Partnering with Patients and Families in the Medical Home 2011 CME Webinar Series brought to you by the National Center for Medical Home Implementation The Role of the Medical Home in Care of Children with Complex Chronic Conditions Dennis Z. Kuo, MD, MHS, FAAP UAMS / Arkansas Children’s Hospital Jane Sneed, MD, FAAP The Children’s Clinic, Jonesboro, AR June 2, 2011

Partnering with Patients and Families in the Medical Home 2011 CME Webinar Series brought to you by the National Center for Medical Home Implementation.
Dec 25, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Partnering with Patients and Families
in the Medical Home
2011 CME Webinar Series brought to you by the National Center for Medical Home Implementation
The Role of the Medical Home in Care of Children with Complex Chronic
Conditions
Dennis Z. Kuo, MD, MHS, FAAPUAMS / Arkansas Children’s Hospital
Jane Sneed, MD, FAAPThe Children’s Clinic, Jonesboro, AR
June 2, 2011
Disclosures
Neither Dr. Kuo or Dr. Sneed have any relevant financial relationships with the manufacturers(s) of any commercial products(s) and/or provider of commercial services discussed in this CME activity.
We do not intend to discuss an unapproved/investigative use of a commercial product/device in our presentation.
Looking Back…
The first and second webinars of this series:
History of medical home modelHealth care teams, family/professional partnerships, Bright Futures, quality improvementCare management of chronic condition (asthma)
Webinar Objectives
By the end of this webinar, the participant will be able to:
Illustrate the importance of building and maintaining multi-specialty teams in the provision of care for children and youth with complex chronic conditions Explore strategies for enhancing complex co-management working partnerships between specialty and primary care clinicians Explain how to effectively work with clinical teams and patients/families for successful and appropriate care transition planning from pediatric to adult care
Alex (name is changed)
Alex is a 3 month old child you have seen since birth. In the nursery, you noticed dysmorphic facies, low tone, undescended testes, and a heart murmur. He developed heart failure shortly after and required surgery to repair a large VSD.
Today, you suspect craniosynostosis on exam. He is developmentally delayed and small for age.
Alex’s needs
What specialists does he need? Cardiology, neurosurgery, urology, GI, genetics when older: ENT, developmental, neurology
What therapists does he need? Speech, swallowing, OT, PT, developmental
What is the role of his primary care provider? Checkups? Nutrition? Care coordination? Immunizations?
What is the role of his family? Should this have gone at the top of the list?
Complex Chronic Conditions
“Medically fragile” or “Medical Complexity”Usually described by:
Multiple subspecialists Technology dependence for basic health needs Frequent visits to tertiary care centers
High prevalence of neurodevelopmental disabilities and genetic disorders
Srivastava 2005; Cohen 2011, Pediatrics
Why consider these children separately?
Highest risk for adverse outcomes Medical, growth, developmental, social Tend to “fall through the cracks”
Most challengingMost satisfying?
The role of the Medical Home (on steroids?)
Bending the cost curve
Medicaid projected growth rate: 8.8% - higher than Medicare or national health spending Bend the curve: slowing the rate of increase
A small number of children are responsible for a majority of health care costs Medicaid: 10% of children = 72% of costs 0.4-1% of children = 12-15% of total costs, 20-25% of
hospitalized patients, and 45-50% of hospital days
Shortell (2009), JAMA; Kenney (2009), Health Affairs; Neff (2004); Berry (2011) unpublished, by permission
The high resource utilizers
The vast majority of the high resource utilizers have “complex” and “chronic” conditions Children who “fall through the cracks” Majority of costs are inpatient
Need to coordinate care and improve quality Integrated, organized systems Fundamental payment reform
Neff (2004); Fisher (2009) NEJM; Berry (2011), J Peds; Cohen (2011)
Building and maintaining multi-specialty teams for children with complex chronic
conditions
Consider: The components of care How the components work together The role of the Medical Home
How the Medical Home can initiate and lead co-management
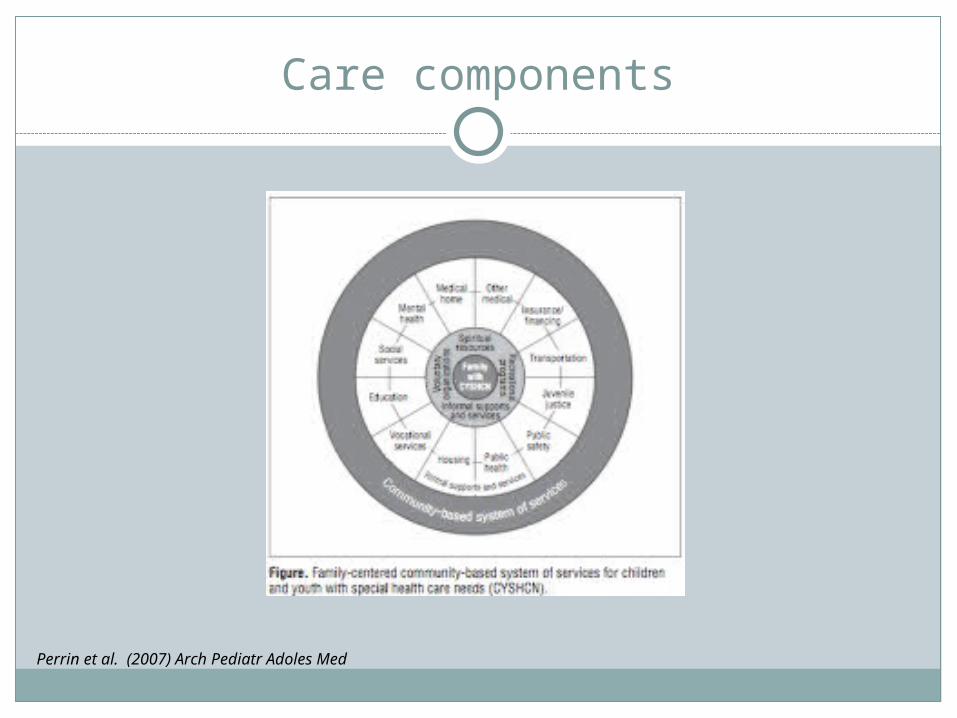
Care components
Perrin et al. (2007) Arch Pediatr Adoles Med
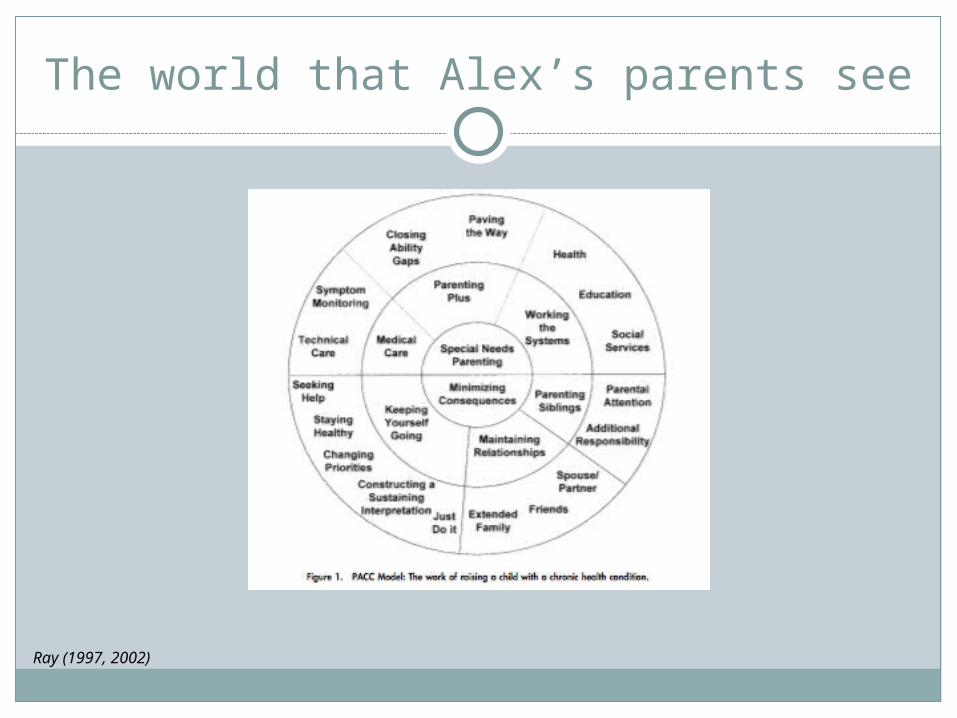
The world that Alex’s parents see
Ray (1997, 2002)
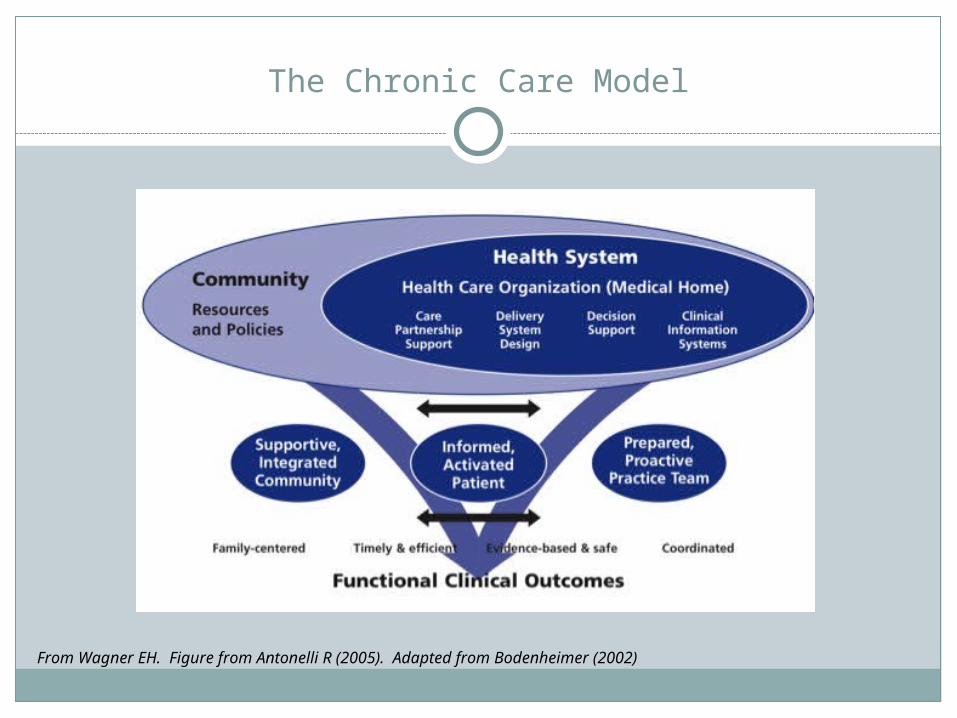
The Chronic Care Model
From Wagner EH. Figure from Antonelli R (2005). Adapted from Bodenheimer (2002)

Chronic Care Model components
Care partnership supportDelivery system designDecision supportClinical information systems
When comprehensive care works
48% decrease in the number of hospital days and a $10.7 million decrease in payments to the tertiary care center Gordon JB Pediatr Adol Med 2007
55% reduction in ED visits Klitzner TS J pediatr 2010
40% reduction in inpatient costs, 27% decrease in hospital stays Casey PH Arch Pediatr Adolesc Med 2011
Courtesy of D. Bergman

Putting it all together: Co-management
Multiple health care professionals partner with families to provide a consistent direction of care
For children with complex chronic conditions: Integrates all components of care Reinforces the active role of the
PCP/Medical Home
Stille (2009)

Partners
Specialty care = straightforward Does not address all needs
Primary care = first point of access, immunizations, continuity Primary care sometimes not fulfilled when
child has multiple visits to specialty services Assumption that needs are being met
Community-based services Not always consistent
Families!Haggerty (2011). Academic Pediatrics

Primary care “Medical Home” as hub of coordination partnership
PCP Family
Specialist
Specialist
Specialist
Medical Home “functions”: explainer, interpreter, advisor, coordinator
PCP= the child’s Primary Care PRACTICE(not just one provider)
Slide courtesy of Chris Stille, MD

Spectrum of co-management
PCP as primary manager, specialist as consultant Less complex, few specialty needs
Specialist as primary manager, PCP less involved Appropriate for high complexity and if comprehensive
service exists at tertiary care centerCo-management
Medical Home has higher responsibility Medical Home acts as care coordinator Some children with complex chronic conditions have no
subspecialty “home”
Hack, Pediatric Annals 1997; Antonelli, 2005; adopted from C. Stille (2009)

Making co-management work
Define your roles Primary care physician has higher
responsibility Specialty provider provides decision
making support
Primary care physician can learn to care for higher complexity over time
Most PCPs welcome co-managementDon’t forget families!
Antonelli (2005); Kuo (2007); Kisker (1997)
Take the initiative
Recognize the components of comprehensive care that only PCP can deliver
PCP determines the additional level of involvement, due to varying experience PCP can provide improved access, continuity, and care
coordination for children and families Higher level of co-management likely improves care
outcomes due to improved accessInitiate communication with specialty colleagues
Determine your roles and be specific for what you needComfort will increase over time
Care partnership: Family-Centered Care
Essential, yet frequently misunderstood
Associated with more efficient use of health care resources for CYSHCN
Principles: Partnership approach to care Respect for diversity Information sharing is open and unbiased Care plans may be negotiated
Kuo (2011) MCHJ; Kuhlthau (2011) Acad Pediatr
Delivery System Design: Define Roles
Medical Home: ALWAYS good primary care First point of contact Anticipatory guidance Immunizations Care hub / care coordination Verify/Initiate Early Intervention
Act as “eyes and ears” for specialty teams Remind families that you can be first point of
contact
Additional roles
With good communication with specialty colleagues, may consider: Labs Medication initiation / adjustment Referrals to community services
Consider designating office staff (such as nurse) to be single point of contact Additional roles for office staff
Help families define their roles Foster children/families likely require extra attention
Kuo (2007). Pediatrics
Decision making support
Clinical care guidelines (e.g. AAP)Be familiar with common issues of
condition(s) High prevalence of neurodevelopmental
disabilities Recognize that many children have
feeding/growth issues, dysphagia, respiratory issues
Learn from specialty colleagues Regular communication; they will teach
you Eyes and ears / red flags
Define communication lines
Keep updated and continuous care plan Consider separate forms and someone to maintain
Methods of communication Email? Fax? Phone call? What will be communicated? – ask specialists Timing and frequency of communication Health care portals
If all else fails, encourage family to contact you and / or schedule regular follow-up visits
Clinical Information Systems
Track your children with special needs Particularly children with complex chronic conditions Quality of care measures
Utilize communication lines, including email, fax, phone
Clinical decision making tools
Conclusions
Comprehensive care can improve health outcomes and reduce utilization
Medical Home must take the lead to develop comprehensive care for children with complex and chronic health conditions
Co-management increases PCP involvement and can lead to improved outcomes

Thank you!
Questions?
Got Medical Home?
Have a specific question or need regarding medical home?
Contact us!
[email protected]/433-9016 ext 7605
Related Documents











