-120 65.54 2.01 12.85 Verbalizing 41 8-40 25.42 1.12 7.16
Identifying 41 8-40 20.83 1.00 6.40 Analyzing 41 8-40 19.29 0.70 4.46
Affective Domain 41 16-80 45.22 1.46 9.33 Emotionalizing 41 8-40 22.44 0.71 4.52
Fantasizing 41 8-40 22.78 1.09 6.98 Total 41 40-200 110.76 2.33 14.89 Neuropsychological Assessment Battery – Screener (Standard Scores)
Attention 41 72.73 2.59 16.59
Language 41 100.49 3.10 19.82
Memory 41 80.63 2.58 16.49
Spatial Ability 41 89.10 2.79 17.86
Executive Functioning 41 88.15 2.39 15.32
Total 41 79.88 2.65 16.95
Trail Making Test
Trails A 41 44.17 3.35 21.46
Trails B 34 98.65 7.56 44.06
Facial Emotion Identification Task
Proportion Correctly Identified - Overall 41 0-1 0.56 0.03 0.21
Happy 41 0-1 0.85 0.05 0.30
Sad 41 0-1 0.50 0.06 0.38
Angry 41 0-1 0.64 0.05 0.33
Ashamed 41 0-1 0.34 0.05 0.30
Afraid 41 0-1 0.46 0.04 0.26
Surprised 41 0-1 0.76 0.05 0.32 Benton Facial Recognition Test 41 0-54 40.95 0.94 6.00
Social Functioning Scale
Social Engagement 38 0-15 10.66 0.38 2.35
Interpersonal Behavior 38 0-9 6.97 0.29 1.76 Prosocial Activities 38 0-39 17.18 1.52 9.36
Recreation 38 0-45 19.08 0.80 4.96 Independence – Competence 38 0-66 34.29 1.00 6.17
Independence – Performance 38 0-39 29.26 1.01 6.21
Employment/Occupation 38 0-10 5.45 0.54 3.36
Total 38 0-223 122.89 2.82 17.41
Multnomah Community Ability Scale
Health 38 5-25 19.34 0.52 3.35
Adaptation 38 3-15 11.37 0.40 2.57
Social Skills 38 5-25 17.98 0.64 4.12
Behavior 38 4-20 18.05 0.37 2.40
Total 38 17-85 66.73 1.47 9.41

52
Instrument n Scale Range M SE SD
Multnomah Community Ability Scale – Self Report
Health 38 5-25 18.71 0.61 3.74 Adaptation 38 3-15 11.21 0.35 2.17
Social Skills 38 5-25 18.03 0.63 3.87 Behavior 38 4-20 18.34 0.29 1.77
Total 38 17-85 66.29 1.39 8.58
Social Cognition and Interaction Training
Participated 14
Not Participated 25
Progress Rating (Maximum) 14 0-10 8.36 0.37 1.39
Integrated Psychological Therapy
Participated 24
Not Participated 15
Progress Rating (Average) 24 0-10 6.66 0.26 1.29
Total scores were analyzed for each of the 15 instruments administered. Outliers
were considered total scores greater than 2.5 standard deviations from the grand mean.
The population under investigation is in part defined by departure from the mean.
Consistent with this idea, 12 participants (29%) had an outlying score on one instrument,
and 1 additional participant had outlying scores on three instruments. Given that 29% of
the participants had an outlying score on one instrument in the data set, this pattern of
responding was considered normative for the population being studied and the scores
were not removed. An exception is a score on Trails B that was more than 4 standard
deviations from the mean; this score was removed from the data set. The participant with
three outlying scores was removed from the data set entirely for having multiple outlying
scores and not representing the larger population.
Performance on the Brief Psychiatric Rating Scale indicates participants’
symptoms were generally in the “not present” to “very mild” range (average item score =
1.81, SD = 0.40 on scale from 1 to 7). Symptoms related to affective flattening were the

53
most severe, in the “very mild” to “mild” range on average (average item score = 2.47,
SD = 1.18), followed by symptoms related to anergia (average item score = 2.38, SD =
0.77). Positive symptoms of psychosis and symptoms of disorganization were the least
severe on average (Thought disorder average item score = 1.82, SD = 0.76;
Disorganization average item score = 1.62, SD = 0.68).
Participants with a diagnosis of an affective disorder (i.e., Schizoaffective
Disorder, Bipolar Disorder, or Major Depressive Disorder) had more severe psychiatric
symptoms (M = 45.75, SD = 9.46) than participants with a diagnosis of schizophrenia
(i.e., Schizophrenia Paranoid Type, Disorganized Type, or Undifferentiated Type) (M =
39.87, SD = 7.90) to a degree approaching clinical significance, t(37) = 2.01, p = .052 .
There were no significant differences between the groups on severity of positive
symptoms [t(36) = 1.63, p = .112], affective symptoms [t(37) = 1.67, p = .103], or
disorganization [t(37) = 1.04, p = .307]. However, participants with a diagnosis of
schizophrenia had significantly more severe symptoms of anergia, t(37) = 2.28, p = .029.
Performance on the Researcher and Consumer Emotion Regulation Scale
indicated emotion regulation abilities were in about the average range. The grand mean
was 108.35 (SD = 15.95), and scores on this instrument range from 30 to 180, with higher
scores reflecting greater emotion regulation. There were no significant differences across
diagnostic categories on this instrument, t < 1.
The grand mean on the Difficulties with Emotion Regulation Scale was 84.47 (SD
= 23.95), and scores on this instrument range from 36 to 180, with higher scores
reflecting more difficulties with emotion regulation. Overall, scores were comparable to
those received by patients with schizophrenia in other studies (e.g., Westermann &

54
Lincoln, 2011). On a 5-point scale (1 = almost never use this strategy; 5 = almost always
use this strategy), average item scores ranged from 2.04 (SD = 0.81) on the Impulse
Control subscale to 2.98 (SD = 1.29) on the Nonacceptance of Emotions subscale. This
indicated that participants had difficulty with regulating emotions “sometimes” to “about
half the time.”
Participants with a diagnosis of an affective disorder had more difficulties with
emotion regulation (M = 92.36, SD = 26.31) than participants with a diagnosis of
schizophrenia (M = 78.13, SD = 14.92) to a degree approaching clinical significance,
t(35) = 1.89, p = .067 . Participants with a diagnosis of an affective disorder had
significantly more difficulties than participants with a diagnosis of schizophrenia with
Acceptance of Emotional Responses [t(35) = 2.17, p = .037] and Engaging in Goal-
Directed Behavior [t(35) = 2.36, p = .024]. There were no significant differences across
diagnostic categories on the remaining subscales (Impulse Control Difficulties; Lack of
Emotional Awareness; Limited Access to Emotion Regulation Strategies; and Lack of
Emotional Clarity).
Performance on the Emotion Regulation Questionnaire indicated that participants
tended to slightly agree that they used both suppression and reappraisal as emotion
regulation strategies. On a 7-point scale (1 = strongly disagree to using the strategy; 7 =
strongly agree to using the strategy), participants rated their use of reappraisal strategies
on average a 4.83 (SD = 1.15) and their use of suppression strategies on average a 4.11
(SD = 1.14). These results are consistent with previous research (e.g., Livingstone et al.,
2009). The sample agreed to using reappraisal more than they agreed to using

55
suppression, t(37) = 3.52, p = .001. There were no significant differences across
diagnostic categories on this instrument, t < 1.
The grand mean on the Bermond-Vorst Alexithymia Questionnaire was 110.76
(SD = 14.89), and scores on this instrument range from 40 to 200, with higher scores
reflecting greater alexithymia. Overall, scores were comparable to those received by
patients with schizophrenia in other studies (e.g., van’t Wout et al., 2007). On a 5-point
scale (1 = This definitely applies; 5 = This in no way applies), participants rated equally
the affective and cognitive factors. The affective factor describes the degree to which one
tries to explain personal emotional states, degree of ability to describe the nature of one’s
own emotions, and degree of ability to verbally communicate about emotional states, and
participants rated these items on average a 2.83 (SD = 0.58). The cognitive factor
describes the degree of arousal from emotional stimuli and degree of likelihood to
fantasize about virtual matters, and participants rated these items on average a 2.73 (SD =
0.54). There were no significant differences across diagnostic categories in degree of
alexithymia (t < 1). However, participants with a diagnosis of an affective disorder had
significantly more difficulty verbally communicating about emotional states (M = 27.44,
SD = 7.27) than participants with a diagnosis of schizophrenia (M = 23.13, SD = 4.85),
t(38) = 2.03, p = .049 .
The standard scores for the Neuropsychological Assessment Battery – Screener
indicate that participants scored 1.34 standard deviations below average (age- and
education-matched controls) on the total battery. Whereas their performance was average
in the Language domain, performance was most impaired in all other domains, with the
greatest impairment in the Attention domain (1.82 standard deviations below average).

56
Participants with a diagnosis of an affective disorder had higher scores on the Memory
domain (M = 84.16, SD = 18.07) than participants with a diagnosis of schizophrenia (M =
74.27, SD = 12.17) to a degree approaching significance, t(38) = 1.88, p = .068 . They
also performed significantly better tasks of immediate verbal memory [t(38) = 2.25, p =
.030] and verbal fluency and generativity [t(38) = 2.69, p = .010]. There were no
significant differences across diagnostic categories on the remaining domains or tasks of
the NAB-Screener.
On average, participants completed Trails A in 44.2 seconds (SD = 21.46
seconds) and Trails B in 98.62 seconds (SD = 44.06 seconds), a statistically significant
time difference, t(33) = 10.66, p < .001. This is consistent with previous findings in
schizophrenia of 40.9 seconds to complete Trails A and 97.5 seconds to complete Trails
B (Perianez et al., 2007). Of the participants who completed Trails A, 7 were unable to
complete Trails B because of frustration with the task or requiring more time than the
task allowed. There were no significant differences across diagnostic categories on these
instruments.
Overall, participants identified 56% of facial emotions correctly on the Facial
Emotion Identification Task. This is consistent with previous findings in schizophrenia of
correct identification of 57% (Mueser et al., 1996). Participants were most successful at
identifying happy faces (85% identified correctly) and least successful at identifying
ashamed faces (34% identified correctly). On average, they correctly identified
significantly more positive facial expressions (M = 80.5%, SD = 27.7) than negative
facial expressions (M = 48.3%, SD = 22.1%), t(40) = 8.11, p <.001. There were no
significant differences across diagnostic categories on this instrument, t < 1.

57
Performance on the Benton Facial Recognition Test indicated participants
correctly identified 40.95 faces on average (SD = 2.35). This is comparable to, though
slightly higher than, previous findings in schizophrenia of correct identification of
approximately 36 faces (Mueser et al., 1996). There were no significant differences
across diagnostic categories on this instrument, t < 1.
The grand mean on the Social Functioning Scale was 122.89 (SD = 17.41), and
scores on this instrument range from 0 to 223, with higher scores reflecting better social
functioning. This score is comparable to previous reports in schizophrenia of total scores
of 122.6 (Addington & Addington, 1999). Greatest performances were in the
Interpersonal Behavior (M = 6.97, SD = 1.76) and Independence – Performance (M =
29.26, SD = 6.21) domains. Weakest performances were in the Prosocial Activities (M =
17.18, SD = 9.36) and Recreation (M = 19.08, SD = 4.96) domains. There were no
significant differences across diagnostic categories on overall social functioning, t < 1,
but participants with a diagnosis of an affective disorder engaged in significantly more
prosocial activities than individuals with schizophrenia, t(35) = 2.18, p = .036.
The grand mean on the Multnomah Community Ability Scale was 66.73 (SD =
9.41), and scores on this instrument range from 17 to 85, with higher scores reflecting
better community ability. This score is comparable to previous reports in schizophrenia
of total scores of 66.5 (Prouteau et al., 2004). Participants’ ability was generally in the
“slightly impaired” to “moderately impaired” range (average item score = 3.93, SD =
1.08 on scale from 1 to 5, with 5 representing “no impairment”). Greatest performance
was in the Behavior domain (M = 18.05, SD = 2.40), and weakest performance was in the
Social Skills domain (M = 17.98, SD = 4.12), but there was no significant difference

58
between performance in these domains, t(40) < 1. There were no significant differences
across diagnostic categories on overall community ability, t(38) = 1.42, p = .163, but
participants with a diagnosis of an affective disorder had significantly more impairment
in health behaviors (including mood regulation and stress management) than individuals
with schizophrenia, t(38) = 2.52, p = .016.
The grand mean on the Multnomah Community Ability Scale – Self Report
version was 66.29 (SD = 8.58), and scores on this instrument range from 17 to 85, with
higher scores reflecting better community ability. Participants’ ability was generally in
the “slightly impaired” to “moderately impaired” range (average item score = 3.91, SD =
1.10 on scale from 1 to 5, with 5 representing “no impairment”). Greatest performance
was in the Behavior domain (M = 18.34, SD = 1.77), and weakest performance was in the
Social Skills domain (M = 18.03, SD = 3.87) , but there was no significant difference
between performance in these domains, t(37) < 1. There were no significant differences
between clinicans’ ratings of participants’ community ability on the MCAS and
participants’ self-reported ratings on the MCAS-SR (p > .10 in all cases). There were no
significant differences across diagnostic categories on this instrument.
There were 14 participants who had completed Social Cognition and Interaction
Training and 24 who had completed Integrated Psychological Therapy. Of these, 12 had
completed both SCIT and IPT and 15 participants who had completed neither SCIT nor
IPT. Whereas 12 participants had completed IPT but not SCIT, only 2 participants had
completed SCIT but not IPT. The overall pattern in the distribution was X²(1) = 5.39, p =
.020, indicating that fewer people had completed SCIT but not IPT than expected. The
sample was evenly divided across diagnostic categories (participants with a diagnosis of

59
an affective disorder vs. participants with a diagnosis of schizophrenia) in participation in
SCIT [X²(1) =0.74, p = .391] and IPT [X²(1) = 0.11, p = .744].
The correlation matrix of the variables included in the analyses indicated that
there was no systematic variation among variables that would theoretically be more
versus less related (see Appendices A-C). This precluded composition of composite latent
variables such as an Emotion Regulation variable that includes all of the measures of
emotion regulation in the study. Therefore, each hypothesis is tested with a series of
models examining the results of various measures to determine whether the same kinds of
predictive relationships hold for each of the measures of the relevant constructs.
Variables were centered at the mean score for regression analyses. The categorical
variable representing history of self-harm (DSHI) was coded such that 0 represented no
history of self-harm and 1 represented a history of self-harm.
Hypothesis 1: Symptom Severity and Emotion Regulation
Hypothesis 1 predicted that more severe positive symptoms of psychosis would
be associated with greater use of suppression as a regulatory strategy. Positive symptoms
were tested with the Thought Disorder factor of the Brief Psychiatric Rating Scale
(BPRS), and suppression was tested with the Suppression subscale of the Emotion
Regulation Questionnaire (ERQ). Correlation analyses were conducted to examine the
relationship between severity of positive symptoms and use of suppression as a
regulatory strategy. As shown in Table 7.2, positive symptom severity and suppression
were not significantly correlated (r = .11, p = .521), indicating that suppression did not
contribute to predicting positive symptom severity.

60
The same analysis was repeated to examine the relationship between severity of
positive symptoms and other indicators of emotion regulation. All measures of emotion
regulation were non-significantly correlated with positive symptom severity, except
greater emotion dysregulation as measured by the Difficulties with Emotion Regulation
Scale (DERS) predicted more severe positive symptoms (r = .36, p = .025). Table 7.2
summarizes the analysis results.
The analyses were repeated to examine the relationship between global
psychiatric symptom severity and indicators of emotion regulation. Again, suppression
did not contribute to predicting global symptom severity (r = .14, p = .388). However,
greater overall emotion dysregulation as measured by the DERS predicted more severe
psychiatric symptoms (r = .60, p < .001), and this relationship approached significance
as measured by RACERS (r = -.29, p = .083). Finally, individuals with a history of self-
harm tended to have more severe psychiatric symptoms than individuals with no history
of self-harm (r = .44, p = .005). Table 7.2 summarizes the analysis results.
Table 7.2. Correlation Matrix for Measures of Emotion Regulation and Symptom
Severity
Emotion Regulation Measure Positive Symptom Severity Global Symptom Severity
ERQ
Suppression .11 .14
Reappraisal -.13 -.21
RACERS -.22 -.29*
DERS .36** .60***
BVAQ .02 -.08
DSHI 0 = no history of self-harm 1 = history of self-harm
.11 .44***
Note.
Bold values are p < .05.
* Correlation is approaching significance at the 0.10 level (2-tailed).
** Correlation is significant at the 0.05 level (2-tailed).
*** Correlation is significant at the 0.01 level (2-tailed).
Positive Symptom Severity = Thought Disorder factor of BPRS.
Global Symptom Severity = Total BPRS score.

61
ERQ = Emotion Regulation Questionnaire; higher scores = more use of that strategy.
RACERS = Researcher and Consumer Emotion Regulation Scale; higher scores = better emotion
regulation.
DERS = Difficulties with Emotion Regulation Scale; higher scores = worse emotion regulation.
BVAQ = Bermond-Vorst Alexithymia Questionnaire; higher scores = more alexithymia.
DSHI = Deliberate Self-Harm Inventory; 0 = no history of self-harm; 1 = history of self-harm.
Overall, there was no evidence specifically supporting a relationship between
positive symptoms of psychosis and suppression as a regulatory strategy. However, there
is some evidence of a broader relationship between more global psychiatric symptoms
and more global emotion dysregulation.
Examination of the descriptive statistics indicated differences approaching
significance between participants with diagnoses of affective disorders versus
participants with a diagnosis of schizophrenia on overall symptom severity [t(37) =
2.01, p = .052] and global emotion dysregulation as measured by the DERS [t(35) = 1.89,
p = .067]. This indicates that an interaction may exist that accounts for some of the
relationship between symptom severity and emotion regulation. A multiple regression
analysis was conducted to examine the interaction between emotion regulation (as
measured by the DERS), symptom severity (as measured by the BPRS total score), and
diagnostic category (as measured by binary grouping of affective diagnoses, coded 0,
versus non-affective diagnoses, coded 1). In the regression, variables were centered at
the mean prior to the analysis. The first model included symptom severity as a predictor
of DERS total score; the second model added diagnostic category as a predictor; and a
third model added the interaction between symptom severity and diagnostic category as a
predictor, computed as the product of these variables.

62
The multiple regression model predicting emotion regulation from symptom
severity (BPRS) produced R2 = .33, F(1, 35) = 17.14, p < .001. Adding diagnostic
category as a predictor did not significantly improve the model fit (R2Δ = .02, p = .276),
nor did including the interaction between symptom severity and diagnostic category (R2Δ
= .01, p = .398). The final model produced R2 = .37, F (3, 33) = 6.35, p = .002. In the
final model, symptom severity had a significant positive regression weight (β = .62, p =
.002). Diagnostic category had a non-significant regression weight (β = -.17, p = .245), as
did the interaction between symptom severity and diagnostic category (β = -.15, p =
.398). Overall, it does not appear that a distinction between affective and non-affective
diagnoses is responsible for the relationship between symptom severity and emotion
regulation.
Hypothesis 2: Neurocognition and Emotion Regulation
Hypothesis 2 predicted that individuals with better emotion regulation would have
higher scores on neurocognitive assessments of attention, memory, and executive
functioning. A series of analyses were used to test this hypothesis, using the following
measures of emotion regulation: Deliberate Self-Harm Inventory (DSHI), Researcher and
Consumer Emotion Regulation Scale (RACERS), Difficulties with Emotion Regulation
Scale (DERS), Emotion Regulation Questionnaire (ERQ Reappraisal and Suppression
subscales), and the Bermond-Vorst Alexithymia Questionnaire (BVAQ). Measures of
neurocognition were separated into those measuring attention (NAB-Screener Attention
domain and Trail Making Test A), memory (NAB-Screener Memory domain), and
executive functioning (NAB-Screener Executive Functioning domain and Trail Making
Test B). Correlations between each of these domains and the various assessments of

63
emotion regulation will be discussed individually. Table 7.3 summarizes the correlation
results.
Table 7.3. Correlation Matrix for Measures of Emotion Regulation and Neurocognition
Emotion Regulation
Measure
Neurocognition Measure
NAB-Screener Domain Trail Making Test
Attention Memory Executive
Functioning
A B
RACERS .05 .10 .07 -.13 .08
DERS
Nonacceptance .21 -.08 .30* -.21 -.39**
Goals -.002 .03 .09 .03 -.14
Awareness .03 -.04 .06 -.08 -.14
Strategies -.03 -.12 .03 -.08 -.32*
Clarity .02 .03 -.05 .13 -.12
Impulse -.34** -.21 -.21 .22 -.02
Total -.02 -.10 .07 -.03 -.28
ERQ
Reappraisal -.08 .24 -.21 .32** .10
Suppression -.21 -.08 -.28* .30* -.01
BVAQ
Cognitive Domain .16 .08 .01 -.07 -.25
Verbalizing .31* .22 .07 -.13 -.39**
Identifying .02 -.02 -.03 .01 -.03
Analyzing -.07 -.08 -.02 .003 -.07
Affective Domain .10 -.09 -.20 .16 .39**
Emotionalizing .08 .04 .06 .04 .37**
Fantasizing .08 -.15 -.31** .19 .29*
Total .19 .01 -.12 .04 .03
DSHI 0 = no history of self-
harm 1 = history of self-harm
.05 .04 -.03
-.25 -.26
Note.
Bold values are p < .05.
* Correlation is approaching significance at the 0.10 level (2-tailed).
** Correlation is significant at the 0.05 level (2-tailed).
RACERS = Researcher and Consumer Emotion Regulation Scale; higher scores = better emotion
regulation.
DERS = Difficulties with Emotion Regulation Scale; higher scores = worse emotion regulation.
ERQ = Emotion Regulation Questionnaire; higher scores = more use of that strategy.
BVAQ = Bermond-Vorst Alexithymia Questionnaire; higher scores = more alexithymia.
DSHI = Deliberate Self-Harm Inventory; 0 = no history of self-harm; 1 = history of self-harm.

64
Correlations between emotion regulation and attention. The NAB-Screener
Attention domain was not significantly correlated with any of the measures of emotion
regulation. However, it was significantly correlated with the Impulse Control subscale of
the DERS (r = .34, p = .034). This indicates that individuals with higher attention scores
tend to have better impulse control, though this relationship does not extend to the more
global measure of emotion dysregulation.
Trail Making Test A was only significantly correlated with the Reappraisal
subscale of the ERQ (r = .32, p = .05). This indicates that individuals with higher
processing speed tend to rely on reappraisal as an emotion regulation strategy. The
correlation between Trail Making Test A and the Suppression subscale of the ERQ was
approaching significance (r = .30, p = .068), indicating that individuals with higher
processing speed may also tend to use suppression as an emotion regulation strategy.
Correlations between emotion regulation and memory. There were no
significant correlations between the NAB-Screener Memory domain and any of the
measures of emotion regulation, indicating the absence of a relationship between these
constructs. Although participants with a diagnosis of an affective disorder had higher
scores on the Memory domain than participants with a diagnosis of schizophrenia to a
degree approaching significance, t(38) = 1.88, p = .068, controlling for diagnostic
category did not bring any of the correlations between the NAB-Screener Memory
domain and any of the measures of emotion regulation to significance, p > .05 in all
instances. Therefore, the absence of a relationship between these constructs exists for
participants with affective and non-affective diagnoses.

65
Correlations between emotion regulation and executive functioning. The
NAB-Screener Executive Functioning domain was only significantly correlated with
the Fantasizing subscale of the BVAQ (r = -.31, p = .047). This indicates that
individuals with higher executive functioning scores are more likely to fantasize about
virtual matters. The correlation between the NAB-Screener Executive Functioning
domain and the Nonacceptance subscale of the DERS was approaching significance (r
= .30, p = .071), indicating that individuals with higher executive functioning scores
may be less likely to have an accepting attitude toward their emotional responses. The
correlation between the NAB-Screener Executive Functioning domain and the
Suppression subscale of the ERQ was also approaching significance (r = .30, p = .068),
indicating that individuals with higher executive functioning scores may be more likely
to use suppression as an emotion regulation strategy.
Trail Making Test B was significantly correlated with the Nonacceptance subscale
of the DERS (r = -.39, p = .031) and its correlation with the Strategies subscale of the
DERS was approaching significance (r = -.32, p = .084). This indicates that individuals
with greater ability to switch cognitive sets tend to be more accepting of their emotional
responses but may have poorer access to emotion regulation strategies.
Trail Making Test B was significantly correlated with the Affective domain of the
BVAQ (r = .39, p = .023), indicating that individuals with greater ability to switch
cognitive sets are more likely to experience arousal from emotional stimuli (r = .37, p =
.031). Trail Making Test B was also significantly correlated with the Verbalizing
subscale of the BVAQ (r = -.39, p = .023), indicating that individuals with greater ability

66
to switch cognitive sets are less able to verbally communicate about their emotional
states.
Multiple regression analyses predicting emotion regulation from
neurocognition. Next, a series of multiple regression analyses were conducted to
examine the relationship between emotion regulation and neurocognition. In each
analysis, the five domains of the NAB-Screener (attention, language ability, memory,
spatial ability, and executive functioning) were centered at the mean and simultaneously
entered into the model predicting one of the measures of emotion regulation (DSHI,
RACERS, DERS, Reappraisal (ERQ), Suppression (ERQ), or BVAQ). In total, six
analyses were conducted. The results are summarized in Table 7.4. Consistent with the
limitations found in the correlation matrix, only one model approached significance: the
model predicting alexithymia (BVAQ). The model produced R2 = .26, F(5, 35) = 2.47, p
= .051. Significant regression weights included attention (β = .67, p = .007) and executive
functioning (β = -.45, p = .034), indicating that these neurocognitive domains contribute
to predicting alexithymia, after controlling for performance in other neurocognitive
domains.

67
Table 7.4. Multiple Regression Models Predicting Emotion Regulation from
Neurocognition
Predictors Model
Criterion
Constant Attention Language Memory Spatial
Ability
Executive
Function
R2 p (F)
DSHI
β
.084 .106 -.002 -.027 -.117 .017 .988
p < .001 .765 .645 .991 .892 .642 RACERS
β
-.195 .297 -.051 .139 .093 .096 .625
p .956 .471 .185 .797 .464 .701 DERS
β
.050 -.235 .019 -.248 .177 .129 .463
p .927 .853 .282 .920 .186 .465 ERQ Reappraisal
β
.089 -.056 .372 -.135 -.330 .165 .303
p .730 .736 .792 .055 .457 .169 ERQ Suppression
β
.002 -.017 .022 -.060 -.263 .080 .730
p .937 .995 .939 .913 .754 .294 BVAQ
β
.669 -.243 .045 -.233 -.451 .261 .051
p .999 .007 .216 .793 .151 .034 Note.
Bold values are p < .05.
Each criterion represents a single regression equation with 5 predictors (the five domains of the NAB-
Screener: attention, language ability, memory, spatial ability, and executive functioning). Thus, this
table represents the results of 6 independent regression equations.
DSHI = Deliberate Self-Harm Inventory; 0 = no history of self-harm; 1 = history of self-harm.
RACERS = Researcher and Consumer Emotion Regulation Scale; higher scores = better emotion
regulation. DERS = Difficulties with Emotion Regulation Scale; higher scores = worse emotion regulation.
ERQ = Emotion Regulation Questionnaire; higher scores = more use of that strategy.
BVAQ = Bermond-Vorst Alexithymia Questionnaire; higher scores = more alexithymia.
Summary. Overall, neurocognition appears to explain very little of the variance
in emotion regulation. However, as predicted, attention and executive functioning do
have the greatest contribution to predicting emotion regulation. Moreover, they provide a
unique contribution to predicting emotion regulation after controlling for other aspects of
neurocognitive functioning.

68
Hypothesis 3: Social and Community Functioning and Emotion Regulation
Correlations between social and community functioning and emotion
regulation. Hypothesis 3a predicted that individuals with better emotion regulation will
have higher scores on assessments of social and community functioning. Again, a series
of analyses were used to test this hypothesis, using the five measures of emotion
regulation [Deliberate Self-Harm Inventory (DSHI), Researcher and Consumer Emotion
Regulation Scale (RACERS), Difficulties with Emotion Regulation Scale (DERS),
Emotion Regulation Questionnaire (ERQ Reappraisal and Suppression subscales), and
the Bermond-Vorst Alexithymia Questionnaire (BVAQ)] and the three measures of social
and community functioning [Social Functioning Scale (SFS), Multnomah Community
Ability Scale (MCAS), and Multnomah Community Ability Scale-Self Report (MCAS-
SR)]. The results are summarized in Table 7.5.
Social functioning as measured by the Social Functioning Scale was correlated
with measures of emotion regulation. Greater use of reappraisal (an indicator of good
emotion regulation) as measured by the ERQ was correlated with better social
functioning as measured by the SFS (r = .49, p = .002), with a particularly strong
relationship with the Prosocial Activities (r = .52, p = .001) subscale. Individuals who
had engaged in self-injury in the past (an indicator of poor emotion regulation) tended to
have lower social functioning (r = -.56, p < .001), with particularly strong relationships to
the interpersonal communication (r = -.60, p < .001) and prosocial activities (r = -.38, p =
.019) subscales. Self-reported difficulties with emotion regulation as measured by the
DERS were correlated with lower social functioning to a degree approaching significance
(r = -.31, p = .056), and significantly correlated with the Social Engagement (r = -.39, p =

69
.016) and Interpersonal Communication (r = -.45, p = .005) subscales. Social functioning
as measured by the SFS was not significantly correlated with emotion regulation as
measured by RACERS (r = .08, p = .622), use of suppression as a regulatory strategy (r
=-.06, p = .729), or alexithymia (r =-.11, p = .526).
Social functioning as measured by the clinician version of the Multnomah
Community Ability Scale was marginally related to difficulties with emotion regulation
as measured by the DERS (r = -.29, p = .076) such that individuals with more difficulties
with emotion regulation tended to have poorer community ability. Clinician-rated
community ability was not correlated with a history of self-injury (r = -.02, p = .913), use
of reappraisal as a regulatory strategy (r = .26, p = .119), use of suppression as a
regulatory strategy (r = -.12, p = .475), emotion regulation as measured by RACERS (r =
.08, p = .645), or alexithymia (r = .18, p = .259).
Social functioning as measured by the self-report version of the Multnomah
Community Ability Scale was correlated with measures of emotion regulation.
Individuals with a history of self-injury tended to rate their overall community ability as
lower (r = -.47, p = .003), and in particular their social skills (r = -.53, p = .001). Self-
reported community ability was also strongly correlated with self-reported emotion
regulation as measured by RACERS (r = .38, p = .019). This relationship extended to the
Adaptation (r = .42, p = .009) and Behavior (r = .33, p = .043) subscales. Difficulties
with emotion regulation as measured by the DERS were strongly related to poorer
community ability (r = -.64, p < .001), which extended to the Health (r = -.49, p = .002),
Social Skills (r = -.55, p < .001), and Behavior (r = -.54, p < .001) subscales of the
MCAS-SR. There was no relationship between use of reappraisal or suppression as

70
regulatory strategies and self-reported community ability (Reappraisal: r = .23, p = .157;
Suppression: r = -.05, p = .752). Nor was there a relationship between alexithymia and
self-reported community ability (r = -.21, p = .218).
Table 7.5. Correlation Matrix for Measures of Emotion Regulation and Social and
Community Functioning
Emotion Regulation Measure
Social and Community Functioning Measure
SFS MCAS MCAS-SR
RACERS .083 .076 .380**
DERS -.313* -.291* -.639***
ERQ
Reappraisal .492*** .258 .234
Suppression -.058 -.119 -.053
BVAQ -.106 .180 -.205
DSHI 0 = no history of self-harm 1 = history of self-harm
-.561*** -.018 -.468***
Note. Bold values are p < .05.
* Correlation is approaching significance at the 0.10 level (2-tailed).
** Correlation is significant at the 0.05 level (2-tailed).
*** Correlation is significant at the 0.01 level (2-tailed).
RACERS = Researcher and Consumer Emotion Regulation Scale; higher scores = better emotion regulation.
DERS = Difficulties with Emotion Regulation Scale; higher scores = worse emotion regulation.
ERQ = Emotion Regulation Questionnaire; higher scores = more use of that strategy.
BVAQ = Bermond-Vorst Alexithymia Questionnaire; higher scores = more alexithymia.
DSHI = Deliberate Self-Harm Inventory; 0 = no history of self-harm; 1 = history of self-harm.
SFS = Social Functioning Scale; higher scores = better social functioning.
MCAS = Multnomah Community Ability Scale; higher scores = better community ability.
MCAS-SR = Multnomah Community Ability Scale – Self-Report; higher scores = better community
ability.
Interaction with severity of positive psychotic symptoms. Hypothesis 3b
predicted that the relationship between emotion regulation and social and community
functioning would interact with severity of positive psychotic symptoms. Multiple
regression analyses were conducted to examine the interaction between emotion
regulation, social functioning, and positive psychotic symptoms. Table 7.6 summarizes
the correlation matrix between positive symptom severity and measures of social and

71
community functioning. Correlations between positive symptom severity and measures
of emotion regulation were noted above, see Table 7.2.
Positive symptom severity was significantly correlated with social functioning as
measured by the SFS (r = -.31, p = .030) and MCAS-SR (r = -.29, p = .039), but not as
measured by the MCAS (r = -.21, p = .102).
Table 7.6. Correlation Matrix for Positive Symptom Severity and Social and
Community Functioning
Positive Symptom Severity
SFS -.31**
MCAS -.21
MCAS-SR -.29** Note. Bold values are p < .05.
* Correlation is approaching significance at the 0.10 level (2-tailed). ** Correlation is significant at the 0.05 level (2-tailed).
*** Correlation is significant at the 0.01 level (2-tailed).
SFS = Social Functioning Scale; higher scores = better social functioning.
MCAS = Multnomah Community Ability Scale; higher scores = better community ability.
MCAS-SR = Multnomah Community Ability Scale – Self-Report; higher scores = better community
ability.
In all regression models reported below, variables were centered at the mean prior
to the analysis. Each analysis followed a similar pattern of evaluating the interaction
hypothesized in Hypothesis 3b: the first model includes a single measure of social
functioning as a predictor for a single measure of emotion regulation; the second model
adds positive symptom severity as a predictor; and the third model adds the interaction
between positive symptom severity and social functioning as a predictor, computed as the
product of these variables.
Social Functioning Scale as predictor. As shown in Table 7.7, consistent with
the correlation matrix, most of the multiple regression models predicting various
measures of emotion regulation from social functioning (as measured by the Social
Functioning Scale) produced nonsignficant models. The fit of these models was improved

72
neither by including positive symptom severity as a predictor nor by including the
interaction between positive symptom severity and social functioning.
Table 7.7. Hierarchical Multiple Regression Analyses Predicting Emotion Regulation
from Social Functioning, Positive Symptom Severity, and the Interaction between Social
Functioning and Positive Symptom Severity
Social
Functioning Predictor
Model 1 Model 2 Model 3
Criterion R2
F p R2Δ
p (FΔ) R
2Δ
p (FΔ)
SFS
DSHI .315 16.571 <.001 .005 .631 .000 .938 RACERS .007 0.248 .622 .043 .215 .120 .033 DERS .098 3.914 .056 .079 .076 .080 .065 Reappraisal (ERQ) .242 11.480 .002 .000 .892 .000 .947 Suppression (ERQ) .003 0.122 .729 .009 .579 .006 .646 BVAQ .011 0.411 .526 .019 .411 .001 .836
MCAS
DSHI .002 0.070 .793 .015 .477 .005 .691 RACERS .014 0.501 .484 .041 .224 .000 .953 DERS .085 3.335 .076 .095 .051 .000 .897 Reappraisal (ERQ) .066 2.557 .119 .006 .628 .059 .137 Suppression (ERQ) .014 0.521 .475 .007 .618 .011 .545 BVAQ .037 1.416 .242 .009 .567 .102 .048
MCAS-SR
DSHI .219 10.116 .003 .001 .852 .010 .513 RACERS .144 6.058 .019 .014 .449 .015 .433 DERS .409 24.880 <.001 .035 .148 .005 .573 Reappraisal (ERQ) .055 2.094 .157 .005 .684 .068 .113 Suppression (ERQ) .003 0.101 .752 .009 .571 .024 .367 BVAQ .205 1.571 .218 .015 .507 .003 .760
Note.
Bold values are p < .05. Each row represents a single regression equation with a single predictor (either SFS, MCAS, or MCAS-SR)
for Model 1.
In Model 2, each row represents the regression equation from Model 1 with an additional predictor
(positive symptom severity).
In Model 3, each row represents the regression equation from Model 2 with an additional predictor
(interaction between a single measure of social functioning and positive symptom severity).
Thus, this table represents the results of 54 independent regression equations.
DSHI = Deliberate Self-Harm Inventory; 0 = no history of self-harm; 1 = history of self-harm.
RACERS = Researcher and Consumer Emotion Regulation Scale; higher scores = better emotion
regulation.
DERS = Difficulties with Emotion Regulation Scale; higher scores = worse emotion regulation. ERQ = Emotion Regulation Questionnaire; higher scores = more use of that strategy.
BVAQ = Bermond-Vorst Alexithymia Questionnaire; higher scores = more alexithymia.
SFS = Social Functioning Scale; higher scores = better social functioning.
MCAS = Multnomah Community Ability Scale; higher scores = better community ability.

73
MCAS-SR = Multnomah Community Ability Scale – Self-Report; higher scores = better community
ability.
There are two noteworthy exceptions. The multiple regression model predicting
emotion regulation as measured by RACERS from social functioning (SFS) produced R2
= .01, F < 1. Adding positive symptom severity to the model did not significantly
improve the model fit (R2Δ = .04, p = .215). However, including the interaction between
positive symptom severity and social functioning significantly improved the model fit
(R2Δ = .12, p = .033). The final model produced R
2 = .17, F (3, 34) = 2.33, p = .092. In
the final model, social functioning had a non-significant regression weight (β = .14, p =
.440) and positive symptom severity had a regression weight approaching significance (β
= -.32, p = .071). The interaction between social functioning and positive symptom
severity had a significant negative regression weight (β = -.39, p = .033), indicating that
the relationship between social functioning and emotion regulation becomes less positive
as symptom severity increases. Figure 7.1 shows the interaction graphically.
When social functioning is above average (high), there is a significant relationship
between positive symptom severity and emotion regulation such that individuals who
have more severe positive symptoms tend to have worse emotion regulation than
individuals with less severe positive symptoms (β = -.62, p = .016). The relationship
between positive symptom severity and emotion regulation is somewhat smaller for
individuals with average social functioning (β = -.32, p = .071), and it becomes zero for
individuals with below average social functioning (β = -.02, p = .926).
In general, there is a non-significantly positive relationship between social
functioning and emotion regulation for individuals with few positive symptoms (β = .43,

74
p = .092), there is a non-significantly positive relationship for individuals with an average
level of positive symptoms (β = .14, p = .440), and there is a non-significantly negative
relationship for individuals with very severe positive symptoms (β = -.16, p = .377).
Overall, positive symptoms have the greatest impact on the relationship between emotion
regulation and social functioning when social functioning is high.
Figure 7.1. Positive Symptoms Moderate Relationship between SFS and RACERS
* Mean difference is p < .05
RACERS scores are centered such that 0 represents the grand mean. Low = individuals with scores one standard deviation below the grand mean.
Medium = individuals with scores at the grand mean.
High = individuals with scores one standard deviation above the grand mean.
RACERS = Researcher and Consumer Emotion Regulation Scale; higher scores = better emotion
regulation.
SFS = Social Functioning Scale; higher scores = better social functioning.
Positive Symptoms = measured by Thought Disorder Factor of BPRS; higher scores = more severe positive
symptoms
Additionally, the multiple regression model predicting difficulties in emotion
regulation as measured by DERS from social functioning (SFS) produced R2 = .10, F(1,
-78
-58
-38
-18
2
22
42
62
Low (-1 std) Medium High (+1 std)
RA
CE
RS
Score
0 =
Gra
nd
Mea
n
Hig
her S
cores
= B
ett
er E
moti
on
Reg
ula
tion
Social Functioning Scale
Low (-1 std) Medium High (+1 std) Positive Symptom Severity
*
*

75
36) = 3.91, p = .056. Adding positive symptom severity to the model improved the model
fit to a degree approaching significance (R2Δ = .08, p = .076). Similarly, including the
interaction between positive symptom severity and social functioning improved the
model fit to a degree approaching significance (R2Δ = .08, p = .065). In the final model,
social functioning had a negative regression weight approaching significance (β = -.32, p
= .059), positive symptom severity had a significant positive regression weight (β = .38, p
= .026), and their interaction had a regression weight approaching significance (β = .32, p
= .065). Figure 7.2 shows the interaction graphically.
When social functioning is above average (high), there is a significant relationship
between positive symptom severity and emotion regulation such that individuals who
have more severe positive symptoms tend to have worse emotion regulation than
individuals with less severe positive symptoms (β = .62, p = .011). The relationship
between positive symptom severity and emotion regulation is somewhat smaller for
individuals with average social functioning (β = .38, p = .026), and it becomes non-
significant for individuals with below average social functioning (β = .13, p = .464).
In general, there is a significant positive relationship between social functioning
and emotion regulation for individuals with few positive symptoms (β = -.56, p = .023),
such that fewer symptoms are associated with better emotion regulation as social
functioning increases. There is also a positive relationship approaching significance for
individuals with an average level of positive symptoms (β = -.38, p = .059), such that
fewer symptoms are associated with better emotion regulation as social functioning
increases. And there is no relationship between emotion regulation and social functioning
for individuals with severe positive symptoms (β = -.08, p = .661). Overall, consistent

76
with the results obtained with RACERS, positive symptoms have the greatest impact on
the relationship between emotion regulation and social functioning when social
functioning is high.
Figure 7.2. Positive Symptoms Moderate Relationship between SFS and DERS * Mean difference is p < .05
DERS scores are centered such that 0 represents the grand mean.
Sx = Positive Symptoms as measured by Thought Disorder Factor of BPRS.
Low = individuals with scores one standard deviation below the grand mean.
Medium = individuals with scores at the grand mean.
High = individuals with scores one standard deviation above the grand mean.
DERS = Difficulties with Emotion Regulation Scale; higher scores = worse emotion regulation.
SFS = Social Functioning Scale; higher scores = better social functioning.
Multnomah Community Ability Scale as predictor. Similar to the results
obtained for the SFS as a predictor, most of the multiple regression models predicting
various measures of emotion regulation from the MCAS produced nonsignficant models,
-50
-30
-10
10
30
50
70
90
Low (-1 std) Medium High (+1 std)
DE
RS
Score
0 =
Gra
nd
Mean
Low
er S
cores
= B
ett
er E
moti
on
Regu
lati
on
Social Functioning Scale
Low (-1 std) Medium High (+1 std) Positive Symptom Severity
* *
*
*

77
the fit of which was not improved by including positive symptom severity as a predictor
nor by including the interaction between positive symptom severity and community
ability. Again, there are two noteworthy exceptions.
The multiple regression model predicting difficulties in emotion regulation as
measured by DERS from community ability (MCAS) produced R2 = .09, F(1, 36) = 3.34,
p = .076. Adding positive symptom severity to the model improved the model fit to a
degree approaching significance (R2Δ = .10, p = .051). However, including the
interaction between positive symptom severity and social functioning did not
significantly improve model fit (R2Δ = .00, p = .897). Nevertheless, positive symptom
severity does appear to account for some of the relationship between emotion regulation
and community ability.
Additionally, the multiple regression model predicting alexithymia (BVAQ) as a
proxy of emotion regulation from community ability (MCAS) produced R2 = .04, F(1,
36) = 1.42, p = .242. Adding positive symptom severity to the model did not improve
model fit (R2Δ = .01, p = .567). However, adding the interaction between positive
symptom severity and social functioning did significantly improve model fit (R2Δ = .10,
p = .048). In the final model, community ability had a non-significant regression weight
(β = .22, p = .202) and positive symptom severity had a non-significant regression weight
(β = .20, p = .254). The interaction between community ability and positive symptom
severity had a significant positive regression weight (β = .34, p = .048), indicating that
the relationship between social functioning and emotion regulation becomes more
positive as symptom severity increases. Figure 7.3 shows the interaction graphically.

78
When community ability is below average (low), there is no relationship between
positive symptom severity and alexithymia (β = -.04, p = .839). The relationship becomes
more positive for individuals with average community ability (β = .20, p = .254) and it
approaches significance for individuals with above average community ability (β = .44, p
= .070), such that individuals with more severe positive symptoms tend to have more
alexithymia than individuals with less severe positive symptoms.
There is no relationship between community ability and alexithymia for
individuals with few positive symptoms (β = -.04, p = .917). The relationship becomes
more positive for individuals with an average level of positive symptoms (β = .37, p =
.202), and it becomes significantly positive for individuals with above average levels of
positive psychotic symptoms (β = .78, p = .029). Overall, consistent with the previous
interaction results, positive symptoms have the greatest impact on the relationship
between emotion regulation and community ability when community ability is high.

79
Figure 7.3. Positive Symptoms Moderate Relationship between MCAS and BVAQ BVAQ scores are centered such that 0 represents the grand mean.
Sx = Positive Symptoms as measured by Thought Disorder Factor of BPRS.
Low = individuals with scores one standard deviation below the grand mean.
Medium = individuals with scores at the grand mean.
High = individuals with scores one standard deviation above the grand mean.
BVAQ = Bermond-Vorst Alexithymia Questionnaire; higher scores = more alexithymia.
MCAS = Multnomah Community Ability Scale; higher scores = better community ability.
Multnomah Community Ability Scale - Self Report version as predictor. Similar
to the results obtained for the SFS and MCAS as predictors, most of the multiple
regression models predicting various measures of emotion regulation from the MCAS
produced nonsignficant models. None of the models were improved by including positive
symptom severity as a predictor nor including the interaction between positive symptom
severity and community ability.
-71
-51
-31
-11
9
29
49
69
89
Low (-1 std) Medium High (+1 std)
BV
AQ
Score
0 =
Gran
d M
ean
Low
er S
cores
≈B
ett
er E
moti
on
Regu
lati
on
Multnomah Community Ability Scale
Low (-1 std) Medium High (+1 std) Positive Symptom Severity

80
Summary. Overall, there are strong relationships between emotion regulation and
social and community functioning, such that better social and community functioning is
associated with better emotion regulation. This holds across multiple measures.
Moreover, this relationship interacts with severity of positive symptoms. The relationship
between emotion regulation and positive symptom severity becomes greater as social
functioning increases. Individuals with below average social functioning have difficulties
with emotion regulation, regardless of the severity of their positive symptoms; but
individuals with average and above average social functioning have many fewer
difficulties with emotion regulation if their symptoms are well controlled than if their
symptoms are severe. In addition, the relationship between emotion regulation and social
functioning becomes greater as positive symptom severity decreases. People with very
severe positive symptoms have difficulties with emotion regulation, regardless of how
well they function in the community; but individuals with very few positive symptoms
have fewer difficulties with emotion regulation as their social functioning improves. . . . .
. . . . .
Hypothesis 4: Group Treatment Participation and Emotion Regulation
Hypothesis 4a predicted that individuals who have completed group treatment
modalities will have better emotion regulation than those who have not. In the total
sample, 26 individuals had completed a group treatment modality (SCIT and/or IPT). A
series of one-way ANOVAS were conducted to determine if scores on various measures
of emotion regulation differed between these groups. As shown in Table 7.8, there were
no significant differences between the groups on any of the measures of emotion
regulation.

81
Table 7.8. Group Means for Emotion Regulation by Completion of Group Skills Training
Modalities
Emotion Regulation Measure
Group Skills Training Completion
Yes (n = 26) No (n = 15) ANOVA
M SD M SD F p df
RACERS 110.10 16.90 104.85 13.80 < 1
DERS 80.96 22.54 95.25 24.95 3.086 .087 1, 36
ERQ
Reappraisal 29.92 7.41 26.92 5.28 1.591 . 215 1, 36
Suppression 16.08 5.18 17.25 2.93 < 1
BVAQ 111.42 16.16 109.60 12.84 < 1 Note.
Yes = Participants have completed Social Cognition and Interaction Training (SCIT) and/or Integrated
Psychological Therapy (IPT).
No = Participants have completed neither SCIT nor IPT.
RACERS = Researcher and Consumer Emotion Regulation Scale; higher scores = better emotion
regulation.
DERS = Difficulties with Emotion Regulation Scale; higher scores = worse emotion regulation.
ERQ = Emotion Regulation Questionnaire; higher scores = more use of that strategy.
BVAQ = Bermond-Vorst Alexithymia Questionnaire; higher scores = more alexithymia.
Hypothesis 4b predicted that individuals who have completed a group treatment
modality based on the specific deficit hypothesis (e.g., SCIT) will have better emotion
regulation than individuals who have completed a group treatment modality based on the
generalized deficit hypothesis (e.g., IPT).
In the total sample, 2 individuals had completed only SCIT, 12 individuals had
completed only IPT, and 12 individuals had completed both groups. The group of
individuals who had completed a group treatment modality based on the specific deficit
hypothesis was insufficient to compare to the group of individuals who had completed a
group treatment modality based on the generalized deficit hypothesis.
Overall, there is little evidence to support the hypothesis that group treatment
participation is associated with better emotion regulation. However, as the means were all
in the expected direction, increasing statistical power may provide evidence in support of
this hypothesis.

82
Hypothesis 5: Emotion Regulation Pathways to Clinical Outcome
A path analysis was conducted in Mplus to test the fit of the hypothesized model
(see Figure 5.3) to the obtained data. Mplus allows for specification of simultaneous
regression equations and therefore implies a very specific covariance matrix that better
approximates the data than sequential regression equations. As composite variables were
not created, it was necessary to choose individual measures to represent the constructs
being studied.
The NAB-Screener total score was chosen to represent the construct of
neurocognition because it measured the broadest range of neurocognitive abilities. The
FEIT total score was chosen to represent the construct of emotion perception because it
was the only measure of this construct included in the battery. A binary variable was
created to represent participation in group treatment modalities. Selection of other
representative constructs was informed by the correlation matrix as follows.
There were four predicted pathways to social functioning: from emotion
perception, emotion regulation, symptom severity, and participation in group treatment
modalities. There was a significant relationship between emotion perception and social
functioning as measured by the SFS (r = -.48, p = .003). There were three significant
relationships between emotion regulation and social functioning: between RACERS and
MCAS-SR (r = .38, p = .019), between DERS and MCAS-SR (r = -.64, p < .001), and
between ERQ Reappraisal and SFS (r = .49, p = .002). There were four significant
relationships between symptom severity and social functioning: between positive
symptoms and MCAS (r = -.37, p = .019), between total symptoms and SFS (r = -.49, p =
.002), between total symptoms and MCAS (r = -.423, p = .006), and between total

83
symptoms and MCAS-SR (r = -.48, p = .003). Finally, there were two significant
relationships between participation in group treatment modalities and social functioning,
as measured by the SFS (r = .39, p = .016) and as measured by MCAS-SR (r = .33, p =
.042). As there were relationships between all four constructs (i.e., emotion perception,
emotion regulation, symptom severity, and participation in group treatment modalities)
and SFS as a measure of social functioning, this measure was chosen to represent the
construct of social functioning. ERQ Reappraisal was the only emotion regulation
measure to correlate significantly with SFS, so that measure came to represent emotion
regulation in the model. As total symptoms correlated with SFS whereas positive
symptoms did not, total symptoms came to represent symptom severity in the model.
Figure 7.4 represents the proposed model after the correlation analysis and including the
instruments chosen to represent the constructs.

84
Figure 7.4. Hypothesized Path Model with Representative Measures NAB-Screener Total = Neuropsychological Assessment Battery Screening Total Score.
FEIT = Facial Emotion Identification Test proportion correctly identified.
IPT, SCIT Participation = Group Skills Training Participation; 0 = Participation in Social Cognition and
Interaction Training (SCIT) and/or Integrated Psychological Therapy (IPT); 1 = Participation in neither
SCIT nor IPT.
BPRS Total = Brief Psychiatric Rating Scale Total Score.
ERQ Reappraisal = Emotion Regulation Questionnaire Reappraisal Score; higher scores = more use of
reappraisal.
DSHI = Deliberate Self-Harm Inventory; 0 = no history of self-harm; 1 = history of self-harm.
SFS Total = Social Functioning Scale Total Score; higher scores = better social functioning.
Next, a path analysis was conducted to evaluate the proposed model. As shown in
Table 7.9, the hypothesized model did not adequately fit the data according to any of the
fit statistics. Therefore, the model was revised on the basis of conceptual and theoretical
foundations and empirical guidance (i.e., the normalized residuals for the covariances,
NAB-Screener Total
FEIT
BPRS Total
ERQ Reappraisal
SFS Total
DSHI - Binary
IPT, SCIT Participation -
Binary

85
correlations, and residual correlations of the models; modification indices; and model
estimate results).

86
Table 7.9. Parameters of the Hypothesized Path Model
Independent Variable Dependent Variable Estimate SE p
NAB BPRS
-.137 .160 .392 NAB FEIT
.363 .139 .009 Group Skills Training FEIT
.021 .150 .890
NAB Reappraisal .212 .160 .186
FEIT Reappraisal -.503 .164 .002
DSHI Reappraisal -.236 .142 .096 BPRS SFS
-.401 .118 .001
FEIT SFS -.440 .125 <.001 Reappraisal SFS
.240 .127 .059 Group Skills Training SFS
.214 .122 .080
Intercepts
BPRS
-.101 .161 .533
FEIT
.047 .259 .855
Reappraisal
.297 .182 .103
SFS -.281 .206 .172
Residual Variances BPRS
.981 .044 <.001
FEIT
.867 .101 <.001
Reappraisal
.707 .135 <.001
SFS
.467 .104 <.001
R2
BPRS
.019 .044 .669
FEIT
.133 .101 .188
Reappraisal
.273 .135 .043
SFS
.533 .104 <.001
Model Fit Number of Free Parameters
18
Loglikelihood, This model
-505.658
Loglikelihood, Saturated (unstructured) model
-498.335
AIC
1047
BIC
1078 Chi-Square Test of Model Fit df = 6 (criterion: p>.05) 14.648 .066
Root Mean Square Error of Approximation (criterion: <.05) .146
CFI (criterion: >.95) .851
TLI (criterion: >.95) .664
Standardized Root Mean Square Residual (criterion: <.08) .122 Note. Bold values are p < .05.
Estimates represent standardized estimates where appropriate.
Criteria for the model fit statistics represent the accepted standards for adequate fit.

87
NAB = Neuropsychological Assessment Battery Screening Total Score.
BPRS = Brief Psychiatric Rating Scale Total Score.
FEIT = Facial Emotion Identification Test proportion correctly identified.
Group Skills Training = Group Skills Training Participation; 0 = Participation in Social Cognition and
Interaction Training (SCIT) and/or Integrated Psychological Therapy (IPT); 1 = Participation in neither
SCIT nor IPT.
Reappraisal = Emotion Regulation Questionnaire Reappraisal Score; higher scores = more use of
reappraisal.
DSHI = Deliberate Self-Harm Inventory; 0 = no history of self-harm; 1 = history of self-harm.
SFS = Social Functioning Scale Total Score; higher scores = better social functioning.
The final model is represented in Figure 7.5 and summarized in Table 7.10. It has
8 direct paths, 4 residual variances, 1 exogenous covariance, and 4 endogenous variable
intercepts. The equation of this final model is as follows:
where the variables represent the intercepts and slopes for person i.

88
Neurocognition(NAB-Screener
Total)
Emotion Perception
(FEIT)
Symptom Severity
(BPRS Total)
Emotion Regulation
(ERQ Reappraisal)Social
Functioning(SFS)
Self-Harm (DSHI – Binary)
0.370.41
0.80
0.87
0.77
Figure 7.5. Final Path Model NAB-Screener Total = Neuropsychological Assessment Battery Screening Total Score.
FEIT = Facial Emotion Identification Test proportion correctly identified.
BPRS Total = Brief Psychiatric Rating Scale Total Score.
ERQ Reappraisal = Emotion Regulation Questionnaire Reappraisal Score; higher scores = more use of
reappraisal.
DSHI = Deliberate Self-Harm Inventory; 0 = no history of self-harm; 1 = history of self-harm.
SFS = Social Functioning Scale Total Score; higher scores = better social functioning.
Direct effect (β), p < .05
Direct effect (β), p > .05
Exogenous Covariance (σ)
Residual (Endogenous) Variance ( )

89
Table 7.10. Parameters of the Revised Path Model Independent Variable Dependent Variable Estimate SE p
DSHI BPRS
.445 .130 .001 NAB FEIT
.365 .139 .009 FEIT Reappraisal -.502 .164 .002 DSHI Reappraisal -.236 .141 .095 BPRS SFS
-.318 .115 .006 FEIT SFS -.398 .122 .001 Reappraisal SFS
.205 .120 .088 DSHI SFS
-.301 .122 .013
Covariance
NAB, Reappraisal
.242 .182 .184
Intercepts
BPRS
-.494 .182 .007
FEIT
.077 .149 .608
Reappraisal
.295 .185 .111
SFS .301 .152 .047
Residual Variances
BPRS
.802 .116 <.001
FEIT
.867 .101 <.001
Reappraisal
.770 .121 <.001
SFS
.409 .095 <.001
R
2
BPRS
.198 .116 .087
FEIT
.133 .101 .189
Reappraisal
.230 .121 .058
SFS
.591 .095 <.001
Model Fit
Number of Free Parameters
19 Loglikelihood, This model
-666.663
Loglikelihood, Saturated (unstructured) model
-665.524
AIC
1371
BIC
1403
Chi-Square Test of Model Fit df = 6 (criterion: p>.05) 2.279 .892
Root Mean Square Error of Approximation (criterion: <.05) <.001
CFI (criterion: >.95) 1.000
TLI (criterion: >.95) 1.188
Standardized Root Mean Square Residual (criterion: <.08) .037 Note.
Bold values are p < .05 and fit statistics that meet or exceed the accepted criterion for adequate fit.
Estimates represent standardized estimates where appropriate.

90
Criteria for the model fit statistics represent the accepted standards for adequate fit.
NAB = Neuropsychological Assessment Battery Screening Total Score.
BPRS = Brief Psychiatric Rating Scale Total Score.
FEIT = Facial Emotion Identification Test proportion correctly identified.
Group Skills Training = Group Skills Training Participation; 0 = Participation in Social Cognition and
Interaction Training (SCIT) and/or Integrated Psychological Therapy (IPT); 1 = Participation in neither
SCIT nor IPT.
Reappraisal = Emotion Regulation Questionnaire Reappraisal Score; higher scores = more use of
reappraisal.
DSHI = Deliberate Self-Harm Inventory; 0 = no history of self-harm; 1 = history of self-harm.
SFS = Social Functioning Scale Total Score; higher scores = better social functioning.
In developing the final model, several pathways remained from the
hypothesized model whereas several new pathways were created. The hypothesized
pathways from neurocognition to social functioning via emotion perception followed
from the results of Brekke et al., 2005 and were supported in the final model. The
hypothesized pathway from neurocognition to social functioning via symptom severity
followed from the results of Lipkovich et al., 2009. The hypothesized pathway from
neurocognition to symptom severity did not remain in the model because of the absence
of a correlation among these variables. However, the hypothesized pathway from
symptom severity to social functioning was supported in the final model.
The hypothesized pathways from participation in group treatment modalities to
emotion perception and social functioning followed from Hypothesis 4. Neither
pathway was included in the final model because of a failure to account for a sufficient
portion of the variance.
The hypothesized pathway from neurocognition to reappraisal followed from
Hypothesis 2 but was eliminated from the model because of the absence of a correlation
between the variables. However, a non-significant covariance did improve the fit of the
model. Similarly, the pathways from self-harm to reappraisal and from reappraisal to

91
social functioning had non-significant contributions to the final model. However, both
remained in the model because these pathways improved the model fit.
A couple of pathways exist in the final model that were not hypothesized: a
direct pathway from self-harm to social functioning and an indirect pathway from self-
harm to social functioning via symptom severity. Of note, the hypothesized pathway
from emotion regulation to social functioning had a non-significant contribution to the
model, but a pathway from self-harm to social functioning did significantly contribute
to the model.
The final model predicts two pathways from self-harm to social functioning: a
direct pathway (DSHI to SFS) and an indirect pathway via symptom severity. Symptom
severity did not significantly mediate the relationship between self-harm and social
functioning (p = .068).
The final model fit the data as well as a saturated (unstructured) model, which has
all variance, covariances, and means estimated. The loglikelihood of the final model was
-666.66, which closely approximates the loglikelihood of the saturated (unstructured)
model, -665.52, indicating the final model accounts for the variances and covariances as
well as the saturated (unstructured) model. The AIC was estimated to be 1371.33 and the
BIC was estimated to be 1402.93, both indicating good fit. The chi-square test of model
fit provides a likelihood ratio test comparing the final model to the saturated
(unstructured) model and indicated that the final model fit equivalently to the saturated
(unstructured) model, χ2(6) = 2.279, p = 0.89. The root mean square error of
approximation is an index of model fit based on the approximated covariance matrix,
where 0 indicates perfect fit. The estimate for the final model was less than 0.001,

92
indicating that the final model fits the data well. The Comparative Fit Index, comparing
fit to an independence model of uncorrelated variables, was estimated to be 1.000, and
the Tucker Lewis Index was estimated to be 1.188, both indicating good model fit (above
0.95). Finally, the standardized root mean square residual provides the average
standardized difference between the observed correlations and the model-predicted
correlations. The estimate was 0.037, which is less than the criterion of 0.08, indicating
the model fit the data well. In sum, all fit indices indicated the model fit the data well.
In the final model, the unstandardized intercepts represent the expected means,
centered at 0. Therefore, the mean emotion perception for individuals with average
reappraisal, symptom severity, and social functioning is expected to be 0.28 units above
average; the mean reappraisal for individuals with average emotion perception, symptom
severity, and social functioning is expected to be 2.05 units above average; the mean
symptom severity for individuals with average emotion perception, reappraisal, and
social functioning is expected to be 4.2 units below average; and the mean social
functioning for individuals with average emotion perception, reappraisal, and symptom
severity is expected to be 5.17 units above average.
The standardized pathways represent the slopes for predicting the dependent
variables. A significant pathway from self-harm to symptom severity was found, such
that for every one standard deviation increase in self-harm, symptom severity was
expected to be higher by 0.45 standard deviations. The unstandardized coefficient
indicates that individuals who have histories of self-harm have an average symptom
severity 7.59 units higher than individuals who have no history of self-harm. A
significant pathway from neurocognition to emotion perception was found, such that for

93
every one standard deviation increase in neurocognition, emotion perception was
expected to be higher by 0.37 standard deviations. A significant pathway from emotion
perception to reappraisal was found, such that for every one standard deviation increase
in emotion perception, use of reappraisal was expected to be lower by 0.50 standard
deviations, for individuals with no history of self-harm; and a non-significant pathway
from self-harm to reappraisal was found, such that for every one standard deviation
increase in self-harm, use of reappraisal was expected to be lower by 0.24 standard
deviations, for individuals with an average emotion perception ability. The
unstandardized coefficient indicates that individuals who have histories of self-harm have
an average use of reappraisal 3.29 units lower than individuals who have no history of
self-harm. Three significant pathways to social functioning were found, from emotion
perception, symptom severity, and self-harm; and one non-significant pathway was
found, from reappraisal. For every one standard deviation increase in emotion perception,
social functioning was expected to be lower by 0.40 standard deviations, for individuals
who have never self-harmed and who have average symptom severity and use of
reappraisal. For every one standard deviation increase in symptom severity, social
functioning was expected to be lower by 0.32 standard deviations, for individuals who
have never self-harmed and who have average emotion perception and use of reappraisal.
For every one standard deviation increase in self-harm, social functioning was expected
to be lower by 0.30 standard deviations, for individuals who have average emotion
perception, symptom severity, and use of reappraisal. The unstandardized coefficient
indicates that individuals who have histories of self-harm have an average social
functioning 10.38 units lower than individuals who have no history of self-harm, among

94
those with average emotion perception abilities, symptom severity, and use of
reappraisal. Finally, for every one standard deviation increase in use of reappraisal, social
functioning was expected to be non-significantly higher by 0.21 standard deviations, for
individuals who have never self-harmed and who have average emotion perception and
symptom severity.
The model explained 13.3% of the variance of emotion perception abilities;
19.8% of the variance in symptom severity; 23.0% of the variance in use of reappraisal;
and 59.1% of the variance in social functioning.
Overall, the hypothesis that emotion regulation can be incorporated in pathways
to clinical outcome was supported.

95
CHAPTER 8
DISCUSSION
Results Summary
Emotion dysregulation was hypothesized to be associated with more severe
positive symptoms, poorer neurocognitive functioning, and poorer social and community
functioning. The results were mixed across the various assessments of these domains.
Difficulties with processing emotions were observed in the sample, consistent
with previous research. These included difficulties expressing emotions, identifying
facial emotions, and regulating emotions. Many participants presented with flat affect,
indicating a deficit in expressing emotions. However, the sample did not necessarily
indicate reduced emotional experience, as an assessment of alexithymia produced a
normal distribution comparable to non-clinical populations. Consistent with previous
research, participants also had difficulty perceiving facial emotions. Whereas they were
relatively successful at identifying positive facial expressions such as happiness, they had
the most difficulty with negative facial expressions, particularly ashamed faces.
Participants also demonstrated difficulty regulating emotions on a variety of assessments.
Of interest, they reported relying more on reappraisal strategies than suppression
strategies to regulate their emotions. This appears inconsistent with the literature, which
suggests that this population has a preference for strategies like suppression. However,
the scores obtained for use of reappraisal and suppression in this study are consistent with
earlier studies (e.g., Livingstone et al., 2009; van der Meer et al., 2009). It is important to
note that, like healthy controls, this population tends to use reappraisal more than
suppression to regulate their emotions. However, this population tends to use reappraisal

96
less than controls and suppression more than controls. Thus, in both populations, the
overall preference is for reappraisal, although healthy controls have a much stronger
preference for that particular regulatory strategy. This study is consistent with those
results.
The possibility remains that participants use emotion regulation strategies to alter
their perception of their emotional experiences, thereby perceiving their abnormal
emotional experiences as normal. However, the obtained results suggest that the emotion
paradox is present in this population (i.e., the population tends to demonstrate reduced
emotional expressiveness while reporting normal emotional experiences). The sample
included in this study had relatively few psychiatric symptoms, including mood
symptoms. It remains unclear whether a pathological excess of negative emotion (e.g., as
seen in affective disorders) is associated with underutilization of strategies to induce
positive emotional changes or with overuse of strategies to induce negative emotional
changes. This important question about how this population regulates emotions during
times of affective crisis is a critical finding that will have implications for treatment
development.
Contrary to previous research (e.g., Gross & John, 2003; Henry et al., 2008), use
of suppression as a regulatory strategy was significantly associated with neither positive
symptom severity nor global psychiatric symptom severity. Only one measure of
emotion regulation (DERS) predicted positive symptom severity, such that greater
emotion dysregulation was associated with more severe positive symptoms. Half of the
measures of emotion regulation predicted global psychiatric symptom severity, such
that greater emotion dysregulation was associated with more severe psychiatric

97
symptoms. The evidence was not strong enough to specifically link suppression as a
regulatory strategy to psychiatric symptom severity; however, there was some evidence
that there may be a relationship between psychiatric symptom severity and broader
emotion dysregulation.
In general, the sample had few psychiatric symptoms, especially positive
symptoms, and this may have limited the associations that could be found between
symptoms and emotion regulation. On the other hand, a sample whose symptoms are well
controlled with pharmacological and behavioral interventions may be representative of
the larger population, particularly those engaged in services founded on principles of
rehabilitation and recovery. In that case, there may be a weaker relationship between
these functional domains.
Overall, there were few relationships between emotion regulation and
neurocognitive abilities. A measure of attention was associated with use of reappraisal
and suppression as regulatory strategies, and a measure of executive functioning was
marginally associated with use of suppression, but there were no relationships between
memory and any of the measures of emotion regulation. That there were no
relationships between memory impairment and reappraisal is consistent with previous
research (e.g., Gross & John, 2002; Richards & Gross, 2000). Of note, none of the
measures of global emotion dysregulation (e.g., RACERS, DERS) significantly
correlated with any of the measures of attention, memory, or executive functioning,
suggesting that a relationship between these constructs might be specific to the
regulatory strategies used and may not extend to more global indicators of emotion

98
regulation and dysregulation. In general, overall neurocognition appears to explain very
little of the variance in emotion regulation in this population.
With respect to social and community functioning, individuals with poorer
emotion regulation, as measured by a variety of instruments, tended to have poorer self-
reported social functioning. Consistent with previous work (e.g., John & Gross, 2004),
greater reliance on reappraisal as a regulatory strategy was associated with better social
functioning, whereas no relationship was found between use of suppression and social
functioning. Perhaps most interesting about these findings is that the strongest
relationships between emotion dysregulation and social functioning were on the self-
report measures of social functioning (i.e., SFS and MCAS-SR). The measure of social
functioning completed by practitioners familiar with the individuals’ functioning in the
community did not significantly relate to any of the measures of emotion regulation.
This could reflect an artifact of the instruments used or could represent a modicum of
insight on the part of the participants regarding the impact of emotion regulation on
social and community functioning.
It was also hypothesized that positive symptom severity would account for some
of the variance in the relationship between emotion regulation and social functioning. A
few of the models indeed indicated this was the case. The interaction models indicated
that positive symptoms have the greatest impact on emotion regulation when social
functioning is above average and that social functioning has the greatest impact on
emotion regulation when positive symptoms are below average. This suggests that
individuals with SMI are best able to regulate their emotions during times of few
psychotic symptoms and good social functioning. . . . . . . . . .

99
Finally, contrary to what was hypothesized, having participated in group skills
training was not related to better emotion regulation. The failure to find a relationship
between skills training and emotion regulation may be attributable to insufficient
statistical power. Indeed, the means were in the expected direction, indicating that
group skills training may have an impact on improving emotion regulation or the skills
required for more effectively regulating emotions.
A path model summarized the relationships among the constructs of interest.
Consistent with the theory that functional neurocognition is a prerequisite for any more
molar biosystemic domain (including emotion regulation), the path model begins with
neurocognition. The hypothesized pathway from neurocognition to emotion regulation
did not remain in the model because of the absence of a correlation among these
domains. However, that a covariance between these constructs improved the fit of the
model indicates that neurocognitive abilities do account for some of the variance in use
of reappraisal as a regulatory strategy, which may be mostly attributable to variance in
the attention domain. These results are supportive of developing interventions based on
the specific deficit hypothesis. Because neurocognition only accounted for a small
proportion of the variance in emotion regulation, interventions based on the generalized
deficit hypothesis may only result in slight improvements in emotion regulation. These
results suggest that a more targeted intervention specifically aimed at remediating
emotion processing deficits may demonstrate greater improvements.
The pathway from emotion perception to emotion regulation with a negative
regression weight is inconsistent with the emotion paradox, which implies that these
constructs might have a positive relationship.

100
Non-significant pathways from self-harm to social functioning via emotion
regulation remained in the model because of contributions to overall model fit,
indicating that self-harm accounts for some of the variance in emotion regulation
strategies, and that emotion regulation strategies in turn account for some of the
variance in social functioning.
In addition, pathways exist in the final model that were not hypothesized. A path
between self-harm and social functioning via symptom severity is consistent with the
regression models reported above indicating that symptom severity accounts for some
of the variance in the relationship between emotion regulation and social functioning.
However, symptom severity did not significantly mediate the relationship between self-
harm and social functioning, owing to its accounting for a small proportion of the
variance. Finally, the hypothesized pathway from emotion regulation to social
functioning had a non-significant contribution to the model, but a pathway from self-
harm to social functioning did significantly contribute to the model. It may be that a
behavioral proxy of emotion regulation (i.e., self-harm) better accounts for variance in
social functioning than the cognitive strategies used to regulate emotions (i.e.,
reappraisal).
Overall, in the final model, better neurocognitive abilities were associated with
better emotion perception abilities. However, better emotion perception was associated
with poorer emotion regulation (i.e., less use of reappraisal) and poorer social
functioning. These unanticipated relationships are in fact among the strongest
relationships in the model. A history of self-harm predicted more severe psychiatric
symptoms, poorer emotion regulation, and poorer social functioning. The model

101
indicates that more severe psychiatric symptoms and poorer emotion regulation both
predict poorer social functioning, but recall that an interaction was found among these
domains that indicates this is a complicated relationship. Such interactions are not
adequately represented in the path model.
Limitations
There are two major limitations to this study: the sample size and the assessment
instruments. The failure to consistently find the hypothesized relationships between the
constructs of interest is likely due in no small part to insufficient statistical power. This
is particularly true for the hypotheses regarding the impact of group skills training on
emotion regulation. In such a heterogeneous population, a larger sample size will more
effectively stabilize estimates of the mean and variance, resulting in more accurate
representations of the relationships among the constructs of interest. The multivariate
interactions investigated in this study demonstrate that there are important relationships
among subgroups of individuals and measures, but insufficient power conceals their
significance.
However, there is also a significant problem in validly and reliably measuring
these constructs in this population, in particular the construct of emotion regulation.
There is only one measure of emotion regulation specifically designed for this
population (RACERS), and it has major limitations owing to its being recently
developed and not having undergone the rigorous psychometric testing and revision
necessary to improve its validity and reliability. The other measures of emotion
regulation included in the battery have undergone more rigorous psychometric testing

102
but were not developed for the SMI population and therefore may not accurately
measure emotion regulation in that population.
Further understanding of emotion regulation in SMI will require that methods
are developed for measuring the latent construct validly and reliably with enough
sensitivity to detect longitudinal changes over the course of the illness. A
conceptualization of emotion regulation as a multidimensional and dynamic construct
requires that measurement also be multidimensional and dynamic. Integrating measures
of multiple aspects of emotion regulation, such as behavioral, cognitive, and emotional
measures from multiple sources (e.g., self-report, clinicians, family, direct observation,
etc.), would be consistent with this approach.
In addition to those limitations, the statistical analyses, including the path
analysis, assumed all variables to be continuous, multivariate normal, and measured with
perfect reliability. In reality, none of these conditions were met by the data. Therefore,
the analysis presented in this manuscript is intended to be an initial hypothesis reflecting
the relationships among the variables of interest. Further analyses using more
sophisticated statistical techniques that more accurately represent the limitations of the
data will result in a more accurate representation of the connections between and among
the functional domains in SMI.
Conclusions
This study evaluated the multivariate relationships between emotion regulation
and other biosystemic domains in outpatients with SMI. The results indicate that emotion
regulation is a central domain in understanding neurocognitive functioning, social
cognitive functioning, psychiatric symptom severity, and social functioning in this

103
population. Many questions remain unanswered, such as more specifically detailing the
nature of the relationships among these domains, including potential interactions among
the domains that more accurately represent variance. The population of interest in this
study is heterogeneous, and the domain of emotion regulation is heterogeneous. The
inconsistencies among the results are indicative of the many individual differences in
abilities in this domain.
Although the sample reported using antecedent-focused strategies to regulate
their emotions, their preference for these strategies remained below what is found in
healthy controls. That they tend to also rely on more maladaptive skills such as
response-focused strategies indicates that skill training may be a beneficial treatment
target. Nevertheless, it is critical to consider that no single regulatory strategy is
inherently adaptive or maladaptive. Therefore, that response-focused strategies tend to
be maladaptive in healthy controls does not necessarily indicate this is the case in the
SMI population or in any particular individual. This highlights the need for valid
assessment.
The path model summarizing the results is consistent with the biosystemic
theory of serious mental illness, which posits that the various processes are independent
yet casually linked throughout the biosystem. Emotional responses entail coordinated
and interrelated systemic changes in thoughts, behavior, and physiology. Thus,
dysfunctional emotional responses will likely require intervention throughout the
biosystem. The independence of the functional domains, as highlighted by their largely
orthogonal relationships in this study, requires individual attention in clinical
assessment and compels the development of separate, specific treatment and

104
rehabilitation interventions. Resolving questions such as the types of emotion
regulation that are ongoing during affective crises in this population will also inform
the skills such training modalities should target. An effective emotion regulation skills
training modality would begin with assessment of adaptive strategies and follow with
improving performance of skills individuals already possess while building their
competence in alternative antecedent-focused strategies and their flexibility of
emotional responses. While innovative and comprehensive modalities are being
developed, utilizing existing treatment strategies in the psychiatric rehabilitation toolkit
such as exercise and relaxation may prove beneficial.
This research joins previous exploratory research in finding that schizophrenia
and related disorders have a major affective component, despite their not being
classified as affective disorders. The deficits and impairments in SMI extend to
regulating emotional experiences, which has implications independent functioning,
particularly interpersonal and occupational functioning. Further characterization of the
emotional component of serious mental illnesses will inform treatment development
and thereby contribute to the recovery of this population.

105
REFERENCES
Addington, J., & Addington, D. (1999). Neurocognitive and social functioning in
schizophrenia. Schizophrenia Bulletin, 25(1), 173-182.
Addington, J., Saeedi, H., & Addington, D. (2006). Facial affect recognition: A mediator
between cognitive and social functioning in schizophrenia? Schizophrenia
Research, 85 (1), 142-150.
Adolphs, R. (2002). Recognizing emotion from facial expressions: Psychological and
neurological mechanisms. Behavioral and Cognitive Neuroscience Reviews, 1 (1),
21-62.
Adolphs, R. (2003). Is the human amygdala specialized for processing social
information? Annals of the New York Academy of Sciences, 985 (1), 326-340.
Aleman, A., & Kahn, R. S. (2005). Strange feelings: Do amygdala abnormalities
dysregulate the emotional brain in schizophrenia? Progress in Neurobiology, 77
(5), 283-298.
Allman, J. M., Hakeem, A., Erwin, J. M., Nimchinsky, E., & Hof, P. (2001). The anterior
cingulate cortex: The evolution of an interface between emotion and cognition.
Annals of the New York Academy of Sciences, 935, 107-117.
American Psychiatric Association. (2000). Diagnostic and statistical manual of mental
disorders (4th
ed., Text Revision). Washington, DC: American Psychiatric
Association.
Archer, J., Hay, D. C., & Young, A. W. (1992). Face processing in psychiatric
conditions. British Journal of Clinical Psychology, 31, 45-61.

106
Badcock, J. C., Paulik, G., & Maybery, M. T. (2011). The role of emotion regulation in
auditory hallucinations. Psychiatry Research, 185, 303-308.
Bak, M., Krabbendam, L., Delespaul, P., Huistra, K., Walraven, W., & van Os, J. (2008).
Executive function does not predict coping with symptoms in stable patients with
a diagnosis of schizophrenia. BMC Psychiatry, 8 (39).
Banich, M. T., Mackiewicz, K. L., Depue, B. E., Whitmer, A. J., Miller, G. A., & Heller,
W. (2009). Cognitive control mechanisms, emotion and memory: A neural
perspective with implications for psychopathology. Neuroscience and
Biobehavioral Reviews, 33, 613-630.
Barker, S., McFarland, B., & O’Malia, L. (2004). Multnomah community ability scale:
Self-report user’s manual. Portland, OR: Network Ventures, Inc.
Barker, S., Barron, N., McFarland, B. H., & Bigelow, D. A. (1994). A community ability
scale for chronically mentally ill consumers: Part I. Reliability and validity.
Community Mental Health Journal, 30 (4), 363-383.
Beevers, C. G., Wenzlaff, R. M., Hayes, A. M., & Scott, W. D. (1999). Depression and
the ironic effects of thought suppression: Therapeutic strategies for improving
mental control. Clinical Psychology: Science and Practice, 6 (2), 133-148.
Bellack, A. S., Blanchard, J. J., & Mueser, K. T. (1996). Cue availability and affect
perception in schizophrenia. Schizophrenia Bulletin, 22 (3), 535-544.
Benton, A. L., Hamsher, K. de S., Varney, N. R., & Spreen, O. (1983). Contributions to
neuropsychological assessment. A clinical manual. New York: Oxford University
Press.

107
Berenbaum, H., & Oltmanns, T. F. (1992). Emotional experience and expression in
schizophrenia and depression. Journal of Abnormal Psychology, 101 (1), 37-44.
Birchwood, M., Smith, J., Cochrane, R., Wetton, S., & Copestake, S. (1990). The social
functioning scale: The development and validation of a new scale of social
adjustment for use in family intervention programmes with schizophrenic
patients. British Journal of Psychiatry, 157, 853-859.
Bleuler, E. (1950). Dementia praecox or the group of schizophrenias. (J. Zinkin, Trans.)
New York: International University Press.
Bloch, L., Moran, E. K., & Kring, A. M. (2010). On the need for conceptual and
definitional clarity in emotion regulation research on psychopathology. In A. M.
Kring, & D. M. Sloan (Eds.), Emotion regulation and psychopathology (pp. 88-
104). New York: The Guilford Press.
Borkovec, T. D., & Costello, E. (1993). Efficacy of applied relaxation and cognitive-
behavioral therapy in the treatment of Generalized Anxiety Disorder. Journal of
Consulting and Clinical Psychology, 61 (4), 611-619.
Borod, J. C., Martin, C. C., Alpert, M. M., Brozgold, A., & Welkowitz, J. (1993).
Perception of facial emotion in schizophrenic and right brain-damaged patients.
Journal of Nervous & Mental Disease, 181 (8), 494-502.
Borod, J. C., Welkowitz, J., Alpert, M., Brozgold, A. Z., Martin, C., Peselow, E., &
Diller, L. (1990). Parameters of emotional processing in neuropsychiatric
disorders: Conceptual issues and a battery of tests. Journal of Communication
Disorders, 23, 247-271.

108
Bottoms, H. C. (2011). Collaborative development and initial validation of the
Researcher and Consumer Emotion Regulation Scale for serious mental illness.
University of Nebraska, Lincoln, NE.
Bozikas, V., Kosmidis, M., Anezoulaki, D., Giannakou, M., Andreou, C., & Karavatos,
A. (2006). Impaired perception of affective prosody in schizophrenia. Journal of
Neuropsychiatry and Clinical Neurosciences, 18 (1), 81-85.
Brekke, J. S., Kay, D. D., Lee, K. S., & Green, M. F. (2005). Biosocial pathways to
functional outcome in schizophrenia. Schizophrenia Research, 80, 213-225.
Brenner, H. D., Hodel, B., Roder, V., & Corrigan, P. (1992). Treatment of cognitive
dysfunctions and behavioral deficits in schizophrenia. Schizophrenia Bulletin, 18
(1), 21-26.
Brunet-Gouet, E., & Decety, J. (2006). Social brain dysfunctions in schizophrenia: A
review of neuroimaging studies. Psychiatry Research: Neuroimaging, 148 (2-3),
75-92.
Bryson, G., Bell, M., & Lysaker, P. (1997). Affect recognition in schizophrenia: A
function of global impairment or a specific cognitive deficit. Psychiatry Research,
71 (2), 105-113.
Bush, G., Luu, P., & Posner, M. I. (2000). Cognitive and emotional influences in anterior
cingulate cortex. Trends in Cognitive Sciences, 4 (6), 215-222.
Butler, E. A., Egloff, B., Wilhelm, F. H., Smith, N. C., Erickson, E. A., & Gross, J. J.
(2003). The social consequences of expressive suppression. Emotion, 3 (1), 48-67.
Calder, A. J., Lawrence, A. D., & Young, A. W. (2001). Neuropsychology of fear and
loathing. Nature Reviews Neuroscience, 2, 352-363.

109
Cannon, W. (1932). The wisdom of the body. New York: Norton.
Combs, D. R., Adams, S. D., Penn, D. L., Roberts, D., Tiegreen, J., & Stem, P. (2007).
Social cognition and interaction training (SCIT) for inpatients with schizophrenia
spectrum disorders: Preliminary findings. Schizophrenia Research, 91 (1-3), 112-
116.
Corrigan, P. W., & Penn, D. L. (2001a). Introduction: Framing models of social cognition
and schizophrenia. In P. W. Corrigan, & D. L. Penn (Eds.), Social cognition and
schizophrenia (pp. 3-37). Washington, DC: American Psychological Association.
Corrigan, P. W., & Penn, D. L. (Eds.). (2001b). Social cognition and schizophrenia.
Washington, DC: American Psychological Association.
Corrigan, P. W., & Toomey, R. (1995). Interpersonal problem solving and information
processing in schizophrenia. Schizophrenia Bulletin, 21 (3), 395-403.
Couture, S. M., Penn, D. L., & Roberts, D. L. (2006). The functional significance of
social cognition in schizophrenia: A review. Schizophrenia Bulletin, 32 (Suppl1),
S44-S63.
Das, P., Kemp, A. H., Flynn, G., Harris, A. W. F., Liddell, B. J., Whitford, T. J., …
Williams, L. M. (2007). Functional disconnections in the direct and indirect
amygdala pathways for fear processing in schizophrenia. Schizophrenia Research,
90, 284-294.
Davidson, R. J., & Irwin, W. (1999). The functional neuroanatomy of emotion and
affective style. Trends in Cognitive Science, 3 (1), 11-21.

110
Davidson, R. J., Jackson, D. C., & Kalin, N. H. (2000). Emotion, plasticity, context, and
regulation: Perspectives from affective neuroscience. Psychological Bulletin, 126
(6), 890-909.
Declerck, C. H., Boone, C., & De Brabander, B. (2006). On feeling in control: A
biological theory for individual differences in control perception. Brain and
Cognition, 62 (2), 143-176.
Denny, B. T., Silvers, J. A., & Ochsner, K. N. (2010). How we heal what we don't want
to feel: The functional neural architecture of emotion regulation. In A. M. Kring,
& D. M. Sloan (Eds.), Emotion regulation and psychopathology: A
transdiagnostic approach to etiology and treatment (pp. 59-87). New York: The
Guilford Press.
Dougherty, P. E., Bartlett, E. S., & Izard, C. E. (1974). Responses of schizophrenics to
expressions of fundamental emotions. Journal of Clinical Psychology, 30, 243-
246.
Dudley, R. E. J., John, C. H., Young, A. W., & Over, D. E. (1997a). Normal and
abnormal reasoning in people with delusions. British Journal of Clinical
Psychology, 36, 243-258.
Dudley, R. E. J., John, C. H., Young, A. W., & Over, D. E. (1997b). The effect of self-
referent material on the reasoning of people with delusions. British Journal of
Clinical Psychology, 36, 575-584.
Earnst, K. S., Kring, A. M., Kadar, M. A., Salem, J. E., Shepard, D. A., & Loosen, P. T.
(1996). Facial expression in schizophrenia. Biological Psychiatry, 40, 556-558.

111
Edwards, J., Jackson, H. J., & Pattison, P. E. (2002). Emotion recognition via facial
expression and affective prosody in schizophrenia. Clinical Psychology Review,
22 (6), 789-832.
Edwards, J., Pattison, P. E., Jackson, H. J., & Wales, R. J. (2001). Facial affect and
affective prosody recognition in first-episode schizophrenia. Schizophrenia
Research, 48, 235-253.
Eisenberg, N., Fabes, R. A., Murphy, B., Maszk, P., Smith, M., & Karbon, M. (1995).
The role of emotionality and regulation in children’s social functioning: A
longitudinal study. Child Development, 66, 1360-1384.
Ekman, P. (1976). Pictures of facial affect. Palo Alto, CA: Consulting Psychologists
Press.
Ellgring, H., & Smith, M. (1998). Affect regulation during psychosis. In W. F. Flack, &
J. D. Laird (Eds.), Emotions in psychopathology: Theory and research (pp. 323-
335). New York, NY: Oxford University Press.
Feinberg, T. E., Rifkin, A., Schaffer, C., & Walker, E. (1986). Facial discrimination and
emotional recognition in schizophrenia and affective disorders. Archives of
General Psychiatry, 43 (3), 276-279.
Freeman, D. (2007). Suspicious minds: The psychology of persecutory delusions.
Clinical Psychology Review, 27 (4), 425-457.
Frommann, N., Streit, M., & Wölwer, W. (2003). Remediation of facial affect
recognition impairments in patients with schziophrenia: A new training program.
Psychiatry Research, 117, 281-284.

112
Gaebel, W., & Wölwer, W. (1992). Facial expression and emotional face recognition in
schizophrenia and depression. European Archives of Psychiatry and Clinical
Neuroscience, 242, 46-52.
Gottheil, E., Paredes, A., Exline, R. V., & Winkelmayer, R. (1970). Communication of
affect in schizophrenia. Archives of General Psychiatry, 23, 439-444.
Gottheil, E., Thornton, C. C., & Exline, R. V. (1976). Appropriate and background affect
in facial displays of emotion comparison of schizophrenic and normal males.
Archives of General Psychiatry, 33, 565-568.
Gratz, K. L. (2001). Measurement of deliberate self-harm: Preliminary data on the
Deliberate Self-Harm Inventory. Journal of Psychopathology and Behavioral
Assessment, 23(4), 253-263.
Gratz, K. L., & Roemer, L. (2004). Multidimensional assessment of emotion regulation
and dys-regulation: Development, factor structure, and initial validation of the
Difficulties in Emotion Regulation Scale. Journal of Psychopathology and
Behavioral Assessment, 26 (1), 41-54.
Green, M. J., & Malhi, G. S. (2006). Neural mechanisms of the cognitive control of
emotion. Acta Neuropsychiatrica, 18, 144-153.
Greenberg, L. S. (2004). Emotion-focused therapy. Clinical Psychology and
Psychotherapy, 11, 3-16.
Greenberg, L. S., & Bolger, E. (2001). An emotion-focused approach to the
overregulation of emotion and emotional pain. Journal of Clinical Psychology, 57
(2), 197-211.

113
Gross, J. J. (1998). Antecedent- and response-focused emotion regulation: Divergent
consequences for experience, expression, and physiology. Journal of Personality
and Social Psychology, 74 (1), 224-237.
Gross, J. J. (2001). Emotion regulation in adulthood: Timing is everything. Current
Directions in Psychological Science, 10, 214-219.
Gross, J. J. (2002). Emotion regulation: Affective, cognitive, and social consequences.
Psychophysiology, 39, 281-291.
Gross, J. J., & John, O. P. (2002). Wise emotion regulation. In L. F. Barrett, & P. Salovey
(Eds.), The wisdom of feelings: Psychological processes in emotional intelligence
(pp. 297-318). New York: The Guilford Press.
Gross, J. J., & John, O. P. (2003). Individual differences in two emotion regulation
processes: Implications for affect, relationships, and well-being. Journal of
Personality and Social Psychology, 85 (2), 348-362.
Gross, J. J., & Muñoz, R. F. (1995). Emotion regulation and mental health. Clinical
Psychology: Science and Practice, 2 (2), 151-164.
Gross, J. J., & Thompson, R. A. (2009). Emotion regulation: Conceptual foundations. In
J. J. Gross (Ed.), Handbook of emotion regulation (pp. 3-24). New York: The
Guilford Press.
Gur, R. E., Kohler, C. G., Ragland, J. D., Siegel, S. J., Lesko, K., Bilker, W. B., & Gur,
R. C. (2006). Flat affect in schizophrenia: Relation to emotion processing and
neurocognitive measures. Schizophrenia Bulletin, 32 (2), 279-287.
Gyurak, A., Goodkind, M. S., Madan, A., Kramer, J. H., Miller, B. L., & Levenson, R.
W. (2009). Do tests of executive functioning predict ability to downregulate

114
emotions spontaneously and when instructed to suppress? Cognitive, Affective &
Behavioral Neuroscience, 9 (2), 144-152.
Habel, U., Koch, K., Kellermann, T., Reske, M., Frommann, N., Wölwer, W., …
Schneider, F. (2010). Training of affect recognition in schizophrenia:
Neurobiological correlates. Social Neuroscience, 5 (1), 92-104.
Heimberg, C., Gur, R. E., Erwin, R. J., Shtasel, D. L., & Gur, R. C. (1992). Facial
emotion discrimination: III. Behavioral findings in schizophrenia. Psychiatry
Research, 42 (3), 253-265.
Hendryx, M., Dyck, D. G., McBride, D., & Whitbeck, J. (2001). A test of the reliability
and validity of the Multnomah Community Ability Scale. Community Mental
Health Journal, 37 (2), 157-168.
Henry, J. D., Green, M. J., de Lucia, A., Restuccia, C., McDonald, S., & O'Donnell, M.
(2007). Emotion dysregulation in schizophrenia: Reduced amplification of
emotional expression is associated with emotional blunting. Schizophrenia
Research, 95, 197-204.
Henry, J. D., Rendell, P. G., Green, M. J., McDonald, S., & O'Donnell, M. (2008).
Emotion regulation in schizophrenia: Affective, social and clinical correlates of
suppression and reappraisal. Journal of Abnormal Psychology, 117 (2), 473-478.
Hodel, B., & Brenner, H. D. (1997). A new development in integrated psychological
therapy for schizophrenic patients (IPT): First results of emotional management
training. In H. D. Brenner, W. Boker, & R. Genner (Eds.), Towards a
comprehensive therapy of schizophrenia (pp. 118-134). Bern, Switzerland:
Hogrefe & Huber Publishing.

115
Hodel, B., & Brenner, H. D. (2002). A training program for coping with maladaptive
emotions: Further development to the Integrated Psychological Therapy for
schizophrenic patients. In M. C. G. Merlo, C. Perris, & H. D. Brenner (Eds.),
Cognitive therapy with schizophrenic patients: The evolution of a new treatment
approach (pp. 125-135). Cambridge, MA: Hogrefe & Huber Publishers.
Hodge, M. A., Siciliano, D., Withey, P., Moss, B., Moore, G., Judd, G., … Harris, A.
(2010). A randomized controlled trial of cognitive remediation in schizophrenia.
Schizophrenia Bulletin, 36 (2), 419-427.
Holt, D. J., Kunkel, L., Weiss, A. P., Goff, D. C., Wright, C. I., Shin, L. M., … Heckers,
S. (2006). Increased medial temporal lobe activation during the passive viewing
of emotional and neutral facial expressions in schizophrenia. Schizophrenia
Research, 82, 153-162.
Hooker, C., & Park, S. (2002). Emotion processing and its relationship to social
functioning in schizophrenia patients. Psychiatry Research, 112, 41-50.
Horan, W. P., Kring, A. M., & Blanchard, J. J. (2006). Anhedonia in schizophrenia: A
review of assessment strategies. Schizophrenia Bulletin, 32 (2), 259-273.
Huang, J., Xu, T., & Chan, R. C. (2011). Do patients with schizophrenia have a general
or specific deficit in the perception of social threat? A meta-analytic study.
Psychiatry Research, 185, 1-8.
Ihnen, G. H., Penn, D. L., Corrigan, P. W., & Martin, J. (1998). Social perception and
social skill in schizophrenia. Schizophrenia Research, 80, 275-286.
Izard, C. E. (1971). The face of emotion. New York: Appleton-Century-Crofts.
James, W. (1884). What is an emotion? Mind, 9 (34), 188-205.

116
James, W. (1890). The principles of psychology. New York: Holt.
John, O. P., & Gross, J. J. (2004). Healthy and unhealthy emotion regulation: Personality
processes, individual differences, and life span development. Journal of
Personality, 72 (6), 1301-1334.
John, O. P., & Gross, J. J. (2009). Individual differences in emotion regulation. In J. J.
Gross (Ed.), Handbook of emotion regulation (pp. 351-372). New York: The
Guilford Press.
Johnston, P. J., Katsikitis, M., & Carr, V. J. (2001). A generalised deficit can account for
problems in facial emotion recognition in schizophrenia. Biological Psychology,
58, 203-227.
Kee, K. S., Green, M. F., Mintz, J., & Brekke, J. S. (2003). Is emotional processing a
predictor of functional outcome in schizophrenia? Schizophrenia Bulletin, 29 (3),
487-497.
Kern, R. S., Wallace, C. J., Hellman, S. G., Womack, L. M., & Green, M. F. (1996). A
training procedure for remediating WCST deficits in chronic psychotic patients:
An adaptation of errorless learning principles. Journal of Psychiatric Research,
30 (4), 283-294.
Kerr, S. L., & Neale, J. M. (1993). Emotion perception in schizophrenia: Specific deficit
or further evidence of generalized poor performance? Journal of Abnormal
Psychology, 102 (2), 312-318.
Kim, J., Doop, M. L., Blake, R., & Park, S. (2005). Impaired visual recognition of
biological motion in schizophrenia. Schizophrenia Research, 77, 299-307.

117
Kirkpatrick, B., Fenton, W. S., Carpenter, J. W., & Marder, S. R. (2006). The NIMH-
MATRICS consensus statement on negative symptoms. Schizophrenia Bulletin,
32 (2), 214-219.
Kleinginna, P. R., Jr., & Kleinginna, A. M. (1981). A categorized list of emotion
definitions, with suggestions for a consensual definition. Motivation and Emotion,
5 (4), 345-379.
Kleinlein, P. (2010). Social Cognition and Interaction Training (SCIT) for individuals
with schizophrenia spectrum disorders in outpatient treatment settings
(Unpublished doctoral dissertation). University of Nebraska, Lincoln, NE.
Kohler, C. G., Turner, T. H., Bilker, W. B., Brensinger, C. M., Siegel, S. J., Kanes, S. J.,
… Gur, R. C. (2003). Facial emotion recognition in schizophrenia: Intensity
effects and error pattern. American Journal of Psychiatry, 160 (10), 1768-1774.
Kosaka, H., Omori, M., Murata, T., Iidaka, T., Yamada, H., Okada, T., … Wada, Y.
(2002). Differential amygdala response during facial recognition in patients with
schizophrenia: An fMRI study. Schizophrenia Research, 57, 57-95.
Kosmidis, M. H., Bozikas, V. P., Giannakou, M., Anezoulaki, D., Fantie, B. D., &
Karavatos, A. (2007). Impaired emotion perception in schizophrenia: A
differential deficit. Psychiatry Research, 149, 279-284.
Kraepelin, E. (1919). Dementia praecox and paraphrenia. (R. M. Barclay, Trans.)
Chicago: Chicago Medical Book Co.
Kring, A. M., & Neale, J. M. (1996). Do schizophrenic patients show a disjunctive
relationship among expressive, experiential, and psychophysiological components
of emotion? Journal of Abnormal Psychology, 105 (2), 249-257.

118
Kring, A. M., & Werner, K. H. (2004). Emotion regulation and psychopathology. In P.
Philippot, & R. S. Feldman (Eds.), The regulation of emotion (pp. 359-385).
Mahwah, NJ: Lawrence Erlbaum Associates Publishers.
Kring, A. M., Kerr, S. L., & Earnst, K. S. (1999). Schizophrenic patients show facial
reactions to emotional facial expressions. Psychophysiology, 36, 186-192.
LeDoux, J. E. (2000). Emotion circuits in the brain. Annual Review of Neuroscience, 23,
155-184.
Lincoln, T. M., Lange, J., Burau, J., Exner, C., & Moritz, S. (2010). The effect of state
anxiety on paranoid ideation and jumping to conclusions: An experimental
investigation. Schizophrenia Bulletin, 36 (6), 1140-1148.
Linehan, M. (1993). Cognitive-behavioral treatment of borderline personality disorder.
New York: Guilford Press.
Lipkovich, I. A., Deberdt, W., Csernansky, J. G., Sabbe, B., Keefe, R. S. E., & Kollack-
Walker, S. (2009). Relationships among neurocognition, symptoms and
functioning in patients with schizophrenia: a path-analytic approach for
associations at baseline and following 24 weeks of antipsychotic drug therapy.
BMC Psychiatry, 9(44). doi:10.1186/1471-244X-9-44
Livingstone, K., Harper, S., & Gillanders, D. (2009). An exploration of emotion
regulation in psychosis. Clinical Psychology and Psychotherapy, 16, 418-430.
Long, J.D., & Brekke, J. S. (1999). Longitudinal factor structure of the Brief Psychiatric
Rating Scale in schizophrenia. Psychological Assessment, 11(4), 498-506.

119
Lysaker, P. H., & Salyers, M. P. (2007). Anxiety symptoms in schizophrenia spectrum
disorders: Assocations with social function, positive and negative symptoms,
hope and trauma history. Acta Psychiatrica Scandinavica, 116, 290-298.
Mandal, M. K., & Palchoudhury, S. (1985). Decoding of facial affect in schizophrenia.
Psychological Reports, 56, 651-652.
Mandal, M. K., Pandey, R., & Prasad, A. B. (1998). Facial expressions of emotions and
schizophrenia: A review. Schizophrenia Bulletin, 24 (3), 399-412.
Martin, C. C., Borod, J. C., Alpert, M., Brozgold, A., & Welkowitz, J. (1990).
Spontaneous expression of facial emotion in schizophrenic and right brain
damaged patients. Journal of Communication Disorder, 23, 287-301.
Mathews, J. R., & Barch, D. M. (2010). Emotion responsivity, social cognition, and
functional outcome in schizophrenia. Journal of Abnormal Psychology, 119 (1),
50-59.
Mazza, M., Lucci, G., Pacitti, F., Pino, M. C., Mariano, M., Casacchia, M., & Roncone,
R. (2010). Could schizophrenic subjects improve their social cognition abilities
only with observation and imitation of social situations? Neuropsychological
Rehabilitation, 20 (5), 675-703.
McDonald, A. J. (1998). Cortical pathways to the mammalian amygdala. Progress in
Neurobiology, 55 (3), 257-332.
Modinos, G., Ormel, J., & Aleman, A. (2010). Altered activation and functional
connectivity of neural systems supporting cognitive control of emotion in
psychosis proneness. Schizophrenia Research, 118, 88-97.

120
Morris, W. N., & Reilly, N. P. (1987). Toward the self-regulation of mood: Theory and
research. Motivation and Emotion, 11 (3), 215-249.
Mueser, K. T., Curran, P. J., & McHugo, G. J. (1997). Factor structure of the Brief
Psychiatric Rating Scale in schizophrenia. Psychological Assessment, 9(3), 196-
204.
Mueser, K. T., Doonan, R., Penn, D. L., Blanchard, J. J., Bellack, A. S., Nishith, P., &
DeLeon, J. (1996). Emotion recognition and social competence in chronic
schizophrenia. Journal of Abnormal Psychology, 105 (2), 271-275.
Muzekari, L. H., & Bates, M. E. (1977). Judgment of emotion among chronic
schizophrenics. Journal of Clinical Psychology, 32, 662-666.
Myin-Germeys, I., Delespaul, P., & Van Os, J. (2005). Behavioural sensitization to daily
life stress in psychosis. Psychological Medicine, 35, 733-741.
Novic, J., Daniel, L., & Perline, R. (1984). Facial affect recognition in schiozphrenia: Is
there a differential deficit? British Journal of Psychiatry, 144, 533-537.
Ochsner, K. N., & Gross, J. J. (2005). The cognitive control of emotion. Trends in
Cognitive Sciences, 9 (5), 242-249.
Ochsner, K. N., & Gross, J. J. (2009). The neural architecture of emotion regulation. In J.
J. Gross (Ed.), Handbook of emotion regulation (pp. 87-109). New York: The
Guilford Press.
Ochsner, K. N., Ray, R. D., Cooper, J. C., Robertson, E. R., Chopra, S., Gabrieli, J. D. E.,
& Gross, J. J. (2004). For better or for worse: Neural systems supporting the
cognitive down- and up-regulation of negative emotion. NeuroImage, 23, 483-
499.

121
Penn, D. L., & Combs, D. (2000). Modification of affect perception deficits in
schizophrenia. Schizophrenia Research, 46, 217-229.
Penn, D. L., Roberts, D. L., Combs, D., & Sterne, A. (2007). The development of the
Social Cognition and Interaction Training program for schizophrenia spectrum
disorders. Psychiatric Services, 58 (4), 449-451.
Penn, D. L., Sanna, L. J., & Roberts, D. L. (2008). Social cognition in schizophrenia: An
overview. Schizophrenia Bulletin, 34 (3), 408-411.
Penn, D. L., van der Does, A. W., Spaulding, W. D., Garbin, C. P., Linszen, D., &
Dingemans, P. (1993). Information processing and social cognitive problem
solving in schizophrenia: Assessment of interrelationships and changes over time.
Journal of Nervous and Mental Disease, 181 (1), 13-20.
Periáñez, J. A., Ríos-Lago, M., Rodríguez-Sánchez, J. M., Androver-Roig, D., Sánchez-
Cubillo, I., Crespo-Facorro, B., … Barceló, F. (2007). Trail Making Test in
traumatic brain injury, schizophrenia, and normal ageing: Sample comparisons
and normative data. Archives of Clinical Neuropscyhology, 22(4), 433-447.
Phillips, L. K., & Seidman, L. J. (2008). Emotion processing in persons at risk for
schizophrenia. Schizophrenia Bulletin, 34 (5), 888-903.
Pinkham, A. E., & Penn, D. L. (2006). Neurocognitive and social cognitive predictors of
interpersonal skill in schizophrenia. Psychiatry Research, 143, 167-178.
Pomarol-Clotet, E., Hynes, F., Ashwin, C., Bullmore, E. T., McKenna, P. J., & Laws, K.
R. (2010). Facial emotion processing in schizophrenia: A non-specific
neuropsychological deficit? Psychological Medicine, 40, 911-919.

122
Poole, J. H., Tobias, F. C., & Vinogradov, S. (2000). The functional relevance of affect
recognition errors in schizophrenia. Journal of the International
Neuropsychological Society, 6, 649-658.
Prouteau, A., Verdoux, H., Briand, C., Lesage, A., Lalonde, P., Nicole, L., … Stip, E.
(2004). The cruicial role of sustained attention in community functioning in
outpatients with schizophrenia. Psychiatry Research, 129, 171-177.
Purdon, C. (1999). Thought suppression and psychopathology. Behaviour Research and
Therapy, 37, 1029-1054.
Raine, A. (2006). Schizotypal peresonality: Neurodevelopmental and psychosocial
tranectories. Annual Review of Clinical Psychology, 2, 291-326.
Reeder, C., Newton, E., Frangou, S., & Wykes, T. (2004). Which executive skills should
we target to affect social functioning and symptom change? A study of cognitive
remediation therapy program. Schizophrenia Bulletin, 30 (1), 87-100.
Reitan, R. M. & Davidson, L. A. (1974). Clinical neuropsychology: Current status and
applications. Washington: V. H. Winston & Sons.
Reske, M., Kellermann, T., Habel, U., Shah, N. J., Backes, V., von Wilmsdorff, M., …
Schneider, F. (2007). Stability of emotional dysfunctions? A long-term fMRI
study in first-episode schizophrenia. Journal of Psychiatric Research, 41, 918-
927.
Richards, J. M., & Gross, J. J. (2000). Emotion regulation and memory: The cognitive
costs of keeping one's cool. Personality Processes and Individual Differences, 79
(3), 410-424.

123
Richards, J. M., & Gross, J. J. (2006). Personality and emotional memory: How
regulating emotion impairs memory for emotional events. Journal of Research in
Personality, 40, 631-651.
Roberts, D. L., & Penn, D. L. (2009). Social cognition and interaction training (SCIT) for
outpatients with schizophrenia: A preliminary study. Psychiatry Research, 166 (2-
3), 141-147.
Roder, V., Mueller, D. R., Brenner, H. D., & Spaulding, W. D. (2010). Integrated
Psychological Therapy (IPT). Bern: Hogrefe Publishing.
Roder, V., Mueller, D. R., Mueser, K. T., & Brenner, H. D. (2006). Integrated
psychological therapy (IPT) for schizophrenia: Is it effective? Schizophrenia
Bulletin, 32 (Suppl 1), S81-S93.
Russell, T. A., Chu, E., & Phillips, M. L. (2006). A pilot study to investigate the
effectiveness of emotion recognition remediation in schizophrenia using the
micro-expression training tool. British Journal of Clinical Psychology, 45, 579-
583.
Sachs, G., Steger-Wuchse, D., Kryspin-Exner, I., Gur, R. C., & Katschnig, H. (2004).
Facial recognition deficits and cognition in schizophrenia. Schizophrenia
Research, 68, 27-35.
Salem, J. E., Kring, A. M., & Kerr, S. L. (1996). More evidence for generalized poor
performance in facial emotion perception in schizophrenia. Journal of Abnormal
Psychology, 105, 480-483.
Salters-Pedneault, K., Steenkamp, M., & Litz, B. T. (2010). Suppression. In A. M. Kring,
& D. M. Sloan (Eds.), Emotion regulation and psychopathology: A

124
transdiagnostic approach to etiology and treatment (pp. 137-156). New York:
The Guilford Press.
Schachter, S., & Singer, J. E. (1962). Cognitive, social, and physiological determinants of
emotional state. Psychological Review, 69, 379-399.
Schneider, F., Gur, R. C., Gur, R. E., & Shtasel, D. L. (1995). Emotional processing in
schizophrenia: Neurobehavioral probes in relation to psychopathology.
Schizophrenia Research, 17, 67-75.
Schwartz, B. L., Mastropaolo, J., Rosse, R. B., Mathis, G., & Deutsch, S. I. (2006).
Imitation of facial expressions in schizophrenia. Psychiatry Research, 145, 87-94.
Scott, D. J., Heltzeg, M. M., Koeppe, R. A., Stohler, C. S., & Zubetla, J. K. (2006).
Variations in the human pain stress experience mediated by ventral and dorsal
basal ganglia dopamine activity. The Journal of Neuroscience, 26 (42), 10789-
10795.
Shaw, R. J., Dong, M., Lim, K. O., Faustman, W. O., Pouget, E. R., & Alpert, M. (1999).
The relationship between affect expression and affect recognition in
schizophrenia. Schizophrenia Research, 37 (3), 245-250.
Silver, H., & Shlomo, N. (2001). Perception of facial emotions in chronic schizophrenia
does not correlate with negative symptoms but correlates with cognitive and
motor dysfunction. Schizophrenia Research, 52, 265-273.
Silver, H., Bilker, W., & Goodman, C. (2009). Impaired recognition of happy, sad and
neutral expressions in schizophrenia is emotion, but not valence, specific and
context dependent. Psychiatry Research, 169, 101-106.

125
Silver, H., Shlomo, N., Turner, T., & Gur, R. C. (2002). Perception of happy and sad
facial expressions in chronic schizophrenia: Evidence for two evaluative systems.
Schizophrenia Research, 55, 171-177.
Solomon, R. C. (2010). The philosophy of emotions. In M. Lewis, J. M. Haviland-Jones,
& L. F. Barrett (Eds.), Handbook of emotions (3rd ed., pp. 3-16). New York: The
Guilford Press.
Spaulding, W. D., & Poland, J. S. (2001). Cognitive rehabilitation for schizophrenia:
Enhancing social cognition by strengthening neurocognitive functioning. In P. W.
Corrigan, & D. L. Penn (Eds.), Social cognition and schizophrenia (pp. 217-248).
Washington, DC: American Psychological Association.
Spaulding, W. D., Reed, D., Sullivan, M., Richardson, C., & Weiler, M. (1999). Effects
of cognitive treatment in psychiatric rehabilitation. Schizophrenia Bulletin, 25 (4),
657-676.
Spaulding, W., Sullivan, M., & Poland, J. (2003). Treatment and rehabilitation for severe
mental illness. New York: Guilford Press.
Stern R. A., & White, T. (2003). Neuropsychological Assessment Battery. Lutz, FL:
Psychological Assessment Resources.
Straube, T., & Miltner, W. H. R. (2011). Attention to aversive emotion and specific
activation of the right insula and right somatosensory cortex. NeuroImage, 54 (3),
2534-2538.
Strauss, E., Sherman, E. M. S., & Spreen, O. (2006). Trail Making Test. In E. Strauss, E.
M. Sherman, & O. Spreen, A compendium of neuropsychological tests:

126
Administration, norms, and commentary (3rd ed., pp. 655-677). New York:
Oxford University Press.
Suslow, T., Roestel, C., Ohrmann, P., & Arolt, V. (2003). The experience of basic
emotions in schizophrenia with and without affective negative symptoms.
Comprehensive Psychiatry, 44 (4), 303-310.
Taylor, S. F., Liberzon, I., Decker, L. R., & Koeppe, R. A. (2002). A functional anatomic
study of emotion in schizophrenia. Schizophrenia Research, 58, 159-172.
Thayer, R. E., Newman, J. R., & McClain, T. M. (1994). Self-regulation of mood:
Strategies for changing a bad mood, raising energy, and reducing tension. Journal
of Personality and Social Psychology, 67 (5), 910-925.
Thompson, R. A. (1994). Emotion regulation: A theme in search of definition.
Monographs of the Society for Research in Child Development, 59 (2/3), 25-52.
Thompson, R. A., & Calkins, S. D. (1996). The double-edged sword: Emotional
regulation for children at-risk. Development and Psychopathology, 8 (1), 163-182.
Trauer, T. (2001). Symptom severity and personal functioning among patients with
schizophrenia discharged from long-term hospital care into the community.
Community Mental Health Journal, 37 (2), 145-155.
Tremeau, F., Malaspina, D., Duval, F., Correa, H., Hager-Budny, M., Coin-Bariou, L., …
Gorman, J. M. (2005). Facial expressiveness in patients with schizophrenia
compared to depressed patients and nonpatient comparison subjects. American
Journal of Psychiatry, 162 (1), 92-101.

127
van den Bosch, R. J., van Asma, M. J. O., Rombouts, R., & Louwerens, J. W. (1992).
Coping style and cognitive dysfunction in schizophrenic patients. British Journal
of Psychiatry, 161 (Suppl. 18), 123-128.
van der Gaag, M., Kern, R. S., van den Bosch, R. J., & Liberman, R. P. (2002). A
controlled trial of cognitive remediation in schizophrenia. Schizophrenia Bulletin,
28 (1), 167-176.
van der Meer, L., van't Wout, M., & Aleman, A. (2009). Emotion regulation strategies in
patients with schizophrenia. Psychiatry Research, 170, 108-113.
van Rijn, S., Aleman, A., & Kahn, R. S. (2005). Neurobiology of emotion and high risk
for schizophrenia: Role of the amygdala and the X-chromosome. Neuroscience &
Biobehavioral Reviews, 29 (3), 385-397.
Van’t Wout, M., Aleman, A., Kessels, R. P., Cahn, W., de Haan, E. H., & Kahn, R. S.
(2007). Exploring the nature of facial affect processing deficits in schizophrenia.
Psychiatry Research, 150 (3), 227-235.
Vaskinn, A., Sunder, K., Friis, S., Simonsen, C., Birkenaes, A. B., Engh, J. A., …
Andreassen, O. A. (2007). The effect of gender on emotion perception in
schizophrenia and bipolar disorder. Acta Psychiatrica Scandinavica, 116, 263-
270.
Ventura, J., Lukoff, D., Nuechterlein, K. H., Liberman, R. P., Green, M. F., & Shaner, A.
(1993). A manual for the expanded Brief Psychiatric Rating Scale. International
Journal of Methods in Psychiatric Research, 3, 227-244.

128
Vorst, H. C., & Bermond, B. (2001). Validity and reliability of the Bermond-Vorst
Alexithymia Questionnaire. Personality and Individual Differences, 30 (3), 413-
434.
Walker, E. F., McGuire, M., & Bettes, B. (1984). Recognition and identification of facial
stimuli by schizophrenics and patients with affective disorders. British Journal of
Clinical Psychology, 23, 37-44.
Wallace, C. J., Nelson, C. J., Liberman, R. P., Aitchison, R. A., Lukoff, D., Elder, J. P., &
Ferris, C. (1980). A review and critique of social skills training with
schizophrenic patients. Schizophrenia Bulletin, 6 (1), 42-63.
Watson, D., & Naragon-Gainey, K. (2010). On the specificity of positive emotional
dysfunction in psychopathology: Evidence from the mood and anxiety disorders
and schizophrenia/schizotypy. Clinical Psychology Review, 30 (7), 839-848.
Wölwer, W., Frommann, N., Halfmann, S., Piaszek, A., Streit, M., & Gaebel, W. (2005).
Remediation of impairments in facial affect recognition in schizophrenia:
Efficacy and specificity of a new training program. Schizophrenia Research, 80,
295-303.
Zani, B., McFarland, B., Wachal, M., Barker, S., & Barron, N. (1999). Statewide
replication of predictive validation for the Multnomah Community Ability Scale.
Community Mental Health Journal, 35 (3), 223-229.
Zimmer, M., Duncan, A. V., Laitano, D., Ferreira, E. E., & Belmonte-de-Abreu, P.
(2007). A twelve-week randomized controlled study of the cognitive-behavioral
Integrated Psychological Therapy program: Positive effect on the social

129
functioning of schizophrenic patients. Revista Brasileira de Psiquiatria, 29 (2),
140-147.
Zuroff, D. C., & Colussy, S. A. (1986). Emotion recognition in schizophrenic and
depressed inpatients. Journal of Clinical Psychology, 48, 411-417.

130
FOOTNOTES
1 It is important to note that some emotion regulation strategies may overlap with
social skills, interpersonal problem solving skills, and so on. Indeed, stress management
curricula often include training in those types of skills in addition to skills more
obviously linked to managing stress and emotions. The distinction between stress
management and emotion regulation is not clearly articulated in the literature. However,
it can be argued that stress management is a broader term, including general lifestyle
management as well as managing emotional reactions to environmental stressors,
whereas emotion regulation refers specifically to strategies intended to change the type,
timing, experience, or expression of emotions. This dissertation focuses on emotion
regulation, as opposed to stress management.
2 Note that neurocognition here refers to neuropsychological processes, or the
poorly understood processes responsible for performance on particular
neuropsychological tasks. In other disciplines of psychology, neurocognition refers more
specifically to molecular cognitive processes and their brain-based mechanisms.

131
APPENDIX

132
Appendix A: Correlation Matrix for
Emotion Regulation by Symptoms, Neurocognition, Social Cognition, and Social Functioning
Symptoms
BPRS
Total -.285 .440**
.471**
.346* .548
** .378
* .398
* .596
** -.206 .144 .255 -.307 -.518
** .143 -.480
** .259 -.078
Neurocognition
Trails
A -.134 -.207 .031 -.084 -.079 .130 .223 -.025 .320* .300 -.130 .194 .037 .003 .163 -.068 .043
B .075 -.389* -.137 -.141 -.315 -.119 -.021 -.282 .095 -.005 -.388
* .291 .371
* -.071 .389
* -.248 .032
NAB
Attention .052 .206 -.002 .027 -.033 .021 -.344* -.016 -.080 -.207 .305 .078 .077 -.066 .095 .155 .194
Lang .256 -.053 -.068 -.178 -.183 -.088 -.438**
-.225 -.016 -.128 .137 -.012 .021 -.112 .001 -.076 -.065
Memory .102 -.083 .029 -.043 -.117 .030 -.212 -.101 .239 -.082 .219 -.148 .036 -.084 -.093 .083 .013
Spt Abil .209 -.184 -.080 -.176 -.171 -.259 -.358* -.271 -.087 -.125 -.103 -.163 .189 -.098 -.031 -.291 -.270
Exe Fnc .072 .296 .089 .064 .029 -.052 -.207 .068 -.214 -.277 .066 -.312* .059 -.015 -.204 .014 -.116
Total .168 .073 .016 -.051 -.093 -.075 -.399* -.111 -.039 -.188 .196 -.168 .085 -.104 -.084 -.016 -.067
Social Cognition
FEIT
Total .286 -.130 -.066 -.123 -.229 -.363* -.318 -.271 -.378
* -.451
** -.141 -.114 .046 -.276 -.063 -.308 -.305
BFRT
Total .331* -.194 -.118 -.166 -.039 -.313 -.345
* -.243 -.036 -.294 .046 -.032 -.031 -.168 -.039 -.128 -.135
RACERS DERS ERQ BVAQ
Tota
l
Nonac
cepta
nce
Goal
s
Aw
aren
ess
Str
ateg
ies
Cla
rity
Impuls
e
Tota
l
Rea
ppra
isal
Suppre
ssio
n
Ver
bal
izin
g
Fan
tasi
zing
Em
oti
onal
izin
g
Anal
yzi
ng
Aff
ecti
ve
Cognit
ive
Tota
l

133
Social Functioning
RACERS DERS ERQ BVAQ T
ota
l
Nonac
cepta
nce
Goal
s
Aw
aren
ess
Str
ateg
ies
Cla
rity
Impuls
e
Tota
l
Rea
ppra
isal
Suppre
ssio
n
Ver
bal
izin
g
Fan
tasi
zing
Em
oti
onal
izin
g
Anal
yzi
ng
Aff
ecti
ve
Cognit
ive
Tota
l
SFS
SocEng .128 -.257 -.354* -.304 -.244 -.412
* -.222 -.389
* .065 -.139 -.287 .082 .232 .076 .171 -.320 -.167
IntCom .121 -.344* -.351
* -.211 -.367
* -.442
** -.260 -.445
** .165 -.005 -.483
** .010 .188 .008 .096 -.437
** -.317
IndepC .119 -.211 -.426**
-.023 -.170 -.062 -.319 -.271 .050 -.167 .179 .196 .212 .160 .246 .074 .224
IndepP .049 -.125 -.383* -.057 -.175 -.037 -.223 -.224 .096 -.258 -.372
* -.049 .160 .021 .039 -.219 -.164
Recreat .173 -.155 -.039 -.198 -.050 -.290 -.054 -.164 .260 -.188 -.445**
-.098 -.046 -.247 -.095 -.327* -.345
*
Prosoc -.037 -.122 .132 -.211 -.050 .093 .122 -.026 .523**
.293 -.107 .117 .141 -.139 .153 -.052 .054
Employ -.186 .300 -.098 .146 .137 -.080 -.069 .108 .306 .045 .092 -.144 .156 .068 -.033 .005 -.017
Total .083 -.241 -.330* -.232 -.207 -.184 -.212 -.313 .492
** -.058 -.323
* .071 .276 -.057 .183 -.259 -.106
MCAS
Health .146 -.105 -.133 .002 -.085 -.195 -.254 -.164 .152 -.157 -.021 .206 .500**
.060 .396* .074 .312
*
Adapt .229 -.037 -.088 -.221 -.339* -.237 -.285 -.277 -.022 -.295 -.102 .012 .309
* -.132 .158 -.131 -.014
SocSk -.211 -.029 -.158 -.317 -.154 -.033 -.044 -.164 .385* .175 -.251 -.044 .379
* .111 .151 -.030 .068
Behavior .276 -.294 -.077 -.233 -.316 -.301 -.198 -.332* .150 -.266 -.188 .223 .432
** -.081 .376
* -.077 .169
Total .076 -.125 -.162 -.271 -.276 -.220 -.235 -.291 .258 -.119 -.193 .114 .539**
.013 .346* -.042 .180
MCAS-Self Report
Health .261 -.393* -.420
** -.120 -.452
** -.295 -.422
** -.489
** .121 -.038 -.286 .026 .291 -.025 .157 -.315 -.172
Adapt .416**
-.216 -.179 -.138 -.182 -.100 -.357* -.267 .085 -.148 -.190 .069 .045 -.171 .073 -.283 -.199
SocSk .205 -.602**
-.298 -.345* -.437
** -.309 -.336
* -.547
** .286 .001 -.531
** .170 .117 .024 .182 -.272 -.118
Behavior .330* -.430
** -.220 -.456
** -.432
** -.284 -.533
** -.542
** .149 .004 -.213 .201 .094 -.117 .194 -.290 -.126
Total .380* -.586
** -.408
* -.337
* -.529
** -.352
* -.536
** -.639
** .234 -.053 -.456
** .147 .211 -.068 .209 -.392
* -.205
Note: Bold values are p < .05. ** Correlation is significant at the 0.01 level.
* Correlation is significant at the 0.05 level.
Spt Abil = Spatial Ability; Exe Fnc = Executive Functions; SocEng = Social Engagement; IntCom = Interpersonal Communication; IndepC = Independence – Competence; IndepP = Independence – Performance; Recreat = Recreation; Prosoc = Prosocial Behavior; Employ = Employment; Adapt = Adaptation; SocSk = Social Skills

134
Appendix B: Correlation Matrix for Neurocognition by Symptoms, Social Cognition, and Social Functioning
Trails NAB-Screener
A B Attention Language Memory Spatial Ability Exec Functions Total
Symptoms
BPRS
Total .037 -.313 .012 -.076 -.058 -.224 -.060 -.109
Social Cognition
FEIT
Total -.167 .021 .154 .307 -.026 .421** .171 .308
BFRT
Total -.256 -.214 .277 .263 .019 .391* .210 .328
*
Social Functioning
SFS
Social Engagement .120 .262 -.216 -.019 .136 .299 -.101 .019
Interpersonal Communication .137 .210 -.322* -.302 -.036 .305 -.153 -.148
Independence – Competence -.124 -.151 .213 .106 .034 -.002 .058 .114
Independence - Performance -.240 -.027 -.036 -.121 .015 .057 .255 .016
Recreation .210 .187 -.312 -.393* -.218 -.279 -.123 -.375
*
Prosocial Behavior .624** .377
* -.328* -.293 .019 -.217 -.239 -.299
Employment -.048 -.332 .145 -.147 -.086 -.083 .293 .014
Total .287 .218 -.236 -.336* -.036 -.121 -.024 -.231
MCAS
Health -.235 -.142 .196 .017 -.182 .265 .244 .139
Adaptation -.086 -.076 .200 .180 .145 .084 .333* .224
Social Skills .102 .216 -.005 -.041 -.077 .097 .092 .011
Behavior -.089 -.107 .007 -.229 -.251 .163 .203 -.054
Total -.085 -.013 .124 -.021 -.123 .201 .270 .102

135
Trails NAB-Screener
A B Attention Language Memory Spatial Ability Exec Functions Total
MCAS-SR
Health .000 .172 -.015 .021 .200 .302 -.038 .113
Adaptation -.347* -.198 .196 .131 .121 .207 .318 .278
Social Skills .147 .287 -.214 -.228 -.037 .104 -.152 -.158
Behavior .122 -.003 .069 .202 .218 .404* .014 .223
Total .003 .151 -.039 -.019 .146 .314 -.002 .094 Note: Bold values are p < .05.
** Correlation is significant at the 0.01 level.
* Correlation is significant at the 0.05 level.
Exec Functions = Executive Functions

136
Appendix C: Correlation Matrix for
Symptoms and Social Cognition by Social Functioning
Symptoms Social Cognition
BPRS FEIT BFRT
Social Functioning Measure
SFS
Social Engagement -.420**
.021 -.060
Interpersonal Communication -.368* -.065 .162
Independence – Competence -.294 -.204 -.066 Independence - Performance -.110 -.212 .133
Recreation -.188 -.485**
-.144
Prosocial Behavior -.391* -.071 .150
Employment -.107 -.272 .061
Total -.491**
-.475**
.010
MCAS Health -.503
** .140 .135
Adaptation -.043 .195 -.106
Social Skills -.267 .164 .002
Behavior -.434**
.217 .009 Total -.425
** .230 .022
MCAS-SR
Health -.363* -.008 .005
Adaptation -.201 .111 .204
Social Skills -.512**
-.309 .061
Behavior -.168 .028 .026
Total -.475**
-.109 .087 Note: Bold values are p < .05.
** Correlation is significant at the 0.01 level.
* Correlation is significant at the 0.05 level.
Related Documents