EMEDICINE Background: Parkinson disease (PD) is a progressive neurodegenerative disorder associated with a loss of dopaminergic nigrostriatal neurons. It is named after James Parkinson, the English physician who described the shaking palsy in 1817. PD is recognized as one of the most common neurological disorders, affecting approximately 1% of individuals older than 60 years. Cardinal features include resting tremor, rigidity, bradykinesia, and postural instability. Pathophysiology: The major neuropathologic findings in PD are a loss of pigmented dopaminergic neurons in the substantia nigra and the presence of Lewy bodies. The loss of dopaminergic neurons occurs most prominently in the ventral lateral substantia nigra. Approximately 60-80% of dopaminergic neurons are lost before the motor signs of PD emerge. Lewy bodies are concentric, eosinophilic, cytoplasmic inclusions with peripheral halos and dense cores. The presence of Lewy bodies within pigmented neurons of the substantia nigra is characteristic, but not pathognomonic, of idiopathic PD. Lewy bodies also are found in the cortex, nucleus basalis, locus ceruleus, intermediolateral column of the spinal cord, and other areas. Lewy bodies are not specific to PD, as they are found in some cases of atypical parkinsonism, Hallervorden-Spatz disease, and other disorders. Incidental Lewy bodies are found at postmortem in patients without clinical signs of parkinsonism. The prevalence of incidental Lewy bodies increases with age. Incidental Lewy bodies have been hypothesized to represent the presymptomatic phase of PD. No standard criteria exist for the neuropathologic diagnosis of PD, as the specificity and sensitivity of the characteristic findings have not been established clearly. Individuals presenting with primary dementia may exhibit neuropathologic features indistinguishable from those of PD. Alpha-synuclein recently was discovered to be a major structural component of Lewy bodies. All Lewy bodies stain for alpha-synuclein and most also stain for ubiquitin.

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

EMEDICINE
Background: Parkinson disease (PD) is a progressive neurodegenerative disorder associated with a loss of dopaminergic nigrostriatal neurons. It is named after James Parkinson, the English physician who described the shaking palsy in 1817.
PD is recognized as one of the most common neurological disorders, affecting approximately 1% of individuals older than 60 years. Cardinal features include resting tremor, rigidity, bradykinesia, and postural instability.
Pathophysiology: The major neuropathologic findings in PD are a loss of pigmented dopaminergic neurons in the substantia nigra and the presence of Lewy bodies. The loss of dopaminergic neurons occurs most prominently in the ventral lateral substantia nigra. Approximately 60-80% of dopaminergic neurons are lost before the motor signs of PD emerge.
Lewy bodies are concentric, eosinophilic, cytoplasmic inclusions with peripheral halos and dense cores. The presence of Lewy bodies within pigmented neurons of the substantia nigra is characteristic, but not pathognomonic, of idiopathic PD. Lewy bodies also are found in the cortex, nucleus basalis, locus ceruleus, intermediolateral column of the spinal cord, and other areas. Lewy bodies are not specific to PD, as they are found in some cases of atypical parkinsonism, Hallervorden-Spatz disease, and other disorders. Incidental Lewy bodies are found at postmortem in patients without clinical signs of parkinsonism. The prevalence of incidental Lewy bodies increases with age. Incidental Lewy bodies have been hypothesized to represent the presymptomatic phase of PD.
No standard criteria exist for the neuropathologic diagnosis of PD, as the specificity and sensitivity of the characteristic findings have not been established clearly. Individuals presenting with primary dementia may exhibit neuropathologic features indistinguishable from those of PD.
Alpha-synuclein recently was discovered to be a major structural component of Lewy bodies. All Lewy bodies stain for alpha-synuclein and most also stain for ubiquitin.
Motor circuit in Parkinson disease
The basal ganglia motor circuit modulates cortical output necessary for normal movement (see Image 1). Signals from the cerebral cortex are processed through the basal ganglia-thalamocortical motor circuit and return to the same area via a feedback pathway. Output from the motor circuit is directed through the internal segment of the globus pallidus (GPi) and the substantia nigra pars reticulata (SNr). This inhibitory output is directed to the thalamocortical pathway and suppresses movement.
Two pathways exist within the basal ganglia circuit; they are referred to as the direct and indirect pathways. In the direct pathway, outflow from the striatum directly inhibits GPi and SNr. The indirect pathway comprises inhibitory connections between the striatum and the external segment of the globus pallidus (GPe) and the GPe and the subthalamic nucleus (STN). The subthalamic nucleus exerts an excitatory influence on the GPi and SNr. The GPi/SNr sends inhibitory output to the ventral lateral (VL) nucleus of the thalamus. Striatal neurons containing D1 receptors constitute the direct pathway and project to the GPi/SNr.

Striatal neurons containing D2 receptors are part of the indirect pathway and project to the GPe.
Dopamine is released from nigrostriatal (SNc) neurons to activate the direct pathway and inhibit the indirect pathway. In PD, decreased striatal dopamine causes increased inhibitory output from the GPi/SNr (see Image 2). This increased inhibition of the thalamocortical pathway suppresses movement. Via the direct pathway, decreased striatal dopamine stimulation causes decreased inhibition of the GPi/SNr. Via the indirect pathway, decreased dopamine inhibition causes increased inhibition of the GPe, resulting in disinhibition of the STN. Increased STN output increases GPi/SNr inhibitory output to the thalamus.
Frequency:
Internationally: The incidence has been estimated to be 4.5-21 cases per 100,000 population per year. Estimates of PD prevalence range from 18-328 per 100,000 population, with most studies yielding a prevalence of approximately 120 per 100,000.
Sex: PD is about 1.5 times more common in men than in women.
Age: The incidence and prevalence of PD increase with age. The average age of onset is approximately 60 years. Onset in persons younger than 40 years is relatively uncommon.
CLINICAL Section 3 of 11
Author Information Introduction Clinical Differentials Workup Treatment Medication Follow-up Miscellaneous Pictures Bibliography
History: Onset of PD is typically asymmetric, with the most common initial finding being an asymmetric resting tremor in an upper extremity. About 20% of patients first experience clumsiness in one hand. Over time, patients notice symptoms related to progressive bradykinesia, rigidity, and gait difficulty.
Tremor usually begins in one upper extremity and initially may be intermittent. As with most tremors, the amplitude increases with stress and resolves during sleep. After several months or as much as a few years, the tremor may affect the extremities on the other side, but asymmetry usually is maintained. PD tremor may also involve the tongue, lips, or chin.
The initial symptoms of PD may be nonspecific and include fatigue, depression, constipation, and sleep problems.
Some patients experience a subtle decrease in dexterity and may notice a lack of coordination with activities such as playing golf or dressing.
Some patients complain of aching or tightness in the calf or shoulder region.

The first affected arm may not swing fully when walking, and the foot on the same side may scrape the floor.
Over time, axial posture becomes progressively flexed and strides become shorter.
Decreased swallowing may lead to excess saliva in the mouth and ultimately drooling.
Symptoms of autonomic dysfunction are common and include constipation, sweating abnormalities, sexual dysfunction, and seborrheic dermatitis.
Sleep disturbances are common.
The best clinical predictors of a pathologic diagnosis of PD are the following:
o Asymmetry
o Presence of resting tremor
o Good response to dopamine replacement therapy
Physical: The 3 cardinal signs of PD are resting tremor, rigidity, and bradykinesia. Of these cardinal features, 2 of 3 are required to make the clinical diagnosis. Postural instability is the fourth cardinal sign, but it emerges late in the disease, usually after 8 years or more.
The characteristic PD tremor is present and most prominent with the limb at rest.
o The usual frequency is 3-5 Hz.
o The tremor may appear as a pill-rolling motion of the hand or a simple oscillation of the hand or arm.
o The same tremor may be observed with the arms outstretched (position of postural maintenance) and a less prominent, higher frequency kinetic tremor is also common.
Rigidity refers to an increase in resistance to passive movement about a joint.
o The resistance can be either smooth (lead pipe) or oscillating (cogwheeling).
o Cogwheeling is thought to reflect tremor rather than rigidity and may be appreciated in tremors not associated with an increase in tone (ie, essential tremor).
o Rigidity usually is tested by flexing and extending the patient's relaxed wrist.
o Rigidity can be made more obvious with voluntary movement in the contralateral limb.
Bradykinesia refers to slowness of movement but also includes a paucity of spontaneous movements and decreased amplitude of movement. Bradykinesia also is

expressed as micrographia (small handwriting), hypomimia (decreased facial expression), decreased blink rate, and hypophonia (soft speech).
Postural instability refers to imbalance and loss of righting reflexes. Its emergence is an important milestone, because it is poorly amenable to treatment and a common source of disability in late disease.
Patients may experience freezing when starting to walk (start-hesitation), during turning, or while crossing a threshold, such as going through a doorway.
Dementia generally occurs late in PD and affects 15-30% of patients. Short-term memory and visuospatial function may be impaired, but aphasia is not present. Cognitive dysfunction within a year of onset of motor features suggests a diagnosis of Lewy body disease, a disease closely related to PD and marked by the presence of cortical Lewy bodies.
Causes: Most cases of idiopathic PD are believed to be due to a combination of genetic and environmental factors. At both ends of the spectrum are rare cases that appear to be due solely to one or the other.
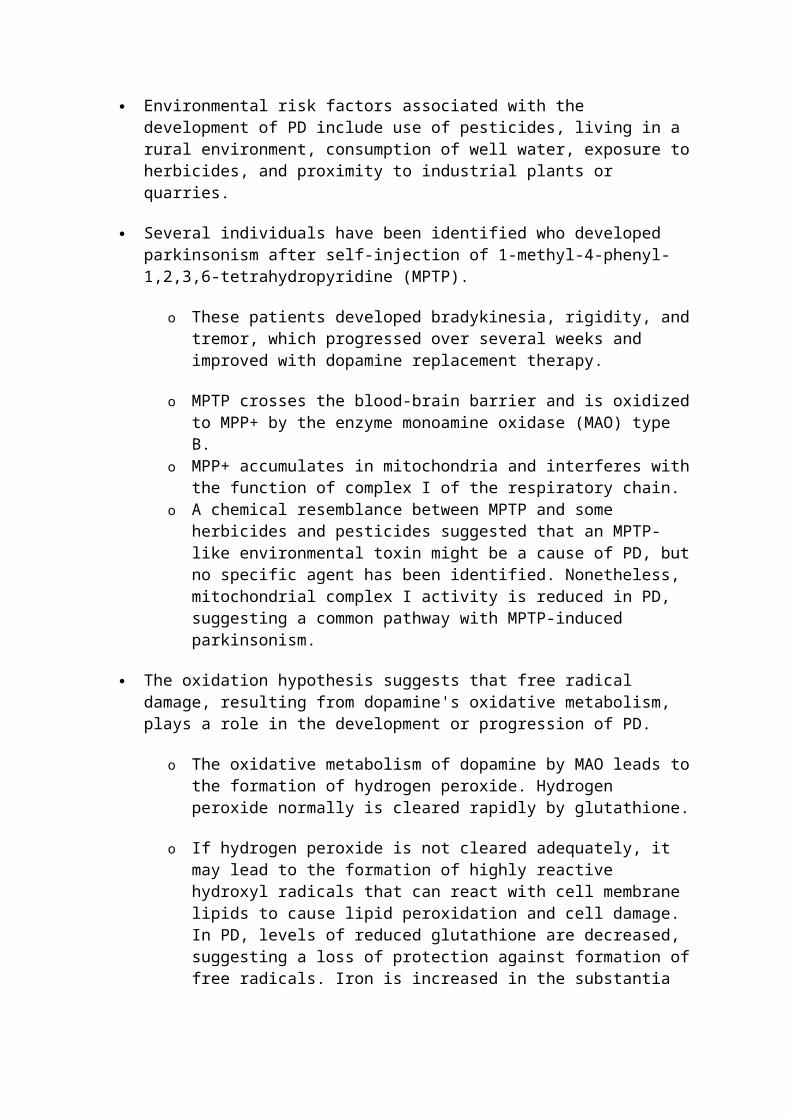
Environmental risk factors associated with the development of PD include use of pesticides, living in a rural environment, consumption of well water, exposure to herbicides, and proximity to industrial plants or quarries.
Several individuals have been identified who developed parkinsonism after self-injection of 1-methyl-4-phenyl-1,2,3,6-tetrahydropyridine (MPTP).
o These patients developed bradykinesia, rigidity, and tremor, which progressed over several weeks and improved with dopamine replacement therapy.
o MPTP crosses the blood-brain barrier and is oxidized to MPP+ by the enzyme monoamine oxidase (MAO) type B.
o MPP+ accumulates in mitochondria and interferes with the function of complex I of the respiratory chain.
o A chemical resemblance between MPTP and some herbicides and pesticides suggested that an MPTP-like environmental toxin might be a cause of PD, but no specific agent has been identified. Nonetheless, mitochondrial complex I activity is reduced in PD, suggesting a common pathway with MPTP-induced parkinsonism.
The oxidation hypothesis suggests that free radical damage, resulting from dopamine's oxidative metabolism, plays a role in the development or progression of PD.
o The oxidative metabolism of dopamine by MAO leads to the formation of hydrogen peroxide. Hydrogen peroxide normally is cleared rapidly by glutathione.
o If hydrogen peroxide is not cleared adequately, it may lead to the formation of highly reactive hydroxyl radicals that can react with cell membrane lipids to cause lipid peroxidation and cell damage. In PD, levels of reduced glutathione

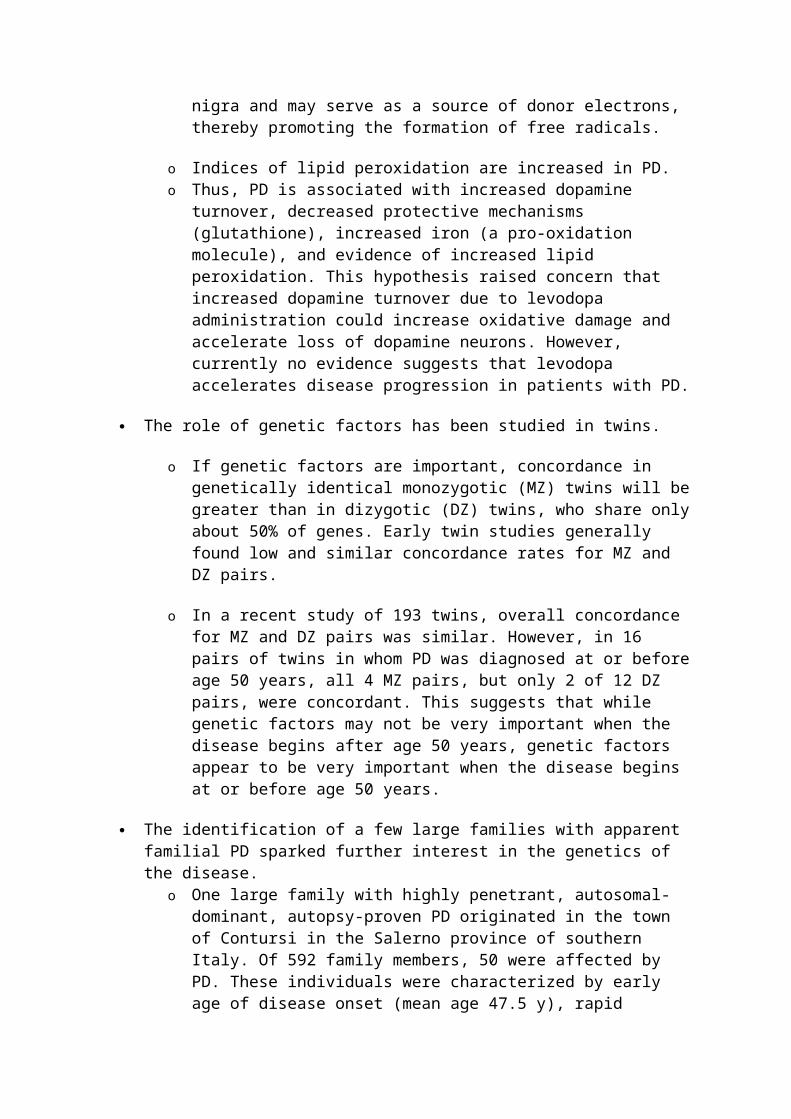
are decreased, suggesting a loss of protection against formation of free radicals. Iron is increased in the substantia nigra and may serve as a source of donor electrons, thereby promoting the formation of free radicals.
o Indices of lipid peroxidation are increased in PD. o Thus, PD is associated with increased dopamine turnover, decreased
protective mechanisms (glutathione), increased iron (a pro-oxidation molecule), and evidence of increased lipid peroxidation. This hypothesis raised concern that increased dopamine turnover due to levodopa administration could increase oxidative damage and accelerate loss of dopamine neurons. However, currently no evidence suggests that levodopa accelerates disease progression in patients with PD.
The role of genetic factors has been studied in twins.
o If genetic factors are important, concordance in genetically identical monozygotic (MZ) twins will be greater than in dizygotic (DZ) twins, who share only about 50% of genes. Early twin studies generally found low and similar concordance rates for MZ and DZ pairs.
o In a recent study of 193 twins, overall concordance for MZ and DZ pairs was similar. However, in 16 pairs of twins in whom PD was diagnosed at or before age 50 years, all 4 MZ pairs, but only 2 of 12 DZ pairs, were concordant. This suggests that while genetic factors may not be very important when the disease begins after age 50 years, genetic factors appear to be very important when the disease begins at or before age 50 years.
The identification of a few large families with apparent familial PD sparked further interest in the genetics of the disease.
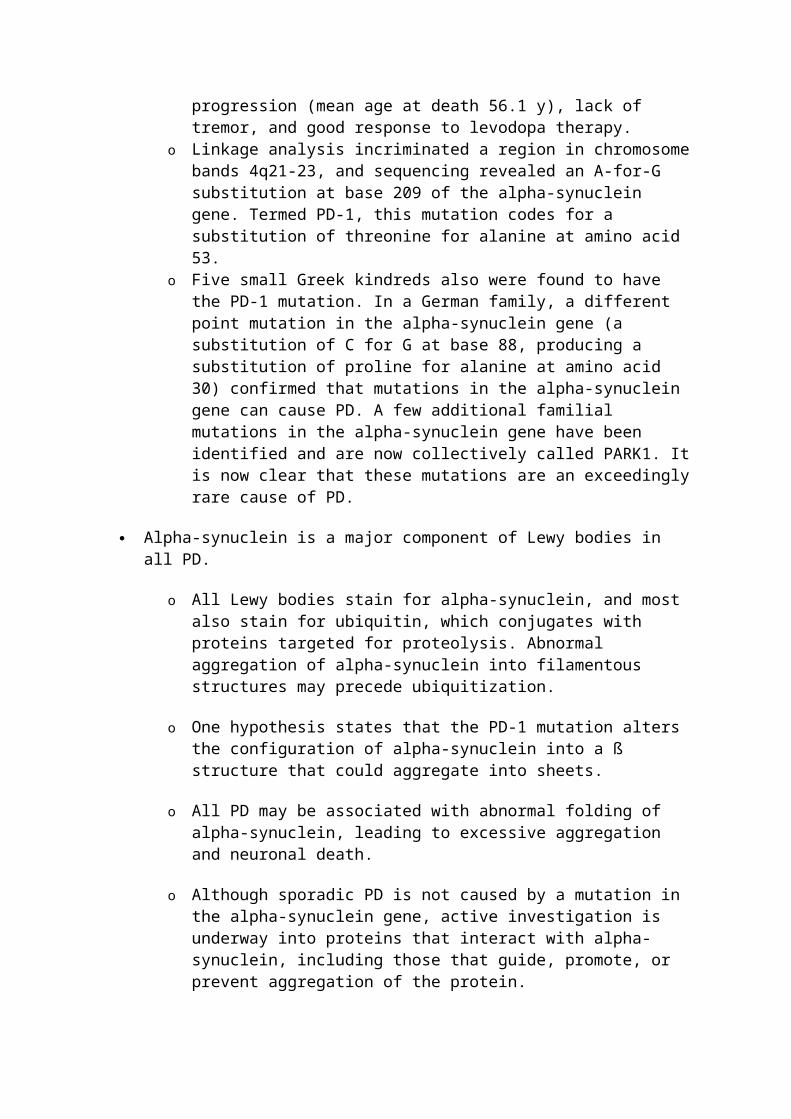
o One large family with highly penetrant, autosomal-dominant, autopsy-proven PD originated in the town of Contursi in the Salerno province of southern Italy. Of 592 family members, 50 were affected by PD. These individuals were characterized by early age of disease onset (mean age 47.5 y), rapid progression (mean age at death 56.1 y), lack of tremor, and good response to levodopa therapy.
o Linkage analysis incriminated a region in chromosome bands 4q21-23, and sequencing revealed an A-for-G substitution at base 209 of the alpha-synuclein gene. Termed PD-1, this mutation codes for a substitution of threonine for alanine at amino acid 53.
o Five small Greek kindreds also were found to have the PD-1 mutation. In a German family, a different point mutation in the alpha-synuclein gene (a substitution of C for G at base 88, producing a substitution of proline for alanine at amino acid 30) confirmed that mutations in the alpha-synuclein gene can cause PD. A few additional familial mutations in the alpha-synuclein gene have been identified and are now collectively called PARK1. It is now clear that these mutations are an exceedingly rare cause of PD.
Alpha-synuclein is a major component of Lewy bodies in all PD.
o All Lewy bodies stain for alpha-synuclein, and most also stain for ubiquitin, which conjugates with proteins targeted for proteolysis. Abnormal aggregation of alpha-synuclein into filamentous structures may precede ubiquitization.
o One hypothesis states that the PD-1 mutation alters the configuration of alpha-synuclein into a ß structure that could aggregate into sheets.
o All PD may be associated with abnormal folding of alpha-synuclein, leading to excessive aggregation and neuronal death.
o Although sporadic PD is not caused by a mutation in the alpha-synuclein gene, active investigation is underway into proteins that interact with alpha-synuclein, including those that guide, promote, or prevent aggregation of the protein.
o As PD, dementia with Lewy bodies, and multiple system atrophy (MSA) all exhibit Lewy bodies that stain for alpha-synuclein, they have been designated “alpha-synucleinopathies.”
A recent hypothesis suggests that PD is caused by abnormalities of the proteosome system, which is responsible for clearing abnormal proteins.
Several homozygous deletions in a gene dubbed Parkin (Park2), which is located on chromosome 6, have been found to cause autosomal-recessive juvenile parkinsonism (AR-JP). This form of parkinsonism differs pathologically from PD in that no Lewy bodies are found in the substantia nigra.
Several other gene abnormalities have been identified in families with PD and these are designated Park3-Park12.
It has been estimated that all currently known genetic causes of PD account for less than 5% of PD cases.
DIFFERENTIALS Section 4 of 11
Author Information Introduction Clinical Differentials Workup Treatment Medication Follow-up Miscellaneous Pictures Bibliography
Alzheimer Disease Cardioembolic Stroke Cortical Basal Ganglionic Degeneration Essential Tremor Hallervorden-Spatz Disease Lacunar Syndromes Multiple System Atrophy Normal Pressure Hydrocephalus Parkinson-Plus Syndromes Progressive Supranuclear Palsy Striatonigral Degeneration
Other Problems to be Considered:
Jakob-Creutzfeldt and other prion diseases
Parkinsonism can be caused by a variety of degenerative disorders, as well as toxins, infections, and vascular or structural lesions.
Parkinsonism also can be induced by medications that block dopamine receptors (eg, neuroleptics, antiemetics) or deplete intraneuronal dopamine stores (eg, reserpine, tetrabenazine).
Quick Find
Author InformationIntroductionClinicalDifferentialsWorkupTreatmentMedicationFollow-upMiscellaneousPicturesBibliography
Click for related images.
Related Articles
Alzheimer Disease
Cardioembolic Stroke
Cortical Basal Ganglionic Degeneration
Essential Tremor
Hallervorden-Spatz Disease
Lacunar Syndromes
Multiple System Atrophy
Normal Pressure Hydrocephalus
Parkinson-Plus Syndromes
Progressive Supranuclear Palsy
Striatonigral Degeneration
Continuing Education
CME available for this topic. Click here to take this CME.
Patient Education
Dementia Center
Parkinson Disease Overview
Parkinson Disease Causes
Parkinson Disease Symptoms
Parkinson Disease Treatment
Parkinson Disease Dementia Overview
WORKUP Section 5 of 11
Author Information Introduction Clinical Differentials Workup Treatment Medication Follow-up Miscellaneous Pictures Bibliography

Lab Studies:
No laboratory biomarkers exist for PD.
Serum ceruloplasmin concentration is obtained as a screening test for Wilson disease. It should be obtained in patients who present with parkinsonian symptoms when younger than 40 years. In cases in which Wilson disease is suspected, 24-hour urinary copper and slit lamp examination of the eyes also should be obtained.
Imaging Studies:
Magnetic resonance imaging (MRI) and computed tomography (CT) scan are unremarkable in PD.
o No imaging study is required in patients with a typical presentation. Such patients are aged 55 years or older; have a slowly progressive, asymmetric parkinsonism with resting tremor and bradykinesia or rigidity; and demonstrate a good response to dopamine replacement therapy.
o MRI is useful to exclude multi-infarct state, hydrocephalus, and the lesions of Wilson disease.
o MRI should be obtained in patients whose clinical presentation does not allow a high degree of diagnostic certainty, including those who lack tremor, have an acute or stepwise progression, or are younger than 55 years.
Positron emission tomography (PET) and single photon emission CT (SPECT) are useful diagnostic imaging studies. They are not widely available and may not be covered by insurance. Moreover, they are not needed for routine clinical diagnosis in patients with a typical presentation.
o At the onset of symptoms, PD patients show an approximately 30% decrease in 18F-dopa uptake in the contralateral putamen.
o 18F-dopa is taken up by the terminals of dopamine neurons and converted to 18F-dopamine. The rate of striatal 18F accumulation reflects transport of 18F-dopa into dopamine neurons and its decarboxylation to 18F-dopamine.
o 11C-Nomifensine and cocaine analogues such as 123I-Beta-CIT bind to dopamine reuptake sites on nigrostriatal terminals and provide an index of the integrity of nigrostriatal projections.
TREATMENT Section 6 of 11
Author Information Introduction Clinical Differentials Workup Treatment Medication Follow-up Miscellaneous Pictures Bibliography
Medical Care: The goal of medical management of PD is to provide control of signs and symptoms for as long as possible while minimizing adverse effects. Medications usually provide good symptomatic control for 4-6 years. After this, disability progresses despite best medical management, and many patients develop long-term motor complications including
fluctuations and dyskinesia. Additional causes of disability in late disease include postural instability (balance difficulty) and dementia.
Putative neuroprotective therapy: Neuroprotective therapies are defined as those that slow the underlying loss of dopamine neurons. Currently, no proven neuroprotective therapies exist for PD.
o If a neuroprotective therapy were available for PD, it would be administered from the time of diagnosis onward.
o Selegiline is the medication that first has garnered interest as a possible neuroprotective agent.
o Laboratory investigations continue to provide evidence that selegiline affords a neuroprotective effect for dopamine neurons independent of MAO-B inhibition.
o Selegiline has been demonstrated to protect cultured dopamine neurons from MPP+ toxicity, an effect that cannot be attributed to MAO-B inhibition. Tatton and Greenwood demonstrated that selegiline protects dopamine cells in mice from MPTP toxicity even when administered after a delay sufficient to allow the oxidation of MPTP to MPP+.
o In cell-culture systems, selegiline's neuroprotective effect is mediated by new protein synthesis. Selegiline induces transcriptional events that result in increased synthesis of antioxidant and anti-apoptotic proteins. Recent evidence indicates that one of selegiline's metabolites, desmethylselegiline, is the active agent for neuroprotection.
o Selegiline's amphetamine metabolites may interfere with its neuroprotective actions.
o In the clinical study called deprenyl (selegiline) and tocopherol (vitamin E) antioxidative therapy of parkinsonism (DATATOP), the Parkinson Study Group evaluated the ability of these 2 medications to delay progression of clinical disability in early PD. Eight hundred patients were randomized to receive selegiline (10 mg/d) or placebo and tocopherol (2000 IU/d) or placebo. Patients assigned to receive selegiline, with placebo or with tocopherol, experienced a significant delay in the need for levodopa therapy (hazard ratio = 0.50, P <0.001). Patients assigned to receive placebo required levodopa at a projected median of 15 months from enrollment, while those who received selegiline required levodopa at a projected median of 24 months after enrollment. Tocopherol had no effect on progression of disability.
o The study conclusively demonstrated that selegiline delays the need for levodopa therapy in early PD; this result is consistent with the hypothesis that selegiline may slow disease progression. However, the study also found that selegiline provided a small symptom-relieving effect, and whether the delay in the need for levodopa was due entirely or in part to this modest effect is not clear.
o In one study, selegiline was associated with increased mortality rate in patients with PD. The Parkinson's Disease Research Group of the United Kingdom reported a 57% higher mortality rate in patients assigned to receive selegiline plus levodopa than in those who received levodopa alone (mortality ratio = 1.57, 95% confidence interval 1.09-2.30, P = 0.015). The difference in mortality rate emerged between the third and fifth years of treatment, and no obvious explanation regarding its cause was identified.

o Many questions have been raised regarding the results and methodology of this study. Mortality rates were not significantly different between groups when the analysis was based on what patients actually were taking and not on intention to treat. In addition, the mortality rate was unusually high in both groups (28% in patients receiving selegiline, 18% in those not receiving selegiline).
o Rasagiline is a new MAO-B inhibitor that exhibits neuroprotective effects in cell culture and animal models. In a clinical trial (TEMPO), treatment with rasagiline for 1 year provided significantly greater improvement than treatment with placebo for 6 months followed by rasagiline for 6 months.
o Co-enzyme Q10 is another drug of interest. It is a scavenger of free radicals. In a preliminary study, co-enzyme Q10 1200 mg/d slowed progression of PD disability.
o Further studies of rasagiline and co-enzyme Q10 are required.
Symptomatic therapy o Levodopa, coupled with a peripheral decarboxylase inhibitor (PDI), remains
the standard of symptomatic treatment for PD. It provides the greatest antiparkinsonian benefit with the fewest adverse effects in the short term.
o Dopamine agonists provide symptomatic benefit comparable to levodopa/PDI in early disease but lack sufficient efficacy to control signs and symptoms by themselves in later disease.
o Dopamine agonists cause more sleepiness, hallucinations, and edema than levodopa.
o Prospective, double-blind studies have demonstrated that initial treatment with a dopamine agonist, to which levodopa can be added as necessary, causes less motor fluctuations and dyskinesias than levodopa alone.
o Dopamine agonists can be used as initial symptomatic therapy in early disease, rather than levodopa/PDI, to delay the onset of motor fluctuations and dyskinesia. This strategy is usually reserved for younger individuals (<65-70 y) who are cognitively intact.
Levodopa and motor complications o As PD progresses, fewer dopamine neurons are available to store and release
levodopa-derived dopamine. The patient's clinical status begins to fluctuate more and more closely in concert with plasma levodopa levels. Exposing striatal dopamine receptors to fluctuating dopamine concentrations may cause a hypersensitivity that is expressed clinically as peak-dose dyskinesia (twisting, turning movements). Fluctuating levodopa-derived dopamine concentrations in association with advancing disease therefore may be responsible for development of motor fluctuations and dyskinesia.
o The Continuous Dopaminergic Stimulation (CDS) hypothesis posits that pulsatile dopamine receptor stimulation induces dyskinesia, whereas smoother more continuous dopamine receptor stimulation causes less dyskinesia.
o In contrast to levodopa, the long-acting dopamine agonists (ie, bromocriptine, pergolide, pramipexole, ropinirole, cabergoline) provide relatively smooth and sustained receptor stimulation. In marmosets with MPTP-induced parkinsonism, levodopa administration causes significantly more dyskinesia than bromocriptine or ropinirole.

o Prospective clinical trials have demonstrated that initial treatment with a dopamine agonist to which levodopa can be added causes less motor fluctuations and dyskinesia than levodopa alone.
o A recent MPTP marmoset study found that the addition of entacapone (which increases the half-life of levodopa) was associated with less motor fluctuations and less dyskinesia than treatment with the same regimen of levodopa alone. This finding is consistent with the CDS hypothesis. A clinical trial (STRIDE-PD) is now underway to determine if levodopa plus entacapone (levodopa/carbidopa/entacapone) delays the occurrence of dyskinesia compared with levodopa/carbidopa when levodopa is first required.
Early disease treatment strategies o The younger the patient, the more emphasis the authors place on long-term
considerations to guide early treatment. Young patients have a longer life expectancy and are more likely to develop motor fluctuations and dyskinesias.
o For older patients and those with cognitive impairment, less emphasis is placed on long-term considerations; the focus is on providing adequate symptomatic benefit in the near term with as few adverse effects as possible.
o At the time of diagnosis, a discussion is initiated to review current information regarding possible neuroprotective agents currently under study.
o The younger the patient, the more critical the need for neuroprotection, and the more likely the authors are to recommend a possible neuroprotective agent.
o Symptomatic therapy is introduced when the patient experiences functional disability. The selection of medication depends in part on the nature and cause of the disability.
o If disability is due solely to tremor, a tremor-specific medication, such as an anticholinergic agent, can be used. Anticholinergic medications provide good tremor relief in approximately 50% of patients but do not improve bradykinesia or rigidity. Because tremor may respond to one anticholinergic medication and not another, a second anticholinergic usually is tried if the first is not successful. These medications should be introduced at a low dose and escalated slowly to minimize adverse effects, which include memory difficulty, confusion, and hallucinations. Adverse cognitive effects are relatively common, especially in the elderly.
o If disability is due to a dopamine-responsive symptom such as bradykinesia, rigidity, decreased dexterity, slow speech, or shuffling gait, a dopaminergic medication, such as an MAO-B inhibitor, amantadine, dopamine agonist, or levodopa, should be introduced. MAO-B inhibitors provide mild symptomatic improvement but have few side effects. Amantadine also provides mild symptomatic improvement but may cause cognitive side effects or hallucinations, especially in older individuals and those with cognitive dysfunction. Dopamine agonists provide moderate benefit and cause less fluctuations and dyskinesias, but they have more side effects including sleepiness, hallucinations, and edema. Levodopa is the strongest symptomatic agent but its long-term use is associated with the development of fluctuations and dyskinesias.
o Symptomatic medications are started at a low dose, escalated slowly, and titrated to control symptoms. Most patients require symptomatic dopaminergic therapy to ameliorate bradykinesia and rigidity within 1-2 years after diagnosis.
o For patients younger than 65 years, the authors often utilize a dopamine agonist and then add levodopa/PDI when the dopamine agonist alone no longer controls symptoms adequately. Dopamine agonists provide antiparkinsonian efficacy comparable to levodopa/PDI for 6-18 months or longer and may control symptoms adequately for several years.
o When the dopamine agonist no longer provides adequate symptomatic control despite titration to the usual maximum or highest tolerated dose, levodopa/PDI is added. The relatively sustained dopamine receptor stimulation provided by the dopamine agonist may buffer receptors from fluctuating levodopa-derived dopamine concentrations and afford a lower incidence of motor fluctuations and dyskinesia.
o For patients who are demented or those older than 70 years, who may be prone to adverse effects from dopamine agonists, and for those likely to require treatment for only a few years, the authors may elect not to use a dopamine agonist and depend on levodopa/PDI as primary symptomatic therapy.
o For patients aged 65-70 years, the authors make a judgment based on general health and cognitive status. The more robust and cognitively intact the patient, the more likely the authors are to start symptomatic treatment with a dopamine agonist and add levodopa/PDI when necessary.
o When introducing a dopamine agonist, starting at a low dose and escalating slowly is important. The dose should be titrated upward until symptoms are controlled, the maximum dose is reached, or adverse effects become intolerable. The most common adverse effects of dopamine agonists are nausea, orthostatic hypotension, hallucinations, and somnolence. Nausea usually can be reduced by having the patient take the medication after meals. Domperidone, a peripheral dopamine agonist available outside the US, is very helpful in relieving refractory nausea.
o Levodopa/PDI is introduced at a low dose and escalated slowly. Currently available levodopa preparations in the United States include levodopa/carbidopa, levodopa/carbidopa CR, levodopa/carbidopa orally disintegrating tablet, and levodopa/carbidopa/entacapone. The orally disintegrating tablet is bioequivalent to oral levodopa/carbidopa but dissolves on the tongue without the need to swallow it with water.
o The levodopa dose is titrated to control clinical symptoms; most patients experience a good response on a daily dosage of 400-600 mg/d for 3-5 years or more. Doses higher than those necessary to control symptoms adequately should be avoided.
o If nausea occurs, the dose may be taken following a meal. Additional measures to alleviate nausea include adding extra carbidopa or introducing domperidone.
Advanced disease treatment strategies o Patients initially experience stable, sustained benefit through the day in
response to levodopa medications. However, after several months to years, many patients notice that the benefit from immediate release levodopa/carbidopa wears off after 4-5 hours. Over time, this shortened duration of response becomes more fleeting, and clinical status fluctuates more and more closely in concert with peripheral levodopa concentration. Ultimately, benefit lasts only 1-2 hours. The time when medication is

providing benefit for bradykinesia, rigidity, and tremor is called “on” time, and the time when medication is not providing benefit is called “off” time.
o By several months to years after the introduction of levodopa, many patients develop peak-dose dyskinesia consisting of choreiform, twisting/turning movements that occur when levodopa-derived dopamine levels are peaking. At this point, increasing dopamine stimulation is likely to worsen peak-dose dyskinesias. Over time, the therapeutic window narrows because of a progressive decrease in the threshold for peak-dose dyskinesia. The therapeutic window lies above the threshold required to improve symptoms (on threshold) and below the threshold for peak-dose dyskinesia (dyskinesia threshold).
o Although many patients prefer dyskinesia to off time, the clinician should recognize that dyskinesias can be sufficiently severe to be troublesome to the patient, either by interfering with activities or because of discomfort. Asking patients how they feel during both off time and time with dyskinesia is important in titrating medication optimally. Having patients fill out a diary may be helpful; the diary should be divided into half-hour time periods on which patients denote whether they are off, on without dyskinesia, on with nontroublesome dyskinesia, or on with troublesome dyskinesia (see Image 3). The goal of medical management is to minimize off time and time on with troublesome dyskinesia.
o Treating motor fluctuations in the absence of peak-dose dyskinesia is relatively easy. Several different strategies, either alone or in combination, can be used to provide more sustained dopaminergic therapy. Possible strategies include adding a dopamine agonist, catechol-O-methyltransferase (COMT) inhibitor, or MAO-B inhibitor; dosing levodopa more frequently; increasing the levodopa dose; or switching from immediate release to CR levodopa or levodopa/carbidopa/entacapone. Unless limited by the emergence of peak-dose symptoms such as dyskinesia or hallucinations, dopaminergic therapy should be increased until off time is eliminated.
o The treatment of patients with both motor fluctuations and troublesome peak-dose dyskinesia can be difficult. The goal of treatment in this situation is to provide as much good functional time through the day as possible. This is accomplished by maximizing on time without troublesome dyskinesia. An attempt is made to reduce both off time and time with troublesome or disabling dyskinesia. Unfortunately, a decrease in dopaminergic therapy may increase off time and an increase in dopaminergic therapy may worsen peak-dose dyskinesia.
o For patients with severe fluctuations and dyskinesia, the best balance between off time and troublesome dyskinesia is sought. The patient's relative preference for off time versus dyskinesia needs to be taken into account.
o For patients with motor fluctuations and dyskinesia on levodopa/PDI, the addition of a dopamine agonist, COMT inhibitor, or MAO-B inhibitor may be helpful. Dyskinesia may increase when these medications are added, necessitating the downward titration of levodopa.
o For patients on CR levodopa, switching to immediate release levodopa/carbidopa often provides a more consistent and predictable dosing cycle and allows finer titration. In general, smaller levodopa doses are administered more frequently. A dose should be sought that is sufficient to provide benefit without causing troublesome dyskinesia. The time to wearing-

off then determines the appropriate interdose interval. The extreme of this strategy is using liquid levodopa, a solution with which the dose can be titrated finely and administered every hour. Amantadine may be of benefit to reduce dyskinesia.
o COMT inhibitors inhibit the peripheral metabolism of levodopa to 3-O-methyldopa (3-OMD), thereby prolonging the levodopa half-life and making more levodopa available for transport across the blood-brain barrier over a longer time.
o Tolcapone was the first COMT inhibitor available for clinical use. Because of the potential risk of hepatotoxicity, liver function test monitoring is required, and it should be used only in patients who are experiencing motor fluctuations on levodopa that cannot be adequately controlled with other medications.
o If dyskinesia emerges, the levodopa dose should be reduced. In patients who already have dyskinesia, the levodopa dose often is reduced by 30-50% at the time tolcapone is introduced.
o Entacapone is a COMT inhibitor that does not cause hepatotoxicity; liver function tests are not required with this medication. A combination tablet of levodopa/carbidopa/entacapone is now available.
o Levodopa/PDI, dopamine agonists, and anticholinergics each provide good benefit for tremor in approximately 50% of patients. If a patient is experiencing troublesome tremor and symptoms are not controlled adequately with one medication, another should be tried. If the tremor is not controlled adequately with medication, thalamotomy or thalamic stimulation surgery may be considered at any time during the disease.
Surgical Care: Stereotactic surgery has made a resurgence in the treatment of PD, largely due to long-term complications of levodopa therapy resulting in significant disability despite optimal medical management.
A better understanding of basal ganglia physiology and circuitry and improvements in surgical techniques, neuroimaging, and electrophysiologic recording have allowed surgical procedures to be performed more accurately and with lower morbidity.
Lesion surgeries involve the destruction of targeted areas of the brain to control the symptoms of PD.
o Thalamotomy involves destruction of a part of the thalamus, generally the ventral intermediate (VIM) nucleus, to relieve tremor. Thalamotomy has little effect on bradykinesia, rigidity, motor fluctuations, or dyskinesia.
o The mechanisms of action of thalamotomy are not known; its effects may be due to destruction of autonomous neural activity (synchronous bursts) at the same frequency as limb tremor.
o More than 90% of patients with PD who undergo thalamotomy have significant improvement in tremor of the limbs contralateral to the side of the lesion.
o Complications from bilateral thalamotomy are common; more than 25% of patients experience speech impairment. Mental changes also can persist after bilateral surgery. Therefore, bilateral thalamotomies are generally avoided.
o Pallidotomy involves destruction of a part of the globus pallidus interna (GPi), which is overactive in PD.

o Results from pallidotomy studies have demonstrated significant improvements in each of the cardinal symptoms of PD (tremor, rigidity, bradykinesia) as well as a significant reduction in dyskinesia.
o Bilateral pallidotomy is not recommended. Although bilateral pallidotomy has been shown to significantly reduce levodopa-induced dyskinesia, complications are relatively common and include speech difficulties, dysphagia, and cognitive impairment.
o Subthalamotomy involves destruction of a part of the subthalamic nucleus (STN), which is also hyperactive in PD.
o Initial results of subthalamotomy have shown significant improvements in the cardinal features of PD as well as the reduction of motor fluctuations and dyskinesia.
o Lesion surgeries for PD have largely been replaced by deep brain stimulation (DBS) that does not involve a permanent lesion in the brain making the procedure reversible and the device can be adjusted to accommodate for disease progression and side effects. In addition, bilateral procedures can be performed without the morbidity seen with bilateral lesion surgeries.
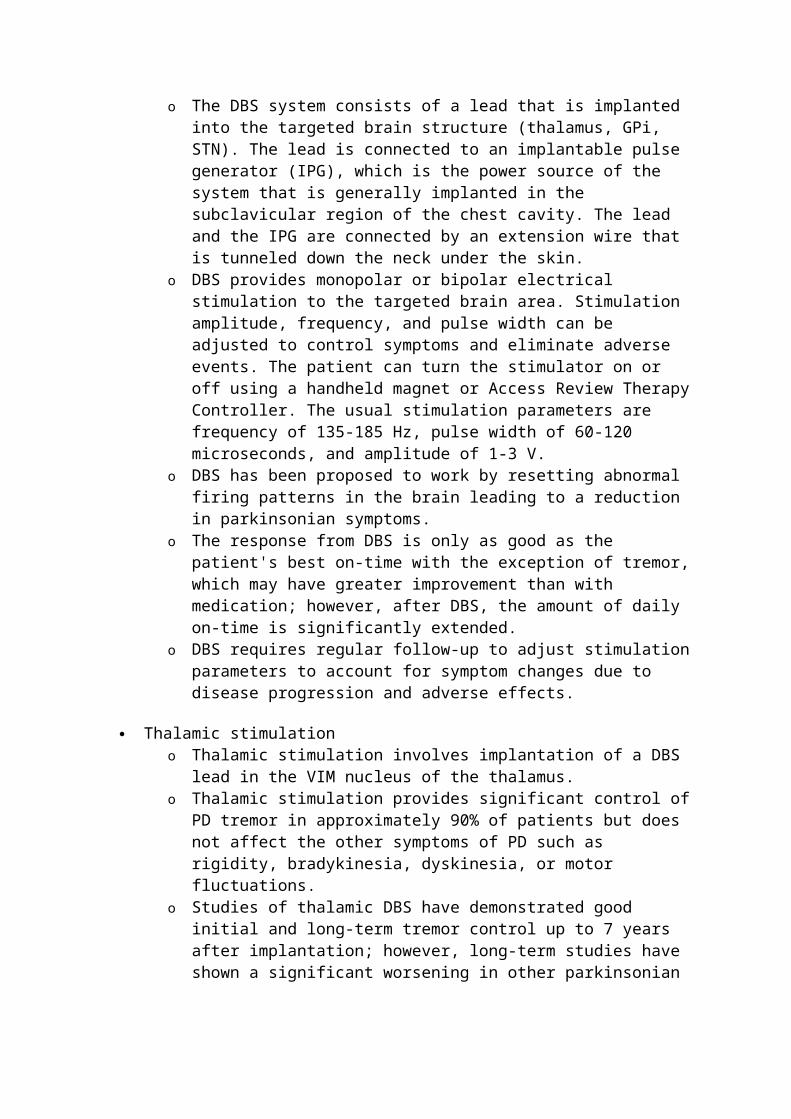
Deep brain stimulation o DBS is an FDA-approved treatment for PD. o The DBS system consists of a lead that is implanted into the targeted brain
structure (thalamus, GPi, STN). The lead is connected to an implantable pulse generator (IPG), which is the power source of the system that is generally implanted in the subclavicular region of the chest cavity. The lead and the IPG are connected by an extension wire that is tunneled down the neck under the skin.
o DBS provides monopolar or bipolar electrical stimulation to the targeted brain area. Stimulation amplitude, frequency, and pulse width can be adjusted to control symptoms and eliminate adverse events. The patient can turn the stimulator on or off using a handheld magnet or Access Review Therapy Controller. The usual stimulation parameters are frequency of 135-185 Hz, pulse width of 60-120 microseconds, and amplitude of 1-3 V.
o DBS has been proposed to work by resetting abnormal firing patterns in the brain leading to a reduction in parkinsonian symptoms.
o The response from DBS is only as good as the patient's best on-time with the exception of tremor, which may have greater improvement than with medication; however, after DBS, the amount of daily on-time is significantly extended.
o DBS requires regular follow-up to adjust stimulation parameters to account for symptom changes due to disease progression and adverse effects.
Thalamic stimulation o Thalamic stimulation involves implantation of a DBS lead in the VIM nucleus
of the thalamus. o Thalamic stimulation provides significant control of PD tremor in
approximately 90% of patients but does not affect the other symptoms of PD such as rigidity, bradykinesia, dyskinesia, or motor fluctuations.
o Studies of thalamic DBS have demonstrated good initial and long-term tremor control up to 7 years after implantation; however, long-term studies have

shown a significant worsening in other parkinsonian symptoms such as bradykinesia, rigidity, and worsening of gait leading to major disability.
o Candidates for thalamic DBS are patients with disabling medication-resistant tremor who have minimal rigidity or bradykinesia. They should not have significant cognitive impairment, mood or behavioral disturbances, or other factors that may increase the risk of surgery.
o The role of thalamic DBS is limited in PD.
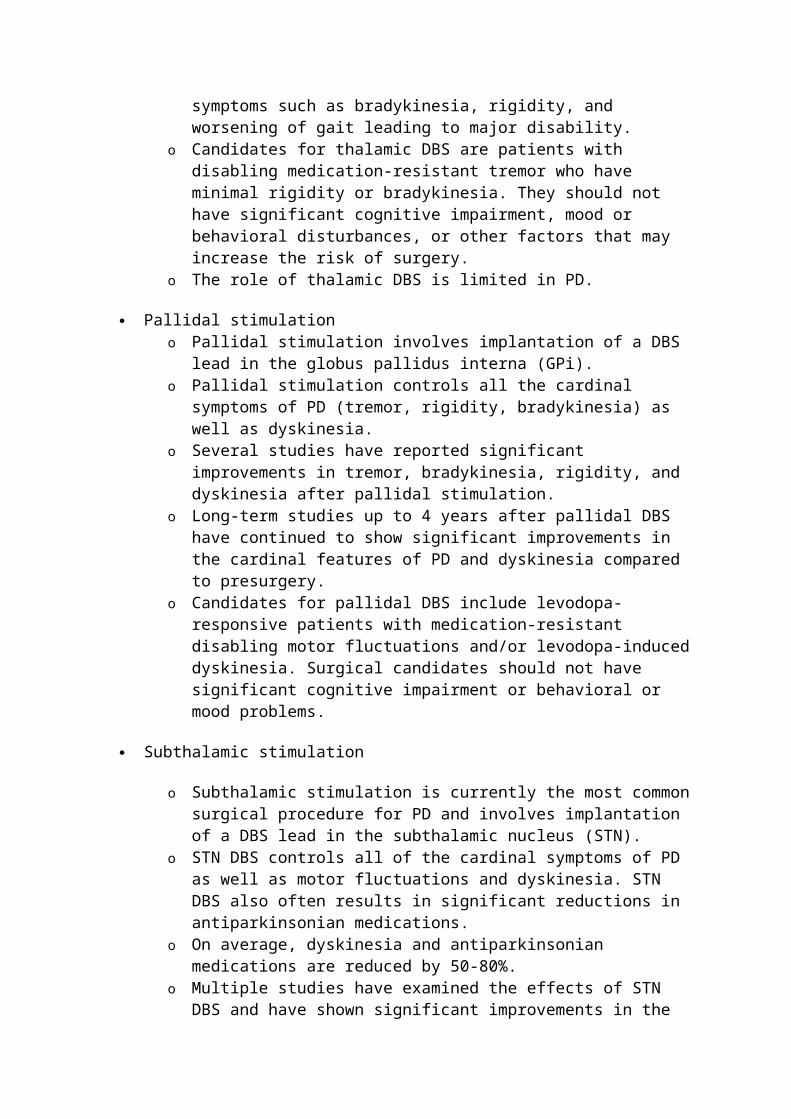
Pallidal stimulation o Pallidal stimulation involves implantation of a DBS lead in the globus pallidus
interna (GPi). o Pallidal stimulation controls all the cardinal symptoms of PD (tremor, rigidity,
bradykinesia) as well as dyskinesia. o Several studies have reported significant improvements in tremor,
bradykinesia, rigidity, and dyskinesia after pallidal stimulation. o Long-term studies up to 4 years after pallidal DBS have continued to show
significant improvements in the cardinal features of PD and dyskinesia compared to presurgery.
o Candidates for pallidal DBS include levodopa-responsive patients with medication-resistant disabling motor fluctuations and/or levodopa-induced dyskinesia. Surgical candidates should not have significant cognitive impairment or behavioral or mood problems.
Subthalamic stimulation
o Subthalamic stimulation is currently the most common surgical procedure for PD and involves implantation of a DBS lead in the subthalamic nucleus (STN).
o STN DBS controls all of the cardinal symptoms of PD as well as motor fluctuations and dyskinesia. STN DBS also often results in significant reductions in antiparkinsonian medications.
o On average, dyskinesia and antiparkinsonian medications are reduced by 50-80%.
o Multiple studies have examined the effects of STN DBS and have shown significant improvements in the motor symptoms of tremor, rigidity, and bradykinesia as well as activities of daily living.
o Long-term follow-up reports have demonstrated that significant improvements in motor function and activities of daily living are maintained for up to 5 years after surgery.
o Candidates for STN DBS include levodopa-responsive patients with medication-resistant disabling motor fluctuations and/or levodopa-induced dyskinesia. Surgical candidates should not have significant cognitive impairment or behavioral or mood problems.
Pallidal stimulation versus subthalamic stimulation o No large controlled trials have been completed comparing STN and GPi
stimulation; however, a large well-designed study is currently underway. o Several small uncontrolled studies have compared STN and GPi stimulation.
Most studies have shown greater improvement after STN DBS compared with GPi DBS, and antiparkinsonian medications were reduced only after STN

DBS. Therefore, STN DBS is currently the surgical procedure of choice for PD.
Complications of DBS o Complications can be separated into surgical complications occurring within
30 days of the procedure; complications related to the components of the DBS system; and complications from the stimulation, which generally can be resolved by adjustments of the stimulation parameters.
o Surgical complications are comparable to those seen with other neurosurgical procedures. Serious adverse events such hemorrhage, ischemic lesions, seizures, or death occur in 1-2% of patients. Infection occurs in approximately 3-5% of patients and may require explantation of the device until the infection is resolved.
o Misplacement of the lead may also occur in approximately 10% of patients requiring additional surgery to correct lead placement.
o Device-related complications include malfunction of the IPG, displacement of the lead, skin erosion, and device fractures. These complications can occur in up to 25% of patients and generally require additional surgery.
o Stimulation side effects include paresthesia, muscle spasms, visual disturbances, mood changes, and pain. These side effects are generally easily resolved with adjustments to the stimulation parameters.
o Although not considered a complication, the IPG (battery) is generally replaced every 3-5 years and requires additional outpatient surgery.
Transplantation o Neural transplantation is a potential treatment for PD because the neuronal
degeneration is site and type specific (ie, dopaminergic), the target area is well defined (ie, striatum), postsynaptic receptors are relatively intact, and the neurons provide tonic stimulation of the receptors and appear to serve a modulatory function.
o Multiple sources of dopamine-producing cells, including fetal nigral cells, sympathetic ganglia, carotid body glomus cells, PC-12 cells, and neuroblastoma cells, have been studied.
o Transplantation of autologous adrenal medullary cells and fetal porcine cells were not found to be effective in double-blind studies and have been abandoned.
o A double-blind study of GDNF demonstrated that it was not superior to placebo in controlling the symptoms of PD and, therefore, due to the lack of benefit and concerns regarding adverse events, clinical trials have been discontinued.
o Double-blind studies demonstrated that transplanted fetal mesencephalic cells can survive transplantation. However, these studies showed only minimal benefit in measures of PD symptoms and often resulted in the development of dyskinesia even in the absence of antiparkinsonian medications.
o Transplanted cultured human retinal pigment epithelial cells (RPE) are currently being evaluated in double-blind studies as a treatment for PD.
o Several studies have recently been initiated to evaluate gene therapy as a treatment for PD. The goal of these studies is to modify genes involved in the development of PD.

o In the laboratory, the use of stem cells is being investigated.
Consultations:
Consider physical therapy, occupational therapy, and speech therapy consultations.
Consider neurosurgical consultation for patients with medically refractory tremor or troublesome dyskinesia and/or motor fluctuations that cannot be controlled with medication adjustments. Patients with dementia or significant psychiatric or behavioral problems are not candidates for the current neurosurgical treatments for PD.
MEDICATION Section 7 of 11
Author Information Introduction Clinical Differentials Workup Treatment Medication Follow-up Miscellaneous Pictures Bibliography
The cornerstone of symptomatic treatment for PD is dopamine replacement therapy.
The criterion standard of symptomatic therapy is levodopa (L-dopa), the metabolic precursor of dopamine, in combination with a peripheral decarboxylase inhibitor (PDI). This combination provides the greatest symptomatic benefit with the fewest short-term adverse effects.
Anticholinergic drugs can be used as an alternative to L-dopa for treating resting tremor. However, they are not highly effective against bradykinesia, gait disturbance, or other features of advanced parkinsonism.
Dopamine agonists (bromocriptine, pergolide, pramipexole, ropinirole) can be used as monotherapy to improve symptoms in early disease or as adjuncts to levodopa in patients whose response to L-dopa is deteriorating and those who are experiencing fluctuations in their response to L-dopa.
MAO-B inhibitors provide symptomatic benefit as monotherapy in early disease and as adjuncts to levodopa in patients experiencing motor fluctuations.
Rasagiline is a second-generation MAO-B inhibitor. Unlike selegiline, rasagiline does not have amphetamine metabolites. It is effective as monotherapy in early PD and as an adjunct to levodopa in patients with motor fluctuations. It is not yet approved by the FDA but is available in some countries. Rasagiline has been studied at 0.5-2 mg/d. Recommended dose is 1 mg/d. Pending final review from the FDA.
COMT inhibitors increase the peripheral half-life of levodopa, thereby delivering more levodopa to the brain over a longer time.
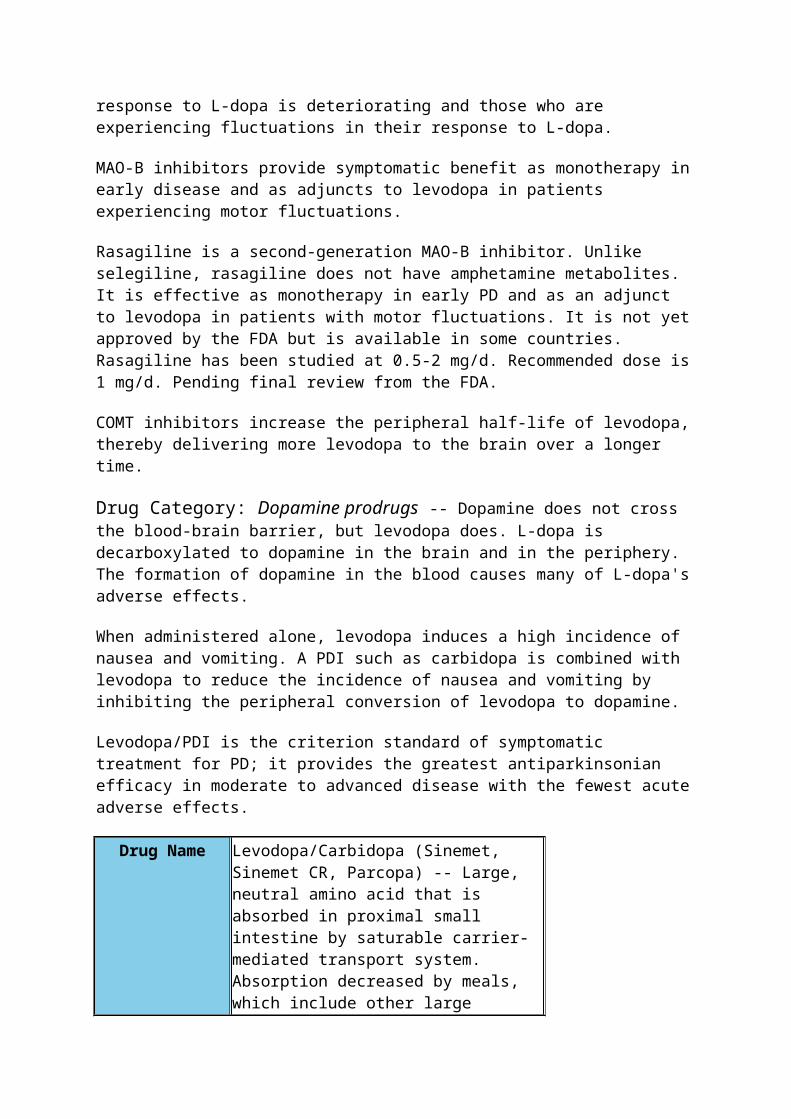
Drug Category: Dopamine prodrugs -- Dopamine does not cross the blood-brain barrier, but levodopa does. L-dopa is decarboxylated to dopamine in the brain and in the periphery. The formation of dopamine in the blood causes many of L-dopa's adverse effects.
When administered alone, levodopa induces a high incidence of nausea and vomiting. A PDI such as carbidopa is combined with levodopa to reduce the incidence of nausea and vomiting by inhibiting the peripheral conversion of levodopa to dopamine.
Levodopa/PDI is the criterion standard of symptomatic treatment for PD; it provides the greatest antiparkinsonian efficacy in moderate to advanced disease with the fewest acute adverse effects.
Drug Name
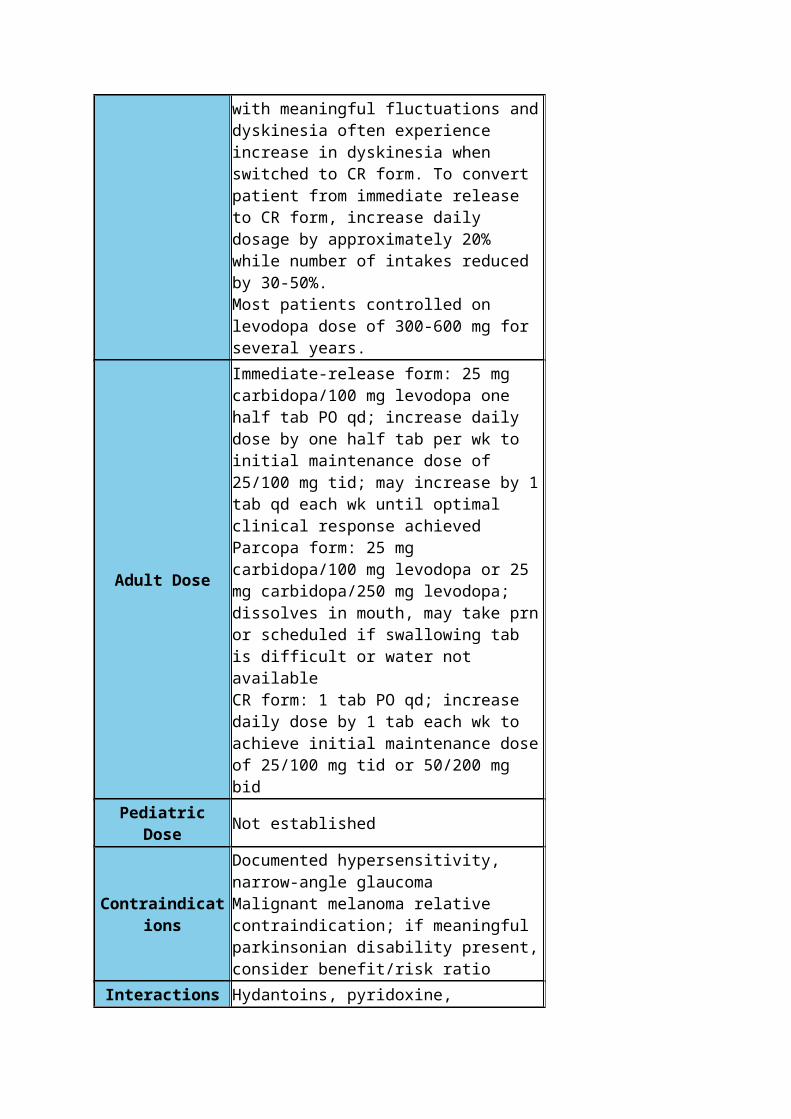
Levodopa/Carbidopa (Sinemet, Sinemet CR, Parcopa) -- Large, neutral amino acid that is absorbed in proximal small intestine by saturable carrier-mediated transport system. Absorption decreased by meals, which include other large neutral amino acids. Only patients with meaningful motor fluctuations must consider a low-protein or protein-redistributed diet. Greater consistency of absorption achieved when levodopa taken 30 min or more before or 1 h or more after meals. Nausea often reduced if L-dopa taken immediately following meals. Some patients with nausea benefit from additional carbidopa in doses up to 200 mg/d.No maximal dose per se. Patients should receive lowest dose that provides good control of parkinsonian symptoms. If parkinsonian disability present, dose should be escalated until adequate control achieved or adverse effects become intolerable. Some patients require 2000 mg or more per d.Half-life of levodopa/carbidopa approximately 2.5 h.CR formulation more slowly absorbed and provides more sustained levodopa levels than immediate release form. CR form as effective as immediate release form when levodopa first required and may be more convenient when fewer intakes are required. Patients with wearing-off motor fluctuations (and no dyskinesia) often benefit from prolongation of short duration response when switched from immediate release to CR form. However, patients with meaningful fluctuations and dyskinesia often experience increase in dyskinesia when switched to CR form. To convert patient from immediate release to CR form, increase daily dosage by approximately 20% while number of intakes reduced by 30-50%.Most patients controlled on levodopa dose of 300-600 mg for several years.
Adult Dose
Immediate-release form: 25 mg carbidopa/100 mg levodopa one half tab PO qd; increase daily dose by one half tab per wk to initial maintenance dose of 25/100 mg tid; may increase by 1 tab qd each wk until optimal clinical response achievedParcopa form: 25 mg carbidopa/100 mg levodopa or 25 mg carbidopa/250 mg levodopa; dissolves in mouth, may take prn or scheduled if swallowing tab is difficult or water not availableCR form: 1 tab PO qd; increase daily dose by 1 tab each wk to achieve initial maintenance dose of 25/100 mg tid or 50/200 mg bid
Pediatric Dose Not established
Contraindications
Documented hypersensitivity, narrow-angle glaucomaMalignant melanoma relative contraindication; if meaningful parkinsonian disability present, consider benefit/risk ratio
Interactions
Hydantoins, pyridoxine, phenothiazine, and hypotensive agents may decrease effects of levodopa; concurrent antacids or nonspecific MAOIs increase levodopa toxicity
PregnancyC - Safety for use during pregnancy has not been established.
Precautions
Most common acute adverse effects are nausea, hypotension, or hallucinations; long-term adverse effects include motor fluctuations and dyskinesia (chorea); for patients experiencing motor fluctuations, dietary protein can be distributed evenly throughout day or redistributed to evening to minimize fluctuations in levodopa absorptionAbrupt withdrawal of treatment may result in neuroleptic malignant syndrome (NMS); use cautiously in patients with history of MI, arrhythmias, asthma, or peptic ulcer disease
Drug Category: Dopamine agonists -- Dopamine agonists directly stimulate postsynaptic dopamine receptors to provide antiparkinsonian benefit. All available dopamine agonists stimulate D2 receptors--an action that is thought to be clinically beneficial. The role of other dopamine receptors is currently unclear.
Dopamine agonists are effective as monotherapy in early PD and as adjuncts to levodopa/PDI in moderate to advanced disease. They provide antiparkinsonian efficacy approximately equal to levodopa/PDI when symptomatic therapy is first required.
After 6 months to a few years, they are not as effective as levodopa/PDI. For patients with motor fluctuations on levodopa/PDI, the addition of a dopamine agonist reduces off time, improves motor function, and allows lower levodopa doses.
Dopamine agonists have been proven to reduce the development of motor fluctuations and dyskinesias when used as an initial therapy and continued once levodopa is added.
Dopamine agonists may slow disease progression based on changes in PET scans, but the evidence is not yet conclusive.
Drug Name
Apomorphine (Apokyn) -- Short-acting dopamine agonist approved in the United States for SC injection as a rescue agent to treat acute immobility episodes (hypomobility or "off-periods") in PD. These episodes consist of inability to rise from a chair, speak, or walk and may occur toward the end of the dose interval or may be spontaneous and unpredictable in onset.
Adult Dose
Dosage is individualizedTest dose: 2 mg (0.2 mL) SC for 1 dose initially during hypomobility, if tolerated (ie, blood pressure remains stable), may use for subsequent hypomobility episodesEstablishing dose: If patient tolerates test dose and hypomobility responds, 2 mg is the dose to use for subsequent hypomobility episodesIf patient tolerates test dose, but hypomobility does not respond to test dose, may increase dose by 1 mg (0.1 mL) q2-3 d until response is observed; not to exceed 6 mg (0.6 mL)/doseNote: Administer only 1 dose per hypomobility episode, do not repeat dose; administer with antiemetic drug
Pediatric Dose Not established
ContraindicationsDocumented hypersensitivity to apomorphine or metabisulfite
Interactions
Coadministration with 5HT3 antagonists used for emesis or irritable bowel syndrome (eg, ondansetron, dolasetron, granisetron, palonosetron, alosetron) may cause hypotension and loss of consciousness; coadministration with drugs that increase QTC interval (eg, thioridazine, quinidine, sotalol, erythromycin, dofetilide) may increase arrhythmia potential; metabolized by catechol-o-methyltransferase (COMT), coadministration with COMT inhibitors (eg, entacapone, tolcapone) may decrease elimination
Pregnancy C - Safety for use during pregnancy has not

been established.
Precautions
Causes severe nausea and vomiting and must be administered with an antiemetic drug (but not with antiemetic agents that are 5HT3 antagonists); may cause orthostatic hypotension, faintness, hallucinations, fluid retention, chest pain, increased sweating, flushing, pallor, dyskinesia, rhinorrhea, and extreme drowsiness (may fall asleep during waking hours without warning)
Drug Name
Bromocriptine (Parlodel) -- Semisynthetic ergot alkaloid derivative that is strong D2 receptor agonist and weak D1 receptor antagonist. FDA approved as adjunct to levodopa/carbidopa; less effective than other dopamine agonists. May relieve akinesia, rigidity, and tremor in PD. Mechanism of therapeutic effect is direct stimulation of dopamine receptors in corpus striatum.Approximately 28% absorbed from GI tract and metabolized in liver. Elimination half-life approximately 50 h with 85% excreted in feces and 3-6% eliminated in urine.Initiate at low dosage and individualize. Increase daily dosage slowly until maximum therapeutic response achieved. If possible, maintain the dosage of levodopa during this introductory period. Assess dosage titrations q2wk to ensure that lowest dosage producing optimal therapeutic response is not exceeded. If adverse reactions mandate, reduce dose gradually in 2.5-mg increments.
Adult Dose
1.25 mg (one half of a 2.5 mg tab) PO qd; increase by 1.25 mg/d per wk to 1.25 mg tid with meals; increase q2-4wk by 2.5 mg/d with meals; usual range 10-40 mg/d divided tid/qid; safety has not been demonstrated in dosages that exceed 100 mg/d
Pediatric Dose Not established
ContraindicationsDocumented hypersensitivity, ischemic heart disease, peripheral vascular disorders
Interactions
Ergot alkaloids increase toxicity; amitriptyline, butyrophenone, imipramine, methyldopa, phenothiazine, and reserpine may decrease effects
PregnancyC - Safety for use during pregnancy has not been established.
Precautions Adverse effects include nausea, hypotension,

hallucinations, and somnolence; use cautiously in patients with renal or hepatic disease
Drug Name
Pergolide (Permax) -- Potent dopamine receptor agonist at both D1 and D2 receptor sites, approximately 10 times more potent than bromocriptine on a mg per mg basis. In PD, pergolide believed to exert its therapeutic effect by directly stimulating postsynaptic dopamine receptors in striatum.Usually administered in divided doses tid.
Adult Dose
0.05 mg PO qd days 1 and 2; gradually increase by 0.1 or 0.15 mg/d q3d over next 12 d, followed by incremental increases of 0.25 mg/d q3d until optimal therapeutic dose achieved; usual maximum dose 3-6 mg/d; usually administered in divided doses tid
Pediatric Dose Not established
Contraindications Documented hypersensitivity
Interactions
Concurrent use of pergolide and levodopa may cause or exacerbate preexisting states of confusion and hallucinations or dyskinesiaDopamine antagonists such as neuroleptics (eg, phenothiazine, butyrophenone, thioxanthenes, metoclopramide) may diminish effectiveness of pergolide; because pergolide mesylate is >90% bound to plasma proteins, exercise caution in coadministering with other drugs known to affect protein binding
PregnancyB - Usually safe but benefits must outweigh the risks.
Precautions
May cause valvular heart disease (yearly echocardiograms recommended for patients on chronic therapy); Inhibits secretion of prolactin; causes transient rise in serum concentrations of growth hormone and decrease in serum concentrations of luteinizing hormone; adverse effects include nausea, hypotension, hallucinations, and somnolence; use caution in patients who have been treated for cardiac dysrhythmias.
Drug Name Pramipexole (Mirapex) -- Nonergot dopamine agonist with specificity for D2 dopamine receptor. Also binds to D3 and D4 receptors. Readily absorbed from GI tract with >90% bioavailability, minimally metabolized in liver with half-life of approximately 8-12 h. Primarily excreted in urine; for patients with CrCl 35-60 mL/min, administer bid (max 1.5 mg bid); for
CrCl 15-35 mL/min, administer qd (not to exceed 1.5 mg/d).FDA approved as monotherapy in early disease and as adjunct to levodopa/PDI in more advanced stages.
Adult Dose
Week 1: 0.125 mg PO tid; week 2: 0.25 mg tid; week 3: 0.5 mg tid; continue escalating by 0.25 mg tid each week as clinically appropriate; usual range 1.5–4.5 mg/d
Pediatric Dose Not established
Contraindications Documented hypersensitivity
InteractionsCimetidine may increase toxicity; increases levels of levodopa if given concurrently
PregnancyC - Safety for use during pregnancy has not been established.
Precautions
Adverse effects include nausea, hallucinations, and somnolence; somnolence may emerge even after administration at stable dose for many months; some patients experience relatively sudden waves of irresistible sleepiness; patients should be warned not to drive if experiencing drowsiness; somnolence usually resolves with dose reduction or discontinuation; use caution in patients with renal insufficiency and preexisting dyskinesias
Drug Name Ropinirole (Requip) -- Nonergot dopamine agonist that has high relative in vitro specificity and full intrinsic activity at D2 subfamily of dopamine receptors; binds with higher affinity to D3 than to D2 or D4 receptor subtypes. Has moderate affinity for opioid receptors, and its metabolites have negligible affinity for dopamine D1, 5HT 1, 5HT 2, benzodiazepine, GABA, muscarinic, alpha 1-, alpha 2- and beta-adrenoreceptors. Mechanism of action is stimulation of dopamine receptors in striatum.Discontinue gradually over 7-d period. Decrease frequency of administration from tid to bid for 4 d. For remaining 3 d, decrease frequency to qd prior to complete withdrawal.When administered as adjunct to levodopa, concurrent dose of levodopa may be decreased gradually as tolerated. FDA approved as monotherapy in early disease and as adjunct to levodopa/PDI in more advanced disease.Readily absorbed from GI tract with 55% bioavailability and metabolized to inactive metabolites in liver by CYP1A2. Half-life
approximately 6 h with inactive metabolites primarily excreted in urine.
Adult Dose
Week 1: 0.25 mg PO tid; week 2: 0.5 mg tid; week 3: 0.75 mg tid; after week 4, if necessary, increase by 1.5 mg/d on a weekly basis up to 9 mg/d, and then by 3 mg/d weekly to total dose as high as 24 mg/d
Contraindications Documented hypersensitivity
Interactions
Estrogens may reduce clearance by 36% (adjust ropinirole dose if estrogen therapy stopped or started during treatment); substrates or inhibitors of CYP1A2 (eg, quinolone antibiotics, erythromycin, cimetidine, diltiazem, fluvoxamine, mexiletine, tacrine) may alter clearance (adjust ropinirole dose if therapy with potent CYP1A2 inhibitor stopped or started during treatment); dopamine antagonists (eg, phenothiazines, butyrophenones, thioxanthenes, metoclopramide, neuroleptics) may diminish effectiveness; CNS depressants may have additive sedative effects
PregnancyC - Safety for use during pregnancy has not been established.
Precautions
Adverse effects include nausea, hypotension, hallucinations, and somnolence; patients should be warned not to drive if experiencing drowsiness; somnolence usually resolves with dose reduction or discontinuationDopamine receptor agonists may potentiate dopaminergic effects of levodopa and may cause or exacerbate preexisting dyskinesia; decreasing dose of levodopa may ameliorate this effectCases of retroperitoneal fibrosis, pulmonary infiltrates, pleural effusion, and pleural thickening have been reported; these complications do not always resolve completely upon drug cessationUse caution in patients taking CNS depressants; monitor for signs and symptoms of orthostatic hypotensionCases of rhabdomyolysis have been reported
Drug Category: Catechol-O-methyltransferase (COMT) inhibitors -- These agents inhibit the peripheral metabolism of levodopa, making more levodopa available for transport across the blood-brain barrier over a longer time. For patients with motor fluctuations on levodopa/carbidopa, the addition of a COMT inhibitor decreases off time, improves motor function, and allows lower levodopa doses. Patients who already have dyskinesia on

levodopa/PDI are likely to experience a worsening of dyskinesia, thereby necessitating a levodopa dose reduction. In such patients, consider reducing levodopa dose at the time of introduction, especially with tolcapone.
Drug Name
Tolcapone (Tasmar) -- Adjunct to levodopa/carbidopa therapy in PD. Mechanism related to its ability to inhibit COMT and alter plasma pharmacokinetics of levodopa. When tolcapone given in conjunction with levodopa and an aromatic amino acid decarboxylase inhibitor (eg, carbidopa), plasma levels of levodopa are more sustained than after administration of levodopa and an aromatic amino acid decarboxylase inhibitor alone. These sustained plasma levels of levodopa may result in more constant dopaminergic stimulation in brain, possibly leading to greater effects on signs and symptoms of PD as well as increased adverse effects of levodopa (which sometimes require levodopa dose decrease). Enters CNS to a minimal extent but has been shown to inhibit central COMT activity in animals. FDA approved as adjunct to levodopa/carbidopa for patients who are experiencing motor fluctuations.Because of risk of hepatotoxicity, it is reserved for patients who have not responded adequately to or are not appropriate candidates for other adjunctive medications. Patients should sign informed consent; strict liver function test monitoring required. If improvement not apparent within 3 wk, medication should be withdrawn. Bioavailability following PO administration about 65%; extensively metabolized before excretion. Main metabolic pathway is glucuronidation. Half-life is approximately 2-3 h with 60% of metabolites excreted in urine and 40% in feces.Patients with levodopa-induced dyskinesia often experience increase in dyskinesia, necessitating 25-50% reduction in levodopa dose. Alternatively, levodopa dose can be reduced by 25-50% when tolcapone introduced, then titrated as clinically indicated.
Adult Dose100 mg PO tid; may increase to 200 mg tid only if anticipated incremental clinical benefit justifies possible risk of hepatotoxicity
Contraindications Documented hypersensitivity, liver disease, ALT/AST levels 2 times >reference range or

higher, patients withdrawn from tolcapone because of induced hepatotoxicity
Interactions
Because of its affinity to cytochrome P450 2C9 in vitro, may interfere with drugs such as tolbutamide and warfarin; may influence pharmacokinetics of drugs metabolized by COMT; when administered with levodopa/carbidopa, increases relative bioavailability (AUC) of levodopa by approximately 2-fold; patients should not be treated ordinarily with combination of tolcapone and MAO-A or nonspecific MAO inhibitor; can be taken concomitantly with selective MAO-B inhibitor
PregnancyC - Safety for use during pregnancy has not been established.
Precautions
Liver function tests required at baseline, q2wk for first 6 mo and then prn; discontinue tolcapone if ALT/AST levels are > 2X ULN; in controlled trials, elevations usually occurred within 6 wk to 6 mo of starting treatment; periodic monitoring of liver enzymes may not prevent fulminant liver failureDiarrhea occurs in 16-18% of patients and is severe enough to necessitate medication withdrawal in 3-4%; typically begins 6-12 wk after therapy, but may occur as early as 2 wk or as late as many moUse caution in patients with troublesome dyskinesia and in those with dementia or hallucinations
Drug Name Entacapone (Comtan) -- Adjunct to levodopa/carbidopa therapy to treat the signs and symptoms of wearing off.Mechanism related to its ability to inhibit COMT and alter plasma pharmacokinetics of levodopa. When given in conjunction with levodopa and an aromatic amino acid decarboxylase inhibitor (eg, carbidopa), plasma levels of levodopa are more sustained than after administration of levodopa and an aromatic amino acid decarboxylase inhibitor alone. These sustained plasma levels of levodopa may result in more constant dopaminergic stimulation in brain. This may lead to greater effects on signs and symptoms of PD, as well as increased levodopa adverse effects (which sometimes require levodopa dose decrease). FDA approved as adjunct to levodopa/carbidopa for patients
who are experiencing motor fluctuations.Bioavailability following PO administration about 35%; extensively metabolized before excretion. Main metabolic pathway is glucuronidation and half-life approximately 0.4-0.7 h with 10% of metabolites excreted in urine and 90% in feces.
Adult Dose200 mg PO with each levodopa/carbidopa intake; not to exceed 8 times daily (1600 mg/d)
Contraindications Documented hypersensitivity
Interactions
When administered with levodopa/carbidopa, increases relative bioavailability (AUC) of levodopa by approximately 35%; patients should not be treated ordinarily with combination of entacapone and MAO-A or nonspecific MAO inhibitor; can be taken concomitantly with selective MAO-B inhibitors; drugs known to be metabolized by COMT (eg, isoproterenol, epinephrine, norepinephrine, dopamine, dobutamine, alpha-methyldopa, apomorphine, isoetharine, bitolterol) should be administered with caution regardless of route of administration
PregnancyC - Safety for use during pregnancy has not been established.
Precautions
Diarrhea occurs in approximately 10% of patients, typically within 4-12 wk after starting treatment; usually mild to moderate in severity, and generally resolves with discontinuation of entacapone; advise patients that entacapone may cause a brownish-orange discoloration of urine in approximately 10% of patients that is not clinically relevant
Drug Name Levodopa, carbidopa, and entacapone (Stalevo) -- Levodopa, carbidopa, and entacapone combination for treating PD. Carbidopa inhibits dopa decarboxylation; thus, allows more complete levodopa distribution to the CNS. Levodopa is a dopamine precursor capable of crossing the blood-brain barrier (BBB), thereby increases CNS dopamine following conversion. Entacapone inhibits catechol-O-methyltransferase (COMT), another enzyme that metabolizes levodopa. COMT inhibition increases and sustains levodopa plasma levels enabling more BBB penetration.Used as a substitute for patients stabilized on equivalent doses of carbidopa/levodopa
(Sinemet) and entacapone (Comtan), or those stabilized on carbidopa/levodopa and initiating entacapone.Available as tab, each contains entacapone 200 mg with immediate-release carbidopa-levodopa 1:4 ratio (ie, 12.5 mg/50 mg, 25 mg/100 mg, 37.5 mg/150 mg).
Adult DoseOptimum dose must be carefully titrated; not to exceed 8 tab/24 h (ie, entacapone 1600 mg/24 h)
ContraindicationsDocumented hypersensitivity; narrow-angle glaucoma; malignant melanoma; undiagnosed skin lesions
Interactions
Levodopa/carbidopa: Hydantoins, pyridoxine, phenothiazine, and hypotensive agents may decrease effects of levodopa; levodopa toxicity increases with antacids and MAO inhibitorsEntacapone: When administered with levodopa/carbidopa, increases relative levodopa bioavailability (AUC) by approximately 35%; do not administer with MAO-A or nonspecific MAO inhibitor (may cause hypertensive crisis); can be taken concomitantly with selective MAO-B inhibitor (eg, selegiline); other drugs metabolized by COMT (eg, isoproterenol, epinephrine, norepinephrine, dopamine, dobutamine, methyldopa, apomorphine, isoetharine, bitolterol) should be administered with caution regardless of administration route
PregnancyC - Safety for use during pregnancy has not been established.
Precautions Levodopa/carbidopa: Certain adverse CNS effects (eg, dyskinesias) may occur at lower dosages and earlier in therapy with SR form; caution in patients with history of myocardial infarction, arrhythmias, asthma, and peptic ulcer disease; sudden discontinuation of levodopa may cause worsening of PD; high protein diets should be distributed throughout the day to avoid fluctuations in levodopa absorptionEntacapone: May cause diarrhea within 4-12 wk after starting treatment in 10% of patients (severity typically mild to moderate and generally resolves when drug discontinued); may cause urine discoloration (brownish orange) in approximately 10% of patients that is not clinically relevant; abrupt withdrawal may aggravate PD symptoms; hepatic impairment may require dose reduction; monitor for enhanced dopaminergic effect (eg, hypotension,

syncope, hallucinations, dyskinesia)
Drug Category: Anticholinergics -- These agents provide benefit for tremor in approximately 50% of patients but do not improve bradykinesia or rigidity. If one anticholinergic does not work, try another.
Drug Name
Trihexyphenidyl (Artane, Trihexy) -- Synthetic tertiary amine anticholinergic agent, reduces incidence and severity (by 20%) of akinesia, rigidity, and tremor and secondary symptoms such as drooling. In addition to suppressing central cholinergic activity, also may inhibit reuptake and storage of dopamine at central dopamine receptors, thereby prolonging action of dopamine.
Adult Dose
1-2 mg/d PO; increase by 2 mg/d at intervals of 3-5 d; usual range 4-15 mg/d divided tid/qid; young adults may tolerate 15-20 mg/d divided tid/qid; older individuals may tolerate no more than 4-8 mg/d
Contraindications
Documented hypersensitivity; glaucoma, particularly angle-closure glaucoma; pyloric or duodenal obstruction, stenosing peptic ulcers; prostatic hypertrophy or bladder neck obstructions; achalasia (megaesophagus); myasthenia gravis; megacolon
InteractionsDecreases effects of levodopa; increases effects of narcotic analgesics, phenothiazines, tricyclic antidepressants, quinidine, and anticholinergics
PregnancyC - Safety for use during pregnancy has not been established.
Precautions
Adverse effects include dry mouth and dry eyes, memory difficulty, confusion, and rarely urinary retention; use caution in patients with tachycardia, cardiac arrhythmias, hypertension, hypotension, prostatic hypertrophy (particularly in elderly), or any tendency toward urinary retention, liver or kidney disorders, or obstructive disease of GI or GU tract; when used to treat extrapyramidal reactions that result from phenothiazines in psychiatric patients, antiparkinson agents may exacerbate mental symptoms and precipitate toxic psychosis
Drug NameBenztropine mesylate (Cogentin) -- Partially blocks striatal cholinergic receptors to help balance cholinergic and dopaminergic activity.
Adult Dose 0.5-6 mg/d PO qd or divided bid; start elderly patients at lower dose; titrate in 0.5-mg
increments at 5- to 6-d intervals; not to exceed 6 mg/d
Contraindications
Documented hypersensitivity; glaucoma, particularly angle-closure glaucoma; pyloric or duodenal obstruction, stenosing peptic ulcers; prostatic hypertrophy or bladder neck obstructions; achalasia (megaesophagus); myasthenia gravis; megacolon
InteractionsDecreases effects of levodopa; increases effects of narcotic analgesics, phenothiazines, tricyclic antidepressants, quinidine, and anticholinergics
PregnancyC - Safety for use during pregnancy has not been established.
Precautions
Adverse effects include dry mouth and dry eyes, memory difficulty, confusion, and rarely urinary retention; use cautiously in patients with tachycardia, cardiac arrhythmias, hypertension, hypotension, prostatic hypertrophy (particularly in elderly); or any tendency toward urinary retention, liver or kidney disorders, or obstructive disease of GI or GU tract; when used to treat extrapyramidal reactions that result from phenothiazines in psychiatric patients, antiparkinson agents may exacerbate mental symptoms and precipitate toxic psychosis
Drug Category: MAO-B inhibitors -- These agents inhibit the activity of MAO-B oxidases that are responsible for inactivating dopamine and possibly the conversion of compounds into neurotoxic types.
Drug Name Selegiline (Eldepryl) -- An irreversible inhibitor of MAO, it acts as a "suicide" substrate for enzyme; MAO converts it to an active moiety which combines irreversibly with active site or enzyme's essential FAD cofactor. Blocks breakdown of dopamine and extends duration of action of each dose of L-dopa. Often allows L-dopa dose reduction that is needed for optimal effect. Because selegiline has greater affinity for type B than for type A active sites, it can serve as selective inhibitor of MAO type B at recommended dose. However, doses higher than 10 mg/d may inhibit MAO-A sites significantly. Its metabolites, amphetamine and methamphetamine, may inhibit dopamine reuptake and enhance dopamine release.FDA approved as adjunct to levodopa/carbidopa in patients who exhibit deterioration in response
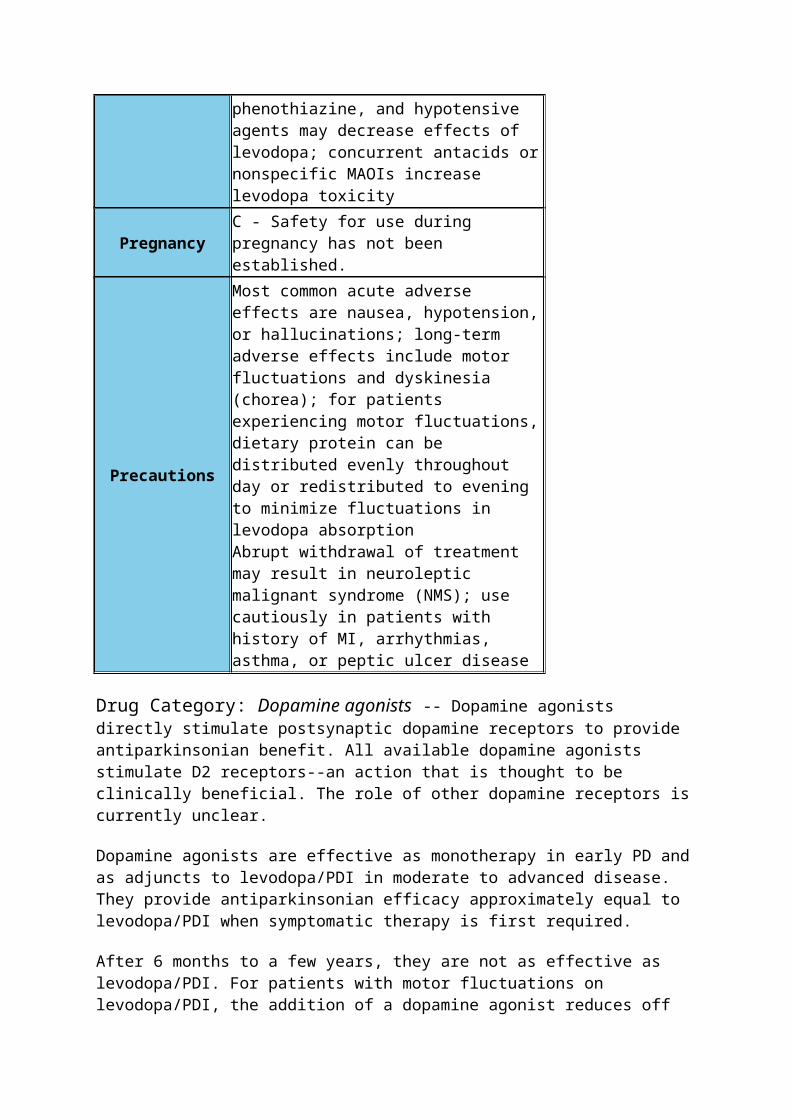
to that therapy. For patients who are experiencing motor fluctuations on levodopa/carbidopa, addition of selegiline reduces off time, improves motor function, and allows levodopa dose reductions. If patient experiences increase in troublesome dyskinesia, reduce levodopa dose.Rapidly absorbed and has 73% bioavailability. Metabolized in liver to N-desmethylselegiline, L-amphetamine, and L-methamphetamine. Half-life approximately 10 h; metabolites excreted in urine.Because inhibition of MAO-B is irreversible, loss of activity is function of new protein synthesis and may last several months. No evidence of additional benefit from doses >10 mg/d.After 2-3 days of treatment, attempt to reduce dose of levodopa/carbidopa. Reduction of 10-30% appears typical. Further reductions of levodopa/carbidopa may be possible during continued selegiline therapy.
Adult Dose5 mg PO bid with breakfast and lunch; not to exceed 10 mg/d
Contraindications
Documented hypersensitivity; concomitant meperidine or other opioids; concomitant tricyclic or serotonin reuptake inhibitor antidepressants (relative contraindication)
Interactions
Concurrent meperidine may cause stupor, muscular rigidity, severe agitation, and elevated temperature; concurrent tricyclic or serotonin reuptake inhibitor antidepressant may cause severe toxicity; one case of hypertensive crisis in a patient taking selegiline and ephedrine has been reported
PregnancyC - Safety for use during pregnancy has not been established.
Precautions
Risks associated with dose >10 mg/d are associated with nonselective inhibition of MAO; concurrent tyramine-containing foods and other indirect-acting sympathomimetics may cause hypertensive crisis
Drug Name Rasagiline (Azilect) -- Irreversible MAO-B inhibitor that blocks dopamine degradation. Not metabolized to amphetamine derivatives. Main metabolite, aminoindan, has some activity and has been shown to improve motor and cognitive functions in experimental models. Indicated for
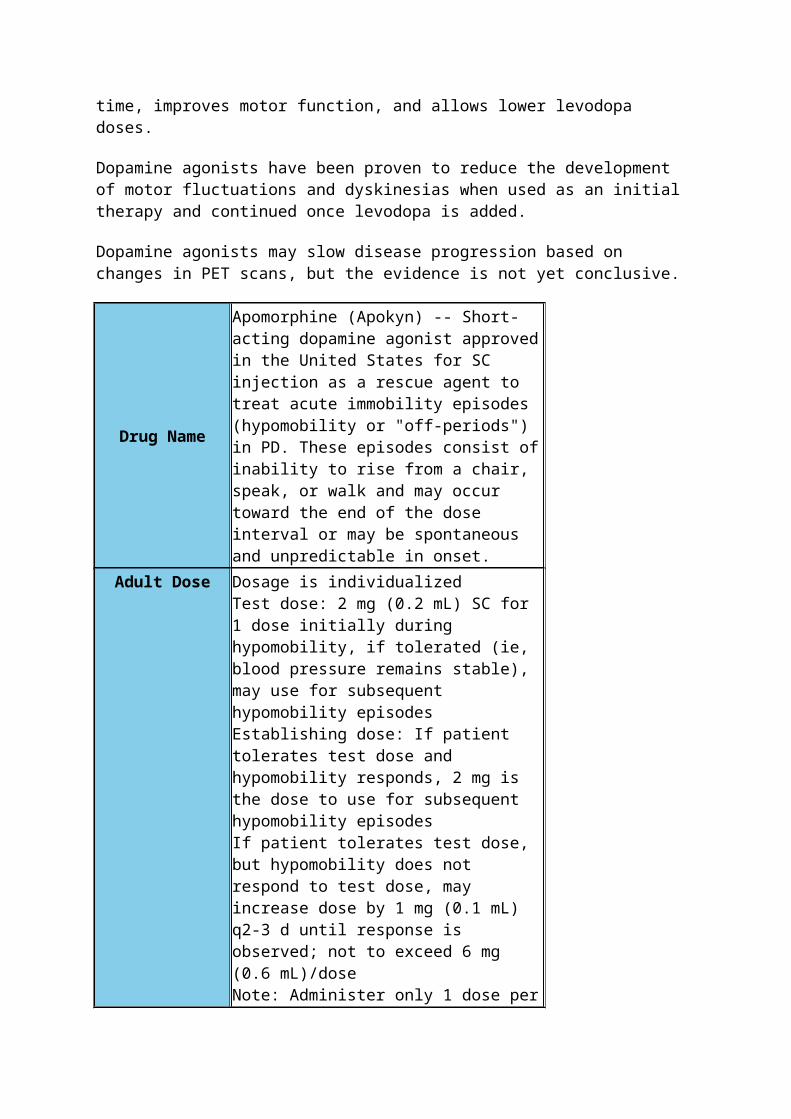
Parkinson disease as initial monotherapy or as adjunctive therapy with levodopa.
Adult Dose
Monotherapy: 1 mg PO qdAdjunctive therapy with levodopa: 0.5 mg PO qd; may increase to 1 mg PO qd Mild hepatic impairment or coadministration with CYP1A2 inhibitors: 0.5 mg PO qd
Contraindications
Documented hypersensitivity; moderate-to-severe hepatic impairment (Child-Pugh score >6); concurrent use with meperidine, tramadol, methadone, propoxyphene; dextromethorphan, St. John's wort, mirtazapine, cyclobenzaprine, sympathomimetic amines (eg, pseudoephedrine, cocaine, ephedrine), other MAOIs, or local anesthetics containing epinephrine; pheochromocytoma
Interactions
P450 CYP1A2 substrate; coadministration with drugs that inhibit CYP1A2 (eg, cimetidine, clarithromycin, erythromycin) may decrease elimination and increase toxicity; coadministration with TCAs, SSRIs, serotonin-norepinephrine reuptake inhibitors (SNRIs), nonselective MAOIs, or selective MAO-B inhibitors has caused severe CNS toxicity associated with hyperpyrexia and death; consuming tyramine-rich foods (eg, cheese, red wine, beer, sausage, avocado) may cause hypertensive crisis; also see Contraindications
PregnancyC - Safety for use during pregnancy has not been established.
Precautions
May cause dyskinesias, hallucinations, or hypotension; if emergent surgery is necessary, benzodiazepines, mivacurium, rapacuronium, fentanyl, morphine, or codeine may be used cautiously; melanoma may develop more frequently in those taking rasagiline than in matched controls
Drug Category: N-methyl-D-aspartic acid (NMDA) receptor inhibitors -- Increases dopaminergic activity in peripheral and central nervous system by augmenting dopamine release and inhibiting cellular reuptake.
Drug Name Amantadine (Symmetrel) -- Inhibits the N-methyl-D-aspartic acid (NMDA) receptor-mediated stimulation of acetylcholine release in rat striatum. May also enhance dopamine release, inhibit dopamine reuptake, stimulate postsynaptic dopamine receptors, or enhance
dopamine receptor sensitivity. Efficacy as monotherapy and as adjunct to levodopa/PDI in treating PD. Provides some benefit for tremor, rigidity, and bradykinesia.Readily and almost completely absorbed from GI tract; is not metabolized. Half-life approximately 9-37 h and prolonged in renal insufficiency. Excreted 90% unchanged in urine.
Adult Dose100 mg PO in am; increase by 100 mg/d each wk prn; not to exceed 100 mg qid
Contraindications Documented hypersensitivity
Interactions
Drugs with anticholinergic or CNS stimulant activity increase toxicity; concurrent hydrochlorothiazide plus triamterene may decrease urinary excretion of amantadine with subsequent increased plasma concentrations
PregnancyC - Safety for use during pregnancy has not been established.
Precautions
Common adverse effects are confusion and hallucinations; use caution in patients with liver disease, history of recurrent and eczematoid dermatitis, uncontrolled psychosis, seizures, and in those receiving CNS stimulant drugs; reduce dose in renal disease when treating PD; do not discontinue medication abruptly
FOLLOW-UP Section 8 of 11
Author Information Introduction Clinical Differentials Workup Treatment Medication Follow-up Miscellaneous Pictures Bibliography
Patient Education:
For excellent patient education resources, visit eMedicine's Dementia Center. Also, see eMedicine's patient education articles Parkinson Disease and Parkinson Disease Dementia.
Related Documents