86ournal of Neurology, Neurosurgery, and Psychiatry 1992;55:836-837 LESSON OF THE MONTH Paraplegia due to a ruptured aneurysm of the distal posterior inferior cerebellar artery Shiro Kashiwagi, Eiji Tsuchida, Yujiro Shiroyama, Haruhide Ito, Tetsuo Yamashita Abstract A case of paraplegia was due to a ruptured aneurysm of the distal posterior inferior cerebellar artery. The paraplegia was caused by a unilateral lesion located bet- ween the cervicomedullary junction and the C2 level, where it involved both crossed and uncrossed pyramidal fibres projecting to the lower extremities. Since a vascular lesion near the cervicomedul- lary junction is likely to be missed, special attention should be paid to this region when investigating subarachnoid haemor- rhage with paraplegia. (7 Neurol Neurosurg Psychiatry 1992;55:836-837) Paraplegia is usually a sign of bilateral involve- ment of the corticospinal tract in the thoracic or lumbar region, or the medial motor cortex in the interhemispheric fissure. When seen in patients with subarachnoid haemorrhage (SAH), it is most probably due to rupture of an aneurysm or arteriovenous malformation (AVM) in the distribution of the anterior cerebral artery causing mechanical com- pression by a haematoma in the interhemi- spheric cistern or ischaemia resulting from vasospasm of the anterior cerebral arteries. Our patient with SAH presented with para- plegia due to a ruptured aneurysm of the distal posterior inferior cerebellar artery (PICA). Department of Neurosurgery, Yamaguchi University School of Medicine S Kashiwagi E Tsuchida Y Shiroyama H Ito T Yamashita Correspondence to: Dr Kashiwagi, Department of Neurosurgery, Yamaguchi University School of Medicine, 1144 Kogushi Ube Yamaguchi, 755 Japan Received 3 March 1992. Accepted 29 April 1992 Case report The patient, a 57 year old woman, had been well until the morning of 23 December 1990, when she was found lying unconscious on the street. She was taken to a local hospital. On arrival at the emergency room, she was semi- comatose with shallow, irregular breathing. The pupils were miotic, and there was tran- sient skew deviation. She was able to move the upper limbs, better on the left side, but did not move the lower limbs in response to painful stimuli. With respiratory support by bag and face mask, her breathing improved and she began to open her eyes in response to pain. CT scan showed diffuse subarachnoid haemor- rhage in both the supra- and infratentorial regions with haemorrhage in the fourth ven- tricle and the posterior horn of the left lateral ventricle. She was transferred to our hospital. On admission, her blood pressure was 140/90, pulse rate 92/min, respiration rate 36/min, and body temperature 37 6°C. She opened her eyes in response to pain. The pupils were isocoric and responded to light. She moved the upper limbs and was able to localise pain on both sides, better on the left, but did not move the lower extremities in response to painful stimuli. Deep tendon reflexes were + + in the upper limbs and + in the lower extremities. The plantar responses were extensor. The three vessel angiography on 23 Decem- ber failed to reveal any aneurysm or other vascular lesions that might be the source of the subarachnoid haemorrhage. She continued to be stuporous with paraparesis over the follow- ing three weeks, and gradually improved in the fourth week. The strength of the lower limbs had recovered to 4/5 on the right and 5/5 on the left by the end of the sixth week after the attack, at which time sensory examination revealed normal response to pain, touch and vibration in the upper and lower limbs. No lower cranial nerve palsy was noted. Reflexes were +2 in the upper and + 3 in the lower extremities. MRI with a 1 5-T superconducting coil was carried out on 22 January 1991, and showed a vascular lesion in the subarachnoid space adjacent to the spinal cord at the level of Cl (fig A). Cerebral angiography was repeated, and right vertebral angiograms revealed an aneurysm in the anterior medullary segment of the right posterior inferior cerebellar artery (PICA) (fig B). On 18 February a right suboccipital cranio- tomy and Cl laminectomy was performed. A saccular aneurysm, 2-5 x 6-0 mm, arose from the anterior medullary segment of the PICA. The dome of the aneurysm was located antero-lateral to the spinal cord just rostral to the Cl roots. There was yellowish pigmenta- tion on the surface of the spinal cord, suggest- ing previous haemorrhage. The neck of the aneurysm was clipped with a slightly curved aneurysm clip. The patient did well post- operatively. She regained the ability to walk, and was discharged from hospital on 11 April 1991. She returned to work three months later. Discussion Distal PICA aneurysm is rare, accounting for less than 0-5% of all intracranial aneurysms.` There are no specific neurological deficits associated with rupture of distal PICA 836 on 15 March 2019 by guest. Protected by copyright. http://jnnp.bmj.com/ J Neurol Neurosurg Psychiatry: first published as 10.1136/jnnp.55.9.836 on 1 September 1992. Downloaded from

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

86ournal of Neurology, Neurosurgery, and Psychiatry 1992;55:836-837
LESSON OFTHE MONTH
Paraplegia due to a ruptured aneurysm of thedistal posterior inferior cerebellar artery
Shiro Kashiwagi, Eiji Tsuchida, Yujiro Shiroyama, Haruhide Ito, Tetsuo Yamashita
AbstractA case ofparaplegia was due to a rupturedaneurysm of the distal posterior inferiorcerebellar artery. The paraplegia wascaused by a unilateral lesion located bet-ween the cervicomedullary junction andthe C2 level, where it involved bothcrossed and uncrossed pyramidal fibresprojecting to the lower extremities. Sincea vascular lesion near the cervicomedul-lary junction is likely to be missed, specialattention should be paid to this regionwhen investigating subarachnoid haemor-rhage with paraplegia.
(7 Neurol Neurosurg Psychiatry 1992;55:836-837)
Paraplegia is usually a sign of bilateral involve-ment of the corticospinal tract in the thoracicor lumbar region, or the medial motor cortexin the interhemispheric fissure. When seen inpatients with subarachnoid haemorrhage(SAH), it is most probably due to rupture ofan aneurysm or arteriovenous malformation(AVM) in the distribution of the anteriorcerebral artery causing mechanical com-pression by a haematoma in the interhemi-spheric cistern or ischaemia resulting fromvasospasm of the anterior cerebral arteries.Our patient with SAH presented with para-
plegia due to a ruptured aneurysm of the distalposterior inferior cerebellar artery (PICA).
Department ofNeurosurgery,Yamaguchi UniversitySchool of MedicineS KashiwagiE TsuchidaY ShiroyamaH ItoT YamashitaCorrespondence to:Dr Kashiwagi, Departmentof Neurosurgery, YamaguchiUniversity School ofMedicine, 1144 KogushiUbe Yamaguchi, 755 JapanReceived 3 March 1992.Accepted 29 April 1992
Case reportThe patient, a 57 year old woman, had beenwell until the morning of 23 December 1990,when she was found lying unconscious on thestreet. She was taken to a local hospital. Onarrival at the emergency room, she was semi-comatose with shallow, irregular breathing.The pupils were miotic, and there was tran-sient skew deviation. She was able to move theupper limbs, better on the left side, but did notmove the lower limbs in response to painfulstimuli. With respiratory support by bag andface mask, her breathing improved and shebegan to open her eyes in response to pain. CTscan showed diffuse subarachnoid haemor-rhage in both the supra- and infratentorialregions with haemorrhage in the fourth ven-
tricle and the posterior horn of the left lateralventricle. She was transferred to our hospital.On admission, her blood pressure was
140/90, pulse rate 92/min, respiration rate
36/min, and body temperature 37 6°C. Sheopened her eyes in response to pain. The pupilswere isocoric and responded to light. Shemoved the upper limbs and was able to localisepain on both sides, better on the left, but didnot move the lower extremities in response topainful stimuli. Deep tendon reflexes were+ + in the upper limbs and + in the lowerextremities. The plantar responses wereextensor.The three vessel angiography on 23 Decem-
ber failed to reveal any aneurysm or othervascular lesions that might be the source of thesubarachnoid haemorrhage. She continued tobe stuporous with paraparesis over the follow-ing three weeks, and gradually improved in thefourth week. The strength of the lower limbshad recovered to 4/5 on the right and 5/5 onthe left by the end of the sixth week after theattack, at which time sensory examinationrevealed normal response to pain, touch andvibration in the upper and lower limbs. Nolower cranial nerve palsy was noted. Reflexeswere +2 in the upper and + 3 in the lowerextremities.MRI with a 1 5-T superconducting coil was
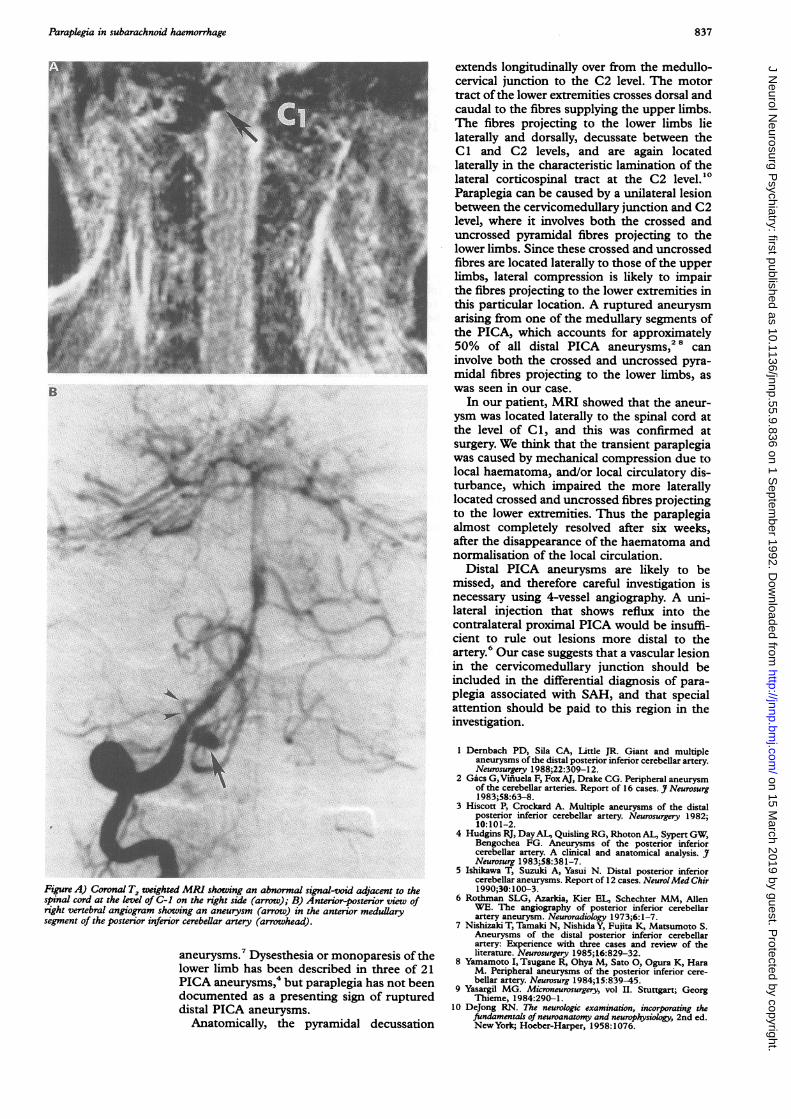
carried out on 22 January 1991, and showed avascular lesion in the subarachnoid spaceadjacent to the spinal cord at the level of Cl(fig A). Cerebral angiography was repeated,and right vertebral angiograms revealed ananeurysm in the anterior medullary segment ofthe right posterior inferior cerebellar artery(PICA) (fig B).On 18 February a right suboccipital cranio-
tomy and Cl laminectomy was performed.A saccular aneurysm, 2-5 x 6-0 mm, arosefrom the anterior medullary segment of thePICA. The dome of the aneurysm was locatedantero-lateral to the spinal cord just rostral tothe Cl roots. There was yellowish pigmenta-tion on the surface of the spinal cord, suggest-ing previous haemorrhage. The neck of theaneurysm was clipped with a slightly curvedaneurysm clip. The patient did well post-operatively. She regained the ability to walk,and was discharged from hospital on 11 April1991. She returned to work three monthslater.
DiscussionDistal PICA aneurysm is rare, accounting forless than 0-5% of all intracranial aneurysms.`There are no specific neurological deficitsassociated with rupture of distal PICA
836 on 15 M
arch 2019 by guest. Protected by copyright.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.55.9.836 on 1 Septem
ber 1992. Dow
nloaded from
Paraplegia in subarachnoid haemorrhage
Figure A) Coronal T, weighted MRI showing an abnormal signal-void adjacen~spinal cord at the levl of C-i on the right side (arrow); B) Anterior-posteriortright vertebral angiogram showing an aneurysm (arrow) in the anterior meduli
segment of the posterior inferior cerebellar artery (arrowhead).
aneurysms.' Dysesthesia or monopare,,lower limb has been described in thr
PICA aneurysms,' but paraplegia has
documented as a presenting sign ofrdistal PICA aneurysms.
Anatomically, the pyramidal dec-
extends longitudinally over from the medullo-cervical junction to the C2 level. The motortract ofthe lower extremities crosses dorsal andcaudal to the fibres supplying the upper limbs.The fibres projecting to the lower limbs lielaterally and dorsally, decussate between theC 1 and C2 levels, and are again locatedlaterally in the characteristic lamination of thelateral corticospinal tract at the C2 level.'0Paraplegia can be caused by a unilateral lesionbetween the cervicomedullary junction and C2level, where it involves both the crossed anduncrossed pyramidal fibres projecting to thelower limbs. Since these crossed and uncrossedfibres are located laterally to those of the upperlimbs, lateral compression is likely to impairthe fibres projecting to the lower extremities inthis particular location. A ruptured aneurysmarising from one of the medullary segments ofthe PICA, which accounts for approximately50% of all distal PICA aneurysms,2 8 caninvolve both the crossed and uncrossed pyra-midal fibres projecting to the lower limbs, aswas seen in our case.
In our patient, MRI showed that the aneur-ysm was located laterally to the spinal cord atthe level of C1, and this was confirmed atsurgery. We think that the transient paraplegiawas caused by mechanical compression due tolocal haematoma, and/or local circulatory dis-turbance, which impaired the more laterallylocated crossed and uncrossed fibres projectingto the lower extremities. Thus the paraplegiaalmost completely resolved after six weeks,after the disappearance of the haematoma andnormalisation of the local circulation.
Distal PICA aneurysms are likely to bemissed, and therefore careful investigation isnecessary using 4-vessel angiography. A uni-lateral injection that shows reflux into thecontralateral proximal PICA would be insuffi-cient to rule out lesions more distal to theartery.6 Our case suggests that a vascular lesionin the cervicomedullary junction should beincluded in the differential diagnosis of para-plegia associated with SAH, and that specialattention should be paid to this region in theinvestigation.
1 Dernbach PD, Sila CA, Little JR. Giant and multipleaneurysms ofthe distal posterior inferior cerebellar artery.Neurosurgery 1988;22:309-12.
2 Gacs G, Viniuela F, Fox AJ, Drake CG. Peripheral aneurysmof the cerebellar arteries. Report of 16 cases. J Neurosurg1 983;58:63-8.
3 Hiscott P, Crockard A. Multiple aneurysms of the distalposterior inferior cerebellar artery. Neurosurgery 1982;10:101-2.
4 Hudgins RJ, DayAL, Quisling RG, Rhoton AL, Sypert GW,Bengochea FG. Aneurysms of the posterior inferiorcerebellar artery. A clinical and anatomical analysis. JNeurosurg 1983;58:381-7.
5 Ishikawa T, Suzuki A, Yasui N. Distal posterior inferiorcerebellar aneurysms. Report of 12 cases. NeurolMed Chir
It to the 1990;30:100-3.view of 6 Rothman SLG, Azarkia, Kier EL, Schechter MM, Allenary 'WE. The angiography of posterior inferior cerebellar
artery aneurysm. Neuroradiology 1973;6:1-7.7 Nishizaki T, Tamaki N, Nishida Y, Fujita K, Matsumoto S.
Aneurysms of the distal posterior inferior cerebellarartery: Experience with three cases and review of the
sis of the literature. Neurosurgery 1985;16:829-32.8 Yamamoto I, Tsugane R, Ohya M, Sato 0, Ogura K, Haraee of 21 M. Peripheral aneurysms of the posterior inferior cere-not been bellar artery. Neurosurg 1984;15:839-45.
9 Yasargil MG. Microneurosurgery, vol II. Stuttgart; Georgruptured Thieme, 1984:290-1.10 DeJong RN. The neurologic examination, incorporating the
fundamentals of neuroanatomy and neurophysiology, 2nd ed.russation New York; Hoeber-Harper, 1958:1076.
837 on 15 M
arch 2019 by guest. Protected by copyright.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.55.9.836 on 1 Septem
ber 1992. Dow
nloaded from
Related Documents











