Journal of the European Academy of Dermatology and Venereology ELSEVIER 6(1996)246-251 Case report Papillon-Lefevre syndrome associated with albinism. Clinical and immunological study Mohammed Amer ^•% Fawzia Farag Mostafa ', Zenab Tosson \ Ahmmed Hegazi ^ From the Department of Dermalology. Unirersity of Zagazig. Faculty of Medicine. Zagazig. Egypt ' National Research Center Dokki, Cairo, Egypt Abstract Background: We report the first association of Papillon-Lefevre syndrome (PLS) with tyrosinase-nega- tivc albinism in two brothers. Also, we studied T-lymphocytes and mononuclear celi activity in them and in two other cases of PLS not associated with albinism. Objective: To recognize clinical and immunological correlation. Methods: Four PLS patients from 3 different families were studied clinically and immunologically. Two brothers (albino) in one family had recurrent infections. The other two patients from two other families had no infection. The patients' healthy parents were also included in the study. Results: A decreased lymphocyte proliferative response to phytohaemaglutinin and in mononuclear cell activities were detected not only in the PLS patients with recurrent pyogenic infection, but also in their healthy parents. Further investigations of these patients showed impaired humoral and cellular immune response. PLS patients with no infection and their parents showed normal immunoiogic parameters. Conclusion: We suggest dividing PLS on clinical and immunological bases into two variants: PLS with pyogenic infections and the other variety without such infection. PLS with pyogenic infections is associated with immunologic dysfunction. Periodontosis could not be explained on an immunological basis. Keywords: Papillon-lefevre; Keratosis palmoplantaris 1. Introduction and Lefevre [1] in 1924. The syndrome is inher- ited as an autosomal recessive trait and its frc- The syndrome of keratosis palmoplantaris with quency has been estimated at approximately one periodontopathy, was first described by Papillon to four per million persons in the general popula- tion [2,3]. There is evidence that this syndrome is associated with increased susceptibility to infec- tions in about 20% of patients [3]. No cases of • Corresponding author. pigment abnormalities have been reported in the 0926-9959/96/513,00 £ 1996 Eisevier Science B.V. All rights reserved SSDI 0926-9959(95)00165-4

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Journal of the European Academy of Dermatology and VenereologyELSEVIER 6(1996)246-251
Case report
Papillon-Lefevre syndrome associated with albinism.Clinical and immunological study
Mohammed Amer •̂% Fawzia Farag Mostafa ', Zenab Tosson \ Ahmmed Hegazi^ From the Department of Dermalology. Unirersity of Zagazig. Faculty of Medicine. Zagazig. Egypt
' National Research Center Dokki, Cairo, Egypt
Abstract
Background: We report the first association of Papillon-Lefevre syndrome (PLS) with tyrosinase-nega-tivc albinism in two brothers. Also, we studied T-lymphocytes and mononuclear celi activity in them andin two other cases of PLS not associated with albinism.
Objective: To recognize clinical and immunological correlation.Methods: Four PLS patients from 3 different families were studied clinically and immunologically.
Two brothers (albino) in one family had recurrent infections. The other two patients from two otherfamilies had no infection. The patients' healthy parents were also included in the study.
Results: A decreased lymphocyte proliferative response to phytohaemaglutinin and in mononuclearcell activities were detected not only in the PLS patients with recurrent pyogenic infection, but also intheir healthy parents. Further investigations of these patients showed impaired humoral and cellularimmune response. PLS patients with no infection and their parents showed normal immunoiogicparameters.
Conclusion: We suggest dividing PLS on clinical and immunological bases into two variants: PLS withpyogenic infections and the other variety without such infection. PLS with pyogenic infections isassociated with immunologic dysfunction. Periodontosis could not be explained on an immunologicalbasis.
Keywords: Papillon-lefevre; Keratosis palmoplantaris
1. Introduction and Lefevre [1] in 1924. The syndrome is inher-ited as an autosomal recessive trait and its frc-
The syndrome of keratosis palmoplantaris with quency has been estimated at approximately oneperiodontopathy, was first described by Papillon to four per million persons in the general popula-
tion [2,3]. There is evidence that this syndrome isassociated with increased susceptibility to infec-tions in about 20% of patients [3]. No cases of
• Corresponding author. pigment abnormalities have been reported in the
0926-9959/96/513,00 £ 1996 Eisevier Science B.V. All rights reservedSSDI 0926-9959(95)00165-4
M. Amer et al. /J. Eur Acad. Dermatol. Venereol. 6 (1996) 246-251 247
literature to date. T-lymphocyte, mononuclear cellactivities and other immunologic parameters werestudied in order to recognize their roles in thepathogenesis of periodontosis and recurrent in-fection if any in PLS.
2. Report of Cases
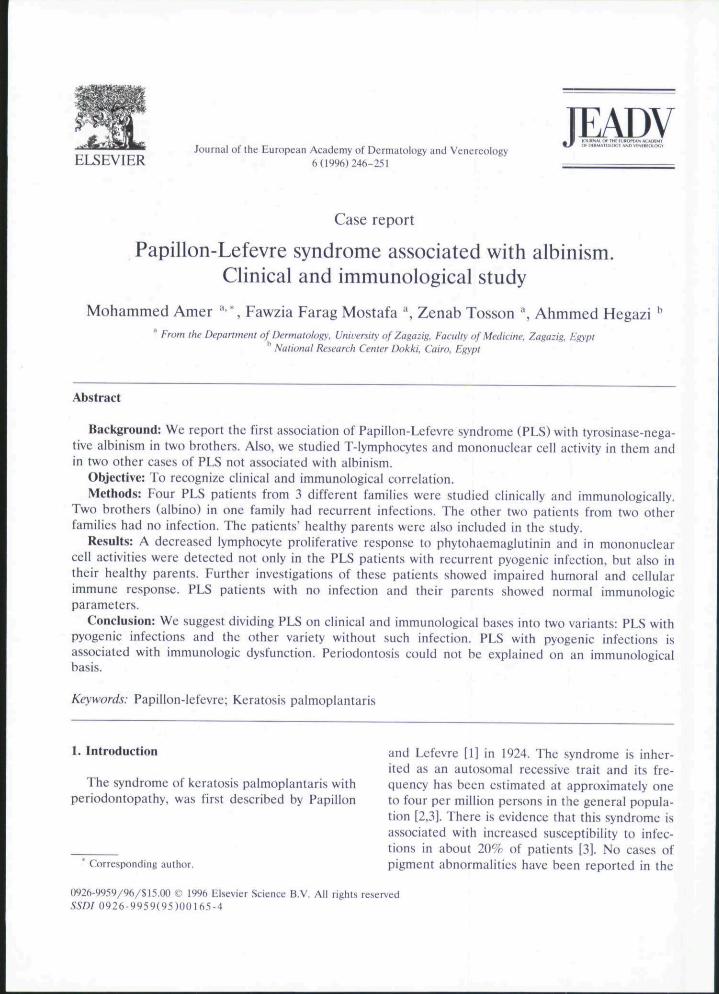
Case 1. An 18 year-old male patient was re-ferred to us from Chest Outpatient Clinic wherehe had been under observation and follow-up formany years. Past history of the patient revealedthat he was suffering from recurrent massive pyo-genic chest and cutaneous infection. He had beenhospitalized most of the time since infancy. Afterhe had taken massive antibiotic therapy and fre-quent chest aspiration his chest became free. Buthe still had recurrent cutaneous infections. Onexamination we found that the patient's skincolour was pink, his hair sparse and white, andthe iris of his eye was red. He had irregularnystagmus, with head nodding and diffuse welldemarcated, yellowish, palmoplantar kerato-derma with extension of the keratosis to the sidesof the hands, and feet up to the Achilles tendon.Symmetric, psoriasiform plaques were observed.Stomatologic examination showed loss of most ofthe teeth. Heavy crusted skin lesions were seenon the chest, thighs and lower limbs.Roentgenograms of the skull failed to reveal ec-topic intracranial calcification. Staphylococcus au-reus was the only organism isolated from cuta-neous lesions. Past history of the patient's familyrevealed that his brother and his great-grand-father had the same association of dyschromia,loss of teeth, keratotic changes and recurrentcutaneous infections.
Case 2. A 14 year-old male patient, brother ofthe first propositus complained of recurrent cuta-neous infections. On examination, the patient'sskin colour was pink, his hair sparse and whiteand the iris of his eye was red. He also hadirregular nystagmus with head nodding. His skinshowed a diffuse well demarcated yellowish pal-moplantar keratoderma. Symmetric psoriasiformplaques were obsereved on both elbows andknees. Stomatologic examination showed loss of
most teeth. Thick crusted lesions were seen onhis lower limbs only. History of previous internalinfection was irrelevant. Staphylococcus aureuswas the only organism isolated from the skin.Roentgenogram of the skull was normal.
Case 3. A 20 year-old male showed palmoplan-tar keratoderma with keratotic lesions on thedorsal aspects of the hands and feet. Keratoticplaques were present on the elbows, knees andAchilles tendons. Oral examination revealed lossof all teeth. Skull roentgenogram was normal.History of infection in this patient was irrelevant.
Case 4. A 17 year-old male presented withpremature loss of all teeth. Skin examinationshowed extensive palmoplantar keratoderma, alsoon the dorsal aspects of the hands and feet.Psoriasiform plaques were present on elbows andknees. Increased susceptibility to infection in hispast or present history was irrelevant; skullroentgenogram was normal.
3. Methods
Parental consanguinity was present in all cases.Roentgenogram of jawbone was done in all cases.Cases 1 and 2 were brothers but cases 3 and 4were from two other families. Hair bulb test wasperformed [4,5] in order to determine the type ofalbinism. Blood samples were taken from all casesand their parents. To evaluate lymphocyte andmononuclear cell activities the following testswere done.
Lymphocyte transformation test according toHall and Gordon [6]: blood was collected byvenesection into sterile gamma irradiated vactain-ers containing 20 units of phenol-free heparin perml of blood. After the blood was mixed, an ali-quant was removed for determination ofmononuclear cells count. Viable lymphocyteswere analysed with haemocytometer (improvedNeu Bauer 1/400 mm" 1/10 mm deep. LevyUlone, Adams, New York, USA); viability shouldexhibit 95%. Cell concentration was adjusted to10'' cells/ml. The lymphocyte cultures were per-formed with addition of phytohaemagglutinin toobtain the mitogenic stimulation. The mitogenicratio as well as stimulation index were calculated
248 M. Amer et al. /J. Fur Acad. Dermatol. Venereol. 6 (1996) 246-25!
after the lymphocyte culture was pulsed with[^'H]thymidinc.
Separation of peripheral blood mononuclearcells, according to Thorsby and Bratile [7]. 10 mlblood was collected by venesection; after mixingin ratio of 1:3 Ficoll the blood was centrifuged at2000 rpm for 30 min. The supernatant was de-canted and the leucocyte layer was collected. Theleucocytes were washed 3 times in PRMl-1640medium, then incubated in a glass Pitery dish forcollection of glass adherent cells. These cells af-ter collection were used for bactericidal activityof E. coli according to Hegazi et al. [8].
Further evaluation of case 1 and 2 include:total serum protein, latex agglutination testagainst staphylococcus aureus, antistreptolysin Otitre and tuberculin test according to Doumus [9],Dickson and Marples [10], Curickshank et al. [11]and Seaton et al., [12] respectively. Flow cytomet-ric study was carried out on these patients using afacscan (Becton Dickinson) according to Abdel-Naser et al. [13].
4. Results
Cases 1 and 2 brothers and both had PLSassociated with tyrosinase negative albinism (Figs.1,2). This is confirmed when incubation of pluckedanagen hair bulbs in a solution of dopa fromthese patients does not darken in comparisonwith control. Family history revealed that their
Table 1Results of lymphocyte transformation and bactericidal activity
Table 2Further immunologic evaluation
Parameters Control Case
1
Stimulation index(patients)
MotherFather% of mononuclear
cell aclivity(patients)
MotherFather
f).4
6.36.8
86
3.1 4.3 f i . 6.3
5.4" 5.430 37
42'45'
4245
6.2 6.46.6 6.0
75 80
81 8379 76
Parameters
Total serum proteinLatex agglutination testAntistreptolysin O titreTuberculin test
T cells subsetTotal T cellsTotal B cells
Suppressor/cytotoxic cellsHelper/inducer cellsHelp/supp. RatioActivated T cellsNK cells
Control
6.21/320+ vt;+ ve
83%16'7f
33%51%1.59%7%
Case
1
3.61/8U-v c- ve
84%.6%39%.48%L27%]()%
1
3.«1/160-ve-ve
70%16%28%48%1.713%13%
Brothers.Father and mother are the same in cases 1 and 2.
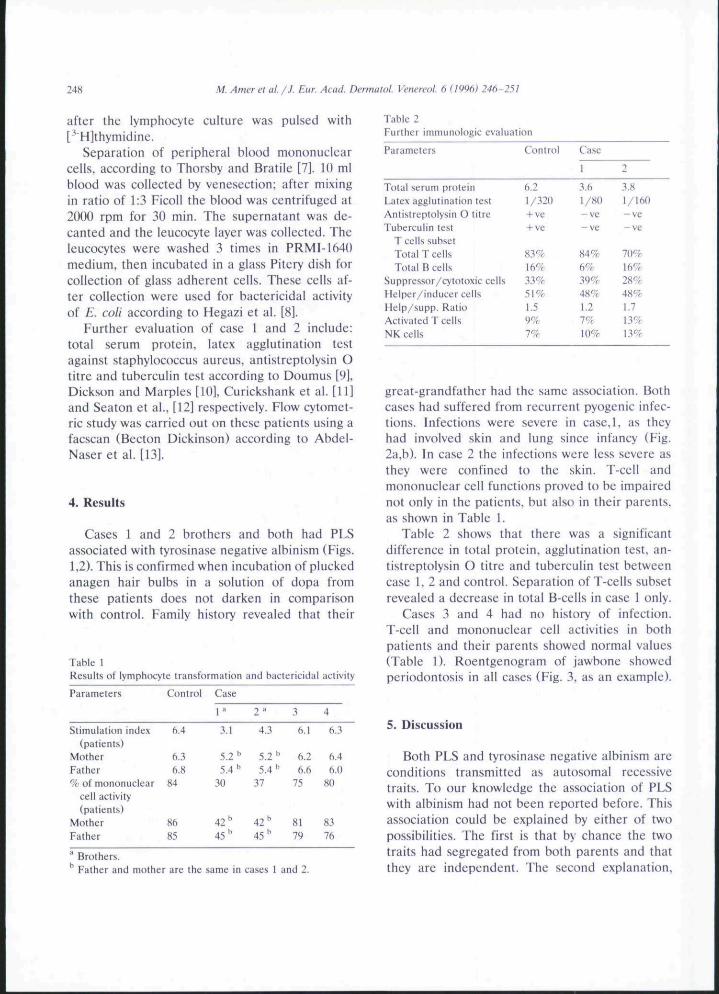
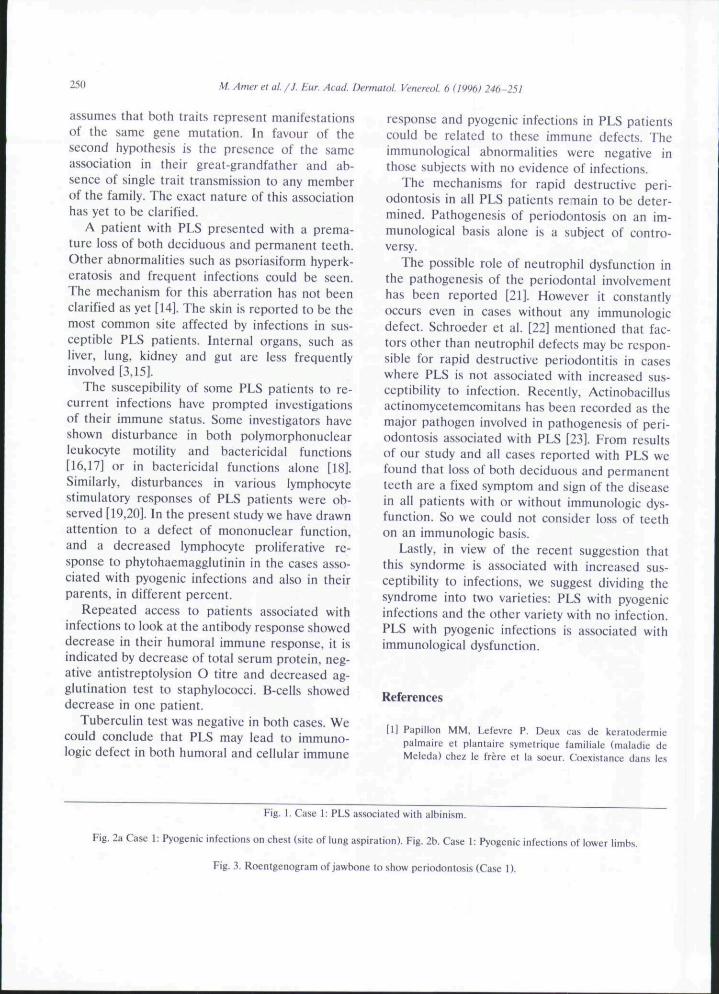
great-grandfather had the same association. Bothcases had suffered from recurrent pyogenic infec-tions. Infections were severe in case,l, as theyhad involved skin and lung since infancy (Fig.2a,b). In case 2 the infections were less severe asthey were confined to the skin. T-cell andmononuclear cell functions proved to be impairednot only in the patients, but also in their parents,as shown in Table 1.
Table 2 shows that there was a significantdifference in total protein, agglutination test, an-tistreptolysin O titre and tuberculin test betweencase 1, 2 and control. Separation of T-cells subsetrevealed a decrease in total B-ce!ls in case 1 only.
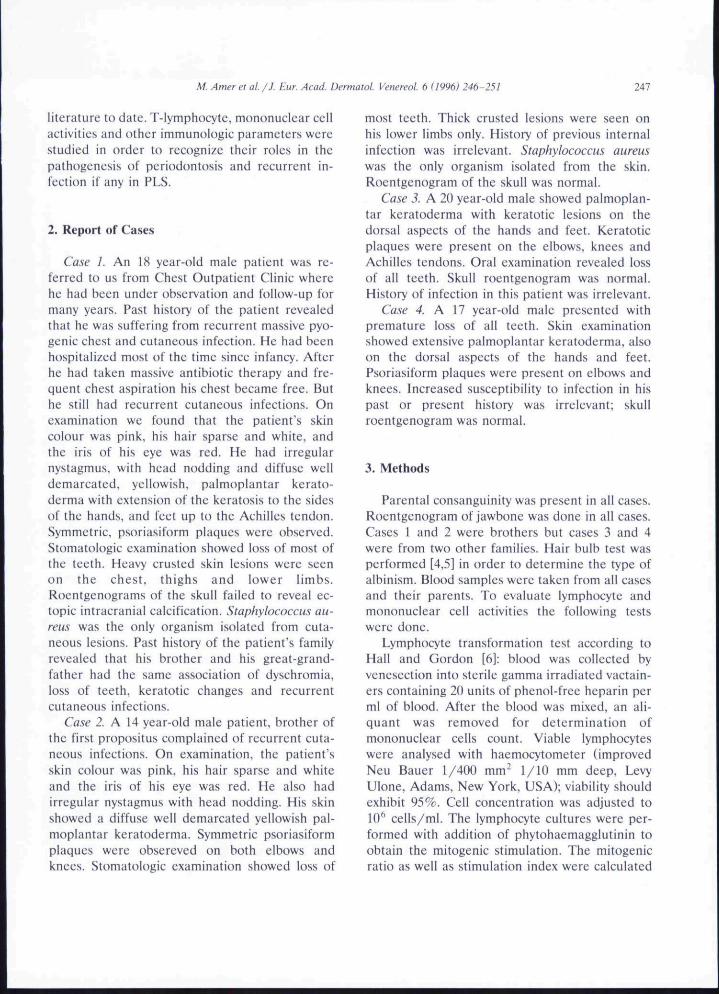
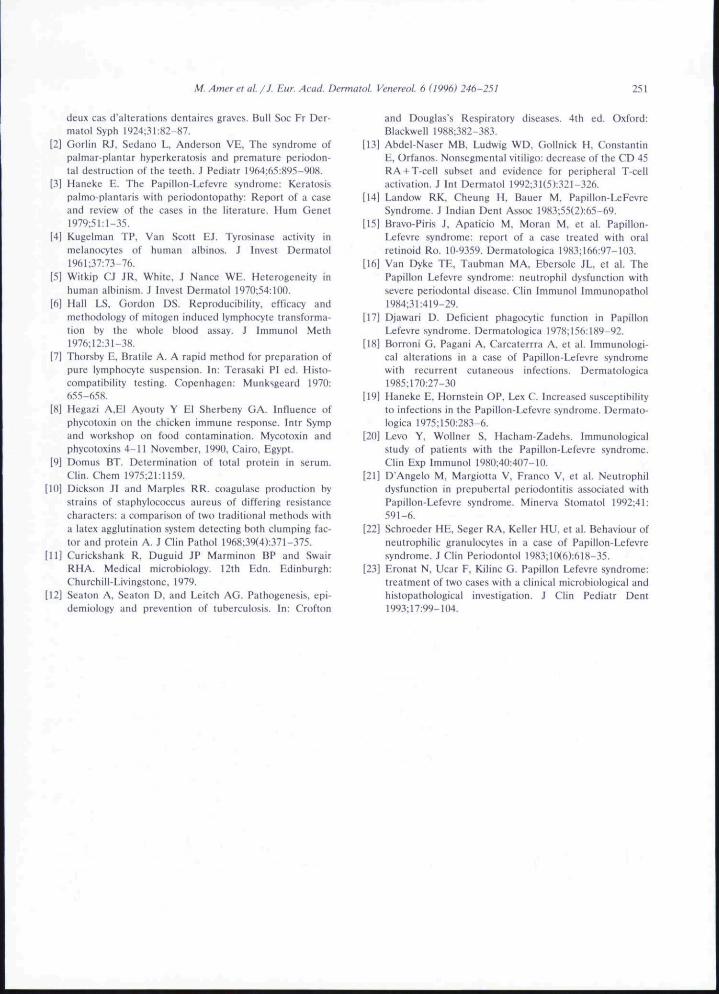
Cases 3 and 4 had no history of infection.T-cell and mononuelear cell activities in bothpatients and their parents showed normal values(Table 1). Roentgenogram of jawbone showedperiodontosis in all cases (Fig. 3, as an example).
5. Discussion
Both PLS and tyrosinase negative albinism areconditions transmitted as autosomal recessivetraits. To our knowledge the association of PLSwith albinism had not been reported before. Thisassociation could be explained by either of twopossibilities. The first is that by chance the twotraits had segregated from both parents and thatthey are independent. The second explanation.
M. Amer et al. /J. Eur Acad. Dermatol Venereot. 6 (1996) 246-251 249
250 M. Amer et al /J. Fur. Acad. Dermatol Venereot. 6 (1996) 246-251
assumes that both traits represent manifestationsof the same gene mutation. In favour of thesecond hypothesis is the presence of the sameassociation in their great-grandfather and ab-sence of single trait transmission to any memberof the family. The exact nature of this associationhas yet to be clarified.
A patient with PLS presented with a prema-ture loss of both deciduous and permanent teeth.Other abnormalities such as psoriasiform hyperk-eratosis and frequent infections could be seen.The mechanism for this aberration has not beenclarified as yet [14]. The skin is reported to be themost common site affected by infections in sus-ceptible PLS patients. Internal organs, such asliver, lung, kidney and gut are less frequentlyinvolved [3,15].
The suscepibility of some PLS patients to re-current infections have prompted investigationsof their immune status. Some investigators haveshown disturbance in both polymorphonuclearleukocyte motility and bactericidal functions[16,17] or in bactericidal functions alone [18].Similarly, disturbances in various lymphocytestimulatory responses of PLS patients were ob-served [19,20]. In the present study we have drawnattention to a defect of mononuelear function,and a decreased lymphocyte proliferative re-sponse to phytohaemagglutinin in the cases asso-ciated with pyogenic infections and also in theirparents, in different percent.
Repeated access to patients associated withinfections to look at the antibody response showeddecrease in their humoral immune response, it isindicated by decrease of total serum protein, neg-ative antistreptolysion O titre and decreased ag-glutination test to staphylococci. B-cells showeddecrease in one patient.
Tuberculin test was negative in both cases. Wecould conclude that PLS may lead to immuno-logic defect in both humoral and cellular immune
response and pyogenic infections in PLS patientscould be related to these immune defects. Theimmunological abnormalities were negative inthose subjects with no evidence of infections.
The mechanisms for rapid destructive peri-odontosis in all PLS patients remain to be deter-mined. Pathogenesis of periodontosis on an im-munological basis alone is a subject of contro-versy.
The possible role of neutrophil dysfunction inthe pathogenesis of the periodontal involvementhas been reported [21]. However it constantlyoccurs even in cases without any immunologicdefect. Schroeder et al. [22] mentioned that fac-tors other than neutrophil defects may be respon-sible for rapid destructive periodontitis in caseswhere PLS is not associated with increased sus-ceptibility to infection. Recently, Actinobacillusactinomycetemcomitans has been reeorded as themajor pathogen involved in pathogenesis of peri-odontosis assoeiated with PLS [23]. From resultsof our study and all cases reported with PLS wefound that loss of both deciduous and permanentteeth are a fixed symptom and sign of the diseasein all patients with or without immunologic dys-function. So we could not consider loss of teethon an immunologie basis.
Lastly, in view of the recent suggestion thatthis syndorme is associated with increased sus-ceptibility to infections, we suggest dividing thesyndrome into two varieties: PLS with pyogenicinfections and the other variety with no infection.PLS with pyogenie infections is associated withimmunological dysfunction.
References
[I] Papillon MM, Lefevre P, Deux cas de keratodermiepalmaire el plantaire symetrique iamiliale (maladie deMeleda) chez le frere et la soeur. Coexislance dans les
Fig. I. Case 1: PLS associated with albinism.
Fig. 2a Case 1: Pyogenic infections on chest (site of lung aspiration). Fig. 2b. Case 1: Pyogenic infections of lower limbs.
Fig. 3. Roentgenogram of jawbone to show periodontosis (Case 1).
M. Amer et al. /J. Fur Acad. Dermatol. Venereol- 6 (1996) 246-251 251
deux cas d alterations dentaires graves. Bull Soc Fr Der-matol Syph 1924:31 ;82-87.
[2] Gorlin RJ, Sedano L, Anderson VE. The syndrome ofpalmiir-planlar hyperkeratosis and premature periodon-tal destruclion of the teeth. J Pediatr l%4:65:8q5-908.
[31 Haneke E. The Papillon-Lelevre syndrome: Keratosispalmo-plantaris with periodontopathy: Report of a caseand review of (he cases in the literature. Hum Genetl979;51:l-35.
[4] Kugelman TP, Van Scott EJ. Tyrosinase activity inmelanocytes of human albinos. J Invest Dermatoll%l:37:73-76.
[5] Witkip CJ JR, White, J Nance WE. Heterogeneity inhuman albinism. J Invest Dermatoi 197();54:inO.
[fl] I lall LS, Gordon DS. Reproducibility, efficacy andmethodology of niilogen induced lymphocyte transforma-tion by the whole blood assay. J Immunol Meth1976;12:31-3«.
[7] Thorsby E, Bratile A. A rapid method for preparation ofpure lymphocyte suspension. In: Terasaki PI ed. Histo-compatibility testing. Copenhagen: Munksgeard 197(1:655-658.
[8] Hegazi A.El Ayouty Y El Sherbeny GA. Influence ofphycotoxin on the chicken immune response, lntr Sympand workshop on food contamination. Mycotoxin andphycotoxins 4-11 November. 1990. Cairo, Egypt.
[9] Domus BT. Determination of total protein in serum.Clin. Chem 1975;21:n59.
[10] Dickson Jl and Marples RR. coagulase production bystrains of staphylococcus aureus of differing resistancecharacters: a comparison of two traditional methods witha latex agglutination system detecting both clumping fac-tor and prolein A. J Clin Patho! 1968:39(4):371-375.
[II] Curickshank R, Duguid JP Marminon BP and SwairRHA. Medical microbiology. 12th Edn. Edinburgh:Churchill-Livingstone, 1979,
[12] Scatun A, Seaton D, and Leitch AG. Pathogenesis, epi-demiology and prevention of tuberculosis. In: Crofton
and Douglas's Respiratory diseases, 4th ed, Oxford:Blackwell l988;382-383.
[13] Abdel-Naser MB. Ludwig WD. Gollnick H, ConstantinE, Orftinos, Nonsegmenlal vitiligo: decrease of the CD 45RA +T-cell subset and evidence for peripheral T-cellactivation, J Int Dermatol 1992:31{5):321-326.
[14] Landow RK, Cheung H, Bauer M. Papillon-LeFevreSyndrome. J Indian Dent Assoc 1983;55(2):65-69,
[15] Bravo-Piris J. Apaticio M, Moran M, et al, Papillon-Lefevre syndrome: report of a case treated with oralretinoid Ro. 10-9359. Dermatologica 1983:166:97-103,
[16] Van Dyke TE, Taubman MA, Ebersole JL. et al. ThePapillon Lefevre syndrome: neutrophil dysfunction withsevere periodontal disease, Clin Immunol Immtinopathol1984:31:419-29.
[17] Djawari D. Deficient phagocytic function in PapillonLefevre syndrome. Dermatologica 1978;156:l89-92.
[18] Borroni G, Pagani A, Carcaterrra A, et al. Immunologi-cal alterations in a case of Papillon-Lefevre syndromewith recurrent cutaneous infections. Dermatologica1985:170:27-30
[19] Haneke E, Hornstein OP. Lex C. Increased susceptibilityto infections in the Papillon-Lefevre syndrome, Dermato-logica 1975;150:283-6.
[20] Levo Y. Wollner S, Hacham-Zadehs, Immunologicalstudy of patients with the Papillon-Lefevre syndrome.Clin Exp Immunol 1980;4n:407-]fl,
[21] D'Angelo M. Margiolta V, Franco V, et al, Neutrophildysfunction in prepubertal periodontitis associaled withPapillon-Lefevre syndrome. Minerva Stomatol 1992;41:591-6.
[22] Schroeder HE, Seger RA, Keller HU, el al. Behaviour ofneutrophilic granulocytes in a case of Papillon-Lefevresyndrome. J Clin Pcriodonlol 1983;HX6):6l8-35,
123] Eronat N, Ucar F, Kilinc G. Papillon Lefevre syndrome:treatment of two cases with a clinical microbiological andhistopathological investigation. J Clin Pediatr Dent1993;I7:99-1O4.

Related Documents











