Chiaki Nakaseko, MD, PhD Department of Hematology Chiba University Hospital Pathophysiology and Management of Peripheral Neuropathy in Multiple Myeloma and Other Plasma Cell Dyscasias The 40th Annual Meeting of the Japanese Society of Myeloma Kumamoto, May 16, 2015

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Chiaki Nakaseko, MD, PhD
Department of HematologyChiba University Hospital
Pathophysiology and Management of
Peripheral Neuropathy in Multiple Myeloma
and Other Plasma Cell Dyscasias
The 40th Annual Meeting of the Japanese Society of Myeloma Kumamoto, May 16, 2015
Paraproteinemic Neuropathies and Neurological Problems in Plasma Cell Dyscrasias
Peripheral neuropathy (PN) is one of the most
important complications of multiple myeloma and other
plasma cell dyscrasias.
PN can be caused by the disease itself, either by the
effects of the monoclonal protein or in the form of
radiculopathy from direct compression,
and particularly by certain therapies, including
bortezomib and thalidomide.
PN significantly affects patients’ QoL and treatment.
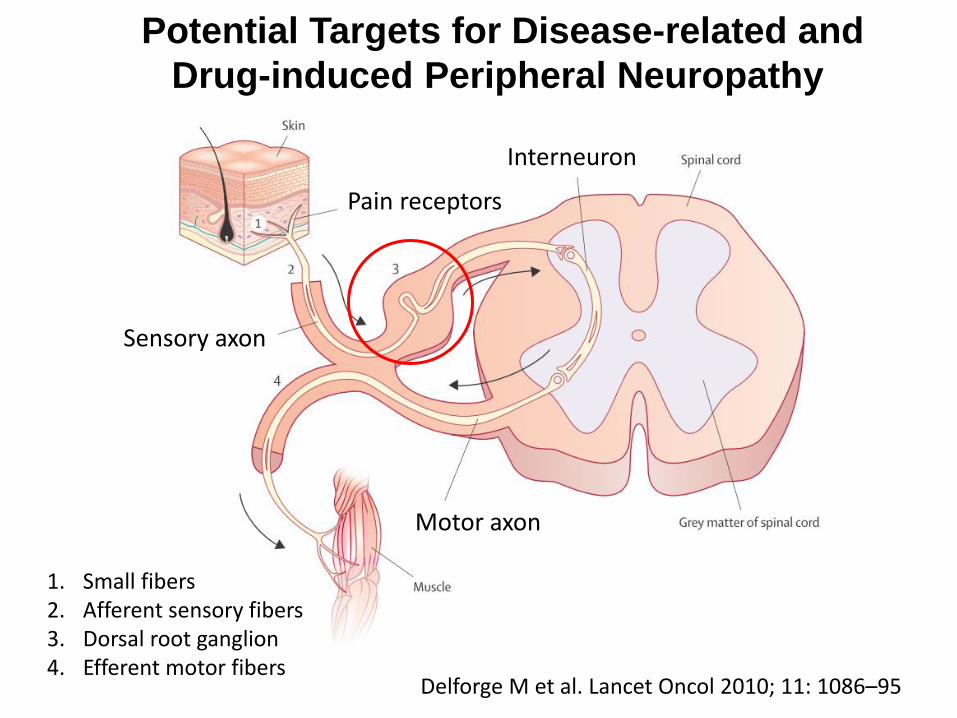
Potential Targets for Disease-related and
Drug-induced Peripheral Neuropathy
Delforge M et al. Lancet Oncol 2010; 11: 1086–95
1. Small fibers2. Afferent sensory fibers3. Dorsal root ganglion4. Efferent motor fibers
Sensory axon
Motor axon
Pain receptors
Interneuron

Demyelination and Axonal Degeneration in Peripheral Neuropathy
MGUS-related Neuropathy
Approximately 10% of patients with cryptogenic
polyneuropathy are secondary to a monoclonal
gammopathy.
Although IgG are the most common M-proteins found in
general population, peripheral neuropathies are more
commonly associated with IgM monoclonal gammopathy
(IgM 60%, IgG 30%, IgA 10%).
Half the patients with IgM MGUS-related peripheral
neuropathy have anti-myelin-associated glycoprotein
(MAG) antibodies and also against other cross-reacting
glycoproteins in myelin.
Ropper AH. N Engl J Med 1998;338:1601-7
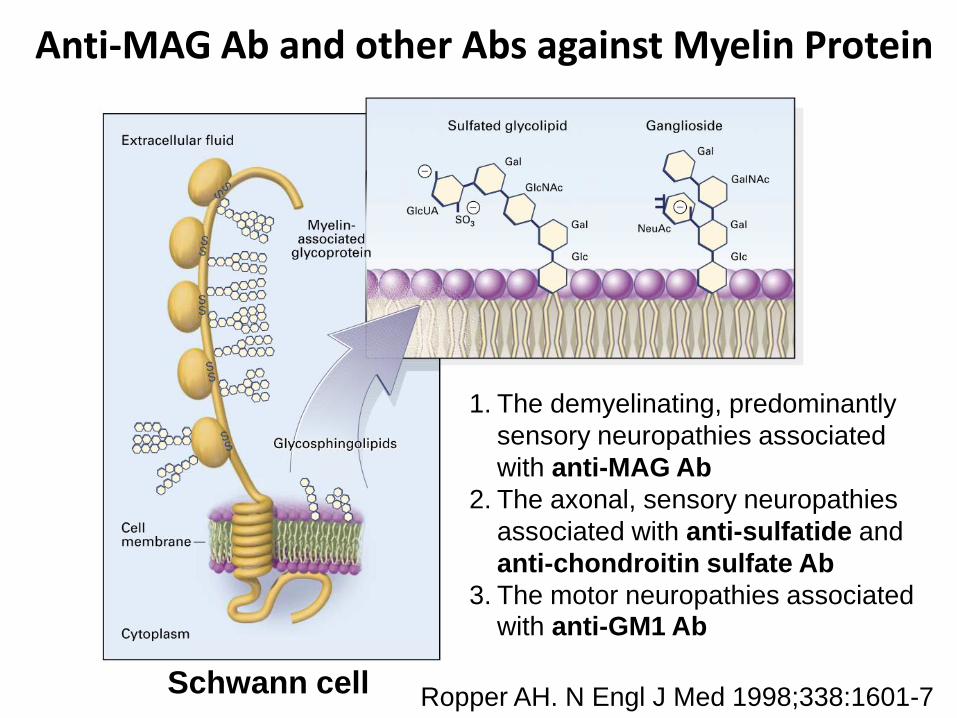
Anti-MAG Ab and other Abs against Myelin Protein
Ropper AH. N Engl J Med 1998;338:1601-7
1. The demyelinating, predominantly
sensory neuropathies associated
with anti-MAG Ab
2. The axonal, sensory neuropathies
associated with anti-sulfatide and
anti-chondroitin sulfate Ab
3. The motor neuropathies associated with anti-GM1 Ab
Schwann cell
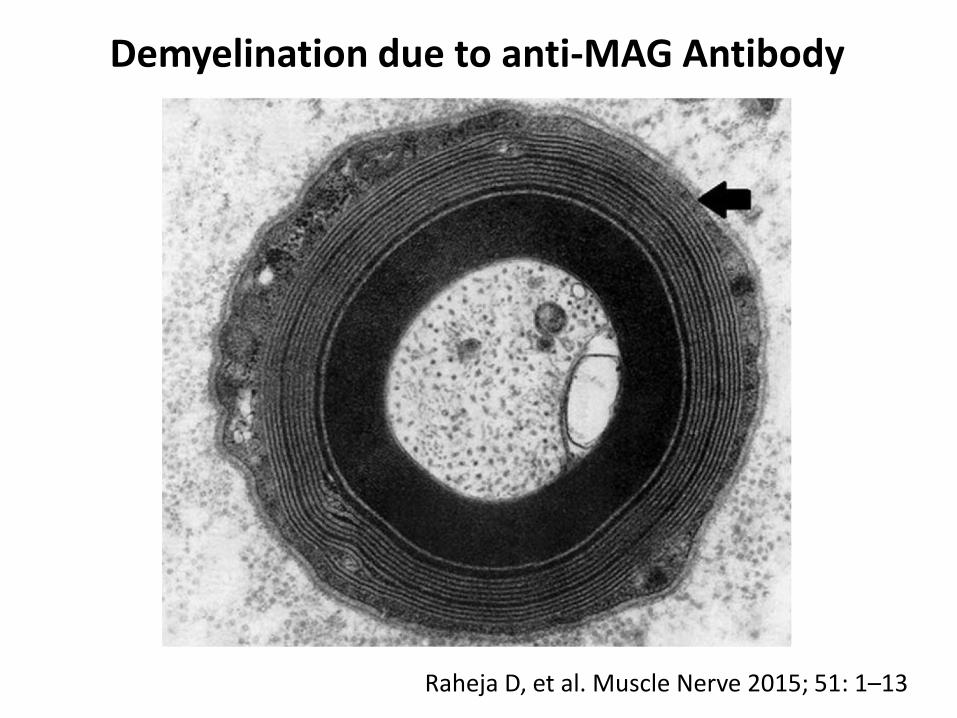
Raheja D, et al. Muscle Nerve 2015; 51: 1–13
Demyelination due to anti-MAG Antibody

Left Median Nerve Electrophysiological Study
MNCV, motor nerve conduction velocity; CB, conduction block; DML, distal motor latency; TLI, terminal latency index
Rajabally YA. Eur J Neurology 2011, 18: 1291–8
A. Anti-MAG Neuropathy B. CIDP associated with IgG MGUS
Conduction block
Wrist
Elbow
Axilla
ERB’s

Placebo-Controlled Trial of Rituximab in IgM anti-MAG Ab Demyelinating Neuropathy
Dakaras MC et al. Ann Neurol 2009;65:286–93
A. IgM B. Anti-MAG AbPlacebo (n=13)
Rituximab (n=13)
Placebo (n=13)
Rituximab (n=13)

Placebo-Controlled Trial of Rituximab in IgM anti-MAG Ab Demyelinating Neuropathy
Dakaras MC et al. Ann Neurol 2009;65:286–93
A. Neuropathy Leg Score B. 10m walk time
Placebo
Rituximab

Paraproteinemia and Neurological Disorder (1)
Clinical Electrodiagnostic Nerve biopsy
IgM MGUS Slowly progressive, distally predominant, and sensory more than motor
Demyelinating.Markedly prolongeddistal motor latencies.Reduced TLI.
IgM, and complementdeposits on myelin.Widening of myelinlamellae
IgG and IgA MGUS
Distally predominantsensorimotor orproximal weaknessas in CIDP
Axonal or acquireddemyelinating(as in CIDP).
Endoneurial Ig deposits.Widening of myelinlamellae. Endoneurialinclusions in IgA.
WM Neuropathy slowlyprogressive, distal,and sensory > motor
Similar to IgM MGUS.Rarely axonal or mixed.
See IgM MGUS
★CIDP: chronic inflammatory demyelinating polyneuropathy
Raheja D, et al. Muscle Nerve 2015; 51: 1–13

Systemic Amyloidosis

Merlini et al. J Clin Oncol 2011; 29:1924-33
Type Abbre-
viation
Precursor Site of
Synthesis
Syndrome and Organ Involved
Immunoglobulin
light chain
amyloidosis
AL Monoclonal
light chain
BM
plasma
cells
・Primary amyloidosis
・10-15% of MM
・Involvement of heart, kidneys, liver,
GI tract, peripheral nerves, autonomic
nerves, soft tissues
Reactive
amyloidosis
AA Serum
amyloid A
Liver ・Secondary to chronic inflammation,
infection, or certain neoplasia
・Involvement of kidneys, GI tract,
spleen, liver, autonomic nerves
Senile systemic
amyloidosis
SSA Transthyretin
wild type
Liver ・Age-related, usually males
・Primarily cardiac involvement
Transthyretin
amyloidosis
ATTR Variant
transthyretin
Liver ・Hereditary
・Involvement of peripheral nerves,
autonomic nerves, heart, eye,
leptomeninges, rarely kidneys
Most Common Types of Systemic Amyloidoses
★To date, at least 28 different proteins have been identified as
causative agents of amyloid diseases

Clinical manifestations at diagnosis in 202
Japanese Patients with systemic AL amyloidosis
Matsuda M et al. Intern Med 2014; 53: 403-12
(n)

Amyloid Neuropathy
Raheja D, et al. Muscle Nerve 2015; 51: 1–13
Congo red stain Viewed with polarized light
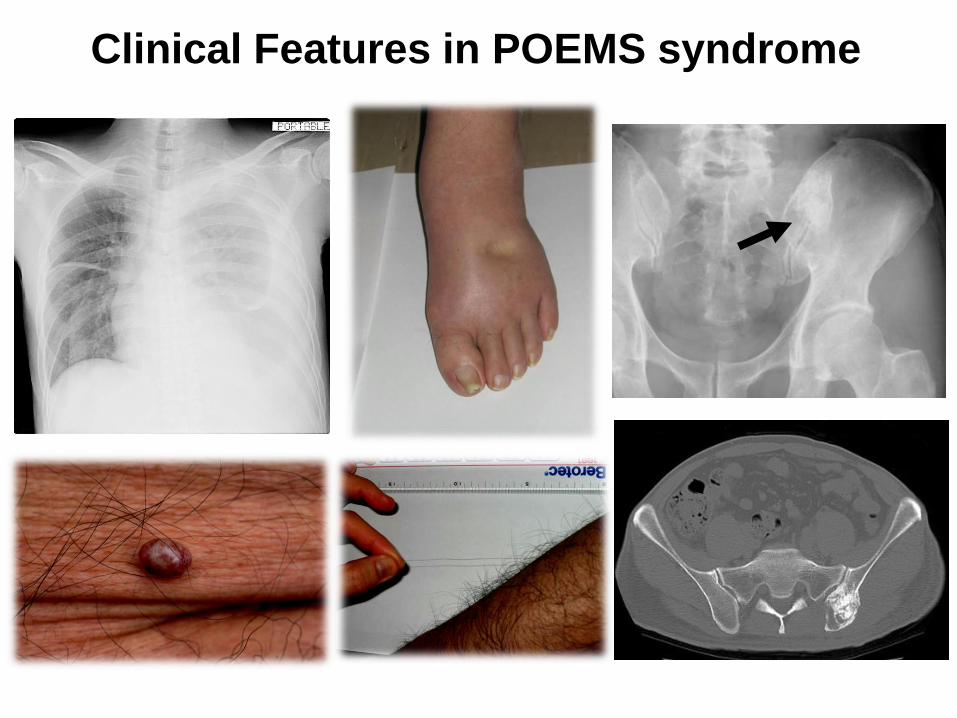
POEMS syndrome
16
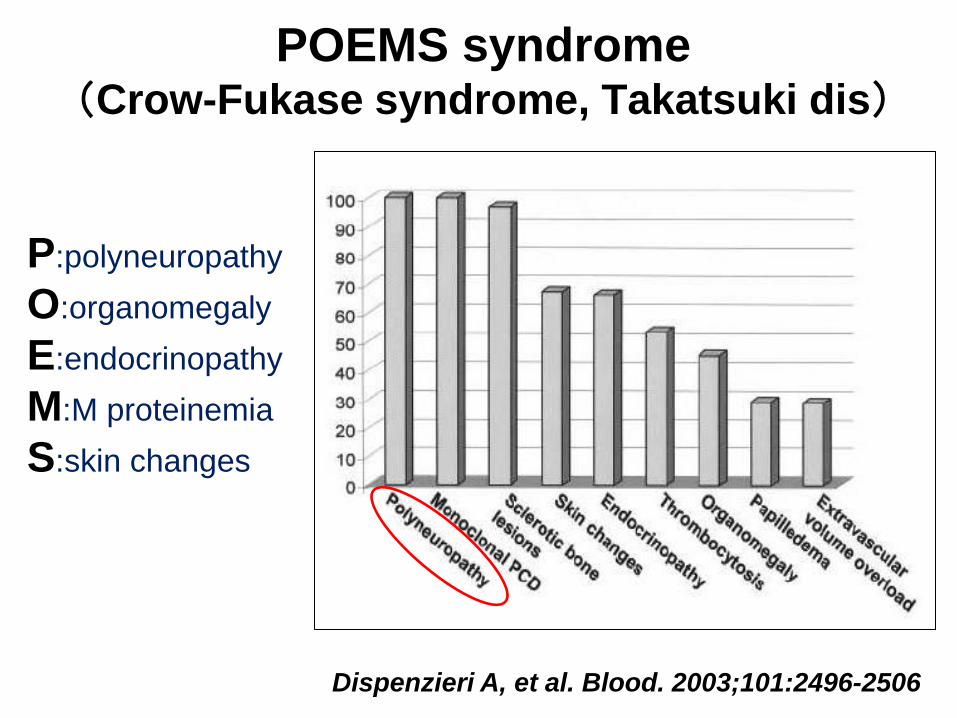
P:polyneuropathy
O:organomegaly
E:endocrinopathy
M:M proteinemia
S:skin changes
Dispenzieri A, et al. Blood. 2003;101:2496-2506
POEMS syndrome (Crow-Fukase syndrome, Takatsuki dis)
18
Clinical Features in POEMS syndrome
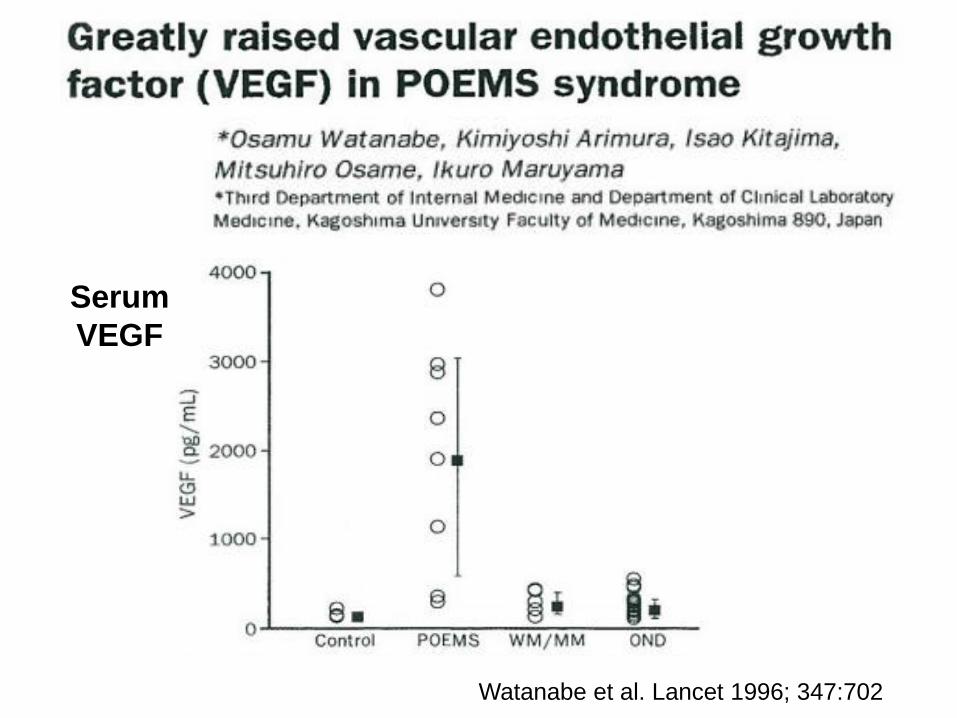
Watanabe et al. Lancet 1996; 347:702
Serum
VEGF
20
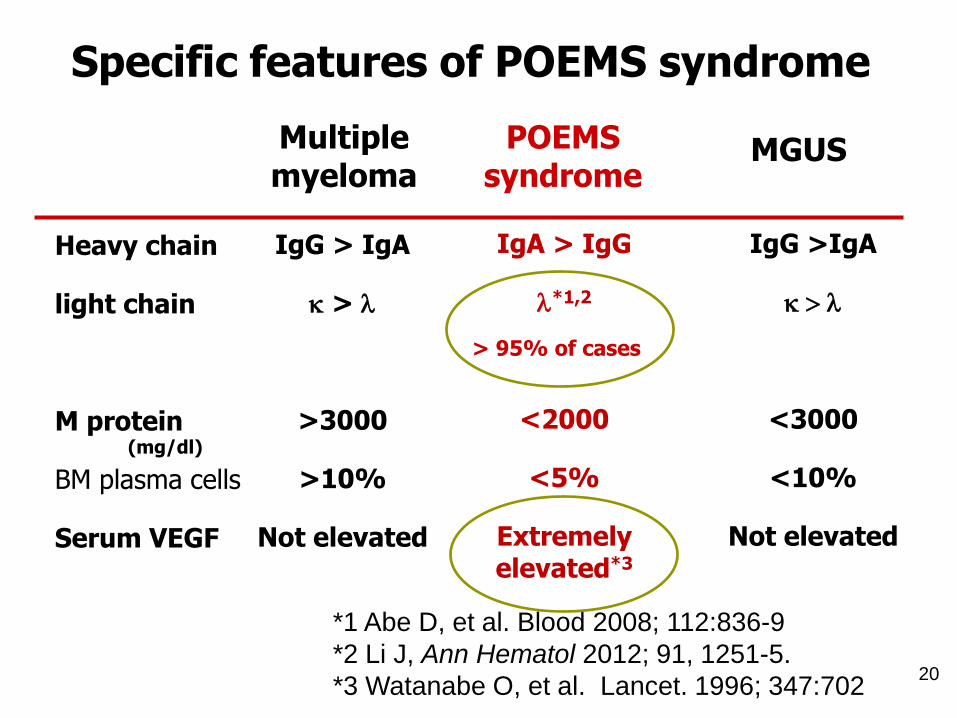
Specific features of POEMS syndrome
Heavy chain
light chain
M protein
BM plasma cells
Serum VEGF
IgA > IgG
l*1,2
<2000
<5%
Extremely elevated*3
IgG > IgA
k > l
>3000
>10%
Not elevated
> 95% of cases
POEMSsyndrome
Multiple myeloma
(mg/dl)
IgG >IgA
k > l
<3000
<10%
Not elevated
MGUS
*1 Abe D, et al. Blood 2008; 112:836-9
*2 Li J, Ann Hematol 2012; 91, 1251-5.
*3 Watanabe O, et al. Lancet. 1996; 347:702

Revised Diagnostic Criteria of POEMS syndrome
Mandatory major criteria
1. Polyneuropathy (typically demyelinating)2. Monoclonal plasma cell-proliferative disorder (almost always λ)
Other major criteria(one required)
3. Castleman disease4. Sclerotic bone lesions5. Vascular endothelial growth factor (VEGF) elevation
Minor criteria 6. Organomegaly (splenomegaly, hepatomegaly, lymphadenopathy)7. Extravascular volume overload (edema, pleural effusion, ascites)8. Endocrinopathy (adrenal, thyroid, pituitary, gonadal, parathyroid, pancreatic)9. Skin changes (hyperpigmentation, hypertrichosis, glomeruloid hemangiomata, plethora, white nails)10. Papilledema11. Thrombocytosis/polycythemia
Other symptoms and signs
Clubbing、weight loss, hyperhidrosis, pulmonary hypertension, restrictive lung disease, thrombotic diathesis, diarrhea, low vitamin B12 values
Dispenzieri A. Ann Hematol 2012: 87:805–14
Severe Peripheral Neuropathy in POEMS Syndrome
Patients initially present with sensory deficits, including paresthesias and coldness, starting distally.
Motor symptoms usually follow, beginning in the distal lower extremities and ascending, and eventually affecting both proximal and distal muscles in a pattern similar to CIDP, leads to greater disability.
Cranial neuropathies are usually absent except for papilledema, and autonomic symptoms are rare.
22
Severe Peripheral Neuropathy in POEMS Syndrome
Electrodiagnostic studies commonly demonstrate both axonal and demyelinating features.
Conduction block, which is common in CIDP, is rare in POEMS.
Nerve biopsies usually reveal features of both axonal degeneration and demyelination. Inflammatory infiltrates may be seen in the epineurium and endoneurium.
In addition to demyelination, nerve edema induced by upregulated VEGF, and upregulated inflammatory cytokines could modulate profiles of POEMS neuropathy.
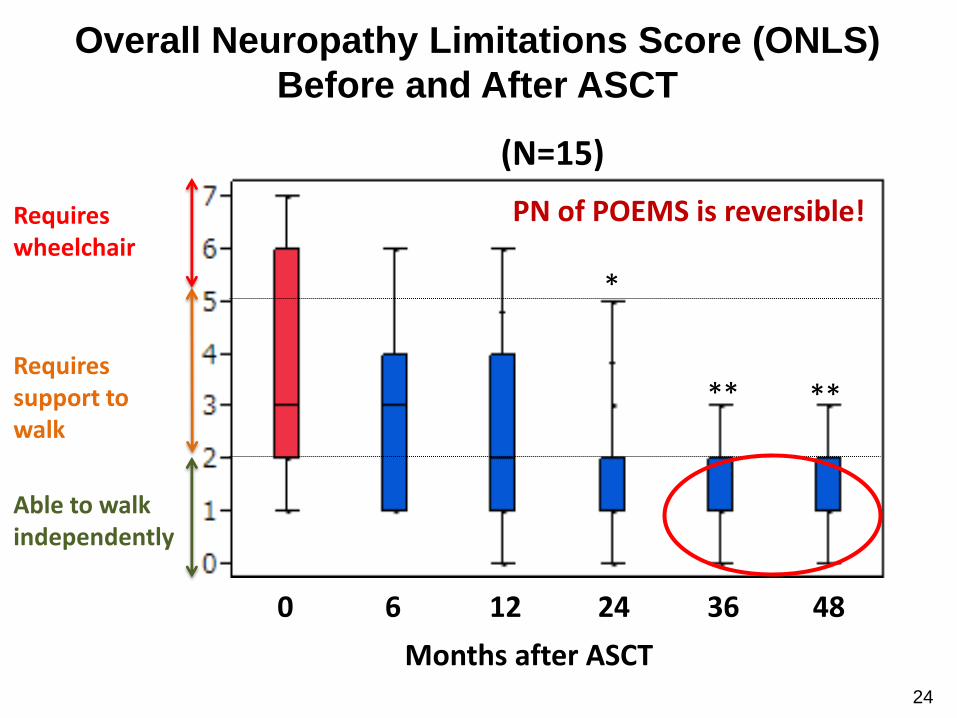
*
** **
Overall Neuropathy Limitations Score (ONLS)
Before and After ASCT
Requires support to walk
Requires wheelchair
Able to walk independently
Months after ASCT
0 12 24 36 486
(N=15)
24
PN of POEMS is reversible!

Arm ONLS score Leg ONLS score
Neurological improvement after ASCTJapanese Society of Stem Cell Transplantation TRUMP Database
*** ***
***
Multiple Myeloma
26
Kosturakis AK, et al. J Clin Oncol 2014; 32:3156-62
27
Kosturakis AK, et al. J Clin Oncol 2014; 32:3156-62
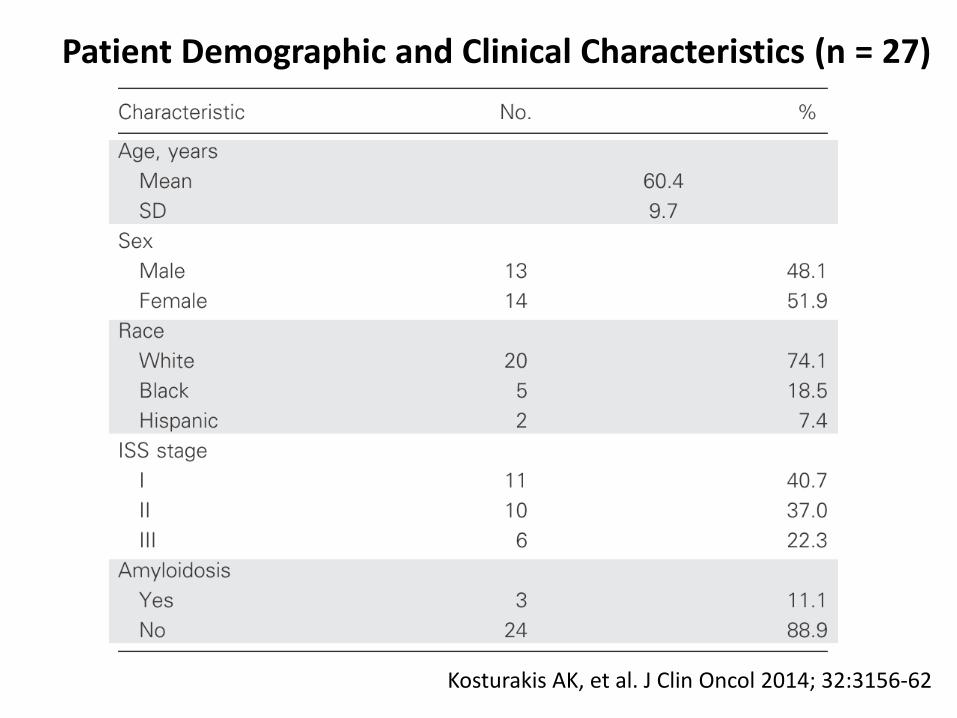
Patient Demographic and Clinical Characteristics (n = 27)

Kosturakis AK, et al. J Clin Oncol 2014; 32:3156-62
Reduced Innervation Density and Sensory Function in Patients With MM
Touch Detection Thresholds Bumps Detection
Kosturakis AK, et al. J Clin Oncol 2014; 32:3156-62
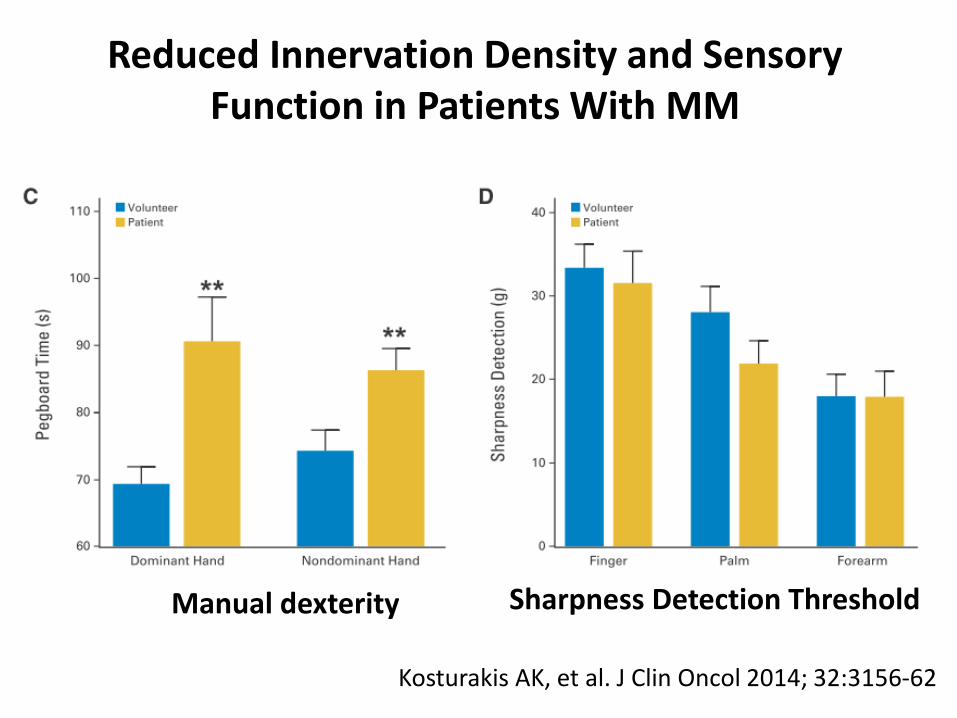
Reduced Innervation Density and Sensory Function in Patients With MM
Manual dexterity Sharpness Detection Threshold
Kosturakis AK, et al. J Clin Oncol 2014; 32:3156-62
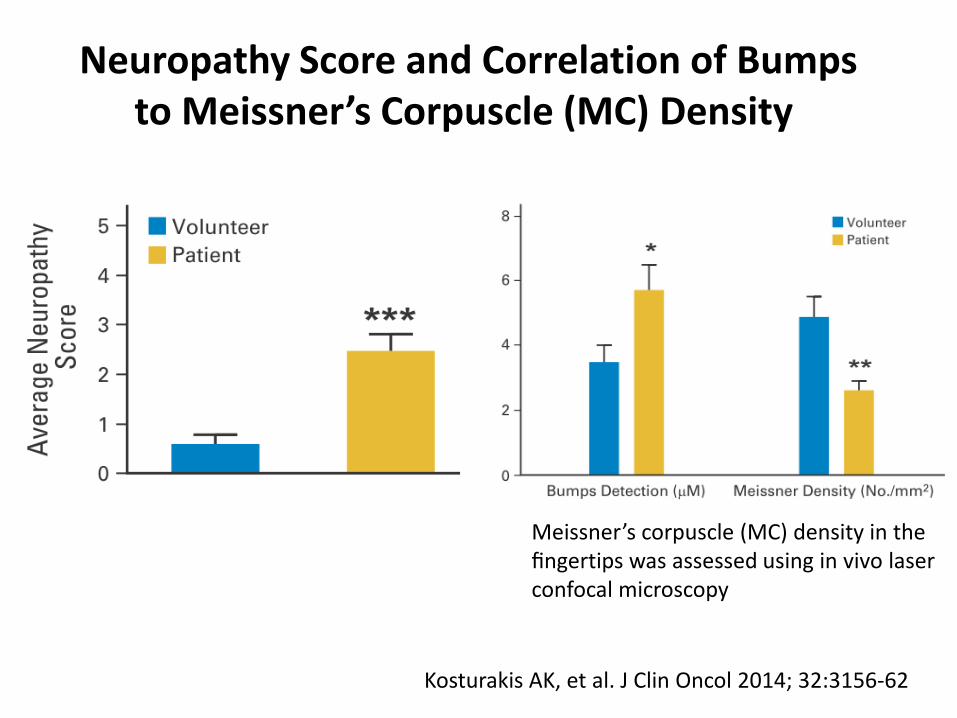
Neuropathy Score and Correlation of Bumps to Meissner’s Corpuscle (MC) Density
Meissner’s corpuscle (MC) density in the fingertips was assessed using in vivo laser confocal microscopy

Paraproteinemia and Neurological Disorder (2)
Clinical Electrodiagnostic Nerve biopsy
PrimaryAmyloidosis
Neuropathy painful andSensorimotorDysautonomia
Axonal sensorimotorneuropathy. Carpal tunnel syndrome.
Amyloid on Congo-red staining. Light chains on immuno-histochemistry.
POEMS Syndrome
Ascending sensorimotorsymptoms. Weaknesseventually predominating
Mixed axonal, demyelinating. No conduction blockor dispersion. Normal TLI.
Axonal degeneration.Loss of myelinatedfibers. Inflammationand uncompactedmyelin lamellae
MultipleMyeloma
Neuropathiesare heterogeneous
Almost always axonal,but very rarelydemyelinating.
Axonal degeneration.May show amyloiddeposits.
Raheja D, et al. Muscle Nerve 2015; 51: 1–13

Therapy-related neuropathy
33
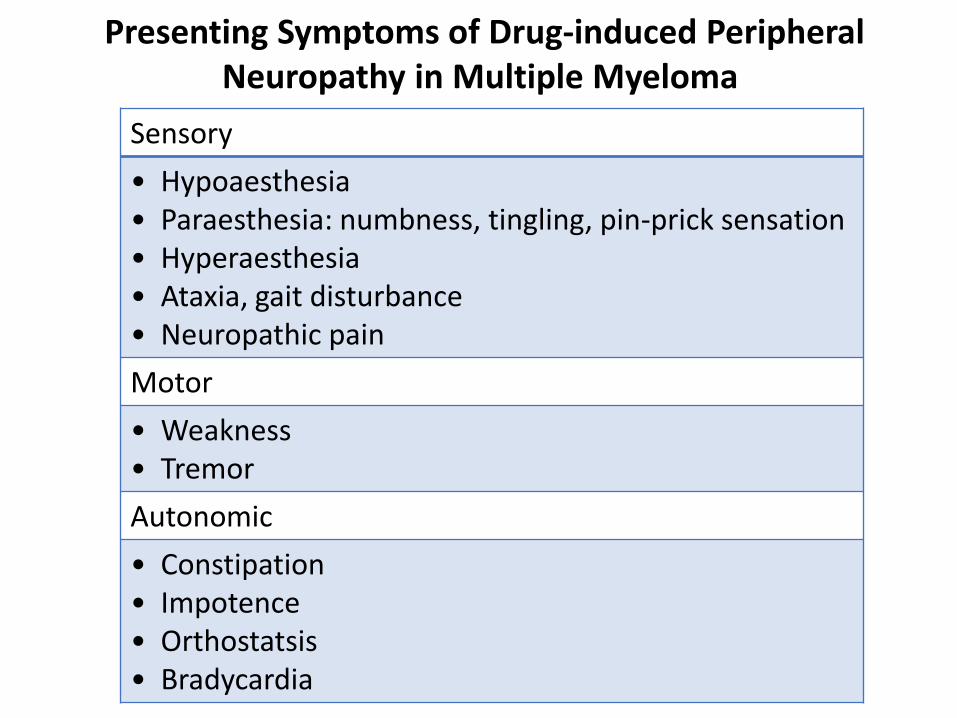
Presenting Symptoms of Drug-induced Peripheral Neuropathy in Multiple Myeloma
Sensory
• Hypoaesthesia• Paraesthesia: numbness, tingling, pin-prick sensation• Hyperaesthesia• Ataxia, gait disturbance• Neuropathic pain
Motor
• Weakness• Tremor
Autonomic
• Constipation• Impotence• Orthostatsis • Bradycardia
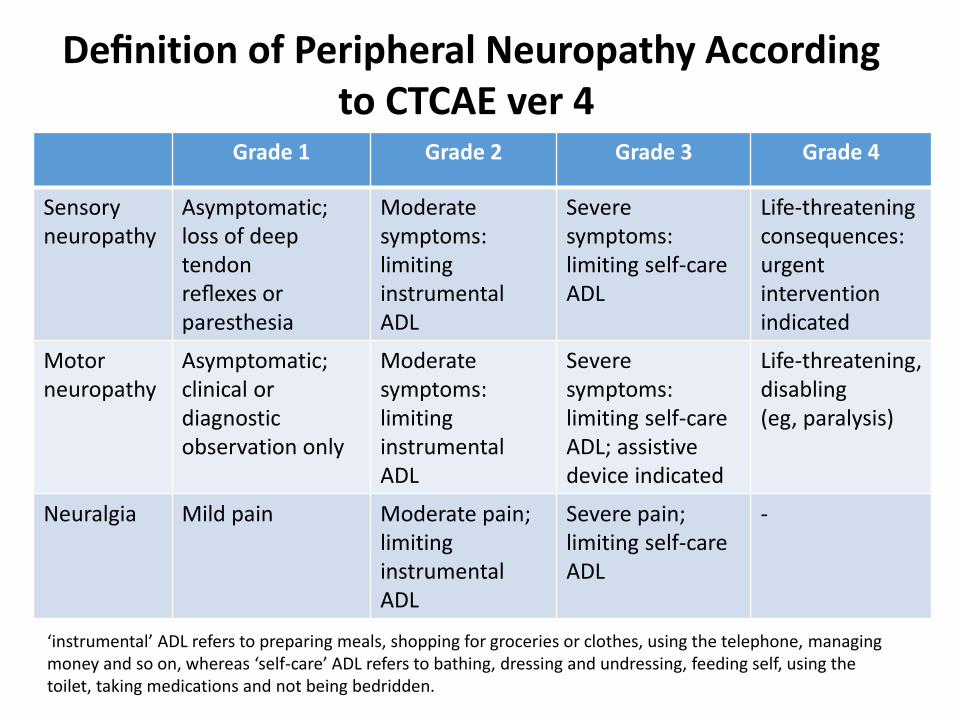
Grade 1 Grade 2 Grade 3 Grade 4
Sensory neuropathy
Asymptomatic; loss of deep tendon reflexes or paresthesia
Moderate symptoms: limitinginstrumental ADL
Severe symptoms: limiting self-care ADL
Life-threateningconsequences: urgent intervention indicated
Motor neuropathy
Asymptomatic; clinical or diagnosticobservation only
Moderate symptoms: limitinginstrumental ADL
Severe symptoms: limiting self-care ADL; assistive device indicated
Life-threatening, disabling (eg, paralysis)
Neuralgia Mild pain Moderate pain; limitinginstrumental ADL
Severe pain; limiting self-care ADL
-
Definition of Peripheral Neuropathy According to CTCAE ver 4
‘instrumental’ ADL refers to preparing meals, shopping for groceries or clothes, using the telephone, managing money and so on, whereas ‘self-care’ ADL refers to bathing, dressing and undressing, feeding self, using the toilet, taking medications and not being bedridden.

Treatment of Neuropathic Pain
Groups Specific drug
Gabapentinoids Gabapentin, Pregabalin
Tricyclic antidepressants Amitriptyline, Nortriptyline, Imipramine
SNRI Paroxetine, Duloxetine, Venlafaxine
Anti-epileptics Carbamazepine, Oxcarbazepine
Narcotis Morphine, Oxicodon, Fentanyl
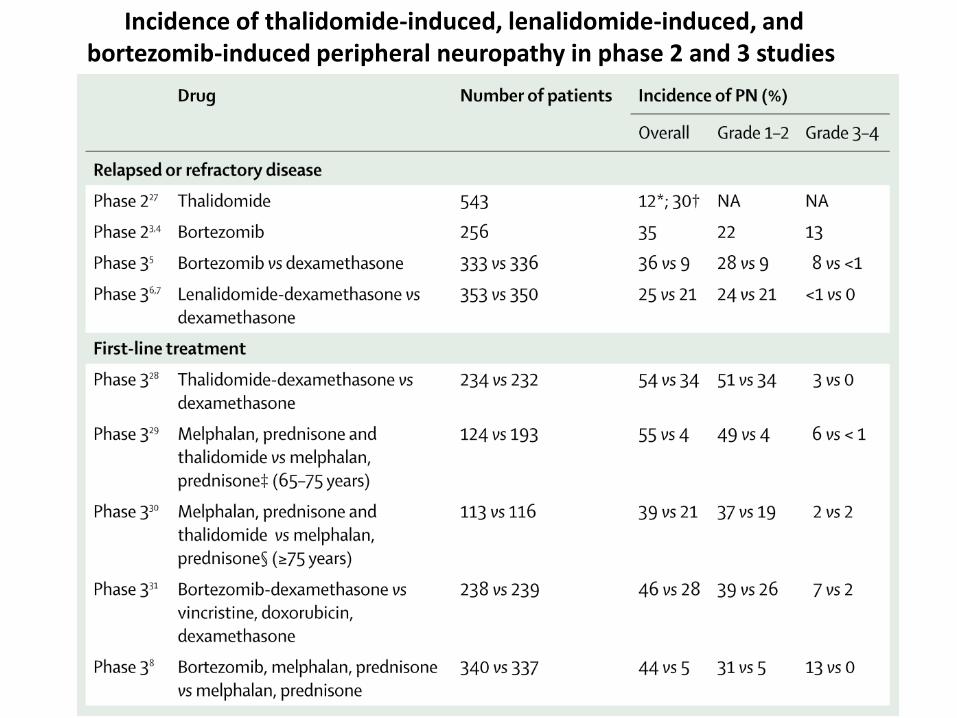
Incidence of thalidomide-induced, lenalidomide-induced, and bortezomib-induced peripheral neuropathy in phase 2 and 3 studies
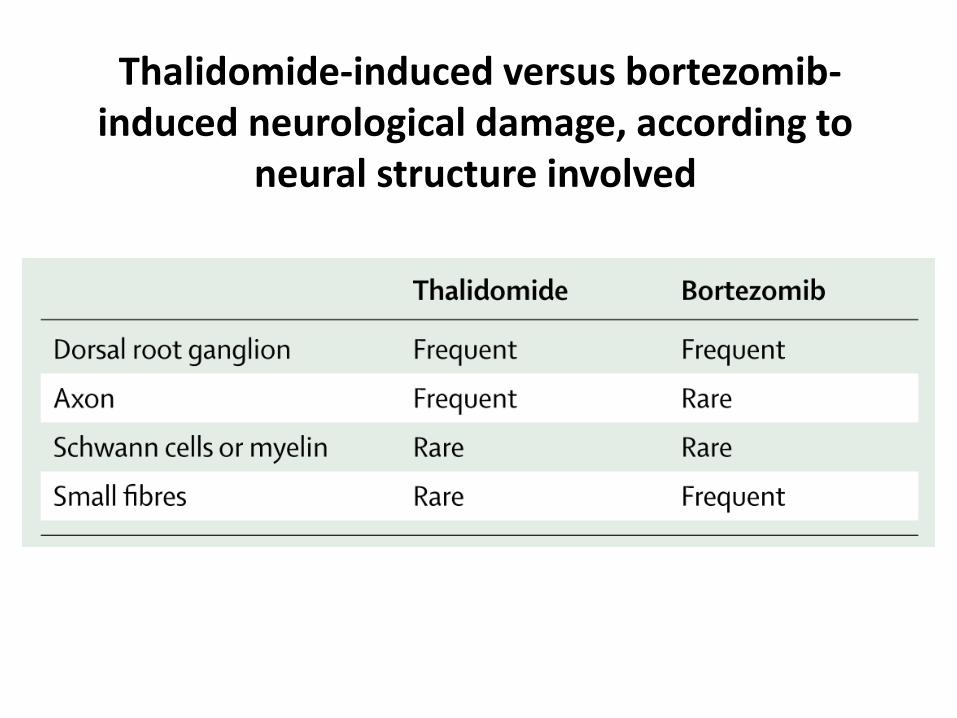
Thalidomide-induced versus bortezomib-induced neurological damage, according to
neural structure involved
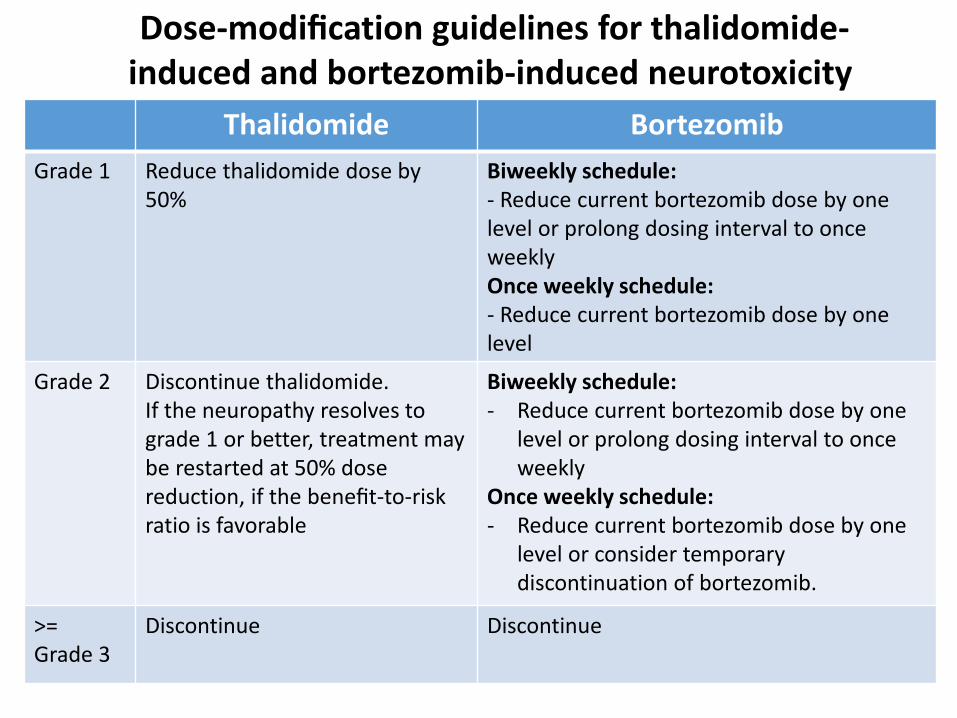
Dose-modification guidelines for thalidomide-induced and bortezomib-induced neurotoxicity
Thalidomide Bortezomib
Grade 1 Reduce thalidomide dose by 50%
Biweekly schedule: - Reduce current bortezomib dose by one level or prolong dosing interval to once weeklyOnce weekly schedule: - Reduce current bortezomib dose by one level
Grade 2 Discontinue thalidomide. If the neuropathy resolves to grade 1 or better, treatment may be restarted at 50% dose reduction, if the benefit-to-risk ratio is favorable
Biweekly schedule: - Reduce current bortezomib dose by one
level or prolong dosing interval to once weekly
Once weekly schedule: - Reduce current bortezomib dose by one
level or consider temporary discontinuation of bortezomib.
>= Grade 3
Discontinue Discontinue

Bortezomib s.c.
Moreau P. et al. Lancet Oncol 2011; 12:431-40
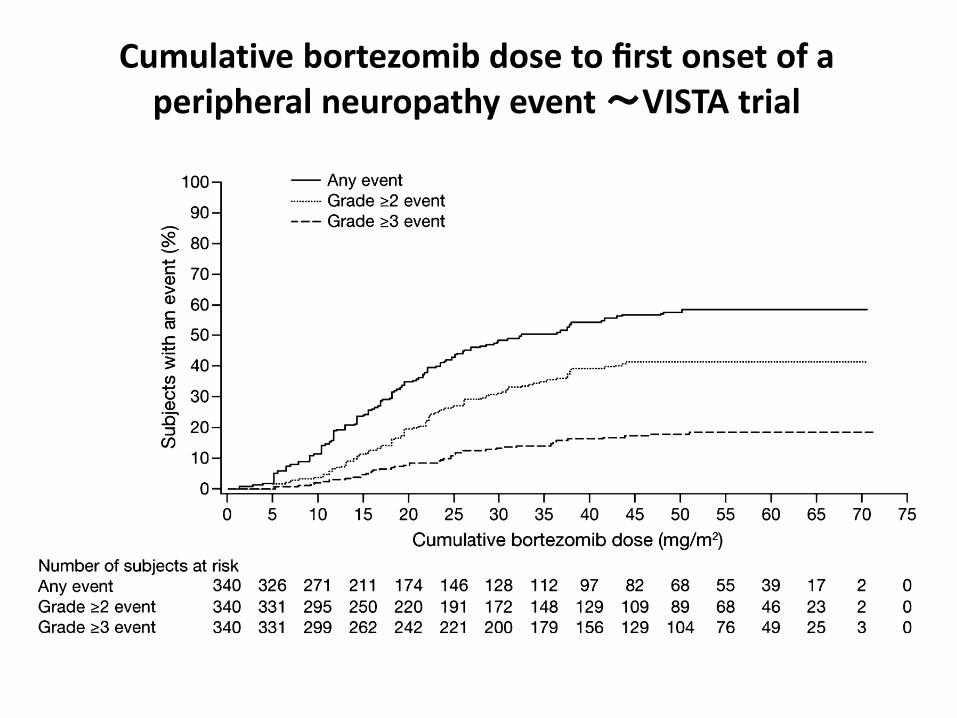
Cumulative bortezomib dose to first onset of a peripheral neuropathy event ~VISTA trial

Nasu S, et al. Clin Neurophysiol. 2014;125:381-7.
Bortezomib-induced neuropathy: Axonal membrane depolarization precedes development of neuropathy

Nasu S, et al. Clin Neurophysiol. 2014;125:381-7.
Study designClinical and neurophysiological assessment was performed at
baseline, prior to every cycle, and at treatment completion

Flow chart of patient involvement

Patient characteristics
Nasu S, et al. Clin Neurophysiol. 2014;125:381-7.
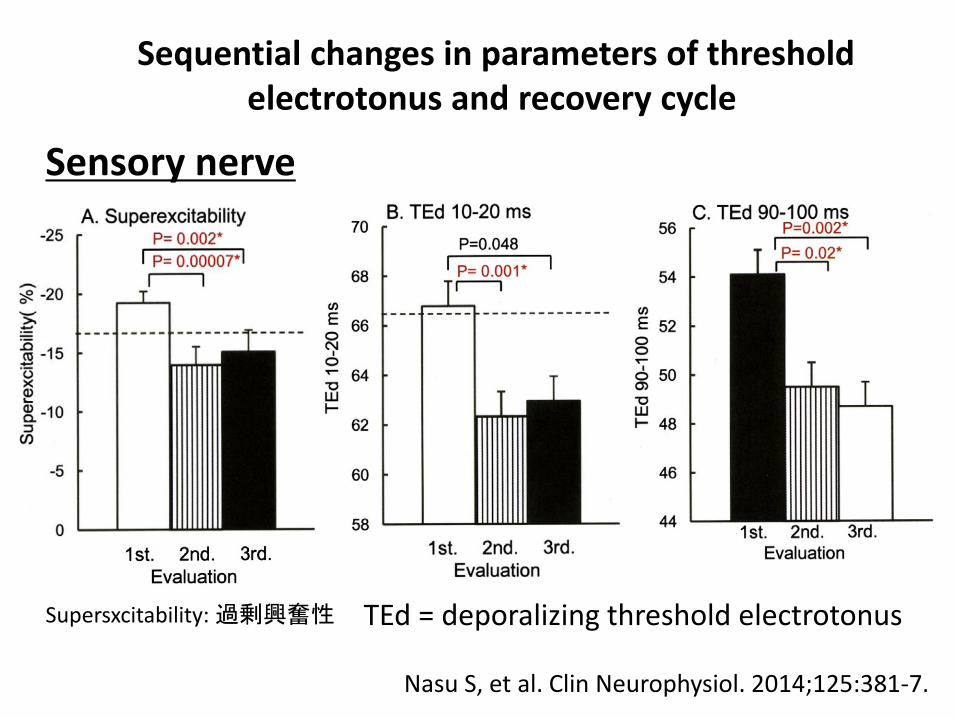
Sequential changes in parameters of threshold electrotonus and recovery cycle
Nasu S, et al. Clin Neurophysiol. 2014;125:381-7.
TEd = deporalizing threshold electrotonus
Sensory nerve
Supersxcitability: 過剰興奮性
Nasu S, et al. Clin Neurophysiol. 2014;125:381-7.
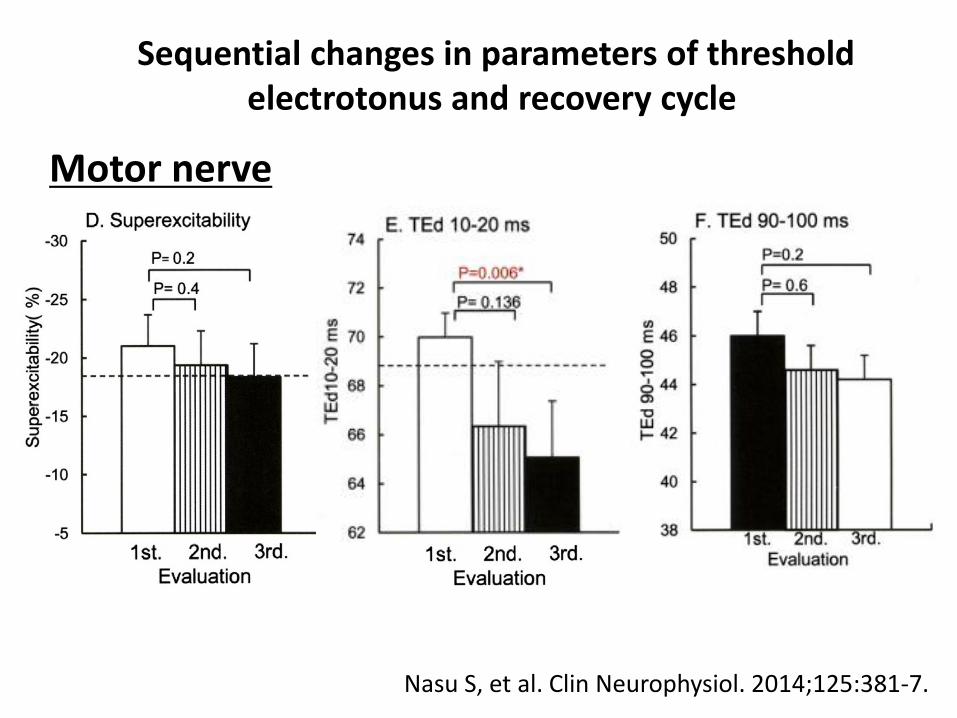
Sequential changes in parameters of threshold electrotonus and recovery cycle
Motor nerve
Nasu S, et al. Clin Neurophysiol. 2014;125:381-7.
Our results show that bortezomib induces sensory-dominant
axonal depolarization prior to the development of axonal
degeneration.
Membrane depolarization can lead to nerve hyperexcitability, consistent with positive symptoms such as pain and paresthesia.
Axonal excitability studies have a potential role in the early diagnosis of neurotoxicity and can provide insights into targets of therapeutic intervention; changes in excitability indices can be detected at the earliest phase of bortezomib-induced neuropathy, when obvious axonal loss has not yet developed.
Results
Conclusions
We should aware that the incidence of paraprotein-
associated peripheral neuropathy is significantly high.
Most of PN are reversible by plasma cell-targeting
therapies.
Collaborative approach with neurologists and
physiatrists from the diagnosis is necessary.
An appropriate evaluation and effective management of
treatment-emergent PN is critical to minimize the
incidence and severity of this complication in patients
with plasma cell dyscrasias.
Related Documents











