Partogram and Partogram and Obstructed Labour Obstructed Labour H. Gee MD, FRCOG H. Gee MD, FRCOG Consultant Obstetrician Consultant Obstetrician

Partogram and Obstructed Labour H. Gee MD, FRCOG Consultant Obstetrician.
Dec 26, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Partogram and Obstructed Partogram and Obstructed LabourLabour
H. Gee MD, FRCOGH. Gee MD, FRCOGConsultant ObstetricianConsultant Obstetrician

When is a Woman in When is a Woman in Labour?Labour?

Good Management ofLabour
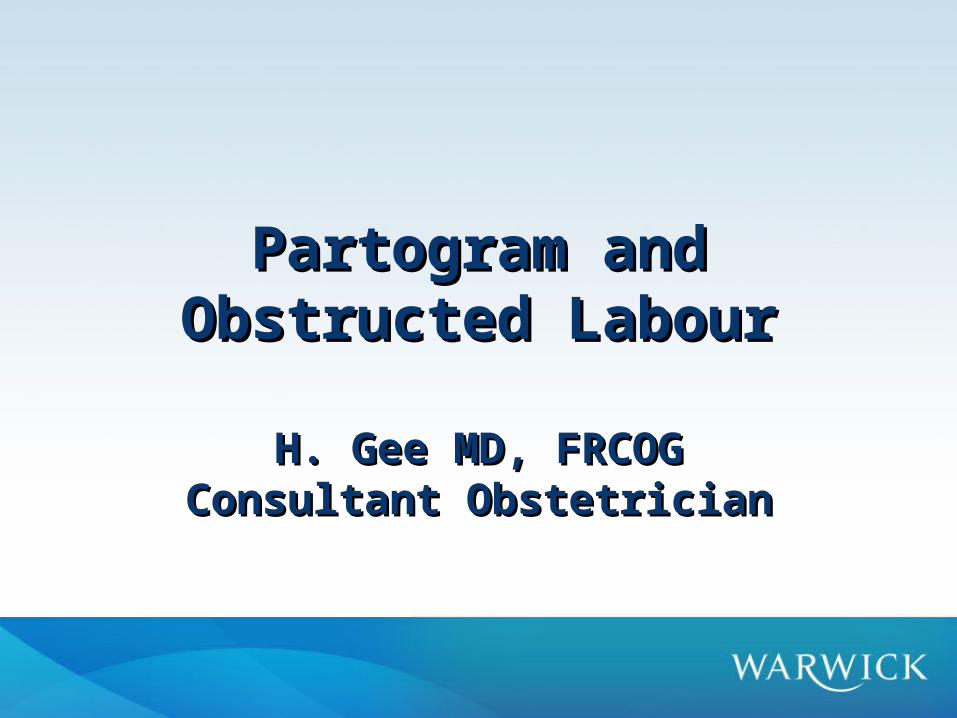
First StagePatterns of First StagePatterns of AberranceAberrance

Patterns of AberrancePatterns of Aberrance• Prolonged Latent Phase
– Slow cervical dilatation before Active Phase established– 20 hrs Nullips & 14 hrs Multips
• Primary Dysfunctional Labour– Progress< 1 cm/hr before Active Phase slope established– Incidence: Nullips 26%, Multips 8%
• Secondary Arrest– Cessation after normal active phase dilatation– Incidence: Nullips 6%, Multips 2%

PARTOGRAM- EAST AFRICA’S PARTOGRAM- EAST AFRICA’S GIFT TO THE WORLDGIFT TO THE WORLD
• Invented in Africa 1960’s
• Identify delay
• Identify increasing risk
• To determine place of delivery
• No comparative or controlled trials
• Common sense value recognised

Active Phase Cervicograms Active Phase Cervicograms - Philpott & Castle- Philpott & Castle
0 2 4 6 8 10
10
8
6
4
2
Alert L
ine
Cer
vica
l Dil
atat
ion
(cm
s,)
Time (hrs.)
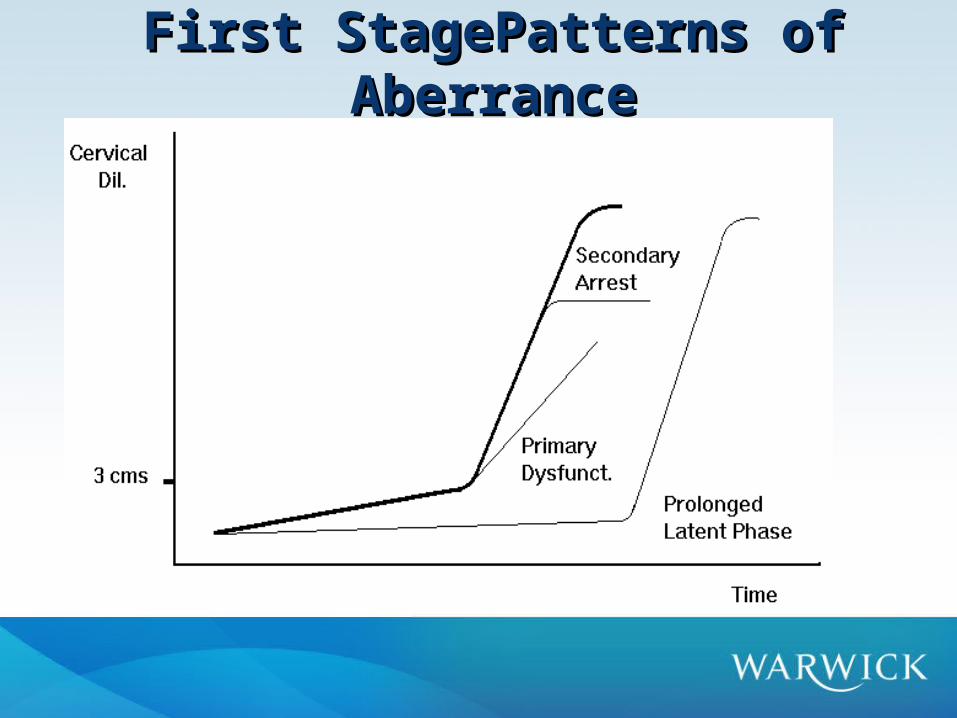
WHO Partograph StudyWHO Partograph Study• Reduced incidence of prolonged
labour (8.3% vs 4.5%)
• Decreased need for augmentation (32% vs 13%)
• Increased spont vag del (74% vs 78%)
• Decreased caesarean section (9.8% vs 6.8%) *
* not Statistically Sig Lancet 1994343;1399-1404 (Nullips)

Why not done?Why not done?Result from Malawi auditResult from Malawi audit

Partograph assessment by progress of labour and augmentation, by type of facilityPartograph assessment by progress of labour and augmentation, by type of facilityResults from Malawi auditResults from Malawi audit
Second Stage Second Stage
• Descent
• Rotation
• Duration– Passive– Active(Pushing)

Current situationCurrent situation
• Midwife tells you CS needed– Problems
• Is she right?• Do you understand the problem & implications.• Are there alternatives?
– e.g. forceps/vacuum in second stage

New situationNew situation
• You are team leader because of this course– When called
• You assess patient
– Power/passages /passenger– You improve care by whole team

Parity & ObstructionParity & Obstruction
• Nulliparous– Inertia
• Multiparous– Uterine Rupture
COMPONENTS OF LABOURCOMPONENTS OF LABOUR
• The powersUterine contractions
• The passagesbony pelvis, and soft
tissues
• The passengerfetus

PowersPowers• Essential for good progress
– Cervical Dilatation– Flexion– Rotation
• Assessed by Palpation– Frequency 3-5 in 10 min.
• Augmented by Oxytocin & Amniotomy

The PassagesThe Passages
• Bony pelvis– Absolute cephalo-pelvic disproportion
• Kyphosis, Scoliosis, poliomyelitis, maternal dwarfism, ricketts, pelvic fracture.
• Soft tissue• fibroids, ovarian tumour, pelvic kidney, fat, cervical
stenosis, cervical cancer, vaginal\vulval atresia, vaginal septum.

The PassagesThe Passages
Disproportion
•Head Not Engaged– > 4/5 Palpable abdominally– VE: high head, caput+++, moulding+++
•CS essential
•PPH – Risk increased in Prolonged/Obstructed
labour

The Passenger-1The Passenger-1
– Large Fetus • Idiopathic
– Increasing Parity
• Pathologic macrosomia, – diabetes
• Fetal abnormalities– hydrocephalus– conjoined twins – hydrops fetalis

The Passenger-2The Passenger-2
• Malposition– Occipito-Posterior– Mento-Posterior
• Malpresentation• compound presentations• shoulder• brow• face
Signs of ObstructionSigns of Obstruction
• Maternal– Tachycardia– Pyrexia– Ketosis– Dehydration
• Fetal– Fetal heart rate abnormalities
TreatmentTreatment
• General– Re-hydration– Anti-biotics (if infection suspected)
• Specific– According to diagnosis
• Caesarean section

Caesarean Section in Caesarean Section in ObstructionObstruction
• Cesarean Section Problems– Impacted head – dis-impact before start– PPH
• IV sytno/ergometrine/misoprostol ready
– Bladder Injury• Leave catheter in for 10 days if blood stained
– Infection • IV antibiotics

Post deliveryPost delivery
• Reflective practise- team leader
• Critical incident review – WHY Poor Outcome?
• NO TRAINING• NO EQUIPTMENT• POOR COMMUNICATION• MATERNAL HEALTH VERY POOR

Improve Partogram UseImprove Partogram Use
• 4 hourly ward rounds/teaching
• Critical incident review– What was wrong?
• Audit
• Change
• Re-audit
Related Documents