-
8/16/2019 Part06 Ch14 Copy
1/13
© 2011 Decker Intellectual Properties
VASCULAR SYSTEM MESENTERIC REVASCULARIZATION PROCEDURES — 1
DOI 10.2310/7800.2109
11/11
MESENTERIC REVASCULARIZA-TION PROCEDURES
Ravi Dhanisetty, MD, Scott Musicant, MD, Lloyd M. Taylor, Jr, MD, FACS, and Gregory L. Moneta, MD
artery stenosis associated with chronic mesenteric ischemia.3,4
Although it is a technically difficult examination to perform,
in experienced hands, the sensitivity of duplex scanning for
detecting lesions in the superior mesenteric artery (SMA) and
celiac artery is 92% and 87%, respectively. When compared
with catheter-based angiography, the overall accuracy for
detection of a 70% lesion in the SMA and celiac artery
was 96% and 82%, respectively.5 By itself, however, duplex
scanning is not sufficient for planning a mesenteric revascu-
larization procedure.
Multidetector CT angiography is the most frequently used
technique for the diagnosis of mesenteric artery stenosis or
occlusions consistent with mesenteric ischemia. Multidetec-
tor CT angiography has in many cases replaced other modal-
ities as the imaging study of choice for evaluation of chronic
mesenteric ischemia [see Figure 2]. It can accurately identifysignificant stenosis in the celiac artery and SMA, identify
significant visceral collaterals, and exclude other potential
intra-abdominal processes.6,7 CT angiography has higher spa-
tial resolution and allows for assessment of visceral branches,
including the inferior mesenteric artery, with greater accuracy
than contrast-enhanced magnetic resonance angiography.8,9
Mesenteric ischemia is encountered infrequently. To date,
there have been no randomized, controlled trials comparing
treatment modalities for either acute or chronic mesenteric
ischemia. Consequently, decisions on how to treat this con-
dition must be based on a few large case series in which a
variety of procedures were used.
Overall evaluation and management of acute mesenteric
ischemia are addressed more fully elsewhere. In what follows,
we focus specifically on the operative techniques used to treat
mesenteric ischemia (whether chronic or acute) and discuss
the available literature supporting their use. The appropriate
technique for a particular patient varies according to the
individual anatomy and intraoperative findings. The relevant
surgical procedures may be conveniently divided into those
employed for chronic mesenteric ischemia and those employed
for acute ischemia.
Procedures for Chronic Intestinal Ischemia
In 1936, J. E. Dunphy was the first to suggest that timely
diagnosis and intervention for mesenteric artery occlusive
disease may prevent intestinal infarction.1 It is now clear that
optimal treatment of mesenteric ischemia depends on prompt
diagnosis and that a high index of suspicion is vital.
Patients with chronic intestinal ischemia generally, but not
always, report experiencing colicky, dull, or aching abdomi-
nal pain, primarily located in the epigastrium but occasionally
radiating to the back. Symptoms typically begin 15 to 30
minutes after eating and may last as long as 3 to 4 hours.
Peritonitis is not a characteristic of reversible intestinal isch-
emia; rather, it is indicative of intestinal infarction. Chronic
postprandial abdominal symptoms result in markedly reduced
food intake (so-called food fear),2 which generally leads to
weight loss.
Physical examination often yields no significant abdominal
findings. Abdominal bruits may be audible but are a non-
specific finding. Patients often, but not always, show evidence
of atherosclerotic disease in other vascular territories. Bowel
habits vary, ranging from normal elimination to diarrhea or
constipation.
Mesenteric ischemia is a clinical diagnosis. Imaging studies
are therefore used to confirm mesenteric artery stenosis orocclusion, supportive of a diagnosis of mesenteric ischemia.
Useful imaging modalities include duplex ultrasonography,
contrast angiography, multi-detector computed tomographic
(CT) angiography, and magnetic resonance angiography.
Duplex scanning is effective in detecting visceral artery steno-
sis [see Figure 1] and may allow earlier detection of visceral
Figure 1 Example of a duplex spectral waveform with
comparative arteriography in a patient with superior
mesenteric artery (SMA) stenosis. The peak systolic
velocity (> 550 cm/s) is dramatically increased over normal
(< 275 cm/s).
American SurgeryScientific
-
8/16/2019 Part06 Ch14 Copy
2/13
MESENTERIC REVASCULARIZATION PROCEDURES — 2
11/11
dangerous. Appropriate magnification views generally allow
characterization of the proximal SMA beyond its origin, even
without selective catheterization of the SMA. Intra-arterial
digital subtraction techniques are usually adequate for lateral
views and require less contrast material than other techniques.
Arteriography also demonstrates coexisting lesions of the
aorta and of the renal and iliac arteries that may be important
in planning revascularization.
Essentially all patients with peripheral artery disease have
some degree of concomitant coronary artery disease (CAD).
Although no symptoms of CAD may be evident, care must
still be taken to provide perioperative cardiac protection.
Perioperative beta blockade, antiplatelet therapy, and statin
medications should be routinely employed whenever possible
in patients undergoing elective arterial reconstructive
procedures.
If the patient is undergoing a bypass procedure, the choice
of graft material should be addressed. In general, prosthetic
grafts work well for mesenteric artery bypasses. However, the
entire abdomen and both legs should still be included in the
operative field in case autologous vein proves necessaryfor the bypass conduit. Autologous vein is often required in
cases involving bowel resection and may also be preferable
for bypasses to smaller visceral vessels. If an autologous vein
bypass procedure is planned, preoperative duplex scanning of
the greater saphenous and femoral veins is recommended to
facilitate selection of the best available vein for the conduit.
Together with noncontrast images, CT, in many cases, offers
enough anatomic details to plan open procedures. Limita-
tions include contrast-related nephropathy, hypersensitivity
reactions, and inaccurate timing of contrast infusion that may
lead to an indeterminate study and delayed diagnosis.
Arteriography is the traditional imaging technique employed
in planning mesenteric revascularization for chronic intestinal
ischemia [see Figure 3 and Figure 4]. Lateral and anteroposte-
rior views of the aorta are required for full evaluation of the
severity of visceral stenosis or occlusion and the extent of col-
lateral development. In most cases, a transfemoral Seldinger
technique is suitable, although in the setting of iliofemoral
occlusive disease, a transaxillary approach is occasionallyrequired. Between 60 and 100 mL of contrast material is
required for appropriate lateral and anteroposterior views of
the abdominal aorta. Visceral artery lesions are usually ostial
but may extend beyond the orifice of the vessel as a posterior
plaque, especially in the SMA. Selective catheterization of
the main intestinal arteries is rarely necessary and may be
Figure 2 Computed tomographic angiography is being used
more frequently to demonstrate mesenteric artery lesions.
With three-dimensional reconstruction, segmental stenosis
or occlusions can be demonstrated in mesenteric arteries.
Above is an example of proximal occlusion (arrow) of the
superior mesenteric artery with distal reconstitution via
collaterals.
Figure 3 A lateral aortogram clearly shows severe stenosis
of the superior mesenteric artery (arrow) in a patient with
intestinal ischemia.
© 2011 Decker Intellectual Properties
VASCULAR SYSTEM
American SurgeryScientific
-
8/16/2019 Part06 Ch14 Copy
3/13
MESENTERIC REVASCULARIZATION PROCEDURES — 3
11/11
Visceral Endarterectomy
Visceral endarterectomy for treatment of mesenteric isch-
emia was first described in 1958 by Shaw and Maynard,10
who performed endarterectomy of the SMA in a blind,
retrograde fashion through a distal arteriotomy. At present,
retrograde endarterectomy cannot be recommended.
The SMA can be approached directly once control of the
supraceliac aorta has been obtained.11 A longitudinal incision
is made across the origin of the SMA, and an endarterectomy
is performed. In most patients, the exposure is limited.
This direct approach may be considered when the SMA is
widely separated from the renal arteries and the visceral
aorta is relatively free of disease; however, this scenario is
uncommon.A more versatile endarterectomy technique is transaortic
endarterectomy.12 This procedure involves a posterolateral
approach to the aorta, in which the aorta is exposed trans-
peritoneally with medial visceral rotation. Alternatively, a
completely retroperitoneal approach may be taken. The main
disadvantage of the retroperitoneal approach is that it restricts
the surgeon’s ability to assess the bowel at the completion of
revascularization.
Transaortic endarterectomy Step 1: incision and initial
approach A midline incision is recommended. A complete
medial visceral rotation is performed, with the left kidney left
in its bed.
Step 2: exposure The lateral aorta is exposed, and theceliac artery and the SMA may be identified anteriorly; the
left renal artery lies posteriorly.
Step 3: endarterectomy A trapdoor incision is made in the
aortic wall in such a way as to encompass the orifices of the
SMA and the celiac artery. Partial occlusion of the aorta with
a clamp is sometimes possible, but in most cases, complete
aortic occlusion is required. If necessary, the aortotomy can
be extended distally and posteriorly to include the renal artery
orifices as well.
Among the advantages of this operation are that it permits
simultaneous endarterectomy of the aorta and all visceral
vessel orifices and that it does not require the use of
prosthetic material [see Figure 4]. The disadvantages include
the potential risks associated with suprarenal clamping (e.g.,
cardiac overload, renal and lower extremity embolization,
and ischemia). Because of these risks, the need for more
extensive dissection, and the unfamiliarity of most surgeons
with this procedure, arterial bypass procedures are generally
preferred for treatment of chronic mesenteric ischemia.
Mesenteric Arterial Bypass
Technical considerations Single-vessel versus multiple-
vessel revascularization There are two schools of thought
on the extent of revascularization for chronic mesenteric
ischemia. Proponents of so-called complete revascularization
advocate revascularization of both the celiac artery and the
SMA and suggest that this approach makes recurrent isch-
emia less likely should one graft or graft limb undergo throm-
bosis.13 In a 1992 study, overall graft patency and survival
were better in patients who underwent multiple-vessel bypassthan in those who underwent single-vessel bypass. The inves-
tigators concluded that multiple-vessel bypass patients were
likely to remain asymptomatic because of the presence of
additional grafts or graft limbs that remained patent.13
Others maintain that the critical vessel involved in chronic
mesenteric ischemia is the SMA and argue that bypass to
the SMA alone is a relatively simple procedure that relieves
symptoms of mesenteric ischemia. In a 2000 study evaluating
49 patients who underwent bypass to the SMA alone, the
9-year primary assisted graft patency rate was 79% and the
5-year survival rate was 61%14 —results equivalent to those
noted in contemporary studies of multiple-vessel revascular-
ization for chronic intestinal ischemia.15
Antegrade versus retrograde bypass Mesenteric bypass grafts
may originate either above or below the renal arteries. Bypassgrafts are considered antegrade if they originate on the ante-
rior surface of the abdominal aorta cephalad to the celiac
artery and retrograde if they originate from the infrarenal
aorta or a common iliac artery. The distal thoracic aorta can
also serve as an inflow site for antegrade mesenteric bypass.
Antegrade bypass from the supraceliac aorta, using either
Figure 4 Lateral aortogram showing so-called coral reef
atheroma involving the visceral aorta with occlusion of the
origin of the superior mesenteric artery. A patient with
mesenteric ischemia and this angiogram may be best treated
with transaortic endarterectomy.
© 2011 Decker Intellectual Properties
VASCULAR SYSTEM
American SurgeryScientific
-
8/16/2019 Part06 Ch14 Copy
4/13
MESENTERIC REVASCULARIZATION PROCEDURES — 4
11/11
prosthetic material or autologous vein, has certain advan-
tages, including a straight graft configuration that minimizes
turbulence and graft kinking. Typically, there is also reduced
atherosclerotic calcification in the supraceliac aorta.16 The
disadvantages of antegrade bypass are similar to those of
visceral endarterectomy and derive from the need to clamp
the supraceliac aorta for the proximal anastomosis. As with
visceral endarterectomy, partial occlusion clamping is theo-
retically possible but not always practical. Clamping of the
supraceliac aorta may increase the risk of cardiac events,
visceral or renal emboli, and ischemia. One prerequisite for
use of the supraceliac aorta in an antegrade bypass is that the
vessel must be angiographically normal to ensure that it can
safely be clamped. It should also be kept in mind that reop-
eration on the supraceliac aorta is difficult: once this site has
been used, reexposure generally is not safe.
Antegrade bypass Step 1: incision and initial approach
Supraceliac aorta–visceral artery bypass is performed through
an upper midline incision. Self-retaining retractors are very
helpful.
Step 2: exposure The dissection begins with division of the
gastrohepatic ligament and retraction of the left lobe of the
liver to the right, followed by incision of the diaphragmaticcrus and exposure of the anterior aspect of the aorta.
Step 3: choice of graft In clean cases with no intestinal
necrosis or perforation, we use woven Dacron grafts. If a
single-vessel bypass is to be performed, a single limb is cut
from the bifurcated graft, incorporating a flange of the main
body of the bifurcated graft for the proximal anastomosis.
Autologous vein grafts are usually reserved for contaminated
cases. The femoral vein is an excellent autogenous conduit
for mesenteric arterial bypass.
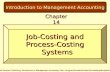
Step 4: anastomosis of graft to supraceliac aorta and visceral
artery If the celiac artery alone is to be revascularized, the
usual procedure is to perform an end-to-side proximal
anastomosis to the aorta, followed by an end-to-side distal
anastomosis to the common hepatic artery. If the SMA alone
is to be revascularized, it is generally necessary to tunnel thegraft beneath the pancreas to the inferior border of the pan-
creas and then perform an end-to-side anastomosis to the
SMA at that level [see Figure 5a]. Extreme care must be
exercised in developing the retropancreatic tunnel. If this area
appears too narrow or is scarred as a result of previous
pancreatic inflammation, the graft should be tunneled ante-
rior to the pancreas to ensure that it is not compressed and
to avoid causing bleeding from disrupted pancreatic veins.17
If a prepancreatic tunnel is required, an autogenous conduit
should be considered because the graft will be lying adjacent
to the posterior wall of the stomach. If both the celiac artery
and the SMA are to be revascularized from the supraceliac
aorta, a bifurcated prosthetic graft is attached to the suprace-
liac aorta proximally, with one distal limb anastomosed to the
hepatic artery and the other to the SMA [see Figure 5b].
Retrograde bypass In a retrograde bypass, the infrarenal
aorta or, more commonly, common iliac artery is used as the
inflow vessel. One clear advantage of this procedure is that
the approach to the infrarenal aorta is more familiar to most
surgeons. Another is that dissection and clamping of the infra-
renal aorta are less risky than dissection and clamping of the
supraceliac aorta. Yet another is that the surgeon can work
within a single operative field. Once the self-retaining retrac-
tor is placed, the operation on the infrarenal aorta and the
SMA can be performed without further adjustment of the
retractor. The main disadvantage is the potential for graft
kinking.
Step 1: incision and initial approach Here, too, a midline
incision and a transperitoneal approach are preferred. The
transverse mesocolon is retracted upward, and the ligament
of Treitz is divided.
Step 2: exposure After division of the ligament of Treitz,
the duodenum and the small bowel are retracted to the right.
The SMA may then be identified arising from beneath the
inferior border of the pancreas. The retroperitoneum is
divided distally along the aorta to a point just beyond the
level of the aortic bifurcation. The distal aorta and both
common iliac arteries are assessed to allow determination of
the optimal location for the proximal anastomosis.
Step 3: choice of graft As a rule, grafts made of Dacron or
of ringed, reinforced expanded polytetrafluoroethylene
(ePTFE) are preferred. Problems may arise when retrograde
bypasses are performed with autologous vein grafts, in that
such grafts are prone to kinking when the viscera are replaced.
When a retrograde vein bypass is performed, the graft may bebrought straight up from the right iliac artery so that it lies
between the aorta and the duodenum and then anastomosed
to the posteromedial wall of the SMA.
Step 4: anastomosis to infrarenal aorta or common iliac artery
and SMA Our preference is to use the area near the junction
of the aorta with the right common iliac artery for the proxi-
mal anastomosis. (Short grafts originating from the midpor-
tion of the infrarenal aorta, although commonly described,
are prone to kinking when the viscera are returned to their
normal position.) The graft to the SMA is passed cephalad,
turned anteriorly and inferiorly 180°, and anastomosed to the
anterior wall of the SMA just beyond the inferior border of
the pancreas.17 In this manner, a gentle C loop is formed that,
if placed correctly, keeps the graft from kinking when the
viscera are restored to their anatomic position after retractorremoval [see Figure 6 ]. The ligament of Treitz and the parietal
and mesenteric peritoneum are closed over the graft to
exclude it from the peritoneal cavity.
Endovascular Techniques
Endovascular techniques, usually a combination of angio-
plasty and stent placement, are being used with greater
frequency for chronic mesenteric ischemia [see Figure 7 ]. By
2002, endovascular procedures (angioplasty/stent) surpassed
all surgical procedures performed for chronic mesenteric
ischemia, with decreased 30-day mortality compared with
open procedures (4 versus 13%).18 Early reports describing
the use of percutaneous transluminal angioplasty (PTA) to
treat visceral atherosclerotic lesions indicated that initial tech-
nical success rates were as high as 80% but that recurrence
rates ranged from 20 to 40%.17,19 Recent reports of endovas-cular therapy for chronic mesenteric ischemia showed no
difference in in-hospital morbidity or mortality or 2-year sur-
vival. Also, there was no difference in symptomatic (23 versus
22%) or radiographic (32 versus 37%) recurrence. However,
radiographic primary patency (58 versus 90%) and primary
assisted patency (65 versus 96%) were significantly lower
© 2011 Decker Intellectual Properties
VASCULAR SYSTEM
American SurgeryScientific
-
8/16/2019 Part06 Ch14 Copy
5/13
MESENTERIC REVASCULARIZATION PROCEDURES — 5
11/11
in the patients who received endovascular treatment.20
Another study with longer follow-up showed 3-year actuarial
patency of 63%. About 30% of patients required reinterven-
tion for recurrent symptoms. The median time to reinterven-
tion for symptom recurrence was 15 months. Because of thishigh rate of restenosis and symptom recurrence, close follow-
up is mandatory in all patients treated with mesenteric artery
stents. Most importantly, initial endovascular treatment did
not preclude any future surgical bypass options.21 These early
results indicate that an endovascular approach to chronic
mesenteric ischemia is a viable option in carefully selected
patients.
Technical
The main technical complication of mesenteric bypass is
acute graft thrombosis. This event is rare, but when it occurs,
prompt recognition is essential to prevent intestinal infarc-
tion. Kinking and compression of the graft are the most
common causes of this condition. If the retrograde graft is toolong, the redundancy makes it more susceptible to kinking.
Similarly, if the graft is not positioned so as to form a gentle
C loop, it is at risk for kinking when the viscera are returned
to their normal position. An antegrade graft that is too long
is equally at risk for kinking and occlusion. When an ante-
grade bypass is tunneled behind the pancreas, an adequate
amount of space must be present to ensure that the graft
is not compressed. In general, prosthetic grafts are more
resistant to kinking and compression than vein grafts are.
Identification of perioperative graft occlusion is hindered
by postoperative incisional pain, fluid shifts, fever, and leuko-cytosis, all of which are common in the postoperative period
and may mask signs of intestinal ischemia. Patients with
chronic mesenteric ischemia often have symptoms only when
eating and thus may be asymptomatic in the postoperative
period until they resume oral feeding. For these reasons,
we advocate evaluating the graft early in the postoperative
period with either conventional contrast angiography or CT
angiography [see Outcome Evaluation, below].
Additional technical complications may occur as a result
of clamp placement. Clamping of the supraceliac aorta can
lead to renal atheroemboli or ischemia. These problems can
be minimized by using a supraceliac clamp only on an
angiographically normal aorta.
Systemic
Myocardial infarction is the most common cause of mor-tality in patients treated for mesenteric ischemia. Pulmonary
compromise is also a common systemic complication of mes-
enteric revascularization. Renal failure after mesenteric revas-
cularization is more common in patients with preoperative
renal insufficiency.22 Mortality is markedly increased when
renal failure occurs postoperatively.22 Postoperative renal
Figure 5 Arterial bypass: antegrade. Shown is bypass from the supraceliac aorta to the superior mesenteric artery (SMA) alone
(a) or to the hepatic artery and the SMA (b).39
a b
© 2011 Decker Intellectual Properties
VASCULAR SYSTEM
American SurgeryScientific
-
8/16/2019 Part06 Ch14 Copy
6/13
MESENTERIC REVASCULARIZATION PROCEDURES — 6
11/11
insufficiency can be minimized by administering mannitol,
furosemide, and, possibly, vasodilators intraoperatively.
Patients who undergo mesenteric revascularization occa-
sionally experience a profound reperfusion syndrome
manifested by acidosis, pulmonary compromise, and coagu-
lopathy. We recommend administering sodium bicarbonate
(to minimize the effects of metabolic acidosis) and mannitol
(for its free radical–scavenging properties) before restoring
intestinal perfusion.
Restoration of pulsatile flow to the small bowel usually
results in immediate active peristalsis and intestinal edema.
The technical success of surgical revascularization is assessed
intraoperatively through visual examination of the intestine
and continuous-wave Doppler examination of the distal
mesenteric vasculature and the bowel wall. Doppler signals
should be detected along the antimesenteric border, and
pulses should be palpable in the mesentery. Intraoperativeduplex scanning may also be used to visualize anastomotic
sites directly.23
Electromagnetic flow measurements can be helpful in
evaluating the adequacy of mesenteric revascularization. Such
measurements must be made after all packs and retractors
have been removed. In most cases, the flow rate through the
graft should be between 500 and 800 mL/min, but flow rates
as high as 1,000 mL/min may be recorded.17
To confirm technical success after mesenteric revascular-
ization, we advocate routine postoperative imaging of the
graft. Ideally, this is done early in the postoperative period.
Catheter-based contrast angiography is optimal for evaluating
the bypass graft and the distal vasculature, allowing identifi-
cation of anastomotic stenoses, kinking [see Figure 8a], or,
in the case of autologous grafts, narrowing caused by valves.
If a technical defect is discovered, reoperation and correction
are required to ensure prolonged patency. In the past few
years, we have started evaluating selected patients periopera-
tively with CT angiography. This modality is less invasive
than traditional contrast angiography but still requires
administration of contrast material and exposure to radiation
[see Figure 8b].
Duplex ultrasonography has been used for postoperative
graft surveillance after mesenteric revascularization.24
Although it can be difficult in the early postoperative period
because of incisional tenderness and postoperative ileus,
it has proven to be a valuable tool to follow bypass grafts.
A retrospective study at our institution has defined normal
duplex ultrasonography–derived velocity characteristics of
mesenteric artery bypass grafts. The anastomotic and mid-graft peak systolic velocities are not affected by the orienta-
tion of the graft. Mean peak systemic velocity for most grafts
is between 140 and 200 cm/s and remains relatively stable on
repeat examinations. Serial duplex examinations can be used
to assess the patency of bypass grafts to mesenteric arteries.25
We routinely use postoperative duplex scanning to establish
Figure 6 Arterial bypass: retrograde. Shown is bypass from
the right common iliac artery to the superior mesenteric
artery.39 The inset shows a method of graft preparation using
the main body of a bifurcated graft to provide a flange for the
proximal anastomosis.
Figure 7 Computed tomographic angiogram showing a stent
in a superior mesenteric artery. Mesenteric artery stents are
being used with increasing frequency as an alternative to
bypass for treatment for chronic visceral ischemia in
higher-risk patients.
© 2011 Decker Intellectual Properties
VASCULAR SYSTEM
American SurgeryScientific
-
8/16/2019 Part06 Ch14 Copy
7/13
MESENTERIC REVASCULARIZATION PROCEDURES — 7
11/11
baseline values and to permit comparisons for follow-up
evaluation of graft patency. If markedly elevated focal peak
systolic velocities (> 300 cm/s) are recorded, especially if
they increase on serial examinations, secondary imaging (CT
or conventional angiography) should be obtained to confirm
graft stenosis and to possibly plan intervention.
Procedures for Acute Intestinal Ischemia
As in the evaluation of patients with chronic mesenteric
ischemia, a high index of suspicion is of primary importance
in the evaluation of patients with possible acute mesenteric
ischemia. Most cases of acute intestinal ischemia result either
from thrombosis of a preexisting stenotic lesion or from
embolization (most frequently to the SMA).26 Cardiac emboli
are the most common variety, although tumor emboli27 and
atheroemboli are seen as well. Atheroemboli generally result
from iatrogenically induced cholesterol embolization caused
by aortic catheterization. The prognosis for acute intestinal
ischemia of embolic origin is more favorable than that for
acute ischemia of thrombotic origin. Emboli typically lodge
distally in the SMA distribution; therefore, the proximalintestine is still partially perfused.26 In contrast, thrombotic
occlusion occurs at the origin of the vessel, resulting in
complete interruption of midgut perfusion.
Acute, severe abdominal pain that is out of proportion to
the physical findings is the classic manifestation and is strongly
suggestive of intestinal ischemia. The duration of symptoms
Figure 8 Routine postoperative imaging is performed to confirm technical success after revascularization. (a) A postoperative
arteriogram shows a iliac artery–superior mesenteric artery (SMA) saphenous vein graft with a kink ( arrow). This problem was
asymptomatic and was corrected by reoperation on postoperative day 5. (b) A postoperative computed tomographic arteriogram
shows a retrograde iliac artery–SMA prosthetic graft. C (hook) configuration of distal anastomosis provides antegrade flow into
the SMA.
a b
© 2011 Decker Intellectual Properties
VASCULAR SYSTEM
American SurgeryScientific
-
8/16/2019 Part06 Ch14 Copy
8/13
MESENTERIC REVASCULARIZATION PROCEDURES — 8
11/11
does not appear to correlate with the degree of intestinal
infarction.28 Peritonitis is initially absent, but vomiting and
diarrhea may be present, and occult gastric or rectal bleeding
may be identified in as many as 25% of patients.28
There are no reliable serum markers for acute intestinal
ischemia. Leukocytosis, hyperamylasemia, or elevated lactate
levels may be present, but these findings are insensitive and
inconsistent. Abdominal radiographs may reveal dilated
bowel loops and, occasionally, thickened bowel wall, but
these findings are similarly inconsistent. In theory, duplex
ultrasonography may be helpful, but in practice, its applica-
bility is often limited by the gaseous visceral distention
frequently associated with acute intestinal ischemia.
Acute intestinal ischemia is a true surgical emergency. Any
evidence of acute abdomen should result in prompt operative
intervention. In stable patients suspected of having acute
mesenteric ischemia, the paradigm for diagnostic workup
has been slowly shifting toward the use of multidetector CT
angiography. Multidetector CT angiography uses thinner
collimation and overlapping data acquisition, which reduces
the amount of volume averaging and creates higher quality
volume sets for three-dimensional reconstruction. There
are several advantages to CT angiography, including near-
universal 24-hour access to a high-resolution scanner. With
three-dimensional reconstruction, mesenteric vessels can be
evaluated for embolus or thrombotic occlusion with accuracy.
Also, bowel can be evaluated concomitantly to support or
refute the diagnosis, and other intra-abdominal pathology can
be evaluated. A prospective study compared preoperative
radiographic findings with operative findings in 62 patients
suspected of acute myocardial infarction. Initial radiologist
interpretation had a sensitivity of 100% and a specificity of
89%.29 A subsequent study using CT angiography had similar
results in terms of accuracy.30 Significant limitations include
the need for proper timing of the contrast to evaluate
the vasculature and that the modality does not offer any
therapeutic options.
The use of preoperative arteriography to diagnose acute
ischemia is controversial. Delaying treatment to perform
arteriography could result in further intestinal infarction.Angiography may be considered in patients who have abdom-
inal pain without any other signs or symptoms of systemic
illness [see Figure 9 ]. In patients who have rebound tender-
ness, rigidity, or evidence of toxicity or shock, emergency
exploration is indicated.
Patients with acute intestinal ischemia who present with
evidence of toxicity must be resuscitated expeditiously to
ensure that surgical intervention is not delayed. Once it
is determined that surgery is indicated, no further delay is
justified. The patient is placed supine on the operating table,
and the entire abdomen and both legs are prepared. As in
operative treatment of chronic intestinal ischemia, the possi-
bility that autologous vein will be needed for bypass grafting
must be anticipated.
Intraoperative Considerations
Mesenteric revascularization and bowel resection
The goals of surgical therapy are to restore normal pulsatile
inflow, to ensure that questionably viable bowel is adequately
perfused, and to resect any clearly nonviable bowel. During
abdominal exploration, the viability of the intestine and the
status of the blood flow to the SMA are assessed with an eye
to determining the appropriate treatment. The surgeon should
be prepared to perform both intestinal revascularization and
intestinal resection. Segments of clearly viable bowel are often
interspersed with segments of marginally viable bowel and
segments of necrotic bowel. Acutely ischemic bowel that is
not yet necrotic may appear deceptively normal. Mildly to
moderately ischemic bowel may exhibit loss of normal sheen,
absence of peristalsis, and dull-gray discoloration. Other
objective signs of ischemia are the absence of a palpable pulse
in the SMA or in its distal branches, the absence of visible
pulsations in the mesentery, and the absence of flow on
continuous-wave Doppler examination of the vessels of the
bowel wall. The small bowel may be deeply cyanotic yet still
viable. In most cases, bowel resection should not be performed
until after revascularization.
The distribution of ischemic changes provides valuable
information about the cause of the ischemia. SMA thrombo-
sis often results in ischemia to the entire small bowel, with
the stomach, the duodenum, and the distal colon spared; in
severe cases, however, the entire foregut may be ischemic.
In contrast, ischemia secondary to SMA embolism generally
spares the stomach, the duodenum, and the proximal jeju-
num because the emboli tend to lodge at the level of the
middle colic artery rather than at the origin of the SMA. The
choice of operation for revascularizing the bowel depends onthe underlying causative condition. Embolectomy is indicated
for arterial embolism, whereas bypass is indicated for throm-
botic occlusion.
Revascularization of the acutely ischemic intestine
Patients with very advanced intestinal ischemia may have
Figure 9 Preoperative arteriogram shows embolic occlusion
of the superior mesenteric artery distal to its origin.
© 2011 Decker Intellectual Properties
VASCULAR SYSTEM
American SurgeryScientific
-
8/16/2019 Part06 Ch14 Copy
9/13
MESENTERIC REVASCULARIZATION PROCEDURES — 9
11/11
obvious widespread bowel necrosis. This situation almost
invariably proves fatal; thus, revascularization is not likely
indicated. In many patients, however, substantial portions of
the bowel are ischemic but not frankly necrotic. Whether
such bowel segments can be restored to viability cannot be
accurately predicted. In most instances, therefore, revascular-
ization should precede resection.
Restoration of normal flow to the SMA can produce
remarkable changes in an ischemic bowel. Because these
changes do not always occur immediately, it is often neces-
sary to preserve questionably viable portions of the bowel
initially and then perform a second-look laparotomy within
12 to 36 hours. If the questionably viable bowel is not in
significantly better condition at the time of the second-look
operation, it should be resected. Occasionally, however, even
a third look is prudent. Revascularized intestine that was
profoundly ischemic may swell dramatically. Temporary
abdominal closure with mesh or leaving the abdomen open
with a temporary closure device may permit tension-free
abdominal “closure,” prevent abdominal compartment syn-
drome, and perhaps even improve intestinal perfusion by
reducing intra-abdominal pressure.
Superior Mesenteric Artery Embolectomy
Step 1: incision and initial approach A midline
incision and transperitoneal approach is used.
Step 2: exposure of SMA at root of mesentery The
SMA is exposed after division of the ligament of Treitz at the
base of the transverse colon mesentery. The duodenum and
the small bowel are retracted to the right [see Figure 10 ]. The
visceral peritoneum is incised above the ligament of Treitz,
just cephalad to the third portion of the duodenum. The SMA
should be readily palpable in this location as it crosses over the
third portion of the duodenum. The dissection is continued to
obtain sufficient proximal and distal control of the vessel.
Heparin is administered, and the vessel is clamped proximally
and distally.
Step 3: arteriotomy An arteriotomy is then made in theSMA. The incision may be either transverse or longitudinal.
We prefer to perform a longitudinal arteriotomy if there is any
possibility that a bypass graft may be needed. The arteriotomy
should be made approximately 2 to 3 cm distal to the origin of
the SMA, although alternative placements may be appropriate
on occasion, depending on the anatomy and the estimated
location of the occlusion [see Figure 11, a and b].
Step 4: embolectomy Proximal embolectomy should be
performed first to ensure adequate inflow. A 3 or 4 French
balloon catheter is sufficient in most cases. If very good pulsa-
tile inflow is not achieved after embolectomy, then thrombosis
of a stenotic lesion is likely to be the underlying cause of the
acute intestinal ischemia, and a bypass graft should be placed.
Even when inflow is apparently adequate, a bypass should
be strongly considered if the proximal SMA is palpably
abnormal.
The narrowness and fragility of the distal SMA and its
branches can make distal embolectomy particularly challeng-
ing. It is best to use a 2 French embolectomy catheter for this
procedure. The catheter must be passed gently, without
undue force.
Step 5: closure Once all possible thrombus has been
removed, the arteriotomy is closed. A transverse arteriotomy
may be closed primarily with interrupted monofilament
sutures [see Figure 11c]; however, a longitudinal arteriotomy
frequently must be closed with an autologous vein patch. If
adequate flow is not restored after the clamps are removed,
the arteriotomy is used as the distal anastomotic site of a
bypass graft.
Superior Mesenteric Artery Bypass
Patients with SMA thrombosis who are seen early enough
and who have no intestinal necrosis may undergo SMA
bypass grafting with a prosthetic conduit. At exploration,
many of these patients have fluid within the peritoneal cavity.
This finding is not, in itself, a contraindication to the use
of a prosthetic graft. However, if the patient has necrotic
bowel that must be resected or if perforation has occurred,
a prosthetic graft should not be used. In these situations, an
autologous vein graft is preferred. A good-quality vein is
mandatory; if the saphenous vein is inadequate, the femoral
vein may be used instead.
The techniques of mesenteric bypass for acute intestinal
ischemia are identical to those for chronic intestinal ischemia.
Because these patients are often acutely ill, it is vital toperform the operation rapidly and efficiently. In the acute
setting, bypass to the SMA alone is strongly preferred [see
Figure 12]. As a rule, a retrograde approach, using the infra-
renal aorta or a common iliac artery for inflow, is best; the
supraceliac aorta is used for inflow only if the infrarenal
vessels are unsuitable for this purpose. Even highly calcified
iliac arteries can be used for inflow provided that there is no
significant pressure gradient and that the surgeon is familiar
with intraluminal balloon occlusion techniques for proximal
and distal control.
Hybrid Technique: Retrograde Open Mesenteric Stenting
Recently, a hybrid technique has been described that
combines the attributes of both endovascular and open
procedures. It allows for both endovascular treatment of mes-
enteric vessels and thorough assessment of bowel viability.
Initial results show a 100% initial success and a lower
in-hospital mortality rate of 17% compared with surgical
bypass or endovascular treatment.31,32
Step 1: Incision and exposure A patient suspected of
acute myocardial infarction is brought directly to the operat-
ing room with ongoing resuscitation. The left arm is abducted
and prepared along with standard preparation for potential
brachial access. Once the diagnosis is confirmed, initial mid-
line exploration and control of the infracolic SMA is obtained
as described for an SMA embolectomy procedure.
Step 2: Patch angioplasty and cannulation of infra-
colic SMA Once exposure and control of infracolic SMA
are obtained, the patient is fully heparinized to activatedclotting time of more than 300 seconds. The artery is incised
longitudinally, and a local thromboendarterectomy with patch
angioplasty is performed. Either bovine pericardium or saphe-
nous vein can be used for the patch. A purse-string suture is
placed in the patch, through which a 6 French sheath is placed
into the SMA in retrograde fashion through the distal end of
© 2011 Decker Intellectual Properties
VASCULAR SYSTEM
American SurgeryScientific
-
8/16/2019 Part06 Ch14 Copy
10/13
MESENTERIC REVASCULARIZATION PROCEDURES — 10
11/11
SMA
DividedLigament of Treitz
IMA
Figure 10 Superior mesenteric
artery (SMA) embolectomy.
Exposure of the infrarenal aorta,
proximal right common iliac
artery, and proximal SMA is
achieved by intestinal retraction
and division of the posterior
peritoneum, ligament of Treitz,
and base of small bowel
mesentery.40 IMA = inferior
mesenteric artery.
a
b c
Figure 11 Superior mesenteric artery (SMA) embolectomy.
(a) The location of embolus within the SMA is identified.
(b) Transverse (as shown) or longitudinal arteriotomy is
performed, and the embolus is extracted with a balloon
catheter. (c) Arteriotomy is closed. Primary closure (as
shown) suffices for transverse arteriotomy, but a vein patch is
usually required for closure of longitudinal arteriotomy.40
© 2011 Decker Intellectual Properties
VASCULAR SYSTEM
American SurgeryScientific
-
8/16/2019 Part06 Ch14 Copy
11/13
MESENTERIC REVASCULARIZATION PROCEDURES — 11
11/11
the patch. This allows for placement and removal of the sheath
without clamping of the vessel. Once the sheath is in place,
all metal retractors are removed. The sheath should be long
enough to allow the surgeon to work out of the wound and
away from the image intensifier.
Step 3: Crossing the lesion with a guidewire Initially,
hand-injected, retrograde, lateral angiography is performed to
delineate the lesion. This angiogram is used as a road map
to cross the lesion with a 0.035-inch glidewire. This is then
catheter exchanged for a lower profile 0.018- or 0.014-inch
platform.
Step 4: Predilatation and stent deployment The
lesion is then predilated with a 2 or 3 mm angioplasty balloon.
A 5 to 7 mm low-profile balloon-expandable stent is deployedin a retrograde fashion. The proximal-most stent is allowed
to protrude 1 to 2 mm into the aortic lumen. More than one
stent may be required to cross the entire length of the lesion.
Completion angiography in the anteroposterior and lateral
projections and pressure measurements are performed across
the lesion.
Step 5: Sheath removal and assessment of bowel
viability After completion angiography is performed, the
sheath is removed and the puncture site in the patch is
repaired. The entire bowel is thoroughly examined, and
any grossly necrotic bowel is expeditiously resected. Final
assessment and reanastomosis are usually delayed for 24 to
48 hours.
Endovascular Techniques
Purely endovascular techniques have a limited role in the
treatment of acute mesenteric ischemia as they do not offer
assessment of ischemic bowel. General surgical principles of
thorough abdominal exploration, along with sepsis control
and routine second-look operations, must be honored in all
patients with acute mesenteric ischemia to optimize favorable
outcomes. It would seem reasonable that endovasculartherapies might come to play a role in the treatment of acute
intestinal ischemia, given that preoperative angiography is
usually feasible in stable patients. Several groups have reported
treating acute arterial embolism with intra-arterial thrombol-
ysis33,34; others have reported treating acute embolism, as well
as thrombotic occlusion, with PTA.35,36 Although a degree
a b
Figure 12 Superior mesenteric artery (SMA) bypass. (a) Iliac artery–SMA bypass with a prosthetic graft is suitable for cases in
which SMA thrombosis produces ischemic but salvageable bowel. (b) Iliac artery–SMA bypass with a saphenous vein is suitable
for cases in which some segments of necrotic or perforated bowel must be resected.40
© 2011 Decker Intellectual Properties
VASCULAR SYSTEM
American SurgeryScientific
-
8/16/2019 Part06 Ch14 Copy
12/13
MESENTERIC REVASCULARIZATION PROCEDURES — 12
10/11
of anecdotal success with these techniques has been achieved
in selected cases, it should be kept in mind that reliance on
endovascular therapy alone for presumed acute intestinal
ischemia runs the risk of missing bowel necrosis. After endo-
vascular therapy, frequent clinical reevaluation is necessary
to identify patients with persistent intestinal ischemia.
Abdominal exploration should be very strongly considered
in most cases, even if the angiographic result of the endovas-
cular procedure is good.
Occasionally, patients present with emboli that have lodged
in the small arterial branches of the SMA. These vessels are
often too small to allow the passage of embolectomy cathe-
ters, and bypass beyond the point of obstruction frequently is
not possible. In these situations, resection of marginally viable
bowel is the best option.
As noted (see above), avoidance of graft kinking is crucial
for preventing early graft failure. Graft failure can have an
even greater adverse effect on bowel viability in the setting
of acute ischemia than in the setting of chronic intestinal
ischemia.
Recovery after revascularization is often prolonged.
Early and prolonged parenteral nutrition may be necessaryin patients with extensive bowel infarction. Only rarely,
however, is lifelong parenteral nutrition required.
The techniques employed to evaluate the success of mes-
enteric revascularization for acute ischemia include clinical
inspection, continuous-wave Doppler ultrasonography,
and intravenous (IV) administration of fluorescein. Clinical
inspection entails visual assessment of pulsatile flow in the
mesenteric arcades, peristalsis, bleeding from cut surfaces,
and, of course, color. In one study, clinical parameters
were found to be 82% sensitive and 91% specific for bowel
viability.37
We routinely use a sterile continuous-wave Doppler ultra-
sonography to evaluate pulsatile flow on the bowel surface.Grossly discolored bowel with no Doppler signal after a
period of observation should be resected; marginal bowel
with no Doppler signal is an indication for second-look
laparotomy.
With the fluorescein fluorescence method, 10 to 15 mg/kg
of fluorescein is injected intravenously, and the intestine is
inspected with a Wood lamp. A complete absence of fluores-
cence is diagnostic of nonviability; rapid, confluent, bright
fluorescence indicates viability. There is, however, a large
gray area between these two extremes in which interpretation
is subjective. In one study, the IV fluorescein method was
found to be 100% sensitive and specific for detecting non-
viable bowel.38 The disadvantages of this technique are that
it requires special equipment and that it exposes the critically
ill patient to the risk of an adverse reaction to the dye.Other assessment methods (e.g., surface oximetry, infrared
photoplethysmography, and laser Doppler velocimetry) are
available, but at present, they are mostly experimental and
are not in general use for evaluation of bowel viability in a
clinical setting.
Financial Disclosures: None Reported
References
1. Dunphy JE. Abdominal pain of vascular
origin. Am J Med Sci 1936;192:109.
2. Moneta GL. Diagnosis of intestinal ischemia.
In: Rutherford RB, editor. Vascular surgery.
Philadelphia: WB Saunders; 2000. p. 1501.
3. Moneta GL, Yeager RA, Dalman R, et al.
Duplex ultrasound criteria for diagnosis of
splanchnic artery stenosis or occlusion. J Vasc
Surg 1991;14:511.
4. Nicholls SC, Kohler TR, Martin RL, et al.
Use of hemodynamic parameters in the diag-
nosis of mesenteric insufficiency. J Vasc Surg
1986;3:507.
5. Moneta GL, Lee RW, Yeager RA, et al.
Mesenteric duplex scanning: a blinded pro-
spective study. J Vasc Surg 1993;17:79–84.
6. Cademartiri F, Raaijmakers RH, Kuiper JW,
et al. Multi-detector row CT angiography
in patients with abdominal angina. Radio-
graphics 2004;24:969–84.
7. Wildermuth S, Leschka S, Alkadhi H,
Marincek B. Multislice CT in the pre- and
postinterventional evaluation of mesenteric
perfusion. Eur Radiol 2005;15:1203–10.
8. Shih MC, Hagspiel KD. CTA and MRA in
mesenteric ischemia: part 1, role in diagnosis
and differential diagnosis. AJR Am J Roent-
genol 2007;188:452–61.
9. Shih MC, Angle JF, Leung DA, et al. CTA
and MRA in mesenteric ischemia: part 2,
normal findings and complications after sur-
gical and endovascular treatment. AJR Am J
Roentgenol 2007;188:462–71.
10. Shaw RS, Maynard EP III. Acute and
chronic thrombosis of the mesenteric arteries
associated with malabsorption: a report of
two cases successfully treated by thromboen-
darterectomy. N Engl J Med 1958;258:874.
11. Hansen HJB. Abdominal angina: results ofarterial reconstruction in 12 patients. ActaChir Scand 1976;142:319.
12. Stoney RJ, Ehrenfeld WK, Wylie EJ. Revas-
cularization methods in chronic visceralischemia. Ann Surg 1977;186:468.
13. McAfee MK, Cherry KJ, Naessens JM, et al.Influence of complete revascularizationon chronic mesenteric ischemia. Am J Surg1992;164:220.
14. Foley MI, Moneta GL, Abou-Zamzam AM,et al. Revascularization of the superior mes-enteric artery alone for treatment of intestinalischemia. J Vasc Surg 2000;32:37.
15. Park WM, Cherry KJ, Chua HK, et al. Cur-rent results of open revascularization forchronic mesenteric ischemia: a standard forcomparison. J Vasc Surg 2002;35:853.
16. Murray SP, Ramos TK, Stoney RJ. Surgeryof the celiac and mesenteric arteries. In:Ascher E, editor. Haimovici’s vascular sur-
gery. Malden (MA): Blackwell Publishing;2004. p. 861.
17. Taylor LM, Moneta GL, Porter JM.Treatment of chronic visceral ischemia. In:
Rutherford RB, editor. Vascular surgery.Philadelphia: WB Saunders; 2000. p. 1532.18. Schemerhorn ML, Giles KA, Hamdan AD,
et al. Mesenteric revascularization: manage-ment and outcomes in United States 1988– 2006. J Vasc Surg 2009;50:341–8.
19. Odurny A, Sniderman KW, Colapinto RF.Intestinal angina: percutaneous transluminal
angioplasty of the celiac and superior mesen-
teric arteries. Radiology 1988;167:59.
20. Atkins MD, Kwolek CJ, LaMuraglia GM,
et al. Surgical revascularization versus
endovascular therapy for chronic mesenteric
ischemia: a comparative experience. J Vasc
Surg 2007;45:1162–71.
21. Peck MA, Conrad MF, Kwolek CJ, et al.
Intermediate-term outcomes of endovascular
treatment for symptomatic chronic mesen-
teric ischemia. Vasc Surg 2010;51:140–
7.e1–2.
22. Mateo RB, O’Hara PJ, Hertzer NR, et al.
Elective surgical treatment of symptomatic
chronic mesenteric occlusive disease: early
results and late outcomes. J Vasc Surg
1999;29:821.
23. Leke MA, Hood DB, Rowe VL, et al. Techni-
cal consideration in the management of
chronic mesenteric ischemia. Am Surg 2002;
68:1088.
24. Nicoloff AD, Williamson WK, Moneta GL,
et al. Duplex ultrasonography in evaluation of
splanchnic artery stenosis. Surg Clin North
Am 1997;77:339.
25. Liem TK, Segall JA, Wei W, et al. Duplex
scan characteristics of bypass grafts to mesen-
teric arteries. J Vasc Surg 2007;45:922–7.
26. Taylor LM, Moneta GL, Porter JM.Treatment of acute intestinal ischemia caused
by arterial occlusions. In: Rutherford RB,
editor. Vascular surgery. Philadelphia: WB
Saunders; 2000. p. 1512.
27. Low DE, Frenkel VJ, Manley PN, et al.
Embolic mesenteric infarction: a unique
initial manifestation of renal cell carcinoma.
Surgery 1989;106:925.
© 2011 Decker Intellectual Properties
VASCULAR SYSTEM
American SurgeryScientific
-
8/16/2019 Part06 Ch14 Copy
13/13
MESENTERIC REVASCULARIZATION PROCEDURES — 13
10/11
28. Ottinger LW. The surgical management of
acute occlusion of the superior mesenteric
artery. Ann Surg 1978;188:72L.
29. Kirkpatrick ID, Kroeker MA, Greenberg
HM. Biphasic CT with mesenteric CT angi-
ography in the evaluation of acute mesenteric
ischemia: initial experience. Radiology 2003;
229:91–8.
30. Aschoff AJ, Stuber G, Becker BW, et al. Eval-
uation of acute mesenteric ischemia: accuracy
of biphasic mesenteric multi-detector CTangiography. Abdom Imaging 2009;34:
345–57.
31. Milner R, Woo EY, Carpenter JP. Superior
mesenteric artery angioplasty and stenting via
a retrograde approach in a patient with bowel
ischemia—a case report. Vasc Endovasc Surg
2004;38:89–91.
32. Wyers MC, Powell RJ, Nolan BW, Cro-
nenwett JL. Retrograde mesenteric stenting
during laparotomy for acute occlusive mesen-
teric ischemia. J Vasc Surg 2007;45:269–75.33. Calin GA, Calin S, Ionescu R, et al. Success-
ful local fibrinolytic treatment and balloonangioplasty in superior mesenteric arterialembolism: a case report and literature review.
Hepatogastroenterology 2003;50:732.34. Michel C, Laffy P, Leblanc G, et al.
Intra-arterial fibrinolytic therapy for acutemesenteric ischemia. J Radiol 2001;82:55.
35. Yilmaz S, Gurkan A, Erdogan O, et al.
Endovascular treatment of an acute superiormesenteric artery occlusion following failedsurgical embolectomy. J Endovasc Ther2003;10:386.
36. Brountzos EN, Critselis A, Magoulas D, et al.
Emergency endovascular treatment of a supe-rior mesenteric artery occlusion. CardiovascIntervent Radiol 2001;24:57.
37. Bulkley GB, Zuidema GD, Hamilton SR,et al. Intraoperative determination of small
bowel viability following ischemic injury:
a prospective, controlled trial of two adjuvant
methods (Doppler and fluorescein) compared
with standard clinical judgment. Ann Surg
1981;193:628.
38. Carter MS, Fantini GA, Sammartano RJ,
et al. Qualitative and quantitative fluorescein
fluorescence in determining intestinal viabi-
lity. Am J Surg 1984;147:117.
39. Taylor LM Jr, Porter JM. Treatment of
chronic intestinal ischemia. Semin Vasc Surg1990;3:186.
40. Kazmers A. Operative management of acute
mesenteric ischemia. Ann Vasc Surg 1998;
12:187.
Acknowledgment
Figures 5, 6, 10, 11, and 12 Alice Y. Chen
© 2011 Decker Intellectual Properties
VASCULAR SYSTEM
American SurgeryScientific