Parental Behaviors During Family Interactions Predict Changes in Depression and Anxiety Symptoms During Adolescence Orli S. Schwartz & Paul Dudgeon & Lisa B. Sheeber & Marie B. H. Yap & Julian G. Simmons & Nicholas B. Allen Published online: 26 July 2011 # Springer Science+Business Media, LLC 2011 Abstract This study investigated the prospective, longitu- dinal relations between parental behaviors observed during parent-adolescent interactions, and the development of depression and anxiety symptoms in a community-based sample of 194 adolescents. Positive and negative parental behaviors were examined, with negative behaviors operation- alized to distinguish between observed parental expressions of aggression and dysphoria. Results showed that higher levels of parental aggression prospectively predicted higher levels of both depression and anxiety symptoms in adoles- cents over two-and-a-half years, whereas higher levels of positive parental behaviors prospectively predicted lower levels of depression symptoms only. Parental dysphoric behavior was not related to changes in either symptom dimension. These results suggest that patterns of parental behaviors may be differentially associated with depressive versus anxious outcomes in adolescents, and highlight the potential role for family-focused prevention or treatment interventions aimed at reducing an escalation of depression and anxiety symptoms in adolescence. Keywords Parenting . Adolescence . Depression . Anxiety . Longitudinal Introduction The current study investigated the prospective influence of both positive parental behaviors that convey acceptance, affection or happiness, and negative parental behaviors that convey aggression or dysphoria, on the development of symptoms of depression and anxiety during adolescence. A better under- standing of the development of internalizing symptoms in adolescence is important because elevated levels of such symptoms have been found to significantly increase risk for the development of depression and anxiety disorders over time (e.g., Klein et al. 2009; Pine et al. 1999). Furthermore, there is evidence to suggest that children and adolescents with elevated levels of depression and anxiety symptoms experi- ence significant disability even when their symptoms do not meet criteria for a diagnosis (Angold et al. 1999). Adolescence is a significant period of development in which to study the effects of parenting behavior on the emergence of depression and anxiety symptoms. The biolog- ical, psychological, and social changes that occur during adolescence render it a time of particular vulnerability for the emergence of symptoms and disorder (Masten 2004), and despite the increased salience of peer relationships during this phase of life, parents continue to have a significant influence on development (Steinberg and Morris 2001). The emotional and interactional quality of parenting behaviors is thought to shape the emotional climate of the family, and thus play an important role in young people’ s This research was supported by grants from the Colonial Foundation, the National Health and Medical Research Council (NHMRC; Australia; Program Grant350241) and the Australian Research Council (Discovery Grant DP0878136). O. S. Schwartz : P. Dudgeon : N. B. Allen (*) Department of Psychological Sciences, University of Melbourne, Victoria, Australia e-mail: [email protected] L. B. Sheeber Oregon Research Institute, Eugene, OR, USA O. S. Schwartz : M. B. H. Yap : J. G. Simmons : N. B. Allen Orygen Youth Health Research Centre, Centre for Youth Mental Health, University of Melbourne, Victoria, Australia J Abnorm Child Psychol (2012) 40:59–71 DOI 10.1007/s10802-011-9542-2

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Parental Behaviors During Family Interactions PredictChanges in Depression and Anxiety SymptomsDuring Adolescence
Orli S. Schwartz & Paul Dudgeon & Lisa B. Sheeber &
Marie B. H. Yap & Julian G. Simmons & Nicholas B. Allen
Published online: 26 July 2011# Springer Science+Business Media, LLC 2011
Abstract This study investigated the prospective, longitu-dinal relations between parental behaviors observed duringparent-adolescent interactions, and the development ofdepression and anxiety symptoms in a community-basedsample of 194 adolescents. Positive and negative parentalbehaviors were examined, with negative behaviors operation-alized to distinguish between observed parental expressionsof aggression and dysphoria. Results showed that higherlevels of parental aggression prospectively predicted higherlevels of both depression and anxiety symptoms in adoles-cents over two-and-a-half years, whereas higher levels ofpositive parental behaviors prospectively predicted lowerlevels of depression symptoms only. Parental dysphoricbehavior was not related to changes in either symptomdimension. These results suggest that patterns of parentalbehaviors may be differentially associated with depressiveversus anxious outcomes in adolescents, and highlight thepotential role for family-focused prevention or treatment
interventions aimed at reducing an escalation of depressionand anxiety symptoms in adolescence.
Keywords Parenting . Adolescence . Depression . Anxiety .
Longitudinal
Introduction
The current study investigated the prospective influence of bothpositive parental behaviors that convey acceptance, affection orhappiness, and negative parental behaviors that conveyaggression or dysphoria, on the development of symptoms ofdepression and anxiety during adolescence. A better under-standing of the development of internalizing symptoms inadolescence is important because elevated levels of suchsymptoms have been found to significantly increase risk forthe development of depression and anxiety disorders over time(e.g., Klein et al. 2009; Pine et al. 1999). Furthermore, there isevidence to suggest that children and adolescents withelevated levels of depression and anxiety symptoms experi-ence significant disability even when their symptoms do notmeet criteria for a diagnosis (Angold et al. 1999).
Adolescence is a significant period of development inwhich to study the effects of parenting behavior on theemergence of depression and anxiety symptoms. The biolog-ical, psychological, and social changes that occur duringadolescence render it a time of particular vulnerability for theemergence of symptoms and disorder (Masten 2004), anddespite the increased salience of peer relationships duringthis phase of life, parents continue to have a significantinfluence on development (Steinberg and Morris 2001).
The emotional and interactional quality of parentingbehaviors is thought to shape the emotional climate of thefamily, and thus play an important role in young people’s
This research was supported by grants from the Colonial Foundation,the National Health and Medical Research Council (NHMRC;Australia; Program Grant350241) and the Australian ResearchCouncil (Discovery Grant DP0878136).
O. S. Schwartz : P. Dudgeon :N. B. Allen (*)Department of Psychological Sciences,University of Melbourne,Victoria, Australiae-mail: [email protected]
L. B. SheeberOregon Research Institute,Eugene, OR, USA
O. S. Schwartz :M. B. H. Yap : J. G. Simmons :N. B. AllenOrygen Youth Health Research Centre,Centre for Youth Mental Health,University of Melbourne,Victoria, Australia
J Abnorm Child Psychol (2012) 40:59–71DOI 10.1007/s10802-011-9542-2

psychosocial development. Specifically, it has been arguedthat through the observation, modelling, and socialreferencing of parental expressions of emotion, childrenlearn about the nature of different emotions, the way inwhich emotions are elicited by different stimuli, and thecontextual appropriateness of emotion expression. In turn,this knowledge is thought to influence the way that childrencome to experience, regulate and express their ownemotions (Eisenberg et al. 1998; Morris et al. 2007).
In the current study, we examined the influence ofparental expressions of positive and negative emotions. Inexamining negative emotional expressions, we distin-guished between dominant (aggressive) and submissive(dysphoric) expressions, as they have divergent socialfunctions and could thus be expected to differentiallypredict symptomatology.
One of the social functions of aggression is to evoke fearand submission responses in others (Keltner and Kring1998). Thus, frequent exposure to parental aggression couldelicit fear responses in adolescents that could contribute tothe development of anxiety symptoms, or it could elicitfeelings of rejection, worthlessness or helplessness, thuscontributing to the development of depression symptoms(Rodriguez 2003). Parental expressions of dysphoric (sadand anxious) behaviors, on the other hand, may confer riskfor internalizing symptoms through modeling or emotioncontagion processes, in which the expression of an emotionby an individual elicits the reciprocation of that emotion byanother (Campos et al. 1994). In addition, one of the socialfunctions of submissive emotions is to elicit support andreassurance from others (Keltner and Kring 1998). Thus,parental expressions of dysphoria may leave childrenfeeling unsupported, or may draw them into a parentingrole, which may also place them at risk for internalizingproblems (Jacobvitz et al. 2004). In contrast, adolescentswho are exposed to positive parental emotions may feelaccepted, loved and secure, which could thus protect themfrom the development of internalizing symptoms (Blatt andHomann 1992).
The current study utilized an observational assessment ofparenting behaviors. In developmental behavior research,observational assessments have been considered the goldstandard (Zeman et al. 2007) because they capture arelatively ‘natural’ sampling of behavior, may be lessinfluenced by social desirability than self-reports, andenable the recording of behavior of which participantsmay not be consciously aware or able to report, such asnon-verbal expressions (Morris et al. 2006). In the currentstudy, observational data was collected as parents andadolescents participated in an event-planning interaction, inwhich the dyads planned an enjoyable event/s to dotogether, and a problem-solving interaction, in which thedyads discussed topics that generate conflict in their
relationship. Though we expected positive, aggressive anddysphoric parental behaviors to be observed in bothinteractions, we anticipated that the event-planning taskwould elicit a greater frequency of positive behaviors andthat the problem-solving task would elicit a greaterfrequency of negative behaviors, due to the nature of thetask demands. In addition, the two tasks were chosen toenable the exploration of the influence of parental expres-sions of negative behaviors in a task designed to elicitpositive behaviors, and positive behaviors in a taskdesigned to elicit negative behaviors.
Studies Examining Parenting and Depression
Observational research on parent-child interactions hasidentified a link between depression symptoms in childrenand adolescents and high rates of negative parentalbehaviors, as well as low rates of positive parentalbehaviors. For example, in a community sample, Messerand Gross (1995) found that the parents of children withhigh levels depression symptoms displayed fewer positivebehaviors, more negative behaviors, and were moredisengaged when interacting in their home environment,compared to the parents of children with low levels ofdepression symptoms. Similar findings have been reportedusing clinical samples, in which the parents of depressedadolescents have been found to display more depressive(Sheeber and Sorensen 1998) and aggressive (Sheeber et al.2007) behaviors, and fewer positive behaviors (Sheeber etal. 2007; Sheeber and Sorensen 1998) than the parents ofnon-depressed adolescents, and such findings have beenreplicated using self-report methodologies (Prange et al.1992; Stark et al. 1990).
There is also evidence suggesting that such parentingbehaviors may play an etiological role in the developmentof depression symptoms. A prospective study conducted bySheeber et al. (1997) followed a community sample ofadolescents over 1 year. Supportive and conflictual parentalbehaviors were found to prospectively predict respectivelylower and higher levels of adolescent depression symptomsat follow-up, after controlling for baseline symptoms.Another longitudinal study reported that maternal nega-tivity and disengagement during an interaction with theirchild predicted higher levels of depression symptoms inchildren 6 months later (Burge and Hammen 1991). Nostudies could be identified that have investigated theprospective influence of dysphoric parenting behaviors ondepression symptoms in adolescence.
Studies Examining Parenting and Anxiety
Research on family processes relevant to childhood anxietydisorders has focused largely on the dimensions of parental
60 J Abnorm Child Psychol (2012) 40:59–71

control/autonomy and positivity/negativity (Rapee 1997).Cross-sectional (Gar and Hudson 2008; Hudson and Rapee2001; Siqueland et al. 1996; Whaley et al. 1999) andlongitudinal (Bayer et al. 2006) studies using observationaldesigns have consistently found evidence indicating highlevels of controlling behavior in the parents of anxiouschildren. The evidence regarding the influence of parentalpositivity/negativity has been mixed, with some studiesreporting lower levels of warmth (Hudson and Rapee 2001)and higher levels of criticism (Gar and Hudson 2008) inthe parental behaviors of anxious children, and othersreporting null effects (Siqueland et al. 1996; Whaley et al.1999). One of the very few studies to examine theindependent influence of positive and negative parentalbehaviors found that parents of boys (but not girls) withanxiety disorders displayed more negative affect and lesspositive affect than the parents of boys without anxietydisorders (Suveg et al. 2008).
Longitudinal studies have also found evidence thatparental behaviors predict anxiety symptoms over time.Rubin et al. (2002) conducted one of very few longitudinalstudies using observational parenting data, but focused onsocial inhibition outcomes rather than anxiety per se. Theyfound that when mothers of inhibited children behaved ineither a controlling or derisive manner at age two, theirchildren exhibited social reticence 2 years later. Otherlongitudinal studies using self-report measures of parentingin early and middle childhood samples have found aprospective relationship between parental controllingbehaviors, low warmth, and negative emotional expressivityand childhood anxiety symptoms (Duchesne et al. 2010;Volbrecht and Hill Goldsmith 2010). Longitudinal studiesbased on adolescents’ reports of parental behaviors havefound that perceived overprotective, rejecting and anxiousparenting predicts an increase in adolescents’ anxietysymptoms over time (Lieb et al. 2000; Rapee 2009).
Overall, it has been suggested that there is consistentevidence for the association between controlling parentalbehaviors and anxiety in their children (McLeod et al.2007; Rapee 1997). There has been less research examiningparental affective behaviors, which are the focus of thecurrent study. However, recent reviews have suggested thatthe existing evidence base more strongly links negativeparental behaviors (such as criticism and hostility) tochildhood anxiety than deficits in positive parental behaviors(Ginsburg et al. 2004; McLeod et al. 2007).
Summary and Limitations of the Existing Literature
In summary, evidence from observational studies hassuggested that high levels of parental negativity (bothaggression and dysphoria) and low levels of parentalpositivity are associated with the development of depres-
sion symptoms in childhood and adolescence. The literaturerelating to the influence of positive and negative parentalbehaviors on anxiety symptoms is more limited. Thestrongest evidence suggests a link between dominantnegative affective behaviors, especially criticism, andanxiety symptoms in young people, and there is a smallerevidence base associating low levels of parental positivitywith anxiety outcomes.
The existing literature has a number of limitations.Firstly, most studies examining relations between observa-tional measures of parenting behaviors and child/adolescentoutcomes have been cross-sectional in design. The findingsof such studies cannot elucidate whether such parentalbehaviors prospectively increase the risk of symptoms inchildren and adolescents, or whether these findings reflectdisruptions in the family environment attributable toconcurrent emotional or behavioral problems in childrenand adolescents.
Secondly, most existing studies have focused on asingle outcome (i.e., depression or anxiety symptoms)and no research could be identified that comparedobserved parental behaviors in the prediction of depres-sion and anxiety symptoms measured separately. It isimportant to examine multiple symptom outcomes so thatthe specificity of the role of particular parental behaviorsin the development of specific syndromes can beevaluated.
Thirdly, relatively few studies have explored the rela-tionship between parental behaviors and symptoms duringadolescence, as opposed to childhood. As discussedpreviously, adolescence is a period of particular sensitivityfor the development of both depression and anxiety, and is aperiod in which the parent-child relationship undergoeschange. In particular, a normative increase in mild conflictand a decrease in closeness has been noted as familiesnegotiate the establishment of their adolescents’ autonomy,before a more egalitarian parent-child relationship isdeveloped in later adolescence (Steinberg and Morris2001). As a result, it is important to understand theinfluence of parental behaviors on the emergence ofsymptoms during adolescence specifically.
Finally, studies examining negative parental emotionalbehaviors have generally focused on dominant negativebehaviors (i.e., criticism and hostility), whereas relativelyfew have examined the influence of submissive negativebehaviors (i.e., sadness and anxiety). Recent reviews (e.g.Morris et al. 2007) have suggested that parental expressionsof dominant negative emotions have been more consistentlyassociated with negative outcomes in children than havesubmissive negative emotions, however the nature of therelationships between different parental behaviors andsymptomatic outcomes in adolescents remains to beclarified.
J Abnorm Child Psychol (2012) 40:59–71 61

The Current Study
Addressing the limitations outlined above, the current studyinvestigated the longitudinal relations between parentalbehaviors and the development of depression and anxietysymptoms in a community-based sample of adolescents.Positive and negative parental behaviors were examined,with negative parental behaviors operationalized to distin-guish between observed parental expressions of aggressiveversus dysphoric behaviors.
Based on the existing research, it was hypothesized that:(i) more frequent aggressive and dysphoric parentalbehaviors would prospectively predict more depressionsymptoms in adolescents; (ii) more frequent aggressiveparental behavior would prospectively predict more anxietysymptoms in adolescence, and (iii) more frequent positiveparental behavior would prospectively predict fewer de-pression and anxiety symptoms.
Method
The data presented here was drawn from the AdolescentDevelopment Study (ADS); a large, ongoing longitudi-nal study conducted in Melbourne, Australia. This studydrew on two waves of ADS data collection: the firstwave of intensive data collection (T1), included afamily-interaction assessment and a psychosocial assess-ment that included the collection of adolescent-ratedquestionnaires; the second wave of intensive datacollection (T2) was conducted approximately two-and-a-half years after T1, and comprised a psychosocialassessment including the collection of adolescent-ratedquestionnaires.
Recruitment and Screening of Participants
The screening sample was drawn from the target populationof final year primary school students (Grade 6; agedapproximately 10–12 years) enrolled in generalist primaryschools in metropolitan Melbourne, Australia. The aim ofthe screening was to identify a sample representing the fullspectrum of risk for psychopathology as a function oftemperament, as measured by the Early Adolescent Tem-perament Questionnaire—Revised (EATQ-R; Ellis andRothbart 2001). A total of 2453 Grade 6 students (53.5%of the total sampling population; 52% female; mean age11.62 years) participated, and the assessment was con-ducted in the classroom in groups of 18–25 students.Participants provided demographic information and com-pleted the EATQ-R. Socio-economic status (SES) wasderived from participants’ home addresses using theAustralian Bureau of Statistics’ Socio-Economic Indexes
for Areas (SEIFA) scores (Australian Bureau of Statistics2008) which rank geographic areas across Australia interms of their socio-economic characteristics. Following thescreening, a sample of 415 students was selected on thebasis of their EATQ-R scores on the Negative Affectivityfactor, which includes items that measure tendency forfrustration, and the Effortful Control factor, which includesitems relating to capacity for attention and self-regulation.High and low scores on these scales, respectively, havebeen associated with depressive and anxiety symptoms inadolescents (Ellis and Rothbart 2001; Muris and Meesters2009). The selected sample of 415 students was comprisedof equal numbers of male and female students who hadEATQ-R scores that were 0–1, 1–2, 2–2.5, and greaterthan 2.5 standard deviations above and below the mean onthe higher order factors of Negative Affectivity andEffortful Control. Thus, adolescents with scores in thetails of the distribution were over-represented in theselected sample.
Of the 415 students selected, 245 agreed to participate inthe T1 intensive data phase, and 199 completed both thepsychosocial assessment and the family interaction tasks.Videorecorded family interaction data was corrupted andthus unusable for two families. In addition, three femaleadolescents with complete family interaction data werediagnosed with major depressive disorder (MDD) usingthe Schedule for Affective Disorders and Schizophreniafor School-Age Children, Present and Lifetime version(K-SADS-PL; Kaufman et al. 1997) at the psychosocialassessment at T1. These participants were excluded toenable a focus on increases in internalizing symptomsprior to the onset of mood disorders, leaving a total sampleof 194 families (95 females). There were no differencesbetween these 194 participants and the remaining 221 ofthe 415 selected participants according to gender, χ2(1)=1.18, ns, age, t[405]=−0.13, ns, socio-economic status, t[405]=−1.29, ns, or scores on Negative Affectivity, t[413]=−0.08, ns, and Effortful Control, t[413]=−0.17, ns.Adolescents in the final sample had a mean age of12.47 years (range 11.38–13.61) at the psychosocial assess-ment phase of T1.
Procedures
Psychosocial Assessment at T1
Families completed the T1 psychosocial assessment anaverage of 10.14 months (range 3.90–17.30) after adoles-cents took part in the school screening. In most instances,the assessment was completed in a single home visit, andincluded the administration of an adolescent-rated batteryof questionnaires. Adolescents were reimbursed for theirtime.
62 J Abnorm Child Psychol (2012) 40:59–71

Family Interaction Assessment at T1
Adolescents and one parent (159 mothers and 35 fathers)completed the lab-based family interaction assessment,which occurred a mean duration of 1.96 months (range0.03–8.04) following the psychosocial assessment at T1.No restrictions were placed on which parent/caregiverparticipated in the study in order to facilitate parentalparticipation. Families completed two 20-minute interactiontasks that were videorecorded for subsequent coding. Thefirst task was an event-planning interaction and the secondwas a problem-solving interaction. The tasks were intendedto differentially elicit positive and negative behavior,respectively. The ordering of tasks was fixed because ofconcern that negative affective states, which are harder toshift out of than positive states (Gilboa and Revelle 1994),had the potential persist into the event-planning task if itwere conducted second.
For the event-planning interaction, parents and adoles-cents were instructed to plan one or more pleasant events,with up to five topics for discussion chosen based onevents that both the parent and adolescent rated asbeing ‘very pleasant’ on the Pleasant Events Schedule(MacPhillamy and Lewinsohn 1976). For the problem-solving interaction, the interviewer selected up to fiveissues for discussion that both the parent and adolescentendorsed as occurring the most frequently and generatingthe highest intensity of anger on the Issues Checklist(Prinz et al. 1979). One family completed only the event-planning interaction, and not the problem-solving interac-tion. Parents and adolescents were reimbursed for theirtime and travel expenses.
Psychosocial Assessment at T2
Of the 194 participants, 178 (91.8%; 48.9% female)completed the T2 psychosocial assessments, which wereconducted a mean of 31.12 months (range 21.17–41.20)following the T1 psychosocial assessments, when adoles-cents had a mean age of 15.04 years (range 13.73–16.19).Adolescents completed a battery of questionnaires,amongst other assessments, and were reimbursed for theirtime.
Measures
Centre for Epidemiological Studies—Depression (CES-D)
The CES-D (Radloff 1977) is a 20-item self-reportquestionnaire designed to measure depression symptomsin the general population. A higher score indicates greaterfrequency and number of depression symptoms. The CES-D has an established validation history of use in adolescent
populations (Radloff 1991). In this study, Cronbach’s alphafor the CES-D was 0.885 at T1 and 0.888 at T2.
Beck Anxiety Inventory (BAI)
The Beck Anxiety Inventory (Beck et al. 1988) is a self-report questionnaire measuring clinical symptoms ofanxiety. It consists of 21 common anxiety symptoms thatwere chosen to avoid overlap with depression symptoms(Beck et al. 1988). The BAI has been commonly used withadolescent populations and has been found to haveadequate reliability and validity (Osman et al. 2002). Inthe current study, Cronbach’s alpha for the BAI was 0.902at T1 and 0.904 T2.
Living in Family Environments (LIFE) Coding System
The LIFE (Hops et al. 1995) is an observational codingsystem that enables a detailed analysis of individual familymembers’ behaviors. The LIFE consists of 10 nonverbalaffect codes (contempt, anger, anxious, dysphoric, pleasant,neutral, happy, caring, whine, and belligerence) and 27verbal content codes (e.g., validation, complaint, provoke).Coding of videorecorded interactions uses an event-basedprotocol in which new codes are entered each time theaffect or content of one of the interactants changes. The 10affect and 27 content codes are used to develop compositebehavior constructs. In this study, the constructs wereAggressive, Dysphoric and Positive behavior. Aggressivebehavior included all codes with contemptuous, angry, orbelligerent affect, as well as cruel, provocative, annoying/disruptive, or argumentative verbal statements made withneutral affect. Dysphoric behavior consisted of all codeswith dysphoric, anxious, or whining affect, as well ascomplaints and self-derogatory verbal comments made withneutral affect. Positive behavior included all codes withhappy, pleasant, and caring affect as well as approving,validating, affectionate or humorous comments made withneutral affect. The LIFE data was used to construct rate perminute (RPM) variables for each of the parental behaviorconstructs in both the event-planning and problem-solvinginteractions, representing the average number of times aparent expressed each behavior type per minute over thecourse of each interaction task.
Coders were extensively trained and blind to theclinical and demographic characteristics of the partic-ipants. Approximately 20% of the interactions were coded bya second observer to provide an estimate of observeragreement. Random pairs of observers were assigned to theinteractions to minimize ‘drift’ between any two observersand to ensure that all observers met minimal criteria foracceptable observations. Inter-observer agreement wasassessed using Kappa, a conservative index that controls for
J Abnorm Child Psychol (2012) 40:59–71 63
chance agreement (Hops et al. 1995). Kappa coefficients forthe Aggressive, Dysphoric, and Positive behavior constructswere, respectively, 0.70, 0.57, and 0.86 for mothers, and0.77, 0.54, and 0.84 for fathers. The average pairwise intra-class correlations among four raters for the Aversive,Dysphoric and Positive RPM variables (over EPI and PSItasks and parents) were 0.81, 0.52. and 0.78, respectively.The validity of the LIFE system as a measure of familyprocesses has been established in numerous studies (e.g.,Katz and Hunter 2007; Sheeber et al. 2007).
Results
Missing Data Imputation
The proportion of missing questionnaire data was 7.22%for the CES-D and 3.61% for the BAI at T1, and 10.82%for the CES-D and 9.79% of the BAI at T2. The data weremissing as a result of incomplete filling out of question-naires at T1 and/or T2, and non-participation in the T2assessment. The data were missing completely at random(MCAR) according to Little’s MCAR test, χ2(65)=71.31,p=0.28, so it was considered appropriate to impute themissing data. All missing questionnaire data was imputedusing the expectation-maximization (EM) algorithm inSPSS (SPSS Inc. 2007). Missing parent behavior data forthe one family that did not complete the problem-solvinginteraction was not imputed.
Descriptive Analyses
Results in Table 1 show that parents displayed Aggressivebehaviors significantly more frequently during the problem-solving interaction compared to the event-planning interac-tion, F(1, 192)=356.08, p<0.01, ηp
2=0.65, and displayedPositive behaviors significantly less frequently, F(1, 192)=186.59.14, p<0.01, ηp
2=0.01. There was little variation inrates of parental Dysphoric behaviors across the two tasks,
F(1, 192)=1.18, p=0.28, ηp2=0.49. Univariate analyses
revealed no parent or adolescent gender differences in anyof the parent RPM behavior constructs in either the event-planning interaction or the problem-solving interaction.
Table 2 shows the levels of depression and anxietysymptoms amongst the adolescents at T1 and T2. Scores onthe CES-D declined slightly from T1 to T2, F(1, 193)=8.14, p<0.01, ηp
2=0.04. A decline in self-reported depres-sion across repeated administration has been commonlyobserved, and evidence suggests that this may be due tomeasurement effects, rather than to a true decline insymptoms (Twenge and Nolen-Hoeksema 2002). Therewas no significant difference between the T1 and T2 scoreson the BAI, F(1, 193)=1.36, p=0.25 ηp
2<0.01.
Design of Path Analyses
Two path analyses were specified, each using data fromeither the event-planning interaction or problem-solvinginteraction. Both models tested the prospective influence ofthe three parental behavior constructs on depression andanxiety symptoms reported by adolescents. Path analyseswere run using Mplus software (Muthén and Muthén 2007)and maximum likelihood estimation. In both models, T1depression and anxiety scores were included as predictorsof the corresponding T2 scores. Parent gender was includedas a predictor of each parent RPM variable in both modelsto control for any parent gender differences (see Fig. 1).
Analysis of Adolescent Gender
A multiple group analysis was employed to test theinvariance of regression parameters across adolescentgender (Muthén and Muthén 1998–2007). Initially, allparameter estimates corresponding to regression coeffi-cients were constrained to be equal across groups. Follow-ing the procedure recommended by Muthén and Muthén(1998–2007), constrained parameters with a modificationindex (MI) of approximately three or above in both theboys and girls groups were sequentially released and themodel re-run, with a chi-square difference test used toTable 1 Descriptives for parental behavior constructs
Mean Standard deviation Range
Event-planning interaction
Aggressive RPM 0.59 0.40 0.00–1.93
Dysphoric RPM 0.57 0.38 0.00–1.97
Positive RPM 2.30 0.52 0.88–4.03
Problem-solving interaction
Aggressive RPM 1.30 0.60 0.10–2.81
Dysphoric RPM 0.53 0.31 0.00–1.41
Positive RPM 1.68 0.69 0.33–3.58
RPM rate per minute
Table 2 Descriptives for adolescent self-report measures
Mean Standard deviation Range
Adolescent self-report measures
CES-D T1 11.49 9.31 0–55
CES-D T2 9.62 7.97 0–43
BAI T1 8.31 8.64 0–45
BAI T2 9.16 8.72 0–45
CES-D Centre for Epidemiological Studies—Depression, BAI BeckAnxiety Inventory, T1 Time 1, T2 Time 2
64 J Abnorm Child Psychol (2012) 40:59–71
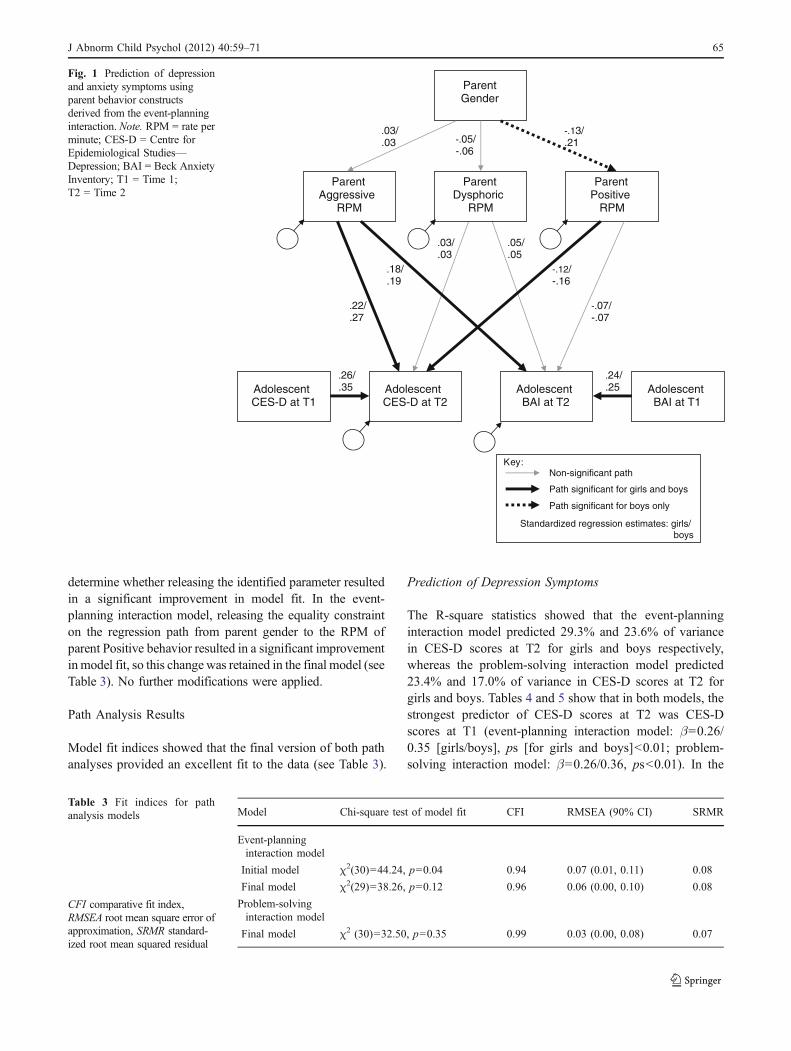
determine whether releasing the identified parameter resultedin a significant improvement in model fit. In the event-planning interaction model, releasing the equality constrainton the regression path from parent gender to the RPM ofparent Positive behavior resulted in a significant improvementinmodel fit, so this change was retained in the final model (seeTable 3). No further modifications were applied.
Path Analysis Results
Model fit indices showed that the final version of both pathanalyses provided an excellent fit to the data (see Table 3).
Prediction of Depression Symptoms
The R-square statistics showed that the event-planninginteraction model predicted 29.3% and 23.6% of variancein CES-D scores at T2 for girls and boys respectively,whereas the problem-solving interaction model predicted23.4% and 17.0% of variance in CES-D scores at T2 forgirls and boys. Tables 4 and 5 show that in both models, thestrongest predictor of CES-D scores at T2 was CES-Dscores at T1 (event-planning interaction model: β=0.26/0.35 [girls/boys], ps [for girls and boys]<0.01; problem-solving interaction model: β=0.26/0.36, ps<0.01). In the
:yeKNon-significant path
.05/
.05 .03/ .03
-.07/ -.07
-.12/ -.16
.18/
.19
.22/
.27
.24/
.25 .26/ .35
-.13/ .21 -.05/
-.06
.03/
.03
Parent Gender
Parent Aggressive
RPM
Parent Dysphoric
RPM
Parent Positive
RPM
Adolescent BAI at T2
Adolescent BAI at T1
Adolescent CES-D at T1
Adolescent CES-D at T2
Path significant for girls and boys
Path significant for boys only
Standardized regression estimates: girls/ boys
Fig. 1 Prediction of depressionand anxiety symptoms usingparent behavior constructsderived from the event-planninginteraction. Note. RPM = rate perminute; CES-D = Centre forEpidemiological Studies—Depression; BAI = Beck AnxietyInventory; T1 = Time 1;T2 = Time 2
Model Chi-square test of model fit CFI RMSEA (90% CI) SRMR
Event-planninginteraction model
Initial model χ2(30)=44.24, p=0.04 0.94 0.07 (0.01, 0.11) 0.08
Final model χ2(29)=38.26, p=0.12 0.96 0.06 (0.00, 0.10) 0.08
Problem-solvinginteraction model
Final model χ2 (30)=32.50, p=0.35 0.99 0.03 (0.00, 0.08) 0.07
Table 3 Fit indices for pathanalysis models
CFI comparative fit index,RMSEA root mean square error ofapproximation, SRMR standard-ized root mean squared residual
J Abnorm Child Psychol (2012) 40:59–71 65
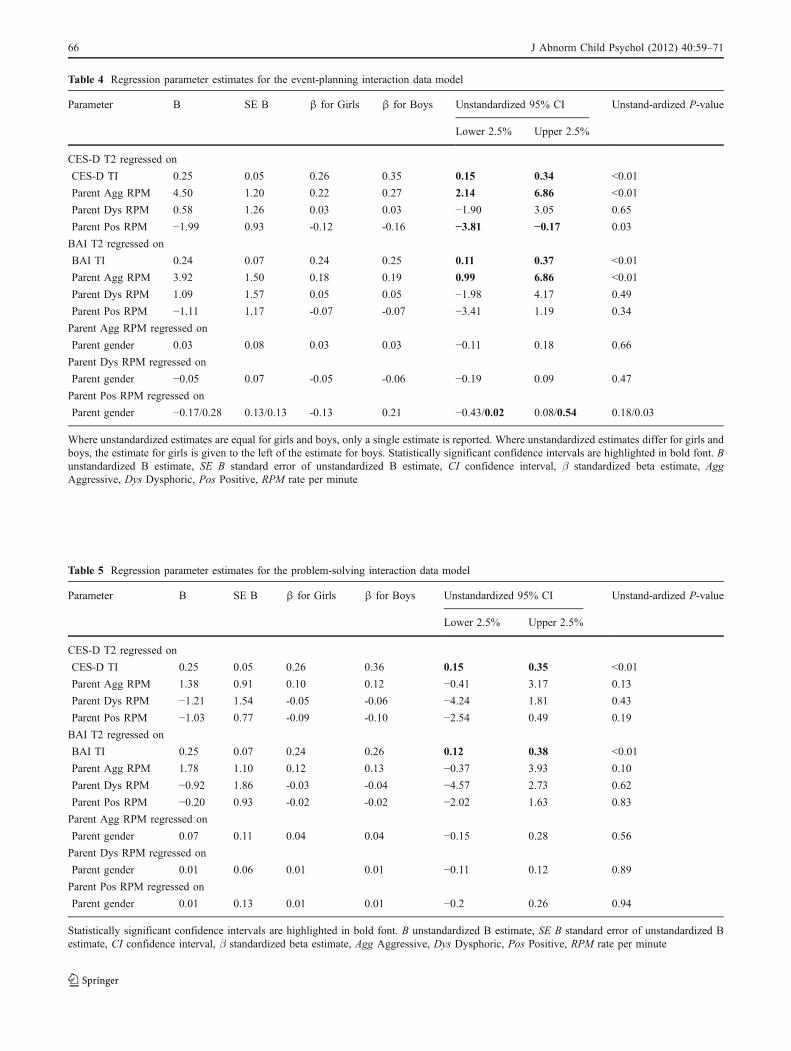
Table 4 Regression parameter estimates for the event-planning interaction data model
Parameter B SE B β for Girls β for Boys Unstandardized 95% CI Unstand-ardized P-value
Lower 2.5% Upper 2.5%
CES-D T2 regressed on
CES-D TI 0.25 0.05 0.26 0.35 0.15 0.34 <0.01
Parent Agg RPM 4.50 1.20 0.22 0.27 2.14 6.86 <0.01
Parent Dys RPM 0.58 1.26 0.03 0.03 −1.90 3.05 0.65
Parent Pos RPM −1.99 0.93 -0.12 -0.16 −3.81 −0.17 0.03
BAI T2 regressed on
BAI TI 0.24 0.07 0.24 0.25 0.11 0.37 <0.01
Parent Agg RPM 3.92 1.50 0.18 0.19 0.99 6.86 <0.01
Parent Dys RPM 1.09 1.57 0.05 0.05 −1.98 4.17 0.49
Parent Pos RPM −1.11 1.17 -0.07 -0.07 −3.41 1.19 0.34
Parent Agg RPM regressed on
Parent gender 0.03 0.08 0.03 0.03 −0.11 0.18 0.66
Parent Dys RPM regressed on
Parent gender −0.05 0.07 -0.05 -0.06 −0.19 0.09 0.47
Parent Pos RPM regressed on
Parent gender −0.17/0.28 0.13/0.13 -0.13 0.21 −0.43/0.02 0.08/0.54 0.18/0.03
Where unstandardized estimates are equal for girls and boys, only a single estimate is reported. Where unstandardized estimates differ for girls andboys, the estimate for girls is given to the left of the estimate for boys. Statistically significant confidence intervals are highlighted in bold font. Bunstandardized B estimate, SE B standard error of unstandardized B estimate, CI confidence interval, β standardized beta estimate, AggAggressive, Dys Dysphoric, Pos Positive, RPM rate per minute
Table 5 Regression parameter estimates for the problem-solving interaction data model
Parameter B SE B β for Girls β for Boys Unstandardized 95% CI Unstand-ardized P-value
Lower 2.5% Upper 2.5%
CES-D T2 regressed on
CES-D TI 0.25 0.05 0.26 0.36 0.15 0.35 <0.01
Parent Agg RPM 1.38 0.91 0.10 0.12 −0.41 3.17 0.13
Parent Dys RPM −1.21 1.54 -0.05 -0.06 −4.24 1.81 0.43
Parent Pos RPM −1.03 0.77 -0.09 -0.10 −2.54 0.49 0.19
BAI T2 regressed on
BAI TI 0.25 0.07 0.24 0.26 0.12 0.38 <0.01
Parent Agg RPM 1.78 1.10 0.12 0.13 −0.37 3.93 0.10
Parent Dys RPM −0.92 1.86 -0.03 -0.04 −4.57 2.73 0.62
Parent Pos RPM −0.20 0.93 -0.02 -0.02 −2.02 1.63 0.83
Parent Agg RPM regressed on
Parent gender 0.07 0.11 0.04 0.04 −0.15 0.28 0.56
Parent Dys RPM regressed on
Parent gender 0.01 0.06 0.01 0.01 −0.11 0.12 0.89
Parent Pos RPM regressed on
Parent gender 0.01 0.13 0.01 0.01 −0.2 0.26 0.94
Statistically significant confidence intervals are highlighted in bold font. B unstandardized B estimate, SE B standard error of unstandardized Bestimate, CI confidence interval, β standardized beta estimate, Agg Aggressive, Dys Dysphoric, Pos Positive, RPM rate per minute
66 J Abnorm Child Psychol (2012) 40:59–71

event-planning interaction model, after controlling forbaseline symptoms, higher levels of depression symptomsat T2 were predicted by higher rates of parental Aggressivebehavior, β=0.22/0.27, ps<0.01, and lower rates ofparental Positive behavior, β=−0.12/-0.16 , ps<0.05 . Noneof the parental behavior variables derived from theproblem-solving interaction significantly predicted CES-Dscores at T2, and parental Dysphoric behavior did notpredict depression symptom outcomes in either model.
Prediction of Anxiety Symptoms
According to the R-square statistics, the event-planninginteraction model predicted 11.2% of variance in BAIscores at T2 for both girls and boys, and the problem-solving interaction model predicted 7.9% and 8.6% ofvariance in BAI scores at T2 for girls and boys,respectively. As with the CES-D scores, the strongestpredictor of anxiety symptoms at T2 was anxiety symptomsat T1 in both the event-planning interaction and problem-solving interaction models (event-planning interactionmodel: β=0.24/0.25, ps<0.01; problem-solving interactionmodel: β=0.24/0.26, ps<0.01). Table 4 shows that in theevent-planning interaction model, after controlling forbaseline symptoms, higher levels of anxiety symptoms atT2 were predicted by higher rates of parental Aggressivebehavior only, β=0.18/0.19, ps<0.01. The parental behaviorvariables derived from the problem-solving interaction did notsignificantly predict BAI scores at T2 (see Table 5), andparental Dysphoric behavior did not predict anxiety symp-tom outcomes in either model.
Parent Gender
In the model using event-planning interaction data (see resultsin Table 4), a significant parent gender effect was observed inthe prediction of the RPM of parent Positive behavior, in thatfathers exhibited a lower rate of this behavior than mothersin interactions with their sons, β=−0.13/0.21, p=0.18/0.03(girls/boys). In the problem-solving interaction model, noneof the parent gender effects had confidence intervals thatexcluded zero.
Discussion
In support of our hypotheses, the results showed that higherlevels of parental aggressive behavior during the event-planning interaction prospectively predicted higher levelsof both depression and anxiety symptoms in adolescents,and higher levels of parental positive behavior during theevent-planning interaction prospectively predicted lowerlevels of depression symptoms. However, there was no
evidence to suggest a prospective relationship betweenpositive parental behaviors and anxiety symptoms inadolescents. Thus, the results suggest that different patternsof parental behaviors may be differentially associated withdepressive versus anxious outcomes in adolescents. Therewas no evidence to suggest that parental expressions ofsubmissive negative emotions (i.e., dysphoric behavior) hadany predictive influence on either symptom outcome inadolescents. Unexpectedly, there were also no significantfindings based on parent behaviors observed during theproblem-solving interaction.
The findings that depression symptoms were predictedby both aggressive and positive parental behaviors areconsistent with the small number of longitudinal studiesusing observational data that have associated negativeand positive parental behaviors with higher and lowerlevels of depression symptoms, respectively (Burge andHammen 1991; Sheeber et al. 1997). Thus, these findingsadd to the evidence base indicating that aggressive andpositive parenting behaviors may respectively increaseand decrease the risk of developing depression symptomsduring adolescence.
With regard to the development of anxiety symptoms,our results extend previous findings that parents of anxiouschildren are more critical (Gar and Hudson 2008), andlongitudinal findings that derisive parental comments(Rubin et al. 2002) and negative parental affectiveexpressivity (Volbrecht and Hill Goldsmith 2010) areassociated with anxiety symptoms over time. To the bestof our knowledge, no previous research has identified aprospective relationship between parental aggression andadolescent anxiety symptoms, and these findings areparticularly notable as they were obtained using anobservational measure of parenting behavior.
In addition, we could not identify any previous researchthat examined the influence of parental behaviors on bothdepression and anxiety symptoms over time, and it isinteresting to observe a different pattern of findings in theprediction of these two outcomes. While positive parentalbehavior was found to significantly predict depression butnot anxiety symptoms in adolescents over time in the event-planning interaction model, a more stringent test of thisdifferential effect is to compare the magnitude of the tworegression paths. Using the method suggested by Paternos-ter and colleagues (1998), the difference between theregression paths from positive parental behavior predictingdepression and anxiety symptoms at T2 was not signifi-cantly different, z=-0.06, p=0.28. Further research directlyexamining this issue would help to clarify whether deficitsin positive parental behaviors are specifically related todepression outcomes in adolescents.
While there is some evidence that dominant negativeparental behaviors may have greater influence on child
J Abnorm Child Psychol (2012) 40:59–71 67

development than submissive behaviors (Eisenberg et al.1998), no previous research has examined the longitudinalinfluence of both aggressive and dysphoric parentalbehaviors on internalizing symptoms in adolescence. Inthe current study, although aggressive and dysphoricbehaviors were expressed by parents with roughly the samefrequency during the event-planning interaction, aggressiveparental behaviors more strongly predicted the developmentof internalizing symptoms. One of the theoretical implica-tions of these findings is that aggressive parental behaviorsmay have a more destabilizing impact on adolescents’mental states than dysphoric parental behaviors. This maybe because aggressive behaviors are likley to be perceivedas threatening and may elicit fear and/or submission. Suchyielding responses to aggression have been theorised to beone of the key functions of depressive behavior (Price et al.1994). In contrast, dysphoric parental behaviors aresubmissive and may be perceived as less threatening, andthus may have a lesser impact on their children (Keltnerand Kring 1998). However, it is unknown whether thecurrent findings would generalize to adolescents living infamily environments in which parents’ expressions ofdysphoric (and/or aggressive) behaviors are more perva-sive, such as when parents are suffering from depressive oranxiety disorders.
No adolescent gender differences emerged in this study,suggesting that parental behaviors influence the develop-ment of internalizing symptoms in male and femaleadolescents in a similar fashion. With regard to parentgender differences, there was evidence to suggest thatfathers displayed lower rates of positive behavior ininteractions with their sons than did mothers in the event-planning task. While this finding is potentially interesting,replication will be required before firm conclusions aredrawn, due to the small number of fathers in the study.
To the best of our knowledge, our research is the first tohave observed parent-adolescent behaviors during an event-planning interaction (Yap et al. 2010), and the currentresults provide a unique insight into the predictive validityof parental expressions of both positive and negativebehaviors in a task designed to elicit positive behaviorson the development of internalizing symptoms over time inadolescence. In contrast, the absence of significant resultsderived from parent behaviors during the problem-solvingtask was puzzling, given the findings obtained fromprevious studies using a similar paradigm (Burge andHammen 1991; Sheeber et al. 2007; Sheeber et al. 1997;Slesnick and Waldron 1997). In the current study, parentsdisplayed relatively high rates of positive behavior duringthe event-planning interaction, and relatively low rates ofaggressive and dysphoric behaviors, whereas higher rates ofaggressive behavior were observed during the problem-solving interaction. A possible explanation for our findings
is that negative behaviors exhibited during the event-planning interaction—a task designed to elicit positiveemotions—may have particular salience. Relatively highlevels of aggressive parental behaviors during the event-planning interaction may represent a particularly intractabletendency of these parents to behave in this way, given thatthe task does not specifically elicit these kinds of behaviors.The occurrence of aggressive parental behaviors during theproblem-solving interaction—a task designed to elicitnegative emotions—may be more normative given the taskdemands, and thus less discriminatory in regards to risk fordepression and anxiety symptoms.
Using the same rationale, it might have been expectedthat positive parental behaviors during the problem-solvinginteraction would be predictive of adolescent outcomes. Apossible explanation for why such findings were notobserved may be that parents’ capacity to display appro-priately high levels of positivity in a task designed to elicitpositive behavior (i.e., the event-planning interaction) maybe more important for the prediction of depressionsymptoms than their display of positive emotions during aproblem-solving task.
Another possible explanation for why all the significantfindings in this study emerged from parental behaviorsobserved during the event-planning task is that theemotional tone of this task may be more representative ofthe normative family environment than the problem-solvinginteraction. Thus, parental behavior during the event-planning interaction may have more predictive power foradolescent outcomes. Alternatively, the fact that the event-planning interaction was completed first may have influ-enced the pattern of results. As previously noted, theordering of tasks was fixed to prevent negative affectivestates elicited by the problem-solving interaction spillingover into the event-planning interaction (Gilboa andRevelle 1994). It may be that behavior observed duringthe first task was more representative of the participants’typical behavior, whereas factors such as fatigue may haveinfluenced participants’ behavior during the second task,thus limiting the potential for observing significant effectsduring the problem-solving interaction.
Clinically, the findings suggest a potential role forfamily-focused prevention or treatment interventions aimedat reducing the escalation of depression and anxietysymptoms and the onset of internalizing disorders inadolescence. To date, there have been few preventiveinterventions targeting parenting behaviors (Gillham et al.2000; Horowitz and Garber 2006), and those that haveincluded such a component have been limited by lowparental participation rates (e.g. Shochet et al. 2001). Basedon the current findings, specific parental behaviors duringparent-adolescent interactions could be addressed as a focusof preventive interventions. In particular, interventions
68 J Abnorm Child Psychol (2012) 40:59–71

targeting behaviors that lead to parent-adolescent conflict,or that help families develop effective conflict resolutionskills, may be beneficial with regard to addressing harshparenting behaviors, thus potentially reducing risk forincreases in internalzing symptoms in adolescents. Withregard to encouragement of warm and supportive parentingbehaviors, interventions that bring behavioral activationstrategies into the family context, motivating both conjointpleasant activities and parental instrumental support ofadolescent activities may be facilitative, particularly inregard to the prevention of depression symptoms. Moregenerally, interventions to help parents develop skills formaintaining developmentally appropriate parent-child con-nections during the period when adolescents both craveautonomy and need engagement for healthy emotionaldevelopment may be protective for adolescent mental health.
A number of limitations in the current study can benoted. All task-based behavioral observation paradigms canbe criticized for lacking external validity; however, it hasbeen found that more naturalistic assessments, such as thosecarried out in the family home, may be characterized by thepreponderance of neutral and solitary behaviors (e.g.,Messer and Gross 1995). Thus, it is necessary to conductnaturalistic observations for a considerably longer period oftime in order to obtain a reliable representation of behavior,which poses a number of practical difficulties.
In addition, it is possible that parental behavior in thecurrent study may have been influenced by a number offactors, such as the behavior of adolescents during theinteraction, and the presence of parental psychopathology.These and other unmeasured factors could have confoundedthe relationships between observed parental behaviors andsymptom outcomes in the adolescents.
As previously noted, a further limitation was theunder-representation of fathers (18%) compared to moth-ers in this study, rendering it difficult to meaningfullycompare the influence of mothers’ and fathers’ parentingbehaviors on the development of adolescent outcomes.The importance of investigating a range of family relation-ships (e.g., mother-child, father-child, and mother-fatherrelationships) in the prediction of child outcomes has beennoted by previous researchers (e.g. Mathijssen et al. 1998),and we acknowledge our inability to do this as a limitation inthis work.
Finally, in order to determine whether distinct parentalbehaviors differentially predict depression and anxietysymptoms in adolescents, it may have been useful toinclude an assessment of parental control behaviors.Parental control behaviors have been linked with thedevelopment of anxiety symptoms in particular (e.g. Rapee1997; Siqueland et al. 1996), and so including suchvariables in the models may have increased the predictivepower. At the time of data coding, the LIFE system did not
have codes that reflected this dimension of parentingbehavior. It is recommended that future research assess thepositive, negative and control dimensions of parentalbehavior in the prediction of internalizing symptoms inadolescents.
There were also important methodological strengths ofthis study. Firstly we used a longitudinal design in order tomore convincingly investigate the directionality of influ-ence than can be obtained using cross-sectional designs,and secondly, a multi-method approach to measurementwas utilized, reducing the possibility of making Type Ierrors due to shared method variance effects. Both thesedesign features enable the findings regarding the prospec-tive influence of parental behaviors on adolescent internal-izing symptom outcomes to be interpreted as plausiblyetiological in nature. Though it is not possible to inferdefinitive causal relationships on the basis of this type ofresearch design, as other unmeasured variables or relation-ships may have accounted for the findings, the design ofthis research allows for greater confidence in the signifi-cance of the findings. This study also recruited a relativelylarge sample of adolescents representing a broad range ofrisk for the development of psychopathology.
In conclusion, the results of this study suggest thatparental aggressive behaviors may place adolescents atincreased risk of developing symptoms of both depressionand anxiety, whereas parental positive behaviors mayprotect against the development of depression symptomsin adolescence. Clinically, these findings suggest a role forpreventive family interventions targeting parents’ aggres-sive and positive behaviors in reducing the increase ininternalizing symptoms commonly seen in adolescence.
References
Angold, A., Costello, E. J., Farmer, E. M. Z., Burns, B. J., & Erkanli,A. (1999). Impaired but undiagnosed. Journal of the AmericanAcademy of Child and Adolescent Psychiatry, 38, 129–137.
Australian Bureau of Statistics. (2008). SEIFA: Socio-EconomicIndexes for Areas. Retrieved 25/08/2010, from http://www.abs.gov.au/websitedbs/D3310114.nsf/home/Seifa_entry_page
Bayer, J. K., Sanson, A. V., & Hemphill, S. A. (2006). Parentinfluences on early childhood internalizing difficulties. Journal ofApplied Developmental Psychology, 27, 542–559.
Beck, A. T., Epstein, N., Brown, G., & Steer, R. A. (1988). Aninventory for measurment clinical anxiety: psychometric proper-ties. Journal of Consulting and Clinical Psychology, 56, 893–897.
Blatt, S. J., & Homann, E. (1992). Parent-child interaction in theetiology of dependent and self-critical depression. ClinicalPsychology Review, 12, 47–92.
Burge, D., & Hammen, C. (1991). Maternal communication:Predictors of outcome at follow-up in a sample of children athigh and low risk for depression. Journal of AbnormalPsychology, 100(2), 174–180.
J Abnorm Child Psychol (2012) 40:59–71 69
Campos, J. J., Mumme, D. L., Kermoian, R., & Campos, R. G.(1994). A functionalist perspective on the nature of emotion.Monographs of the Society for Research in Child Development,59(2/3), 284–303.
Duchesne, S., Larose, S., Vitaro, F., & Tremblay, R. (2010).Trajectories of anxiety in a population sample of children:clarifying the role of children’s behavioral characteristics andmaternal parenting. Development and Psychopathology, 22, 361–373.
Eisenberg, N., Cumberland, A., & Spinrad, T. L. (1998). Parentalsocialization of emotion. Psychological Inquiry, 9(4), 241–273.
Ellis, L. K., & Rothbart, M. K. (2001). Revision of the Early AdolescentTemperament Questionnaire. Paper presented at the BiennialMeeting of the Society for Research in Child Development,Minneapolis, Minnesota.
Gar, N. S., & Hudson, J. L. (2008). An examination of the interactionsbetween mothers and children with anxiety disorders. BehaviourResearch and Therapy, 46, 1266–1274.
Gilboa, E., & Revelle, W. (1994). Personality and the structure ofaffective responses. In S. H. M. Van Goozen, N. E. Van de Poll, &J. A. Sergeant (Eds.), Emotions: Essays on emotion theory.Hillsdale: Erlbaum.
Gillham, J. E., Shatté, A. J., & Freres, D. R. (2000). Preventingdepression: a review of cognitive-behavioral and family inter-ventions. Applied & Preventive Psychology, 9, 63–88.
Ginsburg, G. S., Siqueland, L., Masia-Warner, C., & Hedtke, K. A.(2004). Anxiety disorders in chidlren: family matters. Cognitiveand Behavioral Practice, 11, 28–43.
Hops, H., Biglan, A., Tolman, A., Arthur, J., & Longoria, N. (1995).LIFE: Living in family environments coding system manual.Eugene: Oregon Research Institute.
Hops, H., Davis, B., & Longoria, N. (1995). Methodological issues indirect observation: illustration with the Living in FamilialEnvironments (LIFE) coding system. Journal of Clinical ChildPsychology, 24, 193–203.
Horowitz, J. L., & Garber, J. (2006). The prevention of depressivesymptoms in children and adolescents: a meta-analytic review.Journal of Consulting and Clinical Psychology, 74, 401–415.
Hudson, J. L., & Rapee, R. M. (2001). Parent-child interactions andanxiety disroders: an observational study. Behaviour Researchand Therapy, 39, 1411–1427.
Jacobvitz, D., Hazen, N., Curran, M., & Hitchens, K. (2004).Observations of early triadic family interactions: boundarydisturbances in the family predict symptoms of depression,anxiety and attention-deficit/hyperactivity disorder in middlechildhood. Development and Psychopathology, 16, 577–592.
Katz, L. F., & Hunter, E. C. (2007). Maternal meta-emotionphilosophy and adolescent depressive symptomatology. SocialDevelopment, 16, 343–360.
Kaufman, J., Birmaher, B., Brent, D., Rao, U., Flynn, C., Moreci, P., etal. (1997). Schedule for affective disorders and schizophrenia forschool-age children-present and lifetime version (K-SADS-PL):Initial reliability and validity data. Journal of the AmericanAcademy of Child and Adolescent Psychiatry, 36(7), 980–988.
Keltner, D., & Kring, A. M. (1998). Emotion, social function, andpsychopathology. Review of General Psychology, 2, 320–342.
Klein, D. N., Shankman, S. A., Lewinsohn, P. M., & Seeley, J. R. (2009).Subthreshold depressive disorder in adolescents: predictors ofescalation to full-syndrome depressive disorders. Journal of theAmerican Academy of Child & Adolescent Psychiatry, 48, 703–710.
Lieb, R., Wittchen, H.-U., Hofler, M., Fuetsch, M., Stein, M. B., &Merikangas, K. R. (2000). Parental psychopathology, parentingstyles, and the risk of social phobia in offspring. Archives ofGeneral Psychiatry, 57, 859–866.
MacPhillamy, D. J., & Lewinsohn, P. M. (1976). Manual for thepleasant events schedule. Eugene: University of Oregon.
Masten, A. S. (2004). Regulatory processes, risk and resilience inadolescent development. Annals of the New York Academy ofSciences, 1021, 310–319.
Mathijssen, J. J. J. P., Koot, H. M., Verhulst, F. C., De Bruyn, E. E. J., &Oud, J. H. L. (1998). The relationship between mutual familyrelations and child psychopathology. Journal of Child Psychologyand Psychiatry, 39, 477–487.
McLeod, B. D., Wood, J. J., & Weisz, J. R. (2007). Examining theassociation between parenting and childhood anxiety: a meta-analysis. Clinical Psychology Review, 27, 155–175.
Messer, S. C., & Gross, A. M. (1995). Childhood depression andfamily interaction: a naturalistic observation study. Journal ofClinical Child Psychology, 24, 77–88.
Morris, A. S., Robinson, L. R., & Eisenberg, N. (2006). Applying amultimethod perspective to the study of developmental psychology.In M. Eid & E. Diener (Eds.), Handbook of multimethodmeasurement in psychology (pp. 371–384). Washington: AmericanPsychological Association.
Morris, A. S., Silk, J. S., Steinberg, L., Myers, S. S., & Robinson, L.R. (2007). The role of family context in the development ofemotion regulation. Social Development, 16, 361–388.
Muris, P., & Meesters, C. (2009). Reactive and regulative temperamentin youths: psychometric evaluation of the early adolescenttemperament questionnaire-revised. Journal of Psychopathologyand Behavioral Assessment, 31, 7–19.
Muthén, L. K., & Muthén, B. O. (1998–2007). Mplus user’s guide(Fifth ed.). Los Angeles, CA: Muthén & Muthén.
Muthén, L. K., & Muthén, B. O. (2007). Mplus (Version 5.1). LosAngeles, California: Muthén & Muthén.
Osman, A., Hoffman, J. P., Barrios, F. X., Kopper, B. A., Breitenstein,J. L., & Hahn, S. K. (2002). Factor structure, reliability, andvalidity of the Beck anxiety inventory in adolescent psychiatricinpatients. Journal of Clinical Psychology, 58, 443–456.
Paternoster, R., Brame, R., Mazerolle, P., & Piquero, A. (1998). Using thecorrect statistical test for the equality of regression coefficients.Criminology, 36, 859–866.
Pine, D. S., Cohen, E. C., Cohen, P., & Brook, J. (1999). Adolescentdepressive symptoms as predictors of adult depression: moodi-ness or mood disorder? American Journal of Psychiatry, 156,133–135.
Prange, M. E., Greengaum, P. E., Silver, S. E., Friedman, R. M., Kutash,K., & Duchnowski, A. J. (1992). Family functioning and psycho-pathology among adolescents with severe emotional disturbances.Journal of Abnormal Child Psychology, 20, 83–102.
Price, J., Sloman, L., Gardner, R., Gilbert, P., & Rohde, P. (1994). Thesocial competition hypothesis of depression. British Journal ofPsychiatry, 164, 309–315.
Prinz, R. J., Foster, S. L., Kent, R. N., & O'Leary, K. D. (1979).Multivariate assessment of conflict in distressed and nondis-tressed mother-adolescent dyads. Journal of Applied BehaviorAnalysis, 12, 691–700.
Radloff, L. S. (1977). The CES-D scale: a self-report depression scalefor research in the general population. Applied PsychologicalMeasurement, 1, 385–401.
Radloff, L. S. (1991). The use of the centre for epidemiologic studiesdepression scale in adolescents and young adults. Journal ofYouth and Adolescence, 20, 149–166.
Rapee, R. M. (1997). Potential role of childrearing practices in thedevelopment of anxiety and depression. Clinical PsychologyReview, 17, 47–67.
Rapee, R. M. (2009). Early adolescents' perceptions of their mother’sanxious parenting as a predictor of anxiety symptoms 12 monthslater. Journal of Abnormal Child Psychology, 37, 1103–1112.
Rodriguez, C. M. (2003). Parental discipline and abuse potentialaffects on child depression, anxiety and attributions. Journal ofMarriage and Family, 65, 809–817.
70 J Abnorm Child Psychol (2012) 40:59–71

Rubin, K. H., Burgess, K. B., & Hastings, P. D. (2002). Stability andsocial-behavioral consequences of toddlers' inhibited temperamentand parenting behaviors. Child Development, 73, 483–495.
Sheeber, L., Davis, B., Leve, C., Hops, H., & Tildesley, E. (2007).Adolescents’ relationships with their mothers and fathers:associations with depressive disorder and subdiagnostic symp-tomatology. Journal of Abnormal Psychology, 116, 114–154.
Sheeber, L., Hops, H., Alpert, A., Davis, B., & Andrews, J. (1997).Family support and conflict: prospective relations to adolescentdepression. Journal of Abnormal Child Psychology, 25, 333–344.
Sheeber, L., & Sorensen, E. (1998). Family relationships of depressedadolescents: a multimethod assessment. Journal of Clinical ChildPsychology, 27, 268–277.
Shochet, I. M., Dadds, M. R., Holland, D., Whitefield, K., Harnett, P.H., & Osgarby, S. M. (2001). The efficacy of a universal school-based program to prevent adolescent depression. Journal ofClinical Child Psychology, 30, 303–315.
Siqueland, L., Kendall, P. C., & Steinberg, L. (1996). Anxiety inchildren: perceived family environments and observed familyinteraction. Journal of Clinical Child Psychology, 25, 225–237.
Slesnick, N., & Waldron, H. B. (1997). Interpersonal problem-solvinginteractions of depressed adolescents and their parents. Journal ofFamily Psychology, 11, 234–245.
SPSS Inc. (2007). SPSS for Windows (Version 16.0.2).Stark, K. D., Humphrey, L. L., Crook, K., & Lewis, K. (1990).
Perceived family environments of depressed and anxious
children: child’s and maternal figure's perspectives. Journal ofAbnormal Child Psychology, 18, 527–547.
Steinberg, L., & Morris, A. S. (2001). Adolescent development.Annual Review of Psychology, 52, 83–110.
Suveg, C., Sood, E., Barmish, A., Tiwari, S., Hudson, L., & Kendall,P. C. (2008). “I’d rather not talk about it”: emotion parenting infamilies of children with an anxiety disorder. Journal of FamilyPsychology, 22, 875–884.
Twenge, J. M., & Nolen-Hoeksema, S. (2002). Age, gender, race,socioeconomic status, and birth cohort differences on the child-ren’s depression inventory: a meta-analysis. Journal of AbnormalPsychology, 111, 578–588.
Volbrecht, M. V., & Hill Goldsmith, H. (2010). Early temperamentaland family predictors of shyness and anxiety. DevelopmentalPsychology, 46, 1192–1205.
Whaley, S. E., Pinto, A., & Sigman, M. (1999). Characterizinginteractions between anxious mothers and their children. Journalof Consulting and Clinical Psychology, 67, 826–836.
Yap, M. B. H., Schwartz, O. S., Byrne, M. L., Simmons, J. G., &Allen, N. B. (2010). Maternal positive and negative interactionbehaviors and early adolescents' depressive symptoms: adoles-cent emotion regulation as a mediator. Journal of Research onAdolescence, 20, 1014–1043.
Zeman, J., Klimes-Dougan, B., Cassano, M., & Adrian, M. (2007).Measurement issues in emotion research with children and adoles-cents. Clinical Psychology: Science and Practice, 14, 377–401.
J Abnorm Child Psychol (2012) 40:59–71 71
Related Documents