pathology of Granulomatous Lung Disease With Bacterial Cause Mihan pourabdollah MD.AP.CP.NRITLD

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

pathology of Granulomatous
Lung Disease With Bacterial
Cause
Mihan pourabdollah
MD.AP.CP.NRITLD

Context
• Granulomas are among the most commonly
encountered abnormalities in pulmonary
pathology and often pose a diagnostic
challenge.

DEFINITION AND TERMINOLOGY
• A granuloma is a compact aggregate of
histiocytes (macrophages).
• The histiocytes in granulomas are often
described as ‘‘epithelioid.’
• Epithelioid histiocytes have indistinct cell
borders and elongated, sole-shaped nucle.

DEFINITION AND
TERMINOLOGY
• Aggregation of histiocytes is the minimum
requirement of a granuloma.
• Regardless of whether the lesion also
contains necrosis, lymphocytes, plasma cells,
or multinucleated giant cells.

.

Step 1: Identifying Organisms
• Infection is the most common cause of
pulmonary granulomas.
• Carefully exclude an infectious etiology
before diagnosing a noninfectious
granulomatous lung disease.

APPROACH TO THE DIFFERENTIAL DIAGNOSIS OF
GRANULOMATOUS LUNG DISEASE
• Step 1: Attempt to identify an organism.
• Step 2: Look for histologic features of
noninfectious granulomatous diseases
(Table 2).


Organisms in Pulmonary
Granulomas:
What to Expect.
• The bacterial organism most commonly found
in granulomas of the lung are mycobacteria .
• Mycobacterium tuberculosis
• Nontuberculous mycobacteria (NTM) .

Organisms in Pulmonary
Granulomas:
What to Expect
• Other bacteria (Nocardia,actinomycetes and
Burkholderia ,brucella) may also rarely
cause granulomatous lung disease

MYCOBACTERIUM
Tuberculosis

MYCOBACTERIA
Tuberculosis
• The granulomas of tuberculosis are typically
necrotizing , but may be nonnecrotizing or a mix
of both types.
• poorly formed granuloma or less organized
macrophage infiltrate in immunocompromised
host.
• Small numbers of neutrophils may be present.

Nonnecrotizing granuloma

Necrotizing granuloma

Caseous Necrosis


MYCOBACTERIUM
Tuberculosis
• The granulomas of tuberculosis may be
randomly located or;
bronchiolocentric,bronchocentric,perivascular,
interstitial or alveolar .
• Involvement of blood vessels, less frequently
than in sarcoidosis.
• The histologic appearance of tuberculous
granulomas may be indistinguishable from those
of nontuberculous mycobacterial infection

Bronchiolocentric granuloma


MYCOBACTERIA
Tuberculosis
• Because the histologic features of
tuberculosis are not organism-specific,
the diagnosis rests on detection (and
subsequent speciation) of mycobacteria.

Acid fast stain


Nontuberculous Mycobacteria

Nontuberculous Mycobacteria
• Mycobacteria other than M.TB complex
• More than 140 species
• A wide range of organ involvement
• Pulmonary infections ,most frequent
• Caused by
MAC(90%)and,abscessus,kansasii,fortuitum
complex,chelonei complex,malmoense

Nontuberculous Mycobacteria
• NTM-related lung disease also occurs in
immunocompetent individuals without
preexisting lung disease.

Nontuberculous Mycobacteria In
immunocompromised patients
• collections of mycobacteria laden foamy histiocytes.
• poorly formed granulomas.
• the lack of any significant inflammatory response.
• Neutrophilic infiltrate may predominate
Mycobacteria in this form of NTM disease are numerous
and easy to find, and culture results are usually positive.

Nontuberculous Mycobacteria

The hallmark of MAC infectionsin patients with HIV is abundant acid-fast bacilli within macrophages

Nontuberculous Mycobacteria
In immunocompetent patients
• Granulomatous inflammation indistinguishable from
tuberculosis .
• Like tuberculosis, both necrotizing and nonnecrotizing
granulomas .
• Variable numbers of neutrophils may be present with central
necrosis
• The granulomas may be peribronchiolar.
• Cases with non granulomatous inflammation have also been
described.

Mycobacteria fortuitum and
chelonei
• Patients who take mineral oil for constipation
• Aspiration of these organism from gastric
contents where they are present.
• Cavitary exogenous lipoid pneumonia with
granulomatous inflammation and lipid and
mycobacterium laden giant cells in microscopy.
• Aggressive pneumonia , may need surgical
resection.

Middle lobe syndrome
• Middle lobe of right lung or lingula.
• Middle aged to eldery nonsmoker females.
• Macrophage receptor defect suppressing
phagocytosis of NTM colonizing these areas.
• Peribronchiolar granulomatous inflammation
associated with bronchiectasis.
• Acid fast bacilli are difficult to find

Middle lobe syndrome

Hot Tub Lung
• Young, immunocompetent.
• Significant long standing hot tub exposure.
• Pathology is that of hypersensitivity
pneumonitis.
• Nonnecrotizing granuloma around the airways.
• More areas of an exudative to organizing
pneumonia .
• Cultures of sputum and tub water are positive
for MAC.

Hot Tub Lung

Recommendations,Problems and
pitfalls

Using the Tissue Reaction as a
Clue
• Organisms must be sought in both necrotizing and
nonnecrotizing granulomas since they may be found in either
type.
• The search must be especially thorough in necrotizing
granulomas since these are more likely to yield an organism.
•
• Organisms are by far more common in the center of the necrosis
but may occasionally be found in the periphery of the necrosis
or even within the cellular granulomatous rim.

Histochemical Special Stains
for Organisms.
• GMS for fungi.
•
• ZN (cold kinyon modification) for mycobacteria.
• Modified acid fast such as Fite-Faraco for mycobacteria
and nonmycobacterial acid fast organisms
(nocardia,rhodococcus ,legionella micdadei).
• Tissue Gram stain

Examining Special Stains for
Organisms.
• Regarding the ZN stain, in most cases, mycobacteria are few
and difficult to find, partly because of the use of xylene in
routine processing.(over 100/ml is necessary) .
• Spending at least a few minutes at high magnification (x10
ocular lens, x40 objective) .
• constantly adjusting the fine focus to ensure detection of
organisms that appear only on certain planes.
• Others go further and use a high-power oil immersion
objective
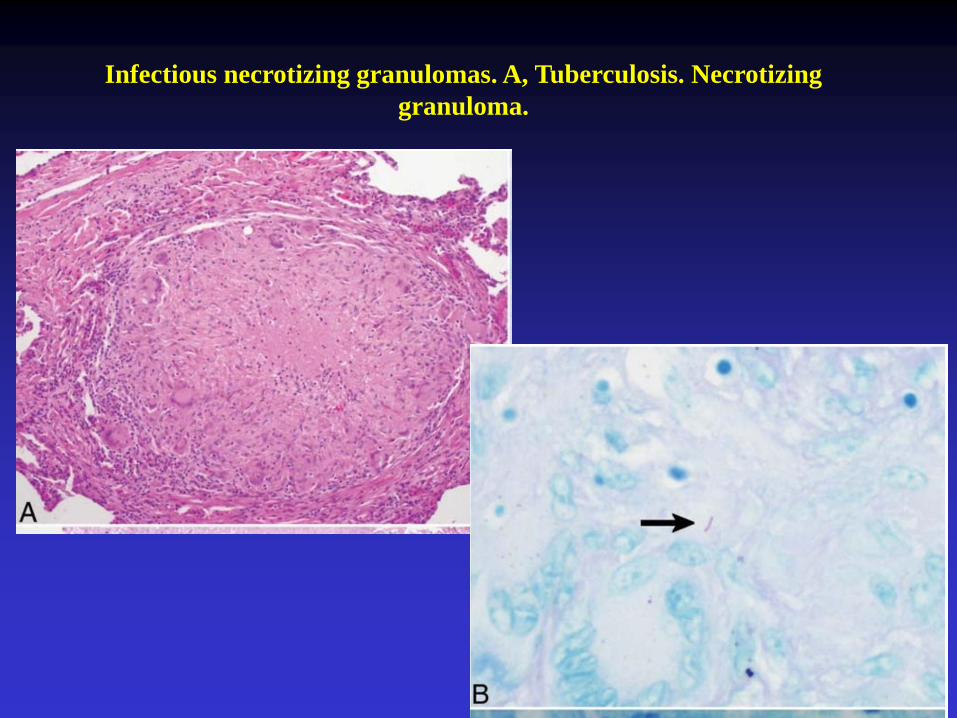
Infectious necrotizing granulomas. A, Tuberculosis. Necrotizing
granuloma.

Examining Special Stains for
Organisms
• Mycobacterial organisms may occasionally be
seen with GMS stains in certain cases and
should not be dismissed as an artifact.
• ‘Infarctlike’’ necrosis may be seen in
granulomas caused by M tuberculosis.

Mycobacterium TB stained with
GMS

Examining Special Stains for
Organisms.
• Immunohistochemical techniques are more
sensitive and specific but have their limitations.
• The auramine/auramine-rhodamine
fluorescence technique, more sensitive than
conventional acid-fast stains but positive result
sould be cofirmed by acid fast stain.

Immunohistochemistery

Fluorescent stain

How to Report the Presence of
Organisms

• The subtyping of infectious mycobacterial or
fungal disease ( progressive primary tuberculosis
versus secondary tuberculosis, etc.) often
requires clinical and radiographic information
that is usually unavailable to the pathologist.
•
• Therefore, for the purposes of the pathology
report, describing the tissue reaction and stating
the organism present is sufficient in most
instances.

differentiation between tuberculous
and nontuberculous mycobacteria
• Unfortunately, the morphologic appearance of
mycobacteria on histologic sections is not reliable for
speciation.
• The published literature on speciation of mycobacteria
by using microscopic morphologic features of the
organisms is based mostly on smears made from
microbiologic cultures rather than formalin-fixed,
paraffin embedded histologic material

differentiation between tuberculous and
nontuberculous mycobacteria
• Currently, the only definitive methods of mycobacterial
speciation are microbiologic culture and molecular methods
such as the polymerase chain reaction (PCR) .
• In most cases, speciation is not a problem because culture
test results are also positive , even when special staining of
histologic material shows negative results..

Eight Week Growth of Mycobacterium
tuberculosis on Lowenstein-Jensen Agar

differentiation between tuberculous
and nontuberculous mycobacteria
• When results with histologic special stains are
positive but those of cultures are negative, or
when biopsied tissue was not submitted for
culture, PCR is the only means

What should we do if special
stains are negative

Special Stain negative
granulomas
• Often, organisms are not found within granulomas
despite a meticulous search. Even in necrotizing
granulomas, this is a fairly frequent scenario.
• Special stain negative cases might represent infectious
granulomas in which the organism has been killed or
removed by immune system

Special Stain negative
granulomas
• The most productive next step for the pathologist is ;
• to reevaluate the special stains.
• If the necrotic portion of the granuloma is not represented on
the slide with the special stain, it may be productive to recut
the block and repeat the stain.
• If some blocks with necrosis are not initially stained with
special stains, staining these may also be productive.
• Ulbright and Katzenstein showed that examining 2 blocks with
necrosis is adequate in most cases.

How to report special staining
negative granulomas

Special Stain negative
granulomas
• In such cases, we recommend issuing a descriptive diagnosis
including the presence/absence of necrosis and the absence of
identifiable organisms.
• In the case of necrotizing granulomas, a comment such as ‘‘the
etiology is most likely infectious despite negative special stains’’
may be appropriate


Role of PCR and Other Molecular Methods
for Detection and Speciation of
Mycobacteria.
• Molecular test is at least as sensitive as
microbiologic cultures for the detection of
mycobacteria in formalin-fixed tissues and is
more sensitive than ZN staining
• It is also possible to determine the species of
organisms by this method.

Pulmonary
nocardiosis

Nocardia• Genus : aerobic Actinomyctes
G+ branching filamentous bacteria
• Subgroup: aerobic nocardiform
actinomycetes
-Mycobacterium
-Corynebacterium
-Nocardia-Rhodococcus
-Gordona
-TsukamurellaDr.T.V.RaoMD
59

Dr.T.V.RaoMD
60
What are Nocardia
• Nocardia is a genus of weakly
staining Gram-positive, catalase-
positive, rod- shaped bacteria. It
forms partially acid- fast beaded
branching filaments.




Nocardia stained with GMS

Diagnosis
Respir Med 2003; 97:709-717

Stellate Granuloma

Nocardia

Nocardia

Microbiology
• Branching,
beaded,
filamentous
bacteria
• Can cause
"Sulfur
granules" like
actinomycosis,
in nocardial
mycetomas.
• Stains acid fast
Actinomyce
s.
Dr.T.V.Rao
MD
8

Microscopy and Culturing essential
for establishing Diagnosis
Dr.T.V.RaoMD
70

Pulmonary melioidosis

Introduction
• Melioidosis is an infectious disease caused by a Gram-negative bacterium.
• Melioidosis, also called Whitmore's disease, is an infectious disease caused by the bacterium Burkholderia pseudomallei.
• Melioidosis is primarily a disease of rats, but also occurs in guinea pigs and rabbits.

Clinical manifestation
• Pulmonary infection
• Skin ulceration
• Lymphadenopathy
• Manifestations are exacerbated long after the exposure; hence called as Vietnam time bomb disease.

Types of melioidosis
a. Acute melioidosis:
• It is characterized by development of a nodule at the site of inoculation of the bacteria in the skin.
• The bacteria can subsequently spread, causing secondary lymphangitis, regional lymphangitis, fever, and myalgia.
• Acute melioidosis may progress rapidly to acute septicemia with high mortality rate.
• Acute blood stream infection is most commonly seen in patients with HIV, diabetes, renal failure, etc. The condition results in septic shock.

b. Pulmonary infection:
1. The condition is associated with high fever, headache, chest pain, anorexia, and general myalgia.
2. Nonproductive or productive cough with normal sputum is typical manifestation of this condition.
c. Chronic suppurative infection
1. It is associated with multiple caseous or suppurative foci of infection in several organs including joints, skin, lymph nodes, spleen, lungs, liver, and brain.
2. It manifests as mild bronchitis to severe pneumonia.
3. Bacteria remain as intracellular pathogens of the reticuloendothelial system, which contributes to long latency and reactivation of the infection.



Gram stain
• Gram stain:
• B. pseudomallei is a Gram-negative bacillus.
• Measures about 2–5 μm in length and 0.4–0.8 μm in diameter.
• It frequently does not show bipolar-staining on Gram stain, but it is often pleomorphic and usually stains slightly unevenly.

Culture
• B. pseudomallei is not fastidious and grows on a large variety of culture media (bloodagar, Chocolate agar, MacConkey agar, etc.).
• Ashdown's medium may be used for selective isolation.
• Cultures typically become positive in 24 to 48 hours

Colony morphology:
• Smooth, creamy, white colonies on BA at 24 hrs
• Some may be mucoid or become dry and wrinkled at 48 - 72 hrs
• Pink colonies on MA agar at 24 - 48 hrs or colorless colonies at 48 hrs

Selective medium (Ashdown medium)
• Contains crystal violet and gentamicin as selectiveagents.
• It is also enriched with 4% glycerol, which isrequired by some strains of B. pseudomallei togrow.
• It usually produces flat wrinkled purple colonies.
• Colonies will also exhibit an earthy odor.
• The colony appears irregular-edge, rough and palepurple.

Biochemical test
• Catalase = Positive
• Oxidase = Positive
• Indole = Negative
• Motility = Positive
• Triple Sugar Iron (TSI) = K/NC
• Colistin/Polymyxin B = Resistant (no zone)

Thank You
Related Documents