1 Participating in the Webinar All attendees will be muted and will remain in Listen Only Mode. Type your questions here so that the moderator can see them. Not all questions will be answered but we will get to as many as possible. How to Receive CME and MOC Points LIVE VIRTUAL GRAND ROUNDS WEBINAR ACG will send a link to a CME & MOC evaluation to all attendees on the live webinar. ABIM Board Certified physicians need to complete their MOC activities by December 31, 2021 in order for the MOC points to count toward any MOC requirements that are due by the end of the year. No MOC credit may be awarded after March 1, 2022 for this activity. 1 2 American College of Gastroenterology

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

1
Participating in the Webinar
All attendees will be muted and will remain in Listen Only Mode.
Type your questions here so that the moderator can see them. Not all questions will be answered but we will get to as many as possible.
How to Receive CME and MOC Points
LIVE VIRTUAL GRAND ROUNDS WEBINAR
ACG will send a link to a CME & MOC evaluation to all attendees on the live webinar.
ABIM Board Certified physicians need to complete their MOC activities by December 31, 2021 in order for the MOC points to count toward any MOC requirements that are due by the end of the year. No MOC credit may be awarded after March 1, 2022 for this activity.
1
2
American College of Gastroenterology

2
MOC QUESTION
If you plan to claim MOC Points for this activity, you will be asked to: Please list specific changes you will make in your
practice as a result of the information you received from this activity.
Include specific strategies or changes that you plan to implement.THESE ANSWERS WILL BE REVIEWED.
ACG Virtual Grand RoundsJoin us for upcoming Virtual Grand Rounds!
Visit gi.org/ACGVGR to Register
Week 31, 2021Screening for Barrett’s Esophagus : Beyond Upper EndoscopyPrasad G. Iyer, MD, MS, FACGAugust 12, 2021 at Noon Eastern
Week 30, 2021Post‐ERCP Pancreatitis: Past, Present and FutureMohammad Yaghoobi, MD, FACGAugust 5, 2021 at Noon Eastern
3
4
American College of Gastroenterology

3
Disclosures:
Speaker: C. Prakash Gyawali, MD, MRCP, FACGConsulting: Medtronic, Diversatek, Ironwood, Takeda, IsoThrive, Quintiles
Moderator: Amit Patel, MD, FACGDr. Patel, faculty for this educational event, has no relevant financial relationship(s) with ineligible companies to disclose.
*All of the relevant financial relationships listed for these individuals have been mitigated
ACG 2020 Clinical GuidelinesClinical Use of Esophageal Physiologic Testing
C. Prakash Gyawali, M.D.
Professor of Medicine
Division of Gastroenterology
July 2021
5
6
American College of Gastroenterology
4
Objectives
1. Describe indications for currently available esophageal physiologic tests
2. Understand performance characteristics of esophageal physiologic tests
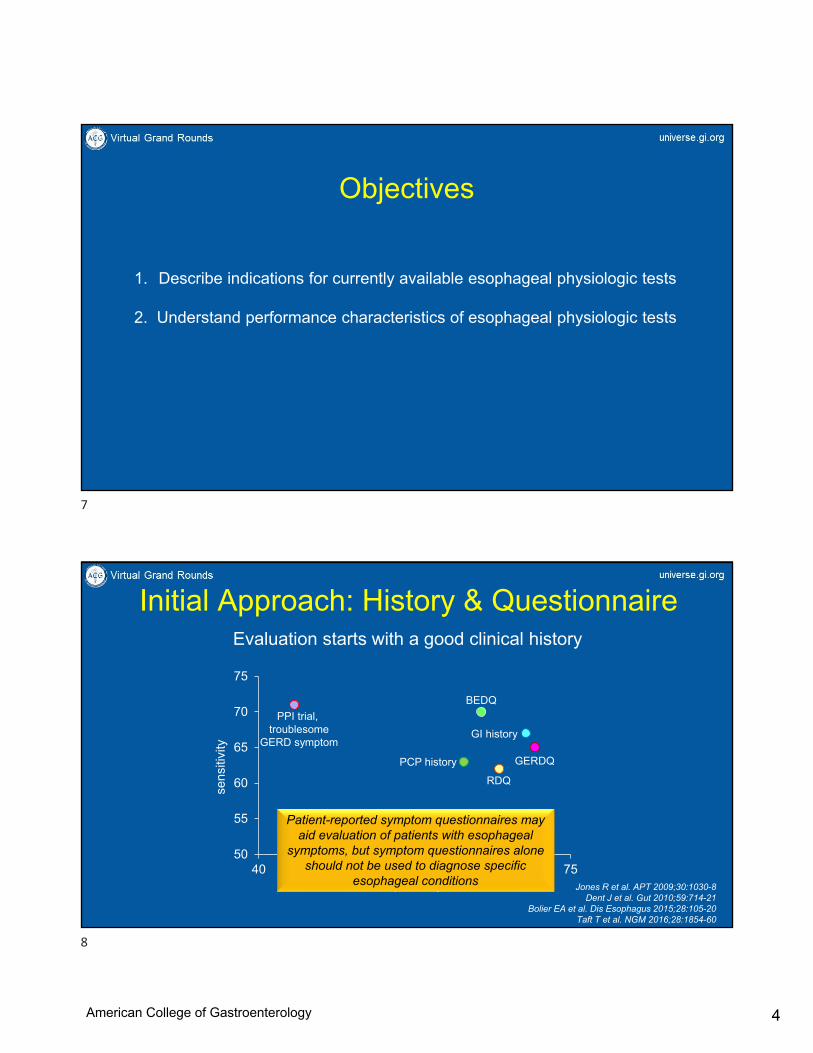
Initial Approach: History & Questionnaire
50
55
60
65
70
75
40 45 50 55 60 65 70 75
PCP history
RDQ
GI history
GERDQ
specificity
sens
itivi
ty
Jones R et al. APT 2009;30:1030-8Dent J et al. Gut 2010;59:714-21
Bolier EA et al. Dis Esophagus 2015;28:105-20Taft T et al. NGM 2016;28:1854-60
PPI trial, foregut symptom
PPI trial, troublesome
GERD symptom
BEDQ
Patient-reported symptom questionnaires may aid evaluation of patients with esophageal
symptoms, but symptom questionnaires alone should not be used to diagnose specific
esophageal conditions
Evaluation starts with a good clinical history
7
8
American College of Gastroenterology

5
A
B
C
D
Gyawali CP, NGM 2012;24(Suppl1):2-4
HRM
UES and LES visible in the same window
Real time visualization of catheter positionCurled catheter can be identified and rectified
Three dimensional assessment of esophageal peristalsisIntuitive depiction of motor functionPatterns of abnormal motility can be easily recognized
Software tools can be used to assess sphincter functionVigor and timing of peristalsis can be assessed
Location of LES can be quickly identified for pH probe placement
HRM vs. Conventional Manometry
Improved diagnostic yield for achalasia compared to conventional manometry
Superior inter-rater agreement for motor diagnoses compared to conventional manometry
Learners favor HRM over conventional manometry
Roman S et al, Am J Gastroenterol 2016;111:372-80Carlson DA et al, Am J Gastroenterol 2015;110:967-77
Soudagar AS et al, Gut 2012;61:798-803
HRM is recommended for evaluation of obstructive esophageal symptoms without a
mechanical cause
HRM is recommended over conventional manometry
HRM
When to request a high-resolution manometry
Transit symptoms (dysphagia, regurgitation) not explained on EGD and/or barium swallow
Suspected esophageal motor disorder
As part of pH monitoring
Unexplained esophageal symptoms
Post fundoplication dysphagia
Dysphagia localized to upper esophageal sphincter
9
10
American College of Gastroenterology

6
Adjunctive HRM Measures
z1
z2
Penagini R, Gyawali CP. J Clin Gastroenterol 2019;53:322-330Rogers B, Gyawali CP. Gastroenterol Clin North Am 2020;49:411-426
ImpedanceRapid Drink Challenge (RDC)Multiple Rapid Swallows (MRS) Utilization of supplementary/provocative
maneuvers with HRM improves the diagnostic yield of esophageal motility disorders in
patients with obstructive esophageal symptoms
DISORDERS OF PERISTALSIS
DISORDERS OF EGJ FUNCTION
10 wet swallows (supine/upright)
Abnormal median IRP
All swallows fail or premature
All swallows fail, no PEP
All swallows fail, 20% PEP
20% premature swallows
Alternate position swallowsRDC/MRS
Abnormal IRP persistsAbnormal RDC/MRS
Abnormal BE or FLIP
Achalasia type 1
Achalasia type 2
Achalasia type 3
EGJOO
Abnormal median IRP Abnormal RDC/MRS
20% premature swallows
All swallows fail, no PEP
20% hypercontractile
>70% ineffective and/or ≥50% failed
Absent contractility
DES
Hypercontractile
IEMNO EGJOO
NO DISORDER OF PERISTALSIS
Consider meal challenges if appropriate
Yadlapati R et al, CCv4.0, Neurogastroenterol Motil 2021
Y
Y
Y
N
N
N
Y
Alternate position swallowsRDC/MRS
N
N
Chicago Classification 4.0
11
12
American College of Gastroenterology
7
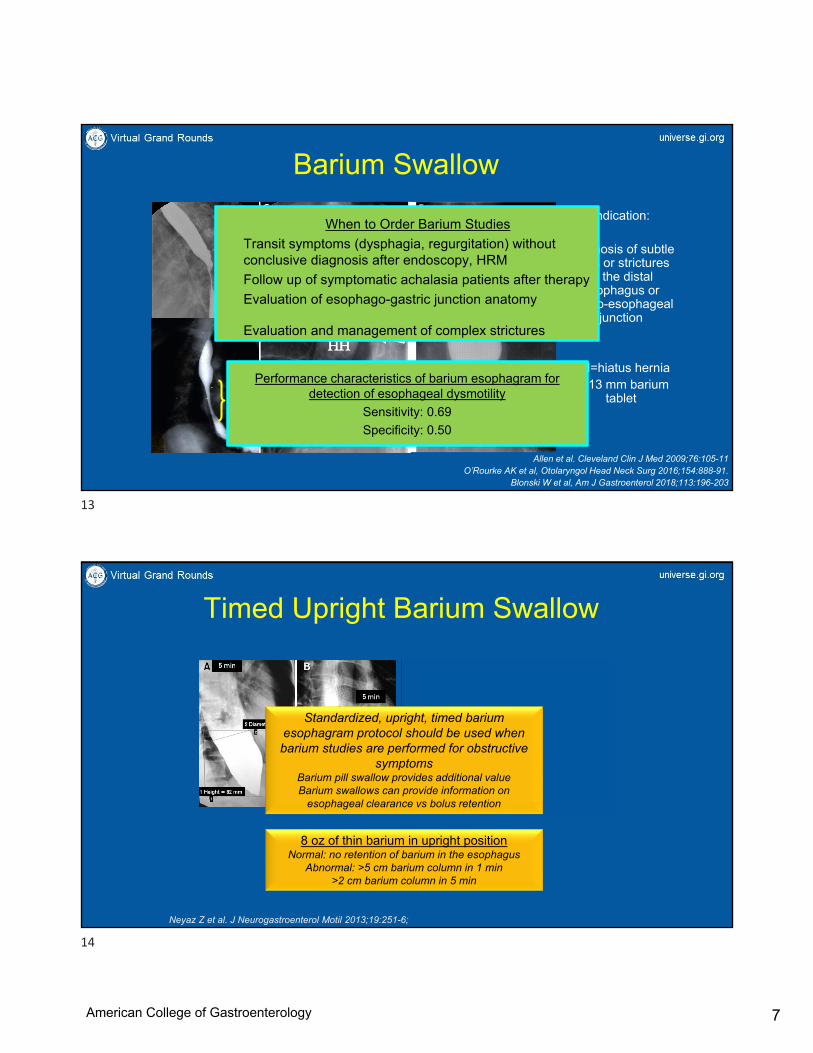
Allen et al. Cleveland Clin J Med 2009;76:105-11O’Rourke AK et al, Otolaryngol Head Neck Surg 2016;154:888-91.
Blonski W et al, Am J Gastroenterol 2018;113:196-203
Barium Swallow
Indication:
Diagnosis of subtle rings or strictures
in the distal esophagus or
gastro-esophageal junction
HH=hiatus herniaT=13 mm barium
tablet
When to Order Barium Studies
Transit symptoms (dysphagia, regurgitation) without conclusive diagnosis after endoscopy, HRM
Follow up of symptomatic achalasia patients after therapy
Evaluation of esophago-gastric junction anatomy
Evaluation and management of complex strictures
Liquid Barium vs. 13 mm Barium PillBoth abnormal in 75% of achalasia patients
Abnormal pill swallow but normal barium swallow in 49% of EGJOOBoth normal in 61% of non-achalasia patients
Performance characteristics of barium esophagram for detection of esophageal dysmotility
Sensitivity: 0.69
Specificity: 0.50
Timed Upright Barium Swallow
Neyaz Z et al. J Neurogastroenterol Motil 2013;19:251-6;
8 oz of thin barium in upright positionNormal: no retention of barium in the esophagus
Abnormal: >5 cm barium column in 1 min>2 cm barium column in 5 min
Standardized, upright, timed barium esophagram protocol should be used when barium studies are performed for obstructive
symptomsBarium pill swallow provides additional valueBarium swallows can provide information on
esophageal clearance vs bolus retention
13
14
American College of Gastroenterology

8
Diameter 6.3 mmCross sectional area: 30 mm2
Distensibility index:1.1
• Placed trans-orally during sedated upper endoscopy
• Positioned with 2-3 channels beyond the waist identified as the EGJ
• Step-wise volumetric distension from 20 to 70 ml
Stomach
16-cm
Functional Lumen Imaging Probe
Carlson D et al, Gastroenterology 2016Carlson D et al, AJG 2021 (in press)
Diameter 10.6 mmCross sectional area: 88 mm2
Distensibility index:5.8
Comparison of FLIP metrics (EGJ-DI, diameter) and HRM metrics
(IRP) to gold standard of esophageal emptying on timed upright barium swallow and/or
barium pill swallow in patients with dysphagia
sIRP15
uIRP12
DI2.0
Diameter13
sens 0.79 0.82 0.81 0.79
spec 0.61 0.55 0.76 0.85
AUC 0.79 0.79 0.84 0.88
FLIP 2.0: Panometry
Carlson D et al, Am J Gastroenterol 2016;111:1726; DDW 2018
When to order a FLIP study
Transit symptoms (dysphagia, regurgitation) not explained on EGD, HRM and/or barium swallow
Suspected esophageal motor disorder
Unexplained esophageal symptoms
Dysphagia despite myotomy, PD or POEM
Post fundoplication dysphagia
Evaluation of the pyloric sphincter
FLIP complements HRM for diagnosis of esophageal motility disorders
Patients in whom manometry cannot be completed Measurement of EGJ cross-sectional area or
distensibility during and following achalasia treatment
Measurement of cross-sectional area or distensibility to assess fibrostenotic remodeling in EoE
15
16
American College of Gastroenterology

9
Dysphagia ± chest pain and bland regurgitationGERD symptoms not responsive to PPI therapy
Upper endoscopy
Normal Esophageal dilation, EGJ resistanceretained food, diverticulum
Mechanical obstruction/esophagitistreat appropriately
HRMPROVOCATIVE MANEUVERS
Vaezi MF et al, ACG Guidelines, Am J Gastroenterol 2020;115:1393-1411
Approach: Obstructive Pathway
TIMED UPRIGHT BARIUM RADIOGRAPH
SECOND OPINION ENDOSCOPY FUNCTIONAL LUMEN IMAGING PROBE
Gyawali CP et al, ACG Guidelines, Am J Gastroenterol 2020;115:1412-1428
DilateBotulinum toxin
ObserveBehavioral therapy
Definitive therapy
Reflux Symptoms: Definitions Are Important!
Refractory Heartburn
Heartburn not responding to stable PPI therapy over 12 weeks
Refractory GERD
Symptoms caused by reflux of gastric content not responding to stable PPI therapy over 12 weeks
Fass R, Sifrim D. Gut 2009;58:295-309Sifrim D, Zerbib F. Gut 2012;61:1340-54
Implication: symptoms may or may not be from reflux
Implication: symptoms are from inadequate management of reflux
Unproven GERD
Proven GERD
No GERD
17
18
American College of Gastroenterology

10
Empiric PPI Therapy for Typical GERD
Jonasson C et al. APT 2012;35:1290-1300
Similar symptom relief
cost savings: €146/$160
Primary care referral: 347 pts
R
GERDQblinded
GERDQblinded
GERDQblinded
EGD/pH-metry
GERDQ GERDQ GERDQStratification
Rx
Rx
Rx
Rx
baseline 4 weeks 8 weeks
symptom basedn=174
test basedn=173
86.5%
80.1%
esophageal symptomsNNT for PPI response
Heartburn: 2Regurgitation: 5.6Chest pain: 4-7
Gyawali CP, Fass R. Gastroenterology 2018;154:302-318
Atypical and Extra-Esophageal Symptoms
Empiric Treatment
QD BID success$1972-4339
BID failure positive pH-impnegative HRM$3296-5721
BID failure negative pH-imp
positive HRM$2906-4880
BID failure negative pH-impnegative HRM$2773-4748
BID success$2998
Up-Front Testing
positive pH-impnegative HRMBID success
$3946
positive pHnegative HRM
BID failure$2581
negative pH-impnegative HRM
$877
negative pH-imppositive HRM
$1020
positive pH-impnegative HRM
surgical referral$1411
Carroll TL et al, Laryngoscope 2017;127:S1-13
Extra-Esophageal symptomsNNT for PPI response
Cough 11.4Hoarseness & sore throat 79.2
Gyawali CP, Fass R. Gastroenterology 2018;154:302-318
Up-front esophageal testing, preferably with pH-impedance monitoring off PPI and HRM, has value over laryngoscopy and empiric PPI trials for the evaluation of extra-esophageal
symptoms when GERD is suspected
19
20
American College of Gastroenterology

11
Approach: Reflux PathwayReflux suspected
Esophagealheartburn
regurgitationchest pain
Extraesophagealcough
hoarsenesssore throat
UPPER GI ENDOSCOPYTo evaluate for conclusive reflux evidence
To evaluate for confounding diagnoses
Alarm symptomsLack of PPI response
treat as reflux?escalate management
conclusiveevidence
Unproven GERD
Proven GERD
obstructive symptomssuspicion for achalasia, motor disorders
motordisorder
Obstructive/atypical pathway
Obstructive/atypical pathway
Gyawali CP et al, ACG Guidelines, Am J Gastroenterol 2020;115:1412-1428
Adkamar K et al, Gastrointest Endosc 1986;32:78-80Takashima T et al, Digestion 2012;86:55-58
Zagari RM et al, Gut 2008;57:1354-9
Yield of Endoscopy
Poh CH et al, Gastrointest Endosc 2010;71:28-34
0
10
20
30
40
erosiveesophagitis
Barrett'sesophagus
hiatus hernia stricture
PPI failure
no treatment
*
0
5
10
15
20
LA grade A LA grade B LA grade C LA grade D
* *
*p≤0.01105 with PPI failure, EGD on PPI91 with no treatment≥3 heartburn episodes a week
%Almost never seen in
asymptomatic controls
Seen in up to 8% of asymptomatic controls
LA Grade A LA Grade B
LA Grade C LA Grade D
Hill grade of EGJ on retroflexion
Hill LD et al, GIE 1996;44:541-4; Osman A et al, DDS 2021;66:151-5
I II
III IV
Endoscopy has high specificity but low sensitivity for findings of conclusive GERD
Bredenoord AJ et al, Neurogastroenterol Motil 2009;21:807-12
21
22
American College of Gastroenterology

12
Reflux Monitoring
swallow acid reflux episode non-acid reflux episode
pH-impedance monitoring• higher sensitivity for detection of reflux episodes• higher potential for reflux-symptom association• acid reflux episodes become non-acid with PPI therapy
When to order ambulatory reflux monitoring
Esophageal symptoms persisting despite PPI
Prior to antireflux surgery or invasive GERD therapy
Persisting symptoms despite antireflux surgery
Symptoms following LES disruption, e.g., myotomy, POEM
Investigation of belching and regurgitation syndromes
Acid Exposure Time (AET)Cumulative time pH<4 as a percentage of the duration of recording
Abnormal pH PatternsReflux episodes
heartburn2 min
Reflux-symptom correlation
23
24
American College of Gastroenterology

13
18.8 Schindlbeck 1987
Kasapidis 1993 3.9
13.6 Mattioli 1989
Vitale 1984 7.2
Johnsson 1987 3.4
Masclee 1990 4.0
Esophageal acid exposure (% time pH<4.0)
Upper limit of normal
Richter 1992 5.8Mattioli 1989,,Smout 1989 5.0
Schindlbeck 1987 7.0
GERD with esophagitis (mean)
9.6 Vitale 1984
12.6 Masclee 1984
27.6-29.8 Mattioli 1989
31.7 Kasapidis 1993
Kahrilas & Quigley Gastro 1996;110:1982-96
10.2 Schindlbeck 1987
6.4 Masclee 1984
11.6 Kasapidis 1993GERD without esophagitis (mean)
4.0
6.0
4.9 Ayazi 20094.4 Wenner 2005
5.9 Pandolfino 20035.8 Vitale 1984
Wireless pH monitoring
pH thresholds are partly based on evidence, but mostly arbitrary and based on consensus
agegender
study off PPI
typical symptoms
abnormal AET*
abnormal RET
SAP (acid reflux)
SAP (all reflux)**
number of reflux events
0 1 2 3 4 5 6
Predictors of GERD Symptom ImprovementpH-impedance in a ‘real world’ setting
Patel A, Sayuk GS, Gyawali CP. CGH 2015;13:884-891.
*p=0.002-0.014**p=0.026-0.05
n=18753.8±0.9 yrs
70.6% female
50.3% tested off PPI61% typical symptoms39.9 ±1.3 mo follow-up
GLOBAL SYMPTOM SEVERITY (GSS) CHANGE
0
20
40
60
8076
69
57
47
Strong Good RH Equivocalp<0.001 across groupsAET+/SAP+ AET+/SAP- SAP+ neither
Abnormal acid exposure time (AET) is a predictor of symptom improvement following
GERD management, including antirefluxsurgery
25
26
American College of Gastroenterology

14
Clinical Value of Prolonged pH Monitoring
NERD
Penagini R et al, J Neurogastroenterol Motil 2015;21:265-72
50 patients 35 patients
Symptom Response to Antireflux Therapy
NERD: 77%FH: 45%
Diagnosis may shift to non-erosive reflux disease when prolonged pH monitoring is utilized
Clinical Value of Prolonged pH MonitoringGERD symptoms
with incomplete response to PPIn=142
EGD off PPI96-hour wireless pH monitoring
n=128
Able to discontinue PPIn=34 (34.0%)
AET 6.6 [SD 3.6]*80% with ≥2 days abnormal AET*
Completed studyn=100
Unable to discontinue PPIn=66 (66.0%)
AET 4.3 [SD 3.6]*67% with 0 days abnormal AET*
RESQ-eD 17.8 [SD 11.7]*GERDQ 9.3 [SD 4.6]*
RESQ-eD 12.0 [SD 9.6]*GERDQ 7.2 [SD 3.0]*
Yadlapati R, Masihi M, Gyawali CP, et al. Gastroenterology 2021;160:174-182
Stopping PPI with 0 vs 4d of AET<4.0% OR 10 (95% CI 2.70-43.32), p<0.01
Continuing PPI with ≥2d of AET>4.0%OR 5.31 (95% CI 2.91-13.44), p<0.01
*p<0.05
14 did not meet inclusion criteria12 had EoE
3 had advanced grade esophagitis7 had insufficient reflux monitoring time
6 were lost to follow up
Physiologic AET on multiple consecutive days rules out pathologic GERD and allows PPI discontinuation
27
28
American College of Gastroenterology

15
Newer Metrics: Markers of Longitudinal Injury
Kessing et al, Am J Gastroenterol 2011;106:2093-7
Baseline Mucosal Impedance
Impedance signature of a bolus passing across a pair of sensors
baseline impedance
Patel A, Gyawali CP et al, APT 2016
Pearson’s r= -0.5
acid exposure time25 20 15 10 5 0
dist
al M
NB
I
CONCLUSIVE EVIDENCE FOR PATHOLOGIC REFLUX
EVIDENCE AGAINST PATHOLOGIC REFLUX
BORDERLINE OR INCONCLUSIVE EVIDENCE
ENDOSCOPY pH or pH-IMPEDANCE
ADJUNCTIVE OR SUPPORTIVE EVIDENCE*
LA grades C&D esophagitisLong segment Barrett’s mucosa
Peptic esophageal stricture
HRM
LA grades A&B esophagitis
Histopathology (score)Electron microscopy (DIS)Low mucosal impedance
AET>6%
AET<4%Reflux episodes<40
AET 4-6%Reflux episodes 40-80
Reflux-symptom associationReflux episodes>80
Low MNBILow PSPWI
Hypotensive EGJHiatus hernia
Esophageal hypomotility
*factors that increase confidence for presence of pathologic reflux when evidence is otherwise borderline or inconclusive
Gyawali CP et al, Lyon Consensus, Gut 2018
Ambulatory reflux monitoring is superior to history, questionnaires, PPI trial and
inconclusive endoscopy for the diagnosis of pathologic GERD
Ambulatory reflux monitoring is performed off PPI in patients without prior conclusive
evidence for GERD
29
30
American College of Gastroenterology

16
Subsequent ApproachReflux suspected
Esophagealheartburn
regurgitationchest pain
Extraesophagealcough
hoarsenesssore throat
UPPER GI ENDOSCOPYTo evaluate for conclusive reflux evidence
To evaluate for confounding diagnoses
treat as reflux?escalate management
?other diagnosestreat as functional
negative
Alarm symptomsLack of PPI response
negative or equivocal evidence
equivocal evidence
treat as reflux?escalate management
conclusiveevidence
ADJUNCTIVE METRICSbaseline impedance, PSPW, mucosal integrity, HRM
conclusiveevidence
AMBULATORY REFLUX MONITORINGTo evaluate for conclusive reflux evidence
Unproven GERD
Proven GERD
Proven GERD
No GERD
negative GERD less likelyGERD likely positive
Wireless pH vs. pH-Impedance Testing
Wireless pH (off PPI)
• Catheter intolerance
• Infrequent symptoms, needing reflux-symptom association
• High clinical suspicion of GERD with negative 24-hour reflux monitoring
• Very low clinical suspicion of GERD
pH-impedance (off PPI, rarely on PPI)
• Refractory typical or atypical symptoms in patients with proven GERD (on PPI)
• Respiratory symptoms or cough in patients with pulmonary disease (off PPI)
• Repetitive belching in patients with and without reflux symptoms (off PPI)
• Suspicion of rumination syndrome (off PPI)
• Persistent reflux or increased belching following antireflux procedures (off PPI)
• High pre-test likelihood of GERD, prior to invasive antireflux procedures
• Investigation of persisting reflux symptoms despite empiric PPI trial
Either option (off PPI)
Sifrim D, Gyawali CP. Am J Gastroenterol 2020;115:1150-1152
31
32
American College of Gastroenterology

17
Using Pre-Test Probability of RefluxTypical Symptoms
heartburnExtra-Esophageal Symptoms
cough hoarseness
asthmaNo response to BID PPI
HAs-BEER toolHeartburn=1Asthma=1BMI>25=1Cough=0
Hoarseness=0
HAs-BEER toolscore of 3:
97.8% sensitivity for AET>5.5%92% positive predictive value
HAs-BEER toolscore of ≤2
80% negative predictive value
pH monitoring off PPIProlonged wireless pH monitoring
pH-impedance monitoring on PPIReflux episodes, non-acid reflux
Patel DA….Vaezi MF et al, Gastroenterology 2018;155:1729-40
<10% of atypical
symptoms
0
5
10
15
20
25
30
35
pre intervention offPPI
pre intervention onPPI
post intervention 6months
post intervention 12months
BID PPI arm
MSA arm
*
GE
RD
HR
QL
scor
e
*
Reflux Episodes Predict GERD Response
Sen
sitiv
ity
1-Specificity
Satisfaction with therapy GERD HRQL
sensitivity 0.64 specificity 0.67 AUC 0.76
sensitivity 0.64 specificity 0.59 AUC 0.71
Rogers BD….Crowell M, Vela MF et al, Gut 2020 (in press)
Randomized Study Comparing BID PPI to MSA
Refractory regurgitation123 patients
age 46.9±1.2 yr43% female
35 reflux episodes 35 reflux episodes
MSA: magnetic sphincter augmentation
>80 reflux episodes pre-crossover to MSApredicted improvement from MSA
Magnetic sphincter augmentation device
33
34
American College of Gastroenterology

18
AETReflux episodes
40 reflux episodessensitivity 0.80specificity 0.51
AUC 0.70
AET 0.5%sensitivity 0.62specificity 0.51
AUC 0.58
Healthy volunteers given BID PPI
European heartburn-predominant cohortn=43
Patients with proven GERDtreated with BID PPI
n=66
North American regurgitation-predominant cohort n=42
pH-impedance monitoring on
BID PPI
Median values in healthy volunteers
median AET 0.0% median reflux episodes 16 median 5 cm MNBI 2400 ohms
Gyawali CP….Sifrim D et al, Gastro 2021 (in press)
Studies ‘on PPI’
AET>4%AET<0.5%
episodes<40
10 4 0 10 4 14
3 10 4 19 2 2
14 patients
2 patients
Abnormal reflux burden and/or abnormal mucosal integrity Parameters based on new thresholds Normal study
Heartburn-Predominant
EuropeanCohort
Regurgitation-Predominant
North AmericanCohort
cumulative n
cumulative n
n
n
Total 14 patients (32.6%)
Total 17 (40.5%) patients
1
2
Hypervigilance
Total 1 patient (2.3%)
Total 2 patients (4.8%)
Total 14 patients (32.6%)
Total 21 (50.0%) patients
10 with AET>4%; 7 with episodes>80; 5 with MNBI<1500 ohms; 2 with episodes 40-80;
4 with RSA; 14 with PSPW index <50%
3 with AET>4%; 12 with episodes>80; 9 with MNBI<1500 ohms; 9 with episodes 40-80; 10
with RSA
10 with episodes 40-80; 8 with AET 0.5-4%; 2 with RSA; 13 with
PSPW index <50%
19 with episodes 40-80; 13 with AET 0.5-4%; 12 with RSA
Escalate reflux management Escalate reflux managementif other supportive features
e.g. hiatus hernia
Neuromodulators
GERD Evidence: Studies ‘on PPI’
Gyawali CP….Sifrim D et al, Gastro 2021 (in press)
57.1% non-responders 28.6% non-responders 100% NR 71.4% R
82.4% non-responders 81.0% non-responders 50% NR 50% R
RSA: reflux-symptom association
MNBI<1500episodes>80 episodes 40-80 AET 0.5-4% RSA
Overall 79% Heartburn 60%
Regurgitation 83%
Response to Surgical Management
Overall 85% Heartburn 60%
Regurgitation 93%
In patients with proven GERD, ambulatory reflux monitoring performed on PPI therapy can be useful in identifying persistent GERD that might benefit from surgical management
35
36
American College of Gastroenterology

19
Role of HRM in GERD
Chan WW et al, Surg Endosc 2011;25:2943
1.0-2.5% of ‘GERD’ referred for anti-reflux
surgery
Predictors of post-fundoplication dysphagia Univariate Multivariate
n=157, 2.1 yr follow up OR 95% CI OR 95 % CI
Age (years) 0.99 0.96, 1.02 0.97 0.92, 1.02
Gender (F) 2.10 0.75, 5.92 1.12 0.25, 4.95
Pre-fundoplication dysphagia 2.95 1.25, 6.98 1.15 0.34, 3.87
Early post-fundoplication dysphagia 3.10 1.23, 7.76 1.40 0.34, 5.83
Dysmotility on post-fundoplication barium swallow
2.17 0.89, 5.24 1.43 0.19, 10.67
Recurrent Hernia on barium swallow 3.45 1.12, 10.63 3.37 0.36, 31.50
Absent contraction reserve 3.37 1.12, 10.59 3.73 1.11,12.56
In patients with persistent reflux symptoms, HRM rules out motor disorders, and assesses
esophageal peristaltic performance
TYPE 2
TYPE 1
TYPE 3
TYPE 3DIAPHRAGM NOT TRAVERSED
0
40
80
0
40
80
0
40
80
Reflux burden: █ normal █ abnormal
Pandolfino JE, et al. Am J Gastroenterol 2007; 102:1056-63Rengarajan A, Gyawali CP. J Clin Gastroenterol 2020;54:22:27
Rogers BD et al. Neurogastroenterol Motil 2020
Healthy controlsn=484
GERD patientsn=482
97.1% 61.8%
2.9% 25.9%
0 12.2%
HRM complements EGD and barium studies in increasing diagnostic yield of hiatus hernia
Tolone et al, UEG Journal 2018
HRM had sensitivity of 94.3% and specificity of 91.5% in detecting hiatus hernia using hernia size at surgery as gold standard compared to endoscopy (96.2%, 74.5%) andbarium radiography (69.8%, 97.9%)
37
38
American College of Gastroenterology

20
LES level
Crural level
Barium Radiography20 patients with reflux symptoms50% had ‘reflux’ on esophagramGold standard: pH impedance
Saleh CMG et al, NGM 2015;27:195-200
sensitivity 46%specificity 44%PPV: 50%, NPV: 40%
Reflux observed during barium studies cannot be used as evidence supporting pathologic
reflux
REFRACTORY REFLUX SYMPTOMSDESPITE PPI THERAPY
PROVEN GERDREFRACTORY GERD SYMPTOMS
LA Grades C/D EsophagitisBarrett’s Esophagus >1 cmPeptic StrictureAcid Exposure Time >6%
ENDOSCOPYHIGH RESOLUTION MANOMETRY
pH OR pH IMPEDANCE MONITORING OFF PPI
ENDOSCOPYHIGH RESOLUTION MANOMETRY
pH IMPEDANCE MONITORING ON PPI**
GERD EVIDENCE*
REFRACTORY GERDPersistent Acid Reflux
Persistent Weakly-Acid Reflux
NO GERD EVIDENCE*NO ONGOING
GERD EVIDENCE*
*according to Lyon Consensus criteria
Persistent symptoms
Repeat endoscopy and high-resolution manometry on case-by-case basis
**pH impedance on PPI not essential in patients with large hiatal hernia and proven GERD with refractory GERD
symptomsZerbib F et al, Neurogastroenterol Motil 2020
UNPROVEN GERD
GERD EVIDENCE*
39
40
American College of Gastroenterology
21
‘r’ wave
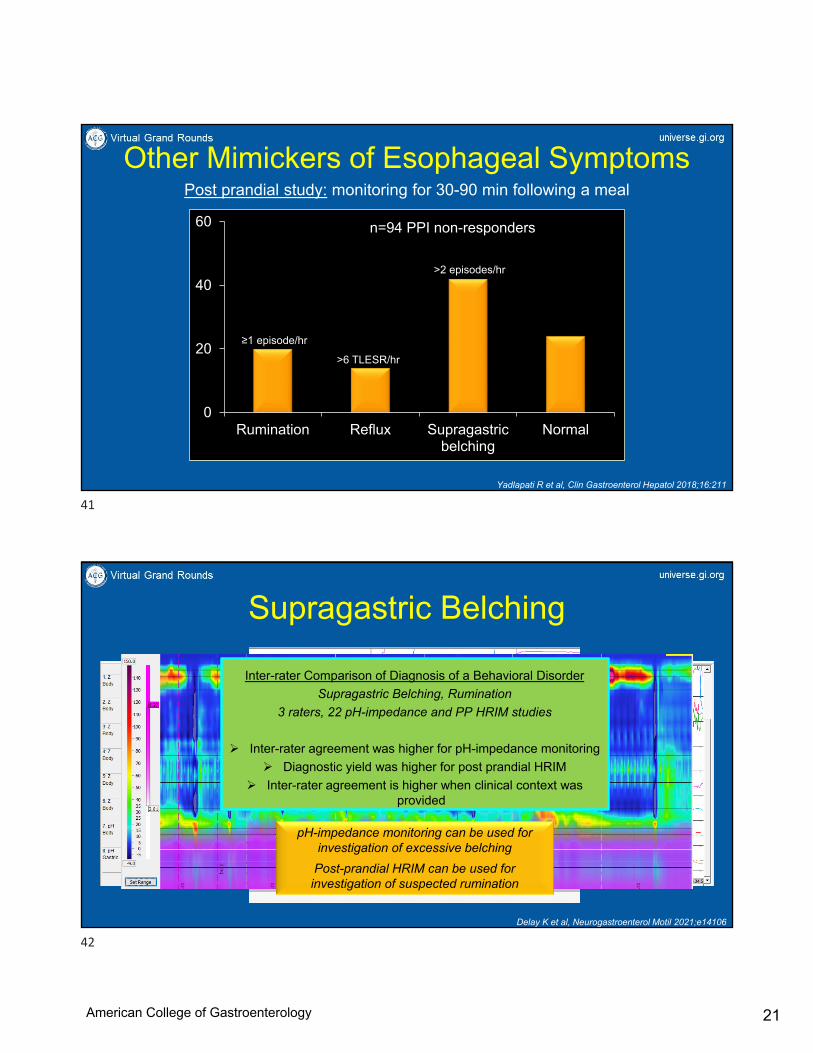
Other Mimickers of Esophageal SymptomsPost prandial study: monitoring for 30-90 min following a meal
Rumination Syndrome
Yadlapati R et al, Clin Gastroenterol Hepatol 2018;16:211
Transient LES RelaxationSupragastric Belching
0
20
40
60
Rumination Reflux Supragastricbelching
Normal
n=94 PPI non-responders
>6 TLESR/hr
≥1 episode/hr
>2 episodes/hr
Supragastric Belching
Inter-rater Comparison of Diagnosis of a Behavioral Disorder
Supragastric Belching, Rumination
3 raters, 22 pH-impedance and PP HRIM studies
Inter-rater agreement was higher for pH-impedance monitoring
Diagnostic yield was higher for post prandial HRIM
Inter-rater agreement is higher when clinical context was provided
Delay K et al, Neurogastroenterol Motil 2021;e14106
pH-impedance monitoring can be used for investigation of excessive belching
Post-prandial HRIM can be used for investigation of suspected rumination
41
42
American College of Gastroenterology
22
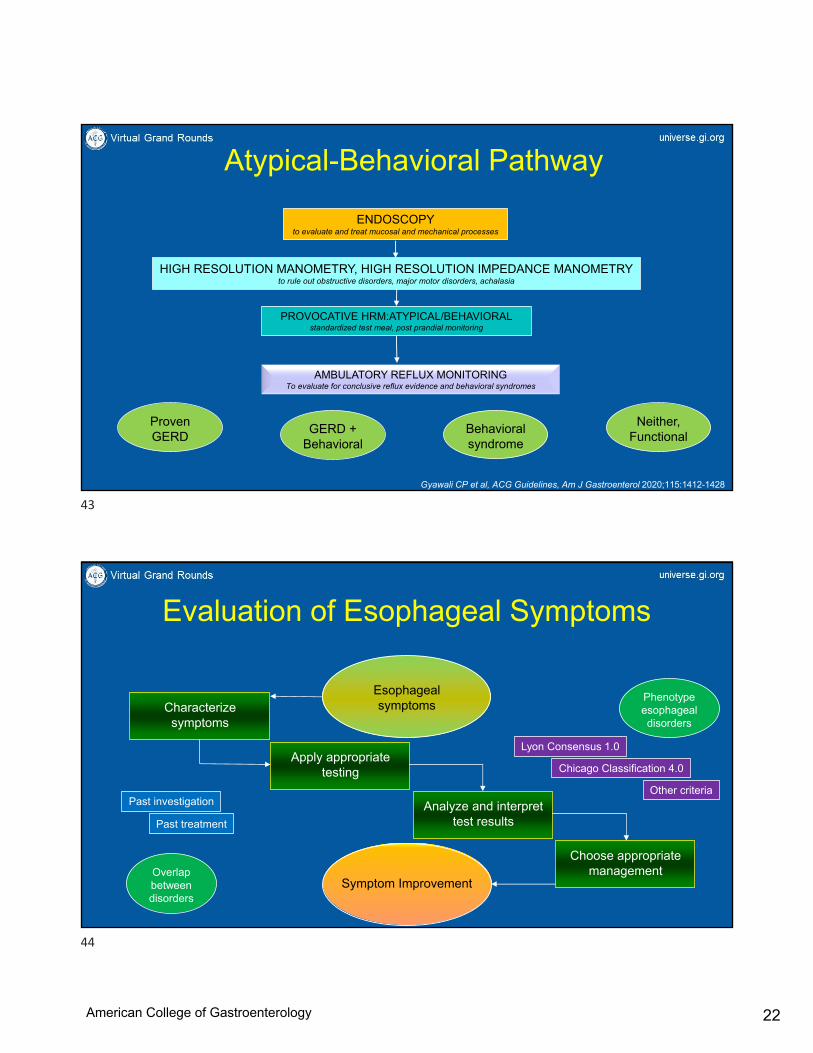
HIGH RESOLUTION MANOMETRY, HIGH RESOLUTION IMPEDANCE MANOMETRYto rule out obstructive disorders, major motor disorders, achalasia
PROVOCATIVE HRM:ATYPICAL/BEHAVIORALstandardized test meal, post prandial monitoring
ENDOSCOPY to evaluate and treat mucosal and mechanical processes
Atypical-Behavioral Pathway
Gyawali CP et al, ACG Guidelines, Am J Gastroenterol 2020;115:1412-1428
AMBULATORY REFLUX MONITORINGTo evaluate for conclusive reflux evidence and behavioral syndromes
Proven GERD
GERD + Behavioral
Behavioral syndrome
Neither, Functional
Evaluation of Esophageal Symptoms
Esophageal symptoms
Symptom Improvement
Characterize symptoms
Apply appropriate testing
Analyze and interpret test results
Choose appropriate management
Lyon Consensus 1.0
Chicago Classification 4.0
Other criteriaPast investigation
Past treatment
Overlap between disorders
Phenotype esophageal disorders
43
44
American College of Gastroenterology

23
Take Home Points
• Start with a good history, which can direct investigation
• EGD, HRM, barium esophagram and FLIP, usually performed in sequence, leads to a diagnosis of obstructive symptoms
• PPI trial is a reasonable starting point for typical reflux symptoms
• Up front esophageal testing is cost effective for atypical symptoms
• Concept of unproven vs. proven GERD determines reflux monitoring off vs. on PPI therapy; interpretation paradigms differ
• Behavioral syndromes are diagnosed using pH-impedance monitoring and post prandial HRIM
Birthplace of High-Resolution ManometrySt. Louis, Missouri, USA
45
46
American College of Gastroenterology

24
Questions?
Speaker: C. Prakash Gyawali, MD, MRCP, FACG
Moderator: Amit Patel, MD, FACG
47
48
American College of Gastroenterology
Related Documents











