Part II – Melanoma: Novel Pathways and Agents Tuesday, June 21, 2011 7:30 PM – 8:30 PM ET RTP TV: An 8-Part Live CME Webcast Series

Part II – Melanoma: Novel Pathways and Agents Tuesday, June 21, 2011 7:30 PM – 8:30 PM ET RTP TV: An 8-Part Live CME Webcast Series.
Dec 30, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Part II – Melanoma: Novel Pathways and AgentsTuesday, June 21, 20117:30 PM – 8:30 PM ET
RTP TV: An 8-Part Live CME Webcast Series

Keith T Flaherty, MDAssociate ProfessorHarvard Medical SchoolDirector of Developmental TherapeuticsMassachusetts General Hospital Cancer CenterBoston, Massachusetts
Jeffrey Weber, MD, PhDSenior Member, H Lee Moffitt Cancer Center Director, Donald A Adam Comprehensive Melanoma Research Center Tampa, Florida
Neil Love, MDResearch To PracticeMiami, Florida
Disclosures for Moderator Neil Love, MD
Dr Love is president and CEO of Research To Practice, which receives funds in the form of educational grants to develop CME activities from the following commercial interests: Allos Therapeutics, Amgen Inc, AstraZeneca Pharmaceuticals LP, Aureon Laboratories Inc, Bayer HealthCare Pharmaceuticals/Onyx Pharmaceuticals Inc, Biogen Idec, Boehringer Ingelheim Pharmaceuticals Inc, Bristol-Myers Squibb Company, Celgene Corporation, Cephalon Inc, Daiichi Sankyo Inc, Dendreon Corporation, Eisai Inc, EMD Serono Inc, Genentech BioOncology, Genomic Health Inc, ImClone Systems, a wholly owned subsidiary of Eli Lilly and Company, Lilly USA LLC, Millennium — The Takeda Oncology Company, Mundipharma International Limited, Myriad Genetics Inc, Novartis Pharmaceuticals Corporation, OSI Oncology, Sanofi and Seattle Genetics.
Disclosures for Keith T Flaherty, MD
Advisory CommitteeBristol-Myers Squibb Company, Eisai Inc, Genentech BioOncology
Consulting Agreements Cephalon Inc, GlaxoSmithKline

Disclosures for Jeffrey Weber MD, PhD
Advisory Committee
Bristol-Myers Squibb Company, Celldex Inc, Genentech BioOncology, Novartis Pharmaceuticals Corporation
Consulting Agreement Bristol-Myers Squibb Company
Stock Ownership Celldex Inc
Pathology Video Primer Adriano Piris, MD
Dermatopathologist, Massachusetts General HospitalDirector, Quality and Safety Division, MGH DermatopathologyInstructor of Pathology, Harvard Medical SchoolBoston, Massachusetts
No financial interests or affiliations to disclose
Agenda
• Overview: Melanoma in current practice
• ASCO 2011 plenary/NEJM
– Dacarbazine + ipilimumab
– Vemurafenib vs dacarbazine
• Faculty cases
• Adjuvant update
– Pathology video primer (Adriano Piris, MD)

Survey of 100 Practicing Oncologists April 15-28, 2011
• 5 — Median number of new patients with melanoma
evaluated in the past year
• Fraction of oncologists who in the past year…
– Referred a melanoma patient to tertiary center: 76%
– Enrolled a melanoma patient on a clinical trial: 57%
– Had melanoma patients tested for BRAF mutation: 47%
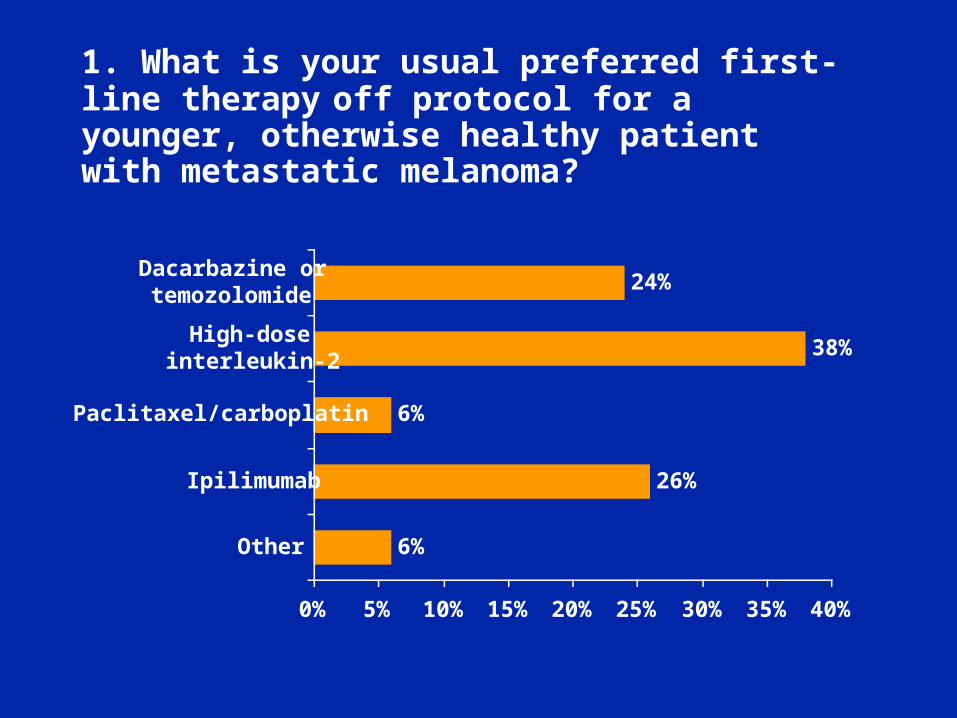
1. What is your usual preferred first-line therapy
off protocol for a younger, otherwise healthy patient with metastatic melanoma?
6%
26%
6%
38%
24%
0% 5% 10% 15% 20% 25% 30% 35% 40%
Other
Ipilimumab
Paclitaxel/carboplatin
High-doseinterleukin-2
Dacarbazine ortemozolomide
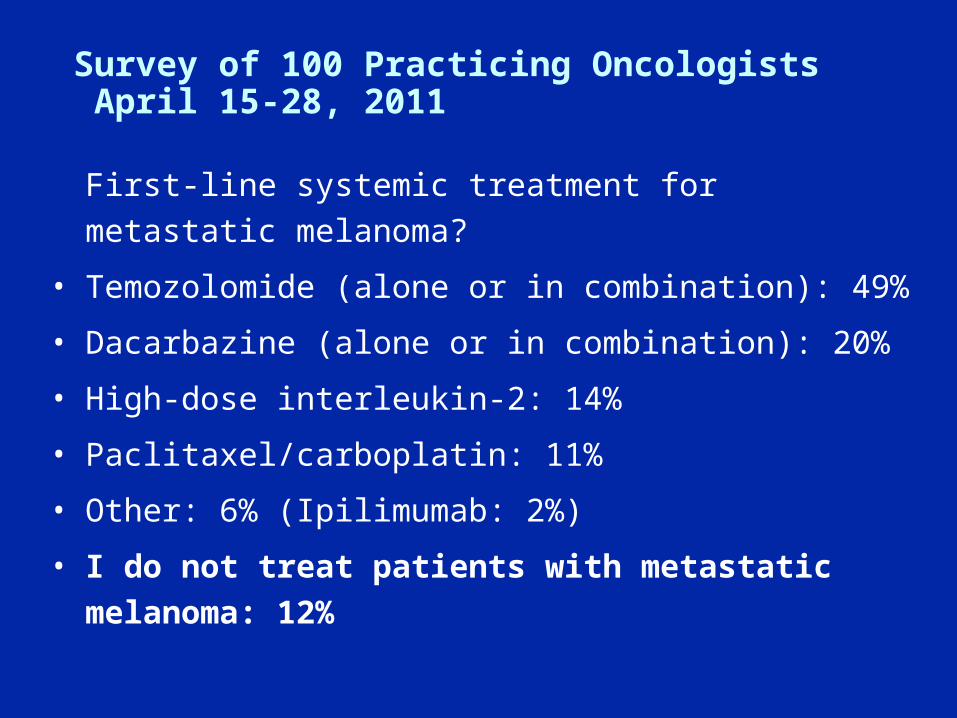
Survey of 100 Practicing Oncologists April 15-28, 2011
First-line systemic treatment for metastatic melanoma?
• Temozolomide (alone or in combination): 49%
• Dacarbazine (alone or in combination): 20%
• High-dose interleukin-2: 14%
• Paclitaxel/carboplatin: 11%
• Other: 6% (Ipilimumab: 2%)
• I do not treat patients with metastatic melanoma: 12%
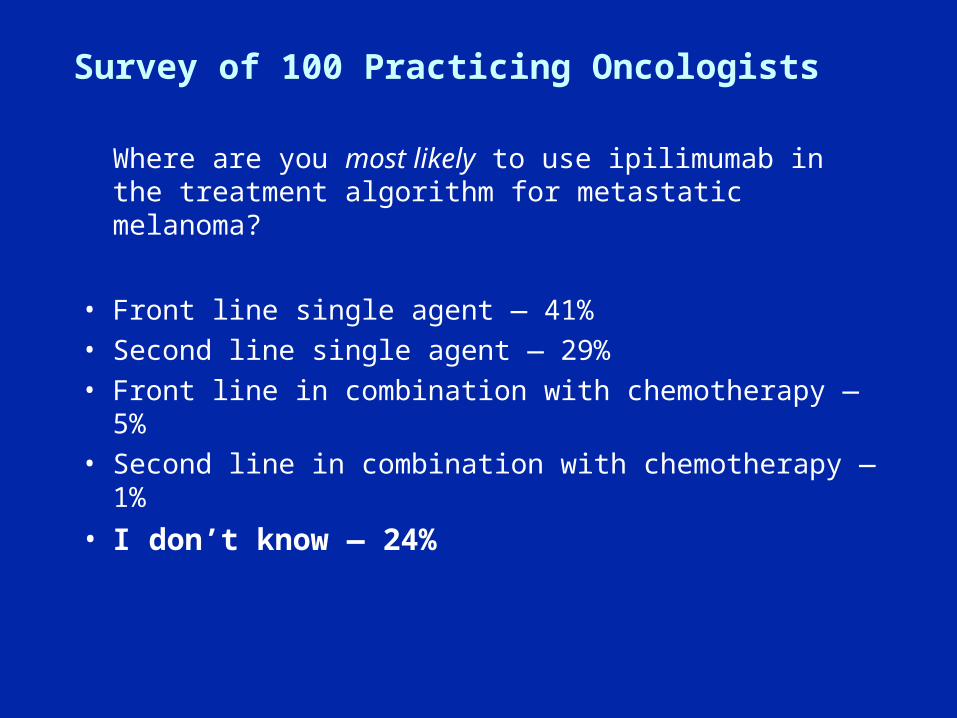
Survey of 100 Practicing Oncologists
Where are you most likely to use ipilimumab in the treatment algorithm for metastatic melanoma?
• Front line single agent — 41%• Second line single agent — 29%• Front line in combination with chemotherapy — 5%• Second line in combination with chemotherapy — 1%
• I don’t know — 24%
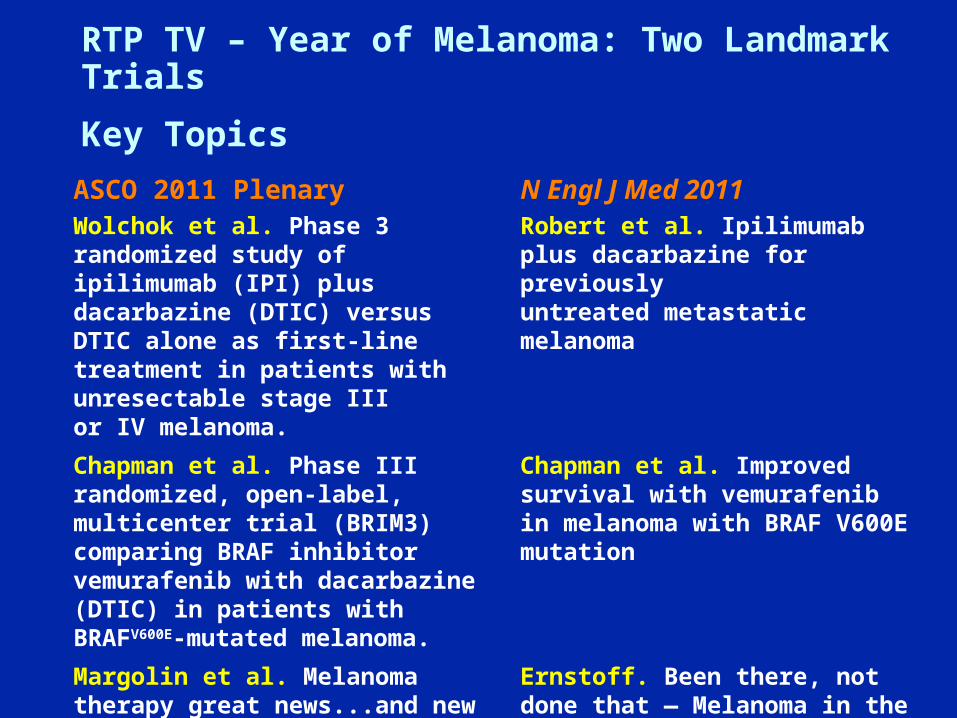
RTP TV – Year of Melanoma: Two Landmark Trials
Key Topics
ASCO 2011 PlenaryWolchok et al. Phase 3 randomized study of ipilimumab (IPI) plus dacarbazine (DTIC) versus DTIC alone as first-line treatment in patients with unresectable stage III or IV melanoma.
N Engl J Med 2011Robert et al. Ipilimumab plus dacarbazine for previouslyuntreated metastatic melanoma
Chapman et al. Phase III randomized, open-label, multicenter trial (BRIM3) comparing BRAF inhibitor vemurafenib with dacarbazine (DTIC) in patients with BRAFV600E-mutated melanoma.
Chapman et al. Improved survival with vemurafenib in melanoma with BRAF V600E mutation
Margolin et al. Melanoma therapy great news...and new challenges
Ernstoff. Been there, not done that — Melanoma in the age of molecular therapy
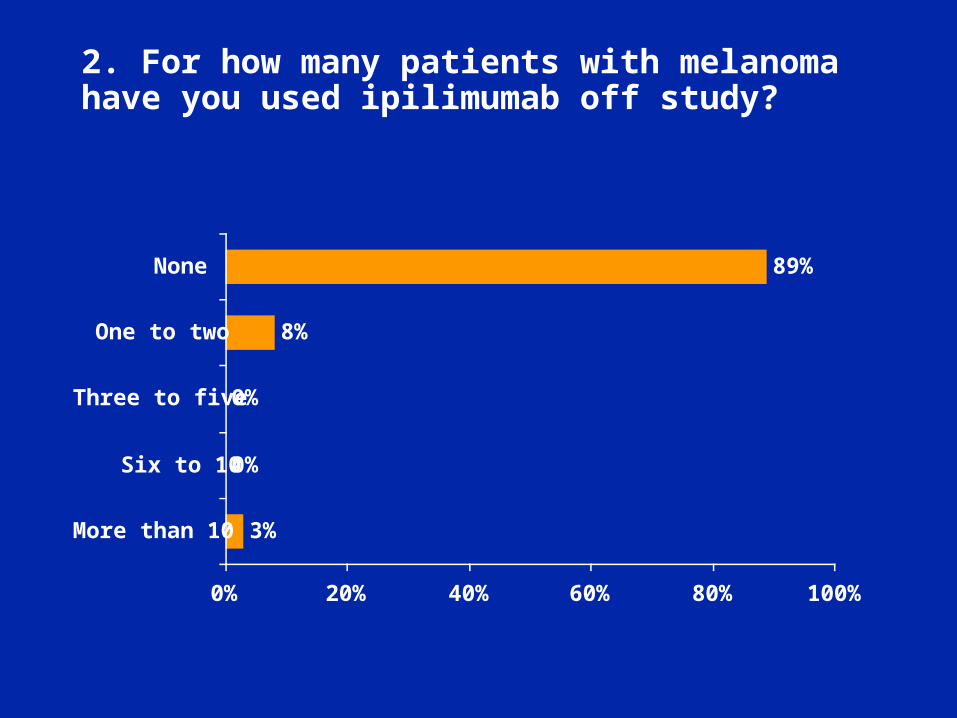
2. For how many patients with melanoma have you used ipilimumab off study?
3%
0%
0%
8%
89%
0% 20% 40% 60% 80% 100%
More than 10
Six to 10
Three to five
One to two
None
Wolchok J et al.
Proc ASCO 2011;Abstract LBA5.
Phase 3 Randomized Study of Ipilimumab (IPI) Plus Dacarbazine (DTIC) vs DTIC Alone as First-Line Treatment in Patients With Unresectable Stage III or IV Melanoma
Robert C et al. N Engl J Med 2011 Jun 5;[Epub ahead of print].
Hodi FS et al. N Engl J Med 2010;363(8):711-23. Hwu P. N Engl J Med 2010;363(8):779-81.
ASCO: June 5, 2010Published: Aug 19, 2010
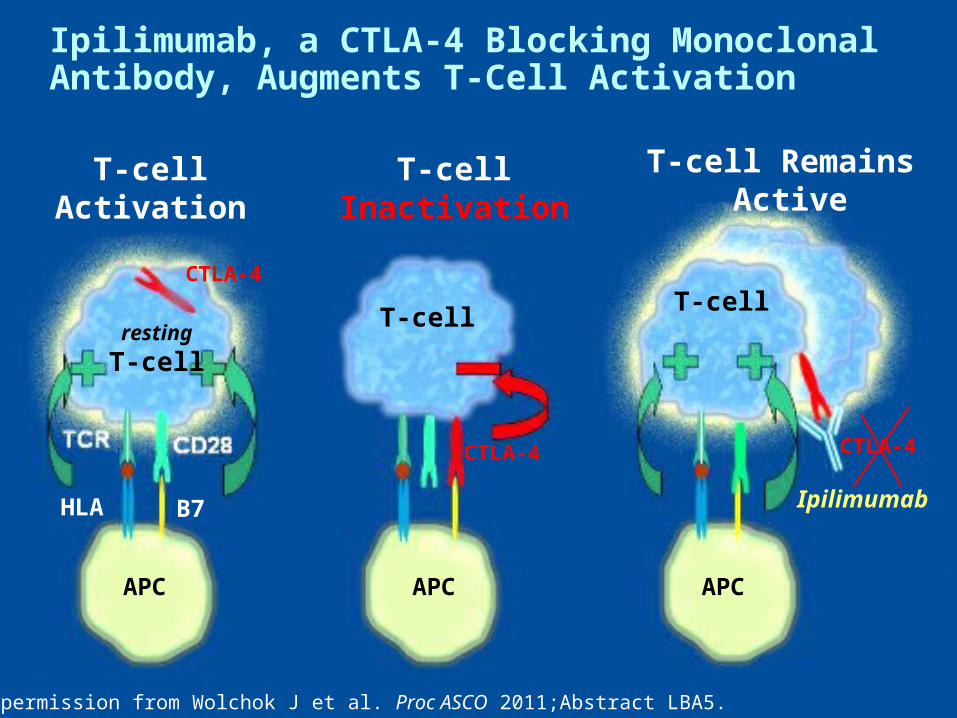
With permission from Wolchok J et al. Proc ASCO 2011;Abstract LBA5.
T-cellActivation
T-cellInactivation
T-cell Remains Active
resting
T-cell
T-cellT-cell
CTLA-4
HLA B7
APC APC APC
Ipilimumab
Ipilimumab, a CTLA-4 Blocking Monoclonal Antibody, Augments T-Cell Activation
CTLA-4
CTLA-4
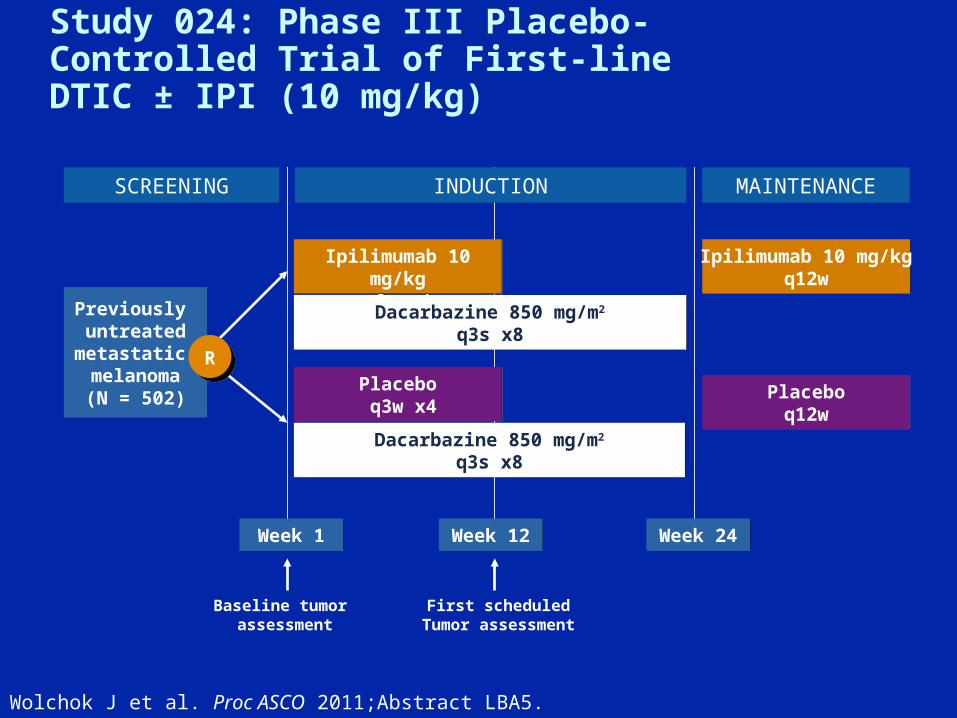
Wolchok J et al. Proc ASCO 2011;Abstract LBA5.
Study 024: Phase III Placebo-Controlled Trial of First-line DTIC ± IPI (10 mg/kg)
SCREENING INDUCTION MAINTENANCE
Previously untreated
metastatic melanoma(N = 502)
Previously untreated
metastatic melanoma(N = 502)
Ipilimumab 10 mg/kgq3w x4
Ipilimumab 10 mg/kgq3w x4
Placebo q3w x4Placebo q3w x4
Ipilimumab 10 mg/kgq12w
Ipilimumab 10 mg/kgq12w
Placeboq12w
Placeboq12w
Week 1Week 1
Dacarbazine 850 mg/m2
q3s x8Dacarbazine 850 mg/m2
q3s x8
Dacarbazine 850 mg/m2
q3s x8Dacarbazine 850 mg/m2
q3s x8
Week 12Week 12 Week 24Week 24
Baseline tumor assessment
First scheduledTumor assessment
R
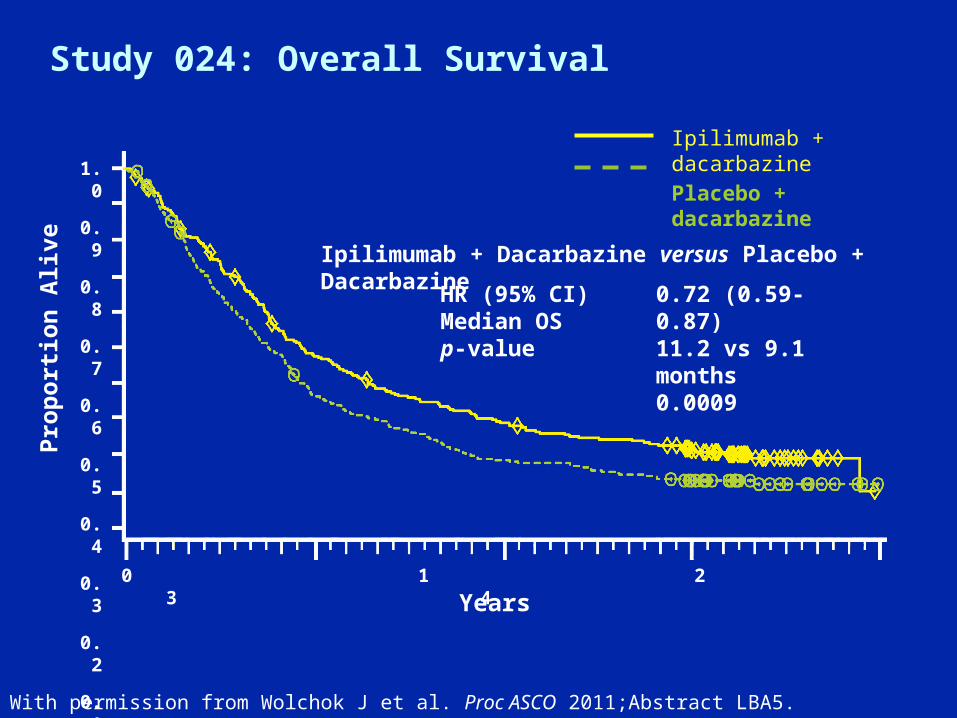
Study 024: Overall Survival
With permission from Wolchok J et al. Proc ASCO 2011;Abstract LBA5.
Ipilimumab + Dacarbazine versus Placebo + Dacarbazine
HR (95% CI)Median OSp-value
0.72 (0.59-0.87)11.2 vs 9.1 months0.0009
Pro
po
rtio
n A
live
Years
1.0
0.9
0.8
0.7
0.6
0.5
0.4
0.3
0.2
0.1
0.0
0 1 2 3 4
Ipilimumab + dacarbazinePlacebo + dacarbazine

Years
Study 024: Overall Survival
With permission from Wolchok J et al. Proc ASCO 2011;Abstract LBA5.
Pro
po
rtio
n A
live
Estimated Survival Rate
1 year 2 year 3 year*
Ipilimumab + dacarbazinen = 250
47.3 28.5 20.8
Placebo + dacarbazinen = 252
36.3 17.9 12.2
Ipilimumab + dacarbazinePlacebo + dacarbazine
1.0
0.9
0.8
0.7
0.6
0.5
0.4
0.3
0.2
0.1
0.0
0 1 2 3 4
*3-year survival was a post-hoc analysis
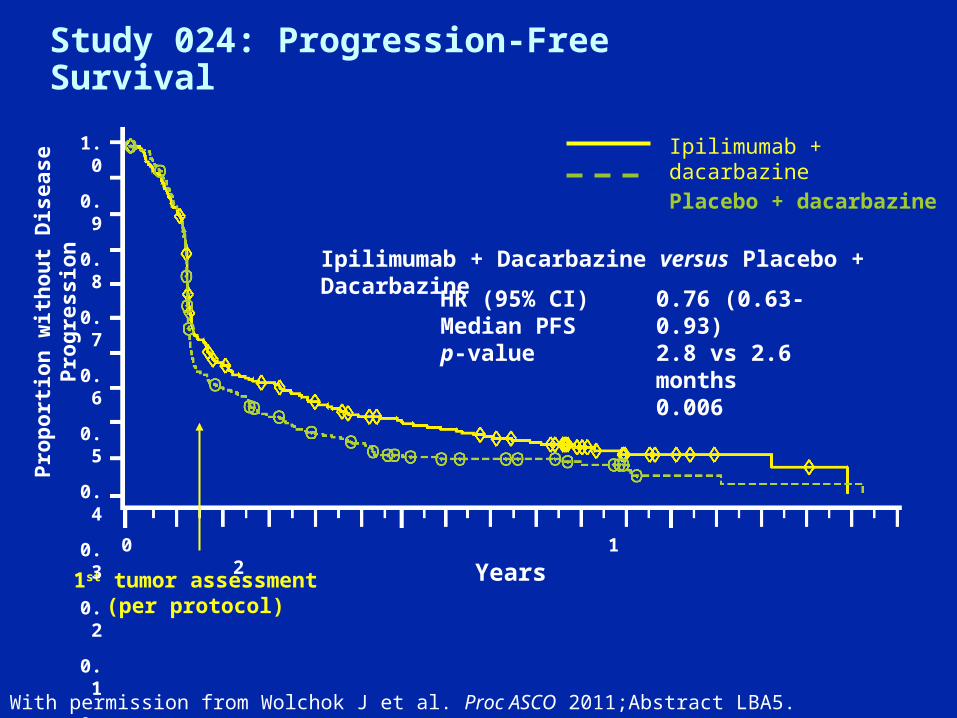
Study 024: Progression-Free Survival
With permission from Wolchok J et al. Proc ASCO 2011;Abstract LBA5.
Ipilimumab + Dacarbazine versus Placebo + Dacarbazine
HR (95% CI)Median PFSp-value
0.76 (0.63-0.93)2.8 vs 2.6 months0.006
Ipilimumab + dacarbazinePlacebo + dacarbazine
1st tumor assessment(per protocol)
Pro
po
rtio
n w
ith
ou
t D
isea
se P
rog
ress
ion
Years
1.0
0.9
0.8
0.7
0.6
0.5
0.4
0.3
0.2
0.1
0.0
0 1 2
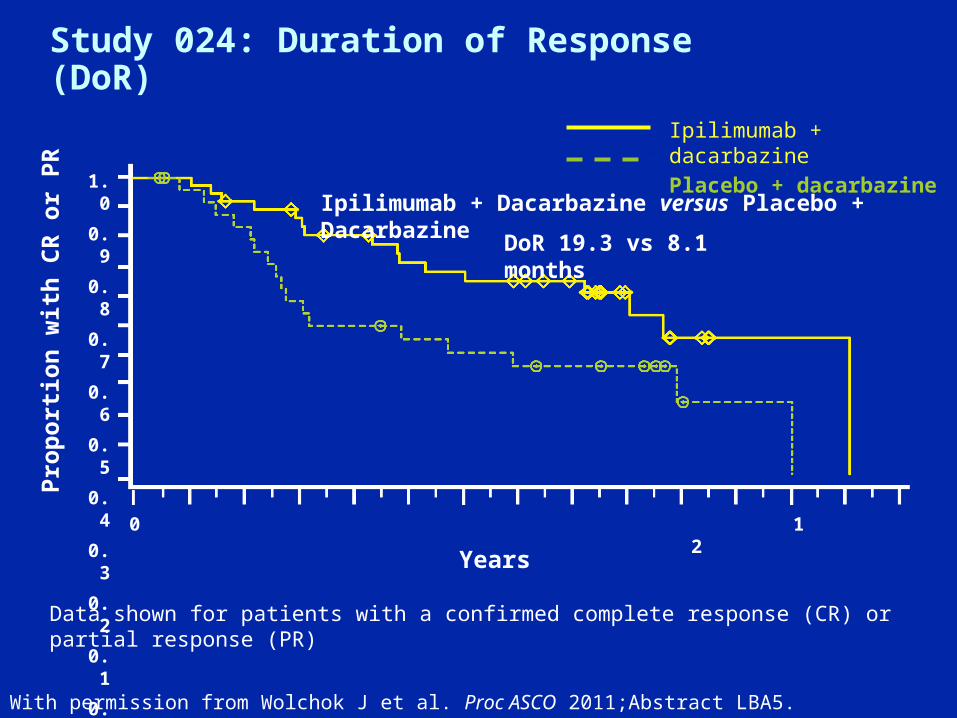
Study 024: Duration of Response (DoR)
With permission from Wolchok J et al. Proc ASCO 2011;Abstract LBA5.
Ipilimumab + dacarbazinePlacebo + dacarbazine
Pro
po
rtio
n w
ith
CR
or
PR
Years
1.0
0.9
0.8
0.7
0.6
0.5
0.4
0.3
0.2
0.1
0.0
0 1 2
Data shown for patients with a confirmed complete response (CR) or partial response (PR)
Ipilimumab + Dacarbazine versus Placebo + Dacarbazine
DoR 19.3 vs 8.1 months

Study 024: Safety Summary
• Types of adverse events associated with IPI consistent with previous studies
– Mainly affect skin, GI tract, liver, endocrine system
• Mechanism (immune)-based:
– Managed with established guidelines
– Generally response to dose interruptions/discontinuation, corticosteroids and/or other immunosuppressants
• Rates of high-grade events different from observed in Phase II
– Elevated AST and ALT rates – higher
– Diarrhea and colitis rates – lower
– No GI perforations
Wolchok J et al. Proc ASCO 2011;Abstract LBA5.

How Should IPI Be Studied Next?
• Single agent questions– Dose and duration of therapy– Biomarkers of activity and of toxicity– Predictive immuno-molecular markers
• Combinations, sequences (ongoing or planned)– Cytotoxic agents– Molecularly targeted agents including vemurafenib– Immunomodulators– VEGF receptor blockade (Hodi et al. Proc ASCO
2011, Abstract 8511.)• Multi-checkpoint blockade (e.g. PD-1 axis)
Margolin K et al. Proc ASCO 2011; Discussant.
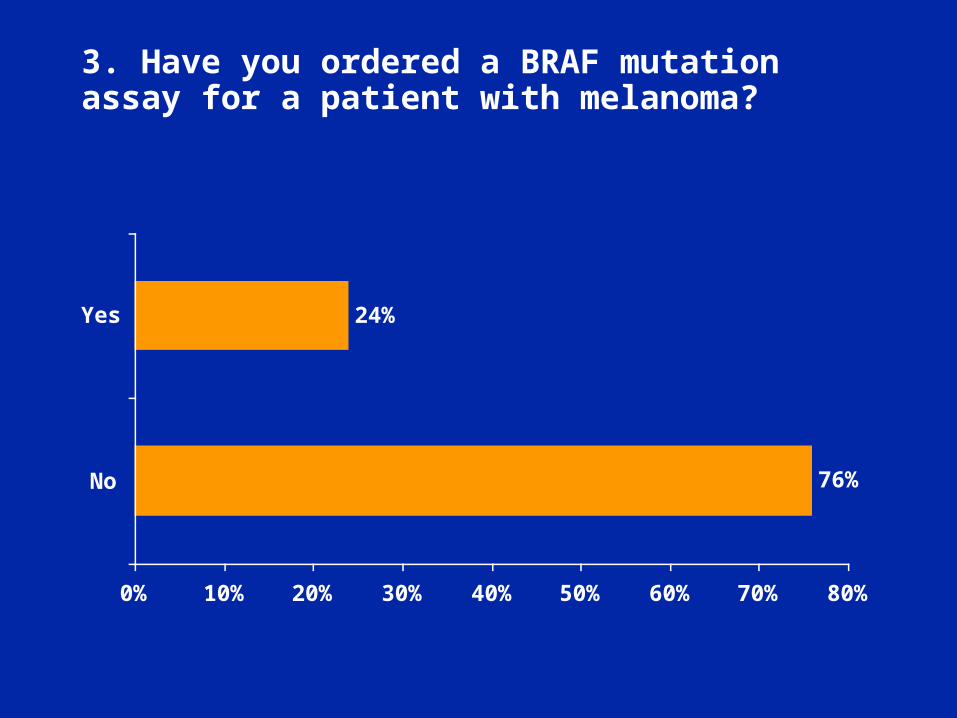
3. Have you ordered a BRAF mutation assay for a patient with melanoma?
76%
24%
0% 10% 20% 30% 40% 50% 60% 70% 80%
No
Yes

Long GV et al. J Clin Oncol 2011;29(10):1239-46. Flaherty KT. J Clin Oncol 2011;9(10):1229-30.
BRAF Mutations in Melanoma
• Roughly 40-60% of cutaneous melanomas are positive for mutations in the BRAF gene1,2.
• BRAF V600E mutation comprises approximately 90% of BRAF mutations3.
1Davies H et al. Nature 2002;417(6892):949-54; 2Curtin JA et al. N Engl J Med 2005;353(20):2135-47; 3Chapman PB et al. N Engl J Med 2011;[Epub ahead of print];
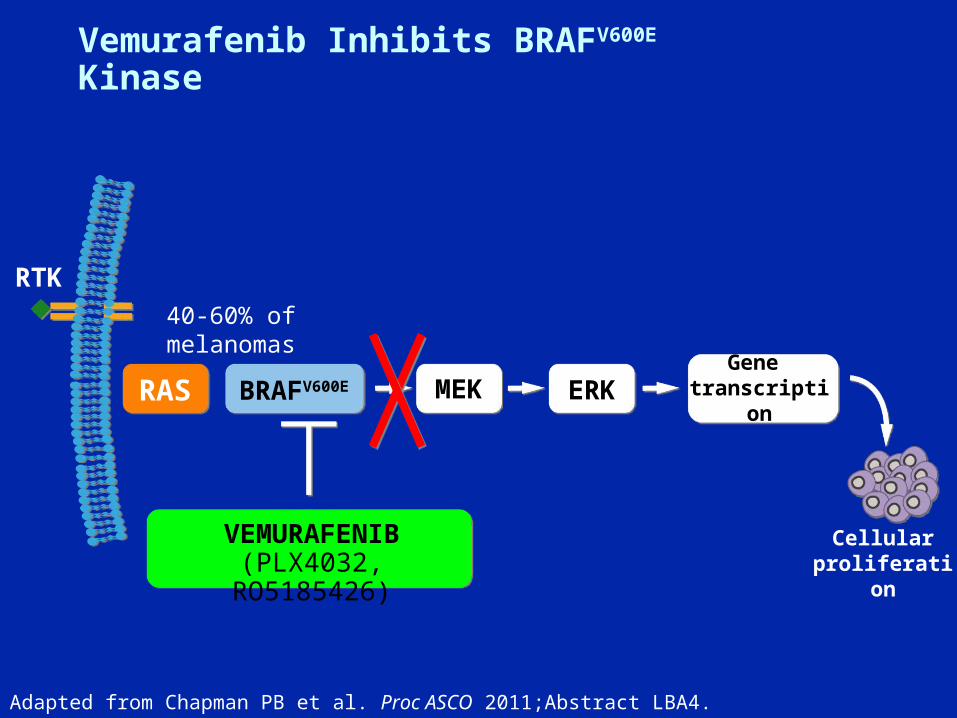
Vemurafenib Inhibits BRAFV600E Kinase
RTK
VEMURAFENIB(PLX4032, RO5185426)
RAS BRAFV600E MEK ERKGene
transcription
40-60% of melanomas
Adapted from Chapman PB et al. Proc ASCO 2011;Abstract LBA4.
Cellular proliferation
Chapman PB et al.
Proc ASCO 2011;Abstract LBA4.
Phase III Randomized, Open-Label, Multicenter Trial (BRIM3) Comparing BRAF Inhibitor Vemurafenib with Dacarbazine in Patients with BRAFV600E-Mutated Melanoma
Chapman PB et al. N Engl J Med 2011 Jun 5;[Epub ahead of print].

BRIM2: An Open-Label, Multicenter Phase II Study of Vemurafenib (PLX4032, RG7204) in Previously Treated Patients with BRAFV600E Mutation-Positive Metastatic Melanoma
Ribas A et al. Proc ASCO 2011;Abstract 8509.
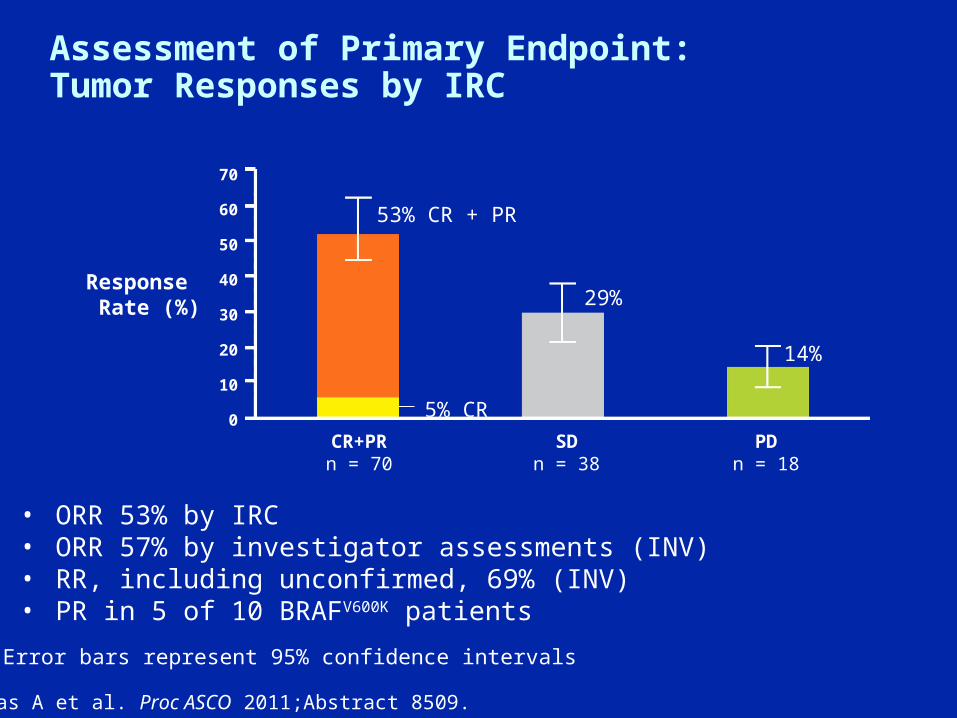
Assessment of Primary Endpoint: Tumor Responses by IRC
• ORR 53% by IRC• ORR 57% by investigator assessments (INV)• RR, including unconfirmed, 69% (INV)• PR in 5 of 10 BRAFV600K patients
Response Rate (%)
70
60
50
40
30
20
10
0CR+PRn = 70
SDn = 38
PDn = 18
53% CR + PR
5% CR
29%
14%
Error bars represent 95% confidence intervals
Ribas A et al. Proc ASCO 2011;Abstract 8509.
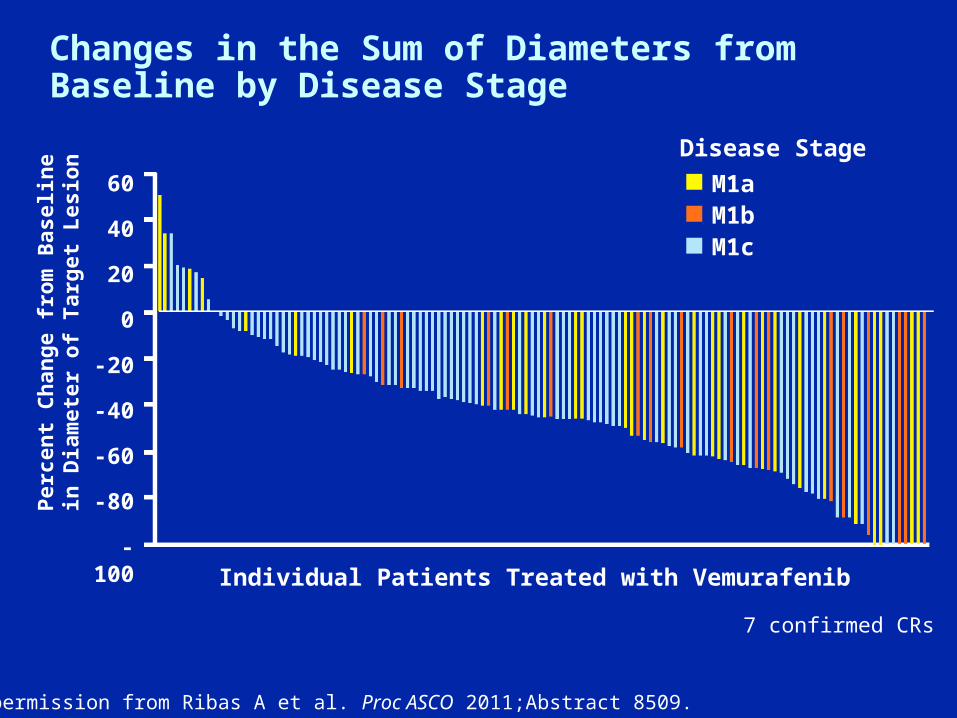
Changes in the Sum of Diameters from Baseline by Disease Stage
60
40
20
0
-20
-40
-60
-80
-100Individual Patients Treated with Vemurafenib
Per
cen
t C
han
ge
fro
m B
asel
ine
in D
iam
eter
of
Tar
get
Les
ion
Disease Stage
M1aM1bM1c
7 confirmed CRs
With permission from Ribas A et al. Proc ASCO 2011;Abstract 8509.
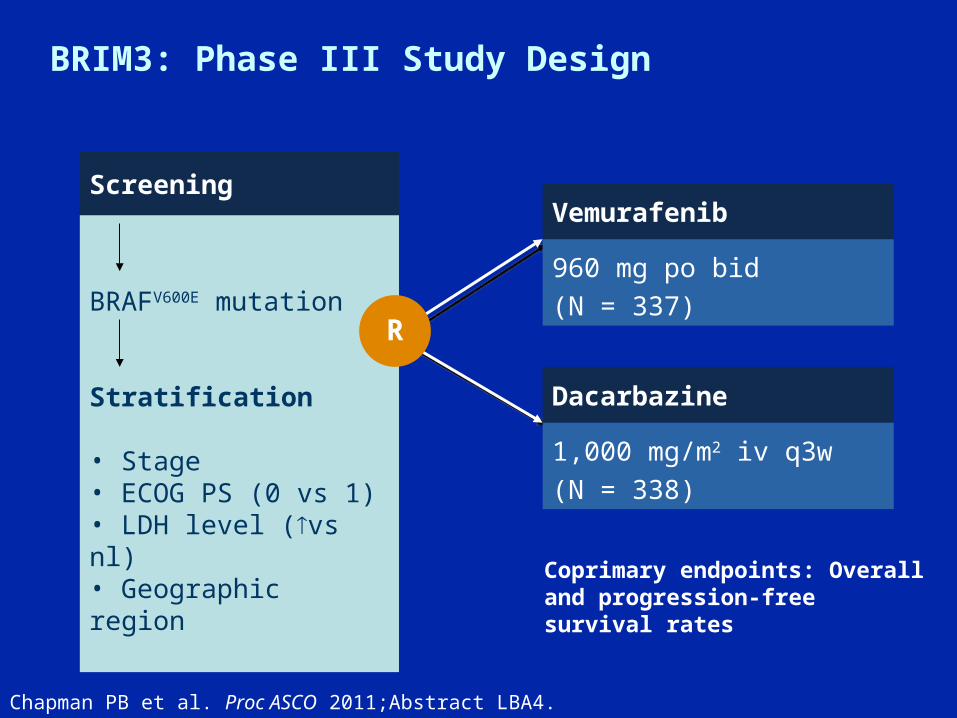
BRIM3: Phase III Study Design
Chapman PB et al. Proc ASCO 2011;Abstract LBA4.
Screening
BRAFV600E mutation
Stratification
• Stage• ECOG PS (0 vs 1)• LDH level (vs nl)• Geographic region
R
Vemurafenib
960 mg po bid
(N = 337)
Dacarbazine
1,000 mg/m2 iv q3w
(N = 338)
Coprimary endpoints: Overall and progression-free survival rates
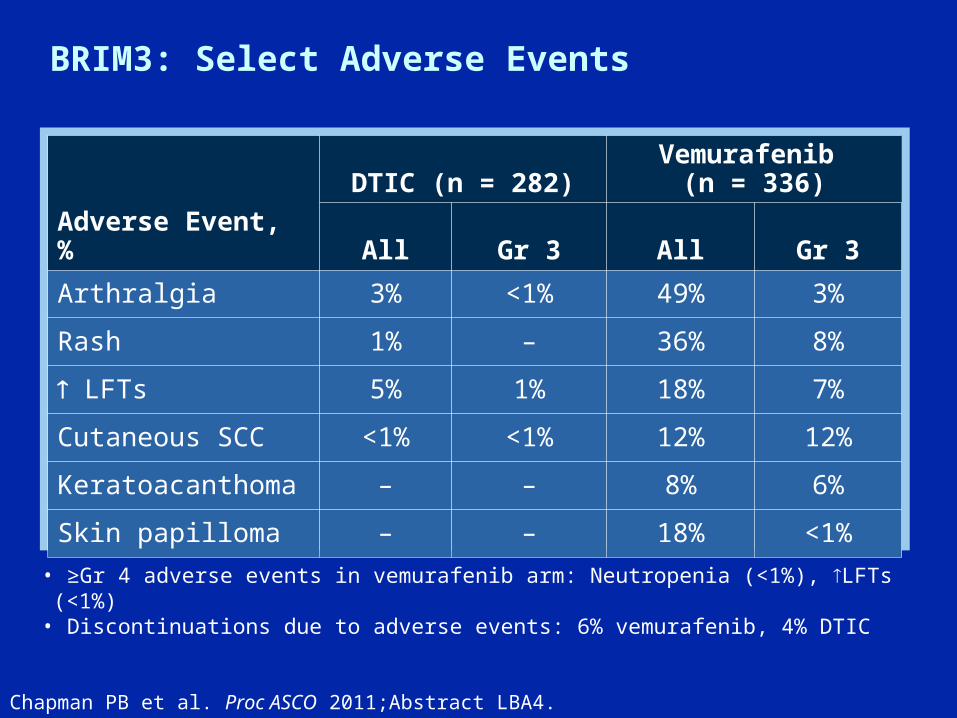
BRIM3: Select Adverse Events
Chapman PB et al. Proc ASCO 2011;Abstract LBA4.
Adverse Event, %
DTIC (n = 282)Vemurafenib
(n = 336)
All Gr 3 All Gr 3
Arthralgia 3% <1% 49% 3%
Rash 1% – 36% 8%
LFTs 5% 1% 18% 7%
Cutaneous SCC <1% <1% 12% 12%
Keratoacanthoma – – 8% 6%
Skin papilloma – – 18% <1%
• ≥Gr 4 adverse events in vemurafenib arm: Neutropenia (<1%), LFTs (<1%)• Discontinuations due to adverse events: 6% vemurafenib, 4% DTIC
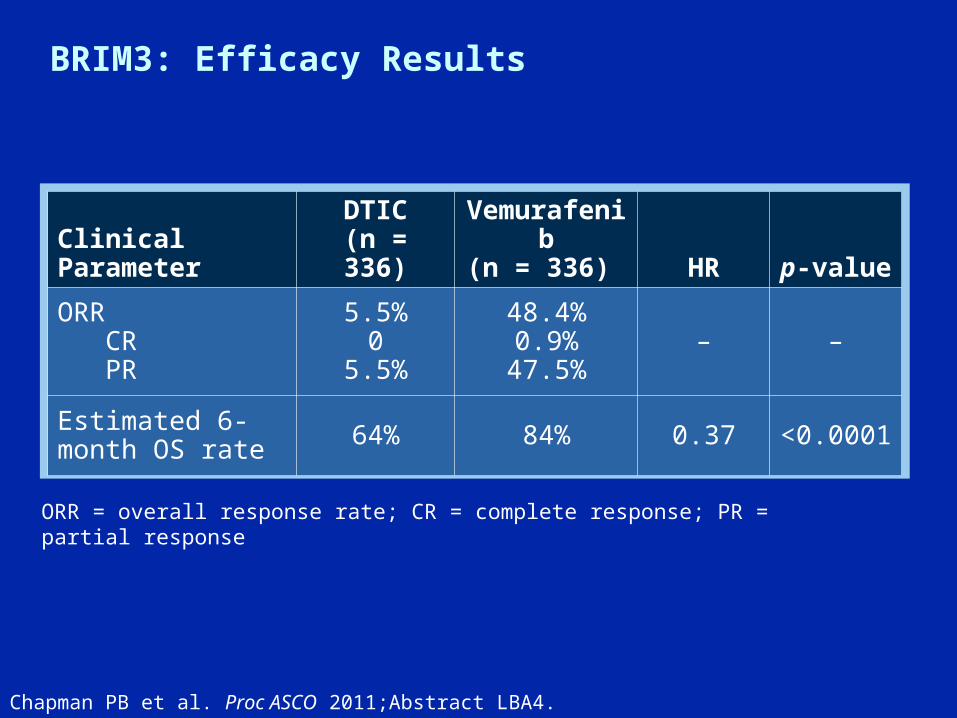
BRIM3: Efficacy Results
Chapman PB et al. Proc ASCO 2011;Abstract LBA4.
Clinical Parameter
DTIC(n = 336)
Vemurafenib(n = 336) HR p-value
ORR CR PR
5.5%0
5.5%
48.4%0.9%
47.5%– –
Estimated 6-month OS rate 64% 84% 0.37 <0.0001
ORR = overall response rate; CR = complete response; PR = partial response

BRIM3: Maximal Tumor Response
Chapman PB et al. N Engl J Med 2011. Jun 5 [Epub ahead of print]. Copyright © 2011 Massachusetts Medical Society. All rights reserved.
Vemurafenib
Dacarbazine
Per
cen
t C
han
ge
fro
m B
ase
lin
e in
Su
m o
f T
um
or
Dia
met
ers
>100
50
0
-50
100
>100
50
0
-50
100

BRIM3: Efficacy Results
Clinical Parameter
DTIC(n = 336)
Vemurafenib(n = 336) HR p-value
ORR CR PR
5.5%0
5.5%
48.4%0.9%
47.5%– –
Estimated 6-month OS rate 64% 84% 0.37 <0.0001
ORR = overall response rate; CR = complete response; PR = partial response
Chapman PB et al. Proc ASCO 2011;Abstract LBA4.

BRIM3: Maximal Tumor Response
Chapman PB et al. N Engl J Med 2011. Jun 5 [Epub ahead of print]. Copyright © 2011 Massachusetts Medical Society. All rights reserved.
Vemurafenib
Dacarbazine
Per
cen
t C
han
ge
fro
m B
ase
lin
e in
Su
m o
f T
um
or
Dia
met
ers
>100
50
0
-50
100
>100
50
0
-50
100
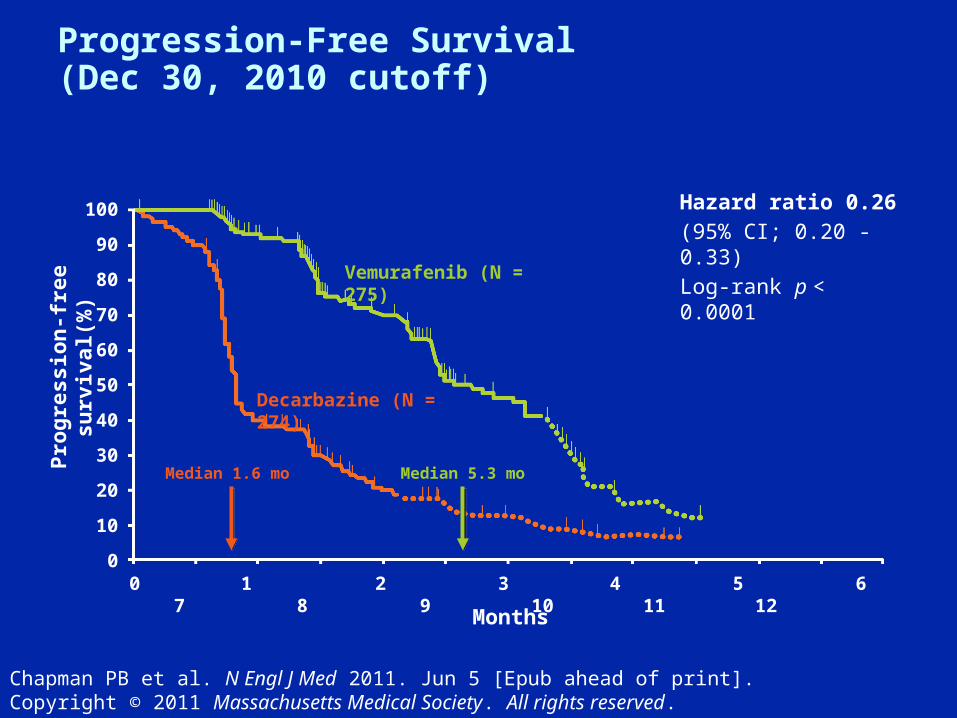
Progression-Free Survival (Dec 30, 2010 cutoff)
Pro
gre
ssio
n-f
ree
surv
ival
(%)
Months
Hazard ratio 0.26(95% CI; 0.20 - 0.33)Log-rank p < 0.0001Vemurafenib (N = 275)
Decarbazine (N = 274)
Median 5.3 moMedian 1.6 mo
100
90
80
70
60
50
40
30
20
10
00 1 2 3 4 5 6 7 8 9 10 11 12
Chapman PB et al. N Engl J Med 2011. Jun 5 [Epub ahead of print]. Copyright © 2011 Massachusetts Medical Society. All rights reserved.
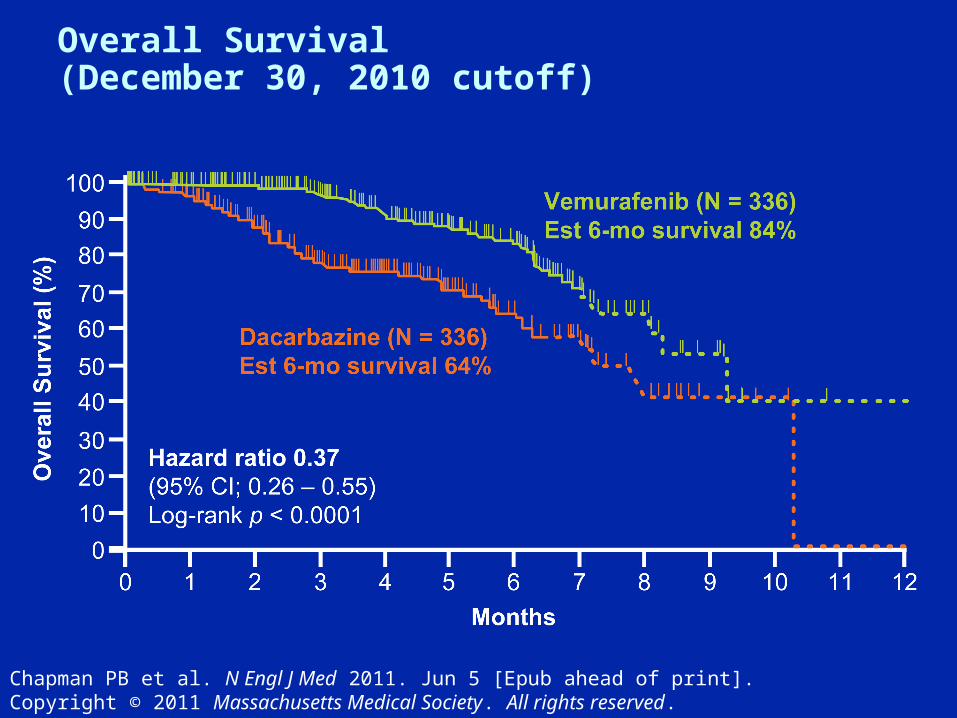
Chapman PB et al. N Engl J Med 2011. Jun 5 [Epub ahead of print]. Copyright © 2011 Massachusetts Medical Society. All rights reserved.
Overall Survival(December 30, 2010 cutoff)
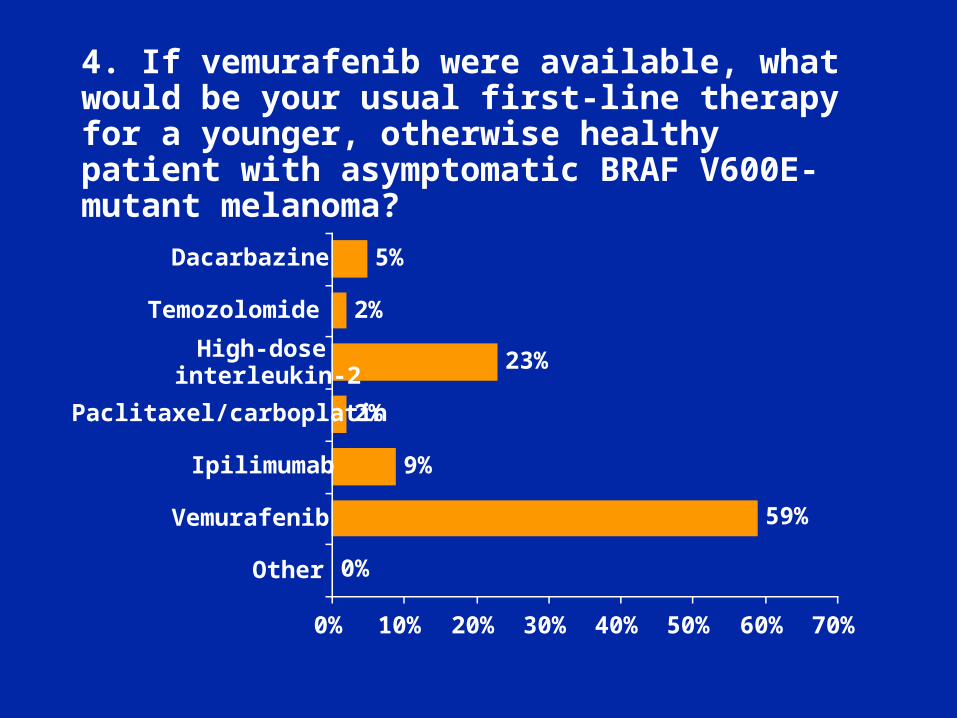
4. If vemurafenib were available, what would be your usual first-line therapy for a younger, otherwise healthy patient with asymptomatic BRAF V600E-mutant melanoma?
59%
9%
2%
23%
2%
5%
0%
0% 10% 20% 30% 40% 50% 60% 70%
Other
Vemurafenib
Ipilimumab
Paclitaxel/carboplatin
High-doseinterleukin-2
Temozolomide
Dacarbazine
Future Research Directions with Vemurafenib
• Biomarkers of resistance/escape
• Predictors of toxicity/management
• Combinations and sequences
– MEK inhibitors
– PI3K and mTOR inhibitors
– IGFR inhibitors
– Immunomodulators
– Cytotoxic agents
Margolin K et al. Proc ASCO 2011; Discussant.
Case 1 (Dr Weber)
• 55 yo man with bulky, unresectable left lower extremity and para-aortic disease
– Treated with the BRAF inhibitor vemurafenib (PLX4032)
– Rapid disease regression, near CR after 16 weeks
– On therapy 12 more months
• Relapses with subcutaneous lesion in involved left leg
– Resected
– PET/CT and MRI: NED
– Remains on vemurafenib
– Alive and disease-free 12 months later
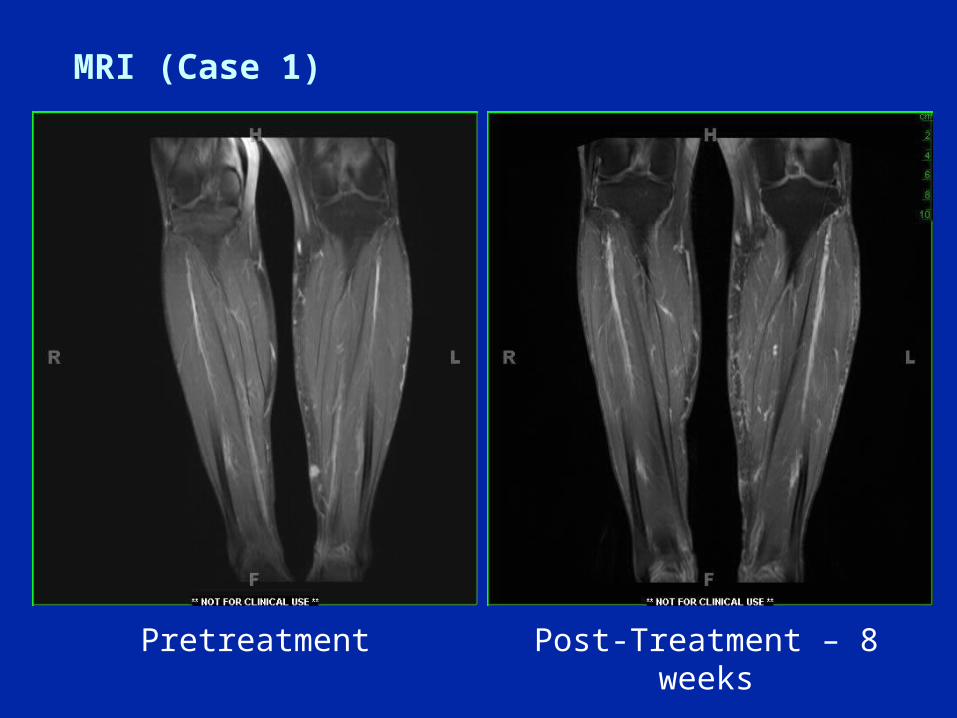
MRI (Case 1)
Pretreatment Post-Treatment – 8 weeks
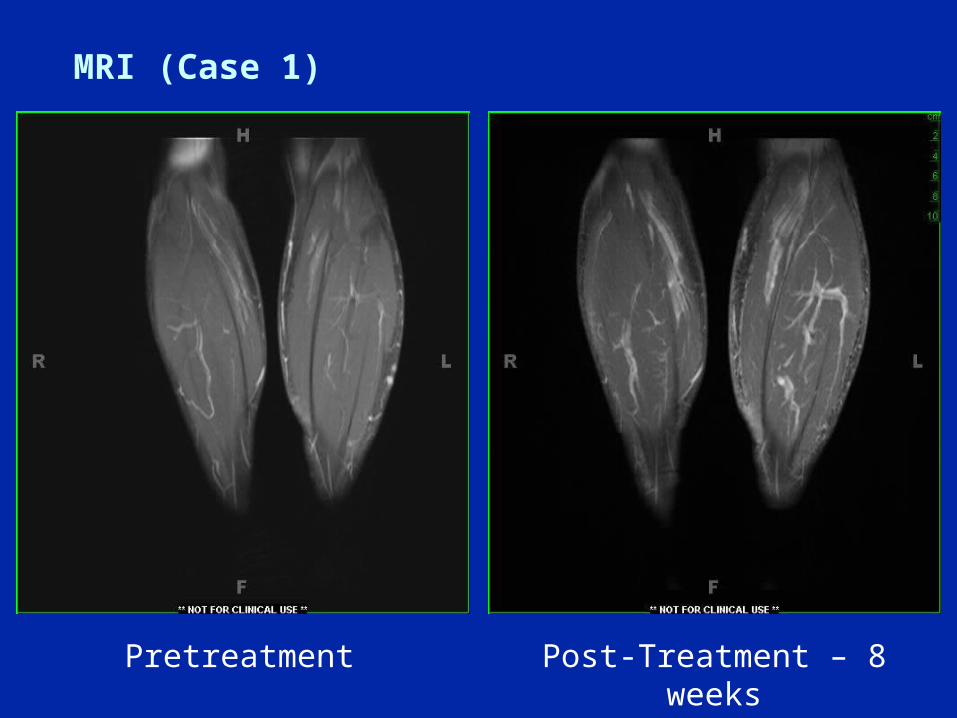
MRI (Case 1)
Pretreatment Post-Treatment – 8 weeks

Case 2 (Dr Flaherty)
• 62 yo man with T4, N1b melanoma resected in 2008 with primary on right arm and involved palpable lymph node in right axilla– Received one year of high-dose interferon
• May 2011: Palpable right supraclavicular lymph node – FNA: Melanoma
• Staging CT scans – Several enlarged right supraclavicular and mediastinal
lymph nodes– Lung and liver lesions– LDH 2x upper limit of normal
• Tumor block from 2008 lymphadenectomy– V600E mutation present
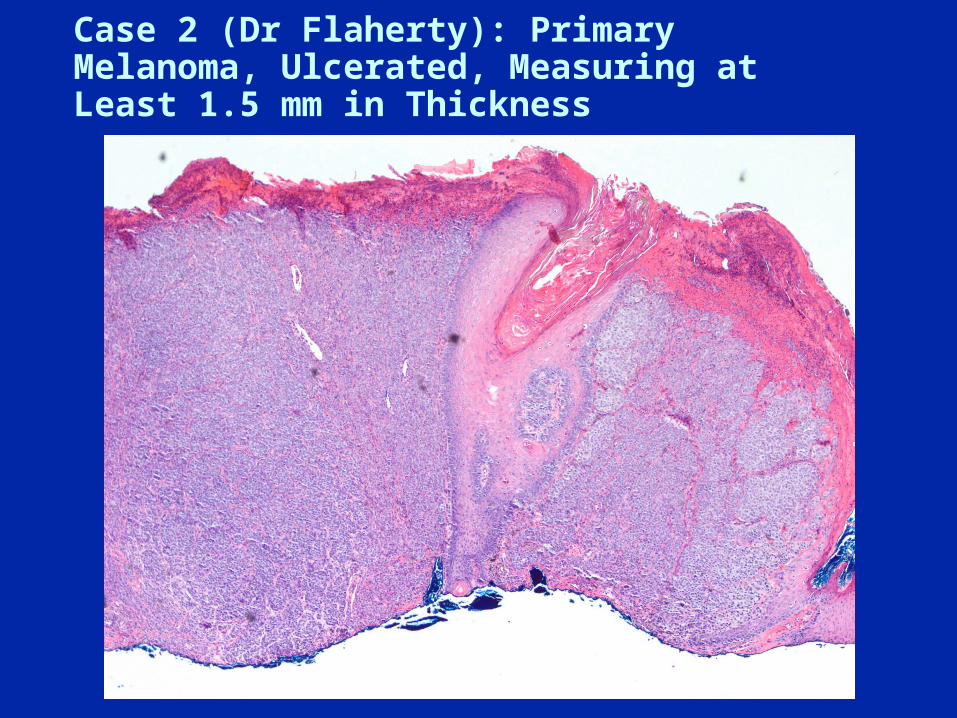
Case 2 (Dr Flaherty): Primary Melanoma, Ulcerated, Measuring at Least 1.5 mm in Thickness
Case 2 (Dr Flaherty)
Case 3 (Dr Weber)
• 72 yo man with lung, liver and bony disease
– Failed carbo/paclitaxel/sorafenib on protocol
– Failed high-dose IL2
– Failed PD-1 antibody
• Ipilimumab off protocol
– Develops itchy rash and hypothyroidism (corrected)
– Continues therapy and has SD at week 12 evaluation
– Slow regression over next 12 months with 90% PR
– Tapered off synthroid with minimal disease via CT
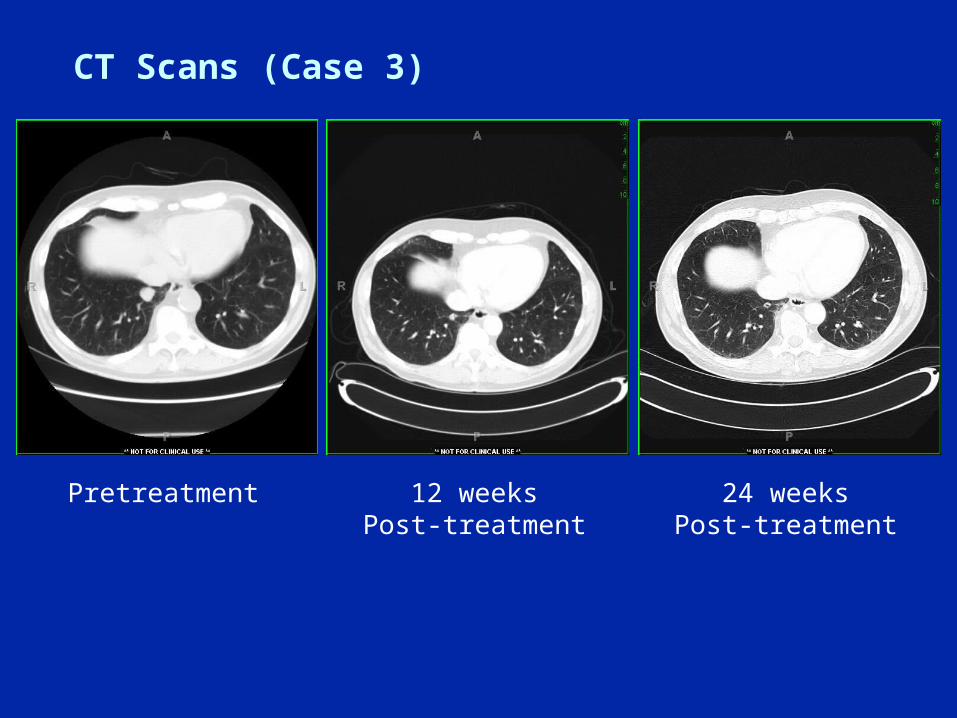
CT Scans (Case 3)
Pretreatment 12 weeks Post-treatment
24 weeks Post-treatment
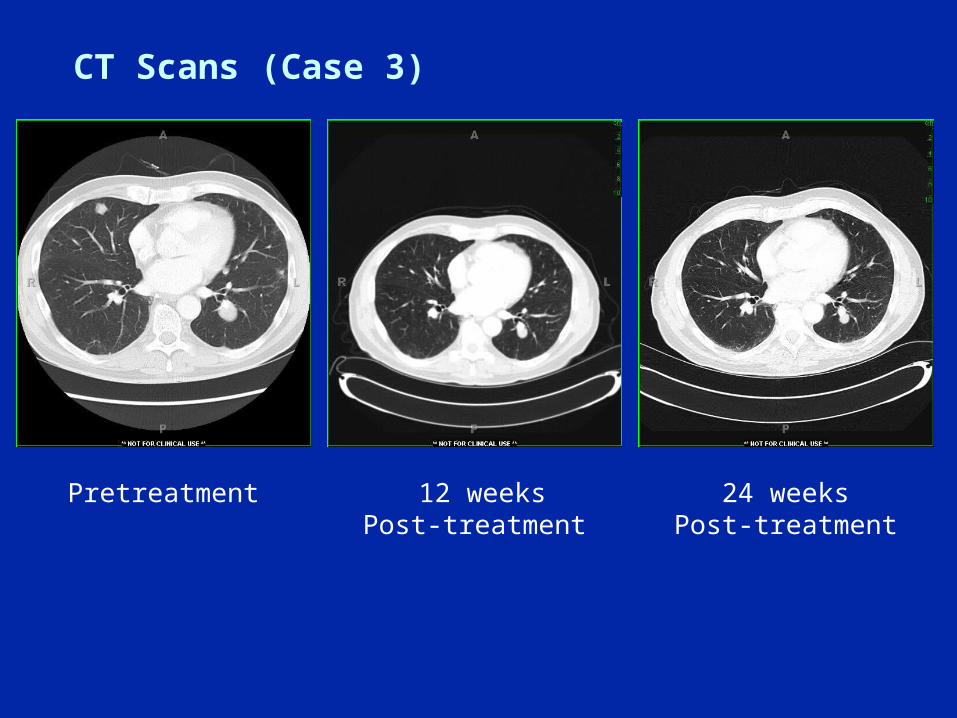
CT Scans (Case 3)
Pretreatment 12 weeksPost-treatment
24 weeks Post-treatment

Case 4 (Dr Flaherty)
• 54 yo man with 2.0 mm, at least level IV, non-ulcerated, melanoma
– 4 mitoses/mm2 on scalp
– Two palpable lymph nodes, total of 10 out of 77 necks nodes positive for melanoma
• Received one year of high-dose interferon
• June 2011: Seizure
– Brain MRI: Two dominant brain metastases and several smaller ones
• Tumor block from 2010 lymphadenectomy
– BRAF mutation testing requested

Case 4 (Dr Flaherty)
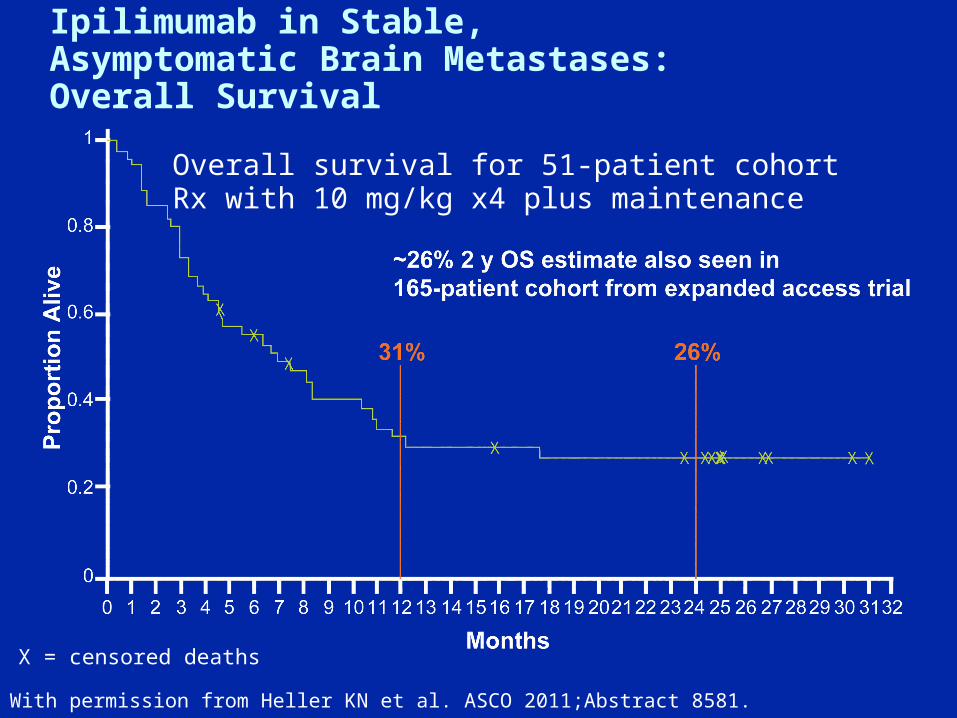
Ipilimumab in Stable, Asymptomatic Brain Metastases: Overall Survival
With permission from Heller KN et al. ASCO 2011;Abstract 8581.
X = censored deaths
Overall survival for 51-patient cohortRx with 10 mg/kg x4 plus maintenance

Case 5 (Dr Weber)
• 32 yo man with lung and intra-abdominal disease
– Treated with biochemotherapy, but increased intra-abdominal disease
– Receives ipilimumab
– Acute abdomen with evidence of free air
– Perforation: Area repaired, with no real disease observed by the surgeon
• Disease regresses at first evaluation
– Patient continues to have diminution of disease
– CR after one year
• Patient is alive and well 8 years later
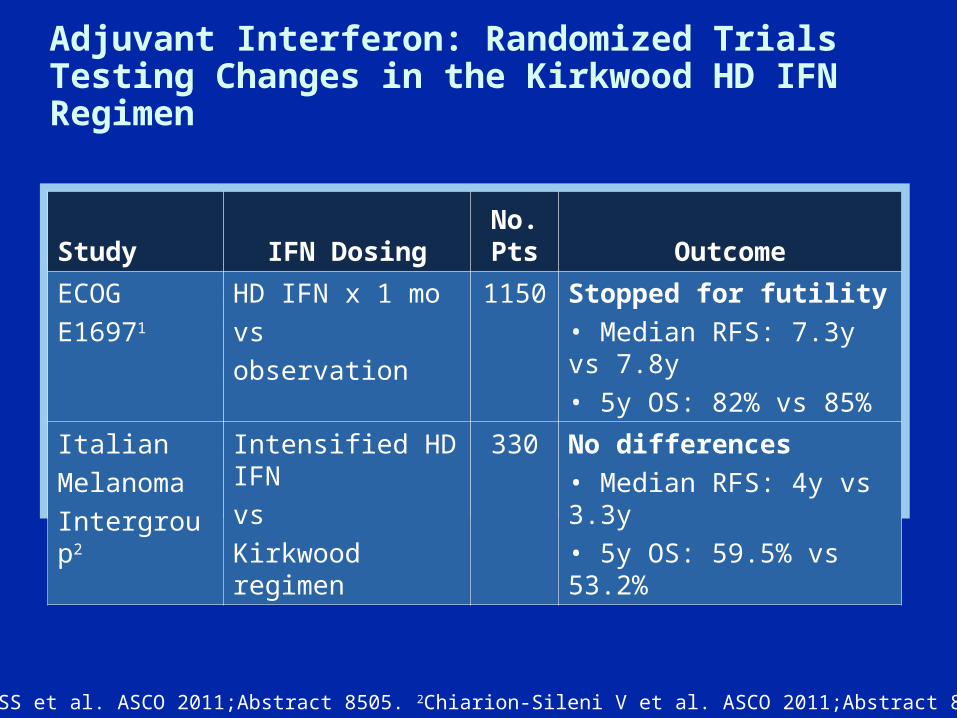
1Agarwala SS et al. ASCO 2011;Abstract 8505. 2Chiarion-Sileni V et al. ASCO 2011;Abstract 8506.
Study IFN DosingNo. Pts Outcome
ECOG
E16971
HD IFN x 1 mo
vs
observation
1150 Stopped for futility
• Median RFS: 7.3y vs 7.8y
• 5y OS: 82% vs 85%
Italian
Melanoma
Intergroup2
Intensified HD IFN
vs
Kirkwood regimen
330 No differences
• Median RFS: 4y vs 3.3y
• 5y OS: 59.5% vs 53.2%
Adjuvant Interferon: Randomized Trials Testing Changes in the Kirkwood HD IFN Regimen
EORTC 18991 Phase III Trial: Long-Term Adjuvant Pegylated Interferon-α2b (PEG-IFN) versus Observation in Resected Stage III Melanoma: Long-Term Results at 7.6-Years Follow-Up
Eggermont AM et al. Proc ASCO 2011;Abstract 8506b.

Eggermont AM et al. ASCO 2011;Abstract 8506b.
RFS DMFS OS
All patients
(N = 1,256)
Obs PEG-IFN Obs PEG-IFN
Obs PEG-IFN
7-year rates 35% 39% 40% 42% 46% 48%
Median, years 2.2 3.0 3.2 3.9 5.6 6.2
Hazard ratiop-value
HR = 0.87
p = 0.05
HR = 0.93
p = 0.33
HR = 0.96
p = 0.57
N1+, ulcerated
(n = 186)
HR = 0.72
p = 0.06
HR = 0.65
p = 0.02
HR = 0.59
p = 0.006
Survival Benefits of PEG-IFN in Resected Stage III Melanoma
Schedule of Events
Tuesday, June 28 Non-Small Cell Lung CancerLucian R Chirieac, MD Thomas J Lynch Jr, MDLecia V Sequist, MD, MPH
Tuesday, July 5Multiple MyelomaNikhil C Munshi, MDA Keith Stewart, MBChB
Tuesday, July 12Gastric CancerCharles S Fuchs, MD, MPHDavid H Ilson, MD, PhDLaura H Tang, MD, PhD
Tuesday, July 19Triple-Negative Breast Cancer: Current Clinical Management
Harold J Burstein, MD, PhDCharles E Geyer Jr, MD
Tuesday, July 26Non-Hodgkin’s Lymphoma/Chronic Lymphocytic LeukemiaStephanie A Gregory, MDJohn P Leonard, MD
Tuesday, August 2Chronic Myeloid LeukemiaSusan M O’Brien, MDNeil P Shah, MD, PhD
Related Documents