Pathogen Inactivation for Platelet Concentrates: What are some of the important clinical issues? William Reed, MD Cerus Dublin, May 2011

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Pathogen Inactivation for Platelet Concentrates:
What are some of the important clinical issues?
William Reed, MDCerusDublin, May 2011

Objectives
➤ Cerus technology: robust PI that targets nucleic acids
➤ Safety and vulnerabilities inherent in the current
methods for blood collection, processing, and distribution
➤ The nature of current risk: patient-specific, non-linear
➤ Some advantages current users of PI are finding
➤ How much inactivation is enough?

French Experience: Active HV 2006-09
PC Transfused Transfusion-related sepsis (TRS) cases
Conventional PC 991,471 31
INTERCEPT PC 67,571 0
Agence Francaise de Securite Sanitaire des Produits de Sante (2006-2009). Rapport Hemovigilance 2006. Paris, Afssaps.
Kientz et al. 13th International Haemovigilance Seminar (IHS) Amsterdam, The Netherlands February 9 - 11th, 2011

Mechanism of Action: Nucleic Acid Targeting
Targeting
Amotosalen(S-59)
Intercalation Crosslinking
Helical region of single-or double-stranded DNA or RNA
UVA Illumination
O
NH2
O
OO
Multiple crosslinks block strand separation and replication

Amotosalen-UVA Pathogen Inactivation: Independent of Active Oxygen Species Generation

Infectivity Log Reduction
Lin et al: Transfusion 2005;45:580-590 and Singh et al: Transfusion 2006;46:1168-1177
Platelets PlasmaHIV-1, cell-free > 6.2 > 6.8
HIV-1, cell-associated > 6.1 > 6.4
HBV > 5.5 > 4.5
HCV > 4.5 > 4.5
HTLV-I, cell associated 4.7 ≥ 4.5
HTLV-II, cell associated 5.1 > 5.7
CMV, cell-associated > 5.9
WNV > 6.0 ≥ 6.8
SARS (Corona Virus) > 6.2 ≥ 5.5
Vaccinia > 5.2
Chikungunya > 6.4 ≥ 7.6
Enveloped
H5N1 > 5.9 >5.7
Non-enveloped Bluetongue Virus 6.1 – 6.4 5.1
Calicivirus 1.7 – 2.4
SV 15 0.7 – 2.3
B19 3.5 – >5.0 1.8
Human Adenovirus 5 > 5.7 ≥ 6.9
Inactivation of Viruses

Log Reduction Log Reduction
Lin et al: Transfusion 2004;44:1496-1504 and Singh et al: Transfusion 2006;46:1168-1177
Gram-positive (Aerobes and Anaerobes) Platelets Plasma Gram-negative Platelets Plasma
Staphylococcus epidermidis > 6.6 > 7.3 Escherichia coli > 6.4
Staphylococcus aureus 6.6 Serratia marcescens > 6.7
Streptococcus pyogenes > 6.8 Klebsiella pneumoniae > 5.6 > 7.4
Listeria monocytogenes > 6.3 Pseudomonas aeruginosa 4.5
Corynebacterium minutissimum > 6.3 Salmonella choleraesuis > 6.2
Bacillus cereus (vegetative) > 6.0 Yersinia enterocolitica > 5.9 > 7.3
Lactobacillus sp > 6.9 Enterobacter cloacae 5.9
Bifidobacterium adolescentis > 6.5 Spirochetes
Propionibacterium acnes > 6.7 Treponema pallidum 6.8 - 7.0 > 5.9
Clostridium perfringens > 7.0 Borrelia burgdorferi > 6.8 > 10.6
Inactivation of Bacteria

Infectivity Log Reduction
Van Voorhis et al: Antimicrobial Agents and Chemotherapy 2003;47:475-479 and Greiller et al: Transfusion 2008;48:1676-1684
Inactivation of Protozoa
Platelets Plasma
Trypanosoma cruzi > 5.3 > 5.0
Plasmodium falciparum ≥ 6.0 ≥ 6.9
Leishmania mexicana > 5.0
Leishmania major > 4.3
Babesia microti > 5.3 > 5.3

Levels of safety – traditional
➤ Volunteer donors
➤ Donor history questionnaire
➤ Physical examination
➤ Laboratory screening
➤ Component manufacture and release
➤ Post-donation information (PDI)
➤ Hemovigilance

Levels of Safety – Vulnerabilities
Vulnerability
Volunteer donors test-seeking, magnet effect, donor incentives, peer pressure, therapeutic phlebotomy
Donor history Truthfulness, complex travel deferrals, live virus vaccinesmany others
Physical exam Pre-symptomatic infection, skin pitting or infection
Lab testing Window period, altered virus, selective testing, unknown agents,known agents without a good test
Manufacture & release
Closed system opened, wrong component ordered (patient need not recognized or information not transmitted), infectious unit released (auto or allo)
PDI Failure of timely call back, failure of donor to recognize the significance of a symptoms
Hemovigilance Passive reporting, incentive not to report can exist

Some TTD Safety Measures:Blood Donation vs. Plasma Fractionation
Blood Donation
Plasma Fractionation
Donor history Y YDonor physical exam Y Y
Standard serologic testing Y YStandard NAT testing Y Y
HAV & Parvo B19 NAT N YManufacturing pool release test n/a Y
Viral inactivation N YNano-filtration N Y
Residual TTD risk Small to moderate risk, multiple agents
Asymptotically small
Residual risk reducible? Likely with existing technology
Not likely with current technology

Example: Problems with Bacterial Screening of Platelets
➤Complex and expensive
➤False positives, indeterminants, false negatives – Follow-up of suspect products
➤ Limited effectiveness: low levels present initially, delayed log-phase growth
➤Equipment failure

~1 in 1,500 Apheresis PC Contains Bacteria
Study and Citation Surveillance Cultures at Expiration
Number of PC Tested
Day Cultured Prevalence of Contamination
Passport(Dumont, Kleinman et al. 2010)
6,039 Day 8: 1/1,509 or 0.062%
Irish Blood Transfusion Service(Murphy, Foley et al. 2008)
8,282 Beyond Day 5Day 4
1/1,200 or 0.083%1/3,310 or 0.030%
Welch Blood Transfusion Service(Pearce, Rowe et al. 2011)
6,438 Beyond Day 5: 1/1,073 or 0.093%
Pan genera detection (Verax)(Jacobs 2010)
18,449 Not specified 1/2,050 or 0.049%
German Working Group on Bacterial Safety in Transfusion(Walther-Wenke, Wirsing von Konig et al. 2010)
11,452 Day 5-8 1/877 or 0.114% (in the absence of day 1
culture)

Example: Transfusion-associated GVHD
➤Near universally fatal – prevention is essential
➤Only some patients are at risk
➤Can be effectively prevented through gamma irradiation of the component – inactivate donor T-lymphocytes
➤Gamma irradiation damages the component and can limit shelf life
➤Not deployed universally (some children’s hospitals)

➤ Initially, risk wholly unrecognized “post-operative erythroderma”(Shimoda 1955)
➤ Possibility of a shared HLA haplotype not initially appreciated(Thaler et al. NEJM 1989;321:25)
➤ Fludarabine treated patients – depth and significance of immunosuppression not initially appreciated(Briz et al. Br J Haematol 1995;91:409)
➤ Aplastic anemia – 2010 BJH;150:365
➤ Unrecognized severe immune deficiency – still a problem(Triulzi et al. Transfusion 2006;46(6):885)(Ness & Lipton, Transfusion 2001;41(5):713)(Sebnem Kilic et al. J Inv Allergol Clin Immunol 2010;20(2):153)(Neves et al. Transfusion 2010 epub ahead of print)
Chronology: which patients need irradiated blood?

2,500 cGy
INTERCEPT Blood System Gamma-irradiation (2,500 cGy)> 5.4 logs > 5.0 logs
No loss of inactivation even when amotosalen concentration is reduced by >1,500-fold
Small reduction in dose results in significant loss of efficacy
Inactivation of Leukocytes (T Cells)

Are Interventions Working?
➤ Not optimal technically:– Bacterial testing (PPV ~27%)
➤ Not optimal operationally (*“selective transfusion protocol”):– Gamma irradiation (‘right product, right patient’ is
challenging, *“selective transfusion” presents a challenge)
➤ Optimal neither technically nor operationally:– CMV testing (residual risk ~1%, “selective transfusion”
presents a challenge)*Ness et al. 2010:Transfusion 41(5): 713-5

What is the Nature of Infectious Risk?
➤ There are recognized discrete risks: HBV, HCV, HIV etc.
➤ Reported on a “per unit” basis – blood center perspective
➤ Case ascertainment depends on passive reporting
➤ Exposure to many donors over long periods of time:– Elective surgery (brief exposure, few donors)– Significant trauma, liver transplant (brief, many donors)– Cancer treatment (months to years, many donors)– Thalassemia major (lifetime, hundreds or thousands of donors)

Total Risk is greater than the sum of known risks
=TotalRSum of knownrisks
Cumulative stochastic risk for a new agent entering the blood supply
PLUS
linear non-linear

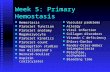
Risk and Total Exposure
EExtent of Exposure (number of units and duration exposed)
Risk
Sum of known risk (linear)
New agent risk (non-linear)

So Why Are Centers Introducing PI?
➤ Primary: Reduction in risk of transfusion-transmitted infections by broad spectrum inactivation of bacteria, viruses, protozoa and leukocytes
➤ Logistics and economics can become favorable with routine use
➤ Secondary reasons for adopting PI:– Replacement of ineffective bacterial detection– Replacement of gamma to prevent TA-GVHD (all products)– Replacement of CMV serology testing (all products)– Reduction of platelet wastage – false pos/neg bacterial testing– Reduction of transfusion reactions– Consistency – PI for plasma and platelets (RBC in the future)– Possible future changes of donor deferrals, PDI procedures– Increase blood component availability - 7 day PC:
» earlier release possible
» longer shelf life possible

High Level Inactivation of Emerging Pathogens
Pathogen Inactivation In PC (Log10)West Nile virus > 6.0
Chikungunya virus > 6.4H1N1 virus > 4.1H5N1 virus > 5.9
Dengue virus > 5.0O. Tsutsugamushi (Q Fever) > 5.5
XMRV > 4.0T. cruzi > 5.3
B. microti > 5.3L. mexicana > 5.0

Reactive Safety Approach Requires Continual Addition of Costly New Tests
HIV-1 Ab
HBc, ALT
HTLV-I
HCV 1.0 HIV-1/2,HCV 2.0
HIV-1 p24
Widespread Leukoreduction
HIV-1/HCV NAT
Chagas’ TestWNV NAT
1985 1990 1995 2000 2005 2010 2015
$100
$150
$200
$250
RBC price data adapted from B Custer & JS Hoch, Transfusion Medicine Reviews, Vol 23, No 1 (January), 2009: pp 1-12
FVIII
Other plasma factors, IVIG
Plasma for transfusion
Platelets
Introduction of PI could stop and even reverse the cycle of additions
25 years of testing, partial protection against just 7 agents:HIV, Hepatitis B, Hepatitis C, HTLV, leukocytes, West Nile virus, Chagas’ disease
Aver
age
RBC
Uni
t C
harg
e(Am
eric
a’s
Bloo
d C
ente
rs)
Introductionof Pathogen Inactivation
Babesia?Borrelia?
Others?Dengue?

Conclusions
➤ “PI” is more than “PI” – it is a different way of thinking about how blood is collected, processed, distributed
➤ Each of our current layers of safety also has corresponding vulnerabilities – impossible to address these with iterative application of the present paradigm
➤ Viewed from the patient’s perspective, risk accumulates over time and is greater that the sum of the per-unit risks
➤ A robust ability to inactivate WBCs and pathogenic micro-organisms is of primary importance
Related Documents