Paraproteinemic Maculopathy Ahmad M. Mansour, MD, 1 J. Fernando Arevalo, MD, 2 Josep Badal, MD, 3 Ramana S. Moorthy, MD, 4 Gaurav K. Shah, MD, 6 Hernando Zegarra, MD, 5 Jose S. Pulido, MD, 7 Abdulrazzak Charbaji, PhD, 8 Luis Amselem, MD, 3 Alejandro Jose Lavaque, MD, 9 Antonio Casella, MD, 10 Baseer Ahmad, MD, 6 Joshua G. Paschall, MD, 4 Antonio Caimi, MD, 11 Giovanni Staurenghi, MD 11 Purpose: Paraproteinemia relates to monoclonal gammopathy-producing pathologic antibodies with serous macular detachment being an uncommon ocular manifestation. We ascertained the clinical course of maculopathy in paraproteinemia and investigated the effect of various therapeutic methods on the resolution of subretinal deposits. Design: Multicenter, retrospective, observational case series. Participants: The records of patients with paraproteinemia with optical coherence tomography (OCT) documentation of serous macular detachment were reviewed. Methods: Data collection included coexisting morbidity, rheology data (immunoglobulin level, hematocrit, and blood viscosity), clinical examination results, and OCT findings. Main Outcome Measures: Best-corrected visual acuity (BCVA), height and basal area of the serous macular detachment, and systemic versus local therapies. Results: A total of 33 cases were collected: 10 new and 23 previously reported in the literature. Diabetes was present in 7 patients, systemic hypertension in 9 patients, and anemia in 18. Mean initial immunoglobulin level was 6497 mg/dl, and mean serum viscosity was 5.5 centipoise (cP). Mean logarithm of the minimum angle of resolution initial vs. final BCVA was 0.55 (Snellen equivalent, 20/71) vs. 0.45 (20/56) in the right eye and 0.38 (20/48) vs. 0.50 (20/63) in the left eye. After mean follow-up of 7 months (range, 0-51 months). Systemic therapies included plasmapheresis (18), chemotherapy (30), blood transfusions (2), transplantation of progenitor hemato- poietic cells (2), and oral rituximab (10). Immunoglobulin levels normalized in 8 patients and were unchanged in 1 after plasmapheresis, chemotherapy, or both. Ocular therapy in 8 patients included vitrectomy (1), laser photo- coagulation (4), intravitreal bevacizumab (5), intravitreal triamcinolone (2), intravitreal dexamethasone implant (1), intravitreal rituximab (1), and sub-Tenon corticosteroid (1). The maculopathy resolved partially or completely in 17 patients and worsened or remained unchanged in 14 patients over median follow-up of 7 months. Maculopathy was unilateral in 9 cases and occurred at a lower initial immunoglobulin level in diabetics. There was a positive correlation between area of the detachment and serum viscosity. Conclusions: Paraproteinemic maculopathy can be unilateral. Decreasing the blood immunoglobulin level is the primary goal of therapy for paraproteinemic maculopathy, and this can be achieved by a systemic route. Coexisting diabetes facilitates leakage of immunoglobulins at lower levels than in nondiabetics. Ophthalmology 2014;- :1e8 ª 2014 by the American Academy of Ophthalmology. Supplemental material is available at www.aaojournal.org. Paraproteinemia, or monoclonal gammopathy, is the presence of excessive amounts of a single monoclonal g-globulin (or paraprotein) in the blood. Monoclonal paraproteins are detected in the sera of 1% of the general population. 1 This is usually the result of an underlying immunoproliferative disorder that includes multiple myeloma (MM), immu- nocytoma, and Waldenström macroglobulinemia (WM). Waldenström macroglobulinemia is a non-Hodgkin’s B-cell lymphoplasmacytic lymphoma affecting 3.8 per 1 million people annually, approximately 2% of all hematologic malignancies, and involving the elderly with onset around 63 years of age. This monoclonal immunoglobulin M (IgM) paraproteinemia is characterized clinically by signs and symptoms of serum hyperviscosity and hemorrhagic tendency. Ocular manifestations of WM include venous stasis retinopathy, immunoprotein deposition in the cornea and pars plana, and IgM deposits in all layers of the retina. A rare peculiar serous macular detachment in paraproteinemia has been described. 2e10 Herein, we review our case series and the literature to attempt to understand the causative factors involved in this maculopathy. Methods The institutional review board approved the retrospective analysis of data for this observational case series. The records of patients with paraproteinemia and macular pathologic features were reviewed. The following data were collected: Snellen best- corrected visual acuity (BCVA; translated into logarithm of the minimum angle of resolution [logMAR] units), immunoglobulin 1 Ó 2014 by the American Academy of Ophthalmology ISSN 0161-6420/14/$ - see front matter Published by Elsevier Inc. http://dx.doi.org/10.1016/j.ophtha.2014.04.007

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Paraproteinemic Maculopathy
Ahmad M Mansour MD1 J Fernando Arevalo MD2 Josep Badal MD3 Ramana S Moorthy MD4
Gaurav K Shah MD6 Hernando Zegarra MD5 Jose S Pulido MD7 Abdulrazzak Charbaji PhD8
Luis Amselem MD3 Alejandro Jose Lavaque MD9 Antonio Casella MD10 Baseer Ahmad MD6
Joshua G Paschall MD4 Antonio Caimi MD11 Giovanni Staurenghi MD11
Purpose Paraproteinemia relates to monoclonal gammopathy-producing pathologic antibodies withserous macular detachment being an uncommon ocular manifestation We ascertained the clinical course ofmaculopathy in paraproteinemia and investigated the effect of various therapeutic methods on the resolution ofsubretinal deposits
Design Multicenter retrospective observational case seriesParticipants The records of patients with paraproteinemia with optical coherence tomography (OCT)
documentation of serous macular detachment were reviewedMethods Data collection included coexisting morbidity rheology data (immunoglobulin level hematocrit
and blood viscosity) clinical examination results and OCT findingsMain Outcome Measures Best-corrected visual acuity (BCVA) height and basal area of the serous macular
detachment and systemic versus local therapiesResults A total of 33 cases were collected 10 new and 23 previously reported in the literature Diabetes was
present in 7 patients systemic hypertension in 9 patients and anemia in 18 Mean initial immunoglobulin levelwas 6497 mgdl and mean serum viscosity was 55 centipoise (cP) Mean logarithm of the minimum angle ofresolution initial vs final BCVA was 055 (Snellen equivalent 2071) vs 045 (2056) in the right eye and 038(2048) vs 050 (2063) in the left eye After mean follow-up of 7 months (range 0-51 months) Systemic therapiesincluded plasmapheresis (18) chemotherapy (30) blood transfusions (2) transplantation of progenitor hemato-poietic cells (2) and oral rituximab (10) Immunoglobulin levels normalized in 8 patients and were unchanged in 1after plasmapheresis chemotherapy or both Ocular therapy in 8 patients included vitrectomy (1) laser photo-coagulation (4) intravitreal bevacizumab (5) intravitreal triamcinolone (2) intravitreal dexamethasone implant (1)intravitreal rituximab (1) and sub-Tenon corticosteroid (1) The maculopathy resolved partially or completely in 17patients and worsened or remained unchanged in 14 patients over median follow-up of 7 months Maculopathywas unilateral in 9 cases and occurred at a lower initial immunoglobulin level in diabetics There was a positivecorrelation between area of the detachment and serum viscosity
Conclusions Paraproteinemicmaculopathy can be unilateral Decreasing the blood immunoglobulin level is theprimary goal of therapy for paraproteinemic maculopathy and this can be achieved by a systemic route Coexistingdiabetes facilitates leakage of immunoglobulins at lower levels than in nondiabetics Ophthalmology 2014-1e8 ordf 2014 by the American Academy of Ophthalmology
Supplemental material is available at wwwaaojournalorg
Paraproteinemia or monoclonal gammopathy is the presenceof excessive amounts of a single monoclonal g-globulin (orparaprotein) in the blood Monoclonal paraproteins aredetected in the sera of 1 of the general population1 This isusually the result of an underlying immunoproliferativedisorder that includes multiple myeloma (MM) immu-nocytoma and Waldenstroumlm macroglobulinemia (WM)Waldenstroumlm macroglobulinemia is a non-Hodgkinrsquos B-celllymphoplasmacytic lymphoma affecting 38 per 1 millionpeople annually approximately 2 of all hematologicmalignancies and involving the elderly with onset around63 years of age This monoclonal immunoglobulin M(IgM) paraproteinemia is characterized clinically by signsand symptoms of serum hyperviscosity and hemorrhagictendency Ocular manifestations of WM include venous
2014 by the American Academy of OphthalmologyPublished by Elsevier Inc
stasis retinopathy immunoprotein deposition in the corneaand pars plana and IgM deposits in all layers of theretina A rare peculiar serous macular detachment inparaproteinemia has been described2e10 Herein we reviewour case series and the literature to attempt to understand thecausative factors involved in this maculopathy
Methods
The institutional review board approved the retrospective analysisof data for this observational case series The records of patientswith paraproteinemia and macular pathologic features werereviewed The following data were collected Snellen best-corrected visual acuity (BCVA translated into logarithm of theminimum angle of resolution [logMAR] units) immunoglobulin
1ISSN 0161-642014$ - see front matterhttpdxdoiorg101016jophtha201404007
Ophthalmology Volume - Number - Month 2014
level hematocrit blood viscosity associated systemic and ocularcomorbidities and treatment methods and their effects as assessedon optical coherence tomography (OCT) Therapies includedvarious combinations of plasmapheresis (plasma exchange)chemotherapy intravitreal bevacizumab (off label) triamcinoloneor rituximab (off label) and laser photocoagulation after informedconsent was obtained
We also collected from the literature cases of paraproteinemicmaculopathy using Scopus Google Scholar and Medline searchesthrough October 2013 searching for macula AND MM WM andparaproteinemia including polyneuropathy organomegaly endo-crinopathy M-protein and skin abnormalities syndrome and light-chain deposition disease Hypertension is defined as a systolicblood pressure of 140 mmHg or more or a diastolic blood pressureof 90 mmHg or more Anemia is defined as hematocrit of less than40 for males and less than 35 for females Correlation wascarried out using correlation coefficient-adjusted r2 1-way analysisof variance and standardized b regression coefficients using SPSSStatistics for Windows version 210 (IBM Corp Armonk NY)Area of the maculopathy and height were measured on fundusphotography (reference being vertical disc diameter [DD]) andOCT (caliper tool in older machines with no calipers the macularretinal thickness was assumed at 300 mm) respectively The hor-izontal and vertical diameters of the sensory detachment weremeasured and the longest of the 2 measurements was taken as thearea Similarly on OCT the height of the sensory detachment wasmeasured on the vertical and horizontal scans through the foveolaand the largest value was adopted for the height
Results
The current retrospective series included 10 subjects (Table 1available at wwwaaojournalorg) comprising 7 men and 3 women
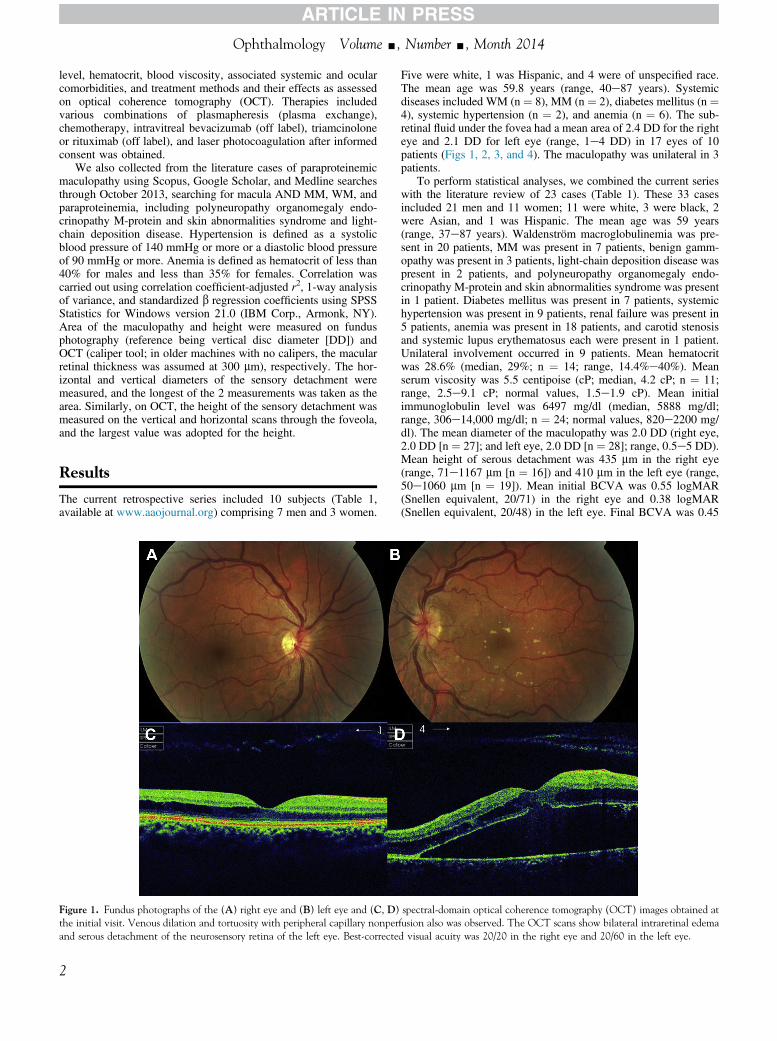
Figure 1 Fundus photographs of the (A) right eye and (B) left eye and (C D)the initial visit Venous dilation and tortuosity with peripheral capillary nonperand serous detachment of the neurosensory retina of the left eye Best-correcte
2
Five were white 1 was Hispanic and 4 were of unspecified raceThe mean age was 598 years (range 40e87 years) Systemicdiseases included WM (n frac14 8) MM (n frac14 2) diabetes mellitus (n frac144) systemic hypertension (n frac14 2) and anemia (n frac14 6) The sub-retinal fluid under the fovea had a mean area of 24 DD for the righteye and 21 DD for left eye (range 1e4 DD) in 17 eyes of 10patients (Figs 1 2 3 and 4) The maculopathy was unilateral in 3patients
To perform statistical analyses we combined the current serieswith the literature review of 23 cases (Table 1) These 33 casesincluded 21 men and 11 women 11 were white 3 were black 2were Asian and 1 was Hispanic The mean age was 59 years(range 37e87 years) Waldenstroumlm macroglobulinemia was pre-sent in 20 patients MM was present in 7 patients benign gamm-opathy was present in 3 patients light-chain deposition disease waspresent in 2 patients and polyneuropathy organomegaly endo-crinopathy M-protein and skin abnormalities syndrome was presentin 1 patient Diabetes mellitus was present in 7 patients systemichypertension was present in 9 patients renal failure was present in5 patients anemia was present in 18 patients and carotid stenosisand systemic lupus erythematosus each were present in 1 patientUnilateral involvement occurred in 9 patients Mean hematocritwas 286 (median 29 n frac14 14 range 144e40) Meanserum viscosity was 55 centipoise (cP median 42 cP n frac14 11range 25e91 cP normal values 15e19 cP) Mean initialimmunoglobulin level was 6497 mgdl (median 5888 mgdlrange 306e14000 mgdl n frac14 24 normal values 820e2200 mgdl) The mean diameter of the maculopathy was 20 DD (right eye20 DD [n frac14 27] and left eye 20 DD [n frac14 28] range 05e5 DD)Mean height of serous detachment was 435 mm in the right eye(range 71e1167 mm [n frac14 16]) and 410 mm in the left eye (range50e1060 mm [n frac14 19]) Mean initial BCVA was 055 logMAR(Snellen equivalent 2071) in the right eye and 038 logMAR(Snellen equivalent 2048) in the left eye Final BCVA was 045
spectral-domain optical coherence tomography (OCT) images obtained atfusion also was observed The OCT scans show bilateral intraretinal edemad visual acuity was 2020 in the right eye and 2060 in the left eye
Figure 3 After 3 monthly 25-mg01-ml bevacizumab injections (A B) fundus photographs and (C D) spectral-domain optical coherence tomography(SD OCT) images showed a mild reduction of both intraretinal and subretinal fluid in both eyes The SD OCT images show refractory edema Best-correctedvisual acuity remained 2060 in the right eye and 20200 in the left eye The SD OCT image from the right eye (C) shows unique stalactite-like projectionsof the outer retina
Figure 2 After 6 weeks (A C) serous macular detachment with overlying cystoid macular edema was observed in the right eye and (B D) an increase inthe subretinal fluid was observed in the left eye Best-corrected visual acuity dropped to 2060 in the right eye and 20200 in the left eye
Mansour et al Paraproteinemic Maculopathy
3
Figure 4 Schematic diagram showing the pathogenesis of paraproteinemic maculopathy BM frac14 Bruchrsquos membrane CC frac14 choriocapillaris IgM frac14immunoglobulin M RPE frac14 retinal pigment epithelium
Ophthalmology Volume - Number - Month 2014
logMAR (Snellen equivalent 2056) in the right eye and 050logMAR (Snellen equivalent 2063) in the left eye (Table 1)
Regarding therapy for the 33 patients plasmapheresis wasadministered in 18 patients chemotherapy was administered in30 patients blood transfusions were administered in 2 patientsand transplant of progenitor hematopoietic cells was performedin 2 patients Oral rituximab was used in 10 patients Immuno-globulin levels normalized in 8 patients and were unchanged in 1patient after plasmapheresis chemotherapy or both Ocular ther-apy in 8 patients included vitrectomy in 1 patient laser photoco-agulation in 4 patients intravitreal bevacizumab in 5 patients(Fig 3) intravitreal triamcinolone in 2 patients intravitrealdexamethasone implant in 1 patient intravitreal rituximab in 1patient (Fig 3) and sub-Tenon corticosteroid in 1 patient (Ta-ble 1) The maculopathy resolved partially or completely in 17patients and worsened or stayed unchanged in 14 patients over amedian follow-up of 7 months (mean 19 months 2 patients had nofollow-up) Immunoglobulins were unchanged in 1 patient andlikewise for maculopathy after therapy in 1 case Immunoglobulindecreased markedly but maculopathy did not improve in 3 pa-tients Immunoglobulin decreased and maculopathy improved in 5patients
There was a strong positive correlation between level ofimmunoglobulin and serum viscosity (P frac14 0007) No correlationwas present between level of immunoglobulin and hematocritdiabetes (P frac14 010) initial BCVA area (P frac14 033 for the right eyeand P frac14 034 for the left eye) and height of the macular detach-ment There was no correlation between area of the detachment andpresence of diabetes age or initial BCVA There was a positivecorrelation between area of the detachment and serum viscosity(P frac14 0017 for the right eye and P frac14 0022 for the left eye) Therewas no correlation between initial BCVA and height or area of themacular detachment Visual gain correlated with initial BCVA
4
(P frac14 0001 for the right eye and P frac14 0021 for the left eye) and didnot correlate with immunoglobulin level serum viscosity hemat-ocrit age diabetes or area or height of the detachment Diabeticsversus nondiabetics had the following mean values age 670versus 567 years (P frac14 004) immunoglobulin level of 4115versus 7306 mgdl (P frac14 010 normal values 820e2200 mgdl)area of macular detachment 22 versus 20 DD in the right eye(P frac14 043) and 183 versus 198 DD in the left eye (P frac14 040) andhematocrit 286 versus 288 (P frac14 050) Additional causesof leakage into the subretinal space included (1) disc edema in1 patient (patient 32) (2) severe ischemic diabetic retinopathy in 1patient (patient 10) (3) occlusive choroidal and retinal disease in 1patient (hence failure of the retinal pigment epithelium [RPE]pump patient 4) and (4) deep retinal leakage sites in 2 patients (2sites in patient 8 and 1 site in patient 6) possibly related to outerretinal defects as seen in patient 9 Of note is a peculiar finding ofstalactite-like projections in the outer retina in macula of patient 9(see ldquoCase Reportrdquo Fig 3C)
Case Report
A 47-year-old white man with no significant medical history wasreferred to our clinic for blurry vision in the left eye BaselineBCVA was 2020 in the right eye and 2060 in the left eye Slit-lamp biomicroscopy results were unremarkable and intraocularpressure was 12 mmHg in the right eye and 14 mmHg in the lefteye Fundus examination showed mild venous dilation and tortu-osity in both eyes and a serous macular detachment with yellowsubretinal exudates in the left eye (Fig 1) Optical coherencetomography revealed bilateral cystoid macular edema anddetachment of the neurosensory retina Fluorescein angiographyshowed peripheral vaso-occlusive disease with significant capil-lary nonperfusion Six weeks after initial presentation BCVA
Mansour et al Paraproteinemic Maculopathy
decreased to 2060 in the right eye and 20200 in the left eye andOCT showed neurosensory detachment with overlying cystoidmacular edema and bilateral disruption of the outer retina (Fig 2)The patientrsquos blood pressure was 13090 mmHg Hyperviscositysyndrome was suspected and blood tests revealed severe anemia(hemoglobin 79 mgdl normal values 135e175 mgdl) and atotal serum protein level of 192 mgdl (normal values 60e80mgdl) with elevated monoclonal IgM of 10 500 mgdl (normalvalues 45e153 mgdl) Bone marrow biopsy showed massivelymphoplasmacytoid infiltration A diagnosis of WM wasmade Computed tomography of the abdomen showed multipleretroperitoneal lymphadenopathies (iliac and inguinal) Plasma-pheresis was performed followed by 8 cycles of systemicpolychemotherapy with rituximab cyclophosphamide doxoru-bicin vincristine and steroids and 2 cycles of cladribineSystemic rituximab was not given until IgM levels decreased toless than 50 mgdl because rituximab is associated with suddenincrease in IgM levels and should be avoided in patients withhyperviscosity Simultaneously 3 monthly 25-mg01-ml intra-vitreal bevacizumab injections were administered in both eyesBest-corrected visual acuity remained 2060 in the right eye and20200 in the left eye and OCT demonstrated a slight bilateraldecrease in neurosensory detachment (Fig 3) At that time the IgMlevel dropped to 3925 mgdl Two months after the last intravitrealbevacizumab injection 3 monthly intravitreal injections ofrituximab (1 mg01 ml) were administered in both eyes Best-corrected visual acuity remained unchanged and OCT demon-strated a slight bilateral decrease in the amount of subretinal fluid(Fig 3) At that time the IgM level dropped to 2943 mgdl After 2years of follow-up complete remission was not reached BCVAwas 2060 in the right eye and 20400 in the left eye and OCTshowed no significant improvement
Discussion
Serous macular detachment is an uncommon ocular mani-festation of paraproteinemia2e27 The absence of angio-graphic leakage within the macular detachment does notsupport the theory of angiographic exudation from the retinalor choroidal vasculature In a few cases there was leakage inthe deep retina (Table 1) Some investigators have focused onthe presence of IgM in the subretinal space1112 suggestingthat an increased osmotic gradient causes fluid accumulationunder the retina In support of this hypothesis several his-topathologic reports documented immunoglobulins in thesubretinal space11e13 High-molecular-weight immunoglob-ulins lead to an osmotic gradient Because IgM antibodies arethe largest antibodies found in the blood and the lymph fluidthey rarely accumulate in pericardial peritoneal and pleuraleffusions2829 Immunoglobulin M antibodies consist of aheavy chain a light chain and 5 base units with a molecularmass of 970 kDa in its pentamer form (molecular weight06e1 000 000 kDa) Because IgM antibodies are very largemolecules and cannot diffuse well they are found in theinterstitium in extremely low quantities When such largepositively charged IgM molecules are present in excess theybind electrostatically to red cells aggregating and formingrouleaux with subsequent increase in the blood viscosity Asthe IgM protein concentration in the serum increases theblood viscosity increases exponentially It is somewhatintriguing to explain how IgM antibodies reach the subretinalspace (Fig 4) According to Klaassen et al30 the central
mechanism of the altered blooderetinal barrier results fromthe altered permeability of retinal endothelial cells causedby elevated levels of growth factors (such as vascularendothelial growth factor) cytokines and loss of pericytes(as occurs in diabetes) Subsequently both paracellular andtranscellular transport across the retinal vascular wall increasevia opening of the endothelial intercellular junctions andincrease in endothelial caveolar transcellular transport Thereis histologic evidence that the bloodeneural barrier (which issimilar to the blooderetinal barrier) is affected inparaproteinemia Kanda et al31 reported the pathologicfindings in a patient with sensorimotor neuropathy associatedwith WM and monoclonal IgM particularly in relation tobloodenerve barrier defects A sural nerve biopsy specimenrevealed gaps between adjacent endothelial cells of smallendoneurial vessels as well as the absence of some of thetight junctions between adjacent endothelial cells Similarlyin a sural nerve biopsy from a patient with benignmonoclonal IgM k gammopathy and sensorimotor demyeli-native neuropathy Lash et al32 found that many endoneurialcapillaries were lined by fenestrated endothelium indicatingthe breakdown of the normal bloodenerve barrier Theendoneurium contained large amounts of extracellularproteinaceous material containing IgM k g-globulin
Brody et al10 suggested thatmacular exudative detachmentsfrom diabetic maculopathy can lead to increased leakage ofimmunoglobulins into the subretinal space In a case withpolyneuropathy organomegaly endocrinopathy M-proteinand skin abnormalities syndrome Okada et al3 proposed thatthe high vascular endothelial growth factor level probablyinduced the retinal microvascular hyperpermeability leadingto leakage of immunoglobulin in the subretinal space Themaculopathy resolved 1 month after hematopoietic surgerywhen serum vascular endothelial growth factor leveldecreased in response to autologous peripheral blood stemcells The sera of WM patients are known to be associatedwith increased levels of angiogenic cytokines such asangiogenin vascular endothelial growth factor and basicfibroblast growth factor33 In normal bone marrowangiopoietin-1 consistently activates tyrosine kinase withimmunoglobulin-like and epidermal growth factor-like do-mains-2 and stabilizes vessels by promoting interactionsbetween endothelial cells and surrounding pericytes Onthe contrary during the malignant process in WMincreased angiopoietin-2 levels block tyrosine kinase with theimmunoglobulin-like and epidermal growth factor-like do-mains-2 receptor and lead to vessel destabilization by loos-ening endothelialeperiendothelial cell interactions anddegrading the extracellular matrix The primary source ofangiopoietin-2 is endothelial cells because angiopoietin-2 isstored in vesicles known as Weibel-Palade bodies and isreleased rapidly in response to hyperglycemia and ischemiaAngiopoietin-2 seems to be an important mediator in thealteration of the blooderetinal barrier in diabetes and otherretinal vascular disorders30
Ashton34 aswell as Foos andAllen35were among the first todescribe retinal and RPE detachment histologically in patientswith MM The subpigment epithelial fluid is derived fromchoroidal vessels The platelets can no longer fulfill theirnormal function of maintenance of endothelium because they
5
Ophthalmology Volume - Number - Month 2014
become covered by paraprotein Moreover the hyperviscositycan cause stasis and hypoxia leading to endotheliumdecompensation There is secondary breakdown of theblooderetinal barrier in addition to the RPE decompensationfrom the underlying deposit and hypoxia Coexisting anemiadiabetes and hypertension are additional risk factors forretinal vascular endothelial damage and ischemic injuryenhancing leakage and breakdown of the blooderetinalbarrier Dumas et al36 explored the contribution of plasmaviscosity and the endothelial cell monolayer to oxygenmolecular transport processes using a fluorescence inhibitionmethod They found hypoxia induced by hyperviscosityplasmas from patients with WM to have increasedintercellular adhesion molecule 1 expression on the surface ofendothelial cells which could be the cause of vasculardisorders through the implication of polymorphonuclearneutrophils
Baker et al2 demonstrated complete disruption of theouter retina within the detachment and proposed that thesefocal outer retinal defects (Figs 2 and 3) slowly progressover time eventually allowing a so-called track for intra-retinal IgM Our study was not aimed at estimating thepresence of such outer retinal defects A pathologiccommunication between the optic disc the subarachnoidspace and the subretinal space was proposed by Feigl et al16
and Khan et al19 Feigl et al16 found a finger-like extensionto the optic disc from the macular detachment by indoc-yanine angiography and proposed the disc as the cause ofthe macular detachment similar to optic pit maculopathy
There is a lot of overlap between the pathogenesis ofcentral serous retinopathy (CSR) and paraproteinemic mac-ulopathy Unilaterality of the maculopathy is one commonfinding in paraproteinemia and CSR as found in the currentseries In CSR Pruumlnte and Flammer37 detected capillary orvenous congestion after ischemia in 1 or more choroidallobules and this finding may be the reason for choroidalhyperpermeability Nicholson et al38 documented thepresence of a thickened and engorged choroid in CSRby enhanced depth OCT and proposed that thesehyperpermeable choroidal vessels produce increased tissuehydrostatic pressure promoting the formation of RPEdetachments overwhelming the barrier function of theRPE and leading to fluid accumulation between the retinaand the RPE Optical coherence tomography also mayshow an anatomic defect (microrip) in the RPE associatedwith fluid that is leaking into the subretinal spaceLikewise there is venous congestion in the choroid andretina in paraproteinemia leading to choroidal ischemiaand hyperpermeability which leads to CSR (Fig 4) Zamirand Chowers39 reported a patient with paraproteinemia whohad CSR in the right eye and branch retinal vein occlusionin the left eye with normal maculae Although CSR couldbe the primary cause of the ocular condition one couldargue that paraproteinemia could have induced a CSR-likecondition as previously discussed
Early treatment is necessary to prevent irreversible visualloss especially with the currently lengthened expected lifespan Paraproteinemic maculopathy becomes symptomaticwhen IgM levels exceed 4000 mgdl in diabetics and 7000mgdl in nondiabetics (Table 1) and serum viscosity exceeds
6
55 cP Prompt referral to a hematologist or oncologist isnecessary for systemic monitoring and treatment The visualloss in paraproteinemic maculopathy may be similar to thevisual loss in CSR with proteinaceous subretinal fluid40
Landa et al40 found a correlation between the subfovealthickness of the protein deposit layer and visual acuity atbaseline in 38 patients with CSR No such relation wasfound in our series possibly because of the retrospectivenature of the study and the small size of the study group
Usually no treatment is indicated for asymptomatic dis-ease Indications for initiating treatment include bloodhyperviscosity and ocular disturbance The cardinal therapiesinclude plasmapheresis (for patients with symptomatichyperviscosity) rituximab (anti-CD20 antibody that isgenetically engineered human monoclonal antibody directedagainst the CD20 antigen found on the surface of normal andmalignant B lymphocytes) and chemotherapy (purinenucleoside analogs alkylating agents thalidomide and bor-tezomib) Plasmapheresis is very useful in reducing serumhyperviscosity and rapidly improving most ocular manifes-tations According to Menke et al41 plasmapheresis resultedin significant reductions in serum IgM (by 465) and serumviscosity (by 447) and venous stasis retinopathy improvedin all patients after plasmapheresis Paraproteinemia-relatedvenous stasis retinopathy mimics a central retinal veinocclusion-like appearance (no thrombus) with normal retinalblood flow In our review the area of the macular detachmentcorrelated with serum viscosity and many eyes did notdemonstrate resolution of the maculopathy despite improve-ment in both the serum viscosity and the venous stasis reti-nopathy One possible reason could be the short follow-upin the current review these immunoglobulins need a longtime to resolve42 Besides plasmapheresis chemotherapyespecially with rituximab remains the mainstay of therapyVarious intravitreal injections (bevacizumab triamcinolonerituximab43) failed to show a definite benefit in the currentseries
In conclusion this case series along with the literaturereview provide further evidence of the direct correlationbetween IgM levels in the blood and the degree of subretinalfluid accumulation under the fovea in these patients Clinicalimprovement clearly correlated with a decrease in serumIgM Maculopathy of paraproteinemia can mimic diabeticretinopathy adult vitelliform dystrophy and CSR espe-cially in the many patients with diabetes Unilateral local-ized macular detachment is noted commonly in patients withelevated serum IgM levels associated with WM Para-proteinemic maculopathy often becomes symptomatic whenIgM levels exceed 7000 mgdl (4000 mgdl in diabetics) andserum viscosity exceeds 55 cP Therapy should be directedtoward decreasing the serum immunoglobulin level and theserum viscosity
References
1 Saleun JP Vicariot M Deroff P Morin JF Monoclonalgammopathies in the adult population of Finistere FranceJ Clin Pathol 19823563ndash8
Mansour et al Paraproteinemic Maculopathy
2 Baker PS Garg SJ Fineman MS et al Serous maculardetachment in Waldenstroumlm macroglobulinemia a report offour cases Am J Ophthalmol 2013155448ndash55
3 Okada K Yamamoto S Tsuyama Y Mizunoya S Case ofPOEMS syndrome associated with bilateral macular detach-ment resolved by autologous peripheral blood stem celltransplantation [letter] Jpn J Ophthalmol 200751237ndash8
4 Pilon AF Rhee PS Messner LV Bilateral persistent serousmacular detachments with Waldenstroumlmrsquos macroglobulinemiaOptom Vis Sci 200582573ndash8
5 Ho AC Benson WE Wong J Unusual immunogammopathymaculopathy Ophthalmology 20001071099ndash103
6 Ogata N Ida H Takahashi K et al Occult retinal pigmentepithelial detachment in hyperviscosity syndrome OphthalmicSurg Lasers 200031248ndash52
7 Cohen SM Kokame GT Gass JD Paraproteinemias associ-ated with serous detachments of the retinal pigment epitheliumand neurosensory retina Retina 199616467ndash73
8 Spielberg LH Heckenlively JR Leys AM Retinal pigmentepithelial detachments and tears and progressive retinaldegeneration in light chain deposition disease Br J Oph-thalmol 201397627ndash31
9 Leys AM Vandenberghe P Serous macular detachments in apatient with IgM paraproteinemia an optical coherence to-mography study Arch Ophthalmol 2001119911ndash3
10 Brody JM Butrus SI Ashraf MF et al Multiple myelomapresenting with bilateral exudative macular detachments ActaOphthalmol Scand 19957381ndash2
11 Berta A Beck P Mikita J IgM paraprotein in the subretinal fluidof a patient with recurrent retinal detachment andWaldenstroumlmrsquosmacroglobulinaemia Acta Med Hung 198542179ndash86
12 Khouri GG Murphy RP Kuhajda FP Green WR Clinico-pathologic features in two cases of multiple myeloma Retina19866169ndash75
13 Freidman AH Marchevsky A Odel JG et al Immunofluo-rescent studies of the eye in Waldenstroumlmrsquos macroglobuli-nemia Arch Ophthalmol 198098743ndash6
14 Thomas EL Olk RJ Markman M et al Irreversible visual lossin Waldenstroumlmrsquos macroglobulinaemia Br J Ophthalmol198367102ndash6
15 Sen HN Chan C-C Caruso RC et al Waldenstroumlmrsquosmacroglobulinemia-associated retinopathy Ophthalmology2004111535ndash9
16 Feigl B Sill H Haas A Serous detection of the neuroretina inWaldenstroumlm disease A case report [in German] Klin MonblAugenheilkd 199921564ndash7
17 Bernard A Rousselie F Macular manifestations of mono-clonal dysgammaglobulinemias Apropos of 3 cases [inFrench] J Fr Ophtalmol 19869805ndash10
18 Quhill F Khan I Rashid A Bilateral serous macular de-tachments in Waldenstroumlmrsquos macroglobulinaemia PostgradMed J 200985382
19 Khan JM McBain V Santiago C Lois N Bilateral lsquovitelli-form-likersquo macular lesions in a patient with multiple myelomaBMJ Case Rep [serial online] 20102010 bcr0520103049Available at httpwwwncbinlmnihgovpmcarticlesPMC3028543 Accessed April 4 2014
20 Brolly A Janon C Precausta F et al Pseudovitelliform sub-foveal deposit in Waldenstroumlmrsquos macroglobulinemia CaseRep Ophthalmol [serial online] 20123236ndash9 Available athttpwwwkargercomArticleAbstract339988 AccessedApril 4 2014
21 Daicker BC Mihatsch MJ Stroslashm EH Fogazzi GB Ocularpathology in light chain deposition disease Eur J Ophthalmol1995575ndash81
22 Ardouin M Urvoy M Gastard J Aspect of the dysproteinemicfundus oculi (microaneurysms and retinal detachment) in acase of Waldenstromrsquos disease [in French] Bull Soc Ophtal-mol Fr 196666129ndash32
23 Lin CJ Chiu YM Chen SN et al Unusual maculopathysecondary to hypergammaglobulinemia in a patient with sys-temic lupus erythematosus Retin Cases Brief Rep 2012627ndash9
24 Besirli CG Johnson MW Immunogammopathy maculopathyassociated with Waldenstrom macroglobulinemia is refractoryto conventional interventions for macular edema Retin CasesBrief Rep 20137319ndash24
25 Gil Hernandez MA Abreu Reyes P Bahaya Alvarez Y AcostaAcosta B Bilateral serous detachment of the neurosensory retinaassociated with light-chain deposition disease [in Spanish] ArchSoc Canaria Oftalmol 200819 Available at wwwoftalmocomscorevista-1919sco09htm Accessed April 4 2014
26 Shah AR Zaidi A Brucker AJ Serous retinal detachmentsassociated with light chain deposition disease Retin CasesBrief Rep 20137236ndash41
27 Fenicia V Balestrieri M Perdicchi A et al Intravitreal injectionof dexamethasone implant in serous macular detachment asso-ciated withWaldenstroumlmrsquos disease Case Rep Ophthalmol [serialonline] 2013464ndash9 Available at httpwwwkargercomArti-cleFullText354066 Accessed April 4 2014
28 Mansoor A Wagner RP DePalma L Waldenstrom macro-globulinemia presenting as a pleural effusion Arch Pathol LabMed 2000124891ndash3
29 Kavuru MS Tubbs ML Miller L Wiedemann P Immuno-cytometry and gene rearrangement analysis in the diagnosis oflymphoma in an idiopathic pleural effusion Am Rev RespirDis 1992145209ndash11
30 Klaassen I Van Noorden CJF Schlingemann RO Molecularbasis of the inner blood-retinal barrier and its breakdown indiabetic macular edema and other pathological conditionsProg Retin Eye Res 20133419ndash48
31 Kanda T Usui S Beppu H et al Blood-nerve barrier in IgMparaproteinemic neuropathy a clinicopathologic assessmentActa Neuropathol 199895184ndash92
32 Lach B Rippstein P Atack D et al Immunoelectron micro-scopic localization of monoclonal IgM antibodies in gamm-opathy associated with peripheral demyelinative neuropathyActa Neuropathol 199385298ndash307
33 Terpos E Tasidou A Kastritis E et al Angiogenesis in Wal-denstroumlmrsquos macroglobulinemia Clin Lymphoma Myeloma2009946ndash9
34 Ashton N Ocular changes in multiple myelomatosis ArchOphthalmol 196573487ndash94
35 Foos RY Allen RA Opaque cysts of the ciliary body (parsciliaris retinae) Arch Ophthalmol 196777559ndash68
36 Dumas D Viriot ML Boura C et al Permeability oxygenthrough endothelial cells monolayer using time-resolvedfluorescence microscopy Effect of human plasma viscosityIn Periasamy A So PT eds Multiphoton Microscopy in theBiomedical Sciences II Bellingham WA Society of Photo-optical Instrumentation Engineers 2002293e301 Pro-ceedings of SPIE Vol 4620
37 Pruumlnte C Flammer J Choroidal capillary and venouscongestion in central serous chorioretinopathy Am JOphthalmol 199612126ndash34
38 Nicholson B Noble J Forooghian F Meyerle C Centralserous chorioretinopathy update on pathophysiology andtreatment Surv Ophthalmol 201358103ndash26
39 Zamir E Chowers I Central serous chorioretinopathy in a patientwith cryoglobulinaemia [letter] Eye (Lond) 199913265ndash6
7
Ophthalmology Volume - Number - Month 2014
40 Landa G Barnett JA Garcia PM et al Quantitative andqualitative spectral domain optical coherence tomographyanalysis of subretinal deposits in patients with acutecentral serous retinopathy Ophthalmologica 201323062ndash8
41 Menke MN Feke GT McMeel JW Treon SP Effect ofplasmapheresis on hyperviscosity-related retinopathy andretinal hemodynamics in patients with Waldenstromrsquos
8
macroglobulinemia Invest Ophthalmol Vis Sci 2008491157ndash60
42 Negi A Marmor MF Effects of subretinal and systemicosmolality on the rate of subretinal fluid resorption InvestOphthalmol Vis Sci 198425616ndash20
43 Larkin KL Saboo US Comer GM et al Use of intravitrealrituximab for treatment of vitreoretinal lymphoma Br J Oph-thalmol 20149899ndash103
Footnotes and Financial Disclosures
Originally received January 22 2014Final revision March 6 2014Accepted April 9 2014Available online --- Manuscript no 2014-1191 Departments of Ophthalmology American University of Beirut and RaficHariri University Hospital Beirut Lebanon2 Retina Departments The King Khaled Eye Specialist Hospital RiyadhKingdom of Saudi Arabia and Wilmer Eye Institute The Johns HopkinsUniversity Baltimore Maryland3 Department of Ophthalmology Hospital Moises Broggi Sant Joan DespiBarcelona Spain4 Associated Vitreoretinal and Uveitis Consultants Department ofOphthalmology Indiana University School of Medicine IndianapolisIndiana5 Retina Associates of Cleveland Beachwood Ohio6 The Retina Institute St Louis Missouri7 Department of Ophthalmology Mayo Clinic Rochester Minnesota8 Department of Statistics and Research Methodology Lebanese AmericanUniversity and Lebanese University Beirut Lebanon9 Retina Service at Oftalmologica San Miguel de Tucumaacuten Argentina10 Department of Ophthalmology Universidade Estadual de LondrinaParana Brazil
11 Department of Clinical Science ldquoLuigi Saccordquo Sacco Hospital Univer-sity of Milan Milan Italy
Financial Disclosure(s)The author(s) have no proprietary or commercial interest in any materialsdiscussed in this article
JFA Consultant - Second Sight LLC Alcon Labs Lecturer - IridexOptos Inc Speakers Bureau - Novartis Pharmaceuticals Alimera SciencesInc Royalties - Springer SBM LLC
GS Consultant - Heidelberg Engineering Zeiss QLT GSK AlconAllergan Bayer Boheringer Genentech Roche Novartis Speakers Bureaue Zeiss Heidelberg Engineering Novartis GSK Patents - Ocular In-struments Novartis
AM Consultant Lecturer - Bayer
Abbreviations and AcronymsBCVA frac14 best-corrected visual acuity cP frac14 centipoise CSR frac14 centralserous retinopathy DD frac14 disc diameter IgM frac14 immunoglobulin MlogMAR frac14 logarithm of the minimum angle of resolution MM frac14 multiplemyeloma OCT frac14 optical coherence tomography RPE frac14 retinal pigmentepithelium WM frac14 Waldenstroumlm macroglobulinemia
CorrespondenceAhmad M Mansour MD Department of Ophthalmology AmericanUniversity of Beirut PO Box 1136044 Beirut Lebanon E-mailammansourmdgmailcom
Ophthalmology Volume - Number - Month 2014
level hematocrit blood viscosity associated systemic and ocularcomorbidities and treatment methods and their effects as assessedon optical coherence tomography (OCT) Therapies includedvarious combinations of plasmapheresis (plasma exchange)chemotherapy intravitreal bevacizumab (off label) triamcinoloneor rituximab (off label) and laser photocoagulation after informedconsent was obtained
We also collected from the literature cases of paraproteinemicmaculopathy using Scopus Google Scholar and Medline searchesthrough October 2013 searching for macula AND MM WM andparaproteinemia including polyneuropathy organomegaly endo-crinopathy M-protein and skin abnormalities syndrome and light-chain deposition disease Hypertension is defined as a systolicblood pressure of 140 mmHg or more or a diastolic blood pressureof 90 mmHg or more Anemia is defined as hematocrit of less than40 for males and less than 35 for females Correlation wascarried out using correlation coefficient-adjusted r2 1-way analysisof variance and standardized b regression coefficients using SPSSStatistics for Windows version 210 (IBM Corp Armonk NY)Area of the maculopathy and height were measured on fundusphotography (reference being vertical disc diameter [DD]) andOCT (caliper tool in older machines with no calipers the macularretinal thickness was assumed at 300 mm) respectively The hor-izontal and vertical diameters of the sensory detachment weremeasured and the longest of the 2 measurements was taken as thearea Similarly on OCT the height of the sensory detachment wasmeasured on the vertical and horizontal scans through the foveolaand the largest value was adopted for the height
Results
The current retrospective series included 10 subjects (Table 1available at wwwaaojournalorg) comprising 7 men and 3 women
Figure 1 Fundus photographs of the (A) right eye and (B) left eye and (C D)the initial visit Venous dilation and tortuosity with peripheral capillary nonperand serous detachment of the neurosensory retina of the left eye Best-correcte
2
Five were white 1 was Hispanic and 4 were of unspecified raceThe mean age was 598 years (range 40e87 years) Systemicdiseases included WM (n frac14 8) MM (n frac14 2) diabetes mellitus (n frac144) systemic hypertension (n frac14 2) and anemia (n frac14 6) The sub-retinal fluid under the fovea had a mean area of 24 DD for the righteye and 21 DD for left eye (range 1e4 DD) in 17 eyes of 10patients (Figs 1 2 3 and 4) The maculopathy was unilateral in 3patients
To perform statistical analyses we combined the current serieswith the literature review of 23 cases (Table 1) These 33 casesincluded 21 men and 11 women 11 were white 3 were black 2were Asian and 1 was Hispanic The mean age was 59 years(range 37e87 years) Waldenstroumlm macroglobulinemia was pre-sent in 20 patients MM was present in 7 patients benign gamm-opathy was present in 3 patients light-chain deposition disease waspresent in 2 patients and polyneuropathy organomegaly endo-crinopathy M-protein and skin abnormalities syndrome was presentin 1 patient Diabetes mellitus was present in 7 patients systemichypertension was present in 9 patients renal failure was present in5 patients anemia was present in 18 patients and carotid stenosisand systemic lupus erythematosus each were present in 1 patientUnilateral involvement occurred in 9 patients Mean hematocritwas 286 (median 29 n frac14 14 range 144e40) Meanserum viscosity was 55 centipoise (cP median 42 cP n frac14 11range 25e91 cP normal values 15e19 cP) Mean initialimmunoglobulin level was 6497 mgdl (median 5888 mgdlrange 306e14000 mgdl n frac14 24 normal values 820e2200 mgdl) The mean diameter of the maculopathy was 20 DD (right eye20 DD [n frac14 27] and left eye 20 DD [n frac14 28] range 05e5 DD)Mean height of serous detachment was 435 mm in the right eye(range 71e1167 mm [n frac14 16]) and 410 mm in the left eye (range50e1060 mm [n frac14 19]) Mean initial BCVA was 055 logMAR(Snellen equivalent 2071) in the right eye and 038 logMAR(Snellen equivalent 2048) in the left eye Final BCVA was 045
spectral-domain optical coherence tomography (OCT) images obtained atfusion also was observed The OCT scans show bilateral intraretinal edemad visual acuity was 2020 in the right eye and 2060 in the left eye
Figure 3 After 3 monthly 25-mg01-ml bevacizumab injections (A B) fundus photographs and (C D) spectral-domain optical coherence tomography(SD OCT) images showed a mild reduction of both intraretinal and subretinal fluid in both eyes The SD OCT images show refractory edema Best-correctedvisual acuity remained 2060 in the right eye and 20200 in the left eye The SD OCT image from the right eye (C) shows unique stalactite-like projectionsof the outer retina
Figure 2 After 6 weeks (A C) serous macular detachment with overlying cystoid macular edema was observed in the right eye and (B D) an increase inthe subretinal fluid was observed in the left eye Best-corrected visual acuity dropped to 2060 in the right eye and 20200 in the left eye
Mansour et al Paraproteinemic Maculopathy
3
Figure 4 Schematic diagram showing the pathogenesis of paraproteinemic maculopathy BM frac14 Bruchrsquos membrane CC frac14 choriocapillaris IgM frac14immunoglobulin M RPE frac14 retinal pigment epithelium
Ophthalmology Volume - Number - Month 2014
logMAR (Snellen equivalent 2056) in the right eye and 050logMAR (Snellen equivalent 2063) in the left eye (Table 1)
Regarding therapy for the 33 patients plasmapheresis wasadministered in 18 patients chemotherapy was administered in30 patients blood transfusions were administered in 2 patientsand transplant of progenitor hematopoietic cells was performedin 2 patients Oral rituximab was used in 10 patients Immuno-globulin levels normalized in 8 patients and were unchanged in 1patient after plasmapheresis chemotherapy or both Ocular ther-apy in 8 patients included vitrectomy in 1 patient laser photoco-agulation in 4 patients intravitreal bevacizumab in 5 patients(Fig 3) intravitreal triamcinolone in 2 patients intravitrealdexamethasone implant in 1 patient intravitreal rituximab in 1patient (Fig 3) and sub-Tenon corticosteroid in 1 patient (Ta-ble 1) The maculopathy resolved partially or completely in 17patients and worsened or stayed unchanged in 14 patients over amedian follow-up of 7 months (mean 19 months 2 patients had nofollow-up) Immunoglobulins were unchanged in 1 patient andlikewise for maculopathy after therapy in 1 case Immunoglobulindecreased markedly but maculopathy did not improve in 3 pa-tients Immunoglobulin decreased and maculopathy improved in 5patients
There was a strong positive correlation between level ofimmunoglobulin and serum viscosity (P frac14 0007) No correlationwas present between level of immunoglobulin and hematocritdiabetes (P frac14 010) initial BCVA area (P frac14 033 for the right eyeand P frac14 034 for the left eye) and height of the macular detach-ment There was no correlation between area of the detachment andpresence of diabetes age or initial BCVA There was a positivecorrelation between area of the detachment and serum viscosity(P frac14 0017 for the right eye and P frac14 0022 for the left eye) Therewas no correlation between initial BCVA and height or area of themacular detachment Visual gain correlated with initial BCVA
4
(P frac14 0001 for the right eye and P frac14 0021 for the left eye) and didnot correlate with immunoglobulin level serum viscosity hemat-ocrit age diabetes or area or height of the detachment Diabeticsversus nondiabetics had the following mean values age 670versus 567 years (P frac14 004) immunoglobulin level of 4115versus 7306 mgdl (P frac14 010 normal values 820e2200 mgdl)area of macular detachment 22 versus 20 DD in the right eye(P frac14 043) and 183 versus 198 DD in the left eye (P frac14 040) andhematocrit 286 versus 288 (P frac14 050) Additional causesof leakage into the subretinal space included (1) disc edema in1 patient (patient 32) (2) severe ischemic diabetic retinopathy in 1patient (patient 10) (3) occlusive choroidal and retinal disease in 1patient (hence failure of the retinal pigment epithelium [RPE]pump patient 4) and (4) deep retinal leakage sites in 2 patients (2sites in patient 8 and 1 site in patient 6) possibly related to outerretinal defects as seen in patient 9 Of note is a peculiar finding ofstalactite-like projections in the outer retina in macula of patient 9(see ldquoCase Reportrdquo Fig 3C)
Case Report
A 47-year-old white man with no significant medical history wasreferred to our clinic for blurry vision in the left eye BaselineBCVA was 2020 in the right eye and 2060 in the left eye Slit-lamp biomicroscopy results were unremarkable and intraocularpressure was 12 mmHg in the right eye and 14 mmHg in the lefteye Fundus examination showed mild venous dilation and tortu-osity in both eyes and a serous macular detachment with yellowsubretinal exudates in the left eye (Fig 1) Optical coherencetomography revealed bilateral cystoid macular edema anddetachment of the neurosensory retina Fluorescein angiographyshowed peripheral vaso-occlusive disease with significant capil-lary nonperfusion Six weeks after initial presentation BCVA
Mansour et al Paraproteinemic Maculopathy
decreased to 2060 in the right eye and 20200 in the left eye andOCT showed neurosensory detachment with overlying cystoidmacular edema and bilateral disruption of the outer retina (Fig 2)The patientrsquos blood pressure was 13090 mmHg Hyperviscositysyndrome was suspected and blood tests revealed severe anemia(hemoglobin 79 mgdl normal values 135e175 mgdl) and atotal serum protein level of 192 mgdl (normal values 60e80mgdl) with elevated monoclonal IgM of 10 500 mgdl (normalvalues 45e153 mgdl) Bone marrow biopsy showed massivelymphoplasmacytoid infiltration A diagnosis of WM wasmade Computed tomography of the abdomen showed multipleretroperitoneal lymphadenopathies (iliac and inguinal) Plasma-pheresis was performed followed by 8 cycles of systemicpolychemotherapy with rituximab cyclophosphamide doxoru-bicin vincristine and steroids and 2 cycles of cladribineSystemic rituximab was not given until IgM levels decreased toless than 50 mgdl because rituximab is associated with suddenincrease in IgM levels and should be avoided in patients withhyperviscosity Simultaneously 3 monthly 25-mg01-ml intra-vitreal bevacizumab injections were administered in both eyesBest-corrected visual acuity remained 2060 in the right eye and20200 in the left eye and OCT demonstrated a slight bilateraldecrease in neurosensory detachment (Fig 3) At that time the IgMlevel dropped to 3925 mgdl Two months after the last intravitrealbevacizumab injection 3 monthly intravitreal injections ofrituximab (1 mg01 ml) were administered in both eyes Best-corrected visual acuity remained unchanged and OCT demon-strated a slight bilateral decrease in the amount of subretinal fluid(Fig 3) At that time the IgM level dropped to 2943 mgdl After 2years of follow-up complete remission was not reached BCVAwas 2060 in the right eye and 20400 in the left eye and OCTshowed no significant improvement
Discussion
Serous macular detachment is an uncommon ocular mani-festation of paraproteinemia2e27 The absence of angio-graphic leakage within the macular detachment does notsupport the theory of angiographic exudation from the retinalor choroidal vasculature In a few cases there was leakage inthe deep retina (Table 1) Some investigators have focused onthe presence of IgM in the subretinal space1112 suggestingthat an increased osmotic gradient causes fluid accumulationunder the retina In support of this hypothesis several his-topathologic reports documented immunoglobulins in thesubretinal space11e13 High-molecular-weight immunoglob-ulins lead to an osmotic gradient Because IgM antibodies arethe largest antibodies found in the blood and the lymph fluidthey rarely accumulate in pericardial peritoneal and pleuraleffusions2829 Immunoglobulin M antibodies consist of aheavy chain a light chain and 5 base units with a molecularmass of 970 kDa in its pentamer form (molecular weight06e1 000 000 kDa) Because IgM antibodies are very largemolecules and cannot diffuse well they are found in theinterstitium in extremely low quantities When such largepositively charged IgM molecules are present in excess theybind electrostatically to red cells aggregating and formingrouleaux with subsequent increase in the blood viscosity Asthe IgM protein concentration in the serum increases theblood viscosity increases exponentially It is somewhatintriguing to explain how IgM antibodies reach the subretinalspace (Fig 4) According to Klaassen et al30 the central
mechanism of the altered blooderetinal barrier results fromthe altered permeability of retinal endothelial cells causedby elevated levels of growth factors (such as vascularendothelial growth factor) cytokines and loss of pericytes(as occurs in diabetes) Subsequently both paracellular andtranscellular transport across the retinal vascular wall increasevia opening of the endothelial intercellular junctions andincrease in endothelial caveolar transcellular transport Thereis histologic evidence that the bloodeneural barrier (which issimilar to the blooderetinal barrier) is affected inparaproteinemia Kanda et al31 reported the pathologicfindings in a patient with sensorimotor neuropathy associatedwith WM and monoclonal IgM particularly in relation tobloodenerve barrier defects A sural nerve biopsy specimenrevealed gaps between adjacent endothelial cells of smallendoneurial vessels as well as the absence of some of thetight junctions between adjacent endothelial cells Similarlyin a sural nerve biopsy from a patient with benignmonoclonal IgM k gammopathy and sensorimotor demyeli-native neuropathy Lash et al32 found that many endoneurialcapillaries were lined by fenestrated endothelium indicatingthe breakdown of the normal bloodenerve barrier Theendoneurium contained large amounts of extracellularproteinaceous material containing IgM k g-globulin
Brody et al10 suggested thatmacular exudative detachmentsfrom diabetic maculopathy can lead to increased leakage ofimmunoglobulins into the subretinal space In a case withpolyneuropathy organomegaly endocrinopathy M-proteinand skin abnormalities syndrome Okada et al3 proposed thatthe high vascular endothelial growth factor level probablyinduced the retinal microvascular hyperpermeability leadingto leakage of immunoglobulin in the subretinal space Themaculopathy resolved 1 month after hematopoietic surgerywhen serum vascular endothelial growth factor leveldecreased in response to autologous peripheral blood stemcells The sera of WM patients are known to be associatedwith increased levels of angiogenic cytokines such asangiogenin vascular endothelial growth factor and basicfibroblast growth factor33 In normal bone marrowangiopoietin-1 consistently activates tyrosine kinase withimmunoglobulin-like and epidermal growth factor-like do-mains-2 and stabilizes vessels by promoting interactionsbetween endothelial cells and surrounding pericytes Onthe contrary during the malignant process in WMincreased angiopoietin-2 levels block tyrosine kinase with theimmunoglobulin-like and epidermal growth factor-like do-mains-2 receptor and lead to vessel destabilization by loos-ening endothelialeperiendothelial cell interactions anddegrading the extracellular matrix The primary source ofangiopoietin-2 is endothelial cells because angiopoietin-2 isstored in vesicles known as Weibel-Palade bodies and isreleased rapidly in response to hyperglycemia and ischemiaAngiopoietin-2 seems to be an important mediator in thealteration of the blooderetinal barrier in diabetes and otherretinal vascular disorders30
Ashton34 aswell as Foos andAllen35were among the first todescribe retinal and RPE detachment histologically in patientswith MM The subpigment epithelial fluid is derived fromchoroidal vessels The platelets can no longer fulfill theirnormal function of maintenance of endothelium because they
5
Ophthalmology Volume - Number - Month 2014
become covered by paraprotein Moreover the hyperviscositycan cause stasis and hypoxia leading to endotheliumdecompensation There is secondary breakdown of theblooderetinal barrier in addition to the RPE decompensationfrom the underlying deposit and hypoxia Coexisting anemiadiabetes and hypertension are additional risk factors forretinal vascular endothelial damage and ischemic injuryenhancing leakage and breakdown of the blooderetinalbarrier Dumas et al36 explored the contribution of plasmaviscosity and the endothelial cell monolayer to oxygenmolecular transport processes using a fluorescence inhibitionmethod They found hypoxia induced by hyperviscosityplasmas from patients with WM to have increasedintercellular adhesion molecule 1 expression on the surface ofendothelial cells which could be the cause of vasculardisorders through the implication of polymorphonuclearneutrophils
Baker et al2 demonstrated complete disruption of theouter retina within the detachment and proposed that thesefocal outer retinal defects (Figs 2 and 3) slowly progressover time eventually allowing a so-called track for intra-retinal IgM Our study was not aimed at estimating thepresence of such outer retinal defects A pathologiccommunication between the optic disc the subarachnoidspace and the subretinal space was proposed by Feigl et al16
and Khan et al19 Feigl et al16 found a finger-like extensionto the optic disc from the macular detachment by indoc-yanine angiography and proposed the disc as the cause ofthe macular detachment similar to optic pit maculopathy
There is a lot of overlap between the pathogenesis ofcentral serous retinopathy (CSR) and paraproteinemic mac-ulopathy Unilaterality of the maculopathy is one commonfinding in paraproteinemia and CSR as found in the currentseries In CSR Pruumlnte and Flammer37 detected capillary orvenous congestion after ischemia in 1 or more choroidallobules and this finding may be the reason for choroidalhyperpermeability Nicholson et al38 documented thepresence of a thickened and engorged choroid in CSRby enhanced depth OCT and proposed that thesehyperpermeable choroidal vessels produce increased tissuehydrostatic pressure promoting the formation of RPEdetachments overwhelming the barrier function of theRPE and leading to fluid accumulation between the retinaand the RPE Optical coherence tomography also mayshow an anatomic defect (microrip) in the RPE associatedwith fluid that is leaking into the subretinal spaceLikewise there is venous congestion in the choroid andretina in paraproteinemia leading to choroidal ischemiaand hyperpermeability which leads to CSR (Fig 4) Zamirand Chowers39 reported a patient with paraproteinemia whohad CSR in the right eye and branch retinal vein occlusionin the left eye with normal maculae Although CSR couldbe the primary cause of the ocular condition one couldargue that paraproteinemia could have induced a CSR-likecondition as previously discussed
Early treatment is necessary to prevent irreversible visualloss especially with the currently lengthened expected lifespan Paraproteinemic maculopathy becomes symptomaticwhen IgM levels exceed 4000 mgdl in diabetics and 7000mgdl in nondiabetics (Table 1) and serum viscosity exceeds
6
55 cP Prompt referral to a hematologist or oncologist isnecessary for systemic monitoring and treatment The visualloss in paraproteinemic maculopathy may be similar to thevisual loss in CSR with proteinaceous subretinal fluid40
Landa et al40 found a correlation between the subfovealthickness of the protein deposit layer and visual acuity atbaseline in 38 patients with CSR No such relation wasfound in our series possibly because of the retrospectivenature of the study and the small size of the study group
Usually no treatment is indicated for asymptomatic dis-ease Indications for initiating treatment include bloodhyperviscosity and ocular disturbance The cardinal therapiesinclude plasmapheresis (for patients with symptomatichyperviscosity) rituximab (anti-CD20 antibody that isgenetically engineered human monoclonal antibody directedagainst the CD20 antigen found on the surface of normal andmalignant B lymphocytes) and chemotherapy (purinenucleoside analogs alkylating agents thalidomide and bor-tezomib) Plasmapheresis is very useful in reducing serumhyperviscosity and rapidly improving most ocular manifes-tations According to Menke et al41 plasmapheresis resultedin significant reductions in serum IgM (by 465) and serumviscosity (by 447) and venous stasis retinopathy improvedin all patients after plasmapheresis Paraproteinemia-relatedvenous stasis retinopathy mimics a central retinal veinocclusion-like appearance (no thrombus) with normal retinalblood flow In our review the area of the macular detachmentcorrelated with serum viscosity and many eyes did notdemonstrate resolution of the maculopathy despite improve-ment in both the serum viscosity and the venous stasis reti-nopathy One possible reason could be the short follow-upin the current review these immunoglobulins need a longtime to resolve42 Besides plasmapheresis chemotherapyespecially with rituximab remains the mainstay of therapyVarious intravitreal injections (bevacizumab triamcinolonerituximab43) failed to show a definite benefit in the currentseries
In conclusion this case series along with the literaturereview provide further evidence of the direct correlationbetween IgM levels in the blood and the degree of subretinalfluid accumulation under the fovea in these patients Clinicalimprovement clearly correlated with a decrease in serumIgM Maculopathy of paraproteinemia can mimic diabeticretinopathy adult vitelliform dystrophy and CSR espe-cially in the many patients with diabetes Unilateral local-ized macular detachment is noted commonly in patients withelevated serum IgM levels associated with WM Para-proteinemic maculopathy often becomes symptomatic whenIgM levels exceed 7000 mgdl (4000 mgdl in diabetics) andserum viscosity exceeds 55 cP Therapy should be directedtoward decreasing the serum immunoglobulin level and theserum viscosity
References
1 Saleun JP Vicariot M Deroff P Morin JF Monoclonalgammopathies in the adult population of Finistere FranceJ Clin Pathol 19823563ndash8
Mansour et al Paraproteinemic Maculopathy
2 Baker PS Garg SJ Fineman MS et al Serous maculardetachment in Waldenstroumlm macroglobulinemia a report offour cases Am J Ophthalmol 2013155448ndash55
3 Okada K Yamamoto S Tsuyama Y Mizunoya S Case ofPOEMS syndrome associated with bilateral macular detach-ment resolved by autologous peripheral blood stem celltransplantation [letter] Jpn J Ophthalmol 200751237ndash8
4 Pilon AF Rhee PS Messner LV Bilateral persistent serousmacular detachments with Waldenstroumlmrsquos macroglobulinemiaOptom Vis Sci 200582573ndash8
5 Ho AC Benson WE Wong J Unusual immunogammopathymaculopathy Ophthalmology 20001071099ndash103
6 Ogata N Ida H Takahashi K et al Occult retinal pigmentepithelial detachment in hyperviscosity syndrome OphthalmicSurg Lasers 200031248ndash52
7 Cohen SM Kokame GT Gass JD Paraproteinemias associ-ated with serous detachments of the retinal pigment epitheliumand neurosensory retina Retina 199616467ndash73
8 Spielberg LH Heckenlively JR Leys AM Retinal pigmentepithelial detachments and tears and progressive retinaldegeneration in light chain deposition disease Br J Oph-thalmol 201397627ndash31
9 Leys AM Vandenberghe P Serous macular detachments in apatient with IgM paraproteinemia an optical coherence to-mography study Arch Ophthalmol 2001119911ndash3
10 Brody JM Butrus SI Ashraf MF et al Multiple myelomapresenting with bilateral exudative macular detachments ActaOphthalmol Scand 19957381ndash2
11 Berta A Beck P Mikita J IgM paraprotein in the subretinal fluidof a patient with recurrent retinal detachment andWaldenstroumlmrsquosmacroglobulinaemia Acta Med Hung 198542179ndash86
12 Khouri GG Murphy RP Kuhajda FP Green WR Clinico-pathologic features in two cases of multiple myeloma Retina19866169ndash75
13 Freidman AH Marchevsky A Odel JG et al Immunofluo-rescent studies of the eye in Waldenstroumlmrsquos macroglobuli-nemia Arch Ophthalmol 198098743ndash6
14 Thomas EL Olk RJ Markman M et al Irreversible visual lossin Waldenstroumlmrsquos macroglobulinaemia Br J Ophthalmol198367102ndash6
15 Sen HN Chan C-C Caruso RC et al Waldenstroumlmrsquosmacroglobulinemia-associated retinopathy Ophthalmology2004111535ndash9
16 Feigl B Sill H Haas A Serous detection of the neuroretina inWaldenstroumlm disease A case report [in German] Klin MonblAugenheilkd 199921564ndash7
17 Bernard A Rousselie F Macular manifestations of mono-clonal dysgammaglobulinemias Apropos of 3 cases [inFrench] J Fr Ophtalmol 19869805ndash10
18 Quhill F Khan I Rashid A Bilateral serous macular de-tachments in Waldenstroumlmrsquos macroglobulinaemia PostgradMed J 200985382
19 Khan JM McBain V Santiago C Lois N Bilateral lsquovitelli-form-likersquo macular lesions in a patient with multiple myelomaBMJ Case Rep [serial online] 20102010 bcr0520103049Available at httpwwwncbinlmnihgovpmcarticlesPMC3028543 Accessed April 4 2014
20 Brolly A Janon C Precausta F et al Pseudovitelliform sub-foveal deposit in Waldenstroumlmrsquos macroglobulinemia CaseRep Ophthalmol [serial online] 20123236ndash9 Available athttpwwwkargercomArticleAbstract339988 AccessedApril 4 2014
21 Daicker BC Mihatsch MJ Stroslashm EH Fogazzi GB Ocularpathology in light chain deposition disease Eur J Ophthalmol1995575ndash81
22 Ardouin M Urvoy M Gastard J Aspect of the dysproteinemicfundus oculi (microaneurysms and retinal detachment) in acase of Waldenstromrsquos disease [in French] Bull Soc Ophtal-mol Fr 196666129ndash32
23 Lin CJ Chiu YM Chen SN et al Unusual maculopathysecondary to hypergammaglobulinemia in a patient with sys-temic lupus erythematosus Retin Cases Brief Rep 2012627ndash9
24 Besirli CG Johnson MW Immunogammopathy maculopathyassociated with Waldenstrom macroglobulinemia is refractoryto conventional interventions for macular edema Retin CasesBrief Rep 20137319ndash24
25 Gil Hernandez MA Abreu Reyes P Bahaya Alvarez Y AcostaAcosta B Bilateral serous detachment of the neurosensory retinaassociated with light-chain deposition disease [in Spanish] ArchSoc Canaria Oftalmol 200819 Available at wwwoftalmocomscorevista-1919sco09htm Accessed April 4 2014
26 Shah AR Zaidi A Brucker AJ Serous retinal detachmentsassociated with light chain deposition disease Retin CasesBrief Rep 20137236ndash41
27 Fenicia V Balestrieri M Perdicchi A et al Intravitreal injectionof dexamethasone implant in serous macular detachment asso-ciated withWaldenstroumlmrsquos disease Case Rep Ophthalmol [serialonline] 2013464ndash9 Available at httpwwwkargercomArti-cleFullText354066 Accessed April 4 2014
28 Mansoor A Wagner RP DePalma L Waldenstrom macro-globulinemia presenting as a pleural effusion Arch Pathol LabMed 2000124891ndash3
29 Kavuru MS Tubbs ML Miller L Wiedemann P Immuno-cytometry and gene rearrangement analysis in the diagnosis oflymphoma in an idiopathic pleural effusion Am Rev RespirDis 1992145209ndash11
30 Klaassen I Van Noorden CJF Schlingemann RO Molecularbasis of the inner blood-retinal barrier and its breakdown indiabetic macular edema and other pathological conditionsProg Retin Eye Res 20133419ndash48
31 Kanda T Usui S Beppu H et al Blood-nerve barrier in IgMparaproteinemic neuropathy a clinicopathologic assessmentActa Neuropathol 199895184ndash92
32 Lach B Rippstein P Atack D et al Immunoelectron micro-scopic localization of monoclonal IgM antibodies in gamm-opathy associated with peripheral demyelinative neuropathyActa Neuropathol 199385298ndash307
33 Terpos E Tasidou A Kastritis E et al Angiogenesis in Wal-denstroumlmrsquos macroglobulinemia Clin Lymphoma Myeloma2009946ndash9
34 Ashton N Ocular changes in multiple myelomatosis ArchOphthalmol 196573487ndash94
35 Foos RY Allen RA Opaque cysts of the ciliary body (parsciliaris retinae) Arch Ophthalmol 196777559ndash68
36 Dumas D Viriot ML Boura C et al Permeability oxygenthrough endothelial cells monolayer using time-resolvedfluorescence microscopy Effect of human plasma viscosityIn Periasamy A So PT eds Multiphoton Microscopy in theBiomedical Sciences II Bellingham WA Society of Photo-optical Instrumentation Engineers 2002293e301 Pro-ceedings of SPIE Vol 4620
37 Pruumlnte C Flammer J Choroidal capillary and venouscongestion in central serous chorioretinopathy Am JOphthalmol 199612126ndash34
38 Nicholson B Noble J Forooghian F Meyerle C Centralserous chorioretinopathy update on pathophysiology andtreatment Surv Ophthalmol 201358103ndash26
39 Zamir E Chowers I Central serous chorioretinopathy in a patientwith cryoglobulinaemia [letter] Eye (Lond) 199913265ndash6
7
Ophthalmology Volume - Number - Month 2014
40 Landa G Barnett JA Garcia PM et al Quantitative andqualitative spectral domain optical coherence tomographyanalysis of subretinal deposits in patients with acutecentral serous retinopathy Ophthalmologica 201323062ndash8
41 Menke MN Feke GT McMeel JW Treon SP Effect ofplasmapheresis on hyperviscosity-related retinopathy andretinal hemodynamics in patients with Waldenstromrsquos
8
macroglobulinemia Invest Ophthalmol Vis Sci 2008491157ndash60
42 Negi A Marmor MF Effects of subretinal and systemicosmolality on the rate of subretinal fluid resorption InvestOphthalmol Vis Sci 198425616ndash20
43 Larkin KL Saboo US Comer GM et al Use of intravitrealrituximab for treatment of vitreoretinal lymphoma Br J Oph-thalmol 20149899ndash103
Footnotes and Financial Disclosures
Originally received January 22 2014Final revision March 6 2014Accepted April 9 2014Available online --- Manuscript no 2014-1191 Departments of Ophthalmology American University of Beirut and RaficHariri University Hospital Beirut Lebanon2 Retina Departments The King Khaled Eye Specialist Hospital RiyadhKingdom of Saudi Arabia and Wilmer Eye Institute The Johns HopkinsUniversity Baltimore Maryland3 Department of Ophthalmology Hospital Moises Broggi Sant Joan DespiBarcelona Spain4 Associated Vitreoretinal and Uveitis Consultants Department ofOphthalmology Indiana University School of Medicine IndianapolisIndiana5 Retina Associates of Cleveland Beachwood Ohio6 The Retina Institute St Louis Missouri7 Department of Ophthalmology Mayo Clinic Rochester Minnesota8 Department of Statistics and Research Methodology Lebanese AmericanUniversity and Lebanese University Beirut Lebanon9 Retina Service at Oftalmologica San Miguel de Tucumaacuten Argentina10 Department of Ophthalmology Universidade Estadual de LondrinaParana Brazil
11 Department of Clinical Science ldquoLuigi Saccordquo Sacco Hospital Univer-sity of Milan Milan Italy
Financial Disclosure(s)The author(s) have no proprietary or commercial interest in any materialsdiscussed in this article
JFA Consultant - Second Sight LLC Alcon Labs Lecturer - IridexOptos Inc Speakers Bureau - Novartis Pharmaceuticals Alimera SciencesInc Royalties - Springer SBM LLC
GS Consultant - Heidelberg Engineering Zeiss QLT GSK AlconAllergan Bayer Boheringer Genentech Roche Novartis Speakers Bureaue Zeiss Heidelberg Engineering Novartis GSK Patents - Ocular In-struments Novartis
AM Consultant Lecturer - Bayer
Abbreviations and AcronymsBCVA frac14 best-corrected visual acuity cP frac14 centipoise CSR frac14 centralserous retinopathy DD frac14 disc diameter IgM frac14 immunoglobulin MlogMAR frac14 logarithm of the minimum angle of resolution MM frac14 multiplemyeloma OCT frac14 optical coherence tomography RPE frac14 retinal pigmentepithelium WM frac14 Waldenstroumlm macroglobulinemia
CorrespondenceAhmad M Mansour MD Department of Ophthalmology AmericanUniversity of Beirut PO Box 1136044 Beirut Lebanon E-mailammansourmdgmailcom

Figure 3 After 3 monthly 25-mg01-ml bevacizumab injections (A B) fundus photographs and (C D) spectral-domain optical coherence tomography(SD OCT) images showed a mild reduction of both intraretinal and subretinal fluid in both eyes The SD OCT images show refractory edema Best-correctedvisual acuity remained 2060 in the right eye and 20200 in the left eye The SD OCT image from the right eye (C) shows unique stalactite-like projectionsof the outer retina
Figure 2 After 6 weeks (A C) serous macular detachment with overlying cystoid macular edema was observed in the right eye and (B D) an increase inthe subretinal fluid was observed in the left eye Best-corrected visual acuity dropped to 2060 in the right eye and 20200 in the left eye
Mansour et al Paraproteinemic Maculopathy
3
Figure 4 Schematic diagram showing the pathogenesis of paraproteinemic maculopathy BM frac14 Bruchrsquos membrane CC frac14 choriocapillaris IgM frac14immunoglobulin M RPE frac14 retinal pigment epithelium
Ophthalmology Volume - Number - Month 2014
logMAR (Snellen equivalent 2056) in the right eye and 050logMAR (Snellen equivalent 2063) in the left eye (Table 1)
Regarding therapy for the 33 patients plasmapheresis wasadministered in 18 patients chemotherapy was administered in30 patients blood transfusions were administered in 2 patientsand transplant of progenitor hematopoietic cells was performedin 2 patients Oral rituximab was used in 10 patients Immuno-globulin levels normalized in 8 patients and were unchanged in 1patient after plasmapheresis chemotherapy or both Ocular ther-apy in 8 patients included vitrectomy in 1 patient laser photoco-agulation in 4 patients intravitreal bevacizumab in 5 patients(Fig 3) intravitreal triamcinolone in 2 patients intravitrealdexamethasone implant in 1 patient intravitreal rituximab in 1patient (Fig 3) and sub-Tenon corticosteroid in 1 patient (Ta-ble 1) The maculopathy resolved partially or completely in 17patients and worsened or stayed unchanged in 14 patients over amedian follow-up of 7 months (mean 19 months 2 patients had nofollow-up) Immunoglobulins were unchanged in 1 patient andlikewise for maculopathy after therapy in 1 case Immunoglobulindecreased markedly but maculopathy did not improve in 3 pa-tients Immunoglobulin decreased and maculopathy improved in 5patients
There was a strong positive correlation between level ofimmunoglobulin and serum viscosity (P frac14 0007) No correlationwas present between level of immunoglobulin and hematocritdiabetes (P frac14 010) initial BCVA area (P frac14 033 for the right eyeand P frac14 034 for the left eye) and height of the macular detach-ment There was no correlation between area of the detachment andpresence of diabetes age or initial BCVA There was a positivecorrelation between area of the detachment and serum viscosity(P frac14 0017 for the right eye and P frac14 0022 for the left eye) Therewas no correlation between initial BCVA and height or area of themacular detachment Visual gain correlated with initial BCVA
4
(P frac14 0001 for the right eye and P frac14 0021 for the left eye) and didnot correlate with immunoglobulin level serum viscosity hemat-ocrit age diabetes or area or height of the detachment Diabeticsversus nondiabetics had the following mean values age 670versus 567 years (P frac14 004) immunoglobulin level of 4115versus 7306 mgdl (P frac14 010 normal values 820e2200 mgdl)area of macular detachment 22 versus 20 DD in the right eye(P frac14 043) and 183 versus 198 DD in the left eye (P frac14 040) andhematocrit 286 versus 288 (P frac14 050) Additional causesof leakage into the subretinal space included (1) disc edema in1 patient (patient 32) (2) severe ischemic diabetic retinopathy in 1patient (patient 10) (3) occlusive choroidal and retinal disease in 1patient (hence failure of the retinal pigment epithelium [RPE]pump patient 4) and (4) deep retinal leakage sites in 2 patients (2sites in patient 8 and 1 site in patient 6) possibly related to outerretinal defects as seen in patient 9 Of note is a peculiar finding ofstalactite-like projections in the outer retina in macula of patient 9(see ldquoCase Reportrdquo Fig 3C)
Case Report
A 47-year-old white man with no significant medical history wasreferred to our clinic for blurry vision in the left eye BaselineBCVA was 2020 in the right eye and 2060 in the left eye Slit-lamp biomicroscopy results were unremarkable and intraocularpressure was 12 mmHg in the right eye and 14 mmHg in the lefteye Fundus examination showed mild venous dilation and tortu-osity in both eyes and a serous macular detachment with yellowsubretinal exudates in the left eye (Fig 1) Optical coherencetomography revealed bilateral cystoid macular edema anddetachment of the neurosensory retina Fluorescein angiographyshowed peripheral vaso-occlusive disease with significant capil-lary nonperfusion Six weeks after initial presentation BCVA
Mansour et al Paraproteinemic Maculopathy
decreased to 2060 in the right eye and 20200 in the left eye andOCT showed neurosensory detachment with overlying cystoidmacular edema and bilateral disruption of the outer retina (Fig 2)The patientrsquos blood pressure was 13090 mmHg Hyperviscositysyndrome was suspected and blood tests revealed severe anemia(hemoglobin 79 mgdl normal values 135e175 mgdl) and atotal serum protein level of 192 mgdl (normal values 60e80mgdl) with elevated monoclonal IgM of 10 500 mgdl (normalvalues 45e153 mgdl) Bone marrow biopsy showed massivelymphoplasmacytoid infiltration A diagnosis of WM wasmade Computed tomography of the abdomen showed multipleretroperitoneal lymphadenopathies (iliac and inguinal) Plasma-pheresis was performed followed by 8 cycles of systemicpolychemotherapy with rituximab cyclophosphamide doxoru-bicin vincristine and steroids and 2 cycles of cladribineSystemic rituximab was not given until IgM levels decreased toless than 50 mgdl because rituximab is associated with suddenincrease in IgM levels and should be avoided in patients withhyperviscosity Simultaneously 3 monthly 25-mg01-ml intra-vitreal bevacizumab injections were administered in both eyesBest-corrected visual acuity remained 2060 in the right eye and20200 in the left eye and OCT demonstrated a slight bilateraldecrease in neurosensory detachment (Fig 3) At that time the IgMlevel dropped to 3925 mgdl Two months after the last intravitrealbevacizumab injection 3 monthly intravitreal injections ofrituximab (1 mg01 ml) were administered in both eyes Best-corrected visual acuity remained unchanged and OCT demon-strated a slight bilateral decrease in the amount of subretinal fluid(Fig 3) At that time the IgM level dropped to 2943 mgdl After 2years of follow-up complete remission was not reached BCVAwas 2060 in the right eye and 20400 in the left eye and OCTshowed no significant improvement
Discussion
Serous macular detachment is an uncommon ocular mani-festation of paraproteinemia2e27 The absence of angio-graphic leakage within the macular detachment does notsupport the theory of angiographic exudation from the retinalor choroidal vasculature In a few cases there was leakage inthe deep retina (Table 1) Some investigators have focused onthe presence of IgM in the subretinal space1112 suggestingthat an increased osmotic gradient causes fluid accumulationunder the retina In support of this hypothesis several his-topathologic reports documented immunoglobulins in thesubretinal space11e13 High-molecular-weight immunoglob-ulins lead to an osmotic gradient Because IgM antibodies arethe largest antibodies found in the blood and the lymph fluidthey rarely accumulate in pericardial peritoneal and pleuraleffusions2829 Immunoglobulin M antibodies consist of aheavy chain a light chain and 5 base units with a molecularmass of 970 kDa in its pentamer form (molecular weight06e1 000 000 kDa) Because IgM antibodies are very largemolecules and cannot diffuse well they are found in theinterstitium in extremely low quantities When such largepositively charged IgM molecules are present in excess theybind electrostatically to red cells aggregating and formingrouleaux with subsequent increase in the blood viscosity Asthe IgM protein concentration in the serum increases theblood viscosity increases exponentially It is somewhatintriguing to explain how IgM antibodies reach the subretinalspace (Fig 4) According to Klaassen et al30 the central
mechanism of the altered blooderetinal barrier results fromthe altered permeability of retinal endothelial cells causedby elevated levels of growth factors (such as vascularendothelial growth factor) cytokines and loss of pericytes(as occurs in diabetes) Subsequently both paracellular andtranscellular transport across the retinal vascular wall increasevia opening of the endothelial intercellular junctions andincrease in endothelial caveolar transcellular transport Thereis histologic evidence that the bloodeneural barrier (which issimilar to the blooderetinal barrier) is affected inparaproteinemia Kanda et al31 reported the pathologicfindings in a patient with sensorimotor neuropathy associatedwith WM and monoclonal IgM particularly in relation tobloodenerve barrier defects A sural nerve biopsy specimenrevealed gaps between adjacent endothelial cells of smallendoneurial vessels as well as the absence of some of thetight junctions between adjacent endothelial cells Similarlyin a sural nerve biopsy from a patient with benignmonoclonal IgM k gammopathy and sensorimotor demyeli-native neuropathy Lash et al32 found that many endoneurialcapillaries were lined by fenestrated endothelium indicatingthe breakdown of the normal bloodenerve barrier Theendoneurium contained large amounts of extracellularproteinaceous material containing IgM k g-globulin
Brody et al10 suggested thatmacular exudative detachmentsfrom diabetic maculopathy can lead to increased leakage ofimmunoglobulins into the subretinal space In a case withpolyneuropathy organomegaly endocrinopathy M-proteinand skin abnormalities syndrome Okada et al3 proposed thatthe high vascular endothelial growth factor level probablyinduced the retinal microvascular hyperpermeability leadingto leakage of immunoglobulin in the subretinal space Themaculopathy resolved 1 month after hematopoietic surgerywhen serum vascular endothelial growth factor leveldecreased in response to autologous peripheral blood stemcells The sera of WM patients are known to be associatedwith increased levels of angiogenic cytokines such asangiogenin vascular endothelial growth factor and basicfibroblast growth factor33 In normal bone marrowangiopoietin-1 consistently activates tyrosine kinase withimmunoglobulin-like and epidermal growth factor-like do-mains-2 and stabilizes vessels by promoting interactionsbetween endothelial cells and surrounding pericytes Onthe contrary during the malignant process in WMincreased angiopoietin-2 levels block tyrosine kinase with theimmunoglobulin-like and epidermal growth factor-like do-mains-2 receptor and lead to vessel destabilization by loos-ening endothelialeperiendothelial cell interactions anddegrading the extracellular matrix The primary source ofangiopoietin-2 is endothelial cells because angiopoietin-2 isstored in vesicles known as Weibel-Palade bodies and isreleased rapidly in response to hyperglycemia and ischemiaAngiopoietin-2 seems to be an important mediator in thealteration of the blooderetinal barrier in diabetes and otherretinal vascular disorders30
Ashton34 aswell as Foos andAllen35were among the first todescribe retinal and RPE detachment histologically in patientswith MM The subpigment epithelial fluid is derived fromchoroidal vessels The platelets can no longer fulfill theirnormal function of maintenance of endothelium because they
5
Ophthalmology Volume - Number - Month 2014
become covered by paraprotein Moreover the hyperviscositycan cause stasis and hypoxia leading to endotheliumdecompensation There is secondary breakdown of theblooderetinal barrier in addition to the RPE decompensationfrom the underlying deposit and hypoxia Coexisting anemiadiabetes and hypertension are additional risk factors forretinal vascular endothelial damage and ischemic injuryenhancing leakage and breakdown of the blooderetinalbarrier Dumas et al36 explored the contribution of plasmaviscosity and the endothelial cell monolayer to oxygenmolecular transport processes using a fluorescence inhibitionmethod They found hypoxia induced by hyperviscosityplasmas from patients with WM to have increasedintercellular adhesion molecule 1 expression on the surface ofendothelial cells which could be the cause of vasculardisorders through the implication of polymorphonuclearneutrophils
Baker et al2 demonstrated complete disruption of theouter retina within the detachment and proposed that thesefocal outer retinal defects (Figs 2 and 3) slowly progressover time eventually allowing a so-called track for intra-retinal IgM Our study was not aimed at estimating thepresence of such outer retinal defects A pathologiccommunication between the optic disc the subarachnoidspace and the subretinal space was proposed by Feigl et al16
and Khan et al19 Feigl et al16 found a finger-like extensionto the optic disc from the macular detachment by indoc-yanine angiography and proposed the disc as the cause ofthe macular detachment similar to optic pit maculopathy
There is a lot of overlap between the pathogenesis ofcentral serous retinopathy (CSR) and paraproteinemic mac-ulopathy Unilaterality of the maculopathy is one commonfinding in paraproteinemia and CSR as found in the currentseries In CSR Pruumlnte and Flammer37 detected capillary orvenous congestion after ischemia in 1 or more choroidallobules and this finding may be the reason for choroidalhyperpermeability Nicholson et al38 documented thepresence of a thickened and engorged choroid in CSRby enhanced depth OCT and proposed that thesehyperpermeable choroidal vessels produce increased tissuehydrostatic pressure promoting the formation of RPEdetachments overwhelming the barrier function of theRPE and leading to fluid accumulation between the retinaand the RPE Optical coherence tomography also mayshow an anatomic defect (microrip) in the RPE associatedwith fluid that is leaking into the subretinal spaceLikewise there is venous congestion in the choroid andretina in paraproteinemia leading to choroidal ischemiaand hyperpermeability which leads to CSR (Fig 4) Zamirand Chowers39 reported a patient with paraproteinemia whohad CSR in the right eye and branch retinal vein occlusionin the left eye with normal maculae Although CSR couldbe the primary cause of the ocular condition one couldargue that paraproteinemia could have induced a CSR-likecondition as previously discussed
Early treatment is necessary to prevent irreversible visualloss especially with the currently lengthened expected lifespan Paraproteinemic maculopathy becomes symptomaticwhen IgM levels exceed 4000 mgdl in diabetics and 7000mgdl in nondiabetics (Table 1) and serum viscosity exceeds
6
55 cP Prompt referral to a hematologist or oncologist isnecessary for systemic monitoring and treatment The visualloss in paraproteinemic maculopathy may be similar to thevisual loss in CSR with proteinaceous subretinal fluid40
Landa et al40 found a correlation between the subfovealthickness of the protein deposit layer and visual acuity atbaseline in 38 patients with CSR No such relation wasfound in our series possibly because of the retrospectivenature of the study and the small size of the study group
Usually no treatment is indicated for asymptomatic dis-ease Indications for initiating treatment include bloodhyperviscosity and ocular disturbance The cardinal therapiesinclude plasmapheresis (for patients with symptomatichyperviscosity) rituximab (anti-CD20 antibody that isgenetically engineered human monoclonal antibody directedagainst the CD20 antigen found on the surface of normal andmalignant B lymphocytes) and chemotherapy (purinenucleoside analogs alkylating agents thalidomide and bor-tezomib) Plasmapheresis is very useful in reducing serumhyperviscosity and rapidly improving most ocular manifes-tations According to Menke et al41 plasmapheresis resultedin significant reductions in serum IgM (by 465) and serumviscosity (by 447) and venous stasis retinopathy improvedin all patients after plasmapheresis Paraproteinemia-relatedvenous stasis retinopathy mimics a central retinal veinocclusion-like appearance (no thrombus) with normal retinalblood flow In our review the area of the macular detachmentcorrelated with serum viscosity and many eyes did notdemonstrate resolution of the maculopathy despite improve-ment in both the serum viscosity and the venous stasis reti-nopathy One possible reason could be the short follow-upin the current review these immunoglobulins need a longtime to resolve42 Besides plasmapheresis chemotherapyespecially with rituximab remains the mainstay of therapyVarious intravitreal injections (bevacizumab triamcinolonerituximab43) failed to show a definite benefit in the currentseries
In conclusion this case series along with the literaturereview provide further evidence of the direct correlationbetween IgM levels in the blood and the degree of subretinalfluid accumulation under the fovea in these patients Clinicalimprovement clearly correlated with a decrease in serumIgM Maculopathy of paraproteinemia can mimic diabeticretinopathy adult vitelliform dystrophy and CSR espe-cially in the many patients with diabetes Unilateral local-ized macular detachment is noted commonly in patients withelevated serum IgM levels associated with WM Para-proteinemic maculopathy often becomes symptomatic whenIgM levels exceed 7000 mgdl (4000 mgdl in diabetics) andserum viscosity exceeds 55 cP Therapy should be directedtoward decreasing the serum immunoglobulin level and theserum viscosity
References
1 Saleun JP Vicariot M Deroff P Morin JF Monoclonalgammopathies in the adult population of Finistere FranceJ Clin Pathol 19823563ndash8
Mansour et al Paraproteinemic Maculopathy
2 Baker PS Garg SJ Fineman MS et al Serous maculardetachment in Waldenstroumlm macroglobulinemia a report offour cases Am J Ophthalmol 2013155448ndash55
3 Okada K Yamamoto S Tsuyama Y Mizunoya S Case ofPOEMS syndrome associated with bilateral macular detach-ment resolved by autologous peripheral blood stem celltransplantation [letter] Jpn J Ophthalmol 200751237ndash8
4 Pilon AF Rhee PS Messner LV Bilateral persistent serousmacular detachments with Waldenstroumlmrsquos macroglobulinemiaOptom Vis Sci 200582573ndash8
5 Ho AC Benson WE Wong J Unusual immunogammopathymaculopathy Ophthalmology 20001071099ndash103
6 Ogata N Ida H Takahashi K et al Occult retinal pigmentepithelial detachment in hyperviscosity syndrome OphthalmicSurg Lasers 200031248ndash52
7 Cohen SM Kokame GT Gass JD Paraproteinemias associ-ated with serous detachments of the retinal pigment epitheliumand neurosensory retina Retina 199616467ndash73
8 Spielberg LH Heckenlively JR Leys AM Retinal pigmentepithelial detachments and tears and progressive retinaldegeneration in light chain deposition disease Br J Oph-thalmol 201397627ndash31
9 Leys AM Vandenberghe P Serous macular detachments in apatient with IgM paraproteinemia an optical coherence to-mography study Arch Ophthalmol 2001119911ndash3
10 Brody JM Butrus SI Ashraf MF et al Multiple myelomapresenting with bilateral exudative macular detachments ActaOphthalmol Scand 19957381ndash2
11 Berta A Beck P Mikita J IgM paraprotein in the subretinal fluidof a patient with recurrent retinal detachment andWaldenstroumlmrsquosmacroglobulinaemia Acta Med Hung 198542179ndash86
12 Khouri GG Murphy RP Kuhajda FP Green WR Clinico-pathologic features in two cases of multiple myeloma Retina19866169ndash75
13 Freidman AH Marchevsky A Odel JG et al Immunofluo-rescent studies of the eye in Waldenstroumlmrsquos macroglobuli-nemia Arch Ophthalmol 198098743ndash6
14 Thomas EL Olk RJ Markman M et al Irreversible visual lossin Waldenstroumlmrsquos macroglobulinaemia Br J Ophthalmol198367102ndash6
15 Sen HN Chan C-C Caruso RC et al Waldenstroumlmrsquosmacroglobulinemia-associated retinopathy Ophthalmology2004111535ndash9
16 Feigl B Sill H Haas A Serous detection of the neuroretina inWaldenstroumlm disease A case report [in German] Klin MonblAugenheilkd 199921564ndash7
17 Bernard A Rousselie F Macular manifestations of mono-clonal dysgammaglobulinemias Apropos of 3 cases [inFrench] J Fr Ophtalmol 19869805ndash10
18 Quhill F Khan I Rashid A Bilateral serous macular de-tachments in Waldenstroumlmrsquos macroglobulinaemia PostgradMed J 200985382
19 Khan JM McBain V Santiago C Lois N Bilateral lsquovitelli-form-likersquo macular lesions in a patient with multiple myelomaBMJ Case Rep [serial online] 20102010 bcr0520103049Available at httpwwwncbinlmnihgovpmcarticlesPMC3028543 Accessed April 4 2014
20 Brolly A Janon C Precausta F et al Pseudovitelliform sub-foveal deposit in Waldenstroumlmrsquos macroglobulinemia CaseRep Ophthalmol [serial online] 20123236ndash9 Available athttpwwwkargercomArticleAbstract339988 AccessedApril 4 2014
21 Daicker BC Mihatsch MJ Stroslashm EH Fogazzi GB Ocularpathology in light chain deposition disease Eur J Ophthalmol1995575ndash81
22 Ardouin M Urvoy M Gastard J Aspect of the dysproteinemicfundus oculi (microaneurysms and retinal detachment) in acase of Waldenstromrsquos disease [in French] Bull Soc Ophtal-mol Fr 196666129ndash32
23 Lin CJ Chiu YM Chen SN et al Unusual maculopathysecondary to hypergammaglobulinemia in a patient with sys-temic lupus erythematosus Retin Cases Brief Rep 2012627ndash9
24 Besirli CG Johnson MW Immunogammopathy maculopathyassociated with Waldenstrom macroglobulinemia is refractoryto conventional interventions for macular edema Retin CasesBrief Rep 20137319ndash24
25 Gil Hernandez MA Abreu Reyes P Bahaya Alvarez Y AcostaAcosta B Bilateral serous detachment of the neurosensory retinaassociated with light-chain deposition disease [in Spanish] ArchSoc Canaria Oftalmol 200819 Available at wwwoftalmocomscorevista-1919sco09htm Accessed April 4 2014
26 Shah AR Zaidi A Brucker AJ Serous retinal detachmentsassociated with light chain deposition disease Retin CasesBrief Rep 20137236ndash41
27 Fenicia V Balestrieri M Perdicchi A et al Intravitreal injectionof dexamethasone implant in serous macular detachment asso-ciated withWaldenstroumlmrsquos disease Case Rep Ophthalmol [serialonline] 2013464ndash9 Available at httpwwwkargercomArti-cleFullText354066 Accessed April 4 2014
28 Mansoor A Wagner RP DePalma L Waldenstrom macro-globulinemia presenting as a pleural effusion Arch Pathol LabMed 2000124891ndash3
29 Kavuru MS Tubbs ML Miller L Wiedemann P Immuno-cytometry and gene rearrangement analysis in the diagnosis oflymphoma in an idiopathic pleural effusion Am Rev RespirDis 1992145209ndash11
30 Klaassen I Van Noorden CJF Schlingemann RO Molecularbasis of the inner blood-retinal barrier and its breakdown indiabetic macular edema and other pathological conditionsProg Retin Eye Res 20133419ndash48
31 Kanda T Usui S Beppu H et al Blood-nerve barrier in IgMparaproteinemic neuropathy a clinicopathologic assessmentActa Neuropathol 199895184ndash92
32 Lach B Rippstein P Atack D et al Immunoelectron micro-scopic localization of monoclonal IgM antibodies in gamm-opathy associated with peripheral demyelinative neuropathyActa Neuropathol 199385298ndash307
33 Terpos E Tasidou A Kastritis E et al Angiogenesis in Wal-denstroumlmrsquos macroglobulinemia Clin Lymphoma Myeloma2009946ndash9
34 Ashton N Ocular changes in multiple myelomatosis ArchOphthalmol 196573487ndash94
35 Foos RY Allen RA Opaque cysts of the ciliary body (parsciliaris retinae) Arch Ophthalmol 196777559ndash68
36 Dumas D Viriot ML Boura C et al Permeability oxygenthrough endothelial cells monolayer using time-resolvedfluorescence microscopy Effect of human plasma viscosityIn Periasamy A So PT eds Multiphoton Microscopy in theBiomedical Sciences II Bellingham WA Society of Photo-optical Instrumentation Engineers 2002293e301 Pro-ceedings of SPIE Vol 4620
37 Pruumlnte C Flammer J Choroidal capillary and venouscongestion in central serous chorioretinopathy Am JOphthalmol 199612126ndash34
38 Nicholson B Noble J Forooghian F Meyerle C Centralserous chorioretinopathy update on pathophysiology andtreatment Surv Ophthalmol 201358103ndash26
39 Zamir E Chowers I Central serous chorioretinopathy in a patientwith cryoglobulinaemia [letter] Eye (Lond) 199913265ndash6
7
Ophthalmology Volume - Number - Month 2014
40 Landa G Barnett JA Garcia PM et al Quantitative andqualitative spectral domain optical coherence tomographyanalysis of subretinal deposits in patients with acutecentral serous retinopathy Ophthalmologica 201323062ndash8
41 Menke MN Feke GT McMeel JW Treon SP Effect ofplasmapheresis on hyperviscosity-related retinopathy andretinal hemodynamics in patients with Waldenstromrsquos
8
macroglobulinemia Invest Ophthalmol Vis Sci 2008491157ndash60
42 Negi A Marmor MF Effects of subretinal and systemicosmolality on the rate of subretinal fluid resorption InvestOphthalmol Vis Sci 198425616ndash20
43 Larkin KL Saboo US Comer GM et al Use of intravitrealrituximab for treatment of vitreoretinal lymphoma Br J Oph-thalmol 20149899ndash103
Footnotes and Financial Disclosures
Originally received January 22 2014Final revision March 6 2014Accepted April 9 2014Available online --- Manuscript no 2014-1191 Departments of Ophthalmology American University of Beirut and RaficHariri University Hospital Beirut Lebanon2 Retina Departments The King Khaled Eye Specialist Hospital RiyadhKingdom of Saudi Arabia and Wilmer Eye Institute The Johns HopkinsUniversity Baltimore Maryland3 Department of Ophthalmology Hospital Moises Broggi Sant Joan DespiBarcelona Spain4 Associated Vitreoretinal and Uveitis Consultants Department ofOphthalmology Indiana University School of Medicine IndianapolisIndiana5 Retina Associates of Cleveland Beachwood Ohio6 The Retina Institute St Louis Missouri7 Department of Ophthalmology Mayo Clinic Rochester Minnesota8 Department of Statistics and Research Methodology Lebanese AmericanUniversity and Lebanese University Beirut Lebanon9 Retina Service at Oftalmologica San Miguel de Tucumaacuten Argentina10 Department of Ophthalmology Universidade Estadual de LondrinaParana Brazil
11 Department of Clinical Science ldquoLuigi Saccordquo Sacco Hospital Univer-sity of Milan Milan Italy
Financial Disclosure(s)The author(s) have no proprietary or commercial interest in any materialsdiscussed in this article
JFA Consultant - Second Sight LLC Alcon Labs Lecturer - IridexOptos Inc Speakers Bureau - Novartis Pharmaceuticals Alimera SciencesInc Royalties - Springer SBM LLC
GS Consultant - Heidelberg Engineering Zeiss QLT GSK AlconAllergan Bayer Boheringer Genentech Roche Novartis Speakers Bureaue Zeiss Heidelberg Engineering Novartis GSK Patents - Ocular In-struments Novartis
AM Consultant Lecturer - Bayer
Abbreviations and AcronymsBCVA frac14 best-corrected visual acuity cP frac14 centipoise CSR frac14 centralserous retinopathy DD frac14 disc diameter IgM frac14 immunoglobulin MlogMAR frac14 logarithm of the minimum angle of resolution MM frac14 multiplemyeloma OCT frac14 optical coherence tomography RPE frac14 retinal pigmentepithelium WM frac14 Waldenstroumlm macroglobulinemia
CorrespondenceAhmad M Mansour MD Department of Ophthalmology AmericanUniversity of Beirut PO Box 1136044 Beirut Lebanon E-mailammansourmdgmailcom

Figure 4 Schematic diagram showing the pathogenesis of paraproteinemic maculopathy BM frac14 Bruchrsquos membrane CC frac14 choriocapillaris IgM frac14immunoglobulin M RPE frac14 retinal pigment epithelium
Ophthalmology Volume - Number - Month 2014
logMAR (Snellen equivalent 2056) in the right eye and 050logMAR (Snellen equivalent 2063) in the left eye (Table 1)
Regarding therapy for the 33 patients plasmapheresis wasadministered in 18 patients chemotherapy was administered in30 patients blood transfusions were administered in 2 patientsand transplant of progenitor hematopoietic cells was performedin 2 patients Oral rituximab was used in 10 patients Immuno-globulin levels normalized in 8 patients and were unchanged in 1patient after plasmapheresis chemotherapy or both Ocular ther-apy in 8 patients included vitrectomy in 1 patient laser photoco-agulation in 4 patients intravitreal bevacizumab in 5 patients(Fig 3) intravitreal triamcinolone in 2 patients intravitrealdexamethasone implant in 1 patient intravitreal rituximab in 1patient (Fig 3) and sub-Tenon corticosteroid in 1 patient (Ta-ble 1) The maculopathy resolved partially or completely in 17patients and worsened or stayed unchanged in 14 patients over amedian follow-up of 7 months (mean 19 months 2 patients had nofollow-up) Immunoglobulins were unchanged in 1 patient andlikewise for maculopathy after therapy in 1 case Immunoglobulindecreased markedly but maculopathy did not improve in 3 pa-tients Immunoglobulin decreased and maculopathy improved in 5patients
There was a strong positive correlation between level ofimmunoglobulin and serum viscosity (P frac14 0007) No correlationwas present between level of immunoglobulin and hematocritdiabetes (P frac14 010) initial BCVA area (P frac14 033 for the right eyeand P frac14 034 for the left eye) and height of the macular detach-ment There was no correlation between area of the detachment andpresence of diabetes age or initial BCVA There was a positivecorrelation between area of the detachment and serum viscosity(P frac14 0017 for the right eye and P frac14 0022 for the left eye) Therewas no correlation between initial BCVA and height or area of themacular detachment Visual gain correlated with initial BCVA
4
(P frac14 0001 for the right eye and P frac14 0021 for the left eye) and didnot correlate with immunoglobulin level serum viscosity hemat-ocrit age diabetes or area or height of the detachment Diabeticsversus nondiabetics had the following mean values age 670versus 567 years (P frac14 004) immunoglobulin level of 4115versus 7306 mgdl (P frac14 010 normal values 820e2200 mgdl)area of macular detachment 22 versus 20 DD in the right eye(P frac14 043) and 183 versus 198 DD in the left eye (P frac14 040) andhematocrit 286 versus 288 (P frac14 050) Additional causesof leakage into the subretinal space included (1) disc edema in1 patient (patient 32) (2) severe ischemic diabetic retinopathy in 1patient (patient 10) (3) occlusive choroidal and retinal disease in 1patient (hence failure of the retinal pigment epithelium [RPE]pump patient 4) and (4) deep retinal leakage sites in 2 patients (2sites in patient 8 and 1 site in patient 6) possibly related to outerretinal defects as seen in patient 9 Of note is a peculiar finding ofstalactite-like projections in the outer retina in macula of patient 9(see ldquoCase Reportrdquo Fig 3C)
Case Report
A 47-year-old white man with no significant medical history wasreferred to our clinic for blurry vision in the left eye BaselineBCVA was 2020 in the right eye and 2060 in the left eye Slit-lamp biomicroscopy results were unremarkable and intraocularpressure was 12 mmHg in the right eye and 14 mmHg in the lefteye Fundus examination showed mild venous dilation and tortu-osity in both eyes and a serous macular detachment with yellowsubretinal exudates in the left eye (Fig 1) Optical coherencetomography revealed bilateral cystoid macular edema anddetachment of the neurosensory retina Fluorescein angiographyshowed peripheral vaso-occlusive disease with significant capil-lary nonperfusion Six weeks after initial presentation BCVA
Mansour et al Paraproteinemic Maculopathy
decreased to 2060 in the right eye and 20200 in the left eye andOCT showed neurosensory detachment with overlying cystoidmacular edema and bilateral disruption of the outer retina (Fig 2)The patientrsquos blood pressure was 13090 mmHg Hyperviscositysyndrome was suspected and blood tests revealed severe anemia(hemoglobin 79 mgdl normal values 135e175 mgdl) and atotal serum protein level of 192 mgdl (normal values 60e80mgdl) with elevated monoclonal IgM of 10 500 mgdl (normalvalues 45e153 mgdl) Bone marrow biopsy showed massivelymphoplasmacytoid infiltration A diagnosis of WM wasmade Computed tomography of the abdomen showed multipleretroperitoneal lymphadenopathies (iliac and inguinal) Plasma-pheresis was performed followed by 8 cycles of systemicpolychemotherapy with rituximab cyclophosphamide doxoru-bicin vincristine and steroids and 2 cycles of cladribineSystemic rituximab was not given until IgM levels decreased toless than 50 mgdl because rituximab is associated with suddenincrease in IgM levels and should be avoided in patients withhyperviscosity Simultaneously 3 monthly 25-mg01-ml intra-vitreal bevacizumab injections were administered in both eyesBest-corrected visual acuity remained 2060 in the right eye and20200 in the left eye and OCT demonstrated a slight bilateraldecrease in neurosensory detachment (Fig 3) At that time the IgMlevel dropped to 3925 mgdl Two months after the last intravitrealbevacizumab injection 3 monthly intravitreal injections ofrituximab (1 mg01 ml) were administered in both eyes Best-corrected visual acuity remained unchanged and OCT demon-strated a slight bilateral decrease in the amount of subretinal fluid(Fig 3) At that time the IgM level dropped to 2943 mgdl After 2years of follow-up complete remission was not reached BCVAwas 2060 in the right eye and 20400 in the left eye and OCTshowed no significant improvement
Discussion
Serous macular detachment is an uncommon ocular mani-festation of paraproteinemia2e27 The absence of angio-graphic leakage within the macular detachment does notsupport the theory of angiographic exudation from the retinalor choroidal vasculature In a few cases there was leakage inthe deep retina (Table 1) Some investigators have focused onthe presence of IgM in the subretinal space1112 suggestingthat an increased osmotic gradient causes fluid accumulationunder the retina In support of this hypothesis several his-topathologic reports documented immunoglobulins in thesubretinal space11e13 High-molecular-weight immunoglob-ulins lead to an osmotic gradient Because IgM antibodies arethe largest antibodies found in the blood and the lymph fluidthey rarely accumulate in pericardial peritoneal and pleuraleffusions2829 Immunoglobulin M antibodies consist of aheavy chain a light chain and 5 base units with a molecularmass of 970 kDa in its pentamer form (molecular weight06e1 000 000 kDa) Because IgM antibodies are very largemolecules and cannot diffuse well they are found in theinterstitium in extremely low quantities When such largepositively charged IgM molecules are present in excess theybind electrostatically to red cells aggregating and formingrouleaux with subsequent increase in the blood viscosity Asthe IgM protein concentration in the serum increases theblood viscosity increases exponentially It is somewhatintriguing to explain how IgM antibodies reach the subretinalspace (Fig 4) According to Klaassen et al30 the central
mechanism of the altered blooderetinal barrier results fromthe altered permeability of retinal endothelial cells causedby elevated levels of growth factors (such as vascularendothelial growth factor) cytokines and loss of pericytes(as occurs in diabetes) Subsequently both paracellular andtranscellular transport across the retinal vascular wall increasevia opening of the endothelial intercellular junctions andincrease in endothelial caveolar transcellular transport Thereis histologic evidence that the bloodeneural barrier (which issimilar to the blooderetinal barrier) is affected inparaproteinemia Kanda et al31 reported the pathologicfindings in a patient with sensorimotor neuropathy associatedwith WM and monoclonal IgM particularly in relation tobloodenerve barrier defects A sural nerve biopsy specimenrevealed gaps between adjacent endothelial cells of smallendoneurial vessels as well as the absence of some of thetight junctions between adjacent endothelial cells Similarlyin a sural nerve biopsy from a patient with benignmonoclonal IgM k gammopathy and sensorimotor demyeli-native neuropathy Lash et al32 found that many endoneurialcapillaries were lined by fenestrated endothelium indicatingthe breakdown of the normal bloodenerve barrier Theendoneurium contained large amounts of extracellularproteinaceous material containing IgM k g-globulin
Brody et al10 suggested thatmacular exudative detachmentsfrom diabetic maculopathy can lead to increased leakage ofimmunoglobulins into the subretinal space In a case withpolyneuropathy organomegaly endocrinopathy M-proteinand skin abnormalities syndrome Okada et al3 proposed thatthe high vascular endothelial growth factor level probablyinduced the retinal microvascular hyperpermeability leadingto leakage of immunoglobulin in the subretinal space Themaculopathy resolved 1 month after hematopoietic surgerywhen serum vascular endothelial growth factor leveldecreased in response to autologous peripheral blood stemcells The sera of WM patients are known to be associatedwith increased levels of angiogenic cytokines such asangiogenin vascular endothelial growth factor and basicfibroblast growth factor33 In normal bone marrowangiopoietin-1 consistently activates tyrosine kinase withimmunoglobulin-like and epidermal growth factor-like do-mains-2 and stabilizes vessels by promoting interactionsbetween endothelial cells and surrounding pericytes Onthe contrary during the malignant process in WMincreased angiopoietin-2 levels block tyrosine kinase with theimmunoglobulin-like and epidermal growth factor-like do-mains-2 receptor and lead to vessel destabilization by loos-ening endothelialeperiendothelial cell interactions anddegrading the extracellular matrix The primary source ofangiopoietin-2 is endothelial cells because angiopoietin-2 isstored in vesicles known as Weibel-Palade bodies and isreleased rapidly in response to hyperglycemia and ischemiaAngiopoietin-2 seems to be an important mediator in thealteration of the blooderetinal barrier in diabetes and otherretinal vascular disorders30
Ashton34 aswell as Foos andAllen35were among the first todescribe retinal and RPE detachment histologically in patientswith MM The subpigment epithelial fluid is derived fromchoroidal vessels The platelets can no longer fulfill theirnormal function of maintenance of endothelium because they
5
Ophthalmology Volume - Number - Month 2014
become covered by paraprotein Moreover the hyperviscositycan cause stasis and hypoxia leading to endotheliumdecompensation There is secondary breakdown of theblooderetinal barrier in addition to the RPE decompensationfrom the underlying deposit and hypoxia Coexisting anemiadiabetes and hypertension are additional risk factors forretinal vascular endothelial damage and ischemic injuryenhancing leakage and breakdown of the blooderetinalbarrier Dumas et al36 explored the contribution of plasmaviscosity and the endothelial cell monolayer to oxygenmolecular transport processes using a fluorescence inhibitionmethod They found hypoxia induced by hyperviscosityplasmas from patients with WM to have increasedintercellular adhesion molecule 1 expression on the surface ofendothelial cells which could be the cause of vasculardisorders through the implication of polymorphonuclearneutrophils
Baker et al2 demonstrated complete disruption of theouter retina within the detachment and proposed that thesefocal outer retinal defects (Figs 2 and 3) slowly progressover time eventually allowing a so-called track for intra-retinal IgM Our study was not aimed at estimating thepresence of such outer retinal defects A pathologiccommunication between the optic disc the subarachnoidspace and the subretinal space was proposed by Feigl et al16
and Khan et al19 Feigl et al16 found a finger-like extensionto the optic disc from the macular detachment by indoc-yanine angiography and proposed the disc as the cause ofthe macular detachment similar to optic pit maculopathy
There is a lot of overlap between the pathogenesis ofcentral serous retinopathy (CSR) and paraproteinemic mac-ulopathy Unilaterality of the maculopathy is one commonfinding in paraproteinemia and CSR as found in the currentseries In CSR Pruumlnte and Flammer37 detected capillary orvenous congestion after ischemia in 1 or more choroidallobules and this finding may be the reason for choroidalhyperpermeability Nicholson et al38 documented thepresence of a thickened and engorged choroid in CSRby enhanced depth OCT and proposed that thesehyperpermeable choroidal vessels produce increased tissuehydrostatic pressure promoting the formation of RPEdetachments overwhelming the barrier function of theRPE and leading to fluid accumulation between the retinaand the RPE Optical coherence tomography also mayshow an anatomic defect (microrip) in the RPE associatedwith fluid that is leaking into the subretinal spaceLikewise there is venous congestion in the choroid andretina in paraproteinemia leading to choroidal ischemiaand hyperpermeability which leads to CSR (Fig 4) Zamirand Chowers39 reported a patient with paraproteinemia whohad CSR in the right eye and branch retinal vein occlusionin the left eye with normal maculae Although CSR couldbe the primary cause of the ocular condition one couldargue that paraproteinemia could have induced a CSR-likecondition as previously discussed
Early treatment is necessary to prevent irreversible visualloss especially with the currently lengthened expected lifespan Paraproteinemic maculopathy becomes symptomaticwhen IgM levels exceed 4000 mgdl in diabetics and 7000mgdl in nondiabetics (Table 1) and serum viscosity exceeds
6
55 cP Prompt referral to a hematologist or oncologist isnecessary for systemic monitoring and treatment The visualloss in paraproteinemic maculopathy may be similar to thevisual loss in CSR with proteinaceous subretinal fluid40
Landa et al40 found a correlation between the subfovealthickness of the protein deposit layer and visual acuity atbaseline in 38 patients with CSR No such relation wasfound in our series possibly because of the retrospectivenature of the study and the small size of the study group
Usually no treatment is indicated for asymptomatic dis-ease Indications for initiating treatment include bloodhyperviscosity and ocular disturbance The cardinal therapiesinclude plasmapheresis (for patients with symptomatichyperviscosity) rituximab (anti-CD20 antibody that isgenetically engineered human monoclonal antibody directedagainst the CD20 antigen found on the surface of normal andmalignant B lymphocytes) and chemotherapy (purinenucleoside analogs alkylating agents thalidomide and bor-tezomib) Plasmapheresis is very useful in reducing serumhyperviscosity and rapidly improving most ocular manifes-tations According to Menke et al41 plasmapheresis resultedin significant reductions in serum IgM (by 465) and serumviscosity (by 447) and venous stasis retinopathy improvedin all patients after plasmapheresis Paraproteinemia-relatedvenous stasis retinopathy mimics a central retinal veinocclusion-like appearance (no thrombus) with normal retinalblood flow In our review the area of the macular detachmentcorrelated with serum viscosity and many eyes did notdemonstrate resolution of the maculopathy despite improve-ment in both the serum viscosity and the venous stasis reti-nopathy One possible reason could be the short follow-upin the current review these immunoglobulins need a longtime to resolve42 Besides plasmapheresis chemotherapyespecially with rituximab remains the mainstay of therapyVarious intravitreal injections (bevacizumab triamcinolonerituximab43) failed to show a definite benefit in the currentseries
In conclusion this case series along with the literaturereview provide further evidence of the direct correlationbetween IgM levels in the blood and the degree of subretinalfluid accumulation under the fovea in these patients Clinicalimprovement clearly correlated with a decrease in serumIgM Maculopathy of paraproteinemia can mimic diabeticretinopathy adult vitelliform dystrophy and CSR espe-cially in the many patients with diabetes Unilateral local-ized macular detachment is noted commonly in patients withelevated serum IgM levels associated with WM Para-proteinemic maculopathy often becomes symptomatic whenIgM levels exceed 7000 mgdl (4000 mgdl in diabetics) andserum viscosity exceeds 55 cP Therapy should be directedtoward decreasing the serum immunoglobulin level and theserum viscosity
References
1 Saleun JP Vicariot M Deroff P Morin JF Monoclonalgammopathies in the adult population of Finistere FranceJ Clin Pathol 19823563ndash8
Mansour et al Paraproteinemic Maculopathy
2 Baker PS Garg SJ Fineman MS et al Serous maculardetachment in Waldenstroumlm macroglobulinemia a report offour cases Am J Ophthalmol 2013155448ndash55
3 Okada K Yamamoto S Tsuyama Y Mizunoya S Case ofPOEMS syndrome associated with bilateral macular detach-ment resolved by autologous peripheral blood stem celltransplantation [letter] Jpn J Ophthalmol 200751237ndash8
4 Pilon AF Rhee PS Messner LV Bilateral persistent serousmacular detachments with Waldenstroumlmrsquos macroglobulinemiaOptom Vis Sci 200582573ndash8
5 Ho AC Benson WE Wong J Unusual immunogammopathymaculopathy Ophthalmology 20001071099ndash103
6 Ogata N Ida H Takahashi K et al Occult retinal pigmentepithelial detachment in hyperviscosity syndrome OphthalmicSurg Lasers 200031248ndash52
7 Cohen SM Kokame GT Gass JD Paraproteinemias associ-ated with serous detachments of the retinal pigment epitheliumand neurosensory retina Retina 199616467ndash73
8 Spielberg LH Heckenlively JR Leys AM Retinal pigmentepithelial detachments and tears and progressive retinaldegeneration in light chain deposition disease Br J Oph-thalmol 201397627ndash31
9 Leys AM Vandenberghe P Serous macular detachments in apatient with IgM paraproteinemia an optical coherence to-mography study Arch Ophthalmol 2001119911ndash3
10 Brody JM Butrus SI Ashraf MF et al Multiple myelomapresenting with bilateral exudative macular detachments ActaOphthalmol Scand 19957381ndash2
11 Berta A Beck P Mikita J IgM paraprotein in the subretinal fluidof a patient with recurrent retinal detachment andWaldenstroumlmrsquosmacroglobulinaemia Acta Med Hung 198542179ndash86
12 Khouri GG Murphy RP Kuhajda FP Green WR Clinico-pathologic features in two cases of multiple myeloma Retina19866169ndash75
13 Freidman AH Marchevsky A Odel JG et al Immunofluo-rescent studies of the eye in Waldenstroumlmrsquos macroglobuli-nemia Arch Ophthalmol 198098743ndash6
14 Thomas EL Olk RJ Markman M et al Irreversible visual lossin Waldenstroumlmrsquos macroglobulinaemia Br J Ophthalmol198367102ndash6
15 Sen HN Chan C-C Caruso RC et al Waldenstroumlmrsquosmacroglobulinemia-associated retinopathy Ophthalmology2004111535ndash9
16 Feigl B Sill H Haas A Serous detection of the neuroretina inWaldenstroumlm disease A case report [in German] Klin MonblAugenheilkd 199921564ndash7
17 Bernard A Rousselie F Macular manifestations of mono-clonal dysgammaglobulinemias Apropos of 3 cases [inFrench] J Fr Ophtalmol 19869805ndash10
18 Quhill F Khan I Rashid A Bilateral serous macular de-tachments in Waldenstroumlmrsquos macroglobulinaemia PostgradMed J 200985382
19 Khan JM McBain V Santiago C Lois N Bilateral lsquovitelli-form-likersquo macular lesions in a patient with multiple myelomaBMJ Case Rep [serial online] 20102010 bcr0520103049Available at httpwwwncbinlmnihgovpmcarticlesPMC3028543 Accessed April 4 2014
20 Brolly A Janon C Precausta F et al Pseudovitelliform sub-foveal deposit in Waldenstroumlmrsquos macroglobulinemia CaseRep Ophthalmol [serial online] 20123236ndash9 Available athttpwwwkargercomArticleAbstract339988 AccessedApril 4 2014
21 Daicker BC Mihatsch MJ Stroslashm EH Fogazzi GB Ocularpathology in light chain deposition disease Eur J Ophthalmol1995575ndash81
22 Ardouin M Urvoy M Gastard J Aspect of the dysproteinemicfundus oculi (microaneurysms and retinal detachment) in acase of Waldenstromrsquos disease [in French] Bull Soc Ophtal-mol Fr 196666129ndash32
23 Lin CJ Chiu YM Chen SN et al Unusual maculopathysecondary to hypergammaglobulinemia in a patient with sys-temic lupus erythematosus Retin Cases Brief Rep 2012627ndash9
24 Besirli CG Johnson MW Immunogammopathy maculopathyassociated with Waldenstrom macroglobulinemia is refractoryto conventional interventions for macular edema Retin CasesBrief Rep 20137319ndash24
25 Gil Hernandez MA Abreu Reyes P Bahaya Alvarez Y AcostaAcosta B Bilateral serous detachment of the neurosensory retinaassociated with light-chain deposition disease [in Spanish] ArchSoc Canaria Oftalmol 200819 Available at wwwoftalmocomscorevista-1919sco09htm Accessed April 4 2014
26 Shah AR Zaidi A Brucker AJ Serous retinal detachmentsassociated with light chain deposition disease Retin CasesBrief Rep 20137236ndash41
27 Fenicia V Balestrieri M Perdicchi A et al Intravitreal injectionof dexamethasone implant in serous macular detachment asso-ciated withWaldenstroumlmrsquos disease Case Rep Ophthalmol [serialonline] 2013464ndash9 Available at httpwwwkargercomArti-cleFullText354066 Accessed April 4 2014
28 Mansoor A Wagner RP DePalma L Waldenstrom macro-globulinemia presenting as a pleural effusion Arch Pathol LabMed 2000124891ndash3
29 Kavuru MS Tubbs ML Miller L Wiedemann P Immuno-cytometry and gene rearrangement analysis in the diagnosis oflymphoma in an idiopathic pleural effusion Am Rev RespirDis 1992145209ndash11
30 Klaassen I Van Noorden CJF Schlingemann RO Molecularbasis of the inner blood-retinal barrier and its breakdown indiabetic macular edema and other pathological conditionsProg Retin Eye Res 20133419ndash48
31 Kanda T Usui S Beppu H et al Blood-nerve barrier in IgMparaproteinemic neuropathy a clinicopathologic assessmentActa Neuropathol 199895184ndash92
32 Lach B Rippstein P Atack D et al Immunoelectron micro-scopic localization of monoclonal IgM antibodies in gamm-opathy associated with peripheral demyelinative neuropathyActa Neuropathol 199385298ndash307
33 Terpos E Tasidou A Kastritis E et al Angiogenesis in Wal-denstroumlmrsquos macroglobulinemia Clin Lymphoma Myeloma2009946ndash9
34 Ashton N Ocular changes in multiple myelomatosis ArchOphthalmol 196573487ndash94
35 Foos RY Allen RA Opaque cysts of the ciliary body (parsciliaris retinae) Arch Ophthalmol 196777559ndash68
36 Dumas D Viriot ML Boura C et al Permeability oxygenthrough endothelial cells monolayer using time-resolvedfluorescence microscopy Effect of human plasma viscosityIn Periasamy A So PT eds Multiphoton Microscopy in theBiomedical Sciences II Bellingham WA Society of Photo-optical Instrumentation Engineers 2002293e301 Pro-ceedings of SPIE Vol 4620
37 Pruumlnte C Flammer J Choroidal capillary and venouscongestion in central serous chorioretinopathy Am JOphthalmol 199612126ndash34
38 Nicholson B Noble J Forooghian F Meyerle C Centralserous chorioretinopathy update on pathophysiology andtreatment Surv Ophthalmol 201358103ndash26
39 Zamir E Chowers I Central serous chorioretinopathy in a patientwith cryoglobulinaemia [letter] Eye (Lond) 199913265ndash6
7
Ophthalmology Volume - Number - Month 2014
40 Landa G Barnett JA Garcia PM et al Quantitative andqualitative spectral domain optical coherence tomographyanalysis of subretinal deposits in patients with acutecentral serous retinopathy Ophthalmologica 201323062ndash8
41 Menke MN Feke GT McMeel JW Treon SP Effect ofplasmapheresis on hyperviscosity-related retinopathy andretinal hemodynamics in patients with Waldenstromrsquos
8
macroglobulinemia Invest Ophthalmol Vis Sci 2008491157ndash60
42 Negi A Marmor MF Effects of subretinal and systemicosmolality on the rate of subretinal fluid resorption InvestOphthalmol Vis Sci 198425616ndash20
43 Larkin KL Saboo US Comer GM et al Use of intravitrealrituximab for treatment of vitreoretinal lymphoma Br J Oph-thalmol 20149899ndash103
Footnotes and Financial Disclosures
Originally received January 22 2014Final revision March 6 2014Accepted April 9 2014Available online --- Manuscript no 2014-1191 Departments of Ophthalmology American University of Beirut and RaficHariri University Hospital Beirut Lebanon2 Retina Departments The King Khaled Eye Specialist Hospital RiyadhKingdom of Saudi Arabia and Wilmer Eye Institute The Johns HopkinsUniversity Baltimore Maryland3 Department of Ophthalmology Hospital Moises Broggi Sant Joan DespiBarcelona Spain4 Associated Vitreoretinal and Uveitis Consultants Department ofOphthalmology Indiana University School of Medicine IndianapolisIndiana5 Retina Associates of Cleveland Beachwood Ohio6 The Retina Institute St Louis Missouri7 Department of Ophthalmology Mayo Clinic Rochester Minnesota8 Department of Statistics and Research Methodology Lebanese AmericanUniversity and Lebanese University Beirut Lebanon9 Retina Service at Oftalmologica San Miguel de Tucumaacuten Argentina10 Department of Ophthalmology Universidade Estadual de LondrinaParana Brazil
11 Department of Clinical Science ldquoLuigi Saccordquo Sacco Hospital Univer-sity of Milan Milan Italy
Financial Disclosure(s)The author(s) have no proprietary or commercial interest in any materialsdiscussed in this article
JFA Consultant - Second Sight LLC Alcon Labs Lecturer - IridexOptos Inc Speakers Bureau - Novartis Pharmaceuticals Alimera SciencesInc Royalties - Springer SBM LLC
GS Consultant - Heidelberg Engineering Zeiss QLT GSK AlconAllergan Bayer Boheringer Genentech Roche Novartis Speakers Bureaue Zeiss Heidelberg Engineering Novartis GSK Patents - Ocular In-struments Novartis
AM Consultant Lecturer - Bayer
Abbreviations and AcronymsBCVA frac14 best-corrected visual acuity cP frac14 centipoise CSR frac14 centralserous retinopathy DD frac14 disc diameter IgM frac14 immunoglobulin MlogMAR frac14 logarithm of the minimum angle of resolution MM frac14 multiplemyeloma OCT frac14 optical coherence tomography RPE frac14 retinal pigmentepithelium WM frac14 Waldenstroumlm macroglobulinemia
CorrespondenceAhmad M Mansour MD Department of Ophthalmology AmericanUniversity of Beirut PO Box 1136044 Beirut Lebanon E-mailammansourmdgmailcom

Mansour et al Paraproteinemic Maculopathy
decreased to 2060 in the right eye and 20200 in the left eye andOCT showed neurosensory detachment with overlying cystoidmacular edema and bilateral disruption of the outer retina (Fig 2)The patientrsquos blood pressure was 13090 mmHg Hyperviscositysyndrome was suspected and blood tests revealed severe anemia(hemoglobin 79 mgdl normal values 135e175 mgdl) and atotal serum protein level of 192 mgdl (normal values 60e80mgdl) with elevated monoclonal IgM of 10 500 mgdl (normalvalues 45e153 mgdl) Bone marrow biopsy showed massivelymphoplasmacytoid infiltration A diagnosis of WM wasmade Computed tomography of the abdomen showed multipleretroperitoneal lymphadenopathies (iliac and inguinal) Plasma-pheresis was performed followed by 8 cycles of systemicpolychemotherapy with rituximab cyclophosphamide doxoru-bicin vincristine and steroids and 2 cycles of cladribineSystemic rituximab was not given until IgM levels decreased toless than 50 mgdl because rituximab is associated with suddenincrease in IgM levels and should be avoided in patients withhyperviscosity Simultaneously 3 monthly 25-mg01-ml intra-vitreal bevacizumab injections were administered in both eyesBest-corrected visual acuity remained 2060 in the right eye and20200 in the left eye and OCT demonstrated a slight bilateraldecrease in neurosensory detachment (Fig 3) At that time the IgMlevel dropped to 3925 mgdl Two months after the last intravitrealbevacizumab injection 3 monthly intravitreal injections ofrituximab (1 mg01 ml) were administered in both eyes Best-corrected visual acuity remained unchanged and OCT demon-strated a slight bilateral decrease in the amount of subretinal fluid(Fig 3) At that time the IgM level dropped to 2943 mgdl After 2years of follow-up complete remission was not reached BCVAwas 2060 in the right eye and 20400 in the left eye and OCTshowed no significant improvement
Discussion
Serous macular detachment is an uncommon ocular mani-festation of paraproteinemia2e27 The absence of angio-graphic leakage within the macular detachment does notsupport the theory of angiographic exudation from the retinalor choroidal vasculature In a few cases there was leakage inthe deep retina (Table 1) Some investigators have focused onthe presence of IgM in the subretinal space1112 suggestingthat an increased osmotic gradient causes fluid accumulationunder the retina In support of this hypothesis several his-topathologic reports documented immunoglobulins in thesubretinal space11e13 High-molecular-weight immunoglob-ulins lead to an osmotic gradient Because IgM antibodies arethe largest antibodies found in the blood and the lymph fluidthey rarely accumulate in pericardial peritoneal and pleuraleffusions2829 Immunoglobulin M antibodies consist of aheavy chain a light chain and 5 base units with a molecularmass of 970 kDa in its pentamer form (molecular weight06e1 000 000 kDa) Because IgM antibodies are very largemolecules and cannot diffuse well they are found in theinterstitium in extremely low quantities When such largepositively charged IgM molecules are present in excess theybind electrostatically to red cells aggregating and formingrouleaux with subsequent increase in the blood viscosity Asthe IgM protein concentration in the serum increases theblood viscosity increases exponentially It is somewhatintriguing to explain how IgM antibodies reach the subretinalspace (Fig 4) According to Klaassen et al30 the central
mechanism of the altered blooderetinal barrier results fromthe altered permeability of retinal endothelial cells causedby elevated levels of growth factors (such as vascularendothelial growth factor) cytokines and loss of pericytes(as occurs in diabetes) Subsequently both paracellular andtranscellular transport across the retinal vascular wall increasevia opening of the endothelial intercellular junctions andincrease in endothelial caveolar transcellular transport Thereis histologic evidence that the bloodeneural barrier (which issimilar to the blooderetinal barrier) is affected inparaproteinemia Kanda et al31 reported the pathologicfindings in a patient with sensorimotor neuropathy associatedwith WM and monoclonal IgM particularly in relation tobloodenerve barrier defects A sural nerve biopsy specimenrevealed gaps between adjacent endothelial cells of smallendoneurial vessels as well as the absence of some of thetight junctions between adjacent endothelial cells Similarlyin a sural nerve biopsy from a patient with benignmonoclonal IgM k gammopathy and sensorimotor demyeli-native neuropathy Lash et al32 found that many endoneurialcapillaries were lined by fenestrated endothelium indicatingthe breakdown of the normal bloodenerve barrier Theendoneurium contained large amounts of extracellularproteinaceous material containing IgM k g-globulin
Brody et al10 suggested thatmacular exudative detachmentsfrom diabetic maculopathy can lead to increased leakage ofimmunoglobulins into the subretinal space In a case withpolyneuropathy organomegaly endocrinopathy M-proteinand skin abnormalities syndrome Okada et al3 proposed thatthe high vascular endothelial growth factor level probablyinduced the retinal microvascular hyperpermeability leadingto leakage of immunoglobulin in the subretinal space Themaculopathy resolved 1 month after hematopoietic surgerywhen serum vascular endothelial growth factor leveldecreased in response to autologous peripheral blood stemcells The sera of WM patients are known to be associatedwith increased levels of angiogenic cytokines such asangiogenin vascular endothelial growth factor and basicfibroblast growth factor33 In normal bone marrowangiopoietin-1 consistently activates tyrosine kinase withimmunoglobulin-like and epidermal growth factor-like do-mains-2 and stabilizes vessels by promoting interactionsbetween endothelial cells and surrounding pericytes Onthe contrary during the malignant process in WMincreased angiopoietin-2 levels block tyrosine kinase with theimmunoglobulin-like and epidermal growth factor-like do-mains-2 receptor and lead to vessel destabilization by loos-ening endothelialeperiendothelial cell interactions anddegrading the extracellular matrix The primary source ofangiopoietin-2 is endothelial cells because angiopoietin-2 isstored in vesicles known as Weibel-Palade bodies and isreleased rapidly in response to hyperglycemia and ischemiaAngiopoietin-2 seems to be an important mediator in thealteration of the blooderetinal barrier in diabetes and otherretinal vascular disorders30
Ashton34 aswell as Foos andAllen35were among the first todescribe retinal and RPE detachment histologically in patientswith MM The subpigment epithelial fluid is derived fromchoroidal vessels The platelets can no longer fulfill theirnormal function of maintenance of endothelium because they
5
Ophthalmology Volume - Number - Month 2014
become covered by paraprotein Moreover the hyperviscositycan cause stasis and hypoxia leading to endotheliumdecompensation There is secondary breakdown of theblooderetinal barrier in addition to the RPE decompensationfrom the underlying deposit and hypoxia Coexisting anemiadiabetes and hypertension are additional risk factors forretinal vascular endothelial damage and ischemic injuryenhancing leakage and breakdown of the blooderetinalbarrier Dumas et al36 explored the contribution of plasmaviscosity and the endothelial cell monolayer to oxygenmolecular transport processes using a fluorescence inhibitionmethod They found hypoxia induced by hyperviscosityplasmas from patients with WM to have increasedintercellular adhesion molecule 1 expression on the surface ofendothelial cells which could be the cause of vasculardisorders through the implication of polymorphonuclearneutrophils
Baker et al2 demonstrated complete disruption of theouter retina within the detachment and proposed that thesefocal outer retinal defects (Figs 2 and 3) slowly progressover time eventually allowing a so-called track for intra-retinal IgM Our study was not aimed at estimating thepresence of such outer retinal defects A pathologiccommunication between the optic disc the subarachnoidspace and the subretinal space was proposed by Feigl et al16
and Khan et al19 Feigl et al16 found a finger-like extensionto the optic disc from the macular detachment by indoc-yanine angiography and proposed the disc as the cause ofthe macular detachment similar to optic pit maculopathy
There is a lot of overlap between the pathogenesis ofcentral serous retinopathy (CSR) and paraproteinemic mac-ulopathy Unilaterality of the maculopathy is one commonfinding in paraproteinemia and CSR as found in the currentseries In CSR Pruumlnte and Flammer37 detected capillary orvenous congestion after ischemia in 1 or more choroidallobules and this finding may be the reason for choroidalhyperpermeability Nicholson et al38 documented thepresence of a thickened and engorged choroid in CSRby enhanced depth OCT and proposed that thesehyperpermeable choroidal vessels produce increased tissuehydrostatic pressure promoting the formation of RPEdetachments overwhelming the barrier function of theRPE and leading to fluid accumulation between the retinaand the RPE Optical coherence tomography also mayshow an anatomic defect (microrip) in the RPE associatedwith fluid that is leaking into the subretinal spaceLikewise there is venous congestion in the choroid andretina in paraproteinemia leading to choroidal ischemiaand hyperpermeability which leads to CSR (Fig 4) Zamirand Chowers39 reported a patient with paraproteinemia whohad CSR in the right eye and branch retinal vein occlusionin the left eye with normal maculae Although CSR couldbe the primary cause of the ocular condition one couldargue that paraproteinemia could have induced a CSR-likecondition as previously discussed
Early treatment is necessary to prevent irreversible visualloss especially with the currently lengthened expected lifespan Paraproteinemic maculopathy becomes symptomaticwhen IgM levels exceed 4000 mgdl in diabetics and 7000mgdl in nondiabetics (Table 1) and serum viscosity exceeds
6
55 cP Prompt referral to a hematologist or oncologist isnecessary for systemic monitoring and treatment The visualloss in paraproteinemic maculopathy may be similar to thevisual loss in CSR with proteinaceous subretinal fluid40
Landa et al40 found a correlation between the subfovealthickness of the protein deposit layer and visual acuity atbaseline in 38 patients with CSR No such relation wasfound in our series possibly because of the retrospectivenature of the study and the small size of the study group
Usually no treatment is indicated for asymptomatic dis-ease Indications for initiating treatment include bloodhyperviscosity and ocular disturbance The cardinal therapiesinclude plasmapheresis (for patients with symptomatichyperviscosity) rituximab (anti-CD20 antibody that isgenetically engineered human monoclonal antibody directedagainst the CD20 antigen found on the surface of normal andmalignant B lymphocytes) and chemotherapy (purinenucleoside analogs alkylating agents thalidomide and bor-tezomib) Plasmapheresis is very useful in reducing serumhyperviscosity and rapidly improving most ocular manifes-tations According to Menke et al41 plasmapheresis resultedin significant reductions in serum IgM (by 465) and serumviscosity (by 447) and venous stasis retinopathy improvedin all patients after plasmapheresis Paraproteinemia-relatedvenous stasis retinopathy mimics a central retinal veinocclusion-like appearance (no thrombus) with normal retinalblood flow In our review the area of the macular detachmentcorrelated with serum viscosity and many eyes did notdemonstrate resolution of the maculopathy despite improve-ment in both the serum viscosity and the venous stasis reti-nopathy One possible reason could be the short follow-upin the current review these immunoglobulins need a longtime to resolve42 Besides plasmapheresis chemotherapyespecially with rituximab remains the mainstay of therapyVarious intravitreal injections (bevacizumab triamcinolonerituximab43) failed to show a definite benefit in the currentseries
In conclusion this case series along with the literaturereview provide further evidence of the direct correlationbetween IgM levels in the blood and the degree of subretinalfluid accumulation under the fovea in these patients Clinicalimprovement clearly correlated with a decrease in serumIgM Maculopathy of paraproteinemia can mimic diabeticretinopathy adult vitelliform dystrophy and CSR espe-cially in the many patients with diabetes Unilateral local-ized macular detachment is noted commonly in patients withelevated serum IgM levels associated with WM Para-proteinemic maculopathy often becomes symptomatic whenIgM levels exceed 7000 mgdl (4000 mgdl in diabetics) andserum viscosity exceeds 55 cP Therapy should be directedtoward decreasing the serum immunoglobulin level and theserum viscosity
References
1 Saleun JP Vicariot M Deroff P Morin JF Monoclonalgammopathies in the adult population of Finistere FranceJ Clin Pathol 19823563ndash8
Mansour et al Paraproteinemic Maculopathy
2 Baker PS Garg SJ Fineman MS et al Serous maculardetachment in Waldenstroumlm macroglobulinemia a report offour cases Am J Ophthalmol 2013155448ndash55
3 Okada K Yamamoto S Tsuyama Y Mizunoya S Case ofPOEMS syndrome associated with bilateral macular detach-ment resolved by autologous peripheral blood stem celltransplantation [letter] Jpn J Ophthalmol 200751237ndash8
4 Pilon AF Rhee PS Messner LV Bilateral persistent serousmacular detachments with Waldenstroumlmrsquos macroglobulinemiaOptom Vis Sci 200582573ndash8
5 Ho AC Benson WE Wong J Unusual immunogammopathymaculopathy Ophthalmology 20001071099ndash103
6 Ogata N Ida H Takahashi K et al Occult retinal pigmentepithelial detachment in hyperviscosity syndrome OphthalmicSurg Lasers 200031248ndash52
7 Cohen SM Kokame GT Gass JD Paraproteinemias associ-ated with serous detachments of the retinal pigment epitheliumand neurosensory retina Retina 199616467ndash73
8 Spielberg LH Heckenlively JR Leys AM Retinal pigmentepithelial detachments and tears and progressive retinaldegeneration in light chain deposition disease Br J Oph-thalmol 201397627ndash31
9 Leys AM Vandenberghe P Serous macular detachments in apatient with IgM paraproteinemia an optical coherence to-mography study Arch Ophthalmol 2001119911ndash3
10 Brody JM Butrus SI Ashraf MF et al Multiple myelomapresenting with bilateral exudative macular detachments ActaOphthalmol Scand 19957381ndash2
11 Berta A Beck P Mikita J IgM paraprotein in the subretinal fluidof a patient with recurrent retinal detachment andWaldenstroumlmrsquosmacroglobulinaemia Acta Med Hung 198542179ndash86
12 Khouri GG Murphy RP Kuhajda FP Green WR Clinico-pathologic features in two cases of multiple myeloma Retina19866169ndash75
13 Freidman AH Marchevsky A Odel JG et al Immunofluo-rescent studies of the eye in Waldenstroumlmrsquos macroglobuli-nemia Arch Ophthalmol 198098743ndash6
14 Thomas EL Olk RJ Markman M et al Irreversible visual lossin Waldenstroumlmrsquos macroglobulinaemia Br J Ophthalmol198367102ndash6
15 Sen HN Chan C-C Caruso RC et al Waldenstroumlmrsquosmacroglobulinemia-associated retinopathy Ophthalmology2004111535ndash9
16 Feigl B Sill H Haas A Serous detection of the neuroretina inWaldenstroumlm disease A case report [in German] Klin MonblAugenheilkd 199921564ndash7
17 Bernard A Rousselie F Macular manifestations of mono-clonal dysgammaglobulinemias Apropos of 3 cases [inFrench] J Fr Ophtalmol 19869805ndash10
18 Quhill F Khan I Rashid A Bilateral serous macular de-tachments in Waldenstroumlmrsquos macroglobulinaemia PostgradMed J 200985382
19 Khan JM McBain V Santiago C Lois N Bilateral lsquovitelli-form-likersquo macular lesions in a patient with multiple myelomaBMJ Case Rep [serial online] 20102010 bcr0520103049Available at httpwwwncbinlmnihgovpmcarticlesPMC3028543 Accessed April 4 2014
20 Brolly A Janon C Precausta F et al Pseudovitelliform sub-foveal deposit in Waldenstroumlmrsquos macroglobulinemia CaseRep Ophthalmol [serial online] 20123236ndash9 Available athttpwwwkargercomArticleAbstract339988 AccessedApril 4 2014
21 Daicker BC Mihatsch MJ Stroslashm EH Fogazzi GB Ocularpathology in light chain deposition disease Eur J Ophthalmol1995575ndash81
22 Ardouin M Urvoy M Gastard J Aspect of the dysproteinemicfundus oculi (microaneurysms and retinal detachment) in acase of Waldenstromrsquos disease [in French] Bull Soc Ophtal-mol Fr 196666129ndash32
23 Lin CJ Chiu YM Chen SN et al Unusual maculopathysecondary to hypergammaglobulinemia in a patient with sys-temic lupus erythematosus Retin Cases Brief Rep 2012627ndash9
24 Besirli CG Johnson MW Immunogammopathy maculopathyassociated with Waldenstrom macroglobulinemia is refractoryto conventional interventions for macular edema Retin CasesBrief Rep 20137319ndash24
25 Gil Hernandez MA Abreu Reyes P Bahaya Alvarez Y AcostaAcosta B Bilateral serous detachment of the neurosensory retinaassociated with light-chain deposition disease [in Spanish] ArchSoc Canaria Oftalmol 200819 Available at wwwoftalmocomscorevista-1919sco09htm Accessed April 4 2014
26 Shah AR Zaidi A Brucker AJ Serous retinal detachmentsassociated with light chain deposition disease Retin CasesBrief Rep 20137236ndash41
27 Fenicia V Balestrieri M Perdicchi A et al Intravitreal injectionof dexamethasone implant in serous macular detachment asso-ciated withWaldenstroumlmrsquos disease Case Rep Ophthalmol [serialonline] 2013464ndash9 Available at httpwwwkargercomArti-cleFullText354066 Accessed April 4 2014
28 Mansoor A Wagner RP DePalma L Waldenstrom macro-globulinemia presenting as a pleural effusion Arch Pathol LabMed 2000124891ndash3
29 Kavuru MS Tubbs ML Miller L Wiedemann P Immuno-cytometry and gene rearrangement analysis in the diagnosis oflymphoma in an idiopathic pleural effusion Am Rev RespirDis 1992145209ndash11
30 Klaassen I Van Noorden CJF Schlingemann RO Molecularbasis of the inner blood-retinal barrier and its breakdown indiabetic macular edema and other pathological conditionsProg Retin Eye Res 20133419ndash48
31 Kanda T Usui S Beppu H et al Blood-nerve barrier in IgMparaproteinemic neuropathy a clinicopathologic assessmentActa Neuropathol 199895184ndash92
32 Lach B Rippstein P Atack D et al Immunoelectron micro-scopic localization of monoclonal IgM antibodies in gamm-opathy associated with peripheral demyelinative neuropathyActa Neuropathol 199385298ndash307
33 Terpos E Tasidou A Kastritis E et al Angiogenesis in Wal-denstroumlmrsquos macroglobulinemia Clin Lymphoma Myeloma2009946ndash9
34 Ashton N Ocular changes in multiple myelomatosis ArchOphthalmol 196573487ndash94
35 Foos RY Allen RA Opaque cysts of the ciliary body (parsciliaris retinae) Arch Ophthalmol 196777559ndash68
36 Dumas D Viriot ML Boura C et al Permeability oxygenthrough endothelial cells monolayer using time-resolvedfluorescence microscopy Effect of human plasma viscosityIn Periasamy A So PT eds Multiphoton Microscopy in theBiomedical Sciences II Bellingham WA Society of Photo-optical Instrumentation Engineers 2002293e301 Pro-ceedings of SPIE Vol 4620
37 Pruumlnte C Flammer J Choroidal capillary and venouscongestion in central serous chorioretinopathy Am JOphthalmol 199612126ndash34
38 Nicholson B Noble J Forooghian F Meyerle C Centralserous chorioretinopathy update on pathophysiology andtreatment Surv Ophthalmol 201358103ndash26
39 Zamir E Chowers I Central serous chorioretinopathy in a patientwith cryoglobulinaemia [letter] Eye (Lond) 199913265ndash6
7
Ophthalmology Volume - Number - Month 2014
40 Landa G Barnett JA Garcia PM et al Quantitative andqualitative spectral domain optical coherence tomographyanalysis of subretinal deposits in patients with acutecentral serous retinopathy Ophthalmologica 201323062ndash8
41 Menke MN Feke GT McMeel JW Treon SP Effect ofplasmapheresis on hyperviscosity-related retinopathy andretinal hemodynamics in patients with Waldenstromrsquos
8
macroglobulinemia Invest Ophthalmol Vis Sci 2008491157ndash60
42 Negi A Marmor MF Effects of subretinal and systemicosmolality on the rate of subretinal fluid resorption InvestOphthalmol Vis Sci 198425616ndash20
43 Larkin KL Saboo US Comer GM et al Use of intravitrealrituximab for treatment of vitreoretinal lymphoma Br J Oph-thalmol 20149899ndash103
Footnotes and Financial Disclosures
Originally received January 22 2014Final revision March 6 2014Accepted April 9 2014Available online --- Manuscript no 2014-1191 Departments of Ophthalmology American University of Beirut and RaficHariri University Hospital Beirut Lebanon2 Retina Departments The King Khaled Eye Specialist Hospital RiyadhKingdom of Saudi Arabia and Wilmer Eye Institute The Johns HopkinsUniversity Baltimore Maryland3 Department of Ophthalmology Hospital Moises Broggi Sant Joan DespiBarcelona Spain4 Associated Vitreoretinal and Uveitis Consultants Department ofOphthalmology Indiana University School of Medicine IndianapolisIndiana5 Retina Associates of Cleveland Beachwood Ohio6 The Retina Institute St Louis Missouri7 Department of Ophthalmology Mayo Clinic Rochester Minnesota8 Department of Statistics and Research Methodology Lebanese AmericanUniversity and Lebanese University Beirut Lebanon9 Retina Service at Oftalmologica San Miguel de Tucumaacuten Argentina10 Department of Ophthalmology Universidade Estadual de LondrinaParana Brazil
11 Department of Clinical Science ldquoLuigi Saccordquo Sacco Hospital Univer-sity of Milan Milan Italy
Financial Disclosure(s)The author(s) have no proprietary or commercial interest in any materialsdiscussed in this article
JFA Consultant - Second Sight LLC Alcon Labs Lecturer - IridexOptos Inc Speakers Bureau - Novartis Pharmaceuticals Alimera SciencesInc Royalties - Springer SBM LLC
GS Consultant - Heidelberg Engineering Zeiss QLT GSK AlconAllergan Bayer Boheringer Genentech Roche Novartis Speakers Bureaue Zeiss Heidelberg Engineering Novartis GSK Patents - Ocular In-struments Novartis
AM Consultant Lecturer - Bayer
Abbreviations and AcronymsBCVA frac14 best-corrected visual acuity cP frac14 centipoise CSR frac14 centralserous retinopathy DD frac14 disc diameter IgM frac14 immunoglobulin MlogMAR frac14 logarithm of the minimum angle of resolution MM frac14 multiplemyeloma OCT frac14 optical coherence tomography RPE frac14 retinal pigmentepithelium WM frac14 Waldenstroumlm macroglobulinemia
CorrespondenceAhmad M Mansour MD Department of Ophthalmology AmericanUniversity of Beirut PO Box 1136044 Beirut Lebanon E-mailammansourmdgmailcom

Ophthalmology Volume - Number - Month 2014
become covered by paraprotein Moreover the hyperviscositycan cause stasis and hypoxia leading to endotheliumdecompensation There is secondary breakdown of theblooderetinal barrier in addition to the RPE decompensationfrom the underlying deposit and hypoxia Coexisting anemiadiabetes and hypertension are additional risk factors forretinal vascular endothelial damage and ischemic injuryenhancing leakage and breakdown of the blooderetinalbarrier Dumas et al36 explored the contribution of plasmaviscosity and the endothelial cell monolayer to oxygenmolecular transport processes using a fluorescence inhibitionmethod They found hypoxia induced by hyperviscosityplasmas from patients with WM to have increasedintercellular adhesion molecule 1 expression on the surface ofendothelial cells which could be the cause of vasculardisorders through the implication of polymorphonuclearneutrophils
Baker et al2 demonstrated complete disruption of theouter retina within the detachment and proposed that thesefocal outer retinal defects (Figs 2 and 3) slowly progressover time eventually allowing a so-called track for intra-retinal IgM Our study was not aimed at estimating thepresence of such outer retinal defects A pathologiccommunication between the optic disc the subarachnoidspace and the subretinal space was proposed by Feigl et al16
and Khan et al19 Feigl et al16 found a finger-like extensionto the optic disc from the macular detachment by indoc-yanine angiography and proposed the disc as the cause ofthe macular detachment similar to optic pit maculopathy
There is a lot of overlap between the pathogenesis ofcentral serous retinopathy (CSR) and paraproteinemic mac-ulopathy Unilaterality of the maculopathy is one commonfinding in paraproteinemia and CSR as found in the currentseries In CSR Pruumlnte and Flammer37 detected capillary orvenous congestion after ischemia in 1 or more choroidallobules and this finding may be the reason for choroidalhyperpermeability Nicholson et al38 documented thepresence of a thickened and engorged choroid in CSRby enhanced depth OCT and proposed that thesehyperpermeable choroidal vessels produce increased tissuehydrostatic pressure promoting the formation of RPEdetachments overwhelming the barrier function of theRPE and leading to fluid accumulation between the retinaand the RPE Optical coherence tomography also mayshow an anatomic defect (microrip) in the RPE associatedwith fluid that is leaking into the subretinal spaceLikewise there is venous congestion in the choroid andretina in paraproteinemia leading to choroidal ischemiaand hyperpermeability which leads to CSR (Fig 4) Zamirand Chowers39 reported a patient with paraproteinemia whohad CSR in the right eye and branch retinal vein occlusionin the left eye with normal maculae Although CSR couldbe the primary cause of the ocular condition one couldargue that paraproteinemia could have induced a CSR-likecondition as previously discussed
Early treatment is necessary to prevent irreversible visualloss especially with the currently lengthened expected lifespan Paraproteinemic maculopathy becomes symptomaticwhen IgM levels exceed 4000 mgdl in diabetics and 7000mgdl in nondiabetics (Table 1) and serum viscosity exceeds
6
55 cP Prompt referral to a hematologist or oncologist isnecessary for systemic monitoring and treatment The visualloss in paraproteinemic maculopathy may be similar to thevisual loss in CSR with proteinaceous subretinal fluid40
Landa et al40 found a correlation between the subfovealthickness of the protein deposit layer and visual acuity atbaseline in 38 patients with CSR No such relation wasfound in our series possibly because of the retrospectivenature of the study and the small size of the study group
Usually no treatment is indicated for asymptomatic dis-ease Indications for initiating treatment include bloodhyperviscosity and ocular disturbance The cardinal therapiesinclude plasmapheresis (for patients with symptomatichyperviscosity) rituximab (anti-CD20 antibody that isgenetically engineered human monoclonal antibody directedagainst the CD20 antigen found on the surface of normal andmalignant B lymphocytes) and chemotherapy (purinenucleoside analogs alkylating agents thalidomide and bor-tezomib) Plasmapheresis is very useful in reducing serumhyperviscosity and rapidly improving most ocular manifes-tations According to Menke et al41 plasmapheresis resultedin significant reductions in serum IgM (by 465) and serumviscosity (by 447) and venous stasis retinopathy improvedin all patients after plasmapheresis Paraproteinemia-relatedvenous stasis retinopathy mimics a central retinal veinocclusion-like appearance (no thrombus) with normal retinalblood flow In our review the area of the macular detachmentcorrelated with serum viscosity and many eyes did notdemonstrate resolution of the maculopathy despite improve-ment in both the serum viscosity and the venous stasis reti-nopathy One possible reason could be the short follow-upin the current review these immunoglobulins need a longtime to resolve42 Besides plasmapheresis chemotherapyespecially with rituximab remains the mainstay of therapyVarious intravitreal injections (bevacizumab triamcinolonerituximab43) failed to show a definite benefit in the currentseries
In conclusion this case series along with the literaturereview provide further evidence of the direct correlationbetween IgM levels in the blood and the degree of subretinalfluid accumulation under the fovea in these patients Clinicalimprovement clearly correlated with a decrease in serumIgM Maculopathy of paraproteinemia can mimic diabeticretinopathy adult vitelliform dystrophy and CSR espe-cially in the many patients with diabetes Unilateral local-ized macular detachment is noted commonly in patients withelevated serum IgM levels associated with WM Para-proteinemic maculopathy often becomes symptomatic whenIgM levels exceed 7000 mgdl (4000 mgdl in diabetics) andserum viscosity exceeds 55 cP Therapy should be directedtoward decreasing the serum immunoglobulin level and theserum viscosity
References
1 Saleun JP Vicariot M Deroff P Morin JF Monoclonalgammopathies in the adult population of Finistere FranceJ Clin Pathol 19823563ndash8
Mansour et al Paraproteinemic Maculopathy
2 Baker PS Garg SJ Fineman MS et al Serous maculardetachment in Waldenstroumlm macroglobulinemia a report offour cases Am J Ophthalmol 2013155448ndash55
3 Okada K Yamamoto S Tsuyama Y Mizunoya S Case ofPOEMS syndrome associated with bilateral macular detach-ment resolved by autologous peripheral blood stem celltransplantation [letter] Jpn J Ophthalmol 200751237ndash8
4 Pilon AF Rhee PS Messner LV Bilateral persistent serousmacular detachments with Waldenstroumlmrsquos macroglobulinemiaOptom Vis Sci 200582573ndash8
5 Ho AC Benson WE Wong J Unusual immunogammopathymaculopathy Ophthalmology 20001071099ndash103
6 Ogata N Ida H Takahashi K et al Occult retinal pigmentepithelial detachment in hyperviscosity syndrome OphthalmicSurg Lasers 200031248ndash52
7 Cohen SM Kokame GT Gass JD Paraproteinemias associ-ated with serous detachments of the retinal pigment epitheliumand neurosensory retina Retina 199616467ndash73
8 Spielberg LH Heckenlively JR Leys AM Retinal pigmentepithelial detachments and tears and progressive retinaldegeneration in light chain deposition disease Br J Oph-thalmol 201397627ndash31
9 Leys AM Vandenberghe P Serous macular detachments in apatient with IgM paraproteinemia an optical coherence to-mography study Arch Ophthalmol 2001119911ndash3
10 Brody JM Butrus SI Ashraf MF et al Multiple myelomapresenting with bilateral exudative macular detachments ActaOphthalmol Scand 19957381ndash2
11 Berta A Beck P Mikita J IgM paraprotein in the subretinal fluidof a patient with recurrent retinal detachment andWaldenstroumlmrsquosmacroglobulinaemia Acta Med Hung 198542179ndash86
12 Khouri GG Murphy RP Kuhajda FP Green WR Clinico-pathologic features in two cases of multiple myeloma Retina19866169ndash75
13 Freidman AH Marchevsky A Odel JG et al Immunofluo-rescent studies of the eye in Waldenstroumlmrsquos macroglobuli-nemia Arch Ophthalmol 198098743ndash6
14 Thomas EL Olk RJ Markman M et al Irreversible visual lossin Waldenstroumlmrsquos macroglobulinaemia Br J Ophthalmol198367102ndash6
15 Sen HN Chan C-C Caruso RC et al Waldenstroumlmrsquosmacroglobulinemia-associated retinopathy Ophthalmology2004111535ndash9
16 Feigl B Sill H Haas A Serous detection of the neuroretina inWaldenstroumlm disease A case report [in German] Klin MonblAugenheilkd 199921564ndash7
17 Bernard A Rousselie F Macular manifestations of mono-clonal dysgammaglobulinemias Apropos of 3 cases [inFrench] J Fr Ophtalmol 19869805ndash10
18 Quhill F Khan I Rashid A Bilateral serous macular de-tachments in Waldenstroumlmrsquos macroglobulinaemia PostgradMed J 200985382
19 Khan JM McBain V Santiago C Lois N Bilateral lsquovitelli-form-likersquo macular lesions in a patient with multiple myelomaBMJ Case Rep [serial online] 20102010 bcr0520103049Available at httpwwwncbinlmnihgovpmcarticlesPMC3028543 Accessed April 4 2014
20 Brolly A Janon C Precausta F et al Pseudovitelliform sub-foveal deposit in Waldenstroumlmrsquos macroglobulinemia CaseRep Ophthalmol [serial online] 20123236ndash9 Available athttpwwwkargercomArticleAbstract339988 AccessedApril 4 2014
21 Daicker BC Mihatsch MJ Stroslashm EH Fogazzi GB Ocularpathology in light chain deposition disease Eur J Ophthalmol1995575ndash81
22 Ardouin M Urvoy M Gastard J Aspect of the dysproteinemicfundus oculi (microaneurysms and retinal detachment) in acase of Waldenstromrsquos disease [in French] Bull Soc Ophtal-mol Fr 196666129ndash32
23 Lin CJ Chiu YM Chen SN et al Unusual maculopathysecondary to hypergammaglobulinemia in a patient with sys-temic lupus erythematosus Retin Cases Brief Rep 2012627ndash9
24 Besirli CG Johnson MW Immunogammopathy maculopathyassociated with Waldenstrom macroglobulinemia is refractoryto conventional interventions for macular edema Retin CasesBrief Rep 20137319ndash24
25 Gil Hernandez MA Abreu Reyes P Bahaya Alvarez Y AcostaAcosta B Bilateral serous detachment of the neurosensory retinaassociated with light-chain deposition disease [in Spanish] ArchSoc Canaria Oftalmol 200819 Available at wwwoftalmocomscorevista-1919sco09htm Accessed April 4 2014
26 Shah AR Zaidi A Brucker AJ Serous retinal detachmentsassociated with light chain deposition disease Retin CasesBrief Rep 20137236ndash41
27 Fenicia V Balestrieri M Perdicchi A et al Intravitreal injectionof dexamethasone implant in serous macular detachment asso-ciated withWaldenstroumlmrsquos disease Case Rep Ophthalmol [serialonline] 2013464ndash9 Available at httpwwwkargercomArti-cleFullText354066 Accessed April 4 2014
28 Mansoor A Wagner RP DePalma L Waldenstrom macro-globulinemia presenting as a pleural effusion Arch Pathol LabMed 2000124891ndash3
29 Kavuru MS Tubbs ML Miller L Wiedemann P Immuno-cytometry and gene rearrangement analysis in the diagnosis oflymphoma in an idiopathic pleural effusion Am Rev RespirDis 1992145209ndash11
30 Klaassen I Van Noorden CJF Schlingemann RO Molecularbasis of the inner blood-retinal barrier and its breakdown indiabetic macular edema and other pathological conditionsProg Retin Eye Res 20133419ndash48
31 Kanda T Usui S Beppu H et al Blood-nerve barrier in IgMparaproteinemic neuropathy a clinicopathologic assessmentActa Neuropathol 199895184ndash92
32 Lach B Rippstein P Atack D et al Immunoelectron micro-scopic localization of monoclonal IgM antibodies in gamm-opathy associated with peripheral demyelinative neuropathyActa Neuropathol 199385298ndash307
33 Terpos E Tasidou A Kastritis E et al Angiogenesis in Wal-denstroumlmrsquos macroglobulinemia Clin Lymphoma Myeloma2009946ndash9
34 Ashton N Ocular changes in multiple myelomatosis ArchOphthalmol 196573487ndash94
35 Foos RY Allen RA Opaque cysts of the ciliary body (parsciliaris retinae) Arch Ophthalmol 196777559ndash68
36 Dumas D Viriot ML Boura C et al Permeability oxygenthrough endothelial cells monolayer using time-resolvedfluorescence microscopy Effect of human plasma viscosityIn Periasamy A So PT eds Multiphoton Microscopy in theBiomedical Sciences II Bellingham WA Society of Photo-optical Instrumentation Engineers 2002293e301 Pro-ceedings of SPIE Vol 4620
37 Pruumlnte C Flammer J Choroidal capillary and venouscongestion in central serous chorioretinopathy Am JOphthalmol 199612126ndash34
38 Nicholson B Noble J Forooghian F Meyerle C Centralserous chorioretinopathy update on pathophysiology andtreatment Surv Ophthalmol 201358103ndash26
39 Zamir E Chowers I Central serous chorioretinopathy in a patientwith cryoglobulinaemia [letter] Eye (Lond) 199913265ndash6
7
Ophthalmology Volume - Number - Month 2014
40 Landa G Barnett JA Garcia PM et al Quantitative andqualitative spectral domain optical coherence tomographyanalysis of subretinal deposits in patients with acutecentral serous retinopathy Ophthalmologica 201323062ndash8
41 Menke MN Feke GT McMeel JW Treon SP Effect ofplasmapheresis on hyperviscosity-related retinopathy andretinal hemodynamics in patients with Waldenstromrsquos
8
macroglobulinemia Invest Ophthalmol Vis Sci 2008491157ndash60
42 Negi A Marmor MF Effects of subretinal and systemicosmolality on the rate of subretinal fluid resorption InvestOphthalmol Vis Sci 198425616ndash20
43 Larkin KL Saboo US Comer GM et al Use of intravitrealrituximab for treatment of vitreoretinal lymphoma Br J Oph-thalmol 20149899ndash103
Footnotes and Financial Disclosures
Originally received January 22 2014Final revision March 6 2014Accepted April 9 2014Available online --- Manuscript no 2014-1191 Departments of Ophthalmology American University of Beirut and RaficHariri University Hospital Beirut Lebanon2 Retina Departments The King Khaled Eye Specialist Hospital RiyadhKingdom of Saudi Arabia and Wilmer Eye Institute The Johns HopkinsUniversity Baltimore Maryland3 Department of Ophthalmology Hospital Moises Broggi Sant Joan DespiBarcelona Spain4 Associated Vitreoretinal and Uveitis Consultants Department ofOphthalmology Indiana University School of Medicine IndianapolisIndiana5 Retina Associates of Cleveland Beachwood Ohio6 The Retina Institute St Louis Missouri7 Department of Ophthalmology Mayo Clinic Rochester Minnesota8 Department of Statistics and Research Methodology Lebanese AmericanUniversity and Lebanese University Beirut Lebanon9 Retina Service at Oftalmologica San Miguel de Tucumaacuten Argentina10 Department of Ophthalmology Universidade Estadual de LondrinaParana Brazil
11 Department of Clinical Science ldquoLuigi Saccordquo Sacco Hospital Univer-sity of Milan Milan Italy
Financial Disclosure(s)The author(s) have no proprietary or commercial interest in any materialsdiscussed in this article
JFA Consultant - Second Sight LLC Alcon Labs Lecturer - IridexOptos Inc Speakers Bureau - Novartis Pharmaceuticals Alimera SciencesInc Royalties - Springer SBM LLC
GS Consultant - Heidelberg Engineering Zeiss QLT GSK AlconAllergan Bayer Boheringer Genentech Roche Novartis Speakers Bureaue Zeiss Heidelberg Engineering Novartis GSK Patents - Ocular In-struments Novartis
AM Consultant Lecturer - Bayer
Abbreviations and AcronymsBCVA frac14 best-corrected visual acuity cP frac14 centipoise CSR frac14 centralserous retinopathy DD frac14 disc diameter IgM frac14 immunoglobulin MlogMAR frac14 logarithm of the minimum angle of resolution MM frac14 multiplemyeloma OCT frac14 optical coherence tomography RPE frac14 retinal pigmentepithelium WM frac14 Waldenstroumlm macroglobulinemia
CorrespondenceAhmad M Mansour MD Department of Ophthalmology AmericanUniversity of Beirut PO Box 1136044 Beirut Lebanon E-mailammansourmdgmailcom

Mansour et al Paraproteinemic Maculopathy
2 Baker PS Garg SJ Fineman MS et al Serous maculardetachment in Waldenstroumlm macroglobulinemia a report offour cases Am J Ophthalmol 2013155448ndash55
3 Okada K Yamamoto S Tsuyama Y Mizunoya S Case ofPOEMS syndrome associated with bilateral macular detach-ment resolved by autologous peripheral blood stem celltransplantation [letter] Jpn J Ophthalmol 200751237ndash8
4 Pilon AF Rhee PS Messner LV Bilateral persistent serousmacular detachments with Waldenstroumlmrsquos macroglobulinemiaOptom Vis Sci 200582573ndash8
5 Ho AC Benson WE Wong J Unusual immunogammopathymaculopathy Ophthalmology 20001071099ndash103
6 Ogata N Ida H Takahashi K et al Occult retinal pigmentepithelial detachment in hyperviscosity syndrome OphthalmicSurg Lasers 200031248ndash52
7 Cohen SM Kokame GT Gass JD Paraproteinemias associ-ated with serous detachments of the retinal pigment epitheliumand neurosensory retina Retina 199616467ndash73
8 Spielberg LH Heckenlively JR Leys AM Retinal pigmentepithelial detachments and tears and progressive retinaldegeneration in light chain deposition disease Br J Oph-thalmol 201397627ndash31
9 Leys AM Vandenberghe P Serous macular detachments in apatient with IgM paraproteinemia an optical coherence to-mography study Arch Ophthalmol 2001119911ndash3
10 Brody JM Butrus SI Ashraf MF et al Multiple myelomapresenting with bilateral exudative macular detachments ActaOphthalmol Scand 19957381ndash2
11 Berta A Beck P Mikita J IgM paraprotein in the subretinal fluidof a patient with recurrent retinal detachment andWaldenstroumlmrsquosmacroglobulinaemia Acta Med Hung 198542179ndash86
12 Khouri GG Murphy RP Kuhajda FP Green WR Clinico-pathologic features in two cases of multiple myeloma Retina19866169ndash75
13 Freidman AH Marchevsky A Odel JG et al Immunofluo-rescent studies of the eye in Waldenstroumlmrsquos macroglobuli-nemia Arch Ophthalmol 198098743ndash6
14 Thomas EL Olk RJ Markman M et al Irreversible visual lossin Waldenstroumlmrsquos macroglobulinaemia Br J Ophthalmol198367102ndash6
15 Sen HN Chan C-C Caruso RC et al Waldenstroumlmrsquosmacroglobulinemia-associated retinopathy Ophthalmology2004111535ndash9
16 Feigl B Sill H Haas A Serous detection of the neuroretina inWaldenstroumlm disease A case report [in German] Klin MonblAugenheilkd 199921564ndash7
17 Bernard A Rousselie F Macular manifestations of mono-clonal dysgammaglobulinemias Apropos of 3 cases [inFrench] J Fr Ophtalmol 19869805ndash10
18 Quhill F Khan I Rashid A Bilateral serous macular de-tachments in Waldenstroumlmrsquos macroglobulinaemia PostgradMed J 200985382
19 Khan JM McBain V Santiago C Lois N Bilateral lsquovitelli-form-likersquo macular lesions in a patient with multiple myelomaBMJ Case Rep [serial online] 20102010 bcr0520103049Available at httpwwwncbinlmnihgovpmcarticlesPMC3028543 Accessed April 4 2014
20 Brolly A Janon C Precausta F et al Pseudovitelliform sub-foveal deposit in Waldenstroumlmrsquos macroglobulinemia CaseRep Ophthalmol [serial online] 20123236ndash9 Available athttpwwwkargercomArticleAbstract339988 AccessedApril 4 2014
21 Daicker BC Mihatsch MJ Stroslashm EH Fogazzi GB Ocularpathology in light chain deposition disease Eur J Ophthalmol1995575ndash81
22 Ardouin M Urvoy M Gastard J Aspect of the dysproteinemicfundus oculi (microaneurysms and retinal detachment) in acase of Waldenstromrsquos disease [in French] Bull Soc Ophtal-mol Fr 196666129ndash32
23 Lin CJ Chiu YM Chen SN et al Unusual maculopathysecondary to hypergammaglobulinemia in a patient with sys-temic lupus erythematosus Retin Cases Brief Rep 2012627ndash9
24 Besirli CG Johnson MW Immunogammopathy maculopathyassociated with Waldenstrom macroglobulinemia is refractoryto conventional interventions for macular edema Retin CasesBrief Rep 20137319ndash24
25 Gil Hernandez MA Abreu Reyes P Bahaya Alvarez Y AcostaAcosta B Bilateral serous detachment of the neurosensory retinaassociated with light-chain deposition disease [in Spanish] ArchSoc Canaria Oftalmol 200819 Available at wwwoftalmocomscorevista-1919sco09htm Accessed April 4 2014
26 Shah AR Zaidi A Brucker AJ Serous retinal detachmentsassociated with light chain deposition disease Retin CasesBrief Rep 20137236ndash41
27 Fenicia V Balestrieri M Perdicchi A et al Intravitreal injectionof dexamethasone implant in serous macular detachment asso-ciated withWaldenstroumlmrsquos disease Case Rep Ophthalmol [serialonline] 2013464ndash9 Available at httpwwwkargercomArti-cleFullText354066 Accessed April 4 2014
28 Mansoor A Wagner RP DePalma L Waldenstrom macro-globulinemia presenting as a pleural effusion Arch Pathol LabMed 2000124891ndash3
29 Kavuru MS Tubbs ML Miller L Wiedemann P Immuno-cytometry and gene rearrangement analysis in the diagnosis oflymphoma in an idiopathic pleural effusion Am Rev RespirDis 1992145209ndash11
30 Klaassen I Van Noorden CJF Schlingemann RO Molecularbasis of the inner blood-retinal barrier and its breakdown indiabetic macular edema and other pathological conditionsProg Retin Eye Res 20133419ndash48
31 Kanda T Usui S Beppu H et al Blood-nerve barrier in IgMparaproteinemic neuropathy a clinicopathologic assessmentActa Neuropathol 199895184ndash92
32 Lach B Rippstein P Atack D et al Immunoelectron micro-scopic localization of monoclonal IgM antibodies in gamm-opathy associated with peripheral demyelinative neuropathyActa Neuropathol 199385298ndash307
33 Terpos E Tasidou A Kastritis E et al Angiogenesis in Wal-denstroumlmrsquos macroglobulinemia Clin Lymphoma Myeloma2009946ndash9
34 Ashton N Ocular changes in multiple myelomatosis ArchOphthalmol 196573487ndash94
35 Foos RY Allen RA Opaque cysts of the ciliary body (parsciliaris retinae) Arch Ophthalmol 196777559ndash68
36 Dumas D Viriot ML Boura C et al Permeability oxygenthrough endothelial cells monolayer using time-resolvedfluorescence microscopy Effect of human plasma viscosityIn Periasamy A So PT eds Multiphoton Microscopy in theBiomedical Sciences II Bellingham WA Society of Photo-optical Instrumentation Engineers 2002293e301 Pro-ceedings of SPIE Vol 4620
37 Pruumlnte C Flammer J Choroidal capillary and venouscongestion in central serous chorioretinopathy Am JOphthalmol 199612126ndash34
38 Nicholson B Noble J Forooghian F Meyerle C Centralserous chorioretinopathy update on pathophysiology andtreatment Surv Ophthalmol 201358103ndash26
39 Zamir E Chowers I Central serous chorioretinopathy in a patientwith cryoglobulinaemia [letter] Eye (Lond) 199913265ndash6
7
Ophthalmology Volume - Number - Month 2014
40 Landa G Barnett JA Garcia PM et al Quantitative andqualitative spectral domain optical coherence tomographyanalysis of subretinal deposits in patients with acutecentral serous retinopathy Ophthalmologica 201323062ndash8
41 Menke MN Feke GT McMeel JW Treon SP Effect ofplasmapheresis on hyperviscosity-related retinopathy andretinal hemodynamics in patients with Waldenstromrsquos
8
macroglobulinemia Invest Ophthalmol Vis Sci 2008491157ndash60
42 Negi A Marmor MF Effects of subretinal and systemicosmolality on the rate of subretinal fluid resorption InvestOphthalmol Vis Sci 198425616ndash20
43 Larkin KL Saboo US Comer GM et al Use of intravitrealrituximab for treatment of vitreoretinal lymphoma Br J Oph-thalmol 20149899ndash103
Footnotes and Financial Disclosures
Originally received January 22 2014Final revision March 6 2014Accepted April 9 2014Available online --- Manuscript no 2014-1191 Departments of Ophthalmology American University of Beirut and RaficHariri University Hospital Beirut Lebanon2 Retina Departments The King Khaled Eye Specialist Hospital RiyadhKingdom of Saudi Arabia and Wilmer Eye Institute The Johns HopkinsUniversity Baltimore Maryland3 Department of Ophthalmology Hospital Moises Broggi Sant Joan DespiBarcelona Spain4 Associated Vitreoretinal and Uveitis Consultants Department ofOphthalmology Indiana University School of Medicine IndianapolisIndiana5 Retina Associates of Cleveland Beachwood Ohio6 The Retina Institute St Louis Missouri7 Department of Ophthalmology Mayo Clinic Rochester Minnesota8 Department of Statistics and Research Methodology Lebanese AmericanUniversity and Lebanese University Beirut Lebanon9 Retina Service at Oftalmologica San Miguel de Tucumaacuten Argentina10 Department of Ophthalmology Universidade Estadual de LondrinaParana Brazil
11 Department of Clinical Science ldquoLuigi Saccordquo Sacco Hospital Univer-sity of Milan Milan Italy
Financial Disclosure(s)The author(s) have no proprietary or commercial interest in any materialsdiscussed in this article
JFA Consultant - Second Sight LLC Alcon Labs Lecturer - IridexOptos Inc Speakers Bureau - Novartis Pharmaceuticals Alimera SciencesInc Royalties - Springer SBM LLC
GS Consultant - Heidelberg Engineering Zeiss QLT GSK AlconAllergan Bayer Boheringer Genentech Roche Novartis Speakers Bureaue Zeiss Heidelberg Engineering Novartis GSK Patents - Ocular In-struments Novartis
AM Consultant Lecturer - Bayer
Abbreviations and AcronymsBCVA frac14 best-corrected visual acuity cP frac14 centipoise CSR frac14 centralserous retinopathy DD frac14 disc diameter IgM frac14 immunoglobulin MlogMAR frac14 logarithm of the minimum angle of resolution MM frac14 multiplemyeloma OCT frac14 optical coherence tomography RPE frac14 retinal pigmentepithelium WM frac14 Waldenstroumlm macroglobulinemia
CorrespondenceAhmad M Mansour MD Department of Ophthalmology AmericanUniversity of Beirut PO Box 1136044 Beirut Lebanon E-mailammansourmdgmailcom

Ophthalmology Volume - Number - Month 2014
40 Landa G Barnett JA Garcia PM et al Quantitative andqualitative spectral domain optical coherence tomographyanalysis of subretinal deposits in patients with acutecentral serous retinopathy Ophthalmologica 201323062ndash8
41 Menke MN Feke GT McMeel JW Treon SP Effect ofplasmapheresis on hyperviscosity-related retinopathy andretinal hemodynamics in patients with Waldenstromrsquos
8
macroglobulinemia Invest Ophthalmol Vis Sci 2008491157ndash60
42 Negi A Marmor MF Effects of subretinal and systemicosmolality on the rate of subretinal fluid resorption InvestOphthalmol Vis Sci 198425616ndash20
43 Larkin KL Saboo US Comer GM et al Use of intravitrealrituximab for treatment of vitreoretinal lymphoma Br J Oph-thalmol 20149899ndash103
Footnotes and Financial Disclosures
Originally received January 22 2014Final revision March 6 2014Accepted April 9 2014Available online --- Manuscript no 2014-1191 Departments of Ophthalmology American University of Beirut and RaficHariri University Hospital Beirut Lebanon2 Retina Departments The King Khaled Eye Specialist Hospital RiyadhKingdom of Saudi Arabia and Wilmer Eye Institute The Johns HopkinsUniversity Baltimore Maryland3 Department of Ophthalmology Hospital Moises Broggi Sant Joan DespiBarcelona Spain4 Associated Vitreoretinal and Uveitis Consultants Department ofOphthalmology Indiana University School of Medicine IndianapolisIndiana5 Retina Associates of Cleveland Beachwood Ohio6 The Retina Institute St Louis Missouri7 Department of Ophthalmology Mayo Clinic Rochester Minnesota8 Department of Statistics and Research Methodology Lebanese AmericanUniversity and Lebanese University Beirut Lebanon9 Retina Service at Oftalmologica San Miguel de Tucumaacuten Argentina10 Department of Ophthalmology Universidade Estadual de LondrinaParana Brazil
11 Department of Clinical Science ldquoLuigi Saccordquo Sacco Hospital Univer-sity of Milan Milan Italy
Financial Disclosure(s)The author(s) have no proprietary or commercial interest in any materialsdiscussed in this article
JFA Consultant - Second Sight LLC Alcon Labs Lecturer - IridexOptos Inc Speakers Bureau - Novartis Pharmaceuticals Alimera SciencesInc Royalties - Springer SBM LLC
GS Consultant - Heidelberg Engineering Zeiss QLT GSK AlconAllergan Bayer Boheringer Genentech Roche Novartis Speakers Bureaue Zeiss Heidelberg Engineering Novartis GSK Patents - Ocular In-struments Novartis
AM Consultant Lecturer - Bayer
Abbreviations and AcronymsBCVA frac14 best-corrected visual acuity cP frac14 centipoise CSR frac14 centralserous retinopathy DD frac14 disc diameter IgM frac14 immunoglobulin MlogMAR frac14 logarithm of the minimum angle of resolution MM frac14 multiplemyeloma OCT frac14 optical coherence tomography RPE frac14 retinal pigmentepithelium WM frac14 Waldenstroumlm macroglobulinemia
CorrespondenceAhmad M Mansour MD Department of Ophthalmology AmericanUniversity of Beirut PO Box 1136044 Beirut Lebanon E-mailammansourmdgmailcom
Related Documents











