PANTHER-IPF PREDNISONE, AZATHIOPRINE, AND N-ACETYLCYSTEINE: A STUDY THAT EVALUATES RESPONSE IN IDIOPATHIC PULMONARY FIBROSIS A RANDOMIZED, DOUBLE-BLIND, PLACEBO-CONTROLLED TRIAL Compiled by: The PANTHER-IPF Protocol Committee Version Date: May 19, 2009 Amendment 1 Date: May 28, 2010 Amendment 2 Date: December 6, 2011 Distributed by: The IPFnet Coordinating Center Duke Clinical Research Institute Duke University PO Box 17969 Durham, NC 27715

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
PANTHER-IPF
PREDNISONE AZATHIOPRINE
AND N-ACETYLCYSTEINE
A STUDY THAT EVALUATES RESPONSE IN
IDIOPATHIC PULMONARY FIBROSIS
A RANDOMIZED DOUBLE-BLIND PLACEBO-CONTROLLED TRIAL
Compiled by
The PANTHER-IPF Protocol Committee
Version Date May 19 2009
Amendment 1 Date May 28 2010
Amendment 2 Date December 6 2011
Distributed by The IPFnet Coordinating Center Duke Clinical Research Institute
Duke University PO Box 17969
Durham NC 27715
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Protocol Summary
PRODUCT N-acetylcysteine
CLINICALTRIALSGOV NUMBER NCT00650091
PROTOCOL TITLE Prednisone Azathioprine and N-acetylcysteine A Study THat Evaluates Response in Idiopathic Pulmonary Fibrosis (PANTHER-IPF)
DIAGNOSIS AND MAIN CRITERIA FOR INCLUSION
Confirmed idiopathic pulmonary fibrosis diagnosed within 48 months of enrollment forced vital capacity ge 50 predicted hemoglobin adjusted diffusing capacity of the lung ge 30 predicted
STUDY OBJECTIVES To assess the safety and efficacy of N-acetylcysteine in subjects with newly diagnosed idiopathic pulmonary fibrosis
STUDY DESIGN Multi-center randomized double-blind placebo-controlled
TREATMENT REGIMENS 1) N-acetylcysteine (600 mg TID) or 2) placebo
ROUTE OF ADMINISTRATION Oral
TIME BETWEEN FIRST AND LAST DOSES OF ACTIVE STUDY AGENT
Maximum of 60 weeks
NUMBER OF SUBJECTS Approximately 130 NAC 130 placebo (11)
NUMBER OF CLINICAL CENTERS Approximately 26 US sites
PRIMARY ENDPOINT Change in longitudinal forced vital capacity measurements over 60 weeks
INTERIM ANALYSIS Completed October 2011
2
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Study Sponsor National Heart Lung and Blood Institute
Acting Steering Group Chair Marvin I Schwarz MD University of Colorado - Denver
Project Officer
Gail Weinmann MD National Heart Lung and Blood Institute Bethesda MD
Protocol Committee Cochairs
Ganesh Raghu MD University of Washington
Fernando J Martinez MD University of Michigan
Data Coordinating Center
Duke Clinical Research Institute Duke University
3
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Table of Contents
List of Tables 7
List of Figures 7
List of Abbreviations 8
1 Summary 12
2 Hypotheses and Specific Aims 13 21 Null Hypothesis 13 22 Specific Aim 1 13 23 Specific Aim 2 13 24 Prespecified Subgroups of Interest 14
3 Background and Significance 15 31 Idiopathic Pulmonary Fibrosis is the Most Common Interstitial Lung Disease15 32 Rationale for Placebo Control 15 33 Rationale for N-acetylcysteine 16 35 Rationale for N-acetylcysteine as a Stand-alone Therapy 17 36 Rationale for the Study Design and Primary Endpoint 18 37 Rationale for Blinding of Treatments 19
4 Methods 21 41 Inclusion Criteria 21
411 Subjects Shown to Have Usual Interstitial Pneumonia Pattern on Surgical Lung Biopsy 21 412 Subjects Who Have Not Undergone a Surgical Lung Biopsy 21
42 Diagnosis of IPF 21 43 Exclusion Criteria 26 44 Study Design and Study Visit 27
441 Study Design Summary 27 442 Study Visits 28
4421 Screening 28 4422 Enrollment 29 4423 Week 15 30 4424 Week 30 31 4425 Week 45 31 4426 Week 60 (Early Withdrawal or Final Treatment Visit) 32 4427 Final Site Visit ndash FVC drop confirmation 33 4428 Final Visit ndash Telephone Follow-up 33 4429 Phone Contact Between Visits 33
45 Dose Justification 35 451 Rationale for N-acetylcysteine Dosing 35
4511 Dosing of N-acetylcysteineplacebo 35 4512 Reasons to Discontinue N-acetylcysteineplacebo 35
452 Dosage Algorithms 37 46 Contraindications Precautions and Side Effects of Study Medications 39
461 Contraindication 39 462 Precautions 39 463 Side Effects 39
47 Recruitment Procedures 40 48 Study Procedures 41
481 Biological Specimen Management 41 4811 Biological Specimen Sample Management 41
49 Concomitant Medications 42 410 Laboratory Testing 42 411 Blinding of Study Drugs 43
4
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
5 Study Endpoints 44 51 Primary Study Endpoint 44 52 Secondary Study Endpoints 44
521 Time to Disease-progression 44 522 Acute Exacerbations 44 523 Respiratory Infections 47 524 Maintained FVC Response 48
6 Safety Evaluations and Procedures 49 61 Adverse Events 49
611 Definitions 49 612 Adverse Event (AE) Reporting 50
6121 Serious Adverse Events (SAE) Reporting 50 6122 Regulatory Reporting 51
62 Clinical Medical Monitoring 52 63 Unblinding Procedures 52
7 Study Drug Procedures 53
8 Data Management 54 81 Hardware and Software Configuration 54
811 Hardware and Database Software 54 812 Statistical Software 54 813 Access Control and Confidentiality Procedures 54 814 Security 54 815 Back-up Procedures 55 816 Virus Protection 55
82 Sources of Data 55 821 Design and Development 55 822 Data Collection Forms 55 823 Data Acquisition and Entry 56 824 Data Center Responsibilities 56 825 Data Editing 56 826 Training 56
9 Study Design and Data Analysis 57 91 General Analytic Considerations 57 92 Randomization Blinding and Reporting of Results 57 93 Stratification 58 94 Specification of the Primary Analyses 58 95 Analysis of Longitudinal Endpoints 58 96 Analysis of Binary Time-to-Event and Time-Lagged Endpoints 59 97 Power Analysis 60
971 Primary Analyses 60 972 Power Analysis for Secondary Endpoints 61
10 Study Administration 62 101 Cooperative Agreement Mechanism 62 102 IPFnet Steering Group 64 103 Data and Safety Monitoring Board 64 104 Recommendations on Interim Monitoring of Efficacy Safety and Futility 64
11 Investigator and Sponsor Obligations 66 111 Monitoring 66 112 Cost and Payment 66 113 Confidentiality and Health Insurance Portability and Accountability Act Considerations 66 114 Informed Consent Procedures 67 115 Institutional Review Boards 67
5
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
12 Investigator Agreement 68
13 References 69
6
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
List of Tables Table 1 Operating Characteristics of Local HRCT Review for Diagnosis of UIP (24)
Table 2 Combining HRCT and Pathology Interpretations to Determine if IPF is Present (25)
Table 3 Schedule of Assessments (34)
Table 4 Side Effects of NAC (40)
Table 5 Final Diagnoses in Evaluation of Suspected Acute Exacerbations (46)
Table 6 Hypothetical Values of Mean FVC (L) Change from Baseline (61)
Table 7 Detectable Differences in Treatment Means for Selected Endpoint Measurements (61)
List of FiguresFigure 1 Changes in Forced Vital Capacity from Baseline in Prior IPF Clinical Trials (19)
Figure 2 Diagnosis of Idiopathic Pulmonary Fibrosis in the IPFnet (22)
Figure 3 Pathology Flow Chart Surgical Lung Biopsy Diagnosis (23)
Figure 4 Acute Exacerbation Flow Chart (47)
7
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
List of Abbreviations
6MWT 6-minute walk test
A-aPO2 alveolar-arterial PO2 difference
ABG arterial blood gas
AE adverse event
AEx acute exacerbation
AG albuminglobulin
ALT alanine aminotransferase
AST aspartate aminotransferase
ATS American Thoracic Society
AZA azathioprine
BAL bronchoalveolar lavage
BUN blood urea nitrogen
CBC complete blood count
cGMP Current Good Manufacturing Practice
CPI Composite Physiologic Index
CPK creatine phosphokinase
CT computed tomography
DCC Data Coordinating Center
DCRI Duke Clinical Research Institute
8
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
DLCO diffusing capacity of the lung for carbon monoxide
DLCOpred diffusing capacity of the lung for carbon monoxide percent predicted
DSMB data and safety monitoring board
eCRF Electronic case report form
ERS European Respiratory Society
FDA Food and Drug Administration (US)
FEV1 forced expiratory volume in 1 second
FSH follicle-stimulating hormone
FVC forced vital capacity
FVCpred forced vital capacity percent predicted
GGT gamma glutamyl transferase
GSH glutathione
HAD Hospital Anxiety and Depression
HHS Health amp Human Services (US Dept of)
HIPAA Health Insurance Portability and Accountability Act
HRCT high-resolution computed tomography
IBW ideal body weight
ICE CAP Investigating Choice Experiments for Preferences of Older People Capability Instrument
ILD interstitial lung disease
IPF idiopathic pulmonary fibrosis
9
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
IPFnet Idiopathic Pulmonary Fibrosis Clinical Research Network
IRB institutional review board
ITT intent to treat
IV intravenous
IVRS interactive voice response system
LDH lactate dehydrogenase
LFT liver function test
LOCF last observation carried forward
LSD Least Significant Difference
MAR missing at random
MCAR missing completely at random
MMRM mixed model repeated measures
MOOP manual of operating procedures
NAC N-acetylcysteine
NHLBI National Heart Lung and Blood Institute (US)
NIH National Institutes of Health (US)
NSIP nonspecific interstitial pneumonia
PaO2 partial pressure of arterial oxygen
PCP primary care provider
PFT pulmonary function test
10
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
PHS Public Health Service (US)
PI principal investigator
PL placebo
PLT platelet
PRED prednisone
QOL quality of life
SAE serious adverse event
SAP statistical analysis plan
SGRQ St Georgersquos Respiratory Questionnaire
SpO2 oxygen saturation by pulse oximetry
TPMT thiopurine methyl transferase
UCSD SOBQ University of California at San Diego Shortness of Breath Questionnaire
UIP usual interstitial pneumonia
ULN upper limit of normal
USP United States Pharmacopoeia
VC vital capacity
WBC white blood cell
11
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
PREDNISONE AZATHIOPRINE AND N-ACETYLCYSTEINE A STUDY
THAT EVALUATES RESPONSE IN IDIOPATHIC PULMONARY FIBROSIS
1 Summary
There are currently no drug therapies that have proven to be effective in the treatment of idiopathic pulmonary
fibrosis (IPF) Previous clinical drug trials have been difficult to interpret due to lack of true placebo (PL)
controls or other methodological concerns Clinical efficacy of immunosuppressive therapies and agents that
reduce oxidative stress remains controversial The IPF Clinical Research Network (IPFnet) is conducting a
randomized double-blind placebo-controlled trial designed to assess the safety and efficacy of
N-acetylcysteine (NAC) as monotherapy in subjects with mild or moderate IPF
The study initially employed a 3-arm design with 111 randomization to NAC azathioprine (AZA)-prednisone
(PRED)-NAC and PL with each subject to be treated up to a maximum of 60 weeks followed by a tapering of
PREDPL and a 4-week period for safety evaluation Approximately 390 subjects who have mild to moderate
IPF (defined as forced vital capacity percent predicted [FVCpred] ge 50 and diffusing capacity of the lung
for carbon monoxide percent predicted [DLCOpred] 30) diagnosed within the past 48 months were to be
enrolled
At the pre-specified interim analysis the DSMB recommended termination of the prednisone-azathioprine-
NAC arm of the study No additional patients will be randomized to that arm However the NAC and placebo
arms remain open for enrollment and we will enroll approximately 130 subjects in each arm (inclusive of the
subjects enrolled at the time of the interim analysis) Follow up for subjects enrolled into the two arms will
continue for 60 weeks
The primary endpoint is the change in longitudinal measurements of FVC over the study period The primary
goal of this study to establish an evidence-based standard of care and clarify myths from facts for
pharmacotherapy of IPF has been met in part by demonstrating that the widely used triple therapy was harmful
to patients with IPF (NHLBI press release Oct 21 2011) To determine the potential therapeutic benefits of
NAC alone the study will continue to enroll patients as a two-arm double-blind placebo-controlled study from
this point on (NAC vs placebo) as recommended by the DSMB following the pre-specified interim analysis
12
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
2 Hypotheses and Specific Aims 21 Null Hypothesis
Treatment with NAC will provide the same efficacy as PL as measured by longitudinal changes in FVC
22 Specific Aim 1
This study is designed to assess the safety and efficacy of NAC in subjects with newly diagnosed IPF
23 Specific Aim 2
Secondary goals of this study are to assess differences between treatment groups for the following
1 Mortality
2 Time to death
3 Frequency of acute exacerbations (AExs)
4 Frequency of maintained FVC response
5 Time-to-disease progression
6 Change in DLCO
7 Change in Composite Physiologic Index (CPI)
8 Change in resting alveolar-arterial oxygen gradient
9 Change in 6-minute walk test (6MWT) distance
10 Change in 6MWT oxygen saturation area under the curve
11 Change in 6MWT distance to desaturation lt 80
12 Change in 6MWT minutes walked
13 Changes in health status as measured by the SF-36 EuroQol and St Georgersquos Respiratory
Questionnaire (SGRQ)
14 Changes in dyspnea as measured by the University of California at San Diego Shortness of Breath
Questionnaire (UCSD SOBQ)
15 Frequency and types of adverse events (AEs)
16 Frequency and types of respiratory complications both infectious and noninfectious
17 Frequency of hospitalizations both all-cause and respiratory-related
13
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
24 Prespecified Subgroups of Interest
Treatment effects will be estimated and compared within key subgroups
Higher enrollment FVC12
Typical vs atypical high-resolution computed tomography (HRCT) reading at baseline3
Recent vs more remote diagnosis (time from initial diagnosis of IPF le 1 year and gt 1 year)
Lower CPI score at enrollment4
Medical therapy for gastroesophageal reflux5
Ethnic background
Sex
Smoking history (current or ex-smoker vs never smoker) given potential impact on oxidant status6
Presence of emphysema gt 25 on HRCT
14
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
3 Background and Significance
31 Idiopathic Pulmonary Fibrosis is the Most Common Interstitial Lung Disease
IPF is the most common interstitial lung disease (ILD) of unknown etiology The current incidence and
prevalence of IPF in the United States are not known A 1994 study of a population-based registry of subjects in
Bernalillo County New Mexico USA estimated an incidence of 107 cases per 100000 per year for males and
74 cases per 100000 per year for females the prevalence of IPF was estimated at 20 per 100000 for males and
13 per 100000 for females7 Extrapolating from a large healthcare claims database a more recent review
estimated the prevalence of IPF in the United States at 427 per 100000 (incidence estimated at 163 per
100000 per year)8 Recent epidemiological studies indicate increasing mortality rates from IPF in the United
States and other industrialized nations9-12
Approximately two-thirds of subjects with IPF are over the age of 60 at the time of presentation and the
incidence increases with age13 IPF has no distinct geographical distribution and predilection by race or
ethnicity has not been identified13 Individual subjects may remain relatively stable for prolonged periods
experience very slow declines in lung function with progression of radiographic abnormalities for a period of
months to years or experience more rapid declines and subsequent death Only 20 to 30 of IPF patients
survive for 5 years following diagnosis
There is currently no proven effective pharmacological treatment for IPF13 Anti-inflammatory and
immunosuppressive agents have been the traditional approach to the management of patients with IPF Based
on the results of the interim analysis of the PANTHER-IPF trial this lsquotraditional approachrsquo will be aborted
However it remains unknown if NAC alone will prove beneficial in IPF patients The primary goal of the
modified study is to establish an evidence-based standard of care and clarify the role of this specific antioxidant
pharmacotherapy for IPF
32 Rationale for Placebo Control
IPF is a disorder for which there is no proven efficacious therapy A major objective of this trial is to test to the
greatest degree possible a proposed standard of care for patients with IPF The current traditional therapy
15
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
employs immunosuppressive and corticosteroid drugs Interim review of the original PANTHER-IPF study has
documented increased adverse events and lack of efficacy for AZA-PRED-NAC compared to placebo
suggesting that this therapeutic approach should not be employed Whether this applies to NAC alone which
has been advocated by international societies has not been proven in well-designed well-powered clinical
trials The recommendations made in the recently published evidence guidelines for NAC monotherapy was
weak based on low quality13 Thus this continued clinical trial randomizing patients to receive NAC or placebo
is pivotal and will answer the important question of the potential therapeutic benefits of NAC monotherapy with
grade A evidence In this prospective randomized clinical trial the inclusion of a PL arm is therefore vital to
adequately test the benefits of NAC in well-characterized subjects with IPF
If NAC has no true efficacy then its role as standard of care will be refuted If a benefit compared with PL is
confirmed it will establish a benchmark against which future novel therapies for IPF will be safely compared
As there is no currently accepted therapy for IPF there is an increasing body of published literature supporting
the concept of no treatment as the ldquobest carerdquo option for IPF13
Post hoc analyses of PL-controlled trials suggest that subjects with milder disease may be more amenable to
therapy12 It is notable that a recent international prospective randomized trial of interferon-gamma for IPF
also included a PL arm the study was terminated early by the data and safety monitoring board (DSMB) due to
lack of treatment effect1415 This underscores the belief that a proven effective therapy for IPF does not
currently exist and that true placebo-controlled trials remain the gold standard Similarly recently completed
trials of etanercept everolimus bosentan and BIPF 1120 in IPF have included PL-treated arms16-19 In three of
these trials the treated subjects showed little if any objective improvement Based on this evidence and the
current status of IPF therapy and therapeutic trials we believe that clinicians and subjects will continue to enroll
in a PL-controlled study
33 Rationale for N-acetylcysteine
NAC is a derivative of the amino acid L-cysteine NAC has been shown to augment levels of the naturally
occurring antioxidant glutathione (GSH ) (glutathione γ-glutamyl cysteinyl glycine) both in vitro and in
vivo2021 GSH is present in all eukaryotic cells and may play an important role in protecting alveolar epithelial
cells against oxidant injury The concentration of GSH in the bronchoalveolar lavage (BAL) fluid in patients
16
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
with IPF is markedly diminished compared with normal subjects This GSH deficiency may be corrected by
exogenous administration of NAC2122
There is evidence of enhanced production of oxidants in an IPF lung Both inflammatory cells and
myofibroblasts derived from patients with IPF generate increased amounts of extracellular oxidants including
hydrogen peroxide2324 Secretion of hydrogen peroxide by activated myofibroblasts may induce the death of
adjacent lung epithelial cells by paracrine mechanisms24 Additionally generation of oxidants by myofibroblasts
induces oxidative crosslinking of extracellular matrix proteins25 a potential mechanism for aberrant matrix
remodeling Thus an oxidant-antioxidant imbalance exists in the lungs of IPF patients26 NAC may confer
protection against this imbalance by augmenting GSH levels in addition to its more direct free-radical
scavenging activity
Intravenous (IV) NAC therapy has been shown to increase total BAL GSH in 8 IPF subjects27 Oral NAC (600
mg 3 times per day) has been shown to decrease markers of oxidant injury and improve both total and reduced
GSH levels in the epithelial lining fluid of subjects with IPF in a small uncontrolled study22 pulmonary
function improved modestly with therapy A similar study in 18 IPF subjects confirmed increased intracellular
GSH concentration after 12 weeks of NAC (600 mg 3 times per day)2228 no clinical correlates were reported
Inhaled NAC was suggested to improve pulmonary function in an open label study29
35 Rationale for N-acetylcysteine as a Stand-alone Therapy
Results of a double-blind multi-center European clinical trial of 150 IPF subjects testing combinations of AZAshy
PRED vs AZA-PRED-NAC have been reported30 NAC added to AZA-PRED (ldquoconventional therapyrdquo) had a
significant positive effect on DLCO (p lt 0005) and vital capacity (VC) (p lt 005) at the end of 1 year30 The
recent ATSERS position statement after much discussion concluded that NAC alone should not be considered
in the majority of patients with IPF without additional data from well-designed studies
The interpretation of these data has been quite controversial Some have suggested that the magnitude of the
treatment effect although statistically significant is modest31 Others have suggested that NAC may be
modulating potential toxic effects of AZA-PRED alone32 supporting the investigation of NAC as stand-alone
therapy
17
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
The IPFnet is now completing the PANTHER-IPF trial with a 11 randomization (NAC vs placebo) and a
simple practical feasible and scientifically rational design that will establish standard of care with NAC for
IPF based on a currently available therapeutic agent and the existing data to support its use We anticipate that
all future clinical trials of novel therapeutic agents will be tested against this to-be-established standard of care
36 Rationale for the Study Design and Primary Endpoint
The optimal study design of a therapeutic trial in IPF would include survival as a primary endpoint The
published results of the IFN-γ 1b Phase 3 (GIPF-001) trial suggested a survival benefit in subjects with milder
disease in retrospective analyses1 although the trial was underpowered to address this question This was likely
related to the limited mortality in the PL arm of the study which included IPF subjects with mild to moderate
disease This study documents that an IPF study powered to improve survival in a patient population with mild
disease requires a larger sample size andor duration of study In fact the recently aborted Phase 3 IFN-γ 1b
(GIPF-007 INSPIRE) study was a survival-based study and recruited more than 800 subjects at 75 centers
worldwide1415 As such within the context of the current IPFnet trial survival is an impractical primary
endpoint variable
Several groups have published data defining an appropriate surrogate outcome variable a 10 decrement in
FVC during 6 to 12 months is a powerful predictor of survival in IPF33-36 Furthermore additional evidence
suggests a similar predictive ability for a 10 decrement in FVC during 3 months of follow-up37 With strong
supportive evidence of FVC progression being related to mortality on a per-subject basis this study will use
FVC changes in liters between treatment groups as the primary endpoint Previously published IPF studies have
shown a steady decline in FVC (and FVCpred) among control group subjects230 The GIPF-001 study
suggested a 48-week decrease in FVC of 016 L in the PL-treated subjects The IFIGENIA study demonstrated
a decline in FVC of approximately 019 L over 52 weeks in the subjects randomized to the control treatment
Figure 1 depicts the change in FVC for control groups from previously published IPF studies38 Based on these
data we expect that the PL group will have a decline of 020 L over the 60-week study period The IPFnet
Steering Group determined that a clinically meaningful improvement would be the preservation of the majority
of the 020-L FVC decline Therefore a mean treatment difference of 015 L in mean FVC over the 60-week
study period was determined to be a clinically meaningful difference
18
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Δ f
rom
bas
elin
e (i
n L
)
01
005
0
-005
-01
-015 Projected Δ for placebo
-02
-025
-019
-016
-013 Pirfenidone GIPF001
NAC
Placebo
4 8 12 16 20 24 28 32 36 40 44 48 52 56 60
Week
Figure 1 Changes in FVC From Baseline in Prior IPF Clinical Trials
Recent data suggest that various patient subgroups would be expected to potentially exhibit differential response
to therapy These parameters will be used to a priori separate patients by a series of baseline characteristics
including
1 Higher enrollment FVC12
2 Typical vs atypical high-resolution computed tomography (HRCT) reading at baseline3
3 Recent vs more remote diagnosis (time from initial diagnosis of IPF le 1 year and gt 1 year)
4 Lower CPI score at enrollment4
5 Medical therapy for gastroesophageal reflux5
6 Ethnic background
7 Sex
8 Smoking history (current or ex-smoker vs never smoker) given potential impact on oxidant status6
9 Presence of emphysema gt 25 on HRCT
37 Rationale for Blinding of Treatments
The issue of treatment blinding was given a great deal of consideration with subject safety being the primary
concern After discussion among the Steering Group members it was decided that as long as subject safety
could be ensured blinding was necessary Blinding allows the study to
Have optimal scientific validity and potential to impact the standard of care for subjects
19
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Make objective assessments of treatment effects
Maintain clinical equipoise among investigators
Encourage subjects to have similar levels of contact with the medical community
Minimize the differential dropout rates across study arms
20
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
4 Methods 41 Inclusion Criteria
1 Age 35 to 85 years inclusive
2 FVC ge 50 of predicted (post-bronchodilator measurement from the screening visit)
3 DLCO ge 30 of predicted (hemoglobin corrected and altitude corrected if gt4000 ft above sea level)
4 Ability to understand and provide informed consent
5 Diagnosis of IPF according to a modified version of the ATS criteria le 48 months from enrollment The
date of diagnosis is defined as the date of the first available HRCT or surgical lung biopsy characteristic
of definite UIP
411 Subjects Shown to Have Usual Interstitial Pneumonia Pattern on Surgical Lung Biopsy
Subjects who have been shown to have UIP pattern on lung biopsy must have all of the following
1 Exclusion of other known causes of ILD such as drug toxicity clinically significant environmental
exposures or diagnosis of connective tissue diseases
2 Bibasilar reticular abnormalities with minimal ground glass opacities on HRCT scan
412 Subjects Who Have Not Undergone a Surgical Lung Biopsy
In addition to the criteria above these subjects must have radiological findings considered to be definite for the
diagnosis of UIPIPF
1 Bibasilar reticular abnormalities with minimal ground glass opacities
2 Honeycombing as the predominant feature and located in the peripheral lung bases
42 Diagnosis of IPF
Only subjects with definite IPF will be eligible for enrollment in this study We will utilize a combination of
clinicalphysiologic features HRCT and review of a clinically obtained surgical lung biopsy specimen to
establish the diagnosis of IPF An algorithm for the diagnosis is provided to guide entry into the protocol as
outlined in the inclusion and exclusion criteria (Figures 2 and 3) This multi-disciplinary approach uses
21
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
expertise from clinicians radiologists and pathologists Investigators at each site in conjunction with central
pathology will work together to establish the diagnosis of IPF This interactive approach to the diagnosis of IPF
increases the level of agreement between observers39
A subject with suspected ILD should be evaluated for secondary causes including but not limited to
environmental exposures drugs and systemic diseases Presence of any of these findings felt to be significant
enough to cause an ILD should disqualify the subject from entry into the trial
If secondary causes are absent an HRCT scan may be obtained If an HRCT of sufficiently high quality has
been obtained within the last 3 months that scan may be used for diagnosis In the appropriate clinical setting
the diagnosis of IPF can be made by the demonstration of a typical radiographic pattern on HRCT or by
demonstration of UIP pattern on a surgical lung biopsy The following criteria for a radiographic (ie
nonsurgical) diagnosis will be used In the absence of known exposures andor clinical associations attributable
to pulmonary fibrosis and in the appropriate clinical setting the presence of definite UIP pattern in HRCT
images is required to meet study criteria for the diagnosis of IPF
Figure 2 Diagnosis of Idiopathic Pulmonary Fibrosis in the IPFnet
22
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Figure 3 Pathology Flow Chart Surgical Lung Biopsy Diagnosis
Requirement for diagnosis
1 Clinical exclusion of other known causes (connective tissue diseases environmental and drug
exposures) of ILD
2 Radiographic HRCT with bibasilar reticular abnormality and honeycomb change with minimal
ground glass opacities
Appropriate clinical setting
1 Age gt 50 years
2 Insidious onset of unexplained dyspnea
3 Duration of illness for ge 3 months
4 Bibasilar inspiratory crackles
23
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Unlike the ATSERS consensus criteria published in 2000 bronchoscopy will not be required for diagnosis
This decision was made based on the experience of the IPFnet Steering Group members regarding the utility of
bronchoscopy in the diagnosis of IPF The presence of an atypical HRCT finding will require documentation of
a definitive diagnosis by surgical lung biopsy In fact this is in keeping with the recently published evidence
based guidelines for diagnosis and management of IPF13 As shown in Figure 3 central review of the pathology
data will be required for a diagnosis of IPF
We will not require central review of HRCT as several studies have shown that a confident local interpretation
of clinicalHRCT criteria as definite IPFUIP is associated with a high positive predictive value for finding UIP
at surgical lung biopsy (see Table 1) Differences in sensitivity in these series likely reflect subject selection as
Flaherty et al3 evaluated only UIP and nonspecific interstitial pneumonia (NSIP) while Raghu et al40 and
Hunninghake et al41 included a broader range of ILD
Table 1 Operating Characteristics of Local HRCT Review for Diagnosis of UIP
Researcher of Subjects Sensitivity () Specificity () PPV () NPV ()
Raghu et al 40
59 (29 UIP by SLB) 78 90 88 82
Hunninghake et al 41 91 (54 UIP by SLB)
74 81 85 67
Flaherty et al 3 96 (only NSIP amp UIP)
37 100 100 30
Abbreviations PPV positive predictive value NPV negative predictive value UIP usual interstitial pneumonia SLB surgical lung biopsy and NSIP nonspecific interstitial pneumonia
Furthermore an analysis of the HRCT scans from subjects enrolled in the GIPF-001 trial confirmed that local
site interpretations have a high congruity to a central radiology core In this multi-center study 263 HRCT
scans were read as definite IPF and a retrospective central radiology core review found 932 to be consistent
with IPF 42 We will also take several additional steps to insure that the local HRCT reads are accurate
including
1 A detailed training module has been developed and must be completed by each site radiologist before
site initiation
2 Clinical centers are to mail all HRCT scans to the HRCT core lab The first 10 HRCT scans from
subjects enrolled at each enrolling clinical center will be reviewed centrally to be certain that local reads
24
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
25
are congruent with a central interpretation If discrepancies are identified additional education will be
provided and HRCT scans will continue to be reviewed centrally until the central radiology core is
confident that the local center is performing appropriately
3 Random scans will be obtained from each center throughout the study to confirm that the local read
continues to agree with central interpretation If discrepancies are identified they will be addressed as in
2 above
In all cases if a subject has a surgical lung biopsy sample that sample will be reviewed by the local and central
pathologists Therefore the only cases that would not be subject to a direct central review process are those
where the HRCT meets the centrally defined criteria for an unequivocal diagnosis and a lung biopsy sample is
not available Table 2 below summarizes the possible combinations for making a diagnosis
Table 2 Combining HRCT and Pathology Interpretations to Determine if IPF is Present
HRCT Diagnosis Pathology Diagnosis Diagnosis of IPF
Definite UIP Definite UIP Yes
Definite UIP Probable UIP Yes
Definite UIP Possible UIP Yes
Definite UIP Not UIP No
Definite UIP Unavailable Yes
Consistent with UIP Definite UIP Yes
Consistent with UIP Probable UIP Yes
Consistent with UIP Possible UIP No
Consistent with UIP Not UIP No
Consistent with UIP Unavailable No
Inconsistent with UIP Any No
Abbreviations HRCT high-resolution computed tomography IPF idiopathic pulmonary fibrosis
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
UIP usual interstitial pneumonia Dx diagnosis 43 Exclusion Criteria
1 History of clinically significant environmental exposure known to cause pulmonary fibrosis
Occupational exposures such as asbestos or environmental exposure to organic dust such as occurs in
pigeon breeders may at times mimic the clinical and radiographic findings of IPF
2 Diagnosis of connective tissue disease felt by the principal investigator (PI) to be the etiology of the
interstitial disease Diagnosis of collagen-vascular conditions will be according to the published
American College of Rheumatology criteria As such the presence of any documented collagen-vascular
disorder or the presence of any suspicious symptom complex whether or not associated with
significantly abnormal rheumatological serologies will exclude the subject at the discretion of the PI
3 Extent of emphysema greater than the extent of fibrotic change (honeycombing reticular changes) on
HRCT scan
4 Forced expiratory volume in 1 second (FEV1)FVC ratio lt 065 at screening (postbronchodilator)
5 Partial pressure of arterial oxygen (PaO2) on room air lt 55 mm Hg (lt 50 mm Hg at Denver site)
6 Residual volume gt 120 predicted at screening (postbronchodilator)
7 Evidence of active infection
8 Significant bronchodilator response on screening spirometry defined as a change in FEV1 ge 12 and
absolute change gt 200 mL OR change in FVC ge 12 and absolute change gt 200 mL The percent
difference between the FVC (or FEV1) values will be calculated by taking the absolute value of the
difference and dividing it by the larger of the two FVC (or FEV1) values
9 Screening and enrollment post-bronchodilator FVC measurements (in liters) differing by gt 11 The
percent difference between the FVC values will be calculated by taking the absolute value of the
difference and dividing it by the larger of the two FVC values (eg the percent difference between FVC
measurements of 19 and 20 liters would be determined by taking the difference between the two (01
liters) and dividing by the larger of the two (20 liters) So 0120 = 5 and these FVC measurements
would not exclude the subject
10 Listed for lung transplantation ie the patient has completed the evaluation process has been accepted
as a candidate for transplantation at an appropriate center and is waiting to receive notification of an
available donor organ
11 History of unstable or deteriorating cardiac disease
12 Myocardial infarction coronary artery bypass or angioplasty within 6 months of screening
26
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
13 Unstable angina pectoris or congestive heart failure requiring hospitalization within 6 months of
screening
14 Uncontrolled arrhythmia
15 Severe uncontrolled hypertension
16 Known HIV or hepatitis C
17 Known cirrhosis and chronic active hepatitis
18 Active substance andor alcohol abuse (as determined by site PI)
19 Pregnancy or lactation (subjects who are pregnant or breastfeeding)
20 Known hypersensitivity to study medication
21 Any condition other than IPF that in the opinion of the site PI is likely to result in the death of the
subject within the next year
22 Any condition that in the judgment of the PI might cause participation in this study to be detrimental to
the subject or that the PI deems makes the subject a poor candidate
23 Any therapy directed at pulmonary fibrosis (excepting triple therapy of prednisone plus azathioprine
plus NAC) requires a 30-day washout period before randomized Triple therapy of lt= 12 weeks duration
in the past 4 years requires a 30-day washout period before randomization
24 History of triple therapy of prednisone plus azathioprine plus NAC for gt 12 weeksrsquo duration in the past
4 years or previous enrollment in the triple-therapy arm of the PANTHER-IPF study
44 Study Design and Study Visit
441 Study Design Summary
This study will be a randomized double-blind PL-controlled trial designed to assess the safety and efficacy of
NAC in subjects with newly diagnosed IPF
Subjects with mild to moderate IPF (defined as FVCpred ge 50 and DLCOpred ge 30) diagnosed within
the past 48 months will be enrolled Screening will continue until April 30 2012
27
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
The study will employ a 2-arm design with 11 randomization to NAC or PL Once enrolled subjects will visit
the clinical center at 15 weeks and 15-week intervals thereafter Each subject will be treated and followed for a
maximum of 60 weeks
During the 60-week visit subjects will be taken off all study agents Approximately four weeks after the final
dose of study agent is taken subjects will receive a safety phone call from the study site
442 Study Visits
Subjects who meet entry criteria will review the informed consent a written description of the purpose
procedures and risks of the study with the PI co-investigator or study coordinator and all questions will be
answered The informed consent form will be signed by the subject at screening No protocol-specific
procedures will be performed until the subject has signed and dated an informed consent form This includes the
screening procedures
4421 Screening
Once informed consent is obtained subjects may immediately begin the screening process or may return within
28 days of consent In the event a study subject has been clinically evaluated at the study site by an IPFnet study
physician and has performed testing within three weeks for this clinical evaluation that meets guidelines
provided in the IPFnet PANTHER-IPF Manual of Operating Procedures (MOOP) this testing may be used to
satisfy the following screening criteria medical history physical exam arterial blood gas (ABG) with A-a
gradient vital signs with oximetry body height and weight spirometry DLCO lung volumes and HRCT scan
Allowing the use of previously performed test results that meet study guidelines for the screening visit is
intended to permit subjects easier access to study entry to prevent subjects from repeating testing that has been
performed within the study window and to decrease risks to subjects from repeated exposure to procedures
such as arterial puncture and HRCT
The following procedures will be performed at screening
Medical history and a physical examination
28
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Measure height and weight
Serum pregnancy test (if applicable)
Measure vital signs including oximetry
Blood draws performed and the following analyses conducted
o Hematology (red cell count white cell count hemoglobin hematocrit cell indices differential
platelet count)
o Blood chemistries according to central laboratory protocol (see Section 410 Laboratory
Testing)
o Beta human chorionic gonadotropin (serum) pregnancy test (in women of childbearing potential)
o Urinalysis
Pulmonary Function Tests (PFTs) including spirometry pre- and post- bronchodilator and postshy
bronchodilator measurement of lung volumes and measurement of hemoglobin adjusted diffusing
capacity
Measure ABGs
HRCT if a satisfactory scan has not been performed on the subject within 3 months of screening (see
PANTHER-IPF MOOP for more details)
Surgical lung biopsies (if applicable) reviewed by local and central pathology departments
Current medications If required a washout period discussed with the subject and initiated at this visit
4422 Enrollment
The enrollment visit is expected to take place within eight weeks of the screening visit Enrollment visit
activities include
Measure vital signs including oximetry
Measure height and weight
Serum pregnancy test (if applicable)
If consent has been given blood will be drawn and a urine specimen collected for the bio-specimen
repository
Spirometry (post-bronchodilator)
Measure 6MWT with Borg Dyspnea Scale
29
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Collect Quality-of-life (QOL) data using the SF-36 EuroQol Investigating Choice Experiments for
Preferences of Older People Capability Instrument (ICE CAP) and SGRQ
Female subjects complete Gender Substudy questionnaire
Dyspnea status collected using the UCSD SOBQ
Evaluate Acute Exacerbation (AEx)
Review of any Adverse Events (AEs)
Review of concomitant medications
Subject receives diary and instructions on its purpose and proper use
Subject receives supply of study drug sufficient to last until his or her 15-week study visit
See the Schedule of Assessments (Table 3) for more details Subjects with screening and enrollment postshy
bronchodilator FVC measurements (in liters) differing by more than 11 are not eligible to be enrolled in the
study
Subjects will be asked to provide a physician of record This physician will be considered the subjectrsquos primary
care provider (PCP) and if the subject agrees the PCP will be informed by letter of the subjectrsquos enrollment in
the trial The subject will be informed that his or her ongoing medical care should be received from the PCP
The PCP will be informed of any safety issues identified by the study staff The PCP will also be given
information regarding communication with study personnel about pertinent health issues or clinic encounters
the subject may have
4423 Week 15
The week 15 visit is expected to occur within +- 14 days of the subjectrsquos scheduled visit time (eg the week 15
visit should occur anytime between 13 and 17 weeks after starting study drug Week 15 activities include
Measure vital signs with oximetry
Measurement height and weight
Serum pregnancy test (if applicable)
Spirometry (post-bronchodilator) measurement
Review of AEs
Evaluate for AEx
30
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Review concomitant medications
If consented draw blood and collect urine specimen for the biospecimen repository
Subjects return used and unused study drug for the visit
Review study diary and a new study diary will be given
Provide additional supply of study drug sufficient to last until the next scheduled visit
4424 Week 30
The week 30 visit is expected to occur within +- 14 days of the subjectrsquos scheduled visit time (eg the week 30
visit should occur anytime between 28 and 32 weeks after starting study drug) Week 30 activities include
Physical examination
Measure vital signs with oximetry
Measure height and weight
Laboratory values (complete blood count [CBC] and serum chemistries)
Serum pregnancy test (if applicable)
Measure spirometry (post-bronchodilator)
6MWT with Borg scale
DLCO
Review of AEs
Evaluate for AEx
Review concomitant medications
Complete all QOL and dyspnea questionnaires (EuroQol ICE CAP SF-36 SGRQ and UCSD SOBQ)
If consent has been given blood will be drawn and a urine specimen collected for the biospecimen
repository
Review study diary
Subjects return used and unused study drug for the visit
Provide additional supply of study drug sufficient to last until the next scheduled visit
4425 Week 45
31
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
The week 45 visit is expected to occur within +- 14 days of the subjectrsquos scheduled visit time (eg the week 45
visit should occur anytime between 43 and 47 weeks after starting study drug) Week 45 activities include
Measure vital signs with oximetry
Measure height and weight
Serum pregnancy test (if applicable)
Measure spirometry (post-bronchodilator)
Review of AEs
Evaluate for AEx
Review concomitant medications
If consent has been given blood will be drawn and a urine specimen collected for the biospecimen
repository
Subjects return used and unused study drug for the visit
Study diary reviewed
Provide additional supply of study drug sufficient to last until the next scheduled visit
4426 Week 60 (Early Withdrawal or Final Treatment Visit)
At week 60 or at subject withdrawal from the study (premature by study doctor or subjectrsquos decision) a final
treatment visit will occur At this final treatment visit subjects will discontinue NACPL abruptly Week 60
activities also include
Physical examination
Measure vital signs with oximetry
Measure height and weight
Laboratory values (complete blood count [CBC] and serum chemistries)
Spirometry (post-bronchodilator) measurement
6MWT with Borg scale measurement
DLCO
Lung volumes
ABG
Review of AEs
32
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Evaluate for AEx
Review concomitant medications
Subjects will complete all QOL and dyspnea questionnaires (EuroQol ICE CAP SF-36 SGRQ and
UCSD SOBQ)
If consent has been given blood will be drawn and a urine specimen collected for the biospecimen
repository
Subjects return used and unused study drug for the visit
Study diary reviewed
4427 Final Site Visit ndash FVC drop confirmation
In the event that the subject has a recorded FVC drop of gt10 from baseline at the final treatment visit and the
subject has not had a confirmation of such a drop at a previous study visit the subject should return to the
clinical site 6 to 8 weeks after the final treatment visit During this visit a post-bronchodilator spirometry test
will be performed This FVC measurement will be evaluated according to section 521 of this protocol
4428 Final Visit ndash Telephone Follow-up
Four weeks following the final dose of study medication subjects will receive a telephone call from the study
coordinator to ensure that there are no side effects and to follow up on any ongoing adverse events (AEs)
4429 Phone Contact Between Visits
At week 2 and each month that a subject does not have a scheduled clinical center visit his or her study
coordinator will contact him or her at least once by telephone to
Inquire if the subject has had any hospitalizations events that might be considered an AE or any events
significant enough to warrant an out-of-cycle visit to the clinical center
Remind subjects of their current dosage levels and confirm that the subject understands them
Address any questions or concerns the subject might have regarding other aspects of the study
Assess adherence to the treatment regimen by reviewing diary data verbal review of medications taken
including nutritional supplements
33
34
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Table 3 Schedule of Assessments
Procedure Screening Visit 0
Enrollment Visit 1
Week 15 Visit 2
Week 30Visit 3
Week 45 Visit 4
Week 60 Early
Withdrawal Visit 5
Final1
Visit (via phone)
Informed consent X
Medical history X
Inclusionexclusion criteria X
Serum pregnancy test (if applicable) X X X X X
Review of lung biopsy X
Arterial Blood Gas X X
6-Minute Walk Test
X
X X
Physical examination X X X
Vital signs with oximetry X X X X X X
Body height and weight X X X X X X
Complete Blood Count X X X
Chemistry panel X X X
Monitor Lab Values X X X
Urinalysis X Specimen repository substudy blood draw and urine collection (if consented)
X
X X X X
HRCT (if not completed within three months) X
Spirometry (pre- and post-bronchodilator) X
Spirometry (post-bronchodilator only) X X X X X
DLCO (post-bronchodilator only) X X X
Lung volumes (post-bronchodilator only) X
X
Evaluate for acute exacerbation X X X X X
Review Adverse Events X X X X X X
Review concomitant meds X X X X X X
Dispense subject diary X X X X
Review subject diary X X X X X
Dispense study agent X X X X
Gender Substudy questionnaire (female subjects only) X
EuroQol ICECAP UCSD SOBQ SGRQ SF-36 X X X
Abbreviations DLCO diffusing capacity of the lung for carbon monoxide QOL Quality of Life ICECAP Investigating Choice Experiments for Preferences of Older People UCSD SOBQ University of California Shortness of Breath Questionnaire SGRQ St Georgersquos Respiratory Questionnaire SF-36 Short Form 36 Health Survey
1Follow-up visit via phone will occur four weeks after final dose of study medication
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
45 Dose Justification
The general philosophy for determining dosing levels was to apply previously examined
treatment regimens With the focus of the study being to establish a standard of care for
mildmoderate IPF subjects the goal was to develop flexible yet standardized treatment rules that
allow for the temporary or permanent withholding of one or more components of treatment when
necessary Subjects developing laboratory abnormalities or symptoms that result in
discontinuation of one or more components of study treatment may continue on the other
components as long as there is no contraindication for this Complete follow-up is important for
the validity of any study As a strategy to maintain protocol adherence we are using a treatment
regimen that will detect potential side effects and prompt interventions proactively in the interest
of patient safety In addition subjects who permanently stop study medications during the course
of the study are encouraged to continue in the study completing all scheduled visits and tests
451 Rationale for N-acetylcysteine Dosing
To our knowledge there have been no IPF studies to correlate clinical outcome measures with
different dosages for NAC The dosage chosen is based on the IFIGENIA study However BAL
lung GSH levels from subjects with IPF have been augmented with the use of oral NAC at 600
mg 3 times per day In addition lung GSH levels have been associated with improved
PFTs212227 The dose chosen for this study was based on previous data including the IFIGENIA
study30
4511 Dosing of N-acetylcysteineplacebo
Dosing of NACPL will be 600 mg orally 3 times a day (1800 mgday)
4512 Reasons to Discontinue N-acetylcysteineplacebo
NACPL may be temporarily or permanently discontinued for the duration of the study for
gastrointestinal symptoms or dermatologic reactions
35
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Temporarily discontinue (hold) oral NACPL for subjects requiring inpatient admission for acute
exacerbation (AEx) or other conditions Resume NACPL after discharge
36
37
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
452 Dosage Algorithms
Dosage Adjustment Algorithm 1 NACPL Dose Modifications for Gastrointestinal Symptoms Nausea Vomiting Abdominal Discomfort Diarrhea
GI Symptoms determined by the PI to be clinically significant Nausea Vomiting Abdominal Discomfort Diarrhea
NACPL Temporarily dc (HOLD) x 3 Days
Monitor symptoms intervene as clinically indicated (eg fluid replacement antidiarrhea or antinausea medication)
Monitor or lab PRN
Are symptoms resolving after 3 days NO
Symptoms NOT resolving after 3 days of holding study medication Assessmentmanagement per clinical
discretion of investigator
Likely not study medication discuss resuming study medication with medical monitor when symptoms resolved
YES
Temporarily dc (HOLD) NACPL for 4 additional days (total hold 1 week) then NACPL Resume 600 MG TID
Did symptoms recur
YES
STOP NACPL for
duration of study
NO
NACPL No Change
38
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Dosage Adjustment Algorithm 2 NACPL Dose Modifications For Dermatologic Reactions
Dermatologic Reactions (Not Acneiform) ge Grade 2 Grading per Common Terminology Criteria for
Adverse Events V30 (httpctepcancergov) For example Grade 1 RASHDESQUAMATION Macular or papular eruption or erythema without associated symptoms Grade 2 RASHDESQUAMATION Macular or popular eruption or erythema with pruritus or other associated symptoms localized desquamation or other lesions covering lt50 of body surface area
NACPL Temporarily dc (HOLD) x 3 days
Are symptoms resolving after 3 days
NO Symptoms not resolving after 3 days of holding study medication Assessmentmanagement per clinical discretion of investigator Likely not study medication Discuss resuming study medication with medical monitor when symptoms
resolved YES
Temporarily dc (HOLD) NACPL for 4 additional days (total hold 1 week) then NACPL resume 600 MG TID
Did symptoms recur
YES
STOP NACPL for
duration of study
NO
NACPL No change
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
46 Contraindications Precautions and Side Effects of Study Medications
461 Contraindication
Contraindication to NAC is known hypersensitivity to it
462 Precautions
Concomitant administration of oral NAC and antibiotics has shown a slightly reduced absorption
of cephalexin and a slight increase in erythromycin serum levels NAC contains free sulfhydryl
groups There is no evidence that individuals sensitive to sulfa drugs are sensitive to NAC
The NAC preparation being administered in this study contains 20 mg of aspartame Because of
the phenylalanine component of aspartame individuals with phenylketonuria should avoid or
restrict aspartame intake to avoid increased blood levels of phenylalanine Because of this risk
labeling is required on all products containing aspartame
463 Side Effects
Side effects of NAC range from common to serious See Table 4
39
40
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Table 4 Side Effects of NAC
Undesirable Effects
System-organ class Uncommon
(gt11000 lt1100)
Rare
(gt110000 lt11000)
Very rare
(lt110000) Not known
Immune system disorders Hypersensitivity Anaphylactic shock
reaction
Nervous system disorders Headache
Ear and labyrinth disorders Tinnitus
Cardiac disorders Tachycardia
Vascular disorders Hemorrhage
Respiratory thoracic and
mediastinal disorders
Bronchospasm
Dyspnea
Gastrointestinal disorders
Vomiting diarrhea
stomatitis abdominal
pain nausea
Dyspepsia
Skin and subcutaneous tissue
disorders
Urticaria rash
angioedema itching
General disorders and
administration site conditions Pyrexia
Investigations Reduced arterial
pressure Face edema
In very rare cases the onset of severe skin reactions such as Stevens-Johnson syndrome and Lyell syndrome was reported to have a temporal relationship with N-acetylcysteine administration Although in most cases at least another suspect drug probably most involved in the genesis of the above mentioned mucocutaneous syndromes has been identified in case of mucocutaneous alterations it is appropriate to contact onersquos doctor and the administration of N-acetylcysteine should be immediately discontinued
Some studies confirmed a reduction of platelet aggregation during N-acetylcysteine administration The clinical significance of these findings has not been defined yet [Source Fluimucil Investigator Brochure]
47 Recruitment Procedures
Subjects recruited for this study will be established patients of the investigators or physician- or
self-referred to participating clinical centers in the IPFnet Each clinical center within IPFnet has
a well-developed infrastructure of local pulmonologists within the surrounding geographic area
These pulmonologists are kept informed of ongoing IPF clinical trials and regularly refer
subjects to studies conducted at IPFnet clinical centers
Additional steps will be taken to inform clinicians of the trials in progress within IPFnet
including presentations at faculty staff meetings at local hospitals medical grand rounds and
national conferences direct mail notification monthly faxes and advertisement of network trials
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
in pulmonary journals Clinical center patients previously diagnosed with IPF will be notified of
the trials by mail whenever possible
Recruitment of minorities and women will be monitored by the DCC and DSMB If necessary
additional recruitment efforts will be made at specific centers to ensure that the aggregate subject
sample contains appropriate representation of women and minorities
48 Study Procedures
The following procedures are detailed in the PANTHER-IPF MOOP accompanying this
protocol
1 PFT
2 ABG
3 HRCT scan of the chest (including imaging of pulmonary arteries)
4 CBC and serum chemistries
5 Pregnancy test
6 6MWTBorg Dyspnea Scale
7 QOL questionnaires (EuroQol HAD SF-36 SGRQ and ICE CAP)
8 UCSD SOBQ
9 Gender Substudy Questionnaire
All assessments of PFTs will be conducted by study personnel not directly involved in the
treatment of the subjects
481 Biological Specimen Management
4811 Biological Specimen Sample Management
Subjects at clinical centers participating in the specimen repository substudy who consent to
having blood drawn for research purposes and for the banking of blood blood components and
other biologic specimens (urine and BAL fluid) will have approximately 405 mL of blood
41
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
drawn 17 mL blood drawn for DNA and 20 mL of urine collected at enrollment visit Subjects
will have approximately 50 mL of blood drawn and 20 mL of urine collected at each 15-week
follow-up visit Blood specimens will be separated according to PANTHER-IPF MOOP
guidelines into the following components for banking in the repository serum plasma and
DNA Coding of all biologic specimens for the repository will be performed by study staff at the
clinical center The samples will be processed per PANTHER-IPF MOOP guidelines aliquoted
labeled with barcode labels and stored at -70degC at the clinical center and shipped to the central
repository
The only subject identifiers will be a sample ID number and subject initials This sample ID will
be linked in the IPFnet DCC clinical database to subject information No subject information will
be transferred to the biological-specimen database
The subjectrsquos samples may be used for approved sub-studies relating to human disease
including but not limited to IPF The studies for which an individualrsquos samples will be made
available will be determined by the subjectrsquos answers to questions on the biological-sample
informed consent form The subjects can choose to make their samples available for all options
or any combination Samples will be made available to researchers only with IPFnet Steering
Group approval until such time as the samples are made public through the NHLBI repository
49 Concomitant Medications
Concurrent treatment with FDA-approved therapy for IPF is allowed Colchicine may be used
for treatment of gout Temporary treatment with oral or IV corticosteroids for clinical worsening
or suspected AEx is permitted Nutritional supplements containing NAC are not allowed
410 Laboratory Testing
Clinical laboratory parameters will be assessed at screening and at the end of the study The
following tests will be performed at the two time points specified in the protocol chemistry (AG
ratio ALT [SGPT] AST [SGOT] albumin alkaline phosphatase amylase bilirubin-direct
42
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
bilirubin-indirect bilirubin-total BUN BUNcreatinine ratio calcium carbon dioxide
cholesterol-total chloride CPK-total creatinine GGT globulin glucose iron-total LDH
lipase magnesium phosphorus-inorganic potassium protein-total sodium TIBC triglycerides
uric acid) and hematology (red blood cell count WBC count hemoglobin hematocrit cell
indices differential platelet count)
411 Blinding of Study Drugs
Subjects and caregivers will be blinded to study treatment Every subject will receive NAC or
matching PLs at every study visit from the baseline visit to the week-45 visit No study agent
will be dispensed at the week-60 visit
43
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
5 Study Endpoints
51 Primary Study Endpoint
The primary endpoint will be the change in serial measurements of FVC over the study period
52 Secondary Study Endpoints
521 Time to Disease-progression
The time-to-death or a 10 decline in FVC will be defined as the time-to-disease progression
The 10 decline in FVC from enrollment must be confirmed on 2 consecutive visits no less than
6 weeks apart For subjects with 2 consecutive visits with a 10 decline in FVC the time-toshy
disease progression will be defined as the time interval between enrollment and the initial visit
with a 10 FVC decline For subjects who experience disease progression the study doctor will
determine whether or not the subject will remain in the study
522 Acute Exacerbations
The following 3 criteria will define AEx in subjects with acute worsening of their respiratory
conditions
1 Clinical (all of the following required)
A) Unexplained worsening of dyspnea or cough within 30 days triggering unscheduled
medical care (eg emergency room clinic study visit hospitalization)
B) No clinical suspicion or overt evidence of cardiac event pulmonary embolism or deep
venous thrombosis to explain acute worsening of dyspnea
C) No pneumothorax
44
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
2 RadiologicPhysiologic (A and B required)
A) New ground glass opacity or consolidation computed tomography (CT) scan OR new
alveolar opacities on chest x-ray
B) Decline of ge 5 in resting room air SpO2 from last recorded level OR decline of ge 8 mm
Hg in resting room air PaO2 from last recorded level
3 Microbiologic (all of the following required)
A) No clinical evidence for infection (ie absence of grossly purulent sputum fever gt 39degC
orally)
B) Lack of positive microbiological results (if done) from lower respiratory tract defined as
(1) Clinically significant bacterial growth on sputum or endotracheal aspirate cultures
(2) Quantitative culture by protected brush specimen ge 103 cfumL or BAL ge 104 cfumL
(3) The presence of specific pathogens on stains of any of the above
C) Lack of positive pathogen in blood cultures (if done)
Identification of Acute Exacerbations
All subjects will be educated about the importance of identifying AExs At the time of
enrollment subjects will be told about the possibility of developing acute symptomatic
worsening that might represent an AEx of IPF and instructed to contact their study clinical
center coordinator within 48 to 72 hours of the apparent event
All subjects will be contacted by phone monthly and questioned about any change in dyspnea or
cough and any interim clinic visits or hospitalizations Finally as part of the IPFnet outreach to
community referring physicians the importance of AExs will be emphasized When a subject is
identified who meets criterion 1A this will trigger the collection of additional clinical data to
evaluate a suspected AEx These data will be collected as part of standard clinical care (ie this
protocol does not require collection of all items) The additional items to be collected for
suspected AEx include
IPFnet AEx case report form (eCRF) (required)
45
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Chest x-ray CT scan withwithout pulmonary angiogram (reports should be faxed and
followed by the hard copiesdiscs)
Oxygen saturation (pulse oximetry)
ABG
Respiratory cultures (sputum endotracheal aspirate lavage)
Blood cultures
Clinichospital records related to the event
All potential cases of AEx will be reviewed by the clinical center PI first and a decision on
whether the case may represent an AEx will be made If AEx is suspected the case will be sent
to the IPFnet adjudication committee which will assign a final diagnosis (see Table 5) If there is
disagreement among members the majority opinion will be recorded
During episodes of suspected AEx as determined by the individual clinical center investigator
subjects will remain blinded and in the study
Table 5 Final Diagnoses in Evaluation of Suspected Acute Exacerbations
Definite acute exacerbation All criteria met no alternative etiology
Unclassifiable acute worsening
Insufficient data to evaluate all criteria no alternative etiology
Not acute exacerbation Alternative etiology identified that explains acute worsening
Management of the suspected AEx will be at the discretion of the treating physician Standard of
care generally involves evaluation for respiratory infection pulmonary embolism cardiac events
and pneumothorax and treatment with IV corticosteroids
Study drugs will be resumed at pre-suspected AEx doses after subjects clinically improve as
confirmed by the local PI All subjects should be seen at the clinical center within 2 to 4 weeks
of recovery for measurement of post-bronchodilator FVC (see Figure 4) Subjects unable to
return to the clinical center after suspected AEx due to medical frailty (eg continued
46
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
institutionalization progressive disability) will be categorized as failing to maintain FVC
response in secondary analyses
Suspected AEx (PI determined)
Hold study drug Treat AEx
(Attending physician determined)
Alive but unable to continue due to
medical frailty
Dead
Alive and able to continue
Site reviewvisit
Restart study drug
FVC within 2-4 weeks
Figure 4 Acute Exacerbation Flow Chart
523 Respiratory Infections
An upper respiratory infection will be defined as
Change in sputum discoloration
Increased cough of no more than 14 daysrsquo duration
A lower-respiratory infection (pneumonia) will be defined as new segmental or lobar airspace
opacities visualized by image studies (chest radiograph or HRCT) in addition to any of the
following
Positive pathogencultures in good sample of sputum or lower-airway secretions retrieved
by fiberoptic bronchoscope
Fever gt 39degC or gt 100degF
Leukocytosis gt 12000 (unexplained no increase in dose of corticosteroids)
47
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
524 Maintained FVC Response
Subjects with follow-up FVCpred measurements at or above their baseline FVCpred level
will be classified as having maintained FVC response Subjects with reduced FVCpred levels
or missing data for any reason including death or medical frailty will be classified as having not
maintained FVC response The FVCpred value is used because unadjusted FVC measurements
are expected to decline with age
48
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
6 Safety Evaluations and Procedures
61 Adverse Events
During a clinical trial the reporting of adverse experience information can lead to important
changes in the way a new treatment is developed as well as provide integral safety data
611 Definitions
An adverse event (AE) is any untoward medical occurrence in a subject or clinical investigation
subject who was administered a pharmaceutical product The AE does not necessarily have to
have a causal relationship with the drug administered An AE can be any unfavorable and
unintended sign (including an abnormal laboratory finding) symptom or disease temporarily
associated with the use of a medicinal product whether or not considered to be related to the
medicinal product Diseases signs symptoms or laboratory abnormalities already existing at
enrollment are not considered AEs unless they worsen (ie increase in intensity or frequency)
Surgical procedures themselves are not AEs they are therapeutic measures for conditions that
require surgery The condition for which the surgery is required may be an AE Surgical
procedures planned before randomization and the conditions necessitating the surgery are not
AEs
A serious adverse event is any untoward event that
Is fatal
Is life-threatening
Requires inpatient hospitalization or prolongation of existing hospitalization with the
following exceptions
o Preplanned (before the study) hospital admissions unless the hospitalization is
prolonged
o Planned admissions (as part of a study eg routine biopsies)
o Hospitalization lasting lt 24 hours
49
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
o Hospitalization for elective procedure
o Emergency room visits
Results in persistent or significant disability or incapacity
Is a congenital anomaly or birth defect
Important medical events that may not result in death be life-threatening or require
inpatient hospitalization may be considered serious adverse events (SAEs) when based
on appropriate medical judgment they may jeopardize the subject and may require
medical or surgical intervention to prevent one of the outcomes listed above
Life-threatening means that the subject was in the view of the investigator at immediate risk of
death from the AE as it occurred It does not include an AE that had it occurred in a more severe
form might have caused death
Persistent or significant disabilityincapacity means that the event resulted in permanent or
significant and substantial disruption of the subjectrsquos ability to carry out normal life functions
Causality
A reasonable possibility means the AE may have been caused byrelated to the study drug A
perceived or real lack of efficacy does not satisfy the definition of relatedness
612 Adverse Event (AE) Reporting
For the PANTHER-IPF trial all AEs (serious and nonserious) occurring from randomization
through final study visit (4 weeks after final dose of all study medication) will be recorded on the
AE page of the case report form (CRF)
6121 Serious Adverse Events (SAE) Reporting
For this trial all deaths and all SAEs which occur from randomization through final study visit
must be entered within the EDC system via the SAE eCRF page within 24 hours of the
investigative sitersquos knowledge of the event It is the responsibility of the clinical center
50
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
investigator to provide a causality assessment of the event for each study medications based upon
the information available at the time of the report It is understood that complete information
about the event may not be known at the time the initial report is submitted In the event the EDC
system is not accessible to the site at the time of event reporting investigative sites will complete
and forward a paper back-up SAE form to DCRI Safety Surveillance for processing
DCRI Safety Surveillance
Telephone 1-919-668-8624 or 1-866-668-7799 (toll free)
Fax 1-919-668-7138 or 1-866-668-7138 (toll free)
The investigator must complete and submit follow-up SAE information via the eCRF when
important new or follow-up information (eg final diagnosis outcome results of specific
investigations) becomes available Follow-up information should be submitted according to the
same process used for reporting the initial event as described above All SAEs will be followed
until resolution stabilization or 30 days after the subject has completed the final visit (4 weeks
after the final dose of study medication) whichever occurs first The investigator is responsible
for reporting SAEs to their institutional review board (IRB) per site specific IRB reporting
guidelines
6122 Regulatory Reporting
AEs that are serious study drug related and unexpected will be reported to the regulatory
authorities The DCRI Safety Surveillance medical monitor will perform a medical review of all
SAEs submitted and evaluate for ldquounexpectednessrdquo DCRI Safety Surveillance will prepare
MedWatch reports for those events identified as serious study drug related and unexpected as
determined by Safety Medical Monitor
DCRI Regulatory Services will submit all unexpected study drug-related SAEs as per 21 CFR
32 DCRI Safety Surveillance will provide a safety alert letter to the NHLBI DSMB and DCC
clinical operation (for distribution to sites) within 15 days of initial receipt of the information
51
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Investigators are responsible for promptly reporting these events to their reviewing IRBs
according to site specific IRB reporting guidelines
62 Clinical Medical Monitoring
There will be an unblinded physician at the IPFnet DCC serving as medical monitor The
medical monitor will be available to assist with questions about dosage adjustments of study
medications including discontinuation or resumption of medications
63 Unblinding Procedures
Unblinding of subjects or investigators to subject treatment is strongly discouraged For ongoing
clinical management all subjects should be presumed to be receiving ldquoactiverdquo study drug To
ensure the subjectrsquos safety the study treatment will be dose-adjusted based on laboratory test
results clinical findings and symptoms
The IPFnet DCC medical monitor and PANTHER-IPF co-chairs Drs Ganesh Raghu and
Fernando Martinez will be available to the study physicians to discuss study drug management
on a case-by-case basis Un-blinding will be considered ONLY when the knowledge of subject
treatment assignment is ABSOLUTELY ESSENTIAL for subject safety and after discussion of
the subjectrsquos case with the medical monitor and either Dr Raghu or Dr Martinez Unblinding of
study treatment should be minimized during the conduct of the trial In those cases where it is
felt to be medically necessary the DCC medical officer will communicate directly with the
managing physician to minimize unblinding of study personnel
52
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
7 Study Drug Procedures
At the baseline 15-week 30-week and 45-week study visits subjects will receive a supply of
study drug sufficient to last until the next visit at which study drug will be dispensed
53
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
8 Data Management
81 Hardware and Software Configuration
811 Hardware and Database Software
Data will be stored in an Oracle database system Oracle has advantages of processing efficiency
and smooth linkage with other software systems The application and database will be hosted on
Solaris Unix servers at the IPFnet DCC
812 Statistical Software
SAS will be used as the principal application for the management of analysis data files and
statistical computations S-Plus will be used to provide supplementary functions as needed
813 Access Control and Confidentiality Procedures
Access to databases will be controlled centrally by the IPFnet DCC through user passwords
linked to appropriate privileges This protects the data from unauthorized changes and
inadvertent loss or damage
814 Security
Database and Web servers will be secured by a firewall and through controlled physical access
Oracle has many security features to ensure that any staff member accessing the database has the
proper authority to perform the functions he or she requests of the system Within the secondary
SAS databases Unix group-access control maintains similar security The Sun workstation login
is secured by extensive user-password facilities under Unix
54
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
815 Back-up Procedures
Database back-up will be performed automatically every day and standard IPFnet DCC policies
and procedures will be applied to dictate tape rotation and retention practices
816 Virus Protection
All disk drives that provide network services and all user computers will be protected using
virus-scanning software Standard IPFnet DCC policies will be applied to update these protection
systems periodically through the study
82 Sources of Data
821 Design and Development
The IPFnet DCC will be responsible for development of the electronic case report forms
(eCRFs) development and validation of the clinical study database ensuring data integrity and
training clinical center staff on applicable data management procedures A web-based distributed
data entry model will be implemented This system will be developed to ensure that guidelines
and regulations surrounding the use of computerized systems used in clinical trials are upheld
The remainder of this section provides an overview of the data management plan associated with
this protocol
822 Data Collection Forms
The data collection process consists of direct data entry at the study clinical centers into the EDC
system(s) provided by the DCC A data collection worksheet will be provided to clinical centers
for recording data in the event the EDC system is unavailable Data entry of the eCRFs should
be completed according to the instructions provided and project specific training The
investigator is responsible for maintaining accurate complete and up-to-date records and for
ensuring the completion of the eCRFs for each research participant
55
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
823 Data Acquisition and Entry
Data entry into eCRFs shall be performed by authorized individuals Selected eCRFs may also
require the investigatorrsquos written signature or electronic signature as appropriate Electronic
CRFs will be monitored for completeness accuracy and attention to detail during the study
824 Data Center Responsibilities
The IPFnet DCC will 1) develop a data management plan and will conduct data management
activities 2) provide final eCRFs for the collection of all data required by the study 3) develop
data dictionaries for each eCRF that will comprehensively define each data element 4) conduct
ongoing data monitoring activities on study data 5) monitor any preliminary analysis data
cleanup activities and 6) rigorously monitor final study data clean up
825 Data Editing
Completed data will be entered into the IPFnet DCC automated data acquisition and
management system If incomplete or inaccurate data are found a data clarification request will
be generated and distributed to clinical centers for a response Clinical centers will resolve data
inconsistencies and errors and enter all corrections and changes into the IPFnet DCC automated
data acquisition and management system
826 Training
The training plan for clinical center staff includes provisions for training on assessments eCRF
completion guidelines data management procedures and the use of computerized systems
56
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
9 Study Design and Data Analysis
91 General Analytic Considerations
All primary analyses will be based on intent-to-treat (ITT) principles using all randomized
subjects Baseline factors across groups will be compared using mean (standard deviation) and
median (25th and 75th percentiles) summary measures Kaplan-Meier curves will be used to
display event rates Due to clinical interest in departures from both sides of the null hypothesis
all test statistics will be 2-sided
Reasonable caution needs to be taken when conducting multiple analyses on key clinical
subgroups For subgroup analyses a conservative significance level of 0001 will be used for all
interaction tests Thus subgroup comparisons will be considered exploratory unless the p-value
from the interaction test is smaller than 0001
92 Randomization Blinding and Reporting of Results
A permuted block-randomization scheme will be created with varying block sizes stratified by
clinical center Once a subject has completed the screening and baseline period and evaluation
for inclusionexclusion criteria the randomization process will begin Subjects will be
randomized to receive NAC or matching placebo with equal probability (11) via telephone
contact with a central interactive voice response system (IVRS) using a toll-free randomization
number On the day of randomization after the subject has successfully met all inclusion and
exclusion criteria the investigator or designee will call the central randomization number to
obtain the assigned kit randomization numbers for that subject At each subject visit the
investigator or designee will call the central randomization number to obtain the new kit
randomization numbers for resupply of the subject For resupply of the clinical center the IVRS
will monitor minimal volume of a kit type andor expiration date and will automatically notify
the pharmacy
57
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
The trial results will be reported according to guidelines specified in the CONSORT statement
A flow diagram describing screening recruitment randomization dropout and vital status will
be included in the primary manuscript AEs and efficacy data will be presented for all treatment
groups Adherence dropout and lost to follow-up will be carefully examined across all treatment
groups Analyses of safety will be based on data from all randomized subjects who received at
least one dose of study drug
93 Stratification
Subjects will be distributed to the two treatment arms in a 11 allocation ratio Stratification
blocks will be based on clinical centers
94 Specification of the Primary Analyses
A mixed model repeated measures (MMRM) analysis described in section 95 will be used to
compare differences in the slope of FVC measurements across the treatment groups Response
variables are values of the FVC measured at baseline and every 15 weeks until study completion
Variables in the model will include treatment time and time by treatment age sex race and
height Contrast estimates of differences in slopes of treatment over time (along with confidence
intervals) will be used to estimate the treatment effect The validity of this model in terms of
meeting modeling assumptions will be assessed via standard modeling diagnostics and goodness-
of-fit measures Based on the MMRM framework missing FVC data will not be imputed for the
primary analysis
95 Analysis of Longitudinal Endpoints
A common goal in clinical trials is to specify models that are easily implemented and
reproducible by independent data analysts On the other hand the models should have proper
statistical behavior in terms of low bias and high precision Many common approaches to
longitudinal data analysis including last observation carried forward (LOCF) imputation rely on
the missing completely at random (MCAR) assumption However the MCAR assumption is
58
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
unlikely to hold in many clinical trials because missing data are often related to disease
progression and prognosis A more reasonable assumption missing at random (MAR) specifies
that the complete data distribution can be modeled using only the observed data The likelihood-
based MMRM approach is valid under the more general MAR assumptions These models will
be applied to analyze the longitudinal data secondary endpoints
The advantages of MMRM analysis are that all important characteristics of the model can be preshy
specified standard software can be used to implement the models and results are based on ITT
principles43 In addition the MMRM approach offers superior control of Type I and Type II
errors compared with the LOCF approach
Response variables are values of the PFTs measured at enrollment and every 15 weeks until
study completion and 6MWT values measured at baseline week 30 and week 60 Covariates are
treatment time time by treatment and key baseline risk factors Contrasts (along with
confidence intervals) of treatment by time will be used to estimate the treatment effect
The correlation structure involves multiple pieces including measurement errors random
variation and interindividual variability For the longitudinal data analyses an unstructured
correlation matrix for within-subject errors will be assumed Other correlation structures
including compound symmetry will be examined as needed A careful examination of reasons
for study discontinuation will be conducted to assess the validity of MCAR Sensitivity analyses
will be used to examine the untestable assumption that the observed data violate the MAR
assumption The MMRM models will be implemented using PROC MIXED in SAS
96 Analysis of Binary Time-to-Event and Time-Lagged Endpoints
Regression modeling approaches using either the logistic regression model or Cox proportional
hazards regression model will be employed when appropriate The validity of these models will
be assessed via standard modeling diagnostics and goodness-of-fit measures Estimates of
cumulative frequencies for more general time-lagged responses will be calculated using the
partitioned version of the Bang-Tsiatis estimator44 The partitions will be set at 15-week intervals
59
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
to correspond with the data-collection process Covariate adjusted event rates will be calculated
using inverse probability-weighted regression estimates45
97 Power Analysis
971 Primary Analyses
Based on previously published IPF clinical trials the PL group is expected to experience a drop
in FVC of approximately 020 L over the study period (see Figure 1) The IPFnet Steering Group
determined a clinically important difference would be to preserve the majority of the decline
relative to PL over the study period In particular a treatment effect of 015 L was determined to
be a clinically meaningful difference Potential dropout is a key factor in the proposed study The
drop-out process assumed 5 lost to follow-up after every study visit Only 80 of subjects
were assumed to be followed for the entire study period All models assumed a compound
symmetry structure for the covariance matrix Power calculations were performed using a SAS
IML program for designing repeated measures studies46 Based on preliminary reviews of the
data from the University of Michigan the covariance matrix parameters were estimated at
approximately σ2 = 0757 (variance parameter) and ρ = 0936 (correlation parameter) To be
conservative the power calculations for the primary analysis were performed with parameter
setting of σ2 = 0810 (variance parameter) and ρ = 0925 (correlation parameter)
The power calculations assume a correction for imperfect compliance proposed by Lachin and
Foulkes to allow for 2 noncompliance for each of the treatment arms47 Thus the sample size
of 130 subjects per arm would be reduced to an adjusted sample size of 130(1-002-002)2 =
1198 or 120 subjects per arm
Under the assumed Type I error rate of 005 with a correlation parameter of 0925 and standard
deviation of 090 the difference of 015 L (or 00025 Lweek) shown in Table 6 would have
power of 93
60
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Table 6 Hypothetical Values of Mean FVC (L) Change from Baseline
Week 15 Week 30 Week 45 Week 60
NAC 00125 00250 00375 00500
Placebo 00500 01000 01500 02000
Difference 00375 00750 01125 01500
Abbreviations FVC forced vital capacity PL placebo
972 Power Analysis for Secondary Endpoints
Power calculations for secondary endpoint measurements are shown in Table 7 Standard
deviations are based on unpublished data provided by the University of Michigan The
calculations are based on a 2-sample t-test with Type I error rate set at 005 These calculations
are likely to be conservative because the statistical approach described in section 95 for
analyzing these endpoints will incorporate incomplete observations as well as intermediate data
points
Table 7 Detectable Differences in Treatment Means for Selected Endpoint Measurements
Secondary Endpoints Std Dev
of the Baseline Score
Detectable Difference for 80 Power
Std Dev of the Change Score
Difference Detectable for
80 Power
DLCOpred 166 58 91 32
6MWT Area Under the Desaturation Curve
219 76 175 61
6MWT Distance to Desaturation 224 78 315 110
6MWT Minutes Walked 210 073 205 071
Abbreviations Std Dev standard deviation DLCOpred diffusing capacity of the lung for carbon monoxide percent predicted 6MWT 6-minute walk test
61
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
10 Study Administration
101 Cooperative Agreement Mechanism
The administrative and funding mechanism used to undertake this project is a ldquocooperative
agreementrdquo (U01) which is an assistance mechanism Under the cooperative agreement the
NHLBI assists supports andor stimulates the project and is substantially involved with
investigators in conducting the study by facilitating performance of the effort in a ldquopartnerrdquo role
The NHLBI project scientist serves on the IPFnet Steering Group and he or another NHLBI
scientist may serve on other project committees when appropriate At the same time however
NHLBI does not assume a dominant role direction or prime responsibility for this research
program
As described below governance of the project is conducted through the IPFnet Steering Group
Principal investigators have lead responsibilities in all aspects of their trials and the project
including any modification of trial designs conduct of the trials quality control data analysis
and interpretation preparation of publications and collaboration with other investigators unless
otherwise provided for by the IPFnet Steering Group
PIs retain custody of and have primary rights to their center-specific and collaborative data
subject to government rights-of-access consistent with current Health amp Human Services (HHS)
Public Health Service (PHS) and National Institutes of Health policies The protocols and
governance policies call for the continual submission of data centrally to the IPFnet DCC for the
collaborative database which at a minimum will contain the key variables selected by the IPFnet
Steering Group for standardization across all clinical centers the submission of copies of the
collaborative datasets to each PI upon completion of the project procedures for data analysis
reporting and publication and procedures to protect and ensure the privacy of medical and
genetic data and records of individuals The NHLBI project scientist on behalf of the NHLBI
will have the same access privileges and responsibilities regarding the collaborative data as the
other members of the Steering Group
62
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
PIs are also encouraged to publish and to publicly release and disseminate results data and other
products of the project concordant with the project protocols and governance and the approved
plan for making data and materials available to the scientific community and to the NHLBI
However during the 3 years after the ending date of NHLBI project support unpublished data
unpublished results data sets not previously released and other study materials or products are
to be made available to any third party only with the approval of the IPFnet Steering Group
Upon completion of the project PIs are expected to put their intervention materials and
procedure manuals into the public domain andor make them available to other investigators
according to the approved plan for making data and materials available to the scientific
community and the NHLBI for the conduct of research at no charge other than the costs of
reproduction and distribution
The NHLBI reserves the right to terminate or curtail the project (or an individual award) in the
event of (a) failure to develop or implement mutually agreeable collaborative measurement
subject eligibility and data management sections of the protocols (b) substantial shortfall in
subject recruitment follow-up data reporting or quality control or other major breach of
protocol (c) substantive changes in the agreed-upon protocols with which NHLBI cannot
concur (d) reaching a major project outcome with persuasive statistical significance
substantially before schedule or (e) human subject ethical issues that may dictate a premature
termination
Any disagreement that may arise in scientificprogrammatic matters (within the scope of the
award) between award recipients and the NHLBI may be brought to arbitration An arbitration
panel will be composed of 3 membersmdash1 selected by the IPFnet Steering Group (with the
NHLBI member not voting) or by the individual PI in the event of an individual disagreement a
second selected by NHLBI and the third selected by the other 2 members This special
arbitration procedure in no way affects the PIrsquos right to appeal an adverse action that is otherwise
appealable in accordance with the PHS regulations at 42 CFR part 50 Subpart D and HHS
63
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
regulation at 45 CFR part 16 or the rights of the NHLBI under applicable statutes regulations
and terms of the award
102 IPFnet Steering Group
The IPFnet Steering Group is the main governing body of the project It is composed of the PIs
of the clinical centers the PI of the DCC and the NHLBI project scientist The clinical centers
the IPFnet DCC and the NHLBI each have 1 vote on the IPFnet Steering Group All decisions
are determined by majority vote
All major scientific decisions are determined by the IPFnet Steering Group It assumes overall
responsibility for the design and conduct of the trial It appoints (and disbands) committees and
subcommittees as the need arises designs approves and implements the study protocols
oversees the development of the MOOP monitors subject recruitment and treatment delivery
evaluates data collection and management oversees quality assurance procedures and
implements changes and enhancements to the study as required It also has primary responsibility
for facilitating the conduct of the trials and reporting the projectrsquos results
103 Data and Safety Monitoring Board
The NHLBI will establish a DSMB in accordance with established policies (see
httpwwwnhlbinihgovfundingpoliciesdsmb_insthtm) to ensure data quality and subject
safety and to provide independent advice to the NHLBI regarding progress and the
appropriateness of study continuation
104 Recommendations on Interim Monitoring of Efficacy Safety and Futility
First and foremost the role of the DSMB will be to review subject safety and trial conduct at
periodic points during the study The DSMB may require analyses of the primary endpoint
results for comparing the benefit and risks of treatment strategies The benefit of collecting
additional data on key secondary endpoints with extended follow-up and establishing a robust
64
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
evidence base for determining a standard of care will need to be carefully considered before
early termination of one or more treatment arms After careful consideration the IPFnet Steering
Group recommends conservative thresholds for the early examinations of the safety and efficacy
data
The DSMB will be expected to meet approximately every 6 months until trial completion to
review safety and toxicity data The DSMB may recommend stopping the study based on these
reviews Because the DSMB could stop the trial for safety concerns as well as for a large
efficacy benefit there could be multiple opportunities to reject the null hypothesis (no difference
in event rates between the PL and NAC groups) A Bonferroni approximation will be applied
during the one planned interim analysis for efficacy
Before locking the database a statistical analysis plan (SAP) will be developed to provide
complete details on the statistical analysis The SAP will include the specifics for how and when
the DSMB will be notified for AEs The IPFnet DCC will deliver to the DSMB all FDA-defined
AEs at 3-month intervals The IPFnet DCC will prepare narrative SAE reports in real time for
DSMB review including recommendations and analysis of similar events for each SAE
submitted to the FDA
65
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
11 Investigator and Sponsor Obligations
111 Monitoring
All monitoring activities for US clinical centers will be performed in accordance with DCRI
standard operating procedures Information regarding the types of visits will be outlined in the
PANTHER-IPF MOOP
112 Cost and Payment
There will be no cost to subjects enrolled in this trial Study-related procedures will be paid for
by the IPFnet
Subjects may be eligible for reimbursement for travel to the clinical center Details of payment
will be explained to each subject during the consent process
113 Confidentiality and Health Insurance Portability and Accountability Act
Considerations
Subject confidentiality will be protected throughout the study All subject data will be kept
strictly confidential and no subject-identifying information will be released to anyone outside
the project Confidentiality will be assured through several mechanisms First each subject will
be assigned an anonymous study ID which will then be used on all study forms Second any
study forms blood samples and paper records that contain subject information (eg address lists
phone lists) will be kept at the clinical centers in secured locked areas coded by number Once
blood is collected there will be no subject identifiers placed on blood samplesmdashonly the study
ID number and the date of sample collection Third access to all subject data and information
including laboratory specimens will be restricted to authorized personnel In the case of
computerized data this restricted access will be assured through user logon IDs and password
protection
66
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
At the IPFnet DCC only authorized personnel will have access to the data files containing study
data Security will be assured through user logon IDs passwords and appropriate access
privileges All study subjects will be identified only by their IPFnet ID numbers and no personal
identifying information such as name address or Social Security number will be entered into
the IPFnet DCC database Any subject-specific data reported to the IPFnet Steering Group will
be identified only by the IPFnet ID number
Finally subjects will not be identified by name in any reports or publications nor will the data
be presented in such a way that the identity of individual subjects can be inferred Analysis files
created for further study by the scientific community will have no subject identifiers These data
files will be created in accordance with the Ancillary Studies and Publication Policy of the
IPFnet
114 Informed Consent Procedures
All IPFnet subjects will provide written informed consent using procedures reviewed and
approved by each clinical centerrsquos IRB Informed consent will be undertaken by study personnel
in-person with the subject The subject has the option of declining further participation in the
study at that point No further study procedures will be conducted until the signed documents
have been provided to the IPFnet clinical center
115 Institutional Review Boards
Before initiating this study the protocol clinical center-specific informed consent forms Health
Insurance Portability and Accountability Act (HIPAA) forms recruitment materials and other
relevant information will be reviewed by a properly constituted IRB at each participating clinical
center A copy of the signed and dated IRB approval at each clinical center will be retrieved prior
to or during the site initiation visit and archived at the IPFnet DCC Any amendments to the
protocol other than simple administrative and typographical changes must be approved by each
IRB before they are implemented The clinical centers will seek annual renewals of their IRB
approvals in accordance with local procedures
67
__________________________________________ ________________
__________________________________________
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
12 Investigator Agreement
I have read the foregoing protocol PANTHER-IPF and agree that it contains all necessary
details for carrying out this study I will conduct the study as outlined herein and will complete
the study within the time designated
I will provide copies of the protocol and all pertinent information to all individuals responsible to
me who assist in the conduct of this study I will discuss this material with them to ensure they
are fully informed regarding the drug and the conduct of the study
I will fulfill all responsibilities for submitting pertinent information to the local IRB if
applicable that is responsible for this study
I further agree that NHLBI andor DCRI will have access to any source documents from which
eCRF information may have been generated
Signature of Principal Investigator Date
Name of Principal Investigator (printed or typed)
Protocol version date May 19 2009
Protocol Amendment 1 version date May 28 2010
Protocol Amendment 2 version date December 6 2011
68
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
13 References
1 Raghu G Brown KK Bradford WZ et al A placebo-controlled trial of interferon gamma-1b in patients with idiopathic pulmonary fibrosis N Engl J Med 2004350125-33 2 King TE Jr Safrin S Starko KM et al Analyses of efficacy end points in a controlled trial of interferon-gamma1b for idiopathic pulmonary fibrosis Chest 2005127171-7 3 Flaherty KR Thwaite EL Kazerooni EA et al Radiological versus histological diagnosis in UIP and NSIP survival implications Thorax 200358143-8 4 Wells AU Desai SR Rubens MB et al Idiopathic pulmonary fibrosis a composite physiologic index derived from disease extent observed by computed tomography Am J Respir Crit Care Med 2003167962-9 5 Raghu G Freudenberger TD Yang S et al High prevalence of abnormal acid gastroshyoesophageal reflux in idiopathic pulmonary fibrosis Eur Respir J 200627136-42 6 Kinnula VL Focus on antioxidant enzymes and antioxidant strategies in smoking related airway diseases Thorax 200560693-700 7 Coultas DB Zumwalt RE Black WC Sobonya RE The epidemiology of interstitial lung diseases Am J Respir Crit Care Med 1994150967-72 8 Raghu G Weycker D Edelsberg J Bradford WZ Oster G Incidence and prevalence of idiopathic pulmonary fibrosis Am J Respir Crit Care Med 2006174810-6 9 Olson AL Swigris JJ Lezotte DC Norris JM Wilson CG Brown KK Mortality from pulmonary fibrosis increased in the United States from 1992 to 2003 Am J Respir Crit Care Med 2007176277-84 10 Mannino DM Etzel RA Parrish RG Pulmonary fibrosis deaths in the United States 1979shy1991 An analysis of multiple-cause mortality data Am J Respir Crit Care Med 19961531548shy52 11 Hubbard R Johnston I Coultas DB Britton J Mortality rates from cryptogenic fibrosing alveolitis in seven countries Thorax 199651711-6 12 Johnston I Britton J Kinnear W Logan R Rising mortality from cryptogenic fibrosing alveolitis Bmj 19903011017-21 13 Raghu G Collard HR Egan JJ et al An official ATSERSJRSALAT statement idiopathic pulmonary fibrosis evidence-based guidelines for diagnosis and management Am J Respir Crit Care Med 2011183788-824 14 (USA) FDA FDA Public Health Advisory Interferon gamma-1b (marketed as Actimmune) In 2007 15 King TE Jr Pardo A Selman M Idiopathic pulmonary fibrosis Lancet 2011 16 Raghu G Brown KK Costabel U et al Treatment of idiopathic pulmonary fibrosis with etanercept an exploratory placebo-controlled trial Am J Respir Crit Care Med 2008178948shy55 17 Malouf MA Hopkins P Snell G Glanville AR An investigator-driven study of everolimus in surgical lung biopsy confirmed idiopathic pulmonary fibrosis Respirology 201116776-83 18 King TE Jr Behr J Brown KK et al BUILD-1 a randomized placebo-controlled trial of bosentan in idiopathic pulmonary fibrosis Am J Respir Crit Care Med 200817775-81 19 Richeldi L Costabel U Selman M et al Efficacy of a tyrosine kinase inhibitor in idiopathic pulmonary fibrosis N Engl J Med 20113651079-87
69
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
20 Borok Z Buhl R Grimes GJ et al Effect of glutathione aerosol on oxidant-antioxidant imbalance in idiopathic pulmonary fibrosis Lancet 1991338215-6 21 Meyer A Buhl R Magnussen H The effect of oral N-acetylcysteine on lung glutathione levels in idiopathic pulmonary fibrosis Eur Respir J 19947431-6 22 Behr J Maier K Degenkolb B Krombach F Vogelmeier C Antioxidative and clinical effects of high-dose N-acetylcysteine in fibrosing alveolitis Adjunctive therapy to maintenance immunosuppression Am J Respir Crit Care Med 19971561897-901 23 Cantin AM North SL Fells GA Hubbard RC Crystal RG Oxidant-mediated epithelial cell injury in idiopathic pulmonary fibrosis J Clin Invest 1987791665-73 24 Waghray M Cui Z Horowitz JC et al Hydrogen peroxide is a diffusible paracrine signal for the induction of epithelial cell death by activated myofibroblasts Faseb J 200519854-6 25 Larios JM Budhiraja R Fanburg BL Thannickal VJ Oxidative protein cross-linking reactions involving L-tyrosine in transforming growth factor-beta1-stimulated fibroblasts J Biol Chem 200127617437-41 26 Kinnula VL Fattman CL Tan RJ Oury TD Oxidative stress in pulmonary fibrosis a possible role for redox modulatory therapy Am J Respir Crit Care Med 2005172417-22 27 Meyer A Buhl R Kampf S Magnussen H Intravenous N-acetylcysteine and lung glutathione of patients with pulmonary fibrosis and normals Am J Respir Crit Care Med 19951521055-60 28 Behr J Degenkolb B Krombach F Vogelmeier C Intracellular glutathione and bronchoalveolar cells in fibrosing alveolitis effects of N-acetylcysteine Eur Respir J 200219906-11 29 Bando M Hosono T Mato N et al Long-term efficacy of inhaled N-acetylcysteine in patients with idiopathic pulmonary fibrosis Intern Med 2010492289-96 30 Demedts M Behr J Buhl R et al High-dose acetylcysteine in idiopathic pulmonary fibrosis N Engl J Med 20053532229-42 31 Toma TP Bhowmik A Rajakulasingam R Acetylcysteine in pulmonary fibrosis N Engl J Med 20063541086-9 author reply -9 32 Hunninghake GW Antioxidant therapy for idiopathic pulmonary fibrosis N Engl J Med 20053532285-7 33 Flaherty KR Mumford JA Murray S et al Prognostic implications of physiologic and radiographic changes in idiopathic interstitial pneumonia Am J Respir Crit Care Med 2003168543-8 34 Latsi PI du Bois RM Nicholson AG et al Fibrotic idiopathic interstitial pneumonia the prognostic value of longitudinal functional trends Am J Respir Crit Care Med 2003168531-7 35 Collard HR King TE Jr Bartelson BB Vourlekis JS Schwarz MI Brown KK Changes in clinical and physiologic variables predict survival in idiopathic pulmonary fibrosis Am J Respir Crit Care Med 2003168538-42 36 Jegal Y Kim DS Shim TS et al Physiology is a stronger predictor of survival than pathology in fibrotic interstitial pneumonia Am J Respir Crit Care Med 2005171639-44 37 Martinez FJ Safrin S Weycker D et al The clinical course of patients with idiopathic pulmonary fibrosis Ann Intern Med 2005142963-7 38 Hull JH Acetylcysteine in pulmonary fibrosis N Engl J Med 20063541089-91 author reply -91
70
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
39 Flaherty KR King TE Jr Raghu G et al Idiopathic interstitial pneumonia what is the effect of a multidisciplinary approach to diagnosis Am J Respir Crit Care Med 2004170904shy10 40 Raghu G Johnson WC Lockhart D Mageto Y Treatment of idiopathic pulmonary fibrosis with a new antifibrotic agent pirfenidone results of a prospective open-label Phase II study Am J Respir Crit Care Med 19991591061-9 41 Hunninghake GW Lynch DA Galvin JR et al Radiologic findings are strongly associated with a pathologic diagnosis of usual interstitial pneumonia Chest 20031241215-23 42 Lynch D Godwin J Safrin S et al High-resolution computed tomography in idiopathic pulmonary fibrosis diagnosis and prognosis Am J Respir Crit Care Med 2005172488-93 43 Mallinckrodt CH Watkin JG Molenberghs G Carroll RJ Choice of the primary analysis in longitudinal clinical trials Pharmaceutical Statistics 20043161-9 44 Bang H Tsiatis A Estimating medical costs with censored data Biometrika 200087329shy43 45 Lin DY Regression analysis of incomplete medical cost data Stat Med 2003221181-200 46 Rochon J Application of GEE procedures for sample size calculations in repeated measures experiments Stat Med 1998171643-58 47 Lachin JM Foulkes MA Evaluation of sample size and power for analyses of survival with allowance for nonuniform patient entry losses to follow-up noncompliance and stratification Biometrics 198642507-19
71
- PANTHER-IPFPREDNISONE AZATHIOPRINEAND N-ACETYLCYSTEINEA STUDY THAT EVALUATES RESPONSE INIDIOPATHIC PULMONARY FIBROSIS
-
- Protocol Summary
- Table of Contents
- List of Tables
- List of Figures
- List of Abbreviations
- 1 Summary
- 2 Hypotheses and Specific Aims
-
- 21 Null Hypothesis
- 22 Specific Aim 1
- 23 Specific Aim 2
- 24 Prespecified Subgroups of Interest
-
- 3 Background and Significance
-
- 31 Idiopathic Pulmonary Fibrosis is the Most Common Interstitial Lung Disease
- 32 Rationale for Placebo Control
- 33 Rationale for N-acetylcysteine
- 35 Rationale for N-acetylcysteine as a Stand-alone Therapy
- 36 Rationale for the Study Design and Primary Endpoint
- 37 Rationale for Blinding of Treatments
-
- 4 Methods
-
- 41 Inclusion Criteria
- 42 Diagnosis of IPF
- 43 Exclusion Criteria
- 44 Study Design and Study Visit
- 45 Dose Justification
- 46 Contraindications Precautions and Side Effects of Study Medications
- 47 Recruitment Procedures
- 48 Study Procedures
- 49 Concomitant Medications
- 410 Laboratory Testing
- 411 Blinding of Study Drugs
-
- 5 Study Endpoints
-
- 51 Primary Study Endpoint
- 52 Secondary Study Endpoints
-
- 6 Safety Evaluations and Procedures
-
- 61 Adverse Events
- 62 Clinical Medical Monitoring
- 63 Unblinding Procedures
-
- 7 Study Drug Procedures
- 8 Data Management
-
- 81 Hardware and Software Configuration
- 82 Sources of Data
-
- 9 Study Design and Data Analysis
-
- 91 General Analytic Considerations
- 92 Randomization Blinding and Reporting of Results
- 93 Stratification
- 94 Specification of the Primary Analyses
- 95 Analysis of Longitudinal Endpoints
- 96 Analysis of Binary Time-to-Event and Time-Lagged Endpoints
- 97 Power Analysis
-
- 10 Study Administration
-
- 101 Cooperative Agreement Mechanism
- 102 IPFnet Steering Group
- 103 Data and Safety Monitoring Board
- 104 Recommendations on Interim Monitoring of Efficacy Safety and Futility
-
- 11 Investigator and Sponsor Obligations
-
- 111 Monitoring
- 112 Cost and Payment
- 113 Confidentiality and Health Insurance Portability and Accountability ActConsiderations
- 114 Informed Consent Procedures
- 115 Institutional Review Boards
-
- 12 Investigator Agreement
- 13 References
-

PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Protocol Summary
PRODUCT N-acetylcysteine
CLINICALTRIALSGOV NUMBER NCT00650091
PROTOCOL TITLE Prednisone Azathioprine and N-acetylcysteine A Study THat Evaluates Response in Idiopathic Pulmonary Fibrosis (PANTHER-IPF)
DIAGNOSIS AND MAIN CRITERIA FOR INCLUSION
Confirmed idiopathic pulmonary fibrosis diagnosed within 48 months of enrollment forced vital capacity ge 50 predicted hemoglobin adjusted diffusing capacity of the lung ge 30 predicted
STUDY OBJECTIVES To assess the safety and efficacy of N-acetylcysteine in subjects with newly diagnosed idiopathic pulmonary fibrosis
STUDY DESIGN Multi-center randomized double-blind placebo-controlled
TREATMENT REGIMENS 1) N-acetylcysteine (600 mg TID) or 2) placebo
ROUTE OF ADMINISTRATION Oral
TIME BETWEEN FIRST AND LAST DOSES OF ACTIVE STUDY AGENT
Maximum of 60 weeks
NUMBER OF SUBJECTS Approximately 130 NAC 130 placebo (11)
NUMBER OF CLINICAL CENTERS Approximately 26 US sites
PRIMARY ENDPOINT Change in longitudinal forced vital capacity measurements over 60 weeks
INTERIM ANALYSIS Completed October 2011
2
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Study Sponsor National Heart Lung and Blood Institute
Acting Steering Group Chair Marvin I Schwarz MD University of Colorado - Denver
Project Officer
Gail Weinmann MD National Heart Lung and Blood Institute Bethesda MD
Protocol Committee Cochairs
Ganesh Raghu MD University of Washington
Fernando J Martinez MD University of Michigan
Data Coordinating Center
Duke Clinical Research Institute Duke University
3
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Table of Contents
List of Tables 7
List of Figures 7
List of Abbreviations 8
1 Summary 12
2 Hypotheses and Specific Aims 13 21 Null Hypothesis 13 22 Specific Aim 1 13 23 Specific Aim 2 13 24 Prespecified Subgroups of Interest 14
3 Background and Significance 15 31 Idiopathic Pulmonary Fibrosis is the Most Common Interstitial Lung Disease15 32 Rationale for Placebo Control 15 33 Rationale for N-acetylcysteine 16 35 Rationale for N-acetylcysteine as a Stand-alone Therapy 17 36 Rationale for the Study Design and Primary Endpoint 18 37 Rationale for Blinding of Treatments 19
4 Methods 21 41 Inclusion Criteria 21
411 Subjects Shown to Have Usual Interstitial Pneumonia Pattern on Surgical Lung Biopsy 21 412 Subjects Who Have Not Undergone a Surgical Lung Biopsy 21
42 Diagnosis of IPF 21 43 Exclusion Criteria 26 44 Study Design and Study Visit 27
441 Study Design Summary 27 442 Study Visits 28
4421 Screening 28 4422 Enrollment 29 4423 Week 15 30 4424 Week 30 31 4425 Week 45 31 4426 Week 60 (Early Withdrawal or Final Treatment Visit) 32 4427 Final Site Visit ndash FVC drop confirmation 33 4428 Final Visit ndash Telephone Follow-up 33 4429 Phone Contact Between Visits 33
45 Dose Justification 35 451 Rationale for N-acetylcysteine Dosing 35
4511 Dosing of N-acetylcysteineplacebo 35 4512 Reasons to Discontinue N-acetylcysteineplacebo 35
452 Dosage Algorithms 37 46 Contraindications Precautions and Side Effects of Study Medications 39
461 Contraindication 39 462 Precautions 39 463 Side Effects 39
47 Recruitment Procedures 40 48 Study Procedures 41
481 Biological Specimen Management 41 4811 Biological Specimen Sample Management 41
49 Concomitant Medications 42 410 Laboratory Testing 42 411 Blinding of Study Drugs 43
4
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
5 Study Endpoints 44 51 Primary Study Endpoint 44 52 Secondary Study Endpoints 44
521 Time to Disease-progression 44 522 Acute Exacerbations 44 523 Respiratory Infections 47 524 Maintained FVC Response 48
6 Safety Evaluations and Procedures 49 61 Adverse Events 49
611 Definitions 49 612 Adverse Event (AE) Reporting 50
6121 Serious Adverse Events (SAE) Reporting 50 6122 Regulatory Reporting 51
62 Clinical Medical Monitoring 52 63 Unblinding Procedures 52
7 Study Drug Procedures 53
8 Data Management 54 81 Hardware and Software Configuration 54
811 Hardware and Database Software 54 812 Statistical Software 54 813 Access Control and Confidentiality Procedures 54 814 Security 54 815 Back-up Procedures 55 816 Virus Protection 55
82 Sources of Data 55 821 Design and Development 55 822 Data Collection Forms 55 823 Data Acquisition and Entry 56 824 Data Center Responsibilities 56 825 Data Editing 56 826 Training 56
9 Study Design and Data Analysis 57 91 General Analytic Considerations 57 92 Randomization Blinding and Reporting of Results 57 93 Stratification 58 94 Specification of the Primary Analyses 58 95 Analysis of Longitudinal Endpoints 58 96 Analysis of Binary Time-to-Event and Time-Lagged Endpoints 59 97 Power Analysis 60
971 Primary Analyses 60 972 Power Analysis for Secondary Endpoints 61
10 Study Administration 62 101 Cooperative Agreement Mechanism 62 102 IPFnet Steering Group 64 103 Data and Safety Monitoring Board 64 104 Recommendations on Interim Monitoring of Efficacy Safety and Futility 64
11 Investigator and Sponsor Obligations 66 111 Monitoring 66 112 Cost and Payment 66 113 Confidentiality and Health Insurance Portability and Accountability Act Considerations 66 114 Informed Consent Procedures 67 115 Institutional Review Boards 67
5
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
12 Investigator Agreement 68
13 References 69
6
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
List of Tables Table 1 Operating Characteristics of Local HRCT Review for Diagnosis of UIP (24)
Table 2 Combining HRCT and Pathology Interpretations to Determine if IPF is Present (25)
Table 3 Schedule of Assessments (34)
Table 4 Side Effects of NAC (40)
Table 5 Final Diagnoses in Evaluation of Suspected Acute Exacerbations (46)
Table 6 Hypothetical Values of Mean FVC (L) Change from Baseline (61)
Table 7 Detectable Differences in Treatment Means for Selected Endpoint Measurements (61)
List of FiguresFigure 1 Changes in Forced Vital Capacity from Baseline in Prior IPF Clinical Trials (19)
Figure 2 Diagnosis of Idiopathic Pulmonary Fibrosis in the IPFnet (22)
Figure 3 Pathology Flow Chart Surgical Lung Biopsy Diagnosis (23)
Figure 4 Acute Exacerbation Flow Chart (47)
7
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
List of Abbreviations
6MWT 6-minute walk test
A-aPO2 alveolar-arterial PO2 difference
ABG arterial blood gas
AE adverse event
AEx acute exacerbation
AG albuminglobulin
ALT alanine aminotransferase
AST aspartate aminotransferase
ATS American Thoracic Society
AZA azathioprine
BAL bronchoalveolar lavage
BUN blood urea nitrogen
CBC complete blood count
cGMP Current Good Manufacturing Practice
CPI Composite Physiologic Index
CPK creatine phosphokinase
CT computed tomography
DCC Data Coordinating Center
DCRI Duke Clinical Research Institute
8
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
DLCO diffusing capacity of the lung for carbon monoxide
DLCOpred diffusing capacity of the lung for carbon monoxide percent predicted
DSMB data and safety monitoring board
eCRF Electronic case report form
ERS European Respiratory Society
FDA Food and Drug Administration (US)
FEV1 forced expiratory volume in 1 second
FSH follicle-stimulating hormone
FVC forced vital capacity
FVCpred forced vital capacity percent predicted
GGT gamma glutamyl transferase
GSH glutathione
HAD Hospital Anxiety and Depression
HHS Health amp Human Services (US Dept of)
HIPAA Health Insurance Portability and Accountability Act
HRCT high-resolution computed tomography
IBW ideal body weight
ICE CAP Investigating Choice Experiments for Preferences of Older People Capability Instrument
ILD interstitial lung disease
IPF idiopathic pulmonary fibrosis
9
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
IPFnet Idiopathic Pulmonary Fibrosis Clinical Research Network
IRB institutional review board
ITT intent to treat
IV intravenous
IVRS interactive voice response system
LDH lactate dehydrogenase
LFT liver function test
LOCF last observation carried forward
LSD Least Significant Difference
MAR missing at random
MCAR missing completely at random
MMRM mixed model repeated measures
MOOP manual of operating procedures
NAC N-acetylcysteine
NHLBI National Heart Lung and Blood Institute (US)
NIH National Institutes of Health (US)
NSIP nonspecific interstitial pneumonia
PaO2 partial pressure of arterial oxygen
PCP primary care provider
PFT pulmonary function test
10
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
PHS Public Health Service (US)
PI principal investigator
PL placebo
PLT platelet
PRED prednisone
QOL quality of life
SAE serious adverse event
SAP statistical analysis plan
SGRQ St Georgersquos Respiratory Questionnaire
SpO2 oxygen saturation by pulse oximetry
TPMT thiopurine methyl transferase
UCSD SOBQ University of California at San Diego Shortness of Breath Questionnaire
UIP usual interstitial pneumonia
ULN upper limit of normal
USP United States Pharmacopoeia
VC vital capacity
WBC white blood cell
11
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
PREDNISONE AZATHIOPRINE AND N-ACETYLCYSTEINE A STUDY
THAT EVALUATES RESPONSE IN IDIOPATHIC PULMONARY FIBROSIS
1 Summary
There are currently no drug therapies that have proven to be effective in the treatment of idiopathic pulmonary
fibrosis (IPF) Previous clinical drug trials have been difficult to interpret due to lack of true placebo (PL)
controls or other methodological concerns Clinical efficacy of immunosuppressive therapies and agents that
reduce oxidative stress remains controversial The IPF Clinical Research Network (IPFnet) is conducting a
randomized double-blind placebo-controlled trial designed to assess the safety and efficacy of
N-acetylcysteine (NAC) as monotherapy in subjects with mild or moderate IPF
The study initially employed a 3-arm design with 111 randomization to NAC azathioprine (AZA)-prednisone
(PRED)-NAC and PL with each subject to be treated up to a maximum of 60 weeks followed by a tapering of
PREDPL and a 4-week period for safety evaluation Approximately 390 subjects who have mild to moderate
IPF (defined as forced vital capacity percent predicted [FVCpred] ge 50 and diffusing capacity of the lung
for carbon monoxide percent predicted [DLCOpred] 30) diagnosed within the past 48 months were to be
enrolled
At the pre-specified interim analysis the DSMB recommended termination of the prednisone-azathioprine-
NAC arm of the study No additional patients will be randomized to that arm However the NAC and placebo
arms remain open for enrollment and we will enroll approximately 130 subjects in each arm (inclusive of the
subjects enrolled at the time of the interim analysis) Follow up for subjects enrolled into the two arms will
continue for 60 weeks
The primary endpoint is the change in longitudinal measurements of FVC over the study period The primary
goal of this study to establish an evidence-based standard of care and clarify myths from facts for
pharmacotherapy of IPF has been met in part by demonstrating that the widely used triple therapy was harmful
to patients with IPF (NHLBI press release Oct 21 2011) To determine the potential therapeutic benefits of
NAC alone the study will continue to enroll patients as a two-arm double-blind placebo-controlled study from
this point on (NAC vs placebo) as recommended by the DSMB following the pre-specified interim analysis
12
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
2 Hypotheses and Specific Aims 21 Null Hypothesis
Treatment with NAC will provide the same efficacy as PL as measured by longitudinal changes in FVC
22 Specific Aim 1
This study is designed to assess the safety and efficacy of NAC in subjects with newly diagnosed IPF
23 Specific Aim 2
Secondary goals of this study are to assess differences between treatment groups for the following
1 Mortality
2 Time to death
3 Frequency of acute exacerbations (AExs)
4 Frequency of maintained FVC response
5 Time-to-disease progression
6 Change in DLCO
7 Change in Composite Physiologic Index (CPI)
8 Change in resting alveolar-arterial oxygen gradient
9 Change in 6-minute walk test (6MWT) distance
10 Change in 6MWT oxygen saturation area under the curve
11 Change in 6MWT distance to desaturation lt 80
12 Change in 6MWT minutes walked
13 Changes in health status as measured by the SF-36 EuroQol and St Georgersquos Respiratory
Questionnaire (SGRQ)
14 Changes in dyspnea as measured by the University of California at San Diego Shortness of Breath
Questionnaire (UCSD SOBQ)
15 Frequency and types of adverse events (AEs)
16 Frequency and types of respiratory complications both infectious and noninfectious
17 Frequency of hospitalizations both all-cause and respiratory-related
13
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
24 Prespecified Subgroups of Interest
Treatment effects will be estimated and compared within key subgroups
Higher enrollment FVC12
Typical vs atypical high-resolution computed tomography (HRCT) reading at baseline3
Recent vs more remote diagnosis (time from initial diagnosis of IPF le 1 year and gt 1 year)
Lower CPI score at enrollment4
Medical therapy for gastroesophageal reflux5
Ethnic background
Sex
Smoking history (current or ex-smoker vs never smoker) given potential impact on oxidant status6
Presence of emphysema gt 25 on HRCT
14
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
3 Background and Significance
31 Idiopathic Pulmonary Fibrosis is the Most Common Interstitial Lung Disease
IPF is the most common interstitial lung disease (ILD) of unknown etiology The current incidence and
prevalence of IPF in the United States are not known A 1994 study of a population-based registry of subjects in
Bernalillo County New Mexico USA estimated an incidence of 107 cases per 100000 per year for males and
74 cases per 100000 per year for females the prevalence of IPF was estimated at 20 per 100000 for males and
13 per 100000 for females7 Extrapolating from a large healthcare claims database a more recent review
estimated the prevalence of IPF in the United States at 427 per 100000 (incidence estimated at 163 per
100000 per year)8 Recent epidemiological studies indicate increasing mortality rates from IPF in the United
States and other industrialized nations9-12
Approximately two-thirds of subjects with IPF are over the age of 60 at the time of presentation and the
incidence increases with age13 IPF has no distinct geographical distribution and predilection by race or
ethnicity has not been identified13 Individual subjects may remain relatively stable for prolonged periods
experience very slow declines in lung function with progression of radiographic abnormalities for a period of
months to years or experience more rapid declines and subsequent death Only 20 to 30 of IPF patients
survive for 5 years following diagnosis
There is currently no proven effective pharmacological treatment for IPF13 Anti-inflammatory and
immunosuppressive agents have been the traditional approach to the management of patients with IPF Based
on the results of the interim analysis of the PANTHER-IPF trial this lsquotraditional approachrsquo will be aborted
However it remains unknown if NAC alone will prove beneficial in IPF patients The primary goal of the
modified study is to establish an evidence-based standard of care and clarify the role of this specific antioxidant
pharmacotherapy for IPF
32 Rationale for Placebo Control
IPF is a disorder for which there is no proven efficacious therapy A major objective of this trial is to test to the
greatest degree possible a proposed standard of care for patients with IPF The current traditional therapy
15
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
employs immunosuppressive and corticosteroid drugs Interim review of the original PANTHER-IPF study has
documented increased adverse events and lack of efficacy for AZA-PRED-NAC compared to placebo
suggesting that this therapeutic approach should not be employed Whether this applies to NAC alone which
has been advocated by international societies has not been proven in well-designed well-powered clinical
trials The recommendations made in the recently published evidence guidelines for NAC monotherapy was
weak based on low quality13 Thus this continued clinical trial randomizing patients to receive NAC or placebo
is pivotal and will answer the important question of the potential therapeutic benefits of NAC monotherapy with
grade A evidence In this prospective randomized clinical trial the inclusion of a PL arm is therefore vital to
adequately test the benefits of NAC in well-characterized subjects with IPF
If NAC has no true efficacy then its role as standard of care will be refuted If a benefit compared with PL is
confirmed it will establish a benchmark against which future novel therapies for IPF will be safely compared
As there is no currently accepted therapy for IPF there is an increasing body of published literature supporting
the concept of no treatment as the ldquobest carerdquo option for IPF13
Post hoc analyses of PL-controlled trials suggest that subjects with milder disease may be more amenable to
therapy12 It is notable that a recent international prospective randomized trial of interferon-gamma for IPF
also included a PL arm the study was terminated early by the data and safety monitoring board (DSMB) due to
lack of treatment effect1415 This underscores the belief that a proven effective therapy for IPF does not
currently exist and that true placebo-controlled trials remain the gold standard Similarly recently completed
trials of etanercept everolimus bosentan and BIPF 1120 in IPF have included PL-treated arms16-19 In three of
these trials the treated subjects showed little if any objective improvement Based on this evidence and the
current status of IPF therapy and therapeutic trials we believe that clinicians and subjects will continue to enroll
in a PL-controlled study
33 Rationale for N-acetylcysteine
NAC is a derivative of the amino acid L-cysteine NAC has been shown to augment levels of the naturally
occurring antioxidant glutathione (GSH ) (glutathione γ-glutamyl cysteinyl glycine) both in vitro and in
vivo2021 GSH is present in all eukaryotic cells and may play an important role in protecting alveolar epithelial
cells against oxidant injury The concentration of GSH in the bronchoalveolar lavage (BAL) fluid in patients
16
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
with IPF is markedly diminished compared with normal subjects This GSH deficiency may be corrected by
exogenous administration of NAC2122
There is evidence of enhanced production of oxidants in an IPF lung Both inflammatory cells and
myofibroblasts derived from patients with IPF generate increased amounts of extracellular oxidants including
hydrogen peroxide2324 Secretion of hydrogen peroxide by activated myofibroblasts may induce the death of
adjacent lung epithelial cells by paracrine mechanisms24 Additionally generation of oxidants by myofibroblasts
induces oxidative crosslinking of extracellular matrix proteins25 a potential mechanism for aberrant matrix
remodeling Thus an oxidant-antioxidant imbalance exists in the lungs of IPF patients26 NAC may confer
protection against this imbalance by augmenting GSH levels in addition to its more direct free-radical
scavenging activity
Intravenous (IV) NAC therapy has been shown to increase total BAL GSH in 8 IPF subjects27 Oral NAC (600
mg 3 times per day) has been shown to decrease markers of oxidant injury and improve both total and reduced
GSH levels in the epithelial lining fluid of subjects with IPF in a small uncontrolled study22 pulmonary
function improved modestly with therapy A similar study in 18 IPF subjects confirmed increased intracellular
GSH concentration after 12 weeks of NAC (600 mg 3 times per day)2228 no clinical correlates were reported
Inhaled NAC was suggested to improve pulmonary function in an open label study29
35 Rationale for N-acetylcysteine as a Stand-alone Therapy
Results of a double-blind multi-center European clinical trial of 150 IPF subjects testing combinations of AZAshy
PRED vs AZA-PRED-NAC have been reported30 NAC added to AZA-PRED (ldquoconventional therapyrdquo) had a
significant positive effect on DLCO (p lt 0005) and vital capacity (VC) (p lt 005) at the end of 1 year30 The
recent ATSERS position statement after much discussion concluded that NAC alone should not be considered
in the majority of patients with IPF without additional data from well-designed studies
The interpretation of these data has been quite controversial Some have suggested that the magnitude of the
treatment effect although statistically significant is modest31 Others have suggested that NAC may be
modulating potential toxic effects of AZA-PRED alone32 supporting the investigation of NAC as stand-alone
therapy
17
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
The IPFnet is now completing the PANTHER-IPF trial with a 11 randomization (NAC vs placebo) and a
simple practical feasible and scientifically rational design that will establish standard of care with NAC for
IPF based on a currently available therapeutic agent and the existing data to support its use We anticipate that
all future clinical trials of novel therapeutic agents will be tested against this to-be-established standard of care
36 Rationale for the Study Design and Primary Endpoint
The optimal study design of a therapeutic trial in IPF would include survival as a primary endpoint The
published results of the IFN-γ 1b Phase 3 (GIPF-001) trial suggested a survival benefit in subjects with milder
disease in retrospective analyses1 although the trial was underpowered to address this question This was likely
related to the limited mortality in the PL arm of the study which included IPF subjects with mild to moderate
disease This study documents that an IPF study powered to improve survival in a patient population with mild
disease requires a larger sample size andor duration of study In fact the recently aborted Phase 3 IFN-γ 1b
(GIPF-007 INSPIRE) study was a survival-based study and recruited more than 800 subjects at 75 centers
worldwide1415 As such within the context of the current IPFnet trial survival is an impractical primary
endpoint variable
Several groups have published data defining an appropriate surrogate outcome variable a 10 decrement in
FVC during 6 to 12 months is a powerful predictor of survival in IPF33-36 Furthermore additional evidence
suggests a similar predictive ability for a 10 decrement in FVC during 3 months of follow-up37 With strong
supportive evidence of FVC progression being related to mortality on a per-subject basis this study will use
FVC changes in liters between treatment groups as the primary endpoint Previously published IPF studies have
shown a steady decline in FVC (and FVCpred) among control group subjects230 The GIPF-001 study
suggested a 48-week decrease in FVC of 016 L in the PL-treated subjects The IFIGENIA study demonstrated
a decline in FVC of approximately 019 L over 52 weeks in the subjects randomized to the control treatment
Figure 1 depicts the change in FVC for control groups from previously published IPF studies38 Based on these
data we expect that the PL group will have a decline of 020 L over the 60-week study period The IPFnet
Steering Group determined that a clinically meaningful improvement would be the preservation of the majority
of the 020-L FVC decline Therefore a mean treatment difference of 015 L in mean FVC over the 60-week
study period was determined to be a clinically meaningful difference
18
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Δ f
rom
bas
elin
e (i
n L
)
01
005
0
-005
-01
-015 Projected Δ for placebo
-02
-025
-019
-016
-013 Pirfenidone GIPF001
NAC
Placebo
4 8 12 16 20 24 28 32 36 40 44 48 52 56 60
Week
Figure 1 Changes in FVC From Baseline in Prior IPF Clinical Trials
Recent data suggest that various patient subgroups would be expected to potentially exhibit differential response
to therapy These parameters will be used to a priori separate patients by a series of baseline characteristics
including
1 Higher enrollment FVC12
2 Typical vs atypical high-resolution computed tomography (HRCT) reading at baseline3
3 Recent vs more remote diagnosis (time from initial diagnosis of IPF le 1 year and gt 1 year)
4 Lower CPI score at enrollment4
5 Medical therapy for gastroesophageal reflux5
6 Ethnic background
7 Sex
8 Smoking history (current or ex-smoker vs never smoker) given potential impact on oxidant status6
9 Presence of emphysema gt 25 on HRCT
37 Rationale for Blinding of Treatments
The issue of treatment blinding was given a great deal of consideration with subject safety being the primary
concern After discussion among the Steering Group members it was decided that as long as subject safety
could be ensured blinding was necessary Blinding allows the study to
Have optimal scientific validity and potential to impact the standard of care for subjects
19
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Make objective assessments of treatment effects
Maintain clinical equipoise among investigators
Encourage subjects to have similar levels of contact with the medical community
Minimize the differential dropout rates across study arms
20
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
4 Methods 41 Inclusion Criteria
1 Age 35 to 85 years inclusive
2 FVC ge 50 of predicted (post-bronchodilator measurement from the screening visit)
3 DLCO ge 30 of predicted (hemoglobin corrected and altitude corrected if gt4000 ft above sea level)
4 Ability to understand and provide informed consent
5 Diagnosis of IPF according to a modified version of the ATS criteria le 48 months from enrollment The
date of diagnosis is defined as the date of the first available HRCT or surgical lung biopsy characteristic
of definite UIP
411 Subjects Shown to Have Usual Interstitial Pneumonia Pattern on Surgical Lung Biopsy
Subjects who have been shown to have UIP pattern on lung biopsy must have all of the following
1 Exclusion of other known causes of ILD such as drug toxicity clinically significant environmental
exposures or diagnosis of connective tissue diseases
2 Bibasilar reticular abnormalities with minimal ground glass opacities on HRCT scan
412 Subjects Who Have Not Undergone a Surgical Lung Biopsy
In addition to the criteria above these subjects must have radiological findings considered to be definite for the
diagnosis of UIPIPF
1 Bibasilar reticular abnormalities with minimal ground glass opacities
2 Honeycombing as the predominant feature and located in the peripheral lung bases
42 Diagnosis of IPF
Only subjects with definite IPF will be eligible for enrollment in this study We will utilize a combination of
clinicalphysiologic features HRCT and review of a clinically obtained surgical lung biopsy specimen to
establish the diagnosis of IPF An algorithm for the diagnosis is provided to guide entry into the protocol as
outlined in the inclusion and exclusion criteria (Figures 2 and 3) This multi-disciplinary approach uses
21
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
expertise from clinicians radiologists and pathologists Investigators at each site in conjunction with central
pathology will work together to establish the diagnosis of IPF This interactive approach to the diagnosis of IPF
increases the level of agreement between observers39
A subject with suspected ILD should be evaluated for secondary causes including but not limited to
environmental exposures drugs and systemic diseases Presence of any of these findings felt to be significant
enough to cause an ILD should disqualify the subject from entry into the trial
If secondary causes are absent an HRCT scan may be obtained If an HRCT of sufficiently high quality has
been obtained within the last 3 months that scan may be used for diagnosis In the appropriate clinical setting
the diagnosis of IPF can be made by the demonstration of a typical radiographic pattern on HRCT or by
demonstration of UIP pattern on a surgical lung biopsy The following criteria for a radiographic (ie
nonsurgical) diagnosis will be used In the absence of known exposures andor clinical associations attributable
to pulmonary fibrosis and in the appropriate clinical setting the presence of definite UIP pattern in HRCT
images is required to meet study criteria for the diagnosis of IPF
Figure 2 Diagnosis of Idiopathic Pulmonary Fibrosis in the IPFnet
22
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Figure 3 Pathology Flow Chart Surgical Lung Biopsy Diagnosis
Requirement for diagnosis
1 Clinical exclusion of other known causes (connective tissue diseases environmental and drug
exposures) of ILD
2 Radiographic HRCT with bibasilar reticular abnormality and honeycomb change with minimal
ground glass opacities
Appropriate clinical setting
1 Age gt 50 years
2 Insidious onset of unexplained dyspnea
3 Duration of illness for ge 3 months
4 Bibasilar inspiratory crackles
23
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Unlike the ATSERS consensus criteria published in 2000 bronchoscopy will not be required for diagnosis
This decision was made based on the experience of the IPFnet Steering Group members regarding the utility of
bronchoscopy in the diagnosis of IPF The presence of an atypical HRCT finding will require documentation of
a definitive diagnosis by surgical lung biopsy In fact this is in keeping with the recently published evidence
based guidelines for diagnosis and management of IPF13 As shown in Figure 3 central review of the pathology
data will be required for a diagnosis of IPF
We will not require central review of HRCT as several studies have shown that a confident local interpretation
of clinicalHRCT criteria as definite IPFUIP is associated with a high positive predictive value for finding UIP
at surgical lung biopsy (see Table 1) Differences in sensitivity in these series likely reflect subject selection as
Flaherty et al3 evaluated only UIP and nonspecific interstitial pneumonia (NSIP) while Raghu et al40 and
Hunninghake et al41 included a broader range of ILD
Table 1 Operating Characteristics of Local HRCT Review for Diagnosis of UIP
Researcher of Subjects Sensitivity () Specificity () PPV () NPV ()
Raghu et al 40
59 (29 UIP by SLB) 78 90 88 82
Hunninghake et al 41 91 (54 UIP by SLB)
74 81 85 67
Flaherty et al 3 96 (only NSIP amp UIP)
37 100 100 30
Abbreviations PPV positive predictive value NPV negative predictive value UIP usual interstitial pneumonia SLB surgical lung biopsy and NSIP nonspecific interstitial pneumonia
Furthermore an analysis of the HRCT scans from subjects enrolled in the GIPF-001 trial confirmed that local
site interpretations have a high congruity to a central radiology core In this multi-center study 263 HRCT
scans were read as definite IPF and a retrospective central radiology core review found 932 to be consistent
with IPF 42 We will also take several additional steps to insure that the local HRCT reads are accurate
including
1 A detailed training module has been developed and must be completed by each site radiologist before
site initiation
2 Clinical centers are to mail all HRCT scans to the HRCT core lab The first 10 HRCT scans from
subjects enrolled at each enrolling clinical center will be reviewed centrally to be certain that local reads
24
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
25
are congruent with a central interpretation If discrepancies are identified additional education will be
provided and HRCT scans will continue to be reviewed centrally until the central radiology core is
confident that the local center is performing appropriately
3 Random scans will be obtained from each center throughout the study to confirm that the local read
continues to agree with central interpretation If discrepancies are identified they will be addressed as in
2 above
In all cases if a subject has a surgical lung biopsy sample that sample will be reviewed by the local and central
pathologists Therefore the only cases that would not be subject to a direct central review process are those
where the HRCT meets the centrally defined criteria for an unequivocal diagnosis and a lung biopsy sample is
not available Table 2 below summarizes the possible combinations for making a diagnosis
Table 2 Combining HRCT and Pathology Interpretations to Determine if IPF is Present
HRCT Diagnosis Pathology Diagnosis Diagnosis of IPF
Definite UIP Definite UIP Yes
Definite UIP Probable UIP Yes
Definite UIP Possible UIP Yes
Definite UIP Not UIP No
Definite UIP Unavailable Yes
Consistent with UIP Definite UIP Yes
Consistent with UIP Probable UIP Yes
Consistent with UIP Possible UIP No
Consistent with UIP Not UIP No
Consistent with UIP Unavailable No
Inconsistent with UIP Any No
Abbreviations HRCT high-resolution computed tomography IPF idiopathic pulmonary fibrosis
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
UIP usual interstitial pneumonia Dx diagnosis 43 Exclusion Criteria
1 History of clinically significant environmental exposure known to cause pulmonary fibrosis
Occupational exposures such as asbestos or environmental exposure to organic dust such as occurs in
pigeon breeders may at times mimic the clinical and radiographic findings of IPF
2 Diagnosis of connective tissue disease felt by the principal investigator (PI) to be the etiology of the
interstitial disease Diagnosis of collagen-vascular conditions will be according to the published
American College of Rheumatology criteria As such the presence of any documented collagen-vascular
disorder or the presence of any suspicious symptom complex whether or not associated with
significantly abnormal rheumatological serologies will exclude the subject at the discretion of the PI
3 Extent of emphysema greater than the extent of fibrotic change (honeycombing reticular changes) on
HRCT scan
4 Forced expiratory volume in 1 second (FEV1)FVC ratio lt 065 at screening (postbronchodilator)
5 Partial pressure of arterial oxygen (PaO2) on room air lt 55 mm Hg (lt 50 mm Hg at Denver site)
6 Residual volume gt 120 predicted at screening (postbronchodilator)
7 Evidence of active infection
8 Significant bronchodilator response on screening spirometry defined as a change in FEV1 ge 12 and
absolute change gt 200 mL OR change in FVC ge 12 and absolute change gt 200 mL The percent
difference between the FVC (or FEV1) values will be calculated by taking the absolute value of the
difference and dividing it by the larger of the two FVC (or FEV1) values
9 Screening and enrollment post-bronchodilator FVC measurements (in liters) differing by gt 11 The
percent difference between the FVC values will be calculated by taking the absolute value of the
difference and dividing it by the larger of the two FVC values (eg the percent difference between FVC
measurements of 19 and 20 liters would be determined by taking the difference between the two (01
liters) and dividing by the larger of the two (20 liters) So 0120 = 5 and these FVC measurements
would not exclude the subject
10 Listed for lung transplantation ie the patient has completed the evaluation process has been accepted
as a candidate for transplantation at an appropriate center and is waiting to receive notification of an
available donor organ
11 History of unstable or deteriorating cardiac disease
12 Myocardial infarction coronary artery bypass or angioplasty within 6 months of screening
26
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
13 Unstable angina pectoris or congestive heart failure requiring hospitalization within 6 months of
screening
14 Uncontrolled arrhythmia
15 Severe uncontrolled hypertension
16 Known HIV or hepatitis C
17 Known cirrhosis and chronic active hepatitis
18 Active substance andor alcohol abuse (as determined by site PI)
19 Pregnancy or lactation (subjects who are pregnant or breastfeeding)
20 Known hypersensitivity to study medication
21 Any condition other than IPF that in the opinion of the site PI is likely to result in the death of the
subject within the next year
22 Any condition that in the judgment of the PI might cause participation in this study to be detrimental to
the subject or that the PI deems makes the subject a poor candidate
23 Any therapy directed at pulmonary fibrosis (excepting triple therapy of prednisone plus azathioprine
plus NAC) requires a 30-day washout period before randomized Triple therapy of lt= 12 weeks duration
in the past 4 years requires a 30-day washout period before randomization
24 History of triple therapy of prednisone plus azathioprine plus NAC for gt 12 weeksrsquo duration in the past
4 years or previous enrollment in the triple-therapy arm of the PANTHER-IPF study
44 Study Design and Study Visit
441 Study Design Summary
This study will be a randomized double-blind PL-controlled trial designed to assess the safety and efficacy of
NAC in subjects with newly diagnosed IPF
Subjects with mild to moderate IPF (defined as FVCpred ge 50 and DLCOpred ge 30) diagnosed within
the past 48 months will be enrolled Screening will continue until April 30 2012
27
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
The study will employ a 2-arm design with 11 randomization to NAC or PL Once enrolled subjects will visit
the clinical center at 15 weeks and 15-week intervals thereafter Each subject will be treated and followed for a
maximum of 60 weeks
During the 60-week visit subjects will be taken off all study agents Approximately four weeks after the final
dose of study agent is taken subjects will receive a safety phone call from the study site
442 Study Visits
Subjects who meet entry criteria will review the informed consent a written description of the purpose
procedures and risks of the study with the PI co-investigator or study coordinator and all questions will be
answered The informed consent form will be signed by the subject at screening No protocol-specific
procedures will be performed until the subject has signed and dated an informed consent form This includes the
screening procedures
4421 Screening
Once informed consent is obtained subjects may immediately begin the screening process or may return within
28 days of consent In the event a study subject has been clinically evaluated at the study site by an IPFnet study
physician and has performed testing within three weeks for this clinical evaluation that meets guidelines
provided in the IPFnet PANTHER-IPF Manual of Operating Procedures (MOOP) this testing may be used to
satisfy the following screening criteria medical history physical exam arterial blood gas (ABG) with A-a
gradient vital signs with oximetry body height and weight spirometry DLCO lung volumes and HRCT scan
Allowing the use of previously performed test results that meet study guidelines for the screening visit is
intended to permit subjects easier access to study entry to prevent subjects from repeating testing that has been
performed within the study window and to decrease risks to subjects from repeated exposure to procedures
such as arterial puncture and HRCT
The following procedures will be performed at screening
Medical history and a physical examination
28
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Measure height and weight
Serum pregnancy test (if applicable)
Measure vital signs including oximetry
Blood draws performed and the following analyses conducted
o Hematology (red cell count white cell count hemoglobin hematocrit cell indices differential
platelet count)
o Blood chemistries according to central laboratory protocol (see Section 410 Laboratory
Testing)
o Beta human chorionic gonadotropin (serum) pregnancy test (in women of childbearing potential)
o Urinalysis
Pulmonary Function Tests (PFTs) including spirometry pre- and post- bronchodilator and postshy
bronchodilator measurement of lung volumes and measurement of hemoglobin adjusted diffusing
capacity
Measure ABGs
HRCT if a satisfactory scan has not been performed on the subject within 3 months of screening (see
PANTHER-IPF MOOP for more details)
Surgical lung biopsies (if applicable) reviewed by local and central pathology departments
Current medications If required a washout period discussed with the subject and initiated at this visit
4422 Enrollment
The enrollment visit is expected to take place within eight weeks of the screening visit Enrollment visit
activities include
Measure vital signs including oximetry
Measure height and weight
Serum pregnancy test (if applicable)
If consent has been given blood will be drawn and a urine specimen collected for the bio-specimen
repository
Spirometry (post-bronchodilator)
Measure 6MWT with Borg Dyspnea Scale
29
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Collect Quality-of-life (QOL) data using the SF-36 EuroQol Investigating Choice Experiments for
Preferences of Older People Capability Instrument (ICE CAP) and SGRQ
Female subjects complete Gender Substudy questionnaire
Dyspnea status collected using the UCSD SOBQ
Evaluate Acute Exacerbation (AEx)
Review of any Adverse Events (AEs)
Review of concomitant medications
Subject receives diary and instructions on its purpose and proper use
Subject receives supply of study drug sufficient to last until his or her 15-week study visit
See the Schedule of Assessments (Table 3) for more details Subjects with screening and enrollment postshy
bronchodilator FVC measurements (in liters) differing by more than 11 are not eligible to be enrolled in the
study
Subjects will be asked to provide a physician of record This physician will be considered the subjectrsquos primary
care provider (PCP) and if the subject agrees the PCP will be informed by letter of the subjectrsquos enrollment in
the trial The subject will be informed that his or her ongoing medical care should be received from the PCP
The PCP will be informed of any safety issues identified by the study staff The PCP will also be given
information regarding communication with study personnel about pertinent health issues or clinic encounters
the subject may have
4423 Week 15
The week 15 visit is expected to occur within +- 14 days of the subjectrsquos scheduled visit time (eg the week 15
visit should occur anytime between 13 and 17 weeks after starting study drug Week 15 activities include
Measure vital signs with oximetry
Measurement height and weight
Serum pregnancy test (if applicable)
Spirometry (post-bronchodilator) measurement
Review of AEs
Evaluate for AEx
30
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Review concomitant medications
If consented draw blood and collect urine specimen for the biospecimen repository
Subjects return used and unused study drug for the visit
Review study diary and a new study diary will be given
Provide additional supply of study drug sufficient to last until the next scheduled visit
4424 Week 30
The week 30 visit is expected to occur within +- 14 days of the subjectrsquos scheduled visit time (eg the week 30
visit should occur anytime between 28 and 32 weeks after starting study drug) Week 30 activities include
Physical examination
Measure vital signs with oximetry
Measure height and weight
Laboratory values (complete blood count [CBC] and serum chemistries)
Serum pregnancy test (if applicable)
Measure spirometry (post-bronchodilator)
6MWT with Borg scale
DLCO
Review of AEs
Evaluate for AEx
Review concomitant medications
Complete all QOL and dyspnea questionnaires (EuroQol ICE CAP SF-36 SGRQ and UCSD SOBQ)
If consent has been given blood will be drawn and a urine specimen collected for the biospecimen
repository
Review study diary
Subjects return used and unused study drug for the visit
Provide additional supply of study drug sufficient to last until the next scheduled visit
4425 Week 45
31
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
The week 45 visit is expected to occur within +- 14 days of the subjectrsquos scheduled visit time (eg the week 45
visit should occur anytime between 43 and 47 weeks after starting study drug) Week 45 activities include
Measure vital signs with oximetry
Measure height and weight
Serum pregnancy test (if applicable)
Measure spirometry (post-bronchodilator)
Review of AEs
Evaluate for AEx
Review concomitant medications
If consent has been given blood will be drawn and a urine specimen collected for the biospecimen
repository
Subjects return used and unused study drug for the visit
Study diary reviewed
Provide additional supply of study drug sufficient to last until the next scheduled visit
4426 Week 60 (Early Withdrawal or Final Treatment Visit)
At week 60 or at subject withdrawal from the study (premature by study doctor or subjectrsquos decision) a final
treatment visit will occur At this final treatment visit subjects will discontinue NACPL abruptly Week 60
activities also include
Physical examination
Measure vital signs with oximetry
Measure height and weight
Laboratory values (complete blood count [CBC] and serum chemistries)
Spirometry (post-bronchodilator) measurement
6MWT with Borg scale measurement
DLCO
Lung volumes
ABG
Review of AEs
32
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Evaluate for AEx
Review concomitant medications
Subjects will complete all QOL and dyspnea questionnaires (EuroQol ICE CAP SF-36 SGRQ and
UCSD SOBQ)
If consent has been given blood will be drawn and a urine specimen collected for the biospecimen
repository
Subjects return used and unused study drug for the visit
Study diary reviewed
4427 Final Site Visit ndash FVC drop confirmation
In the event that the subject has a recorded FVC drop of gt10 from baseline at the final treatment visit and the
subject has not had a confirmation of such a drop at a previous study visit the subject should return to the
clinical site 6 to 8 weeks after the final treatment visit During this visit a post-bronchodilator spirometry test
will be performed This FVC measurement will be evaluated according to section 521 of this protocol
4428 Final Visit ndash Telephone Follow-up
Four weeks following the final dose of study medication subjects will receive a telephone call from the study
coordinator to ensure that there are no side effects and to follow up on any ongoing adverse events (AEs)
4429 Phone Contact Between Visits
At week 2 and each month that a subject does not have a scheduled clinical center visit his or her study
coordinator will contact him or her at least once by telephone to
Inquire if the subject has had any hospitalizations events that might be considered an AE or any events
significant enough to warrant an out-of-cycle visit to the clinical center
Remind subjects of their current dosage levels and confirm that the subject understands them
Address any questions or concerns the subject might have regarding other aspects of the study
Assess adherence to the treatment regimen by reviewing diary data verbal review of medications taken
including nutritional supplements
33
34
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Table 3 Schedule of Assessments
Procedure Screening Visit 0
Enrollment Visit 1
Week 15 Visit 2
Week 30Visit 3
Week 45 Visit 4
Week 60 Early
Withdrawal Visit 5
Final1
Visit (via phone)
Informed consent X
Medical history X
Inclusionexclusion criteria X
Serum pregnancy test (if applicable) X X X X X
Review of lung biopsy X
Arterial Blood Gas X X
6-Minute Walk Test
X
X X
Physical examination X X X
Vital signs with oximetry X X X X X X
Body height and weight X X X X X X
Complete Blood Count X X X
Chemistry panel X X X
Monitor Lab Values X X X
Urinalysis X Specimen repository substudy blood draw and urine collection (if consented)
X
X X X X
HRCT (if not completed within three months) X
Spirometry (pre- and post-bronchodilator) X
Spirometry (post-bronchodilator only) X X X X X
DLCO (post-bronchodilator only) X X X
Lung volumes (post-bronchodilator only) X
X
Evaluate for acute exacerbation X X X X X
Review Adverse Events X X X X X X
Review concomitant meds X X X X X X
Dispense subject diary X X X X
Review subject diary X X X X X
Dispense study agent X X X X
Gender Substudy questionnaire (female subjects only) X
EuroQol ICECAP UCSD SOBQ SGRQ SF-36 X X X
Abbreviations DLCO diffusing capacity of the lung for carbon monoxide QOL Quality of Life ICECAP Investigating Choice Experiments for Preferences of Older People UCSD SOBQ University of California Shortness of Breath Questionnaire SGRQ St Georgersquos Respiratory Questionnaire SF-36 Short Form 36 Health Survey
1Follow-up visit via phone will occur four weeks after final dose of study medication
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
45 Dose Justification
The general philosophy for determining dosing levels was to apply previously examined
treatment regimens With the focus of the study being to establish a standard of care for
mildmoderate IPF subjects the goal was to develop flexible yet standardized treatment rules that
allow for the temporary or permanent withholding of one or more components of treatment when
necessary Subjects developing laboratory abnormalities or symptoms that result in
discontinuation of one or more components of study treatment may continue on the other
components as long as there is no contraindication for this Complete follow-up is important for
the validity of any study As a strategy to maintain protocol adherence we are using a treatment
regimen that will detect potential side effects and prompt interventions proactively in the interest
of patient safety In addition subjects who permanently stop study medications during the course
of the study are encouraged to continue in the study completing all scheduled visits and tests
451 Rationale for N-acetylcysteine Dosing
To our knowledge there have been no IPF studies to correlate clinical outcome measures with
different dosages for NAC The dosage chosen is based on the IFIGENIA study However BAL
lung GSH levels from subjects with IPF have been augmented with the use of oral NAC at 600
mg 3 times per day In addition lung GSH levels have been associated with improved
PFTs212227 The dose chosen for this study was based on previous data including the IFIGENIA
study30
4511 Dosing of N-acetylcysteineplacebo
Dosing of NACPL will be 600 mg orally 3 times a day (1800 mgday)
4512 Reasons to Discontinue N-acetylcysteineplacebo
NACPL may be temporarily or permanently discontinued for the duration of the study for
gastrointestinal symptoms or dermatologic reactions
35
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Temporarily discontinue (hold) oral NACPL for subjects requiring inpatient admission for acute
exacerbation (AEx) or other conditions Resume NACPL after discharge
36
37
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
452 Dosage Algorithms
Dosage Adjustment Algorithm 1 NACPL Dose Modifications for Gastrointestinal Symptoms Nausea Vomiting Abdominal Discomfort Diarrhea
GI Symptoms determined by the PI to be clinically significant Nausea Vomiting Abdominal Discomfort Diarrhea
NACPL Temporarily dc (HOLD) x 3 Days
Monitor symptoms intervene as clinically indicated (eg fluid replacement antidiarrhea or antinausea medication)
Monitor or lab PRN
Are symptoms resolving after 3 days NO
Symptoms NOT resolving after 3 days of holding study medication Assessmentmanagement per clinical
discretion of investigator
Likely not study medication discuss resuming study medication with medical monitor when symptoms resolved
YES
Temporarily dc (HOLD) NACPL for 4 additional days (total hold 1 week) then NACPL Resume 600 MG TID
Did symptoms recur
YES
STOP NACPL for
duration of study
NO
NACPL No Change
38
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Dosage Adjustment Algorithm 2 NACPL Dose Modifications For Dermatologic Reactions
Dermatologic Reactions (Not Acneiform) ge Grade 2 Grading per Common Terminology Criteria for
Adverse Events V30 (httpctepcancergov) For example Grade 1 RASHDESQUAMATION Macular or papular eruption or erythema without associated symptoms Grade 2 RASHDESQUAMATION Macular or popular eruption or erythema with pruritus or other associated symptoms localized desquamation or other lesions covering lt50 of body surface area
NACPL Temporarily dc (HOLD) x 3 days
Are symptoms resolving after 3 days
NO Symptoms not resolving after 3 days of holding study medication Assessmentmanagement per clinical discretion of investigator Likely not study medication Discuss resuming study medication with medical monitor when symptoms
resolved YES
Temporarily dc (HOLD) NACPL for 4 additional days (total hold 1 week) then NACPL resume 600 MG TID
Did symptoms recur
YES
STOP NACPL for
duration of study
NO
NACPL No change
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
46 Contraindications Precautions and Side Effects of Study Medications
461 Contraindication
Contraindication to NAC is known hypersensitivity to it
462 Precautions
Concomitant administration of oral NAC and antibiotics has shown a slightly reduced absorption
of cephalexin and a slight increase in erythromycin serum levels NAC contains free sulfhydryl
groups There is no evidence that individuals sensitive to sulfa drugs are sensitive to NAC
The NAC preparation being administered in this study contains 20 mg of aspartame Because of
the phenylalanine component of aspartame individuals with phenylketonuria should avoid or
restrict aspartame intake to avoid increased blood levels of phenylalanine Because of this risk
labeling is required on all products containing aspartame
463 Side Effects
Side effects of NAC range from common to serious See Table 4
39
40
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Table 4 Side Effects of NAC
Undesirable Effects
System-organ class Uncommon
(gt11000 lt1100)
Rare
(gt110000 lt11000)
Very rare
(lt110000) Not known
Immune system disorders Hypersensitivity Anaphylactic shock
reaction
Nervous system disorders Headache
Ear and labyrinth disorders Tinnitus
Cardiac disorders Tachycardia
Vascular disorders Hemorrhage
Respiratory thoracic and
mediastinal disorders
Bronchospasm
Dyspnea
Gastrointestinal disorders
Vomiting diarrhea
stomatitis abdominal
pain nausea
Dyspepsia
Skin and subcutaneous tissue
disorders
Urticaria rash
angioedema itching
General disorders and
administration site conditions Pyrexia
Investigations Reduced arterial
pressure Face edema
In very rare cases the onset of severe skin reactions such as Stevens-Johnson syndrome and Lyell syndrome was reported to have a temporal relationship with N-acetylcysteine administration Although in most cases at least another suspect drug probably most involved in the genesis of the above mentioned mucocutaneous syndromes has been identified in case of mucocutaneous alterations it is appropriate to contact onersquos doctor and the administration of N-acetylcysteine should be immediately discontinued
Some studies confirmed a reduction of platelet aggregation during N-acetylcysteine administration The clinical significance of these findings has not been defined yet [Source Fluimucil Investigator Brochure]
47 Recruitment Procedures
Subjects recruited for this study will be established patients of the investigators or physician- or
self-referred to participating clinical centers in the IPFnet Each clinical center within IPFnet has
a well-developed infrastructure of local pulmonologists within the surrounding geographic area
These pulmonologists are kept informed of ongoing IPF clinical trials and regularly refer
subjects to studies conducted at IPFnet clinical centers
Additional steps will be taken to inform clinicians of the trials in progress within IPFnet
including presentations at faculty staff meetings at local hospitals medical grand rounds and
national conferences direct mail notification monthly faxes and advertisement of network trials
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
in pulmonary journals Clinical center patients previously diagnosed with IPF will be notified of
the trials by mail whenever possible
Recruitment of minorities and women will be monitored by the DCC and DSMB If necessary
additional recruitment efforts will be made at specific centers to ensure that the aggregate subject
sample contains appropriate representation of women and minorities
48 Study Procedures
The following procedures are detailed in the PANTHER-IPF MOOP accompanying this
protocol
1 PFT
2 ABG
3 HRCT scan of the chest (including imaging of pulmonary arteries)
4 CBC and serum chemistries
5 Pregnancy test
6 6MWTBorg Dyspnea Scale
7 QOL questionnaires (EuroQol HAD SF-36 SGRQ and ICE CAP)
8 UCSD SOBQ
9 Gender Substudy Questionnaire
All assessments of PFTs will be conducted by study personnel not directly involved in the
treatment of the subjects
481 Biological Specimen Management
4811 Biological Specimen Sample Management
Subjects at clinical centers participating in the specimen repository substudy who consent to
having blood drawn for research purposes and for the banking of blood blood components and
other biologic specimens (urine and BAL fluid) will have approximately 405 mL of blood
41
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
drawn 17 mL blood drawn for DNA and 20 mL of urine collected at enrollment visit Subjects
will have approximately 50 mL of blood drawn and 20 mL of urine collected at each 15-week
follow-up visit Blood specimens will be separated according to PANTHER-IPF MOOP
guidelines into the following components for banking in the repository serum plasma and
DNA Coding of all biologic specimens for the repository will be performed by study staff at the
clinical center The samples will be processed per PANTHER-IPF MOOP guidelines aliquoted
labeled with barcode labels and stored at -70degC at the clinical center and shipped to the central
repository
The only subject identifiers will be a sample ID number and subject initials This sample ID will
be linked in the IPFnet DCC clinical database to subject information No subject information will
be transferred to the biological-specimen database
The subjectrsquos samples may be used for approved sub-studies relating to human disease
including but not limited to IPF The studies for which an individualrsquos samples will be made
available will be determined by the subjectrsquos answers to questions on the biological-sample
informed consent form The subjects can choose to make their samples available for all options
or any combination Samples will be made available to researchers only with IPFnet Steering
Group approval until such time as the samples are made public through the NHLBI repository
49 Concomitant Medications
Concurrent treatment with FDA-approved therapy for IPF is allowed Colchicine may be used
for treatment of gout Temporary treatment with oral or IV corticosteroids for clinical worsening
or suspected AEx is permitted Nutritional supplements containing NAC are not allowed
410 Laboratory Testing
Clinical laboratory parameters will be assessed at screening and at the end of the study The
following tests will be performed at the two time points specified in the protocol chemistry (AG
ratio ALT [SGPT] AST [SGOT] albumin alkaline phosphatase amylase bilirubin-direct
42
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
bilirubin-indirect bilirubin-total BUN BUNcreatinine ratio calcium carbon dioxide
cholesterol-total chloride CPK-total creatinine GGT globulin glucose iron-total LDH
lipase magnesium phosphorus-inorganic potassium protein-total sodium TIBC triglycerides
uric acid) and hematology (red blood cell count WBC count hemoglobin hematocrit cell
indices differential platelet count)
411 Blinding of Study Drugs
Subjects and caregivers will be blinded to study treatment Every subject will receive NAC or
matching PLs at every study visit from the baseline visit to the week-45 visit No study agent
will be dispensed at the week-60 visit
43
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
5 Study Endpoints
51 Primary Study Endpoint
The primary endpoint will be the change in serial measurements of FVC over the study period
52 Secondary Study Endpoints
521 Time to Disease-progression
The time-to-death or a 10 decline in FVC will be defined as the time-to-disease progression
The 10 decline in FVC from enrollment must be confirmed on 2 consecutive visits no less than
6 weeks apart For subjects with 2 consecutive visits with a 10 decline in FVC the time-toshy
disease progression will be defined as the time interval between enrollment and the initial visit
with a 10 FVC decline For subjects who experience disease progression the study doctor will
determine whether or not the subject will remain in the study
522 Acute Exacerbations
The following 3 criteria will define AEx in subjects with acute worsening of their respiratory
conditions
1 Clinical (all of the following required)
A) Unexplained worsening of dyspnea or cough within 30 days triggering unscheduled
medical care (eg emergency room clinic study visit hospitalization)
B) No clinical suspicion or overt evidence of cardiac event pulmonary embolism or deep
venous thrombosis to explain acute worsening of dyspnea
C) No pneumothorax
44
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
2 RadiologicPhysiologic (A and B required)
A) New ground glass opacity or consolidation computed tomography (CT) scan OR new
alveolar opacities on chest x-ray
B) Decline of ge 5 in resting room air SpO2 from last recorded level OR decline of ge 8 mm
Hg in resting room air PaO2 from last recorded level
3 Microbiologic (all of the following required)
A) No clinical evidence for infection (ie absence of grossly purulent sputum fever gt 39degC
orally)
B) Lack of positive microbiological results (if done) from lower respiratory tract defined as
(1) Clinically significant bacterial growth on sputum or endotracheal aspirate cultures
(2) Quantitative culture by protected brush specimen ge 103 cfumL or BAL ge 104 cfumL
(3) The presence of specific pathogens on stains of any of the above
C) Lack of positive pathogen in blood cultures (if done)
Identification of Acute Exacerbations
All subjects will be educated about the importance of identifying AExs At the time of
enrollment subjects will be told about the possibility of developing acute symptomatic
worsening that might represent an AEx of IPF and instructed to contact their study clinical
center coordinator within 48 to 72 hours of the apparent event
All subjects will be contacted by phone monthly and questioned about any change in dyspnea or
cough and any interim clinic visits or hospitalizations Finally as part of the IPFnet outreach to
community referring physicians the importance of AExs will be emphasized When a subject is
identified who meets criterion 1A this will trigger the collection of additional clinical data to
evaluate a suspected AEx These data will be collected as part of standard clinical care (ie this
protocol does not require collection of all items) The additional items to be collected for
suspected AEx include
IPFnet AEx case report form (eCRF) (required)
45
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Chest x-ray CT scan withwithout pulmonary angiogram (reports should be faxed and
followed by the hard copiesdiscs)
Oxygen saturation (pulse oximetry)
ABG
Respiratory cultures (sputum endotracheal aspirate lavage)
Blood cultures
Clinichospital records related to the event
All potential cases of AEx will be reviewed by the clinical center PI first and a decision on
whether the case may represent an AEx will be made If AEx is suspected the case will be sent
to the IPFnet adjudication committee which will assign a final diagnosis (see Table 5) If there is
disagreement among members the majority opinion will be recorded
During episodes of suspected AEx as determined by the individual clinical center investigator
subjects will remain blinded and in the study
Table 5 Final Diagnoses in Evaluation of Suspected Acute Exacerbations
Definite acute exacerbation All criteria met no alternative etiology
Unclassifiable acute worsening
Insufficient data to evaluate all criteria no alternative etiology
Not acute exacerbation Alternative etiology identified that explains acute worsening
Management of the suspected AEx will be at the discretion of the treating physician Standard of
care generally involves evaluation for respiratory infection pulmonary embolism cardiac events
and pneumothorax and treatment with IV corticosteroids
Study drugs will be resumed at pre-suspected AEx doses after subjects clinically improve as
confirmed by the local PI All subjects should be seen at the clinical center within 2 to 4 weeks
of recovery for measurement of post-bronchodilator FVC (see Figure 4) Subjects unable to
return to the clinical center after suspected AEx due to medical frailty (eg continued
46
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
institutionalization progressive disability) will be categorized as failing to maintain FVC
response in secondary analyses
Suspected AEx (PI determined)
Hold study drug Treat AEx
(Attending physician determined)
Alive but unable to continue due to
medical frailty
Dead
Alive and able to continue
Site reviewvisit
Restart study drug
FVC within 2-4 weeks
Figure 4 Acute Exacerbation Flow Chart
523 Respiratory Infections
An upper respiratory infection will be defined as
Change in sputum discoloration
Increased cough of no more than 14 daysrsquo duration
A lower-respiratory infection (pneumonia) will be defined as new segmental or lobar airspace
opacities visualized by image studies (chest radiograph or HRCT) in addition to any of the
following
Positive pathogencultures in good sample of sputum or lower-airway secretions retrieved
by fiberoptic bronchoscope
Fever gt 39degC or gt 100degF
Leukocytosis gt 12000 (unexplained no increase in dose of corticosteroids)
47
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
524 Maintained FVC Response
Subjects with follow-up FVCpred measurements at or above their baseline FVCpred level
will be classified as having maintained FVC response Subjects with reduced FVCpred levels
or missing data for any reason including death or medical frailty will be classified as having not
maintained FVC response The FVCpred value is used because unadjusted FVC measurements
are expected to decline with age
48
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
6 Safety Evaluations and Procedures
61 Adverse Events
During a clinical trial the reporting of adverse experience information can lead to important
changes in the way a new treatment is developed as well as provide integral safety data
611 Definitions
An adverse event (AE) is any untoward medical occurrence in a subject or clinical investigation
subject who was administered a pharmaceutical product The AE does not necessarily have to
have a causal relationship with the drug administered An AE can be any unfavorable and
unintended sign (including an abnormal laboratory finding) symptom or disease temporarily
associated with the use of a medicinal product whether or not considered to be related to the
medicinal product Diseases signs symptoms or laboratory abnormalities already existing at
enrollment are not considered AEs unless they worsen (ie increase in intensity or frequency)
Surgical procedures themselves are not AEs they are therapeutic measures for conditions that
require surgery The condition for which the surgery is required may be an AE Surgical
procedures planned before randomization and the conditions necessitating the surgery are not
AEs
A serious adverse event is any untoward event that
Is fatal
Is life-threatening
Requires inpatient hospitalization or prolongation of existing hospitalization with the
following exceptions
o Preplanned (before the study) hospital admissions unless the hospitalization is
prolonged
o Planned admissions (as part of a study eg routine biopsies)
o Hospitalization lasting lt 24 hours
49
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
o Hospitalization for elective procedure
o Emergency room visits
Results in persistent or significant disability or incapacity
Is a congenital anomaly or birth defect
Important medical events that may not result in death be life-threatening or require
inpatient hospitalization may be considered serious adverse events (SAEs) when based
on appropriate medical judgment they may jeopardize the subject and may require
medical or surgical intervention to prevent one of the outcomes listed above
Life-threatening means that the subject was in the view of the investigator at immediate risk of
death from the AE as it occurred It does not include an AE that had it occurred in a more severe
form might have caused death
Persistent or significant disabilityincapacity means that the event resulted in permanent or
significant and substantial disruption of the subjectrsquos ability to carry out normal life functions
Causality
A reasonable possibility means the AE may have been caused byrelated to the study drug A
perceived or real lack of efficacy does not satisfy the definition of relatedness
612 Adverse Event (AE) Reporting
For the PANTHER-IPF trial all AEs (serious and nonserious) occurring from randomization
through final study visit (4 weeks after final dose of all study medication) will be recorded on the
AE page of the case report form (CRF)
6121 Serious Adverse Events (SAE) Reporting
For this trial all deaths and all SAEs which occur from randomization through final study visit
must be entered within the EDC system via the SAE eCRF page within 24 hours of the
investigative sitersquos knowledge of the event It is the responsibility of the clinical center
50
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
investigator to provide a causality assessment of the event for each study medications based upon
the information available at the time of the report It is understood that complete information
about the event may not be known at the time the initial report is submitted In the event the EDC
system is not accessible to the site at the time of event reporting investigative sites will complete
and forward a paper back-up SAE form to DCRI Safety Surveillance for processing
DCRI Safety Surveillance
Telephone 1-919-668-8624 or 1-866-668-7799 (toll free)
Fax 1-919-668-7138 or 1-866-668-7138 (toll free)
The investigator must complete and submit follow-up SAE information via the eCRF when
important new or follow-up information (eg final diagnosis outcome results of specific
investigations) becomes available Follow-up information should be submitted according to the
same process used for reporting the initial event as described above All SAEs will be followed
until resolution stabilization or 30 days after the subject has completed the final visit (4 weeks
after the final dose of study medication) whichever occurs first The investigator is responsible
for reporting SAEs to their institutional review board (IRB) per site specific IRB reporting
guidelines
6122 Regulatory Reporting
AEs that are serious study drug related and unexpected will be reported to the regulatory
authorities The DCRI Safety Surveillance medical monitor will perform a medical review of all
SAEs submitted and evaluate for ldquounexpectednessrdquo DCRI Safety Surveillance will prepare
MedWatch reports for those events identified as serious study drug related and unexpected as
determined by Safety Medical Monitor
DCRI Regulatory Services will submit all unexpected study drug-related SAEs as per 21 CFR
32 DCRI Safety Surveillance will provide a safety alert letter to the NHLBI DSMB and DCC
clinical operation (for distribution to sites) within 15 days of initial receipt of the information
51
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Investigators are responsible for promptly reporting these events to their reviewing IRBs
according to site specific IRB reporting guidelines
62 Clinical Medical Monitoring
There will be an unblinded physician at the IPFnet DCC serving as medical monitor The
medical monitor will be available to assist with questions about dosage adjustments of study
medications including discontinuation or resumption of medications
63 Unblinding Procedures
Unblinding of subjects or investigators to subject treatment is strongly discouraged For ongoing
clinical management all subjects should be presumed to be receiving ldquoactiverdquo study drug To
ensure the subjectrsquos safety the study treatment will be dose-adjusted based on laboratory test
results clinical findings and symptoms
The IPFnet DCC medical monitor and PANTHER-IPF co-chairs Drs Ganesh Raghu and
Fernando Martinez will be available to the study physicians to discuss study drug management
on a case-by-case basis Un-blinding will be considered ONLY when the knowledge of subject
treatment assignment is ABSOLUTELY ESSENTIAL for subject safety and after discussion of
the subjectrsquos case with the medical monitor and either Dr Raghu or Dr Martinez Unblinding of
study treatment should be minimized during the conduct of the trial In those cases where it is
felt to be medically necessary the DCC medical officer will communicate directly with the
managing physician to minimize unblinding of study personnel
52
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
7 Study Drug Procedures
At the baseline 15-week 30-week and 45-week study visits subjects will receive a supply of
study drug sufficient to last until the next visit at which study drug will be dispensed
53
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
8 Data Management
81 Hardware and Software Configuration
811 Hardware and Database Software
Data will be stored in an Oracle database system Oracle has advantages of processing efficiency
and smooth linkage with other software systems The application and database will be hosted on
Solaris Unix servers at the IPFnet DCC
812 Statistical Software
SAS will be used as the principal application for the management of analysis data files and
statistical computations S-Plus will be used to provide supplementary functions as needed
813 Access Control and Confidentiality Procedures
Access to databases will be controlled centrally by the IPFnet DCC through user passwords
linked to appropriate privileges This protects the data from unauthorized changes and
inadvertent loss or damage
814 Security
Database and Web servers will be secured by a firewall and through controlled physical access
Oracle has many security features to ensure that any staff member accessing the database has the
proper authority to perform the functions he or she requests of the system Within the secondary
SAS databases Unix group-access control maintains similar security The Sun workstation login
is secured by extensive user-password facilities under Unix
54
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
815 Back-up Procedures
Database back-up will be performed automatically every day and standard IPFnet DCC policies
and procedures will be applied to dictate tape rotation and retention practices
816 Virus Protection
All disk drives that provide network services and all user computers will be protected using
virus-scanning software Standard IPFnet DCC policies will be applied to update these protection
systems periodically through the study
82 Sources of Data
821 Design and Development
The IPFnet DCC will be responsible for development of the electronic case report forms
(eCRFs) development and validation of the clinical study database ensuring data integrity and
training clinical center staff on applicable data management procedures A web-based distributed
data entry model will be implemented This system will be developed to ensure that guidelines
and regulations surrounding the use of computerized systems used in clinical trials are upheld
The remainder of this section provides an overview of the data management plan associated with
this protocol
822 Data Collection Forms
The data collection process consists of direct data entry at the study clinical centers into the EDC
system(s) provided by the DCC A data collection worksheet will be provided to clinical centers
for recording data in the event the EDC system is unavailable Data entry of the eCRFs should
be completed according to the instructions provided and project specific training The
investigator is responsible for maintaining accurate complete and up-to-date records and for
ensuring the completion of the eCRFs for each research participant
55
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
823 Data Acquisition and Entry
Data entry into eCRFs shall be performed by authorized individuals Selected eCRFs may also
require the investigatorrsquos written signature or electronic signature as appropriate Electronic
CRFs will be monitored for completeness accuracy and attention to detail during the study
824 Data Center Responsibilities
The IPFnet DCC will 1) develop a data management plan and will conduct data management
activities 2) provide final eCRFs for the collection of all data required by the study 3) develop
data dictionaries for each eCRF that will comprehensively define each data element 4) conduct
ongoing data monitoring activities on study data 5) monitor any preliminary analysis data
cleanup activities and 6) rigorously monitor final study data clean up
825 Data Editing
Completed data will be entered into the IPFnet DCC automated data acquisition and
management system If incomplete or inaccurate data are found a data clarification request will
be generated and distributed to clinical centers for a response Clinical centers will resolve data
inconsistencies and errors and enter all corrections and changes into the IPFnet DCC automated
data acquisition and management system
826 Training
The training plan for clinical center staff includes provisions for training on assessments eCRF
completion guidelines data management procedures and the use of computerized systems
56
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
9 Study Design and Data Analysis
91 General Analytic Considerations
All primary analyses will be based on intent-to-treat (ITT) principles using all randomized
subjects Baseline factors across groups will be compared using mean (standard deviation) and
median (25th and 75th percentiles) summary measures Kaplan-Meier curves will be used to
display event rates Due to clinical interest in departures from both sides of the null hypothesis
all test statistics will be 2-sided
Reasonable caution needs to be taken when conducting multiple analyses on key clinical
subgroups For subgroup analyses a conservative significance level of 0001 will be used for all
interaction tests Thus subgroup comparisons will be considered exploratory unless the p-value
from the interaction test is smaller than 0001
92 Randomization Blinding and Reporting of Results
A permuted block-randomization scheme will be created with varying block sizes stratified by
clinical center Once a subject has completed the screening and baseline period and evaluation
for inclusionexclusion criteria the randomization process will begin Subjects will be
randomized to receive NAC or matching placebo with equal probability (11) via telephone
contact with a central interactive voice response system (IVRS) using a toll-free randomization
number On the day of randomization after the subject has successfully met all inclusion and
exclusion criteria the investigator or designee will call the central randomization number to
obtain the assigned kit randomization numbers for that subject At each subject visit the
investigator or designee will call the central randomization number to obtain the new kit
randomization numbers for resupply of the subject For resupply of the clinical center the IVRS
will monitor minimal volume of a kit type andor expiration date and will automatically notify
the pharmacy
57
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
The trial results will be reported according to guidelines specified in the CONSORT statement
A flow diagram describing screening recruitment randomization dropout and vital status will
be included in the primary manuscript AEs and efficacy data will be presented for all treatment
groups Adherence dropout and lost to follow-up will be carefully examined across all treatment
groups Analyses of safety will be based on data from all randomized subjects who received at
least one dose of study drug
93 Stratification
Subjects will be distributed to the two treatment arms in a 11 allocation ratio Stratification
blocks will be based on clinical centers
94 Specification of the Primary Analyses
A mixed model repeated measures (MMRM) analysis described in section 95 will be used to
compare differences in the slope of FVC measurements across the treatment groups Response
variables are values of the FVC measured at baseline and every 15 weeks until study completion
Variables in the model will include treatment time and time by treatment age sex race and
height Contrast estimates of differences in slopes of treatment over time (along with confidence
intervals) will be used to estimate the treatment effect The validity of this model in terms of
meeting modeling assumptions will be assessed via standard modeling diagnostics and goodness-
of-fit measures Based on the MMRM framework missing FVC data will not be imputed for the
primary analysis
95 Analysis of Longitudinal Endpoints
A common goal in clinical trials is to specify models that are easily implemented and
reproducible by independent data analysts On the other hand the models should have proper
statistical behavior in terms of low bias and high precision Many common approaches to
longitudinal data analysis including last observation carried forward (LOCF) imputation rely on
the missing completely at random (MCAR) assumption However the MCAR assumption is
58
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
unlikely to hold in many clinical trials because missing data are often related to disease
progression and prognosis A more reasonable assumption missing at random (MAR) specifies
that the complete data distribution can be modeled using only the observed data The likelihood-
based MMRM approach is valid under the more general MAR assumptions These models will
be applied to analyze the longitudinal data secondary endpoints
The advantages of MMRM analysis are that all important characteristics of the model can be preshy
specified standard software can be used to implement the models and results are based on ITT
principles43 In addition the MMRM approach offers superior control of Type I and Type II
errors compared with the LOCF approach
Response variables are values of the PFTs measured at enrollment and every 15 weeks until
study completion and 6MWT values measured at baseline week 30 and week 60 Covariates are
treatment time time by treatment and key baseline risk factors Contrasts (along with
confidence intervals) of treatment by time will be used to estimate the treatment effect
The correlation structure involves multiple pieces including measurement errors random
variation and interindividual variability For the longitudinal data analyses an unstructured
correlation matrix for within-subject errors will be assumed Other correlation structures
including compound symmetry will be examined as needed A careful examination of reasons
for study discontinuation will be conducted to assess the validity of MCAR Sensitivity analyses
will be used to examine the untestable assumption that the observed data violate the MAR
assumption The MMRM models will be implemented using PROC MIXED in SAS
96 Analysis of Binary Time-to-Event and Time-Lagged Endpoints
Regression modeling approaches using either the logistic regression model or Cox proportional
hazards regression model will be employed when appropriate The validity of these models will
be assessed via standard modeling diagnostics and goodness-of-fit measures Estimates of
cumulative frequencies for more general time-lagged responses will be calculated using the
partitioned version of the Bang-Tsiatis estimator44 The partitions will be set at 15-week intervals
59
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
to correspond with the data-collection process Covariate adjusted event rates will be calculated
using inverse probability-weighted regression estimates45
97 Power Analysis
971 Primary Analyses
Based on previously published IPF clinical trials the PL group is expected to experience a drop
in FVC of approximately 020 L over the study period (see Figure 1) The IPFnet Steering Group
determined a clinically important difference would be to preserve the majority of the decline
relative to PL over the study period In particular a treatment effect of 015 L was determined to
be a clinically meaningful difference Potential dropout is a key factor in the proposed study The
drop-out process assumed 5 lost to follow-up after every study visit Only 80 of subjects
were assumed to be followed for the entire study period All models assumed a compound
symmetry structure for the covariance matrix Power calculations were performed using a SAS
IML program for designing repeated measures studies46 Based on preliminary reviews of the
data from the University of Michigan the covariance matrix parameters were estimated at
approximately σ2 = 0757 (variance parameter) and ρ = 0936 (correlation parameter) To be
conservative the power calculations for the primary analysis were performed with parameter
setting of σ2 = 0810 (variance parameter) and ρ = 0925 (correlation parameter)
The power calculations assume a correction for imperfect compliance proposed by Lachin and
Foulkes to allow for 2 noncompliance for each of the treatment arms47 Thus the sample size
of 130 subjects per arm would be reduced to an adjusted sample size of 130(1-002-002)2 =
1198 or 120 subjects per arm
Under the assumed Type I error rate of 005 with a correlation parameter of 0925 and standard
deviation of 090 the difference of 015 L (or 00025 Lweek) shown in Table 6 would have
power of 93
60
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Table 6 Hypothetical Values of Mean FVC (L) Change from Baseline
Week 15 Week 30 Week 45 Week 60
NAC 00125 00250 00375 00500
Placebo 00500 01000 01500 02000
Difference 00375 00750 01125 01500
Abbreviations FVC forced vital capacity PL placebo
972 Power Analysis for Secondary Endpoints
Power calculations for secondary endpoint measurements are shown in Table 7 Standard
deviations are based on unpublished data provided by the University of Michigan The
calculations are based on a 2-sample t-test with Type I error rate set at 005 These calculations
are likely to be conservative because the statistical approach described in section 95 for
analyzing these endpoints will incorporate incomplete observations as well as intermediate data
points
Table 7 Detectable Differences in Treatment Means for Selected Endpoint Measurements
Secondary Endpoints Std Dev
of the Baseline Score
Detectable Difference for 80 Power
Std Dev of the Change Score
Difference Detectable for
80 Power
DLCOpred 166 58 91 32
6MWT Area Under the Desaturation Curve
219 76 175 61
6MWT Distance to Desaturation 224 78 315 110
6MWT Minutes Walked 210 073 205 071
Abbreviations Std Dev standard deviation DLCOpred diffusing capacity of the lung for carbon monoxide percent predicted 6MWT 6-minute walk test
61
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
10 Study Administration
101 Cooperative Agreement Mechanism
The administrative and funding mechanism used to undertake this project is a ldquocooperative
agreementrdquo (U01) which is an assistance mechanism Under the cooperative agreement the
NHLBI assists supports andor stimulates the project and is substantially involved with
investigators in conducting the study by facilitating performance of the effort in a ldquopartnerrdquo role
The NHLBI project scientist serves on the IPFnet Steering Group and he or another NHLBI
scientist may serve on other project committees when appropriate At the same time however
NHLBI does not assume a dominant role direction or prime responsibility for this research
program
As described below governance of the project is conducted through the IPFnet Steering Group
Principal investigators have lead responsibilities in all aspects of their trials and the project
including any modification of trial designs conduct of the trials quality control data analysis
and interpretation preparation of publications and collaboration with other investigators unless
otherwise provided for by the IPFnet Steering Group
PIs retain custody of and have primary rights to their center-specific and collaborative data
subject to government rights-of-access consistent with current Health amp Human Services (HHS)
Public Health Service (PHS) and National Institutes of Health policies The protocols and
governance policies call for the continual submission of data centrally to the IPFnet DCC for the
collaborative database which at a minimum will contain the key variables selected by the IPFnet
Steering Group for standardization across all clinical centers the submission of copies of the
collaborative datasets to each PI upon completion of the project procedures for data analysis
reporting and publication and procedures to protect and ensure the privacy of medical and
genetic data and records of individuals The NHLBI project scientist on behalf of the NHLBI
will have the same access privileges and responsibilities regarding the collaborative data as the
other members of the Steering Group
62
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
PIs are also encouraged to publish and to publicly release and disseminate results data and other
products of the project concordant with the project protocols and governance and the approved
plan for making data and materials available to the scientific community and to the NHLBI
However during the 3 years after the ending date of NHLBI project support unpublished data
unpublished results data sets not previously released and other study materials or products are
to be made available to any third party only with the approval of the IPFnet Steering Group
Upon completion of the project PIs are expected to put their intervention materials and
procedure manuals into the public domain andor make them available to other investigators
according to the approved plan for making data and materials available to the scientific
community and the NHLBI for the conduct of research at no charge other than the costs of
reproduction and distribution
The NHLBI reserves the right to terminate or curtail the project (or an individual award) in the
event of (a) failure to develop or implement mutually agreeable collaborative measurement
subject eligibility and data management sections of the protocols (b) substantial shortfall in
subject recruitment follow-up data reporting or quality control or other major breach of
protocol (c) substantive changes in the agreed-upon protocols with which NHLBI cannot
concur (d) reaching a major project outcome with persuasive statistical significance
substantially before schedule or (e) human subject ethical issues that may dictate a premature
termination
Any disagreement that may arise in scientificprogrammatic matters (within the scope of the
award) between award recipients and the NHLBI may be brought to arbitration An arbitration
panel will be composed of 3 membersmdash1 selected by the IPFnet Steering Group (with the
NHLBI member not voting) or by the individual PI in the event of an individual disagreement a
second selected by NHLBI and the third selected by the other 2 members This special
arbitration procedure in no way affects the PIrsquos right to appeal an adverse action that is otherwise
appealable in accordance with the PHS regulations at 42 CFR part 50 Subpart D and HHS
63
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
regulation at 45 CFR part 16 or the rights of the NHLBI under applicable statutes regulations
and terms of the award
102 IPFnet Steering Group
The IPFnet Steering Group is the main governing body of the project It is composed of the PIs
of the clinical centers the PI of the DCC and the NHLBI project scientist The clinical centers
the IPFnet DCC and the NHLBI each have 1 vote on the IPFnet Steering Group All decisions
are determined by majority vote
All major scientific decisions are determined by the IPFnet Steering Group It assumes overall
responsibility for the design and conduct of the trial It appoints (and disbands) committees and
subcommittees as the need arises designs approves and implements the study protocols
oversees the development of the MOOP monitors subject recruitment and treatment delivery
evaluates data collection and management oversees quality assurance procedures and
implements changes and enhancements to the study as required It also has primary responsibility
for facilitating the conduct of the trials and reporting the projectrsquos results
103 Data and Safety Monitoring Board
The NHLBI will establish a DSMB in accordance with established policies (see
httpwwwnhlbinihgovfundingpoliciesdsmb_insthtm) to ensure data quality and subject
safety and to provide independent advice to the NHLBI regarding progress and the
appropriateness of study continuation
104 Recommendations on Interim Monitoring of Efficacy Safety and Futility
First and foremost the role of the DSMB will be to review subject safety and trial conduct at
periodic points during the study The DSMB may require analyses of the primary endpoint
results for comparing the benefit and risks of treatment strategies The benefit of collecting
additional data on key secondary endpoints with extended follow-up and establishing a robust
64
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
evidence base for determining a standard of care will need to be carefully considered before
early termination of one or more treatment arms After careful consideration the IPFnet Steering
Group recommends conservative thresholds for the early examinations of the safety and efficacy
data
The DSMB will be expected to meet approximately every 6 months until trial completion to
review safety and toxicity data The DSMB may recommend stopping the study based on these
reviews Because the DSMB could stop the trial for safety concerns as well as for a large
efficacy benefit there could be multiple opportunities to reject the null hypothesis (no difference
in event rates between the PL and NAC groups) A Bonferroni approximation will be applied
during the one planned interim analysis for efficacy
Before locking the database a statistical analysis plan (SAP) will be developed to provide
complete details on the statistical analysis The SAP will include the specifics for how and when
the DSMB will be notified for AEs The IPFnet DCC will deliver to the DSMB all FDA-defined
AEs at 3-month intervals The IPFnet DCC will prepare narrative SAE reports in real time for
DSMB review including recommendations and analysis of similar events for each SAE
submitted to the FDA
65
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
11 Investigator and Sponsor Obligations
111 Monitoring
All monitoring activities for US clinical centers will be performed in accordance with DCRI
standard operating procedures Information regarding the types of visits will be outlined in the
PANTHER-IPF MOOP
112 Cost and Payment
There will be no cost to subjects enrolled in this trial Study-related procedures will be paid for
by the IPFnet
Subjects may be eligible for reimbursement for travel to the clinical center Details of payment
will be explained to each subject during the consent process
113 Confidentiality and Health Insurance Portability and Accountability Act
Considerations
Subject confidentiality will be protected throughout the study All subject data will be kept
strictly confidential and no subject-identifying information will be released to anyone outside
the project Confidentiality will be assured through several mechanisms First each subject will
be assigned an anonymous study ID which will then be used on all study forms Second any
study forms blood samples and paper records that contain subject information (eg address lists
phone lists) will be kept at the clinical centers in secured locked areas coded by number Once
blood is collected there will be no subject identifiers placed on blood samplesmdashonly the study
ID number and the date of sample collection Third access to all subject data and information
including laboratory specimens will be restricted to authorized personnel In the case of
computerized data this restricted access will be assured through user logon IDs and password
protection
66
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
At the IPFnet DCC only authorized personnel will have access to the data files containing study
data Security will be assured through user logon IDs passwords and appropriate access
privileges All study subjects will be identified only by their IPFnet ID numbers and no personal
identifying information such as name address or Social Security number will be entered into
the IPFnet DCC database Any subject-specific data reported to the IPFnet Steering Group will
be identified only by the IPFnet ID number
Finally subjects will not be identified by name in any reports or publications nor will the data
be presented in such a way that the identity of individual subjects can be inferred Analysis files
created for further study by the scientific community will have no subject identifiers These data
files will be created in accordance with the Ancillary Studies and Publication Policy of the
IPFnet
114 Informed Consent Procedures
All IPFnet subjects will provide written informed consent using procedures reviewed and
approved by each clinical centerrsquos IRB Informed consent will be undertaken by study personnel
in-person with the subject The subject has the option of declining further participation in the
study at that point No further study procedures will be conducted until the signed documents
have been provided to the IPFnet clinical center
115 Institutional Review Boards
Before initiating this study the protocol clinical center-specific informed consent forms Health
Insurance Portability and Accountability Act (HIPAA) forms recruitment materials and other
relevant information will be reviewed by a properly constituted IRB at each participating clinical
center A copy of the signed and dated IRB approval at each clinical center will be retrieved prior
to or during the site initiation visit and archived at the IPFnet DCC Any amendments to the
protocol other than simple administrative and typographical changes must be approved by each
IRB before they are implemented The clinical centers will seek annual renewals of their IRB
approvals in accordance with local procedures
67
__________________________________________ ________________
__________________________________________
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
12 Investigator Agreement
I have read the foregoing protocol PANTHER-IPF and agree that it contains all necessary
details for carrying out this study I will conduct the study as outlined herein and will complete
the study within the time designated
I will provide copies of the protocol and all pertinent information to all individuals responsible to
me who assist in the conduct of this study I will discuss this material with them to ensure they
are fully informed regarding the drug and the conduct of the study
I will fulfill all responsibilities for submitting pertinent information to the local IRB if
applicable that is responsible for this study
I further agree that NHLBI andor DCRI will have access to any source documents from which
eCRF information may have been generated
Signature of Principal Investigator Date
Name of Principal Investigator (printed or typed)
Protocol version date May 19 2009
Protocol Amendment 1 version date May 28 2010
Protocol Amendment 2 version date December 6 2011
68
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
13 References
1 Raghu G Brown KK Bradford WZ et al A placebo-controlled trial of interferon gamma-1b in patients with idiopathic pulmonary fibrosis N Engl J Med 2004350125-33 2 King TE Jr Safrin S Starko KM et al Analyses of efficacy end points in a controlled trial of interferon-gamma1b for idiopathic pulmonary fibrosis Chest 2005127171-7 3 Flaherty KR Thwaite EL Kazerooni EA et al Radiological versus histological diagnosis in UIP and NSIP survival implications Thorax 200358143-8 4 Wells AU Desai SR Rubens MB et al Idiopathic pulmonary fibrosis a composite physiologic index derived from disease extent observed by computed tomography Am J Respir Crit Care Med 2003167962-9 5 Raghu G Freudenberger TD Yang S et al High prevalence of abnormal acid gastroshyoesophageal reflux in idiopathic pulmonary fibrosis Eur Respir J 200627136-42 6 Kinnula VL Focus on antioxidant enzymes and antioxidant strategies in smoking related airway diseases Thorax 200560693-700 7 Coultas DB Zumwalt RE Black WC Sobonya RE The epidemiology of interstitial lung diseases Am J Respir Crit Care Med 1994150967-72 8 Raghu G Weycker D Edelsberg J Bradford WZ Oster G Incidence and prevalence of idiopathic pulmonary fibrosis Am J Respir Crit Care Med 2006174810-6 9 Olson AL Swigris JJ Lezotte DC Norris JM Wilson CG Brown KK Mortality from pulmonary fibrosis increased in the United States from 1992 to 2003 Am J Respir Crit Care Med 2007176277-84 10 Mannino DM Etzel RA Parrish RG Pulmonary fibrosis deaths in the United States 1979shy1991 An analysis of multiple-cause mortality data Am J Respir Crit Care Med 19961531548shy52 11 Hubbard R Johnston I Coultas DB Britton J Mortality rates from cryptogenic fibrosing alveolitis in seven countries Thorax 199651711-6 12 Johnston I Britton J Kinnear W Logan R Rising mortality from cryptogenic fibrosing alveolitis Bmj 19903011017-21 13 Raghu G Collard HR Egan JJ et al An official ATSERSJRSALAT statement idiopathic pulmonary fibrosis evidence-based guidelines for diagnosis and management Am J Respir Crit Care Med 2011183788-824 14 (USA) FDA FDA Public Health Advisory Interferon gamma-1b (marketed as Actimmune) In 2007 15 King TE Jr Pardo A Selman M Idiopathic pulmonary fibrosis Lancet 2011 16 Raghu G Brown KK Costabel U et al Treatment of idiopathic pulmonary fibrosis with etanercept an exploratory placebo-controlled trial Am J Respir Crit Care Med 2008178948shy55 17 Malouf MA Hopkins P Snell G Glanville AR An investigator-driven study of everolimus in surgical lung biopsy confirmed idiopathic pulmonary fibrosis Respirology 201116776-83 18 King TE Jr Behr J Brown KK et al BUILD-1 a randomized placebo-controlled trial of bosentan in idiopathic pulmonary fibrosis Am J Respir Crit Care Med 200817775-81 19 Richeldi L Costabel U Selman M et al Efficacy of a tyrosine kinase inhibitor in idiopathic pulmonary fibrosis N Engl J Med 20113651079-87
69
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
20 Borok Z Buhl R Grimes GJ et al Effect of glutathione aerosol on oxidant-antioxidant imbalance in idiopathic pulmonary fibrosis Lancet 1991338215-6 21 Meyer A Buhl R Magnussen H The effect of oral N-acetylcysteine on lung glutathione levels in idiopathic pulmonary fibrosis Eur Respir J 19947431-6 22 Behr J Maier K Degenkolb B Krombach F Vogelmeier C Antioxidative and clinical effects of high-dose N-acetylcysteine in fibrosing alveolitis Adjunctive therapy to maintenance immunosuppression Am J Respir Crit Care Med 19971561897-901 23 Cantin AM North SL Fells GA Hubbard RC Crystal RG Oxidant-mediated epithelial cell injury in idiopathic pulmonary fibrosis J Clin Invest 1987791665-73 24 Waghray M Cui Z Horowitz JC et al Hydrogen peroxide is a diffusible paracrine signal for the induction of epithelial cell death by activated myofibroblasts Faseb J 200519854-6 25 Larios JM Budhiraja R Fanburg BL Thannickal VJ Oxidative protein cross-linking reactions involving L-tyrosine in transforming growth factor-beta1-stimulated fibroblasts J Biol Chem 200127617437-41 26 Kinnula VL Fattman CL Tan RJ Oury TD Oxidative stress in pulmonary fibrosis a possible role for redox modulatory therapy Am J Respir Crit Care Med 2005172417-22 27 Meyer A Buhl R Kampf S Magnussen H Intravenous N-acetylcysteine and lung glutathione of patients with pulmonary fibrosis and normals Am J Respir Crit Care Med 19951521055-60 28 Behr J Degenkolb B Krombach F Vogelmeier C Intracellular glutathione and bronchoalveolar cells in fibrosing alveolitis effects of N-acetylcysteine Eur Respir J 200219906-11 29 Bando M Hosono T Mato N et al Long-term efficacy of inhaled N-acetylcysteine in patients with idiopathic pulmonary fibrosis Intern Med 2010492289-96 30 Demedts M Behr J Buhl R et al High-dose acetylcysteine in idiopathic pulmonary fibrosis N Engl J Med 20053532229-42 31 Toma TP Bhowmik A Rajakulasingam R Acetylcysteine in pulmonary fibrosis N Engl J Med 20063541086-9 author reply -9 32 Hunninghake GW Antioxidant therapy for idiopathic pulmonary fibrosis N Engl J Med 20053532285-7 33 Flaherty KR Mumford JA Murray S et al Prognostic implications of physiologic and radiographic changes in idiopathic interstitial pneumonia Am J Respir Crit Care Med 2003168543-8 34 Latsi PI du Bois RM Nicholson AG et al Fibrotic idiopathic interstitial pneumonia the prognostic value of longitudinal functional trends Am J Respir Crit Care Med 2003168531-7 35 Collard HR King TE Jr Bartelson BB Vourlekis JS Schwarz MI Brown KK Changes in clinical and physiologic variables predict survival in idiopathic pulmonary fibrosis Am J Respir Crit Care Med 2003168538-42 36 Jegal Y Kim DS Shim TS et al Physiology is a stronger predictor of survival than pathology in fibrotic interstitial pneumonia Am J Respir Crit Care Med 2005171639-44 37 Martinez FJ Safrin S Weycker D et al The clinical course of patients with idiopathic pulmonary fibrosis Ann Intern Med 2005142963-7 38 Hull JH Acetylcysteine in pulmonary fibrosis N Engl J Med 20063541089-91 author reply -91
70
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
39 Flaherty KR King TE Jr Raghu G et al Idiopathic interstitial pneumonia what is the effect of a multidisciplinary approach to diagnosis Am J Respir Crit Care Med 2004170904shy10 40 Raghu G Johnson WC Lockhart D Mageto Y Treatment of idiopathic pulmonary fibrosis with a new antifibrotic agent pirfenidone results of a prospective open-label Phase II study Am J Respir Crit Care Med 19991591061-9 41 Hunninghake GW Lynch DA Galvin JR et al Radiologic findings are strongly associated with a pathologic diagnosis of usual interstitial pneumonia Chest 20031241215-23 42 Lynch D Godwin J Safrin S et al High-resolution computed tomography in idiopathic pulmonary fibrosis diagnosis and prognosis Am J Respir Crit Care Med 2005172488-93 43 Mallinckrodt CH Watkin JG Molenberghs G Carroll RJ Choice of the primary analysis in longitudinal clinical trials Pharmaceutical Statistics 20043161-9 44 Bang H Tsiatis A Estimating medical costs with censored data Biometrika 200087329shy43 45 Lin DY Regression analysis of incomplete medical cost data Stat Med 2003221181-200 46 Rochon J Application of GEE procedures for sample size calculations in repeated measures experiments Stat Med 1998171643-58 47 Lachin JM Foulkes MA Evaluation of sample size and power for analyses of survival with allowance for nonuniform patient entry losses to follow-up noncompliance and stratification Biometrics 198642507-19
71
- PANTHER-IPFPREDNISONE AZATHIOPRINEAND N-ACETYLCYSTEINEA STUDY THAT EVALUATES RESPONSE INIDIOPATHIC PULMONARY FIBROSIS
-
- Protocol Summary
- Table of Contents
- List of Tables
- List of Figures
- List of Abbreviations
- 1 Summary
- 2 Hypotheses and Specific Aims
-
- 21 Null Hypothesis
- 22 Specific Aim 1
- 23 Specific Aim 2
- 24 Prespecified Subgroups of Interest
-
- 3 Background and Significance
-
- 31 Idiopathic Pulmonary Fibrosis is the Most Common Interstitial Lung Disease
- 32 Rationale for Placebo Control
- 33 Rationale for N-acetylcysteine
- 35 Rationale for N-acetylcysteine as a Stand-alone Therapy
- 36 Rationale for the Study Design and Primary Endpoint
- 37 Rationale for Blinding of Treatments
-
- 4 Methods
-
- 41 Inclusion Criteria
- 42 Diagnosis of IPF
- 43 Exclusion Criteria
- 44 Study Design and Study Visit
- 45 Dose Justification
- 46 Contraindications Precautions and Side Effects of Study Medications
- 47 Recruitment Procedures
- 48 Study Procedures
- 49 Concomitant Medications
- 410 Laboratory Testing
- 411 Blinding of Study Drugs
-
- 5 Study Endpoints
-
- 51 Primary Study Endpoint
- 52 Secondary Study Endpoints
-
- 6 Safety Evaluations and Procedures
-
- 61 Adverse Events
- 62 Clinical Medical Monitoring
- 63 Unblinding Procedures
-
- 7 Study Drug Procedures
- 8 Data Management
-
- 81 Hardware and Software Configuration
- 82 Sources of Data
-
- 9 Study Design and Data Analysis
-
- 91 General Analytic Considerations
- 92 Randomization Blinding and Reporting of Results
- 93 Stratification
- 94 Specification of the Primary Analyses
- 95 Analysis of Longitudinal Endpoints
- 96 Analysis of Binary Time-to-Event and Time-Lagged Endpoints
- 97 Power Analysis
-
- 10 Study Administration
-
- 101 Cooperative Agreement Mechanism
- 102 IPFnet Steering Group
- 103 Data and Safety Monitoring Board
- 104 Recommendations on Interim Monitoring of Efficacy Safety and Futility
-
- 11 Investigator and Sponsor Obligations
-
- 111 Monitoring
- 112 Cost and Payment
- 113 Confidentiality and Health Insurance Portability and Accountability ActConsiderations
- 114 Informed Consent Procedures
- 115 Institutional Review Boards
-
- 12 Investigator Agreement
- 13 References
-
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Study Sponsor National Heart Lung and Blood Institute
Acting Steering Group Chair Marvin I Schwarz MD University of Colorado - Denver
Project Officer
Gail Weinmann MD National Heart Lung and Blood Institute Bethesda MD
Protocol Committee Cochairs
Ganesh Raghu MD University of Washington
Fernando J Martinez MD University of Michigan
Data Coordinating Center
Duke Clinical Research Institute Duke University
3
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Table of Contents
List of Tables 7
List of Figures 7
List of Abbreviations 8
1 Summary 12
2 Hypotheses and Specific Aims 13 21 Null Hypothesis 13 22 Specific Aim 1 13 23 Specific Aim 2 13 24 Prespecified Subgroups of Interest 14
3 Background and Significance 15 31 Idiopathic Pulmonary Fibrosis is the Most Common Interstitial Lung Disease15 32 Rationale for Placebo Control 15 33 Rationale for N-acetylcysteine 16 35 Rationale for N-acetylcysteine as a Stand-alone Therapy 17 36 Rationale for the Study Design and Primary Endpoint 18 37 Rationale for Blinding of Treatments 19
4 Methods 21 41 Inclusion Criteria 21
411 Subjects Shown to Have Usual Interstitial Pneumonia Pattern on Surgical Lung Biopsy 21 412 Subjects Who Have Not Undergone a Surgical Lung Biopsy 21
42 Diagnosis of IPF 21 43 Exclusion Criteria 26 44 Study Design and Study Visit 27
441 Study Design Summary 27 442 Study Visits 28
4421 Screening 28 4422 Enrollment 29 4423 Week 15 30 4424 Week 30 31 4425 Week 45 31 4426 Week 60 (Early Withdrawal or Final Treatment Visit) 32 4427 Final Site Visit ndash FVC drop confirmation 33 4428 Final Visit ndash Telephone Follow-up 33 4429 Phone Contact Between Visits 33
45 Dose Justification 35 451 Rationale for N-acetylcysteine Dosing 35
4511 Dosing of N-acetylcysteineplacebo 35 4512 Reasons to Discontinue N-acetylcysteineplacebo 35
452 Dosage Algorithms 37 46 Contraindications Precautions and Side Effects of Study Medications 39
461 Contraindication 39 462 Precautions 39 463 Side Effects 39
47 Recruitment Procedures 40 48 Study Procedures 41
481 Biological Specimen Management 41 4811 Biological Specimen Sample Management 41
49 Concomitant Medications 42 410 Laboratory Testing 42 411 Blinding of Study Drugs 43
4
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
5 Study Endpoints 44 51 Primary Study Endpoint 44 52 Secondary Study Endpoints 44
521 Time to Disease-progression 44 522 Acute Exacerbations 44 523 Respiratory Infections 47 524 Maintained FVC Response 48
6 Safety Evaluations and Procedures 49 61 Adverse Events 49
611 Definitions 49 612 Adverse Event (AE) Reporting 50
6121 Serious Adverse Events (SAE) Reporting 50 6122 Regulatory Reporting 51
62 Clinical Medical Monitoring 52 63 Unblinding Procedures 52
7 Study Drug Procedures 53
8 Data Management 54 81 Hardware and Software Configuration 54
811 Hardware and Database Software 54 812 Statistical Software 54 813 Access Control and Confidentiality Procedures 54 814 Security 54 815 Back-up Procedures 55 816 Virus Protection 55
82 Sources of Data 55 821 Design and Development 55 822 Data Collection Forms 55 823 Data Acquisition and Entry 56 824 Data Center Responsibilities 56 825 Data Editing 56 826 Training 56
9 Study Design and Data Analysis 57 91 General Analytic Considerations 57 92 Randomization Blinding and Reporting of Results 57 93 Stratification 58 94 Specification of the Primary Analyses 58 95 Analysis of Longitudinal Endpoints 58 96 Analysis of Binary Time-to-Event and Time-Lagged Endpoints 59 97 Power Analysis 60
971 Primary Analyses 60 972 Power Analysis for Secondary Endpoints 61
10 Study Administration 62 101 Cooperative Agreement Mechanism 62 102 IPFnet Steering Group 64 103 Data and Safety Monitoring Board 64 104 Recommendations on Interim Monitoring of Efficacy Safety and Futility 64
11 Investigator and Sponsor Obligations 66 111 Monitoring 66 112 Cost and Payment 66 113 Confidentiality and Health Insurance Portability and Accountability Act Considerations 66 114 Informed Consent Procedures 67 115 Institutional Review Boards 67
5
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
12 Investigator Agreement 68
13 References 69
6
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
List of Tables Table 1 Operating Characteristics of Local HRCT Review for Diagnosis of UIP (24)
Table 2 Combining HRCT and Pathology Interpretations to Determine if IPF is Present (25)
Table 3 Schedule of Assessments (34)
Table 4 Side Effects of NAC (40)
Table 5 Final Diagnoses in Evaluation of Suspected Acute Exacerbations (46)
Table 6 Hypothetical Values of Mean FVC (L) Change from Baseline (61)
Table 7 Detectable Differences in Treatment Means for Selected Endpoint Measurements (61)
List of FiguresFigure 1 Changes in Forced Vital Capacity from Baseline in Prior IPF Clinical Trials (19)
Figure 2 Diagnosis of Idiopathic Pulmonary Fibrosis in the IPFnet (22)
Figure 3 Pathology Flow Chart Surgical Lung Biopsy Diagnosis (23)
Figure 4 Acute Exacerbation Flow Chart (47)
7
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
List of Abbreviations
6MWT 6-minute walk test
A-aPO2 alveolar-arterial PO2 difference
ABG arterial blood gas
AE adverse event
AEx acute exacerbation
AG albuminglobulin
ALT alanine aminotransferase
AST aspartate aminotransferase
ATS American Thoracic Society
AZA azathioprine
BAL bronchoalveolar lavage
BUN blood urea nitrogen
CBC complete blood count
cGMP Current Good Manufacturing Practice
CPI Composite Physiologic Index
CPK creatine phosphokinase
CT computed tomography
DCC Data Coordinating Center
DCRI Duke Clinical Research Institute
8
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
DLCO diffusing capacity of the lung for carbon monoxide
DLCOpred diffusing capacity of the lung for carbon monoxide percent predicted
DSMB data and safety monitoring board
eCRF Electronic case report form
ERS European Respiratory Society
FDA Food and Drug Administration (US)
FEV1 forced expiratory volume in 1 second
FSH follicle-stimulating hormone
FVC forced vital capacity
FVCpred forced vital capacity percent predicted
GGT gamma glutamyl transferase
GSH glutathione
HAD Hospital Anxiety and Depression
HHS Health amp Human Services (US Dept of)
HIPAA Health Insurance Portability and Accountability Act
HRCT high-resolution computed tomography
IBW ideal body weight
ICE CAP Investigating Choice Experiments for Preferences of Older People Capability Instrument
ILD interstitial lung disease
IPF idiopathic pulmonary fibrosis
9
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
IPFnet Idiopathic Pulmonary Fibrosis Clinical Research Network
IRB institutional review board
ITT intent to treat
IV intravenous
IVRS interactive voice response system
LDH lactate dehydrogenase
LFT liver function test
LOCF last observation carried forward
LSD Least Significant Difference
MAR missing at random
MCAR missing completely at random
MMRM mixed model repeated measures
MOOP manual of operating procedures
NAC N-acetylcysteine
NHLBI National Heart Lung and Blood Institute (US)
NIH National Institutes of Health (US)
NSIP nonspecific interstitial pneumonia
PaO2 partial pressure of arterial oxygen
PCP primary care provider
PFT pulmonary function test
10
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
PHS Public Health Service (US)
PI principal investigator
PL placebo
PLT platelet
PRED prednisone
QOL quality of life
SAE serious adverse event
SAP statistical analysis plan
SGRQ St Georgersquos Respiratory Questionnaire
SpO2 oxygen saturation by pulse oximetry
TPMT thiopurine methyl transferase
UCSD SOBQ University of California at San Diego Shortness of Breath Questionnaire
UIP usual interstitial pneumonia
ULN upper limit of normal
USP United States Pharmacopoeia
VC vital capacity
WBC white blood cell
11
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
PREDNISONE AZATHIOPRINE AND N-ACETYLCYSTEINE A STUDY
THAT EVALUATES RESPONSE IN IDIOPATHIC PULMONARY FIBROSIS
1 Summary
There are currently no drug therapies that have proven to be effective in the treatment of idiopathic pulmonary
fibrosis (IPF) Previous clinical drug trials have been difficult to interpret due to lack of true placebo (PL)
controls or other methodological concerns Clinical efficacy of immunosuppressive therapies and agents that
reduce oxidative stress remains controversial The IPF Clinical Research Network (IPFnet) is conducting a
randomized double-blind placebo-controlled trial designed to assess the safety and efficacy of
N-acetylcysteine (NAC) as monotherapy in subjects with mild or moderate IPF
The study initially employed a 3-arm design with 111 randomization to NAC azathioprine (AZA)-prednisone
(PRED)-NAC and PL with each subject to be treated up to a maximum of 60 weeks followed by a tapering of
PREDPL and a 4-week period for safety evaluation Approximately 390 subjects who have mild to moderate
IPF (defined as forced vital capacity percent predicted [FVCpred] ge 50 and diffusing capacity of the lung
for carbon monoxide percent predicted [DLCOpred] 30) diagnosed within the past 48 months were to be
enrolled
At the pre-specified interim analysis the DSMB recommended termination of the prednisone-azathioprine-
NAC arm of the study No additional patients will be randomized to that arm However the NAC and placebo
arms remain open for enrollment and we will enroll approximately 130 subjects in each arm (inclusive of the
subjects enrolled at the time of the interim analysis) Follow up for subjects enrolled into the two arms will
continue for 60 weeks
The primary endpoint is the change in longitudinal measurements of FVC over the study period The primary
goal of this study to establish an evidence-based standard of care and clarify myths from facts for
pharmacotherapy of IPF has been met in part by demonstrating that the widely used triple therapy was harmful
to patients with IPF (NHLBI press release Oct 21 2011) To determine the potential therapeutic benefits of
NAC alone the study will continue to enroll patients as a two-arm double-blind placebo-controlled study from
this point on (NAC vs placebo) as recommended by the DSMB following the pre-specified interim analysis
12
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
2 Hypotheses and Specific Aims 21 Null Hypothesis
Treatment with NAC will provide the same efficacy as PL as measured by longitudinal changes in FVC
22 Specific Aim 1
This study is designed to assess the safety and efficacy of NAC in subjects with newly diagnosed IPF
23 Specific Aim 2
Secondary goals of this study are to assess differences between treatment groups for the following
1 Mortality
2 Time to death
3 Frequency of acute exacerbations (AExs)
4 Frequency of maintained FVC response
5 Time-to-disease progression
6 Change in DLCO
7 Change in Composite Physiologic Index (CPI)
8 Change in resting alveolar-arterial oxygen gradient
9 Change in 6-minute walk test (6MWT) distance
10 Change in 6MWT oxygen saturation area under the curve
11 Change in 6MWT distance to desaturation lt 80
12 Change in 6MWT minutes walked
13 Changes in health status as measured by the SF-36 EuroQol and St Georgersquos Respiratory
Questionnaire (SGRQ)
14 Changes in dyspnea as measured by the University of California at San Diego Shortness of Breath
Questionnaire (UCSD SOBQ)
15 Frequency and types of adverse events (AEs)
16 Frequency and types of respiratory complications both infectious and noninfectious
17 Frequency of hospitalizations both all-cause and respiratory-related
13
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
24 Prespecified Subgroups of Interest
Treatment effects will be estimated and compared within key subgroups
Higher enrollment FVC12
Typical vs atypical high-resolution computed tomography (HRCT) reading at baseline3
Recent vs more remote diagnosis (time from initial diagnosis of IPF le 1 year and gt 1 year)
Lower CPI score at enrollment4
Medical therapy for gastroesophageal reflux5
Ethnic background
Sex
Smoking history (current or ex-smoker vs never smoker) given potential impact on oxidant status6
Presence of emphysema gt 25 on HRCT
14
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
3 Background and Significance
31 Idiopathic Pulmonary Fibrosis is the Most Common Interstitial Lung Disease
IPF is the most common interstitial lung disease (ILD) of unknown etiology The current incidence and
prevalence of IPF in the United States are not known A 1994 study of a population-based registry of subjects in
Bernalillo County New Mexico USA estimated an incidence of 107 cases per 100000 per year for males and
74 cases per 100000 per year for females the prevalence of IPF was estimated at 20 per 100000 for males and
13 per 100000 for females7 Extrapolating from a large healthcare claims database a more recent review
estimated the prevalence of IPF in the United States at 427 per 100000 (incidence estimated at 163 per
100000 per year)8 Recent epidemiological studies indicate increasing mortality rates from IPF in the United
States and other industrialized nations9-12
Approximately two-thirds of subjects with IPF are over the age of 60 at the time of presentation and the
incidence increases with age13 IPF has no distinct geographical distribution and predilection by race or
ethnicity has not been identified13 Individual subjects may remain relatively stable for prolonged periods
experience very slow declines in lung function with progression of radiographic abnormalities for a period of
months to years or experience more rapid declines and subsequent death Only 20 to 30 of IPF patients
survive for 5 years following diagnosis
There is currently no proven effective pharmacological treatment for IPF13 Anti-inflammatory and
immunosuppressive agents have been the traditional approach to the management of patients with IPF Based
on the results of the interim analysis of the PANTHER-IPF trial this lsquotraditional approachrsquo will be aborted
However it remains unknown if NAC alone will prove beneficial in IPF patients The primary goal of the
modified study is to establish an evidence-based standard of care and clarify the role of this specific antioxidant
pharmacotherapy for IPF
32 Rationale for Placebo Control
IPF is a disorder for which there is no proven efficacious therapy A major objective of this trial is to test to the
greatest degree possible a proposed standard of care for patients with IPF The current traditional therapy
15
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
employs immunosuppressive and corticosteroid drugs Interim review of the original PANTHER-IPF study has
documented increased adverse events and lack of efficacy for AZA-PRED-NAC compared to placebo
suggesting that this therapeutic approach should not be employed Whether this applies to NAC alone which
has been advocated by international societies has not been proven in well-designed well-powered clinical
trials The recommendations made in the recently published evidence guidelines for NAC monotherapy was
weak based on low quality13 Thus this continued clinical trial randomizing patients to receive NAC or placebo
is pivotal and will answer the important question of the potential therapeutic benefits of NAC monotherapy with
grade A evidence In this prospective randomized clinical trial the inclusion of a PL arm is therefore vital to
adequately test the benefits of NAC in well-characterized subjects with IPF
If NAC has no true efficacy then its role as standard of care will be refuted If a benefit compared with PL is
confirmed it will establish a benchmark against which future novel therapies for IPF will be safely compared
As there is no currently accepted therapy for IPF there is an increasing body of published literature supporting
the concept of no treatment as the ldquobest carerdquo option for IPF13
Post hoc analyses of PL-controlled trials suggest that subjects with milder disease may be more amenable to
therapy12 It is notable that a recent international prospective randomized trial of interferon-gamma for IPF
also included a PL arm the study was terminated early by the data and safety monitoring board (DSMB) due to
lack of treatment effect1415 This underscores the belief that a proven effective therapy for IPF does not
currently exist and that true placebo-controlled trials remain the gold standard Similarly recently completed
trials of etanercept everolimus bosentan and BIPF 1120 in IPF have included PL-treated arms16-19 In three of
these trials the treated subjects showed little if any objective improvement Based on this evidence and the
current status of IPF therapy and therapeutic trials we believe that clinicians and subjects will continue to enroll
in a PL-controlled study
33 Rationale for N-acetylcysteine
NAC is a derivative of the amino acid L-cysteine NAC has been shown to augment levels of the naturally
occurring antioxidant glutathione (GSH ) (glutathione γ-glutamyl cysteinyl glycine) both in vitro and in
vivo2021 GSH is present in all eukaryotic cells and may play an important role in protecting alveolar epithelial
cells against oxidant injury The concentration of GSH in the bronchoalveolar lavage (BAL) fluid in patients
16
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
with IPF is markedly diminished compared with normal subjects This GSH deficiency may be corrected by
exogenous administration of NAC2122
There is evidence of enhanced production of oxidants in an IPF lung Both inflammatory cells and
myofibroblasts derived from patients with IPF generate increased amounts of extracellular oxidants including
hydrogen peroxide2324 Secretion of hydrogen peroxide by activated myofibroblasts may induce the death of
adjacent lung epithelial cells by paracrine mechanisms24 Additionally generation of oxidants by myofibroblasts
induces oxidative crosslinking of extracellular matrix proteins25 a potential mechanism for aberrant matrix
remodeling Thus an oxidant-antioxidant imbalance exists in the lungs of IPF patients26 NAC may confer
protection against this imbalance by augmenting GSH levels in addition to its more direct free-radical
scavenging activity
Intravenous (IV) NAC therapy has been shown to increase total BAL GSH in 8 IPF subjects27 Oral NAC (600
mg 3 times per day) has been shown to decrease markers of oxidant injury and improve both total and reduced
GSH levels in the epithelial lining fluid of subjects with IPF in a small uncontrolled study22 pulmonary
function improved modestly with therapy A similar study in 18 IPF subjects confirmed increased intracellular
GSH concentration after 12 weeks of NAC (600 mg 3 times per day)2228 no clinical correlates were reported
Inhaled NAC was suggested to improve pulmonary function in an open label study29
35 Rationale for N-acetylcysteine as a Stand-alone Therapy
Results of a double-blind multi-center European clinical trial of 150 IPF subjects testing combinations of AZAshy
PRED vs AZA-PRED-NAC have been reported30 NAC added to AZA-PRED (ldquoconventional therapyrdquo) had a
significant positive effect on DLCO (p lt 0005) and vital capacity (VC) (p lt 005) at the end of 1 year30 The
recent ATSERS position statement after much discussion concluded that NAC alone should not be considered
in the majority of patients with IPF without additional data from well-designed studies
The interpretation of these data has been quite controversial Some have suggested that the magnitude of the
treatment effect although statistically significant is modest31 Others have suggested that NAC may be
modulating potential toxic effects of AZA-PRED alone32 supporting the investigation of NAC as stand-alone
therapy
17
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
The IPFnet is now completing the PANTHER-IPF trial with a 11 randomization (NAC vs placebo) and a
simple practical feasible and scientifically rational design that will establish standard of care with NAC for
IPF based on a currently available therapeutic agent and the existing data to support its use We anticipate that
all future clinical trials of novel therapeutic agents will be tested against this to-be-established standard of care
36 Rationale for the Study Design and Primary Endpoint
The optimal study design of a therapeutic trial in IPF would include survival as a primary endpoint The
published results of the IFN-γ 1b Phase 3 (GIPF-001) trial suggested a survival benefit in subjects with milder
disease in retrospective analyses1 although the trial was underpowered to address this question This was likely
related to the limited mortality in the PL arm of the study which included IPF subjects with mild to moderate
disease This study documents that an IPF study powered to improve survival in a patient population with mild
disease requires a larger sample size andor duration of study In fact the recently aborted Phase 3 IFN-γ 1b
(GIPF-007 INSPIRE) study was a survival-based study and recruited more than 800 subjects at 75 centers
worldwide1415 As such within the context of the current IPFnet trial survival is an impractical primary
endpoint variable
Several groups have published data defining an appropriate surrogate outcome variable a 10 decrement in
FVC during 6 to 12 months is a powerful predictor of survival in IPF33-36 Furthermore additional evidence
suggests a similar predictive ability for a 10 decrement in FVC during 3 months of follow-up37 With strong
supportive evidence of FVC progression being related to mortality on a per-subject basis this study will use
FVC changes in liters between treatment groups as the primary endpoint Previously published IPF studies have
shown a steady decline in FVC (and FVCpred) among control group subjects230 The GIPF-001 study
suggested a 48-week decrease in FVC of 016 L in the PL-treated subjects The IFIGENIA study demonstrated
a decline in FVC of approximately 019 L over 52 weeks in the subjects randomized to the control treatment
Figure 1 depicts the change in FVC for control groups from previously published IPF studies38 Based on these
data we expect that the PL group will have a decline of 020 L over the 60-week study period The IPFnet
Steering Group determined that a clinically meaningful improvement would be the preservation of the majority
of the 020-L FVC decline Therefore a mean treatment difference of 015 L in mean FVC over the 60-week
study period was determined to be a clinically meaningful difference
18
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Δ f
rom
bas
elin
e (i
n L
)
01
005
0
-005
-01
-015 Projected Δ for placebo
-02
-025
-019
-016
-013 Pirfenidone GIPF001
NAC
Placebo
4 8 12 16 20 24 28 32 36 40 44 48 52 56 60
Week
Figure 1 Changes in FVC From Baseline in Prior IPF Clinical Trials
Recent data suggest that various patient subgroups would be expected to potentially exhibit differential response
to therapy These parameters will be used to a priori separate patients by a series of baseline characteristics
including
1 Higher enrollment FVC12
2 Typical vs atypical high-resolution computed tomography (HRCT) reading at baseline3
3 Recent vs more remote diagnosis (time from initial diagnosis of IPF le 1 year and gt 1 year)
4 Lower CPI score at enrollment4
5 Medical therapy for gastroesophageal reflux5
6 Ethnic background
7 Sex
8 Smoking history (current or ex-smoker vs never smoker) given potential impact on oxidant status6
9 Presence of emphysema gt 25 on HRCT
37 Rationale for Blinding of Treatments
The issue of treatment blinding was given a great deal of consideration with subject safety being the primary
concern After discussion among the Steering Group members it was decided that as long as subject safety
could be ensured blinding was necessary Blinding allows the study to
Have optimal scientific validity and potential to impact the standard of care for subjects
19
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Make objective assessments of treatment effects
Maintain clinical equipoise among investigators
Encourage subjects to have similar levels of contact with the medical community
Minimize the differential dropout rates across study arms
20
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
4 Methods 41 Inclusion Criteria
1 Age 35 to 85 years inclusive
2 FVC ge 50 of predicted (post-bronchodilator measurement from the screening visit)
3 DLCO ge 30 of predicted (hemoglobin corrected and altitude corrected if gt4000 ft above sea level)
4 Ability to understand and provide informed consent
5 Diagnosis of IPF according to a modified version of the ATS criteria le 48 months from enrollment The
date of diagnosis is defined as the date of the first available HRCT or surgical lung biopsy characteristic
of definite UIP
411 Subjects Shown to Have Usual Interstitial Pneumonia Pattern on Surgical Lung Biopsy
Subjects who have been shown to have UIP pattern on lung biopsy must have all of the following
1 Exclusion of other known causes of ILD such as drug toxicity clinically significant environmental
exposures or diagnosis of connective tissue diseases
2 Bibasilar reticular abnormalities with minimal ground glass opacities on HRCT scan
412 Subjects Who Have Not Undergone a Surgical Lung Biopsy
In addition to the criteria above these subjects must have radiological findings considered to be definite for the
diagnosis of UIPIPF
1 Bibasilar reticular abnormalities with minimal ground glass opacities
2 Honeycombing as the predominant feature and located in the peripheral lung bases
42 Diagnosis of IPF
Only subjects with definite IPF will be eligible for enrollment in this study We will utilize a combination of
clinicalphysiologic features HRCT and review of a clinically obtained surgical lung biopsy specimen to
establish the diagnosis of IPF An algorithm for the diagnosis is provided to guide entry into the protocol as
outlined in the inclusion and exclusion criteria (Figures 2 and 3) This multi-disciplinary approach uses
21
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
expertise from clinicians radiologists and pathologists Investigators at each site in conjunction with central
pathology will work together to establish the diagnosis of IPF This interactive approach to the diagnosis of IPF
increases the level of agreement between observers39
A subject with suspected ILD should be evaluated for secondary causes including but not limited to
environmental exposures drugs and systemic diseases Presence of any of these findings felt to be significant
enough to cause an ILD should disqualify the subject from entry into the trial
If secondary causes are absent an HRCT scan may be obtained If an HRCT of sufficiently high quality has
been obtained within the last 3 months that scan may be used for diagnosis In the appropriate clinical setting
the diagnosis of IPF can be made by the demonstration of a typical radiographic pattern on HRCT or by
demonstration of UIP pattern on a surgical lung biopsy The following criteria for a radiographic (ie
nonsurgical) diagnosis will be used In the absence of known exposures andor clinical associations attributable
to pulmonary fibrosis and in the appropriate clinical setting the presence of definite UIP pattern in HRCT
images is required to meet study criteria for the diagnosis of IPF
Figure 2 Diagnosis of Idiopathic Pulmonary Fibrosis in the IPFnet
22
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Figure 3 Pathology Flow Chart Surgical Lung Biopsy Diagnosis
Requirement for diagnosis
1 Clinical exclusion of other known causes (connective tissue diseases environmental and drug
exposures) of ILD
2 Radiographic HRCT with bibasilar reticular abnormality and honeycomb change with minimal
ground glass opacities
Appropriate clinical setting
1 Age gt 50 years
2 Insidious onset of unexplained dyspnea
3 Duration of illness for ge 3 months
4 Bibasilar inspiratory crackles
23
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Unlike the ATSERS consensus criteria published in 2000 bronchoscopy will not be required for diagnosis
This decision was made based on the experience of the IPFnet Steering Group members regarding the utility of
bronchoscopy in the diagnosis of IPF The presence of an atypical HRCT finding will require documentation of
a definitive diagnosis by surgical lung biopsy In fact this is in keeping with the recently published evidence
based guidelines for diagnosis and management of IPF13 As shown in Figure 3 central review of the pathology
data will be required for a diagnosis of IPF
We will not require central review of HRCT as several studies have shown that a confident local interpretation
of clinicalHRCT criteria as definite IPFUIP is associated with a high positive predictive value for finding UIP
at surgical lung biopsy (see Table 1) Differences in sensitivity in these series likely reflect subject selection as
Flaherty et al3 evaluated only UIP and nonspecific interstitial pneumonia (NSIP) while Raghu et al40 and
Hunninghake et al41 included a broader range of ILD
Table 1 Operating Characteristics of Local HRCT Review for Diagnosis of UIP
Researcher of Subjects Sensitivity () Specificity () PPV () NPV ()
Raghu et al 40
59 (29 UIP by SLB) 78 90 88 82
Hunninghake et al 41 91 (54 UIP by SLB)
74 81 85 67
Flaherty et al 3 96 (only NSIP amp UIP)
37 100 100 30
Abbreviations PPV positive predictive value NPV negative predictive value UIP usual interstitial pneumonia SLB surgical lung biopsy and NSIP nonspecific interstitial pneumonia
Furthermore an analysis of the HRCT scans from subjects enrolled in the GIPF-001 trial confirmed that local
site interpretations have a high congruity to a central radiology core In this multi-center study 263 HRCT
scans were read as definite IPF and a retrospective central radiology core review found 932 to be consistent
with IPF 42 We will also take several additional steps to insure that the local HRCT reads are accurate
including
1 A detailed training module has been developed and must be completed by each site radiologist before
site initiation
2 Clinical centers are to mail all HRCT scans to the HRCT core lab The first 10 HRCT scans from
subjects enrolled at each enrolling clinical center will be reviewed centrally to be certain that local reads
24
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
25
are congruent with a central interpretation If discrepancies are identified additional education will be
provided and HRCT scans will continue to be reviewed centrally until the central radiology core is
confident that the local center is performing appropriately
3 Random scans will be obtained from each center throughout the study to confirm that the local read
continues to agree with central interpretation If discrepancies are identified they will be addressed as in
2 above
In all cases if a subject has a surgical lung biopsy sample that sample will be reviewed by the local and central
pathologists Therefore the only cases that would not be subject to a direct central review process are those
where the HRCT meets the centrally defined criteria for an unequivocal diagnosis and a lung biopsy sample is
not available Table 2 below summarizes the possible combinations for making a diagnosis
Table 2 Combining HRCT and Pathology Interpretations to Determine if IPF is Present
HRCT Diagnosis Pathology Diagnosis Diagnosis of IPF
Definite UIP Definite UIP Yes
Definite UIP Probable UIP Yes
Definite UIP Possible UIP Yes
Definite UIP Not UIP No
Definite UIP Unavailable Yes
Consistent with UIP Definite UIP Yes
Consistent with UIP Probable UIP Yes
Consistent with UIP Possible UIP No
Consistent with UIP Not UIP No
Consistent with UIP Unavailable No
Inconsistent with UIP Any No
Abbreviations HRCT high-resolution computed tomography IPF idiopathic pulmonary fibrosis
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
UIP usual interstitial pneumonia Dx diagnosis 43 Exclusion Criteria
1 History of clinically significant environmental exposure known to cause pulmonary fibrosis
Occupational exposures such as asbestos or environmental exposure to organic dust such as occurs in
pigeon breeders may at times mimic the clinical and radiographic findings of IPF
2 Diagnosis of connective tissue disease felt by the principal investigator (PI) to be the etiology of the
interstitial disease Diagnosis of collagen-vascular conditions will be according to the published
American College of Rheumatology criteria As such the presence of any documented collagen-vascular
disorder or the presence of any suspicious symptom complex whether or not associated with
significantly abnormal rheumatological serologies will exclude the subject at the discretion of the PI
3 Extent of emphysema greater than the extent of fibrotic change (honeycombing reticular changes) on
HRCT scan
4 Forced expiratory volume in 1 second (FEV1)FVC ratio lt 065 at screening (postbronchodilator)
5 Partial pressure of arterial oxygen (PaO2) on room air lt 55 mm Hg (lt 50 mm Hg at Denver site)
6 Residual volume gt 120 predicted at screening (postbronchodilator)
7 Evidence of active infection
8 Significant bronchodilator response on screening spirometry defined as a change in FEV1 ge 12 and
absolute change gt 200 mL OR change in FVC ge 12 and absolute change gt 200 mL The percent
difference between the FVC (or FEV1) values will be calculated by taking the absolute value of the
difference and dividing it by the larger of the two FVC (or FEV1) values
9 Screening and enrollment post-bronchodilator FVC measurements (in liters) differing by gt 11 The
percent difference between the FVC values will be calculated by taking the absolute value of the
difference and dividing it by the larger of the two FVC values (eg the percent difference between FVC
measurements of 19 and 20 liters would be determined by taking the difference between the two (01
liters) and dividing by the larger of the two (20 liters) So 0120 = 5 and these FVC measurements
would not exclude the subject
10 Listed for lung transplantation ie the patient has completed the evaluation process has been accepted
as a candidate for transplantation at an appropriate center and is waiting to receive notification of an
available donor organ
11 History of unstable or deteriorating cardiac disease
12 Myocardial infarction coronary artery bypass or angioplasty within 6 months of screening
26
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
13 Unstable angina pectoris or congestive heart failure requiring hospitalization within 6 months of
screening
14 Uncontrolled arrhythmia
15 Severe uncontrolled hypertension
16 Known HIV or hepatitis C
17 Known cirrhosis and chronic active hepatitis
18 Active substance andor alcohol abuse (as determined by site PI)
19 Pregnancy or lactation (subjects who are pregnant or breastfeeding)
20 Known hypersensitivity to study medication
21 Any condition other than IPF that in the opinion of the site PI is likely to result in the death of the
subject within the next year
22 Any condition that in the judgment of the PI might cause participation in this study to be detrimental to
the subject or that the PI deems makes the subject a poor candidate
23 Any therapy directed at pulmonary fibrosis (excepting triple therapy of prednisone plus azathioprine
plus NAC) requires a 30-day washout period before randomized Triple therapy of lt= 12 weeks duration
in the past 4 years requires a 30-day washout period before randomization
24 History of triple therapy of prednisone plus azathioprine plus NAC for gt 12 weeksrsquo duration in the past
4 years or previous enrollment in the triple-therapy arm of the PANTHER-IPF study
44 Study Design and Study Visit
441 Study Design Summary
This study will be a randomized double-blind PL-controlled trial designed to assess the safety and efficacy of
NAC in subjects with newly diagnosed IPF
Subjects with mild to moderate IPF (defined as FVCpred ge 50 and DLCOpred ge 30) diagnosed within
the past 48 months will be enrolled Screening will continue until April 30 2012
27
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
The study will employ a 2-arm design with 11 randomization to NAC or PL Once enrolled subjects will visit
the clinical center at 15 weeks and 15-week intervals thereafter Each subject will be treated and followed for a
maximum of 60 weeks
During the 60-week visit subjects will be taken off all study agents Approximately four weeks after the final
dose of study agent is taken subjects will receive a safety phone call from the study site
442 Study Visits
Subjects who meet entry criteria will review the informed consent a written description of the purpose
procedures and risks of the study with the PI co-investigator or study coordinator and all questions will be
answered The informed consent form will be signed by the subject at screening No protocol-specific
procedures will be performed until the subject has signed and dated an informed consent form This includes the
screening procedures
4421 Screening
Once informed consent is obtained subjects may immediately begin the screening process or may return within
28 days of consent In the event a study subject has been clinically evaluated at the study site by an IPFnet study
physician and has performed testing within three weeks for this clinical evaluation that meets guidelines
provided in the IPFnet PANTHER-IPF Manual of Operating Procedures (MOOP) this testing may be used to
satisfy the following screening criteria medical history physical exam arterial blood gas (ABG) with A-a
gradient vital signs with oximetry body height and weight spirometry DLCO lung volumes and HRCT scan
Allowing the use of previously performed test results that meet study guidelines for the screening visit is
intended to permit subjects easier access to study entry to prevent subjects from repeating testing that has been
performed within the study window and to decrease risks to subjects from repeated exposure to procedures
such as arterial puncture and HRCT
The following procedures will be performed at screening
Medical history and a physical examination
28
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Measure height and weight
Serum pregnancy test (if applicable)
Measure vital signs including oximetry
Blood draws performed and the following analyses conducted
o Hematology (red cell count white cell count hemoglobin hematocrit cell indices differential
platelet count)
o Blood chemistries according to central laboratory protocol (see Section 410 Laboratory
Testing)
o Beta human chorionic gonadotropin (serum) pregnancy test (in women of childbearing potential)
o Urinalysis
Pulmonary Function Tests (PFTs) including spirometry pre- and post- bronchodilator and postshy
bronchodilator measurement of lung volumes and measurement of hemoglobin adjusted diffusing
capacity
Measure ABGs
HRCT if a satisfactory scan has not been performed on the subject within 3 months of screening (see
PANTHER-IPF MOOP for more details)
Surgical lung biopsies (if applicable) reviewed by local and central pathology departments
Current medications If required a washout period discussed with the subject and initiated at this visit
4422 Enrollment
The enrollment visit is expected to take place within eight weeks of the screening visit Enrollment visit
activities include
Measure vital signs including oximetry
Measure height and weight
Serum pregnancy test (if applicable)
If consent has been given blood will be drawn and a urine specimen collected for the bio-specimen
repository
Spirometry (post-bronchodilator)
Measure 6MWT with Borg Dyspnea Scale
29
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Collect Quality-of-life (QOL) data using the SF-36 EuroQol Investigating Choice Experiments for
Preferences of Older People Capability Instrument (ICE CAP) and SGRQ
Female subjects complete Gender Substudy questionnaire
Dyspnea status collected using the UCSD SOBQ
Evaluate Acute Exacerbation (AEx)
Review of any Adverse Events (AEs)
Review of concomitant medications
Subject receives diary and instructions on its purpose and proper use
Subject receives supply of study drug sufficient to last until his or her 15-week study visit
See the Schedule of Assessments (Table 3) for more details Subjects with screening and enrollment postshy
bronchodilator FVC measurements (in liters) differing by more than 11 are not eligible to be enrolled in the
study
Subjects will be asked to provide a physician of record This physician will be considered the subjectrsquos primary
care provider (PCP) and if the subject agrees the PCP will be informed by letter of the subjectrsquos enrollment in
the trial The subject will be informed that his or her ongoing medical care should be received from the PCP
The PCP will be informed of any safety issues identified by the study staff The PCP will also be given
information regarding communication with study personnel about pertinent health issues or clinic encounters
the subject may have
4423 Week 15
The week 15 visit is expected to occur within +- 14 days of the subjectrsquos scheduled visit time (eg the week 15
visit should occur anytime between 13 and 17 weeks after starting study drug Week 15 activities include
Measure vital signs with oximetry
Measurement height and weight
Serum pregnancy test (if applicable)
Spirometry (post-bronchodilator) measurement
Review of AEs
Evaluate for AEx
30
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Review concomitant medications
If consented draw blood and collect urine specimen for the biospecimen repository
Subjects return used and unused study drug for the visit
Review study diary and a new study diary will be given
Provide additional supply of study drug sufficient to last until the next scheduled visit
4424 Week 30
The week 30 visit is expected to occur within +- 14 days of the subjectrsquos scheduled visit time (eg the week 30
visit should occur anytime between 28 and 32 weeks after starting study drug) Week 30 activities include
Physical examination
Measure vital signs with oximetry
Measure height and weight
Laboratory values (complete blood count [CBC] and serum chemistries)
Serum pregnancy test (if applicable)
Measure spirometry (post-bronchodilator)
6MWT with Borg scale
DLCO
Review of AEs
Evaluate for AEx
Review concomitant medications
Complete all QOL and dyspnea questionnaires (EuroQol ICE CAP SF-36 SGRQ and UCSD SOBQ)
If consent has been given blood will be drawn and a urine specimen collected for the biospecimen
repository
Review study diary
Subjects return used and unused study drug for the visit
Provide additional supply of study drug sufficient to last until the next scheduled visit
4425 Week 45
31
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
The week 45 visit is expected to occur within +- 14 days of the subjectrsquos scheduled visit time (eg the week 45
visit should occur anytime between 43 and 47 weeks after starting study drug) Week 45 activities include
Measure vital signs with oximetry
Measure height and weight
Serum pregnancy test (if applicable)
Measure spirometry (post-bronchodilator)
Review of AEs
Evaluate for AEx
Review concomitant medications
If consent has been given blood will be drawn and a urine specimen collected for the biospecimen
repository
Subjects return used and unused study drug for the visit
Study diary reviewed
Provide additional supply of study drug sufficient to last until the next scheduled visit
4426 Week 60 (Early Withdrawal or Final Treatment Visit)
At week 60 or at subject withdrawal from the study (premature by study doctor or subjectrsquos decision) a final
treatment visit will occur At this final treatment visit subjects will discontinue NACPL abruptly Week 60
activities also include
Physical examination
Measure vital signs with oximetry
Measure height and weight
Laboratory values (complete blood count [CBC] and serum chemistries)
Spirometry (post-bronchodilator) measurement
6MWT with Borg scale measurement
DLCO
Lung volumes
ABG
Review of AEs
32
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Evaluate for AEx
Review concomitant medications
Subjects will complete all QOL and dyspnea questionnaires (EuroQol ICE CAP SF-36 SGRQ and
UCSD SOBQ)
If consent has been given blood will be drawn and a urine specimen collected for the biospecimen
repository
Subjects return used and unused study drug for the visit
Study diary reviewed
4427 Final Site Visit ndash FVC drop confirmation
In the event that the subject has a recorded FVC drop of gt10 from baseline at the final treatment visit and the
subject has not had a confirmation of such a drop at a previous study visit the subject should return to the
clinical site 6 to 8 weeks after the final treatment visit During this visit a post-bronchodilator spirometry test
will be performed This FVC measurement will be evaluated according to section 521 of this protocol
4428 Final Visit ndash Telephone Follow-up
Four weeks following the final dose of study medication subjects will receive a telephone call from the study
coordinator to ensure that there are no side effects and to follow up on any ongoing adverse events (AEs)
4429 Phone Contact Between Visits
At week 2 and each month that a subject does not have a scheduled clinical center visit his or her study
coordinator will contact him or her at least once by telephone to
Inquire if the subject has had any hospitalizations events that might be considered an AE or any events
significant enough to warrant an out-of-cycle visit to the clinical center
Remind subjects of their current dosage levels and confirm that the subject understands them
Address any questions or concerns the subject might have regarding other aspects of the study
Assess adherence to the treatment regimen by reviewing diary data verbal review of medications taken
including nutritional supplements
33
34
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Table 3 Schedule of Assessments
Procedure Screening Visit 0
Enrollment Visit 1
Week 15 Visit 2
Week 30Visit 3
Week 45 Visit 4
Week 60 Early
Withdrawal Visit 5
Final1
Visit (via phone)
Informed consent X
Medical history X
Inclusionexclusion criteria X
Serum pregnancy test (if applicable) X X X X X
Review of lung biopsy X
Arterial Blood Gas X X
6-Minute Walk Test
X
X X
Physical examination X X X
Vital signs with oximetry X X X X X X
Body height and weight X X X X X X
Complete Blood Count X X X
Chemistry panel X X X
Monitor Lab Values X X X
Urinalysis X Specimen repository substudy blood draw and urine collection (if consented)
X
X X X X
HRCT (if not completed within three months) X
Spirometry (pre- and post-bronchodilator) X
Spirometry (post-bronchodilator only) X X X X X
DLCO (post-bronchodilator only) X X X
Lung volumes (post-bronchodilator only) X
X
Evaluate for acute exacerbation X X X X X
Review Adverse Events X X X X X X
Review concomitant meds X X X X X X
Dispense subject diary X X X X
Review subject diary X X X X X
Dispense study agent X X X X
Gender Substudy questionnaire (female subjects only) X
EuroQol ICECAP UCSD SOBQ SGRQ SF-36 X X X
Abbreviations DLCO diffusing capacity of the lung for carbon monoxide QOL Quality of Life ICECAP Investigating Choice Experiments for Preferences of Older People UCSD SOBQ University of California Shortness of Breath Questionnaire SGRQ St Georgersquos Respiratory Questionnaire SF-36 Short Form 36 Health Survey
1Follow-up visit via phone will occur four weeks after final dose of study medication
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
45 Dose Justification
The general philosophy for determining dosing levels was to apply previously examined
treatment regimens With the focus of the study being to establish a standard of care for
mildmoderate IPF subjects the goal was to develop flexible yet standardized treatment rules that
allow for the temporary or permanent withholding of one or more components of treatment when
necessary Subjects developing laboratory abnormalities or symptoms that result in
discontinuation of one or more components of study treatment may continue on the other
components as long as there is no contraindication for this Complete follow-up is important for
the validity of any study As a strategy to maintain protocol adherence we are using a treatment
regimen that will detect potential side effects and prompt interventions proactively in the interest
of patient safety In addition subjects who permanently stop study medications during the course
of the study are encouraged to continue in the study completing all scheduled visits and tests
451 Rationale for N-acetylcysteine Dosing
To our knowledge there have been no IPF studies to correlate clinical outcome measures with
different dosages for NAC The dosage chosen is based on the IFIGENIA study However BAL
lung GSH levels from subjects with IPF have been augmented with the use of oral NAC at 600
mg 3 times per day In addition lung GSH levels have been associated with improved
PFTs212227 The dose chosen for this study was based on previous data including the IFIGENIA
study30
4511 Dosing of N-acetylcysteineplacebo
Dosing of NACPL will be 600 mg orally 3 times a day (1800 mgday)
4512 Reasons to Discontinue N-acetylcysteineplacebo
NACPL may be temporarily or permanently discontinued for the duration of the study for
gastrointestinal symptoms or dermatologic reactions
35
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Temporarily discontinue (hold) oral NACPL for subjects requiring inpatient admission for acute
exacerbation (AEx) or other conditions Resume NACPL after discharge
36
37
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
452 Dosage Algorithms
Dosage Adjustment Algorithm 1 NACPL Dose Modifications for Gastrointestinal Symptoms Nausea Vomiting Abdominal Discomfort Diarrhea
GI Symptoms determined by the PI to be clinically significant Nausea Vomiting Abdominal Discomfort Diarrhea
NACPL Temporarily dc (HOLD) x 3 Days
Monitor symptoms intervene as clinically indicated (eg fluid replacement antidiarrhea or antinausea medication)
Monitor or lab PRN
Are symptoms resolving after 3 days NO
Symptoms NOT resolving after 3 days of holding study medication Assessmentmanagement per clinical
discretion of investigator
Likely not study medication discuss resuming study medication with medical monitor when symptoms resolved
YES
Temporarily dc (HOLD) NACPL for 4 additional days (total hold 1 week) then NACPL Resume 600 MG TID
Did symptoms recur
YES
STOP NACPL for
duration of study
NO
NACPL No Change
38
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Dosage Adjustment Algorithm 2 NACPL Dose Modifications For Dermatologic Reactions
Dermatologic Reactions (Not Acneiform) ge Grade 2 Grading per Common Terminology Criteria for
Adverse Events V30 (httpctepcancergov) For example Grade 1 RASHDESQUAMATION Macular or papular eruption or erythema without associated symptoms Grade 2 RASHDESQUAMATION Macular or popular eruption or erythema with pruritus or other associated symptoms localized desquamation or other lesions covering lt50 of body surface area
NACPL Temporarily dc (HOLD) x 3 days
Are symptoms resolving after 3 days
NO Symptoms not resolving after 3 days of holding study medication Assessmentmanagement per clinical discretion of investigator Likely not study medication Discuss resuming study medication with medical monitor when symptoms
resolved YES
Temporarily dc (HOLD) NACPL for 4 additional days (total hold 1 week) then NACPL resume 600 MG TID
Did symptoms recur
YES
STOP NACPL for
duration of study
NO
NACPL No change
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
46 Contraindications Precautions and Side Effects of Study Medications
461 Contraindication
Contraindication to NAC is known hypersensitivity to it
462 Precautions
Concomitant administration of oral NAC and antibiotics has shown a slightly reduced absorption
of cephalexin and a slight increase in erythromycin serum levels NAC contains free sulfhydryl
groups There is no evidence that individuals sensitive to sulfa drugs are sensitive to NAC
The NAC preparation being administered in this study contains 20 mg of aspartame Because of
the phenylalanine component of aspartame individuals with phenylketonuria should avoid or
restrict aspartame intake to avoid increased blood levels of phenylalanine Because of this risk
labeling is required on all products containing aspartame
463 Side Effects
Side effects of NAC range from common to serious See Table 4
39
40
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Table 4 Side Effects of NAC
Undesirable Effects
System-organ class Uncommon
(gt11000 lt1100)
Rare
(gt110000 lt11000)
Very rare
(lt110000) Not known
Immune system disorders Hypersensitivity Anaphylactic shock
reaction
Nervous system disorders Headache
Ear and labyrinth disorders Tinnitus
Cardiac disorders Tachycardia
Vascular disorders Hemorrhage
Respiratory thoracic and
mediastinal disorders
Bronchospasm
Dyspnea
Gastrointestinal disorders
Vomiting diarrhea
stomatitis abdominal
pain nausea
Dyspepsia
Skin and subcutaneous tissue
disorders
Urticaria rash
angioedema itching
General disorders and
administration site conditions Pyrexia
Investigations Reduced arterial
pressure Face edema
In very rare cases the onset of severe skin reactions such as Stevens-Johnson syndrome and Lyell syndrome was reported to have a temporal relationship with N-acetylcysteine administration Although in most cases at least another suspect drug probably most involved in the genesis of the above mentioned mucocutaneous syndromes has been identified in case of mucocutaneous alterations it is appropriate to contact onersquos doctor and the administration of N-acetylcysteine should be immediately discontinued
Some studies confirmed a reduction of platelet aggregation during N-acetylcysteine administration The clinical significance of these findings has not been defined yet [Source Fluimucil Investigator Brochure]
47 Recruitment Procedures
Subjects recruited for this study will be established patients of the investigators or physician- or
self-referred to participating clinical centers in the IPFnet Each clinical center within IPFnet has
a well-developed infrastructure of local pulmonologists within the surrounding geographic area
These pulmonologists are kept informed of ongoing IPF clinical trials and regularly refer
subjects to studies conducted at IPFnet clinical centers
Additional steps will be taken to inform clinicians of the trials in progress within IPFnet
including presentations at faculty staff meetings at local hospitals medical grand rounds and
national conferences direct mail notification monthly faxes and advertisement of network trials
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
in pulmonary journals Clinical center patients previously diagnosed with IPF will be notified of
the trials by mail whenever possible
Recruitment of minorities and women will be monitored by the DCC and DSMB If necessary
additional recruitment efforts will be made at specific centers to ensure that the aggregate subject
sample contains appropriate representation of women and minorities
48 Study Procedures
The following procedures are detailed in the PANTHER-IPF MOOP accompanying this
protocol
1 PFT
2 ABG
3 HRCT scan of the chest (including imaging of pulmonary arteries)
4 CBC and serum chemistries
5 Pregnancy test
6 6MWTBorg Dyspnea Scale
7 QOL questionnaires (EuroQol HAD SF-36 SGRQ and ICE CAP)
8 UCSD SOBQ
9 Gender Substudy Questionnaire
All assessments of PFTs will be conducted by study personnel not directly involved in the
treatment of the subjects
481 Biological Specimen Management
4811 Biological Specimen Sample Management
Subjects at clinical centers participating in the specimen repository substudy who consent to
having blood drawn for research purposes and for the banking of blood blood components and
other biologic specimens (urine and BAL fluid) will have approximately 405 mL of blood
41
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
drawn 17 mL blood drawn for DNA and 20 mL of urine collected at enrollment visit Subjects
will have approximately 50 mL of blood drawn and 20 mL of urine collected at each 15-week
follow-up visit Blood specimens will be separated according to PANTHER-IPF MOOP
guidelines into the following components for banking in the repository serum plasma and
DNA Coding of all biologic specimens for the repository will be performed by study staff at the
clinical center The samples will be processed per PANTHER-IPF MOOP guidelines aliquoted
labeled with barcode labels and stored at -70degC at the clinical center and shipped to the central
repository
The only subject identifiers will be a sample ID number and subject initials This sample ID will
be linked in the IPFnet DCC clinical database to subject information No subject information will
be transferred to the biological-specimen database
The subjectrsquos samples may be used for approved sub-studies relating to human disease
including but not limited to IPF The studies for which an individualrsquos samples will be made
available will be determined by the subjectrsquos answers to questions on the biological-sample
informed consent form The subjects can choose to make their samples available for all options
or any combination Samples will be made available to researchers only with IPFnet Steering
Group approval until such time as the samples are made public through the NHLBI repository
49 Concomitant Medications
Concurrent treatment with FDA-approved therapy for IPF is allowed Colchicine may be used
for treatment of gout Temporary treatment with oral or IV corticosteroids for clinical worsening
or suspected AEx is permitted Nutritional supplements containing NAC are not allowed
410 Laboratory Testing
Clinical laboratory parameters will be assessed at screening and at the end of the study The
following tests will be performed at the two time points specified in the protocol chemistry (AG
ratio ALT [SGPT] AST [SGOT] albumin alkaline phosphatase amylase bilirubin-direct
42
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
bilirubin-indirect bilirubin-total BUN BUNcreatinine ratio calcium carbon dioxide
cholesterol-total chloride CPK-total creatinine GGT globulin glucose iron-total LDH
lipase magnesium phosphorus-inorganic potassium protein-total sodium TIBC triglycerides
uric acid) and hematology (red blood cell count WBC count hemoglobin hematocrit cell
indices differential platelet count)
411 Blinding of Study Drugs
Subjects and caregivers will be blinded to study treatment Every subject will receive NAC or
matching PLs at every study visit from the baseline visit to the week-45 visit No study agent
will be dispensed at the week-60 visit
43
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
5 Study Endpoints
51 Primary Study Endpoint
The primary endpoint will be the change in serial measurements of FVC over the study period
52 Secondary Study Endpoints
521 Time to Disease-progression
The time-to-death or a 10 decline in FVC will be defined as the time-to-disease progression
The 10 decline in FVC from enrollment must be confirmed on 2 consecutive visits no less than
6 weeks apart For subjects with 2 consecutive visits with a 10 decline in FVC the time-toshy
disease progression will be defined as the time interval between enrollment and the initial visit
with a 10 FVC decline For subjects who experience disease progression the study doctor will
determine whether or not the subject will remain in the study
522 Acute Exacerbations
The following 3 criteria will define AEx in subjects with acute worsening of their respiratory
conditions
1 Clinical (all of the following required)
A) Unexplained worsening of dyspnea or cough within 30 days triggering unscheduled
medical care (eg emergency room clinic study visit hospitalization)
B) No clinical suspicion or overt evidence of cardiac event pulmonary embolism or deep
venous thrombosis to explain acute worsening of dyspnea
C) No pneumothorax
44
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
2 RadiologicPhysiologic (A and B required)
A) New ground glass opacity or consolidation computed tomography (CT) scan OR new
alveolar opacities on chest x-ray
B) Decline of ge 5 in resting room air SpO2 from last recorded level OR decline of ge 8 mm
Hg in resting room air PaO2 from last recorded level
3 Microbiologic (all of the following required)
A) No clinical evidence for infection (ie absence of grossly purulent sputum fever gt 39degC
orally)
B) Lack of positive microbiological results (if done) from lower respiratory tract defined as
(1) Clinically significant bacterial growth on sputum or endotracheal aspirate cultures
(2) Quantitative culture by protected brush specimen ge 103 cfumL or BAL ge 104 cfumL
(3) The presence of specific pathogens on stains of any of the above
C) Lack of positive pathogen in blood cultures (if done)
Identification of Acute Exacerbations
All subjects will be educated about the importance of identifying AExs At the time of
enrollment subjects will be told about the possibility of developing acute symptomatic
worsening that might represent an AEx of IPF and instructed to contact their study clinical
center coordinator within 48 to 72 hours of the apparent event
All subjects will be contacted by phone monthly and questioned about any change in dyspnea or
cough and any interim clinic visits or hospitalizations Finally as part of the IPFnet outreach to
community referring physicians the importance of AExs will be emphasized When a subject is
identified who meets criterion 1A this will trigger the collection of additional clinical data to
evaluate a suspected AEx These data will be collected as part of standard clinical care (ie this
protocol does not require collection of all items) The additional items to be collected for
suspected AEx include
IPFnet AEx case report form (eCRF) (required)
45
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Chest x-ray CT scan withwithout pulmonary angiogram (reports should be faxed and
followed by the hard copiesdiscs)
Oxygen saturation (pulse oximetry)
ABG
Respiratory cultures (sputum endotracheal aspirate lavage)
Blood cultures
Clinichospital records related to the event
All potential cases of AEx will be reviewed by the clinical center PI first and a decision on
whether the case may represent an AEx will be made If AEx is suspected the case will be sent
to the IPFnet adjudication committee which will assign a final diagnosis (see Table 5) If there is
disagreement among members the majority opinion will be recorded
During episodes of suspected AEx as determined by the individual clinical center investigator
subjects will remain blinded and in the study
Table 5 Final Diagnoses in Evaluation of Suspected Acute Exacerbations
Definite acute exacerbation All criteria met no alternative etiology
Unclassifiable acute worsening
Insufficient data to evaluate all criteria no alternative etiology
Not acute exacerbation Alternative etiology identified that explains acute worsening
Management of the suspected AEx will be at the discretion of the treating physician Standard of
care generally involves evaluation for respiratory infection pulmonary embolism cardiac events
and pneumothorax and treatment with IV corticosteroids
Study drugs will be resumed at pre-suspected AEx doses after subjects clinically improve as
confirmed by the local PI All subjects should be seen at the clinical center within 2 to 4 weeks
of recovery for measurement of post-bronchodilator FVC (see Figure 4) Subjects unable to
return to the clinical center after suspected AEx due to medical frailty (eg continued
46
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
institutionalization progressive disability) will be categorized as failing to maintain FVC
response in secondary analyses
Suspected AEx (PI determined)
Hold study drug Treat AEx
(Attending physician determined)
Alive but unable to continue due to
medical frailty
Dead
Alive and able to continue
Site reviewvisit
Restart study drug
FVC within 2-4 weeks
Figure 4 Acute Exacerbation Flow Chart
523 Respiratory Infections
An upper respiratory infection will be defined as
Change in sputum discoloration
Increased cough of no more than 14 daysrsquo duration
A lower-respiratory infection (pneumonia) will be defined as new segmental or lobar airspace
opacities visualized by image studies (chest radiograph or HRCT) in addition to any of the
following
Positive pathogencultures in good sample of sputum or lower-airway secretions retrieved
by fiberoptic bronchoscope
Fever gt 39degC or gt 100degF
Leukocytosis gt 12000 (unexplained no increase in dose of corticosteroids)
47
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
524 Maintained FVC Response
Subjects with follow-up FVCpred measurements at or above their baseline FVCpred level
will be classified as having maintained FVC response Subjects with reduced FVCpred levels
or missing data for any reason including death or medical frailty will be classified as having not
maintained FVC response The FVCpred value is used because unadjusted FVC measurements
are expected to decline with age
48
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
6 Safety Evaluations and Procedures
61 Adverse Events
During a clinical trial the reporting of adverse experience information can lead to important
changes in the way a new treatment is developed as well as provide integral safety data
611 Definitions
An adverse event (AE) is any untoward medical occurrence in a subject or clinical investigation
subject who was administered a pharmaceutical product The AE does not necessarily have to
have a causal relationship with the drug administered An AE can be any unfavorable and
unintended sign (including an abnormal laboratory finding) symptom or disease temporarily
associated with the use of a medicinal product whether or not considered to be related to the
medicinal product Diseases signs symptoms or laboratory abnormalities already existing at
enrollment are not considered AEs unless they worsen (ie increase in intensity or frequency)
Surgical procedures themselves are not AEs they are therapeutic measures for conditions that
require surgery The condition for which the surgery is required may be an AE Surgical
procedures planned before randomization and the conditions necessitating the surgery are not
AEs
A serious adverse event is any untoward event that
Is fatal
Is life-threatening
Requires inpatient hospitalization or prolongation of existing hospitalization with the
following exceptions
o Preplanned (before the study) hospital admissions unless the hospitalization is
prolonged
o Planned admissions (as part of a study eg routine biopsies)
o Hospitalization lasting lt 24 hours
49
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
o Hospitalization for elective procedure
o Emergency room visits
Results in persistent or significant disability or incapacity
Is a congenital anomaly or birth defect
Important medical events that may not result in death be life-threatening or require
inpatient hospitalization may be considered serious adverse events (SAEs) when based
on appropriate medical judgment they may jeopardize the subject and may require
medical or surgical intervention to prevent one of the outcomes listed above
Life-threatening means that the subject was in the view of the investigator at immediate risk of
death from the AE as it occurred It does not include an AE that had it occurred in a more severe
form might have caused death
Persistent or significant disabilityincapacity means that the event resulted in permanent or
significant and substantial disruption of the subjectrsquos ability to carry out normal life functions
Causality
A reasonable possibility means the AE may have been caused byrelated to the study drug A
perceived or real lack of efficacy does not satisfy the definition of relatedness
612 Adverse Event (AE) Reporting
For the PANTHER-IPF trial all AEs (serious and nonserious) occurring from randomization
through final study visit (4 weeks after final dose of all study medication) will be recorded on the
AE page of the case report form (CRF)
6121 Serious Adverse Events (SAE) Reporting
For this trial all deaths and all SAEs which occur from randomization through final study visit
must be entered within the EDC system via the SAE eCRF page within 24 hours of the
investigative sitersquos knowledge of the event It is the responsibility of the clinical center
50
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
investigator to provide a causality assessment of the event for each study medications based upon
the information available at the time of the report It is understood that complete information
about the event may not be known at the time the initial report is submitted In the event the EDC
system is not accessible to the site at the time of event reporting investigative sites will complete
and forward a paper back-up SAE form to DCRI Safety Surveillance for processing
DCRI Safety Surveillance
Telephone 1-919-668-8624 or 1-866-668-7799 (toll free)
Fax 1-919-668-7138 or 1-866-668-7138 (toll free)
The investigator must complete and submit follow-up SAE information via the eCRF when
important new or follow-up information (eg final diagnosis outcome results of specific
investigations) becomes available Follow-up information should be submitted according to the
same process used for reporting the initial event as described above All SAEs will be followed
until resolution stabilization or 30 days after the subject has completed the final visit (4 weeks
after the final dose of study medication) whichever occurs first The investigator is responsible
for reporting SAEs to their institutional review board (IRB) per site specific IRB reporting
guidelines
6122 Regulatory Reporting
AEs that are serious study drug related and unexpected will be reported to the regulatory
authorities The DCRI Safety Surveillance medical monitor will perform a medical review of all
SAEs submitted and evaluate for ldquounexpectednessrdquo DCRI Safety Surveillance will prepare
MedWatch reports for those events identified as serious study drug related and unexpected as
determined by Safety Medical Monitor
DCRI Regulatory Services will submit all unexpected study drug-related SAEs as per 21 CFR
32 DCRI Safety Surveillance will provide a safety alert letter to the NHLBI DSMB and DCC
clinical operation (for distribution to sites) within 15 days of initial receipt of the information
51
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Investigators are responsible for promptly reporting these events to their reviewing IRBs
according to site specific IRB reporting guidelines
62 Clinical Medical Monitoring
There will be an unblinded physician at the IPFnet DCC serving as medical monitor The
medical monitor will be available to assist with questions about dosage adjustments of study
medications including discontinuation or resumption of medications
63 Unblinding Procedures
Unblinding of subjects or investigators to subject treatment is strongly discouraged For ongoing
clinical management all subjects should be presumed to be receiving ldquoactiverdquo study drug To
ensure the subjectrsquos safety the study treatment will be dose-adjusted based on laboratory test
results clinical findings and symptoms
The IPFnet DCC medical monitor and PANTHER-IPF co-chairs Drs Ganesh Raghu and
Fernando Martinez will be available to the study physicians to discuss study drug management
on a case-by-case basis Un-blinding will be considered ONLY when the knowledge of subject
treatment assignment is ABSOLUTELY ESSENTIAL for subject safety and after discussion of
the subjectrsquos case with the medical monitor and either Dr Raghu or Dr Martinez Unblinding of
study treatment should be minimized during the conduct of the trial In those cases where it is
felt to be medically necessary the DCC medical officer will communicate directly with the
managing physician to minimize unblinding of study personnel
52
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
7 Study Drug Procedures
At the baseline 15-week 30-week and 45-week study visits subjects will receive a supply of
study drug sufficient to last until the next visit at which study drug will be dispensed
53
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
8 Data Management
81 Hardware and Software Configuration
811 Hardware and Database Software
Data will be stored in an Oracle database system Oracle has advantages of processing efficiency
and smooth linkage with other software systems The application and database will be hosted on
Solaris Unix servers at the IPFnet DCC
812 Statistical Software
SAS will be used as the principal application for the management of analysis data files and
statistical computations S-Plus will be used to provide supplementary functions as needed
813 Access Control and Confidentiality Procedures
Access to databases will be controlled centrally by the IPFnet DCC through user passwords
linked to appropriate privileges This protects the data from unauthorized changes and
inadvertent loss or damage
814 Security
Database and Web servers will be secured by a firewall and through controlled physical access
Oracle has many security features to ensure that any staff member accessing the database has the
proper authority to perform the functions he or she requests of the system Within the secondary
SAS databases Unix group-access control maintains similar security The Sun workstation login
is secured by extensive user-password facilities under Unix
54
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
815 Back-up Procedures
Database back-up will be performed automatically every day and standard IPFnet DCC policies
and procedures will be applied to dictate tape rotation and retention practices
816 Virus Protection
All disk drives that provide network services and all user computers will be protected using
virus-scanning software Standard IPFnet DCC policies will be applied to update these protection
systems periodically through the study
82 Sources of Data
821 Design and Development
The IPFnet DCC will be responsible for development of the electronic case report forms
(eCRFs) development and validation of the clinical study database ensuring data integrity and
training clinical center staff on applicable data management procedures A web-based distributed
data entry model will be implemented This system will be developed to ensure that guidelines
and regulations surrounding the use of computerized systems used in clinical trials are upheld
The remainder of this section provides an overview of the data management plan associated with
this protocol
822 Data Collection Forms
The data collection process consists of direct data entry at the study clinical centers into the EDC
system(s) provided by the DCC A data collection worksheet will be provided to clinical centers
for recording data in the event the EDC system is unavailable Data entry of the eCRFs should
be completed according to the instructions provided and project specific training The
investigator is responsible for maintaining accurate complete and up-to-date records and for
ensuring the completion of the eCRFs for each research participant
55
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
823 Data Acquisition and Entry
Data entry into eCRFs shall be performed by authorized individuals Selected eCRFs may also
require the investigatorrsquos written signature or electronic signature as appropriate Electronic
CRFs will be monitored for completeness accuracy and attention to detail during the study
824 Data Center Responsibilities
The IPFnet DCC will 1) develop a data management plan and will conduct data management
activities 2) provide final eCRFs for the collection of all data required by the study 3) develop
data dictionaries for each eCRF that will comprehensively define each data element 4) conduct
ongoing data monitoring activities on study data 5) monitor any preliminary analysis data
cleanup activities and 6) rigorously monitor final study data clean up
825 Data Editing
Completed data will be entered into the IPFnet DCC automated data acquisition and
management system If incomplete or inaccurate data are found a data clarification request will
be generated and distributed to clinical centers for a response Clinical centers will resolve data
inconsistencies and errors and enter all corrections and changes into the IPFnet DCC automated
data acquisition and management system
826 Training
The training plan for clinical center staff includes provisions for training on assessments eCRF
completion guidelines data management procedures and the use of computerized systems
56
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
9 Study Design and Data Analysis
91 General Analytic Considerations
All primary analyses will be based on intent-to-treat (ITT) principles using all randomized
subjects Baseline factors across groups will be compared using mean (standard deviation) and
median (25th and 75th percentiles) summary measures Kaplan-Meier curves will be used to
display event rates Due to clinical interest in departures from both sides of the null hypothesis
all test statistics will be 2-sided
Reasonable caution needs to be taken when conducting multiple analyses on key clinical
subgroups For subgroup analyses a conservative significance level of 0001 will be used for all
interaction tests Thus subgroup comparisons will be considered exploratory unless the p-value
from the interaction test is smaller than 0001
92 Randomization Blinding and Reporting of Results
A permuted block-randomization scheme will be created with varying block sizes stratified by
clinical center Once a subject has completed the screening and baseline period and evaluation
for inclusionexclusion criteria the randomization process will begin Subjects will be
randomized to receive NAC or matching placebo with equal probability (11) via telephone
contact with a central interactive voice response system (IVRS) using a toll-free randomization
number On the day of randomization after the subject has successfully met all inclusion and
exclusion criteria the investigator or designee will call the central randomization number to
obtain the assigned kit randomization numbers for that subject At each subject visit the
investigator or designee will call the central randomization number to obtain the new kit
randomization numbers for resupply of the subject For resupply of the clinical center the IVRS
will monitor minimal volume of a kit type andor expiration date and will automatically notify
the pharmacy
57
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
The trial results will be reported according to guidelines specified in the CONSORT statement
A flow diagram describing screening recruitment randomization dropout and vital status will
be included in the primary manuscript AEs and efficacy data will be presented for all treatment
groups Adherence dropout and lost to follow-up will be carefully examined across all treatment
groups Analyses of safety will be based on data from all randomized subjects who received at
least one dose of study drug
93 Stratification
Subjects will be distributed to the two treatment arms in a 11 allocation ratio Stratification
blocks will be based on clinical centers
94 Specification of the Primary Analyses
A mixed model repeated measures (MMRM) analysis described in section 95 will be used to
compare differences in the slope of FVC measurements across the treatment groups Response
variables are values of the FVC measured at baseline and every 15 weeks until study completion
Variables in the model will include treatment time and time by treatment age sex race and
height Contrast estimates of differences in slopes of treatment over time (along with confidence
intervals) will be used to estimate the treatment effect The validity of this model in terms of
meeting modeling assumptions will be assessed via standard modeling diagnostics and goodness-
of-fit measures Based on the MMRM framework missing FVC data will not be imputed for the
primary analysis
95 Analysis of Longitudinal Endpoints
A common goal in clinical trials is to specify models that are easily implemented and
reproducible by independent data analysts On the other hand the models should have proper
statistical behavior in terms of low bias and high precision Many common approaches to
longitudinal data analysis including last observation carried forward (LOCF) imputation rely on
the missing completely at random (MCAR) assumption However the MCAR assumption is
58
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
unlikely to hold in many clinical trials because missing data are often related to disease
progression and prognosis A more reasonable assumption missing at random (MAR) specifies
that the complete data distribution can be modeled using only the observed data The likelihood-
based MMRM approach is valid under the more general MAR assumptions These models will
be applied to analyze the longitudinal data secondary endpoints
The advantages of MMRM analysis are that all important characteristics of the model can be preshy
specified standard software can be used to implement the models and results are based on ITT
principles43 In addition the MMRM approach offers superior control of Type I and Type II
errors compared with the LOCF approach
Response variables are values of the PFTs measured at enrollment and every 15 weeks until
study completion and 6MWT values measured at baseline week 30 and week 60 Covariates are
treatment time time by treatment and key baseline risk factors Contrasts (along with
confidence intervals) of treatment by time will be used to estimate the treatment effect
The correlation structure involves multiple pieces including measurement errors random
variation and interindividual variability For the longitudinal data analyses an unstructured
correlation matrix for within-subject errors will be assumed Other correlation structures
including compound symmetry will be examined as needed A careful examination of reasons
for study discontinuation will be conducted to assess the validity of MCAR Sensitivity analyses
will be used to examine the untestable assumption that the observed data violate the MAR
assumption The MMRM models will be implemented using PROC MIXED in SAS
96 Analysis of Binary Time-to-Event and Time-Lagged Endpoints
Regression modeling approaches using either the logistic regression model or Cox proportional
hazards regression model will be employed when appropriate The validity of these models will
be assessed via standard modeling diagnostics and goodness-of-fit measures Estimates of
cumulative frequencies for more general time-lagged responses will be calculated using the
partitioned version of the Bang-Tsiatis estimator44 The partitions will be set at 15-week intervals
59
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
to correspond with the data-collection process Covariate adjusted event rates will be calculated
using inverse probability-weighted regression estimates45
97 Power Analysis
971 Primary Analyses
Based on previously published IPF clinical trials the PL group is expected to experience a drop
in FVC of approximately 020 L over the study period (see Figure 1) The IPFnet Steering Group
determined a clinically important difference would be to preserve the majority of the decline
relative to PL over the study period In particular a treatment effect of 015 L was determined to
be a clinically meaningful difference Potential dropout is a key factor in the proposed study The
drop-out process assumed 5 lost to follow-up after every study visit Only 80 of subjects
were assumed to be followed for the entire study period All models assumed a compound
symmetry structure for the covariance matrix Power calculations were performed using a SAS
IML program for designing repeated measures studies46 Based on preliminary reviews of the
data from the University of Michigan the covariance matrix parameters were estimated at
approximately σ2 = 0757 (variance parameter) and ρ = 0936 (correlation parameter) To be
conservative the power calculations for the primary analysis were performed with parameter
setting of σ2 = 0810 (variance parameter) and ρ = 0925 (correlation parameter)
The power calculations assume a correction for imperfect compliance proposed by Lachin and
Foulkes to allow for 2 noncompliance for each of the treatment arms47 Thus the sample size
of 130 subjects per arm would be reduced to an adjusted sample size of 130(1-002-002)2 =
1198 or 120 subjects per arm
Under the assumed Type I error rate of 005 with a correlation parameter of 0925 and standard
deviation of 090 the difference of 015 L (or 00025 Lweek) shown in Table 6 would have
power of 93
60
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Table 6 Hypothetical Values of Mean FVC (L) Change from Baseline
Week 15 Week 30 Week 45 Week 60
NAC 00125 00250 00375 00500
Placebo 00500 01000 01500 02000
Difference 00375 00750 01125 01500
Abbreviations FVC forced vital capacity PL placebo
972 Power Analysis for Secondary Endpoints
Power calculations for secondary endpoint measurements are shown in Table 7 Standard
deviations are based on unpublished data provided by the University of Michigan The
calculations are based on a 2-sample t-test with Type I error rate set at 005 These calculations
are likely to be conservative because the statistical approach described in section 95 for
analyzing these endpoints will incorporate incomplete observations as well as intermediate data
points
Table 7 Detectable Differences in Treatment Means for Selected Endpoint Measurements
Secondary Endpoints Std Dev
of the Baseline Score
Detectable Difference for 80 Power
Std Dev of the Change Score
Difference Detectable for
80 Power
DLCOpred 166 58 91 32
6MWT Area Under the Desaturation Curve
219 76 175 61
6MWT Distance to Desaturation 224 78 315 110
6MWT Minutes Walked 210 073 205 071
Abbreviations Std Dev standard deviation DLCOpred diffusing capacity of the lung for carbon monoxide percent predicted 6MWT 6-minute walk test
61
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
10 Study Administration
101 Cooperative Agreement Mechanism
The administrative and funding mechanism used to undertake this project is a ldquocooperative
agreementrdquo (U01) which is an assistance mechanism Under the cooperative agreement the
NHLBI assists supports andor stimulates the project and is substantially involved with
investigators in conducting the study by facilitating performance of the effort in a ldquopartnerrdquo role
The NHLBI project scientist serves on the IPFnet Steering Group and he or another NHLBI
scientist may serve on other project committees when appropriate At the same time however
NHLBI does not assume a dominant role direction or prime responsibility for this research
program
As described below governance of the project is conducted through the IPFnet Steering Group
Principal investigators have lead responsibilities in all aspects of their trials and the project
including any modification of trial designs conduct of the trials quality control data analysis
and interpretation preparation of publications and collaboration with other investigators unless
otherwise provided for by the IPFnet Steering Group
PIs retain custody of and have primary rights to their center-specific and collaborative data
subject to government rights-of-access consistent with current Health amp Human Services (HHS)
Public Health Service (PHS) and National Institutes of Health policies The protocols and
governance policies call for the continual submission of data centrally to the IPFnet DCC for the
collaborative database which at a minimum will contain the key variables selected by the IPFnet
Steering Group for standardization across all clinical centers the submission of copies of the
collaborative datasets to each PI upon completion of the project procedures for data analysis
reporting and publication and procedures to protect and ensure the privacy of medical and
genetic data and records of individuals The NHLBI project scientist on behalf of the NHLBI
will have the same access privileges and responsibilities regarding the collaborative data as the
other members of the Steering Group
62
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
PIs are also encouraged to publish and to publicly release and disseminate results data and other
products of the project concordant with the project protocols and governance and the approved
plan for making data and materials available to the scientific community and to the NHLBI
However during the 3 years after the ending date of NHLBI project support unpublished data
unpublished results data sets not previously released and other study materials or products are
to be made available to any third party only with the approval of the IPFnet Steering Group
Upon completion of the project PIs are expected to put their intervention materials and
procedure manuals into the public domain andor make them available to other investigators
according to the approved plan for making data and materials available to the scientific
community and the NHLBI for the conduct of research at no charge other than the costs of
reproduction and distribution
The NHLBI reserves the right to terminate or curtail the project (or an individual award) in the
event of (a) failure to develop or implement mutually agreeable collaborative measurement
subject eligibility and data management sections of the protocols (b) substantial shortfall in
subject recruitment follow-up data reporting or quality control or other major breach of
protocol (c) substantive changes in the agreed-upon protocols with which NHLBI cannot
concur (d) reaching a major project outcome with persuasive statistical significance
substantially before schedule or (e) human subject ethical issues that may dictate a premature
termination
Any disagreement that may arise in scientificprogrammatic matters (within the scope of the
award) between award recipients and the NHLBI may be brought to arbitration An arbitration
panel will be composed of 3 membersmdash1 selected by the IPFnet Steering Group (with the
NHLBI member not voting) or by the individual PI in the event of an individual disagreement a
second selected by NHLBI and the third selected by the other 2 members This special
arbitration procedure in no way affects the PIrsquos right to appeal an adverse action that is otherwise
appealable in accordance with the PHS regulations at 42 CFR part 50 Subpart D and HHS
63
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
regulation at 45 CFR part 16 or the rights of the NHLBI under applicable statutes regulations
and terms of the award
102 IPFnet Steering Group
The IPFnet Steering Group is the main governing body of the project It is composed of the PIs
of the clinical centers the PI of the DCC and the NHLBI project scientist The clinical centers
the IPFnet DCC and the NHLBI each have 1 vote on the IPFnet Steering Group All decisions
are determined by majority vote
All major scientific decisions are determined by the IPFnet Steering Group It assumes overall
responsibility for the design and conduct of the trial It appoints (and disbands) committees and
subcommittees as the need arises designs approves and implements the study protocols
oversees the development of the MOOP monitors subject recruitment and treatment delivery
evaluates data collection and management oversees quality assurance procedures and
implements changes and enhancements to the study as required It also has primary responsibility
for facilitating the conduct of the trials and reporting the projectrsquos results
103 Data and Safety Monitoring Board
The NHLBI will establish a DSMB in accordance with established policies (see
httpwwwnhlbinihgovfundingpoliciesdsmb_insthtm) to ensure data quality and subject
safety and to provide independent advice to the NHLBI regarding progress and the
appropriateness of study continuation
104 Recommendations on Interim Monitoring of Efficacy Safety and Futility
First and foremost the role of the DSMB will be to review subject safety and trial conduct at
periodic points during the study The DSMB may require analyses of the primary endpoint
results for comparing the benefit and risks of treatment strategies The benefit of collecting
additional data on key secondary endpoints with extended follow-up and establishing a robust
64
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
evidence base for determining a standard of care will need to be carefully considered before
early termination of one or more treatment arms After careful consideration the IPFnet Steering
Group recommends conservative thresholds for the early examinations of the safety and efficacy
data
The DSMB will be expected to meet approximately every 6 months until trial completion to
review safety and toxicity data The DSMB may recommend stopping the study based on these
reviews Because the DSMB could stop the trial for safety concerns as well as for a large
efficacy benefit there could be multiple opportunities to reject the null hypothesis (no difference
in event rates between the PL and NAC groups) A Bonferroni approximation will be applied
during the one planned interim analysis for efficacy
Before locking the database a statistical analysis plan (SAP) will be developed to provide
complete details on the statistical analysis The SAP will include the specifics for how and when
the DSMB will be notified for AEs The IPFnet DCC will deliver to the DSMB all FDA-defined
AEs at 3-month intervals The IPFnet DCC will prepare narrative SAE reports in real time for
DSMB review including recommendations and analysis of similar events for each SAE
submitted to the FDA
65
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
11 Investigator and Sponsor Obligations
111 Monitoring
All monitoring activities for US clinical centers will be performed in accordance with DCRI
standard operating procedures Information regarding the types of visits will be outlined in the
PANTHER-IPF MOOP
112 Cost and Payment
There will be no cost to subjects enrolled in this trial Study-related procedures will be paid for
by the IPFnet
Subjects may be eligible for reimbursement for travel to the clinical center Details of payment
will be explained to each subject during the consent process
113 Confidentiality and Health Insurance Portability and Accountability Act
Considerations
Subject confidentiality will be protected throughout the study All subject data will be kept
strictly confidential and no subject-identifying information will be released to anyone outside
the project Confidentiality will be assured through several mechanisms First each subject will
be assigned an anonymous study ID which will then be used on all study forms Second any
study forms blood samples and paper records that contain subject information (eg address lists
phone lists) will be kept at the clinical centers in secured locked areas coded by number Once
blood is collected there will be no subject identifiers placed on blood samplesmdashonly the study
ID number and the date of sample collection Third access to all subject data and information
including laboratory specimens will be restricted to authorized personnel In the case of
computerized data this restricted access will be assured through user logon IDs and password
protection
66
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
At the IPFnet DCC only authorized personnel will have access to the data files containing study
data Security will be assured through user logon IDs passwords and appropriate access
privileges All study subjects will be identified only by their IPFnet ID numbers and no personal
identifying information such as name address or Social Security number will be entered into
the IPFnet DCC database Any subject-specific data reported to the IPFnet Steering Group will
be identified only by the IPFnet ID number
Finally subjects will not be identified by name in any reports or publications nor will the data
be presented in such a way that the identity of individual subjects can be inferred Analysis files
created for further study by the scientific community will have no subject identifiers These data
files will be created in accordance with the Ancillary Studies and Publication Policy of the
IPFnet
114 Informed Consent Procedures
All IPFnet subjects will provide written informed consent using procedures reviewed and
approved by each clinical centerrsquos IRB Informed consent will be undertaken by study personnel
in-person with the subject The subject has the option of declining further participation in the
study at that point No further study procedures will be conducted until the signed documents
have been provided to the IPFnet clinical center
115 Institutional Review Boards
Before initiating this study the protocol clinical center-specific informed consent forms Health
Insurance Portability and Accountability Act (HIPAA) forms recruitment materials and other
relevant information will be reviewed by a properly constituted IRB at each participating clinical
center A copy of the signed and dated IRB approval at each clinical center will be retrieved prior
to or during the site initiation visit and archived at the IPFnet DCC Any amendments to the
protocol other than simple administrative and typographical changes must be approved by each
IRB before they are implemented The clinical centers will seek annual renewals of their IRB
approvals in accordance with local procedures
67
__________________________________________ ________________
__________________________________________
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
12 Investigator Agreement
I have read the foregoing protocol PANTHER-IPF and agree that it contains all necessary
details for carrying out this study I will conduct the study as outlined herein and will complete
the study within the time designated
I will provide copies of the protocol and all pertinent information to all individuals responsible to
me who assist in the conduct of this study I will discuss this material with them to ensure they
are fully informed regarding the drug and the conduct of the study
I will fulfill all responsibilities for submitting pertinent information to the local IRB if
applicable that is responsible for this study
I further agree that NHLBI andor DCRI will have access to any source documents from which
eCRF information may have been generated
Signature of Principal Investigator Date
Name of Principal Investigator (printed or typed)
Protocol version date May 19 2009
Protocol Amendment 1 version date May 28 2010
Protocol Amendment 2 version date December 6 2011
68
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
13 References
1 Raghu G Brown KK Bradford WZ et al A placebo-controlled trial of interferon gamma-1b in patients with idiopathic pulmonary fibrosis N Engl J Med 2004350125-33 2 King TE Jr Safrin S Starko KM et al Analyses of efficacy end points in a controlled trial of interferon-gamma1b for idiopathic pulmonary fibrosis Chest 2005127171-7 3 Flaherty KR Thwaite EL Kazerooni EA et al Radiological versus histological diagnosis in UIP and NSIP survival implications Thorax 200358143-8 4 Wells AU Desai SR Rubens MB et al Idiopathic pulmonary fibrosis a composite physiologic index derived from disease extent observed by computed tomography Am J Respir Crit Care Med 2003167962-9 5 Raghu G Freudenberger TD Yang S et al High prevalence of abnormal acid gastroshyoesophageal reflux in idiopathic pulmonary fibrosis Eur Respir J 200627136-42 6 Kinnula VL Focus on antioxidant enzymes and antioxidant strategies in smoking related airway diseases Thorax 200560693-700 7 Coultas DB Zumwalt RE Black WC Sobonya RE The epidemiology of interstitial lung diseases Am J Respir Crit Care Med 1994150967-72 8 Raghu G Weycker D Edelsberg J Bradford WZ Oster G Incidence and prevalence of idiopathic pulmonary fibrosis Am J Respir Crit Care Med 2006174810-6 9 Olson AL Swigris JJ Lezotte DC Norris JM Wilson CG Brown KK Mortality from pulmonary fibrosis increased in the United States from 1992 to 2003 Am J Respir Crit Care Med 2007176277-84 10 Mannino DM Etzel RA Parrish RG Pulmonary fibrosis deaths in the United States 1979shy1991 An analysis of multiple-cause mortality data Am J Respir Crit Care Med 19961531548shy52 11 Hubbard R Johnston I Coultas DB Britton J Mortality rates from cryptogenic fibrosing alveolitis in seven countries Thorax 199651711-6 12 Johnston I Britton J Kinnear W Logan R Rising mortality from cryptogenic fibrosing alveolitis Bmj 19903011017-21 13 Raghu G Collard HR Egan JJ et al An official ATSERSJRSALAT statement idiopathic pulmonary fibrosis evidence-based guidelines for diagnosis and management Am J Respir Crit Care Med 2011183788-824 14 (USA) FDA FDA Public Health Advisory Interferon gamma-1b (marketed as Actimmune) In 2007 15 King TE Jr Pardo A Selman M Idiopathic pulmonary fibrosis Lancet 2011 16 Raghu G Brown KK Costabel U et al Treatment of idiopathic pulmonary fibrosis with etanercept an exploratory placebo-controlled trial Am J Respir Crit Care Med 2008178948shy55 17 Malouf MA Hopkins P Snell G Glanville AR An investigator-driven study of everolimus in surgical lung biopsy confirmed idiopathic pulmonary fibrosis Respirology 201116776-83 18 King TE Jr Behr J Brown KK et al BUILD-1 a randomized placebo-controlled trial of bosentan in idiopathic pulmonary fibrosis Am J Respir Crit Care Med 200817775-81 19 Richeldi L Costabel U Selman M et al Efficacy of a tyrosine kinase inhibitor in idiopathic pulmonary fibrosis N Engl J Med 20113651079-87
69
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
20 Borok Z Buhl R Grimes GJ et al Effect of glutathione aerosol on oxidant-antioxidant imbalance in idiopathic pulmonary fibrosis Lancet 1991338215-6 21 Meyer A Buhl R Magnussen H The effect of oral N-acetylcysteine on lung glutathione levels in idiopathic pulmonary fibrosis Eur Respir J 19947431-6 22 Behr J Maier K Degenkolb B Krombach F Vogelmeier C Antioxidative and clinical effects of high-dose N-acetylcysteine in fibrosing alveolitis Adjunctive therapy to maintenance immunosuppression Am J Respir Crit Care Med 19971561897-901 23 Cantin AM North SL Fells GA Hubbard RC Crystal RG Oxidant-mediated epithelial cell injury in idiopathic pulmonary fibrosis J Clin Invest 1987791665-73 24 Waghray M Cui Z Horowitz JC et al Hydrogen peroxide is a diffusible paracrine signal for the induction of epithelial cell death by activated myofibroblasts Faseb J 200519854-6 25 Larios JM Budhiraja R Fanburg BL Thannickal VJ Oxidative protein cross-linking reactions involving L-tyrosine in transforming growth factor-beta1-stimulated fibroblasts J Biol Chem 200127617437-41 26 Kinnula VL Fattman CL Tan RJ Oury TD Oxidative stress in pulmonary fibrosis a possible role for redox modulatory therapy Am J Respir Crit Care Med 2005172417-22 27 Meyer A Buhl R Kampf S Magnussen H Intravenous N-acetylcysteine and lung glutathione of patients with pulmonary fibrosis and normals Am J Respir Crit Care Med 19951521055-60 28 Behr J Degenkolb B Krombach F Vogelmeier C Intracellular glutathione and bronchoalveolar cells in fibrosing alveolitis effects of N-acetylcysteine Eur Respir J 200219906-11 29 Bando M Hosono T Mato N et al Long-term efficacy of inhaled N-acetylcysteine in patients with idiopathic pulmonary fibrosis Intern Med 2010492289-96 30 Demedts M Behr J Buhl R et al High-dose acetylcysteine in idiopathic pulmonary fibrosis N Engl J Med 20053532229-42 31 Toma TP Bhowmik A Rajakulasingam R Acetylcysteine in pulmonary fibrosis N Engl J Med 20063541086-9 author reply -9 32 Hunninghake GW Antioxidant therapy for idiopathic pulmonary fibrosis N Engl J Med 20053532285-7 33 Flaherty KR Mumford JA Murray S et al Prognostic implications of physiologic and radiographic changes in idiopathic interstitial pneumonia Am J Respir Crit Care Med 2003168543-8 34 Latsi PI du Bois RM Nicholson AG et al Fibrotic idiopathic interstitial pneumonia the prognostic value of longitudinal functional trends Am J Respir Crit Care Med 2003168531-7 35 Collard HR King TE Jr Bartelson BB Vourlekis JS Schwarz MI Brown KK Changes in clinical and physiologic variables predict survival in idiopathic pulmonary fibrosis Am J Respir Crit Care Med 2003168538-42 36 Jegal Y Kim DS Shim TS et al Physiology is a stronger predictor of survival than pathology in fibrotic interstitial pneumonia Am J Respir Crit Care Med 2005171639-44 37 Martinez FJ Safrin S Weycker D et al The clinical course of patients with idiopathic pulmonary fibrosis Ann Intern Med 2005142963-7 38 Hull JH Acetylcysteine in pulmonary fibrosis N Engl J Med 20063541089-91 author reply -91
70
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
39 Flaherty KR King TE Jr Raghu G et al Idiopathic interstitial pneumonia what is the effect of a multidisciplinary approach to diagnosis Am J Respir Crit Care Med 2004170904shy10 40 Raghu G Johnson WC Lockhart D Mageto Y Treatment of idiopathic pulmonary fibrosis with a new antifibrotic agent pirfenidone results of a prospective open-label Phase II study Am J Respir Crit Care Med 19991591061-9 41 Hunninghake GW Lynch DA Galvin JR et al Radiologic findings are strongly associated with a pathologic diagnosis of usual interstitial pneumonia Chest 20031241215-23 42 Lynch D Godwin J Safrin S et al High-resolution computed tomography in idiopathic pulmonary fibrosis diagnosis and prognosis Am J Respir Crit Care Med 2005172488-93 43 Mallinckrodt CH Watkin JG Molenberghs G Carroll RJ Choice of the primary analysis in longitudinal clinical trials Pharmaceutical Statistics 20043161-9 44 Bang H Tsiatis A Estimating medical costs with censored data Biometrika 200087329shy43 45 Lin DY Regression analysis of incomplete medical cost data Stat Med 2003221181-200 46 Rochon J Application of GEE procedures for sample size calculations in repeated measures experiments Stat Med 1998171643-58 47 Lachin JM Foulkes MA Evaluation of sample size and power for analyses of survival with allowance for nonuniform patient entry losses to follow-up noncompliance and stratification Biometrics 198642507-19
71
- PANTHER-IPFPREDNISONE AZATHIOPRINEAND N-ACETYLCYSTEINEA STUDY THAT EVALUATES RESPONSE INIDIOPATHIC PULMONARY FIBROSIS
-
- Protocol Summary
- Table of Contents
- List of Tables
- List of Figures
- List of Abbreviations
- 1 Summary
- 2 Hypotheses and Specific Aims
-
- 21 Null Hypothesis
- 22 Specific Aim 1
- 23 Specific Aim 2
- 24 Prespecified Subgroups of Interest
-
- 3 Background and Significance
-
- 31 Idiopathic Pulmonary Fibrosis is the Most Common Interstitial Lung Disease
- 32 Rationale for Placebo Control
- 33 Rationale for N-acetylcysteine
- 35 Rationale for N-acetylcysteine as a Stand-alone Therapy
- 36 Rationale for the Study Design and Primary Endpoint
- 37 Rationale for Blinding of Treatments
-
- 4 Methods
-
- 41 Inclusion Criteria
- 42 Diagnosis of IPF
- 43 Exclusion Criteria
- 44 Study Design and Study Visit
- 45 Dose Justification
- 46 Contraindications Precautions and Side Effects of Study Medications
- 47 Recruitment Procedures
- 48 Study Procedures
- 49 Concomitant Medications
- 410 Laboratory Testing
- 411 Blinding of Study Drugs
-
- 5 Study Endpoints
-
- 51 Primary Study Endpoint
- 52 Secondary Study Endpoints
-
- 6 Safety Evaluations and Procedures
-
- 61 Adverse Events
- 62 Clinical Medical Monitoring
- 63 Unblinding Procedures
-
- 7 Study Drug Procedures
- 8 Data Management
-
- 81 Hardware and Software Configuration
- 82 Sources of Data
-
- 9 Study Design and Data Analysis
-
- 91 General Analytic Considerations
- 92 Randomization Blinding and Reporting of Results
- 93 Stratification
- 94 Specification of the Primary Analyses
- 95 Analysis of Longitudinal Endpoints
- 96 Analysis of Binary Time-to-Event and Time-Lagged Endpoints
- 97 Power Analysis
-
- 10 Study Administration
-
- 101 Cooperative Agreement Mechanism
- 102 IPFnet Steering Group
- 103 Data and Safety Monitoring Board
- 104 Recommendations on Interim Monitoring of Efficacy Safety and Futility
-
- 11 Investigator and Sponsor Obligations
-
- 111 Monitoring
- 112 Cost and Payment
- 113 Confidentiality and Health Insurance Portability and Accountability ActConsiderations
- 114 Informed Consent Procedures
- 115 Institutional Review Boards
-
- 12 Investigator Agreement
- 13 References
-

PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Table of Contents
List of Tables 7
List of Figures 7
List of Abbreviations 8
1 Summary 12
2 Hypotheses and Specific Aims 13 21 Null Hypothesis 13 22 Specific Aim 1 13 23 Specific Aim 2 13 24 Prespecified Subgroups of Interest 14
3 Background and Significance 15 31 Idiopathic Pulmonary Fibrosis is the Most Common Interstitial Lung Disease15 32 Rationale for Placebo Control 15 33 Rationale for N-acetylcysteine 16 35 Rationale for N-acetylcysteine as a Stand-alone Therapy 17 36 Rationale for the Study Design and Primary Endpoint 18 37 Rationale for Blinding of Treatments 19
4 Methods 21 41 Inclusion Criteria 21
411 Subjects Shown to Have Usual Interstitial Pneumonia Pattern on Surgical Lung Biopsy 21 412 Subjects Who Have Not Undergone a Surgical Lung Biopsy 21
42 Diagnosis of IPF 21 43 Exclusion Criteria 26 44 Study Design and Study Visit 27
441 Study Design Summary 27 442 Study Visits 28
4421 Screening 28 4422 Enrollment 29 4423 Week 15 30 4424 Week 30 31 4425 Week 45 31 4426 Week 60 (Early Withdrawal or Final Treatment Visit) 32 4427 Final Site Visit ndash FVC drop confirmation 33 4428 Final Visit ndash Telephone Follow-up 33 4429 Phone Contact Between Visits 33
45 Dose Justification 35 451 Rationale for N-acetylcysteine Dosing 35
4511 Dosing of N-acetylcysteineplacebo 35 4512 Reasons to Discontinue N-acetylcysteineplacebo 35
452 Dosage Algorithms 37 46 Contraindications Precautions and Side Effects of Study Medications 39
461 Contraindication 39 462 Precautions 39 463 Side Effects 39
47 Recruitment Procedures 40 48 Study Procedures 41
481 Biological Specimen Management 41 4811 Biological Specimen Sample Management 41
49 Concomitant Medications 42 410 Laboratory Testing 42 411 Blinding of Study Drugs 43
4
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
5 Study Endpoints 44 51 Primary Study Endpoint 44 52 Secondary Study Endpoints 44
521 Time to Disease-progression 44 522 Acute Exacerbations 44 523 Respiratory Infections 47 524 Maintained FVC Response 48
6 Safety Evaluations and Procedures 49 61 Adverse Events 49
611 Definitions 49 612 Adverse Event (AE) Reporting 50
6121 Serious Adverse Events (SAE) Reporting 50 6122 Regulatory Reporting 51
62 Clinical Medical Monitoring 52 63 Unblinding Procedures 52
7 Study Drug Procedures 53
8 Data Management 54 81 Hardware and Software Configuration 54
811 Hardware and Database Software 54 812 Statistical Software 54 813 Access Control and Confidentiality Procedures 54 814 Security 54 815 Back-up Procedures 55 816 Virus Protection 55
82 Sources of Data 55 821 Design and Development 55 822 Data Collection Forms 55 823 Data Acquisition and Entry 56 824 Data Center Responsibilities 56 825 Data Editing 56 826 Training 56
9 Study Design and Data Analysis 57 91 General Analytic Considerations 57 92 Randomization Blinding and Reporting of Results 57 93 Stratification 58 94 Specification of the Primary Analyses 58 95 Analysis of Longitudinal Endpoints 58 96 Analysis of Binary Time-to-Event and Time-Lagged Endpoints 59 97 Power Analysis 60
971 Primary Analyses 60 972 Power Analysis for Secondary Endpoints 61
10 Study Administration 62 101 Cooperative Agreement Mechanism 62 102 IPFnet Steering Group 64 103 Data and Safety Monitoring Board 64 104 Recommendations on Interim Monitoring of Efficacy Safety and Futility 64
11 Investigator and Sponsor Obligations 66 111 Monitoring 66 112 Cost and Payment 66 113 Confidentiality and Health Insurance Portability and Accountability Act Considerations 66 114 Informed Consent Procedures 67 115 Institutional Review Boards 67
5
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
12 Investigator Agreement 68
13 References 69
6
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
List of Tables Table 1 Operating Characteristics of Local HRCT Review for Diagnosis of UIP (24)
Table 2 Combining HRCT and Pathology Interpretations to Determine if IPF is Present (25)
Table 3 Schedule of Assessments (34)
Table 4 Side Effects of NAC (40)
Table 5 Final Diagnoses in Evaluation of Suspected Acute Exacerbations (46)
Table 6 Hypothetical Values of Mean FVC (L) Change from Baseline (61)
Table 7 Detectable Differences in Treatment Means for Selected Endpoint Measurements (61)
List of FiguresFigure 1 Changes in Forced Vital Capacity from Baseline in Prior IPF Clinical Trials (19)
Figure 2 Diagnosis of Idiopathic Pulmonary Fibrosis in the IPFnet (22)
Figure 3 Pathology Flow Chart Surgical Lung Biopsy Diagnosis (23)
Figure 4 Acute Exacerbation Flow Chart (47)
7
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
List of Abbreviations
6MWT 6-minute walk test
A-aPO2 alveolar-arterial PO2 difference
ABG arterial blood gas
AE adverse event
AEx acute exacerbation
AG albuminglobulin
ALT alanine aminotransferase
AST aspartate aminotransferase
ATS American Thoracic Society
AZA azathioprine
BAL bronchoalveolar lavage
BUN blood urea nitrogen
CBC complete blood count
cGMP Current Good Manufacturing Practice
CPI Composite Physiologic Index
CPK creatine phosphokinase
CT computed tomography
DCC Data Coordinating Center
DCRI Duke Clinical Research Institute
8
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
DLCO diffusing capacity of the lung for carbon monoxide
DLCOpred diffusing capacity of the lung for carbon monoxide percent predicted
DSMB data and safety monitoring board
eCRF Electronic case report form
ERS European Respiratory Society
FDA Food and Drug Administration (US)
FEV1 forced expiratory volume in 1 second
FSH follicle-stimulating hormone
FVC forced vital capacity
FVCpred forced vital capacity percent predicted
GGT gamma glutamyl transferase
GSH glutathione
HAD Hospital Anxiety and Depression
HHS Health amp Human Services (US Dept of)
HIPAA Health Insurance Portability and Accountability Act
HRCT high-resolution computed tomography
IBW ideal body weight
ICE CAP Investigating Choice Experiments for Preferences of Older People Capability Instrument
ILD interstitial lung disease
IPF idiopathic pulmonary fibrosis
9
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
IPFnet Idiopathic Pulmonary Fibrosis Clinical Research Network
IRB institutional review board
ITT intent to treat
IV intravenous
IVRS interactive voice response system
LDH lactate dehydrogenase
LFT liver function test
LOCF last observation carried forward
LSD Least Significant Difference
MAR missing at random
MCAR missing completely at random
MMRM mixed model repeated measures
MOOP manual of operating procedures
NAC N-acetylcysteine
NHLBI National Heart Lung and Blood Institute (US)
NIH National Institutes of Health (US)
NSIP nonspecific interstitial pneumonia
PaO2 partial pressure of arterial oxygen
PCP primary care provider
PFT pulmonary function test
10
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
PHS Public Health Service (US)
PI principal investigator
PL placebo
PLT platelet
PRED prednisone
QOL quality of life
SAE serious adverse event
SAP statistical analysis plan
SGRQ St Georgersquos Respiratory Questionnaire
SpO2 oxygen saturation by pulse oximetry
TPMT thiopurine methyl transferase
UCSD SOBQ University of California at San Diego Shortness of Breath Questionnaire
UIP usual interstitial pneumonia
ULN upper limit of normal
USP United States Pharmacopoeia
VC vital capacity
WBC white blood cell
11
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
PREDNISONE AZATHIOPRINE AND N-ACETYLCYSTEINE A STUDY
THAT EVALUATES RESPONSE IN IDIOPATHIC PULMONARY FIBROSIS
1 Summary
There are currently no drug therapies that have proven to be effective in the treatment of idiopathic pulmonary
fibrosis (IPF) Previous clinical drug trials have been difficult to interpret due to lack of true placebo (PL)
controls or other methodological concerns Clinical efficacy of immunosuppressive therapies and agents that
reduce oxidative stress remains controversial The IPF Clinical Research Network (IPFnet) is conducting a
randomized double-blind placebo-controlled trial designed to assess the safety and efficacy of
N-acetylcysteine (NAC) as monotherapy in subjects with mild or moderate IPF
The study initially employed a 3-arm design with 111 randomization to NAC azathioprine (AZA)-prednisone
(PRED)-NAC and PL with each subject to be treated up to a maximum of 60 weeks followed by a tapering of
PREDPL and a 4-week period for safety evaluation Approximately 390 subjects who have mild to moderate
IPF (defined as forced vital capacity percent predicted [FVCpred] ge 50 and diffusing capacity of the lung
for carbon monoxide percent predicted [DLCOpred] 30) diagnosed within the past 48 months were to be
enrolled
At the pre-specified interim analysis the DSMB recommended termination of the prednisone-azathioprine-
NAC arm of the study No additional patients will be randomized to that arm However the NAC and placebo
arms remain open for enrollment and we will enroll approximately 130 subjects in each arm (inclusive of the
subjects enrolled at the time of the interim analysis) Follow up for subjects enrolled into the two arms will
continue for 60 weeks
The primary endpoint is the change in longitudinal measurements of FVC over the study period The primary
goal of this study to establish an evidence-based standard of care and clarify myths from facts for
pharmacotherapy of IPF has been met in part by demonstrating that the widely used triple therapy was harmful
to patients with IPF (NHLBI press release Oct 21 2011) To determine the potential therapeutic benefits of
NAC alone the study will continue to enroll patients as a two-arm double-blind placebo-controlled study from
this point on (NAC vs placebo) as recommended by the DSMB following the pre-specified interim analysis
12
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
2 Hypotheses and Specific Aims 21 Null Hypothesis
Treatment with NAC will provide the same efficacy as PL as measured by longitudinal changes in FVC
22 Specific Aim 1
This study is designed to assess the safety and efficacy of NAC in subjects with newly diagnosed IPF
23 Specific Aim 2
Secondary goals of this study are to assess differences between treatment groups for the following
1 Mortality
2 Time to death
3 Frequency of acute exacerbations (AExs)
4 Frequency of maintained FVC response
5 Time-to-disease progression
6 Change in DLCO
7 Change in Composite Physiologic Index (CPI)
8 Change in resting alveolar-arterial oxygen gradient
9 Change in 6-minute walk test (6MWT) distance
10 Change in 6MWT oxygen saturation area under the curve
11 Change in 6MWT distance to desaturation lt 80
12 Change in 6MWT minutes walked
13 Changes in health status as measured by the SF-36 EuroQol and St Georgersquos Respiratory
Questionnaire (SGRQ)
14 Changes in dyspnea as measured by the University of California at San Diego Shortness of Breath
Questionnaire (UCSD SOBQ)
15 Frequency and types of adverse events (AEs)
16 Frequency and types of respiratory complications both infectious and noninfectious
17 Frequency of hospitalizations both all-cause and respiratory-related
13
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
24 Prespecified Subgroups of Interest
Treatment effects will be estimated and compared within key subgroups
Higher enrollment FVC12
Typical vs atypical high-resolution computed tomography (HRCT) reading at baseline3
Recent vs more remote diagnosis (time from initial diagnosis of IPF le 1 year and gt 1 year)
Lower CPI score at enrollment4
Medical therapy for gastroesophageal reflux5
Ethnic background
Sex
Smoking history (current or ex-smoker vs never smoker) given potential impact on oxidant status6
Presence of emphysema gt 25 on HRCT
14
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
3 Background and Significance
31 Idiopathic Pulmonary Fibrosis is the Most Common Interstitial Lung Disease
IPF is the most common interstitial lung disease (ILD) of unknown etiology The current incidence and
prevalence of IPF in the United States are not known A 1994 study of a population-based registry of subjects in
Bernalillo County New Mexico USA estimated an incidence of 107 cases per 100000 per year for males and
74 cases per 100000 per year for females the prevalence of IPF was estimated at 20 per 100000 for males and
13 per 100000 for females7 Extrapolating from a large healthcare claims database a more recent review
estimated the prevalence of IPF in the United States at 427 per 100000 (incidence estimated at 163 per
100000 per year)8 Recent epidemiological studies indicate increasing mortality rates from IPF in the United
States and other industrialized nations9-12
Approximately two-thirds of subjects with IPF are over the age of 60 at the time of presentation and the
incidence increases with age13 IPF has no distinct geographical distribution and predilection by race or
ethnicity has not been identified13 Individual subjects may remain relatively stable for prolonged periods
experience very slow declines in lung function with progression of radiographic abnormalities for a period of
months to years or experience more rapid declines and subsequent death Only 20 to 30 of IPF patients
survive for 5 years following diagnosis
There is currently no proven effective pharmacological treatment for IPF13 Anti-inflammatory and
immunosuppressive agents have been the traditional approach to the management of patients with IPF Based
on the results of the interim analysis of the PANTHER-IPF trial this lsquotraditional approachrsquo will be aborted
However it remains unknown if NAC alone will prove beneficial in IPF patients The primary goal of the
modified study is to establish an evidence-based standard of care and clarify the role of this specific antioxidant
pharmacotherapy for IPF
32 Rationale for Placebo Control
IPF is a disorder for which there is no proven efficacious therapy A major objective of this trial is to test to the
greatest degree possible a proposed standard of care for patients with IPF The current traditional therapy
15
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
employs immunosuppressive and corticosteroid drugs Interim review of the original PANTHER-IPF study has
documented increased adverse events and lack of efficacy for AZA-PRED-NAC compared to placebo
suggesting that this therapeutic approach should not be employed Whether this applies to NAC alone which
has been advocated by international societies has not been proven in well-designed well-powered clinical
trials The recommendations made in the recently published evidence guidelines for NAC monotherapy was
weak based on low quality13 Thus this continued clinical trial randomizing patients to receive NAC or placebo
is pivotal and will answer the important question of the potential therapeutic benefits of NAC monotherapy with
grade A evidence In this prospective randomized clinical trial the inclusion of a PL arm is therefore vital to
adequately test the benefits of NAC in well-characterized subjects with IPF
If NAC has no true efficacy then its role as standard of care will be refuted If a benefit compared with PL is
confirmed it will establish a benchmark against which future novel therapies for IPF will be safely compared
As there is no currently accepted therapy for IPF there is an increasing body of published literature supporting
the concept of no treatment as the ldquobest carerdquo option for IPF13
Post hoc analyses of PL-controlled trials suggest that subjects with milder disease may be more amenable to
therapy12 It is notable that a recent international prospective randomized trial of interferon-gamma for IPF
also included a PL arm the study was terminated early by the data and safety monitoring board (DSMB) due to
lack of treatment effect1415 This underscores the belief that a proven effective therapy for IPF does not
currently exist and that true placebo-controlled trials remain the gold standard Similarly recently completed
trials of etanercept everolimus bosentan and BIPF 1120 in IPF have included PL-treated arms16-19 In three of
these trials the treated subjects showed little if any objective improvement Based on this evidence and the
current status of IPF therapy and therapeutic trials we believe that clinicians and subjects will continue to enroll
in a PL-controlled study
33 Rationale for N-acetylcysteine
NAC is a derivative of the amino acid L-cysteine NAC has been shown to augment levels of the naturally
occurring antioxidant glutathione (GSH ) (glutathione γ-glutamyl cysteinyl glycine) both in vitro and in
vivo2021 GSH is present in all eukaryotic cells and may play an important role in protecting alveolar epithelial
cells against oxidant injury The concentration of GSH in the bronchoalveolar lavage (BAL) fluid in patients
16
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
with IPF is markedly diminished compared with normal subjects This GSH deficiency may be corrected by
exogenous administration of NAC2122
There is evidence of enhanced production of oxidants in an IPF lung Both inflammatory cells and
myofibroblasts derived from patients with IPF generate increased amounts of extracellular oxidants including
hydrogen peroxide2324 Secretion of hydrogen peroxide by activated myofibroblasts may induce the death of
adjacent lung epithelial cells by paracrine mechanisms24 Additionally generation of oxidants by myofibroblasts
induces oxidative crosslinking of extracellular matrix proteins25 a potential mechanism for aberrant matrix
remodeling Thus an oxidant-antioxidant imbalance exists in the lungs of IPF patients26 NAC may confer
protection against this imbalance by augmenting GSH levels in addition to its more direct free-radical
scavenging activity
Intravenous (IV) NAC therapy has been shown to increase total BAL GSH in 8 IPF subjects27 Oral NAC (600
mg 3 times per day) has been shown to decrease markers of oxidant injury and improve both total and reduced
GSH levels in the epithelial lining fluid of subjects with IPF in a small uncontrolled study22 pulmonary
function improved modestly with therapy A similar study in 18 IPF subjects confirmed increased intracellular
GSH concentration after 12 weeks of NAC (600 mg 3 times per day)2228 no clinical correlates were reported
Inhaled NAC was suggested to improve pulmonary function in an open label study29
35 Rationale for N-acetylcysteine as a Stand-alone Therapy
Results of a double-blind multi-center European clinical trial of 150 IPF subjects testing combinations of AZAshy
PRED vs AZA-PRED-NAC have been reported30 NAC added to AZA-PRED (ldquoconventional therapyrdquo) had a
significant positive effect on DLCO (p lt 0005) and vital capacity (VC) (p lt 005) at the end of 1 year30 The
recent ATSERS position statement after much discussion concluded that NAC alone should not be considered
in the majority of patients with IPF without additional data from well-designed studies
The interpretation of these data has been quite controversial Some have suggested that the magnitude of the
treatment effect although statistically significant is modest31 Others have suggested that NAC may be
modulating potential toxic effects of AZA-PRED alone32 supporting the investigation of NAC as stand-alone
therapy
17
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
The IPFnet is now completing the PANTHER-IPF trial with a 11 randomization (NAC vs placebo) and a
simple practical feasible and scientifically rational design that will establish standard of care with NAC for
IPF based on a currently available therapeutic agent and the existing data to support its use We anticipate that
all future clinical trials of novel therapeutic agents will be tested against this to-be-established standard of care
36 Rationale for the Study Design and Primary Endpoint
The optimal study design of a therapeutic trial in IPF would include survival as a primary endpoint The
published results of the IFN-γ 1b Phase 3 (GIPF-001) trial suggested a survival benefit in subjects with milder
disease in retrospective analyses1 although the trial was underpowered to address this question This was likely
related to the limited mortality in the PL arm of the study which included IPF subjects with mild to moderate
disease This study documents that an IPF study powered to improve survival in a patient population with mild
disease requires a larger sample size andor duration of study In fact the recently aborted Phase 3 IFN-γ 1b
(GIPF-007 INSPIRE) study was a survival-based study and recruited more than 800 subjects at 75 centers
worldwide1415 As such within the context of the current IPFnet trial survival is an impractical primary
endpoint variable
Several groups have published data defining an appropriate surrogate outcome variable a 10 decrement in
FVC during 6 to 12 months is a powerful predictor of survival in IPF33-36 Furthermore additional evidence
suggests a similar predictive ability for a 10 decrement in FVC during 3 months of follow-up37 With strong
supportive evidence of FVC progression being related to mortality on a per-subject basis this study will use
FVC changes in liters between treatment groups as the primary endpoint Previously published IPF studies have
shown a steady decline in FVC (and FVCpred) among control group subjects230 The GIPF-001 study
suggested a 48-week decrease in FVC of 016 L in the PL-treated subjects The IFIGENIA study demonstrated
a decline in FVC of approximately 019 L over 52 weeks in the subjects randomized to the control treatment
Figure 1 depicts the change in FVC for control groups from previously published IPF studies38 Based on these
data we expect that the PL group will have a decline of 020 L over the 60-week study period The IPFnet
Steering Group determined that a clinically meaningful improvement would be the preservation of the majority
of the 020-L FVC decline Therefore a mean treatment difference of 015 L in mean FVC over the 60-week
study period was determined to be a clinically meaningful difference
18
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Δ f
rom
bas
elin
e (i
n L
)
01
005
0
-005
-01
-015 Projected Δ for placebo
-02
-025
-019
-016
-013 Pirfenidone GIPF001
NAC
Placebo
4 8 12 16 20 24 28 32 36 40 44 48 52 56 60
Week
Figure 1 Changes in FVC From Baseline in Prior IPF Clinical Trials
Recent data suggest that various patient subgroups would be expected to potentially exhibit differential response
to therapy These parameters will be used to a priori separate patients by a series of baseline characteristics
including
1 Higher enrollment FVC12
2 Typical vs atypical high-resolution computed tomography (HRCT) reading at baseline3
3 Recent vs more remote diagnosis (time from initial diagnosis of IPF le 1 year and gt 1 year)
4 Lower CPI score at enrollment4
5 Medical therapy for gastroesophageal reflux5
6 Ethnic background
7 Sex
8 Smoking history (current or ex-smoker vs never smoker) given potential impact on oxidant status6
9 Presence of emphysema gt 25 on HRCT
37 Rationale for Blinding of Treatments
The issue of treatment blinding was given a great deal of consideration with subject safety being the primary
concern After discussion among the Steering Group members it was decided that as long as subject safety
could be ensured blinding was necessary Blinding allows the study to
Have optimal scientific validity and potential to impact the standard of care for subjects
19
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Make objective assessments of treatment effects
Maintain clinical equipoise among investigators
Encourage subjects to have similar levels of contact with the medical community
Minimize the differential dropout rates across study arms
20
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
4 Methods 41 Inclusion Criteria
1 Age 35 to 85 years inclusive
2 FVC ge 50 of predicted (post-bronchodilator measurement from the screening visit)
3 DLCO ge 30 of predicted (hemoglobin corrected and altitude corrected if gt4000 ft above sea level)
4 Ability to understand and provide informed consent
5 Diagnosis of IPF according to a modified version of the ATS criteria le 48 months from enrollment The
date of diagnosis is defined as the date of the first available HRCT or surgical lung biopsy characteristic
of definite UIP
411 Subjects Shown to Have Usual Interstitial Pneumonia Pattern on Surgical Lung Biopsy
Subjects who have been shown to have UIP pattern on lung biopsy must have all of the following
1 Exclusion of other known causes of ILD such as drug toxicity clinically significant environmental
exposures or diagnosis of connective tissue diseases
2 Bibasilar reticular abnormalities with minimal ground glass opacities on HRCT scan
412 Subjects Who Have Not Undergone a Surgical Lung Biopsy
In addition to the criteria above these subjects must have radiological findings considered to be definite for the
diagnosis of UIPIPF
1 Bibasilar reticular abnormalities with minimal ground glass opacities
2 Honeycombing as the predominant feature and located in the peripheral lung bases
42 Diagnosis of IPF
Only subjects with definite IPF will be eligible for enrollment in this study We will utilize a combination of
clinicalphysiologic features HRCT and review of a clinically obtained surgical lung biopsy specimen to
establish the diagnosis of IPF An algorithm for the diagnosis is provided to guide entry into the protocol as
outlined in the inclusion and exclusion criteria (Figures 2 and 3) This multi-disciplinary approach uses
21
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
expertise from clinicians radiologists and pathologists Investigators at each site in conjunction with central
pathology will work together to establish the diagnosis of IPF This interactive approach to the diagnosis of IPF
increases the level of agreement between observers39
A subject with suspected ILD should be evaluated for secondary causes including but not limited to
environmental exposures drugs and systemic diseases Presence of any of these findings felt to be significant
enough to cause an ILD should disqualify the subject from entry into the trial
If secondary causes are absent an HRCT scan may be obtained If an HRCT of sufficiently high quality has
been obtained within the last 3 months that scan may be used for diagnosis In the appropriate clinical setting
the diagnosis of IPF can be made by the demonstration of a typical radiographic pattern on HRCT or by
demonstration of UIP pattern on a surgical lung biopsy The following criteria for a radiographic (ie
nonsurgical) diagnosis will be used In the absence of known exposures andor clinical associations attributable
to pulmonary fibrosis and in the appropriate clinical setting the presence of definite UIP pattern in HRCT
images is required to meet study criteria for the diagnosis of IPF
Figure 2 Diagnosis of Idiopathic Pulmonary Fibrosis in the IPFnet
22
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Figure 3 Pathology Flow Chart Surgical Lung Biopsy Diagnosis
Requirement for diagnosis
1 Clinical exclusion of other known causes (connective tissue diseases environmental and drug
exposures) of ILD
2 Radiographic HRCT with bibasilar reticular abnormality and honeycomb change with minimal
ground glass opacities
Appropriate clinical setting
1 Age gt 50 years
2 Insidious onset of unexplained dyspnea
3 Duration of illness for ge 3 months
4 Bibasilar inspiratory crackles
23
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Unlike the ATSERS consensus criteria published in 2000 bronchoscopy will not be required for diagnosis
This decision was made based on the experience of the IPFnet Steering Group members regarding the utility of
bronchoscopy in the diagnosis of IPF The presence of an atypical HRCT finding will require documentation of
a definitive diagnosis by surgical lung biopsy In fact this is in keeping with the recently published evidence
based guidelines for diagnosis and management of IPF13 As shown in Figure 3 central review of the pathology
data will be required for a diagnosis of IPF
We will not require central review of HRCT as several studies have shown that a confident local interpretation
of clinicalHRCT criteria as definite IPFUIP is associated with a high positive predictive value for finding UIP
at surgical lung biopsy (see Table 1) Differences in sensitivity in these series likely reflect subject selection as
Flaherty et al3 evaluated only UIP and nonspecific interstitial pneumonia (NSIP) while Raghu et al40 and
Hunninghake et al41 included a broader range of ILD
Table 1 Operating Characteristics of Local HRCT Review for Diagnosis of UIP
Researcher of Subjects Sensitivity () Specificity () PPV () NPV ()
Raghu et al 40
59 (29 UIP by SLB) 78 90 88 82
Hunninghake et al 41 91 (54 UIP by SLB)
74 81 85 67
Flaherty et al 3 96 (only NSIP amp UIP)
37 100 100 30
Abbreviations PPV positive predictive value NPV negative predictive value UIP usual interstitial pneumonia SLB surgical lung biopsy and NSIP nonspecific interstitial pneumonia
Furthermore an analysis of the HRCT scans from subjects enrolled in the GIPF-001 trial confirmed that local
site interpretations have a high congruity to a central radiology core In this multi-center study 263 HRCT
scans were read as definite IPF and a retrospective central radiology core review found 932 to be consistent
with IPF 42 We will also take several additional steps to insure that the local HRCT reads are accurate
including
1 A detailed training module has been developed and must be completed by each site radiologist before
site initiation
2 Clinical centers are to mail all HRCT scans to the HRCT core lab The first 10 HRCT scans from
subjects enrolled at each enrolling clinical center will be reviewed centrally to be certain that local reads
24
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
25
are congruent with a central interpretation If discrepancies are identified additional education will be
provided and HRCT scans will continue to be reviewed centrally until the central radiology core is
confident that the local center is performing appropriately
3 Random scans will be obtained from each center throughout the study to confirm that the local read
continues to agree with central interpretation If discrepancies are identified they will be addressed as in
2 above
In all cases if a subject has a surgical lung biopsy sample that sample will be reviewed by the local and central
pathologists Therefore the only cases that would not be subject to a direct central review process are those
where the HRCT meets the centrally defined criteria for an unequivocal diagnosis and a lung biopsy sample is
not available Table 2 below summarizes the possible combinations for making a diagnosis
Table 2 Combining HRCT and Pathology Interpretations to Determine if IPF is Present
HRCT Diagnosis Pathology Diagnosis Diagnosis of IPF
Definite UIP Definite UIP Yes
Definite UIP Probable UIP Yes
Definite UIP Possible UIP Yes
Definite UIP Not UIP No
Definite UIP Unavailable Yes
Consistent with UIP Definite UIP Yes
Consistent with UIP Probable UIP Yes
Consistent with UIP Possible UIP No
Consistent with UIP Not UIP No
Consistent with UIP Unavailable No
Inconsistent with UIP Any No
Abbreviations HRCT high-resolution computed tomography IPF idiopathic pulmonary fibrosis
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
UIP usual interstitial pneumonia Dx diagnosis 43 Exclusion Criteria
1 History of clinically significant environmental exposure known to cause pulmonary fibrosis
Occupational exposures such as asbestos or environmental exposure to organic dust such as occurs in
pigeon breeders may at times mimic the clinical and radiographic findings of IPF
2 Diagnosis of connective tissue disease felt by the principal investigator (PI) to be the etiology of the
interstitial disease Diagnosis of collagen-vascular conditions will be according to the published
American College of Rheumatology criteria As such the presence of any documented collagen-vascular
disorder or the presence of any suspicious symptom complex whether or not associated with
significantly abnormal rheumatological serologies will exclude the subject at the discretion of the PI
3 Extent of emphysema greater than the extent of fibrotic change (honeycombing reticular changes) on
HRCT scan
4 Forced expiratory volume in 1 second (FEV1)FVC ratio lt 065 at screening (postbronchodilator)
5 Partial pressure of arterial oxygen (PaO2) on room air lt 55 mm Hg (lt 50 mm Hg at Denver site)
6 Residual volume gt 120 predicted at screening (postbronchodilator)
7 Evidence of active infection
8 Significant bronchodilator response on screening spirometry defined as a change in FEV1 ge 12 and
absolute change gt 200 mL OR change in FVC ge 12 and absolute change gt 200 mL The percent
difference between the FVC (or FEV1) values will be calculated by taking the absolute value of the
difference and dividing it by the larger of the two FVC (or FEV1) values
9 Screening and enrollment post-bronchodilator FVC measurements (in liters) differing by gt 11 The
percent difference between the FVC values will be calculated by taking the absolute value of the
difference and dividing it by the larger of the two FVC values (eg the percent difference between FVC
measurements of 19 and 20 liters would be determined by taking the difference between the two (01
liters) and dividing by the larger of the two (20 liters) So 0120 = 5 and these FVC measurements
would not exclude the subject
10 Listed for lung transplantation ie the patient has completed the evaluation process has been accepted
as a candidate for transplantation at an appropriate center and is waiting to receive notification of an
available donor organ
11 History of unstable or deteriorating cardiac disease
12 Myocardial infarction coronary artery bypass or angioplasty within 6 months of screening
26
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
13 Unstable angina pectoris or congestive heart failure requiring hospitalization within 6 months of
screening
14 Uncontrolled arrhythmia
15 Severe uncontrolled hypertension
16 Known HIV or hepatitis C
17 Known cirrhosis and chronic active hepatitis
18 Active substance andor alcohol abuse (as determined by site PI)
19 Pregnancy or lactation (subjects who are pregnant or breastfeeding)
20 Known hypersensitivity to study medication
21 Any condition other than IPF that in the opinion of the site PI is likely to result in the death of the
subject within the next year
22 Any condition that in the judgment of the PI might cause participation in this study to be detrimental to
the subject or that the PI deems makes the subject a poor candidate
23 Any therapy directed at pulmonary fibrosis (excepting triple therapy of prednisone plus azathioprine
plus NAC) requires a 30-day washout period before randomized Triple therapy of lt= 12 weeks duration
in the past 4 years requires a 30-day washout period before randomization
24 History of triple therapy of prednisone plus azathioprine plus NAC for gt 12 weeksrsquo duration in the past
4 years or previous enrollment in the triple-therapy arm of the PANTHER-IPF study
44 Study Design and Study Visit
441 Study Design Summary
This study will be a randomized double-blind PL-controlled trial designed to assess the safety and efficacy of
NAC in subjects with newly diagnosed IPF
Subjects with mild to moderate IPF (defined as FVCpred ge 50 and DLCOpred ge 30) diagnosed within
the past 48 months will be enrolled Screening will continue until April 30 2012
27
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
The study will employ a 2-arm design with 11 randomization to NAC or PL Once enrolled subjects will visit
the clinical center at 15 weeks and 15-week intervals thereafter Each subject will be treated and followed for a
maximum of 60 weeks
During the 60-week visit subjects will be taken off all study agents Approximately four weeks after the final
dose of study agent is taken subjects will receive a safety phone call from the study site
442 Study Visits
Subjects who meet entry criteria will review the informed consent a written description of the purpose
procedures and risks of the study with the PI co-investigator or study coordinator and all questions will be
answered The informed consent form will be signed by the subject at screening No protocol-specific
procedures will be performed until the subject has signed and dated an informed consent form This includes the
screening procedures
4421 Screening
Once informed consent is obtained subjects may immediately begin the screening process or may return within
28 days of consent In the event a study subject has been clinically evaluated at the study site by an IPFnet study
physician and has performed testing within three weeks for this clinical evaluation that meets guidelines
provided in the IPFnet PANTHER-IPF Manual of Operating Procedures (MOOP) this testing may be used to
satisfy the following screening criteria medical history physical exam arterial blood gas (ABG) with A-a
gradient vital signs with oximetry body height and weight spirometry DLCO lung volumes and HRCT scan
Allowing the use of previously performed test results that meet study guidelines for the screening visit is
intended to permit subjects easier access to study entry to prevent subjects from repeating testing that has been
performed within the study window and to decrease risks to subjects from repeated exposure to procedures
such as arterial puncture and HRCT
The following procedures will be performed at screening
Medical history and a physical examination
28
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Measure height and weight
Serum pregnancy test (if applicable)
Measure vital signs including oximetry
Blood draws performed and the following analyses conducted
o Hematology (red cell count white cell count hemoglobin hematocrit cell indices differential
platelet count)
o Blood chemistries according to central laboratory protocol (see Section 410 Laboratory
Testing)
o Beta human chorionic gonadotropin (serum) pregnancy test (in women of childbearing potential)
o Urinalysis
Pulmonary Function Tests (PFTs) including spirometry pre- and post- bronchodilator and postshy
bronchodilator measurement of lung volumes and measurement of hemoglobin adjusted diffusing
capacity
Measure ABGs
HRCT if a satisfactory scan has not been performed on the subject within 3 months of screening (see
PANTHER-IPF MOOP for more details)
Surgical lung biopsies (if applicable) reviewed by local and central pathology departments
Current medications If required a washout period discussed with the subject and initiated at this visit
4422 Enrollment
The enrollment visit is expected to take place within eight weeks of the screening visit Enrollment visit
activities include
Measure vital signs including oximetry
Measure height and weight
Serum pregnancy test (if applicable)
If consent has been given blood will be drawn and a urine specimen collected for the bio-specimen
repository
Spirometry (post-bronchodilator)
Measure 6MWT with Borg Dyspnea Scale
29
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Collect Quality-of-life (QOL) data using the SF-36 EuroQol Investigating Choice Experiments for
Preferences of Older People Capability Instrument (ICE CAP) and SGRQ
Female subjects complete Gender Substudy questionnaire
Dyspnea status collected using the UCSD SOBQ
Evaluate Acute Exacerbation (AEx)
Review of any Adverse Events (AEs)
Review of concomitant medications
Subject receives diary and instructions on its purpose and proper use
Subject receives supply of study drug sufficient to last until his or her 15-week study visit
See the Schedule of Assessments (Table 3) for more details Subjects with screening and enrollment postshy
bronchodilator FVC measurements (in liters) differing by more than 11 are not eligible to be enrolled in the
study
Subjects will be asked to provide a physician of record This physician will be considered the subjectrsquos primary
care provider (PCP) and if the subject agrees the PCP will be informed by letter of the subjectrsquos enrollment in
the trial The subject will be informed that his or her ongoing medical care should be received from the PCP
The PCP will be informed of any safety issues identified by the study staff The PCP will also be given
information regarding communication with study personnel about pertinent health issues or clinic encounters
the subject may have
4423 Week 15
The week 15 visit is expected to occur within +- 14 days of the subjectrsquos scheduled visit time (eg the week 15
visit should occur anytime between 13 and 17 weeks after starting study drug Week 15 activities include
Measure vital signs with oximetry
Measurement height and weight
Serum pregnancy test (if applicable)
Spirometry (post-bronchodilator) measurement
Review of AEs
Evaluate for AEx
30
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Review concomitant medications
If consented draw blood and collect urine specimen for the biospecimen repository
Subjects return used and unused study drug for the visit
Review study diary and a new study diary will be given
Provide additional supply of study drug sufficient to last until the next scheduled visit
4424 Week 30
The week 30 visit is expected to occur within +- 14 days of the subjectrsquos scheduled visit time (eg the week 30
visit should occur anytime between 28 and 32 weeks after starting study drug) Week 30 activities include
Physical examination
Measure vital signs with oximetry
Measure height and weight
Laboratory values (complete blood count [CBC] and serum chemistries)
Serum pregnancy test (if applicable)
Measure spirometry (post-bronchodilator)
6MWT with Borg scale
DLCO
Review of AEs
Evaluate for AEx
Review concomitant medications
Complete all QOL and dyspnea questionnaires (EuroQol ICE CAP SF-36 SGRQ and UCSD SOBQ)
If consent has been given blood will be drawn and a urine specimen collected for the biospecimen
repository
Review study diary
Subjects return used and unused study drug for the visit
Provide additional supply of study drug sufficient to last until the next scheduled visit
4425 Week 45
31
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
The week 45 visit is expected to occur within +- 14 days of the subjectrsquos scheduled visit time (eg the week 45
visit should occur anytime between 43 and 47 weeks after starting study drug) Week 45 activities include
Measure vital signs with oximetry
Measure height and weight
Serum pregnancy test (if applicable)
Measure spirometry (post-bronchodilator)
Review of AEs
Evaluate for AEx
Review concomitant medications
If consent has been given blood will be drawn and a urine specimen collected for the biospecimen
repository
Subjects return used and unused study drug for the visit
Study diary reviewed
Provide additional supply of study drug sufficient to last until the next scheduled visit
4426 Week 60 (Early Withdrawal or Final Treatment Visit)
At week 60 or at subject withdrawal from the study (premature by study doctor or subjectrsquos decision) a final
treatment visit will occur At this final treatment visit subjects will discontinue NACPL abruptly Week 60
activities also include
Physical examination
Measure vital signs with oximetry
Measure height and weight
Laboratory values (complete blood count [CBC] and serum chemistries)
Spirometry (post-bronchodilator) measurement
6MWT with Borg scale measurement
DLCO
Lung volumes
ABG
Review of AEs
32
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Evaluate for AEx
Review concomitant medications
Subjects will complete all QOL and dyspnea questionnaires (EuroQol ICE CAP SF-36 SGRQ and
UCSD SOBQ)
If consent has been given blood will be drawn and a urine specimen collected for the biospecimen
repository
Subjects return used and unused study drug for the visit
Study diary reviewed
4427 Final Site Visit ndash FVC drop confirmation
In the event that the subject has a recorded FVC drop of gt10 from baseline at the final treatment visit and the
subject has not had a confirmation of such a drop at a previous study visit the subject should return to the
clinical site 6 to 8 weeks after the final treatment visit During this visit a post-bronchodilator spirometry test
will be performed This FVC measurement will be evaluated according to section 521 of this protocol
4428 Final Visit ndash Telephone Follow-up
Four weeks following the final dose of study medication subjects will receive a telephone call from the study
coordinator to ensure that there are no side effects and to follow up on any ongoing adverse events (AEs)
4429 Phone Contact Between Visits
At week 2 and each month that a subject does not have a scheduled clinical center visit his or her study
coordinator will contact him or her at least once by telephone to
Inquire if the subject has had any hospitalizations events that might be considered an AE or any events
significant enough to warrant an out-of-cycle visit to the clinical center
Remind subjects of their current dosage levels and confirm that the subject understands them
Address any questions or concerns the subject might have regarding other aspects of the study
Assess adherence to the treatment regimen by reviewing diary data verbal review of medications taken
including nutritional supplements
33
34
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Table 3 Schedule of Assessments
Procedure Screening Visit 0
Enrollment Visit 1
Week 15 Visit 2
Week 30Visit 3
Week 45 Visit 4
Week 60 Early
Withdrawal Visit 5
Final1
Visit (via phone)
Informed consent X
Medical history X
Inclusionexclusion criteria X
Serum pregnancy test (if applicable) X X X X X
Review of lung biopsy X
Arterial Blood Gas X X
6-Minute Walk Test
X
X X
Physical examination X X X
Vital signs with oximetry X X X X X X
Body height and weight X X X X X X
Complete Blood Count X X X
Chemistry panel X X X
Monitor Lab Values X X X
Urinalysis X Specimen repository substudy blood draw and urine collection (if consented)
X
X X X X
HRCT (if not completed within three months) X
Spirometry (pre- and post-bronchodilator) X
Spirometry (post-bronchodilator only) X X X X X
DLCO (post-bronchodilator only) X X X
Lung volumes (post-bronchodilator only) X
X
Evaluate for acute exacerbation X X X X X
Review Adverse Events X X X X X X
Review concomitant meds X X X X X X
Dispense subject diary X X X X
Review subject diary X X X X X
Dispense study agent X X X X
Gender Substudy questionnaire (female subjects only) X
EuroQol ICECAP UCSD SOBQ SGRQ SF-36 X X X
Abbreviations DLCO diffusing capacity of the lung for carbon monoxide QOL Quality of Life ICECAP Investigating Choice Experiments for Preferences of Older People UCSD SOBQ University of California Shortness of Breath Questionnaire SGRQ St Georgersquos Respiratory Questionnaire SF-36 Short Form 36 Health Survey
1Follow-up visit via phone will occur four weeks after final dose of study medication
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
45 Dose Justification
The general philosophy for determining dosing levels was to apply previously examined
treatment regimens With the focus of the study being to establish a standard of care for
mildmoderate IPF subjects the goal was to develop flexible yet standardized treatment rules that
allow for the temporary or permanent withholding of one or more components of treatment when
necessary Subjects developing laboratory abnormalities or symptoms that result in
discontinuation of one or more components of study treatment may continue on the other
components as long as there is no contraindication for this Complete follow-up is important for
the validity of any study As a strategy to maintain protocol adherence we are using a treatment
regimen that will detect potential side effects and prompt interventions proactively in the interest
of patient safety In addition subjects who permanently stop study medications during the course
of the study are encouraged to continue in the study completing all scheduled visits and tests
451 Rationale for N-acetylcysteine Dosing
To our knowledge there have been no IPF studies to correlate clinical outcome measures with
different dosages for NAC The dosage chosen is based on the IFIGENIA study However BAL
lung GSH levels from subjects with IPF have been augmented with the use of oral NAC at 600
mg 3 times per day In addition lung GSH levels have been associated with improved
PFTs212227 The dose chosen for this study was based on previous data including the IFIGENIA
study30
4511 Dosing of N-acetylcysteineplacebo
Dosing of NACPL will be 600 mg orally 3 times a day (1800 mgday)
4512 Reasons to Discontinue N-acetylcysteineplacebo
NACPL may be temporarily or permanently discontinued for the duration of the study for
gastrointestinal symptoms or dermatologic reactions
35
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Temporarily discontinue (hold) oral NACPL for subjects requiring inpatient admission for acute
exacerbation (AEx) or other conditions Resume NACPL after discharge
36
37
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
452 Dosage Algorithms
Dosage Adjustment Algorithm 1 NACPL Dose Modifications for Gastrointestinal Symptoms Nausea Vomiting Abdominal Discomfort Diarrhea
GI Symptoms determined by the PI to be clinically significant Nausea Vomiting Abdominal Discomfort Diarrhea
NACPL Temporarily dc (HOLD) x 3 Days
Monitor symptoms intervene as clinically indicated (eg fluid replacement antidiarrhea or antinausea medication)
Monitor or lab PRN
Are symptoms resolving after 3 days NO
Symptoms NOT resolving after 3 days of holding study medication Assessmentmanagement per clinical
discretion of investigator
Likely not study medication discuss resuming study medication with medical monitor when symptoms resolved
YES
Temporarily dc (HOLD) NACPL for 4 additional days (total hold 1 week) then NACPL Resume 600 MG TID
Did symptoms recur
YES
STOP NACPL for
duration of study
NO
NACPL No Change
38
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Dosage Adjustment Algorithm 2 NACPL Dose Modifications For Dermatologic Reactions
Dermatologic Reactions (Not Acneiform) ge Grade 2 Grading per Common Terminology Criteria for
Adverse Events V30 (httpctepcancergov) For example Grade 1 RASHDESQUAMATION Macular or papular eruption or erythema without associated symptoms Grade 2 RASHDESQUAMATION Macular or popular eruption or erythema with pruritus or other associated symptoms localized desquamation or other lesions covering lt50 of body surface area
NACPL Temporarily dc (HOLD) x 3 days
Are symptoms resolving after 3 days
NO Symptoms not resolving after 3 days of holding study medication Assessmentmanagement per clinical discretion of investigator Likely not study medication Discuss resuming study medication with medical monitor when symptoms
resolved YES
Temporarily dc (HOLD) NACPL for 4 additional days (total hold 1 week) then NACPL resume 600 MG TID
Did symptoms recur
YES
STOP NACPL for
duration of study
NO
NACPL No change
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
46 Contraindications Precautions and Side Effects of Study Medications
461 Contraindication
Contraindication to NAC is known hypersensitivity to it
462 Precautions
Concomitant administration of oral NAC and antibiotics has shown a slightly reduced absorption
of cephalexin and a slight increase in erythromycin serum levels NAC contains free sulfhydryl
groups There is no evidence that individuals sensitive to sulfa drugs are sensitive to NAC
The NAC preparation being administered in this study contains 20 mg of aspartame Because of
the phenylalanine component of aspartame individuals with phenylketonuria should avoid or
restrict aspartame intake to avoid increased blood levels of phenylalanine Because of this risk
labeling is required on all products containing aspartame
463 Side Effects
Side effects of NAC range from common to serious See Table 4
39
40
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Table 4 Side Effects of NAC
Undesirable Effects
System-organ class Uncommon
(gt11000 lt1100)
Rare
(gt110000 lt11000)
Very rare
(lt110000) Not known
Immune system disorders Hypersensitivity Anaphylactic shock
reaction
Nervous system disorders Headache
Ear and labyrinth disorders Tinnitus
Cardiac disorders Tachycardia
Vascular disorders Hemorrhage
Respiratory thoracic and
mediastinal disorders
Bronchospasm
Dyspnea
Gastrointestinal disorders
Vomiting diarrhea
stomatitis abdominal
pain nausea
Dyspepsia
Skin and subcutaneous tissue
disorders
Urticaria rash
angioedema itching
General disorders and
administration site conditions Pyrexia
Investigations Reduced arterial
pressure Face edema
In very rare cases the onset of severe skin reactions such as Stevens-Johnson syndrome and Lyell syndrome was reported to have a temporal relationship with N-acetylcysteine administration Although in most cases at least another suspect drug probably most involved in the genesis of the above mentioned mucocutaneous syndromes has been identified in case of mucocutaneous alterations it is appropriate to contact onersquos doctor and the administration of N-acetylcysteine should be immediately discontinued
Some studies confirmed a reduction of platelet aggregation during N-acetylcysteine administration The clinical significance of these findings has not been defined yet [Source Fluimucil Investigator Brochure]
47 Recruitment Procedures
Subjects recruited for this study will be established patients of the investigators or physician- or
self-referred to participating clinical centers in the IPFnet Each clinical center within IPFnet has
a well-developed infrastructure of local pulmonologists within the surrounding geographic area
These pulmonologists are kept informed of ongoing IPF clinical trials and regularly refer
subjects to studies conducted at IPFnet clinical centers
Additional steps will be taken to inform clinicians of the trials in progress within IPFnet
including presentations at faculty staff meetings at local hospitals medical grand rounds and
national conferences direct mail notification monthly faxes and advertisement of network trials
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
in pulmonary journals Clinical center patients previously diagnosed with IPF will be notified of
the trials by mail whenever possible
Recruitment of minorities and women will be monitored by the DCC and DSMB If necessary
additional recruitment efforts will be made at specific centers to ensure that the aggregate subject
sample contains appropriate representation of women and minorities
48 Study Procedures
The following procedures are detailed in the PANTHER-IPF MOOP accompanying this
protocol
1 PFT
2 ABG
3 HRCT scan of the chest (including imaging of pulmonary arteries)
4 CBC and serum chemistries
5 Pregnancy test
6 6MWTBorg Dyspnea Scale
7 QOL questionnaires (EuroQol HAD SF-36 SGRQ and ICE CAP)
8 UCSD SOBQ
9 Gender Substudy Questionnaire
All assessments of PFTs will be conducted by study personnel not directly involved in the
treatment of the subjects
481 Biological Specimen Management
4811 Biological Specimen Sample Management
Subjects at clinical centers participating in the specimen repository substudy who consent to
having blood drawn for research purposes and for the banking of blood blood components and
other biologic specimens (urine and BAL fluid) will have approximately 405 mL of blood
41
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
drawn 17 mL blood drawn for DNA and 20 mL of urine collected at enrollment visit Subjects
will have approximately 50 mL of blood drawn and 20 mL of urine collected at each 15-week
follow-up visit Blood specimens will be separated according to PANTHER-IPF MOOP
guidelines into the following components for banking in the repository serum plasma and
DNA Coding of all biologic specimens for the repository will be performed by study staff at the
clinical center The samples will be processed per PANTHER-IPF MOOP guidelines aliquoted
labeled with barcode labels and stored at -70degC at the clinical center and shipped to the central
repository
The only subject identifiers will be a sample ID number and subject initials This sample ID will
be linked in the IPFnet DCC clinical database to subject information No subject information will
be transferred to the biological-specimen database
The subjectrsquos samples may be used for approved sub-studies relating to human disease
including but not limited to IPF The studies for which an individualrsquos samples will be made
available will be determined by the subjectrsquos answers to questions on the biological-sample
informed consent form The subjects can choose to make their samples available for all options
or any combination Samples will be made available to researchers only with IPFnet Steering
Group approval until such time as the samples are made public through the NHLBI repository
49 Concomitant Medications
Concurrent treatment with FDA-approved therapy for IPF is allowed Colchicine may be used
for treatment of gout Temporary treatment with oral or IV corticosteroids for clinical worsening
or suspected AEx is permitted Nutritional supplements containing NAC are not allowed
410 Laboratory Testing
Clinical laboratory parameters will be assessed at screening and at the end of the study The
following tests will be performed at the two time points specified in the protocol chemistry (AG
ratio ALT [SGPT] AST [SGOT] albumin alkaline phosphatase amylase bilirubin-direct
42
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
bilirubin-indirect bilirubin-total BUN BUNcreatinine ratio calcium carbon dioxide
cholesterol-total chloride CPK-total creatinine GGT globulin glucose iron-total LDH
lipase magnesium phosphorus-inorganic potassium protein-total sodium TIBC triglycerides
uric acid) and hematology (red blood cell count WBC count hemoglobin hematocrit cell
indices differential platelet count)
411 Blinding of Study Drugs
Subjects and caregivers will be blinded to study treatment Every subject will receive NAC or
matching PLs at every study visit from the baseline visit to the week-45 visit No study agent
will be dispensed at the week-60 visit
43
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
5 Study Endpoints
51 Primary Study Endpoint
The primary endpoint will be the change in serial measurements of FVC over the study period
52 Secondary Study Endpoints
521 Time to Disease-progression
The time-to-death or a 10 decline in FVC will be defined as the time-to-disease progression
The 10 decline in FVC from enrollment must be confirmed on 2 consecutive visits no less than
6 weeks apart For subjects with 2 consecutive visits with a 10 decline in FVC the time-toshy
disease progression will be defined as the time interval between enrollment and the initial visit
with a 10 FVC decline For subjects who experience disease progression the study doctor will
determine whether or not the subject will remain in the study
522 Acute Exacerbations
The following 3 criteria will define AEx in subjects with acute worsening of their respiratory
conditions
1 Clinical (all of the following required)
A) Unexplained worsening of dyspnea or cough within 30 days triggering unscheduled
medical care (eg emergency room clinic study visit hospitalization)
B) No clinical suspicion or overt evidence of cardiac event pulmonary embolism or deep
venous thrombosis to explain acute worsening of dyspnea
C) No pneumothorax
44
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
2 RadiologicPhysiologic (A and B required)
A) New ground glass opacity or consolidation computed tomography (CT) scan OR new
alveolar opacities on chest x-ray
B) Decline of ge 5 in resting room air SpO2 from last recorded level OR decline of ge 8 mm
Hg in resting room air PaO2 from last recorded level
3 Microbiologic (all of the following required)
A) No clinical evidence for infection (ie absence of grossly purulent sputum fever gt 39degC
orally)
B) Lack of positive microbiological results (if done) from lower respiratory tract defined as
(1) Clinically significant bacterial growth on sputum or endotracheal aspirate cultures
(2) Quantitative culture by protected brush specimen ge 103 cfumL or BAL ge 104 cfumL
(3) The presence of specific pathogens on stains of any of the above
C) Lack of positive pathogen in blood cultures (if done)
Identification of Acute Exacerbations
All subjects will be educated about the importance of identifying AExs At the time of
enrollment subjects will be told about the possibility of developing acute symptomatic
worsening that might represent an AEx of IPF and instructed to contact their study clinical
center coordinator within 48 to 72 hours of the apparent event
All subjects will be contacted by phone monthly and questioned about any change in dyspnea or
cough and any interim clinic visits or hospitalizations Finally as part of the IPFnet outreach to
community referring physicians the importance of AExs will be emphasized When a subject is
identified who meets criterion 1A this will trigger the collection of additional clinical data to
evaluate a suspected AEx These data will be collected as part of standard clinical care (ie this
protocol does not require collection of all items) The additional items to be collected for
suspected AEx include
IPFnet AEx case report form (eCRF) (required)
45
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Chest x-ray CT scan withwithout pulmonary angiogram (reports should be faxed and
followed by the hard copiesdiscs)
Oxygen saturation (pulse oximetry)
ABG
Respiratory cultures (sputum endotracheal aspirate lavage)
Blood cultures
Clinichospital records related to the event
All potential cases of AEx will be reviewed by the clinical center PI first and a decision on
whether the case may represent an AEx will be made If AEx is suspected the case will be sent
to the IPFnet adjudication committee which will assign a final diagnosis (see Table 5) If there is
disagreement among members the majority opinion will be recorded
During episodes of suspected AEx as determined by the individual clinical center investigator
subjects will remain blinded and in the study
Table 5 Final Diagnoses in Evaluation of Suspected Acute Exacerbations
Definite acute exacerbation All criteria met no alternative etiology
Unclassifiable acute worsening
Insufficient data to evaluate all criteria no alternative etiology
Not acute exacerbation Alternative etiology identified that explains acute worsening
Management of the suspected AEx will be at the discretion of the treating physician Standard of
care generally involves evaluation for respiratory infection pulmonary embolism cardiac events
and pneumothorax and treatment with IV corticosteroids
Study drugs will be resumed at pre-suspected AEx doses after subjects clinically improve as
confirmed by the local PI All subjects should be seen at the clinical center within 2 to 4 weeks
of recovery for measurement of post-bronchodilator FVC (see Figure 4) Subjects unable to
return to the clinical center after suspected AEx due to medical frailty (eg continued
46
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
institutionalization progressive disability) will be categorized as failing to maintain FVC
response in secondary analyses
Suspected AEx (PI determined)
Hold study drug Treat AEx
(Attending physician determined)
Alive but unable to continue due to
medical frailty
Dead
Alive and able to continue
Site reviewvisit
Restart study drug
FVC within 2-4 weeks
Figure 4 Acute Exacerbation Flow Chart
523 Respiratory Infections
An upper respiratory infection will be defined as
Change in sputum discoloration
Increased cough of no more than 14 daysrsquo duration
A lower-respiratory infection (pneumonia) will be defined as new segmental or lobar airspace
opacities visualized by image studies (chest radiograph or HRCT) in addition to any of the
following
Positive pathogencultures in good sample of sputum or lower-airway secretions retrieved
by fiberoptic bronchoscope
Fever gt 39degC or gt 100degF
Leukocytosis gt 12000 (unexplained no increase in dose of corticosteroids)
47
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
524 Maintained FVC Response
Subjects with follow-up FVCpred measurements at or above their baseline FVCpred level
will be classified as having maintained FVC response Subjects with reduced FVCpred levels
or missing data for any reason including death or medical frailty will be classified as having not
maintained FVC response The FVCpred value is used because unadjusted FVC measurements
are expected to decline with age
48
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
6 Safety Evaluations and Procedures
61 Adverse Events
During a clinical trial the reporting of adverse experience information can lead to important
changes in the way a new treatment is developed as well as provide integral safety data
611 Definitions
An adverse event (AE) is any untoward medical occurrence in a subject or clinical investigation
subject who was administered a pharmaceutical product The AE does not necessarily have to
have a causal relationship with the drug administered An AE can be any unfavorable and
unintended sign (including an abnormal laboratory finding) symptom or disease temporarily
associated with the use of a medicinal product whether or not considered to be related to the
medicinal product Diseases signs symptoms or laboratory abnormalities already existing at
enrollment are not considered AEs unless they worsen (ie increase in intensity or frequency)
Surgical procedures themselves are not AEs they are therapeutic measures for conditions that
require surgery The condition for which the surgery is required may be an AE Surgical
procedures planned before randomization and the conditions necessitating the surgery are not
AEs
A serious adverse event is any untoward event that
Is fatal
Is life-threatening
Requires inpatient hospitalization or prolongation of existing hospitalization with the
following exceptions
o Preplanned (before the study) hospital admissions unless the hospitalization is
prolonged
o Planned admissions (as part of a study eg routine biopsies)
o Hospitalization lasting lt 24 hours
49
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
o Hospitalization for elective procedure
o Emergency room visits
Results in persistent or significant disability or incapacity
Is a congenital anomaly or birth defect
Important medical events that may not result in death be life-threatening or require
inpatient hospitalization may be considered serious adverse events (SAEs) when based
on appropriate medical judgment they may jeopardize the subject and may require
medical or surgical intervention to prevent one of the outcomes listed above
Life-threatening means that the subject was in the view of the investigator at immediate risk of
death from the AE as it occurred It does not include an AE that had it occurred in a more severe
form might have caused death
Persistent or significant disabilityincapacity means that the event resulted in permanent or
significant and substantial disruption of the subjectrsquos ability to carry out normal life functions
Causality
A reasonable possibility means the AE may have been caused byrelated to the study drug A
perceived or real lack of efficacy does not satisfy the definition of relatedness
612 Adverse Event (AE) Reporting
For the PANTHER-IPF trial all AEs (serious and nonserious) occurring from randomization
through final study visit (4 weeks after final dose of all study medication) will be recorded on the
AE page of the case report form (CRF)
6121 Serious Adverse Events (SAE) Reporting
For this trial all deaths and all SAEs which occur from randomization through final study visit
must be entered within the EDC system via the SAE eCRF page within 24 hours of the
investigative sitersquos knowledge of the event It is the responsibility of the clinical center
50
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
investigator to provide a causality assessment of the event for each study medications based upon
the information available at the time of the report It is understood that complete information
about the event may not be known at the time the initial report is submitted In the event the EDC
system is not accessible to the site at the time of event reporting investigative sites will complete
and forward a paper back-up SAE form to DCRI Safety Surveillance for processing
DCRI Safety Surveillance
Telephone 1-919-668-8624 or 1-866-668-7799 (toll free)
Fax 1-919-668-7138 or 1-866-668-7138 (toll free)
The investigator must complete and submit follow-up SAE information via the eCRF when
important new or follow-up information (eg final diagnosis outcome results of specific
investigations) becomes available Follow-up information should be submitted according to the
same process used for reporting the initial event as described above All SAEs will be followed
until resolution stabilization or 30 days after the subject has completed the final visit (4 weeks
after the final dose of study medication) whichever occurs first The investigator is responsible
for reporting SAEs to their institutional review board (IRB) per site specific IRB reporting
guidelines
6122 Regulatory Reporting
AEs that are serious study drug related and unexpected will be reported to the regulatory
authorities The DCRI Safety Surveillance medical monitor will perform a medical review of all
SAEs submitted and evaluate for ldquounexpectednessrdquo DCRI Safety Surveillance will prepare
MedWatch reports for those events identified as serious study drug related and unexpected as
determined by Safety Medical Monitor
DCRI Regulatory Services will submit all unexpected study drug-related SAEs as per 21 CFR
32 DCRI Safety Surveillance will provide a safety alert letter to the NHLBI DSMB and DCC
clinical operation (for distribution to sites) within 15 days of initial receipt of the information
51
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Investigators are responsible for promptly reporting these events to their reviewing IRBs
according to site specific IRB reporting guidelines
62 Clinical Medical Monitoring
There will be an unblinded physician at the IPFnet DCC serving as medical monitor The
medical monitor will be available to assist with questions about dosage adjustments of study
medications including discontinuation or resumption of medications
63 Unblinding Procedures
Unblinding of subjects or investigators to subject treatment is strongly discouraged For ongoing
clinical management all subjects should be presumed to be receiving ldquoactiverdquo study drug To
ensure the subjectrsquos safety the study treatment will be dose-adjusted based on laboratory test
results clinical findings and symptoms
The IPFnet DCC medical monitor and PANTHER-IPF co-chairs Drs Ganesh Raghu and
Fernando Martinez will be available to the study physicians to discuss study drug management
on a case-by-case basis Un-blinding will be considered ONLY when the knowledge of subject
treatment assignment is ABSOLUTELY ESSENTIAL for subject safety and after discussion of
the subjectrsquos case with the medical monitor and either Dr Raghu or Dr Martinez Unblinding of
study treatment should be minimized during the conduct of the trial In those cases where it is
felt to be medically necessary the DCC medical officer will communicate directly with the
managing physician to minimize unblinding of study personnel
52
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
7 Study Drug Procedures
At the baseline 15-week 30-week and 45-week study visits subjects will receive a supply of
study drug sufficient to last until the next visit at which study drug will be dispensed
53
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
8 Data Management
81 Hardware and Software Configuration
811 Hardware and Database Software
Data will be stored in an Oracle database system Oracle has advantages of processing efficiency
and smooth linkage with other software systems The application and database will be hosted on
Solaris Unix servers at the IPFnet DCC
812 Statistical Software
SAS will be used as the principal application for the management of analysis data files and
statistical computations S-Plus will be used to provide supplementary functions as needed
813 Access Control and Confidentiality Procedures
Access to databases will be controlled centrally by the IPFnet DCC through user passwords
linked to appropriate privileges This protects the data from unauthorized changes and
inadvertent loss or damage
814 Security
Database and Web servers will be secured by a firewall and through controlled physical access
Oracle has many security features to ensure that any staff member accessing the database has the
proper authority to perform the functions he or she requests of the system Within the secondary
SAS databases Unix group-access control maintains similar security The Sun workstation login
is secured by extensive user-password facilities under Unix
54
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
815 Back-up Procedures
Database back-up will be performed automatically every day and standard IPFnet DCC policies
and procedures will be applied to dictate tape rotation and retention practices
816 Virus Protection
All disk drives that provide network services and all user computers will be protected using
virus-scanning software Standard IPFnet DCC policies will be applied to update these protection
systems periodically through the study
82 Sources of Data
821 Design and Development
The IPFnet DCC will be responsible for development of the electronic case report forms
(eCRFs) development and validation of the clinical study database ensuring data integrity and
training clinical center staff on applicable data management procedures A web-based distributed
data entry model will be implemented This system will be developed to ensure that guidelines
and regulations surrounding the use of computerized systems used in clinical trials are upheld
The remainder of this section provides an overview of the data management plan associated with
this protocol
822 Data Collection Forms
The data collection process consists of direct data entry at the study clinical centers into the EDC
system(s) provided by the DCC A data collection worksheet will be provided to clinical centers
for recording data in the event the EDC system is unavailable Data entry of the eCRFs should
be completed according to the instructions provided and project specific training The
investigator is responsible for maintaining accurate complete and up-to-date records and for
ensuring the completion of the eCRFs for each research participant
55
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
823 Data Acquisition and Entry
Data entry into eCRFs shall be performed by authorized individuals Selected eCRFs may also
require the investigatorrsquos written signature or electronic signature as appropriate Electronic
CRFs will be monitored for completeness accuracy and attention to detail during the study
824 Data Center Responsibilities
The IPFnet DCC will 1) develop a data management plan and will conduct data management
activities 2) provide final eCRFs for the collection of all data required by the study 3) develop
data dictionaries for each eCRF that will comprehensively define each data element 4) conduct
ongoing data monitoring activities on study data 5) monitor any preliminary analysis data
cleanup activities and 6) rigorously monitor final study data clean up
825 Data Editing
Completed data will be entered into the IPFnet DCC automated data acquisition and
management system If incomplete or inaccurate data are found a data clarification request will
be generated and distributed to clinical centers for a response Clinical centers will resolve data
inconsistencies and errors and enter all corrections and changes into the IPFnet DCC automated
data acquisition and management system
826 Training
The training plan for clinical center staff includes provisions for training on assessments eCRF
completion guidelines data management procedures and the use of computerized systems
56
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
9 Study Design and Data Analysis
91 General Analytic Considerations
All primary analyses will be based on intent-to-treat (ITT) principles using all randomized
subjects Baseline factors across groups will be compared using mean (standard deviation) and
median (25th and 75th percentiles) summary measures Kaplan-Meier curves will be used to
display event rates Due to clinical interest in departures from both sides of the null hypothesis
all test statistics will be 2-sided
Reasonable caution needs to be taken when conducting multiple analyses on key clinical
subgroups For subgroup analyses a conservative significance level of 0001 will be used for all
interaction tests Thus subgroup comparisons will be considered exploratory unless the p-value
from the interaction test is smaller than 0001
92 Randomization Blinding and Reporting of Results
A permuted block-randomization scheme will be created with varying block sizes stratified by
clinical center Once a subject has completed the screening and baseline period and evaluation
for inclusionexclusion criteria the randomization process will begin Subjects will be
randomized to receive NAC or matching placebo with equal probability (11) via telephone
contact with a central interactive voice response system (IVRS) using a toll-free randomization
number On the day of randomization after the subject has successfully met all inclusion and
exclusion criteria the investigator or designee will call the central randomization number to
obtain the assigned kit randomization numbers for that subject At each subject visit the
investigator or designee will call the central randomization number to obtain the new kit
randomization numbers for resupply of the subject For resupply of the clinical center the IVRS
will monitor minimal volume of a kit type andor expiration date and will automatically notify
the pharmacy
57
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
The trial results will be reported according to guidelines specified in the CONSORT statement
A flow diagram describing screening recruitment randomization dropout and vital status will
be included in the primary manuscript AEs and efficacy data will be presented for all treatment
groups Adherence dropout and lost to follow-up will be carefully examined across all treatment
groups Analyses of safety will be based on data from all randomized subjects who received at
least one dose of study drug
93 Stratification
Subjects will be distributed to the two treatment arms in a 11 allocation ratio Stratification
blocks will be based on clinical centers
94 Specification of the Primary Analyses
A mixed model repeated measures (MMRM) analysis described in section 95 will be used to
compare differences in the slope of FVC measurements across the treatment groups Response
variables are values of the FVC measured at baseline and every 15 weeks until study completion
Variables in the model will include treatment time and time by treatment age sex race and
height Contrast estimates of differences in slopes of treatment over time (along with confidence
intervals) will be used to estimate the treatment effect The validity of this model in terms of
meeting modeling assumptions will be assessed via standard modeling diagnostics and goodness-
of-fit measures Based on the MMRM framework missing FVC data will not be imputed for the
primary analysis
95 Analysis of Longitudinal Endpoints
A common goal in clinical trials is to specify models that are easily implemented and
reproducible by independent data analysts On the other hand the models should have proper
statistical behavior in terms of low bias and high precision Many common approaches to
longitudinal data analysis including last observation carried forward (LOCF) imputation rely on
the missing completely at random (MCAR) assumption However the MCAR assumption is
58
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
unlikely to hold in many clinical trials because missing data are often related to disease
progression and prognosis A more reasonable assumption missing at random (MAR) specifies
that the complete data distribution can be modeled using only the observed data The likelihood-
based MMRM approach is valid under the more general MAR assumptions These models will
be applied to analyze the longitudinal data secondary endpoints
The advantages of MMRM analysis are that all important characteristics of the model can be preshy
specified standard software can be used to implement the models and results are based on ITT
principles43 In addition the MMRM approach offers superior control of Type I and Type II
errors compared with the LOCF approach
Response variables are values of the PFTs measured at enrollment and every 15 weeks until
study completion and 6MWT values measured at baseline week 30 and week 60 Covariates are
treatment time time by treatment and key baseline risk factors Contrasts (along with
confidence intervals) of treatment by time will be used to estimate the treatment effect
The correlation structure involves multiple pieces including measurement errors random
variation and interindividual variability For the longitudinal data analyses an unstructured
correlation matrix for within-subject errors will be assumed Other correlation structures
including compound symmetry will be examined as needed A careful examination of reasons
for study discontinuation will be conducted to assess the validity of MCAR Sensitivity analyses
will be used to examine the untestable assumption that the observed data violate the MAR
assumption The MMRM models will be implemented using PROC MIXED in SAS
96 Analysis of Binary Time-to-Event and Time-Lagged Endpoints
Regression modeling approaches using either the logistic regression model or Cox proportional
hazards regression model will be employed when appropriate The validity of these models will
be assessed via standard modeling diagnostics and goodness-of-fit measures Estimates of
cumulative frequencies for more general time-lagged responses will be calculated using the
partitioned version of the Bang-Tsiatis estimator44 The partitions will be set at 15-week intervals
59
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
to correspond with the data-collection process Covariate adjusted event rates will be calculated
using inverse probability-weighted regression estimates45
97 Power Analysis
971 Primary Analyses
Based on previously published IPF clinical trials the PL group is expected to experience a drop
in FVC of approximately 020 L over the study period (see Figure 1) The IPFnet Steering Group
determined a clinically important difference would be to preserve the majority of the decline
relative to PL over the study period In particular a treatment effect of 015 L was determined to
be a clinically meaningful difference Potential dropout is a key factor in the proposed study The
drop-out process assumed 5 lost to follow-up after every study visit Only 80 of subjects
were assumed to be followed for the entire study period All models assumed a compound
symmetry structure for the covariance matrix Power calculations were performed using a SAS
IML program for designing repeated measures studies46 Based on preliminary reviews of the
data from the University of Michigan the covariance matrix parameters were estimated at
approximately σ2 = 0757 (variance parameter) and ρ = 0936 (correlation parameter) To be
conservative the power calculations for the primary analysis were performed with parameter
setting of σ2 = 0810 (variance parameter) and ρ = 0925 (correlation parameter)
The power calculations assume a correction for imperfect compliance proposed by Lachin and
Foulkes to allow for 2 noncompliance for each of the treatment arms47 Thus the sample size
of 130 subjects per arm would be reduced to an adjusted sample size of 130(1-002-002)2 =
1198 or 120 subjects per arm
Under the assumed Type I error rate of 005 with a correlation parameter of 0925 and standard
deviation of 090 the difference of 015 L (or 00025 Lweek) shown in Table 6 would have
power of 93
60
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Table 6 Hypothetical Values of Mean FVC (L) Change from Baseline
Week 15 Week 30 Week 45 Week 60
NAC 00125 00250 00375 00500
Placebo 00500 01000 01500 02000
Difference 00375 00750 01125 01500
Abbreviations FVC forced vital capacity PL placebo
972 Power Analysis for Secondary Endpoints
Power calculations for secondary endpoint measurements are shown in Table 7 Standard
deviations are based on unpublished data provided by the University of Michigan The
calculations are based on a 2-sample t-test with Type I error rate set at 005 These calculations
are likely to be conservative because the statistical approach described in section 95 for
analyzing these endpoints will incorporate incomplete observations as well as intermediate data
points
Table 7 Detectable Differences in Treatment Means for Selected Endpoint Measurements
Secondary Endpoints Std Dev
of the Baseline Score
Detectable Difference for 80 Power
Std Dev of the Change Score
Difference Detectable for
80 Power
DLCOpred 166 58 91 32
6MWT Area Under the Desaturation Curve
219 76 175 61
6MWT Distance to Desaturation 224 78 315 110
6MWT Minutes Walked 210 073 205 071
Abbreviations Std Dev standard deviation DLCOpred diffusing capacity of the lung for carbon monoxide percent predicted 6MWT 6-minute walk test
61
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
10 Study Administration
101 Cooperative Agreement Mechanism
The administrative and funding mechanism used to undertake this project is a ldquocooperative
agreementrdquo (U01) which is an assistance mechanism Under the cooperative agreement the
NHLBI assists supports andor stimulates the project and is substantially involved with
investigators in conducting the study by facilitating performance of the effort in a ldquopartnerrdquo role
The NHLBI project scientist serves on the IPFnet Steering Group and he or another NHLBI
scientist may serve on other project committees when appropriate At the same time however
NHLBI does not assume a dominant role direction or prime responsibility for this research
program
As described below governance of the project is conducted through the IPFnet Steering Group
Principal investigators have lead responsibilities in all aspects of their trials and the project
including any modification of trial designs conduct of the trials quality control data analysis
and interpretation preparation of publications and collaboration with other investigators unless
otherwise provided for by the IPFnet Steering Group
PIs retain custody of and have primary rights to their center-specific and collaborative data
subject to government rights-of-access consistent with current Health amp Human Services (HHS)
Public Health Service (PHS) and National Institutes of Health policies The protocols and
governance policies call for the continual submission of data centrally to the IPFnet DCC for the
collaborative database which at a minimum will contain the key variables selected by the IPFnet
Steering Group for standardization across all clinical centers the submission of copies of the
collaborative datasets to each PI upon completion of the project procedures for data analysis
reporting and publication and procedures to protect and ensure the privacy of medical and
genetic data and records of individuals The NHLBI project scientist on behalf of the NHLBI
will have the same access privileges and responsibilities regarding the collaborative data as the
other members of the Steering Group
62
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
PIs are also encouraged to publish and to publicly release and disseminate results data and other
products of the project concordant with the project protocols and governance and the approved
plan for making data and materials available to the scientific community and to the NHLBI
However during the 3 years after the ending date of NHLBI project support unpublished data
unpublished results data sets not previously released and other study materials or products are
to be made available to any third party only with the approval of the IPFnet Steering Group
Upon completion of the project PIs are expected to put their intervention materials and
procedure manuals into the public domain andor make them available to other investigators
according to the approved plan for making data and materials available to the scientific
community and the NHLBI for the conduct of research at no charge other than the costs of
reproduction and distribution
The NHLBI reserves the right to terminate or curtail the project (or an individual award) in the
event of (a) failure to develop or implement mutually agreeable collaborative measurement
subject eligibility and data management sections of the protocols (b) substantial shortfall in
subject recruitment follow-up data reporting or quality control or other major breach of
protocol (c) substantive changes in the agreed-upon protocols with which NHLBI cannot
concur (d) reaching a major project outcome with persuasive statistical significance
substantially before schedule or (e) human subject ethical issues that may dictate a premature
termination
Any disagreement that may arise in scientificprogrammatic matters (within the scope of the
award) between award recipients and the NHLBI may be brought to arbitration An arbitration
panel will be composed of 3 membersmdash1 selected by the IPFnet Steering Group (with the
NHLBI member not voting) or by the individual PI in the event of an individual disagreement a
second selected by NHLBI and the third selected by the other 2 members This special
arbitration procedure in no way affects the PIrsquos right to appeal an adverse action that is otherwise
appealable in accordance with the PHS regulations at 42 CFR part 50 Subpart D and HHS
63
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
regulation at 45 CFR part 16 or the rights of the NHLBI under applicable statutes regulations
and terms of the award
102 IPFnet Steering Group
The IPFnet Steering Group is the main governing body of the project It is composed of the PIs
of the clinical centers the PI of the DCC and the NHLBI project scientist The clinical centers
the IPFnet DCC and the NHLBI each have 1 vote on the IPFnet Steering Group All decisions
are determined by majority vote
All major scientific decisions are determined by the IPFnet Steering Group It assumes overall
responsibility for the design and conduct of the trial It appoints (and disbands) committees and
subcommittees as the need arises designs approves and implements the study protocols
oversees the development of the MOOP monitors subject recruitment and treatment delivery
evaluates data collection and management oversees quality assurance procedures and
implements changes and enhancements to the study as required It also has primary responsibility
for facilitating the conduct of the trials and reporting the projectrsquos results
103 Data and Safety Monitoring Board
The NHLBI will establish a DSMB in accordance with established policies (see
httpwwwnhlbinihgovfundingpoliciesdsmb_insthtm) to ensure data quality and subject
safety and to provide independent advice to the NHLBI regarding progress and the
appropriateness of study continuation
104 Recommendations on Interim Monitoring of Efficacy Safety and Futility
First and foremost the role of the DSMB will be to review subject safety and trial conduct at
periodic points during the study The DSMB may require analyses of the primary endpoint
results for comparing the benefit and risks of treatment strategies The benefit of collecting
additional data on key secondary endpoints with extended follow-up and establishing a robust
64
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
evidence base for determining a standard of care will need to be carefully considered before
early termination of one or more treatment arms After careful consideration the IPFnet Steering
Group recommends conservative thresholds for the early examinations of the safety and efficacy
data
The DSMB will be expected to meet approximately every 6 months until trial completion to
review safety and toxicity data The DSMB may recommend stopping the study based on these
reviews Because the DSMB could stop the trial for safety concerns as well as for a large
efficacy benefit there could be multiple opportunities to reject the null hypothesis (no difference
in event rates between the PL and NAC groups) A Bonferroni approximation will be applied
during the one planned interim analysis for efficacy
Before locking the database a statistical analysis plan (SAP) will be developed to provide
complete details on the statistical analysis The SAP will include the specifics for how and when
the DSMB will be notified for AEs The IPFnet DCC will deliver to the DSMB all FDA-defined
AEs at 3-month intervals The IPFnet DCC will prepare narrative SAE reports in real time for
DSMB review including recommendations and analysis of similar events for each SAE
submitted to the FDA
65
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
11 Investigator and Sponsor Obligations
111 Monitoring
All monitoring activities for US clinical centers will be performed in accordance with DCRI
standard operating procedures Information regarding the types of visits will be outlined in the
PANTHER-IPF MOOP
112 Cost and Payment
There will be no cost to subjects enrolled in this trial Study-related procedures will be paid for
by the IPFnet
Subjects may be eligible for reimbursement for travel to the clinical center Details of payment
will be explained to each subject during the consent process
113 Confidentiality and Health Insurance Portability and Accountability Act
Considerations
Subject confidentiality will be protected throughout the study All subject data will be kept
strictly confidential and no subject-identifying information will be released to anyone outside
the project Confidentiality will be assured through several mechanisms First each subject will
be assigned an anonymous study ID which will then be used on all study forms Second any
study forms blood samples and paper records that contain subject information (eg address lists
phone lists) will be kept at the clinical centers in secured locked areas coded by number Once
blood is collected there will be no subject identifiers placed on blood samplesmdashonly the study
ID number and the date of sample collection Third access to all subject data and information
including laboratory specimens will be restricted to authorized personnel In the case of
computerized data this restricted access will be assured through user logon IDs and password
protection
66
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
At the IPFnet DCC only authorized personnel will have access to the data files containing study
data Security will be assured through user logon IDs passwords and appropriate access
privileges All study subjects will be identified only by their IPFnet ID numbers and no personal
identifying information such as name address or Social Security number will be entered into
the IPFnet DCC database Any subject-specific data reported to the IPFnet Steering Group will
be identified only by the IPFnet ID number
Finally subjects will not be identified by name in any reports or publications nor will the data
be presented in such a way that the identity of individual subjects can be inferred Analysis files
created for further study by the scientific community will have no subject identifiers These data
files will be created in accordance with the Ancillary Studies and Publication Policy of the
IPFnet
114 Informed Consent Procedures
All IPFnet subjects will provide written informed consent using procedures reviewed and
approved by each clinical centerrsquos IRB Informed consent will be undertaken by study personnel
in-person with the subject The subject has the option of declining further participation in the
study at that point No further study procedures will be conducted until the signed documents
have been provided to the IPFnet clinical center
115 Institutional Review Boards
Before initiating this study the protocol clinical center-specific informed consent forms Health
Insurance Portability and Accountability Act (HIPAA) forms recruitment materials and other
relevant information will be reviewed by a properly constituted IRB at each participating clinical
center A copy of the signed and dated IRB approval at each clinical center will be retrieved prior
to or during the site initiation visit and archived at the IPFnet DCC Any amendments to the
protocol other than simple administrative and typographical changes must be approved by each
IRB before they are implemented The clinical centers will seek annual renewals of their IRB
approvals in accordance with local procedures
67
__________________________________________ ________________
__________________________________________
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
12 Investigator Agreement
I have read the foregoing protocol PANTHER-IPF and agree that it contains all necessary
details for carrying out this study I will conduct the study as outlined herein and will complete
the study within the time designated
I will provide copies of the protocol and all pertinent information to all individuals responsible to
me who assist in the conduct of this study I will discuss this material with them to ensure they
are fully informed regarding the drug and the conduct of the study
I will fulfill all responsibilities for submitting pertinent information to the local IRB if
applicable that is responsible for this study
I further agree that NHLBI andor DCRI will have access to any source documents from which
eCRF information may have been generated
Signature of Principal Investigator Date
Name of Principal Investigator (printed or typed)
Protocol version date May 19 2009
Protocol Amendment 1 version date May 28 2010
Protocol Amendment 2 version date December 6 2011
68
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
13 References
1 Raghu G Brown KK Bradford WZ et al A placebo-controlled trial of interferon gamma-1b in patients with idiopathic pulmonary fibrosis N Engl J Med 2004350125-33 2 King TE Jr Safrin S Starko KM et al Analyses of efficacy end points in a controlled trial of interferon-gamma1b for idiopathic pulmonary fibrosis Chest 2005127171-7 3 Flaherty KR Thwaite EL Kazerooni EA et al Radiological versus histological diagnosis in UIP and NSIP survival implications Thorax 200358143-8 4 Wells AU Desai SR Rubens MB et al Idiopathic pulmonary fibrosis a composite physiologic index derived from disease extent observed by computed tomography Am J Respir Crit Care Med 2003167962-9 5 Raghu G Freudenberger TD Yang S et al High prevalence of abnormal acid gastroshyoesophageal reflux in idiopathic pulmonary fibrosis Eur Respir J 200627136-42 6 Kinnula VL Focus on antioxidant enzymes and antioxidant strategies in smoking related airway diseases Thorax 200560693-700 7 Coultas DB Zumwalt RE Black WC Sobonya RE The epidemiology of interstitial lung diseases Am J Respir Crit Care Med 1994150967-72 8 Raghu G Weycker D Edelsberg J Bradford WZ Oster G Incidence and prevalence of idiopathic pulmonary fibrosis Am J Respir Crit Care Med 2006174810-6 9 Olson AL Swigris JJ Lezotte DC Norris JM Wilson CG Brown KK Mortality from pulmonary fibrosis increased in the United States from 1992 to 2003 Am J Respir Crit Care Med 2007176277-84 10 Mannino DM Etzel RA Parrish RG Pulmonary fibrosis deaths in the United States 1979shy1991 An analysis of multiple-cause mortality data Am J Respir Crit Care Med 19961531548shy52 11 Hubbard R Johnston I Coultas DB Britton J Mortality rates from cryptogenic fibrosing alveolitis in seven countries Thorax 199651711-6 12 Johnston I Britton J Kinnear W Logan R Rising mortality from cryptogenic fibrosing alveolitis Bmj 19903011017-21 13 Raghu G Collard HR Egan JJ et al An official ATSERSJRSALAT statement idiopathic pulmonary fibrosis evidence-based guidelines for diagnosis and management Am J Respir Crit Care Med 2011183788-824 14 (USA) FDA FDA Public Health Advisory Interferon gamma-1b (marketed as Actimmune) In 2007 15 King TE Jr Pardo A Selman M Idiopathic pulmonary fibrosis Lancet 2011 16 Raghu G Brown KK Costabel U et al Treatment of idiopathic pulmonary fibrosis with etanercept an exploratory placebo-controlled trial Am J Respir Crit Care Med 2008178948shy55 17 Malouf MA Hopkins P Snell G Glanville AR An investigator-driven study of everolimus in surgical lung biopsy confirmed idiopathic pulmonary fibrosis Respirology 201116776-83 18 King TE Jr Behr J Brown KK et al BUILD-1 a randomized placebo-controlled trial of bosentan in idiopathic pulmonary fibrosis Am J Respir Crit Care Med 200817775-81 19 Richeldi L Costabel U Selman M et al Efficacy of a tyrosine kinase inhibitor in idiopathic pulmonary fibrosis N Engl J Med 20113651079-87
69
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
20 Borok Z Buhl R Grimes GJ et al Effect of glutathione aerosol on oxidant-antioxidant imbalance in idiopathic pulmonary fibrosis Lancet 1991338215-6 21 Meyer A Buhl R Magnussen H The effect of oral N-acetylcysteine on lung glutathione levels in idiopathic pulmonary fibrosis Eur Respir J 19947431-6 22 Behr J Maier K Degenkolb B Krombach F Vogelmeier C Antioxidative and clinical effects of high-dose N-acetylcysteine in fibrosing alveolitis Adjunctive therapy to maintenance immunosuppression Am J Respir Crit Care Med 19971561897-901 23 Cantin AM North SL Fells GA Hubbard RC Crystal RG Oxidant-mediated epithelial cell injury in idiopathic pulmonary fibrosis J Clin Invest 1987791665-73 24 Waghray M Cui Z Horowitz JC et al Hydrogen peroxide is a diffusible paracrine signal for the induction of epithelial cell death by activated myofibroblasts Faseb J 200519854-6 25 Larios JM Budhiraja R Fanburg BL Thannickal VJ Oxidative protein cross-linking reactions involving L-tyrosine in transforming growth factor-beta1-stimulated fibroblasts J Biol Chem 200127617437-41 26 Kinnula VL Fattman CL Tan RJ Oury TD Oxidative stress in pulmonary fibrosis a possible role for redox modulatory therapy Am J Respir Crit Care Med 2005172417-22 27 Meyer A Buhl R Kampf S Magnussen H Intravenous N-acetylcysteine and lung glutathione of patients with pulmonary fibrosis and normals Am J Respir Crit Care Med 19951521055-60 28 Behr J Degenkolb B Krombach F Vogelmeier C Intracellular glutathione and bronchoalveolar cells in fibrosing alveolitis effects of N-acetylcysteine Eur Respir J 200219906-11 29 Bando M Hosono T Mato N et al Long-term efficacy of inhaled N-acetylcysteine in patients with idiopathic pulmonary fibrosis Intern Med 2010492289-96 30 Demedts M Behr J Buhl R et al High-dose acetylcysteine in idiopathic pulmonary fibrosis N Engl J Med 20053532229-42 31 Toma TP Bhowmik A Rajakulasingam R Acetylcysteine in pulmonary fibrosis N Engl J Med 20063541086-9 author reply -9 32 Hunninghake GW Antioxidant therapy for idiopathic pulmonary fibrosis N Engl J Med 20053532285-7 33 Flaherty KR Mumford JA Murray S et al Prognostic implications of physiologic and radiographic changes in idiopathic interstitial pneumonia Am J Respir Crit Care Med 2003168543-8 34 Latsi PI du Bois RM Nicholson AG et al Fibrotic idiopathic interstitial pneumonia the prognostic value of longitudinal functional trends Am J Respir Crit Care Med 2003168531-7 35 Collard HR King TE Jr Bartelson BB Vourlekis JS Schwarz MI Brown KK Changes in clinical and physiologic variables predict survival in idiopathic pulmonary fibrosis Am J Respir Crit Care Med 2003168538-42 36 Jegal Y Kim DS Shim TS et al Physiology is a stronger predictor of survival than pathology in fibrotic interstitial pneumonia Am J Respir Crit Care Med 2005171639-44 37 Martinez FJ Safrin S Weycker D et al The clinical course of patients with idiopathic pulmonary fibrosis Ann Intern Med 2005142963-7 38 Hull JH Acetylcysteine in pulmonary fibrosis N Engl J Med 20063541089-91 author reply -91
70
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
39 Flaherty KR King TE Jr Raghu G et al Idiopathic interstitial pneumonia what is the effect of a multidisciplinary approach to diagnosis Am J Respir Crit Care Med 2004170904shy10 40 Raghu G Johnson WC Lockhart D Mageto Y Treatment of idiopathic pulmonary fibrosis with a new antifibrotic agent pirfenidone results of a prospective open-label Phase II study Am J Respir Crit Care Med 19991591061-9 41 Hunninghake GW Lynch DA Galvin JR et al Radiologic findings are strongly associated with a pathologic diagnosis of usual interstitial pneumonia Chest 20031241215-23 42 Lynch D Godwin J Safrin S et al High-resolution computed tomography in idiopathic pulmonary fibrosis diagnosis and prognosis Am J Respir Crit Care Med 2005172488-93 43 Mallinckrodt CH Watkin JG Molenberghs G Carroll RJ Choice of the primary analysis in longitudinal clinical trials Pharmaceutical Statistics 20043161-9 44 Bang H Tsiatis A Estimating medical costs with censored data Biometrika 200087329shy43 45 Lin DY Regression analysis of incomplete medical cost data Stat Med 2003221181-200 46 Rochon J Application of GEE procedures for sample size calculations in repeated measures experiments Stat Med 1998171643-58 47 Lachin JM Foulkes MA Evaluation of sample size and power for analyses of survival with allowance for nonuniform patient entry losses to follow-up noncompliance and stratification Biometrics 198642507-19
71
- PANTHER-IPFPREDNISONE AZATHIOPRINEAND N-ACETYLCYSTEINEA STUDY THAT EVALUATES RESPONSE INIDIOPATHIC PULMONARY FIBROSIS
-
- Protocol Summary
- Table of Contents
- List of Tables
- List of Figures
- List of Abbreviations
- 1 Summary
- 2 Hypotheses and Specific Aims
-
- 21 Null Hypothesis
- 22 Specific Aim 1
- 23 Specific Aim 2
- 24 Prespecified Subgroups of Interest
-
- 3 Background and Significance
-
- 31 Idiopathic Pulmonary Fibrosis is the Most Common Interstitial Lung Disease
- 32 Rationale for Placebo Control
- 33 Rationale for N-acetylcysteine
- 35 Rationale for N-acetylcysteine as a Stand-alone Therapy
- 36 Rationale for the Study Design and Primary Endpoint
- 37 Rationale for Blinding of Treatments
-
- 4 Methods
-
- 41 Inclusion Criteria
- 42 Diagnosis of IPF
- 43 Exclusion Criteria
- 44 Study Design and Study Visit
- 45 Dose Justification
- 46 Contraindications Precautions and Side Effects of Study Medications
- 47 Recruitment Procedures
- 48 Study Procedures
- 49 Concomitant Medications
- 410 Laboratory Testing
- 411 Blinding of Study Drugs
-
- 5 Study Endpoints
-
- 51 Primary Study Endpoint
- 52 Secondary Study Endpoints
-
- 6 Safety Evaluations and Procedures
-
- 61 Adverse Events
- 62 Clinical Medical Monitoring
- 63 Unblinding Procedures
-
- 7 Study Drug Procedures
- 8 Data Management
-
- 81 Hardware and Software Configuration
- 82 Sources of Data
-
- 9 Study Design and Data Analysis
-
- 91 General Analytic Considerations
- 92 Randomization Blinding and Reporting of Results
- 93 Stratification
- 94 Specification of the Primary Analyses
- 95 Analysis of Longitudinal Endpoints
- 96 Analysis of Binary Time-to-Event and Time-Lagged Endpoints
- 97 Power Analysis
-
- 10 Study Administration
-
- 101 Cooperative Agreement Mechanism
- 102 IPFnet Steering Group
- 103 Data and Safety Monitoring Board
- 104 Recommendations on Interim Monitoring of Efficacy Safety and Futility
-
- 11 Investigator and Sponsor Obligations
-
- 111 Monitoring
- 112 Cost and Payment
- 113 Confidentiality and Health Insurance Portability and Accountability ActConsiderations
- 114 Informed Consent Procedures
- 115 Institutional Review Boards
-
- 12 Investigator Agreement
- 13 References
-

PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
5 Study Endpoints 44 51 Primary Study Endpoint 44 52 Secondary Study Endpoints 44
521 Time to Disease-progression 44 522 Acute Exacerbations 44 523 Respiratory Infections 47 524 Maintained FVC Response 48
6 Safety Evaluations and Procedures 49 61 Adverse Events 49
611 Definitions 49 612 Adverse Event (AE) Reporting 50
6121 Serious Adverse Events (SAE) Reporting 50 6122 Regulatory Reporting 51
62 Clinical Medical Monitoring 52 63 Unblinding Procedures 52
7 Study Drug Procedures 53
8 Data Management 54 81 Hardware and Software Configuration 54
811 Hardware and Database Software 54 812 Statistical Software 54 813 Access Control and Confidentiality Procedures 54 814 Security 54 815 Back-up Procedures 55 816 Virus Protection 55
82 Sources of Data 55 821 Design and Development 55 822 Data Collection Forms 55 823 Data Acquisition and Entry 56 824 Data Center Responsibilities 56 825 Data Editing 56 826 Training 56
9 Study Design and Data Analysis 57 91 General Analytic Considerations 57 92 Randomization Blinding and Reporting of Results 57 93 Stratification 58 94 Specification of the Primary Analyses 58 95 Analysis of Longitudinal Endpoints 58 96 Analysis of Binary Time-to-Event and Time-Lagged Endpoints 59 97 Power Analysis 60
971 Primary Analyses 60 972 Power Analysis for Secondary Endpoints 61
10 Study Administration 62 101 Cooperative Agreement Mechanism 62 102 IPFnet Steering Group 64 103 Data and Safety Monitoring Board 64 104 Recommendations on Interim Monitoring of Efficacy Safety and Futility 64
11 Investigator and Sponsor Obligations 66 111 Monitoring 66 112 Cost and Payment 66 113 Confidentiality and Health Insurance Portability and Accountability Act Considerations 66 114 Informed Consent Procedures 67 115 Institutional Review Boards 67
5
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
12 Investigator Agreement 68
13 References 69
6
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
List of Tables Table 1 Operating Characteristics of Local HRCT Review for Diagnosis of UIP (24)
Table 2 Combining HRCT and Pathology Interpretations to Determine if IPF is Present (25)
Table 3 Schedule of Assessments (34)
Table 4 Side Effects of NAC (40)
Table 5 Final Diagnoses in Evaluation of Suspected Acute Exacerbations (46)
Table 6 Hypothetical Values of Mean FVC (L) Change from Baseline (61)
Table 7 Detectable Differences in Treatment Means for Selected Endpoint Measurements (61)
List of FiguresFigure 1 Changes in Forced Vital Capacity from Baseline in Prior IPF Clinical Trials (19)
Figure 2 Diagnosis of Idiopathic Pulmonary Fibrosis in the IPFnet (22)
Figure 3 Pathology Flow Chart Surgical Lung Biopsy Diagnosis (23)
Figure 4 Acute Exacerbation Flow Chart (47)
7
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
List of Abbreviations
6MWT 6-minute walk test
A-aPO2 alveolar-arterial PO2 difference
ABG arterial blood gas
AE adverse event
AEx acute exacerbation
AG albuminglobulin
ALT alanine aminotransferase
AST aspartate aminotransferase
ATS American Thoracic Society
AZA azathioprine
BAL bronchoalveolar lavage
BUN blood urea nitrogen
CBC complete blood count
cGMP Current Good Manufacturing Practice
CPI Composite Physiologic Index
CPK creatine phosphokinase
CT computed tomography
DCC Data Coordinating Center
DCRI Duke Clinical Research Institute
8
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
DLCO diffusing capacity of the lung for carbon monoxide
DLCOpred diffusing capacity of the lung for carbon monoxide percent predicted
DSMB data and safety monitoring board
eCRF Electronic case report form
ERS European Respiratory Society
FDA Food and Drug Administration (US)
FEV1 forced expiratory volume in 1 second
FSH follicle-stimulating hormone
FVC forced vital capacity
FVCpred forced vital capacity percent predicted
GGT gamma glutamyl transferase
GSH glutathione
HAD Hospital Anxiety and Depression
HHS Health amp Human Services (US Dept of)
HIPAA Health Insurance Portability and Accountability Act
HRCT high-resolution computed tomography
IBW ideal body weight
ICE CAP Investigating Choice Experiments for Preferences of Older People Capability Instrument
ILD interstitial lung disease
IPF idiopathic pulmonary fibrosis
9
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
IPFnet Idiopathic Pulmonary Fibrosis Clinical Research Network
IRB institutional review board
ITT intent to treat
IV intravenous
IVRS interactive voice response system
LDH lactate dehydrogenase
LFT liver function test
LOCF last observation carried forward
LSD Least Significant Difference
MAR missing at random
MCAR missing completely at random
MMRM mixed model repeated measures
MOOP manual of operating procedures
NAC N-acetylcysteine
NHLBI National Heart Lung and Blood Institute (US)
NIH National Institutes of Health (US)
NSIP nonspecific interstitial pneumonia
PaO2 partial pressure of arterial oxygen
PCP primary care provider
PFT pulmonary function test
10
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
PHS Public Health Service (US)
PI principal investigator
PL placebo
PLT platelet
PRED prednisone
QOL quality of life
SAE serious adverse event
SAP statistical analysis plan
SGRQ St Georgersquos Respiratory Questionnaire
SpO2 oxygen saturation by pulse oximetry
TPMT thiopurine methyl transferase
UCSD SOBQ University of California at San Diego Shortness of Breath Questionnaire
UIP usual interstitial pneumonia
ULN upper limit of normal
USP United States Pharmacopoeia
VC vital capacity
WBC white blood cell
11
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
PREDNISONE AZATHIOPRINE AND N-ACETYLCYSTEINE A STUDY
THAT EVALUATES RESPONSE IN IDIOPATHIC PULMONARY FIBROSIS
1 Summary
There are currently no drug therapies that have proven to be effective in the treatment of idiopathic pulmonary
fibrosis (IPF) Previous clinical drug trials have been difficult to interpret due to lack of true placebo (PL)
controls or other methodological concerns Clinical efficacy of immunosuppressive therapies and agents that
reduce oxidative stress remains controversial The IPF Clinical Research Network (IPFnet) is conducting a
randomized double-blind placebo-controlled trial designed to assess the safety and efficacy of
N-acetylcysteine (NAC) as monotherapy in subjects with mild or moderate IPF
The study initially employed a 3-arm design with 111 randomization to NAC azathioprine (AZA)-prednisone
(PRED)-NAC and PL with each subject to be treated up to a maximum of 60 weeks followed by a tapering of
PREDPL and a 4-week period for safety evaluation Approximately 390 subjects who have mild to moderate
IPF (defined as forced vital capacity percent predicted [FVCpred] ge 50 and diffusing capacity of the lung
for carbon monoxide percent predicted [DLCOpred] 30) diagnosed within the past 48 months were to be
enrolled
At the pre-specified interim analysis the DSMB recommended termination of the prednisone-azathioprine-
NAC arm of the study No additional patients will be randomized to that arm However the NAC and placebo
arms remain open for enrollment and we will enroll approximately 130 subjects in each arm (inclusive of the
subjects enrolled at the time of the interim analysis) Follow up for subjects enrolled into the two arms will
continue for 60 weeks
The primary endpoint is the change in longitudinal measurements of FVC over the study period The primary
goal of this study to establish an evidence-based standard of care and clarify myths from facts for
pharmacotherapy of IPF has been met in part by demonstrating that the widely used triple therapy was harmful
to patients with IPF (NHLBI press release Oct 21 2011) To determine the potential therapeutic benefits of
NAC alone the study will continue to enroll patients as a two-arm double-blind placebo-controlled study from
this point on (NAC vs placebo) as recommended by the DSMB following the pre-specified interim analysis
12
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
2 Hypotheses and Specific Aims 21 Null Hypothesis
Treatment with NAC will provide the same efficacy as PL as measured by longitudinal changes in FVC
22 Specific Aim 1
This study is designed to assess the safety and efficacy of NAC in subjects with newly diagnosed IPF
23 Specific Aim 2
Secondary goals of this study are to assess differences between treatment groups for the following
1 Mortality
2 Time to death
3 Frequency of acute exacerbations (AExs)
4 Frequency of maintained FVC response
5 Time-to-disease progression
6 Change in DLCO
7 Change in Composite Physiologic Index (CPI)
8 Change in resting alveolar-arterial oxygen gradient
9 Change in 6-minute walk test (6MWT) distance
10 Change in 6MWT oxygen saturation area under the curve
11 Change in 6MWT distance to desaturation lt 80
12 Change in 6MWT minutes walked
13 Changes in health status as measured by the SF-36 EuroQol and St Georgersquos Respiratory
Questionnaire (SGRQ)
14 Changes in dyspnea as measured by the University of California at San Diego Shortness of Breath
Questionnaire (UCSD SOBQ)
15 Frequency and types of adverse events (AEs)
16 Frequency and types of respiratory complications both infectious and noninfectious
17 Frequency of hospitalizations both all-cause and respiratory-related
13
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
24 Prespecified Subgroups of Interest
Treatment effects will be estimated and compared within key subgroups
Higher enrollment FVC12
Typical vs atypical high-resolution computed tomography (HRCT) reading at baseline3
Recent vs more remote diagnosis (time from initial diagnosis of IPF le 1 year and gt 1 year)
Lower CPI score at enrollment4
Medical therapy for gastroesophageal reflux5
Ethnic background
Sex
Smoking history (current or ex-smoker vs never smoker) given potential impact on oxidant status6
Presence of emphysema gt 25 on HRCT
14
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
3 Background and Significance
31 Idiopathic Pulmonary Fibrosis is the Most Common Interstitial Lung Disease
IPF is the most common interstitial lung disease (ILD) of unknown etiology The current incidence and
prevalence of IPF in the United States are not known A 1994 study of a population-based registry of subjects in
Bernalillo County New Mexico USA estimated an incidence of 107 cases per 100000 per year for males and
74 cases per 100000 per year for females the prevalence of IPF was estimated at 20 per 100000 for males and
13 per 100000 for females7 Extrapolating from a large healthcare claims database a more recent review
estimated the prevalence of IPF in the United States at 427 per 100000 (incidence estimated at 163 per
100000 per year)8 Recent epidemiological studies indicate increasing mortality rates from IPF in the United
States and other industrialized nations9-12
Approximately two-thirds of subjects with IPF are over the age of 60 at the time of presentation and the
incidence increases with age13 IPF has no distinct geographical distribution and predilection by race or
ethnicity has not been identified13 Individual subjects may remain relatively stable for prolonged periods
experience very slow declines in lung function with progression of radiographic abnormalities for a period of
months to years or experience more rapid declines and subsequent death Only 20 to 30 of IPF patients
survive for 5 years following diagnosis
There is currently no proven effective pharmacological treatment for IPF13 Anti-inflammatory and
immunosuppressive agents have been the traditional approach to the management of patients with IPF Based
on the results of the interim analysis of the PANTHER-IPF trial this lsquotraditional approachrsquo will be aborted
However it remains unknown if NAC alone will prove beneficial in IPF patients The primary goal of the
modified study is to establish an evidence-based standard of care and clarify the role of this specific antioxidant
pharmacotherapy for IPF
32 Rationale for Placebo Control
IPF is a disorder for which there is no proven efficacious therapy A major objective of this trial is to test to the
greatest degree possible a proposed standard of care for patients with IPF The current traditional therapy
15
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
employs immunosuppressive and corticosteroid drugs Interim review of the original PANTHER-IPF study has
documented increased adverse events and lack of efficacy for AZA-PRED-NAC compared to placebo
suggesting that this therapeutic approach should not be employed Whether this applies to NAC alone which
has been advocated by international societies has not been proven in well-designed well-powered clinical
trials The recommendations made in the recently published evidence guidelines for NAC monotherapy was
weak based on low quality13 Thus this continued clinical trial randomizing patients to receive NAC or placebo
is pivotal and will answer the important question of the potential therapeutic benefits of NAC monotherapy with
grade A evidence In this prospective randomized clinical trial the inclusion of a PL arm is therefore vital to
adequately test the benefits of NAC in well-characterized subjects with IPF
If NAC has no true efficacy then its role as standard of care will be refuted If a benefit compared with PL is
confirmed it will establish a benchmark against which future novel therapies for IPF will be safely compared
As there is no currently accepted therapy for IPF there is an increasing body of published literature supporting
the concept of no treatment as the ldquobest carerdquo option for IPF13
Post hoc analyses of PL-controlled trials suggest that subjects with milder disease may be more amenable to
therapy12 It is notable that a recent international prospective randomized trial of interferon-gamma for IPF
also included a PL arm the study was terminated early by the data and safety monitoring board (DSMB) due to
lack of treatment effect1415 This underscores the belief that a proven effective therapy for IPF does not
currently exist and that true placebo-controlled trials remain the gold standard Similarly recently completed
trials of etanercept everolimus bosentan and BIPF 1120 in IPF have included PL-treated arms16-19 In three of
these trials the treated subjects showed little if any objective improvement Based on this evidence and the
current status of IPF therapy and therapeutic trials we believe that clinicians and subjects will continue to enroll
in a PL-controlled study
33 Rationale for N-acetylcysteine
NAC is a derivative of the amino acid L-cysteine NAC has been shown to augment levels of the naturally
occurring antioxidant glutathione (GSH ) (glutathione γ-glutamyl cysteinyl glycine) both in vitro and in
vivo2021 GSH is present in all eukaryotic cells and may play an important role in protecting alveolar epithelial
cells against oxidant injury The concentration of GSH in the bronchoalveolar lavage (BAL) fluid in patients
16
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
with IPF is markedly diminished compared with normal subjects This GSH deficiency may be corrected by
exogenous administration of NAC2122
There is evidence of enhanced production of oxidants in an IPF lung Both inflammatory cells and
myofibroblasts derived from patients with IPF generate increased amounts of extracellular oxidants including
hydrogen peroxide2324 Secretion of hydrogen peroxide by activated myofibroblasts may induce the death of
adjacent lung epithelial cells by paracrine mechanisms24 Additionally generation of oxidants by myofibroblasts
induces oxidative crosslinking of extracellular matrix proteins25 a potential mechanism for aberrant matrix
remodeling Thus an oxidant-antioxidant imbalance exists in the lungs of IPF patients26 NAC may confer
protection against this imbalance by augmenting GSH levels in addition to its more direct free-radical
scavenging activity
Intravenous (IV) NAC therapy has been shown to increase total BAL GSH in 8 IPF subjects27 Oral NAC (600
mg 3 times per day) has been shown to decrease markers of oxidant injury and improve both total and reduced
GSH levels in the epithelial lining fluid of subjects with IPF in a small uncontrolled study22 pulmonary
function improved modestly with therapy A similar study in 18 IPF subjects confirmed increased intracellular
GSH concentration after 12 weeks of NAC (600 mg 3 times per day)2228 no clinical correlates were reported
Inhaled NAC was suggested to improve pulmonary function in an open label study29
35 Rationale for N-acetylcysteine as a Stand-alone Therapy
Results of a double-blind multi-center European clinical trial of 150 IPF subjects testing combinations of AZAshy
PRED vs AZA-PRED-NAC have been reported30 NAC added to AZA-PRED (ldquoconventional therapyrdquo) had a
significant positive effect on DLCO (p lt 0005) and vital capacity (VC) (p lt 005) at the end of 1 year30 The
recent ATSERS position statement after much discussion concluded that NAC alone should not be considered
in the majority of patients with IPF without additional data from well-designed studies
The interpretation of these data has been quite controversial Some have suggested that the magnitude of the
treatment effect although statistically significant is modest31 Others have suggested that NAC may be
modulating potential toxic effects of AZA-PRED alone32 supporting the investigation of NAC as stand-alone
therapy
17
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
The IPFnet is now completing the PANTHER-IPF trial with a 11 randomization (NAC vs placebo) and a
simple practical feasible and scientifically rational design that will establish standard of care with NAC for
IPF based on a currently available therapeutic agent and the existing data to support its use We anticipate that
all future clinical trials of novel therapeutic agents will be tested against this to-be-established standard of care
36 Rationale for the Study Design and Primary Endpoint
The optimal study design of a therapeutic trial in IPF would include survival as a primary endpoint The
published results of the IFN-γ 1b Phase 3 (GIPF-001) trial suggested a survival benefit in subjects with milder
disease in retrospective analyses1 although the trial was underpowered to address this question This was likely
related to the limited mortality in the PL arm of the study which included IPF subjects with mild to moderate
disease This study documents that an IPF study powered to improve survival in a patient population with mild
disease requires a larger sample size andor duration of study In fact the recently aborted Phase 3 IFN-γ 1b
(GIPF-007 INSPIRE) study was a survival-based study and recruited more than 800 subjects at 75 centers
worldwide1415 As such within the context of the current IPFnet trial survival is an impractical primary
endpoint variable
Several groups have published data defining an appropriate surrogate outcome variable a 10 decrement in
FVC during 6 to 12 months is a powerful predictor of survival in IPF33-36 Furthermore additional evidence
suggests a similar predictive ability for a 10 decrement in FVC during 3 months of follow-up37 With strong
supportive evidence of FVC progression being related to mortality on a per-subject basis this study will use
FVC changes in liters between treatment groups as the primary endpoint Previously published IPF studies have
shown a steady decline in FVC (and FVCpred) among control group subjects230 The GIPF-001 study
suggested a 48-week decrease in FVC of 016 L in the PL-treated subjects The IFIGENIA study demonstrated
a decline in FVC of approximately 019 L over 52 weeks in the subjects randomized to the control treatment
Figure 1 depicts the change in FVC for control groups from previously published IPF studies38 Based on these
data we expect that the PL group will have a decline of 020 L over the 60-week study period The IPFnet
Steering Group determined that a clinically meaningful improvement would be the preservation of the majority
of the 020-L FVC decline Therefore a mean treatment difference of 015 L in mean FVC over the 60-week
study period was determined to be a clinically meaningful difference
18
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Δ f
rom
bas
elin
e (i
n L
)
01
005
0
-005
-01
-015 Projected Δ for placebo
-02
-025
-019
-016
-013 Pirfenidone GIPF001
NAC
Placebo
4 8 12 16 20 24 28 32 36 40 44 48 52 56 60
Week
Figure 1 Changes in FVC From Baseline in Prior IPF Clinical Trials
Recent data suggest that various patient subgroups would be expected to potentially exhibit differential response
to therapy These parameters will be used to a priori separate patients by a series of baseline characteristics
including
1 Higher enrollment FVC12
2 Typical vs atypical high-resolution computed tomography (HRCT) reading at baseline3
3 Recent vs more remote diagnosis (time from initial diagnosis of IPF le 1 year and gt 1 year)
4 Lower CPI score at enrollment4
5 Medical therapy for gastroesophageal reflux5
6 Ethnic background
7 Sex
8 Smoking history (current or ex-smoker vs never smoker) given potential impact on oxidant status6
9 Presence of emphysema gt 25 on HRCT
37 Rationale for Blinding of Treatments
The issue of treatment blinding was given a great deal of consideration with subject safety being the primary
concern After discussion among the Steering Group members it was decided that as long as subject safety
could be ensured blinding was necessary Blinding allows the study to
Have optimal scientific validity and potential to impact the standard of care for subjects
19
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Make objective assessments of treatment effects
Maintain clinical equipoise among investigators
Encourage subjects to have similar levels of contact with the medical community
Minimize the differential dropout rates across study arms
20
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
4 Methods 41 Inclusion Criteria
1 Age 35 to 85 years inclusive
2 FVC ge 50 of predicted (post-bronchodilator measurement from the screening visit)
3 DLCO ge 30 of predicted (hemoglobin corrected and altitude corrected if gt4000 ft above sea level)
4 Ability to understand and provide informed consent
5 Diagnosis of IPF according to a modified version of the ATS criteria le 48 months from enrollment The
date of diagnosis is defined as the date of the first available HRCT or surgical lung biopsy characteristic
of definite UIP
411 Subjects Shown to Have Usual Interstitial Pneumonia Pattern on Surgical Lung Biopsy
Subjects who have been shown to have UIP pattern on lung biopsy must have all of the following
1 Exclusion of other known causes of ILD such as drug toxicity clinically significant environmental
exposures or diagnosis of connective tissue diseases
2 Bibasilar reticular abnormalities with minimal ground glass opacities on HRCT scan
412 Subjects Who Have Not Undergone a Surgical Lung Biopsy
In addition to the criteria above these subjects must have radiological findings considered to be definite for the
diagnosis of UIPIPF
1 Bibasilar reticular abnormalities with minimal ground glass opacities
2 Honeycombing as the predominant feature and located in the peripheral lung bases
42 Diagnosis of IPF
Only subjects with definite IPF will be eligible for enrollment in this study We will utilize a combination of
clinicalphysiologic features HRCT and review of a clinically obtained surgical lung biopsy specimen to
establish the diagnosis of IPF An algorithm for the diagnosis is provided to guide entry into the protocol as
outlined in the inclusion and exclusion criteria (Figures 2 and 3) This multi-disciplinary approach uses
21
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
expertise from clinicians radiologists and pathologists Investigators at each site in conjunction with central
pathology will work together to establish the diagnosis of IPF This interactive approach to the diagnosis of IPF
increases the level of agreement between observers39
A subject with suspected ILD should be evaluated for secondary causes including but not limited to
environmental exposures drugs and systemic diseases Presence of any of these findings felt to be significant
enough to cause an ILD should disqualify the subject from entry into the trial
If secondary causes are absent an HRCT scan may be obtained If an HRCT of sufficiently high quality has
been obtained within the last 3 months that scan may be used for diagnosis In the appropriate clinical setting
the diagnosis of IPF can be made by the demonstration of a typical radiographic pattern on HRCT or by
demonstration of UIP pattern on a surgical lung biopsy The following criteria for a radiographic (ie
nonsurgical) diagnosis will be used In the absence of known exposures andor clinical associations attributable
to pulmonary fibrosis and in the appropriate clinical setting the presence of definite UIP pattern in HRCT
images is required to meet study criteria for the diagnosis of IPF
Figure 2 Diagnosis of Idiopathic Pulmonary Fibrosis in the IPFnet
22
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Figure 3 Pathology Flow Chart Surgical Lung Biopsy Diagnosis
Requirement for diagnosis
1 Clinical exclusion of other known causes (connective tissue diseases environmental and drug
exposures) of ILD
2 Radiographic HRCT with bibasilar reticular abnormality and honeycomb change with minimal
ground glass opacities
Appropriate clinical setting
1 Age gt 50 years
2 Insidious onset of unexplained dyspnea
3 Duration of illness for ge 3 months
4 Bibasilar inspiratory crackles
23
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Unlike the ATSERS consensus criteria published in 2000 bronchoscopy will not be required for diagnosis
This decision was made based on the experience of the IPFnet Steering Group members regarding the utility of
bronchoscopy in the diagnosis of IPF The presence of an atypical HRCT finding will require documentation of
a definitive diagnosis by surgical lung biopsy In fact this is in keeping with the recently published evidence
based guidelines for diagnosis and management of IPF13 As shown in Figure 3 central review of the pathology
data will be required for a diagnosis of IPF
We will not require central review of HRCT as several studies have shown that a confident local interpretation
of clinicalHRCT criteria as definite IPFUIP is associated with a high positive predictive value for finding UIP
at surgical lung biopsy (see Table 1) Differences in sensitivity in these series likely reflect subject selection as
Flaherty et al3 evaluated only UIP and nonspecific interstitial pneumonia (NSIP) while Raghu et al40 and
Hunninghake et al41 included a broader range of ILD
Table 1 Operating Characteristics of Local HRCT Review for Diagnosis of UIP
Researcher of Subjects Sensitivity () Specificity () PPV () NPV ()
Raghu et al 40
59 (29 UIP by SLB) 78 90 88 82
Hunninghake et al 41 91 (54 UIP by SLB)
74 81 85 67
Flaherty et al 3 96 (only NSIP amp UIP)
37 100 100 30
Abbreviations PPV positive predictive value NPV negative predictive value UIP usual interstitial pneumonia SLB surgical lung biopsy and NSIP nonspecific interstitial pneumonia
Furthermore an analysis of the HRCT scans from subjects enrolled in the GIPF-001 trial confirmed that local
site interpretations have a high congruity to a central radiology core In this multi-center study 263 HRCT
scans were read as definite IPF and a retrospective central radiology core review found 932 to be consistent
with IPF 42 We will also take several additional steps to insure that the local HRCT reads are accurate
including
1 A detailed training module has been developed and must be completed by each site radiologist before
site initiation
2 Clinical centers are to mail all HRCT scans to the HRCT core lab The first 10 HRCT scans from
subjects enrolled at each enrolling clinical center will be reviewed centrally to be certain that local reads
24
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
25
are congruent with a central interpretation If discrepancies are identified additional education will be
provided and HRCT scans will continue to be reviewed centrally until the central radiology core is
confident that the local center is performing appropriately
3 Random scans will be obtained from each center throughout the study to confirm that the local read
continues to agree with central interpretation If discrepancies are identified they will be addressed as in
2 above
In all cases if a subject has a surgical lung biopsy sample that sample will be reviewed by the local and central
pathologists Therefore the only cases that would not be subject to a direct central review process are those
where the HRCT meets the centrally defined criteria for an unequivocal diagnosis and a lung biopsy sample is
not available Table 2 below summarizes the possible combinations for making a diagnosis
Table 2 Combining HRCT and Pathology Interpretations to Determine if IPF is Present
HRCT Diagnosis Pathology Diagnosis Diagnosis of IPF
Definite UIP Definite UIP Yes
Definite UIP Probable UIP Yes
Definite UIP Possible UIP Yes
Definite UIP Not UIP No
Definite UIP Unavailable Yes
Consistent with UIP Definite UIP Yes
Consistent with UIP Probable UIP Yes
Consistent with UIP Possible UIP No
Consistent with UIP Not UIP No
Consistent with UIP Unavailable No
Inconsistent with UIP Any No
Abbreviations HRCT high-resolution computed tomography IPF idiopathic pulmonary fibrosis
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
UIP usual interstitial pneumonia Dx diagnosis 43 Exclusion Criteria
1 History of clinically significant environmental exposure known to cause pulmonary fibrosis
Occupational exposures such as asbestos or environmental exposure to organic dust such as occurs in
pigeon breeders may at times mimic the clinical and radiographic findings of IPF
2 Diagnosis of connective tissue disease felt by the principal investigator (PI) to be the etiology of the
interstitial disease Diagnosis of collagen-vascular conditions will be according to the published
American College of Rheumatology criteria As such the presence of any documented collagen-vascular
disorder or the presence of any suspicious symptom complex whether or not associated with
significantly abnormal rheumatological serologies will exclude the subject at the discretion of the PI
3 Extent of emphysema greater than the extent of fibrotic change (honeycombing reticular changes) on
HRCT scan
4 Forced expiratory volume in 1 second (FEV1)FVC ratio lt 065 at screening (postbronchodilator)
5 Partial pressure of arterial oxygen (PaO2) on room air lt 55 mm Hg (lt 50 mm Hg at Denver site)
6 Residual volume gt 120 predicted at screening (postbronchodilator)
7 Evidence of active infection
8 Significant bronchodilator response on screening spirometry defined as a change in FEV1 ge 12 and
absolute change gt 200 mL OR change in FVC ge 12 and absolute change gt 200 mL The percent
difference between the FVC (or FEV1) values will be calculated by taking the absolute value of the
difference and dividing it by the larger of the two FVC (or FEV1) values
9 Screening and enrollment post-bronchodilator FVC measurements (in liters) differing by gt 11 The
percent difference between the FVC values will be calculated by taking the absolute value of the
difference and dividing it by the larger of the two FVC values (eg the percent difference between FVC
measurements of 19 and 20 liters would be determined by taking the difference between the two (01
liters) and dividing by the larger of the two (20 liters) So 0120 = 5 and these FVC measurements
would not exclude the subject
10 Listed for lung transplantation ie the patient has completed the evaluation process has been accepted
as a candidate for transplantation at an appropriate center and is waiting to receive notification of an
available donor organ
11 History of unstable or deteriorating cardiac disease
12 Myocardial infarction coronary artery bypass or angioplasty within 6 months of screening
26
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
13 Unstable angina pectoris or congestive heart failure requiring hospitalization within 6 months of
screening
14 Uncontrolled arrhythmia
15 Severe uncontrolled hypertension
16 Known HIV or hepatitis C
17 Known cirrhosis and chronic active hepatitis
18 Active substance andor alcohol abuse (as determined by site PI)
19 Pregnancy or lactation (subjects who are pregnant or breastfeeding)
20 Known hypersensitivity to study medication
21 Any condition other than IPF that in the opinion of the site PI is likely to result in the death of the
subject within the next year
22 Any condition that in the judgment of the PI might cause participation in this study to be detrimental to
the subject or that the PI deems makes the subject a poor candidate
23 Any therapy directed at pulmonary fibrosis (excepting triple therapy of prednisone plus azathioprine
plus NAC) requires a 30-day washout period before randomized Triple therapy of lt= 12 weeks duration
in the past 4 years requires a 30-day washout period before randomization
24 History of triple therapy of prednisone plus azathioprine plus NAC for gt 12 weeksrsquo duration in the past
4 years or previous enrollment in the triple-therapy arm of the PANTHER-IPF study
44 Study Design and Study Visit
441 Study Design Summary
This study will be a randomized double-blind PL-controlled trial designed to assess the safety and efficacy of
NAC in subjects with newly diagnosed IPF
Subjects with mild to moderate IPF (defined as FVCpred ge 50 and DLCOpred ge 30) diagnosed within
the past 48 months will be enrolled Screening will continue until April 30 2012
27
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
The study will employ a 2-arm design with 11 randomization to NAC or PL Once enrolled subjects will visit
the clinical center at 15 weeks and 15-week intervals thereafter Each subject will be treated and followed for a
maximum of 60 weeks
During the 60-week visit subjects will be taken off all study agents Approximately four weeks after the final
dose of study agent is taken subjects will receive a safety phone call from the study site
442 Study Visits
Subjects who meet entry criteria will review the informed consent a written description of the purpose
procedures and risks of the study with the PI co-investigator or study coordinator and all questions will be
answered The informed consent form will be signed by the subject at screening No protocol-specific
procedures will be performed until the subject has signed and dated an informed consent form This includes the
screening procedures
4421 Screening
Once informed consent is obtained subjects may immediately begin the screening process or may return within
28 days of consent In the event a study subject has been clinically evaluated at the study site by an IPFnet study
physician and has performed testing within three weeks for this clinical evaluation that meets guidelines
provided in the IPFnet PANTHER-IPF Manual of Operating Procedures (MOOP) this testing may be used to
satisfy the following screening criteria medical history physical exam arterial blood gas (ABG) with A-a
gradient vital signs with oximetry body height and weight spirometry DLCO lung volumes and HRCT scan
Allowing the use of previously performed test results that meet study guidelines for the screening visit is
intended to permit subjects easier access to study entry to prevent subjects from repeating testing that has been
performed within the study window and to decrease risks to subjects from repeated exposure to procedures
such as arterial puncture and HRCT
The following procedures will be performed at screening
Medical history and a physical examination
28
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Measure height and weight
Serum pregnancy test (if applicable)
Measure vital signs including oximetry
Blood draws performed and the following analyses conducted
o Hematology (red cell count white cell count hemoglobin hematocrit cell indices differential
platelet count)
o Blood chemistries according to central laboratory protocol (see Section 410 Laboratory
Testing)
o Beta human chorionic gonadotropin (serum) pregnancy test (in women of childbearing potential)
o Urinalysis
Pulmonary Function Tests (PFTs) including spirometry pre- and post- bronchodilator and postshy
bronchodilator measurement of lung volumes and measurement of hemoglobin adjusted diffusing
capacity
Measure ABGs
HRCT if a satisfactory scan has not been performed on the subject within 3 months of screening (see
PANTHER-IPF MOOP for more details)
Surgical lung biopsies (if applicable) reviewed by local and central pathology departments
Current medications If required a washout period discussed with the subject and initiated at this visit
4422 Enrollment
The enrollment visit is expected to take place within eight weeks of the screening visit Enrollment visit
activities include
Measure vital signs including oximetry
Measure height and weight
Serum pregnancy test (if applicable)
If consent has been given blood will be drawn and a urine specimen collected for the bio-specimen
repository
Spirometry (post-bronchodilator)
Measure 6MWT with Borg Dyspnea Scale
29
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Collect Quality-of-life (QOL) data using the SF-36 EuroQol Investigating Choice Experiments for
Preferences of Older People Capability Instrument (ICE CAP) and SGRQ
Female subjects complete Gender Substudy questionnaire
Dyspnea status collected using the UCSD SOBQ
Evaluate Acute Exacerbation (AEx)
Review of any Adverse Events (AEs)
Review of concomitant medications
Subject receives diary and instructions on its purpose and proper use
Subject receives supply of study drug sufficient to last until his or her 15-week study visit
See the Schedule of Assessments (Table 3) for more details Subjects with screening and enrollment postshy
bronchodilator FVC measurements (in liters) differing by more than 11 are not eligible to be enrolled in the
study
Subjects will be asked to provide a physician of record This physician will be considered the subjectrsquos primary
care provider (PCP) and if the subject agrees the PCP will be informed by letter of the subjectrsquos enrollment in
the trial The subject will be informed that his or her ongoing medical care should be received from the PCP
The PCP will be informed of any safety issues identified by the study staff The PCP will also be given
information regarding communication with study personnel about pertinent health issues or clinic encounters
the subject may have
4423 Week 15
The week 15 visit is expected to occur within +- 14 days of the subjectrsquos scheduled visit time (eg the week 15
visit should occur anytime between 13 and 17 weeks after starting study drug Week 15 activities include
Measure vital signs with oximetry
Measurement height and weight
Serum pregnancy test (if applicable)
Spirometry (post-bronchodilator) measurement
Review of AEs
Evaluate for AEx
30
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Review concomitant medications
If consented draw blood and collect urine specimen for the biospecimen repository
Subjects return used and unused study drug for the visit
Review study diary and a new study diary will be given
Provide additional supply of study drug sufficient to last until the next scheduled visit
4424 Week 30
The week 30 visit is expected to occur within +- 14 days of the subjectrsquos scheduled visit time (eg the week 30
visit should occur anytime between 28 and 32 weeks after starting study drug) Week 30 activities include
Physical examination
Measure vital signs with oximetry
Measure height and weight
Laboratory values (complete blood count [CBC] and serum chemistries)
Serum pregnancy test (if applicable)
Measure spirometry (post-bronchodilator)
6MWT with Borg scale
DLCO
Review of AEs
Evaluate for AEx
Review concomitant medications
Complete all QOL and dyspnea questionnaires (EuroQol ICE CAP SF-36 SGRQ and UCSD SOBQ)
If consent has been given blood will be drawn and a urine specimen collected for the biospecimen
repository
Review study diary
Subjects return used and unused study drug for the visit
Provide additional supply of study drug sufficient to last until the next scheduled visit
4425 Week 45
31
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
The week 45 visit is expected to occur within +- 14 days of the subjectrsquos scheduled visit time (eg the week 45
visit should occur anytime between 43 and 47 weeks after starting study drug) Week 45 activities include
Measure vital signs with oximetry
Measure height and weight
Serum pregnancy test (if applicable)
Measure spirometry (post-bronchodilator)
Review of AEs
Evaluate for AEx
Review concomitant medications
If consent has been given blood will be drawn and a urine specimen collected for the biospecimen
repository
Subjects return used and unused study drug for the visit
Study diary reviewed
Provide additional supply of study drug sufficient to last until the next scheduled visit
4426 Week 60 (Early Withdrawal or Final Treatment Visit)
At week 60 or at subject withdrawal from the study (premature by study doctor or subjectrsquos decision) a final
treatment visit will occur At this final treatment visit subjects will discontinue NACPL abruptly Week 60
activities also include
Physical examination
Measure vital signs with oximetry
Measure height and weight
Laboratory values (complete blood count [CBC] and serum chemistries)
Spirometry (post-bronchodilator) measurement
6MWT with Borg scale measurement
DLCO
Lung volumes
ABG
Review of AEs
32
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Evaluate for AEx
Review concomitant medications
Subjects will complete all QOL and dyspnea questionnaires (EuroQol ICE CAP SF-36 SGRQ and
UCSD SOBQ)
If consent has been given blood will be drawn and a urine specimen collected for the biospecimen
repository
Subjects return used and unused study drug for the visit
Study diary reviewed
4427 Final Site Visit ndash FVC drop confirmation
In the event that the subject has a recorded FVC drop of gt10 from baseline at the final treatment visit and the
subject has not had a confirmation of such a drop at a previous study visit the subject should return to the
clinical site 6 to 8 weeks after the final treatment visit During this visit a post-bronchodilator spirometry test
will be performed This FVC measurement will be evaluated according to section 521 of this protocol
4428 Final Visit ndash Telephone Follow-up
Four weeks following the final dose of study medication subjects will receive a telephone call from the study
coordinator to ensure that there are no side effects and to follow up on any ongoing adverse events (AEs)
4429 Phone Contact Between Visits
At week 2 and each month that a subject does not have a scheduled clinical center visit his or her study
coordinator will contact him or her at least once by telephone to
Inquire if the subject has had any hospitalizations events that might be considered an AE or any events
significant enough to warrant an out-of-cycle visit to the clinical center
Remind subjects of their current dosage levels and confirm that the subject understands them
Address any questions or concerns the subject might have regarding other aspects of the study
Assess adherence to the treatment regimen by reviewing diary data verbal review of medications taken
including nutritional supplements
33
34
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Table 3 Schedule of Assessments
Procedure Screening Visit 0
Enrollment Visit 1
Week 15 Visit 2
Week 30Visit 3
Week 45 Visit 4
Week 60 Early
Withdrawal Visit 5
Final1
Visit (via phone)
Informed consent X
Medical history X
Inclusionexclusion criteria X
Serum pregnancy test (if applicable) X X X X X
Review of lung biopsy X
Arterial Blood Gas X X
6-Minute Walk Test
X
X X
Physical examination X X X
Vital signs with oximetry X X X X X X
Body height and weight X X X X X X
Complete Blood Count X X X
Chemistry panel X X X
Monitor Lab Values X X X
Urinalysis X Specimen repository substudy blood draw and urine collection (if consented)
X
X X X X
HRCT (if not completed within three months) X
Spirometry (pre- and post-bronchodilator) X
Spirometry (post-bronchodilator only) X X X X X
DLCO (post-bronchodilator only) X X X
Lung volumes (post-bronchodilator only) X
X
Evaluate for acute exacerbation X X X X X
Review Adverse Events X X X X X X
Review concomitant meds X X X X X X
Dispense subject diary X X X X
Review subject diary X X X X X
Dispense study agent X X X X
Gender Substudy questionnaire (female subjects only) X
EuroQol ICECAP UCSD SOBQ SGRQ SF-36 X X X
Abbreviations DLCO diffusing capacity of the lung for carbon monoxide QOL Quality of Life ICECAP Investigating Choice Experiments for Preferences of Older People UCSD SOBQ University of California Shortness of Breath Questionnaire SGRQ St Georgersquos Respiratory Questionnaire SF-36 Short Form 36 Health Survey
1Follow-up visit via phone will occur four weeks after final dose of study medication
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
45 Dose Justification
The general philosophy for determining dosing levels was to apply previously examined
treatment regimens With the focus of the study being to establish a standard of care for
mildmoderate IPF subjects the goal was to develop flexible yet standardized treatment rules that
allow for the temporary or permanent withholding of one or more components of treatment when
necessary Subjects developing laboratory abnormalities or symptoms that result in
discontinuation of one or more components of study treatment may continue on the other
components as long as there is no contraindication for this Complete follow-up is important for
the validity of any study As a strategy to maintain protocol adherence we are using a treatment
regimen that will detect potential side effects and prompt interventions proactively in the interest
of patient safety In addition subjects who permanently stop study medications during the course
of the study are encouraged to continue in the study completing all scheduled visits and tests
451 Rationale for N-acetylcysteine Dosing
To our knowledge there have been no IPF studies to correlate clinical outcome measures with
different dosages for NAC The dosage chosen is based on the IFIGENIA study However BAL
lung GSH levels from subjects with IPF have been augmented with the use of oral NAC at 600
mg 3 times per day In addition lung GSH levels have been associated with improved
PFTs212227 The dose chosen for this study was based on previous data including the IFIGENIA
study30
4511 Dosing of N-acetylcysteineplacebo
Dosing of NACPL will be 600 mg orally 3 times a day (1800 mgday)
4512 Reasons to Discontinue N-acetylcysteineplacebo
NACPL may be temporarily or permanently discontinued for the duration of the study for
gastrointestinal symptoms or dermatologic reactions
35
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Temporarily discontinue (hold) oral NACPL for subjects requiring inpatient admission for acute
exacerbation (AEx) or other conditions Resume NACPL after discharge
36
37
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
452 Dosage Algorithms
Dosage Adjustment Algorithm 1 NACPL Dose Modifications for Gastrointestinal Symptoms Nausea Vomiting Abdominal Discomfort Diarrhea
GI Symptoms determined by the PI to be clinically significant Nausea Vomiting Abdominal Discomfort Diarrhea
NACPL Temporarily dc (HOLD) x 3 Days
Monitor symptoms intervene as clinically indicated (eg fluid replacement antidiarrhea or antinausea medication)
Monitor or lab PRN
Are symptoms resolving after 3 days NO
Symptoms NOT resolving after 3 days of holding study medication Assessmentmanagement per clinical
discretion of investigator
Likely not study medication discuss resuming study medication with medical monitor when symptoms resolved
YES
Temporarily dc (HOLD) NACPL for 4 additional days (total hold 1 week) then NACPL Resume 600 MG TID
Did symptoms recur
YES
STOP NACPL for
duration of study
NO
NACPL No Change
38
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Dosage Adjustment Algorithm 2 NACPL Dose Modifications For Dermatologic Reactions
Dermatologic Reactions (Not Acneiform) ge Grade 2 Grading per Common Terminology Criteria for
Adverse Events V30 (httpctepcancergov) For example Grade 1 RASHDESQUAMATION Macular or papular eruption or erythema without associated symptoms Grade 2 RASHDESQUAMATION Macular or popular eruption or erythema with pruritus or other associated symptoms localized desquamation or other lesions covering lt50 of body surface area
NACPL Temporarily dc (HOLD) x 3 days
Are symptoms resolving after 3 days
NO Symptoms not resolving after 3 days of holding study medication Assessmentmanagement per clinical discretion of investigator Likely not study medication Discuss resuming study medication with medical monitor when symptoms
resolved YES
Temporarily dc (HOLD) NACPL for 4 additional days (total hold 1 week) then NACPL resume 600 MG TID
Did symptoms recur
YES
STOP NACPL for
duration of study
NO
NACPL No change
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
46 Contraindications Precautions and Side Effects of Study Medications
461 Contraindication
Contraindication to NAC is known hypersensitivity to it
462 Precautions
Concomitant administration of oral NAC and antibiotics has shown a slightly reduced absorption
of cephalexin and a slight increase in erythromycin serum levels NAC contains free sulfhydryl
groups There is no evidence that individuals sensitive to sulfa drugs are sensitive to NAC
The NAC preparation being administered in this study contains 20 mg of aspartame Because of
the phenylalanine component of aspartame individuals with phenylketonuria should avoid or
restrict aspartame intake to avoid increased blood levels of phenylalanine Because of this risk
labeling is required on all products containing aspartame
463 Side Effects
Side effects of NAC range from common to serious See Table 4
39
40
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Table 4 Side Effects of NAC
Undesirable Effects
System-organ class Uncommon
(gt11000 lt1100)
Rare
(gt110000 lt11000)
Very rare
(lt110000) Not known
Immune system disorders Hypersensitivity Anaphylactic shock
reaction
Nervous system disorders Headache
Ear and labyrinth disorders Tinnitus
Cardiac disorders Tachycardia
Vascular disorders Hemorrhage
Respiratory thoracic and
mediastinal disorders
Bronchospasm
Dyspnea
Gastrointestinal disorders
Vomiting diarrhea
stomatitis abdominal
pain nausea
Dyspepsia
Skin and subcutaneous tissue
disorders
Urticaria rash
angioedema itching
General disorders and
administration site conditions Pyrexia
Investigations Reduced arterial
pressure Face edema
In very rare cases the onset of severe skin reactions such as Stevens-Johnson syndrome and Lyell syndrome was reported to have a temporal relationship with N-acetylcysteine administration Although in most cases at least another suspect drug probably most involved in the genesis of the above mentioned mucocutaneous syndromes has been identified in case of mucocutaneous alterations it is appropriate to contact onersquos doctor and the administration of N-acetylcysteine should be immediately discontinued
Some studies confirmed a reduction of platelet aggregation during N-acetylcysteine administration The clinical significance of these findings has not been defined yet [Source Fluimucil Investigator Brochure]
47 Recruitment Procedures
Subjects recruited for this study will be established patients of the investigators or physician- or
self-referred to participating clinical centers in the IPFnet Each clinical center within IPFnet has
a well-developed infrastructure of local pulmonologists within the surrounding geographic area
These pulmonologists are kept informed of ongoing IPF clinical trials and regularly refer
subjects to studies conducted at IPFnet clinical centers
Additional steps will be taken to inform clinicians of the trials in progress within IPFnet
including presentations at faculty staff meetings at local hospitals medical grand rounds and
national conferences direct mail notification monthly faxes and advertisement of network trials
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
in pulmonary journals Clinical center patients previously diagnosed with IPF will be notified of
the trials by mail whenever possible
Recruitment of minorities and women will be monitored by the DCC and DSMB If necessary
additional recruitment efforts will be made at specific centers to ensure that the aggregate subject
sample contains appropriate representation of women and minorities
48 Study Procedures
The following procedures are detailed in the PANTHER-IPF MOOP accompanying this
protocol
1 PFT
2 ABG
3 HRCT scan of the chest (including imaging of pulmonary arteries)
4 CBC and serum chemistries
5 Pregnancy test
6 6MWTBorg Dyspnea Scale
7 QOL questionnaires (EuroQol HAD SF-36 SGRQ and ICE CAP)
8 UCSD SOBQ
9 Gender Substudy Questionnaire
All assessments of PFTs will be conducted by study personnel not directly involved in the
treatment of the subjects
481 Biological Specimen Management
4811 Biological Specimen Sample Management
Subjects at clinical centers participating in the specimen repository substudy who consent to
having blood drawn for research purposes and for the banking of blood blood components and
other biologic specimens (urine and BAL fluid) will have approximately 405 mL of blood
41
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
drawn 17 mL blood drawn for DNA and 20 mL of urine collected at enrollment visit Subjects
will have approximately 50 mL of blood drawn and 20 mL of urine collected at each 15-week
follow-up visit Blood specimens will be separated according to PANTHER-IPF MOOP
guidelines into the following components for banking in the repository serum plasma and
DNA Coding of all biologic specimens for the repository will be performed by study staff at the
clinical center The samples will be processed per PANTHER-IPF MOOP guidelines aliquoted
labeled with barcode labels and stored at -70degC at the clinical center and shipped to the central
repository
The only subject identifiers will be a sample ID number and subject initials This sample ID will
be linked in the IPFnet DCC clinical database to subject information No subject information will
be transferred to the biological-specimen database
The subjectrsquos samples may be used for approved sub-studies relating to human disease
including but not limited to IPF The studies for which an individualrsquos samples will be made
available will be determined by the subjectrsquos answers to questions on the biological-sample
informed consent form The subjects can choose to make their samples available for all options
or any combination Samples will be made available to researchers only with IPFnet Steering
Group approval until such time as the samples are made public through the NHLBI repository
49 Concomitant Medications
Concurrent treatment with FDA-approved therapy for IPF is allowed Colchicine may be used
for treatment of gout Temporary treatment with oral or IV corticosteroids for clinical worsening
or suspected AEx is permitted Nutritional supplements containing NAC are not allowed
410 Laboratory Testing
Clinical laboratory parameters will be assessed at screening and at the end of the study The
following tests will be performed at the two time points specified in the protocol chemistry (AG
ratio ALT [SGPT] AST [SGOT] albumin alkaline phosphatase amylase bilirubin-direct
42
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
bilirubin-indirect bilirubin-total BUN BUNcreatinine ratio calcium carbon dioxide
cholesterol-total chloride CPK-total creatinine GGT globulin glucose iron-total LDH
lipase magnesium phosphorus-inorganic potassium protein-total sodium TIBC triglycerides
uric acid) and hematology (red blood cell count WBC count hemoglobin hematocrit cell
indices differential platelet count)
411 Blinding of Study Drugs
Subjects and caregivers will be blinded to study treatment Every subject will receive NAC or
matching PLs at every study visit from the baseline visit to the week-45 visit No study agent
will be dispensed at the week-60 visit
43
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
5 Study Endpoints
51 Primary Study Endpoint
The primary endpoint will be the change in serial measurements of FVC over the study period
52 Secondary Study Endpoints
521 Time to Disease-progression
The time-to-death or a 10 decline in FVC will be defined as the time-to-disease progression
The 10 decline in FVC from enrollment must be confirmed on 2 consecutive visits no less than
6 weeks apart For subjects with 2 consecutive visits with a 10 decline in FVC the time-toshy
disease progression will be defined as the time interval between enrollment and the initial visit
with a 10 FVC decline For subjects who experience disease progression the study doctor will
determine whether or not the subject will remain in the study
522 Acute Exacerbations
The following 3 criteria will define AEx in subjects with acute worsening of their respiratory
conditions
1 Clinical (all of the following required)
A) Unexplained worsening of dyspnea or cough within 30 days triggering unscheduled
medical care (eg emergency room clinic study visit hospitalization)
B) No clinical suspicion or overt evidence of cardiac event pulmonary embolism or deep
venous thrombosis to explain acute worsening of dyspnea
C) No pneumothorax
44
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
2 RadiologicPhysiologic (A and B required)
A) New ground glass opacity or consolidation computed tomography (CT) scan OR new
alveolar opacities on chest x-ray
B) Decline of ge 5 in resting room air SpO2 from last recorded level OR decline of ge 8 mm
Hg in resting room air PaO2 from last recorded level
3 Microbiologic (all of the following required)
A) No clinical evidence for infection (ie absence of grossly purulent sputum fever gt 39degC
orally)
B) Lack of positive microbiological results (if done) from lower respiratory tract defined as
(1) Clinically significant bacterial growth on sputum or endotracheal aspirate cultures
(2) Quantitative culture by protected brush specimen ge 103 cfumL or BAL ge 104 cfumL
(3) The presence of specific pathogens on stains of any of the above
C) Lack of positive pathogen in blood cultures (if done)
Identification of Acute Exacerbations
All subjects will be educated about the importance of identifying AExs At the time of
enrollment subjects will be told about the possibility of developing acute symptomatic
worsening that might represent an AEx of IPF and instructed to contact their study clinical
center coordinator within 48 to 72 hours of the apparent event
All subjects will be contacted by phone monthly and questioned about any change in dyspnea or
cough and any interim clinic visits or hospitalizations Finally as part of the IPFnet outreach to
community referring physicians the importance of AExs will be emphasized When a subject is
identified who meets criterion 1A this will trigger the collection of additional clinical data to
evaluate a suspected AEx These data will be collected as part of standard clinical care (ie this
protocol does not require collection of all items) The additional items to be collected for
suspected AEx include
IPFnet AEx case report form (eCRF) (required)
45
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Chest x-ray CT scan withwithout pulmonary angiogram (reports should be faxed and
followed by the hard copiesdiscs)
Oxygen saturation (pulse oximetry)
ABG
Respiratory cultures (sputum endotracheal aspirate lavage)
Blood cultures
Clinichospital records related to the event
All potential cases of AEx will be reviewed by the clinical center PI first and a decision on
whether the case may represent an AEx will be made If AEx is suspected the case will be sent
to the IPFnet adjudication committee which will assign a final diagnosis (see Table 5) If there is
disagreement among members the majority opinion will be recorded
During episodes of suspected AEx as determined by the individual clinical center investigator
subjects will remain blinded and in the study
Table 5 Final Diagnoses in Evaluation of Suspected Acute Exacerbations
Definite acute exacerbation All criteria met no alternative etiology
Unclassifiable acute worsening
Insufficient data to evaluate all criteria no alternative etiology
Not acute exacerbation Alternative etiology identified that explains acute worsening
Management of the suspected AEx will be at the discretion of the treating physician Standard of
care generally involves evaluation for respiratory infection pulmonary embolism cardiac events
and pneumothorax and treatment with IV corticosteroids
Study drugs will be resumed at pre-suspected AEx doses after subjects clinically improve as
confirmed by the local PI All subjects should be seen at the clinical center within 2 to 4 weeks
of recovery for measurement of post-bronchodilator FVC (see Figure 4) Subjects unable to
return to the clinical center after suspected AEx due to medical frailty (eg continued
46
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
institutionalization progressive disability) will be categorized as failing to maintain FVC
response in secondary analyses
Suspected AEx (PI determined)
Hold study drug Treat AEx
(Attending physician determined)
Alive but unable to continue due to
medical frailty
Dead
Alive and able to continue
Site reviewvisit
Restart study drug
FVC within 2-4 weeks
Figure 4 Acute Exacerbation Flow Chart
523 Respiratory Infections
An upper respiratory infection will be defined as
Change in sputum discoloration
Increased cough of no more than 14 daysrsquo duration
A lower-respiratory infection (pneumonia) will be defined as new segmental or lobar airspace
opacities visualized by image studies (chest radiograph or HRCT) in addition to any of the
following
Positive pathogencultures in good sample of sputum or lower-airway secretions retrieved
by fiberoptic bronchoscope
Fever gt 39degC or gt 100degF
Leukocytosis gt 12000 (unexplained no increase in dose of corticosteroids)
47
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
524 Maintained FVC Response
Subjects with follow-up FVCpred measurements at or above their baseline FVCpred level
will be classified as having maintained FVC response Subjects with reduced FVCpred levels
or missing data for any reason including death or medical frailty will be classified as having not
maintained FVC response The FVCpred value is used because unadjusted FVC measurements
are expected to decline with age
48
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
6 Safety Evaluations and Procedures
61 Adverse Events
During a clinical trial the reporting of adverse experience information can lead to important
changes in the way a new treatment is developed as well as provide integral safety data
611 Definitions
An adverse event (AE) is any untoward medical occurrence in a subject or clinical investigation
subject who was administered a pharmaceutical product The AE does not necessarily have to
have a causal relationship with the drug administered An AE can be any unfavorable and
unintended sign (including an abnormal laboratory finding) symptom or disease temporarily
associated with the use of a medicinal product whether or not considered to be related to the
medicinal product Diseases signs symptoms or laboratory abnormalities already existing at
enrollment are not considered AEs unless they worsen (ie increase in intensity or frequency)
Surgical procedures themselves are not AEs they are therapeutic measures for conditions that
require surgery The condition for which the surgery is required may be an AE Surgical
procedures planned before randomization and the conditions necessitating the surgery are not
AEs
A serious adverse event is any untoward event that
Is fatal
Is life-threatening
Requires inpatient hospitalization or prolongation of existing hospitalization with the
following exceptions
o Preplanned (before the study) hospital admissions unless the hospitalization is
prolonged
o Planned admissions (as part of a study eg routine biopsies)
o Hospitalization lasting lt 24 hours
49
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
o Hospitalization for elective procedure
o Emergency room visits
Results in persistent or significant disability or incapacity
Is a congenital anomaly or birth defect
Important medical events that may not result in death be life-threatening or require
inpatient hospitalization may be considered serious adverse events (SAEs) when based
on appropriate medical judgment they may jeopardize the subject and may require
medical or surgical intervention to prevent one of the outcomes listed above
Life-threatening means that the subject was in the view of the investigator at immediate risk of
death from the AE as it occurred It does not include an AE that had it occurred in a more severe
form might have caused death
Persistent or significant disabilityincapacity means that the event resulted in permanent or
significant and substantial disruption of the subjectrsquos ability to carry out normal life functions
Causality
A reasonable possibility means the AE may have been caused byrelated to the study drug A
perceived or real lack of efficacy does not satisfy the definition of relatedness
612 Adverse Event (AE) Reporting
For the PANTHER-IPF trial all AEs (serious and nonserious) occurring from randomization
through final study visit (4 weeks after final dose of all study medication) will be recorded on the
AE page of the case report form (CRF)
6121 Serious Adverse Events (SAE) Reporting
For this trial all deaths and all SAEs which occur from randomization through final study visit
must be entered within the EDC system via the SAE eCRF page within 24 hours of the
investigative sitersquos knowledge of the event It is the responsibility of the clinical center
50
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
investigator to provide a causality assessment of the event for each study medications based upon
the information available at the time of the report It is understood that complete information
about the event may not be known at the time the initial report is submitted In the event the EDC
system is not accessible to the site at the time of event reporting investigative sites will complete
and forward a paper back-up SAE form to DCRI Safety Surveillance for processing
DCRI Safety Surveillance
Telephone 1-919-668-8624 or 1-866-668-7799 (toll free)
Fax 1-919-668-7138 or 1-866-668-7138 (toll free)
The investigator must complete and submit follow-up SAE information via the eCRF when
important new or follow-up information (eg final diagnosis outcome results of specific
investigations) becomes available Follow-up information should be submitted according to the
same process used for reporting the initial event as described above All SAEs will be followed
until resolution stabilization or 30 days after the subject has completed the final visit (4 weeks
after the final dose of study medication) whichever occurs first The investigator is responsible
for reporting SAEs to their institutional review board (IRB) per site specific IRB reporting
guidelines
6122 Regulatory Reporting
AEs that are serious study drug related and unexpected will be reported to the regulatory
authorities The DCRI Safety Surveillance medical monitor will perform a medical review of all
SAEs submitted and evaluate for ldquounexpectednessrdquo DCRI Safety Surveillance will prepare
MedWatch reports for those events identified as serious study drug related and unexpected as
determined by Safety Medical Monitor
DCRI Regulatory Services will submit all unexpected study drug-related SAEs as per 21 CFR
32 DCRI Safety Surveillance will provide a safety alert letter to the NHLBI DSMB and DCC
clinical operation (for distribution to sites) within 15 days of initial receipt of the information
51
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Investigators are responsible for promptly reporting these events to their reviewing IRBs
according to site specific IRB reporting guidelines
62 Clinical Medical Monitoring
There will be an unblinded physician at the IPFnet DCC serving as medical monitor The
medical monitor will be available to assist with questions about dosage adjustments of study
medications including discontinuation or resumption of medications
63 Unblinding Procedures
Unblinding of subjects or investigators to subject treatment is strongly discouraged For ongoing
clinical management all subjects should be presumed to be receiving ldquoactiverdquo study drug To
ensure the subjectrsquos safety the study treatment will be dose-adjusted based on laboratory test
results clinical findings and symptoms
The IPFnet DCC medical monitor and PANTHER-IPF co-chairs Drs Ganesh Raghu and
Fernando Martinez will be available to the study physicians to discuss study drug management
on a case-by-case basis Un-blinding will be considered ONLY when the knowledge of subject
treatment assignment is ABSOLUTELY ESSENTIAL for subject safety and after discussion of
the subjectrsquos case with the medical monitor and either Dr Raghu or Dr Martinez Unblinding of
study treatment should be minimized during the conduct of the trial In those cases where it is
felt to be medically necessary the DCC medical officer will communicate directly with the
managing physician to minimize unblinding of study personnel
52
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
7 Study Drug Procedures
At the baseline 15-week 30-week and 45-week study visits subjects will receive a supply of
study drug sufficient to last until the next visit at which study drug will be dispensed
53
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
8 Data Management
81 Hardware and Software Configuration
811 Hardware and Database Software
Data will be stored in an Oracle database system Oracle has advantages of processing efficiency
and smooth linkage with other software systems The application and database will be hosted on
Solaris Unix servers at the IPFnet DCC
812 Statistical Software
SAS will be used as the principal application for the management of analysis data files and
statistical computations S-Plus will be used to provide supplementary functions as needed
813 Access Control and Confidentiality Procedures
Access to databases will be controlled centrally by the IPFnet DCC through user passwords
linked to appropriate privileges This protects the data from unauthorized changes and
inadvertent loss or damage
814 Security
Database and Web servers will be secured by a firewall and through controlled physical access
Oracle has many security features to ensure that any staff member accessing the database has the
proper authority to perform the functions he or she requests of the system Within the secondary
SAS databases Unix group-access control maintains similar security The Sun workstation login
is secured by extensive user-password facilities under Unix
54
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
815 Back-up Procedures
Database back-up will be performed automatically every day and standard IPFnet DCC policies
and procedures will be applied to dictate tape rotation and retention practices
816 Virus Protection
All disk drives that provide network services and all user computers will be protected using
virus-scanning software Standard IPFnet DCC policies will be applied to update these protection
systems periodically through the study
82 Sources of Data
821 Design and Development
The IPFnet DCC will be responsible for development of the electronic case report forms
(eCRFs) development and validation of the clinical study database ensuring data integrity and
training clinical center staff on applicable data management procedures A web-based distributed
data entry model will be implemented This system will be developed to ensure that guidelines
and regulations surrounding the use of computerized systems used in clinical trials are upheld
The remainder of this section provides an overview of the data management plan associated with
this protocol
822 Data Collection Forms
The data collection process consists of direct data entry at the study clinical centers into the EDC
system(s) provided by the DCC A data collection worksheet will be provided to clinical centers
for recording data in the event the EDC system is unavailable Data entry of the eCRFs should
be completed according to the instructions provided and project specific training The
investigator is responsible for maintaining accurate complete and up-to-date records and for
ensuring the completion of the eCRFs for each research participant
55
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
823 Data Acquisition and Entry
Data entry into eCRFs shall be performed by authorized individuals Selected eCRFs may also
require the investigatorrsquos written signature or electronic signature as appropriate Electronic
CRFs will be monitored for completeness accuracy and attention to detail during the study
824 Data Center Responsibilities
The IPFnet DCC will 1) develop a data management plan and will conduct data management
activities 2) provide final eCRFs for the collection of all data required by the study 3) develop
data dictionaries for each eCRF that will comprehensively define each data element 4) conduct
ongoing data monitoring activities on study data 5) monitor any preliminary analysis data
cleanup activities and 6) rigorously monitor final study data clean up
825 Data Editing
Completed data will be entered into the IPFnet DCC automated data acquisition and
management system If incomplete or inaccurate data are found a data clarification request will
be generated and distributed to clinical centers for a response Clinical centers will resolve data
inconsistencies and errors and enter all corrections and changes into the IPFnet DCC automated
data acquisition and management system
826 Training
The training plan for clinical center staff includes provisions for training on assessments eCRF
completion guidelines data management procedures and the use of computerized systems
56
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
9 Study Design and Data Analysis
91 General Analytic Considerations
All primary analyses will be based on intent-to-treat (ITT) principles using all randomized
subjects Baseline factors across groups will be compared using mean (standard deviation) and
median (25th and 75th percentiles) summary measures Kaplan-Meier curves will be used to
display event rates Due to clinical interest in departures from both sides of the null hypothesis
all test statistics will be 2-sided
Reasonable caution needs to be taken when conducting multiple analyses on key clinical
subgroups For subgroup analyses a conservative significance level of 0001 will be used for all
interaction tests Thus subgroup comparisons will be considered exploratory unless the p-value
from the interaction test is smaller than 0001
92 Randomization Blinding and Reporting of Results
A permuted block-randomization scheme will be created with varying block sizes stratified by
clinical center Once a subject has completed the screening and baseline period and evaluation
for inclusionexclusion criteria the randomization process will begin Subjects will be
randomized to receive NAC or matching placebo with equal probability (11) via telephone
contact with a central interactive voice response system (IVRS) using a toll-free randomization
number On the day of randomization after the subject has successfully met all inclusion and
exclusion criteria the investigator or designee will call the central randomization number to
obtain the assigned kit randomization numbers for that subject At each subject visit the
investigator or designee will call the central randomization number to obtain the new kit
randomization numbers for resupply of the subject For resupply of the clinical center the IVRS
will monitor minimal volume of a kit type andor expiration date and will automatically notify
the pharmacy
57
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
The trial results will be reported according to guidelines specified in the CONSORT statement
A flow diagram describing screening recruitment randomization dropout and vital status will
be included in the primary manuscript AEs and efficacy data will be presented for all treatment
groups Adherence dropout and lost to follow-up will be carefully examined across all treatment
groups Analyses of safety will be based on data from all randomized subjects who received at
least one dose of study drug
93 Stratification
Subjects will be distributed to the two treatment arms in a 11 allocation ratio Stratification
blocks will be based on clinical centers
94 Specification of the Primary Analyses
A mixed model repeated measures (MMRM) analysis described in section 95 will be used to
compare differences in the slope of FVC measurements across the treatment groups Response
variables are values of the FVC measured at baseline and every 15 weeks until study completion
Variables in the model will include treatment time and time by treatment age sex race and
height Contrast estimates of differences in slopes of treatment over time (along with confidence
intervals) will be used to estimate the treatment effect The validity of this model in terms of
meeting modeling assumptions will be assessed via standard modeling diagnostics and goodness-
of-fit measures Based on the MMRM framework missing FVC data will not be imputed for the
primary analysis
95 Analysis of Longitudinal Endpoints
A common goal in clinical trials is to specify models that are easily implemented and
reproducible by independent data analysts On the other hand the models should have proper
statistical behavior in terms of low bias and high precision Many common approaches to
longitudinal data analysis including last observation carried forward (LOCF) imputation rely on
the missing completely at random (MCAR) assumption However the MCAR assumption is
58
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
unlikely to hold in many clinical trials because missing data are often related to disease
progression and prognosis A more reasonable assumption missing at random (MAR) specifies
that the complete data distribution can be modeled using only the observed data The likelihood-
based MMRM approach is valid under the more general MAR assumptions These models will
be applied to analyze the longitudinal data secondary endpoints
The advantages of MMRM analysis are that all important characteristics of the model can be preshy
specified standard software can be used to implement the models and results are based on ITT
principles43 In addition the MMRM approach offers superior control of Type I and Type II
errors compared with the LOCF approach
Response variables are values of the PFTs measured at enrollment and every 15 weeks until
study completion and 6MWT values measured at baseline week 30 and week 60 Covariates are
treatment time time by treatment and key baseline risk factors Contrasts (along with
confidence intervals) of treatment by time will be used to estimate the treatment effect
The correlation structure involves multiple pieces including measurement errors random
variation and interindividual variability For the longitudinal data analyses an unstructured
correlation matrix for within-subject errors will be assumed Other correlation structures
including compound symmetry will be examined as needed A careful examination of reasons
for study discontinuation will be conducted to assess the validity of MCAR Sensitivity analyses
will be used to examine the untestable assumption that the observed data violate the MAR
assumption The MMRM models will be implemented using PROC MIXED in SAS
96 Analysis of Binary Time-to-Event and Time-Lagged Endpoints
Regression modeling approaches using either the logistic regression model or Cox proportional
hazards regression model will be employed when appropriate The validity of these models will
be assessed via standard modeling diagnostics and goodness-of-fit measures Estimates of
cumulative frequencies for more general time-lagged responses will be calculated using the
partitioned version of the Bang-Tsiatis estimator44 The partitions will be set at 15-week intervals
59
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
to correspond with the data-collection process Covariate adjusted event rates will be calculated
using inverse probability-weighted regression estimates45
97 Power Analysis
971 Primary Analyses
Based on previously published IPF clinical trials the PL group is expected to experience a drop
in FVC of approximately 020 L over the study period (see Figure 1) The IPFnet Steering Group
determined a clinically important difference would be to preserve the majority of the decline
relative to PL over the study period In particular a treatment effect of 015 L was determined to
be a clinically meaningful difference Potential dropout is a key factor in the proposed study The
drop-out process assumed 5 lost to follow-up after every study visit Only 80 of subjects
were assumed to be followed for the entire study period All models assumed a compound
symmetry structure for the covariance matrix Power calculations were performed using a SAS
IML program for designing repeated measures studies46 Based on preliminary reviews of the
data from the University of Michigan the covariance matrix parameters were estimated at
approximately σ2 = 0757 (variance parameter) and ρ = 0936 (correlation parameter) To be
conservative the power calculations for the primary analysis were performed with parameter
setting of σ2 = 0810 (variance parameter) and ρ = 0925 (correlation parameter)
The power calculations assume a correction for imperfect compliance proposed by Lachin and
Foulkes to allow for 2 noncompliance for each of the treatment arms47 Thus the sample size
of 130 subjects per arm would be reduced to an adjusted sample size of 130(1-002-002)2 =
1198 or 120 subjects per arm
Under the assumed Type I error rate of 005 with a correlation parameter of 0925 and standard
deviation of 090 the difference of 015 L (or 00025 Lweek) shown in Table 6 would have
power of 93
60
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Table 6 Hypothetical Values of Mean FVC (L) Change from Baseline
Week 15 Week 30 Week 45 Week 60
NAC 00125 00250 00375 00500
Placebo 00500 01000 01500 02000
Difference 00375 00750 01125 01500
Abbreviations FVC forced vital capacity PL placebo
972 Power Analysis for Secondary Endpoints
Power calculations for secondary endpoint measurements are shown in Table 7 Standard
deviations are based on unpublished data provided by the University of Michigan The
calculations are based on a 2-sample t-test with Type I error rate set at 005 These calculations
are likely to be conservative because the statistical approach described in section 95 for
analyzing these endpoints will incorporate incomplete observations as well as intermediate data
points
Table 7 Detectable Differences in Treatment Means for Selected Endpoint Measurements
Secondary Endpoints Std Dev
of the Baseline Score
Detectable Difference for 80 Power
Std Dev of the Change Score
Difference Detectable for
80 Power
DLCOpred 166 58 91 32
6MWT Area Under the Desaturation Curve
219 76 175 61
6MWT Distance to Desaturation 224 78 315 110
6MWT Minutes Walked 210 073 205 071
Abbreviations Std Dev standard deviation DLCOpred diffusing capacity of the lung for carbon monoxide percent predicted 6MWT 6-minute walk test
61
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
10 Study Administration
101 Cooperative Agreement Mechanism
The administrative and funding mechanism used to undertake this project is a ldquocooperative
agreementrdquo (U01) which is an assistance mechanism Under the cooperative agreement the
NHLBI assists supports andor stimulates the project and is substantially involved with
investigators in conducting the study by facilitating performance of the effort in a ldquopartnerrdquo role
The NHLBI project scientist serves on the IPFnet Steering Group and he or another NHLBI
scientist may serve on other project committees when appropriate At the same time however
NHLBI does not assume a dominant role direction or prime responsibility for this research
program
As described below governance of the project is conducted through the IPFnet Steering Group
Principal investigators have lead responsibilities in all aspects of their trials and the project
including any modification of trial designs conduct of the trials quality control data analysis
and interpretation preparation of publications and collaboration with other investigators unless
otherwise provided for by the IPFnet Steering Group
PIs retain custody of and have primary rights to their center-specific and collaborative data
subject to government rights-of-access consistent with current Health amp Human Services (HHS)
Public Health Service (PHS) and National Institutes of Health policies The protocols and
governance policies call for the continual submission of data centrally to the IPFnet DCC for the
collaborative database which at a minimum will contain the key variables selected by the IPFnet
Steering Group for standardization across all clinical centers the submission of copies of the
collaborative datasets to each PI upon completion of the project procedures for data analysis
reporting and publication and procedures to protect and ensure the privacy of medical and
genetic data and records of individuals The NHLBI project scientist on behalf of the NHLBI
will have the same access privileges and responsibilities regarding the collaborative data as the
other members of the Steering Group
62
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
PIs are also encouraged to publish and to publicly release and disseminate results data and other
products of the project concordant with the project protocols and governance and the approved
plan for making data and materials available to the scientific community and to the NHLBI
However during the 3 years after the ending date of NHLBI project support unpublished data
unpublished results data sets not previously released and other study materials or products are
to be made available to any third party only with the approval of the IPFnet Steering Group
Upon completion of the project PIs are expected to put their intervention materials and
procedure manuals into the public domain andor make them available to other investigators
according to the approved plan for making data and materials available to the scientific
community and the NHLBI for the conduct of research at no charge other than the costs of
reproduction and distribution
The NHLBI reserves the right to terminate or curtail the project (or an individual award) in the
event of (a) failure to develop or implement mutually agreeable collaborative measurement
subject eligibility and data management sections of the protocols (b) substantial shortfall in
subject recruitment follow-up data reporting or quality control or other major breach of
protocol (c) substantive changes in the agreed-upon protocols with which NHLBI cannot
concur (d) reaching a major project outcome with persuasive statistical significance
substantially before schedule or (e) human subject ethical issues that may dictate a premature
termination
Any disagreement that may arise in scientificprogrammatic matters (within the scope of the
award) between award recipients and the NHLBI may be brought to arbitration An arbitration
panel will be composed of 3 membersmdash1 selected by the IPFnet Steering Group (with the
NHLBI member not voting) or by the individual PI in the event of an individual disagreement a
second selected by NHLBI and the third selected by the other 2 members This special
arbitration procedure in no way affects the PIrsquos right to appeal an adverse action that is otherwise
appealable in accordance with the PHS regulations at 42 CFR part 50 Subpart D and HHS
63
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
regulation at 45 CFR part 16 or the rights of the NHLBI under applicable statutes regulations
and terms of the award
102 IPFnet Steering Group
The IPFnet Steering Group is the main governing body of the project It is composed of the PIs
of the clinical centers the PI of the DCC and the NHLBI project scientist The clinical centers
the IPFnet DCC and the NHLBI each have 1 vote on the IPFnet Steering Group All decisions
are determined by majority vote
All major scientific decisions are determined by the IPFnet Steering Group It assumes overall
responsibility for the design and conduct of the trial It appoints (and disbands) committees and
subcommittees as the need arises designs approves and implements the study protocols
oversees the development of the MOOP monitors subject recruitment and treatment delivery
evaluates data collection and management oversees quality assurance procedures and
implements changes and enhancements to the study as required It also has primary responsibility
for facilitating the conduct of the trials and reporting the projectrsquos results
103 Data and Safety Monitoring Board
The NHLBI will establish a DSMB in accordance with established policies (see
httpwwwnhlbinihgovfundingpoliciesdsmb_insthtm) to ensure data quality and subject
safety and to provide independent advice to the NHLBI regarding progress and the
appropriateness of study continuation
104 Recommendations on Interim Monitoring of Efficacy Safety and Futility
First and foremost the role of the DSMB will be to review subject safety and trial conduct at
periodic points during the study The DSMB may require analyses of the primary endpoint
results for comparing the benefit and risks of treatment strategies The benefit of collecting
additional data on key secondary endpoints with extended follow-up and establishing a robust
64
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
evidence base for determining a standard of care will need to be carefully considered before
early termination of one or more treatment arms After careful consideration the IPFnet Steering
Group recommends conservative thresholds for the early examinations of the safety and efficacy
data
The DSMB will be expected to meet approximately every 6 months until trial completion to
review safety and toxicity data The DSMB may recommend stopping the study based on these
reviews Because the DSMB could stop the trial for safety concerns as well as for a large
efficacy benefit there could be multiple opportunities to reject the null hypothesis (no difference
in event rates between the PL and NAC groups) A Bonferroni approximation will be applied
during the one planned interim analysis for efficacy
Before locking the database a statistical analysis plan (SAP) will be developed to provide
complete details on the statistical analysis The SAP will include the specifics for how and when
the DSMB will be notified for AEs The IPFnet DCC will deliver to the DSMB all FDA-defined
AEs at 3-month intervals The IPFnet DCC will prepare narrative SAE reports in real time for
DSMB review including recommendations and analysis of similar events for each SAE
submitted to the FDA
65
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
11 Investigator and Sponsor Obligations
111 Monitoring
All monitoring activities for US clinical centers will be performed in accordance with DCRI
standard operating procedures Information regarding the types of visits will be outlined in the
PANTHER-IPF MOOP
112 Cost and Payment
There will be no cost to subjects enrolled in this trial Study-related procedures will be paid for
by the IPFnet
Subjects may be eligible for reimbursement for travel to the clinical center Details of payment
will be explained to each subject during the consent process
113 Confidentiality and Health Insurance Portability and Accountability Act
Considerations
Subject confidentiality will be protected throughout the study All subject data will be kept
strictly confidential and no subject-identifying information will be released to anyone outside
the project Confidentiality will be assured through several mechanisms First each subject will
be assigned an anonymous study ID which will then be used on all study forms Second any
study forms blood samples and paper records that contain subject information (eg address lists
phone lists) will be kept at the clinical centers in secured locked areas coded by number Once
blood is collected there will be no subject identifiers placed on blood samplesmdashonly the study
ID number and the date of sample collection Third access to all subject data and information
including laboratory specimens will be restricted to authorized personnel In the case of
computerized data this restricted access will be assured through user logon IDs and password
protection
66
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
At the IPFnet DCC only authorized personnel will have access to the data files containing study
data Security will be assured through user logon IDs passwords and appropriate access
privileges All study subjects will be identified only by their IPFnet ID numbers and no personal
identifying information such as name address or Social Security number will be entered into
the IPFnet DCC database Any subject-specific data reported to the IPFnet Steering Group will
be identified only by the IPFnet ID number
Finally subjects will not be identified by name in any reports or publications nor will the data
be presented in such a way that the identity of individual subjects can be inferred Analysis files
created for further study by the scientific community will have no subject identifiers These data
files will be created in accordance with the Ancillary Studies and Publication Policy of the
IPFnet
114 Informed Consent Procedures
All IPFnet subjects will provide written informed consent using procedures reviewed and
approved by each clinical centerrsquos IRB Informed consent will be undertaken by study personnel
in-person with the subject The subject has the option of declining further participation in the
study at that point No further study procedures will be conducted until the signed documents
have been provided to the IPFnet clinical center
115 Institutional Review Boards
Before initiating this study the protocol clinical center-specific informed consent forms Health
Insurance Portability and Accountability Act (HIPAA) forms recruitment materials and other
relevant information will be reviewed by a properly constituted IRB at each participating clinical
center A copy of the signed and dated IRB approval at each clinical center will be retrieved prior
to or during the site initiation visit and archived at the IPFnet DCC Any amendments to the
protocol other than simple administrative and typographical changes must be approved by each
IRB before they are implemented The clinical centers will seek annual renewals of their IRB
approvals in accordance with local procedures
67
__________________________________________ ________________
__________________________________________
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
12 Investigator Agreement
I have read the foregoing protocol PANTHER-IPF and agree that it contains all necessary
details for carrying out this study I will conduct the study as outlined herein and will complete
the study within the time designated
I will provide copies of the protocol and all pertinent information to all individuals responsible to
me who assist in the conduct of this study I will discuss this material with them to ensure they
are fully informed regarding the drug and the conduct of the study
I will fulfill all responsibilities for submitting pertinent information to the local IRB if
applicable that is responsible for this study
I further agree that NHLBI andor DCRI will have access to any source documents from which
eCRF information may have been generated
Signature of Principal Investigator Date
Name of Principal Investigator (printed or typed)
Protocol version date May 19 2009
Protocol Amendment 1 version date May 28 2010
Protocol Amendment 2 version date December 6 2011
68
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
13 References
1 Raghu G Brown KK Bradford WZ et al A placebo-controlled trial of interferon gamma-1b in patients with idiopathic pulmonary fibrosis N Engl J Med 2004350125-33 2 King TE Jr Safrin S Starko KM et al Analyses of efficacy end points in a controlled trial of interferon-gamma1b for idiopathic pulmonary fibrosis Chest 2005127171-7 3 Flaherty KR Thwaite EL Kazerooni EA et al Radiological versus histological diagnosis in UIP and NSIP survival implications Thorax 200358143-8 4 Wells AU Desai SR Rubens MB et al Idiopathic pulmonary fibrosis a composite physiologic index derived from disease extent observed by computed tomography Am J Respir Crit Care Med 2003167962-9 5 Raghu G Freudenberger TD Yang S et al High prevalence of abnormal acid gastroshyoesophageal reflux in idiopathic pulmonary fibrosis Eur Respir J 200627136-42 6 Kinnula VL Focus on antioxidant enzymes and antioxidant strategies in smoking related airway diseases Thorax 200560693-700 7 Coultas DB Zumwalt RE Black WC Sobonya RE The epidemiology of interstitial lung diseases Am J Respir Crit Care Med 1994150967-72 8 Raghu G Weycker D Edelsberg J Bradford WZ Oster G Incidence and prevalence of idiopathic pulmonary fibrosis Am J Respir Crit Care Med 2006174810-6 9 Olson AL Swigris JJ Lezotte DC Norris JM Wilson CG Brown KK Mortality from pulmonary fibrosis increased in the United States from 1992 to 2003 Am J Respir Crit Care Med 2007176277-84 10 Mannino DM Etzel RA Parrish RG Pulmonary fibrosis deaths in the United States 1979shy1991 An analysis of multiple-cause mortality data Am J Respir Crit Care Med 19961531548shy52 11 Hubbard R Johnston I Coultas DB Britton J Mortality rates from cryptogenic fibrosing alveolitis in seven countries Thorax 199651711-6 12 Johnston I Britton J Kinnear W Logan R Rising mortality from cryptogenic fibrosing alveolitis Bmj 19903011017-21 13 Raghu G Collard HR Egan JJ et al An official ATSERSJRSALAT statement idiopathic pulmonary fibrosis evidence-based guidelines for diagnosis and management Am J Respir Crit Care Med 2011183788-824 14 (USA) FDA FDA Public Health Advisory Interferon gamma-1b (marketed as Actimmune) In 2007 15 King TE Jr Pardo A Selman M Idiopathic pulmonary fibrosis Lancet 2011 16 Raghu G Brown KK Costabel U et al Treatment of idiopathic pulmonary fibrosis with etanercept an exploratory placebo-controlled trial Am J Respir Crit Care Med 2008178948shy55 17 Malouf MA Hopkins P Snell G Glanville AR An investigator-driven study of everolimus in surgical lung biopsy confirmed idiopathic pulmonary fibrosis Respirology 201116776-83 18 King TE Jr Behr J Brown KK et al BUILD-1 a randomized placebo-controlled trial of bosentan in idiopathic pulmonary fibrosis Am J Respir Crit Care Med 200817775-81 19 Richeldi L Costabel U Selman M et al Efficacy of a tyrosine kinase inhibitor in idiopathic pulmonary fibrosis N Engl J Med 20113651079-87
69
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
20 Borok Z Buhl R Grimes GJ et al Effect of glutathione aerosol on oxidant-antioxidant imbalance in idiopathic pulmonary fibrosis Lancet 1991338215-6 21 Meyer A Buhl R Magnussen H The effect of oral N-acetylcysteine on lung glutathione levels in idiopathic pulmonary fibrosis Eur Respir J 19947431-6 22 Behr J Maier K Degenkolb B Krombach F Vogelmeier C Antioxidative and clinical effects of high-dose N-acetylcysteine in fibrosing alveolitis Adjunctive therapy to maintenance immunosuppression Am J Respir Crit Care Med 19971561897-901 23 Cantin AM North SL Fells GA Hubbard RC Crystal RG Oxidant-mediated epithelial cell injury in idiopathic pulmonary fibrosis J Clin Invest 1987791665-73 24 Waghray M Cui Z Horowitz JC et al Hydrogen peroxide is a diffusible paracrine signal for the induction of epithelial cell death by activated myofibroblasts Faseb J 200519854-6 25 Larios JM Budhiraja R Fanburg BL Thannickal VJ Oxidative protein cross-linking reactions involving L-tyrosine in transforming growth factor-beta1-stimulated fibroblasts J Biol Chem 200127617437-41 26 Kinnula VL Fattman CL Tan RJ Oury TD Oxidative stress in pulmonary fibrosis a possible role for redox modulatory therapy Am J Respir Crit Care Med 2005172417-22 27 Meyer A Buhl R Kampf S Magnussen H Intravenous N-acetylcysteine and lung glutathione of patients with pulmonary fibrosis and normals Am J Respir Crit Care Med 19951521055-60 28 Behr J Degenkolb B Krombach F Vogelmeier C Intracellular glutathione and bronchoalveolar cells in fibrosing alveolitis effects of N-acetylcysteine Eur Respir J 200219906-11 29 Bando M Hosono T Mato N et al Long-term efficacy of inhaled N-acetylcysteine in patients with idiopathic pulmonary fibrosis Intern Med 2010492289-96 30 Demedts M Behr J Buhl R et al High-dose acetylcysteine in idiopathic pulmonary fibrosis N Engl J Med 20053532229-42 31 Toma TP Bhowmik A Rajakulasingam R Acetylcysteine in pulmonary fibrosis N Engl J Med 20063541086-9 author reply -9 32 Hunninghake GW Antioxidant therapy for idiopathic pulmonary fibrosis N Engl J Med 20053532285-7 33 Flaherty KR Mumford JA Murray S et al Prognostic implications of physiologic and radiographic changes in idiopathic interstitial pneumonia Am J Respir Crit Care Med 2003168543-8 34 Latsi PI du Bois RM Nicholson AG et al Fibrotic idiopathic interstitial pneumonia the prognostic value of longitudinal functional trends Am J Respir Crit Care Med 2003168531-7 35 Collard HR King TE Jr Bartelson BB Vourlekis JS Schwarz MI Brown KK Changes in clinical and physiologic variables predict survival in idiopathic pulmonary fibrosis Am J Respir Crit Care Med 2003168538-42 36 Jegal Y Kim DS Shim TS et al Physiology is a stronger predictor of survival than pathology in fibrotic interstitial pneumonia Am J Respir Crit Care Med 2005171639-44 37 Martinez FJ Safrin S Weycker D et al The clinical course of patients with idiopathic pulmonary fibrosis Ann Intern Med 2005142963-7 38 Hull JH Acetylcysteine in pulmonary fibrosis N Engl J Med 20063541089-91 author reply -91
70
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
39 Flaherty KR King TE Jr Raghu G et al Idiopathic interstitial pneumonia what is the effect of a multidisciplinary approach to diagnosis Am J Respir Crit Care Med 2004170904shy10 40 Raghu G Johnson WC Lockhart D Mageto Y Treatment of idiopathic pulmonary fibrosis with a new antifibrotic agent pirfenidone results of a prospective open-label Phase II study Am J Respir Crit Care Med 19991591061-9 41 Hunninghake GW Lynch DA Galvin JR et al Radiologic findings are strongly associated with a pathologic diagnosis of usual interstitial pneumonia Chest 20031241215-23 42 Lynch D Godwin J Safrin S et al High-resolution computed tomography in idiopathic pulmonary fibrosis diagnosis and prognosis Am J Respir Crit Care Med 2005172488-93 43 Mallinckrodt CH Watkin JG Molenberghs G Carroll RJ Choice of the primary analysis in longitudinal clinical trials Pharmaceutical Statistics 20043161-9 44 Bang H Tsiatis A Estimating medical costs with censored data Biometrika 200087329shy43 45 Lin DY Regression analysis of incomplete medical cost data Stat Med 2003221181-200 46 Rochon J Application of GEE procedures for sample size calculations in repeated measures experiments Stat Med 1998171643-58 47 Lachin JM Foulkes MA Evaluation of sample size and power for analyses of survival with allowance for nonuniform patient entry losses to follow-up noncompliance and stratification Biometrics 198642507-19
71
- PANTHER-IPFPREDNISONE AZATHIOPRINEAND N-ACETYLCYSTEINEA STUDY THAT EVALUATES RESPONSE INIDIOPATHIC PULMONARY FIBROSIS
-
- Protocol Summary
- Table of Contents
- List of Tables
- List of Figures
- List of Abbreviations
- 1 Summary
- 2 Hypotheses and Specific Aims
-
- 21 Null Hypothesis
- 22 Specific Aim 1
- 23 Specific Aim 2
- 24 Prespecified Subgroups of Interest
-
- 3 Background and Significance
-
- 31 Idiopathic Pulmonary Fibrosis is the Most Common Interstitial Lung Disease
- 32 Rationale for Placebo Control
- 33 Rationale for N-acetylcysteine
- 35 Rationale for N-acetylcysteine as a Stand-alone Therapy
- 36 Rationale for the Study Design and Primary Endpoint
- 37 Rationale for Blinding of Treatments
-
- 4 Methods
-
- 41 Inclusion Criteria
- 42 Diagnosis of IPF
- 43 Exclusion Criteria
- 44 Study Design and Study Visit
- 45 Dose Justification
- 46 Contraindications Precautions and Side Effects of Study Medications
- 47 Recruitment Procedures
- 48 Study Procedures
- 49 Concomitant Medications
- 410 Laboratory Testing
- 411 Blinding of Study Drugs
-
- 5 Study Endpoints
-
- 51 Primary Study Endpoint
- 52 Secondary Study Endpoints
-
- 6 Safety Evaluations and Procedures
-
- 61 Adverse Events
- 62 Clinical Medical Monitoring
- 63 Unblinding Procedures
-
- 7 Study Drug Procedures
- 8 Data Management
-
- 81 Hardware and Software Configuration
- 82 Sources of Data
-
- 9 Study Design and Data Analysis
-
- 91 General Analytic Considerations
- 92 Randomization Blinding and Reporting of Results
- 93 Stratification
- 94 Specification of the Primary Analyses
- 95 Analysis of Longitudinal Endpoints
- 96 Analysis of Binary Time-to-Event and Time-Lagged Endpoints
- 97 Power Analysis
-
- 10 Study Administration
-
- 101 Cooperative Agreement Mechanism
- 102 IPFnet Steering Group
- 103 Data and Safety Monitoring Board
- 104 Recommendations on Interim Monitoring of Efficacy Safety and Futility
-
- 11 Investigator and Sponsor Obligations
-
- 111 Monitoring
- 112 Cost and Payment
- 113 Confidentiality and Health Insurance Portability and Accountability ActConsiderations
- 114 Informed Consent Procedures
- 115 Institutional Review Boards
-
- 12 Investigator Agreement
- 13 References
-

PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
12 Investigator Agreement 68
13 References 69
6
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
List of Tables Table 1 Operating Characteristics of Local HRCT Review for Diagnosis of UIP (24)
Table 2 Combining HRCT and Pathology Interpretations to Determine if IPF is Present (25)
Table 3 Schedule of Assessments (34)
Table 4 Side Effects of NAC (40)
Table 5 Final Diagnoses in Evaluation of Suspected Acute Exacerbations (46)
Table 6 Hypothetical Values of Mean FVC (L) Change from Baseline (61)
Table 7 Detectable Differences in Treatment Means for Selected Endpoint Measurements (61)
List of FiguresFigure 1 Changes in Forced Vital Capacity from Baseline in Prior IPF Clinical Trials (19)
Figure 2 Diagnosis of Idiopathic Pulmonary Fibrosis in the IPFnet (22)
Figure 3 Pathology Flow Chart Surgical Lung Biopsy Diagnosis (23)
Figure 4 Acute Exacerbation Flow Chart (47)
7
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
List of Abbreviations
6MWT 6-minute walk test
A-aPO2 alveolar-arterial PO2 difference
ABG arterial blood gas
AE adverse event
AEx acute exacerbation
AG albuminglobulin
ALT alanine aminotransferase
AST aspartate aminotransferase
ATS American Thoracic Society
AZA azathioprine
BAL bronchoalveolar lavage
BUN blood urea nitrogen
CBC complete blood count
cGMP Current Good Manufacturing Practice
CPI Composite Physiologic Index
CPK creatine phosphokinase
CT computed tomography
DCC Data Coordinating Center
DCRI Duke Clinical Research Institute
8
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
DLCO diffusing capacity of the lung for carbon monoxide
DLCOpred diffusing capacity of the lung for carbon monoxide percent predicted
DSMB data and safety monitoring board
eCRF Electronic case report form
ERS European Respiratory Society
FDA Food and Drug Administration (US)
FEV1 forced expiratory volume in 1 second
FSH follicle-stimulating hormone
FVC forced vital capacity
FVCpred forced vital capacity percent predicted
GGT gamma glutamyl transferase
GSH glutathione
HAD Hospital Anxiety and Depression
HHS Health amp Human Services (US Dept of)
HIPAA Health Insurance Portability and Accountability Act
HRCT high-resolution computed tomography
IBW ideal body weight
ICE CAP Investigating Choice Experiments for Preferences of Older People Capability Instrument
ILD interstitial lung disease
IPF idiopathic pulmonary fibrosis
9
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
IPFnet Idiopathic Pulmonary Fibrosis Clinical Research Network
IRB institutional review board
ITT intent to treat
IV intravenous
IVRS interactive voice response system
LDH lactate dehydrogenase
LFT liver function test
LOCF last observation carried forward
LSD Least Significant Difference
MAR missing at random
MCAR missing completely at random
MMRM mixed model repeated measures
MOOP manual of operating procedures
NAC N-acetylcysteine
NHLBI National Heart Lung and Blood Institute (US)
NIH National Institutes of Health (US)
NSIP nonspecific interstitial pneumonia
PaO2 partial pressure of arterial oxygen
PCP primary care provider
PFT pulmonary function test
10
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
PHS Public Health Service (US)
PI principal investigator
PL placebo
PLT platelet
PRED prednisone
QOL quality of life
SAE serious adverse event
SAP statistical analysis plan
SGRQ St Georgersquos Respiratory Questionnaire
SpO2 oxygen saturation by pulse oximetry
TPMT thiopurine methyl transferase
UCSD SOBQ University of California at San Diego Shortness of Breath Questionnaire
UIP usual interstitial pneumonia
ULN upper limit of normal
USP United States Pharmacopoeia
VC vital capacity
WBC white blood cell
11
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
PREDNISONE AZATHIOPRINE AND N-ACETYLCYSTEINE A STUDY
THAT EVALUATES RESPONSE IN IDIOPATHIC PULMONARY FIBROSIS
1 Summary
There are currently no drug therapies that have proven to be effective in the treatment of idiopathic pulmonary
fibrosis (IPF) Previous clinical drug trials have been difficult to interpret due to lack of true placebo (PL)
controls or other methodological concerns Clinical efficacy of immunosuppressive therapies and agents that
reduce oxidative stress remains controversial The IPF Clinical Research Network (IPFnet) is conducting a
randomized double-blind placebo-controlled trial designed to assess the safety and efficacy of
N-acetylcysteine (NAC) as monotherapy in subjects with mild or moderate IPF
The study initially employed a 3-arm design with 111 randomization to NAC azathioprine (AZA)-prednisone
(PRED)-NAC and PL with each subject to be treated up to a maximum of 60 weeks followed by a tapering of
PREDPL and a 4-week period for safety evaluation Approximately 390 subjects who have mild to moderate
IPF (defined as forced vital capacity percent predicted [FVCpred] ge 50 and diffusing capacity of the lung
for carbon monoxide percent predicted [DLCOpred] 30) diagnosed within the past 48 months were to be
enrolled
At the pre-specified interim analysis the DSMB recommended termination of the prednisone-azathioprine-
NAC arm of the study No additional patients will be randomized to that arm However the NAC and placebo
arms remain open for enrollment and we will enroll approximately 130 subjects in each arm (inclusive of the
subjects enrolled at the time of the interim analysis) Follow up for subjects enrolled into the two arms will
continue for 60 weeks
The primary endpoint is the change in longitudinal measurements of FVC over the study period The primary
goal of this study to establish an evidence-based standard of care and clarify myths from facts for
pharmacotherapy of IPF has been met in part by demonstrating that the widely used triple therapy was harmful
to patients with IPF (NHLBI press release Oct 21 2011) To determine the potential therapeutic benefits of
NAC alone the study will continue to enroll patients as a two-arm double-blind placebo-controlled study from
this point on (NAC vs placebo) as recommended by the DSMB following the pre-specified interim analysis
12
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
2 Hypotheses and Specific Aims 21 Null Hypothesis
Treatment with NAC will provide the same efficacy as PL as measured by longitudinal changes in FVC
22 Specific Aim 1
This study is designed to assess the safety and efficacy of NAC in subjects with newly diagnosed IPF
23 Specific Aim 2
Secondary goals of this study are to assess differences between treatment groups for the following
1 Mortality
2 Time to death
3 Frequency of acute exacerbations (AExs)
4 Frequency of maintained FVC response
5 Time-to-disease progression
6 Change in DLCO
7 Change in Composite Physiologic Index (CPI)
8 Change in resting alveolar-arterial oxygen gradient
9 Change in 6-minute walk test (6MWT) distance
10 Change in 6MWT oxygen saturation area under the curve
11 Change in 6MWT distance to desaturation lt 80
12 Change in 6MWT minutes walked
13 Changes in health status as measured by the SF-36 EuroQol and St Georgersquos Respiratory
Questionnaire (SGRQ)
14 Changes in dyspnea as measured by the University of California at San Diego Shortness of Breath
Questionnaire (UCSD SOBQ)
15 Frequency and types of adverse events (AEs)
16 Frequency and types of respiratory complications both infectious and noninfectious
17 Frequency of hospitalizations both all-cause and respiratory-related
13
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
24 Prespecified Subgroups of Interest
Treatment effects will be estimated and compared within key subgroups
Higher enrollment FVC12
Typical vs atypical high-resolution computed tomography (HRCT) reading at baseline3
Recent vs more remote diagnosis (time from initial diagnosis of IPF le 1 year and gt 1 year)
Lower CPI score at enrollment4
Medical therapy for gastroesophageal reflux5
Ethnic background
Sex
Smoking history (current or ex-smoker vs never smoker) given potential impact on oxidant status6
Presence of emphysema gt 25 on HRCT
14
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
3 Background and Significance
31 Idiopathic Pulmonary Fibrosis is the Most Common Interstitial Lung Disease
IPF is the most common interstitial lung disease (ILD) of unknown etiology The current incidence and
prevalence of IPF in the United States are not known A 1994 study of a population-based registry of subjects in
Bernalillo County New Mexico USA estimated an incidence of 107 cases per 100000 per year for males and
74 cases per 100000 per year for females the prevalence of IPF was estimated at 20 per 100000 for males and
13 per 100000 for females7 Extrapolating from a large healthcare claims database a more recent review
estimated the prevalence of IPF in the United States at 427 per 100000 (incidence estimated at 163 per
100000 per year)8 Recent epidemiological studies indicate increasing mortality rates from IPF in the United
States and other industrialized nations9-12
Approximately two-thirds of subjects with IPF are over the age of 60 at the time of presentation and the
incidence increases with age13 IPF has no distinct geographical distribution and predilection by race or
ethnicity has not been identified13 Individual subjects may remain relatively stable for prolonged periods
experience very slow declines in lung function with progression of radiographic abnormalities for a period of
months to years or experience more rapid declines and subsequent death Only 20 to 30 of IPF patients
survive for 5 years following diagnosis
There is currently no proven effective pharmacological treatment for IPF13 Anti-inflammatory and
immunosuppressive agents have been the traditional approach to the management of patients with IPF Based
on the results of the interim analysis of the PANTHER-IPF trial this lsquotraditional approachrsquo will be aborted
However it remains unknown if NAC alone will prove beneficial in IPF patients The primary goal of the
modified study is to establish an evidence-based standard of care and clarify the role of this specific antioxidant
pharmacotherapy for IPF
32 Rationale for Placebo Control
IPF is a disorder for which there is no proven efficacious therapy A major objective of this trial is to test to the
greatest degree possible a proposed standard of care for patients with IPF The current traditional therapy
15
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
employs immunosuppressive and corticosteroid drugs Interim review of the original PANTHER-IPF study has
documented increased adverse events and lack of efficacy for AZA-PRED-NAC compared to placebo
suggesting that this therapeutic approach should not be employed Whether this applies to NAC alone which
has been advocated by international societies has not been proven in well-designed well-powered clinical
trials The recommendations made in the recently published evidence guidelines for NAC monotherapy was
weak based on low quality13 Thus this continued clinical trial randomizing patients to receive NAC or placebo
is pivotal and will answer the important question of the potential therapeutic benefits of NAC monotherapy with
grade A evidence In this prospective randomized clinical trial the inclusion of a PL arm is therefore vital to
adequately test the benefits of NAC in well-characterized subjects with IPF
If NAC has no true efficacy then its role as standard of care will be refuted If a benefit compared with PL is
confirmed it will establish a benchmark against which future novel therapies for IPF will be safely compared
As there is no currently accepted therapy for IPF there is an increasing body of published literature supporting
the concept of no treatment as the ldquobest carerdquo option for IPF13
Post hoc analyses of PL-controlled trials suggest that subjects with milder disease may be more amenable to
therapy12 It is notable that a recent international prospective randomized trial of interferon-gamma for IPF
also included a PL arm the study was terminated early by the data and safety monitoring board (DSMB) due to
lack of treatment effect1415 This underscores the belief that a proven effective therapy for IPF does not
currently exist and that true placebo-controlled trials remain the gold standard Similarly recently completed
trials of etanercept everolimus bosentan and BIPF 1120 in IPF have included PL-treated arms16-19 In three of
these trials the treated subjects showed little if any objective improvement Based on this evidence and the
current status of IPF therapy and therapeutic trials we believe that clinicians and subjects will continue to enroll
in a PL-controlled study
33 Rationale for N-acetylcysteine
NAC is a derivative of the amino acid L-cysteine NAC has been shown to augment levels of the naturally
occurring antioxidant glutathione (GSH ) (glutathione γ-glutamyl cysteinyl glycine) both in vitro and in
vivo2021 GSH is present in all eukaryotic cells and may play an important role in protecting alveolar epithelial
cells against oxidant injury The concentration of GSH in the bronchoalveolar lavage (BAL) fluid in patients
16
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
with IPF is markedly diminished compared with normal subjects This GSH deficiency may be corrected by
exogenous administration of NAC2122
There is evidence of enhanced production of oxidants in an IPF lung Both inflammatory cells and
myofibroblasts derived from patients with IPF generate increased amounts of extracellular oxidants including
hydrogen peroxide2324 Secretion of hydrogen peroxide by activated myofibroblasts may induce the death of
adjacent lung epithelial cells by paracrine mechanisms24 Additionally generation of oxidants by myofibroblasts
induces oxidative crosslinking of extracellular matrix proteins25 a potential mechanism for aberrant matrix
remodeling Thus an oxidant-antioxidant imbalance exists in the lungs of IPF patients26 NAC may confer
protection against this imbalance by augmenting GSH levels in addition to its more direct free-radical
scavenging activity
Intravenous (IV) NAC therapy has been shown to increase total BAL GSH in 8 IPF subjects27 Oral NAC (600
mg 3 times per day) has been shown to decrease markers of oxidant injury and improve both total and reduced
GSH levels in the epithelial lining fluid of subjects with IPF in a small uncontrolled study22 pulmonary
function improved modestly with therapy A similar study in 18 IPF subjects confirmed increased intracellular
GSH concentration after 12 weeks of NAC (600 mg 3 times per day)2228 no clinical correlates were reported
Inhaled NAC was suggested to improve pulmonary function in an open label study29
35 Rationale for N-acetylcysteine as a Stand-alone Therapy
Results of a double-blind multi-center European clinical trial of 150 IPF subjects testing combinations of AZAshy
PRED vs AZA-PRED-NAC have been reported30 NAC added to AZA-PRED (ldquoconventional therapyrdquo) had a
significant positive effect on DLCO (p lt 0005) and vital capacity (VC) (p lt 005) at the end of 1 year30 The
recent ATSERS position statement after much discussion concluded that NAC alone should not be considered
in the majority of patients with IPF without additional data from well-designed studies
The interpretation of these data has been quite controversial Some have suggested that the magnitude of the
treatment effect although statistically significant is modest31 Others have suggested that NAC may be
modulating potential toxic effects of AZA-PRED alone32 supporting the investigation of NAC as stand-alone
therapy
17
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
The IPFnet is now completing the PANTHER-IPF trial with a 11 randomization (NAC vs placebo) and a
simple practical feasible and scientifically rational design that will establish standard of care with NAC for
IPF based on a currently available therapeutic agent and the existing data to support its use We anticipate that
all future clinical trials of novel therapeutic agents will be tested against this to-be-established standard of care
36 Rationale for the Study Design and Primary Endpoint
The optimal study design of a therapeutic trial in IPF would include survival as a primary endpoint The
published results of the IFN-γ 1b Phase 3 (GIPF-001) trial suggested a survival benefit in subjects with milder
disease in retrospective analyses1 although the trial was underpowered to address this question This was likely
related to the limited mortality in the PL arm of the study which included IPF subjects with mild to moderate
disease This study documents that an IPF study powered to improve survival in a patient population with mild
disease requires a larger sample size andor duration of study In fact the recently aborted Phase 3 IFN-γ 1b
(GIPF-007 INSPIRE) study was a survival-based study and recruited more than 800 subjects at 75 centers
worldwide1415 As such within the context of the current IPFnet trial survival is an impractical primary
endpoint variable
Several groups have published data defining an appropriate surrogate outcome variable a 10 decrement in
FVC during 6 to 12 months is a powerful predictor of survival in IPF33-36 Furthermore additional evidence
suggests a similar predictive ability for a 10 decrement in FVC during 3 months of follow-up37 With strong
supportive evidence of FVC progression being related to mortality on a per-subject basis this study will use
FVC changes in liters between treatment groups as the primary endpoint Previously published IPF studies have
shown a steady decline in FVC (and FVCpred) among control group subjects230 The GIPF-001 study
suggested a 48-week decrease in FVC of 016 L in the PL-treated subjects The IFIGENIA study demonstrated
a decline in FVC of approximately 019 L over 52 weeks in the subjects randomized to the control treatment
Figure 1 depicts the change in FVC for control groups from previously published IPF studies38 Based on these
data we expect that the PL group will have a decline of 020 L over the 60-week study period The IPFnet
Steering Group determined that a clinically meaningful improvement would be the preservation of the majority
of the 020-L FVC decline Therefore a mean treatment difference of 015 L in mean FVC over the 60-week
study period was determined to be a clinically meaningful difference
18
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Δ f
rom
bas
elin
e (i
n L
)
01
005
0
-005
-01
-015 Projected Δ for placebo
-02
-025
-019
-016
-013 Pirfenidone GIPF001
NAC
Placebo
4 8 12 16 20 24 28 32 36 40 44 48 52 56 60
Week
Figure 1 Changes in FVC From Baseline in Prior IPF Clinical Trials
Recent data suggest that various patient subgroups would be expected to potentially exhibit differential response
to therapy These parameters will be used to a priori separate patients by a series of baseline characteristics
including
1 Higher enrollment FVC12
2 Typical vs atypical high-resolution computed tomography (HRCT) reading at baseline3
3 Recent vs more remote diagnosis (time from initial diagnosis of IPF le 1 year and gt 1 year)
4 Lower CPI score at enrollment4
5 Medical therapy for gastroesophageal reflux5
6 Ethnic background
7 Sex
8 Smoking history (current or ex-smoker vs never smoker) given potential impact on oxidant status6
9 Presence of emphysema gt 25 on HRCT
37 Rationale for Blinding of Treatments
The issue of treatment blinding was given a great deal of consideration with subject safety being the primary
concern After discussion among the Steering Group members it was decided that as long as subject safety
could be ensured blinding was necessary Blinding allows the study to
Have optimal scientific validity and potential to impact the standard of care for subjects
19
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Make objective assessments of treatment effects
Maintain clinical equipoise among investigators
Encourage subjects to have similar levels of contact with the medical community
Minimize the differential dropout rates across study arms
20
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
4 Methods 41 Inclusion Criteria
1 Age 35 to 85 years inclusive
2 FVC ge 50 of predicted (post-bronchodilator measurement from the screening visit)
3 DLCO ge 30 of predicted (hemoglobin corrected and altitude corrected if gt4000 ft above sea level)
4 Ability to understand and provide informed consent
5 Diagnosis of IPF according to a modified version of the ATS criteria le 48 months from enrollment The
date of diagnosis is defined as the date of the first available HRCT or surgical lung biopsy characteristic
of definite UIP
411 Subjects Shown to Have Usual Interstitial Pneumonia Pattern on Surgical Lung Biopsy
Subjects who have been shown to have UIP pattern on lung biopsy must have all of the following
1 Exclusion of other known causes of ILD such as drug toxicity clinically significant environmental
exposures or diagnosis of connective tissue diseases
2 Bibasilar reticular abnormalities with minimal ground glass opacities on HRCT scan
412 Subjects Who Have Not Undergone a Surgical Lung Biopsy
In addition to the criteria above these subjects must have radiological findings considered to be definite for the
diagnosis of UIPIPF
1 Bibasilar reticular abnormalities with minimal ground glass opacities
2 Honeycombing as the predominant feature and located in the peripheral lung bases
42 Diagnosis of IPF
Only subjects with definite IPF will be eligible for enrollment in this study We will utilize a combination of
clinicalphysiologic features HRCT and review of a clinically obtained surgical lung biopsy specimen to
establish the diagnosis of IPF An algorithm for the diagnosis is provided to guide entry into the protocol as
outlined in the inclusion and exclusion criteria (Figures 2 and 3) This multi-disciplinary approach uses
21
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
expertise from clinicians radiologists and pathologists Investigators at each site in conjunction with central
pathology will work together to establish the diagnosis of IPF This interactive approach to the diagnosis of IPF
increases the level of agreement between observers39
A subject with suspected ILD should be evaluated for secondary causes including but not limited to
environmental exposures drugs and systemic diseases Presence of any of these findings felt to be significant
enough to cause an ILD should disqualify the subject from entry into the trial
If secondary causes are absent an HRCT scan may be obtained If an HRCT of sufficiently high quality has
been obtained within the last 3 months that scan may be used for diagnosis In the appropriate clinical setting
the diagnosis of IPF can be made by the demonstration of a typical radiographic pattern on HRCT or by
demonstration of UIP pattern on a surgical lung biopsy The following criteria for a radiographic (ie
nonsurgical) diagnosis will be used In the absence of known exposures andor clinical associations attributable
to pulmonary fibrosis and in the appropriate clinical setting the presence of definite UIP pattern in HRCT
images is required to meet study criteria for the diagnosis of IPF
Figure 2 Diagnosis of Idiopathic Pulmonary Fibrosis in the IPFnet
22
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Figure 3 Pathology Flow Chart Surgical Lung Biopsy Diagnosis
Requirement for diagnosis
1 Clinical exclusion of other known causes (connective tissue diseases environmental and drug
exposures) of ILD
2 Radiographic HRCT with bibasilar reticular abnormality and honeycomb change with minimal
ground glass opacities
Appropriate clinical setting
1 Age gt 50 years
2 Insidious onset of unexplained dyspnea
3 Duration of illness for ge 3 months
4 Bibasilar inspiratory crackles
23
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Unlike the ATSERS consensus criteria published in 2000 bronchoscopy will not be required for diagnosis
This decision was made based on the experience of the IPFnet Steering Group members regarding the utility of
bronchoscopy in the diagnosis of IPF The presence of an atypical HRCT finding will require documentation of
a definitive diagnosis by surgical lung biopsy In fact this is in keeping with the recently published evidence
based guidelines for diagnosis and management of IPF13 As shown in Figure 3 central review of the pathology
data will be required for a diagnosis of IPF
We will not require central review of HRCT as several studies have shown that a confident local interpretation
of clinicalHRCT criteria as definite IPFUIP is associated with a high positive predictive value for finding UIP
at surgical lung biopsy (see Table 1) Differences in sensitivity in these series likely reflect subject selection as
Flaherty et al3 evaluated only UIP and nonspecific interstitial pneumonia (NSIP) while Raghu et al40 and
Hunninghake et al41 included a broader range of ILD
Table 1 Operating Characteristics of Local HRCT Review for Diagnosis of UIP
Researcher of Subjects Sensitivity () Specificity () PPV () NPV ()
Raghu et al 40
59 (29 UIP by SLB) 78 90 88 82
Hunninghake et al 41 91 (54 UIP by SLB)
74 81 85 67
Flaherty et al 3 96 (only NSIP amp UIP)
37 100 100 30
Abbreviations PPV positive predictive value NPV negative predictive value UIP usual interstitial pneumonia SLB surgical lung biopsy and NSIP nonspecific interstitial pneumonia
Furthermore an analysis of the HRCT scans from subjects enrolled in the GIPF-001 trial confirmed that local
site interpretations have a high congruity to a central radiology core In this multi-center study 263 HRCT
scans were read as definite IPF and a retrospective central radiology core review found 932 to be consistent
with IPF 42 We will also take several additional steps to insure that the local HRCT reads are accurate
including
1 A detailed training module has been developed and must be completed by each site radiologist before
site initiation
2 Clinical centers are to mail all HRCT scans to the HRCT core lab The first 10 HRCT scans from
subjects enrolled at each enrolling clinical center will be reviewed centrally to be certain that local reads
24
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
25
are congruent with a central interpretation If discrepancies are identified additional education will be
provided and HRCT scans will continue to be reviewed centrally until the central radiology core is
confident that the local center is performing appropriately
3 Random scans will be obtained from each center throughout the study to confirm that the local read
continues to agree with central interpretation If discrepancies are identified they will be addressed as in
2 above
In all cases if a subject has a surgical lung biopsy sample that sample will be reviewed by the local and central
pathologists Therefore the only cases that would not be subject to a direct central review process are those
where the HRCT meets the centrally defined criteria for an unequivocal diagnosis and a lung biopsy sample is
not available Table 2 below summarizes the possible combinations for making a diagnosis
Table 2 Combining HRCT and Pathology Interpretations to Determine if IPF is Present
HRCT Diagnosis Pathology Diagnosis Diagnosis of IPF
Definite UIP Definite UIP Yes
Definite UIP Probable UIP Yes
Definite UIP Possible UIP Yes
Definite UIP Not UIP No
Definite UIP Unavailable Yes
Consistent with UIP Definite UIP Yes
Consistent with UIP Probable UIP Yes
Consistent with UIP Possible UIP No
Consistent with UIP Not UIP No
Consistent with UIP Unavailable No
Inconsistent with UIP Any No
Abbreviations HRCT high-resolution computed tomography IPF idiopathic pulmonary fibrosis
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
UIP usual interstitial pneumonia Dx diagnosis 43 Exclusion Criteria
1 History of clinically significant environmental exposure known to cause pulmonary fibrosis
Occupational exposures such as asbestos or environmental exposure to organic dust such as occurs in
pigeon breeders may at times mimic the clinical and radiographic findings of IPF
2 Diagnosis of connective tissue disease felt by the principal investigator (PI) to be the etiology of the
interstitial disease Diagnosis of collagen-vascular conditions will be according to the published
American College of Rheumatology criteria As such the presence of any documented collagen-vascular
disorder or the presence of any suspicious symptom complex whether or not associated with
significantly abnormal rheumatological serologies will exclude the subject at the discretion of the PI
3 Extent of emphysema greater than the extent of fibrotic change (honeycombing reticular changes) on
HRCT scan
4 Forced expiratory volume in 1 second (FEV1)FVC ratio lt 065 at screening (postbronchodilator)
5 Partial pressure of arterial oxygen (PaO2) on room air lt 55 mm Hg (lt 50 mm Hg at Denver site)
6 Residual volume gt 120 predicted at screening (postbronchodilator)
7 Evidence of active infection
8 Significant bronchodilator response on screening spirometry defined as a change in FEV1 ge 12 and
absolute change gt 200 mL OR change in FVC ge 12 and absolute change gt 200 mL The percent
difference between the FVC (or FEV1) values will be calculated by taking the absolute value of the
difference and dividing it by the larger of the two FVC (or FEV1) values
9 Screening and enrollment post-bronchodilator FVC measurements (in liters) differing by gt 11 The
percent difference between the FVC values will be calculated by taking the absolute value of the
difference and dividing it by the larger of the two FVC values (eg the percent difference between FVC
measurements of 19 and 20 liters would be determined by taking the difference between the two (01
liters) and dividing by the larger of the two (20 liters) So 0120 = 5 and these FVC measurements
would not exclude the subject
10 Listed for lung transplantation ie the patient has completed the evaluation process has been accepted
as a candidate for transplantation at an appropriate center and is waiting to receive notification of an
available donor organ
11 History of unstable or deteriorating cardiac disease
12 Myocardial infarction coronary artery bypass or angioplasty within 6 months of screening
26
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
13 Unstable angina pectoris or congestive heart failure requiring hospitalization within 6 months of
screening
14 Uncontrolled arrhythmia
15 Severe uncontrolled hypertension
16 Known HIV or hepatitis C
17 Known cirrhosis and chronic active hepatitis
18 Active substance andor alcohol abuse (as determined by site PI)
19 Pregnancy or lactation (subjects who are pregnant or breastfeeding)
20 Known hypersensitivity to study medication
21 Any condition other than IPF that in the opinion of the site PI is likely to result in the death of the
subject within the next year
22 Any condition that in the judgment of the PI might cause participation in this study to be detrimental to
the subject or that the PI deems makes the subject a poor candidate
23 Any therapy directed at pulmonary fibrosis (excepting triple therapy of prednisone plus azathioprine
plus NAC) requires a 30-day washout period before randomized Triple therapy of lt= 12 weeks duration
in the past 4 years requires a 30-day washout period before randomization
24 History of triple therapy of prednisone plus azathioprine plus NAC for gt 12 weeksrsquo duration in the past
4 years or previous enrollment in the triple-therapy arm of the PANTHER-IPF study
44 Study Design and Study Visit
441 Study Design Summary
This study will be a randomized double-blind PL-controlled trial designed to assess the safety and efficacy of
NAC in subjects with newly diagnosed IPF
Subjects with mild to moderate IPF (defined as FVCpred ge 50 and DLCOpred ge 30) diagnosed within
the past 48 months will be enrolled Screening will continue until April 30 2012
27
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
The study will employ a 2-arm design with 11 randomization to NAC or PL Once enrolled subjects will visit
the clinical center at 15 weeks and 15-week intervals thereafter Each subject will be treated and followed for a
maximum of 60 weeks
During the 60-week visit subjects will be taken off all study agents Approximately four weeks after the final
dose of study agent is taken subjects will receive a safety phone call from the study site
442 Study Visits
Subjects who meet entry criteria will review the informed consent a written description of the purpose
procedures and risks of the study with the PI co-investigator or study coordinator and all questions will be
answered The informed consent form will be signed by the subject at screening No protocol-specific
procedures will be performed until the subject has signed and dated an informed consent form This includes the
screening procedures
4421 Screening
Once informed consent is obtained subjects may immediately begin the screening process or may return within
28 days of consent In the event a study subject has been clinically evaluated at the study site by an IPFnet study
physician and has performed testing within three weeks for this clinical evaluation that meets guidelines
provided in the IPFnet PANTHER-IPF Manual of Operating Procedures (MOOP) this testing may be used to
satisfy the following screening criteria medical history physical exam arterial blood gas (ABG) with A-a
gradient vital signs with oximetry body height and weight spirometry DLCO lung volumes and HRCT scan
Allowing the use of previously performed test results that meet study guidelines for the screening visit is
intended to permit subjects easier access to study entry to prevent subjects from repeating testing that has been
performed within the study window and to decrease risks to subjects from repeated exposure to procedures
such as arterial puncture and HRCT
The following procedures will be performed at screening
Medical history and a physical examination
28
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Measure height and weight
Serum pregnancy test (if applicable)
Measure vital signs including oximetry
Blood draws performed and the following analyses conducted
o Hematology (red cell count white cell count hemoglobin hematocrit cell indices differential
platelet count)
o Blood chemistries according to central laboratory protocol (see Section 410 Laboratory
Testing)
o Beta human chorionic gonadotropin (serum) pregnancy test (in women of childbearing potential)
o Urinalysis
Pulmonary Function Tests (PFTs) including spirometry pre- and post- bronchodilator and postshy
bronchodilator measurement of lung volumes and measurement of hemoglobin adjusted diffusing
capacity
Measure ABGs
HRCT if a satisfactory scan has not been performed on the subject within 3 months of screening (see
PANTHER-IPF MOOP for more details)
Surgical lung biopsies (if applicable) reviewed by local and central pathology departments
Current medications If required a washout period discussed with the subject and initiated at this visit
4422 Enrollment
The enrollment visit is expected to take place within eight weeks of the screening visit Enrollment visit
activities include
Measure vital signs including oximetry
Measure height and weight
Serum pregnancy test (if applicable)
If consent has been given blood will be drawn and a urine specimen collected for the bio-specimen
repository
Spirometry (post-bronchodilator)
Measure 6MWT with Borg Dyspnea Scale
29
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Collect Quality-of-life (QOL) data using the SF-36 EuroQol Investigating Choice Experiments for
Preferences of Older People Capability Instrument (ICE CAP) and SGRQ
Female subjects complete Gender Substudy questionnaire
Dyspnea status collected using the UCSD SOBQ
Evaluate Acute Exacerbation (AEx)
Review of any Adverse Events (AEs)
Review of concomitant medications
Subject receives diary and instructions on its purpose and proper use
Subject receives supply of study drug sufficient to last until his or her 15-week study visit
See the Schedule of Assessments (Table 3) for more details Subjects with screening and enrollment postshy
bronchodilator FVC measurements (in liters) differing by more than 11 are not eligible to be enrolled in the
study
Subjects will be asked to provide a physician of record This physician will be considered the subjectrsquos primary
care provider (PCP) and if the subject agrees the PCP will be informed by letter of the subjectrsquos enrollment in
the trial The subject will be informed that his or her ongoing medical care should be received from the PCP
The PCP will be informed of any safety issues identified by the study staff The PCP will also be given
information regarding communication with study personnel about pertinent health issues or clinic encounters
the subject may have
4423 Week 15
The week 15 visit is expected to occur within +- 14 days of the subjectrsquos scheduled visit time (eg the week 15
visit should occur anytime between 13 and 17 weeks after starting study drug Week 15 activities include
Measure vital signs with oximetry
Measurement height and weight
Serum pregnancy test (if applicable)
Spirometry (post-bronchodilator) measurement
Review of AEs
Evaluate for AEx
30
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Review concomitant medications
If consented draw blood and collect urine specimen for the biospecimen repository
Subjects return used and unused study drug for the visit
Review study diary and a new study diary will be given
Provide additional supply of study drug sufficient to last until the next scheduled visit
4424 Week 30
The week 30 visit is expected to occur within +- 14 days of the subjectrsquos scheduled visit time (eg the week 30
visit should occur anytime between 28 and 32 weeks after starting study drug) Week 30 activities include
Physical examination
Measure vital signs with oximetry
Measure height and weight
Laboratory values (complete blood count [CBC] and serum chemistries)
Serum pregnancy test (if applicable)
Measure spirometry (post-bronchodilator)
6MWT with Borg scale
DLCO
Review of AEs
Evaluate for AEx
Review concomitant medications
Complete all QOL and dyspnea questionnaires (EuroQol ICE CAP SF-36 SGRQ and UCSD SOBQ)
If consent has been given blood will be drawn and a urine specimen collected for the biospecimen
repository
Review study diary
Subjects return used and unused study drug for the visit
Provide additional supply of study drug sufficient to last until the next scheduled visit
4425 Week 45
31
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
The week 45 visit is expected to occur within +- 14 days of the subjectrsquos scheduled visit time (eg the week 45
visit should occur anytime between 43 and 47 weeks after starting study drug) Week 45 activities include
Measure vital signs with oximetry
Measure height and weight
Serum pregnancy test (if applicable)
Measure spirometry (post-bronchodilator)
Review of AEs
Evaluate for AEx
Review concomitant medications
If consent has been given blood will be drawn and a urine specimen collected for the biospecimen
repository
Subjects return used and unused study drug for the visit
Study diary reviewed
Provide additional supply of study drug sufficient to last until the next scheduled visit
4426 Week 60 (Early Withdrawal or Final Treatment Visit)
At week 60 or at subject withdrawal from the study (premature by study doctor or subjectrsquos decision) a final
treatment visit will occur At this final treatment visit subjects will discontinue NACPL abruptly Week 60
activities also include
Physical examination
Measure vital signs with oximetry
Measure height and weight
Laboratory values (complete blood count [CBC] and serum chemistries)
Spirometry (post-bronchodilator) measurement
6MWT with Borg scale measurement
DLCO
Lung volumes
ABG
Review of AEs
32
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Evaluate for AEx
Review concomitant medications
Subjects will complete all QOL and dyspnea questionnaires (EuroQol ICE CAP SF-36 SGRQ and
UCSD SOBQ)
If consent has been given blood will be drawn and a urine specimen collected for the biospecimen
repository
Subjects return used and unused study drug for the visit
Study diary reviewed
4427 Final Site Visit ndash FVC drop confirmation
In the event that the subject has a recorded FVC drop of gt10 from baseline at the final treatment visit and the
subject has not had a confirmation of such a drop at a previous study visit the subject should return to the
clinical site 6 to 8 weeks after the final treatment visit During this visit a post-bronchodilator spirometry test
will be performed This FVC measurement will be evaluated according to section 521 of this protocol
4428 Final Visit ndash Telephone Follow-up
Four weeks following the final dose of study medication subjects will receive a telephone call from the study
coordinator to ensure that there are no side effects and to follow up on any ongoing adverse events (AEs)
4429 Phone Contact Between Visits
At week 2 and each month that a subject does not have a scheduled clinical center visit his or her study
coordinator will contact him or her at least once by telephone to
Inquire if the subject has had any hospitalizations events that might be considered an AE or any events
significant enough to warrant an out-of-cycle visit to the clinical center
Remind subjects of their current dosage levels and confirm that the subject understands them
Address any questions or concerns the subject might have regarding other aspects of the study
Assess adherence to the treatment regimen by reviewing diary data verbal review of medications taken
including nutritional supplements
33
34
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Table 3 Schedule of Assessments
Procedure Screening Visit 0
Enrollment Visit 1
Week 15 Visit 2
Week 30Visit 3
Week 45 Visit 4
Week 60 Early
Withdrawal Visit 5
Final1
Visit (via phone)
Informed consent X
Medical history X
Inclusionexclusion criteria X
Serum pregnancy test (if applicable) X X X X X
Review of lung biopsy X
Arterial Blood Gas X X
6-Minute Walk Test
X
X X
Physical examination X X X
Vital signs with oximetry X X X X X X
Body height and weight X X X X X X
Complete Blood Count X X X
Chemistry panel X X X
Monitor Lab Values X X X
Urinalysis X Specimen repository substudy blood draw and urine collection (if consented)
X
X X X X
HRCT (if not completed within three months) X
Spirometry (pre- and post-bronchodilator) X
Spirometry (post-bronchodilator only) X X X X X
DLCO (post-bronchodilator only) X X X
Lung volumes (post-bronchodilator only) X
X
Evaluate for acute exacerbation X X X X X
Review Adverse Events X X X X X X
Review concomitant meds X X X X X X
Dispense subject diary X X X X
Review subject diary X X X X X
Dispense study agent X X X X
Gender Substudy questionnaire (female subjects only) X
EuroQol ICECAP UCSD SOBQ SGRQ SF-36 X X X
Abbreviations DLCO diffusing capacity of the lung for carbon monoxide QOL Quality of Life ICECAP Investigating Choice Experiments for Preferences of Older People UCSD SOBQ University of California Shortness of Breath Questionnaire SGRQ St Georgersquos Respiratory Questionnaire SF-36 Short Form 36 Health Survey
1Follow-up visit via phone will occur four weeks after final dose of study medication
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
45 Dose Justification
The general philosophy for determining dosing levels was to apply previously examined
treatment regimens With the focus of the study being to establish a standard of care for
mildmoderate IPF subjects the goal was to develop flexible yet standardized treatment rules that
allow for the temporary or permanent withholding of one or more components of treatment when
necessary Subjects developing laboratory abnormalities or symptoms that result in
discontinuation of one or more components of study treatment may continue on the other
components as long as there is no contraindication for this Complete follow-up is important for
the validity of any study As a strategy to maintain protocol adherence we are using a treatment
regimen that will detect potential side effects and prompt interventions proactively in the interest
of patient safety In addition subjects who permanently stop study medications during the course
of the study are encouraged to continue in the study completing all scheduled visits and tests
451 Rationale for N-acetylcysteine Dosing
To our knowledge there have been no IPF studies to correlate clinical outcome measures with
different dosages for NAC The dosage chosen is based on the IFIGENIA study However BAL
lung GSH levels from subjects with IPF have been augmented with the use of oral NAC at 600
mg 3 times per day In addition lung GSH levels have been associated with improved
PFTs212227 The dose chosen for this study was based on previous data including the IFIGENIA
study30
4511 Dosing of N-acetylcysteineplacebo
Dosing of NACPL will be 600 mg orally 3 times a day (1800 mgday)
4512 Reasons to Discontinue N-acetylcysteineplacebo
NACPL may be temporarily or permanently discontinued for the duration of the study for
gastrointestinal symptoms or dermatologic reactions
35
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Temporarily discontinue (hold) oral NACPL for subjects requiring inpatient admission for acute
exacerbation (AEx) or other conditions Resume NACPL after discharge
36
37
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
452 Dosage Algorithms
Dosage Adjustment Algorithm 1 NACPL Dose Modifications for Gastrointestinal Symptoms Nausea Vomiting Abdominal Discomfort Diarrhea
GI Symptoms determined by the PI to be clinically significant Nausea Vomiting Abdominal Discomfort Diarrhea
NACPL Temporarily dc (HOLD) x 3 Days
Monitor symptoms intervene as clinically indicated (eg fluid replacement antidiarrhea or antinausea medication)
Monitor or lab PRN
Are symptoms resolving after 3 days NO
Symptoms NOT resolving after 3 days of holding study medication Assessmentmanagement per clinical
discretion of investigator
Likely not study medication discuss resuming study medication with medical monitor when symptoms resolved
YES
Temporarily dc (HOLD) NACPL for 4 additional days (total hold 1 week) then NACPL Resume 600 MG TID
Did symptoms recur
YES
STOP NACPL for
duration of study
NO
NACPL No Change
38
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Dosage Adjustment Algorithm 2 NACPL Dose Modifications For Dermatologic Reactions
Dermatologic Reactions (Not Acneiform) ge Grade 2 Grading per Common Terminology Criteria for
Adverse Events V30 (httpctepcancergov) For example Grade 1 RASHDESQUAMATION Macular or papular eruption or erythema without associated symptoms Grade 2 RASHDESQUAMATION Macular or popular eruption or erythema with pruritus or other associated symptoms localized desquamation or other lesions covering lt50 of body surface area
NACPL Temporarily dc (HOLD) x 3 days
Are symptoms resolving after 3 days
NO Symptoms not resolving after 3 days of holding study medication Assessmentmanagement per clinical discretion of investigator Likely not study medication Discuss resuming study medication with medical monitor when symptoms
resolved YES
Temporarily dc (HOLD) NACPL for 4 additional days (total hold 1 week) then NACPL resume 600 MG TID
Did symptoms recur
YES
STOP NACPL for
duration of study
NO
NACPL No change
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
46 Contraindications Precautions and Side Effects of Study Medications
461 Contraindication
Contraindication to NAC is known hypersensitivity to it
462 Precautions
Concomitant administration of oral NAC and antibiotics has shown a slightly reduced absorption
of cephalexin and a slight increase in erythromycin serum levels NAC contains free sulfhydryl
groups There is no evidence that individuals sensitive to sulfa drugs are sensitive to NAC
The NAC preparation being administered in this study contains 20 mg of aspartame Because of
the phenylalanine component of aspartame individuals with phenylketonuria should avoid or
restrict aspartame intake to avoid increased blood levels of phenylalanine Because of this risk
labeling is required on all products containing aspartame
463 Side Effects
Side effects of NAC range from common to serious See Table 4
39
40
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Table 4 Side Effects of NAC
Undesirable Effects
System-organ class Uncommon
(gt11000 lt1100)
Rare
(gt110000 lt11000)
Very rare
(lt110000) Not known
Immune system disorders Hypersensitivity Anaphylactic shock
reaction
Nervous system disorders Headache
Ear and labyrinth disorders Tinnitus
Cardiac disorders Tachycardia
Vascular disorders Hemorrhage
Respiratory thoracic and
mediastinal disorders
Bronchospasm
Dyspnea
Gastrointestinal disorders
Vomiting diarrhea
stomatitis abdominal
pain nausea
Dyspepsia
Skin and subcutaneous tissue
disorders
Urticaria rash
angioedema itching
General disorders and
administration site conditions Pyrexia
Investigations Reduced arterial
pressure Face edema
In very rare cases the onset of severe skin reactions such as Stevens-Johnson syndrome and Lyell syndrome was reported to have a temporal relationship with N-acetylcysteine administration Although in most cases at least another suspect drug probably most involved in the genesis of the above mentioned mucocutaneous syndromes has been identified in case of mucocutaneous alterations it is appropriate to contact onersquos doctor and the administration of N-acetylcysteine should be immediately discontinued
Some studies confirmed a reduction of platelet aggregation during N-acetylcysteine administration The clinical significance of these findings has not been defined yet [Source Fluimucil Investigator Brochure]
47 Recruitment Procedures
Subjects recruited for this study will be established patients of the investigators or physician- or
self-referred to participating clinical centers in the IPFnet Each clinical center within IPFnet has
a well-developed infrastructure of local pulmonologists within the surrounding geographic area
These pulmonologists are kept informed of ongoing IPF clinical trials and regularly refer
subjects to studies conducted at IPFnet clinical centers
Additional steps will be taken to inform clinicians of the trials in progress within IPFnet
including presentations at faculty staff meetings at local hospitals medical grand rounds and
national conferences direct mail notification monthly faxes and advertisement of network trials
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
in pulmonary journals Clinical center patients previously diagnosed with IPF will be notified of
the trials by mail whenever possible
Recruitment of minorities and women will be monitored by the DCC and DSMB If necessary
additional recruitment efforts will be made at specific centers to ensure that the aggregate subject
sample contains appropriate representation of women and minorities
48 Study Procedures
The following procedures are detailed in the PANTHER-IPF MOOP accompanying this
protocol
1 PFT
2 ABG
3 HRCT scan of the chest (including imaging of pulmonary arteries)
4 CBC and serum chemistries
5 Pregnancy test
6 6MWTBorg Dyspnea Scale
7 QOL questionnaires (EuroQol HAD SF-36 SGRQ and ICE CAP)
8 UCSD SOBQ
9 Gender Substudy Questionnaire
All assessments of PFTs will be conducted by study personnel not directly involved in the
treatment of the subjects
481 Biological Specimen Management
4811 Biological Specimen Sample Management
Subjects at clinical centers participating in the specimen repository substudy who consent to
having blood drawn for research purposes and for the banking of blood blood components and
other biologic specimens (urine and BAL fluid) will have approximately 405 mL of blood
41
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
drawn 17 mL blood drawn for DNA and 20 mL of urine collected at enrollment visit Subjects
will have approximately 50 mL of blood drawn and 20 mL of urine collected at each 15-week
follow-up visit Blood specimens will be separated according to PANTHER-IPF MOOP
guidelines into the following components for banking in the repository serum plasma and
DNA Coding of all biologic specimens for the repository will be performed by study staff at the
clinical center The samples will be processed per PANTHER-IPF MOOP guidelines aliquoted
labeled with barcode labels and stored at -70degC at the clinical center and shipped to the central
repository
The only subject identifiers will be a sample ID number and subject initials This sample ID will
be linked in the IPFnet DCC clinical database to subject information No subject information will
be transferred to the biological-specimen database
The subjectrsquos samples may be used for approved sub-studies relating to human disease
including but not limited to IPF The studies for which an individualrsquos samples will be made
available will be determined by the subjectrsquos answers to questions on the biological-sample
informed consent form The subjects can choose to make their samples available for all options
or any combination Samples will be made available to researchers only with IPFnet Steering
Group approval until such time as the samples are made public through the NHLBI repository
49 Concomitant Medications
Concurrent treatment with FDA-approved therapy for IPF is allowed Colchicine may be used
for treatment of gout Temporary treatment with oral or IV corticosteroids for clinical worsening
or suspected AEx is permitted Nutritional supplements containing NAC are not allowed
410 Laboratory Testing
Clinical laboratory parameters will be assessed at screening and at the end of the study The
following tests will be performed at the two time points specified in the protocol chemistry (AG
ratio ALT [SGPT] AST [SGOT] albumin alkaline phosphatase amylase bilirubin-direct
42
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
bilirubin-indirect bilirubin-total BUN BUNcreatinine ratio calcium carbon dioxide
cholesterol-total chloride CPK-total creatinine GGT globulin glucose iron-total LDH
lipase magnesium phosphorus-inorganic potassium protein-total sodium TIBC triglycerides
uric acid) and hematology (red blood cell count WBC count hemoglobin hematocrit cell
indices differential platelet count)
411 Blinding of Study Drugs
Subjects and caregivers will be blinded to study treatment Every subject will receive NAC or
matching PLs at every study visit from the baseline visit to the week-45 visit No study agent
will be dispensed at the week-60 visit
43
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
5 Study Endpoints
51 Primary Study Endpoint
The primary endpoint will be the change in serial measurements of FVC over the study period
52 Secondary Study Endpoints
521 Time to Disease-progression
The time-to-death or a 10 decline in FVC will be defined as the time-to-disease progression
The 10 decline in FVC from enrollment must be confirmed on 2 consecutive visits no less than
6 weeks apart For subjects with 2 consecutive visits with a 10 decline in FVC the time-toshy
disease progression will be defined as the time interval between enrollment and the initial visit
with a 10 FVC decline For subjects who experience disease progression the study doctor will
determine whether or not the subject will remain in the study
522 Acute Exacerbations
The following 3 criteria will define AEx in subjects with acute worsening of their respiratory
conditions
1 Clinical (all of the following required)
A) Unexplained worsening of dyspnea or cough within 30 days triggering unscheduled
medical care (eg emergency room clinic study visit hospitalization)
B) No clinical suspicion or overt evidence of cardiac event pulmonary embolism or deep
venous thrombosis to explain acute worsening of dyspnea
C) No pneumothorax
44
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
2 RadiologicPhysiologic (A and B required)
A) New ground glass opacity or consolidation computed tomography (CT) scan OR new
alveolar opacities on chest x-ray
B) Decline of ge 5 in resting room air SpO2 from last recorded level OR decline of ge 8 mm
Hg in resting room air PaO2 from last recorded level
3 Microbiologic (all of the following required)
A) No clinical evidence for infection (ie absence of grossly purulent sputum fever gt 39degC
orally)
B) Lack of positive microbiological results (if done) from lower respiratory tract defined as
(1) Clinically significant bacterial growth on sputum or endotracheal aspirate cultures
(2) Quantitative culture by protected brush specimen ge 103 cfumL or BAL ge 104 cfumL
(3) The presence of specific pathogens on stains of any of the above
C) Lack of positive pathogen in blood cultures (if done)
Identification of Acute Exacerbations
All subjects will be educated about the importance of identifying AExs At the time of
enrollment subjects will be told about the possibility of developing acute symptomatic
worsening that might represent an AEx of IPF and instructed to contact their study clinical
center coordinator within 48 to 72 hours of the apparent event
All subjects will be contacted by phone monthly and questioned about any change in dyspnea or
cough and any interim clinic visits or hospitalizations Finally as part of the IPFnet outreach to
community referring physicians the importance of AExs will be emphasized When a subject is
identified who meets criterion 1A this will trigger the collection of additional clinical data to
evaluate a suspected AEx These data will be collected as part of standard clinical care (ie this
protocol does not require collection of all items) The additional items to be collected for
suspected AEx include
IPFnet AEx case report form (eCRF) (required)
45
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Chest x-ray CT scan withwithout pulmonary angiogram (reports should be faxed and
followed by the hard copiesdiscs)
Oxygen saturation (pulse oximetry)
ABG
Respiratory cultures (sputum endotracheal aspirate lavage)
Blood cultures
Clinichospital records related to the event
All potential cases of AEx will be reviewed by the clinical center PI first and a decision on
whether the case may represent an AEx will be made If AEx is suspected the case will be sent
to the IPFnet adjudication committee which will assign a final diagnosis (see Table 5) If there is
disagreement among members the majority opinion will be recorded
During episodes of suspected AEx as determined by the individual clinical center investigator
subjects will remain blinded and in the study
Table 5 Final Diagnoses in Evaluation of Suspected Acute Exacerbations
Definite acute exacerbation All criteria met no alternative etiology
Unclassifiable acute worsening
Insufficient data to evaluate all criteria no alternative etiology
Not acute exacerbation Alternative etiology identified that explains acute worsening
Management of the suspected AEx will be at the discretion of the treating physician Standard of
care generally involves evaluation for respiratory infection pulmonary embolism cardiac events
and pneumothorax and treatment with IV corticosteroids
Study drugs will be resumed at pre-suspected AEx doses after subjects clinically improve as
confirmed by the local PI All subjects should be seen at the clinical center within 2 to 4 weeks
of recovery for measurement of post-bronchodilator FVC (see Figure 4) Subjects unable to
return to the clinical center after suspected AEx due to medical frailty (eg continued
46
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
institutionalization progressive disability) will be categorized as failing to maintain FVC
response in secondary analyses
Suspected AEx (PI determined)
Hold study drug Treat AEx
(Attending physician determined)
Alive but unable to continue due to
medical frailty
Dead
Alive and able to continue
Site reviewvisit
Restart study drug
FVC within 2-4 weeks
Figure 4 Acute Exacerbation Flow Chart
523 Respiratory Infections
An upper respiratory infection will be defined as
Change in sputum discoloration
Increased cough of no more than 14 daysrsquo duration
A lower-respiratory infection (pneumonia) will be defined as new segmental or lobar airspace
opacities visualized by image studies (chest radiograph or HRCT) in addition to any of the
following
Positive pathogencultures in good sample of sputum or lower-airway secretions retrieved
by fiberoptic bronchoscope
Fever gt 39degC or gt 100degF
Leukocytosis gt 12000 (unexplained no increase in dose of corticosteroids)
47
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
524 Maintained FVC Response
Subjects with follow-up FVCpred measurements at or above their baseline FVCpred level
will be classified as having maintained FVC response Subjects with reduced FVCpred levels
or missing data for any reason including death or medical frailty will be classified as having not
maintained FVC response The FVCpred value is used because unadjusted FVC measurements
are expected to decline with age
48
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
6 Safety Evaluations and Procedures
61 Adverse Events
During a clinical trial the reporting of adverse experience information can lead to important
changes in the way a new treatment is developed as well as provide integral safety data
611 Definitions
An adverse event (AE) is any untoward medical occurrence in a subject or clinical investigation
subject who was administered a pharmaceutical product The AE does not necessarily have to
have a causal relationship with the drug administered An AE can be any unfavorable and
unintended sign (including an abnormal laboratory finding) symptom or disease temporarily
associated with the use of a medicinal product whether or not considered to be related to the
medicinal product Diseases signs symptoms or laboratory abnormalities already existing at
enrollment are not considered AEs unless they worsen (ie increase in intensity or frequency)
Surgical procedures themselves are not AEs they are therapeutic measures for conditions that
require surgery The condition for which the surgery is required may be an AE Surgical
procedures planned before randomization and the conditions necessitating the surgery are not
AEs
A serious adverse event is any untoward event that
Is fatal
Is life-threatening
Requires inpatient hospitalization or prolongation of existing hospitalization with the
following exceptions
o Preplanned (before the study) hospital admissions unless the hospitalization is
prolonged
o Planned admissions (as part of a study eg routine biopsies)
o Hospitalization lasting lt 24 hours
49
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
o Hospitalization for elective procedure
o Emergency room visits
Results in persistent or significant disability or incapacity
Is a congenital anomaly or birth defect
Important medical events that may not result in death be life-threatening or require
inpatient hospitalization may be considered serious adverse events (SAEs) when based
on appropriate medical judgment they may jeopardize the subject and may require
medical or surgical intervention to prevent one of the outcomes listed above
Life-threatening means that the subject was in the view of the investigator at immediate risk of
death from the AE as it occurred It does not include an AE that had it occurred in a more severe
form might have caused death
Persistent or significant disabilityincapacity means that the event resulted in permanent or
significant and substantial disruption of the subjectrsquos ability to carry out normal life functions
Causality
A reasonable possibility means the AE may have been caused byrelated to the study drug A
perceived or real lack of efficacy does not satisfy the definition of relatedness
612 Adverse Event (AE) Reporting
For the PANTHER-IPF trial all AEs (serious and nonserious) occurring from randomization
through final study visit (4 weeks after final dose of all study medication) will be recorded on the
AE page of the case report form (CRF)
6121 Serious Adverse Events (SAE) Reporting
For this trial all deaths and all SAEs which occur from randomization through final study visit
must be entered within the EDC system via the SAE eCRF page within 24 hours of the
investigative sitersquos knowledge of the event It is the responsibility of the clinical center
50
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
investigator to provide a causality assessment of the event for each study medications based upon
the information available at the time of the report It is understood that complete information
about the event may not be known at the time the initial report is submitted In the event the EDC
system is not accessible to the site at the time of event reporting investigative sites will complete
and forward a paper back-up SAE form to DCRI Safety Surveillance for processing
DCRI Safety Surveillance
Telephone 1-919-668-8624 or 1-866-668-7799 (toll free)
Fax 1-919-668-7138 or 1-866-668-7138 (toll free)
The investigator must complete and submit follow-up SAE information via the eCRF when
important new or follow-up information (eg final diagnosis outcome results of specific
investigations) becomes available Follow-up information should be submitted according to the
same process used for reporting the initial event as described above All SAEs will be followed
until resolution stabilization or 30 days after the subject has completed the final visit (4 weeks
after the final dose of study medication) whichever occurs first The investigator is responsible
for reporting SAEs to their institutional review board (IRB) per site specific IRB reporting
guidelines
6122 Regulatory Reporting
AEs that are serious study drug related and unexpected will be reported to the regulatory
authorities The DCRI Safety Surveillance medical monitor will perform a medical review of all
SAEs submitted and evaluate for ldquounexpectednessrdquo DCRI Safety Surveillance will prepare
MedWatch reports for those events identified as serious study drug related and unexpected as
determined by Safety Medical Monitor
DCRI Regulatory Services will submit all unexpected study drug-related SAEs as per 21 CFR
32 DCRI Safety Surveillance will provide a safety alert letter to the NHLBI DSMB and DCC
clinical operation (for distribution to sites) within 15 days of initial receipt of the information
51
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Investigators are responsible for promptly reporting these events to their reviewing IRBs
according to site specific IRB reporting guidelines
62 Clinical Medical Monitoring
There will be an unblinded physician at the IPFnet DCC serving as medical monitor The
medical monitor will be available to assist with questions about dosage adjustments of study
medications including discontinuation or resumption of medications
63 Unblinding Procedures
Unblinding of subjects or investigators to subject treatment is strongly discouraged For ongoing
clinical management all subjects should be presumed to be receiving ldquoactiverdquo study drug To
ensure the subjectrsquos safety the study treatment will be dose-adjusted based on laboratory test
results clinical findings and symptoms
The IPFnet DCC medical monitor and PANTHER-IPF co-chairs Drs Ganesh Raghu and
Fernando Martinez will be available to the study physicians to discuss study drug management
on a case-by-case basis Un-blinding will be considered ONLY when the knowledge of subject
treatment assignment is ABSOLUTELY ESSENTIAL for subject safety and after discussion of
the subjectrsquos case with the medical monitor and either Dr Raghu or Dr Martinez Unblinding of
study treatment should be minimized during the conduct of the trial In those cases where it is
felt to be medically necessary the DCC medical officer will communicate directly with the
managing physician to minimize unblinding of study personnel
52
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
7 Study Drug Procedures
At the baseline 15-week 30-week and 45-week study visits subjects will receive a supply of
study drug sufficient to last until the next visit at which study drug will be dispensed
53
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
8 Data Management
81 Hardware and Software Configuration
811 Hardware and Database Software
Data will be stored in an Oracle database system Oracle has advantages of processing efficiency
and smooth linkage with other software systems The application and database will be hosted on
Solaris Unix servers at the IPFnet DCC
812 Statistical Software
SAS will be used as the principal application for the management of analysis data files and
statistical computations S-Plus will be used to provide supplementary functions as needed
813 Access Control and Confidentiality Procedures
Access to databases will be controlled centrally by the IPFnet DCC through user passwords
linked to appropriate privileges This protects the data from unauthorized changes and
inadvertent loss or damage
814 Security
Database and Web servers will be secured by a firewall and through controlled physical access
Oracle has many security features to ensure that any staff member accessing the database has the
proper authority to perform the functions he or she requests of the system Within the secondary
SAS databases Unix group-access control maintains similar security The Sun workstation login
is secured by extensive user-password facilities under Unix
54
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
815 Back-up Procedures
Database back-up will be performed automatically every day and standard IPFnet DCC policies
and procedures will be applied to dictate tape rotation and retention practices
816 Virus Protection
All disk drives that provide network services and all user computers will be protected using
virus-scanning software Standard IPFnet DCC policies will be applied to update these protection
systems periodically through the study
82 Sources of Data
821 Design and Development
The IPFnet DCC will be responsible for development of the electronic case report forms
(eCRFs) development and validation of the clinical study database ensuring data integrity and
training clinical center staff on applicable data management procedures A web-based distributed
data entry model will be implemented This system will be developed to ensure that guidelines
and regulations surrounding the use of computerized systems used in clinical trials are upheld
The remainder of this section provides an overview of the data management plan associated with
this protocol
822 Data Collection Forms
The data collection process consists of direct data entry at the study clinical centers into the EDC
system(s) provided by the DCC A data collection worksheet will be provided to clinical centers
for recording data in the event the EDC system is unavailable Data entry of the eCRFs should
be completed according to the instructions provided and project specific training The
investigator is responsible for maintaining accurate complete and up-to-date records and for
ensuring the completion of the eCRFs for each research participant
55
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
823 Data Acquisition and Entry
Data entry into eCRFs shall be performed by authorized individuals Selected eCRFs may also
require the investigatorrsquos written signature or electronic signature as appropriate Electronic
CRFs will be monitored for completeness accuracy and attention to detail during the study
824 Data Center Responsibilities
The IPFnet DCC will 1) develop a data management plan and will conduct data management
activities 2) provide final eCRFs for the collection of all data required by the study 3) develop
data dictionaries for each eCRF that will comprehensively define each data element 4) conduct
ongoing data monitoring activities on study data 5) monitor any preliminary analysis data
cleanup activities and 6) rigorously monitor final study data clean up
825 Data Editing
Completed data will be entered into the IPFnet DCC automated data acquisition and
management system If incomplete or inaccurate data are found a data clarification request will
be generated and distributed to clinical centers for a response Clinical centers will resolve data
inconsistencies and errors and enter all corrections and changes into the IPFnet DCC automated
data acquisition and management system
826 Training
The training plan for clinical center staff includes provisions for training on assessments eCRF
completion guidelines data management procedures and the use of computerized systems
56
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
9 Study Design and Data Analysis
91 General Analytic Considerations
All primary analyses will be based on intent-to-treat (ITT) principles using all randomized
subjects Baseline factors across groups will be compared using mean (standard deviation) and
median (25th and 75th percentiles) summary measures Kaplan-Meier curves will be used to
display event rates Due to clinical interest in departures from both sides of the null hypothesis
all test statistics will be 2-sided
Reasonable caution needs to be taken when conducting multiple analyses on key clinical
subgroups For subgroup analyses a conservative significance level of 0001 will be used for all
interaction tests Thus subgroup comparisons will be considered exploratory unless the p-value
from the interaction test is smaller than 0001
92 Randomization Blinding and Reporting of Results
A permuted block-randomization scheme will be created with varying block sizes stratified by
clinical center Once a subject has completed the screening and baseline period and evaluation
for inclusionexclusion criteria the randomization process will begin Subjects will be
randomized to receive NAC or matching placebo with equal probability (11) via telephone
contact with a central interactive voice response system (IVRS) using a toll-free randomization
number On the day of randomization after the subject has successfully met all inclusion and
exclusion criteria the investigator or designee will call the central randomization number to
obtain the assigned kit randomization numbers for that subject At each subject visit the
investigator or designee will call the central randomization number to obtain the new kit
randomization numbers for resupply of the subject For resupply of the clinical center the IVRS
will monitor minimal volume of a kit type andor expiration date and will automatically notify
the pharmacy
57
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
The trial results will be reported according to guidelines specified in the CONSORT statement
A flow diagram describing screening recruitment randomization dropout and vital status will
be included in the primary manuscript AEs and efficacy data will be presented for all treatment
groups Adherence dropout and lost to follow-up will be carefully examined across all treatment
groups Analyses of safety will be based on data from all randomized subjects who received at
least one dose of study drug
93 Stratification
Subjects will be distributed to the two treatment arms in a 11 allocation ratio Stratification
blocks will be based on clinical centers
94 Specification of the Primary Analyses
A mixed model repeated measures (MMRM) analysis described in section 95 will be used to
compare differences in the slope of FVC measurements across the treatment groups Response
variables are values of the FVC measured at baseline and every 15 weeks until study completion
Variables in the model will include treatment time and time by treatment age sex race and
height Contrast estimates of differences in slopes of treatment over time (along with confidence
intervals) will be used to estimate the treatment effect The validity of this model in terms of
meeting modeling assumptions will be assessed via standard modeling diagnostics and goodness-
of-fit measures Based on the MMRM framework missing FVC data will not be imputed for the
primary analysis
95 Analysis of Longitudinal Endpoints
A common goal in clinical trials is to specify models that are easily implemented and
reproducible by independent data analysts On the other hand the models should have proper
statistical behavior in terms of low bias and high precision Many common approaches to
longitudinal data analysis including last observation carried forward (LOCF) imputation rely on
the missing completely at random (MCAR) assumption However the MCAR assumption is
58
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
unlikely to hold in many clinical trials because missing data are often related to disease
progression and prognosis A more reasonable assumption missing at random (MAR) specifies
that the complete data distribution can be modeled using only the observed data The likelihood-
based MMRM approach is valid under the more general MAR assumptions These models will
be applied to analyze the longitudinal data secondary endpoints
The advantages of MMRM analysis are that all important characteristics of the model can be preshy
specified standard software can be used to implement the models and results are based on ITT
principles43 In addition the MMRM approach offers superior control of Type I and Type II
errors compared with the LOCF approach
Response variables are values of the PFTs measured at enrollment and every 15 weeks until
study completion and 6MWT values measured at baseline week 30 and week 60 Covariates are
treatment time time by treatment and key baseline risk factors Contrasts (along with
confidence intervals) of treatment by time will be used to estimate the treatment effect
The correlation structure involves multiple pieces including measurement errors random
variation and interindividual variability For the longitudinal data analyses an unstructured
correlation matrix for within-subject errors will be assumed Other correlation structures
including compound symmetry will be examined as needed A careful examination of reasons
for study discontinuation will be conducted to assess the validity of MCAR Sensitivity analyses
will be used to examine the untestable assumption that the observed data violate the MAR
assumption The MMRM models will be implemented using PROC MIXED in SAS
96 Analysis of Binary Time-to-Event and Time-Lagged Endpoints
Regression modeling approaches using either the logistic regression model or Cox proportional
hazards regression model will be employed when appropriate The validity of these models will
be assessed via standard modeling diagnostics and goodness-of-fit measures Estimates of
cumulative frequencies for more general time-lagged responses will be calculated using the
partitioned version of the Bang-Tsiatis estimator44 The partitions will be set at 15-week intervals
59
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
to correspond with the data-collection process Covariate adjusted event rates will be calculated
using inverse probability-weighted regression estimates45
97 Power Analysis
971 Primary Analyses
Based on previously published IPF clinical trials the PL group is expected to experience a drop
in FVC of approximately 020 L over the study period (see Figure 1) The IPFnet Steering Group
determined a clinically important difference would be to preserve the majority of the decline
relative to PL over the study period In particular a treatment effect of 015 L was determined to
be a clinically meaningful difference Potential dropout is a key factor in the proposed study The
drop-out process assumed 5 lost to follow-up after every study visit Only 80 of subjects
were assumed to be followed for the entire study period All models assumed a compound
symmetry structure for the covariance matrix Power calculations were performed using a SAS
IML program for designing repeated measures studies46 Based on preliminary reviews of the
data from the University of Michigan the covariance matrix parameters were estimated at
approximately σ2 = 0757 (variance parameter) and ρ = 0936 (correlation parameter) To be
conservative the power calculations for the primary analysis were performed with parameter
setting of σ2 = 0810 (variance parameter) and ρ = 0925 (correlation parameter)
The power calculations assume a correction for imperfect compliance proposed by Lachin and
Foulkes to allow for 2 noncompliance for each of the treatment arms47 Thus the sample size
of 130 subjects per arm would be reduced to an adjusted sample size of 130(1-002-002)2 =
1198 or 120 subjects per arm
Under the assumed Type I error rate of 005 with a correlation parameter of 0925 and standard
deviation of 090 the difference of 015 L (or 00025 Lweek) shown in Table 6 would have
power of 93
60
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Table 6 Hypothetical Values of Mean FVC (L) Change from Baseline
Week 15 Week 30 Week 45 Week 60
NAC 00125 00250 00375 00500
Placebo 00500 01000 01500 02000
Difference 00375 00750 01125 01500
Abbreviations FVC forced vital capacity PL placebo
972 Power Analysis for Secondary Endpoints
Power calculations for secondary endpoint measurements are shown in Table 7 Standard
deviations are based on unpublished data provided by the University of Michigan The
calculations are based on a 2-sample t-test with Type I error rate set at 005 These calculations
are likely to be conservative because the statistical approach described in section 95 for
analyzing these endpoints will incorporate incomplete observations as well as intermediate data
points
Table 7 Detectable Differences in Treatment Means for Selected Endpoint Measurements
Secondary Endpoints Std Dev
of the Baseline Score
Detectable Difference for 80 Power
Std Dev of the Change Score
Difference Detectable for
80 Power
DLCOpred 166 58 91 32
6MWT Area Under the Desaturation Curve
219 76 175 61
6MWT Distance to Desaturation 224 78 315 110
6MWT Minutes Walked 210 073 205 071
Abbreviations Std Dev standard deviation DLCOpred diffusing capacity of the lung for carbon monoxide percent predicted 6MWT 6-minute walk test
61
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
10 Study Administration
101 Cooperative Agreement Mechanism
The administrative and funding mechanism used to undertake this project is a ldquocooperative
agreementrdquo (U01) which is an assistance mechanism Under the cooperative agreement the
NHLBI assists supports andor stimulates the project and is substantially involved with
investigators in conducting the study by facilitating performance of the effort in a ldquopartnerrdquo role
The NHLBI project scientist serves on the IPFnet Steering Group and he or another NHLBI
scientist may serve on other project committees when appropriate At the same time however
NHLBI does not assume a dominant role direction or prime responsibility for this research
program
As described below governance of the project is conducted through the IPFnet Steering Group
Principal investigators have lead responsibilities in all aspects of their trials and the project
including any modification of trial designs conduct of the trials quality control data analysis
and interpretation preparation of publications and collaboration with other investigators unless
otherwise provided for by the IPFnet Steering Group
PIs retain custody of and have primary rights to their center-specific and collaborative data
subject to government rights-of-access consistent with current Health amp Human Services (HHS)
Public Health Service (PHS) and National Institutes of Health policies The protocols and
governance policies call for the continual submission of data centrally to the IPFnet DCC for the
collaborative database which at a minimum will contain the key variables selected by the IPFnet
Steering Group for standardization across all clinical centers the submission of copies of the
collaborative datasets to each PI upon completion of the project procedures for data analysis
reporting and publication and procedures to protect and ensure the privacy of medical and
genetic data and records of individuals The NHLBI project scientist on behalf of the NHLBI
will have the same access privileges and responsibilities regarding the collaborative data as the
other members of the Steering Group
62
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
PIs are also encouraged to publish and to publicly release and disseminate results data and other
products of the project concordant with the project protocols and governance and the approved
plan for making data and materials available to the scientific community and to the NHLBI
However during the 3 years after the ending date of NHLBI project support unpublished data
unpublished results data sets not previously released and other study materials or products are
to be made available to any third party only with the approval of the IPFnet Steering Group
Upon completion of the project PIs are expected to put their intervention materials and
procedure manuals into the public domain andor make them available to other investigators
according to the approved plan for making data and materials available to the scientific
community and the NHLBI for the conduct of research at no charge other than the costs of
reproduction and distribution
The NHLBI reserves the right to terminate or curtail the project (or an individual award) in the
event of (a) failure to develop or implement mutually agreeable collaborative measurement
subject eligibility and data management sections of the protocols (b) substantial shortfall in
subject recruitment follow-up data reporting or quality control or other major breach of
protocol (c) substantive changes in the agreed-upon protocols with which NHLBI cannot
concur (d) reaching a major project outcome with persuasive statistical significance
substantially before schedule or (e) human subject ethical issues that may dictate a premature
termination
Any disagreement that may arise in scientificprogrammatic matters (within the scope of the
award) between award recipients and the NHLBI may be brought to arbitration An arbitration
panel will be composed of 3 membersmdash1 selected by the IPFnet Steering Group (with the
NHLBI member not voting) or by the individual PI in the event of an individual disagreement a
second selected by NHLBI and the third selected by the other 2 members This special
arbitration procedure in no way affects the PIrsquos right to appeal an adverse action that is otherwise
appealable in accordance with the PHS regulations at 42 CFR part 50 Subpart D and HHS
63
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
regulation at 45 CFR part 16 or the rights of the NHLBI under applicable statutes regulations
and terms of the award
102 IPFnet Steering Group
The IPFnet Steering Group is the main governing body of the project It is composed of the PIs
of the clinical centers the PI of the DCC and the NHLBI project scientist The clinical centers
the IPFnet DCC and the NHLBI each have 1 vote on the IPFnet Steering Group All decisions
are determined by majority vote
All major scientific decisions are determined by the IPFnet Steering Group It assumes overall
responsibility for the design and conduct of the trial It appoints (and disbands) committees and
subcommittees as the need arises designs approves and implements the study protocols
oversees the development of the MOOP monitors subject recruitment and treatment delivery
evaluates data collection and management oversees quality assurance procedures and
implements changes and enhancements to the study as required It also has primary responsibility
for facilitating the conduct of the trials and reporting the projectrsquos results
103 Data and Safety Monitoring Board
The NHLBI will establish a DSMB in accordance with established policies (see
httpwwwnhlbinihgovfundingpoliciesdsmb_insthtm) to ensure data quality and subject
safety and to provide independent advice to the NHLBI regarding progress and the
appropriateness of study continuation
104 Recommendations on Interim Monitoring of Efficacy Safety and Futility
First and foremost the role of the DSMB will be to review subject safety and trial conduct at
periodic points during the study The DSMB may require analyses of the primary endpoint
results for comparing the benefit and risks of treatment strategies The benefit of collecting
additional data on key secondary endpoints with extended follow-up and establishing a robust
64
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
evidence base for determining a standard of care will need to be carefully considered before
early termination of one or more treatment arms After careful consideration the IPFnet Steering
Group recommends conservative thresholds for the early examinations of the safety and efficacy
data
The DSMB will be expected to meet approximately every 6 months until trial completion to
review safety and toxicity data The DSMB may recommend stopping the study based on these
reviews Because the DSMB could stop the trial for safety concerns as well as for a large
efficacy benefit there could be multiple opportunities to reject the null hypothesis (no difference
in event rates between the PL and NAC groups) A Bonferroni approximation will be applied
during the one planned interim analysis for efficacy
Before locking the database a statistical analysis plan (SAP) will be developed to provide
complete details on the statistical analysis The SAP will include the specifics for how and when
the DSMB will be notified for AEs The IPFnet DCC will deliver to the DSMB all FDA-defined
AEs at 3-month intervals The IPFnet DCC will prepare narrative SAE reports in real time for
DSMB review including recommendations and analysis of similar events for each SAE
submitted to the FDA
65
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
11 Investigator and Sponsor Obligations
111 Monitoring
All monitoring activities for US clinical centers will be performed in accordance with DCRI
standard operating procedures Information regarding the types of visits will be outlined in the
PANTHER-IPF MOOP
112 Cost and Payment
There will be no cost to subjects enrolled in this trial Study-related procedures will be paid for
by the IPFnet
Subjects may be eligible for reimbursement for travel to the clinical center Details of payment
will be explained to each subject during the consent process
113 Confidentiality and Health Insurance Portability and Accountability Act
Considerations
Subject confidentiality will be protected throughout the study All subject data will be kept
strictly confidential and no subject-identifying information will be released to anyone outside
the project Confidentiality will be assured through several mechanisms First each subject will
be assigned an anonymous study ID which will then be used on all study forms Second any
study forms blood samples and paper records that contain subject information (eg address lists
phone lists) will be kept at the clinical centers in secured locked areas coded by number Once
blood is collected there will be no subject identifiers placed on blood samplesmdashonly the study
ID number and the date of sample collection Third access to all subject data and information
including laboratory specimens will be restricted to authorized personnel In the case of
computerized data this restricted access will be assured through user logon IDs and password
protection
66
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
At the IPFnet DCC only authorized personnel will have access to the data files containing study
data Security will be assured through user logon IDs passwords and appropriate access
privileges All study subjects will be identified only by their IPFnet ID numbers and no personal
identifying information such as name address or Social Security number will be entered into
the IPFnet DCC database Any subject-specific data reported to the IPFnet Steering Group will
be identified only by the IPFnet ID number
Finally subjects will not be identified by name in any reports or publications nor will the data
be presented in such a way that the identity of individual subjects can be inferred Analysis files
created for further study by the scientific community will have no subject identifiers These data
files will be created in accordance with the Ancillary Studies and Publication Policy of the
IPFnet
114 Informed Consent Procedures
All IPFnet subjects will provide written informed consent using procedures reviewed and
approved by each clinical centerrsquos IRB Informed consent will be undertaken by study personnel
in-person with the subject The subject has the option of declining further participation in the
study at that point No further study procedures will be conducted until the signed documents
have been provided to the IPFnet clinical center
115 Institutional Review Boards
Before initiating this study the protocol clinical center-specific informed consent forms Health
Insurance Portability and Accountability Act (HIPAA) forms recruitment materials and other
relevant information will be reviewed by a properly constituted IRB at each participating clinical
center A copy of the signed and dated IRB approval at each clinical center will be retrieved prior
to or during the site initiation visit and archived at the IPFnet DCC Any amendments to the
protocol other than simple administrative and typographical changes must be approved by each
IRB before they are implemented The clinical centers will seek annual renewals of their IRB
approvals in accordance with local procedures
67
__________________________________________ ________________
__________________________________________
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
12 Investigator Agreement
I have read the foregoing protocol PANTHER-IPF and agree that it contains all necessary
details for carrying out this study I will conduct the study as outlined herein and will complete
the study within the time designated
I will provide copies of the protocol and all pertinent information to all individuals responsible to
me who assist in the conduct of this study I will discuss this material with them to ensure they
are fully informed regarding the drug and the conduct of the study
I will fulfill all responsibilities for submitting pertinent information to the local IRB if
applicable that is responsible for this study
I further agree that NHLBI andor DCRI will have access to any source documents from which
eCRF information may have been generated
Signature of Principal Investigator Date
Name of Principal Investigator (printed or typed)
Protocol version date May 19 2009
Protocol Amendment 1 version date May 28 2010
Protocol Amendment 2 version date December 6 2011
68
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
13 References
1 Raghu G Brown KK Bradford WZ et al A placebo-controlled trial of interferon gamma-1b in patients with idiopathic pulmonary fibrosis N Engl J Med 2004350125-33 2 King TE Jr Safrin S Starko KM et al Analyses of efficacy end points in a controlled trial of interferon-gamma1b for idiopathic pulmonary fibrosis Chest 2005127171-7 3 Flaherty KR Thwaite EL Kazerooni EA et al Radiological versus histological diagnosis in UIP and NSIP survival implications Thorax 200358143-8 4 Wells AU Desai SR Rubens MB et al Idiopathic pulmonary fibrosis a composite physiologic index derived from disease extent observed by computed tomography Am J Respir Crit Care Med 2003167962-9 5 Raghu G Freudenberger TD Yang S et al High prevalence of abnormal acid gastroshyoesophageal reflux in idiopathic pulmonary fibrosis Eur Respir J 200627136-42 6 Kinnula VL Focus on antioxidant enzymes and antioxidant strategies in smoking related airway diseases Thorax 200560693-700 7 Coultas DB Zumwalt RE Black WC Sobonya RE The epidemiology of interstitial lung diseases Am J Respir Crit Care Med 1994150967-72 8 Raghu G Weycker D Edelsberg J Bradford WZ Oster G Incidence and prevalence of idiopathic pulmonary fibrosis Am J Respir Crit Care Med 2006174810-6 9 Olson AL Swigris JJ Lezotte DC Norris JM Wilson CG Brown KK Mortality from pulmonary fibrosis increased in the United States from 1992 to 2003 Am J Respir Crit Care Med 2007176277-84 10 Mannino DM Etzel RA Parrish RG Pulmonary fibrosis deaths in the United States 1979shy1991 An analysis of multiple-cause mortality data Am J Respir Crit Care Med 19961531548shy52 11 Hubbard R Johnston I Coultas DB Britton J Mortality rates from cryptogenic fibrosing alveolitis in seven countries Thorax 199651711-6 12 Johnston I Britton J Kinnear W Logan R Rising mortality from cryptogenic fibrosing alveolitis Bmj 19903011017-21 13 Raghu G Collard HR Egan JJ et al An official ATSERSJRSALAT statement idiopathic pulmonary fibrosis evidence-based guidelines for diagnosis and management Am J Respir Crit Care Med 2011183788-824 14 (USA) FDA FDA Public Health Advisory Interferon gamma-1b (marketed as Actimmune) In 2007 15 King TE Jr Pardo A Selman M Idiopathic pulmonary fibrosis Lancet 2011 16 Raghu G Brown KK Costabel U et al Treatment of idiopathic pulmonary fibrosis with etanercept an exploratory placebo-controlled trial Am J Respir Crit Care Med 2008178948shy55 17 Malouf MA Hopkins P Snell G Glanville AR An investigator-driven study of everolimus in surgical lung biopsy confirmed idiopathic pulmonary fibrosis Respirology 201116776-83 18 King TE Jr Behr J Brown KK et al BUILD-1 a randomized placebo-controlled trial of bosentan in idiopathic pulmonary fibrosis Am J Respir Crit Care Med 200817775-81 19 Richeldi L Costabel U Selman M et al Efficacy of a tyrosine kinase inhibitor in idiopathic pulmonary fibrosis N Engl J Med 20113651079-87
69
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
20 Borok Z Buhl R Grimes GJ et al Effect of glutathione aerosol on oxidant-antioxidant imbalance in idiopathic pulmonary fibrosis Lancet 1991338215-6 21 Meyer A Buhl R Magnussen H The effect of oral N-acetylcysteine on lung glutathione levels in idiopathic pulmonary fibrosis Eur Respir J 19947431-6 22 Behr J Maier K Degenkolb B Krombach F Vogelmeier C Antioxidative and clinical effects of high-dose N-acetylcysteine in fibrosing alveolitis Adjunctive therapy to maintenance immunosuppression Am J Respir Crit Care Med 19971561897-901 23 Cantin AM North SL Fells GA Hubbard RC Crystal RG Oxidant-mediated epithelial cell injury in idiopathic pulmonary fibrosis J Clin Invest 1987791665-73 24 Waghray M Cui Z Horowitz JC et al Hydrogen peroxide is a diffusible paracrine signal for the induction of epithelial cell death by activated myofibroblasts Faseb J 200519854-6 25 Larios JM Budhiraja R Fanburg BL Thannickal VJ Oxidative protein cross-linking reactions involving L-tyrosine in transforming growth factor-beta1-stimulated fibroblasts J Biol Chem 200127617437-41 26 Kinnula VL Fattman CL Tan RJ Oury TD Oxidative stress in pulmonary fibrosis a possible role for redox modulatory therapy Am J Respir Crit Care Med 2005172417-22 27 Meyer A Buhl R Kampf S Magnussen H Intravenous N-acetylcysteine and lung glutathione of patients with pulmonary fibrosis and normals Am J Respir Crit Care Med 19951521055-60 28 Behr J Degenkolb B Krombach F Vogelmeier C Intracellular glutathione and bronchoalveolar cells in fibrosing alveolitis effects of N-acetylcysteine Eur Respir J 200219906-11 29 Bando M Hosono T Mato N et al Long-term efficacy of inhaled N-acetylcysteine in patients with idiopathic pulmonary fibrosis Intern Med 2010492289-96 30 Demedts M Behr J Buhl R et al High-dose acetylcysteine in idiopathic pulmonary fibrosis N Engl J Med 20053532229-42 31 Toma TP Bhowmik A Rajakulasingam R Acetylcysteine in pulmonary fibrosis N Engl J Med 20063541086-9 author reply -9 32 Hunninghake GW Antioxidant therapy for idiopathic pulmonary fibrosis N Engl J Med 20053532285-7 33 Flaherty KR Mumford JA Murray S et al Prognostic implications of physiologic and radiographic changes in idiopathic interstitial pneumonia Am J Respir Crit Care Med 2003168543-8 34 Latsi PI du Bois RM Nicholson AG et al Fibrotic idiopathic interstitial pneumonia the prognostic value of longitudinal functional trends Am J Respir Crit Care Med 2003168531-7 35 Collard HR King TE Jr Bartelson BB Vourlekis JS Schwarz MI Brown KK Changes in clinical and physiologic variables predict survival in idiopathic pulmonary fibrosis Am J Respir Crit Care Med 2003168538-42 36 Jegal Y Kim DS Shim TS et al Physiology is a stronger predictor of survival than pathology in fibrotic interstitial pneumonia Am J Respir Crit Care Med 2005171639-44 37 Martinez FJ Safrin S Weycker D et al The clinical course of patients with idiopathic pulmonary fibrosis Ann Intern Med 2005142963-7 38 Hull JH Acetylcysteine in pulmonary fibrosis N Engl J Med 20063541089-91 author reply -91
70
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
39 Flaherty KR King TE Jr Raghu G et al Idiopathic interstitial pneumonia what is the effect of a multidisciplinary approach to diagnosis Am J Respir Crit Care Med 2004170904shy10 40 Raghu G Johnson WC Lockhart D Mageto Y Treatment of idiopathic pulmonary fibrosis with a new antifibrotic agent pirfenidone results of a prospective open-label Phase II study Am J Respir Crit Care Med 19991591061-9 41 Hunninghake GW Lynch DA Galvin JR et al Radiologic findings are strongly associated with a pathologic diagnosis of usual interstitial pneumonia Chest 20031241215-23 42 Lynch D Godwin J Safrin S et al High-resolution computed tomography in idiopathic pulmonary fibrosis diagnosis and prognosis Am J Respir Crit Care Med 2005172488-93 43 Mallinckrodt CH Watkin JG Molenberghs G Carroll RJ Choice of the primary analysis in longitudinal clinical trials Pharmaceutical Statistics 20043161-9 44 Bang H Tsiatis A Estimating medical costs with censored data Biometrika 200087329shy43 45 Lin DY Regression analysis of incomplete medical cost data Stat Med 2003221181-200 46 Rochon J Application of GEE procedures for sample size calculations in repeated measures experiments Stat Med 1998171643-58 47 Lachin JM Foulkes MA Evaluation of sample size and power for analyses of survival with allowance for nonuniform patient entry losses to follow-up noncompliance and stratification Biometrics 198642507-19
71
- PANTHER-IPFPREDNISONE AZATHIOPRINEAND N-ACETYLCYSTEINEA STUDY THAT EVALUATES RESPONSE INIDIOPATHIC PULMONARY FIBROSIS
-
- Protocol Summary
- Table of Contents
- List of Tables
- List of Figures
- List of Abbreviations
- 1 Summary
- 2 Hypotheses and Specific Aims
-
- 21 Null Hypothesis
- 22 Specific Aim 1
- 23 Specific Aim 2
- 24 Prespecified Subgroups of Interest
-
- 3 Background and Significance
-
- 31 Idiopathic Pulmonary Fibrosis is the Most Common Interstitial Lung Disease
- 32 Rationale for Placebo Control
- 33 Rationale for N-acetylcysteine
- 35 Rationale for N-acetylcysteine as a Stand-alone Therapy
- 36 Rationale for the Study Design and Primary Endpoint
- 37 Rationale for Blinding of Treatments
-
- 4 Methods
-
- 41 Inclusion Criteria
- 42 Diagnosis of IPF
- 43 Exclusion Criteria
- 44 Study Design and Study Visit
- 45 Dose Justification
- 46 Contraindications Precautions and Side Effects of Study Medications
- 47 Recruitment Procedures
- 48 Study Procedures
- 49 Concomitant Medications
- 410 Laboratory Testing
- 411 Blinding of Study Drugs
-
- 5 Study Endpoints
-
- 51 Primary Study Endpoint
- 52 Secondary Study Endpoints
-
- 6 Safety Evaluations and Procedures
-
- 61 Adverse Events
- 62 Clinical Medical Monitoring
- 63 Unblinding Procedures
-
- 7 Study Drug Procedures
- 8 Data Management
-
- 81 Hardware and Software Configuration
- 82 Sources of Data
-
- 9 Study Design and Data Analysis
-
- 91 General Analytic Considerations
- 92 Randomization Blinding and Reporting of Results
- 93 Stratification
- 94 Specification of the Primary Analyses
- 95 Analysis of Longitudinal Endpoints
- 96 Analysis of Binary Time-to-Event and Time-Lagged Endpoints
- 97 Power Analysis
-
- 10 Study Administration
-
- 101 Cooperative Agreement Mechanism
- 102 IPFnet Steering Group
- 103 Data and Safety Monitoring Board
- 104 Recommendations on Interim Monitoring of Efficacy Safety and Futility
-
- 11 Investigator and Sponsor Obligations
-
- 111 Monitoring
- 112 Cost and Payment
- 113 Confidentiality and Health Insurance Portability and Accountability ActConsiderations
- 114 Informed Consent Procedures
- 115 Institutional Review Boards
-
- 12 Investigator Agreement
- 13 References
-

PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
List of Tables Table 1 Operating Characteristics of Local HRCT Review for Diagnosis of UIP (24)
Table 2 Combining HRCT and Pathology Interpretations to Determine if IPF is Present (25)
Table 3 Schedule of Assessments (34)
Table 4 Side Effects of NAC (40)
Table 5 Final Diagnoses in Evaluation of Suspected Acute Exacerbations (46)
Table 6 Hypothetical Values of Mean FVC (L) Change from Baseline (61)
Table 7 Detectable Differences in Treatment Means for Selected Endpoint Measurements (61)
List of FiguresFigure 1 Changes in Forced Vital Capacity from Baseline in Prior IPF Clinical Trials (19)
Figure 2 Diagnosis of Idiopathic Pulmonary Fibrosis in the IPFnet (22)
Figure 3 Pathology Flow Chart Surgical Lung Biopsy Diagnosis (23)
Figure 4 Acute Exacerbation Flow Chart (47)
7
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
List of Abbreviations
6MWT 6-minute walk test
A-aPO2 alveolar-arterial PO2 difference
ABG arterial blood gas
AE adverse event
AEx acute exacerbation
AG albuminglobulin
ALT alanine aminotransferase
AST aspartate aminotransferase
ATS American Thoracic Society
AZA azathioprine
BAL bronchoalveolar lavage
BUN blood urea nitrogen
CBC complete blood count
cGMP Current Good Manufacturing Practice
CPI Composite Physiologic Index
CPK creatine phosphokinase
CT computed tomography
DCC Data Coordinating Center
DCRI Duke Clinical Research Institute
8
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
DLCO diffusing capacity of the lung for carbon monoxide
DLCOpred diffusing capacity of the lung for carbon monoxide percent predicted
DSMB data and safety monitoring board
eCRF Electronic case report form
ERS European Respiratory Society
FDA Food and Drug Administration (US)
FEV1 forced expiratory volume in 1 second
FSH follicle-stimulating hormone
FVC forced vital capacity
FVCpred forced vital capacity percent predicted
GGT gamma glutamyl transferase
GSH glutathione
HAD Hospital Anxiety and Depression
HHS Health amp Human Services (US Dept of)
HIPAA Health Insurance Portability and Accountability Act
HRCT high-resolution computed tomography
IBW ideal body weight
ICE CAP Investigating Choice Experiments for Preferences of Older People Capability Instrument
ILD interstitial lung disease
IPF idiopathic pulmonary fibrosis
9
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
IPFnet Idiopathic Pulmonary Fibrosis Clinical Research Network
IRB institutional review board
ITT intent to treat
IV intravenous
IVRS interactive voice response system
LDH lactate dehydrogenase
LFT liver function test
LOCF last observation carried forward
LSD Least Significant Difference
MAR missing at random
MCAR missing completely at random
MMRM mixed model repeated measures
MOOP manual of operating procedures
NAC N-acetylcysteine
NHLBI National Heart Lung and Blood Institute (US)
NIH National Institutes of Health (US)
NSIP nonspecific interstitial pneumonia
PaO2 partial pressure of arterial oxygen
PCP primary care provider
PFT pulmonary function test
10
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
PHS Public Health Service (US)
PI principal investigator
PL placebo
PLT platelet
PRED prednisone
QOL quality of life
SAE serious adverse event
SAP statistical analysis plan
SGRQ St Georgersquos Respiratory Questionnaire
SpO2 oxygen saturation by pulse oximetry
TPMT thiopurine methyl transferase
UCSD SOBQ University of California at San Diego Shortness of Breath Questionnaire
UIP usual interstitial pneumonia
ULN upper limit of normal
USP United States Pharmacopoeia
VC vital capacity
WBC white blood cell
11
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
PREDNISONE AZATHIOPRINE AND N-ACETYLCYSTEINE A STUDY
THAT EVALUATES RESPONSE IN IDIOPATHIC PULMONARY FIBROSIS
1 Summary
There are currently no drug therapies that have proven to be effective in the treatment of idiopathic pulmonary
fibrosis (IPF) Previous clinical drug trials have been difficult to interpret due to lack of true placebo (PL)
controls or other methodological concerns Clinical efficacy of immunosuppressive therapies and agents that
reduce oxidative stress remains controversial The IPF Clinical Research Network (IPFnet) is conducting a
randomized double-blind placebo-controlled trial designed to assess the safety and efficacy of
N-acetylcysteine (NAC) as monotherapy in subjects with mild or moderate IPF
The study initially employed a 3-arm design with 111 randomization to NAC azathioprine (AZA)-prednisone
(PRED)-NAC and PL with each subject to be treated up to a maximum of 60 weeks followed by a tapering of
PREDPL and a 4-week period for safety evaluation Approximately 390 subjects who have mild to moderate
IPF (defined as forced vital capacity percent predicted [FVCpred] ge 50 and diffusing capacity of the lung
for carbon monoxide percent predicted [DLCOpred] 30) diagnosed within the past 48 months were to be
enrolled
At the pre-specified interim analysis the DSMB recommended termination of the prednisone-azathioprine-
NAC arm of the study No additional patients will be randomized to that arm However the NAC and placebo
arms remain open for enrollment and we will enroll approximately 130 subjects in each arm (inclusive of the
subjects enrolled at the time of the interim analysis) Follow up for subjects enrolled into the two arms will
continue for 60 weeks
The primary endpoint is the change in longitudinal measurements of FVC over the study period The primary
goal of this study to establish an evidence-based standard of care and clarify myths from facts for
pharmacotherapy of IPF has been met in part by demonstrating that the widely used triple therapy was harmful
to patients with IPF (NHLBI press release Oct 21 2011) To determine the potential therapeutic benefits of
NAC alone the study will continue to enroll patients as a two-arm double-blind placebo-controlled study from
this point on (NAC vs placebo) as recommended by the DSMB following the pre-specified interim analysis
12
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
2 Hypotheses and Specific Aims 21 Null Hypothesis
Treatment with NAC will provide the same efficacy as PL as measured by longitudinal changes in FVC
22 Specific Aim 1
This study is designed to assess the safety and efficacy of NAC in subjects with newly diagnosed IPF
23 Specific Aim 2
Secondary goals of this study are to assess differences between treatment groups for the following
1 Mortality
2 Time to death
3 Frequency of acute exacerbations (AExs)
4 Frequency of maintained FVC response
5 Time-to-disease progression
6 Change in DLCO
7 Change in Composite Physiologic Index (CPI)
8 Change in resting alveolar-arterial oxygen gradient
9 Change in 6-minute walk test (6MWT) distance
10 Change in 6MWT oxygen saturation area under the curve
11 Change in 6MWT distance to desaturation lt 80
12 Change in 6MWT minutes walked
13 Changes in health status as measured by the SF-36 EuroQol and St Georgersquos Respiratory
Questionnaire (SGRQ)
14 Changes in dyspnea as measured by the University of California at San Diego Shortness of Breath
Questionnaire (UCSD SOBQ)
15 Frequency and types of adverse events (AEs)
16 Frequency and types of respiratory complications both infectious and noninfectious
17 Frequency of hospitalizations both all-cause and respiratory-related
13
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
24 Prespecified Subgroups of Interest
Treatment effects will be estimated and compared within key subgroups
Higher enrollment FVC12
Typical vs atypical high-resolution computed tomography (HRCT) reading at baseline3
Recent vs more remote diagnosis (time from initial diagnosis of IPF le 1 year and gt 1 year)
Lower CPI score at enrollment4
Medical therapy for gastroesophageal reflux5
Ethnic background
Sex
Smoking history (current or ex-smoker vs never smoker) given potential impact on oxidant status6
Presence of emphysema gt 25 on HRCT
14
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
3 Background and Significance
31 Idiopathic Pulmonary Fibrosis is the Most Common Interstitial Lung Disease
IPF is the most common interstitial lung disease (ILD) of unknown etiology The current incidence and
prevalence of IPF in the United States are not known A 1994 study of a population-based registry of subjects in
Bernalillo County New Mexico USA estimated an incidence of 107 cases per 100000 per year for males and
74 cases per 100000 per year for females the prevalence of IPF was estimated at 20 per 100000 for males and
13 per 100000 for females7 Extrapolating from a large healthcare claims database a more recent review
estimated the prevalence of IPF in the United States at 427 per 100000 (incidence estimated at 163 per
100000 per year)8 Recent epidemiological studies indicate increasing mortality rates from IPF in the United
States and other industrialized nations9-12
Approximately two-thirds of subjects with IPF are over the age of 60 at the time of presentation and the
incidence increases with age13 IPF has no distinct geographical distribution and predilection by race or
ethnicity has not been identified13 Individual subjects may remain relatively stable for prolonged periods
experience very slow declines in lung function with progression of radiographic abnormalities for a period of
months to years or experience more rapid declines and subsequent death Only 20 to 30 of IPF patients
survive for 5 years following diagnosis
There is currently no proven effective pharmacological treatment for IPF13 Anti-inflammatory and
immunosuppressive agents have been the traditional approach to the management of patients with IPF Based
on the results of the interim analysis of the PANTHER-IPF trial this lsquotraditional approachrsquo will be aborted
However it remains unknown if NAC alone will prove beneficial in IPF patients The primary goal of the
modified study is to establish an evidence-based standard of care and clarify the role of this specific antioxidant
pharmacotherapy for IPF
32 Rationale for Placebo Control
IPF is a disorder for which there is no proven efficacious therapy A major objective of this trial is to test to the
greatest degree possible a proposed standard of care for patients with IPF The current traditional therapy
15
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
employs immunosuppressive and corticosteroid drugs Interim review of the original PANTHER-IPF study has
documented increased adverse events and lack of efficacy for AZA-PRED-NAC compared to placebo
suggesting that this therapeutic approach should not be employed Whether this applies to NAC alone which
has been advocated by international societies has not been proven in well-designed well-powered clinical
trials The recommendations made in the recently published evidence guidelines for NAC monotherapy was
weak based on low quality13 Thus this continued clinical trial randomizing patients to receive NAC or placebo
is pivotal and will answer the important question of the potential therapeutic benefits of NAC monotherapy with
grade A evidence In this prospective randomized clinical trial the inclusion of a PL arm is therefore vital to
adequately test the benefits of NAC in well-characterized subjects with IPF
If NAC has no true efficacy then its role as standard of care will be refuted If a benefit compared with PL is
confirmed it will establish a benchmark against which future novel therapies for IPF will be safely compared
As there is no currently accepted therapy for IPF there is an increasing body of published literature supporting
the concept of no treatment as the ldquobest carerdquo option for IPF13
Post hoc analyses of PL-controlled trials suggest that subjects with milder disease may be more amenable to
therapy12 It is notable that a recent international prospective randomized trial of interferon-gamma for IPF
also included a PL arm the study was terminated early by the data and safety monitoring board (DSMB) due to
lack of treatment effect1415 This underscores the belief that a proven effective therapy for IPF does not
currently exist and that true placebo-controlled trials remain the gold standard Similarly recently completed
trials of etanercept everolimus bosentan and BIPF 1120 in IPF have included PL-treated arms16-19 In three of
these trials the treated subjects showed little if any objective improvement Based on this evidence and the
current status of IPF therapy and therapeutic trials we believe that clinicians and subjects will continue to enroll
in a PL-controlled study
33 Rationale for N-acetylcysteine
NAC is a derivative of the amino acid L-cysteine NAC has been shown to augment levels of the naturally
occurring antioxidant glutathione (GSH ) (glutathione γ-glutamyl cysteinyl glycine) both in vitro and in
vivo2021 GSH is present in all eukaryotic cells and may play an important role in protecting alveolar epithelial
cells against oxidant injury The concentration of GSH in the bronchoalveolar lavage (BAL) fluid in patients
16
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
with IPF is markedly diminished compared with normal subjects This GSH deficiency may be corrected by
exogenous administration of NAC2122
There is evidence of enhanced production of oxidants in an IPF lung Both inflammatory cells and
myofibroblasts derived from patients with IPF generate increased amounts of extracellular oxidants including
hydrogen peroxide2324 Secretion of hydrogen peroxide by activated myofibroblasts may induce the death of
adjacent lung epithelial cells by paracrine mechanisms24 Additionally generation of oxidants by myofibroblasts
induces oxidative crosslinking of extracellular matrix proteins25 a potential mechanism for aberrant matrix
remodeling Thus an oxidant-antioxidant imbalance exists in the lungs of IPF patients26 NAC may confer
protection against this imbalance by augmenting GSH levels in addition to its more direct free-radical
scavenging activity
Intravenous (IV) NAC therapy has been shown to increase total BAL GSH in 8 IPF subjects27 Oral NAC (600
mg 3 times per day) has been shown to decrease markers of oxidant injury and improve both total and reduced
GSH levels in the epithelial lining fluid of subjects with IPF in a small uncontrolled study22 pulmonary
function improved modestly with therapy A similar study in 18 IPF subjects confirmed increased intracellular
GSH concentration after 12 weeks of NAC (600 mg 3 times per day)2228 no clinical correlates were reported
Inhaled NAC was suggested to improve pulmonary function in an open label study29
35 Rationale for N-acetylcysteine as a Stand-alone Therapy
Results of a double-blind multi-center European clinical trial of 150 IPF subjects testing combinations of AZAshy
PRED vs AZA-PRED-NAC have been reported30 NAC added to AZA-PRED (ldquoconventional therapyrdquo) had a
significant positive effect on DLCO (p lt 0005) and vital capacity (VC) (p lt 005) at the end of 1 year30 The
recent ATSERS position statement after much discussion concluded that NAC alone should not be considered
in the majority of patients with IPF without additional data from well-designed studies
The interpretation of these data has been quite controversial Some have suggested that the magnitude of the
treatment effect although statistically significant is modest31 Others have suggested that NAC may be
modulating potential toxic effects of AZA-PRED alone32 supporting the investigation of NAC as stand-alone
therapy
17
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
The IPFnet is now completing the PANTHER-IPF trial with a 11 randomization (NAC vs placebo) and a
simple practical feasible and scientifically rational design that will establish standard of care with NAC for
IPF based on a currently available therapeutic agent and the existing data to support its use We anticipate that
all future clinical trials of novel therapeutic agents will be tested against this to-be-established standard of care
36 Rationale for the Study Design and Primary Endpoint
The optimal study design of a therapeutic trial in IPF would include survival as a primary endpoint The
published results of the IFN-γ 1b Phase 3 (GIPF-001) trial suggested a survival benefit in subjects with milder
disease in retrospective analyses1 although the trial was underpowered to address this question This was likely
related to the limited mortality in the PL arm of the study which included IPF subjects with mild to moderate
disease This study documents that an IPF study powered to improve survival in a patient population with mild
disease requires a larger sample size andor duration of study In fact the recently aborted Phase 3 IFN-γ 1b
(GIPF-007 INSPIRE) study was a survival-based study and recruited more than 800 subjects at 75 centers
worldwide1415 As such within the context of the current IPFnet trial survival is an impractical primary
endpoint variable
Several groups have published data defining an appropriate surrogate outcome variable a 10 decrement in
FVC during 6 to 12 months is a powerful predictor of survival in IPF33-36 Furthermore additional evidence
suggests a similar predictive ability for a 10 decrement in FVC during 3 months of follow-up37 With strong
supportive evidence of FVC progression being related to mortality on a per-subject basis this study will use
FVC changes in liters between treatment groups as the primary endpoint Previously published IPF studies have
shown a steady decline in FVC (and FVCpred) among control group subjects230 The GIPF-001 study
suggested a 48-week decrease in FVC of 016 L in the PL-treated subjects The IFIGENIA study demonstrated
a decline in FVC of approximately 019 L over 52 weeks in the subjects randomized to the control treatment
Figure 1 depicts the change in FVC for control groups from previously published IPF studies38 Based on these
data we expect that the PL group will have a decline of 020 L over the 60-week study period The IPFnet
Steering Group determined that a clinically meaningful improvement would be the preservation of the majority
of the 020-L FVC decline Therefore a mean treatment difference of 015 L in mean FVC over the 60-week
study period was determined to be a clinically meaningful difference
18
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Δ f
rom
bas
elin
e (i
n L
)
01
005
0
-005
-01
-015 Projected Δ for placebo
-02
-025
-019
-016
-013 Pirfenidone GIPF001
NAC
Placebo
4 8 12 16 20 24 28 32 36 40 44 48 52 56 60
Week
Figure 1 Changes in FVC From Baseline in Prior IPF Clinical Trials
Recent data suggest that various patient subgroups would be expected to potentially exhibit differential response
to therapy These parameters will be used to a priori separate patients by a series of baseline characteristics
including
1 Higher enrollment FVC12
2 Typical vs atypical high-resolution computed tomography (HRCT) reading at baseline3
3 Recent vs more remote diagnosis (time from initial diagnosis of IPF le 1 year and gt 1 year)
4 Lower CPI score at enrollment4
5 Medical therapy for gastroesophageal reflux5
6 Ethnic background
7 Sex
8 Smoking history (current or ex-smoker vs never smoker) given potential impact on oxidant status6
9 Presence of emphysema gt 25 on HRCT
37 Rationale for Blinding of Treatments
The issue of treatment blinding was given a great deal of consideration with subject safety being the primary
concern After discussion among the Steering Group members it was decided that as long as subject safety
could be ensured blinding was necessary Blinding allows the study to
Have optimal scientific validity and potential to impact the standard of care for subjects
19
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Make objective assessments of treatment effects
Maintain clinical equipoise among investigators
Encourage subjects to have similar levels of contact with the medical community
Minimize the differential dropout rates across study arms
20
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
4 Methods 41 Inclusion Criteria
1 Age 35 to 85 years inclusive
2 FVC ge 50 of predicted (post-bronchodilator measurement from the screening visit)
3 DLCO ge 30 of predicted (hemoglobin corrected and altitude corrected if gt4000 ft above sea level)
4 Ability to understand and provide informed consent
5 Diagnosis of IPF according to a modified version of the ATS criteria le 48 months from enrollment The
date of diagnosis is defined as the date of the first available HRCT or surgical lung biopsy characteristic
of definite UIP
411 Subjects Shown to Have Usual Interstitial Pneumonia Pattern on Surgical Lung Biopsy
Subjects who have been shown to have UIP pattern on lung biopsy must have all of the following
1 Exclusion of other known causes of ILD such as drug toxicity clinically significant environmental
exposures or diagnosis of connective tissue diseases
2 Bibasilar reticular abnormalities with minimal ground glass opacities on HRCT scan
412 Subjects Who Have Not Undergone a Surgical Lung Biopsy
In addition to the criteria above these subjects must have radiological findings considered to be definite for the
diagnosis of UIPIPF
1 Bibasilar reticular abnormalities with minimal ground glass opacities
2 Honeycombing as the predominant feature and located in the peripheral lung bases
42 Diagnosis of IPF
Only subjects with definite IPF will be eligible for enrollment in this study We will utilize a combination of
clinicalphysiologic features HRCT and review of a clinically obtained surgical lung biopsy specimen to
establish the diagnosis of IPF An algorithm for the diagnosis is provided to guide entry into the protocol as
outlined in the inclusion and exclusion criteria (Figures 2 and 3) This multi-disciplinary approach uses
21
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
expertise from clinicians radiologists and pathologists Investigators at each site in conjunction with central
pathology will work together to establish the diagnosis of IPF This interactive approach to the diagnosis of IPF
increases the level of agreement between observers39
A subject with suspected ILD should be evaluated for secondary causes including but not limited to
environmental exposures drugs and systemic diseases Presence of any of these findings felt to be significant
enough to cause an ILD should disqualify the subject from entry into the trial
If secondary causes are absent an HRCT scan may be obtained If an HRCT of sufficiently high quality has
been obtained within the last 3 months that scan may be used for diagnosis In the appropriate clinical setting
the diagnosis of IPF can be made by the demonstration of a typical radiographic pattern on HRCT or by
demonstration of UIP pattern on a surgical lung biopsy The following criteria for a radiographic (ie
nonsurgical) diagnosis will be used In the absence of known exposures andor clinical associations attributable
to pulmonary fibrosis and in the appropriate clinical setting the presence of definite UIP pattern in HRCT
images is required to meet study criteria for the diagnosis of IPF
Figure 2 Diagnosis of Idiopathic Pulmonary Fibrosis in the IPFnet
22
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Figure 3 Pathology Flow Chart Surgical Lung Biopsy Diagnosis
Requirement for diagnosis
1 Clinical exclusion of other known causes (connective tissue diseases environmental and drug
exposures) of ILD
2 Radiographic HRCT with bibasilar reticular abnormality and honeycomb change with minimal
ground glass opacities
Appropriate clinical setting
1 Age gt 50 years
2 Insidious onset of unexplained dyspnea
3 Duration of illness for ge 3 months
4 Bibasilar inspiratory crackles
23
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Unlike the ATSERS consensus criteria published in 2000 bronchoscopy will not be required for diagnosis
This decision was made based on the experience of the IPFnet Steering Group members regarding the utility of
bronchoscopy in the diagnosis of IPF The presence of an atypical HRCT finding will require documentation of
a definitive diagnosis by surgical lung biopsy In fact this is in keeping with the recently published evidence
based guidelines for diagnosis and management of IPF13 As shown in Figure 3 central review of the pathology
data will be required for a diagnosis of IPF
We will not require central review of HRCT as several studies have shown that a confident local interpretation
of clinicalHRCT criteria as definite IPFUIP is associated with a high positive predictive value for finding UIP
at surgical lung biopsy (see Table 1) Differences in sensitivity in these series likely reflect subject selection as
Flaherty et al3 evaluated only UIP and nonspecific interstitial pneumonia (NSIP) while Raghu et al40 and
Hunninghake et al41 included a broader range of ILD
Table 1 Operating Characteristics of Local HRCT Review for Diagnosis of UIP
Researcher of Subjects Sensitivity () Specificity () PPV () NPV ()
Raghu et al 40
59 (29 UIP by SLB) 78 90 88 82
Hunninghake et al 41 91 (54 UIP by SLB)
74 81 85 67
Flaherty et al 3 96 (only NSIP amp UIP)
37 100 100 30
Abbreviations PPV positive predictive value NPV negative predictive value UIP usual interstitial pneumonia SLB surgical lung biopsy and NSIP nonspecific interstitial pneumonia
Furthermore an analysis of the HRCT scans from subjects enrolled in the GIPF-001 trial confirmed that local
site interpretations have a high congruity to a central radiology core In this multi-center study 263 HRCT
scans were read as definite IPF and a retrospective central radiology core review found 932 to be consistent
with IPF 42 We will also take several additional steps to insure that the local HRCT reads are accurate
including
1 A detailed training module has been developed and must be completed by each site radiologist before
site initiation
2 Clinical centers are to mail all HRCT scans to the HRCT core lab The first 10 HRCT scans from
subjects enrolled at each enrolling clinical center will be reviewed centrally to be certain that local reads
24
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
25
are congruent with a central interpretation If discrepancies are identified additional education will be
provided and HRCT scans will continue to be reviewed centrally until the central radiology core is
confident that the local center is performing appropriately
3 Random scans will be obtained from each center throughout the study to confirm that the local read
continues to agree with central interpretation If discrepancies are identified they will be addressed as in
2 above
In all cases if a subject has a surgical lung biopsy sample that sample will be reviewed by the local and central
pathologists Therefore the only cases that would not be subject to a direct central review process are those
where the HRCT meets the centrally defined criteria for an unequivocal diagnosis and a lung biopsy sample is
not available Table 2 below summarizes the possible combinations for making a diagnosis
Table 2 Combining HRCT and Pathology Interpretations to Determine if IPF is Present
HRCT Diagnosis Pathology Diagnosis Diagnosis of IPF
Definite UIP Definite UIP Yes
Definite UIP Probable UIP Yes
Definite UIP Possible UIP Yes
Definite UIP Not UIP No
Definite UIP Unavailable Yes
Consistent with UIP Definite UIP Yes
Consistent with UIP Probable UIP Yes
Consistent with UIP Possible UIP No
Consistent with UIP Not UIP No
Consistent with UIP Unavailable No
Inconsistent with UIP Any No
Abbreviations HRCT high-resolution computed tomography IPF idiopathic pulmonary fibrosis
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
UIP usual interstitial pneumonia Dx diagnosis 43 Exclusion Criteria
1 History of clinically significant environmental exposure known to cause pulmonary fibrosis
Occupational exposures such as asbestos or environmental exposure to organic dust such as occurs in
pigeon breeders may at times mimic the clinical and radiographic findings of IPF
2 Diagnosis of connective tissue disease felt by the principal investigator (PI) to be the etiology of the
interstitial disease Diagnosis of collagen-vascular conditions will be according to the published
American College of Rheumatology criteria As such the presence of any documented collagen-vascular
disorder or the presence of any suspicious symptom complex whether or not associated with
significantly abnormal rheumatological serologies will exclude the subject at the discretion of the PI
3 Extent of emphysema greater than the extent of fibrotic change (honeycombing reticular changes) on
HRCT scan
4 Forced expiratory volume in 1 second (FEV1)FVC ratio lt 065 at screening (postbronchodilator)
5 Partial pressure of arterial oxygen (PaO2) on room air lt 55 mm Hg (lt 50 mm Hg at Denver site)
6 Residual volume gt 120 predicted at screening (postbronchodilator)
7 Evidence of active infection
8 Significant bronchodilator response on screening spirometry defined as a change in FEV1 ge 12 and
absolute change gt 200 mL OR change in FVC ge 12 and absolute change gt 200 mL The percent
difference between the FVC (or FEV1) values will be calculated by taking the absolute value of the
difference and dividing it by the larger of the two FVC (or FEV1) values
9 Screening and enrollment post-bronchodilator FVC measurements (in liters) differing by gt 11 The
percent difference between the FVC values will be calculated by taking the absolute value of the
difference and dividing it by the larger of the two FVC values (eg the percent difference between FVC
measurements of 19 and 20 liters would be determined by taking the difference between the two (01
liters) and dividing by the larger of the two (20 liters) So 0120 = 5 and these FVC measurements
would not exclude the subject
10 Listed for lung transplantation ie the patient has completed the evaluation process has been accepted
as a candidate for transplantation at an appropriate center and is waiting to receive notification of an
available donor organ
11 History of unstable or deteriorating cardiac disease
12 Myocardial infarction coronary artery bypass or angioplasty within 6 months of screening
26
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
13 Unstable angina pectoris or congestive heart failure requiring hospitalization within 6 months of
screening
14 Uncontrolled arrhythmia
15 Severe uncontrolled hypertension
16 Known HIV or hepatitis C
17 Known cirrhosis and chronic active hepatitis
18 Active substance andor alcohol abuse (as determined by site PI)
19 Pregnancy or lactation (subjects who are pregnant or breastfeeding)
20 Known hypersensitivity to study medication
21 Any condition other than IPF that in the opinion of the site PI is likely to result in the death of the
subject within the next year
22 Any condition that in the judgment of the PI might cause participation in this study to be detrimental to
the subject or that the PI deems makes the subject a poor candidate
23 Any therapy directed at pulmonary fibrosis (excepting triple therapy of prednisone plus azathioprine
plus NAC) requires a 30-day washout period before randomized Triple therapy of lt= 12 weeks duration
in the past 4 years requires a 30-day washout period before randomization
24 History of triple therapy of prednisone plus azathioprine plus NAC for gt 12 weeksrsquo duration in the past
4 years or previous enrollment in the triple-therapy arm of the PANTHER-IPF study
44 Study Design and Study Visit
441 Study Design Summary
This study will be a randomized double-blind PL-controlled trial designed to assess the safety and efficacy of
NAC in subjects with newly diagnosed IPF
Subjects with mild to moderate IPF (defined as FVCpred ge 50 and DLCOpred ge 30) diagnosed within
the past 48 months will be enrolled Screening will continue until April 30 2012
27
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
The study will employ a 2-arm design with 11 randomization to NAC or PL Once enrolled subjects will visit
the clinical center at 15 weeks and 15-week intervals thereafter Each subject will be treated and followed for a
maximum of 60 weeks
During the 60-week visit subjects will be taken off all study agents Approximately four weeks after the final
dose of study agent is taken subjects will receive a safety phone call from the study site
442 Study Visits
Subjects who meet entry criteria will review the informed consent a written description of the purpose
procedures and risks of the study with the PI co-investigator or study coordinator and all questions will be
answered The informed consent form will be signed by the subject at screening No protocol-specific
procedures will be performed until the subject has signed and dated an informed consent form This includes the
screening procedures
4421 Screening
Once informed consent is obtained subjects may immediately begin the screening process or may return within
28 days of consent In the event a study subject has been clinically evaluated at the study site by an IPFnet study
physician and has performed testing within three weeks for this clinical evaluation that meets guidelines
provided in the IPFnet PANTHER-IPF Manual of Operating Procedures (MOOP) this testing may be used to
satisfy the following screening criteria medical history physical exam arterial blood gas (ABG) with A-a
gradient vital signs with oximetry body height and weight spirometry DLCO lung volumes and HRCT scan
Allowing the use of previously performed test results that meet study guidelines for the screening visit is
intended to permit subjects easier access to study entry to prevent subjects from repeating testing that has been
performed within the study window and to decrease risks to subjects from repeated exposure to procedures
such as arterial puncture and HRCT
The following procedures will be performed at screening
Medical history and a physical examination
28
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Measure height and weight
Serum pregnancy test (if applicable)
Measure vital signs including oximetry
Blood draws performed and the following analyses conducted
o Hematology (red cell count white cell count hemoglobin hematocrit cell indices differential
platelet count)
o Blood chemistries according to central laboratory protocol (see Section 410 Laboratory
Testing)
o Beta human chorionic gonadotropin (serum) pregnancy test (in women of childbearing potential)
o Urinalysis
Pulmonary Function Tests (PFTs) including spirometry pre- and post- bronchodilator and postshy
bronchodilator measurement of lung volumes and measurement of hemoglobin adjusted diffusing
capacity
Measure ABGs
HRCT if a satisfactory scan has not been performed on the subject within 3 months of screening (see
PANTHER-IPF MOOP for more details)
Surgical lung biopsies (if applicable) reviewed by local and central pathology departments
Current medications If required a washout period discussed with the subject and initiated at this visit
4422 Enrollment
The enrollment visit is expected to take place within eight weeks of the screening visit Enrollment visit
activities include
Measure vital signs including oximetry
Measure height and weight
Serum pregnancy test (if applicable)
If consent has been given blood will be drawn and a urine specimen collected for the bio-specimen
repository
Spirometry (post-bronchodilator)
Measure 6MWT with Borg Dyspnea Scale
29
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Collect Quality-of-life (QOL) data using the SF-36 EuroQol Investigating Choice Experiments for
Preferences of Older People Capability Instrument (ICE CAP) and SGRQ
Female subjects complete Gender Substudy questionnaire
Dyspnea status collected using the UCSD SOBQ
Evaluate Acute Exacerbation (AEx)
Review of any Adverse Events (AEs)
Review of concomitant medications
Subject receives diary and instructions on its purpose and proper use
Subject receives supply of study drug sufficient to last until his or her 15-week study visit
See the Schedule of Assessments (Table 3) for more details Subjects with screening and enrollment postshy
bronchodilator FVC measurements (in liters) differing by more than 11 are not eligible to be enrolled in the
study
Subjects will be asked to provide a physician of record This physician will be considered the subjectrsquos primary
care provider (PCP) and if the subject agrees the PCP will be informed by letter of the subjectrsquos enrollment in
the trial The subject will be informed that his or her ongoing medical care should be received from the PCP
The PCP will be informed of any safety issues identified by the study staff The PCP will also be given
information regarding communication with study personnel about pertinent health issues or clinic encounters
the subject may have
4423 Week 15
The week 15 visit is expected to occur within +- 14 days of the subjectrsquos scheduled visit time (eg the week 15
visit should occur anytime between 13 and 17 weeks after starting study drug Week 15 activities include
Measure vital signs with oximetry
Measurement height and weight
Serum pregnancy test (if applicable)
Spirometry (post-bronchodilator) measurement
Review of AEs
Evaluate for AEx
30
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Review concomitant medications
If consented draw blood and collect urine specimen for the biospecimen repository
Subjects return used and unused study drug for the visit
Review study diary and a new study diary will be given
Provide additional supply of study drug sufficient to last until the next scheduled visit
4424 Week 30
The week 30 visit is expected to occur within +- 14 days of the subjectrsquos scheduled visit time (eg the week 30
visit should occur anytime between 28 and 32 weeks after starting study drug) Week 30 activities include
Physical examination
Measure vital signs with oximetry
Measure height and weight
Laboratory values (complete blood count [CBC] and serum chemistries)
Serum pregnancy test (if applicable)
Measure spirometry (post-bronchodilator)
6MWT with Borg scale
DLCO
Review of AEs
Evaluate for AEx
Review concomitant medications
Complete all QOL and dyspnea questionnaires (EuroQol ICE CAP SF-36 SGRQ and UCSD SOBQ)
If consent has been given blood will be drawn and a urine specimen collected for the biospecimen
repository
Review study diary
Subjects return used and unused study drug for the visit
Provide additional supply of study drug sufficient to last until the next scheduled visit
4425 Week 45
31
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
The week 45 visit is expected to occur within +- 14 days of the subjectrsquos scheduled visit time (eg the week 45
visit should occur anytime between 43 and 47 weeks after starting study drug) Week 45 activities include
Measure vital signs with oximetry
Measure height and weight
Serum pregnancy test (if applicable)
Measure spirometry (post-bronchodilator)
Review of AEs
Evaluate for AEx
Review concomitant medications
If consent has been given blood will be drawn and a urine specimen collected for the biospecimen
repository
Subjects return used and unused study drug for the visit
Study diary reviewed
Provide additional supply of study drug sufficient to last until the next scheduled visit
4426 Week 60 (Early Withdrawal or Final Treatment Visit)
At week 60 or at subject withdrawal from the study (premature by study doctor or subjectrsquos decision) a final
treatment visit will occur At this final treatment visit subjects will discontinue NACPL abruptly Week 60
activities also include
Physical examination
Measure vital signs with oximetry
Measure height and weight
Laboratory values (complete blood count [CBC] and serum chemistries)
Spirometry (post-bronchodilator) measurement
6MWT with Borg scale measurement
DLCO
Lung volumes
ABG
Review of AEs
32
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Evaluate for AEx
Review concomitant medications
Subjects will complete all QOL and dyspnea questionnaires (EuroQol ICE CAP SF-36 SGRQ and
UCSD SOBQ)
If consent has been given blood will be drawn and a urine specimen collected for the biospecimen
repository
Subjects return used and unused study drug for the visit
Study diary reviewed
4427 Final Site Visit ndash FVC drop confirmation
In the event that the subject has a recorded FVC drop of gt10 from baseline at the final treatment visit and the
subject has not had a confirmation of such a drop at a previous study visit the subject should return to the
clinical site 6 to 8 weeks after the final treatment visit During this visit a post-bronchodilator spirometry test
will be performed This FVC measurement will be evaluated according to section 521 of this protocol
4428 Final Visit ndash Telephone Follow-up
Four weeks following the final dose of study medication subjects will receive a telephone call from the study
coordinator to ensure that there are no side effects and to follow up on any ongoing adverse events (AEs)
4429 Phone Contact Between Visits
At week 2 and each month that a subject does not have a scheduled clinical center visit his or her study
coordinator will contact him or her at least once by telephone to
Inquire if the subject has had any hospitalizations events that might be considered an AE or any events
significant enough to warrant an out-of-cycle visit to the clinical center
Remind subjects of their current dosage levels and confirm that the subject understands them
Address any questions or concerns the subject might have regarding other aspects of the study
Assess adherence to the treatment regimen by reviewing diary data verbal review of medications taken
including nutritional supplements
33
34
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Table 3 Schedule of Assessments
Procedure Screening Visit 0
Enrollment Visit 1
Week 15 Visit 2
Week 30Visit 3
Week 45 Visit 4
Week 60 Early
Withdrawal Visit 5
Final1
Visit (via phone)
Informed consent X
Medical history X
Inclusionexclusion criteria X
Serum pregnancy test (if applicable) X X X X X
Review of lung biopsy X
Arterial Blood Gas X X
6-Minute Walk Test
X
X X
Physical examination X X X
Vital signs with oximetry X X X X X X
Body height and weight X X X X X X
Complete Blood Count X X X
Chemistry panel X X X
Monitor Lab Values X X X
Urinalysis X Specimen repository substudy blood draw and urine collection (if consented)
X
X X X X
HRCT (if not completed within three months) X
Spirometry (pre- and post-bronchodilator) X
Spirometry (post-bronchodilator only) X X X X X
DLCO (post-bronchodilator only) X X X
Lung volumes (post-bronchodilator only) X
X
Evaluate for acute exacerbation X X X X X
Review Adverse Events X X X X X X
Review concomitant meds X X X X X X
Dispense subject diary X X X X
Review subject diary X X X X X
Dispense study agent X X X X
Gender Substudy questionnaire (female subjects only) X
EuroQol ICECAP UCSD SOBQ SGRQ SF-36 X X X
Abbreviations DLCO diffusing capacity of the lung for carbon monoxide QOL Quality of Life ICECAP Investigating Choice Experiments for Preferences of Older People UCSD SOBQ University of California Shortness of Breath Questionnaire SGRQ St Georgersquos Respiratory Questionnaire SF-36 Short Form 36 Health Survey
1Follow-up visit via phone will occur four weeks after final dose of study medication
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
45 Dose Justification
The general philosophy for determining dosing levels was to apply previously examined
treatment regimens With the focus of the study being to establish a standard of care for
mildmoderate IPF subjects the goal was to develop flexible yet standardized treatment rules that
allow for the temporary or permanent withholding of one or more components of treatment when
necessary Subjects developing laboratory abnormalities or symptoms that result in
discontinuation of one or more components of study treatment may continue on the other
components as long as there is no contraindication for this Complete follow-up is important for
the validity of any study As a strategy to maintain protocol adherence we are using a treatment
regimen that will detect potential side effects and prompt interventions proactively in the interest
of patient safety In addition subjects who permanently stop study medications during the course
of the study are encouraged to continue in the study completing all scheduled visits and tests
451 Rationale for N-acetylcysteine Dosing
To our knowledge there have been no IPF studies to correlate clinical outcome measures with
different dosages for NAC The dosage chosen is based on the IFIGENIA study However BAL
lung GSH levels from subjects with IPF have been augmented with the use of oral NAC at 600
mg 3 times per day In addition lung GSH levels have been associated with improved
PFTs212227 The dose chosen for this study was based on previous data including the IFIGENIA
study30
4511 Dosing of N-acetylcysteineplacebo
Dosing of NACPL will be 600 mg orally 3 times a day (1800 mgday)
4512 Reasons to Discontinue N-acetylcysteineplacebo
NACPL may be temporarily or permanently discontinued for the duration of the study for
gastrointestinal symptoms or dermatologic reactions
35
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Temporarily discontinue (hold) oral NACPL for subjects requiring inpatient admission for acute
exacerbation (AEx) or other conditions Resume NACPL after discharge
36
37
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
452 Dosage Algorithms
Dosage Adjustment Algorithm 1 NACPL Dose Modifications for Gastrointestinal Symptoms Nausea Vomiting Abdominal Discomfort Diarrhea
GI Symptoms determined by the PI to be clinically significant Nausea Vomiting Abdominal Discomfort Diarrhea
NACPL Temporarily dc (HOLD) x 3 Days
Monitor symptoms intervene as clinically indicated (eg fluid replacement antidiarrhea or antinausea medication)
Monitor or lab PRN
Are symptoms resolving after 3 days NO
Symptoms NOT resolving after 3 days of holding study medication Assessmentmanagement per clinical
discretion of investigator
Likely not study medication discuss resuming study medication with medical monitor when symptoms resolved
YES
Temporarily dc (HOLD) NACPL for 4 additional days (total hold 1 week) then NACPL Resume 600 MG TID
Did symptoms recur
YES
STOP NACPL for
duration of study
NO
NACPL No Change
38
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Dosage Adjustment Algorithm 2 NACPL Dose Modifications For Dermatologic Reactions
Dermatologic Reactions (Not Acneiform) ge Grade 2 Grading per Common Terminology Criteria for
Adverse Events V30 (httpctepcancergov) For example Grade 1 RASHDESQUAMATION Macular or papular eruption or erythema without associated symptoms Grade 2 RASHDESQUAMATION Macular or popular eruption or erythema with pruritus or other associated symptoms localized desquamation or other lesions covering lt50 of body surface area
NACPL Temporarily dc (HOLD) x 3 days
Are symptoms resolving after 3 days
NO Symptoms not resolving after 3 days of holding study medication Assessmentmanagement per clinical discretion of investigator Likely not study medication Discuss resuming study medication with medical monitor when symptoms
resolved YES
Temporarily dc (HOLD) NACPL for 4 additional days (total hold 1 week) then NACPL resume 600 MG TID
Did symptoms recur
YES
STOP NACPL for
duration of study
NO
NACPL No change
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
46 Contraindications Precautions and Side Effects of Study Medications
461 Contraindication
Contraindication to NAC is known hypersensitivity to it
462 Precautions
Concomitant administration of oral NAC and antibiotics has shown a slightly reduced absorption
of cephalexin and a slight increase in erythromycin serum levels NAC contains free sulfhydryl
groups There is no evidence that individuals sensitive to sulfa drugs are sensitive to NAC
The NAC preparation being administered in this study contains 20 mg of aspartame Because of
the phenylalanine component of aspartame individuals with phenylketonuria should avoid or
restrict aspartame intake to avoid increased blood levels of phenylalanine Because of this risk
labeling is required on all products containing aspartame
463 Side Effects
Side effects of NAC range from common to serious See Table 4
39
40
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Table 4 Side Effects of NAC
Undesirable Effects
System-organ class Uncommon
(gt11000 lt1100)
Rare
(gt110000 lt11000)
Very rare
(lt110000) Not known
Immune system disorders Hypersensitivity Anaphylactic shock
reaction
Nervous system disorders Headache
Ear and labyrinth disorders Tinnitus
Cardiac disorders Tachycardia
Vascular disorders Hemorrhage
Respiratory thoracic and
mediastinal disorders
Bronchospasm
Dyspnea
Gastrointestinal disorders
Vomiting diarrhea
stomatitis abdominal
pain nausea
Dyspepsia
Skin and subcutaneous tissue
disorders
Urticaria rash
angioedema itching
General disorders and
administration site conditions Pyrexia
Investigations Reduced arterial
pressure Face edema
In very rare cases the onset of severe skin reactions such as Stevens-Johnson syndrome and Lyell syndrome was reported to have a temporal relationship with N-acetylcysteine administration Although in most cases at least another suspect drug probably most involved in the genesis of the above mentioned mucocutaneous syndromes has been identified in case of mucocutaneous alterations it is appropriate to contact onersquos doctor and the administration of N-acetylcysteine should be immediately discontinued
Some studies confirmed a reduction of platelet aggregation during N-acetylcysteine administration The clinical significance of these findings has not been defined yet [Source Fluimucil Investigator Brochure]
47 Recruitment Procedures
Subjects recruited for this study will be established patients of the investigators or physician- or
self-referred to participating clinical centers in the IPFnet Each clinical center within IPFnet has
a well-developed infrastructure of local pulmonologists within the surrounding geographic area
These pulmonologists are kept informed of ongoing IPF clinical trials and regularly refer
subjects to studies conducted at IPFnet clinical centers
Additional steps will be taken to inform clinicians of the trials in progress within IPFnet
including presentations at faculty staff meetings at local hospitals medical grand rounds and
national conferences direct mail notification monthly faxes and advertisement of network trials
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
in pulmonary journals Clinical center patients previously diagnosed with IPF will be notified of
the trials by mail whenever possible
Recruitment of minorities and women will be monitored by the DCC and DSMB If necessary
additional recruitment efforts will be made at specific centers to ensure that the aggregate subject
sample contains appropriate representation of women and minorities
48 Study Procedures
The following procedures are detailed in the PANTHER-IPF MOOP accompanying this
protocol
1 PFT
2 ABG
3 HRCT scan of the chest (including imaging of pulmonary arteries)
4 CBC and serum chemistries
5 Pregnancy test
6 6MWTBorg Dyspnea Scale
7 QOL questionnaires (EuroQol HAD SF-36 SGRQ and ICE CAP)
8 UCSD SOBQ
9 Gender Substudy Questionnaire
All assessments of PFTs will be conducted by study personnel not directly involved in the
treatment of the subjects
481 Biological Specimen Management
4811 Biological Specimen Sample Management
Subjects at clinical centers participating in the specimen repository substudy who consent to
having blood drawn for research purposes and for the banking of blood blood components and
other biologic specimens (urine and BAL fluid) will have approximately 405 mL of blood
41
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
drawn 17 mL blood drawn for DNA and 20 mL of urine collected at enrollment visit Subjects
will have approximately 50 mL of blood drawn and 20 mL of urine collected at each 15-week
follow-up visit Blood specimens will be separated according to PANTHER-IPF MOOP
guidelines into the following components for banking in the repository serum plasma and
DNA Coding of all biologic specimens for the repository will be performed by study staff at the
clinical center The samples will be processed per PANTHER-IPF MOOP guidelines aliquoted
labeled with barcode labels and stored at -70degC at the clinical center and shipped to the central
repository
The only subject identifiers will be a sample ID number and subject initials This sample ID will
be linked in the IPFnet DCC clinical database to subject information No subject information will
be transferred to the biological-specimen database
The subjectrsquos samples may be used for approved sub-studies relating to human disease
including but not limited to IPF The studies for which an individualrsquos samples will be made
available will be determined by the subjectrsquos answers to questions on the biological-sample
informed consent form The subjects can choose to make their samples available for all options
or any combination Samples will be made available to researchers only with IPFnet Steering
Group approval until such time as the samples are made public through the NHLBI repository
49 Concomitant Medications
Concurrent treatment with FDA-approved therapy for IPF is allowed Colchicine may be used
for treatment of gout Temporary treatment with oral or IV corticosteroids for clinical worsening
or suspected AEx is permitted Nutritional supplements containing NAC are not allowed
410 Laboratory Testing
Clinical laboratory parameters will be assessed at screening and at the end of the study The
following tests will be performed at the two time points specified in the protocol chemistry (AG
ratio ALT [SGPT] AST [SGOT] albumin alkaline phosphatase amylase bilirubin-direct
42
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
bilirubin-indirect bilirubin-total BUN BUNcreatinine ratio calcium carbon dioxide
cholesterol-total chloride CPK-total creatinine GGT globulin glucose iron-total LDH
lipase magnesium phosphorus-inorganic potassium protein-total sodium TIBC triglycerides
uric acid) and hematology (red blood cell count WBC count hemoglobin hematocrit cell
indices differential platelet count)
411 Blinding of Study Drugs
Subjects and caregivers will be blinded to study treatment Every subject will receive NAC or
matching PLs at every study visit from the baseline visit to the week-45 visit No study agent
will be dispensed at the week-60 visit
43
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
5 Study Endpoints
51 Primary Study Endpoint
The primary endpoint will be the change in serial measurements of FVC over the study period
52 Secondary Study Endpoints
521 Time to Disease-progression
The time-to-death or a 10 decline in FVC will be defined as the time-to-disease progression
The 10 decline in FVC from enrollment must be confirmed on 2 consecutive visits no less than
6 weeks apart For subjects with 2 consecutive visits with a 10 decline in FVC the time-toshy
disease progression will be defined as the time interval between enrollment and the initial visit
with a 10 FVC decline For subjects who experience disease progression the study doctor will
determine whether or not the subject will remain in the study
522 Acute Exacerbations
The following 3 criteria will define AEx in subjects with acute worsening of their respiratory
conditions
1 Clinical (all of the following required)
A) Unexplained worsening of dyspnea or cough within 30 days triggering unscheduled
medical care (eg emergency room clinic study visit hospitalization)
B) No clinical suspicion or overt evidence of cardiac event pulmonary embolism or deep
venous thrombosis to explain acute worsening of dyspnea
C) No pneumothorax
44
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
2 RadiologicPhysiologic (A and B required)
A) New ground glass opacity or consolidation computed tomography (CT) scan OR new
alveolar opacities on chest x-ray
B) Decline of ge 5 in resting room air SpO2 from last recorded level OR decline of ge 8 mm
Hg in resting room air PaO2 from last recorded level
3 Microbiologic (all of the following required)
A) No clinical evidence for infection (ie absence of grossly purulent sputum fever gt 39degC
orally)
B) Lack of positive microbiological results (if done) from lower respiratory tract defined as
(1) Clinically significant bacterial growth on sputum or endotracheal aspirate cultures
(2) Quantitative culture by protected brush specimen ge 103 cfumL or BAL ge 104 cfumL
(3) The presence of specific pathogens on stains of any of the above
C) Lack of positive pathogen in blood cultures (if done)
Identification of Acute Exacerbations
All subjects will be educated about the importance of identifying AExs At the time of
enrollment subjects will be told about the possibility of developing acute symptomatic
worsening that might represent an AEx of IPF and instructed to contact their study clinical
center coordinator within 48 to 72 hours of the apparent event
All subjects will be contacted by phone monthly and questioned about any change in dyspnea or
cough and any interim clinic visits or hospitalizations Finally as part of the IPFnet outreach to
community referring physicians the importance of AExs will be emphasized When a subject is
identified who meets criterion 1A this will trigger the collection of additional clinical data to
evaluate a suspected AEx These data will be collected as part of standard clinical care (ie this
protocol does not require collection of all items) The additional items to be collected for
suspected AEx include
IPFnet AEx case report form (eCRF) (required)
45
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Chest x-ray CT scan withwithout pulmonary angiogram (reports should be faxed and
followed by the hard copiesdiscs)
Oxygen saturation (pulse oximetry)
ABG
Respiratory cultures (sputum endotracheal aspirate lavage)
Blood cultures
Clinichospital records related to the event
All potential cases of AEx will be reviewed by the clinical center PI first and a decision on
whether the case may represent an AEx will be made If AEx is suspected the case will be sent
to the IPFnet adjudication committee which will assign a final diagnosis (see Table 5) If there is
disagreement among members the majority opinion will be recorded
During episodes of suspected AEx as determined by the individual clinical center investigator
subjects will remain blinded and in the study
Table 5 Final Diagnoses in Evaluation of Suspected Acute Exacerbations
Definite acute exacerbation All criteria met no alternative etiology
Unclassifiable acute worsening
Insufficient data to evaluate all criteria no alternative etiology
Not acute exacerbation Alternative etiology identified that explains acute worsening
Management of the suspected AEx will be at the discretion of the treating physician Standard of
care generally involves evaluation for respiratory infection pulmonary embolism cardiac events
and pneumothorax and treatment with IV corticosteroids
Study drugs will be resumed at pre-suspected AEx doses after subjects clinically improve as
confirmed by the local PI All subjects should be seen at the clinical center within 2 to 4 weeks
of recovery for measurement of post-bronchodilator FVC (see Figure 4) Subjects unable to
return to the clinical center after suspected AEx due to medical frailty (eg continued
46
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
institutionalization progressive disability) will be categorized as failing to maintain FVC
response in secondary analyses
Suspected AEx (PI determined)
Hold study drug Treat AEx
(Attending physician determined)
Alive but unable to continue due to
medical frailty
Dead
Alive and able to continue
Site reviewvisit
Restart study drug
FVC within 2-4 weeks
Figure 4 Acute Exacerbation Flow Chart
523 Respiratory Infections
An upper respiratory infection will be defined as
Change in sputum discoloration
Increased cough of no more than 14 daysrsquo duration
A lower-respiratory infection (pneumonia) will be defined as new segmental or lobar airspace
opacities visualized by image studies (chest radiograph or HRCT) in addition to any of the
following
Positive pathogencultures in good sample of sputum or lower-airway secretions retrieved
by fiberoptic bronchoscope
Fever gt 39degC or gt 100degF
Leukocytosis gt 12000 (unexplained no increase in dose of corticosteroids)
47
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
524 Maintained FVC Response
Subjects with follow-up FVCpred measurements at or above their baseline FVCpred level
will be classified as having maintained FVC response Subjects with reduced FVCpred levels
or missing data for any reason including death or medical frailty will be classified as having not
maintained FVC response The FVCpred value is used because unadjusted FVC measurements
are expected to decline with age
48
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
6 Safety Evaluations and Procedures
61 Adverse Events
During a clinical trial the reporting of adverse experience information can lead to important
changes in the way a new treatment is developed as well as provide integral safety data
611 Definitions
An adverse event (AE) is any untoward medical occurrence in a subject or clinical investigation
subject who was administered a pharmaceutical product The AE does not necessarily have to
have a causal relationship with the drug administered An AE can be any unfavorable and
unintended sign (including an abnormal laboratory finding) symptom or disease temporarily
associated with the use of a medicinal product whether or not considered to be related to the
medicinal product Diseases signs symptoms or laboratory abnormalities already existing at
enrollment are not considered AEs unless they worsen (ie increase in intensity or frequency)
Surgical procedures themselves are not AEs they are therapeutic measures for conditions that
require surgery The condition for which the surgery is required may be an AE Surgical
procedures planned before randomization and the conditions necessitating the surgery are not
AEs
A serious adverse event is any untoward event that
Is fatal
Is life-threatening
Requires inpatient hospitalization or prolongation of existing hospitalization with the
following exceptions
o Preplanned (before the study) hospital admissions unless the hospitalization is
prolonged
o Planned admissions (as part of a study eg routine biopsies)
o Hospitalization lasting lt 24 hours
49
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
o Hospitalization for elective procedure
o Emergency room visits
Results in persistent or significant disability or incapacity
Is a congenital anomaly or birth defect
Important medical events that may not result in death be life-threatening or require
inpatient hospitalization may be considered serious adverse events (SAEs) when based
on appropriate medical judgment they may jeopardize the subject and may require
medical or surgical intervention to prevent one of the outcomes listed above
Life-threatening means that the subject was in the view of the investigator at immediate risk of
death from the AE as it occurred It does not include an AE that had it occurred in a more severe
form might have caused death
Persistent or significant disabilityincapacity means that the event resulted in permanent or
significant and substantial disruption of the subjectrsquos ability to carry out normal life functions
Causality
A reasonable possibility means the AE may have been caused byrelated to the study drug A
perceived or real lack of efficacy does not satisfy the definition of relatedness
612 Adverse Event (AE) Reporting
For the PANTHER-IPF trial all AEs (serious and nonserious) occurring from randomization
through final study visit (4 weeks after final dose of all study medication) will be recorded on the
AE page of the case report form (CRF)
6121 Serious Adverse Events (SAE) Reporting
For this trial all deaths and all SAEs which occur from randomization through final study visit
must be entered within the EDC system via the SAE eCRF page within 24 hours of the
investigative sitersquos knowledge of the event It is the responsibility of the clinical center
50
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
investigator to provide a causality assessment of the event for each study medications based upon
the information available at the time of the report It is understood that complete information
about the event may not be known at the time the initial report is submitted In the event the EDC
system is not accessible to the site at the time of event reporting investigative sites will complete
and forward a paper back-up SAE form to DCRI Safety Surveillance for processing
DCRI Safety Surveillance
Telephone 1-919-668-8624 or 1-866-668-7799 (toll free)
Fax 1-919-668-7138 or 1-866-668-7138 (toll free)
The investigator must complete and submit follow-up SAE information via the eCRF when
important new or follow-up information (eg final diagnosis outcome results of specific
investigations) becomes available Follow-up information should be submitted according to the
same process used for reporting the initial event as described above All SAEs will be followed
until resolution stabilization or 30 days after the subject has completed the final visit (4 weeks
after the final dose of study medication) whichever occurs first The investigator is responsible
for reporting SAEs to their institutional review board (IRB) per site specific IRB reporting
guidelines
6122 Regulatory Reporting
AEs that are serious study drug related and unexpected will be reported to the regulatory
authorities The DCRI Safety Surveillance medical monitor will perform a medical review of all
SAEs submitted and evaluate for ldquounexpectednessrdquo DCRI Safety Surveillance will prepare
MedWatch reports for those events identified as serious study drug related and unexpected as
determined by Safety Medical Monitor
DCRI Regulatory Services will submit all unexpected study drug-related SAEs as per 21 CFR
32 DCRI Safety Surveillance will provide a safety alert letter to the NHLBI DSMB and DCC
clinical operation (for distribution to sites) within 15 days of initial receipt of the information
51
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Investigators are responsible for promptly reporting these events to their reviewing IRBs
according to site specific IRB reporting guidelines
62 Clinical Medical Monitoring
There will be an unblinded physician at the IPFnet DCC serving as medical monitor The
medical monitor will be available to assist with questions about dosage adjustments of study
medications including discontinuation or resumption of medications
63 Unblinding Procedures
Unblinding of subjects or investigators to subject treatment is strongly discouraged For ongoing
clinical management all subjects should be presumed to be receiving ldquoactiverdquo study drug To
ensure the subjectrsquos safety the study treatment will be dose-adjusted based on laboratory test
results clinical findings and symptoms
The IPFnet DCC medical monitor and PANTHER-IPF co-chairs Drs Ganesh Raghu and
Fernando Martinez will be available to the study physicians to discuss study drug management
on a case-by-case basis Un-blinding will be considered ONLY when the knowledge of subject
treatment assignment is ABSOLUTELY ESSENTIAL for subject safety and after discussion of
the subjectrsquos case with the medical monitor and either Dr Raghu or Dr Martinez Unblinding of
study treatment should be minimized during the conduct of the trial In those cases where it is
felt to be medically necessary the DCC medical officer will communicate directly with the
managing physician to minimize unblinding of study personnel
52
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
7 Study Drug Procedures
At the baseline 15-week 30-week and 45-week study visits subjects will receive a supply of
study drug sufficient to last until the next visit at which study drug will be dispensed
53
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
8 Data Management
81 Hardware and Software Configuration
811 Hardware and Database Software
Data will be stored in an Oracle database system Oracle has advantages of processing efficiency
and smooth linkage with other software systems The application and database will be hosted on
Solaris Unix servers at the IPFnet DCC
812 Statistical Software
SAS will be used as the principal application for the management of analysis data files and
statistical computations S-Plus will be used to provide supplementary functions as needed
813 Access Control and Confidentiality Procedures
Access to databases will be controlled centrally by the IPFnet DCC through user passwords
linked to appropriate privileges This protects the data from unauthorized changes and
inadvertent loss or damage
814 Security
Database and Web servers will be secured by a firewall and through controlled physical access
Oracle has many security features to ensure that any staff member accessing the database has the
proper authority to perform the functions he or she requests of the system Within the secondary
SAS databases Unix group-access control maintains similar security The Sun workstation login
is secured by extensive user-password facilities under Unix
54
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
815 Back-up Procedures
Database back-up will be performed automatically every day and standard IPFnet DCC policies
and procedures will be applied to dictate tape rotation and retention practices
816 Virus Protection
All disk drives that provide network services and all user computers will be protected using
virus-scanning software Standard IPFnet DCC policies will be applied to update these protection
systems periodically through the study
82 Sources of Data
821 Design and Development
The IPFnet DCC will be responsible for development of the electronic case report forms
(eCRFs) development and validation of the clinical study database ensuring data integrity and
training clinical center staff on applicable data management procedures A web-based distributed
data entry model will be implemented This system will be developed to ensure that guidelines
and regulations surrounding the use of computerized systems used in clinical trials are upheld
The remainder of this section provides an overview of the data management plan associated with
this protocol
822 Data Collection Forms
The data collection process consists of direct data entry at the study clinical centers into the EDC
system(s) provided by the DCC A data collection worksheet will be provided to clinical centers
for recording data in the event the EDC system is unavailable Data entry of the eCRFs should
be completed according to the instructions provided and project specific training The
investigator is responsible for maintaining accurate complete and up-to-date records and for
ensuring the completion of the eCRFs for each research participant
55
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
823 Data Acquisition and Entry
Data entry into eCRFs shall be performed by authorized individuals Selected eCRFs may also
require the investigatorrsquos written signature or electronic signature as appropriate Electronic
CRFs will be monitored for completeness accuracy and attention to detail during the study
824 Data Center Responsibilities
The IPFnet DCC will 1) develop a data management plan and will conduct data management
activities 2) provide final eCRFs for the collection of all data required by the study 3) develop
data dictionaries for each eCRF that will comprehensively define each data element 4) conduct
ongoing data monitoring activities on study data 5) monitor any preliminary analysis data
cleanup activities and 6) rigorously monitor final study data clean up
825 Data Editing
Completed data will be entered into the IPFnet DCC automated data acquisition and
management system If incomplete or inaccurate data are found a data clarification request will
be generated and distributed to clinical centers for a response Clinical centers will resolve data
inconsistencies and errors and enter all corrections and changes into the IPFnet DCC automated
data acquisition and management system
826 Training
The training plan for clinical center staff includes provisions for training on assessments eCRF
completion guidelines data management procedures and the use of computerized systems
56
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
9 Study Design and Data Analysis
91 General Analytic Considerations
All primary analyses will be based on intent-to-treat (ITT) principles using all randomized
subjects Baseline factors across groups will be compared using mean (standard deviation) and
median (25th and 75th percentiles) summary measures Kaplan-Meier curves will be used to
display event rates Due to clinical interest in departures from both sides of the null hypothesis
all test statistics will be 2-sided
Reasonable caution needs to be taken when conducting multiple analyses on key clinical
subgroups For subgroup analyses a conservative significance level of 0001 will be used for all
interaction tests Thus subgroup comparisons will be considered exploratory unless the p-value
from the interaction test is smaller than 0001
92 Randomization Blinding and Reporting of Results
A permuted block-randomization scheme will be created with varying block sizes stratified by
clinical center Once a subject has completed the screening and baseline period and evaluation
for inclusionexclusion criteria the randomization process will begin Subjects will be
randomized to receive NAC or matching placebo with equal probability (11) via telephone
contact with a central interactive voice response system (IVRS) using a toll-free randomization
number On the day of randomization after the subject has successfully met all inclusion and
exclusion criteria the investigator or designee will call the central randomization number to
obtain the assigned kit randomization numbers for that subject At each subject visit the
investigator or designee will call the central randomization number to obtain the new kit
randomization numbers for resupply of the subject For resupply of the clinical center the IVRS
will monitor minimal volume of a kit type andor expiration date and will automatically notify
the pharmacy
57
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
The trial results will be reported according to guidelines specified in the CONSORT statement
A flow diagram describing screening recruitment randomization dropout and vital status will
be included in the primary manuscript AEs and efficacy data will be presented for all treatment
groups Adherence dropout and lost to follow-up will be carefully examined across all treatment
groups Analyses of safety will be based on data from all randomized subjects who received at
least one dose of study drug
93 Stratification
Subjects will be distributed to the two treatment arms in a 11 allocation ratio Stratification
blocks will be based on clinical centers
94 Specification of the Primary Analyses
A mixed model repeated measures (MMRM) analysis described in section 95 will be used to
compare differences in the slope of FVC measurements across the treatment groups Response
variables are values of the FVC measured at baseline and every 15 weeks until study completion
Variables in the model will include treatment time and time by treatment age sex race and
height Contrast estimates of differences in slopes of treatment over time (along with confidence
intervals) will be used to estimate the treatment effect The validity of this model in terms of
meeting modeling assumptions will be assessed via standard modeling diagnostics and goodness-
of-fit measures Based on the MMRM framework missing FVC data will not be imputed for the
primary analysis
95 Analysis of Longitudinal Endpoints
A common goal in clinical trials is to specify models that are easily implemented and
reproducible by independent data analysts On the other hand the models should have proper
statistical behavior in terms of low bias and high precision Many common approaches to
longitudinal data analysis including last observation carried forward (LOCF) imputation rely on
the missing completely at random (MCAR) assumption However the MCAR assumption is
58
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
unlikely to hold in many clinical trials because missing data are often related to disease
progression and prognosis A more reasonable assumption missing at random (MAR) specifies
that the complete data distribution can be modeled using only the observed data The likelihood-
based MMRM approach is valid under the more general MAR assumptions These models will
be applied to analyze the longitudinal data secondary endpoints
The advantages of MMRM analysis are that all important characteristics of the model can be preshy
specified standard software can be used to implement the models and results are based on ITT
principles43 In addition the MMRM approach offers superior control of Type I and Type II
errors compared with the LOCF approach
Response variables are values of the PFTs measured at enrollment and every 15 weeks until
study completion and 6MWT values measured at baseline week 30 and week 60 Covariates are
treatment time time by treatment and key baseline risk factors Contrasts (along with
confidence intervals) of treatment by time will be used to estimate the treatment effect
The correlation structure involves multiple pieces including measurement errors random
variation and interindividual variability For the longitudinal data analyses an unstructured
correlation matrix for within-subject errors will be assumed Other correlation structures
including compound symmetry will be examined as needed A careful examination of reasons
for study discontinuation will be conducted to assess the validity of MCAR Sensitivity analyses
will be used to examine the untestable assumption that the observed data violate the MAR
assumption The MMRM models will be implemented using PROC MIXED in SAS
96 Analysis of Binary Time-to-Event and Time-Lagged Endpoints
Regression modeling approaches using either the logistic regression model or Cox proportional
hazards regression model will be employed when appropriate The validity of these models will
be assessed via standard modeling diagnostics and goodness-of-fit measures Estimates of
cumulative frequencies for more general time-lagged responses will be calculated using the
partitioned version of the Bang-Tsiatis estimator44 The partitions will be set at 15-week intervals
59
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
to correspond with the data-collection process Covariate adjusted event rates will be calculated
using inverse probability-weighted regression estimates45
97 Power Analysis
971 Primary Analyses
Based on previously published IPF clinical trials the PL group is expected to experience a drop
in FVC of approximately 020 L over the study period (see Figure 1) The IPFnet Steering Group
determined a clinically important difference would be to preserve the majority of the decline
relative to PL over the study period In particular a treatment effect of 015 L was determined to
be a clinically meaningful difference Potential dropout is a key factor in the proposed study The
drop-out process assumed 5 lost to follow-up after every study visit Only 80 of subjects
were assumed to be followed for the entire study period All models assumed a compound
symmetry structure for the covariance matrix Power calculations were performed using a SAS
IML program for designing repeated measures studies46 Based on preliminary reviews of the
data from the University of Michigan the covariance matrix parameters were estimated at
approximately σ2 = 0757 (variance parameter) and ρ = 0936 (correlation parameter) To be
conservative the power calculations for the primary analysis were performed with parameter
setting of σ2 = 0810 (variance parameter) and ρ = 0925 (correlation parameter)
The power calculations assume a correction for imperfect compliance proposed by Lachin and
Foulkes to allow for 2 noncompliance for each of the treatment arms47 Thus the sample size
of 130 subjects per arm would be reduced to an adjusted sample size of 130(1-002-002)2 =
1198 or 120 subjects per arm
Under the assumed Type I error rate of 005 with a correlation parameter of 0925 and standard
deviation of 090 the difference of 015 L (or 00025 Lweek) shown in Table 6 would have
power of 93
60
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Table 6 Hypothetical Values of Mean FVC (L) Change from Baseline
Week 15 Week 30 Week 45 Week 60
NAC 00125 00250 00375 00500
Placebo 00500 01000 01500 02000
Difference 00375 00750 01125 01500
Abbreviations FVC forced vital capacity PL placebo
972 Power Analysis for Secondary Endpoints
Power calculations for secondary endpoint measurements are shown in Table 7 Standard
deviations are based on unpublished data provided by the University of Michigan The
calculations are based on a 2-sample t-test with Type I error rate set at 005 These calculations
are likely to be conservative because the statistical approach described in section 95 for
analyzing these endpoints will incorporate incomplete observations as well as intermediate data
points
Table 7 Detectable Differences in Treatment Means for Selected Endpoint Measurements
Secondary Endpoints Std Dev
of the Baseline Score
Detectable Difference for 80 Power
Std Dev of the Change Score
Difference Detectable for
80 Power
DLCOpred 166 58 91 32
6MWT Area Under the Desaturation Curve
219 76 175 61
6MWT Distance to Desaturation 224 78 315 110
6MWT Minutes Walked 210 073 205 071
Abbreviations Std Dev standard deviation DLCOpred diffusing capacity of the lung for carbon monoxide percent predicted 6MWT 6-minute walk test
61
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
10 Study Administration
101 Cooperative Agreement Mechanism
The administrative and funding mechanism used to undertake this project is a ldquocooperative
agreementrdquo (U01) which is an assistance mechanism Under the cooperative agreement the
NHLBI assists supports andor stimulates the project and is substantially involved with
investigators in conducting the study by facilitating performance of the effort in a ldquopartnerrdquo role
The NHLBI project scientist serves on the IPFnet Steering Group and he or another NHLBI
scientist may serve on other project committees when appropriate At the same time however
NHLBI does not assume a dominant role direction or prime responsibility for this research
program
As described below governance of the project is conducted through the IPFnet Steering Group
Principal investigators have lead responsibilities in all aspects of their trials and the project
including any modification of trial designs conduct of the trials quality control data analysis
and interpretation preparation of publications and collaboration with other investigators unless
otherwise provided for by the IPFnet Steering Group
PIs retain custody of and have primary rights to their center-specific and collaborative data
subject to government rights-of-access consistent with current Health amp Human Services (HHS)
Public Health Service (PHS) and National Institutes of Health policies The protocols and
governance policies call for the continual submission of data centrally to the IPFnet DCC for the
collaborative database which at a minimum will contain the key variables selected by the IPFnet
Steering Group for standardization across all clinical centers the submission of copies of the
collaborative datasets to each PI upon completion of the project procedures for data analysis
reporting and publication and procedures to protect and ensure the privacy of medical and
genetic data and records of individuals The NHLBI project scientist on behalf of the NHLBI
will have the same access privileges and responsibilities regarding the collaborative data as the
other members of the Steering Group
62
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
PIs are also encouraged to publish and to publicly release and disseminate results data and other
products of the project concordant with the project protocols and governance and the approved
plan for making data and materials available to the scientific community and to the NHLBI
However during the 3 years after the ending date of NHLBI project support unpublished data
unpublished results data sets not previously released and other study materials or products are
to be made available to any third party only with the approval of the IPFnet Steering Group
Upon completion of the project PIs are expected to put their intervention materials and
procedure manuals into the public domain andor make them available to other investigators
according to the approved plan for making data and materials available to the scientific
community and the NHLBI for the conduct of research at no charge other than the costs of
reproduction and distribution
The NHLBI reserves the right to terminate or curtail the project (or an individual award) in the
event of (a) failure to develop or implement mutually agreeable collaborative measurement
subject eligibility and data management sections of the protocols (b) substantial shortfall in
subject recruitment follow-up data reporting or quality control or other major breach of
protocol (c) substantive changes in the agreed-upon protocols with which NHLBI cannot
concur (d) reaching a major project outcome with persuasive statistical significance
substantially before schedule or (e) human subject ethical issues that may dictate a premature
termination
Any disagreement that may arise in scientificprogrammatic matters (within the scope of the
award) between award recipients and the NHLBI may be brought to arbitration An arbitration
panel will be composed of 3 membersmdash1 selected by the IPFnet Steering Group (with the
NHLBI member not voting) or by the individual PI in the event of an individual disagreement a
second selected by NHLBI and the third selected by the other 2 members This special
arbitration procedure in no way affects the PIrsquos right to appeal an adverse action that is otherwise
appealable in accordance with the PHS regulations at 42 CFR part 50 Subpart D and HHS
63
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
regulation at 45 CFR part 16 or the rights of the NHLBI under applicable statutes regulations
and terms of the award
102 IPFnet Steering Group
The IPFnet Steering Group is the main governing body of the project It is composed of the PIs
of the clinical centers the PI of the DCC and the NHLBI project scientist The clinical centers
the IPFnet DCC and the NHLBI each have 1 vote on the IPFnet Steering Group All decisions
are determined by majority vote
All major scientific decisions are determined by the IPFnet Steering Group It assumes overall
responsibility for the design and conduct of the trial It appoints (and disbands) committees and
subcommittees as the need arises designs approves and implements the study protocols
oversees the development of the MOOP monitors subject recruitment and treatment delivery
evaluates data collection and management oversees quality assurance procedures and
implements changes and enhancements to the study as required It also has primary responsibility
for facilitating the conduct of the trials and reporting the projectrsquos results
103 Data and Safety Monitoring Board
The NHLBI will establish a DSMB in accordance with established policies (see
httpwwwnhlbinihgovfundingpoliciesdsmb_insthtm) to ensure data quality and subject
safety and to provide independent advice to the NHLBI regarding progress and the
appropriateness of study continuation
104 Recommendations on Interim Monitoring of Efficacy Safety and Futility
First and foremost the role of the DSMB will be to review subject safety and trial conduct at
periodic points during the study The DSMB may require analyses of the primary endpoint
results for comparing the benefit and risks of treatment strategies The benefit of collecting
additional data on key secondary endpoints with extended follow-up and establishing a robust
64
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
evidence base for determining a standard of care will need to be carefully considered before
early termination of one or more treatment arms After careful consideration the IPFnet Steering
Group recommends conservative thresholds for the early examinations of the safety and efficacy
data
The DSMB will be expected to meet approximately every 6 months until trial completion to
review safety and toxicity data The DSMB may recommend stopping the study based on these
reviews Because the DSMB could stop the trial for safety concerns as well as for a large
efficacy benefit there could be multiple opportunities to reject the null hypothesis (no difference
in event rates between the PL and NAC groups) A Bonferroni approximation will be applied
during the one planned interim analysis for efficacy
Before locking the database a statistical analysis plan (SAP) will be developed to provide
complete details on the statistical analysis The SAP will include the specifics for how and when
the DSMB will be notified for AEs The IPFnet DCC will deliver to the DSMB all FDA-defined
AEs at 3-month intervals The IPFnet DCC will prepare narrative SAE reports in real time for
DSMB review including recommendations and analysis of similar events for each SAE
submitted to the FDA
65
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
11 Investigator and Sponsor Obligations
111 Monitoring
All monitoring activities for US clinical centers will be performed in accordance with DCRI
standard operating procedures Information regarding the types of visits will be outlined in the
PANTHER-IPF MOOP
112 Cost and Payment
There will be no cost to subjects enrolled in this trial Study-related procedures will be paid for
by the IPFnet
Subjects may be eligible for reimbursement for travel to the clinical center Details of payment
will be explained to each subject during the consent process
113 Confidentiality and Health Insurance Portability and Accountability Act
Considerations
Subject confidentiality will be protected throughout the study All subject data will be kept
strictly confidential and no subject-identifying information will be released to anyone outside
the project Confidentiality will be assured through several mechanisms First each subject will
be assigned an anonymous study ID which will then be used on all study forms Second any
study forms blood samples and paper records that contain subject information (eg address lists
phone lists) will be kept at the clinical centers in secured locked areas coded by number Once
blood is collected there will be no subject identifiers placed on blood samplesmdashonly the study
ID number and the date of sample collection Third access to all subject data and information
including laboratory specimens will be restricted to authorized personnel In the case of
computerized data this restricted access will be assured through user logon IDs and password
protection
66
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
At the IPFnet DCC only authorized personnel will have access to the data files containing study
data Security will be assured through user logon IDs passwords and appropriate access
privileges All study subjects will be identified only by their IPFnet ID numbers and no personal
identifying information such as name address or Social Security number will be entered into
the IPFnet DCC database Any subject-specific data reported to the IPFnet Steering Group will
be identified only by the IPFnet ID number
Finally subjects will not be identified by name in any reports or publications nor will the data
be presented in such a way that the identity of individual subjects can be inferred Analysis files
created for further study by the scientific community will have no subject identifiers These data
files will be created in accordance with the Ancillary Studies and Publication Policy of the
IPFnet
114 Informed Consent Procedures
All IPFnet subjects will provide written informed consent using procedures reviewed and
approved by each clinical centerrsquos IRB Informed consent will be undertaken by study personnel
in-person with the subject The subject has the option of declining further participation in the
study at that point No further study procedures will be conducted until the signed documents
have been provided to the IPFnet clinical center
115 Institutional Review Boards
Before initiating this study the protocol clinical center-specific informed consent forms Health
Insurance Portability and Accountability Act (HIPAA) forms recruitment materials and other
relevant information will be reviewed by a properly constituted IRB at each participating clinical
center A copy of the signed and dated IRB approval at each clinical center will be retrieved prior
to or during the site initiation visit and archived at the IPFnet DCC Any amendments to the
protocol other than simple administrative and typographical changes must be approved by each
IRB before they are implemented The clinical centers will seek annual renewals of their IRB
approvals in accordance with local procedures
67
__________________________________________ ________________
__________________________________________
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
12 Investigator Agreement
I have read the foregoing protocol PANTHER-IPF and agree that it contains all necessary
details for carrying out this study I will conduct the study as outlined herein and will complete
the study within the time designated
I will provide copies of the protocol and all pertinent information to all individuals responsible to
me who assist in the conduct of this study I will discuss this material with them to ensure they
are fully informed regarding the drug and the conduct of the study
I will fulfill all responsibilities for submitting pertinent information to the local IRB if
applicable that is responsible for this study
I further agree that NHLBI andor DCRI will have access to any source documents from which
eCRF information may have been generated
Signature of Principal Investigator Date
Name of Principal Investigator (printed or typed)
Protocol version date May 19 2009
Protocol Amendment 1 version date May 28 2010
Protocol Amendment 2 version date December 6 2011
68
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
13 References
1 Raghu G Brown KK Bradford WZ et al A placebo-controlled trial of interferon gamma-1b in patients with idiopathic pulmonary fibrosis N Engl J Med 2004350125-33 2 King TE Jr Safrin S Starko KM et al Analyses of efficacy end points in a controlled trial of interferon-gamma1b for idiopathic pulmonary fibrosis Chest 2005127171-7 3 Flaherty KR Thwaite EL Kazerooni EA et al Radiological versus histological diagnosis in UIP and NSIP survival implications Thorax 200358143-8 4 Wells AU Desai SR Rubens MB et al Idiopathic pulmonary fibrosis a composite physiologic index derived from disease extent observed by computed tomography Am J Respir Crit Care Med 2003167962-9 5 Raghu G Freudenberger TD Yang S et al High prevalence of abnormal acid gastroshyoesophageal reflux in idiopathic pulmonary fibrosis Eur Respir J 200627136-42 6 Kinnula VL Focus on antioxidant enzymes and antioxidant strategies in smoking related airway diseases Thorax 200560693-700 7 Coultas DB Zumwalt RE Black WC Sobonya RE The epidemiology of interstitial lung diseases Am J Respir Crit Care Med 1994150967-72 8 Raghu G Weycker D Edelsberg J Bradford WZ Oster G Incidence and prevalence of idiopathic pulmonary fibrosis Am J Respir Crit Care Med 2006174810-6 9 Olson AL Swigris JJ Lezotte DC Norris JM Wilson CG Brown KK Mortality from pulmonary fibrosis increased in the United States from 1992 to 2003 Am J Respir Crit Care Med 2007176277-84 10 Mannino DM Etzel RA Parrish RG Pulmonary fibrosis deaths in the United States 1979shy1991 An analysis of multiple-cause mortality data Am J Respir Crit Care Med 19961531548shy52 11 Hubbard R Johnston I Coultas DB Britton J Mortality rates from cryptogenic fibrosing alveolitis in seven countries Thorax 199651711-6 12 Johnston I Britton J Kinnear W Logan R Rising mortality from cryptogenic fibrosing alveolitis Bmj 19903011017-21 13 Raghu G Collard HR Egan JJ et al An official ATSERSJRSALAT statement idiopathic pulmonary fibrosis evidence-based guidelines for diagnosis and management Am J Respir Crit Care Med 2011183788-824 14 (USA) FDA FDA Public Health Advisory Interferon gamma-1b (marketed as Actimmune) In 2007 15 King TE Jr Pardo A Selman M Idiopathic pulmonary fibrosis Lancet 2011 16 Raghu G Brown KK Costabel U et al Treatment of idiopathic pulmonary fibrosis with etanercept an exploratory placebo-controlled trial Am J Respir Crit Care Med 2008178948shy55 17 Malouf MA Hopkins P Snell G Glanville AR An investigator-driven study of everolimus in surgical lung biopsy confirmed idiopathic pulmonary fibrosis Respirology 201116776-83 18 King TE Jr Behr J Brown KK et al BUILD-1 a randomized placebo-controlled trial of bosentan in idiopathic pulmonary fibrosis Am J Respir Crit Care Med 200817775-81 19 Richeldi L Costabel U Selman M et al Efficacy of a tyrosine kinase inhibitor in idiopathic pulmonary fibrosis N Engl J Med 20113651079-87
69
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
20 Borok Z Buhl R Grimes GJ et al Effect of glutathione aerosol on oxidant-antioxidant imbalance in idiopathic pulmonary fibrosis Lancet 1991338215-6 21 Meyer A Buhl R Magnussen H The effect of oral N-acetylcysteine on lung glutathione levels in idiopathic pulmonary fibrosis Eur Respir J 19947431-6 22 Behr J Maier K Degenkolb B Krombach F Vogelmeier C Antioxidative and clinical effects of high-dose N-acetylcysteine in fibrosing alveolitis Adjunctive therapy to maintenance immunosuppression Am J Respir Crit Care Med 19971561897-901 23 Cantin AM North SL Fells GA Hubbard RC Crystal RG Oxidant-mediated epithelial cell injury in idiopathic pulmonary fibrosis J Clin Invest 1987791665-73 24 Waghray M Cui Z Horowitz JC et al Hydrogen peroxide is a diffusible paracrine signal for the induction of epithelial cell death by activated myofibroblasts Faseb J 200519854-6 25 Larios JM Budhiraja R Fanburg BL Thannickal VJ Oxidative protein cross-linking reactions involving L-tyrosine in transforming growth factor-beta1-stimulated fibroblasts J Biol Chem 200127617437-41 26 Kinnula VL Fattman CL Tan RJ Oury TD Oxidative stress in pulmonary fibrosis a possible role for redox modulatory therapy Am J Respir Crit Care Med 2005172417-22 27 Meyer A Buhl R Kampf S Magnussen H Intravenous N-acetylcysteine and lung glutathione of patients with pulmonary fibrosis and normals Am J Respir Crit Care Med 19951521055-60 28 Behr J Degenkolb B Krombach F Vogelmeier C Intracellular glutathione and bronchoalveolar cells in fibrosing alveolitis effects of N-acetylcysteine Eur Respir J 200219906-11 29 Bando M Hosono T Mato N et al Long-term efficacy of inhaled N-acetylcysteine in patients with idiopathic pulmonary fibrosis Intern Med 2010492289-96 30 Demedts M Behr J Buhl R et al High-dose acetylcysteine in idiopathic pulmonary fibrosis N Engl J Med 20053532229-42 31 Toma TP Bhowmik A Rajakulasingam R Acetylcysteine in pulmonary fibrosis N Engl J Med 20063541086-9 author reply -9 32 Hunninghake GW Antioxidant therapy for idiopathic pulmonary fibrosis N Engl J Med 20053532285-7 33 Flaherty KR Mumford JA Murray S et al Prognostic implications of physiologic and radiographic changes in idiopathic interstitial pneumonia Am J Respir Crit Care Med 2003168543-8 34 Latsi PI du Bois RM Nicholson AG et al Fibrotic idiopathic interstitial pneumonia the prognostic value of longitudinal functional trends Am J Respir Crit Care Med 2003168531-7 35 Collard HR King TE Jr Bartelson BB Vourlekis JS Schwarz MI Brown KK Changes in clinical and physiologic variables predict survival in idiopathic pulmonary fibrosis Am J Respir Crit Care Med 2003168538-42 36 Jegal Y Kim DS Shim TS et al Physiology is a stronger predictor of survival than pathology in fibrotic interstitial pneumonia Am J Respir Crit Care Med 2005171639-44 37 Martinez FJ Safrin S Weycker D et al The clinical course of patients with idiopathic pulmonary fibrosis Ann Intern Med 2005142963-7 38 Hull JH Acetylcysteine in pulmonary fibrosis N Engl J Med 20063541089-91 author reply -91
70
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
39 Flaherty KR King TE Jr Raghu G et al Idiopathic interstitial pneumonia what is the effect of a multidisciplinary approach to diagnosis Am J Respir Crit Care Med 2004170904shy10 40 Raghu G Johnson WC Lockhart D Mageto Y Treatment of idiopathic pulmonary fibrosis with a new antifibrotic agent pirfenidone results of a prospective open-label Phase II study Am J Respir Crit Care Med 19991591061-9 41 Hunninghake GW Lynch DA Galvin JR et al Radiologic findings are strongly associated with a pathologic diagnosis of usual interstitial pneumonia Chest 20031241215-23 42 Lynch D Godwin J Safrin S et al High-resolution computed tomography in idiopathic pulmonary fibrosis diagnosis and prognosis Am J Respir Crit Care Med 2005172488-93 43 Mallinckrodt CH Watkin JG Molenberghs G Carroll RJ Choice of the primary analysis in longitudinal clinical trials Pharmaceutical Statistics 20043161-9 44 Bang H Tsiatis A Estimating medical costs with censored data Biometrika 200087329shy43 45 Lin DY Regression analysis of incomplete medical cost data Stat Med 2003221181-200 46 Rochon J Application of GEE procedures for sample size calculations in repeated measures experiments Stat Med 1998171643-58 47 Lachin JM Foulkes MA Evaluation of sample size and power for analyses of survival with allowance for nonuniform patient entry losses to follow-up noncompliance and stratification Biometrics 198642507-19
71
- PANTHER-IPFPREDNISONE AZATHIOPRINEAND N-ACETYLCYSTEINEA STUDY THAT EVALUATES RESPONSE INIDIOPATHIC PULMONARY FIBROSIS
-
- Protocol Summary
- Table of Contents
- List of Tables
- List of Figures
- List of Abbreviations
- 1 Summary
- 2 Hypotheses and Specific Aims
-
- 21 Null Hypothesis
- 22 Specific Aim 1
- 23 Specific Aim 2
- 24 Prespecified Subgroups of Interest
-
- 3 Background and Significance
-
- 31 Idiopathic Pulmonary Fibrosis is the Most Common Interstitial Lung Disease
- 32 Rationale for Placebo Control
- 33 Rationale for N-acetylcysteine
- 35 Rationale for N-acetylcysteine as a Stand-alone Therapy
- 36 Rationale for the Study Design and Primary Endpoint
- 37 Rationale for Blinding of Treatments
-
- 4 Methods
-
- 41 Inclusion Criteria
- 42 Diagnosis of IPF
- 43 Exclusion Criteria
- 44 Study Design and Study Visit
- 45 Dose Justification
- 46 Contraindications Precautions and Side Effects of Study Medications
- 47 Recruitment Procedures
- 48 Study Procedures
- 49 Concomitant Medications
- 410 Laboratory Testing
- 411 Blinding of Study Drugs
-
- 5 Study Endpoints
-
- 51 Primary Study Endpoint
- 52 Secondary Study Endpoints
-
- 6 Safety Evaluations and Procedures
-
- 61 Adverse Events
- 62 Clinical Medical Monitoring
- 63 Unblinding Procedures
-
- 7 Study Drug Procedures
- 8 Data Management
-
- 81 Hardware and Software Configuration
- 82 Sources of Data
-
- 9 Study Design and Data Analysis
-
- 91 General Analytic Considerations
- 92 Randomization Blinding and Reporting of Results
- 93 Stratification
- 94 Specification of the Primary Analyses
- 95 Analysis of Longitudinal Endpoints
- 96 Analysis of Binary Time-to-Event and Time-Lagged Endpoints
- 97 Power Analysis
-
- 10 Study Administration
-
- 101 Cooperative Agreement Mechanism
- 102 IPFnet Steering Group
- 103 Data and Safety Monitoring Board
- 104 Recommendations on Interim Monitoring of Efficacy Safety and Futility
-
- 11 Investigator and Sponsor Obligations
-
- 111 Monitoring
- 112 Cost and Payment
- 113 Confidentiality and Health Insurance Portability and Accountability ActConsiderations
- 114 Informed Consent Procedures
- 115 Institutional Review Boards
-
- 12 Investigator Agreement
- 13 References
-

PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
List of Abbreviations
6MWT 6-minute walk test
A-aPO2 alveolar-arterial PO2 difference
ABG arterial blood gas
AE adverse event
AEx acute exacerbation
AG albuminglobulin
ALT alanine aminotransferase
AST aspartate aminotransferase
ATS American Thoracic Society
AZA azathioprine
BAL bronchoalveolar lavage
BUN blood urea nitrogen
CBC complete blood count
cGMP Current Good Manufacturing Practice
CPI Composite Physiologic Index
CPK creatine phosphokinase
CT computed tomography
DCC Data Coordinating Center
DCRI Duke Clinical Research Institute
8
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
DLCO diffusing capacity of the lung for carbon monoxide
DLCOpred diffusing capacity of the lung for carbon monoxide percent predicted
DSMB data and safety monitoring board
eCRF Electronic case report form
ERS European Respiratory Society
FDA Food and Drug Administration (US)
FEV1 forced expiratory volume in 1 second
FSH follicle-stimulating hormone
FVC forced vital capacity
FVCpred forced vital capacity percent predicted
GGT gamma glutamyl transferase
GSH glutathione
HAD Hospital Anxiety and Depression
HHS Health amp Human Services (US Dept of)
HIPAA Health Insurance Portability and Accountability Act
HRCT high-resolution computed tomography
IBW ideal body weight
ICE CAP Investigating Choice Experiments for Preferences of Older People Capability Instrument
ILD interstitial lung disease
IPF idiopathic pulmonary fibrosis
9
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
IPFnet Idiopathic Pulmonary Fibrosis Clinical Research Network
IRB institutional review board
ITT intent to treat
IV intravenous
IVRS interactive voice response system
LDH lactate dehydrogenase
LFT liver function test
LOCF last observation carried forward
LSD Least Significant Difference
MAR missing at random
MCAR missing completely at random
MMRM mixed model repeated measures
MOOP manual of operating procedures
NAC N-acetylcysteine
NHLBI National Heart Lung and Blood Institute (US)
NIH National Institutes of Health (US)
NSIP nonspecific interstitial pneumonia
PaO2 partial pressure of arterial oxygen
PCP primary care provider
PFT pulmonary function test
10
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
PHS Public Health Service (US)
PI principal investigator
PL placebo
PLT platelet
PRED prednisone
QOL quality of life
SAE serious adverse event
SAP statistical analysis plan
SGRQ St Georgersquos Respiratory Questionnaire
SpO2 oxygen saturation by pulse oximetry
TPMT thiopurine methyl transferase
UCSD SOBQ University of California at San Diego Shortness of Breath Questionnaire
UIP usual interstitial pneumonia
ULN upper limit of normal
USP United States Pharmacopoeia
VC vital capacity
WBC white blood cell
11
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
PREDNISONE AZATHIOPRINE AND N-ACETYLCYSTEINE A STUDY
THAT EVALUATES RESPONSE IN IDIOPATHIC PULMONARY FIBROSIS
1 Summary
There are currently no drug therapies that have proven to be effective in the treatment of idiopathic pulmonary
fibrosis (IPF) Previous clinical drug trials have been difficult to interpret due to lack of true placebo (PL)
controls or other methodological concerns Clinical efficacy of immunosuppressive therapies and agents that
reduce oxidative stress remains controversial The IPF Clinical Research Network (IPFnet) is conducting a
randomized double-blind placebo-controlled trial designed to assess the safety and efficacy of
N-acetylcysteine (NAC) as monotherapy in subjects with mild or moderate IPF
The study initially employed a 3-arm design with 111 randomization to NAC azathioprine (AZA)-prednisone
(PRED)-NAC and PL with each subject to be treated up to a maximum of 60 weeks followed by a tapering of
PREDPL and a 4-week period for safety evaluation Approximately 390 subjects who have mild to moderate
IPF (defined as forced vital capacity percent predicted [FVCpred] ge 50 and diffusing capacity of the lung
for carbon monoxide percent predicted [DLCOpred] 30) diagnosed within the past 48 months were to be
enrolled
At the pre-specified interim analysis the DSMB recommended termination of the prednisone-azathioprine-
NAC arm of the study No additional patients will be randomized to that arm However the NAC and placebo
arms remain open for enrollment and we will enroll approximately 130 subjects in each arm (inclusive of the
subjects enrolled at the time of the interim analysis) Follow up for subjects enrolled into the two arms will
continue for 60 weeks
The primary endpoint is the change in longitudinal measurements of FVC over the study period The primary
goal of this study to establish an evidence-based standard of care and clarify myths from facts for
pharmacotherapy of IPF has been met in part by demonstrating that the widely used triple therapy was harmful
to patients with IPF (NHLBI press release Oct 21 2011) To determine the potential therapeutic benefits of
NAC alone the study will continue to enroll patients as a two-arm double-blind placebo-controlled study from
this point on (NAC vs placebo) as recommended by the DSMB following the pre-specified interim analysis
12
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
2 Hypotheses and Specific Aims 21 Null Hypothesis
Treatment with NAC will provide the same efficacy as PL as measured by longitudinal changes in FVC
22 Specific Aim 1
This study is designed to assess the safety and efficacy of NAC in subjects with newly diagnosed IPF
23 Specific Aim 2
Secondary goals of this study are to assess differences between treatment groups for the following
1 Mortality
2 Time to death
3 Frequency of acute exacerbations (AExs)
4 Frequency of maintained FVC response
5 Time-to-disease progression
6 Change in DLCO
7 Change in Composite Physiologic Index (CPI)
8 Change in resting alveolar-arterial oxygen gradient
9 Change in 6-minute walk test (6MWT) distance
10 Change in 6MWT oxygen saturation area under the curve
11 Change in 6MWT distance to desaturation lt 80
12 Change in 6MWT minutes walked
13 Changes in health status as measured by the SF-36 EuroQol and St Georgersquos Respiratory
Questionnaire (SGRQ)
14 Changes in dyspnea as measured by the University of California at San Diego Shortness of Breath
Questionnaire (UCSD SOBQ)
15 Frequency and types of adverse events (AEs)
16 Frequency and types of respiratory complications both infectious and noninfectious
17 Frequency of hospitalizations both all-cause and respiratory-related
13
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
24 Prespecified Subgroups of Interest
Treatment effects will be estimated and compared within key subgroups
Higher enrollment FVC12
Typical vs atypical high-resolution computed tomography (HRCT) reading at baseline3
Recent vs more remote diagnosis (time from initial diagnosis of IPF le 1 year and gt 1 year)
Lower CPI score at enrollment4
Medical therapy for gastroesophageal reflux5
Ethnic background
Sex
Smoking history (current or ex-smoker vs never smoker) given potential impact on oxidant status6
Presence of emphysema gt 25 on HRCT
14
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
3 Background and Significance
31 Idiopathic Pulmonary Fibrosis is the Most Common Interstitial Lung Disease
IPF is the most common interstitial lung disease (ILD) of unknown etiology The current incidence and
prevalence of IPF in the United States are not known A 1994 study of a population-based registry of subjects in
Bernalillo County New Mexico USA estimated an incidence of 107 cases per 100000 per year for males and
74 cases per 100000 per year for females the prevalence of IPF was estimated at 20 per 100000 for males and
13 per 100000 for females7 Extrapolating from a large healthcare claims database a more recent review
estimated the prevalence of IPF in the United States at 427 per 100000 (incidence estimated at 163 per
100000 per year)8 Recent epidemiological studies indicate increasing mortality rates from IPF in the United
States and other industrialized nations9-12
Approximately two-thirds of subjects with IPF are over the age of 60 at the time of presentation and the
incidence increases with age13 IPF has no distinct geographical distribution and predilection by race or
ethnicity has not been identified13 Individual subjects may remain relatively stable for prolonged periods
experience very slow declines in lung function with progression of radiographic abnormalities for a period of
months to years or experience more rapid declines and subsequent death Only 20 to 30 of IPF patients
survive for 5 years following diagnosis
There is currently no proven effective pharmacological treatment for IPF13 Anti-inflammatory and
immunosuppressive agents have been the traditional approach to the management of patients with IPF Based
on the results of the interim analysis of the PANTHER-IPF trial this lsquotraditional approachrsquo will be aborted
However it remains unknown if NAC alone will prove beneficial in IPF patients The primary goal of the
modified study is to establish an evidence-based standard of care and clarify the role of this specific antioxidant
pharmacotherapy for IPF
32 Rationale for Placebo Control
IPF is a disorder for which there is no proven efficacious therapy A major objective of this trial is to test to the
greatest degree possible a proposed standard of care for patients with IPF The current traditional therapy
15
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
employs immunosuppressive and corticosteroid drugs Interim review of the original PANTHER-IPF study has
documented increased adverse events and lack of efficacy for AZA-PRED-NAC compared to placebo
suggesting that this therapeutic approach should not be employed Whether this applies to NAC alone which
has been advocated by international societies has not been proven in well-designed well-powered clinical
trials The recommendations made in the recently published evidence guidelines for NAC monotherapy was
weak based on low quality13 Thus this continued clinical trial randomizing patients to receive NAC or placebo
is pivotal and will answer the important question of the potential therapeutic benefits of NAC monotherapy with
grade A evidence In this prospective randomized clinical trial the inclusion of a PL arm is therefore vital to
adequately test the benefits of NAC in well-characterized subjects with IPF
If NAC has no true efficacy then its role as standard of care will be refuted If a benefit compared with PL is
confirmed it will establish a benchmark against which future novel therapies for IPF will be safely compared
As there is no currently accepted therapy for IPF there is an increasing body of published literature supporting
the concept of no treatment as the ldquobest carerdquo option for IPF13
Post hoc analyses of PL-controlled trials suggest that subjects with milder disease may be more amenable to
therapy12 It is notable that a recent international prospective randomized trial of interferon-gamma for IPF
also included a PL arm the study was terminated early by the data and safety monitoring board (DSMB) due to
lack of treatment effect1415 This underscores the belief that a proven effective therapy for IPF does not
currently exist and that true placebo-controlled trials remain the gold standard Similarly recently completed
trials of etanercept everolimus bosentan and BIPF 1120 in IPF have included PL-treated arms16-19 In three of
these trials the treated subjects showed little if any objective improvement Based on this evidence and the
current status of IPF therapy and therapeutic trials we believe that clinicians and subjects will continue to enroll
in a PL-controlled study
33 Rationale for N-acetylcysteine
NAC is a derivative of the amino acid L-cysteine NAC has been shown to augment levels of the naturally
occurring antioxidant glutathione (GSH ) (glutathione γ-glutamyl cysteinyl glycine) both in vitro and in
vivo2021 GSH is present in all eukaryotic cells and may play an important role in protecting alveolar epithelial
cells against oxidant injury The concentration of GSH in the bronchoalveolar lavage (BAL) fluid in patients
16
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
with IPF is markedly diminished compared with normal subjects This GSH deficiency may be corrected by
exogenous administration of NAC2122
There is evidence of enhanced production of oxidants in an IPF lung Both inflammatory cells and
myofibroblasts derived from patients with IPF generate increased amounts of extracellular oxidants including
hydrogen peroxide2324 Secretion of hydrogen peroxide by activated myofibroblasts may induce the death of
adjacent lung epithelial cells by paracrine mechanisms24 Additionally generation of oxidants by myofibroblasts
induces oxidative crosslinking of extracellular matrix proteins25 a potential mechanism for aberrant matrix
remodeling Thus an oxidant-antioxidant imbalance exists in the lungs of IPF patients26 NAC may confer
protection against this imbalance by augmenting GSH levels in addition to its more direct free-radical
scavenging activity
Intravenous (IV) NAC therapy has been shown to increase total BAL GSH in 8 IPF subjects27 Oral NAC (600
mg 3 times per day) has been shown to decrease markers of oxidant injury and improve both total and reduced
GSH levels in the epithelial lining fluid of subjects with IPF in a small uncontrolled study22 pulmonary
function improved modestly with therapy A similar study in 18 IPF subjects confirmed increased intracellular
GSH concentration after 12 weeks of NAC (600 mg 3 times per day)2228 no clinical correlates were reported
Inhaled NAC was suggested to improve pulmonary function in an open label study29
35 Rationale for N-acetylcysteine as a Stand-alone Therapy
Results of a double-blind multi-center European clinical trial of 150 IPF subjects testing combinations of AZAshy
PRED vs AZA-PRED-NAC have been reported30 NAC added to AZA-PRED (ldquoconventional therapyrdquo) had a
significant positive effect on DLCO (p lt 0005) and vital capacity (VC) (p lt 005) at the end of 1 year30 The
recent ATSERS position statement after much discussion concluded that NAC alone should not be considered
in the majority of patients with IPF without additional data from well-designed studies
The interpretation of these data has been quite controversial Some have suggested that the magnitude of the
treatment effect although statistically significant is modest31 Others have suggested that NAC may be
modulating potential toxic effects of AZA-PRED alone32 supporting the investigation of NAC as stand-alone
therapy
17
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
The IPFnet is now completing the PANTHER-IPF trial with a 11 randomization (NAC vs placebo) and a
simple practical feasible and scientifically rational design that will establish standard of care with NAC for
IPF based on a currently available therapeutic agent and the existing data to support its use We anticipate that
all future clinical trials of novel therapeutic agents will be tested against this to-be-established standard of care
36 Rationale for the Study Design and Primary Endpoint
The optimal study design of a therapeutic trial in IPF would include survival as a primary endpoint The
published results of the IFN-γ 1b Phase 3 (GIPF-001) trial suggested a survival benefit in subjects with milder
disease in retrospective analyses1 although the trial was underpowered to address this question This was likely
related to the limited mortality in the PL arm of the study which included IPF subjects with mild to moderate
disease This study documents that an IPF study powered to improve survival in a patient population with mild
disease requires a larger sample size andor duration of study In fact the recently aborted Phase 3 IFN-γ 1b
(GIPF-007 INSPIRE) study was a survival-based study and recruited more than 800 subjects at 75 centers
worldwide1415 As such within the context of the current IPFnet trial survival is an impractical primary
endpoint variable
Several groups have published data defining an appropriate surrogate outcome variable a 10 decrement in
FVC during 6 to 12 months is a powerful predictor of survival in IPF33-36 Furthermore additional evidence
suggests a similar predictive ability for a 10 decrement in FVC during 3 months of follow-up37 With strong
supportive evidence of FVC progression being related to mortality on a per-subject basis this study will use
FVC changes in liters between treatment groups as the primary endpoint Previously published IPF studies have
shown a steady decline in FVC (and FVCpred) among control group subjects230 The GIPF-001 study
suggested a 48-week decrease in FVC of 016 L in the PL-treated subjects The IFIGENIA study demonstrated
a decline in FVC of approximately 019 L over 52 weeks in the subjects randomized to the control treatment
Figure 1 depicts the change in FVC for control groups from previously published IPF studies38 Based on these
data we expect that the PL group will have a decline of 020 L over the 60-week study period The IPFnet
Steering Group determined that a clinically meaningful improvement would be the preservation of the majority
of the 020-L FVC decline Therefore a mean treatment difference of 015 L in mean FVC over the 60-week
study period was determined to be a clinically meaningful difference
18
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Δ f
rom
bas
elin
e (i
n L
)
01
005
0
-005
-01
-015 Projected Δ for placebo
-02
-025
-019
-016
-013 Pirfenidone GIPF001
NAC
Placebo
4 8 12 16 20 24 28 32 36 40 44 48 52 56 60
Week
Figure 1 Changes in FVC From Baseline in Prior IPF Clinical Trials
Recent data suggest that various patient subgroups would be expected to potentially exhibit differential response
to therapy These parameters will be used to a priori separate patients by a series of baseline characteristics
including
1 Higher enrollment FVC12
2 Typical vs atypical high-resolution computed tomography (HRCT) reading at baseline3
3 Recent vs more remote diagnosis (time from initial diagnosis of IPF le 1 year and gt 1 year)
4 Lower CPI score at enrollment4
5 Medical therapy for gastroesophageal reflux5
6 Ethnic background
7 Sex
8 Smoking history (current or ex-smoker vs never smoker) given potential impact on oxidant status6
9 Presence of emphysema gt 25 on HRCT
37 Rationale for Blinding of Treatments
The issue of treatment blinding was given a great deal of consideration with subject safety being the primary
concern After discussion among the Steering Group members it was decided that as long as subject safety
could be ensured blinding was necessary Blinding allows the study to
Have optimal scientific validity and potential to impact the standard of care for subjects
19
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Make objective assessments of treatment effects
Maintain clinical equipoise among investigators
Encourage subjects to have similar levels of contact with the medical community
Minimize the differential dropout rates across study arms
20
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
4 Methods 41 Inclusion Criteria
1 Age 35 to 85 years inclusive
2 FVC ge 50 of predicted (post-bronchodilator measurement from the screening visit)
3 DLCO ge 30 of predicted (hemoglobin corrected and altitude corrected if gt4000 ft above sea level)
4 Ability to understand and provide informed consent
5 Diagnosis of IPF according to a modified version of the ATS criteria le 48 months from enrollment The
date of diagnosis is defined as the date of the first available HRCT or surgical lung biopsy characteristic
of definite UIP
411 Subjects Shown to Have Usual Interstitial Pneumonia Pattern on Surgical Lung Biopsy
Subjects who have been shown to have UIP pattern on lung biopsy must have all of the following
1 Exclusion of other known causes of ILD such as drug toxicity clinically significant environmental
exposures or diagnosis of connective tissue diseases
2 Bibasilar reticular abnormalities with minimal ground glass opacities on HRCT scan
412 Subjects Who Have Not Undergone a Surgical Lung Biopsy
In addition to the criteria above these subjects must have radiological findings considered to be definite for the
diagnosis of UIPIPF
1 Bibasilar reticular abnormalities with minimal ground glass opacities
2 Honeycombing as the predominant feature and located in the peripheral lung bases
42 Diagnosis of IPF
Only subjects with definite IPF will be eligible for enrollment in this study We will utilize a combination of
clinicalphysiologic features HRCT and review of a clinically obtained surgical lung biopsy specimen to
establish the diagnosis of IPF An algorithm for the diagnosis is provided to guide entry into the protocol as
outlined in the inclusion and exclusion criteria (Figures 2 and 3) This multi-disciplinary approach uses
21
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
expertise from clinicians radiologists and pathologists Investigators at each site in conjunction with central
pathology will work together to establish the diagnosis of IPF This interactive approach to the diagnosis of IPF
increases the level of agreement between observers39
A subject with suspected ILD should be evaluated for secondary causes including but not limited to
environmental exposures drugs and systemic diseases Presence of any of these findings felt to be significant
enough to cause an ILD should disqualify the subject from entry into the trial
If secondary causes are absent an HRCT scan may be obtained If an HRCT of sufficiently high quality has
been obtained within the last 3 months that scan may be used for diagnosis In the appropriate clinical setting
the diagnosis of IPF can be made by the demonstration of a typical radiographic pattern on HRCT or by
demonstration of UIP pattern on a surgical lung biopsy The following criteria for a radiographic (ie
nonsurgical) diagnosis will be used In the absence of known exposures andor clinical associations attributable
to pulmonary fibrosis and in the appropriate clinical setting the presence of definite UIP pattern in HRCT
images is required to meet study criteria for the diagnosis of IPF
Figure 2 Diagnosis of Idiopathic Pulmonary Fibrosis in the IPFnet
22
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Figure 3 Pathology Flow Chart Surgical Lung Biopsy Diagnosis
Requirement for diagnosis
1 Clinical exclusion of other known causes (connective tissue diseases environmental and drug
exposures) of ILD
2 Radiographic HRCT with bibasilar reticular abnormality and honeycomb change with minimal
ground glass opacities
Appropriate clinical setting
1 Age gt 50 years
2 Insidious onset of unexplained dyspnea
3 Duration of illness for ge 3 months
4 Bibasilar inspiratory crackles
23
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Unlike the ATSERS consensus criteria published in 2000 bronchoscopy will not be required for diagnosis
This decision was made based on the experience of the IPFnet Steering Group members regarding the utility of
bronchoscopy in the diagnosis of IPF The presence of an atypical HRCT finding will require documentation of
a definitive diagnosis by surgical lung biopsy In fact this is in keeping with the recently published evidence
based guidelines for diagnosis and management of IPF13 As shown in Figure 3 central review of the pathology
data will be required for a diagnosis of IPF
We will not require central review of HRCT as several studies have shown that a confident local interpretation
of clinicalHRCT criteria as definite IPFUIP is associated with a high positive predictive value for finding UIP
at surgical lung biopsy (see Table 1) Differences in sensitivity in these series likely reflect subject selection as
Flaherty et al3 evaluated only UIP and nonspecific interstitial pneumonia (NSIP) while Raghu et al40 and
Hunninghake et al41 included a broader range of ILD
Table 1 Operating Characteristics of Local HRCT Review for Diagnosis of UIP
Researcher of Subjects Sensitivity () Specificity () PPV () NPV ()
Raghu et al 40
59 (29 UIP by SLB) 78 90 88 82
Hunninghake et al 41 91 (54 UIP by SLB)
74 81 85 67
Flaherty et al 3 96 (only NSIP amp UIP)
37 100 100 30
Abbreviations PPV positive predictive value NPV negative predictive value UIP usual interstitial pneumonia SLB surgical lung biopsy and NSIP nonspecific interstitial pneumonia
Furthermore an analysis of the HRCT scans from subjects enrolled in the GIPF-001 trial confirmed that local
site interpretations have a high congruity to a central radiology core In this multi-center study 263 HRCT
scans were read as definite IPF and a retrospective central radiology core review found 932 to be consistent
with IPF 42 We will also take several additional steps to insure that the local HRCT reads are accurate
including
1 A detailed training module has been developed and must be completed by each site radiologist before
site initiation
2 Clinical centers are to mail all HRCT scans to the HRCT core lab The first 10 HRCT scans from
subjects enrolled at each enrolling clinical center will be reviewed centrally to be certain that local reads
24
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
25
are congruent with a central interpretation If discrepancies are identified additional education will be
provided and HRCT scans will continue to be reviewed centrally until the central radiology core is
confident that the local center is performing appropriately
3 Random scans will be obtained from each center throughout the study to confirm that the local read
continues to agree with central interpretation If discrepancies are identified they will be addressed as in
2 above
In all cases if a subject has a surgical lung biopsy sample that sample will be reviewed by the local and central
pathologists Therefore the only cases that would not be subject to a direct central review process are those
where the HRCT meets the centrally defined criteria for an unequivocal diagnosis and a lung biopsy sample is
not available Table 2 below summarizes the possible combinations for making a diagnosis
Table 2 Combining HRCT and Pathology Interpretations to Determine if IPF is Present
HRCT Diagnosis Pathology Diagnosis Diagnosis of IPF
Definite UIP Definite UIP Yes
Definite UIP Probable UIP Yes
Definite UIP Possible UIP Yes
Definite UIP Not UIP No
Definite UIP Unavailable Yes
Consistent with UIP Definite UIP Yes
Consistent with UIP Probable UIP Yes
Consistent with UIP Possible UIP No
Consistent with UIP Not UIP No
Consistent with UIP Unavailable No
Inconsistent with UIP Any No
Abbreviations HRCT high-resolution computed tomography IPF idiopathic pulmonary fibrosis
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
UIP usual interstitial pneumonia Dx diagnosis 43 Exclusion Criteria
1 History of clinically significant environmental exposure known to cause pulmonary fibrosis
Occupational exposures such as asbestos or environmental exposure to organic dust such as occurs in
pigeon breeders may at times mimic the clinical and radiographic findings of IPF
2 Diagnosis of connective tissue disease felt by the principal investigator (PI) to be the etiology of the
interstitial disease Diagnosis of collagen-vascular conditions will be according to the published
American College of Rheumatology criteria As such the presence of any documented collagen-vascular
disorder or the presence of any suspicious symptom complex whether or not associated with
significantly abnormal rheumatological serologies will exclude the subject at the discretion of the PI
3 Extent of emphysema greater than the extent of fibrotic change (honeycombing reticular changes) on
HRCT scan
4 Forced expiratory volume in 1 second (FEV1)FVC ratio lt 065 at screening (postbronchodilator)
5 Partial pressure of arterial oxygen (PaO2) on room air lt 55 mm Hg (lt 50 mm Hg at Denver site)
6 Residual volume gt 120 predicted at screening (postbronchodilator)
7 Evidence of active infection
8 Significant bronchodilator response on screening spirometry defined as a change in FEV1 ge 12 and
absolute change gt 200 mL OR change in FVC ge 12 and absolute change gt 200 mL The percent
difference between the FVC (or FEV1) values will be calculated by taking the absolute value of the
difference and dividing it by the larger of the two FVC (or FEV1) values
9 Screening and enrollment post-bronchodilator FVC measurements (in liters) differing by gt 11 The
percent difference between the FVC values will be calculated by taking the absolute value of the
difference and dividing it by the larger of the two FVC values (eg the percent difference between FVC
measurements of 19 and 20 liters would be determined by taking the difference between the two (01
liters) and dividing by the larger of the two (20 liters) So 0120 = 5 and these FVC measurements
would not exclude the subject
10 Listed for lung transplantation ie the patient has completed the evaluation process has been accepted
as a candidate for transplantation at an appropriate center and is waiting to receive notification of an
available donor organ
11 History of unstable or deteriorating cardiac disease
12 Myocardial infarction coronary artery bypass or angioplasty within 6 months of screening
26
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
13 Unstable angina pectoris or congestive heart failure requiring hospitalization within 6 months of
screening
14 Uncontrolled arrhythmia
15 Severe uncontrolled hypertension
16 Known HIV or hepatitis C
17 Known cirrhosis and chronic active hepatitis
18 Active substance andor alcohol abuse (as determined by site PI)
19 Pregnancy or lactation (subjects who are pregnant or breastfeeding)
20 Known hypersensitivity to study medication
21 Any condition other than IPF that in the opinion of the site PI is likely to result in the death of the
subject within the next year
22 Any condition that in the judgment of the PI might cause participation in this study to be detrimental to
the subject or that the PI deems makes the subject a poor candidate
23 Any therapy directed at pulmonary fibrosis (excepting triple therapy of prednisone plus azathioprine
plus NAC) requires a 30-day washout period before randomized Triple therapy of lt= 12 weeks duration
in the past 4 years requires a 30-day washout period before randomization
24 History of triple therapy of prednisone plus azathioprine plus NAC for gt 12 weeksrsquo duration in the past
4 years or previous enrollment in the triple-therapy arm of the PANTHER-IPF study
44 Study Design and Study Visit
441 Study Design Summary
This study will be a randomized double-blind PL-controlled trial designed to assess the safety and efficacy of
NAC in subjects with newly diagnosed IPF
Subjects with mild to moderate IPF (defined as FVCpred ge 50 and DLCOpred ge 30) diagnosed within
the past 48 months will be enrolled Screening will continue until April 30 2012
27
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
The study will employ a 2-arm design with 11 randomization to NAC or PL Once enrolled subjects will visit
the clinical center at 15 weeks and 15-week intervals thereafter Each subject will be treated and followed for a
maximum of 60 weeks
During the 60-week visit subjects will be taken off all study agents Approximately four weeks after the final
dose of study agent is taken subjects will receive a safety phone call from the study site
442 Study Visits
Subjects who meet entry criteria will review the informed consent a written description of the purpose
procedures and risks of the study with the PI co-investigator or study coordinator and all questions will be
answered The informed consent form will be signed by the subject at screening No protocol-specific
procedures will be performed until the subject has signed and dated an informed consent form This includes the
screening procedures
4421 Screening
Once informed consent is obtained subjects may immediately begin the screening process or may return within
28 days of consent In the event a study subject has been clinically evaluated at the study site by an IPFnet study
physician and has performed testing within three weeks for this clinical evaluation that meets guidelines
provided in the IPFnet PANTHER-IPF Manual of Operating Procedures (MOOP) this testing may be used to
satisfy the following screening criteria medical history physical exam arterial blood gas (ABG) with A-a
gradient vital signs with oximetry body height and weight spirometry DLCO lung volumes and HRCT scan
Allowing the use of previously performed test results that meet study guidelines for the screening visit is
intended to permit subjects easier access to study entry to prevent subjects from repeating testing that has been
performed within the study window and to decrease risks to subjects from repeated exposure to procedures
such as arterial puncture and HRCT
The following procedures will be performed at screening
Medical history and a physical examination
28
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Measure height and weight
Serum pregnancy test (if applicable)
Measure vital signs including oximetry
Blood draws performed and the following analyses conducted
o Hematology (red cell count white cell count hemoglobin hematocrit cell indices differential
platelet count)
o Blood chemistries according to central laboratory protocol (see Section 410 Laboratory
Testing)
o Beta human chorionic gonadotropin (serum) pregnancy test (in women of childbearing potential)
o Urinalysis
Pulmonary Function Tests (PFTs) including spirometry pre- and post- bronchodilator and postshy
bronchodilator measurement of lung volumes and measurement of hemoglobin adjusted diffusing
capacity
Measure ABGs
HRCT if a satisfactory scan has not been performed on the subject within 3 months of screening (see
PANTHER-IPF MOOP for more details)
Surgical lung biopsies (if applicable) reviewed by local and central pathology departments
Current medications If required a washout period discussed with the subject and initiated at this visit
4422 Enrollment
The enrollment visit is expected to take place within eight weeks of the screening visit Enrollment visit
activities include
Measure vital signs including oximetry
Measure height and weight
Serum pregnancy test (if applicable)
If consent has been given blood will be drawn and a urine specimen collected for the bio-specimen
repository
Spirometry (post-bronchodilator)
Measure 6MWT with Borg Dyspnea Scale
29
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Collect Quality-of-life (QOL) data using the SF-36 EuroQol Investigating Choice Experiments for
Preferences of Older People Capability Instrument (ICE CAP) and SGRQ
Female subjects complete Gender Substudy questionnaire
Dyspnea status collected using the UCSD SOBQ
Evaluate Acute Exacerbation (AEx)
Review of any Adverse Events (AEs)
Review of concomitant medications
Subject receives diary and instructions on its purpose and proper use
Subject receives supply of study drug sufficient to last until his or her 15-week study visit
See the Schedule of Assessments (Table 3) for more details Subjects with screening and enrollment postshy
bronchodilator FVC measurements (in liters) differing by more than 11 are not eligible to be enrolled in the
study
Subjects will be asked to provide a physician of record This physician will be considered the subjectrsquos primary
care provider (PCP) and if the subject agrees the PCP will be informed by letter of the subjectrsquos enrollment in
the trial The subject will be informed that his or her ongoing medical care should be received from the PCP
The PCP will be informed of any safety issues identified by the study staff The PCP will also be given
information regarding communication with study personnel about pertinent health issues or clinic encounters
the subject may have
4423 Week 15
The week 15 visit is expected to occur within +- 14 days of the subjectrsquos scheduled visit time (eg the week 15
visit should occur anytime between 13 and 17 weeks after starting study drug Week 15 activities include
Measure vital signs with oximetry
Measurement height and weight
Serum pregnancy test (if applicable)
Spirometry (post-bronchodilator) measurement
Review of AEs
Evaluate for AEx
30
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Review concomitant medications
If consented draw blood and collect urine specimen for the biospecimen repository
Subjects return used and unused study drug for the visit
Review study diary and a new study diary will be given
Provide additional supply of study drug sufficient to last until the next scheduled visit
4424 Week 30
The week 30 visit is expected to occur within +- 14 days of the subjectrsquos scheduled visit time (eg the week 30
visit should occur anytime between 28 and 32 weeks after starting study drug) Week 30 activities include
Physical examination
Measure vital signs with oximetry
Measure height and weight
Laboratory values (complete blood count [CBC] and serum chemistries)
Serum pregnancy test (if applicable)
Measure spirometry (post-bronchodilator)
6MWT with Borg scale
DLCO
Review of AEs
Evaluate for AEx
Review concomitant medications
Complete all QOL and dyspnea questionnaires (EuroQol ICE CAP SF-36 SGRQ and UCSD SOBQ)
If consent has been given blood will be drawn and a urine specimen collected for the biospecimen
repository
Review study diary
Subjects return used and unused study drug for the visit
Provide additional supply of study drug sufficient to last until the next scheduled visit
4425 Week 45
31
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
The week 45 visit is expected to occur within +- 14 days of the subjectrsquos scheduled visit time (eg the week 45
visit should occur anytime between 43 and 47 weeks after starting study drug) Week 45 activities include
Measure vital signs with oximetry
Measure height and weight
Serum pregnancy test (if applicable)
Measure spirometry (post-bronchodilator)
Review of AEs
Evaluate for AEx
Review concomitant medications
If consent has been given blood will be drawn and a urine specimen collected for the biospecimen
repository
Subjects return used and unused study drug for the visit
Study diary reviewed
Provide additional supply of study drug sufficient to last until the next scheduled visit
4426 Week 60 (Early Withdrawal or Final Treatment Visit)
At week 60 or at subject withdrawal from the study (premature by study doctor or subjectrsquos decision) a final
treatment visit will occur At this final treatment visit subjects will discontinue NACPL abruptly Week 60
activities also include
Physical examination
Measure vital signs with oximetry
Measure height and weight
Laboratory values (complete blood count [CBC] and serum chemistries)
Spirometry (post-bronchodilator) measurement
6MWT with Borg scale measurement
DLCO
Lung volumes
ABG
Review of AEs
32
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Evaluate for AEx
Review concomitant medications
Subjects will complete all QOL and dyspnea questionnaires (EuroQol ICE CAP SF-36 SGRQ and
UCSD SOBQ)
If consent has been given blood will be drawn and a urine specimen collected for the biospecimen
repository
Subjects return used and unused study drug for the visit
Study diary reviewed
4427 Final Site Visit ndash FVC drop confirmation
In the event that the subject has a recorded FVC drop of gt10 from baseline at the final treatment visit and the
subject has not had a confirmation of such a drop at a previous study visit the subject should return to the
clinical site 6 to 8 weeks after the final treatment visit During this visit a post-bronchodilator spirometry test
will be performed This FVC measurement will be evaluated according to section 521 of this protocol
4428 Final Visit ndash Telephone Follow-up
Four weeks following the final dose of study medication subjects will receive a telephone call from the study
coordinator to ensure that there are no side effects and to follow up on any ongoing adverse events (AEs)
4429 Phone Contact Between Visits
At week 2 and each month that a subject does not have a scheduled clinical center visit his or her study
coordinator will contact him or her at least once by telephone to
Inquire if the subject has had any hospitalizations events that might be considered an AE or any events
significant enough to warrant an out-of-cycle visit to the clinical center
Remind subjects of their current dosage levels and confirm that the subject understands them
Address any questions or concerns the subject might have regarding other aspects of the study
Assess adherence to the treatment regimen by reviewing diary data verbal review of medications taken
including nutritional supplements
33
34
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Table 3 Schedule of Assessments
Procedure Screening Visit 0
Enrollment Visit 1
Week 15 Visit 2
Week 30Visit 3
Week 45 Visit 4
Week 60 Early
Withdrawal Visit 5
Final1
Visit (via phone)
Informed consent X
Medical history X
Inclusionexclusion criteria X
Serum pregnancy test (if applicable) X X X X X
Review of lung biopsy X
Arterial Blood Gas X X
6-Minute Walk Test
X
X X
Physical examination X X X
Vital signs with oximetry X X X X X X
Body height and weight X X X X X X
Complete Blood Count X X X
Chemistry panel X X X
Monitor Lab Values X X X
Urinalysis X Specimen repository substudy blood draw and urine collection (if consented)
X
X X X X
HRCT (if not completed within three months) X
Spirometry (pre- and post-bronchodilator) X
Spirometry (post-bronchodilator only) X X X X X
DLCO (post-bronchodilator only) X X X
Lung volumes (post-bronchodilator only) X
X
Evaluate for acute exacerbation X X X X X
Review Adverse Events X X X X X X
Review concomitant meds X X X X X X
Dispense subject diary X X X X
Review subject diary X X X X X
Dispense study agent X X X X
Gender Substudy questionnaire (female subjects only) X
EuroQol ICECAP UCSD SOBQ SGRQ SF-36 X X X
Abbreviations DLCO diffusing capacity of the lung for carbon monoxide QOL Quality of Life ICECAP Investigating Choice Experiments for Preferences of Older People UCSD SOBQ University of California Shortness of Breath Questionnaire SGRQ St Georgersquos Respiratory Questionnaire SF-36 Short Form 36 Health Survey
1Follow-up visit via phone will occur four weeks after final dose of study medication
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
45 Dose Justification
The general philosophy for determining dosing levels was to apply previously examined
treatment regimens With the focus of the study being to establish a standard of care for
mildmoderate IPF subjects the goal was to develop flexible yet standardized treatment rules that
allow for the temporary or permanent withholding of one or more components of treatment when
necessary Subjects developing laboratory abnormalities or symptoms that result in
discontinuation of one or more components of study treatment may continue on the other
components as long as there is no contraindication for this Complete follow-up is important for
the validity of any study As a strategy to maintain protocol adherence we are using a treatment
regimen that will detect potential side effects and prompt interventions proactively in the interest
of patient safety In addition subjects who permanently stop study medications during the course
of the study are encouraged to continue in the study completing all scheduled visits and tests
451 Rationale for N-acetylcysteine Dosing
To our knowledge there have been no IPF studies to correlate clinical outcome measures with
different dosages for NAC The dosage chosen is based on the IFIGENIA study However BAL
lung GSH levels from subjects with IPF have been augmented with the use of oral NAC at 600
mg 3 times per day In addition lung GSH levels have been associated with improved
PFTs212227 The dose chosen for this study was based on previous data including the IFIGENIA
study30
4511 Dosing of N-acetylcysteineplacebo
Dosing of NACPL will be 600 mg orally 3 times a day (1800 mgday)
4512 Reasons to Discontinue N-acetylcysteineplacebo
NACPL may be temporarily or permanently discontinued for the duration of the study for
gastrointestinal symptoms or dermatologic reactions
35
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Temporarily discontinue (hold) oral NACPL for subjects requiring inpatient admission for acute
exacerbation (AEx) or other conditions Resume NACPL after discharge
36
37
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
452 Dosage Algorithms
Dosage Adjustment Algorithm 1 NACPL Dose Modifications for Gastrointestinal Symptoms Nausea Vomiting Abdominal Discomfort Diarrhea
GI Symptoms determined by the PI to be clinically significant Nausea Vomiting Abdominal Discomfort Diarrhea
NACPL Temporarily dc (HOLD) x 3 Days
Monitor symptoms intervene as clinically indicated (eg fluid replacement antidiarrhea or antinausea medication)
Monitor or lab PRN
Are symptoms resolving after 3 days NO
Symptoms NOT resolving after 3 days of holding study medication Assessmentmanagement per clinical
discretion of investigator
Likely not study medication discuss resuming study medication with medical monitor when symptoms resolved
YES
Temporarily dc (HOLD) NACPL for 4 additional days (total hold 1 week) then NACPL Resume 600 MG TID
Did symptoms recur
YES
STOP NACPL for
duration of study
NO
NACPL No Change
38
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Dosage Adjustment Algorithm 2 NACPL Dose Modifications For Dermatologic Reactions
Dermatologic Reactions (Not Acneiform) ge Grade 2 Grading per Common Terminology Criteria for
Adverse Events V30 (httpctepcancergov) For example Grade 1 RASHDESQUAMATION Macular or papular eruption or erythema without associated symptoms Grade 2 RASHDESQUAMATION Macular or popular eruption or erythema with pruritus or other associated symptoms localized desquamation or other lesions covering lt50 of body surface area
NACPL Temporarily dc (HOLD) x 3 days
Are symptoms resolving after 3 days
NO Symptoms not resolving after 3 days of holding study medication Assessmentmanagement per clinical discretion of investigator Likely not study medication Discuss resuming study medication with medical monitor when symptoms
resolved YES
Temporarily dc (HOLD) NACPL for 4 additional days (total hold 1 week) then NACPL resume 600 MG TID
Did symptoms recur
YES
STOP NACPL for
duration of study
NO
NACPL No change
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
46 Contraindications Precautions and Side Effects of Study Medications
461 Contraindication
Contraindication to NAC is known hypersensitivity to it
462 Precautions
Concomitant administration of oral NAC and antibiotics has shown a slightly reduced absorption
of cephalexin and a slight increase in erythromycin serum levels NAC contains free sulfhydryl
groups There is no evidence that individuals sensitive to sulfa drugs are sensitive to NAC
The NAC preparation being administered in this study contains 20 mg of aspartame Because of
the phenylalanine component of aspartame individuals with phenylketonuria should avoid or
restrict aspartame intake to avoid increased blood levels of phenylalanine Because of this risk
labeling is required on all products containing aspartame
463 Side Effects
Side effects of NAC range from common to serious See Table 4
39
40
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Table 4 Side Effects of NAC
Undesirable Effects
System-organ class Uncommon
(gt11000 lt1100)
Rare
(gt110000 lt11000)
Very rare
(lt110000) Not known
Immune system disorders Hypersensitivity Anaphylactic shock
reaction
Nervous system disorders Headache
Ear and labyrinth disorders Tinnitus
Cardiac disorders Tachycardia
Vascular disorders Hemorrhage
Respiratory thoracic and
mediastinal disorders
Bronchospasm
Dyspnea
Gastrointestinal disorders
Vomiting diarrhea
stomatitis abdominal
pain nausea
Dyspepsia
Skin and subcutaneous tissue
disorders
Urticaria rash
angioedema itching
General disorders and
administration site conditions Pyrexia
Investigations Reduced arterial
pressure Face edema
In very rare cases the onset of severe skin reactions such as Stevens-Johnson syndrome and Lyell syndrome was reported to have a temporal relationship with N-acetylcysteine administration Although in most cases at least another suspect drug probably most involved in the genesis of the above mentioned mucocutaneous syndromes has been identified in case of mucocutaneous alterations it is appropriate to contact onersquos doctor and the administration of N-acetylcysteine should be immediately discontinued
Some studies confirmed a reduction of platelet aggregation during N-acetylcysteine administration The clinical significance of these findings has not been defined yet [Source Fluimucil Investigator Brochure]
47 Recruitment Procedures
Subjects recruited for this study will be established patients of the investigators or physician- or
self-referred to participating clinical centers in the IPFnet Each clinical center within IPFnet has
a well-developed infrastructure of local pulmonologists within the surrounding geographic area
These pulmonologists are kept informed of ongoing IPF clinical trials and regularly refer
subjects to studies conducted at IPFnet clinical centers
Additional steps will be taken to inform clinicians of the trials in progress within IPFnet
including presentations at faculty staff meetings at local hospitals medical grand rounds and
national conferences direct mail notification monthly faxes and advertisement of network trials
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
in pulmonary journals Clinical center patients previously diagnosed with IPF will be notified of
the trials by mail whenever possible
Recruitment of minorities and women will be monitored by the DCC and DSMB If necessary
additional recruitment efforts will be made at specific centers to ensure that the aggregate subject
sample contains appropriate representation of women and minorities
48 Study Procedures
The following procedures are detailed in the PANTHER-IPF MOOP accompanying this
protocol
1 PFT
2 ABG
3 HRCT scan of the chest (including imaging of pulmonary arteries)
4 CBC and serum chemistries
5 Pregnancy test
6 6MWTBorg Dyspnea Scale
7 QOL questionnaires (EuroQol HAD SF-36 SGRQ and ICE CAP)
8 UCSD SOBQ
9 Gender Substudy Questionnaire
All assessments of PFTs will be conducted by study personnel not directly involved in the
treatment of the subjects
481 Biological Specimen Management
4811 Biological Specimen Sample Management
Subjects at clinical centers participating in the specimen repository substudy who consent to
having blood drawn for research purposes and for the banking of blood blood components and
other biologic specimens (urine and BAL fluid) will have approximately 405 mL of blood
41
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
drawn 17 mL blood drawn for DNA and 20 mL of urine collected at enrollment visit Subjects
will have approximately 50 mL of blood drawn and 20 mL of urine collected at each 15-week
follow-up visit Blood specimens will be separated according to PANTHER-IPF MOOP
guidelines into the following components for banking in the repository serum plasma and
DNA Coding of all biologic specimens for the repository will be performed by study staff at the
clinical center The samples will be processed per PANTHER-IPF MOOP guidelines aliquoted
labeled with barcode labels and stored at -70degC at the clinical center and shipped to the central
repository
The only subject identifiers will be a sample ID number and subject initials This sample ID will
be linked in the IPFnet DCC clinical database to subject information No subject information will
be transferred to the biological-specimen database
The subjectrsquos samples may be used for approved sub-studies relating to human disease
including but not limited to IPF The studies for which an individualrsquos samples will be made
available will be determined by the subjectrsquos answers to questions on the biological-sample
informed consent form The subjects can choose to make their samples available for all options
or any combination Samples will be made available to researchers only with IPFnet Steering
Group approval until such time as the samples are made public through the NHLBI repository
49 Concomitant Medications
Concurrent treatment with FDA-approved therapy for IPF is allowed Colchicine may be used
for treatment of gout Temporary treatment with oral or IV corticosteroids for clinical worsening
or suspected AEx is permitted Nutritional supplements containing NAC are not allowed
410 Laboratory Testing
Clinical laboratory parameters will be assessed at screening and at the end of the study The
following tests will be performed at the two time points specified in the protocol chemistry (AG
ratio ALT [SGPT] AST [SGOT] albumin alkaline phosphatase amylase bilirubin-direct
42
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
bilirubin-indirect bilirubin-total BUN BUNcreatinine ratio calcium carbon dioxide
cholesterol-total chloride CPK-total creatinine GGT globulin glucose iron-total LDH
lipase magnesium phosphorus-inorganic potassium protein-total sodium TIBC triglycerides
uric acid) and hematology (red blood cell count WBC count hemoglobin hematocrit cell
indices differential platelet count)
411 Blinding of Study Drugs
Subjects and caregivers will be blinded to study treatment Every subject will receive NAC or
matching PLs at every study visit from the baseline visit to the week-45 visit No study agent
will be dispensed at the week-60 visit
43
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
5 Study Endpoints
51 Primary Study Endpoint
The primary endpoint will be the change in serial measurements of FVC over the study period
52 Secondary Study Endpoints
521 Time to Disease-progression
The time-to-death or a 10 decline in FVC will be defined as the time-to-disease progression
The 10 decline in FVC from enrollment must be confirmed on 2 consecutive visits no less than
6 weeks apart For subjects with 2 consecutive visits with a 10 decline in FVC the time-toshy
disease progression will be defined as the time interval between enrollment and the initial visit
with a 10 FVC decline For subjects who experience disease progression the study doctor will
determine whether or not the subject will remain in the study
522 Acute Exacerbations
The following 3 criteria will define AEx in subjects with acute worsening of their respiratory
conditions
1 Clinical (all of the following required)
A) Unexplained worsening of dyspnea or cough within 30 days triggering unscheduled
medical care (eg emergency room clinic study visit hospitalization)
B) No clinical suspicion or overt evidence of cardiac event pulmonary embolism or deep
venous thrombosis to explain acute worsening of dyspnea
C) No pneumothorax
44
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
2 RadiologicPhysiologic (A and B required)
A) New ground glass opacity or consolidation computed tomography (CT) scan OR new
alveolar opacities on chest x-ray
B) Decline of ge 5 in resting room air SpO2 from last recorded level OR decline of ge 8 mm
Hg in resting room air PaO2 from last recorded level
3 Microbiologic (all of the following required)
A) No clinical evidence for infection (ie absence of grossly purulent sputum fever gt 39degC
orally)
B) Lack of positive microbiological results (if done) from lower respiratory tract defined as
(1) Clinically significant bacterial growth on sputum or endotracheal aspirate cultures
(2) Quantitative culture by protected brush specimen ge 103 cfumL or BAL ge 104 cfumL
(3) The presence of specific pathogens on stains of any of the above
C) Lack of positive pathogen in blood cultures (if done)
Identification of Acute Exacerbations
All subjects will be educated about the importance of identifying AExs At the time of
enrollment subjects will be told about the possibility of developing acute symptomatic
worsening that might represent an AEx of IPF and instructed to contact their study clinical
center coordinator within 48 to 72 hours of the apparent event
All subjects will be contacted by phone monthly and questioned about any change in dyspnea or
cough and any interim clinic visits or hospitalizations Finally as part of the IPFnet outreach to
community referring physicians the importance of AExs will be emphasized When a subject is
identified who meets criterion 1A this will trigger the collection of additional clinical data to
evaluate a suspected AEx These data will be collected as part of standard clinical care (ie this
protocol does not require collection of all items) The additional items to be collected for
suspected AEx include
IPFnet AEx case report form (eCRF) (required)
45
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Chest x-ray CT scan withwithout pulmonary angiogram (reports should be faxed and
followed by the hard copiesdiscs)
Oxygen saturation (pulse oximetry)
ABG
Respiratory cultures (sputum endotracheal aspirate lavage)
Blood cultures
Clinichospital records related to the event
All potential cases of AEx will be reviewed by the clinical center PI first and a decision on
whether the case may represent an AEx will be made If AEx is suspected the case will be sent
to the IPFnet adjudication committee which will assign a final diagnosis (see Table 5) If there is
disagreement among members the majority opinion will be recorded
During episodes of suspected AEx as determined by the individual clinical center investigator
subjects will remain blinded and in the study
Table 5 Final Diagnoses in Evaluation of Suspected Acute Exacerbations
Definite acute exacerbation All criteria met no alternative etiology
Unclassifiable acute worsening
Insufficient data to evaluate all criteria no alternative etiology
Not acute exacerbation Alternative etiology identified that explains acute worsening
Management of the suspected AEx will be at the discretion of the treating physician Standard of
care generally involves evaluation for respiratory infection pulmonary embolism cardiac events
and pneumothorax and treatment with IV corticosteroids
Study drugs will be resumed at pre-suspected AEx doses after subjects clinically improve as
confirmed by the local PI All subjects should be seen at the clinical center within 2 to 4 weeks
of recovery for measurement of post-bronchodilator FVC (see Figure 4) Subjects unable to
return to the clinical center after suspected AEx due to medical frailty (eg continued
46
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
institutionalization progressive disability) will be categorized as failing to maintain FVC
response in secondary analyses
Suspected AEx (PI determined)
Hold study drug Treat AEx
(Attending physician determined)
Alive but unable to continue due to
medical frailty
Dead
Alive and able to continue
Site reviewvisit
Restart study drug
FVC within 2-4 weeks
Figure 4 Acute Exacerbation Flow Chart
523 Respiratory Infections
An upper respiratory infection will be defined as
Change in sputum discoloration
Increased cough of no more than 14 daysrsquo duration
A lower-respiratory infection (pneumonia) will be defined as new segmental or lobar airspace
opacities visualized by image studies (chest radiograph or HRCT) in addition to any of the
following
Positive pathogencultures in good sample of sputum or lower-airway secretions retrieved
by fiberoptic bronchoscope
Fever gt 39degC or gt 100degF
Leukocytosis gt 12000 (unexplained no increase in dose of corticosteroids)
47
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
524 Maintained FVC Response
Subjects with follow-up FVCpred measurements at or above their baseline FVCpred level
will be classified as having maintained FVC response Subjects with reduced FVCpred levels
or missing data for any reason including death or medical frailty will be classified as having not
maintained FVC response The FVCpred value is used because unadjusted FVC measurements
are expected to decline with age
48
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
6 Safety Evaluations and Procedures
61 Adverse Events
During a clinical trial the reporting of adverse experience information can lead to important
changes in the way a new treatment is developed as well as provide integral safety data
611 Definitions
An adverse event (AE) is any untoward medical occurrence in a subject or clinical investigation
subject who was administered a pharmaceutical product The AE does not necessarily have to
have a causal relationship with the drug administered An AE can be any unfavorable and
unintended sign (including an abnormal laboratory finding) symptom or disease temporarily
associated with the use of a medicinal product whether or not considered to be related to the
medicinal product Diseases signs symptoms or laboratory abnormalities already existing at
enrollment are not considered AEs unless they worsen (ie increase in intensity or frequency)
Surgical procedures themselves are not AEs they are therapeutic measures for conditions that
require surgery The condition for which the surgery is required may be an AE Surgical
procedures planned before randomization and the conditions necessitating the surgery are not
AEs
A serious adverse event is any untoward event that
Is fatal
Is life-threatening
Requires inpatient hospitalization or prolongation of existing hospitalization with the
following exceptions
o Preplanned (before the study) hospital admissions unless the hospitalization is
prolonged
o Planned admissions (as part of a study eg routine biopsies)
o Hospitalization lasting lt 24 hours
49
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
o Hospitalization for elective procedure
o Emergency room visits
Results in persistent or significant disability or incapacity
Is a congenital anomaly or birth defect
Important medical events that may not result in death be life-threatening or require
inpatient hospitalization may be considered serious adverse events (SAEs) when based
on appropriate medical judgment they may jeopardize the subject and may require
medical or surgical intervention to prevent one of the outcomes listed above
Life-threatening means that the subject was in the view of the investigator at immediate risk of
death from the AE as it occurred It does not include an AE that had it occurred in a more severe
form might have caused death
Persistent or significant disabilityincapacity means that the event resulted in permanent or
significant and substantial disruption of the subjectrsquos ability to carry out normal life functions
Causality
A reasonable possibility means the AE may have been caused byrelated to the study drug A
perceived or real lack of efficacy does not satisfy the definition of relatedness
612 Adverse Event (AE) Reporting
For the PANTHER-IPF trial all AEs (serious and nonserious) occurring from randomization
through final study visit (4 weeks after final dose of all study medication) will be recorded on the
AE page of the case report form (CRF)
6121 Serious Adverse Events (SAE) Reporting
For this trial all deaths and all SAEs which occur from randomization through final study visit
must be entered within the EDC system via the SAE eCRF page within 24 hours of the
investigative sitersquos knowledge of the event It is the responsibility of the clinical center
50
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
investigator to provide a causality assessment of the event for each study medications based upon
the information available at the time of the report It is understood that complete information
about the event may not be known at the time the initial report is submitted In the event the EDC
system is not accessible to the site at the time of event reporting investigative sites will complete
and forward a paper back-up SAE form to DCRI Safety Surveillance for processing
DCRI Safety Surveillance
Telephone 1-919-668-8624 or 1-866-668-7799 (toll free)
Fax 1-919-668-7138 or 1-866-668-7138 (toll free)
The investigator must complete and submit follow-up SAE information via the eCRF when
important new or follow-up information (eg final diagnosis outcome results of specific
investigations) becomes available Follow-up information should be submitted according to the
same process used for reporting the initial event as described above All SAEs will be followed
until resolution stabilization or 30 days after the subject has completed the final visit (4 weeks
after the final dose of study medication) whichever occurs first The investigator is responsible
for reporting SAEs to their institutional review board (IRB) per site specific IRB reporting
guidelines
6122 Regulatory Reporting
AEs that are serious study drug related and unexpected will be reported to the regulatory
authorities The DCRI Safety Surveillance medical monitor will perform a medical review of all
SAEs submitted and evaluate for ldquounexpectednessrdquo DCRI Safety Surveillance will prepare
MedWatch reports for those events identified as serious study drug related and unexpected as
determined by Safety Medical Monitor
DCRI Regulatory Services will submit all unexpected study drug-related SAEs as per 21 CFR
32 DCRI Safety Surveillance will provide a safety alert letter to the NHLBI DSMB and DCC
clinical operation (for distribution to sites) within 15 days of initial receipt of the information
51
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Investigators are responsible for promptly reporting these events to their reviewing IRBs
according to site specific IRB reporting guidelines
62 Clinical Medical Monitoring
There will be an unblinded physician at the IPFnet DCC serving as medical monitor The
medical monitor will be available to assist with questions about dosage adjustments of study
medications including discontinuation or resumption of medications
63 Unblinding Procedures
Unblinding of subjects or investigators to subject treatment is strongly discouraged For ongoing
clinical management all subjects should be presumed to be receiving ldquoactiverdquo study drug To
ensure the subjectrsquos safety the study treatment will be dose-adjusted based on laboratory test
results clinical findings and symptoms
The IPFnet DCC medical monitor and PANTHER-IPF co-chairs Drs Ganesh Raghu and
Fernando Martinez will be available to the study physicians to discuss study drug management
on a case-by-case basis Un-blinding will be considered ONLY when the knowledge of subject
treatment assignment is ABSOLUTELY ESSENTIAL for subject safety and after discussion of
the subjectrsquos case with the medical monitor and either Dr Raghu or Dr Martinez Unblinding of
study treatment should be minimized during the conduct of the trial In those cases where it is
felt to be medically necessary the DCC medical officer will communicate directly with the
managing physician to minimize unblinding of study personnel
52
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
7 Study Drug Procedures
At the baseline 15-week 30-week and 45-week study visits subjects will receive a supply of
study drug sufficient to last until the next visit at which study drug will be dispensed
53
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
8 Data Management
81 Hardware and Software Configuration
811 Hardware and Database Software
Data will be stored in an Oracle database system Oracle has advantages of processing efficiency
and smooth linkage with other software systems The application and database will be hosted on
Solaris Unix servers at the IPFnet DCC
812 Statistical Software
SAS will be used as the principal application for the management of analysis data files and
statistical computations S-Plus will be used to provide supplementary functions as needed
813 Access Control and Confidentiality Procedures
Access to databases will be controlled centrally by the IPFnet DCC through user passwords
linked to appropriate privileges This protects the data from unauthorized changes and
inadvertent loss or damage
814 Security
Database and Web servers will be secured by a firewall and through controlled physical access
Oracle has many security features to ensure that any staff member accessing the database has the
proper authority to perform the functions he or she requests of the system Within the secondary
SAS databases Unix group-access control maintains similar security The Sun workstation login
is secured by extensive user-password facilities under Unix
54
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
815 Back-up Procedures
Database back-up will be performed automatically every day and standard IPFnet DCC policies
and procedures will be applied to dictate tape rotation and retention practices
816 Virus Protection
All disk drives that provide network services and all user computers will be protected using
virus-scanning software Standard IPFnet DCC policies will be applied to update these protection
systems periodically through the study
82 Sources of Data
821 Design and Development
The IPFnet DCC will be responsible for development of the electronic case report forms
(eCRFs) development and validation of the clinical study database ensuring data integrity and
training clinical center staff on applicable data management procedures A web-based distributed
data entry model will be implemented This system will be developed to ensure that guidelines
and regulations surrounding the use of computerized systems used in clinical trials are upheld
The remainder of this section provides an overview of the data management plan associated with
this protocol
822 Data Collection Forms
The data collection process consists of direct data entry at the study clinical centers into the EDC
system(s) provided by the DCC A data collection worksheet will be provided to clinical centers
for recording data in the event the EDC system is unavailable Data entry of the eCRFs should
be completed according to the instructions provided and project specific training The
investigator is responsible for maintaining accurate complete and up-to-date records and for
ensuring the completion of the eCRFs for each research participant
55
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
823 Data Acquisition and Entry
Data entry into eCRFs shall be performed by authorized individuals Selected eCRFs may also
require the investigatorrsquos written signature or electronic signature as appropriate Electronic
CRFs will be monitored for completeness accuracy and attention to detail during the study
824 Data Center Responsibilities
The IPFnet DCC will 1) develop a data management plan and will conduct data management
activities 2) provide final eCRFs for the collection of all data required by the study 3) develop
data dictionaries for each eCRF that will comprehensively define each data element 4) conduct
ongoing data monitoring activities on study data 5) monitor any preliminary analysis data
cleanup activities and 6) rigorously monitor final study data clean up
825 Data Editing
Completed data will be entered into the IPFnet DCC automated data acquisition and
management system If incomplete or inaccurate data are found a data clarification request will
be generated and distributed to clinical centers for a response Clinical centers will resolve data
inconsistencies and errors and enter all corrections and changes into the IPFnet DCC automated
data acquisition and management system
826 Training
The training plan for clinical center staff includes provisions for training on assessments eCRF
completion guidelines data management procedures and the use of computerized systems
56
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
9 Study Design and Data Analysis
91 General Analytic Considerations
All primary analyses will be based on intent-to-treat (ITT) principles using all randomized
subjects Baseline factors across groups will be compared using mean (standard deviation) and
median (25th and 75th percentiles) summary measures Kaplan-Meier curves will be used to
display event rates Due to clinical interest in departures from both sides of the null hypothesis
all test statistics will be 2-sided
Reasonable caution needs to be taken when conducting multiple analyses on key clinical
subgroups For subgroup analyses a conservative significance level of 0001 will be used for all
interaction tests Thus subgroup comparisons will be considered exploratory unless the p-value
from the interaction test is smaller than 0001
92 Randomization Blinding and Reporting of Results
A permuted block-randomization scheme will be created with varying block sizes stratified by
clinical center Once a subject has completed the screening and baseline period and evaluation
for inclusionexclusion criteria the randomization process will begin Subjects will be
randomized to receive NAC or matching placebo with equal probability (11) via telephone
contact with a central interactive voice response system (IVRS) using a toll-free randomization
number On the day of randomization after the subject has successfully met all inclusion and
exclusion criteria the investigator or designee will call the central randomization number to
obtain the assigned kit randomization numbers for that subject At each subject visit the
investigator or designee will call the central randomization number to obtain the new kit
randomization numbers for resupply of the subject For resupply of the clinical center the IVRS
will monitor minimal volume of a kit type andor expiration date and will automatically notify
the pharmacy
57
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
The trial results will be reported according to guidelines specified in the CONSORT statement
A flow diagram describing screening recruitment randomization dropout and vital status will
be included in the primary manuscript AEs and efficacy data will be presented for all treatment
groups Adherence dropout and lost to follow-up will be carefully examined across all treatment
groups Analyses of safety will be based on data from all randomized subjects who received at
least one dose of study drug
93 Stratification
Subjects will be distributed to the two treatment arms in a 11 allocation ratio Stratification
blocks will be based on clinical centers
94 Specification of the Primary Analyses
A mixed model repeated measures (MMRM) analysis described in section 95 will be used to
compare differences in the slope of FVC measurements across the treatment groups Response
variables are values of the FVC measured at baseline and every 15 weeks until study completion
Variables in the model will include treatment time and time by treatment age sex race and
height Contrast estimates of differences in slopes of treatment over time (along with confidence
intervals) will be used to estimate the treatment effect The validity of this model in terms of
meeting modeling assumptions will be assessed via standard modeling diagnostics and goodness-
of-fit measures Based on the MMRM framework missing FVC data will not be imputed for the
primary analysis
95 Analysis of Longitudinal Endpoints
A common goal in clinical trials is to specify models that are easily implemented and
reproducible by independent data analysts On the other hand the models should have proper
statistical behavior in terms of low bias and high precision Many common approaches to
longitudinal data analysis including last observation carried forward (LOCF) imputation rely on
the missing completely at random (MCAR) assumption However the MCAR assumption is
58
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
unlikely to hold in many clinical trials because missing data are often related to disease
progression and prognosis A more reasonable assumption missing at random (MAR) specifies
that the complete data distribution can be modeled using only the observed data The likelihood-
based MMRM approach is valid under the more general MAR assumptions These models will
be applied to analyze the longitudinal data secondary endpoints
The advantages of MMRM analysis are that all important characteristics of the model can be preshy
specified standard software can be used to implement the models and results are based on ITT
principles43 In addition the MMRM approach offers superior control of Type I and Type II
errors compared with the LOCF approach
Response variables are values of the PFTs measured at enrollment and every 15 weeks until
study completion and 6MWT values measured at baseline week 30 and week 60 Covariates are
treatment time time by treatment and key baseline risk factors Contrasts (along with
confidence intervals) of treatment by time will be used to estimate the treatment effect
The correlation structure involves multiple pieces including measurement errors random
variation and interindividual variability For the longitudinal data analyses an unstructured
correlation matrix for within-subject errors will be assumed Other correlation structures
including compound symmetry will be examined as needed A careful examination of reasons
for study discontinuation will be conducted to assess the validity of MCAR Sensitivity analyses
will be used to examine the untestable assumption that the observed data violate the MAR
assumption The MMRM models will be implemented using PROC MIXED in SAS
96 Analysis of Binary Time-to-Event and Time-Lagged Endpoints
Regression modeling approaches using either the logistic regression model or Cox proportional
hazards regression model will be employed when appropriate The validity of these models will
be assessed via standard modeling diagnostics and goodness-of-fit measures Estimates of
cumulative frequencies for more general time-lagged responses will be calculated using the
partitioned version of the Bang-Tsiatis estimator44 The partitions will be set at 15-week intervals
59
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
to correspond with the data-collection process Covariate adjusted event rates will be calculated
using inverse probability-weighted regression estimates45
97 Power Analysis
971 Primary Analyses
Based on previously published IPF clinical trials the PL group is expected to experience a drop
in FVC of approximately 020 L over the study period (see Figure 1) The IPFnet Steering Group
determined a clinically important difference would be to preserve the majority of the decline
relative to PL over the study period In particular a treatment effect of 015 L was determined to
be a clinically meaningful difference Potential dropout is a key factor in the proposed study The
drop-out process assumed 5 lost to follow-up after every study visit Only 80 of subjects
were assumed to be followed for the entire study period All models assumed a compound
symmetry structure for the covariance matrix Power calculations were performed using a SAS
IML program for designing repeated measures studies46 Based on preliminary reviews of the
data from the University of Michigan the covariance matrix parameters were estimated at
approximately σ2 = 0757 (variance parameter) and ρ = 0936 (correlation parameter) To be
conservative the power calculations for the primary analysis were performed with parameter
setting of σ2 = 0810 (variance parameter) and ρ = 0925 (correlation parameter)
The power calculations assume a correction for imperfect compliance proposed by Lachin and
Foulkes to allow for 2 noncompliance for each of the treatment arms47 Thus the sample size
of 130 subjects per arm would be reduced to an adjusted sample size of 130(1-002-002)2 =
1198 or 120 subjects per arm
Under the assumed Type I error rate of 005 with a correlation parameter of 0925 and standard
deviation of 090 the difference of 015 L (or 00025 Lweek) shown in Table 6 would have
power of 93
60
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Table 6 Hypothetical Values of Mean FVC (L) Change from Baseline
Week 15 Week 30 Week 45 Week 60
NAC 00125 00250 00375 00500
Placebo 00500 01000 01500 02000
Difference 00375 00750 01125 01500
Abbreviations FVC forced vital capacity PL placebo
972 Power Analysis for Secondary Endpoints
Power calculations for secondary endpoint measurements are shown in Table 7 Standard
deviations are based on unpublished data provided by the University of Michigan The
calculations are based on a 2-sample t-test with Type I error rate set at 005 These calculations
are likely to be conservative because the statistical approach described in section 95 for
analyzing these endpoints will incorporate incomplete observations as well as intermediate data
points
Table 7 Detectable Differences in Treatment Means for Selected Endpoint Measurements
Secondary Endpoints Std Dev
of the Baseline Score
Detectable Difference for 80 Power
Std Dev of the Change Score
Difference Detectable for
80 Power
DLCOpred 166 58 91 32
6MWT Area Under the Desaturation Curve
219 76 175 61
6MWT Distance to Desaturation 224 78 315 110
6MWT Minutes Walked 210 073 205 071
Abbreviations Std Dev standard deviation DLCOpred diffusing capacity of the lung for carbon monoxide percent predicted 6MWT 6-minute walk test
61
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
10 Study Administration
101 Cooperative Agreement Mechanism
The administrative and funding mechanism used to undertake this project is a ldquocooperative
agreementrdquo (U01) which is an assistance mechanism Under the cooperative agreement the
NHLBI assists supports andor stimulates the project and is substantially involved with
investigators in conducting the study by facilitating performance of the effort in a ldquopartnerrdquo role
The NHLBI project scientist serves on the IPFnet Steering Group and he or another NHLBI
scientist may serve on other project committees when appropriate At the same time however
NHLBI does not assume a dominant role direction or prime responsibility for this research
program
As described below governance of the project is conducted through the IPFnet Steering Group
Principal investigators have lead responsibilities in all aspects of their trials and the project
including any modification of trial designs conduct of the trials quality control data analysis
and interpretation preparation of publications and collaboration with other investigators unless
otherwise provided for by the IPFnet Steering Group
PIs retain custody of and have primary rights to their center-specific and collaborative data
subject to government rights-of-access consistent with current Health amp Human Services (HHS)
Public Health Service (PHS) and National Institutes of Health policies The protocols and
governance policies call for the continual submission of data centrally to the IPFnet DCC for the
collaborative database which at a minimum will contain the key variables selected by the IPFnet
Steering Group for standardization across all clinical centers the submission of copies of the
collaborative datasets to each PI upon completion of the project procedures for data analysis
reporting and publication and procedures to protect and ensure the privacy of medical and
genetic data and records of individuals The NHLBI project scientist on behalf of the NHLBI
will have the same access privileges and responsibilities regarding the collaborative data as the
other members of the Steering Group
62
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
PIs are also encouraged to publish and to publicly release and disseminate results data and other
products of the project concordant with the project protocols and governance and the approved
plan for making data and materials available to the scientific community and to the NHLBI
However during the 3 years after the ending date of NHLBI project support unpublished data
unpublished results data sets not previously released and other study materials or products are
to be made available to any third party only with the approval of the IPFnet Steering Group
Upon completion of the project PIs are expected to put their intervention materials and
procedure manuals into the public domain andor make them available to other investigators
according to the approved plan for making data and materials available to the scientific
community and the NHLBI for the conduct of research at no charge other than the costs of
reproduction and distribution
The NHLBI reserves the right to terminate or curtail the project (or an individual award) in the
event of (a) failure to develop or implement mutually agreeable collaborative measurement
subject eligibility and data management sections of the protocols (b) substantial shortfall in
subject recruitment follow-up data reporting or quality control or other major breach of
protocol (c) substantive changes in the agreed-upon protocols with which NHLBI cannot
concur (d) reaching a major project outcome with persuasive statistical significance
substantially before schedule or (e) human subject ethical issues that may dictate a premature
termination
Any disagreement that may arise in scientificprogrammatic matters (within the scope of the
award) between award recipients and the NHLBI may be brought to arbitration An arbitration
panel will be composed of 3 membersmdash1 selected by the IPFnet Steering Group (with the
NHLBI member not voting) or by the individual PI in the event of an individual disagreement a
second selected by NHLBI and the third selected by the other 2 members This special
arbitration procedure in no way affects the PIrsquos right to appeal an adverse action that is otherwise
appealable in accordance with the PHS regulations at 42 CFR part 50 Subpart D and HHS
63
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
regulation at 45 CFR part 16 or the rights of the NHLBI under applicable statutes regulations
and terms of the award
102 IPFnet Steering Group
The IPFnet Steering Group is the main governing body of the project It is composed of the PIs
of the clinical centers the PI of the DCC and the NHLBI project scientist The clinical centers
the IPFnet DCC and the NHLBI each have 1 vote on the IPFnet Steering Group All decisions
are determined by majority vote
All major scientific decisions are determined by the IPFnet Steering Group It assumes overall
responsibility for the design and conduct of the trial It appoints (and disbands) committees and
subcommittees as the need arises designs approves and implements the study protocols
oversees the development of the MOOP monitors subject recruitment and treatment delivery
evaluates data collection and management oversees quality assurance procedures and
implements changes and enhancements to the study as required It also has primary responsibility
for facilitating the conduct of the trials and reporting the projectrsquos results
103 Data and Safety Monitoring Board
The NHLBI will establish a DSMB in accordance with established policies (see
httpwwwnhlbinihgovfundingpoliciesdsmb_insthtm) to ensure data quality and subject
safety and to provide independent advice to the NHLBI regarding progress and the
appropriateness of study continuation
104 Recommendations on Interim Monitoring of Efficacy Safety and Futility
First and foremost the role of the DSMB will be to review subject safety and trial conduct at
periodic points during the study The DSMB may require analyses of the primary endpoint
results for comparing the benefit and risks of treatment strategies The benefit of collecting
additional data on key secondary endpoints with extended follow-up and establishing a robust
64
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
evidence base for determining a standard of care will need to be carefully considered before
early termination of one or more treatment arms After careful consideration the IPFnet Steering
Group recommends conservative thresholds for the early examinations of the safety and efficacy
data
The DSMB will be expected to meet approximately every 6 months until trial completion to
review safety and toxicity data The DSMB may recommend stopping the study based on these
reviews Because the DSMB could stop the trial for safety concerns as well as for a large
efficacy benefit there could be multiple opportunities to reject the null hypothesis (no difference
in event rates between the PL and NAC groups) A Bonferroni approximation will be applied
during the one planned interim analysis for efficacy
Before locking the database a statistical analysis plan (SAP) will be developed to provide
complete details on the statistical analysis The SAP will include the specifics for how and when
the DSMB will be notified for AEs The IPFnet DCC will deliver to the DSMB all FDA-defined
AEs at 3-month intervals The IPFnet DCC will prepare narrative SAE reports in real time for
DSMB review including recommendations and analysis of similar events for each SAE
submitted to the FDA
65
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
11 Investigator and Sponsor Obligations
111 Monitoring
All monitoring activities for US clinical centers will be performed in accordance with DCRI
standard operating procedures Information regarding the types of visits will be outlined in the
PANTHER-IPF MOOP
112 Cost and Payment
There will be no cost to subjects enrolled in this trial Study-related procedures will be paid for
by the IPFnet
Subjects may be eligible for reimbursement for travel to the clinical center Details of payment
will be explained to each subject during the consent process
113 Confidentiality and Health Insurance Portability and Accountability Act
Considerations
Subject confidentiality will be protected throughout the study All subject data will be kept
strictly confidential and no subject-identifying information will be released to anyone outside
the project Confidentiality will be assured through several mechanisms First each subject will
be assigned an anonymous study ID which will then be used on all study forms Second any
study forms blood samples and paper records that contain subject information (eg address lists
phone lists) will be kept at the clinical centers in secured locked areas coded by number Once
blood is collected there will be no subject identifiers placed on blood samplesmdashonly the study
ID number and the date of sample collection Third access to all subject data and information
including laboratory specimens will be restricted to authorized personnel In the case of
computerized data this restricted access will be assured through user logon IDs and password
protection
66
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
At the IPFnet DCC only authorized personnel will have access to the data files containing study
data Security will be assured through user logon IDs passwords and appropriate access
privileges All study subjects will be identified only by their IPFnet ID numbers and no personal
identifying information such as name address or Social Security number will be entered into
the IPFnet DCC database Any subject-specific data reported to the IPFnet Steering Group will
be identified only by the IPFnet ID number
Finally subjects will not be identified by name in any reports or publications nor will the data
be presented in such a way that the identity of individual subjects can be inferred Analysis files
created for further study by the scientific community will have no subject identifiers These data
files will be created in accordance with the Ancillary Studies and Publication Policy of the
IPFnet
114 Informed Consent Procedures
All IPFnet subjects will provide written informed consent using procedures reviewed and
approved by each clinical centerrsquos IRB Informed consent will be undertaken by study personnel
in-person with the subject The subject has the option of declining further participation in the
study at that point No further study procedures will be conducted until the signed documents
have been provided to the IPFnet clinical center
115 Institutional Review Boards
Before initiating this study the protocol clinical center-specific informed consent forms Health
Insurance Portability and Accountability Act (HIPAA) forms recruitment materials and other
relevant information will be reviewed by a properly constituted IRB at each participating clinical
center A copy of the signed and dated IRB approval at each clinical center will be retrieved prior
to or during the site initiation visit and archived at the IPFnet DCC Any amendments to the
protocol other than simple administrative and typographical changes must be approved by each
IRB before they are implemented The clinical centers will seek annual renewals of their IRB
approvals in accordance with local procedures
67
__________________________________________ ________________
__________________________________________
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
12 Investigator Agreement
I have read the foregoing protocol PANTHER-IPF and agree that it contains all necessary
details for carrying out this study I will conduct the study as outlined herein and will complete
the study within the time designated
I will provide copies of the protocol and all pertinent information to all individuals responsible to
me who assist in the conduct of this study I will discuss this material with them to ensure they
are fully informed regarding the drug and the conduct of the study
I will fulfill all responsibilities for submitting pertinent information to the local IRB if
applicable that is responsible for this study
I further agree that NHLBI andor DCRI will have access to any source documents from which
eCRF information may have been generated
Signature of Principal Investigator Date
Name of Principal Investigator (printed or typed)
Protocol version date May 19 2009
Protocol Amendment 1 version date May 28 2010
Protocol Amendment 2 version date December 6 2011
68
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
13 References
1 Raghu G Brown KK Bradford WZ et al A placebo-controlled trial of interferon gamma-1b in patients with idiopathic pulmonary fibrosis N Engl J Med 2004350125-33 2 King TE Jr Safrin S Starko KM et al Analyses of efficacy end points in a controlled trial of interferon-gamma1b for idiopathic pulmonary fibrosis Chest 2005127171-7 3 Flaherty KR Thwaite EL Kazerooni EA et al Radiological versus histological diagnosis in UIP and NSIP survival implications Thorax 200358143-8 4 Wells AU Desai SR Rubens MB et al Idiopathic pulmonary fibrosis a composite physiologic index derived from disease extent observed by computed tomography Am J Respir Crit Care Med 2003167962-9 5 Raghu G Freudenberger TD Yang S et al High prevalence of abnormal acid gastroshyoesophageal reflux in idiopathic pulmonary fibrosis Eur Respir J 200627136-42 6 Kinnula VL Focus on antioxidant enzymes and antioxidant strategies in smoking related airway diseases Thorax 200560693-700 7 Coultas DB Zumwalt RE Black WC Sobonya RE The epidemiology of interstitial lung diseases Am J Respir Crit Care Med 1994150967-72 8 Raghu G Weycker D Edelsberg J Bradford WZ Oster G Incidence and prevalence of idiopathic pulmonary fibrosis Am J Respir Crit Care Med 2006174810-6 9 Olson AL Swigris JJ Lezotte DC Norris JM Wilson CG Brown KK Mortality from pulmonary fibrosis increased in the United States from 1992 to 2003 Am J Respir Crit Care Med 2007176277-84 10 Mannino DM Etzel RA Parrish RG Pulmonary fibrosis deaths in the United States 1979shy1991 An analysis of multiple-cause mortality data Am J Respir Crit Care Med 19961531548shy52 11 Hubbard R Johnston I Coultas DB Britton J Mortality rates from cryptogenic fibrosing alveolitis in seven countries Thorax 199651711-6 12 Johnston I Britton J Kinnear W Logan R Rising mortality from cryptogenic fibrosing alveolitis Bmj 19903011017-21 13 Raghu G Collard HR Egan JJ et al An official ATSERSJRSALAT statement idiopathic pulmonary fibrosis evidence-based guidelines for diagnosis and management Am J Respir Crit Care Med 2011183788-824 14 (USA) FDA FDA Public Health Advisory Interferon gamma-1b (marketed as Actimmune) In 2007 15 King TE Jr Pardo A Selman M Idiopathic pulmonary fibrosis Lancet 2011 16 Raghu G Brown KK Costabel U et al Treatment of idiopathic pulmonary fibrosis with etanercept an exploratory placebo-controlled trial Am J Respir Crit Care Med 2008178948shy55 17 Malouf MA Hopkins P Snell G Glanville AR An investigator-driven study of everolimus in surgical lung biopsy confirmed idiopathic pulmonary fibrosis Respirology 201116776-83 18 King TE Jr Behr J Brown KK et al BUILD-1 a randomized placebo-controlled trial of bosentan in idiopathic pulmonary fibrosis Am J Respir Crit Care Med 200817775-81 19 Richeldi L Costabel U Selman M et al Efficacy of a tyrosine kinase inhibitor in idiopathic pulmonary fibrosis N Engl J Med 20113651079-87
69
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
20 Borok Z Buhl R Grimes GJ et al Effect of glutathione aerosol on oxidant-antioxidant imbalance in idiopathic pulmonary fibrosis Lancet 1991338215-6 21 Meyer A Buhl R Magnussen H The effect of oral N-acetylcysteine on lung glutathione levels in idiopathic pulmonary fibrosis Eur Respir J 19947431-6 22 Behr J Maier K Degenkolb B Krombach F Vogelmeier C Antioxidative and clinical effects of high-dose N-acetylcysteine in fibrosing alveolitis Adjunctive therapy to maintenance immunosuppression Am J Respir Crit Care Med 19971561897-901 23 Cantin AM North SL Fells GA Hubbard RC Crystal RG Oxidant-mediated epithelial cell injury in idiopathic pulmonary fibrosis J Clin Invest 1987791665-73 24 Waghray M Cui Z Horowitz JC et al Hydrogen peroxide is a diffusible paracrine signal for the induction of epithelial cell death by activated myofibroblasts Faseb J 200519854-6 25 Larios JM Budhiraja R Fanburg BL Thannickal VJ Oxidative protein cross-linking reactions involving L-tyrosine in transforming growth factor-beta1-stimulated fibroblasts J Biol Chem 200127617437-41 26 Kinnula VL Fattman CL Tan RJ Oury TD Oxidative stress in pulmonary fibrosis a possible role for redox modulatory therapy Am J Respir Crit Care Med 2005172417-22 27 Meyer A Buhl R Kampf S Magnussen H Intravenous N-acetylcysteine and lung glutathione of patients with pulmonary fibrosis and normals Am J Respir Crit Care Med 19951521055-60 28 Behr J Degenkolb B Krombach F Vogelmeier C Intracellular glutathione and bronchoalveolar cells in fibrosing alveolitis effects of N-acetylcysteine Eur Respir J 200219906-11 29 Bando M Hosono T Mato N et al Long-term efficacy of inhaled N-acetylcysteine in patients with idiopathic pulmonary fibrosis Intern Med 2010492289-96 30 Demedts M Behr J Buhl R et al High-dose acetylcysteine in idiopathic pulmonary fibrosis N Engl J Med 20053532229-42 31 Toma TP Bhowmik A Rajakulasingam R Acetylcysteine in pulmonary fibrosis N Engl J Med 20063541086-9 author reply -9 32 Hunninghake GW Antioxidant therapy for idiopathic pulmonary fibrosis N Engl J Med 20053532285-7 33 Flaherty KR Mumford JA Murray S et al Prognostic implications of physiologic and radiographic changes in idiopathic interstitial pneumonia Am J Respir Crit Care Med 2003168543-8 34 Latsi PI du Bois RM Nicholson AG et al Fibrotic idiopathic interstitial pneumonia the prognostic value of longitudinal functional trends Am J Respir Crit Care Med 2003168531-7 35 Collard HR King TE Jr Bartelson BB Vourlekis JS Schwarz MI Brown KK Changes in clinical and physiologic variables predict survival in idiopathic pulmonary fibrosis Am J Respir Crit Care Med 2003168538-42 36 Jegal Y Kim DS Shim TS et al Physiology is a stronger predictor of survival than pathology in fibrotic interstitial pneumonia Am J Respir Crit Care Med 2005171639-44 37 Martinez FJ Safrin S Weycker D et al The clinical course of patients with idiopathic pulmonary fibrosis Ann Intern Med 2005142963-7 38 Hull JH Acetylcysteine in pulmonary fibrosis N Engl J Med 20063541089-91 author reply -91
70
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
39 Flaherty KR King TE Jr Raghu G et al Idiopathic interstitial pneumonia what is the effect of a multidisciplinary approach to diagnosis Am J Respir Crit Care Med 2004170904shy10 40 Raghu G Johnson WC Lockhart D Mageto Y Treatment of idiopathic pulmonary fibrosis with a new antifibrotic agent pirfenidone results of a prospective open-label Phase II study Am J Respir Crit Care Med 19991591061-9 41 Hunninghake GW Lynch DA Galvin JR et al Radiologic findings are strongly associated with a pathologic diagnosis of usual interstitial pneumonia Chest 20031241215-23 42 Lynch D Godwin J Safrin S et al High-resolution computed tomography in idiopathic pulmonary fibrosis diagnosis and prognosis Am J Respir Crit Care Med 2005172488-93 43 Mallinckrodt CH Watkin JG Molenberghs G Carroll RJ Choice of the primary analysis in longitudinal clinical trials Pharmaceutical Statistics 20043161-9 44 Bang H Tsiatis A Estimating medical costs with censored data Biometrika 200087329shy43 45 Lin DY Regression analysis of incomplete medical cost data Stat Med 2003221181-200 46 Rochon J Application of GEE procedures for sample size calculations in repeated measures experiments Stat Med 1998171643-58 47 Lachin JM Foulkes MA Evaluation of sample size and power for analyses of survival with allowance for nonuniform patient entry losses to follow-up noncompliance and stratification Biometrics 198642507-19
71
- PANTHER-IPFPREDNISONE AZATHIOPRINEAND N-ACETYLCYSTEINEA STUDY THAT EVALUATES RESPONSE INIDIOPATHIC PULMONARY FIBROSIS
-
- Protocol Summary
- Table of Contents
- List of Tables
- List of Figures
- List of Abbreviations
- 1 Summary
- 2 Hypotheses and Specific Aims
-
- 21 Null Hypothesis
- 22 Specific Aim 1
- 23 Specific Aim 2
- 24 Prespecified Subgroups of Interest
-
- 3 Background and Significance
-
- 31 Idiopathic Pulmonary Fibrosis is the Most Common Interstitial Lung Disease
- 32 Rationale for Placebo Control
- 33 Rationale for N-acetylcysteine
- 35 Rationale for N-acetylcysteine as a Stand-alone Therapy
- 36 Rationale for the Study Design and Primary Endpoint
- 37 Rationale for Blinding of Treatments
-
- 4 Methods
-
- 41 Inclusion Criteria
- 42 Diagnosis of IPF
- 43 Exclusion Criteria
- 44 Study Design and Study Visit
- 45 Dose Justification
- 46 Contraindications Precautions and Side Effects of Study Medications
- 47 Recruitment Procedures
- 48 Study Procedures
- 49 Concomitant Medications
- 410 Laboratory Testing
- 411 Blinding of Study Drugs
-
- 5 Study Endpoints
-
- 51 Primary Study Endpoint
- 52 Secondary Study Endpoints
-
- 6 Safety Evaluations and Procedures
-
- 61 Adverse Events
- 62 Clinical Medical Monitoring
- 63 Unblinding Procedures
-
- 7 Study Drug Procedures
- 8 Data Management
-
- 81 Hardware and Software Configuration
- 82 Sources of Data
-
- 9 Study Design and Data Analysis
-
- 91 General Analytic Considerations
- 92 Randomization Blinding and Reporting of Results
- 93 Stratification
- 94 Specification of the Primary Analyses
- 95 Analysis of Longitudinal Endpoints
- 96 Analysis of Binary Time-to-Event and Time-Lagged Endpoints
- 97 Power Analysis
-
- 10 Study Administration
-
- 101 Cooperative Agreement Mechanism
- 102 IPFnet Steering Group
- 103 Data and Safety Monitoring Board
- 104 Recommendations on Interim Monitoring of Efficacy Safety and Futility
-
- 11 Investigator and Sponsor Obligations
-
- 111 Monitoring
- 112 Cost and Payment
- 113 Confidentiality and Health Insurance Portability and Accountability ActConsiderations
- 114 Informed Consent Procedures
- 115 Institutional Review Boards
-
- 12 Investigator Agreement
- 13 References
-

PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
DLCO diffusing capacity of the lung for carbon monoxide
DLCOpred diffusing capacity of the lung for carbon monoxide percent predicted
DSMB data and safety monitoring board
eCRF Electronic case report form
ERS European Respiratory Society
FDA Food and Drug Administration (US)
FEV1 forced expiratory volume in 1 second
FSH follicle-stimulating hormone
FVC forced vital capacity
FVCpred forced vital capacity percent predicted
GGT gamma glutamyl transferase
GSH glutathione
HAD Hospital Anxiety and Depression
HHS Health amp Human Services (US Dept of)
HIPAA Health Insurance Portability and Accountability Act
HRCT high-resolution computed tomography
IBW ideal body weight
ICE CAP Investigating Choice Experiments for Preferences of Older People Capability Instrument
ILD interstitial lung disease
IPF idiopathic pulmonary fibrosis
9
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
IPFnet Idiopathic Pulmonary Fibrosis Clinical Research Network
IRB institutional review board
ITT intent to treat
IV intravenous
IVRS interactive voice response system
LDH lactate dehydrogenase
LFT liver function test
LOCF last observation carried forward
LSD Least Significant Difference
MAR missing at random
MCAR missing completely at random
MMRM mixed model repeated measures
MOOP manual of operating procedures
NAC N-acetylcysteine
NHLBI National Heart Lung and Blood Institute (US)
NIH National Institutes of Health (US)
NSIP nonspecific interstitial pneumonia
PaO2 partial pressure of arterial oxygen
PCP primary care provider
PFT pulmonary function test
10
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
PHS Public Health Service (US)
PI principal investigator
PL placebo
PLT platelet
PRED prednisone
QOL quality of life
SAE serious adverse event
SAP statistical analysis plan
SGRQ St Georgersquos Respiratory Questionnaire
SpO2 oxygen saturation by pulse oximetry
TPMT thiopurine methyl transferase
UCSD SOBQ University of California at San Diego Shortness of Breath Questionnaire
UIP usual interstitial pneumonia
ULN upper limit of normal
USP United States Pharmacopoeia
VC vital capacity
WBC white blood cell
11
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
PREDNISONE AZATHIOPRINE AND N-ACETYLCYSTEINE A STUDY
THAT EVALUATES RESPONSE IN IDIOPATHIC PULMONARY FIBROSIS
1 Summary
There are currently no drug therapies that have proven to be effective in the treatment of idiopathic pulmonary
fibrosis (IPF) Previous clinical drug trials have been difficult to interpret due to lack of true placebo (PL)
controls or other methodological concerns Clinical efficacy of immunosuppressive therapies and agents that
reduce oxidative stress remains controversial The IPF Clinical Research Network (IPFnet) is conducting a
randomized double-blind placebo-controlled trial designed to assess the safety and efficacy of
N-acetylcysteine (NAC) as monotherapy in subjects with mild or moderate IPF
The study initially employed a 3-arm design with 111 randomization to NAC azathioprine (AZA)-prednisone
(PRED)-NAC and PL with each subject to be treated up to a maximum of 60 weeks followed by a tapering of
PREDPL and a 4-week period for safety evaluation Approximately 390 subjects who have mild to moderate
IPF (defined as forced vital capacity percent predicted [FVCpred] ge 50 and diffusing capacity of the lung
for carbon monoxide percent predicted [DLCOpred] 30) diagnosed within the past 48 months were to be
enrolled
At the pre-specified interim analysis the DSMB recommended termination of the prednisone-azathioprine-
NAC arm of the study No additional patients will be randomized to that arm However the NAC and placebo
arms remain open for enrollment and we will enroll approximately 130 subjects in each arm (inclusive of the
subjects enrolled at the time of the interim analysis) Follow up for subjects enrolled into the two arms will
continue for 60 weeks
The primary endpoint is the change in longitudinal measurements of FVC over the study period The primary
goal of this study to establish an evidence-based standard of care and clarify myths from facts for
pharmacotherapy of IPF has been met in part by demonstrating that the widely used triple therapy was harmful
to patients with IPF (NHLBI press release Oct 21 2011) To determine the potential therapeutic benefits of
NAC alone the study will continue to enroll patients as a two-arm double-blind placebo-controlled study from
this point on (NAC vs placebo) as recommended by the DSMB following the pre-specified interim analysis
12
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
2 Hypotheses and Specific Aims 21 Null Hypothesis
Treatment with NAC will provide the same efficacy as PL as measured by longitudinal changes in FVC
22 Specific Aim 1
This study is designed to assess the safety and efficacy of NAC in subjects with newly diagnosed IPF
23 Specific Aim 2
Secondary goals of this study are to assess differences between treatment groups for the following
1 Mortality
2 Time to death
3 Frequency of acute exacerbations (AExs)
4 Frequency of maintained FVC response
5 Time-to-disease progression
6 Change in DLCO
7 Change in Composite Physiologic Index (CPI)
8 Change in resting alveolar-arterial oxygen gradient
9 Change in 6-minute walk test (6MWT) distance
10 Change in 6MWT oxygen saturation area under the curve
11 Change in 6MWT distance to desaturation lt 80
12 Change in 6MWT minutes walked
13 Changes in health status as measured by the SF-36 EuroQol and St Georgersquos Respiratory
Questionnaire (SGRQ)
14 Changes in dyspnea as measured by the University of California at San Diego Shortness of Breath
Questionnaire (UCSD SOBQ)
15 Frequency and types of adverse events (AEs)
16 Frequency and types of respiratory complications both infectious and noninfectious
17 Frequency of hospitalizations both all-cause and respiratory-related
13
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
24 Prespecified Subgroups of Interest
Treatment effects will be estimated and compared within key subgroups
Higher enrollment FVC12
Typical vs atypical high-resolution computed tomography (HRCT) reading at baseline3
Recent vs more remote diagnosis (time from initial diagnosis of IPF le 1 year and gt 1 year)
Lower CPI score at enrollment4
Medical therapy for gastroesophageal reflux5
Ethnic background
Sex
Smoking history (current or ex-smoker vs never smoker) given potential impact on oxidant status6
Presence of emphysema gt 25 on HRCT
14
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
3 Background and Significance
31 Idiopathic Pulmonary Fibrosis is the Most Common Interstitial Lung Disease
IPF is the most common interstitial lung disease (ILD) of unknown etiology The current incidence and
prevalence of IPF in the United States are not known A 1994 study of a population-based registry of subjects in
Bernalillo County New Mexico USA estimated an incidence of 107 cases per 100000 per year for males and
74 cases per 100000 per year for females the prevalence of IPF was estimated at 20 per 100000 for males and
13 per 100000 for females7 Extrapolating from a large healthcare claims database a more recent review
estimated the prevalence of IPF in the United States at 427 per 100000 (incidence estimated at 163 per
100000 per year)8 Recent epidemiological studies indicate increasing mortality rates from IPF in the United
States and other industrialized nations9-12
Approximately two-thirds of subjects with IPF are over the age of 60 at the time of presentation and the
incidence increases with age13 IPF has no distinct geographical distribution and predilection by race or
ethnicity has not been identified13 Individual subjects may remain relatively stable for prolonged periods
experience very slow declines in lung function with progression of radiographic abnormalities for a period of
months to years or experience more rapid declines and subsequent death Only 20 to 30 of IPF patients
survive for 5 years following diagnosis
There is currently no proven effective pharmacological treatment for IPF13 Anti-inflammatory and
immunosuppressive agents have been the traditional approach to the management of patients with IPF Based
on the results of the interim analysis of the PANTHER-IPF trial this lsquotraditional approachrsquo will be aborted
However it remains unknown if NAC alone will prove beneficial in IPF patients The primary goal of the
modified study is to establish an evidence-based standard of care and clarify the role of this specific antioxidant
pharmacotherapy for IPF
32 Rationale for Placebo Control
IPF is a disorder for which there is no proven efficacious therapy A major objective of this trial is to test to the
greatest degree possible a proposed standard of care for patients with IPF The current traditional therapy
15
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
employs immunosuppressive and corticosteroid drugs Interim review of the original PANTHER-IPF study has
documented increased adverse events and lack of efficacy for AZA-PRED-NAC compared to placebo
suggesting that this therapeutic approach should not be employed Whether this applies to NAC alone which
has been advocated by international societies has not been proven in well-designed well-powered clinical
trials The recommendations made in the recently published evidence guidelines for NAC monotherapy was
weak based on low quality13 Thus this continued clinical trial randomizing patients to receive NAC or placebo
is pivotal and will answer the important question of the potential therapeutic benefits of NAC monotherapy with
grade A evidence In this prospective randomized clinical trial the inclusion of a PL arm is therefore vital to
adequately test the benefits of NAC in well-characterized subjects with IPF
If NAC has no true efficacy then its role as standard of care will be refuted If a benefit compared with PL is
confirmed it will establish a benchmark against which future novel therapies for IPF will be safely compared
As there is no currently accepted therapy for IPF there is an increasing body of published literature supporting
the concept of no treatment as the ldquobest carerdquo option for IPF13
Post hoc analyses of PL-controlled trials suggest that subjects with milder disease may be more amenable to
therapy12 It is notable that a recent international prospective randomized trial of interferon-gamma for IPF
also included a PL arm the study was terminated early by the data and safety monitoring board (DSMB) due to
lack of treatment effect1415 This underscores the belief that a proven effective therapy for IPF does not
currently exist and that true placebo-controlled trials remain the gold standard Similarly recently completed
trials of etanercept everolimus bosentan and BIPF 1120 in IPF have included PL-treated arms16-19 In three of
these trials the treated subjects showed little if any objective improvement Based on this evidence and the
current status of IPF therapy and therapeutic trials we believe that clinicians and subjects will continue to enroll
in a PL-controlled study
33 Rationale for N-acetylcysteine
NAC is a derivative of the amino acid L-cysteine NAC has been shown to augment levels of the naturally
occurring antioxidant glutathione (GSH ) (glutathione γ-glutamyl cysteinyl glycine) both in vitro and in
vivo2021 GSH is present in all eukaryotic cells and may play an important role in protecting alveolar epithelial
cells against oxidant injury The concentration of GSH in the bronchoalveolar lavage (BAL) fluid in patients
16
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
with IPF is markedly diminished compared with normal subjects This GSH deficiency may be corrected by
exogenous administration of NAC2122
There is evidence of enhanced production of oxidants in an IPF lung Both inflammatory cells and
myofibroblasts derived from patients with IPF generate increased amounts of extracellular oxidants including
hydrogen peroxide2324 Secretion of hydrogen peroxide by activated myofibroblasts may induce the death of
adjacent lung epithelial cells by paracrine mechanisms24 Additionally generation of oxidants by myofibroblasts
induces oxidative crosslinking of extracellular matrix proteins25 a potential mechanism for aberrant matrix
remodeling Thus an oxidant-antioxidant imbalance exists in the lungs of IPF patients26 NAC may confer
protection against this imbalance by augmenting GSH levels in addition to its more direct free-radical
scavenging activity
Intravenous (IV) NAC therapy has been shown to increase total BAL GSH in 8 IPF subjects27 Oral NAC (600
mg 3 times per day) has been shown to decrease markers of oxidant injury and improve both total and reduced
GSH levels in the epithelial lining fluid of subjects with IPF in a small uncontrolled study22 pulmonary
function improved modestly with therapy A similar study in 18 IPF subjects confirmed increased intracellular
GSH concentration after 12 weeks of NAC (600 mg 3 times per day)2228 no clinical correlates were reported
Inhaled NAC was suggested to improve pulmonary function in an open label study29
35 Rationale for N-acetylcysteine as a Stand-alone Therapy
Results of a double-blind multi-center European clinical trial of 150 IPF subjects testing combinations of AZAshy
PRED vs AZA-PRED-NAC have been reported30 NAC added to AZA-PRED (ldquoconventional therapyrdquo) had a
significant positive effect on DLCO (p lt 0005) and vital capacity (VC) (p lt 005) at the end of 1 year30 The
recent ATSERS position statement after much discussion concluded that NAC alone should not be considered
in the majority of patients with IPF without additional data from well-designed studies
The interpretation of these data has been quite controversial Some have suggested that the magnitude of the
treatment effect although statistically significant is modest31 Others have suggested that NAC may be
modulating potential toxic effects of AZA-PRED alone32 supporting the investigation of NAC as stand-alone
therapy
17
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
The IPFnet is now completing the PANTHER-IPF trial with a 11 randomization (NAC vs placebo) and a
simple practical feasible and scientifically rational design that will establish standard of care with NAC for
IPF based on a currently available therapeutic agent and the existing data to support its use We anticipate that
all future clinical trials of novel therapeutic agents will be tested against this to-be-established standard of care
36 Rationale for the Study Design and Primary Endpoint
The optimal study design of a therapeutic trial in IPF would include survival as a primary endpoint The
published results of the IFN-γ 1b Phase 3 (GIPF-001) trial suggested a survival benefit in subjects with milder
disease in retrospective analyses1 although the trial was underpowered to address this question This was likely
related to the limited mortality in the PL arm of the study which included IPF subjects with mild to moderate
disease This study documents that an IPF study powered to improve survival in a patient population with mild
disease requires a larger sample size andor duration of study In fact the recently aborted Phase 3 IFN-γ 1b
(GIPF-007 INSPIRE) study was a survival-based study and recruited more than 800 subjects at 75 centers
worldwide1415 As such within the context of the current IPFnet trial survival is an impractical primary
endpoint variable
Several groups have published data defining an appropriate surrogate outcome variable a 10 decrement in
FVC during 6 to 12 months is a powerful predictor of survival in IPF33-36 Furthermore additional evidence
suggests a similar predictive ability for a 10 decrement in FVC during 3 months of follow-up37 With strong
supportive evidence of FVC progression being related to mortality on a per-subject basis this study will use
FVC changes in liters between treatment groups as the primary endpoint Previously published IPF studies have
shown a steady decline in FVC (and FVCpred) among control group subjects230 The GIPF-001 study
suggested a 48-week decrease in FVC of 016 L in the PL-treated subjects The IFIGENIA study demonstrated
a decline in FVC of approximately 019 L over 52 weeks in the subjects randomized to the control treatment
Figure 1 depicts the change in FVC for control groups from previously published IPF studies38 Based on these
data we expect that the PL group will have a decline of 020 L over the 60-week study period The IPFnet
Steering Group determined that a clinically meaningful improvement would be the preservation of the majority
of the 020-L FVC decline Therefore a mean treatment difference of 015 L in mean FVC over the 60-week
study period was determined to be a clinically meaningful difference
18
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Δ f
rom
bas
elin
e (i
n L
)
01
005
0
-005
-01
-015 Projected Δ for placebo
-02
-025
-019
-016
-013 Pirfenidone GIPF001
NAC
Placebo
4 8 12 16 20 24 28 32 36 40 44 48 52 56 60
Week
Figure 1 Changes in FVC From Baseline in Prior IPF Clinical Trials
Recent data suggest that various patient subgroups would be expected to potentially exhibit differential response
to therapy These parameters will be used to a priori separate patients by a series of baseline characteristics
including
1 Higher enrollment FVC12
2 Typical vs atypical high-resolution computed tomography (HRCT) reading at baseline3
3 Recent vs more remote diagnosis (time from initial diagnosis of IPF le 1 year and gt 1 year)
4 Lower CPI score at enrollment4
5 Medical therapy for gastroesophageal reflux5
6 Ethnic background
7 Sex
8 Smoking history (current or ex-smoker vs never smoker) given potential impact on oxidant status6
9 Presence of emphysema gt 25 on HRCT
37 Rationale for Blinding of Treatments
The issue of treatment blinding was given a great deal of consideration with subject safety being the primary
concern After discussion among the Steering Group members it was decided that as long as subject safety
could be ensured blinding was necessary Blinding allows the study to
Have optimal scientific validity and potential to impact the standard of care for subjects
19
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Make objective assessments of treatment effects
Maintain clinical equipoise among investigators
Encourage subjects to have similar levels of contact with the medical community
Minimize the differential dropout rates across study arms
20
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
4 Methods 41 Inclusion Criteria
1 Age 35 to 85 years inclusive
2 FVC ge 50 of predicted (post-bronchodilator measurement from the screening visit)
3 DLCO ge 30 of predicted (hemoglobin corrected and altitude corrected if gt4000 ft above sea level)
4 Ability to understand and provide informed consent
5 Diagnosis of IPF according to a modified version of the ATS criteria le 48 months from enrollment The
date of diagnosis is defined as the date of the first available HRCT or surgical lung biopsy characteristic
of definite UIP
411 Subjects Shown to Have Usual Interstitial Pneumonia Pattern on Surgical Lung Biopsy
Subjects who have been shown to have UIP pattern on lung biopsy must have all of the following
1 Exclusion of other known causes of ILD such as drug toxicity clinically significant environmental
exposures or diagnosis of connective tissue diseases
2 Bibasilar reticular abnormalities with minimal ground glass opacities on HRCT scan
412 Subjects Who Have Not Undergone a Surgical Lung Biopsy
In addition to the criteria above these subjects must have radiological findings considered to be definite for the
diagnosis of UIPIPF
1 Bibasilar reticular abnormalities with minimal ground glass opacities
2 Honeycombing as the predominant feature and located in the peripheral lung bases
42 Diagnosis of IPF
Only subjects with definite IPF will be eligible for enrollment in this study We will utilize a combination of
clinicalphysiologic features HRCT and review of a clinically obtained surgical lung biopsy specimen to
establish the diagnosis of IPF An algorithm for the diagnosis is provided to guide entry into the protocol as
outlined in the inclusion and exclusion criteria (Figures 2 and 3) This multi-disciplinary approach uses
21
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
expertise from clinicians radiologists and pathologists Investigators at each site in conjunction with central
pathology will work together to establish the diagnosis of IPF This interactive approach to the diagnosis of IPF
increases the level of agreement between observers39
A subject with suspected ILD should be evaluated for secondary causes including but not limited to
environmental exposures drugs and systemic diseases Presence of any of these findings felt to be significant
enough to cause an ILD should disqualify the subject from entry into the trial
If secondary causes are absent an HRCT scan may be obtained If an HRCT of sufficiently high quality has
been obtained within the last 3 months that scan may be used for diagnosis In the appropriate clinical setting
the diagnosis of IPF can be made by the demonstration of a typical radiographic pattern on HRCT or by
demonstration of UIP pattern on a surgical lung biopsy The following criteria for a radiographic (ie
nonsurgical) diagnosis will be used In the absence of known exposures andor clinical associations attributable
to pulmonary fibrosis and in the appropriate clinical setting the presence of definite UIP pattern in HRCT
images is required to meet study criteria for the diagnosis of IPF
Figure 2 Diagnosis of Idiopathic Pulmonary Fibrosis in the IPFnet
22
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Figure 3 Pathology Flow Chart Surgical Lung Biopsy Diagnosis
Requirement for diagnosis
1 Clinical exclusion of other known causes (connective tissue diseases environmental and drug
exposures) of ILD
2 Radiographic HRCT with bibasilar reticular abnormality and honeycomb change with minimal
ground glass opacities
Appropriate clinical setting
1 Age gt 50 years
2 Insidious onset of unexplained dyspnea
3 Duration of illness for ge 3 months
4 Bibasilar inspiratory crackles
23
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Unlike the ATSERS consensus criteria published in 2000 bronchoscopy will not be required for diagnosis
This decision was made based on the experience of the IPFnet Steering Group members regarding the utility of
bronchoscopy in the diagnosis of IPF The presence of an atypical HRCT finding will require documentation of
a definitive diagnosis by surgical lung biopsy In fact this is in keeping with the recently published evidence
based guidelines for diagnosis and management of IPF13 As shown in Figure 3 central review of the pathology
data will be required for a diagnosis of IPF
We will not require central review of HRCT as several studies have shown that a confident local interpretation
of clinicalHRCT criteria as definite IPFUIP is associated with a high positive predictive value for finding UIP
at surgical lung biopsy (see Table 1) Differences in sensitivity in these series likely reflect subject selection as
Flaherty et al3 evaluated only UIP and nonspecific interstitial pneumonia (NSIP) while Raghu et al40 and
Hunninghake et al41 included a broader range of ILD
Table 1 Operating Characteristics of Local HRCT Review for Diagnosis of UIP
Researcher of Subjects Sensitivity () Specificity () PPV () NPV ()
Raghu et al 40
59 (29 UIP by SLB) 78 90 88 82
Hunninghake et al 41 91 (54 UIP by SLB)
74 81 85 67
Flaherty et al 3 96 (only NSIP amp UIP)
37 100 100 30
Abbreviations PPV positive predictive value NPV negative predictive value UIP usual interstitial pneumonia SLB surgical lung biopsy and NSIP nonspecific interstitial pneumonia
Furthermore an analysis of the HRCT scans from subjects enrolled in the GIPF-001 trial confirmed that local
site interpretations have a high congruity to a central radiology core In this multi-center study 263 HRCT
scans were read as definite IPF and a retrospective central radiology core review found 932 to be consistent
with IPF 42 We will also take several additional steps to insure that the local HRCT reads are accurate
including
1 A detailed training module has been developed and must be completed by each site radiologist before
site initiation
2 Clinical centers are to mail all HRCT scans to the HRCT core lab The first 10 HRCT scans from
subjects enrolled at each enrolling clinical center will be reviewed centrally to be certain that local reads
24
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
25
are congruent with a central interpretation If discrepancies are identified additional education will be
provided and HRCT scans will continue to be reviewed centrally until the central radiology core is
confident that the local center is performing appropriately
3 Random scans will be obtained from each center throughout the study to confirm that the local read
continues to agree with central interpretation If discrepancies are identified they will be addressed as in
2 above
In all cases if a subject has a surgical lung biopsy sample that sample will be reviewed by the local and central
pathologists Therefore the only cases that would not be subject to a direct central review process are those
where the HRCT meets the centrally defined criteria for an unequivocal diagnosis and a lung biopsy sample is
not available Table 2 below summarizes the possible combinations for making a diagnosis
Table 2 Combining HRCT and Pathology Interpretations to Determine if IPF is Present
HRCT Diagnosis Pathology Diagnosis Diagnosis of IPF
Definite UIP Definite UIP Yes
Definite UIP Probable UIP Yes
Definite UIP Possible UIP Yes
Definite UIP Not UIP No
Definite UIP Unavailable Yes
Consistent with UIP Definite UIP Yes
Consistent with UIP Probable UIP Yes
Consistent with UIP Possible UIP No
Consistent with UIP Not UIP No
Consistent with UIP Unavailable No
Inconsistent with UIP Any No
Abbreviations HRCT high-resolution computed tomography IPF idiopathic pulmonary fibrosis
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
UIP usual interstitial pneumonia Dx diagnosis 43 Exclusion Criteria
1 History of clinically significant environmental exposure known to cause pulmonary fibrosis
Occupational exposures such as asbestos or environmental exposure to organic dust such as occurs in
pigeon breeders may at times mimic the clinical and radiographic findings of IPF
2 Diagnosis of connective tissue disease felt by the principal investigator (PI) to be the etiology of the
interstitial disease Diagnosis of collagen-vascular conditions will be according to the published
American College of Rheumatology criteria As such the presence of any documented collagen-vascular
disorder or the presence of any suspicious symptom complex whether or not associated with
significantly abnormal rheumatological serologies will exclude the subject at the discretion of the PI
3 Extent of emphysema greater than the extent of fibrotic change (honeycombing reticular changes) on
HRCT scan
4 Forced expiratory volume in 1 second (FEV1)FVC ratio lt 065 at screening (postbronchodilator)
5 Partial pressure of arterial oxygen (PaO2) on room air lt 55 mm Hg (lt 50 mm Hg at Denver site)
6 Residual volume gt 120 predicted at screening (postbronchodilator)
7 Evidence of active infection
8 Significant bronchodilator response on screening spirometry defined as a change in FEV1 ge 12 and
absolute change gt 200 mL OR change in FVC ge 12 and absolute change gt 200 mL The percent
difference between the FVC (or FEV1) values will be calculated by taking the absolute value of the
difference and dividing it by the larger of the two FVC (or FEV1) values
9 Screening and enrollment post-bronchodilator FVC measurements (in liters) differing by gt 11 The
percent difference between the FVC values will be calculated by taking the absolute value of the
difference and dividing it by the larger of the two FVC values (eg the percent difference between FVC
measurements of 19 and 20 liters would be determined by taking the difference between the two (01
liters) and dividing by the larger of the two (20 liters) So 0120 = 5 and these FVC measurements
would not exclude the subject
10 Listed for lung transplantation ie the patient has completed the evaluation process has been accepted
as a candidate for transplantation at an appropriate center and is waiting to receive notification of an
available donor organ
11 History of unstable or deteriorating cardiac disease
12 Myocardial infarction coronary artery bypass or angioplasty within 6 months of screening
26
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
13 Unstable angina pectoris or congestive heart failure requiring hospitalization within 6 months of
screening
14 Uncontrolled arrhythmia
15 Severe uncontrolled hypertension
16 Known HIV or hepatitis C
17 Known cirrhosis and chronic active hepatitis
18 Active substance andor alcohol abuse (as determined by site PI)
19 Pregnancy or lactation (subjects who are pregnant or breastfeeding)
20 Known hypersensitivity to study medication
21 Any condition other than IPF that in the opinion of the site PI is likely to result in the death of the
subject within the next year
22 Any condition that in the judgment of the PI might cause participation in this study to be detrimental to
the subject or that the PI deems makes the subject a poor candidate
23 Any therapy directed at pulmonary fibrosis (excepting triple therapy of prednisone plus azathioprine
plus NAC) requires a 30-day washout period before randomized Triple therapy of lt= 12 weeks duration
in the past 4 years requires a 30-day washout period before randomization
24 History of triple therapy of prednisone plus azathioprine plus NAC for gt 12 weeksrsquo duration in the past
4 years or previous enrollment in the triple-therapy arm of the PANTHER-IPF study
44 Study Design and Study Visit
441 Study Design Summary
This study will be a randomized double-blind PL-controlled trial designed to assess the safety and efficacy of
NAC in subjects with newly diagnosed IPF
Subjects with mild to moderate IPF (defined as FVCpred ge 50 and DLCOpred ge 30) diagnosed within
the past 48 months will be enrolled Screening will continue until April 30 2012
27
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
The study will employ a 2-arm design with 11 randomization to NAC or PL Once enrolled subjects will visit
the clinical center at 15 weeks and 15-week intervals thereafter Each subject will be treated and followed for a
maximum of 60 weeks
During the 60-week visit subjects will be taken off all study agents Approximately four weeks after the final
dose of study agent is taken subjects will receive a safety phone call from the study site
442 Study Visits
Subjects who meet entry criteria will review the informed consent a written description of the purpose
procedures and risks of the study with the PI co-investigator or study coordinator and all questions will be
answered The informed consent form will be signed by the subject at screening No protocol-specific
procedures will be performed until the subject has signed and dated an informed consent form This includes the
screening procedures
4421 Screening
Once informed consent is obtained subjects may immediately begin the screening process or may return within
28 days of consent In the event a study subject has been clinically evaluated at the study site by an IPFnet study
physician and has performed testing within three weeks for this clinical evaluation that meets guidelines
provided in the IPFnet PANTHER-IPF Manual of Operating Procedures (MOOP) this testing may be used to
satisfy the following screening criteria medical history physical exam arterial blood gas (ABG) with A-a
gradient vital signs with oximetry body height and weight spirometry DLCO lung volumes and HRCT scan
Allowing the use of previously performed test results that meet study guidelines for the screening visit is
intended to permit subjects easier access to study entry to prevent subjects from repeating testing that has been
performed within the study window and to decrease risks to subjects from repeated exposure to procedures
such as arterial puncture and HRCT
The following procedures will be performed at screening
Medical history and a physical examination
28
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Measure height and weight
Serum pregnancy test (if applicable)
Measure vital signs including oximetry
Blood draws performed and the following analyses conducted
o Hematology (red cell count white cell count hemoglobin hematocrit cell indices differential
platelet count)
o Blood chemistries according to central laboratory protocol (see Section 410 Laboratory
Testing)
o Beta human chorionic gonadotropin (serum) pregnancy test (in women of childbearing potential)
o Urinalysis
Pulmonary Function Tests (PFTs) including spirometry pre- and post- bronchodilator and postshy
bronchodilator measurement of lung volumes and measurement of hemoglobin adjusted diffusing
capacity
Measure ABGs
HRCT if a satisfactory scan has not been performed on the subject within 3 months of screening (see
PANTHER-IPF MOOP for more details)
Surgical lung biopsies (if applicable) reviewed by local and central pathology departments
Current medications If required a washout period discussed with the subject and initiated at this visit
4422 Enrollment
The enrollment visit is expected to take place within eight weeks of the screening visit Enrollment visit
activities include
Measure vital signs including oximetry
Measure height and weight
Serum pregnancy test (if applicable)
If consent has been given blood will be drawn and a urine specimen collected for the bio-specimen
repository
Spirometry (post-bronchodilator)
Measure 6MWT with Borg Dyspnea Scale
29
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Collect Quality-of-life (QOL) data using the SF-36 EuroQol Investigating Choice Experiments for
Preferences of Older People Capability Instrument (ICE CAP) and SGRQ
Female subjects complete Gender Substudy questionnaire
Dyspnea status collected using the UCSD SOBQ
Evaluate Acute Exacerbation (AEx)
Review of any Adverse Events (AEs)
Review of concomitant medications
Subject receives diary and instructions on its purpose and proper use
Subject receives supply of study drug sufficient to last until his or her 15-week study visit
See the Schedule of Assessments (Table 3) for more details Subjects with screening and enrollment postshy
bronchodilator FVC measurements (in liters) differing by more than 11 are not eligible to be enrolled in the
study
Subjects will be asked to provide a physician of record This physician will be considered the subjectrsquos primary
care provider (PCP) and if the subject agrees the PCP will be informed by letter of the subjectrsquos enrollment in
the trial The subject will be informed that his or her ongoing medical care should be received from the PCP
The PCP will be informed of any safety issues identified by the study staff The PCP will also be given
information regarding communication with study personnel about pertinent health issues or clinic encounters
the subject may have
4423 Week 15
The week 15 visit is expected to occur within +- 14 days of the subjectrsquos scheduled visit time (eg the week 15
visit should occur anytime between 13 and 17 weeks after starting study drug Week 15 activities include
Measure vital signs with oximetry
Measurement height and weight
Serum pregnancy test (if applicable)
Spirometry (post-bronchodilator) measurement
Review of AEs
Evaluate for AEx
30
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Review concomitant medications
If consented draw blood and collect urine specimen for the biospecimen repository
Subjects return used and unused study drug for the visit
Review study diary and a new study diary will be given
Provide additional supply of study drug sufficient to last until the next scheduled visit
4424 Week 30
The week 30 visit is expected to occur within +- 14 days of the subjectrsquos scheduled visit time (eg the week 30
visit should occur anytime between 28 and 32 weeks after starting study drug) Week 30 activities include
Physical examination
Measure vital signs with oximetry
Measure height and weight
Laboratory values (complete blood count [CBC] and serum chemistries)
Serum pregnancy test (if applicable)
Measure spirometry (post-bronchodilator)
6MWT with Borg scale
DLCO
Review of AEs
Evaluate for AEx
Review concomitant medications
Complete all QOL and dyspnea questionnaires (EuroQol ICE CAP SF-36 SGRQ and UCSD SOBQ)
If consent has been given blood will be drawn and a urine specimen collected for the biospecimen
repository
Review study diary
Subjects return used and unused study drug for the visit
Provide additional supply of study drug sufficient to last until the next scheduled visit
4425 Week 45
31
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
The week 45 visit is expected to occur within +- 14 days of the subjectrsquos scheduled visit time (eg the week 45
visit should occur anytime between 43 and 47 weeks after starting study drug) Week 45 activities include
Measure vital signs with oximetry
Measure height and weight
Serum pregnancy test (if applicable)
Measure spirometry (post-bronchodilator)
Review of AEs
Evaluate for AEx
Review concomitant medications
If consent has been given blood will be drawn and a urine specimen collected for the biospecimen
repository
Subjects return used and unused study drug for the visit
Study diary reviewed
Provide additional supply of study drug sufficient to last until the next scheduled visit
4426 Week 60 (Early Withdrawal or Final Treatment Visit)
At week 60 or at subject withdrawal from the study (premature by study doctor or subjectrsquos decision) a final
treatment visit will occur At this final treatment visit subjects will discontinue NACPL abruptly Week 60
activities also include
Physical examination
Measure vital signs with oximetry
Measure height and weight
Laboratory values (complete blood count [CBC] and serum chemistries)
Spirometry (post-bronchodilator) measurement
6MWT with Borg scale measurement
DLCO
Lung volumes
ABG
Review of AEs
32
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Evaluate for AEx
Review concomitant medications
Subjects will complete all QOL and dyspnea questionnaires (EuroQol ICE CAP SF-36 SGRQ and
UCSD SOBQ)
If consent has been given blood will be drawn and a urine specimen collected for the biospecimen
repository
Subjects return used and unused study drug for the visit
Study diary reviewed
4427 Final Site Visit ndash FVC drop confirmation
In the event that the subject has a recorded FVC drop of gt10 from baseline at the final treatment visit and the
subject has not had a confirmation of such a drop at a previous study visit the subject should return to the
clinical site 6 to 8 weeks after the final treatment visit During this visit a post-bronchodilator spirometry test
will be performed This FVC measurement will be evaluated according to section 521 of this protocol
4428 Final Visit ndash Telephone Follow-up
Four weeks following the final dose of study medication subjects will receive a telephone call from the study
coordinator to ensure that there are no side effects and to follow up on any ongoing adverse events (AEs)
4429 Phone Contact Between Visits
At week 2 and each month that a subject does not have a scheduled clinical center visit his or her study
coordinator will contact him or her at least once by telephone to
Inquire if the subject has had any hospitalizations events that might be considered an AE or any events
significant enough to warrant an out-of-cycle visit to the clinical center
Remind subjects of their current dosage levels and confirm that the subject understands them
Address any questions or concerns the subject might have regarding other aspects of the study
Assess adherence to the treatment regimen by reviewing diary data verbal review of medications taken
including nutritional supplements
33
34
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Table 3 Schedule of Assessments
Procedure Screening Visit 0
Enrollment Visit 1
Week 15 Visit 2
Week 30Visit 3
Week 45 Visit 4
Week 60 Early
Withdrawal Visit 5
Final1
Visit (via phone)
Informed consent X
Medical history X
Inclusionexclusion criteria X
Serum pregnancy test (if applicable) X X X X X
Review of lung biopsy X
Arterial Blood Gas X X
6-Minute Walk Test
X
X X
Physical examination X X X
Vital signs with oximetry X X X X X X
Body height and weight X X X X X X
Complete Blood Count X X X
Chemistry panel X X X
Monitor Lab Values X X X
Urinalysis X Specimen repository substudy blood draw and urine collection (if consented)
X
X X X X
HRCT (if not completed within three months) X
Spirometry (pre- and post-bronchodilator) X
Spirometry (post-bronchodilator only) X X X X X
DLCO (post-bronchodilator only) X X X
Lung volumes (post-bronchodilator only) X
X
Evaluate for acute exacerbation X X X X X
Review Adverse Events X X X X X X
Review concomitant meds X X X X X X
Dispense subject diary X X X X
Review subject diary X X X X X
Dispense study agent X X X X
Gender Substudy questionnaire (female subjects only) X
EuroQol ICECAP UCSD SOBQ SGRQ SF-36 X X X
Abbreviations DLCO diffusing capacity of the lung for carbon monoxide QOL Quality of Life ICECAP Investigating Choice Experiments for Preferences of Older People UCSD SOBQ University of California Shortness of Breath Questionnaire SGRQ St Georgersquos Respiratory Questionnaire SF-36 Short Form 36 Health Survey
1Follow-up visit via phone will occur four weeks after final dose of study medication
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
45 Dose Justification
The general philosophy for determining dosing levels was to apply previously examined
treatment regimens With the focus of the study being to establish a standard of care for
mildmoderate IPF subjects the goal was to develop flexible yet standardized treatment rules that
allow for the temporary or permanent withholding of one or more components of treatment when
necessary Subjects developing laboratory abnormalities or symptoms that result in
discontinuation of one or more components of study treatment may continue on the other
components as long as there is no contraindication for this Complete follow-up is important for
the validity of any study As a strategy to maintain protocol adherence we are using a treatment
regimen that will detect potential side effects and prompt interventions proactively in the interest
of patient safety In addition subjects who permanently stop study medications during the course
of the study are encouraged to continue in the study completing all scheduled visits and tests
451 Rationale for N-acetylcysteine Dosing
To our knowledge there have been no IPF studies to correlate clinical outcome measures with
different dosages for NAC The dosage chosen is based on the IFIGENIA study However BAL
lung GSH levels from subjects with IPF have been augmented with the use of oral NAC at 600
mg 3 times per day In addition lung GSH levels have been associated with improved
PFTs212227 The dose chosen for this study was based on previous data including the IFIGENIA
study30
4511 Dosing of N-acetylcysteineplacebo
Dosing of NACPL will be 600 mg orally 3 times a day (1800 mgday)
4512 Reasons to Discontinue N-acetylcysteineplacebo
NACPL may be temporarily or permanently discontinued for the duration of the study for
gastrointestinal symptoms or dermatologic reactions
35
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Temporarily discontinue (hold) oral NACPL for subjects requiring inpatient admission for acute
exacerbation (AEx) or other conditions Resume NACPL after discharge
36
37
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
452 Dosage Algorithms
Dosage Adjustment Algorithm 1 NACPL Dose Modifications for Gastrointestinal Symptoms Nausea Vomiting Abdominal Discomfort Diarrhea
GI Symptoms determined by the PI to be clinically significant Nausea Vomiting Abdominal Discomfort Diarrhea
NACPL Temporarily dc (HOLD) x 3 Days
Monitor symptoms intervene as clinically indicated (eg fluid replacement antidiarrhea or antinausea medication)
Monitor or lab PRN
Are symptoms resolving after 3 days NO
Symptoms NOT resolving after 3 days of holding study medication Assessmentmanagement per clinical
discretion of investigator
Likely not study medication discuss resuming study medication with medical monitor when symptoms resolved
YES
Temporarily dc (HOLD) NACPL for 4 additional days (total hold 1 week) then NACPL Resume 600 MG TID
Did symptoms recur
YES
STOP NACPL for
duration of study
NO
NACPL No Change
38
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Dosage Adjustment Algorithm 2 NACPL Dose Modifications For Dermatologic Reactions
Dermatologic Reactions (Not Acneiform) ge Grade 2 Grading per Common Terminology Criteria for
Adverse Events V30 (httpctepcancergov) For example Grade 1 RASHDESQUAMATION Macular or papular eruption or erythema without associated symptoms Grade 2 RASHDESQUAMATION Macular or popular eruption or erythema with pruritus or other associated symptoms localized desquamation or other lesions covering lt50 of body surface area
NACPL Temporarily dc (HOLD) x 3 days
Are symptoms resolving after 3 days
NO Symptoms not resolving after 3 days of holding study medication Assessmentmanagement per clinical discretion of investigator Likely not study medication Discuss resuming study medication with medical monitor when symptoms
resolved YES
Temporarily dc (HOLD) NACPL for 4 additional days (total hold 1 week) then NACPL resume 600 MG TID
Did symptoms recur
YES
STOP NACPL for
duration of study
NO
NACPL No change
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
46 Contraindications Precautions and Side Effects of Study Medications
461 Contraindication
Contraindication to NAC is known hypersensitivity to it
462 Precautions
Concomitant administration of oral NAC and antibiotics has shown a slightly reduced absorption
of cephalexin and a slight increase in erythromycin serum levels NAC contains free sulfhydryl
groups There is no evidence that individuals sensitive to sulfa drugs are sensitive to NAC
The NAC preparation being administered in this study contains 20 mg of aspartame Because of
the phenylalanine component of aspartame individuals with phenylketonuria should avoid or
restrict aspartame intake to avoid increased blood levels of phenylalanine Because of this risk
labeling is required on all products containing aspartame
463 Side Effects
Side effects of NAC range from common to serious See Table 4
39
40
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Table 4 Side Effects of NAC
Undesirable Effects
System-organ class Uncommon
(gt11000 lt1100)
Rare
(gt110000 lt11000)
Very rare
(lt110000) Not known
Immune system disorders Hypersensitivity Anaphylactic shock
reaction
Nervous system disorders Headache
Ear and labyrinth disorders Tinnitus
Cardiac disorders Tachycardia
Vascular disorders Hemorrhage
Respiratory thoracic and
mediastinal disorders
Bronchospasm
Dyspnea
Gastrointestinal disorders
Vomiting diarrhea
stomatitis abdominal
pain nausea
Dyspepsia
Skin and subcutaneous tissue
disorders
Urticaria rash
angioedema itching
General disorders and
administration site conditions Pyrexia
Investigations Reduced arterial
pressure Face edema
In very rare cases the onset of severe skin reactions such as Stevens-Johnson syndrome and Lyell syndrome was reported to have a temporal relationship with N-acetylcysteine administration Although in most cases at least another suspect drug probably most involved in the genesis of the above mentioned mucocutaneous syndromes has been identified in case of mucocutaneous alterations it is appropriate to contact onersquos doctor and the administration of N-acetylcysteine should be immediately discontinued
Some studies confirmed a reduction of platelet aggregation during N-acetylcysteine administration The clinical significance of these findings has not been defined yet [Source Fluimucil Investigator Brochure]
47 Recruitment Procedures
Subjects recruited for this study will be established patients of the investigators or physician- or
self-referred to participating clinical centers in the IPFnet Each clinical center within IPFnet has
a well-developed infrastructure of local pulmonologists within the surrounding geographic area
These pulmonologists are kept informed of ongoing IPF clinical trials and regularly refer
subjects to studies conducted at IPFnet clinical centers
Additional steps will be taken to inform clinicians of the trials in progress within IPFnet
including presentations at faculty staff meetings at local hospitals medical grand rounds and
national conferences direct mail notification monthly faxes and advertisement of network trials
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
in pulmonary journals Clinical center patients previously diagnosed with IPF will be notified of
the trials by mail whenever possible
Recruitment of minorities and women will be monitored by the DCC and DSMB If necessary
additional recruitment efforts will be made at specific centers to ensure that the aggregate subject
sample contains appropriate representation of women and minorities
48 Study Procedures
The following procedures are detailed in the PANTHER-IPF MOOP accompanying this
protocol
1 PFT
2 ABG
3 HRCT scan of the chest (including imaging of pulmonary arteries)
4 CBC and serum chemistries
5 Pregnancy test
6 6MWTBorg Dyspnea Scale
7 QOL questionnaires (EuroQol HAD SF-36 SGRQ and ICE CAP)
8 UCSD SOBQ
9 Gender Substudy Questionnaire
All assessments of PFTs will be conducted by study personnel not directly involved in the
treatment of the subjects
481 Biological Specimen Management
4811 Biological Specimen Sample Management
Subjects at clinical centers participating in the specimen repository substudy who consent to
having blood drawn for research purposes and for the banking of blood blood components and
other biologic specimens (urine and BAL fluid) will have approximately 405 mL of blood
41
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
drawn 17 mL blood drawn for DNA and 20 mL of urine collected at enrollment visit Subjects
will have approximately 50 mL of blood drawn and 20 mL of urine collected at each 15-week
follow-up visit Blood specimens will be separated according to PANTHER-IPF MOOP
guidelines into the following components for banking in the repository serum plasma and
DNA Coding of all biologic specimens for the repository will be performed by study staff at the
clinical center The samples will be processed per PANTHER-IPF MOOP guidelines aliquoted
labeled with barcode labels and stored at -70degC at the clinical center and shipped to the central
repository
The only subject identifiers will be a sample ID number and subject initials This sample ID will
be linked in the IPFnet DCC clinical database to subject information No subject information will
be transferred to the biological-specimen database
The subjectrsquos samples may be used for approved sub-studies relating to human disease
including but not limited to IPF The studies for which an individualrsquos samples will be made
available will be determined by the subjectrsquos answers to questions on the biological-sample
informed consent form The subjects can choose to make their samples available for all options
or any combination Samples will be made available to researchers only with IPFnet Steering
Group approval until such time as the samples are made public through the NHLBI repository
49 Concomitant Medications
Concurrent treatment with FDA-approved therapy for IPF is allowed Colchicine may be used
for treatment of gout Temporary treatment with oral or IV corticosteroids for clinical worsening
or suspected AEx is permitted Nutritional supplements containing NAC are not allowed
410 Laboratory Testing
Clinical laboratory parameters will be assessed at screening and at the end of the study The
following tests will be performed at the two time points specified in the protocol chemistry (AG
ratio ALT [SGPT] AST [SGOT] albumin alkaline phosphatase amylase bilirubin-direct
42
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
bilirubin-indirect bilirubin-total BUN BUNcreatinine ratio calcium carbon dioxide
cholesterol-total chloride CPK-total creatinine GGT globulin glucose iron-total LDH
lipase magnesium phosphorus-inorganic potassium protein-total sodium TIBC triglycerides
uric acid) and hematology (red blood cell count WBC count hemoglobin hematocrit cell
indices differential platelet count)
411 Blinding of Study Drugs
Subjects and caregivers will be blinded to study treatment Every subject will receive NAC or
matching PLs at every study visit from the baseline visit to the week-45 visit No study agent
will be dispensed at the week-60 visit
43
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
5 Study Endpoints
51 Primary Study Endpoint
The primary endpoint will be the change in serial measurements of FVC over the study period
52 Secondary Study Endpoints
521 Time to Disease-progression
The time-to-death or a 10 decline in FVC will be defined as the time-to-disease progression
The 10 decline in FVC from enrollment must be confirmed on 2 consecutive visits no less than
6 weeks apart For subjects with 2 consecutive visits with a 10 decline in FVC the time-toshy
disease progression will be defined as the time interval between enrollment and the initial visit
with a 10 FVC decline For subjects who experience disease progression the study doctor will
determine whether or not the subject will remain in the study
522 Acute Exacerbations
The following 3 criteria will define AEx in subjects with acute worsening of their respiratory
conditions
1 Clinical (all of the following required)
A) Unexplained worsening of dyspnea or cough within 30 days triggering unscheduled
medical care (eg emergency room clinic study visit hospitalization)
B) No clinical suspicion or overt evidence of cardiac event pulmonary embolism or deep
venous thrombosis to explain acute worsening of dyspnea
C) No pneumothorax
44
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
2 RadiologicPhysiologic (A and B required)
A) New ground glass opacity or consolidation computed tomography (CT) scan OR new
alveolar opacities on chest x-ray
B) Decline of ge 5 in resting room air SpO2 from last recorded level OR decline of ge 8 mm
Hg in resting room air PaO2 from last recorded level
3 Microbiologic (all of the following required)
A) No clinical evidence for infection (ie absence of grossly purulent sputum fever gt 39degC
orally)
B) Lack of positive microbiological results (if done) from lower respiratory tract defined as
(1) Clinically significant bacterial growth on sputum or endotracheal aspirate cultures
(2) Quantitative culture by protected brush specimen ge 103 cfumL or BAL ge 104 cfumL
(3) The presence of specific pathogens on stains of any of the above
C) Lack of positive pathogen in blood cultures (if done)
Identification of Acute Exacerbations
All subjects will be educated about the importance of identifying AExs At the time of
enrollment subjects will be told about the possibility of developing acute symptomatic
worsening that might represent an AEx of IPF and instructed to contact their study clinical
center coordinator within 48 to 72 hours of the apparent event
All subjects will be contacted by phone monthly and questioned about any change in dyspnea or
cough and any interim clinic visits or hospitalizations Finally as part of the IPFnet outreach to
community referring physicians the importance of AExs will be emphasized When a subject is
identified who meets criterion 1A this will trigger the collection of additional clinical data to
evaluate a suspected AEx These data will be collected as part of standard clinical care (ie this
protocol does not require collection of all items) The additional items to be collected for
suspected AEx include
IPFnet AEx case report form (eCRF) (required)
45
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Chest x-ray CT scan withwithout pulmonary angiogram (reports should be faxed and
followed by the hard copiesdiscs)
Oxygen saturation (pulse oximetry)
ABG
Respiratory cultures (sputum endotracheal aspirate lavage)
Blood cultures
Clinichospital records related to the event
All potential cases of AEx will be reviewed by the clinical center PI first and a decision on
whether the case may represent an AEx will be made If AEx is suspected the case will be sent
to the IPFnet adjudication committee which will assign a final diagnosis (see Table 5) If there is
disagreement among members the majority opinion will be recorded
During episodes of suspected AEx as determined by the individual clinical center investigator
subjects will remain blinded and in the study
Table 5 Final Diagnoses in Evaluation of Suspected Acute Exacerbations
Definite acute exacerbation All criteria met no alternative etiology
Unclassifiable acute worsening
Insufficient data to evaluate all criteria no alternative etiology
Not acute exacerbation Alternative etiology identified that explains acute worsening
Management of the suspected AEx will be at the discretion of the treating physician Standard of
care generally involves evaluation for respiratory infection pulmonary embolism cardiac events
and pneumothorax and treatment with IV corticosteroids
Study drugs will be resumed at pre-suspected AEx doses after subjects clinically improve as
confirmed by the local PI All subjects should be seen at the clinical center within 2 to 4 weeks
of recovery for measurement of post-bronchodilator FVC (see Figure 4) Subjects unable to
return to the clinical center after suspected AEx due to medical frailty (eg continued
46
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
institutionalization progressive disability) will be categorized as failing to maintain FVC
response in secondary analyses
Suspected AEx (PI determined)
Hold study drug Treat AEx
(Attending physician determined)
Alive but unable to continue due to
medical frailty
Dead
Alive and able to continue
Site reviewvisit
Restart study drug
FVC within 2-4 weeks
Figure 4 Acute Exacerbation Flow Chart
523 Respiratory Infections
An upper respiratory infection will be defined as
Change in sputum discoloration
Increased cough of no more than 14 daysrsquo duration
A lower-respiratory infection (pneumonia) will be defined as new segmental or lobar airspace
opacities visualized by image studies (chest radiograph or HRCT) in addition to any of the
following
Positive pathogencultures in good sample of sputum or lower-airway secretions retrieved
by fiberoptic bronchoscope
Fever gt 39degC or gt 100degF
Leukocytosis gt 12000 (unexplained no increase in dose of corticosteroids)
47
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
524 Maintained FVC Response
Subjects with follow-up FVCpred measurements at or above their baseline FVCpred level
will be classified as having maintained FVC response Subjects with reduced FVCpred levels
or missing data for any reason including death or medical frailty will be classified as having not
maintained FVC response The FVCpred value is used because unadjusted FVC measurements
are expected to decline with age
48
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
6 Safety Evaluations and Procedures
61 Adverse Events
During a clinical trial the reporting of adverse experience information can lead to important
changes in the way a new treatment is developed as well as provide integral safety data
611 Definitions
An adverse event (AE) is any untoward medical occurrence in a subject or clinical investigation
subject who was administered a pharmaceutical product The AE does not necessarily have to
have a causal relationship with the drug administered An AE can be any unfavorable and
unintended sign (including an abnormal laboratory finding) symptom or disease temporarily
associated with the use of a medicinal product whether or not considered to be related to the
medicinal product Diseases signs symptoms or laboratory abnormalities already existing at
enrollment are not considered AEs unless they worsen (ie increase in intensity or frequency)
Surgical procedures themselves are not AEs they are therapeutic measures for conditions that
require surgery The condition for which the surgery is required may be an AE Surgical
procedures planned before randomization and the conditions necessitating the surgery are not
AEs
A serious adverse event is any untoward event that
Is fatal
Is life-threatening
Requires inpatient hospitalization or prolongation of existing hospitalization with the
following exceptions
o Preplanned (before the study) hospital admissions unless the hospitalization is
prolonged
o Planned admissions (as part of a study eg routine biopsies)
o Hospitalization lasting lt 24 hours
49
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
o Hospitalization for elective procedure
o Emergency room visits
Results in persistent or significant disability or incapacity
Is a congenital anomaly or birth defect
Important medical events that may not result in death be life-threatening or require
inpatient hospitalization may be considered serious adverse events (SAEs) when based
on appropriate medical judgment they may jeopardize the subject and may require
medical or surgical intervention to prevent one of the outcomes listed above
Life-threatening means that the subject was in the view of the investigator at immediate risk of
death from the AE as it occurred It does not include an AE that had it occurred in a more severe
form might have caused death
Persistent or significant disabilityincapacity means that the event resulted in permanent or
significant and substantial disruption of the subjectrsquos ability to carry out normal life functions
Causality
A reasonable possibility means the AE may have been caused byrelated to the study drug A
perceived or real lack of efficacy does not satisfy the definition of relatedness
612 Adverse Event (AE) Reporting
For the PANTHER-IPF trial all AEs (serious and nonserious) occurring from randomization
through final study visit (4 weeks after final dose of all study medication) will be recorded on the
AE page of the case report form (CRF)
6121 Serious Adverse Events (SAE) Reporting
For this trial all deaths and all SAEs which occur from randomization through final study visit
must be entered within the EDC system via the SAE eCRF page within 24 hours of the
investigative sitersquos knowledge of the event It is the responsibility of the clinical center
50
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
investigator to provide a causality assessment of the event for each study medications based upon
the information available at the time of the report It is understood that complete information
about the event may not be known at the time the initial report is submitted In the event the EDC
system is not accessible to the site at the time of event reporting investigative sites will complete
and forward a paper back-up SAE form to DCRI Safety Surveillance for processing
DCRI Safety Surveillance
Telephone 1-919-668-8624 or 1-866-668-7799 (toll free)
Fax 1-919-668-7138 or 1-866-668-7138 (toll free)
The investigator must complete and submit follow-up SAE information via the eCRF when
important new or follow-up information (eg final diagnosis outcome results of specific
investigations) becomes available Follow-up information should be submitted according to the
same process used for reporting the initial event as described above All SAEs will be followed
until resolution stabilization or 30 days after the subject has completed the final visit (4 weeks
after the final dose of study medication) whichever occurs first The investigator is responsible
for reporting SAEs to their institutional review board (IRB) per site specific IRB reporting
guidelines
6122 Regulatory Reporting
AEs that are serious study drug related and unexpected will be reported to the regulatory
authorities The DCRI Safety Surveillance medical monitor will perform a medical review of all
SAEs submitted and evaluate for ldquounexpectednessrdquo DCRI Safety Surveillance will prepare
MedWatch reports for those events identified as serious study drug related and unexpected as
determined by Safety Medical Monitor
DCRI Regulatory Services will submit all unexpected study drug-related SAEs as per 21 CFR
32 DCRI Safety Surveillance will provide a safety alert letter to the NHLBI DSMB and DCC
clinical operation (for distribution to sites) within 15 days of initial receipt of the information
51
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Investigators are responsible for promptly reporting these events to their reviewing IRBs
according to site specific IRB reporting guidelines
62 Clinical Medical Monitoring
There will be an unblinded physician at the IPFnet DCC serving as medical monitor The
medical monitor will be available to assist with questions about dosage adjustments of study
medications including discontinuation or resumption of medications
63 Unblinding Procedures
Unblinding of subjects or investigators to subject treatment is strongly discouraged For ongoing
clinical management all subjects should be presumed to be receiving ldquoactiverdquo study drug To
ensure the subjectrsquos safety the study treatment will be dose-adjusted based on laboratory test
results clinical findings and symptoms
The IPFnet DCC medical monitor and PANTHER-IPF co-chairs Drs Ganesh Raghu and
Fernando Martinez will be available to the study physicians to discuss study drug management
on a case-by-case basis Un-blinding will be considered ONLY when the knowledge of subject
treatment assignment is ABSOLUTELY ESSENTIAL for subject safety and after discussion of
the subjectrsquos case with the medical monitor and either Dr Raghu or Dr Martinez Unblinding of
study treatment should be minimized during the conduct of the trial In those cases where it is
felt to be medically necessary the DCC medical officer will communicate directly with the
managing physician to minimize unblinding of study personnel
52
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
7 Study Drug Procedures
At the baseline 15-week 30-week and 45-week study visits subjects will receive a supply of
study drug sufficient to last until the next visit at which study drug will be dispensed
53
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
8 Data Management
81 Hardware and Software Configuration
811 Hardware and Database Software
Data will be stored in an Oracle database system Oracle has advantages of processing efficiency
and smooth linkage with other software systems The application and database will be hosted on
Solaris Unix servers at the IPFnet DCC
812 Statistical Software
SAS will be used as the principal application for the management of analysis data files and
statistical computations S-Plus will be used to provide supplementary functions as needed
813 Access Control and Confidentiality Procedures
Access to databases will be controlled centrally by the IPFnet DCC through user passwords
linked to appropriate privileges This protects the data from unauthorized changes and
inadvertent loss or damage
814 Security
Database and Web servers will be secured by a firewall and through controlled physical access
Oracle has many security features to ensure that any staff member accessing the database has the
proper authority to perform the functions he or she requests of the system Within the secondary
SAS databases Unix group-access control maintains similar security The Sun workstation login
is secured by extensive user-password facilities under Unix
54
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
815 Back-up Procedures
Database back-up will be performed automatically every day and standard IPFnet DCC policies
and procedures will be applied to dictate tape rotation and retention practices
816 Virus Protection
All disk drives that provide network services and all user computers will be protected using
virus-scanning software Standard IPFnet DCC policies will be applied to update these protection
systems periodically through the study
82 Sources of Data
821 Design and Development
The IPFnet DCC will be responsible for development of the electronic case report forms
(eCRFs) development and validation of the clinical study database ensuring data integrity and
training clinical center staff on applicable data management procedures A web-based distributed
data entry model will be implemented This system will be developed to ensure that guidelines
and regulations surrounding the use of computerized systems used in clinical trials are upheld
The remainder of this section provides an overview of the data management plan associated with
this protocol
822 Data Collection Forms
The data collection process consists of direct data entry at the study clinical centers into the EDC
system(s) provided by the DCC A data collection worksheet will be provided to clinical centers
for recording data in the event the EDC system is unavailable Data entry of the eCRFs should
be completed according to the instructions provided and project specific training The
investigator is responsible for maintaining accurate complete and up-to-date records and for
ensuring the completion of the eCRFs for each research participant
55
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
823 Data Acquisition and Entry
Data entry into eCRFs shall be performed by authorized individuals Selected eCRFs may also
require the investigatorrsquos written signature or electronic signature as appropriate Electronic
CRFs will be monitored for completeness accuracy and attention to detail during the study
824 Data Center Responsibilities
The IPFnet DCC will 1) develop a data management plan and will conduct data management
activities 2) provide final eCRFs for the collection of all data required by the study 3) develop
data dictionaries for each eCRF that will comprehensively define each data element 4) conduct
ongoing data monitoring activities on study data 5) monitor any preliminary analysis data
cleanup activities and 6) rigorously monitor final study data clean up
825 Data Editing
Completed data will be entered into the IPFnet DCC automated data acquisition and
management system If incomplete or inaccurate data are found a data clarification request will
be generated and distributed to clinical centers for a response Clinical centers will resolve data
inconsistencies and errors and enter all corrections and changes into the IPFnet DCC automated
data acquisition and management system
826 Training
The training plan for clinical center staff includes provisions for training on assessments eCRF
completion guidelines data management procedures and the use of computerized systems
56
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
9 Study Design and Data Analysis
91 General Analytic Considerations
All primary analyses will be based on intent-to-treat (ITT) principles using all randomized
subjects Baseline factors across groups will be compared using mean (standard deviation) and
median (25th and 75th percentiles) summary measures Kaplan-Meier curves will be used to
display event rates Due to clinical interest in departures from both sides of the null hypothesis
all test statistics will be 2-sided
Reasonable caution needs to be taken when conducting multiple analyses on key clinical
subgroups For subgroup analyses a conservative significance level of 0001 will be used for all
interaction tests Thus subgroup comparisons will be considered exploratory unless the p-value
from the interaction test is smaller than 0001
92 Randomization Blinding and Reporting of Results
A permuted block-randomization scheme will be created with varying block sizes stratified by
clinical center Once a subject has completed the screening and baseline period and evaluation
for inclusionexclusion criteria the randomization process will begin Subjects will be
randomized to receive NAC or matching placebo with equal probability (11) via telephone
contact with a central interactive voice response system (IVRS) using a toll-free randomization
number On the day of randomization after the subject has successfully met all inclusion and
exclusion criteria the investigator or designee will call the central randomization number to
obtain the assigned kit randomization numbers for that subject At each subject visit the
investigator or designee will call the central randomization number to obtain the new kit
randomization numbers for resupply of the subject For resupply of the clinical center the IVRS
will monitor minimal volume of a kit type andor expiration date and will automatically notify
the pharmacy
57
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
The trial results will be reported according to guidelines specified in the CONSORT statement
A flow diagram describing screening recruitment randomization dropout and vital status will
be included in the primary manuscript AEs and efficacy data will be presented for all treatment
groups Adherence dropout and lost to follow-up will be carefully examined across all treatment
groups Analyses of safety will be based on data from all randomized subjects who received at
least one dose of study drug
93 Stratification
Subjects will be distributed to the two treatment arms in a 11 allocation ratio Stratification
blocks will be based on clinical centers
94 Specification of the Primary Analyses
A mixed model repeated measures (MMRM) analysis described in section 95 will be used to
compare differences in the slope of FVC measurements across the treatment groups Response
variables are values of the FVC measured at baseline and every 15 weeks until study completion
Variables in the model will include treatment time and time by treatment age sex race and
height Contrast estimates of differences in slopes of treatment over time (along with confidence
intervals) will be used to estimate the treatment effect The validity of this model in terms of
meeting modeling assumptions will be assessed via standard modeling diagnostics and goodness-
of-fit measures Based on the MMRM framework missing FVC data will not be imputed for the
primary analysis
95 Analysis of Longitudinal Endpoints
A common goal in clinical trials is to specify models that are easily implemented and
reproducible by independent data analysts On the other hand the models should have proper
statistical behavior in terms of low bias and high precision Many common approaches to
longitudinal data analysis including last observation carried forward (LOCF) imputation rely on
the missing completely at random (MCAR) assumption However the MCAR assumption is
58
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
unlikely to hold in many clinical trials because missing data are often related to disease
progression and prognosis A more reasonable assumption missing at random (MAR) specifies
that the complete data distribution can be modeled using only the observed data The likelihood-
based MMRM approach is valid under the more general MAR assumptions These models will
be applied to analyze the longitudinal data secondary endpoints
The advantages of MMRM analysis are that all important characteristics of the model can be preshy
specified standard software can be used to implement the models and results are based on ITT
principles43 In addition the MMRM approach offers superior control of Type I and Type II
errors compared with the LOCF approach
Response variables are values of the PFTs measured at enrollment and every 15 weeks until
study completion and 6MWT values measured at baseline week 30 and week 60 Covariates are
treatment time time by treatment and key baseline risk factors Contrasts (along with
confidence intervals) of treatment by time will be used to estimate the treatment effect
The correlation structure involves multiple pieces including measurement errors random
variation and interindividual variability For the longitudinal data analyses an unstructured
correlation matrix for within-subject errors will be assumed Other correlation structures
including compound symmetry will be examined as needed A careful examination of reasons
for study discontinuation will be conducted to assess the validity of MCAR Sensitivity analyses
will be used to examine the untestable assumption that the observed data violate the MAR
assumption The MMRM models will be implemented using PROC MIXED in SAS
96 Analysis of Binary Time-to-Event and Time-Lagged Endpoints
Regression modeling approaches using either the logistic regression model or Cox proportional
hazards regression model will be employed when appropriate The validity of these models will
be assessed via standard modeling diagnostics and goodness-of-fit measures Estimates of
cumulative frequencies for more general time-lagged responses will be calculated using the
partitioned version of the Bang-Tsiatis estimator44 The partitions will be set at 15-week intervals
59
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
to correspond with the data-collection process Covariate adjusted event rates will be calculated
using inverse probability-weighted regression estimates45
97 Power Analysis
971 Primary Analyses
Based on previously published IPF clinical trials the PL group is expected to experience a drop
in FVC of approximately 020 L over the study period (see Figure 1) The IPFnet Steering Group
determined a clinically important difference would be to preserve the majority of the decline
relative to PL over the study period In particular a treatment effect of 015 L was determined to
be a clinically meaningful difference Potential dropout is a key factor in the proposed study The
drop-out process assumed 5 lost to follow-up after every study visit Only 80 of subjects
were assumed to be followed for the entire study period All models assumed a compound
symmetry structure for the covariance matrix Power calculations were performed using a SAS
IML program for designing repeated measures studies46 Based on preliminary reviews of the
data from the University of Michigan the covariance matrix parameters were estimated at
approximately σ2 = 0757 (variance parameter) and ρ = 0936 (correlation parameter) To be
conservative the power calculations for the primary analysis were performed with parameter
setting of σ2 = 0810 (variance parameter) and ρ = 0925 (correlation parameter)
The power calculations assume a correction for imperfect compliance proposed by Lachin and
Foulkes to allow for 2 noncompliance for each of the treatment arms47 Thus the sample size
of 130 subjects per arm would be reduced to an adjusted sample size of 130(1-002-002)2 =
1198 or 120 subjects per arm
Under the assumed Type I error rate of 005 with a correlation parameter of 0925 and standard
deviation of 090 the difference of 015 L (or 00025 Lweek) shown in Table 6 would have
power of 93
60
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Table 6 Hypothetical Values of Mean FVC (L) Change from Baseline
Week 15 Week 30 Week 45 Week 60
NAC 00125 00250 00375 00500
Placebo 00500 01000 01500 02000
Difference 00375 00750 01125 01500
Abbreviations FVC forced vital capacity PL placebo
972 Power Analysis for Secondary Endpoints
Power calculations for secondary endpoint measurements are shown in Table 7 Standard
deviations are based on unpublished data provided by the University of Michigan The
calculations are based on a 2-sample t-test with Type I error rate set at 005 These calculations
are likely to be conservative because the statistical approach described in section 95 for
analyzing these endpoints will incorporate incomplete observations as well as intermediate data
points
Table 7 Detectable Differences in Treatment Means for Selected Endpoint Measurements
Secondary Endpoints Std Dev
of the Baseline Score
Detectable Difference for 80 Power
Std Dev of the Change Score
Difference Detectable for
80 Power
DLCOpred 166 58 91 32
6MWT Area Under the Desaturation Curve
219 76 175 61
6MWT Distance to Desaturation 224 78 315 110
6MWT Minutes Walked 210 073 205 071
Abbreviations Std Dev standard deviation DLCOpred diffusing capacity of the lung for carbon monoxide percent predicted 6MWT 6-minute walk test
61
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
10 Study Administration
101 Cooperative Agreement Mechanism
The administrative and funding mechanism used to undertake this project is a ldquocooperative
agreementrdquo (U01) which is an assistance mechanism Under the cooperative agreement the
NHLBI assists supports andor stimulates the project and is substantially involved with
investigators in conducting the study by facilitating performance of the effort in a ldquopartnerrdquo role
The NHLBI project scientist serves on the IPFnet Steering Group and he or another NHLBI
scientist may serve on other project committees when appropriate At the same time however
NHLBI does not assume a dominant role direction or prime responsibility for this research
program
As described below governance of the project is conducted through the IPFnet Steering Group
Principal investigators have lead responsibilities in all aspects of their trials and the project
including any modification of trial designs conduct of the trials quality control data analysis
and interpretation preparation of publications and collaboration with other investigators unless
otherwise provided for by the IPFnet Steering Group
PIs retain custody of and have primary rights to their center-specific and collaborative data
subject to government rights-of-access consistent with current Health amp Human Services (HHS)
Public Health Service (PHS) and National Institutes of Health policies The protocols and
governance policies call for the continual submission of data centrally to the IPFnet DCC for the
collaborative database which at a minimum will contain the key variables selected by the IPFnet
Steering Group for standardization across all clinical centers the submission of copies of the
collaborative datasets to each PI upon completion of the project procedures for data analysis
reporting and publication and procedures to protect and ensure the privacy of medical and
genetic data and records of individuals The NHLBI project scientist on behalf of the NHLBI
will have the same access privileges and responsibilities regarding the collaborative data as the
other members of the Steering Group
62
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
PIs are also encouraged to publish and to publicly release and disseminate results data and other
products of the project concordant with the project protocols and governance and the approved
plan for making data and materials available to the scientific community and to the NHLBI
However during the 3 years after the ending date of NHLBI project support unpublished data
unpublished results data sets not previously released and other study materials or products are
to be made available to any third party only with the approval of the IPFnet Steering Group
Upon completion of the project PIs are expected to put their intervention materials and
procedure manuals into the public domain andor make them available to other investigators
according to the approved plan for making data and materials available to the scientific
community and the NHLBI for the conduct of research at no charge other than the costs of
reproduction and distribution
The NHLBI reserves the right to terminate or curtail the project (or an individual award) in the
event of (a) failure to develop or implement mutually agreeable collaborative measurement
subject eligibility and data management sections of the protocols (b) substantial shortfall in
subject recruitment follow-up data reporting or quality control or other major breach of
protocol (c) substantive changes in the agreed-upon protocols with which NHLBI cannot
concur (d) reaching a major project outcome with persuasive statistical significance
substantially before schedule or (e) human subject ethical issues that may dictate a premature
termination
Any disagreement that may arise in scientificprogrammatic matters (within the scope of the
award) between award recipients and the NHLBI may be brought to arbitration An arbitration
panel will be composed of 3 membersmdash1 selected by the IPFnet Steering Group (with the
NHLBI member not voting) or by the individual PI in the event of an individual disagreement a
second selected by NHLBI and the third selected by the other 2 members This special
arbitration procedure in no way affects the PIrsquos right to appeal an adverse action that is otherwise
appealable in accordance with the PHS regulations at 42 CFR part 50 Subpart D and HHS
63
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
regulation at 45 CFR part 16 or the rights of the NHLBI under applicable statutes regulations
and terms of the award
102 IPFnet Steering Group
The IPFnet Steering Group is the main governing body of the project It is composed of the PIs
of the clinical centers the PI of the DCC and the NHLBI project scientist The clinical centers
the IPFnet DCC and the NHLBI each have 1 vote on the IPFnet Steering Group All decisions
are determined by majority vote
All major scientific decisions are determined by the IPFnet Steering Group It assumes overall
responsibility for the design and conduct of the trial It appoints (and disbands) committees and
subcommittees as the need arises designs approves and implements the study protocols
oversees the development of the MOOP monitors subject recruitment and treatment delivery
evaluates data collection and management oversees quality assurance procedures and
implements changes and enhancements to the study as required It also has primary responsibility
for facilitating the conduct of the trials and reporting the projectrsquos results
103 Data and Safety Monitoring Board
The NHLBI will establish a DSMB in accordance with established policies (see
httpwwwnhlbinihgovfundingpoliciesdsmb_insthtm) to ensure data quality and subject
safety and to provide independent advice to the NHLBI regarding progress and the
appropriateness of study continuation
104 Recommendations on Interim Monitoring of Efficacy Safety and Futility
First and foremost the role of the DSMB will be to review subject safety and trial conduct at
periodic points during the study The DSMB may require analyses of the primary endpoint
results for comparing the benefit and risks of treatment strategies The benefit of collecting
additional data on key secondary endpoints with extended follow-up and establishing a robust
64
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
evidence base for determining a standard of care will need to be carefully considered before
early termination of one or more treatment arms After careful consideration the IPFnet Steering
Group recommends conservative thresholds for the early examinations of the safety and efficacy
data
The DSMB will be expected to meet approximately every 6 months until trial completion to
review safety and toxicity data The DSMB may recommend stopping the study based on these
reviews Because the DSMB could stop the trial for safety concerns as well as for a large
efficacy benefit there could be multiple opportunities to reject the null hypothesis (no difference
in event rates between the PL and NAC groups) A Bonferroni approximation will be applied
during the one planned interim analysis for efficacy
Before locking the database a statistical analysis plan (SAP) will be developed to provide
complete details on the statistical analysis The SAP will include the specifics for how and when
the DSMB will be notified for AEs The IPFnet DCC will deliver to the DSMB all FDA-defined
AEs at 3-month intervals The IPFnet DCC will prepare narrative SAE reports in real time for
DSMB review including recommendations and analysis of similar events for each SAE
submitted to the FDA
65
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
11 Investigator and Sponsor Obligations
111 Monitoring
All monitoring activities for US clinical centers will be performed in accordance with DCRI
standard operating procedures Information regarding the types of visits will be outlined in the
PANTHER-IPF MOOP
112 Cost and Payment
There will be no cost to subjects enrolled in this trial Study-related procedures will be paid for
by the IPFnet
Subjects may be eligible for reimbursement for travel to the clinical center Details of payment
will be explained to each subject during the consent process
113 Confidentiality and Health Insurance Portability and Accountability Act
Considerations
Subject confidentiality will be protected throughout the study All subject data will be kept
strictly confidential and no subject-identifying information will be released to anyone outside
the project Confidentiality will be assured through several mechanisms First each subject will
be assigned an anonymous study ID which will then be used on all study forms Second any
study forms blood samples and paper records that contain subject information (eg address lists
phone lists) will be kept at the clinical centers in secured locked areas coded by number Once
blood is collected there will be no subject identifiers placed on blood samplesmdashonly the study
ID number and the date of sample collection Third access to all subject data and information
including laboratory specimens will be restricted to authorized personnel In the case of
computerized data this restricted access will be assured through user logon IDs and password
protection
66
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
At the IPFnet DCC only authorized personnel will have access to the data files containing study
data Security will be assured through user logon IDs passwords and appropriate access
privileges All study subjects will be identified only by their IPFnet ID numbers and no personal
identifying information such as name address or Social Security number will be entered into
the IPFnet DCC database Any subject-specific data reported to the IPFnet Steering Group will
be identified only by the IPFnet ID number
Finally subjects will not be identified by name in any reports or publications nor will the data
be presented in such a way that the identity of individual subjects can be inferred Analysis files
created for further study by the scientific community will have no subject identifiers These data
files will be created in accordance with the Ancillary Studies and Publication Policy of the
IPFnet
114 Informed Consent Procedures
All IPFnet subjects will provide written informed consent using procedures reviewed and
approved by each clinical centerrsquos IRB Informed consent will be undertaken by study personnel
in-person with the subject The subject has the option of declining further participation in the
study at that point No further study procedures will be conducted until the signed documents
have been provided to the IPFnet clinical center
115 Institutional Review Boards
Before initiating this study the protocol clinical center-specific informed consent forms Health
Insurance Portability and Accountability Act (HIPAA) forms recruitment materials and other
relevant information will be reviewed by a properly constituted IRB at each participating clinical
center A copy of the signed and dated IRB approval at each clinical center will be retrieved prior
to or during the site initiation visit and archived at the IPFnet DCC Any amendments to the
protocol other than simple administrative and typographical changes must be approved by each
IRB before they are implemented The clinical centers will seek annual renewals of their IRB
approvals in accordance with local procedures
67
__________________________________________ ________________
__________________________________________
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
12 Investigator Agreement
I have read the foregoing protocol PANTHER-IPF and agree that it contains all necessary
details for carrying out this study I will conduct the study as outlined herein and will complete
the study within the time designated
I will provide copies of the protocol and all pertinent information to all individuals responsible to
me who assist in the conduct of this study I will discuss this material with them to ensure they
are fully informed regarding the drug and the conduct of the study
I will fulfill all responsibilities for submitting pertinent information to the local IRB if
applicable that is responsible for this study
I further agree that NHLBI andor DCRI will have access to any source documents from which
eCRF information may have been generated
Signature of Principal Investigator Date
Name of Principal Investigator (printed or typed)
Protocol version date May 19 2009
Protocol Amendment 1 version date May 28 2010
Protocol Amendment 2 version date December 6 2011
68
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
13 References
1 Raghu G Brown KK Bradford WZ et al A placebo-controlled trial of interferon gamma-1b in patients with idiopathic pulmonary fibrosis N Engl J Med 2004350125-33 2 King TE Jr Safrin S Starko KM et al Analyses of efficacy end points in a controlled trial of interferon-gamma1b for idiopathic pulmonary fibrosis Chest 2005127171-7 3 Flaherty KR Thwaite EL Kazerooni EA et al Radiological versus histological diagnosis in UIP and NSIP survival implications Thorax 200358143-8 4 Wells AU Desai SR Rubens MB et al Idiopathic pulmonary fibrosis a composite physiologic index derived from disease extent observed by computed tomography Am J Respir Crit Care Med 2003167962-9 5 Raghu G Freudenberger TD Yang S et al High prevalence of abnormal acid gastroshyoesophageal reflux in idiopathic pulmonary fibrosis Eur Respir J 200627136-42 6 Kinnula VL Focus on antioxidant enzymes and antioxidant strategies in smoking related airway diseases Thorax 200560693-700 7 Coultas DB Zumwalt RE Black WC Sobonya RE The epidemiology of interstitial lung diseases Am J Respir Crit Care Med 1994150967-72 8 Raghu G Weycker D Edelsberg J Bradford WZ Oster G Incidence and prevalence of idiopathic pulmonary fibrosis Am J Respir Crit Care Med 2006174810-6 9 Olson AL Swigris JJ Lezotte DC Norris JM Wilson CG Brown KK Mortality from pulmonary fibrosis increased in the United States from 1992 to 2003 Am J Respir Crit Care Med 2007176277-84 10 Mannino DM Etzel RA Parrish RG Pulmonary fibrosis deaths in the United States 1979shy1991 An analysis of multiple-cause mortality data Am J Respir Crit Care Med 19961531548shy52 11 Hubbard R Johnston I Coultas DB Britton J Mortality rates from cryptogenic fibrosing alveolitis in seven countries Thorax 199651711-6 12 Johnston I Britton J Kinnear W Logan R Rising mortality from cryptogenic fibrosing alveolitis Bmj 19903011017-21 13 Raghu G Collard HR Egan JJ et al An official ATSERSJRSALAT statement idiopathic pulmonary fibrosis evidence-based guidelines for diagnosis and management Am J Respir Crit Care Med 2011183788-824 14 (USA) FDA FDA Public Health Advisory Interferon gamma-1b (marketed as Actimmune) In 2007 15 King TE Jr Pardo A Selman M Idiopathic pulmonary fibrosis Lancet 2011 16 Raghu G Brown KK Costabel U et al Treatment of idiopathic pulmonary fibrosis with etanercept an exploratory placebo-controlled trial Am J Respir Crit Care Med 2008178948shy55 17 Malouf MA Hopkins P Snell G Glanville AR An investigator-driven study of everolimus in surgical lung biopsy confirmed idiopathic pulmonary fibrosis Respirology 201116776-83 18 King TE Jr Behr J Brown KK et al BUILD-1 a randomized placebo-controlled trial of bosentan in idiopathic pulmonary fibrosis Am J Respir Crit Care Med 200817775-81 19 Richeldi L Costabel U Selman M et al Efficacy of a tyrosine kinase inhibitor in idiopathic pulmonary fibrosis N Engl J Med 20113651079-87
69
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
20 Borok Z Buhl R Grimes GJ et al Effect of glutathione aerosol on oxidant-antioxidant imbalance in idiopathic pulmonary fibrosis Lancet 1991338215-6 21 Meyer A Buhl R Magnussen H The effect of oral N-acetylcysteine on lung glutathione levels in idiopathic pulmonary fibrosis Eur Respir J 19947431-6 22 Behr J Maier K Degenkolb B Krombach F Vogelmeier C Antioxidative and clinical effects of high-dose N-acetylcysteine in fibrosing alveolitis Adjunctive therapy to maintenance immunosuppression Am J Respir Crit Care Med 19971561897-901 23 Cantin AM North SL Fells GA Hubbard RC Crystal RG Oxidant-mediated epithelial cell injury in idiopathic pulmonary fibrosis J Clin Invest 1987791665-73 24 Waghray M Cui Z Horowitz JC et al Hydrogen peroxide is a diffusible paracrine signal for the induction of epithelial cell death by activated myofibroblasts Faseb J 200519854-6 25 Larios JM Budhiraja R Fanburg BL Thannickal VJ Oxidative protein cross-linking reactions involving L-tyrosine in transforming growth factor-beta1-stimulated fibroblasts J Biol Chem 200127617437-41 26 Kinnula VL Fattman CL Tan RJ Oury TD Oxidative stress in pulmonary fibrosis a possible role for redox modulatory therapy Am J Respir Crit Care Med 2005172417-22 27 Meyer A Buhl R Kampf S Magnussen H Intravenous N-acetylcysteine and lung glutathione of patients with pulmonary fibrosis and normals Am J Respir Crit Care Med 19951521055-60 28 Behr J Degenkolb B Krombach F Vogelmeier C Intracellular glutathione and bronchoalveolar cells in fibrosing alveolitis effects of N-acetylcysteine Eur Respir J 200219906-11 29 Bando M Hosono T Mato N et al Long-term efficacy of inhaled N-acetylcysteine in patients with idiopathic pulmonary fibrosis Intern Med 2010492289-96 30 Demedts M Behr J Buhl R et al High-dose acetylcysteine in idiopathic pulmonary fibrosis N Engl J Med 20053532229-42 31 Toma TP Bhowmik A Rajakulasingam R Acetylcysteine in pulmonary fibrosis N Engl J Med 20063541086-9 author reply -9 32 Hunninghake GW Antioxidant therapy for idiopathic pulmonary fibrosis N Engl J Med 20053532285-7 33 Flaherty KR Mumford JA Murray S et al Prognostic implications of physiologic and radiographic changes in idiopathic interstitial pneumonia Am J Respir Crit Care Med 2003168543-8 34 Latsi PI du Bois RM Nicholson AG et al Fibrotic idiopathic interstitial pneumonia the prognostic value of longitudinal functional trends Am J Respir Crit Care Med 2003168531-7 35 Collard HR King TE Jr Bartelson BB Vourlekis JS Schwarz MI Brown KK Changes in clinical and physiologic variables predict survival in idiopathic pulmonary fibrosis Am J Respir Crit Care Med 2003168538-42 36 Jegal Y Kim DS Shim TS et al Physiology is a stronger predictor of survival than pathology in fibrotic interstitial pneumonia Am J Respir Crit Care Med 2005171639-44 37 Martinez FJ Safrin S Weycker D et al The clinical course of patients with idiopathic pulmonary fibrosis Ann Intern Med 2005142963-7 38 Hull JH Acetylcysteine in pulmonary fibrosis N Engl J Med 20063541089-91 author reply -91
70
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
39 Flaherty KR King TE Jr Raghu G et al Idiopathic interstitial pneumonia what is the effect of a multidisciplinary approach to diagnosis Am J Respir Crit Care Med 2004170904shy10 40 Raghu G Johnson WC Lockhart D Mageto Y Treatment of idiopathic pulmonary fibrosis with a new antifibrotic agent pirfenidone results of a prospective open-label Phase II study Am J Respir Crit Care Med 19991591061-9 41 Hunninghake GW Lynch DA Galvin JR et al Radiologic findings are strongly associated with a pathologic diagnosis of usual interstitial pneumonia Chest 20031241215-23 42 Lynch D Godwin J Safrin S et al High-resolution computed tomography in idiopathic pulmonary fibrosis diagnosis and prognosis Am J Respir Crit Care Med 2005172488-93 43 Mallinckrodt CH Watkin JG Molenberghs G Carroll RJ Choice of the primary analysis in longitudinal clinical trials Pharmaceutical Statistics 20043161-9 44 Bang H Tsiatis A Estimating medical costs with censored data Biometrika 200087329shy43 45 Lin DY Regression analysis of incomplete medical cost data Stat Med 2003221181-200 46 Rochon J Application of GEE procedures for sample size calculations in repeated measures experiments Stat Med 1998171643-58 47 Lachin JM Foulkes MA Evaluation of sample size and power for analyses of survival with allowance for nonuniform patient entry losses to follow-up noncompliance and stratification Biometrics 198642507-19
71
- PANTHER-IPFPREDNISONE AZATHIOPRINEAND N-ACETYLCYSTEINEA STUDY THAT EVALUATES RESPONSE INIDIOPATHIC PULMONARY FIBROSIS
-
- Protocol Summary
- Table of Contents
- List of Tables
- List of Figures
- List of Abbreviations
- 1 Summary
- 2 Hypotheses and Specific Aims
-
- 21 Null Hypothesis
- 22 Specific Aim 1
- 23 Specific Aim 2
- 24 Prespecified Subgroups of Interest
-
- 3 Background and Significance
-
- 31 Idiopathic Pulmonary Fibrosis is the Most Common Interstitial Lung Disease
- 32 Rationale for Placebo Control
- 33 Rationale for N-acetylcysteine
- 35 Rationale for N-acetylcysteine as a Stand-alone Therapy
- 36 Rationale for the Study Design and Primary Endpoint
- 37 Rationale for Blinding of Treatments
-
- 4 Methods
-
- 41 Inclusion Criteria
- 42 Diagnosis of IPF
- 43 Exclusion Criteria
- 44 Study Design and Study Visit
- 45 Dose Justification
- 46 Contraindications Precautions and Side Effects of Study Medications
- 47 Recruitment Procedures
- 48 Study Procedures
- 49 Concomitant Medications
- 410 Laboratory Testing
- 411 Blinding of Study Drugs
-
- 5 Study Endpoints
-
- 51 Primary Study Endpoint
- 52 Secondary Study Endpoints
-
- 6 Safety Evaluations and Procedures
-
- 61 Adverse Events
- 62 Clinical Medical Monitoring
- 63 Unblinding Procedures
-
- 7 Study Drug Procedures
- 8 Data Management
-
- 81 Hardware and Software Configuration
- 82 Sources of Data
-
- 9 Study Design and Data Analysis
-
- 91 General Analytic Considerations
- 92 Randomization Blinding and Reporting of Results
- 93 Stratification
- 94 Specification of the Primary Analyses
- 95 Analysis of Longitudinal Endpoints
- 96 Analysis of Binary Time-to-Event and Time-Lagged Endpoints
- 97 Power Analysis
-
- 10 Study Administration
-
- 101 Cooperative Agreement Mechanism
- 102 IPFnet Steering Group
- 103 Data and Safety Monitoring Board
- 104 Recommendations on Interim Monitoring of Efficacy Safety and Futility
-
- 11 Investigator and Sponsor Obligations
-
- 111 Monitoring
- 112 Cost and Payment
- 113 Confidentiality and Health Insurance Portability and Accountability ActConsiderations
- 114 Informed Consent Procedures
- 115 Institutional Review Boards
-
- 12 Investigator Agreement
- 13 References
-

PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
IPFnet Idiopathic Pulmonary Fibrosis Clinical Research Network
IRB institutional review board
ITT intent to treat
IV intravenous
IVRS interactive voice response system
LDH lactate dehydrogenase
LFT liver function test
LOCF last observation carried forward
LSD Least Significant Difference
MAR missing at random
MCAR missing completely at random
MMRM mixed model repeated measures
MOOP manual of operating procedures
NAC N-acetylcysteine
NHLBI National Heart Lung and Blood Institute (US)
NIH National Institutes of Health (US)
NSIP nonspecific interstitial pneumonia
PaO2 partial pressure of arterial oxygen
PCP primary care provider
PFT pulmonary function test
10
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
PHS Public Health Service (US)
PI principal investigator
PL placebo
PLT platelet
PRED prednisone
QOL quality of life
SAE serious adverse event
SAP statistical analysis plan
SGRQ St Georgersquos Respiratory Questionnaire
SpO2 oxygen saturation by pulse oximetry
TPMT thiopurine methyl transferase
UCSD SOBQ University of California at San Diego Shortness of Breath Questionnaire
UIP usual interstitial pneumonia
ULN upper limit of normal
USP United States Pharmacopoeia
VC vital capacity
WBC white blood cell
11
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
PREDNISONE AZATHIOPRINE AND N-ACETYLCYSTEINE A STUDY
THAT EVALUATES RESPONSE IN IDIOPATHIC PULMONARY FIBROSIS
1 Summary
There are currently no drug therapies that have proven to be effective in the treatment of idiopathic pulmonary
fibrosis (IPF) Previous clinical drug trials have been difficult to interpret due to lack of true placebo (PL)
controls or other methodological concerns Clinical efficacy of immunosuppressive therapies and agents that
reduce oxidative stress remains controversial The IPF Clinical Research Network (IPFnet) is conducting a
randomized double-blind placebo-controlled trial designed to assess the safety and efficacy of
N-acetylcysteine (NAC) as monotherapy in subjects with mild or moderate IPF
The study initially employed a 3-arm design with 111 randomization to NAC azathioprine (AZA)-prednisone
(PRED)-NAC and PL with each subject to be treated up to a maximum of 60 weeks followed by a tapering of
PREDPL and a 4-week period for safety evaluation Approximately 390 subjects who have mild to moderate
IPF (defined as forced vital capacity percent predicted [FVCpred] ge 50 and diffusing capacity of the lung
for carbon monoxide percent predicted [DLCOpred] 30) diagnosed within the past 48 months were to be
enrolled
At the pre-specified interim analysis the DSMB recommended termination of the prednisone-azathioprine-
NAC arm of the study No additional patients will be randomized to that arm However the NAC and placebo
arms remain open for enrollment and we will enroll approximately 130 subjects in each arm (inclusive of the
subjects enrolled at the time of the interim analysis) Follow up for subjects enrolled into the two arms will
continue for 60 weeks
The primary endpoint is the change in longitudinal measurements of FVC over the study period The primary
goal of this study to establish an evidence-based standard of care and clarify myths from facts for
pharmacotherapy of IPF has been met in part by demonstrating that the widely used triple therapy was harmful
to patients with IPF (NHLBI press release Oct 21 2011) To determine the potential therapeutic benefits of
NAC alone the study will continue to enroll patients as a two-arm double-blind placebo-controlled study from
this point on (NAC vs placebo) as recommended by the DSMB following the pre-specified interim analysis
12
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
2 Hypotheses and Specific Aims 21 Null Hypothesis
Treatment with NAC will provide the same efficacy as PL as measured by longitudinal changes in FVC
22 Specific Aim 1
This study is designed to assess the safety and efficacy of NAC in subjects with newly diagnosed IPF
23 Specific Aim 2
Secondary goals of this study are to assess differences between treatment groups for the following
1 Mortality
2 Time to death
3 Frequency of acute exacerbations (AExs)
4 Frequency of maintained FVC response
5 Time-to-disease progression
6 Change in DLCO
7 Change in Composite Physiologic Index (CPI)
8 Change in resting alveolar-arterial oxygen gradient
9 Change in 6-minute walk test (6MWT) distance
10 Change in 6MWT oxygen saturation area under the curve
11 Change in 6MWT distance to desaturation lt 80
12 Change in 6MWT minutes walked
13 Changes in health status as measured by the SF-36 EuroQol and St Georgersquos Respiratory
Questionnaire (SGRQ)
14 Changes in dyspnea as measured by the University of California at San Diego Shortness of Breath
Questionnaire (UCSD SOBQ)
15 Frequency and types of adverse events (AEs)
16 Frequency and types of respiratory complications both infectious and noninfectious
17 Frequency of hospitalizations both all-cause and respiratory-related
13
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
24 Prespecified Subgroups of Interest
Treatment effects will be estimated and compared within key subgroups
Higher enrollment FVC12
Typical vs atypical high-resolution computed tomography (HRCT) reading at baseline3
Recent vs more remote diagnosis (time from initial diagnosis of IPF le 1 year and gt 1 year)
Lower CPI score at enrollment4
Medical therapy for gastroesophageal reflux5
Ethnic background
Sex
Smoking history (current or ex-smoker vs never smoker) given potential impact on oxidant status6
Presence of emphysema gt 25 on HRCT
14
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
3 Background and Significance
31 Idiopathic Pulmonary Fibrosis is the Most Common Interstitial Lung Disease
IPF is the most common interstitial lung disease (ILD) of unknown etiology The current incidence and
prevalence of IPF in the United States are not known A 1994 study of a population-based registry of subjects in
Bernalillo County New Mexico USA estimated an incidence of 107 cases per 100000 per year for males and
74 cases per 100000 per year for females the prevalence of IPF was estimated at 20 per 100000 for males and
13 per 100000 for females7 Extrapolating from a large healthcare claims database a more recent review
estimated the prevalence of IPF in the United States at 427 per 100000 (incidence estimated at 163 per
100000 per year)8 Recent epidemiological studies indicate increasing mortality rates from IPF in the United
States and other industrialized nations9-12
Approximately two-thirds of subjects with IPF are over the age of 60 at the time of presentation and the
incidence increases with age13 IPF has no distinct geographical distribution and predilection by race or
ethnicity has not been identified13 Individual subjects may remain relatively stable for prolonged periods
experience very slow declines in lung function with progression of radiographic abnormalities for a period of
months to years or experience more rapid declines and subsequent death Only 20 to 30 of IPF patients
survive for 5 years following diagnosis
There is currently no proven effective pharmacological treatment for IPF13 Anti-inflammatory and
immunosuppressive agents have been the traditional approach to the management of patients with IPF Based
on the results of the interim analysis of the PANTHER-IPF trial this lsquotraditional approachrsquo will be aborted
However it remains unknown if NAC alone will prove beneficial in IPF patients The primary goal of the
modified study is to establish an evidence-based standard of care and clarify the role of this specific antioxidant
pharmacotherapy for IPF
32 Rationale for Placebo Control
IPF is a disorder for which there is no proven efficacious therapy A major objective of this trial is to test to the
greatest degree possible a proposed standard of care for patients with IPF The current traditional therapy
15
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
employs immunosuppressive and corticosteroid drugs Interim review of the original PANTHER-IPF study has
documented increased adverse events and lack of efficacy for AZA-PRED-NAC compared to placebo
suggesting that this therapeutic approach should not be employed Whether this applies to NAC alone which
has been advocated by international societies has not been proven in well-designed well-powered clinical
trials The recommendations made in the recently published evidence guidelines for NAC monotherapy was
weak based on low quality13 Thus this continued clinical trial randomizing patients to receive NAC or placebo
is pivotal and will answer the important question of the potential therapeutic benefits of NAC monotherapy with
grade A evidence In this prospective randomized clinical trial the inclusion of a PL arm is therefore vital to
adequately test the benefits of NAC in well-characterized subjects with IPF
If NAC has no true efficacy then its role as standard of care will be refuted If a benefit compared with PL is
confirmed it will establish a benchmark against which future novel therapies for IPF will be safely compared
As there is no currently accepted therapy for IPF there is an increasing body of published literature supporting
the concept of no treatment as the ldquobest carerdquo option for IPF13
Post hoc analyses of PL-controlled trials suggest that subjects with milder disease may be more amenable to
therapy12 It is notable that a recent international prospective randomized trial of interferon-gamma for IPF
also included a PL arm the study was terminated early by the data and safety monitoring board (DSMB) due to
lack of treatment effect1415 This underscores the belief that a proven effective therapy for IPF does not
currently exist and that true placebo-controlled trials remain the gold standard Similarly recently completed
trials of etanercept everolimus bosentan and BIPF 1120 in IPF have included PL-treated arms16-19 In three of
these trials the treated subjects showed little if any objective improvement Based on this evidence and the
current status of IPF therapy and therapeutic trials we believe that clinicians and subjects will continue to enroll
in a PL-controlled study
33 Rationale for N-acetylcysteine
NAC is a derivative of the amino acid L-cysteine NAC has been shown to augment levels of the naturally
occurring antioxidant glutathione (GSH ) (glutathione γ-glutamyl cysteinyl glycine) both in vitro and in
vivo2021 GSH is present in all eukaryotic cells and may play an important role in protecting alveolar epithelial
cells against oxidant injury The concentration of GSH in the bronchoalveolar lavage (BAL) fluid in patients
16
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
with IPF is markedly diminished compared with normal subjects This GSH deficiency may be corrected by
exogenous administration of NAC2122
There is evidence of enhanced production of oxidants in an IPF lung Both inflammatory cells and
myofibroblasts derived from patients with IPF generate increased amounts of extracellular oxidants including
hydrogen peroxide2324 Secretion of hydrogen peroxide by activated myofibroblasts may induce the death of
adjacent lung epithelial cells by paracrine mechanisms24 Additionally generation of oxidants by myofibroblasts
induces oxidative crosslinking of extracellular matrix proteins25 a potential mechanism for aberrant matrix
remodeling Thus an oxidant-antioxidant imbalance exists in the lungs of IPF patients26 NAC may confer
protection against this imbalance by augmenting GSH levels in addition to its more direct free-radical
scavenging activity
Intravenous (IV) NAC therapy has been shown to increase total BAL GSH in 8 IPF subjects27 Oral NAC (600
mg 3 times per day) has been shown to decrease markers of oxidant injury and improve both total and reduced
GSH levels in the epithelial lining fluid of subjects with IPF in a small uncontrolled study22 pulmonary
function improved modestly with therapy A similar study in 18 IPF subjects confirmed increased intracellular
GSH concentration after 12 weeks of NAC (600 mg 3 times per day)2228 no clinical correlates were reported
Inhaled NAC was suggested to improve pulmonary function in an open label study29
35 Rationale for N-acetylcysteine as a Stand-alone Therapy
Results of a double-blind multi-center European clinical trial of 150 IPF subjects testing combinations of AZAshy
PRED vs AZA-PRED-NAC have been reported30 NAC added to AZA-PRED (ldquoconventional therapyrdquo) had a
significant positive effect on DLCO (p lt 0005) and vital capacity (VC) (p lt 005) at the end of 1 year30 The
recent ATSERS position statement after much discussion concluded that NAC alone should not be considered
in the majority of patients with IPF without additional data from well-designed studies
The interpretation of these data has been quite controversial Some have suggested that the magnitude of the
treatment effect although statistically significant is modest31 Others have suggested that NAC may be
modulating potential toxic effects of AZA-PRED alone32 supporting the investigation of NAC as stand-alone
therapy
17
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
The IPFnet is now completing the PANTHER-IPF trial with a 11 randomization (NAC vs placebo) and a
simple practical feasible and scientifically rational design that will establish standard of care with NAC for
IPF based on a currently available therapeutic agent and the existing data to support its use We anticipate that
all future clinical trials of novel therapeutic agents will be tested against this to-be-established standard of care
36 Rationale for the Study Design and Primary Endpoint
The optimal study design of a therapeutic trial in IPF would include survival as a primary endpoint The
published results of the IFN-γ 1b Phase 3 (GIPF-001) trial suggested a survival benefit in subjects with milder
disease in retrospective analyses1 although the trial was underpowered to address this question This was likely
related to the limited mortality in the PL arm of the study which included IPF subjects with mild to moderate
disease This study documents that an IPF study powered to improve survival in a patient population with mild
disease requires a larger sample size andor duration of study In fact the recently aborted Phase 3 IFN-γ 1b
(GIPF-007 INSPIRE) study was a survival-based study and recruited more than 800 subjects at 75 centers
worldwide1415 As such within the context of the current IPFnet trial survival is an impractical primary
endpoint variable
Several groups have published data defining an appropriate surrogate outcome variable a 10 decrement in
FVC during 6 to 12 months is a powerful predictor of survival in IPF33-36 Furthermore additional evidence
suggests a similar predictive ability for a 10 decrement in FVC during 3 months of follow-up37 With strong
supportive evidence of FVC progression being related to mortality on a per-subject basis this study will use
FVC changes in liters between treatment groups as the primary endpoint Previously published IPF studies have
shown a steady decline in FVC (and FVCpred) among control group subjects230 The GIPF-001 study
suggested a 48-week decrease in FVC of 016 L in the PL-treated subjects The IFIGENIA study demonstrated
a decline in FVC of approximately 019 L over 52 weeks in the subjects randomized to the control treatment
Figure 1 depicts the change in FVC for control groups from previously published IPF studies38 Based on these
data we expect that the PL group will have a decline of 020 L over the 60-week study period The IPFnet
Steering Group determined that a clinically meaningful improvement would be the preservation of the majority
of the 020-L FVC decline Therefore a mean treatment difference of 015 L in mean FVC over the 60-week
study period was determined to be a clinically meaningful difference
18
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Δ f
rom
bas
elin
e (i
n L
)
01
005
0
-005
-01
-015 Projected Δ for placebo
-02
-025
-019
-016
-013 Pirfenidone GIPF001
NAC
Placebo
4 8 12 16 20 24 28 32 36 40 44 48 52 56 60
Week
Figure 1 Changes in FVC From Baseline in Prior IPF Clinical Trials
Recent data suggest that various patient subgroups would be expected to potentially exhibit differential response
to therapy These parameters will be used to a priori separate patients by a series of baseline characteristics
including
1 Higher enrollment FVC12
2 Typical vs atypical high-resolution computed tomography (HRCT) reading at baseline3
3 Recent vs more remote diagnosis (time from initial diagnosis of IPF le 1 year and gt 1 year)
4 Lower CPI score at enrollment4
5 Medical therapy for gastroesophageal reflux5
6 Ethnic background
7 Sex
8 Smoking history (current or ex-smoker vs never smoker) given potential impact on oxidant status6
9 Presence of emphysema gt 25 on HRCT
37 Rationale for Blinding of Treatments
The issue of treatment blinding was given a great deal of consideration with subject safety being the primary
concern After discussion among the Steering Group members it was decided that as long as subject safety
could be ensured blinding was necessary Blinding allows the study to
Have optimal scientific validity and potential to impact the standard of care for subjects
19
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Make objective assessments of treatment effects
Maintain clinical equipoise among investigators
Encourage subjects to have similar levels of contact with the medical community
Minimize the differential dropout rates across study arms
20
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
4 Methods 41 Inclusion Criteria
1 Age 35 to 85 years inclusive
2 FVC ge 50 of predicted (post-bronchodilator measurement from the screening visit)
3 DLCO ge 30 of predicted (hemoglobin corrected and altitude corrected if gt4000 ft above sea level)
4 Ability to understand and provide informed consent
5 Diagnosis of IPF according to a modified version of the ATS criteria le 48 months from enrollment The
date of diagnosis is defined as the date of the first available HRCT or surgical lung biopsy characteristic
of definite UIP
411 Subjects Shown to Have Usual Interstitial Pneumonia Pattern on Surgical Lung Biopsy
Subjects who have been shown to have UIP pattern on lung biopsy must have all of the following
1 Exclusion of other known causes of ILD such as drug toxicity clinically significant environmental
exposures or diagnosis of connective tissue diseases
2 Bibasilar reticular abnormalities with minimal ground glass opacities on HRCT scan
412 Subjects Who Have Not Undergone a Surgical Lung Biopsy
In addition to the criteria above these subjects must have radiological findings considered to be definite for the
diagnosis of UIPIPF
1 Bibasilar reticular abnormalities with minimal ground glass opacities
2 Honeycombing as the predominant feature and located in the peripheral lung bases
42 Diagnosis of IPF
Only subjects with definite IPF will be eligible for enrollment in this study We will utilize a combination of
clinicalphysiologic features HRCT and review of a clinically obtained surgical lung biopsy specimen to
establish the diagnosis of IPF An algorithm for the diagnosis is provided to guide entry into the protocol as
outlined in the inclusion and exclusion criteria (Figures 2 and 3) This multi-disciplinary approach uses
21
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
expertise from clinicians radiologists and pathologists Investigators at each site in conjunction with central
pathology will work together to establish the diagnosis of IPF This interactive approach to the diagnosis of IPF
increases the level of agreement between observers39
A subject with suspected ILD should be evaluated for secondary causes including but not limited to
environmental exposures drugs and systemic diseases Presence of any of these findings felt to be significant
enough to cause an ILD should disqualify the subject from entry into the trial
If secondary causes are absent an HRCT scan may be obtained If an HRCT of sufficiently high quality has
been obtained within the last 3 months that scan may be used for diagnosis In the appropriate clinical setting
the diagnosis of IPF can be made by the demonstration of a typical radiographic pattern on HRCT or by
demonstration of UIP pattern on a surgical lung biopsy The following criteria for a radiographic (ie
nonsurgical) diagnosis will be used In the absence of known exposures andor clinical associations attributable
to pulmonary fibrosis and in the appropriate clinical setting the presence of definite UIP pattern in HRCT
images is required to meet study criteria for the diagnosis of IPF
Figure 2 Diagnosis of Idiopathic Pulmonary Fibrosis in the IPFnet
22
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Figure 3 Pathology Flow Chart Surgical Lung Biopsy Diagnosis
Requirement for diagnosis
1 Clinical exclusion of other known causes (connective tissue diseases environmental and drug
exposures) of ILD
2 Radiographic HRCT with bibasilar reticular abnormality and honeycomb change with minimal
ground glass opacities
Appropriate clinical setting
1 Age gt 50 years
2 Insidious onset of unexplained dyspnea
3 Duration of illness for ge 3 months
4 Bibasilar inspiratory crackles
23
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Unlike the ATSERS consensus criteria published in 2000 bronchoscopy will not be required for diagnosis
This decision was made based on the experience of the IPFnet Steering Group members regarding the utility of
bronchoscopy in the diagnosis of IPF The presence of an atypical HRCT finding will require documentation of
a definitive diagnosis by surgical lung biopsy In fact this is in keeping with the recently published evidence
based guidelines for diagnosis and management of IPF13 As shown in Figure 3 central review of the pathology
data will be required for a diagnosis of IPF
We will not require central review of HRCT as several studies have shown that a confident local interpretation
of clinicalHRCT criteria as definite IPFUIP is associated with a high positive predictive value for finding UIP
at surgical lung biopsy (see Table 1) Differences in sensitivity in these series likely reflect subject selection as
Flaherty et al3 evaluated only UIP and nonspecific interstitial pneumonia (NSIP) while Raghu et al40 and
Hunninghake et al41 included a broader range of ILD
Table 1 Operating Characteristics of Local HRCT Review for Diagnosis of UIP
Researcher of Subjects Sensitivity () Specificity () PPV () NPV ()
Raghu et al 40
59 (29 UIP by SLB) 78 90 88 82
Hunninghake et al 41 91 (54 UIP by SLB)
74 81 85 67
Flaherty et al 3 96 (only NSIP amp UIP)
37 100 100 30
Abbreviations PPV positive predictive value NPV negative predictive value UIP usual interstitial pneumonia SLB surgical lung biopsy and NSIP nonspecific interstitial pneumonia
Furthermore an analysis of the HRCT scans from subjects enrolled in the GIPF-001 trial confirmed that local
site interpretations have a high congruity to a central radiology core In this multi-center study 263 HRCT
scans were read as definite IPF and a retrospective central radiology core review found 932 to be consistent
with IPF 42 We will also take several additional steps to insure that the local HRCT reads are accurate
including
1 A detailed training module has been developed and must be completed by each site radiologist before
site initiation
2 Clinical centers are to mail all HRCT scans to the HRCT core lab The first 10 HRCT scans from
subjects enrolled at each enrolling clinical center will be reviewed centrally to be certain that local reads
24
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
25
are congruent with a central interpretation If discrepancies are identified additional education will be
provided and HRCT scans will continue to be reviewed centrally until the central radiology core is
confident that the local center is performing appropriately
3 Random scans will be obtained from each center throughout the study to confirm that the local read
continues to agree with central interpretation If discrepancies are identified they will be addressed as in
2 above
In all cases if a subject has a surgical lung biopsy sample that sample will be reviewed by the local and central
pathologists Therefore the only cases that would not be subject to a direct central review process are those
where the HRCT meets the centrally defined criteria for an unequivocal diagnosis and a lung biopsy sample is
not available Table 2 below summarizes the possible combinations for making a diagnosis
Table 2 Combining HRCT and Pathology Interpretations to Determine if IPF is Present
HRCT Diagnosis Pathology Diagnosis Diagnosis of IPF
Definite UIP Definite UIP Yes
Definite UIP Probable UIP Yes
Definite UIP Possible UIP Yes
Definite UIP Not UIP No
Definite UIP Unavailable Yes
Consistent with UIP Definite UIP Yes
Consistent with UIP Probable UIP Yes
Consistent with UIP Possible UIP No
Consistent with UIP Not UIP No
Consistent with UIP Unavailable No
Inconsistent with UIP Any No
Abbreviations HRCT high-resolution computed tomography IPF idiopathic pulmonary fibrosis
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
UIP usual interstitial pneumonia Dx diagnosis 43 Exclusion Criteria
1 History of clinically significant environmental exposure known to cause pulmonary fibrosis
Occupational exposures such as asbestos or environmental exposure to organic dust such as occurs in
pigeon breeders may at times mimic the clinical and radiographic findings of IPF
2 Diagnosis of connective tissue disease felt by the principal investigator (PI) to be the etiology of the
interstitial disease Diagnosis of collagen-vascular conditions will be according to the published
American College of Rheumatology criteria As such the presence of any documented collagen-vascular
disorder or the presence of any suspicious symptom complex whether or not associated with
significantly abnormal rheumatological serologies will exclude the subject at the discretion of the PI
3 Extent of emphysema greater than the extent of fibrotic change (honeycombing reticular changes) on
HRCT scan
4 Forced expiratory volume in 1 second (FEV1)FVC ratio lt 065 at screening (postbronchodilator)
5 Partial pressure of arterial oxygen (PaO2) on room air lt 55 mm Hg (lt 50 mm Hg at Denver site)
6 Residual volume gt 120 predicted at screening (postbronchodilator)
7 Evidence of active infection
8 Significant bronchodilator response on screening spirometry defined as a change in FEV1 ge 12 and
absolute change gt 200 mL OR change in FVC ge 12 and absolute change gt 200 mL The percent
difference between the FVC (or FEV1) values will be calculated by taking the absolute value of the
difference and dividing it by the larger of the two FVC (or FEV1) values
9 Screening and enrollment post-bronchodilator FVC measurements (in liters) differing by gt 11 The
percent difference between the FVC values will be calculated by taking the absolute value of the
difference and dividing it by the larger of the two FVC values (eg the percent difference between FVC
measurements of 19 and 20 liters would be determined by taking the difference between the two (01
liters) and dividing by the larger of the two (20 liters) So 0120 = 5 and these FVC measurements
would not exclude the subject
10 Listed for lung transplantation ie the patient has completed the evaluation process has been accepted
as a candidate for transplantation at an appropriate center and is waiting to receive notification of an
available donor organ
11 History of unstable or deteriorating cardiac disease
12 Myocardial infarction coronary artery bypass or angioplasty within 6 months of screening
26
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
13 Unstable angina pectoris or congestive heart failure requiring hospitalization within 6 months of
screening
14 Uncontrolled arrhythmia
15 Severe uncontrolled hypertension
16 Known HIV or hepatitis C
17 Known cirrhosis and chronic active hepatitis
18 Active substance andor alcohol abuse (as determined by site PI)
19 Pregnancy or lactation (subjects who are pregnant or breastfeeding)
20 Known hypersensitivity to study medication
21 Any condition other than IPF that in the opinion of the site PI is likely to result in the death of the
subject within the next year
22 Any condition that in the judgment of the PI might cause participation in this study to be detrimental to
the subject or that the PI deems makes the subject a poor candidate
23 Any therapy directed at pulmonary fibrosis (excepting triple therapy of prednisone plus azathioprine
plus NAC) requires a 30-day washout period before randomized Triple therapy of lt= 12 weeks duration
in the past 4 years requires a 30-day washout period before randomization
24 History of triple therapy of prednisone plus azathioprine plus NAC for gt 12 weeksrsquo duration in the past
4 years or previous enrollment in the triple-therapy arm of the PANTHER-IPF study
44 Study Design and Study Visit
441 Study Design Summary
This study will be a randomized double-blind PL-controlled trial designed to assess the safety and efficacy of
NAC in subjects with newly diagnosed IPF
Subjects with mild to moderate IPF (defined as FVCpred ge 50 and DLCOpred ge 30) diagnosed within
the past 48 months will be enrolled Screening will continue until April 30 2012
27
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
The study will employ a 2-arm design with 11 randomization to NAC or PL Once enrolled subjects will visit
the clinical center at 15 weeks and 15-week intervals thereafter Each subject will be treated and followed for a
maximum of 60 weeks
During the 60-week visit subjects will be taken off all study agents Approximately four weeks after the final
dose of study agent is taken subjects will receive a safety phone call from the study site
442 Study Visits
Subjects who meet entry criteria will review the informed consent a written description of the purpose
procedures and risks of the study with the PI co-investigator or study coordinator and all questions will be
answered The informed consent form will be signed by the subject at screening No protocol-specific
procedures will be performed until the subject has signed and dated an informed consent form This includes the
screening procedures
4421 Screening
Once informed consent is obtained subjects may immediately begin the screening process or may return within
28 days of consent In the event a study subject has been clinically evaluated at the study site by an IPFnet study
physician and has performed testing within three weeks for this clinical evaluation that meets guidelines
provided in the IPFnet PANTHER-IPF Manual of Operating Procedures (MOOP) this testing may be used to
satisfy the following screening criteria medical history physical exam arterial blood gas (ABG) with A-a
gradient vital signs with oximetry body height and weight spirometry DLCO lung volumes and HRCT scan
Allowing the use of previously performed test results that meet study guidelines for the screening visit is
intended to permit subjects easier access to study entry to prevent subjects from repeating testing that has been
performed within the study window and to decrease risks to subjects from repeated exposure to procedures
such as arterial puncture and HRCT
The following procedures will be performed at screening
Medical history and a physical examination
28
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Measure height and weight
Serum pregnancy test (if applicable)
Measure vital signs including oximetry
Blood draws performed and the following analyses conducted
o Hematology (red cell count white cell count hemoglobin hematocrit cell indices differential
platelet count)
o Blood chemistries according to central laboratory protocol (see Section 410 Laboratory
Testing)
o Beta human chorionic gonadotropin (serum) pregnancy test (in women of childbearing potential)
o Urinalysis
Pulmonary Function Tests (PFTs) including spirometry pre- and post- bronchodilator and postshy
bronchodilator measurement of lung volumes and measurement of hemoglobin adjusted diffusing
capacity
Measure ABGs
HRCT if a satisfactory scan has not been performed on the subject within 3 months of screening (see
PANTHER-IPF MOOP for more details)
Surgical lung biopsies (if applicable) reviewed by local and central pathology departments
Current medications If required a washout period discussed with the subject and initiated at this visit
4422 Enrollment
The enrollment visit is expected to take place within eight weeks of the screening visit Enrollment visit
activities include
Measure vital signs including oximetry
Measure height and weight
Serum pregnancy test (if applicable)
If consent has been given blood will be drawn and a urine specimen collected for the bio-specimen
repository
Spirometry (post-bronchodilator)
Measure 6MWT with Borg Dyspnea Scale
29
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Collect Quality-of-life (QOL) data using the SF-36 EuroQol Investigating Choice Experiments for
Preferences of Older People Capability Instrument (ICE CAP) and SGRQ
Female subjects complete Gender Substudy questionnaire
Dyspnea status collected using the UCSD SOBQ
Evaluate Acute Exacerbation (AEx)
Review of any Adverse Events (AEs)
Review of concomitant medications
Subject receives diary and instructions on its purpose and proper use
Subject receives supply of study drug sufficient to last until his or her 15-week study visit
See the Schedule of Assessments (Table 3) for more details Subjects with screening and enrollment postshy
bronchodilator FVC measurements (in liters) differing by more than 11 are not eligible to be enrolled in the
study
Subjects will be asked to provide a physician of record This physician will be considered the subjectrsquos primary
care provider (PCP) and if the subject agrees the PCP will be informed by letter of the subjectrsquos enrollment in
the trial The subject will be informed that his or her ongoing medical care should be received from the PCP
The PCP will be informed of any safety issues identified by the study staff The PCP will also be given
information regarding communication with study personnel about pertinent health issues or clinic encounters
the subject may have
4423 Week 15
The week 15 visit is expected to occur within +- 14 days of the subjectrsquos scheduled visit time (eg the week 15
visit should occur anytime between 13 and 17 weeks after starting study drug Week 15 activities include
Measure vital signs with oximetry
Measurement height and weight
Serum pregnancy test (if applicable)
Spirometry (post-bronchodilator) measurement
Review of AEs
Evaluate for AEx
30
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Review concomitant medications
If consented draw blood and collect urine specimen for the biospecimen repository
Subjects return used and unused study drug for the visit
Review study diary and a new study diary will be given
Provide additional supply of study drug sufficient to last until the next scheduled visit
4424 Week 30
The week 30 visit is expected to occur within +- 14 days of the subjectrsquos scheduled visit time (eg the week 30
visit should occur anytime between 28 and 32 weeks after starting study drug) Week 30 activities include
Physical examination
Measure vital signs with oximetry
Measure height and weight
Laboratory values (complete blood count [CBC] and serum chemistries)
Serum pregnancy test (if applicable)
Measure spirometry (post-bronchodilator)
6MWT with Borg scale
DLCO
Review of AEs
Evaluate for AEx
Review concomitant medications
Complete all QOL and dyspnea questionnaires (EuroQol ICE CAP SF-36 SGRQ and UCSD SOBQ)
If consent has been given blood will be drawn and a urine specimen collected for the biospecimen
repository
Review study diary
Subjects return used and unused study drug for the visit
Provide additional supply of study drug sufficient to last until the next scheduled visit
4425 Week 45
31
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
The week 45 visit is expected to occur within +- 14 days of the subjectrsquos scheduled visit time (eg the week 45
visit should occur anytime between 43 and 47 weeks after starting study drug) Week 45 activities include
Measure vital signs with oximetry
Measure height and weight
Serum pregnancy test (if applicable)
Measure spirometry (post-bronchodilator)
Review of AEs
Evaluate for AEx
Review concomitant medications
If consent has been given blood will be drawn and a urine specimen collected for the biospecimen
repository
Subjects return used and unused study drug for the visit
Study diary reviewed
Provide additional supply of study drug sufficient to last until the next scheduled visit
4426 Week 60 (Early Withdrawal or Final Treatment Visit)
At week 60 or at subject withdrawal from the study (premature by study doctor or subjectrsquos decision) a final
treatment visit will occur At this final treatment visit subjects will discontinue NACPL abruptly Week 60
activities also include
Physical examination
Measure vital signs with oximetry
Measure height and weight
Laboratory values (complete blood count [CBC] and serum chemistries)
Spirometry (post-bronchodilator) measurement
6MWT with Borg scale measurement
DLCO
Lung volumes
ABG
Review of AEs
32
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Evaluate for AEx
Review concomitant medications
Subjects will complete all QOL and dyspnea questionnaires (EuroQol ICE CAP SF-36 SGRQ and
UCSD SOBQ)
If consent has been given blood will be drawn and a urine specimen collected for the biospecimen
repository
Subjects return used and unused study drug for the visit
Study diary reviewed
4427 Final Site Visit ndash FVC drop confirmation
In the event that the subject has a recorded FVC drop of gt10 from baseline at the final treatment visit and the
subject has not had a confirmation of such a drop at a previous study visit the subject should return to the
clinical site 6 to 8 weeks after the final treatment visit During this visit a post-bronchodilator spirometry test
will be performed This FVC measurement will be evaluated according to section 521 of this protocol
4428 Final Visit ndash Telephone Follow-up
Four weeks following the final dose of study medication subjects will receive a telephone call from the study
coordinator to ensure that there are no side effects and to follow up on any ongoing adverse events (AEs)
4429 Phone Contact Between Visits
At week 2 and each month that a subject does not have a scheduled clinical center visit his or her study
coordinator will contact him or her at least once by telephone to
Inquire if the subject has had any hospitalizations events that might be considered an AE or any events
significant enough to warrant an out-of-cycle visit to the clinical center
Remind subjects of their current dosage levels and confirm that the subject understands them
Address any questions or concerns the subject might have regarding other aspects of the study
Assess adherence to the treatment regimen by reviewing diary data verbal review of medications taken
including nutritional supplements
33
34
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Table 3 Schedule of Assessments
Procedure Screening Visit 0
Enrollment Visit 1
Week 15 Visit 2
Week 30Visit 3
Week 45 Visit 4
Week 60 Early
Withdrawal Visit 5
Final1
Visit (via phone)
Informed consent X
Medical history X
Inclusionexclusion criteria X
Serum pregnancy test (if applicable) X X X X X
Review of lung biopsy X
Arterial Blood Gas X X
6-Minute Walk Test
X
X X
Physical examination X X X
Vital signs with oximetry X X X X X X
Body height and weight X X X X X X
Complete Blood Count X X X
Chemistry panel X X X
Monitor Lab Values X X X
Urinalysis X Specimen repository substudy blood draw and urine collection (if consented)
X
X X X X
HRCT (if not completed within three months) X
Spirometry (pre- and post-bronchodilator) X
Spirometry (post-bronchodilator only) X X X X X
DLCO (post-bronchodilator only) X X X
Lung volumes (post-bronchodilator only) X
X
Evaluate for acute exacerbation X X X X X
Review Adverse Events X X X X X X
Review concomitant meds X X X X X X
Dispense subject diary X X X X
Review subject diary X X X X X
Dispense study agent X X X X
Gender Substudy questionnaire (female subjects only) X
EuroQol ICECAP UCSD SOBQ SGRQ SF-36 X X X
Abbreviations DLCO diffusing capacity of the lung for carbon monoxide QOL Quality of Life ICECAP Investigating Choice Experiments for Preferences of Older People UCSD SOBQ University of California Shortness of Breath Questionnaire SGRQ St Georgersquos Respiratory Questionnaire SF-36 Short Form 36 Health Survey
1Follow-up visit via phone will occur four weeks after final dose of study medication
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
45 Dose Justification
The general philosophy for determining dosing levels was to apply previously examined
treatment regimens With the focus of the study being to establish a standard of care for
mildmoderate IPF subjects the goal was to develop flexible yet standardized treatment rules that
allow for the temporary or permanent withholding of one or more components of treatment when
necessary Subjects developing laboratory abnormalities or symptoms that result in
discontinuation of one or more components of study treatment may continue on the other
components as long as there is no contraindication for this Complete follow-up is important for
the validity of any study As a strategy to maintain protocol adherence we are using a treatment
regimen that will detect potential side effects and prompt interventions proactively in the interest
of patient safety In addition subjects who permanently stop study medications during the course
of the study are encouraged to continue in the study completing all scheduled visits and tests
451 Rationale for N-acetylcysteine Dosing
To our knowledge there have been no IPF studies to correlate clinical outcome measures with
different dosages for NAC The dosage chosen is based on the IFIGENIA study However BAL
lung GSH levels from subjects with IPF have been augmented with the use of oral NAC at 600
mg 3 times per day In addition lung GSH levels have been associated with improved
PFTs212227 The dose chosen for this study was based on previous data including the IFIGENIA
study30
4511 Dosing of N-acetylcysteineplacebo
Dosing of NACPL will be 600 mg orally 3 times a day (1800 mgday)
4512 Reasons to Discontinue N-acetylcysteineplacebo
NACPL may be temporarily or permanently discontinued for the duration of the study for
gastrointestinal symptoms or dermatologic reactions
35
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Temporarily discontinue (hold) oral NACPL for subjects requiring inpatient admission for acute
exacerbation (AEx) or other conditions Resume NACPL after discharge
36
37
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
452 Dosage Algorithms
Dosage Adjustment Algorithm 1 NACPL Dose Modifications for Gastrointestinal Symptoms Nausea Vomiting Abdominal Discomfort Diarrhea
GI Symptoms determined by the PI to be clinically significant Nausea Vomiting Abdominal Discomfort Diarrhea
NACPL Temporarily dc (HOLD) x 3 Days
Monitor symptoms intervene as clinically indicated (eg fluid replacement antidiarrhea or antinausea medication)
Monitor or lab PRN
Are symptoms resolving after 3 days NO
Symptoms NOT resolving after 3 days of holding study medication Assessmentmanagement per clinical
discretion of investigator
Likely not study medication discuss resuming study medication with medical monitor when symptoms resolved
YES
Temporarily dc (HOLD) NACPL for 4 additional days (total hold 1 week) then NACPL Resume 600 MG TID
Did symptoms recur
YES
STOP NACPL for
duration of study
NO
NACPL No Change
38
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Dosage Adjustment Algorithm 2 NACPL Dose Modifications For Dermatologic Reactions
Dermatologic Reactions (Not Acneiform) ge Grade 2 Grading per Common Terminology Criteria for
Adverse Events V30 (httpctepcancergov) For example Grade 1 RASHDESQUAMATION Macular or papular eruption or erythema without associated symptoms Grade 2 RASHDESQUAMATION Macular or popular eruption or erythema with pruritus or other associated symptoms localized desquamation or other lesions covering lt50 of body surface area
NACPL Temporarily dc (HOLD) x 3 days
Are symptoms resolving after 3 days
NO Symptoms not resolving after 3 days of holding study medication Assessmentmanagement per clinical discretion of investigator Likely not study medication Discuss resuming study medication with medical monitor when symptoms
resolved YES
Temporarily dc (HOLD) NACPL for 4 additional days (total hold 1 week) then NACPL resume 600 MG TID
Did symptoms recur
YES
STOP NACPL for
duration of study
NO
NACPL No change
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
46 Contraindications Precautions and Side Effects of Study Medications
461 Contraindication
Contraindication to NAC is known hypersensitivity to it
462 Precautions
Concomitant administration of oral NAC and antibiotics has shown a slightly reduced absorption
of cephalexin and a slight increase in erythromycin serum levels NAC contains free sulfhydryl
groups There is no evidence that individuals sensitive to sulfa drugs are sensitive to NAC
The NAC preparation being administered in this study contains 20 mg of aspartame Because of
the phenylalanine component of aspartame individuals with phenylketonuria should avoid or
restrict aspartame intake to avoid increased blood levels of phenylalanine Because of this risk
labeling is required on all products containing aspartame
463 Side Effects
Side effects of NAC range from common to serious See Table 4
39
40
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Table 4 Side Effects of NAC
Undesirable Effects
System-organ class Uncommon
(gt11000 lt1100)
Rare
(gt110000 lt11000)
Very rare
(lt110000) Not known
Immune system disorders Hypersensitivity Anaphylactic shock
reaction
Nervous system disorders Headache
Ear and labyrinth disorders Tinnitus
Cardiac disorders Tachycardia
Vascular disorders Hemorrhage
Respiratory thoracic and
mediastinal disorders
Bronchospasm
Dyspnea
Gastrointestinal disorders
Vomiting diarrhea
stomatitis abdominal
pain nausea
Dyspepsia
Skin and subcutaneous tissue
disorders
Urticaria rash
angioedema itching
General disorders and
administration site conditions Pyrexia
Investigations Reduced arterial
pressure Face edema
In very rare cases the onset of severe skin reactions such as Stevens-Johnson syndrome and Lyell syndrome was reported to have a temporal relationship with N-acetylcysteine administration Although in most cases at least another suspect drug probably most involved in the genesis of the above mentioned mucocutaneous syndromes has been identified in case of mucocutaneous alterations it is appropriate to contact onersquos doctor and the administration of N-acetylcysteine should be immediately discontinued
Some studies confirmed a reduction of platelet aggregation during N-acetylcysteine administration The clinical significance of these findings has not been defined yet [Source Fluimucil Investigator Brochure]
47 Recruitment Procedures
Subjects recruited for this study will be established patients of the investigators or physician- or
self-referred to participating clinical centers in the IPFnet Each clinical center within IPFnet has
a well-developed infrastructure of local pulmonologists within the surrounding geographic area
These pulmonologists are kept informed of ongoing IPF clinical trials and regularly refer
subjects to studies conducted at IPFnet clinical centers
Additional steps will be taken to inform clinicians of the trials in progress within IPFnet
including presentations at faculty staff meetings at local hospitals medical grand rounds and
national conferences direct mail notification monthly faxes and advertisement of network trials
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
in pulmonary journals Clinical center patients previously diagnosed with IPF will be notified of
the trials by mail whenever possible
Recruitment of minorities and women will be monitored by the DCC and DSMB If necessary
additional recruitment efforts will be made at specific centers to ensure that the aggregate subject
sample contains appropriate representation of women and minorities
48 Study Procedures
The following procedures are detailed in the PANTHER-IPF MOOP accompanying this
protocol
1 PFT
2 ABG
3 HRCT scan of the chest (including imaging of pulmonary arteries)
4 CBC and serum chemistries
5 Pregnancy test
6 6MWTBorg Dyspnea Scale
7 QOL questionnaires (EuroQol HAD SF-36 SGRQ and ICE CAP)
8 UCSD SOBQ
9 Gender Substudy Questionnaire
All assessments of PFTs will be conducted by study personnel not directly involved in the
treatment of the subjects
481 Biological Specimen Management
4811 Biological Specimen Sample Management
Subjects at clinical centers participating in the specimen repository substudy who consent to
having blood drawn for research purposes and for the banking of blood blood components and
other biologic specimens (urine and BAL fluid) will have approximately 405 mL of blood
41
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
drawn 17 mL blood drawn for DNA and 20 mL of urine collected at enrollment visit Subjects
will have approximately 50 mL of blood drawn and 20 mL of urine collected at each 15-week
follow-up visit Blood specimens will be separated according to PANTHER-IPF MOOP
guidelines into the following components for banking in the repository serum plasma and
DNA Coding of all biologic specimens for the repository will be performed by study staff at the
clinical center The samples will be processed per PANTHER-IPF MOOP guidelines aliquoted
labeled with barcode labels and stored at -70degC at the clinical center and shipped to the central
repository
The only subject identifiers will be a sample ID number and subject initials This sample ID will
be linked in the IPFnet DCC clinical database to subject information No subject information will
be transferred to the biological-specimen database
The subjectrsquos samples may be used for approved sub-studies relating to human disease
including but not limited to IPF The studies for which an individualrsquos samples will be made
available will be determined by the subjectrsquos answers to questions on the biological-sample
informed consent form The subjects can choose to make their samples available for all options
or any combination Samples will be made available to researchers only with IPFnet Steering
Group approval until such time as the samples are made public through the NHLBI repository
49 Concomitant Medications
Concurrent treatment with FDA-approved therapy for IPF is allowed Colchicine may be used
for treatment of gout Temporary treatment with oral or IV corticosteroids for clinical worsening
or suspected AEx is permitted Nutritional supplements containing NAC are not allowed
410 Laboratory Testing
Clinical laboratory parameters will be assessed at screening and at the end of the study The
following tests will be performed at the two time points specified in the protocol chemistry (AG
ratio ALT [SGPT] AST [SGOT] albumin alkaline phosphatase amylase bilirubin-direct
42
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
bilirubin-indirect bilirubin-total BUN BUNcreatinine ratio calcium carbon dioxide
cholesterol-total chloride CPK-total creatinine GGT globulin glucose iron-total LDH
lipase magnesium phosphorus-inorganic potassium protein-total sodium TIBC triglycerides
uric acid) and hematology (red blood cell count WBC count hemoglobin hematocrit cell
indices differential platelet count)
411 Blinding of Study Drugs
Subjects and caregivers will be blinded to study treatment Every subject will receive NAC or
matching PLs at every study visit from the baseline visit to the week-45 visit No study agent
will be dispensed at the week-60 visit
43
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
5 Study Endpoints
51 Primary Study Endpoint
The primary endpoint will be the change in serial measurements of FVC over the study period
52 Secondary Study Endpoints
521 Time to Disease-progression
The time-to-death or a 10 decline in FVC will be defined as the time-to-disease progression
The 10 decline in FVC from enrollment must be confirmed on 2 consecutive visits no less than
6 weeks apart For subjects with 2 consecutive visits with a 10 decline in FVC the time-toshy
disease progression will be defined as the time interval between enrollment and the initial visit
with a 10 FVC decline For subjects who experience disease progression the study doctor will
determine whether or not the subject will remain in the study
522 Acute Exacerbations
The following 3 criteria will define AEx in subjects with acute worsening of their respiratory
conditions
1 Clinical (all of the following required)
A) Unexplained worsening of dyspnea or cough within 30 days triggering unscheduled
medical care (eg emergency room clinic study visit hospitalization)
B) No clinical suspicion or overt evidence of cardiac event pulmonary embolism or deep
venous thrombosis to explain acute worsening of dyspnea
C) No pneumothorax
44
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
2 RadiologicPhysiologic (A and B required)
A) New ground glass opacity or consolidation computed tomography (CT) scan OR new
alveolar opacities on chest x-ray
B) Decline of ge 5 in resting room air SpO2 from last recorded level OR decline of ge 8 mm
Hg in resting room air PaO2 from last recorded level
3 Microbiologic (all of the following required)
A) No clinical evidence for infection (ie absence of grossly purulent sputum fever gt 39degC
orally)
B) Lack of positive microbiological results (if done) from lower respiratory tract defined as
(1) Clinically significant bacterial growth on sputum or endotracheal aspirate cultures
(2) Quantitative culture by protected brush specimen ge 103 cfumL or BAL ge 104 cfumL
(3) The presence of specific pathogens on stains of any of the above
C) Lack of positive pathogen in blood cultures (if done)
Identification of Acute Exacerbations
All subjects will be educated about the importance of identifying AExs At the time of
enrollment subjects will be told about the possibility of developing acute symptomatic
worsening that might represent an AEx of IPF and instructed to contact their study clinical
center coordinator within 48 to 72 hours of the apparent event
All subjects will be contacted by phone monthly and questioned about any change in dyspnea or
cough and any interim clinic visits or hospitalizations Finally as part of the IPFnet outreach to
community referring physicians the importance of AExs will be emphasized When a subject is
identified who meets criterion 1A this will trigger the collection of additional clinical data to
evaluate a suspected AEx These data will be collected as part of standard clinical care (ie this
protocol does not require collection of all items) The additional items to be collected for
suspected AEx include
IPFnet AEx case report form (eCRF) (required)
45
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Chest x-ray CT scan withwithout pulmonary angiogram (reports should be faxed and
followed by the hard copiesdiscs)
Oxygen saturation (pulse oximetry)
ABG
Respiratory cultures (sputum endotracheal aspirate lavage)
Blood cultures
Clinichospital records related to the event
All potential cases of AEx will be reviewed by the clinical center PI first and a decision on
whether the case may represent an AEx will be made If AEx is suspected the case will be sent
to the IPFnet adjudication committee which will assign a final diagnosis (see Table 5) If there is
disagreement among members the majority opinion will be recorded
During episodes of suspected AEx as determined by the individual clinical center investigator
subjects will remain blinded and in the study
Table 5 Final Diagnoses in Evaluation of Suspected Acute Exacerbations
Definite acute exacerbation All criteria met no alternative etiology
Unclassifiable acute worsening
Insufficient data to evaluate all criteria no alternative etiology
Not acute exacerbation Alternative etiology identified that explains acute worsening
Management of the suspected AEx will be at the discretion of the treating physician Standard of
care generally involves evaluation for respiratory infection pulmonary embolism cardiac events
and pneumothorax and treatment with IV corticosteroids
Study drugs will be resumed at pre-suspected AEx doses after subjects clinically improve as
confirmed by the local PI All subjects should be seen at the clinical center within 2 to 4 weeks
of recovery for measurement of post-bronchodilator FVC (see Figure 4) Subjects unable to
return to the clinical center after suspected AEx due to medical frailty (eg continued
46
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
institutionalization progressive disability) will be categorized as failing to maintain FVC
response in secondary analyses
Suspected AEx (PI determined)
Hold study drug Treat AEx
(Attending physician determined)
Alive but unable to continue due to
medical frailty
Dead
Alive and able to continue
Site reviewvisit
Restart study drug
FVC within 2-4 weeks
Figure 4 Acute Exacerbation Flow Chart
523 Respiratory Infections
An upper respiratory infection will be defined as
Change in sputum discoloration
Increased cough of no more than 14 daysrsquo duration
A lower-respiratory infection (pneumonia) will be defined as new segmental or lobar airspace
opacities visualized by image studies (chest radiograph or HRCT) in addition to any of the
following
Positive pathogencultures in good sample of sputum or lower-airway secretions retrieved
by fiberoptic bronchoscope
Fever gt 39degC or gt 100degF
Leukocytosis gt 12000 (unexplained no increase in dose of corticosteroids)
47
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
524 Maintained FVC Response
Subjects with follow-up FVCpred measurements at or above their baseline FVCpred level
will be classified as having maintained FVC response Subjects with reduced FVCpred levels
or missing data for any reason including death or medical frailty will be classified as having not
maintained FVC response The FVCpred value is used because unadjusted FVC measurements
are expected to decline with age
48
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
6 Safety Evaluations and Procedures
61 Adverse Events
During a clinical trial the reporting of adverse experience information can lead to important
changes in the way a new treatment is developed as well as provide integral safety data
611 Definitions
An adverse event (AE) is any untoward medical occurrence in a subject or clinical investigation
subject who was administered a pharmaceutical product The AE does not necessarily have to
have a causal relationship with the drug administered An AE can be any unfavorable and
unintended sign (including an abnormal laboratory finding) symptom or disease temporarily
associated with the use of a medicinal product whether or not considered to be related to the
medicinal product Diseases signs symptoms or laboratory abnormalities already existing at
enrollment are not considered AEs unless they worsen (ie increase in intensity or frequency)
Surgical procedures themselves are not AEs they are therapeutic measures for conditions that
require surgery The condition for which the surgery is required may be an AE Surgical
procedures planned before randomization and the conditions necessitating the surgery are not
AEs
A serious adverse event is any untoward event that
Is fatal
Is life-threatening
Requires inpatient hospitalization or prolongation of existing hospitalization with the
following exceptions
o Preplanned (before the study) hospital admissions unless the hospitalization is
prolonged
o Planned admissions (as part of a study eg routine biopsies)
o Hospitalization lasting lt 24 hours
49
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
o Hospitalization for elective procedure
o Emergency room visits
Results in persistent or significant disability or incapacity
Is a congenital anomaly or birth defect
Important medical events that may not result in death be life-threatening or require
inpatient hospitalization may be considered serious adverse events (SAEs) when based
on appropriate medical judgment they may jeopardize the subject and may require
medical or surgical intervention to prevent one of the outcomes listed above
Life-threatening means that the subject was in the view of the investigator at immediate risk of
death from the AE as it occurred It does not include an AE that had it occurred in a more severe
form might have caused death
Persistent or significant disabilityincapacity means that the event resulted in permanent or
significant and substantial disruption of the subjectrsquos ability to carry out normal life functions
Causality
A reasonable possibility means the AE may have been caused byrelated to the study drug A
perceived or real lack of efficacy does not satisfy the definition of relatedness
612 Adverse Event (AE) Reporting
For the PANTHER-IPF trial all AEs (serious and nonserious) occurring from randomization
through final study visit (4 weeks after final dose of all study medication) will be recorded on the
AE page of the case report form (CRF)
6121 Serious Adverse Events (SAE) Reporting
For this trial all deaths and all SAEs which occur from randomization through final study visit
must be entered within the EDC system via the SAE eCRF page within 24 hours of the
investigative sitersquos knowledge of the event It is the responsibility of the clinical center
50
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
investigator to provide a causality assessment of the event for each study medications based upon
the information available at the time of the report It is understood that complete information
about the event may not be known at the time the initial report is submitted In the event the EDC
system is not accessible to the site at the time of event reporting investigative sites will complete
and forward a paper back-up SAE form to DCRI Safety Surveillance for processing
DCRI Safety Surveillance
Telephone 1-919-668-8624 or 1-866-668-7799 (toll free)
Fax 1-919-668-7138 or 1-866-668-7138 (toll free)
The investigator must complete and submit follow-up SAE information via the eCRF when
important new or follow-up information (eg final diagnosis outcome results of specific
investigations) becomes available Follow-up information should be submitted according to the
same process used for reporting the initial event as described above All SAEs will be followed
until resolution stabilization or 30 days after the subject has completed the final visit (4 weeks
after the final dose of study medication) whichever occurs first The investigator is responsible
for reporting SAEs to their institutional review board (IRB) per site specific IRB reporting
guidelines
6122 Regulatory Reporting
AEs that are serious study drug related and unexpected will be reported to the regulatory
authorities The DCRI Safety Surveillance medical monitor will perform a medical review of all
SAEs submitted and evaluate for ldquounexpectednessrdquo DCRI Safety Surveillance will prepare
MedWatch reports for those events identified as serious study drug related and unexpected as
determined by Safety Medical Monitor
DCRI Regulatory Services will submit all unexpected study drug-related SAEs as per 21 CFR
32 DCRI Safety Surveillance will provide a safety alert letter to the NHLBI DSMB and DCC
clinical operation (for distribution to sites) within 15 days of initial receipt of the information
51
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Investigators are responsible for promptly reporting these events to their reviewing IRBs
according to site specific IRB reporting guidelines
62 Clinical Medical Monitoring
There will be an unblinded physician at the IPFnet DCC serving as medical monitor The
medical monitor will be available to assist with questions about dosage adjustments of study
medications including discontinuation or resumption of medications
63 Unblinding Procedures
Unblinding of subjects or investigators to subject treatment is strongly discouraged For ongoing
clinical management all subjects should be presumed to be receiving ldquoactiverdquo study drug To
ensure the subjectrsquos safety the study treatment will be dose-adjusted based on laboratory test
results clinical findings and symptoms
The IPFnet DCC medical monitor and PANTHER-IPF co-chairs Drs Ganesh Raghu and
Fernando Martinez will be available to the study physicians to discuss study drug management
on a case-by-case basis Un-blinding will be considered ONLY when the knowledge of subject
treatment assignment is ABSOLUTELY ESSENTIAL for subject safety and after discussion of
the subjectrsquos case with the medical monitor and either Dr Raghu or Dr Martinez Unblinding of
study treatment should be minimized during the conduct of the trial In those cases where it is
felt to be medically necessary the DCC medical officer will communicate directly with the
managing physician to minimize unblinding of study personnel
52
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
7 Study Drug Procedures
At the baseline 15-week 30-week and 45-week study visits subjects will receive a supply of
study drug sufficient to last until the next visit at which study drug will be dispensed
53
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
8 Data Management
81 Hardware and Software Configuration
811 Hardware and Database Software
Data will be stored in an Oracle database system Oracle has advantages of processing efficiency
and smooth linkage with other software systems The application and database will be hosted on
Solaris Unix servers at the IPFnet DCC
812 Statistical Software
SAS will be used as the principal application for the management of analysis data files and
statistical computations S-Plus will be used to provide supplementary functions as needed
813 Access Control and Confidentiality Procedures
Access to databases will be controlled centrally by the IPFnet DCC through user passwords
linked to appropriate privileges This protects the data from unauthorized changes and
inadvertent loss or damage
814 Security
Database and Web servers will be secured by a firewall and through controlled physical access
Oracle has many security features to ensure that any staff member accessing the database has the
proper authority to perform the functions he or she requests of the system Within the secondary
SAS databases Unix group-access control maintains similar security The Sun workstation login
is secured by extensive user-password facilities under Unix
54
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
815 Back-up Procedures
Database back-up will be performed automatically every day and standard IPFnet DCC policies
and procedures will be applied to dictate tape rotation and retention practices
816 Virus Protection
All disk drives that provide network services and all user computers will be protected using
virus-scanning software Standard IPFnet DCC policies will be applied to update these protection
systems periodically through the study
82 Sources of Data
821 Design and Development
The IPFnet DCC will be responsible for development of the electronic case report forms
(eCRFs) development and validation of the clinical study database ensuring data integrity and
training clinical center staff on applicable data management procedures A web-based distributed
data entry model will be implemented This system will be developed to ensure that guidelines
and regulations surrounding the use of computerized systems used in clinical trials are upheld
The remainder of this section provides an overview of the data management plan associated with
this protocol
822 Data Collection Forms
The data collection process consists of direct data entry at the study clinical centers into the EDC
system(s) provided by the DCC A data collection worksheet will be provided to clinical centers
for recording data in the event the EDC system is unavailable Data entry of the eCRFs should
be completed according to the instructions provided and project specific training The
investigator is responsible for maintaining accurate complete and up-to-date records and for
ensuring the completion of the eCRFs for each research participant
55
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
823 Data Acquisition and Entry
Data entry into eCRFs shall be performed by authorized individuals Selected eCRFs may also
require the investigatorrsquos written signature or electronic signature as appropriate Electronic
CRFs will be monitored for completeness accuracy and attention to detail during the study
824 Data Center Responsibilities
The IPFnet DCC will 1) develop a data management plan and will conduct data management
activities 2) provide final eCRFs for the collection of all data required by the study 3) develop
data dictionaries for each eCRF that will comprehensively define each data element 4) conduct
ongoing data monitoring activities on study data 5) monitor any preliminary analysis data
cleanup activities and 6) rigorously monitor final study data clean up
825 Data Editing
Completed data will be entered into the IPFnet DCC automated data acquisition and
management system If incomplete or inaccurate data are found a data clarification request will
be generated and distributed to clinical centers for a response Clinical centers will resolve data
inconsistencies and errors and enter all corrections and changes into the IPFnet DCC automated
data acquisition and management system
826 Training
The training plan for clinical center staff includes provisions for training on assessments eCRF
completion guidelines data management procedures and the use of computerized systems
56
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
9 Study Design and Data Analysis
91 General Analytic Considerations
All primary analyses will be based on intent-to-treat (ITT) principles using all randomized
subjects Baseline factors across groups will be compared using mean (standard deviation) and
median (25th and 75th percentiles) summary measures Kaplan-Meier curves will be used to
display event rates Due to clinical interest in departures from both sides of the null hypothesis
all test statistics will be 2-sided
Reasonable caution needs to be taken when conducting multiple analyses on key clinical
subgroups For subgroup analyses a conservative significance level of 0001 will be used for all
interaction tests Thus subgroup comparisons will be considered exploratory unless the p-value
from the interaction test is smaller than 0001
92 Randomization Blinding and Reporting of Results
A permuted block-randomization scheme will be created with varying block sizes stratified by
clinical center Once a subject has completed the screening and baseline period and evaluation
for inclusionexclusion criteria the randomization process will begin Subjects will be
randomized to receive NAC or matching placebo with equal probability (11) via telephone
contact with a central interactive voice response system (IVRS) using a toll-free randomization
number On the day of randomization after the subject has successfully met all inclusion and
exclusion criteria the investigator or designee will call the central randomization number to
obtain the assigned kit randomization numbers for that subject At each subject visit the
investigator or designee will call the central randomization number to obtain the new kit
randomization numbers for resupply of the subject For resupply of the clinical center the IVRS
will monitor minimal volume of a kit type andor expiration date and will automatically notify
the pharmacy
57
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
The trial results will be reported according to guidelines specified in the CONSORT statement
A flow diagram describing screening recruitment randomization dropout and vital status will
be included in the primary manuscript AEs and efficacy data will be presented for all treatment
groups Adherence dropout and lost to follow-up will be carefully examined across all treatment
groups Analyses of safety will be based on data from all randomized subjects who received at
least one dose of study drug
93 Stratification
Subjects will be distributed to the two treatment arms in a 11 allocation ratio Stratification
blocks will be based on clinical centers
94 Specification of the Primary Analyses
A mixed model repeated measures (MMRM) analysis described in section 95 will be used to
compare differences in the slope of FVC measurements across the treatment groups Response
variables are values of the FVC measured at baseline and every 15 weeks until study completion
Variables in the model will include treatment time and time by treatment age sex race and
height Contrast estimates of differences in slopes of treatment over time (along with confidence
intervals) will be used to estimate the treatment effect The validity of this model in terms of
meeting modeling assumptions will be assessed via standard modeling diagnostics and goodness-
of-fit measures Based on the MMRM framework missing FVC data will not be imputed for the
primary analysis
95 Analysis of Longitudinal Endpoints
A common goal in clinical trials is to specify models that are easily implemented and
reproducible by independent data analysts On the other hand the models should have proper
statistical behavior in terms of low bias and high precision Many common approaches to
longitudinal data analysis including last observation carried forward (LOCF) imputation rely on
the missing completely at random (MCAR) assumption However the MCAR assumption is
58
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
unlikely to hold in many clinical trials because missing data are often related to disease
progression and prognosis A more reasonable assumption missing at random (MAR) specifies
that the complete data distribution can be modeled using only the observed data The likelihood-
based MMRM approach is valid under the more general MAR assumptions These models will
be applied to analyze the longitudinal data secondary endpoints
The advantages of MMRM analysis are that all important characteristics of the model can be preshy
specified standard software can be used to implement the models and results are based on ITT
principles43 In addition the MMRM approach offers superior control of Type I and Type II
errors compared with the LOCF approach
Response variables are values of the PFTs measured at enrollment and every 15 weeks until
study completion and 6MWT values measured at baseline week 30 and week 60 Covariates are
treatment time time by treatment and key baseline risk factors Contrasts (along with
confidence intervals) of treatment by time will be used to estimate the treatment effect
The correlation structure involves multiple pieces including measurement errors random
variation and interindividual variability For the longitudinal data analyses an unstructured
correlation matrix for within-subject errors will be assumed Other correlation structures
including compound symmetry will be examined as needed A careful examination of reasons
for study discontinuation will be conducted to assess the validity of MCAR Sensitivity analyses
will be used to examine the untestable assumption that the observed data violate the MAR
assumption The MMRM models will be implemented using PROC MIXED in SAS
96 Analysis of Binary Time-to-Event and Time-Lagged Endpoints
Regression modeling approaches using either the logistic regression model or Cox proportional
hazards regression model will be employed when appropriate The validity of these models will
be assessed via standard modeling diagnostics and goodness-of-fit measures Estimates of
cumulative frequencies for more general time-lagged responses will be calculated using the
partitioned version of the Bang-Tsiatis estimator44 The partitions will be set at 15-week intervals
59
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
to correspond with the data-collection process Covariate adjusted event rates will be calculated
using inverse probability-weighted regression estimates45
97 Power Analysis
971 Primary Analyses
Based on previously published IPF clinical trials the PL group is expected to experience a drop
in FVC of approximately 020 L over the study period (see Figure 1) The IPFnet Steering Group
determined a clinically important difference would be to preserve the majority of the decline
relative to PL over the study period In particular a treatment effect of 015 L was determined to
be a clinically meaningful difference Potential dropout is a key factor in the proposed study The
drop-out process assumed 5 lost to follow-up after every study visit Only 80 of subjects
were assumed to be followed for the entire study period All models assumed a compound
symmetry structure for the covariance matrix Power calculations were performed using a SAS
IML program for designing repeated measures studies46 Based on preliminary reviews of the
data from the University of Michigan the covariance matrix parameters were estimated at
approximately σ2 = 0757 (variance parameter) and ρ = 0936 (correlation parameter) To be
conservative the power calculations for the primary analysis were performed with parameter
setting of σ2 = 0810 (variance parameter) and ρ = 0925 (correlation parameter)
The power calculations assume a correction for imperfect compliance proposed by Lachin and
Foulkes to allow for 2 noncompliance for each of the treatment arms47 Thus the sample size
of 130 subjects per arm would be reduced to an adjusted sample size of 130(1-002-002)2 =
1198 or 120 subjects per arm
Under the assumed Type I error rate of 005 with a correlation parameter of 0925 and standard
deviation of 090 the difference of 015 L (or 00025 Lweek) shown in Table 6 would have
power of 93
60
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Table 6 Hypothetical Values of Mean FVC (L) Change from Baseline
Week 15 Week 30 Week 45 Week 60
NAC 00125 00250 00375 00500
Placebo 00500 01000 01500 02000
Difference 00375 00750 01125 01500
Abbreviations FVC forced vital capacity PL placebo
972 Power Analysis for Secondary Endpoints
Power calculations for secondary endpoint measurements are shown in Table 7 Standard
deviations are based on unpublished data provided by the University of Michigan The
calculations are based on a 2-sample t-test with Type I error rate set at 005 These calculations
are likely to be conservative because the statistical approach described in section 95 for
analyzing these endpoints will incorporate incomplete observations as well as intermediate data
points
Table 7 Detectable Differences in Treatment Means for Selected Endpoint Measurements
Secondary Endpoints Std Dev
of the Baseline Score
Detectable Difference for 80 Power
Std Dev of the Change Score
Difference Detectable for
80 Power
DLCOpred 166 58 91 32
6MWT Area Under the Desaturation Curve
219 76 175 61
6MWT Distance to Desaturation 224 78 315 110
6MWT Minutes Walked 210 073 205 071
Abbreviations Std Dev standard deviation DLCOpred diffusing capacity of the lung for carbon monoxide percent predicted 6MWT 6-minute walk test
61
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
10 Study Administration
101 Cooperative Agreement Mechanism
The administrative and funding mechanism used to undertake this project is a ldquocooperative
agreementrdquo (U01) which is an assistance mechanism Under the cooperative agreement the
NHLBI assists supports andor stimulates the project and is substantially involved with
investigators in conducting the study by facilitating performance of the effort in a ldquopartnerrdquo role
The NHLBI project scientist serves on the IPFnet Steering Group and he or another NHLBI
scientist may serve on other project committees when appropriate At the same time however
NHLBI does not assume a dominant role direction or prime responsibility for this research
program
As described below governance of the project is conducted through the IPFnet Steering Group
Principal investigators have lead responsibilities in all aspects of their trials and the project
including any modification of trial designs conduct of the trials quality control data analysis
and interpretation preparation of publications and collaboration with other investigators unless
otherwise provided for by the IPFnet Steering Group
PIs retain custody of and have primary rights to their center-specific and collaborative data
subject to government rights-of-access consistent with current Health amp Human Services (HHS)
Public Health Service (PHS) and National Institutes of Health policies The protocols and
governance policies call for the continual submission of data centrally to the IPFnet DCC for the
collaborative database which at a minimum will contain the key variables selected by the IPFnet
Steering Group for standardization across all clinical centers the submission of copies of the
collaborative datasets to each PI upon completion of the project procedures for data analysis
reporting and publication and procedures to protect and ensure the privacy of medical and
genetic data and records of individuals The NHLBI project scientist on behalf of the NHLBI
will have the same access privileges and responsibilities regarding the collaborative data as the
other members of the Steering Group
62
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
PIs are also encouraged to publish and to publicly release and disseminate results data and other
products of the project concordant with the project protocols and governance and the approved
plan for making data and materials available to the scientific community and to the NHLBI
However during the 3 years after the ending date of NHLBI project support unpublished data
unpublished results data sets not previously released and other study materials or products are
to be made available to any third party only with the approval of the IPFnet Steering Group
Upon completion of the project PIs are expected to put their intervention materials and
procedure manuals into the public domain andor make them available to other investigators
according to the approved plan for making data and materials available to the scientific
community and the NHLBI for the conduct of research at no charge other than the costs of
reproduction and distribution
The NHLBI reserves the right to terminate or curtail the project (or an individual award) in the
event of (a) failure to develop or implement mutually agreeable collaborative measurement
subject eligibility and data management sections of the protocols (b) substantial shortfall in
subject recruitment follow-up data reporting or quality control or other major breach of
protocol (c) substantive changes in the agreed-upon protocols with which NHLBI cannot
concur (d) reaching a major project outcome with persuasive statistical significance
substantially before schedule or (e) human subject ethical issues that may dictate a premature
termination
Any disagreement that may arise in scientificprogrammatic matters (within the scope of the
award) between award recipients and the NHLBI may be brought to arbitration An arbitration
panel will be composed of 3 membersmdash1 selected by the IPFnet Steering Group (with the
NHLBI member not voting) or by the individual PI in the event of an individual disagreement a
second selected by NHLBI and the third selected by the other 2 members This special
arbitration procedure in no way affects the PIrsquos right to appeal an adverse action that is otherwise
appealable in accordance with the PHS regulations at 42 CFR part 50 Subpart D and HHS
63
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
regulation at 45 CFR part 16 or the rights of the NHLBI under applicable statutes regulations
and terms of the award
102 IPFnet Steering Group
The IPFnet Steering Group is the main governing body of the project It is composed of the PIs
of the clinical centers the PI of the DCC and the NHLBI project scientist The clinical centers
the IPFnet DCC and the NHLBI each have 1 vote on the IPFnet Steering Group All decisions
are determined by majority vote
All major scientific decisions are determined by the IPFnet Steering Group It assumes overall
responsibility for the design and conduct of the trial It appoints (and disbands) committees and
subcommittees as the need arises designs approves and implements the study protocols
oversees the development of the MOOP monitors subject recruitment and treatment delivery
evaluates data collection and management oversees quality assurance procedures and
implements changes and enhancements to the study as required It also has primary responsibility
for facilitating the conduct of the trials and reporting the projectrsquos results
103 Data and Safety Monitoring Board
The NHLBI will establish a DSMB in accordance with established policies (see
httpwwwnhlbinihgovfundingpoliciesdsmb_insthtm) to ensure data quality and subject
safety and to provide independent advice to the NHLBI regarding progress and the
appropriateness of study continuation
104 Recommendations on Interim Monitoring of Efficacy Safety and Futility
First and foremost the role of the DSMB will be to review subject safety and trial conduct at
periodic points during the study The DSMB may require analyses of the primary endpoint
results for comparing the benefit and risks of treatment strategies The benefit of collecting
additional data on key secondary endpoints with extended follow-up and establishing a robust
64
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
evidence base for determining a standard of care will need to be carefully considered before
early termination of one or more treatment arms After careful consideration the IPFnet Steering
Group recommends conservative thresholds for the early examinations of the safety and efficacy
data
The DSMB will be expected to meet approximately every 6 months until trial completion to
review safety and toxicity data The DSMB may recommend stopping the study based on these
reviews Because the DSMB could stop the trial for safety concerns as well as for a large
efficacy benefit there could be multiple opportunities to reject the null hypothesis (no difference
in event rates between the PL and NAC groups) A Bonferroni approximation will be applied
during the one planned interim analysis for efficacy
Before locking the database a statistical analysis plan (SAP) will be developed to provide
complete details on the statistical analysis The SAP will include the specifics for how and when
the DSMB will be notified for AEs The IPFnet DCC will deliver to the DSMB all FDA-defined
AEs at 3-month intervals The IPFnet DCC will prepare narrative SAE reports in real time for
DSMB review including recommendations and analysis of similar events for each SAE
submitted to the FDA
65
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
11 Investigator and Sponsor Obligations
111 Monitoring
All monitoring activities for US clinical centers will be performed in accordance with DCRI
standard operating procedures Information regarding the types of visits will be outlined in the
PANTHER-IPF MOOP
112 Cost and Payment
There will be no cost to subjects enrolled in this trial Study-related procedures will be paid for
by the IPFnet
Subjects may be eligible for reimbursement for travel to the clinical center Details of payment
will be explained to each subject during the consent process
113 Confidentiality and Health Insurance Portability and Accountability Act
Considerations
Subject confidentiality will be protected throughout the study All subject data will be kept
strictly confidential and no subject-identifying information will be released to anyone outside
the project Confidentiality will be assured through several mechanisms First each subject will
be assigned an anonymous study ID which will then be used on all study forms Second any
study forms blood samples and paper records that contain subject information (eg address lists
phone lists) will be kept at the clinical centers in secured locked areas coded by number Once
blood is collected there will be no subject identifiers placed on blood samplesmdashonly the study
ID number and the date of sample collection Third access to all subject data and information
including laboratory specimens will be restricted to authorized personnel In the case of
computerized data this restricted access will be assured through user logon IDs and password
protection
66
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
At the IPFnet DCC only authorized personnel will have access to the data files containing study
data Security will be assured through user logon IDs passwords and appropriate access
privileges All study subjects will be identified only by their IPFnet ID numbers and no personal
identifying information such as name address or Social Security number will be entered into
the IPFnet DCC database Any subject-specific data reported to the IPFnet Steering Group will
be identified only by the IPFnet ID number
Finally subjects will not be identified by name in any reports or publications nor will the data
be presented in such a way that the identity of individual subjects can be inferred Analysis files
created for further study by the scientific community will have no subject identifiers These data
files will be created in accordance with the Ancillary Studies and Publication Policy of the
IPFnet
114 Informed Consent Procedures
All IPFnet subjects will provide written informed consent using procedures reviewed and
approved by each clinical centerrsquos IRB Informed consent will be undertaken by study personnel
in-person with the subject The subject has the option of declining further participation in the
study at that point No further study procedures will be conducted until the signed documents
have been provided to the IPFnet clinical center
115 Institutional Review Boards
Before initiating this study the protocol clinical center-specific informed consent forms Health
Insurance Portability and Accountability Act (HIPAA) forms recruitment materials and other
relevant information will be reviewed by a properly constituted IRB at each participating clinical
center A copy of the signed and dated IRB approval at each clinical center will be retrieved prior
to or during the site initiation visit and archived at the IPFnet DCC Any amendments to the
protocol other than simple administrative and typographical changes must be approved by each
IRB before they are implemented The clinical centers will seek annual renewals of their IRB
approvals in accordance with local procedures
67
__________________________________________ ________________
__________________________________________
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
12 Investigator Agreement
I have read the foregoing protocol PANTHER-IPF and agree that it contains all necessary
details for carrying out this study I will conduct the study as outlined herein and will complete
the study within the time designated
I will provide copies of the protocol and all pertinent information to all individuals responsible to
me who assist in the conduct of this study I will discuss this material with them to ensure they
are fully informed regarding the drug and the conduct of the study
I will fulfill all responsibilities for submitting pertinent information to the local IRB if
applicable that is responsible for this study
I further agree that NHLBI andor DCRI will have access to any source documents from which
eCRF information may have been generated
Signature of Principal Investigator Date
Name of Principal Investigator (printed or typed)
Protocol version date May 19 2009
Protocol Amendment 1 version date May 28 2010
Protocol Amendment 2 version date December 6 2011
68
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
13 References
1 Raghu G Brown KK Bradford WZ et al A placebo-controlled trial of interferon gamma-1b in patients with idiopathic pulmonary fibrosis N Engl J Med 2004350125-33 2 King TE Jr Safrin S Starko KM et al Analyses of efficacy end points in a controlled trial of interferon-gamma1b for idiopathic pulmonary fibrosis Chest 2005127171-7 3 Flaherty KR Thwaite EL Kazerooni EA et al Radiological versus histological diagnosis in UIP and NSIP survival implications Thorax 200358143-8 4 Wells AU Desai SR Rubens MB et al Idiopathic pulmonary fibrosis a composite physiologic index derived from disease extent observed by computed tomography Am J Respir Crit Care Med 2003167962-9 5 Raghu G Freudenberger TD Yang S et al High prevalence of abnormal acid gastroshyoesophageal reflux in idiopathic pulmonary fibrosis Eur Respir J 200627136-42 6 Kinnula VL Focus on antioxidant enzymes and antioxidant strategies in smoking related airway diseases Thorax 200560693-700 7 Coultas DB Zumwalt RE Black WC Sobonya RE The epidemiology of interstitial lung diseases Am J Respir Crit Care Med 1994150967-72 8 Raghu G Weycker D Edelsberg J Bradford WZ Oster G Incidence and prevalence of idiopathic pulmonary fibrosis Am J Respir Crit Care Med 2006174810-6 9 Olson AL Swigris JJ Lezotte DC Norris JM Wilson CG Brown KK Mortality from pulmonary fibrosis increased in the United States from 1992 to 2003 Am J Respir Crit Care Med 2007176277-84 10 Mannino DM Etzel RA Parrish RG Pulmonary fibrosis deaths in the United States 1979shy1991 An analysis of multiple-cause mortality data Am J Respir Crit Care Med 19961531548shy52 11 Hubbard R Johnston I Coultas DB Britton J Mortality rates from cryptogenic fibrosing alveolitis in seven countries Thorax 199651711-6 12 Johnston I Britton J Kinnear W Logan R Rising mortality from cryptogenic fibrosing alveolitis Bmj 19903011017-21 13 Raghu G Collard HR Egan JJ et al An official ATSERSJRSALAT statement idiopathic pulmonary fibrosis evidence-based guidelines for diagnosis and management Am J Respir Crit Care Med 2011183788-824 14 (USA) FDA FDA Public Health Advisory Interferon gamma-1b (marketed as Actimmune) In 2007 15 King TE Jr Pardo A Selman M Idiopathic pulmonary fibrosis Lancet 2011 16 Raghu G Brown KK Costabel U et al Treatment of idiopathic pulmonary fibrosis with etanercept an exploratory placebo-controlled trial Am J Respir Crit Care Med 2008178948shy55 17 Malouf MA Hopkins P Snell G Glanville AR An investigator-driven study of everolimus in surgical lung biopsy confirmed idiopathic pulmonary fibrosis Respirology 201116776-83 18 King TE Jr Behr J Brown KK et al BUILD-1 a randomized placebo-controlled trial of bosentan in idiopathic pulmonary fibrosis Am J Respir Crit Care Med 200817775-81 19 Richeldi L Costabel U Selman M et al Efficacy of a tyrosine kinase inhibitor in idiopathic pulmonary fibrosis N Engl J Med 20113651079-87
69
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
20 Borok Z Buhl R Grimes GJ et al Effect of glutathione aerosol on oxidant-antioxidant imbalance in idiopathic pulmonary fibrosis Lancet 1991338215-6 21 Meyer A Buhl R Magnussen H The effect of oral N-acetylcysteine on lung glutathione levels in idiopathic pulmonary fibrosis Eur Respir J 19947431-6 22 Behr J Maier K Degenkolb B Krombach F Vogelmeier C Antioxidative and clinical effects of high-dose N-acetylcysteine in fibrosing alveolitis Adjunctive therapy to maintenance immunosuppression Am J Respir Crit Care Med 19971561897-901 23 Cantin AM North SL Fells GA Hubbard RC Crystal RG Oxidant-mediated epithelial cell injury in idiopathic pulmonary fibrosis J Clin Invest 1987791665-73 24 Waghray M Cui Z Horowitz JC et al Hydrogen peroxide is a diffusible paracrine signal for the induction of epithelial cell death by activated myofibroblasts Faseb J 200519854-6 25 Larios JM Budhiraja R Fanburg BL Thannickal VJ Oxidative protein cross-linking reactions involving L-tyrosine in transforming growth factor-beta1-stimulated fibroblasts J Biol Chem 200127617437-41 26 Kinnula VL Fattman CL Tan RJ Oury TD Oxidative stress in pulmonary fibrosis a possible role for redox modulatory therapy Am J Respir Crit Care Med 2005172417-22 27 Meyer A Buhl R Kampf S Magnussen H Intravenous N-acetylcysteine and lung glutathione of patients with pulmonary fibrosis and normals Am J Respir Crit Care Med 19951521055-60 28 Behr J Degenkolb B Krombach F Vogelmeier C Intracellular glutathione and bronchoalveolar cells in fibrosing alveolitis effects of N-acetylcysteine Eur Respir J 200219906-11 29 Bando M Hosono T Mato N et al Long-term efficacy of inhaled N-acetylcysteine in patients with idiopathic pulmonary fibrosis Intern Med 2010492289-96 30 Demedts M Behr J Buhl R et al High-dose acetylcysteine in idiopathic pulmonary fibrosis N Engl J Med 20053532229-42 31 Toma TP Bhowmik A Rajakulasingam R Acetylcysteine in pulmonary fibrosis N Engl J Med 20063541086-9 author reply -9 32 Hunninghake GW Antioxidant therapy for idiopathic pulmonary fibrosis N Engl J Med 20053532285-7 33 Flaherty KR Mumford JA Murray S et al Prognostic implications of physiologic and radiographic changes in idiopathic interstitial pneumonia Am J Respir Crit Care Med 2003168543-8 34 Latsi PI du Bois RM Nicholson AG et al Fibrotic idiopathic interstitial pneumonia the prognostic value of longitudinal functional trends Am J Respir Crit Care Med 2003168531-7 35 Collard HR King TE Jr Bartelson BB Vourlekis JS Schwarz MI Brown KK Changes in clinical and physiologic variables predict survival in idiopathic pulmonary fibrosis Am J Respir Crit Care Med 2003168538-42 36 Jegal Y Kim DS Shim TS et al Physiology is a stronger predictor of survival than pathology in fibrotic interstitial pneumonia Am J Respir Crit Care Med 2005171639-44 37 Martinez FJ Safrin S Weycker D et al The clinical course of patients with idiopathic pulmonary fibrosis Ann Intern Med 2005142963-7 38 Hull JH Acetylcysteine in pulmonary fibrosis N Engl J Med 20063541089-91 author reply -91
70
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
39 Flaherty KR King TE Jr Raghu G et al Idiopathic interstitial pneumonia what is the effect of a multidisciplinary approach to diagnosis Am J Respir Crit Care Med 2004170904shy10 40 Raghu G Johnson WC Lockhart D Mageto Y Treatment of idiopathic pulmonary fibrosis with a new antifibrotic agent pirfenidone results of a prospective open-label Phase II study Am J Respir Crit Care Med 19991591061-9 41 Hunninghake GW Lynch DA Galvin JR et al Radiologic findings are strongly associated with a pathologic diagnosis of usual interstitial pneumonia Chest 20031241215-23 42 Lynch D Godwin J Safrin S et al High-resolution computed tomography in idiopathic pulmonary fibrosis diagnosis and prognosis Am J Respir Crit Care Med 2005172488-93 43 Mallinckrodt CH Watkin JG Molenberghs G Carroll RJ Choice of the primary analysis in longitudinal clinical trials Pharmaceutical Statistics 20043161-9 44 Bang H Tsiatis A Estimating medical costs with censored data Biometrika 200087329shy43 45 Lin DY Regression analysis of incomplete medical cost data Stat Med 2003221181-200 46 Rochon J Application of GEE procedures for sample size calculations in repeated measures experiments Stat Med 1998171643-58 47 Lachin JM Foulkes MA Evaluation of sample size and power for analyses of survival with allowance for nonuniform patient entry losses to follow-up noncompliance and stratification Biometrics 198642507-19
71
- PANTHER-IPFPREDNISONE AZATHIOPRINEAND N-ACETYLCYSTEINEA STUDY THAT EVALUATES RESPONSE INIDIOPATHIC PULMONARY FIBROSIS
-
- Protocol Summary
- Table of Contents
- List of Tables
- List of Figures
- List of Abbreviations
- 1 Summary
- 2 Hypotheses and Specific Aims
-
- 21 Null Hypothesis
- 22 Specific Aim 1
- 23 Specific Aim 2
- 24 Prespecified Subgroups of Interest
-
- 3 Background and Significance
-
- 31 Idiopathic Pulmonary Fibrosis is the Most Common Interstitial Lung Disease
- 32 Rationale for Placebo Control
- 33 Rationale for N-acetylcysteine
- 35 Rationale for N-acetylcysteine as a Stand-alone Therapy
- 36 Rationale for the Study Design and Primary Endpoint
- 37 Rationale for Blinding of Treatments
-
- 4 Methods
-
- 41 Inclusion Criteria
- 42 Diagnosis of IPF
- 43 Exclusion Criteria
- 44 Study Design and Study Visit
- 45 Dose Justification
- 46 Contraindications Precautions and Side Effects of Study Medications
- 47 Recruitment Procedures
- 48 Study Procedures
- 49 Concomitant Medications
- 410 Laboratory Testing
- 411 Blinding of Study Drugs
-
- 5 Study Endpoints
-
- 51 Primary Study Endpoint
- 52 Secondary Study Endpoints
-
- 6 Safety Evaluations and Procedures
-
- 61 Adverse Events
- 62 Clinical Medical Monitoring
- 63 Unblinding Procedures
-
- 7 Study Drug Procedures
- 8 Data Management
-
- 81 Hardware and Software Configuration
- 82 Sources of Data
-
- 9 Study Design and Data Analysis
-
- 91 General Analytic Considerations
- 92 Randomization Blinding and Reporting of Results
- 93 Stratification
- 94 Specification of the Primary Analyses
- 95 Analysis of Longitudinal Endpoints
- 96 Analysis of Binary Time-to-Event and Time-Lagged Endpoints
- 97 Power Analysis
-
- 10 Study Administration
-
- 101 Cooperative Agreement Mechanism
- 102 IPFnet Steering Group
- 103 Data and Safety Monitoring Board
- 104 Recommendations on Interim Monitoring of Efficacy Safety and Futility
-
- 11 Investigator and Sponsor Obligations
-
- 111 Monitoring
- 112 Cost and Payment
- 113 Confidentiality and Health Insurance Portability and Accountability ActConsiderations
- 114 Informed Consent Procedures
- 115 Institutional Review Boards
-
- 12 Investigator Agreement
- 13 References
-

PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
PHS Public Health Service (US)
PI principal investigator
PL placebo
PLT platelet
PRED prednisone
QOL quality of life
SAE serious adverse event
SAP statistical analysis plan
SGRQ St Georgersquos Respiratory Questionnaire
SpO2 oxygen saturation by pulse oximetry
TPMT thiopurine methyl transferase
UCSD SOBQ University of California at San Diego Shortness of Breath Questionnaire
UIP usual interstitial pneumonia
ULN upper limit of normal
USP United States Pharmacopoeia
VC vital capacity
WBC white blood cell
11
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
PREDNISONE AZATHIOPRINE AND N-ACETYLCYSTEINE A STUDY
THAT EVALUATES RESPONSE IN IDIOPATHIC PULMONARY FIBROSIS
1 Summary
There are currently no drug therapies that have proven to be effective in the treatment of idiopathic pulmonary
fibrosis (IPF) Previous clinical drug trials have been difficult to interpret due to lack of true placebo (PL)
controls or other methodological concerns Clinical efficacy of immunosuppressive therapies and agents that
reduce oxidative stress remains controversial The IPF Clinical Research Network (IPFnet) is conducting a
randomized double-blind placebo-controlled trial designed to assess the safety and efficacy of
N-acetylcysteine (NAC) as monotherapy in subjects with mild or moderate IPF
The study initially employed a 3-arm design with 111 randomization to NAC azathioprine (AZA)-prednisone
(PRED)-NAC and PL with each subject to be treated up to a maximum of 60 weeks followed by a tapering of
PREDPL and a 4-week period for safety evaluation Approximately 390 subjects who have mild to moderate
IPF (defined as forced vital capacity percent predicted [FVCpred] ge 50 and diffusing capacity of the lung
for carbon monoxide percent predicted [DLCOpred] 30) diagnosed within the past 48 months were to be
enrolled
At the pre-specified interim analysis the DSMB recommended termination of the prednisone-azathioprine-
NAC arm of the study No additional patients will be randomized to that arm However the NAC and placebo
arms remain open for enrollment and we will enroll approximately 130 subjects in each arm (inclusive of the
subjects enrolled at the time of the interim analysis) Follow up for subjects enrolled into the two arms will
continue for 60 weeks
The primary endpoint is the change in longitudinal measurements of FVC over the study period The primary
goal of this study to establish an evidence-based standard of care and clarify myths from facts for
pharmacotherapy of IPF has been met in part by demonstrating that the widely used triple therapy was harmful
to patients with IPF (NHLBI press release Oct 21 2011) To determine the potential therapeutic benefits of
NAC alone the study will continue to enroll patients as a two-arm double-blind placebo-controlled study from
this point on (NAC vs placebo) as recommended by the DSMB following the pre-specified interim analysis
12
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
2 Hypotheses and Specific Aims 21 Null Hypothesis
Treatment with NAC will provide the same efficacy as PL as measured by longitudinal changes in FVC
22 Specific Aim 1
This study is designed to assess the safety and efficacy of NAC in subjects with newly diagnosed IPF
23 Specific Aim 2
Secondary goals of this study are to assess differences between treatment groups for the following
1 Mortality
2 Time to death
3 Frequency of acute exacerbations (AExs)
4 Frequency of maintained FVC response
5 Time-to-disease progression
6 Change in DLCO
7 Change in Composite Physiologic Index (CPI)
8 Change in resting alveolar-arterial oxygen gradient
9 Change in 6-minute walk test (6MWT) distance
10 Change in 6MWT oxygen saturation area under the curve
11 Change in 6MWT distance to desaturation lt 80
12 Change in 6MWT minutes walked
13 Changes in health status as measured by the SF-36 EuroQol and St Georgersquos Respiratory
Questionnaire (SGRQ)
14 Changes in dyspnea as measured by the University of California at San Diego Shortness of Breath
Questionnaire (UCSD SOBQ)
15 Frequency and types of adverse events (AEs)
16 Frequency and types of respiratory complications both infectious and noninfectious
17 Frequency of hospitalizations both all-cause and respiratory-related
13
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
24 Prespecified Subgroups of Interest
Treatment effects will be estimated and compared within key subgroups
Higher enrollment FVC12
Typical vs atypical high-resolution computed tomography (HRCT) reading at baseline3
Recent vs more remote diagnosis (time from initial diagnosis of IPF le 1 year and gt 1 year)
Lower CPI score at enrollment4
Medical therapy for gastroesophageal reflux5
Ethnic background
Sex
Smoking history (current or ex-smoker vs never smoker) given potential impact on oxidant status6
Presence of emphysema gt 25 on HRCT
14
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
3 Background and Significance
31 Idiopathic Pulmonary Fibrosis is the Most Common Interstitial Lung Disease
IPF is the most common interstitial lung disease (ILD) of unknown etiology The current incidence and
prevalence of IPF in the United States are not known A 1994 study of a population-based registry of subjects in
Bernalillo County New Mexico USA estimated an incidence of 107 cases per 100000 per year for males and
74 cases per 100000 per year for females the prevalence of IPF was estimated at 20 per 100000 for males and
13 per 100000 for females7 Extrapolating from a large healthcare claims database a more recent review
estimated the prevalence of IPF in the United States at 427 per 100000 (incidence estimated at 163 per
100000 per year)8 Recent epidemiological studies indicate increasing mortality rates from IPF in the United
States and other industrialized nations9-12
Approximately two-thirds of subjects with IPF are over the age of 60 at the time of presentation and the
incidence increases with age13 IPF has no distinct geographical distribution and predilection by race or
ethnicity has not been identified13 Individual subjects may remain relatively stable for prolonged periods
experience very slow declines in lung function with progression of radiographic abnormalities for a period of
months to years or experience more rapid declines and subsequent death Only 20 to 30 of IPF patients
survive for 5 years following diagnosis
There is currently no proven effective pharmacological treatment for IPF13 Anti-inflammatory and
immunosuppressive agents have been the traditional approach to the management of patients with IPF Based
on the results of the interim analysis of the PANTHER-IPF trial this lsquotraditional approachrsquo will be aborted
However it remains unknown if NAC alone will prove beneficial in IPF patients The primary goal of the
modified study is to establish an evidence-based standard of care and clarify the role of this specific antioxidant
pharmacotherapy for IPF
32 Rationale for Placebo Control
IPF is a disorder for which there is no proven efficacious therapy A major objective of this trial is to test to the
greatest degree possible a proposed standard of care for patients with IPF The current traditional therapy
15
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
employs immunosuppressive and corticosteroid drugs Interim review of the original PANTHER-IPF study has
documented increased adverse events and lack of efficacy for AZA-PRED-NAC compared to placebo
suggesting that this therapeutic approach should not be employed Whether this applies to NAC alone which
has been advocated by international societies has not been proven in well-designed well-powered clinical
trials The recommendations made in the recently published evidence guidelines for NAC monotherapy was
weak based on low quality13 Thus this continued clinical trial randomizing patients to receive NAC or placebo
is pivotal and will answer the important question of the potential therapeutic benefits of NAC monotherapy with
grade A evidence In this prospective randomized clinical trial the inclusion of a PL arm is therefore vital to
adequately test the benefits of NAC in well-characterized subjects with IPF
If NAC has no true efficacy then its role as standard of care will be refuted If a benefit compared with PL is
confirmed it will establish a benchmark against which future novel therapies for IPF will be safely compared
As there is no currently accepted therapy for IPF there is an increasing body of published literature supporting
the concept of no treatment as the ldquobest carerdquo option for IPF13
Post hoc analyses of PL-controlled trials suggest that subjects with milder disease may be more amenable to
therapy12 It is notable that a recent international prospective randomized trial of interferon-gamma for IPF
also included a PL arm the study was terminated early by the data and safety monitoring board (DSMB) due to
lack of treatment effect1415 This underscores the belief that a proven effective therapy for IPF does not
currently exist and that true placebo-controlled trials remain the gold standard Similarly recently completed
trials of etanercept everolimus bosentan and BIPF 1120 in IPF have included PL-treated arms16-19 In three of
these trials the treated subjects showed little if any objective improvement Based on this evidence and the
current status of IPF therapy and therapeutic trials we believe that clinicians and subjects will continue to enroll
in a PL-controlled study
33 Rationale for N-acetylcysteine
NAC is a derivative of the amino acid L-cysteine NAC has been shown to augment levels of the naturally
occurring antioxidant glutathione (GSH ) (glutathione γ-glutamyl cysteinyl glycine) both in vitro and in
vivo2021 GSH is present in all eukaryotic cells and may play an important role in protecting alveolar epithelial
cells against oxidant injury The concentration of GSH in the bronchoalveolar lavage (BAL) fluid in patients
16
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
with IPF is markedly diminished compared with normal subjects This GSH deficiency may be corrected by
exogenous administration of NAC2122
There is evidence of enhanced production of oxidants in an IPF lung Both inflammatory cells and
myofibroblasts derived from patients with IPF generate increased amounts of extracellular oxidants including
hydrogen peroxide2324 Secretion of hydrogen peroxide by activated myofibroblasts may induce the death of
adjacent lung epithelial cells by paracrine mechanisms24 Additionally generation of oxidants by myofibroblasts
induces oxidative crosslinking of extracellular matrix proteins25 a potential mechanism for aberrant matrix
remodeling Thus an oxidant-antioxidant imbalance exists in the lungs of IPF patients26 NAC may confer
protection against this imbalance by augmenting GSH levels in addition to its more direct free-radical
scavenging activity
Intravenous (IV) NAC therapy has been shown to increase total BAL GSH in 8 IPF subjects27 Oral NAC (600
mg 3 times per day) has been shown to decrease markers of oxidant injury and improve both total and reduced
GSH levels in the epithelial lining fluid of subjects with IPF in a small uncontrolled study22 pulmonary
function improved modestly with therapy A similar study in 18 IPF subjects confirmed increased intracellular
GSH concentration after 12 weeks of NAC (600 mg 3 times per day)2228 no clinical correlates were reported
Inhaled NAC was suggested to improve pulmonary function in an open label study29
35 Rationale for N-acetylcysteine as a Stand-alone Therapy
Results of a double-blind multi-center European clinical trial of 150 IPF subjects testing combinations of AZAshy
PRED vs AZA-PRED-NAC have been reported30 NAC added to AZA-PRED (ldquoconventional therapyrdquo) had a
significant positive effect on DLCO (p lt 0005) and vital capacity (VC) (p lt 005) at the end of 1 year30 The
recent ATSERS position statement after much discussion concluded that NAC alone should not be considered
in the majority of patients with IPF without additional data from well-designed studies
The interpretation of these data has been quite controversial Some have suggested that the magnitude of the
treatment effect although statistically significant is modest31 Others have suggested that NAC may be
modulating potential toxic effects of AZA-PRED alone32 supporting the investigation of NAC as stand-alone
therapy
17
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
The IPFnet is now completing the PANTHER-IPF trial with a 11 randomization (NAC vs placebo) and a
simple practical feasible and scientifically rational design that will establish standard of care with NAC for
IPF based on a currently available therapeutic agent and the existing data to support its use We anticipate that
all future clinical trials of novel therapeutic agents will be tested against this to-be-established standard of care
36 Rationale for the Study Design and Primary Endpoint
The optimal study design of a therapeutic trial in IPF would include survival as a primary endpoint The
published results of the IFN-γ 1b Phase 3 (GIPF-001) trial suggested a survival benefit in subjects with milder
disease in retrospective analyses1 although the trial was underpowered to address this question This was likely
related to the limited mortality in the PL arm of the study which included IPF subjects with mild to moderate
disease This study documents that an IPF study powered to improve survival in a patient population with mild
disease requires a larger sample size andor duration of study In fact the recently aborted Phase 3 IFN-γ 1b
(GIPF-007 INSPIRE) study was a survival-based study and recruited more than 800 subjects at 75 centers
worldwide1415 As such within the context of the current IPFnet trial survival is an impractical primary
endpoint variable
Several groups have published data defining an appropriate surrogate outcome variable a 10 decrement in
FVC during 6 to 12 months is a powerful predictor of survival in IPF33-36 Furthermore additional evidence
suggests a similar predictive ability for a 10 decrement in FVC during 3 months of follow-up37 With strong
supportive evidence of FVC progression being related to mortality on a per-subject basis this study will use
FVC changes in liters between treatment groups as the primary endpoint Previously published IPF studies have
shown a steady decline in FVC (and FVCpred) among control group subjects230 The GIPF-001 study
suggested a 48-week decrease in FVC of 016 L in the PL-treated subjects The IFIGENIA study demonstrated
a decline in FVC of approximately 019 L over 52 weeks in the subjects randomized to the control treatment
Figure 1 depicts the change in FVC for control groups from previously published IPF studies38 Based on these
data we expect that the PL group will have a decline of 020 L over the 60-week study period The IPFnet
Steering Group determined that a clinically meaningful improvement would be the preservation of the majority
of the 020-L FVC decline Therefore a mean treatment difference of 015 L in mean FVC over the 60-week
study period was determined to be a clinically meaningful difference
18
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Δ f
rom
bas
elin
e (i
n L
)
01
005
0
-005
-01
-015 Projected Δ for placebo
-02
-025
-019
-016
-013 Pirfenidone GIPF001
NAC
Placebo
4 8 12 16 20 24 28 32 36 40 44 48 52 56 60
Week
Figure 1 Changes in FVC From Baseline in Prior IPF Clinical Trials
Recent data suggest that various patient subgroups would be expected to potentially exhibit differential response
to therapy These parameters will be used to a priori separate patients by a series of baseline characteristics
including
1 Higher enrollment FVC12
2 Typical vs atypical high-resolution computed tomography (HRCT) reading at baseline3
3 Recent vs more remote diagnosis (time from initial diagnosis of IPF le 1 year and gt 1 year)
4 Lower CPI score at enrollment4
5 Medical therapy for gastroesophageal reflux5
6 Ethnic background
7 Sex
8 Smoking history (current or ex-smoker vs never smoker) given potential impact on oxidant status6
9 Presence of emphysema gt 25 on HRCT
37 Rationale for Blinding of Treatments
The issue of treatment blinding was given a great deal of consideration with subject safety being the primary
concern After discussion among the Steering Group members it was decided that as long as subject safety
could be ensured blinding was necessary Blinding allows the study to
Have optimal scientific validity and potential to impact the standard of care for subjects
19
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Make objective assessments of treatment effects
Maintain clinical equipoise among investigators
Encourage subjects to have similar levels of contact with the medical community
Minimize the differential dropout rates across study arms
20
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
4 Methods 41 Inclusion Criteria
1 Age 35 to 85 years inclusive
2 FVC ge 50 of predicted (post-bronchodilator measurement from the screening visit)
3 DLCO ge 30 of predicted (hemoglobin corrected and altitude corrected if gt4000 ft above sea level)
4 Ability to understand and provide informed consent
5 Diagnosis of IPF according to a modified version of the ATS criteria le 48 months from enrollment The
date of diagnosis is defined as the date of the first available HRCT or surgical lung biopsy characteristic
of definite UIP
411 Subjects Shown to Have Usual Interstitial Pneumonia Pattern on Surgical Lung Biopsy
Subjects who have been shown to have UIP pattern on lung biopsy must have all of the following
1 Exclusion of other known causes of ILD such as drug toxicity clinically significant environmental
exposures or diagnosis of connective tissue diseases
2 Bibasilar reticular abnormalities with minimal ground glass opacities on HRCT scan
412 Subjects Who Have Not Undergone a Surgical Lung Biopsy
In addition to the criteria above these subjects must have radiological findings considered to be definite for the
diagnosis of UIPIPF
1 Bibasilar reticular abnormalities with minimal ground glass opacities
2 Honeycombing as the predominant feature and located in the peripheral lung bases
42 Diagnosis of IPF
Only subjects with definite IPF will be eligible for enrollment in this study We will utilize a combination of
clinicalphysiologic features HRCT and review of a clinically obtained surgical lung biopsy specimen to
establish the diagnosis of IPF An algorithm for the diagnosis is provided to guide entry into the protocol as
outlined in the inclusion and exclusion criteria (Figures 2 and 3) This multi-disciplinary approach uses
21
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
expertise from clinicians radiologists and pathologists Investigators at each site in conjunction with central
pathology will work together to establish the diagnosis of IPF This interactive approach to the diagnosis of IPF
increases the level of agreement between observers39
A subject with suspected ILD should be evaluated for secondary causes including but not limited to
environmental exposures drugs and systemic diseases Presence of any of these findings felt to be significant
enough to cause an ILD should disqualify the subject from entry into the trial
If secondary causes are absent an HRCT scan may be obtained If an HRCT of sufficiently high quality has
been obtained within the last 3 months that scan may be used for diagnosis In the appropriate clinical setting
the diagnosis of IPF can be made by the demonstration of a typical radiographic pattern on HRCT or by
demonstration of UIP pattern on a surgical lung biopsy The following criteria for a radiographic (ie
nonsurgical) diagnosis will be used In the absence of known exposures andor clinical associations attributable
to pulmonary fibrosis and in the appropriate clinical setting the presence of definite UIP pattern in HRCT
images is required to meet study criteria for the diagnosis of IPF
Figure 2 Diagnosis of Idiopathic Pulmonary Fibrosis in the IPFnet
22
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Figure 3 Pathology Flow Chart Surgical Lung Biopsy Diagnosis
Requirement for diagnosis
1 Clinical exclusion of other known causes (connective tissue diseases environmental and drug
exposures) of ILD
2 Radiographic HRCT with bibasilar reticular abnormality and honeycomb change with minimal
ground glass opacities
Appropriate clinical setting
1 Age gt 50 years
2 Insidious onset of unexplained dyspnea
3 Duration of illness for ge 3 months
4 Bibasilar inspiratory crackles
23
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Unlike the ATSERS consensus criteria published in 2000 bronchoscopy will not be required for diagnosis
This decision was made based on the experience of the IPFnet Steering Group members regarding the utility of
bronchoscopy in the diagnosis of IPF The presence of an atypical HRCT finding will require documentation of
a definitive diagnosis by surgical lung biopsy In fact this is in keeping with the recently published evidence
based guidelines for diagnosis and management of IPF13 As shown in Figure 3 central review of the pathology
data will be required for a diagnosis of IPF
We will not require central review of HRCT as several studies have shown that a confident local interpretation
of clinicalHRCT criteria as definite IPFUIP is associated with a high positive predictive value for finding UIP
at surgical lung biopsy (see Table 1) Differences in sensitivity in these series likely reflect subject selection as
Flaherty et al3 evaluated only UIP and nonspecific interstitial pneumonia (NSIP) while Raghu et al40 and
Hunninghake et al41 included a broader range of ILD
Table 1 Operating Characteristics of Local HRCT Review for Diagnosis of UIP
Researcher of Subjects Sensitivity () Specificity () PPV () NPV ()
Raghu et al 40
59 (29 UIP by SLB) 78 90 88 82
Hunninghake et al 41 91 (54 UIP by SLB)
74 81 85 67
Flaherty et al 3 96 (only NSIP amp UIP)
37 100 100 30
Abbreviations PPV positive predictive value NPV negative predictive value UIP usual interstitial pneumonia SLB surgical lung biopsy and NSIP nonspecific interstitial pneumonia
Furthermore an analysis of the HRCT scans from subjects enrolled in the GIPF-001 trial confirmed that local
site interpretations have a high congruity to a central radiology core In this multi-center study 263 HRCT
scans were read as definite IPF and a retrospective central radiology core review found 932 to be consistent
with IPF 42 We will also take several additional steps to insure that the local HRCT reads are accurate
including
1 A detailed training module has been developed and must be completed by each site radiologist before
site initiation
2 Clinical centers are to mail all HRCT scans to the HRCT core lab The first 10 HRCT scans from
subjects enrolled at each enrolling clinical center will be reviewed centrally to be certain that local reads
24
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
25
are congruent with a central interpretation If discrepancies are identified additional education will be
provided and HRCT scans will continue to be reviewed centrally until the central radiology core is
confident that the local center is performing appropriately
3 Random scans will be obtained from each center throughout the study to confirm that the local read
continues to agree with central interpretation If discrepancies are identified they will be addressed as in
2 above
In all cases if a subject has a surgical lung biopsy sample that sample will be reviewed by the local and central
pathologists Therefore the only cases that would not be subject to a direct central review process are those
where the HRCT meets the centrally defined criteria for an unequivocal diagnosis and a lung biopsy sample is
not available Table 2 below summarizes the possible combinations for making a diagnosis
Table 2 Combining HRCT and Pathology Interpretations to Determine if IPF is Present
HRCT Diagnosis Pathology Diagnosis Diagnosis of IPF
Definite UIP Definite UIP Yes
Definite UIP Probable UIP Yes
Definite UIP Possible UIP Yes
Definite UIP Not UIP No
Definite UIP Unavailable Yes
Consistent with UIP Definite UIP Yes
Consistent with UIP Probable UIP Yes
Consistent with UIP Possible UIP No
Consistent with UIP Not UIP No
Consistent with UIP Unavailable No
Inconsistent with UIP Any No
Abbreviations HRCT high-resolution computed tomography IPF idiopathic pulmonary fibrosis
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
UIP usual interstitial pneumonia Dx diagnosis 43 Exclusion Criteria
1 History of clinically significant environmental exposure known to cause pulmonary fibrosis
Occupational exposures such as asbestos or environmental exposure to organic dust such as occurs in
pigeon breeders may at times mimic the clinical and radiographic findings of IPF
2 Diagnosis of connective tissue disease felt by the principal investigator (PI) to be the etiology of the
interstitial disease Diagnosis of collagen-vascular conditions will be according to the published
American College of Rheumatology criteria As such the presence of any documented collagen-vascular
disorder or the presence of any suspicious symptom complex whether or not associated with
significantly abnormal rheumatological serologies will exclude the subject at the discretion of the PI
3 Extent of emphysema greater than the extent of fibrotic change (honeycombing reticular changes) on
HRCT scan
4 Forced expiratory volume in 1 second (FEV1)FVC ratio lt 065 at screening (postbronchodilator)
5 Partial pressure of arterial oxygen (PaO2) on room air lt 55 mm Hg (lt 50 mm Hg at Denver site)
6 Residual volume gt 120 predicted at screening (postbronchodilator)
7 Evidence of active infection
8 Significant bronchodilator response on screening spirometry defined as a change in FEV1 ge 12 and
absolute change gt 200 mL OR change in FVC ge 12 and absolute change gt 200 mL The percent
difference between the FVC (or FEV1) values will be calculated by taking the absolute value of the
difference and dividing it by the larger of the two FVC (or FEV1) values
9 Screening and enrollment post-bronchodilator FVC measurements (in liters) differing by gt 11 The
percent difference between the FVC values will be calculated by taking the absolute value of the
difference and dividing it by the larger of the two FVC values (eg the percent difference between FVC
measurements of 19 and 20 liters would be determined by taking the difference between the two (01
liters) and dividing by the larger of the two (20 liters) So 0120 = 5 and these FVC measurements
would not exclude the subject
10 Listed for lung transplantation ie the patient has completed the evaluation process has been accepted
as a candidate for transplantation at an appropriate center and is waiting to receive notification of an
available donor organ
11 History of unstable or deteriorating cardiac disease
12 Myocardial infarction coronary artery bypass or angioplasty within 6 months of screening
26
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
13 Unstable angina pectoris or congestive heart failure requiring hospitalization within 6 months of
screening
14 Uncontrolled arrhythmia
15 Severe uncontrolled hypertension
16 Known HIV or hepatitis C
17 Known cirrhosis and chronic active hepatitis
18 Active substance andor alcohol abuse (as determined by site PI)
19 Pregnancy or lactation (subjects who are pregnant or breastfeeding)
20 Known hypersensitivity to study medication
21 Any condition other than IPF that in the opinion of the site PI is likely to result in the death of the
subject within the next year
22 Any condition that in the judgment of the PI might cause participation in this study to be detrimental to
the subject or that the PI deems makes the subject a poor candidate
23 Any therapy directed at pulmonary fibrosis (excepting triple therapy of prednisone plus azathioprine
plus NAC) requires a 30-day washout period before randomized Triple therapy of lt= 12 weeks duration
in the past 4 years requires a 30-day washout period before randomization
24 History of triple therapy of prednisone plus azathioprine plus NAC for gt 12 weeksrsquo duration in the past
4 years or previous enrollment in the triple-therapy arm of the PANTHER-IPF study
44 Study Design and Study Visit
441 Study Design Summary
This study will be a randomized double-blind PL-controlled trial designed to assess the safety and efficacy of
NAC in subjects with newly diagnosed IPF
Subjects with mild to moderate IPF (defined as FVCpred ge 50 and DLCOpred ge 30) diagnosed within
the past 48 months will be enrolled Screening will continue until April 30 2012
27
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
The study will employ a 2-arm design with 11 randomization to NAC or PL Once enrolled subjects will visit
the clinical center at 15 weeks and 15-week intervals thereafter Each subject will be treated and followed for a
maximum of 60 weeks
During the 60-week visit subjects will be taken off all study agents Approximately four weeks after the final
dose of study agent is taken subjects will receive a safety phone call from the study site
442 Study Visits
Subjects who meet entry criteria will review the informed consent a written description of the purpose
procedures and risks of the study with the PI co-investigator or study coordinator and all questions will be
answered The informed consent form will be signed by the subject at screening No protocol-specific
procedures will be performed until the subject has signed and dated an informed consent form This includes the
screening procedures
4421 Screening
Once informed consent is obtained subjects may immediately begin the screening process or may return within
28 days of consent In the event a study subject has been clinically evaluated at the study site by an IPFnet study
physician and has performed testing within three weeks for this clinical evaluation that meets guidelines
provided in the IPFnet PANTHER-IPF Manual of Operating Procedures (MOOP) this testing may be used to
satisfy the following screening criteria medical history physical exam arterial blood gas (ABG) with A-a
gradient vital signs with oximetry body height and weight spirometry DLCO lung volumes and HRCT scan
Allowing the use of previously performed test results that meet study guidelines for the screening visit is
intended to permit subjects easier access to study entry to prevent subjects from repeating testing that has been
performed within the study window and to decrease risks to subjects from repeated exposure to procedures
such as arterial puncture and HRCT
The following procedures will be performed at screening
Medical history and a physical examination
28
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Measure height and weight
Serum pregnancy test (if applicable)
Measure vital signs including oximetry
Blood draws performed and the following analyses conducted
o Hematology (red cell count white cell count hemoglobin hematocrit cell indices differential
platelet count)
o Blood chemistries according to central laboratory protocol (see Section 410 Laboratory
Testing)
o Beta human chorionic gonadotropin (serum) pregnancy test (in women of childbearing potential)
o Urinalysis
Pulmonary Function Tests (PFTs) including spirometry pre- and post- bronchodilator and postshy
bronchodilator measurement of lung volumes and measurement of hemoglobin adjusted diffusing
capacity
Measure ABGs
HRCT if a satisfactory scan has not been performed on the subject within 3 months of screening (see
PANTHER-IPF MOOP for more details)
Surgical lung biopsies (if applicable) reviewed by local and central pathology departments
Current medications If required a washout period discussed with the subject and initiated at this visit
4422 Enrollment
The enrollment visit is expected to take place within eight weeks of the screening visit Enrollment visit
activities include
Measure vital signs including oximetry
Measure height and weight
Serum pregnancy test (if applicable)
If consent has been given blood will be drawn and a urine specimen collected for the bio-specimen
repository
Spirometry (post-bronchodilator)
Measure 6MWT with Borg Dyspnea Scale
29
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Collect Quality-of-life (QOL) data using the SF-36 EuroQol Investigating Choice Experiments for
Preferences of Older People Capability Instrument (ICE CAP) and SGRQ
Female subjects complete Gender Substudy questionnaire
Dyspnea status collected using the UCSD SOBQ
Evaluate Acute Exacerbation (AEx)
Review of any Adverse Events (AEs)
Review of concomitant medications
Subject receives diary and instructions on its purpose and proper use
Subject receives supply of study drug sufficient to last until his or her 15-week study visit
See the Schedule of Assessments (Table 3) for more details Subjects with screening and enrollment postshy
bronchodilator FVC measurements (in liters) differing by more than 11 are not eligible to be enrolled in the
study
Subjects will be asked to provide a physician of record This physician will be considered the subjectrsquos primary
care provider (PCP) and if the subject agrees the PCP will be informed by letter of the subjectrsquos enrollment in
the trial The subject will be informed that his or her ongoing medical care should be received from the PCP
The PCP will be informed of any safety issues identified by the study staff The PCP will also be given
information regarding communication with study personnel about pertinent health issues or clinic encounters
the subject may have
4423 Week 15
The week 15 visit is expected to occur within +- 14 days of the subjectrsquos scheduled visit time (eg the week 15
visit should occur anytime between 13 and 17 weeks after starting study drug Week 15 activities include
Measure vital signs with oximetry
Measurement height and weight
Serum pregnancy test (if applicable)
Spirometry (post-bronchodilator) measurement
Review of AEs
Evaluate for AEx
30
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Review concomitant medications
If consented draw blood and collect urine specimen for the biospecimen repository
Subjects return used and unused study drug for the visit
Review study diary and a new study diary will be given
Provide additional supply of study drug sufficient to last until the next scheduled visit
4424 Week 30
The week 30 visit is expected to occur within +- 14 days of the subjectrsquos scheduled visit time (eg the week 30
visit should occur anytime between 28 and 32 weeks after starting study drug) Week 30 activities include
Physical examination
Measure vital signs with oximetry
Measure height and weight
Laboratory values (complete blood count [CBC] and serum chemistries)
Serum pregnancy test (if applicable)
Measure spirometry (post-bronchodilator)
6MWT with Borg scale
DLCO
Review of AEs
Evaluate for AEx
Review concomitant medications
Complete all QOL and dyspnea questionnaires (EuroQol ICE CAP SF-36 SGRQ and UCSD SOBQ)
If consent has been given blood will be drawn and a urine specimen collected for the biospecimen
repository
Review study diary
Subjects return used and unused study drug for the visit
Provide additional supply of study drug sufficient to last until the next scheduled visit
4425 Week 45
31
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
The week 45 visit is expected to occur within +- 14 days of the subjectrsquos scheduled visit time (eg the week 45
visit should occur anytime between 43 and 47 weeks after starting study drug) Week 45 activities include
Measure vital signs with oximetry
Measure height and weight
Serum pregnancy test (if applicable)
Measure spirometry (post-bronchodilator)
Review of AEs
Evaluate for AEx
Review concomitant medications
If consent has been given blood will be drawn and a urine specimen collected for the biospecimen
repository
Subjects return used and unused study drug for the visit
Study diary reviewed
Provide additional supply of study drug sufficient to last until the next scheduled visit
4426 Week 60 (Early Withdrawal or Final Treatment Visit)
At week 60 or at subject withdrawal from the study (premature by study doctor or subjectrsquos decision) a final
treatment visit will occur At this final treatment visit subjects will discontinue NACPL abruptly Week 60
activities also include
Physical examination
Measure vital signs with oximetry
Measure height and weight
Laboratory values (complete blood count [CBC] and serum chemistries)
Spirometry (post-bronchodilator) measurement
6MWT with Borg scale measurement
DLCO
Lung volumes
ABG
Review of AEs
32
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Evaluate for AEx
Review concomitant medications
Subjects will complete all QOL and dyspnea questionnaires (EuroQol ICE CAP SF-36 SGRQ and
UCSD SOBQ)
If consent has been given blood will be drawn and a urine specimen collected for the biospecimen
repository
Subjects return used and unused study drug for the visit
Study diary reviewed
4427 Final Site Visit ndash FVC drop confirmation
In the event that the subject has a recorded FVC drop of gt10 from baseline at the final treatment visit and the
subject has not had a confirmation of such a drop at a previous study visit the subject should return to the
clinical site 6 to 8 weeks after the final treatment visit During this visit a post-bronchodilator spirometry test
will be performed This FVC measurement will be evaluated according to section 521 of this protocol
4428 Final Visit ndash Telephone Follow-up
Four weeks following the final dose of study medication subjects will receive a telephone call from the study
coordinator to ensure that there are no side effects and to follow up on any ongoing adverse events (AEs)
4429 Phone Contact Between Visits
At week 2 and each month that a subject does not have a scheduled clinical center visit his or her study
coordinator will contact him or her at least once by telephone to
Inquire if the subject has had any hospitalizations events that might be considered an AE or any events
significant enough to warrant an out-of-cycle visit to the clinical center
Remind subjects of their current dosage levels and confirm that the subject understands them
Address any questions or concerns the subject might have regarding other aspects of the study
Assess adherence to the treatment regimen by reviewing diary data verbal review of medications taken
including nutritional supplements
33
34
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Table 3 Schedule of Assessments
Procedure Screening Visit 0
Enrollment Visit 1
Week 15 Visit 2
Week 30Visit 3
Week 45 Visit 4
Week 60 Early
Withdrawal Visit 5
Final1
Visit (via phone)
Informed consent X
Medical history X
Inclusionexclusion criteria X
Serum pregnancy test (if applicable) X X X X X
Review of lung biopsy X
Arterial Blood Gas X X
6-Minute Walk Test
X
X X
Physical examination X X X
Vital signs with oximetry X X X X X X
Body height and weight X X X X X X
Complete Blood Count X X X
Chemistry panel X X X
Monitor Lab Values X X X
Urinalysis X Specimen repository substudy blood draw and urine collection (if consented)
X
X X X X
HRCT (if not completed within three months) X
Spirometry (pre- and post-bronchodilator) X
Spirometry (post-bronchodilator only) X X X X X
DLCO (post-bronchodilator only) X X X
Lung volumes (post-bronchodilator only) X
X
Evaluate for acute exacerbation X X X X X
Review Adverse Events X X X X X X
Review concomitant meds X X X X X X
Dispense subject diary X X X X
Review subject diary X X X X X
Dispense study agent X X X X
Gender Substudy questionnaire (female subjects only) X
EuroQol ICECAP UCSD SOBQ SGRQ SF-36 X X X
Abbreviations DLCO diffusing capacity of the lung for carbon monoxide QOL Quality of Life ICECAP Investigating Choice Experiments for Preferences of Older People UCSD SOBQ University of California Shortness of Breath Questionnaire SGRQ St Georgersquos Respiratory Questionnaire SF-36 Short Form 36 Health Survey
1Follow-up visit via phone will occur four weeks after final dose of study medication
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
45 Dose Justification
The general philosophy for determining dosing levels was to apply previously examined
treatment regimens With the focus of the study being to establish a standard of care for
mildmoderate IPF subjects the goal was to develop flexible yet standardized treatment rules that
allow for the temporary or permanent withholding of one or more components of treatment when
necessary Subjects developing laboratory abnormalities or symptoms that result in
discontinuation of one or more components of study treatment may continue on the other
components as long as there is no contraindication for this Complete follow-up is important for
the validity of any study As a strategy to maintain protocol adherence we are using a treatment
regimen that will detect potential side effects and prompt interventions proactively in the interest
of patient safety In addition subjects who permanently stop study medications during the course
of the study are encouraged to continue in the study completing all scheduled visits and tests
451 Rationale for N-acetylcysteine Dosing
To our knowledge there have been no IPF studies to correlate clinical outcome measures with
different dosages for NAC The dosage chosen is based on the IFIGENIA study However BAL
lung GSH levels from subjects with IPF have been augmented with the use of oral NAC at 600
mg 3 times per day In addition lung GSH levels have been associated with improved
PFTs212227 The dose chosen for this study was based on previous data including the IFIGENIA
study30
4511 Dosing of N-acetylcysteineplacebo
Dosing of NACPL will be 600 mg orally 3 times a day (1800 mgday)
4512 Reasons to Discontinue N-acetylcysteineplacebo
NACPL may be temporarily or permanently discontinued for the duration of the study for
gastrointestinal symptoms or dermatologic reactions
35
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Temporarily discontinue (hold) oral NACPL for subjects requiring inpatient admission for acute
exacerbation (AEx) or other conditions Resume NACPL after discharge
36
37
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
452 Dosage Algorithms
Dosage Adjustment Algorithm 1 NACPL Dose Modifications for Gastrointestinal Symptoms Nausea Vomiting Abdominal Discomfort Diarrhea
GI Symptoms determined by the PI to be clinically significant Nausea Vomiting Abdominal Discomfort Diarrhea
NACPL Temporarily dc (HOLD) x 3 Days
Monitor symptoms intervene as clinically indicated (eg fluid replacement antidiarrhea or antinausea medication)
Monitor or lab PRN
Are symptoms resolving after 3 days NO
Symptoms NOT resolving after 3 days of holding study medication Assessmentmanagement per clinical
discretion of investigator
Likely not study medication discuss resuming study medication with medical monitor when symptoms resolved
YES
Temporarily dc (HOLD) NACPL for 4 additional days (total hold 1 week) then NACPL Resume 600 MG TID
Did symptoms recur
YES
STOP NACPL for
duration of study
NO
NACPL No Change
38
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Dosage Adjustment Algorithm 2 NACPL Dose Modifications For Dermatologic Reactions
Dermatologic Reactions (Not Acneiform) ge Grade 2 Grading per Common Terminology Criteria for
Adverse Events V30 (httpctepcancergov) For example Grade 1 RASHDESQUAMATION Macular or papular eruption or erythema without associated symptoms Grade 2 RASHDESQUAMATION Macular or popular eruption or erythema with pruritus or other associated symptoms localized desquamation or other lesions covering lt50 of body surface area
NACPL Temporarily dc (HOLD) x 3 days
Are symptoms resolving after 3 days
NO Symptoms not resolving after 3 days of holding study medication Assessmentmanagement per clinical discretion of investigator Likely not study medication Discuss resuming study medication with medical monitor when symptoms
resolved YES
Temporarily dc (HOLD) NACPL for 4 additional days (total hold 1 week) then NACPL resume 600 MG TID
Did symptoms recur
YES
STOP NACPL for
duration of study
NO
NACPL No change
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
46 Contraindications Precautions and Side Effects of Study Medications
461 Contraindication
Contraindication to NAC is known hypersensitivity to it
462 Precautions
Concomitant administration of oral NAC and antibiotics has shown a slightly reduced absorption
of cephalexin and a slight increase in erythromycin serum levels NAC contains free sulfhydryl
groups There is no evidence that individuals sensitive to sulfa drugs are sensitive to NAC
The NAC preparation being administered in this study contains 20 mg of aspartame Because of
the phenylalanine component of aspartame individuals with phenylketonuria should avoid or
restrict aspartame intake to avoid increased blood levels of phenylalanine Because of this risk
labeling is required on all products containing aspartame
463 Side Effects
Side effects of NAC range from common to serious See Table 4
39
40
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Table 4 Side Effects of NAC
Undesirable Effects
System-organ class Uncommon
(gt11000 lt1100)
Rare
(gt110000 lt11000)
Very rare
(lt110000) Not known
Immune system disorders Hypersensitivity Anaphylactic shock
reaction
Nervous system disorders Headache
Ear and labyrinth disorders Tinnitus
Cardiac disorders Tachycardia
Vascular disorders Hemorrhage
Respiratory thoracic and
mediastinal disorders
Bronchospasm
Dyspnea
Gastrointestinal disorders
Vomiting diarrhea
stomatitis abdominal
pain nausea
Dyspepsia
Skin and subcutaneous tissue
disorders
Urticaria rash
angioedema itching
General disorders and
administration site conditions Pyrexia
Investigations Reduced arterial
pressure Face edema
In very rare cases the onset of severe skin reactions such as Stevens-Johnson syndrome and Lyell syndrome was reported to have a temporal relationship with N-acetylcysteine administration Although in most cases at least another suspect drug probably most involved in the genesis of the above mentioned mucocutaneous syndromes has been identified in case of mucocutaneous alterations it is appropriate to contact onersquos doctor and the administration of N-acetylcysteine should be immediately discontinued
Some studies confirmed a reduction of platelet aggregation during N-acetylcysteine administration The clinical significance of these findings has not been defined yet [Source Fluimucil Investigator Brochure]
47 Recruitment Procedures
Subjects recruited for this study will be established patients of the investigators or physician- or
self-referred to participating clinical centers in the IPFnet Each clinical center within IPFnet has
a well-developed infrastructure of local pulmonologists within the surrounding geographic area
These pulmonologists are kept informed of ongoing IPF clinical trials and regularly refer
subjects to studies conducted at IPFnet clinical centers
Additional steps will be taken to inform clinicians of the trials in progress within IPFnet
including presentations at faculty staff meetings at local hospitals medical grand rounds and
national conferences direct mail notification monthly faxes and advertisement of network trials
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
in pulmonary journals Clinical center patients previously diagnosed with IPF will be notified of
the trials by mail whenever possible
Recruitment of minorities and women will be monitored by the DCC and DSMB If necessary
additional recruitment efforts will be made at specific centers to ensure that the aggregate subject
sample contains appropriate representation of women and minorities
48 Study Procedures
The following procedures are detailed in the PANTHER-IPF MOOP accompanying this
protocol
1 PFT
2 ABG
3 HRCT scan of the chest (including imaging of pulmonary arteries)
4 CBC and serum chemistries
5 Pregnancy test
6 6MWTBorg Dyspnea Scale
7 QOL questionnaires (EuroQol HAD SF-36 SGRQ and ICE CAP)
8 UCSD SOBQ
9 Gender Substudy Questionnaire
All assessments of PFTs will be conducted by study personnel not directly involved in the
treatment of the subjects
481 Biological Specimen Management
4811 Biological Specimen Sample Management
Subjects at clinical centers participating in the specimen repository substudy who consent to
having blood drawn for research purposes and for the banking of blood blood components and
other biologic specimens (urine and BAL fluid) will have approximately 405 mL of blood
41
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
drawn 17 mL blood drawn for DNA and 20 mL of urine collected at enrollment visit Subjects
will have approximately 50 mL of blood drawn and 20 mL of urine collected at each 15-week
follow-up visit Blood specimens will be separated according to PANTHER-IPF MOOP
guidelines into the following components for banking in the repository serum plasma and
DNA Coding of all biologic specimens for the repository will be performed by study staff at the
clinical center The samples will be processed per PANTHER-IPF MOOP guidelines aliquoted
labeled with barcode labels and stored at -70degC at the clinical center and shipped to the central
repository
The only subject identifiers will be a sample ID number and subject initials This sample ID will
be linked in the IPFnet DCC clinical database to subject information No subject information will
be transferred to the biological-specimen database
The subjectrsquos samples may be used for approved sub-studies relating to human disease
including but not limited to IPF The studies for which an individualrsquos samples will be made
available will be determined by the subjectrsquos answers to questions on the biological-sample
informed consent form The subjects can choose to make their samples available for all options
or any combination Samples will be made available to researchers only with IPFnet Steering
Group approval until such time as the samples are made public through the NHLBI repository
49 Concomitant Medications
Concurrent treatment with FDA-approved therapy for IPF is allowed Colchicine may be used
for treatment of gout Temporary treatment with oral or IV corticosteroids for clinical worsening
or suspected AEx is permitted Nutritional supplements containing NAC are not allowed
410 Laboratory Testing
Clinical laboratory parameters will be assessed at screening and at the end of the study The
following tests will be performed at the two time points specified in the protocol chemistry (AG
ratio ALT [SGPT] AST [SGOT] albumin alkaline phosphatase amylase bilirubin-direct
42
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
bilirubin-indirect bilirubin-total BUN BUNcreatinine ratio calcium carbon dioxide
cholesterol-total chloride CPK-total creatinine GGT globulin glucose iron-total LDH
lipase magnesium phosphorus-inorganic potassium protein-total sodium TIBC triglycerides
uric acid) and hematology (red blood cell count WBC count hemoglobin hematocrit cell
indices differential platelet count)
411 Blinding of Study Drugs
Subjects and caregivers will be blinded to study treatment Every subject will receive NAC or
matching PLs at every study visit from the baseline visit to the week-45 visit No study agent
will be dispensed at the week-60 visit
43
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
5 Study Endpoints
51 Primary Study Endpoint
The primary endpoint will be the change in serial measurements of FVC over the study period
52 Secondary Study Endpoints
521 Time to Disease-progression
The time-to-death or a 10 decline in FVC will be defined as the time-to-disease progression
The 10 decline in FVC from enrollment must be confirmed on 2 consecutive visits no less than
6 weeks apart For subjects with 2 consecutive visits with a 10 decline in FVC the time-toshy
disease progression will be defined as the time interval between enrollment and the initial visit
with a 10 FVC decline For subjects who experience disease progression the study doctor will
determine whether or not the subject will remain in the study
522 Acute Exacerbations
The following 3 criteria will define AEx in subjects with acute worsening of their respiratory
conditions
1 Clinical (all of the following required)
A) Unexplained worsening of dyspnea or cough within 30 days triggering unscheduled
medical care (eg emergency room clinic study visit hospitalization)
B) No clinical suspicion or overt evidence of cardiac event pulmonary embolism or deep
venous thrombosis to explain acute worsening of dyspnea
C) No pneumothorax
44
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
2 RadiologicPhysiologic (A and B required)
A) New ground glass opacity or consolidation computed tomography (CT) scan OR new
alveolar opacities on chest x-ray
B) Decline of ge 5 in resting room air SpO2 from last recorded level OR decline of ge 8 mm
Hg in resting room air PaO2 from last recorded level
3 Microbiologic (all of the following required)
A) No clinical evidence for infection (ie absence of grossly purulent sputum fever gt 39degC
orally)
B) Lack of positive microbiological results (if done) from lower respiratory tract defined as
(1) Clinically significant bacterial growth on sputum or endotracheal aspirate cultures
(2) Quantitative culture by protected brush specimen ge 103 cfumL or BAL ge 104 cfumL
(3) The presence of specific pathogens on stains of any of the above
C) Lack of positive pathogen in blood cultures (if done)
Identification of Acute Exacerbations
All subjects will be educated about the importance of identifying AExs At the time of
enrollment subjects will be told about the possibility of developing acute symptomatic
worsening that might represent an AEx of IPF and instructed to contact their study clinical
center coordinator within 48 to 72 hours of the apparent event
All subjects will be contacted by phone monthly and questioned about any change in dyspnea or
cough and any interim clinic visits or hospitalizations Finally as part of the IPFnet outreach to
community referring physicians the importance of AExs will be emphasized When a subject is
identified who meets criterion 1A this will trigger the collection of additional clinical data to
evaluate a suspected AEx These data will be collected as part of standard clinical care (ie this
protocol does not require collection of all items) The additional items to be collected for
suspected AEx include
IPFnet AEx case report form (eCRF) (required)
45
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Chest x-ray CT scan withwithout pulmonary angiogram (reports should be faxed and
followed by the hard copiesdiscs)
Oxygen saturation (pulse oximetry)
ABG
Respiratory cultures (sputum endotracheal aspirate lavage)
Blood cultures
Clinichospital records related to the event
All potential cases of AEx will be reviewed by the clinical center PI first and a decision on
whether the case may represent an AEx will be made If AEx is suspected the case will be sent
to the IPFnet adjudication committee which will assign a final diagnosis (see Table 5) If there is
disagreement among members the majority opinion will be recorded
During episodes of suspected AEx as determined by the individual clinical center investigator
subjects will remain blinded and in the study
Table 5 Final Diagnoses in Evaluation of Suspected Acute Exacerbations
Definite acute exacerbation All criteria met no alternative etiology
Unclassifiable acute worsening
Insufficient data to evaluate all criteria no alternative etiology
Not acute exacerbation Alternative etiology identified that explains acute worsening
Management of the suspected AEx will be at the discretion of the treating physician Standard of
care generally involves evaluation for respiratory infection pulmonary embolism cardiac events
and pneumothorax and treatment with IV corticosteroids
Study drugs will be resumed at pre-suspected AEx doses after subjects clinically improve as
confirmed by the local PI All subjects should be seen at the clinical center within 2 to 4 weeks
of recovery for measurement of post-bronchodilator FVC (see Figure 4) Subjects unable to
return to the clinical center after suspected AEx due to medical frailty (eg continued
46
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
institutionalization progressive disability) will be categorized as failing to maintain FVC
response in secondary analyses
Suspected AEx (PI determined)
Hold study drug Treat AEx
(Attending physician determined)
Alive but unable to continue due to
medical frailty
Dead
Alive and able to continue
Site reviewvisit
Restart study drug
FVC within 2-4 weeks
Figure 4 Acute Exacerbation Flow Chart
523 Respiratory Infections
An upper respiratory infection will be defined as
Change in sputum discoloration
Increased cough of no more than 14 daysrsquo duration
A lower-respiratory infection (pneumonia) will be defined as new segmental or lobar airspace
opacities visualized by image studies (chest radiograph or HRCT) in addition to any of the
following
Positive pathogencultures in good sample of sputum or lower-airway secretions retrieved
by fiberoptic bronchoscope
Fever gt 39degC or gt 100degF
Leukocytosis gt 12000 (unexplained no increase in dose of corticosteroids)
47
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
524 Maintained FVC Response
Subjects with follow-up FVCpred measurements at or above their baseline FVCpred level
will be classified as having maintained FVC response Subjects with reduced FVCpred levels
or missing data for any reason including death or medical frailty will be classified as having not
maintained FVC response The FVCpred value is used because unadjusted FVC measurements
are expected to decline with age
48
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
6 Safety Evaluations and Procedures
61 Adverse Events
During a clinical trial the reporting of adverse experience information can lead to important
changes in the way a new treatment is developed as well as provide integral safety data
611 Definitions
An adverse event (AE) is any untoward medical occurrence in a subject or clinical investigation
subject who was administered a pharmaceutical product The AE does not necessarily have to
have a causal relationship with the drug administered An AE can be any unfavorable and
unintended sign (including an abnormal laboratory finding) symptom or disease temporarily
associated with the use of a medicinal product whether or not considered to be related to the
medicinal product Diseases signs symptoms or laboratory abnormalities already existing at
enrollment are not considered AEs unless they worsen (ie increase in intensity or frequency)
Surgical procedures themselves are not AEs they are therapeutic measures for conditions that
require surgery The condition for which the surgery is required may be an AE Surgical
procedures planned before randomization and the conditions necessitating the surgery are not
AEs
A serious adverse event is any untoward event that
Is fatal
Is life-threatening
Requires inpatient hospitalization or prolongation of existing hospitalization with the
following exceptions
o Preplanned (before the study) hospital admissions unless the hospitalization is
prolonged
o Planned admissions (as part of a study eg routine biopsies)
o Hospitalization lasting lt 24 hours
49
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
o Hospitalization for elective procedure
o Emergency room visits
Results in persistent or significant disability or incapacity
Is a congenital anomaly or birth defect
Important medical events that may not result in death be life-threatening or require
inpatient hospitalization may be considered serious adverse events (SAEs) when based
on appropriate medical judgment they may jeopardize the subject and may require
medical or surgical intervention to prevent one of the outcomes listed above
Life-threatening means that the subject was in the view of the investigator at immediate risk of
death from the AE as it occurred It does not include an AE that had it occurred in a more severe
form might have caused death
Persistent or significant disabilityincapacity means that the event resulted in permanent or
significant and substantial disruption of the subjectrsquos ability to carry out normal life functions
Causality
A reasonable possibility means the AE may have been caused byrelated to the study drug A
perceived or real lack of efficacy does not satisfy the definition of relatedness
612 Adverse Event (AE) Reporting
For the PANTHER-IPF trial all AEs (serious and nonserious) occurring from randomization
through final study visit (4 weeks after final dose of all study medication) will be recorded on the
AE page of the case report form (CRF)
6121 Serious Adverse Events (SAE) Reporting
For this trial all deaths and all SAEs which occur from randomization through final study visit
must be entered within the EDC system via the SAE eCRF page within 24 hours of the
investigative sitersquos knowledge of the event It is the responsibility of the clinical center
50
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
investigator to provide a causality assessment of the event for each study medications based upon
the information available at the time of the report It is understood that complete information
about the event may not be known at the time the initial report is submitted In the event the EDC
system is not accessible to the site at the time of event reporting investigative sites will complete
and forward a paper back-up SAE form to DCRI Safety Surveillance for processing
DCRI Safety Surveillance
Telephone 1-919-668-8624 or 1-866-668-7799 (toll free)
Fax 1-919-668-7138 or 1-866-668-7138 (toll free)
The investigator must complete and submit follow-up SAE information via the eCRF when
important new or follow-up information (eg final diagnosis outcome results of specific
investigations) becomes available Follow-up information should be submitted according to the
same process used for reporting the initial event as described above All SAEs will be followed
until resolution stabilization or 30 days after the subject has completed the final visit (4 weeks
after the final dose of study medication) whichever occurs first The investigator is responsible
for reporting SAEs to their institutional review board (IRB) per site specific IRB reporting
guidelines
6122 Regulatory Reporting
AEs that are serious study drug related and unexpected will be reported to the regulatory
authorities The DCRI Safety Surveillance medical monitor will perform a medical review of all
SAEs submitted and evaluate for ldquounexpectednessrdquo DCRI Safety Surveillance will prepare
MedWatch reports for those events identified as serious study drug related and unexpected as
determined by Safety Medical Monitor
DCRI Regulatory Services will submit all unexpected study drug-related SAEs as per 21 CFR
32 DCRI Safety Surveillance will provide a safety alert letter to the NHLBI DSMB and DCC
clinical operation (for distribution to sites) within 15 days of initial receipt of the information
51
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Investigators are responsible for promptly reporting these events to their reviewing IRBs
according to site specific IRB reporting guidelines
62 Clinical Medical Monitoring
There will be an unblinded physician at the IPFnet DCC serving as medical monitor The
medical monitor will be available to assist with questions about dosage adjustments of study
medications including discontinuation or resumption of medications
63 Unblinding Procedures
Unblinding of subjects or investigators to subject treatment is strongly discouraged For ongoing
clinical management all subjects should be presumed to be receiving ldquoactiverdquo study drug To
ensure the subjectrsquos safety the study treatment will be dose-adjusted based on laboratory test
results clinical findings and symptoms
The IPFnet DCC medical monitor and PANTHER-IPF co-chairs Drs Ganesh Raghu and
Fernando Martinez will be available to the study physicians to discuss study drug management
on a case-by-case basis Un-blinding will be considered ONLY when the knowledge of subject
treatment assignment is ABSOLUTELY ESSENTIAL for subject safety and after discussion of
the subjectrsquos case with the medical monitor and either Dr Raghu or Dr Martinez Unblinding of
study treatment should be minimized during the conduct of the trial In those cases where it is
felt to be medically necessary the DCC medical officer will communicate directly with the
managing physician to minimize unblinding of study personnel
52
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
7 Study Drug Procedures
At the baseline 15-week 30-week and 45-week study visits subjects will receive a supply of
study drug sufficient to last until the next visit at which study drug will be dispensed
53
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
8 Data Management
81 Hardware and Software Configuration
811 Hardware and Database Software
Data will be stored in an Oracle database system Oracle has advantages of processing efficiency
and smooth linkage with other software systems The application and database will be hosted on
Solaris Unix servers at the IPFnet DCC
812 Statistical Software
SAS will be used as the principal application for the management of analysis data files and
statistical computations S-Plus will be used to provide supplementary functions as needed
813 Access Control and Confidentiality Procedures
Access to databases will be controlled centrally by the IPFnet DCC through user passwords
linked to appropriate privileges This protects the data from unauthorized changes and
inadvertent loss or damage
814 Security
Database and Web servers will be secured by a firewall and through controlled physical access
Oracle has many security features to ensure that any staff member accessing the database has the
proper authority to perform the functions he or she requests of the system Within the secondary
SAS databases Unix group-access control maintains similar security The Sun workstation login
is secured by extensive user-password facilities under Unix
54
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
815 Back-up Procedures
Database back-up will be performed automatically every day and standard IPFnet DCC policies
and procedures will be applied to dictate tape rotation and retention practices
816 Virus Protection
All disk drives that provide network services and all user computers will be protected using
virus-scanning software Standard IPFnet DCC policies will be applied to update these protection
systems periodically through the study
82 Sources of Data
821 Design and Development
The IPFnet DCC will be responsible for development of the electronic case report forms
(eCRFs) development and validation of the clinical study database ensuring data integrity and
training clinical center staff on applicable data management procedures A web-based distributed
data entry model will be implemented This system will be developed to ensure that guidelines
and regulations surrounding the use of computerized systems used in clinical trials are upheld
The remainder of this section provides an overview of the data management plan associated with
this protocol
822 Data Collection Forms
The data collection process consists of direct data entry at the study clinical centers into the EDC
system(s) provided by the DCC A data collection worksheet will be provided to clinical centers
for recording data in the event the EDC system is unavailable Data entry of the eCRFs should
be completed according to the instructions provided and project specific training The
investigator is responsible for maintaining accurate complete and up-to-date records and for
ensuring the completion of the eCRFs for each research participant
55
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
823 Data Acquisition and Entry
Data entry into eCRFs shall be performed by authorized individuals Selected eCRFs may also
require the investigatorrsquos written signature or electronic signature as appropriate Electronic
CRFs will be monitored for completeness accuracy and attention to detail during the study
824 Data Center Responsibilities
The IPFnet DCC will 1) develop a data management plan and will conduct data management
activities 2) provide final eCRFs for the collection of all data required by the study 3) develop
data dictionaries for each eCRF that will comprehensively define each data element 4) conduct
ongoing data monitoring activities on study data 5) monitor any preliminary analysis data
cleanup activities and 6) rigorously monitor final study data clean up
825 Data Editing
Completed data will be entered into the IPFnet DCC automated data acquisition and
management system If incomplete or inaccurate data are found a data clarification request will
be generated and distributed to clinical centers for a response Clinical centers will resolve data
inconsistencies and errors and enter all corrections and changes into the IPFnet DCC automated
data acquisition and management system
826 Training
The training plan for clinical center staff includes provisions for training on assessments eCRF
completion guidelines data management procedures and the use of computerized systems
56
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
9 Study Design and Data Analysis
91 General Analytic Considerations
All primary analyses will be based on intent-to-treat (ITT) principles using all randomized
subjects Baseline factors across groups will be compared using mean (standard deviation) and
median (25th and 75th percentiles) summary measures Kaplan-Meier curves will be used to
display event rates Due to clinical interest in departures from both sides of the null hypothesis
all test statistics will be 2-sided
Reasonable caution needs to be taken when conducting multiple analyses on key clinical
subgroups For subgroup analyses a conservative significance level of 0001 will be used for all
interaction tests Thus subgroup comparisons will be considered exploratory unless the p-value
from the interaction test is smaller than 0001
92 Randomization Blinding and Reporting of Results
A permuted block-randomization scheme will be created with varying block sizes stratified by
clinical center Once a subject has completed the screening and baseline period and evaluation
for inclusionexclusion criteria the randomization process will begin Subjects will be
randomized to receive NAC or matching placebo with equal probability (11) via telephone
contact with a central interactive voice response system (IVRS) using a toll-free randomization
number On the day of randomization after the subject has successfully met all inclusion and
exclusion criteria the investigator or designee will call the central randomization number to
obtain the assigned kit randomization numbers for that subject At each subject visit the
investigator or designee will call the central randomization number to obtain the new kit
randomization numbers for resupply of the subject For resupply of the clinical center the IVRS
will monitor minimal volume of a kit type andor expiration date and will automatically notify
the pharmacy
57
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
The trial results will be reported according to guidelines specified in the CONSORT statement
A flow diagram describing screening recruitment randomization dropout and vital status will
be included in the primary manuscript AEs and efficacy data will be presented for all treatment
groups Adherence dropout and lost to follow-up will be carefully examined across all treatment
groups Analyses of safety will be based on data from all randomized subjects who received at
least one dose of study drug
93 Stratification
Subjects will be distributed to the two treatment arms in a 11 allocation ratio Stratification
blocks will be based on clinical centers
94 Specification of the Primary Analyses
A mixed model repeated measures (MMRM) analysis described in section 95 will be used to
compare differences in the slope of FVC measurements across the treatment groups Response
variables are values of the FVC measured at baseline and every 15 weeks until study completion
Variables in the model will include treatment time and time by treatment age sex race and
height Contrast estimates of differences in slopes of treatment over time (along with confidence
intervals) will be used to estimate the treatment effect The validity of this model in terms of
meeting modeling assumptions will be assessed via standard modeling diagnostics and goodness-
of-fit measures Based on the MMRM framework missing FVC data will not be imputed for the
primary analysis
95 Analysis of Longitudinal Endpoints
A common goal in clinical trials is to specify models that are easily implemented and
reproducible by independent data analysts On the other hand the models should have proper
statistical behavior in terms of low bias and high precision Many common approaches to
longitudinal data analysis including last observation carried forward (LOCF) imputation rely on
the missing completely at random (MCAR) assumption However the MCAR assumption is
58
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
unlikely to hold in many clinical trials because missing data are often related to disease
progression and prognosis A more reasonable assumption missing at random (MAR) specifies
that the complete data distribution can be modeled using only the observed data The likelihood-
based MMRM approach is valid under the more general MAR assumptions These models will
be applied to analyze the longitudinal data secondary endpoints
The advantages of MMRM analysis are that all important characteristics of the model can be preshy
specified standard software can be used to implement the models and results are based on ITT
principles43 In addition the MMRM approach offers superior control of Type I and Type II
errors compared with the LOCF approach
Response variables are values of the PFTs measured at enrollment and every 15 weeks until
study completion and 6MWT values measured at baseline week 30 and week 60 Covariates are
treatment time time by treatment and key baseline risk factors Contrasts (along with
confidence intervals) of treatment by time will be used to estimate the treatment effect
The correlation structure involves multiple pieces including measurement errors random
variation and interindividual variability For the longitudinal data analyses an unstructured
correlation matrix for within-subject errors will be assumed Other correlation structures
including compound symmetry will be examined as needed A careful examination of reasons
for study discontinuation will be conducted to assess the validity of MCAR Sensitivity analyses
will be used to examine the untestable assumption that the observed data violate the MAR
assumption The MMRM models will be implemented using PROC MIXED in SAS
96 Analysis of Binary Time-to-Event and Time-Lagged Endpoints
Regression modeling approaches using either the logistic regression model or Cox proportional
hazards regression model will be employed when appropriate The validity of these models will
be assessed via standard modeling diagnostics and goodness-of-fit measures Estimates of
cumulative frequencies for more general time-lagged responses will be calculated using the
partitioned version of the Bang-Tsiatis estimator44 The partitions will be set at 15-week intervals
59
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
to correspond with the data-collection process Covariate adjusted event rates will be calculated
using inverse probability-weighted regression estimates45
97 Power Analysis
971 Primary Analyses
Based on previously published IPF clinical trials the PL group is expected to experience a drop
in FVC of approximately 020 L over the study period (see Figure 1) The IPFnet Steering Group
determined a clinically important difference would be to preserve the majority of the decline
relative to PL over the study period In particular a treatment effect of 015 L was determined to
be a clinically meaningful difference Potential dropout is a key factor in the proposed study The
drop-out process assumed 5 lost to follow-up after every study visit Only 80 of subjects
were assumed to be followed for the entire study period All models assumed a compound
symmetry structure for the covariance matrix Power calculations were performed using a SAS
IML program for designing repeated measures studies46 Based on preliminary reviews of the
data from the University of Michigan the covariance matrix parameters were estimated at
approximately σ2 = 0757 (variance parameter) and ρ = 0936 (correlation parameter) To be
conservative the power calculations for the primary analysis were performed with parameter
setting of σ2 = 0810 (variance parameter) and ρ = 0925 (correlation parameter)
The power calculations assume a correction for imperfect compliance proposed by Lachin and
Foulkes to allow for 2 noncompliance for each of the treatment arms47 Thus the sample size
of 130 subjects per arm would be reduced to an adjusted sample size of 130(1-002-002)2 =
1198 or 120 subjects per arm
Under the assumed Type I error rate of 005 with a correlation parameter of 0925 and standard
deviation of 090 the difference of 015 L (or 00025 Lweek) shown in Table 6 would have
power of 93
60
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Table 6 Hypothetical Values of Mean FVC (L) Change from Baseline
Week 15 Week 30 Week 45 Week 60
NAC 00125 00250 00375 00500
Placebo 00500 01000 01500 02000
Difference 00375 00750 01125 01500
Abbreviations FVC forced vital capacity PL placebo
972 Power Analysis for Secondary Endpoints
Power calculations for secondary endpoint measurements are shown in Table 7 Standard
deviations are based on unpublished data provided by the University of Michigan The
calculations are based on a 2-sample t-test with Type I error rate set at 005 These calculations
are likely to be conservative because the statistical approach described in section 95 for
analyzing these endpoints will incorporate incomplete observations as well as intermediate data
points
Table 7 Detectable Differences in Treatment Means for Selected Endpoint Measurements
Secondary Endpoints Std Dev
of the Baseline Score
Detectable Difference for 80 Power
Std Dev of the Change Score
Difference Detectable for
80 Power
DLCOpred 166 58 91 32
6MWT Area Under the Desaturation Curve
219 76 175 61
6MWT Distance to Desaturation 224 78 315 110
6MWT Minutes Walked 210 073 205 071
Abbreviations Std Dev standard deviation DLCOpred diffusing capacity of the lung for carbon monoxide percent predicted 6MWT 6-minute walk test
61
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
10 Study Administration
101 Cooperative Agreement Mechanism
The administrative and funding mechanism used to undertake this project is a ldquocooperative
agreementrdquo (U01) which is an assistance mechanism Under the cooperative agreement the
NHLBI assists supports andor stimulates the project and is substantially involved with
investigators in conducting the study by facilitating performance of the effort in a ldquopartnerrdquo role
The NHLBI project scientist serves on the IPFnet Steering Group and he or another NHLBI
scientist may serve on other project committees when appropriate At the same time however
NHLBI does not assume a dominant role direction or prime responsibility for this research
program
As described below governance of the project is conducted through the IPFnet Steering Group
Principal investigators have lead responsibilities in all aspects of their trials and the project
including any modification of trial designs conduct of the trials quality control data analysis
and interpretation preparation of publications and collaboration with other investigators unless
otherwise provided for by the IPFnet Steering Group
PIs retain custody of and have primary rights to their center-specific and collaborative data
subject to government rights-of-access consistent with current Health amp Human Services (HHS)
Public Health Service (PHS) and National Institutes of Health policies The protocols and
governance policies call for the continual submission of data centrally to the IPFnet DCC for the
collaborative database which at a minimum will contain the key variables selected by the IPFnet
Steering Group for standardization across all clinical centers the submission of copies of the
collaborative datasets to each PI upon completion of the project procedures for data analysis
reporting and publication and procedures to protect and ensure the privacy of medical and
genetic data and records of individuals The NHLBI project scientist on behalf of the NHLBI
will have the same access privileges and responsibilities regarding the collaborative data as the
other members of the Steering Group
62
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
PIs are also encouraged to publish and to publicly release and disseminate results data and other
products of the project concordant with the project protocols and governance and the approved
plan for making data and materials available to the scientific community and to the NHLBI
However during the 3 years after the ending date of NHLBI project support unpublished data
unpublished results data sets not previously released and other study materials or products are
to be made available to any third party only with the approval of the IPFnet Steering Group
Upon completion of the project PIs are expected to put their intervention materials and
procedure manuals into the public domain andor make them available to other investigators
according to the approved plan for making data and materials available to the scientific
community and the NHLBI for the conduct of research at no charge other than the costs of
reproduction and distribution
The NHLBI reserves the right to terminate or curtail the project (or an individual award) in the
event of (a) failure to develop or implement mutually agreeable collaborative measurement
subject eligibility and data management sections of the protocols (b) substantial shortfall in
subject recruitment follow-up data reporting or quality control or other major breach of
protocol (c) substantive changes in the agreed-upon protocols with which NHLBI cannot
concur (d) reaching a major project outcome with persuasive statistical significance
substantially before schedule or (e) human subject ethical issues that may dictate a premature
termination
Any disagreement that may arise in scientificprogrammatic matters (within the scope of the
award) between award recipients and the NHLBI may be brought to arbitration An arbitration
panel will be composed of 3 membersmdash1 selected by the IPFnet Steering Group (with the
NHLBI member not voting) or by the individual PI in the event of an individual disagreement a
second selected by NHLBI and the third selected by the other 2 members This special
arbitration procedure in no way affects the PIrsquos right to appeal an adverse action that is otherwise
appealable in accordance with the PHS regulations at 42 CFR part 50 Subpart D and HHS
63
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
regulation at 45 CFR part 16 or the rights of the NHLBI under applicable statutes regulations
and terms of the award
102 IPFnet Steering Group
The IPFnet Steering Group is the main governing body of the project It is composed of the PIs
of the clinical centers the PI of the DCC and the NHLBI project scientist The clinical centers
the IPFnet DCC and the NHLBI each have 1 vote on the IPFnet Steering Group All decisions
are determined by majority vote
All major scientific decisions are determined by the IPFnet Steering Group It assumes overall
responsibility for the design and conduct of the trial It appoints (and disbands) committees and
subcommittees as the need arises designs approves and implements the study protocols
oversees the development of the MOOP monitors subject recruitment and treatment delivery
evaluates data collection and management oversees quality assurance procedures and
implements changes and enhancements to the study as required It also has primary responsibility
for facilitating the conduct of the trials and reporting the projectrsquos results
103 Data and Safety Monitoring Board
The NHLBI will establish a DSMB in accordance with established policies (see
httpwwwnhlbinihgovfundingpoliciesdsmb_insthtm) to ensure data quality and subject
safety and to provide independent advice to the NHLBI regarding progress and the
appropriateness of study continuation
104 Recommendations on Interim Monitoring of Efficacy Safety and Futility
First and foremost the role of the DSMB will be to review subject safety and trial conduct at
periodic points during the study The DSMB may require analyses of the primary endpoint
results for comparing the benefit and risks of treatment strategies The benefit of collecting
additional data on key secondary endpoints with extended follow-up and establishing a robust
64
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
evidence base for determining a standard of care will need to be carefully considered before
early termination of one or more treatment arms After careful consideration the IPFnet Steering
Group recommends conservative thresholds for the early examinations of the safety and efficacy
data
The DSMB will be expected to meet approximately every 6 months until trial completion to
review safety and toxicity data The DSMB may recommend stopping the study based on these
reviews Because the DSMB could stop the trial for safety concerns as well as for a large
efficacy benefit there could be multiple opportunities to reject the null hypothesis (no difference
in event rates between the PL and NAC groups) A Bonferroni approximation will be applied
during the one planned interim analysis for efficacy
Before locking the database a statistical analysis plan (SAP) will be developed to provide
complete details on the statistical analysis The SAP will include the specifics for how and when
the DSMB will be notified for AEs The IPFnet DCC will deliver to the DSMB all FDA-defined
AEs at 3-month intervals The IPFnet DCC will prepare narrative SAE reports in real time for
DSMB review including recommendations and analysis of similar events for each SAE
submitted to the FDA
65
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
11 Investigator and Sponsor Obligations
111 Monitoring
All monitoring activities for US clinical centers will be performed in accordance with DCRI
standard operating procedures Information regarding the types of visits will be outlined in the
PANTHER-IPF MOOP
112 Cost and Payment
There will be no cost to subjects enrolled in this trial Study-related procedures will be paid for
by the IPFnet
Subjects may be eligible for reimbursement for travel to the clinical center Details of payment
will be explained to each subject during the consent process
113 Confidentiality and Health Insurance Portability and Accountability Act
Considerations
Subject confidentiality will be protected throughout the study All subject data will be kept
strictly confidential and no subject-identifying information will be released to anyone outside
the project Confidentiality will be assured through several mechanisms First each subject will
be assigned an anonymous study ID which will then be used on all study forms Second any
study forms blood samples and paper records that contain subject information (eg address lists
phone lists) will be kept at the clinical centers in secured locked areas coded by number Once
blood is collected there will be no subject identifiers placed on blood samplesmdashonly the study
ID number and the date of sample collection Third access to all subject data and information
including laboratory specimens will be restricted to authorized personnel In the case of
computerized data this restricted access will be assured through user logon IDs and password
protection
66
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
At the IPFnet DCC only authorized personnel will have access to the data files containing study
data Security will be assured through user logon IDs passwords and appropriate access
privileges All study subjects will be identified only by their IPFnet ID numbers and no personal
identifying information such as name address or Social Security number will be entered into
the IPFnet DCC database Any subject-specific data reported to the IPFnet Steering Group will
be identified only by the IPFnet ID number
Finally subjects will not be identified by name in any reports or publications nor will the data
be presented in such a way that the identity of individual subjects can be inferred Analysis files
created for further study by the scientific community will have no subject identifiers These data
files will be created in accordance with the Ancillary Studies and Publication Policy of the
IPFnet
114 Informed Consent Procedures
All IPFnet subjects will provide written informed consent using procedures reviewed and
approved by each clinical centerrsquos IRB Informed consent will be undertaken by study personnel
in-person with the subject The subject has the option of declining further participation in the
study at that point No further study procedures will be conducted until the signed documents
have been provided to the IPFnet clinical center
115 Institutional Review Boards
Before initiating this study the protocol clinical center-specific informed consent forms Health
Insurance Portability and Accountability Act (HIPAA) forms recruitment materials and other
relevant information will be reviewed by a properly constituted IRB at each participating clinical
center A copy of the signed and dated IRB approval at each clinical center will be retrieved prior
to or during the site initiation visit and archived at the IPFnet DCC Any amendments to the
protocol other than simple administrative and typographical changes must be approved by each
IRB before they are implemented The clinical centers will seek annual renewals of their IRB
approvals in accordance with local procedures
67
__________________________________________ ________________
__________________________________________
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
12 Investigator Agreement
I have read the foregoing protocol PANTHER-IPF and agree that it contains all necessary
details for carrying out this study I will conduct the study as outlined herein and will complete
the study within the time designated
I will provide copies of the protocol and all pertinent information to all individuals responsible to
me who assist in the conduct of this study I will discuss this material with them to ensure they
are fully informed regarding the drug and the conduct of the study
I will fulfill all responsibilities for submitting pertinent information to the local IRB if
applicable that is responsible for this study
I further agree that NHLBI andor DCRI will have access to any source documents from which
eCRF information may have been generated
Signature of Principal Investigator Date
Name of Principal Investigator (printed or typed)
Protocol version date May 19 2009
Protocol Amendment 1 version date May 28 2010
Protocol Amendment 2 version date December 6 2011
68
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
13 References
1 Raghu G Brown KK Bradford WZ et al A placebo-controlled trial of interferon gamma-1b in patients with idiopathic pulmonary fibrosis N Engl J Med 2004350125-33 2 King TE Jr Safrin S Starko KM et al Analyses of efficacy end points in a controlled trial of interferon-gamma1b for idiopathic pulmonary fibrosis Chest 2005127171-7 3 Flaherty KR Thwaite EL Kazerooni EA et al Radiological versus histological diagnosis in UIP and NSIP survival implications Thorax 200358143-8 4 Wells AU Desai SR Rubens MB et al Idiopathic pulmonary fibrosis a composite physiologic index derived from disease extent observed by computed tomography Am J Respir Crit Care Med 2003167962-9 5 Raghu G Freudenberger TD Yang S et al High prevalence of abnormal acid gastroshyoesophageal reflux in idiopathic pulmonary fibrosis Eur Respir J 200627136-42 6 Kinnula VL Focus on antioxidant enzymes and antioxidant strategies in smoking related airway diseases Thorax 200560693-700 7 Coultas DB Zumwalt RE Black WC Sobonya RE The epidemiology of interstitial lung diseases Am J Respir Crit Care Med 1994150967-72 8 Raghu G Weycker D Edelsberg J Bradford WZ Oster G Incidence and prevalence of idiopathic pulmonary fibrosis Am J Respir Crit Care Med 2006174810-6 9 Olson AL Swigris JJ Lezotte DC Norris JM Wilson CG Brown KK Mortality from pulmonary fibrosis increased in the United States from 1992 to 2003 Am J Respir Crit Care Med 2007176277-84 10 Mannino DM Etzel RA Parrish RG Pulmonary fibrosis deaths in the United States 1979shy1991 An analysis of multiple-cause mortality data Am J Respir Crit Care Med 19961531548shy52 11 Hubbard R Johnston I Coultas DB Britton J Mortality rates from cryptogenic fibrosing alveolitis in seven countries Thorax 199651711-6 12 Johnston I Britton J Kinnear W Logan R Rising mortality from cryptogenic fibrosing alveolitis Bmj 19903011017-21 13 Raghu G Collard HR Egan JJ et al An official ATSERSJRSALAT statement idiopathic pulmonary fibrosis evidence-based guidelines for diagnosis and management Am J Respir Crit Care Med 2011183788-824 14 (USA) FDA FDA Public Health Advisory Interferon gamma-1b (marketed as Actimmune) In 2007 15 King TE Jr Pardo A Selman M Idiopathic pulmonary fibrosis Lancet 2011 16 Raghu G Brown KK Costabel U et al Treatment of idiopathic pulmonary fibrosis with etanercept an exploratory placebo-controlled trial Am J Respir Crit Care Med 2008178948shy55 17 Malouf MA Hopkins P Snell G Glanville AR An investigator-driven study of everolimus in surgical lung biopsy confirmed idiopathic pulmonary fibrosis Respirology 201116776-83 18 King TE Jr Behr J Brown KK et al BUILD-1 a randomized placebo-controlled trial of bosentan in idiopathic pulmonary fibrosis Am J Respir Crit Care Med 200817775-81 19 Richeldi L Costabel U Selman M et al Efficacy of a tyrosine kinase inhibitor in idiopathic pulmonary fibrosis N Engl J Med 20113651079-87
69
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
20 Borok Z Buhl R Grimes GJ et al Effect of glutathione aerosol on oxidant-antioxidant imbalance in idiopathic pulmonary fibrosis Lancet 1991338215-6 21 Meyer A Buhl R Magnussen H The effect of oral N-acetylcysteine on lung glutathione levels in idiopathic pulmonary fibrosis Eur Respir J 19947431-6 22 Behr J Maier K Degenkolb B Krombach F Vogelmeier C Antioxidative and clinical effects of high-dose N-acetylcysteine in fibrosing alveolitis Adjunctive therapy to maintenance immunosuppression Am J Respir Crit Care Med 19971561897-901 23 Cantin AM North SL Fells GA Hubbard RC Crystal RG Oxidant-mediated epithelial cell injury in idiopathic pulmonary fibrosis J Clin Invest 1987791665-73 24 Waghray M Cui Z Horowitz JC et al Hydrogen peroxide is a diffusible paracrine signal for the induction of epithelial cell death by activated myofibroblasts Faseb J 200519854-6 25 Larios JM Budhiraja R Fanburg BL Thannickal VJ Oxidative protein cross-linking reactions involving L-tyrosine in transforming growth factor-beta1-stimulated fibroblasts J Biol Chem 200127617437-41 26 Kinnula VL Fattman CL Tan RJ Oury TD Oxidative stress in pulmonary fibrosis a possible role for redox modulatory therapy Am J Respir Crit Care Med 2005172417-22 27 Meyer A Buhl R Kampf S Magnussen H Intravenous N-acetylcysteine and lung glutathione of patients with pulmonary fibrosis and normals Am J Respir Crit Care Med 19951521055-60 28 Behr J Degenkolb B Krombach F Vogelmeier C Intracellular glutathione and bronchoalveolar cells in fibrosing alveolitis effects of N-acetylcysteine Eur Respir J 200219906-11 29 Bando M Hosono T Mato N et al Long-term efficacy of inhaled N-acetylcysteine in patients with idiopathic pulmonary fibrosis Intern Med 2010492289-96 30 Demedts M Behr J Buhl R et al High-dose acetylcysteine in idiopathic pulmonary fibrosis N Engl J Med 20053532229-42 31 Toma TP Bhowmik A Rajakulasingam R Acetylcysteine in pulmonary fibrosis N Engl J Med 20063541086-9 author reply -9 32 Hunninghake GW Antioxidant therapy for idiopathic pulmonary fibrosis N Engl J Med 20053532285-7 33 Flaherty KR Mumford JA Murray S et al Prognostic implications of physiologic and radiographic changes in idiopathic interstitial pneumonia Am J Respir Crit Care Med 2003168543-8 34 Latsi PI du Bois RM Nicholson AG et al Fibrotic idiopathic interstitial pneumonia the prognostic value of longitudinal functional trends Am J Respir Crit Care Med 2003168531-7 35 Collard HR King TE Jr Bartelson BB Vourlekis JS Schwarz MI Brown KK Changes in clinical and physiologic variables predict survival in idiopathic pulmonary fibrosis Am J Respir Crit Care Med 2003168538-42 36 Jegal Y Kim DS Shim TS et al Physiology is a stronger predictor of survival than pathology in fibrotic interstitial pneumonia Am J Respir Crit Care Med 2005171639-44 37 Martinez FJ Safrin S Weycker D et al The clinical course of patients with idiopathic pulmonary fibrosis Ann Intern Med 2005142963-7 38 Hull JH Acetylcysteine in pulmonary fibrosis N Engl J Med 20063541089-91 author reply -91
70
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
39 Flaherty KR King TE Jr Raghu G et al Idiopathic interstitial pneumonia what is the effect of a multidisciplinary approach to diagnosis Am J Respir Crit Care Med 2004170904shy10 40 Raghu G Johnson WC Lockhart D Mageto Y Treatment of idiopathic pulmonary fibrosis with a new antifibrotic agent pirfenidone results of a prospective open-label Phase II study Am J Respir Crit Care Med 19991591061-9 41 Hunninghake GW Lynch DA Galvin JR et al Radiologic findings are strongly associated with a pathologic diagnosis of usual interstitial pneumonia Chest 20031241215-23 42 Lynch D Godwin J Safrin S et al High-resolution computed tomography in idiopathic pulmonary fibrosis diagnosis and prognosis Am J Respir Crit Care Med 2005172488-93 43 Mallinckrodt CH Watkin JG Molenberghs G Carroll RJ Choice of the primary analysis in longitudinal clinical trials Pharmaceutical Statistics 20043161-9 44 Bang H Tsiatis A Estimating medical costs with censored data Biometrika 200087329shy43 45 Lin DY Regression analysis of incomplete medical cost data Stat Med 2003221181-200 46 Rochon J Application of GEE procedures for sample size calculations in repeated measures experiments Stat Med 1998171643-58 47 Lachin JM Foulkes MA Evaluation of sample size and power for analyses of survival with allowance for nonuniform patient entry losses to follow-up noncompliance and stratification Biometrics 198642507-19
71
- PANTHER-IPFPREDNISONE AZATHIOPRINEAND N-ACETYLCYSTEINEA STUDY THAT EVALUATES RESPONSE INIDIOPATHIC PULMONARY FIBROSIS
-
- Protocol Summary
- Table of Contents
- List of Tables
- List of Figures
- List of Abbreviations
- 1 Summary
- 2 Hypotheses and Specific Aims
-
- 21 Null Hypothesis
- 22 Specific Aim 1
- 23 Specific Aim 2
- 24 Prespecified Subgroups of Interest
-
- 3 Background and Significance
-
- 31 Idiopathic Pulmonary Fibrosis is the Most Common Interstitial Lung Disease
- 32 Rationale for Placebo Control
- 33 Rationale for N-acetylcysteine
- 35 Rationale for N-acetylcysteine as a Stand-alone Therapy
- 36 Rationale for the Study Design and Primary Endpoint
- 37 Rationale for Blinding of Treatments
-
- 4 Methods
-
- 41 Inclusion Criteria
- 42 Diagnosis of IPF
- 43 Exclusion Criteria
- 44 Study Design and Study Visit
- 45 Dose Justification
- 46 Contraindications Precautions and Side Effects of Study Medications
- 47 Recruitment Procedures
- 48 Study Procedures
- 49 Concomitant Medications
- 410 Laboratory Testing
- 411 Blinding of Study Drugs
-
- 5 Study Endpoints
-
- 51 Primary Study Endpoint
- 52 Secondary Study Endpoints
-
- 6 Safety Evaluations and Procedures
-
- 61 Adverse Events
- 62 Clinical Medical Monitoring
- 63 Unblinding Procedures
-
- 7 Study Drug Procedures
- 8 Data Management
-
- 81 Hardware and Software Configuration
- 82 Sources of Data
-
- 9 Study Design and Data Analysis
-
- 91 General Analytic Considerations
- 92 Randomization Blinding and Reporting of Results
- 93 Stratification
- 94 Specification of the Primary Analyses
- 95 Analysis of Longitudinal Endpoints
- 96 Analysis of Binary Time-to-Event and Time-Lagged Endpoints
- 97 Power Analysis
-
- 10 Study Administration
-
- 101 Cooperative Agreement Mechanism
- 102 IPFnet Steering Group
- 103 Data and Safety Monitoring Board
- 104 Recommendations on Interim Monitoring of Efficacy Safety and Futility
-
- 11 Investigator and Sponsor Obligations
-
- 111 Monitoring
- 112 Cost and Payment
- 113 Confidentiality and Health Insurance Portability and Accountability ActConsiderations
- 114 Informed Consent Procedures
- 115 Institutional Review Boards
-
- 12 Investigator Agreement
- 13 References
-

PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
PREDNISONE AZATHIOPRINE AND N-ACETYLCYSTEINE A STUDY
THAT EVALUATES RESPONSE IN IDIOPATHIC PULMONARY FIBROSIS
1 Summary
There are currently no drug therapies that have proven to be effective in the treatment of idiopathic pulmonary
fibrosis (IPF) Previous clinical drug trials have been difficult to interpret due to lack of true placebo (PL)
controls or other methodological concerns Clinical efficacy of immunosuppressive therapies and agents that
reduce oxidative stress remains controversial The IPF Clinical Research Network (IPFnet) is conducting a
randomized double-blind placebo-controlled trial designed to assess the safety and efficacy of
N-acetylcysteine (NAC) as monotherapy in subjects with mild or moderate IPF
The study initially employed a 3-arm design with 111 randomization to NAC azathioprine (AZA)-prednisone
(PRED)-NAC and PL with each subject to be treated up to a maximum of 60 weeks followed by a tapering of
PREDPL and a 4-week period for safety evaluation Approximately 390 subjects who have mild to moderate
IPF (defined as forced vital capacity percent predicted [FVCpred] ge 50 and diffusing capacity of the lung
for carbon monoxide percent predicted [DLCOpred] 30) diagnosed within the past 48 months were to be
enrolled
At the pre-specified interim analysis the DSMB recommended termination of the prednisone-azathioprine-
NAC arm of the study No additional patients will be randomized to that arm However the NAC and placebo
arms remain open for enrollment and we will enroll approximately 130 subjects in each arm (inclusive of the
subjects enrolled at the time of the interim analysis) Follow up for subjects enrolled into the two arms will
continue for 60 weeks
The primary endpoint is the change in longitudinal measurements of FVC over the study period The primary
goal of this study to establish an evidence-based standard of care and clarify myths from facts for
pharmacotherapy of IPF has been met in part by demonstrating that the widely used triple therapy was harmful
to patients with IPF (NHLBI press release Oct 21 2011) To determine the potential therapeutic benefits of
NAC alone the study will continue to enroll patients as a two-arm double-blind placebo-controlled study from
this point on (NAC vs placebo) as recommended by the DSMB following the pre-specified interim analysis
12
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
2 Hypotheses and Specific Aims 21 Null Hypothesis
Treatment with NAC will provide the same efficacy as PL as measured by longitudinal changes in FVC
22 Specific Aim 1
This study is designed to assess the safety and efficacy of NAC in subjects with newly diagnosed IPF
23 Specific Aim 2
Secondary goals of this study are to assess differences between treatment groups for the following
1 Mortality
2 Time to death
3 Frequency of acute exacerbations (AExs)
4 Frequency of maintained FVC response
5 Time-to-disease progression
6 Change in DLCO
7 Change in Composite Physiologic Index (CPI)
8 Change in resting alveolar-arterial oxygen gradient
9 Change in 6-minute walk test (6MWT) distance
10 Change in 6MWT oxygen saturation area under the curve
11 Change in 6MWT distance to desaturation lt 80
12 Change in 6MWT minutes walked
13 Changes in health status as measured by the SF-36 EuroQol and St Georgersquos Respiratory
Questionnaire (SGRQ)
14 Changes in dyspnea as measured by the University of California at San Diego Shortness of Breath
Questionnaire (UCSD SOBQ)
15 Frequency and types of adverse events (AEs)
16 Frequency and types of respiratory complications both infectious and noninfectious
17 Frequency of hospitalizations both all-cause and respiratory-related
13
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
24 Prespecified Subgroups of Interest
Treatment effects will be estimated and compared within key subgroups
Higher enrollment FVC12
Typical vs atypical high-resolution computed tomography (HRCT) reading at baseline3
Recent vs more remote diagnosis (time from initial diagnosis of IPF le 1 year and gt 1 year)
Lower CPI score at enrollment4
Medical therapy for gastroesophageal reflux5
Ethnic background
Sex
Smoking history (current or ex-smoker vs never smoker) given potential impact on oxidant status6
Presence of emphysema gt 25 on HRCT
14
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
3 Background and Significance
31 Idiopathic Pulmonary Fibrosis is the Most Common Interstitial Lung Disease
IPF is the most common interstitial lung disease (ILD) of unknown etiology The current incidence and
prevalence of IPF in the United States are not known A 1994 study of a population-based registry of subjects in
Bernalillo County New Mexico USA estimated an incidence of 107 cases per 100000 per year for males and
74 cases per 100000 per year for females the prevalence of IPF was estimated at 20 per 100000 for males and
13 per 100000 for females7 Extrapolating from a large healthcare claims database a more recent review
estimated the prevalence of IPF in the United States at 427 per 100000 (incidence estimated at 163 per
100000 per year)8 Recent epidemiological studies indicate increasing mortality rates from IPF in the United
States and other industrialized nations9-12
Approximately two-thirds of subjects with IPF are over the age of 60 at the time of presentation and the
incidence increases with age13 IPF has no distinct geographical distribution and predilection by race or
ethnicity has not been identified13 Individual subjects may remain relatively stable for prolonged periods
experience very slow declines in lung function with progression of radiographic abnormalities for a period of
months to years or experience more rapid declines and subsequent death Only 20 to 30 of IPF patients
survive for 5 years following diagnosis
There is currently no proven effective pharmacological treatment for IPF13 Anti-inflammatory and
immunosuppressive agents have been the traditional approach to the management of patients with IPF Based
on the results of the interim analysis of the PANTHER-IPF trial this lsquotraditional approachrsquo will be aborted
However it remains unknown if NAC alone will prove beneficial in IPF patients The primary goal of the
modified study is to establish an evidence-based standard of care and clarify the role of this specific antioxidant
pharmacotherapy for IPF
32 Rationale for Placebo Control
IPF is a disorder for which there is no proven efficacious therapy A major objective of this trial is to test to the
greatest degree possible a proposed standard of care for patients with IPF The current traditional therapy
15
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
employs immunosuppressive and corticosteroid drugs Interim review of the original PANTHER-IPF study has
documented increased adverse events and lack of efficacy for AZA-PRED-NAC compared to placebo
suggesting that this therapeutic approach should not be employed Whether this applies to NAC alone which
has been advocated by international societies has not been proven in well-designed well-powered clinical
trials The recommendations made in the recently published evidence guidelines for NAC monotherapy was
weak based on low quality13 Thus this continued clinical trial randomizing patients to receive NAC or placebo
is pivotal and will answer the important question of the potential therapeutic benefits of NAC monotherapy with
grade A evidence In this prospective randomized clinical trial the inclusion of a PL arm is therefore vital to
adequately test the benefits of NAC in well-characterized subjects with IPF
If NAC has no true efficacy then its role as standard of care will be refuted If a benefit compared with PL is
confirmed it will establish a benchmark against which future novel therapies for IPF will be safely compared
As there is no currently accepted therapy for IPF there is an increasing body of published literature supporting
the concept of no treatment as the ldquobest carerdquo option for IPF13
Post hoc analyses of PL-controlled trials suggest that subjects with milder disease may be more amenable to
therapy12 It is notable that a recent international prospective randomized trial of interferon-gamma for IPF
also included a PL arm the study was terminated early by the data and safety monitoring board (DSMB) due to
lack of treatment effect1415 This underscores the belief that a proven effective therapy for IPF does not
currently exist and that true placebo-controlled trials remain the gold standard Similarly recently completed
trials of etanercept everolimus bosentan and BIPF 1120 in IPF have included PL-treated arms16-19 In three of
these trials the treated subjects showed little if any objective improvement Based on this evidence and the
current status of IPF therapy and therapeutic trials we believe that clinicians and subjects will continue to enroll
in a PL-controlled study
33 Rationale for N-acetylcysteine
NAC is a derivative of the amino acid L-cysteine NAC has been shown to augment levels of the naturally
occurring antioxidant glutathione (GSH ) (glutathione γ-glutamyl cysteinyl glycine) both in vitro and in
vivo2021 GSH is present in all eukaryotic cells and may play an important role in protecting alveolar epithelial
cells against oxidant injury The concentration of GSH in the bronchoalveolar lavage (BAL) fluid in patients
16
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
with IPF is markedly diminished compared with normal subjects This GSH deficiency may be corrected by
exogenous administration of NAC2122
There is evidence of enhanced production of oxidants in an IPF lung Both inflammatory cells and
myofibroblasts derived from patients with IPF generate increased amounts of extracellular oxidants including
hydrogen peroxide2324 Secretion of hydrogen peroxide by activated myofibroblasts may induce the death of
adjacent lung epithelial cells by paracrine mechanisms24 Additionally generation of oxidants by myofibroblasts
induces oxidative crosslinking of extracellular matrix proteins25 a potential mechanism for aberrant matrix
remodeling Thus an oxidant-antioxidant imbalance exists in the lungs of IPF patients26 NAC may confer
protection against this imbalance by augmenting GSH levels in addition to its more direct free-radical
scavenging activity
Intravenous (IV) NAC therapy has been shown to increase total BAL GSH in 8 IPF subjects27 Oral NAC (600
mg 3 times per day) has been shown to decrease markers of oxidant injury and improve both total and reduced
GSH levels in the epithelial lining fluid of subjects with IPF in a small uncontrolled study22 pulmonary
function improved modestly with therapy A similar study in 18 IPF subjects confirmed increased intracellular
GSH concentration after 12 weeks of NAC (600 mg 3 times per day)2228 no clinical correlates were reported
Inhaled NAC was suggested to improve pulmonary function in an open label study29
35 Rationale for N-acetylcysteine as a Stand-alone Therapy
Results of a double-blind multi-center European clinical trial of 150 IPF subjects testing combinations of AZAshy
PRED vs AZA-PRED-NAC have been reported30 NAC added to AZA-PRED (ldquoconventional therapyrdquo) had a
significant positive effect on DLCO (p lt 0005) and vital capacity (VC) (p lt 005) at the end of 1 year30 The
recent ATSERS position statement after much discussion concluded that NAC alone should not be considered
in the majority of patients with IPF without additional data from well-designed studies
The interpretation of these data has been quite controversial Some have suggested that the magnitude of the
treatment effect although statistically significant is modest31 Others have suggested that NAC may be
modulating potential toxic effects of AZA-PRED alone32 supporting the investigation of NAC as stand-alone
therapy
17
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
The IPFnet is now completing the PANTHER-IPF trial with a 11 randomization (NAC vs placebo) and a
simple practical feasible and scientifically rational design that will establish standard of care with NAC for
IPF based on a currently available therapeutic agent and the existing data to support its use We anticipate that
all future clinical trials of novel therapeutic agents will be tested against this to-be-established standard of care
36 Rationale for the Study Design and Primary Endpoint
The optimal study design of a therapeutic trial in IPF would include survival as a primary endpoint The
published results of the IFN-γ 1b Phase 3 (GIPF-001) trial suggested a survival benefit in subjects with milder
disease in retrospective analyses1 although the trial was underpowered to address this question This was likely
related to the limited mortality in the PL arm of the study which included IPF subjects with mild to moderate
disease This study documents that an IPF study powered to improve survival in a patient population with mild
disease requires a larger sample size andor duration of study In fact the recently aborted Phase 3 IFN-γ 1b
(GIPF-007 INSPIRE) study was a survival-based study and recruited more than 800 subjects at 75 centers
worldwide1415 As such within the context of the current IPFnet trial survival is an impractical primary
endpoint variable
Several groups have published data defining an appropriate surrogate outcome variable a 10 decrement in
FVC during 6 to 12 months is a powerful predictor of survival in IPF33-36 Furthermore additional evidence
suggests a similar predictive ability for a 10 decrement in FVC during 3 months of follow-up37 With strong
supportive evidence of FVC progression being related to mortality on a per-subject basis this study will use
FVC changes in liters between treatment groups as the primary endpoint Previously published IPF studies have
shown a steady decline in FVC (and FVCpred) among control group subjects230 The GIPF-001 study
suggested a 48-week decrease in FVC of 016 L in the PL-treated subjects The IFIGENIA study demonstrated
a decline in FVC of approximately 019 L over 52 weeks in the subjects randomized to the control treatment
Figure 1 depicts the change in FVC for control groups from previously published IPF studies38 Based on these
data we expect that the PL group will have a decline of 020 L over the 60-week study period The IPFnet
Steering Group determined that a clinically meaningful improvement would be the preservation of the majority
of the 020-L FVC decline Therefore a mean treatment difference of 015 L in mean FVC over the 60-week
study period was determined to be a clinically meaningful difference
18
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Δ f
rom
bas
elin
e (i
n L
)
01
005
0
-005
-01
-015 Projected Δ for placebo
-02
-025
-019
-016
-013 Pirfenidone GIPF001
NAC
Placebo
4 8 12 16 20 24 28 32 36 40 44 48 52 56 60
Week
Figure 1 Changes in FVC From Baseline in Prior IPF Clinical Trials
Recent data suggest that various patient subgroups would be expected to potentially exhibit differential response
to therapy These parameters will be used to a priori separate patients by a series of baseline characteristics
including
1 Higher enrollment FVC12
2 Typical vs atypical high-resolution computed tomography (HRCT) reading at baseline3
3 Recent vs more remote diagnosis (time from initial diagnosis of IPF le 1 year and gt 1 year)
4 Lower CPI score at enrollment4
5 Medical therapy for gastroesophageal reflux5
6 Ethnic background
7 Sex
8 Smoking history (current or ex-smoker vs never smoker) given potential impact on oxidant status6
9 Presence of emphysema gt 25 on HRCT
37 Rationale for Blinding of Treatments
The issue of treatment blinding was given a great deal of consideration with subject safety being the primary
concern After discussion among the Steering Group members it was decided that as long as subject safety
could be ensured blinding was necessary Blinding allows the study to
Have optimal scientific validity and potential to impact the standard of care for subjects
19
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Make objective assessments of treatment effects
Maintain clinical equipoise among investigators
Encourage subjects to have similar levels of contact with the medical community
Minimize the differential dropout rates across study arms
20
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
4 Methods 41 Inclusion Criteria
1 Age 35 to 85 years inclusive
2 FVC ge 50 of predicted (post-bronchodilator measurement from the screening visit)
3 DLCO ge 30 of predicted (hemoglobin corrected and altitude corrected if gt4000 ft above sea level)
4 Ability to understand and provide informed consent
5 Diagnosis of IPF according to a modified version of the ATS criteria le 48 months from enrollment The
date of diagnosis is defined as the date of the first available HRCT or surgical lung biopsy characteristic
of definite UIP
411 Subjects Shown to Have Usual Interstitial Pneumonia Pattern on Surgical Lung Biopsy
Subjects who have been shown to have UIP pattern on lung biopsy must have all of the following
1 Exclusion of other known causes of ILD such as drug toxicity clinically significant environmental
exposures or diagnosis of connective tissue diseases
2 Bibasilar reticular abnormalities with minimal ground glass opacities on HRCT scan
412 Subjects Who Have Not Undergone a Surgical Lung Biopsy
In addition to the criteria above these subjects must have radiological findings considered to be definite for the
diagnosis of UIPIPF
1 Bibasilar reticular abnormalities with minimal ground glass opacities
2 Honeycombing as the predominant feature and located in the peripheral lung bases
42 Diagnosis of IPF
Only subjects with definite IPF will be eligible for enrollment in this study We will utilize a combination of
clinicalphysiologic features HRCT and review of a clinically obtained surgical lung biopsy specimen to
establish the diagnosis of IPF An algorithm for the diagnosis is provided to guide entry into the protocol as
outlined in the inclusion and exclusion criteria (Figures 2 and 3) This multi-disciplinary approach uses
21
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
expertise from clinicians radiologists and pathologists Investigators at each site in conjunction with central
pathology will work together to establish the diagnosis of IPF This interactive approach to the diagnosis of IPF
increases the level of agreement between observers39
A subject with suspected ILD should be evaluated for secondary causes including but not limited to
environmental exposures drugs and systemic diseases Presence of any of these findings felt to be significant
enough to cause an ILD should disqualify the subject from entry into the trial
If secondary causes are absent an HRCT scan may be obtained If an HRCT of sufficiently high quality has
been obtained within the last 3 months that scan may be used for diagnosis In the appropriate clinical setting
the diagnosis of IPF can be made by the demonstration of a typical radiographic pattern on HRCT or by
demonstration of UIP pattern on a surgical lung biopsy The following criteria for a radiographic (ie
nonsurgical) diagnosis will be used In the absence of known exposures andor clinical associations attributable
to pulmonary fibrosis and in the appropriate clinical setting the presence of definite UIP pattern in HRCT
images is required to meet study criteria for the diagnosis of IPF
Figure 2 Diagnosis of Idiopathic Pulmonary Fibrosis in the IPFnet
22
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Figure 3 Pathology Flow Chart Surgical Lung Biopsy Diagnosis
Requirement for diagnosis
1 Clinical exclusion of other known causes (connective tissue diseases environmental and drug
exposures) of ILD
2 Radiographic HRCT with bibasilar reticular abnormality and honeycomb change with minimal
ground glass opacities
Appropriate clinical setting
1 Age gt 50 years
2 Insidious onset of unexplained dyspnea
3 Duration of illness for ge 3 months
4 Bibasilar inspiratory crackles
23
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Unlike the ATSERS consensus criteria published in 2000 bronchoscopy will not be required for diagnosis
This decision was made based on the experience of the IPFnet Steering Group members regarding the utility of
bronchoscopy in the diagnosis of IPF The presence of an atypical HRCT finding will require documentation of
a definitive diagnosis by surgical lung biopsy In fact this is in keeping with the recently published evidence
based guidelines for diagnosis and management of IPF13 As shown in Figure 3 central review of the pathology
data will be required for a diagnosis of IPF
We will not require central review of HRCT as several studies have shown that a confident local interpretation
of clinicalHRCT criteria as definite IPFUIP is associated with a high positive predictive value for finding UIP
at surgical lung biopsy (see Table 1) Differences in sensitivity in these series likely reflect subject selection as
Flaherty et al3 evaluated only UIP and nonspecific interstitial pneumonia (NSIP) while Raghu et al40 and
Hunninghake et al41 included a broader range of ILD
Table 1 Operating Characteristics of Local HRCT Review for Diagnosis of UIP
Researcher of Subjects Sensitivity () Specificity () PPV () NPV ()
Raghu et al 40
59 (29 UIP by SLB) 78 90 88 82
Hunninghake et al 41 91 (54 UIP by SLB)
74 81 85 67
Flaherty et al 3 96 (only NSIP amp UIP)
37 100 100 30
Abbreviations PPV positive predictive value NPV negative predictive value UIP usual interstitial pneumonia SLB surgical lung biopsy and NSIP nonspecific interstitial pneumonia
Furthermore an analysis of the HRCT scans from subjects enrolled in the GIPF-001 trial confirmed that local
site interpretations have a high congruity to a central radiology core In this multi-center study 263 HRCT
scans were read as definite IPF and a retrospective central radiology core review found 932 to be consistent
with IPF 42 We will also take several additional steps to insure that the local HRCT reads are accurate
including
1 A detailed training module has been developed and must be completed by each site radiologist before
site initiation
2 Clinical centers are to mail all HRCT scans to the HRCT core lab The first 10 HRCT scans from
subjects enrolled at each enrolling clinical center will be reviewed centrally to be certain that local reads
24
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
25
are congruent with a central interpretation If discrepancies are identified additional education will be
provided and HRCT scans will continue to be reviewed centrally until the central radiology core is
confident that the local center is performing appropriately
3 Random scans will be obtained from each center throughout the study to confirm that the local read
continues to agree with central interpretation If discrepancies are identified they will be addressed as in
2 above
In all cases if a subject has a surgical lung biopsy sample that sample will be reviewed by the local and central
pathologists Therefore the only cases that would not be subject to a direct central review process are those
where the HRCT meets the centrally defined criteria for an unequivocal diagnosis and a lung biopsy sample is
not available Table 2 below summarizes the possible combinations for making a diagnosis
Table 2 Combining HRCT and Pathology Interpretations to Determine if IPF is Present
HRCT Diagnosis Pathology Diagnosis Diagnosis of IPF
Definite UIP Definite UIP Yes
Definite UIP Probable UIP Yes
Definite UIP Possible UIP Yes
Definite UIP Not UIP No
Definite UIP Unavailable Yes
Consistent with UIP Definite UIP Yes
Consistent with UIP Probable UIP Yes
Consistent with UIP Possible UIP No
Consistent with UIP Not UIP No
Consistent with UIP Unavailable No
Inconsistent with UIP Any No
Abbreviations HRCT high-resolution computed tomography IPF idiopathic pulmonary fibrosis
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
UIP usual interstitial pneumonia Dx diagnosis 43 Exclusion Criteria
1 History of clinically significant environmental exposure known to cause pulmonary fibrosis
Occupational exposures such as asbestos or environmental exposure to organic dust such as occurs in
pigeon breeders may at times mimic the clinical and radiographic findings of IPF
2 Diagnosis of connective tissue disease felt by the principal investigator (PI) to be the etiology of the
interstitial disease Diagnosis of collagen-vascular conditions will be according to the published
American College of Rheumatology criteria As such the presence of any documented collagen-vascular
disorder or the presence of any suspicious symptom complex whether or not associated with
significantly abnormal rheumatological serologies will exclude the subject at the discretion of the PI
3 Extent of emphysema greater than the extent of fibrotic change (honeycombing reticular changes) on
HRCT scan
4 Forced expiratory volume in 1 second (FEV1)FVC ratio lt 065 at screening (postbronchodilator)
5 Partial pressure of arterial oxygen (PaO2) on room air lt 55 mm Hg (lt 50 mm Hg at Denver site)
6 Residual volume gt 120 predicted at screening (postbronchodilator)
7 Evidence of active infection
8 Significant bronchodilator response on screening spirometry defined as a change in FEV1 ge 12 and
absolute change gt 200 mL OR change in FVC ge 12 and absolute change gt 200 mL The percent
difference between the FVC (or FEV1) values will be calculated by taking the absolute value of the
difference and dividing it by the larger of the two FVC (or FEV1) values
9 Screening and enrollment post-bronchodilator FVC measurements (in liters) differing by gt 11 The
percent difference between the FVC values will be calculated by taking the absolute value of the
difference and dividing it by the larger of the two FVC values (eg the percent difference between FVC
measurements of 19 and 20 liters would be determined by taking the difference between the two (01
liters) and dividing by the larger of the two (20 liters) So 0120 = 5 and these FVC measurements
would not exclude the subject
10 Listed for lung transplantation ie the patient has completed the evaluation process has been accepted
as a candidate for transplantation at an appropriate center and is waiting to receive notification of an
available donor organ
11 History of unstable or deteriorating cardiac disease
12 Myocardial infarction coronary artery bypass or angioplasty within 6 months of screening
26
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
13 Unstable angina pectoris or congestive heart failure requiring hospitalization within 6 months of
screening
14 Uncontrolled arrhythmia
15 Severe uncontrolled hypertension
16 Known HIV or hepatitis C
17 Known cirrhosis and chronic active hepatitis
18 Active substance andor alcohol abuse (as determined by site PI)
19 Pregnancy or lactation (subjects who are pregnant or breastfeeding)
20 Known hypersensitivity to study medication
21 Any condition other than IPF that in the opinion of the site PI is likely to result in the death of the
subject within the next year
22 Any condition that in the judgment of the PI might cause participation in this study to be detrimental to
the subject or that the PI deems makes the subject a poor candidate
23 Any therapy directed at pulmonary fibrosis (excepting triple therapy of prednisone plus azathioprine
plus NAC) requires a 30-day washout period before randomized Triple therapy of lt= 12 weeks duration
in the past 4 years requires a 30-day washout period before randomization
24 History of triple therapy of prednisone plus azathioprine plus NAC for gt 12 weeksrsquo duration in the past
4 years or previous enrollment in the triple-therapy arm of the PANTHER-IPF study
44 Study Design and Study Visit
441 Study Design Summary
This study will be a randomized double-blind PL-controlled trial designed to assess the safety and efficacy of
NAC in subjects with newly diagnosed IPF
Subjects with mild to moderate IPF (defined as FVCpred ge 50 and DLCOpred ge 30) diagnosed within
the past 48 months will be enrolled Screening will continue until April 30 2012
27
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
The study will employ a 2-arm design with 11 randomization to NAC or PL Once enrolled subjects will visit
the clinical center at 15 weeks and 15-week intervals thereafter Each subject will be treated and followed for a
maximum of 60 weeks
During the 60-week visit subjects will be taken off all study agents Approximately four weeks after the final
dose of study agent is taken subjects will receive a safety phone call from the study site
442 Study Visits
Subjects who meet entry criteria will review the informed consent a written description of the purpose
procedures and risks of the study with the PI co-investigator or study coordinator and all questions will be
answered The informed consent form will be signed by the subject at screening No protocol-specific
procedures will be performed until the subject has signed and dated an informed consent form This includes the
screening procedures
4421 Screening
Once informed consent is obtained subjects may immediately begin the screening process or may return within
28 days of consent In the event a study subject has been clinically evaluated at the study site by an IPFnet study
physician and has performed testing within three weeks for this clinical evaluation that meets guidelines
provided in the IPFnet PANTHER-IPF Manual of Operating Procedures (MOOP) this testing may be used to
satisfy the following screening criteria medical history physical exam arterial blood gas (ABG) with A-a
gradient vital signs with oximetry body height and weight spirometry DLCO lung volumes and HRCT scan
Allowing the use of previously performed test results that meet study guidelines for the screening visit is
intended to permit subjects easier access to study entry to prevent subjects from repeating testing that has been
performed within the study window and to decrease risks to subjects from repeated exposure to procedures
such as arterial puncture and HRCT
The following procedures will be performed at screening
Medical history and a physical examination
28
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Measure height and weight
Serum pregnancy test (if applicable)
Measure vital signs including oximetry
Blood draws performed and the following analyses conducted
o Hematology (red cell count white cell count hemoglobin hematocrit cell indices differential
platelet count)
o Blood chemistries according to central laboratory protocol (see Section 410 Laboratory
Testing)
o Beta human chorionic gonadotropin (serum) pregnancy test (in women of childbearing potential)
o Urinalysis
Pulmonary Function Tests (PFTs) including spirometry pre- and post- bronchodilator and postshy
bronchodilator measurement of lung volumes and measurement of hemoglobin adjusted diffusing
capacity
Measure ABGs
HRCT if a satisfactory scan has not been performed on the subject within 3 months of screening (see
PANTHER-IPF MOOP for more details)
Surgical lung biopsies (if applicable) reviewed by local and central pathology departments
Current medications If required a washout period discussed with the subject and initiated at this visit
4422 Enrollment
The enrollment visit is expected to take place within eight weeks of the screening visit Enrollment visit
activities include
Measure vital signs including oximetry
Measure height and weight
Serum pregnancy test (if applicable)
If consent has been given blood will be drawn and a urine specimen collected for the bio-specimen
repository
Spirometry (post-bronchodilator)
Measure 6MWT with Borg Dyspnea Scale
29
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Collect Quality-of-life (QOL) data using the SF-36 EuroQol Investigating Choice Experiments for
Preferences of Older People Capability Instrument (ICE CAP) and SGRQ
Female subjects complete Gender Substudy questionnaire
Dyspnea status collected using the UCSD SOBQ
Evaluate Acute Exacerbation (AEx)
Review of any Adverse Events (AEs)
Review of concomitant medications
Subject receives diary and instructions on its purpose and proper use
Subject receives supply of study drug sufficient to last until his or her 15-week study visit
See the Schedule of Assessments (Table 3) for more details Subjects with screening and enrollment postshy
bronchodilator FVC measurements (in liters) differing by more than 11 are not eligible to be enrolled in the
study
Subjects will be asked to provide a physician of record This physician will be considered the subjectrsquos primary
care provider (PCP) and if the subject agrees the PCP will be informed by letter of the subjectrsquos enrollment in
the trial The subject will be informed that his or her ongoing medical care should be received from the PCP
The PCP will be informed of any safety issues identified by the study staff The PCP will also be given
information regarding communication with study personnel about pertinent health issues or clinic encounters
the subject may have
4423 Week 15
The week 15 visit is expected to occur within +- 14 days of the subjectrsquos scheduled visit time (eg the week 15
visit should occur anytime between 13 and 17 weeks after starting study drug Week 15 activities include
Measure vital signs with oximetry
Measurement height and weight
Serum pregnancy test (if applicable)
Spirometry (post-bronchodilator) measurement
Review of AEs
Evaluate for AEx
30
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Review concomitant medications
If consented draw blood and collect urine specimen for the biospecimen repository
Subjects return used and unused study drug for the visit
Review study diary and a new study diary will be given
Provide additional supply of study drug sufficient to last until the next scheduled visit
4424 Week 30
The week 30 visit is expected to occur within +- 14 days of the subjectrsquos scheduled visit time (eg the week 30
visit should occur anytime between 28 and 32 weeks after starting study drug) Week 30 activities include
Physical examination
Measure vital signs with oximetry
Measure height and weight
Laboratory values (complete blood count [CBC] and serum chemistries)
Serum pregnancy test (if applicable)
Measure spirometry (post-bronchodilator)
6MWT with Borg scale
DLCO
Review of AEs
Evaluate for AEx
Review concomitant medications
Complete all QOL and dyspnea questionnaires (EuroQol ICE CAP SF-36 SGRQ and UCSD SOBQ)
If consent has been given blood will be drawn and a urine specimen collected for the biospecimen
repository
Review study diary
Subjects return used and unused study drug for the visit
Provide additional supply of study drug sufficient to last until the next scheduled visit
4425 Week 45
31
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
The week 45 visit is expected to occur within +- 14 days of the subjectrsquos scheduled visit time (eg the week 45
visit should occur anytime between 43 and 47 weeks after starting study drug) Week 45 activities include
Measure vital signs with oximetry
Measure height and weight
Serum pregnancy test (if applicable)
Measure spirometry (post-bronchodilator)
Review of AEs
Evaluate for AEx
Review concomitant medications
If consent has been given blood will be drawn and a urine specimen collected for the biospecimen
repository
Subjects return used and unused study drug for the visit
Study diary reviewed
Provide additional supply of study drug sufficient to last until the next scheduled visit
4426 Week 60 (Early Withdrawal or Final Treatment Visit)
At week 60 or at subject withdrawal from the study (premature by study doctor or subjectrsquos decision) a final
treatment visit will occur At this final treatment visit subjects will discontinue NACPL abruptly Week 60
activities also include
Physical examination
Measure vital signs with oximetry
Measure height and weight
Laboratory values (complete blood count [CBC] and serum chemistries)
Spirometry (post-bronchodilator) measurement
6MWT with Borg scale measurement
DLCO
Lung volumes
ABG
Review of AEs
32
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Evaluate for AEx
Review concomitant medications
Subjects will complete all QOL and dyspnea questionnaires (EuroQol ICE CAP SF-36 SGRQ and
UCSD SOBQ)
If consent has been given blood will be drawn and a urine specimen collected for the biospecimen
repository
Subjects return used and unused study drug for the visit
Study diary reviewed
4427 Final Site Visit ndash FVC drop confirmation
In the event that the subject has a recorded FVC drop of gt10 from baseline at the final treatment visit and the
subject has not had a confirmation of such a drop at a previous study visit the subject should return to the
clinical site 6 to 8 weeks after the final treatment visit During this visit a post-bronchodilator spirometry test
will be performed This FVC measurement will be evaluated according to section 521 of this protocol
4428 Final Visit ndash Telephone Follow-up
Four weeks following the final dose of study medication subjects will receive a telephone call from the study
coordinator to ensure that there are no side effects and to follow up on any ongoing adverse events (AEs)
4429 Phone Contact Between Visits
At week 2 and each month that a subject does not have a scheduled clinical center visit his or her study
coordinator will contact him or her at least once by telephone to
Inquire if the subject has had any hospitalizations events that might be considered an AE or any events
significant enough to warrant an out-of-cycle visit to the clinical center
Remind subjects of their current dosage levels and confirm that the subject understands them
Address any questions or concerns the subject might have regarding other aspects of the study
Assess adherence to the treatment regimen by reviewing diary data verbal review of medications taken
including nutritional supplements
33
34
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Table 3 Schedule of Assessments
Procedure Screening Visit 0
Enrollment Visit 1
Week 15 Visit 2
Week 30Visit 3
Week 45 Visit 4
Week 60 Early
Withdrawal Visit 5
Final1
Visit (via phone)
Informed consent X
Medical history X
Inclusionexclusion criteria X
Serum pregnancy test (if applicable) X X X X X
Review of lung biopsy X
Arterial Blood Gas X X
6-Minute Walk Test
X
X X
Physical examination X X X
Vital signs with oximetry X X X X X X
Body height and weight X X X X X X
Complete Blood Count X X X
Chemistry panel X X X
Monitor Lab Values X X X
Urinalysis X Specimen repository substudy blood draw and urine collection (if consented)
X
X X X X
HRCT (if not completed within three months) X
Spirometry (pre- and post-bronchodilator) X
Spirometry (post-bronchodilator only) X X X X X
DLCO (post-bronchodilator only) X X X
Lung volumes (post-bronchodilator only) X
X
Evaluate for acute exacerbation X X X X X
Review Adverse Events X X X X X X
Review concomitant meds X X X X X X
Dispense subject diary X X X X
Review subject diary X X X X X
Dispense study agent X X X X
Gender Substudy questionnaire (female subjects only) X
EuroQol ICECAP UCSD SOBQ SGRQ SF-36 X X X
Abbreviations DLCO diffusing capacity of the lung for carbon monoxide QOL Quality of Life ICECAP Investigating Choice Experiments for Preferences of Older People UCSD SOBQ University of California Shortness of Breath Questionnaire SGRQ St Georgersquos Respiratory Questionnaire SF-36 Short Form 36 Health Survey
1Follow-up visit via phone will occur four weeks after final dose of study medication
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
45 Dose Justification
The general philosophy for determining dosing levels was to apply previously examined
treatment regimens With the focus of the study being to establish a standard of care for
mildmoderate IPF subjects the goal was to develop flexible yet standardized treatment rules that
allow for the temporary or permanent withholding of one or more components of treatment when
necessary Subjects developing laboratory abnormalities or symptoms that result in
discontinuation of one or more components of study treatment may continue on the other
components as long as there is no contraindication for this Complete follow-up is important for
the validity of any study As a strategy to maintain protocol adherence we are using a treatment
regimen that will detect potential side effects and prompt interventions proactively in the interest
of patient safety In addition subjects who permanently stop study medications during the course
of the study are encouraged to continue in the study completing all scheduled visits and tests
451 Rationale for N-acetylcysteine Dosing
To our knowledge there have been no IPF studies to correlate clinical outcome measures with
different dosages for NAC The dosage chosen is based on the IFIGENIA study However BAL
lung GSH levels from subjects with IPF have been augmented with the use of oral NAC at 600
mg 3 times per day In addition lung GSH levels have been associated with improved
PFTs212227 The dose chosen for this study was based on previous data including the IFIGENIA
study30
4511 Dosing of N-acetylcysteineplacebo
Dosing of NACPL will be 600 mg orally 3 times a day (1800 mgday)
4512 Reasons to Discontinue N-acetylcysteineplacebo
NACPL may be temporarily or permanently discontinued for the duration of the study for
gastrointestinal symptoms or dermatologic reactions
35
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Temporarily discontinue (hold) oral NACPL for subjects requiring inpatient admission for acute
exacerbation (AEx) or other conditions Resume NACPL after discharge
36
37
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
452 Dosage Algorithms
Dosage Adjustment Algorithm 1 NACPL Dose Modifications for Gastrointestinal Symptoms Nausea Vomiting Abdominal Discomfort Diarrhea
GI Symptoms determined by the PI to be clinically significant Nausea Vomiting Abdominal Discomfort Diarrhea
NACPL Temporarily dc (HOLD) x 3 Days
Monitor symptoms intervene as clinically indicated (eg fluid replacement antidiarrhea or antinausea medication)
Monitor or lab PRN
Are symptoms resolving after 3 days NO
Symptoms NOT resolving after 3 days of holding study medication Assessmentmanagement per clinical
discretion of investigator
Likely not study medication discuss resuming study medication with medical monitor when symptoms resolved
YES
Temporarily dc (HOLD) NACPL for 4 additional days (total hold 1 week) then NACPL Resume 600 MG TID
Did symptoms recur
YES
STOP NACPL for
duration of study
NO
NACPL No Change
38
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Dosage Adjustment Algorithm 2 NACPL Dose Modifications For Dermatologic Reactions
Dermatologic Reactions (Not Acneiform) ge Grade 2 Grading per Common Terminology Criteria for
Adverse Events V30 (httpctepcancergov) For example Grade 1 RASHDESQUAMATION Macular or papular eruption or erythema without associated symptoms Grade 2 RASHDESQUAMATION Macular or popular eruption or erythema with pruritus or other associated symptoms localized desquamation or other lesions covering lt50 of body surface area
NACPL Temporarily dc (HOLD) x 3 days
Are symptoms resolving after 3 days
NO Symptoms not resolving after 3 days of holding study medication Assessmentmanagement per clinical discretion of investigator Likely not study medication Discuss resuming study medication with medical monitor when symptoms
resolved YES
Temporarily dc (HOLD) NACPL for 4 additional days (total hold 1 week) then NACPL resume 600 MG TID
Did symptoms recur
YES
STOP NACPL for
duration of study
NO
NACPL No change
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
46 Contraindications Precautions and Side Effects of Study Medications
461 Contraindication
Contraindication to NAC is known hypersensitivity to it
462 Precautions
Concomitant administration of oral NAC and antibiotics has shown a slightly reduced absorption
of cephalexin and a slight increase in erythromycin serum levels NAC contains free sulfhydryl
groups There is no evidence that individuals sensitive to sulfa drugs are sensitive to NAC
The NAC preparation being administered in this study contains 20 mg of aspartame Because of
the phenylalanine component of aspartame individuals with phenylketonuria should avoid or
restrict aspartame intake to avoid increased blood levels of phenylalanine Because of this risk
labeling is required on all products containing aspartame
463 Side Effects
Side effects of NAC range from common to serious See Table 4
39
40
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Table 4 Side Effects of NAC
Undesirable Effects
System-organ class Uncommon
(gt11000 lt1100)
Rare
(gt110000 lt11000)
Very rare
(lt110000) Not known
Immune system disorders Hypersensitivity Anaphylactic shock
reaction
Nervous system disorders Headache
Ear and labyrinth disorders Tinnitus
Cardiac disorders Tachycardia
Vascular disorders Hemorrhage
Respiratory thoracic and
mediastinal disorders
Bronchospasm
Dyspnea
Gastrointestinal disorders
Vomiting diarrhea
stomatitis abdominal
pain nausea
Dyspepsia
Skin and subcutaneous tissue
disorders
Urticaria rash
angioedema itching
General disorders and
administration site conditions Pyrexia
Investigations Reduced arterial
pressure Face edema
In very rare cases the onset of severe skin reactions such as Stevens-Johnson syndrome and Lyell syndrome was reported to have a temporal relationship with N-acetylcysteine administration Although in most cases at least another suspect drug probably most involved in the genesis of the above mentioned mucocutaneous syndromes has been identified in case of mucocutaneous alterations it is appropriate to contact onersquos doctor and the administration of N-acetylcysteine should be immediately discontinued
Some studies confirmed a reduction of platelet aggregation during N-acetylcysteine administration The clinical significance of these findings has not been defined yet [Source Fluimucil Investigator Brochure]
47 Recruitment Procedures
Subjects recruited for this study will be established patients of the investigators or physician- or
self-referred to participating clinical centers in the IPFnet Each clinical center within IPFnet has
a well-developed infrastructure of local pulmonologists within the surrounding geographic area
These pulmonologists are kept informed of ongoing IPF clinical trials and regularly refer
subjects to studies conducted at IPFnet clinical centers
Additional steps will be taken to inform clinicians of the trials in progress within IPFnet
including presentations at faculty staff meetings at local hospitals medical grand rounds and
national conferences direct mail notification monthly faxes and advertisement of network trials
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
in pulmonary journals Clinical center patients previously diagnosed with IPF will be notified of
the trials by mail whenever possible
Recruitment of minorities and women will be monitored by the DCC and DSMB If necessary
additional recruitment efforts will be made at specific centers to ensure that the aggregate subject
sample contains appropriate representation of women and minorities
48 Study Procedures
The following procedures are detailed in the PANTHER-IPF MOOP accompanying this
protocol
1 PFT
2 ABG
3 HRCT scan of the chest (including imaging of pulmonary arteries)
4 CBC and serum chemistries
5 Pregnancy test
6 6MWTBorg Dyspnea Scale
7 QOL questionnaires (EuroQol HAD SF-36 SGRQ and ICE CAP)
8 UCSD SOBQ
9 Gender Substudy Questionnaire
All assessments of PFTs will be conducted by study personnel not directly involved in the
treatment of the subjects
481 Biological Specimen Management
4811 Biological Specimen Sample Management
Subjects at clinical centers participating in the specimen repository substudy who consent to
having blood drawn for research purposes and for the banking of blood blood components and
other biologic specimens (urine and BAL fluid) will have approximately 405 mL of blood
41
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
drawn 17 mL blood drawn for DNA and 20 mL of urine collected at enrollment visit Subjects
will have approximately 50 mL of blood drawn and 20 mL of urine collected at each 15-week
follow-up visit Blood specimens will be separated according to PANTHER-IPF MOOP
guidelines into the following components for banking in the repository serum plasma and
DNA Coding of all biologic specimens for the repository will be performed by study staff at the
clinical center The samples will be processed per PANTHER-IPF MOOP guidelines aliquoted
labeled with barcode labels and stored at -70degC at the clinical center and shipped to the central
repository
The only subject identifiers will be a sample ID number and subject initials This sample ID will
be linked in the IPFnet DCC clinical database to subject information No subject information will
be transferred to the biological-specimen database
The subjectrsquos samples may be used for approved sub-studies relating to human disease
including but not limited to IPF The studies for which an individualrsquos samples will be made
available will be determined by the subjectrsquos answers to questions on the biological-sample
informed consent form The subjects can choose to make their samples available for all options
or any combination Samples will be made available to researchers only with IPFnet Steering
Group approval until such time as the samples are made public through the NHLBI repository
49 Concomitant Medications
Concurrent treatment with FDA-approved therapy for IPF is allowed Colchicine may be used
for treatment of gout Temporary treatment with oral or IV corticosteroids for clinical worsening
or suspected AEx is permitted Nutritional supplements containing NAC are not allowed
410 Laboratory Testing
Clinical laboratory parameters will be assessed at screening and at the end of the study The
following tests will be performed at the two time points specified in the protocol chemistry (AG
ratio ALT [SGPT] AST [SGOT] albumin alkaline phosphatase amylase bilirubin-direct
42
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
bilirubin-indirect bilirubin-total BUN BUNcreatinine ratio calcium carbon dioxide
cholesterol-total chloride CPK-total creatinine GGT globulin glucose iron-total LDH
lipase magnesium phosphorus-inorganic potassium protein-total sodium TIBC triglycerides
uric acid) and hematology (red blood cell count WBC count hemoglobin hematocrit cell
indices differential platelet count)
411 Blinding of Study Drugs
Subjects and caregivers will be blinded to study treatment Every subject will receive NAC or
matching PLs at every study visit from the baseline visit to the week-45 visit No study agent
will be dispensed at the week-60 visit
43
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
5 Study Endpoints
51 Primary Study Endpoint
The primary endpoint will be the change in serial measurements of FVC over the study period
52 Secondary Study Endpoints
521 Time to Disease-progression
The time-to-death or a 10 decline in FVC will be defined as the time-to-disease progression
The 10 decline in FVC from enrollment must be confirmed on 2 consecutive visits no less than
6 weeks apart For subjects with 2 consecutive visits with a 10 decline in FVC the time-toshy
disease progression will be defined as the time interval between enrollment and the initial visit
with a 10 FVC decline For subjects who experience disease progression the study doctor will
determine whether or not the subject will remain in the study
522 Acute Exacerbations
The following 3 criteria will define AEx in subjects with acute worsening of their respiratory
conditions
1 Clinical (all of the following required)
A) Unexplained worsening of dyspnea or cough within 30 days triggering unscheduled
medical care (eg emergency room clinic study visit hospitalization)
B) No clinical suspicion or overt evidence of cardiac event pulmonary embolism or deep
venous thrombosis to explain acute worsening of dyspnea
C) No pneumothorax
44
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
2 RadiologicPhysiologic (A and B required)
A) New ground glass opacity or consolidation computed tomography (CT) scan OR new
alveolar opacities on chest x-ray
B) Decline of ge 5 in resting room air SpO2 from last recorded level OR decline of ge 8 mm
Hg in resting room air PaO2 from last recorded level
3 Microbiologic (all of the following required)
A) No clinical evidence for infection (ie absence of grossly purulent sputum fever gt 39degC
orally)
B) Lack of positive microbiological results (if done) from lower respiratory tract defined as
(1) Clinically significant bacterial growth on sputum or endotracheal aspirate cultures
(2) Quantitative culture by protected brush specimen ge 103 cfumL or BAL ge 104 cfumL
(3) The presence of specific pathogens on stains of any of the above
C) Lack of positive pathogen in blood cultures (if done)
Identification of Acute Exacerbations
All subjects will be educated about the importance of identifying AExs At the time of
enrollment subjects will be told about the possibility of developing acute symptomatic
worsening that might represent an AEx of IPF and instructed to contact their study clinical
center coordinator within 48 to 72 hours of the apparent event
All subjects will be contacted by phone monthly and questioned about any change in dyspnea or
cough and any interim clinic visits or hospitalizations Finally as part of the IPFnet outreach to
community referring physicians the importance of AExs will be emphasized When a subject is
identified who meets criterion 1A this will trigger the collection of additional clinical data to
evaluate a suspected AEx These data will be collected as part of standard clinical care (ie this
protocol does not require collection of all items) The additional items to be collected for
suspected AEx include
IPFnet AEx case report form (eCRF) (required)
45
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Chest x-ray CT scan withwithout pulmonary angiogram (reports should be faxed and
followed by the hard copiesdiscs)
Oxygen saturation (pulse oximetry)
ABG
Respiratory cultures (sputum endotracheal aspirate lavage)
Blood cultures
Clinichospital records related to the event
All potential cases of AEx will be reviewed by the clinical center PI first and a decision on
whether the case may represent an AEx will be made If AEx is suspected the case will be sent
to the IPFnet adjudication committee which will assign a final diagnosis (see Table 5) If there is
disagreement among members the majority opinion will be recorded
During episodes of suspected AEx as determined by the individual clinical center investigator
subjects will remain blinded and in the study
Table 5 Final Diagnoses in Evaluation of Suspected Acute Exacerbations
Definite acute exacerbation All criteria met no alternative etiology
Unclassifiable acute worsening
Insufficient data to evaluate all criteria no alternative etiology
Not acute exacerbation Alternative etiology identified that explains acute worsening
Management of the suspected AEx will be at the discretion of the treating physician Standard of
care generally involves evaluation for respiratory infection pulmonary embolism cardiac events
and pneumothorax and treatment with IV corticosteroids
Study drugs will be resumed at pre-suspected AEx doses after subjects clinically improve as
confirmed by the local PI All subjects should be seen at the clinical center within 2 to 4 weeks
of recovery for measurement of post-bronchodilator FVC (see Figure 4) Subjects unable to
return to the clinical center after suspected AEx due to medical frailty (eg continued
46
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
institutionalization progressive disability) will be categorized as failing to maintain FVC
response in secondary analyses
Suspected AEx (PI determined)
Hold study drug Treat AEx
(Attending physician determined)
Alive but unable to continue due to
medical frailty
Dead
Alive and able to continue
Site reviewvisit
Restart study drug
FVC within 2-4 weeks
Figure 4 Acute Exacerbation Flow Chart
523 Respiratory Infections
An upper respiratory infection will be defined as
Change in sputum discoloration
Increased cough of no more than 14 daysrsquo duration
A lower-respiratory infection (pneumonia) will be defined as new segmental or lobar airspace
opacities visualized by image studies (chest radiograph or HRCT) in addition to any of the
following
Positive pathogencultures in good sample of sputum or lower-airway secretions retrieved
by fiberoptic bronchoscope
Fever gt 39degC or gt 100degF
Leukocytosis gt 12000 (unexplained no increase in dose of corticosteroids)
47
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
524 Maintained FVC Response
Subjects with follow-up FVCpred measurements at or above their baseline FVCpred level
will be classified as having maintained FVC response Subjects with reduced FVCpred levels
or missing data for any reason including death or medical frailty will be classified as having not
maintained FVC response The FVCpred value is used because unadjusted FVC measurements
are expected to decline with age
48
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
6 Safety Evaluations and Procedures
61 Adverse Events
During a clinical trial the reporting of adverse experience information can lead to important
changes in the way a new treatment is developed as well as provide integral safety data
611 Definitions
An adverse event (AE) is any untoward medical occurrence in a subject or clinical investigation
subject who was administered a pharmaceutical product The AE does not necessarily have to
have a causal relationship with the drug administered An AE can be any unfavorable and
unintended sign (including an abnormal laboratory finding) symptom or disease temporarily
associated with the use of a medicinal product whether or not considered to be related to the
medicinal product Diseases signs symptoms or laboratory abnormalities already existing at
enrollment are not considered AEs unless they worsen (ie increase in intensity or frequency)
Surgical procedures themselves are not AEs they are therapeutic measures for conditions that
require surgery The condition for which the surgery is required may be an AE Surgical
procedures planned before randomization and the conditions necessitating the surgery are not
AEs
A serious adverse event is any untoward event that
Is fatal
Is life-threatening
Requires inpatient hospitalization or prolongation of existing hospitalization with the
following exceptions
o Preplanned (before the study) hospital admissions unless the hospitalization is
prolonged
o Planned admissions (as part of a study eg routine biopsies)
o Hospitalization lasting lt 24 hours
49
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
o Hospitalization for elective procedure
o Emergency room visits
Results in persistent or significant disability or incapacity
Is a congenital anomaly or birth defect
Important medical events that may not result in death be life-threatening or require
inpatient hospitalization may be considered serious adverse events (SAEs) when based
on appropriate medical judgment they may jeopardize the subject and may require
medical or surgical intervention to prevent one of the outcomes listed above
Life-threatening means that the subject was in the view of the investigator at immediate risk of
death from the AE as it occurred It does not include an AE that had it occurred in a more severe
form might have caused death
Persistent or significant disabilityincapacity means that the event resulted in permanent or
significant and substantial disruption of the subjectrsquos ability to carry out normal life functions
Causality
A reasonable possibility means the AE may have been caused byrelated to the study drug A
perceived or real lack of efficacy does not satisfy the definition of relatedness
612 Adverse Event (AE) Reporting
For the PANTHER-IPF trial all AEs (serious and nonserious) occurring from randomization
through final study visit (4 weeks after final dose of all study medication) will be recorded on the
AE page of the case report form (CRF)
6121 Serious Adverse Events (SAE) Reporting
For this trial all deaths and all SAEs which occur from randomization through final study visit
must be entered within the EDC system via the SAE eCRF page within 24 hours of the
investigative sitersquos knowledge of the event It is the responsibility of the clinical center
50
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
investigator to provide a causality assessment of the event for each study medications based upon
the information available at the time of the report It is understood that complete information
about the event may not be known at the time the initial report is submitted In the event the EDC
system is not accessible to the site at the time of event reporting investigative sites will complete
and forward a paper back-up SAE form to DCRI Safety Surveillance for processing
DCRI Safety Surveillance
Telephone 1-919-668-8624 or 1-866-668-7799 (toll free)
Fax 1-919-668-7138 or 1-866-668-7138 (toll free)
The investigator must complete and submit follow-up SAE information via the eCRF when
important new or follow-up information (eg final diagnosis outcome results of specific
investigations) becomes available Follow-up information should be submitted according to the
same process used for reporting the initial event as described above All SAEs will be followed
until resolution stabilization or 30 days after the subject has completed the final visit (4 weeks
after the final dose of study medication) whichever occurs first The investigator is responsible
for reporting SAEs to their institutional review board (IRB) per site specific IRB reporting
guidelines
6122 Regulatory Reporting
AEs that are serious study drug related and unexpected will be reported to the regulatory
authorities The DCRI Safety Surveillance medical monitor will perform a medical review of all
SAEs submitted and evaluate for ldquounexpectednessrdquo DCRI Safety Surveillance will prepare
MedWatch reports for those events identified as serious study drug related and unexpected as
determined by Safety Medical Monitor
DCRI Regulatory Services will submit all unexpected study drug-related SAEs as per 21 CFR
32 DCRI Safety Surveillance will provide a safety alert letter to the NHLBI DSMB and DCC
clinical operation (for distribution to sites) within 15 days of initial receipt of the information
51
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Investigators are responsible for promptly reporting these events to their reviewing IRBs
according to site specific IRB reporting guidelines
62 Clinical Medical Monitoring
There will be an unblinded physician at the IPFnet DCC serving as medical monitor The
medical monitor will be available to assist with questions about dosage adjustments of study
medications including discontinuation or resumption of medications
63 Unblinding Procedures
Unblinding of subjects or investigators to subject treatment is strongly discouraged For ongoing
clinical management all subjects should be presumed to be receiving ldquoactiverdquo study drug To
ensure the subjectrsquos safety the study treatment will be dose-adjusted based on laboratory test
results clinical findings and symptoms
The IPFnet DCC medical monitor and PANTHER-IPF co-chairs Drs Ganesh Raghu and
Fernando Martinez will be available to the study physicians to discuss study drug management
on a case-by-case basis Un-blinding will be considered ONLY when the knowledge of subject
treatment assignment is ABSOLUTELY ESSENTIAL for subject safety and after discussion of
the subjectrsquos case with the medical monitor and either Dr Raghu or Dr Martinez Unblinding of
study treatment should be minimized during the conduct of the trial In those cases where it is
felt to be medically necessary the DCC medical officer will communicate directly with the
managing physician to minimize unblinding of study personnel
52
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
7 Study Drug Procedures
At the baseline 15-week 30-week and 45-week study visits subjects will receive a supply of
study drug sufficient to last until the next visit at which study drug will be dispensed
53
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
8 Data Management
81 Hardware and Software Configuration
811 Hardware and Database Software
Data will be stored in an Oracle database system Oracle has advantages of processing efficiency
and smooth linkage with other software systems The application and database will be hosted on
Solaris Unix servers at the IPFnet DCC
812 Statistical Software
SAS will be used as the principal application for the management of analysis data files and
statistical computations S-Plus will be used to provide supplementary functions as needed
813 Access Control and Confidentiality Procedures
Access to databases will be controlled centrally by the IPFnet DCC through user passwords
linked to appropriate privileges This protects the data from unauthorized changes and
inadvertent loss or damage
814 Security
Database and Web servers will be secured by a firewall and through controlled physical access
Oracle has many security features to ensure that any staff member accessing the database has the
proper authority to perform the functions he or she requests of the system Within the secondary
SAS databases Unix group-access control maintains similar security The Sun workstation login
is secured by extensive user-password facilities under Unix
54
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
815 Back-up Procedures
Database back-up will be performed automatically every day and standard IPFnet DCC policies
and procedures will be applied to dictate tape rotation and retention practices
816 Virus Protection
All disk drives that provide network services and all user computers will be protected using
virus-scanning software Standard IPFnet DCC policies will be applied to update these protection
systems periodically through the study
82 Sources of Data
821 Design and Development
The IPFnet DCC will be responsible for development of the electronic case report forms
(eCRFs) development and validation of the clinical study database ensuring data integrity and
training clinical center staff on applicable data management procedures A web-based distributed
data entry model will be implemented This system will be developed to ensure that guidelines
and regulations surrounding the use of computerized systems used in clinical trials are upheld
The remainder of this section provides an overview of the data management plan associated with
this protocol
822 Data Collection Forms
The data collection process consists of direct data entry at the study clinical centers into the EDC
system(s) provided by the DCC A data collection worksheet will be provided to clinical centers
for recording data in the event the EDC system is unavailable Data entry of the eCRFs should
be completed according to the instructions provided and project specific training The
investigator is responsible for maintaining accurate complete and up-to-date records and for
ensuring the completion of the eCRFs for each research participant
55
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
823 Data Acquisition and Entry
Data entry into eCRFs shall be performed by authorized individuals Selected eCRFs may also
require the investigatorrsquos written signature or electronic signature as appropriate Electronic
CRFs will be monitored for completeness accuracy and attention to detail during the study
824 Data Center Responsibilities
The IPFnet DCC will 1) develop a data management plan and will conduct data management
activities 2) provide final eCRFs for the collection of all data required by the study 3) develop
data dictionaries for each eCRF that will comprehensively define each data element 4) conduct
ongoing data monitoring activities on study data 5) monitor any preliminary analysis data
cleanup activities and 6) rigorously monitor final study data clean up
825 Data Editing
Completed data will be entered into the IPFnet DCC automated data acquisition and
management system If incomplete or inaccurate data are found a data clarification request will
be generated and distributed to clinical centers for a response Clinical centers will resolve data
inconsistencies and errors and enter all corrections and changes into the IPFnet DCC automated
data acquisition and management system
826 Training
The training plan for clinical center staff includes provisions for training on assessments eCRF
completion guidelines data management procedures and the use of computerized systems
56
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
9 Study Design and Data Analysis
91 General Analytic Considerations
All primary analyses will be based on intent-to-treat (ITT) principles using all randomized
subjects Baseline factors across groups will be compared using mean (standard deviation) and
median (25th and 75th percentiles) summary measures Kaplan-Meier curves will be used to
display event rates Due to clinical interest in departures from both sides of the null hypothesis
all test statistics will be 2-sided
Reasonable caution needs to be taken when conducting multiple analyses on key clinical
subgroups For subgroup analyses a conservative significance level of 0001 will be used for all
interaction tests Thus subgroup comparisons will be considered exploratory unless the p-value
from the interaction test is smaller than 0001
92 Randomization Blinding and Reporting of Results
A permuted block-randomization scheme will be created with varying block sizes stratified by
clinical center Once a subject has completed the screening and baseline period and evaluation
for inclusionexclusion criteria the randomization process will begin Subjects will be
randomized to receive NAC or matching placebo with equal probability (11) via telephone
contact with a central interactive voice response system (IVRS) using a toll-free randomization
number On the day of randomization after the subject has successfully met all inclusion and
exclusion criteria the investigator or designee will call the central randomization number to
obtain the assigned kit randomization numbers for that subject At each subject visit the
investigator or designee will call the central randomization number to obtain the new kit
randomization numbers for resupply of the subject For resupply of the clinical center the IVRS
will monitor minimal volume of a kit type andor expiration date and will automatically notify
the pharmacy
57
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
The trial results will be reported according to guidelines specified in the CONSORT statement
A flow diagram describing screening recruitment randomization dropout and vital status will
be included in the primary manuscript AEs and efficacy data will be presented for all treatment
groups Adherence dropout and lost to follow-up will be carefully examined across all treatment
groups Analyses of safety will be based on data from all randomized subjects who received at
least one dose of study drug
93 Stratification
Subjects will be distributed to the two treatment arms in a 11 allocation ratio Stratification
blocks will be based on clinical centers
94 Specification of the Primary Analyses
A mixed model repeated measures (MMRM) analysis described in section 95 will be used to
compare differences in the slope of FVC measurements across the treatment groups Response
variables are values of the FVC measured at baseline and every 15 weeks until study completion
Variables in the model will include treatment time and time by treatment age sex race and
height Contrast estimates of differences in slopes of treatment over time (along with confidence
intervals) will be used to estimate the treatment effect The validity of this model in terms of
meeting modeling assumptions will be assessed via standard modeling diagnostics and goodness-
of-fit measures Based on the MMRM framework missing FVC data will not be imputed for the
primary analysis
95 Analysis of Longitudinal Endpoints
A common goal in clinical trials is to specify models that are easily implemented and
reproducible by independent data analysts On the other hand the models should have proper
statistical behavior in terms of low bias and high precision Many common approaches to
longitudinal data analysis including last observation carried forward (LOCF) imputation rely on
the missing completely at random (MCAR) assumption However the MCAR assumption is
58
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
unlikely to hold in many clinical trials because missing data are often related to disease
progression and prognosis A more reasonable assumption missing at random (MAR) specifies
that the complete data distribution can be modeled using only the observed data The likelihood-
based MMRM approach is valid under the more general MAR assumptions These models will
be applied to analyze the longitudinal data secondary endpoints
The advantages of MMRM analysis are that all important characteristics of the model can be preshy
specified standard software can be used to implement the models and results are based on ITT
principles43 In addition the MMRM approach offers superior control of Type I and Type II
errors compared with the LOCF approach
Response variables are values of the PFTs measured at enrollment and every 15 weeks until
study completion and 6MWT values measured at baseline week 30 and week 60 Covariates are
treatment time time by treatment and key baseline risk factors Contrasts (along with
confidence intervals) of treatment by time will be used to estimate the treatment effect
The correlation structure involves multiple pieces including measurement errors random
variation and interindividual variability For the longitudinal data analyses an unstructured
correlation matrix for within-subject errors will be assumed Other correlation structures
including compound symmetry will be examined as needed A careful examination of reasons
for study discontinuation will be conducted to assess the validity of MCAR Sensitivity analyses
will be used to examine the untestable assumption that the observed data violate the MAR
assumption The MMRM models will be implemented using PROC MIXED in SAS
96 Analysis of Binary Time-to-Event and Time-Lagged Endpoints
Regression modeling approaches using either the logistic regression model or Cox proportional
hazards regression model will be employed when appropriate The validity of these models will
be assessed via standard modeling diagnostics and goodness-of-fit measures Estimates of
cumulative frequencies for more general time-lagged responses will be calculated using the
partitioned version of the Bang-Tsiatis estimator44 The partitions will be set at 15-week intervals
59
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
to correspond with the data-collection process Covariate adjusted event rates will be calculated
using inverse probability-weighted regression estimates45
97 Power Analysis
971 Primary Analyses
Based on previously published IPF clinical trials the PL group is expected to experience a drop
in FVC of approximately 020 L over the study period (see Figure 1) The IPFnet Steering Group
determined a clinically important difference would be to preserve the majority of the decline
relative to PL over the study period In particular a treatment effect of 015 L was determined to
be a clinically meaningful difference Potential dropout is a key factor in the proposed study The
drop-out process assumed 5 lost to follow-up after every study visit Only 80 of subjects
were assumed to be followed for the entire study period All models assumed a compound
symmetry structure for the covariance matrix Power calculations were performed using a SAS
IML program for designing repeated measures studies46 Based on preliminary reviews of the
data from the University of Michigan the covariance matrix parameters were estimated at
approximately σ2 = 0757 (variance parameter) and ρ = 0936 (correlation parameter) To be
conservative the power calculations for the primary analysis were performed with parameter
setting of σ2 = 0810 (variance parameter) and ρ = 0925 (correlation parameter)
The power calculations assume a correction for imperfect compliance proposed by Lachin and
Foulkes to allow for 2 noncompliance for each of the treatment arms47 Thus the sample size
of 130 subjects per arm would be reduced to an adjusted sample size of 130(1-002-002)2 =
1198 or 120 subjects per arm
Under the assumed Type I error rate of 005 with a correlation parameter of 0925 and standard
deviation of 090 the difference of 015 L (or 00025 Lweek) shown in Table 6 would have
power of 93
60
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Table 6 Hypothetical Values of Mean FVC (L) Change from Baseline
Week 15 Week 30 Week 45 Week 60
NAC 00125 00250 00375 00500
Placebo 00500 01000 01500 02000
Difference 00375 00750 01125 01500
Abbreviations FVC forced vital capacity PL placebo
972 Power Analysis for Secondary Endpoints
Power calculations for secondary endpoint measurements are shown in Table 7 Standard
deviations are based on unpublished data provided by the University of Michigan The
calculations are based on a 2-sample t-test with Type I error rate set at 005 These calculations
are likely to be conservative because the statistical approach described in section 95 for
analyzing these endpoints will incorporate incomplete observations as well as intermediate data
points
Table 7 Detectable Differences in Treatment Means for Selected Endpoint Measurements
Secondary Endpoints Std Dev
of the Baseline Score
Detectable Difference for 80 Power
Std Dev of the Change Score
Difference Detectable for
80 Power
DLCOpred 166 58 91 32
6MWT Area Under the Desaturation Curve
219 76 175 61
6MWT Distance to Desaturation 224 78 315 110
6MWT Minutes Walked 210 073 205 071
Abbreviations Std Dev standard deviation DLCOpred diffusing capacity of the lung for carbon monoxide percent predicted 6MWT 6-minute walk test
61
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
10 Study Administration
101 Cooperative Agreement Mechanism
The administrative and funding mechanism used to undertake this project is a ldquocooperative
agreementrdquo (U01) which is an assistance mechanism Under the cooperative agreement the
NHLBI assists supports andor stimulates the project and is substantially involved with
investigators in conducting the study by facilitating performance of the effort in a ldquopartnerrdquo role
The NHLBI project scientist serves on the IPFnet Steering Group and he or another NHLBI
scientist may serve on other project committees when appropriate At the same time however
NHLBI does not assume a dominant role direction or prime responsibility for this research
program
As described below governance of the project is conducted through the IPFnet Steering Group
Principal investigators have lead responsibilities in all aspects of their trials and the project
including any modification of trial designs conduct of the trials quality control data analysis
and interpretation preparation of publications and collaboration with other investigators unless
otherwise provided for by the IPFnet Steering Group
PIs retain custody of and have primary rights to their center-specific and collaborative data
subject to government rights-of-access consistent with current Health amp Human Services (HHS)
Public Health Service (PHS) and National Institutes of Health policies The protocols and
governance policies call for the continual submission of data centrally to the IPFnet DCC for the
collaborative database which at a minimum will contain the key variables selected by the IPFnet
Steering Group for standardization across all clinical centers the submission of copies of the
collaborative datasets to each PI upon completion of the project procedures for data analysis
reporting and publication and procedures to protect and ensure the privacy of medical and
genetic data and records of individuals The NHLBI project scientist on behalf of the NHLBI
will have the same access privileges and responsibilities regarding the collaborative data as the
other members of the Steering Group
62
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
PIs are also encouraged to publish and to publicly release and disseminate results data and other
products of the project concordant with the project protocols and governance and the approved
plan for making data and materials available to the scientific community and to the NHLBI
However during the 3 years after the ending date of NHLBI project support unpublished data
unpublished results data sets not previously released and other study materials or products are
to be made available to any third party only with the approval of the IPFnet Steering Group
Upon completion of the project PIs are expected to put their intervention materials and
procedure manuals into the public domain andor make them available to other investigators
according to the approved plan for making data and materials available to the scientific
community and the NHLBI for the conduct of research at no charge other than the costs of
reproduction and distribution
The NHLBI reserves the right to terminate or curtail the project (or an individual award) in the
event of (a) failure to develop or implement mutually agreeable collaborative measurement
subject eligibility and data management sections of the protocols (b) substantial shortfall in
subject recruitment follow-up data reporting or quality control or other major breach of
protocol (c) substantive changes in the agreed-upon protocols with which NHLBI cannot
concur (d) reaching a major project outcome with persuasive statistical significance
substantially before schedule or (e) human subject ethical issues that may dictate a premature
termination
Any disagreement that may arise in scientificprogrammatic matters (within the scope of the
award) between award recipients and the NHLBI may be brought to arbitration An arbitration
panel will be composed of 3 membersmdash1 selected by the IPFnet Steering Group (with the
NHLBI member not voting) or by the individual PI in the event of an individual disagreement a
second selected by NHLBI and the third selected by the other 2 members This special
arbitration procedure in no way affects the PIrsquos right to appeal an adverse action that is otherwise
appealable in accordance with the PHS regulations at 42 CFR part 50 Subpart D and HHS
63
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
regulation at 45 CFR part 16 or the rights of the NHLBI under applicable statutes regulations
and terms of the award
102 IPFnet Steering Group
The IPFnet Steering Group is the main governing body of the project It is composed of the PIs
of the clinical centers the PI of the DCC and the NHLBI project scientist The clinical centers
the IPFnet DCC and the NHLBI each have 1 vote on the IPFnet Steering Group All decisions
are determined by majority vote
All major scientific decisions are determined by the IPFnet Steering Group It assumes overall
responsibility for the design and conduct of the trial It appoints (and disbands) committees and
subcommittees as the need arises designs approves and implements the study protocols
oversees the development of the MOOP monitors subject recruitment and treatment delivery
evaluates data collection and management oversees quality assurance procedures and
implements changes and enhancements to the study as required It also has primary responsibility
for facilitating the conduct of the trials and reporting the projectrsquos results
103 Data and Safety Monitoring Board
The NHLBI will establish a DSMB in accordance with established policies (see
httpwwwnhlbinihgovfundingpoliciesdsmb_insthtm) to ensure data quality and subject
safety and to provide independent advice to the NHLBI regarding progress and the
appropriateness of study continuation
104 Recommendations on Interim Monitoring of Efficacy Safety and Futility
First and foremost the role of the DSMB will be to review subject safety and trial conduct at
periodic points during the study The DSMB may require analyses of the primary endpoint
results for comparing the benefit and risks of treatment strategies The benefit of collecting
additional data on key secondary endpoints with extended follow-up and establishing a robust
64
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
evidence base for determining a standard of care will need to be carefully considered before
early termination of one or more treatment arms After careful consideration the IPFnet Steering
Group recommends conservative thresholds for the early examinations of the safety and efficacy
data
The DSMB will be expected to meet approximately every 6 months until trial completion to
review safety and toxicity data The DSMB may recommend stopping the study based on these
reviews Because the DSMB could stop the trial for safety concerns as well as for a large
efficacy benefit there could be multiple opportunities to reject the null hypothesis (no difference
in event rates between the PL and NAC groups) A Bonferroni approximation will be applied
during the one planned interim analysis for efficacy
Before locking the database a statistical analysis plan (SAP) will be developed to provide
complete details on the statistical analysis The SAP will include the specifics for how and when
the DSMB will be notified for AEs The IPFnet DCC will deliver to the DSMB all FDA-defined
AEs at 3-month intervals The IPFnet DCC will prepare narrative SAE reports in real time for
DSMB review including recommendations and analysis of similar events for each SAE
submitted to the FDA
65
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
11 Investigator and Sponsor Obligations
111 Monitoring
All monitoring activities for US clinical centers will be performed in accordance with DCRI
standard operating procedures Information regarding the types of visits will be outlined in the
PANTHER-IPF MOOP
112 Cost and Payment
There will be no cost to subjects enrolled in this trial Study-related procedures will be paid for
by the IPFnet
Subjects may be eligible for reimbursement for travel to the clinical center Details of payment
will be explained to each subject during the consent process
113 Confidentiality and Health Insurance Portability and Accountability Act
Considerations
Subject confidentiality will be protected throughout the study All subject data will be kept
strictly confidential and no subject-identifying information will be released to anyone outside
the project Confidentiality will be assured through several mechanisms First each subject will
be assigned an anonymous study ID which will then be used on all study forms Second any
study forms blood samples and paper records that contain subject information (eg address lists
phone lists) will be kept at the clinical centers in secured locked areas coded by number Once
blood is collected there will be no subject identifiers placed on blood samplesmdashonly the study
ID number and the date of sample collection Third access to all subject data and information
including laboratory specimens will be restricted to authorized personnel In the case of
computerized data this restricted access will be assured through user logon IDs and password
protection
66
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
At the IPFnet DCC only authorized personnel will have access to the data files containing study
data Security will be assured through user logon IDs passwords and appropriate access
privileges All study subjects will be identified only by their IPFnet ID numbers and no personal
identifying information such as name address or Social Security number will be entered into
the IPFnet DCC database Any subject-specific data reported to the IPFnet Steering Group will
be identified only by the IPFnet ID number
Finally subjects will not be identified by name in any reports or publications nor will the data
be presented in such a way that the identity of individual subjects can be inferred Analysis files
created for further study by the scientific community will have no subject identifiers These data
files will be created in accordance with the Ancillary Studies and Publication Policy of the
IPFnet
114 Informed Consent Procedures
All IPFnet subjects will provide written informed consent using procedures reviewed and
approved by each clinical centerrsquos IRB Informed consent will be undertaken by study personnel
in-person with the subject The subject has the option of declining further participation in the
study at that point No further study procedures will be conducted until the signed documents
have been provided to the IPFnet clinical center
115 Institutional Review Boards
Before initiating this study the protocol clinical center-specific informed consent forms Health
Insurance Portability and Accountability Act (HIPAA) forms recruitment materials and other
relevant information will be reviewed by a properly constituted IRB at each participating clinical
center A copy of the signed and dated IRB approval at each clinical center will be retrieved prior
to or during the site initiation visit and archived at the IPFnet DCC Any amendments to the
protocol other than simple administrative and typographical changes must be approved by each
IRB before they are implemented The clinical centers will seek annual renewals of their IRB
approvals in accordance with local procedures
67
__________________________________________ ________________
__________________________________________
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
12 Investigator Agreement
I have read the foregoing protocol PANTHER-IPF and agree that it contains all necessary
details for carrying out this study I will conduct the study as outlined herein and will complete
the study within the time designated
I will provide copies of the protocol and all pertinent information to all individuals responsible to
me who assist in the conduct of this study I will discuss this material with them to ensure they
are fully informed regarding the drug and the conduct of the study
I will fulfill all responsibilities for submitting pertinent information to the local IRB if
applicable that is responsible for this study
I further agree that NHLBI andor DCRI will have access to any source documents from which
eCRF information may have been generated
Signature of Principal Investigator Date
Name of Principal Investigator (printed or typed)
Protocol version date May 19 2009
Protocol Amendment 1 version date May 28 2010
Protocol Amendment 2 version date December 6 2011
68
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
13 References
1 Raghu G Brown KK Bradford WZ et al A placebo-controlled trial of interferon gamma-1b in patients with idiopathic pulmonary fibrosis N Engl J Med 2004350125-33 2 King TE Jr Safrin S Starko KM et al Analyses of efficacy end points in a controlled trial of interferon-gamma1b for idiopathic pulmonary fibrosis Chest 2005127171-7 3 Flaherty KR Thwaite EL Kazerooni EA et al Radiological versus histological diagnosis in UIP and NSIP survival implications Thorax 200358143-8 4 Wells AU Desai SR Rubens MB et al Idiopathic pulmonary fibrosis a composite physiologic index derived from disease extent observed by computed tomography Am J Respir Crit Care Med 2003167962-9 5 Raghu G Freudenberger TD Yang S et al High prevalence of abnormal acid gastroshyoesophageal reflux in idiopathic pulmonary fibrosis Eur Respir J 200627136-42 6 Kinnula VL Focus on antioxidant enzymes and antioxidant strategies in smoking related airway diseases Thorax 200560693-700 7 Coultas DB Zumwalt RE Black WC Sobonya RE The epidemiology of interstitial lung diseases Am J Respir Crit Care Med 1994150967-72 8 Raghu G Weycker D Edelsberg J Bradford WZ Oster G Incidence and prevalence of idiopathic pulmonary fibrosis Am J Respir Crit Care Med 2006174810-6 9 Olson AL Swigris JJ Lezotte DC Norris JM Wilson CG Brown KK Mortality from pulmonary fibrosis increased in the United States from 1992 to 2003 Am J Respir Crit Care Med 2007176277-84 10 Mannino DM Etzel RA Parrish RG Pulmonary fibrosis deaths in the United States 1979shy1991 An analysis of multiple-cause mortality data Am J Respir Crit Care Med 19961531548shy52 11 Hubbard R Johnston I Coultas DB Britton J Mortality rates from cryptogenic fibrosing alveolitis in seven countries Thorax 199651711-6 12 Johnston I Britton J Kinnear W Logan R Rising mortality from cryptogenic fibrosing alveolitis Bmj 19903011017-21 13 Raghu G Collard HR Egan JJ et al An official ATSERSJRSALAT statement idiopathic pulmonary fibrosis evidence-based guidelines for diagnosis and management Am J Respir Crit Care Med 2011183788-824 14 (USA) FDA FDA Public Health Advisory Interferon gamma-1b (marketed as Actimmune) In 2007 15 King TE Jr Pardo A Selman M Idiopathic pulmonary fibrosis Lancet 2011 16 Raghu G Brown KK Costabel U et al Treatment of idiopathic pulmonary fibrosis with etanercept an exploratory placebo-controlled trial Am J Respir Crit Care Med 2008178948shy55 17 Malouf MA Hopkins P Snell G Glanville AR An investigator-driven study of everolimus in surgical lung biopsy confirmed idiopathic pulmonary fibrosis Respirology 201116776-83 18 King TE Jr Behr J Brown KK et al BUILD-1 a randomized placebo-controlled trial of bosentan in idiopathic pulmonary fibrosis Am J Respir Crit Care Med 200817775-81 19 Richeldi L Costabel U Selman M et al Efficacy of a tyrosine kinase inhibitor in idiopathic pulmonary fibrosis N Engl J Med 20113651079-87
69
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
20 Borok Z Buhl R Grimes GJ et al Effect of glutathione aerosol on oxidant-antioxidant imbalance in idiopathic pulmonary fibrosis Lancet 1991338215-6 21 Meyer A Buhl R Magnussen H The effect of oral N-acetylcysteine on lung glutathione levels in idiopathic pulmonary fibrosis Eur Respir J 19947431-6 22 Behr J Maier K Degenkolb B Krombach F Vogelmeier C Antioxidative and clinical effects of high-dose N-acetylcysteine in fibrosing alveolitis Adjunctive therapy to maintenance immunosuppression Am J Respir Crit Care Med 19971561897-901 23 Cantin AM North SL Fells GA Hubbard RC Crystal RG Oxidant-mediated epithelial cell injury in idiopathic pulmonary fibrosis J Clin Invest 1987791665-73 24 Waghray M Cui Z Horowitz JC et al Hydrogen peroxide is a diffusible paracrine signal for the induction of epithelial cell death by activated myofibroblasts Faseb J 200519854-6 25 Larios JM Budhiraja R Fanburg BL Thannickal VJ Oxidative protein cross-linking reactions involving L-tyrosine in transforming growth factor-beta1-stimulated fibroblasts J Biol Chem 200127617437-41 26 Kinnula VL Fattman CL Tan RJ Oury TD Oxidative stress in pulmonary fibrosis a possible role for redox modulatory therapy Am J Respir Crit Care Med 2005172417-22 27 Meyer A Buhl R Kampf S Magnussen H Intravenous N-acetylcysteine and lung glutathione of patients with pulmonary fibrosis and normals Am J Respir Crit Care Med 19951521055-60 28 Behr J Degenkolb B Krombach F Vogelmeier C Intracellular glutathione and bronchoalveolar cells in fibrosing alveolitis effects of N-acetylcysteine Eur Respir J 200219906-11 29 Bando M Hosono T Mato N et al Long-term efficacy of inhaled N-acetylcysteine in patients with idiopathic pulmonary fibrosis Intern Med 2010492289-96 30 Demedts M Behr J Buhl R et al High-dose acetylcysteine in idiopathic pulmonary fibrosis N Engl J Med 20053532229-42 31 Toma TP Bhowmik A Rajakulasingam R Acetylcysteine in pulmonary fibrosis N Engl J Med 20063541086-9 author reply -9 32 Hunninghake GW Antioxidant therapy for idiopathic pulmonary fibrosis N Engl J Med 20053532285-7 33 Flaherty KR Mumford JA Murray S et al Prognostic implications of physiologic and radiographic changes in idiopathic interstitial pneumonia Am J Respir Crit Care Med 2003168543-8 34 Latsi PI du Bois RM Nicholson AG et al Fibrotic idiopathic interstitial pneumonia the prognostic value of longitudinal functional trends Am J Respir Crit Care Med 2003168531-7 35 Collard HR King TE Jr Bartelson BB Vourlekis JS Schwarz MI Brown KK Changes in clinical and physiologic variables predict survival in idiopathic pulmonary fibrosis Am J Respir Crit Care Med 2003168538-42 36 Jegal Y Kim DS Shim TS et al Physiology is a stronger predictor of survival than pathology in fibrotic interstitial pneumonia Am J Respir Crit Care Med 2005171639-44 37 Martinez FJ Safrin S Weycker D et al The clinical course of patients with idiopathic pulmonary fibrosis Ann Intern Med 2005142963-7 38 Hull JH Acetylcysteine in pulmonary fibrosis N Engl J Med 20063541089-91 author reply -91
70
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
39 Flaherty KR King TE Jr Raghu G et al Idiopathic interstitial pneumonia what is the effect of a multidisciplinary approach to diagnosis Am J Respir Crit Care Med 2004170904shy10 40 Raghu G Johnson WC Lockhart D Mageto Y Treatment of idiopathic pulmonary fibrosis with a new antifibrotic agent pirfenidone results of a prospective open-label Phase II study Am J Respir Crit Care Med 19991591061-9 41 Hunninghake GW Lynch DA Galvin JR et al Radiologic findings are strongly associated with a pathologic diagnosis of usual interstitial pneumonia Chest 20031241215-23 42 Lynch D Godwin J Safrin S et al High-resolution computed tomography in idiopathic pulmonary fibrosis diagnosis and prognosis Am J Respir Crit Care Med 2005172488-93 43 Mallinckrodt CH Watkin JG Molenberghs G Carroll RJ Choice of the primary analysis in longitudinal clinical trials Pharmaceutical Statistics 20043161-9 44 Bang H Tsiatis A Estimating medical costs with censored data Biometrika 200087329shy43 45 Lin DY Regression analysis of incomplete medical cost data Stat Med 2003221181-200 46 Rochon J Application of GEE procedures for sample size calculations in repeated measures experiments Stat Med 1998171643-58 47 Lachin JM Foulkes MA Evaluation of sample size and power for analyses of survival with allowance for nonuniform patient entry losses to follow-up noncompliance and stratification Biometrics 198642507-19
71
- PANTHER-IPFPREDNISONE AZATHIOPRINEAND N-ACETYLCYSTEINEA STUDY THAT EVALUATES RESPONSE INIDIOPATHIC PULMONARY FIBROSIS
-
- Protocol Summary
- Table of Contents
- List of Tables
- List of Figures
- List of Abbreviations
- 1 Summary
- 2 Hypotheses and Specific Aims
-
- 21 Null Hypothesis
- 22 Specific Aim 1
- 23 Specific Aim 2
- 24 Prespecified Subgroups of Interest
-
- 3 Background and Significance
-
- 31 Idiopathic Pulmonary Fibrosis is the Most Common Interstitial Lung Disease
- 32 Rationale for Placebo Control
- 33 Rationale for N-acetylcysteine
- 35 Rationale for N-acetylcysteine as a Stand-alone Therapy
- 36 Rationale for the Study Design and Primary Endpoint
- 37 Rationale for Blinding of Treatments
-
- 4 Methods
-
- 41 Inclusion Criteria
- 42 Diagnosis of IPF
- 43 Exclusion Criteria
- 44 Study Design and Study Visit
- 45 Dose Justification
- 46 Contraindications Precautions and Side Effects of Study Medications
- 47 Recruitment Procedures
- 48 Study Procedures
- 49 Concomitant Medications
- 410 Laboratory Testing
- 411 Blinding of Study Drugs
-
- 5 Study Endpoints
-
- 51 Primary Study Endpoint
- 52 Secondary Study Endpoints
-
- 6 Safety Evaluations and Procedures
-
- 61 Adverse Events
- 62 Clinical Medical Monitoring
- 63 Unblinding Procedures
-
- 7 Study Drug Procedures
- 8 Data Management
-
- 81 Hardware and Software Configuration
- 82 Sources of Data
-
- 9 Study Design and Data Analysis
-
- 91 General Analytic Considerations
- 92 Randomization Blinding and Reporting of Results
- 93 Stratification
- 94 Specification of the Primary Analyses
- 95 Analysis of Longitudinal Endpoints
- 96 Analysis of Binary Time-to-Event and Time-Lagged Endpoints
- 97 Power Analysis
-
- 10 Study Administration
-
- 101 Cooperative Agreement Mechanism
- 102 IPFnet Steering Group
- 103 Data and Safety Monitoring Board
- 104 Recommendations on Interim Monitoring of Efficacy Safety and Futility
-
- 11 Investigator and Sponsor Obligations
-
- 111 Monitoring
- 112 Cost and Payment
- 113 Confidentiality and Health Insurance Portability and Accountability ActConsiderations
- 114 Informed Consent Procedures
- 115 Institutional Review Boards
-
- 12 Investigator Agreement
- 13 References
-

PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
2 Hypotheses and Specific Aims 21 Null Hypothesis
Treatment with NAC will provide the same efficacy as PL as measured by longitudinal changes in FVC
22 Specific Aim 1
This study is designed to assess the safety and efficacy of NAC in subjects with newly diagnosed IPF
23 Specific Aim 2
Secondary goals of this study are to assess differences between treatment groups for the following
1 Mortality
2 Time to death
3 Frequency of acute exacerbations (AExs)
4 Frequency of maintained FVC response
5 Time-to-disease progression
6 Change in DLCO
7 Change in Composite Physiologic Index (CPI)
8 Change in resting alveolar-arterial oxygen gradient
9 Change in 6-minute walk test (6MWT) distance
10 Change in 6MWT oxygen saturation area under the curve
11 Change in 6MWT distance to desaturation lt 80
12 Change in 6MWT minutes walked
13 Changes in health status as measured by the SF-36 EuroQol and St Georgersquos Respiratory
Questionnaire (SGRQ)
14 Changes in dyspnea as measured by the University of California at San Diego Shortness of Breath
Questionnaire (UCSD SOBQ)
15 Frequency and types of adverse events (AEs)
16 Frequency and types of respiratory complications both infectious and noninfectious
17 Frequency of hospitalizations both all-cause and respiratory-related
13
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
24 Prespecified Subgroups of Interest
Treatment effects will be estimated and compared within key subgroups
Higher enrollment FVC12
Typical vs atypical high-resolution computed tomography (HRCT) reading at baseline3
Recent vs more remote diagnosis (time from initial diagnosis of IPF le 1 year and gt 1 year)
Lower CPI score at enrollment4
Medical therapy for gastroesophageal reflux5
Ethnic background
Sex
Smoking history (current or ex-smoker vs never smoker) given potential impact on oxidant status6
Presence of emphysema gt 25 on HRCT
14
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
3 Background and Significance
31 Idiopathic Pulmonary Fibrosis is the Most Common Interstitial Lung Disease
IPF is the most common interstitial lung disease (ILD) of unknown etiology The current incidence and
prevalence of IPF in the United States are not known A 1994 study of a population-based registry of subjects in
Bernalillo County New Mexico USA estimated an incidence of 107 cases per 100000 per year for males and
74 cases per 100000 per year for females the prevalence of IPF was estimated at 20 per 100000 for males and
13 per 100000 for females7 Extrapolating from a large healthcare claims database a more recent review
estimated the prevalence of IPF in the United States at 427 per 100000 (incidence estimated at 163 per
100000 per year)8 Recent epidemiological studies indicate increasing mortality rates from IPF in the United
States and other industrialized nations9-12
Approximately two-thirds of subjects with IPF are over the age of 60 at the time of presentation and the
incidence increases with age13 IPF has no distinct geographical distribution and predilection by race or
ethnicity has not been identified13 Individual subjects may remain relatively stable for prolonged periods
experience very slow declines in lung function with progression of radiographic abnormalities for a period of
months to years or experience more rapid declines and subsequent death Only 20 to 30 of IPF patients
survive for 5 years following diagnosis
There is currently no proven effective pharmacological treatment for IPF13 Anti-inflammatory and
immunosuppressive agents have been the traditional approach to the management of patients with IPF Based
on the results of the interim analysis of the PANTHER-IPF trial this lsquotraditional approachrsquo will be aborted
However it remains unknown if NAC alone will prove beneficial in IPF patients The primary goal of the
modified study is to establish an evidence-based standard of care and clarify the role of this specific antioxidant
pharmacotherapy for IPF
32 Rationale for Placebo Control
IPF is a disorder for which there is no proven efficacious therapy A major objective of this trial is to test to the
greatest degree possible a proposed standard of care for patients with IPF The current traditional therapy
15
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
employs immunosuppressive and corticosteroid drugs Interim review of the original PANTHER-IPF study has
documented increased adverse events and lack of efficacy for AZA-PRED-NAC compared to placebo
suggesting that this therapeutic approach should not be employed Whether this applies to NAC alone which
has been advocated by international societies has not been proven in well-designed well-powered clinical
trials The recommendations made in the recently published evidence guidelines for NAC monotherapy was
weak based on low quality13 Thus this continued clinical trial randomizing patients to receive NAC or placebo
is pivotal and will answer the important question of the potential therapeutic benefits of NAC monotherapy with
grade A evidence In this prospective randomized clinical trial the inclusion of a PL arm is therefore vital to
adequately test the benefits of NAC in well-characterized subjects with IPF
If NAC has no true efficacy then its role as standard of care will be refuted If a benefit compared with PL is
confirmed it will establish a benchmark against which future novel therapies for IPF will be safely compared
As there is no currently accepted therapy for IPF there is an increasing body of published literature supporting
the concept of no treatment as the ldquobest carerdquo option for IPF13
Post hoc analyses of PL-controlled trials suggest that subjects with milder disease may be more amenable to
therapy12 It is notable that a recent international prospective randomized trial of interferon-gamma for IPF
also included a PL arm the study was terminated early by the data and safety monitoring board (DSMB) due to
lack of treatment effect1415 This underscores the belief that a proven effective therapy for IPF does not
currently exist and that true placebo-controlled trials remain the gold standard Similarly recently completed
trials of etanercept everolimus bosentan and BIPF 1120 in IPF have included PL-treated arms16-19 In three of
these trials the treated subjects showed little if any objective improvement Based on this evidence and the
current status of IPF therapy and therapeutic trials we believe that clinicians and subjects will continue to enroll
in a PL-controlled study
33 Rationale for N-acetylcysteine
NAC is a derivative of the amino acid L-cysteine NAC has been shown to augment levels of the naturally
occurring antioxidant glutathione (GSH ) (glutathione γ-glutamyl cysteinyl glycine) both in vitro and in
vivo2021 GSH is present in all eukaryotic cells and may play an important role in protecting alveolar epithelial
cells against oxidant injury The concentration of GSH in the bronchoalveolar lavage (BAL) fluid in patients
16
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
with IPF is markedly diminished compared with normal subjects This GSH deficiency may be corrected by
exogenous administration of NAC2122
There is evidence of enhanced production of oxidants in an IPF lung Both inflammatory cells and
myofibroblasts derived from patients with IPF generate increased amounts of extracellular oxidants including
hydrogen peroxide2324 Secretion of hydrogen peroxide by activated myofibroblasts may induce the death of
adjacent lung epithelial cells by paracrine mechanisms24 Additionally generation of oxidants by myofibroblasts
induces oxidative crosslinking of extracellular matrix proteins25 a potential mechanism for aberrant matrix
remodeling Thus an oxidant-antioxidant imbalance exists in the lungs of IPF patients26 NAC may confer
protection against this imbalance by augmenting GSH levels in addition to its more direct free-radical
scavenging activity
Intravenous (IV) NAC therapy has been shown to increase total BAL GSH in 8 IPF subjects27 Oral NAC (600
mg 3 times per day) has been shown to decrease markers of oxidant injury and improve both total and reduced
GSH levels in the epithelial lining fluid of subjects with IPF in a small uncontrolled study22 pulmonary
function improved modestly with therapy A similar study in 18 IPF subjects confirmed increased intracellular
GSH concentration after 12 weeks of NAC (600 mg 3 times per day)2228 no clinical correlates were reported
Inhaled NAC was suggested to improve pulmonary function in an open label study29
35 Rationale for N-acetylcysteine as a Stand-alone Therapy
Results of a double-blind multi-center European clinical trial of 150 IPF subjects testing combinations of AZAshy
PRED vs AZA-PRED-NAC have been reported30 NAC added to AZA-PRED (ldquoconventional therapyrdquo) had a
significant positive effect on DLCO (p lt 0005) and vital capacity (VC) (p lt 005) at the end of 1 year30 The
recent ATSERS position statement after much discussion concluded that NAC alone should not be considered
in the majority of patients with IPF without additional data from well-designed studies
The interpretation of these data has been quite controversial Some have suggested that the magnitude of the
treatment effect although statistically significant is modest31 Others have suggested that NAC may be
modulating potential toxic effects of AZA-PRED alone32 supporting the investigation of NAC as stand-alone
therapy
17
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
The IPFnet is now completing the PANTHER-IPF trial with a 11 randomization (NAC vs placebo) and a
simple practical feasible and scientifically rational design that will establish standard of care with NAC for
IPF based on a currently available therapeutic agent and the existing data to support its use We anticipate that
all future clinical trials of novel therapeutic agents will be tested against this to-be-established standard of care
36 Rationale for the Study Design and Primary Endpoint
The optimal study design of a therapeutic trial in IPF would include survival as a primary endpoint The
published results of the IFN-γ 1b Phase 3 (GIPF-001) trial suggested a survival benefit in subjects with milder
disease in retrospective analyses1 although the trial was underpowered to address this question This was likely
related to the limited mortality in the PL arm of the study which included IPF subjects with mild to moderate
disease This study documents that an IPF study powered to improve survival in a patient population with mild
disease requires a larger sample size andor duration of study In fact the recently aborted Phase 3 IFN-γ 1b
(GIPF-007 INSPIRE) study was a survival-based study and recruited more than 800 subjects at 75 centers
worldwide1415 As such within the context of the current IPFnet trial survival is an impractical primary
endpoint variable
Several groups have published data defining an appropriate surrogate outcome variable a 10 decrement in
FVC during 6 to 12 months is a powerful predictor of survival in IPF33-36 Furthermore additional evidence
suggests a similar predictive ability for a 10 decrement in FVC during 3 months of follow-up37 With strong
supportive evidence of FVC progression being related to mortality on a per-subject basis this study will use
FVC changes in liters between treatment groups as the primary endpoint Previously published IPF studies have
shown a steady decline in FVC (and FVCpred) among control group subjects230 The GIPF-001 study
suggested a 48-week decrease in FVC of 016 L in the PL-treated subjects The IFIGENIA study demonstrated
a decline in FVC of approximately 019 L over 52 weeks in the subjects randomized to the control treatment
Figure 1 depicts the change in FVC for control groups from previously published IPF studies38 Based on these
data we expect that the PL group will have a decline of 020 L over the 60-week study period The IPFnet
Steering Group determined that a clinically meaningful improvement would be the preservation of the majority
of the 020-L FVC decline Therefore a mean treatment difference of 015 L in mean FVC over the 60-week
study period was determined to be a clinically meaningful difference
18
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Δ f
rom
bas
elin
e (i
n L
)
01
005
0
-005
-01
-015 Projected Δ for placebo
-02
-025
-019
-016
-013 Pirfenidone GIPF001
NAC
Placebo
4 8 12 16 20 24 28 32 36 40 44 48 52 56 60
Week
Figure 1 Changes in FVC From Baseline in Prior IPF Clinical Trials
Recent data suggest that various patient subgroups would be expected to potentially exhibit differential response
to therapy These parameters will be used to a priori separate patients by a series of baseline characteristics
including
1 Higher enrollment FVC12
2 Typical vs atypical high-resolution computed tomography (HRCT) reading at baseline3
3 Recent vs more remote diagnosis (time from initial diagnosis of IPF le 1 year and gt 1 year)
4 Lower CPI score at enrollment4
5 Medical therapy for gastroesophageal reflux5
6 Ethnic background
7 Sex
8 Smoking history (current or ex-smoker vs never smoker) given potential impact on oxidant status6
9 Presence of emphysema gt 25 on HRCT
37 Rationale for Blinding of Treatments
The issue of treatment blinding was given a great deal of consideration with subject safety being the primary
concern After discussion among the Steering Group members it was decided that as long as subject safety
could be ensured blinding was necessary Blinding allows the study to
Have optimal scientific validity and potential to impact the standard of care for subjects
19
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Make objective assessments of treatment effects
Maintain clinical equipoise among investigators
Encourage subjects to have similar levels of contact with the medical community
Minimize the differential dropout rates across study arms
20
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
4 Methods 41 Inclusion Criteria
1 Age 35 to 85 years inclusive
2 FVC ge 50 of predicted (post-bronchodilator measurement from the screening visit)
3 DLCO ge 30 of predicted (hemoglobin corrected and altitude corrected if gt4000 ft above sea level)
4 Ability to understand and provide informed consent
5 Diagnosis of IPF according to a modified version of the ATS criteria le 48 months from enrollment The
date of diagnosis is defined as the date of the first available HRCT or surgical lung biopsy characteristic
of definite UIP
411 Subjects Shown to Have Usual Interstitial Pneumonia Pattern on Surgical Lung Biopsy
Subjects who have been shown to have UIP pattern on lung biopsy must have all of the following
1 Exclusion of other known causes of ILD such as drug toxicity clinically significant environmental
exposures or diagnosis of connective tissue diseases
2 Bibasilar reticular abnormalities with minimal ground glass opacities on HRCT scan
412 Subjects Who Have Not Undergone a Surgical Lung Biopsy
In addition to the criteria above these subjects must have radiological findings considered to be definite for the
diagnosis of UIPIPF
1 Bibasilar reticular abnormalities with minimal ground glass opacities
2 Honeycombing as the predominant feature and located in the peripheral lung bases
42 Diagnosis of IPF
Only subjects with definite IPF will be eligible for enrollment in this study We will utilize a combination of
clinicalphysiologic features HRCT and review of a clinically obtained surgical lung biopsy specimen to
establish the diagnosis of IPF An algorithm for the diagnosis is provided to guide entry into the protocol as
outlined in the inclusion and exclusion criteria (Figures 2 and 3) This multi-disciplinary approach uses
21
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
expertise from clinicians radiologists and pathologists Investigators at each site in conjunction with central
pathology will work together to establish the diagnosis of IPF This interactive approach to the diagnosis of IPF
increases the level of agreement between observers39
A subject with suspected ILD should be evaluated for secondary causes including but not limited to
environmental exposures drugs and systemic diseases Presence of any of these findings felt to be significant
enough to cause an ILD should disqualify the subject from entry into the trial
If secondary causes are absent an HRCT scan may be obtained If an HRCT of sufficiently high quality has
been obtained within the last 3 months that scan may be used for diagnosis In the appropriate clinical setting
the diagnosis of IPF can be made by the demonstration of a typical radiographic pattern on HRCT or by
demonstration of UIP pattern on a surgical lung biopsy The following criteria for a radiographic (ie
nonsurgical) diagnosis will be used In the absence of known exposures andor clinical associations attributable
to pulmonary fibrosis and in the appropriate clinical setting the presence of definite UIP pattern in HRCT
images is required to meet study criteria for the diagnosis of IPF
Figure 2 Diagnosis of Idiopathic Pulmonary Fibrosis in the IPFnet
22
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Figure 3 Pathology Flow Chart Surgical Lung Biopsy Diagnosis
Requirement for diagnosis
1 Clinical exclusion of other known causes (connective tissue diseases environmental and drug
exposures) of ILD
2 Radiographic HRCT with bibasilar reticular abnormality and honeycomb change with minimal
ground glass opacities
Appropriate clinical setting
1 Age gt 50 years
2 Insidious onset of unexplained dyspnea
3 Duration of illness for ge 3 months
4 Bibasilar inspiratory crackles
23
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Unlike the ATSERS consensus criteria published in 2000 bronchoscopy will not be required for diagnosis
This decision was made based on the experience of the IPFnet Steering Group members regarding the utility of
bronchoscopy in the diagnosis of IPF The presence of an atypical HRCT finding will require documentation of
a definitive diagnosis by surgical lung biopsy In fact this is in keeping with the recently published evidence
based guidelines for diagnosis and management of IPF13 As shown in Figure 3 central review of the pathology
data will be required for a diagnosis of IPF
We will not require central review of HRCT as several studies have shown that a confident local interpretation
of clinicalHRCT criteria as definite IPFUIP is associated with a high positive predictive value for finding UIP
at surgical lung biopsy (see Table 1) Differences in sensitivity in these series likely reflect subject selection as
Flaherty et al3 evaluated only UIP and nonspecific interstitial pneumonia (NSIP) while Raghu et al40 and
Hunninghake et al41 included a broader range of ILD
Table 1 Operating Characteristics of Local HRCT Review for Diagnosis of UIP
Researcher of Subjects Sensitivity () Specificity () PPV () NPV ()
Raghu et al 40
59 (29 UIP by SLB) 78 90 88 82
Hunninghake et al 41 91 (54 UIP by SLB)
74 81 85 67
Flaherty et al 3 96 (only NSIP amp UIP)
37 100 100 30
Abbreviations PPV positive predictive value NPV negative predictive value UIP usual interstitial pneumonia SLB surgical lung biopsy and NSIP nonspecific interstitial pneumonia
Furthermore an analysis of the HRCT scans from subjects enrolled in the GIPF-001 trial confirmed that local
site interpretations have a high congruity to a central radiology core In this multi-center study 263 HRCT
scans were read as definite IPF and a retrospective central radiology core review found 932 to be consistent
with IPF 42 We will also take several additional steps to insure that the local HRCT reads are accurate
including
1 A detailed training module has been developed and must be completed by each site radiologist before
site initiation
2 Clinical centers are to mail all HRCT scans to the HRCT core lab The first 10 HRCT scans from
subjects enrolled at each enrolling clinical center will be reviewed centrally to be certain that local reads
24
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
25
are congruent with a central interpretation If discrepancies are identified additional education will be
provided and HRCT scans will continue to be reviewed centrally until the central radiology core is
confident that the local center is performing appropriately
3 Random scans will be obtained from each center throughout the study to confirm that the local read
continues to agree with central interpretation If discrepancies are identified they will be addressed as in
2 above
In all cases if a subject has a surgical lung biopsy sample that sample will be reviewed by the local and central
pathologists Therefore the only cases that would not be subject to a direct central review process are those
where the HRCT meets the centrally defined criteria for an unequivocal diagnosis and a lung biopsy sample is
not available Table 2 below summarizes the possible combinations for making a diagnosis
Table 2 Combining HRCT and Pathology Interpretations to Determine if IPF is Present
HRCT Diagnosis Pathology Diagnosis Diagnosis of IPF
Definite UIP Definite UIP Yes
Definite UIP Probable UIP Yes
Definite UIP Possible UIP Yes
Definite UIP Not UIP No
Definite UIP Unavailable Yes
Consistent with UIP Definite UIP Yes
Consistent with UIP Probable UIP Yes
Consistent with UIP Possible UIP No
Consistent with UIP Not UIP No
Consistent with UIP Unavailable No
Inconsistent with UIP Any No
Abbreviations HRCT high-resolution computed tomography IPF idiopathic pulmonary fibrosis
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
UIP usual interstitial pneumonia Dx diagnosis 43 Exclusion Criteria
1 History of clinically significant environmental exposure known to cause pulmonary fibrosis
Occupational exposures such as asbestos or environmental exposure to organic dust such as occurs in
pigeon breeders may at times mimic the clinical and radiographic findings of IPF
2 Diagnosis of connective tissue disease felt by the principal investigator (PI) to be the etiology of the
interstitial disease Diagnosis of collagen-vascular conditions will be according to the published
American College of Rheumatology criteria As such the presence of any documented collagen-vascular
disorder or the presence of any suspicious symptom complex whether or not associated with
significantly abnormal rheumatological serologies will exclude the subject at the discretion of the PI
3 Extent of emphysema greater than the extent of fibrotic change (honeycombing reticular changes) on
HRCT scan
4 Forced expiratory volume in 1 second (FEV1)FVC ratio lt 065 at screening (postbronchodilator)
5 Partial pressure of arterial oxygen (PaO2) on room air lt 55 mm Hg (lt 50 mm Hg at Denver site)
6 Residual volume gt 120 predicted at screening (postbronchodilator)
7 Evidence of active infection
8 Significant bronchodilator response on screening spirometry defined as a change in FEV1 ge 12 and
absolute change gt 200 mL OR change in FVC ge 12 and absolute change gt 200 mL The percent
difference between the FVC (or FEV1) values will be calculated by taking the absolute value of the
difference and dividing it by the larger of the two FVC (or FEV1) values
9 Screening and enrollment post-bronchodilator FVC measurements (in liters) differing by gt 11 The
percent difference between the FVC values will be calculated by taking the absolute value of the
difference and dividing it by the larger of the two FVC values (eg the percent difference between FVC
measurements of 19 and 20 liters would be determined by taking the difference between the two (01
liters) and dividing by the larger of the two (20 liters) So 0120 = 5 and these FVC measurements
would not exclude the subject
10 Listed for lung transplantation ie the patient has completed the evaluation process has been accepted
as a candidate for transplantation at an appropriate center and is waiting to receive notification of an
available donor organ
11 History of unstable or deteriorating cardiac disease
12 Myocardial infarction coronary artery bypass or angioplasty within 6 months of screening
26
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
13 Unstable angina pectoris or congestive heart failure requiring hospitalization within 6 months of
screening
14 Uncontrolled arrhythmia
15 Severe uncontrolled hypertension
16 Known HIV or hepatitis C
17 Known cirrhosis and chronic active hepatitis
18 Active substance andor alcohol abuse (as determined by site PI)
19 Pregnancy or lactation (subjects who are pregnant or breastfeeding)
20 Known hypersensitivity to study medication
21 Any condition other than IPF that in the opinion of the site PI is likely to result in the death of the
subject within the next year
22 Any condition that in the judgment of the PI might cause participation in this study to be detrimental to
the subject or that the PI deems makes the subject a poor candidate
23 Any therapy directed at pulmonary fibrosis (excepting triple therapy of prednisone plus azathioprine
plus NAC) requires a 30-day washout period before randomized Triple therapy of lt= 12 weeks duration
in the past 4 years requires a 30-day washout period before randomization
24 History of triple therapy of prednisone plus azathioprine plus NAC for gt 12 weeksrsquo duration in the past
4 years or previous enrollment in the triple-therapy arm of the PANTHER-IPF study
44 Study Design and Study Visit
441 Study Design Summary
This study will be a randomized double-blind PL-controlled trial designed to assess the safety and efficacy of
NAC in subjects with newly diagnosed IPF
Subjects with mild to moderate IPF (defined as FVCpred ge 50 and DLCOpred ge 30) diagnosed within
the past 48 months will be enrolled Screening will continue until April 30 2012
27
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
The study will employ a 2-arm design with 11 randomization to NAC or PL Once enrolled subjects will visit
the clinical center at 15 weeks and 15-week intervals thereafter Each subject will be treated and followed for a
maximum of 60 weeks
During the 60-week visit subjects will be taken off all study agents Approximately four weeks after the final
dose of study agent is taken subjects will receive a safety phone call from the study site
442 Study Visits
Subjects who meet entry criteria will review the informed consent a written description of the purpose
procedures and risks of the study with the PI co-investigator or study coordinator and all questions will be
answered The informed consent form will be signed by the subject at screening No protocol-specific
procedures will be performed until the subject has signed and dated an informed consent form This includes the
screening procedures
4421 Screening
Once informed consent is obtained subjects may immediately begin the screening process or may return within
28 days of consent In the event a study subject has been clinically evaluated at the study site by an IPFnet study
physician and has performed testing within three weeks for this clinical evaluation that meets guidelines
provided in the IPFnet PANTHER-IPF Manual of Operating Procedures (MOOP) this testing may be used to
satisfy the following screening criteria medical history physical exam arterial blood gas (ABG) with A-a
gradient vital signs with oximetry body height and weight spirometry DLCO lung volumes and HRCT scan
Allowing the use of previously performed test results that meet study guidelines for the screening visit is
intended to permit subjects easier access to study entry to prevent subjects from repeating testing that has been
performed within the study window and to decrease risks to subjects from repeated exposure to procedures
such as arterial puncture and HRCT
The following procedures will be performed at screening
Medical history and a physical examination
28
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Measure height and weight
Serum pregnancy test (if applicable)
Measure vital signs including oximetry
Blood draws performed and the following analyses conducted
o Hematology (red cell count white cell count hemoglobin hematocrit cell indices differential
platelet count)
o Blood chemistries according to central laboratory protocol (see Section 410 Laboratory
Testing)
o Beta human chorionic gonadotropin (serum) pregnancy test (in women of childbearing potential)
o Urinalysis
Pulmonary Function Tests (PFTs) including spirometry pre- and post- bronchodilator and postshy
bronchodilator measurement of lung volumes and measurement of hemoglobin adjusted diffusing
capacity
Measure ABGs
HRCT if a satisfactory scan has not been performed on the subject within 3 months of screening (see
PANTHER-IPF MOOP for more details)
Surgical lung biopsies (if applicable) reviewed by local and central pathology departments
Current medications If required a washout period discussed with the subject and initiated at this visit
4422 Enrollment
The enrollment visit is expected to take place within eight weeks of the screening visit Enrollment visit
activities include
Measure vital signs including oximetry
Measure height and weight
Serum pregnancy test (if applicable)
If consent has been given blood will be drawn and a urine specimen collected for the bio-specimen
repository
Spirometry (post-bronchodilator)
Measure 6MWT with Borg Dyspnea Scale
29
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Collect Quality-of-life (QOL) data using the SF-36 EuroQol Investigating Choice Experiments for
Preferences of Older People Capability Instrument (ICE CAP) and SGRQ
Female subjects complete Gender Substudy questionnaire
Dyspnea status collected using the UCSD SOBQ
Evaluate Acute Exacerbation (AEx)
Review of any Adverse Events (AEs)
Review of concomitant medications
Subject receives diary and instructions on its purpose and proper use
Subject receives supply of study drug sufficient to last until his or her 15-week study visit
See the Schedule of Assessments (Table 3) for more details Subjects with screening and enrollment postshy
bronchodilator FVC measurements (in liters) differing by more than 11 are not eligible to be enrolled in the
study
Subjects will be asked to provide a physician of record This physician will be considered the subjectrsquos primary
care provider (PCP) and if the subject agrees the PCP will be informed by letter of the subjectrsquos enrollment in
the trial The subject will be informed that his or her ongoing medical care should be received from the PCP
The PCP will be informed of any safety issues identified by the study staff The PCP will also be given
information regarding communication with study personnel about pertinent health issues or clinic encounters
the subject may have
4423 Week 15
The week 15 visit is expected to occur within +- 14 days of the subjectrsquos scheduled visit time (eg the week 15
visit should occur anytime between 13 and 17 weeks after starting study drug Week 15 activities include
Measure vital signs with oximetry
Measurement height and weight
Serum pregnancy test (if applicable)
Spirometry (post-bronchodilator) measurement
Review of AEs
Evaluate for AEx
30
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Review concomitant medications
If consented draw blood and collect urine specimen for the biospecimen repository
Subjects return used and unused study drug for the visit
Review study diary and a new study diary will be given
Provide additional supply of study drug sufficient to last until the next scheduled visit
4424 Week 30
The week 30 visit is expected to occur within +- 14 days of the subjectrsquos scheduled visit time (eg the week 30
visit should occur anytime between 28 and 32 weeks after starting study drug) Week 30 activities include
Physical examination
Measure vital signs with oximetry
Measure height and weight
Laboratory values (complete blood count [CBC] and serum chemistries)
Serum pregnancy test (if applicable)
Measure spirometry (post-bronchodilator)
6MWT with Borg scale
DLCO
Review of AEs
Evaluate for AEx
Review concomitant medications
Complete all QOL and dyspnea questionnaires (EuroQol ICE CAP SF-36 SGRQ and UCSD SOBQ)
If consent has been given blood will be drawn and a urine specimen collected for the biospecimen
repository
Review study diary
Subjects return used and unused study drug for the visit
Provide additional supply of study drug sufficient to last until the next scheduled visit
4425 Week 45
31
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
The week 45 visit is expected to occur within +- 14 days of the subjectrsquos scheduled visit time (eg the week 45
visit should occur anytime between 43 and 47 weeks after starting study drug) Week 45 activities include
Measure vital signs with oximetry
Measure height and weight
Serum pregnancy test (if applicable)
Measure spirometry (post-bronchodilator)
Review of AEs
Evaluate for AEx
Review concomitant medications
If consent has been given blood will be drawn and a urine specimen collected for the biospecimen
repository
Subjects return used and unused study drug for the visit
Study diary reviewed
Provide additional supply of study drug sufficient to last until the next scheduled visit
4426 Week 60 (Early Withdrawal or Final Treatment Visit)
At week 60 or at subject withdrawal from the study (premature by study doctor or subjectrsquos decision) a final
treatment visit will occur At this final treatment visit subjects will discontinue NACPL abruptly Week 60
activities also include
Physical examination
Measure vital signs with oximetry
Measure height and weight
Laboratory values (complete blood count [CBC] and serum chemistries)
Spirometry (post-bronchodilator) measurement
6MWT with Borg scale measurement
DLCO
Lung volumes
ABG
Review of AEs
32
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Evaluate for AEx
Review concomitant medications
Subjects will complete all QOL and dyspnea questionnaires (EuroQol ICE CAP SF-36 SGRQ and
UCSD SOBQ)
If consent has been given blood will be drawn and a urine specimen collected for the biospecimen
repository
Subjects return used and unused study drug for the visit
Study diary reviewed
4427 Final Site Visit ndash FVC drop confirmation
In the event that the subject has a recorded FVC drop of gt10 from baseline at the final treatment visit and the
subject has not had a confirmation of such a drop at a previous study visit the subject should return to the
clinical site 6 to 8 weeks after the final treatment visit During this visit a post-bronchodilator spirometry test
will be performed This FVC measurement will be evaluated according to section 521 of this protocol
4428 Final Visit ndash Telephone Follow-up
Four weeks following the final dose of study medication subjects will receive a telephone call from the study
coordinator to ensure that there are no side effects and to follow up on any ongoing adverse events (AEs)
4429 Phone Contact Between Visits
At week 2 and each month that a subject does not have a scheduled clinical center visit his or her study
coordinator will contact him or her at least once by telephone to
Inquire if the subject has had any hospitalizations events that might be considered an AE or any events
significant enough to warrant an out-of-cycle visit to the clinical center
Remind subjects of their current dosage levels and confirm that the subject understands them
Address any questions or concerns the subject might have regarding other aspects of the study
Assess adherence to the treatment regimen by reviewing diary data verbal review of medications taken
including nutritional supplements
33
34
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Table 3 Schedule of Assessments
Procedure Screening Visit 0
Enrollment Visit 1
Week 15 Visit 2
Week 30Visit 3
Week 45 Visit 4
Week 60 Early
Withdrawal Visit 5
Final1
Visit (via phone)
Informed consent X
Medical history X
Inclusionexclusion criteria X
Serum pregnancy test (if applicable) X X X X X
Review of lung biopsy X
Arterial Blood Gas X X
6-Minute Walk Test
X
X X
Physical examination X X X
Vital signs with oximetry X X X X X X
Body height and weight X X X X X X
Complete Blood Count X X X
Chemistry panel X X X
Monitor Lab Values X X X
Urinalysis X Specimen repository substudy blood draw and urine collection (if consented)
X
X X X X
HRCT (if not completed within three months) X
Spirometry (pre- and post-bronchodilator) X
Spirometry (post-bronchodilator only) X X X X X
DLCO (post-bronchodilator only) X X X
Lung volumes (post-bronchodilator only) X
X
Evaluate for acute exacerbation X X X X X
Review Adverse Events X X X X X X
Review concomitant meds X X X X X X
Dispense subject diary X X X X
Review subject diary X X X X X
Dispense study agent X X X X
Gender Substudy questionnaire (female subjects only) X
EuroQol ICECAP UCSD SOBQ SGRQ SF-36 X X X
Abbreviations DLCO diffusing capacity of the lung for carbon monoxide QOL Quality of Life ICECAP Investigating Choice Experiments for Preferences of Older People UCSD SOBQ University of California Shortness of Breath Questionnaire SGRQ St Georgersquos Respiratory Questionnaire SF-36 Short Form 36 Health Survey
1Follow-up visit via phone will occur four weeks after final dose of study medication
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
45 Dose Justification
The general philosophy for determining dosing levels was to apply previously examined
treatment regimens With the focus of the study being to establish a standard of care for
mildmoderate IPF subjects the goal was to develop flexible yet standardized treatment rules that
allow for the temporary or permanent withholding of one or more components of treatment when
necessary Subjects developing laboratory abnormalities or symptoms that result in
discontinuation of one or more components of study treatment may continue on the other
components as long as there is no contraindication for this Complete follow-up is important for
the validity of any study As a strategy to maintain protocol adherence we are using a treatment
regimen that will detect potential side effects and prompt interventions proactively in the interest
of patient safety In addition subjects who permanently stop study medications during the course
of the study are encouraged to continue in the study completing all scheduled visits and tests
451 Rationale for N-acetylcysteine Dosing
To our knowledge there have been no IPF studies to correlate clinical outcome measures with
different dosages for NAC The dosage chosen is based on the IFIGENIA study However BAL
lung GSH levels from subjects with IPF have been augmented with the use of oral NAC at 600
mg 3 times per day In addition lung GSH levels have been associated with improved
PFTs212227 The dose chosen for this study was based on previous data including the IFIGENIA
study30
4511 Dosing of N-acetylcysteineplacebo
Dosing of NACPL will be 600 mg orally 3 times a day (1800 mgday)
4512 Reasons to Discontinue N-acetylcysteineplacebo
NACPL may be temporarily or permanently discontinued for the duration of the study for
gastrointestinal symptoms or dermatologic reactions
35
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Temporarily discontinue (hold) oral NACPL for subjects requiring inpatient admission for acute
exacerbation (AEx) or other conditions Resume NACPL after discharge
36
37
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
452 Dosage Algorithms
Dosage Adjustment Algorithm 1 NACPL Dose Modifications for Gastrointestinal Symptoms Nausea Vomiting Abdominal Discomfort Diarrhea
GI Symptoms determined by the PI to be clinically significant Nausea Vomiting Abdominal Discomfort Diarrhea
NACPL Temporarily dc (HOLD) x 3 Days
Monitor symptoms intervene as clinically indicated (eg fluid replacement antidiarrhea or antinausea medication)
Monitor or lab PRN
Are symptoms resolving after 3 days NO
Symptoms NOT resolving after 3 days of holding study medication Assessmentmanagement per clinical
discretion of investigator
Likely not study medication discuss resuming study medication with medical monitor when symptoms resolved
YES
Temporarily dc (HOLD) NACPL for 4 additional days (total hold 1 week) then NACPL Resume 600 MG TID
Did symptoms recur
YES
STOP NACPL for
duration of study
NO
NACPL No Change
38
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Dosage Adjustment Algorithm 2 NACPL Dose Modifications For Dermatologic Reactions
Dermatologic Reactions (Not Acneiform) ge Grade 2 Grading per Common Terminology Criteria for
Adverse Events V30 (httpctepcancergov) For example Grade 1 RASHDESQUAMATION Macular or papular eruption or erythema without associated symptoms Grade 2 RASHDESQUAMATION Macular or popular eruption or erythema with pruritus or other associated symptoms localized desquamation or other lesions covering lt50 of body surface area
NACPL Temporarily dc (HOLD) x 3 days
Are symptoms resolving after 3 days
NO Symptoms not resolving after 3 days of holding study medication Assessmentmanagement per clinical discretion of investigator Likely not study medication Discuss resuming study medication with medical monitor when symptoms
resolved YES
Temporarily dc (HOLD) NACPL for 4 additional days (total hold 1 week) then NACPL resume 600 MG TID
Did symptoms recur
YES
STOP NACPL for
duration of study
NO
NACPL No change
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
46 Contraindications Precautions and Side Effects of Study Medications
461 Contraindication
Contraindication to NAC is known hypersensitivity to it
462 Precautions
Concomitant administration of oral NAC and antibiotics has shown a slightly reduced absorption
of cephalexin and a slight increase in erythromycin serum levels NAC contains free sulfhydryl
groups There is no evidence that individuals sensitive to sulfa drugs are sensitive to NAC
The NAC preparation being administered in this study contains 20 mg of aspartame Because of
the phenylalanine component of aspartame individuals with phenylketonuria should avoid or
restrict aspartame intake to avoid increased blood levels of phenylalanine Because of this risk
labeling is required on all products containing aspartame
463 Side Effects
Side effects of NAC range from common to serious See Table 4
39
40
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Table 4 Side Effects of NAC
Undesirable Effects
System-organ class Uncommon
(gt11000 lt1100)
Rare
(gt110000 lt11000)
Very rare
(lt110000) Not known
Immune system disorders Hypersensitivity Anaphylactic shock
reaction
Nervous system disorders Headache
Ear and labyrinth disorders Tinnitus
Cardiac disorders Tachycardia
Vascular disorders Hemorrhage
Respiratory thoracic and
mediastinal disorders
Bronchospasm
Dyspnea
Gastrointestinal disorders
Vomiting diarrhea
stomatitis abdominal
pain nausea
Dyspepsia
Skin and subcutaneous tissue
disorders
Urticaria rash
angioedema itching
General disorders and
administration site conditions Pyrexia
Investigations Reduced arterial
pressure Face edema
In very rare cases the onset of severe skin reactions such as Stevens-Johnson syndrome and Lyell syndrome was reported to have a temporal relationship with N-acetylcysteine administration Although in most cases at least another suspect drug probably most involved in the genesis of the above mentioned mucocutaneous syndromes has been identified in case of mucocutaneous alterations it is appropriate to contact onersquos doctor and the administration of N-acetylcysteine should be immediately discontinued
Some studies confirmed a reduction of platelet aggregation during N-acetylcysteine administration The clinical significance of these findings has not been defined yet [Source Fluimucil Investigator Brochure]
47 Recruitment Procedures
Subjects recruited for this study will be established patients of the investigators or physician- or
self-referred to participating clinical centers in the IPFnet Each clinical center within IPFnet has
a well-developed infrastructure of local pulmonologists within the surrounding geographic area
These pulmonologists are kept informed of ongoing IPF clinical trials and regularly refer
subjects to studies conducted at IPFnet clinical centers
Additional steps will be taken to inform clinicians of the trials in progress within IPFnet
including presentations at faculty staff meetings at local hospitals medical grand rounds and
national conferences direct mail notification monthly faxes and advertisement of network trials
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
in pulmonary journals Clinical center patients previously diagnosed with IPF will be notified of
the trials by mail whenever possible
Recruitment of minorities and women will be monitored by the DCC and DSMB If necessary
additional recruitment efforts will be made at specific centers to ensure that the aggregate subject
sample contains appropriate representation of women and minorities
48 Study Procedures
The following procedures are detailed in the PANTHER-IPF MOOP accompanying this
protocol
1 PFT
2 ABG
3 HRCT scan of the chest (including imaging of pulmonary arteries)
4 CBC and serum chemistries
5 Pregnancy test
6 6MWTBorg Dyspnea Scale
7 QOL questionnaires (EuroQol HAD SF-36 SGRQ and ICE CAP)
8 UCSD SOBQ
9 Gender Substudy Questionnaire
All assessments of PFTs will be conducted by study personnel not directly involved in the
treatment of the subjects
481 Biological Specimen Management
4811 Biological Specimen Sample Management
Subjects at clinical centers participating in the specimen repository substudy who consent to
having blood drawn for research purposes and for the banking of blood blood components and
other biologic specimens (urine and BAL fluid) will have approximately 405 mL of blood
41
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
drawn 17 mL blood drawn for DNA and 20 mL of urine collected at enrollment visit Subjects
will have approximately 50 mL of blood drawn and 20 mL of urine collected at each 15-week
follow-up visit Blood specimens will be separated according to PANTHER-IPF MOOP
guidelines into the following components for banking in the repository serum plasma and
DNA Coding of all biologic specimens for the repository will be performed by study staff at the
clinical center The samples will be processed per PANTHER-IPF MOOP guidelines aliquoted
labeled with barcode labels and stored at -70degC at the clinical center and shipped to the central
repository
The only subject identifiers will be a sample ID number and subject initials This sample ID will
be linked in the IPFnet DCC clinical database to subject information No subject information will
be transferred to the biological-specimen database
The subjectrsquos samples may be used for approved sub-studies relating to human disease
including but not limited to IPF The studies for which an individualrsquos samples will be made
available will be determined by the subjectrsquos answers to questions on the biological-sample
informed consent form The subjects can choose to make their samples available for all options
or any combination Samples will be made available to researchers only with IPFnet Steering
Group approval until such time as the samples are made public through the NHLBI repository
49 Concomitant Medications
Concurrent treatment with FDA-approved therapy for IPF is allowed Colchicine may be used
for treatment of gout Temporary treatment with oral or IV corticosteroids for clinical worsening
or suspected AEx is permitted Nutritional supplements containing NAC are not allowed
410 Laboratory Testing
Clinical laboratory parameters will be assessed at screening and at the end of the study The
following tests will be performed at the two time points specified in the protocol chemistry (AG
ratio ALT [SGPT] AST [SGOT] albumin alkaline phosphatase amylase bilirubin-direct
42
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
bilirubin-indirect bilirubin-total BUN BUNcreatinine ratio calcium carbon dioxide
cholesterol-total chloride CPK-total creatinine GGT globulin glucose iron-total LDH
lipase magnesium phosphorus-inorganic potassium protein-total sodium TIBC triglycerides
uric acid) and hematology (red blood cell count WBC count hemoglobin hematocrit cell
indices differential platelet count)
411 Blinding of Study Drugs
Subjects and caregivers will be blinded to study treatment Every subject will receive NAC or
matching PLs at every study visit from the baseline visit to the week-45 visit No study agent
will be dispensed at the week-60 visit
43
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
5 Study Endpoints
51 Primary Study Endpoint
The primary endpoint will be the change in serial measurements of FVC over the study period
52 Secondary Study Endpoints
521 Time to Disease-progression
The time-to-death or a 10 decline in FVC will be defined as the time-to-disease progression
The 10 decline in FVC from enrollment must be confirmed on 2 consecutive visits no less than
6 weeks apart For subjects with 2 consecutive visits with a 10 decline in FVC the time-toshy
disease progression will be defined as the time interval between enrollment and the initial visit
with a 10 FVC decline For subjects who experience disease progression the study doctor will
determine whether or not the subject will remain in the study
522 Acute Exacerbations
The following 3 criteria will define AEx in subjects with acute worsening of their respiratory
conditions
1 Clinical (all of the following required)
A) Unexplained worsening of dyspnea or cough within 30 days triggering unscheduled
medical care (eg emergency room clinic study visit hospitalization)
B) No clinical suspicion or overt evidence of cardiac event pulmonary embolism or deep
venous thrombosis to explain acute worsening of dyspnea
C) No pneumothorax
44
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
2 RadiologicPhysiologic (A and B required)
A) New ground glass opacity or consolidation computed tomography (CT) scan OR new
alveolar opacities on chest x-ray
B) Decline of ge 5 in resting room air SpO2 from last recorded level OR decline of ge 8 mm
Hg in resting room air PaO2 from last recorded level
3 Microbiologic (all of the following required)
A) No clinical evidence for infection (ie absence of grossly purulent sputum fever gt 39degC
orally)
B) Lack of positive microbiological results (if done) from lower respiratory tract defined as
(1) Clinically significant bacterial growth on sputum or endotracheal aspirate cultures
(2) Quantitative culture by protected brush specimen ge 103 cfumL or BAL ge 104 cfumL
(3) The presence of specific pathogens on stains of any of the above
C) Lack of positive pathogen in blood cultures (if done)
Identification of Acute Exacerbations
All subjects will be educated about the importance of identifying AExs At the time of
enrollment subjects will be told about the possibility of developing acute symptomatic
worsening that might represent an AEx of IPF and instructed to contact their study clinical
center coordinator within 48 to 72 hours of the apparent event
All subjects will be contacted by phone monthly and questioned about any change in dyspnea or
cough and any interim clinic visits or hospitalizations Finally as part of the IPFnet outreach to
community referring physicians the importance of AExs will be emphasized When a subject is
identified who meets criterion 1A this will trigger the collection of additional clinical data to
evaluate a suspected AEx These data will be collected as part of standard clinical care (ie this
protocol does not require collection of all items) The additional items to be collected for
suspected AEx include
IPFnet AEx case report form (eCRF) (required)
45
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Chest x-ray CT scan withwithout pulmonary angiogram (reports should be faxed and
followed by the hard copiesdiscs)
Oxygen saturation (pulse oximetry)
ABG
Respiratory cultures (sputum endotracheal aspirate lavage)
Blood cultures
Clinichospital records related to the event
All potential cases of AEx will be reviewed by the clinical center PI first and a decision on
whether the case may represent an AEx will be made If AEx is suspected the case will be sent
to the IPFnet adjudication committee which will assign a final diagnosis (see Table 5) If there is
disagreement among members the majority opinion will be recorded
During episodes of suspected AEx as determined by the individual clinical center investigator
subjects will remain blinded and in the study
Table 5 Final Diagnoses in Evaluation of Suspected Acute Exacerbations
Definite acute exacerbation All criteria met no alternative etiology
Unclassifiable acute worsening
Insufficient data to evaluate all criteria no alternative etiology
Not acute exacerbation Alternative etiology identified that explains acute worsening
Management of the suspected AEx will be at the discretion of the treating physician Standard of
care generally involves evaluation for respiratory infection pulmonary embolism cardiac events
and pneumothorax and treatment with IV corticosteroids
Study drugs will be resumed at pre-suspected AEx doses after subjects clinically improve as
confirmed by the local PI All subjects should be seen at the clinical center within 2 to 4 weeks
of recovery for measurement of post-bronchodilator FVC (see Figure 4) Subjects unable to
return to the clinical center after suspected AEx due to medical frailty (eg continued
46
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
institutionalization progressive disability) will be categorized as failing to maintain FVC
response in secondary analyses
Suspected AEx (PI determined)
Hold study drug Treat AEx
(Attending physician determined)
Alive but unable to continue due to
medical frailty
Dead
Alive and able to continue
Site reviewvisit
Restart study drug
FVC within 2-4 weeks
Figure 4 Acute Exacerbation Flow Chart
523 Respiratory Infections
An upper respiratory infection will be defined as
Change in sputum discoloration
Increased cough of no more than 14 daysrsquo duration
A lower-respiratory infection (pneumonia) will be defined as new segmental or lobar airspace
opacities visualized by image studies (chest radiograph or HRCT) in addition to any of the
following
Positive pathogencultures in good sample of sputum or lower-airway secretions retrieved
by fiberoptic bronchoscope
Fever gt 39degC or gt 100degF
Leukocytosis gt 12000 (unexplained no increase in dose of corticosteroids)
47
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
524 Maintained FVC Response
Subjects with follow-up FVCpred measurements at or above their baseline FVCpred level
will be classified as having maintained FVC response Subjects with reduced FVCpred levels
or missing data for any reason including death or medical frailty will be classified as having not
maintained FVC response The FVCpred value is used because unadjusted FVC measurements
are expected to decline with age
48
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
6 Safety Evaluations and Procedures
61 Adverse Events
During a clinical trial the reporting of adverse experience information can lead to important
changes in the way a new treatment is developed as well as provide integral safety data
611 Definitions
An adverse event (AE) is any untoward medical occurrence in a subject or clinical investigation
subject who was administered a pharmaceutical product The AE does not necessarily have to
have a causal relationship with the drug administered An AE can be any unfavorable and
unintended sign (including an abnormal laboratory finding) symptom or disease temporarily
associated with the use of a medicinal product whether or not considered to be related to the
medicinal product Diseases signs symptoms or laboratory abnormalities already existing at
enrollment are not considered AEs unless they worsen (ie increase in intensity or frequency)
Surgical procedures themselves are not AEs they are therapeutic measures for conditions that
require surgery The condition for which the surgery is required may be an AE Surgical
procedures planned before randomization and the conditions necessitating the surgery are not
AEs
A serious adverse event is any untoward event that
Is fatal
Is life-threatening
Requires inpatient hospitalization or prolongation of existing hospitalization with the
following exceptions
o Preplanned (before the study) hospital admissions unless the hospitalization is
prolonged
o Planned admissions (as part of a study eg routine biopsies)
o Hospitalization lasting lt 24 hours
49
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
o Hospitalization for elective procedure
o Emergency room visits
Results in persistent or significant disability or incapacity
Is a congenital anomaly or birth defect
Important medical events that may not result in death be life-threatening or require
inpatient hospitalization may be considered serious adverse events (SAEs) when based
on appropriate medical judgment they may jeopardize the subject and may require
medical or surgical intervention to prevent one of the outcomes listed above
Life-threatening means that the subject was in the view of the investigator at immediate risk of
death from the AE as it occurred It does not include an AE that had it occurred in a more severe
form might have caused death
Persistent or significant disabilityincapacity means that the event resulted in permanent or
significant and substantial disruption of the subjectrsquos ability to carry out normal life functions
Causality
A reasonable possibility means the AE may have been caused byrelated to the study drug A
perceived or real lack of efficacy does not satisfy the definition of relatedness
612 Adverse Event (AE) Reporting
For the PANTHER-IPF trial all AEs (serious and nonserious) occurring from randomization
through final study visit (4 weeks after final dose of all study medication) will be recorded on the
AE page of the case report form (CRF)
6121 Serious Adverse Events (SAE) Reporting
For this trial all deaths and all SAEs which occur from randomization through final study visit
must be entered within the EDC system via the SAE eCRF page within 24 hours of the
investigative sitersquos knowledge of the event It is the responsibility of the clinical center
50
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
investigator to provide a causality assessment of the event for each study medications based upon
the information available at the time of the report It is understood that complete information
about the event may not be known at the time the initial report is submitted In the event the EDC
system is not accessible to the site at the time of event reporting investigative sites will complete
and forward a paper back-up SAE form to DCRI Safety Surveillance for processing
DCRI Safety Surveillance
Telephone 1-919-668-8624 or 1-866-668-7799 (toll free)
Fax 1-919-668-7138 or 1-866-668-7138 (toll free)
The investigator must complete and submit follow-up SAE information via the eCRF when
important new or follow-up information (eg final diagnosis outcome results of specific
investigations) becomes available Follow-up information should be submitted according to the
same process used for reporting the initial event as described above All SAEs will be followed
until resolution stabilization or 30 days after the subject has completed the final visit (4 weeks
after the final dose of study medication) whichever occurs first The investigator is responsible
for reporting SAEs to their institutional review board (IRB) per site specific IRB reporting
guidelines
6122 Regulatory Reporting
AEs that are serious study drug related and unexpected will be reported to the regulatory
authorities The DCRI Safety Surveillance medical monitor will perform a medical review of all
SAEs submitted and evaluate for ldquounexpectednessrdquo DCRI Safety Surveillance will prepare
MedWatch reports for those events identified as serious study drug related and unexpected as
determined by Safety Medical Monitor
DCRI Regulatory Services will submit all unexpected study drug-related SAEs as per 21 CFR
32 DCRI Safety Surveillance will provide a safety alert letter to the NHLBI DSMB and DCC
clinical operation (for distribution to sites) within 15 days of initial receipt of the information
51
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Investigators are responsible for promptly reporting these events to their reviewing IRBs
according to site specific IRB reporting guidelines
62 Clinical Medical Monitoring
There will be an unblinded physician at the IPFnet DCC serving as medical monitor The
medical monitor will be available to assist with questions about dosage adjustments of study
medications including discontinuation or resumption of medications
63 Unblinding Procedures
Unblinding of subjects or investigators to subject treatment is strongly discouraged For ongoing
clinical management all subjects should be presumed to be receiving ldquoactiverdquo study drug To
ensure the subjectrsquos safety the study treatment will be dose-adjusted based on laboratory test
results clinical findings and symptoms
The IPFnet DCC medical monitor and PANTHER-IPF co-chairs Drs Ganesh Raghu and
Fernando Martinez will be available to the study physicians to discuss study drug management
on a case-by-case basis Un-blinding will be considered ONLY when the knowledge of subject
treatment assignment is ABSOLUTELY ESSENTIAL for subject safety and after discussion of
the subjectrsquos case with the medical monitor and either Dr Raghu or Dr Martinez Unblinding of
study treatment should be minimized during the conduct of the trial In those cases where it is
felt to be medically necessary the DCC medical officer will communicate directly with the
managing physician to minimize unblinding of study personnel
52
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
7 Study Drug Procedures
At the baseline 15-week 30-week and 45-week study visits subjects will receive a supply of
study drug sufficient to last until the next visit at which study drug will be dispensed
53
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
8 Data Management
81 Hardware and Software Configuration
811 Hardware and Database Software
Data will be stored in an Oracle database system Oracle has advantages of processing efficiency
and smooth linkage with other software systems The application and database will be hosted on
Solaris Unix servers at the IPFnet DCC
812 Statistical Software
SAS will be used as the principal application for the management of analysis data files and
statistical computations S-Plus will be used to provide supplementary functions as needed
813 Access Control and Confidentiality Procedures
Access to databases will be controlled centrally by the IPFnet DCC through user passwords
linked to appropriate privileges This protects the data from unauthorized changes and
inadvertent loss or damage
814 Security
Database and Web servers will be secured by a firewall and through controlled physical access
Oracle has many security features to ensure that any staff member accessing the database has the
proper authority to perform the functions he or she requests of the system Within the secondary
SAS databases Unix group-access control maintains similar security The Sun workstation login
is secured by extensive user-password facilities under Unix
54
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
815 Back-up Procedures
Database back-up will be performed automatically every day and standard IPFnet DCC policies
and procedures will be applied to dictate tape rotation and retention practices
816 Virus Protection
All disk drives that provide network services and all user computers will be protected using
virus-scanning software Standard IPFnet DCC policies will be applied to update these protection
systems periodically through the study
82 Sources of Data
821 Design and Development
The IPFnet DCC will be responsible for development of the electronic case report forms
(eCRFs) development and validation of the clinical study database ensuring data integrity and
training clinical center staff on applicable data management procedures A web-based distributed
data entry model will be implemented This system will be developed to ensure that guidelines
and regulations surrounding the use of computerized systems used in clinical trials are upheld
The remainder of this section provides an overview of the data management plan associated with
this protocol
822 Data Collection Forms
The data collection process consists of direct data entry at the study clinical centers into the EDC
system(s) provided by the DCC A data collection worksheet will be provided to clinical centers
for recording data in the event the EDC system is unavailable Data entry of the eCRFs should
be completed according to the instructions provided and project specific training The
investigator is responsible for maintaining accurate complete and up-to-date records and for
ensuring the completion of the eCRFs for each research participant
55
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
823 Data Acquisition and Entry
Data entry into eCRFs shall be performed by authorized individuals Selected eCRFs may also
require the investigatorrsquos written signature or electronic signature as appropriate Electronic
CRFs will be monitored for completeness accuracy and attention to detail during the study
824 Data Center Responsibilities
The IPFnet DCC will 1) develop a data management plan and will conduct data management
activities 2) provide final eCRFs for the collection of all data required by the study 3) develop
data dictionaries for each eCRF that will comprehensively define each data element 4) conduct
ongoing data monitoring activities on study data 5) monitor any preliminary analysis data
cleanup activities and 6) rigorously monitor final study data clean up
825 Data Editing
Completed data will be entered into the IPFnet DCC automated data acquisition and
management system If incomplete or inaccurate data are found a data clarification request will
be generated and distributed to clinical centers for a response Clinical centers will resolve data
inconsistencies and errors and enter all corrections and changes into the IPFnet DCC automated
data acquisition and management system
826 Training
The training plan for clinical center staff includes provisions for training on assessments eCRF
completion guidelines data management procedures and the use of computerized systems
56
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
9 Study Design and Data Analysis
91 General Analytic Considerations
All primary analyses will be based on intent-to-treat (ITT) principles using all randomized
subjects Baseline factors across groups will be compared using mean (standard deviation) and
median (25th and 75th percentiles) summary measures Kaplan-Meier curves will be used to
display event rates Due to clinical interest in departures from both sides of the null hypothesis
all test statistics will be 2-sided
Reasonable caution needs to be taken when conducting multiple analyses on key clinical
subgroups For subgroup analyses a conservative significance level of 0001 will be used for all
interaction tests Thus subgroup comparisons will be considered exploratory unless the p-value
from the interaction test is smaller than 0001
92 Randomization Blinding and Reporting of Results
A permuted block-randomization scheme will be created with varying block sizes stratified by
clinical center Once a subject has completed the screening and baseline period and evaluation
for inclusionexclusion criteria the randomization process will begin Subjects will be
randomized to receive NAC or matching placebo with equal probability (11) via telephone
contact with a central interactive voice response system (IVRS) using a toll-free randomization
number On the day of randomization after the subject has successfully met all inclusion and
exclusion criteria the investigator or designee will call the central randomization number to
obtain the assigned kit randomization numbers for that subject At each subject visit the
investigator or designee will call the central randomization number to obtain the new kit
randomization numbers for resupply of the subject For resupply of the clinical center the IVRS
will monitor minimal volume of a kit type andor expiration date and will automatically notify
the pharmacy
57
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
The trial results will be reported according to guidelines specified in the CONSORT statement
A flow diagram describing screening recruitment randomization dropout and vital status will
be included in the primary manuscript AEs and efficacy data will be presented for all treatment
groups Adherence dropout and lost to follow-up will be carefully examined across all treatment
groups Analyses of safety will be based on data from all randomized subjects who received at
least one dose of study drug
93 Stratification
Subjects will be distributed to the two treatment arms in a 11 allocation ratio Stratification
blocks will be based on clinical centers
94 Specification of the Primary Analyses
A mixed model repeated measures (MMRM) analysis described in section 95 will be used to
compare differences in the slope of FVC measurements across the treatment groups Response
variables are values of the FVC measured at baseline and every 15 weeks until study completion
Variables in the model will include treatment time and time by treatment age sex race and
height Contrast estimates of differences in slopes of treatment over time (along with confidence
intervals) will be used to estimate the treatment effect The validity of this model in terms of
meeting modeling assumptions will be assessed via standard modeling diagnostics and goodness-
of-fit measures Based on the MMRM framework missing FVC data will not be imputed for the
primary analysis
95 Analysis of Longitudinal Endpoints
A common goal in clinical trials is to specify models that are easily implemented and
reproducible by independent data analysts On the other hand the models should have proper
statistical behavior in terms of low bias and high precision Many common approaches to
longitudinal data analysis including last observation carried forward (LOCF) imputation rely on
the missing completely at random (MCAR) assumption However the MCAR assumption is
58
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
unlikely to hold in many clinical trials because missing data are often related to disease
progression and prognosis A more reasonable assumption missing at random (MAR) specifies
that the complete data distribution can be modeled using only the observed data The likelihood-
based MMRM approach is valid under the more general MAR assumptions These models will
be applied to analyze the longitudinal data secondary endpoints
The advantages of MMRM analysis are that all important characteristics of the model can be preshy
specified standard software can be used to implement the models and results are based on ITT
principles43 In addition the MMRM approach offers superior control of Type I and Type II
errors compared with the LOCF approach
Response variables are values of the PFTs measured at enrollment and every 15 weeks until
study completion and 6MWT values measured at baseline week 30 and week 60 Covariates are
treatment time time by treatment and key baseline risk factors Contrasts (along with
confidence intervals) of treatment by time will be used to estimate the treatment effect
The correlation structure involves multiple pieces including measurement errors random
variation and interindividual variability For the longitudinal data analyses an unstructured
correlation matrix for within-subject errors will be assumed Other correlation structures
including compound symmetry will be examined as needed A careful examination of reasons
for study discontinuation will be conducted to assess the validity of MCAR Sensitivity analyses
will be used to examine the untestable assumption that the observed data violate the MAR
assumption The MMRM models will be implemented using PROC MIXED in SAS
96 Analysis of Binary Time-to-Event and Time-Lagged Endpoints
Regression modeling approaches using either the logistic regression model or Cox proportional
hazards regression model will be employed when appropriate The validity of these models will
be assessed via standard modeling diagnostics and goodness-of-fit measures Estimates of
cumulative frequencies for more general time-lagged responses will be calculated using the
partitioned version of the Bang-Tsiatis estimator44 The partitions will be set at 15-week intervals
59
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
to correspond with the data-collection process Covariate adjusted event rates will be calculated
using inverse probability-weighted regression estimates45
97 Power Analysis
971 Primary Analyses
Based on previously published IPF clinical trials the PL group is expected to experience a drop
in FVC of approximately 020 L over the study period (see Figure 1) The IPFnet Steering Group
determined a clinically important difference would be to preserve the majority of the decline
relative to PL over the study period In particular a treatment effect of 015 L was determined to
be a clinically meaningful difference Potential dropout is a key factor in the proposed study The
drop-out process assumed 5 lost to follow-up after every study visit Only 80 of subjects
were assumed to be followed for the entire study period All models assumed a compound
symmetry structure for the covariance matrix Power calculations were performed using a SAS
IML program for designing repeated measures studies46 Based on preliminary reviews of the
data from the University of Michigan the covariance matrix parameters were estimated at
approximately σ2 = 0757 (variance parameter) and ρ = 0936 (correlation parameter) To be
conservative the power calculations for the primary analysis were performed with parameter
setting of σ2 = 0810 (variance parameter) and ρ = 0925 (correlation parameter)
The power calculations assume a correction for imperfect compliance proposed by Lachin and
Foulkes to allow for 2 noncompliance for each of the treatment arms47 Thus the sample size
of 130 subjects per arm would be reduced to an adjusted sample size of 130(1-002-002)2 =
1198 or 120 subjects per arm
Under the assumed Type I error rate of 005 with a correlation parameter of 0925 and standard
deviation of 090 the difference of 015 L (or 00025 Lweek) shown in Table 6 would have
power of 93
60
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Table 6 Hypothetical Values of Mean FVC (L) Change from Baseline
Week 15 Week 30 Week 45 Week 60
NAC 00125 00250 00375 00500
Placebo 00500 01000 01500 02000
Difference 00375 00750 01125 01500
Abbreviations FVC forced vital capacity PL placebo
972 Power Analysis for Secondary Endpoints
Power calculations for secondary endpoint measurements are shown in Table 7 Standard
deviations are based on unpublished data provided by the University of Michigan The
calculations are based on a 2-sample t-test with Type I error rate set at 005 These calculations
are likely to be conservative because the statistical approach described in section 95 for
analyzing these endpoints will incorporate incomplete observations as well as intermediate data
points
Table 7 Detectable Differences in Treatment Means for Selected Endpoint Measurements
Secondary Endpoints Std Dev
of the Baseline Score
Detectable Difference for 80 Power
Std Dev of the Change Score
Difference Detectable for
80 Power
DLCOpred 166 58 91 32
6MWT Area Under the Desaturation Curve
219 76 175 61
6MWT Distance to Desaturation 224 78 315 110
6MWT Minutes Walked 210 073 205 071
Abbreviations Std Dev standard deviation DLCOpred diffusing capacity of the lung for carbon monoxide percent predicted 6MWT 6-minute walk test
61
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
10 Study Administration
101 Cooperative Agreement Mechanism
The administrative and funding mechanism used to undertake this project is a ldquocooperative
agreementrdquo (U01) which is an assistance mechanism Under the cooperative agreement the
NHLBI assists supports andor stimulates the project and is substantially involved with
investigators in conducting the study by facilitating performance of the effort in a ldquopartnerrdquo role
The NHLBI project scientist serves on the IPFnet Steering Group and he or another NHLBI
scientist may serve on other project committees when appropriate At the same time however
NHLBI does not assume a dominant role direction or prime responsibility for this research
program
As described below governance of the project is conducted through the IPFnet Steering Group
Principal investigators have lead responsibilities in all aspects of their trials and the project
including any modification of trial designs conduct of the trials quality control data analysis
and interpretation preparation of publications and collaboration with other investigators unless
otherwise provided for by the IPFnet Steering Group
PIs retain custody of and have primary rights to their center-specific and collaborative data
subject to government rights-of-access consistent with current Health amp Human Services (HHS)
Public Health Service (PHS) and National Institutes of Health policies The protocols and
governance policies call for the continual submission of data centrally to the IPFnet DCC for the
collaborative database which at a minimum will contain the key variables selected by the IPFnet
Steering Group for standardization across all clinical centers the submission of copies of the
collaborative datasets to each PI upon completion of the project procedures for data analysis
reporting and publication and procedures to protect and ensure the privacy of medical and
genetic data and records of individuals The NHLBI project scientist on behalf of the NHLBI
will have the same access privileges and responsibilities regarding the collaborative data as the
other members of the Steering Group
62
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
PIs are also encouraged to publish and to publicly release and disseminate results data and other
products of the project concordant with the project protocols and governance and the approved
plan for making data and materials available to the scientific community and to the NHLBI
However during the 3 years after the ending date of NHLBI project support unpublished data
unpublished results data sets not previously released and other study materials or products are
to be made available to any third party only with the approval of the IPFnet Steering Group
Upon completion of the project PIs are expected to put their intervention materials and
procedure manuals into the public domain andor make them available to other investigators
according to the approved plan for making data and materials available to the scientific
community and the NHLBI for the conduct of research at no charge other than the costs of
reproduction and distribution
The NHLBI reserves the right to terminate or curtail the project (or an individual award) in the
event of (a) failure to develop or implement mutually agreeable collaborative measurement
subject eligibility and data management sections of the protocols (b) substantial shortfall in
subject recruitment follow-up data reporting or quality control or other major breach of
protocol (c) substantive changes in the agreed-upon protocols with which NHLBI cannot
concur (d) reaching a major project outcome with persuasive statistical significance
substantially before schedule or (e) human subject ethical issues that may dictate a premature
termination
Any disagreement that may arise in scientificprogrammatic matters (within the scope of the
award) between award recipients and the NHLBI may be brought to arbitration An arbitration
panel will be composed of 3 membersmdash1 selected by the IPFnet Steering Group (with the
NHLBI member not voting) or by the individual PI in the event of an individual disagreement a
second selected by NHLBI and the third selected by the other 2 members This special
arbitration procedure in no way affects the PIrsquos right to appeal an adverse action that is otherwise
appealable in accordance with the PHS regulations at 42 CFR part 50 Subpart D and HHS
63
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
regulation at 45 CFR part 16 or the rights of the NHLBI under applicable statutes regulations
and terms of the award
102 IPFnet Steering Group
The IPFnet Steering Group is the main governing body of the project It is composed of the PIs
of the clinical centers the PI of the DCC and the NHLBI project scientist The clinical centers
the IPFnet DCC and the NHLBI each have 1 vote on the IPFnet Steering Group All decisions
are determined by majority vote
All major scientific decisions are determined by the IPFnet Steering Group It assumes overall
responsibility for the design and conduct of the trial It appoints (and disbands) committees and
subcommittees as the need arises designs approves and implements the study protocols
oversees the development of the MOOP monitors subject recruitment and treatment delivery
evaluates data collection and management oversees quality assurance procedures and
implements changes and enhancements to the study as required It also has primary responsibility
for facilitating the conduct of the trials and reporting the projectrsquos results
103 Data and Safety Monitoring Board
The NHLBI will establish a DSMB in accordance with established policies (see
httpwwwnhlbinihgovfundingpoliciesdsmb_insthtm) to ensure data quality and subject
safety and to provide independent advice to the NHLBI regarding progress and the
appropriateness of study continuation
104 Recommendations on Interim Monitoring of Efficacy Safety and Futility
First and foremost the role of the DSMB will be to review subject safety and trial conduct at
periodic points during the study The DSMB may require analyses of the primary endpoint
results for comparing the benefit and risks of treatment strategies The benefit of collecting
additional data on key secondary endpoints with extended follow-up and establishing a robust
64
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
evidence base for determining a standard of care will need to be carefully considered before
early termination of one or more treatment arms After careful consideration the IPFnet Steering
Group recommends conservative thresholds for the early examinations of the safety and efficacy
data
The DSMB will be expected to meet approximately every 6 months until trial completion to
review safety and toxicity data The DSMB may recommend stopping the study based on these
reviews Because the DSMB could stop the trial for safety concerns as well as for a large
efficacy benefit there could be multiple opportunities to reject the null hypothesis (no difference
in event rates between the PL and NAC groups) A Bonferroni approximation will be applied
during the one planned interim analysis for efficacy
Before locking the database a statistical analysis plan (SAP) will be developed to provide
complete details on the statistical analysis The SAP will include the specifics for how and when
the DSMB will be notified for AEs The IPFnet DCC will deliver to the DSMB all FDA-defined
AEs at 3-month intervals The IPFnet DCC will prepare narrative SAE reports in real time for
DSMB review including recommendations and analysis of similar events for each SAE
submitted to the FDA
65
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
11 Investigator and Sponsor Obligations
111 Monitoring
All monitoring activities for US clinical centers will be performed in accordance with DCRI
standard operating procedures Information regarding the types of visits will be outlined in the
PANTHER-IPF MOOP
112 Cost and Payment
There will be no cost to subjects enrolled in this trial Study-related procedures will be paid for
by the IPFnet
Subjects may be eligible for reimbursement for travel to the clinical center Details of payment
will be explained to each subject during the consent process
113 Confidentiality and Health Insurance Portability and Accountability Act
Considerations
Subject confidentiality will be protected throughout the study All subject data will be kept
strictly confidential and no subject-identifying information will be released to anyone outside
the project Confidentiality will be assured through several mechanisms First each subject will
be assigned an anonymous study ID which will then be used on all study forms Second any
study forms blood samples and paper records that contain subject information (eg address lists
phone lists) will be kept at the clinical centers in secured locked areas coded by number Once
blood is collected there will be no subject identifiers placed on blood samplesmdashonly the study
ID number and the date of sample collection Third access to all subject data and information
including laboratory specimens will be restricted to authorized personnel In the case of
computerized data this restricted access will be assured through user logon IDs and password
protection
66
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
At the IPFnet DCC only authorized personnel will have access to the data files containing study
data Security will be assured through user logon IDs passwords and appropriate access
privileges All study subjects will be identified only by their IPFnet ID numbers and no personal
identifying information such as name address or Social Security number will be entered into
the IPFnet DCC database Any subject-specific data reported to the IPFnet Steering Group will
be identified only by the IPFnet ID number
Finally subjects will not be identified by name in any reports or publications nor will the data
be presented in such a way that the identity of individual subjects can be inferred Analysis files
created for further study by the scientific community will have no subject identifiers These data
files will be created in accordance with the Ancillary Studies and Publication Policy of the
IPFnet
114 Informed Consent Procedures
All IPFnet subjects will provide written informed consent using procedures reviewed and
approved by each clinical centerrsquos IRB Informed consent will be undertaken by study personnel
in-person with the subject The subject has the option of declining further participation in the
study at that point No further study procedures will be conducted until the signed documents
have been provided to the IPFnet clinical center
115 Institutional Review Boards
Before initiating this study the protocol clinical center-specific informed consent forms Health
Insurance Portability and Accountability Act (HIPAA) forms recruitment materials and other
relevant information will be reviewed by a properly constituted IRB at each participating clinical
center A copy of the signed and dated IRB approval at each clinical center will be retrieved prior
to or during the site initiation visit and archived at the IPFnet DCC Any amendments to the
protocol other than simple administrative and typographical changes must be approved by each
IRB before they are implemented The clinical centers will seek annual renewals of their IRB
approvals in accordance with local procedures
67
__________________________________________ ________________
__________________________________________
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
12 Investigator Agreement
I have read the foregoing protocol PANTHER-IPF and agree that it contains all necessary
details for carrying out this study I will conduct the study as outlined herein and will complete
the study within the time designated
I will provide copies of the protocol and all pertinent information to all individuals responsible to
me who assist in the conduct of this study I will discuss this material with them to ensure they
are fully informed regarding the drug and the conduct of the study
I will fulfill all responsibilities for submitting pertinent information to the local IRB if
applicable that is responsible for this study
I further agree that NHLBI andor DCRI will have access to any source documents from which
eCRF information may have been generated
Signature of Principal Investigator Date
Name of Principal Investigator (printed or typed)
Protocol version date May 19 2009
Protocol Amendment 1 version date May 28 2010
Protocol Amendment 2 version date December 6 2011
68
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
13 References
1 Raghu G Brown KK Bradford WZ et al A placebo-controlled trial of interferon gamma-1b in patients with idiopathic pulmonary fibrosis N Engl J Med 2004350125-33 2 King TE Jr Safrin S Starko KM et al Analyses of efficacy end points in a controlled trial of interferon-gamma1b for idiopathic pulmonary fibrosis Chest 2005127171-7 3 Flaherty KR Thwaite EL Kazerooni EA et al Radiological versus histological diagnosis in UIP and NSIP survival implications Thorax 200358143-8 4 Wells AU Desai SR Rubens MB et al Idiopathic pulmonary fibrosis a composite physiologic index derived from disease extent observed by computed tomography Am J Respir Crit Care Med 2003167962-9 5 Raghu G Freudenberger TD Yang S et al High prevalence of abnormal acid gastroshyoesophageal reflux in idiopathic pulmonary fibrosis Eur Respir J 200627136-42 6 Kinnula VL Focus on antioxidant enzymes and antioxidant strategies in smoking related airway diseases Thorax 200560693-700 7 Coultas DB Zumwalt RE Black WC Sobonya RE The epidemiology of interstitial lung diseases Am J Respir Crit Care Med 1994150967-72 8 Raghu G Weycker D Edelsberg J Bradford WZ Oster G Incidence and prevalence of idiopathic pulmonary fibrosis Am J Respir Crit Care Med 2006174810-6 9 Olson AL Swigris JJ Lezotte DC Norris JM Wilson CG Brown KK Mortality from pulmonary fibrosis increased in the United States from 1992 to 2003 Am J Respir Crit Care Med 2007176277-84 10 Mannino DM Etzel RA Parrish RG Pulmonary fibrosis deaths in the United States 1979shy1991 An analysis of multiple-cause mortality data Am J Respir Crit Care Med 19961531548shy52 11 Hubbard R Johnston I Coultas DB Britton J Mortality rates from cryptogenic fibrosing alveolitis in seven countries Thorax 199651711-6 12 Johnston I Britton J Kinnear W Logan R Rising mortality from cryptogenic fibrosing alveolitis Bmj 19903011017-21 13 Raghu G Collard HR Egan JJ et al An official ATSERSJRSALAT statement idiopathic pulmonary fibrosis evidence-based guidelines for diagnosis and management Am J Respir Crit Care Med 2011183788-824 14 (USA) FDA FDA Public Health Advisory Interferon gamma-1b (marketed as Actimmune) In 2007 15 King TE Jr Pardo A Selman M Idiopathic pulmonary fibrosis Lancet 2011 16 Raghu G Brown KK Costabel U et al Treatment of idiopathic pulmonary fibrosis with etanercept an exploratory placebo-controlled trial Am J Respir Crit Care Med 2008178948shy55 17 Malouf MA Hopkins P Snell G Glanville AR An investigator-driven study of everolimus in surgical lung biopsy confirmed idiopathic pulmonary fibrosis Respirology 201116776-83 18 King TE Jr Behr J Brown KK et al BUILD-1 a randomized placebo-controlled trial of bosentan in idiopathic pulmonary fibrosis Am J Respir Crit Care Med 200817775-81 19 Richeldi L Costabel U Selman M et al Efficacy of a tyrosine kinase inhibitor in idiopathic pulmonary fibrosis N Engl J Med 20113651079-87
69
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
20 Borok Z Buhl R Grimes GJ et al Effect of glutathione aerosol on oxidant-antioxidant imbalance in idiopathic pulmonary fibrosis Lancet 1991338215-6 21 Meyer A Buhl R Magnussen H The effect of oral N-acetylcysteine on lung glutathione levels in idiopathic pulmonary fibrosis Eur Respir J 19947431-6 22 Behr J Maier K Degenkolb B Krombach F Vogelmeier C Antioxidative and clinical effects of high-dose N-acetylcysteine in fibrosing alveolitis Adjunctive therapy to maintenance immunosuppression Am J Respir Crit Care Med 19971561897-901 23 Cantin AM North SL Fells GA Hubbard RC Crystal RG Oxidant-mediated epithelial cell injury in idiopathic pulmonary fibrosis J Clin Invest 1987791665-73 24 Waghray M Cui Z Horowitz JC et al Hydrogen peroxide is a diffusible paracrine signal for the induction of epithelial cell death by activated myofibroblasts Faseb J 200519854-6 25 Larios JM Budhiraja R Fanburg BL Thannickal VJ Oxidative protein cross-linking reactions involving L-tyrosine in transforming growth factor-beta1-stimulated fibroblasts J Biol Chem 200127617437-41 26 Kinnula VL Fattman CL Tan RJ Oury TD Oxidative stress in pulmonary fibrosis a possible role for redox modulatory therapy Am J Respir Crit Care Med 2005172417-22 27 Meyer A Buhl R Kampf S Magnussen H Intravenous N-acetylcysteine and lung glutathione of patients with pulmonary fibrosis and normals Am J Respir Crit Care Med 19951521055-60 28 Behr J Degenkolb B Krombach F Vogelmeier C Intracellular glutathione and bronchoalveolar cells in fibrosing alveolitis effects of N-acetylcysteine Eur Respir J 200219906-11 29 Bando M Hosono T Mato N et al Long-term efficacy of inhaled N-acetylcysteine in patients with idiopathic pulmonary fibrosis Intern Med 2010492289-96 30 Demedts M Behr J Buhl R et al High-dose acetylcysteine in idiopathic pulmonary fibrosis N Engl J Med 20053532229-42 31 Toma TP Bhowmik A Rajakulasingam R Acetylcysteine in pulmonary fibrosis N Engl J Med 20063541086-9 author reply -9 32 Hunninghake GW Antioxidant therapy for idiopathic pulmonary fibrosis N Engl J Med 20053532285-7 33 Flaherty KR Mumford JA Murray S et al Prognostic implications of physiologic and radiographic changes in idiopathic interstitial pneumonia Am J Respir Crit Care Med 2003168543-8 34 Latsi PI du Bois RM Nicholson AG et al Fibrotic idiopathic interstitial pneumonia the prognostic value of longitudinal functional trends Am J Respir Crit Care Med 2003168531-7 35 Collard HR King TE Jr Bartelson BB Vourlekis JS Schwarz MI Brown KK Changes in clinical and physiologic variables predict survival in idiopathic pulmonary fibrosis Am J Respir Crit Care Med 2003168538-42 36 Jegal Y Kim DS Shim TS et al Physiology is a stronger predictor of survival than pathology in fibrotic interstitial pneumonia Am J Respir Crit Care Med 2005171639-44 37 Martinez FJ Safrin S Weycker D et al The clinical course of patients with idiopathic pulmonary fibrosis Ann Intern Med 2005142963-7 38 Hull JH Acetylcysteine in pulmonary fibrosis N Engl J Med 20063541089-91 author reply -91
70
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
39 Flaherty KR King TE Jr Raghu G et al Idiopathic interstitial pneumonia what is the effect of a multidisciplinary approach to diagnosis Am J Respir Crit Care Med 2004170904shy10 40 Raghu G Johnson WC Lockhart D Mageto Y Treatment of idiopathic pulmonary fibrosis with a new antifibrotic agent pirfenidone results of a prospective open-label Phase II study Am J Respir Crit Care Med 19991591061-9 41 Hunninghake GW Lynch DA Galvin JR et al Radiologic findings are strongly associated with a pathologic diagnosis of usual interstitial pneumonia Chest 20031241215-23 42 Lynch D Godwin J Safrin S et al High-resolution computed tomography in idiopathic pulmonary fibrosis diagnosis and prognosis Am J Respir Crit Care Med 2005172488-93 43 Mallinckrodt CH Watkin JG Molenberghs G Carroll RJ Choice of the primary analysis in longitudinal clinical trials Pharmaceutical Statistics 20043161-9 44 Bang H Tsiatis A Estimating medical costs with censored data Biometrika 200087329shy43 45 Lin DY Regression analysis of incomplete medical cost data Stat Med 2003221181-200 46 Rochon J Application of GEE procedures for sample size calculations in repeated measures experiments Stat Med 1998171643-58 47 Lachin JM Foulkes MA Evaluation of sample size and power for analyses of survival with allowance for nonuniform patient entry losses to follow-up noncompliance and stratification Biometrics 198642507-19
71
- PANTHER-IPFPREDNISONE AZATHIOPRINEAND N-ACETYLCYSTEINEA STUDY THAT EVALUATES RESPONSE INIDIOPATHIC PULMONARY FIBROSIS
-
- Protocol Summary
- Table of Contents
- List of Tables
- List of Figures
- List of Abbreviations
- 1 Summary
- 2 Hypotheses and Specific Aims
-
- 21 Null Hypothesis
- 22 Specific Aim 1
- 23 Specific Aim 2
- 24 Prespecified Subgroups of Interest
-
- 3 Background and Significance
-
- 31 Idiopathic Pulmonary Fibrosis is the Most Common Interstitial Lung Disease
- 32 Rationale for Placebo Control
- 33 Rationale for N-acetylcysteine
- 35 Rationale for N-acetylcysteine as a Stand-alone Therapy
- 36 Rationale for the Study Design and Primary Endpoint
- 37 Rationale for Blinding of Treatments
-
- 4 Methods
-
- 41 Inclusion Criteria
- 42 Diagnosis of IPF
- 43 Exclusion Criteria
- 44 Study Design and Study Visit
- 45 Dose Justification
- 46 Contraindications Precautions and Side Effects of Study Medications
- 47 Recruitment Procedures
- 48 Study Procedures
- 49 Concomitant Medications
- 410 Laboratory Testing
- 411 Blinding of Study Drugs
-
- 5 Study Endpoints
-
- 51 Primary Study Endpoint
- 52 Secondary Study Endpoints
-
- 6 Safety Evaluations and Procedures
-
- 61 Adverse Events
- 62 Clinical Medical Monitoring
- 63 Unblinding Procedures
-
- 7 Study Drug Procedures
- 8 Data Management
-
- 81 Hardware and Software Configuration
- 82 Sources of Data
-
- 9 Study Design and Data Analysis
-
- 91 General Analytic Considerations
- 92 Randomization Blinding and Reporting of Results
- 93 Stratification
- 94 Specification of the Primary Analyses
- 95 Analysis of Longitudinal Endpoints
- 96 Analysis of Binary Time-to-Event and Time-Lagged Endpoints
- 97 Power Analysis
-
- 10 Study Administration
-
- 101 Cooperative Agreement Mechanism
- 102 IPFnet Steering Group
- 103 Data and Safety Monitoring Board
- 104 Recommendations on Interim Monitoring of Efficacy Safety and Futility
-
- 11 Investigator and Sponsor Obligations
-
- 111 Monitoring
- 112 Cost and Payment
- 113 Confidentiality and Health Insurance Portability and Accountability ActConsiderations
- 114 Informed Consent Procedures
- 115 Institutional Review Boards
-
- 12 Investigator Agreement
- 13 References
-

PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
24 Prespecified Subgroups of Interest
Treatment effects will be estimated and compared within key subgroups
Higher enrollment FVC12
Typical vs atypical high-resolution computed tomography (HRCT) reading at baseline3
Recent vs more remote diagnosis (time from initial diagnosis of IPF le 1 year and gt 1 year)
Lower CPI score at enrollment4
Medical therapy for gastroesophageal reflux5
Ethnic background
Sex
Smoking history (current or ex-smoker vs never smoker) given potential impact on oxidant status6
Presence of emphysema gt 25 on HRCT
14
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
3 Background and Significance
31 Idiopathic Pulmonary Fibrosis is the Most Common Interstitial Lung Disease
IPF is the most common interstitial lung disease (ILD) of unknown etiology The current incidence and
prevalence of IPF in the United States are not known A 1994 study of a population-based registry of subjects in
Bernalillo County New Mexico USA estimated an incidence of 107 cases per 100000 per year for males and
74 cases per 100000 per year for females the prevalence of IPF was estimated at 20 per 100000 for males and
13 per 100000 for females7 Extrapolating from a large healthcare claims database a more recent review
estimated the prevalence of IPF in the United States at 427 per 100000 (incidence estimated at 163 per
100000 per year)8 Recent epidemiological studies indicate increasing mortality rates from IPF in the United
States and other industrialized nations9-12
Approximately two-thirds of subjects with IPF are over the age of 60 at the time of presentation and the
incidence increases with age13 IPF has no distinct geographical distribution and predilection by race or
ethnicity has not been identified13 Individual subjects may remain relatively stable for prolonged periods
experience very slow declines in lung function with progression of radiographic abnormalities for a period of
months to years or experience more rapid declines and subsequent death Only 20 to 30 of IPF patients
survive for 5 years following diagnosis
There is currently no proven effective pharmacological treatment for IPF13 Anti-inflammatory and
immunosuppressive agents have been the traditional approach to the management of patients with IPF Based
on the results of the interim analysis of the PANTHER-IPF trial this lsquotraditional approachrsquo will be aborted
However it remains unknown if NAC alone will prove beneficial in IPF patients The primary goal of the
modified study is to establish an evidence-based standard of care and clarify the role of this specific antioxidant
pharmacotherapy for IPF
32 Rationale for Placebo Control
IPF is a disorder for which there is no proven efficacious therapy A major objective of this trial is to test to the
greatest degree possible a proposed standard of care for patients with IPF The current traditional therapy
15
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
employs immunosuppressive and corticosteroid drugs Interim review of the original PANTHER-IPF study has
documented increased adverse events and lack of efficacy for AZA-PRED-NAC compared to placebo
suggesting that this therapeutic approach should not be employed Whether this applies to NAC alone which
has been advocated by international societies has not been proven in well-designed well-powered clinical
trials The recommendations made in the recently published evidence guidelines for NAC monotherapy was
weak based on low quality13 Thus this continued clinical trial randomizing patients to receive NAC or placebo
is pivotal and will answer the important question of the potential therapeutic benefits of NAC monotherapy with
grade A evidence In this prospective randomized clinical trial the inclusion of a PL arm is therefore vital to
adequately test the benefits of NAC in well-characterized subjects with IPF
If NAC has no true efficacy then its role as standard of care will be refuted If a benefit compared with PL is
confirmed it will establish a benchmark against which future novel therapies for IPF will be safely compared
As there is no currently accepted therapy for IPF there is an increasing body of published literature supporting
the concept of no treatment as the ldquobest carerdquo option for IPF13
Post hoc analyses of PL-controlled trials suggest that subjects with milder disease may be more amenable to
therapy12 It is notable that a recent international prospective randomized trial of interferon-gamma for IPF
also included a PL arm the study was terminated early by the data and safety monitoring board (DSMB) due to
lack of treatment effect1415 This underscores the belief that a proven effective therapy for IPF does not
currently exist and that true placebo-controlled trials remain the gold standard Similarly recently completed
trials of etanercept everolimus bosentan and BIPF 1120 in IPF have included PL-treated arms16-19 In three of
these trials the treated subjects showed little if any objective improvement Based on this evidence and the
current status of IPF therapy and therapeutic trials we believe that clinicians and subjects will continue to enroll
in a PL-controlled study
33 Rationale for N-acetylcysteine
NAC is a derivative of the amino acid L-cysteine NAC has been shown to augment levels of the naturally
occurring antioxidant glutathione (GSH ) (glutathione γ-glutamyl cysteinyl glycine) both in vitro and in
vivo2021 GSH is present in all eukaryotic cells and may play an important role in protecting alveolar epithelial
cells against oxidant injury The concentration of GSH in the bronchoalveolar lavage (BAL) fluid in patients
16
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
with IPF is markedly diminished compared with normal subjects This GSH deficiency may be corrected by
exogenous administration of NAC2122
There is evidence of enhanced production of oxidants in an IPF lung Both inflammatory cells and
myofibroblasts derived from patients with IPF generate increased amounts of extracellular oxidants including
hydrogen peroxide2324 Secretion of hydrogen peroxide by activated myofibroblasts may induce the death of
adjacent lung epithelial cells by paracrine mechanisms24 Additionally generation of oxidants by myofibroblasts
induces oxidative crosslinking of extracellular matrix proteins25 a potential mechanism for aberrant matrix
remodeling Thus an oxidant-antioxidant imbalance exists in the lungs of IPF patients26 NAC may confer
protection against this imbalance by augmenting GSH levels in addition to its more direct free-radical
scavenging activity
Intravenous (IV) NAC therapy has been shown to increase total BAL GSH in 8 IPF subjects27 Oral NAC (600
mg 3 times per day) has been shown to decrease markers of oxidant injury and improve both total and reduced
GSH levels in the epithelial lining fluid of subjects with IPF in a small uncontrolled study22 pulmonary
function improved modestly with therapy A similar study in 18 IPF subjects confirmed increased intracellular
GSH concentration after 12 weeks of NAC (600 mg 3 times per day)2228 no clinical correlates were reported
Inhaled NAC was suggested to improve pulmonary function in an open label study29
35 Rationale for N-acetylcysteine as a Stand-alone Therapy
Results of a double-blind multi-center European clinical trial of 150 IPF subjects testing combinations of AZAshy
PRED vs AZA-PRED-NAC have been reported30 NAC added to AZA-PRED (ldquoconventional therapyrdquo) had a
significant positive effect on DLCO (p lt 0005) and vital capacity (VC) (p lt 005) at the end of 1 year30 The
recent ATSERS position statement after much discussion concluded that NAC alone should not be considered
in the majority of patients with IPF without additional data from well-designed studies
The interpretation of these data has been quite controversial Some have suggested that the magnitude of the
treatment effect although statistically significant is modest31 Others have suggested that NAC may be
modulating potential toxic effects of AZA-PRED alone32 supporting the investigation of NAC as stand-alone
therapy
17
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
The IPFnet is now completing the PANTHER-IPF trial with a 11 randomization (NAC vs placebo) and a
simple practical feasible and scientifically rational design that will establish standard of care with NAC for
IPF based on a currently available therapeutic agent and the existing data to support its use We anticipate that
all future clinical trials of novel therapeutic agents will be tested against this to-be-established standard of care
36 Rationale for the Study Design and Primary Endpoint
The optimal study design of a therapeutic trial in IPF would include survival as a primary endpoint The
published results of the IFN-γ 1b Phase 3 (GIPF-001) trial suggested a survival benefit in subjects with milder
disease in retrospective analyses1 although the trial was underpowered to address this question This was likely
related to the limited mortality in the PL arm of the study which included IPF subjects with mild to moderate
disease This study documents that an IPF study powered to improve survival in a patient population with mild
disease requires a larger sample size andor duration of study In fact the recently aborted Phase 3 IFN-γ 1b
(GIPF-007 INSPIRE) study was a survival-based study and recruited more than 800 subjects at 75 centers
worldwide1415 As such within the context of the current IPFnet trial survival is an impractical primary
endpoint variable
Several groups have published data defining an appropriate surrogate outcome variable a 10 decrement in
FVC during 6 to 12 months is a powerful predictor of survival in IPF33-36 Furthermore additional evidence
suggests a similar predictive ability for a 10 decrement in FVC during 3 months of follow-up37 With strong
supportive evidence of FVC progression being related to mortality on a per-subject basis this study will use
FVC changes in liters between treatment groups as the primary endpoint Previously published IPF studies have
shown a steady decline in FVC (and FVCpred) among control group subjects230 The GIPF-001 study
suggested a 48-week decrease in FVC of 016 L in the PL-treated subjects The IFIGENIA study demonstrated
a decline in FVC of approximately 019 L over 52 weeks in the subjects randomized to the control treatment
Figure 1 depicts the change in FVC for control groups from previously published IPF studies38 Based on these
data we expect that the PL group will have a decline of 020 L over the 60-week study period The IPFnet
Steering Group determined that a clinically meaningful improvement would be the preservation of the majority
of the 020-L FVC decline Therefore a mean treatment difference of 015 L in mean FVC over the 60-week
study period was determined to be a clinically meaningful difference
18
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Δ f
rom
bas
elin
e (i
n L
)
01
005
0
-005
-01
-015 Projected Δ for placebo
-02
-025
-019
-016
-013 Pirfenidone GIPF001
NAC
Placebo
4 8 12 16 20 24 28 32 36 40 44 48 52 56 60
Week
Figure 1 Changes in FVC From Baseline in Prior IPF Clinical Trials
Recent data suggest that various patient subgroups would be expected to potentially exhibit differential response
to therapy These parameters will be used to a priori separate patients by a series of baseline characteristics
including
1 Higher enrollment FVC12
2 Typical vs atypical high-resolution computed tomography (HRCT) reading at baseline3
3 Recent vs more remote diagnosis (time from initial diagnosis of IPF le 1 year and gt 1 year)
4 Lower CPI score at enrollment4
5 Medical therapy for gastroesophageal reflux5
6 Ethnic background
7 Sex
8 Smoking history (current or ex-smoker vs never smoker) given potential impact on oxidant status6
9 Presence of emphysema gt 25 on HRCT
37 Rationale for Blinding of Treatments
The issue of treatment blinding was given a great deal of consideration with subject safety being the primary
concern After discussion among the Steering Group members it was decided that as long as subject safety
could be ensured blinding was necessary Blinding allows the study to
Have optimal scientific validity and potential to impact the standard of care for subjects
19
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Make objective assessments of treatment effects
Maintain clinical equipoise among investigators
Encourage subjects to have similar levels of contact with the medical community
Minimize the differential dropout rates across study arms
20
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
4 Methods 41 Inclusion Criteria
1 Age 35 to 85 years inclusive
2 FVC ge 50 of predicted (post-bronchodilator measurement from the screening visit)
3 DLCO ge 30 of predicted (hemoglobin corrected and altitude corrected if gt4000 ft above sea level)
4 Ability to understand and provide informed consent
5 Diagnosis of IPF according to a modified version of the ATS criteria le 48 months from enrollment The
date of diagnosis is defined as the date of the first available HRCT or surgical lung biopsy characteristic
of definite UIP
411 Subjects Shown to Have Usual Interstitial Pneumonia Pattern on Surgical Lung Biopsy
Subjects who have been shown to have UIP pattern on lung biopsy must have all of the following
1 Exclusion of other known causes of ILD such as drug toxicity clinically significant environmental
exposures or diagnosis of connective tissue diseases
2 Bibasilar reticular abnormalities with minimal ground glass opacities on HRCT scan
412 Subjects Who Have Not Undergone a Surgical Lung Biopsy
In addition to the criteria above these subjects must have radiological findings considered to be definite for the
diagnosis of UIPIPF
1 Bibasilar reticular abnormalities with minimal ground glass opacities
2 Honeycombing as the predominant feature and located in the peripheral lung bases
42 Diagnosis of IPF
Only subjects with definite IPF will be eligible for enrollment in this study We will utilize a combination of
clinicalphysiologic features HRCT and review of a clinically obtained surgical lung biopsy specimen to
establish the diagnosis of IPF An algorithm for the diagnosis is provided to guide entry into the protocol as
outlined in the inclusion and exclusion criteria (Figures 2 and 3) This multi-disciplinary approach uses
21
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
expertise from clinicians radiologists and pathologists Investigators at each site in conjunction with central
pathology will work together to establish the diagnosis of IPF This interactive approach to the diagnosis of IPF
increases the level of agreement between observers39
A subject with suspected ILD should be evaluated for secondary causes including but not limited to
environmental exposures drugs and systemic diseases Presence of any of these findings felt to be significant
enough to cause an ILD should disqualify the subject from entry into the trial
If secondary causes are absent an HRCT scan may be obtained If an HRCT of sufficiently high quality has
been obtained within the last 3 months that scan may be used for diagnosis In the appropriate clinical setting
the diagnosis of IPF can be made by the demonstration of a typical radiographic pattern on HRCT or by
demonstration of UIP pattern on a surgical lung biopsy The following criteria for a radiographic (ie
nonsurgical) diagnosis will be used In the absence of known exposures andor clinical associations attributable
to pulmonary fibrosis and in the appropriate clinical setting the presence of definite UIP pattern in HRCT
images is required to meet study criteria for the diagnosis of IPF
Figure 2 Diagnosis of Idiopathic Pulmonary Fibrosis in the IPFnet
22
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Figure 3 Pathology Flow Chart Surgical Lung Biopsy Diagnosis
Requirement for diagnosis
1 Clinical exclusion of other known causes (connective tissue diseases environmental and drug
exposures) of ILD
2 Radiographic HRCT with bibasilar reticular abnormality and honeycomb change with minimal
ground glass opacities
Appropriate clinical setting
1 Age gt 50 years
2 Insidious onset of unexplained dyspnea
3 Duration of illness for ge 3 months
4 Bibasilar inspiratory crackles
23
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Unlike the ATSERS consensus criteria published in 2000 bronchoscopy will not be required for diagnosis
This decision was made based on the experience of the IPFnet Steering Group members regarding the utility of
bronchoscopy in the diagnosis of IPF The presence of an atypical HRCT finding will require documentation of
a definitive diagnosis by surgical lung biopsy In fact this is in keeping with the recently published evidence
based guidelines for diagnosis and management of IPF13 As shown in Figure 3 central review of the pathology
data will be required for a diagnosis of IPF
We will not require central review of HRCT as several studies have shown that a confident local interpretation
of clinicalHRCT criteria as definite IPFUIP is associated with a high positive predictive value for finding UIP
at surgical lung biopsy (see Table 1) Differences in sensitivity in these series likely reflect subject selection as
Flaherty et al3 evaluated only UIP and nonspecific interstitial pneumonia (NSIP) while Raghu et al40 and
Hunninghake et al41 included a broader range of ILD
Table 1 Operating Characteristics of Local HRCT Review for Diagnosis of UIP
Researcher of Subjects Sensitivity () Specificity () PPV () NPV ()
Raghu et al 40
59 (29 UIP by SLB) 78 90 88 82
Hunninghake et al 41 91 (54 UIP by SLB)
74 81 85 67
Flaherty et al 3 96 (only NSIP amp UIP)
37 100 100 30
Abbreviations PPV positive predictive value NPV negative predictive value UIP usual interstitial pneumonia SLB surgical lung biopsy and NSIP nonspecific interstitial pneumonia
Furthermore an analysis of the HRCT scans from subjects enrolled in the GIPF-001 trial confirmed that local
site interpretations have a high congruity to a central radiology core In this multi-center study 263 HRCT
scans were read as definite IPF and a retrospective central radiology core review found 932 to be consistent
with IPF 42 We will also take several additional steps to insure that the local HRCT reads are accurate
including
1 A detailed training module has been developed and must be completed by each site radiologist before
site initiation
2 Clinical centers are to mail all HRCT scans to the HRCT core lab The first 10 HRCT scans from
subjects enrolled at each enrolling clinical center will be reviewed centrally to be certain that local reads
24
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
25
are congruent with a central interpretation If discrepancies are identified additional education will be
provided and HRCT scans will continue to be reviewed centrally until the central radiology core is
confident that the local center is performing appropriately
3 Random scans will be obtained from each center throughout the study to confirm that the local read
continues to agree with central interpretation If discrepancies are identified they will be addressed as in
2 above
In all cases if a subject has a surgical lung biopsy sample that sample will be reviewed by the local and central
pathologists Therefore the only cases that would not be subject to a direct central review process are those
where the HRCT meets the centrally defined criteria for an unequivocal diagnosis and a lung biopsy sample is
not available Table 2 below summarizes the possible combinations for making a diagnosis
Table 2 Combining HRCT and Pathology Interpretations to Determine if IPF is Present
HRCT Diagnosis Pathology Diagnosis Diagnosis of IPF
Definite UIP Definite UIP Yes
Definite UIP Probable UIP Yes
Definite UIP Possible UIP Yes
Definite UIP Not UIP No
Definite UIP Unavailable Yes
Consistent with UIP Definite UIP Yes
Consistent with UIP Probable UIP Yes
Consistent with UIP Possible UIP No
Consistent with UIP Not UIP No
Consistent with UIP Unavailable No
Inconsistent with UIP Any No
Abbreviations HRCT high-resolution computed tomography IPF idiopathic pulmonary fibrosis
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
UIP usual interstitial pneumonia Dx diagnosis 43 Exclusion Criteria
1 History of clinically significant environmental exposure known to cause pulmonary fibrosis
Occupational exposures such as asbestos or environmental exposure to organic dust such as occurs in
pigeon breeders may at times mimic the clinical and radiographic findings of IPF
2 Diagnosis of connective tissue disease felt by the principal investigator (PI) to be the etiology of the
interstitial disease Diagnosis of collagen-vascular conditions will be according to the published
American College of Rheumatology criteria As such the presence of any documented collagen-vascular
disorder or the presence of any suspicious symptom complex whether or not associated with
significantly abnormal rheumatological serologies will exclude the subject at the discretion of the PI
3 Extent of emphysema greater than the extent of fibrotic change (honeycombing reticular changes) on
HRCT scan
4 Forced expiratory volume in 1 second (FEV1)FVC ratio lt 065 at screening (postbronchodilator)
5 Partial pressure of arterial oxygen (PaO2) on room air lt 55 mm Hg (lt 50 mm Hg at Denver site)
6 Residual volume gt 120 predicted at screening (postbronchodilator)
7 Evidence of active infection
8 Significant bronchodilator response on screening spirometry defined as a change in FEV1 ge 12 and
absolute change gt 200 mL OR change in FVC ge 12 and absolute change gt 200 mL The percent
difference between the FVC (or FEV1) values will be calculated by taking the absolute value of the
difference and dividing it by the larger of the two FVC (or FEV1) values
9 Screening and enrollment post-bronchodilator FVC measurements (in liters) differing by gt 11 The
percent difference between the FVC values will be calculated by taking the absolute value of the
difference and dividing it by the larger of the two FVC values (eg the percent difference between FVC
measurements of 19 and 20 liters would be determined by taking the difference between the two (01
liters) and dividing by the larger of the two (20 liters) So 0120 = 5 and these FVC measurements
would not exclude the subject
10 Listed for lung transplantation ie the patient has completed the evaluation process has been accepted
as a candidate for transplantation at an appropriate center and is waiting to receive notification of an
available donor organ
11 History of unstable or deteriorating cardiac disease
12 Myocardial infarction coronary artery bypass or angioplasty within 6 months of screening
26
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
13 Unstable angina pectoris or congestive heart failure requiring hospitalization within 6 months of
screening
14 Uncontrolled arrhythmia
15 Severe uncontrolled hypertension
16 Known HIV or hepatitis C
17 Known cirrhosis and chronic active hepatitis
18 Active substance andor alcohol abuse (as determined by site PI)
19 Pregnancy or lactation (subjects who are pregnant or breastfeeding)
20 Known hypersensitivity to study medication
21 Any condition other than IPF that in the opinion of the site PI is likely to result in the death of the
subject within the next year
22 Any condition that in the judgment of the PI might cause participation in this study to be detrimental to
the subject or that the PI deems makes the subject a poor candidate
23 Any therapy directed at pulmonary fibrosis (excepting triple therapy of prednisone plus azathioprine
plus NAC) requires a 30-day washout period before randomized Triple therapy of lt= 12 weeks duration
in the past 4 years requires a 30-day washout period before randomization
24 History of triple therapy of prednisone plus azathioprine plus NAC for gt 12 weeksrsquo duration in the past
4 years or previous enrollment in the triple-therapy arm of the PANTHER-IPF study
44 Study Design and Study Visit
441 Study Design Summary
This study will be a randomized double-blind PL-controlled trial designed to assess the safety and efficacy of
NAC in subjects with newly diagnosed IPF
Subjects with mild to moderate IPF (defined as FVCpred ge 50 and DLCOpred ge 30) diagnosed within
the past 48 months will be enrolled Screening will continue until April 30 2012
27
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
The study will employ a 2-arm design with 11 randomization to NAC or PL Once enrolled subjects will visit
the clinical center at 15 weeks and 15-week intervals thereafter Each subject will be treated and followed for a
maximum of 60 weeks
During the 60-week visit subjects will be taken off all study agents Approximately four weeks after the final
dose of study agent is taken subjects will receive a safety phone call from the study site
442 Study Visits
Subjects who meet entry criteria will review the informed consent a written description of the purpose
procedures and risks of the study with the PI co-investigator or study coordinator and all questions will be
answered The informed consent form will be signed by the subject at screening No protocol-specific
procedures will be performed until the subject has signed and dated an informed consent form This includes the
screening procedures
4421 Screening
Once informed consent is obtained subjects may immediately begin the screening process or may return within
28 days of consent In the event a study subject has been clinically evaluated at the study site by an IPFnet study
physician and has performed testing within three weeks for this clinical evaluation that meets guidelines
provided in the IPFnet PANTHER-IPF Manual of Operating Procedures (MOOP) this testing may be used to
satisfy the following screening criteria medical history physical exam arterial blood gas (ABG) with A-a
gradient vital signs with oximetry body height and weight spirometry DLCO lung volumes and HRCT scan
Allowing the use of previously performed test results that meet study guidelines for the screening visit is
intended to permit subjects easier access to study entry to prevent subjects from repeating testing that has been
performed within the study window and to decrease risks to subjects from repeated exposure to procedures
such as arterial puncture and HRCT
The following procedures will be performed at screening
Medical history and a physical examination
28
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Measure height and weight
Serum pregnancy test (if applicable)
Measure vital signs including oximetry
Blood draws performed and the following analyses conducted
o Hematology (red cell count white cell count hemoglobin hematocrit cell indices differential
platelet count)
o Blood chemistries according to central laboratory protocol (see Section 410 Laboratory
Testing)
o Beta human chorionic gonadotropin (serum) pregnancy test (in women of childbearing potential)
o Urinalysis
Pulmonary Function Tests (PFTs) including spirometry pre- and post- bronchodilator and postshy
bronchodilator measurement of lung volumes and measurement of hemoglobin adjusted diffusing
capacity
Measure ABGs
HRCT if a satisfactory scan has not been performed on the subject within 3 months of screening (see
PANTHER-IPF MOOP for more details)
Surgical lung biopsies (if applicable) reviewed by local and central pathology departments
Current medications If required a washout period discussed with the subject and initiated at this visit
4422 Enrollment
The enrollment visit is expected to take place within eight weeks of the screening visit Enrollment visit
activities include
Measure vital signs including oximetry
Measure height and weight
Serum pregnancy test (if applicable)
If consent has been given blood will be drawn and a urine specimen collected for the bio-specimen
repository
Spirometry (post-bronchodilator)
Measure 6MWT with Borg Dyspnea Scale
29
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Collect Quality-of-life (QOL) data using the SF-36 EuroQol Investigating Choice Experiments for
Preferences of Older People Capability Instrument (ICE CAP) and SGRQ
Female subjects complete Gender Substudy questionnaire
Dyspnea status collected using the UCSD SOBQ
Evaluate Acute Exacerbation (AEx)
Review of any Adverse Events (AEs)
Review of concomitant medications
Subject receives diary and instructions on its purpose and proper use
Subject receives supply of study drug sufficient to last until his or her 15-week study visit
See the Schedule of Assessments (Table 3) for more details Subjects with screening and enrollment postshy
bronchodilator FVC measurements (in liters) differing by more than 11 are not eligible to be enrolled in the
study
Subjects will be asked to provide a physician of record This physician will be considered the subjectrsquos primary
care provider (PCP) and if the subject agrees the PCP will be informed by letter of the subjectrsquos enrollment in
the trial The subject will be informed that his or her ongoing medical care should be received from the PCP
The PCP will be informed of any safety issues identified by the study staff The PCP will also be given
information regarding communication with study personnel about pertinent health issues or clinic encounters
the subject may have
4423 Week 15
The week 15 visit is expected to occur within +- 14 days of the subjectrsquos scheduled visit time (eg the week 15
visit should occur anytime between 13 and 17 weeks after starting study drug Week 15 activities include
Measure vital signs with oximetry
Measurement height and weight
Serum pregnancy test (if applicable)
Spirometry (post-bronchodilator) measurement
Review of AEs
Evaluate for AEx
30
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Review concomitant medications
If consented draw blood and collect urine specimen for the biospecimen repository
Subjects return used and unused study drug for the visit
Review study diary and a new study diary will be given
Provide additional supply of study drug sufficient to last until the next scheduled visit
4424 Week 30
The week 30 visit is expected to occur within +- 14 days of the subjectrsquos scheduled visit time (eg the week 30
visit should occur anytime between 28 and 32 weeks after starting study drug) Week 30 activities include
Physical examination
Measure vital signs with oximetry
Measure height and weight
Laboratory values (complete blood count [CBC] and serum chemistries)
Serum pregnancy test (if applicable)
Measure spirometry (post-bronchodilator)
6MWT with Borg scale
DLCO
Review of AEs
Evaluate for AEx
Review concomitant medications
Complete all QOL and dyspnea questionnaires (EuroQol ICE CAP SF-36 SGRQ and UCSD SOBQ)
If consent has been given blood will be drawn and a urine specimen collected for the biospecimen
repository
Review study diary
Subjects return used and unused study drug for the visit
Provide additional supply of study drug sufficient to last until the next scheduled visit
4425 Week 45
31
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
The week 45 visit is expected to occur within +- 14 days of the subjectrsquos scheduled visit time (eg the week 45
visit should occur anytime between 43 and 47 weeks after starting study drug) Week 45 activities include
Measure vital signs with oximetry
Measure height and weight
Serum pregnancy test (if applicable)
Measure spirometry (post-bronchodilator)
Review of AEs
Evaluate for AEx
Review concomitant medications
If consent has been given blood will be drawn and a urine specimen collected for the biospecimen
repository
Subjects return used and unused study drug for the visit
Study diary reviewed
Provide additional supply of study drug sufficient to last until the next scheduled visit
4426 Week 60 (Early Withdrawal or Final Treatment Visit)
At week 60 or at subject withdrawal from the study (premature by study doctor or subjectrsquos decision) a final
treatment visit will occur At this final treatment visit subjects will discontinue NACPL abruptly Week 60
activities also include
Physical examination
Measure vital signs with oximetry
Measure height and weight
Laboratory values (complete blood count [CBC] and serum chemistries)
Spirometry (post-bronchodilator) measurement
6MWT with Borg scale measurement
DLCO
Lung volumes
ABG
Review of AEs
32
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Evaluate for AEx
Review concomitant medications
Subjects will complete all QOL and dyspnea questionnaires (EuroQol ICE CAP SF-36 SGRQ and
UCSD SOBQ)
If consent has been given blood will be drawn and a urine specimen collected for the biospecimen
repository
Subjects return used and unused study drug for the visit
Study diary reviewed
4427 Final Site Visit ndash FVC drop confirmation
In the event that the subject has a recorded FVC drop of gt10 from baseline at the final treatment visit and the
subject has not had a confirmation of such a drop at a previous study visit the subject should return to the
clinical site 6 to 8 weeks after the final treatment visit During this visit a post-bronchodilator spirometry test
will be performed This FVC measurement will be evaluated according to section 521 of this protocol
4428 Final Visit ndash Telephone Follow-up
Four weeks following the final dose of study medication subjects will receive a telephone call from the study
coordinator to ensure that there are no side effects and to follow up on any ongoing adverse events (AEs)
4429 Phone Contact Between Visits
At week 2 and each month that a subject does not have a scheduled clinical center visit his or her study
coordinator will contact him or her at least once by telephone to
Inquire if the subject has had any hospitalizations events that might be considered an AE or any events
significant enough to warrant an out-of-cycle visit to the clinical center
Remind subjects of their current dosage levels and confirm that the subject understands them
Address any questions or concerns the subject might have regarding other aspects of the study
Assess adherence to the treatment regimen by reviewing diary data verbal review of medications taken
including nutritional supplements
33
34
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Table 3 Schedule of Assessments
Procedure Screening Visit 0
Enrollment Visit 1
Week 15 Visit 2
Week 30Visit 3
Week 45 Visit 4
Week 60 Early
Withdrawal Visit 5
Final1
Visit (via phone)
Informed consent X
Medical history X
Inclusionexclusion criteria X
Serum pregnancy test (if applicable) X X X X X
Review of lung biopsy X
Arterial Blood Gas X X
6-Minute Walk Test
X
X X
Physical examination X X X
Vital signs with oximetry X X X X X X
Body height and weight X X X X X X
Complete Blood Count X X X
Chemistry panel X X X
Monitor Lab Values X X X
Urinalysis X Specimen repository substudy blood draw and urine collection (if consented)
X
X X X X
HRCT (if not completed within three months) X
Spirometry (pre- and post-bronchodilator) X
Spirometry (post-bronchodilator only) X X X X X
DLCO (post-bronchodilator only) X X X
Lung volumes (post-bronchodilator only) X
X
Evaluate for acute exacerbation X X X X X
Review Adverse Events X X X X X X
Review concomitant meds X X X X X X
Dispense subject diary X X X X
Review subject diary X X X X X
Dispense study agent X X X X
Gender Substudy questionnaire (female subjects only) X
EuroQol ICECAP UCSD SOBQ SGRQ SF-36 X X X
Abbreviations DLCO diffusing capacity of the lung for carbon monoxide QOL Quality of Life ICECAP Investigating Choice Experiments for Preferences of Older People UCSD SOBQ University of California Shortness of Breath Questionnaire SGRQ St Georgersquos Respiratory Questionnaire SF-36 Short Form 36 Health Survey
1Follow-up visit via phone will occur four weeks after final dose of study medication
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
45 Dose Justification
The general philosophy for determining dosing levels was to apply previously examined
treatment regimens With the focus of the study being to establish a standard of care for
mildmoderate IPF subjects the goal was to develop flexible yet standardized treatment rules that
allow for the temporary or permanent withholding of one or more components of treatment when
necessary Subjects developing laboratory abnormalities or symptoms that result in
discontinuation of one or more components of study treatment may continue on the other
components as long as there is no contraindication for this Complete follow-up is important for
the validity of any study As a strategy to maintain protocol adherence we are using a treatment
regimen that will detect potential side effects and prompt interventions proactively in the interest
of patient safety In addition subjects who permanently stop study medications during the course
of the study are encouraged to continue in the study completing all scheduled visits and tests
451 Rationale for N-acetylcysteine Dosing
To our knowledge there have been no IPF studies to correlate clinical outcome measures with
different dosages for NAC The dosage chosen is based on the IFIGENIA study However BAL
lung GSH levels from subjects with IPF have been augmented with the use of oral NAC at 600
mg 3 times per day In addition lung GSH levels have been associated with improved
PFTs212227 The dose chosen for this study was based on previous data including the IFIGENIA
study30
4511 Dosing of N-acetylcysteineplacebo
Dosing of NACPL will be 600 mg orally 3 times a day (1800 mgday)
4512 Reasons to Discontinue N-acetylcysteineplacebo
NACPL may be temporarily or permanently discontinued for the duration of the study for
gastrointestinal symptoms or dermatologic reactions
35
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Temporarily discontinue (hold) oral NACPL for subjects requiring inpatient admission for acute
exacerbation (AEx) or other conditions Resume NACPL after discharge
36
37
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
452 Dosage Algorithms
Dosage Adjustment Algorithm 1 NACPL Dose Modifications for Gastrointestinal Symptoms Nausea Vomiting Abdominal Discomfort Diarrhea
GI Symptoms determined by the PI to be clinically significant Nausea Vomiting Abdominal Discomfort Diarrhea
NACPL Temporarily dc (HOLD) x 3 Days
Monitor symptoms intervene as clinically indicated (eg fluid replacement antidiarrhea or antinausea medication)
Monitor or lab PRN
Are symptoms resolving after 3 days NO
Symptoms NOT resolving after 3 days of holding study medication Assessmentmanagement per clinical
discretion of investigator
Likely not study medication discuss resuming study medication with medical monitor when symptoms resolved
YES
Temporarily dc (HOLD) NACPL for 4 additional days (total hold 1 week) then NACPL Resume 600 MG TID
Did symptoms recur
YES
STOP NACPL for
duration of study
NO
NACPL No Change
38
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Dosage Adjustment Algorithm 2 NACPL Dose Modifications For Dermatologic Reactions
Dermatologic Reactions (Not Acneiform) ge Grade 2 Grading per Common Terminology Criteria for
Adverse Events V30 (httpctepcancergov) For example Grade 1 RASHDESQUAMATION Macular or papular eruption or erythema without associated symptoms Grade 2 RASHDESQUAMATION Macular or popular eruption or erythema with pruritus or other associated symptoms localized desquamation or other lesions covering lt50 of body surface area
NACPL Temporarily dc (HOLD) x 3 days
Are symptoms resolving after 3 days
NO Symptoms not resolving after 3 days of holding study medication Assessmentmanagement per clinical discretion of investigator Likely not study medication Discuss resuming study medication with medical monitor when symptoms
resolved YES
Temporarily dc (HOLD) NACPL for 4 additional days (total hold 1 week) then NACPL resume 600 MG TID
Did symptoms recur
YES
STOP NACPL for
duration of study
NO
NACPL No change
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
46 Contraindications Precautions and Side Effects of Study Medications
461 Contraindication
Contraindication to NAC is known hypersensitivity to it
462 Precautions
Concomitant administration of oral NAC and antibiotics has shown a slightly reduced absorption
of cephalexin and a slight increase in erythromycin serum levels NAC contains free sulfhydryl
groups There is no evidence that individuals sensitive to sulfa drugs are sensitive to NAC
The NAC preparation being administered in this study contains 20 mg of aspartame Because of
the phenylalanine component of aspartame individuals with phenylketonuria should avoid or
restrict aspartame intake to avoid increased blood levels of phenylalanine Because of this risk
labeling is required on all products containing aspartame
463 Side Effects
Side effects of NAC range from common to serious See Table 4
39
40
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Table 4 Side Effects of NAC
Undesirable Effects
System-organ class Uncommon
(gt11000 lt1100)
Rare
(gt110000 lt11000)
Very rare
(lt110000) Not known
Immune system disorders Hypersensitivity Anaphylactic shock
reaction
Nervous system disorders Headache
Ear and labyrinth disorders Tinnitus
Cardiac disorders Tachycardia
Vascular disorders Hemorrhage
Respiratory thoracic and
mediastinal disorders
Bronchospasm
Dyspnea
Gastrointestinal disorders
Vomiting diarrhea
stomatitis abdominal
pain nausea
Dyspepsia
Skin and subcutaneous tissue
disorders
Urticaria rash
angioedema itching
General disorders and
administration site conditions Pyrexia
Investigations Reduced arterial
pressure Face edema
In very rare cases the onset of severe skin reactions such as Stevens-Johnson syndrome and Lyell syndrome was reported to have a temporal relationship with N-acetylcysteine administration Although in most cases at least another suspect drug probably most involved in the genesis of the above mentioned mucocutaneous syndromes has been identified in case of mucocutaneous alterations it is appropriate to contact onersquos doctor and the administration of N-acetylcysteine should be immediately discontinued
Some studies confirmed a reduction of platelet aggregation during N-acetylcysteine administration The clinical significance of these findings has not been defined yet [Source Fluimucil Investigator Brochure]
47 Recruitment Procedures
Subjects recruited for this study will be established patients of the investigators or physician- or
self-referred to participating clinical centers in the IPFnet Each clinical center within IPFnet has
a well-developed infrastructure of local pulmonologists within the surrounding geographic area
These pulmonologists are kept informed of ongoing IPF clinical trials and regularly refer
subjects to studies conducted at IPFnet clinical centers
Additional steps will be taken to inform clinicians of the trials in progress within IPFnet
including presentations at faculty staff meetings at local hospitals medical grand rounds and
national conferences direct mail notification monthly faxes and advertisement of network trials
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
in pulmonary journals Clinical center patients previously diagnosed with IPF will be notified of
the trials by mail whenever possible
Recruitment of minorities and women will be monitored by the DCC and DSMB If necessary
additional recruitment efforts will be made at specific centers to ensure that the aggregate subject
sample contains appropriate representation of women and minorities
48 Study Procedures
The following procedures are detailed in the PANTHER-IPF MOOP accompanying this
protocol
1 PFT
2 ABG
3 HRCT scan of the chest (including imaging of pulmonary arteries)
4 CBC and serum chemistries
5 Pregnancy test
6 6MWTBorg Dyspnea Scale
7 QOL questionnaires (EuroQol HAD SF-36 SGRQ and ICE CAP)
8 UCSD SOBQ
9 Gender Substudy Questionnaire
All assessments of PFTs will be conducted by study personnel not directly involved in the
treatment of the subjects
481 Biological Specimen Management
4811 Biological Specimen Sample Management
Subjects at clinical centers participating in the specimen repository substudy who consent to
having blood drawn for research purposes and for the banking of blood blood components and
other biologic specimens (urine and BAL fluid) will have approximately 405 mL of blood
41
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
drawn 17 mL blood drawn for DNA and 20 mL of urine collected at enrollment visit Subjects
will have approximately 50 mL of blood drawn and 20 mL of urine collected at each 15-week
follow-up visit Blood specimens will be separated according to PANTHER-IPF MOOP
guidelines into the following components for banking in the repository serum plasma and
DNA Coding of all biologic specimens for the repository will be performed by study staff at the
clinical center The samples will be processed per PANTHER-IPF MOOP guidelines aliquoted
labeled with barcode labels and stored at -70degC at the clinical center and shipped to the central
repository
The only subject identifiers will be a sample ID number and subject initials This sample ID will
be linked in the IPFnet DCC clinical database to subject information No subject information will
be transferred to the biological-specimen database
The subjectrsquos samples may be used for approved sub-studies relating to human disease
including but not limited to IPF The studies for which an individualrsquos samples will be made
available will be determined by the subjectrsquos answers to questions on the biological-sample
informed consent form The subjects can choose to make their samples available for all options
or any combination Samples will be made available to researchers only with IPFnet Steering
Group approval until such time as the samples are made public through the NHLBI repository
49 Concomitant Medications
Concurrent treatment with FDA-approved therapy for IPF is allowed Colchicine may be used
for treatment of gout Temporary treatment with oral or IV corticosteroids for clinical worsening
or suspected AEx is permitted Nutritional supplements containing NAC are not allowed
410 Laboratory Testing
Clinical laboratory parameters will be assessed at screening and at the end of the study The
following tests will be performed at the two time points specified in the protocol chemistry (AG
ratio ALT [SGPT] AST [SGOT] albumin alkaline phosphatase amylase bilirubin-direct
42
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
bilirubin-indirect bilirubin-total BUN BUNcreatinine ratio calcium carbon dioxide
cholesterol-total chloride CPK-total creatinine GGT globulin glucose iron-total LDH
lipase magnesium phosphorus-inorganic potassium protein-total sodium TIBC triglycerides
uric acid) and hematology (red blood cell count WBC count hemoglobin hematocrit cell
indices differential platelet count)
411 Blinding of Study Drugs
Subjects and caregivers will be blinded to study treatment Every subject will receive NAC or
matching PLs at every study visit from the baseline visit to the week-45 visit No study agent
will be dispensed at the week-60 visit
43
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
5 Study Endpoints
51 Primary Study Endpoint
The primary endpoint will be the change in serial measurements of FVC over the study period
52 Secondary Study Endpoints
521 Time to Disease-progression
The time-to-death or a 10 decline in FVC will be defined as the time-to-disease progression
The 10 decline in FVC from enrollment must be confirmed on 2 consecutive visits no less than
6 weeks apart For subjects with 2 consecutive visits with a 10 decline in FVC the time-toshy
disease progression will be defined as the time interval between enrollment and the initial visit
with a 10 FVC decline For subjects who experience disease progression the study doctor will
determine whether or not the subject will remain in the study
522 Acute Exacerbations
The following 3 criteria will define AEx in subjects with acute worsening of their respiratory
conditions
1 Clinical (all of the following required)
A) Unexplained worsening of dyspnea or cough within 30 days triggering unscheduled
medical care (eg emergency room clinic study visit hospitalization)
B) No clinical suspicion or overt evidence of cardiac event pulmonary embolism or deep
venous thrombosis to explain acute worsening of dyspnea
C) No pneumothorax
44
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
2 RadiologicPhysiologic (A and B required)
A) New ground glass opacity or consolidation computed tomography (CT) scan OR new
alveolar opacities on chest x-ray
B) Decline of ge 5 in resting room air SpO2 from last recorded level OR decline of ge 8 mm
Hg in resting room air PaO2 from last recorded level
3 Microbiologic (all of the following required)
A) No clinical evidence for infection (ie absence of grossly purulent sputum fever gt 39degC
orally)
B) Lack of positive microbiological results (if done) from lower respiratory tract defined as
(1) Clinically significant bacterial growth on sputum or endotracheal aspirate cultures
(2) Quantitative culture by protected brush specimen ge 103 cfumL or BAL ge 104 cfumL
(3) The presence of specific pathogens on stains of any of the above
C) Lack of positive pathogen in blood cultures (if done)
Identification of Acute Exacerbations
All subjects will be educated about the importance of identifying AExs At the time of
enrollment subjects will be told about the possibility of developing acute symptomatic
worsening that might represent an AEx of IPF and instructed to contact their study clinical
center coordinator within 48 to 72 hours of the apparent event
All subjects will be contacted by phone monthly and questioned about any change in dyspnea or
cough and any interim clinic visits or hospitalizations Finally as part of the IPFnet outreach to
community referring physicians the importance of AExs will be emphasized When a subject is
identified who meets criterion 1A this will trigger the collection of additional clinical data to
evaluate a suspected AEx These data will be collected as part of standard clinical care (ie this
protocol does not require collection of all items) The additional items to be collected for
suspected AEx include
IPFnet AEx case report form (eCRF) (required)
45
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Chest x-ray CT scan withwithout pulmonary angiogram (reports should be faxed and
followed by the hard copiesdiscs)
Oxygen saturation (pulse oximetry)
ABG
Respiratory cultures (sputum endotracheal aspirate lavage)
Blood cultures
Clinichospital records related to the event
All potential cases of AEx will be reviewed by the clinical center PI first and a decision on
whether the case may represent an AEx will be made If AEx is suspected the case will be sent
to the IPFnet adjudication committee which will assign a final diagnosis (see Table 5) If there is
disagreement among members the majority opinion will be recorded
During episodes of suspected AEx as determined by the individual clinical center investigator
subjects will remain blinded and in the study
Table 5 Final Diagnoses in Evaluation of Suspected Acute Exacerbations
Definite acute exacerbation All criteria met no alternative etiology
Unclassifiable acute worsening
Insufficient data to evaluate all criteria no alternative etiology
Not acute exacerbation Alternative etiology identified that explains acute worsening
Management of the suspected AEx will be at the discretion of the treating physician Standard of
care generally involves evaluation for respiratory infection pulmonary embolism cardiac events
and pneumothorax and treatment with IV corticosteroids
Study drugs will be resumed at pre-suspected AEx doses after subjects clinically improve as
confirmed by the local PI All subjects should be seen at the clinical center within 2 to 4 weeks
of recovery for measurement of post-bronchodilator FVC (see Figure 4) Subjects unable to
return to the clinical center after suspected AEx due to medical frailty (eg continued
46
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
institutionalization progressive disability) will be categorized as failing to maintain FVC
response in secondary analyses
Suspected AEx (PI determined)
Hold study drug Treat AEx
(Attending physician determined)
Alive but unable to continue due to
medical frailty
Dead
Alive and able to continue
Site reviewvisit
Restart study drug
FVC within 2-4 weeks
Figure 4 Acute Exacerbation Flow Chart
523 Respiratory Infections
An upper respiratory infection will be defined as
Change in sputum discoloration
Increased cough of no more than 14 daysrsquo duration
A lower-respiratory infection (pneumonia) will be defined as new segmental or lobar airspace
opacities visualized by image studies (chest radiograph or HRCT) in addition to any of the
following
Positive pathogencultures in good sample of sputum or lower-airway secretions retrieved
by fiberoptic bronchoscope
Fever gt 39degC or gt 100degF
Leukocytosis gt 12000 (unexplained no increase in dose of corticosteroids)
47
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
524 Maintained FVC Response
Subjects with follow-up FVCpred measurements at or above their baseline FVCpred level
will be classified as having maintained FVC response Subjects with reduced FVCpred levels
or missing data for any reason including death or medical frailty will be classified as having not
maintained FVC response The FVCpred value is used because unadjusted FVC measurements
are expected to decline with age
48
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
6 Safety Evaluations and Procedures
61 Adverse Events
During a clinical trial the reporting of adverse experience information can lead to important
changes in the way a new treatment is developed as well as provide integral safety data
611 Definitions
An adverse event (AE) is any untoward medical occurrence in a subject or clinical investigation
subject who was administered a pharmaceutical product The AE does not necessarily have to
have a causal relationship with the drug administered An AE can be any unfavorable and
unintended sign (including an abnormal laboratory finding) symptom or disease temporarily
associated with the use of a medicinal product whether or not considered to be related to the
medicinal product Diseases signs symptoms or laboratory abnormalities already existing at
enrollment are not considered AEs unless they worsen (ie increase in intensity or frequency)
Surgical procedures themselves are not AEs they are therapeutic measures for conditions that
require surgery The condition for which the surgery is required may be an AE Surgical
procedures planned before randomization and the conditions necessitating the surgery are not
AEs
A serious adverse event is any untoward event that
Is fatal
Is life-threatening
Requires inpatient hospitalization or prolongation of existing hospitalization with the
following exceptions
o Preplanned (before the study) hospital admissions unless the hospitalization is
prolonged
o Planned admissions (as part of a study eg routine biopsies)
o Hospitalization lasting lt 24 hours
49
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
o Hospitalization for elective procedure
o Emergency room visits
Results in persistent or significant disability or incapacity
Is a congenital anomaly or birth defect
Important medical events that may not result in death be life-threatening or require
inpatient hospitalization may be considered serious adverse events (SAEs) when based
on appropriate medical judgment they may jeopardize the subject and may require
medical or surgical intervention to prevent one of the outcomes listed above
Life-threatening means that the subject was in the view of the investigator at immediate risk of
death from the AE as it occurred It does not include an AE that had it occurred in a more severe
form might have caused death
Persistent or significant disabilityincapacity means that the event resulted in permanent or
significant and substantial disruption of the subjectrsquos ability to carry out normal life functions
Causality
A reasonable possibility means the AE may have been caused byrelated to the study drug A
perceived or real lack of efficacy does not satisfy the definition of relatedness
612 Adverse Event (AE) Reporting
For the PANTHER-IPF trial all AEs (serious and nonserious) occurring from randomization
through final study visit (4 weeks after final dose of all study medication) will be recorded on the
AE page of the case report form (CRF)
6121 Serious Adverse Events (SAE) Reporting
For this trial all deaths and all SAEs which occur from randomization through final study visit
must be entered within the EDC system via the SAE eCRF page within 24 hours of the
investigative sitersquos knowledge of the event It is the responsibility of the clinical center
50
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
investigator to provide a causality assessment of the event for each study medications based upon
the information available at the time of the report It is understood that complete information
about the event may not be known at the time the initial report is submitted In the event the EDC
system is not accessible to the site at the time of event reporting investigative sites will complete
and forward a paper back-up SAE form to DCRI Safety Surveillance for processing
DCRI Safety Surveillance
Telephone 1-919-668-8624 or 1-866-668-7799 (toll free)
Fax 1-919-668-7138 or 1-866-668-7138 (toll free)
The investigator must complete and submit follow-up SAE information via the eCRF when
important new or follow-up information (eg final diagnosis outcome results of specific
investigations) becomes available Follow-up information should be submitted according to the
same process used for reporting the initial event as described above All SAEs will be followed
until resolution stabilization or 30 days after the subject has completed the final visit (4 weeks
after the final dose of study medication) whichever occurs first The investigator is responsible
for reporting SAEs to their institutional review board (IRB) per site specific IRB reporting
guidelines
6122 Regulatory Reporting
AEs that are serious study drug related and unexpected will be reported to the regulatory
authorities The DCRI Safety Surveillance medical monitor will perform a medical review of all
SAEs submitted and evaluate for ldquounexpectednessrdquo DCRI Safety Surveillance will prepare
MedWatch reports for those events identified as serious study drug related and unexpected as
determined by Safety Medical Monitor
DCRI Regulatory Services will submit all unexpected study drug-related SAEs as per 21 CFR
32 DCRI Safety Surveillance will provide a safety alert letter to the NHLBI DSMB and DCC
clinical operation (for distribution to sites) within 15 days of initial receipt of the information
51
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Investigators are responsible for promptly reporting these events to their reviewing IRBs
according to site specific IRB reporting guidelines
62 Clinical Medical Monitoring
There will be an unblinded physician at the IPFnet DCC serving as medical monitor The
medical monitor will be available to assist with questions about dosage adjustments of study
medications including discontinuation or resumption of medications
63 Unblinding Procedures
Unblinding of subjects or investigators to subject treatment is strongly discouraged For ongoing
clinical management all subjects should be presumed to be receiving ldquoactiverdquo study drug To
ensure the subjectrsquos safety the study treatment will be dose-adjusted based on laboratory test
results clinical findings and symptoms
The IPFnet DCC medical monitor and PANTHER-IPF co-chairs Drs Ganesh Raghu and
Fernando Martinez will be available to the study physicians to discuss study drug management
on a case-by-case basis Un-blinding will be considered ONLY when the knowledge of subject
treatment assignment is ABSOLUTELY ESSENTIAL for subject safety and after discussion of
the subjectrsquos case with the medical monitor and either Dr Raghu or Dr Martinez Unblinding of
study treatment should be minimized during the conduct of the trial In those cases where it is
felt to be medically necessary the DCC medical officer will communicate directly with the
managing physician to minimize unblinding of study personnel
52
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
7 Study Drug Procedures
At the baseline 15-week 30-week and 45-week study visits subjects will receive a supply of
study drug sufficient to last until the next visit at which study drug will be dispensed
53
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
8 Data Management
81 Hardware and Software Configuration
811 Hardware and Database Software
Data will be stored in an Oracle database system Oracle has advantages of processing efficiency
and smooth linkage with other software systems The application and database will be hosted on
Solaris Unix servers at the IPFnet DCC
812 Statistical Software
SAS will be used as the principal application for the management of analysis data files and
statistical computations S-Plus will be used to provide supplementary functions as needed
813 Access Control and Confidentiality Procedures
Access to databases will be controlled centrally by the IPFnet DCC through user passwords
linked to appropriate privileges This protects the data from unauthorized changes and
inadvertent loss or damage
814 Security
Database and Web servers will be secured by a firewall and through controlled physical access
Oracle has many security features to ensure that any staff member accessing the database has the
proper authority to perform the functions he or she requests of the system Within the secondary
SAS databases Unix group-access control maintains similar security The Sun workstation login
is secured by extensive user-password facilities under Unix
54
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
815 Back-up Procedures
Database back-up will be performed automatically every day and standard IPFnet DCC policies
and procedures will be applied to dictate tape rotation and retention practices
816 Virus Protection
All disk drives that provide network services and all user computers will be protected using
virus-scanning software Standard IPFnet DCC policies will be applied to update these protection
systems periodically through the study
82 Sources of Data
821 Design and Development
The IPFnet DCC will be responsible for development of the electronic case report forms
(eCRFs) development and validation of the clinical study database ensuring data integrity and
training clinical center staff on applicable data management procedures A web-based distributed
data entry model will be implemented This system will be developed to ensure that guidelines
and regulations surrounding the use of computerized systems used in clinical trials are upheld
The remainder of this section provides an overview of the data management plan associated with
this protocol
822 Data Collection Forms
The data collection process consists of direct data entry at the study clinical centers into the EDC
system(s) provided by the DCC A data collection worksheet will be provided to clinical centers
for recording data in the event the EDC system is unavailable Data entry of the eCRFs should
be completed according to the instructions provided and project specific training The
investigator is responsible for maintaining accurate complete and up-to-date records and for
ensuring the completion of the eCRFs for each research participant
55
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
823 Data Acquisition and Entry
Data entry into eCRFs shall be performed by authorized individuals Selected eCRFs may also
require the investigatorrsquos written signature or electronic signature as appropriate Electronic
CRFs will be monitored for completeness accuracy and attention to detail during the study
824 Data Center Responsibilities
The IPFnet DCC will 1) develop a data management plan and will conduct data management
activities 2) provide final eCRFs for the collection of all data required by the study 3) develop
data dictionaries for each eCRF that will comprehensively define each data element 4) conduct
ongoing data monitoring activities on study data 5) monitor any preliminary analysis data
cleanup activities and 6) rigorously monitor final study data clean up
825 Data Editing
Completed data will be entered into the IPFnet DCC automated data acquisition and
management system If incomplete or inaccurate data are found a data clarification request will
be generated and distributed to clinical centers for a response Clinical centers will resolve data
inconsistencies and errors and enter all corrections and changes into the IPFnet DCC automated
data acquisition and management system
826 Training
The training plan for clinical center staff includes provisions for training on assessments eCRF
completion guidelines data management procedures and the use of computerized systems
56
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
9 Study Design and Data Analysis
91 General Analytic Considerations
All primary analyses will be based on intent-to-treat (ITT) principles using all randomized
subjects Baseline factors across groups will be compared using mean (standard deviation) and
median (25th and 75th percentiles) summary measures Kaplan-Meier curves will be used to
display event rates Due to clinical interest in departures from both sides of the null hypothesis
all test statistics will be 2-sided
Reasonable caution needs to be taken when conducting multiple analyses on key clinical
subgroups For subgroup analyses a conservative significance level of 0001 will be used for all
interaction tests Thus subgroup comparisons will be considered exploratory unless the p-value
from the interaction test is smaller than 0001
92 Randomization Blinding and Reporting of Results
A permuted block-randomization scheme will be created with varying block sizes stratified by
clinical center Once a subject has completed the screening and baseline period and evaluation
for inclusionexclusion criteria the randomization process will begin Subjects will be
randomized to receive NAC or matching placebo with equal probability (11) via telephone
contact with a central interactive voice response system (IVRS) using a toll-free randomization
number On the day of randomization after the subject has successfully met all inclusion and
exclusion criteria the investigator or designee will call the central randomization number to
obtain the assigned kit randomization numbers for that subject At each subject visit the
investigator or designee will call the central randomization number to obtain the new kit
randomization numbers for resupply of the subject For resupply of the clinical center the IVRS
will monitor minimal volume of a kit type andor expiration date and will automatically notify
the pharmacy
57
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
The trial results will be reported according to guidelines specified in the CONSORT statement
A flow diagram describing screening recruitment randomization dropout and vital status will
be included in the primary manuscript AEs and efficacy data will be presented for all treatment
groups Adherence dropout and lost to follow-up will be carefully examined across all treatment
groups Analyses of safety will be based on data from all randomized subjects who received at
least one dose of study drug
93 Stratification
Subjects will be distributed to the two treatment arms in a 11 allocation ratio Stratification
blocks will be based on clinical centers
94 Specification of the Primary Analyses
A mixed model repeated measures (MMRM) analysis described in section 95 will be used to
compare differences in the slope of FVC measurements across the treatment groups Response
variables are values of the FVC measured at baseline and every 15 weeks until study completion
Variables in the model will include treatment time and time by treatment age sex race and
height Contrast estimates of differences in slopes of treatment over time (along with confidence
intervals) will be used to estimate the treatment effect The validity of this model in terms of
meeting modeling assumptions will be assessed via standard modeling diagnostics and goodness-
of-fit measures Based on the MMRM framework missing FVC data will not be imputed for the
primary analysis
95 Analysis of Longitudinal Endpoints
A common goal in clinical trials is to specify models that are easily implemented and
reproducible by independent data analysts On the other hand the models should have proper
statistical behavior in terms of low bias and high precision Many common approaches to
longitudinal data analysis including last observation carried forward (LOCF) imputation rely on
the missing completely at random (MCAR) assumption However the MCAR assumption is
58
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
unlikely to hold in many clinical trials because missing data are often related to disease
progression and prognosis A more reasonable assumption missing at random (MAR) specifies
that the complete data distribution can be modeled using only the observed data The likelihood-
based MMRM approach is valid under the more general MAR assumptions These models will
be applied to analyze the longitudinal data secondary endpoints
The advantages of MMRM analysis are that all important characteristics of the model can be preshy
specified standard software can be used to implement the models and results are based on ITT
principles43 In addition the MMRM approach offers superior control of Type I and Type II
errors compared with the LOCF approach
Response variables are values of the PFTs measured at enrollment and every 15 weeks until
study completion and 6MWT values measured at baseline week 30 and week 60 Covariates are
treatment time time by treatment and key baseline risk factors Contrasts (along with
confidence intervals) of treatment by time will be used to estimate the treatment effect
The correlation structure involves multiple pieces including measurement errors random
variation and interindividual variability For the longitudinal data analyses an unstructured
correlation matrix for within-subject errors will be assumed Other correlation structures
including compound symmetry will be examined as needed A careful examination of reasons
for study discontinuation will be conducted to assess the validity of MCAR Sensitivity analyses
will be used to examine the untestable assumption that the observed data violate the MAR
assumption The MMRM models will be implemented using PROC MIXED in SAS
96 Analysis of Binary Time-to-Event and Time-Lagged Endpoints
Regression modeling approaches using either the logistic regression model or Cox proportional
hazards regression model will be employed when appropriate The validity of these models will
be assessed via standard modeling diagnostics and goodness-of-fit measures Estimates of
cumulative frequencies for more general time-lagged responses will be calculated using the
partitioned version of the Bang-Tsiatis estimator44 The partitions will be set at 15-week intervals
59
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
to correspond with the data-collection process Covariate adjusted event rates will be calculated
using inverse probability-weighted regression estimates45
97 Power Analysis
971 Primary Analyses
Based on previously published IPF clinical trials the PL group is expected to experience a drop
in FVC of approximately 020 L over the study period (see Figure 1) The IPFnet Steering Group
determined a clinically important difference would be to preserve the majority of the decline
relative to PL over the study period In particular a treatment effect of 015 L was determined to
be a clinically meaningful difference Potential dropout is a key factor in the proposed study The
drop-out process assumed 5 lost to follow-up after every study visit Only 80 of subjects
were assumed to be followed for the entire study period All models assumed a compound
symmetry structure for the covariance matrix Power calculations were performed using a SAS
IML program for designing repeated measures studies46 Based on preliminary reviews of the
data from the University of Michigan the covariance matrix parameters were estimated at
approximately σ2 = 0757 (variance parameter) and ρ = 0936 (correlation parameter) To be
conservative the power calculations for the primary analysis were performed with parameter
setting of σ2 = 0810 (variance parameter) and ρ = 0925 (correlation parameter)
The power calculations assume a correction for imperfect compliance proposed by Lachin and
Foulkes to allow for 2 noncompliance for each of the treatment arms47 Thus the sample size
of 130 subjects per arm would be reduced to an adjusted sample size of 130(1-002-002)2 =
1198 or 120 subjects per arm
Under the assumed Type I error rate of 005 with a correlation parameter of 0925 and standard
deviation of 090 the difference of 015 L (or 00025 Lweek) shown in Table 6 would have
power of 93
60
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Table 6 Hypothetical Values of Mean FVC (L) Change from Baseline
Week 15 Week 30 Week 45 Week 60
NAC 00125 00250 00375 00500
Placebo 00500 01000 01500 02000
Difference 00375 00750 01125 01500
Abbreviations FVC forced vital capacity PL placebo
972 Power Analysis for Secondary Endpoints
Power calculations for secondary endpoint measurements are shown in Table 7 Standard
deviations are based on unpublished data provided by the University of Michigan The
calculations are based on a 2-sample t-test with Type I error rate set at 005 These calculations
are likely to be conservative because the statistical approach described in section 95 for
analyzing these endpoints will incorporate incomplete observations as well as intermediate data
points
Table 7 Detectable Differences in Treatment Means for Selected Endpoint Measurements
Secondary Endpoints Std Dev
of the Baseline Score
Detectable Difference for 80 Power
Std Dev of the Change Score
Difference Detectable for
80 Power
DLCOpred 166 58 91 32
6MWT Area Under the Desaturation Curve
219 76 175 61
6MWT Distance to Desaturation 224 78 315 110
6MWT Minutes Walked 210 073 205 071
Abbreviations Std Dev standard deviation DLCOpred diffusing capacity of the lung for carbon monoxide percent predicted 6MWT 6-minute walk test
61
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
10 Study Administration
101 Cooperative Agreement Mechanism
The administrative and funding mechanism used to undertake this project is a ldquocooperative
agreementrdquo (U01) which is an assistance mechanism Under the cooperative agreement the
NHLBI assists supports andor stimulates the project and is substantially involved with
investigators in conducting the study by facilitating performance of the effort in a ldquopartnerrdquo role
The NHLBI project scientist serves on the IPFnet Steering Group and he or another NHLBI
scientist may serve on other project committees when appropriate At the same time however
NHLBI does not assume a dominant role direction or prime responsibility for this research
program
As described below governance of the project is conducted through the IPFnet Steering Group
Principal investigators have lead responsibilities in all aspects of their trials and the project
including any modification of trial designs conduct of the trials quality control data analysis
and interpretation preparation of publications and collaboration with other investigators unless
otherwise provided for by the IPFnet Steering Group
PIs retain custody of and have primary rights to their center-specific and collaborative data
subject to government rights-of-access consistent with current Health amp Human Services (HHS)
Public Health Service (PHS) and National Institutes of Health policies The protocols and
governance policies call for the continual submission of data centrally to the IPFnet DCC for the
collaborative database which at a minimum will contain the key variables selected by the IPFnet
Steering Group for standardization across all clinical centers the submission of copies of the
collaborative datasets to each PI upon completion of the project procedures for data analysis
reporting and publication and procedures to protect and ensure the privacy of medical and
genetic data and records of individuals The NHLBI project scientist on behalf of the NHLBI
will have the same access privileges and responsibilities regarding the collaborative data as the
other members of the Steering Group
62
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
PIs are also encouraged to publish and to publicly release and disseminate results data and other
products of the project concordant with the project protocols and governance and the approved
plan for making data and materials available to the scientific community and to the NHLBI
However during the 3 years after the ending date of NHLBI project support unpublished data
unpublished results data sets not previously released and other study materials or products are
to be made available to any third party only with the approval of the IPFnet Steering Group
Upon completion of the project PIs are expected to put their intervention materials and
procedure manuals into the public domain andor make them available to other investigators
according to the approved plan for making data and materials available to the scientific
community and the NHLBI for the conduct of research at no charge other than the costs of
reproduction and distribution
The NHLBI reserves the right to terminate or curtail the project (or an individual award) in the
event of (a) failure to develop or implement mutually agreeable collaborative measurement
subject eligibility and data management sections of the protocols (b) substantial shortfall in
subject recruitment follow-up data reporting or quality control or other major breach of
protocol (c) substantive changes in the agreed-upon protocols with which NHLBI cannot
concur (d) reaching a major project outcome with persuasive statistical significance
substantially before schedule or (e) human subject ethical issues that may dictate a premature
termination
Any disagreement that may arise in scientificprogrammatic matters (within the scope of the
award) between award recipients and the NHLBI may be brought to arbitration An arbitration
panel will be composed of 3 membersmdash1 selected by the IPFnet Steering Group (with the
NHLBI member not voting) or by the individual PI in the event of an individual disagreement a
second selected by NHLBI and the third selected by the other 2 members This special
arbitration procedure in no way affects the PIrsquos right to appeal an adverse action that is otherwise
appealable in accordance with the PHS regulations at 42 CFR part 50 Subpart D and HHS
63
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
regulation at 45 CFR part 16 or the rights of the NHLBI under applicable statutes regulations
and terms of the award
102 IPFnet Steering Group
The IPFnet Steering Group is the main governing body of the project It is composed of the PIs
of the clinical centers the PI of the DCC and the NHLBI project scientist The clinical centers
the IPFnet DCC and the NHLBI each have 1 vote on the IPFnet Steering Group All decisions
are determined by majority vote
All major scientific decisions are determined by the IPFnet Steering Group It assumes overall
responsibility for the design and conduct of the trial It appoints (and disbands) committees and
subcommittees as the need arises designs approves and implements the study protocols
oversees the development of the MOOP monitors subject recruitment and treatment delivery
evaluates data collection and management oversees quality assurance procedures and
implements changes and enhancements to the study as required It also has primary responsibility
for facilitating the conduct of the trials and reporting the projectrsquos results
103 Data and Safety Monitoring Board
The NHLBI will establish a DSMB in accordance with established policies (see
httpwwwnhlbinihgovfundingpoliciesdsmb_insthtm) to ensure data quality and subject
safety and to provide independent advice to the NHLBI regarding progress and the
appropriateness of study continuation
104 Recommendations on Interim Monitoring of Efficacy Safety and Futility
First and foremost the role of the DSMB will be to review subject safety and trial conduct at
periodic points during the study The DSMB may require analyses of the primary endpoint
results for comparing the benefit and risks of treatment strategies The benefit of collecting
additional data on key secondary endpoints with extended follow-up and establishing a robust
64
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
evidence base for determining a standard of care will need to be carefully considered before
early termination of one or more treatment arms After careful consideration the IPFnet Steering
Group recommends conservative thresholds for the early examinations of the safety and efficacy
data
The DSMB will be expected to meet approximately every 6 months until trial completion to
review safety and toxicity data The DSMB may recommend stopping the study based on these
reviews Because the DSMB could stop the trial for safety concerns as well as for a large
efficacy benefit there could be multiple opportunities to reject the null hypothesis (no difference
in event rates between the PL and NAC groups) A Bonferroni approximation will be applied
during the one planned interim analysis for efficacy
Before locking the database a statistical analysis plan (SAP) will be developed to provide
complete details on the statistical analysis The SAP will include the specifics for how and when
the DSMB will be notified for AEs The IPFnet DCC will deliver to the DSMB all FDA-defined
AEs at 3-month intervals The IPFnet DCC will prepare narrative SAE reports in real time for
DSMB review including recommendations and analysis of similar events for each SAE
submitted to the FDA
65
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
11 Investigator and Sponsor Obligations
111 Monitoring
All monitoring activities for US clinical centers will be performed in accordance with DCRI
standard operating procedures Information regarding the types of visits will be outlined in the
PANTHER-IPF MOOP
112 Cost and Payment
There will be no cost to subjects enrolled in this trial Study-related procedures will be paid for
by the IPFnet
Subjects may be eligible for reimbursement for travel to the clinical center Details of payment
will be explained to each subject during the consent process
113 Confidentiality and Health Insurance Portability and Accountability Act
Considerations
Subject confidentiality will be protected throughout the study All subject data will be kept
strictly confidential and no subject-identifying information will be released to anyone outside
the project Confidentiality will be assured through several mechanisms First each subject will
be assigned an anonymous study ID which will then be used on all study forms Second any
study forms blood samples and paper records that contain subject information (eg address lists
phone lists) will be kept at the clinical centers in secured locked areas coded by number Once
blood is collected there will be no subject identifiers placed on blood samplesmdashonly the study
ID number and the date of sample collection Third access to all subject data and information
including laboratory specimens will be restricted to authorized personnel In the case of
computerized data this restricted access will be assured through user logon IDs and password
protection
66
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
At the IPFnet DCC only authorized personnel will have access to the data files containing study
data Security will be assured through user logon IDs passwords and appropriate access
privileges All study subjects will be identified only by their IPFnet ID numbers and no personal
identifying information such as name address or Social Security number will be entered into
the IPFnet DCC database Any subject-specific data reported to the IPFnet Steering Group will
be identified only by the IPFnet ID number
Finally subjects will not be identified by name in any reports or publications nor will the data
be presented in such a way that the identity of individual subjects can be inferred Analysis files
created for further study by the scientific community will have no subject identifiers These data
files will be created in accordance with the Ancillary Studies and Publication Policy of the
IPFnet
114 Informed Consent Procedures
All IPFnet subjects will provide written informed consent using procedures reviewed and
approved by each clinical centerrsquos IRB Informed consent will be undertaken by study personnel
in-person with the subject The subject has the option of declining further participation in the
study at that point No further study procedures will be conducted until the signed documents
have been provided to the IPFnet clinical center
115 Institutional Review Boards
Before initiating this study the protocol clinical center-specific informed consent forms Health
Insurance Portability and Accountability Act (HIPAA) forms recruitment materials and other
relevant information will be reviewed by a properly constituted IRB at each participating clinical
center A copy of the signed and dated IRB approval at each clinical center will be retrieved prior
to or during the site initiation visit and archived at the IPFnet DCC Any amendments to the
protocol other than simple administrative and typographical changes must be approved by each
IRB before they are implemented The clinical centers will seek annual renewals of their IRB
approvals in accordance with local procedures
67
__________________________________________ ________________
__________________________________________
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
12 Investigator Agreement
I have read the foregoing protocol PANTHER-IPF and agree that it contains all necessary
details for carrying out this study I will conduct the study as outlined herein and will complete
the study within the time designated
I will provide copies of the protocol and all pertinent information to all individuals responsible to
me who assist in the conduct of this study I will discuss this material with them to ensure they
are fully informed regarding the drug and the conduct of the study
I will fulfill all responsibilities for submitting pertinent information to the local IRB if
applicable that is responsible for this study
I further agree that NHLBI andor DCRI will have access to any source documents from which
eCRF information may have been generated
Signature of Principal Investigator Date
Name of Principal Investigator (printed or typed)
Protocol version date May 19 2009
Protocol Amendment 1 version date May 28 2010
Protocol Amendment 2 version date December 6 2011
68
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
13 References
1 Raghu G Brown KK Bradford WZ et al A placebo-controlled trial of interferon gamma-1b in patients with idiopathic pulmonary fibrosis N Engl J Med 2004350125-33 2 King TE Jr Safrin S Starko KM et al Analyses of efficacy end points in a controlled trial of interferon-gamma1b for idiopathic pulmonary fibrosis Chest 2005127171-7 3 Flaherty KR Thwaite EL Kazerooni EA et al Radiological versus histological diagnosis in UIP and NSIP survival implications Thorax 200358143-8 4 Wells AU Desai SR Rubens MB et al Idiopathic pulmonary fibrosis a composite physiologic index derived from disease extent observed by computed tomography Am J Respir Crit Care Med 2003167962-9 5 Raghu G Freudenberger TD Yang S et al High prevalence of abnormal acid gastroshyoesophageal reflux in idiopathic pulmonary fibrosis Eur Respir J 200627136-42 6 Kinnula VL Focus on antioxidant enzymes and antioxidant strategies in smoking related airway diseases Thorax 200560693-700 7 Coultas DB Zumwalt RE Black WC Sobonya RE The epidemiology of interstitial lung diseases Am J Respir Crit Care Med 1994150967-72 8 Raghu G Weycker D Edelsberg J Bradford WZ Oster G Incidence and prevalence of idiopathic pulmonary fibrosis Am J Respir Crit Care Med 2006174810-6 9 Olson AL Swigris JJ Lezotte DC Norris JM Wilson CG Brown KK Mortality from pulmonary fibrosis increased in the United States from 1992 to 2003 Am J Respir Crit Care Med 2007176277-84 10 Mannino DM Etzel RA Parrish RG Pulmonary fibrosis deaths in the United States 1979shy1991 An analysis of multiple-cause mortality data Am J Respir Crit Care Med 19961531548shy52 11 Hubbard R Johnston I Coultas DB Britton J Mortality rates from cryptogenic fibrosing alveolitis in seven countries Thorax 199651711-6 12 Johnston I Britton J Kinnear W Logan R Rising mortality from cryptogenic fibrosing alveolitis Bmj 19903011017-21 13 Raghu G Collard HR Egan JJ et al An official ATSERSJRSALAT statement idiopathic pulmonary fibrosis evidence-based guidelines for diagnosis and management Am J Respir Crit Care Med 2011183788-824 14 (USA) FDA FDA Public Health Advisory Interferon gamma-1b (marketed as Actimmune) In 2007 15 King TE Jr Pardo A Selman M Idiopathic pulmonary fibrosis Lancet 2011 16 Raghu G Brown KK Costabel U et al Treatment of idiopathic pulmonary fibrosis with etanercept an exploratory placebo-controlled trial Am J Respir Crit Care Med 2008178948shy55 17 Malouf MA Hopkins P Snell G Glanville AR An investigator-driven study of everolimus in surgical lung biopsy confirmed idiopathic pulmonary fibrosis Respirology 201116776-83 18 King TE Jr Behr J Brown KK et al BUILD-1 a randomized placebo-controlled trial of bosentan in idiopathic pulmonary fibrosis Am J Respir Crit Care Med 200817775-81 19 Richeldi L Costabel U Selman M et al Efficacy of a tyrosine kinase inhibitor in idiopathic pulmonary fibrosis N Engl J Med 20113651079-87
69
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
20 Borok Z Buhl R Grimes GJ et al Effect of glutathione aerosol on oxidant-antioxidant imbalance in idiopathic pulmonary fibrosis Lancet 1991338215-6 21 Meyer A Buhl R Magnussen H The effect of oral N-acetylcysteine on lung glutathione levels in idiopathic pulmonary fibrosis Eur Respir J 19947431-6 22 Behr J Maier K Degenkolb B Krombach F Vogelmeier C Antioxidative and clinical effects of high-dose N-acetylcysteine in fibrosing alveolitis Adjunctive therapy to maintenance immunosuppression Am J Respir Crit Care Med 19971561897-901 23 Cantin AM North SL Fells GA Hubbard RC Crystal RG Oxidant-mediated epithelial cell injury in idiopathic pulmonary fibrosis J Clin Invest 1987791665-73 24 Waghray M Cui Z Horowitz JC et al Hydrogen peroxide is a diffusible paracrine signal for the induction of epithelial cell death by activated myofibroblasts Faseb J 200519854-6 25 Larios JM Budhiraja R Fanburg BL Thannickal VJ Oxidative protein cross-linking reactions involving L-tyrosine in transforming growth factor-beta1-stimulated fibroblasts J Biol Chem 200127617437-41 26 Kinnula VL Fattman CL Tan RJ Oury TD Oxidative stress in pulmonary fibrosis a possible role for redox modulatory therapy Am J Respir Crit Care Med 2005172417-22 27 Meyer A Buhl R Kampf S Magnussen H Intravenous N-acetylcysteine and lung glutathione of patients with pulmonary fibrosis and normals Am J Respir Crit Care Med 19951521055-60 28 Behr J Degenkolb B Krombach F Vogelmeier C Intracellular glutathione and bronchoalveolar cells in fibrosing alveolitis effects of N-acetylcysteine Eur Respir J 200219906-11 29 Bando M Hosono T Mato N et al Long-term efficacy of inhaled N-acetylcysteine in patients with idiopathic pulmonary fibrosis Intern Med 2010492289-96 30 Demedts M Behr J Buhl R et al High-dose acetylcysteine in idiopathic pulmonary fibrosis N Engl J Med 20053532229-42 31 Toma TP Bhowmik A Rajakulasingam R Acetylcysteine in pulmonary fibrosis N Engl J Med 20063541086-9 author reply -9 32 Hunninghake GW Antioxidant therapy for idiopathic pulmonary fibrosis N Engl J Med 20053532285-7 33 Flaherty KR Mumford JA Murray S et al Prognostic implications of physiologic and radiographic changes in idiopathic interstitial pneumonia Am J Respir Crit Care Med 2003168543-8 34 Latsi PI du Bois RM Nicholson AG et al Fibrotic idiopathic interstitial pneumonia the prognostic value of longitudinal functional trends Am J Respir Crit Care Med 2003168531-7 35 Collard HR King TE Jr Bartelson BB Vourlekis JS Schwarz MI Brown KK Changes in clinical and physiologic variables predict survival in idiopathic pulmonary fibrosis Am J Respir Crit Care Med 2003168538-42 36 Jegal Y Kim DS Shim TS et al Physiology is a stronger predictor of survival than pathology in fibrotic interstitial pneumonia Am J Respir Crit Care Med 2005171639-44 37 Martinez FJ Safrin S Weycker D et al The clinical course of patients with idiopathic pulmonary fibrosis Ann Intern Med 2005142963-7 38 Hull JH Acetylcysteine in pulmonary fibrosis N Engl J Med 20063541089-91 author reply -91
70
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
39 Flaherty KR King TE Jr Raghu G et al Idiopathic interstitial pneumonia what is the effect of a multidisciplinary approach to diagnosis Am J Respir Crit Care Med 2004170904shy10 40 Raghu G Johnson WC Lockhart D Mageto Y Treatment of idiopathic pulmonary fibrosis with a new antifibrotic agent pirfenidone results of a prospective open-label Phase II study Am J Respir Crit Care Med 19991591061-9 41 Hunninghake GW Lynch DA Galvin JR et al Radiologic findings are strongly associated with a pathologic diagnosis of usual interstitial pneumonia Chest 20031241215-23 42 Lynch D Godwin J Safrin S et al High-resolution computed tomography in idiopathic pulmonary fibrosis diagnosis and prognosis Am J Respir Crit Care Med 2005172488-93 43 Mallinckrodt CH Watkin JG Molenberghs G Carroll RJ Choice of the primary analysis in longitudinal clinical trials Pharmaceutical Statistics 20043161-9 44 Bang H Tsiatis A Estimating medical costs with censored data Biometrika 200087329shy43 45 Lin DY Regression analysis of incomplete medical cost data Stat Med 2003221181-200 46 Rochon J Application of GEE procedures for sample size calculations in repeated measures experiments Stat Med 1998171643-58 47 Lachin JM Foulkes MA Evaluation of sample size and power for analyses of survival with allowance for nonuniform patient entry losses to follow-up noncompliance and stratification Biometrics 198642507-19
71
- PANTHER-IPFPREDNISONE AZATHIOPRINEAND N-ACETYLCYSTEINEA STUDY THAT EVALUATES RESPONSE INIDIOPATHIC PULMONARY FIBROSIS
-
- Protocol Summary
- Table of Contents
- List of Tables
- List of Figures
- List of Abbreviations
- 1 Summary
- 2 Hypotheses and Specific Aims
-
- 21 Null Hypothesis
- 22 Specific Aim 1
- 23 Specific Aim 2
- 24 Prespecified Subgroups of Interest
-
- 3 Background and Significance
-
- 31 Idiopathic Pulmonary Fibrosis is the Most Common Interstitial Lung Disease
- 32 Rationale for Placebo Control
- 33 Rationale for N-acetylcysteine
- 35 Rationale for N-acetylcysteine as a Stand-alone Therapy
- 36 Rationale for the Study Design and Primary Endpoint
- 37 Rationale for Blinding of Treatments
-
- 4 Methods
-
- 41 Inclusion Criteria
- 42 Diagnosis of IPF
- 43 Exclusion Criteria
- 44 Study Design and Study Visit
- 45 Dose Justification
- 46 Contraindications Precautions and Side Effects of Study Medications
- 47 Recruitment Procedures
- 48 Study Procedures
- 49 Concomitant Medications
- 410 Laboratory Testing
- 411 Blinding of Study Drugs
-
- 5 Study Endpoints
-
- 51 Primary Study Endpoint
- 52 Secondary Study Endpoints
-
- 6 Safety Evaluations and Procedures
-
- 61 Adverse Events
- 62 Clinical Medical Monitoring
- 63 Unblinding Procedures
-
- 7 Study Drug Procedures
- 8 Data Management
-
- 81 Hardware and Software Configuration
- 82 Sources of Data
-
- 9 Study Design and Data Analysis
-
- 91 General Analytic Considerations
- 92 Randomization Blinding and Reporting of Results
- 93 Stratification
- 94 Specification of the Primary Analyses
- 95 Analysis of Longitudinal Endpoints
- 96 Analysis of Binary Time-to-Event and Time-Lagged Endpoints
- 97 Power Analysis
-
- 10 Study Administration
-
- 101 Cooperative Agreement Mechanism
- 102 IPFnet Steering Group
- 103 Data and Safety Monitoring Board
- 104 Recommendations on Interim Monitoring of Efficacy Safety and Futility
-
- 11 Investigator and Sponsor Obligations
-
- 111 Monitoring
- 112 Cost and Payment
- 113 Confidentiality and Health Insurance Portability and Accountability ActConsiderations
- 114 Informed Consent Procedures
- 115 Institutional Review Boards
-
- 12 Investigator Agreement
- 13 References
-

PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
3 Background and Significance
31 Idiopathic Pulmonary Fibrosis is the Most Common Interstitial Lung Disease
IPF is the most common interstitial lung disease (ILD) of unknown etiology The current incidence and
prevalence of IPF in the United States are not known A 1994 study of a population-based registry of subjects in
Bernalillo County New Mexico USA estimated an incidence of 107 cases per 100000 per year for males and
74 cases per 100000 per year for females the prevalence of IPF was estimated at 20 per 100000 for males and
13 per 100000 for females7 Extrapolating from a large healthcare claims database a more recent review
estimated the prevalence of IPF in the United States at 427 per 100000 (incidence estimated at 163 per
100000 per year)8 Recent epidemiological studies indicate increasing mortality rates from IPF in the United
States and other industrialized nations9-12
Approximately two-thirds of subjects with IPF are over the age of 60 at the time of presentation and the
incidence increases with age13 IPF has no distinct geographical distribution and predilection by race or
ethnicity has not been identified13 Individual subjects may remain relatively stable for prolonged periods
experience very slow declines in lung function with progression of radiographic abnormalities for a period of
months to years or experience more rapid declines and subsequent death Only 20 to 30 of IPF patients
survive for 5 years following diagnosis
There is currently no proven effective pharmacological treatment for IPF13 Anti-inflammatory and
immunosuppressive agents have been the traditional approach to the management of patients with IPF Based
on the results of the interim analysis of the PANTHER-IPF trial this lsquotraditional approachrsquo will be aborted
However it remains unknown if NAC alone will prove beneficial in IPF patients The primary goal of the
modified study is to establish an evidence-based standard of care and clarify the role of this specific antioxidant
pharmacotherapy for IPF
32 Rationale for Placebo Control
IPF is a disorder for which there is no proven efficacious therapy A major objective of this trial is to test to the
greatest degree possible a proposed standard of care for patients with IPF The current traditional therapy
15
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
employs immunosuppressive and corticosteroid drugs Interim review of the original PANTHER-IPF study has
documented increased adverse events and lack of efficacy for AZA-PRED-NAC compared to placebo
suggesting that this therapeutic approach should not be employed Whether this applies to NAC alone which
has been advocated by international societies has not been proven in well-designed well-powered clinical
trials The recommendations made in the recently published evidence guidelines for NAC monotherapy was
weak based on low quality13 Thus this continued clinical trial randomizing patients to receive NAC or placebo
is pivotal and will answer the important question of the potential therapeutic benefits of NAC monotherapy with
grade A evidence In this prospective randomized clinical trial the inclusion of a PL arm is therefore vital to
adequately test the benefits of NAC in well-characterized subjects with IPF
If NAC has no true efficacy then its role as standard of care will be refuted If a benefit compared with PL is
confirmed it will establish a benchmark against which future novel therapies for IPF will be safely compared
As there is no currently accepted therapy for IPF there is an increasing body of published literature supporting
the concept of no treatment as the ldquobest carerdquo option for IPF13
Post hoc analyses of PL-controlled trials suggest that subjects with milder disease may be more amenable to
therapy12 It is notable that a recent international prospective randomized trial of interferon-gamma for IPF
also included a PL arm the study was terminated early by the data and safety monitoring board (DSMB) due to
lack of treatment effect1415 This underscores the belief that a proven effective therapy for IPF does not
currently exist and that true placebo-controlled trials remain the gold standard Similarly recently completed
trials of etanercept everolimus bosentan and BIPF 1120 in IPF have included PL-treated arms16-19 In three of
these trials the treated subjects showed little if any objective improvement Based on this evidence and the
current status of IPF therapy and therapeutic trials we believe that clinicians and subjects will continue to enroll
in a PL-controlled study
33 Rationale for N-acetylcysteine
NAC is a derivative of the amino acid L-cysteine NAC has been shown to augment levels of the naturally
occurring antioxidant glutathione (GSH ) (glutathione γ-glutamyl cysteinyl glycine) both in vitro and in
vivo2021 GSH is present in all eukaryotic cells and may play an important role in protecting alveolar epithelial
cells against oxidant injury The concentration of GSH in the bronchoalveolar lavage (BAL) fluid in patients
16
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
with IPF is markedly diminished compared with normal subjects This GSH deficiency may be corrected by
exogenous administration of NAC2122
There is evidence of enhanced production of oxidants in an IPF lung Both inflammatory cells and
myofibroblasts derived from patients with IPF generate increased amounts of extracellular oxidants including
hydrogen peroxide2324 Secretion of hydrogen peroxide by activated myofibroblasts may induce the death of
adjacent lung epithelial cells by paracrine mechanisms24 Additionally generation of oxidants by myofibroblasts
induces oxidative crosslinking of extracellular matrix proteins25 a potential mechanism for aberrant matrix
remodeling Thus an oxidant-antioxidant imbalance exists in the lungs of IPF patients26 NAC may confer
protection against this imbalance by augmenting GSH levels in addition to its more direct free-radical
scavenging activity
Intravenous (IV) NAC therapy has been shown to increase total BAL GSH in 8 IPF subjects27 Oral NAC (600
mg 3 times per day) has been shown to decrease markers of oxidant injury and improve both total and reduced
GSH levels in the epithelial lining fluid of subjects with IPF in a small uncontrolled study22 pulmonary
function improved modestly with therapy A similar study in 18 IPF subjects confirmed increased intracellular
GSH concentration after 12 weeks of NAC (600 mg 3 times per day)2228 no clinical correlates were reported
Inhaled NAC was suggested to improve pulmonary function in an open label study29
35 Rationale for N-acetylcysteine as a Stand-alone Therapy
Results of a double-blind multi-center European clinical trial of 150 IPF subjects testing combinations of AZAshy
PRED vs AZA-PRED-NAC have been reported30 NAC added to AZA-PRED (ldquoconventional therapyrdquo) had a
significant positive effect on DLCO (p lt 0005) and vital capacity (VC) (p lt 005) at the end of 1 year30 The
recent ATSERS position statement after much discussion concluded that NAC alone should not be considered
in the majority of patients with IPF without additional data from well-designed studies
The interpretation of these data has been quite controversial Some have suggested that the magnitude of the
treatment effect although statistically significant is modest31 Others have suggested that NAC may be
modulating potential toxic effects of AZA-PRED alone32 supporting the investigation of NAC as stand-alone
therapy
17
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
The IPFnet is now completing the PANTHER-IPF trial with a 11 randomization (NAC vs placebo) and a
simple practical feasible and scientifically rational design that will establish standard of care with NAC for
IPF based on a currently available therapeutic agent and the existing data to support its use We anticipate that
all future clinical trials of novel therapeutic agents will be tested against this to-be-established standard of care
36 Rationale for the Study Design and Primary Endpoint
The optimal study design of a therapeutic trial in IPF would include survival as a primary endpoint The
published results of the IFN-γ 1b Phase 3 (GIPF-001) trial suggested a survival benefit in subjects with milder
disease in retrospective analyses1 although the trial was underpowered to address this question This was likely
related to the limited mortality in the PL arm of the study which included IPF subjects with mild to moderate
disease This study documents that an IPF study powered to improve survival in a patient population with mild
disease requires a larger sample size andor duration of study In fact the recently aborted Phase 3 IFN-γ 1b
(GIPF-007 INSPIRE) study was a survival-based study and recruited more than 800 subjects at 75 centers
worldwide1415 As such within the context of the current IPFnet trial survival is an impractical primary
endpoint variable
Several groups have published data defining an appropriate surrogate outcome variable a 10 decrement in
FVC during 6 to 12 months is a powerful predictor of survival in IPF33-36 Furthermore additional evidence
suggests a similar predictive ability for a 10 decrement in FVC during 3 months of follow-up37 With strong
supportive evidence of FVC progression being related to mortality on a per-subject basis this study will use
FVC changes in liters between treatment groups as the primary endpoint Previously published IPF studies have
shown a steady decline in FVC (and FVCpred) among control group subjects230 The GIPF-001 study
suggested a 48-week decrease in FVC of 016 L in the PL-treated subjects The IFIGENIA study demonstrated
a decline in FVC of approximately 019 L over 52 weeks in the subjects randomized to the control treatment
Figure 1 depicts the change in FVC for control groups from previously published IPF studies38 Based on these
data we expect that the PL group will have a decline of 020 L over the 60-week study period The IPFnet
Steering Group determined that a clinically meaningful improvement would be the preservation of the majority
of the 020-L FVC decline Therefore a mean treatment difference of 015 L in mean FVC over the 60-week
study period was determined to be a clinically meaningful difference
18
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Δ f
rom
bas
elin
e (i
n L
)
01
005
0
-005
-01
-015 Projected Δ for placebo
-02
-025
-019
-016
-013 Pirfenidone GIPF001
NAC
Placebo
4 8 12 16 20 24 28 32 36 40 44 48 52 56 60
Week
Figure 1 Changes in FVC From Baseline in Prior IPF Clinical Trials
Recent data suggest that various patient subgroups would be expected to potentially exhibit differential response
to therapy These parameters will be used to a priori separate patients by a series of baseline characteristics
including
1 Higher enrollment FVC12
2 Typical vs atypical high-resolution computed tomography (HRCT) reading at baseline3
3 Recent vs more remote diagnosis (time from initial diagnosis of IPF le 1 year and gt 1 year)
4 Lower CPI score at enrollment4
5 Medical therapy for gastroesophageal reflux5
6 Ethnic background
7 Sex
8 Smoking history (current or ex-smoker vs never smoker) given potential impact on oxidant status6
9 Presence of emphysema gt 25 on HRCT
37 Rationale for Blinding of Treatments
The issue of treatment blinding was given a great deal of consideration with subject safety being the primary
concern After discussion among the Steering Group members it was decided that as long as subject safety
could be ensured blinding was necessary Blinding allows the study to
Have optimal scientific validity and potential to impact the standard of care for subjects
19
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Make objective assessments of treatment effects
Maintain clinical equipoise among investigators
Encourage subjects to have similar levels of contact with the medical community
Minimize the differential dropout rates across study arms
20
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
4 Methods 41 Inclusion Criteria
1 Age 35 to 85 years inclusive
2 FVC ge 50 of predicted (post-bronchodilator measurement from the screening visit)
3 DLCO ge 30 of predicted (hemoglobin corrected and altitude corrected if gt4000 ft above sea level)
4 Ability to understand and provide informed consent
5 Diagnosis of IPF according to a modified version of the ATS criteria le 48 months from enrollment The
date of diagnosis is defined as the date of the first available HRCT or surgical lung biopsy characteristic
of definite UIP
411 Subjects Shown to Have Usual Interstitial Pneumonia Pattern on Surgical Lung Biopsy
Subjects who have been shown to have UIP pattern on lung biopsy must have all of the following
1 Exclusion of other known causes of ILD such as drug toxicity clinically significant environmental
exposures or diagnosis of connective tissue diseases
2 Bibasilar reticular abnormalities with minimal ground glass opacities on HRCT scan
412 Subjects Who Have Not Undergone a Surgical Lung Biopsy
In addition to the criteria above these subjects must have radiological findings considered to be definite for the
diagnosis of UIPIPF
1 Bibasilar reticular abnormalities with minimal ground glass opacities
2 Honeycombing as the predominant feature and located in the peripheral lung bases
42 Diagnosis of IPF
Only subjects with definite IPF will be eligible for enrollment in this study We will utilize a combination of
clinicalphysiologic features HRCT and review of a clinically obtained surgical lung biopsy specimen to
establish the diagnosis of IPF An algorithm for the diagnosis is provided to guide entry into the protocol as
outlined in the inclusion and exclusion criteria (Figures 2 and 3) This multi-disciplinary approach uses
21
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
expertise from clinicians radiologists and pathologists Investigators at each site in conjunction with central
pathology will work together to establish the diagnosis of IPF This interactive approach to the diagnosis of IPF
increases the level of agreement between observers39
A subject with suspected ILD should be evaluated for secondary causes including but not limited to
environmental exposures drugs and systemic diseases Presence of any of these findings felt to be significant
enough to cause an ILD should disqualify the subject from entry into the trial
If secondary causes are absent an HRCT scan may be obtained If an HRCT of sufficiently high quality has
been obtained within the last 3 months that scan may be used for diagnosis In the appropriate clinical setting
the diagnosis of IPF can be made by the demonstration of a typical radiographic pattern on HRCT or by
demonstration of UIP pattern on a surgical lung biopsy The following criteria for a radiographic (ie
nonsurgical) diagnosis will be used In the absence of known exposures andor clinical associations attributable
to pulmonary fibrosis and in the appropriate clinical setting the presence of definite UIP pattern in HRCT
images is required to meet study criteria for the diagnosis of IPF
Figure 2 Diagnosis of Idiopathic Pulmonary Fibrosis in the IPFnet
22
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Figure 3 Pathology Flow Chart Surgical Lung Biopsy Diagnosis
Requirement for diagnosis
1 Clinical exclusion of other known causes (connective tissue diseases environmental and drug
exposures) of ILD
2 Radiographic HRCT with bibasilar reticular abnormality and honeycomb change with minimal
ground glass opacities
Appropriate clinical setting
1 Age gt 50 years
2 Insidious onset of unexplained dyspnea
3 Duration of illness for ge 3 months
4 Bibasilar inspiratory crackles
23
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Unlike the ATSERS consensus criteria published in 2000 bronchoscopy will not be required for diagnosis
This decision was made based on the experience of the IPFnet Steering Group members regarding the utility of
bronchoscopy in the diagnosis of IPF The presence of an atypical HRCT finding will require documentation of
a definitive diagnosis by surgical lung biopsy In fact this is in keeping with the recently published evidence
based guidelines for diagnosis and management of IPF13 As shown in Figure 3 central review of the pathology
data will be required for a diagnosis of IPF
We will not require central review of HRCT as several studies have shown that a confident local interpretation
of clinicalHRCT criteria as definite IPFUIP is associated with a high positive predictive value for finding UIP
at surgical lung biopsy (see Table 1) Differences in sensitivity in these series likely reflect subject selection as
Flaherty et al3 evaluated only UIP and nonspecific interstitial pneumonia (NSIP) while Raghu et al40 and
Hunninghake et al41 included a broader range of ILD
Table 1 Operating Characteristics of Local HRCT Review for Diagnosis of UIP
Researcher of Subjects Sensitivity () Specificity () PPV () NPV ()
Raghu et al 40
59 (29 UIP by SLB) 78 90 88 82
Hunninghake et al 41 91 (54 UIP by SLB)
74 81 85 67
Flaherty et al 3 96 (only NSIP amp UIP)
37 100 100 30
Abbreviations PPV positive predictive value NPV negative predictive value UIP usual interstitial pneumonia SLB surgical lung biopsy and NSIP nonspecific interstitial pneumonia
Furthermore an analysis of the HRCT scans from subjects enrolled in the GIPF-001 trial confirmed that local
site interpretations have a high congruity to a central radiology core In this multi-center study 263 HRCT
scans were read as definite IPF and a retrospective central radiology core review found 932 to be consistent
with IPF 42 We will also take several additional steps to insure that the local HRCT reads are accurate
including
1 A detailed training module has been developed and must be completed by each site radiologist before
site initiation
2 Clinical centers are to mail all HRCT scans to the HRCT core lab The first 10 HRCT scans from
subjects enrolled at each enrolling clinical center will be reviewed centrally to be certain that local reads
24
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
25
are congruent with a central interpretation If discrepancies are identified additional education will be
provided and HRCT scans will continue to be reviewed centrally until the central radiology core is
confident that the local center is performing appropriately
3 Random scans will be obtained from each center throughout the study to confirm that the local read
continues to agree with central interpretation If discrepancies are identified they will be addressed as in
2 above
In all cases if a subject has a surgical lung biopsy sample that sample will be reviewed by the local and central
pathologists Therefore the only cases that would not be subject to a direct central review process are those
where the HRCT meets the centrally defined criteria for an unequivocal diagnosis and a lung biopsy sample is
not available Table 2 below summarizes the possible combinations for making a diagnosis
Table 2 Combining HRCT and Pathology Interpretations to Determine if IPF is Present
HRCT Diagnosis Pathology Diagnosis Diagnosis of IPF
Definite UIP Definite UIP Yes
Definite UIP Probable UIP Yes
Definite UIP Possible UIP Yes
Definite UIP Not UIP No
Definite UIP Unavailable Yes
Consistent with UIP Definite UIP Yes
Consistent with UIP Probable UIP Yes
Consistent with UIP Possible UIP No
Consistent with UIP Not UIP No
Consistent with UIP Unavailable No
Inconsistent with UIP Any No
Abbreviations HRCT high-resolution computed tomography IPF idiopathic pulmonary fibrosis
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
UIP usual interstitial pneumonia Dx diagnosis 43 Exclusion Criteria
1 History of clinically significant environmental exposure known to cause pulmonary fibrosis
Occupational exposures such as asbestos or environmental exposure to organic dust such as occurs in
pigeon breeders may at times mimic the clinical and radiographic findings of IPF
2 Diagnosis of connective tissue disease felt by the principal investigator (PI) to be the etiology of the
interstitial disease Diagnosis of collagen-vascular conditions will be according to the published
American College of Rheumatology criteria As such the presence of any documented collagen-vascular
disorder or the presence of any suspicious symptom complex whether or not associated with
significantly abnormal rheumatological serologies will exclude the subject at the discretion of the PI
3 Extent of emphysema greater than the extent of fibrotic change (honeycombing reticular changes) on
HRCT scan
4 Forced expiratory volume in 1 second (FEV1)FVC ratio lt 065 at screening (postbronchodilator)
5 Partial pressure of arterial oxygen (PaO2) on room air lt 55 mm Hg (lt 50 mm Hg at Denver site)
6 Residual volume gt 120 predicted at screening (postbronchodilator)
7 Evidence of active infection
8 Significant bronchodilator response on screening spirometry defined as a change in FEV1 ge 12 and
absolute change gt 200 mL OR change in FVC ge 12 and absolute change gt 200 mL The percent
difference between the FVC (or FEV1) values will be calculated by taking the absolute value of the
difference and dividing it by the larger of the two FVC (or FEV1) values
9 Screening and enrollment post-bronchodilator FVC measurements (in liters) differing by gt 11 The
percent difference between the FVC values will be calculated by taking the absolute value of the
difference and dividing it by the larger of the two FVC values (eg the percent difference between FVC
measurements of 19 and 20 liters would be determined by taking the difference between the two (01
liters) and dividing by the larger of the two (20 liters) So 0120 = 5 and these FVC measurements
would not exclude the subject
10 Listed for lung transplantation ie the patient has completed the evaluation process has been accepted
as a candidate for transplantation at an appropriate center and is waiting to receive notification of an
available donor organ
11 History of unstable or deteriorating cardiac disease
12 Myocardial infarction coronary artery bypass or angioplasty within 6 months of screening
26
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
13 Unstable angina pectoris or congestive heart failure requiring hospitalization within 6 months of
screening
14 Uncontrolled arrhythmia
15 Severe uncontrolled hypertension
16 Known HIV or hepatitis C
17 Known cirrhosis and chronic active hepatitis
18 Active substance andor alcohol abuse (as determined by site PI)
19 Pregnancy or lactation (subjects who are pregnant or breastfeeding)
20 Known hypersensitivity to study medication
21 Any condition other than IPF that in the opinion of the site PI is likely to result in the death of the
subject within the next year
22 Any condition that in the judgment of the PI might cause participation in this study to be detrimental to
the subject or that the PI deems makes the subject a poor candidate
23 Any therapy directed at pulmonary fibrosis (excepting triple therapy of prednisone plus azathioprine
plus NAC) requires a 30-day washout period before randomized Triple therapy of lt= 12 weeks duration
in the past 4 years requires a 30-day washout period before randomization
24 History of triple therapy of prednisone plus azathioprine plus NAC for gt 12 weeksrsquo duration in the past
4 years or previous enrollment in the triple-therapy arm of the PANTHER-IPF study
44 Study Design and Study Visit
441 Study Design Summary
This study will be a randomized double-blind PL-controlled trial designed to assess the safety and efficacy of
NAC in subjects with newly diagnosed IPF
Subjects with mild to moderate IPF (defined as FVCpred ge 50 and DLCOpred ge 30) diagnosed within
the past 48 months will be enrolled Screening will continue until April 30 2012
27
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
The study will employ a 2-arm design with 11 randomization to NAC or PL Once enrolled subjects will visit
the clinical center at 15 weeks and 15-week intervals thereafter Each subject will be treated and followed for a
maximum of 60 weeks
During the 60-week visit subjects will be taken off all study agents Approximately four weeks after the final
dose of study agent is taken subjects will receive a safety phone call from the study site
442 Study Visits
Subjects who meet entry criteria will review the informed consent a written description of the purpose
procedures and risks of the study with the PI co-investigator or study coordinator and all questions will be
answered The informed consent form will be signed by the subject at screening No protocol-specific
procedures will be performed until the subject has signed and dated an informed consent form This includes the
screening procedures
4421 Screening
Once informed consent is obtained subjects may immediately begin the screening process or may return within
28 days of consent In the event a study subject has been clinically evaluated at the study site by an IPFnet study
physician and has performed testing within three weeks for this clinical evaluation that meets guidelines
provided in the IPFnet PANTHER-IPF Manual of Operating Procedures (MOOP) this testing may be used to
satisfy the following screening criteria medical history physical exam arterial blood gas (ABG) with A-a
gradient vital signs with oximetry body height and weight spirometry DLCO lung volumes and HRCT scan
Allowing the use of previously performed test results that meet study guidelines for the screening visit is
intended to permit subjects easier access to study entry to prevent subjects from repeating testing that has been
performed within the study window and to decrease risks to subjects from repeated exposure to procedures
such as arterial puncture and HRCT
The following procedures will be performed at screening
Medical history and a physical examination
28
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Measure height and weight
Serum pregnancy test (if applicable)
Measure vital signs including oximetry
Blood draws performed and the following analyses conducted
o Hematology (red cell count white cell count hemoglobin hematocrit cell indices differential
platelet count)
o Blood chemistries according to central laboratory protocol (see Section 410 Laboratory
Testing)
o Beta human chorionic gonadotropin (serum) pregnancy test (in women of childbearing potential)
o Urinalysis
Pulmonary Function Tests (PFTs) including spirometry pre- and post- bronchodilator and postshy
bronchodilator measurement of lung volumes and measurement of hemoglobin adjusted diffusing
capacity
Measure ABGs
HRCT if a satisfactory scan has not been performed on the subject within 3 months of screening (see
PANTHER-IPF MOOP for more details)
Surgical lung biopsies (if applicable) reviewed by local and central pathology departments
Current medications If required a washout period discussed with the subject and initiated at this visit
4422 Enrollment
The enrollment visit is expected to take place within eight weeks of the screening visit Enrollment visit
activities include
Measure vital signs including oximetry
Measure height and weight
Serum pregnancy test (if applicable)
If consent has been given blood will be drawn and a urine specimen collected for the bio-specimen
repository
Spirometry (post-bronchodilator)
Measure 6MWT with Borg Dyspnea Scale
29
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Collect Quality-of-life (QOL) data using the SF-36 EuroQol Investigating Choice Experiments for
Preferences of Older People Capability Instrument (ICE CAP) and SGRQ
Female subjects complete Gender Substudy questionnaire
Dyspnea status collected using the UCSD SOBQ
Evaluate Acute Exacerbation (AEx)
Review of any Adverse Events (AEs)
Review of concomitant medications
Subject receives diary and instructions on its purpose and proper use
Subject receives supply of study drug sufficient to last until his or her 15-week study visit
See the Schedule of Assessments (Table 3) for more details Subjects with screening and enrollment postshy
bronchodilator FVC measurements (in liters) differing by more than 11 are not eligible to be enrolled in the
study
Subjects will be asked to provide a physician of record This physician will be considered the subjectrsquos primary
care provider (PCP) and if the subject agrees the PCP will be informed by letter of the subjectrsquos enrollment in
the trial The subject will be informed that his or her ongoing medical care should be received from the PCP
The PCP will be informed of any safety issues identified by the study staff The PCP will also be given
information regarding communication with study personnel about pertinent health issues or clinic encounters
the subject may have
4423 Week 15
The week 15 visit is expected to occur within +- 14 days of the subjectrsquos scheduled visit time (eg the week 15
visit should occur anytime between 13 and 17 weeks after starting study drug Week 15 activities include
Measure vital signs with oximetry
Measurement height and weight
Serum pregnancy test (if applicable)
Spirometry (post-bronchodilator) measurement
Review of AEs
Evaluate for AEx
30
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Review concomitant medications
If consented draw blood and collect urine specimen for the biospecimen repository
Subjects return used and unused study drug for the visit
Review study diary and a new study diary will be given
Provide additional supply of study drug sufficient to last until the next scheduled visit
4424 Week 30
The week 30 visit is expected to occur within +- 14 days of the subjectrsquos scheduled visit time (eg the week 30
visit should occur anytime between 28 and 32 weeks after starting study drug) Week 30 activities include
Physical examination
Measure vital signs with oximetry
Measure height and weight
Laboratory values (complete blood count [CBC] and serum chemistries)
Serum pregnancy test (if applicable)
Measure spirometry (post-bronchodilator)
6MWT with Borg scale
DLCO
Review of AEs
Evaluate for AEx
Review concomitant medications
Complete all QOL and dyspnea questionnaires (EuroQol ICE CAP SF-36 SGRQ and UCSD SOBQ)
If consent has been given blood will be drawn and a urine specimen collected for the biospecimen
repository
Review study diary
Subjects return used and unused study drug for the visit
Provide additional supply of study drug sufficient to last until the next scheduled visit
4425 Week 45
31
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
The week 45 visit is expected to occur within +- 14 days of the subjectrsquos scheduled visit time (eg the week 45
visit should occur anytime between 43 and 47 weeks after starting study drug) Week 45 activities include
Measure vital signs with oximetry
Measure height and weight
Serum pregnancy test (if applicable)
Measure spirometry (post-bronchodilator)
Review of AEs
Evaluate for AEx
Review concomitant medications
If consent has been given blood will be drawn and a urine specimen collected for the biospecimen
repository
Subjects return used and unused study drug for the visit
Study diary reviewed
Provide additional supply of study drug sufficient to last until the next scheduled visit
4426 Week 60 (Early Withdrawal or Final Treatment Visit)
At week 60 or at subject withdrawal from the study (premature by study doctor or subjectrsquos decision) a final
treatment visit will occur At this final treatment visit subjects will discontinue NACPL abruptly Week 60
activities also include
Physical examination
Measure vital signs with oximetry
Measure height and weight
Laboratory values (complete blood count [CBC] and serum chemistries)
Spirometry (post-bronchodilator) measurement
6MWT with Borg scale measurement
DLCO
Lung volumes
ABG
Review of AEs
32
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Evaluate for AEx
Review concomitant medications
Subjects will complete all QOL and dyspnea questionnaires (EuroQol ICE CAP SF-36 SGRQ and
UCSD SOBQ)
If consent has been given blood will be drawn and a urine specimen collected for the biospecimen
repository
Subjects return used and unused study drug for the visit
Study diary reviewed
4427 Final Site Visit ndash FVC drop confirmation
In the event that the subject has a recorded FVC drop of gt10 from baseline at the final treatment visit and the
subject has not had a confirmation of such a drop at a previous study visit the subject should return to the
clinical site 6 to 8 weeks after the final treatment visit During this visit a post-bronchodilator spirometry test
will be performed This FVC measurement will be evaluated according to section 521 of this protocol
4428 Final Visit ndash Telephone Follow-up
Four weeks following the final dose of study medication subjects will receive a telephone call from the study
coordinator to ensure that there are no side effects and to follow up on any ongoing adverse events (AEs)
4429 Phone Contact Between Visits
At week 2 and each month that a subject does not have a scheduled clinical center visit his or her study
coordinator will contact him or her at least once by telephone to
Inquire if the subject has had any hospitalizations events that might be considered an AE or any events
significant enough to warrant an out-of-cycle visit to the clinical center
Remind subjects of their current dosage levels and confirm that the subject understands them
Address any questions or concerns the subject might have regarding other aspects of the study
Assess adherence to the treatment regimen by reviewing diary data verbal review of medications taken
including nutritional supplements
33
34
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Table 3 Schedule of Assessments
Procedure Screening Visit 0
Enrollment Visit 1
Week 15 Visit 2
Week 30Visit 3
Week 45 Visit 4
Week 60 Early
Withdrawal Visit 5
Final1
Visit (via phone)
Informed consent X
Medical history X
Inclusionexclusion criteria X
Serum pregnancy test (if applicable) X X X X X
Review of lung biopsy X
Arterial Blood Gas X X
6-Minute Walk Test
X
X X
Physical examination X X X
Vital signs with oximetry X X X X X X
Body height and weight X X X X X X
Complete Blood Count X X X
Chemistry panel X X X
Monitor Lab Values X X X
Urinalysis X Specimen repository substudy blood draw and urine collection (if consented)
X
X X X X
HRCT (if not completed within three months) X
Spirometry (pre- and post-bronchodilator) X
Spirometry (post-bronchodilator only) X X X X X
DLCO (post-bronchodilator only) X X X
Lung volumes (post-bronchodilator only) X
X
Evaluate for acute exacerbation X X X X X
Review Adverse Events X X X X X X
Review concomitant meds X X X X X X
Dispense subject diary X X X X
Review subject diary X X X X X
Dispense study agent X X X X
Gender Substudy questionnaire (female subjects only) X
EuroQol ICECAP UCSD SOBQ SGRQ SF-36 X X X
Abbreviations DLCO diffusing capacity of the lung for carbon monoxide QOL Quality of Life ICECAP Investigating Choice Experiments for Preferences of Older People UCSD SOBQ University of California Shortness of Breath Questionnaire SGRQ St Georgersquos Respiratory Questionnaire SF-36 Short Form 36 Health Survey
1Follow-up visit via phone will occur four weeks after final dose of study medication
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
45 Dose Justification
The general philosophy for determining dosing levels was to apply previously examined
treatment regimens With the focus of the study being to establish a standard of care for
mildmoderate IPF subjects the goal was to develop flexible yet standardized treatment rules that
allow for the temporary or permanent withholding of one or more components of treatment when
necessary Subjects developing laboratory abnormalities or symptoms that result in
discontinuation of one or more components of study treatment may continue on the other
components as long as there is no contraindication for this Complete follow-up is important for
the validity of any study As a strategy to maintain protocol adherence we are using a treatment
regimen that will detect potential side effects and prompt interventions proactively in the interest
of patient safety In addition subjects who permanently stop study medications during the course
of the study are encouraged to continue in the study completing all scheduled visits and tests
451 Rationale for N-acetylcysteine Dosing
To our knowledge there have been no IPF studies to correlate clinical outcome measures with
different dosages for NAC The dosage chosen is based on the IFIGENIA study However BAL
lung GSH levels from subjects with IPF have been augmented with the use of oral NAC at 600
mg 3 times per day In addition lung GSH levels have been associated with improved
PFTs212227 The dose chosen for this study was based on previous data including the IFIGENIA
study30
4511 Dosing of N-acetylcysteineplacebo
Dosing of NACPL will be 600 mg orally 3 times a day (1800 mgday)
4512 Reasons to Discontinue N-acetylcysteineplacebo
NACPL may be temporarily or permanently discontinued for the duration of the study for
gastrointestinal symptoms or dermatologic reactions
35
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Temporarily discontinue (hold) oral NACPL for subjects requiring inpatient admission for acute
exacerbation (AEx) or other conditions Resume NACPL after discharge
36
37
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
452 Dosage Algorithms
Dosage Adjustment Algorithm 1 NACPL Dose Modifications for Gastrointestinal Symptoms Nausea Vomiting Abdominal Discomfort Diarrhea
GI Symptoms determined by the PI to be clinically significant Nausea Vomiting Abdominal Discomfort Diarrhea
NACPL Temporarily dc (HOLD) x 3 Days
Monitor symptoms intervene as clinically indicated (eg fluid replacement antidiarrhea or antinausea medication)
Monitor or lab PRN
Are symptoms resolving after 3 days NO
Symptoms NOT resolving after 3 days of holding study medication Assessmentmanagement per clinical
discretion of investigator
Likely not study medication discuss resuming study medication with medical monitor when symptoms resolved
YES
Temporarily dc (HOLD) NACPL for 4 additional days (total hold 1 week) then NACPL Resume 600 MG TID
Did symptoms recur
YES
STOP NACPL for
duration of study
NO
NACPL No Change
38
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Dosage Adjustment Algorithm 2 NACPL Dose Modifications For Dermatologic Reactions
Dermatologic Reactions (Not Acneiform) ge Grade 2 Grading per Common Terminology Criteria for
Adverse Events V30 (httpctepcancergov) For example Grade 1 RASHDESQUAMATION Macular or papular eruption or erythema without associated symptoms Grade 2 RASHDESQUAMATION Macular or popular eruption or erythema with pruritus or other associated symptoms localized desquamation or other lesions covering lt50 of body surface area
NACPL Temporarily dc (HOLD) x 3 days
Are symptoms resolving after 3 days
NO Symptoms not resolving after 3 days of holding study medication Assessmentmanagement per clinical discretion of investigator Likely not study medication Discuss resuming study medication with medical monitor when symptoms
resolved YES
Temporarily dc (HOLD) NACPL for 4 additional days (total hold 1 week) then NACPL resume 600 MG TID
Did symptoms recur
YES
STOP NACPL for
duration of study
NO
NACPL No change
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
46 Contraindications Precautions and Side Effects of Study Medications
461 Contraindication
Contraindication to NAC is known hypersensitivity to it
462 Precautions
Concomitant administration of oral NAC and antibiotics has shown a slightly reduced absorption
of cephalexin and a slight increase in erythromycin serum levels NAC contains free sulfhydryl
groups There is no evidence that individuals sensitive to sulfa drugs are sensitive to NAC
The NAC preparation being administered in this study contains 20 mg of aspartame Because of
the phenylalanine component of aspartame individuals with phenylketonuria should avoid or
restrict aspartame intake to avoid increased blood levels of phenylalanine Because of this risk
labeling is required on all products containing aspartame
463 Side Effects
Side effects of NAC range from common to serious See Table 4
39
40
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Table 4 Side Effects of NAC
Undesirable Effects
System-organ class Uncommon
(gt11000 lt1100)
Rare
(gt110000 lt11000)
Very rare
(lt110000) Not known
Immune system disorders Hypersensitivity Anaphylactic shock
reaction
Nervous system disorders Headache
Ear and labyrinth disorders Tinnitus
Cardiac disorders Tachycardia
Vascular disorders Hemorrhage
Respiratory thoracic and
mediastinal disorders
Bronchospasm
Dyspnea
Gastrointestinal disorders
Vomiting diarrhea
stomatitis abdominal
pain nausea
Dyspepsia
Skin and subcutaneous tissue
disorders
Urticaria rash
angioedema itching
General disorders and
administration site conditions Pyrexia
Investigations Reduced arterial
pressure Face edema
In very rare cases the onset of severe skin reactions such as Stevens-Johnson syndrome and Lyell syndrome was reported to have a temporal relationship with N-acetylcysteine administration Although in most cases at least another suspect drug probably most involved in the genesis of the above mentioned mucocutaneous syndromes has been identified in case of mucocutaneous alterations it is appropriate to contact onersquos doctor and the administration of N-acetylcysteine should be immediately discontinued
Some studies confirmed a reduction of platelet aggregation during N-acetylcysteine administration The clinical significance of these findings has not been defined yet [Source Fluimucil Investigator Brochure]
47 Recruitment Procedures
Subjects recruited for this study will be established patients of the investigators or physician- or
self-referred to participating clinical centers in the IPFnet Each clinical center within IPFnet has
a well-developed infrastructure of local pulmonologists within the surrounding geographic area
These pulmonologists are kept informed of ongoing IPF clinical trials and regularly refer
subjects to studies conducted at IPFnet clinical centers
Additional steps will be taken to inform clinicians of the trials in progress within IPFnet
including presentations at faculty staff meetings at local hospitals medical grand rounds and
national conferences direct mail notification monthly faxes and advertisement of network trials
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
in pulmonary journals Clinical center patients previously diagnosed with IPF will be notified of
the trials by mail whenever possible
Recruitment of minorities and women will be monitored by the DCC and DSMB If necessary
additional recruitment efforts will be made at specific centers to ensure that the aggregate subject
sample contains appropriate representation of women and minorities
48 Study Procedures
The following procedures are detailed in the PANTHER-IPF MOOP accompanying this
protocol
1 PFT
2 ABG
3 HRCT scan of the chest (including imaging of pulmonary arteries)
4 CBC and serum chemistries
5 Pregnancy test
6 6MWTBorg Dyspnea Scale
7 QOL questionnaires (EuroQol HAD SF-36 SGRQ and ICE CAP)
8 UCSD SOBQ
9 Gender Substudy Questionnaire
All assessments of PFTs will be conducted by study personnel not directly involved in the
treatment of the subjects
481 Biological Specimen Management
4811 Biological Specimen Sample Management
Subjects at clinical centers participating in the specimen repository substudy who consent to
having blood drawn for research purposes and for the banking of blood blood components and
other biologic specimens (urine and BAL fluid) will have approximately 405 mL of blood
41
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
drawn 17 mL blood drawn for DNA and 20 mL of urine collected at enrollment visit Subjects
will have approximately 50 mL of blood drawn and 20 mL of urine collected at each 15-week
follow-up visit Blood specimens will be separated according to PANTHER-IPF MOOP
guidelines into the following components for banking in the repository serum plasma and
DNA Coding of all biologic specimens for the repository will be performed by study staff at the
clinical center The samples will be processed per PANTHER-IPF MOOP guidelines aliquoted
labeled with barcode labels and stored at -70degC at the clinical center and shipped to the central
repository
The only subject identifiers will be a sample ID number and subject initials This sample ID will
be linked in the IPFnet DCC clinical database to subject information No subject information will
be transferred to the biological-specimen database
The subjectrsquos samples may be used for approved sub-studies relating to human disease
including but not limited to IPF The studies for which an individualrsquos samples will be made
available will be determined by the subjectrsquos answers to questions on the biological-sample
informed consent form The subjects can choose to make their samples available for all options
or any combination Samples will be made available to researchers only with IPFnet Steering
Group approval until such time as the samples are made public through the NHLBI repository
49 Concomitant Medications
Concurrent treatment with FDA-approved therapy for IPF is allowed Colchicine may be used
for treatment of gout Temporary treatment with oral or IV corticosteroids for clinical worsening
or suspected AEx is permitted Nutritional supplements containing NAC are not allowed
410 Laboratory Testing
Clinical laboratory parameters will be assessed at screening and at the end of the study The
following tests will be performed at the two time points specified in the protocol chemistry (AG
ratio ALT [SGPT] AST [SGOT] albumin alkaline phosphatase amylase bilirubin-direct
42
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
bilirubin-indirect bilirubin-total BUN BUNcreatinine ratio calcium carbon dioxide
cholesterol-total chloride CPK-total creatinine GGT globulin glucose iron-total LDH
lipase magnesium phosphorus-inorganic potassium protein-total sodium TIBC triglycerides
uric acid) and hematology (red blood cell count WBC count hemoglobin hematocrit cell
indices differential platelet count)
411 Blinding of Study Drugs
Subjects and caregivers will be blinded to study treatment Every subject will receive NAC or
matching PLs at every study visit from the baseline visit to the week-45 visit No study agent
will be dispensed at the week-60 visit
43
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
5 Study Endpoints
51 Primary Study Endpoint
The primary endpoint will be the change in serial measurements of FVC over the study period
52 Secondary Study Endpoints
521 Time to Disease-progression
The time-to-death or a 10 decline in FVC will be defined as the time-to-disease progression
The 10 decline in FVC from enrollment must be confirmed on 2 consecutive visits no less than
6 weeks apart For subjects with 2 consecutive visits with a 10 decline in FVC the time-toshy
disease progression will be defined as the time interval between enrollment and the initial visit
with a 10 FVC decline For subjects who experience disease progression the study doctor will
determine whether or not the subject will remain in the study
522 Acute Exacerbations
The following 3 criteria will define AEx in subjects with acute worsening of their respiratory
conditions
1 Clinical (all of the following required)
A) Unexplained worsening of dyspnea or cough within 30 days triggering unscheduled
medical care (eg emergency room clinic study visit hospitalization)
B) No clinical suspicion or overt evidence of cardiac event pulmonary embolism or deep
venous thrombosis to explain acute worsening of dyspnea
C) No pneumothorax
44
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
2 RadiologicPhysiologic (A and B required)
A) New ground glass opacity or consolidation computed tomography (CT) scan OR new
alveolar opacities on chest x-ray
B) Decline of ge 5 in resting room air SpO2 from last recorded level OR decline of ge 8 mm
Hg in resting room air PaO2 from last recorded level
3 Microbiologic (all of the following required)
A) No clinical evidence for infection (ie absence of grossly purulent sputum fever gt 39degC
orally)
B) Lack of positive microbiological results (if done) from lower respiratory tract defined as
(1) Clinically significant bacterial growth on sputum or endotracheal aspirate cultures
(2) Quantitative culture by protected brush specimen ge 103 cfumL or BAL ge 104 cfumL
(3) The presence of specific pathogens on stains of any of the above
C) Lack of positive pathogen in blood cultures (if done)
Identification of Acute Exacerbations
All subjects will be educated about the importance of identifying AExs At the time of
enrollment subjects will be told about the possibility of developing acute symptomatic
worsening that might represent an AEx of IPF and instructed to contact their study clinical
center coordinator within 48 to 72 hours of the apparent event
All subjects will be contacted by phone monthly and questioned about any change in dyspnea or
cough and any interim clinic visits or hospitalizations Finally as part of the IPFnet outreach to
community referring physicians the importance of AExs will be emphasized When a subject is
identified who meets criterion 1A this will trigger the collection of additional clinical data to
evaluate a suspected AEx These data will be collected as part of standard clinical care (ie this
protocol does not require collection of all items) The additional items to be collected for
suspected AEx include
IPFnet AEx case report form (eCRF) (required)
45
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Chest x-ray CT scan withwithout pulmonary angiogram (reports should be faxed and
followed by the hard copiesdiscs)
Oxygen saturation (pulse oximetry)
ABG
Respiratory cultures (sputum endotracheal aspirate lavage)
Blood cultures
Clinichospital records related to the event
All potential cases of AEx will be reviewed by the clinical center PI first and a decision on
whether the case may represent an AEx will be made If AEx is suspected the case will be sent
to the IPFnet adjudication committee which will assign a final diagnosis (see Table 5) If there is
disagreement among members the majority opinion will be recorded
During episodes of suspected AEx as determined by the individual clinical center investigator
subjects will remain blinded and in the study
Table 5 Final Diagnoses in Evaluation of Suspected Acute Exacerbations
Definite acute exacerbation All criteria met no alternative etiology
Unclassifiable acute worsening
Insufficient data to evaluate all criteria no alternative etiology
Not acute exacerbation Alternative etiology identified that explains acute worsening
Management of the suspected AEx will be at the discretion of the treating physician Standard of
care generally involves evaluation for respiratory infection pulmonary embolism cardiac events
and pneumothorax and treatment with IV corticosteroids
Study drugs will be resumed at pre-suspected AEx doses after subjects clinically improve as
confirmed by the local PI All subjects should be seen at the clinical center within 2 to 4 weeks
of recovery for measurement of post-bronchodilator FVC (see Figure 4) Subjects unable to
return to the clinical center after suspected AEx due to medical frailty (eg continued
46
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
institutionalization progressive disability) will be categorized as failing to maintain FVC
response in secondary analyses
Suspected AEx (PI determined)
Hold study drug Treat AEx
(Attending physician determined)
Alive but unable to continue due to
medical frailty
Dead
Alive and able to continue
Site reviewvisit
Restart study drug
FVC within 2-4 weeks
Figure 4 Acute Exacerbation Flow Chart
523 Respiratory Infections
An upper respiratory infection will be defined as
Change in sputum discoloration
Increased cough of no more than 14 daysrsquo duration
A lower-respiratory infection (pneumonia) will be defined as new segmental or lobar airspace
opacities visualized by image studies (chest radiograph or HRCT) in addition to any of the
following
Positive pathogencultures in good sample of sputum or lower-airway secretions retrieved
by fiberoptic bronchoscope
Fever gt 39degC or gt 100degF
Leukocytosis gt 12000 (unexplained no increase in dose of corticosteroids)
47
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
524 Maintained FVC Response
Subjects with follow-up FVCpred measurements at or above their baseline FVCpred level
will be classified as having maintained FVC response Subjects with reduced FVCpred levels
or missing data for any reason including death or medical frailty will be classified as having not
maintained FVC response The FVCpred value is used because unadjusted FVC measurements
are expected to decline with age
48
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
6 Safety Evaluations and Procedures
61 Adverse Events
During a clinical trial the reporting of adverse experience information can lead to important
changes in the way a new treatment is developed as well as provide integral safety data
611 Definitions
An adverse event (AE) is any untoward medical occurrence in a subject or clinical investigation
subject who was administered a pharmaceutical product The AE does not necessarily have to
have a causal relationship with the drug administered An AE can be any unfavorable and
unintended sign (including an abnormal laboratory finding) symptom or disease temporarily
associated with the use of a medicinal product whether or not considered to be related to the
medicinal product Diseases signs symptoms or laboratory abnormalities already existing at
enrollment are not considered AEs unless they worsen (ie increase in intensity or frequency)
Surgical procedures themselves are not AEs they are therapeutic measures for conditions that
require surgery The condition for which the surgery is required may be an AE Surgical
procedures planned before randomization and the conditions necessitating the surgery are not
AEs
A serious adverse event is any untoward event that
Is fatal
Is life-threatening
Requires inpatient hospitalization or prolongation of existing hospitalization with the
following exceptions
o Preplanned (before the study) hospital admissions unless the hospitalization is
prolonged
o Planned admissions (as part of a study eg routine biopsies)
o Hospitalization lasting lt 24 hours
49
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
o Hospitalization for elective procedure
o Emergency room visits
Results in persistent or significant disability or incapacity
Is a congenital anomaly or birth defect
Important medical events that may not result in death be life-threatening or require
inpatient hospitalization may be considered serious adverse events (SAEs) when based
on appropriate medical judgment they may jeopardize the subject and may require
medical or surgical intervention to prevent one of the outcomes listed above
Life-threatening means that the subject was in the view of the investigator at immediate risk of
death from the AE as it occurred It does not include an AE that had it occurred in a more severe
form might have caused death
Persistent or significant disabilityincapacity means that the event resulted in permanent or
significant and substantial disruption of the subjectrsquos ability to carry out normal life functions
Causality
A reasonable possibility means the AE may have been caused byrelated to the study drug A
perceived or real lack of efficacy does not satisfy the definition of relatedness
612 Adverse Event (AE) Reporting
For the PANTHER-IPF trial all AEs (serious and nonserious) occurring from randomization
through final study visit (4 weeks after final dose of all study medication) will be recorded on the
AE page of the case report form (CRF)
6121 Serious Adverse Events (SAE) Reporting
For this trial all deaths and all SAEs which occur from randomization through final study visit
must be entered within the EDC system via the SAE eCRF page within 24 hours of the
investigative sitersquos knowledge of the event It is the responsibility of the clinical center
50
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
investigator to provide a causality assessment of the event for each study medications based upon
the information available at the time of the report It is understood that complete information
about the event may not be known at the time the initial report is submitted In the event the EDC
system is not accessible to the site at the time of event reporting investigative sites will complete
and forward a paper back-up SAE form to DCRI Safety Surveillance for processing
DCRI Safety Surveillance
Telephone 1-919-668-8624 or 1-866-668-7799 (toll free)
Fax 1-919-668-7138 or 1-866-668-7138 (toll free)
The investigator must complete and submit follow-up SAE information via the eCRF when
important new or follow-up information (eg final diagnosis outcome results of specific
investigations) becomes available Follow-up information should be submitted according to the
same process used for reporting the initial event as described above All SAEs will be followed
until resolution stabilization or 30 days after the subject has completed the final visit (4 weeks
after the final dose of study medication) whichever occurs first The investigator is responsible
for reporting SAEs to their institutional review board (IRB) per site specific IRB reporting
guidelines
6122 Regulatory Reporting
AEs that are serious study drug related and unexpected will be reported to the regulatory
authorities The DCRI Safety Surveillance medical monitor will perform a medical review of all
SAEs submitted and evaluate for ldquounexpectednessrdquo DCRI Safety Surveillance will prepare
MedWatch reports for those events identified as serious study drug related and unexpected as
determined by Safety Medical Monitor
DCRI Regulatory Services will submit all unexpected study drug-related SAEs as per 21 CFR
32 DCRI Safety Surveillance will provide a safety alert letter to the NHLBI DSMB and DCC
clinical operation (for distribution to sites) within 15 days of initial receipt of the information
51
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Investigators are responsible for promptly reporting these events to their reviewing IRBs
according to site specific IRB reporting guidelines
62 Clinical Medical Monitoring
There will be an unblinded physician at the IPFnet DCC serving as medical monitor The
medical monitor will be available to assist with questions about dosage adjustments of study
medications including discontinuation or resumption of medications
63 Unblinding Procedures
Unblinding of subjects or investigators to subject treatment is strongly discouraged For ongoing
clinical management all subjects should be presumed to be receiving ldquoactiverdquo study drug To
ensure the subjectrsquos safety the study treatment will be dose-adjusted based on laboratory test
results clinical findings and symptoms
The IPFnet DCC medical monitor and PANTHER-IPF co-chairs Drs Ganesh Raghu and
Fernando Martinez will be available to the study physicians to discuss study drug management
on a case-by-case basis Un-blinding will be considered ONLY when the knowledge of subject
treatment assignment is ABSOLUTELY ESSENTIAL for subject safety and after discussion of
the subjectrsquos case with the medical monitor and either Dr Raghu or Dr Martinez Unblinding of
study treatment should be minimized during the conduct of the trial In those cases where it is
felt to be medically necessary the DCC medical officer will communicate directly with the
managing physician to minimize unblinding of study personnel
52
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
7 Study Drug Procedures
At the baseline 15-week 30-week and 45-week study visits subjects will receive a supply of
study drug sufficient to last until the next visit at which study drug will be dispensed
53
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
8 Data Management
81 Hardware and Software Configuration
811 Hardware and Database Software
Data will be stored in an Oracle database system Oracle has advantages of processing efficiency
and smooth linkage with other software systems The application and database will be hosted on
Solaris Unix servers at the IPFnet DCC
812 Statistical Software
SAS will be used as the principal application for the management of analysis data files and
statistical computations S-Plus will be used to provide supplementary functions as needed
813 Access Control and Confidentiality Procedures
Access to databases will be controlled centrally by the IPFnet DCC through user passwords
linked to appropriate privileges This protects the data from unauthorized changes and
inadvertent loss or damage
814 Security
Database and Web servers will be secured by a firewall and through controlled physical access
Oracle has many security features to ensure that any staff member accessing the database has the
proper authority to perform the functions he or she requests of the system Within the secondary
SAS databases Unix group-access control maintains similar security The Sun workstation login
is secured by extensive user-password facilities under Unix
54
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
815 Back-up Procedures
Database back-up will be performed automatically every day and standard IPFnet DCC policies
and procedures will be applied to dictate tape rotation and retention practices
816 Virus Protection
All disk drives that provide network services and all user computers will be protected using
virus-scanning software Standard IPFnet DCC policies will be applied to update these protection
systems periodically through the study
82 Sources of Data
821 Design and Development
The IPFnet DCC will be responsible for development of the electronic case report forms
(eCRFs) development and validation of the clinical study database ensuring data integrity and
training clinical center staff on applicable data management procedures A web-based distributed
data entry model will be implemented This system will be developed to ensure that guidelines
and regulations surrounding the use of computerized systems used in clinical trials are upheld
The remainder of this section provides an overview of the data management plan associated with
this protocol
822 Data Collection Forms
The data collection process consists of direct data entry at the study clinical centers into the EDC
system(s) provided by the DCC A data collection worksheet will be provided to clinical centers
for recording data in the event the EDC system is unavailable Data entry of the eCRFs should
be completed according to the instructions provided and project specific training The
investigator is responsible for maintaining accurate complete and up-to-date records and for
ensuring the completion of the eCRFs for each research participant
55
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
823 Data Acquisition and Entry
Data entry into eCRFs shall be performed by authorized individuals Selected eCRFs may also
require the investigatorrsquos written signature or electronic signature as appropriate Electronic
CRFs will be monitored for completeness accuracy and attention to detail during the study
824 Data Center Responsibilities
The IPFnet DCC will 1) develop a data management plan and will conduct data management
activities 2) provide final eCRFs for the collection of all data required by the study 3) develop
data dictionaries for each eCRF that will comprehensively define each data element 4) conduct
ongoing data monitoring activities on study data 5) monitor any preliminary analysis data
cleanup activities and 6) rigorously monitor final study data clean up
825 Data Editing
Completed data will be entered into the IPFnet DCC automated data acquisition and
management system If incomplete or inaccurate data are found a data clarification request will
be generated and distributed to clinical centers for a response Clinical centers will resolve data
inconsistencies and errors and enter all corrections and changes into the IPFnet DCC automated
data acquisition and management system
826 Training
The training plan for clinical center staff includes provisions for training on assessments eCRF
completion guidelines data management procedures and the use of computerized systems
56
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
9 Study Design and Data Analysis
91 General Analytic Considerations
All primary analyses will be based on intent-to-treat (ITT) principles using all randomized
subjects Baseline factors across groups will be compared using mean (standard deviation) and
median (25th and 75th percentiles) summary measures Kaplan-Meier curves will be used to
display event rates Due to clinical interest in departures from both sides of the null hypothesis
all test statistics will be 2-sided
Reasonable caution needs to be taken when conducting multiple analyses on key clinical
subgroups For subgroup analyses a conservative significance level of 0001 will be used for all
interaction tests Thus subgroup comparisons will be considered exploratory unless the p-value
from the interaction test is smaller than 0001
92 Randomization Blinding and Reporting of Results
A permuted block-randomization scheme will be created with varying block sizes stratified by
clinical center Once a subject has completed the screening and baseline period and evaluation
for inclusionexclusion criteria the randomization process will begin Subjects will be
randomized to receive NAC or matching placebo with equal probability (11) via telephone
contact with a central interactive voice response system (IVRS) using a toll-free randomization
number On the day of randomization after the subject has successfully met all inclusion and
exclusion criteria the investigator or designee will call the central randomization number to
obtain the assigned kit randomization numbers for that subject At each subject visit the
investigator or designee will call the central randomization number to obtain the new kit
randomization numbers for resupply of the subject For resupply of the clinical center the IVRS
will monitor minimal volume of a kit type andor expiration date and will automatically notify
the pharmacy
57
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
The trial results will be reported according to guidelines specified in the CONSORT statement
A flow diagram describing screening recruitment randomization dropout and vital status will
be included in the primary manuscript AEs and efficacy data will be presented for all treatment
groups Adherence dropout and lost to follow-up will be carefully examined across all treatment
groups Analyses of safety will be based on data from all randomized subjects who received at
least one dose of study drug
93 Stratification
Subjects will be distributed to the two treatment arms in a 11 allocation ratio Stratification
blocks will be based on clinical centers
94 Specification of the Primary Analyses
A mixed model repeated measures (MMRM) analysis described in section 95 will be used to
compare differences in the slope of FVC measurements across the treatment groups Response
variables are values of the FVC measured at baseline and every 15 weeks until study completion
Variables in the model will include treatment time and time by treatment age sex race and
height Contrast estimates of differences in slopes of treatment over time (along with confidence
intervals) will be used to estimate the treatment effect The validity of this model in terms of
meeting modeling assumptions will be assessed via standard modeling diagnostics and goodness-
of-fit measures Based on the MMRM framework missing FVC data will not be imputed for the
primary analysis
95 Analysis of Longitudinal Endpoints
A common goal in clinical trials is to specify models that are easily implemented and
reproducible by independent data analysts On the other hand the models should have proper
statistical behavior in terms of low bias and high precision Many common approaches to
longitudinal data analysis including last observation carried forward (LOCF) imputation rely on
the missing completely at random (MCAR) assumption However the MCAR assumption is
58
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
unlikely to hold in many clinical trials because missing data are often related to disease
progression and prognosis A more reasonable assumption missing at random (MAR) specifies
that the complete data distribution can be modeled using only the observed data The likelihood-
based MMRM approach is valid under the more general MAR assumptions These models will
be applied to analyze the longitudinal data secondary endpoints
The advantages of MMRM analysis are that all important characteristics of the model can be preshy
specified standard software can be used to implement the models and results are based on ITT
principles43 In addition the MMRM approach offers superior control of Type I and Type II
errors compared with the LOCF approach
Response variables are values of the PFTs measured at enrollment and every 15 weeks until
study completion and 6MWT values measured at baseline week 30 and week 60 Covariates are
treatment time time by treatment and key baseline risk factors Contrasts (along with
confidence intervals) of treatment by time will be used to estimate the treatment effect
The correlation structure involves multiple pieces including measurement errors random
variation and interindividual variability For the longitudinal data analyses an unstructured
correlation matrix for within-subject errors will be assumed Other correlation structures
including compound symmetry will be examined as needed A careful examination of reasons
for study discontinuation will be conducted to assess the validity of MCAR Sensitivity analyses
will be used to examine the untestable assumption that the observed data violate the MAR
assumption The MMRM models will be implemented using PROC MIXED in SAS
96 Analysis of Binary Time-to-Event and Time-Lagged Endpoints
Regression modeling approaches using either the logistic regression model or Cox proportional
hazards regression model will be employed when appropriate The validity of these models will
be assessed via standard modeling diagnostics and goodness-of-fit measures Estimates of
cumulative frequencies for more general time-lagged responses will be calculated using the
partitioned version of the Bang-Tsiatis estimator44 The partitions will be set at 15-week intervals
59
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
to correspond with the data-collection process Covariate adjusted event rates will be calculated
using inverse probability-weighted regression estimates45
97 Power Analysis
971 Primary Analyses
Based on previously published IPF clinical trials the PL group is expected to experience a drop
in FVC of approximately 020 L over the study period (see Figure 1) The IPFnet Steering Group
determined a clinically important difference would be to preserve the majority of the decline
relative to PL over the study period In particular a treatment effect of 015 L was determined to
be a clinically meaningful difference Potential dropout is a key factor in the proposed study The
drop-out process assumed 5 lost to follow-up after every study visit Only 80 of subjects
were assumed to be followed for the entire study period All models assumed a compound
symmetry structure for the covariance matrix Power calculations were performed using a SAS
IML program for designing repeated measures studies46 Based on preliminary reviews of the
data from the University of Michigan the covariance matrix parameters were estimated at
approximately σ2 = 0757 (variance parameter) and ρ = 0936 (correlation parameter) To be
conservative the power calculations for the primary analysis were performed with parameter
setting of σ2 = 0810 (variance parameter) and ρ = 0925 (correlation parameter)
The power calculations assume a correction for imperfect compliance proposed by Lachin and
Foulkes to allow for 2 noncompliance for each of the treatment arms47 Thus the sample size
of 130 subjects per arm would be reduced to an adjusted sample size of 130(1-002-002)2 =
1198 or 120 subjects per arm
Under the assumed Type I error rate of 005 with a correlation parameter of 0925 and standard
deviation of 090 the difference of 015 L (or 00025 Lweek) shown in Table 6 would have
power of 93
60
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Table 6 Hypothetical Values of Mean FVC (L) Change from Baseline
Week 15 Week 30 Week 45 Week 60
NAC 00125 00250 00375 00500
Placebo 00500 01000 01500 02000
Difference 00375 00750 01125 01500
Abbreviations FVC forced vital capacity PL placebo
972 Power Analysis for Secondary Endpoints
Power calculations for secondary endpoint measurements are shown in Table 7 Standard
deviations are based on unpublished data provided by the University of Michigan The
calculations are based on a 2-sample t-test with Type I error rate set at 005 These calculations
are likely to be conservative because the statistical approach described in section 95 for
analyzing these endpoints will incorporate incomplete observations as well as intermediate data
points
Table 7 Detectable Differences in Treatment Means for Selected Endpoint Measurements
Secondary Endpoints Std Dev
of the Baseline Score
Detectable Difference for 80 Power
Std Dev of the Change Score
Difference Detectable for
80 Power
DLCOpred 166 58 91 32
6MWT Area Under the Desaturation Curve
219 76 175 61
6MWT Distance to Desaturation 224 78 315 110
6MWT Minutes Walked 210 073 205 071
Abbreviations Std Dev standard deviation DLCOpred diffusing capacity of the lung for carbon monoxide percent predicted 6MWT 6-minute walk test
61
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
10 Study Administration
101 Cooperative Agreement Mechanism
The administrative and funding mechanism used to undertake this project is a ldquocooperative
agreementrdquo (U01) which is an assistance mechanism Under the cooperative agreement the
NHLBI assists supports andor stimulates the project and is substantially involved with
investigators in conducting the study by facilitating performance of the effort in a ldquopartnerrdquo role
The NHLBI project scientist serves on the IPFnet Steering Group and he or another NHLBI
scientist may serve on other project committees when appropriate At the same time however
NHLBI does not assume a dominant role direction or prime responsibility for this research
program
As described below governance of the project is conducted through the IPFnet Steering Group
Principal investigators have lead responsibilities in all aspects of their trials and the project
including any modification of trial designs conduct of the trials quality control data analysis
and interpretation preparation of publications and collaboration with other investigators unless
otherwise provided for by the IPFnet Steering Group
PIs retain custody of and have primary rights to their center-specific and collaborative data
subject to government rights-of-access consistent with current Health amp Human Services (HHS)
Public Health Service (PHS) and National Institutes of Health policies The protocols and
governance policies call for the continual submission of data centrally to the IPFnet DCC for the
collaborative database which at a minimum will contain the key variables selected by the IPFnet
Steering Group for standardization across all clinical centers the submission of copies of the
collaborative datasets to each PI upon completion of the project procedures for data analysis
reporting and publication and procedures to protect and ensure the privacy of medical and
genetic data and records of individuals The NHLBI project scientist on behalf of the NHLBI
will have the same access privileges and responsibilities regarding the collaborative data as the
other members of the Steering Group
62
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
PIs are also encouraged to publish and to publicly release and disseminate results data and other
products of the project concordant with the project protocols and governance and the approved
plan for making data and materials available to the scientific community and to the NHLBI
However during the 3 years after the ending date of NHLBI project support unpublished data
unpublished results data sets not previously released and other study materials or products are
to be made available to any third party only with the approval of the IPFnet Steering Group
Upon completion of the project PIs are expected to put their intervention materials and
procedure manuals into the public domain andor make them available to other investigators
according to the approved plan for making data and materials available to the scientific
community and the NHLBI for the conduct of research at no charge other than the costs of
reproduction and distribution
The NHLBI reserves the right to terminate or curtail the project (or an individual award) in the
event of (a) failure to develop or implement mutually agreeable collaborative measurement
subject eligibility and data management sections of the protocols (b) substantial shortfall in
subject recruitment follow-up data reporting or quality control or other major breach of
protocol (c) substantive changes in the agreed-upon protocols with which NHLBI cannot
concur (d) reaching a major project outcome with persuasive statistical significance
substantially before schedule or (e) human subject ethical issues that may dictate a premature
termination
Any disagreement that may arise in scientificprogrammatic matters (within the scope of the
award) between award recipients and the NHLBI may be brought to arbitration An arbitration
panel will be composed of 3 membersmdash1 selected by the IPFnet Steering Group (with the
NHLBI member not voting) or by the individual PI in the event of an individual disagreement a
second selected by NHLBI and the third selected by the other 2 members This special
arbitration procedure in no way affects the PIrsquos right to appeal an adverse action that is otherwise
appealable in accordance with the PHS regulations at 42 CFR part 50 Subpart D and HHS
63
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
regulation at 45 CFR part 16 or the rights of the NHLBI under applicable statutes regulations
and terms of the award
102 IPFnet Steering Group
The IPFnet Steering Group is the main governing body of the project It is composed of the PIs
of the clinical centers the PI of the DCC and the NHLBI project scientist The clinical centers
the IPFnet DCC and the NHLBI each have 1 vote on the IPFnet Steering Group All decisions
are determined by majority vote
All major scientific decisions are determined by the IPFnet Steering Group It assumes overall
responsibility for the design and conduct of the trial It appoints (and disbands) committees and
subcommittees as the need arises designs approves and implements the study protocols
oversees the development of the MOOP monitors subject recruitment and treatment delivery
evaluates data collection and management oversees quality assurance procedures and
implements changes and enhancements to the study as required It also has primary responsibility
for facilitating the conduct of the trials and reporting the projectrsquos results
103 Data and Safety Monitoring Board
The NHLBI will establish a DSMB in accordance with established policies (see
httpwwwnhlbinihgovfundingpoliciesdsmb_insthtm) to ensure data quality and subject
safety and to provide independent advice to the NHLBI regarding progress and the
appropriateness of study continuation
104 Recommendations on Interim Monitoring of Efficacy Safety and Futility
First and foremost the role of the DSMB will be to review subject safety and trial conduct at
periodic points during the study The DSMB may require analyses of the primary endpoint
results for comparing the benefit and risks of treatment strategies The benefit of collecting
additional data on key secondary endpoints with extended follow-up and establishing a robust
64
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
evidence base for determining a standard of care will need to be carefully considered before
early termination of one or more treatment arms After careful consideration the IPFnet Steering
Group recommends conservative thresholds for the early examinations of the safety and efficacy
data
The DSMB will be expected to meet approximately every 6 months until trial completion to
review safety and toxicity data The DSMB may recommend stopping the study based on these
reviews Because the DSMB could stop the trial for safety concerns as well as for a large
efficacy benefit there could be multiple opportunities to reject the null hypothesis (no difference
in event rates between the PL and NAC groups) A Bonferroni approximation will be applied
during the one planned interim analysis for efficacy
Before locking the database a statistical analysis plan (SAP) will be developed to provide
complete details on the statistical analysis The SAP will include the specifics for how and when
the DSMB will be notified for AEs The IPFnet DCC will deliver to the DSMB all FDA-defined
AEs at 3-month intervals The IPFnet DCC will prepare narrative SAE reports in real time for
DSMB review including recommendations and analysis of similar events for each SAE
submitted to the FDA
65
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
11 Investigator and Sponsor Obligations
111 Monitoring
All monitoring activities for US clinical centers will be performed in accordance with DCRI
standard operating procedures Information regarding the types of visits will be outlined in the
PANTHER-IPF MOOP
112 Cost and Payment
There will be no cost to subjects enrolled in this trial Study-related procedures will be paid for
by the IPFnet
Subjects may be eligible for reimbursement for travel to the clinical center Details of payment
will be explained to each subject during the consent process
113 Confidentiality and Health Insurance Portability and Accountability Act
Considerations
Subject confidentiality will be protected throughout the study All subject data will be kept
strictly confidential and no subject-identifying information will be released to anyone outside
the project Confidentiality will be assured through several mechanisms First each subject will
be assigned an anonymous study ID which will then be used on all study forms Second any
study forms blood samples and paper records that contain subject information (eg address lists
phone lists) will be kept at the clinical centers in secured locked areas coded by number Once
blood is collected there will be no subject identifiers placed on blood samplesmdashonly the study
ID number and the date of sample collection Third access to all subject data and information
including laboratory specimens will be restricted to authorized personnel In the case of
computerized data this restricted access will be assured through user logon IDs and password
protection
66
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
At the IPFnet DCC only authorized personnel will have access to the data files containing study
data Security will be assured through user logon IDs passwords and appropriate access
privileges All study subjects will be identified only by their IPFnet ID numbers and no personal
identifying information such as name address or Social Security number will be entered into
the IPFnet DCC database Any subject-specific data reported to the IPFnet Steering Group will
be identified only by the IPFnet ID number
Finally subjects will not be identified by name in any reports or publications nor will the data
be presented in such a way that the identity of individual subjects can be inferred Analysis files
created for further study by the scientific community will have no subject identifiers These data
files will be created in accordance with the Ancillary Studies and Publication Policy of the
IPFnet
114 Informed Consent Procedures
All IPFnet subjects will provide written informed consent using procedures reviewed and
approved by each clinical centerrsquos IRB Informed consent will be undertaken by study personnel
in-person with the subject The subject has the option of declining further participation in the
study at that point No further study procedures will be conducted until the signed documents
have been provided to the IPFnet clinical center
115 Institutional Review Boards
Before initiating this study the protocol clinical center-specific informed consent forms Health
Insurance Portability and Accountability Act (HIPAA) forms recruitment materials and other
relevant information will be reviewed by a properly constituted IRB at each participating clinical
center A copy of the signed and dated IRB approval at each clinical center will be retrieved prior
to or during the site initiation visit and archived at the IPFnet DCC Any amendments to the
protocol other than simple administrative and typographical changes must be approved by each
IRB before they are implemented The clinical centers will seek annual renewals of their IRB
approvals in accordance with local procedures
67
__________________________________________ ________________
__________________________________________
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
12 Investigator Agreement
I have read the foregoing protocol PANTHER-IPF and agree that it contains all necessary
details for carrying out this study I will conduct the study as outlined herein and will complete
the study within the time designated
I will provide copies of the protocol and all pertinent information to all individuals responsible to
me who assist in the conduct of this study I will discuss this material with them to ensure they
are fully informed regarding the drug and the conduct of the study
I will fulfill all responsibilities for submitting pertinent information to the local IRB if
applicable that is responsible for this study
I further agree that NHLBI andor DCRI will have access to any source documents from which
eCRF information may have been generated
Signature of Principal Investigator Date
Name of Principal Investigator (printed or typed)
Protocol version date May 19 2009
Protocol Amendment 1 version date May 28 2010
Protocol Amendment 2 version date December 6 2011
68
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
13 References
1 Raghu G Brown KK Bradford WZ et al A placebo-controlled trial of interferon gamma-1b in patients with idiopathic pulmonary fibrosis N Engl J Med 2004350125-33 2 King TE Jr Safrin S Starko KM et al Analyses of efficacy end points in a controlled trial of interferon-gamma1b for idiopathic pulmonary fibrosis Chest 2005127171-7 3 Flaherty KR Thwaite EL Kazerooni EA et al Radiological versus histological diagnosis in UIP and NSIP survival implications Thorax 200358143-8 4 Wells AU Desai SR Rubens MB et al Idiopathic pulmonary fibrosis a composite physiologic index derived from disease extent observed by computed tomography Am J Respir Crit Care Med 2003167962-9 5 Raghu G Freudenberger TD Yang S et al High prevalence of abnormal acid gastroshyoesophageal reflux in idiopathic pulmonary fibrosis Eur Respir J 200627136-42 6 Kinnula VL Focus on antioxidant enzymes and antioxidant strategies in smoking related airway diseases Thorax 200560693-700 7 Coultas DB Zumwalt RE Black WC Sobonya RE The epidemiology of interstitial lung diseases Am J Respir Crit Care Med 1994150967-72 8 Raghu G Weycker D Edelsberg J Bradford WZ Oster G Incidence and prevalence of idiopathic pulmonary fibrosis Am J Respir Crit Care Med 2006174810-6 9 Olson AL Swigris JJ Lezotte DC Norris JM Wilson CG Brown KK Mortality from pulmonary fibrosis increased in the United States from 1992 to 2003 Am J Respir Crit Care Med 2007176277-84 10 Mannino DM Etzel RA Parrish RG Pulmonary fibrosis deaths in the United States 1979shy1991 An analysis of multiple-cause mortality data Am J Respir Crit Care Med 19961531548shy52 11 Hubbard R Johnston I Coultas DB Britton J Mortality rates from cryptogenic fibrosing alveolitis in seven countries Thorax 199651711-6 12 Johnston I Britton J Kinnear W Logan R Rising mortality from cryptogenic fibrosing alveolitis Bmj 19903011017-21 13 Raghu G Collard HR Egan JJ et al An official ATSERSJRSALAT statement idiopathic pulmonary fibrosis evidence-based guidelines for diagnosis and management Am J Respir Crit Care Med 2011183788-824 14 (USA) FDA FDA Public Health Advisory Interferon gamma-1b (marketed as Actimmune) In 2007 15 King TE Jr Pardo A Selman M Idiopathic pulmonary fibrosis Lancet 2011 16 Raghu G Brown KK Costabel U et al Treatment of idiopathic pulmonary fibrosis with etanercept an exploratory placebo-controlled trial Am J Respir Crit Care Med 2008178948shy55 17 Malouf MA Hopkins P Snell G Glanville AR An investigator-driven study of everolimus in surgical lung biopsy confirmed idiopathic pulmonary fibrosis Respirology 201116776-83 18 King TE Jr Behr J Brown KK et al BUILD-1 a randomized placebo-controlled trial of bosentan in idiopathic pulmonary fibrosis Am J Respir Crit Care Med 200817775-81 19 Richeldi L Costabel U Selman M et al Efficacy of a tyrosine kinase inhibitor in idiopathic pulmonary fibrosis N Engl J Med 20113651079-87
69
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
20 Borok Z Buhl R Grimes GJ et al Effect of glutathione aerosol on oxidant-antioxidant imbalance in idiopathic pulmonary fibrosis Lancet 1991338215-6 21 Meyer A Buhl R Magnussen H The effect of oral N-acetylcysteine on lung glutathione levels in idiopathic pulmonary fibrosis Eur Respir J 19947431-6 22 Behr J Maier K Degenkolb B Krombach F Vogelmeier C Antioxidative and clinical effects of high-dose N-acetylcysteine in fibrosing alveolitis Adjunctive therapy to maintenance immunosuppression Am J Respir Crit Care Med 19971561897-901 23 Cantin AM North SL Fells GA Hubbard RC Crystal RG Oxidant-mediated epithelial cell injury in idiopathic pulmonary fibrosis J Clin Invest 1987791665-73 24 Waghray M Cui Z Horowitz JC et al Hydrogen peroxide is a diffusible paracrine signal for the induction of epithelial cell death by activated myofibroblasts Faseb J 200519854-6 25 Larios JM Budhiraja R Fanburg BL Thannickal VJ Oxidative protein cross-linking reactions involving L-tyrosine in transforming growth factor-beta1-stimulated fibroblasts J Biol Chem 200127617437-41 26 Kinnula VL Fattman CL Tan RJ Oury TD Oxidative stress in pulmonary fibrosis a possible role for redox modulatory therapy Am J Respir Crit Care Med 2005172417-22 27 Meyer A Buhl R Kampf S Magnussen H Intravenous N-acetylcysteine and lung glutathione of patients with pulmonary fibrosis and normals Am J Respir Crit Care Med 19951521055-60 28 Behr J Degenkolb B Krombach F Vogelmeier C Intracellular glutathione and bronchoalveolar cells in fibrosing alveolitis effects of N-acetylcysteine Eur Respir J 200219906-11 29 Bando M Hosono T Mato N et al Long-term efficacy of inhaled N-acetylcysteine in patients with idiopathic pulmonary fibrosis Intern Med 2010492289-96 30 Demedts M Behr J Buhl R et al High-dose acetylcysteine in idiopathic pulmonary fibrosis N Engl J Med 20053532229-42 31 Toma TP Bhowmik A Rajakulasingam R Acetylcysteine in pulmonary fibrosis N Engl J Med 20063541086-9 author reply -9 32 Hunninghake GW Antioxidant therapy for idiopathic pulmonary fibrosis N Engl J Med 20053532285-7 33 Flaherty KR Mumford JA Murray S et al Prognostic implications of physiologic and radiographic changes in idiopathic interstitial pneumonia Am J Respir Crit Care Med 2003168543-8 34 Latsi PI du Bois RM Nicholson AG et al Fibrotic idiopathic interstitial pneumonia the prognostic value of longitudinal functional trends Am J Respir Crit Care Med 2003168531-7 35 Collard HR King TE Jr Bartelson BB Vourlekis JS Schwarz MI Brown KK Changes in clinical and physiologic variables predict survival in idiopathic pulmonary fibrosis Am J Respir Crit Care Med 2003168538-42 36 Jegal Y Kim DS Shim TS et al Physiology is a stronger predictor of survival than pathology in fibrotic interstitial pneumonia Am J Respir Crit Care Med 2005171639-44 37 Martinez FJ Safrin S Weycker D et al The clinical course of patients with idiopathic pulmonary fibrosis Ann Intern Med 2005142963-7 38 Hull JH Acetylcysteine in pulmonary fibrosis N Engl J Med 20063541089-91 author reply -91
70
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
39 Flaherty KR King TE Jr Raghu G et al Idiopathic interstitial pneumonia what is the effect of a multidisciplinary approach to diagnosis Am J Respir Crit Care Med 2004170904shy10 40 Raghu G Johnson WC Lockhart D Mageto Y Treatment of idiopathic pulmonary fibrosis with a new antifibrotic agent pirfenidone results of a prospective open-label Phase II study Am J Respir Crit Care Med 19991591061-9 41 Hunninghake GW Lynch DA Galvin JR et al Radiologic findings are strongly associated with a pathologic diagnosis of usual interstitial pneumonia Chest 20031241215-23 42 Lynch D Godwin J Safrin S et al High-resolution computed tomography in idiopathic pulmonary fibrosis diagnosis and prognosis Am J Respir Crit Care Med 2005172488-93 43 Mallinckrodt CH Watkin JG Molenberghs G Carroll RJ Choice of the primary analysis in longitudinal clinical trials Pharmaceutical Statistics 20043161-9 44 Bang H Tsiatis A Estimating medical costs with censored data Biometrika 200087329shy43 45 Lin DY Regression analysis of incomplete medical cost data Stat Med 2003221181-200 46 Rochon J Application of GEE procedures for sample size calculations in repeated measures experiments Stat Med 1998171643-58 47 Lachin JM Foulkes MA Evaluation of sample size and power for analyses of survival with allowance for nonuniform patient entry losses to follow-up noncompliance and stratification Biometrics 198642507-19
71
- PANTHER-IPFPREDNISONE AZATHIOPRINEAND N-ACETYLCYSTEINEA STUDY THAT EVALUATES RESPONSE INIDIOPATHIC PULMONARY FIBROSIS
-
- Protocol Summary
- Table of Contents
- List of Tables
- List of Figures
- List of Abbreviations
- 1 Summary
- 2 Hypotheses and Specific Aims
-
- 21 Null Hypothesis
- 22 Specific Aim 1
- 23 Specific Aim 2
- 24 Prespecified Subgroups of Interest
-
- 3 Background and Significance
-
- 31 Idiopathic Pulmonary Fibrosis is the Most Common Interstitial Lung Disease
- 32 Rationale for Placebo Control
- 33 Rationale for N-acetylcysteine
- 35 Rationale for N-acetylcysteine as a Stand-alone Therapy
- 36 Rationale for the Study Design and Primary Endpoint
- 37 Rationale for Blinding of Treatments
-
- 4 Methods
-
- 41 Inclusion Criteria
- 42 Diagnosis of IPF
- 43 Exclusion Criteria
- 44 Study Design and Study Visit
- 45 Dose Justification
- 46 Contraindications Precautions and Side Effects of Study Medications
- 47 Recruitment Procedures
- 48 Study Procedures
- 49 Concomitant Medications
- 410 Laboratory Testing
- 411 Blinding of Study Drugs
-
- 5 Study Endpoints
-
- 51 Primary Study Endpoint
- 52 Secondary Study Endpoints
-
- 6 Safety Evaluations and Procedures
-
- 61 Adverse Events
- 62 Clinical Medical Monitoring
- 63 Unblinding Procedures
-
- 7 Study Drug Procedures
- 8 Data Management
-
- 81 Hardware and Software Configuration
- 82 Sources of Data
-
- 9 Study Design and Data Analysis
-
- 91 General Analytic Considerations
- 92 Randomization Blinding and Reporting of Results
- 93 Stratification
- 94 Specification of the Primary Analyses
- 95 Analysis of Longitudinal Endpoints
- 96 Analysis of Binary Time-to-Event and Time-Lagged Endpoints
- 97 Power Analysis
-
- 10 Study Administration
-
- 101 Cooperative Agreement Mechanism
- 102 IPFnet Steering Group
- 103 Data and Safety Monitoring Board
- 104 Recommendations on Interim Monitoring of Efficacy Safety and Futility
-
- 11 Investigator and Sponsor Obligations
-
- 111 Monitoring
- 112 Cost and Payment
- 113 Confidentiality and Health Insurance Portability and Accountability ActConsiderations
- 114 Informed Consent Procedures
- 115 Institutional Review Boards
-
- 12 Investigator Agreement
- 13 References
-

PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
employs immunosuppressive and corticosteroid drugs Interim review of the original PANTHER-IPF study has
documented increased adverse events and lack of efficacy for AZA-PRED-NAC compared to placebo
suggesting that this therapeutic approach should not be employed Whether this applies to NAC alone which
has been advocated by international societies has not been proven in well-designed well-powered clinical
trials The recommendations made in the recently published evidence guidelines for NAC monotherapy was
weak based on low quality13 Thus this continued clinical trial randomizing patients to receive NAC or placebo
is pivotal and will answer the important question of the potential therapeutic benefits of NAC monotherapy with
grade A evidence In this prospective randomized clinical trial the inclusion of a PL arm is therefore vital to
adequately test the benefits of NAC in well-characterized subjects with IPF
If NAC has no true efficacy then its role as standard of care will be refuted If a benefit compared with PL is
confirmed it will establish a benchmark against which future novel therapies for IPF will be safely compared
As there is no currently accepted therapy for IPF there is an increasing body of published literature supporting
the concept of no treatment as the ldquobest carerdquo option for IPF13
Post hoc analyses of PL-controlled trials suggest that subjects with milder disease may be more amenable to
therapy12 It is notable that a recent international prospective randomized trial of interferon-gamma for IPF
also included a PL arm the study was terminated early by the data and safety monitoring board (DSMB) due to
lack of treatment effect1415 This underscores the belief that a proven effective therapy for IPF does not
currently exist and that true placebo-controlled trials remain the gold standard Similarly recently completed
trials of etanercept everolimus bosentan and BIPF 1120 in IPF have included PL-treated arms16-19 In three of
these trials the treated subjects showed little if any objective improvement Based on this evidence and the
current status of IPF therapy and therapeutic trials we believe that clinicians and subjects will continue to enroll
in a PL-controlled study
33 Rationale for N-acetylcysteine
NAC is a derivative of the amino acid L-cysteine NAC has been shown to augment levels of the naturally
occurring antioxidant glutathione (GSH ) (glutathione γ-glutamyl cysteinyl glycine) both in vitro and in
vivo2021 GSH is present in all eukaryotic cells and may play an important role in protecting alveolar epithelial
cells against oxidant injury The concentration of GSH in the bronchoalveolar lavage (BAL) fluid in patients
16
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
with IPF is markedly diminished compared with normal subjects This GSH deficiency may be corrected by
exogenous administration of NAC2122
There is evidence of enhanced production of oxidants in an IPF lung Both inflammatory cells and
myofibroblasts derived from patients with IPF generate increased amounts of extracellular oxidants including
hydrogen peroxide2324 Secretion of hydrogen peroxide by activated myofibroblasts may induce the death of
adjacent lung epithelial cells by paracrine mechanisms24 Additionally generation of oxidants by myofibroblasts
induces oxidative crosslinking of extracellular matrix proteins25 a potential mechanism for aberrant matrix
remodeling Thus an oxidant-antioxidant imbalance exists in the lungs of IPF patients26 NAC may confer
protection against this imbalance by augmenting GSH levels in addition to its more direct free-radical
scavenging activity
Intravenous (IV) NAC therapy has been shown to increase total BAL GSH in 8 IPF subjects27 Oral NAC (600
mg 3 times per day) has been shown to decrease markers of oxidant injury and improve both total and reduced
GSH levels in the epithelial lining fluid of subjects with IPF in a small uncontrolled study22 pulmonary
function improved modestly with therapy A similar study in 18 IPF subjects confirmed increased intracellular
GSH concentration after 12 weeks of NAC (600 mg 3 times per day)2228 no clinical correlates were reported
Inhaled NAC was suggested to improve pulmonary function in an open label study29
35 Rationale for N-acetylcysteine as a Stand-alone Therapy
Results of a double-blind multi-center European clinical trial of 150 IPF subjects testing combinations of AZAshy
PRED vs AZA-PRED-NAC have been reported30 NAC added to AZA-PRED (ldquoconventional therapyrdquo) had a
significant positive effect on DLCO (p lt 0005) and vital capacity (VC) (p lt 005) at the end of 1 year30 The
recent ATSERS position statement after much discussion concluded that NAC alone should not be considered
in the majority of patients with IPF without additional data from well-designed studies
The interpretation of these data has been quite controversial Some have suggested that the magnitude of the
treatment effect although statistically significant is modest31 Others have suggested that NAC may be
modulating potential toxic effects of AZA-PRED alone32 supporting the investigation of NAC as stand-alone
therapy
17
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
The IPFnet is now completing the PANTHER-IPF trial with a 11 randomization (NAC vs placebo) and a
simple practical feasible and scientifically rational design that will establish standard of care with NAC for
IPF based on a currently available therapeutic agent and the existing data to support its use We anticipate that
all future clinical trials of novel therapeutic agents will be tested against this to-be-established standard of care
36 Rationale for the Study Design and Primary Endpoint
The optimal study design of a therapeutic trial in IPF would include survival as a primary endpoint The
published results of the IFN-γ 1b Phase 3 (GIPF-001) trial suggested a survival benefit in subjects with milder
disease in retrospective analyses1 although the trial was underpowered to address this question This was likely
related to the limited mortality in the PL arm of the study which included IPF subjects with mild to moderate
disease This study documents that an IPF study powered to improve survival in a patient population with mild
disease requires a larger sample size andor duration of study In fact the recently aborted Phase 3 IFN-γ 1b
(GIPF-007 INSPIRE) study was a survival-based study and recruited more than 800 subjects at 75 centers
worldwide1415 As such within the context of the current IPFnet trial survival is an impractical primary
endpoint variable
Several groups have published data defining an appropriate surrogate outcome variable a 10 decrement in
FVC during 6 to 12 months is a powerful predictor of survival in IPF33-36 Furthermore additional evidence
suggests a similar predictive ability for a 10 decrement in FVC during 3 months of follow-up37 With strong
supportive evidence of FVC progression being related to mortality on a per-subject basis this study will use
FVC changes in liters between treatment groups as the primary endpoint Previously published IPF studies have
shown a steady decline in FVC (and FVCpred) among control group subjects230 The GIPF-001 study
suggested a 48-week decrease in FVC of 016 L in the PL-treated subjects The IFIGENIA study demonstrated
a decline in FVC of approximately 019 L over 52 weeks in the subjects randomized to the control treatment
Figure 1 depicts the change in FVC for control groups from previously published IPF studies38 Based on these
data we expect that the PL group will have a decline of 020 L over the 60-week study period The IPFnet
Steering Group determined that a clinically meaningful improvement would be the preservation of the majority
of the 020-L FVC decline Therefore a mean treatment difference of 015 L in mean FVC over the 60-week
study period was determined to be a clinically meaningful difference
18
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Δ f
rom
bas
elin
e (i
n L
)
01
005
0
-005
-01
-015 Projected Δ for placebo
-02
-025
-019
-016
-013 Pirfenidone GIPF001
NAC
Placebo
4 8 12 16 20 24 28 32 36 40 44 48 52 56 60
Week
Figure 1 Changes in FVC From Baseline in Prior IPF Clinical Trials
Recent data suggest that various patient subgroups would be expected to potentially exhibit differential response
to therapy These parameters will be used to a priori separate patients by a series of baseline characteristics
including
1 Higher enrollment FVC12
2 Typical vs atypical high-resolution computed tomography (HRCT) reading at baseline3
3 Recent vs more remote diagnosis (time from initial diagnosis of IPF le 1 year and gt 1 year)
4 Lower CPI score at enrollment4
5 Medical therapy for gastroesophageal reflux5
6 Ethnic background
7 Sex
8 Smoking history (current or ex-smoker vs never smoker) given potential impact on oxidant status6
9 Presence of emphysema gt 25 on HRCT
37 Rationale for Blinding of Treatments
The issue of treatment blinding was given a great deal of consideration with subject safety being the primary
concern After discussion among the Steering Group members it was decided that as long as subject safety
could be ensured blinding was necessary Blinding allows the study to
Have optimal scientific validity and potential to impact the standard of care for subjects
19
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Make objective assessments of treatment effects
Maintain clinical equipoise among investigators
Encourage subjects to have similar levels of contact with the medical community
Minimize the differential dropout rates across study arms
20
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
4 Methods 41 Inclusion Criteria
1 Age 35 to 85 years inclusive
2 FVC ge 50 of predicted (post-bronchodilator measurement from the screening visit)
3 DLCO ge 30 of predicted (hemoglobin corrected and altitude corrected if gt4000 ft above sea level)
4 Ability to understand and provide informed consent
5 Diagnosis of IPF according to a modified version of the ATS criteria le 48 months from enrollment The
date of diagnosis is defined as the date of the first available HRCT or surgical lung biopsy characteristic
of definite UIP
411 Subjects Shown to Have Usual Interstitial Pneumonia Pattern on Surgical Lung Biopsy
Subjects who have been shown to have UIP pattern on lung biopsy must have all of the following
1 Exclusion of other known causes of ILD such as drug toxicity clinically significant environmental
exposures or diagnosis of connective tissue diseases
2 Bibasilar reticular abnormalities with minimal ground glass opacities on HRCT scan
412 Subjects Who Have Not Undergone a Surgical Lung Biopsy
In addition to the criteria above these subjects must have radiological findings considered to be definite for the
diagnosis of UIPIPF
1 Bibasilar reticular abnormalities with minimal ground glass opacities
2 Honeycombing as the predominant feature and located in the peripheral lung bases
42 Diagnosis of IPF
Only subjects with definite IPF will be eligible for enrollment in this study We will utilize a combination of
clinicalphysiologic features HRCT and review of a clinically obtained surgical lung biopsy specimen to
establish the diagnosis of IPF An algorithm for the diagnosis is provided to guide entry into the protocol as
outlined in the inclusion and exclusion criteria (Figures 2 and 3) This multi-disciplinary approach uses
21
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
expertise from clinicians radiologists and pathologists Investigators at each site in conjunction with central
pathology will work together to establish the diagnosis of IPF This interactive approach to the diagnosis of IPF
increases the level of agreement between observers39
A subject with suspected ILD should be evaluated for secondary causes including but not limited to
environmental exposures drugs and systemic diseases Presence of any of these findings felt to be significant
enough to cause an ILD should disqualify the subject from entry into the trial
If secondary causes are absent an HRCT scan may be obtained If an HRCT of sufficiently high quality has
been obtained within the last 3 months that scan may be used for diagnosis In the appropriate clinical setting
the diagnosis of IPF can be made by the demonstration of a typical radiographic pattern on HRCT or by
demonstration of UIP pattern on a surgical lung biopsy The following criteria for a radiographic (ie
nonsurgical) diagnosis will be used In the absence of known exposures andor clinical associations attributable
to pulmonary fibrosis and in the appropriate clinical setting the presence of definite UIP pattern in HRCT
images is required to meet study criteria for the diagnosis of IPF
Figure 2 Diagnosis of Idiopathic Pulmonary Fibrosis in the IPFnet
22
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Figure 3 Pathology Flow Chart Surgical Lung Biopsy Diagnosis
Requirement for diagnosis
1 Clinical exclusion of other known causes (connective tissue diseases environmental and drug
exposures) of ILD
2 Radiographic HRCT with bibasilar reticular abnormality and honeycomb change with minimal
ground glass opacities
Appropriate clinical setting
1 Age gt 50 years
2 Insidious onset of unexplained dyspnea
3 Duration of illness for ge 3 months
4 Bibasilar inspiratory crackles
23
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Unlike the ATSERS consensus criteria published in 2000 bronchoscopy will not be required for diagnosis
This decision was made based on the experience of the IPFnet Steering Group members regarding the utility of
bronchoscopy in the diagnosis of IPF The presence of an atypical HRCT finding will require documentation of
a definitive diagnosis by surgical lung biopsy In fact this is in keeping with the recently published evidence
based guidelines for diagnosis and management of IPF13 As shown in Figure 3 central review of the pathology
data will be required for a diagnosis of IPF
We will not require central review of HRCT as several studies have shown that a confident local interpretation
of clinicalHRCT criteria as definite IPFUIP is associated with a high positive predictive value for finding UIP
at surgical lung biopsy (see Table 1) Differences in sensitivity in these series likely reflect subject selection as
Flaherty et al3 evaluated only UIP and nonspecific interstitial pneumonia (NSIP) while Raghu et al40 and
Hunninghake et al41 included a broader range of ILD
Table 1 Operating Characteristics of Local HRCT Review for Diagnosis of UIP
Researcher of Subjects Sensitivity () Specificity () PPV () NPV ()
Raghu et al 40
59 (29 UIP by SLB) 78 90 88 82
Hunninghake et al 41 91 (54 UIP by SLB)
74 81 85 67
Flaherty et al 3 96 (only NSIP amp UIP)
37 100 100 30
Abbreviations PPV positive predictive value NPV negative predictive value UIP usual interstitial pneumonia SLB surgical lung biopsy and NSIP nonspecific interstitial pneumonia
Furthermore an analysis of the HRCT scans from subjects enrolled in the GIPF-001 trial confirmed that local
site interpretations have a high congruity to a central radiology core In this multi-center study 263 HRCT
scans were read as definite IPF and a retrospective central radiology core review found 932 to be consistent
with IPF 42 We will also take several additional steps to insure that the local HRCT reads are accurate
including
1 A detailed training module has been developed and must be completed by each site radiologist before
site initiation
2 Clinical centers are to mail all HRCT scans to the HRCT core lab The first 10 HRCT scans from
subjects enrolled at each enrolling clinical center will be reviewed centrally to be certain that local reads
24
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
25
are congruent with a central interpretation If discrepancies are identified additional education will be
provided and HRCT scans will continue to be reviewed centrally until the central radiology core is
confident that the local center is performing appropriately
3 Random scans will be obtained from each center throughout the study to confirm that the local read
continues to agree with central interpretation If discrepancies are identified they will be addressed as in
2 above
In all cases if a subject has a surgical lung biopsy sample that sample will be reviewed by the local and central
pathologists Therefore the only cases that would not be subject to a direct central review process are those
where the HRCT meets the centrally defined criteria for an unequivocal diagnosis and a lung biopsy sample is
not available Table 2 below summarizes the possible combinations for making a diagnosis
Table 2 Combining HRCT and Pathology Interpretations to Determine if IPF is Present
HRCT Diagnosis Pathology Diagnosis Diagnosis of IPF
Definite UIP Definite UIP Yes
Definite UIP Probable UIP Yes
Definite UIP Possible UIP Yes
Definite UIP Not UIP No
Definite UIP Unavailable Yes
Consistent with UIP Definite UIP Yes
Consistent with UIP Probable UIP Yes
Consistent with UIP Possible UIP No
Consistent with UIP Not UIP No
Consistent with UIP Unavailable No
Inconsistent with UIP Any No
Abbreviations HRCT high-resolution computed tomography IPF idiopathic pulmonary fibrosis
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
UIP usual interstitial pneumonia Dx diagnosis 43 Exclusion Criteria
1 History of clinically significant environmental exposure known to cause pulmonary fibrosis
Occupational exposures such as asbestos or environmental exposure to organic dust such as occurs in
pigeon breeders may at times mimic the clinical and radiographic findings of IPF
2 Diagnosis of connective tissue disease felt by the principal investigator (PI) to be the etiology of the
interstitial disease Diagnosis of collagen-vascular conditions will be according to the published
American College of Rheumatology criteria As such the presence of any documented collagen-vascular
disorder or the presence of any suspicious symptom complex whether or not associated with
significantly abnormal rheumatological serologies will exclude the subject at the discretion of the PI
3 Extent of emphysema greater than the extent of fibrotic change (honeycombing reticular changes) on
HRCT scan
4 Forced expiratory volume in 1 second (FEV1)FVC ratio lt 065 at screening (postbronchodilator)
5 Partial pressure of arterial oxygen (PaO2) on room air lt 55 mm Hg (lt 50 mm Hg at Denver site)
6 Residual volume gt 120 predicted at screening (postbronchodilator)
7 Evidence of active infection
8 Significant bronchodilator response on screening spirometry defined as a change in FEV1 ge 12 and
absolute change gt 200 mL OR change in FVC ge 12 and absolute change gt 200 mL The percent
difference between the FVC (or FEV1) values will be calculated by taking the absolute value of the
difference and dividing it by the larger of the two FVC (or FEV1) values
9 Screening and enrollment post-bronchodilator FVC measurements (in liters) differing by gt 11 The
percent difference between the FVC values will be calculated by taking the absolute value of the
difference and dividing it by the larger of the two FVC values (eg the percent difference between FVC
measurements of 19 and 20 liters would be determined by taking the difference between the two (01
liters) and dividing by the larger of the two (20 liters) So 0120 = 5 and these FVC measurements
would not exclude the subject
10 Listed for lung transplantation ie the patient has completed the evaluation process has been accepted
as a candidate for transplantation at an appropriate center and is waiting to receive notification of an
available donor organ
11 History of unstable or deteriorating cardiac disease
12 Myocardial infarction coronary artery bypass or angioplasty within 6 months of screening
26
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
13 Unstable angina pectoris or congestive heart failure requiring hospitalization within 6 months of
screening
14 Uncontrolled arrhythmia
15 Severe uncontrolled hypertension
16 Known HIV or hepatitis C
17 Known cirrhosis and chronic active hepatitis
18 Active substance andor alcohol abuse (as determined by site PI)
19 Pregnancy or lactation (subjects who are pregnant or breastfeeding)
20 Known hypersensitivity to study medication
21 Any condition other than IPF that in the opinion of the site PI is likely to result in the death of the
subject within the next year
22 Any condition that in the judgment of the PI might cause participation in this study to be detrimental to
the subject or that the PI deems makes the subject a poor candidate
23 Any therapy directed at pulmonary fibrosis (excepting triple therapy of prednisone plus azathioprine
plus NAC) requires a 30-day washout period before randomized Triple therapy of lt= 12 weeks duration
in the past 4 years requires a 30-day washout period before randomization
24 History of triple therapy of prednisone plus azathioprine plus NAC for gt 12 weeksrsquo duration in the past
4 years or previous enrollment in the triple-therapy arm of the PANTHER-IPF study
44 Study Design and Study Visit
441 Study Design Summary
This study will be a randomized double-blind PL-controlled trial designed to assess the safety and efficacy of
NAC in subjects with newly diagnosed IPF
Subjects with mild to moderate IPF (defined as FVCpred ge 50 and DLCOpred ge 30) diagnosed within
the past 48 months will be enrolled Screening will continue until April 30 2012
27
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
The study will employ a 2-arm design with 11 randomization to NAC or PL Once enrolled subjects will visit
the clinical center at 15 weeks and 15-week intervals thereafter Each subject will be treated and followed for a
maximum of 60 weeks
During the 60-week visit subjects will be taken off all study agents Approximately four weeks after the final
dose of study agent is taken subjects will receive a safety phone call from the study site
442 Study Visits
Subjects who meet entry criteria will review the informed consent a written description of the purpose
procedures and risks of the study with the PI co-investigator or study coordinator and all questions will be
answered The informed consent form will be signed by the subject at screening No protocol-specific
procedures will be performed until the subject has signed and dated an informed consent form This includes the
screening procedures
4421 Screening
Once informed consent is obtained subjects may immediately begin the screening process or may return within
28 days of consent In the event a study subject has been clinically evaluated at the study site by an IPFnet study
physician and has performed testing within three weeks for this clinical evaluation that meets guidelines
provided in the IPFnet PANTHER-IPF Manual of Operating Procedures (MOOP) this testing may be used to
satisfy the following screening criteria medical history physical exam arterial blood gas (ABG) with A-a
gradient vital signs with oximetry body height and weight spirometry DLCO lung volumes and HRCT scan
Allowing the use of previously performed test results that meet study guidelines for the screening visit is
intended to permit subjects easier access to study entry to prevent subjects from repeating testing that has been
performed within the study window and to decrease risks to subjects from repeated exposure to procedures
such as arterial puncture and HRCT
The following procedures will be performed at screening
Medical history and a physical examination
28
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Measure height and weight
Serum pregnancy test (if applicable)
Measure vital signs including oximetry
Blood draws performed and the following analyses conducted
o Hematology (red cell count white cell count hemoglobin hematocrit cell indices differential
platelet count)
o Blood chemistries according to central laboratory protocol (see Section 410 Laboratory
Testing)
o Beta human chorionic gonadotropin (serum) pregnancy test (in women of childbearing potential)
o Urinalysis
Pulmonary Function Tests (PFTs) including spirometry pre- and post- bronchodilator and postshy
bronchodilator measurement of lung volumes and measurement of hemoglobin adjusted diffusing
capacity
Measure ABGs
HRCT if a satisfactory scan has not been performed on the subject within 3 months of screening (see
PANTHER-IPF MOOP for more details)
Surgical lung biopsies (if applicable) reviewed by local and central pathology departments
Current medications If required a washout period discussed with the subject and initiated at this visit
4422 Enrollment
The enrollment visit is expected to take place within eight weeks of the screening visit Enrollment visit
activities include
Measure vital signs including oximetry
Measure height and weight
Serum pregnancy test (if applicable)
If consent has been given blood will be drawn and a urine specimen collected for the bio-specimen
repository
Spirometry (post-bronchodilator)
Measure 6MWT with Borg Dyspnea Scale
29
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Collect Quality-of-life (QOL) data using the SF-36 EuroQol Investigating Choice Experiments for
Preferences of Older People Capability Instrument (ICE CAP) and SGRQ
Female subjects complete Gender Substudy questionnaire
Dyspnea status collected using the UCSD SOBQ
Evaluate Acute Exacerbation (AEx)
Review of any Adverse Events (AEs)
Review of concomitant medications
Subject receives diary and instructions on its purpose and proper use
Subject receives supply of study drug sufficient to last until his or her 15-week study visit
See the Schedule of Assessments (Table 3) for more details Subjects with screening and enrollment postshy
bronchodilator FVC measurements (in liters) differing by more than 11 are not eligible to be enrolled in the
study
Subjects will be asked to provide a physician of record This physician will be considered the subjectrsquos primary
care provider (PCP) and if the subject agrees the PCP will be informed by letter of the subjectrsquos enrollment in
the trial The subject will be informed that his or her ongoing medical care should be received from the PCP
The PCP will be informed of any safety issues identified by the study staff The PCP will also be given
information regarding communication with study personnel about pertinent health issues or clinic encounters
the subject may have
4423 Week 15
The week 15 visit is expected to occur within +- 14 days of the subjectrsquos scheduled visit time (eg the week 15
visit should occur anytime between 13 and 17 weeks after starting study drug Week 15 activities include
Measure vital signs with oximetry
Measurement height and weight
Serum pregnancy test (if applicable)
Spirometry (post-bronchodilator) measurement
Review of AEs
Evaluate for AEx
30
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Review concomitant medications
If consented draw blood and collect urine specimen for the biospecimen repository
Subjects return used and unused study drug for the visit
Review study diary and a new study diary will be given
Provide additional supply of study drug sufficient to last until the next scheduled visit
4424 Week 30
The week 30 visit is expected to occur within +- 14 days of the subjectrsquos scheduled visit time (eg the week 30
visit should occur anytime between 28 and 32 weeks after starting study drug) Week 30 activities include
Physical examination
Measure vital signs with oximetry
Measure height and weight
Laboratory values (complete blood count [CBC] and serum chemistries)
Serum pregnancy test (if applicable)
Measure spirometry (post-bronchodilator)
6MWT with Borg scale
DLCO
Review of AEs
Evaluate for AEx
Review concomitant medications
Complete all QOL and dyspnea questionnaires (EuroQol ICE CAP SF-36 SGRQ and UCSD SOBQ)
If consent has been given blood will be drawn and a urine specimen collected for the biospecimen
repository
Review study diary
Subjects return used and unused study drug for the visit
Provide additional supply of study drug sufficient to last until the next scheduled visit
4425 Week 45
31
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
The week 45 visit is expected to occur within +- 14 days of the subjectrsquos scheduled visit time (eg the week 45
visit should occur anytime between 43 and 47 weeks after starting study drug) Week 45 activities include
Measure vital signs with oximetry
Measure height and weight
Serum pregnancy test (if applicable)
Measure spirometry (post-bronchodilator)
Review of AEs
Evaluate for AEx
Review concomitant medications
If consent has been given blood will be drawn and a urine specimen collected for the biospecimen
repository
Subjects return used and unused study drug for the visit
Study diary reviewed
Provide additional supply of study drug sufficient to last until the next scheduled visit
4426 Week 60 (Early Withdrawal or Final Treatment Visit)
At week 60 or at subject withdrawal from the study (premature by study doctor or subjectrsquos decision) a final
treatment visit will occur At this final treatment visit subjects will discontinue NACPL abruptly Week 60
activities also include
Physical examination
Measure vital signs with oximetry
Measure height and weight
Laboratory values (complete blood count [CBC] and serum chemistries)
Spirometry (post-bronchodilator) measurement
6MWT with Borg scale measurement
DLCO
Lung volumes
ABG
Review of AEs
32
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Evaluate for AEx
Review concomitant medications
Subjects will complete all QOL and dyspnea questionnaires (EuroQol ICE CAP SF-36 SGRQ and
UCSD SOBQ)
If consent has been given blood will be drawn and a urine specimen collected for the biospecimen
repository
Subjects return used and unused study drug for the visit
Study diary reviewed
4427 Final Site Visit ndash FVC drop confirmation
In the event that the subject has a recorded FVC drop of gt10 from baseline at the final treatment visit and the
subject has not had a confirmation of such a drop at a previous study visit the subject should return to the
clinical site 6 to 8 weeks after the final treatment visit During this visit a post-bronchodilator spirometry test
will be performed This FVC measurement will be evaluated according to section 521 of this protocol
4428 Final Visit ndash Telephone Follow-up
Four weeks following the final dose of study medication subjects will receive a telephone call from the study
coordinator to ensure that there are no side effects and to follow up on any ongoing adverse events (AEs)
4429 Phone Contact Between Visits
At week 2 and each month that a subject does not have a scheduled clinical center visit his or her study
coordinator will contact him or her at least once by telephone to
Inquire if the subject has had any hospitalizations events that might be considered an AE or any events
significant enough to warrant an out-of-cycle visit to the clinical center
Remind subjects of their current dosage levels and confirm that the subject understands them
Address any questions or concerns the subject might have regarding other aspects of the study
Assess adherence to the treatment regimen by reviewing diary data verbal review of medications taken
including nutritional supplements
33
34
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Table 3 Schedule of Assessments
Procedure Screening Visit 0
Enrollment Visit 1
Week 15 Visit 2
Week 30Visit 3
Week 45 Visit 4
Week 60 Early
Withdrawal Visit 5
Final1
Visit (via phone)
Informed consent X
Medical history X
Inclusionexclusion criteria X
Serum pregnancy test (if applicable) X X X X X
Review of lung biopsy X
Arterial Blood Gas X X
6-Minute Walk Test
X
X X
Physical examination X X X
Vital signs with oximetry X X X X X X
Body height and weight X X X X X X
Complete Blood Count X X X
Chemistry panel X X X
Monitor Lab Values X X X
Urinalysis X Specimen repository substudy blood draw and urine collection (if consented)
X
X X X X
HRCT (if not completed within three months) X
Spirometry (pre- and post-bronchodilator) X
Spirometry (post-bronchodilator only) X X X X X
DLCO (post-bronchodilator only) X X X
Lung volumes (post-bronchodilator only) X
X
Evaluate for acute exacerbation X X X X X
Review Adverse Events X X X X X X
Review concomitant meds X X X X X X
Dispense subject diary X X X X
Review subject diary X X X X X
Dispense study agent X X X X
Gender Substudy questionnaire (female subjects only) X
EuroQol ICECAP UCSD SOBQ SGRQ SF-36 X X X
Abbreviations DLCO diffusing capacity of the lung for carbon monoxide QOL Quality of Life ICECAP Investigating Choice Experiments for Preferences of Older People UCSD SOBQ University of California Shortness of Breath Questionnaire SGRQ St Georgersquos Respiratory Questionnaire SF-36 Short Form 36 Health Survey
1Follow-up visit via phone will occur four weeks after final dose of study medication
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
45 Dose Justification
The general philosophy for determining dosing levels was to apply previously examined
treatment regimens With the focus of the study being to establish a standard of care for
mildmoderate IPF subjects the goal was to develop flexible yet standardized treatment rules that
allow for the temporary or permanent withholding of one or more components of treatment when
necessary Subjects developing laboratory abnormalities or symptoms that result in
discontinuation of one or more components of study treatment may continue on the other
components as long as there is no contraindication for this Complete follow-up is important for
the validity of any study As a strategy to maintain protocol adherence we are using a treatment
regimen that will detect potential side effects and prompt interventions proactively in the interest
of patient safety In addition subjects who permanently stop study medications during the course
of the study are encouraged to continue in the study completing all scheduled visits and tests
451 Rationale for N-acetylcysteine Dosing
To our knowledge there have been no IPF studies to correlate clinical outcome measures with
different dosages for NAC The dosage chosen is based on the IFIGENIA study However BAL
lung GSH levels from subjects with IPF have been augmented with the use of oral NAC at 600
mg 3 times per day In addition lung GSH levels have been associated with improved
PFTs212227 The dose chosen for this study was based on previous data including the IFIGENIA
study30
4511 Dosing of N-acetylcysteineplacebo
Dosing of NACPL will be 600 mg orally 3 times a day (1800 mgday)
4512 Reasons to Discontinue N-acetylcysteineplacebo
NACPL may be temporarily or permanently discontinued for the duration of the study for
gastrointestinal symptoms or dermatologic reactions
35
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Temporarily discontinue (hold) oral NACPL for subjects requiring inpatient admission for acute
exacerbation (AEx) or other conditions Resume NACPL after discharge
36
37
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
452 Dosage Algorithms
Dosage Adjustment Algorithm 1 NACPL Dose Modifications for Gastrointestinal Symptoms Nausea Vomiting Abdominal Discomfort Diarrhea
GI Symptoms determined by the PI to be clinically significant Nausea Vomiting Abdominal Discomfort Diarrhea
NACPL Temporarily dc (HOLD) x 3 Days
Monitor symptoms intervene as clinically indicated (eg fluid replacement antidiarrhea or antinausea medication)
Monitor or lab PRN
Are symptoms resolving after 3 days NO
Symptoms NOT resolving after 3 days of holding study medication Assessmentmanagement per clinical
discretion of investigator
Likely not study medication discuss resuming study medication with medical monitor when symptoms resolved
YES
Temporarily dc (HOLD) NACPL for 4 additional days (total hold 1 week) then NACPL Resume 600 MG TID
Did symptoms recur
YES
STOP NACPL for
duration of study
NO
NACPL No Change
38
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Dosage Adjustment Algorithm 2 NACPL Dose Modifications For Dermatologic Reactions
Dermatologic Reactions (Not Acneiform) ge Grade 2 Grading per Common Terminology Criteria for
Adverse Events V30 (httpctepcancergov) For example Grade 1 RASHDESQUAMATION Macular or papular eruption or erythema without associated symptoms Grade 2 RASHDESQUAMATION Macular or popular eruption or erythema with pruritus or other associated symptoms localized desquamation or other lesions covering lt50 of body surface area
NACPL Temporarily dc (HOLD) x 3 days
Are symptoms resolving after 3 days
NO Symptoms not resolving after 3 days of holding study medication Assessmentmanagement per clinical discretion of investigator Likely not study medication Discuss resuming study medication with medical monitor when symptoms
resolved YES
Temporarily dc (HOLD) NACPL for 4 additional days (total hold 1 week) then NACPL resume 600 MG TID
Did symptoms recur
YES
STOP NACPL for
duration of study
NO
NACPL No change
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
46 Contraindications Precautions and Side Effects of Study Medications
461 Contraindication
Contraindication to NAC is known hypersensitivity to it
462 Precautions
Concomitant administration of oral NAC and antibiotics has shown a slightly reduced absorption
of cephalexin and a slight increase in erythromycin serum levels NAC contains free sulfhydryl
groups There is no evidence that individuals sensitive to sulfa drugs are sensitive to NAC
The NAC preparation being administered in this study contains 20 mg of aspartame Because of
the phenylalanine component of aspartame individuals with phenylketonuria should avoid or
restrict aspartame intake to avoid increased blood levels of phenylalanine Because of this risk
labeling is required on all products containing aspartame
463 Side Effects
Side effects of NAC range from common to serious See Table 4
39
40
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Table 4 Side Effects of NAC
Undesirable Effects
System-organ class Uncommon
(gt11000 lt1100)
Rare
(gt110000 lt11000)
Very rare
(lt110000) Not known
Immune system disorders Hypersensitivity Anaphylactic shock
reaction
Nervous system disorders Headache
Ear and labyrinth disorders Tinnitus
Cardiac disorders Tachycardia
Vascular disorders Hemorrhage
Respiratory thoracic and
mediastinal disorders
Bronchospasm
Dyspnea
Gastrointestinal disorders
Vomiting diarrhea
stomatitis abdominal
pain nausea
Dyspepsia
Skin and subcutaneous tissue
disorders
Urticaria rash
angioedema itching
General disorders and
administration site conditions Pyrexia
Investigations Reduced arterial
pressure Face edema
In very rare cases the onset of severe skin reactions such as Stevens-Johnson syndrome and Lyell syndrome was reported to have a temporal relationship with N-acetylcysteine administration Although in most cases at least another suspect drug probably most involved in the genesis of the above mentioned mucocutaneous syndromes has been identified in case of mucocutaneous alterations it is appropriate to contact onersquos doctor and the administration of N-acetylcysteine should be immediately discontinued
Some studies confirmed a reduction of platelet aggregation during N-acetylcysteine administration The clinical significance of these findings has not been defined yet [Source Fluimucil Investigator Brochure]
47 Recruitment Procedures
Subjects recruited for this study will be established patients of the investigators or physician- or
self-referred to participating clinical centers in the IPFnet Each clinical center within IPFnet has
a well-developed infrastructure of local pulmonologists within the surrounding geographic area
These pulmonologists are kept informed of ongoing IPF clinical trials and regularly refer
subjects to studies conducted at IPFnet clinical centers
Additional steps will be taken to inform clinicians of the trials in progress within IPFnet
including presentations at faculty staff meetings at local hospitals medical grand rounds and
national conferences direct mail notification monthly faxes and advertisement of network trials
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
in pulmonary journals Clinical center patients previously diagnosed with IPF will be notified of
the trials by mail whenever possible
Recruitment of minorities and women will be monitored by the DCC and DSMB If necessary
additional recruitment efforts will be made at specific centers to ensure that the aggregate subject
sample contains appropriate representation of women and minorities
48 Study Procedures
The following procedures are detailed in the PANTHER-IPF MOOP accompanying this
protocol
1 PFT
2 ABG
3 HRCT scan of the chest (including imaging of pulmonary arteries)
4 CBC and serum chemistries
5 Pregnancy test
6 6MWTBorg Dyspnea Scale
7 QOL questionnaires (EuroQol HAD SF-36 SGRQ and ICE CAP)
8 UCSD SOBQ
9 Gender Substudy Questionnaire
All assessments of PFTs will be conducted by study personnel not directly involved in the
treatment of the subjects
481 Biological Specimen Management
4811 Biological Specimen Sample Management
Subjects at clinical centers participating in the specimen repository substudy who consent to
having blood drawn for research purposes and for the banking of blood blood components and
other biologic specimens (urine and BAL fluid) will have approximately 405 mL of blood
41
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
drawn 17 mL blood drawn for DNA and 20 mL of urine collected at enrollment visit Subjects
will have approximately 50 mL of blood drawn and 20 mL of urine collected at each 15-week
follow-up visit Blood specimens will be separated according to PANTHER-IPF MOOP
guidelines into the following components for banking in the repository serum plasma and
DNA Coding of all biologic specimens for the repository will be performed by study staff at the
clinical center The samples will be processed per PANTHER-IPF MOOP guidelines aliquoted
labeled with barcode labels and stored at -70degC at the clinical center and shipped to the central
repository
The only subject identifiers will be a sample ID number and subject initials This sample ID will
be linked in the IPFnet DCC clinical database to subject information No subject information will
be transferred to the biological-specimen database
The subjectrsquos samples may be used for approved sub-studies relating to human disease
including but not limited to IPF The studies for which an individualrsquos samples will be made
available will be determined by the subjectrsquos answers to questions on the biological-sample
informed consent form The subjects can choose to make their samples available for all options
or any combination Samples will be made available to researchers only with IPFnet Steering
Group approval until such time as the samples are made public through the NHLBI repository
49 Concomitant Medications
Concurrent treatment with FDA-approved therapy for IPF is allowed Colchicine may be used
for treatment of gout Temporary treatment with oral or IV corticosteroids for clinical worsening
or suspected AEx is permitted Nutritional supplements containing NAC are not allowed
410 Laboratory Testing
Clinical laboratory parameters will be assessed at screening and at the end of the study The
following tests will be performed at the two time points specified in the protocol chemistry (AG
ratio ALT [SGPT] AST [SGOT] albumin alkaline phosphatase amylase bilirubin-direct
42
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
bilirubin-indirect bilirubin-total BUN BUNcreatinine ratio calcium carbon dioxide
cholesterol-total chloride CPK-total creatinine GGT globulin glucose iron-total LDH
lipase magnesium phosphorus-inorganic potassium protein-total sodium TIBC triglycerides
uric acid) and hematology (red blood cell count WBC count hemoglobin hematocrit cell
indices differential platelet count)
411 Blinding of Study Drugs
Subjects and caregivers will be blinded to study treatment Every subject will receive NAC or
matching PLs at every study visit from the baseline visit to the week-45 visit No study agent
will be dispensed at the week-60 visit
43
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
5 Study Endpoints
51 Primary Study Endpoint
The primary endpoint will be the change in serial measurements of FVC over the study period
52 Secondary Study Endpoints
521 Time to Disease-progression
The time-to-death or a 10 decline in FVC will be defined as the time-to-disease progression
The 10 decline in FVC from enrollment must be confirmed on 2 consecutive visits no less than
6 weeks apart For subjects with 2 consecutive visits with a 10 decline in FVC the time-toshy
disease progression will be defined as the time interval between enrollment and the initial visit
with a 10 FVC decline For subjects who experience disease progression the study doctor will
determine whether or not the subject will remain in the study
522 Acute Exacerbations
The following 3 criteria will define AEx in subjects with acute worsening of their respiratory
conditions
1 Clinical (all of the following required)
A) Unexplained worsening of dyspnea or cough within 30 days triggering unscheduled
medical care (eg emergency room clinic study visit hospitalization)
B) No clinical suspicion or overt evidence of cardiac event pulmonary embolism or deep
venous thrombosis to explain acute worsening of dyspnea
C) No pneumothorax
44
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
2 RadiologicPhysiologic (A and B required)
A) New ground glass opacity or consolidation computed tomography (CT) scan OR new
alveolar opacities on chest x-ray
B) Decline of ge 5 in resting room air SpO2 from last recorded level OR decline of ge 8 mm
Hg in resting room air PaO2 from last recorded level
3 Microbiologic (all of the following required)
A) No clinical evidence for infection (ie absence of grossly purulent sputum fever gt 39degC
orally)
B) Lack of positive microbiological results (if done) from lower respiratory tract defined as
(1) Clinically significant bacterial growth on sputum or endotracheal aspirate cultures
(2) Quantitative culture by protected brush specimen ge 103 cfumL or BAL ge 104 cfumL
(3) The presence of specific pathogens on stains of any of the above
C) Lack of positive pathogen in blood cultures (if done)
Identification of Acute Exacerbations
All subjects will be educated about the importance of identifying AExs At the time of
enrollment subjects will be told about the possibility of developing acute symptomatic
worsening that might represent an AEx of IPF and instructed to contact their study clinical
center coordinator within 48 to 72 hours of the apparent event
All subjects will be contacted by phone monthly and questioned about any change in dyspnea or
cough and any interim clinic visits or hospitalizations Finally as part of the IPFnet outreach to
community referring physicians the importance of AExs will be emphasized When a subject is
identified who meets criterion 1A this will trigger the collection of additional clinical data to
evaluate a suspected AEx These data will be collected as part of standard clinical care (ie this
protocol does not require collection of all items) The additional items to be collected for
suspected AEx include
IPFnet AEx case report form (eCRF) (required)
45
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Chest x-ray CT scan withwithout pulmonary angiogram (reports should be faxed and
followed by the hard copiesdiscs)
Oxygen saturation (pulse oximetry)
ABG
Respiratory cultures (sputum endotracheal aspirate lavage)
Blood cultures
Clinichospital records related to the event
All potential cases of AEx will be reviewed by the clinical center PI first and a decision on
whether the case may represent an AEx will be made If AEx is suspected the case will be sent
to the IPFnet adjudication committee which will assign a final diagnosis (see Table 5) If there is
disagreement among members the majority opinion will be recorded
During episodes of suspected AEx as determined by the individual clinical center investigator
subjects will remain blinded and in the study
Table 5 Final Diagnoses in Evaluation of Suspected Acute Exacerbations
Definite acute exacerbation All criteria met no alternative etiology
Unclassifiable acute worsening
Insufficient data to evaluate all criteria no alternative etiology
Not acute exacerbation Alternative etiology identified that explains acute worsening
Management of the suspected AEx will be at the discretion of the treating physician Standard of
care generally involves evaluation for respiratory infection pulmonary embolism cardiac events
and pneumothorax and treatment with IV corticosteroids
Study drugs will be resumed at pre-suspected AEx doses after subjects clinically improve as
confirmed by the local PI All subjects should be seen at the clinical center within 2 to 4 weeks
of recovery for measurement of post-bronchodilator FVC (see Figure 4) Subjects unable to
return to the clinical center after suspected AEx due to medical frailty (eg continued
46
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
institutionalization progressive disability) will be categorized as failing to maintain FVC
response in secondary analyses
Suspected AEx (PI determined)
Hold study drug Treat AEx
(Attending physician determined)
Alive but unable to continue due to
medical frailty
Dead
Alive and able to continue
Site reviewvisit
Restart study drug
FVC within 2-4 weeks
Figure 4 Acute Exacerbation Flow Chart
523 Respiratory Infections
An upper respiratory infection will be defined as
Change in sputum discoloration
Increased cough of no more than 14 daysrsquo duration
A lower-respiratory infection (pneumonia) will be defined as new segmental or lobar airspace
opacities visualized by image studies (chest radiograph or HRCT) in addition to any of the
following
Positive pathogencultures in good sample of sputum or lower-airway secretions retrieved
by fiberoptic bronchoscope
Fever gt 39degC or gt 100degF
Leukocytosis gt 12000 (unexplained no increase in dose of corticosteroids)
47
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
524 Maintained FVC Response
Subjects with follow-up FVCpred measurements at or above their baseline FVCpred level
will be classified as having maintained FVC response Subjects with reduced FVCpred levels
or missing data for any reason including death or medical frailty will be classified as having not
maintained FVC response The FVCpred value is used because unadjusted FVC measurements
are expected to decline with age
48
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
6 Safety Evaluations and Procedures
61 Adverse Events
During a clinical trial the reporting of adverse experience information can lead to important
changes in the way a new treatment is developed as well as provide integral safety data
611 Definitions
An adverse event (AE) is any untoward medical occurrence in a subject or clinical investigation
subject who was administered a pharmaceutical product The AE does not necessarily have to
have a causal relationship with the drug administered An AE can be any unfavorable and
unintended sign (including an abnormal laboratory finding) symptom or disease temporarily
associated with the use of a medicinal product whether or not considered to be related to the
medicinal product Diseases signs symptoms or laboratory abnormalities already existing at
enrollment are not considered AEs unless they worsen (ie increase in intensity or frequency)
Surgical procedures themselves are not AEs they are therapeutic measures for conditions that
require surgery The condition for which the surgery is required may be an AE Surgical
procedures planned before randomization and the conditions necessitating the surgery are not
AEs
A serious adverse event is any untoward event that
Is fatal
Is life-threatening
Requires inpatient hospitalization or prolongation of existing hospitalization with the
following exceptions
o Preplanned (before the study) hospital admissions unless the hospitalization is
prolonged
o Planned admissions (as part of a study eg routine biopsies)
o Hospitalization lasting lt 24 hours
49
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
o Hospitalization for elective procedure
o Emergency room visits
Results in persistent or significant disability or incapacity
Is a congenital anomaly or birth defect
Important medical events that may not result in death be life-threatening or require
inpatient hospitalization may be considered serious adverse events (SAEs) when based
on appropriate medical judgment they may jeopardize the subject and may require
medical or surgical intervention to prevent one of the outcomes listed above
Life-threatening means that the subject was in the view of the investigator at immediate risk of
death from the AE as it occurred It does not include an AE that had it occurred in a more severe
form might have caused death
Persistent or significant disabilityincapacity means that the event resulted in permanent or
significant and substantial disruption of the subjectrsquos ability to carry out normal life functions
Causality
A reasonable possibility means the AE may have been caused byrelated to the study drug A
perceived or real lack of efficacy does not satisfy the definition of relatedness
612 Adverse Event (AE) Reporting
For the PANTHER-IPF trial all AEs (serious and nonserious) occurring from randomization
through final study visit (4 weeks after final dose of all study medication) will be recorded on the
AE page of the case report form (CRF)
6121 Serious Adverse Events (SAE) Reporting
For this trial all deaths and all SAEs which occur from randomization through final study visit
must be entered within the EDC system via the SAE eCRF page within 24 hours of the
investigative sitersquos knowledge of the event It is the responsibility of the clinical center
50
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
investigator to provide a causality assessment of the event for each study medications based upon
the information available at the time of the report It is understood that complete information
about the event may not be known at the time the initial report is submitted In the event the EDC
system is not accessible to the site at the time of event reporting investigative sites will complete
and forward a paper back-up SAE form to DCRI Safety Surveillance for processing
DCRI Safety Surveillance
Telephone 1-919-668-8624 or 1-866-668-7799 (toll free)
Fax 1-919-668-7138 or 1-866-668-7138 (toll free)
The investigator must complete and submit follow-up SAE information via the eCRF when
important new or follow-up information (eg final diagnosis outcome results of specific
investigations) becomes available Follow-up information should be submitted according to the
same process used for reporting the initial event as described above All SAEs will be followed
until resolution stabilization or 30 days after the subject has completed the final visit (4 weeks
after the final dose of study medication) whichever occurs first The investigator is responsible
for reporting SAEs to their institutional review board (IRB) per site specific IRB reporting
guidelines
6122 Regulatory Reporting
AEs that are serious study drug related and unexpected will be reported to the regulatory
authorities The DCRI Safety Surveillance medical monitor will perform a medical review of all
SAEs submitted and evaluate for ldquounexpectednessrdquo DCRI Safety Surveillance will prepare
MedWatch reports for those events identified as serious study drug related and unexpected as
determined by Safety Medical Monitor
DCRI Regulatory Services will submit all unexpected study drug-related SAEs as per 21 CFR
32 DCRI Safety Surveillance will provide a safety alert letter to the NHLBI DSMB and DCC
clinical operation (for distribution to sites) within 15 days of initial receipt of the information
51
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Investigators are responsible for promptly reporting these events to their reviewing IRBs
according to site specific IRB reporting guidelines
62 Clinical Medical Monitoring
There will be an unblinded physician at the IPFnet DCC serving as medical monitor The
medical monitor will be available to assist with questions about dosage adjustments of study
medications including discontinuation or resumption of medications
63 Unblinding Procedures
Unblinding of subjects or investigators to subject treatment is strongly discouraged For ongoing
clinical management all subjects should be presumed to be receiving ldquoactiverdquo study drug To
ensure the subjectrsquos safety the study treatment will be dose-adjusted based on laboratory test
results clinical findings and symptoms
The IPFnet DCC medical monitor and PANTHER-IPF co-chairs Drs Ganesh Raghu and
Fernando Martinez will be available to the study physicians to discuss study drug management
on a case-by-case basis Un-blinding will be considered ONLY when the knowledge of subject
treatment assignment is ABSOLUTELY ESSENTIAL for subject safety and after discussion of
the subjectrsquos case with the medical monitor and either Dr Raghu or Dr Martinez Unblinding of
study treatment should be minimized during the conduct of the trial In those cases where it is
felt to be medically necessary the DCC medical officer will communicate directly with the
managing physician to minimize unblinding of study personnel
52
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
7 Study Drug Procedures
At the baseline 15-week 30-week and 45-week study visits subjects will receive a supply of
study drug sufficient to last until the next visit at which study drug will be dispensed
53
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
8 Data Management
81 Hardware and Software Configuration
811 Hardware and Database Software
Data will be stored in an Oracle database system Oracle has advantages of processing efficiency
and smooth linkage with other software systems The application and database will be hosted on
Solaris Unix servers at the IPFnet DCC
812 Statistical Software
SAS will be used as the principal application for the management of analysis data files and
statistical computations S-Plus will be used to provide supplementary functions as needed
813 Access Control and Confidentiality Procedures
Access to databases will be controlled centrally by the IPFnet DCC through user passwords
linked to appropriate privileges This protects the data from unauthorized changes and
inadvertent loss or damage
814 Security
Database and Web servers will be secured by a firewall and through controlled physical access
Oracle has many security features to ensure that any staff member accessing the database has the
proper authority to perform the functions he or she requests of the system Within the secondary
SAS databases Unix group-access control maintains similar security The Sun workstation login
is secured by extensive user-password facilities under Unix
54
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
815 Back-up Procedures
Database back-up will be performed automatically every day and standard IPFnet DCC policies
and procedures will be applied to dictate tape rotation and retention practices
816 Virus Protection
All disk drives that provide network services and all user computers will be protected using
virus-scanning software Standard IPFnet DCC policies will be applied to update these protection
systems periodically through the study
82 Sources of Data
821 Design and Development
The IPFnet DCC will be responsible for development of the electronic case report forms
(eCRFs) development and validation of the clinical study database ensuring data integrity and
training clinical center staff on applicable data management procedures A web-based distributed
data entry model will be implemented This system will be developed to ensure that guidelines
and regulations surrounding the use of computerized systems used in clinical trials are upheld
The remainder of this section provides an overview of the data management plan associated with
this protocol
822 Data Collection Forms
The data collection process consists of direct data entry at the study clinical centers into the EDC
system(s) provided by the DCC A data collection worksheet will be provided to clinical centers
for recording data in the event the EDC system is unavailable Data entry of the eCRFs should
be completed according to the instructions provided and project specific training The
investigator is responsible for maintaining accurate complete and up-to-date records and for
ensuring the completion of the eCRFs for each research participant
55
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
823 Data Acquisition and Entry
Data entry into eCRFs shall be performed by authorized individuals Selected eCRFs may also
require the investigatorrsquos written signature or electronic signature as appropriate Electronic
CRFs will be monitored for completeness accuracy and attention to detail during the study
824 Data Center Responsibilities
The IPFnet DCC will 1) develop a data management plan and will conduct data management
activities 2) provide final eCRFs for the collection of all data required by the study 3) develop
data dictionaries for each eCRF that will comprehensively define each data element 4) conduct
ongoing data monitoring activities on study data 5) monitor any preliminary analysis data
cleanup activities and 6) rigorously monitor final study data clean up
825 Data Editing
Completed data will be entered into the IPFnet DCC automated data acquisition and
management system If incomplete or inaccurate data are found a data clarification request will
be generated and distributed to clinical centers for a response Clinical centers will resolve data
inconsistencies and errors and enter all corrections and changes into the IPFnet DCC automated
data acquisition and management system
826 Training
The training plan for clinical center staff includes provisions for training on assessments eCRF
completion guidelines data management procedures and the use of computerized systems
56
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
9 Study Design and Data Analysis
91 General Analytic Considerations
All primary analyses will be based on intent-to-treat (ITT) principles using all randomized
subjects Baseline factors across groups will be compared using mean (standard deviation) and
median (25th and 75th percentiles) summary measures Kaplan-Meier curves will be used to
display event rates Due to clinical interest in departures from both sides of the null hypothesis
all test statistics will be 2-sided
Reasonable caution needs to be taken when conducting multiple analyses on key clinical
subgroups For subgroup analyses a conservative significance level of 0001 will be used for all
interaction tests Thus subgroup comparisons will be considered exploratory unless the p-value
from the interaction test is smaller than 0001
92 Randomization Blinding and Reporting of Results
A permuted block-randomization scheme will be created with varying block sizes stratified by
clinical center Once a subject has completed the screening and baseline period and evaluation
for inclusionexclusion criteria the randomization process will begin Subjects will be
randomized to receive NAC or matching placebo with equal probability (11) via telephone
contact with a central interactive voice response system (IVRS) using a toll-free randomization
number On the day of randomization after the subject has successfully met all inclusion and
exclusion criteria the investigator or designee will call the central randomization number to
obtain the assigned kit randomization numbers for that subject At each subject visit the
investigator or designee will call the central randomization number to obtain the new kit
randomization numbers for resupply of the subject For resupply of the clinical center the IVRS
will monitor minimal volume of a kit type andor expiration date and will automatically notify
the pharmacy
57
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
The trial results will be reported according to guidelines specified in the CONSORT statement
A flow diagram describing screening recruitment randomization dropout and vital status will
be included in the primary manuscript AEs and efficacy data will be presented for all treatment
groups Adherence dropout and lost to follow-up will be carefully examined across all treatment
groups Analyses of safety will be based on data from all randomized subjects who received at
least one dose of study drug
93 Stratification
Subjects will be distributed to the two treatment arms in a 11 allocation ratio Stratification
blocks will be based on clinical centers
94 Specification of the Primary Analyses
A mixed model repeated measures (MMRM) analysis described in section 95 will be used to
compare differences in the slope of FVC measurements across the treatment groups Response
variables are values of the FVC measured at baseline and every 15 weeks until study completion
Variables in the model will include treatment time and time by treatment age sex race and
height Contrast estimates of differences in slopes of treatment over time (along with confidence
intervals) will be used to estimate the treatment effect The validity of this model in terms of
meeting modeling assumptions will be assessed via standard modeling diagnostics and goodness-
of-fit measures Based on the MMRM framework missing FVC data will not be imputed for the
primary analysis
95 Analysis of Longitudinal Endpoints
A common goal in clinical trials is to specify models that are easily implemented and
reproducible by independent data analysts On the other hand the models should have proper
statistical behavior in terms of low bias and high precision Many common approaches to
longitudinal data analysis including last observation carried forward (LOCF) imputation rely on
the missing completely at random (MCAR) assumption However the MCAR assumption is
58
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
unlikely to hold in many clinical trials because missing data are often related to disease
progression and prognosis A more reasonable assumption missing at random (MAR) specifies
that the complete data distribution can be modeled using only the observed data The likelihood-
based MMRM approach is valid under the more general MAR assumptions These models will
be applied to analyze the longitudinal data secondary endpoints
The advantages of MMRM analysis are that all important characteristics of the model can be preshy
specified standard software can be used to implement the models and results are based on ITT
principles43 In addition the MMRM approach offers superior control of Type I and Type II
errors compared with the LOCF approach
Response variables are values of the PFTs measured at enrollment and every 15 weeks until
study completion and 6MWT values measured at baseline week 30 and week 60 Covariates are
treatment time time by treatment and key baseline risk factors Contrasts (along with
confidence intervals) of treatment by time will be used to estimate the treatment effect
The correlation structure involves multiple pieces including measurement errors random
variation and interindividual variability For the longitudinal data analyses an unstructured
correlation matrix for within-subject errors will be assumed Other correlation structures
including compound symmetry will be examined as needed A careful examination of reasons
for study discontinuation will be conducted to assess the validity of MCAR Sensitivity analyses
will be used to examine the untestable assumption that the observed data violate the MAR
assumption The MMRM models will be implemented using PROC MIXED in SAS
96 Analysis of Binary Time-to-Event and Time-Lagged Endpoints
Regression modeling approaches using either the logistic regression model or Cox proportional
hazards regression model will be employed when appropriate The validity of these models will
be assessed via standard modeling diagnostics and goodness-of-fit measures Estimates of
cumulative frequencies for more general time-lagged responses will be calculated using the
partitioned version of the Bang-Tsiatis estimator44 The partitions will be set at 15-week intervals
59
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
to correspond with the data-collection process Covariate adjusted event rates will be calculated
using inverse probability-weighted regression estimates45
97 Power Analysis
971 Primary Analyses
Based on previously published IPF clinical trials the PL group is expected to experience a drop
in FVC of approximately 020 L over the study period (see Figure 1) The IPFnet Steering Group
determined a clinically important difference would be to preserve the majority of the decline
relative to PL over the study period In particular a treatment effect of 015 L was determined to
be a clinically meaningful difference Potential dropout is a key factor in the proposed study The
drop-out process assumed 5 lost to follow-up after every study visit Only 80 of subjects
were assumed to be followed for the entire study period All models assumed a compound
symmetry structure for the covariance matrix Power calculations were performed using a SAS
IML program for designing repeated measures studies46 Based on preliminary reviews of the
data from the University of Michigan the covariance matrix parameters were estimated at
approximately σ2 = 0757 (variance parameter) and ρ = 0936 (correlation parameter) To be
conservative the power calculations for the primary analysis were performed with parameter
setting of σ2 = 0810 (variance parameter) and ρ = 0925 (correlation parameter)
The power calculations assume a correction for imperfect compliance proposed by Lachin and
Foulkes to allow for 2 noncompliance for each of the treatment arms47 Thus the sample size
of 130 subjects per arm would be reduced to an adjusted sample size of 130(1-002-002)2 =
1198 or 120 subjects per arm
Under the assumed Type I error rate of 005 with a correlation parameter of 0925 and standard
deviation of 090 the difference of 015 L (or 00025 Lweek) shown in Table 6 would have
power of 93
60
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Table 6 Hypothetical Values of Mean FVC (L) Change from Baseline
Week 15 Week 30 Week 45 Week 60
NAC 00125 00250 00375 00500
Placebo 00500 01000 01500 02000
Difference 00375 00750 01125 01500
Abbreviations FVC forced vital capacity PL placebo
972 Power Analysis for Secondary Endpoints
Power calculations for secondary endpoint measurements are shown in Table 7 Standard
deviations are based on unpublished data provided by the University of Michigan The
calculations are based on a 2-sample t-test with Type I error rate set at 005 These calculations
are likely to be conservative because the statistical approach described in section 95 for
analyzing these endpoints will incorporate incomplete observations as well as intermediate data
points
Table 7 Detectable Differences in Treatment Means for Selected Endpoint Measurements
Secondary Endpoints Std Dev
of the Baseline Score
Detectable Difference for 80 Power
Std Dev of the Change Score
Difference Detectable for
80 Power
DLCOpred 166 58 91 32
6MWT Area Under the Desaturation Curve
219 76 175 61
6MWT Distance to Desaturation 224 78 315 110
6MWT Minutes Walked 210 073 205 071
Abbreviations Std Dev standard deviation DLCOpred diffusing capacity of the lung for carbon monoxide percent predicted 6MWT 6-minute walk test
61
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
10 Study Administration
101 Cooperative Agreement Mechanism
The administrative and funding mechanism used to undertake this project is a ldquocooperative
agreementrdquo (U01) which is an assistance mechanism Under the cooperative agreement the
NHLBI assists supports andor stimulates the project and is substantially involved with
investigators in conducting the study by facilitating performance of the effort in a ldquopartnerrdquo role
The NHLBI project scientist serves on the IPFnet Steering Group and he or another NHLBI
scientist may serve on other project committees when appropriate At the same time however
NHLBI does not assume a dominant role direction or prime responsibility for this research
program
As described below governance of the project is conducted through the IPFnet Steering Group
Principal investigators have lead responsibilities in all aspects of their trials and the project
including any modification of trial designs conduct of the trials quality control data analysis
and interpretation preparation of publications and collaboration with other investigators unless
otherwise provided for by the IPFnet Steering Group
PIs retain custody of and have primary rights to their center-specific and collaborative data
subject to government rights-of-access consistent with current Health amp Human Services (HHS)
Public Health Service (PHS) and National Institutes of Health policies The protocols and
governance policies call for the continual submission of data centrally to the IPFnet DCC for the
collaborative database which at a minimum will contain the key variables selected by the IPFnet
Steering Group for standardization across all clinical centers the submission of copies of the
collaborative datasets to each PI upon completion of the project procedures for data analysis
reporting and publication and procedures to protect and ensure the privacy of medical and
genetic data and records of individuals The NHLBI project scientist on behalf of the NHLBI
will have the same access privileges and responsibilities regarding the collaborative data as the
other members of the Steering Group
62
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
PIs are also encouraged to publish and to publicly release and disseminate results data and other
products of the project concordant with the project protocols and governance and the approved
plan for making data and materials available to the scientific community and to the NHLBI
However during the 3 years after the ending date of NHLBI project support unpublished data
unpublished results data sets not previously released and other study materials or products are
to be made available to any third party only with the approval of the IPFnet Steering Group
Upon completion of the project PIs are expected to put their intervention materials and
procedure manuals into the public domain andor make them available to other investigators
according to the approved plan for making data and materials available to the scientific
community and the NHLBI for the conduct of research at no charge other than the costs of
reproduction and distribution
The NHLBI reserves the right to terminate or curtail the project (or an individual award) in the
event of (a) failure to develop or implement mutually agreeable collaborative measurement
subject eligibility and data management sections of the protocols (b) substantial shortfall in
subject recruitment follow-up data reporting or quality control or other major breach of
protocol (c) substantive changes in the agreed-upon protocols with which NHLBI cannot
concur (d) reaching a major project outcome with persuasive statistical significance
substantially before schedule or (e) human subject ethical issues that may dictate a premature
termination
Any disagreement that may arise in scientificprogrammatic matters (within the scope of the
award) between award recipients and the NHLBI may be brought to arbitration An arbitration
panel will be composed of 3 membersmdash1 selected by the IPFnet Steering Group (with the
NHLBI member not voting) or by the individual PI in the event of an individual disagreement a
second selected by NHLBI and the third selected by the other 2 members This special
arbitration procedure in no way affects the PIrsquos right to appeal an adverse action that is otherwise
appealable in accordance with the PHS regulations at 42 CFR part 50 Subpart D and HHS
63
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
regulation at 45 CFR part 16 or the rights of the NHLBI under applicable statutes regulations
and terms of the award
102 IPFnet Steering Group
The IPFnet Steering Group is the main governing body of the project It is composed of the PIs
of the clinical centers the PI of the DCC and the NHLBI project scientist The clinical centers
the IPFnet DCC and the NHLBI each have 1 vote on the IPFnet Steering Group All decisions
are determined by majority vote
All major scientific decisions are determined by the IPFnet Steering Group It assumes overall
responsibility for the design and conduct of the trial It appoints (and disbands) committees and
subcommittees as the need arises designs approves and implements the study protocols
oversees the development of the MOOP monitors subject recruitment and treatment delivery
evaluates data collection and management oversees quality assurance procedures and
implements changes and enhancements to the study as required It also has primary responsibility
for facilitating the conduct of the trials and reporting the projectrsquos results
103 Data and Safety Monitoring Board
The NHLBI will establish a DSMB in accordance with established policies (see
httpwwwnhlbinihgovfundingpoliciesdsmb_insthtm) to ensure data quality and subject
safety and to provide independent advice to the NHLBI regarding progress and the
appropriateness of study continuation
104 Recommendations on Interim Monitoring of Efficacy Safety and Futility
First and foremost the role of the DSMB will be to review subject safety and trial conduct at
periodic points during the study The DSMB may require analyses of the primary endpoint
results for comparing the benefit and risks of treatment strategies The benefit of collecting
additional data on key secondary endpoints with extended follow-up and establishing a robust
64
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
evidence base for determining a standard of care will need to be carefully considered before
early termination of one or more treatment arms After careful consideration the IPFnet Steering
Group recommends conservative thresholds for the early examinations of the safety and efficacy
data
The DSMB will be expected to meet approximately every 6 months until trial completion to
review safety and toxicity data The DSMB may recommend stopping the study based on these
reviews Because the DSMB could stop the trial for safety concerns as well as for a large
efficacy benefit there could be multiple opportunities to reject the null hypothesis (no difference
in event rates between the PL and NAC groups) A Bonferroni approximation will be applied
during the one planned interim analysis for efficacy
Before locking the database a statistical analysis plan (SAP) will be developed to provide
complete details on the statistical analysis The SAP will include the specifics for how and when
the DSMB will be notified for AEs The IPFnet DCC will deliver to the DSMB all FDA-defined
AEs at 3-month intervals The IPFnet DCC will prepare narrative SAE reports in real time for
DSMB review including recommendations and analysis of similar events for each SAE
submitted to the FDA
65
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
11 Investigator and Sponsor Obligations
111 Monitoring
All monitoring activities for US clinical centers will be performed in accordance with DCRI
standard operating procedures Information regarding the types of visits will be outlined in the
PANTHER-IPF MOOP
112 Cost and Payment
There will be no cost to subjects enrolled in this trial Study-related procedures will be paid for
by the IPFnet
Subjects may be eligible for reimbursement for travel to the clinical center Details of payment
will be explained to each subject during the consent process
113 Confidentiality and Health Insurance Portability and Accountability Act
Considerations
Subject confidentiality will be protected throughout the study All subject data will be kept
strictly confidential and no subject-identifying information will be released to anyone outside
the project Confidentiality will be assured through several mechanisms First each subject will
be assigned an anonymous study ID which will then be used on all study forms Second any
study forms blood samples and paper records that contain subject information (eg address lists
phone lists) will be kept at the clinical centers in secured locked areas coded by number Once
blood is collected there will be no subject identifiers placed on blood samplesmdashonly the study
ID number and the date of sample collection Third access to all subject data and information
including laboratory specimens will be restricted to authorized personnel In the case of
computerized data this restricted access will be assured through user logon IDs and password
protection
66
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
At the IPFnet DCC only authorized personnel will have access to the data files containing study
data Security will be assured through user logon IDs passwords and appropriate access
privileges All study subjects will be identified only by their IPFnet ID numbers and no personal
identifying information such as name address or Social Security number will be entered into
the IPFnet DCC database Any subject-specific data reported to the IPFnet Steering Group will
be identified only by the IPFnet ID number
Finally subjects will not be identified by name in any reports or publications nor will the data
be presented in such a way that the identity of individual subjects can be inferred Analysis files
created for further study by the scientific community will have no subject identifiers These data
files will be created in accordance with the Ancillary Studies and Publication Policy of the
IPFnet
114 Informed Consent Procedures
All IPFnet subjects will provide written informed consent using procedures reviewed and
approved by each clinical centerrsquos IRB Informed consent will be undertaken by study personnel
in-person with the subject The subject has the option of declining further participation in the
study at that point No further study procedures will be conducted until the signed documents
have been provided to the IPFnet clinical center
115 Institutional Review Boards
Before initiating this study the protocol clinical center-specific informed consent forms Health
Insurance Portability and Accountability Act (HIPAA) forms recruitment materials and other
relevant information will be reviewed by a properly constituted IRB at each participating clinical
center A copy of the signed and dated IRB approval at each clinical center will be retrieved prior
to or during the site initiation visit and archived at the IPFnet DCC Any amendments to the
protocol other than simple administrative and typographical changes must be approved by each
IRB before they are implemented The clinical centers will seek annual renewals of their IRB
approvals in accordance with local procedures
67
__________________________________________ ________________
__________________________________________
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
12 Investigator Agreement
I have read the foregoing protocol PANTHER-IPF and agree that it contains all necessary
details for carrying out this study I will conduct the study as outlined herein and will complete
the study within the time designated
I will provide copies of the protocol and all pertinent information to all individuals responsible to
me who assist in the conduct of this study I will discuss this material with them to ensure they
are fully informed regarding the drug and the conduct of the study
I will fulfill all responsibilities for submitting pertinent information to the local IRB if
applicable that is responsible for this study
I further agree that NHLBI andor DCRI will have access to any source documents from which
eCRF information may have been generated
Signature of Principal Investigator Date
Name of Principal Investigator (printed or typed)
Protocol version date May 19 2009
Protocol Amendment 1 version date May 28 2010
Protocol Amendment 2 version date December 6 2011
68
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
13 References
1 Raghu G Brown KK Bradford WZ et al A placebo-controlled trial of interferon gamma-1b in patients with idiopathic pulmonary fibrosis N Engl J Med 2004350125-33 2 King TE Jr Safrin S Starko KM et al Analyses of efficacy end points in a controlled trial of interferon-gamma1b for idiopathic pulmonary fibrosis Chest 2005127171-7 3 Flaherty KR Thwaite EL Kazerooni EA et al Radiological versus histological diagnosis in UIP and NSIP survival implications Thorax 200358143-8 4 Wells AU Desai SR Rubens MB et al Idiopathic pulmonary fibrosis a composite physiologic index derived from disease extent observed by computed tomography Am J Respir Crit Care Med 2003167962-9 5 Raghu G Freudenberger TD Yang S et al High prevalence of abnormal acid gastroshyoesophageal reflux in idiopathic pulmonary fibrosis Eur Respir J 200627136-42 6 Kinnula VL Focus on antioxidant enzymes and antioxidant strategies in smoking related airway diseases Thorax 200560693-700 7 Coultas DB Zumwalt RE Black WC Sobonya RE The epidemiology of interstitial lung diseases Am J Respir Crit Care Med 1994150967-72 8 Raghu G Weycker D Edelsberg J Bradford WZ Oster G Incidence and prevalence of idiopathic pulmonary fibrosis Am J Respir Crit Care Med 2006174810-6 9 Olson AL Swigris JJ Lezotte DC Norris JM Wilson CG Brown KK Mortality from pulmonary fibrosis increased in the United States from 1992 to 2003 Am J Respir Crit Care Med 2007176277-84 10 Mannino DM Etzel RA Parrish RG Pulmonary fibrosis deaths in the United States 1979shy1991 An analysis of multiple-cause mortality data Am J Respir Crit Care Med 19961531548shy52 11 Hubbard R Johnston I Coultas DB Britton J Mortality rates from cryptogenic fibrosing alveolitis in seven countries Thorax 199651711-6 12 Johnston I Britton J Kinnear W Logan R Rising mortality from cryptogenic fibrosing alveolitis Bmj 19903011017-21 13 Raghu G Collard HR Egan JJ et al An official ATSERSJRSALAT statement idiopathic pulmonary fibrosis evidence-based guidelines for diagnosis and management Am J Respir Crit Care Med 2011183788-824 14 (USA) FDA FDA Public Health Advisory Interferon gamma-1b (marketed as Actimmune) In 2007 15 King TE Jr Pardo A Selman M Idiopathic pulmonary fibrosis Lancet 2011 16 Raghu G Brown KK Costabel U et al Treatment of idiopathic pulmonary fibrosis with etanercept an exploratory placebo-controlled trial Am J Respir Crit Care Med 2008178948shy55 17 Malouf MA Hopkins P Snell G Glanville AR An investigator-driven study of everolimus in surgical lung biopsy confirmed idiopathic pulmonary fibrosis Respirology 201116776-83 18 King TE Jr Behr J Brown KK et al BUILD-1 a randomized placebo-controlled trial of bosentan in idiopathic pulmonary fibrosis Am J Respir Crit Care Med 200817775-81 19 Richeldi L Costabel U Selman M et al Efficacy of a tyrosine kinase inhibitor in idiopathic pulmonary fibrosis N Engl J Med 20113651079-87
69
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
20 Borok Z Buhl R Grimes GJ et al Effect of glutathione aerosol on oxidant-antioxidant imbalance in idiopathic pulmonary fibrosis Lancet 1991338215-6 21 Meyer A Buhl R Magnussen H The effect of oral N-acetylcysteine on lung glutathione levels in idiopathic pulmonary fibrosis Eur Respir J 19947431-6 22 Behr J Maier K Degenkolb B Krombach F Vogelmeier C Antioxidative and clinical effects of high-dose N-acetylcysteine in fibrosing alveolitis Adjunctive therapy to maintenance immunosuppression Am J Respir Crit Care Med 19971561897-901 23 Cantin AM North SL Fells GA Hubbard RC Crystal RG Oxidant-mediated epithelial cell injury in idiopathic pulmonary fibrosis J Clin Invest 1987791665-73 24 Waghray M Cui Z Horowitz JC et al Hydrogen peroxide is a diffusible paracrine signal for the induction of epithelial cell death by activated myofibroblasts Faseb J 200519854-6 25 Larios JM Budhiraja R Fanburg BL Thannickal VJ Oxidative protein cross-linking reactions involving L-tyrosine in transforming growth factor-beta1-stimulated fibroblasts J Biol Chem 200127617437-41 26 Kinnula VL Fattman CL Tan RJ Oury TD Oxidative stress in pulmonary fibrosis a possible role for redox modulatory therapy Am J Respir Crit Care Med 2005172417-22 27 Meyer A Buhl R Kampf S Magnussen H Intravenous N-acetylcysteine and lung glutathione of patients with pulmonary fibrosis and normals Am J Respir Crit Care Med 19951521055-60 28 Behr J Degenkolb B Krombach F Vogelmeier C Intracellular glutathione and bronchoalveolar cells in fibrosing alveolitis effects of N-acetylcysteine Eur Respir J 200219906-11 29 Bando M Hosono T Mato N et al Long-term efficacy of inhaled N-acetylcysteine in patients with idiopathic pulmonary fibrosis Intern Med 2010492289-96 30 Demedts M Behr J Buhl R et al High-dose acetylcysteine in idiopathic pulmonary fibrosis N Engl J Med 20053532229-42 31 Toma TP Bhowmik A Rajakulasingam R Acetylcysteine in pulmonary fibrosis N Engl J Med 20063541086-9 author reply -9 32 Hunninghake GW Antioxidant therapy for idiopathic pulmonary fibrosis N Engl J Med 20053532285-7 33 Flaherty KR Mumford JA Murray S et al Prognostic implications of physiologic and radiographic changes in idiopathic interstitial pneumonia Am J Respir Crit Care Med 2003168543-8 34 Latsi PI du Bois RM Nicholson AG et al Fibrotic idiopathic interstitial pneumonia the prognostic value of longitudinal functional trends Am J Respir Crit Care Med 2003168531-7 35 Collard HR King TE Jr Bartelson BB Vourlekis JS Schwarz MI Brown KK Changes in clinical and physiologic variables predict survival in idiopathic pulmonary fibrosis Am J Respir Crit Care Med 2003168538-42 36 Jegal Y Kim DS Shim TS et al Physiology is a stronger predictor of survival than pathology in fibrotic interstitial pneumonia Am J Respir Crit Care Med 2005171639-44 37 Martinez FJ Safrin S Weycker D et al The clinical course of patients with idiopathic pulmonary fibrosis Ann Intern Med 2005142963-7 38 Hull JH Acetylcysteine in pulmonary fibrosis N Engl J Med 20063541089-91 author reply -91
70
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
39 Flaherty KR King TE Jr Raghu G et al Idiopathic interstitial pneumonia what is the effect of a multidisciplinary approach to diagnosis Am J Respir Crit Care Med 2004170904shy10 40 Raghu G Johnson WC Lockhart D Mageto Y Treatment of idiopathic pulmonary fibrosis with a new antifibrotic agent pirfenidone results of a prospective open-label Phase II study Am J Respir Crit Care Med 19991591061-9 41 Hunninghake GW Lynch DA Galvin JR et al Radiologic findings are strongly associated with a pathologic diagnosis of usual interstitial pneumonia Chest 20031241215-23 42 Lynch D Godwin J Safrin S et al High-resolution computed tomography in idiopathic pulmonary fibrosis diagnosis and prognosis Am J Respir Crit Care Med 2005172488-93 43 Mallinckrodt CH Watkin JG Molenberghs G Carroll RJ Choice of the primary analysis in longitudinal clinical trials Pharmaceutical Statistics 20043161-9 44 Bang H Tsiatis A Estimating medical costs with censored data Biometrika 200087329shy43 45 Lin DY Regression analysis of incomplete medical cost data Stat Med 2003221181-200 46 Rochon J Application of GEE procedures for sample size calculations in repeated measures experiments Stat Med 1998171643-58 47 Lachin JM Foulkes MA Evaluation of sample size and power for analyses of survival with allowance for nonuniform patient entry losses to follow-up noncompliance and stratification Biometrics 198642507-19
71
- PANTHER-IPFPREDNISONE AZATHIOPRINEAND N-ACETYLCYSTEINEA STUDY THAT EVALUATES RESPONSE INIDIOPATHIC PULMONARY FIBROSIS
-
- Protocol Summary
- Table of Contents
- List of Tables
- List of Figures
- List of Abbreviations
- 1 Summary
- 2 Hypotheses and Specific Aims
-
- 21 Null Hypothesis
- 22 Specific Aim 1
- 23 Specific Aim 2
- 24 Prespecified Subgroups of Interest
-
- 3 Background and Significance
-
- 31 Idiopathic Pulmonary Fibrosis is the Most Common Interstitial Lung Disease
- 32 Rationale for Placebo Control
- 33 Rationale for N-acetylcysteine
- 35 Rationale for N-acetylcysteine as a Stand-alone Therapy
- 36 Rationale for the Study Design and Primary Endpoint
- 37 Rationale for Blinding of Treatments
-
- 4 Methods
-
- 41 Inclusion Criteria
- 42 Diagnosis of IPF
- 43 Exclusion Criteria
- 44 Study Design and Study Visit
- 45 Dose Justification
- 46 Contraindications Precautions and Side Effects of Study Medications
- 47 Recruitment Procedures
- 48 Study Procedures
- 49 Concomitant Medications
- 410 Laboratory Testing
- 411 Blinding of Study Drugs
-
- 5 Study Endpoints
-
- 51 Primary Study Endpoint
- 52 Secondary Study Endpoints
-
- 6 Safety Evaluations and Procedures
-
- 61 Adverse Events
- 62 Clinical Medical Monitoring
- 63 Unblinding Procedures
-
- 7 Study Drug Procedures
- 8 Data Management
-
- 81 Hardware and Software Configuration
- 82 Sources of Data
-
- 9 Study Design and Data Analysis
-
- 91 General Analytic Considerations
- 92 Randomization Blinding and Reporting of Results
- 93 Stratification
- 94 Specification of the Primary Analyses
- 95 Analysis of Longitudinal Endpoints
- 96 Analysis of Binary Time-to-Event and Time-Lagged Endpoints
- 97 Power Analysis
-
- 10 Study Administration
-
- 101 Cooperative Agreement Mechanism
- 102 IPFnet Steering Group
- 103 Data and Safety Monitoring Board
- 104 Recommendations on Interim Monitoring of Efficacy Safety and Futility
-
- 11 Investigator and Sponsor Obligations
-
- 111 Monitoring
- 112 Cost and Payment
- 113 Confidentiality and Health Insurance Portability and Accountability ActConsiderations
- 114 Informed Consent Procedures
- 115 Institutional Review Boards
-
- 12 Investigator Agreement
- 13 References
-
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
with IPF is markedly diminished compared with normal subjects This GSH deficiency may be corrected by
exogenous administration of NAC2122
There is evidence of enhanced production of oxidants in an IPF lung Both inflammatory cells and
myofibroblasts derived from patients with IPF generate increased amounts of extracellular oxidants including
hydrogen peroxide2324 Secretion of hydrogen peroxide by activated myofibroblasts may induce the death of
adjacent lung epithelial cells by paracrine mechanisms24 Additionally generation of oxidants by myofibroblasts
induces oxidative crosslinking of extracellular matrix proteins25 a potential mechanism for aberrant matrix
remodeling Thus an oxidant-antioxidant imbalance exists in the lungs of IPF patients26 NAC may confer
protection against this imbalance by augmenting GSH levels in addition to its more direct free-radical
scavenging activity
Intravenous (IV) NAC therapy has been shown to increase total BAL GSH in 8 IPF subjects27 Oral NAC (600
mg 3 times per day) has been shown to decrease markers of oxidant injury and improve both total and reduced
GSH levels in the epithelial lining fluid of subjects with IPF in a small uncontrolled study22 pulmonary
function improved modestly with therapy A similar study in 18 IPF subjects confirmed increased intracellular
GSH concentration after 12 weeks of NAC (600 mg 3 times per day)2228 no clinical correlates were reported
Inhaled NAC was suggested to improve pulmonary function in an open label study29
35 Rationale for N-acetylcysteine as a Stand-alone Therapy
Results of a double-blind multi-center European clinical trial of 150 IPF subjects testing combinations of AZAshy
PRED vs AZA-PRED-NAC have been reported30 NAC added to AZA-PRED (ldquoconventional therapyrdquo) had a
significant positive effect on DLCO (p lt 0005) and vital capacity (VC) (p lt 005) at the end of 1 year30 The
recent ATSERS position statement after much discussion concluded that NAC alone should not be considered
in the majority of patients with IPF without additional data from well-designed studies
The interpretation of these data has been quite controversial Some have suggested that the magnitude of the
treatment effect although statistically significant is modest31 Others have suggested that NAC may be
modulating potential toxic effects of AZA-PRED alone32 supporting the investigation of NAC as stand-alone
therapy
17
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
The IPFnet is now completing the PANTHER-IPF trial with a 11 randomization (NAC vs placebo) and a
simple practical feasible and scientifically rational design that will establish standard of care with NAC for
IPF based on a currently available therapeutic agent and the existing data to support its use We anticipate that
all future clinical trials of novel therapeutic agents will be tested against this to-be-established standard of care
36 Rationale for the Study Design and Primary Endpoint
The optimal study design of a therapeutic trial in IPF would include survival as a primary endpoint The
published results of the IFN-γ 1b Phase 3 (GIPF-001) trial suggested a survival benefit in subjects with milder
disease in retrospective analyses1 although the trial was underpowered to address this question This was likely
related to the limited mortality in the PL arm of the study which included IPF subjects with mild to moderate
disease This study documents that an IPF study powered to improve survival in a patient population with mild
disease requires a larger sample size andor duration of study In fact the recently aborted Phase 3 IFN-γ 1b
(GIPF-007 INSPIRE) study was a survival-based study and recruited more than 800 subjects at 75 centers
worldwide1415 As such within the context of the current IPFnet trial survival is an impractical primary
endpoint variable
Several groups have published data defining an appropriate surrogate outcome variable a 10 decrement in
FVC during 6 to 12 months is a powerful predictor of survival in IPF33-36 Furthermore additional evidence
suggests a similar predictive ability for a 10 decrement in FVC during 3 months of follow-up37 With strong
supportive evidence of FVC progression being related to mortality on a per-subject basis this study will use
FVC changes in liters between treatment groups as the primary endpoint Previously published IPF studies have
shown a steady decline in FVC (and FVCpred) among control group subjects230 The GIPF-001 study
suggested a 48-week decrease in FVC of 016 L in the PL-treated subjects The IFIGENIA study demonstrated
a decline in FVC of approximately 019 L over 52 weeks in the subjects randomized to the control treatment
Figure 1 depicts the change in FVC for control groups from previously published IPF studies38 Based on these
data we expect that the PL group will have a decline of 020 L over the 60-week study period The IPFnet
Steering Group determined that a clinically meaningful improvement would be the preservation of the majority
of the 020-L FVC decline Therefore a mean treatment difference of 015 L in mean FVC over the 60-week
study period was determined to be a clinically meaningful difference
18
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Δ f
rom
bas
elin
e (i
n L
)
01
005
0
-005
-01
-015 Projected Δ for placebo
-02
-025
-019
-016
-013 Pirfenidone GIPF001
NAC
Placebo
4 8 12 16 20 24 28 32 36 40 44 48 52 56 60
Week
Figure 1 Changes in FVC From Baseline in Prior IPF Clinical Trials
Recent data suggest that various patient subgroups would be expected to potentially exhibit differential response
to therapy These parameters will be used to a priori separate patients by a series of baseline characteristics
including
1 Higher enrollment FVC12
2 Typical vs atypical high-resolution computed tomography (HRCT) reading at baseline3
3 Recent vs more remote diagnosis (time from initial diagnosis of IPF le 1 year and gt 1 year)
4 Lower CPI score at enrollment4
5 Medical therapy for gastroesophageal reflux5
6 Ethnic background
7 Sex
8 Smoking history (current or ex-smoker vs never smoker) given potential impact on oxidant status6
9 Presence of emphysema gt 25 on HRCT
37 Rationale for Blinding of Treatments
The issue of treatment blinding was given a great deal of consideration with subject safety being the primary
concern After discussion among the Steering Group members it was decided that as long as subject safety
could be ensured blinding was necessary Blinding allows the study to
Have optimal scientific validity and potential to impact the standard of care for subjects
19
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Make objective assessments of treatment effects
Maintain clinical equipoise among investigators
Encourage subjects to have similar levels of contact with the medical community
Minimize the differential dropout rates across study arms
20
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
4 Methods 41 Inclusion Criteria
1 Age 35 to 85 years inclusive
2 FVC ge 50 of predicted (post-bronchodilator measurement from the screening visit)
3 DLCO ge 30 of predicted (hemoglobin corrected and altitude corrected if gt4000 ft above sea level)
4 Ability to understand and provide informed consent
5 Diagnosis of IPF according to a modified version of the ATS criteria le 48 months from enrollment The
date of diagnosis is defined as the date of the first available HRCT or surgical lung biopsy characteristic
of definite UIP
411 Subjects Shown to Have Usual Interstitial Pneumonia Pattern on Surgical Lung Biopsy
Subjects who have been shown to have UIP pattern on lung biopsy must have all of the following
1 Exclusion of other known causes of ILD such as drug toxicity clinically significant environmental
exposures or diagnosis of connective tissue diseases
2 Bibasilar reticular abnormalities with minimal ground glass opacities on HRCT scan
412 Subjects Who Have Not Undergone a Surgical Lung Biopsy
In addition to the criteria above these subjects must have radiological findings considered to be definite for the
diagnosis of UIPIPF
1 Bibasilar reticular abnormalities with minimal ground glass opacities
2 Honeycombing as the predominant feature and located in the peripheral lung bases
42 Diagnosis of IPF
Only subjects with definite IPF will be eligible for enrollment in this study We will utilize a combination of
clinicalphysiologic features HRCT and review of a clinically obtained surgical lung biopsy specimen to
establish the diagnosis of IPF An algorithm for the diagnosis is provided to guide entry into the protocol as
outlined in the inclusion and exclusion criteria (Figures 2 and 3) This multi-disciplinary approach uses
21
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
expertise from clinicians radiologists and pathologists Investigators at each site in conjunction with central
pathology will work together to establish the diagnosis of IPF This interactive approach to the diagnosis of IPF
increases the level of agreement between observers39
A subject with suspected ILD should be evaluated for secondary causes including but not limited to
environmental exposures drugs and systemic diseases Presence of any of these findings felt to be significant
enough to cause an ILD should disqualify the subject from entry into the trial
If secondary causes are absent an HRCT scan may be obtained If an HRCT of sufficiently high quality has
been obtained within the last 3 months that scan may be used for diagnosis In the appropriate clinical setting
the diagnosis of IPF can be made by the demonstration of a typical radiographic pattern on HRCT or by
demonstration of UIP pattern on a surgical lung biopsy The following criteria for a radiographic (ie
nonsurgical) diagnosis will be used In the absence of known exposures andor clinical associations attributable
to pulmonary fibrosis and in the appropriate clinical setting the presence of definite UIP pattern in HRCT
images is required to meet study criteria for the diagnosis of IPF
Figure 2 Diagnosis of Idiopathic Pulmonary Fibrosis in the IPFnet
22
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Figure 3 Pathology Flow Chart Surgical Lung Biopsy Diagnosis
Requirement for diagnosis
1 Clinical exclusion of other known causes (connective tissue diseases environmental and drug
exposures) of ILD
2 Radiographic HRCT with bibasilar reticular abnormality and honeycomb change with minimal
ground glass opacities
Appropriate clinical setting
1 Age gt 50 years
2 Insidious onset of unexplained dyspnea
3 Duration of illness for ge 3 months
4 Bibasilar inspiratory crackles
23
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Unlike the ATSERS consensus criteria published in 2000 bronchoscopy will not be required for diagnosis
This decision was made based on the experience of the IPFnet Steering Group members regarding the utility of
bronchoscopy in the diagnosis of IPF The presence of an atypical HRCT finding will require documentation of
a definitive diagnosis by surgical lung biopsy In fact this is in keeping with the recently published evidence
based guidelines for diagnosis and management of IPF13 As shown in Figure 3 central review of the pathology
data will be required for a diagnosis of IPF
We will not require central review of HRCT as several studies have shown that a confident local interpretation
of clinicalHRCT criteria as definite IPFUIP is associated with a high positive predictive value for finding UIP
at surgical lung biopsy (see Table 1) Differences in sensitivity in these series likely reflect subject selection as
Flaherty et al3 evaluated only UIP and nonspecific interstitial pneumonia (NSIP) while Raghu et al40 and
Hunninghake et al41 included a broader range of ILD
Table 1 Operating Characteristics of Local HRCT Review for Diagnosis of UIP
Researcher of Subjects Sensitivity () Specificity () PPV () NPV ()
Raghu et al 40
59 (29 UIP by SLB) 78 90 88 82
Hunninghake et al 41 91 (54 UIP by SLB)
74 81 85 67
Flaherty et al 3 96 (only NSIP amp UIP)
37 100 100 30
Abbreviations PPV positive predictive value NPV negative predictive value UIP usual interstitial pneumonia SLB surgical lung biopsy and NSIP nonspecific interstitial pneumonia
Furthermore an analysis of the HRCT scans from subjects enrolled in the GIPF-001 trial confirmed that local
site interpretations have a high congruity to a central radiology core In this multi-center study 263 HRCT
scans were read as definite IPF and a retrospective central radiology core review found 932 to be consistent
with IPF 42 We will also take several additional steps to insure that the local HRCT reads are accurate
including
1 A detailed training module has been developed and must be completed by each site radiologist before
site initiation
2 Clinical centers are to mail all HRCT scans to the HRCT core lab The first 10 HRCT scans from
subjects enrolled at each enrolling clinical center will be reviewed centrally to be certain that local reads
24
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
25
are congruent with a central interpretation If discrepancies are identified additional education will be
provided and HRCT scans will continue to be reviewed centrally until the central radiology core is
confident that the local center is performing appropriately
3 Random scans will be obtained from each center throughout the study to confirm that the local read
continues to agree with central interpretation If discrepancies are identified they will be addressed as in
2 above
In all cases if a subject has a surgical lung biopsy sample that sample will be reviewed by the local and central
pathologists Therefore the only cases that would not be subject to a direct central review process are those
where the HRCT meets the centrally defined criteria for an unequivocal diagnosis and a lung biopsy sample is
not available Table 2 below summarizes the possible combinations for making a diagnosis
Table 2 Combining HRCT and Pathology Interpretations to Determine if IPF is Present
HRCT Diagnosis Pathology Diagnosis Diagnosis of IPF
Definite UIP Definite UIP Yes
Definite UIP Probable UIP Yes
Definite UIP Possible UIP Yes
Definite UIP Not UIP No
Definite UIP Unavailable Yes
Consistent with UIP Definite UIP Yes
Consistent with UIP Probable UIP Yes
Consistent with UIP Possible UIP No
Consistent with UIP Not UIP No
Consistent with UIP Unavailable No
Inconsistent with UIP Any No
Abbreviations HRCT high-resolution computed tomography IPF idiopathic pulmonary fibrosis
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
UIP usual interstitial pneumonia Dx diagnosis 43 Exclusion Criteria
1 History of clinically significant environmental exposure known to cause pulmonary fibrosis
Occupational exposures such as asbestos or environmental exposure to organic dust such as occurs in
pigeon breeders may at times mimic the clinical and radiographic findings of IPF
2 Diagnosis of connective tissue disease felt by the principal investigator (PI) to be the etiology of the
interstitial disease Diagnosis of collagen-vascular conditions will be according to the published
American College of Rheumatology criteria As such the presence of any documented collagen-vascular
disorder or the presence of any suspicious symptom complex whether or not associated with
significantly abnormal rheumatological serologies will exclude the subject at the discretion of the PI
3 Extent of emphysema greater than the extent of fibrotic change (honeycombing reticular changes) on
HRCT scan
4 Forced expiratory volume in 1 second (FEV1)FVC ratio lt 065 at screening (postbronchodilator)
5 Partial pressure of arterial oxygen (PaO2) on room air lt 55 mm Hg (lt 50 mm Hg at Denver site)
6 Residual volume gt 120 predicted at screening (postbronchodilator)
7 Evidence of active infection
8 Significant bronchodilator response on screening spirometry defined as a change in FEV1 ge 12 and
absolute change gt 200 mL OR change in FVC ge 12 and absolute change gt 200 mL The percent
difference between the FVC (or FEV1) values will be calculated by taking the absolute value of the
difference and dividing it by the larger of the two FVC (or FEV1) values
9 Screening and enrollment post-bronchodilator FVC measurements (in liters) differing by gt 11 The
percent difference between the FVC values will be calculated by taking the absolute value of the
difference and dividing it by the larger of the two FVC values (eg the percent difference between FVC
measurements of 19 and 20 liters would be determined by taking the difference between the two (01
liters) and dividing by the larger of the two (20 liters) So 0120 = 5 and these FVC measurements
would not exclude the subject
10 Listed for lung transplantation ie the patient has completed the evaluation process has been accepted
as a candidate for transplantation at an appropriate center and is waiting to receive notification of an
available donor organ
11 History of unstable or deteriorating cardiac disease
12 Myocardial infarction coronary artery bypass or angioplasty within 6 months of screening
26
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
13 Unstable angina pectoris or congestive heart failure requiring hospitalization within 6 months of
screening
14 Uncontrolled arrhythmia
15 Severe uncontrolled hypertension
16 Known HIV or hepatitis C
17 Known cirrhosis and chronic active hepatitis
18 Active substance andor alcohol abuse (as determined by site PI)
19 Pregnancy or lactation (subjects who are pregnant or breastfeeding)
20 Known hypersensitivity to study medication
21 Any condition other than IPF that in the opinion of the site PI is likely to result in the death of the
subject within the next year
22 Any condition that in the judgment of the PI might cause participation in this study to be detrimental to
the subject or that the PI deems makes the subject a poor candidate
23 Any therapy directed at pulmonary fibrosis (excepting triple therapy of prednisone plus azathioprine
plus NAC) requires a 30-day washout period before randomized Triple therapy of lt= 12 weeks duration
in the past 4 years requires a 30-day washout period before randomization
24 History of triple therapy of prednisone plus azathioprine plus NAC for gt 12 weeksrsquo duration in the past
4 years or previous enrollment in the triple-therapy arm of the PANTHER-IPF study
44 Study Design and Study Visit
441 Study Design Summary
This study will be a randomized double-blind PL-controlled trial designed to assess the safety and efficacy of
NAC in subjects with newly diagnosed IPF
Subjects with mild to moderate IPF (defined as FVCpred ge 50 and DLCOpred ge 30) diagnosed within
the past 48 months will be enrolled Screening will continue until April 30 2012
27
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
The study will employ a 2-arm design with 11 randomization to NAC or PL Once enrolled subjects will visit
the clinical center at 15 weeks and 15-week intervals thereafter Each subject will be treated and followed for a
maximum of 60 weeks
During the 60-week visit subjects will be taken off all study agents Approximately four weeks after the final
dose of study agent is taken subjects will receive a safety phone call from the study site
442 Study Visits
Subjects who meet entry criteria will review the informed consent a written description of the purpose
procedures and risks of the study with the PI co-investigator or study coordinator and all questions will be
answered The informed consent form will be signed by the subject at screening No protocol-specific
procedures will be performed until the subject has signed and dated an informed consent form This includes the
screening procedures
4421 Screening
Once informed consent is obtained subjects may immediately begin the screening process or may return within
28 days of consent In the event a study subject has been clinically evaluated at the study site by an IPFnet study
physician and has performed testing within three weeks for this clinical evaluation that meets guidelines
provided in the IPFnet PANTHER-IPF Manual of Operating Procedures (MOOP) this testing may be used to
satisfy the following screening criteria medical history physical exam arterial blood gas (ABG) with A-a
gradient vital signs with oximetry body height and weight spirometry DLCO lung volumes and HRCT scan
Allowing the use of previously performed test results that meet study guidelines for the screening visit is
intended to permit subjects easier access to study entry to prevent subjects from repeating testing that has been
performed within the study window and to decrease risks to subjects from repeated exposure to procedures
such as arterial puncture and HRCT
The following procedures will be performed at screening
Medical history and a physical examination
28
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Measure height and weight
Serum pregnancy test (if applicable)
Measure vital signs including oximetry
Blood draws performed and the following analyses conducted
o Hematology (red cell count white cell count hemoglobin hematocrit cell indices differential
platelet count)
o Blood chemistries according to central laboratory protocol (see Section 410 Laboratory
Testing)
o Beta human chorionic gonadotropin (serum) pregnancy test (in women of childbearing potential)
o Urinalysis
Pulmonary Function Tests (PFTs) including spirometry pre- and post- bronchodilator and postshy
bronchodilator measurement of lung volumes and measurement of hemoglobin adjusted diffusing
capacity
Measure ABGs
HRCT if a satisfactory scan has not been performed on the subject within 3 months of screening (see
PANTHER-IPF MOOP for more details)
Surgical lung biopsies (if applicable) reviewed by local and central pathology departments
Current medications If required a washout period discussed with the subject and initiated at this visit
4422 Enrollment
The enrollment visit is expected to take place within eight weeks of the screening visit Enrollment visit
activities include
Measure vital signs including oximetry
Measure height and weight
Serum pregnancy test (if applicable)
If consent has been given blood will be drawn and a urine specimen collected for the bio-specimen
repository
Spirometry (post-bronchodilator)
Measure 6MWT with Borg Dyspnea Scale
29
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Collect Quality-of-life (QOL) data using the SF-36 EuroQol Investigating Choice Experiments for
Preferences of Older People Capability Instrument (ICE CAP) and SGRQ
Female subjects complete Gender Substudy questionnaire
Dyspnea status collected using the UCSD SOBQ
Evaluate Acute Exacerbation (AEx)
Review of any Adverse Events (AEs)
Review of concomitant medications
Subject receives diary and instructions on its purpose and proper use
Subject receives supply of study drug sufficient to last until his or her 15-week study visit
See the Schedule of Assessments (Table 3) for more details Subjects with screening and enrollment postshy
bronchodilator FVC measurements (in liters) differing by more than 11 are not eligible to be enrolled in the
study
Subjects will be asked to provide a physician of record This physician will be considered the subjectrsquos primary
care provider (PCP) and if the subject agrees the PCP will be informed by letter of the subjectrsquos enrollment in
the trial The subject will be informed that his or her ongoing medical care should be received from the PCP
The PCP will be informed of any safety issues identified by the study staff The PCP will also be given
information regarding communication with study personnel about pertinent health issues or clinic encounters
the subject may have
4423 Week 15
The week 15 visit is expected to occur within +- 14 days of the subjectrsquos scheduled visit time (eg the week 15
visit should occur anytime between 13 and 17 weeks after starting study drug Week 15 activities include
Measure vital signs with oximetry
Measurement height and weight
Serum pregnancy test (if applicable)
Spirometry (post-bronchodilator) measurement
Review of AEs
Evaluate for AEx
30
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Review concomitant medications
If consented draw blood and collect urine specimen for the biospecimen repository
Subjects return used and unused study drug for the visit
Review study diary and a new study diary will be given
Provide additional supply of study drug sufficient to last until the next scheduled visit
4424 Week 30
The week 30 visit is expected to occur within +- 14 days of the subjectrsquos scheduled visit time (eg the week 30
visit should occur anytime between 28 and 32 weeks after starting study drug) Week 30 activities include
Physical examination
Measure vital signs with oximetry
Measure height and weight
Laboratory values (complete blood count [CBC] and serum chemistries)
Serum pregnancy test (if applicable)
Measure spirometry (post-bronchodilator)
6MWT with Borg scale
DLCO
Review of AEs
Evaluate for AEx
Review concomitant medications
Complete all QOL and dyspnea questionnaires (EuroQol ICE CAP SF-36 SGRQ and UCSD SOBQ)
If consent has been given blood will be drawn and a urine specimen collected for the biospecimen
repository
Review study diary
Subjects return used and unused study drug for the visit
Provide additional supply of study drug sufficient to last until the next scheduled visit
4425 Week 45
31
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
The week 45 visit is expected to occur within +- 14 days of the subjectrsquos scheduled visit time (eg the week 45
visit should occur anytime between 43 and 47 weeks after starting study drug) Week 45 activities include
Measure vital signs with oximetry
Measure height and weight
Serum pregnancy test (if applicable)
Measure spirometry (post-bronchodilator)
Review of AEs
Evaluate for AEx
Review concomitant medications
If consent has been given blood will be drawn and a urine specimen collected for the biospecimen
repository
Subjects return used and unused study drug for the visit
Study diary reviewed
Provide additional supply of study drug sufficient to last until the next scheduled visit
4426 Week 60 (Early Withdrawal or Final Treatment Visit)
At week 60 or at subject withdrawal from the study (premature by study doctor or subjectrsquos decision) a final
treatment visit will occur At this final treatment visit subjects will discontinue NACPL abruptly Week 60
activities also include
Physical examination
Measure vital signs with oximetry
Measure height and weight
Laboratory values (complete blood count [CBC] and serum chemistries)
Spirometry (post-bronchodilator) measurement
6MWT with Borg scale measurement
DLCO
Lung volumes
ABG
Review of AEs
32
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Evaluate for AEx
Review concomitant medications
Subjects will complete all QOL and dyspnea questionnaires (EuroQol ICE CAP SF-36 SGRQ and
UCSD SOBQ)
If consent has been given blood will be drawn and a urine specimen collected for the biospecimen
repository
Subjects return used and unused study drug for the visit
Study diary reviewed
4427 Final Site Visit ndash FVC drop confirmation
In the event that the subject has a recorded FVC drop of gt10 from baseline at the final treatment visit and the
subject has not had a confirmation of such a drop at a previous study visit the subject should return to the
clinical site 6 to 8 weeks after the final treatment visit During this visit a post-bronchodilator spirometry test
will be performed This FVC measurement will be evaluated according to section 521 of this protocol
4428 Final Visit ndash Telephone Follow-up
Four weeks following the final dose of study medication subjects will receive a telephone call from the study
coordinator to ensure that there are no side effects and to follow up on any ongoing adverse events (AEs)
4429 Phone Contact Between Visits
At week 2 and each month that a subject does not have a scheduled clinical center visit his or her study
coordinator will contact him or her at least once by telephone to
Inquire if the subject has had any hospitalizations events that might be considered an AE or any events
significant enough to warrant an out-of-cycle visit to the clinical center
Remind subjects of their current dosage levels and confirm that the subject understands them
Address any questions or concerns the subject might have regarding other aspects of the study
Assess adherence to the treatment regimen by reviewing diary data verbal review of medications taken
including nutritional supplements
33
34
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Table 3 Schedule of Assessments
Procedure Screening Visit 0
Enrollment Visit 1
Week 15 Visit 2
Week 30Visit 3
Week 45 Visit 4
Week 60 Early
Withdrawal Visit 5
Final1
Visit (via phone)
Informed consent X
Medical history X
Inclusionexclusion criteria X
Serum pregnancy test (if applicable) X X X X X
Review of lung biopsy X
Arterial Blood Gas X X
6-Minute Walk Test
X
X X
Physical examination X X X
Vital signs with oximetry X X X X X X
Body height and weight X X X X X X
Complete Blood Count X X X
Chemistry panel X X X
Monitor Lab Values X X X
Urinalysis X Specimen repository substudy blood draw and urine collection (if consented)
X
X X X X
HRCT (if not completed within three months) X
Spirometry (pre- and post-bronchodilator) X
Spirometry (post-bronchodilator only) X X X X X
DLCO (post-bronchodilator only) X X X
Lung volumes (post-bronchodilator only) X
X
Evaluate for acute exacerbation X X X X X
Review Adverse Events X X X X X X
Review concomitant meds X X X X X X
Dispense subject diary X X X X
Review subject diary X X X X X
Dispense study agent X X X X
Gender Substudy questionnaire (female subjects only) X
EuroQol ICECAP UCSD SOBQ SGRQ SF-36 X X X
Abbreviations DLCO diffusing capacity of the lung for carbon monoxide QOL Quality of Life ICECAP Investigating Choice Experiments for Preferences of Older People UCSD SOBQ University of California Shortness of Breath Questionnaire SGRQ St Georgersquos Respiratory Questionnaire SF-36 Short Form 36 Health Survey
1Follow-up visit via phone will occur four weeks after final dose of study medication
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
45 Dose Justification
The general philosophy for determining dosing levels was to apply previously examined
treatment regimens With the focus of the study being to establish a standard of care for
mildmoderate IPF subjects the goal was to develop flexible yet standardized treatment rules that
allow for the temporary or permanent withholding of one or more components of treatment when
necessary Subjects developing laboratory abnormalities or symptoms that result in
discontinuation of one or more components of study treatment may continue on the other
components as long as there is no contraindication for this Complete follow-up is important for
the validity of any study As a strategy to maintain protocol adherence we are using a treatment
regimen that will detect potential side effects and prompt interventions proactively in the interest
of patient safety In addition subjects who permanently stop study medications during the course
of the study are encouraged to continue in the study completing all scheduled visits and tests
451 Rationale for N-acetylcysteine Dosing
To our knowledge there have been no IPF studies to correlate clinical outcome measures with
different dosages for NAC The dosage chosen is based on the IFIGENIA study However BAL
lung GSH levels from subjects with IPF have been augmented with the use of oral NAC at 600
mg 3 times per day In addition lung GSH levels have been associated with improved
PFTs212227 The dose chosen for this study was based on previous data including the IFIGENIA
study30
4511 Dosing of N-acetylcysteineplacebo
Dosing of NACPL will be 600 mg orally 3 times a day (1800 mgday)
4512 Reasons to Discontinue N-acetylcysteineplacebo
NACPL may be temporarily or permanently discontinued for the duration of the study for
gastrointestinal symptoms or dermatologic reactions
35
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Temporarily discontinue (hold) oral NACPL for subjects requiring inpatient admission for acute
exacerbation (AEx) or other conditions Resume NACPL after discharge
36
37
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
452 Dosage Algorithms
Dosage Adjustment Algorithm 1 NACPL Dose Modifications for Gastrointestinal Symptoms Nausea Vomiting Abdominal Discomfort Diarrhea
GI Symptoms determined by the PI to be clinically significant Nausea Vomiting Abdominal Discomfort Diarrhea
NACPL Temporarily dc (HOLD) x 3 Days
Monitor symptoms intervene as clinically indicated (eg fluid replacement antidiarrhea or antinausea medication)
Monitor or lab PRN
Are symptoms resolving after 3 days NO
Symptoms NOT resolving after 3 days of holding study medication Assessmentmanagement per clinical
discretion of investigator
Likely not study medication discuss resuming study medication with medical monitor when symptoms resolved
YES
Temporarily dc (HOLD) NACPL for 4 additional days (total hold 1 week) then NACPL Resume 600 MG TID
Did symptoms recur
YES
STOP NACPL for
duration of study
NO
NACPL No Change
38
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Dosage Adjustment Algorithm 2 NACPL Dose Modifications For Dermatologic Reactions
Dermatologic Reactions (Not Acneiform) ge Grade 2 Grading per Common Terminology Criteria for
Adverse Events V30 (httpctepcancergov) For example Grade 1 RASHDESQUAMATION Macular or papular eruption or erythema without associated symptoms Grade 2 RASHDESQUAMATION Macular or popular eruption or erythema with pruritus or other associated symptoms localized desquamation or other lesions covering lt50 of body surface area
NACPL Temporarily dc (HOLD) x 3 days
Are symptoms resolving after 3 days
NO Symptoms not resolving after 3 days of holding study medication Assessmentmanagement per clinical discretion of investigator Likely not study medication Discuss resuming study medication with medical monitor when symptoms
resolved YES
Temporarily dc (HOLD) NACPL for 4 additional days (total hold 1 week) then NACPL resume 600 MG TID
Did symptoms recur
YES
STOP NACPL for
duration of study
NO
NACPL No change
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
46 Contraindications Precautions and Side Effects of Study Medications
461 Contraindication
Contraindication to NAC is known hypersensitivity to it
462 Precautions
Concomitant administration of oral NAC and antibiotics has shown a slightly reduced absorption
of cephalexin and a slight increase in erythromycin serum levels NAC contains free sulfhydryl
groups There is no evidence that individuals sensitive to sulfa drugs are sensitive to NAC
The NAC preparation being administered in this study contains 20 mg of aspartame Because of
the phenylalanine component of aspartame individuals with phenylketonuria should avoid or
restrict aspartame intake to avoid increased blood levels of phenylalanine Because of this risk
labeling is required on all products containing aspartame
463 Side Effects
Side effects of NAC range from common to serious See Table 4
39
40
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Table 4 Side Effects of NAC
Undesirable Effects
System-organ class Uncommon
(gt11000 lt1100)
Rare
(gt110000 lt11000)
Very rare
(lt110000) Not known
Immune system disorders Hypersensitivity Anaphylactic shock
reaction
Nervous system disorders Headache
Ear and labyrinth disorders Tinnitus
Cardiac disorders Tachycardia
Vascular disorders Hemorrhage
Respiratory thoracic and
mediastinal disorders
Bronchospasm
Dyspnea
Gastrointestinal disorders
Vomiting diarrhea
stomatitis abdominal
pain nausea
Dyspepsia
Skin and subcutaneous tissue
disorders
Urticaria rash
angioedema itching
General disorders and
administration site conditions Pyrexia
Investigations Reduced arterial
pressure Face edema
In very rare cases the onset of severe skin reactions such as Stevens-Johnson syndrome and Lyell syndrome was reported to have a temporal relationship with N-acetylcysteine administration Although in most cases at least another suspect drug probably most involved in the genesis of the above mentioned mucocutaneous syndromes has been identified in case of mucocutaneous alterations it is appropriate to contact onersquos doctor and the administration of N-acetylcysteine should be immediately discontinued
Some studies confirmed a reduction of platelet aggregation during N-acetylcysteine administration The clinical significance of these findings has not been defined yet [Source Fluimucil Investigator Brochure]
47 Recruitment Procedures
Subjects recruited for this study will be established patients of the investigators or physician- or
self-referred to participating clinical centers in the IPFnet Each clinical center within IPFnet has
a well-developed infrastructure of local pulmonologists within the surrounding geographic area
These pulmonologists are kept informed of ongoing IPF clinical trials and regularly refer
subjects to studies conducted at IPFnet clinical centers
Additional steps will be taken to inform clinicians of the trials in progress within IPFnet
including presentations at faculty staff meetings at local hospitals medical grand rounds and
national conferences direct mail notification monthly faxes and advertisement of network trials
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
in pulmonary journals Clinical center patients previously diagnosed with IPF will be notified of
the trials by mail whenever possible
Recruitment of minorities and women will be monitored by the DCC and DSMB If necessary
additional recruitment efforts will be made at specific centers to ensure that the aggregate subject
sample contains appropriate representation of women and minorities
48 Study Procedures
The following procedures are detailed in the PANTHER-IPF MOOP accompanying this
protocol
1 PFT
2 ABG
3 HRCT scan of the chest (including imaging of pulmonary arteries)
4 CBC and serum chemistries
5 Pregnancy test
6 6MWTBorg Dyspnea Scale
7 QOL questionnaires (EuroQol HAD SF-36 SGRQ and ICE CAP)
8 UCSD SOBQ
9 Gender Substudy Questionnaire
All assessments of PFTs will be conducted by study personnel not directly involved in the
treatment of the subjects
481 Biological Specimen Management
4811 Biological Specimen Sample Management
Subjects at clinical centers participating in the specimen repository substudy who consent to
having blood drawn for research purposes and for the banking of blood blood components and
other biologic specimens (urine and BAL fluid) will have approximately 405 mL of blood
41
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
drawn 17 mL blood drawn for DNA and 20 mL of urine collected at enrollment visit Subjects
will have approximately 50 mL of blood drawn and 20 mL of urine collected at each 15-week
follow-up visit Blood specimens will be separated according to PANTHER-IPF MOOP
guidelines into the following components for banking in the repository serum plasma and
DNA Coding of all biologic specimens for the repository will be performed by study staff at the
clinical center The samples will be processed per PANTHER-IPF MOOP guidelines aliquoted
labeled with barcode labels and stored at -70degC at the clinical center and shipped to the central
repository
The only subject identifiers will be a sample ID number and subject initials This sample ID will
be linked in the IPFnet DCC clinical database to subject information No subject information will
be transferred to the biological-specimen database
The subjectrsquos samples may be used for approved sub-studies relating to human disease
including but not limited to IPF The studies for which an individualrsquos samples will be made
available will be determined by the subjectrsquos answers to questions on the biological-sample
informed consent form The subjects can choose to make their samples available for all options
or any combination Samples will be made available to researchers only with IPFnet Steering
Group approval until such time as the samples are made public through the NHLBI repository
49 Concomitant Medications
Concurrent treatment with FDA-approved therapy for IPF is allowed Colchicine may be used
for treatment of gout Temporary treatment with oral or IV corticosteroids for clinical worsening
or suspected AEx is permitted Nutritional supplements containing NAC are not allowed
410 Laboratory Testing
Clinical laboratory parameters will be assessed at screening and at the end of the study The
following tests will be performed at the two time points specified in the protocol chemistry (AG
ratio ALT [SGPT] AST [SGOT] albumin alkaline phosphatase amylase bilirubin-direct
42
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
bilirubin-indirect bilirubin-total BUN BUNcreatinine ratio calcium carbon dioxide
cholesterol-total chloride CPK-total creatinine GGT globulin glucose iron-total LDH
lipase magnesium phosphorus-inorganic potassium protein-total sodium TIBC triglycerides
uric acid) and hematology (red blood cell count WBC count hemoglobin hematocrit cell
indices differential platelet count)
411 Blinding of Study Drugs
Subjects and caregivers will be blinded to study treatment Every subject will receive NAC or
matching PLs at every study visit from the baseline visit to the week-45 visit No study agent
will be dispensed at the week-60 visit
43
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
5 Study Endpoints
51 Primary Study Endpoint
The primary endpoint will be the change in serial measurements of FVC over the study period
52 Secondary Study Endpoints
521 Time to Disease-progression
The time-to-death or a 10 decline in FVC will be defined as the time-to-disease progression
The 10 decline in FVC from enrollment must be confirmed on 2 consecutive visits no less than
6 weeks apart For subjects with 2 consecutive visits with a 10 decline in FVC the time-toshy
disease progression will be defined as the time interval between enrollment and the initial visit
with a 10 FVC decline For subjects who experience disease progression the study doctor will
determine whether or not the subject will remain in the study
522 Acute Exacerbations
The following 3 criteria will define AEx in subjects with acute worsening of their respiratory
conditions
1 Clinical (all of the following required)
A) Unexplained worsening of dyspnea or cough within 30 days triggering unscheduled
medical care (eg emergency room clinic study visit hospitalization)
B) No clinical suspicion or overt evidence of cardiac event pulmonary embolism or deep
venous thrombosis to explain acute worsening of dyspnea
C) No pneumothorax
44
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
2 RadiologicPhysiologic (A and B required)
A) New ground glass opacity or consolidation computed tomography (CT) scan OR new
alveolar opacities on chest x-ray
B) Decline of ge 5 in resting room air SpO2 from last recorded level OR decline of ge 8 mm
Hg in resting room air PaO2 from last recorded level
3 Microbiologic (all of the following required)
A) No clinical evidence for infection (ie absence of grossly purulent sputum fever gt 39degC
orally)
B) Lack of positive microbiological results (if done) from lower respiratory tract defined as
(1) Clinically significant bacterial growth on sputum or endotracheal aspirate cultures
(2) Quantitative culture by protected brush specimen ge 103 cfumL or BAL ge 104 cfumL
(3) The presence of specific pathogens on stains of any of the above
C) Lack of positive pathogen in blood cultures (if done)
Identification of Acute Exacerbations
All subjects will be educated about the importance of identifying AExs At the time of
enrollment subjects will be told about the possibility of developing acute symptomatic
worsening that might represent an AEx of IPF and instructed to contact their study clinical
center coordinator within 48 to 72 hours of the apparent event
All subjects will be contacted by phone monthly and questioned about any change in dyspnea or
cough and any interim clinic visits or hospitalizations Finally as part of the IPFnet outreach to
community referring physicians the importance of AExs will be emphasized When a subject is
identified who meets criterion 1A this will trigger the collection of additional clinical data to
evaluate a suspected AEx These data will be collected as part of standard clinical care (ie this
protocol does not require collection of all items) The additional items to be collected for
suspected AEx include
IPFnet AEx case report form (eCRF) (required)
45
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Chest x-ray CT scan withwithout pulmonary angiogram (reports should be faxed and
followed by the hard copiesdiscs)
Oxygen saturation (pulse oximetry)
ABG
Respiratory cultures (sputum endotracheal aspirate lavage)
Blood cultures
Clinichospital records related to the event
All potential cases of AEx will be reviewed by the clinical center PI first and a decision on
whether the case may represent an AEx will be made If AEx is suspected the case will be sent
to the IPFnet adjudication committee which will assign a final diagnosis (see Table 5) If there is
disagreement among members the majority opinion will be recorded
During episodes of suspected AEx as determined by the individual clinical center investigator
subjects will remain blinded and in the study
Table 5 Final Diagnoses in Evaluation of Suspected Acute Exacerbations
Definite acute exacerbation All criteria met no alternative etiology
Unclassifiable acute worsening
Insufficient data to evaluate all criteria no alternative etiology
Not acute exacerbation Alternative etiology identified that explains acute worsening
Management of the suspected AEx will be at the discretion of the treating physician Standard of
care generally involves evaluation for respiratory infection pulmonary embolism cardiac events
and pneumothorax and treatment with IV corticosteroids
Study drugs will be resumed at pre-suspected AEx doses after subjects clinically improve as
confirmed by the local PI All subjects should be seen at the clinical center within 2 to 4 weeks
of recovery for measurement of post-bronchodilator FVC (see Figure 4) Subjects unable to
return to the clinical center after suspected AEx due to medical frailty (eg continued
46
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
institutionalization progressive disability) will be categorized as failing to maintain FVC
response in secondary analyses
Suspected AEx (PI determined)
Hold study drug Treat AEx
(Attending physician determined)
Alive but unable to continue due to
medical frailty
Dead
Alive and able to continue
Site reviewvisit
Restart study drug
FVC within 2-4 weeks
Figure 4 Acute Exacerbation Flow Chart
523 Respiratory Infections
An upper respiratory infection will be defined as
Change in sputum discoloration
Increased cough of no more than 14 daysrsquo duration
A lower-respiratory infection (pneumonia) will be defined as new segmental or lobar airspace
opacities visualized by image studies (chest radiograph or HRCT) in addition to any of the
following
Positive pathogencultures in good sample of sputum or lower-airway secretions retrieved
by fiberoptic bronchoscope
Fever gt 39degC or gt 100degF
Leukocytosis gt 12000 (unexplained no increase in dose of corticosteroids)
47
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
524 Maintained FVC Response
Subjects with follow-up FVCpred measurements at or above their baseline FVCpred level
will be classified as having maintained FVC response Subjects with reduced FVCpred levels
or missing data for any reason including death or medical frailty will be classified as having not
maintained FVC response The FVCpred value is used because unadjusted FVC measurements
are expected to decline with age
48
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
6 Safety Evaluations and Procedures
61 Adverse Events
During a clinical trial the reporting of adverse experience information can lead to important
changes in the way a new treatment is developed as well as provide integral safety data
611 Definitions
An adverse event (AE) is any untoward medical occurrence in a subject or clinical investigation
subject who was administered a pharmaceutical product The AE does not necessarily have to
have a causal relationship with the drug administered An AE can be any unfavorable and
unintended sign (including an abnormal laboratory finding) symptom or disease temporarily
associated with the use of a medicinal product whether or not considered to be related to the
medicinal product Diseases signs symptoms or laboratory abnormalities already existing at
enrollment are not considered AEs unless they worsen (ie increase in intensity or frequency)
Surgical procedures themselves are not AEs they are therapeutic measures for conditions that
require surgery The condition for which the surgery is required may be an AE Surgical
procedures planned before randomization and the conditions necessitating the surgery are not
AEs
A serious adverse event is any untoward event that
Is fatal
Is life-threatening
Requires inpatient hospitalization or prolongation of existing hospitalization with the
following exceptions
o Preplanned (before the study) hospital admissions unless the hospitalization is
prolonged
o Planned admissions (as part of a study eg routine biopsies)
o Hospitalization lasting lt 24 hours
49
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
o Hospitalization for elective procedure
o Emergency room visits
Results in persistent or significant disability or incapacity
Is a congenital anomaly or birth defect
Important medical events that may not result in death be life-threatening or require
inpatient hospitalization may be considered serious adverse events (SAEs) when based
on appropriate medical judgment they may jeopardize the subject and may require
medical or surgical intervention to prevent one of the outcomes listed above
Life-threatening means that the subject was in the view of the investigator at immediate risk of
death from the AE as it occurred It does not include an AE that had it occurred in a more severe
form might have caused death
Persistent or significant disabilityincapacity means that the event resulted in permanent or
significant and substantial disruption of the subjectrsquos ability to carry out normal life functions
Causality
A reasonable possibility means the AE may have been caused byrelated to the study drug A
perceived or real lack of efficacy does not satisfy the definition of relatedness
612 Adverse Event (AE) Reporting
For the PANTHER-IPF trial all AEs (serious and nonserious) occurring from randomization
through final study visit (4 weeks after final dose of all study medication) will be recorded on the
AE page of the case report form (CRF)
6121 Serious Adverse Events (SAE) Reporting
For this trial all deaths and all SAEs which occur from randomization through final study visit
must be entered within the EDC system via the SAE eCRF page within 24 hours of the
investigative sitersquos knowledge of the event It is the responsibility of the clinical center
50
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
investigator to provide a causality assessment of the event for each study medications based upon
the information available at the time of the report It is understood that complete information
about the event may not be known at the time the initial report is submitted In the event the EDC
system is not accessible to the site at the time of event reporting investigative sites will complete
and forward a paper back-up SAE form to DCRI Safety Surveillance for processing
DCRI Safety Surveillance
Telephone 1-919-668-8624 or 1-866-668-7799 (toll free)
Fax 1-919-668-7138 or 1-866-668-7138 (toll free)
The investigator must complete and submit follow-up SAE information via the eCRF when
important new or follow-up information (eg final diagnosis outcome results of specific
investigations) becomes available Follow-up information should be submitted according to the
same process used for reporting the initial event as described above All SAEs will be followed
until resolution stabilization or 30 days after the subject has completed the final visit (4 weeks
after the final dose of study medication) whichever occurs first The investigator is responsible
for reporting SAEs to their institutional review board (IRB) per site specific IRB reporting
guidelines
6122 Regulatory Reporting
AEs that are serious study drug related and unexpected will be reported to the regulatory
authorities The DCRI Safety Surveillance medical monitor will perform a medical review of all
SAEs submitted and evaluate for ldquounexpectednessrdquo DCRI Safety Surveillance will prepare
MedWatch reports for those events identified as serious study drug related and unexpected as
determined by Safety Medical Monitor
DCRI Regulatory Services will submit all unexpected study drug-related SAEs as per 21 CFR
32 DCRI Safety Surveillance will provide a safety alert letter to the NHLBI DSMB and DCC
clinical operation (for distribution to sites) within 15 days of initial receipt of the information
51
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Investigators are responsible for promptly reporting these events to their reviewing IRBs
according to site specific IRB reporting guidelines
62 Clinical Medical Monitoring
There will be an unblinded physician at the IPFnet DCC serving as medical monitor The
medical monitor will be available to assist with questions about dosage adjustments of study
medications including discontinuation or resumption of medications
63 Unblinding Procedures
Unblinding of subjects or investigators to subject treatment is strongly discouraged For ongoing
clinical management all subjects should be presumed to be receiving ldquoactiverdquo study drug To
ensure the subjectrsquos safety the study treatment will be dose-adjusted based on laboratory test
results clinical findings and symptoms
The IPFnet DCC medical monitor and PANTHER-IPF co-chairs Drs Ganesh Raghu and
Fernando Martinez will be available to the study physicians to discuss study drug management
on a case-by-case basis Un-blinding will be considered ONLY when the knowledge of subject
treatment assignment is ABSOLUTELY ESSENTIAL for subject safety and after discussion of
the subjectrsquos case with the medical monitor and either Dr Raghu or Dr Martinez Unblinding of
study treatment should be minimized during the conduct of the trial In those cases where it is
felt to be medically necessary the DCC medical officer will communicate directly with the
managing physician to minimize unblinding of study personnel
52
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
7 Study Drug Procedures
At the baseline 15-week 30-week and 45-week study visits subjects will receive a supply of
study drug sufficient to last until the next visit at which study drug will be dispensed
53
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
8 Data Management
81 Hardware and Software Configuration
811 Hardware and Database Software
Data will be stored in an Oracle database system Oracle has advantages of processing efficiency
and smooth linkage with other software systems The application and database will be hosted on
Solaris Unix servers at the IPFnet DCC
812 Statistical Software
SAS will be used as the principal application for the management of analysis data files and
statistical computations S-Plus will be used to provide supplementary functions as needed
813 Access Control and Confidentiality Procedures
Access to databases will be controlled centrally by the IPFnet DCC through user passwords
linked to appropriate privileges This protects the data from unauthorized changes and
inadvertent loss or damage
814 Security
Database and Web servers will be secured by a firewall and through controlled physical access
Oracle has many security features to ensure that any staff member accessing the database has the
proper authority to perform the functions he or she requests of the system Within the secondary
SAS databases Unix group-access control maintains similar security The Sun workstation login
is secured by extensive user-password facilities under Unix
54
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
815 Back-up Procedures
Database back-up will be performed automatically every day and standard IPFnet DCC policies
and procedures will be applied to dictate tape rotation and retention practices
816 Virus Protection
All disk drives that provide network services and all user computers will be protected using
virus-scanning software Standard IPFnet DCC policies will be applied to update these protection
systems periodically through the study
82 Sources of Data
821 Design and Development
The IPFnet DCC will be responsible for development of the electronic case report forms
(eCRFs) development and validation of the clinical study database ensuring data integrity and
training clinical center staff on applicable data management procedures A web-based distributed
data entry model will be implemented This system will be developed to ensure that guidelines
and regulations surrounding the use of computerized systems used in clinical trials are upheld
The remainder of this section provides an overview of the data management plan associated with
this protocol
822 Data Collection Forms
The data collection process consists of direct data entry at the study clinical centers into the EDC
system(s) provided by the DCC A data collection worksheet will be provided to clinical centers
for recording data in the event the EDC system is unavailable Data entry of the eCRFs should
be completed according to the instructions provided and project specific training The
investigator is responsible for maintaining accurate complete and up-to-date records and for
ensuring the completion of the eCRFs for each research participant
55
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
823 Data Acquisition and Entry
Data entry into eCRFs shall be performed by authorized individuals Selected eCRFs may also
require the investigatorrsquos written signature or electronic signature as appropriate Electronic
CRFs will be monitored for completeness accuracy and attention to detail during the study
824 Data Center Responsibilities
The IPFnet DCC will 1) develop a data management plan and will conduct data management
activities 2) provide final eCRFs for the collection of all data required by the study 3) develop
data dictionaries for each eCRF that will comprehensively define each data element 4) conduct
ongoing data monitoring activities on study data 5) monitor any preliminary analysis data
cleanup activities and 6) rigorously monitor final study data clean up
825 Data Editing
Completed data will be entered into the IPFnet DCC automated data acquisition and
management system If incomplete or inaccurate data are found a data clarification request will
be generated and distributed to clinical centers for a response Clinical centers will resolve data
inconsistencies and errors and enter all corrections and changes into the IPFnet DCC automated
data acquisition and management system
826 Training
The training plan for clinical center staff includes provisions for training on assessments eCRF
completion guidelines data management procedures and the use of computerized systems
56
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
9 Study Design and Data Analysis
91 General Analytic Considerations
All primary analyses will be based on intent-to-treat (ITT) principles using all randomized
subjects Baseline factors across groups will be compared using mean (standard deviation) and
median (25th and 75th percentiles) summary measures Kaplan-Meier curves will be used to
display event rates Due to clinical interest in departures from both sides of the null hypothesis
all test statistics will be 2-sided
Reasonable caution needs to be taken when conducting multiple analyses on key clinical
subgroups For subgroup analyses a conservative significance level of 0001 will be used for all
interaction tests Thus subgroup comparisons will be considered exploratory unless the p-value
from the interaction test is smaller than 0001
92 Randomization Blinding and Reporting of Results
A permuted block-randomization scheme will be created with varying block sizes stratified by
clinical center Once a subject has completed the screening and baseline period and evaluation
for inclusionexclusion criteria the randomization process will begin Subjects will be
randomized to receive NAC or matching placebo with equal probability (11) via telephone
contact with a central interactive voice response system (IVRS) using a toll-free randomization
number On the day of randomization after the subject has successfully met all inclusion and
exclusion criteria the investigator or designee will call the central randomization number to
obtain the assigned kit randomization numbers for that subject At each subject visit the
investigator or designee will call the central randomization number to obtain the new kit
randomization numbers for resupply of the subject For resupply of the clinical center the IVRS
will monitor minimal volume of a kit type andor expiration date and will automatically notify
the pharmacy
57
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
The trial results will be reported according to guidelines specified in the CONSORT statement
A flow diagram describing screening recruitment randomization dropout and vital status will
be included in the primary manuscript AEs and efficacy data will be presented for all treatment
groups Adherence dropout and lost to follow-up will be carefully examined across all treatment
groups Analyses of safety will be based on data from all randomized subjects who received at
least one dose of study drug
93 Stratification
Subjects will be distributed to the two treatment arms in a 11 allocation ratio Stratification
blocks will be based on clinical centers
94 Specification of the Primary Analyses
A mixed model repeated measures (MMRM) analysis described in section 95 will be used to
compare differences in the slope of FVC measurements across the treatment groups Response
variables are values of the FVC measured at baseline and every 15 weeks until study completion
Variables in the model will include treatment time and time by treatment age sex race and
height Contrast estimates of differences in slopes of treatment over time (along with confidence
intervals) will be used to estimate the treatment effect The validity of this model in terms of
meeting modeling assumptions will be assessed via standard modeling diagnostics and goodness-
of-fit measures Based on the MMRM framework missing FVC data will not be imputed for the
primary analysis
95 Analysis of Longitudinal Endpoints
A common goal in clinical trials is to specify models that are easily implemented and
reproducible by independent data analysts On the other hand the models should have proper
statistical behavior in terms of low bias and high precision Many common approaches to
longitudinal data analysis including last observation carried forward (LOCF) imputation rely on
the missing completely at random (MCAR) assumption However the MCAR assumption is
58
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
unlikely to hold in many clinical trials because missing data are often related to disease
progression and prognosis A more reasonable assumption missing at random (MAR) specifies
that the complete data distribution can be modeled using only the observed data The likelihood-
based MMRM approach is valid under the more general MAR assumptions These models will
be applied to analyze the longitudinal data secondary endpoints
The advantages of MMRM analysis are that all important characteristics of the model can be preshy
specified standard software can be used to implement the models and results are based on ITT
principles43 In addition the MMRM approach offers superior control of Type I and Type II
errors compared with the LOCF approach
Response variables are values of the PFTs measured at enrollment and every 15 weeks until
study completion and 6MWT values measured at baseline week 30 and week 60 Covariates are
treatment time time by treatment and key baseline risk factors Contrasts (along with
confidence intervals) of treatment by time will be used to estimate the treatment effect
The correlation structure involves multiple pieces including measurement errors random
variation and interindividual variability For the longitudinal data analyses an unstructured
correlation matrix for within-subject errors will be assumed Other correlation structures
including compound symmetry will be examined as needed A careful examination of reasons
for study discontinuation will be conducted to assess the validity of MCAR Sensitivity analyses
will be used to examine the untestable assumption that the observed data violate the MAR
assumption The MMRM models will be implemented using PROC MIXED in SAS
96 Analysis of Binary Time-to-Event and Time-Lagged Endpoints
Regression modeling approaches using either the logistic regression model or Cox proportional
hazards regression model will be employed when appropriate The validity of these models will
be assessed via standard modeling diagnostics and goodness-of-fit measures Estimates of
cumulative frequencies for more general time-lagged responses will be calculated using the
partitioned version of the Bang-Tsiatis estimator44 The partitions will be set at 15-week intervals
59
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
to correspond with the data-collection process Covariate adjusted event rates will be calculated
using inverse probability-weighted regression estimates45
97 Power Analysis
971 Primary Analyses
Based on previously published IPF clinical trials the PL group is expected to experience a drop
in FVC of approximately 020 L over the study period (see Figure 1) The IPFnet Steering Group
determined a clinically important difference would be to preserve the majority of the decline
relative to PL over the study period In particular a treatment effect of 015 L was determined to
be a clinically meaningful difference Potential dropout is a key factor in the proposed study The
drop-out process assumed 5 lost to follow-up after every study visit Only 80 of subjects
were assumed to be followed for the entire study period All models assumed a compound
symmetry structure for the covariance matrix Power calculations were performed using a SAS
IML program for designing repeated measures studies46 Based on preliminary reviews of the
data from the University of Michigan the covariance matrix parameters were estimated at
approximately σ2 = 0757 (variance parameter) and ρ = 0936 (correlation parameter) To be
conservative the power calculations for the primary analysis were performed with parameter
setting of σ2 = 0810 (variance parameter) and ρ = 0925 (correlation parameter)
The power calculations assume a correction for imperfect compliance proposed by Lachin and
Foulkes to allow for 2 noncompliance for each of the treatment arms47 Thus the sample size
of 130 subjects per arm would be reduced to an adjusted sample size of 130(1-002-002)2 =
1198 or 120 subjects per arm
Under the assumed Type I error rate of 005 with a correlation parameter of 0925 and standard
deviation of 090 the difference of 015 L (or 00025 Lweek) shown in Table 6 would have
power of 93
60
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Table 6 Hypothetical Values of Mean FVC (L) Change from Baseline
Week 15 Week 30 Week 45 Week 60
NAC 00125 00250 00375 00500
Placebo 00500 01000 01500 02000
Difference 00375 00750 01125 01500
Abbreviations FVC forced vital capacity PL placebo
972 Power Analysis for Secondary Endpoints
Power calculations for secondary endpoint measurements are shown in Table 7 Standard
deviations are based on unpublished data provided by the University of Michigan The
calculations are based on a 2-sample t-test with Type I error rate set at 005 These calculations
are likely to be conservative because the statistical approach described in section 95 for
analyzing these endpoints will incorporate incomplete observations as well as intermediate data
points
Table 7 Detectable Differences in Treatment Means for Selected Endpoint Measurements
Secondary Endpoints Std Dev
of the Baseline Score
Detectable Difference for 80 Power
Std Dev of the Change Score
Difference Detectable for
80 Power
DLCOpred 166 58 91 32
6MWT Area Under the Desaturation Curve
219 76 175 61
6MWT Distance to Desaturation 224 78 315 110
6MWT Minutes Walked 210 073 205 071
Abbreviations Std Dev standard deviation DLCOpred diffusing capacity of the lung for carbon monoxide percent predicted 6MWT 6-minute walk test
61
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
10 Study Administration
101 Cooperative Agreement Mechanism
The administrative and funding mechanism used to undertake this project is a ldquocooperative
agreementrdquo (U01) which is an assistance mechanism Under the cooperative agreement the
NHLBI assists supports andor stimulates the project and is substantially involved with
investigators in conducting the study by facilitating performance of the effort in a ldquopartnerrdquo role
The NHLBI project scientist serves on the IPFnet Steering Group and he or another NHLBI
scientist may serve on other project committees when appropriate At the same time however
NHLBI does not assume a dominant role direction or prime responsibility for this research
program
As described below governance of the project is conducted through the IPFnet Steering Group
Principal investigators have lead responsibilities in all aspects of their trials and the project
including any modification of trial designs conduct of the trials quality control data analysis
and interpretation preparation of publications and collaboration with other investigators unless
otherwise provided for by the IPFnet Steering Group
PIs retain custody of and have primary rights to their center-specific and collaborative data
subject to government rights-of-access consistent with current Health amp Human Services (HHS)
Public Health Service (PHS) and National Institutes of Health policies The protocols and
governance policies call for the continual submission of data centrally to the IPFnet DCC for the
collaborative database which at a minimum will contain the key variables selected by the IPFnet
Steering Group for standardization across all clinical centers the submission of copies of the
collaborative datasets to each PI upon completion of the project procedures for data analysis
reporting and publication and procedures to protect and ensure the privacy of medical and
genetic data and records of individuals The NHLBI project scientist on behalf of the NHLBI
will have the same access privileges and responsibilities regarding the collaborative data as the
other members of the Steering Group
62
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
PIs are also encouraged to publish and to publicly release and disseminate results data and other
products of the project concordant with the project protocols and governance and the approved
plan for making data and materials available to the scientific community and to the NHLBI
However during the 3 years after the ending date of NHLBI project support unpublished data
unpublished results data sets not previously released and other study materials or products are
to be made available to any third party only with the approval of the IPFnet Steering Group
Upon completion of the project PIs are expected to put their intervention materials and
procedure manuals into the public domain andor make them available to other investigators
according to the approved plan for making data and materials available to the scientific
community and the NHLBI for the conduct of research at no charge other than the costs of
reproduction and distribution
The NHLBI reserves the right to terminate or curtail the project (or an individual award) in the
event of (a) failure to develop or implement mutually agreeable collaborative measurement
subject eligibility and data management sections of the protocols (b) substantial shortfall in
subject recruitment follow-up data reporting or quality control or other major breach of
protocol (c) substantive changes in the agreed-upon protocols with which NHLBI cannot
concur (d) reaching a major project outcome with persuasive statistical significance
substantially before schedule or (e) human subject ethical issues that may dictate a premature
termination
Any disagreement that may arise in scientificprogrammatic matters (within the scope of the
award) between award recipients and the NHLBI may be brought to arbitration An arbitration
panel will be composed of 3 membersmdash1 selected by the IPFnet Steering Group (with the
NHLBI member not voting) or by the individual PI in the event of an individual disagreement a
second selected by NHLBI and the third selected by the other 2 members This special
arbitration procedure in no way affects the PIrsquos right to appeal an adverse action that is otherwise
appealable in accordance with the PHS regulations at 42 CFR part 50 Subpart D and HHS
63
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
regulation at 45 CFR part 16 or the rights of the NHLBI under applicable statutes regulations
and terms of the award
102 IPFnet Steering Group
The IPFnet Steering Group is the main governing body of the project It is composed of the PIs
of the clinical centers the PI of the DCC and the NHLBI project scientist The clinical centers
the IPFnet DCC and the NHLBI each have 1 vote on the IPFnet Steering Group All decisions
are determined by majority vote
All major scientific decisions are determined by the IPFnet Steering Group It assumes overall
responsibility for the design and conduct of the trial It appoints (and disbands) committees and
subcommittees as the need arises designs approves and implements the study protocols
oversees the development of the MOOP monitors subject recruitment and treatment delivery
evaluates data collection and management oversees quality assurance procedures and
implements changes and enhancements to the study as required It also has primary responsibility
for facilitating the conduct of the trials and reporting the projectrsquos results
103 Data and Safety Monitoring Board
The NHLBI will establish a DSMB in accordance with established policies (see
httpwwwnhlbinihgovfundingpoliciesdsmb_insthtm) to ensure data quality and subject
safety and to provide independent advice to the NHLBI regarding progress and the
appropriateness of study continuation
104 Recommendations on Interim Monitoring of Efficacy Safety and Futility
First and foremost the role of the DSMB will be to review subject safety and trial conduct at
periodic points during the study The DSMB may require analyses of the primary endpoint
results for comparing the benefit and risks of treatment strategies The benefit of collecting
additional data on key secondary endpoints with extended follow-up and establishing a robust
64
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
evidence base for determining a standard of care will need to be carefully considered before
early termination of one or more treatment arms After careful consideration the IPFnet Steering
Group recommends conservative thresholds for the early examinations of the safety and efficacy
data
The DSMB will be expected to meet approximately every 6 months until trial completion to
review safety and toxicity data The DSMB may recommend stopping the study based on these
reviews Because the DSMB could stop the trial for safety concerns as well as for a large
efficacy benefit there could be multiple opportunities to reject the null hypothesis (no difference
in event rates between the PL and NAC groups) A Bonferroni approximation will be applied
during the one planned interim analysis for efficacy
Before locking the database a statistical analysis plan (SAP) will be developed to provide
complete details on the statistical analysis The SAP will include the specifics for how and when
the DSMB will be notified for AEs The IPFnet DCC will deliver to the DSMB all FDA-defined
AEs at 3-month intervals The IPFnet DCC will prepare narrative SAE reports in real time for
DSMB review including recommendations and analysis of similar events for each SAE
submitted to the FDA
65
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
11 Investigator and Sponsor Obligations
111 Monitoring
All monitoring activities for US clinical centers will be performed in accordance with DCRI
standard operating procedures Information regarding the types of visits will be outlined in the
PANTHER-IPF MOOP
112 Cost and Payment
There will be no cost to subjects enrolled in this trial Study-related procedures will be paid for
by the IPFnet
Subjects may be eligible for reimbursement for travel to the clinical center Details of payment
will be explained to each subject during the consent process
113 Confidentiality and Health Insurance Portability and Accountability Act
Considerations
Subject confidentiality will be protected throughout the study All subject data will be kept
strictly confidential and no subject-identifying information will be released to anyone outside
the project Confidentiality will be assured through several mechanisms First each subject will
be assigned an anonymous study ID which will then be used on all study forms Second any
study forms blood samples and paper records that contain subject information (eg address lists
phone lists) will be kept at the clinical centers in secured locked areas coded by number Once
blood is collected there will be no subject identifiers placed on blood samplesmdashonly the study
ID number and the date of sample collection Third access to all subject data and information
including laboratory specimens will be restricted to authorized personnel In the case of
computerized data this restricted access will be assured through user logon IDs and password
protection
66
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
At the IPFnet DCC only authorized personnel will have access to the data files containing study
data Security will be assured through user logon IDs passwords and appropriate access
privileges All study subjects will be identified only by their IPFnet ID numbers and no personal
identifying information such as name address or Social Security number will be entered into
the IPFnet DCC database Any subject-specific data reported to the IPFnet Steering Group will
be identified only by the IPFnet ID number
Finally subjects will not be identified by name in any reports or publications nor will the data
be presented in such a way that the identity of individual subjects can be inferred Analysis files
created for further study by the scientific community will have no subject identifiers These data
files will be created in accordance with the Ancillary Studies and Publication Policy of the
IPFnet
114 Informed Consent Procedures
All IPFnet subjects will provide written informed consent using procedures reviewed and
approved by each clinical centerrsquos IRB Informed consent will be undertaken by study personnel
in-person with the subject The subject has the option of declining further participation in the
study at that point No further study procedures will be conducted until the signed documents
have been provided to the IPFnet clinical center
115 Institutional Review Boards
Before initiating this study the protocol clinical center-specific informed consent forms Health
Insurance Portability and Accountability Act (HIPAA) forms recruitment materials and other
relevant information will be reviewed by a properly constituted IRB at each participating clinical
center A copy of the signed and dated IRB approval at each clinical center will be retrieved prior
to or during the site initiation visit and archived at the IPFnet DCC Any amendments to the
protocol other than simple administrative and typographical changes must be approved by each
IRB before they are implemented The clinical centers will seek annual renewals of their IRB
approvals in accordance with local procedures
67
__________________________________________ ________________
__________________________________________
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
12 Investigator Agreement
I have read the foregoing protocol PANTHER-IPF and agree that it contains all necessary
details for carrying out this study I will conduct the study as outlined herein and will complete
the study within the time designated
I will provide copies of the protocol and all pertinent information to all individuals responsible to
me who assist in the conduct of this study I will discuss this material with them to ensure they
are fully informed regarding the drug and the conduct of the study
I will fulfill all responsibilities for submitting pertinent information to the local IRB if
applicable that is responsible for this study
I further agree that NHLBI andor DCRI will have access to any source documents from which
eCRF information may have been generated
Signature of Principal Investigator Date
Name of Principal Investigator (printed or typed)
Protocol version date May 19 2009
Protocol Amendment 1 version date May 28 2010
Protocol Amendment 2 version date December 6 2011
68
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
13 References
1 Raghu G Brown KK Bradford WZ et al A placebo-controlled trial of interferon gamma-1b in patients with idiopathic pulmonary fibrosis N Engl J Med 2004350125-33 2 King TE Jr Safrin S Starko KM et al Analyses of efficacy end points in a controlled trial of interferon-gamma1b for idiopathic pulmonary fibrosis Chest 2005127171-7 3 Flaherty KR Thwaite EL Kazerooni EA et al Radiological versus histological diagnosis in UIP and NSIP survival implications Thorax 200358143-8 4 Wells AU Desai SR Rubens MB et al Idiopathic pulmonary fibrosis a composite physiologic index derived from disease extent observed by computed tomography Am J Respir Crit Care Med 2003167962-9 5 Raghu G Freudenberger TD Yang S et al High prevalence of abnormal acid gastroshyoesophageal reflux in idiopathic pulmonary fibrosis Eur Respir J 200627136-42 6 Kinnula VL Focus on antioxidant enzymes and antioxidant strategies in smoking related airway diseases Thorax 200560693-700 7 Coultas DB Zumwalt RE Black WC Sobonya RE The epidemiology of interstitial lung diseases Am J Respir Crit Care Med 1994150967-72 8 Raghu G Weycker D Edelsberg J Bradford WZ Oster G Incidence and prevalence of idiopathic pulmonary fibrosis Am J Respir Crit Care Med 2006174810-6 9 Olson AL Swigris JJ Lezotte DC Norris JM Wilson CG Brown KK Mortality from pulmonary fibrosis increased in the United States from 1992 to 2003 Am J Respir Crit Care Med 2007176277-84 10 Mannino DM Etzel RA Parrish RG Pulmonary fibrosis deaths in the United States 1979shy1991 An analysis of multiple-cause mortality data Am J Respir Crit Care Med 19961531548shy52 11 Hubbard R Johnston I Coultas DB Britton J Mortality rates from cryptogenic fibrosing alveolitis in seven countries Thorax 199651711-6 12 Johnston I Britton J Kinnear W Logan R Rising mortality from cryptogenic fibrosing alveolitis Bmj 19903011017-21 13 Raghu G Collard HR Egan JJ et al An official ATSERSJRSALAT statement idiopathic pulmonary fibrosis evidence-based guidelines for diagnosis and management Am J Respir Crit Care Med 2011183788-824 14 (USA) FDA FDA Public Health Advisory Interferon gamma-1b (marketed as Actimmune) In 2007 15 King TE Jr Pardo A Selman M Idiopathic pulmonary fibrosis Lancet 2011 16 Raghu G Brown KK Costabel U et al Treatment of idiopathic pulmonary fibrosis with etanercept an exploratory placebo-controlled trial Am J Respir Crit Care Med 2008178948shy55 17 Malouf MA Hopkins P Snell G Glanville AR An investigator-driven study of everolimus in surgical lung biopsy confirmed idiopathic pulmonary fibrosis Respirology 201116776-83 18 King TE Jr Behr J Brown KK et al BUILD-1 a randomized placebo-controlled trial of bosentan in idiopathic pulmonary fibrosis Am J Respir Crit Care Med 200817775-81 19 Richeldi L Costabel U Selman M et al Efficacy of a tyrosine kinase inhibitor in idiopathic pulmonary fibrosis N Engl J Med 20113651079-87
69
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
20 Borok Z Buhl R Grimes GJ et al Effect of glutathione aerosol on oxidant-antioxidant imbalance in idiopathic pulmonary fibrosis Lancet 1991338215-6 21 Meyer A Buhl R Magnussen H The effect of oral N-acetylcysteine on lung glutathione levels in idiopathic pulmonary fibrosis Eur Respir J 19947431-6 22 Behr J Maier K Degenkolb B Krombach F Vogelmeier C Antioxidative and clinical effects of high-dose N-acetylcysteine in fibrosing alveolitis Adjunctive therapy to maintenance immunosuppression Am J Respir Crit Care Med 19971561897-901 23 Cantin AM North SL Fells GA Hubbard RC Crystal RG Oxidant-mediated epithelial cell injury in idiopathic pulmonary fibrosis J Clin Invest 1987791665-73 24 Waghray M Cui Z Horowitz JC et al Hydrogen peroxide is a diffusible paracrine signal for the induction of epithelial cell death by activated myofibroblasts Faseb J 200519854-6 25 Larios JM Budhiraja R Fanburg BL Thannickal VJ Oxidative protein cross-linking reactions involving L-tyrosine in transforming growth factor-beta1-stimulated fibroblasts J Biol Chem 200127617437-41 26 Kinnula VL Fattman CL Tan RJ Oury TD Oxidative stress in pulmonary fibrosis a possible role for redox modulatory therapy Am J Respir Crit Care Med 2005172417-22 27 Meyer A Buhl R Kampf S Magnussen H Intravenous N-acetylcysteine and lung glutathione of patients with pulmonary fibrosis and normals Am J Respir Crit Care Med 19951521055-60 28 Behr J Degenkolb B Krombach F Vogelmeier C Intracellular glutathione and bronchoalveolar cells in fibrosing alveolitis effects of N-acetylcysteine Eur Respir J 200219906-11 29 Bando M Hosono T Mato N et al Long-term efficacy of inhaled N-acetylcysteine in patients with idiopathic pulmonary fibrosis Intern Med 2010492289-96 30 Demedts M Behr J Buhl R et al High-dose acetylcysteine in idiopathic pulmonary fibrosis N Engl J Med 20053532229-42 31 Toma TP Bhowmik A Rajakulasingam R Acetylcysteine in pulmonary fibrosis N Engl J Med 20063541086-9 author reply -9 32 Hunninghake GW Antioxidant therapy for idiopathic pulmonary fibrosis N Engl J Med 20053532285-7 33 Flaherty KR Mumford JA Murray S et al Prognostic implications of physiologic and radiographic changes in idiopathic interstitial pneumonia Am J Respir Crit Care Med 2003168543-8 34 Latsi PI du Bois RM Nicholson AG et al Fibrotic idiopathic interstitial pneumonia the prognostic value of longitudinal functional trends Am J Respir Crit Care Med 2003168531-7 35 Collard HR King TE Jr Bartelson BB Vourlekis JS Schwarz MI Brown KK Changes in clinical and physiologic variables predict survival in idiopathic pulmonary fibrosis Am J Respir Crit Care Med 2003168538-42 36 Jegal Y Kim DS Shim TS et al Physiology is a stronger predictor of survival than pathology in fibrotic interstitial pneumonia Am J Respir Crit Care Med 2005171639-44 37 Martinez FJ Safrin S Weycker D et al The clinical course of patients with idiopathic pulmonary fibrosis Ann Intern Med 2005142963-7 38 Hull JH Acetylcysteine in pulmonary fibrosis N Engl J Med 20063541089-91 author reply -91
70
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
39 Flaherty KR King TE Jr Raghu G et al Idiopathic interstitial pneumonia what is the effect of a multidisciplinary approach to diagnosis Am J Respir Crit Care Med 2004170904shy10 40 Raghu G Johnson WC Lockhart D Mageto Y Treatment of idiopathic pulmonary fibrosis with a new antifibrotic agent pirfenidone results of a prospective open-label Phase II study Am J Respir Crit Care Med 19991591061-9 41 Hunninghake GW Lynch DA Galvin JR et al Radiologic findings are strongly associated with a pathologic diagnosis of usual interstitial pneumonia Chest 20031241215-23 42 Lynch D Godwin J Safrin S et al High-resolution computed tomography in idiopathic pulmonary fibrosis diagnosis and prognosis Am J Respir Crit Care Med 2005172488-93 43 Mallinckrodt CH Watkin JG Molenberghs G Carroll RJ Choice of the primary analysis in longitudinal clinical trials Pharmaceutical Statistics 20043161-9 44 Bang H Tsiatis A Estimating medical costs with censored data Biometrika 200087329shy43 45 Lin DY Regression analysis of incomplete medical cost data Stat Med 2003221181-200 46 Rochon J Application of GEE procedures for sample size calculations in repeated measures experiments Stat Med 1998171643-58 47 Lachin JM Foulkes MA Evaluation of sample size and power for analyses of survival with allowance for nonuniform patient entry losses to follow-up noncompliance and stratification Biometrics 198642507-19
71
- PANTHER-IPFPREDNISONE AZATHIOPRINEAND N-ACETYLCYSTEINEA STUDY THAT EVALUATES RESPONSE INIDIOPATHIC PULMONARY FIBROSIS
-
- Protocol Summary
- Table of Contents
- List of Tables
- List of Figures
- List of Abbreviations
- 1 Summary
- 2 Hypotheses and Specific Aims
-
- 21 Null Hypothesis
- 22 Specific Aim 1
- 23 Specific Aim 2
- 24 Prespecified Subgroups of Interest
-
- 3 Background and Significance
-
- 31 Idiopathic Pulmonary Fibrosis is the Most Common Interstitial Lung Disease
- 32 Rationale for Placebo Control
- 33 Rationale for N-acetylcysteine
- 35 Rationale for N-acetylcysteine as a Stand-alone Therapy
- 36 Rationale for the Study Design and Primary Endpoint
- 37 Rationale for Blinding of Treatments
-
- 4 Methods
-
- 41 Inclusion Criteria
- 42 Diagnosis of IPF
- 43 Exclusion Criteria
- 44 Study Design and Study Visit
- 45 Dose Justification
- 46 Contraindications Precautions and Side Effects of Study Medications
- 47 Recruitment Procedures
- 48 Study Procedures
- 49 Concomitant Medications
- 410 Laboratory Testing
- 411 Blinding of Study Drugs
-
- 5 Study Endpoints
-
- 51 Primary Study Endpoint
- 52 Secondary Study Endpoints
-
- 6 Safety Evaluations and Procedures
-
- 61 Adverse Events
- 62 Clinical Medical Monitoring
- 63 Unblinding Procedures
-
- 7 Study Drug Procedures
- 8 Data Management
-
- 81 Hardware and Software Configuration
- 82 Sources of Data
-
- 9 Study Design and Data Analysis
-
- 91 General Analytic Considerations
- 92 Randomization Blinding and Reporting of Results
- 93 Stratification
- 94 Specification of the Primary Analyses
- 95 Analysis of Longitudinal Endpoints
- 96 Analysis of Binary Time-to-Event and Time-Lagged Endpoints
- 97 Power Analysis
-
- 10 Study Administration
-
- 101 Cooperative Agreement Mechanism
- 102 IPFnet Steering Group
- 103 Data and Safety Monitoring Board
- 104 Recommendations on Interim Monitoring of Efficacy Safety and Futility
-
- 11 Investigator and Sponsor Obligations
-
- 111 Monitoring
- 112 Cost and Payment
- 113 Confidentiality and Health Insurance Portability and Accountability ActConsiderations
- 114 Informed Consent Procedures
- 115 Institutional Review Boards
-
- 12 Investigator Agreement
- 13 References
-
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
The IPFnet is now completing the PANTHER-IPF trial with a 11 randomization (NAC vs placebo) and a
simple practical feasible and scientifically rational design that will establish standard of care with NAC for
IPF based on a currently available therapeutic agent and the existing data to support its use We anticipate that
all future clinical trials of novel therapeutic agents will be tested against this to-be-established standard of care
36 Rationale for the Study Design and Primary Endpoint
The optimal study design of a therapeutic trial in IPF would include survival as a primary endpoint The
published results of the IFN-γ 1b Phase 3 (GIPF-001) trial suggested a survival benefit in subjects with milder
disease in retrospective analyses1 although the trial was underpowered to address this question This was likely
related to the limited mortality in the PL arm of the study which included IPF subjects with mild to moderate
disease This study documents that an IPF study powered to improve survival in a patient population with mild
disease requires a larger sample size andor duration of study In fact the recently aborted Phase 3 IFN-γ 1b
(GIPF-007 INSPIRE) study was a survival-based study and recruited more than 800 subjects at 75 centers
worldwide1415 As such within the context of the current IPFnet trial survival is an impractical primary
endpoint variable
Several groups have published data defining an appropriate surrogate outcome variable a 10 decrement in
FVC during 6 to 12 months is a powerful predictor of survival in IPF33-36 Furthermore additional evidence
suggests a similar predictive ability for a 10 decrement in FVC during 3 months of follow-up37 With strong
supportive evidence of FVC progression being related to mortality on a per-subject basis this study will use
FVC changes in liters between treatment groups as the primary endpoint Previously published IPF studies have
shown a steady decline in FVC (and FVCpred) among control group subjects230 The GIPF-001 study
suggested a 48-week decrease in FVC of 016 L in the PL-treated subjects The IFIGENIA study demonstrated
a decline in FVC of approximately 019 L over 52 weeks in the subjects randomized to the control treatment
Figure 1 depicts the change in FVC for control groups from previously published IPF studies38 Based on these
data we expect that the PL group will have a decline of 020 L over the 60-week study period The IPFnet
Steering Group determined that a clinically meaningful improvement would be the preservation of the majority
of the 020-L FVC decline Therefore a mean treatment difference of 015 L in mean FVC over the 60-week
study period was determined to be a clinically meaningful difference
18
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Δ f
rom
bas
elin
e (i
n L
)
01
005
0
-005
-01
-015 Projected Δ for placebo
-02
-025
-019
-016
-013 Pirfenidone GIPF001
NAC
Placebo
4 8 12 16 20 24 28 32 36 40 44 48 52 56 60
Week
Figure 1 Changes in FVC From Baseline in Prior IPF Clinical Trials
Recent data suggest that various patient subgroups would be expected to potentially exhibit differential response
to therapy These parameters will be used to a priori separate patients by a series of baseline characteristics
including
1 Higher enrollment FVC12
2 Typical vs atypical high-resolution computed tomography (HRCT) reading at baseline3
3 Recent vs more remote diagnosis (time from initial diagnosis of IPF le 1 year and gt 1 year)
4 Lower CPI score at enrollment4
5 Medical therapy for gastroesophageal reflux5
6 Ethnic background
7 Sex
8 Smoking history (current or ex-smoker vs never smoker) given potential impact on oxidant status6
9 Presence of emphysema gt 25 on HRCT
37 Rationale for Blinding of Treatments
The issue of treatment blinding was given a great deal of consideration with subject safety being the primary
concern After discussion among the Steering Group members it was decided that as long as subject safety
could be ensured blinding was necessary Blinding allows the study to
Have optimal scientific validity and potential to impact the standard of care for subjects
19
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Make objective assessments of treatment effects
Maintain clinical equipoise among investigators
Encourage subjects to have similar levels of contact with the medical community
Minimize the differential dropout rates across study arms
20
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
4 Methods 41 Inclusion Criteria
1 Age 35 to 85 years inclusive
2 FVC ge 50 of predicted (post-bronchodilator measurement from the screening visit)
3 DLCO ge 30 of predicted (hemoglobin corrected and altitude corrected if gt4000 ft above sea level)
4 Ability to understand and provide informed consent
5 Diagnosis of IPF according to a modified version of the ATS criteria le 48 months from enrollment The
date of diagnosis is defined as the date of the first available HRCT or surgical lung biopsy characteristic
of definite UIP
411 Subjects Shown to Have Usual Interstitial Pneumonia Pattern on Surgical Lung Biopsy
Subjects who have been shown to have UIP pattern on lung biopsy must have all of the following
1 Exclusion of other known causes of ILD such as drug toxicity clinically significant environmental
exposures or diagnosis of connective tissue diseases
2 Bibasilar reticular abnormalities with minimal ground glass opacities on HRCT scan
412 Subjects Who Have Not Undergone a Surgical Lung Biopsy
In addition to the criteria above these subjects must have radiological findings considered to be definite for the
diagnosis of UIPIPF
1 Bibasilar reticular abnormalities with minimal ground glass opacities
2 Honeycombing as the predominant feature and located in the peripheral lung bases
42 Diagnosis of IPF
Only subjects with definite IPF will be eligible for enrollment in this study We will utilize a combination of
clinicalphysiologic features HRCT and review of a clinically obtained surgical lung biopsy specimen to
establish the diagnosis of IPF An algorithm for the diagnosis is provided to guide entry into the protocol as
outlined in the inclusion and exclusion criteria (Figures 2 and 3) This multi-disciplinary approach uses
21
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
expertise from clinicians radiologists and pathologists Investigators at each site in conjunction with central
pathology will work together to establish the diagnosis of IPF This interactive approach to the diagnosis of IPF
increases the level of agreement between observers39
A subject with suspected ILD should be evaluated for secondary causes including but not limited to
environmental exposures drugs and systemic diseases Presence of any of these findings felt to be significant
enough to cause an ILD should disqualify the subject from entry into the trial
If secondary causes are absent an HRCT scan may be obtained If an HRCT of sufficiently high quality has
been obtained within the last 3 months that scan may be used for diagnosis In the appropriate clinical setting
the diagnosis of IPF can be made by the demonstration of a typical radiographic pattern on HRCT or by
demonstration of UIP pattern on a surgical lung biopsy The following criteria for a radiographic (ie
nonsurgical) diagnosis will be used In the absence of known exposures andor clinical associations attributable
to pulmonary fibrosis and in the appropriate clinical setting the presence of definite UIP pattern in HRCT
images is required to meet study criteria for the diagnosis of IPF
Figure 2 Diagnosis of Idiopathic Pulmonary Fibrosis in the IPFnet
22
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Figure 3 Pathology Flow Chart Surgical Lung Biopsy Diagnosis
Requirement for diagnosis
1 Clinical exclusion of other known causes (connective tissue diseases environmental and drug
exposures) of ILD
2 Radiographic HRCT with bibasilar reticular abnormality and honeycomb change with minimal
ground glass opacities
Appropriate clinical setting
1 Age gt 50 years
2 Insidious onset of unexplained dyspnea
3 Duration of illness for ge 3 months
4 Bibasilar inspiratory crackles
23
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Unlike the ATSERS consensus criteria published in 2000 bronchoscopy will not be required for diagnosis
This decision was made based on the experience of the IPFnet Steering Group members regarding the utility of
bronchoscopy in the diagnosis of IPF The presence of an atypical HRCT finding will require documentation of
a definitive diagnosis by surgical lung biopsy In fact this is in keeping with the recently published evidence
based guidelines for diagnosis and management of IPF13 As shown in Figure 3 central review of the pathology
data will be required for a diagnosis of IPF
We will not require central review of HRCT as several studies have shown that a confident local interpretation
of clinicalHRCT criteria as definite IPFUIP is associated with a high positive predictive value for finding UIP
at surgical lung biopsy (see Table 1) Differences in sensitivity in these series likely reflect subject selection as
Flaherty et al3 evaluated only UIP and nonspecific interstitial pneumonia (NSIP) while Raghu et al40 and
Hunninghake et al41 included a broader range of ILD
Table 1 Operating Characteristics of Local HRCT Review for Diagnosis of UIP
Researcher of Subjects Sensitivity () Specificity () PPV () NPV ()
Raghu et al 40
59 (29 UIP by SLB) 78 90 88 82
Hunninghake et al 41 91 (54 UIP by SLB)
74 81 85 67
Flaherty et al 3 96 (only NSIP amp UIP)
37 100 100 30
Abbreviations PPV positive predictive value NPV negative predictive value UIP usual interstitial pneumonia SLB surgical lung biopsy and NSIP nonspecific interstitial pneumonia
Furthermore an analysis of the HRCT scans from subjects enrolled in the GIPF-001 trial confirmed that local
site interpretations have a high congruity to a central radiology core In this multi-center study 263 HRCT
scans were read as definite IPF and a retrospective central radiology core review found 932 to be consistent
with IPF 42 We will also take several additional steps to insure that the local HRCT reads are accurate
including
1 A detailed training module has been developed and must be completed by each site radiologist before
site initiation
2 Clinical centers are to mail all HRCT scans to the HRCT core lab The first 10 HRCT scans from
subjects enrolled at each enrolling clinical center will be reviewed centrally to be certain that local reads
24
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
25
are congruent with a central interpretation If discrepancies are identified additional education will be
provided and HRCT scans will continue to be reviewed centrally until the central radiology core is
confident that the local center is performing appropriately
3 Random scans will be obtained from each center throughout the study to confirm that the local read
continues to agree with central interpretation If discrepancies are identified they will be addressed as in
2 above
In all cases if a subject has a surgical lung biopsy sample that sample will be reviewed by the local and central
pathologists Therefore the only cases that would not be subject to a direct central review process are those
where the HRCT meets the centrally defined criteria for an unequivocal diagnosis and a lung biopsy sample is
not available Table 2 below summarizes the possible combinations for making a diagnosis
Table 2 Combining HRCT and Pathology Interpretations to Determine if IPF is Present
HRCT Diagnosis Pathology Diagnosis Diagnosis of IPF
Definite UIP Definite UIP Yes
Definite UIP Probable UIP Yes
Definite UIP Possible UIP Yes
Definite UIP Not UIP No
Definite UIP Unavailable Yes
Consistent with UIP Definite UIP Yes
Consistent with UIP Probable UIP Yes
Consistent with UIP Possible UIP No
Consistent with UIP Not UIP No
Consistent with UIP Unavailable No
Inconsistent with UIP Any No
Abbreviations HRCT high-resolution computed tomography IPF idiopathic pulmonary fibrosis
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
UIP usual interstitial pneumonia Dx diagnosis 43 Exclusion Criteria
1 History of clinically significant environmental exposure known to cause pulmonary fibrosis
Occupational exposures such as asbestos or environmental exposure to organic dust such as occurs in
pigeon breeders may at times mimic the clinical and radiographic findings of IPF
2 Diagnosis of connective tissue disease felt by the principal investigator (PI) to be the etiology of the
interstitial disease Diagnosis of collagen-vascular conditions will be according to the published
American College of Rheumatology criteria As such the presence of any documented collagen-vascular
disorder or the presence of any suspicious symptom complex whether or not associated with
significantly abnormal rheumatological serologies will exclude the subject at the discretion of the PI
3 Extent of emphysema greater than the extent of fibrotic change (honeycombing reticular changes) on
HRCT scan
4 Forced expiratory volume in 1 second (FEV1)FVC ratio lt 065 at screening (postbronchodilator)
5 Partial pressure of arterial oxygen (PaO2) on room air lt 55 mm Hg (lt 50 mm Hg at Denver site)
6 Residual volume gt 120 predicted at screening (postbronchodilator)
7 Evidence of active infection
8 Significant bronchodilator response on screening spirometry defined as a change in FEV1 ge 12 and
absolute change gt 200 mL OR change in FVC ge 12 and absolute change gt 200 mL The percent
difference between the FVC (or FEV1) values will be calculated by taking the absolute value of the
difference and dividing it by the larger of the two FVC (or FEV1) values
9 Screening and enrollment post-bronchodilator FVC measurements (in liters) differing by gt 11 The
percent difference between the FVC values will be calculated by taking the absolute value of the
difference and dividing it by the larger of the two FVC values (eg the percent difference between FVC
measurements of 19 and 20 liters would be determined by taking the difference between the two (01
liters) and dividing by the larger of the two (20 liters) So 0120 = 5 and these FVC measurements
would not exclude the subject
10 Listed for lung transplantation ie the patient has completed the evaluation process has been accepted
as a candidate for transplantation at an appropriate center and is waiting to receive notification of an
available donor organ
11 History of unstable or deteriorating cardiac disease
12 Myocardial infarction coronary artery bypass or angioplasty within 6 months of screening
26
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
13 Unstable angina pectoris or congestive heart failure requiring hospitalization within 6 months of
screening
14 Uncontrolled arrhythmia
15 Severe uncontrolled hypertension
16 Known HIV or hepatitis C
17 Known cirrhosis and chronic active hepatitis
18 Active substance andor alcohol abuse (as determined by site PI)
19 Pregnancy or lactation (subjects who are pregnant or breastfeeding)
20 Known hypersensitivity to study medication
21 Any condition other than IPF that in the opinion of the site PI is likely to result in the death of the
subject within the next year
22 Any condition that in the judgment of the PI might cause participation in this study to be detrimental to
the subject or that the PI deems makes the subject a poor candidate
23 Any therapy directed at pulmonary fibrosis (excepting triple therapy of prednisone plus azathioprine
plus NAC) requires a 30-day washout period before randomized Triple therapy of lt= 12 weeks duration
in the past 4 years requires a 30-day washout period before randomization
24 History of triple therapy of prednisone plus azathioprine plus NAC for gt 12 weeksrsquo duration in the past
4 years or previous enrollment in the triple-therapy arm of the PANTHER-IPF study
44 Study Design and Study Visit
441 Study Design Summary
This study will be a randomized double-blind PL-controlled trial designed to assess the safety and efficacy of
NAC in subjects with newly diagnosed IPF
Subjects with mild to moderate IPF (defined as FVCpred ge 50 and DLCOpred ge 30) diagnosed within
the past 48 months will be enrolled Screening will continue until April 30 2012
27
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
The study will employ a 2-arm design with 11 randomization to NAC or PL Once enrolled subjects will visit
the clinical center at 15 weeks and 15-week intervals thereafter Each subject will be treated and followed for a
maximum of 60 weeks
During the 60-week visit subjects will be taken off all study agents Approximately four weeks after the final
dose of study agent is taken subjects will receive a safety phone call from the study site
442 Study Visits
Subjects who meet entry criteria will review the informed consent a written description of the purpose
procedures and risks of the study with the PI co-investigator or study coordinator and all questions will be
answered The informed consent form will be signed by the subject at screening No protocol-specific
procedures will be performed until the subject has signed and dated an informed consent form This includes the
screening procedures
4421 Screening
Once informed consent is obtained subjects may immediately begin the screening process or may return within
28 days of consent In the event a study subject has been clinically evaluated at the study site by an IPFnet study
physician and has performed testing within three weeks for this clinical evaluation that meets guidelines
provided in the IPFnet PANTHER-IPF Manual of Operating Procedures (MOOP) this testing may be used to
satisfy the following screening criteria medical history physical exam arterial blood gas (ABG) with A-a
gradient vital signs with oximetry body height and weight spirometry DLCO lung volumes and HRCT scan
Allowing the use of previously performed test results that meet study guidelines for the screening visit is
intended to permit subjects easier access to study entry to prevent subjects from repeating testing that has been
performed within the study window and to decrease risks to subjects from repeated exposure to procedures
such as arterial puncture and HRCT
The following procedures will be performed at screening
Medical history and a physical examination
28
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Measure height and weight
Serum pregnancy test (if applicable)
Measure vital signs including oximetry
Blood draws performed and the following analyses conducted
o Hematology (red cell count white cell count hemoglobin hematocrit cell indices differential
platelet count)
o Blood chemistries according to central laboratory protocol (see Section 410 Laboratory
Testing)
o Beta human chorionic gonadotropin (serum) pregnancy test (in women of childbearing potential)
o Urinalysis
Pulmonary Function Tests (PFTs) including spirometry pre- and post- bronchodilator and postshy
bronchodilator measurement of lung volumes and measurement of hemoglobin adjusted diffusing
capacity
Measure ABGs
HRCT if a satisfactory scan has not been performed on the subject within 3 months of screening (see
PANTHER-IPF MOOP for more details)
Surgical lung biopsies (if applicable) reviewed by local and central pathology departments
Current medications If required a washout period discussed with the subject and initiated at this visit
4422 Enrollment
The enrollment visit is expected to take place within eight weeks of the screening visit Enrollment visit
activities include
Measure vital signs including oximetry
Measure height and weight
Serum pregnancy test (if applicable)
If consent has been given blood will be drawn and a urine specimen collected for the bio-specimen
repository
Spirometry (post-bronchodilator)
Measure 6MWT with Borg Dyspnea Scale
29
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Collect Quality-of-life (QOL) data using the SF-36 EuroQol Investigating Choice Experiments for
Preferences of Older People Capability Instrument (ICE CAP) and SGRQ
Female subjects complete Gender Substudy questionnaire
Dyspnea status collected using the UCSD SOBQ
Evaluate Acute Exacerbation (AEx)
Review of any Adverse Events (AEs)
Review of concomitant medications
Subject receives diary and instructions on its purpose and proper use
Subject receives supply of study drug sufficient to last until his or her 15-week study visit
See the Schedule of Assessments (Table 3) for more details Subjects with screening and enrollment postshy
bronchodilator FVC measurements (in liters) differing by more than 11 are not eligible to be enrolled in the
study
Subjects will be asked to provide a physician of record This physician will be considered the subjectrsquos primary
care provider (PCP) and if the subject agrees the PCP will be informed by letter of the subjectrsquos enrollment in
the trial The subject will be informed that his or her ongoing medical care should be received from the PCP
The PCP will be informed of any safety issues identified by the study staff The PCP will also be given
information regarding communication with study personnel about pertinent health issues or clinic encounters
the subject may have
4423 Week 15
The week 15 visit is expected to occur within +- 14 days of the subjectrsquos scheduled visit time (eg the week 15
visit should occur anytime between 13 and 17 weeks after starting study drug Week 15 activities include
Measure vital signs with oximetry
Measurement height and weight
Serum pregnancy test (if applicable)
Spirometry (post-bronchodilator) measurement
Review of AEs
Evaluate for AEx
30
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Review concomitant medications
If consented draw blood and collect urine specimen for the biospecimen repository
Subjects return used and unused study drug for the visit
Review study diary and a new study diary will be given
Provide additional supply of study drug sufficient to last until the next scheduled visit
4424 Week 30
The week 30 visit is expected to occur within +- 14 days of the subjectrsquos scheduled visit time (eg the week 30
visit should occur anytime between 28 and 32 weeks after starting study drug) Week 30 activities include
Physical examination
Measure vital signs with oximetry
Measure height and weight
Laboratory values (complete blood count [CBC] and serum chemistries)
Serum pregnancy test (if applicable)
Measure spirometry (post-bronchodilator)
6MWT with Borg scale
DLCO
Review of AEs
Evaluate for AEx
Review concomitant medications
Complete all QOL and dyspnea questionnaires (EuroQol ICE CAP SF-36 SGRQ and UCSD SOBQ)
If consent has been given blood will be drawn and a urine specimen collected for the biospecimen
repository
Review study diary
Subjects return used and unused study drug for the visit
Provide additional supply of study drug sufficient to last until the next scheduled visit
4425 Week 45
31
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
The week 45 visit is expected to occur within +- 14 days of the subjectrsquos scheduled visit time (eg the week 45
visit should occur anytime between 43 and 47 weeks after starting study drug) Week 45 activities include
Measure vital signs with oximetry
Measure height and weight
Serum pregnancy test (if applicable)
Measure spirometry (post-bronchodilator)
Review of AEs
Evaluate for AEx
Review concomitant medications
If consent has been given blood will be drawn and a urine specimen collected for the biospecimen
repository
Subjects return used and unused study drug for the visit
Study diary reviewed
Provide additional supply of study drug sufficient to last until the next scheduled visit
4426 Week 60 (Early Withdrawal or Final Treatment Visit)
At week 60 or at subject withdrawal from the study (premature by study doctor or subjectrsquos decision) a final
treatment visit will occur At this final treatment visit subjects will discontinue NACPL abruptly Week 60
activities also include
Physical examination
Measure vital signs with oximetry
Measure height and weight
Laboratory values (complete blood count [CBC] and serum chemistries)
Spirometry (post-bronchodilator) measurement
6MWT with Borg scale measurement
DLCO
Lung volumes
ABG
Review of AEs
32
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Evaluate for AEx
Review concomitant medications
Subjects will complete all QOL and dyspnea questionnaires (EuroQol ICE CAP SF-36 SGRQ and
UCSD SOBQ)
If consent has been given blood will be drawn and a urine specimen collected for the biospecimen
repository
Subjects return used and unused study drug for the visit
Study diary reviewed
4427 Final Site Visit ndash FVC drop confirmation
In the event that the subject has a recorded FVC drop of gt10 from baseline at the final treatment visit and the
subject has not had a confirmation of such a drop at a previous study visit the subject should return to the
clinical site 6 to 8 weeks after the final treatment visit During this visit a post-bronchodilator spirometry test
will be performed This FVC measurement will be evaluated according to section 521 of this protocol
4428 Final Visit ndash Telephone Follow-up
Four weeks following the final dose of study medication subjects will receive a telephone call from the study
coordinator to ensure that there are no side effects and to follow up on any ongoing adverse events (AEs)
4429 Phone Contact Between Visits
At week 2 and each month that a subject does not have a scheduled clinical center visit his or her study
coordinator will contact him or her at least once by telephone to
Inquire if the subject has had any hospitalizations events that might be considered an AE or any events
significant enough to warrant an out-of-cycle visit to the clinical center
Remind subjects of their current dosage levels and confirm that the subject understands them
Address any questions or concerns the subject might have regarding other aspects of the study
Assess adherence to the treatment regimen by reviewing diary data verbal review of medications taken
including nutritional supplements
33
34
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Table 3 Schedule of Assessments
Procedure Screening Visit 0
Enrollment Visit 1
Week 15 Visit 2
Week 30Visit 3
Week 45 Visit 4
Week 60 Early
Withdrawal Visit 5
Final1
Visit (via phone)
Informed consent X
Medical history X
Inclusionexclusion criteria X
Serum pregnancy test (if applicable) X X X X X
Review of lung biopsy X
Arterial Blood Gas X X
6-Minute Walk Test
X
X X
Physical examination X X X
Vital signs with oximetry X X X X X X
Body height and weight X X X X X X
Complete Blood Count X X X
Chemistry panel X X X
Monitor Lab Values X X X
Urinalysis X Specimen repository substudy blood draw and urine collection (if consented)
X
X X X X
HRCT (if not completed within three months) X
Spirometry (pre- and post-bronchodilator) X
Spirometry (post-bronchodilator only) X X X X X
DLCO (post-bronchodilator only) X X X
Lung volumes (post-bronchodilator only) X
X
Evaluate for acute exacerbation X X X X X
Review Adverse Events X X X X X X
Review concomitant meds X X X X X X
Dispense subject diary X X X X
Review subject diary X X X X X
Dispense study agent X X X X
Gender Substudy questionnaire (female subjects only) X
EuroQol ICECAP UCSD SOBQ SGRQ SF-36 X X X
Abbreviations DLCO diffusing capacity of the lung for carbon monoxide QOL Quality of Life ICECAP Investigating Choice Experiments for Preferences of Older People UCSD SOBQ University of California Shortness of Breath Questionnaire SGRQ St Georgersquos Respiratory Questionnaire SF-36 Short Form 36 Health Survey
1Follow-up visit via phone will occur four weeks after final dose of study medication
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
45 Dose Justification
The general philosophy for determining dosing levels was to apply previously examined
treatment regimens With the focus of the study being to establish a standard of care for
mildmoderate IPF subjects the goal was to develop flexible yet standardized treatment rules that
allow for the temporary or permanent withholding of one or more components of treatment when
necessary Subjects developing laboratory abnormalities or symptoms that result in
discontinuation of one or more components of study treatment may continue on the other
components as long as there is no contraindication for this Complete follow-up is important for
the validity of any study As a strategy to maintain protocol adherence we are using a treatment
regimen that will detect potential side effects and prompt interventions proactively in the interest
of patient safety In addition subjects who permanently stop study medications during the course
of the study are encouraged to continue in the study completing all scheduled visits and tests
451 Rationale for N-acetylcysteine Dosing
To our knowledge there have been no IPF studies to correlate clinical outcome measures with
different dosages for NAC The dosage chosen is based on the IFIGENIA study However BAL
lung GSH levels from subjects with IPF have been augmented with the use of oral NAC at 600
mg 3 times per day In addition lung GSH levels have been associated with improved
PFTs212227 The dose chosen for this study was based on previous data including the IFIGENIA
study30
4511 Dosing of N-acetylcysteineplacebo
Dosing of NACPL will be 600 mg orally 3 times a day (1800 mgday)
4512 Reasons to Discontinue N-acetylcysteineplacebo
NACPL may be temporarily or permanently discontinued for the duration of the study for
gastrointestinal symptoms or dermatologic reactions
35
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Temporarily discontinue (hold) oral NACPL for subjects requiring inpatient admission for acute
exacerbation (AEx) or other conditions Resume NACPL after discharge
36
37
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
452 Dosage Algorithms
Dosage Adjustment Algorithm 1 NACPL Dose Modifications for Gastrointestinal Symptoms Nausea Vomiting Abdominal Discomfort Diarrhea
GI Symptoms determined by the PI to be clinically significant Nausea Vomiting Abdominal Discomfort Diarrhea
NACPL Temporarily dc (HOLD) x 3 Days
Monitor symptoms intervene as clinically indicated (eg fluid replacement antidiarrhea or antinausea medication)
Monitor or lab PRN
Are symptoms resolving after 3 days NO
Symptoms NOT resolving after 3 days of holding study medication Assessmentmanagement per clinical
discretion of investigator
Likely not study medication discuss resuming study medication with medical monitor when symptoms resolved
YES
Temporarily dc (HOLD) NACPL for 4 additional days (total hold 1 week) then NACPL Resume 600 MG TID
Did symptoms recur
YES
STOP NACPL for
duration of study
NO
NACPL No Change
38
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Dosage Adjustment Algorithm 2 NACPL Dose Modifications For Dermatologic Reactions
Dermatologic Reactions (Not Acneiform) ge Grade 2 Grading per Common Terminology Criteria for
Adverse Events V30 (httpctepcancergov) For example Grade 1 RASHDESQUAMATION Macular or papular eruption or erythema without associated symptoms Grade 2 RASHDESQUAMATION Macular or popular eruption or erythema with pruritus or other associated symptoms localized desquamation or other lesions covering lt50 of body surface area
NACPL Temporarily dc (HOLD) x 3 days
Are symptoms resolving after 3 days
NO Symptoms not resolving after 3 days of holding study medication Assessmentmanagement per clinical discretion of investigator Likely not study medication Discuss resuming study medication with medical monitor when symptoms
resolved YES
Temporarily dc (HOLD) NACPL for 4 additional days (total hold 1 week) then NACPL resume 600 MG TID
Did symptoms recur
YES
STOP NACPL for
duration of study
NO
NACPL No change
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
46 Contraindications Precautions and Side Effects of Study Medications
461 Contraindication
Contraindication to NAC is known hypersensitivity to it
462 Precautions
Concomitant administration of oral NAC and antibiotics has shown a slightly reduced absorption
of cephalexin and a slight increase in erythromycin serum levels NAC contains free sulfhydryl
groups There is no evidence that individuals sensitive to sulfa drugs are sensitive to NAC
The NAC preparation being administered in this study contains 20 mg of aspartame Because of
the phenylalanine component of aspartame individuals with phenylketonuria should avoid or
restrict aspartame intake to avoid increased blood levels of phenylalanine Because of this risk
labeling is required on all products containing aspartame
463 Side Effects
Side effects of NAC range from common to serious See Table 4
39
40
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Table 4 Side Effects of NAC
Undesirable Effects
System-organ class Uncommon
(gt11000 lt1100)
Rare
(gt110000 lt11000)
Very rare
(lt110000) Not known
Immune system disorders Hypersensitivity Anaphylactic shock
reaction
Nervous system disorders Headache
Ear and labyrinth disorders Tinnitus
Cardiac disorders Tachycardia
Vascular disorders Hemorrhage
Respiratory thoracic and
mediastinal disorders
Bronchospasm
Dyspnea
Gastrointestinal disorders
Vomiting diarrhea
stomatitis abdominal
pain nausea
Dyspepsia
Skin and subcutaneous tissue
disorders
Urticaria rash
angioedema itching
General disorders and
administration site conditions Pyrexia
Investigations Reduced arterial
pressure Face edema
In very rare cases the onset of severe skin reactions such as Stevens-Johnson syndrome and Lyell syndrome was reported to have a temporal relationship with N-acetylcysteine administration Although in most cases at least another suspect drug probably most involved in the genesis of the above mentioned mucocutaneous syndromes has been identified in case of mucocutaneous alterations it is appropriate to contact onersquos doctor and the administration of N-acetylcysteine should be immediately discontinued
Some studies confirmed a reduction of platelet aggregation during N-acetylcysteine administration The clinical significance of these findings has not been defined yet [Source Fluimucil Investigator Brochure]
47 Recruitment Procedures
Subjects recruited for this study will be established patients of the investigators or physician- or
self-referred to participating clinical centers in the IPFnet Each clinical center within IPFnet has
a well-developed infrastructure of local pulmonologists within the surrounding geographic area
These pulmonologists are kept informed of ongoing IPF clinical trials and regularly refer
subjects to studies conducted at IPFnet clinical centers
Additional steps will be taken to inform clinicians of the trials in progress within IPFnet
including presentations at faculty staff meetings at local hospitals medical grand rounds and
national conferences direct mail notification monthly faxes and advertisement of network trials
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
in pulmonary journals Clinical center patients previously diagnosed with IPF will be notified of
the trials by mail whenever possible
Recruitment of minorities and women will be monitored by the DCC and DSMB If necessary
additional recruitment efforts will be made at specific centers to ensure that the aggregate subject
sample contains appropriate representation of women and minorities
48 Study Procedures
The following procedures are detailed in the PANTHER-IPF MOOP accompanying this
protocol
1 PFT
2 ABG
3 HRCT scan of the chest (including imaging of pulmonary arteries)
4 CBC and serum chemistries
5 Pregnancy test
6 6MWTBorg Dyspnea Scale
7 QOL questionnaires (EuroQol HAD SF-36 SGRQ and ICE CAP)
8 UCSD SOBQ
9 Gender Substudy Questionnaire
All assessments of PFTs will be conducted by study personnel not directly involved in the
treatment of the subjects
481 Biological Specimen Management
4811 Biological Specimen Sample Management
Subjects at clinical centers participating in the specimen repository substudy who consent to
having blood drawn for research purposes and for the banking of blood blood components and
other biologic specimens (urine and BAL fluid) will have approximately 405 mL of blood
41
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
drawn 17 mL blood drawn for DNA and 20 mL of urine collected at enrollment visit Subjects
will have approximately 50 mL of blood drawn and 20 mL of urine collected at each 15-week
follow-up visit Blood specimens will be separated according to PANTHER-IPF MOOP
guidelines into the following components for banking in the repository serum plasma and
DNA Coding of all biologic specimens for the repository will be performed by study staff at the
clinical center The samples will be processed per PANTHER-IPF MOOP guidelines aliquoted
labeled with barcode labels and stored at -70degC at the clinical center and shipped to the central
repository
The only subject identifiers will be a sample ID number and subject initials This sample ID will
be linked in the IPFnet DCC clinical database to subject information No subject information will
be transferred to the biological-specimen database
The subjectrsquos samples may be used for approved sub-studies relating to human disease
including but not limited to IPF The studies for which an individualrsquos samples will be made
available will be determined by the subjectrsquos answers to questions on the biological-sample
informed consent form The subjects can choose to make their samples available for all options
or any combination Samples will be made available to researchers only with IPFnet Steering
Group approval until such time as the samples are made public through the NHLBI repository
49 Concomitant Medications
Concurrent treatment with FDA-approved therapy for IPF is allowed Colchicine may be used
for treatment of gout Temporary treatment with oral or IV corticosteroids for clinical worsening
or suspected AEx is permitted Nutritional supplements containing NAC are not allowed
410 Laboratory Testing
Clinical laboratory parameters will be assessed at screening and at the end of the study The
following tests will be performed at the two time points specified in the protocol chemistry (AG
ratio ALT [SGPT] AST [SGOT] albumin alkaline phosphatase amylase bilirubin-direct
42
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
bilirubin-indirect bilirubin-total BUN BUNcreatinine ratio calcium carbon dioxide
cholesterol-total chloride CPK-total creatinine GGT globulin glucose iron-total LDH
lipase magnesium phosphorus-inorganic potassium protein-total sodium TIBC triglycerides
uric acid) and hematology (red blood cell count WBC count hemoglobin hematocrit cell
indices differential platelet count)
411 Blinding of Study Drugs
Subjects and caregivers will be blinded to study treatment Every subject will receive NAC or
matching PLs at every study visit from the baseline visit to the week-45 visit No study agent
will be dispensed at the week-60 visit
43
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
5 Study Endpoints
51 Primary Study Endpoint
The primary endpoint will be the change in serial measurements of FVC over the study period
52 Secondary Study Endpoints
521 Time to Disease-progression
The time-to-death or a 10 decline in FVC will be defined as the time-to-disease progression
The 10 decline in FVC from enrollment must be confirmed on 2 consecutive visits no less than
6 weeks apart For subjects with 2 consecutive visits with a 10 decline in FVC the time-toshy
disease progression will be defined as the time interval between enrollment and the initial visit
with a 10 FVC decline For subjects who experience disease progression the study doctor will
determine whether or not the subject will remain in the study
522 Acute Exacerbations
The following 3 criteria will define AEx in subjects with acute worsening of their respiratory
conditions
1 Clinical (all of the following required)
A) Unexplained worsening of dyspnea or cough within 30 days triggering unscheduled
medical care (eg emergency room clinic study visit hospitalization)
B) No clinical suspicion or overt evidence of cardiac event pulmonary embolism or deep
venous thrombosis to explain acute worsening of dyspnea
C) No pneumothorax
44
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
2 RadiologicPhysiologic (A and B required)
A) New ground glass opacity or consolidation computed tomography (CT) scan OR new
alveolar opacities on chest x-ray
B) Decline of ge 5 in resting room air SpO2 from last recorded level OR decline of ge 8 mm
Hg in resting room air PaO2 from last recorded level
3 Microbiologic (all of the following required)
A) No clinical evidence for infection (ie absence of grossly purulent sputum fever gt 39degC
orally)
B) Lack of positive microbiological results (if done) from lower respiratory tract defined as
(1) Clinically significant bacterial growth on sputum or endotracheal aspirate cultures
(2) Quantitative culture by protected brush specimen ge 103 cfumL or BAL ge 104 cfumL
(3) The presence of specific pathogens on stains of any of the above
C) Lack of positive pathogen in blood cultures (if done)
Identification of Acute Exacerbations
All subjects will be educated about the importance of identifying AExs At the time of
enrollment subjects will be told about the possibility of developing acute symptomatic
worsening that might represent an AEx of IPF and instructed to contact their study clinical
center coordinator within 48 to 72 hours of the apparent event
All subjects will be contacted by phone monthly and questioned about any change in dyspnea or
cough and any interim clinic visits or hospitalizations Finally as part of the IPFnet outreach to
community referring physicians the importance of AExs will be emphasized When a subject is
identified who meets criterion 1A this will trigger the collection of additional clinical data to
evaluate a suspected AEx These data will be collected as part of standard clinical care (ie this
protocol does not require collection of all items) The additional items to be collected for
suspected AEx include
IPFnet AEx case report form (eCRF) (required)
45
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Chest x-ray CT scan withwithout pulmonary angiogram (reports should be faxed and
followed by the hard copiesdiscs)
Oxygen saturation (pulse oximetry)
ABG
Respiratory cultures (sputum endotracheal aspirate lavage)
Blood cultures
Clinichospital records related to the event
All potential cases of AEx will be reviewed by the clinical center PI first and a decision on
whether the case may represent an AEx will be made If AEx is suspected the case will be sent
to the IPFnet adjudication committee which will assign a final diagnosis (see Table 5) If there is
disagreement among members the majority opinion will be recorded
During episodes of suspected AEx as determined by the individual clinical center investigator
subjects will remain blinded and in the study
Table 5 Final Diagnoses in Evaluation of Suspected Acute Exacerbations
Definite acute exacerbation All criteria met no alternative etiology
Unclassifiable acute worsening
Insufficient data to evaluate all criteria no alternative etiology
Not acute exacerbation Alternative etiology identified that explains acute worsening
Management of the suspected AEx will be at the discretion of the treating physician Standard of
care generally involves evaluation for respiratory infection pulmonary embolism cardiac events
and pneumothorax and treatment with IV corticosteroids
Study drugs will be resumed at pre-suspected AEx doses after subjects clinically improve as
confirmed by the local PI All subjects should be seen at the clinical center within 2 to 4 weeks
of recovery for measurement of post-bronchodilator FVC (see Figure 4) Subjects unable to
return to the clinical center after suspected AEx due to medical frailty (eg continued
46
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
institutionalization progressive disability) will be categorized as failing to maintain FVC
response in secondary analyses
Suspected AEx (PI determined)
Hold study drug Treat AEx
(Attending physician determined)
Alive but unable to continue due to
medical frailty
Dead
Alive and able to continue
Site reviewvisit
Restart study drug
FVC within 2-4 weeks
Figure 4 Acute Exacerbation Flow Chart
523 Respiratory Infections
An upper respiratory infection will be defined as
Change in sputum discoloration
Increased cough of no more than 14 daysrsquo duration
A lower-respiratory infection (pneumonia) will be defined as new segmental or lobar airspace
opacities visualized by image studies (chest radiograph or HRCT) in addition to any of the
following
Positive pathogencultures in good sample of sputum or lower-airway secretions retrieved
by fiberoptic bronchoscope
Fever gt 39degC or gt 100degF
Leukocytosis gt 12000 (unexplained no increase in dose of corticosteroids)
47
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
524 Maintained FVC Response
Subjects with follow-up FVCpred measurements at or above their baseline FVCpred level
will be classified as having maintained FVC response Subjects with reduced FVCpred levels
or missing data for any reason including death or medical frailty will be classified as having not
maintained FVC response The FVCpred value is used because unadjusted FVC measurements
are expected to decline with age
48
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
6 Safety Evaluations and Procedures
61 Adverse Events
During a clinical trial the reporting of adverse experience information can lead to important
changes in the way a new treatment is developed as well as provide integral safety data
611 Definitions
An adverse event (AE) is any untoward medical occurrence in a subject or clinical investigation
subject who was administered a pharmaceutical product The AE does not necessarily have to
have a causal relationship with the drug administered An AE can be any unfavorable and
unintended sign (including an abnormal laboratory finding) symptom or disease temporarily
associated with the use of a medicinal product whether or not considered to be related to the
medicinal product Diseases signs symptoms or laboratory abnormalities already existing at
enrollment are not considered AEs unless they worsen (ie increase in intensity or frequency)
Surgical procedures themselves are not AEs they are therapeutic measures for conditions that
require surgery The condition for which the surgery is required may be an AE Surgical
procedures planned before randomization and the conditions necessitating the surgery are not
AEs
A serious adverse event is any untoward event that
Is fatal
Is life-threatening
Requires inpatient hospitalization or prolongation of existing hospitalization with the
following exceptions
o Preplanned (before the study) hospital admissions unless the hospitalization is
prolonged
o Planned admissions (as part of a study eg routine biopsies)
o Hospitalization lasting lt 24 hours
49
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
o Hospitalization for elective procedure
o Emergency room visits
Results in persistent or significant disability or incapacity
Is a congenital anomaly or birth defect
Important medical events that may not result in death be life-threatening or require
inpatient hospitalization may be considered serious adverse events (SAEs) when based
on appropriate medical judgment they may jeopardize the subject and may require
medical or surgical intervention to prevent one of the outcomes listed above
Life-threatening means that the subject was in the view of the investigator at immediate risk of
death from the AE as it occurred It does not include an AE that had it occurred in a more severe
form might have caused death
Persistent or significant disabilityincapacity means that the event resulted in permanent or
significant and substantial disruption of the subjectrsquos ability to carry out normal life functions
Causality
A reasonable possibility means the AE may have been caused byrelated to the study drug A
perceived or real lack of efficacy does not satisfy the definition of relatedness
612 Adverse Event (AE) Reporting
For the PANTHER-IPF trial all AEs (serious and nonserious) occurring from randomization
through final study visit (4 weeks after final dose of all study medication) will be recorded on the
AE page of the case report form (CRF)
6121 Serious Adverse Events (SAE) Reporting
For this trial all deaths and all SAEs which occur from randomization through final study visit
must be entered within the EDC system via the SAE eCRF page within 24 hours of the
investigative sitersquos knowledge of the event It is the responsibility of the clinical center
50
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
investigator to provide a causality assessment of the event for each study medications based upon
the information available at the time of the report It is understood that complete information
about the event may not be known at the time the initial report is submitted In the event the EDC
system is not accessible to the site at the time of event reporting investigative sites will complete
and forward a paper back-up SAE form to DCRI Safety Surveillance for processing
DCRI Safety Surveillance
Telephone 1-919-668-8624 or 1-866-668-7799 (toll free)
Fax 1-919-668-7138 or 1-866-668-7138 (toll free)
The investigator must complete and submit follow-up SAE information via the eCRF when
important new or follow-up information (eg final diagnosis outcome results of specific
investigations) becomes available Follow-up information should be submitted according to the
same process used for reporting the initial event as described above All SAEs will be followed
until resolution stabilization or 30 days after the subject has completed the final visit (4 weeks
after the final dose of study medication) whichever occurs first The investigator is responsible
for reporting SAEs to their institutional review board (IRB) per site specific IRB reporting
guidelines
6122 Regulatory Reporting
AEs that are serious study drug related and unexpected will be reported to the regulatory
authorities The DCRI Safety Surveillance medical monitor will perform a medical review of all
SAEs submitted and evaluate for ldquounexpectednessrdquo DCRI Safety Surveillance will prepare
MedWatch reports for those events identified as serious study drug related and unexpected as
determined by Safety Medical Monitor
DCRI Regulatory Services will submit all unexpected study drug-related SAEs as per 21 CFR
32 DCRI Safety Surveillance will provide a safety alert letter to the NHLBI DSMB and DCC
clinical operation (for distribution to sites) within 15 days of initial receipt of the information
51
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Investigators are responsible for promptly reporting these events to their reviewing IRBs
according to site specific IRB reporting guidelines
62 Clinical Medical Monitoring
There will be an unblinded physician at the IPFnet DCC serving as medical monitor The
medical monitor will be available to assist with questions about dosage adjustments of study
medications including discontinuation or resumption of medications
63 Unblinding Procedures
Unblinding of subjects or investigators to subject treatment is strongly discouraged For ongoing
clinical management all subjects should be presumed to be receiving ldquoactiverdquo study drug To
ensure the subjectrsquos safety the study treatment will be dose-adjusted based on laboratory test
results clinical findings and symptoms
The IPFnet DCC medical monitor and PANTHER-IPF co-chairs Drs Ganesh Raghu and
Fernando Martinez will be available to the study physicians to discuss study drug management
on a case-by-case basis Un-blinding will be considered ONLY when the knowledge of subject
treatment assignment is ABSOLUTELY ESSENTIAL for subject safety and after discussion of
the subjectrsquos case with the medical monitor and either Dr Raghu or Dr Martinez Unblinding of
study treatment should be minimized during the conduct of the trial In those cases where it is
felt to be medically necessary the DCC medical officer will communicate directly with the
managing physician to minimize unblinding of study personnel
52
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
7 Study Drug Procedures
At the baseline 15-week 30-week and 45-week study visits subjects will receive a supply of
study drug sufficient to last until the next visit at which study drug will be dispensed
53
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
8 Data Management
81 Hardware and Software Configuration
811 Hardware and Database Software
Data will be stored in an Oracle database system Oracle has advantages of processing efficiency
and smooth linkage with other software systems The application and database will be hosted on
Solaris Unix servers at the IPFnet DCC
812 Statistical Software
SAS will be used as the principal application for the management of analysis data files and
statistical computations S-Plus will be used to provide supplementary functions as needed
813 Access Control and Confidentiality Procedures
Access to databases will be controlled centrally by the IPFnet DCC through user passwords
linked to appropriate privileges This protects the data from unauthorized changes and
inadvertent loss or damage
814 Security
Database and Web servers will be secured by a firewall and through controlled physical access
Oracle has many security features to ensure that any staff member accessing the database has the
proper authority to perform the functions he or she requests of the system Within the secondary
SAS databases Unix group-access control maintains similar security The Sun workstation login
is secured by extensive user-password facilities under Unix
54
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
815 Back-up Procedures
Database back-up will be performed automatically every day and standard IPFnet DCC policies
and procedures will be applied to dictate tape rotation and retention practices
816 Virus Protection
All disk drives that provide network services and all user computers will be protected using
virus-scanning software Standard IPFnet DCC policies will be applied to update these protection
systems periodically through the study
82 Sources of Data
821 Design and Development
The IPFnet DCC will be responsible for development of the electronic case report forms
(eCRFs) development and validation of the clinical study database ensuring data integrity and
training clinical center staff on applicable data management procedures A web-based distributed
data entry model will be implemented This system will be developed to ensure that guidelines
and regulations surrounding the use of computerized systems used in clinical trials are upheld
The remainder of this section provides an overview of the data management plan associated with
this protocol
822 Data Collection Forms
The data collection process consists of direct data entry at the study clinical centers into the EDC
system(s) provided by the DCC A data collection worksheet will be provided to clinical centers
for recording data in the event the EDC system is unavailable Data entry of the eCRFs should
be completed according to the instructions provided and project specific training The
investigator is responsible for maintaining accurate complete and up-to-date records and for
ensuring the completion of the eCRFs for each research participant
55
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
823 Data Acquisition and Entry
Data entry into eCRFs shall be performed by authorized individuals Selected eCRFs may also
require the investigatorrsquos written signature or electronic signature as appropriate Electronic
CRFs will be monitored for completeness accuracy and attention to detail during the study
824 Data Center Responsibilities
The IPFnet DCC will 1) develop a data management plan and will conduct data management
activities 2) provide final eCRFs for the collection of all data required by the study 3) develop
data dictionaries for each eCRF that will comprehensively define each data element 4) conduct
ongoing data monitoring activities on study data 5) monitor any preliminary analysis data
cleanup activities and 6) rigorously monitor final study data clean up
825 Data Editing
Completed data will be entered into the IPFnet DCC automated data acquisition and
management system If incomplete or inaccurate data are found a data clarification request will
be generated and distributed to clinical centers for a response Clinical centers will resolve data
inconsistencies and errors and enter all corrections and changes into the IPFnet DCC automated
data acquisition and management system
826 Training
The training plan for clinical center staff includes provisions for training on assessments eCRF
completion guidelines data management procedures and the use of computerized systems
56
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
9 Study Design and Data Analysis
91 General Analytic Considerations
All primary analyses will be based on intent-to-treat (ITT) principles using all randomized
subjects Baseline factors across groups will be compared using mean (standard deviation) and
median (25th and 75th percentiles) summary measures Kaplan-Meier curves will be used to
display event rates Due to clinical interest in departures from both sides of the null hypothesis
all test statistics will be 2-sided
Reasonable caution needs to be taken when conducting multiple analyses on key clinical
subgroups For subgroup analyses a conservative significance level of 0001 will be used for all
interaction tests Thus subgroup comparisons will be considered exploratory unless the p-value
from the interaction test is smaller than 0001
92 Randomization Blinding and Reporting of Results
A permuted block-randomization scheme will be created with varying block sizes stratified by
clinical center Once a subject has completed the screening and baseline period and evaluation
for inclusionexclusion criteria the randomization process will begin Subjects will be
randomized to receive NAC or matching placebo with equal probability (11) via telephone
contact with a central interactive voice response system (IVRS) using a toll-free randomization
number On the day of randomization after the subject has successfully met all inclusion and
exclusion criteria the investigator or designee will call the central randomization number to
obtain the assigned kit randomization numbers for that subject At each subject visit the
investigator or designee will call the central randomization number to obtain the new kit
randomization numbers for resupply of the subject For resupply of the clinical center the IVRS
will monitor minimal volume of a kit type andor expiration date and will automatically notify
the pharmacy
57
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
The trial results will be reported according to guidelines specified in the CONSORT statement
A flow diagram describing screening recruitment randomization dropout and vital status will
be included in the primary manuscript AEs and efficacy data will be presented for all treatment
groups Adherence dropout and lost to follow-up will be carefully examined across all treatment
groups Analyses of safety will be based on data from all randomized subjects who received at
least one dose of study drug
93 Stratification
Subjects will be distributed to the two treatment arms in a 11 allocation ratio Stratification
blocks will be based on clinical centers
94 Specification of the Primary Analyses
A mixed model repeated measures (MMRM) analysis described in section 95 will be used to
compare differences in the slope of FVC measurements across the treatment groups Response
variables are values of the FVC measured at baseline and every 15 weeks until study completion
Variables in the model will include treatment time and time by treatment age sex race and
height Contrast estimates of differences in slopes of treatment over time (along with confidence
intervals) will be used to estimate the treatment effect The validity of this model in terms of
meeting modeling assumptions will be assessed via standard modeling diagnostics and goodness-
of-fit measures Based on the MMRM framework missing FVC data will not be imputed for the
primary analysis
95 Analysis of Longitudinal Endpoints
A common goal in clinical trials is to specify models that are easily implemented and
reproducible by independent data analysts On the other hand the models should have proper
statistical behavior in terms of low bias and high precision Many common approaches to
longitudinal data analysis including last observation carried forward (LOCF) imputation rely on
the missing completely at random (MCAR) assumption However the MCAR assumption is
58
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
unlikely to hold in many clinical trials because missing data are often related to disease
progression and prognosis A more reasonable assumption missing at random (MAR) specifies
that the complete data distribution can be modeled using only the observed data The likelihood-
based MMRM approach is valid under the more general MAR assumptions These models will
be applied to analyze the longitudinal data secondary endpoints
The advantages of MMRM analysis are that all important characteristics of the model can be preshy
specified standard software can be used to implement the models and results are based on ITT
principles43 In addition the MMRM approach offers superior control of Type I and Type II
errors compared with the LOCF approach
Response variables are values of the PFTs measured at enrollment and every 15 weeks until
study completion and 6MWT values measured at baseline week 30 and week 60 Covariates are
treatment time time by treatment and key baseline risk factors Contrasts (along with
confidence intervals) of treatment by time will be used to estimate the treatment effect
The correlation structure involves multiple pieces including measurement errors random
variation and interindividual variability For the longitudinal data analyses an unstructured
correlation matrix for within-subject errors will be assumed Other correlation structures
including compound symmetry will be examined as needed A careful examination of reasons
for study discontinuation will be conducted to assess the validity of MCAR Sensitivity analyses
will be used to examine the untestable assumption that the observed data violate the MAR
assumption The MMRM models will be implemented using PROC MIXED in SAS
96 Analysis of Binary Time-to-Event and Time-Lagged Endpoints
Regression modeling approaches using either the logistic regression model or Cox proportional
hazards regression model will be employed when appropriate The validity of these models will
be assessed via standard modeling diagnostics and goodness-of-fit measures Estimates of
cumulative frequencies for more general time-lagged responses will be calculated using the
partitioned version of the Bang-Tsiatis estimator44 The partitions will be set at 15-week intervals
59
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
to correspond with the data-collection process Covariate adjusted event rates will be calculated
using inverse probability-weighted regression estimates45
97 Power Analysis
971 Primary Analyses
Based on previously published IPF clinical trials the PL group is expected to experience a drop
in FVC of approximately 020 L over the study period (see Figure 1) The IPFnet Steering Group
determined a clinically important difference would be to preserve the majority of the decline
relative to PL over the study period In particular a treatment effect of 015 L was determined to
be a clinically meaningful difference Potential dropout is a key factor in the proposed study The
drop-out process assumed 5 lost to follow-up after every study visit Only 80 of subjects
were assumed to be followed for the entire study period All models assumed a compound
symmetry structure for the covariance matrix Power calculations were performed using a SAS
IML program for designing repeated measures studies46 Based on preliminary reviews of the
data from the University of Michigan the covariance matrix parameters were estimated at
approximately σ2 = 0757 (variance parameter) and ρ = 0936 (correlation parameter) To be
conservative the power calculations for the primary analysis were performed with parameter
setting of σ2 = 0810 (variance parameter) and ρ = 0925 (correlation parameter)
The power calculations assume a correction for imperfect compliance proposed by Lachin and
Foulkes to allow for 2 noncompliance for each of the treatment arms47 Thus the sample size
of 130 subjects per arm would be reduced to an adjusted sample size of 130(1-002-002)2 =
1198 or 120 subjects per arm
Under the assumed Type I error rate of 005 with a correlation parameter of 0925 and standard
deviation of 090 the difference of 015 L (or 00025 Lweek) shown in Table 6 would have
power of 93
60
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Table 6 Hypothetical Values of Mean FVC (L) Change from Baseline
Week 15 Week 30 Week 45 Week 60
NAC 00125 00250 00375 00500
Placebo 00500 01000 01500 02000
Difference 00375 00750 01125 01500
Abbreviations FVC forced vital capacity PL placebo
972 Power Analysis for Secondary Endpoints
Power calculations for secondary endpoint measurements are shown in Table 7 Standard
deviations are based on unpublished data provided by the University of Michigan The
calculations are based on a 2-sample t-test with Type I error rate set at 005 These calculations
are likely to be conservative because the statistical approach described in section 95 for
analyzing these endpoints will incorporate incomplete observations as well as intermediate data
points
Table 7 Detectable Differences in Treatment Means for Selected Endpoint Measurements
Secondary Endpoints Std Dev
of the Baseline Score
Detectable Difference for 80 Power
Std Dev of the Change Score
Difference Detectable for
80 Power
DLCOpred 166 58 91 32
6MWT Area Under the Desaturation Curve
219 76 175 61
6MWT Distance to Desaturation 224 78 315 110
6MWT Minutes Walked 210 073 205 071
Abbreviations Std Dev standard deviation DLCOpred diffusing capacity of the lung for carbon monoxide percent predicted 6MWT 6-minute walk test
61
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
10 Study Administration
101 Cooperative Agreement Mechanism
The administrative and funding mechanism used to undertake this project is a ldquocooperative
agreementrdquo (U01) which is an assistance mechanism Under the cooperative agreement the
NHLBI assists supports andor stimulates the project and is substantially involved with
investigators in conducting the study by facilitating performance of the effort in a ldquopartnerrdquo role
The NHLBI project scientist serves on the IPFnet Steering Group and he or another NHLBI
scientist may serve on other project committees when appropriate At the same time however
NHLBI does not assume a dominant role direction or prime responsibility for this research
program
As described below governance of the project is conducted through the IPFnet Steering Group
Principal investigators have lead responsibilities in all aspects of their trials and the project
including any modification of trial designs conduct of the trials quality control data analysis
and interpretation preparation of publications and collaboration with other investigators unless
otherwise provided for by the IPFnet Steering Group
PIs retain custody of and have primary rights to their center-specific and collaborative data
subject to government rights-of-access consistent with current Health amp Human Services (HHS)
Public Health Service (PHS) and National Institutes of Health policies The protocols and
governance policies call for the continual submission of data centrally to the IPFnet DCC for the
collaborative database which at a minimum will contain the key variables selected by the IPFnet
Steering Group for standardization across all clinical centers the submission of copies of the
collaborative datasets to each PI upon completion of the project procedures for data analysis
reporting and publication and procedures to protect and ensure the privacy of medical and
genetic data and records of individuals The NHLBI project scientist on behalf of the NHLBI
will have the same access privileges and responsibilities regarding the collaborative data as the
other members of the Steering Group
62
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
PIs are also encouraged to publish and to publicly release and disseminate results data and other
products of the project concordant with the project protocols and governance and the approved
plan for making data and materials available to the scientific community and to the NHLBI
However during the 3 years after the ending date of NHLBI project support unpublished data
unpublished results data sets not previously released and other study materials or products are
to be made available to any third party only with the approval of the IPFnet Steering Group
Upon completion of the project PIs are expected to put their intervention materials and
procedure manuals into the public domain andor make them available to other investigators
according to the approved plan for making data and materials available to the scientific
community and the NHLBI for the conduct of research at no charge other than the costs of
reproduction and distribution
The NHLBI reserves the right to terminate or curtail the project (or an individual award) in the
event of (a) failure to develop or implement mutually agreeable collaborative measurement
subject eligibility and data management sections of the protocols (b) substantial shortfall in
subject recruitment follow-up data reporting or quality control or other major breach of
protocol (c) substantive changes in the agreed-upon protocols with which NHLBI cannot
concur (d) reaching a major project outcome with persuasive statistical significance
substantially before schedule or (e) human subject ethical issues that may dictate a premature
termination
Any disagreement that may arise in scientificprogrammatic matters (within the scope of the
award) between award recipients and the NHLBI may be brought to arbitration An arbitration
panel will be composed of 3 membersmdash1 selected by the IPFnet Steering Group (with the
NHLBI member not voting) or by the individual PI in the event of an individual disagreement a
second selected by NHLBI and the third selected by the other 2 members This special
arbitration procedure in no way affects the PIrsquos right to appeal an adverse action that is otherwise
appealable in accordance with the PHS regulations at 42 CFR part 50 Subpart D and HHS
63
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
regulation at 45 CFR part 16 or the rights of the NHLBI under applicable statutes regulations
and terms of the award
102 IPFnet Steering Group
The IPFnet Steering Group is the main governing body of the project It is composed of the PIs
of the clinical centers the PI of the DCC and the NHLBI project scientist The clinical centers
the IPFnet DCC and the NHLBI each have 1 vote on the IPFnet Steering Group All decisions
are determined by majority vote
All major scientific decisions are determined by the IPFnet Steering Group It assumes overall
responsibility for the design and conduct of the trial It appoints (and disbands) committees and
subcommittees as the need arises designs approves and implements the study protocols
oversees the development of the MOOP monitors subject recruitment and treatment delivery
evaluates data collection and management oversees quality assurance procedures and
implements changes and enhancements to the study as required It also has primary responsibility
for facilitating the conduct of the trials and reporting the projectrsquos results
103 Data and Safety Monitoring Board
The NHLBI will establish a DSMB in accordance with established policies (see
httpwwwnhlbinihgovfundingpoliciesdsmb_insthtm) to ensure data quality and subject
safety and to provide independent advice to the NHLBI regarding progress and the
appropriateness of study continuation
104 Recommendations on Interim Monitoring of Efficacy Safety and Futility
First and foremost the role of the DSMB will be to review subject safety and trial conduct at
periodic points during the study The DSMB may require analyses of the primary endpoint
results for comparing the benefit and risks of treatment strategies The benefit of collecting
additional data on key secondary endpoints with extended follow-up and establishing a robust
64
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
evidence base for determining a standard of care will need to be carefully considered before
early termination of one or more treatment arms After careful consideration the IPFnet Steering
Group recommends conservative thresholds for the early examinations of the safety and efficacy
data
The DSMB will be expected to meet approximately every 6 months until trial completion to
review safety and toxicity data The DSMB may recommend stopping the study based on these
reviews Because the DSMB could stop the trial for safety concerns as well as for a large
efficacy benefit there could be multiple opportunities to reject the null hypothesis (no difference
in event rates between the PL and NAC groups) A Bonferroni approximation will be applied
during the one planned interim analysis for efficacy
Before locking the database a statistical analysis plan (SAP) will be developed to provide
complete details on the statistical analysis The SAP will include the specifics for how and when
the DSMB will be notified for AEs The IPFnet DCC will deliver to the DSMB all FDA-defined
AEs at 3-month intervals The IPFnet DCC will prepare narrative SAE reports in real time for
DSMB review including recommendations and analysis of similar events for each SAE
submitted to the FDA
65
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
11 Investigator and Sponsor Obligations
111 Monitoring
All monitoring activities for US clinical centers will be performed in accordance with DCRI
standard operating procedures Information regarding the types of visits will be outlined in the
PANTHER-IPF MOOP
112 Cost and Payment
There will be no cost to subjects enrolled in this trial Study-related procedures will be paid for
by the IPFnet
Subjects may be eligible for reimbursement for travel to the clinical center Details of payment
will be explained to each subject during the consent process
113 Confidentiality and Health Insurance Portability and Accountability Act
Considerations
Subject confidentiality will be protected throughout the study All subject data will be kept
strictly confidential and no subject-identifying information will be released to anyone outside
the project Confidentiality will be assured through several mechanisms First each subject will
be assigned an anonymous study ID which will then be used on all study forms Second any
study forms blood samples and paper records that contain subject information (eg address lists
phone lists) will be kept at the clinical centers in secured locked areas coded by number Once
blood is collected there will be no subject identifiers placed on blood samplesmdashonly the study
ID number and the date of sample collection Third access to all subject data and information
including laboratory specimens will be restricted to authorized personnel In the case of
computerized data this restricted access will be assured through user logon IDs and password
protection
66
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
At the IPFnet DCC only authorized personnel will have access to the data files containing study
data Security will be assured through user logon IDs passwords and appropriate access
privileges All study subjects will be identified only by their IPFnet ID numbers and no personal
identifying information such as name address or Social Security number will be entered into
the IPFnet DCC database Any subject-specific data reported to the IPFnet Steering Group will
be identified only by the IPFnet ID number
Finally subjects will not be identified by name in any reports or publications nor will the data
be presented in such a way that the identity of individual subjects can be inferred Analysis files
created for further study by the scientific community will have no subject identifiers These data
files will be created in accordance with the Ancillary Studies and Publication Policy of the
IPFnet
114 Informed Consent Procedures
All IPFnet subjects will provide written informed consent using procedures reviewed and
approved by each clinical centerrsquos IRB Informed consent will be undertaken by study personnel
in-person with the subject The subject has the option of declining further participation in the
study at that point No further study procedures will be conducted until the signed documents
have been provided to the IPFnet clinical center
115 Institutional Review Boards
Before initiating this study the protocol clinical center-specific informed consent forms Health
Insurance Portability and Accountability Act (HIPAA) forms recruitment materials and other
relevant information will be reviewed by a properly constituted IRB at each participating clinical
center A copy of the signed and dated IRB approval at each clinical center will be retrieved prior
to or during the site initiation visit and archived at the IPFnet DCC Any amendments to the
protocol other than simple administrative and typographical changes must be approved by each
IRB before they are implemented The clinical centers will seek annual renewals of their IRB
approvals in accordance with local procedures
67
__________________________________________ ________________
__________________________________________
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
12 Investigator Agreement
I have read the foregoing protocol PANTHER-IPF and agree that it contains all necessary
details for carrying out this study I will conduct the study as outlined herein and will complete
the study within the time designated
I will provide copies of the protocol and all pertinent information to all individuals responsible to
me who assist in the conduct of this study I will discuss this material with them to ensure they
are fully informed regarding the drug and the conduct of the study
I will fulfill all responsibilities for submitting pertinent information to the local IRB if
applicable that is responsible for this study
I further agree that NHLBI andor DCRI will have access to any source documents from which
eCRF information may have been generated
Signature of Principal Investigator Date
Name of Principal Investigator (printed or typed)
Protocol version date May 19 2009
Protocol Amendment 1 version date May 28 2010
Protocol Amendment 2 version date December 6 2011
68
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
13 References
1 Raghu G Brown KK Bradford WZ et al A placebo-controlled trial of interferon gamma-1b in patients with idiopathic pulmonary fibrosis N Engl J Med 2004350125-33 2 King TE Jr Safrin S Starko KM et al Analyses of efficacy end points in a controlled trial of interferon-gamma1b for idiopathic pulmonary fibrosis Chest 2005127171-7 3 Flaherty KR Thwaite EL Kazerooni EA et al Radiological versus histological diagnosis in UIP and NSIP survival implications Thorax 200358143-8 4 Wells AU Desai SR Rubens MB et al Idiopathic pulmonary fibrosis a composite physiologic index derived from disease extent observed by computed tomography Am J Respir Crit Care Med 2003167962-9 5 Raghu G Freudenberger TD Yang S et al High prevalence of abnormal acid gastroshyoesophageal reflux in idiopathic pulmonary fibrosis Eur Respir J 200627136-42 6 Kinnula VL Focus on antioxidant enzymes and antioxidant strategies in smoking related airway diseases Thorax 200560693-700 7 Coultas DB Zumwalt RE Black WC Sobonya RE The epidemiology of interstitial lung diseases Am J Respir Crit Care Med 1994150967-72 8 Raghu G Weycker D Edelsberg J Bradford WZ Oster G Incidence and prevalence of idiopathic pulmonary fibrosis Am J Respir Crit Care Med 2006174810-6 9 Olson AL Swigris JJ Lezotte DC Norris JM Wilson CG Brown KK Mortality from pulmonary fibrosis increased in the United States from 1992 to 2003 Am J Respir Crit Care Med 2007176277-84 10 Mannino DM Etzel RA Parrish RG Pulmonary fibrosis deaths in the United States 1979shy1991 An analysis of multiple-cause mortality data Am J Respir Crit Care Med 19961531548shy52 11 Hubbard R Johnston I Coultas DB Britton J Mortality rates from cryptogenic fibrosing alveolitis in seven countries Thorax 199651711-6 12 Johnston I Britton J Kinnear W Logan R Rising mortality from cryptogenic fibrosing alveolitis Bmj 19903011017-21 13 Raghu G Collard HR Egan JJ et al An official ATSERSJRSALAT statement idiopathic pulmonary fibrosis evidence-based guidelines for diagnosis and management Am J Respir Crit Care Med 2011183788-824 14 (USA) FDA FDA Public Health Advisory Interferon gamma-1b (marketed as Actimmune) In 2007 15 King TE Jr Pardo A Selman M Idiopathic pulmonary fibrosis Lancet 2011 16 Raghu G Brown KK Costabel U et al Treatment of idiopathic pulmonary fibrosis with etanercept an exploratory placebo-controlled trial Am J Respir Crit Care Med 2008178948shy55 17 Malouf MA Hopkins P Snell G Glanville AR An investigator-driven study of everolimus in surgical lung biopsy confirmed idiopathic pulmonary fibrosis Respirology 201116776-83 18 King TE Jr Behr J Brown KK et al BUILD-1 a randomized placebo-controlled trial of bosentan in idiopathic pulmonary fibrosis Am J Respir Crit Care Med 200817775-81 19 Richeldi L Costabel U Selman M et al Efficacy of a tyrosine kinase inhibitor in idiopathic pulmonary fibrosis N Engl J Med 20113651079-87
69
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
20 Borok Z Buhl R Grimes GJ et al Effect of glutathione aerosol on oxidant-antioxidant imbalance in idiopathic pulmonary fibrosis Lancet 1991338215-6 21 Meyer A Buhl R Magnussen H The effect of oral N-acetylcysteine on lung glutathione levels in idiopathic pulmonary fibrosis Eur Respir J 19947431-6 22 Behr J Maier K Degenkolb B Krombach F Vogelmeier C Antioxidative and clinical effects of high-dose N-acetylcysteine in fibrosing alveolitis Adjunctive therapy to maintenance immunosuppression Am J Respir Crit Care Med 19971561897-901 23 Cantin AM North SL Fells GA Hubbard RC Crystal RG Oxidant-mediated epithelial cell injury in idiopathic pulmonary fibrosis J Clin Invest 1987791665-73 24 Waghray M Cui Z Horowitz JC et al Hydrogen peroxide is a diffusible paracrine signal for the induction of epithelial cell death by activated myofibroblasts Faseb J 200519854-6 25 Larios JM Budhiraja R Fanburg BL Thannickal VJ Oxidative protein cross-linking reactions involving L-tyrosine in transforming growth factor-beta1-stimulated fibroblasts J Biol Chem 200127617437-41 26 Kinnula VL Fattman CL Tan RJ Oury TD Oxidative stress in pulmonary fibrosis a possible role for redox modulatory therapy Am J Respir Crit Care Med 2005172417-22 27 Meyer A Buhl R Kampf S Magnussen H Intravenous N-acetylcysteine and lung glutathione of patients with pulmonary fibrosis and normals Am J Respir Crit Care Med 19951521055-60 28 Behr J Degenkolb B Krombach F Vogelmeier C Intracellular glutathione and bronchoalveolar cells in fibrosing alveolitis effects of N-acetylcysteine Eur Respir J 200219906-11 29 Bando M Hosono T Mato N et al Long-term efficacy of inhaled N-acetylcysteine in patients with idiopathic pulmonary fibrosis Intern Med 2010492289-96 30 Demedts M Behr J Buhl R et al High-dose acetylcysteine in idiopathic pulmonary fibrosis N Engl J Med 20053532229-42 31 Toma TP Bhowmik A Rajakulasingam R Acetylcysteine in pulmonary fibrosis N Engl J Med 20063541086-9 author reply -9 32 Hunninghake GW Antioxidant therapy for idiopathic pulmonary fibrosis N Engl J Med 20053532285-7 33 Flaherty KR Mumford JA Murray S et al Prognostic implications of physiologic and radiographic changes in idiopathic interstitial pneumonia Am J Respir Crit Care Med 2003168543-8 34 Latsi PI du Bois RM Nicholson AG et al Fibrotic idiopathic interstitial pneumonia the prognostic value of longitudinal functional trends Am J Respir Crit Care Med 2003168531-7 35 Collard HR King TE Jr Bartelson BB Vourlekis JS Schwarz MI Brown KK Changes in clinical and physiologic variables predict survival in idiopathic pulmonary fibrosis Am J Respir Crit Care Med 2003168538-42 36 Jegal Y Kim DS Shim TS et al Physiology is a stronger predictor of survival than pathology in fibrotic interstitial pneumonia Am J Respir Crit Care Med 2005171639-44 37 Martinez FJ Safrin S Weycker D et al The clinical course of patients with idiopathic pulmonary fibrosis Ann Intern Med 2005142963-7 38 Hull JH Acetylcysteine in pulmonary fibrosis N Engl J Med 20063541089-91 author reply -91
70
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
39 Flaherty KR King TE Jr Raghu G et al Idiopathic interstitial pneumonia what is the effect of a multidisciplinary approach to diagnosis Am J Respir Crit Care Med 2004170904shy10 40 Raghu G Johnson WC Lockhart D Mageto Y Treatment of idiopathic pulmonary fibrosis with a new antifibrotic agent pirfenidone results of a prospective open-label Phase II study Am J Respir Crit Care Med 19991591061-9 41 Hunninghake GW Lynch DA Galvin JR et al Radiologic findings are strongly associated with a pathologic diagnosis of usual interstitial pneumonia Chest 20031241215-23 42 Lynch D Godwin J Safrin S et al High-resolution computed tomography in idiopathic pulmonary fibrosis diagnosis and prognosis Am J Respir Crit Care Med 2005172488-93 43 Mallinckrodt CH Watkin JG Molenberghs G Carroll RJ Choice of the primary analysis in longitudinal clinical trials Pharmaceutical Statistics 20043161-9 44 Bang H Tsiatis A Estimating medical costs with censored data Biometrika 200087329shy43 45 Lin DY Regression analysis of incomplete medical cost data Stat Med 2003221181-200 46 Rochon J Application of GEE procedures for sample size calculations in repeated measures experiments Stat Med 1998171643-58 47 Lachin JM Foulkes MA Evaluation of sample size and power for analyses of survival with allowance for nonuniform patient entry losses to follow-up noncompliance and stratification Biometrics 198642507-19
71
- PANTHER-IPFPREDNISONE AZATHIOPRINEAND N-ACETYLCYSTEINEA STUDY THAT EVALUATES RESPONSE INIDIOPATHIC PULMONARY FIBROSIS
-
- Protocol Summary
- Table of Contents
- List of Tables
- List of Figures
- List of Abbreviations
- 1 Summary
- 2 Hypotheses and Specific Aims
-
- 21 Null Hypothesis
- 22 Specific Aim 1
- 23 Specific Aim 2
- 24 Prespecified Subgroups of Interest
-
- 3 Background and Significance
-
- 31 Idiopathic Pulmonary Fibrosis is the Most Common Interstitial Lung Disease
- 32 Rationale for Placebo Control
- 33 Rationale for N-acetylcysteine
- 35 Rationale for N-acetylcysteine as a Stand-alone Therapy
- 36 Rationale for the Study Design and Primary Endpoint
- 37 Rationale for Blinding of Treatments
-
- 4 Methods
-
- 41 Inclusion Criteria
- 42 Diagnosis of IPF
- 43 Exclusion Criteria
- 44 Study Design and Study Visit
- 45 Dose Justification
- 46 Contraindications Precautions and Side Effects of Study Medications
- 47 Recruitment Procedures
- 48 Study Procedures
- 49 Concomitant Medications
- 410 Laboratory Testing
- 411 Blinding of Study Drugs
-
- 5 Study Endpoints
-
- 51 Primary Study Endpoint
- 52 Secondary Study Endpoints
-
- 6 Safety Evaluations and Procedures
-
- 61 Adverse Events
- 62 Clinical Medical Monitoring
- 63 Unblinding Procedures
-
- 7 Study Drug Procedures
- 8 Data Management
-
- 81 Hardware and Software Configuration
- 82 Sources of Data
-
- 9 Study Design and Data Analysis
-
- 91 General Analytic Considerations
- 92 Randomization Blinding and Reporting of Results
- 93 Stratification
- 94 Specification of the Primary Analyses
- 95 Analysis of Longitudinal Endpoints
- 96 Analysis of Binary Time-to-Event and Time-Lagged Endpoints
- 97 Power Analysis
-
- 10 Study Administration
-
- 101 Cooperative Agreement Mechanism
- 102 IPFnet Steering Group
- 103 Data and Safety Monitoring Board
- 104 Recommendations on Interim Monitoring of Efficacy Safety and Futility
-
- 11 Investigator and Sponsor Obligations
-
- 111 Monitoring
- 112 Cost and Payment
- 113 Confidentiality and Health Insurance Portability and Accountability ActConsiderations
- 114 Informed Consent Procedures
- 115 Institutional Review Boards
-
- 12 Investigator Agreement
- 13 References
-
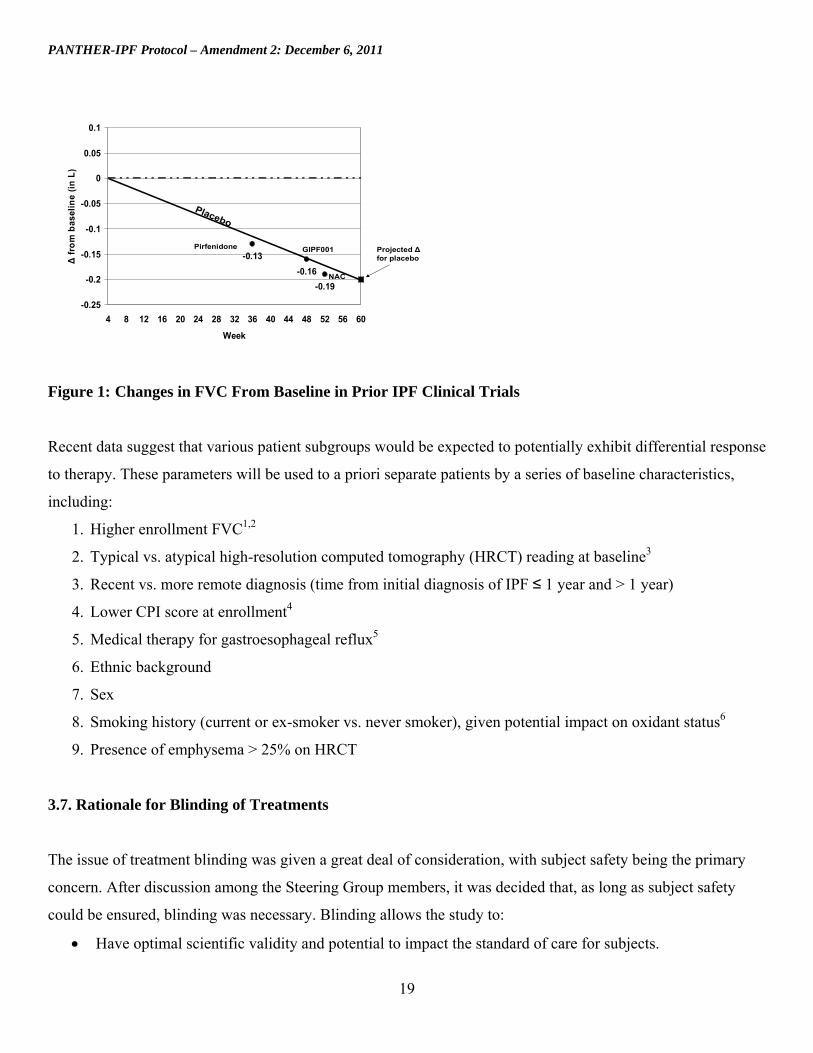
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Δ f
rom
bas
elin
e (i
n L
)
01
005
0
-005
-01
-015 Projected Δ for placebo
-02
-025
-019
-016
-013 Pirfenidone GIPF001
NAC
Placebo
4 8 12 16 20 24 28 32 36 40 44 48 52 56 60
Week
Figure 1 Changes in FVC From Baseline in Prior IPF Clinical Trials
Recent data suggest that various patient subgroups would be expected to potentially exhibit differential response
to therapy These parameters will be used to a priori separate patients by a series of baseline characteristics
including
1 Higher enrollment FVC12
2 Typical vs atypical high-resolution computed tomography (HRCT) reading at baseline3
3 Recent vs more remote diagnosis (time from initial diagnosis of IPF le 1 year and gt 1 year)
4 Lower CPI score at enrollment4
5 Medical therapy for gastroesophageal reflux5
6 Ethnic background
7 Sex
8 Smoking history (current or ex-smoker vs never smoker) given potential impact on oxidant status6
9 Presence of emphysema gt 25 on HRCT
37 Rationale for Blinding of Treatments
The issue of treatment blinding was given a great deal of consideration with subject safety being the primary
concern After discussion among the Steering Group members it was decided that as long as subject safety
could be ensured blinding was necessary Blinding allows the study to
Have optimal scientific validity and potential to impact the standard of care for subjects
19
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Make objective assessments of treatment effects
Maintain clinical equipoise among investigators
Encourage subjects to have similar levels of contact with the medical community
Minimize the differential dropout rates across study arms
20
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
4 Methods 41 Inclusion Criteria
1 Age 35 to 85 years inclusive
2 FVC ge 50 of predicted (post-bronchodilator measurement from the screening visit)
3 DLCO ge 30 of predicted (hemoglobin corrected and altitude corrected if gt4000 ft above sea level)
4 Ability to understand and provide informed consent
5 Diagnosis of IPF according to a modified version of the ATS criteria le 48 months from enrollment The
date of diagnosis is defined as the date of the first available HRCT or surgical lung biopsy characteristic
of definite UIP
411 Subjects Shown to Have Usual Interstitial Pneumonia Pattern on Surgical Lung Biopsy
Subjects who have been shown to have UIP pattern on lung biopsy must have all of the following
1 Exclusion of other known causes of ILD such as drug toxicity clinically significant environmental
exposures or diagnosis of connective tissue diseases
2 Bibasilar reticular abnormalities with minimal ground glass opacities on HRCT scan
412 Subjects Who Have Not Undergone a Surgical Lung Biopsy
In addition to the criteria above these subjects must have radiological findings considered to be definite for the
diagnosis of UIPIPF
1 Bibasilar reticular abnormalities with minimal ground glass opacities
2 Honeycombing as the predominant feature and located in the peripheral lung bases
42 Diagnosis of IPF
Only subjects with definite IPF will be eligible for enrollment in this study We will utilize a combination of
clinicalphysiologic features HRCT and review of a clinically obtained surgical lung biopsy specimen to
establish the diagnosis of IPF An algorithm for the diagnosis is provided to guide entry into the protocol as
outlined in the inclusion and exclusion criteria (Figures 2 and 3) This multi-disciplinary approach uses
21
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
expertise from clinicians radiologists and pathologists Investigators at each site in conjunction with central
pathology will work together to establish the diagnosis of IPF This interactive approach to the diagnosis of IPF
increases the level of agreement between observers39
A subject with suspected ILD should be evaluated for secondary causes including but not limited to
environmental exposures drugs and systemic diseases Presence of any of these findings felt to be significant
enough to cause an ILD should disqualify the subject from entry into the trial
If secondary causes are absent an HRCT scan may be obtained If an HRCT of sufficiently high quality has
been obtained within the last 3 months that scan may be used for diagnosis In the appropriate clinical setting
the diagnosis of IPF can be made by the demonstration of a typical radiographic pattern on HRCT or by
demonstration of UIP pattern on a surgical lung biopsy The following criteria for a radiographic (ie
nonsurgical) diagnosis will be used In the absence of known exposures andor clinical associations attributable
to pulmonary fibrosis and in the appropriate clinical setting the presence of definite UIP pattern in HRCT
images is required to meet study criteria for the diagnosis of IPF
Figure 2 Diagnosis of Idiopathic Pulmonary Fibrosis in the IPFnet
22
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Figure 3 Pathology Flow Chart Surgical Lung Biopsy Diagnosis
Requirement for diagnosis
1 Clinical exclusion of other known causes (connective tissue diseases environmental and drug
exposures) of ILD
2 Radiographic HRCT with bibasilar reticular abnormality and honeycomb change with minimal
ground glass opacities
Appropriate clinical setting
1 Age gt 50 years
2 Insidious onset of unexplained dyspnea
3 Duration of illness for ge 3 months
4 Bibasilar inspiratory crackles
23
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Unlike the ATSERS consensus criteria published in 2000 bronchoscopy will not be required for diagnosis
This decision was made based on the experience of the IPFnet Steering Group members regarding the utility of
bronchoscopy in the diagnosis of IPF The presence of an atypical HRCT finding will require documentation of
a definitive diagnosis by surgical lung biopsy In fact this is in keeping with the recently published evidence
based guidelines for diagnosis and management of IPF13 As shown in Figure 3 central review of the pathology
data will be required for a diagnosis of IPF
We will not require central review of HRCT as several studies have shown that a confident local interpretation
of clinicalHRCT criteria as definite IPFUIP is associated with a high positive predictive value for finding UIP
at surgical lung biopsy (see Table 1) Differences in sensitivity in these series likely reflect subject selection as
Flaherty et al3 evaluated only UIP and nonspecific interstitial pneumonia (NSIP) while Raghu et al40 and
Hunninghake et al41 included a broader range of ILD
Table 1 Operating Characteristics of Local HRCT Review for Diagnosis of UIP
Researcher of Subjects Sensitivity () Specificity () PPV () NPV ()
Raghu et al 40
59 (29 UIP by SLB) 78 90 88 82
Hunninghake et al 41 91 (54 UIP by SLB)
74 81 85 67
Flaherty et al 3 96 (only NSIP amp UIP)
37 100 100 30
Abbreviations PPV positive predictive value NPV negative predictive value UIP usual interstitial pneumonia SLB surgical lung biopsy and NSIP nonspecific interstitial pneumonia
Furthermore an analysis of the HRCT scans from subjects enrolled in the GIPF-001 trial confirmed that local
site interpretations have a high congruity to a central radiology core In this multi-center study 263 HRCT
scans were read as definite IPF and a retrospective central radiology core review found 932 to be consistent
with IPF 42 We will also take several additional steps to insure that the local HRCT reads are accurate
including
1 A detailed training module has been developed and must be completed by each site radiologist before
site initiation
2 Clinical centers are to mail all HRCT scans to the HRCT core lab The first 10 HRCT scans from
subjects enrolled at each enrolling clinical center will be reviewed centrally to be certain that local reads
24
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
25
are congruent with a central interpretation If discrepancies are identified additional education will be
provided and HRCT scans will continue to be reviewed centrally until the central radiology core is
confident that the local center is performing appropriately
3 Random scans will be obtained from each center throughout the study to confirm that the local read
continues to agree with central interpretation If discrepancies are identified they will be addressed as in
2 above
In all cases if a subject has a surgical lung biopsy sample that sample will be reviewed by the local and central
pathologists Therefore the only cases that would not be subject to a direct central review process are those
where the HRCT meets the centrally defined criteria for an unequivocal diagnosis and a lung biopsy sample is
not available Table 2 below summarizes the possible combinations for making a diagnosis
Table 2 Combining HRCT and Pathology Interpretations to Determine if IPF is Present
HRCT Diagnosis Pathology Diagnosis Diagnosis of IPF
Definite UIP Definite UIP Yes
Definite UIP Probable UIP Yes
Definite UIP Possible UIP Yes
Definite UIP Not UIP No
Definite UIP Unavailable Yes
Consistent with UIP Definite UIP Yes
Consistent with UIP Probable UIP Yes
Consistent with UIP Possible UIP No
Consistent with UIP Not UIP No
Consistent with UIP Unavailable No
Inconsistent with UIP Any No
Abbreviations HRCT high-resolution computed tomography IPF idiopathic pulmonary fibrosis
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
UIP usual interstitial pneumonia Dx diagnosis 43 Exclusion Criteria
1 History of clinically significant environmental exposure known to cause pulmonary fibrosis
Occupational exposures such as asbestos or environmental exposure to organic dust such as occurs in
pigeon breeders may at times mimic the clinical and radiographic findings of IPF
2 Diagnosis of connective tissue disease felt by the principal investigator (PI) to be the etiology of the
interstitial disease Diagnosis of collagen-vascular conditions will be according to the published
American College of Rheumatology criteria As such the presence of any documented collagen-vascular
disorder or the presence of any suspicious symptom complex whether or not associated with
significantly abnormal rheumatological serologies will exclude the subject at the discretion of the PI
3 Extent of emphysema greater than the extent of fibrotic change (honeycombing reticular changes) on
HRCT scan
4 Forced expiratory volume in 1 second (FEV1)FVC ratio lt 065 at screening (postbronchodilator)
5 Partial pressure of arterial oxygen (PaO2) on room air lt 55 mm Hg (lt 50 mm Hg at Denver site)
6 Residual volume gt 120 predicted at screening (postbronchodilator)
7 Evidence of active infection
8 Significant bronchodilator response on screening spirometry defined as a change in FEV1 ge 12 and
absolute change gt 200 mL OR change in FVC ge 12 and absolute change gt 200 mL The percent
difference between the FVC (or FEV1) values will be calculated by taking the absolute value of the
difference and dividing it by the larger of the two FVC (or FEV1) values
9 Screening and enrollment post-bronchodilator FVC measurements (in liters) differing by gt 11 The
percent difference between the FVC values will be calculated by taking the absolute value of the
difference and dividing it by the larger of the two FVC values (eg the percent difference between FVC
measurements of 19 and 20 liters would be determined by taking the difference between the two (01
liters) and dividing by the larger of the two (20 liters) So 0120 = 5 and these FVC measurements
would not exclude the subject
10 Listed for lung transplantation ie the patient has completed the evaluation process has been accepted
as a candidate for transplantation at an appropriate center and is waiting to receive notification of an
available donor organ
11 History of unstable or deteriorating cardiac disease
12 Myocardial infarction coronary artery bypass or angioplasty within 6 months of screening
26
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
13 Unstable angina pectoris or congestive heart failure requiring hospitalization within 6 months of
screening
14 Uncontrolled arrhythmia
15 Severe uncontrolled hypertension
16 Known HIV or hepatitis C
17 Known cirrhosis and chronic active hepatitis
18 Active substance andor alcohol abuse (as determined by site PI)
19 Pregnancy or lactation (subjects who are pregnant or breastfeeding)
20 Known hypersensitivity to study medication
21 Any condition other than IPF that in the opinion of the site PI is likely to result in the death of the
subject within the next year
22 Any condition that in the judgment of the PI might cause participation in this study to be detrimental to
the subject or that the PI deems makes the subject a poor candidate
23 Any therapy directed at pulmonary fibrosis (excepting triple therapy of prednisone plus azathioprine
plus NAC) requires a 30-day washout period before randomized Triple therapy of lt= 12 weeks duration
in the past 4 years requires a 30-day washout period before randomization
24 History of triple therapy of prednisone plus azathioprine plus NAC for gt 12 weeksrsquo duration in the past
4 years or previous enrollment in the triple-therapy arm of the PANTHER-IPF study
44 Study Design and Study Visit
441 Study Design Summary
This study will be a randomized double-blind PL-controlled trial designed to assess the safety and efficacy of
NAC in subjects with newly diagnosed IPF
Subjects with mild to moderate IPF (defined as FVCpred ge 50 and DLCOpred ge 30) diagnosed within
the past 48 months will be enrolled Screening will continue until April 30 2012
27
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
The study will employ a 2-arm design with 11 randomization to NAC or PL Once enrolled subjects will visit
the clinical center at 15 weeks and 15-week intervals thereafter Each subject will be treated and followed for a
maximum of 60 weeks
During the 60-week visit subjects will be taken off all study agents Approximately four weeks after the final
dose of study agent is taken subjects will receive a safety phone call from the study site
442 Study Visits
Subjects who meet entry criteria will review the informed consent a written description of the purpose
procedures and risks of the study with the PI co-investigator or study coordinator and all questions will be
answered The informed consent form will be signed by the subject at screening No protocol-specific
procedures will be performed until the subject has signed and dated an informed consent form This includes the
screening procedures
4421 Screening
Once informed consent is obtained subjects may immediately begin the screening process or may return within
28 days of consent In the event a study subject has been clinically evaluated at the study site by an IPFnet study
physician and has performed testing within three weeks for this clinical evaluation that meets guidelines
provided in the IPFnet PANTHER-IPF Manual of Operating Procedures (MOOP) this testing may be used to
satisfy the following screening criteria medical history physical exam arterial blood gas (ABG) with A-a
gradient vital signs with oximetry body height and weight spirometry DLCO lung volumes and HRCT scan
Allowing the use of previously performed test results that meet study guidelines for the screening visit is
intended to permit subjects easier access to study entry to prevent subjects from repeating testing that has been
performed within the study window and to decrease risks to subjects from repeated exposure to procedures
such as arterial puncture and HRCT
The following procedures will be performed at screening
Medical history and a physical examination
28
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Measure height and weight
Serum pregnancy test (if applicable)
Measure vital signs including oximetry
Blood draws performed and the following analyses conducted
o Hematology (red cell count white cell count hemoglobin hematocrit cell indices differential
platelet count)
o Blood chemistries according to central laboratory protocol (see Section 410 Laboratory
Testing)
o Beta human chorionic gonadotropin (serum) pregnancy test (in women of childbearing potential)
o Urinalysis
Pulmonary Function Tests (PFTs) including spirometry pre- and post- bronchodilator and postshy
bronchodilator measurement of lung volumes and measurement of hemoglobin adjusted diffusing
capacity
Measure ABGs
HRCT if a satisfactory scan has not been performed on the subject within 3 months of screening (see
PANTHER-IPF MOOP for more details)
Surgical lung biopsies (if applicable) reviewed by local and central pathology departments
Current medications If required a washout period discussed with the subject and initiated at this visit
4422 Enrollment
The enrollment visit is expected to take place within eight weeks of the screening visit Enrollment visit
activities include
Measure vital signs including oximetry
Measure height and weight
Serum pregnancy test (if applicable)
If consent has been given blood will be drawn and a urine specimen collected for the bio-specimen
repository
Spirometry (post-bronchodilator)
Measure 6MWT with Borg Dyspnea Scale
29
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Collect Quality-of-life (QOL) data using the SF-36 EuroQol Investigating Choice Experiments for
Preferences of Older People Capability Instrument (ICE CAP) and SGRQ
Female subjects complete Gender Substudy questionnaire
Dyspnea status collected using the UCSD SOBQ
Evaluate Acute Exacerbation (AEx)
Review of any Adverse Events (AEs)
Review of concomitant medications
Subject receives diary and instructions on its purpose and proper use
Subject receives supply of study drug sufficient to last until his or her 15-week study visit
See the Schedule of Assessments (Table 3) for more details Subjects with screening and enrollment postshy
bronchodilator FVC measurements (in liters) differing by more than 11 are not eligible to be enrolled in the
study
Subjects will be asked to provide a physician of record This physician will be considered the subjectrsquos primary
care provider (PCP) and if the subject agrees the PCP will be informed by letter of the subjectrsquos enrollment in
the trial The subject will be informed that his or her ongoing medical care should be received from the PCP
The PCP will be informed of any safety issues identified by the study staff The PCP will also be given
information regarding communication with study personnel about pertinent health issues or clinic encounters
the subject may have
4423 Week 15
The week 15 visit is expected to occur within +- 14 days of the subjectrsquos scheduled visit time (eg the week 15
visit should occur anytime between 13 and 17 weeks after starting study drug Week 15 activities include
Measure vital signs with oximetry
Measurement height and weight
Serum pregnancy test (if applicable)
Spirometry (post-bronchodilator) measurement
Review of AEs
Evaluate for AEx
30
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Review concomitant medications
If consented draw blood and collect urine specimen for the biospecimen repository
Subjects return used and unused study drug for the visit
Review study diary and a new study diary will be given
Provide additional supply of study drug sufficient to last until the next scheduled visit
4424 Week 30
The week 30 visit is expected to occur within +- 14 days of the subjectrsquos scheduled visit time (eg the week 30
visit should occur anytime between 28 and 32 weeks after starting study drug) Week 30 activities include
Physical examination
Measure vital signs with oximetry
Measure height and weight
Laboratory values (complete blood count [CBC] and serum chemistries)
Serum pregnancy test (if applicable)
Measure spirometry (post-bronchodilator)
6MWT with Borg scale
DLCO
Review of AEs
Evaluate for AEx
Review concomitant medications
Complete all QOL and dyspnea questionnaires (EuroQol ICE CAP SF-36 SGRQ and UCSD SOBQ)
If consent has been given blood will be drawn and a urine specimen collected for the biospecimen
repository
Review study diary
Subjects return used and unused study drug for the visit
Provide additional supply of study drug sufficient to last until the next scheduled visit
4425 Week 45
31
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
The week 45 visit is expected to occur within +- 14 days of the subjectrsquos scheduled visit time (eg the week 45
visit should occur anytime between 43 and 47 weeks after starting study drug) Week 45 activities include
Measure vital signs with oximetry
Measure height and weight
Serum pregnancy test (if applicable)
Measure spirometry (post-bronchodilator)
Review of AEs
Evaluate for AEx
Review concomitant medications
If consent has been given blood will be drawn and a urine specimen collected for the biospecimen
repository
Subjects return used and unused study drug for the visit
Study diary reviewed
Provide additional supply of study drug sufficient to last until the next scheduled visit
4426 Week 60 (Early Withdrawal or Final Treatment Visit)
At week 60 or at subject withdrawal from the study (premature by study doctor or subjectrsquos decision) a final
treatment visit will occur At this final treatment visit subjects will discontinue NACPL abruptly Week 60
activities also include
Physical examination
Measure vital signs with oximetry
Measure height and weight
Laboratory values (complete blood count [CBC] and serum chemistries)
Spirometry (post-bronchodilator) measurement
6MWT with Borg scale measurement
DLCO
Lung volumes
ABG
Review of AEs
32
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Evaluate for AEx
Review concomitant medications
Subjects will complete all QOL and dyspnea questionnaires (EuroQol ICE CAP SF-36 SGRQ and
UCSD SOBQ)
If consent has been given blood will be drawn and a urine specimen collected for the biospecimen
repository
Subjects return used and unused study drug for the visit
Study diary reviewed
4427 Final Site Visit ndash FVC drop confirmation
In the event that the subject has a recorded FVC drop of gt10 from baseline at the final treatment visit and the
subject has not had a confirmation of such a drop at a previous study visit the subject should return to the
clinical site 6 to 8 weeks after the final treatment visit During this visit a post-bronchodilator spirometry test
will be performed This FVC measurement will be evaluated according to section 521 of this protocol
4428 Final Visit ndash Telephone Follow-up
Four weeks following the final dose of study medication subjects will receive a telephone call from the study
coordinator to ensure that there are no side effects and to follow up on any ongoing adverse events (AEs)
4429 Phone Contact Between Visits
At week 2 and each month that a subject does not have a scheduled clinical center visit his or her study
coordinator will contact him or her at least once by telephone to
Inquire if the subject has had any hospitalizations events that might be considered an AE or any events
significant enough to warrant an out-of-cycle visit to the clinical center
Remind subjects of their current dosage levels and confirm that the subject understands them
Address any questions or concerns the subject might have regarding other aspects of the study
Assess adherence to the treatment regimen by reviewing diary data verbal review of medications taken
including nutritional supplements
33
34
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Table 3 Schedule of Assessments
Procedure Screening Visit 0
Enrollment Visit 1
Week 15 Visit 2
Week 30Visit 3
Week 45 Visit 4
Week 60 Early
Withdrawal Visit 5
Final1
Visit (via phone)
Informed consent X
Medical history X
Inclusionexclusion criteria X
Serum pregnancy test (if applicable) X X X X X
Review of lung biopsy X
Arterial Blood Gas X X
6-Minute Walk Test
X
X X
Physical examination X X X
Vital signs with oximetry X X X X X X
Body height and weight X X X X X X
Complete Blood Count X X X
Chemistry panel X X X
Monitor Lab Values X X X
Urinalysis X Specimen repository substudy blood draw and urine collection (if consented)
X
X X X X
HRCT (if not completed within three months) X
Spirometry (pre- and post-bronchodilator) X
Spirometry (post-bronchodilator only) X X X X X
DLCO (post-bronchodilator only) X X X
Lung volumes (post-bronchodilator only) X
X
Evaluate for acute exacerbation X X X X X
Review Adverse Events X X X X X X
Review concomitant meds X X X X X X
Dispense subject diary X X X X
Review subject diary X X X X X
Dispense study agent X X X X
Gender Substudy questionnaire (female subjects only) X
EuroQol ICECAP UCSD SOBQ SGRQ SF-36 X X X
Abbreviations DLCO diffusing capacity of the lung for carbon monoxide QOL Quality of Life ICECAP Investigating Choice Experiments for Preferences of Older People UCSD SOBQ University of California Shortness of Breath Questionnaire SGRQ St Georgersquos Respiratory Questionnaire SF-36 Short Form 36 Health Survey
1Follow-up visit via phone will occur four weeks after final dose of study medication
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
45 Dose Justification
The general philosophy for determining dosing levels was to apply previously examined
treatment regimens With the focus of the study being to establish a standard of care for
mildmoderate IPF subjects the goal was to develop flexible yet standardized treatment rules that
allow for the temporary or permanent withholding of one or more components of treatment when
necessary Subjects developing laboratory abnormalities or symptoms that result in
discontinuation of one or more components of study treatment may continue on the other
components as long as there is no contraindication for this Complete follow-up is important for
the validity of any study As a strategy to maintain protocol adherence we are using a treatment
regimen that will detect potential side effects and prompt interventions proactively in the interest
of patient safety In addition subjects who permanently stop study medications during the course
of the study are encouraged to continue in the study completing all scheduled visits and tests
451 Rationale for N-acetylcysteine Dosing
To our knowledge there have been no IPF studies to correlate clinical outcome measures with
different dosages for NAC The dosage chosen is based on the IFIGENIA study However BAL
lung GSH levels from subjects with IPF have been augmented with the use of oral NAC at 600
mg 3 times per day In addition lung GSH levels have been associated with improved
PFTs212227 The dose chosen for this study was based on previous data including the IFIGENIA
study30
4511 Dosing of N-acetylcysteineplacebo
Dosing of NACPL will be 600 mg orally 3 times a day (1800 mgday)
4512 Reasons to Discontinue N-acetylcysteineplacebo
NACPL may be temporarily or permanently discontinued for the duration of the study for
gastrointestinal symptoms or dermatologic reactions
35
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Temporarily discontinue (hold) oral NACPL for subjects requiring inpatient admission for acute
exacerbation (AEx) or other conditions Resume NACPL after discharge
36
37
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
452 Dosage Algorithms
Dosage Adjustment Algorithm 1 NACPL Dose Modifications for Gastrointestinal Symptoms Nausea Vomiting Abdominal Discomfort Diarrhea
GI Symptoms determined by the PI to be clinically significant Nausea Vomiting Abdominal Discomfort Diarrhea
NACPL Temporarily dc (HOLD) x 3 Days
Monitor symptoms intervene as clinically indicated (eg fluid replacement antidiarrhea or antinausea medication)
Monitor or lab PRN
Are symptoms resolving after 3 days NO
Symptoms NOT resolving after 3 days of holding study medication Assessmentmanagement per clinical
discretion of investigator
Likely not study medication discuss resuming study medication with medical monitor when symptoms resolved
YES
Temporarily dc (HOLD) NACPL for 4 additional days (total hold 1 week) then NACPL Resume 600 MG TID
Did symptoms recur
YES
STOP NACPL for
duration of study
NO
NACPL No Change
38
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Dosage Adjustment Algorithm 2 NACPL Dose Modifications For Dermatologic Reactions
Dermatologic Reactions (Not Acneiform) ge Grade 2 Grading per Common Terminology Criteria for
Adverse Events V30 (httpctepcancergov) For example Grade 1 RASHDESQUAMATION Macular or papular eruption or erythema without associated symptoms Grade 2 RASHDESQUAMATION Macular or popular eruption or erythema with pruritus or other associated symptoms localized desquamation or other lesions covering lt50 of body surface area
NACPL Temporarily dc (HOLD) x 3 days
Are symptoms resolving after 3 days
NO Symptoms not resolving after 3 days of holding study medication Assessmentmanagement per clinical discretion of investigator Likely not study medication Discuss resuming study medication with medical monitor when symptoms
resolved YES
Temporarily dc (HOLD) NACPL for 4 additional days (total hold 1 week) then NACPL resume 600 MG TID
Did symptoms recur
YES
STOP NACPL for
duration of study
NO
NACPL No change
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
46 Contraindications Precautions and Side Effects of Study Medications
461 Contraindication
Contraindication to NAC is known hypersensitivity to it
462 Precautions
Concomitant administration of oral NAC and antibiotics has shown a slightly reduced absorption
of cephalexin and a slight increase in erythromycin serum levels NAC contains free sulfhydryl
groups There is no evidence that individuals sensitive to sulfa drugs are sensitive to NAC
The NAC preparation being administered in this study contains 20 mg of aspartame Because of
the phenylalanine component of aspartame individuals with phenylketonuria should avoid or
restrict aspartame intake to avoid increased blood levels of phenylalanine Because of this risk
labeling is required on all products containing aspartame
463 Side Effects
Side effects of NAC range from common to serious See Table 4
39
40
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Table 4 Side Effects of NAC
Undesirable Effects
System-organ class Uncommon
(gt11000 lt1100)
Rare
(gt110000 lt11000)
Very rare
(lt110000) Not known
Immune system disorders Hypersensitivity Anaphylactic shock
reaction
Nervous system disorders Headache
Ear and labyrinth disorders Tinnitus
Cardiac disorders Tachycardia
Vascular disorders Hemorrhage
Respiratory thoracic and
mediastinal disorders
Bronchospasm
Dyspnea
Gastrointestinal disorders
Vomiting diarrhea
stomatitis abdominal
pain nausea
Dyspepsia
Skin and subcutaneous tissue
disorders
Urticaria rash
angioedema itching
General disorders and
administration site conditions Pyrexia
Investigations Reduced arterial
pressure Face edema
In very rare cases the onset of severe skin reactions such as Stevens-Johnson syndrome and Lyell syndrome was reported to have a temporal relationship with N-acetylcysteine administration Although in most cases at least another suspect drug probably most involved in the genesis of the above mentioned mucocutaneous syndromes has been identified in case of mucocutaneous alterations it is appropriate to contact onersquos doctor and the administration of N-acetylcysteine should be immediately discontinued
Some studies confirmed a reduction of platelet aggregation during N-acetylcysteine administration The clinical significance of these findings has not been defined yet [Source Fluimucil Investigator Brochure]
47 Recruitment Procedures
Subjects recruited for this study will be established patients of the investigators or physician- or
self-referred to participating clinical centers in the IPFnet Each clinical center within IPFnet has
a well-developed infrastructure of local pulmonologists within the surrounding geographic area
These pulmonologists are kept informed of ongoing IPF clinical trials and regularly refer
subjects to studies conducted at IPFnet clinical centers
Additional steps will be taken to inform clinicians of the trials in progress within IPFnet
including presentations at faculty staff meetings at local hospitals medical grand rounds and
national conferences direct mail notification monthly faxes and advertisement of network trials
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
in pulmonary journals Clinical center patients previously diagnosed with IPF will be notified of
the trials by mail whenever possible
Recruitment of minorities and women will be monitored by the DCC and DSMB If necessary
additional recruitment efforts will be made at specific centers to ensure that the aggregate subject
sample contains appropriate representation of women and minorities
48 Study Procedures
The following procedures are detailed in the PANTHER-IPF MOOP accompanying this
protocol
1 PFT
2 ABG
3 HRCT scan of the chest (including imaging of pulmonary arteries)
4 CBC and serum chemistries
5 Pregnancy test
6 6MWTBorg Dyspnea Scale
7 QOL questionnaires (EuroQol HAD SF-36 SGRQ and ICE CAP)
8 UCSD SOBQ
9 Gender Substudy Questionnaire
All assessments of PFTs will be conducted by study personnel not directly involved in the
treatment of the subjects
481 Biological Specimen Management
4811 Biological Specimen Sample Management
Subjects at clinical centers participating in the specimen repository substudy who consent to
having blood drawn for research purposes and for the banking of blood blood components and
other biologic specimens (urine and BAL fluid) will have approximately 405 mL of blood
41
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
drawn 17 mL blood drawn for DNA and 20 mL of urine collected at enrollment visit Subjects
will have approximately 50 mL of blood drawn and 20 mL of urine collected at each 15-week
follow-up visit Blood specimens will be separated according to PANTHER-IPF MOOP
guidelines into the following components for banking in the repository serum plasma and
DNA Coding of all biologic specimens for the repository will be performed by study staff at the
clinical center The samples will be processed per PANTHER-IPF MOOP guidelines aliquoted
labeled with barcode labels and stored at -70degC at the clinical center and shipped to the central
repository
The only subject identifiers will be a sample ID number and subject initials This sample ID will
be linked in the IPFnet DCC clinical database to subject information No subject information will
be transferred to the biological-specimen database
The subjectrsquos samples may be used for approved sub-studies relating to human disease
including but not limited to IPF The studies for which an individualrsquos samples will be made
available will be determined by the subjectrsquos answers to questions on the biological-sample
informed consent form The subjects can choose to make their samples available for all options
or any combination Samples will be made available to researchers only with IPFnet Steering
Group approval until such time as the samples are made public through the NHLBI repository
49 Concomitant Medications
Concurrent treatment with FDA-approved therapy for IPF is allowed Colchicine may be used
for treatment of gout Temporary treatment with oral or IV corticosteroids for clinical worsening
or suspected AEx is permitted Nutritional supplements containing NAC are not allowed
410 Laboratory Testing
Clinical laboratory parameters will be assessed at screening and at the end of the study The
following tests will be performed at the two time points specified in the protocol chemistry (AG
ratio ALT [SGPT] AST [SGOT] albumin alkaline phosphatase amylase bilirubin-direct
42
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
bilirubin-indirect bilirubin-total BUN BUNcreatinine ratio calcium carbon dioxide
cholesterol-total chloride CPK-total creatinine GGT globulin glucose iron-total LDH
lipase magnesium phosphorus-inorganic potassium protein-total sodium TIBC triglycerides
uric acid) and hematology (red blood cell count WBC count hemoglobin hematocrit cell
indices differential platelet count)
411 Blinding of Study Drugs
Subjects and caregivers will be blinded to study treatment Every subject will receive NAC or
matching PLs at every study visit from the baseline visit to the week-45 visit No study agent
will be dispensed at the week-60 visit
43
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
5 Study Endpoints
51 Primary Study Endpoint
The primary endpoint will be the change in serial measurements of FVC over the study period
52 Secondary Study Endpoints
521 Time to Disease-progression
The time-to-death or a 10 decline in FVC will be defined as the time-to-disease progression
The 10 decline in FVC from enrollment must be confirmed on 2 consecutive visits no less than
6 weeks apart For subjects with 2 consecutive visits with a 10 decline in FVC the time-toshy
disease progression will be defined as the time interval between enrollment and the initial visit
with a 10 FVC decline For subjects who experience disease progression the study doctor will
determine whether or not the subject will remain in the study
522 Acute Exacerbations
The following 3 criteria will define AEx in subjects with acute worsening of their respiratory
conditions
1 Clinical (all of the following required)
A) Unexplained worsening of dyspnea or cough within 30 days triggering unscheduled
medical care (eg emergency room clinic study visit hospitalization)
B) No clinical suspicion or overt evidence of cardiac event pulmonary embolism or deep
venous thrombosis to explain acute worsening of dyspnea
C) No pneumothorax
44
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
2 RadiologicPhysiologic (A and B required)
A) New ground glass opacity or consolidation computed tomography (CT) scan OR new
alveolar opacities on chest x-ray
B) Decline of ge 5 in resting room air SpO2 from last recorded level OR decline of ge 8 mm
Hg in resting room air PaO2 from last recorded level
3 Microbiologic (all of the following required)
A) No clinical evidence for infection (ie absence of grossly purulent sputum fever gt 39degC
orally)
B) Lack of positive microbiological results (if done) from lower respiratory tract defined as
(1) Clinically significant bacterial growth on sputum or endotracheal aspirate cultures
(2) Quantitative culture by protected brush specimen ge 103 cfumL or BAL ge 104 cfumL
(3) The presence of specific pathogens on stains of any of the above
C) Lack of positive pathogen in blood cultures (if done)
Identification of Acute Exacerbations
All subjects will be educated about the importance of identifying AExs At the time of
enrollment subjects will be told about the possibility of developing acute symptomatic
worsening that might represent an AEx of IPF and instructed to contact their study clinical
center coordinator within 48 to 72 hours of the apparent event
All subjects will be contacted by phone monthly and questioned about any change in dyspnea or
cough and any interim clinic visits or hospitalizations Finally as part of the IPFnet outreach to
community referring physicians the importance of AExs will be emphasized When a subject is
identified who meets criterion 1A this will trigger the collection of additional clinical data to
evaluate a suspected AEx These data will be collected as part of standard clinical care (ie this
protocol does not require collection of all items) The additional items to be collected for
suspected AEx include
IPFnet AEx case report form (eCRF) (required)
45
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Chest x-ray CT scan withwithout pulmonary angiogram (reports should be faxed and
followed by the hard copiesdiscs)
Oxygen saturation (pulse oximetry)
ABG
Respiratory cultures (sputum endotracheal aspirate lavage)
Blood cultures
Clinichospital records related to the event
All potential cases of AEx will be reviewed by the clinical center PI first and a decision on
whether the case may represent an AEx will be made If AEx is suspected the case will be sent
to the IPFnet adjudication committee which will assign a final diagnosis (see Table 5) If there is
disagreement among members the majority opinion will be recorded
During episodes of suspected AEx as determined by the individual clinical center investigator
subjects will remain blinded and in the study
Table 5 Final Diagnoses in Evaluation of Suspected Acute Exacerbations
Definite acute exacerbation All criteria met no alternative etiology
Unclassifiable acute worsening
Insufficient data to evaluate all criteria no alternative etiology
Not acute exacerbation Alternative etiology identified that explains acute worsening
Management of the suspected AEx will be at the discretion of the treating physician Standard of
care generally involves evaluation for respiratory infection pulmonary embolism cardiac events
and pneumothorax and treatment with IV corticosteroids
Study drugs will be resumed at pre-suspected AEx doses after subjects clinically improve as
confirmed by the local PI All subjects should be seen at the clinical center within 2 to 4 weeks
of recovery for measurement of post-bronchodilator FVC (see Figure 4) Subjects unable to
return to the clinical center after suspected AEx due to medical frailty (eg continued
46
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
institutionalization progressive disability) will be categorized as failing to maintain FVC
response in secondary analyses
Suspected AEx (PI determined)
Hold study drug Treat AEx
(Attending physician determined)
Alive but unable to continue due to
medical frailty
Dead
Alive and able to continue
Site reviewvisit
Restart study drug
FVC within 2-4 weeks
Figure 4 Acute Exacerbation Flow Chart
523 Respiratory Infections
An upper respiratory infection will be defined as
Change in sputum discoloration
Increased cough of no more than 14 daysrsquo duration
A lower-respiratory infection (pneumonia) will be defined as new segmental or lobar airspace
opacities visualized by image studies (chest radiograph or HRCT) in addition to any of the
following
Positive pathogencultures in good sample of sputum or lower-airway secretions retrieved
by fiberoptic bronchoscope
Fever gt 39degC or gt 100degF
Leukocytosis gt 12000 (unexplained no increase in dose of corticosteroids)
47
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
524 Maintained FVC Response
Subjects with follow-up FVCpred measurements at or above their baseline FVCpred level
will be classified as having maintained FVC response Subjects with reduced FVCpred levels
or missing data for any reason including death or medical frailty will be classified as having not
maintained FVC response The FVCpred value is used because unadjusted FVC measurements
are expected to decline with age
48
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
6 Safety Evaluations and Procedures
61 Adverse Events
During a clinical trial the reporting of adverse experience information can lead to important
changes in the way a new treatment is developed as well as provide integral safety data
611 Definitions
An adverse event (AE) is any untoward medical occurrence in a subject or clinical investigation
subject who was administered a pharmaceutical product The AE does not necessarily have to
have a causal relationship with the drug administered An AE can be any unfavorable and
unintended sign (including an abnormal laboratory finding) symptom or disease temporarily
associated with the use of a medicinal product whether or not considered to be related to the
medicinal product Diseases signs symptoms or laboratory abnormalities already existing at
enrollment are not considered AEs unless they worsen (ie increase in intensity or frequency)
Surgical procedures themselves are not AEs they are therapeutic measures for conditions that
require surgery The condition for which the surgery is required may be an AE Surgical
procedures planned before randomization and the conditions necessitating the surgery are not
AEs
A serious adverse event is any untoward event that
Is fatal
Is life-threatening
Requires inpatient hospitalization or prolongation of existing hospitalization with the
following exceptions
o Preplanned (before the study) hospital admissions unless the hospitalization is
prolonged
o Planned admissions (as part of a study eg routine biopsies)
o Hospitalization lasting lt 24 hours
49
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
o Hospitalization for elective procedure
o Emergency room visits
Results in persistent or significant disability or incapacity
Is a congenital anomaly or birth defect
Important medical events that may not result in death be life-threatening or require
inpatient hospitalization may be considered serious adverse events (SAEs) when based
on appropriate medical judgment they may jeopardize the subject and may require
medical or surgical intervention to prevent one of the outcomes listed above
Life-threatening means that the subject was in the view of the investigator at immediate risk of
death from the AE as it occurred It does not include an AE that had it occurred in a more severe
form might have caused death
Persistent or significant disabilityincapacity means that the event resulted in permanent or
significant and substantial disruption of the subjectrsquos ability to carry out normal life functions
Causality
A reasonable possibility means the AE may have been caused byrelated to the study drug A
perceived or real lack of efficacy does not satisfy the definition of relatedness
612 Adverse Event (AE) Reporting
For the PANTHER-IPF trial all AEs (serious and nonserious) occurring from randomization
through final study visit (4 weeks after final dose of all study medication) will be recorded on the
AE page of the case report form (CRF)
6121 Serious Adverse Events (SAE) Reporting
For this trial all deaths and all SAEs which occur from randomization through final study visit
must be entered within the EDC system via the SAE eCRF page within 24 hours of the
investigative sitersquos knowledge of the event It is the responsibility of the clinical center
50
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
investigator to provide a causality assessment of the event for each study medications based upon
the information available at the time of the report It is understood that complete information
about the event may not be known at the time the initial report is submitted In the event the EDC
system is not accessible to the site at the time of event reporting investigative sites will complete
and forward a paper back-up SAE form to DCRI Safety Surveillance for processing
DCRI Safety Surveillance
Telephone 1-919-668-8624 or 1-866-668-7799 (toll free)
Fax 1-919-668-7138 or 1-866-668-7138 (toll free)
The investigator must complete and submit follow-up SAE information via the eCRF when
important new or follow-up information (eg final diagnosis outcome results of specific
investigations) becomes available Follow-up information should be submitted according to the
same process used for reporting the initial event as described above All SAEs will be followed
until resolution stabilization or 30 days after the subject has completed the final visit (4 weeks
after the final dose of study medication) whichever occurs first The investigator is responsible
for reporting SAEs to their institutional review board (IRB) per site specific IRB reporting
guidelines
6122 Regulatory Reporting
AEs that are serious study drug related and unexpected will be reported to the regulatory
authorities The DCRI Safety Surveillance medical monitor will perform a medical review of all
SAEs submitted and evaluate for ldquounexpectednessrdquo DCRI Safety Surveillance will prepare
MedWatch reports for those events identified as serious study drug related and unexpected as
determined by Safety Medical Monitor
DCRI Regulatory Services will submit all unexpected study drug-related SAEs as per 21 CFR
32 DCRI Safety Surveillance will provide a safety alert letter to the NHLBI DSMB and DCC
clinical operation (for distribution to sites) within 15 days of initial receipt of the information
51
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Investigators are responsible for promptly reporting these events to their reviewing IRBs
according to site specific IRB reporting guidelines
62 Clinical Medical Monitoring
There will be an unblinded physician at the IPFnet DCC serving as medical monitor The
medical monitor will be available to assist with questions about dosage adjustments of study
medications including discontinuation or resumption of medications
63 Unblinding Procedures
Unblinding of subjects or investigators to subject treatment is strongly discouraged For ongoing
clinical management all subjects should be presumed to be receiving ldquoactiverdquo study drug To
ensure the subjectrsquos safety the study treatment will be dose-adjusted based on laboratory test
results clinical findings and symptoms
The IPFnet DCC medical monitor and PANTHER-IPF co-chairs Drs Ganesh Raghu and
Fernando Martinez will be available to the study physicians to discuss study drug management
on a case-by-case basis Un-blinding will be considered ONLY when the knowledge of subject
treatment assignment is ABSOLUTELY ESSENTIAL for subject safety and after discussion of
the subjectrsquos case with the medical monitor and either Dr Raghu or Dr Martinez Unblinding of
study treatment should be minimized during the conduct of the trial In those cases where it is
felt to be medically necessary the DCC medical officer will communicate directly with the
managing physician to minimize unblinding of study personnel
52
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
7 Study Drug Procedures
At the baseline 15-week 30-week and 45-week study visits subjects will receive a supply of
study drug sufficient to last until the next visit at which study drug will be dispensed
53
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
8 Data Management
81 Hardware and Software Configuration
811 Hardware and Database Software
Data will be stored in an Oracle database system Oracle has advantages of processing efficiency
and smooth linkage with other software systems The application and database will be hosted on
Solaris Unix servers at the IPFnet DCC
812 Statistical Software
SAS will be used as the principal application for the management of analysis data files and
statistical computations S-Plus will be used to provide supplementary functions as needed
813 Access Control and Confidentiality Procedures
Access to databases will be controlled centrally by the IPFnet DCC through user passwords
linked to appropriate privileges This protects the data from unauthorized changes and
inadvertent loss or damage
814 Security
Database and Web servers will be secured by a firewall and through controlled physical access
Oracle has many security features to ensure that any staff member accessing the database has the
proper authority to perform the functions he or she requests of the system Within the secondary
SAS databases Unix group-access control maintains similar security The Sun workstation login
is secured by extensive user-password facilities under Unix
54
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
815 Back-up Procedures
Database back-up will be performed automatically every day and standard IPFnet DCC policies
and procedures will be applied to dictate tape rotation and retention practices
816 Virus Protection
All disk drives that provide network services and all user computers will be protected using
virus-scanning software Standard IPFnet DCC policies will be applied to update these protection
systems periodically through the study
82 Sources of Data
821 Design and Development
The IPFnet DCC will be responsible for development of the electronic case report forms
(eCRFs) development and validation of the clinical study database ensuring data integrity and
training clinical center staff on applicable data management procedures A web-based distributed
data entry model will be implemented This system will be developed to ensure that guidelines
and regulations surrounding the use of computerized systems used in clinical trials are upheld
The remainder of this section provides an overview of the data management plan associated with
this protocol
822 Data Collection Forms
The data collection process consists of direct data entry at the study clinical centers into the EDC
system(s) provided by the DCC A data collection worksheet will be provided to clinical centers
for recording data in the event the EDC system is unavailable Data entry of the eCRFs should
be completed according to the instructions provided and project specific training The
investigator is responsible for maintaining accurate complete and up-to-date records and for
ensuring the completion of the eCRFs for each research participant
55
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
823 Data Acquisition and Entry
Data entry into eCRFs shall be performed by authorized individuals Selected eCRFs may also
require the investigatorrsquos written signature or electronic signature as appropriate Electronic
CRFs will be monitored for completeness accuracy and attention to detail during the study
824 Data Center Responsibilities
The IPFnet DCC will 1) develop a data management plan and will conduct data management
activities 2) provide final eCRFs for the collection of all data required by the study 3) develop
data dictionaries for each eCRF that will comprehensively define each data element 4) conduct
ongoing data monitoring activities on study data 5) monitor any preliminary analysis data
cleanup activities and 6) rigorously monitor final study data clean up
825 Data Editing
Completed data will be entered into the IPFnet DCC automated data acquisition and
management system If incomplete or inaccurate data are found a data clarification request will
be generated and distributed to clinical centers for a response Clinical centers will resolve data
inconsistencies and errors and enter all corrections and changes into the IPFnet DCC automated
data acquisition and management system
826 Training
The training plan for clinical center staff includes provisions for training on assessments eCRF
completion guidelines data management procedures and the use of computerized systems
56
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
9 Study Design and Data Analysis
91 General Analytic Considerations
All primary analyses will be based on intent-to-treat (ITT) principles using all randomized
subjects Baseline factors across groups will be compared using mean (standard deviation) and
median (25th and 75th percentiles) summary measures Kaplan-Meier curves will be used to
display event rates Due to clinical interest in departures from both sides of the null hypothesis
all test statistics will be 2-sided
Reasonable caution needs to be taken when conducting multiple analyses on key clinical
subgroups For subgroup analyses a conservative significance level of 0001 will be used for all
interaction tests Thus subgroup comparisons will be considered exploratory unless the p-value
from the interaction test is smaller than 0001
92 Randomization Blinding and Reporting of Results
A permuted block-randomization scheme will be created with varying block sizes stratified by
clinical center Once a subject has completed the screening and baseline period and evaluation
for inclusionexclusion criteria the randomization process will begin Subjects will be
randomized to receive NAC or matching placebo with equal probability (11) via telephone
contact with a central interactive voice response system (IVRS) using a toll-free randomization
number On the day of randomization after the subject has successfully met all inclusion and
exclusion criteria the investigator or designee will call the central randomization number to
obtain the assigned kit randomization numbers for that subject At each subject visit the
investigator or designee will call the central randomization number to obtain the new kit
randomization numbers for resupply of the subject For resupply of the clinical center the IVRS
will monitor minimal volume of a kit type andor expiration date and will automatically notify
the pharmacy
57
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
The trial results will be reported according to guidelines specified in the CONSORT statement
A flow diagram describing screening recruitment randomization dropout and vital status will
be included in the primary manuscript AEs and efficacy data will be presented for all treatment
groups Adherence dropout and lost to follow-up will be carefully examined across all treatment
groups Analyses of safety will be based on data from all randomized subjects who received at
least one dose of study drug
93 Stratification
Subjects will be distributed to the two treatment arms in a 11 allocation ratio Stratification
blocks will be based on clinical centers
94 Specification of the Primary Analyses
A mixed model repeated measures (MMRM) analysis described in section 95 will be used to
compare differences in the slope of FVC measurements across the treatment groups Response
variables are values of the FVC measured at baseline and every 15 weeks until study completion
Variables in the model will include treatment time and time by treatment age sex race and
height Contrast estimates of differences in slopes of treatment over time (along with confidence
intervals) will be used to estimate the treatment effect The validity of this model in terms of
meeting modeling assumptions will be assessed via standard modeling diagnostics and goodness-
of-fit measures Based on the MMRM framework missing FVC data will not be imputed for the
primary analysis
95 Analysis of Longitudinal Endpoints
A common goal in clinical trials is to specify models that are easily implemented and
reproducible by independent data analysts On the other hand the models should have proper
statistical behavior in terms of low bias and high precision Many common approaches to
longitudinal data analysis including last observation carried forward (LOCF) imputation rely on
the missing completely at random (MCAR) assumption However the MCAR assumption is
58
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
unlikely to hold in many clinical trials because missing data are often related to disease
progression and prognosis A more reasonable assumption missing at random (MAR) specifies
that the complete data distribution can be modeled using only the observed data The likelihood-
based MMRM approach is valid under the more general MAR assumptions These models will
be applied to analyze the longitudinal data secondary endpoints
The advantages of MMRM analysis are that all important characteristics of the model can be preshy
specified standard software can be used to implement the models and results are based on ITT
principles43 In addition the MMRM approach offers superior control of Type I and Type II
errors compared with the LOCF approach
Response variables are values of the PFTs measured at enrollment and every 15 weeks until
study completion and 6MWT values measured at baseline week 30 and week 60 Covariates are
treatment time time by treatment and key baseline risk factors Contrasts (along with
confidence intervals) of treatment by time will be used to estimate the treatment effect
The correlation structure involves multiple pieces including measurement errors random
variation and interindividual variability For the longitudinal data analyses an unstructured
correlation matrix for within-subject errors will be assumed Other correlation structures
including compound symmetry will be examined as needed A careful examination of reasons
for study discontinuation will be conducted to assess the validity of MCAR Sensitivity analyses
will be used to examine the untestable assumption that the observed data violate the MAR
assumption The MMRM models will be implemented using PROC MIXED in SAS
96 Analysis of Binary Time-to-Event and Time-Lagged Endpoints
Regression modeling approaches using either the logistic regression model or Cox proportional
hazards regression model will be employed when appropriate The validity of these models will
be assessed via standard modeling diagnostics and goodness-of-fit measures Estimates of
cumulative frequencies for more general time-lagged responses will be calculated using the
partitioned version of the Bang-Tsiatis estimator44 The partitions will be set at 15-week intervals
59
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
to correspond with the data-collection process Covariate adjusted event rates will be calculated
using inverse probability-weighted regression estimates45
97 Power Analysis
971 Primary Analyses
Based on previously published IPF clinical trials the PL group is expected to experience a drop
in FVC of approximately 020 L over the study period (see Figure 1) The IPFnet Steering Group
determined a clinically important difference would be to preserve the majority of the decline
relative to PL over the study period In particular a treatment effect of 015 L was determined to
be a clinically meaningful difference Potential dropout is a key factor in the proposed study The
drop-out process assumed 5 lost to follow-up after every study visit Only 80 of subjects
were assumed to be followed for the entire study period All models assumed a compound
symmetry structure for the covariance matrix Power calculations were performed using a SAS
IML program for designing repeated measures studies46 Based on preliminary reviews of the
data from the University of Michigan the covariance matrix parameters were estimated at
approximately σ2 = 0757 (variance parameter) and ρ = 0936 (correlation parameter) To be
conservative the power calculations for the primary analysis were performed with parameter
setting of σ2 = 0810 (variance parameter) and ρ = 0925 (correlation parameter)
The power calculations assume a correction for imperfect compliance proposed by Lachin and
Foulkes to allow for 2 noncompliance for each of the treatment arms47 Thus the sample size
of 130 subjects per arm would be reduced to an adjusted sample size of 130(1-002-002)2 =
1198 or 120 subjects per arm
Under the assumed Type I error rate of 005 with a correlation parameter of 0925 and standard
deviation of 090 the difference of 015 L (or 00025 Lweek) shown in Table 6 would have
power of 93
60
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Table 6 Hypothetical Values of Mean FVC (L) Change from Baseline
Week 15 Week 30 Week 45 Week 60
NAC 00125 00250 00375 00500
Placebo 00500 01000 01500 02000
Difference 00375 00750 01125 01500
Abbreviations FVC forced vital capacity PL placebo
972 Power Analysis for Secondary Endpoints
Power calculations for secondary endpoint measurements are shown in Table 7 Standard
deviations are based on unpublished data provided by the University of Michigan The
calculations are based on a 2-sample t-test with Type I error rate set at 005 These calculations
are likely to be conservative because the statistical approach described in section 95 for
analyzing these endpoints will incorporate incomplete observations as well as intermediate data
points
Table 7 Detectable Differences in Treatment Means for Selected Endpoint Measurements
Secondary Endpoints Std Dev
of the Baseline Score
Detectable Difference for 80 Power
Std Dev of the Change Score
Difference Detectable for
80 Power
DLCOpred 166 58 91 32
6MWT Area Under the Desaturation Curve
219 76 175 61
6MWT Distance to Desaturation 224 78 315 110
6MWT Minutes Walked 210 073 205 071
Abbreviations Std Dev standard deviation DLCOpred diffusing capacity of the lung for carbon monoxide percent predicted 6MWT 6-minute walk test
61
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
10 Study Administration
101 Cooperative Agreement Mechanism
The administrative and funding mechanism used to undertake this project is a ldquocooperative
agreementrdquo (U01) which is an assistance mechanism Under the cooperative agreement the
NHLBI assists supports andor stimulates the project and is substantially involved with
investigators in conducting the study by facilitating performance of the effort in a ldquopartnerrdquo role
The NHLBI project scientist serves on the IPFnet Steering Group and he or another NHLBI
scientist may serve on other project committees when appropriate At the same time however
NHLBI does not assume a dominant role direction or prime responsibility for this research
program
As described below governance of the project is conducted through the IPFnet Steering Group
Principal investigators have lead responsibilities in all aspects of their trials and the project
including any modification of trial designs conduct of the trials quality control data analysis
and interpretation preparation of publications and collaboration with other investigators unless
otherwise provided for by the IPFnet Steering Group
PIs retain custody of and have primary rights to their center-specific and collaborative data
subject to government rights-of-access consistent with current Health amp Human Services (HHS)
Public Health Service (PHS) and National Institutes of Health policies The protocols and
governance policies call for the continual submission of data centrally to the IPFnet DCC for the
collaborative database which at a minimum will contain the key variables selected by the IPFnet
Steering Group for standardization across all clinical centers the submission of copies of the
collaborative datasets to each PI upon completion of the project procedures for data analysis
reporting and publication and procedures to protect and ensure the privacy of medical and
genetic data and records of individuals The NHLBI project scientist on behalf of the NHLBI
will have the same access privileges and responsibilities regarding the collaborative data as the
other members of the Steering Group
62
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
PIs are also encouraged to publish and to publicly release and disseminate results data and other
products of the project concordant with the project protocols and governance and the approved
plan for making data and materials available to the scientific community and to the NHLBI
However during the 3 years after the ending date of NHLBI project support unpublished data
unpublished results data sets not previously released and other study materials or products are
to be made available to any third party only with the approval of the IPFnet Steering Group
Upon completion of the project PIs are expected to put their intervention materials and
procedure manuals into the public domain andor make them available to other investigators
according to the approved plan for making data and materials available to the scientific
community and the NHLBI for the conduct of research at no charge other than the costs of
reproduction and distribution
The NHLBI reserves the right to terminate or curtail the project (or an individual award) in the
event of (a) failure to develop or implement mutually agreeable collaborative measurement
subject eligibility and data management sections of the protocols (b) substantial shortfall in
subject recruitment follow-up data reporting or quality control or other major breach of
protocol (c) substantive changes in the agreed-upon protocols with which NHLBI cannot
concur (d) reaching a major project outcome with persuasive statistical significance
substantially before schedule or (e) human subject ethical issues that may dictate a premature
termination
Any disagreement that may arise in scientificprogrammatic matters (within the scope of the
award) between award recipients and the NHLBI may be brought to arbitration An arbitration
panel will be composed of 3 membersmdash1 selected by the IPFnet Steering Group (with the
NHLBI member not voting) or by the individual PI in the event of an individual disagreement a
second selected by NHLBI and the third selected by the other 2 members This special
arbitration procedure in no way affects the PIrsquos right to appeal an adverse action that is otherwise
appealable in accordance with the PHS regulations at 42 CFR part 50 Subpart D and HHS
63
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
regulation at 45 CFR part 16 or the rights of the NHLBI under applicable statutes regulations
and terms of the award
102 IPFnet Steering Group
The IPFnet Steering Group is the main governing body of the project It is composed of the PIs
of the clinical centers the PI of the DCC and the NHLBI project scientist The clinical centers
the IPFnet DCC and the NHLBI each have 1 vote on the IPFnet Steering Group All decisions
are determined by majority vote
All major scientific decisions are determined by the IPFnet Steering Group It assumes overall
responsibility for the design and conduct of the trial It appoints (and disbands) committees and
subcommittees as the need arises designs approves and implements the study protocols
oversees the development of the MOOP monitors subject recruitment and treatment delivery
evaluates data collection and management oversees quality assurance procedures and
implements changes and enhancements to the study as required It also has primary responsibility
for facilitating the conduct of the trials and reporting the projectrsquos results
103 Data and Safety Monitoring Board
The NHLBI will establish a DSMB in accordance with established policies (see
httpwwwnhlbinihgovfundingpoliciesdsmb_insthtm) to ensure data quality and subject
safety and to provide independent advice to the NHLBI regarding progress and the
appropriateness of study continuation
104 Recommendations on Interim Monitoring of Efficacy Safety and Futility
First and foremost the role of the DSMB will be to review subject safety and trial conduct at
periodic points during the study The DSMB may require analyses of the primary endpoint
results for comparing the benefit and risks of treatment strategies The benefit of collecting
additional data on key secondary endpoints with extended follow-up and establishing a robust
64
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
evidence base for determining a standard of care will need to be carefully considered before
early termination of one or more treatment arms After careful consideration the IPFnet Steering
Group recommends conservative thresholds for the early examinations of the safety and efficacy
data
The DSMB will be expected to meet approximately every 6 months until trial completion to
review safety and toxicity data The DSMB may recommend stopping the study based on these
reviews Because the DSMB could stop the trial for safety concerns as well as for a large
efficacy benefit there could be multiple opportunities to reject the null hypothesis (no difference
in event rates between the PL and NAC groups) A Bonferroni approximation will be applied
during the one planned interim analysis for efficacy
Before locking the database a statistical analysis plan (SAP) will be developed to provide
complete details on the statistical analysis The SAP will include the specifics for how and when
the DSMB will be notified for AEs The IPFnet DCC will deliver to the DSMB all FDA-defined
AEs at 3-month intervals The IPFnet DCC will prepare narrative SAE reports in real time for
DSMB review including recommendations and analysis of similar events for each SAE
submitted to the FDA
65
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
11 Investigator and Sponsor Obligations
111 Monitoring
All monitoring activities for US clinical centers will be performed in accordance with DCRI
standard operating procedures Information regarding the types of visits will be outlined in the
PANTHER-IPF MOOP
112 Cost and Payment
There will be no cost to subjects enrolled in this trial Study-related procedures will be paid for
by the IPFnet
Subjects may be eligible for reimbursement for travel to the clinical center Details of payment
will be explained to each subject during the consent process
113 Confidentiality and Health Insurance Portability and Accountability Act
Considerations
Subject confidentiality will be protected throughout the study All subject data will be kept
strictly confidential and no subject-identifying information will be released to anyone outside
the project Confidentiality will be assured through several mechanisms First each subject will
be assigned an anonymous study ID which will then be used on all study forms Second any
study forms blood samples and paper records that contain subject information (eg address lists
phone lists) will be kept at the clinical centers in secured locked areas coded by number Once
blood is collected there will be no subject identifiers placed on blood samplesmdashonly the study
ID number and the date of sample collection Third access to all subject data and information
including laboratory specimens will be restricted to authorized personnel In the case of
computerized data this restricted access will be assured through user logon IDs and password
protection
66
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
At the IPFnet DCC only authorized personnel will have access to the data files containing study
data Security will be assured through user logon IDs passwords and appropriate access
privileges All study subjects will be identified only by their IPFnet ID numbers and no personal
identifying information such as name address or Social Security number will be entered into
the IPFnet DCC database Any subject-specific data reported to the IPFnet Steering Group will
be identified only by the IPFnet ID number
Finally subjects will not be identified by name in any reports or publications nor will the data
be presented in such a way that the identity of individual subjects can be inferred Analysis files
created for further study by the scientific community will have no subject identifiers These data
files will be created in accordance with the Ancillary Studies and Publication Policy of the
IPFnet
114 Informed Consent Procedures
All IPFnet subjects will provide written informed consent using procedures reviewed and
approved by each clinical centerrsquos IRB Informed consent will be undertaken by study personnel
in-person with the subject The subject has the option of declining further participation in the
study at that point No further study procedures will be conducted until the signed documents
have been provided to the IPFnet clinical center
115 Institutional Review Boards
Before initiating this study the protocol clinical center-specific informed consent forms Health
Insurance Portability and Accountability Act (HIPAA) forms recruitment materials and other
relevant information will be reviewed by a properly constituted IRB at each participating clinical
center A copy of the signed and dated IRB approval at each clinical center will be retrieved prior
to or during the site initiation visit and archived at the IPFnet DCC Any amendments to the
protocol other than simple administrative and typographical changes must be approved by each
IRB before they are implemented The clinical centers will seek annual renewals of their IRB
approvals in accordance with local procedures
67
__________________________________________ ________________
__________________________________________
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
12 Investigator Agreement
I have read the foregoing protocol PANTHER-IPF and agree that it contains all necessary
details for carrying out this study I will conduct the study as outlined herein and will complete
the study within the time designated
I will provide copies of the protocol and all pertinent information to all individuals responsible to
me who assist in the conduct of this study I will discuss this material with them to ensure they
are fully informed regarding the drug and the conduct of the study
I will fulfill all responsibilities for submitting pertinent information to the local IRB if
applicable that is responsible for this study
I further agree that NHLBI andor DCRI will have access to any source documents from which
eCRF information may have been generated
Signature of Principal Investigator Date
Name of Principal Investigator (printed or typed)
Protocol version date May 19 2009
Protocol Amendment 1 version date May 28 2010
Protocol Amendment 2 version date December 6 2011
68
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
13 References
1 Raghu G Brown KK Bradford WZ et al A placebo-controlled trial of interferon gamma-1b in patients with idiopathic pulmonary fibrosis N Engl J Med 2004350125-33 2 King TE Jr Safrin S Starko KM et al Analyses of efficacy end points in a controlled trial of interferon-gamma1b for idiopathic pulmonary fibrosis Chest 2005127171-7 3 Flaherty KR Thwaite EL Kazerooni EA et al Radiological versus histological diagnosis in UIP and NSIP survival implications Thorax 200358143-8 4 Wells AU Desai SR Rubens MB et al Idiopathic pulmonary fibrosis a composite physiologic index derived from disease extent observed by computed tomography Am J Respir Crit Care Med 2003167962-9 5 Raghu G Freudenberger TD Yang S et al High prevalence of abnormal acid gastroshyoesophageal reflux in idiopathic pulmonary fibrosis Eur Respir J 200627136-42 6 Kinnula VL Focus on antioxidant enzymes and antioxidant strategies in smoking related airway diseases Thorax 200560693-700 7 Coultas DB Zumwalt RE Black WC Sobonya RE The epidemiology of interstitial lung diseases Am J Respir Crit Care Med 1994150967-72 8 Raghu G Weycker D Edelsberg J Bradford WZ Oster G Incidence and prevalence of idiopathic pulmonary fibrosis Am J Respir Crit Care Med 2006174810-6 9 Olson AL Swigris JJ Lezotte DC Norris JM Wilson CG Brown KK Mortality from pulmonary fibrosis increased in the United States from 1992 to 2003 Am J Respir Crit Care Med 2007176277-84 10 Mannino DM Etzel RA Parrish RG Pulmonary fibrosis deaths in the United States 1979shy1991 An analysis of multiple-cause mortality data Am J Respir Crit Care Med 19961531548shy52 11 Hubbard R Johnston I Coultas DB Britton J Mortality rates from cryptogenic fibrosing alveolitis in seven countries Thorax 199651711-6 12 Johnston I Britton J Kinnear W Logan R Rising mortality from cryptogenic fibrosing alveolitis Bmj 19903011017-21 13 Raghu G Collard HR Egan JJ et al An official ATSERSJRSALAT statement idiopathic pulmonary fibrosis evidence-based guidelines for diagnosis and management Am J Respir Crit Care Med 2011183788-824 14 (USA) FDA FDA Public Health Advisory Interferon gamma-1b (marketed as Actimmune) In 2007 15 King TE Jr Pardo A Selman M Idiopathic pulmonary fibrosis Lancet 2011 16 Raghu G Brown KK Costabel U et al Treatment of idiopathic pulmonary fibrosis with etanercept an exploratory placebo-controlled trial Am J Respir Crit Care Med 2008178948shy55 17 Malouf MA Hopkins P Snell G Glanville AR An investigator-driven study of everolimus in surgical lung biopsy confirmed idiopathic pulmonary fibrosis Respirology 201116776-83 18 King TE Jr Behr J Brown KK et al BUILD-1 a randomized placebo-controlled trial of bosentan in idiopathic pulmonary fibrosis Am J Respir Crit Care Med 200817775-81 19 Richeldi L Costabel U Selman M et al Efficacy of a tyrosine kinase inhibitor in idiopathic pulmonary fibrosis N Engl J Med 20113651079-87
69
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
20 Borok Z Buhl R Grimes GJ et al Effect of glutathione aerosol on oxidant-antioxidant imbalance in idiopathic pulmonary fibrosis Lancet 1991338215-6 21 Meyer A Buhl R Magnussen H The effect of oral N-acetylcysteine on lung glutathione levels in idiopathic pulmonary fibrosis Eur Respir J 19947431-6 22 Behr J Maier K Degenkolb B Krombach F Vogelmeier C Antioxidative and clinical effects of high-dose N-acetylcysteine in fibrosing alveolitis Adjunctive therapy to maintenance immunosuppression Am J Respir Crit Care Med 19971561897-901 23 Cantin AM North SL Fells GA Hubbard RC Crystal RG Oxidant-mediated epithelial cell injury in idiopathic pulmonary fibrosis J Clin Invest 1987791665-73 24 Waghray M Cui Z Horowitz JC et al Hydrogen peroxide is a diffusible paracrine signal for the induction of epithelial cell death by activated myofibroblasts Faseb J 200519854-6 25 Larios JM Budhiraja R Fanburg BL Thannickal VJ Oxidative protein cross-linking reactions involving L-tyrosine in transforming growth factor-beta1-stimulated fibroblasts J Biol Chem 200127617437-41 26 Kinnula VL Fattman CL Tan RJ Oury TD Oxidative stress in pulmonary fibrosis a possible role for redox modulatory therapy Am J Respir Crit Care Med 2005172417-22 27 Meyer A Buhl R Kampf S Magnussen H Intravenous N-acetylcysteine and lung glutathione of patients with pulmonary fibrosis and normals Am J Respir Crit Care Med 19951521055-60 28 Behr J Degenkolb B Krombach F Vogelmeier C Intracellular glutathione and bronchoalveolar cells in fibrosing alveolitis effects of N-acetylcysteine Eur Respir J 200219906-11 29 Bando M Hosono T Mato N et al Long-term efficacy of inhaled N-acetylcysteine in patients with idiopathic pulmonary fibrosis Intern Med 2010492289-96 30 Demedts M Behr J Buhl R et al High-dose acetylcysteine in idiopathic pulmonary fibrosis N Engl J Med 20053532229-42 31 Toma TP Bhowmik A Rajakulasingam R Acetylcysteine in pulmonary fibrosis N Engl J Med 20063541086-9 author reply -9 32 Hunninghake GW Antioxidant therapy for idiopathic pulmonary fibrosis N Engl J Med 20053532285-7 33 Flaherty KR Mumford JA Murray S et al Prognostic implications of physiologic and radiographic changes in idiopathic interstitial pneumonia Am J Respir Crit Care Med 2003168543-8 34 Latsi PI du Bois RM Nicholson AG et al Fibrotic idiopathic interstitial pneumonia the prognostic value of longitudinal functional trends Am J Respir Crit Care Med 2003168531-7 35 Collard HR King TE Jr Bartelson BB Vourlekis JS Schwarz MI Brown KK Changes in clinical and physiologic variables predict survival in idiopathic pulmonary fibrosis Am J Respir Crit Care Med 2003168538-42 36 Jegal Y Kim DS Shim TS et al Physiology is a stronger predictor of survival than pathology in fibrotic interstitial pneumonia Am J Respir Crit Care Med 2005171639-44 37 Martinez FJ Safrin S Weycker D et al The clinical course of patients with idiopathic pulmonary fibrosis Ann Intern Med 2005142963-7 38 Hull JH Acetylcysteine in pulmonary fibrosis N Engl J Med 20063541089-91 author reply -91
70
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
39 Flaherty KR King TE Jr Raghu G et al Idiopathic interstitial pneumonia what is the effect of a multidisciplinary approach to diagnosis Am J Respir Crit Care Med 2004170904shy10 40 Raghu G Johnson WC Lockhart D Mageto Y Treatment of idiopathic pulmonary fibrosis with a new antifibrotic agent pirfenidone results of a prospective open-label Phase II study Am J Respir Crit Care Med 19991591061-9 41 Hunninghake GW Lynch DA Galvin JR et al Radiologic findings are strongly associated with a pathologic diagnosis of usual interstitial pneumonia Chest 20031241215-23 42 Lynch D Godwin J Safrin S et al High-resolution computed tomography in idiopathic pulmonary fibrosis diagnosis and prognosis Am J Respir Crit Care Med 2005172488-93 43 Mallinckrodt CH Watkin JG Molenberghs G Carroll RJ Choice of the primary analysis in longitudinal clinical trials Pharmaceutical Statistics 20043161-9 44 Bang H Tsiatis A Estimating medical costs with censored data Biometrika 200087329shy43 45 Lin DY Regression analysis of incomplete medical cost data Stat Med 2003221181-200 46 Rochon J Application of GEE procedures for sample size calculations in repeated measures experiments Stat Med 1998171643-58 47 Lachin JM Foulkes MA Evaluation of sample size and power for analyses of survival with allowance for nonuniform patient entry losses to follow-up noncompliance and stratification Biometrics 198642507-19
71
- PANTHER-IPFPREDNISONE AZATHIOPRINEAND N-ACETYLCYSTEINEA STUDY THAT EVALUATES RESPONSE INIDIOPATHIC PULMONARY FIBROSIS
-
- Protocol Summary
- Table of Contents
- List of Tables
- List of Figures
- List of Abbreviations
- 1 Summary
- 2 Hypotheses and Specific Aims
-
- 21 Null Hypothesis
- 22 Specific Aim 1
- 23 Specific Aim 2
- 24 Prespecified Subgroups of Interest
-
- 3 Background and Significance
-
- 31 Idiopathic Pulmonary Fibrosis is the Most Common Interstitial Lung Disease
- 32 Rationale for Placebo Control
- 33 Rationale for N-acetylcysteine
- 35 Rationale for N-acetylcysteine as a Stand-alone Therapy
- 36 Rationale for the Study Design and Primary Endpoint
- 37 Rationale for Blinding of Treatments
-
- 4 Methods
-
- 41 Inclusion Criteria
- 42 Diagnosis of IPF
- 43 Exclusion Criteria
- 44 Study Design and Study Visit
- 45 Dose Justification
- 46 Contraindications Precautions and Side Effects of Study Medications
- 47 Recruitment Procedures
- 48 Study Procedures
- 49 Concomitant Medications
- 410 Laboratory Testing
- 411 Blinding of Study Drugs
-
- 5 Study Endpoints
-
- 51 Primary Study Endpoint
- 52 Secondary Study Endpoints
-
- 6 Safety Evaluations and Procedures
-
- 61 Adverse Events
- 62 Clinical Medical Monitoring
- 63 Unblinding Procedures
-
- 7 Study Drug Procedures
- 8 Data Management
-
- 81 Hardware and Software Configuration
- 82 Sources of Data
-
- 9 Study Design and Data Analysis
-
- 91 General Analytic Considerations
- 92 Randomization Blinding and Reporting of Results
- 93 Stratification
- 94 Specification of the Primary Analyses
- 95 Analysis of Longitudinal Endpoints
- 96 Analysis of Binary Time-to-Event and Time-Lagged Endpoints
- 97 Power Analysis
-
- 10 Study Administration
-
- 101 Cooperative Agreement Mechanism
- 102 IPFnet Steering Group
- 103 Data and Safety Monitoring Board
- 104 Recommendations on Interim Monitoring of Efficacy Safety and Futility
-
- 11 Investigator and Sponsor Obligations
-
- 111 Monitoring
- 112 Cost and Payment
- 113 Confidentiality and Health Insurance Portability and Accountability ActConsiderations
- 114 Informed Consent Procedures
- 115 Institutional Review Boards
-
- 12 Investigator Agreement
- 13 References
-

PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Make objective assessments of treatment effects
Maintain clinical equipoise among investigators
Encourage subjects to have similar levels of contact with the medical community
Minimize the differential dropout rates across study arms
20
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
4 Methods 41 Inclusion Criteria
1 Age 35 to 85 years inclusive
2 FVC ge 50 of predicted (post-bronchodilator measurement from the screening visit)
3 DLCO ge 30 of predicted (hemoglobin corrected and altitude corrected if gt4000 ft above sea level)
4 Ability to understand and provide informed consent
5 Diagnosis of IPF according to a modified version of the ATS criteria le 48 months from enrollment The
date of diagnosis is defined as the date of the first available HRCT or surgical lung biopsy characteristic
of definite UIP
411 Subjects Shown to Have Usual Interstitial Pneumonia Pattern on Surgical Lung Biopsy
Subjects who have been shown to have UIP pattern on lung biopsy must have all of the following
1 Exclusion of other known causes of ILD such as drug toxicity clinically significant environmental
exposures or diagnosis of connective tissue diseases
2 Bibasilar reticular abnormalities with minimal ground glass opacities on HRCT scan
412 Subjects Who Have Not Undergone a Surgical Lung Biopsy
In addition to the criteria above these subjects must have radiological findings considered to be definite for the
diagnosis of UIPIPF
1 Bibasilar reticular abnormalities with minimal ground glass opacities
2 Honeycombing as the predominant feature and located in the peripheral lung bases
42 Diagnosis of IPF
Only subjects with definite IPF will be eligible for enrollment in this study We will utilize a combination of
clinicalphysiologic features HRCT and review of a clinically obtained surgical lung biopsy specimen to
establish the diagnosis of IPF An algorithm for the diagnosis is provided to guide entry into the protocol as
outlined in the inclusion and exclusion criteria (Figures 2 and 3) This multi-disciplinary approach uses
21
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
expertise from clinicians radiologists and pathologists Investigators at each site in conjunction with central
pathology will work together to establish the diagnosis of IPF This interactive approach to the diagnosis of IPF
increases the level of agreement between observers39
A subject with suspected ILD should be evaluated for secondary causes including but not limited to
environmental exposures drugs and systemic diseases Presence of any of these findings felt to be significant
enough to cause an ILD should disqualify the subject from entry into the trial
If secondary causes are absent an HRCT scan may be obtained If an HRCT of sufficiently high quality has
been obtained within the last 3 months that scan may be used for diagnosis In the appropriate clinical setting
the diagnosis of IPF can be made by the demonstration of a typical radiographic pattern on HRCT or by
demonstration of UIP pattern on a surgical lung biopsy The following criteria for a radiographic (ie
nonsurgical) diagnosis will be used In the absence of known exposures andor clinical associations attributable
to pulmonary fibrosis and in the appropriate clinical setting the presence of definite UIP pattern in HRCT
images is required to meet study criteria for the diagnosis of IPF
Figure 2 Diagnosis of Idiopathic Pulmonary Fibrosis in the IPFnet
22
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Figure 3 Pathology Flow Chart Surgical Lung Biopsy Diagnosis
Requirement for diagnosis
1 Clinical exclusion of other known causes (connective tissue diseases environmental and drug
exposures) of ILD
2 Radiographic HRCT with bibasilar reticular abnormality and honeycomb change with minimal
ground glass opacities
Appropriate clinical setting
1 Age gt 50 years
2 Insidious onset of unexplained dyspnea
3 Duration of illness for ge 3 months
4 Bibasilar inspiratory crackles
23
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Unlike the ATSERS consensus criteria published in 2000 bronchoscopy will not be required for diagnosis
This decision was made based on the experience of the IPFnet Steering Group members regarding the utility of
bronchoscopy in the diagnosis of IPF The presence of an atypical HRCT finding will require documentation of
a definitive diagnosis by surgical lung biopsy In fact this is in keeping with the recently published evidence
based guidelines for diagnosis and management of IPF13 As shown in Figure 3 central review of the pathology
data will be required for a diagnosis of IPF
We will not require central review of HRCT as several studies have shown that a confident local interpretation
of clinicalHRCT criteria as definite IPFUIP is associated with a high positive predictive value for finding UIP
at surgical lung biopsy (see Table 1) Differences in sensitivity in these series likely reflect subject selection as
Flaherty et al3 evaluated only UIP and nonspecific interstitial pneumonia (NSIP) while Raghu et al40 and
Hunninghake et al41 included a broader range of ILD
Table 1 Operating Characteristics of Local HRCT Review for Diagnosis of UIP
Researcher of Subjects Sensitivity () Specificity () PPV () NPV ()
Raghu et al 40
59 (29 UIP by SLB) 78 90 88 82
Hunninghake et al 41 91 (54 UIP by SLB)
74 81 85 67
Flaherty et al 3 96 (only NSIP amp UIP)
37 100 100 30
Abbreviations PPV positive predictive value NPV negative predictive value UIP usual interstitial pneumonia SLB surgical lung biopsy and NSIP nonspecific interstitial pneumonia
Furthermore an analysis of the HRCT scans from subjects enrolled in the GIPF-001 trial confirmed that local
site interpretations have a high congruity to a central radiology core In this multi-center study 263 HRCT
scans were read as definite IPF and a retrospective central radiology core review found 932 to be consistent
with IPF 42 We will also take several additional steps to insure that the local HRCT reads are accurate
including
1 A detailed training module has been developed and must be completed by each site radiologist before
site initiation
2 Clinical centers are to mail all HRCT scans to the HRCT core lab The first 10 HRCT scans from
subjects enrolled at each enrolling clinical center will be reviewed centrally to be certain that local reads
24
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
25
are congruent with a central interpretation If discrepancies are identified additional education will be
provided and HRCT scans will continue to be reviewed centrally until the central radiology core is
confident that the local center is performing appropriately
3 Random scans will be obtained from each center throughout the study to confirm that the local read
continues to agree with central interpretation If discrepancies are identified they will be addressed as in
2 above
In all cases if a subject has a surgical lung biopsy sample that sample will be reviewed by the local and central
pathologists Therefore the only cases that would not be subject to a direct central review process are those
where the HRCT meets the centrally defined criteria for an unequivocal diagnosis and a lung biopsy sample is
not available Table 2 below summarizes the possible combinations for making a diagnosis
Table 2 Combining HRCT and Pathology Interpretations to Determine if IPF is Present
HRCT Diagnosis Pathology Diagnosis Diagnosis of IPF
Definite UIP Definite UIP Yes
Definite UIP Probable UIP Yes
Definite UIP Possible UIP Yes
Definite UIP Not UIP No
Definite UIP Unavailable Yes
Consistent with UIP Definite UIP Yes
Consistent with UIP Probable UIP Yes
Consistent with UIP Possible UIP No
Consistent with UIP Not UIP No
Consistent with UIP Unavailable No
Inconsistent with UIP Any No
Abbreviations HRCT high-resolution computed tomography IPF idiopathic pulmonary fibrosis
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
UIP usual interstitial pneumonia Dx diagnosis 43 Exclusion Criteria
1 History of clinically significant environmental exposure known to cause pulmonary fibrosis
Occupational exposures such as asbestos or environmental exposure to organic dust such as occurs in
pigeon breeders may at times mimic the clinical and radiographic findings of IPF
2 Diagnosis of connective tissue disease felt by the principal investigator (PI) to be the etiology of the
interstitial disease Diagnosis of collagen-vascular conditions will be according to the published
American College of Rheumatology criteria As such the presence of any documented collagen-vascular
disorder or the presence of any suspicious symptom complex whether or not associated with
significantly abnormal rheumatological serologies will exclude the subject at the discretion of the PI
3 Extent of emphysema greater than the extent of fibrotic change (honeycombing reticular changes) on
HRCT scan
4 Forced expiratory volume in 1 second (FEV1)FVC ratio lt 065 at screening (postbronchodilator)
5 Partial pressure of arterial oxygen (PaO2) on room air lt 55 mm Hg (lt 50 mm Hg at Denver site)
6 Residual volume gt 120 predicted at screening (postbronchodilator)
7 Evidence of active infection
8 Significant bronchodilator response on screening spirometry defined as a change in FEV1 ge 12 and
absolute change gt 200 mL OR change in FVC ge 12 and absolute change gt 200 mL The percent
difference between the FVC (or FEV1) values will be calculated by taking the absolute value of the
difference and dividing it by the larger of the two FVC (or FEV1) values
9 Screening and enrollment post-bronchodilator FVC measurements (in liters) differing by gt 11 The
percent difference between the FVC values will be calculated by taking the absolute value of the
difference and dividing it by the larger of the two FVC values (eg the percent difference between FVC
measurements of 19 and 20 liters would be determined by taking the difference between the two (01
liters) and dividing by the larger of the two (20 liters) So 0120 = 5 and these FVC measurements
would not exclude the subject
10 Listed for lung transplantation ie the patient has completed the evaluation process has been accepted
as a candidate for transplantation at an appropriate center and is waiting to receive notification of an
available donor organ
11 History of unstable or deteriorating cardiac disease
12 Myocardial infarction coronary artery bypass or angioplasty within 6 months of screening
26
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
13 Unstable angina pectoris or congestive heart failure requiring hospitalization within 6 months of
screening
14 Uncontrolled arrhythmia
15 Severe uncontrolled hypertension
16 Known HIV or hepatitis C
17 Known cirrhosis and chronic active hepatitis
18 Active substance andor alcohol abuse (as determined by site PI)
19 Pregnancy or lactation (subjects who are pregnant or breastfeeding)
20 Known hypersensitivity to study medication
21 Any condition other than IPF that in the opinion of the site PI is likely to result in the death of the
subject within the next year
22 Any condition that in the judgment of the PI might cause participation in this study to be detrimental to
the subject or that the PI deems makes the subject a poor candidate
23 Any therapy directed at pulmonary fibrosis (excepting triple therapy of prednisone plus azathioprine
plus NAC) requires a 30-day washout period before randomized Triple therapy of lt= 12 weeks duration
in the past 4 years requires a 30-day washout period before randomization
24 History of triple therapy of prednisone plus azathioprine plus NAC for gt 12 weeksrsquo duration in the past
4 years or previous enrollment in the triple-therapy arm of the PANTHER-IPF study
44 Study Design and Study Visit
441 Study Design Summary
This study will be a randomized double-blind PL-controlled trial designed to assess the safety and efficacy of
NAC in subjects with newly diagnosed IPF
Subjects with mild to moderate IPF (defined as FVCpred ge 50 and DLCOpred ge 30) diagnosed within
the past 48 months will be enrolled Screening will continue until April 30 2012
27
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
The study will employ a 2-arm design with 11 randomization to NAC or PL Once enrolled subjects will visit
the clinical center at 15 weeks and 15-week intervals thereafter Each subject will be treated and followed for a
maximum of 60 weeks
During the 60-week visit subjects will be taken off all study agents Approximately four weeks after the final
dose of study agent is taken subjects will receive a safety phone call from the study site
442 Study Visits
Subjects who meet entry criteria will review the informed consent a written description of the purpose
procedures and risks of the study with the PI co-investigator or study coordinator and all questions will be
answered The informed consent form will be signed by the subject at screening No protocol-specific
procedures will be performed until the subject has signed and dated an informed consent form This includes the
screening procedures
4421 Screening
Once informed consent is obtained subjects may immediately begin the screening process or may return within
28 days of consent In the event a study subject has been clinically evaluated at the study site by an IPFnet study
physician and has performed testing within three weeks for this clinical evaluation that meets guidelines
provided in the IPFnet PANTHER-IPF Manual of Operating Procedures (MOOP) this testing may be used to
satisfy the following screening criteria medical history physical exam arterial blood gas (ABG) with A-a
gradient vital signs with oximetry body height and weight spirometry DLCO lung volumes and HRCT scan
Allowing the use of previously performed test results that meet study guidelines for the screening visit is
intended to permit subjects easier access to study entry to prevent subjects from repeating testing that has been
performed within the study window and to decrease risks to subjects from repeated exposure to procedures
such as arterial puncture and HRCT
The following procedures will be performed at screening
Medical history and a physical examination
28
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Measure height and weight
Serum pregnancy test (if applicable)
Measure vital signs including oximetry
Blood draws performed and the following analyses conducted
o Hematology (red cell count white cell count hemoglobin hematocrit cell indices differential
platelet count)
o Blood chemistries according to central laboratory protocol (see Section 410 Laboratory
Testing)
o Beta human chorionic gonadotropin (serum) pregnancy test (in women of childbearing potential)
o Urinalysis
Pulmonary Function Tests (PFTs) including spirometry pre- and post- bronchodilator and postshy
bronchodilator measurement of lung volumes and measurement of hemoglobin adjusted diffusing
capacity
Measure ABGs
HRCT if a satisfactory scan has not been performed on the subject within 3 months of screening (see
PANTHER-IPF MOOP for more details)
Surgical lung biopsies (if applicable) reviewed by local and central pathology departments
Current medications If required a washout period discussed with the subject and initiated at this visit
4422 Enrollment
The enrollment visit is expected to take place within eight weeks of the screening visit Enrollment visit
activities include
Measure vital signs including oximetry
Measure height and weight
Serum pregnancy test (if applicable)
If consent has been given blood will be drawn and a urine specimen collected for the bio-specimen
repository
Spirometry (post-bronchodilator)
Measure 6MWT with Borg Dyspnea Scale
29
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Collect Quality-of-life (QOL) data using the SF-36 EuroQol Investigating Choice Experiments for
Preferences of Older People Capability Instrument (ICE CAP) and SGRQ
Female subjects complete Gender Substudy questionnaire
Dyspnea status collected using the UCSD SOBQ
Evaluate Acute Exacerbation (AEx)
Review of any Adverse Events (AEs)
Review of concomitant medications
Subject receives diary and instructions on its purpose and proper use
Subject receives supply of study drug sufficient to last until his or her 15-week study visit
See the Schedule of Assessments (Table 3) for more details Subjects with screening and enrollment postshy
bronchodilator FVC measurements (in liters) differing by more than 11 are not eligible to be enrolled in the
study
Subjects will be asked to provide a physician of record This physician will be considered the subjectrsquos primary
care provider (PCP) and if the subject agrees the PCP will be informed by letter of the subjectrsquos enrollment in
the trial The subject will be informed that his or her ongoing medical care should be received from the PCP
The PCP will be informed of any safety issues identified by the study staff The PCP will also be given
information regarding communication with study personnel about pertinent health issues or clinic encounters
the subject may have
4423 Week 15
The week 15 visit is expected to occur within +- 14 days of the subjectrsquos scheduled visit time (eg the week 15
visit should occur anytime between 13 and 17 weeks after starting study drug Week 15 activities include
Measure vital signs with oximetry
Measurement height and weight
Serum pregnancy test (if applicable)
Spirometry (post-bronchodilator) measurement
Review of AEs
Evaluate for AEx
30
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Review concomitant medications
If consented draw blood and collect urine specimen for the biospecimen repository
Subjects return used and unused study drug for the visit
Review study diary and a new study diary will be given
Provide additional supply of study drug sufficient to last until the next scheduled visit
4424 Week 30
The week 30 visit is expected to occur within +- 14 days of the subjectrsquos scheduled visit time (eg the week 30
visit should occur anytime between 28 and 32 weeks after starting study drug) Week 30 activities include
Physical examination
Measure vital signs with oximetry
Measure height and weight
Laboratory values (complete blood count [CBC] and serum chemistries)
Serum pregnancy test (if applicable)
Measure spirometry (post-bronchodilator)
6MWT with Borg scale
DLCO
Review of AEs
Evaluate for AEx
Review concomitant medications
Complete all QOL and dyspnea questionnaires (EuroQol ICE CAP SF-36 SGRQ and UCSD SOBQ)
If consent has been given blood will be drawn and a urine specimen collected for the biospecimen
repository
Review study diary
Subjects return used and unused study drug for the visit
Provide additional supply of study drug sufficient to last until the next scheduled visit
4425 Week 45
31
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
The week 45 visit is expected to occur within +- 14 days of the subjectrsquos scheduled visit time (eg the week 45
visit should occur anytime between 43 and 47 weeks after starting study drug) Week 45 activities include
Measure vital signs with oximetry
Measure height and weight
Serum pregnancy test (if applicable)
Measure spirometry (post-bronchodilator)
Review of AEs
Evaluate for AEx
Review concomitant medications
If consent has been given blood will be drawn and a urine specimen collected for the biospecimen
repository
Subjects return used and unused study drug for the visit
Study diary reviewed
Provide additional supply of study drug sufficient to last until the next scheduled visit
4426 Week 60 (Early Withdrawal or Final Treatment Visit)
At week 60 or at subject withdrawal from the study (premature by study doctor or subjectrsquos decision) a final
treatment visit will occur At this final treatment visit subjects will discontinue NACPL abruptly Week 60
activities also include
Physical examination
Measure vital signs with oximetry
Measure height and weight
Laboratory values (complete blood count [CBC] and serum chemistries)
Spirometry (post-bronchodilator) measurement
6MWT with Borg scale measurement
DLCO
Lung volumes
ABG
Review of AEs
32
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Evaluate for AEx
Review concomitant medications
Subjects will complete all QOL and dyspnea questionnaires (EuroQol ICE CAP SF-36 SGRQ and
UCSD SOBQ)
If consent has been given blood will be drawn and a urine specimen collected for the biospecimen
repository
Subjects return used and unused study drug for the visit
Study diary reviewed
4427 Final Site Visit ndash FVC drop confirmation
In the event that the subject has a recorded FVC drop of gt10 from baseline at the final treatment visit and the
subject has not had a confirmation of such a drop at a previous study visit the subject should return to the
clinical site 6 to 8 weeks after the final treatment visit During this visit a post-bronchodilator spirometry test
will be performed This FVC measurement will be evaluated according to section 521 of this protocol
4428 Final Visit ndash Telephone Follow-up
Four weeks following the final dose of study medication subjects will receive a telephone call from the study
coordinator to ensure that there are no side effects and to follow up on any ongoing adverse events (AEs)
4429 Phone Contact Between Visits
At week 2 and each month that a subject does not have a scheduled clinical center visit his or her study
coordinator will contact him or her at least once by telephone to
Inquire if the subject has had any hospitalizations events that might be considered an AE or any events
significant enough to warrant an out-of-cycle visit to the clinical center
Remind subjects of their current dosage levels and confirm that the subject understands them
Address any questions or concerns the subject might have regarding other aspects of the study
Assess adherence to the treatment regimen by reviewing diary data verbal review of medications taken
including nutritional supplements
33
34
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Table 3 Schedule of Assessments
Procedure Screening Visit 0
Enrollment Visit 1
Week 15 Visit 2
Week 30Visit 3
Week 45 Visit 4
Week 60 Early
Withdrawal Visit 5
Final1
Visit (via phone)
Informed consent X
Medical history X
Inclusionexclusion criteria X
Serum pregnancy test (if applicable) X X X X X
Review of lung biopsy X
Arterial Blood Gas X X
6-Minute Walk Test
X
X X
Physical examination X X X
Vital signs with oximetry X X X X X X
Body height and weight X X X X X X
Complete Blood Count X X X
Chemistry panel X X X
Monitor Lab Values X X X
Urinalysis X Specimen repository substudy blood draw and urine collection (if consented)
X
X X X X
HRCT (if not completed within three months) X
Spirometry (pre- and post-bronchodilator) X
Spirometry (post-bronchodilator only) X X X X X
DLCO (post-bronchodilator only) X X X
Lung volumes (post-bronchodilator only) X
X
Evaluate for acute exacerbation X X X X X
Review Adverse Events X X X X X X
Review concomitant meds X X X X X X
Dispense subject diary X X X X
Review subject diary X X X X X
Dispense study agent X X X X
Gender Substudy questionnaire (female subjects only) X
EuroQol ICECAP UCSD SOBQ SGRQ SF-36 X X X
Abbreviations DLCO diffusing capacity of the lung for carbon monoxide QOL Quality of Life ICECAP Investigating Choice Experiments for Preferences of Older People UCSD SOBQ University of California Shortness of Breath Questionnaire SGRQ St Georgersquos Respiratory Questionnaire SF-36 Short Form 36 Health Survey
1Follow-up visit via phone will occur four weeks after final dose of study medication
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
45 Dose Justification
The general philosophy for determining dosing levels was to apply previously examined
treatment regimens With the focus of the study being to establish a standard of care for
mildmoderate IPF subjects the goal was to develop flexible yet standardized treatment rules that
allow for the temporary or permanent withholding of one or more components of treatment when
necessary Subjects developing laboratory abnormalities or symptoms that result in
discontinuation of one or more components of study treatment may continue on the other
components as long as there is no contraindication for this Complete follow-up is important for
the validity of any study As a strategy to maintain protocol adherence we are using a treatment
regimen that will detect potential side effects and prompt interventions proactively in the interest
of patient safety In addition subjects who permanently stop study medications during the course
of the study are encouraged to continue in the study completing all scheduled visits and tests
451 Rationale for N-acetylcysteine Dosing
To our knowledge there have been no IPF studies to correlate clinical outcome measures with
different dosages for NAC The dosage chosen is based on the IFIGENIA study However BAL
lung GSH levels from subjects with IPF have been augmented with the use of oral NAC at 600
mg 3 times per day In addition lung GSH levels have been associated with improved
PFTs212227 The dose chosen for this study was based on previous data including the IFIGENIA
study30
4511 Dosing of N-acetylcysteineplacebo
Dosing of NACPL will be 600 mg orally 3 times a day (1800 mgday)
4512 Reasons to Discontinue N-acetylcysteineplacebo
NACPL may be temporarily or permanently discontinued for the duration of the study for
gastrointestinal symptoms or dermatologic reactions
35
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Temporarily discontinue (hold) oral NACPL for subjects requiring inpatient admission for acute
exacerbation (AEx) or other conditions Resume NACPL after discharge
36
37
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
452 Dosage Algorithms
Dosage Adjustment Algorithm 1 NACPL Dose Modifications for Gastrointestinal Symptoms Nausea Vomiting Abdominal Discomfort Diarrhea
GI Symptoms determined by the PI to be clinically significant Nausea Vomiting Abdominal Discomfort Diarrhea
NACPL Temporarily dc (HOLD) x 3 Days
Monitor symptoms intervene as clinically indicated (eg fluid replacement antidiarrhea or antinausea medication)
Monitor or lab PRN
Are symptoms resolving after 3 days NO
Symptoms NOT resolving after 3 days of holding study medication Assessmentmanagement per clinical
discretion of investigator
Likely not study medication discuss resuming study medication with medical monitor when symptoms resolved
YES
Temporarily dc (HOLD) NACPL for 4 additional days (total hold 1 week) then NACPL Resume 600 MG TID
Did symptoms recur
YES
STOP NACPL for
duration of study
NO
NACPL No Change
38
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Dosage Adjustment Algorithm 2 NACPL Dose Modifications For Dermatologic Reactions
Dermatologic Reactions (Not Acneiform) ge Grade 2 Grading per Common Terminology Criteria for
Adverse Events V30 (httpctepcancergov) For example Grade 1 RASHDESQUAMATION Macular or papular eruption or erythema without associated symptoms Grade 2 RASHDESQUAMATION Macular or popular eruption or erythema with pruritus or other associated symptoms localized desquamation or other lesions covering lt50 of body surface area
NACPL Temporarily dc (HOLD) x 3 days
Are symptoms resolving after 3 days
NO Symptoms not resolving after 3 days of holding study medication Assessmentmanagement per clinical discretion of investigator Likely not study medication Discuss resuming study medication with medical monitor when symptoms
resolved YES
Temporarily dc (HOLD) NACPL for 4 additional days (total hold 1 week) then NACPL resume 600 MG TID
Did symptoms recur
YES
STOP NACPL for
duration of study
NO
NACPL No change
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
46 Contraindications Precautions and Side Effects of Study Medications
461 Contraindication
Contraindication to NAC is known hypersensitivity to it
462 Precautions
Concomitant administration of oral NAC and antibiotics has shown a slightly reduced absorption
of cephalexin and a slight increase in erythromycin serum levels NAC contains free sulfhydryl
groups There is no evidence that individuals sensitive to sulfa drugs are sensitive to NAC
The NAC preparation being administered in this study contains 20 mg of aspartame Because of
the phenylalanine component of aspartame individuals with phenylketonuria should avoid or
restrict aspartame intake to avoid increased blood levels of phenylalanine Because of this risk
labeling is required on all products containing aspartame
463 Side Effects
Side effects of NAC range from common to serious See Table 4
39
40
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Table 4 Side Effects of NAC
Undesirable Effects
System-organ class Uncommon
(gt11000 lt1100)
Rare
(gt110000 lt11000)
Very rare
(lt110000) Not known
Immune system disorders Hypersensitivity Anaphylactic shock
reaction
Nervous system disorders Headache
Ear and labyrinth disorders Tinnitus
Cardiac disorders Tachycardia
Vascular disorders Hemorrhage
Respiratory thoracic and
mediastinal disorders
Bronchospasm
Dyspnea
Gastrointestinal disorders
Vomiting diarrhea
stomatitis abdominal
pain nausea
Dyspepsia
Skin and subcutaneous tissue
disorders
Urticaria rash
angioedema itching
General disorders and
administration site conditions Pyrexia
Investigations Reduced arterial
pressure Face edema
In very rare cases the onset of severe skin reactions such as Stevens-Johnson syndrome and Lyell syndrome was reported to have a temporal relationship with N-acetylcysteine administration Although in most cases at least another suspect drug probably most involved in the genesis of the above mentioned mucocutaneous syndromes has been identified in case of mucocutaneous alterations it is appropriate to contact onersquos doctor and the administration of N-acetylcysteine should be immediately discontinued
Some studies confirmed a reduction of platelet aggregation during N-acetylcysteine administration The clinical significance of these findings has not been defined yet [Source Fluimucil Investigator Brochure]
47 Recruitment Procedures
Subjects recruited for this study will be established patients of the investigators or physician- or
self-referred to participating clinical centers in the IPFnet Each clinical center within IPFnet has
a well-developed infrastructure of local pulmonologists within the surrounding geographic area
These pulmonologists are kept informed of ongoing IPF clinical trials and regularly refer
subjects to studies conducted at IPFnet clinical centers
Additional steps will be taken to inform clinicians of the trials in progress within IPFnet
including presentations at faculty staff meetings at local hospitals medical grand rounds and
national conferences direct mail notification monthly faxes and advertisement of network trials
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
in pulmonary journals Clinical center patients previously diagnosed with IPF will be notified of
the trials by mail whenever possible
Recruitment of minorities and women will be monitored by the DCC and DSMB If necessary
additional recruitment efforts will be made at specific centers to ensure that the aggregate subject
sample contains appropriate representation of women and minorities
48 Study Procedures
The following procedures are detailed in the PANTHER-IPF MOOP accompanying this
protocol
1 PFT
2 ABG
3 HRCT scan of the chest (including imaging of pulmonary arteries)
4 CBC and serum chemistries
5 Pregnancy test
6 6MWTBorg Dyspnea Scale
7 QOL questionnaires (EuroQol HAD SF-36 SGRQ and ICE CAP)
8 UCSD SOBQ
9 Gender Substudy Questionnaire
All assessments of PFTs will be conducted by study personnel not directly involved in the
treatment of the subjects
481 Biological Specimen Management
4811 Biological Specimen Sample Management
Subjects at clinical centers participating in the specimen repository substudy who consent to
having blood drawn for research purposes and for the banking of blood blood components and
other biologic specimens (urine and BAL fluid) will have approximately 405 mL of blood
41
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
drawn 17 mL blood drawn for DNA and 20 mL of urine collected at enrollment visit Subjects
will have approximately 50 mL of blood drawn and 20 mL of urine collected at each 15-week
follow-up visit Blood specimens will be separated according to PANTHER-IPF MOOP
guidelines into the following components for banking in the repository serum plasma and
DNA Coding of all biologic specimens for the repository will be performed by study staff at the
clinical center The samples will be processed per PANTHER-IPF MOOP guidelines aliquoted
labeled with barcode labels and stored at -70degC at the clinical center and shipped to the central
repository
The only subject identifiers will be a sample ID number and subject initials This sample ID will
be linked in the IPFnet DCC clinical database to subject information No subject information will
be transferred to the biological-specimen database
The subjectrsquos samples may be used for approved sub-studies relating to human disease
including but not limited to IPF The studies for which an individualrsquos samples will be made
available will be determined by the subjectrsquos answers to questions on the biological-sample
informed consent form The subjects can choose to make their samples available for all options
or any combination Samples will be made available to researchers only with IPFnet Steering
Group approval until such time as the samples are made public through the NHLBI repository
49 Concomitant Medications
Concurrent treatment with FDA-approved therapy for IPF is allowed Colchicine may be used
for treatment of gout Temporary treatment with oral or IV corticosteroids for clinical worsening
or suspected AEx is permitted Nutritional supplements containing NAC are not allowed
410 Laboratory Testing
Clinical laboratory parameters will be assessed at screening and at the end of the study The
following tests will be performed at the two time points specified in the protocol chemistry (AG
ratio ALT [SGPT] AST [SGOT] albumin alkaline phosphatase amylase bilirubin-direct
42
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
bilirubin-indirect bilirubin-total BUN BUNcreatinine ratio calcium carbon dioxide
cholesterol-total chloride CPK-total creatinine GGT globulin glucose iron-total LDH
lipase magnesium phosphorus-inorganic potassium protein-total sodium TIBC triglycerides
uric acid) and hematology (red blood cell count WBC count hemoglobin hematocrit cell
indices differential platelet count)
411 Blinding of Study Drugs
Subjects and caregivers will be blinded to study treatment Every subject will receive NAC or
matching PLs at every study visit from the baseline visit to the week-45 visit No study agent
will be dispensed at the week-60 visit
43
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
5 Study Endpoints
51 Primary Study Endpoint
The primary endpoint will be the change in serial measurements of FVC over the study period
52 Secondary Study Endpoints
521 Time to Disease-progression
The time-to-death or a 10 decline in FVC will be defined as the time-to-disease progression
The 10 decline in FVC from enrollment must be confirmed on 2 consecutive visits no less than
6 weeks apart For subjects with 2 consecutive visits with a 10 decline in FVC the time-toshy
disease progression will be defined as the time interval between enrollment and the initial visit
with a 10 FVC decline For subjects who experience disease progression the study doctor will
determine whether or not the subject will remain in the study
522 Acute Exacerbations
The following 3 criteria will define AEx in subjects with acute worsening of their respiratory
conditions
1 Clinical (all of the following required)
A) Unexplained worsening of dyspnea or cough within 30 days triggering unscheduled
medical care (eg emergency room clinic study visit hospitalization)
B) No clinical suspicion or overt evidence of cardiac event pulmonary embolism or deep
venous thrombosis to explain acute worsening of dyspnea
C) No pneumothorax
44
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
2 RadiologicPhysiologic (A and B required)
A) New ground glass opacity or consolidation computed tomography (CT) scan OR new
alveolar opacities on chest x-ray
B) Decline of ge 5 in resting room air SpO2 from last recorded level OR decline of ge 8 mm
Hg in resting room air PaO2 from last recorded level
3 Microbiologic (all of the following required)
A) No clinical evidence for infection (ie absence of grossly purulent sputum fever gt 39degC
orally)
B) Lack of positive microbiological results (if done) from lower respiratory tract defined as
(1) Clinically significant bacterial growth on sputum or endotracheal aspirate cultures
(2) Quantitative culture by protected brush specimen ge 103 cfumL or BAL ge 104 cfumL
(3) The presence of specific pathogens on stains of any of the above
C) Lack of positive pathogen in blood cultures (if done)
Identification of Acute Exacerbations
All subjects will be educated about the importance of identifying AExs At the time of
enrollment subjects will be told about the possibility of developing acute symptomatic
worsening that might represent an AEx of IPF and instructed to contact their study clinical
center coordinator within 48 to 72 hours of the apparent event
All subjects will be contacted by phone monthly and questioned about any change in dyspnea or
cough and any interim clinic visits or hospitalizations Finally as part of the IPFnet outreach to
community referring physicians the importance of AExs will be emphasized When a subject is
identified who meets criterion 1A this will trigger the collection of additional clinical data to
evaluate a suspected AEx These data will be collected as part of standard clinical care (ie this
protocol does not require collection of all items) The additional items to be collected for
suspected AEx include
IPFnet AEx case report form (eCRF) (required)
45
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Chest x-ray CT scan withwithout pulmonary angiogram (reports should be faxed and
followed by the hard copiesdiscs)
Oxygen saturation (pulse oximetry)
ABG
Respiratory cultures (sputum endotracheal aspirate lavage)
Blood cultures
Clinichospital records related to the event
All potential cases of AEx will be reviewed by the clinical center PI first and a decision on
whether the case may represent an AEx will be made If AEx is suspected the case will be sent
to the IPFnet adjudication committee which will assign a final diagnosis (see Table 5) If there is
disagreement among members the majority opinion will be recorded
During episodes of suspected AEx as determined by the individual clinical center investigator
subjects will remain blinded and in the study
Table 5 Final Diagnoses in Evaluation of Suspected Acute Exacerbations
Definite acute exacerbation All criteria met no alternative etiology
Unclassifiable acute worsening
Insufficient data to evaluate all criteria no alternative etiology
Not acute exacerbation Alternative etiology identified that explains acute worsening
Management of the suspected AEx will be at the discretion of the treating physician Standard of
care generally involves evaluation for respiratory infection pulmonary embolism cardiac events
and pneumothorax and treatment with IV corticosteroids
Study drugs will be resumed at pre-suspected AEx doses after subjects clinically improve as
confirmed by the local PI All subjects should be seen at the clinical center within 2 to 4 weeks
of recovery for measurement of post-bronchodilator FVC (see Figure 4) Subjects unable to
return to the clinical center after suspected AEx due to medical frailty (eg continued
46
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
institutionalization progressive disability) will be categorized as failing to maintain FVC
response in secondary analyses
Suspected AEx (PI determined)
Hold study drug Treat AEx
(Attending physician determined)
Alive but unable to continue due to
medical frailty
Dead
Alive and able to continue
Site reviewvisit
Restart study drug
FVC within 2-4 weeks
Figure 4 Acute Exacerbation Flow Chart
523 Respiratory Infections
An upper respiratory infection will be defined as
Change in sputum discoloration
Increased cough of no more than 14 daysrsquo duration
A lower-respiratory infection (pneumonia) will be defined as new segmental or lobar airspace
opacities visualized by image studies (chest radiograph or HRCT) in addition to any of the
following
Positive pathogencultures in good sample of sputum or lower-airway secretions retrieved
by fiberoptic bronchoscope
Fever gt 39degC or gt 100degF
Leukocytosis gt 12000 (unexplained no increase in dose of corticosteroids)
47
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
524 Maintained FVC Response
Subjects with follow-up FVCpred measurements at or above their baseline FVCpred level
will be classified as having maintained FVC response Subjects with reduced FVCpred levels
or missing data for any reason including death or medical frailty will be classified as having not
maintained FVC response The FVCpred value is used because unadjusted FVC measurements
are expected to decline with age
48
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
6 Safety Evaluations and Procedures
61 Adverse Events
During a clinical trial the reporting of adverse experience information can lead to important
changes in the way a new treatment is developed as well as provide integral safety data
611 Definitions
An adverse event (AE) is any untoward medical occurrence in a subject or clinical investigation
subject who was administered a pharmaceutical product The AE does not necessarily have to
have a causal relationship with the drug administered An AE can be any unfavorable and
unintended sign (including an abnormal laboratory finding) symptom or disease temporarily
associated with the use of a medicinal product whether or not considered to be related to the
medicinal product Diseases signs symptoms or laboratory abnormalities already existing at
enrollment are not considered AEs unless they worsen (ie increase in intensity or frequency)
Surgical procedures themselves are not AEs they are therapeutic measures for conditions that
require surgery The condition for which the surgery is required may be an AE Surgical
procedures planned before randomization and the conditions necessitating the surgery are not
AEs
A serious adverse event is any untoward event that
Is fatal
Is life-threatening
Requires inpatient hospitalization or prolongation of existing hospitalization with the
following exceptions
o Preplanned (before the study) hospital admissions unless the hospitalization is
prolonged
o Planned admissions (as part of a study eg routine biopsies)
o Hospitalization lasting lt 24 hours
49
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
o Hospitalization for elective procedure
o Emergency room visits
Results in persistent or significant disability or incapacity
Is a congenital anomaly or birth defect
Important medical events that may not result in death be life-threatening or require
inpatient hospitalization may be considered serious adverse events (SAEs) when based
on appropriate medical judgment they may jeopardize the subject and may require
medical or surgical intervention to prevent one of the outcomes listed above
Life-threatening means that the subject was in the view of the investigator at immediate risk of
death from the AE as it occurred It does not include an AE that had it occurred in a more severe
form might have caused death
Persistent or significant disabilityincapacity means that the event resulted in permanent or
significant and substantial disruption of the subjectrsquos ability to carry out normal life functions
Causality
A reasonable possibility means the AE may have been caused byrelated to the study drug A
perceived or real lack of efficacy does not satisfy the definition of relatedness
612 Adverse Event (AE) Reporting
For the PANTHER-IPF trial all AEs (serious and nonserious) occurring from randomization
through final study visit (4 weeks after final dose of all study medication) will be recorded on the
AE page of the case report form (CRF)
6121 Serious Adverse Events (SAE) Reporting
For this trial all deaths and all SAEs which occur from randomization through final study visit
must be entered within the EDC system via the SAE eCRF page within 24 hours of the
investigative sitersquos knowledge of the event It is the responsibility of the clinical center
50
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
investigator to provide a causality assessment of the event for each study medications based upon
the information available at the time of the report It is understood that complete information
about the event may not be known at the time the initial report is submitted In the event the EDC
system is not accessible to the site at the time of event reporting investigative sites will complete
and forward a paper back-up SAE form to DCRI Safety Surveillance for processing
DCRI Safety Surveillance
Telephone 1-919-668-8624 or 1-866-668-7799 (toll free)
Fax 1-919-668-7138 or 1-866-668-7138 (toll free)
The investigator must complete and submit follow-up SAE information via the eCRF when
important new or follow-up information (eg final diagnosis outcome results of specific
investigations) becomes available Follow-up information should be submitted according to the
same process used for reporting the initial event as described above All SAEs will be followed
until resolution stabilization or 30 days after the subject has completed the final visit (4 weeks
after the final dose of study medication) whichever occurs first The investigator is responsible
for reporting SAEs to their institutional review board (IRB) per site specific IRB reporting
guidelines
6122 Regulatory Reporting
AEs that are serious study drug related and unexpected will be reported to the regulatory
authorities The DCRI Safety Surveillance medical monitor will perform a medical review of all
SAEs submitted and evaluate for ldquounexpectednessrdquo DCRI Safety Surveillance will prepare
MedWatch reports for those events identified as serious study drug related and unexpected as
determined by Safety Medical Monitor
DCRI Regulatory Services will submit all unexpected study drug-related SAEs as per 21 CFR
32 DCRI Safety Surveillance will provide a safety alert letter to the NHLBI DSMB and DCC
clinical operation (for distribution to sites) within 15 days of initial receipt of the information
51
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Investigators are responsible for promptly reporting these events to their reviewing IRBs
according to site specific IRB reporting guidelines
62 Clinical Medical Monitoring
There will be an unblinded physician at the IPFnet DCC serving as medical monitor The
medical monitor will be available to assist with questions about dosage adjustments of study
medications including discontinuation or resumption of medications
63 Unblinding Procedures
Unblinding of subjects or investigators to subject treatment is strongly discouraged For ongoing
clinical management all subjects should be presumed to be receiving ldquoactiverdquo study drug To
ensure the subjectrsquos safety the study treatment will be dose-adjusted based on laboratory test
results clinical findings and symptoms
The IPFnet DCC medical monitor and PANTHER-IPF co-chairs Drs Ganesh Raghu and
Fernando Martinez will be available to the study physicians to discuss study drug management
on a case-by-case basis Un-blinding will be considered ONLY when the knowledge of subject
treatment assignment is ABSOLUTELY ESSENTIAL for subject safety and after discussion of
the subjectrsquos case with the medical monitor and either Dr Raghu or Dr Martinez Unblinding of
study treatment should be minimized during the conduct of the trial In those cases where it is
felt to be medically necessary the DCC medical officer will communicate directly with the
managing physician to minimize unblinding of study personnel
52
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
7 Study Drug Procedures
At the baseline 15-week 30-week and 45-week study visits subjects will receive a supply of
study drug sufficient to last until the next visit at which study drug will be dispensed
53
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
8 Data Management
81 Hardware and Software Configuration
811 Hardware and Database Software
Data will be stored in an Oracle database system Oracle has advantages of processing efficiency
and smooth linkage with other software systems The application and database will be hosted on
Solaris Unix servers at the IPFnet DCC
812 Statistical Software
SAS will be used as the principal application for the management of analysis data files and
statistical computations S-Plus will be used to provide supplementary functions as needed
813 Access Control and Confidentiality Procedures
Access to databases will be controlled centrally by the IPFnet DCC through user passwords
linked to appropriate privileges This protects the data from unauthorized changes and
inadvertent loss or damage
814 Security
Database and Web servers will be secured by a firewall and through controlled physical access
Oracle has many security features to ensure that any staff member accessing the database has the
proper authority to perform the functions he or she requests of the system Within the secondary
SAS databases Unix group-access control maintains similar security The Sun workstation login
is secured by extensive user-password facilities under Unix
54
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
815 Back-up Procedures
Database back-up will be performed automatically every day and standard IPFnet DCC policies
and procedures will be applied to dictate tape rotation and retention practices
816 Virus Protection
All disk drives that provide network services and all user computers will be protected using
virus-scanning software Standard IPFnet DCC policies will be applied to update these protection
systems periodically through the study
82 Sources of Data
821 Design and Development
The IPFnet DCC will be responsible for development of the electronic case report forms
(eCRFs) development and validation of the clinical study database ensuring data integrity and
training clinical center staff on applicable data management procedures A web-based distributed
data entry model will be implemented This system will be developed to ensure that guidelines
and regulations surrounding the use of computerized systems used in clinical trials are upheld
The remainder of this section provides an overview of the data management plan associated with
this protocol
822 Data Collection Forms
The data collection process consists of direct data entry at the study clinical centers into the EDC
system(s) provided by the DCC A data collection worksheet will be provided to clinical centers
for recording data in the event the EDC system is unavailable Data entry of the eCRFs should
be completed according to the instructions provided and project specific training The
investigator is responsible for maintaining accurate complete and up-to-date records and for
ensuring the completion of the eCRFs for each research participant
55
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
823 Data Acquisition and Entry
Data entry into eCRFs shall be performed by authorized individuals Selected eCRFs may also
require the investigatorrsquos written signature or electronic signature as appropriate Electronic
CRFs will be monitored for completeness accuracy and attention to detail during the study
824 Data Center Responsibilities
The IPFnet DCC will 1) develop a data management plan and will conduct data management
activities 2) provide final eCRFs for the collection of all data required by the study 3) develop
data dictionaries for each eCRF that will comprehensively define each data element 4) conduct
ongoing data monitoring activities on study data 5) monitor any preliminary analysis data
cleanup activities and 6) rigorously monitor final study data clean up
825 Data Editing
Completed data will be entered into the IPFnet DCC automated data acquisition and
management system If incomplete or inaccurate data are found a data clarification request will
be generated and distributed to clinical centers for a response Clinical centers will resolve data
inconsistencies and errors and enter all corrections and changes into the IPFnet DCC automated
data acquisition and management system
826 Training
The training plan for clinical center staff includes provisions for training on assessments eCRF
completion guidelines data management procedures and the use of computerized systems
56
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
9 Study Design and Data Analysis
91 General Analytic Considerations
All primary analyses will be based on intent-to-treat (ITT) principles using all randomized
subjects Baseline factors across groups will be compared using mean (standard deviation) and
median (25th and 75th percentiles) summary measures Kaplan-Meier curves will be used to
display event rates Due to clinical interest in departures from both sides of the null hypothesis
all test statistics will be 2-sided
Reasonable caution needs to be taken when conducting multiple analyses on key clinical
subgroups For subgroup analyses a conservative significance level of 0001 will be used for all
interaction tests Thus subgroup comparisons will be considered exploratory unless the p-value
from the interaction test is smaller than 0001
92 Randomization Blinding and Reporting of Results
A permuted block-randomization scheme will be created with varying block sizes stratified by
clinical center Once a subject has completed the screening and baseline period and evaluation
for inclusionexclusion criteria the randomization process will begin Subjects will be
randomized to receive NAC or matching placebo with equal probability (11) via telephone
contact with a central interactive voice response system (IVRS) using a toll-free randomization
number On the day of randomization after the subject has successfully met all inclusion and
exclusion criteria the investigator or designee will call the central randomization number to
obtain the assigned kit randomization numbers for that subject At each subject visit the
investigator or designee will call the central randomization number to obtain the new kit
randomization numbers for resupply of the subject For resupply of the clinical center the IVRS
will monitor minimal volume of a kit type andor expiration date and will automatically notify
the pharmacy
57
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
The trial results will be reported according to guidelines specified in the CONSORT statement
A flow diagram describing screening recruitment randomization dropout and vital status will
be included in the primary manuscript AEs and efficacy data will be presented for all treatment
groups Adherence dropout and lost to follow-up will be carefully examined across all treatment
groups Analyses of safety will be based on data from all randomized subjects who received at
least one dose of study drug
93 Stratification
Subjects will be distributed to the two treatment arms in a 11 allocation ratio Stratification
blocks will be based on clinical centers
94 Specification of the Primary Analyses
A mixed model repeated measures (MMRM) analysis described in section 95 will be used to
compare differences in the slope of FVC measurements across the treatment groups Response
variables are values of the FVC measured at baseline and every 15 weeks until study completion
Variables in the model will include treatment time and time by treatment age sex race and
height Contrast estimates of differences in slopes of treatment over time (along with confidence
intervals) will be used to estimate the treatment effect The validity of this model in terms of
meeting modeling assumptions will be assessed via standard modeling diagnostics and goodness-
of-fit measures Based on the MMRM framework missing FVC data will not be imputed for the
primary analysis
95 Analysis of Longitudinal Endpoints
A common goal in clinical trials is to specify models that are easily implemented and
reproducible by independent data analysts On the other hand the models should have proper
statistical behavior in terms of low bias and high precision Many common approaches to
longitudinal data analysis including last observation carried forward (LOCF) imputation rely on
the missing completely at random (MCAR) assumption However the MCAR assumption is
58
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
unlikely to hold in many clinical trials because missing data are often related to disease
progression and prognosis A more reasonable assumption missing at random (MAR) specifies
that the complete data distribution can be modeled using only the observed data The likelihood-
based MMRM approach is valid under the more general MAR assumptions These models will
be applied to analyze the longitudinal data secondary endpoints
The advantages of MMRM analysis are that all important characteristics of the model can be preshy
specified standard software can be used to implement the models and results are based on ITT
principles43 In addition the MMRM approach offers superior control of Type I and Type II
errors compared with the LOCF approach
Response variables are values of the PFTs measured at enrollment and every 15 weeks until
study completion and 6MWT values measured at baseline week 30 and week 60 Covariates are
treatment time time by treatment and key baseline risk factors Contrasts (along with
confidence intervals) of treatment by time will be used to estimate the treatment effect
The correlation structure involves multiple pieces including measurement errors random
variation and interindividual variability For the longitudinal data analyses an unstructured
correlation matrix for within-subject errors will be assumed Other correlation structures
including compound symmetry will be examined as needed A careful examination of reasons
for study discontinuation will be conducted to assess the validity of MCAR Sensitivity analyses
will be used to examine the untestable assumption that the observed data violate the MAR
assumption The MMRM models will be implemented using PROC MIXED in SAS
96 Analysis of Binary Time-to-Event and Time-Lagged Endpoints
Regression modeling approaches using either the logistic regression model or Cox proportional
hazards regression model will be employed when appropriate The validity of these models will
be assessed via standard modeling diagnostics and goodness-of-fit measures Estimates of
cumulative frequencies for more general time-lagged responses will be calculated using the
partitioned version of the Bang-Tsiatis estimator44 The partitions will be set at 15-week intervals
59
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
to correspond with the data-collection process Covariate adjusted event rates will be calculated
using inverse probability-weighted regression estimates45
97 Power Analysis
971 Primary Analyses
Based on previously published IPF clinical trials the PL group is expected to experience a drop
in FVC of approximately 020 L over the study period (see Figure 1) The IPFnet Steering Group
determined a clinically important difference would be to preserve the majority of the decline
relative to PL over the study period In particular a treatment effect of 015 L was determined to
be a clinically meaningful difference Potential dropout is a key factor in the proposed study The
drop-out process assumed 5 lost to follow-up after every study visit Only 80 of subjects
were assumed to be followed for the entire study period All models assumed a compound
symmetry structure for the covariance matrix Power calculations were performed using a SAS
IML program for designing repeated measures studies46 Based on preliminary reviews of the
data from the University of Michigan the covariance matrix parameters were estimated at
approximately σ2 = 0757 (variance parameter) and ρ = 0936 (correlation parameter) To be
conservative the power calculations for the primary analysis were performed with parameter
setting of σ2 = 0810 (variance parameter) and ρ = 0925 (correlation parameter)
The power calculations assume a correction for imperfect compliance proposed by Lachin and
Foulkes to allow for 2 noncompliance for each of the treatment arms47 Thus the sample size
of 130 subjects per arm would be reduced to an adjusted sample size of 130(1-002-002)2 =
1198 or 120 subjects per arm
Under the assumed Type I error rate of 005 with a correlation parameter of 0925 and standard
deviation of 090 the difference of 015 L (or 00025 Lweek) shown in Table 6 would have
power of 93
60
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Table 6 Hypothetical Values of Mean FVC (L) Change from Baseline
Week 15 Week 30 Week 45 Week 60
NAC 00125 00250 00375 00500
Placebo 00500 01000 01500 02000
Difference 00375 00750 01125 01500
Abbreviations FVC forced vital capacity PL placebo
972 Power Analysis for Secondary Endpoints
Power calculations for secondary endpoint measurements are shown in Table 7 Standard
deviations are based on unpublished data provided by the University of Michigan The
calculations are based on a 2-sample t-test with Type I error rate set at 005 These calculations
are likely to be conservative because the statistical approach described in section 95 for
analyzing these endpoints will incorporate incomplete observations as well as intermediate data
points
Table 7 Detectable Differences in Treatment Means for Selected Endpoint Measurements
Secondary Endpoints Std Dev
of the Baseline Score
Detectable Difference for 80 Power
Std Dev of the Change Score
Difference Detectable for
80 Power
DLCOpred 166 58 91 32
6MWT Area Under the Desaturation Curve
219 76 175 61
6MWT Distance to Desaturation 224 78 315 110
6MWT Minutes Walked 210 073 205 071
Abbreviations Std Dev standard deviation DLCOpred diffusing capacity of the lung for carbon monoxide percent predicted 6MWT 6-minute walk test
61
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
10 Study Administration
101 Cooperative Agreement Mechanism
The administrative and funding mechanism used to undertake this project is a ldquocooperative
agreementrdquo (U01) which is an assistance mechanism Under the cooperative agreement the
NHLBI assists supports andor stimulates the project and is substantially involved with
investigators in conducting the study by facilitating performance of the effort in a ldquopartnerrdquo role
The NHLBI project scientist serves on the IPFnet Steering Group and he or another NHLBI
scientist may serve on other project committees when appropriate At the same time however
NHLBI does not assume a dominant role direction or prime responsibility for this research
program
As described below governance of the project is conducted through the IPFnet Steering Group
Principal investigators have lead responsibilities in all aspects of their trials and the project
including any modification of trial designs conduct of the trials quality control data analysis
and interpretation preparation of publications and collaboration with other investigators unless
otherwise provided for by the IPFnet Steering Group
PIs retain custody of and have primary rights to their center-specific and collaborative data
subject to government rights-of-access consistent with current Health amp Human Services (HHS)
Public Health Service (PHS) and National Institutes of Health policies The protocols and
governance policies call for the continual submission of data centrally to the IPFnet DCC for the
collaborative database which at a minimum will contain the key variables selected by the IPFnet
Steering Group for standardization across all clinical centers the submission of copies of the
collaborative datasets to each PI upon completion of the project procedures for data analysis
reporting and publication and procedures to protect and ensure the privacy of medical and
genetic data and records of individuals The NHLBI project scientist on behalf of the NHLBI
will have the same access privileges and responsibilities regarding the collaborative data as the
other members of the Steering Group
62
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
PIs are also encouraged to publish and to publicly release and disseminate results data and other
products of the project concordant with the project protocols and governance and the approved
plan for making data and materials available to the scientific community and to the NHLBI
However during the 3 years after the ending date of NHLBI project support unpublished data
unpublished results data sets not previously released and other study materials or products are
to be made available to any third party only with the approval of the IPFnet Steering Group
Upon completion of the project PIs are expected to put their intervention materials and
procedure manuals into the public domain andor make them available to other investigators
according to the approved plan for making data and materials available to the scientific
community and the NHLBI for the conduct of research at no charge other than the costs of
reproduction and distribution
The NHLBI reserves the right to terminate or curtail the project (or an individual award) in the
event of (a) failure to develop or implement mutually agreeable collaborative measurement
subject eligibility and data management sections of the protocols (b) substantial shortfall in
subject recruitment follow-up data reporting or quality control or other major breach of
protocol (c) substantive changes in the agreed-upon protocols with which NHLBI cannot
concur (d) reaching a major project outcome with persuasive statistical significance
substantially before schedule or (e) human subject ethical issues that may dictate a premature
termination
Any disagreement that may arise in scientificprogrammatic matters (within the scope of the
award) between award recipients and the NHLBI may be brought to arbitration An arbitration
panel will be composed of 3 membersmdash1 selected by the IPFnet Steering Group (with the
NHLBI member not voting) or by the individual PI in the event of an individual disagreement a
second selected by NHLBI and the third selected by the other 2 members This special
arbitration procedure in no way affects the PIrsquos right to appeal an adverse action that is otherwise
appealable in accordance with the PHS regulations at 42 CFR part 50 Subpart D and HHS
63
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
regulation at 45 CFR part 16 or the rights of the NHLBI under applicable statutes regulations
and terms of the award
102 IPFnet Steering Group
The IPFnet Steering Group is the main governing body of the project It is composed of the PIs
of the clinical centers the PI of the DCC and the NHLBI project scientist The clinical centers
the IPFnet DCC and the NHLBI each have 1 vote on the IPFnet Steering Group All decisions
are determined by majority vote
All major scientific decisions are determined by the IPFnet Steering Group It assumes overall
responsibility for the design and conduct of the trial It appoints (and disbands) committees and
subcommittees as the need arises designs approves and implements the study protocols
oversees the development of the MOOP monitors subject recruitment and treatment delivery
evaluates data collection and management oversees quality assurance procedures and
implements changes and enhancements to the study as required It also has primary responsibility
for facilitating the conduct of the trials and reporting the projectrsquos results
103 Data and Safety Monitoring Board
The NHLBI will establish a DSMB in accordance with established policies (see
httpwwwnhlbinihgovfundingpoliciesdsmb_insthtm) to ensure data quality and subject
safety and to provide independent advice to the NHLBI regarding progress and the
appropriateness of study continuation
104 Recommendations on Interim Monitoring of Efficacy Safety and Futility
First and foremost the role of the DSMB will be to review subject safety and trial conduct at
periodic points during the study The DSMB may require analyses of the primary endpoint
results for comparing the benefit and risks of treatment strategies The benefit of collecting
additional data on key secondary endpoints with extended follow-up and establishing a robust
64
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
evidence base for determining a standard of care will need to be carefully considered before
early termination of one or more treatment arms After careful consideration the IPFnet Steering
Group recommends conservative thresholds for the early examinations of the safety and efficacy
data
The DSMB will be expected to meet approximately every 6 months until trial completion to
review safety and toxicity data The DSMB may recommend stopping the study based on these
reviews Because the DSMB could stop the trial for safety concerns as well as for a large
efficacy benefit there could be multiple opportunities to reject the null hypothesis (no difference
in event rates between the PL and NAC groups) A Bonferroni approximation will be applied
during the one planned interim analysis for efficacy
Before locking the database a statistical analysis plan (SAP) will be developed to provide
complete details on the statistical analysis The SAP will include the specifics for how and when
the DSMB will be notified for AEs The IPFnet DCC will deliver to the DSMB all FDA-defined
AEs at 3-month intervals The IPFnet DCC will prepare narrative SAE reports in real time for
DSMB review including recommendations and analysis of similar events for each SAE
submitted to the FDA
65
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
11 Investigator and Sponsor Obligations
111 Monitoring
All monitoring activities for US clinical centers will be performed in accordance with DCRI
standard operating procedures Information regarding the types of visits will be outlined in the
PANTHER-IPF MOOP
112 Cost and Payment
There will be no cost to subjects enrolled in this trial Study-related procedures will be paid for
by the IPFnet
Subjects may be eligible for reimbursement for travel to the clinical center Details of payment
will be explained to each subject during the consent process
113 Confidentiality and Health Insurance Portability and Accountability Act
Considerations
Subject confidentiality will be protected throughout the study All subject data will be kept
strictly confidential and no subject-identifying information will be released to anyone outside
the project Confidentiality will be assured through several mechanisms First each subject will
be assigned an anonymous study ID which will then be used on all study forms Second any
study forms blood samples and paper records that contain subject information (eg address lists
phone lists) will be kept at the clinical centers in secured locked areas coded by number Once
blood is collected there will be no subject identifiers placed on blood samplesmdashonly the study
ID number and the date of sample collection Third access to all subject data and information
including laboratory specimens will be restricted to authorized personnel In the case of
computerized data this restricted access will be assured through user logon IDs and password
protection
66
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
At the IPFnet DCC only authorized personnel will have access to the data files containing study
data Security will be assured through user logon IDs passwords and appropriate access
privileges All study subjects will be identified only by their IPFnet ID numbers and no personal
identifying information such as name address or Social Security number will be entered into
the IPFnet DCC database Any subject-specific data reported to the IPFnet Steering Group will
be identified only by the IPFnet ID number
Finally subjects will not be identified by name in any reports or publications nor will the data
be presented in such a way that the identity of individual subjects can be inferred Analysis files
created for further study by the scientific community will have no subject identifiers These data
files will be created in accordance with the Ancillary Studies and Publication Policy of the
IPFnet
114 Informed Consent Procedures
All IPFnet subjects will provide written informed consent using procedures reviewed and
approved by each clinical centerrsquos IRB Informed consent will be undertaken by study personnel
in-person with the subject The subject has the option of declining further participation in the
study at that point No further study procedures will be conducted until the signed documents
have been provided to the IPFnet clinical center
115 Institutional Review Boards
Before initiating this study the protocol clinical center-specific informed consent forms Health
Insurance Portability and Accountability Act (HIPAA) forms recruitment materials and other
relevant information will be reviewed by a properly constituted IRB at each participating clinical
center A copy of the signed and dated IRB approval at each clinical center will be retrieved prior
to or during the site initiation visit and archived at the IPFnet DCC Any amendments to the
protocol other than simple administrative and typographical changes must be approved by each
IRB before they are implemented The clinical centers will seek annual renewals of their IRB
approvals in accordance with local procedures
67
__________________________________________ ________________
__________________________________________
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
12 Investigator Agreement
I have read the foregoing protocol PANTHER-IPF and agree that it contains all necessary
details for carrying out this study I will conduct the study as outlined herein and will complete
the study within the time designated
I will provide copies of the protocol and all pertinent information to all individuals responsible to
me who assist in the conduct of this study I will discuss this material with them to ensure they
are fully informed regarding the drug and the conduct of the study
I will fulfill all responsibilities for submitting pertinent information to the local IRB if
applicable that is responsible for this study
I further agree that NHLBI andor DCRI will have access to any source documents from which
eCRF information may have been generated
Signature of Principal Investigator Date
Name of Principal Investigator (printed or typed)
Protocol version date May 19 2009
Protocol Amendment 1 version date May 28 2010
Protocol Amendment 2 version date December 6 2011
68
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
13 References
1 Raghu G Brown KK Bradford WZ et al A placebo-controlled trial of interferon gamma-1b in patients with idiopathic pulmonary fibrosis N Engl J Med 2004350125-33 2 King TE Jr Safrin S Starko KM et al Analyses of efficacy end points in a controlled trial of interferon-gamma1b for idiopathic pulmonary fibrosis Chest 2005127171-7 3 Flaherty KR Thwaite EL Kazerooni EA et al Radiological versus histological diagnosis in UIP and NSIP survival implications Thorax 200358143-8 4 Wells AU Desai SR Rubens MB et al Idiopathic pulmonary fibrosis a composite physiologic index derived from disease extent observed by computed tomography Am J Respir Crit Care Med 2003167962-9 5 Raghu G Freudenberger TD Yang S et al High prevalence of abnormal acid gastroshyoesophageal reflux in idiopathic pulmonary fibrosis Eur Respir J 200627136-42 6 Kinnula VL Focus on antioxidant enzymes and antioxidant strategies in smoking related airway diseases Thorax 200560693-700 7 Coultas DB Zumwalt RE Black WC Sobonya RE The epidemiology of interstitial lung diseases Am J Respir Crit Care Med 1994150967-72 8 Raghu G Weycker D Edelsberg J Bradford WZ Oster G Incidence and prevalence of idiopathic pulmonary fibrosis Am J Respir Crit Care Med 2006174810-6 9 Olson AL Swigris JJ Lezotte DC Norris JM Wilson CG Brown KK Mortality from pulmonary fibrosis increased in the United States from 1992 to 2003 Am J Respir Crit Care Med 2007176277-84 10 Mannino DM Etzel RA Parrish RG Pulmonary fibrosis deaths in the United States 1979shy1991 An analysis of multiple-cause mortality data Am J Respir Crit Care Med 19961531548shy52 11 Hubbard R Johnston I Coultas DB Britton J Mortality rates from cryptogenic fibrosing alveolitis in seven countries Thorax 199651711-6 12 Johnston I Britton J Kinnear W Logan R Rising mortality from cryptogenic fibrosing alveolitis Bmj 19903011017-21 13 Raghu G Collard HR Egan JJ et al An official ATSERSJRSALAT statement idiopathic pulmonary fibrosis evidence-based guidelines for diagnosis and management Am J Respir Crit Care Med 2011183788-824 14 (USA) FDA FDA Public Health Advisory Interferon gamma-1b (marketed as Actimmune) In 2007 15 King TE Jr Pardo A Selman M Idiopathic pulmonary fibrosis Lancet 2011 16 Raghu G Brown KK Costabel U et al Treatment of idiopathic pulmonary fibrosis with etanercept an exploratory placebo-controlled trial Am J Respir Crit Care Med 2008178948shy55 17 Malouf MA Hopkins P Snell G Glanville AR An investigator-driven study of everolimus in surgical lung biopsy confirmed idiopathic pulmonary fibrosis Respirology 201116776-83 18 King TE Jr Behr J Brown KK et al BUILD-1 a randomized placebo-controlled trial of bosentan in idiopathic pulmonary fibrosis Am J Respir Crit Care Med 200817775-81 19 Richeldi L Costabel U Selman M et al Efficacy of a tyrosine kinase inhibitor in idiopathic pulmonary fibrosis N Engl J Med 20113651079-87
69
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
20 Borok Z Buhl R Grimes GJ et al Effect of glutathione aerosol on oxidant-antioxidant imbalance in idiopathic pulmonary fibrosis Lancet 1991338215-6 21 Meyer A Buhl R Magnussen H The effect of oral N-acetylcysteine on lung glutathione levels in idiopathic pulmonary fibrosis Eur Respir J 19947431-6 22 Behr J Maier K Degenkolb B Krombach F Vogelmeier C Antioxidative and clinical effects of high-dose N-acetylcysteine in fibrosing alveolitis Adjunctive therapy to maintenance immunosuppression Am J Respir Crit Care Med 19971561897-901 23 Cantin AM North SL Fells GA Hubbard RC Crystal RG Oxidant-mediated epithelial cell injury in idiopathic pulmonary fibrosis J Clin Invest 1987791665-73 24 Waghray M Cui Z Horowitz JC et al Hydrogen peroxide is a diffusible paracrine signal for the induction of epithelial cell death by activated myofibroblasts Faseb J 200519854-6 25 Larios JM Budhiraja R Fanburg BL Thannickal VJ Oxidative protein cross-linking reactions involving L-tyrosine in transforming growth factor-beta1-stimulated fibroblasts J Biol Chem 200127617437-41 26 Kinnula VL Fattman CL Tan RJ Oury TD Oxidative stress in pulmonary fibrosis a possible role for redox modulatory therapy Am J Respir Crit Care Med 2005172417-22 27 Meyer A Buhl R Kampf S Magnussen H Intravenous N-acetylcysteine and lung glutathione of patients with pulmonary fibrosis and normals Am J Respir Crit Care Med 19951521055-60 28 Behr J Degenkolb B Krombach F Vogelmeier C Intracellular glutathione and bronchoalveolar cells in fibrosing alveolitis effects of N-acetylcysteine Eur Respir J 200219906-11 29 Bando M Hosono T Mato N et al Long-term efficacy of inhaled N-acetylcysteine in patients with idiopathic pulmonary fibrosis Intern Med 2010492289-96 30 Demedts M Behr J Buhl R et al High-dose acetylcysteine in idiopathic pulmonary fibrosis N Engl J Med 20053532229-42 31 Toma TP Bhowmik A Rajakulasingam R Acetylcysteine in pulmonary fibrosis N Engl J Med 20063541086-9 author reply -9 32 Hunninghake GW Antioxidant therapy for idiopathic pulmonary fibrosis N Engl J Med 20053532285-7 33 Flaherty KR Mumford JA Murray S et al Prognostic implications of physiologic and radiographic changes in idiopathic interstitial pneumonia Am J Respir Crit Care Med 2003168543-8 34 Latsi PI du Bois RM Nicholson AG et al Fibrotic idiopathic interstitial pneumonia the prognostic value of longitudinal functional trends Am J Respir Crit Care Med 2003168531-7 35 Collard HR King TE Jr Bartelson BB Vourlekis JS Schwarz MI Brown KK Changes in clinical and physiologic variables predict survival in idiopathic pulmonary fibrosis Am J Respir Crit Care Med 2003168538-42 36 Jegal Y Kim DS Shim TS et al Physiology is a stronger predictor of survival than pathology in fibrotic interstitial pneumonia Am J Respir Crit Care Med 2005171639-44 37 Martinez FJ Safrin S Weycker D et al The clinical course of patients with idiopathic pulmonary fibrosis Ann Intern Med 2005142963-7 38 Hull JH Acetylcysteine in pulmonary fibrosis N Engl J Med 20063541089-91 author reply -91
70
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
39 Flaherty KR King TE Jr Raghu G et al Idiopathic interstitial pneumonia what is the effect of a multidisciplinary approach to diagnosis Am J Respir Crit Care Med 2004170904shy10 40 Raghu G Johnson WC Lockhart D Mageto Y Treatment of idiopathic pulmonary fibrosis with a new antifibrotic agent pirfenidone results of a prospective open-label Phase II study Am J Respir Crit Care Med 19991591061-9 41 Hunninghake GW Lynch DA Galvin JR et al Radiologic findings are strongly associated with a pathologic diagnosis of usual interstitial pneumonia Chest 20031241215-23 42 Lynch D Godwin J Safrin S et al High-resolution computed tomography in idiopathic pulmonary fibrosis diagnosis and prognosis Am J Respir Crit Care Med 2005172488-93 43 Mallinckrodt CH Watkin JG Molenberghs G Carroll RJ Choice of the primary analysis in longitudinal clinical trials Pharmaceutical Statistics 20043161-9 44 Bang H Tsiatis A Estimating medical costs with censored data Biometrika 200087329shy43 45 Lin DY Regression analysis of incomplete medical cost data Stat Med 2003221181-200 46 Rochon J Application of GEE procedures for sample size calculations in repeated measures experiments Stat Med 1998171643-58 47 Lachin JM Foulkes MA Evaluation of sample size and power for analyses of survival with allowance for nonuniform patient entry losses to follow-up noncompliance and stratification Biometrics 198642507-19
71
- PANTHER-IPFPREDNISONE AZATHIOPRINEAND N-ACETYLCYSTEINEA STUDY THAT EVALUATES RESPONSE INIDIOPATHIC PULMONARY FIBROSIS
-
- Protocol Summary
- Table of Contents
- List of Tables
- List of Figures
- List of Abbreviations
- 1 Summary
- 2 Hypotheses and Specific Aims
-
- 21 Null Hypothesis
- 22 Specific Aim 1
- 23 Specific Aim 2
- 24 Prespecified Subgroups of Interest
-
- 3 Background and Significance
-
- 31 Idiopathic Pulmonary Fibrosis is the Most Common Interstitial Lung Disease
- 32 Rationale for Placebo Control
- 33 Rationale for N-acetylcysteine
- 35 Rationale for N-acetylcysteine as a Stand-alone Therapy
- 36 Rationale for the Study Design and Primary Endpoint
- 37 Rationale for Blinding of Treatments
-
- 4 Methods
-
- 41 Inclusion Criteria
- 42 Diagnosis of IPF
- 43 Exclusion Criteria
- 44 Study Design and Study Visit
- 45 Dose Justification
- 46 Contraindications Precautions and Side Effects of Study Medications
- 47 Recruitment Procedures
- 48 Study Procedures
- 49 Concomitant Medications
- 410 Laboratory Testing
- 411 Blinding of Study Drugs
-
- 5 Study Endpoints
-
- 51 Primary Study Endpoint
- 52 Secondary Study Endpoints
-
- 6 Safety Evaluations and Procedures
-
- 61 Adverse Events
- 62 Clinical Medical Monitoring
- 63 Unblinding Procedures
-
- 7 Study Drug Procedures
- 8 Data Management
-
- 81 Hardware and Software Configuration
- 82 Sources of Data
-
- 9 Study Design and Data Analysis
-
- 91 General Analytic Considerations
- 92 Randomization Blinding and Reporting of Results
- 93 Stratification
- 94 Specification of the Primary Analyses
- 95 Analysis of Longitudinal Endpoints
- 96 Analysis of Binary Time-to-Event and Time-Lagged Endpoints
- 97 Power Analysis
-
- 10 Study Administration
-
- 101 Cooperative Agreement Mechanism
- 102 IPFnet Steering Group
- 103 Data and Safety Monitoring Board
- 104 Recommendations on Interim Monitoring of Efficacy Safety and Futility
-
- 11 Investigator and Sponsor Obligations
-
- 111 Monitoring
- 112 Cost and Payment
- 113 Confidentiality and Health Insurance Portability and Accountability ActConsiderations
- 114 Informed Consent Procedures
- 115 Institutional Review Boards
-
- 12 Investigator Agreement
- 13 References
-

PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
4 Methods 41 Inclusion Criteria
1 Age 35 to 85 years inclusive
2 FVC ge 50 of predicted (post-bronchodilator measurement from the screening visit)
3 DLCO ge 30 of predicted (hemoglobin corrected and altitude corrected if gt4000 ft above sea level)
4 Ability to understand and provide informed consent
5 Diagnosis of IPF according to a modified version of the ATS criteria le 48 months from enrollment The
date of diagnosis is defined as the date of the first available HRCT or surgical lung biopsy characteristic
of definite UIP
411 Subjects Shown to Have Usual Interstitial Pneumonia Pattern on Surgical Lung Biopsy
Subjects who have been shown to have UIP pattern on lung biopsy must have all of the following
1 Exclusion of other known causes of ILD such as drug toxicity clinically significant environmental
exposures or diagnosis of connective tissue diseases
2 Bibasilar reticular abnormalities with minimal ground glass opacities on HRCT scan
412 Subjects Who Have Not Undergone a Surgical Lung Biopsy
In addition to the criteria above these subjects must have radiological findings considered to be definite for the
diagnosis of UIPIPF
1 Bibasilar reticular abnormalities with minimal ground glass opacities
2 Honeycombing as the predominant feature and located in the peripheral lung bases
42 Diagnosis of IPF
Only subjects with definite IPF will be eligible for enrollment in this study We will utilize a combination of
clinicalphysiologic features HRCT and review of a clinically obtained surgical lung biopsy specimen to
establish the diagnosis of IPF An algorithm for the diagnosis is provided to guide entry into the protocol as
outlined in the inclusion and exclusion criteria (Figures 2 and 3) This multi-disciplinary approach uses
21
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
expertise from clinicians radiologists and pathologists Investigators at each site in conjunction with central
pathology will work together to establish the diagnosis of IPF This interactive approach to the diagnosis of IPF
increases the level of agreement between observers39
A subject with suspected ILD should be evaluated for secondary causes including but not limited to
environmental exposures drugs and systemic diseases Presence of any of these findings felt to be significant
enough to cause an ILD should disqualify the subject from entry into the trial
If secondary causes are absent an HRCT scan may be obtained If an HRCT of sufficiently high quality has
been obtained within the last 3 months that scan may be used for diagnosis In the appropriate clinical setting
the diagnosis of IPF can be made by the demonstration of a typical radiographic pattern on HRCT or by
demonstration of UIP pattern on a surgical lung biopsy The following criteria for a radiographic (ie
nonsurgical) diagnosis will be used In the absence of known exposures andor clinical associations attributable
to pulmonary fibrosis and in the appropriate clinical setting the presence of definite UIP pattern in HRCT
images is required to meet study criteria for the diagnosis of IPF
Figure 2 Diagnosis of Idiopathic Pulmonary Fibrosis in the IPFnet
22
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Figure 3 Pathology Flow Chart Surgical Lung Biopsy Diagnosis
Requirement for diagnosis
1 Clinical exclusion of other known causes (connective tissue diseases environmental and drug
exposures) of ILD
2 Radiographic HRCT with bibasilar reticular abnormality and honeycomb change with minimal
ground glass opacities
Appropriate clinical setting
1 Age gt 50 years
2 Insidious onset of unexplained dyspnea
3 Duration of illness for ge 3 months
4 Bibasilar inspiratory crackles
23
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Unlike the ATSERS consensus criteria published in 2000 bronchoscopy will not be required for diagnosis
This decision was made based on the experience of the IPFnet Steering Group members regarding the utility of
bronchoscopy in the diagnosis of IPF The presence of an atypical HRCT finding will require documentation of
a definitive diagnosis by surgical lung biopsy In fact this is in keeping with the recently published evidence
based guidelines for diagnosis and management of IPF13 As shown in Figure 3 central review of the pathology
data will be required for a diagnosis of IPF
We will not require central review of HRCT as several studies have shown that a confident local interpretation
of clinicalHRCT criteria as definite IPFUIP is associated with a high positive predictive value for finding UIP
at surgical lung biopsy (see Table 1) Differences in sensitivity in these series likely reflect subject selection as
Flaherty et al3 evaluated only UIP and nonspecific interstitial pneumonia (NSIP) while Raghu et al40 and
Hunninghake et al41 included a broader range of ILD
Table 1 Operating Characteristics of Local HRCT Review for Diagnosis of UIP
Researcher of Subjects Sensitivity () Specificity () PPV () NPV ()
Raghu et al 40
59 (29 UIP by SLB) 78 90 88 82
Hunninghake et al 41 91 (54 UIP by SLB)
74 81 85 67
Flaherty et al 3 96 (only NSIP amp UIP)
37 100 100 30
Abbreviations PPV positive predictive value NPV negative predictive value UIP usual interstitial pneumonia SLB surgical lung biopsy and NSIP nonspecific interstitial pneumonia
Furthermore an analysis of the HRCT scans from subjects enrolled in the GIPF-001 trial confirmed that local
site interpretations have a high congruity to a central radiology core In this multi-center study 263 HRCT
scans were read as definite IPF and a retrospective central radiology core review found 932 to be consistent
with IPF 42 We will also take several additional steps to insure that the local HRCT reads are accurate
including
1 A detailed training module has been developed and must be completed by each site radiologist before
site initiation
2 Clinical centers are to mail all HRCT scans to the HRCT core lab The first 10 HRCT scans from
subjects enrolled at each enrolling clinical center will be reviewed centrally to be certain that local reads
24
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
25
are congruent with a central interpretation If discrepancies are identified additional education will be
provided and HRCT scans will continue to be reviewed centrally until the central radiology core is
confident that the local center is performing appropriately
3 Random scans will be obtained from each center throughout the study to confirm that the local read
continues to agree with central interpretation If discrepancies are identified they will be addressed as in
2 above
In all cases if a subject has a surgical lung biopsy sample that sample will be reviewed by the local and central
pathologists Therefore the only cases that would not be subject to a direct central review process are those
where the HRCT meets the centrally defined criteria for an unequivocal diagnosis and a lung biopsy sample is
not available Table 2 below summarizes the possible combinations for making a diagnosis
Table 2 Combining HRCT and Pathology Interpretations to Determine if IPF is Present
HRCT Diagnosis Pathology Diagnosis Diagnosis of IPF
Definite UIP Definite UIP Yes
Definite UIP Probable UIP Yes
Definite UIP Possible UIP Yes
Definite UIP Not UIP No
Definite UIP Unavailable Yes
Consistent with UIP Definite UIP Yes
Consistent with UIP Probable UIP Yes
Consistent with UIP Possible UIP No
Consistent with UIP Not UIP No
Consistent with UIP Unavailable No
Inconsistent with UIP Any No
Abbreviations HRCT high-resolution computed tomography IPF idiopathic pulmonary fibrosis
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
UIP usual interstitial pneumonia Dx diagnosis 43 Exclusion Criteria
1 History of clinically significant environmental exposure known to cause pulmonary fibrosis
Occupational exposures such as asbestos or environmental exposure to organic dust such as occurs in
pigeon breeders may at times mimic the clinical and radiographic findings of IPF
2 Diagnosis of connective tissue disease felt by the principal investigator (PI) to be the etiology of the
interstitial disease Diagnosis of collagen-vascular conditions will be according to the published
American College of Rheumatology criteria As such the presence of any documented collagen-vascular
disorder or the presence of any suspicious symptom complex whether or not associated with
significantly abnormal rheumatological serologies will exclude the subject at the discretion of the PI
3 Extent of emphysema greater than the extent of fibrotic change (honeycombing reticular changes) on
HRCT scan
4 Forced expiratory volume in 1 second (FEV1)FVC ratio lt 065 at screening (postbronchodilator)
5 Partial pressure of arterial oxygen (PaO2) on room air lt 55 mm Hg (lt 50 mm Hg at Denver site)
6 Residual volume gt 120 predicted at screening (postbronchodilator)
7 Evidence of active infection
8 Significant bronchodilator response on screening spirometry defined as a change in FEV1 ge 12 and
absolute change gt 200 mL OR change in FVC ge 12 and absolute change gt 200 mL The percent
difference between the FVC (or FEV1) values will be calculated by taking the absolute value of the
difference and dividing it by the larger of the two FVC (or FEV1) values
9 Screening and enrollment post-bronchodilator FVC measurements (in liters) differing by gt 11 The
percent difference between the FVC values will be calculated by taking the absolute value of the
difference and dividing it by the larger of the two FVC values (eg the percent difference between FVC
measurements of 19 and 20 liters would be determined by taking the difference between the two (01
liters) and dividing by the larger of the two (20 liters) So 0120 = 5 and these FVC measurements
would not exclude the subject
10 Listed for lung transplantation ie the patient has completed the evaluation process has been accepted
as a candidate for transplantation at an appropriate center and is waiting to receive notification of an
available donor organ
11 History of unstable or deteriorating cardiac disease
12 Myocardial infarction coronary artery bypass or angioplasty within 6 months of screening
26
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
13 Unstable angina pectoris or congestive heart failure requiring hospitalization within 6 months of
screening
14 Uncontrolled arrhythmia
15 Severe uncontrolled hypertension
16 Known HIV or hepatitis C
17 Known cirrhosis and chronic active hepatitis
18 Active substance andor alcohol abuse (as determined by site PI)
19 Pregnancy or lactation (subjects who are pregnant or breastfeeding)
20 Known hypersensitivity to study medication
21 Any condition other than IPF that in the opinion of the site PI is likely to result in the death of the
subject within the next year
22 Any condition that in the judgment of the PI might cause participation in this study to be detrimental to
the subject or that the PI deems makes the subject a poor candidate
23 Any therapy directed at pulmonary fibrosis (excepting triple therapy of prednisone plus azathioprine
plus NAC) requires a 30-day washout period before randomized Triple therapy of lt= 12 weeks duration
in the past 4 years requires a 30-day washout period before randomization
24 History of triple therapy of prednisone plus azathioprine plus NAC for gt 12 weeksrsquo duration in the past
4 years or previous enrollment in the triple-therapy arm of the PANTHER-IPF study
44 Study Design and Study Visit
441 Study Design Summary
This study will be a randomized double-blind PL-controlled trial designed to assess the safety and efficacy of
NAC in subjects with newly diagnosed IPF
Subjects with mild to moderate IPF (defined as FVCpred ge 50 and DLCOpred ge 30) diagnosed within
the past 48 months will be enrolled Screening will continue until April 30 2012
27
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
The study will employ a 2-arm design with 11 randomization to NAC or PL Once enrolled subjects will visit
the clinical center at 15 weeks and 15-week intervals thereafter Each subject will be treated and followed for a
maximum of 60 weeks
During the 60-week visit subjects will be taken off all study agents Approximately four weeks after the final
dose of study agent is taken subjects will receive a safety phone call from the study site
442 Study Visits
Subjects who meet entry criteria will review the informed consent a written description of the purpose
procedures and risks of the study with the PI co-investigator or study coordinator and all questions will be
answered The informed consent form will be signed by the subject at screening No protocol-specific
procedures will be performed until the subject has signed and dated an informed consent form This includes the
screening procedures
4421 Screening
Once informed consent is obtained subjects may immediately begin the screening process or may return within
28 days of consent In the event a study subject has been clinically evaluated at the study site by an IPFnet study
physician and has performed testing within three weeks for this clinical evaluation that meets guidelines
provided in the IPFnet PANTHER-IPF Manual of Operating Procedures (MOOP) this testing may be used to
satisfy the following screening criteria medical history physical exam arterial blood gas (ABG) with A-a
gradient vital signs with oximetry body height and weight spirometry DLCO lung volumes and HRCT scan
Allowing the use of previously performed test results that meet study guidelines for the screening visit is
intended to permit subjects easier access to study entry to prevent subjects from repeating testing that has been
performed within the study window and to decrease risks to subjects from repeated exposure to procedures
such as arterial puncture and HRCT
The following procedures will be performed at screening
Medical history and a physical examination
28
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Measure height and weight
Serum pregnancy test (if applicable)
Measure vital signs including oximetry
Blood draws performed and the following analyses conducted
o Hematology (red cell count white cell count hemoglobin hematocrit cell indices differential
platelet count)
o Blood chemistries according to central laboratory protocol (see Section 410 Laboratory
Testing)
o Beta human chorionic gonadotropin (serum) pregnancy test (in women of childbearing potential)
o Urinalysis
Pulmonary Function Tests (PFTs) including spirometry pre- and post- bronchodilator and postshy
bronchodilator measurement of lung volumes and measurement of hemoglobin adjusted diffusing
capacity
Measure ABGs
HRCT if a satisfactory scan has not been performed on the subject within 3 months of screening (see
PANTHER-IPF MOOP for more details)
Surgical lung biopsies (if applicable) reviewed by local and central pathology departments
Current medications If required a washout period discussed with the subject and initiated at this visit
4422 Enrollment
The enrollment visit is expected to take place within eight weeks of the screening visit Enrollment visit
activities include
Measure vital signs including oximetry
Measure height and weight
Serum pregnancy test (if applicable)
If consent has been given blood will be drawn and a urine specimen collected for the bio-specimen
repository
Spirometry (post-bronchodilator)
Measure 6MWT with Borg Dyspnea Scale
29
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Collect Quality-of-life (QOL) data using the SF-36 EuroQol Investigating Choice Experiments for
Preferences of Older People Capability Instrument (ICE CAP) and SGRQ
Female subjects complete Gender Substudy questionnaire
Dyspnea status collected using the UCSD SOBQ
Evaluate Acute Exacerbation (AEx)
Review of any Adverse Events (AEs)
Review of concomitant medications
Subject receives diary and instructions on its purpose and proper use
Subject receives supply of study drug sufficient to last until his or her 15-week study visit
See the Schedule of Assessments (Table 3) for more details Subjects with screening and enrollment postshy
bronchodilator FVC measurements (in liters) differing by more than 11 are not eligible to be enrolled in the
study
Subjects will be asked to provide a physician of record This physician will be considered the subjectrsquos primary
care provider (PCP) and if the subject agrees the PCP will be informed by letter of the subjectrsquos enrollment in
the trial The subject will be informed that his or her ongoing medical care should be received from the PCP
The PCP will be informed of any safety issues identified by the study staff The PCP will also be given
information regarding communication with study personnel about pertinent health issues or clinic encounters
the subject may have
4423 Week 15
The week 15 visit is expected to occur within +- 14 days of the subjectrsquos scheduled visit time (eg the week 15
visit should occur anytime between 13 and 17 weeks after starting study drug Week 15 activities include
Measure vital signs with oximetry
Measurement height and weight
Serum pregnancy test (if applicable)
Spirometry (post-bronchodilator) measurement
Review of AEs
Evaluate for AEx
30
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Review concomitant medications
If consented draw blood and collect urine specimen for the biospecimen repository
Subjects return used and unused study drug for the visit
Review study diary and a new study diary will be given
Provide additional supply of study drug sufficient to last until the next scheduled visit
4424 Week 30
The week 30 visit is expected to occur within +- 14 days of the subjectrsquos scheduled visit time (eg the week 30
visit should occur anytime between 28 and 32 weeks after starting study drug) Week 30 activities include
Physical examination
Measure vital signs with oximetry
Measure height and weight
Laboratory values (complete blood count [CBC] and serum chemistries)
Serum pregnancy test (if applicable)
Measure spirometry (post-bronchodilator)
6MWT with Borg scale
DLCO
Review of AEs
Evaluate for AEx
Review concomitant medications
Complete all QOL and dyspnea questionnaires (EuroQol ICE CAP SF-36 SGRQ and UCSD SOBQ)
If consent has been given blood will be drawn and a urine specimen collected for the biospecimen
repository
Review study diary
Subjects return used and unused study drug for the visit
Provide additional supply of study drug sufficient to last until the next scheduled visit
4425 Week 45
31
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
The week 45 visit is expected to occur within +- 14 days of the subjectrsquos scheduled visit time (eg the week 45
visit should occur anytime between 43 and 47 weeks after starting study drug) Week 45 activities include
Measure vital signs with oximetry
Measure height and weight
Serum pregnancy test (if applicable)
Measure spirometry (post-bronchodilator)
Review of AEs
Evaluate for AEx
Review concomitant medications
If consent has been given blood will be drawn and a urine specimen collected for the biospecimen
repository
Subjects return used and unused study drug for the visit
Study diary reviewed
Provide additional supply of study drug sufficient to last until the next scheduled visit
4426 Week 60 (Early Withdrawal or Final Treatment Visit)
At week 60 or at subject withdrawal from the study (premature by study doctor or subjectrsquos decision) a final
treatment visit will occur At this final treatment visit subjects will discontinue NACPL abruptly Week 60
activities also include
Physical examination
Measure vital signs with oximetry
Measure height and weight
Laboratory values (complete blood count [CBC] and serum chemistries)
Spirometry (post-bronchodilator) measurement
6MWT with Borg scale measurement
DLCO
Lung volumes
ABG
Review of AEs
32
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Evaluate for AEx
Review concomitant medications
Subjects will complete all QOL and dyspnea questionnaires (EuroQol ICE CAP SF-36 SGRQ and
UCSD SOBQ)
If consent has been given blood will be drawn and a urine specimen collected for the biospecimen
repository
Subjects return used and unused study drug for the visit
Study diary reviewed
4427 Final Site Visit ndash FVC drop confirmation
In the event that the subject has a recorded FVC drop of gt10 from baseline at the final treatment visit and the
subject has not had a confirmation of such a drop at a previous study visit the subject should return to the
clinical site 6 to 8 weeks after the final treatment visit During this visit a post-bronchodilator spirometry test
will be performed This FVC measurement will be evaluated according to section 521 of this protocol
4428 Final Visit ndash Telephone Follow-up
Four weeks following the final dose of study medication subjects will receive a telephone call from the study
coordinator to ensure that there are no side effects and to follow up on any ongoing adverse events (AEs)
4429 Phone Contact Between Visits
At week 2 and each month that a subject does not have a scheduled clinical center visit his or her study
coordinator will contact him or her at least once by telephone to
Inquire if the subject has had any hospitalizations events that might be considered an AE or any events
significant enough to warrant an out-of-cycle visit to the clinical center
Remind subjects of their current dosage levels and confirm that the subject understands them
Address any questions or concerns the subject might have regarding other aspects of the study
Assess adherence to the treatment regimen by reviewing diary data verbal review of medications taken
including nutritional supplements
33
34
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Table 3 Schedule of Assessments
Procedure Screening Visit 0
Enrollment Visit 1
Week 15 Visit 2
Week 30Visit 3
Week 45 Visit 4
Week 60 Early
Withdrawal Visit 5
Final1
Visit (via phone)
Informed consent X
Medical history X
Inclusionexclusion criteria X
Serum pregnancy test (if applicable) X X X X X
Review of lung biopsy X
Arterial Blood Gas X X
6-Minute Walk Test
X
X X
Physical examination X X X
Vital signs with oximetry X X X X X X
Body height and weight X X X X X X
Complete Blood Count X X X
Chemistry panel X X X
Monitor Lab Values X X X
Urinalysis X Specimen repository substudy blood draw and urine collection (if consented)
X
X X X X
HRCT (if not completed within three months) X
Spirometry (pre- and post-bronchodilator) X
Spirometry (post-bronchodilator only) X X X X X
DLCO (post-bronchodilator only) X X X
Lung volumes (post-bronchodilator only) X
X
Evaluate for acute exacerbation X X X X X
Review Adverse Events X X X X X X
Review concomitant meds X X X X X X
Dispense subject diary X X X X
Review subject diary X X X X X
Dispense study agent X X X X
Gender Substudy questionnaire (female subjects only) X
EuroQol ICECAP UCSD SOBQ SGRQ SF-36 X X X
Abbreviations DLCO diffusing capacity of the lung for carbon monoxide QOL Quality of Life ICECAP Investigating Choice Experiments for Preferences of Older People UCSD SOBQ University of California Shortness of Breath Questionnaire SGRQ St Georgersquos Respiratory Questionnaire SF-36 Short Form 36 Health Survey
1Follow-up visit via phone will occur four weeks after final dose of study medication
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
45 Dose Justification
The general philosophy for determining dosing levels was to apply previously examined
treatment regimens With the focus of the study being to establish a standard of care for
mildmoderate IPF subjects the goal was to develop flexible yet standardized treatment rules that
allow for the temporary or permanent withholding of one or more components of treatment when
necessary Subjects developing laboratory abnormalities or symptoms that result in
discontinuation of one or more components of study treatment may continue on the other
components as long as there is no contraindication for this Complete follow-up is important for
the validity of any study As a strategy to maintain protocol adherence we are using a treatment
regimen that will detect potential side effects and prompt interventions proactively in the interest
of patient safety In addition subjects who permanently stop study medications during the course
of the study are encouraged to continue in the study completing all scheduled visits and tests
451 Rationale for N-acetylcysteine Dosing
To our knowledge there have been no IPF studies to correlate clinical outcome measures with
different dosages for NAC The dosage chosen is based on the IFIGENIA study However BAL
lung GSH levels from subjects with IPF have been augmented with the use of oral NAC at 600
mg 3 times per day In addition lung GSH levels have been associated with improved
PFTs212227 The dose chosen for this study was based on previous data including the IFIGENIA
study30
4511 Dosing of N-acetylcysteineplacebo
Dosing of NACPL will be 600 mg orally 3 times a day (1800 mgday)
4512 Reasons to Discontinue N-acetylcysteineplacebo
NACPL may be temporarily or permanently discontinued for the duration of the study for
gastrointestinal symptoms or dermatologic reactions
35
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Temporarily discontinue (hold) oral NACPL for subjects requiring inpatient admission for acute
exacerbation (AEx) or other conditions Resume NACPL after discharge
36
37
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
452 Dosage Algorithms
Dosage Adjustment Algorithm 1 NACPL Dose Modifications for Gastrointestinal Symptoms Nausea Vomiting Abdominal Discomfort Diarrhea
GI Symptoms determined by the PI to be clinically significant Nausea Vomiting Abdominal Discomfort Diarrhea
NACPL Temporarily dc (HOLD) x 3 Days
Monitor symptoms intervene as clinically indicated (eg fluid replacement antidiarrhea or antinausea medication)
Monitor or lab PRN
Are symptoms resolving after 3 days NO
Symptoms NOT resolving after 3 days of holding study medication Assessmentmanagement per clinical
discretion of investigator
Likely not study medication discuss resuming study medication with medical monitor when symptoms resolved
YES
Temporarily dc (HOLD) NACPL for 4 additional days (total hold 1 week) then NACPL Resume 600 MG TID
Did symptoms recur
YES
STOP NACPL for
duration of study
NO
NACPL No Change
38
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Dosage Adjustment Algorithm 2 NACPL Dose Modifications For Dermatologic Reactions
Dermatologic Reactions (Not Acneiform) ge Grade 2 Grading per Common Terminology Criteria for
Adverse Events V30 (httpctepcancergov) For example Grade 1 RASHDESQUAMATION Macular or papular eruption or erythema without associated symptoms Grade 2 RASHDESQUAMATION Macular or popular eruption or erythema with pruritus or other associated symptoms localized desquamation or other lesions covering lt50 of body surface area
NACPL Temporarily dc (HOLD) x 3 days
Are symptoms resolving after 3 days
NO Symptoms not resolving after 3 days of holding study medication Assessmentmanagement per clinical discretion of investigator Likely not study medication Discuss resuming study medication with medical monitor when symptoms
resolved YES
Temporarily dc (HOLD) NACPL for 4 additional days (total hold 1 week) then NACPL resume 600 MG TID
Did symptoms recur
YES
STOP NACPL for
duration of study
NO
NACPL No change
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
46 Contraindications Precautions and Side Effects of Study Medications
461 Contraindication
Contraindication to NAC is known hypersensitivity to it
462 Precautions
Concomitant administration of oral NAC and antibiotics has shown a slightly reduced absorption
of cephalexin and a slight increase in erythromycin serum levels NAC contains free sulfhydryl
groups There is no evidence that individuals sensitive to sulfa drugs are sensitive to NAC
The NAC preparation being administered in this study contains 20 mg of aspartame Because of
the phenylalanine component of aspartame individuals with phenylketonuria should avoid or
restrict aspartame intake to avoid increased blood levels of phenylalanine Because of this risk
labeling is required on all products containing aspartame
463 Side Effects
Side effects of NAC range from common to serious See Table 4
39
40
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Table 4 Side Effects of NAC
Undesirable Effects
System-organ class Uncommon
(gt11000 lt1100)
Rare
(gt110000 lt11000)
Very rare
(lt110000) Not known
Immune system disorders Hypersensitivity Anaphylactic shock
reaction
Nervous system disorders Headache
Ear and labyrinth disorders Tinnitus
Cardiac disorders Tachycardia
Vascular disorders Hemorrhage
Respiratory thoracic and
mediastinal disorders
Bronchospasm
Dyspnea
Gastrointestinal disorders
Vomiting diarrhea
stomatitis abdominal
pain nausea
Dyspepsia
Skin and subcutaneous tissue
disorders
Urticaria rash
angioedema itching
General disorders and
administration site conditions Pyrexia
Investigations Reduced arterial
pressure Face edema
In very rare cases the onset of severe skin reactions such as Stevens-Johnson syndrome and Lyell syndrome was reported to have a temporal relationship with N-acetylcysteine administration Although in most cases at least another suspect drug probably most involved in the genesis of the above mentioned mucocutaneous syndromes has been identified in case of mucocutaneous alterations it is appropriate to contact onersquos doctor and the administration of N-acetylcysteine should be immediately discontinued
Some studies confirmed a reduction of platelet aggregation during N-acetylcysteine administration The clinical significance of these findings has not been defined yet [Source Fluimucil Investigator Brochure]
47 Recruitment Procedures
Subjects recruited for this study will be established patients of the investigators or physician- or
self-referred to participating clinical centers in the IPFnet Each clinical center within IPFnet has
a well-developed infrastructure of local pulmonologists within the surrounding geographic area
These pulmonologists are kept informed of ongoing IPF clinical trials and regularly refer
subjects to studies conducted at IPFnet clinical centers
Additional steps will be taken to inform clinicians of the trials in progress within IPFnet
including presentations at faculty staff meetings at local hospitals medical grand rounds and
national conferences direct mail notification monthly faxes and advertisement of network trials
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
in pulmonary journals Clinical center patients previously diagnosed with IPF will be notified of
the trials by mail whenever possible
Recruitment of minorities and women will be monitored by the DCC and DSMB If necessary
additional recruitment efforts will be made at specific centers to ensure that the aggregate subject
sample contains appropriate representation of women and minorities
48 Study Procedures
The following procedures are detailed in the PANTHER-IPF MOOP accompanying this
protocol
1 PFT
2 ABG
3 HRCT scan of the chest (including imaging of pulmonary arteries)
4 CBC and serum chemistries
5 Pregnancy test
6 6MWTBorg Dyspnea Scale
7 QOL questionnaires (EuroQol HAD SF-36 SGRQ and ICE CAP)
8 UCSD SOBQ
9 Gender Substudy Questionnaire
All assessments of PFTs will be conducted by study personnel not directly involved in the
treatment of the subjects
481 Biological Specimen Management
4811 Biological Specimen Sample Management
Subjects at clinical centers participating in the specimen repository substudy who consent to
having blood drawn for research purposes and for the banking of blood blood components and
other biologic specimens (urine and BAL fluid) will have approximately 405 mL of blood
41
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
drawn 17 mL blood drawn for DNA and 20 mL of urine collected at enrollment visit Subjects
will have approximately 50 mL of blood drawn and 20 mL of urine collected at each 15-week
follow-up visit Blood specimens will be separated according to PANTHER-IPF MOOP
guidelines into the following components for banking in the repository serum plasma and
DNA Coding of all biologic specimens for the repository will be performed by study staff at the
clinical center The samples will be processed per PANTHER-IPF MOOP guidelines aliquoted
labeled with barcode labels and stored at -70degC at the clinical center and shipped to the central
repository
The only subject identifiers will be a sample ID number and subject initials This sample ID will
be linked in the IPFnet DCC clinical database to subject information No subject information will
be transferred to the biological-specimen database
The subjectrsquos samples may be used for approved sub-studies relating to human disease
including but not limited to IPF The studies for which an individualrsquos samples will be made
available will be determined by the subjectrsquos answers to questions on the biological-sample
informed consent form The subjects can choose to make their samples available for all options
or any combination Samples will be made available to researchers only with IPFnet Steering
Group approval until such time as the samples are made public through the NHLBI repository
49 Concomitant Medications
Concurrent treatment with FDA-approved therapy for IPF is allowed Colchicine may be used
for treatment of gout Temporary treatment with oral or IV corticosteroids for clinical worsening
or suspected AEx is permitted Nutritional supplements containing NAC are not allowed
410 Laboratory Testing
Clinical laboratory parameters will be assessed at screening and at the end of the study The
following tests will be performed at the two time points specified in the protocol chemistry (AG
ratio ALT [SGPT] AST [SGOT] albumin alkaline phosphatase amylase bilirubin-direct
42
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
bilirubin-indirect bilirubin-total BUN BUNcreatinine ratio calcium carbon dioxide
cholesterol-total chloride CPK-total creatinine GGT globulin glucose iron-total LDH
lipase magnesium phosphorus-inorganic potassium protein-total sodium TIBC triglycerides
uric acid) and hematology (red blood cell count WBC count hemoglobin hematocrit cell
indices differential platelet count)
411 Blinding of Study Drugs
Subjects and caregivers will be blinded to study treatment Every subject will receive NAC or
matching PLs at every study visit from the baseline visit to the week-45 visit No study agent
will be dispensed at the week-60 visit
43
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
5 Study Endpoints
51 Primary Study Endpoint
The primary endpoint will be the change in serial measurements of FVC over the study period
52 Secondary Study Endpoints
521 Time to Disease-progression
The time-to-death or a 10 decline in FVC will be defined as the time-to-disease progression
The 10 decline in FVC from enrollment must be confirmed on 2 consecutive visits no less than
6 weeks apart For subjects with 2 consecutive visits with a 10 decline in FVC the time-toshy
disease progression will be defined as the time interval between enrollment and the initial visit
with a 10 FVC decline For subjects who experience disease progression the study doctor will
determine whether or not the subject will remain in the study
522 Acute Exacerbations
The following 3 criteria will define AEx in subjects with acute worsening of their respiratory
conditions
1 Clinical (all of the following required)
A) Unexplained worsening of dyspnea or cough within 30 days triggering unscheduled
medical care (eg emergency room clinic study visit hospitalization)
B) No clinical suspicion or overt evidence of cardiac event pulmonary embolism or deep
venous thrombosis to explain acute worsening of dyspnea
C) No pneumothorax
44
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
2 RadiologicPhysiologic (A and B required)
A) New ground glass opacity or consolidation computed tomography (CT) scan OR new
alveolar opacities on chest x-ray
B) Decline of ge 5 in resting room air SpO2 from last recorded level OR decline of ge 8 mm
Hg in resting room air PaO2 from last recorded level
3 Microbiologic (all of the following required)
A) No clinical evidence for infection (ie absence of grossly purulent sputum fever gt 39degC
orally)
B) Lack of positive microbiological results (if done) from lower respiratory tract defined as
(1) Clinically significant bacterial growth on sputum or endotracheal aspirate cultures
(2) Quantitative culture by protected brush specimen ge 103 cfumL or BAL ge 104 cfumL
(3) The presence of specific pathogens on stains of any of the above
C) Lack of positive pathogen in blood cultures (if done)
Identification of Acute Exacerbations
All subjects will be educated about the importance of identifying AExs At the time of
enrollment subjects will be told about the possibility of developing acute symptomatic
worsening that might represent an AEx of IPF and instructed to contact their study clinical
center coordinator within 48 to 72 hours of the apparent event
All subjects will be contacted by phone monthly and questioned about any change in dyspnea or
cough and any interim clinic visits or hospitalizations Finally as part of the IPFnet outreach to
community referring physicians the importance of AExs will be emphasized When a subject is
identified who meets criterion 1A this will trigger the collection of additional clinical data to
evaluate a suspected AEx These data will be collected as part of standard clinical care (ie this
protocol does not require collection of all items) The additional items to be collected for
suspected AEx include
IPFnet AEx case report form (eCRF) (required)
45
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Chest x-ray CT scan withwithout pulmonary angiogram (reports should be faxed and
followed by the hard copiesdiscs)
Oxygen saturation (pulse oximetry)
ABG
Respiratory cultures (sputum endotracheal aspirate lavage)
Blood cultures
Clinichospital records related to the event
All potential cases of AEx will be reviewed by the clinical center PI first and a decision on
whether the case may represent an AEx will be made If AEx is suspected the case will be sent
to the IPFnet adjudication committee which will assign a final diagnosis (see Table 5) If there is
disagreement among members the majority opinion will be recorded
During episodes of suspected AEx as determined by the individual clinical center investigator
subjects will remain blinded and in the study
Table 5 Final Diagnoses in Evaluation of Suspected Acute Exacerbations
Definite acute exacerbation All criteria met no alternative etiology
Unclassifiable acute worsening
Insufficient data to evaluate all criteria no alternative etiology
Not acute exacerbation Alternative etiology identified that explains acute worsening
Management of the suspected AEx will be at the discretion of the treating physician Standard of
care generally involves evaluation for respiratory infection pulmonary embolism cardiac events
and pneumothorax and treatment with IV corticosteroids
Study drugs will be resumed at pre-suspected AEx doses after subjects clinically improve as
confirmed by the local PI All subjects should be seen at the clinical center within 2 to 4 weeks
of recovery for measurement of post-bronchodilator FVC (see Figure 4) Subjects unable to
return to the clinical center after suspected AEx due to medical frailty (eg continued
46
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
institutionalization progressive disability) will be categorized as failing to maintain FVC
response in secondary analyses
Suspected AEx (PI determined)
Hold study drug Treat AEx
(Attending physician determined)
Alive but unable to continue due to
medical frailty
Dead
Alive and able to continue
Site reviewvisit
Restart study drug
FVC within 2-4 weeks
Figure 4 Acute Exacerbation Flow Chart
523 Respiratory Infections
An upper respiratory infection will be defined as
Change in sputum discoloration
Increased cough of no more than 14 daysrsquo duration
A lower-respiratory infection (pneumonia) will be defined as new segmental or lobar airspace
opacities visualized by image studies (chest radiograph or HRCT) in addition to any of the
following
Positive pathogencultures in good sample of sputum or lower-airway secretions retrieved
by fiberoptic bronchoscope
Fever gt 39degC or gt 100degF
Leukocytosis gt 12000 (unexplained no increase in dose of corticosteroids)
47
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
524 Maintained FVC Response
Subjects with follow-up FVCpred measurements at or above their baseline FVCpred level
will be classified as having maintained FVC response Subjects with reduced FVCpred levels
or missing data for any reason including death or medical frailty will be classified as having not
maintained FVC response The FVCpred value is used because unadjusted FVC measurements
are expected to decline with age
48
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
6 Safety Evaluations and Procedures
61 Adverse Events
During a clinical trial the reporting of adverse experience information can lead to important
changes in the way a new treatment is developed as well as provide integral safety data
611 Definitions
An adverse event (AE) is any untoward medical occurrence in a subject or clinical investigation
subject who was administered a pharmaceutical product The AE does not necessarily have to
have a causal relationship with the drug administered An AE can be any unfavorable and
unintended sign (including an abnormal laboratory finding) symptom or disease temporarily
associated with the use of a medicinal product whether or not considered to be related to the
medicinal product Diseases signs symptoms or laboratory abnormalities already existing at
enrollment are not considered AEs unless they worsen (ie increase in intensity or frequency)
Surgical procedures themselves are not AEs they are therapeutic measures for conditions that
require surgery The condition for which the surgery is required may be an AE Surgical
procedures planned before randomization and the conditions necessitating the surgery are not
AEs
A serious adverse event is any untoward event that
Is fatal
Is life-threatening
Requires inpatient hospitalization or prolongation of existing hospitalization with the
following exceptions
o Preplanned (before the study) hospital admissions unless the hospitalization is
prolonged
o Planned admissions (as part of a study eg routine biopsies)
o Hospitalization lasting lt 24 hours
49
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
o Hospitalization for elective procedure
o Emergency room visits
Results in persistent or significant disability or incapacity
Is a congenital anomaly or birth defect
Important medical events that may not result in death be life-threatening or require
inpatient hospitalization may be considered serious adverse events (SAEs) when based
on appropriate medical judgment they may jeopardize the subject and may require
medical or surgical intervention to prevent one of the outcomes listed above
Life-threatening means that the subject was in the view of the investigator at immediate risk of
death from the AE as it occurred It does not include an AE that had it occurred in a more severe
form might have caused death
Persistent or significant disabilityincapacity means that the event resulted in permanent or
significant and substantial disruption of the subjectrsquos ability to carry out normal life functions
Causality
A reasonable possibility means the AE may have been caused byrelated to the study drug A
perceived or real lack of efficacy does not satisfy the definition of relatedness
612 Adverse Event (AE) Reporting
For the PANTHER-IPF trial all AEs (serious and nonserious) occurring from randomization
through final study visit (4 weeks after final dose of all study medication) will be recorded on the
AE page of the case report form (CRF)
6121 Serious Adverse Events (SAE) Reporting
For this trial all deaths and all SAEs which occur from randomization through final study visit
must be entered within the EDC system via the SAE eCRF page within 24 hours of the
investigative sitersquos knowledge of the event It is the responsibility of the clinical center
50
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
investigator to provide a causality assessment of the event for each study medications based upon
the information available at the time of the report It is understood that complete information
about the event may not be known at the time the initial report is submitted In the event the EDC
system is not accessible to the site at the time of event reporting investigative sites will complete
and forward a paper back-up SAE form to DCRI Safety Surveillance for processing
DCRI Safety Surveillance
Telephone 1-919-668-8624 or 1-866-668-7799 (toll free)
Fax 1-919-668-7138 or 1-866-668-7138 (toll free)
The investigator must complete and submit follow-up SAE information via the eCRF when
important new or follow-up information (eg final diagnosis outcome results of specific
investigations) becomes available Follow-up information should be submitted according to the
same process used for reporting the initial event as described above All SAEs will be followed
until resolution stabilization or 30 days after the subject has completed the final visit (4 weeks
after the final dose of study medication) whichever occurs first The investigator is responsible
for reporting SAEs to their institutional review board (IRB) per site specific IRB reporting
guidelines
6122 Regulatory Reporting
AEs that are serious study drug related and unexpected will be reported to the regulatory
authorities The DCRI Safety Surveillance medical monitor will perform a medical review of all
SAEs submitted and evaluate for ldquounexpectednessrdquo DCRI Safety Surveillance will prepare
MedWatch reports for those events identified as serious study drug related and unexpected as
determined by Safety Medical Monitor
DCRI Regulatory Services will submit all unexpected study drug-related SAEs as per 21 CFR
32 DCRI Safety Surveillance will provide a safety alert letter to the NHLBI DSMB and DCC
clinical operation (for distribution to sites) within 15 days of initial receipt of the information
51
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Investigators are responsible for promptly reporting these events to their reviewing IRBs
according to site specific IRB reporting guidelines
62 Clinical Medical Monitoring
There will be an unblinded physician at the IPFnet DCC serving as medical monitor The
medical monitor will be available to assist with questions about dosage adjustments of study
medications including discontinuation or resumption of medications
63 Unblinding Procedures
Unblinding of subjects or investigators to subject treatment is strongly discouraged For ongoing
clinical management all subjects should be presumed to be receiving ldquoactiverdquo study drug To
ensure the subjectrsquos safety the study treatment will be dose-adjusted based on laboratory test
results clinical findings and symptoms
The IPFnet DCC medical monitor and PANTHER-IPF co-chairs Drs Ganesh Raghu and
Fernando Martinez will be available to the study physicians to discuss study drug management
on a case-by-case basis Un-blinding will be considered ONLY when the knowledge of subject
treatment assignment is ABSOLUTELY ESSENTIAL for subject safety and after discussion of
the subjectrsquos case with the medical monitor and either Dr Raghu or Dr Martinez Unblinding of
study treatment should be minimized during the conduct of the trial In those cases where it is
felt to be medically necessary the DCC medical officer will communicate directly with the
managing physician to minimize unblinding of study personnel
52
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
7 Study Drug Procedures
At the baseline 15-week 30-week and 45-week study visits subjects will receive a supply of
study drug sufficient to last until the next visit at which study drug will be dispensed
53
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
8 Data Management
81 Hardware and Software Configuration
811 Hardware and Database Software
Data will be stored in an Oracle database system Oracle has advantages of processing efficiency
and smooth linkage with other software systems The application and database will be hosted on
Solaris Unix servers at the IPFnet DCC
812 Statistical Software
SAS will be used as the principal application for the management of analysis data files and
statistical computations S-Plus will be used to provide supplementary functions as needed
813 Access Control and Confidentiality Procedures
Access to databases will be controlled centrally by the IPFnet DCC through user passwords
linked to appropriate privileges This protects the data from unauthorized changes and
inadvertent loss or damage
814 Security
Database and Web servers will be secured by a firewall and through controlled physical access
Oracle has many security features to ensure that any staff member accessing the database has the
proper authority to perform the functions he or she requests of the system Within the secondary
SAS databases Unix group-access control maintains similar security The Sun workstation login
is secured by extensive user-password facilities under Unix
54
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
815 Back-up Procedures
Database back-up will be performed automatically every day and standard IPFnet DCC policies
and procedures will be applied to dictate tape rotation and retention practices
816 Virus Protection
All disk drives that provide network services and all user computers will be protected using
virus-scanning software Standard IPFnet DCC policies will be applied to update these protection
systems periodically through the study
82 Sources of Data
821 Design and Development
The IPFnet DCC will be responsible for development of the electronic case report forms
(eCRFs) development and validation of the clinical study database ensuring data integrity and
training clinical center staff on applicable data management procedures A web-based distributed
data entry model will be implemented This system will be developed to ensure that guidelines
and regulations surrounding the use of computerized systems used in clinical trials are upheld
The remainder of this section provides an overview of the data management plan associated with
this protocol
822 Data Collection Forms
The data collection process consists of direct data entry at the study clinical centers into the EDC
system(s) provided by the DCC A data collection worksheet will be provided to clinical centers
for recording data in the event the EDC system is unavailable Data entry of the eCRFs should
be completed according to the instructions provided and project specific training The
investigator is responsible for maintaining accurate complete and up-to-date records and for
ensuring the completion of the eCRFs for each research participant
55
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
823 Data Acquisition and Entry
Data entry into eCRFs shall be performed by authorized individuals Selected eCRFs may also
require the investigatorrsquos written signature or electronic signature as appropriate Electronic
CRFs will be monitored for completeness accuracy and attention to detail during the study
824 Data Center Responsibilities
The IPFnet DCC will 1) develop a data management plan and will conduct data management
activities 2) provide final eCRFs for the collection of all data required by the study 3) develop
data dictionaries for each eCRF that will comprehensively define each data element 4) conduct
ongoing data monitoring activities on study data 5) monitor any preliminary analysis data
cleanup activities and 6) rigorously monitor final study data clean up
825 Data Editing
Completed data will be entered into the IPFnet DCC automated data acquisition and
management system If incomplete or inaccurate data are found a data clarification request will
be generated and distributed to clinical centers for a response Clinical centers will resolve data
inconsistencies and errors and enter all corrections and changes into the IPFnet DCC automated
data acquisition and management system
826 Training
The training plan for clinical center staff includes provisions for training on assessments eCRF
completion guidelines data management procedures and the use of computerized systems
56
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
9 Study Design and Data Analysis
91 General Analytic Considerations
All primary analyses will be based on intent-to-treat (ITT) principles using all randomized
subjects Baseline factors across groups will be compared using mean (standard deviation) and
median (25th and 75th percentiles) summary measures Kaplan-Meier curves will be used to
display event rates Due to clinical interest in departures from both sides of the null hypothesis
all test statistics will be 2-sided
Reasonable caution needs to be taken when conducting multiple analyses on key clinical
subgroups For subgroup analyses a conservative significance level of 0001 will be used for all
interaction tests Thus subgroup comparisons will be considered exploratory unless the p-value
from the interaction test is smaller than 0001
92 Randomization Blinding and Reporting of Results
A permuted block-randomization scheme will be created with varying block sizes stratified by
clinical center Once a subject has completed the screening and baseline period and evaluation
for inclusionexclusion criteria the randomization process will begin Subjects will be
randomized to receive NAC or matching placebo with equal probability (11) via telephone
contact with a central interactive voice response system (IVRS) using a toll-free randomization
number On the day of randomization after the subject has successfully met all inclusion and
exclusion criteria the investigator or designee will call the central randomization number to
obtain the assigned kit randomization numbers for that subject At each subject visit the
investigator or designee will call the central randomization number to obtain the new kit
randomization numbers for resupply of the subject For resupply of the clinical center the IVRS
will monitor minimal volume of a kit type andor expiration date and will automatically notify
the pharmacy
57
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
The trial results will be reported according to guidelines specified in the CONSORT statement
A flow diagram describing screening recruitment randomization dropout and vital status will
be included in the primary manuscript AEs and efficacy data will be presented for all treatment
groups Adherence dropout and lost to follow-up will be carefully examined across all treatment
groups Analyses of safety will be based on data from all randomized subjects who received at
least one dose of study drug
93 Stratification
Subjects will be distributed to the two treatment arms in a 11 allocation ratio Stratification
blocks will be based on clinical centers
94 Specification of the Primary Analyses
A mixed model repeated measures (MMRM) analysis described in section 95 will be used to
compare differences in the slope of FVC measurements across the treatment groups Response
variables are values of the FVC measured at baseline and every 15 weeks until study completion
Variables in the model will include treatment time and time by treatment age sex race and
height Contrast estimates of differences in slopes of treatment over time (along with confidence
intervals) will be used to estimate the treatment effect The validity of this model in terms of
meeting modeling assumptions will be assessed via standard modeling diagnostics and goodness-
of-fit measures Based on the MMRM framework missing FVC data will not be imputed for the
primary analysis
95 Analysis of Longitudinal Endpoints
A common goal in clinical trials is to specify models that are easily implemented and
reproducible by independent data analysts On the other hand the models should have proper
statistical behavior in terms of low bias and high precision Many common approaches to
longitudinal data analysis including last observation carried forward (LOCF) imputation rely on
the missing completely at random (MCAR) assumption However the MCAR assumption is
58
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
unlikely to hold in many clinical trials because missing data are often related to disease
progression and prognosis A more reasonable assumption missing at random (MAR) specifies
that the complete data distribution can be modeled using only the observed data The likelihood-
based MMRM approach is valid under the more general MAR assumptions These models will
be applied to analyze the longitudinal data secondary endpoints
The advantages of MMRM analysis are that all important characteristics of the model can be preshy
specified standard software can be used to implement the models and results are based on ITT
principles43 In addition the MMRM approach offers superior control of Type I and Type II
errors compared with the LOCF approach
Response variables are values of the PFTs measured at enrollment and every 15 weeks until
study completion and 6MWT values measured at baseline week 30 and week 60 Covariates are
treatment time time by treatment and key baseline risk factors Contrasts (along with
confidence intervals) of treatment by time will be used to estimate the treatment effect
The correlation structure involves multiple pieces including measurement errors random
variation and interindividual variability For the longitudinal data analyses an unstructured
correlation matrix for within-subject errors will be assumed Other correlation structures
including compound symmetry will be examined as needed A careful examination of reasons
for study discontinuation will be conducted to assess the validity of MCAR Sensitivity analyses
will be used to examine the untestable assumption that the observed data violate the MAR
assumption The MMRM models will be implemented using PROC MIXED in SAS
96 Analysis of Binary Time-to-Event and Time-Lagged Endpoints
Regression modeling approaches using either the logistic regression model or Cox proportional
hazards regression model will be employed when appropriate The validity of these models will
be assessed via standard modeling diagnostics and goodness-of-fit measures Estimates of
cumulative frequencies for more general time-lagged responses will be calculated using the
partitioned version of the Bang-Tsiatis estimator44 The partitions will be set at 15-week intervals
59
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
to correspond with the data-collection process Covariate adjusted event rates will be calculated
using inverse probability-weighted regression estimates45
97 Power Analysis
971 Primary Analyses
Based on previously published IPF clinical trials the PL group is expected to experience a drop
in FVC of approximately 020 L over the study period (see Figure 1) The IPFnet Steering Group
determined a clinically important difference would be to preserve the majority of the decline
relative to PL over the study period In particular a treatment effect of 015 L was determined to
be a clinically meaningful difference Potential dropout is a key factor in the proposed study The
drop-out process assumed 5 lost to follow-up after every study visit Only 80 of subjects
were assumed to be followed for the entire study period All models assumed a compound
symmetry structure for the covariance matrix Power calculations were performed using a SAS
IML program for designing repeated measures studies46 Based on preliminary reviews of the
data from the University of Michigan the covariance matrix parameters were estimated at
approximately σ2 = 0757 (variance parameter) and ρ = 0936 (correlation parameter) To be
conservative the power calculations for the primary analysis were performed with parameter
setting of σ2 = 0810 (variance parameter) and ρ = 0925 (correlation parameter)
The power calculations assume a correction for imperfect compliance proposed by Lachin and
Foulkes to allow for 2 noncompliance for each of the treatment arms47 Thus the sample size
of 130 subjects per arm would be reduced to an adjusted sample size of 130(1-002-002)2 =
1198 or 120 subjects per arm
Under the assumed Type I error rate of 005 with a correlation parameter of 0925 and standard
deviation of 090 the difference of 015 L (or 00025 Lweek) shown in Table 6 would have
power of 93
60
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Table 6 Hypothetical Values of Mean FVC (L) Change from Baseline
Week 15 Week 30 Week 45 Week 60
NAC 00125 00250 00375 00500
Placebo 00500 01000 01500 02000
Difference 00375 00750 01125 01500
Abbreviations FVC forced vital capacity PL placebo
972 Power Analysis for Secondary Endpoints
Power calculations for secondary endpoint measurements are shown in Table 7 Standard
deviations are based on unpublished data provided by the University of Michigan The
calculations are based on a 2-sample t-test with Type I error rate set at 005 These calculations
are likely to be conservative because the statistical approach described in section 95 for
analyzing these endpoints will incorporate incomplete observations as well as intermediate data
points
Table 7 Detectable Differences in Treatment Means for Selected Endpoint Measurements
Secondary Endpoints Std Dev
of the Baseline Score
Detectable Difference for 80 Power
Std Dev of the Change Score
Difference Detectable for
80 Power
DLCOpred 166 58 91 32
6MWT Area Under the Desaturation Curve
219 76 175 61
6MWT Distance to Desaturation 224 78 315 110
6MWT Minutes Walked 210 073 205 071
Abbreviations Std Dev standard deviation DLCOpred diffusing capacity of the lung for carbon monoxide percent predicted 6MWT 6-minute walk test
61
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
10 Study Administration
101 Cooperative Agreement Mechanism
The administrative and funding mechanism used to undertake this project is a ldquocooperative
agreementrdquo (U01) which is an assistance mechanism Under the cooperative agreement the
NHLBI assists supports andor stimulates the project and is substantially involved with
investigators in conducting the study by facilitating performance of the effort in a ldquopartnerrdquo role
The NHLBI project scientist serves on the IPFnet Steering Group and he or another NHLBI
scientist may serve on other project committees when appropriate At the same time however
NHLBI does not assume a dominant role direction or prime responsibility for this research
program
As described below governance of the project is conducted through the IPFnet Steering Group
Principal investigators have lead responsibilities in all aspects of their trials and the project
including any modification of trial designs conduct of the trials quality control data analysis
and interpretation preparation of publications and collaboration with other investigators unless
otherwise provided for by the IPFnet Steering Group
PIs retain custody of and have primary rights to their center-specific and collaborative data
subject to government rights-of-access consistent with current Health amp Human Services (HHS)
Public Health Service (PHS) and National Institutes of Health policies The protocols and
governance policies call for the continual submission of data centrally to the IPFnet DCC for the
collaborative database which at a minimum will contain the key variables selected by the IPFnet
Steering Group for standardization across all clinical centers the submission of copies of the
collaborative datasets to each PI upon completion of the project procedures for data analysis
reporting and publication and procedures to protect and ensure the privacy of medical and
genetic data and records of individuals The NHLBI project scientist on behalf of the NHLBI
will have the same access privileges and responsibilities regarding the collaborative data as the
other members of the Steering Group
62
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
PIs are also encouraged to publish and to publicly release and disseminate results data and other
products of the project concordant with the project protocols and governance and the approved
plan for making data and materials available to the scientific community and to the NHLBI
However during the 3 years after the ending date of NHLBI project support unpublished data
unpublished results data sets not previously released and other study materials or products are
to be made available to any third party only with the approval of the IPFnet Steering Group
Upon completion of the project PIs are expected to put their intervention materials and
procedure manuals into the public domain andor make them available to other investigators
according to the approved plan for making data and materials available to the scientific
community and the NHLBI for the conduct of research at no charge other than the costs of
reproduction and distribution
The NHLBI reserves the right to terminate or curtail the project (or an individual award) in the
event of (a) failure to develop or implement mutually agreeable collaborative measurement
subject eligibility and data management sections of the protocols (b) substantial shortfall in
subject recruitment follow-up data reporting or quality control or other major breach of
protocol (c) substantive changes in the agreed-upon protocols with which NHLBI cannot
concur (d) reaching a major project outcome with persuasive statistical significance
substantially before schedule or (e) human subject ethical issues that may dictate a premature
termination
Any disagreement that may arise in scientificprogrammatic matters (within the scope of the
award) between award recipients and the NHLBI may be brought to arbitration An arbitration
panel will be composed of 3 membersmdash1 selected by the IPFnet Steering Group (with the
NHLBI member not voting) or by the individual PI in the event of an individual disagreement a
second selected by NHLBI and the third selected by the other 2 members This special
arbitration procedure in no way affects the PIrsquos right to appeal an adverse action that is otherwise
appealable in accordance with the PHS regulations at 42 CFR part 50 Subpart D and HHS
63
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
regulation at 45 CFR part 16 or the rights of the NHLBI under applicable statutes regulations
and terms of the award
102 IPFnet Steering Group
The IPFnet Steering Group is the main governing body of the project It is composed of the PIs
of the clinical centers the PI of the DCC and the NHLBI project scientist The clinical centers
the IPFnet DCC and the NHLBI each have 1 vote on the IPFnet Steering Group All decisions
are determined by majority vote
All major scientific decisions are determined by the IPFnet Steering Group It assumes overall
responsibility for the design and conduct of the trial It appoints (and disbands) committees and
subcommittees as the need arises designs approves and implements the study protocols
oversees the development of the MOOP monitors subject recruitment and treatment delivery
evaluates data collection and management oversees quality assurance procedures and
implements changes and enhancements to the study as required It also has primary responsibility
for facilitating the conduct of the trials and reporting the projectrsquos results
103 Data and Safety Monitoring Board
The NHLBI will establish a DSMB in accordance with established policies (see
httpwwwnhlbinihgovfundingpoliciesdsmb_insthtm) to ensure data quality and subject
safety and to provide independent advice to the NHLBI regarding progress and the
appropriateness of study continuation
104 Recommendations on Interim Monitoring of Efficacy Safety and Futility
First and foremost the role of the DSMB will be to review subject safety and trial conduct at
periodic points during the study The DSMB may require analyses of the primary endpoint
results for comparing the benefit and risks of treatment strategies The benefit of collecting
additional data on key secondary endpoints with extended follow-up and establishing a robust
64
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
evidence base for determining a standard of care will need to be carefully considered before
early termination of one or more treatment arms After careful consideration the IPFnet Steering
Group recommends conservative thresholds for the early examinations of the safety and efficacy
data
The DSMB will be expected to meet approximately every 6 months until trial completion to
review safety and toxicity data The DSMB may recommend stopping the study based on these
reviews Because the DSMB could stop the trial for safety concerns as well as for a large
efficacy benefit there could be multiple opportunities to reject the null hypothesis (no difference
in event rates between the PL and NAC groups) A Bonferroni approximation will be applied
during the one planned interim analysis for efficacy
Before locking the database a statistical analysis plan (SAP) will be developed to provide
complete details on the statistical analysis The SAP will include the specifics for how and when
the DSMB will be notified for AEs The IPFnet DCC will deliver to the DSMB all FDA-defined
AEs at 3-month intervals The IPFnet DCC will prepare narrative SAE reports in real time for
DSMB review including recommendations and analysis of similar events for each SAE
submitted to the FDA
65
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
11 Investigator and Sponsor Obligations
111 Monitoring
All monitoring activities for US clinical centers will be performed in accordance with DCRI
standard operating procedures Information regarding the types of visits will be outlined in the
PANTHER-IPF MOOP
112 Cost and Payment
There will be no cost to subjects enrolled in this trial Study-related procedures will be paid for
by the IPFnet
Subjects may be eligible for reimbursement for travel to the clinical center Details of payment
will be explained to each subject during the consent process
113 Confidentiality and Health Insurance Portability and Accountability Act
Considerations
Subject confidentiality will be protected throughout the study All subject data will be kept
strictly confidential and no subject-identifying information will be released to anyone outside
the project Confidentiality will be assured through several mechanisms First each subject will
be assigned an anonymous study ID which will then be used on all study forms Second any
study forms blood samples and paper records that contain subject information (eg address lists
phone lists) will be kept at the clinical centers in secured locked areas coded by number Once
blood is collected there will be no subject identifiers placed on blood samplesmdashonly the study
ID number and the date of sample collection Third access to all subject data and information
including laboratory specimens will be restricted to authorized personnel In the case of
computerized data this restricted access will be assured through user logon IDs and password
protection
66
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
At the IPFnet DCC only authorized personnel will have access to the data files containing study
data Security will be assured through user logon IDs passwords and appropriate access
privileges All study subjects will be identified only by their IPFnet ID numbers and no personal
identifying information such as name address or Social Security number will be entered into
the IPFnet DCC database Any subject-specific data reported to the IPFnet Steering Group will
be identified only by the IPFnet ID number
Finally subjects will not be identified by name in any reports or publications nor will the data
be presented in such a way that the identity of individual subjects can be inferred Analysis files
created for further study by the scientific community will have no subject identifiers These data
files will be created in accordance with the Ancillary Studies and Publication Policy of the
IPFnet
114 Informed Consent Procedures
All IPFnet subjects will provide written informed consent using procedures reviewed and
approved by each clinical centerrsquos IRB Informed consent will be undertaken by study personnel
in-person with the subject The subject has the option of declining further participation in the
study at that point No further study procedures will be conducted until the signed documents
have been provided to the IPFnet clinical center
115 Institutional Review Boards
Before initiating this study the protocol clinical center-specific informed consent forms Health
Insurance Portability and Accountability Act (HIPAA) forms recruitment materials and other
relevant information will be reviewed by a properly constituted IRB at each participating clinical
center A copy of the signed and dated IRB approval at each clinical center will be retrieved prior
to or during the site initiation visit and archived at the IPFnet DCC Any amendments to the
protocol other than simple administrative and typographical changes must be approved by each
IRB before they are implemented The clinical centers will seek annual renewals of their IRB
approvals in accordance with local procedures
67
__________________________________________ ________________
__________________________________________
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
12 Investigator Agreement
I have read the foregoing protocol PANTHER-IPF and agree that it contains all necessary
details for carrying out this study I will conduct the study as outlined herein and will complete
the study within the time designated
I will provide copies of the protocol and all pertinent information to all individuals responsible to
me who assist in the conduct of this study I will discuss this material with them to ensure they
are fully informed regarding the drug and the conduct of the study
I will fulfill all responsibilities for submitting pertinent information to the local IRB if
applicable that is responsible for this study
I further agree that NHLBI andor DCRI will have access to any source documents from which
eCRF information may have been generated
Signature of Principal Investigator Date
Name of Principal Investigator (printed or typed)
Protocol version date May 19 2009
Protocol Amendment 1 version date May 28 2010
Protocol Amendment 2 version date December 6 2011
68
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
13 References
1 Raghu G Brown KK Bradford WZ et al A placebo-controlled trial of interferon gamma-1b in patients with idiopathic pulmonary fibrosis N Engl J Med 2004350125-33 2 King TE Jr Safrin S Starko KM et al Analyses of efficacy end points in a controlled trial of interferon-gamma1b for idiopathic pulmonary fibrosis Chest 2005127171-7 3 Flaherty KR Thwaite EL Kazerooni EA et al Radiological versus histological diagnosis in UIP and NSIP survival implications Thorax 200358143-8 4 Wells AU Desai SR Rubens MB et al Idiopathic pulmonary fibrosis a composite physiologic index derived from disease extent observed by computed tomography Am J Respir Crit Care Med 2003167962-9 5 Raghu G Freudenberger TD Yang S et al High prevalence of abnormal acid gastroshyoesophageal reflux in idiopathic pulmonary fibrosis Eur Respir J 200627136-42 6 Kinnula VL Focus on antioxidant enzymes and antioxidant strategies in smoking related airway diseases Thorax 200560693-700 7 Coultas DB Zumwalt RE Black WC Sobonya RE The epidemiology of interstitial lung diseases Am J Respir Crit Care Med 1994150967-72 8 Raghu G Weycker D Edelsberg J Bradford WZ Oster G Incidence and prevalence of idiopathic pulmonary fibrosis Am J Respir Crit Care Med 2006174810-6 9 Olson AL Swigris JJ Lezotte DC Norris JM Wilson CG Brown KK Mortality from pulmonary fibrosis increased in the United States from 1992 to 2003 Am J Respir Crit Care Med 2007176277-84 10 Mannino DM Etzel RA Parrish RG Pulmonary fibrosis deaths in the United States 1979shy1991 An analysis of multiple-cause mortality data Am J Respir Crit Care Med 19961531548shy52 11 Hubbard R Johnston I Coultas DB Britton J Mortality rates from cryptogenic fibrosing alveolitis in seven countries Thorax 199651711-6 12 Johnston I Britton J Kinnear W Logan R Rising mortality from cryptogenic fibrosing alveolitis Bmj 19903011017-21 13 Raghu G Collard HR Egan JJ et al An official ATSERSJRSALAT statement idiopathic pulmonary fibrosis evidence-based guidelines for diagnosis and management Am J Respir Crit Care Med 2011183788-824 14 (USA) FDA FDA Public Health Advisory Interferon gamma-1b (marketed as Actimmune) In 2007 15 King TE Jr Pardo A Selman M Idiopathic pulmonary fibrosis Lancet 2011 16 Raghu G Brown KK Costabel U et al Treatment of idiopathic pulmonary fibrosis with etanercept an exploratory placebo-controlled trial Am J Respir Crit Care Med 2008178948shy55 17 Malouf MA Hopkins P Snell G Glanville AR An investigator-driven study of everolimus in surgical lung biopsy confirmed idiopathic pulmonary fibrosis Respirology 201116776-83 18 King TE Jr Behr J Brown KK et al BUILD-1 a randomized placebo-controlled trial of bosentan in idiopathic pulmonary fibrosis Am J Respir Crit Care Med 200817775-81 19 Richeldi L Costabel U Selman M et al Efficacy of a tyrosine kinase inhibitor in idiopathic pulmonary fibrosis N Engl J Med 20113651079-87
69
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
20 Borok Z Buhl R Grimes GJ et al Effect of glutathione aerosol on oxidant-antioxidant imbalance in idiopathic pulmonary fibrosis Lancet 1991338215-6 21 Meyer A Buhl R Magnussen H The effect of oral N-acetylcysteine on lung glutathione levels in idiopathic pulmonary fibrosis Eur Respir J 19947431-6 22 Behr J Maier K Degenkolb B Krombach F Vogelmeier C Antioxidative and clinical effects of high-dose N-acetylcysteine in fibrosing alveolitis Adjunctive therapy to maintenance immunosuppression Am J Respir Crit Care Med 19971561897-901 23 Cantin AM North SL Fells GA Hubbard RC Crystal RG Oxidant-mediated epithelial cell injury in idiopathic pulmonary fibrosis J Clin Invest 1987791665-73 24 Waghray M Cui Z Horowitz JC et al Hydrogen peroxide is a diffusible paracrine signal for the induction of epithelial cell death by activated myofibroblasts Faseb J 200519854-6 25 Larios JM Budhiraja R Fanburg BL Thannickal VJ Oxidative protein cross-linking reactions involving L-tyrosine in transforming growth factor-beta1-stimulated fibroblasts J Biol Chem 200127617437-41 26 Kinnula VL Fattman CL Tan RJ Oury TD Oxidative stress in pulmonary fibrosis a possible role for redox modulatory therapy Am J Respir Crit Care Med 2005172417-22 27 Meyer A Buhl R Kampf S Magnussen H Intravenous N-acetylcysteine and lung glutathione of patients with pulmonary fibrosis and normals Am J Respir Crit Care Med 19951521055-60 28 Behr J Degenkolb B Krombach F Vogelmeier C Intracellular glutathione and bronchoalveolar cells in fibrosing alveolitis effects of N-acetylcysteine Eur Respir J 200219906-11 29 Bando M Hosono T Mato N et al Long-term efficacy of inhaled N-acetylcysteine in patients with idiopathic pulmonary fibrosis Intern Med 2010492289-96 30 Demedts M Behr J Buhl R et al High-dose acetylcysteine in idiopathic pulmonary fibrosis N Engl J Med 20053532229-42 31 Toma TP Bhowmik A Rajakulasingam R Acetylcysteine in pulmonary fibrosis N Engl J Med 20063541086-9 author reply -9 32 Hunninghake GW Antioxidant therapy for idiopathic pulmonary fibrosis N Engl J Med 20053532285-7 33 Flaherty KR Mumford JA Murray S et al Prognostic implications of physiologic and radiographic changes in idiopathic interstitial pneumonia Am J Respir Crit Care Med 2003168543-8 34 Latsi PI du Bois RM Nicholson AG et al Fibrotic idiopathic interstitial pneumonia the prognostic value of longitudinal functional trends Am J Respir Crit Care Med 2003168531-7 35 Collard HR King TE Jr Bartelson BB Vourlekis JS Schwarz MI Brown KK Changes in clinical and physiologic variables predict survival in idiopathic pulmonary fibrosis Am J Respir Crit Care Med 2003168538-42 36 Jegal Y Kim DS Shim TS et al Physiology is a stronger predictor of survival than pathology in fibrotic interstitial pneumonia Am J Respir Crit Care Med 2005171639-44 37 Martinez FJ Safrin S Weycker D et al The clinical course of patients with idiopathic pulmonary fibrosis Ann Intern Med 2005142963-7 38 Hull JH Acetylcysteine in pulmonary fibrosis N Engl J Med 20063541089-91 author reply -91
70
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
39 Flaherty KR King TE Jr Raghu G et al Idiopathic interstitial pneumonia what is the effect of a multidisciplinary approach to diagnosis Am J Respir Crit Care Med 2004170904shy10 40 Raghu G Johnson WC Lockhart D Mageto Y Treatment of idiopathic pulmonary fibrosis with a new antifibrotic agent pirfenidone results of a prospective open-label Phase II study Am J Respir Crit Care Med 19991591061-9 41 Hunninghake GW Lynch DA Galvin JR et al Radiologic findings are strongly associated with a pathologic diagnosis of usual interstitial pneumonia Chest 20031241215-23 42 Lynch D Godwin J Safrin S et al High-resolution computed tomography in idiopathic pulmonary fibrosis diagnosis and prognosis Am J Respir Crit Care Med 2005172488-93 43 Mallinckrodt CH Watkin JG Molenberghs G Carroll RJ Choice of the primary analysis in longitudinal clinical trials Pharmaceutical Statistics 20043161-9 44 Bang H Tsiatis A Estimating medical costs with censored data Biometrika 200087329shy43 45 Lin DY Regression analysis of incomplete medical cost data Stat Med 2003221181-200 46 Rochon J Application of GEE procedures for sample size calculations in repeated measures experiments Stat Med 1998171643-58 47 Lachin JM Foulkes MA Evaluation of sample size and power for analyses of survival with allowance for nonuniform patient entry losses to follow-up noncompliance and stratification Biometrics 198642507-19
71
- PANTHER-IPFPREDNISONE AZATHIOPRINEAND N-ACETYLCYSTEINEA STUDY THAT EVALUATES RESPONSE INIDIOPATHIC PULMONARY FIBROSIS
-
- Protocol Summary
- Table of Contents
- List of Tables
- List of Figures
- List of Abbreviations
- 1 Summary
- 2 Hypotheses and Specific Aims
-
- 21 Null Hypothesis
- 22 Specific Aim 1
- 23 Specific Aim 2
- 24 Prespecified Subgroups of Interest
-
- 3 Background and Significance
-
- 31 Idiopathic Pulmonary Fibrosis is the Most Common Interstitial Lung Disease
- 32 Rationale for Placebo Control
- 33 Rationale for N-acetylcysteine
- 35 Rationale for N-acetylcysteine as a Stand-alone Therapy
- 36 Rationale for the Study Design and Primary Endpoint
- 37 Rationale for Blinding of Treatments
-
- 4 Methods
-
- 41 Inclusion Criteria
- 42 Diagnosis of IPF
- 43 Exclusion Criteria
- 44 Study Design and Study Visit
- 45 Dose Justification
- 46 Contraindications Precautions and Side Effects of Study Medications
- 47 Recruitment Procedures
- 48 Study Procedures
- 49 Concomitant Medications
- 410 Laboratory Testing
- 411 Blinding of Study Drugs
-
- 5 Study Endpoints
-
- 51 Primary Study Endpoint
- 52 Secondary Study Endpoints
-
- 6 Safety Evaluations and Procedures
-
- 61 Adverse Events
- 62 Clinical Medical Monitoring
- 63 Unblinding Procedures
-
- 7 Study Drug Procedures
- 8 Data Management
-
- 81 Hardware and Software Configuration
- 82 Sources of Data
-
- 9 Study Design and Data Analysis
-
- 91 General Analytic Considerations
- 92 Randomization Blinding and Reporting of Results
- 93 Stratification
- 94 Specification of the Primary Analyses
- 95 Analysis of Longitudinal Endpoints
- 96 Analysis of Binary Time-to-Event and Time-Lagged Endpoints
- 97 Power Analysis
-
- 10 Study Administration
-
- 101 Cooperative Agreement Mechanism
- 102 IPFnet Steering Group
- 103 Data and Safety Monitoring Board
- 104 Recommendations on Interim Monitoring of Efficacy Safety and Futility
-
- 11 Investigator and Sponsor Obligations
-
- 111 Monitoring
- 112 Cost and Payment
- 113 Confidentiality and Health Insurance Portability and Accountability ActConsiderations
- 114 Informed Consent Procedures
- 115 Institutional Review Boards
-
- 12 Investigator Agreement
- 13 References
-

PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
expertise from clinicians radiologists and pathologists Investigators at each site in conjunction with central
pathology will work together to establish the diagnosis of IPF This interactive approach to the diagnosis of IPF
increases the level of agreement between observers39
A subject with suspected ILD should be evaluated for secondary causes including but not limited to
environmental exposures drugs and systemic diseases Presence of any of these findings felt to be significant
enough to cause an ILD should disqualify the subject from entry into the trial
If secondary causes are absent an HRCT scan may be obtained If an HRCT of sufficiently high quality has
been obtained within the last 3 months that scan may be used for diagnosis In the appropriate clinical setting
the diagnosis of IPF can be made by the demonstration of a typical radiographic pattern on HRCT or by
demonstration of UIP pattern on a surgical lung biopsy The following criteria for a radiographic (ie
nonsurgical) diagnosis will be used In the absence of known exposures andor clinical associations attributable
to pulmonary fibrosis and in the appropriate clinical setting the presence of definite UIP pattern in HRCT
images is required to meet study criteria for the diagnosis of IPF
Figure 2 Diagnosis of Idiopathic Pulmonary Fibrosis in the IPFnet
22
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Figure 3 Pathology Flow Chart Surgical Lung Biopsy Diagnosis
Requirement for diagnosis
1 Clinical exclusion of other known causes (connective tissue diseases environmental and drug
exposures) of ILD
2 Radiographic HRCT with bibasilar reticular abnormality and honeycomb change with minimal
ground glass opacities
Appropriate clinical setting
1 Age gt 50 years
2 Insidious onset of unexplained dyspnea
3 Duration of illness for ge 3 months
4 Bibasilar inspiratory crackles
23
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Unlike the ATSERS consensus criteria published in 2000 bronchoscopy will not be required for diagnosis
This decision was made based on the experience of the IPFnet Steering Group members regarding the utility of
bronchoscopy in the diagnosis of IPF The presence of an atypical HRCT finding will require documentation of
a definitive diagnosis by surgical lung biopsy In fact this is in keeping with the recently published evidence
based guidelines for diagnosis and management of IPF13 As shown in Figure 3 central review of the pathology
data will be required for a diagnosis of IPF
We will not require central review of HRCT as several studies have shown that a confident local interpretation
of clinicalHRCT criteria as definite IPFUIP is associated with a high positive predictive value for finding UIP
at surgical lung biopsy (see Table 1) Differences in sensitivity in these series likely reflect subject selection as
Flaherty et al3 evaluated only UIP and nonspecific interstitial pneumonia (NSIP) while Raghu et al40 and
Hunninghake et al41 included a broader range of ILD
Table 1 Operating Characteristics of Local HRCT Review for Diagnosis of UIP
Researcher of Subjects Sensitivity () Specificity () PPV () NPV ()
Raghu et al 40
59 (29 UIP by SLB) 78 90 88 82
Hunninghake et al 41 91 (54 UIP by SLB)
74 81 85 67
Flaherty et al 3 96 (only NSIP amp UIP)
37 100 100 30
Abbreviations PPV positive predictive value NPV negative predictive value UIP usual interstitial pneumonia SLB surgical lung biopsy and NSIP nonspecific interstitial pneumonia
Furthermore an analysis of the HRCT scans from subjects enrolled in the GIPF-001 trial confirmed that local
site interpretations have a high congruity to a central radiology core In this multi-center study 263 HRCT
scans were read as definite IPF and a retrospective central radiology core review found 932 to be consistent
with IPF 42 We will also take several additional steps to insure that the local HRCT reads are accurate
including
1 A detailed training module has been developed and must be completed by each site radiologist before
site initiation
2 Clinical centers are to mail all HRCT scans to the HRCT core lab The first 10 HRCT scans from
subjects enrolled at each enrolling clinical center will be reviewed centrally to be certain that local reads
24
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
25
are congruent with a central interpretation If discrepancies are identified additional education will be
provided and HRCT scans will continue to be reviewed centrally until the central radiology core is
confident that the local center is performing appropriately
3 Random scans will be obtained from each center throughout the study to confirm that the local read
continues to agree with central interpretation If discrepancies are identified they will be addressed as in
2 above
In all cases if a subject has a surgical lung biopsy sample that sample will be reviewed by the local and central
pathologists Therefore the only cases that would not be subject to a direct central review process are those
where the HRCT meets the centrally defined criteria for an unequivocal diagnosis and a lung biopsy sample is
not available Table 2 below summarizes the possible combinations for making a diagnosis
Table 2 Combining HRCT and Pathology Interpretations to Determine if IPF is Present
HRCT Diagnosis Pathology Diagnosis Diagnosis of IPF
Definite UIP Definite UIP Yes
Definite UIP Probable UIP Yes
Definite UIP Possible UIP Yes
Definite UIP Not UIP No
Definite UIP Unavailable Yes
Consistent with UIP Definite UIP Yes
Consistent with UIP Probable UIP Yes
Consistent with UIP Possible UIP No
Consistent with UIP Not UIP No
Consistent with UIP Unavailable No
Inconsistent with UIP Any No
Abbreviations HRCT high-resolution computed tomography IPF idiopathic pulmonary fibrosis
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
UIP usual interstitial pneumonia Dx diagnosis 43 Exclusion Criteria
1 History of clinically significant environmental exposure known to cause pulmonary fibrosis
Occupational exposures such as asbestos or environmental exposure to organic dust such as occurs in
pigeon breeders may at times mimic the clinical and radiographic findings of IPF
2 Diagnosis of connective tissue disease felt by the principal investigator (PI) to be the etiology of the
interstitial disease Diagnosis of collagen-vascular conditions will be according to the published
American College of Rheumatology criteria As such the presence of any documented collagen-vascular
disorder or the presence of any suspicious symptom complex whether or not associated with
significantly abnormal rheumatological serologies will exclude the subject at the discretion of the PI
3 Extent of emphysema greater than the extent of fibrotic change (honeycombing reticular changes) on
HRCT scan
4 Forced expiratory volume in 1 second (FEV1)FVC ratio lt 065 at screening (postbronchodilator)
5 Partial pressure of arterial oxygen (PaO2) on room air lt 55 mm Hg (lt 50 mm Hg at Denver site)
6 Residual volume gt 120 predicted at screening (postbronchodilator)
7 Evidence of active infection
8 Significant bronchodilator response on screening spirometry defined as a change in FEV1 ge 12 and
absolute change gt 200 mL OR change in FVC ge 12 and absolute change gt 200 mL The percent
difference between the FVC (or FEV1) values will be calculated by taking the absolute value of the
difference and dividing it by the larger of the two FVC (or FEV1) values
9 Screening and enrollment post-bronchodilator FVC measurements (in liters) differing by gt 11 The
percent difference between the FVC values will be calculated by taking the absolute value of the
difference and dividing it by the larger of the two FVC values (eg the percent difference between FVC
measurements of 19 and 20 liters would be determined by taking the difference between the two (01
liters) and dividing by the larger of the two (20 liters) So 0120 = 5 and these FVC measurements
would not exclude the subject
10 Listed for lung transplantation ie the patient has completed the evaluation process has been accepted
as a candidate for transplantation at an appropriate center and is waiting to receive notification of an
available donor organ
11 History of unstable or deteriorating cardiac disease
12 Myocardial infarction coronary artery bypass or angioplasty within 6 months of screening
26
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
13 Unstable angina pectoris or congestive heart failure requiring hospitalization within 6 months of
screening
14 Uncontrolled arrhythmia
15 Severe uncontrolled hypertension
16 Known HIV or hepatitis C
17 Known cirrhosis and chronic active hepatitis
18 Active substance andor alcohol abuse (as determined by site PI)
19 Pregnancy or lactation (subjects who are pregnant or breastfeeding)
20 Known hypersensitivity to study medication
21 Any condition other than IPF that in the opinion of the site PI is likely to result in the death of the
subject within the next year
22 Any condition that in the judgment of the PI might cause participation in this study to be detrimental to
the subject or that the PI deems makes the subject a poor candidate
23 Any therapy directed at pulmonary fibrosis (excepting triple therapy of prednisone plus azathioprine
plus NAC) requires a 30-day washout period before randomized Triple therapy of lt= 12 weeks duration
in the past 4 years requires a 30-day washout period before randomization
24 History of triple therapy of prednisone plus azathioprine plus NAC for gt 12 weeksrsquo duration in the past
4 years or previous enrollment in the triple-therapy arm of the PANTHER-IPF study
44 Study Design and Study Visit
441 Study Design Summary
This study will be a randomized double-blind PL-controlled trial designed to assess the safety and efficacy of
NAC in subjects with newly diagnosed IPF
Subjects with mild to moderate IPF (defined as FVCpred ge 50 and DLCOpred ge 30) diagnosed within
the past 48 months will be enrolled Screening will continue until April 30 2012
27
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
The study will employ a 2-arm design with 11 randomization to NAC or PL Once enrolled subjects will visit
the clinical center at 15 weeks and 15-week intervals thereafter Each subject will be treated and followed for a
maximum of 60 weeks
During the 60-week visit subjects will be taken off all study agents Approximately four weeks after the final
dose of study agent is taken subjects will receive a safety phone call from the study site
442 Study Visits
Subjects who meet entry criteria will review the informed consent a written description of the purpose
procedures and risks of the study with the PI co-investigator or study coordinator and all questions will be
answered The informed consent form will be signed by the subject at screening No protocol-specific
procedures will be performed until the subject has signed and dated an informed consent form This includes the
screening procedures
4421 Screening
Once informed consent is obtained subjects may immediately begin the screening process or may return within
28 days of consent In the event a study subject has been clinically evaluated at the study site by an IPFnet study
physician and has performed testing within three weeks for this clinical evaluation that meets guidelines
provided in the IPFnet PANTHER-IPF Manual of Operating Procedures (MOOP) this testing may be used to
satisfy the following screening criteria medical history physical exam arterial blood gas (ABG) with A-a
gradient vital signs with oximetry body height and weight spirometry DLCO lung volumes and HRCT scan
Allowing the use of previously performed test results that meet study guidelines for the screening visit is
intended to permit subjects easier access to study entry to prevent subjects from repeating testing that has been
performed within the study window and to decrease risks to subjects from repeated exposure to procedures
such as arterial puncture and HRCT
The following procedures will be performed at screening
Medical history and a physical examination
28
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Measure height and weight
Serum pregnancy test (if applicable)
Measure vital signs including oximetry
Blood draws performed and the following analyses conducted
o Hematology (red cell count white cell count hemoglobin hematocrit cell indices differential
platelet count)
o Blood chemistries according to central laboratory protocol (see Section 410 Laboratory
Testing)
o Beta human chorionic gonadotropin (serum) pregnancy test (in women of childbearing potential)
o Urinalysis
Pulmonary Function Tests (PFTs) including spirometry pre- and post- bronchodilator and postshy
bronchodilator measurement of lung volumes and measurement of hemoglobin adjusted diffusing
capacity
Measure ABGs
HRCT if a satisfactory scan has not been performed on the subject within 3 months of screening (see
PANTHER-IPF MOOP for more details)
Surgical lung biopsies (if applicable) reviewed by local and central pathology departments
Current medications If required a washout period discussed with the subject and initiated at this visit
4422 Enrollment
The enrollment visit is expected to take place within eight weeks of the screening visit Enrollment visit
activities include
Measure vital signs including oximetry
Measure height and weight
Serum pregnancy test (if applicable)
If consent has been given blood will be drawn and a urine specimen collected for the bio-specimen
repository
Spirometry (post-bronchodilator)
Measure 6MWT with Borg Dyspnea Scale
29
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Collect Quality-of-life (QOL) data using the SF-36 EuroQol Investigating Choice Experiments for
Preferences of Older People Capability Instrument (ICE CAP) and SGRQ
Female subjects complete Gender Substudy questionnaire
Dyspnea status collected using the UCSD SOBQ
Evaluate Acute Exacerbation (AEx)
Review of any Adverse Events (AEs)
Review of concomitant medications
Subject receives diary and instructions on its purpose and proper use
Subject receives supply of study drug sufficient to last until his or her 15-week study visit
See the Schedule of Assessments (Table 3) for more details Subjects with screening and enrollment postshy
bronchodilator FVC measurements (in liters) differing by more than 11 are not eligible to be enrolled in the
study
Subjects will be asked to provide a physician of record This physician will be considered the subjectrsquos primary
care provider (PCP) and if the subject agrees the PCP will be informed by letter of the subjectrsquos enrollment in
the trial The subject will be informed that his or her ongoing medical care should be received from the PCP
The PCP will be informed of any safety issues identified by the study staff The PCP will also be given
information regarding communication with study personnel about pertinent health issues or clinic encounters
the subject may have
4423 Week 15
The week 15 visit is expected to occur within +- 14 days of the subjectrsquos scheduled visit time (eg the week 15
visit should occur anytime between 13 and 17 weeks after starting study drug Week 15 activities include
Measure vital signs with oximetry
Measurement height and weight
Serum pregnancy test (if applicable)
Spirometry (post-bronchodilator) measurement
Review of AEs
Evaluate for AEx
30
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Review concomitant medications
If consented draw blood and collect urine specimen for the biospecimen repository
Subjects return used and unused study drug for the visit
Review study diary and a new study diary will be given
Provide additional supply of study drug sufficient to last until the next scheduled visit
4424 Week 30
The week 30 visit is expected to occur within +- 14 days of the subjectrsquos scheduled visit time (eg the week 30
visit should occur anytime between 28 and 32 weeks after starting study drug) Week 30 activities include
Physical examination
Measure vital signs with oximetry
Measure height and weight
Laboratory values (complete blood count [CBC] and serum chemistries)
Serum pregnancy test (if applicable)
Measure spirometry (post-bronchodilator)
6MWT with Borg scale
DLCO
Review of AEs
Evaluate for AEx
Review concomitant medications
Complete all QOL and dyspnea questionnaires (EuroQol ICE CAP SF-36 SGRQ and UCSD SOBQ)
If consent has been given blood will be drawn and a urine specimen collected for the biospecimen
repository
Review study diary
Subjects return used and unused study drug for the visit
Provide additional supply of study drug sufficient to last until the next scheduled visit
4425 Week 45
31
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
The week 45 visit is expected to occur within +- 14 days of the subjectrsquos scheduled visit time (eg the week 45
visit should occur anytime between 43 and 47 weeks after starting study drug) Week 45 activities include
Measure vital signs with oximetry
Measure height and weight
Serum pregnancy test (if applicable)
Measure spirometry (post-bronchodilator)
Review of AEs
Evaluate for AEx
Review concomitant medications
If consent has been given blood will be drawn and a urine specimen collected for the biospecimen
repository
Subjects return used and unused study drug for the visit
Study diary reviewed
Provide additional supply of study drug sufficient to last until the next scheduled visit
4426 Week 60 (Early Withdrawal or Final Treatment Visit)
At week 60 or at subject withdrawal from the study (premature by study doctor or subjectrsquos decision) a final
treatment visit will occur At this final treatment visit subjects will discontinue NACPL abruptly Week 60
activities also include
Physical examination
Measure vital signs with oximetry
Measure height and weight
Laboratory values (complete blood count [CBC] and serum chemistries)
Spirometry (post-bronchodilator) measurement
6MWT with Borg scale measurement
DLCO
Lung volumes
ABG
Review of AEs
32
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Evaluate for AEx
Review concomitant medications
Subjects will complete all QOL and dyspnea questionnaires (EuroQol ICE CAP SF-36 SGRQ and
UCSD SOBQ)
If consent has been given blood will be drawn and a urine specimen collected for the biospecimen
repository
Subjects return used and unused study drug for the visit
Study diary reviewed
4427 Final Site Visit ndash FVC drop confirmation
In the event that the subject has a recorded FVC drop of gt10 from baseline at the final treatment visit and the
subject has not had a confirmation of such a drop at a previous study visit the subject should return to the
clinical site 6 to 8 weeks after the final treatment visit During this visit a post-bronchodilator spirometry test
will be performed This FVC measurement will be evaluated according to section 521 of this protocol
4428 Final Visit ndash Telephone Follow-up
Four weeks following the final dose of study medication subjects will receive a telephone call from the study
coordinator to ensure that there are no side effects and to follow up on any ongoing adverse events (AEs)
4429 Phone Contact Between Visits
At week 2 and each month that a subject does not have a scheduled clinical center visit his or her study
coordinator will contact him or her at least once by telephone to
Inquire if the subject has had any hospitalizations events that might be considered an AE or any events
significant enough to warrant an out-of-cycle visit to the clinical center
Remind subjects of their current dosage levels and confirm that the subject understands them
Address any questions or concerns the subject might have regarding other aspects of the study
Assess adherence to the treatment regimen by reviewing diary data verbal review of medications taken
including nutritional supplements
33
34
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Table 3 Schedule of Assessments
Procedure Screening Visit 0
Enrollment Visit 1
Week 15 Visit 2
Week 30Visit 3
Week 45 Visit 4
Week 60 Early
Withdrawal Visit 5
Final1
Visit (via phone)
Informed consent X
Medical history X
Inclusionexclusion criteria X
Serum pregnancy test (if applicable) X X X X X
Review of lung biopsy X
Arterial Blood Gas X X
6-Minute Walk Test
X
X X
Physical examination X X X
Vital signs with oximetry X X X X X X
Body height and weight X X X X X X
Complete Blood Count X X X
Chemistry panel X X X
Monitor Lab Values X X X
Urinalysis X Specimen repository substudy blood draw and urine collection (if consented)
X
X X X X
HRCT (if not completed within three months) X
Spirometry (pre- and post-bronchodilator) X
Spirometry (post-bronchodilator only) X X X X X
DLCO (post-bronchodilator only) X X X
Lung volumes (post-bronchodilator only) X
X
Evaluate for acute exacerbation X X X X X
Review Adverse Events X X X X X X
Review concomitant meds X X X X X X
Dispense subject diary X X X X
Review subject diary X X X X X
Dispense study agent X X X X
Gender Substudy questionnaire (female subjects only) X
EuroQol ICECAP UCSD SOBQ SGRQ SF-36 X X X
Abbreviations DLCO diffusing capacity of the lung for carbon monoxide QOL Quality of Life ICECAP Investigating Choice Experiments for Preferences of Older People UCSD SOBQ University of California Shortness of Breath Questionnaire SGRQ St Georgersquos Respiratory Questionnaire SF-36 Short Form 36 Health Survey
1Follow-up visit via phone will occur four weeks after final dose of study medication
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
45 Dose Justification
The general philosophy for determining dosing levels was to apply previously examined
treatment regimens With the focus of the study being to establish a standard of care for
mildmoderate IPF subjects the goal was to develop flexible yet standardized treatment rules that
allow for the temporary or permanent withholding of one or more components of treatment when
necessary Subjects developing laboratory abnormalities or symptoms that result in
discontinuation of one or more components of study treatment may continue on the other
components as long as there is no contraindication for this Complete follow-up is important for
the validity of any study As a strategy to maintain protocol adherence we are using a treatment
regimen that will detect potential side effects and prompt interventions proactively in the interest
of patient safety In addition subjects who permanently stop study medications during the course
of the study are encouraged to continue in the study completing all scheduled visits and tests
451 Rationale for N-acetylcysteine Dosing
To our knowledge there have been no IPF studies to correlate clinical outcome measures with
different dosages for NAC The dosage chosen is based on the IFIGENIA study However BAL
lung GSH levels from subjects with IPF have been augmented with the use of oral NAC at 600
mg 3 times per day In addition lung GSH levels have been associated with improved
PFTs212227 The dose chosen for this study was based on previous data including the IFIGENIA
study30
4511 Dosing of N-acetylcysteineplacebo
Dosing of NACPL will be 600 mg orally 3 times a day (1800 mgday)
4512 Reasons to Discontinue N-acetylcysteineplacebo
NACPL may be temporarily or permanently discontinued for the duration of the study for
gastrointestinal symptoms or dermatologic reactions
35
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Temporarily discontinue (hold) oral NACPL for subjects requiring inpatient admission for acute
exacerbation (AEx) or other conditions Resume NACPL after discharge
36
37
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
452 Dosage Algorithms
Dosage Adjustment Algorithm 1 NACPL Dose Modifications for Gastrointestinal Symptoms Nausea Vomiting Abdominal Discomfort Diarrhea
GI Symptoms determined by the PI to be clinically significant Nausea Vomiting Abdominal Discomfort Diarrhea
NACPL Temporarily dc (HOLD) x 3 Days
Monitor symptoms intervene as clinically indicated (eg fluid replacement antidiarrhea or antinausea medication)
Monitor or lab PRN
Are symptoms resolving after 3 days NO
Symptoms NOT resolving after 3 days of holding study medication Assessmentmanagement per clinical
discretion of investigator
Likely not study medication discuss resuming study medication with medical monitor when symptoms resolved
YES
Temporarily dc (HOLD) NACPL for 4 additional days (total hold 1 week) then NACPL Resume 600 MG TID
Did symptoms recur
YES
STOP NACPL for
duration of study
NO
NACPL No Change
38
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Dosage Adjustment Algorithm 2 NACPL Dose Modifications For Dermatologic Reactions
Dermatologic Reactions (Not Acneiform) ge Grade 2 Grading per Common Terminology Criteria for
Adverse Events V30 (httpctepcancergov) For example Grade 1 RASHDESQUAMATION Macular or papular eruption or erythema without associated symptoms Grade 2 RASHDESQUAMATION Macular or popular eruption or erythema with pruritus or other associated symptoms localized desquamation or other lesions covering lt50 of body surface area
NACPL Temporarily dc (HOLD) x 3 days
Are symptoms resolving after 3 days
NO Symptoms not resolving after 3 days of holding study medication Assessmentmanagement per clinical discretion of investigator Likely not study medication Discuss resuming study medication with medical monitor when symptoms
resolved YES
Temporarily dc (HOLD) NACPL for 4 additional days (total hold 1 week) then NACPL resume 600 MG TID
Did symptoms recur
YES
STOP NACPL for
duration of study
NO
NACPL No change
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
46 Contraindications Precautions and Side Effects of Study Medications
461 Contraindication
Contraindication to NAC is known hypersensitivity to it
462 Precautions
Concomitant administration of oral NAC and antibiotics has shown a slightly reduced absorption
of cephalexin and a slight increase in erythromycin serum levels NAC contains free sulfhydryl
groups There is no evidence that individuals sensitive to sulfa drugs are sensitive to NAC
The NAC preparation being administered in this study contains 20 mg of aspartame Because of
the phenylalanine component of aspartame individuals with phenylketonuria should avoid or
restrict aspartame intake to avoid increased blood levels of phenylalanine Because of this risk
labeling is required on all products containing aspartame
463 Side Effects
Side effects of NAC range from common to serious See Table 4
39
40
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Table 4 Side Effects of NAC
Undesirable Effects
System-organ class Uncommon
(gt11000 lt1100)
Rare
(gt110000 lt11000)
Very rare
(lt110000) Not known
Immune system disorders Hypersensitivity Anaphylactic shock
reaction
Nervous system disorders Headache
Ear and labyrinth disorders Tinnitus
Cardiac disorders Tachycardia
Vascular disorders Hemorrhage
Respiratory thoracic and
mediastinal disorders
Bronchospasm
Dyspnea
Gastrointestinal disorders
Vomiting diarrhea
stomatitis abdominal
pain nausea
Dyspepsia
Skin and subcutaneous tissue
disorders
Urticaria rash
angioedema itching
General disorders and
administration site conditions Pyrexia
Investigations Reduced arterial
pressure Face edema
In very rare cases the onset of severe skin reactions such as Stevens-Johnson syndrome and Lyell syndrome was reported to have a temporal relationship with N-acetylcysteine administration Although in most cases at least another suspect drug probably most involved in the genesis of the above mentioned mucocutaneous syndromes has been identified in case of mucocutaneous alterations it is appropriate to contact onersquos doctor and the administration of N-acetylcysteine should be immediately discontinued
Some studies confirmed a reduction of platelet aggregation during N-acetylcysteine administration The clinical significance of these findings has not been defined yet [Source Fluimucil Investigator Brochure]
47 Recruitment Procedures
Subjects recruited for this study will be established patients of the investigators or physician- or
self-referred to participating clinical centers in the IPFnet Each clinical center within IPFnet has
a well-developed infrastructure of local pulmonologists within the surrounding geographic area
These pulmonologists are kept informed of ongoing IPF clinical trials and regularly refer
subjects to studies conducted at IPFnet clinical centers
Additional steps will be taken to inform clinicians of the trials in progress within IPFnet
including presentations at faculty staff meetings at local hospitals medical grand rounds and
national conferences direct mail notification monthly faxes and advertisement of network trials
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
in pulmonary journals Clinical center patients previously diagnosed with IPF will be notified of
the trials by mail whenever possible
Recruitment of minorities and women will be monitored by the DCC and DSMB If necessary
additional recruitment efforts will be made at specific centers to ensure that the aggregate subject
sample contains appropriate representation of women and minorities
48 Study Procedures
The following procedures are detailed in the PANTHER-IPF MOOP accompanying this
protocol
1 PFT
2 ABG
3 HRCT scan of the chest (including imaging of pulmonary arteries)
4 CBC and serum chemistries
5 Pregnancy test
6 6MWTBorg Dyspnea Scale
7 QOL questionnaires (EuroQol HAD SF-36 SGRQ and ICE CAP)
8 UCSD SOBQ
9 Gender Substudy Questionnaire
All assessments of PFTs will be conducted by study personnel not directly involved in the
treatment of the subjects
481 Biological Specimen Management
4811 Biological Specimen Sample Management
Subjects at clinical centers participating in the specimen repository substudy who consent to
having blood drawn for research purposes and for the banking of blood blood components and
other biologic specimens (urine and BAL fluid) will have approximately 405 mL of blood
41
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
drawn 17 mL blood drawn for DNA and 20 mL of urine collected at enrollment visit Subjects
will have approximately 50 mL of blood drawn and 20 mL of urine collected at each 15-week
follow-up visit Blood specimens will be separated according to PANTHER-IPF MOOP
guidelines into the following components for banking in the repository serum plasma and
DNA Coding of all biologic specimens for the repository will be performed by study staff at the
clinical center The samples will be processed per PANTHER-IPF MOOP guidelines aliquoted
labeled with barcode labels and stored at -70degC at the clinical center and shipped to the central
repository
The only subject identifiers will be a sample ID number and subject initials This sample ID will
be linked in the IPFnet DCC clinical database to subject information No subject information will
be transferred to the biological-specimen database
The subjectrsquos samples may be used for approved sub-studies relating to human disease
including but not limited to IPF The studies for which an individualrsquos samples will be made
available will be determined by the subjectrsquos answers to questions on the biological-sample
informed consent form The subjects can choose to make their samples available for all options
or any combination Samples will be made available to researchers only with IPFnet Steering
Group approval until such time as the samples are made public through the NHLBI repository
49 Concomitant Medications
Concurrent treatment with FDA-approved therapy for IPF is allowed Colchicine may be used
for treatment of gout Temporary treatment with oral or IV corticosteroids for clinical worsening
or suspected AEx is permitted Nutritional supplements containing NAC are not allowed
410 Laboratory Testing
Clinical laboratory parameters will be assessed at screening and at the end of the study The
following tests will be performed at the two time points specified in the protocol chemistry (AG
ratio ALT [SGPT] AST [SGOT] albumin alkaline phosphatase amylase bilirubin-direct
42
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
bilirubin-indirect bilirubin-total BUN BUNcreatinine ratio calcium carbon dioxide
cholesterol-total chloride CPK-total creatinine GGT globulin glucose iron-total LDH
lipase magnesium phosphorus-inorganic potassium protein-total sodium TIBC triglycerides
uric acid) and hematology (red blood cell count WBC count hemoglobin hematocrit cell
indices differential platelet count)
411 Blinding of Study Drugs
Subjects and caregivers will be blinded to study treatment Every subject will receive NAC or
matching PLs at every study visit from the baseline visit to the week-45 visit No study agent
will be dispensed at the week-60 visit
43
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
5 Study Endpoints
51 Primary Study Endpoint
The primary endpoint will be the change in serial measurements of FVC over the study period
52 Secondary Study Endpoints
521 Time to Disease-progression
The time-to-death or a 10 decline in FVC will be defined as the time-to-disease progression
The 10 decline in FVC from enrollment must be confirmed on 2 consecutive visits no less than
6 weeks apart For subjects with 2 consecutive visits with a 10 decline in FVC the time-toshy
disease progression will be defined as the time interval between enrollment and the initial visit
with a 10 FVC decline For subjects who experience disease progression the study doctor will
determine whether or not the subject will remain in the study
522 Acute Exacerbations
The following 3 criteria will define AEx in subjects with acute worsening of their respiratory
conditions
1 Clinical (all of the following required)
A) Unexplained worsening of dyspnea or cough within 30 days triggering unscheduled
medical care (eg emergency room clinic study visit hospitalization)
B) No clinical suspicion or overt evidence of cardiac event pulmonary embolism or deep
venous thrombosis to explain acute worsening of dyspnea
C) No pneumothorax
44
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
2 RadiologicPhysiologic (A and B required)
A) New ground glass opacity or consolidation computed tomography (CT) scan OR new
alveolar opacities on chest x-ray
B) Decline of ge 5 in resting room air SpO2 from last recorded level OR decline of ge 8 mm
Hg in resting room air PaO2 from last recorded level
3 Microbiologic (all of the following required)
A) No clinical evidence for infection (ie absence of grossly purulent sputum fever gt 39degC
orally)
B) Lack of positive microbiological results (if done) from lower respiratory tract defined as
(1) Clinically significant bacterial growth on sputum or endotracheal aspirate cultures
(2) Quantitative culture by protected brush specimen ge 103 cfumL or BAL ge 104 cfumL
(3) The presence of specific pathogens on stains of any of the above
C) Lack of positive pathogen in blood cultures (if done)
Identification of Acute Exacerbations
All subjects will be educated about the importance of identifying AExs At the time of
enrollment subjects will be told about the possibility of developing acute symptomatic
worsening that might represent an AEx of IPF and instructed to contact their study clinical
center coordinator within 48 to 72 hours of the apparent event
All subjects will be contacted by phone monthly and questioned about any change in dyspnea or
cough and any interim clinic visits or hospitalizations Finally as part of the IPFnet outreach to
community referring physicians the importance of AExs will be emphasized When a subject is
identified who meets criterion 1A this will trigger the collection of additional clinical data to
evaluate a suspected AEx These data will be collected as part of standard clinical care (ie this
protocol does not require collection of all items) The additional items to be collected for
suspected AEx include
IPFnet AEx case report form (eCRF) (required)
45
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Chest x-ray CT scan withwithout pulmonary angiogram (reports should be faxed and
followed by the hard copiesdiscs)
Oxygen saturation (pulse oximetry)
ABG
Respiratory cultures (sputum endotracheal aspirate lavage)
Blood cultures
Clinichospital records related to the event
All potential cases of AEx will be reviewed by the clinical center PI first and a decision on
whether the case may represent an AEx will be made If AEx is suspected the case will be sent
to the IPFnet adjudication committee which will assign a final diagnosis (see Table 5) If there is
disagreement among members the majority opinion will be recorded
During episodes of suspected AEx as determined by the individual clinical center investigator
subjects will remain blinded and in the study
Table 5 Final Diagnoses in Evaluation of Suspected Acute Exacerbations
Definite acute exacerbation All criteria met no alternative etiology
Unclassifiable acute worsening
Insufficient data to evaluate all criteria no alternative etiology
Not acute exacerbation Alternative etiology identified that explains acute worsening
Management of the suspected AEx will be at the discretion of the treating physician Standard of
care generally involves evaluation for respiratory infection pulmonary embolism cardiac events
and pneumothorax and treatment with IV corticosteroids
Study drugs will be resumed at pre-suspected AEx doses after subjects clinically improve as
confirmed by the local PI All subjects should be seen at the clinical center within 2 to 4 weeks
of recovery for measurement of post-bronchodilator FVC (see Figure 4) Subjects unable to
return to the clinical center after suspected AEx due to medical frailty (eg continued
46
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
institutionalization progressive disability) will be categorized as failing to maintain FVC
response in secondary analyses
Suspected AEx (PI determined)
Hold study drug Treat AEx
(Attending physician determined)
Alive but unable to continue due to
medical frailty
Dead
Alive and able to continue
Site reviewvisit
Restart study drug
FVC within 2-4 weeks
Figure 4 Acute Exacerbation Flow Chart
523 Respiratory Infections
An upper respiratory infection will be defined as
Change in sputum discoloration
Increased cough of no more than 14 daysrsquo duration
A lower-respiratory infection (pneumonia) will be defined as new segmental or lobar airspace
opacities visualized by image studies (chest radiograph or HRCT) in addition to any of the
following
Positive pathogencultures in good sample of sputum or lower-airway secretions retrieved
by fiberoptic bronchoscope
Fever gt 39degC or gt 100degF
Leukocytosis gt 12000 (unexplained no increase in dose of corticosteroids)
47
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
524 Maintained FVC Response
Subjects with follow-up FVCpred measurements at or above their baseline FVCpred level
will be classified as having maintained FVC response Subjects with reduced FVCpred levels
or missing data for any reason including death or medical frailty will be classified as having not
maintained FVC response The FVCpred value is used because unadjusted FVC measurements
are expected to decline with age
48
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
6 Safety Evaluations and Procedures
61 Adverse Events
During a clinical trial the reporting of adverse experience information can lead to important
changes in the way a new treatment is developed as well as provide integral safety data
611 Definitions
An adverse event (AE) is any untoward medical occurrence in a subject or clinical investigation
subject who was administered a pharmaceutical product The AE does not necessarily have to
have a causal relationship with the drug administered An AE can be any unfavorable and
unintended sign (including an abnormal laboratory finding) symptom or disease temporarily
associated with the use of a medicinal product whether or not considered to be related to the
medicinal product Diseases signs symptoms or laboratory abnormalities already existing at
enrollment are not considered AEs unless they worsen (ie increase in intensity or frequency)
Surgical procedures themselves are not AEs they are therapeutic measures for conditions that
require surgery The condition for which the surgery is required may be an AE Surgical
procedures planned before randomization and the conditions necessitating the surgery are not
AEs
A serious adverse event is any untoward event that
Is fatal
Is life-threatening
Requires inpatient hospitalization or prolongation of existing hospitalization with the
following exceptions
o Preplanned (before the study) hospital admissions unless the hospitalization is
prolonged
o Planned admissions (as part of a study eg routine biopsies)
o Hospitalization lasting lt 24 hours
49
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
o Hospitalization for elective procedure
o Emergency room visits
Results in persistent or significant disability or incapacity
Is a congenital anomaly or birth defect
Important medical events that may not result in death be life-threatening or require
inpatient hospitalization may be considered serious adverse events (SAEs) when based
on appropriate medical judgment they may jeopardize the subject and may require
medical or surgical intervention to prevent one of the outcomes listed above
Life-threatening means that the subject was in the view of the investigator at immediate risk of
death from the AE as it occurred It does not include an AE that had it occurred in a more severe
form might have caused death
Persistent or significant disabilityincapacity means that the event resulted in permanent or
significant and substantial disruption of the subjectrsquos ability to carry out normal life functions
Causality
A reasonable possibility means the AE may have been caused byrelated to the study drug A
perceived or real lack of efficacy does not satisfy the definition of relatedness
612 Adverse Event (AE) Reporting
For the PANTHER-IPF trial all AEs (serious and nonserious) occurring from randomization
through final study visit (4 weeks after final dose of all study medication) will be recorded on the
AE page of the case report form (CRF)
6121 Serious Adverse Events (SAE) Reporting
For this trial all deaths and all SAEs which occur from randomization through final study visit
must be entered within the EDC system via the SAE eCRF page within 24 hours of the
investigative sitersquos knowledge of the event It is the responsibility of the clinical center
50
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
investigator to provide a causality assessment of the event for each study medications based upon
the information available at the time of the report It is understood that complete information
about the event may not be known at the time the initial report is submitted In the event the EDC
system is not accessible to the site at the time of event reporting investigative sites will complete
and forward a paper back-up SAE form to DCRI Safety Surveillance for processing
DCRI Safety Surveillance
Telephone 1-919-668-8624 or 1-866-668-7799 (toll free)
Fax 1-919-668-7138 or 1-866-668-7138 (toll free)
The investigator must complete and submit follow-up SAE information via the eCRF when
important new or follow-up information (eg final diagnosis outcome results of specific
investigations) becomes available Follow-up information should be submitted according to the
same process used for reporting the initial event as described above All SAEs will be followed
until resolution stabilization or 30 days after the subject has completed the final visit (4 weeks
after the final dose of study medication) whichever occurs first The investigator is responsible
for reporting SAEs to their institutional review board (IRB) per site specific IRB reporting
guidelines
6122 Regulatory Reporting
AEs that are serious study drug related and unexpected will be reported to the regulatory
authorities The DCRI Safety Surveillance medical monitor will perform a medical review of all
SAEs submitted and evaluate for ldquounexpectednessrdquo DCRI Safety Surveillance will prepare
MedWatch reports for those events identified as serious study drug related and unexpected as
determined by Safety Medical Monitor
DCRI Regulatory Services will submit all unexpected study drug-related SAEs as per 21 CFR
32 DCRI Safety Surveillance will provide a safety alert letter to the NHLBI DSMB and DCC
clinical operation (for distribution to sites) within 15 days of initial receipt of the information
51
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Investigators are responsible for promptly reporting these events to their reviewing IRBs
according to site specific IRB reporting guidelines
62 Clinical Medical Monitoring
There will be an unblinded physician at the IPFnet DCC serving as medical monitor The
medical monitor will be available to assist with questions about dosage adjustments of study
medications including discontinuation or resumption of medications
63 Unblinding Procedures
Unblinding of subjects or investigators to subject treatment is strongly discouraged For ongoing
clinical management all subjects should be presumed to be receiving ldquoactiverdquo study drug To
ensure the subjectrsquos safety the study treatment will be dose-adjusted based on laboratory test
results clinical findings and symptoms
The IPFnet DCC medical monitor and PANTHER-IPF co-chairs Drs Ganesh Raghu and
Fernando Martinez will be available to the study physicians to discuss study drug management
on a case-by-case basis Un-blinding will be considered ONLY when the knowledge of subject
treatment assignment is ABSOLUTELY ESSENTIAL for subject safety and after discussion of
the subjectrsquos case with the medical monitor and either Dr Raghu or Dr Martinez Unblinding of
study treatment should be minimized during the conduct of the trial In those cases where it is
felt to be medically necessary the DCC medical officer will communicate directly with the
managing physician to minimize unblinding of study personnel
52
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
7 Study Drug Procedures
At the baseline 15-week 30-week and 45-week study visits subjects will receive a supply of
study drug sufficient to last until the next visit at which study drug will be dispensed
53
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
8 Data Management
81 Hardware and Software Configuration
811 Hardware and Database Software
Data will be stored in an Oracle database system Oracle has advantages of processing efficiency
and smooth linkage with other software systems The application and database will be hosted on
Solaris Unix servers at the IPFnet DCC
812 Statistical Software
SAS will be used as the principal application for the management of analysis data files and
statistical computations S-Plus will be used to provide supplementary functions as needed
813 Access Control and Confidentiality Procedures
Access to databases will be controlled centrally by the IPFnet DCC through user passwords
linked to appropriate privileges This protects the data from unauthorized changes and
inadvertent loss or damage
814 Security
Database and Web servers will be secured by a firewall and through controlled physical access
Oracle has many security features to ensure that any staff member accessing the database has the
proper authority to perform the functions he or she requests of the system Within the secondary
SAS databases Unix group-access control maintains similar security The Sun workstation login
is secured by extensive user-password facilities under Unix
54
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
815 Back-up Procedures
Database back-up will be performed automatically every day and standard IPFnet DCC policies
and procedures will be applied to dictate tape rotation and retention practices
816 Virus Protection
All disk drives that provide network services and all user computers will be protected using
virus-scanning software Standard IPFnet DCC policies will be applied to update these protection
systems periodically through the study
82 Sources of Data
821 Design and Development
The IPFnet DCC will be responsible for development of the electronic case report forms
(eCRFs) development and validation of the clinical study database ensuring data integrity and
training clinical center staff on applicable data management procedures A web-based distributed
data entry model will be implemented This system will be developed to ensure that guidelines
and regulations surrounding the use of computerized systems used in clinical trials are upheld
The remainder of this section provides an overview of the data management plan associated with
this protocol
822 Data Collection Forms
The data collection process consists of direct data entry at the study clinical centers into the EDC
system(s) provided by the DCC A data collection worksheet will be provided to clinical centers
for recording data in the event the EDC system is unavailable Data entry of the eCRFs should
be completed according to the instructions provided and project specific training The
investigator is responsible for maintaining accurate complete and up-to-date records and for
ensuring the completion of the eCRFs for each research participant
55
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
823 Data Acquisition and Entry
Data entry into eCRFs shall be performed by authorized individuals Selected eCRFs may also
require the investigatorrsquos written signature or electronic signature as appropriate Electronic
CRFs will be monitored for completeness accuracy and attention to detail during the study
824 Data Center Responsibilities
The IPFnet DCC will 1) develop a data management plan and will conduct data management
activities 2) provide final eCRFs for the collection of all data required by the study 3) develop
data dictionaries for each eCRF that will comprehensively define each data element 4) conduct
ongoing data monitoring activities on study data 5) monitor any preliminary analysis data
cleanup activities and 6) rigorously monitor final study data clean up
825 Data Editing
Completed data will be entered into the IPFnet DCC automated data acquisition and
management system If incomplete or inaccurate data are found a data clarification request will
be generated and distributed to clinical centers for a response Clinical centers will resolve data
inconsistencies and errors and enter all corrections and changes into the IPFnet DCC automated
data acquisition and management system
826 Training
The training plan for clinical center staff includes provisions for training on assessments eCRF
completion guidelines data management procedures and the use of computerized systems
56
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
9 Study Design and Data Analysis
91 General Analytic Considerations
All primary analyses will be based on intent-to-treat (ITT) principles using all randomized
subjects Baseline factors across groups will be compared using mean (standard deviation) and
median (25th and 75th percentiles) summary measures Kaplan-Meier curves will be used to
display event rates Due to clinical interest in departures from both sides of the null hypothesis
all test statistics will be 2-sided
Reasonable caution needs to be taken when conducting multiple analyses on key clinical
subgroups For subgroup analyses a conservative significance level of 0001 will be used for all
interaction tests Thus subgroup comparisons will be considered exploratory unless the p-value
from the interaction test is smaller than 0001
92 Randomization Blinding and Reporting of Results
A permuted block-randomization scheme will be created with varying block sizes stratified by
clinical center Once a subject has completed the screening and baseline period and evaluation
for inclusionexclusion criteria the randomization process will begin Subjects will be
randomized to receive NAC or matching placebo with equal probability (11) via telephone
contact with a central interactive voice response system (IVRS) using a toll-free randomization
number On the day of randomization after the subject has successfully met all inclusion and
exclusion criteria the investigator or designee will call the central randomization number to
obtain the assigned kit randomization numbers for that subject At each subject visit the
investigator or designee will call the central randomization number to obtain the new kit
randomization numbers for resupply of the subject For resupply of the clinical center the IVRS
will monitor minimal volume of a kit type andor expiration date and will automatically notify
the pharmacy
57
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
The trial results will be reported according to guidelines specified in the CONSORT statement
A flow diagram describing screening recruitment randomization dropout and vital status will
be included in the primary manuscript AEs and efficacy data will be presented for all treatment
groups Adherence dropout and lost to follow-up will be carefully examined across all treatment
groups Analyses of safety will be based on data from all randomized subjects who received at
least one dose of study drug
93 Stratification
Subjects will be distributed to the two treatment arms in a 11 allocation ratio Stratification
blocks will be based on clinical centers
94 Specification of the Primary Analyses
A mixed model repeated measures (MMRM) analysis described in section 95 will be used to
compare differences in the slope of FVC measurements across the treatment groups Response
variables are values of the FVC measured at baseline and every 15 weeks until study completion
Variables in the model will include treatment time and time by treatment age sex race and
height Contrast estimates of differences in slopes of treatment over time (along with confidence
intervals) will be used to estimate the treatment effect The validity of this model in terms of
meeting modeling assumptions will be assessed via standard modeling diagnostics and goodness-
of-fit measures Based on the MMRM framework missing FVC data will not be imputed for the
primary analysis
95 Analysis of Longitudinal Endpoints
A common goal in clinical trials is to specify models that are easily implemented and
reproducible by independent data analysts On the other hand the models should have proper
statistical behavior in terms of low bias and high precision Many common approaches to
longitudinal data analysis including last observation carried forward (LOCF) imputation rely on
the missing completely at random (MCAR) assumption However the MCAR assumption is
58
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
unlikely to hold in many clinical trials because missing data are often related to disease
progression and prognosis A more reasonable assumption missing at random (MAR) specifies
that the complete data distribution can be modeled using only the observed data The likelihood-
based MMRM approach is valid under the more general MAR assumptions These models will
be applied to analyze the longitudinal data secondary endpoints
The advantages of MMRM analysis are that all important characteristics of the model can be preshy
specified standard software can be used to implement the models and results are based on ITT
principles43 In addition the MMRM approach offers superior control of Type I and Type II
errors compared with the LOCF approach
Response variables are values of the PFTs measured at enrollment and every 15 weeks until
study completion and 6MWT values measured at baseline week 30 and week 60 Covariates are
treatment time time by treatment and key baseline risk factors Contrasts (along with
confidence intervals) of treatment by time will be used to estimate the treatment effect
The correlation structure involves multiple pieces including measurement errors random
variation and interindividual variability For the longitudinal data analyses an unstructured
correlation matrix for within-subject errors will be assumed Other correlation structures
including compound symmetry will be examined as needed A careful examination of reasons
for study discontinuation will be conducted to assess the validity of MCAR Sensitivity analyses
will be used to examine the untestable assumption that the observed data violate the MAR
assumption The MMRM models will be implemented using PROC MIXED in SAS
96 Analysis of Binary Time-to-Event and Time-Lagged Endpoints
Regression modeling approaches using either the logistic regression model or Cox proportional
hazards regression model will be employed when appropriate The validity of these models will
be assessed via standard modeling diagnostics and goodness-of-fit measures Estimates of
cumulative frequencies for more general time-lagged responses will be calculated using the
partitioned version of the Bang-Tsiatis estimator44 The partitions will be set at 15-week intervals
59
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
to correspond with the data-collection process Covariate adjusted event rates will be calculated
using inverse probability-weighted regression estimates45
97 Power Analysis
971 Primary Analyses
Based on previously published IPF clinical trials the PL group is expected to experience a drop
in FVC of approximately 020 L over the study period (see Figure 1) The IPFnet Steering Group
determined a clinically important difference would be to preserve the majority of the decline
relative to PL over the study period In particular a treatment effect of 015 L was determined to
be a clinically meaningful difference Potential dropout is a key factor in the proposed study The
drop-out process assumed 5 lost to follow-up after every study visit Only 80 of subjects
were assumed to be followed for the entire study period All models assumed a compound
symmetry structure for the covariance matrix Power calculations were performed using a SAS
IML program for designing repeated measures studies46 Based on preliminary reviews of the
data from the University of Michigan the covariance matrix parameters were estimated at
approximately σ2 = 0757 (variance parameter) and ρ = 0936 (correlation parameter) To be
conservative the power calculations for the primary analysis were performed with parameter
setting of σ2 = 0810 (variance parameter) and ρ = 0925 (correlation parameter)
The power calculations assume a correction for imperfect compliance proposed by Lachin and
Foulkes to allow for 2 noncompliance for each of the treatment arms47 Thus the sample size
of 130 subjects per arm would be reduced to an adjusted sample size of 130(1-002-002)2 =
1198 or 120 subjects per arm
Under the assumed Type I error rate of 005 with a correlation parameter of 0925 and standard
deviation of 090 the difference of 015 L (or 00025 Lweek) shown in Table 6 would have
power of 93
60
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Table 6 Hypothetical Values of Mean FVC (L) Change from Baseline
Week 15 Week 30 Week 45 Week 60
NAC 00125 00250 00375 00500
Placebo 00500 01000 01500 02000
Difference 00375 00750 01125 01500
Abbreviations FVC forced vital capacity PL placebo
972 Power Analysis for Secondary Endpoints
Power calculations for secondary endpoint measurements are shown in Table 7 Standard
deviations are based on unpublished data provided by the University of Michigan The
calculations are based on a 2-sample t-test with Type I error rate set at 005 These calculations
are likely to be conservative because the statistical approach described in section 95 for
analyzing these endpoints will incorporate incomplete observations as well as intermediate data
points
Table 7 Detectable Differences in Treatment Means for Selected Endpoint Measurements
Secondary Endpoints Std Dev
of the Baseline Score
Detectable Difference for 80 Power
Std Dev of the Change Score
Difference Detectable for
80 Power
DLCOpred 166 58 91 32
6MWT Area Under the Desaturation Curve
219 76 175 61
6MWT Distance to Desaturation 224 78 315 110
6MWT Minutes Walked 210 073 205 071
Abbreviations Std Dev standard deviation DLCOpred diffusing capacity of the lung for carbon monoxide percent predicted 6MWT 6-minute walk test
61
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
10 Study Administration
101 Cooperative Agreement Mechanism
The administrative and funding mechanism used to undertake this project is a ldquocooperative
agreementrdquo (U01) which is an assistance mechanism Under the cooperative agreement the
NHLBI assists supports andor stimulates the project and is substantially involved with
investigators in conducting the study by facilitating performance of the effort in a ldquopartnerrdquo role
The NHLBI project scientist serves on the IPFnet Steering Group and he or another NHLBI
scientist may serve on other project committees when appropriate At the same time however
NHLBI does not assume a dominant role direction or prime responsibility for this research
program
As described below governance of the project is conducted through the IPFnet Steering Group
Principal investigators have lead responsibilities in all aspects of their trials and the project
including any modification of trial designs conduct of the trials quality control data analysis
and interpretation preparation of publications and collaboration with other investigators unless
otherwise provided for by the IPFnet Steering Group
PIs retain custody of and have primary rights to their center-specific and collaborative data
subject to government rights-of-access consistent with current Health amp Human Services (HHS)
Public Health Service (PHS) and National Institutes of Health policies The protocols and
governance policies call for the continual submission of data centrally to the IPFnet DCC for the
collaborative database which at a minimum will contain the key variables selected by the IPFnet
Steering Group for standardization across all clinical centers the submission of copies of the
collaborative datasets to each PI upon completion of the project procedures for data analysis
reporting and publication and procedures to protect and ensure the privacy of medical and
genetic data and records of individuals The NHLBI project scientist on behalf of the NHLBI
will have the same access privileges and responsibilities regarding the collaborative data as the
other members of the Steering Group
62
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
PIs are also encouraged to publish and to publicly release and disseminate results data and other
products of the project concordant with the project protocols and governance and the approved
plan for making data and materials available to the scientific community and to the NHLBI
However during the 3 years after the ending date of NHLBI project support unpublished data
unpublished results data sets not previously released and other study materials or products are
to be made available to any third party only with the approval of the IPFnet Steering Group
Upon completion of the project PIs are expected to put their intervention materials and
procedure manuals into the public domain andor make them available to other investigators
according to the approved plan for making data and materials available to the scientific
community and the NHLBI for the conduct of research at no charge other than the costs of
reproduction and distribution
The NHLBI reserves the right to terminate or curtail the project (or an individual award) in the
event of (a) failure to develop or implement mutually agreeable collaborative measurement
subject eligibility and data management sections of the protocols (b) substantial shortfall in
subject recruitment follow-up data reporting or quality control or other major breach of
protocol (c) substantive changes in the agreed-upon protocols with which NHLBI cannot
concur (d) reaching a major project outcome with persuasive statistical significance
substantially before schedule or (e) human subject ethical issues that may dictate a premature
termination
Any disagreement that may arise in scientificprogrammatic matters (within the scope of the
award) between award recipients and the NHLBI may be brought to arbitration An arbitration
panel will be composed of 3 membersmdash1 selected by the IPFnet Steering Group (with the
NHLBI member not voting) or by the individual PI in the event of an individual disagreement a
second selected by NHLBI and the third selected by the other 2 members This special
arbitration procedure in no way affects the PIrsquos right to appeal an adverse action that is otherwise
appealable in accordance with the PHS regulations at 42 CFR part 50 Subpart D and HHS
63
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
regulation at 45 CFR part 16 or the rights of the NHLBI under applicable statutes regulations
and terms of the award
102 IPFnet Steering Group
The IPFnet Steering Group is the main governing body of the project It is composed of the PIs
of the clinical centers the PI of the DCC and the NHLBI project scientist The clinical centers
the IPFnet DCC and the NHLBI each have 1 vote on the IPFnet Steering Group All decisions
are determined by majority vote
All major scientific decisions are determined by the IPFnet Steering Group It assumes overall
responsibility for the design and conduct of the trial It appoints (and disbands) committees and
subcommittees as the need arises designs approves and implements the study protocols
oversees the development of the MOOP monitors subject recruitment and treatment delivery
evaluates data collection and management oversees quality assurance procedures and
implements changes and enhancements to the study as required It also has primary responsibility
for facilitating the conduct of the trials and reporting the projectrsquos results
103 Data and Safety Monitoring Board
The NHLBI will establish a DSMB in accordance with established policies (see
httpwwwnhlbinihgovfundingpoliciesdsmb_insthtm) to ensure data quality and subject
safety and to provide independent advice to the NHLBI regarding progress and the
appropriateness of study continuation
104 Recommendations on Interim Monitoring of Efficacy Safety and Futility
First and foremost the role of the DSMB will be to review subject safety and trial conduct at
periodic points during the study The DSMB may require analyses of the primary endpoint
results for comparing the benefit and risks of treatment strategies The benefit of collecting
additional data on key secondary endpoints with extended follow-up and establishing a robust
64
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
evidence base for determining a standard of care will need to be carefully considered before
early termination of one or more treatment arms After careful consideration the IPFnet Steering
Group recommends conservative thresholds for the early examinations of the safety and efficacy
data
The DSMB will be expected to meet approximately every 6 months until trial completion to
review safety and toxicity data The DSMB may recommend stopping the study based on these
reviews Because the DSMB could stop the trial for safety concerns as well as for a large
efficacy benefit there could be multiple opportunities to reject the null hypothesis (no difference
in event rates between the PL and NAC groups) A Bonferroni approximation will be applied
during the one planned interim analysis for efficacy
Before locking the database a statistical analysis plan (SAP) will be developed to provide
complete details on the statistical analysis The SAP will include the specifics for how and when
the DSMB will be notified for AEs The IPFnet DCC will deliver to the DSMB all FDA-defined
AEs at 3-month intervals The IPFnet DCC will prepare narrative SAE reports in real time for
DSMB review including recommendations and analysis of similar events for each SAE
submitted to the FDA
65
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
11 Investigator and Sponsor Obligations
111 Monitoring
All monitoring activities for US clinical centers will be performed in accordance with DCRI
standard operating procedures Information regarding the types of visits will be outlined in the
PANTHER-IPF MOOP
112 Cost and Payment
There will be no cost to subjects enrolled in this trial Study-related procedures will be paid for
by the IPFnet
Subjects may be eligible for reimbursement for travel to the clinical center Details of payment
will be explained to each subject during the consent process
113 Confidentiality and Health Insurance Portability and Accountability Act
Considerations
Subject confidentiality will be protected throughout the study All subject data will be kept
strictly confidential and no subject-identifying information will be released to anyone outside
the project Confidentiality will be assured through several mechanisms First each subject will
be assigned an anonymous study ID which will then be used on all study forms Second any
study forms blood samples and paper records that contain subject information (eg address lists
phone lists) will be kept at the clinical centers in secured locked areas coded by number Once
blood is collected there will be no subject identifiers placed on blood samplesmdashonly the study
ID number and the date of sample collection Third access to all subject data and information
including laboratory specimens will be restricted to authorized personnel In the case of
computerized data this restricted access will be assured through user logon IDs and password
protection
66
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
At the IPFnet DCC only authorized personnel will have access to the data files containing study
data Security will be assured through user logon IDs passwords and appropriate access
privileges All study subjects will be identified only by their IPFnet ID numbers and no personal
identifying information such as name address or Social Security number will be entered into
the IPFnet DCC database Any subject-specific data reported to the IPFnet Steering Group will
be identified only by the IPFnet ID number
Finally subjects will not be identified by name in any reports or publications nor will the data
be presented in such a way that the identity of individual subjects can be inferred Analysis files
created for further study by the scientific community will have no subject identifiers These data
files will be created in accordance with the Ancillary Studies and Publication Policy of the
IPFnet
114 Informed Consent Procedures
All IPFnet subjects will provide written informed consent using procedures reviewed and
approved by each clinical centerrsquos IRB Informed consent will be undertaken by study personnel
in-person with the subject The subject has the option of declining further participation in the
study at that point No further study procedures will be conducted until the signed documents
have been provided to the IPFnet clinical center
115 Institutional Review Boards
Before initiating this study the protocol clinical center-specific informed consent forms Health
Insurance Portability and Accountability Act (HIPAA) forms recruitment materials and other
relevant information will be reviewed by a properly constituted IRB at each participating clinical
center A copy of the signed and dated IRB approval at each clinical center will be retrieved prior
to or during the site initiation visit and archived at the IPFnet DCC Any amendments to the
protocol other than simple administrative and typographical changes must be approved by each
IRB before they are implemented The clinical centers will seek annual renewals of their IRB
approvals in accordance with local procedures
67
__________________________________________ ________________
__________________________________________
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
12 Investigator Agreement
I have read the foregoing protocol PANTHER-IPF and agree that it contains all necessary
details for carrying out this study I will conduct the study as outlined herein and will complete
the study within the time designated
I will provide copies of the protocol and all pertinent information to all individuals responsible to
me who assist in the conduct of this study I will discuss this material with them to ensure they
are fully informed regarding the drug and the conduct of the study
I will fulfill all responsibilities for submitting pertinent information to the local IRB if
applicable that is responsible for this study
I further agree that NHLBI andor DCRI will have access to any source documents from which
eCRF information may have been generated
Signature of Principal Investigator Date
Name of Principal Investigator (printed or typed)
Protocol version date May 19 2009
Protocol Amendment 1 version date May 28 2010
Protocol Amendment 2 version date December 6 2011
68
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
13 References
1 Raghu G Brown KK Bradford WZ et al A placebo-controlled trial of interferon gamma-1b in patients with idiopathic pulmonary fibrosis N Engl J Med 2004350125-33 2 King TE Jr Safrin S Starko KM et al Analyses of efficacy end points in a controlled trial of interferon-gamma1b for idiopathic pulmonary fibrosis Chest 2005127171-7 3 Flaherty KR Thwaite EL Kazerooni EA et al Radiological versus histological diagnosis in UIP and NSIP survival implications Thorax 200358143-8 4 Wells AU Desai SR Rubens MB et al Idiopathic pulmonary fibrosis a composite physiologic index derived from disease extent observed by computed tomography Am J Respir Crit Care Med 2003167962-9 5 Raghu G Freudenberger TD Yang S et al High prevalence of abnormal acid gastroshyoesophageal reflux in idiopathic pulmonary fibrosis Eur Respir J 200627136-42 6 Kinnula VL Focus on antioxidant enzymes and antioxidant strategies in smoking related airway diseases Thorax 200560693-700 7 Coultas DB Zumwalt RE Black WC Sobonya RE The epidemiology of interstitial lung diseases Am J Respir Crit Care Med 1994150967-72 8 Raghu G Weycker D Edelsberg J Bradford WZ Oster G Incidence and prevalence of idiopathic pulmonary fibrosis Am J Respir Crit Care Med 2006174810-6 9 Olson AL Swigris JJ Lezotte DC Norris JM Wilson CG Brown KK Mortality from pulmonary fibrosis increased in the United States from 1992 to 2003 Am J Respir Crit Care Med 2007176277-84 10 Mannino DM Etzel RA Parrish RG Pulmonary fibrosis deaths in the United States 1979shy1991 An analysis of multiple-cause mortality data Am J Respir Crit Care Med 19961531548shy52 11 Hubbard R Johnston I Coultas DB Britton J Mortality rates from cryptogenic fibrosing alveolitis in seven countries Thorax 199651711-6 12 Johnston I Britton J Kinnear W Logan R Rising mortality from cryptogenic fibrosing alveolitis Bmj 19903011017-21 13 Raghu G Collard HR Egan JJ et al An official ATSERSJRSALAT statement idiopathic pulmonary fibrosis evidence-based guidelines for diagnosis and management Am J Respir Crit Care Med 2011183788-824 14 (USA) FDA FDA Public Health Advisory Interferon gamma-1b (marketed as Actimmune) In 2007 15 King TE Jr Pardo A Selman M Idiopathic pulmonary fibrosis Lancet 2011 16 Raghu G Brown KK Costabel U et al Treatment of idiopathic pulmonary fibrosis with etanercept an exploratory placebo-controlled trial Am J Respir Crit Care Med 2008178948shy55 17 Malouf MA Hopkins P Snell G Glanville AR An investigator-driven study of everolimus in surgical lung biopsy confirmed idiopathic pulmonary fibrosis Respirology 201116776-83 18 King TE Jr Behr J Brown KK et al BUILD-1 a randomized placebo-controlled trial of bosentan in idiopathic pulmonary fibrosis Am J Respir Crit Care Med 200817775-81 19 Richeldi L Costabel U Selman M et al Efficacy of a tyrosine kinase inhibitor in idiopathic pulmonary fibrosis N Engl J Med 20113651079-87
69
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
20 Borok Z Buhl R Grimes GJ et al Effect of glutathione aerosol on oxidant-antioxidant imbalance in idiopathic pulmonary fibrosis Lancet 1991338215-6 21 Meyer A Buhl R Magnussen H The effect of oral N-acetylcysteine on lung glutathione levels in idiopathic pulmonary fibrosis Eur Respir J 19947431-6 22 Behr J Maier K Degenkolb B Krombach F Vogelmeier C Antioxidative and clinical effects of high-dose N-acetylcysteine in fibrosing alveolitis Adjunctive therapy to maintenance immunosuppression Am J Respir Crit Care Med 19971561897-901 23 Cantin AM North SL Fells GA Hubbard RC Crystal RG Oxidant-mediated epithelial cell injury in idiopathic pulmonary fibrosis J Clin Invest 1987791665-73 24 Waghray M Cui Z Horowitz JC et al Hydrogen peroxide is a diffusible paracrine signal for the induction of epithelial cell death by activated myofibroblasts Faseb J 200519854-6 25 Larios JM Budhiraja R Fanburg BL Thannickal VJ Oxidative protein cross-linking reactions involving L-tyrosine in transforming growth factor-beta1-stimulated fibroblasts J Biol Chem 200127617437-41 26 Kinnula VL Fattman CL Tan RJ Oury TD Oxidative stress in pulmonary fibrosis a possible role for redox modulatory therapy Am J Respir Crit Care Med 2005172417-22 27 Meyer A Buhl R Kampf S Magnussen H Intravenous N-acetylcysteine and lung glutathione of patients with pulmonary fibrosis and normals Am J Respir Crit Care Med 19951521055-60 28 Behr J Degenkolb B Krombach F Vogelmeier C Intracellular glutathione and bronchoalveolar cells in fibrosing alveolitis effects of N-acetylcysteine Eur Respir J 200219906-11 29 Bando M Hosono T Mato N et al Long-term efficacy of inhaled N-acetylcysteine in patients with idiopathic pulmonary fibrosis Intern Med 2010492289-96 30 Demedts M Behr J Buhl R et al High-dose acetylcysteine in idiopathic pulmonary fibrosis N Engl J Med 20053532229-42 31 Toma TP Bhowmik A Rajakulasingam R Acetylcysteine in pulmonary fibrosis N Engl J Med 20063541086-9 author reply -9 32 Hunninghake GW Antioxidant therapy for idiopathic pulmonary fibrosis N Engl J Med 20053532285-7 33 Flaherty KR Mumford JA Murray S et al Prognostic implications of physiologic and radiographic changes in idiopathic interstitial pneumonia Am J Respir Crit Care Med 2003168543-8 34 Latsi PI du Bois RM Nicholson AG et al Fibrotic idiopathic interstitial pneumonia the prognostic value of longitudinal functional trends Am J Respir Crit Care Med 2003168531-7 35 Collard HR King TE Jr Bartelson BB Vourlekis JS Schwarz MI Brown KK Changes in clinical and physiologic variables predict survival in idiopathic pulmonary fibrosis Am J Respir Crit Care Med 2003168538-42 36 Jegal Y Kim DS Shim TS et al Physiology is a stronger predictor of survival than pathology in fibrotic interstitial pneumonia Am J Respir Crit Care Med 2005171639-44 37 Martinez FJ Safrin S Weycker D et al The clinical course of patients with idiopathic pulmonary fibrosis Ann Intern Med 2005142963-7 38 Hull JH Acetylcysteine in pulmonary fibrosis N Engl J Med 20063541089-91 author reply -91
70
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
39 Flaherty KR King TE Jr Raghu G et al Idiopathic interstitial pneumonia what is the effect of a multidisciplinary approach to diagnosis Am J Respir Crit Care Med 2004170904shy10 40 Raghu G Johnson WC Lockhart D Mageto Y Treatment of idiopathic pulmonary fibrosis with a new antifibrotic agent pirfenidone results of a prospective open-label Phase II study Am J Respir Crit Care Med 19991591061-9 41 Hunninghake GW Lynch DA Galvin JR et al Radiologic findings are strongly associated with a pathologic diagnosis of usual interstitial pneumonia Chest 20031241215-23 42 Lynch D Godwin J Safrin S et al High-resolution computed tomography in idiopathic pulmonary fibrosis diagnosis and prognosis Am J Respir Crit Care Med 2005172488-93 43 Mallinckrodt CH Watkin JG Molenberghs G Carroll RJ Choice of the primary analysis in longitudinal clinical trials Pharmaceutical Statistics 20043161-9 44 Bang H Tsiatis A Estimating medical costs with censored data Biometrika 200087329shy43 45 Lin DY Regression analysis of incomplete medical cost data Stat Med 2003221181-200 46 Rochon J Application of GEE procedures for sample size calculations in repeated measures experiments Stat Med 1998171643-58 47 Lachin JM Foulkes MA Evaluation of sample size and power for analyses of survival with allowance for nonuniform patient entry losses to follow-up noncompliance and stratification Biometrics 198642507-19
71
- PANTHER-IPFPREDNISONE AZATHIOPRINEAND N-ACETYLCYSTEINEA STUDY THAT EVALUATES RESPONSE INIDIOPATHIC PULMONARY FIBROSIS
-
- Protocol Summary
- Table of Contents
- List of Tables
- List of Figures
- List of Abbreviations
- 1 Summary
- 2 Hypotheses and Specific Aims
-
- 21 Null Hypothesis
- 22 Specific Aim 1
- 23 Specific Aim 2
- 24 Prespecified Subgroups of Interest
-
- 3 Background and Significance
-
- 31 Idiopathic Pulmonary Fibrosis is the Most Common Interstitial Lung Disease
- 32 Rationale for Placebo Control
- 33 Rationale for N-acetylcysteine
- 35 Rationale for N-acetylcysteine as a Stand-alone Therapy
- 36 Rationale for the Study Design and Primary Endpoint
- 37 Rationale for Blinding of Treatments
-
- 4 Methods
-
- 41 Inclusion Criteria
- 42 Diagnosis of IPF
- 43 Exclusion Criteria
- 44 Study Design and Study Visit
- 45 Dose Justification
- 46 Contraindications Precautions and Side Effects of Study Medications
- 47 Recruitment Procedures
- 48 Study Procedures
- 49 Concomitant Medications
- 410 Laboratory Testing
- 411 Blinding of Study Drugs
-
- 5 Study Endpoints
-
- 51 Primary Study Endpoint
- 52 Secondary Study Endpoints
-
- 6 Safety Evaluations and Procedures
-
- 61 Adverse Events
- 62 Clinical Medical Monitoring
- 63 Unblinding Procedures
-
- 7 Study Drug Procedures
- 8 Data Management
-
- 81 Hardware and Software Configuration
- 82 Sources of Data
-
- 9 Study Design and Data Analysis
-
- 91 General Analytic Considerations
- 92 Randomization Blinding and Reporting of Results
- 93 Stratification
- 94 Specification of the Primary Analyses
- 95 Analysis of Longitudinal Endpoints
- 96 Analysis of Binary Time-to-Event and Time-Lagged Endpoints
- 97 Power Analysis
-
- 10 Study Administration
-
- 101 Cooperative Agreement Mechanism
- 102 IPFnet Steering Group
- 103 Data and Safety Monitoring Board
- 104 Recommendations on Interim Monitoring of Efficacy Safety and Futility
-
- 11 Investigator and Sponsor Obligations
-
- 111 Monitoring
- 112 Cost and Payment
- 113 Confidentiality and Health Insurance Portability and Accountability ActConsiderations
- 114 Informed Consent Procedures
- 115 Institutional Review Boards
-
- 12 Investigator Agreement
- 13 References
-

PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Figure 3 Pathology Flow Chart Surgical Lung Biopsy Diagnosis
Requirement for diagnosis
1 Clinical exclusion of other known causes (connective tissue diseases environmental and drug
exposures) of ILD
2 Radiographic HRCT with bibasilar reticular abnormality and honeycomb change with minimal
ground glass opacities
Appropriate clinical setting
1 Age gt 50 years
2 Insidious onset of unexplained dyspnea
3 Duration of illness for ge 3 months
4 Bibasilar inspiratory crackles
23
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Unlike the ATSERS consensus criteria published in 2000 bronchoscopy will not be required for diagnosis
This decision was made based on the experience of the IPFnet Steering Group members regarding the utility of
bronchoscopy in the diagnosis of IPF The presence of an atypical HRCT finding will require documentation of
a definitive diagnosis by surgical lung biopsy In fact this is in keeping with the recently published evidence
based guidelines for diagnosis and management of IPF13 As shown in Figure 3 central review of the pathology
data will be required for a diagnosis of IPF
We will not require central review of HRCT as several studies have shown that a confident local interpretation
of clinicalHRCT criteria as definite IPFUIP is associated with a high positive predictive value for finding UIP
at surgical lung biopsy (see Table 1) Differences in sensitivity in these series likely reflect subject selection as
Flaherty et al3 evaluated only UIP and nonspecific interstitial pneumonia (NSIP) while Raghu et al40 and
Hunninghake et al41 included a broader range of ILD
Table 1 Operating Characteristics of Local HRCT Review for Diagnosis of UIP
Researcher of Subjects Sensitivity () Specificity () PPV () NPV ()
Raghu et al 40
59 (29 UIP by SLB) 78 90 88 82
Hunninghake et al 41 91 (54 UIP by SLB)
74 81 85 67
Flaherty et al 3 96 (only NSIP amp UIP)
37 100 100 30
Abbreviations PPV positive predictive value NPV negative predictive value UIP usual interstitial pneumonia SLB surgical lung biopsy and NSIP nonspecific interstitial pneumonia
Furthermore an analysis of the HRCT scans from subjects enrolled in the GIPF-001 trial confirmed that local
site interpretations have a high congruity to a central radiology core In this multi-center study 263 HRCT
scans were read as definite IPF and a retrospective central radiology core review found 932 to be consistent
with IPF 42 We will also take several additional steps to insure that the local HRCT reads are accurate
including
1 A detailed training module has been developed and must be completed by each site radiologist before
site initiation
2 Clinical centers are to mail all HRCT scans to the HRCT core lab The first 10 HRCT scans from
subjects enrolled at each enrolling clinical center will be reviewed centrally to be certain that local reads
24
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
25
are congruent with a central interpretation If discrepancies are identified additional education will be
provided and HRCT scans will continue to be reviewed centrally until the central radiology core is
confident that the local center is performing appropriately
3 Random scans will be obtained from each center throughout the study to confirm that the local read
continues to agree with central interpretation If discrepancies are identified they will be addressed as in
2 above
In all cases if a subject has a surgical lung biopsy sample that sample will be reviewed by the local and central
pathologists Therefore the only cases that would not be subject to a direct central review process are those
where the HRCT meets the centrally defined criteria for an unequivocal diagnosis and a lung biopsy sample is
not available Table 2 below summarizes the possible combinations for making a diagnosis
Table 2 Combining HRCT and Pathology Interpretations to Determine if IPF is Present
HRCT Diagnosis Pathology Diagnosis Diagnosis of IPF
Definite UIP Definite UIP Yes
Definite UIP Probable UIP Yes
Definite UIP Possible UIP Yes
Definite UIP Not UIP No
Definite UIP Unavailable Yes
Consistent with UIP Definite UIP Yes
Consistent with UIP Probable UIP Yes
Consistent with UIP Possible UIP No
Consistent with UIP Not UIP No
Consistent with UIP Unavailable No
Inconsistent with UIP Any No
Abbreviations HRCT high-resolution computed tomography IPF idiopathic pulmonary fibrosis
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
UIP usual interstitial pneumonia Dx diagnosis 43 Exclusion Criteria
1 History of clinically significant environmental exposure known to cause pulmonary fibrosis
Occupational exposures such as asbestos or environmental exposure to organic dust such as occurs in
pigeon breeders may at times mimic the clinical and radiographic findings of IPF
2 Diagnosis of connective tissue disease felt by the principal investigator (PI) to be the etiology of the
interstitial disease Diagnosis of collagen-vascular conditions will be according to the published
American College of Rheumatology criteria As such the presence of any documented collagen-vascular
disorder or the presence of any suspicious symptom complex whether or not associated with
significantly abnormal rheumatological serologies will exclude the subject at the discretion of the PI
3 Extent of emphysema greater than the extent of fibrotic change (honeycombing reticular changes) on
HRCT scan
4 Forced expiratory volume in 1 second (FEV1)FVC ratio lt 065 at screening (postbronchodilator)
5 Partial pressure of arterial oxygen (PaO2) on room air lt 55 mm Hg (lt 50 mm Hg at Denver site)
6 Residual volume gt 120 predicted at screening (postbronchodilator)
7 Evidence of active infection
8 Significant bronchodilator response on screening spirometry defined as a change in FEV1 ge 12 and
absolute change gt 200 mL OR change in FVC ge 12 and absolute change gt 200 mL The percent
difference between the FVC (or FEV1) values will be calculated by taking the absolute value of the
difference and dividing it by the larger of the two FVC (or FEV1) values
9 Screening and enrollment post-bronchodilator FVC measurements (in liters) differing by gt 11 The
percent difference between the FVC values will be calculated by taking the absolute value of the
difference and dividing it by the larger of the two FVC values (eg the percent difference between FVC
measurements of 19 and 20 liters would be determined by taking the difference between the two (01
liters) and dividing by the larger of the two (20 liters) So 0120 = 5 and these FVC measurements
would not exclude the subject
10 Listed for lung transplantation ie the patient has completed the evaluation process has been accepted
as a candidate for transplantation at an appropriate center and is waiting to receive notification of an
available donor organ
11 History of unstable or deteriorating cardiac disease
12 Myocardial infarction coronary artery bypass or angioplasty within 6 months of screening
26
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
13 Unstable angina pectoris or congestive heart failure requiring hospitalization within 6 months of
screening
14 Uncontrolled arrhythmia
15 Severe uncontrolled hypertension
16 Known HIV or hepatitis C
17 Known cirrhosis and chronic active hepatitis
18 Active substance andor alcohol abuse (as determined by site PI)
19 Pregnancy or lactation (subjects who are pregnant or breastfeeding)
20 Known hypersensitivity to study medication
21 Any condition other than IPF that in the opinion of the site PI is likely to result in the death of the
subject within the next year
22 Any condition that in the judgment of the PI might cause participation in this study to be detrimental to
the subject or that the PI deems makes the subject a poor candidate
23 Any therapy directed at pulmonary fibrosis (excepting triple therapy of prednisone plus azathioprine
plus NAC) requires a 30-day washout period before randomized Triple therapy of lt= 12 weeks duration
in the past 4 years requires a 30-day washout period before randomization
24 History of triple therapy of prednisone plus azathioprine plus NAC for gt 12 weeksrsquo duration in the past
4 years or previous enrollment in the triple-therapy arm of the PANTHER-IPF study
44 Study Design and Study Visit
441 Study Design Summary
This study will be a randomized double-blind PL-controlled trial designed to assess the safety and efficacy of
NAC in subjects with newly diagnosed IPF
Subjects with mild to moderate IPF (defined as FVCpred ge 50 and DLCOpred ge 30) diagnosed within
the past 48 months will be enrolled Screening will continue until April 30 2012
27
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
The study will employ a 2-arm design with 11 randomization to NAC or PL Once enrolled subjects will visit
the clinical center at 15 weeks and 15-week intervals thereafter Each subject will be treated and followed for a
maximum of 60 weeks
During the 60-week visit subjects will be taken off all study agents Approximately four weeks after the final
dose of study agent is taken subjects will receive a safety phone call from the study site
442 Study Visits
Subjects who meet entry criteria will review the informed consent a written description of the purpose
procedures and risks of the study with the PI co-investigator or study coordinator and all questions will be
answered The informed consent form will be signed by the subject at screening No protocol-specific
procedures will be performed until the subject has signed and dated an informed consent form This includes the
screening procedures
4421 Screening
Once informed consent is obtained subjects may immediately begin the screening process or may return within
28 days of consent In the event a study subject has been clinically evaluated at the study site by an IPFnet study
physician and has performed testing within three weeks for this clinical evaluation that meets guidelines
provided in the IPFnet PANTHER-IPF Manual of Operating Procedures (MOOP) this testing may be used to
satisfy the following screening criteria medical history physical exam arterial blood gas (ABG) with A-a
gradient vital signs with oximetry body height and weight spirometry DLCO lung volumes and HRCT scan
Allowing the use of previously performed test results that meet study guidelines for the screening visit is
intended to permit subjects easier access to study entry to prevent subjects from repeating testing that has been
performed within the study window and to decrease risks to subjects from repeated exposure to procedures
such as arterial puncture and HRCT
The following procedures will be performed at screening
Medical history and a physical examination
28
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Measure height and weight
Serum pregnancy test (if applicable)
Measure vital signs including oximetry
Blood draws performed and the following analyses conducted
o Hematology (red cell count white cell count hemoglobin hematocrit cell indices differential
platelet count)
o Blood chemistries according to central laboratory protocol (see Section 410 Laboratory
Testing)
o Beta human chorionic gonadotropin (serum) pregnancy test (in women of childbearing potential)
o Urinalysis
Pulmonary Function Tests (PFTs) including spirometry pre- and post- bronchodilator and postshy
bronchodilator measurement of lung volumes and measurement of hemoglobin adjusted diffusing
capacity
Measure ABGs
HRCT if a satisfactory scan has not been performed on the subject within 3 months of screening (see
PANTHER-IPF MOOP for more details)
Surgical lung biopsies (if applicable) reviewed by local and central pathology departments
Current medications If required a washout period discussed with the subject and initiated at this visit
4422 Enrollment
The enrollment visit is expected to take place within eight weeks of the screening visit Enrollment visit
activities include
Measure vital signs including oximetry
Measure height and weight
Serum pregnancy test (if applicable)
If consent has been given blood will be drawn and a urine specimen collected for the bio-specimen
repository
Spirometry (post-bronchodilator)
Measure 6MWT with Borg Dyspnea Scale
29
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Collect Quality-of-life (QOL) data using the SF-36 EuroQol Investigating Choice Experiments for
Preferences of Older People Capability Instrument (ICE CAP) and SGRQ
Female subjects complete Gender Substudy questionnaire
Dyspnea status collected using the UCSD SOBQ
Evaluate Acute Exacerbation (AEx)
Review of any Adverse Events (AEs)
Review of concomitant medications
Subject receives diary and instructions on its purpose and proper use
Subject receives supply of study drug sufficient to last until his or her 15-week study visit
See the Schedule of Assessments (Table 3) for more details Subjects with screening and enrollment postshy
bronchodilator FVC measurements (in liters) differing by more than 11 are not eligible to be enrolled in the
study
Subjects will be asked to provide a physician of record This physician will be considered the subjectrsquos primary
care provider (PCP) and if the subject agrees the PCP will be informed by letter of the subjectrsquos enrollment in
the trial The subject will be informed that his or her ongoing medical care should be received from the PCP
The PCP will be informed of any safety issues identified by the study staff The PCP will also be given
information regarding communication with study personnel about pertinent health issues or clinic encounters
the subject may have
4423 Week 15
The week 15 visit is expected to occur within +- 14 days of the subjectrsquos scheduled visit time (eg the week 15
visit should occur anytime between 13 and 17 weeks after starting study drug Week 15 activities include
Measure vital signs with oximetry
Measurement height and weight
Serum pregnancy test (if applicable)
Spirometry (post-bronchodilator) measurement
Review of AEs
Evaluate for AEx
30
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Review concomitant medications
If consented draw blood and collect urine specimen for the biospecimen repository
Subjects return used and unused study drug for the visit
Review study diary and a new study diary will be given
Provide additional supply of study drug sufficient to last until the next scheduled visit
4424 Week 30
The week 30 visit is expected to occur within +- 14 days of the subjectrsquos scheduled visit time (eg the week 30
visit should occur anytime between 28 and 32 weeks after starting study drug) Week 30 activities include
Physical examination
Measure vital signs with oximetry
Measure height and weight
Laboratory values (complete blood count [CBC] and serum chemistries)
Serum pregnancy test (if applicable)
Measure spirometry (post-bronchodilator)
6MWT with Borg scale
DLCO
Review of AEs
Evaluate for AEx
Review concomitant medications
Complete all QOL and dyspnea questionnaires (EuroQol ICE CAP SF-36 SGRQ and UCSD SOBQ)
If consent has been given blood will be drawn and a urine specimen collected for the biospecimen
repository
Review study diary
Subjects return used and unused study drug for the visit
Provide additional supply of study drug sufficient to last until the next scheduled visit
4425 Week 45
31
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
The week 45 visit is expected to occur within +- 14 days of the subjectrsquos scheduled visit time (eg the week 45
visit should occur anytime between 43 and 47 weeks after starting study drug) Week 45 activities include
Measure vital signs with oximetry
Measure height and weight
Serum pregnancy test (if applicable)
Measure spirometry (post-bronchodilator)
Review of AEs
Evaluate for AEx
Review concomitant medications
If consent has been given blood will be drawn and a urine specimen collected for the biospecimen
repository
Subjects return used and unused study drug for the visit
Study diary reviewed
Provide additional supply of study drug sufficient to last until the next scheduled visit
4426 Week 60 (Early Withdrawal or Final Treatment Visit)
At week 60 or at subject withdrawal from the study (premature by study doctor or subjectrsquos decision) a final
treatment visit will occur At this final treatment visit subjects will discontinue NACPL abruptly Week 60
activities also include
Physical examination
Measure vital signs with oximetry
Measure height and weight
Laboratory values (complete blood count [CBC] and serum chemistries)
Spirometry (post-bronchodilator) measurement
6MWT with Borg scale measurement
DLCO
Lung volumes
ABG
Review of AEs
32
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Evaluate for AEx
Review concomitant medications
Subjects will complete all QOL and dyspnea questionnaires (EuroQol ICE CAP SF-36 SGRQ and
UCSD SOBQ)
If consent has been given blood will be drawn and a urine specimen collected for the biospecimen
repository
Subjects return used and unused study drug for the visit
Study diary reviewed
4427 Final Site Visit ndash FVC drop confirmation
In the event that the subject has a recorded FVC drop of gt10 from baseline at the final treatment visit and the
subject has not had a confirmation of such a drop at a previous study visit the subject should return to the
clinical site 6 to 8 weeks after the final treatment visit During this visit a post-bronchodilator spirometry test
will be performed This FVC measurement will be evaluated according to section 521 of this protocol
4428 Final Visit ndash Telephone Follow-up
Four weeks following the final dose of study medication subjects will receive a telephone call from the study
coordinator to ensure that there are no side effects and to follow up on any ongoing adverse events (AEs)
4429 Phone Contact Between Visits
At week 2 and each month that a subject does not have a scheduled clinical center visit his or her study
coordinator will contact him or her at least once by telephone to
Inquire if the subject has had any hospitalizations events that might be considered an AE or any events
significant enough to warrant an out-of-cycle visit to the clinical center
Remind subjects of their current dosage levels and confirm that the subject understands them
Address any questions or concerns the subject might have regarding other aspects of the study
Assess adherence to the treatment regimen by reviewing diary data verbal review of medications taken
including nutritional supplements
33
34
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Table 3 Schedule of Assessments
Procedure Screening Visit 0
Enrollment Visit 1
Week 15 Visit 2
Week 30Visit 3
Week 45 Visit 4
Week 60 Early
Withdrawal Visit 5
Final1
Visit (via phone)
Informed consent X
Medical history X
Inclusionexclusion criteria X
Serum pregnancy test (if applicable) X X X X X
Review of lung biopsy X
Arterial Blood Gas X X
6-Minute Walk Test
X
X X
Physical examination X X X
Vital signs with oximetry X X X X X X
Body height and weight X X X X X X
Complete Blood Count X X X
Chemistry panel X X X
Monitor Lab Values X X X
Urinalysis X Specimen repository substudy blood draw and urine collection (if consented)
X
X X X X
HRCT (if not completed within three months) X
Spirometry (pre- and post-bronchodilator) X
Spirometry (post-bronchodilator only) X X X X X
DLCO (post-bronchodilator only) X X X
Lung volumes (post-bronchodilator only) X
X
Evaluate for acute exacerbation X X X X X
Review Adverse Events X X X X X X
Review concomitant meds X X X X X X
Dispense subject diary X X X X
Review subject diary X X X X X
Dispense study agent X X X X
Gender Substudy questionnaire (female subjects only) X
EuroQol ICECAP UCSD SOBQ SGRQ SF-36 X X X
Abbreviations DLCO diffusing capacity of the lung for carbon monoxide QOL Quality of Life ICECAP Investigating Choice Experiments for Preferences of Older People UCSD SOBQ University of California Shortness of Breath Questionnaire SGRQ St Georgersquos Respiratory Questionnaire SF-36 Short Form 36 Health Survey
1Follow-up visit via phone will occur four weeks after final dose of study medication
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
45 Dose Justification
The general philosophy for determining dosing levels was to apply previously examined
treatment regimens With the focus of the study being to establish a standard of care for
mildmoderate IPF subjects the goal was to develop flexible yet standardized treatment rules that
allow for the temporary or permanent withholding of one or more components of treatment when
necessary Subjects developing laboratory abnormalities or symptoms that result in
discontinuation of one or more components of study treatment may continue on the other
components as long as there is no contraindication for this Complete follow-up is important for
the validity of any study As a strategy to maintain protocol adherence we are using a treatment
regimen that will detect potential side effects and prompt interventions proactively in the interest
of patient safety In addition subjects who permanently stop study medications during the course
of the study are encouraged to continue in the study completing all scheduled visits and tests
451 Rationale for N-acetylcysteine Dosing
To our knowledge there have been no IPF studies to correlate clinical outcome measures with
different dosages for NAC The dosage chosen is based on the IFIGENIA study However BAL
lung GSH levels from subjects with IPF have been augmented with the use of oral NAC at 600
mg 3 times per day In addition lung GSH levels have been associated with improved
PFTs212227 The dose chosen for this study was based on previous data including the IFIGENIA
study30
4511 Dosing of N-acetylcysteineplacebo
Dosing of NACPL will be 600 mg orally 3 times a day (1800 mgday)
4512 Reasons to Discontinue N-acetylcysteineplacebo
NACPL may be temporarily or permanently discontinued for the duration of the study for
gastrointestinal symptoms or dermatologic reactions
35
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Temporarily discontinue (hold) oral NACPL for subjects requiring inpatient admission for acute
exacerbation (AEx) or other conditions Resume NACPL after discharge
36
37
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
452 Dosage Algorithms
Dosage Adjustment Algorithm 1 NACPL Dose Modifications for Gastrointestinal Symptoms Nausea Vomiting Abdominal Discomfort Diarrhea
GI Symptoms determined by the PI to be clinically significant Nausea Vomiting Abdominal Discomfort Diarrhea
NACPL Temporarily dc (HOLD) x 3 Days
Monitor symptoms intervene as clinically indicated (eg fluid replacement antidiarrhea or antinausea medication)
Monitor or lab PRN
Are symptoms resolving after 3 days NO
Symptoms NOT resolving after 3 days of holding study medication Assessmentmanagement per clinical
discretion of investigator
Likely not study medication discuss resuming study medication with medical monitor when symptoms resolved
YES
Temporarily dc (HOLD) NACPL for 4 additional days (total hold 1 week) then NACPL Resume 600 MG TID
Did symptoms recur
YES
STOP NACPL for
duration of study
NO
NACPL No Change
38
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Dosage Adjustment Algorithm 2 NACPL Dose Modifications For Dermatologic Reactions
Dermatologic Reactions (Not Acneiform) ge Grade 2 Grading per Common Terminology Criteria for
Adverse Events V30 (httpctepcancergov) For example Grade 1 RASHDESQUAMATION Macular or papular eruption or erythema without associated symptoms Grade 2 RASHDESQUAMATION Macular or popular eruption or erythema with pruritus or other associated symptoms localized desquamation or other lesions covering lt50 of body surface area
NACPL Temporarily dc (HOLD) x 3 days
Are symptoms resolving after 3 days
NO Symptoms not resolving after 3 days of holding study medication Assessmentmanagement per clinical discretion of investigator Likely not study medication Discuss resuming study medication with medical monitor when symptoms
resolved YES
Temporarily dc (HOLD) NACPL for 4 additional days (total hold 1 week) then NACPL resume 600 MG TID
Did symptoms recur
YES
STOP NACPL for
duration of study
NO
NACPL No change
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
46 Contraindications Precautions and Side Effects of Study Medications
461 Contraindication
Contraindication to NAC is known hypersensitivity to it
462 Precautions
Concomitant administration of oral NAC and antibiotics has shown a slightly reduced absorption
of cephalexin and a slight increase in erythromycin serum levels NAC contains free sulfhydryl
groups There is no evidence that individuals sensitive to sulfa drugs are sensitive to NAC
The NAC preparation being administered in this study contains 20 mg of aspartame Because of
the phenylalanine component of aspartame individuals with phenylketonuria should avoid or
restrict aspartame intake to avoid increased blood levels of phenylalanine Because of this risk
labeling is required on all products containing aspartame
463 Side Effects
Side effects of NAC range from common to serious See Table 4
39
40
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Table 4 Side Effects of NAC
Undesirable Effects
System-organ class Uncommon
(gt11000 lt1100)
Rare
(gt110000 lt11000)
Very rare
(lt110000) Not known
Immune system disorders Hypersensitivity Anaphylactic shock
reaction
Nervous system disorders Headache
Ear and labyrinth disorders Tinnitus
Cardiac disorders Tachycardia
Vascular disorders Hemorrhage
Respiratory thoracic and
mediastinal disorders
Bronchospasm
Dyspnea
Gastrointestinal disorders
Vomiting diarrhea
stomatitis abdominal
pain nausea
Dyspepsia
Skin and subcutaneous tissue
disorders
Urticaria rash
angioedema itching
General disorders and
administration site conditions Pyrexia
Investigations Reduced arterial
pressure Face edema
In very rare cases the onset of severe skin reactions such as Stevens-Johnson syndrome and Lyell syndrome was reported to have a temporal relationship with N-acetylcysteine administration Although in most cases at least another suspect drug probably most involved in the genesis of the above mentioned mucocutaneous syndromes has been identified in case of mucocutaneous alterations it is appropriate to contact onersquos doctor and the administration of N-acetylcysteine should be immediately discontinued
Some studies confirmed a reduction of platelet aggregation during N-acetylcysteine administration The clinical significance of these findings has not been defined yet [Source Fluimucil Investigator Brochure]
47 Recruitment Procedures
Subjects recruited for this study will be established patients of the investigators or physician- or
self-referred to participating clinical centers in the IPFnet Each clinical center within IPFnet has
a well-developed infrastructure of local pulmonologists within the surrounding geographic area
These pulmonologists are kept informed of ongoing IPF clinical trials and regularly refer
subjects to studies conducted at IPFnet clinical centers
Additional steps will be taken to inform clinicians of the trials in progress within IPFnet
including presentations at faculty staff meetings at local hospitals medical grand rounds and
national conferences direct mail notification monthly faxes and advertisement of network trials
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
in pulmonary journals Clinical center patients previously diagnosed with IPF will be notified of
the trials by mail whenever possible
Recruitment of minorities and women will be monitored by the DCC and DSMB If necessary
additional recruitment efforts will be made at specific centers to ensure that the aggregate subject
sample contains appropriate representation of women and minorities
48 Study Procedures
The following procedures are detailed in the PANTHER-IPF MOOP accompanying this
protocol
1 PFT
2 ABG
3 HRCT scan of the chest (including imaging of pulmonary arteries)
4 CBC and serum chemistries
5 Pregnancy test
6 6MWTBorg Dyspnea Scale
7 QOL questionnaires (EuroQol HAD SF-36 SGRQ and ICE CAP)
8 UCSD SOBQ
9 Gender Substudy Questionnaire
All assessments of PFTs will be conducted by study personnel not directly involved in the
treatment of the subjects
481 Biological Specimen Management
4811 Biological Specimen Sample Management
Subjects at clinical centers participating in the specimen repository substudy who consent to
having blood drawn for research purposes and for the banking of blood blood components and
other biologic specimens (urine and BAL fluid) will have approximately 405 mL of blood
41
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
drawn 17 mL blood drawn for DNA and 20 mL of urine collected at enrollment visit Subjects
will have approximately 50 mL of blood drawn and 20 mL of urine collected at each 15-week
follow-up visit Blood specimens will be separated according to PANTHER-IPF MOOP
guidelines into the following components for banking in the repository serum plasma and
DNA Coding of all biologic specimens for the repository will be performed by study staff at the
clinical center The samples will be processed per PANTHER-IPF MOOP guidelines aliquoted
labeled with barcode labels and stored at -70degC at the clinical center and shipped to the central
repository
The only subject identifiers will be a sample ID number and subject initials This sample ID will
be linked in the IPFnet DCC clinical database to subject information No subject information will
be transferred to the biological-specimen database
The subjectrsquos samples may be used for approved sub-studies relating to human disease
including but not limited to IPF The studies for which an individualrsquos samples will be made
available will be determined by the subjectrsquos answers to questions on the biological-sample
informed consent form The subjects can choose to make their samples available for all options
or any combination Samples will be made available to researchers only with IPFnet Steering
Group approval until such time as the samples are made public through the NHLBI repository
49 Concomitant Medications
Concurrent treatment with FDA-approved therapy for IPF is allowed Colchicine may be used
for treatment of gout Temporary treatment with oral or IV corticosteroids for clinical worsening
or suspected AEx is permitted Nutritional supplements containing NAC are not allowed
410 Laboratory Testing
Clinical laboratory parameters will be assessed at screening and at the end of the study The
following tests will be performed at the two time points specified in the protocol chemistry (AG
ratio ALT [SGPT] AST [SGOT] albumin alkaline phosphatase amylase bilirubin-direct
42
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
bilirubin-indirect bilirubin-total BUN BUNcreatinine ratio calcium carbon dioxide
cholesterol-total chloride CPK-total creatinine GGT globulin glucose iron-total LDH
lipase magnesium phosphorus-inorganic potassium protein-total sodium TIBC triglycerides
uric acid) and hematology (red blood cell count WBC count hemoglobin hematocrit cell
indices differential platelet count)
411 Blinding of Study Drugs
Subjects and caregivers will be blinded to study treatment Every subject will receive NAC or
matching PLs at every study visit from the baseline visit to the week-45 visit No study agent
will be dispensed at the week-60 visit
43
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
5 Study Endpoints
51 Primary Study Endpoint
The primary endpoint will be the change in serial measurements of FVC over the study period
52 Secondary Study Endpoints
521 Time to Disease-progression
The time-to-death or a 10 decline in FVC will be defined as the time-to-disease progression
The 10 decline in FVC from enrollment must be confirmed on 2 consecutive visits no less than
6 weeks apart For subjects with 2 consecutive visits with a 10 decline in FVC the time-toshy
disease progression will be defined as the time interval between enrollment and the initial visit
with a 10 FVC decline For subjects who experience disease progression the study doctor will
determine whether or not the subject will remain in the study
522 Acute Exacerbations
The following 3 criteria will define AEx in subjects with acute worsening of their respiratory
conditions
1 Clinical (all of the following required)
A) Unexplained worsening of dyspnea or cough within 30 days triggering unscheduled
medical care (eg emergency room clinic study visit hospitalization)
B) No clinical suspicion or overt evidence of cardiac event pulmonary embolism or deep
venous thrombosis to explain acute worsening of dyspnea
C) No pneumothorax
44
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
2 RadiologicPhysiologic (A and B required)
A) New ground glass opacity or consolidation computed tomography (CT) scan OR new
alveolar opacities on chest x-ray
B) Decline of ge 5 in resting room air SpO2 from last recorded level OR decline of ge 8 mm
Hg in resting room air PaO2 from last recorded level
3 Microbiologic (all of the following required)
A) No clinical evidence for infection (ie absence of grossly purulent sputum fever gt 39degC
orally)
B) Lack of positive microbiological results (if done) from lower respiratory tract defined as
(1) Clinically significant bacterial growth on sputum or endotracheal aspirate cultures
(2) Quantitative culture by protected brush specimen ge 103 cfumL or BAL ge 104 cfumL
(3) The presence of specific pathogens on stains of any of the above
C) Lack of positive pathogen in blood cultures (if done)
Identification of Acute Exacerbations
All subjects will be educated about the importance of identifying AExs At the time of
enrollment subjects will be told about the possibility of developing acute symptomatic
worsening that might represent an AEx of IPF and instructed to contact their study clinical
center coordinator within 48 to 72 hours of the apparent event
All subjects will be contacted by phone monthly and questioned about any change in dyspnea or
cough and any interim clinic visits or hospitalizations Finally as part of the IPFnet outreach to
community referring physicians the importance of AExs will be emphasized When a subject is
identified who meets criterion 1A this will trigger the collection of additional clinical data to
evaluate a suspected AEx These data will be collected as part of standard clinical care (ie this
protocol does not require collection of all items) The additional items to be collected for
suspected AEx include
IPFnet AEx case report form (eCRF) (required)
45
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Chest x-ray CT scan withwithout pulmonary angiogram (reports should be faxed and
followed by the hard copiesdiscs)
Oxygen saturation (pulse oximetry)
ABG
Respiratory cultures (sputum endotracheal aspirate lavage)
Blood cultures
Clinichospital records related to the event
All potential cases of AEx will be reviewed by the clinical center PI first and a decision on
whether the case may represent an AEx will be made If AEx is suspected the case will be sent
to the IPFnet adjudication committee which will assign a final diagnosis (see Table 5) If there is
disagreement among members the majority opinion will be recorded
During episodes of suspected AEx as determined by the individual clinical center investigator
subjects will remain blinded and in the study
Table 5 Final Diagnoses in Evaluation of Suspected Acute Exacerbations
Definite acute exacerbation All criteria met no alternative etiology
Unclassifiable acute worsening
Insufficient data to evaluate all criteria no alternative etiology
Not acute exacerbation Alternative etiology identified that explains acute worsening
Management of the suspected AEx will be at the discretion of the treating physician Standard of
care generally involves evaluation for respiratory infection pulmonary embolism cardiac events
and pneumothorax and treatment with IV corticosteroids
Study drugs will be resumed at pre-suspected AEx doses after subjects clinically improve as
confirmed by the local PI All subjects should be seen at the clinical center within 2 to 4 weeks
of recovery for measurement of post-bronchodilator FVC (see Figure 4) Subjects unable to
return to the clinical center after suspected AEx due to medical frailty (eg continued
46
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
institutionalization progressive disability) will be categorized as failing to maintain FVC
response in secondary analyses
Suspected AEx (PI determined)
Hold study drug Treat AEx
(Attending physician determined)
Alive but unable to continue due to
medical frailty
Dead
Alive and able to continue
Site reviewvisit
Restart study drug
FVC within 2-4 weeks
Figure 4 Acute Exacerbation Flow Chart
523 Respiratory Infections
An upper respiratory infection will be defined as
Change in sputum discoloration
Increased cough of no more than 14 daysrsquo duration
A lower-respiratory infection (pneumonia) will be defined as new segmental or lobar airspace
opacities visualized by image studies (chest radiograph or HRCT) in addition to any of the
following
Positive pathogencultures in good sample of sputum or lower-airway secretions retrieved
by fiberoptic bronchoscope
Fever gt 39degC or gt 100degF
Leukocytosis gt 12000 (unexplained no increase in dose of corticosteroids)
47
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
524 Maintained FVC Response
Subjects with follow-up FVCpred measurements at or above their baseline FVCpred level
will be classified as having maintained FVC response Subjects with reduced FVCpred levels
or missing data for any reason including death or medical frailty will be classified as having not
maintained FVC response The FVCpred value is used because unadjusted FVC measurements
are expected to decline with age
48
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
6 Safety Evaluations and Procedures
61 Adverse Events
During a clinical trial the reporting of adverse experience information can lead to important
changes in the way a new treatment is developed as well as provide integral safety data
611 Definitions
An adverse event (AE) is any untoward medical occurrence in a subject or clinical investigation
subject who was administered a pharmaceutical product The AE does not necessarily have to
have a causal relationship with the drug administered An AE can be any unfavorable and
unintended sign (including an abnormal laboratory finding) symptom or disease temporarily
associated with the use of a medicinal product whether or not considered to be related to the
medicinal product Diseases signs symptoms or laboratory abnormalities already existing at
enrollment are not considered AEs unless they worsen (ie increase in intensity or frequency)
Surgical procedures themselves are not AEs they are therapeutic measures for conditions that
require surgery The condition for which the surgery is required may be an AE Surgical
procedures planned before randomization and the conditions necessitating the surgery are not
AEs
A serious adverse event is any untoward event that
Is fatal
Is life-threatening
Requires inpatient hospitalization or prolongation of existing hospitalization with the
following exceptions
o Preplanned (before the study) hospital admissions unless the hospitalization is
prolonged
o Planned admissions (as part of a study eg routine biopsies)
o Hospitalization lasting lt 24 hours
49
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
o Hospitalization for elective procedure
o Emergency room visits
Results in persistent or significant disability or incapacity
Is a congenital anomaly or birth defect
Important medical events that may not result in death be life-threatening or require
inpatient hospitalization may be considered serious adverse events (SAEs) when based
on appropriate medical judgment they may jeopardize the subject and may require
medical or surgical intervention to prevent one of the outcomes listed above
Life-threatening means that the subject was in the view of the investigator at immediate risk of
death from the AE as it occurred It does not include an AE that had it occurred in a more severe
form might have caused death
Persistent or significant disabilityincapacity means that the event resulted in permanent or
significant and substantial disruption of the subjectrsquos ability to carry out normal life functions
Causality
A reasonable possibility means the AE may have been caused byrelated to the study drug A
perceived or real lack of efficacy does not satisfy the definition of relatedness
612 Adverse Event (AE) Reporting
For the PANTHER-IPF trial all AEs (serious and nonserious) occurring from randomization
through final study visit (4 weeks after final dose of all study medication) will be recorded on the
AE page of the case report form (CRF)
6121 Serious Adverse Events (SAE) Reporting
For this trial all deaths and all SAEs which occur from randomization through final study visit
must be entered within the EDC system via the SAE eCRF page within 24 hours of the
investigative sitersquos knowledge of the event It is the responsibility of the clinical center
50
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
investigator to provide a causality assessment of the event for each study medications based upon
the information available at the time of the report It is understood that complete information
about the event may not be known at the time the initial report is submitted In the event the EDC
system is not accessible to the site at the time of event reporting investigative sites will complete
and forward a paper back-up SAE form to DCRI Safety Surveillance for processing
DCRI Safety Surveillance
Telephone 1-919-668-8624 or 1-866-668-7799 (toll free)
Fax 1-919-668-7138 or 1-866-668-7138 (toll free)
The investigator must complete and submit follow-up SAE information via the eCRF when
important new or follow-up information (eg final diagnosis outcome results of specific
investigations) becomes available Follow-up information should be submitted according to the
same process used for reporting the initial event as described above All SAEs will be followed
until resolution stabilization or 30 days after the subject has completed the final visit (4 weeks
after the final dose of study medication) whichever occurs first The investigator is responsible
for reporting SAEs to their institutional review board (IRB) per site specific IRB reporting
guidelines
6122 Regulatory Reporting
AEs that are serious study drug related and unexpected will be reported to the regulatory
authorities The DCRI Safety Surveillance medical monitor will perform a medical review of all
SAEs submitted and evaluate for ldquounexpectednessrdquo DCRI Safety Surveillance will prepare
MedWatch reports for those events identified as serious study drug related and unexpected as
determined by Safety Medical Monitor
DCRI Regulatory Services will submit all unexpected study drug-related SAEs as per 21 CFR
32 DCRI Safety Surveillance will provide a safety alert letter to the NHLBI DSMB and DCC
clinical operation (for distribution to sites) within 15 days of initial receipt of the information
51
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Investigators are responsible for promptly reporting these events to their reviewing IRBs
according to site specific IRB reporting guidelines
62 Clinical Medical Monitoring
There will be an unblinded physician at the IPFnet DCC serving as medical monitor The
medical monitor will be available to assist with questions about dosage adjustments of study
medications including discontinuation or resumption of medications
63 Unblinding Procedures
Unblinding of subjects or investigators to subject treatment is strongly discouraged For ongoing
clinical management all subjects should be presumed to be receiving ldquoactiverdquo study drug To
ensure the subjectrsquos safety the study treatment will be dose-adjusted based on laboratory test
results clinical findings and symptoms
The IPFnet DCC medical monitor and PANTHER-IPF co-chairs Drs Ganesh Raghu and
Fernando Martinez will be available to the study physicians to discuss study drug management
on a case-by-case basis Un-blinding will be considered ONLY when the knowledge of subject
treatment assignment is ABSOLUTELY ESSENTIAL for subject safety and after discussion of
the subjectrsquos case with the medical monitor and either Dr Raghu or Dr Martinez Unblinding of
study treatment should be minimized during the conduct of the trial In those cases where it is
felt to be medically necessary the DCC medical officer will communicate directly with the
managing physician to minimize unblinding of study personnel
52
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
7 Study Drug Procedures
At the baseline 15-week 30-week and 45-week study visits subjects will receive a supply of
study drug sufficient to last until the next visit at which study drug will be dispensed
53
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
8 Data Management
81 Hardware and Software Configuration
811 Hardware and Database Software
Data will be stored in an Oracle database system Oracle has advantages of processing efficiency
and smooth linkage with other software systems The application and database will be hosted on
Solaris Unix servers at the IPFnet DCC
812 Statistical Software
SAS will be used as the principal application for the management of analysis data files and
statistical computations S-Plus will be used to provide supplementary functions as needed
813 Access Control and Confidentiality Procedures
Access to databases will be controlled centrally by the IPFnet DCC through user passwords
linked to appropriate privileges This protects the data from unauthorized changes and
inadvertent loss or damage
814 Security
Database and Web servers will be secured by a firewall and through controlled physical access
Oracle has many security features to ensure that any staff member accessing the database has the
proper authority to perform the functions he or she requests of the system Within the secondary
SAS databases Unix group-access control maintains similar security The Sun workstation login
is secured by extensive user-password facilities under Unix
54
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
815 Back-up Procedures
Database back-up will be performed automatically every day and standard IPFnet DCC policies
and procedures will be applied to dictate tape rotation and retention practices
816 Virus Protection
All disk drives that provide network services and all user computers will be protected using
virus-scanning software Standard IPFnet DCC policies will be applied to update these protection
systems periodically through the study
82 Sources of Data
821 Design and Development
The IPFnet DCC will be responsible for development of the electronic case report forms
(eCRFs) development and validation of the clinical study database ensuring data integrity and
training clinical center staff on applicable data management procedures A web-based distributed
data entry model will be implemented This system will be developed to ensure that guidelines
and regulations surrounding the use of computerized systems used in clinical trials are upheld
The remainder of this section provides an overview of the data management plan associated with
this protocol
822 Data Collection Forms
The data collection process consists of direct data entry at the study clinical centers into the EDC
system(s) provided by the DCC A data collection worksheet will be provided to clinical centers
for recording data in the event the EDC system is unavailable Data entry of the eCRFs should
be completed according to the instructions provided and project specific training The
investigator is responsible for maintaining accurate complete and up-to-date records and for
ensuring the completion of the eCRFs for each research participant
55
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
823 Data Acquisition and Entry
Data entry into eCRFs shall be performed by authorized individuals Selected eCRFs may also
require the investigatorrsquos written signature or electronic signature as appropriate Electronic
CRFs will be monitored for completeness accuracy and attention to detail during the study
824 Data Center Responsibilities
The IPFnet DCC will 1) develop a data management plan and will conduct data management
activities 2) provide final eCRFs for the collection of all data required by the study 3) develop
data dictionaries for each eCRF that will comprehensively define each data element 4) conduct
ongoing data monitoring activities on study data 5) monitor any preliminary analysis data
cleanup activities and 6) rigorously monitor final study data clean up
825 Data Editing
Completed data will be entered into the IPFnet DCC automated data acquisition and
management system If incomplete or inaccurate data are found a data clarification request will
be generated and distributed to clinical centers for a response Clinical centers will resolve data
inconsistencies and errors and enter all corrections and changes into the IPFnet DCC automated
data acquisition and management system
826 Training
The training plan for clinical center staff includes provisions for training on assessments eCRF
completion guidelines data management procedures and the use of computerized systems
56
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
9 Study Design and Data Analysis
91 General Analytic Considerations
All primary analyses will be based on intent-to-treat (ITT) principles using all randomized
subjects Baseline factors across groups will be compared using mean (standard deviation) and
median (25th and 75th percentiles) summary measures Kaplan-Meier curves will be used to
display event rates Due to clinical interest in departures from both sides of the null hypothesis
all test statistics will be 2-sided
Reasonable caution needs to be taken when conducting multiple analyses on key clinical
subgroups For subgroup analyses a conservative significance level of 0001 will be used for all
interaction tests Thus subgroup comparisons will be considered exploratory unless the p-value
from the interaction test is smaller than 0001
92 Randomization Blinding and Reporting of Results
A permuted block-randomization scheme will be created with varying block sizes stratified by
clinical center Once a subject has completed the screening and baseline period and evaluation
for inclusionexclusion criteria the randomization process will begin Subjects will be
randomized to receive NAC or matching placebo with equal probability (11) via telephone
contact with a central interactive voice response system (IVRS) using a toll-free randomization
number On the day of randomization after the subject has successfully met all inclusion and
exclusion criteria the investigator or designee will call the central randomization number to
obtain the assigned kit randomization numbers for that subject At each subject visit the
investigator or designee will call the central randomization number to obtain the new kit
randomization numbers for resupply of the subject For resupply of the clinical center the IVRS
will monitor minimal volume of a kit type andor expiration date and will automatically notify
the pharmacy
57
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
The trial results will be reported according to guidelines specified in the CONSORT statement
A flow diagram describing screening recruitment randomization dropout and vital status will
be included in the primary manuscript AEs and efficacy data will be presented for all treatment
groups Adherence dropout and lost to follow-up will be carefully examined across all treatment
groups Analyses of safety will be based on data from all randomized subjects who received at
least one dose of study drug
93 Stratification
Subjects will be distributed to the two treatment arms in a 11 allocation ratio Stratification
blocks will be based on clinical centers
94 Specification of the Primary Analyses
A mixed model repeated measures (MMRM) analysis described in section 95 will be used to
compare differences in the slope of FVC measurements across the treatment groups Response
variables are values of the FVC measured at baseline and every 15 weeks until study completion
Variables in the model will include treatment time and time by treatment age sex race and
height Contrast estimates of differences in slopes of treatment over time (along with confidence
intervals) will be used to estimate the treatment effect The validity of this model in terms of
meeting modeling assumptions will be assessed via standard modeling diagnostics and goodness-
of-fit measures Based on the MMRM framework missing FVC data will not be imputed for the
primary analysis
95 Analysis of Longitudinal Endpoints
A common goal in clinical trials is to specify models that are easily implemented and
reproducible by independent data analysts On the other hand the models should have proper
statistical behavior in terms of low bias and high precision Many common approaches to
longitudinal data analysis including last observation carried forward (LOCF) imputation rely on
the missing completely at random (MCAR) assumption However the MCAR assumption is
58
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
unlikely to hold in many clinical trials because missing data are often related to disease
progression and prognosis A more reasonable assumption missing at random (MAR) specifies
that the complete data distribution can be modeled using only the observed data The likelihood-
based MMRM approach is valid under the more general MAR assumptions These models will
be applied to analyze the longitudinal data secondary endpoints
The advantages of MMRM analysis are that all important characteristics of the model can be preshy
specified standard software can be used to implement the models and results are based on ITT
principles43 In addition the MMRM approach offers superior control of Type I and Type II
errors compared with the LOCF approach
Response variables are values of the PFTs measured at enrollment and every 15 weeks until
study completion and 6MWT values measured at baseline week 30 and week 60 Covariates are
treatment time time by treatment and key baseline risk factors Contrasts (along with
confidence intervals) of treatment by time will be used to estimate the treatment effect
The correlation structure involves multiple pieces including measurement errors random
variation and interindividual variability For the longitudinal data analyses an unstructured
correlation matrix for within-subject errors will be assumed Other correlation structures
including compound symmetry will be examined as needed A careful examination of reasons
for study discontinuation will be conducted to assess the validity of MCAR Sensitivity analyses
will be used to examine the untestable assumption that the observed data violate the MAR
assumption The MMRM models will be implemented using PROC MIXED in SAS
96 Analysis of Binary Time-to-Event and Time-Lagged Endpoints
Regression modeling approaches using either the logistic regression model or Cox proportional
hazards regression model will be employed when appropriate The validity of these models will
be assessed via standard modeling diagnostics and goodness-of-fit measures Estimates of
cumulative frequencies for more general time-lagged responses will be calculated using the
partitioned version of the Bang-Tsiatis estimator44 The partitions will be set at 15-week intervals
59
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
to correspond with the data-collection process Covariate adjusted event rates will be calculated
using inverse probability-weighted regression estimates45
97 Power Analysis
971 Primary Analyses
Based on previously published IPF clinical trials the PL group is expected to experience a drop
in FVC of approximately 020 L over the study period (see Figure 1) The IPFnet Steering Group
determined a clinically important difference would be to preserve the majority of the decline
relative to PL over the study period In particular a treatment effect of 015 L was determined to
be a clinically meaningful difference Potential dropout is a key factor in the proposed study The
drop-out process assumed 5 lost to follow-up after every study visit Only 80 of subjects
were assumed to be followed for the entire study period All models assumed a compound
symmetry structure for the covariance matrix Power calculations were performed using a SAS
IML program for designing repeated measures studies46 Based on preliminary reviews of the
data from the University of Michigan the covariance matrix parameters were estimated at
approximately σ2 = 0757 (variance parameter) and ρ = 0936 (correlation parameter) To be
conservative the power calculations for the primary analysis were performed with parameter
setting of σ2 = 0810 (variance parameter) and ρ = 0925 (correlation parameter)
The power calculations assume a correction for imperfect compliance proposed by Lachin and
Foulkes to allow for 2 noncompliance for each of the treatment arms47 Thus the sample size
of 130 subjects per arm would be reduced to an adjusted sample size of 130(1-002-002)2 =
1198 or 120 subjects per arm
Under the assumed Type I error rate of 005 with a correlation parameter of 0925 and standard
deviation of 090 the difference of 015 L (or 00025 Lweek) shown in Table 6 would have
power of 93
60
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Table 6 Hypothetical Values of Mean FVC (L) Change from Baseline
Week 15 Week 30 Week 45 Week 60
NAC 00125 00250 00375 00500
Placebo 00500 01000 01500 02000
Difference 00375 00750 01125 01500
Abbreviations FVC forced vital capacity PL placebo
972 Power Analysis for Secondary Endpoints
Power calculations for secondary endpoint measurements are shown in Table 7 Standard
deviations are based on unpublished data provided by the University of Michigan The
calculations are based on a 2-sample t-test with Type I error rate set at 005 These calculations
are likely to be conservative because the statistical approach described in section 95 for
analyzing these endpoints will incorporate incomplete observations as well as intermediate data
points
Table 7 Detectable Differences in Treatment Means for Selected Endpoint Measurements
Secondary Endpoints Std Dev
of the Baseline Score
Detectable Difference for 80 Power
Std Dev of the Change Score
Difference Detectable for
80 Power
DLCOpred 166 58 91 32
6MWT Area Under the Desaturation Curve
219 76 175 61
6MWT Distance to Desaturation 224 78 315 110
6MWT Minutes Walked 210 073 205 071
Abbreviations Std Dev standard deviation DLCOpred diffusing capacity of the lung for carbon monoxide percent predicted 6MWT 6-minute walk test
61
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
10 Study Administration
101 Cooperative Agreement Mechanism
The administrative and funding mechanism used to undertake this project is a ldquocooperative
agreementrdquo (U01) which is an assistance mechanism Under the cooperative agreement the
NHLBI assists supports andor stimulates the project and is substantially involved with
investigators in conducting the study by facilitating performance of the effort in a ldquopartnerrdquo role
The NHLBI project scientist serves on the IPFnet Steering Group and he or another NHLBI
scientist may serve on other project committees when appropriate At the same time however
NHLBI does not assume a dominant role direction or prime responsibility for this research
program
As described below governance of the project is conducted through the IPFnet Steering Group
Principal investigators have lead responsibilities in all aspects of their trials and the project
including any modification of trial designs conduct of the trials quality control data analysis
and interpretation preparation of publications and collaboration with other investigators unless
otherwise provided for by the IPFnet Steering Group
PIs retain custody of and have primary rights to their center-specific and collaborative data
subject to government rights-of-access consistent with current Health amp Human Services (HHS)
Public Health Service (PHS) and National Institutes of Health policies The protocols and
governance policies call for the continual submission of data centrally to the IPFnet DCC for the
collaborative database which at a minimum will contain the key variables selected by the IPFnet
Steering Group for standardization across all clinical centers the submission of copies of the
collaborative datasets to each PI upon completion of the project procedures for data analysis
reporting and publication and procedures to protect and ensure the privacy of medical and
genetic data and records of individuals The NHLBI project scientist on behalf of the NHLBI
will have the same access privileges and responsibilities regarding the collaborative data as the
other members of the Steering Group
62
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
PIs are also encouraged to publish and to publicly release and disseminate results data and other
products of the project concordant with the project protocols and governance and the approved
plan for making data and materials available to the scientific community and to the NHLBI
However during the 3 years after the ending date of NHLBI project support unpublished data
unpublished results data sets not previously released and other study materials or products are
to be made available to any third party only with the approval of the IPFnet Steering Group
Upon completion of the project PIs are expected to put their intervention materials and
procedure manuals into the public domain andor make them available to other investigators
according to the approved plan for making data and materials available to the scientific
community and the NHLBI for the conduct of research at no charge other than the costs of
reproduction and distribution
The NHLBI reserves the right to terminate or curtail the project (or an individual award) in the
event of (a) failure to develop or implement mutually agreeable collaborative measurement
subject eligibility and data management sections of the protocols (b) substantial shortfall in
subject recruitment follow-up data reporting or quality control or other major breach of
protocol (c) substantive changes in the agreed-upon protocols with which NHLBI cannot
concur (d) reaching a major project outcome with persuasive statistical significance
substantially before schedule or (e) human subject ethical issues that may dictate a premature
termination
Any disagreement that may arise in scientificprogrammatic matters (within the scope of the
award) between award recipients and the NHLBI may be brought to arbitration An arbitration
panel will be composed of 3 membersmdash1 selected by the IPFnet Steering Group (with the
NHLBI member not voting) or by the individual PI in the event of an individual disagreement a
second selected by NHLBI and the third selected by the other 2 members This special
arbitration procedure in no way affects the PIrsquos right to appeal an adverse action that is otherwise
appealable in accordance with the PHS regulations at 42 CFR part 50 Subpart D and HHS
63
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
regulation at 45 CFR part 16 or the rights of the NHLBI under applicable statutes regulations
and terms of the award
102 IPFnet Steering Group
The IPFnet Steering Group is the main governing body of the project It is composed of the PIs
of the clinical centers the PI of the DCC and the NHLBI project scientist The clinical centers
the IPFnet DCC and the NHLBI each have 1 vote on the IPFnet Steering Group All decisions
are determined by majority vote
All major scientific decisions are determined by the IPFnet Steering Group It assumes overall
responsibility for the design and conduct of the trial It appoints (and disbands) committees and
subcommittees as the need arises designs approves and implements the study protocols
oversees the development of the MOOP monitors subject recruitment and treatment delivery
evaluates data collection and management oversees quality assurance procedures and
implements changes and enhancements to the study as required It also has primary responsibility
for facilitating the conduct of the trials and reporting the projectrsquos results
103 Data and Safety Monitoring Board
The NHLBI will establish a DSMB in accordance with established policies (see
httpwwwnhlbinihgovfundingpoliciesdsmb_insthtm) to ensure data quality and subject
safety and to provide independent advice to the NHLBI regarding progress and the
appropriateness of study continuation
104 Recommendations on Interim Monitoring of Efficacy Safety and Futility
First and foremost the role of the DSMB will be to review subject safety and trial conduct at
periodic points during the study The DSMB may require analyses of the primary endpoint
results for comparing the benefit and risks of treatment strategies The benefit of collecting
additional data on key secondary endpoints with extended follow-up and establishing a robust
64
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
evidence base for determining a standard of care will need to be carefully considered before
early termination of one or more treatment arms After careful consideration the IPFnet Steering
Group recommends conservative thresholds for the early examinations of the safety and efficacy
data
The DSMB will be expected to meet approximately every 6 months until trial completion to
review safety and toxicity data The DSMB may recommend stopping the study based on these
reviews Because the DSMB could stop the trial for safety concerns as well as for a large
efficacy benefit there could be multiple opportunities to reject the null hypothesis (no difference
in event rates between the PL and NAC groups) A Bonferroni approximation will be applied
during the one planned interim analysis for efficacy
Before locking the database a statistical analysis plan (SAP) will be developed to provide
complete details on the statistical analysis The SAP will include the specifics for how and when
the DSMB will be notified for AEs The IPFnet DCC will deliver to the DSMB all FDA-defined
AEs at 3-month intervals The IPFnet DCC will prepare narrative SAE reports in real time for
DSMB review including recommendations and analysis of similar events for each SAE
submitted to the FDA
65
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
11 Investigator and Sponsor Obligations
111 Monitoring
All monitoring activities for US clinical centers will be performed in accordance with DCRI
standard operating procedures Information regarding the types of visits will be outlined in the
PANTHER-IPF MOOP
112 Cost and Payment
There will be no cost to subjects enrolled in this trial Study-related procedures will be paid for
by the IPFnet
Subjects may be eligible for reimbursement for travel to the clinical center Details of payment
will be explained to each subject during the consent process
113 Confidentiality and Health Insurance Portability and Accountability Act
Considerations
Subject confidentiality will be protected throughout the study All subject data will be kept
strictly confidential and no subject-identifying information will be released to anyone outside
the project Confidentiality will be assured through several mechanisms First each subject will
be assigned an anonymous study ID which will then be used on all study forms Second any
study forms blood samples and paper records that contain subject information (eg address lists
phone lists) will be kept at the clinical centers in secured locked areas coded by number Once
blood is collected there will be no subject identifiers placed on blood samplesmdashonly the study
ID number and the date of sample collection Third access to all subject data and information
including laboratory specimens will be restricted to authorized personnel In the case of
computerized data this restricted access will be assured through user logon IDs and password
protection
66
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
At the IPFnet DCC only authorized personnel will have access to the data files containing study
data Security will be assured through user logon IDs passwords and appropriate access
privileges All study subjects will be identified only by their IPFnet ID numbers and no personal
identifying information such as name address or Social Security number will be entered into
the IPFnet DCC database Any subject-specific data reported to the IPFnet Steering Group will
be identified only by the IPFnet ID number
Finally subjects will not be identified by name in any reports or publications nor will the data
be presented in such a way that the identity of individual subjects can be inferred Analysis files
created for further study by the scientific community will have no subject identifiers These data
files will be created in accordance with the Ancillary Studies and Publication Policy of the
IPFnet
114 Informed Consent Procedures
All IPFnet subjects will provide written informed consent using procedures reviewed and
approved by each clinical centerrsquos IRB Informed consent will be undertaken by study personnel
in-person with the subject The subject has the option of declining further participation in the
study at that point No further study procedures will be conducted until the signed documents
have been provided to the IPFnet clinical center
115 Institutional Review Boards
Before initiating this study the protocol clinical center-specific informed consent forms Health
Insurance Portability and Accountability Act (HIPAA) forms recruitment materials and other
relevant information will be reviewed by a properly constituted IRB at each participating clinical
center A copy of the signed and dated IRB approval at each clinical center will be retrieved prior
to or during the site initiation visit and archived at the IPFnet DCC Any amendments to the
protocol other than simple administrative and typographical changes must be approved by each
IRB before they are implemented The clinical centers will seek annual renewals of their IRB
approvals in accordance with local procedures
67
__________________________________________ ________________
__________________________________________
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
12 Investigator Agreement
I have read the foregoing protocol PANTHER-IPF and agree that it contains all necessary
details for carrying out this study I will conduct the study as outlined herein and will complete
the study within the time designated
I will provide copies of the protocol and all pertinent information to all individuals responsible to
me who assist in the conduct of this study I will discuss this material with them to ensure they
are fully informed regarding the drug and the conduct of the study
I will fulfill all responsibilities for submitting pertinent information to the local IRB if
applicable that is responsible for this study
I further agree that NHLBI andor DCRI will have access to any source documents from which
eCRF information may have been generated
Signature of Principal Investigator Date
Name of Principal Investigator (printed or typed)
Protocol version date May 19 2009
Protocol Amendment 1 version date May 28 2010
Protocol Amendment 2 version date December 6 2011
68
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
13 References
1 Raghu G Brown KK Bradford WZ et al A placebo-controlled trial of interferon gamma-1b in patients with idiopathic pulmonary fibrosis N Engl J Med 2004350125-33 2 King TE Jr Safrin S Starko KM et al Analyses of efficacy end points in a controlled trial of interferon-gamma1b for idiopathic pulmonary fibrosis Chest 2005127171-7 3 Flaherty KR Thwaite EL Kazerooni EA et al Radiological versus histological diagnosis in UIP and NSIP survival implications Thorax 200358143-8 4 Wells AU Desai SR Rubens MB et al Idiopathic pulmonary fibrosis a composite physiologic index derived from disease extent observed by computed tomography Am J Respir Crit Care Med 2003167962-9 5 Raghu G Freudenberger TD Yang S et al High prevalence of abnormal acid gastroshyoesophageal reflux in idiopathic pulmonary fibrosis Eur Respir J 200627136-42 6 Kinnula VL Focus on antioxidant enzymes and antioxidant strategies in smoking related airway diseases Thorax 200560693-700 7 Coultas DB Zumwalt RE Black WC Sobonya RE The epidemiology of interstitial lung diseases Am J Respir Crit Care Med 1994150967-72 8 Raghu G Weycker D Edelsberg J Bradford WZ Oster G Incidence and prevalence of idiopathic pulmonary fibrosis Am J Respir Crit Care Med 2006174810-6 9 Olson AL Swigris JJ Lezotte DC Norris JM Wilson CG Brown KK Mortality from pulmonary fibrosis increased in the United States from 1992 to 2003 Am J Respir Crit Care Med 2007176277-84 10 Mannino DM Etzel RA Parrish RG Pulmonary fibrosis deaths in the United States 1979shy1991 An analysis of multiple-cause mortality data Am J Respir Crit Care Med 19961531548shy52 11 Hubbard R Johnston I Coultas DB Britton J Mortality rates from cryptogenic fibrosing alveolitis in seven countries Thorax 199651711-6 12 Johnston I Britton J Kinnear W Logan R Rising mortality from cryptogenic fibrosing alveolitis Bmj 19903011017-21 13 Raghu G Collard HR Egan JJ et al An official ATSERSJRSALAT statement idiopathic pulmonary fibrosis evidence-based guidelines for diagnosis and management Am J Respir Crit Care Med 2011183788-824 14 (USA) FDA FDA Public Health Advisory Interferon gamma-1b (marketed as Actimmune) In 2007 15 King TE Jr Pardo A Selman M Idiopathic pulmonary fibrosis Lancet 2011 16 Raghu G Brown KK Costabel U et al Treatment of idiopathic pulmonary fibrosis with etanercept an exploratory placebo-controlled trial Am J Respir Crit Care Med 2008178948shy55 17 Malouf MA Hopkins P Snell G Glanville AR An investigator-driven study of everolimus in surgical lung biopsy confirmed idiopathic pulmonary fibrosis Respirology 201116776-83 18 King TE Jr Behr J Brown KK et al BUILD-1 a randomized placebo-controlled trial of bosentan in idiopathic pulmonary fibrosis Am J Respir Crit Care Med 200817775-81 19 Richeldi L Costabel U Selman M et al Efficacy of a tyrosine kinase inhibitor in idiopathic pulmonary fibrosis N Engl J Med 20113651079-87
69
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
20 Borok Z Buhl R Grimes GJ et al Effect of glutathione aerosol on oxidant-antioxidant imbalance in idiopathic pulmonary fibrosis Lancet 1991338215-6 21 Meyer A Buhl R Magnussen H The effect of oral N-acetylcysteine on lung glutathione levels in idiopathic pulmonary fibrosis Eur Respir J 19947431-6 22 Behr J Maier K Degenkolb B Krombach F Vogelmeier C Antioxidative and clinical effects of high-dose N-acetylcysteine in fibrosing alveolitis Adjunctive therapy to maintenance immunosuppression Am J Respir Crit Care Med 19971561897-901 23 Cantin AM North SL Fells GA Hubbard RC Crystal RG Oxidant-mediated epithelial cell injury in idiopathic pulmonary fibrosis J Clin Invest 1987791665-73 24 Waghray M Cui Z Horowitz JC et al Hydrogen peroxide is a diffusible paracrine signal for the induction of epithelial cell death by activated myofibroblasts Faseb J 200519854-6 25 Larios JM Budhiraja R Fanburg BL Thannickal VJ Oxidative protein cross-linking reactions involving L-tyrosine in transforming growth factor-beta1-stimulated fibroblasts J Biol Chem 200127617437-41 26 Kinnula VL Fattman CL Tan RJ Oury TD Oxidative stress in pulmonary fibrosis a possible role for redox modulatory therapy Am J Respir Crit Care Med 2005172417-22 27 Meyer A Buhl R Kampf S Magnussen H Intravenous N-acetylcysteine and lung glutathione of patients with pulmonary fibrosis and normals Am J Respir Crit Care Med 19951521055-60 28 Behr J Degenkolb B Krombach F Vogelmeier C Intracellular glutathione and bronchoalveolar cells in fibrosing alveolitis effects of N-acetylcysteine Eur Respir J 200219906-11 29 Bando M Hosono T Mato N et al Long-term efficacy of inhaled N-acetylcysteine in patients with idiopathic pulmonary fibrosis Intern Med 2010492289-96 30 Demedts M Behr J Buhl R et al High-dose acetylcysteine in idiopathic pulmonary fibrosis N Engl J Med 20053532229-42 31 Toma TP Bhowmik A Rajakulasingam R Acetylcysteine in pulmonary fibrosis N Engl J Med 20063541086-9 author reply -9 32 Hunninghake GW Antioxidant therapy for idiopathic pulmonary fibrosis N Engl J Med 20053532285-7 33 Flaherty KR Mumford JA Murray S et al Prognostic implications of physiologic and radiographic changes in idiopathic interstitial pneumonia Am J Respir Crit Care Med 2003168543-8 34 Latsi PI du Bois RM Nicholson AG et al Fibrotic idiopathic interstitial pneumonia the prognostic value of longitudinal functional trends Am J Respir Crit Care Med 2003168531-7 35 Collard HR King TE Jr Bartelson BB Vourlekis JS Schwarz MI Brown KK Changes in clinical and physiologic variables predict survival in idiopathic pulmonary fibrosis Am J Respir Crit Care Med 2003168538-42 36 Jegal Y Kim DS Shim TS et al Physiology is a stronger predictor of survival than pathology in fibrotic interstitial pneumonia Am J Respir Crit Care Med 2005171639-44 37 Martinez FJ Safrin S Weycker D et al The clinical course of patients with idiopathic pulmonary fibrosis Ann Intern Med 2005142963-7 38 Hull JH Acetylcysteine in pulmonary fibrosis N Engl J Med 20063541089-91 author reply -91
70
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
39 Flaherty KR King TE Jr Raghu G et al Idiopathic interstitial pneumonia what is the effect of a multidisciplinary approach to diagnosis Am J Respir Crit Care Med 2004170904shy10 40 Raghu G Johnson WC Lockhart D Mageto Y Treatment of idiopathic pulmonary fibrosis with a new antifibrotic agent pirfenidone results of a prospective open-label Phase II study Am J Respir Crit Care Med 19991591061-9 41 Hunninghake GW Lynch DA Galvin JR et al Radiologic findings are strongly associated with a pathologic diagnosis of usual interstitial pneumonia Chest 20031241215-23 42 Lynch D Godwin J Safrin S et al High-resolution computed tomography in idiopathic pulmonary fibrosis diagnosis and prognosis Am J Respir Crit Care Med 2005172488-93 43 Mallinckrodt CH Watkin JG Molenberghs G Carroll RJ Choice of the primary analysis in longitudinal clinical trials Pharmaceutical Statistics 20043161-9 44 Bang H Tsiatis A Estimating medical costs with censored data Biometrika 200087329shy43 45 Lin DY Regression analysis of incomplete medical cost data Stat Med 2003221181-200 46 Rochon J Application of GEE procedures for sample size calculations in repeated measures experiments Stat Med 1998171643-58 47 Lachin JM Foulkes MA Evaluation of sample size and power for analyses of survival with allowance for nonuniform patient entry losses to follow-up noncompliance and stratification Biometrics 198642507-19
71
- PANTHER-IPFPREDNISONE AZATHIOPRINEAND N-ACETYLCYSTEINEA STUDY THAT EVALUATES RESPONSE INIDIOPATHIC PULMONARY FIBROSIS
-
- Protocol Summary
- Table of Contents
- List of Tables
- List of Figures
- List of Abbreviations
- 1 Summary
- 2 Hypotheses and Specific Aims
-
- 21 Null Hypothesis
- 22 Specific Aim 1
- 23 Specific Aim 2
- 24 Prespecified Subgroups of Interest
-
- 3 Background and Significance
-
- 31 Idiopathic Pulmonary Fibrosis is the Most Common Interstitial Lung Disease
- 32 Rationale for Placebo Control
- 33 Rationale for N-acetylcysteine
- 35 Rationale for N-acetylcysteine as a Stand-alone Therapy
- 36 Rationale for the Study Design and Primary Endpoint
- 37 Rationale for Blinding of Treatments
-
- 4 Methods
-
- 41 Inclusion Criteria
- 42 Diagnosis of IPF
- 43 Exclusion Criteria
- 44 Study Design and Study Visit
- 45 Dose Justification
- 46 Contraindications Precautions and Side Effects of Study Medications
- 47 Recruitment Procedures
- 48 Study Procedures
- 49 Concomitant Medications
- 410 Laboratory Testing
- 411 Blinding of Study Drugs
-
- 5 Study Endpoints
-
- 51 Primary Study Endpoint
- 52 Secondary Study Endpoints
-
- 6 Safety Evaluations and Procedures
-
- 61 Adverse Events
- 62 Clinical Medical Monitoring
- 63 Unblinding Procedures
-
- 7 Study Drug Procedures
- 8 Data Management
-
- 81 Hardware and Software Configuration
- 82 Sources of Data
-
- 9 Study Design and Data Analysis
-
- 91 General Analytic Considerations
- 92 Randomization Blinding and Reporting of Results
- 93 Stratification
- 94 Specification of the Primary Analyses
- 95 Analysis of Longitudinal Endpoints
- 96 Analysis of Binary Time-to-Event and Time-Lagged Endpoints
- 97 Power Analysis
-
- 10 Study Administration
-
- 101 Cooperative Agreement Mechanism
- 102 IPFnet Steering Group
- 103 Data and Safety Monitoring Board
- 104 Recommendations on Interim Monitoring of Efficacy Safety and Futility
-
- 11 Investigator and Sponsor Obligations
-
- 111 Monitoring
- 112 Cost and Payment
- 113 Confidentiality and Health Insurance Portability and Accountability ActConsiderations
- 114 Informed Consent Procedures
- 115 Institutional Review Boards
-
- 12 Investigator Agreement
- 13 References
-

PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Unlike the ATSERS consensus criteria published in 2000 bronchoscopy will not be required for diagnosis
This decision was made based on the experience of the IPFnet Steering Group members regarding the utility of
bronchoscopy in the diagnosis of IPF The presence of an atypical HRCT finding will require documentation of
a definitive diagnosis by surgical lung biopsy In fact this is in keeping with the recently published evidence
based guidelines for diagnosis and management of IPF13 As shown in Figure 3 central review of the pathology
data will be required for a diagnosis of IPF
We will not require central review of HRCT as several studies have shown that a confident local interpretation
of clinicalHRCT criteria as definite IPFUIP is associated with a high positive predictive value for finding UIP
at surgical lung biopsy (see Table 1) Differences in sensitivity in these series likely reflect subject selection as
Flaherty et al3 evaluated only UIP and nonspecific interstitial pneumonia (NSIP) while Raghu et al40 and
Hunninghake et al41 included a broader range of ILD
Table 1 Operating Characteristics of Local HRCT Review for Diagnosis of UIP
Researcher of Subjects Sensitivity () Specificity () PPV () NPV ()
Raghu et al 40
59 (29 UIP by SLB) 78 90 88 82
Hunninghake et al 41 91 (54 UIP by SLB)
74 81 85 67
Flaherty et al 3 96 (only NSIP amp UIP)
37 100 100 30
Abbreviations PPV positive predictive value NPV negative predictive value UIP usual interstitial pneumonia SLB surgical lung biopsy and NSIP nonspecific interstitial pneumonia
Furthermore an analysis of the HRCT scans from subjects enrolled in the GIPF-001 trial confirmed that local
site interpretations have a high congruity to a central radiology core In this multi-center study 263 HRCT
scans were read as definite IPF and a retrospective central radiology core review found 932 to be consistent
with IPF 42 We will also take several additional steps to insure that the local HRCT reads are accurate
including
1 A detailed training module has been developed and must be completed by each site radiologist before
site initiation
2 Clinical centers are to mail all HRCT scans to the HRCT core lab The first 10 HRCT scans from
subjects enrolled at each enrolling clinical center will be reviewed centrally to be certain that local reads
24
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
25
are congruent with a central interpretation If discrepancies are identified additional education will be
provided and HRCT scans will continue to be reviewed centrally until the central radiology core is
confident that the local center is performing appropriately
3 Random scans will be obtained from each center throughout the study to confirm that the local read
continues to agree with central interpretation If discrepancies are identified they will be addressed as in
2 above
In all cases if a subject has a surgical lung biopsy sample that sample will be reviewed by the local and central
pathologists Therefore the only cases that would not be subject to a direct central review process are those
where the HRCT meets the centrally defined criteria for an unequivocal diagnosis and a lung biopsy sample is
not available Table 2 below summarizes the possible combinations for making a diagnosis
Table 2 Combining HRCT and Pathology Interpretations to Determine if IPF is Present
HRCT Diagnosis Pathology Diagnosis Diagnosis of IPF
Definite UIP Definite UIP Yes
Definite UIP Probable UIP Yes
Definite UIP Possible UIP Yes
Definite UIP Not UIP No
Definite UIP Unavailable Yes
Consistent with UIP Definite UIP Yes
Consistent with UIP Probable UIP Yes
Consistent with UIP Possible UIP No
Consistent with UIP Not UIP No
Consistent with UIP Unavailable No
Inconsistent with UIP Any No
Abbreviations HRCT high-resolution computed tomography IPF idiopathic pulmonary fibrosis
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
UIP usual interstitial pneumonia Dx diagnosis 43 Exclusion Criteria
1 History of clinically significant environmental exposure known to cause pulmonary fibrosis
Occupational exposures such as asbestos or environmental exposure to organic dust such as occurs in
pigeon breeders may at times mimic the clinical and radiographic findings of IPF
2 Diagnosis of connective tissue disease felt by the principal investigator (PI) to be the etiology of the
interstitial disease Diagnosis of collagen-vascular conditions will be according to the published
American College of Rheumatology criteria As such the presence of any documented collagen-vascular
disorder or the presence of any suspicious symptom complex whether or not associated with
significantly abnormal rheumatological serologies will exclude the subject at the discretion of the PI
3 Extent of emphysema greater than the extent of fibrotic change (honeycombing reticular changes) on
HRCT scan
4 Forced expiratory volume in 1 second (FEV1)FVC ratio lt 065 at screening (postbronchodilator)
5 Partial pressure of arterial oxygen (PaO2) on room air lt 55 mm Hg (lt 50 mm Hg at Denver site)
6 Residual volume gt 120 predicted at screening (postbronchodilator)
7 Evidence of active infection
8 Significant bronchodilator response on screening spirometry defined as a change in FEV1 ge 12 and
absolute change gt 200 mL OR change in FVC ge 12 and absolute change gt 200 mL The percent
difference between the FVC (or FEV1) values will be calculated by taking the absolute value of the
difference and dividing it by the larger of the two FVC (or FEV1) values
9 Screening and enrollment post-bronchodilator FVC measurements (in liters) differing by gt 11 The
percent difference between the FVC values will be calculated by taking the absolute value of the
difference and dividing it by the larger of the two FVC values (eg the percent difference between FVC
measurements of 19 and 20 liters would be determined by taking the difference between the two (01
liters) and dividing by the larger of the two (20 liters) So 0120 = 5 and these FVC measurements
would not exclude the subject
10 Listed for lung transplantation ie the patient has completed the evaluation process has been accepted
as a candidate for transplantation at an appropriate center and is waiting to receive notification of an
available donor organ
11 History of unstable or deteriorating cardiac disease
12 Myocardial infarction coronary artery bypass or angioplasty within 6 months of screening
26
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
13 Unstable angina pectoris or congestive heart failure requiring hospitalization within 6 months of
screening
14 Uncontrolled arrhythmia
15 Severe uncontrolled hypertension
16 Known HIV or hepatitis C
17 Known cirrhosis and chronic active hepatitis
18 Active substance andor alcohol abuse (as determined by site PI)
19 Pregnancy or lactation (subjects who are pregnant or breastfeeding)
20 Known hypersensitivity to study medication
21 Any condition other than IPF that in the opinion of the site PI is likely to result in the death of the
subject within the next year
22 Any condition that in the judgment of the PI might cause participation in this study to be detrimental to
the subject or that the PI deems makes the subject a poor candidate
23 Any therapy directed at pulmonary fibrosis (excepting triple therapy of prednisone plus azathioprine
plus NAC) requires a 30-day washout period before randomized Triple therapy of lt= 12 weeks duration
in the past 4 years requires a 30-day washout period before randomization
24 History of triple therapy of prednisone plus azathioprine plus NAC for gt 12 weeksrsquo duration in the past
4 years or previous enrollment in the triple-therapy arm of the PANTHER-IPF study
44 Study Design and Study Visit
441 Study Design Summary
This study will be a randomized double-blind PL-controlled trial designed to assess the safety and efficacy of
NAC in subjects with newly diagnosed IPF
Subjects with mild to moderate IPF (defined as FVCpred ge 50 and DLCOpred ge 30) diagnosed within
the past 48 months will be enrolled Screening will continue until April 30 2012
27
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
The study will employ a 2-arm design with 11 randomization to NAC or PL Once enrolled subjects will visit
the clinical center at 15 weeks and 15-week intervals thereafter Each subject will be treated and followed for a
maximum of 60 weeks
During the 60-week visit subjects will be taken off all study agents Approximately four weeks after the final
dose of study agent is taken subjects will receive a safety phone call from the study site
442 Study Visits
Subjects who meet entry criteria will review the informed consent a written description of the purpose
procedures and risks of the study with the PI co-investigator or study coordinator and all questions will be
answered The informed consent form will be signed by the subject at screening No protocol-specific
procedures will be performed until the subject has signed and dated an informed consent form This includes the
screening procedures
4421 Screening
Once informed consent is obtained subjects may immediately begin the screening process or may return within
28 days of consent In the event a study subject has been clinically evaluated at the study site by an IPFnet study
physician and has performed testing within three weeks for this clinical evaluation that meets guidelines
provided in the IPFnet PANTHER-IPF Manual of Operating Procedures (MOOP) this testing may be used to
satisfy the following screening criteria medical history physical exam arterial blood gas (ABG) with A-a
gradient vital signs with oximetry body height and weight spirometry DLCO lung volumes and HRCT scan
Allowing the use of previously performed test results that meet study guidelines for the screening visit is
intended to permit subjects easier access to study entry to prevent subjects from repeating testing that has been
performed within the study window and to decrease risks to subjects from repeated exposure to procedures
such as arterial puncture and HRCT
The following procedures will be performed at screening
Medical history and a physical examination
28
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Measure height and weight
Serum pregnancy test (if applicable)
Measure vital signs including oximetry
Blood draws performed and the following analyses conducted
o Hematology (red cell count white cell count hemoglobin hematocrit cell indices differential
platelet count)
o Blood chemistries according to central laboratory protocol (see Section 410 Laboratory
Testing)
o Beta human chorionic gonadotropin (serum) pregnancy test (in women of childbearing potential)
o Urinalysis
Pulmonary Function Tests (PFTs) including spirometry pre- and post- bronchodilator and postshy
bronchodilator measurement of lung volumes and measurement of hemoglobin adjusted diffusing
capacity
Measure ABGs
HRCT if a satisfactory scan has not been performed on the subject within 3 months of screening (see
PANTHER-IPF MOOP for more details)
Surgical lung biopsies (if applicable) reviewed by local and central pathology departments
Current medications If required a washout period discussed with the subject and initiated at this visit
4422 Enrollment
The enrollment visit is expected to take place within eight weeks of the screening visit Enrollment visit
activities include
Measure vital signs including oximetry
Measure height and weight
Serum pregnancy test (if applicable)
If consent has been given blood will be drawn and a urine specimen collected for the bio-specimen
repository
Spirometry (post-bronchodilator)
Measure 6MWT with Borg Dyspnea Scale
29
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Collect Quality-of-life (QOL) data using the SF-36 EuroQol Investigating Choice Experiments for
Preferences of Older People Capability Instrument (ICE CAP) and SGRQ
Female subjects complete Gender Substudy questionnaire
Dyspnea status collected using the UCSD SOBQ
Evaluate Acute Exacerbation (AEx)
Review of any Adverse Events (AEs)
Review of concomitant medications
Subject receives diary and instructions on its purpose and proper use
Subject receives supply of study drug sufficient to last until his or her 15-week study visit
See the Schedule of Assessments (Table 3) for more details Subjects with screening and enrollment postshy
bronchodilator FVC measurements (in liters) differing by more than 11 are not eligible to be enrolled in the
study
Subjects will be asked to provide a physician of record This physician will be considered the subjectrsquos primary
care provider (PCP) and if the subject agrees the PCP will be informed by letter of the subjectrsquos enrollment in
the trial The subject will be informed that his or her ongoing medical care should be received from the PCP
The PCP will be informed of any safety issues identified by the study staff The PCP will also be given
information regarding communication with study personnel about pertinent health issues or clinic encounters
the subject may have
4423 Week 15
The week 15 visit is expected to occur within +- 14 days of the subjectrsquos scheduled visit time (eg the week 15
visit should occur anytime between 13 and 17 weeks after starting study drug Week 15 activities include
Measure vital signs with oximetry
Measurement height and weight
Serum pregnancy test (if applicable)
Spirometry (post-bronchodilator) measurement
Review of AEs
Evaluate for AEx
30
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Review concomitant medications
If consented draw blood and collect urine specimen for the biospecimen repository
Subjects return used and unused study drug for the visit
Review study diary and a new study diary will be given
Provide additional supply of study drug sufficient to last until the next scheduled visit
4424 Week 30
The week 30 visit is expected to occur within +- 14 days of the subjectrsquos scheduled visit time (eg the week 30
visit should occur anytime between 28 and 32 weeks after starting study drug) Week 30 activities include
Physical examination
Measure vital signs with oximetry
Measure height and weight
Laboratory values (complete blood count [CBC] and serum chemistries)
Serum pregnancy test (if applicable)
Measure spirometry (post-bronchodilator)
6MWT with Borg scale
DLCO
Review of AEs
Evaluate for AEx
Review concomitant medications
Complete all QOL and dyspnea questionnaires (EuroQol ICE CAP SF-36 SGRQ and UCSD SOBQ)
If consent has been given blood will be drawn and a urine specimen collected for the biospecimen
repository
Review study diary
Subjects return used and unused study drug for the visit
Provide additional supply of study drug sufficient to last until the next scheduled visit
4425 Week 45
31
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
The week 45 visit is expected to occur within +- 14 days of the subjectrsquos scheduled visit time (eg the week 45
visit should occur anytime between 43 and 47 weeks after starting study drug) Week 45 activities include
Measure vital signs with oximetry
Measure height and weight
Serum pregnancy test (if applicable)
Measure spirometry (post-bronchodilator)
Review of AEs
Evaluate for AEx
Review concomitant medications
If consent has been given blood will be drawn and a urine specimen collected for the biospecimen
repository
Subjects return used and unused study drug for the visit
Study diary reviewed
Provide additional supply of study drug sufficient to last until the next scheduled visit
4426 Week 60 (Early Withdrawal or Final Treatment Visit)
At week 60 or at subject withdrawal from the study (premature by study doctor or subjectrsquos decision) a final
treatment visit will occur At this final treatment visit subjects will discontinue NACPL abruptly Week 60
activities also include
Physical examination
Measure vital signs with oximetry
Measure height and weight
Laboratory values (complete blood count [CBC] and serum chemistries)
Spirometry (post-bronchodilator) measurement
6MWT with Borg scale measurement
DLCO
Lung volumes
ABG
Review of AEs
32
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Evaluate for AEx
Review concomitant medications
Subjects will complete all QOL and dyspnea questionnaires (EuroQol ICE CAP SF-36 SGRQ and
UCSD SOBQ)
If consent has been given blood will be drawn and a urine specimen collected for the biospecimen
repository
Subjects return used and unused study drug for the visit
Study diary reviewed
4427 Final Site Visit ndash FVC drop confirmation
In the event that the subject has a recorded FVC drop of gt10 from baseline at the final treatment visit and the
subject has not had a confirmation of such a drop at a previous study visit the subject should return to the
clinical site 6 to 8 weeks after the final treatment visit During this visit a post-bronchodilator spirometry test
will be performed This FVC measurement will be evaluated according to section 521 of this protocol
4428 Final Visit ndash Telephone Follow-up
Four weeks following the final dose of study medication subjects will receive a telephone call from the study
coordinator to ensure that there are no side effects and to follow up on any ongoing adverse events (AEs)
4429 Phone Contact Between Visits
At week 2 and each month that a subject does not have a scheduled clinical center visit his or her study
coordinator will contact him or her at least once by telephone to
Inquire if the subject has had any hospitalizations events that might be considered an AE or any events
significant enough to warrant an out-of-cycle visit to the clinical center
Remind subjects of their current dosage levels and confirm that the subject understands them
Address any questions or concerns the subject might have regarding other aspects of the study
Assess adherence to the treatment regimen by reviewing diary data verbal review of medications taken
including nutritional supplements
33
34
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Table 3 Schedule of Assessments
Procedure Screening Visit 0
Enrollment Visit 1
Week 15 Visit 2
Week 30Visit 3
Week 45 Visit 4
Week 60 Early
Withdrawal Visit 5
Final1
Visit (via phone)
Informed consent X
Medical history X
Inclusionexclusion criteria X
Serum pregnancy test (if applicable) X X X X X
Review of lung biopsy X
Arterial Blood Gas X X
6-Minute Walk Test
X
X X
Physical examination X X X
Vital signs with oximetry X X X X X X
Body height and weight X X X X X X
Complete Blood Count X X X
Chemistry panel X X X
Monitor Lab Values X X X
Urinalysis X Specimen repository substudy blood draw and urine collection (if consented)
X
X X X X
HRCT (if not completed within three months) X
Spirometry (pre- and post-bronchodilator) X
Spirometry (post-bronchodilator only) X X X X X
DLCO (post-bronchodilator only) X X X
Lung volumes (post-bronchodilator only) X
X
Evaluate for acute exacerbation X X X X X
Review Adverse Events X X X X X X
Review concomitant meds X X X X X X
Dispense subject diary X X X X
Review subject diary X X X X X
Dispense study agent X X X X
Gender Substudy questionnaire (female subjects only) X
EuroQol ICECAP UCSD SOBQ SGRQ SF-36 X X X
Abbreviations DLCO diffusing capacity of the lung for carbon monoxide QOL Quality of Life ICECAP Investigating Choice Experiments for Preferences of Older People UCSD SOBQ University of California Shortness of Breath Questionnaire SGRQ St Georgersquos Respiratory Questionnaire SF-36 Short Form 36 Health Survey
1Follow-up visit via phone will occur four weeks after final dose of study medication
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
45 Dose Justification
The general philosophy for determining dosing levels was to apply previously examined
treatment regimens With the focus of the study being to establish a standard of care for
mildmoderate IPF subjects the goal was to develop flexible yet standardized treatment rules that
allow for the temporary or permanent withholding of one or more components of treatment when
necessary Subjects developing laboratory abnormalities or symptoms that result in
discontinuation of one or more components of study treatment may continue on the other
components as long as there is no contraindication for this Complete follow-up is important for
the validity of any study As a strategy to maintain protocol adherence we are using a treatment
regimen that will detect potential side effects and prompt interventions proactively in the interest
of patient safety In addition subjects who permanently stop study medications during the course
of the study are encouraged to continue in the study completing all scheduled visits and tests
451 Rationale for N-acetylcysteine Dosing
To our knowledge there have been no IPF studies to correlate clinical outcome measures with
different dosages for NAC The dosage chosen is based on the IFIGENIA study However BAL
lung GSH levels from subjects with IPF have been augmented with the use of oral NAC at 600
mg 3 times per day In addition lung GSH levels have been associated with improved
PFTs212227 The dose chosen for this study was based on previous data including the IFIGENIA
study30
4511 Dosing of N-acetylcysteineplacebo
Dosing of NACPL will be 600 mg orally 3 times a day (1800 mgday)
4512 Reasons to Discontinue N-acetylcysteineplacebo
NACPL may be temporarily or permanently discontinued for the duration of the study for
gastrointestinal symptoms or dermatologic reactions
35
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Temporarily discontinue (hold) oral NACPL for subjects requiring inpatient admission for acute
exacerbation (AEx) or other conditions Resume NACPL after discharge
36
37
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
452 Dosage Algorithms
Dosage Adjustment Algorithm 1 NACPL Dose Modifications for Gastrointestinal Symptoms Nausea Vomiting Abdominal Discomfort Diarrhea
GI Symptoms determined by the PI to be clinically significant Nausea Vomiting Abdominal Discomfort Diarrhea
NACPL Temporarily dc (HOLD) x 3 Days
Monitor symptoms intervene as clinically indicated (eg fluid replacement antidiarrhea or antinausea medication)
Monitor or lab PRN
Are symptoms resolving after 3 days NO
Symptoms NOT resolving after 3 days of holding study medication Assessmentmanagement per clinical
discretion of investigator
Likely not study medication discuss resuming study medication with medical monitor when symptoms resolved
YES
Temporarily dc (HOLD) NACPL for 4 additional days (total hold 1 week) then NACPL Resume 600 MG TID
Did symptoms recur
YES
STOP NACPL for
duration of study
NO
NACPL No Change
38
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Dosage Adjustment Algorithm 2 NACPL Dose Modifications For Dermatologic Reactions
Dermatologic Reactions (Not Acneiform) ge Grade 2 Grading per Common Terminology Criteria for
Adverse Events V30 (httpctepcancergov) For example Grade 1 RASHDESQUAMATION Macular or papular eruption or erythema without associated symptoms Grade 2 RASHDESQUAMATION Macular or popular eruption or erythema with pruritus or other associated symptoms localized desquamation or other lesions covering lt50 of body surface area
NACPL Temporarily dc (HOLD) x 3 days
Are symptoms resolving after 3 days
NO Symptoms not resolving after 3 days of holding study medication Assessmentmanagement per clinical discretion of investigator Likely not study medication Discuss resuming study medication with medical monitor when symptoms
resolved YES
Temporarily dc (HOLD) NACPL for 4 additional days (total hold 1 week) then NACPL resume 600 MG TID
Did symptoms recur
YES
STOP NACPL for
duration of study
NO
NACPL No change
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
46 Contraindications Precautions and Side Effects of Study Medications
461 Contraindication
Contraindication to NAC is known hypersensitivity to it
462 Precautions
Concomitant administration of oral NAC and antibiotics has shown a slightly reduced absorption
of cephalexin and a slight increase in erythromycin serum levels NAC contains free sulfhydryl
groups There is no evidence that individuals sensitive to sulfa drugs are sensitive to NAC
The NAC preparation being administered in this study contains 20 mg of aspartame Because of
the phenylalanine component of aspartame individuals with phenylketonuria should avoid or
restrict aspartame intake to avoid increased blood levels of phenylalanine Because of this risk
labeling is required on all products containing aspartame
463 Side Effects
Side effects of NAC range from common to serious See Table 4
39
40
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Table 4 Side Effects of NAC
Undesirable Effects
System-organ class Uncommon
(gt11000 lt1100)
Rare
(gt110000 lt11000)
Very rare
(lt110000) Not known
Immune system disorders Hypersensitivity Anaphylactic shock
reaction
Nervous system disorders Headache
Ear and labyrinth disorders Tinnitus
Cardiac disorders Tachycardia
Vascular disorders Hemorrhage
Respiratory thoracic and
mediastinal disorders
Bronchospasm
Dyspnea
Gastrointestinal disorders
Vomiting diarrhea
stomatitis abdominal
pain nausea
Dyspepsia
Skin and subcutaneous tissue
disorders
Urticaria rash
angioedema itching
General disorders and
administration site conditions Pyrexia
Investigations Reduced arterial
pressure Face edema
In very rare cases the onset of severe skin reactions such as Stevens-Johnson syndrome and Lyell syndrome was reported to have a temporal relationship with N-acetylcysteine administration Although in most cases at least another suspect drug probably most involved in the genesis of the above mentioned mucocutaneous syndromes has been identified in case of mucocutaneous alterations it is appropriate to contact onersquos doctor and the administration of N-acetylcysteine should be immediately discontinued
Some studies confirmed a reduction of platelet aggregation during N-acetylcysteine administration The clinical significance of these findings has not been defined yet [Source Fluimucil Investigator Brochure]
47 Recruitment Procedures
Subjects recruited for this study will be established patients of the investigators or physician- or
self-referred to participating clinical centers in the IPFnet Each clinical center within IPFnet has
a well-developed infrastructure of local pulmonologists within the surrounding geographic area
These pulmonologists are kept informed of ongoing IPF clinical trials and regularly refer
subjects to studies conducted at IPFnet clinical centers
Additional steps will be taken to inform clinicians of the trials in progress within IPFnet
including presentations at faculty staff meetings at local hospitals medical grand rounds and
national conferences direct mail notification monthly faxes and advertisement of network trials
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
in pulmonary journals Clinical center patients previously diagnosed with IPF will be notified of
the trials by mail whenever possible
Recruitment of minorities and women will be monitored by the DCC and DSMB If necessary
additional recruitment efforts will be made at specific centers to ensure that the aggregate subject
sample contains appropriate representation of women and minorities
48 Study Procedures
The following procedures are detailed in the PANTHER-IPF MOOP accompanying this
protocol
1 PFT
2 ABG
3 HRCT scan of the chest (including imaging of pulmonary arteries)
4 CBC and serum chemistries
5 Pregnancy test
6 6MWTBorg Dyspnea Scale
7 QOL questionnaires (EuroQol HAD SF-36 SGRQ and ICE CAP)
8 UCSD SOBQ
9 Gender Substudy Questionnaire
All assessments of PFTs will be conducted by study personnel not directly involved in the
treatment of the subjects
481 Biological Specimen Management
4811 Biological Specimen Sample Management
Subjects at clinical centers participating in the specimen repository substudy who consent to
having blood drawn for research purposes and for the banking of blood blood components and
other biologic specimens (urine and BAL fluid) will have approximately 405 mL of blood
41
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
drawn 17 mL blood drawn for DNA and 20 mL of urine collected at enrollment visit Subjects
will have approximately 50 mL of blood drawn and 20 mL of urine collected at each 15-week
follow-up visit Blood specimens will be separated according to PANTHER-IPF MOOP
guidelines into the following components for banking in the repository serum plasma and
DNA Coding of all biologic specimens for the repository will be performed by study staff at the
clinical center The samples will be processed per PANTHER-IPF MOOP guidelines aliquoted
labeled with barcode labels and stored at -70degC at the clinical center and shipped to the central
repository
The only subject identifiers will be a sample ID number and subject initials This sample ID will
be linked in the IPFnet DCC clinical database to subject information No subject information will
be transferred to the biological-specimen database
The subjectrsquos samples may be used for approved sub-studies relating to human disease
including but not limited to IPF The studies for which an individualrsquos samples will be made
available will be determined by the subjectrsquos answers to questions on the biological-sample
informed consent form The subjects can choose to make their samples available for all options
or any combination Samples will be made available to researchers only with IPFnet Steering
Group approval until such time as the samples are made public through the NHLBI repository
49 Concomitant Medications
Concurrent treatment with FDA-approved therapy for IPF is allowed Colchicine may be used
for treatment of gout Temporary treatment with oral or IV corticosteroids for clinical worsening
or suspected AEx is permitted Nutritional supplements containing NAC are not allowed
410 Laboratory Testing
Clinical laboratory parameters will be assessed at screening and at the end of the study The
following tests will be performed at the two time points specified in the protocol chemistry (AG
ratio ALT [SGPT] AST [SGOT] albumin alkaline phosphatase amylase bilirubin-direct
42
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
bilirubin-indirect bilirubin-total BUN BUNcreatinine ratio calcium carbon dioxide
cholesterol-total chloride CPK-total creatinine GGT globulin glucose iron-total LDH
lipase magnesium phosphorus-inorganic potassium protein-total sodium TIBC triglycerides
uric acid) and hematology (red blood cell count WBC count hemoglobin hematocrit cell
indices differential platelet count)
411 Blinding of Study Drugs
Subjects and caregivers will be blinded to study treatment Every subject will receive NAC or
matching PLs at every study visit from the baseline visit to the week-45 visit No study agent
will be dispensed at the week-60 visit
43
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
5 Study Endpoints
51 Primary Study Endpoint
The primary endpoint will be the change in serial measurements of FVC over the study period
52 Secondary Study Endpoints
521 Time to Disease-progression
The time-to-death or a 10 decline in FVC will be defined as the time-to-disease progression
The 10 decline in FVC from enrollment must be confirmed on 2 consecutive visits no less than
6 weeks apart For subjects with 2 consecutive visits with a 10 decline in FVC the time-toshy
disease progression will be defined as the time interval between enrollment and the initial visit
with a 10 FVC decline For subjects who experience disease progression the study doctor will
determine whether or not the subject will remain in the study
522 Acute Exacerbations
The following 3 criteria will define AEx in subjects with acute worsening of their respiratory
conditions
1 Clinical (all of the following required)
A) Unexplained worsening of dyspnea or cough within 30 days triggering unscheduled
medical care (eg emergency room clinic study visit hospitalization)
B) No clinical suspicion or overt evidence of cardiac event pulmonary embolism or deep
venous thrombosis to explain acute worsening of dyspnea
C) No pneumothorax
44
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
2 RadiologicPhysiologic (A and B required)
A) New ground glass opacity or consolidation computed tomography (CT) scan OR new
alveolar opacities on chest x-ray
B) Decline of ge 5 in resting room air SpO2 from last recorded level OR decline of ge 8 mm
Hg in resting room air PaO2 from last recorded level
3 Microbiologic (all of the following required)
A) No clinical evidence for infection (ie absence of grossly purulent sputum fever gt 39degC
orally)
B) Lack of positive microbiological results (if done) from lower respiratory tract defined as
(1) Clinically significant bacterial growth on sputum or endotracheal aspirate cultures
(2) Quantitative culture by protected brush specimen ge 103 cfumL or BAL ge 104 cfumL
(3) The presence of specific pathogens on stains of any of the above
C) Lack of positive pathogen in blood cultures (if done)
Identification of Acute Exacerbations
All subjects will be educated about the importance of identifying AExs At the time of
enrollment subjects will be told about the possibility of developing acute symptomatic
worsening that might represent an AEx of IPF and instructed to contact their study clinical
center coordinator within 48 to 72 hours of the apparent event
All subjects will be contacted by phone monthly and questioned about any change in dyspnea or
cough and any interim clinic visits or hospitalizations Finally as part of the IPFnet outreach to
community referring physicians the importance of AExs will be emphasized When a subject is
identified who meets criterion 1A this will trigger the collection of additional clinical data to
evaluate a suspected AEx These data will be collected as part of standard clinical care (ie this
protocol does not require collection of all items) The additional items to be collected for
suspected AEx include
IPFnet AEx case report form (eCRF) (required)
45
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Chest x-ray CT scan withwithout pulmonary angiogram (reports should be faxed and
followed by the hard copiesdiscs)
Oxygen saturation (pulse oximetry)
ABG
Respiratory cultures (sputum endotracheal aspirate lavage)
Blood cultures
Clinichospital records related to the event
All potential cases of AEx will be reviewed by the clinical center PI first and a decision on
whether the case may represent an AEx will be made If AEx is suspected the case will be sent
to the IPFnet adjudication committee which will assign a final diagnosis (see Table 5) If there is
disagreement among members the majority opinion will be recorded
During episodes of suspected AEx as determined by the individual clinical center investigator
subjects will remain blinded and in the study
Table 5 Final Diagnoses in Evaluation of Suspected Acute Exacerbations
Definite acute exacerbation All criteria met no alternative etiology
Unclassifiable acute worsening
Insufficient data to evaluate all criteria no alternative etiology
Not acute exacerbation Alternative etiology identified that explains acute worsening
Management of the suspected AEx will be at the discretion of the treating physician Standard of
care generally involves evaluation for respiratory infection pulmonary embolism cardiac events
and pneumothorax and treatment with IV corticosteroids
Study drugs will be resumed at pre-suspected AEx doses after subjects clinically improve as
confirmed by the local PI All subjects should be seen at the clinical center within 2 to 4 weeks
of recovery for measurement of post-bronchodilator FVC (see Figure 4) Subjects unable to
return to the clinical center after suspected AEx due to medical frailty (eg continued
46
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
institutionalization progressive disability) will be categorized as failing to maintain FVC
response in secondary analyses
Suspected AEx (PI determined)
Hold study drug Treat AEx
(Attending physician determined)
Alive but unable to continue due to
medical frailty
Dead
Alive and able to continue
Site reviewvisit
Restart study drug
FVC within 2-4 weeks
Figure 4 Acute Exacerbation Flow Chart
523 Respiratory Infections
An upper respiratory infection will be defined as
Change in sputum discoloration
Increased cough of no more than 14 daysrsquo duration
A lower-respiratory infection (pneumonia) will be defined as new segmental or lobar airspace
opacities visualized by image studies (chest radiograph or HRCT) in addition to any of the
following
Positive pathogencultures in good sample of sputum or lower-airway secretions retrieved
by fiberoptic bronchoscope
Fever gt 39degC or gt 100degF
Leukocytosis gt 12000 (unexplained no increase in dose of corticosteroids)
47
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
524 Maintained FVC Response
Subjects with follow-up FVCpred measurements at or above their baseline FVCpred level
will be classified as having maintained FVC response Subjects with reduced FVCpred levels
or missing data for any reason including death or medical frailty will be classified as having not
maintained FVC response The FVCpred value is used because unadjusted FVC measurements
are expected to decline with age
48
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
6 Safety Evaluations and Procedures
61 Adverse Events
During a clinical trial the reporting of adverse experience information can lead to important
changes in the way a new treatment is developed as well as provide integral safety data
611 Definitions
An adverse event (AE) is any untoward medical occurrence in a subject or clinical investigation
subject who was administered a pharmaceutical product The AE does not necessarily have to
have a causal relationship with the drug administered An AE can be any unfavorable and
unintended sign (including an abnormal laboratory finding) symptom or disease temporarily
associated with the use of a medicinal product whether or not considered to be related to the
medicinal product Diseases signs symptoms or laboratory abnormalities already existing at
enrollment are not considered AEs unless they worsen (ie increase in intensity or frequency)
Surgical procedures themselves are not AEs they are therapeutic measures for conditions that
require surgery The condition for which the surgery is required may be an AE Surgical
procedures planned before randomization and the conditions necessitating the surgery are not
AEs
A serious adverse event is any untoward event that
Is fatal
Is life-threatening
Requires inpatient hospitalization or prolongation of existing hospitalization with the
following exceptions
o Preplanned (before the study) hospital admissions unless the hospitalization is
prolonged
o Planned admissions (as part of a study eg routine biopsies)
o Hospitalization lasting lt 24 hours
49
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
o Hospitalization for elective procedure
o Emergency room visits
Results in persistent or significant disability or incapacity
Is a congenital anomaly or birth defect
Important medical events that may not result in death be life-threatening or require
inpatient hospitalization may be considered serious adverse events (SAEs) when based
on appropriate medical judgment they may jeopardize the subject and may require
medical or surgical intervention to prevent one of the outcomes listed above
Life-threatening means that the subject was in the view of the investigator at immediate risk of
death from the AE as it occurred It does not include an AE that had it occurred in a more severe
form might have caused death
Persistent or significant disabilityincapacity means that the event resulted in permanent or
significant and substantial disruption of the subjectrsquos ability to carry out normal life functions
Causality
A reasonable possibility means the AE may have been caused byrelated to the study drug A
perceived or real lack of efficacy does not satisfy the definition of relatedness
612 Adverse Event (AE) Reporting
For the PANTHER-IPF trial all AEs (serious and nonserious) occurring from randomization
through final study visit (4 weeks after final dose of all study medication) will be recorded on the
AE page of the case report form (CRF)
6121 Serious Adverse Events (SAE) Reporting
For this trial all deaths and all SAEs which occur from randomization through final study visit
must be entered within the EDC system via the SAE eCRF page within 24 hours of the
investigative sitersquos knowledge of the event It is the responsibility of the clinical center
50
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
investigator to provide a causality assessment of the event for each study medications based upon
the information available at the time of the report It is understood that complete information
about the event may not be known at the time the initial report is submitted In the event the EDC
system is not accessible to the site at the time of event reporting investigative sites will complete
and forward a paper back-up SAE form to DCRI Safety Surveillance for processing
DCRI Safety Surveillance
Telephone 1-919-668-8624 or 1-866-668-7799 (toll free)
Fax 1-919-668-7138 or 1-866-668-7138 (toll free)
The investigator must complete and submit follow-up SAE information via the eCRF when
important new or follow-up information (eg final diagnosis outcome results of specific
investigations) becomes available Follow-up information should be submitted according to the
same process used for reporting the initial event as described above All SAEs will be followed
until resolution stabilization or 30 days after the subject has completed the final visit (4 weeks
after the final dose of study medication) whichever occurs first The investigator is responsible
for reporting SAEs to their institutional review board (IRB) per site specific IRB reporting
guidelines
6122 Regulatory Reporting
AEs that are serious study drug related and unexpected will be reported to the regulatory
authorities The DCRI Safety Surveillance medical monitor will perform a medical review of all
SAEs submitted and evaluate for ldquounexpectednessrdquo DCRI Safety Surveillance will prepare
MedWatch reports for those events identified as serious study drug related and unexpected as
determined by Safety Medical Monitor
DCRI Regulatory Services will submit all unexpected study drug-related SAEs as per 21 CFR
32 DCRI Safety Surveillance will provide a safety alert letter to the NHLBI DSMB and DCC
clinical operation (for distribution to sites) within 15 days of initial receipt of the information
51
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Investigators are responsible for promptly reporting these events to their reviewing IRBs
according to site specific IRB reporting guidelines
62 Clinical Medical Monitoring
There will be an unblinded physician at the IPFnet DCC serving as medical monitor The
medical monitor will be available to assist with questions about dosage adjustments of study
medications including discontinuation or resumption of medications
63 Unblinding Procedures
Unblinding of subjects or investigators to subject treatment is strongly discouraged For ongoing
clinical management all subjects should be presumed to be receiving ldquoactiverdquo study drug To
ensure the subjectrsquos safety the study treatment will be dose-adjusted based on laboratory test
results clinical findings and symptoms
The IPFnet DCC medical monitor and PANTHER-IPF co-chairs Drs Ganesh Raghu and
Fernando Martinez will be available to the study physicians to discuss study drug management
on a case-by-case basis Un-blinding will be considered ONLY when the knowledge of subject
treatment assignment is ABSOLUTELY ESSENTIAL for subject safety and after discussion of
the subjectrsquos case with the medical monitor and either Dr Raghu or Dr Martinez Unblinding of
study treatment should be minimized during the conduct of the trial In those cases where it is
felt to be medically necessary the DCC medical officer will communicate directly with the
managing physician to minimize unblinding of study personnel
52
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
7 Study Drug Procedures
At the baseline 15-week 30-week and 45-week study visits subjects will receive a supply of
study drug sufficient to last until the next visit at which study drug will be dispensed
53
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
8 Data Management
81 Hardware and Software Configuration
811 Hardware and Database Software
Data will be stored in an Oracle database system Oracle has advantages of processing efficiency
and smooth linkage with other software systems The application and database will be hosted on
Solaris Unix servers at the IPFnet DCC
812 Statistical Software
SAS will be used as the principal application for the management of analysis data files and
statistical computations S-Plus will be used to provide supplementary functions as needed
813 Access Control and Confidentiality Procedures
Access to databases will be controlled centrally by the IPFnet DCC through user passwords
linked to appropriate privileges This protects the data from unauthorized changes and
inadvertent loss or damage
814 Security
Database and Web servers will be secured by a firewall and through controlled physical access
Oracle has many security features to ensure that any staff member accessing the database has the
proper authority to perform the functions he or she requests of the system Within the secondary
SAS databases Unix group-access control maintains similar security The Sun workstation login
is secured by extensive user-password facilities under Unix
54
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
815 Back-up Procedures
Database back-up will be performed automatically every day and standard IPFnet DCC policies
and procedures will be applied to dictate tape rotation and retention practices
816 Virus Protection
All disk drives that provide network services and all user computers will be protected using
virus-scanning software Standard IPFnet DCC policies will be applied to update these protection
systems periodically through the study
82 Sources of Data
821 Design and Development
The IPFnet DCC will be responsible for development of the electronic case report forms
(eCRFs) development and validation of the clinical study database ensuring data integrity and
training clinical center staff on applicable data management procedures A web-based distributed
data entry model will be implemented This system will be developed to ensure that guidelines
and regulations surrounding the use of computerized systems used in clinical trials are upheld
The remainder of this section provides an overview of the data management plan associated with
this protocol
822 Data Collection Forms
The data collection process consists of direct data entry at the study clinical centers into the EDC
system(s) provided by the DCC A data collection worksheet will be provided to clinical centers
for recording data in the event the EDC system is unavailable Data entry of the eCRFs should
be completed according to the instructions provided and project specific training The
investigator is responsible for maintaining accurate complete and up-to-date records and for
ensuring the completion of the eCRFs for each research participant
55
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
823 Data Acquisition and Entry
Data entry into eCRFs shall be performed by authorized individuals Selected eCRFs may also
require the investigatorrsquos written signature or electronic signature as appropriate Electronic
CRFs will be monitored for completeness accuracy and attention to detail during the study
824 Data Center Responsibilities
The IPFnet DCC will 1) develop a data management plan and will conduct data management
activities 2) provide final eCRFs for the collection of all data required by the study 3) develop
data dictionaries for each eCRF that will comprehensively define each data element 4) conduct
ongoing data monitoring activities on study data 5) monitor any preliminary analysis data
cleanup activities and 6) rigorously monitor final study data clean up
825 Data Editing
Completed data will be entered into the IPFnet DCC automated data acquisition and
management system If incomplete or inaccurate data are found a data clarification request will
be generated and distributed to clinical centers for a response Clinical centers will resolve data
inconsistencies and errors and enter all corrections and changes into the IPFnet DCC automated
data acquisition and management system
826 Training
The training plan for clinical center staff includes provisions for training on assessments eCRF
completion guidelines data management procedures and the use of computerized systems
56
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
9 Study Design and Data Analysis
91 General Analytic Considerations
All primary analyses will be based on intent-to-treat (ITT) principles using all randomized
subjects Baseline factors across groups will be compared using mean (standard deviation) and
median (25th and 75th percentiles) summary measures Kaplan-Meier curves will be used to
display event rates Due to clinical interest in departures from both sides of the null hypothesis
all test statistics will be 2-sided
Reasonable caution needs to be taken when conducting multiple analyses on key clinical
subgroups For subgroup analyses a conservative significance level of 0001 will be used for all
interaction tests Thus subgroup comparisons will be considered exploratory unless the p-value
from the interaction test is smaller than 0001
92 Randomization Blinding and Reporting of Results
A permuted block-randomization scheme will be created with varying block sizes stratified by
clinical center Once a subject has completed the screening and baseline period and evaluation
for inclusionexclusion criteria the randomization process will begin Subjects will be
randomized to receive NAC or matching placebo with equal probability (11) via telephone
contact with a central interactive voice response system (IVRS) using a toll-free randomization
number On the day of randomization after the subject has successfully met all inclusion and
exclusion criteria the investigator or designee will call the central randomization number to
obtain the assigned kit randomization numbers for that subject At each subject visit the
investigator or designee will call the central randomization number to obtain the new kit
randomization numbers for resupply of the subject For resupply of the clinical center the IVRS
will monitor minimal volume of a kit type andor expiration date and will automatically notify
the pharmacy
57
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
The trial results will be reported according to guidelines specified in the CONSORT statement
A flow diagram describing screening recruitment randomization dropout and vital status will
be included in the primary manuscript AEs and efficacy data will be presented for all treatment
groups Adherence dropout and lost to follow-up will be carefully examined across all treatment
groups Analyses of safety will be based on data from all randomized subjects who received at
least one dose of study drug
93 Stratification
Subjects will be distributed to the two treatment arms in a 11 allocation ratio Stratification
blocks will be based on clinical centers
94 Specification of the Primary Analyses
A mixed model repeated measures (MMRM) analysis described in section 95 will be used to
compare differences in the slope of FVC measurements across the treatment groups Response
variables are values of the FVC measured at baseline and every 15 weeks until study completion
Variables in the model will include treatment time and time by treatment age sex race and
height Contrast estimates of differences in slopes of treatment over time (along with confidence
intervals) will be used to estimate the treatment effect The validity of this model in terms of
meeting modeling assumptions will be assessed via standard modeling diagnostics and goodness-
of-fit measures Based on the MMRM framework missing FVC data will not be imputed for the
primary analysis
95 Analysis of Longitudinal Endpoints
A common goal in clinical trials is to specify models that are easily implemented and
reproducible by independent data analysts On the other hand the models should have proper
statistical behavior in terms of low bias and high precision Many common approaches to
longitudinal data analysis including last observation carried forward (LOCF) imputation rely on
the missing completely at random (MCAR) assumption However the MCAR assumption is
58
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
unlikely to hold in many clinical trials because missing data are often related to disease
progression and prognosis A more reasonable assumption missing at random (MAR) specifies
that the complete data distribution can be modeled using only the observed data The likelihood-
based MMRM approach is valid under the more general MAR assumptions These models will
be applied to analyze the longitudinal data secondary endpoints
The advantages of MMRM analysis are that all important characteristics of the model can be preshy
specified standard software can be used to implement the models and results are based on ITT
principles43 In addition the MMRM approach offers superior control of Type I and Type II
errors compared with the LOCF approach
Response variables are values of the PFTs measured at enrollment and every 15 weeks until
study completion and 6MWT values measured at baseline week 30 and week 60 Covariates are
treatment time time by treatment and key baseline risk factors Contrasts (along with
confidence intervals) of treatment by time will be used to estimate the treatment effect
The correlation structure involves multiple pieces including measurement errors random
variation and interindividual variability For the longitudinal data analyses an unstructured
correlation matrix for within-subject errors will be assumed Other correlation structures
including compound symmetry will be examined as needed A careful examination of reasons
for study discontinuation will be conducted to assess the validity of MCAR Sensitivity analyses
will be used to examine the untestable assumption that the observed data violate the MAR
assumption The MMRM models will be implemented using PROC MIXED in SAS
96 Analysis of Binary Time-to-Event and Time-Lagged Endpoints
Regression modeling approaches using either the logistic regression model or Cox proportional
hazards regression model will be employed when appropriate The validity of these models will
be assessed via standard modeling diagnostics and goodness-of-fit measures Estimates of
cumulative frequencies for more general time-lagged responses will be calculated using the
partitioned version of the Bang-Tsiatis estimator44 The partitions will be set at 15-week intervals
59
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
to correspond with the data-collection process Covariate adjusted event rates will be calculated
using inverse probability-weighted regression estimates45
97 Power Analysis
971 Primary Analyses
Based on previously published IPF clinical trials the PL group is expected to experience a drop
in FVC of approximately 020 L over the study period (see Figure 1) The IPFnet Steering Group
determined a clinically important difference would be to preserve the majority of the decline
relative to PL over the study period In particular a treatment effect of 015 L was determined to
be a clinically meaningful difference Potential dropout is a key factor in the proposed study The
drop-out process assumed 5 lost to follow-up after every study visit Only 80 of subjects
were assumed to be followed for the entire study period All models assumed a compound
symmetry structure for the covariance matrix Power calculations were performed using a SAS
IML program for designing repeated measures studies46 Based on preliminary reviews of the
data from the University of Michigan the covariance matrix parameters were estimated at
approximately σ2 = 0757 (variance parameter) and ρ = 0936 (correlation parameter) To be
conservative the power calculations for the primary analysis were performed with parameter
setting of σ2 = 0810 (variance parameter) and ρ = 0925 (correlation parameter)
The power calculations assume a correction for imperfect compliance proposed by Lachin and
Foulkes to allow for 2 noncompliance for each of the treatment arms47 Thus the sample size
of 130 subjects per arm would be reduced to an adjusted sample size of 130(1-002-002)2 =
1198 or 120 subjects per arm
Under the assumed Type I error rate of 005 with a correlation parameter of 0925 and standard
deviation of 090 the difference of 015 L (or 00025 Lweek) shown in Table 6 would have
power of 93
60
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Table 6 Hypothetical Values of Mean FVC (L) Change from Baseline
Week 15 Week 30 Week 45 Week 60
NAC 00125 00250 00375 00500
Placebo 00500 01000 01500 02000
Difference 00375 00750 01125 01500
Abbreviations FVC forced vital capacity PL placebo
972 Power Analysis for Secondary Endpoints
Power calculations for secondary endpoint measurements are shown in Table 7 Standard
deviations are based on unpublished data provided by the University of Michigan The
calculations are based on a 2-sample t-test with Type I error rate set at 005 These calculations
are likely to be conservative because the statistical approach described in section 95 for
analyzing these endpoints will incorporate incomplete observations as well as intermediate data
points
Table 7 Detectable Differences in Treatment Means for Selected Endpoint Measurements
Secondary Endpoints Std Dev
of the Baseline Score
Detectable Difference for 80 Power
Std Dev of the Change Score
Difference Detectable for
80 Power
DLCOpred 166 58 91 32
6MWT Area Under the Desaturation Curve
219 76 175 61
6MWT Distance to Desaturation 224 78 315 110
6MWT Minutes Walked 210 073 205 071
Abbreviations Std Dev standard deviation DLCOpred diffusing capacity of the lung for carbon monoxide percent predicted 6MWT 6-minute walk test
61
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
10 Study Administration
101 Cooperative Agreement Mechanism
The administrative and funding mechanism used to undertake this project is a ldquocooperative
agreementrdquo (U01) which is an assistance mechanism Under the cooperative agreement the
NHLBI assists supports andor stimulates the project and is substantially involved with
investigators in conducting the study by facilitating performance of the effort in a ldquopartnerrdquo role
The NHLBI project scientist serves on the IPFnet Steering Group and he or another NHLBI
scientist may serve on other project committees when appropriate At the same time however
NHLBI does not assume a dominant role direction or prime responsibility for this research
program
As described below governance of the project is conducted through the IPFnet Steering Group
Principal investigators have lead responsibilities in all aspects of their trials and the project
including any modification of trial designs conduct of the trials quality control data analysis
and interpretation preparation of publications and collaboration with other investigators unless
otherwise provided for by the IPFnet Steering Group
PIs retain custody of and have primary rights to their center-specific and collaborative data
subject to government rights-of-access consistent with current Health amp Human Services (HHS)
Public Health Service (PHS) and National Institutes of Health policies The protocols and
governance policies call for the continual submission of data centrally to the IPFnet DCC for the
collaborative database which at a minimum will contain the key variables selected by the IPFnet
Steering Group for standardization across all clinical centers the submission of copies of the
collaborative datasets to each PI upon completion of the project procedures for data analysis
reporting and publication and procedures to protect and ensure the privacy of medical and
genetic data and records of individuals The NHLBI project scientist on behalf of the NHLBI
will have the same access privileges and responsibilities regarding the collaborative data as the
other members of the Steering Group
62
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
PIs are also encouraged to publish and to publicly release and disseminate results data and other
products of the project concordant with the project protocols and governance and the approved
plan for making data and materials available to the scientific community and to the NHLBI
However during the 3 years after the ending date of NHLBI project support unpublished data
unpublished results data sets not previously released and other study materials or products are
to be made available to any third party only with the approval of the IPFnet Steering Group
Upon completion of the project PIs are expected to put their intervention materials and
procedure manuals into the public domain andor make them available to other investigators
according to the approved plan for making data and materials available to the scientific
community and the NHLBI for the conduct of research at no charge other than the costs of
reproduction and distribution
The NHLBI reserves the right to terminate or curtail the project (or an individual award) in the
event of (a) failure to develop or implement mutually agreeable collaborative measurement
subject eligibility and data management sections of the protocols (b) substantial shortfall in
subject recruitment follow-up data reporting or quality control or other major breach of
protocol (c) substantive changes in the agreed-upon protocols with which NHLBI cannot
concur (d) reaching a major project outcome with persuasive statistical significance
substantially before schedule or (e) human subject ethical issues that may dictate a premature
termination
Any disagreement that may arise in scientificprogrammatic matters (within the scope of the
award) between award recipients and the NHLBI may be brought to arbitration An arbitration
panel will be composed of 3 membersmdash1 selected by the IPFnet Steering Group (with the
NHLBI member not voting) or by the individual PI in the event of an individual disagreement a
second selected by NHLBI and the third selected by the other 2 members This special
arbitration procedure in no way affects the PIrsquos right to appeal an adverse action that is otherwise
appealable in accordance with the PHS regulations at 42 CFR part 50 Subpart D and HHS
63
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
regulation at 45 CFR part 16 or the rights of the NHLBI under applicable statutes regulations
and terms of the award
102 IPFnet Steering Group
The IPFnet Steering Group is the main governing body of the project It is composed of the PIs
of the clinical centers the PI of the DCC and the NHLBI project scientist The clinical centers
the IPFnet DCC and the NHLBI each have 1 vote on the IPFnet Steering Group All decisions
are determined by majority vote
All major scientific decisions are determined by the IPFnet Steering Group It assumes overall
responsibility for the design and conduct of the trial It appoints (and disbands) committees and
subcommittees as the need arises designs approves and implements the study protocols
oversees the development of the MOOP monitors subject recruitment and treatment delivery
evaluates data collection and management oversees quality assurance procedures and
implements changes and enhancements to the study as required It also has primary responsibility
for facilitating the conduct of the trials and reporting the projectrsquos results
103 Data and Safety Monitoring Board
The NHLBI will establish a DSMB in accordance with established policies (see
httpwwwnhlbinihgovfundingpoliciesdsmb_insthtm) to ensure data quality and subject
safety and to provide independent advice to the NHLBI regarding progress and the
appropriateness of study continuation
104 Recommendations on Interim Monitoring of Efficacy Safety and Futility
First and foremost the role of the DSMB will be to review subject safety and trial conduct at
periodic points during the study The DSMB may require analyses of the primary endpoint
results for comparing the benefit and risks of treatment strategies The benefit of collecting
additional data on key secondary endpoints with extended follow-up and establishing a robust
64
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
evidence base for determining a standard of care will need to be carefully considered before
early termination of one or more treatment arms After careful consideration the IPFnet Steering
Group recommends conservative thresholds for the early examinations of the safety and efficacy
data
The DSMB will be expected to meet approximately every 6 months until trial completion to
review safety and toxicity data The DSMB may recommend stopping the study based on these
reviews Because the DSMB could stop the trial for safety concerns as well as for a large
efficacy benefit there could be multiple opportunities to reject the null hypothesis (no difference
in event rates between the PL and NAC groups) A Bonferroni approximation will be applied
during the one planned interim analysis for efficacy
Before locking the database a statistical analysis plan (SAP) will be developed to provide
complete details on the statistical analysis The SAP will include the specifics for how and when
the DSMB will be notified for AEs The IPFnet DCC will deliver to the DSMB all FDA-defined
AEs at 3-month intervals The IPFnet DCC will prepare narrative SAE reports in real time for
DSMB review including recommendations and analysis of similar events for each SAE
submitted to the FDA
65
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
11 Investigator and Sponsor Obligations
111 Monitoring
All monitoring activities for US clinical centers will be performed in accordance with DCRI
standard operating procedures Information regarding the types of visits will be outlined in the
PANTHER-IPF MOOP
112 Cost and Payment
There will be no cost to subjects enrolled in this trial Study-related procedures will be paid for
by the IPFnet
Subjects may be eligible for reimbursement for travel to the clinical center Details of payment
will be explained to each subject during the consent process
113 Confidentiality and Health Insurance Portability and Accountability Act
Considerations
Subject confidentiality will be protected throughout the study All subject data will be kept
strictly confidential and no subject-identifying information will be released to anyone outside
the project Confidentiality will be assured through several mechanisms First each subject will
be assigned an anonymous study ID which will then be used on all study forms Second any
study forms blood samples and paper records that contain subject information (eg address lists
phone lists) will be kept at the clinical centers in secured locked areas coded by number Once
blood is collected there will be no subject identifiers placed on blood samplesmdashonly the study
ID number and the date of sample collection Third access to all subject data and information
including laboratory specimens will be restricted to authorized personnel In the case of
computerized data this restricted access will be assured through user logon IDs and password
protection
66
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
At the IPFnet DCC only authorized personnel will have access to the data files containing study
data Security will be assured through user logon IDs passwords and appropriate access
privileges All study subjects will be identified only by their IPFnet ID numbers and no personal
identifying information such as name address or Social Security number will be entered into
the IPFnet DCC database Any subject-specific data reported to the IPFnet Steering Group will
be identified only by the IPFnet ID number
Finally subjects will not be identified by name in any reports or publications nor will the data
be presented in such a way that the identity of individual subjects can be inferred Analysis files
created for further study by the scientific community will have no subject identifiers These data
files will be created in accordance with the Ancillary Studies and Publication Policy of the
IPFnet
114 Informed Consent Procedures
All IPFnet subjects will provide written informed consent using procedures reviewed and
approved by each clinical centerrsquos IRB Informed consent will be undertaken by study personnel
in-person with the subject The subject has the option of declining further participation in the
study at that point No further study procedures will be conducted until the signed documents
have been provided to the IPFnet clinical center
115 Institutional Review Boards
Before initiating this study the protocol clinical center-specific informed consent forms Health
Insurance Portability and Accountability Act (HIPAA) forms recruitment materials and other
relevant information will be reviewed by a properly constituted IRB at each participating clinical
center A copy of the signed and dated IRB approval at each clinical center will be retrieved prior
to or during the site initiation visit and archived at the IPFnet DCC Any amendments to the
protocol other than simple administrative and typographical changes must be approved by each
IRB before they are implemented The clinical centers will seek annual renewals of their IRB
approvals in accordance with local procedures
67
__________________________________________ ________________
__________________________________________
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
12 Investigator Agreement
I have read the foregoing protocol PANTHER-IPF and agree that it contains all necessary
details for carrying out this study I will conduct the study as outlined herein and will complete
the study within the time designated
I will provide copies of the protocol and all pertinent information to all individuals responsible to
me who assist in the conduct of this study I will discuss this material with them to ensure they
are fully informed regarding the drug and the conduct of the study
I will fulfill all responsibilities for submitting pertinent information to the local IRB if
applicable that is responsible for this study
I further agree that NHLBI andor DCRI will have access to any source documents from which
eCRF information may have been generated
Signature of Principal Investigator Date
Name of Principal Investigator (printed or typed)
Protocol version date May 19 2009
Protocol Amendment 1 version date May 28 2010
Protocol Amendment 2 version date December 6 2011
68
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
13 References
1 Raghu G Brown KK Bradford WZ et al A placebo-controlled trial of interferon gamma-1b in patients with idiopathic pulmonary fibrosis N Engl J Med 2004350125-33 2 King TE Jr Safrin S Starko KM et al Analyses of efficacy end points in a controlled trial of interferon-gamma1b for idiopathic pulmonary fibrosis Chest 2005127171-7 3 Flaherty KR Thwaite EL Kazerooni EA et al Radiological versus histological diagnosis in UIP and NSIP survival implications Thorax 200358143-8 4 Wells AU Desai SR Rubens MB et al Idiopathic pulmonary fibrosis a composite physiologic index derived from disease extent observed by computed tomography Am J Respir Crit Care Med 2003167962-9 5 Raghu G Freudenberger TD Yang S et al High prevalence of abnormal acid gastroshyoesophageal reflux in idiopathic pulmonary fibrosis Eur Respir J 200627136-42 6 Kinnula VL Focus on antioxidant enzymes and antioxidant strategies in smoking related airway diseases Thorax 200560693-700 7 Coultas DB Zumwalt RE Black WC Sobonya RE The epidemiology of interstitial lung diseases Am J Respir Crit Care Med 1994150967-72 8 Raghu G Weycker D Edelsberg J Bradford WZ Oster G Incidence and prevalence of idiopathic pulmonary fibrosis Am J Respir Crit Care Med 2006174810-6 9 Olson AL Swigris JJ Lezotte DC Norris JM Wilson CG Brown KK Mortality from pulmonary fibrosis increased in the United States from 1992 to 2003 Am J Respir Crit Care Med 2007176277-84 10 Mannino DM Etzel RA Parrish RG Pulmonary fibrosis deaths in the United States 1979shy1991 An analysis of multiple-cause mortality data Am J Respir Crit Care Med 19961531548shy52 11 Hubbard R Johnston I Coultas DB Britton J Mortality rates from cryptogenic fibrosing alveolitis in seven countries Thorax 199651711-6 12 Johnston I Britton J Kinnear W Logan R Rising mortality from cryptogenic fibrosing alveolitis Bmj 19903011017-21 13 Raghu G Collard HR Egan JJ et al An official ATSERSJRSALAT statement idiopathic pulmonary fibrosis evidence-based guidelines for diagnosis and management Am J Respir Crit Care Med 2011183788-824 14 (USA) FDA FDA Public Health Advisory Interferon gamma-1b (marketed as Actimmune) In 2007 15 King TE Jr Pardo A Selman M Idiopathic pulmonary fibrosis Lancet 2011 16 Raghu G Brown KK Costabel U et al Treatment of idiopathic pulmonary fibrosis with etanercept an exploratory placebo-controlled trial Am J Respir Crit Care Med 2008178948shy55 17 Malouf MA Hopkins P Snell G Glanville AR An investigator-driven study of everolimus in surgical lung biopsy confirmed idiopathic pulmonary fibrosis Respirology 201116776-83 18 King TE Jr Behr J Brown KK et al BUILD-1 a randomized placebo-controlled trial of bosentan in idiopathic pulmonary fibrosis Am J Respir Crit Care Med 200817775-81 19 Richeldi L Costabel U Selman M et al Efficacy of a tyrosine kinase inhibitor in idiopathic pulmonary fibrosis N Engl J Med 20113651079-87
69
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
20 Borok Z Buhl R Grimes GJ et al Effect of glutathione aerosol on oxidant-antioxidant imbalance in idiopathic pulmonary fibrosis Lancet 1991338215-6 21 Meyer A Buhl R Magnussen H The effect of oral N-acetylcysteine on lung glutathione levels in idiopathic pulmonary fibrosis Eur Respir J 19947431-6 22 Behr J Maier K Degenkolb B Krombach F Vogelmeier C Antioxidative and clinical effects of high-dose N-acetylcysteine in fibrosing alveolitis Adjunctive therapy to maintenance immunosuppression Am J Respir Crit Care Med 19971561897-901 23 Cantin AM North SL Fells GA Hubbard RC Crystal RG Oxidant-mediated epithelial cell injury in idiopathic pulmonary fibrosis J Clin Invest 1987791665-73 24 Waghray M Cui Z Horowitz JC et al Hydrogen peroxide is a diffusible paracrine signal for the induction of epithelial cell death by activated myofibroblasts Faseb J 200519854-6 25 Larios JM Budhiraja R Fanburg BL Thannickal VJ Oxidative protein cross-linking reactions involving L-tyrosine in transforming growth factor-beta1-stimulated fibroblasts J Biol Chem 200127617437-41 26 Kinnula VL Fattman CL Tan RJ Oury TD Oxidative stress in pulmonary fibrosis a possible role for redox modulatory therapy Am J Respir Crit Care Med 2005172417-22 27 Meyer A Buhl R Kampf S Magnussen H Intravenous N-acetylcysteine and lung glutathione of patients with pulmonary fibrosis and normals Am J Respir Crit Care Med 19951521055-60 28 Behr J Degenkolb B Krombach F Vogelmeier C Intracellular glutathione and bronchoalveolar cells in fibrosing alveolitis effects of N-acetylcysteine Eur Respir J 200219906-11 29 Bando M Hosono T Mato N et al Long-term efficacy of inhaled N-acetylcysteine in patients with idiopathic pulmonary fibrosis Intern Med 2010492289-96 30 Demedts M Behr J Buhl R et al High-dose acetylcysteine in idiopathic pulmonary fibrosis N Engl J Med 20053532229-42 31 Toma TP Bhowmik A Rajakulasingam R Acetylcysteine in pulmonary fibrosis N Engl J Med 20063541086-9 author reply -9 32 Hunninghake GW Antioxidant therapy for idiopathic pulmonary fibrosis N Engl J Med 20053532285-7 33 Flaherty KR Mumford JA Murray S et al Prognostic implications of physiologic and radiographic changes in idiopathic interstitial pneumonia Am J Respir Crit Care Med 2003168543-8 34 Latsi PI du Bois RM Nicholson AG et al Fibrotic idiopathic interstitial pneumonia the prognostic value of longitudinal functional trends Am J Respir Crit Care Med 2003168531-7 35 Collard HR King TE Jr Bartelson BB Vourlekis JS Schwarz MI Brown KK Changes in clinical and physiologic variables predict survival in idiopathic pulmonary fibrosis Am J Respir Crit Care Med 2003168538-42 36 Jegal Y Kim DS Shim TS et al Physiology is a stronger predictor of survival than pathology in fibrotic interstitial pneumonia Am J Respir Crit Care Med 2005171639-44 37 Martinez FJ Safrin S Weycker D et al The clinical course of patients with idiopathic pulmonary fibrosis Ann Intern Med 2005142963-7 38 Hull JH Acetylcysteine in pulmonary fibrosis N Engl J Med 20063541089-91 author reply -91
70
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
39 Flaherty KR King TE Jr Raghu G et al Idiopathic interstitial pneumonia what is the effect of a multidisciplinary approach to diagnosis Am J Respir Crit Care Med 2004170904shy10 40 Raghu G Johnson WC Lockhart D Mageto Y Treatment of idiopathic pulmonary fibrosis with a new antifibrotic agent pirfenidone results of a prospective open-label Phase II study Am J Respir Crit Care Med 19991591061-9 41 Hunninghake GW Lynch DA Galvin JR et al Radiologic findings are strongly associated with a pathologic diagnosis of usual interstitial pneumonia Chest 20031241215-23 42 Lynch D Godwin J Safrin S et al High-resolution computed tomography in idiopathic pulmonary fibrosis diagnosis and prognosis Am J Respir Crit Care Med 2005172488-93 43 Mallinckrodt CH Watkin JG Molenberghs G Carroll RJ Choice of the primary analysis in longitudinal clinical trials Pharmaceutical Statistics 20043161-9 44 Bang H Tsiatis A Estimating medical costs with censored data Biometrika 200087329shy43 45 Lin DY Regression analysis of incomplete medical cost data Stat Med 2003221181-200 46 Rochon J Application of GEE procedures for sample size calculations in repeated measures experiments Stat Med 1998171643-58 47 Lachin JM Foulkes MA Evaluation of sample size and power for analyses of survival with allowance for nonuniform patient entry losses to follow-up noncompliance and stratification Biometrics 198642507-19
71
- PANTHER-IPFPREDNISONE AZATHIOPRINEAND N-ACETYLCYSTEINEA STUDY THAT EVALUATES RESPONSE INIDIOPATHIC PULMONARY FIBROSIS
-
- Protocol Summary
- Table of Contents
- List of Tables
- List of Figures
- List of Abbreviations
- 1 Summary
- 2 Hypotheses and Specific Aims
-
- 21 Null Hypothesis
- 22 Specific Aim 1
- 23 Specific Aim 2
- 24 Prespecified Subgroups of Interest
-
- 3 Background and Significance
-
- 31 Idiopathic Pulmonary Fibrosis is the Most Common Interstitial Lung Disease
- 32 Rationale for Placebo Control
- 33 Rationale for N-acetylcysteine
- 35 Rationale for N-acetylcysteine as a Stand-alone Therapy
- 36 Rationale for the Study Design and Primary Endpoint
- 37 Rationale for Blinding of Treatments
-
- 4 Methods
-
- 41 Inclusion Criteria
- 42 Diagnosis of IPF
- 43 Exclusion Criteria
- 44 Study Design and Study Visit
- 45 Dose Justification
- 46 Contraindications Precautions and Side Effects of Study Medications
- 47 Recruitment Procedures
- 48 Study Procedures
- 49 Concomitant Medications
- 410 Laboratory Testing
- 411 Blinding of Study Drugs
-
- 5 Study Endpoints
-
- 51 Primary Study Endpoint
- 52 Secondary Study Endpoints
-
- 6 Safety Evaluations and Procedures
-
- 61 Adverse Events
- 62 Clinical Medical Monitoring
- 63 Unblinding Procedures
-
- 7 Study Drug Procedures
- 8 Data Management
-
- 81 Hardware and Software Configuration
- 82 Sources of Data
-
- 9 Study Design and Data Analysis
-
- 91 General Analytic Considerations
- 92 Randomization Blinding and Reporting of Results
- 93 Stratification
- 94 Specification of the Primary Analyses
- 95 Analysis of Longitudinal Endpoints
- 96 Analysis of Binary Time-to-Event and Time-Lagged Endpoints
- 97 Power Analysis
-
- 10 Study Administration
-
- 101 Cooperative Agreement Mechanism
- 102 IPFnet Steering Group
- 103 Data and Safety Monitoring Board
- 104 Recommendations on Interim Monitoring of Efficacy Safety and Futility
-
- 11 Investigator and Sponsor Obligations
-
- 111 Monitoring
- 112 Cost and Payment
- 113 Confidentiality and Health Insurance Portability and Accountability ActConsiderations
- 114 Informed Consent Procedures
- 115 Institutional Review Boards
-
- 12 Investigator Agreement
- 13 References
-
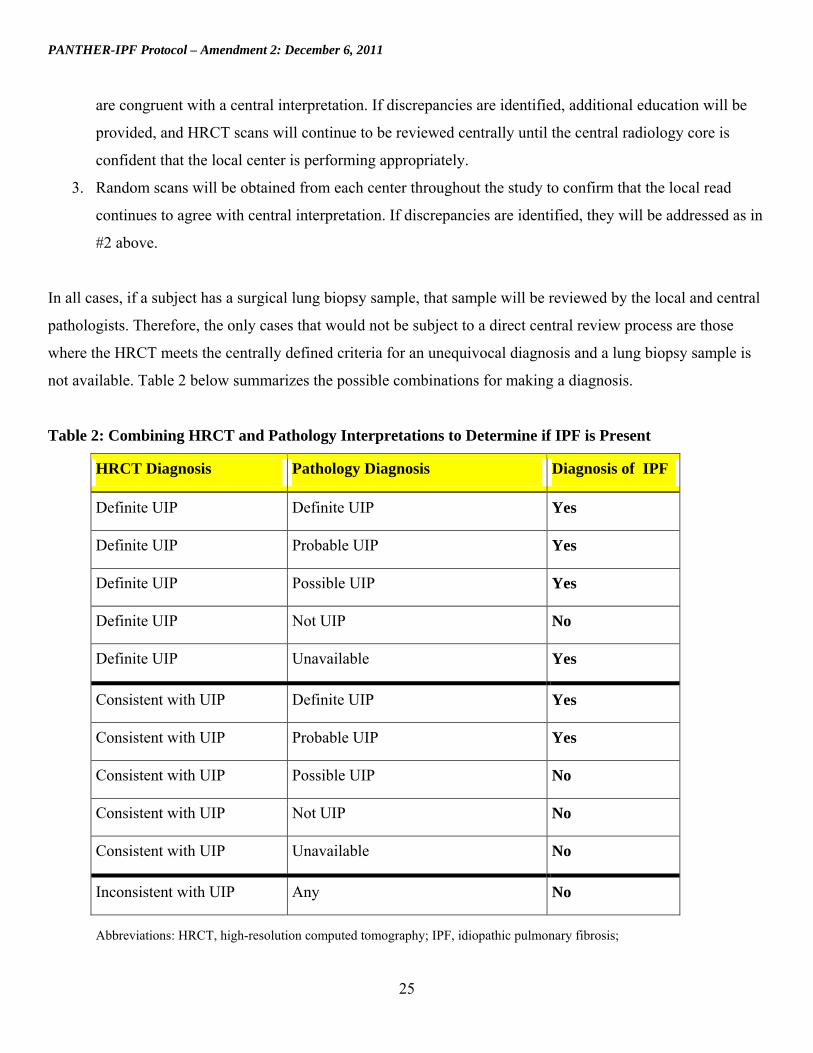
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
25
are congruent with a central interpretation If discrepancies are identified additional education will be
provided and HRCT scans will continue to be reviewed centrally until the central radiology core is
confident that the local center is performing appropriately
3 Random scans will be obtained from each center throughout the study to confirm that the local read
continues to agree with central interpretation If discrepancies are identified they will be addressed as in
2 above
In all cases if a subject has a surgical lung biopsy sample that sample will be reviewed by the local and central
pathologists Therefore the only cases that would not be subject to a direct central review process are those
where the HRCT meets the centrally defined criteria for an unequivocal diagnosis and a lung biopsy sample is
not available Table 2 below summarizes the possible combinations for making a diagnosis
Table 2 Combining HRCT and Pathology Interpretations to Determine if IPF is Present
HRCT Diagnosis Pathology Diagnosis Diagnosis of IPF
Definite UIP Definite UIP Yes
Definite UIP Probable UIP Yes
Definite UIP Possible UIP Yes
Definite UIP Not UIP No
Definite UIP Unavailable Yes
Consistent with UIP Definite UIP Yes
Consistent with UIP Probable UIP Yes
Consistent with UIP Possible UIP No
Consistent with UIP Not UIP No
Consistent with UIP Unavailable No
Inconsistent with UIP Any No
Abbreviations HRCT high-resolution computed tomography IPF idiopathic pulmonary fibrosis
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
UIP usual interstitial pneumonia Dx diagnosis 43 Exclusion Criteria
1 History of clinically significant environmental exposure known to cause pulmonary fibrosis
Occupational exposures such as asbestos or environmental exposure to organic dust such as occurs in
pigeon breeders may at times mimic the clinical and radiographic findings of IPF
2 Diagnosis of connective tissue disease felt by the principal investigator (PI) to be the etiology of the
interstitial disease Diagnosis of collagen-vascular conditions will be according to the published
American College of Rheumatology criteria As such the presence of any documented collagen-vascular
disorder or the presence of any suspicious symptom complex whether or not associated with
significantly abnormal rheumatological serologies will exclude the subject at the discretion of the PI
3 Extent of emphysema greater than the extent of fibrotic change (honeycombing reticular changes) on
HRCT scan
4 Forced expiratory volume in 1 second (FEV1)FVC ratio lt 065 at screening (postbronchodilator)
5 Partial pressure of arterial oxygen (PaO2) on room air lt 55 mm Hg (lt 50 mm Hg at Denver site)
6 Residual volume gt 120 predicted at screening (postbronchodilator)
7 Evidence of active infection
8 Significant bronchodilator response on screening spirometry defined as a change in FEV1 ge 12 and
absolute change gt 200 mL OR change in FVC ge 12 and absolute change gt 200 mL The percent
difference between the FVC (or FEV1) values will be calculated by taking the absolute value of the
difference and dividing it by the larger of the two FVC (or FEV1) values
9 Screening and enrollment post-bronchodilator FVC measurements (in liters) differing by gt 11 The
percent difference between the FVC values will be calculated by taking the absolute value of the
difference and dividing it by the larger of the two FVC values (eg the percent difference between FVC
measurements of 19 and 20 liters would be determined by taking the difference between the two (01
liters) and dividing by the larger of the two (20 liters) So 0120 = 5 and these FVC measurements
would not exclude the subject
10 Listed for lung transplantation ie the patient has completed the evaluation process has been accepted
as a candidate for transplantation at an appropriate center and is waiting to receive notification of an
available donor organ
11 History of unstable or deteriorating cardiac disease
12 Myocardial infarction coronary artery bypass or angioplasty within 6 months of screening
26
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
13 Unstable angina pectoris or congestive heart failure requiring hospitalization within 6 months of
screening
14 Uncontrolled arrhythmia
15 Severe uncontrolled hypertension
16 Known HIV or hepatitis C
17 Known cirrhosis and chronic active hepatitis
18 Active substance andor alcohol abuse (as determined by site PI)
19 Pregnancy or lactation (subjects who are pregnant or breastfeeding)
20 Known hypersensitivity to study medication
21 Any condition other than IPF that in the opinion of the site PI is likely to result in the death of the
subject within the next year
22 Any condition that in the judgment of the PI might cause participation in this study to be detrimental to
the subject or that the PI deems makes the subject a poor candidate
23 Any therapy directed at pulmonary fibrosis (excepting triple therapy of prednisone plus azathioprine
plus NAC) requires a 30-day washout period before randomized Triple therapy of lt= 12 weeks duration
in the past 4 years requires a 30-day washout period before randomization
24 History of triple therapy of prednisone plus azathioprine plus NAC for gt 12 weeksrsquo duration in the past
4 years or previous enrollment in the triple-therapy arm of the PANTHER-IPF study
44 Study Design and Study Visit
441 Study Design Summary
This study will be a randomized double-blind PL-controlled trial designed to assess the safety and efficacy of
NAC in subjects with newly diagnosed IPF
Subjects with mild to moderate IPF (defined as FVCpred ge 50 and DLCOpred ge 30) diagnosed within
the past 48 months will be enrolled Screening will continue until April 30 2012
27
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
The study will employ a 2-arm design with 11 randomization to NAC or PL Once enrolled subjects will visit
the clinical center at 15 weeks and 15-week intervals thereafter Each subject will be treated and followed for a
maximum of 60 weeks
During the 60-week visit subjects will be taken off all study agents Approximately four weeks after the final
dose of study agent is taken subjects will receive a safety phone call from the study site
442 Study Visits
Subjects who meet entry criteria will review the informed consent a written description of the purpose
procedures and risks of the study with the PI co-investigator or study coordinator and all questions will be
answered The informed consent form will be signed by the subject at screening No protocol-specific
procedures will be performed until the subject has signed and dated an informed consent form This includes the
screening procedures
4421 Screening
Once informed consent is obtained subjects may immediately begin the screening process or may return within
28 days of consent In the event a study subject has been clinically evaluated at the study site by an IPFnet study
physician and has performed testing within three weeks for this clinical evaluation that meets guidelines
provided in the IPFnet PANTHER-IPF Manual of Operating Procedures (MOOP) this testing may be used to
satisfy the following screening criteria medical history physical exam arterial blood gas (ABG) with A-a
gradient vital signs with oximetry body height and weight spirometry DLCO lung volumes and HRCT scan
Allowing the use of previously performed test results that meet study guidelines for the screening visit is
intended to permit subjects easier access to study entry to prevent subjects from repeating testing that has been
performed within the study window and to decrease risks to subjects from repeated exposure to procedures
such as arterial puncture and HRCT
The following procedures will be performed at screening
Medical history and a physical examination
28
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Measure height and weight
Serum pregnancy test (if applicable)
Measure vital signs including oximetry
Blood draws performed and the following analyses conducted
o Hematology (red cell count white cell count hemoglobin hematocrit cell indices differential
platelet count)
o Blood chemistries according to central laboratory protocol (see Section 410 Laboratory
Testing)
o Beta human chorionic gonadotropin (serum) pregnancy test (in women of childbearing potential)
o Urinalysis
Pulmonary Function Tests (PFTs) including spirometry pre- and post- bronchodilator and postshy
bronchodilator measurement of lung volumes and measurement of hemoglobin adjusted diffusing
capacity
Measure ABGs
HRCT if a satisfactory scan has not been performed on the subject within 3 months of screening (see
PANTHER-IPF MOOP for more details)
Surgical lung biopsies (if applicable) reviewed by local and central pathology departments
Current medications If required a washout period discussed with the subject and initiated at this visit
4422 Enrollment
The enrollment visit is expected to take place within eight weeks of the screening visit Enrollment visit
activities include
Measure vital signs including oximetry
Measure height and weight
Serum pregnancy test (if applicable)
If consent has been given blood will be drawn and a urine specimen collected for the bio-specimen
repository
Spirometry (post-bronchodilator)
Measure 6MWT with Borg Dyspnea Scale
29
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Collect Quality-of-life (QOL) data using the SF-36 EuroQol Investigating Choice Experiments for
Preferences of Older People Capability Instrument (ICE CAP) and SGRQ
Female subjects complete Gender Substudy questionnaire
Dyspnea status collected using the UCSD SOBQ
Evaluate Acute Exacerbation (AEx)
Review of any Adverse Events (AEs)
Review of concomitant medications
Subject receives diary and instructions on its purpose and proper use
Subject receives supply of study drug sufficient to last until his or her 15-week study visit
See the Schedule of Assessments (Table 3) for more details Subjects with screening and enrollment postshy
bronchodilator FVC measurements (in liters) differing by more than 11 are not eligible to be enrolled in the
study
Subjects will be asked to provide a physician of record This physician will be considered the subjectrsquos primary
care provider (PCP) and if the subject agrees the PCP will be informed by letter of the subjectrsquos enrollment in
the trial The subject will be informed that his or her ongoing medical care should be received from the PCP
The PCP will be informed of any safety issues identified by the study staff The PCP will also be given
information regarding communication with study personnel about pertinent health issues or clinic encounters
the subject may have
4423 Week 15
The week 15 visit is expected to occur within +- 14 days of the subjectrsquos scheduled visit time (eg the week 15
visit should occur anytime between 13 and 17 weeks after starting study drug Week 15 activities include
Measure vital signs with oximetry
Measurement height and weight
Serum pregnancy test (if applicable)
Spirometry (post-bronchodilator) measurement
Review of AEs
Evaluate for AEx
30
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Review concomitant medications
If consented draw blood and collect urine specimen for the biospecimen repository
Subjects return used and unused study drug for the visit
Review study diary and a new study diary will be given
Provide additional supply of study drug sufficient to last until the next scheduled visit
4424 Week 30
The week 30 visit is expected to occur within +- 14 days of the subjectrsquos scheduled visit time (eg the week 30
visit should occur anytime between 28 and 32 weeks after starting study drug) Week 30 activities include
Physical examination
Measure vital signs with oximetry
Measure height and weight
Laboratory values (complete blood count [CBC] and serum chemistries)
Serum pregnancy test (if applicable)
Measure spirometry (post-bronchodilator)
6MWT with Borg scale
DLCO
Review of AEs
Evaluate for AEx
Review concomitant medications
Complete all QOL and dyspnea questionnaires (EuroQol ICE CAP SF-36 SGRQ and UCSD SOBQ)
If consent has been given blood will be drawn and a urine specimen collected for the biospecimen
repository
Review study diary
Subjects return used and unused study drug for the visit
Provide additional supply of study drug sufficient to last until the next scheduled visit
4425 Week 45
31
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
The week 45 visit is expected to occur within +- 14 days of the subjectrsquos scheduled visit time (eg the week 45
visit should occur anytime between 43 and 47 weeks after starting study drug) Week 45 activities include
Measure vital signs with oximetry
Measure height and weight
Serum pregnancy test (if applicable)
Measure spirometry (post-bronchodilator)
Review of AEs
Evaluate for AEx
Review concomitant medications
If consent has been given blood will be drawn and a urine specimen collected for the biospecimen
repository
Subjects return used and unused study drug for the visit
Study diary reviewed
Provide additional supply of study drug sufficient to last until the next scheduled visit
4426 Week 60 (Early Withdrawal or Final Treatment Visit)
At week 60 or at subject withdrawal from the study (premature by study doctor or subjectrsquos decision) a final
treatment visit will occur At this final treatment visit subjects will discontinue NACPL abruptly Week 60
activities also include
Physical examination
Measure vital signs with oximetry
Measure height and weight
Laboratory values (complete blood count [CBC] and serum chemistries)
Spirometry (post-bronchodilator) measurement
6MWT with Borg scale measurement
DLCO
Lung volumes
ABG
Review of AEs
32
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Evaluate for AEx
Review concomitant medications
Subjects will complete all QOL and dyspnea questionnaires (EuroQol ICE CAP SF-36 SGRQ and
UCSD SOBQ)
If consent has been given blood will be drawn and a urine specimen collected for the biospecimen
repository
Subjects return used and unused study drug for the visit
Study diary reviewed
4427 Final Site Visit ndash FVC drop confirmation
In the event that the subject has a recorded FVC drop of gt10 from baseline at the final treatment visit and the
subject has not had a confirmation of such a drop at a previous study visit the subject should return to the
clinical site 6 to 8 weeks after the final treatment visit During this visit a post-bronchodilator spirometry test
will be performed This FVC measurement will be evaluated according to section 521 of this protocol
4428 Final Visit ndash Telephone Follow-up
Four weeks following the final dose of study medication subjects will receive a telephone call from the study
coordinator to ensure that there are no side effects and to follow up on any ongoing adverse events (AEs)
4429 Phone Contact Between Visits
At week 2 and each month that a subject does not have a scheduled clinical center visit his or her study
coordinator will contact him or her at least once by telephone to
Inquire if the subject has had any hospitalizations events that might be considered an AE or any events
significant enough to warrant an out-of-cycle visit to the clinical center
Remind subjects of their current dosage levels and confirm that the subject understands them
Address any questions or concerns the subject might have regarding other aspects of the study
Assess adherence to the treatment regimen by reviewing diary data verbal review of medications taken
including nutritional supplements
33
34
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Table 3 Schedule of Assessments
Procedure Screening Visit 0
Enrollment Visit 1
Week 15 Visit 2
Week 30Visit 3
Week 45 Visit 4
Week 60 Early
Withdrawal Visit 5
Final1
Visit (via phone)
Informed consent X
Medical history X
Inclusionexclusion criteria X
Serum pregnancy test (if applicable) X X X X X
Review of lung biopsy X
Arterial Blood Gas X X
6-Minute Walk Test
X
X X
Physical examination X X X
Vital signs with oximetry X X X X X X
Body height and weight X X X X X X
Complete Blood Count X X X
Chemistry panel X X X
Monitor Lab Values X X X
Urinalysis X Specimen repository substudy blood draw and urine collection (if consented)
X
X X X X
HRCT (if not completed within three months) X
Spirometry (pre- and post-bronchodilator) X
Spirometry (post-bronchodilator only) X X X X X
DLCO (post-bronchodilator only) X X X
Lung volumes (post-bronchodilator only) X
X
Evaluate for acute exacerbation X X X X X
Review Adverse Events X X X X X X
Review concomitant meds X X X X X X
Dispense subject diary X X X X
Review subject diary X X X X X
Dispense study agent X X X X
Gender Substudy questionnaire (female subjects only) X
EuroQol ICECAP UCSD SOBQ SGRQ SF-36 X X X
Abbreviations DLCO diffusing capacity of the lung for carbon monoxide QOL Quality of Life ICECAP Investigating Choice Experiments for Preferences of Older People UCSD SOBQ University of California Shortness of Breath Questionnaire SGRQ St Georgersquos Respiratory Questionnaire SF-36 Short Form 36 Health Survey
1Follow-up visit via phone will occur four weeks after final dose of study medication
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
45 Dose Justification
The general philosophy for determining dosing levels was to apply previously examined
treatment regimens With the focus of the study being to establish a standard of care for
mildmoderate IPF subjects the goal was to develop flexible yet standardized treatment rules that
allow for the temporary or permanent withholding of one or more components of treatment when
necessary Subjects developing laboratory abnormalities or symptoms that result in
discontinuation of one or more components of study treatment may continue on the other
components as long as there is no contraindication for this Complete follow-up is important for
the validity of any study As a strategy to maintain protocol adherence we are using a treatment
regimen that will detect potential side effects and prompt interventions proactively in the interest
of patient safety In addition subjects who permanently stop study medications during the course
of the study are encouraged to continue in the study completing all scheduled visits and tests
451 Rationale for N-acetylcysteine Dosing
To our knowledge there have been no IPF studies to correlate clinical outcome measures with
different dosages for NAC The dosage chosen is based on the IFIGENIA study However BAL
lung GSH levels from subjects with IPF have been augmented with the use of oral NAC at 600
mg 3 times per day In addition lung GSH levels have been associated with improved
PFTs212227 The dose chosen for this study was based on previous data including the IFIGENIA
study30
4511 Dosing of N-acetylcysteineplacebo
Dosing of NACPL will be 600 mg orally 3 times a day (1800 mgday)
4512 Reasons to Discontinue N-acetylcysteineplacebo
NACPL may be temporarily or permanently discontinued for the duration of the study for
gastrointestinal symptoms or dermatologic reactions
35
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Temporarily discontinue (hold) oral NACPL for subjects requiring inpatient admission for acute
exacerbation (AEx) or other conditions Resume NACPL after discharge
36
37
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
452 Dosage Algorithms
Dosage Adjustment Algorithm 1 NACPL Dose Modifications for Gastrointestinal Symptoms Nausea Vomiting Abdominal Discomfort Diarrhea
GI Symptoms determined by the PI to be clinically significant Nausea Vomiting Abdominal Discomfort Diarrhea
NACPL Temporarily dc (HOLD) x 3 Days
Monitor symptoms intervene as clinically indicated (eg fluid replacement antidiarrhea or antinausea medication)
Monitor or lab PRN
Are symptoms resolving after 3 days NO
Symptoms NOT resolving after 3 days of holding study medication Assessmentmanagement per clinical
discretion of investigator
Likely not study medication discuss resuming study medication with medical monitor when symptoms resolved
YES
Temporarily dc (HOLD) NACPL for 4 additional days (total hold 1 week) then NACPL Resume 600 MG TID
Did symptoms recur
YES
STOP NACPL for
duration of study
NO
NACPL No Change
38
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Dosage Adjustment Algorithm 2 NACPL Dose Modifications For Dermatologic Reactions
Dermatologic Reactions (Not Acneiform) ge Grade 2 Grading per Common Terminology Criteria for
Adverse Events V30 (httpctepcancergov) For example Grade 1 RASHDESQUAMATION Macular or papular eruption or erythema without associated symptoms Grade 2 RASHDESQUAMATION Macular or popular eruption or erythema with pruritus or other associated symptoms localized desquamation or other lesions covering lt50 of body surface area
NACPL Temporarily dc (HOLD) x 3 days
Are symptoms resolving after 3 days
NO Symptoms not resolving after 3 days of holding study medication Assessmentmanagement per clinical discretion of investigator Likely not study medication Discuss resuming study medication with medical monitor when symptoms
resolved YES
Temporarily dc (HOLD) NACPL for 4 additional days (total hold 1 week) then NACPL resume 600 MG TID
Did symptoms recur
YES
STOP NACPL for
duration of study
NO
NACPL No change
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
46 Contraindications Precautions and Side Effects of Study Medications
461 Contraindication
Contraindication to NAC is known hypersensitivity to it
462 Precautions
Concomitant administration of oral NAC and antibiotics has shown a slightly reduced absorption
of cephalexin and a slight increase in erythromycin serum levels NAC contains free sulfhydryl
groups There is no evidence that individuals sensitive to sulfa drugs are sensitive to NAC
The NAC preparation being administered in this study contains 20 mg of aspartame Because of
the phenylalanine component of aspartame individuals with phenylketonuria should avoid or
restrict aspartame intake to avoid increased blood levels of phenylalanine Because of this risk
labeling is required on all products containing aspartame
463 Side Effects
Side effects of NAC range from common to serious See Table 4
39
40
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Table 4 Side Effects of NAC
Undesirable Effects
System-organ class Uncommon
(gt11000 lt1100)
Rare
(gt110000 lt11000)
Very rare
(lt110000) Not known
Immune system disorders Hypersensitivity Anaphylactic shock
reaction
Nervous system disorders Headache
Ear and labyrinth disorders Tinnitus
Cardiac disorders Tachycardia
Vascular disorders Hemorrhage
Respiratory thoracic and
mediastinal disorders
Bronchospasm
Dyspnea
Gastrointestinal disorders
Vomiting diarrhea
stomatitis abdominal
pain nausea
Dyspepsia
Skin and subcutaneous tissue
disorders
Urticaria rash
angioedema itching
General disorders and
administration site conditions Pyrexia
Investigations Reduced arterial
pressure Face edema
In very rare cases the onset of severe skin reactions such as Stevens-Johnson syndrome and Lyell syndrome was reported to have a temporal relationship with N-acetylcysteine administration Although in most cases at least another suspect drug probably most involved in the genesis of the above mentioned mucocutaneous syndromes has been identified in case of mucocutaneous alterations it is appropriate to contact onersquos doctor and the administration of N-acetylcysteine should be immediately discontinued
Some studies confirmed a reduction of platelet aggregation during N-acetylcysteine administration The clinical significance of these findings has not been defined yet [Source Fluimucil Investigator Brochure]
47 Recruitment Procedures
Subjects recruited for this study will be established patients of the investigators or physician- or
self-referred to participating clinical centers in the IPFnet Each clinical center within IPFnet has
a well-developed infrastructure of local pulmonologists within the surrounding geographic area
These pulmonologists are kept informed of ongoing IPF clinical trials and regularly refer
subjects to studies conducted at IPFnet clinical centers
Additional steps will be taken to inform clinicians of the trials in progress within IPFnet
including presentations at faculty staff meetings at local hospitals medical grand rounds and
national conferences direct mail notification monthly faxes and advertisement of network trials
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
in pulmonary journals Clinical center patients previously diagnosed with IPF will be notified of
the trials by mail whenever possible
Recruitment of minorities and women will be monitored by the DCC and DSMB If necessary
additional recruitment efforts will be made at specific centers to ensure that the aggregate subject
sample contains appropriate representation of women and minorities
48 Study Procedures
The following procedures are detailed in the PANTHER-IPF MOOP accompanying this
protocol
1 PFT
2 ABG
3 HRCT scan of the chest (including imaging of pulmonary arteries)
4 CBC and serum chemistries
5 Pregnancy test
6 6MWTBorg Dyspnea Scale
7 QOL questionnaires (EuroQol HAD SF-36 SGRQ and ICE CAP)
8 UCSD SOBQ
9 Gender Substudy Questionnaire
All assessments of PFTs will be conducted by study personnel not directly involved in the
treatment of the subjects
481 Biological Specimen Management
4811 Biological Specimen Sample Management
Subjects at clinical centers participating in the specimen repository substudy who consent to
having blood drawn for research purposes and for the banking of blood blood components and
other biologic specimens (urine and BAL fluid) will have approximately 405 mL of blood
41
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
drawn 17 mL blood drawn for DNA and 20 mL of urine collected at enrollment visit Subjects
will have approximately 50 mL of blood drawn and 20 mL of urine collected at each 15-week
follow-up visit Blood specimens will be separated according to PANTHER-IPF MOOP
guidelines into the following components for banking in the repository serum plasma and
DNA Coding of all biologic specimens for the repository will be performed by study staff at the
clinical center The samples will be processed per PANTHER-IPF MOOP guidelines aliquoted
labeled with barcode labels and stored at -70degC at the clinical center and shipped to the central
repository
The only subject identifiers will be a sample ID number and subject initials This sample ID will
be linked in the IPFnet DCC clinical database to subject information No subject information will
be transferred to the biological-specimen database
The subjectrsquos samples may be used for approved sub-studies relating to human disease
including but not limited to IPF The studies for which an individualrsquos samples will be made
available will be determined by the subjectrsquos answers to questions on the biological-sample
informed consent form The subjects can choose to make their samples available for all options
or any combination Samples will be made available to researchers only with IPFnet Steering
Group approval until such time as the samples are made public through the NHLBI repository
49 Concomitant Medications
Concurrent treatment with FDA-approved therapy for IPF is allowed Colchicine may be used
for treatment of gout Temporary treatment with oral or IV corticosteroids for clinical worsening
or suspected AEx is permitted Nutritional supplements containing NAC are not allowed
410 Laboratory Testing
Clinical laboratory parameters will be assessed at screening and at the end of the study The
following tests will be performed at the two time points specified in the protocol chemistry (AG
ratio ALT [SGPT] AST [SGOT] albumin alkaline phosphatase amylase bilirubin-direct
42
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
bilirubin-indirect bilirubin-total BUN BUNcreatinine ratio calcium carbon dioxide
cholesterol-total chloride CPK-total creatinine GGT globulin glucose iron-total LDH
lipase magnesium phosphorus-inorganic potassium protein-total sodium TIBC triglycerides
uric acid) and hematology (red blood cell count WBC count hemoglobin hematocrit cell
indices differential platelet count)
411 Blinding of Study Drugs
Subjects and caregivers will be blinded to study treatment Every subject will receive NAC or
matching PLs at every study visit from the baseline visit to the week-45 visit No study agent
will be dispensed at the week-60 visit
43
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
5 Study Endpoints
51 Primary Study Endpoint
The primary endpoint will be the change in serial measurements of FVC over the study period
52 Secondary Study Endpoints
521 Time to Disease-progression
The time-to-death or a 10 decline in FVC will be defined as the time-to-disease progression
The 10 decline in FVC from enrollment must be confirmed on 2 consecutive visits no less than
6 weeks apart For subjects with 2 consecutive visits with a 10 decline in FVC the time-toshy
disease progression will be defined as the time interval between enrollment and the initial visit
with a 10 FVC decline For subjects who experience disease progression the study doctor will
determine whether or not the subject will remain in the study
522 Acute Exacerbations
The following 3 criteria will define AEx in subjects with acute worsening of their respiratory
conditions
1 Clinical (all of the following required)
A) Unexplained worsening of dyspnea or cough within 30 days triggering unscheduled
medical care (eg emergency room clinic study visit hospitalization)
B) No clinical suspicion or overt evidence of cardiac event pulmonary embolism or deep
venous thrombosis to explain acute worsening of dyspnea
C) No pneumothorax
44
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
2 RadiologicPhysiologic (A and B required)
A) New ground glass opacity or consolidation computed tomography (CT) scan OR new
alveolar opacities on chest x-ray
B) Decline of ge 5 in resting room air SpO2 from last recorded level OR decline of ge 8 mm
Hg in resting room air PaO2 from last recorded level
3 Microbiologic (all of the following required)
A) No clinical evidence for infection (ie absence of grossly purulent sputum fever gt 39degC
orally)
B) Lack of positive microbiological results (if done) from lower respiratory tract defined as
(1) Clinically significant bacterial growth on sputum or endotracheal aspirate cultures
(2) Quantitative culture by protected brush specimen ge 103 cfumL or BAL ge 104 cfumL
(3) The presence of specific pathogens on stains of any of the above
C) Lack of positive pathogen in blood cultures (if done)
Identification of Acute Exacerbations
All subjects will be educated about the importance of identifying AExs At the time of
enrollment subjects will be told about the possibility of developing acute symptomatic
worsening that might represent an AEx of IPF and instructed to contact their study clinical
center coordinator within 48 to 72 hours of the apparent event
All subjects will be contacted by phone monthly and questioned about any change in dyspnea or
cough and any interim clinic visits or hospitalizations Finally as part of the IPFnet outreach to
community referring physicians the importance of AExs will be emphasized When a subject is
identified who meets criterion 1A this will trigger the collection of additional clinical data to
evaluate a suspected AEx These data will be collected as part of standard clinical care (ie this
protocol does not require collection of all items) The additional items to be collected for
suspected AEx include
IPFnet AEx case report form (eCRF) (required)
45
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Chest x-ray CT scan withwithout pulmonary angiogram (reports should be faxed and
followed by the hard copiesdiscs)
Oxygen saturation (pulse oximetry)
ABG
Respiratory cultures (sputum endotracheal aspirate lavage)
Blood cultures
Clinichospital records related to the event
All potential cases of AEx will be reviewed by the clinical center PI first and a decision on
whether the case may represent an AEx will be made If AEx is suspected the case will be sent
to the IPFnet adjudication committee which will assign a final diagnosis (see Table 5) If there is
disagreement among members the majority opinion will be recorded
During episodes of suspected AEx as determined by the individual clinical center investigator
subjects will remain blinded and in the study
Table 5 Final Diagnoses in Evaluation of Suspected Acute Exacerbations
Definite acute exacerbation All criteria met no alternative etiology
Unclassifiable acute worsening
Insufficient data to evaluate all criteria no alternative etiology
Not acute exacerbation Alternative etiology identified that explains acute worsening
Management of the suspected AEx will be at the discretion of the treating physician Standard of
care generally involves evaluation for respiratory infection pulmonary embolism cardiac events
and pneumothorax and treatment with IV corticosteroids
Study drugs will be resumed at pre-suspected AEx doses after subjects clinically improve as
confirmed by the local PI All subjects should be seen at the clinical center within 2 to 4 weeks
of recovery for measurement of post-bronchodilator FVC (see Figure 4) Subjects unable to
return to the clinical center after suspected AEx due to medical frailty (eg continued
46
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
institutionalization progressive disability) will be categorized as failing to maintain FVC
response in secondary analyses
Suspected AEx (PI determined)
Hold study drug Treat AEx
(Attending physician determined)
Alive but unable to continue due to
medical frailty
Dead
Alive and able to continue
Site reviewvisit
Restart study drug
FVC within 2-4 weeks
Figure 4 Acute Exacerbation Flow Chart
523 Respiratory Infections
An upper respiratory infection will be defined as
Change in sputum discoloration
Increased cough of no more than 14 daysrsquo duration
A lower-respiratory infection (pneumonia) will be defined as new segmental or lobar airspace
opacities visualized by image studies (chest radiograph or HRCT) in addition to any of the
following
Positive pathogencultures in good sample of sputum or lower-airway secretions retrieved
by fiberoptic bronchoscope
Fever gt 39degC or gt 100degF
Leukocytosis gt 12000 (unexplained no increase in dose of corticosteroids)
47
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
524 Maintained FVC Response
Subjects with follow-up FVCpred measurements at or above their baseline FVCpred level
will be classified as having maintained FVC response Subjects with reduced FVCpred levels
or missing data for any reason including death or medical frailty will be classified as having not
maintained FVC response The FVCpred value is used because unadjusted FVC measurements
are expected to decline with age
48
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
6 Safety Evaluations and Procedures
61 Adverse Events
During a clinical trial the reporting of adverse experience information can lead to important
changes in the way a new treatment is developed as well as provide integral safety data
611 Definitions
An adverse event (AE) is any untoward medical occurrence in a subject or clinical investigation
subject who was administered a pharmaceutical product The AE does not necessarily have to
have a causal relationship with the drug administered An AE can be any unfavorable and
unintended sign (including an abnormal laboratory finding) symptom or disease temporarily
associated with the use of a medicinal product whether or not considered to be related to the
medicinal product Diseases signs symptoms or laboratory abnormalities already existing at
enrollment are not considered AEs unless they worsen (ie increase in intensity or frequency)
Surgical procedures themselves are not AEs they are therapeutic measures for conditions that
require surgery The condition for which the surgery is required may be an AE Surgical
procedures planned before randomization and the conditions necessitating the surgery are not
AEs
A serious adverse event is any untoward event that
Is fatal
Is life-threatening
Requires inpatient hospitalization or prolongation of existing hospitalization with the
following exceptions
o Preplanned (before the study) hospital admissions unless the hospitalization is
prolonged
o Planned admissions (as part of a study eg routine biopsies)
o Hospitalization lasting lt 24 hours
49
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
o Hospitalization for elective procedure
o Emergency room visits
Results in persistent or significant disability or incapacity
Is a congenital anomaly or birth defect
Important medical events that may not result in death be life-threatening or require
inpatient hospitalization may be considered serious adverse events (SAEs) when based
on appropriate medical judgment they may jeopardize the subject and may require
medical or surgical intervention to prevent one of the outcomes listed above
Life-threatening means that the subject was in the view of the investigator at immediate risk of
death from the AE as it occurred It does not include an AE that had it occurred in a more severe
form might have caused death
Persistent or significant disabilityincapacity means that the event resulted in permanent or
significant and substantial disruption of the subjectrsquos ability to carry out normal life functions
Causality
A reasonable possibility means the AE may have been caused byrelated to the study drug A
perceived or real lack of efficacy does not satisfy the definition of relatedness
612 Adverse Event (AE) Reporting
For the PANTHER-IPF trial all AEs (serious and nonserious) occurring from randomization
through final study visit (4 weeks after final dose of all study medication) will be recorded on the
AE page of the case report form (CRF)
6121 Serious Adverse Events (SAE) Reporting
For this trial all deaths and all SAEs which occur from randomization through final study visit
must be entered within the EDC system via the SAE eCRF page within 24 hours of the
investigative sitersquos knowledge of the event It is the responsibility of the clinical center
50
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
investigator to provide a causality assessment of the event for each study medications based upon
the information available at the time of the report It is understood that complete information
about the event may not be known at the time the initial report is submitted In the event the EDC
system is not accessible to the site at the time of event reporting investigative sites will complete
and forward a paper back-up SAE form to DCRI Safety Surveillance for processing
DCRI Safety Surveillance
Telephone 1-919-668-8624 or 1-866-668-7799 (toll free)
Fax 1-919-668-7138 or 1-866-668-7138 (toll free)
The investigator must complete and submit follow-up SAE information via the eCRF when
important new or follow-up information (eg final diagnosis outcome results of specific
investigations) becomes available Follow-up information should be submitted according to the
same process used for reporting the initial event as described above All SAEs will be followed
until resolution stabilization or 30 days after the subject has completed the final visit (4 weeks
after the final dose of study medication) whichever occurs first The investigator is responsible
for reporting SAEs to their institutional review board (IRB) per site specific IRB reporting
guidelines
6122 Regulatory Reporting
AEs that are serious study drug related and unexpected will be reported to the regulatory
authorities The DCRI Safety Surveillance medical monitor will perform a medical review of all
SAEs submitted and evaluate for ldquounexpectednessrdquo DCRI Safety Surveillance will prepare
MedWatch reports for those events identified as serious study drug related and unexpected as
determined by Safety Medical Monitor
DCRI Regulatory Services will submit all unexpected study drug-related SAEs as per 21 CFR
32 DCRI Safety Surveillance will provide a safety alert letter to the NHLBI DSMB and DCC
clinical operation (for distribution to sites) within 15 days of initial receipt of the information
51
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Investigators are responsible for promptly reporting these events to their reviewing IRBs
according to site specific IRB reporting guidelines
62 Clinical Medical Monitoring
There will be an unblinded physician at the IPFnet DCC serving as medical monitor The
medical monitor will be available to assist with questions about dosage adjustments of study
medications including discontinuation or resumption of medications
63 Unblinding Procedures
Unblinding of subjects or investigators to subject treatment is strongly discouraged For ongoing
clinical management all subjects should be presumed to be receiving ldquoactiverdquo study drug To
ensure the subjectrsquos safety the study treatment will be dose-adjusted based on laboratory test
results clinical findings and symptoms
The IPFnet DCC medical monitor and PANTHER-IPF co-chairs Drs Ganesh Raghu and
Fernando Martinez will be available to the study physicians to discuss study drug management
on a case-by-case basis Un-blinding will be considered ONLY when the knowledge of subject
treatment assignment is ABSOLUTELY ESSENTIAL for subject safety and after discussion of
the subjectrsquos case with the medical monitor and either Dr Raghu or Dr Martinez Unblinding of
study treatment should be minimized during the conduct of the trial In those cases where it is
felt to be medically necessary the DCC medical officer will communicate directly with the
managing physician to minimize unblinding of study personnel
52
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
7 Study Drug Procedures
At the baseline 15-week 30-week and 45-week study visits subjects will receive a supply of
study drug sufficient to last until the next visit at which study drug will be dispensed
53
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
8 Data Management
81 Hardware and Software Configuration
811 Hardware and Database Software
Data will be stored in an Oracle database system Oracle has advantages of processing efficiency
and smooth linkage with other software systems The application and database will be hosted on
Solaris Unix servers at the IPFnet DCC
812 Statistical Software
SAS will be used as the principal application for the management of analysis data files and
statistical computations S-Plus will be used to provide supplementary functions as needed
813 Access Control and Confidentiality Procedures
Access to databases will be controlled centrally by the IPFnet DCC through user passwords
linked to appropriate privileges This protects the data from unauthorized changes and
inadvertent loss or damage
814 Security
Database and Web servers will be secured by a firewall and through controlled physical access
Oracle has many security features to ensure that any staff member accessing the database has the
proper authority to perform the functions he or she requests of the system Within the secondary
SAS databases Unix group-access control maintains similar security The Sun workstation login
is secured by extensive user-password facilities under Unix
54
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
815 Back-up Procedures
Database back-up will be performed automatically every day and standard IPFnet DCC policies
and procedures will be applied to dictate tape rotation and retention practices
816 Virus Protection
All disk drives that provide network services and all user computers will be protected using
virus-scanning software Standard IPFnet DCC policies will be applied to update these protection
systems periodically through the study
82 Sources of Data
821 Design and Development
The IPFnet DCC will be responsible for development of the electronic case report forms
(eCRFs) development and validation of the clinical study database ensuring data integrity and
training clinical center staff on applicable data management procedures A web-based distributed
data entry model will be implemented This system will be developed to ensure that guidelines
and regulations surrounding the use of computerized systems used in clinical trials are upheld
The remainder of this section provides an overview of the data management plan associated with
this protocol
822 Data Collection Forms
The data collection process consists of direct data entry at the study clinical centers into the EDC
system(s) provided by the DCC A data collection worksheet will be provided to clinical centers
for recording data in the event the EDC system is unavailable Data entry of the eCRFs should
be completed according to the instructions provided and project specific training The
investigator is responsible for maintaining accurate complete and up-to-date records and for
ensuring the completion of the eCRFs for each research participant
55
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
823 Data Acquisition and Entry
Data entry into eCRFs shall be performed by authorized individuals Selected eCRFs may also
require the investigatorrsquos written signature or electronic signature as appropriate Electronic
CRFs will be monitored for completeness accuracy and attention to detail during the study
824 Data Center Responsibilities
The IPFnet DCC will 1) develop a data management plan and will conduct data management
activities 2) provide final eCRFs for the collection of all data required by the study 3) develop
data dictionaries for each eCRF that will comprehensively define each data element 4) conduct
ongoing data monitoring activities on study data 5) monitor any preliminary analysis data
cleanup activities and 6) rigorously monitor final study data clean up
825 Data Editing
Completed data will be entered into the IPFnet DCC automated data acquisition and
management system If incomplete or inaccurate data are found a data clarification request will
be generated and distributed to clinical centers for a response Clinical centers will resolve data
inconsistencies and errors and enter all corrections and changes into the IPFnet DCC automated
data acquisition and management system
826 Training
The training plan for clinical center staff includes provisions for training on assessments eCRF
completion guidelines data management procedures and the use of computerized systems
56
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
9 Study Design and Data Analysis
91 General Analytic Considerations
All primary analyses will be based on intent-to-treat (ITT) principles using all randomized
subjects Baseline factors across groups will be compared using mean (standard deviation) and
median (25th and 75th percentiles) summary measures Kaplan-Meier curves will be used to
display event rates Due to clinical interest in departures from both sides of the null hypothesis
all test statistics will be 2-sided
Reasonable caution needs to be taken when conducting multiple analyses on key clinical
subgroups For subgroup analyses a conservative significance level of 0001 will be used for all
interaction tests Thus subgroup comparisons will be considered exploratory unless the p-value
from the interaction test is smaller than 0001
92 Randomization Blinding and Reporting of Results
A permuted block-randomization scheme will be created with varying block sizes stratified by
clinical center Once a subject has completed the screening and baseline period and evaluation
for inclusionexclusion criteria the randomization process will begin Subjects will be
randomized to receive NAC or matching placebo with equal probability (11) via telephone
contact with a central interactive voice response system (IVRS) using a toll-free randomization
number On the day of randomization after the subject has successfully met all inclusion and
exclusion criteria the investigator or designee will call the central randomization number to
obtain the assigned kit randomization numbers for that subject At each subject visit the
investigator or designee will call the central randomization number to obtain the new kit
randomization numbers for resupply of the subject For resupply of the clinical center the IVRS
will monitor minimal volume of a kit type andor expiration date and will automatically notify
the pharmacy
57
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
The trial results will be reported according to guidelines specified in the CONSORT statement
A flow diagram describing screening recruitment randomization dropout and vital status will
be included in the primary manuscript AEs and efficacy data will be presented for all treatment
groups Adherence dropout and lost to follow-up will be carefully examined across all treatment
groups Analyses of safety will be based on data from all randomized subjects who received at
least one dose of study drug
93 Stratification
Subjects will be distributed to the two treatment arms in a 11 allocation ratio Stratification
blocks will be based on clinical centers
94 Specification of the Primary Analyses
A mixed model repeated measures (MMRM) analysis described in section 95 will be used to
compare differences in the slope of FVC measurements across the treatment groups Response
variables are values of the FVC measured at baseline and every 15 weeks until study completion
Variables in the model will include treatment time and time by treatment age sex race and
height Contrast estimates of differences in slopes of treatment over time (along with confidence
intervals) will be used to estimate the treatment effect The validity of this model in terms of
meeting modeling assumptions will be assessed via standard modeling diagnostics and goodness-
of-fit measures Based on the MMRM framework missing FVC data will not be imputed for the
primary analysis
95 Analysis of Longitudinal Endpoints
A common goal in clinical trials is to specify models that are easily implemented and
reproducible by independent data analysts On the other hand the models should have proper
statistical behavior in terms of low bias and high precision Many common approaches to
longitudinal data analysis including last observation carried forward (LOCF) imputation rely on
the missing completely at random (MCAR) assumption However the MCAR assumption is
58
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
unlikely to hold in many clinical trials because missing data are often related to disease
progression and prognosis A more reasonable assumption missing at random (MAR) specifies
that the complete data distribution can be modeled using only the observed data The likelihood-
based MMRM approach is valid under the more general MAR assumptions These models will
be applied to analyze the longitudinal data secondary endpoints
The advantages of MMRM analysis are that all important characteristics of the model can be preshy
specified standard software can be used to implement the models and results are based on ITT
principles43 In addition the MMRM approach offers superior control of Type I and Type II
errors compared with the LOCF approach
Response variables are values of the PFTs measured at enrollment and every 15 weeks until
study completion and 6MWT values measured at baseline week 30 and week 60 Covariates are
treatment time time by treatment and key baseline risk factors Contrasts (along with
confidence intervals) of treatment by time will be used to estimate the treatment effect
The correlation structure involves multiple pieces including measurement errors random
variation and interindividual variability For the longitudinal data analyses an unstructured
correlation matrix for within-subject errors will be assumed Other correlation structures
including compound symmetry will be examined as needed A careful examination of reasons
for study discontinuation will be conducted to assess the validity of MCAR Sensitivity analyses
will be used to examine the untestable assumption that the observed data violate the MAR
assumption The MMRM models will be implemented using PROC MIXED in SAS
96 Analysis of Binary Time-to-Event and Time-Lagged Endpoints
Regression modeling approaches using either the logistic regression model or Cox proportional
hazards regression model will be employed when appropriate The validity of these models will
be assessed via standard modeling diagnostics and goodness-of-fit measures Estimates of
cumulative frequencies for more general time-lagged responses will be calculated using the
partitioned version of the Bang-Tsiatis estimator44 The partitions will be set at 15-week intervals
59
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
to correspond with the data-collection process Covariate adjusted event rates will be calculated
using inverse probability-weighted regression estimates45
97 Power Analysis
971 Primary Analyses
Based on previously published IPF clinical trials the PL group is expected to experience a drop
in FVC of approximately 020 L over the study period (see Figure 1) The IPFnet Steering Group
determined a clinically important difference would be to preserve the majority of the decline
relative to PL over the study period In particular a treatment effect of 015 L was determined to
be a clinically meaningful difference Potential dropout is a key factor in the proposed study The
drop-out process assumed 5 lost to follow-up after every study visit Only 80 of subjects
were assumed to be followed for the entire study period All models assumed a compound
symmetry structure for the covariance matrix Power calculations were performed using a SAS
IML program for designing repeated measures studies46 Based on preliminary reviews of the
data from the University of Michigan the covariance matrix parameters were estimated at
approximately σ2 = 0757 (variance parameter) and ρ = 0936 (correlation parameter) To be
conservative the power calculations for the primary analysis were performed with parameter
setting of σ2 = 0810 (variance parameter) and ρ = 0925 (correlation parameter)
The power calculations assume a correction for imperfect compliance proposed by Lachin and
Foulkes to allow for 2 noncompliance for each of the treatment arms47 Thus the sample size
of 130 subjects per arm would be reduced to an adjusted sample size of 130(1-002-002)2 =
1198 or 120 subjects per arm
Under the assumed Type I error rate of 005 with a correlation parameter of 0925 and standard
deviation of 090 the difference of 015 L (or 00025 Lweek) shown in Table 6 would have
power of 93
60
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Table 6 Hypothetical Values of Mean FVC (L) Change from Baseline
Week 15 Week 30 Week 45 Week 60
NAC 00125 00250 00375 00500
Placebo 00500 01000 01500 02000
Difference 00375 00750 01125 01500
Abbreviations FVC forced vital capacity PL placebo
972 Power Analysis for Secondary Endpoints
Power calculations for secondary endpoint measurements are shown in Table 7 Standard
deviations are based on unpublished data provided by the University of Michigan The
calculations are based on a 2-sample t-test with Type I error rate set at 005 These calculations
are likely to be conservative because the statistical approach described in section 95 for
analyzing these endpoints will incorporate incomplete observations as well as intermediate data
points
Table 7 Detectable Differences in Treatment Means for Selected Endpoint Measurements
Secondary Endpoints Std Dev
of the Baseline Score
Detectable Difference for 80 Power
Std Dev of the Change Score
Difference Detectable for
80 Power
DLCOpred 166 58 91 32
6MWT Area Under the Desaturation Curve
219 76 175 61
6MWT Distance to Desaturation 224 78 315 110
6MWT Minutes Walked 210 073 205 071
Abbreviations Std Dev standard deviation DLCOpred diffusing capacity of the lung for carbon monoxide percent predicted 6MWT 6-minute walk test
61
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
10 Study Administration
101 Cooperative Agreement Mechanism
The administrative and funding mechanism used to undertake this project is a ldquocooperative
agreementrdquo (U01) which is an assistance mechanism Under the cooperative agreement the
NHLBI assists supports andor stimulates the project and is substantially involved with
investigators in conducting the study by facilitating performance of the effort in a ldquopartnerrdquo role
The NHLBI project scientist serves on the IPFnet Steering Group and he or another NHLBI
scientist may serve on other project committees when appropriate At the same time however
NHLBI does not assume a dominant role direction or prime responsibility for this research
program
As described below governance of the project is conducted through the IPFnet Steering Group
Principal investigators have lead responsibilities in all aspects of their trials and the project
including any modification of trial designs conduct of the trials quality control data analysis
and interpretation preparation of publications and collaboration with other investigators unless
otherwise provided for by the IPFnet Steering Group
PIs retain custody of and have primary rights to their center-specific and collaborative data
subject to government rights-of-access consistent with current Health amp Human Services (HHS)
Public Health Service (PHS) and National Institutes of Health policies The protocols and
governance policies call for the continual submission of data centrally to the IPFnet DCC for the
collaborative database which at a minimum will contain the key variables selected by the IPFnet
Steering Group for standardization across all clinical centers the submission of copies of the
collaborative datasets to each PI upon completion of the project procedures for data analysis
reporting and publication and procedures to protect and ensure the privacy of medical and
genetic data and records of individuals The NHLBI project scientist on behalf of the NHLBI
will have the same access privileges and responsibilities regarding the collaborative data as the
other members of the Steering Group
62
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
PIs are also encouraged to publish and to publicly release and disseminate results data and other
products of the project concordant with the project protocols and governance and the approved
plan for making data and materials available to the scientific community and to the NHLBI
However during the 3 years after the ending date of NHLBI project support unpublished data
unpublished results data sets not previously released and other study materials or products are
to be made available to any third party only with the approval of the IPFnet Steering Group
Upon completion of the project PIs are expected to put their intervention materials and
procedure manuals into the public domain andor make them available to other investigators
according to the approved plan for making data and materials available to the scientific
community and the NHLBI for the conduct of research at no charge other than the costs of
reproduction and distribution
The NHLBI reserves the right to terminate or curtail the project (or an individual award) in the
event of (a) failure to develop or implement mutually agreeable collaborative measurement
subject eligibility and data management sections of the protocols (b) substantial shortfall in
subject recruitment follow-up data reporting or quality control or other major breach of
protocol (c) substantive changes in the agreed-upon protocols with which NHLBI cannot
concur (d) reaching a major project outcome with persuasive statistical significance
substantially before schedule or (e) human subject ethical issues that may dictate a premature
termination
Any disagreement that may arise in scientificprogrammatic matters (within the scope of the
award) between award recipients and the NHLBI may be brought to arbitration An arbitration
panel will be composed of 3 membersmdash1 selected by the IPFnet Steering Group (with the
NHLBI member not voting) or by the individual PI in the event of an individual disagreement a
second selected by NHLBI and the third selected by the other 2 members This special
arbitration procedure in no way affects the PIrsquos right to appeal an adverse action that is otherwise
appealable in accordance with the PHS regulations at 42 CFR part 50 Subpart D and HHS
63
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
regulation at 45 CFR part 16 or the rights of the NHLBI under applicable statutes regulations
and terms of the award
102 IPFnet Steering Group
The IPFnet Steering Group is the main governing body of the project It is composed of the PIs
of the clinical centers the PI of the DCC and the NHLBI project scientist The clinical centers
the IPFnet DCC and the NHLBI each have 1 vote on the IPFnet Steering Group All decisions
are determined by majority vote
All major scientific decisions are determined by the IPFnet Steering Group It assumes overall
responsibility for the design and conduct of the trial It appoints (and disbands) committees and
subcommittees as the need arises designs approves and implements the study protocols
oversees the development of the MOOP monitors subject recruitment and treatment delivery
evaluates data collection and management oversees quality assurance procedures and
implements changes and enhancements to the study as required It also has primary responsibility
for facilitating the conduct of the trials and reporting the projectrsquos results
103 Data and Safety Monitoring Board
The NHLBI will establish a DSMB in accordance with established policies (see
httpwwwnhlbinihgovfundingpoliciesdsmb_insthtm) to ensure data quality and subject
safety and to provide independent advice to the NHLBI regarding progress and the
appropriateness of study continuation
104 Recommendations on Interim Monitoring of Efficacy Safety and Futility
First and foremost the role of the DSMB will be to review subject safety and trial conduct at
periodic points during the study The DSMB may require analyses of the primary endpoint
results for comparing the benefit and risks of treatment strategies The benefit of collecting
additional data on key secondary endpoints with extended follow-up and establishing a robust
64
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
evidence base for determining a standard of care will need to be carefully considered before
early termination of one or more treatment arms After careful consideration the IPFnet Steering
Group recommends conservative thresholds for the early examinations of the safety and efficacy
data
The DSMB will be expected to meet approximately every 6 months until trial completion to
review safety and toxicity data The DSMB may recommend stopping the study based on these
reviews Because the DSMB could stop the trial for safety concerns as well as for a large
efficacy benefit there could be multiple opportunities to reject the null hypothesis (no difference
in event rates between the PL and NAC groups) A Bonferroni approximation will be applied
during the one planned interim analysis for efficacy
Before locking the database a statistical analysis plan (SAP) will be developed to provide
complete details on the statistical analysis The SAP will include the specifics for how and when
the DSMB will be notified for AEs The IPFnet DCC will deliver to the DSMB all FDA-defined
AEs at 3-month intervals The IPFnet DCC will prepare narrative SAE reports in real time for
DSMB review including recommendations and analysis of similar events for each SAE
submitted to the FDA
65
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
11 Investigator and Sponsor Obligations
111 Monitoring
All monitoring activities for US clinical centers will be performed in accordance with DCRI
standard operating procedures Information regarding the types of visits will be outlined in the
PANTHER-IPF MOOP
112 Cost and Payment
There will be no cost to subjects enrolled in this trial Study-related procedures will be paid for
by the IPFnet
Subjects may be eligible for reimbursement for travel to the clinical center Details of payment
will be explained to each subject during the consent process
113 Confidentiality and Health Insurance Portability and Accountability Act
Considerations
Subject confidentiality will be protected throughout the study All subject data will be kept
strictly confidential and no subject-identifying information will be released to anyone outside
the project Confidentiality will be assured through several mechanisms First each subject will
be assigned an anonymous study ID which will then be used on all study forms Second any
study forms blood samples and paper records that contain subject information (eg address lists
phone lists) will be kept at the clinical centers in secured locked areas coded by number Once
blood is collected there will be no subject identifiers placed on blood samplesmdashonly the study
ID number and the date of sample collection Third access to all subject data and information
including laboratory specimens will be restricted to authorized personnel In the case of
computerized data this restricted access will be assured through user logon IDs and password
protection
66
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
At the IPFnet DCC only authorized personnel will have access to the data files containing study
data Security will be assured through user logon IDs passwords and appropriate access
privileges All study subjects will be identified only by their IPFnet ID numbers and no personal
identifying information such as name address or Social Security number will be entered into
the IPFnet DCC database Any subject-specific data reported to the IPFnet Steering Group will
be identified only by the IPFnet ID number
Finally subjects will not be identified by name in any reports or publications nor will the data
be presented in such a way that the identity of individual subjects can be inferred Analysis files
created for further study by the scientific community will have no subject identifiers These data
files will be created in accordance with the Ancillary Studies and Publication Policy of the
IPFnet
114 Informed Consent Procedures
All IPFnet subjects will provide written informed consent using procedures reviewed and
approved by each clinical centerrsquos IRB Informed consent will be undertaken by study personnel
in-person with the subject The subject has the option of declining further participation in the
study at that point No further study procedures will be conducted until the signed documents
have been provided to the IPFnet clinical center
115 Institutional Review Boards
Before initiating this study the protocol clinical center-specific informed consent forms Health
Insurance Portability and Accountability Act (HIPAA) forms recruitment materials and other
relevant information will be reviewed by a properly constituted IRB at each participating clinical
center A copy of the signed and dated IRB approval at each clinical center will be retrieved prior
to or during the site initiation visit and archived at the IPFnet DCC Any amendments to the
protocol other than simple administrative and typographical changes must be approved by each
IRB before they are implemented The clinical centers will seek annual renewals of their IRB
approvals in accordance with local procedures
67
__________________________________________ ________________
__________________________________________
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
12 Investigator Agreement
I have read the foregoing protocol PANTHER-IPF and agree that it contains all necessary
details for carrying out this study I will conduct the study as outlined herein and will complete
the study within the time designated
I will provide copies of the protocol and all pertinent information to all individuals responsible to
me who assist in the conduct of this study I will discuss this material with them to ensure they
are fully informed regarding the drug and the conduct of the study
I will fulfill all responsibilities for submitting pertinent information to the local IRB if
applicable that is responsible for this study
I further agree that NHLBI andor DCRI will have access to any source documents from which
eCRF information may have been generated
Signature of Principal Investigator Date
Name of Principal Investigator (printed or typed)
Protocol version date May 19 2009
Protocol Amendment 1 version date May 28 2010
Protocol Amendment 2 version date December 6 2011
68
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
13 References
1 Raghu G Brown KK Bradford WZ et al A placebo-controlled trial of interferon gamma-1b in patients with idiopathic pulmonary fibrosis N Engl J Med 2004350125-33 2 King TE Jr Safrin S Starko KM et al Analyses of efficacy end points in a controlled trial of interferon-gamma1b for idiopathic pulmonary fibrosis Chest 2005127171-7 3 Flaherty KR Thwaite EL Kazerooni EA et al Radiological versus histological diagnosis in UIP and NSIP survival implications Thorax 200358143-8 4 Wells AU Desai SR Rubens MB et al Idiopathic pulmonary fibrosis a composite physiologic index derived from disease extent observed by computed tomography Am J Respir Crit Care Med 2003167962-9 5 Raghu G Freudenberger TD Yang S et al High prevalence of abnormal acid gastroshyoesophageal reflux in idiopathic pulmonary fibrosis Eur Respir J 200627136-42 6 Kinnula VL Focus on antioxidant enzymes and antioxidant strategies in smoking related airway diseases Thorax 200560693-700 7 Coultas DB Zumwalt RE Black WC Sobonya RE The epidemiology of interstitial lung diseases Am J Respir Crit Care Med 1994150967-72 8 Raghu G Weycker D Edelsberg J Bradford WZ Oster G Incidence and prevalence of idiopathic pulmonary fibrosis Am J Respir Crit Care Med 2006174810-6 9 Olson AL Swigris JJ Lezotte DC Norris JM Wilson CG Brown KK Mortality from pulmonary fibrosis increased in the United States from 1992 to 2003 Am J Respir Crit Care Med 2007176277-84 10 Mannino DM Etzel RA Parrish RG Pulmonary fibrosis deaths in the United States 1979shy1991 An analysis of multiple-cause mortality data Am J Respir Crit Care Med 19961531548shy52 11 Hubbard R Johnston I Coultas DB Britton J Mortality rates from cryptogenic fibrosing alveolitis in seven countries Thorax 199651711-6 12 Johnston I Britton J Kinnear W Logan R Rising mortality from cryptogenic fibrosing alveolitis Bmj 19903011017-21 13 Raghu G Collard HR Egan JJ et al An official ATSERSJRSALAT statement idiopathic pulmonary fibrosis evidence-based guidelines for diagnosis and management Am J Respir Crit Care Med 2011183788-824 14 (USA) FDA FDA Public Health Advisory Interferon gamma-1b (marketed as Actimmune) In 2007 15 King TE Jr Pardo A Selman M Idiopathic pulmonary fibrosis Lancet 2011 16 Raghu G Brown KK Costabel U et al Treatment of idiopathic pulmonary fibrosis with etanercept an exploratory placebo-controlled trial Am J Respir Crit Care Med 2008178948shy55 17 Malouf MA Hopkins P Snell G Glanville AR An investigator-driven study of everolimus in surgical lung biopsy confirmed idiopathic pulmonary fibrosis Respirology 201116776-83 18 King TE Jr Behr J Brown KK et al BUILD-1 a randomized placebo-controlled trial of bosentan in idiopathic pulmonary fibrosis Am J Respir Crit Care Med 200817775-81 19 Richeldi L Costabel U Selman M et al Efficacy of a tyrosine kinase inhibitor in idiopathic pulmonary fibrosis N Engl J Med 20113651079-87
69
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
20 Borok Z Buhl R Grimes GJ et al Effect of glutathione aerosol on oxidant-antioxidant imbalance in idiopathic pulmonary fibrosis Lancet 1991338215-6 21 Meyer A Buhl R Magnussen H The effect of oral N-acetylcysteine on lung glutathione levels in idiopathic pulmonary fibrosis Eur Respir J 19947431-6 22 Behr J Maier K Degenkolb B Krombach F Vogelmeier C Antioxidative and clinical effects of high-dose N-acetylcysteine in fibrosing alveolitis Adjunctive therapy to maintenance immunosuppression Am J Respir Crit Care Med 19971561897-901 23 Cantin AM North SL Fells GA Hubbard RC Crystal RG Oxidant-mediated epithelial cell injury in idiopathic pulmonary fibrosis J Clin Invest 1987791665-73 24 Waghray M Cui Z Horowitz JC et al Hydrogen peroxide is a diffusible paracrine signal for the induction of epithelial cell death by activated myofibroblasts Faseb J 200519854-6 25 Larios JM Budhiraja R Fanburg BL Thannickal VJ Oxidative protein cross-linking reactions involving L-tyrosine in transforming growth factor-beta1-stimulated fibroblasts J Biol Chem 200127617437-41 26 Kinnula VL Fattman CL Tan RJ Oury TD Oxidative stress in pulmonary fibrosis a possible role for redox modulatory therapy Am J Respir Crit Care Med 2005172417-22 27 Meyer A Buhl R Kampf S Magnussen H Intravenous N-acetylcysteine and lung glutathione of patients with pulmonary fibrosis and normals Am J Respir Crit Care Med 19951521055-60 28 Behr J Degenkolb B Krombach F Vogelmeier C Intracellular glutathione and bronchoalveolar cells in fibrosing alveolitis effects of N-acetylcysteine Eur Respir J 200219906-11 29 Bando M Hosono T Mato N et al Long-term efficacy of inhaled N-acetylcysteine in patients with idiopathic pulmonary fibrosis Intern Med 2010492289-96 30 Demedts M Behr J Buhl R et al High-dose acetylcysteine in idiopathic pulmonary fibrosis N Engl J Med 20053532229-42 31 Toma TP Bhowmik A Rajakulasingam R Acetylcysteine in pulmonary fibrosis N Engl J Med 20063541086-9 author reply -9 32 Hunninghake GW Antioxidant therapy for idiopathic pulmonary fibrosis N Engl J Med 20053532285-7 33 Flaherty KR Mumford JA Murray S et al Prognostic implications of physiologic and radiographic changes in idiopathic interstitial pneumonia Am J Respir Crit Care Med 2003168543-8 34 Latsi PI du Bois RM Nicholson AG et al Fibrotic idiopathic interstitial pneumonia the prognostic value of longitudinal functional trends Am J Respir Crit Care Med 2003168531-7 35 Collard HR King TE Jr Bartelson BB Vourlekis JS Schwarz MI Brown KK Changes in clinical and physiologic variables predict survival in idiopathic pulmonary fibrosis Am J Respir Crit Care Med 2003168538-42 36 Jegal Y Kim DS Shim TS et al Physiology is a stronger predictor of survival than pathology in fibrotic interstitial pneumonia Am J Respir Crit Care Med 2005171639-44 37 Martinez FJ Safrin S Weycker D et al The clinical course of patients with idiopathic pulmonary fibrosis Ann Intern Med 2005142963-7 38 Hull JH Acetylcysteine in pulmonary fibrosis N Engl J Med 20063541089-91 author reply -91
70
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
39 Flaherty KR King TE Jr Raghu G et al Idiopathic interstitial pneumonia what is the effect of a multidisciplinary approach to diagnosis Am J Respir Crit Care Med 2004170904shy10 40 Raghu G Johnson WC Lockhart D Mageto Y Treatment of idiopathic pulmonary fibrosis with a new antifibrotic agent pirfenidone results of a prospective open-label Phase II study Am J Respir Crit Care Med 19991591061-9 41 Hunninghake GW Lynch DA Galvin JR et al Radiologic findings are strongly associated with a pathologic diagnosis of usual interstitial pneumonia Chest 20031241215-23 42 Lynch D Godwin J Safrin S et al High-resolution computed tomography in idiopathic pulmonary fibrosis diagnosis and prognosis Am J Respir Crit Care Med 2005172488-93 43 Mallinckrodt CH Watkin JG Molenberghs G Carroll RJ Choice of the primary analysis in longitudinal clinical trials Pharmaceutical Statistics 20043161-9 44 Bang H Tsiatis A Estimating medical costs with censored data Biometrika 200087329shy43 45 Lin DY Regression analysis of incomplete medical cost data Stat Med 2003221181-200 46 Rochon J Application of GEE procedures for sample size calculations in repeated measures experiments Stat Med 1998171643-58 47 Lachin JM Foulkes MA Evaluation of sample size and power for analyses of survival with allowance for nonuniform patient entry losses to follow-up noncompliance and stratification Biometrics 198642507-19
71
- PANTHER-IPFPREDNISONE AZATHIOPRINEAND N-ACETYLCYSTEINEA STUDY THAT EVALUATES RESPONSE INIDIOPATHIC PULMONARY FIBROSIS
-
- Protocol Summary
- Table of Contents
- List of Tables
- List of Figures
- List of Abbreviations
- 1 Summary
- 2 Hypotheses and Specific Aims
-
- 21 Null Hypothesis
- 22 Specific Aim 1
- 23 Specific Aim 2
- 24 Prespecified Subgroups of Interest
-
- 3 Background and Significance
-
- 31 Idiopathic Pulmonary Fibrosis is the Most Common Interstitial Lung Disease
- 32 Rationale for Placebo Control
- 33 Rationale for N-acetylcysteine
- 35 Rationale for N-acetylcysteine as a Stand-alone Therapy
- 36 Rationale for the Study Design and Primary Endpoint
- 37 Rationale for Blinding of Treatments
-
- 4 Methods
-
- 41 Inclusion Criteria
- 42 Diagnosis of IPF
- 43 Exclusion Criteria
- 44 Study Design and Study Visit
- 45 Dose Justification
- 46 Contraindications Precautions and Side Effects of Study Medications
- 47 Recruitment Procedures
- 48 Study Procedures
- 49 Concomitant Medications
- 410 Laboratory Testing
- 411 Blinding of Study Drugs
-
- 5 Study Endpoints
-
- 51 Primary Study Endpoint
- 52 Secondary Study Endpoints
-
- 6 Safety Evaluations and Procedures
-
- 61 Adverse Events
- 62 Clinical Medical Monitoring
- 63 Unblinding Procedures
-
- 7 Study Drug Procedures
- 8 Data Management
-
- 81 Hardware and Software Configuration
- 82 Sources of Data
-
- 9 Study Design and Data Analysis
-
- 91 General Analytic Considerations
- 92 Randomization Blinding and Reporting of Results
- 93 Stratification
- 94 Specification of the Primary Analyses
- 95 Analysis of Longitudinal Endpoints
- 96 Analysis of Binary Time-to-Event and Time-Lagged Endpoints
- 97 Power Analysis
-
- 10 Study Administration
-
- 101 Cooperative Agreement Mechanism
- 102 IPFnet Steering Group
- 103 Data and Safety Monitoring Board
- 104 Recommendations on Interim Monitoring of Efficacy Safety and Futility
-
- 11 Investigator and Sponsor Obligations
-
- 111 Monitoring
- 112 Cost and Payment
- 113 Confidentiality and Health Insurance Portability and Accountability ActConsiderations
- 114 Informed Consent Procedures
- 115 Institutional Review Boards
-
- 12 Investigator Agreement
- 13 References
-

PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
UIP usual interstitial pneumonia Dx diagnosis 43 Exclusion Criteria
1 History of clinically significant environmental exposure known to cause pulmonary fibrosis
Occupational exposures such as asbestos or environmental exposure to organic dust such as occurs in
pigeon breeders may at times mimic the clinical and radiographic findings of IPF
2 Diagnosis of connective tissue disease felt by the principal investigator (PI) to be the etiology of the
interstitial disease Diagnosis of collagen-vascular conditions will be according to the published
American College of Rheumatology criteria As such the presence of any documented collagen-vascular
disorder or the presence of any suspicious symptom complex whether or not associated with
significantly abnormal rheumatological serologies will exclude the subject at the discretion of the PI
3 Extent of emphysema greater than the extent of fibrotic change (honeycombing reticular changes) on
HRCT scan
4 Forced expiratory volume in 1 second (FEV1)FVC ratio lt 065 at screening (postbronchodilator)
5 Partial pressure of arterial oxygen (PaO2) on room air lt 55 mm Hg (lt 50 mm Hg at Denver site)
6 Residual volume gt 120 predicted at screening (postbronchodilator)
7 Evidence of active infection
8 Significant bronchodilator response on screening spirometry defined as a change in FEV1 ge 12 and
absolute change gt 200 mL OR change in FVC ge 12 and absolute change gt 200 mL The percent
difference between the FVC (or FEV1) values will be calculated by taking the absolute value of the
difference and dividing it by the larger of the two FVC (or FEV1) values
9 Screening and enrollment post-bronchodilator FVC measurements (in liters) differing by gt 11 The
percent difference between the FVC values will be calculated by taking the absolute value of the
difference and dividing it by the larger of the two FVC values (eg the percent difference between FVC
measurements of 19 and 20 liters would be determined by taking the difference between the two (01
liters) and dividing by the larger of the two (20 liters) So 0120 = 5 and these FVC measurements
would not exclude the subject
10 Listed for lung transplantation ie the patient has completed the evaluation process has been accepted
as a candidate for transplantation at an appropriate center and is waiting to receive notification of an
available donor organ
11 History of unstable or deteriorating cardiac disease
12 Myocardial infarction coronary artery bypass or angioplasty within 6 months of screening
26
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
13 Unstable angina pectoris or congestive heart failure requiring hospitalization within 6 months of
screening
14 Uncontrolled arrhythmia
15 Severe uncontrolled hypertension
16 Known HIV or hepatitis C
17 Known cirrhosis and chronic active hepatitis
18 Active substance andor alcohol abuse (as determined by site PI)
19 Pregnancy or lactation (subjects who are pregnant or breastfeeding)
20 Known hypersensitivity to study medication
21 Any condition other than IPF that in the opinion of the site PI is likely to result in the death of the
subject within the next year
22 Any condition that in the judgment of the PI might cause participation in this study to be detrimental to
the subject or that the PI deems makes the subject a poor candidate
23 Any therapy directed at pulmonary fibrosis (excepting triple therapy of prednisone plus azathioprine
plus NAC) requires a 30-day washout period before randomized Triple therapy of lt= 12 weeks duration
in the past 4 years requires a 30-day washout period before randomization
24 History of triple therapy of prednisone plus azathioprine plus NAC for gt 12 weeksrsquo duration in the past
4 years or previous enrollment in the triple-therapy arm of the PANTHER-IPF study
44 Study Design and Study Visit
441 Study Design Summary
This study will be a randomized double-blind PL-controlled trial designed to assess the safety and efficacy of
NAC in subjects with newly diagnosed IPF
Subjects with mild to moderate IPF (defined as FVCpred ge 50 and DLCOpred ge 30) diagnosed within
the past 48 months will be enrolled Screening will continue until April 30 2012
27
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
The study will employ a 2-arm design with 11 randomization to NAC or PL Once enrolled subjects will visit
the clinical center at 15 weeks and 15-week intervals thereafter Each subject will be treated and followed for a
maximum of 60 weeks
During the 60-week visit subjects will be taken off all study agents Approximately four weeks after the final
dose of study agent is taken subjects will receive a safety phone call from the study site
442 Study Visits
Subjects who meet entry criteria will review the informed consent a written description of the purpose
procedures and risks of the study with the PI co-investigator or study coordinator and all questions will be
answered The informed consent form will be signed by the subject at screening No protocol-specific
procedures will be performed until the subject has signed and dated an informed consent form This includes the
screening procedures
4421 Screening
Once informed consent is obtained subjects may immediately begin the screening process or may return within
28 days of consent In the event a study subject has been clinically evaluated at the study site by an IPFnet study
physician and has performed testing within three weeks for this clinical evaluation that meets guidelines
provided in the IPFnet PANTHER-IPF Manual of Operating Procedures (MOOP) this testing may be used to
satisfy the following screening criteria medical history physical exam arterial blood gas (ABG) with A-a
gradient vital signs with oximetry body height and weight spirometry DLCO lung volumes and HRCT scan
Allowing the use of previously performed test results that meet study guidelines for the screening visit is
intended to permit subjects easier access to study entry to prevent subjects from repeating testing that has been
performed within the study window and to decrease risks to subjects from repeated exposure to procedures
such as arterial puncture and HRCT
The following procedures will be performed at screening
Medical history and a physical examination
28
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Measure height and weight
Serum pregnancy test (if applicable)
Measure vital signs including oximetry
Blood draws performed and the following analyses conducted
o Hematology (red cell count white cell count hemoglobin hematocrit cell indices differential
platelet count)
o Blood chemistries according to central laboratory protocol (see Section 410 Laboratory
Testing)
o Beta human chorionic gonadotropin (serum) pregnancy test (in women of childbearing potential)
o Urinalysis
Pulmonary Function Tests (PFTs) including spirometry pre- and post- bronchodilator and postshy
bronchodilator measurement of lung volumes and measurement of hemoglobin adjusted diffusing
capacity
Measure ABGs
HRCT if a satisfactory scan has not been performed on the subject within 3 months of screening (see
PANTHER-IPF MOOP for more details)
Surgical lung biopsies (if applicable) reviewed by local and central pathology departments
Current medications If required a washout period discussed with the subject and initiated at this visit
4422 Enrollment
The enrollment visit is expected to take place within eight weeks of the screening visit Enrollment visit
activities include
Measure vital signs including oximetry
Measure height and weight
Serum pregnancy test (if applicable)
If consent has been given blood will be drawn and a urine specimen collected for the bio-specimen
repository
Spirometry (post-bronchodilator)
Measure 6MWT with Borg Dyspnea Scale
29
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Collect Quality-of-life (QOL) data using the SF-36 EuroQol Investigating Choice Experiments for
Preferences of Older People Capability Instrument (ICE CAP) and SGRQ
Female subjects complete Gender Substudy questionnaire
Dyspnea status collected using the UCSD SOBQ
Evaluate Acute Exacerbation (AEx)
Review of any Adverse Events (AEs)
Review of concomitant medications
Subject receives diary and instructions on its purpose and proper use
Subject receives supply of study drug sufficient to last until his or her 15-week study visit
See the Schedule of Assessments (Table 3) for more details Subjects with screening and enrollment postshy
bronchodilator FVC measurements (in liters) differing by more than 11 are not eligible to be enrolled in the
study
Subjects will be asked to provide a physician of record This physician will be considered the subjectrsquos primary
care provider (PCP) and if the subject agrees the PCP will be informed by letter of the subjectrsquos enrollment in
the trial The subject will be informed that his or her ongoing medical care should be received from the PCP
The PCP will be informed of any safety issues identified by the study staff The PCP will also be given
information regarding communication with study personnel about pertinent health issues or clinic encounters
the subject may have
4423 Week 15
The week 15 visit is expected to occur within +- 14 days of the subjectrsquos scheduled visit time (eg the week 15
visit should occur anytime between 13 and 17 weeks after starting study drug Week 15 activities include
Measure vital signs with oximetry
Measurement height and weight
Serum pregnancy test (if applicable)
Spirometry (post-bronchodilator) measurement
Review of AEs
Evaluate for AEx
30
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Review concomitant medications
If consented draw blood and collect urine specimen for the biospecimen repository
Subjects return used and unused study drug for the visit
Review study diary and a new study diary will be given
Provide additional supply of study drug sufficient to last until the next scheduled visit
4424 Week 30
The week 30 visit is expected to occur within +- 14 days of the subjectrsquos scheduled visit time (eg the week 30
visit should occur anytime between 28 and 32 weeks after starting study drug) Week 30 activities include
Physical examination
Measure vital signs with oximetry
Measure height and weight
Laboratory values (complete blood count [CBC] and serum chemistries)
Serum pregnancy test (if applicable)
Measure spirometry (post-bronchodilator)
6MWT with Borg scale
DLCO
Review of AEs
Evaluate for AEx
Review concomitant medications
Complete all QOL and dyspnea questionnaires (EuroQol ICE CAP SF-36 SGRQ and UCSD SOBQ)
If consent has been given blood will be drawn and a urine specimen collected for the biospecimen
repository
Review study diary
Subjects return used and unused study drug for the visit
Provide additional supply of study drug sufficient to last until the next scheduled visit
4425 Week 45
31
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
The week 45 visit is expected to occur within +- 14 days of the subjectrsquos scheduled visit time (eg the week 45
visit should occur anytime between 43 and 47 weeks after starting study drug) Week 45 activities include
Measure vital signs with oximetry
Measure height and weight
Serum pregnancy test (if applicable)
Measure spirometry (post-bronchodilator)
Review of AEs
Evaluate for AEx
Review concomitant medications
If consent has been given blood will be drawn and a urine specimen collected for the biospecimen
repository
Subjects return used and unused study drug for the visit
Study diary reviewed
Provide additional supply of study drug sufficient to last until the next scheduled visit
4426 Week 60 (Early Withdrawal or Final Treatment Visit)
At week 60 or at subject withdrawal from the study (premature by study doctor or subjectrsquos decision) a final
treatment visit will occur At this final treatment visit subjects will discontinue NACPL abruptly Week 60
activities also include
Physical examination
Measure vital signs with oximetry
Measure height and weight
Laboratory values (complete blood count [CBC] and serum chemistries)
Spirometry (post-bronchodilator) measurement
6MWT with Borg scale measurement
DLCO
Lung volumes
ABG
Review of AEs
32
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Evaluate for AEx
Review concomitant medications
Subjects will complete all QOL and dyspnea questionnaires (EuroQol ICE CAP SF-36 SGRQ and
UCSD SOBQ)
If consent has been given blood will be drawn and a urine specimen collected for the biospecimen
repository
Subjects return used and unused study drug for the visit
Study diary reviewed
4427 Final Site Visit ndash FVC drop confirmation
In the event that the subject has a recorded FVC drop of gt10 from baseline at the final treatment visit and the
subject has not had a confirmation of such a drop at a previous study visit the subject should return to the
clinical site 6 to 8 weeks after the final treatment visit During this visit a post-bronchodilator spirometry test
will be performed This FVC measurement will be evaluated according to section 521 of this protocol
4428 Final Visit ndash Telephone Follow-up
Four weeks following the final dose of study medication subjects will receive a telephone call from the study
coordinator to ensure that there are no side effects and to follow up on any ongoing adverse events (AEs)
4429 Phone Contact Between Visits
At week 2 and each month that a subject does not have a scheduled clinical center visit his or her study
coordinator will contact him or her at least once by telephone to
Inquire if the subject has had any hospitalizations events that might be considered an AE or any events
significant enough to warrant an out-of-cycle visit to the clinical center
Remind subjects of their current dosage levels and confirm that the subject understands them
Address any questions or concerns the subject might have regarding other aspects of the study
Assess adherence to the treatment regimen by reviewing diary data verbal review of medications taken
including nutritional supplements
33
34
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Table 3 Schedule of Assessments
Procedure Screening Visit 0
Enrollment Visit 1
Week 15 Visit 2
Week 30Visit 3
Week 45 Visit 4
Week 60 Early
Withdrawal Visit 5
Final1
Visit (via phone)
Informed consent X
Medical history X
Inclusionexclusion criteria X
Serum pregnancy test (if applicable) X X X X X
Review of lung biopsy X
Arterial Blood Gas X X
6-Minute Walk Test
X
X X
Physical examination X X X
Vital signs with oximetry X X X X X X
Body height and weight X X X X X X
Complete Blood Count X X X
Chemistry panel X X X
Monitor Lab Values X X X
Urinalysis X Specimen repository substudy blood draw and urine collection (if consented)
X
X X X X
HRCT (if not completed within three months) X
Spirometry (pre- and post-bronchodilator) X
Spirometry (post-bronchodilator only) X X X X X
DLCO (post-bronchodilator only) X X X
Lung volumes (post-bronchodilator only) X
X
Evaluate for acute exacerbation X X X X X
Review Adverse Events X X X X X X
Review concomitant meds X X X X X X
Dispense subject diary X X X X
Review subject diary X X X X X
Dispense study agent X X X X
Gender Substudy questionnaire (female subjects only) X
EuroQol ICECAP UCSD SOBQ SGRQ SF-36 X X X
Abbreviations DLCO diffusing capacity of the lung for carbon monoxide QOL Quality of Life ICECAP Investigating Choice Experiments for Preferences of Older People UCSD SOBQ University of California Shortness of Breath Questionnaire SGRQ St Georgersquos Respiratory Questionnaire SF-36 Short Form 36 Health Survey
1Follow-up visit via phone will occur four weeks after final dose of study medication
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
45 Dose Justification
The general philosophy for determining dosing levels was to apply previously examined
treatment regimens With the focus of the study being to establish a standard of care for
mildmoderate IPF subjects the goal was to develop flexible yet standardized treatment rules that
allow for the temporary or permanent withholding of one or more components of treatment when
necessary Subjects developing laboratory abnormalities or symptoms that result in
discontinuation of one or more components of study treatment may continue on the other
components as long as there is no contraindication for this Complete follow-up is important for
the validity of any study As a strategy to maintain protocol adherence we are using a treatment
regimen that will detect potential side effects and prompt interventions proactively in the interest
of patient safety In addition subjects who permanently stop study medications during the course
of the study are encouraged to continue in the study completing all scheduled visits and tests
451 Rationale for N-acetylcysteine Dosing
To our knowledge there have been no IPF studies to correlate clinical outcome measures with
different dosages for NAC The dosage chosen is based on the IFIGENIA study However BAL
lung GSH levels from subjects with IPF have been augmented with the use of oral NAC at 600
mg 3 times per day In addition lung GSH levels have been associated with improved
PFTs212227 The dose chosen for this study was based on previous data including the IFIGENIA
study30
4511 Dosing of N-acetylcysteineplacebo
Dosing of NACPL will be 600 mg orally 3 times a day (1800 mgday)
4512 Reasons to Discontinue N-acetylcysteineplacebo
NACPL may be temporarily or permanently discontinued for the duration of the study for
gastrointestinal symptoms or dermatologic reactions
35
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Temporarily discontinue (hold) oral NACPL for subjects requiring inpatient admission for acute
exacerbation (AEx) or other conditions Resume NACPL after discharge
36
37
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
452 Dosage Algorithms
Dosage Adjustment Algorithm 1 NACPL Dose Modifications for Gastrointestinal Symptoms Nausea Vomiting Abdominal Discomfort Diarrhea
GI Symptoms determined by the PI to be clinically significant Nausea Vomiting Abdominal Discomfort Diarrhea
NACPL Temporarily dc (HOLD) x 3 Days
Monitor symptoms intervene as clinically indicated (eg fluid replacement antidiarrhea or antinausea medication)
Monitor or lab PRN
Are symptoms resolving after 3 days NO
Symptoms NOT resolving after 3 days of holding study medication Assessmentmanagement per clinical
discretion of investigator
Likely not study medication discuss resuming study medication with medical monitor when symptoms resolved
YES
Temporarily dc (HOLD) NACPL for 4 additional days (total hold 1 week) then NACPL Resume 600 MG TID
Did symptoms recur
YES
STOP NACPL for
duration of study
NO
NACPL No Change
38
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Dosage Adjustment Algorithm 2 NACPL Dose Modifications For Dermatologic Reactions
Dermatologic Reactions (Not Acneiform) ge Grade 2 Grading per Common Terminology Criteria for
Adverse Events V30 (httpctepcancergov) For example Grade 1 RASHDESQUAMATION Macular or papular eruption or erythema without associated symptoms Grade 2 RASHDESQUAMATION Macular or popular eruption or erythema with pruritus or other associated symptoms localized desquamation or other lesions covering lt50 of body surface area
NACPL Temporarily dc (HOLD) x 3 days
Are symptoms resolving after 3 days
NO Symptoms not resolving after 3 days of holding study medication Assessmentmanagement per clinical discretion of investigator Likely not study medication Discuss resuming study medication with medical monitor when symptoms
resolved YES
Temporarily dc (HOLD) NACPL for 4 additional days (total hold 1 week) then NACPL resume 600 MG TID
Did symptoms recur
YES
STOP NACPL for
duration of study
NO
NACPL No change
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
46 Contraindications Precautions and Side Effects of Study Medications
461 Contraindication
Contraindication to NAC is known hypersensitivity to it
462 Precautions
Concomitant administration of oral NAC and antibiotics has shown a slightly reduced absorption
of cephalexin and a slight increase in erythromycin serum levels NAC contains free sulfhydryl
groups There is no evidence that individuals sensitive to sulfa drugs are sensitive to NAC
The NAC preparation being administered in this study contains 20 mg of aspartame Because of
the phenylalanine component of aspartame individuals with phenylketonuria should avoid or
restrict aspartame intake to avoid increased blood levels of phenylalanine Because of this risk
labeling is required on all products containing aspartame
463 Side Effects
Side effects of NAC range from common to serious See Table 4
39
40
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Table 4 Side Effects of NAC
Undesirable Effects
System-organ class Uncommon
(gt11000 lt1100)
Rare
(gt110000 lt11000)
Very rare
(lt110000) Not known
Immune system disorders Hypersensitivity Anaphylactic shock
reaction
Nervous system disorders Headache
Ear and labyrinth disorders Tinnitus
Cardiac disorders Tachycardia
Vascular disorders Hemorrhage
Respiratory thoracic and
mediastinal disorders
Bronchospasm
Dyspnea
Gastrointestinal disorders
Vomiting diarrhea
stomatitis abdominal
pain nausea
Dyspepsia
Skin and subcutaneous tissue
disorders
Urticaria rash
angioedema itching
General disorders and
administration site conditions Pyrexia
Investigations Reduced arterial
pressure Face edema
In very rare cases the onset of severe skin reactions such as Stevens-Johnson syndrome and Lyell syndrome was reported to have a temporal relationship with N-acetylcysteine administration Although in most cases at least another suspect drug probably most involved in the genesis of the above mentioned mucocutaneous syndromes has been identified in case of mucocutaneous alterations it is appropriate to contact onersquos doctor and the administration of N-acetylcysteine should be immediately discontinued
Some studies confirmed a reduction of platelet aggregation during N-acetylcysteine administration The clinical significance of these findings has not been defined yet [Source Fluimucil Investigator Brochure]
47 Recruitment Procedures
Subjects recruited for this study will be established patients of the investigators or physician- or
self-referred to participating clinical centers in the IPFnet Each clinical center within IPFnet has
a well-developed infrastructure of local pulmonologists within the surrounding geographic area
These pulmonologists are kept informed of ongoing IPF clinical trials and regularly refer
subjects to studies conducted at IPFnet clinical centers
Additional steps will be taken to inform clinicians of the trials in progress within IPFnet
including presentations at faculty staff meetings at local hospitals medical grand rounds and
national conferences direct mail notification monthly faxes and advertisement of network trials
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
in pulmonary journals Clinical center patients previously diagnosed with IPF will be notified of
the trials by mail whenever possible
Recruitment of minorities and women will be monitored by the DCC and DSMB If necessary
additional recruitment efforts will be made at specific centers to ensure that the aggregate subject
sample contains appropriate representation of women and minorities
48 Study Procedures
The following procedures are detailed in the PANTHER-IPF MOOP accompanying this
protocol
1 PFT
2 ABG
3 HRCT scan of the chest (including imaging of pulmonary arteries)
4 CBC and serum chemistries
5 Pregnancy test
6 6MWTBorg Dyspnea Scale
7 QOL questionnaires (EuroQol HAD SF-36 SGRQ and ICE CAP)
8 UCSD SOBQ
9 Gender Substudy Questionnaire
All assessments of PFTs will be conducted by study personnel not directly involved in the
treatment of the subjects
481 Biological Specimen Management
4811 Biological Specimen Sample Management
Subjects at clinical centers participating in the specimen repository substudy who consent to
having blood drawn for research purposes and for the banking of blood blood components and
other biologic specimens (urine and BAL fluid) will have approximately 405 mL of blood
41
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
drawn 17 mL blood drawn for DNA and 20 mL of urine collected at enrollment visit Subjects
will have approximately 50 mL of blood drawn and 20 mL of urine collected at each 15-week
follow-up visit Blood specimens will be separated according to PANTHER-IPF MOOP
guidelines into the following components for banking in the repository serum plasma and
DNA Coding of all biologic specimens for the repository will be performed by study staff at the
clinical center The samples will be processed per PANTHER-IPF MOOP guidelines aliquoted
labeled with barcode labels and stored at -70degC at the clinical center and shipped to the central
repository
The only subject identifiers will be a sample ID number and subject initials This sample ID will
be linked in the IPFnet DCC clinical database to subject information No subject information will
be transferred to the biological-specimen database
The subjectrsquos samples may be used for approved sub-studies relating to human disease
including but not limited to IPF The studies for which an individualrsquos samples will be made
available will be determined by the subjectrsquos answers to questions on the biological-sample
informed consent form The subjects can choose to make their samples available for all options
or any combination Samples will be made available to researchers only with IPFnet Steering
Group approval until such time as the samples are made public through the NHLBI repository
49 Concomitant Medications
Concurrent treatment with FDA-approved therapy for IPF is allowed Colchicine may be used
for treatment of gout Temporary treatment with oral or IV corticosteroids for clinical worsening
or suspected AEx is permitted Nutritional supplements containing NAC are not allowed
410 Laboratory Testing
Clinical laboratory parameters will be assessed at screening and at the end of the study The
following tests will be performed at the two time points specified in the protocol chemistry (AG
ratio ALT [SGPT] AST [SGOT] albumin alkaline phosphatase amylase bilirubin-direct
42
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
bilirubin-indirect bilirubin-total BUN BUNcreatinine ratio calcium carbon dioxide
cholesterol-total chloride CPK-total creatinine GGT globulin glucose iron-total LDH
lipase magnesium phosphorus-inorganic potassium protein-total sodium TIBC triglycerides
uric acid) and hematology (red blood cell count WBC count hemoglobin hematocrit cell
indices differential platelet count)
411 Blinding of Study Drugs
Subjects and caregivers will be blinded to study treatment Every subject will receive NAC or
matching PLs at every study visit from the baseline visit to the week-45 visit No study agent
will be dispensed at the week-60 visit
43
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
5 Study Endpoints
51 Primary Study Endpoint
The primary endpoint will be the change in serial measurements of FVC over the study period
52 Secondary Study Endpoints
521 Time to Disease-progression
The time-to-death or a 10 decline in FVC will be defined as the time-to-disease progression
The 10 decline in FVC from enrollment must be confirmed on 2 consecutive visits no less than
6 weeks apart For subjects with 2 consecutive visits with a 10 decline in FVC the time-toshy
disease progression will be defined as the time interval between enrollment and the initial visit
with a 10 FVC decline For subjects who experience disease progression the study doctor will
determine whether or not the subject will remain in the study
522 Acute Exacerbations
The following 3 criteria will define AEx in subjects with acute worsening of their respiratory
conditions
1 Clinical (all of the following required)
A) Unexplained worsening of dyspnea or cough within 30 days triggering unscheduled
medical care (eg emergency room clinic study visit hospitalization)
B) No clinical suspicion or overt evidence of cardiac event pulmonary embolism or deep
venous thrombosis to explain acute worsening of dyspnea
C) No pneumothorax
44
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
2 RadiologicPhysiologic (A and B required)
A) New ground glass opacity or consolidation computed tomography (CT) scan OR new
alveolar opacities on chest x-ray
B) Decline of ge 5 in resting room air SpO2 from last recorded level OR decline of ge 8 mm
Hg in resting room air PaO2 from last recorded level
3 Microbiologic (all of the following required)
A) No clinical evidence for infection (ie absence of grossly purulent sputum fever gt 39degC
orally)
B) Lack of positive microbiological results (if done) from lower respiratory tract defined as
(1) Clinically significant bacterial growth on sputum or endotracheal aspirate cultures
(2) Quantitative culture by protected brush specimen ge 103 cfumL or BAL ge 104 cfumL
(3) The presence of specific pathogens on stains of any of the above
C) Lack of positive pathogen in blood cultures (if done)
Identification of Acute Exacerbations
All subjects will be educated about the importance of identifying AExs At the time of
enrollment subjects will be told about the possibility of developing acute symptomatic
worsening that might represent an AEx of IPF and instructed to contact their study clinical
center coordinator within 48 to 72 hours of the apparent event
All subjects will be contacted by phone monthly and questioned about any change in dyspnea or
cough and any interim clinic visits or hospitalizations Finally as part of the IPFnet outreach to
community referring physicians the importance of AExs will be emphasized When a subject is
identified who meets criterion 1A this will trigger the collection of additional clinical data to
evaluate a suspected AEx These data will be collected as part of standard clinical care (ie this
protocol does not require collection of all items) The additional items to be collected for
suspected AEx include
IPFnet AEx case report form (eCRF) (required)
45
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Chest x-ray CT scan withwithout pulmonary angiogram (reports should be faxed and
followed by the hard copiesdiscs)
Oxygen saturation (pulse oximetry)
ABG
Respiratory cultures (sputum endotracheal aspirate lavage)
Blood cultures
Clinichospital records related to the event
All potential cases of AEx will be reviewed by the clinical center PI first and a decision on
whether the case may represent an AEx will be made If AEx is suspected the case will be sent
to the IPFnet adjudication committee which will assign a final diagnosis (see Table 5) If there is
disagreement among members the majority opinion will be recorded
During episodes of suspected AEx as determined by the individual clinical center investigator
subjects will remain blinded and in the study
Table 5 Final Diagnoses in Evaluation of Suspected Acute Exacerbations
Definite acute exacerbation All criteria met no alternative etiology
Unclassifiable acute worsening
Insufficient data to evaluate all criteria no alternative etiology
Not acute exacerbation Alternative etiology identified that explains acute worsening
Management of the suspected AEx will be at the discretion of the treating physician Standard of
care generally involves evaluation for respiratory infection pulmonary embolism cardiac events
and pneumothorax and treatment with IV corticosteroids
Study drugs will be resumed at pre-suspected AEx doses after subjects clinically improve as
confirmed by the local PI All subjects should be seen at the clinical center within 2 to 4 weeks
of recovery for measurement of post-bronchodilator FVC (see Figure 4) Subjects unable to
return to the clinical center after suspected AEx due to medical frailty (eg continued
46
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
institutionalization progressive disability) will be categorized as failing to maintain FVC
response in secondary analyses
Suspected AEx (PI determined)
Hold study drug Treat AEx
(Attending physician determined)
Alive but unable to continue due to
medical frailty
Dead
Alive and able to continue
Site reviewvisit
Restart study drug
FVC within 2-4 weeks
Figure 4 Acute Exacerbation Flow Chart
523 Respiratory Infections
An upper respiratory infection will be defined as
Change in sputum discoloration
Increased cough of no more than 14 daysrsquo duration
A lower-respiratory infection (pneumonia) will be defined as new segmental or lobar airspace
opacities visualized by image studies (chest radiograph or HRCT) in addition to any of the
following
Positive pathogencultures in good sample of sputum or lower-airway secretions retrieved
by fiberoptic bronchoscope
Fever gt 39degC or gt 100degF
Leukocytosis gt 12000 (unexplained no increase in dose of corticosteroids)
47
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
524 Maintained FVC Response
Subjects with follow-up FVCpred measurements at or above their baseline FVCpred level
will be classified as having maintained FVC response Subjects with reduced FVCpred levels
or missing data for any reason including death or medical frailty will be classified as having not
maintained FVC response The FVCpred value is used because unadjusted FVC measurements
are expected to decline with age
48
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
6 Safety Evaluations and Procedures
61 Adverse Events
During a clinical trial the reporting of adverse experience information can lead to important
changes in the way a new treatment is developed as well as provide integral safety data
611 Definitions
An adverse event (AE) is any untoward medical occurrence in a subject or clinical investigation
subject who was administered a pharmaceutical product The AE does not necessarily have to
have a causal relationship with the drug administered An AE can be any unfavorable and
unintended sign (including an abnormal laboratory finding) symptom or disease temporarily
associated with the use of a medicinal product whether or not considered to be related to the
medicinal product Diseases signs symptoms or laboratory abnormalities already existing at
enrollment are not considered AEs unless they worsen (ie increase in intensity or frequency)
Surgical procedures themselves are not AEs they are therapeutic measures for conditions that
require surgery The condition for which the surgery is required may be an AE Surgical
procedures planned before randomization and the conditions necessitating the surgery are not
AEs
A serious adverse event is any untoward event that
Is fatal
Is life-threatening
Requires inpatient hospitalization or prolongation of existing hospitalization with the
following exceptions
o Preplanned (before the study) hospital admissions unless the hospitalization is
prolonged
o Planned admissions (as part of a study eg routine biopsies)
o Hospitalization lasting lt 24 hours
49
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
o Hospitalization for elective procedure
o Emergency room visits
Results in persistent or significant disability or incapacity
Is a congenital anomaly or birth defect
Important medical events that may not result in death be life-threatening or require
inpatient hospitalization may be considered serious adverse events (SAEs) when based
on appropriate medical judgment they may jeopardize the subject and may require
medical or surgical intervention to prevent one of the outcomes listed above
Life-threatening means that the subject was in the view of the investigator at immediate risk of
death from the AE as it occurred It does not include an AE that had it occurred in a more severe
form might have caused death
Persistent or significant disabilityincapacity means that the event resulted in permanent or
significant and substantial disruption of the subjectrsquos ability to carry out normal life functions
Causality
A reasonable possibility means the AE may have been caused byrelated to the study drug A
perceived or real lack of efficacy does not satisfy the definition of relatedness
612 Adverse Event (AE) Reporting
For the PANTHER-IPF trial all AEs (serious and nonserious) occurring from randomization
through final study visit (4 weeks after final dose of all study medication) will be recorded on the
AE page of the case report form (CRF)
6121 Serious Adverse Events (SAE) Reporting
For this trial all deaths and all SAEs which occur from randomization through final study visit
must be entered within the EDC system via the SAE eCRF page within 24 hours of the
investigative sitersquos knowledge of the event It is the responsibility of the clinical center
50
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
investigator to provide a causality assessment of the event for each study medications based upon
the information available at the time of the report It is understood that complete information
about the event may not be known at the time the initial report is submitted In the event the EDC
system is not accessible to the site at the time of event reporting investigative sites will complete
and forward a paper back-up SAE form to DCRI Safety Surveillance for processing
DCRI Safety Surveillance
Telephone 1-919-668-8624 or 1-866-668-7799 (toll free)
Fax 1-919-668-7138 or 1-866-668-7138 (toll free)
The investigator must complete and submit follow-up SAE information via the eCRF when
important new or follow-up information (eg final diagnosis outcome results of specific
investigations) becomes available Follow-up information should be submitted according to the
same process used for reporting the initial event as described above All SAEs will be followed
until resolution stabilization or 30 days after the subject has completed the final visit (4 weeks
after the final dose of study medication) whichever occurs first The investigator is responsible
for reporting SAEs to their institutional review board (IRB) per site specific IRB reporting
guidelines
6122 Regulatory Reporting
AEs that are serious study drug related and unexpected will be reported to the regulatory
authorities The DCRI Safety Surveillance medical monitor will perform a medical review of all
SAEs submitted and evaluate for ldquounexpectednessrdquo DCRI Safety Surveillance will prepare
MedWatch reports for those events identified as serious study drug related and unexpected as
determined by Safety Medical Monitor
DCRI Regulatory Services will submit all unexpected study drug-related SAEs as per 21 CFR
32 DCRI Safety Surveillance will provide a safety alert letter to the NHLBI DSMB and DCC
clinical operation (for distribution to sites) within 15 days of initial receipt of the information
51
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Investigators are responsible for promptly reporting these events to their reviewing IRBs
according to site specific IRB reporting guidelines
62 Clinical Medical Monitoring
There will be an unblinded physician at the IPFnet DCC serving as medical monitor The
medical monitor will be available to assist with questions about dosage adjustments of study
medications including discontinuation or resumption of medications
63 Unblinding Procedures
Unblinding of subjects or investigators to subject treatment is strongly discouraged For ongoing
clinical management all subjects should be presumed to be receiving ldquoactiverdquo study drug To
ensure the subjectrsquos safety the study treatment will be dose-adjusted based on laboratory test
results clinical findings and symptoms
The IPFnet DCC medical monitor and PANTHER-IPF co-chairs Drs Ganesh Raghu and
Fernando Martinez will be available to the study physicians to discuss study drug management
on a case-by-case basis Un-blinding will be considered ONLY when the knowledge of subject
treatment assignment is ABSOLUTELY ESSENTIAL for subject safety and after discussion of
the subjectrsquos case with the medical monitor and either Dr Raghu or Dr Martinez Unblinding of
study treatment should be minimized during the conduct of the trial In those cases where it is
felt to be medically necessary the DCC medical officer will communicate directly with the
managing physician to minimize unblinding of study personnel
52
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
7 Study Drug Procedures
At the baseline 15-week 30-week and 45-week study visits subjects will receive a supply of
study drug sufficient to last until the next visit at which study drug will be dispensed
53
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
8 Data Management
81 Hardware and Software Configuration
811 Hardware and Database Software
Data will be stored in an Oracle database system Oracle has advantages of processing efficiency
and smooth linkage with other software systems The application and database will be hosted on
Solaris Unix servers at the IPFnet DCC
812 Statistical Software
SAS will be used as the principal application for the management of analysis data files and
statistical computations S-Plus will be used to provide supplementary functions as needed
813 Access Control and Confidentiality Procedures
Access to databases will be controlled centrally by the IPFnet DCC through user passwords
linked to appropriate privileges This protects the data from unauthorized changes and
inadvertent loss or damage
814 Security
Database and Web servers will be secured by a firewall and through controlled physical access
Oracle has many security features to ensure that any staff member accessing the database has the
proper authority to perform the functions he or she requests of the system Within the secondary
SAS databases Unix group-access control maintains similar security The Sun workstation login
is secured by extensive user-password facilities under Unix
54
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
815 Back-up Procedures
Database back-up will be performed automatically every day and standard IPFnet DCC policies
and procedures will be applied to dictate tape rotation and retention practices
816 Virus Protection
All disk drives that provide network services and all user computers will be protected using
virus-scanning software Standard IPFnet DCC policies will be applied to update these protection
systems periodically through the study
82 Sources of Data
821 Design and Development
The IPFnet DCC will be responsible for development of the electronic case report forms
(eCRFs) development and validation of the clinical study database ensuring data integrity and
training clinical center staff on applicable data management procedures A web-based distributed
data entry model will be implemented This system will be developed to ensure that guidelines
and regulations surrounding the use of computerized systems used in clinical trials are upheld
The remainder of this section provides an overview of the data management plan associated with
this protocol
822 Data Collection Forms
The data collection process consists of direct data entry at the study clinical centers into the EDC
system(s) provided by the DCC A data collection worksheet will be provided to clinical centers
for recording data in the event the EDC system is unavailable Data entry of the eCRFs should
be completed according to the instructions provided and project specific training The
investigator is responsible for maintaining accurate complete and up-to-date records and for
ensuring the completion of the eCRFs for each research participant
55
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
823 Data Acquisition and Entry
Data entry into eCRFs shall be performed by authorized individuals Selected eCRFs may also
require the investigatorrsquos written signature or electronic signature as appropriate Electronic
CRFs will be monitored for completeness accuracy and attention to detail during the study
824 Data Center Responsibilities
The IPFnet DCC will 1) develop a data management plan and will conduct data management
activities 2) provide final eCRFs for the collection of all data required by the study 3) develop
data dictionaries for each eCRF that will comprehensively define each data element 4) conduct
ongoing data monitoring activities on study data 5) monitor any preliminary analysis data
cleanup activities and 6) rigorously monitor final study data clean up
825 Data Editing
Completed data will be entered into the IPFnet DCC automated data acquisition and
management system If incomplete or inaccurate data are found a data clarification request will
be generated and distributed to clinical centers for a response Clinical centers will resolve data
inconsistencies and errors and enter all corrections and changes into the IPFnet DCC automated
data acquisition and management system
826 Training
The training plan for clinical center staff includes provisions for training on assessments eCRF
completion guidelines data management procedures and the use of computerized systems
56
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
9 Study Design and Data Analysis
91 General Analytic Considerations
All primary analyses will be based on intent-to-treat (ITT) principles using all randomized
subjects Baseline factors across groups will be compared using mean (standard deviation) and
median (25th and 75th percentiles) summary measures Kaplan-Meier curves will be used to
display event rates Due to clinical interest in departures from both sides of the null hypothesis
all test statistics will be 2-sided
Reasonable caution needs to be taken when conducting multiple analyses on key clinical
subgroups For subgroup analyses a conservative significance level of 0001 will be used for all
interaction tests Thus subgroup comparisons will be considered exploratory unless the p-value
from the interaction test is smaller than 0001
92 Randomization Blinding and Reporting of Results
A permuted block-randomization scheme will be created with varying block sizes stratified by
clinical center Once a subject has completed the screening and baseline period and evaluation
for inclusionexclusion criteria the randomization process will begin Subjects will be
randomized to receive NAC or matching placebo with equal probability (11) via telephone
contact with a central interactive voice response system (IVRS) using a toll-free randomization
number On the day of randomization after the subject has successfully met all inclusion and
exclusion criteria the investigator or designee will call the central randomization number to
obtain the assigned kit randomization numbers for that subject At each subject visit the
investigator or designee will call the central randomization number to obtain the new kit
randomization numbers for resupply of the subject For resupply of the clinical center the IVRS
will monitor minimal volume of a kit type andor expiration date and will automatically notify
the pharmacy
57
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
The trial results will be reported according to guidelines specified in the CONSORT statement
A flow diagram describing screening recruitment randomization dropout and vital status will
be included in the primary manuscript AEs and efficacy data will be presented for all treatment
groups Adherence dropout and lost to follow-up will be carefully examined across all treatment
groups Analyses of safety will be based on data from all randomized subjects who received at
least one dose of study drug
93 Stratification
Subjects will be distributed to the two treatment arms in a 11 allocation ratio Stratification
blocks will be based on clinical centers
94 Specification of the Primary Analyses
A mixed model repeated measures (MMRM) analysis described in section 95 will be used to
compare differences in the slope of FVC measurements across the treatment groups Response
variables are values of the FVC measured at baseline and every 15 weeks until study completion
Variables in the model will include treatment time and time by treatment age sex race and
height Contrast estimates of differences in slopes of treatment over time (along with confidence
intervals) will be used to estimate the treatment effect The validity of this model in terms of
meeting modeling assumptions will be assessed via standard modeling diagnostics and goodness-
of-fit measures Based on the MMRM framework missing FVC data will not be imputed for the
primary analysis
95 Analysis of Longitudinal Endpoints
A common goal in clinical trials is to specify models that are easily implemented and
reproducible by independent data analysts On the other hand the models should have proper
statistical behavior in terms of low bias and high precision Many common approaches to
longitudinal data analysis including last observation carried forward (LOCF) imputation rely on
the missing completely at random (MCAR) assumption However the MCAR assumption is
58
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
unlikely to hold in many clinical trials because missing data are often related to disease
progression and prognosis A more reasonable assumption missing at random (MAR) specifies
that the complete data distribution can be modeled using only the observed data The likelihood-
based MMRM approach is valid under the more general MAR assumptions These models will
be applied to analyze the longitudinal data secondary endpoints
The advantages of MMRM analysis are that all important characteristics of the model can be preshy
specified standard software can be used to implement the models and results are based on ITT
principles43 In addition the MMRM approach offers superior control of Type I and Type II
errors compared with the LOCF approach
Response variables are values of the PFTs measured at enrollment and every 15 weeks until
study completion and 6MWT values measured at baseline week 30 and week 60 Covariates are
treatment time time by treatment and key baseline risk factors Contrasts (along with
confidence intervals) of treatment by time will be used to estimate the treatment effect
The correlation structure involves multiple pieces including measurement errors random
variation and interindividual variability For the longitudinal data analyses an unstructured
correlation matrix for within-subject errors will be assumed Other correlation structures
including compound symmetry will be examined as needed A careful examination of reasons
for study discontinuation will be conducted to assess the validity of MCAR Sensitivity analyses
will be used to examine the untestable assumption that the observed data violate the MAR
assumption The MMRM models will be implemented using PROC MIXED in SAS
96 Analysis of Binary Time-to-Event and Time-Lagged Endpoints
Regression modeling approaches using either the logistic regression model or Cox proportional
hazards regression model will be employed when appropriate The validity of these models will
be assessed via standard modeling diagnostics and goodness-of-fit measures Estimates of
cumulative frequencies for more general time-lagged responses will be calculated using the
partitioned version of the Bang-Tsiatis estimator44 The partitions will be set at 15-week intervals
59
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
to correspond with the data-collection process Covariate adjusted event rates will be calculated
using inverse probability-weighted regression estimates45
97 Power Analysis
971 Primary Analyses
Based on previously published IPF clinical trials the PL group is expected to experience a drop
in FVC of approximately 020 L over the study period (see Figure 1) The IPFnet Steering Group
determined a clinically important difference would be to preserve the majority of the decline
relative to PL over the study period In particular a treatment effect of 015 L was determined to
be a clinically meaningful difference Potential dropout is a key factor in the proposed study The
drop-out process assumed 5 lost to follow-up after every study visit Only 80 of subjects
were assumed to be followed for the entire study period All models assumed a compound
symmetry structure for the covariance matrix Power calculations were performed using a SAS
IML program for designing repeated measures studies46 Based on preliminary reviews of the
data from the University of Michigan the covariance matrix parameters were estimated at
approximately σ2 = 0757 (variance parameter) and ρ = 0936 (correlation parameter) To be
conservative the power calculations for the primary analysis were performed with parameter
setting of σ2 = 0810 (variance parameter) and ρ = 0925 (correlation parameter)
The power calculations assume a correction for imperfect compliance proposed by Lachin and
Foulkes to allow for 2 noncompliance for each of the treatment arms47 Thus the sample size
of 130 subjects per arm would be reduced to an adjusted sample size of 130(1-002-002)2 =
1198 or 120 subjects per arm
Under the assumed Type I error rate of 005 with a correlation parameter of 0925 and standard
deviation of 090 the difference of 015 L (or 00025 Lweek) shown in Table 6 would have
power of 93
60
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Table 6 Hypothetical Values of Mean FVC (L) Change from Baseline
Week 15 Week 30 Week 45 Week 60
NAC 00125 00250 00375 00500
Placebo 00500 01000 01500 02000
Difference 00375 00750 01125 01500
Abbreviations FVC forced vital capacity PL placebo
972 Power Analysis for Secondary Endpoints
Power calculations for secondary endpoint measurements are shown in Table 7 Standard
deviations are based on unpublished data provided by the University of Michigan The
calculations are based on a 2-sample t-test with Type I error rate set at 005 These calculations
are likely to be conservative because the statistical approach described in section 95 for
analyzing these endpoints will incorporate incomplete observations as well as intermediate data
points
Table 7 Detectable Differences in Treatment Means for Selected Endpoint Measurements
Secondary Endpoints Std Dev
of the Baseline Score
Detectable Difference for 80 Power
Std Dev of the Change Score
Difference Detectable for
80 Power
DLCOpred 166 58 91 32
6MWT Area Under the Desaturation Curve
219 76 175 61
6MWT Distance to Desaturation 224 78 315 110
6MWT Minutes Walked 210 073 205 071
Abbreviations Std Dev standard deviation DLCOpred diffusing capacity of the lung for carbon monoxide percent predicted 6MWT 6-minute walk test
61
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
10 Study Administration
101 Cooperative Agreement Mechanism
The administrative and funding mechanism used to undertake this project is a ldquocooperative
agreementrdquo (U01) which is an assistance mechanism Under the cooperative agreement the
NHLBI assists supports andor stimulates the project and is substantially involved with
investigators in conducting the study by facilitating performance of the effort in a ldquopartnerrdquo role
The NHLBI project scientist serves on the IPFnet Steering Group and he or another NHLBI
scientist may serve on other project committees when appropriate At the same time however
NHLBI does not assume a dominant role direction or prime responsibility for this research
program
As described below governance of the project is conducted through the IPFnet Steering Group
Principal investigators have lead responsibilities in all aspects of their trials and the project
including any modification of trial designs conduct of the trials quality control data analysis
and interpretation preparation of publications and collaboration with other investigators unless
otherwise provided for by the IPFnet Steering Group
PIs retain custody of and have primary rights to their center-specific and collaborative data
subject to government rights-of-access consistent with current Health amp Human Services (HHS)
Public Health Service (PHS) and National Institutes of Health policies The protocols and
governance policies call for the continual submission of data centrally to the IPFnet DCC for the
collaborative database which at a minimum will contain the key variables selected by the IPFnet
Steering Group for standardization across all clinical centers the submission of copies of the
collaborative datasets to each PI upon completion of the project procedures for data analysis
reporting and publication and procedures to protect and ensure the privacy of medical and
genetic data and records of individuals The NHLBI project scientist on behalf of the NHLBI
will have the same access privileges and responsibilities regarding the collaborative data as the
other members of the Steering Group
62
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
PIs are also encouraged to publish and to publicly release and disseminate results data and other
products of the project concordant with the project protocols and governance and the approved
plan for making data and materials available to the scientific community and to the NHLBI
However during the 3 years after the ending date of NHLBI project support unpublished data
unpublished results data sets not previously released and other study materials or products are
to be made available to any third party only with the approval of the IPFnet Steering Group
Upon completion of the project PIs are expected to put their intervention materials and
procedure manuals into the public domain andor make them available to other investigators
according to the approved plan for making data and materials available to the scientific
community and the NHLBI for the conduct of research at no charge other than the costs of
reproduction and distribution
The NHLBI reserves the right to terminate or curtail the project (or an individual award) in the
event of (a) failure to develop or implement mutually agreeable collaborative measurement
subject eligibility and data management sections of the protocols (b) substantial shortfall in
subject recruitment follow-up data reporting or quality control or other major breach of
protocol (c) substantive changes in the agreed-upon protocols with which NHLBI cannot
concur (d) reaching a major project outcome with persuasive statistical significance
substantially before schedule or (e) human subject ethical issues that may dictate a premature
termination
Any disagreement that may arise in scientificprogrammatic matters (within the scope of the
award) between award recipients and the NHLBI may be brought to arbitration An arbitration
panel will be composed of 3 membersmdash1 selected by the IPFnet Steering Group (with the
NHLBI member not voting) or by the individual PI in the event of an individual disagreement a
second selected by NHLBI and the third selected by the other 2 members This special
arbitration procedure in no way affects the PIrsquos right to appeal an adverse action that is otherwise
appealable in accordance with the PHS regulations at 42 CFR part 50 Subpart D and HHS
63
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
regulation at 45 CFR part 16 or the rights of the NHLBI under applicable statutes regulations
and terms of the award
102 IPFnet Steering Group
The IPFnet Steering Group is the main governing body of the project It is composed of the PIs
of the clinical centers the PI of the DCC and the NHLBI project scientist The clinical centers
the IPFnet DCC and the NHLBI each have 1 vote on the IPFnet Steering Group All decisions
are determined by majority vote
All major scientific decisions are determined by the IPFnet Steering Group It assumes overall
responsibility for the design and conduct of the trial It appoints (and disbands) committees and
subcommittees as the need arises designs approves and implements the study protocols
oversees the development of the MOOP monitors subject recruitment and treatment delivery
evaluates data collection and management oversees quality assurance procedures and
implements changes and enhancements to the study as required It also has primary responsibility
for facilitating the conduct of the trials and reporting the projectrsquos results
103 Data and Safety Monitoring Board
The NHLBI will establish a DSMB in accordance with established policies (see
httpwwwnhlbinihgovfundingpoliciesdsmb_insthtm) to ensure data quality and subject
safety and to provide independent advice to the NHLBI regarding progress and the
appropriateness of study continuation
104 Recommendations on Interim Monitoring of Efficacy Safety and Futility
First and foremost the role of the DSMB will be to review subject safety and trial conduct at
periodic points during the study The DSMB may require analyses of the primary endpoint
results for comparing the benefit and risks of treatment strategies The benefit of collecting
additional data on key secondary endpoints with extended follow-up and establishing a robust
64
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
evidence base for determining a standard of care will need to be carefully considered before
early termination of one or more treatment arms After careful consideration the IPFnet Steering
Group recommends conservative thresholds for the early examinations of the safety and efficacy
data
The DSMB will be expected to meet approximately every 6 months until trial completion to
review safety and toxicity data The DSMB may recommend stopping the study based on these
reviews Because the DSMB could stop the trial for safety concerns as well as for a large
efficacy benefit there could be multiple opportunities to reject the null hypothesis (no difference
in event rates between the PL and NAC groups) A Bonferroni approximation will be applied
during the one planned interim analysis for efficacy
Before locking the database a statistical analysis plan (SAP) will be developed to provide
complete details on the statistical analysis The SAP will include the specifics for how and when
the DSMB will be notified for AEs The IPFnet DCC will deliver to the DSMB all FDA-defined
AEs at 3-month intervals The IPFnet DCC will prepare narrative SAE reports in real time for
DSMB review including recommendations and analysis of similar events for each SAE
submitted to the FDA
65
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
11 Investigator and Sponsor Obligations
111 Monitoring
All monitoring activities for US clinical centers will be performed in accordance with DCRI
standard operating procedures Information regarding the types of visits will be outlined in the
PANTHER-IPF MOOP
112 Cost and Payment
There will be no cost to subjects enrolled in this trial Study-related procedures will be paid for
by the IPFnet
Subjects may be eligible for reimbursement for travel to the clinical center Details of payment
will be explained to each subject during the consent process
113 Confidentiality and Health Insurance Portability and Accountability Act
Considerations
Subject confidentiality will be protected throughout the study All subject data will be kept
strictly confidential and no subject-identifying information will be released to anyone outside
the project Confidentiality will be assured through several mechanisms First each subject will
be assigned an anonymous study ID which will then be used on all study forms Second any
study forms blood samples and paper records that contain subject information (eg address lists
phone lists) will be kept at the clinical centers in secured locked areas coded by number Once
blood is collected there will be no subject identifiers placed on blood samplesmdashonly the study
ID number and the date of sample collection Third access to all subject data and information
including laboratory specimens will be restricted to authorized personnel In the case of
computerized data this restricted access will be assured through user logon IDs and password
protection
66
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
At the IPFnet DCC only authorized personnel will have access to the data files containing study
data Security will be assured through user logon IDs passwords and appropriate access
privileges All study subjects will be identified only by their IPFnet ID numbers and no personal
identifying information such as name address or Social Security number will be entered into
the IPFnet DCC database Any subject-specific data reported to the IPFnet Steering Group will
be identified only by the IPFnet ID number
Finally subjects will not be identified by name in any reports or publications nor will the data
be presented in such a way that the identity of individual subjects can be inferred Analysis files
created for further study by the scientific community will have no subject identifiers These data
files will be created in accordance with the Ancillary Studies and Publication Policy of the
IPFnet
114 Informed Consent Procedures
All IPFnet subjects will provide written informed consent using procedures reviewed and
approved by each clinical centerrsquos IRB Informed consent will be undertaken by study personnel
in-person with the subject The subject has the option of declining further participation in the
study at that point No further study procedures will be conducted until the signed documents
have been provided to the IPFnet clinical center
115 Institutional Review Boards
Before initiating this study the protocol clinical center-specific informed consent forms Health
Insurance Portability and Accountability Act (HIPAA) forms recruitment materials and other
relevant information will be reviewed by a properly constituted IRB at each participating clinical
center A copy of the signed and dated IRB approval at each clinical center will be retrieved prior
to or during the site initiation visit and archived at the IPFnet DCC Any amendments to the
protocol other than simple administrative and typographical changes must be approved by each
IRB before they are implemented The clinical centers will seek annual renewals of their IRB
approvals in accordance with local procedures
67
__________________________________________ ________________
__________________________________________
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
12 Investigator Agreement
I have read the foregoing protocol PANTHER-IPF and agree that it contains all necessary
details for carrying out this study I will conduct the study as outlined herein and will complete
the study within the time designated
I will provide copies of the protocol and all pertinent information to all individuals responsible to
me who assist in the conduct of this study I will discuss this material with them to ensure they
are fully informed regarding the drug and the conduct of the study
I will fulfill all responsibilities for submitting pertinent information to the local IRB if
applicable that is responsible for this study
I further agree that NHLBI andor DCRI will have access to any source documents from which
eCRF information may have been generated
Signature of Principal Investigator Date
Name of Principal Investigator (printed or typed)
Protocol version date May 19 2009
Protocol Amendment 1 version date May 28 2010
Protocol Amendment 2 version date December 6 2011
68
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
13 References
1 Raghu G Brown KK Bradford WZ et al A placebo-controlled trial of interferon gamma-1b in patients with idiopathic pulmonary fibrosis N Engl J Med 2004350125-33 2 King TE Jr Safrin S Starko KM et al Analyses of efficacy end points in a controlled trial of interferon-gamma1b for idiopathic pulmonary fibrosis Chest 2005127171-7 3 Flaherty KR Thwaite EL Kazerooni EA et al Radiological versus histological diagnosis in UIP and NSIP survival implications Thorax 200358143-8 4 Wells AU Desai SR Rubens MB et al Idiopathic pulmonary fibrosis a composite physiologic index derived from disease extent observed by computed tomography Am J Respir Crit Care Med 2003167962-9 5 Raghu G Freudenberger TD Yang S et al High prevalence of abnormal acid gastroshyoesophageal reflux in idiopathic pulmonary fibrosis Eur Respir J 200627136-42 6 Kinnula VL Focus on antioxidant enzymes and antioxidant strategies in smoking related airway diseases Thorax 200560693-700 7 Coultas DB Zumwalt RE Black WC Sobonya RE The epidemiology of interstitial lung diseases Am J Respir Crit Care Med 1994150967-72 8 Raghu G Weycker D Edelsberg J Bradford WZ Oster G Incidence and prevalence of idiopathic pulmonary fibrosis Am J Respir Crit Care Med 2006174810-6 9 Olson AL Swigris JJ Lezotte DC Norris JM Wilson CG Brown KK Mortality from pulmonary fibrosis increased in the United States from 1992 to 2003 Am J Respir Crit Care Med 2007176277-84 10 Mannino DM Etzel RA Parrish RG Pulmonary fibrosis deaths in the United States 1979shy1991 An analysis of multiple-cause mortality data Am J Respir Crit Care Med 19961531548shy52 11 Hubbard R Johnston I Coultas DB Britton J Mortality rates from cryptogenic fibrosing alveolitis in seven countries Thorax 199651711-6 12 Johnston I Britton J Kinnear W Logan R Rising mortality from cryptogenic fibrosing alveolitis Bmj 19903011017-21 13 Raghu G Collard HR Egan JJ et al An official ATSERSJRSALAT statement idiopathic pulmonary fibrosis evidence-based guidelines for diagnosis and management Am J Respir Crit Care Med 2011183788-824 14 (USA) FDA FDA Public Health Advisory Interferon gamma-1b (marketed as Actimmune) In 2007 15 King TE Jr Pardo A Selman M Idiopathic pulmonary fibrosis Lancet 2011 16 Raghu G Brown KK Costabel U et al Treatment of idiopathic pulmonary fibrosis with etanercept an exploratory placebo-controlled trial Am J Respir Crit Care Med 2008178948shy55 17 Malouf MA Hopkins P Snell G Glanville AR An investigator-driven study of everolimus in surgical lung biopsy confirmed idiopathic pulmonary fibrosis Respirology 201116776-83 18 King TE Jr Behr J Brown KK et al BUILD-1 a randomized placebo-controlled trial of bosentan in idiopathic pulmonary fibrosis Am J Respir Crit Care Med 200817775-81 19 Richeldi L Costabel U Selman M et al Efficacy of a tyrosine kinase inhibitor in idiopathic pulmonary fibrosis N Engl J Med 20113651079-87
69
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
20 Borok Z Buhl R Grimes GJ et al Effect of glutathione aerosol on oxidant-antioxidant imbalance in idiopathic pulmonary fibrosis Lancet 1991338215-6 21 Meyer A Buhl R Magnussen H The effect of oral N-acetylcysteine on lung glutathione levels in idiopathic pulmonary fibrosis Eur Respir J 19947431-6 22 Behr J Maier K Degenkolb B Krombach F Vogelmeier C Antioxidative and clinical effects of high-dose N-acetylcysteine in fibrosing alveolitis Adjunctive therapy to maintenance immunosuppression Am J Respir Crit Care Med 19971561897-901 23 Cantin AM North SL Fells GA Hubbard RC Crystal RG Oxidant-mediated epithelial cell injury in idiopathic pulmonary fibrosis J Clin Invest 1987791665-73 24 Waghray M Cui Z Horowitz JC et al Hydrogen peroxide is a diffusible paracrine signal for the induction of epithelial cell death by activated myofibroblasts Faseb J 200519854-6 25 Larios JM Budhiraja R Fanburg BL Thannickal VJ Oxidative protein cross-linking reactions involving L-tyrosine in transforming growth factor-beta1-stimulated fibroblasts J Biol Chem 200127617437-41 26 Kinnula VL Fattman CL Tan RJ Oury TD Oxidative stress in pulmonary fibrosis a possible role for redox modulatory therapy Am J Respir Crit Care Med 2005172417-22 27 Meyer A Buhl R Kampf S Magnussen H Intravenous N-acetylcysteine and lung glutathione of patients with pulmonary fibrosis and normals Am J Respir Crit Care Med 19951521055-60 28 Behr J Degenkolb B Krombach F Vogelmeier C Intracellular glutathione and bronchoalveolar cells in fibrosing alveolitis effects of N-acetylcysteine Eur Respir J 200219906-11 29 Bando M Hosono T Mato N et al Long-term efficacy of inhaled N-acetylcysteine in patients with idiopathic pulmonary fibrosis Intern Med 2010492289-96 30 Demedts M Behr J Buhl R et al High-dose acetylcysteine in idiopathic pulmonary fibrosis N Engl J Med 20053532229-42 31 Toma TP Bhowmik A Rajakulasingam R Acetylcysteine in pulmonary fibrosis N Engl J Med 20063541086-9 author reply -9 32 Hunninghake GW Antioxidant therapy for idiopathic pulmonary fibrosis N Engl J Med 20053532285-7 33 Flaherty KR Mumford JA Murray S et al Prognostic implications of physiologic and radiographic changes in idiopathic interstitial pneumonia Am J Respir Crit Care Med 2003168543-8 34 Latsi PI du Bois RM Nicholson AG et al Fibrotic idiopathic interstitial pneumonia the prognostic value of longitudinal functional trends Am J Respir Crit Care Med 2003168531-7 35 Collard HR King TE Jr Bartelson BB Vourlekis JS Schwarz MI Brown KK Changes in clinical and physiologic variables predict survival in idiopathic pulmonary fibrosis Am J Respir Crit Care Med 2003168538-42 36 Jegal Y Kim DS Shim TS et al Physiology is a stronger predictor of survival than pathology in fibrotic interstitial pneumonia Am J Respir Crit Care Med 2005171639-44 37 Martinez FJ Safrin S Weycker D et al The clinical course of patients with idiopathic pulmonary fibrosis Ann Intern Med 2005142963-7 38 Hull JH Acetylcysteine in pulmonary fibrosis N Engl J Med 20063541089-91 author reply -91
70
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
39 Flaherty KR King TE Jr Raghu G et al Idiopathic interstitial pneumonia what is the effect of a multidisciplinary approach to diagnosis Am J Respir Crit Care Med 2004170904shy10 40 Raghu G Johnson WC Lockhart D Mageto Y Treatment of idiopathic pulmonary fibrosis with a new antifibrotic agent pirfenidone results of a prospective open-label Phase II study Am J Respir Crit Care Med 19991591061-9 41 Hunninghake GW Lynch DA Galvin JR et al Radiologic findings are strongly associated with a pathologic diagnosis of usual interstitial pneumonia Chest 20031241215-23 42 Lynch D Godwin J Safrin S et al High-resolution computed tomography in idiopathic pulmonary fibrosis diagnosis and prognosis Am J Respir Crit Care Med 2005172488-93 43 Mallinckrodt CH Watkin JG Molenberghs G Carroll RJ Choice of the primary analysis in longitudinal clinical trials Pharmaceutical Statistics 20043161-9 44 Bang H Tsiatis A Estimating medical costs with censored data Biometrika 200087329shy43 45 Lin DY Regression analysis of incomplete medical cost data Stat Med 2003221181-200 46 Rochon J Application of GEE procedures for sample size calculations in repeated measures experiments Stat Med 1998171643-58 47 Lachin JM Foulkes MA Evaluation of sample size and power for analyses of survival with allowance for nonuniform patient entry losses to follow-up noncompliance and stratification Biometrics 198642507-19
71
- PANTHER-IPFPREDNISONE AZATHIOPRINEAND N-ACETYLCYSTEINEA STUDY THAT EVALUATES RESPONSE INIDIOPATHIC PULMONARY FIBROSIS
-
- Protocol Summary
- Table of Contents
- List of Tables
- List of Figures
- List of Abbreviations
- 1 Summary
- 2 Hypotheses and Specific Aims
-
- 21 Null Hypothesis
- 22 Specific Aim 1
- 23 Specific Aim 2
- 24 Prespecified Subgroups of Interest
-
- 3 Background and Significance
-
- 31 Idiopathic Pulmonary Fibrosis is the Most Common Interstitial Lung Disease
- 32 Rationale for Placebo Control
- 33 Rationale for N-acetylcysteine
- 35 Rationale for N-acetylcysteine as a Stand-alone Therapy
- 36 Rationale for the Study Design and Primary Endpoint
- 37 Rationale for Blinding of Treatments
-
- 4 Methods
-
- 41 Inclusion Criteria
- 42 Diagnosis of IPF
- 43 Exclusion Criteria
- 44 Study Design and Study Visit
- 45 Dose Justification
- 46 Contraindications Precautions and Side Effects of Study Medications
- 47 Recruitment Procedures
- 48 Study Procedures
- 49 Concomitant Medications
- 410 Laboratory Testing
- 411 Blinding of Study Drugs
-
- 5 Study Endpoints
-
- 51 Primary Study Endpoint
- 52 Secondary Study Endpoints
-
- 6 Safety Evaluations and Procedures
-
- 61 Adverse Events
- 62 Clinical Medical Monitoring
- 63 Unblinding Procedures
-
- 7 Study Drug Procedures
- 8 Data Management
-
- 81 Hardware and Software Configuration
- 82 Sources of Data
-
- 9 Study Design and Data Analysis
-
- 91 General Analytic Considerations
- 92 Randomization Blinding and Reporting of Results
- 93 Stratification
- 94 Specification of the Primary Analyses
- 95 Analysis of Longitudinal Endpoints
- 96 Analysis of Binary Time-to-Event and Time-Lagged Endpoints
- 97 Power Analysis
-
- 10 Study Administration
-
- 101 Cooperative Agreement Mechanism
- 102 IPFnet Steering Group
- 103 Data and Safety Monitoring Board
- 104 Recommendations on Interim Monitoring of Efficacy Safety and Futility
-
- 11 Investigator and Sponsor Obligations
-
- 111 Monitoring
- 112 Cost and Payment
- 113 Confidentiality and Health Insurance Portability and Accountability ActConsiderations
- 114 Informed Consent Procedures
- 115 Institutional Review Boards
-
- 12 Investigator Agreement
- 13 References
-

PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
13 Unstable angina pectoris or congestive heart failure requiring hospitalization within 6 months of
screening
14 Uncontrolled arrhythmia
15 Severe uncontrolled hypertension
16 Known HIV or hepatitis C
17 Known cirrhosis and chronic active hepatitis
18 Active substance andor alcohol abuse (as determined by site PI)
19 Pregnancy or lactation (subjects who are pregnant or breastfeeding)
20 Known hypersensitivity to study medication
21 Any condition other than IPF that in the opinion of the site PI is likely to result in the death of the
subject within the next year
22 Any condition that in the judgment of the PI might cause participation in this study to be detrimental to
the subject or that the PI deems makes the subject a poor candidate
23 Any therapy directed at pulmonary fibrosis (excepting triple therapy of prednisone plus azathioprine
plus NAC) requires a 30-day washout period before randomized Triple therapy of lt= 12 weeks duration
in the past 4 years requires a 30-day washout period before randomization
24 History of triple therapy of prednisone plus azathioprine plus NAC for gt 12 weeksrsquo duration in the past
4 years or previous enrollment in the triple-therapy arm of the PANTHER-IPF study
44 Study Design and Study Visit
441 Study Design Summary
This study will be a randomized double-blind PL-controlled trial designed to assess the safety and efficacy of
NAC in subjects with newly diagnosed IPF
Subjects with mild to moderate IPF (defined as FVCpred ge 50 and DLCOpred ge 30) diagnosed within
the past 48 months will be enrolled Screening will continue until April 30 2012
27
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
The study will employ a 2-arm design with 11 randomization to NAC or PL Once enrolled subjects will visit
the clinical center at 15 weeks and 15-week intervals thereafter Each subject will be treated and followed for a
maximum of 60 weeks
During the 60-week visit subjects will be taken off all study agents Approximately four weeks after the final
dose of study agent is taken subjects will receive a safety phone call from the study site
442 Study Visits
Subjects who meet entry criteria will review the informed consent a written description of the purpose
procedures and risks of the study with the PI co-investigator or study coordinator and all questions will be
answered The informed consent form will be signed by the subject at screening No protocol-specific
procedures will be performed until the subject has signed and dated an informed consent form This includes the
screening procedures
4421 Screening
Once informed consent is obtained subjects may immediately begin the screening process or may return within
28 days of consent In the event a study subject has been clinically evaluated at the study site by an IPFnet study
physician and has performed testing within three weeks for this clinical evaluation that meets guidelines
provided in the IPFnet PANTHER-IPF Manual of Operating Procedures (MOOP) this testing may be used to
satisfy the following screening criteria medical history physical exam arterial blood gas (ABG) with A-a
gradient vital signs with oximetry body height and weight spirometry DLCO lung volumes and HRCT scan
Allowing the use of previously performed test results that meet study guidelines for the screening visit is
intended to permit subjects easier access to study entry to prevent subjects from repeating testing that has been
performed within the study window and to decrease risks to subjects from repeated exposure to procedures
such as arterial puncture and HRCT
The following procedures will be performed at screening
Medical history and a physical examination
28
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Measure height and weight
Serum pregnancy test (if applicable)
Measure vital signs including oximetry
Blood draws performed and the following analyses conducted
o Hematology (red cell count white cell count hemoglobin hematocrit cell indices differential
platelet count)
o Blood chemistries according to central laboratory protocol (see Section 410 Laboratory
Testing)
o Beta human chorionic gonadotropin (serum) pregnancy test (in women of childbearing potential)
o Urinalysis
Pulmonary Function Tests (PFTs) including spirometry pre- and post- bronchodilator and postshy
bronchodilator measurement of lung volumes and measurement of hemoglobin adjusted diffusing
capacity
Measure ABGs
HRCT if a satisfactory scan has not been performed on the subject within 3 months of screening (see
PANTHER-IPF MOOP for more details)
Surgical lung biopsies (if applicable) reviewed by local and central pathology departments
Current medications If required a washout period discussed with the subject and initiated at this visit
4422 Enrollment
The enrollment visit is expected to take place within eight weeks of the screening visit Enrollment visit
activities include
Measure vital signs including oximetry
Measure height and weight
Serum pregnancy test (if applicable)
If consent has been given blood will be drawn and a urine specimen collected for the bio-specimen
repository
Spirometry (post-bronchodilator)
Measure 6MWT with Borg Dyspnea Scale
29
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Collect Quality-of-life (QOL) data using the SF-36 EuroQol Investigating Choice Experiments for
Preferences of Older People Capability Instrument (ICE CAP) and SGRQ
Female subjects complete Gender Substudy questionnaire
Dyspnea status collected using the UCSD SOBQ
Evaluate Acute Exacerbation (AEx)
Review of any Adverse Events (AEs)
Review of concomitant medications
Subject receives diary and instructions on its purpose and proper use
Subject receives supply of study drug sufficient to last until his or her 15-week study visit
See the Schedule of Assessments (Table 3) for more details Subjects with screening and enrollment postshy
bronchodilator FVC measurements (in liters) differing by more than 11 are not eligible to be enrolled in the
study
Subjects will be asked to provide a physician of record This physician will be considered the subjectrsquos primary
care provider (PCP) and if the subject agrees the PCP will be informed by letter of the subjectrsquos enrollment in
the trial The subject will be informed that his or her ongoing medical care should be received from the PCP
The PCP will be informed of any safety issues identified by the study staff The PCP will also be given
information regarding communication with study personnel about pertinent health issues or clinic encounters
the subject may have
4423 Week 15
The week 15 visit is expected to occur within +- 14 days of the subjectrsquos scheduled visit time (eg the week 15
visit should occur anytime between 13 and 17 weeks after starting study drug Week 15 activities include
Measure vital signs with oximetry
Measurement height and weight
Serum pregnancy test (if applicable)
Spirometry (post-bronchodilator) measurement
Review of AEs
Evaluate for AEx
30
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Review concomitant medications
If consented draw blood and collect urine specimen for the biospecimen repository
Subjects return used and unused study drug for the visit
Review study diary and a new study diary will be given
Provide additional supply of study drug sufficient to last until the next scheduled visit
4424 Week 30
The week 30 visit is expected to occur within +- 14 days of the subjectrsquos scheduled visit time (eg the week 30
visit should occur anytime between 28 and 32 weeks after starting study drug) Week 30 activities include
Physical examination
Measure vital signs with oximetry
Measure height and weight
Laboratory values (complete blood count [CBC] and serum chemistries)
Serum pregnancy test (if applicable)
Measure spirometry (post-bronchodilator)
6MWT with Borg scale
DLCO
Review of AEs
Evaluate for AEx
Review concomitant medications
Complete all QOL and dyspnea questionnaires (EuroQol ICE CAP SF-36 SGRQ and UCSD SOBQ)
If consent has been given blood will be drawn and a urine specimen collected for the biospecimen
repository
Review study diary
Subjects return used and unused study drug for the visit
Provide additional supply of study drug sufficient to last until the next scheduled visit
4425 Week 45
31
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
The week 45 visit is expected to occur within +- 14 days of the subjectrsquos scheduled visit time (eg the week 45
visit should occur anytime between 43 and 47 weeks after starting study drug) Week 45 activities include
Measure vital signs with oximetry
Measure height and weight
Serum pregnancy test (if applicable)
Measure spirometry (post-bronchodilator)
Review of AEs
Evaluate for AEx
Review concomitant medications
If consent has been given blood will be drawn and a urine specimen collected for the biospecimen
repository
Subjects return used and unused study drug for the visit
Study diary reviewed
Provide additional supply of study drug sufficient to last until the next scheduled visit
4426 Week 60 (Early Withdrawal or Final Treatment Visit)
At week 60 or at subject withdrawal from the study (premature by study doctor or subjectrsquos decision) a final
treatment visit will occur At this final treatment visit subjects will discontinue NACPL abruptly Week 60
activities also include
Physical examination
Measure vital signs with oximetry
Measure height and weight
Laboratory values (complete blood count [CBC] and serum chemistries)
Spirometry (post-bronchodilator) measurement
6MWT with Borg scale measurement
DLCO
Lung volumes
ABG
Review of AEs
32
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Evaluate for AEx
Review concomitant medications
Subjects will complete all QOL and dyspnea questionnaires (EuroQol ICE CAP SF-36 SGRQ and
UCSD SOBQ)
If consent has been given blood will be drawn and a urine specimen collected for the biospecimen
repository
Subjects return used and unused study drug for the visit
Study diary reviewed
4427 Final Site Visit ndash FVC drop confirmation
In the event that the subject has a recorded FVC drop of gt10 from baseline at the final treatment visit and the
subject has not had a confirmation of such a drop at a previous study visit the subject should return to the
clinical site 6 to 8 weeks after the final treatment visit During this visit a post-bronchodilator spirometry test
will be performed This FVC measurement will be evaluated according to section 521 of this protocol
4428 Final Visit ndash Telephone Follow-up
Four weeks following the final dose of study medication subjects will receive a telephone call from the study
coordinator to ensure that there are no side effects and to follow up on any ongoing adverse events (AEs)
4429 Phone Contact Between Visits
At week 2 and each month that a subject does not have a scheduled clinical center visit his or her study
coordinator will contact him or her at least once by telephone to
Inquire if the subject has had any hospitalizations events that might be considered an AE or any events
significant enough to warrant an out-of-cycle visit to the clinical center
Remind subjects of their current dosage levels and confirm that the subject understands them
Address any questions or concerns the subject might have regarding other aspects of the study
Assess adherence to the treatment regimen by reviewing diary data verbal review of medications taken
including nutritional supplements
33
34
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Table 3 Schedule of Assessments
Procedure Screening Visit 0
Enrollment Visit 1
Week 15 Visit 2
Week 30Visit 3
Week 45 Visit 4
Week 60 Early
Withdrawal Visit 5
Final1
Visit (via phone)
Informed consent X
Medical history X
Inclusionexclusion criteria X
Serum pregnancy test (if applicable) X X X X X
Review of lung biopsy X
Arterial Blood Gas X X
6-Minute Walk Test
X
X X
Physical examination X X X
Vital signs with oximetry X X X X X X
Body height and weight X X X X X X
Complete Blood Count X X X
Chemistry panel X X X
Monitor Lab Values X X X
Urinalysis X Specimen repository substudy blood draw and urine collection (if consented)
X
X X X X
HRCT (if not completed within three months) X
Spirometry (pre- and post-bronchodilator) X
Spirometry (post-bronchodilator only) X X X X X
DLCO (post-bronchodilator only) X X X
Lung volumes (post-bronchodilator only) X
X
Evaluate for acute exacerbation X X X X X
Review Adverse Events X X X X X X
Review concomitant meds X X X X X X
Dispense subject diary X X X X
Review subject diary X X X X X
Dispense study agent X X X X
Gender Substudy questionnaire (female subjects only) X
EuroQol ICECAP UCSD SOBQ SGRQ SF-36 X X X
Abbreviations DLCO diffusing capacity of the lung for carbon monoxide QOL Quality of Life ICECAP Investigating Choice Experiments for Preferences of Older People UCSD SOBQ University of California Shortness of Breath Questionnaire SGRQ St Georgersquos Respiratory Questionnaire SF-36 Short Form 36 Health Survey
1Follow-up visit via phone will occur four weeks after final dose of study medication
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
45 Dose Justification
The general philosophy for determining dosing levels was to apply previously examined
treatment regimens With the focus of the study being to establish a standard of care for
mildmoderate IPF subjects the goal was to develop flexible yet standardized treatment rules that
allow for the temporary or permanent withholding of one or more components of treatment when
necessary Subjects developing laboratory abnormalities or symptoms that result in
discontinuation of one or more components of study treatment may continue on the other
components as long as there is no contraindication for this Complete follow-up is important for
the validity of any study As a strategy to maintain protocol adherence we are using a treatment
regimen that will detect potential side effects and prompt interventions proactively in the interest
of patient safety In addition subjects who permanently stop study medications during the course
of the study are encouraged to continue in the study completing all scheduled visits and tests
451 Rationale for N-acetylcysteine Dosing
To our knowledge there have been no IPF studies to correlate clinical outcome measures with
different dosages for NAC The dosage chosen is based on the IFIGENIA study However BAL
lung GSH levels from subjects with IPF have been augmented with the use of oral NAC at 600
mg 3 times per day In addition lung GSH levels have been associated with improved
PFTs212227 The dose chosen for this study was based on previous data including the IFIGENIA
study30
4511 Dosing of N-acetylcysteineplacebo
Dosing of NACPL will be 600 mg orally 3 times a day (1800 mgday)
4512 Reasons to Discontinue N-acetylcysteineplacebo
NACPL may be temporarily or permanently discontinued for the duration of the study for
gastrointestinal symptoms or dermatologic reactions
35
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Temporarily discontinue (hold) oral NACPL for subjects requiring inpatient admission for acute
exacerbation (AEx) or other conditions Resume NACPL after discharge
36
37
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
452 Dosage Algorithms
Dosage Adjustment Algorithm 1 NACPL Dose Modifications for Gastrointestinal Symptoms Nausea Vomiting Abdominal Discomfort Diarrhea
GI Symptoms determined by the PI to be clinically significant Nausea Vomiting Abdominal Discomfort Diarrhea
NACPL Temporarily dc (HOLD) x 3 Days
Monitor symptoms intervene as clinically indicated (eg fluid replacement antidiarrhea or antinausea medication)
Monitor or lab PRN
Are symptoms resolving after 3 days NO
Symptoms NOT resolving after 3 days of holding study medication Assessmentmanagement per clinical
discretion of investigator
Likely not study medication discuss resuming study medication with medical monitor when symptoms resolved
YES
Temporarily dc (HOLD) NACPL for 4 additional days (total hold 1 week) then NACPL Resume 600 MG TID
Did symptoms recur
YES
STOP NACPL for
duration of study
NO
NACPL No Change
38
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Dosage Adjustment Algorithm 2 NACPL Dose Modifications For Dermatologic Reactions
Dermatologic Reactions (Not Acneiform) ge Grade 2 Grading per Common Terminology Criteria for
Adverse Events V30 (httpctepcancergov) For example Grade 1 RASHDESQUAMATION Macular or papular eruption or erythema without associated symptoms Grade 2 RASHDESQUAMATION Macular or popular eruption or erythema with pruritus or other associated symptoms localized desquamation or other lesions covering lt50 of body surface area
NACPL Temporarily dc (HOLD) x 3 days
Are symptoms resolving after 3 days
NO Symptoms not resolving after 3 days of holding study medication Assessmentmanagement per clinical discretion of investigator Likely not study medication Discuss resuming study medication with medical monitor when symptoms
resolved YES
Temporarily dc (HOLD) NACPL for 4 additional days (total hold 1 week) then NACPL resume 600 MG TID
Did symptoms recur
YES
STOP NACPL for
duration of study
NO
NACPL No change
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
46 Contraindications Precautions and Side Effects of Study Medications
461 Contraindication
Contraindication to NAC is known hypersensitivity to it
462 Precautions
Concomitant administration of oral NAC and antibiotics has shown a slightly reduced absorption
of cephalexin and a slight increase in erythromycin serum levels NAC contains free sulfhydryl
groups There is no evidence that individuals sensitive to sulfa drugs are sensitive to NAC
The NAC preparation being administered in this study contains 20 mg of aspartame Because of
the phenylalanine component of aspartame individuals with phenylketonuria should avoid or
restrict aspartame intake to avoid increased blood levels of phenylalanine Because of this risk
labeling is required on all products containing aspartame
463 Side Effects
Side effects of NAC range from common to serious See Table 4
39
40
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Table 4 Side Effects of NAC
Undesirable Effects
System-organ class Uncommon
(gt11000 lt1100)
Rare
(gt110000 lt11000)
Very rare
(lt110000) Not known
Immune system disorders Hypersensitivity Anaphylactic shock
reaction
Nervous system disorders Headache
Ear and labyrinth disorders Tinnitus
Cardiac disorders Tachycardia
Vascular disorders Hemorrhage
Respiratory thoracic and
mediastinal disorders
Bronchospasm
Dyspnea
Gastrointestinal disorders
Vomiting diarrhea
stomatitis abdominal
pain nausea
Dyspepsia
Skin and subcutaneous tissue
disorders
Urticaria rash
angioedema itching
General disorders and
administration site conditions Pyrexia
Investigations Reduced arterial
pressure Face edema
In very rare cases the onset of severe skin reactions such as Stevens-Johnson syndrome and Lyell syndrome was reported to have a temporal relationship with N-acetylcysteine administration Although in most cases at least another suspect drug probably most involved in the genesis of the above mentioned mucocutaneous syndromes has been identified in case of mucocutaneous alterations it is appropriate to contact onersquos doctor and the administration of N-acetylcysteine should be immediately discontinued
Some studies confirmed a reduction of platelet aggregation during N-acetylcysteine administration The clinical significance of these findings has not been defined yet [Source Fluimucil Investigator Brochure]
47 Recruitment Procedures
Subjects recruited for this study will be established patients of the investigators or physician- or
self-referred to participating clinical centers in the IPFnet Each clinical center within IPFnet has
a well-developed infrastructure of local pulmonologists within the surrounding geographic area
These pulmonologists are kept informed of ongoing IPF clinical trials and regularly refer
subjects to studies conducted at IPFnet clinical centers
Additional steps will be taken to inform clinicians of the trials in progress within IPFnet
including presentations at faculty staff meetings at local hospitals medical grand rounds and
national conferences direct mail notification monthly faxes and advertisement of network trials
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
in pulmonary journals Clinical center patients previously diagnosed with IPF will be notified of
the trials by mail whenever possible
Recruitment of minorities and women will be monitored by the DCC and DSMB If necessary
additional recruitment efforts will be made at specific centers to ensure that the aggregate subject
sample contains appropriate representation of women and minorities
48 Study Procedures
The following procedures are detailed in the PANTHER-IPF MOOP accompanying this
protocol
1 PFT
2 ABG
3 HRCT scan of the chest (including imaging of pulmonary arteries)
4 CBC and serum chemistries
5 Pregnancy test
6 6MWTBorg Dyspnea Scale
7 QOL questionnaires (EuroQol HAD SF-36 SGRQ and ICE CAP)
8 UCSD SOBQ
9 Gender Substudy Questionnaire
All assessments of PFTs will be conducted by study personnel not directly involved in the
treatment of the subjects
481 Biological Specimen Management
4811 Biological Specimen Sample Management
Subjects at clinical centers participating in the specimen repository substudy who consent to
having blood drawn for research purposes and for the banking of blood blood components and
other biologic specimens (urine and BAL fluid) will have approximately 405 mL of blood
41
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
drawn 17 mL blood drawn for DNA and 20 mL of urine collected at enrollment visit Subjects
will have approximately 50 mL of blood drawn and 20 mL of urine collected at each 15-week
follow-up visit Blood specimens will be separated according to PANTHER-IPF MOOP
guidelines into the following components for banking in the repository serum plasma and
DNA Coding of all biologic specimens for the repository will be performed by study staff at the
clinical center The samples will be processed per PANTHER-IPF MOOP guidelines aliquoted
labeled with barcode labels and stored at -70degC at the clinical center and shipped to the central
repository
The only subject identifiers will be a sample ID number and subject initials This sample ID will
be linked in the IPFnet DCC clinical database to subject information No subject information will
be transferred to the biological-specimen database
The subjectrsquos samples may be used for approved sub-studies relating to human disease
including but not limited to IPF The studies for which an individualrsquos samples will be made
available will be determined by the subjectrsquos answers to questions on the biological-sample
informed consent form The subjects can choose to make their samples available for all options
or any combination Samples will be made available to researchers only with IPFnet Steering
Group approval until such time as the samples are made public through the NHLBI repository
49 Concomitant Medications
Concurrent treatment with FDA-approved therapy for IPF is allowed Colchicine may be used
for treatment of gout Temporary treatment with oral or IV corticosteroids for clinical worsening
or suspected AEx is permitted Nutritional supplements containing NAC are not allowed
410 Laboratory Testing
Clinical laboratory parameters will be assessed at screening and at the end of the study The
following tests will be performed at the two time points specified in the protocol chemistry (AG
ratio ALT [SGPT] AST [SGOT] albumin alkaline phosphatase amylase bilirubin-direct
42
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
bilirubin-indirect bilirubin-total BUN BUNcreatinine ratio calcium carbon dioxide
cholesterol-total chloride CPK-total creatinine GGT globulin glucose iron-total LDH
lipase magnesium phosphorus-inorganic potassium protein-total sodium TIBC triglycerides
uric acid) and hematology (red blood cell count WBC count hemoglobin hematocrit cell
indices differential platelet count)
411 Blinding of Study Drugs
Subjects and caregivers will be blinded to study treatment Every subject will receive NAC or
matching PLs at every study visit from the baseline visit to the week-45 visit No study agent
will be dispensed at the week-60 visit
43
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
5 Study Endpoints
51 Primary Study Endpoint
The primary endpoint will be the change in serial measurements of FVC over the study period
52 Secondary Study Endpoints
521 Time to Disease-progression
The time-to-death or a 10 decline in FVC will be defined as the time-to-disease progression
The 10 decline in FVC from enrollment must be confirmed on 2 consecutive visits no less than
6 weeks apart For subjects with 2 consecutive visits with a 10 decline in FVC the time-toshy
disease progression will be defined as the time interval between enrollment and the initial visit
with a 10 FVC decline For subjects who experience disease progression the study doctor will
determine whether or not the subject will remain in the study
522 Acute Exacerbations
The following 3 criteria will define AEx in subjects with acute worsening of their respiratory
conditions
1 Clinical (all of the following required)
A) Unexplained worsening of dyspnea or cough within 30 days triggering unscheduled
medical care (eg emergency room clinic study visit hospitalization)
B) No clinical suspicion or overt evidence of cardiac event pulmonary embolism or deep
venous thrombosis to explain acute worsening of dyspnea
C) No pneumothorax
44
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
2 RadiologicPhysiologic (A and B required)
A) New ground glass opacity or consolidation computed tomography (CT) scan OR new
alveolar opacities on chest x-ray
B) Decline of ge 5 in resting room air SpO2 from last recorded level OR decline of ge 8 mm
Hg in resting room air PaO2 from last recorded level
3 Microbiologic (all of the following required)
A) No clinical evidence for infection (ie absence of grossly purulent sputum fever gt 39degC
orally)
B) Lack of positive microbiological results (if done) from lower respiratory tract defined as
(1) Clinically significant bacterial growth on sputum or endotracheal aspirate cultures
(2) Quantitative culture by protected brush specimen ge 103 cfumL or BAL ge 104 cfumL
(3) The presence of specific pathogens on stains of any of the above
C) Lack of positive pathogen in blood cultures (if done)
Identification of Acute Exacerbations
All subjects will be educated about the importance of identifying AExs At the time of
enrollment subjects will be told about the possibility of developing acute symptomatic
worsening that might represent an AEx of IPF and instructed to contact their study clinical
center coordinator within 48 to 72 hours of the apparent event
All subjects will be contacted by phone monthly and questioned about any change in dyspnea or
cough and any interim clinic visits or hospitalizations Finally as part of the IPFnet outreach to
community referring physicians the importance of AExs will be emphasized When a subject is
identified who meets criterion 1A this will trigger the collection of additional clinical data to
evaluate a suspected AEx These data will be collected as part of standard clinical care (ie this
protocol does not require collection of all items) The additional items to be collected for
suspected AEx include
IPFnet AEx case report form (eCRF) (required)
45
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Chest x-ray CT scan withwithout pulmonary angiogram (reports should be faxed and
followed by the hard copiesdiscs)
Oxygen saturation (pulse oximetry)
ABG
Respiratory cultures (sputum endotracheal aspirate lavage)
Blood cultures
Clinichospital records related to the event
All potential cases of AEx will be reviewed by the clinical center PI first and a decision on
whether the case may represent an AEx will be made If AEx is suspected the case will be sent
to the IPFnet adjudication committee which will assign a final diagnosis (see Table 5) If there is
disagreement among members the majority opinion will be recorded
During episodes of suspected AEx as determined by the individual clinical center investigator
subjects will remain blinded and in the study
Table 5 Final Diagnoses in Evaluation of Suspected Acute Exacerbations
Definite acute exacerbation All criteria met no alternative etiology
Unclassifiable acute worsening
Insufficient data to evaluate all criteria no alternative etiology
Not acute exacerbation Alternative etiology identified that explains acute worsening
Management of the suspected AEx will be at the discretion of the treating physician Standard of
care generally involves evaluation for respiratory infection pulmonary embolism cardiac events
and pneumothorax and treatment with IV corticosteroids
Study drugs will be resumed at pre-suspected AEx doses after subjects clinically improve as
confirmed by the local PI All subjects should be seen at the clinical center within 2 to 4 weeks
of recovery for measurement of post-bronchodilator FVC (see Figure 4) Subjects unable to
return to the clinical center after suspected AEx due to medical frailty (eg continued
46
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
institutionalization progressive disability) will be categorized as failing to maintain FVC
response in secondary analyses
Suspected AEx (PI determined)
Hold study drug Treat AEx
(Attending physician determined)
Alive but unable to continue due to
medical frailty
Dead
Alive and able to continue
Site reviewvisit
Restart study drug
FVC within 2-4 weeks
Figure 4 Acute Exacerbation Flow Chart
523 Respiratory Infections
An upper respiratory infection will be defined as
Change in sputum discoloration
Increased cough of no more than 14 daysrsquo duration
A lower-respiratory infection (pneumonia) will be defined as new segmental or lobar airspace
opacities visualized by image studies (chest radiograph or HRCT) in addition to any of the
following
Positive pathogencultures in good sample of sputum or lower-airway secretions retrieved
by fiberoptic bronchoscope
Fever gt 39degC or gt 100degF
Leukocytosis gt 12000 (unexplained no increase in dose of corticosteroids)
47
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
524 Maintained FVC Response
Subjects with follow-up FVCpred measurements at or above their baseline FVCpred level
will be classified as having maintained FVC response Subjects with reduced FVCpred levels
or missing data for any reason including death or medical frailty will be classified as having not
maintained FVC response The FVCpred value is used because unadjusted FVC measurements
are expected to decline with age
48
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
6 Safety Evaluations and Procedures
61 Adverse Events
During a clinical trial the reporting of adverse experience information can lead to important
changes in the way a new treatment is developed as well as provide integral safety data
611 Definitions
An adverse event (AE) is any untoward medical occurrence in a subject or clinical investigation
subject who was administered a pharmaceutical product The AE does not necessarily have to
have a causal relationship with the drug administered An AE can be any unfavorable and
unintended sign (including an abnormal laboratory finding) symptom or disease temporarily
associated with the use of a medicinal product whether or not considered to be related to the
medicinal product Diseases signs symptoms or laboratory abnormalities already existing at
enrollment are not considered AEs unless they worsen (ie increase in intensity or frequency)
Surgical procedures themselves are not AEs they are therapeutic measures for conditions that
require surgery The condition for which the surgery is required may be an AE Surgical
procedures planned before randomization and the conditions necessitating the surgery are not
AEs
A serious adverse event is any untoward event that
Is fatal
Is life-threatening
Requires inpatient hospitalization or prolongation of existing hospitalization with the
following exceptions
o Preplanned (before the study) hospital admissions unless the hospitalization is
prolonged
o Planned admissions (as part of a study eg routine biopsies)
o Hospitalization lasting lt 24 hours
49
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
o Hospitalization for elective procedure
o Emergency room visits
Results in persistent or significant disability or incapacity
Is a congenital anomaly or birth defect
Important medical events that may not result in death be life-threatening or require
inpatient hospitalization may be considered serious adverse events (SAEs) when based
on appropriate medical judgment they may jeopardize the subject and may require
medical or surgical intervention to prevent one of the outcomes listed above
Life-threatening means that the subject was in the view of the investigator at immediate risk of
death from the AE as it occurred It does not include an AE that had it occurred in a more severe
form might have caused death
Persistent or significant disabilityincapacity means that the event resulted in permanent or
significant and substantial disruption of the subjectrsquos ability to carry out normal life functions
Causality
A reasonable possibility means the AE may have been caused byrelated to the study drug A
perceived or real lack of efficacy does not satisfy the definition of relatedness
612 Adverse Event (AE) Reporting
For the PANTHER-IPF trial all AEs (serious and nonserious) occurring from randomization
through final study visit (4 weeks after final dose of all study medication) will be recorded on the
AE page of the case report form (CRF)
6121 Serious Adverse Events (SAE) Reporting
For this trial all deaths and all SAEs which occur from randomization through final study visit
must be entered within the EDC system via the SAE eCRF page within 24 hours of the
investigative sitersquos knowledge of the event It is the responsibility of the clinical center
50
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
investigator to provide a causality assessment of the event for each study medications based upon
the information available at the time of the report It is understood that complete information
about the event may not be known at the time the initial report is submitted In the event the EDC
system is not accessible to the site at the time of event reporting investigative sites will complete
and forward a paper back-up SAE form to DCRI Safety Surveillance for processing
DCRI Safety Surveillance
Telephone 1-919-668-8624 or 1-866-668-7799 (toll free)
Fax 1-919-668-7138 or 1-866-668-7138 (toll free)
The investigator must complete and submit follow-up SAE information via the eCRF when
important new or follow-up information (eg final diagnosis outcome results of specific
investigations) becomes available Follow-up information should be submitted according to the
same process used for reporting the initial event as described above All SAEs will be followed
until resolution stabilization or 30 days after the subject has completed the final visit (4 weeks
after the final dose of study medication) whichever occurs first The investigator is responsible
for reporting SAEs to their institutional review board (IRB) per site specific IRB reporting
guidelines
6122 Regulatory Reporting
AEs that are serious study drug related and unexpected will be reported to the regulatory
authorities The DCRI Safety Surveillance medical monitor will perform a medical review of all
SAEs submitted and evaluate for ldquounexpectednessrdquo DCRI Safety Surveillance will prepare
MedWatch reports for those events identified as serious study drug related and unexpected as
determined by Safety Medical Monitor
DCRI Regulatory Services will submit all unexpected study drug-related SAEs as per 21 CFR
32 DCRI Safety Surveillance will provide a safety alert letter to the NHLBI DSMB and DCC
clinical operation (for distribution to sites) within 15 days of initial receipt of the information
51
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Investigators are responsible for promptly reporting these events to their reviewing IRBs
according to site specific IRB reporting guidelines
62 Clinical Medical Monitoring
There will be an unblinded physician at the IPFnet DCC serving as medical monitor The
medical monitor will be available to assist with questions about dosage adjustments of study
medications including discontinuation or resumption of medications
63 Unblinding Procedures
Unblinding of subjects or investigators to subject treatment is strongly discouraged For ongoing
clinical management all subjects should be presumed to be receiving ldquoactiverdquo study drug To
ensure the subjectrsquos safety the study treatment will be dose-adjusted based on laboratory test
results clinical findings and symptoms
The IPFnet DCC medical monitor and PANTHER-IPF co-chairs Drs Ganesh Raghu and
Fernando Martinez will be available to the study physicians to discuss study drug management
on a case-by-case basis Un-blinding will be considered ONLY when the knowledge of subject
treatment assignment is ABSOLUTELY ESSENTIAL for subject safety and after discussion of
the subjectrsquos case with the medical monitor and either Dr Raghu or Dr Martinez Unblinding of
study treatment should be minimized during the conduct of the trial In those cases where it is
felt to be medically necessary the DCC medical officer will communicate directly with the
managing physician to minimize unblinding of study personnel
52
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
7 Study Drug Procedures
At the baseline 15-week 30-week and 45-week study visits subjects will receive a supply of
study drug sufficient to last until the next visit at which study drug will be dispensed
53
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
8 Data Management
81 Hardware and Software Configuration
811 Hardware and Database Software
Data will be stored in an Oracle database system Oracle has advantages of processing efficiency
and smooth linkage with other software systems The application and database will be hosted on
Solaris Unix servers at the IPFnet DCC
812 Statistical Software
SAS will be used as the principal application for the management of analysis data files and
statistical computations S-Plus will be used to provide supplementary functions as needed
813 Access Control and Confidentiality Procedures
Access to databases will be controlled centrally by the IPFnet DCC through user passwords
linked to appropriate privileges This protects the data from unauthorized changes and
inadvertent loss or damage
814 Security
Database and Web servers will be secured by a firewall and through controlled physical access
Oracle has many security features to ensure that any staff member accessing the database has the
proper authority to perform the functions he or she requests of the system Within the secondary
SAS databases Unix group-access control maintains similar security The Sun workstation login
is secured by extensive user-password facilities under Unix
54
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
815 Back-up Procedures
Database back-up will be performed automatically every day and standard IPFnet DCC policies
and procedures will be applied to dictate tape rotation and retention practices
816 Virus Protection
All disk drives that provide network services and all user computers will be protected using
virus-scanning software Standard IPFnet DCC policies will be applied to update these protection
systems periodically through the study
82 Sources of Data
821 Design and Development
The IPFnet DCC will be responsible for development of the electronic case report forms
(eCRFs) development and validation of the clinical study database ensuring data integrity and
training clinical center staff on applicable data management procedures A web-based distributed
data entry model will be implemented This system will be developed to ensure that guidelines
and regulations surrounding the use of computerized systems used in clinical trials are upheld
The remainder of this section provides an overview of the data management plan associated with
this protocol
822 Data Collection Forms
The data collection process consists of direct data entry at the study clinical centers into the EDC
system(s) provided by the DCC A data collection worksheet will be provided to clinical centers
for recording data in the event the EDC system is unavailable Data entry of the eCRFs should
be completed according to the instructions provided and project specific training The
investigator is responsible for maintaining accurate complete and up-to-date records and for
ensuring the completion of the eCRFs for each research participant
55
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
823 Data Acquisition and Entry
Data entry into eCRFs shall be performed by authorized individuals Selected eCRFs may also
require the investigatorrsquos written signature or electronic signature as appropriate Electronic
CRFs will be monitored for completeness accuracy and attention to detail during the study
824 Data Center Responsibilities
The IPFnet DCC will 1) develop a data management plan and will conduct data management
activities 2) provide final eCRFs for the collection of all data required by the study 3) develop
data dictionaries for each eCRF that will comprehensively define each data element 4) conduct
ongoing data monitoring activities on study data 5) monitor any preliminary analysis data
cleanup activities and 6) rigorously monitor final study data clean up
825 Data Editing
Completed data will be entered into the IPFnet DCC automated data acquisition and
management system If incomplete or inaccurate data are found a data clarification request will
be generated and distributed to clinical centers for a response Clinical centers will resolve data
inconsistencies and errors and enter all corrections and changes into the IPFnet DCC automated
data acquisition and management system
826 Training
The training plan for clinical center staff includes provisions for training on assessments eCRF
completion guidelines data management procedures and the use of computerized systems
56
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
9 Study Design and Data Analysis
91 General Analytic Considerations
All primary analyses will be based on intent-to-treat (ITT) principles using all randomized
subjects Baseline factors across groups will be compared using mean (standard deviation) and
median (25th and 75th percentiles) summary measures Kaplan-Meier curves will be used to
display event rates Due to clinical interest in departures from both sides of the null hypothesis
all test statistics will be 2-sided
Reasonable caution needs to be taken when conducting multiple analyses on key clinical
subgroups For subgroup analyses a conservative significance level of 0001 will be used for all
interaction tests Thus subgroup comparisons will be considered exploratory unless the p-value
from the interaction test is smaller than 0001
92 Randomization Blinding and Reporting of Results
A permuted block-randomization scheme will be created with varying block sizes stratified by
clinical center Once a subject has completed the screening and baseline period and evaluation
for inclusionexclusion criteria the randomization process will begin Subjects will be
randomized to receive NAC or matching placebo with equal probability (11) via telephone
contact with a central interactive voice response system (IVRS) using a toll-free randomization
number On the day of randomization after the subject has successfully met all inclusion and
exclusion criteria the investigator or designee will call the central randomization number to
obtain the assigned kit randomization numbers for that subject At each subject visit the
investigator or designee will call the central randomization number to obtain the new kit
randomization numbers for resupply of the subject For resupply of the clinical center the IVRS
will monitor minimal volume of a kit type andor expiration date and will automatically notify
the pharmacy
57
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
The trial results will be reported according to guidelines specified in the CONSORT statement
A flow diagram describing screening recruitment randomization dropout and vital status will
be included in the primary manuscript AEs and efficacy data will be presented for all treatment
groups Adherence dropout and lost to follow-up will be carefully examined across all treatment
groups Analyses of safety will be based on data from all randomized subjects who received at
least one dose of study drug
93 Stratification
Subjects will be distributed to the two treatment arms in a 11 allocation ratio Stratification
blocks will be based on clinical centers
94 Specification of the Primary Analyses
A mixed model repeated measures (MMRM) analysis described in section 95 will be used to
compare differences in the slope of FVC measurements across the treatment groups Response
variables are values of the FVC measured at baseline and every 15 weeks until study completion
Variables in the model will include treatment time and time by treatment age sex race and
height Contrast estimates of differences in slopes of treatment over time (along with confidence
intervals) will be used to estimate the treatment effect The validity of this model in terms of
meeting modeling assumptions will be assessed via standard modeling diagnostics and goodness-
of-fit measures Based on the MMRM framework missing FVC data will not be imputed for the
primary analysis
95 Analysis of Longitudinal Endpoints
A common goal in clinical trials is to specify models that are easily implemented and
reproducible by independent data analysts On the other hand the models should have proper
statistical behavior in terms of low bias and high precision Many common approaches to
longitudinal data analysis including last observation carried forward (LOCF) imputation rely on
the missing completely at random (MCAR) assumption However the MCAR assumption is
58
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
unlikely to hold in many clinical trials because missing data are often related to disease
progression and prognosis A more reasonable assumption missing at random (MAR) specifies
that the complete data distribution can be modeled using only the observed data The likelihood-
based MMRM approach is valid under the more general MAR assumptions These models will
be applied to analyze the longitudinal data secondary endpoints
The advantages of MMRM analysis are that all important characteristics of the model can be preshy
specified standard software can be used to implement the models and results are based on ITT
principles43 In addition the MMRM approach offers superior control of Type I and Type II
errors compared with the LOCF approach
Response variables are values of the PFTs measured at enrollment and every 15 weeks until
study completion and 6MWT values measured at baseline week 30 and week 60 Covariates are
treatment time time by treatment and key baseline risk factors Contrasts (along with
confidence intervals) of treatment by time will be used to estimate the treatment effect
The correlation structure involves multiple pieces including measurement errors random
variation and interindividual variability For the longitudinal data analyses an unstructured
correlation matrix for within-subject errors will be assumed Other correlation structures
including compound symmetry will be examined as needed A careful examination of reasons
for study discontinuation will be conducted to assess the validity of MCAR Sensitivity analyses
will be used to examine the untestable assumption that the observed data violate the MAR
assumption The MMRM models will be implemented using PROC MIXED in SAS
96 Analysis of Binary Time-to-Event and Time-Lagged Endpoints
Regression modeling approaches using either the logistic regression model or Cox proportional
hazards regression model will be employed when appropriate The validity of these models will
be assessed via standard modeling diagnostics and goodness-of-fit measures Estimates of
cumulative frequencies for more general time-lagged responses will be calculated using the
partitioned version of the Bang-Tsiatis estimator44 The partitions will be set at 15-week intervals
59
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
to correspond with the data-collection process Covariate adjusted event rates will be calculated
using inverse probability-weighted regression estimates45
97 Power Analysis
971 Primary Analyses
Based on previously published IPF clinical trials the PL group is expected to experience a drop
in FVC of approximately 020 L over the study period (see Figure 1) The IPFnet Steering Group
determined a clinically important difference would be to preserve the majority of the decline
relative to PL over the study period In particular a treatment effect of 015 L was determined to
be a clinically meaningful difference Potential dropout is a key factor in the proposed study The
drop-out process assumed 5 lost to follow-up after every study visit Only 80 of subjects
were assumed to be followed for the entire study period All models assumed a compound
symmetry structure for the covariance matrix Power calculations were performed using a SAS
IML program for designing repeated measures studies46 Based on preliminary reviews of the
data from the University of Michigan the covariance matrix parameters were estimated at
approximately σ2 = 0757 (variance parameter) and ρ = 0936 (correlation parameter) To be
conservative the power calculations for the primary analysis were performed with parameter
setting of σ2 = 0810 (variance parameter) and ρ = 0925 (correlation parameter)
The power calculations assume a correction for imperfect compliance proposed by Lachin and
Foulkes to allow for 2 noncompliance for each of the treatment arms47 Thus the sample size
of 130 subjects per arm would be reduced to an adjusted sample size of 130(1-002-002)2 =
1198 or 120 subjects per arm
Under the assumed Type I error rate of 005 with a correlation parameter of 0925 and standard
deviation of 090 the difference of 015 L (or 00025 Lweek) shown in Table 6 would have
power of 93
60
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Table 6 Hypothetical Values of Mean FVC (L) Change from Baseline
Week 15 Week 30 Week 45 Week 60
NAC 00125 00250 00375 00500
Placebo 00500 01000 01500 02000
Difference 00375 00750 01125 01500
Abbreviations FVC forced vital capacity PL placebo
972 Power Analysis for Secondary Endpoints
Power calculations for secondary endpoint measurements are shown in Table 7 Standard
deviations are based on unpublished data provided by the University of Michigan The
calculations are based on a 2-sample t-test with Type I error rate set at 005 These calculations
are likely to be conservative because the statistical approach described in section 95 for
analyzing these endpoints will incorporate incomplete observations as well as intermediate data
points
Table 7 Detectable Differences in Treatment Means for Selected Endpoint Measurements
Secondary Endpoints Std Dev
of the Baseline Score
Detectable Difference for 80 Power
Std Dev of the Change Score
Difference Detectable for
80 Power
DLCOpred 166 58 91 32
6MWT Area Under the Desaturation Curve
219 76 175 61
6MWT Distance to Desaturation 224 78 315 110
6MWT Minutes Walked 210 073 205 071
Abbreviations Std Dev standard deviation DLCOpred diffusing capacity of the lung for carbon monoxide percent predicted 6MWT 6-minute walk test
61
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
10 Study Administration
101 Cooperative Agreement Mechanism
The administrative and funding mechanism used to undertake this project is a ldquocooperative
agreementrdquo (U01) which is an assistance mechanism Under the cooperative agreement the
NHLBI assists supports andor stimulates the project and is substantially involved with
investigators in conducting the study by facilitating performance of the effort in a ldquopartnerrdquo role
The NHLBI project scientist serves on the IPFnet Steering Group and he or another NHLBI
scientist may serve on other project committees when appropriate At the same time however
NHLBI does not assume a dominant role direction or prime responsibility for this research
program
As described below governance of the project is conducted through the IPFnet Steering Group
Principal investigators have lead responsibilities in all aspects of their trials and the project
including any modification of trial designs conduct of the trials quality control data analysis
and interpretation preparation of publications and collaboration with other investigators unless
otherwise provided for by the IPFnet Steering Group
PIs retain custody of and have primary rights to their center-specific and collaborative data
subject to government rights-of-access consistent with current Health amp Human Services (HHS)
Public Health Service (PHS) and National Institutes of Health policies The protocols and
governance policies call for the continual submission of data centrally to the IPFnet DCC for the
collaborative database which at a minimum will contain the key variables selected by the IPFnet
Steering Group for standardization across all clinical centers the submission of copies of the
collaborative datasets to each PI upon completion of the project procedures for data analysis
reporting and publication and procedures to protect and ensure the privacy of medical and
genetic data and records of individuals The NHLBI project scientist on behalf of the NHLBI
will have the same access privileges and responsibilities regarding the collaborative data as the
other members of the Steering Group
62
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
PIs are also encouraged to publish and to publicly release and disseminate results data and other
products of the project concordant with the project protocols and governance and the approved
plan for making data and materials available to the scientific community and to the NHLBI
However during the 3 years after the ending date of NHLBI project support unpublished data
unpublished results data sets not previously released and other study materials or products are
to be made available to any third party only with the approval of the IPFnet Steering Group
Upon completion of the project PIs are expected to put their intervention materials and
procedure manuals into the public domain andor make them available to other investigators
according to the approved plan for making data and materials available to the scientific
community and the NHLBI for the conduct of research at no charge other than the costs of
reproduction and distribution
The NHLBI reserves the right to terminate or curtail the project (or an individual award) in the
event of (a) failure to develop or implement mutually agreeable collaborative measurement
subject eligibility and data management sections of the protocols (b) substantial shortfall in
subject recruitment follow-up data reporting or quality control or other major breach of
protocol (c) substantive changes in the agreed-upon protocols with which NHLBI cannot
concur (d) reaching a major project outcome with persuasive statistical significance
substantially before schedule or (e) human subject ethical issues that may dictate a premature
termination
Any disagreement that may arise in scientificprogrammatic matters (within the scope of the
award) between award recipients and the NHLBI may be brought to arbitration An arbitration
panel will be composed of 3 membersmdash1 selected by the IPFnet Steering Group (with the
NHLBI member not voting) or by the individual PI in the event of an individual disagreement a
second selected by NHLBI and the third selected by the other 2 members This special
arbitration procedure in no way affects the PIrsquos right to appeal an adverse action that is otherwise
appealable in accordance with the PHS regulations at 42 CFR part 50 Subpart D and HHS
63
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
regulation at 45 CFR part 16 or the rights of the NHLBI under applicable statutes regulations
and terms of the award
102 IPFnet Steering Group
The IPFnet Steering Group is the main governing body of the project It is composed of the PIs
of the clinical centers the PI of the DCC and the NHLBI project scientist The clinical centers
the IPFnet DCC and the NHLBI each have 1 vote on the IPFnet Steering Group All decisions
are determined by majority vote
All major scientific decisions are determined by the IPFnet Steering Group It assumes overall
responsibility for the design and conduct of the trial It appoints (and disbands) committees and
subcommittees as the need arises designs approves and implements the study protocols
oversees the development of the MOOP monitors subject recruitment and treatment delivery
evaluates data collection and management oversees quality assurance procedures and
implements changes and enhancements to the study as required It also has primary responsibility
for facilitating the conduct of the trials and reporting the projectrsquos results
103 Data and Safety Monitoring Board
The NHLBI will establish a DSMB in accordance with established policies (see
httpwwwnhlbinihgovfundingpoliciesdsmb_insthtm) to ensure data quality and subject
safety and to provide independent advice to the NHLBI regarding progress and the
appropriateness of study continuation
104 Recommendations on Interim Monitoring of Efficacy Safety and Futility
First and foremost the role of the DSMB will be to review subject safety and trial conduct at
periodic points during the study The DSMB may require analyses of the primary endpoint
results for comparing the benefit and risks of treatment strategies The benefit of collecting
additional data on key secondary endpoints with extended follow-up and establishing a robust
64
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
evidence base for determining a standard of care will need to be carefully considered before
early termination of one or more treatment arms After careful consideration the IPFnet Steering
Group recommends conservative thresholds for the early examinations of the safety and efficacy
data
The DSMB will be expected to meet approximately every 6 months until trial completion to
review safety and toxicity data The DSMB may recommend stopping the study based on these
reviews Because the DSMB could stop the trial for safety concerns as well as for a large
efficacy benefit there could be multiple opportunities to reject the null hypothesis (no difference
in event rates between the PL and NAC groups) A Bonferroni approximation will be applied
during the one planned interim analysis for efficacy
Before locking the database a statistical analysis plan (SAP) will be developed to provide
complete details on the statistical analysis The SAP will include the specifics for how and when
the DSMB will be notified for AEs The IPFnet DCC will deliver to the DSMB all FDA-defined
AEs at 3-month intervals The IPFnet DCC will prepare narrative SAE reports in real time for
DSMB review including recommendations and analysis of similar events for each SAE
submitted to the FDA
65
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
11 Investigator and Sponsor Obligations
111 Monitoring
All monitoring activities for US clinical centers will be performed in accordance with DCRI
standard operating procedures Information regarding the types of visits will be outlined in the
PANTHER-IPF MOOP
112 Cost and Payment
There will be no cost to subjects enrolled in this trial Study-related procedures will be paid for
by the IPFnet
Subjects may be eligible for reimbursement for travel to the clinical center Details of payment
will be explained to each subject during the consent process
113 Confidentiality and Health Insurance Portability and Accountability Act
Considerations
Subject confidentiality will be protected throughout the study All subject data will be kept
strictly confidential and no subject-identifying information will be released to anyone outside
the project Confidentiality will be assured through several mechanisms First each subject will
be assigned an anonymous study ID which will then be used on all study forms Second any
study forms blood samples and paper records that contain subject information (eg address lists
phone lists) will be kept at the clinical centers in secured locked areas coded by number Once
blood is collected there will be no subject identifiers placed on blood samplesmdashonly the study
ID number and the date of sample collection Third access to all subject data and information
including laboratory specimens will be restricted to authorized personnel In the case of
computerized data this restricted access will be assured through user logon IDs and password
protection
66
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
At the IPFnet DCC only authorized personnel will have access to the data files containing study
data Security will be assured through user logon IDs passwords and appropriate access
privileges All study subjects will be identified only by their IPFnet ID numbers and no personal
identifying information such as name address or Social Security number will be entered into
the IPFnet DCC database Any subject-specific data reported to the IPFnet Steering Group will
be identified only by the IPFnet ID number
Finally subjects will not be identified by name in any reports or publications nor will the data
be presented in such a way that the identity of individual subjects can be inferred Analysis files
created for further study by the scientific community will have no subject identifiers These data
files will be created in accordance with the Ancillary Studies and Publication Policy of the
IPFnet
114 Informed Consent Procedures
All IPFnet subjects will provide written informed consent using procedures reviewed and
approved by each clinical centerrsquos IRB Informed consent will be undertaken by study personnel
in-person with the subject The subject has the option of declining further participation in the
study at that point No further study procedures will be conducted until the signed documents
have been provided to the IPFnet clinical center
115 Institutional Review Boards
Before initiating this study the protocol clinical center-specific informed consent forms Health
Insurance Portability and Accountability Act (HIPAA) forms recruitment materials and other
relevant information will be reviewed by a properly constituted IRB at each participating clinical
center A copy of the signed and dated IRB approval at each clinical center will be retrieved prior
to or during the site initiation visit and archived at the IPFnet DCC Any amendments to the
protocol other than simple administrative and typographical changes must be approved by each
IRB before they are implemented The clinical centers will seek annual renewals of their IRB
approvals in accordance with local procedures
67
__________________________________________ ________________
__________________________________________
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
12 Investigator Agreement
I have read the foregoing protocol PANTHER-IPF and agree that it contains all necessary
details for carrying out this study I will conduct the study as outlined herein and will complete
the study within the time designated
I will provide copies of the protocol and all pertinent information to all individuals responsible to
me who assist in the conduct of this study I will discuss this material with them to ensure they
are fully informed regarding the drug and the conduct of the study
I will fulfill all responsibilities for submitting pertinent information to the local IRB if
applicable that is responsible for this study
I further agree that NHLBI andor DCRI will have access to any source documents from which
eCRF information may have been generated
Signature of Principal Investigator Date
Name of Principal Investigator (printed or typed)
Protocol version date May 19 2009
Protocol Amendment 1 version date May 28 2010
Protocol Amendment 2 version date December 6 2011
68
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
13 References
1 Raghu G Brown KK Bradford WZ et al A placebo-controlled trial of interferon gamma-1b in patients with idiopathic pulmonary fibrosis N Engl J Med 2004350125-33 2 King TE Jr Safrin S Starko KM et al Analyses of efficacy end points in a controlled trial of interferon-gamma1b for idiopathic pulmonary fibrosis Chest 2005127171-7 3 Flaherty KR Thwaite EL Kazerooni EA et al Radiological versus histological diagnosis in UIP and NSIP survival implications Thorax 200358143-8 4 Wells AU Desai SR Rubens MB et al Idiopathic pulmonary fibrosis a composite physiologic index derived from disease extent observed by computed tomography Am J Respir Crit Care Med 2003167962-9 5 Raghu G Freudenberger TD Yang S et al High prevalence of abnormal acid gastroshyoesophageal reflux in idiopathic pulmonary fibrosis Eur Respir J 200627136-42 6 Kinnula VL Focus on antioxidant enzymes and antioxidant strategies in smoking related airway diseases Thorax 200560693-700 7 Coultas DB Zumwalt RE Black WC Sobonya RE The epidemiology of interstitial lung diseases Am J Respir Crit Care Med 1994150967-72 8 Raghu G Weycker D Edelsberg J Bradford WZ Oster G Incidence and prevalence of idiopathic pulmonary fibrosis Am J Respir Crit Care Med 2006174810-6 9 Olson AL Swigris JJ Lezotte DC Norris JM Wilson CG Brown KK Mortality from pulmonary fibrosis increased in the United States from 1992 to 2003 Am J Respir Crit Care Med 2007176277-84 10 Mannino DM Etzel RA Parrish RG Pulmonary fibrosis deaths in the United States 1979shy1991 An analysis of multiple-cause mortality data Am J Respir Crit Care Med 19961531548shy52 11 Hubbard R Johnston I Coultas DB Britton J Mortality rates from cryptogenic fibrosing alveolitis in seven countries Thorax 199651711-6 12 Johnston I Britton J Kinnear W Logan R Rising mortality from cryptogenic fibrosing alveolitis Bmj 19903011017-21 13 Raghu G Collard HR Egan JJ et al An official ATSERSJRSALAT statement idiopathic pulmonary fibrosis evidence-based guidelines for diagnosis and management Am J Respir Crit Care Med 2011183788-824 14 (USA) FDA FDA Public Health Advisory Interferon gamma-1b (marketed as Actimmune) In 2007 15 King TE Jr Pardo A Selman M Idiopathic pulmonary fibrosis Lancet 2011 16 Raghu G Brown KK Costabel U et al Treatment of idiopathic pulmonary fibrosis with etanercept an exploratory placebo-controlled trial Am J Respir Crit Care Med 2008178948shy55 17 Malouf MA Hopkins P Snell G Glanville AR An investigator-driven study of everolimus in surgical lung biopsy confirmed idiopathic pulmonary fibrosis Respirology 201116776-83 18 King TE Jr Behr J Brown KK et al BUILD-1 a randomized placebo-controlled trial of bosentan in idiopathic pulmonary fibrosis Am J Respir Crit Care Med 200817775-81 19 Richeldi L Costabel U Selman M et al Efficacy of a tyrosine kinase inhibitor in idiopathic pulmonary fibrosis N Engl J Med 20113651079-87
69
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
20 Borok Z Buhl R Grimes GJ et al Effect of glutathione aerosol on oxidant-antioxidant imbalance in idiopathic pulmonary fibrosis Lancet 1991338215-6 21 Meyer A Buhl R Magnussen H The effect of oral N-acetylcysteine on lung glutathione levels in idiopathic pulmonary fibrosis Eur Respir J 19947431-6 22 Behr J Maier K Degenkolb B Krombach F Vogelmeier C Antioxidative and clinical effects of high-dose N-acetylcysteine in fibrosing alveolitis Adjunctive therapy to maintenance immunosuppression Am J Respir Crit Care Med 19971561897-901 23 Cantin AM North SL Fells GA Hubbard RC Crystal RG Oxidant-mediated epithelial cell injury in idiopathic pulmonary fibrosis J Clin Invest 1987791665-73 24 Waghray M Cui Z Horowitz JC et al Hydrogen peroxide is a diffusible paracrine signal for the induction of epithelial cell death by activated myofibroblasts Faseb J 200519854-6 25 Larios JM Budhiraja R Fanburg BL Thannickal VJ Oxidative protein cross-linking reactions involving L-tyrosine in transforming growth factor-beta1-stimulated fibroblasts J Biol Chem 200127617437-41 26 Kinnula VL Fattman CL Tan RJ Oury TD Oxidative stress in pulmonary fibrosis a possible role for redox modulatory therapy Am J Respir Crit Care Med 2005172417-22 27 Meyer A Buhl R Kampf S Magnussen H Intravenous N-acetylcysteine and lung glutathione of patients with pulmonary fibrosis and normals Am J Respir Crit Care Med 19951521055-60 28 Behr J Degenkolb B Krombach F Vogelmeier C Intracellular glutathione and bronchoalveolar cells in fibrosing alveolitis effects of N-acetylcysteine Eur Respir J 200219906-11 29 Bando M Hosono T Mato N et al Long-term efficacy of inhaled N-acetylcysteine in patients with idiopathic pulmonary fibrosis Intern Med 2010492289-96 30 Demedts M Behr J Buhl R et al High-dose acetylcysteine in idiopathic pulmonary fibrosis N Engl J Med 20053532229-42 31 Toma TP Bhowmik A Rajakulasingam R Acetylcysteine in pulmonary fibrosis N Engl J Med 20063541086-9 author reply -9 32 Hunninghake GW Antioxidant therapy for idiopathic pulmonary fibrosis N Engl J Med 20053532285-7 33 Flaherty KR Mumford JA Murray S et al Prognostic implications of physiologic and radiographic changes in idiopathic interstitial pneumonia Am J Respir Crit Care Med 2003168543-8 34 Latsi PI du Bois RM Nicholson AG et al Fibrotic idiopathic interstitial pneumonia the prognostic value of longitudinal functional trends Am J Respir Crit Care Med 2003168531-7 35 Collard HR King TE Jr Bartelson BB Vourlekis JS Schwarz MI Brown KK Changes in clinical and physiologic variables predict survival in idiopathic pulmonary fibrosis Am J Respir Crit Care Med 2003168538-42 36 Jegal Y Kim DS Shim TS et al Physiology is a stronger predictor of survival than pathology in fibrotic interstitial pneumonia Am J Respir Crit Care Med 2005171639-44 37 Martinez FJ Safrin S Weycker D et al The clinical course of patients with idiopathic pulmonary fibrosis Ann Intern Med 2005142963-7 38 Hull JH Acetylcysteine in pulmonary fibrosis N Engl J Med 20063541089-91 author reply -91
70
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
39 Flaherty KR King TE Jr Raghu G et al Idiopathic interstitial pneumonia what is the effect of a multidisciplinary approach to diagnosis Am J Respir Crit Care Med 2004170904shy10 40 Raghu G Johnson WC Lockhart D Mageto Y Treatment of idiopathic pulmonary fibrosis with a new antifibrotic agent pirfenidone results of a prospective open-label Phase II study Am J Respir Crit Care Med 19991591061-9 41 Hunninghake GW Lynch DA Galvin JR et al Radiologic findings are strongly associated with a pathologic diagnosis of usual interstitial pneumonia Chest 20031241215-23 42 Lynch D Godwin J Safrin S et al High-resolution computed tomography in idiopathic pulmonary fibrosis diagnosis and prognosis Am J Respir Crit Care Med 2005172488-93 43 Mallinckrodt CH Watkin JG Molenberghs G Carroll RJ Choice of the primary analysis in longitudinal clinical trials Pharmaceutical Statistics 20043161-9 44 Bang H Tsiatis A Estimating medical costs with censored data Biometrika 200087329shy43 45 Lin DY Regression analysis of incomplete medical cost data Stat Med 2003221181-200 46 Rochon J Application of GEE procedures for sample size calculations in repeated measures experiments Stat Med 1998171643-58 47 Lachin JM Foulkes MA Evaluation of sample size and power for analyses of survival with allowance for nonuniform patient entry losses to follow-up noncompliance and stratification Biometrics 198642507-19
71
- PANTHER-IPFPREDNISONE AZATHIOPRINEAND N-ACETYLCYSTEINEA STUDY THAT EVALUATES RESPONSE INIDIOPATHIC PULMONARY FIBROSIS
-
- Protocol Summary
- Table of Contents
- List of Tables
- List of Figures
- List of Abbreviations
- 1 Summary
- 2 Hypotheses and Specific Aims
-
- 21 Null Hypothesis
- 22 Specific Aim 1
- 23 Specific Aim 2
- 24 Prespecified Subgroups of Interest
-
- 3 Background and Significance
-
- 31 Idiopathic Pulmonary Fibrosis is the Most Common Interstitial Lung Disease
- 32 Rationale for Placebo Control
- 33 Rationale for N-acetylcysteine
- 35 Rationale for N-acetylcysteine as a Stand-alone Therapy
- 36 Rationale for the Study Design and Primary Endpoint
- 37 Rationale for Blinding of Treatments
-
- 4 Methods
-
- 41 Inclusion Criteria
- 42 Diagnosis of IPF
- 43 Exclusion Criteria
- 44 Study Design and Study Visit
- 45 Dose Justification
- 46 Contraindications Precautions and Side Effects of Study Medications
- 47 Recruitment Procedures
- 48 Study Procedures
- 49 Concomitant Medications
- 410 Laboratory Testing
- 411 Blinding of Study Drugs
-
- 5 Study Endpoints
-
- 51 Primary Study Endpoint
- 52 Secondary Study Endpoints
-
- 6 Safety Evaluations and Procedures
-
- 61 Adverse Events
- 62 Clinical Medical Monitoring
- 63 Unblinding Procedures
-
- 7 Study Drug Procedures
- 8 Data Management
-
- 81 Hardware and Software Configuration
- 82 Sources of Data
-
- 9 Study Design and Data Analysis
-
- 91 General Analytic Considerations
- 92 Randomization Blinding and Reporting of Results
- 93 Stratification
- 94 Specification of the Primary Analyses
- 95 Analysis of Longitudinal Endpoints
- 96 Analysis of Binary Time-to-Event and Time-Lagged Endpoints
- 97 Power Analysis
-
- 10 Study Administration
-
- 101 Cooperative Agreement Mechanism
- 102 IPFnet Steering Group
- 103 Data and Safety Monitoring Board
- 104 Recommendations on Interim Monitoring of Efficacy Safety and Futility
-
- 11 Investigator and Sponsor Obligations
-
- 111 Monitoring
- 112 Cost and Payment
- 113 Confidentiality and Health Insurance Portability and Accountability ActConsiderations
- 114 Informed Consent Procedures
- 115 Institutional Review Boards
-
- 12 Investigator Agreement
- 13 References
-

PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
The study will employ a 2-arm design with 11 randomization to NAC or PL Once enrolled subjects will visit
the clinical center at 15 weeks and 15-week intervals thereafter Each subject will be treated and followed for a
maximum of 60 weeks
During the 60-week visit subjects will be taken off all study agents Approximately four weeks after the final
dose of study agent is taken subjects will receive a safety phone call from the study site
442 Study Visits
Subjects who meet entry criteria will review the informed consent a written description of the purpose
procedures and risks of the study with the PI co-investigator or study coordinator and all questions will be
answered The informed consent form will be signed by the subject at screening No protocol-specific
procedures will be performed until the subject has signed and dated an informed consent form This includes the
screening procedures
4421 Screening
Once informed consent is obtained subjects may immediately begin the screening process or may return within
28 days of consent In the event a study subject has been clinically evaluated at the study site by an IPFnet study
physician and has performed testing within three weeks for this clinical evaluation that meets guidelines
provided in the IPFnet PANTHER-IPF Manual of Operating Procedures (MOOP) this testing may be used to
satisfy the following screening criteria medical history physical exam arterial blood gas (ABG) with A-a
gradient vital signs with oximetry body height and weight spirometry DLCO lung volumes and HRCT scan
Allowing the use of previously performed test results that meet study guidelines for the screening visit is
intended to permit subjects easier access to study entry to prevent subjects from repeating testing that has been
performed within the study window and to decrease risks to subjects from repeated exposure to procedures
such as arterial puncture and HRCT
The following procedures will be performed at screening
Medical history and a physical examination
28
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Measure height and weight
Serum pregnancy test (if applicable)
Measure vital signs including oximetry
Blood draws performed and the following analyses conducted
o Hematology (red cell count white cell count hemoglobin hematocrit cell indices differential
platelet count)
o Blood chemistries according to central laboratory protocol (see Section 410 Laboratory
Testing)
o Beta human chorionic gonadotropin (serum) pregnancy test (in women of childbearing potential)
o Urinalysis
Pulmonary Function Tests (PFTs) including spirometry pre- and post- bronchodilator and postshy
bronchodilator measurement of lung volumes and measurement of hemoglobin adjusted diffusing
capacity
Measure ABGs
HRCT if a satisfactory scan has not been performed on the subject within 3 months of screening (see
PANTHER-IPF MOOP for more details)
Surgical lung biopsies (if applicable) reviewed by local and central pathology departments
Current medications If required a washout period discussed with the subject and initiated at this visit
4422 Enrollment
The enrollment visit is expected to take place within eight weeks of the screening visit Enrollment visit
activities include
Measure vital signs including oximetry
Measure height and weight
Serum pregnancy test (if applicable)
If consent has been given blood will be drawn and a urine specimen collected for the bio-specimen
repository
Spirometry (post-bronchodilator)
Measure 6MWT with Borg Dyspnea Scale
29
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Collect Quality-of-life (QOL) data using the SF-36 EuroQol Investigating Choice Experiments for
Preferences of Older People Capability Instrument (ICE CAP) and SGRQ
Female subjects complete Gender Substudy questionnaire
Dyspnea status collected using the UCSD SOBQ
Evaluate Acute Exacerbation (AEx)
Review of any Adverse Events (AEs)
Review of concomitant medications
Subject receives diary and instructions on its purpose and proper use
Subject receives supply of study drug sufficient to last until his or her 15-week study visit
See the Schedule of Assessments (Table 3) for more details Subjects with screening and enrollment postshy
bronchodilator FVC measurements (in liters) differing by more than 11 are not eligible to be enrolled in the
study
Subjects will be asked to provide a physician of record This physician will be considered the subjectrsquos primary
care provider (PCP) and if the subject agrees the PCP will be informed by letter of the subjectrsquos enrollment in
the trial The subject will be informed that his or her ongoing medical care should be received from the PCP
The PCP will be informed of any safety issues identified by the study staff The PCP will also be given
information regarding communication with study personnel about pertinent health issues or clinic encounters
the subject may have
4423 Week 15
The week 15 visit is expected to occur within +- 14 days of the subjectrsquos scheduled visit time (eg the week 15
visit should occur anytime between 13 and 17 weeks after starting study drug Week 15 activities include
Measure vital signs with oximetry
Measurement height and weight
Serum pregnancy test (if applicable)
Spirometry (post-bronchodilator) measurement
Review of AEs
Evaluate for AEx
30
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Review concomitant medications
If consented draw blood and collect urine specimen for the biospecimen repository
Subjects return used and unused study drug for the visit
Review study diary and a new study diary will be given
Provide additional supply of study drug sufficient to last until the next scheduled visit
4424 Week 30
The week 30 visit is expected to occur within +- 14 days of the subjectrsquos scheduled visit time (eg the week 30
visit should occur anytime between 28 and 32 weeks after starting study drug) Week 30 activities include
Physical examination
Measure vital signs with oximetry
Measure height and weight
Laboratory values (complete blood count [CBC] and serum chemistries)
Serum pregnancy test (if applicable)
Measure spirometry (post-bronchodilator)
6MWT with Borg scale
DLCO
Review of AEs
Evaluate for AEx
Review concomitant medications
Complete all QOL and dyspnea questionnaires (EuroQol ICE CAP SF-36 SGRQ and UCSD SOBQ)
If consent has been given blood will be drawn and a urine specimen collected for the biospecimen
repository
Review study diary
Subjects return used and unused study drug for the visit
Provide additional supply of study drug sufficient to last until the next scheduled visit
4425 Week 45
31
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
The week 45 visit is expected to occur within +- 14 days of the subjectrsquos scheduled visit time (eg the week 45
visit should occur anytime between 43 and 47 weeks after starting study drug) Week 45 activities include
Measure vital signs with oximetry
Measure height and weight
Serum pregnancy test (if applicable)
Measure spirometry (post-bronchodilator)
Review of AEs
Evaluate for AEx
Review concomitant medications
If consent has been given blood will be drawn and a urine specimen collected for the biospecimen
repository
Subjects return used and unused study drug for the visit
Study diary reviewed
Provide additional supply of study drug sufficient to last until the next scheduled visit
4426 Week 60 (Early Withdrawal or Final Treatment Visit)
At week 60 or at subject withdrawal from the study (premature by study doctor or subjectrsquos decision) a final
treatment visit will occur At this final treatment visit subjects will discontinue NACPL abruptly Week 60
activities also include
Physical examination
Measure vital signs with oximetry
Measure height and weight
Laboratory values (complete blood count [CBC] and serum chemistries)
Spirometry (post-bronchodilator) measurement
6MWT with Borg scale measurement
DLCO
Lung volumes
ABG
Review of AEs
32
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Evaluate for AEx
Review concomitant medications
Subjects will complete all QOL and dyspnea questionnaires (EuroQol ICE CAP SF-36 SGRQ and
UCSD SOBQ)
If consent has been given blood will be drawn and a urine specimen collected for the biospecimen
repository
Subjects return used and unused study drug for the visit
Study diary reviewed
4427 Final Site Visit ndash FVC drop confirmation
In the event that the subject has a recorded FVC drop of gt10 from baseline at the final treatment visit and the
subject has not had a confirmation of such a drop at a previous study visit the subject should return to the
clinical site 6 to 8 weeks after the final treatment visit During this visit a post-bronchodilator spirometry test
will be performed This FVC measurement will be evaluated according to section 521 of this protocol
4428 Final Visit ndash Telephone Follow-up
Four weeks following the final dose of study medication subjects will receive a telephone call from the study
coordinator to ensure that there are no side effects and to follow up on any ongoing adverse events (AEs)
4429 Phone Contact Between Visits
At week 2 and each month that a subject does not have a scheduled clinical center visit his or her study
coordinator will contact him or her at least once by telephone to
Inquire if the subject has had any hospitalizations events that might be considered an AE or any events
significant enough to warrant an out-of-cycle visit to the clinical center
Remind subjects of their current dosage levels and confirm that the subject understands them
Address any questions or concerns the subject might have regarding other aspects of the study
Assess adherence to the treatment regimen by reviewing diary data verbal review of medications taken
including nutritional supplements
33
34
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Table 3 Schedule of Assessments
Procedure Screening Visit 0
Enrollment Visit 1
Week 15 Visit 2
Week 30Visit 3
Week 45 Visit 4
Week 60 Early
Withdrawal Visit 5
Final1
Visit (via phone)
Informed consent X
Medical history X
Inclusionexclusion criteria X
Serum pregnancy test (if applicable) X X X X X
Review of lung biopsy X
Arterial Blood Gas X X
6-Minute Walk Test
X
X X
Physical examination X X X
Vital signs with oximetry X X X X X X
Body height and weight X X X X X X
Complete Blood Count X X X
Chemistry panel X X X
Monitor Lab Values X X X
Urinalysis X Specimen repository substudy blood draw and urine collection (if consented)
X
X X X X
HRCT (if not completed within three months) X
Spirometry (pre- and post-bronchodilator) X
Spirometry (post-bronchodilator only) X X X X X
DLCO (post-bronchodilator only) X X X
Lung volumes (post-bronchodilator only) X
X
Evaluate for acute exacerbation X X X X X
Review Adverse Events X X X X X X
Review concomitant meds X X X X X X
Dispense subject diary X X X X
Review subject diary X X X X X
Dispense study agent X X X X
Gender Substudy questionnaire (female subjects only) X
EuroQol ICECAP UCSD SOBQ SGRQ SF-36 X X X
Abbreviations DLCO diffusing capacity of the lung for carbon monoxide QOL Quality of Life ICECAP Investigating Choice Experiments for Preferences of Older People UCSD SOBQ University of California Shortness of Breath Questionnaire SGRQ St Georgersquos Respiratory Questionnaire SF-36 Short Form 36 Health Survey
1Follow-up visit via phone will occur four weeks after final dose of study medication
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
45 Dose Justification
The general philosophy for determining dosing levels was to apply previously examined
treatment regimens With the focus of the study being to establish a standard of care for
mildmoderate IPF subjects the goal was to develop flexible yet standardized treatment rules that
allow for the temporary or permanent withholding of one or more components of treatment when
necessary Subjects developing laboratory abnormalities or symptoms that result in
discontinuation of one or more components of study treatment may continue on the other
components as long as there is no contraindication for this Complete follow-up is important for
the validity of any study As a strategy to maintain protocol adherence we are using a treatment
regimen that will detect potential side effects and prompt interventions proactively in the interest
of patient safety In addition subjects who permanently stop study medications during the course
of the study are encouraged to continue in the study completing all scheduled visits and tests
451 Rationale for N-acetylcysteine Dosing
To our knowledge there have been no IPF studies to correlate clinical outcome measures with
different dosages for NAC The dosage chosen is based on the IFIGENIA study However BAL
lung GSH levels from subjects with IPF have been augmented with the use of oral NAC at 600
mg 3 times per day In addition lung GSH levels have been associated with improved
PFTs212227 The dose chosen for this study was based on previous data including the IFIGENIA
study30
4511 Dosing of N-acetylcysteineplacebo
Dosing of NACPL will be 600 mg orally 3 times a day (1800 mgday)
4512 Reasons to Discontinue N-acetylcysteineplacebo
NACPL may be temporarily or permanently discontinued for the duration of the study for
gastrointestinal symptoms or dermatologic reactions
35
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Temporarily discontinue (hold) oral NACPL for subjects requiring inpatient admission for acute
exacerbation (AEx) or other conditions Resume NACPL after discharge
36
37
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
452 Dosage Algorithms
Dosage Adjustment Algorithm 1 NACPL Dose Modifications for Gastrointestinal Symptoms Nausea Vomiting Abdominal Discomfort Diarrhea
GI Symptoms determined by the PI to be clinically significant Nausea Vomiting Abdominal Discomfort Diarrhea
NACPL Temporarily dc (HOLD) x 3 Days
Monitor symptoms intervene as clinically indicated (eg fluid replacement antidiarrhea or antinausea medication)
Monitor or lab PRN
Are symptoms resolving after 3 days NO
Symptoms NOT resolving after 3 days of holding study medication Assessmentmanagement per clinical
discretion of investigator
Likely not study medication discuss resuming study medication with medical monitor when symptoms resolved
YES
Temporarily dc (HOLD) NACPL for 4 additional days (total hold 1 week) then NACPL Resume 600 MG TID
Did symptoms recur
YES
STOP NACPL for
duration of study
NO
NACPL No Change
38
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Dosage Adjustment Algorithm 2 NACPL Dose Modifications For Dermatologic Reactions
Dermatologic Reactions (Not Acneiform) ge Grade 2 Grading per Common Terminology Criteria for
Adverse Events V30 (httpctepcancergov) For example Grade 1 RASHDESQUAMATION Macular or papular eruption or erythema without associated symptoms Grade 2 RASHDESQUAMATION Macular or popular eruption or erythema with pruritus or other associated symptoms localized desquamation or other lesions covering lt50 of body surface area
NACPL Temporarily dc (HOLD) x 3 days
Are symptoms resolving after 3 days
NO Symptoms not resolving after 3 days of holding study medication Assessmentmanagement per clinical discretion of investigator Likely not study medication Discuss resuming study medication with medical monitor when symptoms
resolved YES
Temporarily dc (HOLD) NACPL for 4 additional days (total hold 1 week) then NACPL resume 600 MG TID
Did symptoms recur
YES
STOP NACPL for
duration of study
NO
NACPL No change
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
46 Contraindications Precautions and Side Effects of Study Medications
461 Contraindication
Contraindication to NAC is known hypersensitivity to it
462 Precautions
Concomitant administration of oral NAC and antibiotics has shown a slightly reduced absorption
of cephalexin and a slight increase in erythromycin serum levels NAC contains free sulfhydryl
groups There is no evidence that individuals sensitive to sulfa drugs are sensitive to NAC
The NAC preparation being administered in this study contains 20 mg of aspartame Because of
the phenylalanine component of aspartame individuals with phenylketonuria should avoid or
restrict aspartame intake to avoid increased blood levels of phenylalanine Because of this risk
labeling is required on all products containing aspartame
463 Side Effects
Side effects of NAC range from common to serious See Table 4
39
40
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Table 4 Side Effects of NAC
Undesirable Effects
System-organ class Uncommon
(gt11000 lt1100)
Rare
(gt110000 lt11000)
Very rare
(lt110000) Not known
Immune system disorders Hypersensitivity Anaphylactic shock
reaction
Nervous system disorders Headache
Ear and labyrinth disorders Tinnitus
Cardiac disorders Tachycardia
Vascular disorders Hemorrhage
Respiratory thoracic and
mediastinal disorders
Bronchospasm
Dyspnea
Gastrointestinal disorders
Vomiting diarrhea
stomatitis abdominal
pain nausea
Dyspepsia
Skin and subcutaneous tissue
disorders
Urticaria rash
angioedema itching
General disorders and
administration site conditions Pyrexia
Investigations Reduced arterial
pressure Face edema
In very rare cases the onset of severe skin reactions such as Stevens-Johnson syndrome and Lyell syndrome was reported to have a temporal relationship with N-acetylcysteine administration Although in most cases at least another suspect drug probably most involved in the genesis of the above mentioned mucocutaneous syndromes has been identified in case of mucocutaneous alterations it is appropriate to contact onersquos doctor and the administration of N-acetylcysteine should be immediately discontinued
Some studies confirmed a reduction of platelet aggregation during N-acetylcysteine administration The clinical significance of these findings has not been defined yet [Source Fluimucil Investigator Brochure]
47 Recruitment Procedures
Subjects recruited for this study will be established patients of the investigators or physician- or
self-referred to participating clinical centers in the IPFnet Each clinical center within IPFnet has
a well-developed infrastructure of local pulmonologists within the surrounding geographic area
These pulmonologists are kept informed of ongoing IPF clinical trials and regularly refer
subjects to studies conducted at IPFnet clinical centers
Additional steps will be taken to inform clinicians of the trials in progress within IPFnet
including presentations at faculty staff meetings at local hospitals medical grand rounds and
national conferences direct mail notification monthly faxes and advertisement of network trials
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
in pulmonary journals Clinical center patients previously diagnosed with IPF will be notified of
the trials by mail whenever possible
Recruitment of minorities and women will be monitored by the DCC and DSMB If necessary
additional recruitment efforts will be made at specific centers to ensure that the aggregate subject
sample contains appropriate representation of women and minorities
48 Study Procedures
The following procedures are detailed in the PANTHER-IPF MOOP accompanying this
protocol
1 PFT
2 ABG
3 HRCT scan of the chest (including imaging of pulmonary arteries)
4 CBC and serum chemistries
5 Pregnancy test
6 6MWTBorg Dyspnea Scale
7 QOL questionnaires (EuroQol HAD SF-36 SGRQ and ICE CAP)
8 UCSD SOBQ
9 Gender Substudy Questionnaire
All assessments of PFTs will be conducted by study personnel not directly involved in the
treatment of the subjects
481 Biological Specimen Management
4811 Biological Specimen Sample Management
Subjects at clinical centers participating in the specimen repository substudy who consent to
having blood drawn for research purposes and for the banking of blood blood components and
other biologic specimens (urine and BAL fluid) will have approximately 405 mL of blood
41
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
drawn 17 mL blood drawn for DNA and 20 mL of urine collected at enrollment visit Subjects
will have approximately 50 mL of blood drawn and 20 mL of urine collected at each 15-week
follow-up visit Blood specimens will be separated according to PANTHER-IPF MOOP
guidelines into the following components for banking in the repository serum plasma and
DNA Coding of all biologic specimens for the repository will be performed by study staff at the
clinical center The samples will be processed per PANTHER-IPF MOOP guidelines aliquoted
labeled with barcode labels and stored at -70degC at the clinical center and shipped to the central
repository
The only subject identifiers will be a sample ID number and subject initials This sample ID will
be linked in the IPFnet DCC clinical database to subject information No subject information will
be transferred to the biological-specimen database
The subjectrsquos samples may be used for approved sub-studies relating to human disease
including but not limited to IPF The studies for which an individualrsquos samples will be made
available will be determined by the subjectrsquos answers to questions on the biological-sample
informed consent form The subjects can choose to make their samples available for all options
or any combination Samples will be made available to researchers only with IPFnet Steering
Group approval until such time as the samples are made public through the NHLBI repository
49 Concomitant Medications
Concurrent treatment with FDA-approved therapy for IPF is allowed Colchicine may be used
for treatment of gout Temporary treatment with oral or IV corticosteroids for clinical worsening
or suspected AEx is permitted Nutritional supplements containing NAC are not allowed
410 Laboratory Testing
Clinical laboratory parameters will be assessed at screening and at the end of the study The
following tests will be performed at the two time points specified in the protocol chemistry (AG
ratio ALT [SGPT] AST [SGOT] albumin alkaline phosphatase amylase bilirubin-direct
42
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
bilirubin-indirect bilirubin-total BUN BUNcreatinine ratio calcium carbon dioxide
cholesterol-total chloride CPK-total creatinine GGT globulin glucose iron-total LDH
lipase magnesium phosphorus-inorganic potassium protein-total sodium TIBC triglycerides
uric acid) and hematology (red blood cell count WBC count hemoglobin hematocrit cell
indices differential platelet count)
411 Blinding of Study Drugs
Subjects and caregivers will be blinded to study treatment Every subject will receive NAC or
matching PLs at every study visit from the baseline visit to the week-45 visit No study agent
will be dispensed at the week-60 visit
43
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
5 Study Endpoints
51 Primary Study Endpoint
The primary endpoint will be the change in serial measurements of FVC over the study period
52 Secondary Study Endpoints
521 Time to Disease-progression
The time-to-death or a 10 decline in FVC will be defined as the time-to-disease progression
The 10 decline in FVC from enrollment must be confirmed on 2 consecutive visits no less than
6 weeks apart For subjects with 2 consecutive visits with a 10 decline in FVC the time-toshy
disease progression will be defined as the time interval between enrollment and the initial visit
with a 10 FVC decline For subjects who experience disease progression the study doctor will
determine whether or not the subject will remain in the study
522 Acute Exacerbations
The following 3 criteria will define AEx in subjects with acute worsening of their respiratory
conditions
1 Clinical (all of the following required)
A) Unexplained worsening of dyspnea or cough within 30 days triggering unscheduled
medical care (eg emergency room clinic study visit hospitalization)
B) No clinical suspicion or overt evidence of cardiac event pulmonary embolism or deep
venous thrombosis to explain acute worsening of dyspnea
C) No pneumothorax
44
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
2 RadiologicPhysiologic (A and B required)
A) New ground glass opacity or consolidation computed tomography (CT) scan OR new
alveolar opacities on chest x-ray
B) Decline of ge 5 in resting room air SpO2 from last recorded level OR decline of ge 8 mm
Hg in resting room air PaO2 from last recorded level
3 Microbiologic (all of the following required)
A) No clinical evidence for infection (ie absence of grossly purulent sputum fever gt 39degC
orally)
B) Lack of positive microbiological results (if done) from lower respiratory tract defined as
(1) Clinically significant bacterial growth on sputum or endotracheal aspirate cultures
(2) Quantitative culture by protected brush specimen ge 103 cfumL or BAL ge 104 cfumL
(3) The presence of specific pathogens on stains of any of the above
C) Lack of positive pathogen in blood cultures (if done)
Identification of Acute Exacerbations
All subjects will be educated about the importance of identifying AExs At the time of
enrollment subjects will be told about the possibility of developing acute symptomatic
worsening that might represent an AEx of IPF and instructed to contact their study clinical
center coordinator within 48 to 72 hours of the apparent event
All subjects will be contacted by phone monthly and questioned about any change in dyspnea or
cough and any interim clinic visits or hospitalizations Finally as part of the IPFnet outreach to
community referring physicians the importance of AExs will be emphasized When a subject is
identified who meets criterion 1A this will trigger the collection of additional clinical data to
evaluate a suspected AEx These data will be collected as part of standard clinical care (ie this
protocol does not require collection of all items) The additional items to be collected for
suspected AEx include
IPFnet AEx case report form (eCRF) (required)
45
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Chest x-ray CT scan withwithout pulmonary angiogram (reports should be faxed and
followed by the hard copiesdiscs)
Oxygen saturation (pulse oximetry)
ABG
Respiratory cultures (sputum endotracheal aspirate lavage)
Blood cultures
Clinichospital records related to the event
All potential cases of AEx will be reviewed by the clinical center PI first and a decision on
whether the case may represent an AEx will be made If AEx is suspected the case will be sent
to the IPFnet adjudication committee which will assign a final diagnosis (see Table 5) If there is
disagreement among members the majority opinion will be recorded
During episodes of suspected AEx as determined by the individual clinical center investigator
subjects will remain blinded and in the study
Table 5 Final Diagnoses in Evaluation of Suspected Acute Exacerbations
Definite acute exacerbation All criteria met no alternative etiology
Unclassifiable acute worsening
Insufficient data to evaluate all criteria no alternative etiology
Not acute exacerbation Alternative etiology identified that explains acute worsening
Management of the suspected AEx will be at the discretion of the treating physician Standard of
care generally involves evaluation for respiratory infection pulmonary embolism cardiac events
and pneumothorax and treatment with IV corticosteroids
Study drugs will be resumed at pre-suspected AEx doses after subjects clinically improve as
confirmed by the local PI All subjects should be seen at the clinical center within 2 to 4 weeks
of recovery for measurement of post-bronchodilator FVC (see Figure 4) Subjects unable to
return to the clinical center after suspected AEx due to medical frailty (eg continued
46
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
institutionalization progressive disability) will be categorized as failing to maintain FVC
response in secondary analyses
Suspected AEx (PI determined)
Hold study drug Treat AEx
(Attending physician determined)
Alive but unable to continue due to
medical frailty
Dead
Alive and able to continue
Site reviewvisit
Restart study drug
FVC within 2-4 weeks
Figure 4 Acute Exacerbation Flow Chart
523 Respiratory Infections
An upper respiratory infection will be defined as
Change in sputum discoloration
Increased cough of no more than 14 daysrsquo duration
A lower-respiratory infection (pneumonia) will be defined as new segmental or lobar airspace
opacities visualized by image studies (chest radiograph or HRCT) in addition to any of the
following
Positive pathogencultures in good sample of sputum or lower-airway secretions retrieved
by fiberoptic bronchoscope
Fever gt 39degC or gt 100degF
Leukocytosis gt 12000 (unexplained no increase in dose of corticosteroids)
47
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
524 Maintained FVC Response
Subjects with follow-up FVCpred measurements at or above their baseline FVCpred level
will be classified as having maintained FVC response Subjects with reduced FVCpred levels
or missing data for any reason including death or medical frailty will be classified as having not
maintained FVC response The FVCpred value is used because unadjusted FVC measurements
are expected to decline with age
48
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
6 Safety Evaluations and Procedures
61 Adverse Events
During a clinical trial the reporting of adverse experience information can lead to important
changes in the way a new treatment is developed as well as provide integral safety data
611 Definitions
An adverse event (AE) is any untoward medical occurrence in a subject or clinical investigation
subject who was administered a pharmaceutical product The AE does not necessarily have to
have a causal relationship with the drug administered An AE can be any unfavorable and
unintended sign (including an abnormal laboratory finding) symptom or disease temporarily
associated with the use of a medicinal product whether or not considered to be related to the
medicinal product Diseases signs symptoms or laboratory abnormalities already existing at
enrollment are not considered AEs unless they worsen (ie increase in intensity or frequency)
Surgical procedures themselves are not AEs they are therapeutic measures for conditions that
require surgery The condition for which the surgery is required may be an AE Surgical
procedures planned before randomization and the conditions necessitating the surgery are not
AEs
A serious adverse event is any untoward event that
Is fatal
Is life-threatening
Requires inpatient hospitalization or prolongation of existing hospitalization with the
following exceptions
o Preplanned (before the study) hospital admissions unless the hospitalization is
prolonged
o Planned admissions (as part of a study eg routine biopsies)
o Hospitalization lasting lt 24 hours
49
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
o Hospitalization for elective procedure
o Emergency room visits
Results in persistent or significant disability or incapacity
Is a congenital anomaly or birth defect
Important medical events that may not result in death be life-threatening or require
inpatient hospitalization may be considered serious adverse events (SAEs) when based
on appropriate medical judgment they may jeopardize the subject and may require
medical or surgical intervention to prevent one of the outcomes listed above
Life-threatening means that the subject was in the view of the investigator at immediate risk of
death from the AE as it occurred It does not include an AE that had it occurred in a more severe
form might have caused death
Persistent or significant disabilityincapacity means that the event resulted in permanent or
significant and substantial disruption of the subjectrsquos ability to carry out normal life functions
Causality
A reasonable possibility means the AE may have been caused byrelated to the study drug A
perceived or real lack of efficacy does not satisfy the definition of relatedness
612 Adverse Event (AE) Reporting
For the PANTHER-IPF trial all AEs (serious and nonserious) occurring from randomization
through final study visit (4 weeks after final dose of all study medication) will be recorded on the
AE page of the case report form (CRF)
6121 Serious Adverse Events (SAE) Reporting
For this trial all deaths and all SAEs which occur from randomization through final study visit
must be entered within the EDC system via the SAE eCRF page within 24 hours of the
investigative sitersquos knowledge of the event It is the responsibility of the clinical center
50
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
investigator to provide a causality assessment of the event for each study medications based upon
the information available at the time of the report It is understood that complete information
about the event may not be known at the time the initial report is submitted In the event the EDC
system is not accessible to the site at the time of event reporting investigative sites will complete
and forward a paper back-up SAE form to DCRI Safety Surveillance for processing
DCRI Safety Surveillance
Telephone 1-919-668-8624 or 1-866-668-7799 (toll free)
Fax 1-919-668-7138 or 1-866-668-7138 (toll free)
The investigator must complete and submit follow-up SAE information via the eCRF when
important new or follow-up information (eg final diagnosis outcome results of specific
investigations) becomes available Follow-up information should be submitted according to the
same process used for reporting the initial event as described above All SAEs will be followed
until resolution stabilization or 30 days after the subject has completed the final visit (4 weeks
after the final dose of study medication) whichever occurs first The investigator is responsible
for reporting SAEs to their institutional review board (IRB) per site specific IRB reporting
guidelines
6122 Regulatory Reporting
AEs that are serious study drug related and unexpected will be reported to the regulatory
authorities The DCRI Safety Surveillance medical monitor will perform a medical review of all
SAEs submitted and evaluate for ldquounexpectednessrdquo DCRI Safety Surveillance will prepare
MedWatch reports for those events identified as serious study drug related and unexpected as
determined by Safety Medical Monitor
DCRI Regulatory Services will submit all unexpected study drug-related SAEs as per 21 CFR
32 DCRI Safety Surveillance will provide a safety alert letter to the NHLBI DSMB and DCC
clinical operation (for distribution to sites) within 15 days of initial receipt of the information
51
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Investigators are responsible for promptly reporting these events to their reviewing IRBs
according to site specific IRB reporting guidelines
62 Clinical Medical Monitoring
There will be an unblinded physician at the IPFnet DCC serving as medical monitor The
medical monitor will be available to assist with questions about dosage adjustments of study
medications including discontinuation or resumption of medications
63 Unblinding Procedures
Unblinding of subjects or investigators to subject treatment is strongly discouraged For ongoing
clinical management all subjects should be presumed to be receiving ldquoactiverdquo study drug To
ensure the subjectrsquos safety the study treatment will be dose-adjusted based on laboratory test
results clinical findings and symptoms
The IPFnet DCC medical monitor and PANTHER-IPF co-chairs Drs Ganesh Raghu and
Fernando Martinez will be available to the study physicians to discuss study drug management
on a case-by-case basis Un-blinding will be considered ONLY when the knowledge of subject
treatment assignment is ABSOLUTELY ESSENTIAL for subject safety and after discussion of
the subjectrsquos case with the medical monitor and either Dr Raghu or Dr Martinez Unblinding of
study treatment should be minimized during the conduct of the trial In those cases where it is
felt to be medically necessary the DCC medical officer will communicate directly with the
managing physician to minimize unblinding of study personnel
52
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
7 Study Drug Procedures
At the baseline 15-week 30-week and 45-week study visits subjects will receive a supply of
study drug sufficient to last until the next visit at which study drug will be dispensed
53
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
8 Data Management
81 Hardware and Software Configuration
811 Hardware and Database Software
Data will be stored in an Oracle database system Oracle has advantages of processing efficiency
and smooth linkage with other software systems The application and database will be hosted on
Solaris Unix servers at the IPFnet DCC
812 Statistical Software
SAS will be used as the principal application for the management of analysis data files and
statistical computations S-Plus will be used to provide supplementary functions as needed
813 Access Control and Confidentiality Procedures
Access to databases will be controlled centrally by the IPFnet DCC through user passwords
linked to appropriate privileges This protects the data from unauthorized changes and
inadvertent loss or damage
814 Security
Database and Web servers will be secured by a firewall and through controlled physical access
Oracle has many security features to ensure that any staff member accessing the database has the
proper authority to perform the functions he or she requests of the system Within the secondary
SAS databases Unix group-access control maintains similar security The Sun workstation login
is secured by extensive user-password facilities under Unix
54
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
815 Back-up Procedures
Database back-up will be performed automatically every day and standard IPFnet DCC policies
and procedures will be applied to dictate tape rotation and retention practices
816 Virus Protection
All disk drives that provide network services and all user computers will be protected using
virus-scanning software Standard IPFnet DCC policies will be applied to update these protection
systems periodically through the study
82 Sources of Data
821 Design and Development
The IPFnet DCC will be responsible for development of the electronic case report forms
(eCRFs) development and validation of the clinical study database ensuring data integrity and
training clinical center staff on applicable data management procedures A web-based distributed
data entry model will be implemented This system will be developed to ensure that guidelines
and regulations surrounding the use of computerized systems used in clinical trials are upheld
The remainder of this section provides an overview of the data management plan associated with
this protocol
822 Data Collection Forms
The data collection process consists of direct data entry at the study clinical centers into the EDC
system(s) provided by the DCC A data collection worksheet will be provided to clinical centers
for recording data in the event the EDC system is unavailable Data entry of the eCRFs should
be completed according to the instructions provided and project specific training The
investigator is responsible for maintaining accurate complete and up-to-date records and for
ensuring the completion of the eCRFs for each research participant
55
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
823 Data Acquisition and Entry
Data entry into eCRFs shall be performed by authorized individuals Selected eCRFs may also
require the investigatorrsquos written signature or electronic signature as appropriate Electronic
CRFs will be monitored for completeness accuracy and attention to detail during the study
824 Data Center Responsibilities
The IPFnet DCC will 1) develop a data management plan and will conduct data management
activities 2) provide final eCRFs for the collection of all data required by the study 3) develop
data dictionaries for each eCRF that will comprehensively define each data element 4) conduct
ongoing data monitoring activities on study data 5) monitor any preliminary analysis data
cleanup activities and 6) rigorously monitor final study data clean up
825 Data Editing
Completed data will be entered into the IPFnet DCC automated data acquisition and
management system If incomplete or inaccurate data are found a data clarification request will
be generated and distributed to clinical centers for a response Clinical centers will resolve data
inconsistencies and errors and enter all corrections and changes into the IPFnet DCC automated
data acquisition and management system
826 Training
The training plan for clinical center staff includes provisions for training on assessments eCRF
completion guidelines data management procedures and the use of computerized systems
56
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
9 Study Design and Data Analysis
91 General Analytic Considerations
All primary analyses will be based on intent-to-treat (ITT) principles using all randomized
subjects Baseline factors across groups will be compared using mean (standard deviation) and
median (25th and 75th percentiles) summary measures Kaplan-Meier curves will be used to
display event rates Due to clinical interest in departures from both sides of the null hypothesis
all test statistics will be 2-sided
Reasonable caution needs to be taken when conducting multiple analyses on key clinical
subgroups For subgroup analyses a conservative significance level of 0001 will be used for all
interaction tests Thus subgroup comparisons will be considered exploratory unless the p-value
from the interaction test is smaller than 0001
92 Randomization Blinding and Reporting of Results
A permuted block-randomization scheme will be created with varying block sizes stratified by
clinical center Once a subject has completed the screening and baseline period and evaluation
for inclusionexclusion criteria the randomization process will begin Subjects will be
randomized to receive NAC or matching placebo with equal probability (11) via telephone
contact with a central interactive voice response system (IVRS) using a toll-free randomization
number On the day of randomization after the subject has successfully met all inclusion and
exclusion criteria the investigator or designee will call the central randomization number to
obtain the assigned kit randomization numbers for that subject At each subject visit the
investigator or designee will call the central randomization number to obtain the new kit
randomization numbers for resupply of the subject For resupply of the clinical center the IVRS
will monitor minimal volume of a kit type andor expiration date and will automatically notify
the pharmacy
57
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
The trial results will be reported according to guidelines specified in the CONSORT statement
A flow diagram describing screening recruitment randomization dropout and vital status will
be included in the primary manuscript AEs and efficacy data will be presented for all treatment
groups Adherence dropout and lost to follow-up will be carefully examined across all treatment
groups Analyses of safety will be based on data from all randomized subjects who received at
least one dose of study drug
93 Stratification
Subjects will be distributed to the two treatment arms in a 11 allocation ratio Stratification
blocks will be based on clinical centers
94 Specification of the Primary Analyses
A mixed model repeated measures (MMRM) analysis described in section 95 will be used to
compare differences in the slope of FVC measurements across the treatment groups Response
variables are values of the FVC measured at baseline and every 15 weeks until study completion
Variables in the model will include treatment time and time by treatment age sex race and
height Contrast estimates of differences in slopes of treatment over time (along with confidence
intervals) will be used to estimate the treatment effect The validity of this model in terms of
meeting modeling assumptions will be assessed via standard modeling diagnostics and goodness-
of-fit measures Based on the MMRM framework missing FVC data will not be imputed for the
primary analysis
95 Analysis of Longitudinal Endpoints
A common goal in clinical trials is to specify models that are easily implemented and
reproducible by independent data analysts On the other hand the models should have proper
statistical behavior in terms of low bias and high precision Many common approaches to
longitudinal data analysis including last observation carried forward (LOCF) imputation rely on
the missing completely at random (MCAR) assumption However the MCAR assumption is
58
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
unlikely to hold in many clinical trials because missing data are often related to disease
progression and prognosis A more reasonable assumption missing at random (MAR) specifies
that the complete data distribution can be modeled using only the observed data The likelihood-
based MMRM approach is valid under the more general MAR assumptions These models will
be applied to analyze the longitudinal data secondary endpoints
The advantages of MMRM analysis are that all important characteristics of the model can be preshy
specified standard software can be used to implement the models and results are based on ITT
principles43 In addition the MMRM approach offers superior control of Type I and Type II
errors compared with the LOCF approach
Response variables are values of the PFTs measured at enrollment and every 15 weeks until
study completion and 6MWT values measured at baseline week 30 and week 60 Covariates are
treatment time time by treatment and key baseline risk factors Contrasts (along with
confidence intervals) of treatment by time will be used to estimate the treatment effect
The correlation structure involves multiple pieces including measurement errors random
variation and interindividual variability For the longitudinal data analyses an unstructured
correlation matrix for within-subject errors will be assumed Other correlation structures
including compound symmetry will be examined as needed A careful examination of reasons
for study discontinuation will be conducted to assess the validity of MCAR Sensitivity analyses
will be used to examine the untestable assumption that the observed data violate the MAR
assumption The MMRM models will be implemented using PROC MIXED in SAS
96 Analysis of Binary Time-to-Event and Time-Lagged Endpoints
Regression modeling approaches using either the logistic regression model or Cox proportional
hazards regression model will be employed when appropriate The validity of these models will
be assessed via standard modeling diagnostics and goodness-of-fit measures Estimates of
cumulative frequencies for more general time-lagged responses will be calculated using the
partitioned version of the Bang-Tsiatis estimator44 The partitions will be set at 15-week intervals
59
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
to correspond with the data-collection process Covariate adjusted event rates will be calculated
using inverse probability-weighted regression estimates45
97 Power Analysis
971 Primary Analyses
Based on previously published IPF clinical trials the PL group is expected to experience a drop
in FVC of approximately 020 L over the study period (see Figure 1) The IPFnet Steering Group
determined a clinically important difference would be to preserve the majority of the decline
relative to PL over the study period In particular a treatment effect of 015 L was determined to
be a clinically meaningful difference Potential dropout is a key factor in the proposed study The
drop-out process assumed 5 lost to follow-up after every study visit Only 80 of subjects
were assumed to be followed for the entire study period All models assumed a compound
symmetry structure for the covariance matrix Power calculations were performed using a SAS
IML program for designing repeated measures studies46 Based on preliminary reviews of the
data from the University of Michigan the covariance matrix parameters were estimated at
approximately σ2 = 0757 (variance parameter) and ρ = 0936 (correlation parameter) To be
conservative the power calculations for the primary analysis were performed with parameter
setting of σ2 = 0810 (variance parameter) and ρ = 0925 (correlation parameter)
The power calculations assume a correction for imperfect compliance proposed by Lachin and
Foulkes to allow for 2 noncompliance for each of the treatment arms47 Thus the sample size
of 130 subjects per arm would be reduced to an adjusted sample size of 130(1-002-002)2 =
1198 or 120 subjects per arm
Under the assumed Type I error rate of 005 with a correlation parameter of 0925 and standard
deviation of 090 the difference of 015 L (or 00025 Lweek) shown in Table 6 would have
power of 93
60
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Table 6 Hypothetical Values of Mean FVC (L) Change from Baseline
Week 15 Week 30 Week 45 Week 60
NAC 00125 00250 00375 00500
Placebo 00500 01000 01500 02000
Difference 00375 00750 01125 01500
Abbreviations FVC forced vital capacity PL placebo
972 Power Analysis for Secondary Endpoints
Power calculations for secondary endpoint measurements are shown in Table 7 Standard
deviations are based on unpublished data provided by the University of Michigan The
calculations are based on a 2-sample t-test with Type I error rate set at 005 These calculations
are likely to be conservative because the statistical approach described in section 95 for
analyzing these endpoints will incorporate incomplete observations as well as intermediate data
points
Table 7 Detectable Differences in Treatment Means for Selected Endpoint Measurements
Secondary Endpoints Std Dev
of the Baseline Score
Detectable Difference for 80 Power
Std Dev of the Change Score
Difference Detectable for
80 Power
DLCOpred 166 58 91 32
6MWT Area Under the Desaturation Curve
219 76 175 61
6MWT Distance to Desaturation 224 78 315 110
6MWT Minutes Walked 210 073 205 071
Abbreviations Std Dev standard deviation DLCOpred diffusing capacity of the lung for carbon monoxide percent predicted 6MWT 6-minute walk test
61
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
10 Study Administration
101 Cooperative Agreement Mechanism
The administrative and funding mechanism used to undertake this project is a ldquocooperative
agreementrdquo (U01) which is an assistance mechanism Under the cooperative agreement the
NHLBI assists supports andor stimulates the project and is substantially involved with
investigators in conducting the study by facilitating performance of the effort in a ldquopartnerrdquo role
The NHLBI project scientist serves on the IPFnet Steering Group and he or another NHLBI
scientist may serve on other project committees when appropriate At the same time however
NHLBI does not assume a dominant role direction or prime responsibility for this research
program
As described below governance of the project is conducted through the IPFnet Steering Group
Principal investigators have lead responsibilities in all aspects of their trials and the project
including any modification of trial designs conduct of the trials quality control data analysis
and interpretation preparation of publications and collaboration with other investigators unless
otherwise provided for by the IPFnet Steering Group
PIs retain custody of and have primary rights to their center-specific and collaborative data
subject to government rights-of-access consistent with current Health amp Human Services (HHS)
Public Health Service (PHS) and National Institutes of Health policies The protocols and
governance policies call for the continual submission of data centrally to the IPFnet DCC for the
collaborative database which at a minimum will contain the key variables selected by the IPFnet
Steering Group for standardization across all clinical centers the submission of copies of the
collaborative datasets to each PI upon completion of the project procedures for data analysis
reporting and publication and procedures to protect and ensure the privacy of medical and
genetic data and records of individuals The NHLBI project scientist on behalf of the NHLBI
will have the same access privileges and responsibilities regarding the collaborative data as the
other members of the Steering Group
62
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
PIs are also encouraged to publish and to publicly release and disseminate results data and other
products of the project concordant with the project protocols and governance and the approved
plan for making data and materials available to the scientific community and to the NHLBI
However during the 3 years after the ending date of NHLBI project support unpublished data
unpublished results data sets not previously released and other study materials or products are
to be made available to any third party only with the approval of the IPFnet Steering Group
Upon completion of the project PIs are expected to put their intervention materials and
procedure manuals into the public domain andor make them available to other investigators
according to the approved plan for making data and materials available to the scientific
community and the NHLBI for the conduct of research at no charge other than the costs of
reproduction and distribution
The NHLBI reserves the right to terminate or curtail the project (or an individual award) in the
event of (a) failure to develop or implement mutually agreeable collaborative measurement
subject eligibility and data management sections of the protocols (b) substantial shortfall in
subject recruitment follow-up data reporting or quality control or other major breach of
protocol (c) substantive changes in the agreed-upon protocols with which NHLBI cannot
concur (d) reaching a major project outcome with persuasive statistical significance
substantially before schedule or (e) human subject ethical issues that may dictate a premature
termination
Any disagreement that may arise in scientificprogrammatic matters (within the scope of the
award) between award recipients and the NHLBI may be brought to arbitration An arbitration
panel will be composed of 3 membersmdash1 selected by the IPFnet Steering Group (with the
NHLBI member not voting) or by the individual PI in the event of an individual disagreement a
second selected by NHLBI and the third selected by the other 2 members This special
arbitration procedure in no way affects the PIrsquos right to appeal an adverse action that is otherwise
appealable in accordance with the PHS regulations at 42 CFR part 50 Subpart D and HHS
63
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
regulation at 45 CFR part 16 or the rights of the NHLBI under applicable statutes regulations
and terms of the award
102 IPFnet Steering Group
The IPFnet Steering Group is the main governing body of the project It is composed of the PIs
of the clinical centers the PI of the DCC and the NHLBI project scientist The clinical centers
the IPFnet DCC and the NHLBI each have 1 vote on the IPFnet Steering Group All decisions
are determined by majority vote
All major scientific decisions are determined by the IPFnet Steering Group It assumes overall
responsibility for the design and conduct of the trial It appoints (and disbands) committees and
subcommittees as the need arises designs approves and implements the study protocols
oversees the development of the MOOP monitors subject recruitment and treatment delivery
evaluates data collection and management oversees quality assurance procedures and
implements changes and enhancements to the study as required It also has primary responsibility
for facilitating the conduct of the trials and reporting the projectrsquos results
103 Data and Safety Monitoring Board
The NHLBI will establish a DSMB in accordance with established policies (see
httpwwwnhlbinihgovfundingpoliciesdsmb_insthtm) to ensure data quality and subject
safety and to provide independent advice to the NHLBI regarding progress and the
appropriateness of study continuation
104 Recommendations on Interim Monitoring of Efficacy Safety and Futility
First and foremost the role of the DSMB will be to review subject safety and trial conduct at
periodic points during the study The DSMB may require analyses of the primary endpoint
results for comparing the benefit and risks of treatment strategies The benefit of collecting
additional data on key secondary endpoints with extended follow-up and establishing a robust
64
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
evidence base for determining a standard of care will need to be carefully considered before
early termination of one or more treatment arms After careful consideration the IPFnet Steering
Group recommends conservative thresholds for the early examinations of the safety and efficacy
data
The DSMB will be expected to meet approximately every 6 months until trial completion to
review safety and toxicity data The DSMB may recommend stopping the study based on these
reviews Because the DSMB could stop the trial for safety concerns as well as for a large
efficacy benefit there could be multiple opportunities to reject the null hypothesis (no difference
in event rates between the PL and NAC groups) A Bonferroni approximation will be applied
during the one planned interim analysis for efficacy
Before locking the database a statistical analysis plan (SAP) will be developed to provide
complete details on the statistical analysis The SAP will include the specifics for how and when
the DSMB will be notified for AEs The IPFnet DCC will deliver to the DSMB all FDA-defined
AEs at 3-month intervals The IPFnet DCC will prepare narrative SAE reports in real time for
DSMB review including recommendations and analysis of similar events for each SAE
submitted to the FDA
65
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
11 Investigator and Sponsor Obligations
111 Monitoring
All monitoring activities for US clinical centers will be performed in accordance with DCRI
standard operating procedures Information regarding the types of visits will be outlined in the
PANTHER-IPF MOOP
112 Cost and Payment
There will be no cost to subjects enrolled in this trial Study-related procedures will be paid for
by the IPFnet
Subjects may be eligible for reimbursement for travel to the clinical center Details of payment
will be explained to each subject during the consent process
113 Confidentiality and Health Insurance Portability and Accountability Act
Considerations
Subject confidentiality will be protected throughout the study All subject data will be kept
strictly confidential and no subject-identifying information will be released to anyone outside
the project Confidentiality will be assured through several mechanisms First each subject will
be assigned an anonymous study ID which will then be used on all study forms Second any
study forms blood samples and paper records that contain subject information (eg address lists
phone lists) will be kept at the clinical centers in secured locked areas coded by number Once
blood is collected there will be no subject identifiers placed on blood samplesmdashonly the study
ID number and the date of sample collection Third access to all subject data and information
including laboratory specimens will be restricted to authorized personnel In the case of
computerized data this restricted access will be assured through user logon IDs and password
protection
66
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
At the IPFnet DCC only authorized personnel will have access to the data files containing study
data Security will be assured through user logon IDs passwords and appropriate access
privileges All study subjects will be identified only by their IPFnet ID numbers and no personal
identifying information such as name address or Social Security number will be entered into
the IPFnet DCC database Any subject-specific data reported to the IPFnet Steering Group will
be identified only by the IPFnet ID number
Finally subjects will not be identified by name in any reports or publications nor will the data
be presented in such a way that the identity of individual subjects can be inferred Analysis files
created for further study by the scientific community will have no subject identifiers These data
files will be created in accordance with the Ancillary Studies and Publication Policy of the
IPFnet
114 Informed Consent Procedures
All IPFnet subjects will provide written informed consent using procedures reviewed and
approved by each clinical centerrsquos IRB Informed consent will be undertaken by study personnel
in-person with the subject The subject has the option of declining further participation in the
study at that point No further study procedures will be conducted until the signed documents
have been provided to the IPFnet clinical center
115 Institutional Review Boards
Before initiating this study the protocol clinical center-specific informed consent forms Health
Insurance Portability and Accountability Act (HIPAA) forms recruitment materials and other
relevant information will be reviewed by a properly constituted IRB at each participating clinical
center A copy of the signed and dated IRB approval at each clinical center will be retrieved prior
to or during the site initiation visit and archived at the IPFnet DCC Any amendments to the
protocol other than simple administrative and typographical changes must be approved by each
IRB before they are implemented The clinical centers will seek annual renewals of their IRB
approvals in accordance with local procedures
67
__________________________________________ ________________
__________________________________________
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
12 Investigator Agreement
I have read the foregoing protocol PANTHER-IPF and agree that it contains all necessary
details for carrying out this study I will conduct the study as outlined herein and will complete
the study within the time designated
I will provide copies of the protocol and all pertinent information to all individuals responsible to
me who assist in the conduct of this study I will discuss this material with them to ensure they
are fully informed regarding the drug and the conduct of the study
I will fulfill all responsibilities for submitting pertinent information to the local IRB if
applicable that is responsible for this study
I further agree that NHLBI andor DCRI will have access to any source documents from which
eCRF information may have been generated
Signature of Principal Investigator Date
Name of Principal Investigator (printed or typed)
Protocol version date May 19 2009
Protocol Amendment 1 version date May 28 2010
Protocol Amendment 2 version date December 6 2011
68
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
13 References
1 Raghu G Brown KK Bradford WZ et al A placebo-controlled trial of interferon gamma-1b in patients with idiopathic pulmonary fibrosis N Engl J Med 2004350125-33 2 King TE Jr Safrin S Starko KM et al Analyses of efficacy end points in a controlled trial of interferon-gamma1b for idiopathic pulmonary fibrosis Chest 2005127171-7 3 Flaherty KR Thwaite EL Kazerooni EA et al Radiological versus histological diagnosis in UIP and NSIP survival implications Thorax 200358143-8 4 Wells AU Desai SR Rubens MB et al Idiopathic pulmonary fibrosis a composite physiologic index derived from disease extent observed by computed tomography Am J Respir Crit Care Med 2003167962-9 5 Raghu G Freudenberger TD Yang S et al High prevalence of abnormal acid gastroshyoesophageal reflux in idiopathic pulmonary fibrosis Eur Respir J 200627136-42 6 Kinnula VL Focus on antioxidant enzymes and antioxidant strategies in smoking related airway diseases Thorax 200560693-700 7 Coultas DB Zumwalt RE Black WC Sobonya RE The epidemiology of interstitial lung diseases Am J Respir Crit Care Med 1994150967-72 8 Raghu G Weycker D Edelsberg J Bradford WZ Oster G Incidence and prevalence of idiopathic pulmonary fibrosis Am J Respir Crit Care Med 2006174810-6 9 Olson AL Swigris JJ Lezotte DC Norris JM Wilson CG Brown KK Mortality from pulmonary fibrosis increased in the United States from 1992 to 2003 Am J Respir Crit Care Med 2007176277-84 10 Mannino DM Etzel RA Parrish RG Pulmonary fibrosis deaths in the United States 1979shy1991 An analysis of multiple-cause mortality data Am J Respir Crit Care Med 19961531548shy52 11 Hubbard R Johnston I Coultas DB Britton J Mortality rates from cryptogenic fibrosing alveolitis in seven countries Thorax 199651711-6 12 Johnston I Britton J Kinnear W Logan R Rising mortality from cryptogenic fibrosing alveolitis Bmj 19903011017-21 13 Raghu G Collard HR Egan JJ et al An official ATSERSJRSALAT statement idiopathic pulmonary fibrosis evidence-based guidelines for diagnosis and management Am J Respir Crit Care Med 2011183788-824 14 (USA) FDA FDA Public Health Advisory Interferon gamma-1b (marketed as Actimmune) In 2007 15 King TE Jr Pardo A Selman M Idiopathic pulmonary fibrosis Lancet 2011 16 Raghu G Brown KK Costabel U et al Treatment of idiopathic pulmonary fibrosis with etanercept an exploratory placebo-controlled trial Am J Respir Crit Care Med 2008178948shy55 17 Malouf MA Hopkins P Snell G Glanville AR An investigator-driven study of everolimus in surgical lung biopsy confirmed idiopathic pulmonary fibrosis Respirology 201116776-83 18 King TE Jr Behr J Brown KK et al BUILD-1 a randomized placebo-controlled trial of bosentan in idiopathic pulmonary fibrosis Am J Respir Crit Care Med 200817775-81 19 Richeldi L Costabel U Selman M et al Efficacy of a tyrosine kinase inhibitor in idiopathic pulmonary fibrosis N Engl J Med 20113651079-87
69
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
20 Borok Z Buhl R Grimes GJ et al Effect of glutathione aerosol on oxidant-antioxidant imbalance in idiopathic pulmonary fibrosis Lancet 1991338215-6 21 Meyer A Buhl R Magnussen H The effect of oral N-acetylcysteine on lung glutathione levels in idiopathic pulmonary fibrosis Eur Respir J 19947431-6 22 Behr J Maier K Degenkolb B Krombach F Vogelmeier C Antioxidative and clinical effects of high-dose N-acetylcysteine in fibrosing alveolitis Adjunctive therapy to maintenance immunosuppression Am J Respir Crit Care Med 19971561897-901 23 Cantin AM North SL Fells GA Hubbard RC Crystal RG Oxidant-mediated epithelial cell injury in idiopathic pulmonary fibrosis J Clin Invest 1987791665-73 24 Waghray M Cui Z Horowitz JC et al Hydrogen peroxide is a diffusible paracrine signal for the induction of epithelial cell death by activated myofibroblasts Faseb J 200519854-6 25 Larios JM Budhiraja R Fanburg BL Thannickal VJ Oxidative protein cross-linking reactions involving L-tyrosine in transforming growth factor-beta1-stimulated fibroblasts J Biol Chem 200127617437-41 26 Kinnula VL Fattman CL Tan RJ Oury TD Oxidative stress in pulmonary fibrosis a possible role for redox modulatory therapy Am J Respir Crit Care Med 2005172417-22 27 Meyer A Buhl R Kampf S Magnussen H Intravenous N-acetylcysteine and lung glutathione of patients with pulmonary fibrosis and normals Am J Respir Crit Care Med 19951521055-60 28 Behr J Degenkolb B Krombach F Vogelmeier C Intracellular glutathione and bronchoalveolar cells in fibrosing alveolitis effects of N-acetylcysteine Eur Respir J 200219906-11 29 Bando M Hosono T Mato N et al Long-term efficacy of inhaled N-acetylcysteine in patients with idiopathic pulmonary fibrosis Intern Med 2010492289-96 30 Demedts M Behr J Buhl R et al High-dose acetylcysteine in idiopathic pulmonary fibrosis N Engl J Med 20053532229-42 31 Toma TP Bhowmik A Rajakulasingam R Acetylcysteine in pulmonary fibrosis N Engl J Med 20063541086-9 author reply -9 32 Hunninghake GW Antioxidant therapy for idiopathic pulmonary fibrosis N Engl J Med 20053532285-7 33 Flaherty KR Mumford JA Murray S et al Prognostic implications of physiologic and radiographic changes in idiopathic interstitial pneumonia Am J Respir Crit Care Med 2003168543-8 34 Latsi PI du Bois RM Nicholson AG et al Fibrotic idiopathic interstitial pneumonia the prognostic value of longitudinal functional trends Am J Respir Crit Care Med 2003168531-7 35 Collard HR King TE Jr Bartelson BB Vourlekis JS Schwarz MI Brown KK Changes in clinical and physiologic variables predict survival in idiopathic pulmonary fibrosis Am J Respir Crit Care Med 2003168538-42 36 Jegal Y Kim DS Shim TS et al Physiology is a stronger predictor of survival than pathology in fibrotic interstitial pneumonia Am J Respir Crit Care Med 2005171639-44 37 Martinez FJ Safrin S Weycker D et al The clinical course of patients with idiopathic pulmonary fibrosis Ann Intern Med 2005142963-7 38 Hull JH Acetylcysteine in pulmonary fibrosis N Engl J Med 20063541089-91 author reply -91
70
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
39 Flaherty KR King TE Jr Raghu G et al Idiopathic interstitial pneumonia what is the effect of a multidisciplinary approach to diagnosis Am J Respir Crit Care Med 2004170904shy10 40 Raghu G Johnson WC Lockhart D Mageto Y Treatment of idiopathic pulmonary fibrosis with a new antifibrotic agent pirfenidone results of a prospective open-label Phase II study Am J Respir Crit Care Med 19991591061-9 41 Hunninghake GW Lynch DA Galvin JR et al Radiologic findings are strongly associated with a pathologic diagnosis of usual interstitial pneumonia Chest 20031241215-23 42 Lynch D Godwin J Safrin S et al High-resolution computed tomography in idiopathic pulmonary fibrosis diagnosis and prognosis Am J Respir Crit Care Med 2005172488-93 43 Mallinckrodt CH Watkin JG Molenberghs G Carroll RJ Choice of the primary analysis in longitudinal clinical trials Pharmaceutical Statistics 20043161-9 44 Bang H Tsiatis A Estimating medical costs with censored data Biometrika 200087329shy43 45 Lin DY Regression analysis of incomplete medical cost data Stat Med 2003221181-200 46 Rochon J Application of GEE procedures for sample size calculations in repeated measures experiments Stat Med 1998171643-58 47 Lachin JM Foulkes MA Evaluation of sample size and power for analyses of survival with allowance for nonuniform patient entry losses to follow-up noncompliance and stratification Biometrics 198642507-19
71
- PANTHER-IPFPREDNISONE AZATHIOPRINEAND N-ACETYLCYSTEINEA STUDY THAT EVALUATES RESPONSE INIDIOPATHIC PULMONARY FIBROSIS
-
- Protocol Summary
- Table of Contents
- List of Tables
- List of Figures
- List of Abbreviations
- 1 Summary
- 2 Hypotheses and Specific Aims
-
- 21 Null Hypothesis
- 22 Specific Aim 1
- 23 Specific Aim 2
- 24 Prespecified Subgroups of Interest
-
- 3 Background and Significance
-
- 31 Idiopathic Pulmonary Fibrosis is the Most Common Interstitial Lung Disease
- 32 Rationale for Placebo Control
- 33 Rationale for N-acetylcysteine
- 35 Rationale for N-acetylcysteine as a Stand-alone Therapy
- 36 Rationale for the Study Design and Primary Endpoint
- 37 Rationale for Blinding of Treatments
-
- 4 Methods
-
- 41 Inclusion Criteria
- 42 Diagnosis of IPF
- 43 Exclusion Criteria
- 44 Study Design and Study Visit
- 45 Dose Justification
- 46 Contraindications Precautions and Side Effects of Study Medications
- 47 Recruitment Procedures
- 48 Study Procedures
- 49 Concomitant Medications
- 410 Laboratory Testing
- 411 Blinding of Study Drugs
-
- 5 Study Endpoints
-
- 51 Primary Study Endpoint
- 52 Secondary Study Endpoints
-
- 6 Safety Evaluations and Procedures
-
- 61 Adverse Events
- 62 Clinical Medical Monitoring
- 63 Unblinding Procedures
-
- 7 Study Drug Procedures
- 8 Data Management
-
- 81 Hardware and Software Configuration
- 82 Sources of Data
-
- 9 Study Design and Data Analysis
-
- 91 General Analytic Considerations
- 92 Randomization Blinding and Reporting of Results
- 93 Stratification
- 94 Specification of the Primary Analyses
- 95 Analysis of Longitudinal Endpoints
- 96 Analysis of Binary Time-to-Event and Time-Lagged Endpoints
- 97 Power Analysis
-
- 10 Study Administration
-
- 101 Cooperative Agreement Mechanism
- 102 IPFnet Steering Group
- 103 Data and Safety Monitoring Board
- 104 Recommendations on Interim Monitoring of Efficacy Safety and Futility
-
- 11 Investigator and Sponsor Obligations
-
- 111 Monitoring
- 112 Cost and Payment
- 113 Confidentiality and Health Insurance Portability and Accountability ActConsiderations
- 114 Informed Consent Procedures
- 115 Institutional Review Boards
-
- 12 Investigator Agreement
- 13 References
-

PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Measure height and weight
Serum pregnancy test (if applicable)
Measure vital signs including oximetry
Blood draws performed and the following analyses conducted
o Hematology (red cell count white cell count hemoglobin hematocrit cell indices differential
platelet count)
o Blood chemistries according to central laboratory protocol (see Section 410 Laboratory
Testing)
o Beta human chorionic gonadotropin (serum) pregnancy test (in women of childbearing potential)
o Urinalysis
Pulmonary Function Tests (PFTs) including spirometry pre- and post- bronchodilator and postshy
bronchodilator measurement of lung volumes and measurement of hemoglobin adjusted diffusing
capacity
Measure ABGs
HRCT if a satisfactory scan has not been performed on the subject within 3 months of screening (see
PANTHER-IPF MOOP for more details)
Surgical lung biopsies (if applicable) reviewed by local and central pathology departments
Current medications If required a washout period discussed with the subject and initiated at this visit
4422 Enrollment
The enrollment visit is expected to take place within eight weeks of the screening visit Enrollment visit
activities include
Measure vital signs including oximetry
Measure height and weight
Serum pregnancy test (if applicable)
If consent has been given blood will be drawn and a urine specimen collected for the bio-specimen
repository
Spirometry (post-bronchodilator)
Measure 6MWT with Borg Dyspnea Scale
29
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Collect Quality-of-life (QOL) data using the SF-36 EuroQol Investigating Choice Experiments for
Preferences of Older People Capability Instrument (ICE CAP) and SGRQ
Female subjects complete Gender Substudy questionnaire
Dyspnea status collected using the UCSD SOBQ
Evaluate Acute Exacerbation (AEx)
Review of any Adverse Events (AEs)
Review of concomitant medications
Subject receives diary and instructions on its purpose and proper use
Subject receives supply of study drug sufficient to last until his or her 15-week study visit
See the Schedule of Assessments (Table 3) for more details Subjects with screening and enrollment postshy
bronchodilator FVC measurements (in liters) differing by more than 11 are not eligible to be enrolled in the
study
Subjects will be asked to provide a physician of record This physician will be considered the subjectrsquos primary
care provider (PCP) and if the subject agrees the PCP will be informed by letter of the subjectrsquos enrollment in
the trial The subject will be informed that his or her ongoing medical care should be received from the PCP
The PCP will be informed of any safety issues identified by the study staff The PCP will also be given
information regarding communication with study personnel about pertinent health issues or clinic encounters
the subject may have
4423 Week 15
The week 15 visit is expected to occur within +- 14 days of the subjectrsquos scheduled visit time (eg the week 15
visit should occur anytime between 13 and 17 weeks after starting study drug Week 15 activities include
Measure vital signs with oximetry
Measurement height and weight
Serum pregnancy test (if applicable)
Spirometry (post-bronchodilator) measurement
Review of AEs
Evaluate for AEx
30
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Review concomitant medications
If consented draw blood and collect urine specimen for the biospecimen repository
Subjects return used and unused study drug for the visit
Review study diary and a new study diary will be given
Provide additional supply of study drug sufficient to last until the next scheduled visit
4424 Week 30
The week 30 visit is expected to occur within +- 14 days of the subjectrsquos scheduled visit time (eg the week 30
visit should occur anytime between 28 and 32 weeks after starting study drug) Week 30 activities include
Physical examination
Measure vital signs with oximetry
Measure height and weight
Laboratory values (complete blood count [CBC] and serum chemistries)
Serum pregnancy test (if applicable)
Measure spirometry (post-bronchodilator)
6MWT with Borg scale
DLCO
Review of AEs
Evaluate for AEx
Review concomitant medications
Complete all QOL and dyspnea questionnaires (EuroQol ICE CAP SF-36 SGRQ and UCSD SOBQ)
If consent has been given blood will be drawn and a urine specimen collected for the biospecimen
repository
Review study diary
Subjects return used and unused study drug for the visit
Provide additional supply of study drug sufficient to last until the next scheduled visit
4425 Week 45
31
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
The week 45 visit is expected to occur within +- 14 days of the subjectrsquos scheduled visit time (eg the week 45
visit should occur anytime between 43 and 47 weeks after starting study drug) Week 45 activities include
Measure vital signs with oximetry
Measure height and weight
Serum pregnancy test (if applicable)
Measure spirometry (post-bronchodilator)
Review of AEs
Evaluate for AEx
Review concomitant medications
If consent has been given blood will be drawn and a urine specimen collected for the biospecimen
repository
Subjects return used and unused study drug for the visit
Study diary reviewed
Provide additional supply of study drug sufficient to last until the next scheduled visit
4426 Week 60 (Early Withdrawal or Final Treatment Visit)
At week 60 or at subject withdrawal from the study (premature by study doctor or subjectrsquos decision) a final
treatment visit will occur At this final treatment visit subjects will discontinue NACPL abruptly Week 60
activities also include
Physical examination
Measure vital signs with oximetry
Measure height and weight
Laboratory values (complete blood count [CBC] and serum chemistries)
Spirometry (post-bronchodilator) measurement
6MWT with Borg scale measurement
DLCO
Lung volumes
ABG
Review of AEs
32
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Evaluate for AEx
Review concomitant medications
Subjects will complete all QOL and dyspnea questionnaires (EuroQol ICE CAP SF-36 SGRQ and
UCSD SOBQ)
If consent has been given blood will be drawn and a urine specimen collected for the biospecimen
repository
Subjects return used and unused study drug for the visit
Study diary reviewed
4427 Final Site Visit ndash FVC drop confirmation
In the event that the subject has a recorded FVC drop of gt10 from baseline at the final treatment visit and the
subject has not had a confirmation of such a drop at a previous study visit the subject should return to the
clinical site 6 to 8 weeks after the final treatment visit During this visit a post-bronchodilator spirometry test
will be performed This FVC measurement will be evaluated according to section 521 of this protocol
4428 Final Visit ndash Telephone Follow-up
Four weeks following the final dose of study medication subjects will receive a telephone call from the study
coordinator to ensure that there are no side effects and to follow up on any ongoing adverse events (AEs)
4429 Phone Contact Between Visits
At week 2 and each month that a subject does not have a scheduled clinical center visit his or her study
coordinator will contact him or her at least once by telephone to
Inquire if the subject has had any hospitalizations events that might be considered an AE or any events
significant enough to warrant an out-of-cycle visit to the clinical center
Remind subjects of their current dosage levels and confirm that the subject understands them
Address any questions or concerns the subject might have regarding other aspects of the study
Assess adherence to the treatment regimen by reviewing diary data verbal review of medications taken
including nutritional supplements
33
34
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Table 3 Schedule of Assessments
Procedure Screening Visit 0
Enrollment Visit 1
Week 15 Visit 2
Week 30Visit 3
Week 45 Visit 4
Week 60 Early
Withdrawal Visit 5
Final1
Visit (via phone)
Informed consent X
Medical history X
Inclusionexclusion criteria X
Serum pregnancy test (if applicable) X X X X X
Review of lung biopsy X
Arterial Blood Gas X X
6-Minute Walk Test
X
X X
Physical examination X X X
Vital signs with oximetry X X X X X X
Body height and weight X X X X X X
Complete Blood Count X X X
Chemistry panel X X X
Monitor Lab Values X X X
Urinalysis X Specimen repository substudy blood draw and urine collection (if consented)
X
X X X X
HRCT (if not completed within three months) X
Spirometry (pre- and post-bronchodilator) X
Spirometry (post-bronchodilator only) X X X X X
DLCO (post-bronchodilator only) X X X
Lung volumes (post-bronchodilator only) X
X
Evaluate for acute exacerbation X X X X X
Review Adverse Events X X X X X X
Review concomitant meds X X X X X X
Dispense subject diary X X X X
Review subject diary X X X X X
Dispense study agent X X X X
Gender Substudy questionnaire (female subjects only) X
EuroQol ICECAP UCSD SOBQ SGRQ SF-36 X X X
Abbreviations DLCO diffusing capacity of the lung for carbon monoxide QOL Quality of Life ICECAP Investigating Choice Experiments for Preferences of Older People UCSD SOBQ University of California Shortness of Breath Questionnaire SGRQ St Georgersquos Respiratory Questionnaire SF-36 Short Form 36 Health Survey
1Follow-up visit via phone will occur four weeks after final dose of study medication
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
45 Dose Justification
The general philosophy for determining dosing levels was to apply previously examined
treatment regimens With the focus of the study being to establish a standard of care for
mildmoderate IPF subjects the goal was to develop flexible yet standardized treatment rules that
allow for the temporary or permanent withholding of one or more components of treatment when
necessary Subjects developing laboratory abnormalities or symptoms that result in
discontinuation of one or more components of study treatment may continue on the other
components as long as there is no contraindication for this Complete follow-up is important for
the validity of any study As a strategy to maintain protocol adherence we are using a treatment
regimen that will detect potential side effects and prompt interventions proactively in the interest
of patient safety In addition subjects who permanently stop study medications during the course
of the study are encouraged to continue in the study completing all scheduled visits and tests
451 Rationale for N-acetylcysteine Dosing
To our knowledge there have been no IPF studies to correlate clinical outcome measures with
different dosages for NAC The dosage chosen is based on the IFIGENIA study However BAL
lung GSH levels from subjects with IPF have been augmented with the use of oral NAC at 600
mg 3 times per day In addition lung GSH levels have been associated with improved
PFTs212227 The dose chosen for this study was based on previous data including the IFIGENIA
study30
4511 Dosing of N-acetylcysteineplacebo
Dosing of NACPL will be 600 mg orally 3 times a day (1800 mgday)
4512 Reasons to Discontinue N-acetylcysteineplacebo
NACPL may be temporarily or permanently discontinued for the duration of the study for
gastrointestinal symptoms or dermatologic reactions
35
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Temporarily discontinue (hold) oral NACPL for subjects requiring inpatient admission for acute
exacerbation (AEx) or other conditions Resume NACPL after discharge
36
37
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
452 Dosage Algorithms
Dosage Adjustment Algorithm 1 NACPL Dose Modifications for Gastrointestinal Symptoms Nausea Vomiting Abdominal Discomfort Diarrhea
GI Symptoms determined by the PI to be clinically significant Nausea Vomiting Abdominal Discomfort Diarrhea
NACPL Temporarily dc (HOLD) x 3 Days
Monitor symptoms intervene as clinically indicated (eg fluid replacement antidiarrhea or antinausea medication)
Monitor or lab PRN
Are symptoms resolving after 3 days NO
Symptoms NOT resolving after 3 days of holding study medication Assessmentmanagement per clinical
discretion of investigator
Likely not study medication discuss resuming study medication with medical monitor when symptoms resolved
YES
Temporarily dc (HOLD) NACPL for 4 additional days (total hold 1 week) then NACPL Resume 600 MG TID
Did symptoms recur
YES
STOP NACPL for
duration of study
NO
NACPL No Change
38
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Dosage Adjustment Algorithm 2 NACPL Dose Modifications For Dermatologic Reactions
Dermatologic Reactions (Not Acneiform) ge Grade 2 Grading per Common Terminology Criteria for
Adverse Events V30 (httpctepcancergov) For example Grade 1 RASHDESQUAMATION Macular or papular eruption or erythema without associated symptoms Grade 2 RASHDESQUAMATION Macular or popular eruption or erythema with pruritus or other associated symptoms localized desquamation or other lesions covering lt50 of body surface area
NACPL Temporarily dc (HOLD) x 3 days
Are symptoms resolving after 3 days
NO Symptoms not resolving after 3 days of holding study medication Assessmentmanagement per clinical discretion of investigator Likely not study medication Discuss resuming study medication with medical monitor when symptoms
resolved YES
Temporarily dc (HOLD) NACPL for 4 additional days (total hold 1 week) then NACPL resume 600 MG TID
Did symptoms recur
YES
STOP NACPL for
duration of study
NO
NACPL No change
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
46 Contraindications Precautions and Side Effects of Study Medications
461 Contraindication
Contraindication to NAC is known hypersensitivity to it
462 Precautions
Concomitant administration of oral NAC and antibiotics has shown a slightly reduced absorption
of cephalexin and a slight increase in erythromycin serum levels NAC contains free sulfhydryl
groups There is no evidence that individuals sensitive to sulfa drugs are sensitive to NAC
The NAC preparation being administered in this study contains 20 mg of aspartame Because of
the phenylalanine component of aspartame individuals with phenylketonuria should avoid or
restrict aspartame intake to avoid increased blood levels of phenylalanine Because of this risk
labeling is required on all products containing aspartame
463 Side Effects
Side effects of NAC range from common to serious See Table 4
39
40
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Table 4 Side Effects of NAC
Undesirable Effects
System-organ class Uncommon
(gt11000 lt1100)
Rare
(gt110000 lt11000)
Very rare
(lt110000) Not known
Immune system disorders Hypersensitivity Anaphylactic shock
reaction
Nervous system disorders Headache
Ear and labyrinth disorders Tinnitus
Cardiac disorders Tachycardia
Vascular disorders Hemorrhage
Respiratory thoracic and
mediastinal disorders
Bronchospasm
Dyspnea
Gastrointestinal disorders
Vomiting diarrhea
stomatitis abdominal
pain nausea
Dyspepsia
Skin and subcutaneous tissue
disorders
Urticaria rash
angioedema itching
General disorders and
administration site conditions Pyrexia
Investigations Reduced arterial
pressure Face edema
In very rare cases the onset of severe skin reactions such as Stevens-Johnson syndrome and Lyell syndrome was reported to have a temporal relationship with N-acetylcysteine administration Although in most cases at least another suspect drug probably most involved in the genesis of the above mentioned mucocutaneous syndromes has been identified in case of mucocutaneous alterations it is appropriate to contact onersquos doctor and the administration of N-acetylcysteine should be immediately discontinued
Some studies confirmed a reduction of platelet aggregation during N-acetylcysteine administration The clinical significance of these findings has not been defined yet [Source Fluimucil Investigator Brochure]
47 Recruitment Procedures
Subjects recruited for this study will be established patients of the investigators or physician- or
self-referred to participating clinical centers in the IPFnet Each clinical center within IPFnet has
a well-developed infrastructure of local pulmonologists within the surrounding geographic area
These pulmonologists are kept informed of ongoing IPF clinical trials and regularly refer
subjects to studies conducted at IPFnet clinical centers
Additional steps will be taken to inform clinicians of the trials in progress within IPFnet
including presentations at faculty staff meetings at local hospitals medical grand rounds and
national conferences direct mail notification monthly faxes and advertisement of network trials
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
in pulmonary journals Clinical center patients previously diagnosed with IPF will be notified of
the trials by mail whenever possible
Recruitment of minorities and women will be monitored by the DCC and DSMB If necessary
additional recruitment efforts will be made at specific centers to ensure that the aggregate subject
sample contains appropriate representation of women and minorities
48 Study Procedures
The following procedures are detailed in the PANTHER-IPF MOOP accompanying this
protocol
1 PFT
2 ABG
3 HRCT scan of the chest (including imaging of pulmonary arteries)
4 CBC and serum chemistries
5 Pregnancy test
6 6MWTBorg Dyspnea Scale
7 QOL questionnaires (EuroQol HAD SF-36 SGRQ and ICE CAP)
8 UCSD SOBQ
9 Gender Substudy Questionnaire
All assessments of PFTs will be conducted by study personnel not directly involved in the
treatment of the subjects
481 Biological Specimen Management
4811 Biological Specimen Sample Management
Subjects at clinical centers participating in the specimen repository substudy who consent to
having blood drawn for research purposes and for the banking of blood blood components and
other biologic specimens (urine and BAL fluid) will have approximately 405 mL of blood
41
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
drawn 17 mL blood drawn for DNA and 20 mL of urine collected at enrollment visit Subjects
will have approximately 50 mL of blood drawn and 20 mL of urine collected at each 15-week
follow-up visit Blood specimens will be separated according to PANTHER-IPF MOOP
guidelines into the following components for banking in the repository serum plasma and
DNA Coding of all biologic specimens for the repository will be performed by study staff at the
clinical center The samples will be processed per PANTHER-IPF MOOP guidelines aliquoted
labeled with barcode labels and stored at -70degC at the clinical center and shipped to the central
repository
The only subject identifiers will be a sample ID number and subject initials This sample ID will
be linked in the IPFnet DCC clinical database to subject information No subject information will
be transferred to the biological-specimen database
The subjectrsquos samples may be used for approved sub-studies relating to human disease
including but not limited to IPF The studies for which an individualrsquos samples will be made
available will be determined by the subjectrsquos answers to questions on the biological-sample
informed consent form The subjects can choose to make their samples available for all options
or any combination Samples will be made available to researchers only with IPFnet Steering
Group approval until such time as the samples are made public through the NHLBI repository
49 Concomitant Medications
Concurrent treatment with FDA-approved therapy for IPF is allowed Colchicine may be used
for treatment of gout Temporary treatment with oral or IV corticosteroids for clinical worsening
or suspected AEx is permitted Nutritional supplements containing NAC are not allowed
410 Laboratory Testing
Clinical laboratory parameters will be assessed at screening and at the end of the study The
following tests will be performed at the two time points specified in the protocol chemistry (AG
ratio ALT [SGPT] AST [SGOT] albumin alkaline phosphatase amylase bilirubin-direct
42
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
bilirubin-indirect bilirubin-total BUN BUNcreatinine ratio calcium carbon dioxide
cholesterol-total chloride CPK-total creatinine GGT globulin glucose iron-total LDH
lipase magnesium phosphorus-inorganic potassium protein-total sodium TIBC triglycerides
uric acid) and hematology (red blood cell count WBC count hemoglobin hematocrit cell
indices differential platelet count)
411 Blinding of Study Drugs
Subjects and caregivers will be blinded to study treatment Every subject will receive NAC or
matching PLs at every study visit from the baseline visit to the week-45 visit No study agent
will be dispensed at the week-60 visit
43
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
5 Study Endpoints
51 Primary Study Endpoint
The primary endpoint will be the change in serial measurements of FVC over the study period
52 Secondary Study Endpoints
521 Time to Disease-progression
The time-to-death or a 10 decline in FVC will be defined as the time-to-disease progression
The 10 decline in FVC from enrollment must be confirmed on 2 consecutive visits no less than
6 weeks apart For subjects with 2 consecutive visits with a 10 decline in FVC the time-toshy
disease progression will be defined as the time interval between enrollment and the initial visit
with a 10 FVC decline For subjects who experience disease progression the study doctor will
determine whether or not the subject will remain in the study
522 Acute Exacerbations
The following 3 criteria will define AEx in subjects with acute worsening of their respiratory
conditions
1 Clinical (all of the following required)
A) Unexplained worsening of dyspnea or cough within 30 days triggering unscheduled
medical care (eg emergency room clinic study visit hospitalization)
B) No clinical suspicion or overt evidence of cardiac event pulmonary embolism or deep
venous thrombosis to explain acute worsening of dyspnea
C) No pneumothorax
44
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
2 RadiologicPhysiologic (A and B required)
A) New ground glass opacity or consolidation computed tomography (CT) scan OR new
alveolar opacities on chest x-ray
B) Decline of ge 5 in resting room air SpO2 from last recorded level OR decline of ge 8 mm
Hg in resting room air PaO2 from last recorded level
3 Microbiologic (all of the following required)
A) No clinical evidence for infection (ie absence of grossly purulent sputum fever gt 39degC
orally)
B) Lack of positive microbiological results (if done) from lower respiratory tract defined as
(1) Clinically significant bacterial growth on sputum or endotracheal aspirate cultures
(2) Quantitative culture by protected brush specimen ge 103 cfumL or BAL ge 104 cfumL
(3) The presence of specific pathogens on stains of any of the above
C) Lack of positive pathogen in blood cultures (if done)
Identification of Acute Exacerbations
All subjects will be educated about the importance of identifying AExs At the time of
enrollment subjects will be told about the possibility of developing acute symptomatic
worsening that might represent an AEx of IPF and instructed to contact their study clinical
center coordinator within 48 to 72 hours of the apparent event
All subjects will be contacted by phone monthly and questioned about any change in dyspnea or
cough and any interim clinic visits or hospitalizations Finally as part of the IPFnet outreach to
community referring physicians the importance of AExs will be emphasized When a subject is
identified who meets criterion 1A this will trigger the collection of additional clinical data to
evaluate a suspected AEx These data will be collected as part of standard clinical care (ie this
protocol does not require collection of all items) The additional items to be collected for
suspected AEx include
IPFnet AEx case report form (eCRF) (required)
45
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Chest x-ray CT scan withwithout pulmonary angiogram (reports should be faxed and
followed by the hard copiesdiscs)
Oxygen saturation (pulse oximetry)
ABG
Respiratory cultures (sputum endotracheal aspirate lavage)
Blood cultures
Clinichospital records related to the event
All potential cases of AEx will be reviewed by the clinical center PI first and a decision on
whether the case may represent an AEx will be made If AEx is suspected the case will be sent
to the IPFnet adjudication committee which will assign a final diagnosis (see Table 5) If there is
disagreement among members the majority opinion will be recorded
During episodes of suspected AEx as determined by the individual clinical center investigator
subjects will remain blinded and in the study
Table 5 Final Diagnoses in Evaluation of Suspected Acute Exacerbations
Definite acute exacerbation All criteria met no alternative etiology
Unclassifiable acute worsening
Insufficient data to evaluate all criteria no alternative etiology
Not acute exacerbation Alternative etiology identified that explains acute worsening
Management of the suspected AEx will be at the discretion of the treating physician Standard of
care generally involves evaluation for respiratory infection pulmonary embolism cardiac events
and pneumothorax and treatment with IV corticosteroids
Study drugs will be resumed at pre-suspected AEx doses after subjects clinically improve as
confirmed by the local PI All subjects should be seen at the clinical center within 2 to 4 weeks
of recovery for measurement of post-bronchodilator FVC (see Figure 4) Subjects unable to
return to the clinical center after suspected AEx due to medical frailty (eg continued
46
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
institutionalization progressive disability) will be categorized as failing to maintain FVC
response in secondary analyses
Suspected AEx (PI determined)
Hold study drug Treat AEx
(Attending physician determined)
Alive but unable to continue due to
medical frailty
Dead
Alive and able to continue
Site reviewvisit
Restart study drug
FVC within 2-4 weeks
Figure 4 Acute Exacerbation Flow Chart
523 Respiratory Infections
An upper respiratory infection will be defined as
Change in sputum discoloration
Increased cough of no more than 14 daysrsquo duration
A lower-respiratory infection (pneumonia) will be defined as new segmental or lobar airspace
opacities visualized by image studies (chest radiograph or HRCT) in addition to any of the
following
Positive pathogencultures in good sample of sputum or lower-airway secretions retrieved
by fiberoptic bronchoscope
Fever gt 39degC or gt 100degF
Leukocytosis gt 12000 (unexplained no increase in dose of corticosteroids)
47
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
524 Maintained FVC Response
Subjects with follow-up FVCpred measurements at or above their baseline FVCpred level
will be classified as having maintained FVC response Subjects with reduced FVCpred levels
or missing data for any reason including death or medical frailty will be classified as having not
maintained FVC response The FVCpred value is used because unadjusted FVC measurements
are expected to decline with age
48
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
6 Safety Evaluations and Procedures
61 Adverse Events
During a clinical trial the reporting of adverse experience information can lead to important
changes in the way a new treatment is developed as well as provide integral safety data
611 Definitions
An adverse event (AE) is any untoward medical occurrence in a subject or clinical investigation
subject who was administered a pharmaceutical product The AE does not necessarily have to
have a causal relationship with the drug administered An AE can be any unfavorable and
unintended sign (including an abnormal laboratory finding) symptom or disease temporarily
associated with the use of a medicinal product whether or not considered to be related to the
medicinal product Diseases signs symptoms or laboratory abnormalities already existing at
enrollment are not considered AEs unless they worsen (ie increase in intensity or frequency)
Surgical procedures themselves are not AEs they are therapeutic measures for conditions that
require surgery The condition for which the surgery is required may be an AE Surgical
procedures planned before randomization and the conditions necessitating the surgery are not
AEs
A serious adverse event is any untoward event that
Is fatal
Is life-threatening
Requires inpatient hospitalization or prolongation of existing hospitalization with the
following exceptions
o Preplanned (before the study) hospital admissions unless the hospitalization is
prolonged
o Planned admissions (as part of a study eg routine biopsies)
o Hospitalization lasting lt 24 hours
49
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
o Hospitalization for elective procedure
o Emergency room visits
Results in persistent or significant disability or incapacity
Is a congenital anomaly or birth defect
Important medical events that may not result in death be life-threatening or require
inpatient hospitalization may be considered serious adverse events (SAEs) when based
on appropriate medical judgment they may jeopardize the subject and may require
medical or surgical intervention to prevent one of the outcomes listed above
Life-threatening means that the subject was in the view of the investigator at immediate risk of
death from the AE as it occurred It does not include an AE that had it occurred in a more severe
form might have caused death
Persistent or significant disabilityincapacity means that the event resulted in permanent or
significant and substantial disruption of the subjectrsquos ability to carry out normal life functions
Causality
A reasonable possibility means the AE may have been caused byrelated to the study drug A
perceived or real lack of efficacy does not satisfy the definition of relatedness
612 Adverse Event (AE) Reporting
For the PANTHER-IPF trial all AEs (serious and nonserious) occurring from randomization
through final study visit (4 weeks after final dose of all study medication) will be recorded on the
AE page of the case report form (CRF)
6121 Serious Adverse Events (SAE) Reporting
For this trial all deaths and all SAEs which occur from randomization through final study visit
must be entered within the EDC system via the SAE eCRF page within 24 hours of the
investigative sitersquos knowledge of the event It is the responsibility of the clinical center
50
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
investigator to provide a causality assessment of the event for each study medications based upon
the information available at the time of the report It is understood that complete information
about the event may not be known at the time the initial report is submitted In the event the EDC
system is not accessible to the site at the time of event reporting investigative sites will complete
and forward a paper back-up SAE form to DCRI Safety Surveillance for processing
DCRI Safety Surveillance
Telephone 1-919-668-8624 or 1-866-668-7799 (toll free)
Fax 1-919-668-7138 or 1-866-668-7138 (toll free)
The investigator must complete and submit follow-up SAE information via the eCRF when
important new or follow-up information (eg final diagnosis outcome results of specific
investigations) becomes available Follow-up information should be submitted according to the
same process used for reporting the initial event as described above All SAEs will be followed
until resolution stabilization or 30 days after the subject has completed the final visit (4 weeks
after the final dose of study medication) whichever occurs first The investigator is responsible
for reporting SAEs to their institutional review board (IRB) per site specific IRB reporting
guidelines
6122 Regulatory Reporting
AEs that are serious study drug related and unexpected will be reported to the regulatory
authorities The DCRI Safety Surveillance medical monitor will perform a medical review of all
SAEs submitted and evaluate for ldquounexpectednessrdquo DCRI Safety Surveillance will prepare
MedWatch reports for those events identified as serious study drug related and unexpected as
determined by Safety Medical Monitor
DCRI Regulatory Services will submit all unexpected study drug-related SAEs as per 21 CFR
32 DCRI Safety Surveillance will provide a safety alert letter to the NHLBI DSMB and DCC
clinical operation (for distribution to sites) within 15 days of initial receipt of the information
51
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Investigators are responsible for promptly reporting these events to their reviewing IRBs
according to site specific IRB reporting guidelines
62 Clinical Medical Monitoring
There will be an unblinded physician at the IPFnet DCC serving as medical monitor The
medical monitor will be available to assist with questions about dosage adjustments of study
medications including discontinuation or resumption of medications
63 Unblinding Procedures
Unblinding of subjects or investigators to subject treatment is strongly discouraged For ongoing
clinical management all subjects should be presumed to be receiving ldquoactiverdquo study drug To
ensure the subjectrsquos safety the study treatment will be dose-adjusted based on laboratory test
results clinical findings and symptoms
The IPFnet DCC medical monitor and PANTHER-IPF co-chairs Drs Ganesh Raghu and
Fernando Martinez will be available to the study physicians to discuss study drug management
on a case-by-case basis Un-blinding will be considered ONLY when the knowledge of subject
treatment assignment is ABSOLUTELY ESSENTIAL for subject safety and after discussion of
the subjectrsquos case with the medical monitor and either Dr Raghu or Dr Martinez Unblinding of
study treatment should be minimized during the conduct of the trial In those cases where it is
felt to be medically necessary the DCC medical officer will communicate directly with the
managing physician to minimize unblinding of study personnel
52
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
7 Study Drug Procedures
At the baseline 15-week 30-week and 45-week study visits subjects will receive a supply of
study drug sufficient to last until the next visit at which study drug will be dispensed
53
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
8 Data Management
81 Hardware and Software Configuration
811 Hardware and Database Software
Data will be stored in an Oracle database system Oracle has advantages of processing efficiency
and smooth linkage with other software systems The application and database will be hosted on
Solaris Unix servers at the IPFnet DCC
812 Statistical Software
SAS will be used as the principal application for the management of analysis data files and
statistical computations S-Plus will be used to provide supplementary functions as needed
813 Access Control and Confidentiality Procedures
Access to databases will be controlled centrally by the IPFnet DCC through user passwords
linked to appropriate privileges This protects the data from unauthorized changes and
inadvertent loss or damage
814 Security
Database and Web servers will be secured by a firewall and through controlled physical access
Oracle has many security features to ensure that any staff member accessing the database has the
proper authority to perform the functions he or she requests of the system Within the secondary
SAS databases Unix group-access control maintains similar security The Sun workstation login
is secured by extensive user-password facilities under Unix
54
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
815 Back-up Procedures
Database back-up will be performed automatically every day and standard IPFnet DCC policies
and procedures will be applied to dictate tape rotation and retention practices
816 Virus Protection
All disk drives that provide network services and all user computers will be protected using
virus-scanning software Standard IPFnet DCC policies will be applied to update these protection
systems periodically through the study
82 Sources of Data
821 Design and Development
The IPFnet DCC will be responsible for development of the electronic case report forms
(eCRFs) development and validation of the clinical study database ensuring data integrity and
training clinical center staff on applicable data management procedures A web-based distributed
data entry model will be implemented This system will be developed to ensure that guidelines
and regulations surrounding the use of computerized systems used in clinical trials are upheld
The remainder of this section provides an overview of the data management plan associated with
this protocol
822 Data Collection Forms
The data collection process consists of direct data entry at the study clinical centers into the EDC
system(s) provided by the DCC A data collection worksheet will be provided to clinical centers
for recording data in the event the EDC system is unavailable Data entry of the eCRFs should
be completed according to the instructions provided and project specific training The
investigator is responsible for maintaining accurate complete and up-to-date records and for
ensuring the completion of the eCRFs for each research participant
55
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
823 Data Acquisition and Entry
Data entry into eCRFs shall be performed by authorized individuals Selected eCRFs may also
require the investigatorrsquos written signature or electronic signature as appropriate Electronic
CRFs will be monitored for completeness accuracy and attention to detail during the study
824 Data Center Responsibilities
The IPFnet DCC will 1) develop a data management plan and will conduct data management
activities 2) provide final eCRFs for the collection of all data required by the study 3) develop
data dictionaries for each eCRF that will comprehensively define each data element 4) conduct
ongoing data monitoring activities on study data 5) monitor any preliminary analysis data
cleanup activities and 6) rigorously monitor final study data clean up
825 Data Editing
Completed data will be entered into the IPFnet DCC automated data acquisition and
management system If incomplete or inaccurate data are found a data clarification request will
be generated and distributed to clinical centers for a response Clinical centers will resolve data
inconsistencies and errors and enter all corrections and changes into the IPFnet DCC automated
data acquisition and management system
826 Training
The training plan for clinical center staff includes provisions for training on assessments eCRF
completion guidelines data management procedures and the use of computerized systems
56
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
9 Study Design and Data Analysis
91 General Analytic Considerations
All primary analyses will be based on intent-to-treat (ITT) principles using all randomized
subjects Baseline factors across groups will be compared using mean (standard deviation) and
median (25th and 75th percentiles) summary measures Kaplan-Meier curves will be used to
display event rates Due to clinical interest in departures from both sides of the null hypothesis
all test statistics will be 2-sided
Reasonable caution needs to be taken when conducting multiple analyses on key clinical
subgroups For subgroup analyses a conservative significance level of 0001 will be used for all
interaction tests Thus subgroup comparisons will be considered exploratory unless the p-value
from the interaction test is smaller than 0001
92 Randomization Blinding and Reporting of Results
A permuted block-randomization scheme will be created with varying block sizes stratified by
clinical center Once a subject has completed the screening and baseline period and evaluation
for inclusionexclusion criteria the randomization process will begin Subjects will be
randomized to receive NAC or matching placebo with equal probability (11) via telephone
contact with a central interactive voice response system (IVRS) using a toll-free randomization
number On the day of randomization after the subject has successfully met all inclusion and
exclusion criteria the investigator or designee will call the central randomization number to
obtain the assigned kit randomization numbers for that subject At each subject visit the
investigator or designee will call the central randomization number to obtain the new kit
randomization numbers for resupply of the subject For resupply of the clinical center the IVRS
will monitor minimal volume of a kit type andor expiration date and will automatically notify
the pharmacy
57
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
The trial results will be reported according to guidelines specified in the CONSORT statement
A flow diagram describing screening recruitment randomization dropout and vital status will
be included in the primary manuscript AEs and efficacy data will be presented for all treatment
groups Adherence dropout and lost to follow-up will be carefully examined across all treatment
groups Analyses of safety will be based on data from all randomized subjects who received at
least one dose of study drug
93 Stratification
Subjects will be distributed to the two treatment arms in a 11 allocation ratio Stratification
blocks will be based on clinical centers
94 Specification of the Primary Analyses
A mixed model repeated measures (MMRM) analysis described in section 95 will be used to
compare differences in the slope of FVC measurements across the treatment groups Response
variables are values of the FVC measured at baseline and every 15 weeks until study completion
Variables in the model will include treatment time and time by treatment age sex race and
height Contrast estimates of differences in slopes of treatment over time (along with confidence
intervals) will be used to estimate the treatment effect The validity of this model in terms of
meeting modeling assumptions will be assessed via standard modeling diagnostics and goodness-
of-fit measures Based on the MMRM framework missing FVC data will not be imputed for the
primary analysis
95 Analysis of Longitudinal Endpoints
A common goal in clinical trials is to specify models that are easily implemented and
reproducible by independent data analysts On the other hand the models should have proper
statistical behavior in terms of low bias and high precision Many common approaches to
longitudinal data analysis including last observation carried forward (LOCF) imputation rely on
the missing completely at random (MCAR) assumption However the MCAR assumption is
58
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
unlikely to hold in many clinical trials because missing data are often related to disease
progression and prognosis A more reasonable assumption missing at random (MAR) specifies
that the complete data distribution can be modeled using only the observed data The likelihood-
based MMRM approach is valid under the more general MAR assumptions These models will
be applied to analyze the longitudinal data secondary endpoints
The advantages of MMRM analysis are that all important characteristics of the model can be preshy
specified standard software can be used to implement the models and results are based on ITT
principles43 In addition the MMRM approach offers superior control of Type I and Type II
errors compared with the LOCF approach
Response variables are values of the PFTs measured at enrollment and every 15 weeks until
study completion and 6MWT values measured at baseline week 30 and week 60 Covariates are
treatment time time by treatment and key baseline risk factors Contrasts (along with
confidence intervals) of treatment by time will be used to estimate the treatment effect
The correlation structure involves multiple pieces including measurement errors random
variation and interindividual variability For the longitudinal data analyses an unstructured
correlation matrix for within-subject errors will be assumed Other correlation structures
including compound symmetry will be examined as needed A careful examination of reasons
for study discontinuation will be conducted to assess the validity of MCAR Sensitivity analyses
will be used to examine the untestable assumption that the observed data violate the MAR
assumption The MMRM models will be implemented using PROC MIXED in SAS
96 Analysis of Binary Time-to-Event and Time-Lagged Endpoints
Regression modeling approaches using either the logistic regression model or Cox proportional
hazards regression model will be employed when appropriate The validity of these models will
be assessed via standard modeling diagnostics and goodness-of-fit measures Estimates of
cumulative frequencies for more general time-lagged responses will be calculated using the
partitioned version of the Bang-Tsiatis estimator44 The partitions will be set at 15-week intervals
59
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
to correspond with the data-collection process Covariate adjusted event rates will be calculated
using inverse probability-weighted regression estimates45
97 Power Analysis
971 Primary Analyses
Based on previously published IPF clinical trials the PL group is expected to experience a drop
in FVC of approximately 020 L over the study period (see Figure 1) The IPFnet Steering Group
determined a clinically important difference would be to preserve the majority of the decline
relative to PL over the study period In particular a treatment effect of 015 L was determined to
be a clinically meaningful difference Potential dropout is a key factor in the proposed study The
drop-out process assumed 5 lost to follow-up after every study visit Only 80 of subjects
were assumed to be followed for the entire study period All models assumed a compound
symmetry structure for the covariance matrix Power calculations were performed using a SAS
IML program for designing repeated measures studies46 Based on preliminary reviews of the
data from the University of Michigan the covariance matrix parameters were estimated at
approximately σ2 = 0757 (variance parameter) and ρ = 0936 (correlation parameter) To be
conservative the power calculations for the primary analysis were performed with parameter
setting of σ2 = 0810 (variance parameter) and ρ = 0925 (correlation parameter)
The power calculations assume a correction for imperfect compliance proposed by Lachin and
Foulkes to allow for 2 noncompliance for each of the treatment arms47 Thus the sample size
of 130 subjects per arm would be reduced to an adjusted sample size of 130(1-002-002)2 =
1198 or 120 subjects per arm
Under the assumed Type I error rate of 005 with a correlation parameter of 0925 and standard
deviation of 090 the difference of 015 L (or 00025 Lweek) shown in Table 6 would have
power of 93
60
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Table 6 Hypothetical Values of Mean FVC (L) Change from Baseline
Week 15 Week 30 Week 45 Week 60
NAC 00125 00250 00375 00500
Placebo 00500 01000 01500 02000
Difference 00375 00750 01125 01500
Abbreviations FVC forced vital capacity PL placebo
972 Power Analysis for Secondary Endpoints
Power calculations for secondary endpoint measurements are shown in Table 7 Standard
deviations are based on unpublished data provided by the University of Michigan The
calculations are based on a 2-sample t-test with Type I error rate set at 005 These calculations
are likely to be conservative because the statistical approach described in section 95 for
analyzing these endpoints will incorporate incomplete observations as well as intermediate data
points
Table 7 Detectable Differences in Treatment Means for Selected Endpoint Measurements
Secondary Endpoints Std Dev
of the Baseline Score
Detectable Difference for 80 Power
Std Dev of the Change Score
Difference Detectable for
80 Power
DLCOpred 166 58 91 32
6MWT Area Under the Desaturation Curve
219 76 175 61
6MWT Distance to Desaturation 224 78 315 110
6MWT Minutes Walked 210 073 205 071
Abbreviations Std Dev standard deviation DLCOpred diffusing capacity of the lung for carbon monoxide percent predicted 6MWT 6-minute walk test
61
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
10 Study Administration
101 Cooperative Agreement Mechanism
The administrative and funding mechanism used to undertake this project is a ldquocooperative
agreementrdquo (U01) which is an assistance mechanism Under the cooperative agreement the
NHLBI assists supports andor stimulates the project and is substantially involved with
investigators in conducting the study by facilitating performance of the effort in a ldquopartnerrdquo role
The NHLBI project scientist serves on the IPFnet Steering Group and he or another NHLBI
scientist may serve on other project committees when appropriate At the same time however
NHLBI does not assume a dominant role direction or prime responsibility for this research
program
As described below governance of the project is conducted through the IPFnet Steering Group
Principal investigators have lead responsibilities in all aspects of their trials and the project
including any modification of trial designs conduct of the trials quality control data analysis
and interpretation preparation of publications and collaboration with other investigators unless
otherwise provided for by the IPFnet Steering Group
PIs retain custody of and have primary rights to their center-specific and collaborative data
subject to government rights-of-access consistent with current Health amp Human Services (HHS)
Public Health Service (PHS) and National Institutes of Health policies The protocols and
governance policies call for the continual submission of data centrally to the IPFnet DCC for the
collaborative database which at a minimum will contain the key variables selected by the IPFnet
Steering Group for standardization across all clinical centers the submission of copies of the
collaborative datasets to each PI upon completion of the project procedures for data analysis
reporting and publication and procedures to protect and ensure the privacy of medical and
genetic data and records of individuals The NHLBI project scientist on behalf of the NHLBI
will have the same access privileges and responsibilities regarding the collaborative data as the
other members of the Steering Group
62
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
PIs are also encouraged to publish and to publicly release and disseminate results data and other
products of the project concordant with the project protocols and governance and the approved
plan for making data and materials available to the scientific community and to the NHLBI
However during the 3 years after the ending date of NHLBI project support unpublished data
unpublished results data sets not previously released and other study materials or products are
to be made available to any third party only with the approval of the IPFnet Steering Group
Upon completion of the project PIs are expected to put their intervention materials and
procedure manuals into the public domain andor make them available to other investigators
according to the approved plan for making data and materials available to the scientific
community and the NHLBI for the conduct of research at no charge other than the costs of
reproduction and distribution
The NHLBI reserves the right to terminate or curtail the project (or an individual award) in the
event of (a) failure to develop or implement mutually agreeable collaborative measurement
subject eligibility and data management sections of the protocols (b) substantial shortfall in
subject recruitment follow-up data reporting or quality control or other major breach of
protocol (c) substantive changes in the agreed-upon protocols with which NHLBI cannot
concur (d) reaching a major project outcome with persuasive statistical significance
substantially before schedule or (e) human subject ethical issues that may dictate a premature
termination
Any disagreement that may arise in scientificprogrammatic matters (within the scope of the
award) between award recipients and the NHLBI may be brought to arbitration An arbitration
panel will be composed of 3 membersmdash1 selected by the IPFnet Steering Group (with the
NHLBI member not voting) or by the individual PI in the event of an individual disagreement a
second selected by NHLBI and the third selected by the other 2 members This special
arbitration procedure in no way affects the PIrsquos right to appeal an adverse action that is otherwise
appealable in accordance with the PHS regulations at 42 CFR part 50 Subpart D and HHS
63
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
regulation at 45 CFR part 16 or the rights of the NHLBI under applicable statutes regulations
and terms of the award
102 IPFnet Steering Group
The IPFnet Steering Group is the main governing body of the project It is composed of the PIs
of the clinical centers the PI of the DCC and the NHLBI project scientist The clinical centers
the IPFnet DCC and the NHLBI each have 1 vote on the IPFnet Steering Group All decisions
are determined by majority vote
All major scientific decisions are determined by the IPFnet Steering Group It assumes overall
responsibility for the design and conduct of the trial It appoints (and disbands) committees and
subcommittees as the need arises designs approves and implements the study protocols
oversees the development of the MOOP monitors subject recruitment and treatment delivery
evaluates data collection and management oversees quality assurance procedures and
implements changes and enhancements to the study as required It also has primary responsibility
for facilitating the conduct of the trials and reporting the projectrsquos results
103 Data and Safety Monitoring Board
The NHLBI will establish a DSMB in accordance with established policies (see
httpwwwnhlbinihgovfundingpoliciesdsmb_insthtm) to ensure data quality and subject
safety and to provide independent advice to the NHLBI regarding progress and the
appropriateness of study continuation
104 Recommendations on Interim Monitoring of Efficacy Safety and Futility
First and foremost the role of the DSMB will be to review subject safety and trial conduct at
periodic points during the study The DSMB may require analyses of the primary endpoint
results for comparing the benefit and risks of treatment strategies The benefit of collecting
additional data on key secondary endpoints with extended follow-up and establishing a robust
64
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
evidence base for determining a standard of care will need to be carefully considered before
early termination of one or more treatment arms After careful consideration the IPFnet Steering
Group recommends conservative thresholds for the early examinations of the safety and efficacy
data
The DSMB will be expected to meet approximately every 6 months until trial completion to
review safety and toxicity data The DSMB may recommend stopping the study based on these
reviews Because the DSMB could stop the trial for safety concerns as well as for a large
efficacy benefit there could be multiple opportunities to reject the null hypothesis (no difference
in event rates between the PL and NAC groups) A Bonferroni approximation will be applied
during the one planned interim analysis for efficacy
Before locking the database a statistical analysis plan (SAP) will be developed to provide
complete details on the statistical analysis The SAP will include the specifics for how and when
the DSMB will be notified for AEs The IPFnet DCC will deliver to the DSMB all FDA-defined
AEs at 3-month intervals The IPFnet DCC will prepare narrative SAE reports in real time for
DSMB review including recommendations and analysis of similar events for each SAE
submitted to the FDA
65
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
11 Investigator and Sponsor Obligations
111 Monitoring
All monitoring activities for US clinical centers will be performed in accordance with DCRI
standard operating procedures Information regarding the types of visits will be outlined in the
PANTHER-IPF MOOP
112 Cost and Payment
There will be no cost to subjects enrolled in this trial Study-related procedures will be paid for
by the IPFnet
Subjects may be eligible for reimbursement for travel to the clinical center Details of payment
will be explained to each subject during the consent process
113 Confidentiality and Health Insurance Portability and Accountability Act
Considerations
Subject confidentiality will be protected throughout the study All subject data will be kept
strictly confidential and no subject-identifying information will be released to anyone outside
the project Confidentiality will be assured through several mechanisms First each subject will
be assigned an anonymous study ID which will then be used on all study forms Second any
study forms blood samples and paper records that contain subject information (eg address lists
phone lists) will be kept at the clinical centers in secured locked areas coded by number Once
blood is collected there will be no subject identifiers placed on blood samplesmdashonly the study
ID number and the date of sample collection Third access to all subject data and information
including laboratory specimens will be restricted to authorized personnel In the case of
computerized data this restricted access will be assured through user logon IDs and password
protection
66
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
At the IPFnet DCC only authorized personnel will have access to the data files containing study
data Security will be assured through user logon IDs passwords and appropriate access
privileges All study subjects will be identified only by their IPFnet ID numbers and no personal
identifying information such as name address or Social Security number will be entered into
the IPFnet DCC database Any subject-specific data reported to the IPFnet Steering Group will
be identified only by the IPFnet ID number
Finally subjects will not be identified by name in any reports or publications nor will the data
be presented in such a way that the identity of individual subjects can be inferred Analysis files
created for further study by the scientific community will have no subject identifiers These data
files will be created in accordance with the Ancillary Studies and Publication Policy of the
IPFnet
114 Informed Consent Procedures
All IPFnet subjects will provide written informed consent using procedures reviewed and
approved by each clinical centerrsquos IRB Informed consent will be undertaken by study personnel
in-person with the subject The subject has the option of declining further participation in the
study at that point No further study procedures will be conducted until the signed documents
have been provided to the IPFnet clinical center
115 Institutional Review Boards
Before initiating this study the protocol clinical center-specific informed consent forms Health
Insurance Portability and Accountability Act (HIPAA) forms recruitment materials and other
relevant information will be reviewed by a properly constituted IRB at each participating clinical
center A copy of the signed and dated IRB approval at each clinical center will be retrieved prior
to or during the site initiation visit and archived at the IPFnet DCC Any amendments to the
protocol other than simple administrative and typographical changes must be approved by each
IRB before they are implemented The clinical centers will seek annual renewals of their IRB
approvals in accordance with local procedures
67
__________________________________________ ________________
__________________________________________
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
12 Investigator Agreement
I have read the foregoing protocol PANTHER-IPF and agree that it contains all necessary
details for carrying out this study I will conduct the study as outlined herein and will complete
the study within the time designated
I will provide copies of the protocol and all pertinent information to all individuals responsible to
me who assist in the conduct of this study I will discuss this material with them to ensure they
are fully informed regarding the drug and the conduct of the study
I will fulfill all responsibilities for submitting pertinent information to the local IRB if
applicable that is responsible for this study
I further agree that NHLBI andor DCRI will have access to any source documents from which
eCRF information may have been generated
Signature of Principal Investigator Date
Name of Principal Investigator (printed or typed)
Protocol version date May 19 2009
Protocol Amendment 1 version date May 28 2010
Protocol Amendment 2 version date December 6 2011
68
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
13 References
1 Raghu G Brown KK Bradford WZ et al A placebo-controlled trial of interferon gamma-1b in patients with idiopathic pulmonary fibrosis N Engl J Med 2004350125-33 2 King TE Jr Safrin S Starko KM et al Analyses of efficacy end points in a controlled trial of interferon-gamma1b for idiopathic pulmonary fibrosis Chest 2005127171-7 3 Flaherty KR Thwaite EL Kazerooni EA et al Radiological versus histological diagnosis in UIP and NSIP survival implications Thorax 200358143-8 4 Wells AU Desai SR Rubens MB et al Idiopathic pulmonary fibrosis a composite physiologic index derived from disease extent observed by computed tomography Am J Respir Crit Care Med 2003167962-9 5 Raghu G Freudenberger TD Yang S et al High prevalence of abnormal acid gastroshyoesophageal reflux in idiopathic pulmonary fibrosis Eur Respir J 200627136-42 6 Kinnula VL Focus on antioxidant enzymes and antioxidant strategies in smoking related airway diseases Thorax 200560693-700 7 Coultas DB Zumwalt RE Black WC Sobonya RE The epidemiology of interstitial lung diseases Am J Respir Crit Care Med 1994150967-72 8 Raghu G Weycker D Edelsberg J Bradford WZ Oster G Incidence and prevalence of idiopathic pulmonary fibrosis Am J Respir Crit Care Med 2006174810-6 9 Olson AL Swigris JJ Lezotte DC Norris JM Wilson CG Brown KK Mortality from pulmonary fibrosis increased in the United States from 1992 to 2003 Am J Respir Crit Care Med 2007176277-84 10 Mannino DM Etzel RA Parrish RG Pulmonary fibrosis deaths in the United States 1979shy1991 An analysis of multiple-cause mortality data Am J Respir Crit Care Med 19961531548shy52 11 Hubbard R Johnston I Coultas DB Britton J Mortality rates from cryptogenic fibrosing alveolitis in seven countries Thorax 199651711-6 12 Johnston I Britton J Kinnear W Logan R Rising mortality from cryptogenic fibrosing alveolitis Bmj 19903011017-21 13 Raghu G Collard HR Egan JJ et al An official ATSERSJRSALAT statement idiopathic pulmonary fibrosis evidence-based guidelines for diagnosis and management Am J Respir Crit Care Med 2011183788-824 14 (USA) FDA FDA Public Health Advisory Interferon gamma-1b (marketed as Actimmune) In 2007 15 King TE Jr Pardo A Selman M Idiopathic pulmonary fibrosis Lancet 2011 16 Raghu G Brown KK Costabel U et al Treatment of idiopathic pulmonary fibrosis with etanercept an exploratory placebo-controlled trial Am J Respir Crit Care Med 2008178948shy55 17 Malouf MA Hopkins P Snell G Glanville AR An investigator-driven study of everolimus in surgical lung biopsy confirmed idiopathic pulmonary fibrosis Respirology 201116776-83 18 King TE Jr Behr J Brown KK et al BUILD-1 a randomized placebo-controlled trial of bosentan in idiopathic pulmonary fibrosis Am J Respir Crit Care Med 200817775-81 19 Richeldi L Costabel U Selman M et al Efficacy of a tyrosine kinase inhibitor in idiopathic pulmonary fibrosis N Engl J Med 20113651079-87
69
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
20 Borok Z Buhl R Grimes GJ et al Effect of glutathione aerosol on oxidant-antioxidant imbalance in idiopathic pulmonary fibrosis Lancet 1991338215-6 21 Meyer A Buhl R Magnussen H The effect of oral N-acetylcysteine on lung glutathione levels in idiopathic pulmonary fibrosis Eur Respir J 19947431-6 22 Behr J Maier K Degenkolb B Krombach F Vogelmeier C Antioxidative and clinical effects of high-dose N-acetylcysteine in fibrosing alveolitis Adjunctive therapy to maintenance immunosuppression Am J Respir Crit Care Med 19971561897-901 23 Cantin AM North SL Fells GA Hubbard RC Crystal RG Oxidant-mediated epithelial cell injury in idiopathic pulmonary fibrosis J Clin Invest 1987791665-73 24 Waghray M Cui Z Horowitz JC et al Hydrogen peroxide is a diffusible paracrine signal for the induction of epithelial cell death by activated myofibroblasts Faseb J 200519854-6 25 Larios JM Budhiraja R Fanburg BL Thannickal VJ Oxidative protein cross-linking reactions involving L-tyrosine in transforming growth factor-beta1-stimulated fibroblasts J Biol Chem 200127617437-41 26 Kinnula VL Fattman CL Tan RJ Oury TD Oxidative stress in pulmonary fibrosis a possible role for redox modulatory therapy Am J Respir Crit Care Med 2005172417-22 27 Meyer A Buhl R Kampf S Magnussen H Intravenous N-acetylcysteine and lung glutathione of patients with pulmonary fibrosis and normals Am J Respir Crit Care Med 19951521055-60 28 Behr J Degenkolb B Krombach F Vogelmeier C Intracellular glutathione and bronchoalveolar cells in fibrosing alveolitis effects of N-acetylcysteine Eur Respir J 200219906-11 29 Bando M Hosono T Mato N et al Long-term efficacy of inhaled N-acetylcysteine in patients with idiopathic pulmonary fibrosis Intern Med 2010492289-96 30 Demedts M Behr J Buhl R et al High-dose acetylcysteine in idiopathic pulmonary fibrosis N Engl J Med 20053532229-42 31 Toma TP Bhowmik A Rajakulasingam R Acetylcysteine in pulmonary fibrosis N Engl J Med 20063541086-9 author reply -9 32 Hunninghake GW Antioxidant therapy for idiopathic pulmonary fibrosis N Engl J Med 20053532285-7 33 Flaherty KR Mumford JA Murray S et al Prognostic implications of physiologic and radiographic changes in idiopathic interstitial pneumonia Am J Respir Crit Care Med 2003168543-8 34 Latsi PI du Bois RM Nicholson AG et al Fibrotic idiopathic interstitial pneumonia the prognostic value of longitudinal functional trends Am J Respir Crit Care Med 2003168531-7 35 Collard HR King TE Jr Bartelson BB Vourlekis JS Schwarz MI Brown KK Changes in clinical and physiologic variables predict survival in idiopathic pulmonary fibrosis Am J Respir Crit Care Med 2003168538-42 36 Jegal Y Kim DS Shim TS et al Physiology is a stronger predictor of survival than pathology in fibrotic interstitial pneumonia Am J Respir Crit Care Med 2005171639-44 37 Martinez FJ Safrin S Weycker D et al The clinical course of patients with idiopathic pulmonary fibrosis Ann Intern Med 2005142963-7 38 Hull JH Acetylcysteine in pulmonary fibrosis N Engl J Med 20063541089-91 author reply -91
70
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
39 Flaherty KR King TE Jr Raghu G et al Idiopathic interstitial pneumonia what is the effect of a multidisciplinary approach to diagnosis Am J Respir Crit Care Med 2004170904shy10 40 Raghu G Johnson WC Lockhart D Mageto Y Treatment of idiopathic pulmonary fibrosis with a new antifibrotic agent pirfenidone results of a prospective open-label Phase II study Am J Respir Crit Care Med 19991591061-9 41 Hunninghake GW Lynch DA Galvin JR et al Radiologic findings are strongly associated with a pathologic diagnosis of usual interstitial pneumonia Chest 20031241215-23 42 Lynch D Godwin J Safrin S et al High-resolution computed tomography in idiopathic pulmonary fibrosis diagnosis and prognosis Am J Respir Crit Care Med 2005172488-93 43 Mallinckrodt CH Watkin JG Molenberghs G Carroll RJ Choice of the primary analysis in longitudinal clinical trials Pharmaceutical Statistics 20043161-9 44 Bang H Tsiatis A Estimating medical costs with censored data Biometrika 200087329shy43 45 Lin DY Regression analysis of incomplete medical cost data Stat Med 2003221181-200 46 Rochon J Application of GEE procedures for sample size calculations in repeated measures experiments Stat Med 1998171643-58 47 Lachin JM Foulkes MA Evaluation of sample size and power for analyses of survival with allowance for nonuniform patient entry losses to follow-up noncompliance and stratification Biometrics 198642507-19
71
- PANTHER-IPFPREDNISONE AZATHIOPRINEAND N-ACETYLCYSTEINEA STUDY THAT EVALUATES RESPONSE INIDIOPATHIC PULMONARY FIBROSIS
-
- Protocol Summary
- Table of Contents
- List of Tables
- List of Figures
- List of Abbreviations
- 1 Summary
- 2 Hypotheses and Specific Aims
-
- 21 Null Hypothesis
- 22 Specific Aim 1
- 23 Specific Aim 2
- 24 Prespecified Subgroups of Interest
-
- 3 Background and Significance
-
- 31 Idiopathic Pulmonary Fibrosis is the Most Common Interstitial Lung Disease
- 32 Rationale for Placebo Control
- 33 Rationale for N-acetylcysteine
- 35 Rationale for N-acetylcysteine as a Stand-alone Therapy
- 36 Rationale for the Study Design and Primary Endpoint
- 37 Rationale for Blinding of Treatments
-
- 4 Methods
-
- 41 Inclusion Criteria
- 42 Diagnosis of IPF
- 43 Exclusion Criteria
- 44 Study Design and Study Visit
- 45 Dose Justification
- 46 Contraindications Precautions and Side Effects of Study Medications
- 47 Recruitment Procedures
- 48 Study Procedures
- 49 Concomitant Medications
- 410 Laboratory Testing
- 411 Blinding of Study Drugs
-
- 5 Study Endpoints
-
- 51 Primary Study Endpoint
- 52 Secondary Study Endpoints
-
- 6 Safety Evaluations and Procedures
-
- 61 Adverse Events
- 62 Clinical Medical Monitoring
- 63 Unblinding Procedures
-
- 7 Study Drug Procedures
- 8 Data Management
-
- 81 Hardware and Software Configuration
- 82 Sources of Data
-
- 9 Study Design and Data Analysis
-
- 91 General Analytic Considerations
- 92 Randomization Blinding and Reporting of Results
- 93 Stratification
- 94 Specification of the Primary Analyses
- 95 Analysis of Longitudinal Endpoints
- 96 Analysis of Binary Time-to-Event and Time-Lagged Endpoints
- 97 Power Analysis
-
- 10 Study Administration
-
- 101 Cooperative Agreement Mechanism
- 102 IPFnet Steering Group
- 103 Data and Safety Monitoring Board
- 104 Recommendations on Interim Monitoring of Efficacy Safety and Futility
-
- 11 Investigator and Sponsor Obligations
-
- 111 Monitoring
- 112 Cost and Payment
- 113 Confidentiality and Health Insurance Portability and Accountability ActConsiderations
- 114 Informed Consent Procedures
- 115 Institutional Review Boards
-
- 12 Investigator Agreement
- 13 References
-

PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Collect Quality-of-life (QOL) data using the SF-36 EuroQol Investigating Choice Experiments for
Preferences of Older People Capability Instrument (ICE CAP) and SGRQ
Female subjects complete Gender Substudy questionnaire
Dyspnea status collected using the UCSD SOBQ
Evaluate Acute Exacerbation (AEx)
Review of any Adverse Events (AEs)
Review of concomitant medications
Subject receives diary and instructions on its purpose and proper use
Subject receives supply of study drug sufficient to last until his or her 15-week study visit
See the Schedule of Assessments (Table 3) for more details Subjects with screening and enrollment postshy
bronchodilator FVC measurements (in liters) differing by more than 11 are not eligible to be enrolled in the
study
Subjects will be asked to provide a physician of record This physician will be considered the subjectrsquos primary
care provider (PCP) and if the subject agrees the PCP will be informed by letter of the subjectrsquos enrollment in
the trial The subject will be informed that his or her ongoing medical care should be received from the PCP
The PCP will be informed of any safety issues identified by the study staff The PCP will also be given
information regarding communication with study personnel about pertinent health issues or clinic encounters
the subject may have
4423 Week 15
The week 15 visit is expected to occur within +- 14 days of the subjectrsquos scheduled visit time (eg the week 15
visit should occur anytime between 13 and 17 weeks after starting study drug Week 15 activities include
Measure vital signs with oximetry
Measurement height and weight
Serum pregnancy test (if applicable)
Spirometry (post-bronchodilator) measurement
Review of AEs
Evaluate for AEx
30
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Review concomitant medications
If consented draw blood and collect urine specimen for the biospecimen repository
Subjects return used and unused study drug for the visit
Review study diary and a new study diary will be given
Provide additional supply of study drug sufficient to last until the next scheduled visit
4424 Week 30
The week 30 visit is expected to occur within +- 14 days of the subjectrsquos scheduled visit time (eg the week 30
visit should occur anytime between 28 and 32 weeks after starting study drug) Week 30 activities include
Physical examination
Measure vital signs with oximetry
Measure height and weight
Laboratory values (complete blood count [CBC] and serum chemistries)
Serum pregnancy test (if applicable)
Measure spirometry (post-bronchodilator)
6MWT with Borg scale
DLCO
Review of AEs
Evaluate for AEx
Review concomitant medications
Complete all QOL and dyspnea questionnaires (EuroQol ICE CAP SF-36 SGRQ and UCSD SOBQ)
If consent has been given blood will be drawn and a urine specimen collected for the biospecimen
repository
Review study diary
Subjects return used and unused study drug for the visit
Provide additional supply of study drug sufficient to last until the next scheduled visit
4425 Week 45
31
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
The week 45 visit is expected to occur within +- 14 days of the subjectrsquos scheduled visit time (eg the week 45
visit should occur anytime between 43 and 47 weeks after starting study drug) Week 45 activities include
Measure vital signs with oximetry
Measure height and weight
Serum pregnancy test (if applicable)
Measure spirometry (post-bronchodilator)
Review of AEs
Evaluate for AEx
Review concomitant medications
If consent has been given blood will be drawn and a urine specimen collected for the biospecimen
repository
Subjects return used and unused study drug for the visit
Study diary reviewed
Provide additional supply of study drug sufficient to last until the next scheduled visit
4426 Week 60 (Early Withdrawal or Final Treatment Visit)
At week 60 or at subject withdrawal from the study (premature by study doctor or subjectrsquos decision) a final
treatment visit will occur At this final treatment visit subjects will discontinue NACPL abruptly Week 60
activities also include
Physical examination
Measure vital signs with oximetry
Measure height and weight
Laboratory values (complete blood count [CBC] and serum chemistries)
Spirometry (post-bronchodilator) measurement
6MWT with Borg scale measurement
DLCO
Lung volumes
ABG
Review of AEs
32
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Evaluate for AEx
Review concomitant medications
Subjects will complete all QOL and dyspnea questionnaires (EuroQol ICE CAP SF-36 SGRQ and
UCSD SOBQ)
If consent has been given blood will be drawn and a urine specimen collected for the biospecimen
repository
Subjects return used and unused study drug for the visit
Study diary reviewed
4427 Final Site Visit ndash FVC drop confirmation
In the event that the subject has a recorded FVC drop of gt10 from baseline at the final treatment visit and the
subject has not had a confirmation of such a drop at a previous study visit the subject should return to the
clinical site 6 to 8 weeks after the final treatment visit During this visit a post-bronchodilator spirometry test
will be performed This FVC measurement will be evaluated according to section 521 of this protocol
4428 Final Visit ndash Telephone Follow-up
Four weeks following the final dose of study medication subjects will receive a telephone call from the study
coordinator to ensure that there are no side effects and to follow up on any ongoing adverse events (AEs)
4429 Phone Contact Between Visits
At week 2 and each month that a subject does not have a scheduled clinical center visit his or her study
coordinator will contact him or her at least once by telephone to
Inquire if the subject has had any hospitalizations events that might be considered an AE or any events
significant enough to warrant an out-of-cycle visit to the clinical center
Remind subjects of their current dosage levels and confirm that the subject understands them
Address any questions or concerns the subject might have regarding other aspects of the study
Assess adherence to the treatment regimen by reviewing diary data verbal review of medications taken
including nutritional supplements
33
34
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Table 3 Schedule of Assessments
Procedure Screening Visit 0
Enrollment Visit 1
Week 15 Visit 2
Week 30Visit 3
Week 45 Visit 4
Week 60 Early
Withdrawal Visit 5
Final1
Visit (via phone)
Informed consent X
Medical history X
Inclusionexclusion criteria X
Serum pregnancy test (if applicable) X X X X X
Review of lung biopsy X
Arterial Blood Gas X X
6-Minute Walk Test
X
X X
Physical examination X X X
Vital signs with oximetry X X X X X X
Body height and weight X X X X X X
Complete Blood Count X X X
Chemistry panel X X X
Monitor Lab Values X X X
Urinalysis X Specimen repository substudy blood draw and urine collection (if consented)
X
X X X X
HRCT (if not completed within three months) X
Spirometry (pre- and post-bronchodilator) X
Spirometry (post-bronchodilator only) X X X X X
DLCO (post-bronchodilator only) X X X
Lung volumes (post-bronchodilator only) X
X
Evaluate for acute exacerbation X X X X X
Review Adverse Events X X X X X X
Review concomitant meds X X X X X X
Dispense subject diary X X X X
Review subject diary X X X X X
Dispense study agent X X X X
Gender Substudy questionnaire (female subjects only) X
EuroQol ICECAP UCSD SOBQ SGRQ SF-36 X X X
Abbreviations DLCO diffusing capacity of the lung for carbon monoxide QOL Quality of Life ICECAP Investigating Choice Experiments for Preferences of Older People UCSD SOBQ University of California Shortness of Breath Questionnaire SGRQ St Georgersquos Respiratory Questionnaire SF-36 Short Form 36 Health Survey
1Follow-up visit via phone will occur four weeks after final dose of study medication
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
45 Dose Justification
The general philosophy for determining dosing levels was to apply previously examined
treatment regimens With the focus of the study being to establish a standard of care for
mildmoderate IPF subjects the goal was to develop flexible yet standardized treatment rules that
allow for the temporary or permanent withholding of one or more components of treatment when
necessary Subjects developing laboratory abnormalities or symptoms that result in
discontinuation of one or more components of study treatment may continue on the other
components as long as there is no contraindication for this Complete follow-up is important for
the validity of any study As a strategy to maintain protocol adherence we are using a treatment
regimen that will detect potential side effects and prompt interventions proactively in the interest
of patient safety In addition subjects who permanently stop study medications during the course
of the study are encouraged to continue in the study completing all scheduled visits and tests
451 Rationale for N-acetylcysteine Dosing
To our knowledge there have been no IPF studies to correlate clinical outcome measures with
different dosages for NAC The dosage chosen is based on the IFIGENIA study However BAL
lung GSH levels from subjects with IPF have been augmented with the use of oral NAC at 600
mg 3 times per day In addition lung GSH levels have been associated with improved
PFTs212227 The dose chosen for this study was based on previous data including the IFIGENIA
study30
4511 Dosing of N-acetylcysteineplacebo
Dosing of NACPL will be 600 mg orally 3 times a day (1800 mgday)
4512 Reasons to Discontinue N-acetylcysteineplacebo
NACPL may be temporarily or permanently discontinued for the duration of the study for
gastrointestinal symptoms or dermatologic reactions
35
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Temporarily discontinue (hold) oral NACPL for subjects requiring inpatient admission for acute
exacerbation (AEx) or other conditions Resume NACPL after discharge
36
37
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
452 Dosage Algorithms
Dosage Adjustment Algorithm 1 NACPL Dose Modifications for Gastrointestinal Symptoms Nausea Vomiting Abdominal Discomfort Diarrhea
GI Symptoms determined by the PI to be clinically significant Nausea Vomiting Abdominal Discomfort Diarrhea
NACPL Temporarily dc (HOLD) x 3 Days
Monitor symptoms intervene as clinically indicated (eg fluid replacement antidiarrhea or antinausea medication)
Monitor or lab PRN
Are symptoms resolving after 3 days NO
Symptoms NOT resolving after 3 days of holding study medication Assessmentmanagement per clinical
discretion of investigator
Likely not study medication discuss resuming study medication with medical monitor when symptoms resolved
YES
Temporarily dc (HOLD) NACPL for 4 additional days (total hold 1 week) then NACPL Resume 600 MG TID
Did symptoms recur
YES
STOP NACPL for
duration of study
NO
NACPL No Change
38
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Dosage Adjustment Algorithm 2 NACPL Dose Modifications For Dermatologic Reactions
Dermatologic Reactions (Not Acneiform) ge Grade 2 Grading per Common Terminology Criteria for
Adverse Events V30 (httpctepcancergov) For example Grade 1 RASHDESQUAMATION Macular or papular eruption or erythema without associated symptoms Grade 2 RASHDESQUAMATION Macular or popular eruption or erythema with pruritus or other associated symptoms localized desquamation or other lesions covering lt50 of body surface area
NACPL Temporarily dc (HOLD) x 3 days
Are symptoms resolving after 3 days
NO Symptoms not resolving after 3 days of holding study medication Assessmentmanagement per clinical discretion of investigator Likely not study medication Discuss resuming study medication with medical monitor when symptoms
resolved YES
Temporarily dc (HOLD) NACPL for 4 additional days (total hold 1 week) then NACPL resume 600 MG TID
Did symptoms recur
YES
STOP NACPL for
duration of study
NO
NACPL No change
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
46 Contraindications Precautions and Side Effects of Study Medications
461 Contraindication
Contraindication to NAC is known hypersensitivity to it
462 Precautions
Concomitant administration of oral NAC and antibiotics has shown a slightly reduced absorption
of cephalexin and a slight increase in erythromycin serum levels NAC contains free sulfhydryl
groups There is no evidence that individuals sensitive to sulfa drugs are sensitive to NAC
The NAC preparation being administered in this study contains 20 mg of aspartame Because of
the phenylalanine component of aspartame individuals with phenylketonuria should avoid or
restrict aspartame intake to avoid increased blood levels of phenylalanine Because of this risk
labeling is required on all products containing aspartame
463 Side Effects
Side effects of NAC range from common to serious See Table 4
39
40
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Table 4 Side Effects of NAC
Undesirable Effects
System-organ class Uncommon
(gt11000 lt1100)
Rare
(gt110000 lt11000)
Very rare
(lt110000) Not known
Immune system disorders Hypersensitivity Anaphylactic shock
reaction
Nervous system disorders Headache
Ear and labyrinth disorders Tinnitus
Cardiac disorders Tachycardia
Vascular disorders Hemorrhage
Respiratory thoracic and
mediastinal disorders
Bronchospasm
Dyspnea
Gastrointestinal disorders
Vomiting diarrhea
stomatitis abdominal
pain nausea
Dyspepsia
Skin and subcutaneous tissue
disorders
Urticaria rash
angioedema itching
General disorders and
administration site conditions Pyrexia
Investigations Reduced arterial
pressure Face edema
In very rare cases the onset of severe skin reactions such as Stevens-Johnson syndrome and Lyell syndrome was reported to have a temporal relationship with N-acetylcysteine administration Although in most cases at least another suspect drug probably most involved in the genesis of the above mentioned mucocutaneous syndromes has been identified in case of mucocutaneous alterations it is appropriate to contact onersquos doctor and the administration of N-acetylcysteine should be immediately discontinued
Some studies confirmed a reduction of platelet aggregation during N-acetylcysteine administration The clinical significance of these findings has not been defined yet [Source Fluimucil Investigator Brochure]
47 Recruitment Procedures
Subjects recruited for this study will be established patients of the investigators or physician- or
self-referred to participating clinical centers in the IPFnet Each clinical center within IPFnet has
a well-developed infrastructure of local pulmonologists within the surrounding geographic area
These pulmonologists are kept informed of ongoing IPF clinical trials and regularly refer
subjects to studies conducted at IPFnet clinical centers
Additional steps will be taken to inform clinicians of the trials in progress within IPFnet
including presentations at faculty staff meetings at local hospitals medical grand rounds and
national conferences direct mail notification monthly faxes and advertisement of network trials
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
in pulmonary journals Clinical center patients previously diagnosed with IPF will be notified of
the trials by mail whenever possible
Recruitment of minorities and women will be monitored by the DCC and DSMB If necessary
additional recruitment efforts will be made at specific centers to ensure that the aggregate subject
sample contains appropriate representation of women and minorities
48 Study Procedures
The following procedures are detailed in the PANTHER-IPF MOOP accompanying this
protocol
1 PFT
2 ABG
3 HRCT scan of the chest (including imaging of pulmonary arteries)
4 CBC and serum chemistries
5 Pregnancy test
6 6MWTBorg Dyspnea Scale
7 QOL questionnaires (EuroQol HAD SF-36 SGRQ and ICE CAP)
8 UCSD SOBQ
9 Gender Substudy Questionnaire
All assessments of PFTs will be conducted by study personnel not directly involved in the
treatment of the subjects
481 Biological Specimen Management
4811 Biological Specimen Sample Management
Subjects at clinical centers participating in the specimen repository substudy who consent to
having blood drawn for research purposes and for the banking of blood blood components and
other biologic specimens (urine and BAL fluid) will have approximately 405 mL of blood
41
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
drawn 17 mL blood drawn for DNA and 20 mL of urine collected at enrollment visit Subjects
will have approximately 50 mL of blood drawn and 20 mL of urine collected at each 15-week
follow-up visit Blood specimens will be separated according to PANTHER-IPF MOOP
guidelines into the following components for banking in the repository serum plasma and
DNA Coding of all biologic specimens for the repository will be performed by study staff at the
clinical center The samples will be processed per PANTHER-IPF MOOP guidelines aliquoted
labeled with barcode labels and stored at -70degC at the clinical center and shipped to the central
repository
The only subject identifiers will be a sample ID number and subject initials This sample ID will
be linked in the IPFnet DCC clinical database to subject information No subject information will
be transferred to the biological-specimen database
The subjectrsquos samples may be used for approved sub-studies relating to human disease
including but not limited to IPF The studies for which an individualrsquos samples will be made
available will be determined by the subjectrsquos answers to questions on the biological-sample
informed consent form The subjects can choose to make their samples available for all options
or any combination Samples will be made available to researchers only with IPFnet Steering
Group approval until such time as the samples are made public through the NHLBI repository
49 Concomitant Medications
Concurrent treatment with FDA-approved therapy for IPF is allowed Colchicine may be used
for treatment of gout Temporary treatment with oral or IV corticosteroids for clinical worsening
or suspected AEx is permitted Nutritional supplements containing NAC are not allowed
410 Laboratory Testing
Clinical laboratory parameters will be assessed at screening and at the end of the study The
following tests will be performed at the two time points specified in the protocol chemistry (AG
ratio ALT [SGPT] AST [SGOT] albumin alkaline phosphatase amylase bilirubin-direct
42
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
bilirubin-indirect bilirubin-total BUN BUNcreatinine ratio calcium carbon dioxide
cholesterol-total chloride CPK-total creatinine GGT globulin glucose iron-total LDH
lipase magnesium phosphorus-inorganic potassium protein-total sodium TIBC triglycerides
uric acid) and hematology (red blood cell count WBC count hemoglobin hematocrit cell
indices differential platelet count)
411 Blinding of Study Drugs
Subjects and caregivers will be blinded to study treatment Every subject will receive NAC or
matching PLs at every study visit from the baseline visit to the week-45 visit No study agent
will be dispensed at the week-60 visit
43
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
5 Study Endpoints
51 Primary Study Endpoint
The primary endpoint will be the change in serial measurements of FVC over the study period
52 Secondary Study Endpoints
521 Time to Disease-progression
The time-to-death or a 10 decline in FVC will be defined as the time-to-disease progression
The 10 decline in FVC from enrollment must be confirmed on 2 consecutive visits no less than
6 weeks apart For subjects with 2 consecutive visits with a 10 decline in FVC the time-toshy
disease progression will be defined as the time interval between enrollment and the initial visit
with a 10 FVC decline For subjects who experience disease progression the study doctor will
determine whether or not the subject will remain in the study
522 Acute Exacerbations
The following 3 criteria will define AEx in subjects with acute worsening of their respiratory
conditions
1 Clinical (all of the following required)
A) Unexplained worsening of dyspnea or cough within 30 days triggering unscheduled
medical care (eg emergency room clinic study visit hospitalization)
B) No clinical suspicion or overt evidence of cardiac event pulmonary embolism or deep
venous thrombosis to explain acute worsening of dyspnea
C) No pneumothorax
44
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
2 RadiologicPhysiologic (A and B required)
A) New ground glass opacity or consolidation computed tomography (CT) scan OR new
alveolar opacities on chest x-ray
B) Decline of ge 5 in resting room air SpO2 from last recorded level OR decline of ge 8 mm
Hg in resting room air PaO2 from last recorded level
3 Microbiologic (all of the following required)
A) No clinical evidence for infection (ie absence of grossly purulent sputum fever gt 39degC
orally)
B) Lack of positive microbiological results (if done) from lower respiratory tract defined as
(1) Clinically significant bacterial growth on sputum or endotracheal aspirate cultures
(2) Quantitative culture by protected brush specimen ge 103 cfumL or BAL ge 104 cfumL
(3) The presence of specific pathogens on stains of any of the above
C) Lack of positive pathogen in blood cultures (if done)
Identification of Acute Exacerbations
All subjects will be educated about the importance of identifying AExs At the time of
enrollment subjects will be told about the possibility of developing acute symptomatic
worsening that might represent an AEx of IPF and instructed to contact their study clinical
center coordinator within 48 to 72 hours of the apparent event
All subjects will be contacted by phone monthly and questioned about any change in dyspnea or
cough and any interim clinic visits or hospitalizations Finally as part of the IPFnet outreach to
community referring physicians the importance of AExs will be emphasized When a subject is
identified who meets criterion 1A this will trigger the collection of additional clinical data to
evaluate a suspected AEx These data will be collected as part of standard clinical care (ie this
protocol does not require collection of all items) The additional items to be collected for
suspected AEx include
IPFnet AEx case report form (eCRF) (required)
45
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Chest x-ray CT scan withwithout pulmonary angiogram (reports should be faxed and
followed by the hard copiesdiscs)
Oxygen saturation (pulse oximetry)
ABG
Respiratory cultures (sputum endotracheal aspirate lavage)
Blood cultures
Clinichospital records related to the event
All potential cases of AEx will be reviewed by the clinical center PI first and a decision on
whether the case may represent an AEx will be made If AEx is suspected the case will be sent
to the IPFnet adjudication committee which will assign a final diagnosis (see Table 5) If there is
disagreement among members the majority opinion will be recorded
During episodes of suspected AEx as determined by the individual clinical center investigator
subjects will remain blinded and in the study
Table 5 Final Diagnoses in Evaluation of Suspected Acute Exacerbations
Definite acute exacerbation All criteria met no alternative etiology
Unclassifiable acute worsening
Insufficient data to evaluate all criteria no alternative etiology
Not acute exacerbation Alternative etiology identified that explains acute worsening
Management of the suspected AEx will be at the discretion of the treating physician Standard of
care generally involves evaluation for respiratory infection pulmonary embolism cardiac events
and pneumothorax and treatment with IV corticosteroids
Study drugs will be resumed at pre-suspected AEx doses after subjects clinically improve as
confirmed by the local PI All subjects should be seen at the clinical center within 2 to 4 weeks
of recovery for measurement of post-bronchodilator FVC (see Figure 4) Subjects unable to
return to the clinical center after suspected AEx due to medical frailty (eg continued
46
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
institutionalization progressive disability) will be categorized as failing to maintain FVC
response in secondary analyses
Suspected AEx (PI determined)
Hold study drug Treat AEx
(Attending physician determined)
Alive but unable to continue due to
medical frailty
Dead
Alive and able to continue
Site reviewvisit
Restart study drug
FVC within 2-4 weeks
Figure 4 Acute Exacerbation Flow Chart
523 Respiratory Infections
An upper respiratory infection will be defined as
Change in sputum discoloration
Increased cough of no more than 14 daysrsquo duration
A lower-respiratory infection (pneumonia) will be defined as new segmental or lobar airspace
opacities visualized by image studies (chest radiograph or HRCT) in addition to any of the
following
Positive pathogencultures in good sample of sputum or lower-airway secretions retrieved
by fiberoptic bronchoscope
Fever gt 39degC or gt 100degF
Leukocytosis gt 12000 (unexplained no increase in dose of corticosteroids)
47
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
524 Maintained FVC Response
Subjects with follow-up FVCpred measurements at or above their baseline FVCpred level
will be classified as having maintained FVC response Subjects with reduced FVCpred levels
or missing data for any reason including death or medical frailty will be classified as having not
maintained FVC response The FVCpred value is used because unadjusted FVC measurements
are expected to decline with age
48
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
6 Safety Evaluations and Procedures
61 Adverse Events
During a clinical trial the reporting of adverse experience information can lead to important
changes in the way a new treatment is developed as well as provide integral safety data
611 Definitions
An adverse event (AE) is any untoward medical occurrence in a subject or clinical investigation
subject who was administered a pharmaceutical product The AE does not necessarily have to
have a causal relationship with the drug administered An AE can be any unfavorable and
unintended sign (including an abnormal laboratory finding) symptom or disease temporarily
associated with the use of a medicinal product whether or not considered to be related to the
medicinal product Diseases signs symptoms or laboratory abnormalities already existing at
enrollment are not considered AEs unless they worsen (ie increase in intensity or frequency)
Surgical procedures themselves are not AEs they are therapeutic measures for conditions that
require surgery The condition for which the surgery is required may be an AE Surgical
procedures planned before randomization and the conditions necessitating the surgery are not
AEs
A serious adverse event is any untoward event that
Is fatal
Is life-threatening
Requires inpatient hospitalization or prolongation of existing hospitalization with the
following exceptions
o Preplanned (before the study) hospital admissions unless the hospitalization is
prolonged
o Planned admissions (as part of a study eg routine biopsies)
o Hospitalization lasting lt 24 hours
49
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
o Hospitalization for elective procedure
o Emergency room visits
Results in persistent or significant disability or incapacity
Is a congenital anomaly or birth defect
Important medical events that may not result in death be life-threatening or require
inpatient hospitalization may be considered serious adverse events (SAEs) when based
on appropriate medical judgment they may jeopardize the subject and may require
medical or surgical intervention to prevent one of the outcomes listed above
Life-threatening means that the subject was in the view of the investigator at immediate risk of
death from the AE as it occurred It does not include an AE that had it occurred in a more severe
form might have caused death
Persistent or significant disabilityincapacity means that the event resulted in permanent or
significant and substantial disruption of the subjectrsquos ability to carry out normal life functions
Causality
A reasonable possibility means the AE may have been caused byrelated to the study drug A
perceived or real lack of efficacy does not satisfy the definition of relatedness
612 Adverse Event (AE) Reporting
For the PANTHER-IPF trial all AEs (serious and nonserious) occurring from randomization
through final study visit (4 weeks after final dose of all study medication) will be recorded on the
AE page of the case report form (CRF)
6121 Serious Adverse Events (SAE) Reporting
For this trial all deaths and all SAEs which occur from randomization through final study visit
must be entered within the EDC system via the SAE eCRF page within 24 hours of the
investigative sitersquos knowledge of the event It is the responsibility of the clinical center
50
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
investigator to provide a causality assessment of the event for each study medications based upon
the information available at the time of the report It is understood that complete information
about the event may not be known at the time the initial report is submitted In the event the EDC
system is not accessible to the site at the time of event reporting investigative sites will complete
and forward a paper back-up SAE form to DCRI Safety Surveillance for processing
DCRI Safety Surveillance
Telephone 1-919-668-8624 or 1-866-668-7799 (toll free)
Fax 1-919-668-7138 or 1-866-668-7138 (toll free)
The investigator must complete and submit follow-up SAE information via the eCRF when
important new or follow-up information (eg final diagnosis outcome results of specific
investigations) becomes available Follow-up information should be submitted according to the
same process used for reporting the initial event as described above All SAEs will be followed
until resolution stabilization or 30 days after the subject has completed the final visit (4 weeks
after the final dose of study medication) whichever occurs first The investigator is responsible
for reporting SAEs to their institutional review board (IRB) per site specific IRB reporting
guidelines
6122 Regulatory Reporting
AEs that are serious study drug related and unexpected will be reported to the regulatory
authorities The DCRI Safety Surveillance medical monitor will perform a medical review of all
SAEs submitted and evaluate for ldquounexpectednessrdquo DCRI Safety Surveillance will prepare
MedWatch reports for those events identified as serious study drug related and unexpected as
determined by Safety Medical Monitor
DCRI Regulatory Services will submit all unexpected study drug-related SAEs as per 21 CFR
32 DCRI Safety Surveillance will provide a safety alert letter to the NHLBI DSMB and DCC
clinical operation (for distribution to sites) within 15 days of initial receipt of the information
51
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Investigators are responsible for promptly reporting these events to their reviewing IRBs
according to site specific IRB reporting guidelines
62 Clinical Medical Monitoring
There will be an unblinded physician at the IPFnet DCC serving as medical monitor The
medical monitor will be available to assist with questions about dosage adjustments of study
medications including discontinuation or resumption of medications
63 Unblinding Procedures
Unblinding of subjects or investigators to subject treatment is strongly discouraged For ongoing
clinical management all subjects should be presumed to be receiving ldquoactiverdquo study drug To
ensure the subjectrsquos safety the study treatment will be dose-adjusted based on laboratory test
results clinical findings and symptoms
The IPFnet DCC medical monitor and PANTHER-IPF co-chairs Drs Ganesh Raghu and
Fernando Martinez will be available to the study physicians to discuss study drug management
on a case-by-case basis Un-blinding will be considered ONLY when the knowledge of subject
treatment assignment is ABSOLUTELY ESSENTIAL for subject safety and after discussion of
the subjectrsquos case with the medical monitor and either Dr Raghu or Dr Martinez Unblinding of
study treatment should be minimized during the conduct of the trial In those cases where it is
felt to be medically necessary the DCC medical officer will communicate directly with the
managing physician to minimize unblinding of study personnel
52
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
7 Study Drug Procedures
At the baseline 15-week 30-week and 45-week study visits subjects will receive a supply of
study drug sufficient to last until the next visit at which study drug will be dispensed
53
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
8 Data Management
81 Hardware and Software Configuration
811 Hardware and Database Software
Data will be stored in an Oracle database system Oracle has advantages of processing efficiency
and smooth linkage with other software systems The application and database will be hosted on
Solaris Unix servers at the IPFnet DCC
812 Statistical Software
SAS will be used as the principal application for the management of analysis data files and
statistical computations S-Plus will be used to provide supplementary functions as needed
813 Access Control and Confidentiality Procedures
Access to databases will be controlled centrally by the IPFnet DCC through user passwords
linked to appropriate privileges This protects the data from unauthorized changes and
inadvertent loss or damage
814 Security
Database and Web servers will be secured by a firewall and through controlled physical access
Oracle has many security features to ensure that any staff member accessing the database has the
proper authority to perform the functions he or she requests of the system Within the secondary
SAS databases Unix group-access control maintains similar security The Sun workstation login
is secured by extensive user-password facilities under Unix
54
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
815 Back-up Procedures
Database back-up will be performed automatically every day and standard IPFnet DCC policies
and procedures will be applied to dictate tape rotation and retention practices
816 Virus Protection
All disk drives that provide network services and all user computers will be protected using
virus-scanning software Standard IPFnet DCC policies will be applied to update these protection
systems periodically through the study
82 Sources of Data
821 Design and Development
The IPFnet DCC will be responsible for development of the electronic case report forms
(eCRFs) development and validation of the clinical study database ensuring data integrity and
training clinical center staff on applicable data management procedures A web-based distributed
data entry model will be implemented This system will be developed to ensure that guidelines
and regulations surrounding the use of computerized systems used in clinical trials are upheld
The remainder of this section provides an overview of the data management plan associated with
this protocol
822 Data Collection Forms
The data collection process consists of direct data entry at the study clinical centers into the EDC
system(s) provided by the DCC A data collection worksheet will be provided to clinical centers
for recording data in the event the EDC system is unavailable Data entry of the eCRFs should
be completed according to the instructions provided and project specific training The
investigator is responsible for maintaining accurate complete and up-to-date records and for
ensuring the completion of the eCRFs for each research participant
55
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
823 Data Acquisition and Entry
Data entry into eCRFs shall be performed by authorized individuals Selected eCRFs may also
require the investigatorrsquos written signature or electronic signature as appropriate Electronic
CRFs will be monitored for completeness accuracy and attention to detail during the study
824 Data Center Responsibilities
The IPFnet DCC will 1) develop a data management plan and will conduct data management
activities 2) provide final eCRFs for the collection of all data required by the study 3) develop
data dictionaries for each eCRF that will comprehensively define each data element 4) conduct
ongoing data monitoring activities on study data 5) monitor any preliminary analysis data
cleanup activities and 6) rigorously monitor final study data clean up
825 Data Editing
Completed data will be entered into the IPFnet DCC automated data acquisition and
management system If incomplete or inaccurate data are found a data clarification request will
be generated and distributed to clinical centers for a response Clinical centers will resolve data
inconsistencies and errors and enter all corrections and changes into the IPFnet DCC automated
data acquisition and management system
826 Training
The training plan for clinical center staff includes provisions for training on assessments eCRF
completion guidelines data management procedures and the use of computerized systems
56
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
9 Study Design and Data Analysis
91 General Analytic Considerations
All primary analyses will be based on intent-to-treat (ITT) principles using all randomized
subjects Baseline factors across groups will be compared using mean (standard deviation) and
median (25th and 75th percentiles) summary measures Kaplan-Meier curves will be used to
display event rates Due to clinical interest in departures from both sides of the null hypothesis
all test statistics will be 2-sided
Reasonable caution needs to be taken when conducting multiple analyses on key clinical
subgroups For subgroup analyses a conservative significance level of 0001 will be used for all
interaction tests Thus subgroup comparisons will be considered exploratory unless the p-value
from the interaction test is smaller than 0001
92 Randomization Blinding and Reporting of Results
A permuted block-randomization scheme will be created with varying block sizes stratified by
clinical center Once a subject has completed the screening and baseline period and evaluation
for inclusionexclusion criteria the randomization process will begin Subjects will be
randomized to receive NAC or matching placebo with equal probability (11) via telephone
contact with a central interactive voice response system (IVRS) using a toll-free randomization
number On the day of randomization after the subject has successfully met all inclusion and
exclusion criteria the investigator or designee will call the central randomization number to
obtain the assigned kit randomization numbers for that subject At each subject visit the
investigator or designee will call the central randomization number to obtain the new kit
randomization numbers for resupply of the subject For resupply of the clinical center the IVRS
will monitor minimal volume of a kit type andor expiration date and will automatically notify
the pharmacy
57
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
The trial results will be reported according to guidelines specified in the CONSORT statement
A flow diagram describing screening recruitment randomization dropout and vital status will
be included in the primary manuscript AEs and efficacy data will be presented for all treatment
groups Adherence dropout and lost to follow-up will be carefully examined across all treatment
groups Analyses of safety will be based on data from all randomized subjects who received at
least one dose of study drug
93 Stratification
Subjects will be distributed to the two treatment arms in a 11 allocation ratio Stratification
blocks will be based on clinical centers
94 Specification of the Primary Analyses
A mixed model repeated measures (MMRM) analysis described in section 95 will be used to
compare differences in the slope of FVC measurements across the treatment groups Response
variables are values of the FVC measured at baseline and every 15 weeks until study completion
Variables in the model will include treatment time and time by treatment age sex race and
height Contrast estimates of differences in slopes of treatment over time (along with confidence
intervals) will be used to estimate the treatment effect The validity of this model in terms of
meeting modeling assumptions will be assessed via standard modeling diagnostics and goodness-
of-fit measures Based on the MMRM framework missing FVC data will not be imputed for the
primary analysis
95 Analysis of Longitudinal Endpoints
A common goal in clinical trials is to specify models that are easily implemented and
reproducible by independent data analysts On the other hand the models should have proper
statistical behavior in terms of low bias and high precision Many common approaches to
longitudinal data analysis including last observation carried forward (LOCF) imputation rely on
the missing completely at random (MCAR) assumption However the MCAR assumption is
58
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
unlikely to hold in many clinical trials because missing data are often related to disease
progression and prognosis A more reasonable assumption missing at random (MAR) specifies
that the complete data distribution can be modeled using only the observed data The likelihood-
based MMRM approach is valid under the more general MAR assumptions These models will
be applied to analyze the longitudinal data secondary endpoints
The advantages of MMRM analysis are that all important characteristics of the model can be preshy
specified standard software can be used to implement the models and results are based on ITT
principles43 In addition the MMRM approach offers superior control of Type I and Type II
errors compared with the LOCF approach
Response variables are values of the PFTs measured at enrollment and every 15 weeks until
study completion and 6MWT values measured at baseline week 30 and week 60 Covariates are
treatment time time by treatment and key baseline risk factors Contrasts (along with
confidence intervals) of treatment by time will be used to estimate the treatment effect
The correlation structure involves multiple pieces including measurement errors random
variation and interindividual variability For the longitudinal data analyses an unstructured
correlation matrix for within-subject errors will be assumed Other correlation structures
including compound symmetry will be examined as needed A careful examination of reasons
for study discontinuation will be conducted to assess the validity of MCAR Sensitivity analyses
will be used to examine the untestable assumption that the observed data violate the MAR
assumption The MMRM models will be implemented using PROC MIXED in SAS
96 Analysis of Binary Time-to-Event and Time-Lagged Endpoints
Regression modeling approaches using either the logistic regression model or Cox proportional
hazards regression model will be employed when appropriate The validity of these models will
be assessed via standard modeling diagnostics and goodness-of-fit measures Estimates of
cumulative frequencies for more general time-lagged responses will be calculated using the
partitioned version of the Bang-Tsiatis estimator44 The partitions will be set at 15-week intervals
59
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
to correspond with the data-collection process Covariate adjusted event rates will be calculated
using inverse probability-weighted regression estimates45
97 Power Analysis
971 Primary Analyses
Based on previously published IPF clinical trials the PL group is expected to experience a drop
in FVC of approximately 020 L over the study period (see Figure 1) The IPFnet Steering Group
determined a clinically important difference would be to preserve the majority of the decline
relative to PL over the study period In particular a treatment effect of 015 L was determined to
be a clinically meaningful difference Potential dropout is a key factor in the proposed study The
drop-out process assumed 5 lost to follow-up after every study visit Only 80 of subjects
were assumed to be followed for the entire study period All models assumed a compound
symmetry structure for the covariance matrix Power calculations were performed using a SAS
IML program for designing repeated measures studies46 Based on preliminary reviews of the
data from the University of Michigan the covariance matrix parameters were estimated at
approximately σ2 = 0757 (variance parameter) and ρ = 0936 (correlation parameter) To be
conservative the power calculations for the primary analysis were performed with parameter
setting of σ2 = 0810 (variance parameter) and ρ = 0925 (correlation parameter)
The power calculations assume a correction for imperfect compliance proposed by Lachin and
Foulkes to allow for 2 noncompliance for each of the treatment arms47 Thus the sample size
of 130 subjects per arm would be reduced to an adjusted sample size of 130(1-002-002)2 =
1198 or 120 subjects per arm
Under the assumed Type I error rate of 005 with a correlation parameter of 0925 and standard
deviation of 090 the difference of 015 L (or 00025 Lweek) shown in Table 6 would have
power of 93
60
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Table 6 Hypothetical Values of Mean FVC (L) Change from Baseline
Week 15 Week 30 Week 45 Week 60
NAC 00125 00250 00375 00500
Placebo 00500 01000 01500 02000
Difference 00375 00750 01125 01500
Abbreviations FVC forced vital capacity PL placebo
972 Power Analysis for Secondary Endpoints
Power calculations for secondary endpoint measurements are shown in Table 7 Standard
deviations are based on unpublished data provided by the University of Michigan The
calculations are based on a 2-sample t-test with Type I error rate set at 005 These calculations
are likely to be conservative because the statistical approach described in section 95 for
analyzing these endpoints will incorporate incomplete observations as well as intermediate data
points
Table 7 Detectable Differences in Treatment Means for Selected Endpoint Measurements
Secondary Endpoints Std Dev
of the Baseline Score
Detectable Difference for 80 Power
Std Dev of the Change Score
Difference Detectable for
80 Power
DLCOpred 166 58 91 32
6MWT Area Under the Desaturation Curve
219 76 175 61
6MWT Distance to Desaturation 224 78 315 110
6MWT Minutes Walked 210 073 205 071
Abbreviations Std Dev standard deviation DLCOpred diffusing capacity of the lung for carbon monoxide percent predicted 6MWT 6-minute walk test
61
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
10 Study Administration
101 Cooperative Agreement Mechanism
The administrative and funding mechanism used to undertake this project is a ldquocooperative
agreementrdquo (U01) which is an assistance mechanism Under the cooperative agreement the
NHLBI assists supports andor stimulates the project and is substantially involved with
investigators in conducting the study by facilitating performance of the effort in a ldquopartnerrdquo role
The NHLBI project scientist serves on the IPFnet Steering Group and he or another NHLBI
scientist may serve on other project committees when appropriate At the same time however
NHLBI does not assume a dominant role direction or prime responsibility for this research
program
As described below governance of the project is conducted through the IPFnet Steering Group
Principal investigators have lead responsibilities in all aspects of their trials and the project
including any modification of trial designs conduct of the trials quality control data analysis
and interpretation preparation of publications and collaboration with other investigators unless
otherwise provided for by the IPFnet Steering Group
PIs retain custody of and have primary rights to their center-specific and collaborative data
subject to government rights-of-access consistent with current Health amp Human Services (HHS)
Public Health Service (PHS) and National Institutes of Health policies The protocols and
governance policies call for the continual submission of data centrally to the IPFnet DCC for the
collaborative database which at a minimum will contain the key variables selected by the IPFnet
Steering Group for standardization across all clinical centers the submission of copies of the
collaborative datasets to each PI upon completion of the project procedures for data analysis
reporting and publication and procedures to protect and ensure the privacy of medical and
genetic data and records of individuals The NHLBI project scientist on behalf of the NHLBI
will have the same access privileges and responsibilities regarding the collaborative data as the
other members of the Steering Group
62
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
PIs are also encouraged to publish and to publicly release and disseminate results data and other
products of the project concordant with the project protocols and governance and the approved
plan for making data and materials available to the scientific community and to the NHLBI
However during the 3 years after the ending date of NHLBI project support unpublished data
unpublished results data sets not previously released and other study materials or products are
to be made available to any third party only with the approval of the IPFnet Steering Group
Upon completion of the project PIs are expected to put their intervention materials and
procedure manuals into the public domain andor make them available to other investigators
according to the approved plan for making data and materials available to the scientific
community and the NHLBI for the conduct of research at no charge other than the costs of
reproduction and distribution
The NHLBI reserves the right to terminate or curtail the project (or an individual award) in the
event of (a) failure to develop or implement mutually agreeable collaborative measurement
subject eligibility and data management sections of the protocols (b) substantial shortfall in
subject recruitment follow-up data reporting or quality control or other major breach of
protocol (c) substantive changes in the agreed-upon protocols with which NHLBI cannot
concur (d) reaching a major project outcome with persuasive statistical significance
substantially before schedule or (e) human subject ethical issues that may dictate a premature
termination
Any disagreement that may arise in scientificprogrammatic matters (within the scope of the
award) between award recipients and the NHLBI may be brought to arbitration An arbitration
panel will be composed of 3 membersmdash1 selected by the IPFnet Steering Group (with the
NHLBI member not voting) or by the individual PI in the event of an individual disagreement a
second selected by NHLBI and the third selected by the other 2 members This special
arbitration procedure in no way affects the PIrsquos right to appeal an adverse action that is otherwise
appealable in accordance with the PHS regulations at 42 CFR part 50 Subpart D and HHS
63
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
regulation at 45 CFR part 16 or the rights of the NHLBI under applicable statutes regulations
and terms of the award
102 IPFnet Steering Group
The IPFnet Steering Group is the main governing body of the project It is composed of the PIs
of the clinical centers the PI of the DCC and the NHLBI project scientist The clinical centers
the IPFnet DCC and the NHLBI each have 1 vote on the IPFnet Steering Group All decisions
are determined by majority vote
All major scientific decisions are determined by the IPFnet Steering Group It assumes overall
responsibility for the design and conduct of the trial It appoints (and disbands) committees and
subcommittees as the need arises designs approves and implements the study protocols
oversees the development of the MOOP monitors subject recruitment and treatment delivery
evaluates data collection and management oversees quality assurance procedures and
implements changes and enhancements to the study as required It also has primary responsibility
for facilitating the conduct of the trials and reporting the projectrsquos results
103 Data and Safety Monitoring Board
The NHLBI will establish a DSMB in accordance with established policies (see
httpwwwnhlbinihgovfundingpoliciesdsmb_insthtm) to ensure data quality and subject
safety and to provide independent advice to the NHLBI regarding progress and the
appropriateness of study continuation
104 Recommendations on Interim Monitoring of Efficacy Safety and Futility
First and foremost the role of the DSMB will be to review subject safety and trial conduct at
periodic points during the study The DSMB may require analyses of the primary endpoint
results for comparing the benefit and risks of treatment strategies The benefit of collecting
additional data on key secondary endpoints with extended follow-up and establishing a robust
64
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
evidence base for determining a standard of care will need to be carefully considered before
early termination of one or more treatment arms After careful consideration the IPFnet Steering
Group recommends conservative thresholds for the early examinations of the safety and efficacy
data
The DSMB will be expected to meet approximately every 6 months until trial completion to
review safety and toxicity data The DSMB may recommend stopping the study based on these
reviews Because the DSMB could stop the trial for safety concerns as well as for a large
efficacy benefit there could be multiple opportunities to reject the null hypothesis (no difference
in event rates between the PL and NAC groups) A Bonferroni approximation will be applied
during the one planned interim analysis for efficacy
Before locking the database a statistical analysis plan (SAP) will be developed to provide
complete details on the statistical analysis The SAP will include the specifics for how and when
the DSMB will be notified for AEs The IPFnet DCC will deliver to the DSMB all FDA-defined
AEs at 3-month intervals The IPFnet DCC will prepare narrative SAE reports in real time for
DSMB review including recommendations and analysis of similar events for each SAE
submitted to the FDA
65
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
11 Investigator and Sponsor Obligations
111 Monitoring
All monitoring activities for US clinical centers will be performed in accordance with DCRI
standard operating procedures Information regarding the types of visits will be outlined in the
PANTHER-IPF MOOP
112 Cost and Payment
There will be no cost to subjects enrolled in this trial Study-related procedures will be paid for
by the IPFnet
Subjects may be eligible for reimbursement for travel to the clinical center Details of payment
will be explained to each subject during the consent process
113 Confidentiality and Health Insurance Portability and Accountability Act
Considerations
Subject confidentiality will be protected throughout the study All subject data will be kept
strictly confidential and no subject-identifying information will be released to anyone outside
the project Confidentiality will be assured through several mechanisms First each subject will
be assigned an anonymous study ID which will then be used on all study forms Second any
study forms blood samples and paper records that contain subject information (eg address lists
phone lists) will be kept at the clinical centers in secured locked areas coded by number Once
blood is collected there will be no subject identifiers placed on blood samplesmdashonly the study
ID number and the date of sample collection Third access to all subject data and information
including laboratory specimens will be restricted to authorized personnel In the case of
computerized data this restricted access will be assured through user logon IDs and password
protection
66
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
At the IPFnet DCC only authorized personnel will have access to the data files containing study
data Security will be assured through user logon IDs passwords and appropriate access
privileges All study subjects will be identified only by their IPFnet ID numbers and no personal
identifying information such as name address or Social Security number will be entered into
the IPFnet DCC database Any subject-specific data reported to the IPFnet Steering Group will
be identified only by the IPFnet ID number
Finally subjects will not be identified by name in any reports or publications nor will the data
be presented in such a way that the identity of individual subjects can be inferred Analysis files
created for further study by the scientific community will have no subject identifiers These data
files will be created in accordance with the Ancillary Studies and Publication Policy of the
IPFnet
114 Informed Consent Procedures
All IPFnet subjects will provide written informed consent using procedures reviewed and
approved by each clinical centerrsquos IRB Informed consent will be undertaken by study personnel
in-person with the subject The subject has the option of declining further participation in the
study at that point No further study procedures will be conducted until the signed documents
have been provided to the IPFnet clinical center
115 Institutional Review Boards
Before initiating this study the protocol clinical center-specific informed consent forms Health
Insurance Portability and Accountability Act (HIPAA) forms recruitment materials and other
relevant information will be reviewed by a properly constituted IRB at each participating clinical
center A copy of the signed and dated IRB approval at each clinical center will be retrieved prior
to or during the site initiation visit and archived at the IPFnet DCC Any amendments to the
protocol other than simple administrative and typographical changes must be approved by each
IRB before they are implemented The clinical centers will seek annual renewals of their IRB
approvals in accordance with local procedures
67
__________________________________________ ________________
__________________________________________
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
12 Investigator Agreement
I have read the foregoing protocol PANTHER-IPF and agree that it contains all necessary
details for carrying out this study I will conduct the study as outlined herein and will complete
the study within the time designated
I will provide copies of the protocol and all pertinent information to all individuals responsible to
me who assist in the conduct of this study I will discuss this material with them to ensure they
are fully informed regarding the drug and the conduct of the study
I will fulfill all responsibilities for submitting pertinent information to the local IRB if
applicable that is responsible for this study
I further agree that NHLBI andor DCRI will have access to any source documents from which
eCRF information may have been generated
Signature of Principal Investigator Date
Name of Principal Investigator (printed or typed)
Protocol version date May 19 2009
Protocol Amendment 1 version date May 28 2010
Protocol Amendment 2 version date December 6 2011
68
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
13 References
1 Raghu G Brown KK Bradford WZ et al A placebo-controlled trial of interferon gamma-1b in patients with idiopathic pulmonary fibrosis N Engl J Med 2004350125-33 2 King TE Jr Safrin S Starko KM et al Analyses of efficacy end points in a controlled trial of interferon-gamma1b for idiopathic pulmonary fibrosis Chest 2005127171-7 3 Flaherty KR Thwaite EL Kazerooni EA et al Radiological versus histological diagnosis in UIP and NSIP survival implications Thorax 200358143-8 4 Wells AU Desai SR Rubens MB et al Idiopathic pulmonary fibrosis a composite physiologic index derived from disease extent observed by computed tomography Am J Respir Crit Care Med 2003167962-9 5 Raghu G Freudenberger TD Yang S et al High prevalence of abnormal acid gastroshyoesophageal reflux in idiopathic pulmonary fibrosis Eur Respir J 200627136-42 6 Kinnula VL Focus on antioxidant enzymes and antioxidant strategies in smoking related airway diseases Thorax 200560693-700 7 Coultas DB Zumwalt RE Black WC Sobonya RE The epidemiology of interstitial lung diseases Am J Respir Crit Care Med 1994150967-72 8 Raghu G Weycker D Edelsberg J Bradford WZ Oster G Incidence and prevalence of idiopathic pulmonary fibrosis Am J Respir Crit Care Med 2006174810-6 9 Olson AL Swigris JJ Lezotte DC Norris JM Wilson CG Brown KK Mortality from pulmonary fibrosis increased in the United States from 1992 to 2003 Am J Respir Crit Care Med 2007176277-84 10 Mannino DM Etzel RA Parrish RG Pulmonary fibrosis deaths in the United States 1979shy1991 An analysis of multiple-cause mortality data Am J Respir Crit Care Med 19961531548shy52 11 Hubbard R Johnston I Coultas DB Britton J Mortality rates from cryptogenic fibrosing alveolitis in seven countries Thorax 199651711-6 12 Johnston I Britton J Kinnear W Logan R Rising mortality from cryptogenic fibrosing alveolitis Bmj 19903011017-21 13 Raghu G Collard HR Egan JJ et al An official ATSERSJRSALAT statement idiopathic pulmonary fibrosis evidence-based guidelines for diagnosis and management Am J Respir Crit Care Med 2011183788-824 14 (USA) FDA FDA Public Health Advisory Interferon gamma-1b (marketed as Actimmune) In 2007 15 King TE Jr Pardo A Selman M Idiopathic pulmonary fibrosis Lancet 2011 16 Raghu G Brown KK Costabel U et al Treatment of idiopathic pulmonary fibrosis with etanercept an exploratory placebo-controlled trial Am J Respir Crit Care Med 2008178948shy55 17 Malouf MA Hopkins P Snell G Glanville AR An investigator-driven study of everolimus in surgical lung biopsy confirmed idiopathic pulmonary fibrosis Respirology 201116776-83 18 King TE Jr Behr J Brown KK et al BUILD-1 a randomized placebo-controlled trial of bosentan in idiopathic pulmonary fibrosis Am J Respir Crit Care Med 200817775-81 19 Richeldi L Costabel U Selman M et al Efficacy of a tyrosine kinase inhibitor in idiopathic pulmonary fibrosis N Engl J Med 20113651079-87
69
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
20 Borok Z Buhl R Grimes GJ et al Effect of glutathione aerosol on oxidant-antioxidant imbalance in idiopathic pulmonary fibrosis Lancet 1991338215-6 21 Meyer A Buhl R Magnussen H The effect of oral N-acetylcysteine on lung glutathione levels in idiopathic pulmonary fibrosis Eur Respir J 19947431-6 22 Behr J Maier K Degenkolb B Krombach F Vogelmeier C Antioxidative and clinical effects of high-dose N-acetylcysteine in fibrosing alveolitis Adjunctive therapy to maintenance immunosuppression Am J Respir Crit Care Med 19971561897-901 23 Cantin AM North SL Fells GA Hubbard RC Crystal RG Oxidant-mediated epithelial cell injury in idiopathic pulmonary fibrosis J Clin Invest 1987791665-73 24 Waghray M Cui Z Horowitz JC et al Hydrogen peroxide is a diffusible paracrine signal for the induction of epithelial cell death by activated myofibroblasts Faseb J 200519854-6 25 Larios JM Budhiraja R Fanburg BL Thannickal VJ Oxidative protein cross-linking reactions involving L-tyrosine in transforming growth factor-beta1-stimulated fibroblasts J Biol Chem 200127617437-41 26 Kinnula VL Fattman CL Tan RJ Oury TD Oxidative stress in pulmonary fibrosis a possible role for redox modulatory therapy Am J Respir Crit Care Med 2005172417-22 27 Meyer A Buhl R Kampf S Magnussen H Intravenous N-acetylcysteine and lung glutathione of patients with pulmonary fibrosis and normals Am J Respir Crit Care Med 19951521055-60 28 Behr J Degenkolb B Krombach F Vogelmeier C Intracellular glutathione and bronchoalveolar cells in fibrosing alveolitis effects of N-acetylcysteine Eur Respir J 200219906-11 29 Bando M Hosono T Mato N et al Long-term efficacy of inhaled N-acetylcysteine in patients with idiopathic pulmonary fibrosis Intern Med 2010492289-96 30 Demedts M Behr J Buhl R et al High-dose acetylcysteine in idiopathic pulmonary fibrosis N Engl J Med 20053532229-42 31 Toma TP Bhowmik A Rajakulasingam R Acetylcysteine in pulmonary fibrosis N Engl J Med 20063541086-9 author reply -9 32 Hunninghake GW Antioxidant therapy for idiopathic pulmonary fibrosis N Engl J Med 20053532285-7 33 Flaherty KR Mumford JA Murray S et al Prognostic implications of physiologic and radiographic changes in idiopathic interstitial pneumonia Am J Respir Crit Care Med 2003168543-8 34 Latsi PI du Bois RM Nicholson AG et al Fibrotic idiopathic interstitial pneumonia the prognostic value of longitudinal functional trends Am J Respir Crit Care Med 2003168531-7 35 Collard HR King TE Jr Bartelson BB Vourlekis JS Schwarz MI Brown KK Changes in clinical and physiologic variables predict survival in idiopathic pulmonary fibrosis Am J Respir Crit Care Med 2003168538-42 36 Jegal Y Kim DS Shim TS et al Physiology is a stronger predictor of survival than pathology in fibrotic interstitial pneumonia Am J Respir Crit Care Med 2005171639-44 37 Martinez FJ Safrin S Weycker D et al The clinical course of patients with idiopathic pulmonary fibrosis Ann Intern Med 2005142963-7 38 Hull JH Acetylcysteine in pulmonary fibrosis N Engl J Med 20063541089-91 author reply -91
70
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
39 Flaherty KR King TE Jr Raghu G et al Idiopathic interstitial pneumonia what is the effect of a multidisciplinary approach to diagnosis Am J Respir Crit Care Med 2004170904shy10 40 Raghu G Johnson WC Lockhart D Mageto Y Treatment of idiopathic pulmonary fibrosis with a new antifibrotic agent pirfenidone results of a prospective open-label Phase II study Am J Respir Crit Care Med 19991591061-9 41 Hunninghake GW Lynch DA Galvin JR et al Radiologic findings are strongly associated with a pathologic diagnosis of usual interstitial pneumonia Chest 20031241215-23 42 Lynch D Godwin J Safrin S et al High-resolution computed tomography in idiopathic pulmonary fibrosis diagnosis and prognosis Am J Respir Crit Care Med 2005172488-93 43 Mallinckrodt CH Watkin JG Molenberghs G Carroll RJ Choice of the primary analysis in longitudinal clinical trials Pharmaceutical Statistics 20043161-9 44 Bang H Tsiatis A Estimating medical costs with censored data Biometrika 200087329shy43 45 Lin DY Regression analysis of incomplete medical cost data Stat Med 2003221181-200 46 Rochon J Application of GEE procedures for sample size calculations in repeated measures experiments Stat Med 1998171643-58 47 Lachin JM Foulkes MA Evaluation of sample size and power for analyses of survival with allowance for nonuniform patient entry losses to follow-up noncompliance and stratification Biometrics 198642507-19
71
- PANTHER-IPFPREDNISONE AZATHIOPRINEAND N-ACETYLCYSTEINEA STUDY THAT EVALUATES RESPONSE INIDIOPATHIC PULMONARY FIBROSIS
-
- Protocol Summary
- Table of Contents
- List of Tables
- List of Figures
- List of Abbreviations
- 1 Summary
- 2 Hypotheses and Specific Aims
-
- 21 Null Hypothesis
- 22 Specific Aim 1
- 23 Specific Aim 2
- 24 Prespecified Subgroups of Interest
-
- 3 Background and Significance
-
- 31 Idiopathic Pulmonary Fibrosis is the Most Common Interstitial Lung Disease
- 32 Rationale for Placebo Control
- 33 Rationale for N-acetylcysteine
- 35 Rationale for N-acetylcysteine as a Stand-alone Therapy
- 36 Rationale for the Study Design and Primary Endpoint
- 37 Rationale for Blinding of Treatments
-
- 4 Methods
-
- 41 Inclusion Criteria
- 42 Diagnosis of IPF
- 43 Exclusion Criteria
- 44 Study Design and Study Visit
- 45 Dose Justification
- 46 Contraindications Precautions and Side Effects of Study Medications
- 47 Recruitment Procedures
- 48 Study Procedures
- 49 Concomitant Medications
- 410 Laboratory Testing
- 411 Blinding of Study Drugs
-
- 5 Study Endpoints
-
- 51 Primary Study Endpoint
- 52 Secondary Study Endpoints
-
- 6 Safety Evaluations and Procedures
-
- 61 Adverse Events
- 62 Clinical Medical Monitoring
- 63 Unblinding Procedures
-
- 7 Study Drug Procedures
- 8 Data Management
-
- 81 Hardware and Software Configuration
- 82 Sources of Data
-
- 9 Study Design and Data Analysis
-
- 91 General Analytic Considerations
- 92 Randomization Blinding and Reporting of Results
- 93 Stratification
- 94 Specification of the Primary Analyses
- 95 Analysis of Longitudinal Endpoints
- 96 Analysis of Binary Time-to-Event and Time-Lagged Endpoints
- 97 Power Analysis
-
- 10 Study Administration
-
- 101 Cooperative Agreement Mechanism
- 102 IPFnet Steering Group
- 103 Data and Safety Monitoring Board
- 104 Recommendations on Interim Monitoring of Efficacy Safety and Futility
-
- 11 Investigator and Sponsor Obligations
-
- 111 Monitoring
- 112 Cost and Payment
- 113 Confidentiality and Health Insurance Portability and Accountability ActConsiderations
- 114 Informed Consent Procedures
- 115 Institutional Review Boards
-
- 12 Investigator Agreement
- 13 References
-
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Review concomitant medications
If consented draw blood and collect urine specimen for the biospecimen repository
Subjects return used and unused study drug for the visit
Review study diary and a new study diary will be given
Provide additional supply of study drug sufficient to last until the next scheduled visit
4424 Week 30
The week 30 visit is expected to occur within +- 14 days of the subjectrsquos scheduled visit time (eg the week 30
visit should occur anytime between 28 and 32 weeks after starting study drug) Week 30 activities include
Physical examination
Measure vital signs with oximetry
Measure height and weight
Laboratory values (complete blood count [CBC] and serum chemistries)
Serum pregnancy test (if applicable)
Measure spirometry (post-bronchodilator)
6MWT with Borg scale
DLCO
Review of AEs
Evaluate for AEx
Review concomitant medications
Complete all QOL and dyspnea questionnaires (EuroQol ICE CAP SF-36 SGRQ and UCSD SOBQ)
If consent has been given blood will be drawn and a urine specimen collected for the biospecimen
repository
Review study diary
Subjects return used and unused study drug for the visit
Provide additional supply of study drug sufficient to last until the next scheduled visit
4425 Week 45
31
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
The week 45 visit is expected to occur within +- 14 days of the subjectrsquos scheduled visit time (eg the week 45
visit should occur anytime between 43 and 47 weeks after starting study drug) Week 45 activities include
Measure vital signs with oximetry
Measure height and weight
Serum pregnancy test (if applicable)
Measure spirometry (post-bronchodilator)
Review of AEs
Evaluate for AEx
Review concomitant medications
If consent has been given blood will be drawn and a urine specimen collected for the biospecimen
repository
Subjects return used and unused study drug for the visit
Study diary reviewed
Provide additional supply of study drug sufficient to last until the next scheduled visit
4426 Week 60 (Early Withdrawal or Final Treatment Visit)
At week 60 or at subject withdrawal from the study (premature by study doctor or subjectrsquos decision) a final
treatment visit will occur At this final treatment visit subjects will discontinue NACPL abruptly Week 60
activities also include
Physical examination
Measure vital signs with oximetry
Measure height and weight
Laboratory values (complete blood count [CBC] and serum chemistries)
Spirometry (post-bronchodilator) measurement
6MWT with Borg scale measurement
DLCO
Lung volumes
ABG
Review of AEs
32
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Evaluate for AEx
Review concomitant medications
Subjects will complete all QOL and dyspnea questionnaires (EuroQol ICE CAP SF-36 SGRQ and
UCSD SOBQ)
If consent has been given blood will be drawn and a urine specimen collected for the biospecimen
repository
Subjects return used and unused study drug for the visit
Study diary reviewed
4427 Final Site Visit ndash FVC drop confirmation
In the event that the subject has a recorded FVC drop of gt10 from baseline at the final treatment visit and the
subject has not had a confirmation of such a drop at a previous study visit the subject should return to the
clinical site 6 to 8 weeks after the final treatment visit During this visit a post-bronchodilator spirometry test
will be performed This FVC measurement will be evaluated according to section 521 of this protocol
4428 Final Visit ndash Telephone Follow-up
Four weeks following the final dose of study medication subjects will receive a telephone call from the study
coordinator to ensure that there are no side effects and to follow up on any ongoing adverse events (AEs)
4429 Phone Contact Between Visits
At week 2 and each month that a subject does not have a scheduled clinical center visit his or her study
coordinator will contact him or her at least once by telephone to
Inquire if the subject has had any hospitalizations events that might be considered an AE or any events
significant enough to warrant an out-of-cycle visit to the clinical center
Remind subjects of their current dosage levels and confirm that the subject understands them
Address any questions or concerns the subject might have regarding other aspects of the study
Assess adherence to the treatment regimen by reviewing diary data verbal review of medications taken
including nutritional supplements
33
34
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Table 3 Schedule of Assessments
Procedure Screening Visit 0
Enrollment Visit 1
Week 15 Visit 2
Week 30Visit 3
Week 45 Visit 4
Week 60 Early
Withdrawal Visit 5
Final1
Visit (via phone)
Informed consent X
Medical history X
Inclusionexclusion criteria X
Serum pregnancy test (if applicable) X X X X X
Review of lung biopsy X
Arterial Blood Gas X X
6-Minute Walk Test
X
X X
Physical examination X X X
Vital signs with oximetry X X X X X X
Body height and weight X X X X X X
Complete Blood Count X X X
Chemistry panel X X X
Monitor Lab Values X X X
Urinalysis X Specimen repository substudy blood draw and urine collection (if consented)
X
X X X X
HRCT (if not completed within three months) X
Spirometry (pre- and post-bronchodilator) X
Spirometry (post-bronchodilator only) X X X X X
DLCO (post-bronchodilator only) X X X
Lung volumes (post-bronchodilator only) X
X
Evaluate for acute exacerbation X X X X X
Review Adverse Events X X X X X X
Review concomitant meds X X X X X X
Dispense subject diary X X X X
Review subject diary X X X X X
Dispense study agent X X X X
Gender Substudy questionnaire (female subjects only) X
EuroQol ICECAP UCSD SOBQ SGRQ SF-36 X X X
Abbreviations DLCO diffusing capacity of the lung for carbon monoxide QOL Quality of Life ICECAP Investigating Choice Experiments for Preferences of Older People UCSD SOBQ University of California Shortness of Breath Questionnaire SGRQ St Georgersquos Respiratory Questionnaire SF-36 Short Form 36 Health Survey
1Follow-up visit via phone will occur four weeks after final dose of study medication
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
45 Dose Justification
The general philosophy for determining dosing levels was to apply previously examined
treatment regimens With the focus of the study being to establish a standard of care for
mildmoderate IPF subjects the goal was to develop flexible yet standardized treatment rules that
allow for the temporary or permanent withholding of one or more components of treatment when
necessary Subjects developing laboratory abnormalities or symptoms that result in
discontinuation of one or more components of study treatment may continue on the other
components as long as there is no contraindication for this Complete follow-up is important for
the validity of any study As a strategy to maintain protocol adherence we are using a treatment
regimen that will detect potential side effects and prompt interventions proactively in the interest
of patient safety In addition subjects who permanently stop study medications during the course
of the study are encouraged to continue in the study completing all scheduled visits and tests
451 Rationale for N-acetylcysteine Dosing
To our knowledge there have been no IPF studies to correlate clinical outcome measures with
different dosages for NAC The dosage chosen is based on the IFIGENIA study However BAL
lung GSH levels from subjects with IPF have been augmented with the use of oral NAC at 600
mg 3 times per day In addition lung GSH levels have been associated with improved
PFTs212227 The dose chosen for this study was based on previous data including the IFIGENIA
study30
4511 Dosing of N-acetylcysteineplacebo
Dosing of NACPL will be 600 mg orally 3 times a day (1800 mgday)
4512 Reasons to Discontinue N-acetylcysteineplacebo
NACPL may be temporarily or permanently discontinued for the duration of the study for
gastrointestinal symptoms or dermatologic reactions
35
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Temporarily discontinue (hold) oral NACPL for subjects requiring inpatient admission for acute
exacerbation (AEx) or other conditions Resume NACPL after discharge
36
37
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
452 Dosage Algorithms
Dosage Adjustment Algorithm 1 NACPL Dose Modifications for Gastrointestinal Symptoms Nausea Vomiting Abdominal Discomfort Diarrhea
GI Symptoms determined by the PI to be clinically significant Nausea Vomiting Abdominal Discomfort Diarrhea
NACPL Temporarily dc (HOLD) x 3 Days
Monitor symptoms intervene as clinically indicated (eg fluid replacement antidiarrhea or antinausea medication)
Monitor or lab PRN
Are symptoms resolving after 3 days NO
Symptoms NOT resolving after 3 days of holding study medication Assessmentmanagement per clinical
discretion of investigator
Likely not study medication discuss resuming study medication with medical monitor when symptoms resolved
YES
Temporarily dc (HOLD) NACPL for 4 additional days (total hold 1 week) then NACPL Resume 600 MG TID
Did symptoms recur
YES
STOP NACPL for
duration of study
NO
NACPL No Change
38
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Dosage Adjustment Algorithm 2 NACPL Dose Modifications For Dermatologic Reactions
Dermatologic Reactions (Not Acneiform) ge Grade 2 Grading per Common Terminology Criteria for
Adverse Events V30 (httpctepcancergov) For example Grade 1 RASHDESQUAMATION Macular or papular eruption or erythema without associated symptoms Grade 2 RASHDESQUAMATION Macular or popular eruption or erythema with pruritus or other associated symptoms localized desquamation or other lesions covering lt50 of body surface area
NACPL Temporarily dc (HOLD) x 3 days
Are symptoms resolving after 3 days
NO Symptoms not resolving after 3 days of holding study medication Assessmentmanagement per clinical discretion of investigator Likely not study medication Discuss resuming study medication with medical monitor when symptoms
resolved YES
Temporarily dc (HOLD) NACPL for 4 additional days (total hold 1 week) then NACPL resume 600 MG TID
Did symptoms recur
YES
STOP NACPL for
duration of study
NO
NACPL No change
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
46 Contraindications Precautions and Side Effects of Study Medications
461 Contraindication
Contraindication to NAC is known hypersensitivity to it
462 Precautions
Concomitant administration of oral NAC and antibiotics has shown a slightly reduced absorption
of cephalexin and a slight increase in erythromycin serum levels NAC contains free sulfhydryl
groups There is no evidence that individuals sensitive to sulfa drugs are sensitive to NAC
The NAC preparation being administered in this study contains 20 mg of aspartame Because of
the phenylalanine component of aspartame individuals with phenylketonuria should avoid or
restrict aspartame intake to avoid increased blood levels of phenylalanine Because of this risk
labeling is required on all products containing aspartame
463 Side Effects
Side effects of NAC range from common to serious See Table 4
39
40
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Table 4 Side Effects of NAC
Undesirable Effects
System-organ class Uncommon
(gt11000 lt1100)
Rare
(gt110000 lt11000)
Very rare
(lt110000) Not known
Immune system disorders Hypersensitivity Anaphylactic shock
reaction
Nervous system disorders Headache
Ear and labyrinth disorders Tinnitus
Cardiac disorders Tachycardia
Vascular disorders Hemorrhage
Respiratory thoracic and
mediastinal disorders
Bronchospasm
Dyspnea
Gastrointestinal disorders
Vomiting diarrhea
stomatitis abdominal
pain nausea
Dyspepsia
Skin and subcutaneous tissue
disorders
Urticaria rash
angioedema itching
General disorders and
administration site conditions Pyrexia
Investigations Reduced arterial
pressure Face edema
In very rare cases the onset of severe skin reactions such as Stevens-Johnson syndrome and Lyell syndrome was reported to have a temporal relationship with N-acetylcysteine administration Although in most cases at least another suspect drug probably most involved in the genesis of the above mentioned mucocutaneous syndromes has been identified in case of mucocutaneous alterations it is appropriate to contact onersquos doctor and the administration of N-acetylcysteine should be immediately discontinued
Some studies confirmed a reduction of platelet aggregation during N-acetylcysteine administration The clinical significance of these findings has not been defined yet [Source Fluimucil Investigator Brochure]
47 Recruitment Procedures
Subjects recruited for this study will be established patients of the investigators or physician- or
self-referred to participating clinical centers in the IPFnet Each clinical center within IPFnet has
a well-developed infrastructure of local pulmonologists within the surrounding geographic area
These pulmonologists are kept informed of ongoing IPF clinical trials and regularly refer
subjects to studies conducted at IPFnet clinical centers
Additional steps will be taken to inform clinicians of the trials in progress within IPFnet
including presentations at faculty staff meetings at local hospitals medical grand rounds and
national conferences direct mail notification monthly faxes and advertisement of network trials
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
in pulmonary journals Clinical center patients previously diagnosed with IPF will be notified of
the trials by mail whenever possible
Recruitment of minorities and women will be monitored by the DCC and DSMB If necessary
additional recruitment efforts will be made at specific centers to ensure that the aggregate subject
sample contains appropriate representation of women and minorities
48 Study Procedures
The following procedures are detailed in the PANTHER-IPF MOOP accompanying this
protocol
1 PFT
2 ABG
3 HRCT scan of the chest (including imaging of pulmonary arteries)
4 CBC and serum chemistries
5 Pregnancy test
6 6MWTBorg Dyspnea Scale
7 QOL questionnaires (EuroQol HAD SF-36 SGRQ and ICE CAP)
8 UCSD SOBQ
9 Gender Substudy Questionnaire
All assessments of PFTs will be conducted by study personnel not directly involved in the
treatment of the subjects
481 Biological Specimen Management
4811 Biological Specimen Sample Management
Subjects at clinical centers participating in the specimen repository substudy who consent to
having blood drawn for research purposes and for the banking of blood blood components and
other biologic specimens (urine and BAL fluid) will have approximately 405 mL of blood
41
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
drawn 17 mL blood drawn for DNA and 20 mL of urine collected at enrollment visit Subjects
will have approximately 50 mL of blood drawn and 20 mL of urine collected at each 15-week
follow-up visit Blood specimens will be separated according to PANTHER-IPF MOOP
guidelines into the following components for banking in the repository serum plasma and
DNA Coding of all biologic specimens for the repository will be performed by study staff at the
clinical center The samples will be processed per PANTHER-IPF MOOP guidelines aliquoted
labeled with barcode labels and stored at -70degC at the clinical center and shipped to the central
repository
The only subject identifiers will be a sample ID number and subject initials This sample ID will
be linked in the IPFnet DCC clinical database to subject information No subject information will
be transferred to the biological-specimen database
The subjectrsquos samples may be used for approved sub-studies relating to human disease
including but not limited to IPF The studies for which an individualrsquos samples will be made
available will be determined by the subjectrsquos answers to questions on the biological-sample
informed consent form The subjects can choose to make their samples available for all options
or any combination Samples will be made available to researchers only with IPFnet Steering
Group approval until such time as the samples are made public through the NHLBI repository
49 Concomitant Medications
Concurrent treatment with FDA-approved therapy for IPF is allowed Colchicine may be used
for treatment of gout Temporary treatment with oral or IV corticosteroids for clinical worsening
or suspected AEx is permitted Nutritional supplements containing NAC are not allowed
410 Laboratory Testing
Clinical laboratory parameters will be assessed at screening and at the end of the study The
following tests will be performed at the two time points specified in the protocol chemistry (AG
ratio ALT [SGPT] AST [SGOT] albumin alkaline phosphatase amylase bilirubin-direct
42
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
bilirubin-indirect bilirubin-total BUN BUNcreatinine ratio calcium carbon dioxide
cholesterol-total chloride CPK-total creatinine GGT globulin glucose iron-total LDH
lipase magnesium phosphorus-inorganic potassium protein-total sodium TIBC triglycerides
uric acid) and hematology (red blood cell count WBC count hemoglobin hematocrit cell
indices differential platelet count)
411 Blinding of Study Drugs
Subjects and caregivers will be blinded to study treatment Every subject will receive NAC or
matching PLs at every study visit from the baseline visit to the week-45 visit No study agent
will be dispensed at the week-60 visit
43
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
5 Study Endpoints
51 Primary Study Endpoint
The primary endpoint will be the change in serial measurements of FVC over the study period
52 Secondary Study Endpoints
521 Time to Disease-progression
The time-to-death or a 10 decline in FVC will be defined as the time-to-disease progression
The 10 decline in FVC from enrollment must be confirmed on 2 consecutive visits no less than
6 weeks apart For subjects with 2 consecutive visits with a 10 decline in FVC the time-toshy
disease progression will be defined as the time interval between enrollment and the initial visit
with a 10 FVC decline For subjects who experience disease progression the study doctor will
determine whether or not the subject will remain in the study
522 Acute Exacerbations
The following 3 criteria will define AEx in subjects with acute worsening of their respiratory
conditions
1 Clinical (all of the following required)
A) Unexplained worsening of dyspnea or cough within 30 days triggering unscheduled
medical care (eg emergency room clinic study visit hospitalization)
B) No clinical suspicion or overt evidence of cardiac event pulmonary embolism or deep
venous thrombosis to explain acute worsening of dyspnea
C) No pneumothorax
44
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
2 RadiologicPhysiologic (A and B required)
A) New ground glass opacity or consolidation computed tomography (CT) scan OR new
alveolar opacities on chest x-ray
B) Decline of ge 5 in resting room air SpO2 from last recorded level OR decline of ge 8 mm
Hg in resting room air PaO2 from last recorded level
3 Microbiologic (all of the following required)
A) No clinical evidence for infection (ie absence of grossly purulent sputum fever gt 39degC
orally)
B) Lack of positive microbiological results (if done) from lower respiratory tract defined as
(1) Clinically significant bacterial growth on sputum or endotracheal aspirate cultures
(2) Quantitative culture by protected brush specimen ge 103 cfumL or BAL ge 104 cfumL
(3) The presence of specific pathogens on stains of any of the above
C) Lack of positive pathogen in blood cultures (if done)
Identification of Acute Exacerbations
All subjects will be educated about the importance of identifying AExs At the time of
enrollment subjects will be told about the possibility of developing acute symptomatic
worsening that might represent an AEx of IPF and instructed to contact their study clinical
center coordinator within 48 to 72 hours of the apparent event
All subjects will be contacted by phone monthly and questioned about any change in dyspnea or
cough and any interim clinic visits or hospitalizations Finally as part of the IPFnet outreach to
community referring physicians the importance of AExs will be emphasized When a subject is
identified who meets criterion 1A this will trigger the collection of additional clinical data to
evaluate a suspected AEx These data will be collected as part of standard clinical care (ie this
protocol does not require collection of all items) The additional items to be collected for
suspected AEx include
IPFnet AEx case report form (eCRF) (required)
45
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Chest x-ray CT scan withwithout pulmonary angiogram (reports should be faxed and
followed by the hard copiesdiscs)
Oxygen saturation (pulse oximetry)
ABG
Respiratory cultures (sputum endotracheal aspirate lavage)
Blood cultures
Clinichospital records related to the event
All potential cases of AEx will be reviewed by the clinical center PI first and a decision on
whether the case may represent an AEx will be made If AEx is suspected the case will be sent
to the IPFnet adjudication committee which will assign a final diagnosis (see Table 5) If there is
disagreement among members the majority opinion will be recorded
During episodes of suspected AEx as determined by the individual clinical center investigator
subjects will remain blinded and in the study
Table 5 Final Diagnoses in Evaluation of Suspected Acute Exacerbations
Definite acute exacerbation All criteria met no alternative etiology
Unclassifiable acute worsening
Insufficient data to evaluate all criteria no alternative etiology
Not acute exacerbation Alternative etiology identified that explains acute worsening
Management of the suspected AEx will be at the discretion of the treating physician Standard of
care generally involves evaluation for respiratory infection pulmonary embolism cardiac events
and pneumothorax and treatment with IV corticosteroids
Study drugs will be resumed at pre-suspected AEx doses after subjects clinically improve as
confirmed by the local PI All subjects should be seen at the clinical center within 2 to 4 weeks
of recovery for measurement of post-bronchodilator FVC (see Figure 4) Subjects unable to
return to the clinical center after suspected AEx due to medical frailty (eg continued
46
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
institutionalization progressive disability) will be categorized as failing to maintain FVC
response in secondary analyses
Suspected AEx (PI determined)
Hold study drug Treat AEx
(Attending physician determined)
Alive but unable to continue due to
medical frailty
Dead
Alive and able to continue
Site reviewvisit
Restart study drug
FVC within 2-4 weeks
Figure 4 Acute Exacerbation Flow Chart
523 Respiratory Infections
An upper respiratory infection will be defined as
Change in sputum discoloration
Increased cough of no more than 14 daysrsquo duration
A lower-respiratory infection (pneumonia) will be defined as new segmental or lobar airspace
opacities visualized by image studies (chest radiograph or HRCT) in addition to any of the
following
Positive pathogencultures in good sample of sputum or lower-airway secretions retrieved
by fiberoptic bronchoscope
Fever gt 39degC or gt 100degF
Leukocytosis gt 12000 (unexplained no increase in dose of corticosteroids)
47
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
524 Maintained FVC Response
Subjects with follow-up FVCpred measurements at or above their baseline FVCpred level
will be classified as having maintained FVC response Subjects with reduced FVCpred levels
or missing data for any reason including death or medical frailty will be classified as having not
maintained FVC response The FVCpred value is used because unadjusted FVC measurements
are expected to decline with age
48
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
6 Safety Evaluations and Procedures
61 Adverse Events
During a clinical trial the reporting of adverse experience information can lead to important
changes in the way a new treatment is developed as well as provide integral safety data
611 Definitions
An adverse event (AE) is any untoward medical occurrence in a subject or clinical investigation
subject who was administered a pharmaceutical product The AE does not necessarily have to
have a causal relationship with the drug administered An AE can be any unfavorable and
unintended sign (including an abnormal laboratory finding) symptom or disease temporarily
associated with the use of a medicinal product whether or not considered to be related to the
medicinal product Diseases signs symptoms or laboratory abnormalities already existing at
enrollment are not considered AEs unless they worsen (ie increase in intensity or frequency)
Surgical procedures themselves are not AEs they are therapeutic measures for conditions that
require surgery The condition for which the surgery is required may be an AE Surgical
procedures planned before randomization and the conditions necessitating the surgery are not
AEs
A serious adverse event is any untoward event that
Is fatal
Is life-threatening
Requires inpatient hospitalization or prolongation of existing hospitalization with the
following exceptions
o Preplanned (before the study) hospital admissions unless the hospitalization is
prolonged
o Planned admissions (as part of a study eg routine biopsies)
o Hospitalization lasting lt 24 hours
49
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
o Hospitalization for elective procedure
o Emergency room visits
Results in persistent or significant disability or incapacity
Is a congenital anomaly or birth defect
Important medical events that may not result in death be life-threatening or require
inpatient hospitalization may be considered serious adverse events (SAEs) when based
on appropriate medical judgment they may jeopardize the subject and may require
medical or surgical intervention to prevent one of the outcomes listed above
Life-threatening means that the subject was in the view of the investigator at immediate risk of
death from the AE as it occurred It does not include an AE that had it occurred in a more severe
form might have caused death
Persistent or significant disabilityincapacity means that the event resulted in permanent or
significant and substantial disruption of the subjectrsquos ability to carry out normal life functions
Causality
A reasonable possibility means the AE may have been caused byrelated to the study drug A
perceived or real lack of efficacy does not satisfy the definition of relatedness
612 Adverse Event (AE) Reporting
For the PANTHER-IPF trial all AEs (serious and nonserious) occurring from randomization
through final study visit (4 weeks after final dose of all study medication) will be recorded on the
AE page of the case report form (CRF)
6121 Serious Adverse Events (SAE) Reporting
For this trial all deaths and all SAEs which occur from randomization through final study visit
must be entered within the EDC system via the SAE eCRF page within 24 hours of the
investigative sitersquos knowledge of the event It is the responsibility of the clinical center
50
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
investigator to provide a causality assessment of the event for each study medications based upon
the information available at the time of the report It is understood that complete information
about the event may not be known at the time the initial report is submitted In the event the EDC
system is not accessible to the site at the time of event reporting investigative sites will complete
and forward a paper back-up SAE form to DCRI Safety Surveillance for processing
DCRI Safety Surveillance
Telephone 1-919-668-8624 or 1-866-668-7799 (toll free)
Fax 1-919-668-7138 or 1-866-668-7138 (toll free)
The investigator must complete and submit follow-up SAE information via the eCRF when
important new or follow-up information (eg final diagnosis outcome results of specific
investigations) becomes available Follow-up information should be submitted according to the
same process used for reporting the initial event as described above All SAEs will be followed
until resolution stabilization or 30 days after the subject has completed the final visit (4 weeks
after the final dose of study medication) whichever occurs first The investigator is responsible
for reporting SAEs to their institutional review board (IRB) per site specific IRB reporting
guidelines
6122 Regulatory Reporting
AEs that are serious study drug related and unexpected will be reported to the regulatory
authorities The DCRI Safety Surveillance medical monitor will perform a medical review of all
SAEs submitted and evaluate for ldquounexpectednessrdquo DCRI Safety Surveillance will prepare
MedWatch reports for those events identified as serious study drug related and unexpected as
determined by Safety Medical Monitor
DCRI Regulatory Services will submit all unexpected study drug-related SAEs as per 21 CFR
32 DCRI Safety Surveillance will provide a safety alert letter to the NHLBI DSMB and DCC
clinical operation (for distribution to sites) within 15 days of initial receipt of the information
51
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Investigators are responsible for promptly reporting these events to their reviewing IRBs
according to site specific IRB reporting guidelines
62 Clinical Medical Monitoring
There will be an unblinded physician at the IPFnet DCC serving as medical monitor The
medical monitor will be available to assist with questions about dosage adjustments of study
medications including discontinuation or resumption of medications
63 Unblinding Procedures
Unblinding of subjects or investigators to subject treatment is strongly discouraged For ongoing
clinical management all subjects should be presumed to be receiving ldquoactiverdquo study drug To
ensure the subjectrsquos safety the study treatment will be dose-adjusted based on laboratory test
results clinical findings and symptoms
The IPFnet DCC medical monitor and PANTHER-IPF co-chairs Drs Ganesh Raghu and
Fernando Martinez will be available to the study physicians to discuss study drug management
on a case-by-case basis Un-blinding will be considered ONLY when the knowledge of subject
treatment assignment is ABSOLUTELY ESSENTIAL for subject safety and after discussion of
the subjectrsquos case with the medical monitor and either Dr Raghu or Dr Martinez Unblinding of
study treatment should be minimized during the conduct of the trial In those cases where it is
felt to be medically necessary the DCC medical officer will communicate directly with the
managing physician to minimize unblinding of study personnel
52
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
7 Study Drug Procedures
At the baseline 15-week 30-week and 45-week study visits subjects will receive a supply of
study drug sufficient to last until the next visit at which study drug will be dispensed
53
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
8 Data Management
81 Hardware and Software Configuration
811 Hardware and Database Software
Data will be stored in an Oracle database system Oracle has advantages of processing efficiency
and smooth linkage with other software systems The application and database will be hosted on
Solaris Unix servers at the IPFnet DCC
812 Statistical Software
SAS will be used as the principal application for the management of analysis data files and
statistical computations S-Plus will be used to provide supplementary functions as needed
813 Access Control and Confidentiality Procedures
Access to databases will be controlled centrally by the IPFnet DCC through user passwords
linked to appropriate privileges This protects the data from unauthorized changes and
inadvertent loss or damage
814 Security
Database and Web servers will be secured by a firewall and through controlled physical access
Oracle has many security features to ensure that any staff member accessing the database has the
proper authority to perform the functions he or she requests of the system Within the secondary
SAS databases Unix group-access control maintains similar security The Sun workstation login
is secured by extensive user-password facilities under Unix
54
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
815 Back-up Procedures
Database back-up will be performed automatically every day and standard IPFnet DCC policies
and procedures will be applied to dictate tape rotation and retention practices
816 Virus Protection
All disk drives that provide network services and all user computers will be protected using
virus-scanning software Standard IPFnet DCC policies will be applied to update these protection
systems periodically through the study
82 Sources of Data
821 Design and Development
The IPFnet DCC will be responsible for development of the electronic case report forms
(eCRFs) development and validation of the clinical study database ensuring data integrity and
training clinical center staff on applicable data management procedures A web-based distributed
data entry model will be implemented This system will be developed to ensure that guidelines
and regulations surrounding the use of computerized systems used in clinical trials are upheld
The remainder of this section provides an overview of the data management plan associated with
this protocol
822 Data Collection Forms
The data collection process consists of direct data entry at the study clinical centers into the EDC
system(s) provided by the DCC A data collection worksheet will be provided to clinical centers
for recording data in the event the EDC system is unavailable Data entry of the eCRFs should
be completed according to the instructions provided and project specific training The
investigator is responsible for maintaining accurate complete and up-to-date records and for
ensuring the completion of the eCRFs for each research participant
55
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
823 Data Acquisition and Entry
Data entry into eCRFs shall be performed by authorized individuals Selected eCRFs may also
require the investigatorrsquos written signature or electronic signature as appropriate Electronic
CRFs will be monitored for completeness accuracy and attention to detail during the study
824 Data Center Responsibilities
The IPFnet DCC will 1) develop a data management plan and will conduct data management
activities 2) provide final eCRFs for the collection of all data required by the study 3) develop
data dictionaries for each eCRF that will comprehensively define each data element 4) conduct
ongoing data monitoring activities on study data 5) monitor any preliminary analysis data
cleanup activities and 6) rigorously monitor final study data clean up
825 Data Editing
Completed data will be entered into the IPFnet DCC automated data acquisition and
management system If incomplete or inaccurate data are found a data clarification request will
be generated and distributed to clinical centers for a response Clinical centers will resolve data
inconsistencies and errors and enter all corrections and changes into the IPFnet DCC automated
data acquisition and management system
826 Training
The training plan for clinical center staff includes provisions for training on assessments eCRF
completion guidelines data management procedures and the use of computerized systems
56
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
9 Study Design and Data Analysis
91 General Analytic Considerations
All primary analyses will be based on intent-to-treat (ITT) principles using all randomized
subjects Baseline factors across groups will be compared using mean (standard deviation) and
median (25th and 75th percentiles) summary measures Kaplan-Meier curves will be used to
display event rates Due to clinical interest in departures from both sides of the null hypothesis
all test statistics will be 2-sided
Reasonable caution needs to be taken when conducting multiple analyses on key clinical
subgroups For subgroup analyses a conservative significance level of 0001 will be used for all
interaction tests Thus subgroup comparisons will be considered exploratory unless the p-value
from the interaction test is smaller than 0001
92 Randomization Blinding and Reporting of Results
A permuted block-randomization scheme will be created with varying block sizes stratified by
clinical center Once a subject has completed the screening and baseline period and evaluation
for inclusionexclusion criteria the randomization process will begin Subjects will be
randomized to receive NAC or matching placebo with equal probability (11) via telephone
contact with a central interactive voice response system (IVRS) using a toll-free randomization
number On the day of randomization after the subject has successfully met all inclusion and
exclusion criteria the investigator or designee will call the central randomization number to
obtain the assigned kit randomization numbers for that subject At each subject visit the
investigator or designee will call the central randomization number to obtain the new kit
randomization numbers for resupply of the subject For resupply of the clinical center the IVRS
will monitor minimal volume of a kit type andor expiration date and will automatically notify
the pharmacy
57
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
The trial results will be reported according to guidelines specified in the CONSORT statement
A flow diagram describing screening recruitment randomization dropout and vital status will
be included in the primary manuscript AEs and efficacy data will be presented for all treatment
groups Adherence dropout and lost to follow-up will be carefully examined across all treatment
groups Analyses of safety will be based on data from all randomized subjects who received at
least one dose of study drug
93 Stratification
Subjects will be distributed to the two treatment arms in a 11 allocation ratio Stratification
blocks will be based on clinical centers
94 Specification of the Primary Analyses
A mixed model repeated measures (MMRM) analysis described in section 95 will be used to
compare differences in the slope of FVC measurements across the treatment groups Response
variables are values of the FVC measured at baseline and every 15 weeks until study completion
Variables in the model will include treatment time and time by treatment age sex race and
height Contrast estimates of differences in slopes of treatment over time (along with confidence
intervals) will be used to estimate the treatment effect The validity of this model in terms of
meeting modeling assumptions will be assessed via standard modeling diagnostics and goodness-
of-fit measures Based on the MMRM framework missing FVC data will not be imputed for the
primary analysis
95 Analysis of Longitudinal Endpoints
A common goal in clinical trials is to specify models that are easily implemented and
reproducible by independent data analysts On the other hand the models should have proper
statistical behavior in terms of low bias and high precision Many common approaches to
longitudinal data analysis including last observation carried forward (LOCF) imputation rely on
the missing completely at random (MCAR) assumption However the MCAR assumption is
58
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
unlikely to hold in many clinical trials because missing data are often related to disease
progression and prognosis A more reasonable assumption missing at random (MAR) specifies
that the complete data distribution can be modeled using only the observed data The likelihood-
based MMRM approach is valid under the more general MAR assumptions These models will
be applied to analyze the longitudinal data secondary endpoints
The advantages of MMRM analysis are that all important characteristics of the model can be preshy
specified standard software can be used to implement the models and results are based on ITT
principles43 In addition the MMRM approach offers superior control of Type I and Type II
errors compared with the LOCF approach
Response variables are values of the PFTs measured at enrollment and every 15 weeks until
study completion and 6MWT values measured at baseline week 30 and week 60 Covariates are
treatment time time by treatment and key baseline risk factors Contrasts (along with
confidence intervals) of treatment by time will be used to estimate the treatment effect
The correlation structure involves multiple pieces including measurement errors random
variation and interindividual variability For the longitudinal data analyses an unstructured
correlation matrix for within-subject errors will be assumed Other correlation structures
including compound symmetry will be examined as needed A careful examination of reasons
for study discontinuation will be conducted to assess the validity of MCAR Sensitivity analyses
will be used to examine the untestable assumption that the observed data violate the MAR
assumption The MMRM models will be implemented using PROC MIXED in SAS
96 Analysis of Binary Time-to-Event and Time-Lagged Endpoints
Regression modeling approaches using either the logistic regression model or Cox proportional
hazards regression model will be employed when appropriate The validity of these models will
be assessed via standard modeling diagnostics and goodness-of-fit measures Estimates of
cumulative frequencies for more general time-lagged responses will be calculated using the
partitioned version of the Bang-Tsiatis estimator44 The partitions will be set at 15-week intervals
59
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
to correspond with the data-collection process Covariate adjusted event rates will be calculated
using inverse probability-weighted regression estimates45
97 Power Analysis
971 Primary Analyses
Based on previously published IPF clinical trials the PL group is expected to experience a drop
in FVC of approximately 020 L over the study period (see Figure 1) The IPFnet Steering Group
determined a clinically important difference would be to preserve the majority of the decline
relative to PL over the study period In particular a treatment effect of 015 L was determined to
be a clinically meaningful difference Potential dropout is a key factor in the proposed study The
drop-out process assumed 5 lost to follow-up after every study visit Only 80 of subjects
were assumed to be followed for the entire study period All models assumed a compound
symmetry structure for the covariance matrix Power calculations were performed using a SAS
IML program for designing repeated measures studies46 Based on preliminary reviews of the
data from the University of Michigan the covariance matrix parameters were estimated at
approximately σ2 = 0757 (variance parameter) and ρ = 0936 (correlation parameter) To be
conservative the power calculations for the primary analysis were performed with parameter
setting of σ2 = 0810 (variance parameter) and ρ = 0925 (correlation parameter)
The power calculations assume a correction for imperfect compliance proposed by Lachin and
Foulkes to allow for 2 noncompliance for each of the treatment arms47 Thus the sample size
of 130 subjects per arm would be reduced to an adjusted sample size of 130(1-002-002)2 =
1198 or 120 subjects per arm
Under the assumed Type I error rate of 005 with a correlation parameter of 0925 and standard
deviation of 090 the difference of 015 L (or 00025 Lweek) shown in Table 6 would have
power of 93
60
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Table 6 Hypothetical Values of Mean FVC (L) Change from Baseline
Week 15 Week 30 Week 45 Week 60
NAC 00125 00250 00375 00500
Placebo 00500 01000 01500 02000
Difference 00375 00750 01125 01500
Abbreviations FVC forced vital capacity PL placebo
972 Power Analysis for Secondary Endpoints
Power calculations for secondary endpoint measurements are shown in Table 7 Standard
deviations are based on unpublished data provided by the University of Michigan The
calculations are based on a 2-sample t-test with Type I error rate set at 005 These calculations
are likely to be conservative because the statistical approach described in section 95 for
analyzing these endpoints will incorporate incomplete observations as well as intermediate data
points
Table 7 Detectable Differences in Treatment Means for Selected Endpoint Measurements
Secondary Endpoints Std Dev
of the Baseline Score
Detectable Difference for 80 Power
Std Dev of the Change Score
Difference Detectable for
80 Power
DLCOpred 166 58 91 32
6MWT Area Under the Desaturation Curve
219 76 175 61
6MWT Distance to Desaturation 224 78 315 110
6MWT Minutes Walked 210 073 205 071
Abbreviations Std Dev standard deviation DLCOpred diffusing capacity of the lung for carbon monoxide percent predicted 6MWT 6-minute walk test
61
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
10 Study Administration
101 Cooperative Agreement Mechanism
The administrative and funding mechanism used to undertake this project is a ldquocooperative
agreementrdquo (U01) which is an assistance mechanism Under the cooperative agreement the
NHLBI assists supports andor stimulates the project and is substantially involved with
investigators in conducting the study by facilitating performance of the effort in a ldquopartnerrdquo role
The NHLBI project scientist serves on the IPFnet Steering Group and he or another NHLBI
scientist may serve on other project committees when appropriate At the same time however
NHLBI does not assume a dominant role direction or prime responsibility for this research
program
As described below governance of the project is conducted through the IPFnet Steering Group
Principal investigators have lead responsibilities in all aspects of their trials and the project
including any modification of trial designs conduct of the trials quality control data analysis
and interpretation preparation of publications and collaboration with other investigators unless
otherwise provided for by the IPFnet Steering Group
PIs retain custody of and have primary rights to their center-specific and collaborative data
subject to government rights-of-access consistent with current Health amp Human Services (HHS)
Public Health Service (PHS) and National Institutes of Health policies The protocols and
governance policies call for the continual submission of data centrally to the IPFnet DCC for the
collaborative database which at a minimum will contain the key variables selected by the IPFnet
Steering Group for standardization across all clinical centers the submission of copies of the
collaborative datasets to each PI upon completion of the project procedures for data analysis
reporting and publication and procedures to protect and ensure the privacy of medical and
genetic data and records of individuals The NHLBI project scientist on behalf of the NHLBI
will have the same access privileges and responsibilities regarding the collaborative data as the
other members of the Steering Group
62
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
PIs are also encouraged to publish and to publicly release and disseminate results data and other
products of the project concordant with the project protocols and governance and the approved
plan for making data and materials available to the scientific community and to the NHLBI
However during the 3 years after the ending date of NHLBI project support unpublished data
unpublished results data sets not previously released and other study materials or products are
to be made available to any third party only with the approval of the IPFnet Steering Group
Upon completion of the project PIs are expected to put their intervention materials and
procedure manuals into the public domain andor make them available to other investigators
according to the approved plan for making data and materials available to the scientific
community and the NHLBI for the conduct of research at no charge other than the costs of
reproduction and distribution
The NHLBI reserves the right to terminate or curtail the project (or an individual award) in the
event of (a) failure to develop or implement mutually agreeable collaborative measurement
subject eligibility and data management sections of the protocols (b) substantial shortfall in
subject recruitment follow-up data reporting or quality control or other major breach of
protocol (c) substantive changes in the agreed-upon protocols with which NHLBI cannot
concur (d) reaching a major project outcome with persuasive statistical significance
substantially before schedule or (e) human subject ethical issues that may dictate a premature
termination
Any disagreement that may arise in scientificprogrammatic matters (within the scope of the
award) between award recipients and the NHLBI may be brought to arbitration An arbitration
panel will be composed of 3 membersmdash1 selected by the IPFnet Steering Group (with the
NHLBI member not voting) or by the individual PI in the event of an individual disagreement a
second selected by NHLBI and the third selected by the other 2 members This special
arbitration procedure in no way affects the PIrsquos right to appeal an adverse action that is otherwise
appealable in accordance with the PHS regulations at 42 CFR part 50 Subpart D and HHS
63
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
regulation at 45 CFR part 16 or the rights of the NHLBI under applicable statutes regulations
and terms of the award
102 IPFnet Steering Group
The IPFnet Steering Group is the main governing body of the project It is composed of the PIs
of the clinical centers the PI of the DCC and the NHLBI project scientist The clinical centers
the IPFnet DCC and the NHLBI each have 1 vote on the IPFnet Steering Group All decisions
are determined by majority vote
All major scientific decisions are determined by the IPFnet Steering Group It assumes overall
responsibility for the design and conduct of the trial It appoints (and disbands) committees and
subcommittees as the need arises designs approves and implements the study protocols
oversees the development of the MOOP monitors subject recruitment and treatment delivery
evaluates data collection and management oversees quality assurance procedures and
implements changes and enhancements to the study as required It also has primary responsibility
for facilitating the conduct of the trials and reporting the projectrsquos results
103 Data and Safety Monitoring Board
The NHLBI will establish a DSMB in accordance with established policies (see
httpwwwnhlbinihgovfundingpoliciesdsmb_insthtm) to ensure data quality and subject
safety and to provide independent advice to the NHLBI regarding progress and the
appropriateness of study continuation
104 Recommendations on Interim Monitoring of Efficacy Safety and Futility
First and foremost the role of the DSMB will be to review subject safety and trial conduct at
periodic points during the study The DSMB may require analyses of the primary endpoint
results for comparing the benefit and risks of treatment strategies The benefit of collecting
additional data on key secondary endpoints with extended follow-up and establishing a robust
64
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
evidence base for determining a standard of care will need to be carefully considered before
early termination of one or more treatment arms After careful consideration the IPFnet Steering
Group recommends conservative thresholds for the early examinations of the safety and efficacy
data
The DSMB will be expected to meet approximately every 6 months until trial completion to
review safety and toxicity data The DSMB may recommend stopping the study based on these
reviews Because the DSMB could stop the trial for safety concerns as well as for a large
efficacy benefit there could be multiple opportunities to reject the null hypothesis (no difference
in event rates between the PL and NAC groups) A Bonferroni approximation will be applied
during the one planned interim analysis for efficacy
Before locking the database a statistical analysis plan (SAP) will be developed to provide
complete details on the statistical analysis The SAP will include the specifics for how and when
the DSMB will be notified for AEs The IPFnet DCC will deliver to the DSMB all FDA-defined
AEs at 3-month intervals The IPFnet DCC will prepare narrative SAE reports in real time for
DSMB review including recommendations and analysis of similar events for each SAE
submitted to the FDA
65
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
11 Investigator and Sponsor Obligations
111 Monitoring
All monitoring activities for US clinical centers will be performed in accordance with DCRI
standard operating procedures Information regarding the types of visits will be outlined in the
PANTHER-IPF MOOP
112 Cost and Payment
There will be no cost to subjects enrolled in this trial Study-related procedures will be paid for
by the IPFnet
Subjects may be eligible for reimbursement for travel to the clinical center Details of payment
will be explained to each subject during the consent process
113 Confidentiality and Health Insurance Portability and Accountability Act
Considerations
Subject confidentiality will be protected throughout the study All subject data will be kept
strictly confidential and no subject-identifying information will be released to anyone outside
the project Confidentiality will be assured through several mechanisms First each subject will
be assigned an anonymous study ID which will then be used on all study forms Second any
study forms blood samples and paper records that contain subject information (eg address lists
phone lists) will be kept at the clinical centers in secured locked areas coded by number Once
blood is collected there will be no subject identifiers placed on blood samplesmdashonly the study
ID number and the date of sample collection Third access to all subject data and information
including laboratory specimens will be restricted to authorized personnel In the case of
computerized data this restricted access will be assured through user logon IDs and password
protection
66
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
At the IPFnet DCC only authorized personnel will have access to the data files containing study
data Security will be assured through user logon IDs passwords and appropriate access
privileges All study subjects will be identified only by their IPFnet ID numbers and no personal
identifying information such as name address or Social Security number will be entered into
the IPFnet DCC database Any subject-specific data reported to the IPFnet Steering Group will
be identified only by the IPFnet ID number
Finally subjects will not be identified by name in any reports or publications nor will the data
be presented in such a way that the identity of individual subjects can be inferred Analysis files
created for further study by the scientific community will have no subject identifiers These data
files will be created in accordance with the Ancillary Studies and Publication Policy of the
IPFnet
114 Informed Consent Procedures
All IPFnet subjects will provide written informed consent using procedures reviewed and
approved by each clinical centerrsquos IRB Informed consent will be undertaken by study personnel
in-person with the subject The subject has the option of declining further participation in the
study at that point No further study procedures will be conducted until the signed documents
have been provided to the IPFnet clinical center
115 Institutional Review Boards
Before initiating this study the protocol clinical center-specific informed consent forms Health
Insurance Portability and Accountability Act (HIPAA) forms recruitment materials and other
relevant information will be reviewed by a properly constituted IRB at each participating clinical
center A copy of the signed and dated IRB approval at each clinical center will be retrieved prior
to or during the site initiation visit and archived at the IPFnet DCC Any amendments to the
protocol other than simple administrative and typographical changes must be approved by each
IRB before they are implemented The clinical centers will seek annual renewals of their IRB
approvals in accordance with local procedures
67
__________________________________________ ________________
__________________________________________
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
12 Investigator Agreement
I have read the foregoing protocol PANTHER-IPF and agree that it contains all necessary
details for carrying out this study I will conduct the study as outlined herein and will complete
the study within the time designated
I will provide copies of the protocol and all pertinent information to all individuals responsible to
me who assist in the conduct of this study I will discuss this material with them to ensure they
are fully informed regarding the drug and the conduct of the study
I will fulfill all responsibilities for submitting pertinent information to the local IRB if
applicable that is responsible for this study
I further agree that NHLBI andor DCRI will have access to any source documents from which
eCRF information may have been generated
Signature of Principal Investigator Date
Name of Principal Investigator (printed or typed)
Protocol version date May 19 2009
Protocol Amendment 1 version date May 28 2010
Protocol Amendment 2 version date December 6 2011
68
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
13 References
1 Raghu G Brown KK Bradford WZ et al A placebo-controlled trial of interferon gamma-1b in patients with idiopathic pulmonary fibrosis N Engl J Med 2004350125-33 2 King TE Jr Safrin S Starko KM et al Analyses of efficacy end points in a controlled trial of interferon-gamma1b for idiopathic pulmonary fibrosis Chest 2005127171-7 3 Flaherty KR Thwaite EL Kazerooni EA et al Radiological versus histological diagnosis in UIP and NSIP survival implications Thorax 200358143-8 4 Wells AU Desai SR Rubens MB et al Idiopathic pulmonary fibrosis a composite physiologic index derived from disease extent observed by computed tomography Am J Respir Crit Care Med 2003167962-9 5 Raghu G Freudenberger TD Yang S et al High prevalence of abnormal acid gastroshyoesophageal reflux in idiopathic pulmonary fibrosis Eur Respir J 200627136-42 6 Kinnula VL Focus on antioxidant enzymes and antioxidant strategies in smoking related airway diseases Thorax 200560693-700 7 Coultas DB Zumwalt RE Black WC Sobonya RE The epidemiology of interstitial lung diseases Am J Respir Crit Care Med 1994150967-72 8 Raghu G Weycker D Edelsberg J Bradford WZ Oster G Incidence and prevalence of idiopathic pulmonary fibrosis Am J Respir Crit Care Med 2006174810-6 9 Olson AL Swigris JJ Lezotte DC Norris JM Wilson CG Brown KK Mortality from pulmonary fibrosis increased in the United States from 1992 to 2003 Am J Respir Crit Care Med 2007176277-84 10 Mannino DM Etzel RA Parrish RG Pulmonary fibrosis deaths in the United States 1979shy1991 An analysis of multiple-cause mortality data Am J Respir Crit Care Med 19961531548shy52 11 Hubbard R Johnston I Coultas DB Britton J Mortality rates from cryptogenic fibrosing alveolitis in seven countries Thorax 199651711-6 12 Johnston I Britton J Kinnear W Logan R Rising mortality from cryptogenic fibrosing alveolitis Bmj 19903011017-21 13 Raghu G Collard HR Egan JJ et al An official ATSERSJRSALAT statement idiopathic pulmonary fibrosis evidence-based guidelines for diagnosis and management Am J Respir Crit Care Med 2011183788-824 14 (USA) FDA FDA Public Health Advisory Interferon gamma-1b (marketed as Actimmune) In 2007 15 King TE Jr Pardo A Selman M Idiopathic pulmonary fibrosis Lancet 2011 16 Raghu G Brown KK Costabel U et al Treatment of idiopathic pulmonary fibrosis with etanercept an exploratory placebo-controlled trial Am J Respir Crit Care Med 2008178948shy55 17 Malouf MA Hopkins P Snell G Glanville AR An investigator-driven study of everolimus in surgical lung biopsy confirmed idiopathic pulmonary fibrosis Respirology 201116776-83 18 King TE Jr Behr J Brown KK et al BUILD-1 a randomized placebo-controlled trial of bosentan in idiopathic pulmonary fibrosis Am J Respir Crit Care Med 200817775-81 19 Richeldi L Costabel U Selman M et al Efficacy of a tyrosine kinase inhibitor in idiopathic pulmonary fibrosis N Engl J Med 20113651079-87
69
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
20 Borok Z Buhl R Grimes GJ et al Effect of glutathione aerosol on oxidant-antioxidant imbalance in idiopathic pulmonary fibrosis Lancet 1991338215-6 21 Meyer A Buhl R Magnussen H The effect of oral N-acetylcysteine on lung glutathione levels in idiopathic pulmonary fibrosis Eur Respir J 19947431-6 22 Behr J Maier K Degenkolb B Krombach F Vogelmeier C Antioxidative and clinical effects of high-dose N-acetylcysteine in fibrosing alveolitis Adjunctive therapy to maintenance immunosuppression Am J Respir Crit Care Med 19971561897-901 23 Cantin AM North SL Fells GA Hubbard RC Crystal RG Oxidant-mediated epithelial cell injury in idiopathic pulmonary fibrosis J Clin Invest 1987791665-73 24 Waghray M Cui Z Horowitz JC et al Hydrogen peroxide is a diffusible paracrine signal for the induction of epithelial cell death by activated myofibroblasts Faseb J 200519854-6 25 Larios JM Budhiraja R Fanburg BL Thannickal VJ Oxidative protein cross-linking reactions involving L-tyrosine in transforming growth factor-beta1-stimulated fibroblasts J Biol Chem 200127617437-41 26 Kinnula VL Fattman CL Tan RJ Oury TD Oxidative stress in pulmonary fibrosis a possible role for redox modulatory therapy Am J Respir Crit Care Med 2005172417-22 27 Meyer A Buhl R Kampf S Magnussen H Intravenous N-acetylcysteine and lung glutathione of patients with pulmonary fibrosis and normals Am J Respir Crit Care Med 19951521055-60 28 Behr J Degenkolb B Krombach F Vogelmeier C Intracellular glutathione and bronchoalveolar cells in fibrosing alveolitis effects of N-acetylcysteine Eur Respir J 200219906-11 29 Bando M Hosono T Mato N et al Long-term efficacy of inhaled N-acetylcysteine in patients with idiopathic pulmonary fibrosis Intern Med 2010492289-96 30 Demedts M Behr J Buhl R et al High-dose acetylcysteine in idiopathic pulmonary fibrosis N Engl J Med 20053532229-42 31 Toma TP Bhowmik A Rajakulasingam R Acetylcysteine in pulmonary fibrosis N Engl J Med 20063541086-9 author reply -9 32 Hunninghake GW Antioxidant therapy for idiopathic pulmonary fibrosis N Engl J Med 20053532285-7 33 Flaherty KR Mumford JA Murray S et al Prognostic implications of physiologic and radiographic changes in idiopathic interstitial pneumonia Am J Respir Crit Care Med 2003168543-8 34 Latsi PI du Bois RM Nicholson AG et al Fibrotic idiopathic interstitial pneumonia the prognostic value of longitudinal functional trends Am J Respir Crit Care Med 2003168531-7 35 Collard HR King TE Jr Bartelson BB Vourlekis JS Schwarz MI Brown KK Changes in clinical and physiologic variables predict survival in idiopathic pulmonary fibrosis Am J Respir Crit Care Med 2003168538-42 36 Jegal Y Kim DS Shim TS et al Physiology is a stronger predictor of survival than pathology in fibrotic interstitial pneumonia Am J Respir Crit Care Med 2005171639-44 37 Martinez FJ Safrin S Weycker D et al The clinical course of patients with idiopathic pulmonary fibrosis Ann Intern Med 2005142963-7 38 Hull JH Acetylcysteine in pulmonary fibrosis N Engl J Med 20063541089-91 author reply -91
70
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
39 Flaherty KR King TE Jr Raghu G et al Idiopathic interstitial pneumonia what is the effect of a multidisciplinary approach to diagnosis Am J Respir Crit Care Med 2004170904shy10 40 Raghu G Johnson WC Lockhart D Mageto Y Treatment of idiopathic pulmonary fibrosis with a new antifibrotic agent pirfenidone results of a prospective open-label Phase II study Am J Respir Crit Care Med 19991591061-9 41 Hunninghake GW Lynch DA Galvin JR et al Radiologic findings are strongly associated with a pathologic diagnosis of usual interstitial pneumonia Chest 20031241215-23 42 Lynch D Godwin J Safrin S et al High-resolution computed tomography in idiopathic pulmonary fibrosis diagnosis and prognosis Am J Respir Crit Care Med 2005172488-93 43 Mallinckrodt CH Watkin JG Molenberghs G Carroll RJ Choice of the primary analysis in longitudinal clinical trials Pharmaceutical Statistics 20043161-9 44 Bang H Tsiatis A Estimating medical costs with censored data Biometrika 200087329shy43 45 Lin DY Regression analysis of incomplete medical cost data Stat Med 2003221181-200 46 Rochon J Application of GEE procedures for sample size calculations in repeated measures experiments Stat Med 1998171643-58 47 Lachin JM Foulkes MA Evaluation of sample size and power for analyses of survival with allowance for nonuniform patient entry losses to follow-up noncompliance and stratification Biometrics 198642507-19
71
- PANTHER-IPFPREDNISONE AZATHIOPRINEAND N-ACETYLCYSTEINEA STUDY THAT EVALUATES RESPONSE INIDIOPATHIC PULMONARY FIBROSIS
-
- Protocol Summary
- Table of Contents
- List of Tables
- List of Figures
- List of Abbreviations
- 1 Summary
- 2 Hypotheses and Specific Aims
-
- 21 Null Hypothesis
- 22 Specific Aim 1
- 23 Specific Aim 2
- 24 Prespecified Subgroups of Interest
-
- 3 Background and Significance
-
- 31 Idiopathic Pulmonary Fibrosis is the Most Common Interstitial Lung Disease
- 32 Rationale for Placebo Control
- 33 Rationale for N-acetylcysteine
- 35 Rationale for N-acetylcysteine as a Stand-alone Therapy
- 36 Rationale for the Study Design and Primary Endpoint
- 37 Rationale for Blinding of Treatments
-
- 4 Methods
-
- 41 Inclusion Criteria
- 42 Diagnosis of IPF
- 43 Exclusion Criteria
- 44 Study Design and Study Visit
- 45 Dose Justification
- 46 Contraindications Precautions and Side Effects of Study Medications
- 47 Recruitment Procedures
- 48 Study Procedures
- 49 Concomitant Medications
- 410 Laboratory Testing
- 411 Blinding of Study Drugs
-
- 5 Study Endpoints
-
- 51 Primary Study Endpoint
- 52 Secondary Study Endpoints
-
- 6 Safety Evaluations and Procedures
-
- 61 Adverse Events
- 62 Clinical Medical Monitoring
- 63 Unblinding Procedures
-
- 7 Study Drug Procedures
- 8 Data Management
-
- 81 Hardware and Software Configuration
- 82 Sources of Data
-
- 9 Study Design and Data Analysis
-
- 91 General Analytic Considerations
- 92 Randomization Blinding and Reporting of Results
- 93 Stratification
- 94 Specification of the Primary Analyses
- 95 Analysis of Longitudinal Endpoints
- 96 Analysis of Binary Time-to-Event and Time-Lagged Endpoints
- 97 Power Analysis
-
- 10 Study Administration
-
- 101 Cooperative Agreement Mechanism
- 102 IPFnet Steering Group
- 103 Data and Safety Monitoring Board
- 104 Recommendations on Interim Monitoring of Efficacy Safety and Futility
-
- 11 Investigator and Sponsor Obligations
-
- 111 Monitoring
- 112 Cost and Payment
- 113 Confidentiality and Health Insurance Portability and Accountability ActConsiderations
- 114 Informed Consent Procedures
- 115 Institutional Review Boards
-
- 12 Investigator Agreement
- 13 References
-
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
The week 45 visit is expected to occur within +- 14 days of the subjectrsquos scheduled visit time (eg the week 45
visit should occur anytime between 43 and 47 weeks after starting study drug) Week 45 activities include
Measure vital signs with oximetry
Measure height and weight
Serum pregnancy test (if applicable)
Measure spirometry (post-bronchodilator)
Review of AEs
Evaluate for AEx
Review concomitant medications
If consent has been given blood will be drawn and a urine specimen collected for the biospecimen
repository
Subjects return used and unused study drug for the visit
Study diary reviewed
Provide additional supply of study drug sufficient to last until the next scheduled visit
4426 Week 60 (Early Withdrawal or Final Treatment Visit)
At week 60 or at subject withdrawal from the study (premature by study doctor or subjectrsquos decision) a final
treatment visit will occur At this final treatment visit subjects will discontinue NACPL abruptly Week 60
activities also include
Physical examination
Measure vital signs with oximetry
Measure height and weight
Laboratory values (complete blood count [CBC] and serum chemistries)
Spirometry (post-bronchodilator) measurement
6MWT with Borg scale measurement
DLCO
Lung volumes
ABG
Review of AEs
32
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Evaluate for AEx
Review concomitant medications
Subjects will complete all QOL and dyspnea questionnaires (EuroQol ICE CAP SF-36 SGRQ and
UCSD SOBQ)
If consent has been given blood will be drawn and a urine specimen collected for the biospecimen
repository
Subjects return used and unused study drug for the visit
Study diary reviewed
4427 Final Site Visit ndash FVC drop confirmation
In the event that the subject has a recorded FVC drop of gt10 from baseline at the final treatment visit and the
subject has not had a confirmation of such a drop at a previous study visit the subject should return to the
clinical site 6 to 8 weeks after the final treatment visit During this visit a post-bronchodilator spirometry test
will be performed This FVC measurement will be evaluated according to section 521 of this protocol
4428 Final Visit ndash Telephone Follow-up
Four weeks following the final dose of study medication subjects will receive a telephone call from the study
coordinator to ensure that there are no side effects and to follow up on any ongoing adverse events (AEs)
4429 Phone Contact Between Visits
At week 2 and each month that a subject does not have a scheduled clinical center visit his or her study
coordinator will contact him or her at least once by telephone to
Inquire if the subject has had any hospitalizations events that might be considered an AE or any events
significant enough to warrant an out-of-cycle visit to the clinical center
Remind subjects of their current dosage levels and confirm that the subject understands them
Address any questions or concerns the subject might have regarding other aspects of the study
Assess adherence to the treatment regimen by reviewing diary data verbal review of medications taken
including nutritional supplements
33
34
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Table 3 Schedule of Assessments
Procedure Screening Visit 0
Enrollment Visit 1
Week 15 Visit 2
Week 30Visit 3
Week 45 Visit 4
Week 60 Early
Withdrawal Visit 5
Final1
Visit (via phone)
Informed consent X
Medical history X
Inclusionexclusion criteria X
Serum pregnancy test (if applicable) X X X X X
Review of lung biopsy X
Arterial Blood Gas X X
6-Minute Walk Test
X
X X
Physical examination X X X
Vital signs with oximetry X X X X X X
Body height and weight X X X X X X
Complete Blood Count X X X
Chemistry panel X X X
Monitor Lab Values X X X
Urinalysis X Specimen repository substudy blood draw and urine collection (if consented)
X
X X X X
HRCT (if not completed within three months) X
Spirometry (pre- and post-bronchodilator) X
Spirometry (post-bronchodilator only) X X X X X
DLCO (post-bronchodilator only) X X X
Lung volumes (post-bronchodilator only) X
X
Evaluate for acute exacerbation X X X X X
Review Adverse Events X X X X X X
Review concomitant meds X X X X X X
Dispense subject diary X X X X
Review subject diary X X X X X
Dispense study agent X X X X
Gender Substudy questionnaire (female subjects only) X
EuroQol ICECAP UCSD SOBQ SGRQ SF-36 X X X
Abbreviations DLCO diffusing capacity of the lung for carbon monoxide QOL Quality of Life ICECAP Investigating Choice Experiments for Preferences of Older People UCSD SOBQ University of California Shortness of Breath Questionnaire SGRQ St Georgersquos Respiratory Questionnaire SF-36 Short Form 36 Health Survey
1Follow-up visit via phone will occur four weeks after final dose of study medication
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
45 Dose Justification
The general philosophy for determining dosing levels was to apply previously examined
treatment regimens With the focus of the study being to establish a standard of care for
mildmoderate IPF subjects the goal was to develop flexible yet standardized treatment rules that
allow for the temporary or permanent withholding of one or more components of treatment when
necessary Subjects developing laboratory abnormalities or symptoms that result in
discontinuation of one or more components of study treatment may continue on the other
components as long as there is no contraindication for this Complete follow-up is important for
the validity of any study As a strategy to maintain protocol adherence we are using a treatment
regimen that will detect potential side effects and prompt interventions proactively in the interest
of patient safety In addition subjects who permanently stop study medications during the course
of the study are encouraged to continue in the study completing all scheduled visits and tests
451 Rationale for N-acetylcysteine Dosing
To our knowledge there have been no IPF studies to correlate clinical outcome measures with
different dosages for NAC The dosage chosen is based on the IFIGENIA study However BAL
lung GSH levels from subjects with IPF have been augmented with the use of oral NAC at 600
mg 3 times per day In addition lung GSH levels have been associated with improved
PFTs212227 The dose chosen for this study was based on previous data including the IFIGENIA
study30
4511 Dosing of N-acetylcysteineplacebo
Dosing of NACPL will be 600 mg orally 3 times a day (1800 mgday)
4512 Reasons to Discontinue N-acetylcysteineplacebo
NACPL may be temporarily or permanently discontinued for the duration of the study for
gastrointestinal symptoms or dermatologic reactions
35
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Temporarily discontinue (hold) oral NACPL for subjects requiring inpatient admission for acute
exacerbation (AEx) or other conditions Resume NACPL after discharge
36
37
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
452 Dosage Algorithms
Dosage Adjustment Algorithm 1 NACPL Dose Modifications for Gastrointestinal Symptoms Nausea Vomiting Abdominal Discomfort Diarrhea
GI Symptoms determined by the PI to be clinically significant Nausea Vomiting Abdominal Discomfort Diarrhea
NACPL Temporarily dc (HOLD) x 3 Days
Monitor symptoms intervene as clinically indicated (eg fluid replacement antidiarrhea or antinausea medication)
Monitor or lab PRN
Are symptoms resolving after 3 days NO
Symptoms NOT resolving after 3 days of holding study medication Assessmentmanagement per clinical
discretion of investigator
Likely not study medication discuss resuming study medication with medical monitor when symptoms resolved
YES
Temporarily dc (HOLD) NACPL for 4 additional days (total hold 1 week) then NACPL Resume 600 MG TID
Did symptoms recur
YES
STOP NACPL for
duration of study
NO
NACPL No Change
38
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Dosage Adjustment Algorithm 2 NACPL Dose Modifications For Dermatologic Reactions
Dermatologic Reactions (Not Acneiform) ge Grade 2 Grading per Common Terminology Criteria for
Adverse Events V30 (httpctepcancergov) For example Grade 1 RASHDESQUAMATION Macular or papular eruption or erythema without associated symptoms Grade 2 RASHDESQUAMATION Macular or popular eruption or erythema with pruritus or other associated symptoms localized desquamation or other lesions covering lt50 of body surface area
NACPL Temporarily dc (HOLD) x 3 days
Are symptoms resolving after 3 days
NO Symptoms not resolving after 3 days of holding study medication Assessmentmanagement per clinical discretion of investigator Likely not study medication Discuss resuming study medication with medical monitor when symptoms
resolved YES
Temporarily dc (HOLD) NACPL for 4 additional days (total hold 1 week) then NACPL resume 600 MG TID
Did symptoms recur
YES
STOP NACPL for
duration of study
NO
NACPL No change
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
46 Contraindications Precautions and Side Effects of Study Medications
461 Contraindication
Contraindication to NAC is known hypersensitivity to it
462 Precautions
Concomitant administration of oral NAC and antibiotics has shown a slightly reduced absorption
of cephalexin and a slight increase in erythromycin serum levels NAC contains free sulfhydryl
groups There is no evidence that individuals sensitive to sulfa drugs are sensitive to NAC
The NAC preparation being administered in this study contains 20 mg of aspartame Because of
the phenylalanine component of aspartame individuals with phenylketonuria should avoid or
restrict aspartame intake to avoid increased blood levels of phenylalanine Because of this risk
labeling is required on all products containing aspartame
463 Side Effects
Side effects of NAC range from common to serious See Table 4
39
40
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Table 4 Side Effects of NAC
Undesirable Effects
System-organ class Uncommon
(gt11000 lt1100)
Rare
(gt110000 lt11000)
Very rare
(lt110000) Not known
Immune system disorders Hypersensitivity Anaphylactic shock
reaction
Nervous system disorders Headache
Ear and labyrinth disorders Tinnitus
Cardiac disorders Tachycardia
Vascular disorders Hemorrhage
Respiratory thoracic and
mediastinal disorders
Bronchospasm
Dyspnea
Gastrointestinal disorders
Vomiting diarrhea
stomatitis abdominal
pain nausea
Dyspepsia
Skin and subcutaneous tissue
disorders
Urticaria rash
angioedema itching
General disorders and
administration site conditions Pyrexia
Investigations Reduced arterial
pressure Face edema
In very rare cases the onset of severe skin reactions such as Stevens-Johnson syndrome and Lyell syndrome was reported to have a temporal relationship with N-acetylcysteine administration Although in most cases at least another suspect drug probably most involved in the genesis of the above mentioned mucocutaneous syndromes has been identified in case of mucocutaneous alterations it is appropriate to contact onersquos doctor and the administration of N-acetylcysteine should be immediately discontinued
Some studies confirmed a reduction of platelet aggregation during N-acetylcysteine administration The clinical significance of these findings has not been defined yet [Source Fluimucil Investigator Brochure]
47 Recruitment Procedures
Subjects recruited for this study will be established patients of the investigators or physician- or
self-referred to participating clinical centers in the IPFnet Each clinical center within IPFnet has
a well-developed infrastructure of local pulmonologists within the surrounding geographic area
These pulmonologists are kept informed of ongoing IPF clinical trials and regularly refer
subjects to studies conducted at IPFnet clinical centers
Additional steps will be taken to inform clinicians of the trials in progress within IPFnet
including presentations at faculty staff meetings at local hospitals medical grand rounds and
national conferences direct mail notification monthly faxes and advertisement of network trials
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
in pulmonary journals Clinical center patients previously diagnosed with IPF will be notified of
the trials by mail whenever possible
Recruitment of minorities and women will be monitored by the DCC and DSMB If necessary
additional recruitment efforts will be made at specific centers to ensure that the aggregate subject
sample contains appropriate representation of women and minorities
48 Study Procedures
The following procedures are detailed in the PANTHER-IPF MOOP accompanying this
protocol
1 PFT
2 ABG
3 HRCT scan of the chest (including imaging of pulmonary arteries)
4 CBC and serum chemistries
5 Pregnancy test
6 6MWTBorg Dyspnea Scale
7 QOL questionnaires (EuroQol HAD SF-36 SGRQ and ICE CAP)
8 UCSD SOBQ
9 Gender Substudy Questionnaire
All assessments of PFTs will be conducted by study personnel not directly involved in the
treatment of the subjects
481 Biological Specimen Management
4811 Biological Specimen Sample Management
Subjects at clinical centers participating in the specimen repository substudy who consent to
having blood drawn for research purposes and for the banking of blood blood components and
other biologic specimens (urine and BAL fluid) will have approximately 405 mL of blood
41
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
drawn 17 mL blood drawn for DNA and 20 mL of urine collected at enrollment visit Subjects
will have approximately 50 mL of blood drawn and 20 mL of urine collected at each 15-week
follow-up visit Blood specimens will be separated according to PANTHER-IPF MOOP
guidelines into the following components for banking in the repository serum plasma and
DNA Coding of all biologic specimens for the repository will be performed by study staff at the
clinical center The samples will be processed per PANTHER-IPF MOOP guidelines aliquoted
labeled with barcode labels and stored at -70degC at the clinical center and shipped to the central
repository
The only subject identifiers will be a sample ID number and subject initials This sample ID will
be linked in the IPFnet DCC clinical database to subject information No subject information will
be transferred to the biological-specimen database
The subjectrsquos samples may be used for approved sub-studies relating to human disease
including but not limited to IPF The studies for which an individualrsquos samples will be made
available will be determined by the subjectrsquos answers to questions on the biological-sample
informed consent form The subjects can choose to make their samples available for all options
or any combination Samples will be made available to researchers only with IPFnet Steering
Group approval until such time as the samples are made public through the NHLBI repository
49 Concomitant Medications
Concurrent treatment with FDA-approved therapy for IPF is allowed Colchicine may be used
for treatment of gout Temporary treatment with oral or IV corticosteroids for clinical worsening
or suspected AEx is permitted Nutritional supplements containing NAC are not allowed
410 Laboratory Testing
Clinical laboratory parameters will be assessed at screening and at the end of the study The
following tests will be performed at the two time points specified in the protocol chemistry (AG
ratio ALT [SGPT] AST [SGOT] albumin alkaline phosphatase amylase bilirubin-direct
42
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
bilirubin-indirect bilirubin-total BUN BUNcreatinine ratio calcium carbon dioxide
cholesterol-total chloride CPK-total creatinine GGT globulin glucose iron-total LDH
lipase magnesium phosphorus-inorganic potassium protein-total sodium TIBC triglycerides
uric acid) and hematology (red blood cell count WBC count hemoglobin hematocrit cell
indices differential platelet count)
411 Blinding of Study Drugs
Subjects and caregivers will be blinded to study treatment Every subject will receive NAC or
matching PLs at every study visit from the baseline visit to the week-45 visit No study agent
will be dispensed at the week-60 visit
43
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
5 Study Endpoints
51 Primary Study Endpoint
The primary endpoint will be the change in serial measurements of FVC over the study period
52 Secondary Study Endpoints
521 Time to Disease-progression
The time-to-death or a 10 decline in FVC will be defined as the time-to-disease progression
The 10 decline in FVC from enrollment must be confirmed on 2 consecutive visits no less than
6 weeks apart For subjects with 2 consecutive visits with a 10 decline in FVC the time-toshy
disease progression will be defined as the time interval between enrollment and the initial visit
with a 10 FVC decline For subjects who experience disease progression the study doctor will
determine whether or not the subject will remain in the study
522 Acute Exacerbations
The following 3 criteria will define AEx in subjects with acute worsening of their respiratory
conditions
1 Clinical (all of the following required)
A) Unexplained worsening of dyspnea or cough within 30 days triggering unscheduled
medical care (eg emergency room clinic study visit hospitalization)
B) No clinical suspicion or overt evidence of cardiac event pulmonary embolism or deep
venous thrombosis to explain acute worsening of dyspnea
C) No pneumothorax
44
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
2 RadiologicPhysiologic (A and B required)
A) New ground glass opacity or consolidation computed tomography (CT) scan OR new
alveolar opacities on chest x-ray
B) Decline of ge 5 in resting room air SpO2 from last recorded level OR decline of ge 8 mm
Hg in resting room air PaO2 from last recorded level
3 Microbiologic (all of the following required)
A) No clinical evidence for infection (ie absence of grossly purulent sputum fever gt 39degC
orally)
B) Lack of positive microbiological results (if done) from lower respiratory tract defined as
(1) Clinically significant bacterial growth on sputum or endotracheal aspirate cultures
(2) Quantitative culture by protected brush specimen ge 103 cfumL or BAL ge 104 cfumL
(3) The presence of specific pathogens on stains of any of the above
C) Lack of positive pathogen in blood cultures (if done)
Identification of Acute Exacerbations
All subjects will be educated about the importance of identifying AExs At the time of
enrollment subjects will be told about the possibility of developing acute symptomatic
worsening that might represent an AEx of IPF and instructed to contact their study clinical
center coordinator within 48 to 72 hours of the apparent event
All subjects will be contacted by phone monthly and questioned about any change in dyspnea or
cough and any interim clinic visits or hospitalizations Finally as part of the IPFnet outreach to
community referring physicians the importance of AExs will be emphasized When a subject is
identified who meets criterion 1A this will trigger the collection of additional clinical data to
evaluate a suspected AEx These data will be collected as part of standard clinical care (ie this
protocol does not require collection of all items) The additional items to be collected for
suspected AEx include
IPFnet AEx case report form (eCRF) (required)
45
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Chest x-ray CT scan withwithout pulmonary angiogram (reports should be faxed and
followed by the hard copiesdiscs)
Oxygen saturation (pulse oximetry)
ABG
Respiratory cultures (sputum endotracheal aspirate lavage)
Blood cultures
Clinichospital records related to the event
All potential cases of AEx will be reviewed by the clinical center PI first and a decision on
whether the case may represent an AEx will be made If AEx is suspected the case will be sent
to the IPFnet adjudication committee which will assign a final diagnosis (see Table 5) If there is
disagreement among members the majority opinion will be recorded
During episodes of suspected AEx as determined by the individual clinical center investigator
subjects will remain blinded and in the study
Table 5 Final Diagnoses in Evaluation of Suspected Acute Exacerbations
Definite acute exacerbation All criteria met no alternative etiology
Unclassifiable acute worsening
Insufficient data to evaluate all criteria no alternative etiology
Not acute exacerbation Alternative etiology identified that explains acute worsening
Management of the suspected AEx will be at the discretion of the treating physician Standard of
care generally involves evaluation for respiratory infection pulmonary embolism cardiac events
and pneumothorax and treatment with IV corticosteroids
Study drugs will be resumed at pre-suspected AEx doses after subjects clinically improve as
confirmed by the local PI All subjects should be seen at the clinical center within 2 to 4 weeks
of recovery for measurement of post-bronchodilator FVC (see Figure 4) Subjects unable to
return to the clinical center after suspected AEx due to medical frailty (eg continued
46
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
institutionalization progressive disability) will be categorized as failing to maintain FVC
response in secondary analyses
Suspected AEx (PI determined)
Hold study drug Treat AEx
(Attending physician determined)
Alive but unable to continue due to
medical frailty
Dead
Alive and able to continue
Site reviewvisit
Restart study drug
FVC within 2-4 weeks
Figure 4 Acute Exacerbation Flow Chart
523 Respiratory Infections
An upper respiratory infection will be defined as
Change in sputum discoloration
Increased cough of no more than 14 daysrsquo duration
A lower-respiratory infection (pneumonia) will be defined as new segmental or lobar airspace
opacities visualized by image studies (chest radiograph or HRCT) in addition to any of the
following
Positive pathogencultures in good sample of sputum or lower-airway secretions retrieved
by fiberoptic bronchoscope
Fever gt 39degC or gt 100degF
Leukocytosis gt 12000 (unexplained no increase in dose of corticosteroids)
47
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
524 Maintained FVC Response
Subjects with follow-up FVCpred measurements at or above their baseline FVCpred level
will be classified as having maintained FVC response Subjects with reduced FVCpred levels
or missing data for any reason including death or medical frailty will be classified as having not
maintained FVC response The FVCpred value is used because unadjusted FVC measurements
are expected to decline with age
48
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
6 Safety Evaluations and Procedures
61 Adverse Events
During a clinical trial the reporting of adverse experience information can lead to important
changes in the way a new treatment is developed as well as provide integral safety data
611 Definitions
An adverse event (AE) is any untoward medical occurrence in a subject or clinical investigation
subject who was administered a pharmaceutical product The AE does not necessarily have to
have a causal relationship with the drug administered An AE can be any unfavorable and
unintended sign (including an abnormal laboratory finding) symptom or disease temporarily
associated with the use of a medicinal product whether or not considered to be related to the
medicinal product Diseases signs symptoms or laboratory abnormalities already existing at
enrollment are not considered AEs unless they worsen (ie increase in intensity or frequency)
Surgical procedures themselves are not AEs they are therapeutic measures for conditions that
require surgery The condition for which the surgery is required may be an AE Surgical
procedures planned before randomization and the conditions necessitating the surgery are not
AEs
A serious adverse event is any untoward event that
Is fatal
Is life-threatening
Requires inpatient hospitalization or prolongation of existing hospitalization with the
following exceptions
o Preplanned (before the study) hospital admissions unless the hospitalization is
prolonged
o Planned admissions (as part of a study eg routine biopsies)
o Hospitalization lasting lt 24 hours
49
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
o Hospitalization for elective procedure
o Emergency room visits
Results in persistent or significant disability or incapacity
Is a congenital anomaly or birth defect
Important medical events that may not result in death be life-threatening or require
inpatient hospitalization may be considered serious adverse events (SAEs) when based
on appropriate medical judgment they may jeopardize the subject and may require
medical or surgical intervention to prevent one of the outcomes listed above
Life-threatening means that the subject was in the view of the investigator at immediate risk of
death from the AE as it occurred It does not include an AE that had it occurred in a more severe
form might have caused death
Persistent or significant disabilityincapacity means that the event resulted in permanent or
significant and substantial disruption of the subjectrsquos ability to carry out normal life functions
Causality
A reasonable possibility means the AE may have been caused byrelated to the study drug A
perceived or real lack of efficacy does not satisfy the definition of relatedness
612 Adverse Event (AE) Reporting
For the PANTHER-IPF trial all AEs (serious and nonserious) occurring from randomization
through final study visit (4 weeks after final dose of all study medication) will be recorded on the
AE page of the case report form (CRF)
6121 Serious Adverse Events (SAE) Reporting
For this trial all deaths and all SAEs which occur from randomization through final study visit
must be entered within the EDC system via the SAE eCRF page within 24 hours of the
investigative sitersquos knowledge of the event It is the responsibility of the clinical center
50
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
investigator to provide a causality assessment of the event for each study medications based upon
the information available at the time of the report It is understood that complete information
about the event may not be known at the time the initial report is submitted In the event the EDC
system is not accessible to the site at the time of event reporting investigative sites will complete
and forward a paper back-up SAE form to DCRI Safety Surveillance for processing
DCRI Safety Surveillance
Telephone 1-919-668-8624 or 1-866-668-7799 (toll free)
Fax 1-919-668-7138 or 1-866-668-7138 (toll free)
The investigator must complete and submit follow-up SAE information via the eCRF when
important new or follow-up information (eg final diagnosis outcome results of specific
investigations) becomes available Follow-up information should be submitted according to the
same process used for reporting the initial event as described above All SAEs will be followed
until resolution stabilization or 30 days after the subject has completed the final visit (4 weeks
after the final dose of study medication) whichever occurs first The investigator is responsible
for reporting SAEs to their institutional review board (IRB) per site specific IRB reporting
guidelines
6122 Regulatory Reporting
AEs that are serious study drug related and unexpected will be reported to the regulatory
authorities The DCRI Safety Surveillance medical monitor will perform a medical review of all
SAEs submitted and evaluate for ldquounexpectednessrdquo DCRI Safety Surveillance will prepare
MedWatch reports for those events identified as serious study drug related and unexpected as
determined by Safety Medical Monitor
DCRI Regulatory Services will submit all unexpected study drug-related SAEs as per 21 CFR
32 DCRI Safety Surveillance will provide a safety alert letter to the NHLBI DSMB and DCC
clinical operation (for distribution to sites) within 15 days of initial receipt of the information
51
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Investigators are responsible for promptly reporting these events to their reviewing IRBs
according to site specific IRB reporting guidelines
62 Clinical Medical Monitoring
There will be an unblinded physician at the IPFnet DCC serving as medical monitor The
medical monitor will be available to assist with questions about dosage adjustments of study
medications including discontinuation or resumption of medications
63 Unblinding Procedures
Unblinding of subjects or investigators to subject treatment is strongly discouraged For ongoing
clinical management all subjects should be presumed to be receiving ldquoactiverdquo study drug To
ensure the subjectrsquos safety the study treatment will be dose-adjusted based on laboratory test
results clinical findings and symptoms
The IPFnet DCC medical monitor and PANTHER-IPF co-chairs Drs Ganesh Raghu and
Fernando Martinez will be available to the study physicians to discuss study drug management
on a case-by-case basis Un-blinding will be considered ONLY when the knowledge of subject
treatment assignment is ABSOLUTELY ESSENTIAL for subject safety and after discussion of
the subjectrsquos case with the medical monitor and either Dr Raghu or Dr Martinez Unblinding of
study treatment should be minimized during the conduct of the trial In those cases where it is
felt to be medically necessary the DCC medical officer will communicate directly with the
managing physician to minimize unblinding of study personnel
52
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
7 Study Drug Procedures
At the baseline 15-week 30-week and 45-week study visits subjects will receive a supply of
study drug sufficient to last until the next visit at which study drug will be dispensed
53
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
8 Data Management
81 Hardware and Software Configuration
811 Hardware and Database Software
Data will be stored in an Oracle database system Oracle has advantages of processing efficiency
and smooth linkage with other software systems The application and database will be hosted on
Solaris Unix servers at the IPFnet DCC
812 Statistical Software
SAS will be used as the principal application for the management of analysis data files and
statistical computations S-Plus will be used to provide supplementary functions as needed
813 Access Control and Confidentiality Procedures
Access to databases will be controlled centrally by the IPFnet DCC through user passwords
linked to appropriate privileges This protects the data from unauthorized changes and
inadvertent loss or damage
814 Security
Database and Web servers will be secured by a firewall and through controlled physical access
Oracle has many security features to ensure that any staff member accessing the database has the
proper authority to perform the functions he or she requests of the system Within the secondary
SAS databases Unix group-access control maintains similar security The Sun workstation login
is secured by extensive user-password facilities under Unix
54
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
815 Back-up Procedures
Database back-up will be performed automatically every day and standard IPFnet DCC policies
and procedures will be applied to dictate tape rotation and retention practices
816 Virus Protection
All disk drives that provide network services and all user computers will be protected using
virus-scanning software Standard IPFnet DCC policies will be applied to update these protection
systems periodically through the study
82 Sources of Data
821 Design and Development
The IPFnet DCC will be responsible for development of the electronic case report forms
(eCRFs) development and validation of the clinical study database ensuring data integrity and
training clinical center staff on applicable data management procedures A web-based distributed
data entry model will be implemented This system will be developed to ensure that guidelines
and regulations surrounding the use of computerized systems used in clinical trials are upheld
The remainder of this section provides an overview of the data management plan associated with
this protocol
822 Data Collection Forms
The data collection process consists of direct data entry at the study clinical centers into the EDC
system(s) provided by the DCC A data collection worksheet will be provided to clinical centers
for recording data in the event the EDC system is unavailable Data entry of the eCRFs should
be completed according to the instructions provided and project specific training The
investigator is responsible for maintaining accurate complete and up-to-date records and for
ensuring the completion of the eCRFs for each research participant
55
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
823 Data Acquisition and Entry
Data entry into eCRFs shall be performed by authorized individuals Selected eCRFs may also
require the investigatorrsquos written signature or electronic signature as appropriate Electronic
CRFs will be monitored for completeness accuracy and attention to detail during the study
824 Data Center Responsibilities
The IPFnet DCC will 1) develop a data management plan and will conduct data management
activities 2) provide final eCRFs for the collection of all data required by the study 3) develop
data dictionaries for each eCRF that will comprehensively define each data element 4) conduct
ongoing data monitoring activities on study data 5) monitor any preliminary analysis data
cleanup activities and 6) rigorously monitor final study data clean up
825 Data Editing
Completed data will be entered into the IPFnet DCC automated data acquisition and
management system If incomplete or inaccurate data are found a data clarification request will
be generated and distributed to clinical centers for a response Clinical centers will resolve data
inconsistencies and errors and enter all corrections and changes into the IPFnet DCC automated
data acquisition and management system
826 Training
The training plan for clinical center staff includes provisions for training on assessments eCRF
completion guidelines data management procedures and the use of computerized systems
56
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
9 Study Design and Data Analysis
91 General Analytic Considerations
All primary analyses will be based on intent-to-treat (ITT) principles using all randomized
subjects Baseline factors across groups will be compared using mean (standard deviation) and
median (25th and 75th percentiles) summary measures Kaplan-Meier curves will be used to
display event rates Due to clinical interest in departures from both sides of the null hypothesis
all test statistics will be 2-sided
Reasonable caution needs to be taken when conducting multiple analyses on key clinical
subgroups For subgroup analyses a conservative significance level of 0001 will be used for all
interaction tests Thus subgroup comparisons will be considered exploratory unless the p-value
from the interaction test is smaller than 0001
92 Randomization Blinding and Reporting of Results
A permuted block-randomization scheme will be created with varying block sizes stratified by
clinical center Once a subject has completed the screening and baseline period and evaluation
for inclusionexclusion criteria the randomization process will begin Subjects will be
randomized to receive NAC or matching placebo with equal probability (11) via telephone
contact with a central interactive voice response system (IVRS) using a toll-free randomization
number On the day of randomization after the subject has successfully met all inclusion and
exclusion criteria the investigator or designee will call the central randomization number to
obtain the assigned kit randomization numbers for that subject At each subject visit the
investigator or designee will call the central randomization number to obtain the new kit
randomization numbers for resupply of the subject For resupply of the clinical center the IVRS
will monitor minimal volume of a kit type andor expiration date and will automatically notify
the pharmacy
57
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
The trial results will be reported according to guidelines specified in the CONSORT statement
A flow diagram describing screening recruitment randomization dropout and vital status will
be included in the primary manuscript AEs and efficacy data will be presented for all treatment
groups Adherence dropout and lost to follow-up will be carefully examined across all treatment
groups Analyses of safety will be based on data from all randomized subjects who received at
least one dose of study drug
93 Stratification
Subjects will be distributed to the two treatment arms in a 11 allocation ratio Stratification
blocks will be based on clinical centers
94 Specification of the Primary Analyses
A mixed model repeated measures (MMRM) analysis described in section 95 will be used to
compare differences in the slope of FVC measurements across the treatment groups Response
variables are values of the FVC measured at baseline and every 15 weeks until study completion
Variables in the model will include treatment time and time by treatment age sex race and
height Contrast estimates of differences in slopes of treatment over time (along with confidence
intervals) will be used to estimate the treatment effect The validity of this model in terms of
meeting modeling assumptions will be assessed via standard modeling diagnostics and goodness-
of-fit measures Based on the MMRM framework missing FVC data will not be imputed for the
primary analysis
95 Analysis of Longitudinal Endpoints
A common goal in clinical trials is to specify models that are easily implemented and
reproducible by independent data analysts On the other hand the models should have proper
statistical behavior in terms of low bias and high precision Many common approaches to
longitudinal data analysis including last observation carried forward (LOCF) imputation rely on
the missing completely at random (MCAR) assumption However the MCAR assumption is
58
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
unlikely to hold in many clinical trials because missing data are often related to disease
progression and prognosis A more reasonable assumption missing at random (MAR) specifies
that the complete data distribution can be modeled using only the observed data The likelihood-
based MMRM approach is valid under the more general MAR assumptions These models will
be applied to analyze the longitudinal data secondary endpoints
The advantages of MMRM analysis are that all important characteristics of the model can be preshy
specified standard software can be used to implement the models and results are based on ITT
principles43 In addition the MMRM approach offers superior control of Type I and Type II
errors compared with the LOCF approach
Response variables are values of the PFTs measured at enrollment and every 15 weeks until
study completion and 6MWT values measured at baseline week 30 and week 60 Covariates are
treatment time time by treatment and key baseline risk factors Contrasts (along with
confidence intervals) of treatment by time will be used to estimate the treatment effect
The correlation structure involves multiple pieces including measurement errors random
variation and interindividual variability For the longitudinal data analyses an unstructured
correlation matrix for within-subject errors will be assumed Other correlation structures
including compound symmetry will be examined as needed A careful examination of reasons
for study discontinuation will be conducted to assess the validity of MCAR Sensitivity analyses
will be used to examine the untestable assumption that the observed data violate the MAR
assumption The MMRM models will be implemented using PROC MIXED in SAS
96 Analysis of Binary Time-to-Event and Time-Lagged Endpoints
Regression modeling approaches using either the logistic regression model or Cox proportional
hazards regression model will be employed when appropriate The validity of these models will
be assessed via standard modeling diagnostics and goodness-of-fit measures Estimates of
cumulative frequencies for more general time-lagged responses will be calculated using the
partitioned version of the Bang-Tsiatis estimator44 The partitions will be set at 15-week intervals
59
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
to correspond with the data-collection process Covariate adjusted event rates will be calculated
using inverse probability-weighted regression estimates45
97 Power Analysis
971 Primary Analyses
Based on previously published IPF clinical trials the PL group is expected to experience a drop
in FVC of approximately 020 L over the study period (see Figure 1) The IPFnet Steering Group
determined a clinically important difference would be to preserve the majority of the decline
relative to PL over the study period In particular a treatment effect of 015 L was determined to
be a clinically meaningful difference Potential dropout is a key factor in the proposed study The
drop-out process assumed 5 lost to follow-up after every study visit Only 80 of subjects
were assumed to be followed for the entire study period All models assumed a compound
symmetry structure for the covariance matrix Power calculations were performed using a SAS
IML program for designing repeated measures studies46 Based on preliminary reviews of the
data from the University of Michigan the covariance matrix parameters were estimated at
approximately σ2 = 0757 (variance parameter) and ρ = 0936 (correlation parameter) To be
conservative the power calculations for the primary analysis were performed with parameter
setting of σ2 = 0810 (variance parameter) and ρ = 0925 (correlation parameter)
The power calculations assume a correction for imperfect compliance proposed by Lachin and
Foulkes to allow for 2 noncompliance for each of the treatment arms47 Thus the sample size
of 130 subjects per arm would be reduced to an adjusted sample size of 130(1-002-002)2 =
1198 or 120 subjects per arm
Under the assumed Type I error rate of 005 with a correlation parameter of 0925 and standard
deviation of 090 the difference of 015 L (or 00025 Lweek) shown in Table 6 would have
power of 93
60
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Table 6 Hypothetical Values of Mean FVC (L) Change from Baseline
Week 15 Week 30 Week 45 Week 60
NAC 00125 00250 00375 00500
Placebo 00500 01000 01500 02000
Difference 00375 00750 01125 01500
Abbreviations FVC forced vital capacity PL placebo
972 Power Analysis for Secondary Endpoints
Power calculations for secondary endpoint measurements are shown in Table 7 Standard
deviations are based on unpublished data provided by the University of Michigan The
calculations are based on a 2-sample t-test with Type I error rate set at 005 These calculations
are likely to be conservative because the statistical approach described in section 95 for
analyzing these endpoints will incorporate incomplete observations as well as intermediate data
points
Table 7 Detectable Differences in Treatment Means for Selected Endpoint Measurements
Secondary Endpoints Std Dev
of the Baseline Score
Detectable Difference for 80 Power
Std Dev of the Change Score
Difference Detectable for
80 Power
DLCOpred 166 58 91 32
6MWT Area Under the Desaturation Curve
219 76 175 61
6MWT Distance to Desaturation 224 78 315 110
6MWT Minutes Walked 210 073 205 071
Abbreviations Std Dev standard deviation DLCOpred diffusing capacity of the lung for carbon monoxide percent predicted 6MWT 6-minute walk test
61
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
10 Study Administration
101 Cooperative Agreement Mechanism
The administrative and funding mechanism used to undertake this project is a ldquocooperative
agreementrdquo (U01) which is an assistance mechanism Under the cooperative agreement the
NHLBI assists supports andor stimulates the project and is substantially involved with
investigators in conducting the study by facilitating performance of the effort in a ldquopartnerrdquo role
The NHLBI project scientist serves on the IPFnet Steering Group and he or another NHLBI
scientist may serve on other project committees when appropriate At the same time however
NHLBI does not assume a dominant role direction or prime responsibility for this research
program
As described below governance of the project is conducted through the IPFnet Steering Group
Principal investigators have lead responsibilities in all aspects of their trials and the project
including any modification of trial designs conduct of the trials quality control data analysis
and interpretation preparation of publications and collaboration with other investigators unless
otherwise provided for by the IPFnet Steering Group
PIs retain custody of and have primary rights to their center-specific and collaborative data
subject to government rights-of-access consistent with current Health amp Human Services (HHS)
Public Health Service (PHS) and National Institutes of Health policies The protocols and
governance policies call for the continual submission of data centrally to the IPFnet DCC for the
collaborative database which at a minimum will contain the key variables selected by the IPFnet
Steering Group for standardization across all clinical centers the submission of copies of the
collaborative datasets to each PI upon completion of the project procedures for data analysis
reporting and publication and procedures to protect and ensure the privacy of medical and
genetic data and records of individuals The NHLBI project scientist on behalf of the NHLBI
will have the same access privileges and responsibilities regarding the collaborative data as the
other members of the Steering Group
62
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
PIs are also encouraged to publish and to publicly release and disseminate results data and other
products of the project concordant with the project protocols and governance and the approved
plan for making data and materials available to the scientific community and to the NHLBI
However during the 3 years after the ending date of NHLBI project support unpublished data
unpublished results data sets not previously released and other study materials or products are
to be made available to any third party only with the approval of the IPFnet Steering Group
Upon completion of the project PIs are expected to put their intervention materials and
procedure manuals into the public domain andor make them available to other investigators
according to the approved plan for making data and materials available to the scientific
community and the NHLBI for the conduct of research at no charge other than the costs of
reproduction and distribution
The NHLBI reserves the right to terminate or curtail the project (or an individual award) in the
event of (a) failure to develop or implement mutually agreeable collaborative measurement
subject eligibility and data management sections of the protocols (b) substantial shortfall in
subject recruitment follow-up data reporting or quality control or other major breach of
protocol (c) substantive changes in the agreed-upon protocols with which NHLBI cannot
concur (d) reaching a major project outcome with persuasive statistical significance
substantially before schedule or (e) human subject ethical issues that may dictate a premature
termination
Any disagreement that may arise in scientificprogrammatic matters (within the scope of the
award) between award recipients and the NHLBI may be brought to arbitration An arbitration
panel will be composed of 3 membersmdash1 selected by the IPFnet Steering Group (with the
NHLBI member not voting) or by the individual PI in the event of an individual disagreement a
second selected by NHLBI and the third selected by the other 2 members This special
arbitration procedure in no way affects the PIrsquos right to appeal an adverse action that is otherwise
appealable in accordance with the PHS regulations at 42 CFR part 50 Subpart D and HHS
63
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
regulation at 45 CFR part 16 or the rights of the NHLBI under applicable statutes regulations
and terms of the award
102 IPFnet Steering Group
The IPFnet Steering Group is the main governing body of the project It is composed of the PIs
of the clinical centers the PI of the DCC and the NHLBI project scientist The clinical centers
the IPFnet DCC and the NHLBI each have 1 vote on the IPFnet Steering Group All decisions
are determined by majority vote
All major scientific decisions are determined by the IPFnet Steering Group It assumes overall
responsibility for the design and conduct of the trial It appoints (and disbands) committees and
subcommittees as the need arises designs approves and implements the study protocols
oversees the development of the MOOP monitors subject recruitment and treatment delivery
evaluates data collection and management oversees quality assurance procedures and
implements changes and enhancements to the study as required It also has primary responsibility
for facilitating the conduct of the trials and reporting the projectrsquos results
103 Data and Safety Monitoring Board
The NHLBI will establish a DSMB in accordance with established policies (see
httpwwwnhlbinihgovfundingpoliciesdsmb_insthtm) to ensure data quality and subject
safety and to provide independent advice to the NHLBI regarding progress and the
appropriateness of study continuation
104 Recommendations on Interim Monitoring of Efficacy Safety and Futility
First and foremost the role of the DSMB will be to review subject safety and trial conduct at
periodic points during the study The DSMB may require analyses of the primary endpoint
results for comparing the benefit and risks of treatment strategies The benefit of collecting
additional data on key secondary endpoints with extended follow-up and establishing a robust
64
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
evidence base for determining a standard of care will need to be carefully considered before
early termination of one or more treatment arms After careful consideration the IPFnet Steering
Group recommends conservative thresholds for the early examinations of the safety and efficacy
data
The DSMB will be expected to meet approximately every 6 months until trial completion to
review safety and toxicity data The DSMB may recommend stopping the study based on these
reviews Because the DSMB could stop the trial for safety concerns as well as for a large
efficacy benefit there could be multiple opportunities to reject the null hypothesis (no difference
in event rates between the PL and NAC groups) A Bonferroni approximation will be applied
during the one planned interim analysis for efficacy
Before locking the database a statistical analysis plan (SAP) will be developed to provide
complete details on the statistical analysis The SAP will include the specifics for how and when
the DSMB will be notified for AEs The IPFnet DCC will deliver to the DSMB all FDA-defined
AEs at 3-month intervals The IPFnet DCC will prepare narrative SAE reports in real time for
DSMB review including recommendations and analysis of similar events for each SAE
submitted to the FDA
65
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
11 Investigator and Sponsor Obligations
111 Monitoring
All monitoring activities for US clinical centers will be performed in accordance with DCRI
standard operating procedures Information regarding the types of visits will be outlined in the
PANTHER-IPF MOOP
112 Cost and Payment
There will be no cost to subjects enrolled in this trial Study-related procedures will be paid for
by the IPFnet
Subjects may be eligible for reimbursement for travel to the clinical center Details of payment
will be explained to each subject during the consent process
113 Confidentiality and Health Insurance Portability and Accountability Act
Considerations
Subject confidentiality will be protected throughout the study All subject data will be kept
strictly confidential and no subject-identifying information will be released to anyone outside
the project Confidentiality will be assured through several mechanisms First each subject will
be assigned an anonymous study ID which will then be used on all study forms Second any
study forms blood samples and paper records that contain subject information (eg address lists
phone lists) will be kept at the clinical centers in secured locked areas coded by number Once
blood is collected there will be no subject identifiers placed on blood samplesmdashonly the study
ID number and the date of sample collection Third access to all subject data and information
including laboratory specimens will be restricted to authorized personnel In the case of
computerized data this restricted access will be assured through user logon IDs and password
protection
66
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
At the IPFnet DCC only authorized personnel will have access to the data files containing study
data Security will be assured through user logon IDs passwords and appropriate access
privileges All study subjects will be identified only by their IPFnet ID numbers and no personal
identifying information such as name address or Social Security number will be entered into
the IPFnet DCC database Any subject-specific data reported to the IPFnet Steering Group will
be identified only by the IPFnet ID number
Finally subjects will not be identified by name in any reports or publications nor will the data
be presented in such a way that the identity of individual subjects can be inferred Analysis files
created for further study by the scientific community will have no subject identifiers These data
files will be created in accordance with the Ancillary Studies and Publication Policy of the
IPFnet
114 Informed Consent Procedures
All IPFnet subjects will provide written informed consent using procedures reviewed and
approved by each clinical centerrsquos IRB Informed consent will be undertaken by study personnel
in-person with the subject The subject has the option of declining further participation in the
study at that point No further study procedures will be conducted until the signed documents
have been provided to the IPFnet clinical center
115 Institutional Review Boards
Before initiating this study the protocol clinical center-specific informed consent forms Health
Insurance Portability and Accountability Act (HIPAA) forms recruitment materials and other
relevant information will be reviewed by a properly constituted IRB at each participating clinical
center A copy of the signed and dated IRB approval at each clinical center will be retrieved prior
to or during the site initiation visit and archived at the IPFnet DCC Any amendments to the
protocol other than simple administrative and typographical changes must be approved by each
IRB before they are implemented The clinical centers will seek annual renewals of their IRB
approvals in accordance with local procedures
67
__________________________________________ ________________
__________________________________________
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
12 Investigator Agreement
I have read the foregoing protocol PANTHER-IPF and agree that it contains all necessary
details for carrying out this study I will conduct the study as outlined herein and will complete
the study within the time designated
I will provide copies of the protocol and all pertinent information to all individuals responsible to
me who assist in the conduct of this study I will discuss this material with them to ensure they
are fully informed regarding the drug and the conduct of the study
I will fulfill all responsibilities for submitting pertinent information to the local IRB if
applicable that is responsible for this study
I further agree that NHLBI andor DCRI will have access to any source documents from which
eCRF information may have been generated
Signature of Principal Investigator Date
Name of Principal Investigator (printed or typed)
Protocol version date May 19 2009
Protocol Amendment 1 version date May 28 2010
Protocol Amendment 2 version date December 6 2011
68
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
13 References
1 Raghu G Brown KK Bradford WZ et al A placebo-controlled trial of interferon gamma-1b in patients with idiopathic pulmonary fibrosis N Engl J Med 2004350125-33 2 King TE Jr Safrin S Starko KM et al Analyses of efficacy end points in a controlled trial of interferon-gamma1b for idiopathic pulmonary fibrosis Chest 2005127171-7 3 Flaherty KR Thwaite EL Kazerooni EA et al Radiological versus histological diagnosis in UIP and NSIP survival implications Thorax 200358143-8 4 Wells AU Desai SR Rubens MB et al Idiopathic pulmonary fibrosis a composite physiologic index derived from disease extent observed by computed tomography Am J Respir Crit Care Med 2003167962-9 5 Raghu G Freudenberger TD Yang S et al High prevalence of abnormal acid gastroshyoesophageal reflux in idiopathic pulmonary fibrosis Eur Respir J 200627136-42 6 Kinnula VL Focus on antioxidant enzymes and antioxidant strategies in smoking related airway diseases Thorax 200560693-700 7 Coultas DB Zumwalt RE Black WC Sobonya RE The epidemiology of interstitial lung diseases Am J Respir Crit Care Med 1994150967-72 8 Raghu G Weycker D Edelsberg J Bradford WZ Oster G Incidence and prevalence of idiopathic pulmonary fibrosis Am J Respir Crit Care Med 2006174810-6 9 Olson AL Swigris JJ Lezotte DC Norris JM Wilson CG Brown KK Mortality from pulmonary fibrosis increased in the United States from 1992 to 2003 Am J Respir Crit Care Med 2007176277-84 10 Mannino DM Etzel RA Parrish RG Pulmonary fibrosis deaths in the United States 1979shy1991 An analysis of multiple-cause mortality data Am J Respir Crit Care Med 19961531548shy52 11 Hubbard R Johnston I Coultas DB Britton J Mortality rates from cryptogenic fibrosing alveolitis in seven countries Thorax 199651711-6 12 Johnston I Britton J Kinnear W Logan R Rising mortality from cryptogenic fibrosing alveolitis Bmj 19903011017-21 13 Raghu G Collard HR Egan JJ et al An official ATSERSJRSALAT statement idiopathic pulmonary fibrosis evidence-based guidelines for diagnosis and management Am J Respir Crit Care Med 2011183788-824 14 (USA) FDA FDA Public Health Advisory Interferon gamma-1b (marketed as Actimmune) In 2007 15 King TE Jr Pardo A Selman M Idiopathic pulmonary fibrosis Lancet 2011 16 Raghu G Brown KK Costabel U et al Treatment of idiopathic pulmonary fibrosis with etanercept an exploratory placebo-controlled trial Am J Respir Crit Care Med 2008178948shy55 17 Malouf MA Hopkins P Snell G Glanville AR An investigator-driven study of everolimus in surgical lung biopsy confirmed idiopathic pulmonary fibrosis Respirology 201116776-83 18 King TE Jr Behr J Brown KK et al BUILD-1 a randomized placebo-controlled trial of bosentan in idiopathic pulmonary fibrosis Am J Respir Crit Care Med 200817775-81 19 Richeldi L Costabel U Selman M et al Efficacy of a tyrosine kinase inhibitor in idiopathic pulmonary fibrosis N Engl J Med 20113651079-87
69
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
20 Borok Z Buhl R Grimes GJ et al Effect of glutathione aerosol on oxidant-antioxidant imbalance in idiopathic pulmonary fibrosis Lancet 1991338215-6 21 Meyer A Buhl R Magnussen H The effect of oral N-acetylcysteine on lung glutathione levels in idiopathic pulmonary fibrosis Eur Respir J 19947431-6 22 Behr J Maier K Degenkolb B Krombach F Vogelmeier C Antioxidative and clinical effects of high-dose N-acetylcysteine in fibrosing alveolitis Adjunctive therapy to maintenance immunosuppression Am J Respir Crit Care Med 19971561897-901 23 Cantin AM North SL Fells GA Hubbard RC Crystal RG Oxidant-mediated epithelial cell injury in idiopathic pulmonary fibrosis J Clin Invest 1987791665-73 24 Waghray M Cui Z Horowitz JC et al Hydrogen peroxide is a diffusible paracrine signal for the induction of epithelial cell death by activated myofibroblasts Faseb J 200519854-6 25 Larios JM Budhiraja R Fanburg BL Thannickal VJ Oxidative protein cross-linking reactions involving L-tyrosine in transforming growth factor-beta1-stimulated fibroblasts J Biol Chem 200127617437-41 26 Kinnula VL Fattman CL Tan RJ Oury TD Oxidative stress in pulmonary fibrosis a possible role for redox modulatory therapy Am J Respir Crit Care Med 2005172417-22 27 Meyer A Buhl R Kampf S Magnussen H Intravenous N-acetylcysteine and lung glutathione of patients with pulmonary fibrosis and normals Am J Respir Crit Care Med 19951521055-60 28 Behr J Degenkolb B Krombach F Vogelmeier C Intracellular glutathione and bronchoalveolar cells in fibrosing alveolitis effects of N-acetylcysteine Eur Respir J 200219906-11 29 Bando M Hosono T Mato N et al Long-term efficacy of inhaled N-acetylcysteine in patients with idiopathic pulmonary fibrosis Intern Med 2010492289-96 30 Demedts M Behr J Buhl R et al High-dose acetylcysteine in idiopathic pulmonary fibrosis N Engl J Med 20053532229-42 31 Toma TP Bhowmik A Rajakulasingam R Acetylcysteine in pulmonary fibrosis N Engl J Med 20063541086-9 author reply -9 32 Hunninghake GW Antioxidant therapy for idiopathic pulmonary fibrosis N Engl J Med 20053532285-7 33 Flaherty KR Mumford JA Murray S et al Prognostic implications of physiologic and radiographic changes in idiopathic interstitial pneumonia Am J Respir Crit Care Med 2003168543-8 34 Latsi PI du Bois RM Nicholson AG et al Fibrotic idiopathic interstitial pneumonia the prognostic value of longitudinal functional trends Am J Respir Crit Care Med 2003168531-7 35 Collard HR King TE Jr Bartelson BB Vourlekis JS Schwarz MI Brown KK Changes in clinical and physiologic variables predict survival in idiopathic pulmonary fibrosis Am J Respir Crit Care Med 2003168538-42 36 Jegal Y Kim DS Shim TS et al Physiology is a stronger predictor of survival than pathology in fibrotic interstitial pneumonia Am J Respir Crit Care Med 2005171639-44 37 Martinez FJ Safrin S Weycker D et al The clinical course of patients with idiopathic pulmonary fibrosis Ann Intern Med 2005142963-7 38 Hull JH Acetylcysteine in pulmonary fibrosis N Engl J Med 20063541089-91 author reply -91
70
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
39 Flaherty KR King TE Jr Raghu G et al Idiopathic interstitial pneumonia what is the effect of a multidisciplinary approach to diagnosis Am J Respir Crit Care Med 2004170904shy10 40 Raghu G Johnson WC Lockhart D Mageto Y Treatment of idiopathic pulmonary fibrosis with a new antifibrotic agent pirfenidone results of a prospective open-label Phase II study Am J Respir Crit Care Med 19991591061-9 41 Hunninghake GW Lynch DA Galvin JR et al Radiologic findings are strongly associated with a pathologic diagnosis of usual interstitial pneumonia Chest 20031241215-23 42 Lynch D Godwin J Safrin S et al High-resolution computed tomography in idiopathic pulmonary fibrosis diagnosis and prognosis Am J Respir Crit Care Med 2005172488-93 43 Mallinckrodt CH Watkin JG Molenberghs G Carroll RJ Choice of the primary analysis in longitudinal clinical trials Pharmaceutical Statistics 20043161-9 44 Bang H Tsiatis A Estimating medical costs with censored data Biometrika 200087329shy43 45 Lin DY Regression analysis of incomplete medical cost data Stat Med 2003221181-200 46 Rochon J Application of GEE procedures for sample size calculations in repeated measures experiments Stat Med 1998171643-58 47 Lachin JM Foulkes MA Evaluation of sample size and power for analyses of survival with allowance for nonuniform patient entry losses to follow-up noncompliance and stratification Biometrics 198642507-19
71
- PANTHER-IPFPREDNISONE AZATHIOPRINEAND N-ACETYLCYSTEINEA STUDY THAT EVALUATES RESPONSE INIDIOPATHIC PULMONARY FIBROSIS
-
- Protocol Summary
- Table of Contents
- List of Tables
- List of Figures
- List of Abbreviations
- 1 Summary
- 2 Hypotheses and Specific Aims
-
- 21 Null Hypothesis
- 22 Specific Aim 1
- 23 Specific Aim 2
- 24 Prespecified Subgroups of Interest
-
- 3 Background and Significance
-
- 31 Idiopathic Pulmonary Fibrosis is the Most Common Interstitial Lung Disease
- 32 Rationale for Placebo Control
- 33 Rationale for N-acetylcysteine
- 35 Rationale for N-acetylcysteine as a Stand-alone Therapy
- 36 Rationale for the Study Design and Primary Endpoint
- 37 Rationale for Blinding of Treatments
-
- 4 Methods
-
- 41 Inclusion Criteria
- 42 Diagnosis of IPF
- 43 Exclusion Criteria
- 44 Study Design and Study Visit
- 45 Dose Justification
- 46 Contraindications Precautions and Side Effects of Study Medications
- 47 Recruitment Procedures
- 48 Study Procedures
- 49 Concomitant Medications
- 410 Laboratory Testing
- 411 Blinding of Study Drugs
-
- 5 Study Endpoints
-
- 51 Primary Study Endpoint
- 52 Secondary Study Endpoints
-
- 6 Safety Evaluations and Procedures
-
- 61 Adverse Events
- 62 Clinical Medical Monitoring
- 63 Unblinding Procedures
-
- 7 Study Drug Procedures
- 8 Data Management
-
- 81 Hardware and Software Configuration
- 82 Sources of Data
-
- 9 Study Design and Data Analysis
-
- 91 General Analytic Considerations
- 92 Randomization Blinding and Reporting of Results
- 93 Stratification
- 94 Specification of the Primary Analyses
- 95 Analysis of Longitudinal Endpoints
- 96 Analysis of Binary Time-to-Event and Time-Lagged Endpoints
- 97 Power Analysis
-
- 10 Study Administration
-
- 101 Cooperative Agreement Mechanism
- 102 IPFnet Steering Group
- 103 Data and Safety Monitoring Board
- 104 Recommendations on Interim Monitoring of Efficacy Safety and Futility
-
- 11 Investigator and Sponsor Obligations
-
- 111 Monitoring
- 112 Cost and Payment
- 113 Confidentiality and Health Insurance Portability and Accountability ActConsiderations
- 114 Informed Consent Procedures
- 115 Institutional Review Boards
-
- 12 Investigator Agreement
- 13 References
-
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Evaluate for AEx
Review concomitant medications
Subjects will complete all QOL and dyspnea questionnaires (EuroQol ICE CAP SF-36 SGRQ and
UCSD SOBQ)
If consent has been given blood will be drawn and a urine specimen collected for the biospecimen
repository
Subjects return used and unused study drug for the visit
Study diary reviewed
4427 Final Site Visit ndash FVC drop confirmation
In the event that the subject has a recorded FVC drop of gt10 from baseline at the final treatment visit and the
subject has not had a confirmation of such a drop at a previous study visit the subject should return to the
clinical site 6 to 8 weeks after the final treatment visit During this visit a post-bronchodilator spirometry test
will be performed This FVC measurement will be evaluated according to section 521 of this protocol
4428 Final Visit ndash Telephone Follow-up
Four weeks following the final dose of study medication subjects will receive a telephone call from the study
coordinator to ensure that there are no side effects and to follow up on any ongoing adverse events (AEs)
4429 Phone Contact Between Visits
At week 2 and each month that a subject does not have a scheduled clinical center visit his or her study
coordinator will contact him or her at least once by telephone to
Inquire if the subject has had any hospitalizations events that might be considered an AE or any events
significant enough to warrant an out-of-cycle visit to the clinical center
Remind subjects of their current dosage levels and confirm that the subject understands them
Address any questions or concerns the subject might have regarding other aspects of the study
Assess adherence to the treatment regimen by reviewing diary data verbal review of medications taken
including nutritional supplements
33
34
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Table 3 Schedule of Assessments
Procedure Screening Visit 0
Enrollment Visit 1
Week 15 Visit 2
Week 30Visit 3
Week 45 Visit 4
Week 60 Early
Withdrawal Visit 5
Final1
Visit (via phone)
Informed consent X
Medical history X
Inclusionexclusion criteria X
Serum pregnancy test (if applicable) X X X X X
Review of lung biopsy X
Arterial Blood Gas X X
6-Minute Walk Test
X
X X
Physical examination X X X
Vital signs with oximetry X X X X X X
Body height and weight X X X X X X
Complete Blood Count X X X
Chemistry panel X X X
Monitor Lab Values X X X
Urinalysis X Specimen repository substudy blood draw and urine collection (if consented)
X
X X X X
HRCT (if not completed within three months) X
Spirometry (pre- and post-bronchodilator) X
Spirometry (post-bronchodilator only) X X X X X
DLCO (post-bronchodilator only) X X X
Lung volumes (post-bronchodilator only) X
X
Evaluate for acute exacerbation X X X X X
Review Adverse Events X X X X X X
Review concomitant meds X X X X X X
Dispense subject diary X X X X
Review subject diary X X X X X
Dispense study agent X X X X
Gender Substudy questionnaire (female subjects only) X
EuroQol ICECAP UCSD SOBQ SGRQ SF-36 X X X
Abbreviations DLCO diffusing capacity of the lung for carbon monoxide QOL Quality of Life ICECAP Investigating Choice Experiments for Preferences of Older People UCSD SOBQ University of California Shortness of Breath Questionnaire SGRQ St Georgersquos Respiratory Questionnaire SF-36 Short Form 36 Health Survey
1Follow-up visit via phone will occur four weeks after final dose of study medication
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
45 Dose Justification
The general philosophy for determining dosing levels was to apply previously examined
treatment regimens With the focus of the study being to establish a standard of care for
mildmoderate IPF subjects the goal was to develop flexible yet standardized treatment rules that
allow for the temporary or permanent withholding of one or more components of treatment when
necessary Subjects developing laboratory abnormalities or symptoms that result in
discontinuation of one or more components of study treatment may continue on the other
components as long as there is no contraindication for this Complete follow-up is important for
the validity of any study As a strategy to maintain protocol adherence we are using a treatment
regimen that will detect potential side effects and prompt interventions proactively in the interest
of patient safety In addition subjects who permanently stop study medications during the course
of the study are encouraged to continue in the study completing all scheduled visits and tests
451 Rationale for N-acetylcysteine Dosing
To our knowledge there have been no IPF studies to correlate clinical outcome measures with
different dosages for NAC The dosage chosen is based on the IFIGENIA study However BAL
lung GSH levels from subjects with IPF have been augmented with the use of oral NAC at 600
mg 3 times per day In addition lung GSH levels have been associated with improved
PFTs212227 The dose chosen for this study was based on previous data including the IFIGENIA
study30
4511 Dosing of N-acetylcysteineplacebo
Dosing of NACPL will be 600 mg orally 3 times a day (1800 mgday)
4512 Reasons to Discontinue N-acetylcysteineplacebo
NACPL may be temporarily or permanently discontinued for the duration of the study for
gastrointestinal symptoms or dermatologic reactions
35
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Temporarily discontinue (hold) oral NACPL for subjects requiring inpatient admission for acute
exacerbation (AEx) or other conditions Resume NACPL after discharge
36
37
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
452 Dosage Algorithms
Dosage Adjustment Algorithm 1 NACPL Dose Modifications for Gastrointestinal Symptoms Nausea Vomiting Abdominal Discomfort Diarrhea
GI Symptoms determined by the PI to be clinically significant Nausea Vomiting Abdominal Discomfort Diarrhea
NACPL Temporarily dc (HOLD) x 3 Days
Monitor symptoms intervene as clinically indicated (eg fluid replacement antidiarrhea or antinausea medication)
Monitor or lab PRN
Are symptoms resolving after 3 days NO
Symptoms NOT resolving after 3 days of holding study medication Assessmentmanagement per clinical
discretion of investigator
Likely not study medication discuss resuming study medication with medical monitor when symptoms resolved
YES
Temporarily dc (HOLD) NACPL for 4 additional days (total hold 1 week) then NACPL Resume 600 MG TID
Did symptoms recur
YES
STOP NACPL for
duration of study
NO
NACPL No Change
38
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Dosage Adjustment Algorithm 2 NACPL Dose Modifications For Dermatologic Reactions
Dermatologic Reactions (Not Acneiform) ge Grade 2 Grading per Common Terminology Criteria for
Adverse Events V30 (httpctepcancergov) For example Grade 1 RASHDESQUAMATION Macular or papular eruption or erythema without associated symptoms Grade 2 RASHDESQUAMATION Macular or popular eruption or erythema with pruritus or other associated symptoms localized desquamation or other lesions covering lt50 of body surface area
NACPL Temporarily dc (HOLD) x 3 days
Are symptoms resolving after 3 days
NO Symptoms not resolving after 3 days of holding study medication Assessmentmanagement per clinical discretion of investigator Likely not study medication Discuss resuming study medication with medical monitor when symptoms
resolved YES
Temporarily dc (HOLD) NACPL for 4 additional days (total hold 1 week) then NACPL resume 600 MG TID
Did symptoms recur
YES
STOP NACPL for
duration of study
NO
NACPL No change
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
46 Contraindications Precautions and Side Effects of Study Medications
461 Contraindication
Contraindication to NAC is known hypersensitivity to it
462 Precautions
Concomitant administration of oral NAC and antibiotics has shown a slightly reduced absorption
of cephalexin and a slight increase in erythromycin serum levels NAC contains free sulfhydryl
groups There is no evidence that individuals sensitive to sulfa drugs are sensitive to NAC
The NAC preparation being administered in this study contains 20 mg of aspartame Because of
the phenylalanine component of aspartame individuals with phenylketonuria should avoid or
restrict aspartame intake to avoid increased blood levels of phenylalanine Because of this risk
labeling is required on all products containing aspartame
463 Side Effects
Side effects of NAC range from common to serious See Table 4
39
40
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Table 4 Side Effects of NAC
Undesirable Effects
System-organ class Uncommon
(gt11000 lt1100)
Rare
(gt110000 lt11000)
Very rare
(lt110000) Not known
Immune system disorders Hypersensitivity Anaphylactic shock
reaction
Nervous system disorders Headache
Ear and labyrinth disorders Tinnitus
Cardiac disorders Tachycardia
Vascular disorders Hemorrhage
Respiratory thoracic and
mediastinal disorders
Bronchospasm
Dyspnea
Gastrointestinal disorders
Vomiting diarrhea
stomatitis abdominal
pain nausea
Dyspepsia
Skin and subcutaneous tissue
disorders
Urticaria rash
angioedema itching
General disorders and
administration site conditions Pyrexia
Investigations Reduced arterial
pressure Face edema
In very rare cases the onset of severe skin reactions such as Stevens-Johnson syndrome and Lyell syndrome was reported to have a temporal relationship with N-acetylcysteine administration Although in most cases at least another suspect drug probably most involved in the genesis of the above mentioned mucocutaneous syndromes has been identified in case of mucocutaneous alterations it is appropriate to contact onersquos doctor and the administration of N-acetylcysteine should be immediately discontinued
Some studies confirmed a reduction of platelet aggregation during N-acetylcysteine administration The clinical significance of these findings has not been defined yet [Source Fluimucil Investigator Brochure]
47 Recruitment Procedures
Subjects recruited for this study will be established patients of the investigators or physician- or
self-referred to participating clinical centers in the IPFnet Each clinical center within IPFnet has
a well-developed infrastructure of local pulmonologists within the surrounding geographic area
These pulmonologists are kept informed of ongoing IPF clinical trials and regularly refer
subjects to studies conducted at IPFnet clinical centers
Additional steps will be taken to inform clinicians of the trials in progress within IPFnet
including presentations at faculty staff meetings at local hospitals medical grand rounds and
national conferences direct mail notification monthly faxes and advertisement of network trials
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
in pulmonary journals Clinical center patients previously diagnosed with IPF will be notified of
the trials by mail whenever possible
Recruitment of minorities and women will be monitored by the DCC and DSMB If necessary
additional recruitment efforts will be made at specific centers to ensure that the aggregate subject
sample contains appropriate representation of women and minorities
48 Study Procedures
The following procedures are detailed in the PANTHER-IPF MOOP accompanying this
protocol
1 PFT
2 ABG
3 HRCT scan of the chest (including imaging of pulmonary arteries)
4 CBC and serum chemistries
5 Pregnancy test
6 6MWTBorg Dyspnea Scale
7 QOL questionnaires (EuroQol HAD SF-36 SGRQ and ICE CAP)
8 UCSD SOBQ
9 Gender Substudy Questionnaire
All assessments of PFTs will be conducted by study personnel not directly involved in the
treatment of the subjects
481 Biological Specimen Management
4811 Biological Specimen Sample Management
Subjects at clinical centers participating in the specimen repository substudy who consent to
having blood drawn for research purposes and for the banking of blood blood components and
other biologic specimens (urine and BAL fluid) will have approximately 405 mL of blood
41
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
drawn 17 mL blood drawn for DNA and 20 mL of urine collected at enrollment visit Subjects
will have approximately 50 mL of blood drawn and 20 mL of urine collected at each 15-week
follow-up visit Blood specimens will be separated according to PANTHER-IPF MOOP
guidelines into the following components for banking in the repository serum plasma and
DNA Coding of all biologic specimens for the repository will be performed by study staff at the
clinical center The samples will be processed per PANTHER-IPF MOOP guidelines aliquoted
labeled with barcode labels and stored at -70degC at the clinical center and shipped to the central
repository
The only subject identifiers will be a sample ID number and subject initials This sample ID will
be linked in the IPFnet DCC clinical database to subject information No subject information will
be transferred to the biological-specimen database
The subjectrsquos samples may be used for approved sub-studies relating to human disease
including but not limited to IPF The studies for which an individualrsquos samples will be made
available will be determined by the subjectrsquos answers to questions on the biological-sample
informed consent form The subjects can choose to make their samples available for all options
or any combination Samples will be made available to researchers only with IPFnet Steering
Group approval until such time as the samples are made public through the NHLBI repository
49 Concomitant Medications
Concurrent treatment with FDA-approved therapy for IPF is allowed Colchicine may be used
for treatment of gout Temporary treatment with oral or IV corticosteroids for clinical worsening
or suspected AEx is permitted Nutritional supplements containing NAC are not allowed
410 Laboratory Testing
Clinical laboratory parameters will be assessed at screening and at the end of the study The
following tests will be performed at the two time points specified in the protocol chemistry (AG
ratio ALT [SGPT] AST [SGOT] albumin alkaline phosphatase amylase bilirubin-direct
42
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
bilirubin-indirect bilirubin-total BUN BUNcreatinine ratio calcium carbon dioxide
cholesterol-total chloride CPK-total creatinine GGT globulin glucose iron-total LDH
lipase magnesium phosphorus-inorganic potassium protein-total sodium TIBC triglycerides
uric acid) and hematology (red blood cell count WBC count hemoglobin hematocrit cell
indices differential platelet count)
411 Blinding of Study Drugs
Subjects and caregivers will be blinded to study treatment Every subject will receive NAC or
matching PLs at every study visit from the baseline visit to the week-45 visit No study agent
will be dispensed at the week-60 visit
43
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
5 Study Endpoints
51 Primary Study Endpoint
The primary endpoint will be the change in serial measurements of FVC over the study period
52 Secondary Study Endpoints
521 Time to Disease-progression
The time-to-death or a 10 decline in FVC will be defined as the time-to-disease progression
The 10 decline in FVC from enrollment must be confirmed on 2 consecutive visits no less than
6 weeks apart For subjects with 2 consecutive visits with a 10 decline in FVC the time-toshy
disease progression will be defined as the time interval between enrollment and the initial visit
with a 10 FVC decline For subjects who experience disease progression the study doctor will
determine whether or not the subject will remain in the study
522 Acute Exacerbations
The following 3 criteria will define AEx in subjects with acute worsening of their respiratory
conditions
1 Clinical (all of the following required)
A) Unexplained worsening of dyspnea or cough within 30 days triggering unscheduled
medical care (eg emergency room clinic study visit hospitalization)
B) No clinical suspicion or overt evidence of cardiac event pulmonary embolism or deep
venous thrombosis to explain acute worsening of dyspnea
C) No pneumothorax
44
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
2 RadiologicPhysiologic (A and B required)
A) New ground glass opacity or consolidation computed tomography (CT) scan OR new
alveolar opacities on chest x-ray
B) Decline of ge 5 in resting room air SpO2 from last recorded level OR decline of ge 8 mm
Hg in resting room air PaO2 from last recorded level
3 Microbiologic (all of the following required)
A) No clinical evidence for infection (ie absence of grossly purulent sputum fever gt 39degC
orally)
B) Lack of positive microbiological results (if done) from lower respiratory tract defined as
(1) Clinically significant bacterial growth on sputum or endotracheal aspirate cultures
(2) Quantitative culture by protected brush specimen ge 103 cfumL or BAL ge 104 cfumL
(3) The presence of specific pathogens on stains of any of the above
C) Lack of positive pathogen in blood cultures (if done)
Identification of Acute Exacerbations
All subjects will be educated about the importance of identifying AExs At the time of
enrollment subjects will be told about the possibility of developing acute symptomatic
worsening that might represent an AEx of IPF and instructed to contact their study clinical
center coordinator within 48 to 72 hours of the apparent event
All subjects will be contacted by phone monthly and questioned about any change in dyspnea or
cough and any interim clinic visits or hospitalizations Finally as part of the IPFnet outreach to
community referring physicians the importance of AExs will be emphasized When a subject is
identified who meets criterion 1A this will trigger the collection of additional clinical data to
evaluate a suspected AEx These data will be collected as part of standard clinical care (ie this
protocol does not require collection of all items) The additional items to be collected for
suspected AEx include
IPFnet AEx case report form (eCRF) (required)
45
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Chest x-ray CT scan withwithout pulmonary angiogram (reports should be faxed and
followed by the hard copiesdiscs)
Oxygen saturation (pulse oximetry)
ABG
Respiratory cultures (sputum endotracheal aspirate lavage)
Blood cultures
Clinichospital records related to the event
All potential cases of AEx will be reviewed by the clinical center PI first and a decision on
whether the case may represent an AEx will be made If AEx is suspected the case will be sent
to the IPFnet adjudication committee which will assign a final diagnosis (see Table 5) If there is
disagreement among members the majority opinion will be recorded
During episodes of suspected AEx as determined by the individual clinical center investigator
subjects will remain blinded and in the study
Table 5 Final Diagnoses in Evaluation of Suspected Acute Exacerbations
Definite acute exacerbation All criteria met no alternative etiology
Unclassifiable acute worsening
Insufficient data to evaluate all criteria no alternative etiology
Not acute exacerbation Alternative etiology identified that explains acute worsening
Management of the suspected AEx will be at the discretion of the treating physician Standard of
care generally involves evaluation for respiratory infection pulmonary embolism cardiac events
and pneumothorax and treatment with IV corticosteroids
Study drugs will be resumed at pre-suspected AEx doses after subjects clinically improve as
confirmed by the local PI All subjects should be seen at the clinical center within 2 to 4 weeks
of recovery for measurement of post-bronchodilator FVC (see Figure 4) Subjects unable to
return to the clinical center after suspected AEx due to medical frailty (eg continued
46
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
institutionalization progressive disability) will be categorized as failing to maintain FVC
response in secondary analyses
Suspected AEx (PI determined)
Hold study drug Treat AEx
(Attending physician determined)
Alive but unable to continue due to
medical frailty
Dead
Alive and able to continue
Site reviewvisit
Restart study drug
FVC within 2-4 weeks
Figure 4 Acute Exacerbation Flow Chart
523 Respiratory Infections
An upper respiratory infection will be defined as
Change in sputum discoloration
Increased cough of no more than 14 daysrsquo duration
A lower-respiratory infection (pneumonia) will be defined as new segmental or lobar airspace
opacities visualized by image studies (chest radiograph or HRCT) in addition to any of the
following
Positive pathogencultures in good sample of sputum or lower-airway secretions retrieved
by fiberoptic bronchoscope
Fever gt 39degC or gt 100degF
Leukocytosis gt 12000 (unexplained no increase in dose of corticosteroids)
47
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
524 Maintained FVC Response
Subjects with follow-up FVCpred measurements at or above their baseline FVCpred level
will be classified as having maintained FVC response Subjects with reduced FVCpred levels
or missing data for any reason including death or medical frailty will be classified as having not
maintained FVC response The FVCpred value is used because unadjusted FVC measurements
are expected to decline with age
48
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
6 Safety Evaluations and Procedures
61 Adverse Events
During a clinical trial the reporting of adverse experience information can lead to important
changes in the way a new treatment is developed as well as provide integral safety data
611 Definitions
An adverse event (AE) is any untoward medical occurrence in a subject or clinical investigation
subject who was administered a pharmaceutical product The AE does not necessarily have to
have a causal relationship with the drug administered An AE can be any unfavorable and
unintended sign (including an abnormal laboratory finding) symptom or disease temporarily
associated with the use of a medicinal product whether or not considered to be related to the
medicinal product Diseases signs symptoms or laboratory abnormalities already existing at
enrollment are not considered AEs unless they worsen (ie increase in intensity or frequency)
Surgical procedures themselves are not AEs they are therapeutic measures for conditions that
require surgery The condition for which the surgery is required may be an AE Surgical
procedures planned before randomization and the conditions necessitating the surgery are not
AEs
A serious adverse event is any untoward event that
Is fatal
Is life-threatening
Requires inpatient hospitalization or prolongation of existing hospitalization with the
following exceptions
o Preplanned (before the study) hospital admissions unless the hospitalization is
prolonged
o Planned admissions (as part of a study eg routine biopsies)
o Hospitalization lasting lt 24 hours
49
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
o Hospitalization for elective procedure
o Emergency room visits
Results in persistent or significant disability or incapacity
Is a congenital anomaly or birth defect
Important medical events that may not result in death be life-threatening or require
inpatient hospitalization may be considered serious adverse events (SAEs) when based
on appropriate medical judgment they may jeopardize the subject and may require
medical or surgical intervention to prevent one of the outcomes listed above
Life-threatening means that the subject was in the view of the investigator at immediate risk of
death from the AE as it occurred It does not include an AE that had it occurred in a more severe
form might have caused death
Persistent or significant disabilityincapacity means that the event resulted in permanent or
significant and substantial disruption of the subjectrsquos ability to carry out normal life functions
Causality
A reasonable possibility means the AE may have been caused byrelated to the study drug A
perceived or real lack of efficacy does not satisfy the definition of relatedness
612 Adverse Event (AE) Reporting
For the PANTHER-IPF trial all AEs (serious and nonserious) occurring from randomization
through final study visit (4 weeks after final dose of all study medication) will be recorded on the
AE page of the case report form (CRF)
6121 Serious Adverse Events (SAE) Reporting
For this trial all deaths and all SAEs which occur from randomization through final study visit
must be entered within the EDC system via the SAE eCRF page within 24 hours of the
investigative sitersquos knowledge of the event It is the responsibility of the clinical center
50
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
investigator to provide a causality assessment of the event for each study medications based upon
the information available at the time of the report It is understood that complete information
about the event may not be known at the time the initial report is submitted In the event the EDC
system is not accessible to the site at the time of event reporting investigative sites will complete
and forward a paper back-up SAE form to DCRI Safety Surveillance for processing
DCRI Safety Surveillance
Telephone 1-919-668-8624 or 1-866-668-7799 (toll free)
Fax 1-919-668-7138 or 1-866-668-7138 (toll free)
The investigator must complete and submit follow-up SAE information via the eCRF when
important new or follow-up information (eg final diagnosis outcome results of specific
investigations) becomes available Follow-up information should be submitted according to the
same process used for reporting the initial event as described above All SAEs will be followed
until resolution stabilization or 30 days after the subject has completed the final visit (4 weeks
after the final dose of study medication) whichever occurs first The investigator is responsible
for reporting SAEs to their institutional review board (IRB) per site specific IRB reporting
guidelines
6122 Regulatory Reporting
AEs that are serious study drug related and unexpected will be reported to the regulatory
authorities The DCRI Safety Surveillance medical monitor will perform a medical review of all
SAEs submitted and evaluate for ldquounexpectednessrdquo DCRI Safety Surveillance will prepare
MedWatch reports for those events identified as serious study drug related and unexpected as
determined by Safety Medical Monitor
DCRI Regulatory Services will submit all unexpected study drug-related SAEs as per 21 CFR
32 DCRI Safety Surveillance will provide a safety alert letter to the NHLBI DSMB and DCC
clinical operation (for distribution to sites) within 15 days of initial receipt of the information
51
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Investigators are responsible for promptly reporting these events to their reviewing IRBs
according to site specific IRB reporting guidelines
62 Clinical Medical Monitoring
There will be an unblinded physician at the IPFnet DCC serving as medical monitor The
medical monitor will be available to assist with questions about dosage adjustments of study
medications including discontinuation or resumption of medications
63 Unblinding Procedures
Unblinding of subjects or investigators to subject treatment is strongly discouraged For ongoing
clinical management all subjects should be presumed to be receiving ldquoactiverdquo study drug To
ensure the subjectrsquos safety the study treatment will be dose-adjusted based on laboratory test
results clinical findings and symptoms
The IPFnet DCC medical monitor and PANTHER-IPF co-chairs Drs Ganesh Raghu and
Fernando Martinez will be available to the study physicians to discuss study drug management
on a case-by-case basis Un-blinding will be considered ONLY when the knowledge of subject
treatment assignment is ABSOLUTELY ESSENTIAL for subject safety and after discussion of
the subjectrsquos case with the medical monitor and either Dr Raghu or Dr Martinez Unblinding of
study treatment should be minimized during the conduct of the trial In those cases where it is
felt to be medically necessary the DCC medical officer will communicate directly with the
managing physician to minimize unblinding of study personnel
52
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
7 Study Drug Procedures
At the baseline 15-week 30-week and 45-week study visits subjects will receive a supply of
study drug sufficient to last until the next visit at which study drug will be dispensed
53
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
8 Data Management
81 Hardware and Software Configuration
811 Hardware and Database Software
Data will be stored in an Oracle database system Oracle has advantages of processing efficiency
and smooth linkage with other software systems The application and database will be hosted on
Solaris Unix servers at the IPFnet DCC
812 Statistical Software
SAS will be used as the principal application for the management of analysis data files and
statistical computations S-Plus will be used to provide supplementary functions as needed
813 Access Control and Confidentiality Procedures
Access to databases will be controlled centrally by the IPFnet DCC through user passwords
linked to appropriate privileges This protects the data from unauthorized changes and
inadvertent loss or damage
814 Security
Database and Web servers will be secured by a firewall and through controlled physical access
Oracle has many security features to ensure that any staff member accessing the database has the
proper authority to perform the functions he or she requests of the system Within the secondary
SAS databases Unix group-access control maintains similar security The Sun workstation login
is secured by extensive user-password facilities under Unix
54
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
815 Back-up Procedures
Database back-up will be performed automatically every day and standard IPFnet DCC policies
and procedures will be applied to dictate tape rotation and retention practices
816 Virus Protection
All disk drives that provide network services and all user computers will be protected using
virus-scanning software Standard IPFnet DCC policies will be applied to update these protection
systems periodically through the study
82 Sources of Data
821 Design and Development
The IPFnet DCC will be responsible for development of the electronic case report forms
(eCRFs) development and validation of the clinical study database ensuring data integrity and
training clinical center staff on applicable data management procedures A web-based distributed
data entry model will be implemented This system will be developed to ensure that guidelines
and regulations surrounding the use of computerized systems used in clinical trials are upheld
The remainder of this section provides an overview of the data management plan associated with
this protocol
822 Data Collection Forms
The data collection process consists of direct data entry at the study clinical centers into the EDC
system(s) provided by the DCC A data collection worksheet will be provided to clinical centers
for recording data in the event the EDC system is unavailable Data entry of the eCRFs should
be completed according to the instructions provided and project specific training The
investigator is responsible for maintaining accurate complete and up-to-date records and for
ensuring the completion of the eCRFs for each research participant
55
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
823 Data Acquisition and Entry
Data entry into eCRFs shall be performed by authorized individuals Selected eCRFs may also
require the investigatorrsquos written signature or electronic signature as appropriate Electronic
CRFs will be monitored for completeness accuracy and attention to detail during the study
824 Data Center Responsibilities
The IPFnet DCC will 1) develop a data management plan and will conduct data management
activities 2) provide final eCRFs for the collection of all data required by the study 3) develop
data dictionaries for each eCRF that will comprehensively define each data element 4) conduct
ongoing data monitoring activities on study data 5) monitor any preliminary analysis data
cleanup activities and 6) rigorously monitor final study data clean up
825 Data Editing
Completed data will be entered into the IPFnet DCC automated data acquisition and
management system If incomplete or inaccurate data are found a data clarification request will
be generated and distributed to clinical centers for a response Clinical centers will resolve data
inconsistencies and errors and enter all corrections and changes into the IPFnet DCC automated
data acquisition and management system
826 Training
The training plan for clinical center staff includes provisions for training on assessments eCRF
completion guidelines data management procedures and the use of computerized systems
56
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
9 Study Design and Data Analysis
91 General Analytic Considerations
All primary analyses will be based on intent-to-treat (ITT) principles using all randomized
subjects Baseline factors across groups will be compared using mean (standard deviation) and
median (25th and 75th percentiles) summary measures Kaplan-Meier curves will be used to
display event rates Due to clinical interest in departures from both sides of the null hypothesis
all test statistics will be 2-sided
Reasonable caution needs to be taken when conducting multiple analyses on key clinical
subgroups For subgroup analyses a conservative significance level of 0001 will be used for all
interaction tests Thus subgroup comparisons will be considered exploratory unless the p-value
from the interaction test is smaller than 0001
92 Randomization Blinding and Reporting of Results
A permuted block-randomization scheme will be created with varying block sizes stratified by
clinical center Once a subject has completed the screening and baseline period and evaluation
for inclusionexclusion criteria the randomization process will begin Subjects will be
randomized to receive NAC or matching placebo with equal probability (11) via telephone
contact with a central interactive voice response system (IVRS) using a toll-free randomization
number On the day of randomization after the subject has successfully met all inclusion and
exclusion criteria the investigator or designee will call the central randomization number to
obtain the assigned kit randomization numbers for that subject At each subject visit the
investigator or designee will call the central randomization number to obtain the new kit
randomization numbers for resupply of the subject For resupply of the clinical center the IVRS
will monitor minimal volume of a kit type andor expiration date and will automatically notify
the pharmacy
57
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
The trial results will be reported according to guidelines specified in the CONSORT statement
A flow diagram describing screening recruitment randomization dropout and vital status will
be included in the primary manuscript AEs and efficacy data will be presented for all treatment
groups Adherence dropout and lost to follow-up will be carefully examined across all treatment
groups Analyses of safety will be based on data from all randomized subjects who received at
least one dose of study drug
93 Stratification
Subjects will be distributed to the two treatment arms in a 11 allocation ratio Stratification
blocks will be based on clinical centers
94 Specification of the Primary Analyses
A mixed model repeated measures (MMRM) analysis described in section 95 will be used to
compare differences in the slope of FVC measurements across the treatment groups Response
variables are values of the FVC measured at baseline and every 15 weeks until study completion
Variables in the model will include treatment time and time by treatment age sex race and
height Contrast estimates of differences in slopes of treatment over time (along with confidence
intervals) will be used to estimate the treatment effect The validity of this model in terms of
meeting modeling assumptions will be assessed via standard modeling diagnostics and goodness-
of-fit measures Based on the MMRM framework missing FVC data will not be imputed for the
primary analysis
95 Analysis of Longitudinal Endpoints
A common goal in clinical trials is to specify models that are easily implemented and
reproducible by independent data analysts On the other hand the models should have proper
statistical behavior in terms of low bias and high precision Many common approaches to
longitudinal data analysis including last observation carried forward (LOCF) imputation rely on
the missing completely at random (MCAR) assumption However the MCAR assumption is
58
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
unlikely to hold in many clinical trials because missing data are often related to disease
progression and prognosis A more reasonable assumption missing at random (MAR) specifies
that the complete data distribution can be modeled using only the observed data The likelihood-
based MMRM approach is valid under the more general MAR assumptions These models will
be applied to analyze the longitudinal data secondary endpoints
The advantages of MMRM analysis are that all important characteristics of the model can be preshy
specified standard software can be used to implement the models and results are based on ITT
principles43 In addition the MMRM approach offers superior control of Type I and Type II
errors compared with the LOCF approach
Response variables are values of the PFTs measured at enrollment and every 15 weeks until
study completion and 6MWT values measured at baseline week 30 and week 60 Covariates are
treatment time time by treatment and key baseline risk factors Contrasts (along with
confidence intervals) of treatment by time will be used to estimate the treatment effect
The correlation structure involves multiple pieces including measurement errors random
variation and interindividual variability For the longitudinal data analyses an unstructured
correlation matrix for within-subject errors will be assumed Other correlation structures
including compound symmetry will be examined as needed A careful examination of reasons
for study discontinuation will be conducted to assess the validity of MCAR Sensitivity analyses
will be used to examine the untestable assumption that the observed data violate the MAR
assumption The MMRM models will be implemented using PROC MIXED in SAS
96 Analysis of Binary Time-to-Event and Time-Lagged Endpoints
Regression modeling approaches using either the logistic regression model or Cox proportional
hazards regression model will be employed when appropriate The validity of these models will
be assessed via standard modeling diagnostics and goodness-of-fit measures Estimates of
cumulative frequencies for more general time-lagged responses will be calculated using the
partitioned version of the Bang-Tsiatis estimator44 The partitions will be set at 15-week intervals
59
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
to correspond with the data-collection process Covariate adjusted event rates will be calculated
using inverse probability-weighted regression estimates45
97 Power Analysis
971 Primary Analyses
Based on previously published IPF clinical trials the PL group is expected to experience a drop
in FVC of approximately 020 L over the study period (see Figure 1) The IPFnet Steering Group
determined a clinically important difference would be to preserve the majority of the decline
relative to PL over the study period In particular a treatment effect of 015 L was determined to
be a clinically meaningful difference Potential dropout is a key factor in the proposed study The
drop-out process assumed 5 lost to follow-up after every study visit Only 80 of subjects
were assumed to be followed for the entire study period All models assumed a compound
symmetry structure for the covariance matrix Power calculations were performed using a SAS
IML program for designing repeated measures studies46 Based on preliminary reviews of the
data from the University of Michigan the covariance matrix parameters were estimated at
approximately σ2 = 0757 (variance parameter) and ρ = 0936 (correlation parameter) To be
conservative the power calculations for the primary analysis were performed with parameter
setting of σ2 = 0810 (variance parameter) and ρ = 0925 (correlation parameter)
The power calculations assume a correction for imperfect compliance proposed by Lachin and
Foulkes to allow for 2 noncompliance for each of the treatment arms47 Thus the sample size
of 130 subjects per arm would be reduced to an adjusted sample size of 130(1-002-002)2 =
1198 or 120 subjects per arm
Under the assumed Type I error rate of 005 with a correlation parameter of 0925 and standard
deviation of 090 the difference of 015 L (or 00025 Lweek) shown in Table 6 would have
power of 93
60
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Table 6 Hypothetical Values of Mean FVC (L) Change from Baseline
Week 15 Week 30 Week 45 Week 60
NAC 00125 00250 00375 00500
Placebo 00500 01000 01500 02000
Difference 00375 00750 01125 01500
Abbreviations FVC forced vital capacity PL placebo
972 Power Analysis for Secondary Endpoints
Power calculations for secondary endpoint measurements are shown in Table 7 Standard
deviations are based on unpublished data provided by the University of Michigan The
calculations are based on a 2-sample t-test with Type I error rate set at 005 These calculations
are likely to be conservative because the statistical approach described in section 95 for
analyzing these endpoints will incorporate incomplete observations as well as intermediate data
points
Table 7 Detectable Differences in Treatment Means for Selected Endpoint Measurements
Secondary Endpoints Std Dev
of the Baseline Score
Detectable Difference for 80 Power
Std Dev of the Change Score
Difference Detectable for
80 Power
DLCOpred 166 58 91 32
6MWT Area Under the Desaturation Curve
219 76 175 61
6MWT Distance to Desaturation 224 78 315 110
6MWT Minutes Walked 210 073 205 071
Abbreviations Std Dev standard deviation DLCOpred diffusing capacity of the lung for carbon monoxide percent predicted 6MWT 6-minute walk test
61
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
10 Study Administration
101 Cooperative Agreement Mechanism
The administrative and funding mechanism used to undertake this project is a ldquocooperative
agreementrdquo (U01) which is an assistance mechanism Under the cooperative agreement the
NHLBI assists supports andor stimulates the project and is substantially involved with
investigators in conducting the study by facilitating performance of the effort in a ldquopartnerrdquo role
The NHLBI project scientist serves on the IPFnet Steering Group and he or another NHLBI
scientist may serve on other project committees when appropriate At the same time however
NHLBI does not assume a dominant role direction or prime responsibility for this research
program
As described below governance of the project is conducted through the IPFnet Steering Group
Principal investigators have lead responsibilities in all aspects of their trials and the project
including any modification of trial designs conduct of the trials quality control data analysis
and interpretation preparation of publications and collaboration with other investigators unless
otherwise provided for by the IPFnet Steering Group
PIs retain custody of and have primary rights to their center-specific and collaborative data
subject to government rights-of-access consistent with current Health amp Human Services (HHS)
Public Health Service (PHS) and National Institutes of Health policies The protocols and
governance policies call for the continual submission of data centrally to the IPFnet DCC for the
collaborative database which at a minimum will contain the key variables selected by the IPFnet
Steering Group for standardization across all clinical centers the submission of copies of the
collaborative datasets to each PI upon completion of the project procedures for data analysis
reporting and publication and procedures to protect and ensure the privacy of medical and
genetic data and records of individuals The NHLBI project scientist on behalf of the NHLBI
will have the same access privileges and responsibilities regarding the collaborative data as the
other members of the Steering Group
62
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
PIs are also encouraged to publish and to publicly release and disseminate results data and other
products of the project concordant with the project protocols and governance and the approved
plan for making data and materials available to the scientific community and to the NHLBI
However during the 3 years after the ending date of NHLBI project support unpublished data
unpublished results data sets not previously released and other study materials or products are
to be made available to any third party only with the approval of the IPFnet Steering Group
Upon completion of the project PIs are expected to put their intervention materials and
procedure manuals into the public domain andor make them available to other investigators
according to the approved plan for making data and materials available to the scientific
community and the NHLBI for the conduct of research at no charge other than the costs of
reproduction and distribution
The NHLBI reserves the right to terminate or curtail the project (or an individual award) in the
event of (a) failure to develop or implement mutually agreeable collaborative measurement
subject eligibility and data management sections of the protocols (b) substantial shortfall in
subject recruitment follow-up data reporting or quality control or other major breach of
protocol (c) substantive changes in the agreed-upon protocols with which NHLBI cannot
concur (d) reaching a major project outcome with persuasive statistical significance
substantially before schedule or (e) human subject ethical issues that may dictate a premature
termination
Any disagreement that may arise in scientificprogrammatic matters (within the scope of the
award) between award recipients and the NHLBI may be brought to arbitration An arbitration
panel will be composed of 3 membersmdash1 selected by the IPFnet Steering Group (with the
NHLBI member not voting) or by the individual PI in the event of an individual disagreement a
second selected by NHLBI and the third selected by the other 2 members This special
arbitration procedure in no way affects the PIrsquos right to appeal an adverse action that is otherwise
appealable in accordance with the PHS regulations at 42 CFR part 50 Subpart D and HHS
63
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
regulation at 45 CFR part 16 or the rights of the NHLBI under applicable statutes regulations
and terms of the award
102 IPFnet Steering Group
The IPFnet Steering Group is the main governing body of the project It is composed of the PIs
of the clinical centers the PI of the DCC and the NHLBI project scientist The clinical centers
the IPFnet DCC and the NHLBI each have 1 vote on the IPFnet Steering Group All decisions
are determined by majority vote
All major scientific decisions are determined by the IPFnet Steering Group It assumes overall
responsibility for the design and conduct of the trial It appoints (and disbands) committees and
subcommittees as the need arises designs approves and implements the study protocols
oversees the development of the MOOP monitors subject recruitment and treatment delivery
evaluates data collection and management oversees quality assurance procedures and
implements changes and enhancements to the study as required It also has primary responsibility
for facilitating the conduct of the trials and reporting the projectrsquos results
103 Data and Safety Monitoring Board
The NHLBI will establish a DSMB in accordance with established policies (see
httpwwwnhlbinihgovfundingpoliciesdsmb_insthtm) to ensure data quality and subject
safety and to provide independent advice to the NHLBI regarding progress and the
appropriateness of study continuation
104 Recommendations on Interim Monitoring of Efficacy Safety and Futility
First and foremost the role of the DSMB will be to review subject safety and trial conduct at
periodic points during the study The DSMB may require analyses of the primary endpoint
results for comparing the benefit and risks of treatment strategies The benefit of collecting
additional data on key secondary endpoints with extended follow-up and establishing a robust
64
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
evidence base for determining a standard of care will need to be carefully considered before
early termination of one or more treatment arms After careful consideration the IPFnet Steering
Group recommends conservative thresholds for the early examinations of the safety and efficacy
data
The DSMB will be expected to meet approximately every 6 months until trial completion to
review safety and toxicity data The DSMB may recommend stopping the study based on these
reviews Because the DSMB could stop the trial for safety concerns as well as for a large
efficacy benefit there could be multiple opportunities to reject the null hypothesis (no difference
in event rates between the PL and NAC groups) A Bonferroni approximation will be applied
during the one planned interim analysis for efficacy
Before locking the database a statistical analysis plan (SAP) will be developed to provide
complete details on the statistical analysis The SAP will include the specifics for how and when
the DSMB will be notified for AEs The IPFnet DCC will deliver to the DSMB all FDA-defined
AEs at 3-month intervals The IPFnet DCC will prepare narrative SAE reports in real time for
DSMB review including recommendations and analysis of similar events for each SAE
submitted to the FDA
65
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
11 Investigator and Sponsor Obligations
111 Monitoring
All monitoring activities for US clinical centers will be performed in accordance with DCRI
standard operating procedures Information regarding the types of visits will be outlined in the
PANTHER-IPF MOOP
112 Cost and Payment
There will be no cost to subjects enrolled in this trial Study-related procedures will be paid for
by the IPFnet
Subjects may be eligible for reimbursement for travel to the clinical center Details of payment
will be explained to each subject during the consent process
113 Confidentiality and Health Insurance Portability and Accountability Act
Considerations
Subject confidentiality will be protected throughout the study All subject data will be kept
strictly confidential and no subject-identifying information will be released to anyone outside
the project Confidentiality will be assured through several mechanisms First each subject will
be assigned an anonymous study ID which will then be used on all study forms Second any
study forms blood samples and paper records that contain subject information (eg address lists
phone lists) will be kept at the clinical centers in secured locked areas coded by number Once
blood is collected there will be no subject identifiers placed on blood samplesmdashonly the study
ID number and the date of sample collection Third access to all subject data and information
including laboratory specimens will be restricted to authorized personnel In the case of
computerized data this restricted access will be assured through user logon IDs and password
protection
66
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
At the IPFnet DCC only authorized personnel will have access to the data files containing study
data Security will be assured through user logon IDs passwords and appropriate access
privileges All study subjects will be identified only by their IPFnet ID numbers and no personal
identifying information such as name address or Social Security number will be entered into
the IPFnet DCC database Any subject-specific data reported to the IPFnet Steering Group will
be identified only by the IPFnet ID number
Finally subjects will not be identified by name in any reports or publications nor will the data
be presented in such a way that the identity of individual subjects can be inferred Analysis files
created for further study by the scientific community will have no subject identifiers These data
files will be created in accordance with the Ancillary Studies and Publication Policy of the
IPFnet
114 Informed Consent Procedures
All IPFnet subjects will provide written informed consent using procedures reviewed and
approved by each clinical centerrsquos IRB Informed consent will be undertaken by study personnel
in-person with the subject The subject has the option of declining further participation in the
study at that point No further study procedures will be conducted until the signed documents
have been provided to the IPFnet clinical center
115 Institutional Review Boards
Before initiating this study the protocol clinical center-specific informed consent forms Health
Insurance Portability and Accountability Act (HIPAA) forms recruitment materials and other
relevant information will be reviewed by a properly constituted IRB at each participating clinical
center A copy of the signed and dated IRB approval at each clinical center will be retrieved prior
to or during the site initiation visit and archived at the IPFnet DCC Any amendments to the
protocol other than simple administrative and typographical changes must be approved by each
IRB before they are implemented The clinical centers will seek annual renewals of their IRB
approvals in accordance with local procedures
67
__________________________________________ ________________
__________________________________________
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
12 Investigator Agreement
I have read the foregoing protocol PANTHER-IPF and agree that it contains all necessary
details for carrying out this study I will conduct the study as outlined herein and will complete
the study within the time designated
I will provide copies of the protocol and all pertinent information to all individuals responsible to
me who assist in the conduct of this study I will discuss this material with them to ensure they
are fully informed regarding the drug and the conduct of the study
I will fulfill all responsibilities for submitting pertinent information to the local IRB if
applicable that is responsible for this study
I further agree that NHLBI andor DCRI will have access to any source documents from which
eCRF information may have been generated
Signature of Principal Investigator Date
Name of Principal Investigator (printed or typed)
Protocol version date May 19 2009
Protocol Amendment 1 version date May 28 2010
Protocol Amendment 2 version date December 6 2011
68
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
13 References
1 Raghu G Brown KK Bradford WZ et al A placebo-controlled trial of interferon gamma-1b in patients with idiopathic pulmonary fibrosis N Engl J Med 2004350125-33 2 King TE Jr Safrin S Starko KM et al Analyses of efficacy end points in a controlled trial of interferon-gamma1b for idiopathic pulmonary fibrosis Chest 2005127171-7 3 Flaherty KR Thwaite EL Kazerooni EA et al Radiological versus histological diagnosis in UIP and NSIP survival implications Thorax 200358143-8 4 Wells AU Desai SR Rubens MB et al Idiopathic pulmonary fibrosis a composite physiologic index derived from disease extent observed by computed tomography Am J Respir Crit Care Med 2003167962-9 5 Raghu G Freudenberger TD Yang S et al High prevalence of abnormal acid gastroshyoesophageal reflux in idiopathic pulmonary fibrosis Eur Respir J 200627136-42 6 Kinnula VL Focus on antioxidant enzymes and antioxidant strategies in smoking related airway diseases Thorax 200560693-700 7 Coultas DB Zumwalt RE Black WC Sobonya RE The epidemiology of interstitial lung diseases Am J Respir Crit Care Med 1994150967-72 8 Raghu G Weycker D Edelsberg J Bradford WZ Oster G Incidence and prevalence of idiopathic pulmonary fibrosis Am J Respir Crit Care Med 2006174810-6 9 Olson AL Swigris JJ Lezotte DC Norris JM Wilson CG Brown KK Mortality from pulmonary fibrosis increased in the United States from 1992 to 2003 Am J Respir Crit Care Med 2007176277-84 10 Mannino DM Etzel RA Parrish RG Pulmonary fibrosis deaths in the United States 1979shy1991 An analysis of multiple-cause mortality data Am J Respir Crit Care Med 19961531548shy52 11 Hubbard R Johnston I Coultas DB Britton J Mortality rates from cryptogenic fibrosing alveolitis in seven countries Thorax 199651711-6 12 Johnston I Britton J Kinnear W Logan R Rising mortality from cryptogenic fibrosing alveolitis Bmj 19903011017-21 13 Raghu G Collard HR Egan JJ et al An official ATSERSJRSALAT statement idiopathic pulmonary fibrosis evidence-based guidelines for diagnosis and management Am J Respir Crit Care Med 2011183788-824 14 (USA) FDA FDA Public Health Advisory Interferon gamma-1b (marketed as Actimmune) In 2007 15 King TE Jr Pardo A Selman M Idiopathic pulmonary fibrosis Lancet 2011 16 Raghu G Brown KK Costabel U et al Treatment of idiopathic pulmonary fibrosis with etanercept an exploratory placebo-controlled trial Am J Respir Crit Care Med 2008178948shy55 17 Malouf MA Hopkins P Snell G Glanville AR An investigator-driven study of everolimus in surgical lung biopsy confirmed idiopathic pulmonary fibrosis Respirology 201116776-83 18 King TE Jr Behr J Brown KK et al BUILD-1 a randomized placebo-controlled trial of bosentan in idiopathic pulmonary fibrosis Am J Respir Crit Care Med 200817775-81 19 Richeldi L Costabel U Selman M et al Efficacy of a tyrosine kinase inhibitor in idiopathic pulmonary fibrosis N Engl J Med 20113651079-87
69
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
20 Borok Z Buhl R Grimes GJ et al Effect of glutathione aerosol on oxidant-antioxidant imbalance in idiopathic pulmonary fibrosis Lancet 1991338215-6 21 Meyer A Buhl R Magnussen H The effect of oral N-acetylcysteine on lung glutathione levels in idiopathic pulmonary fibrosis Eur Respir J 19947431-6 22 Behr J Maier K Degenkolb B Krombach F Vogelmeier C Antioxidative and clinical effects of high-dose N-acetylcysteine in fibrosing alveolitis Adjunctive therapy to maintenance immunosuppression Am J Respir Crit Care Med 19971561897-901 23 Cantin AM North SL Fells GA Hubbard RC Crystal RG Oxidant-mediated epithelial cell injury in idiopathic pulmonary fibrosis J Clin Invest 1987791665-73 24 Waghray M Cui Z Horowitz JC et al Hydrogen peroxide is a diffusible paracrine signal for the induction of epithelial cell death by activated myofibroblasts Faseb J 200519854-6 25 Larios JM Budhiraja R Fanburg BL Thannickal VJ Oxidative protein cross-linking reactions involving L-tyrosine in transforming growth factor-beta1-stimulated fibroblasts J Biol Chem 200127617437-41 26 Kinnula VL Fattman CL Tan RJ Oury TD Oxidative stress in pulmonary fibrosis a possible role for redox modulatory therapy Am J Respir Crit Care Med 2005172417-22 27 Meyer A Buhl R Kampf S Magnussen H Intravenous N-acetylcysteine and lung glutathione of patients with pulmonary fibrosis and normals Am J Respir Crit Care Med 19951521055-60 28 Behr J Degenkolb B Krombach F Vogelmeier C Intracellular glutathione and bronchoalveolar cells in fibrosing alveolitis effects of N-acetylcysteine Eur Respir J 200219906-11 29 Bando M Hosono T Mato N et al Long-term efficacy of inhaled N-acetylcysteine in patients with idiopathic pulmonary fibrosis Intern Med 2010492289-96 30 Demedts M Behr J Buhl R et al High-dose acetylcysteine in idiopathic pulmonary fibrosis N Engl J Med 20053532229-42 31 Toma TP Bhowmik A Rajakulasingam R Acetylcysteine in pulmonary fibrosis N Engl J Med 20063541086-9 author reply -9 32 Hunninghake GW Antioxidant therapy for idiopathic pulmonary fibrosis N Engl J Med 20053532285-7 33 Flaherty KR Mumford JA Murray S et al Prognostic implications of physiologic and radiographic changes in idiopathic interstitial pneumonia Am J Respir Crit Care Med 2003168543-8 34 Latsi PI du Bois RM Nicholson AG et al Fibrotic idiopathic interstitial pneumonia the prognostic value of longitudinal functional trends Am J Respir Crit Care Med 2003168531-7 35 Collard HR King TE Jr Bartelson BB Vourlekis JS Schwarz MI Brown KK Changes in clinical and physiologic variables predict survival in idiopathic pulmonary fibrosis Am J Respir Crit Care Med 2003168538-42 36 Jegal Y Kim DS Shim TS et al Physiology is a stronger predictor of survival than pathology in fibrotic interstitial pneumonia Am J Respir Crit Care Med 2005171639-44 37 Martinez FJ Safrin S Weycker D et al The clinical course of patients with idiopathic pulmonary fibrosis Ann Intern Med 2005142963-7 38 Hull JH Acetylcysteine in pulmonary fibrosis N Engl J Med 20063541089-91 author reply -91
70
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
39 Flaherty KR King TE Jr Raghu G et al Idiopathic interstitial pneumonia what is the effect of a multidisciplinary approach to diagnosis Am J Respir Crit Care Med 2004170904shy10 40 Raghu G Johnson WC Lockhart D Mageto Y Treatment of idiopathic pulmonary fibrosis with a new antifibrotic agent pirfenidone results of a prospective open-label Phase II study Am J Respir Crit Care Med 19991591061-9 41 Hunninghake GW Lynch DA Galvin JR et al Radiologic findings are strongly associated with a pathologic diagnosis of usual interstitial pneumonia Chest 20031241215-23 42 Lynch D Godwin J Safrin S et al High-resolution computed tomography in idiopathic pulmonary fibrosis diagnosis and prognosis Am J Respir Crit Care Med 2005172488-93 43 Mallinckrodt CH Watkin JG Molenberghs G Carroll RJ Choice of the primary analysis in longitudinal clinical trials Pharmaceutical Statistics 20043161-9 44 Bang H Tsiatis A Estimating medical costs with censored data Biometrika 200087329shy43 45 Lin DY Regression analysis of incomplete medical cost data Stat Med 2003221181-200 46 Rochon J Application of GEE procedures for sample size calculations in repeated measures experiments Stat Med 1998171643-58 47 Lachin JM Foulkes MA Evaluation of sample size and power for analyses of survival with allowance for nonuniform patient entry losses to follow-up noncompliance and stratification Biometrics 198642507-19
71
- PANTHER-IPFPREDNISONE AZATHIOPRINEAND N-ACETYLCYSTEINEA STUDY THAT EVALUATES RESPONSE INIDIOPATHIC PULMONARY FIBROSIS
-
- Protocol Summary
- Table of Contents
- List of Tables
- List of Figures
- List of Abbreviations
- 1 Summary
- 2 Hypotheses and Specific Aims
-
- 21 Null Hypothesis
- 22 Specific Aim 1
- 23 Specific Aim 2
- 24 Prespecified Subgroups of Interest
-
- 3 Background and Significance
-
- 31 Idiopathic Pulmonary Fibrosis is the Most Common Interstitial Lung Disease
- 32 Rationale for Placebo Control
- 33 Rationale for N-acetylcysteine
- 35 Rationale for N-acetylcysteine as a Stand-alone Therapy
- 36 Rationale for the Study Design and Primary Endpoint
- 37 Rationale for Blinding of Treatments
-
- 4 Methods
-
- 41 Inclusion Criteria
- 42 Diagnosis of IPF
- 43 Exclusion Criteria
- 44 Study Design and Study Visit
- 45 Dose Justification
- 46 Contraindications Precautions and Side Effects of Study Medications
- 47 Recruitment Procedures
- 48 Study Procedures
- 49 Concomitant Medications
- 410 Laboratory Testing
- 411 Blinding of Study Drugs
-
- 5 Study Endpoints
-
- 51 Primary Study Endpoint
- 52 Secondary Study Endpoints
-
- 6 Safety Evaluations and Procedures
-
- 61 Adverse Events
- 62 Clinical Medical Monitoring
- 63 Unblinding Procedures
-
- 7 Study Drug Procedures
- 8 Data Management
-
- 81 Hardware and Software Configuration
- 82 Sources of Data
-
- 9 Study Design and Data Analysis
-
- 91 General Analytic Considerations
- 92 Randomization Blinding and Reporting of Results
- 93 Stratification
- 94 Specification of the Primary Analyses
- 95 Analysis of Longitudinal Endpoints
- 96 Analysis of Binary Time-to-Event and Time-Lagged Endpoints
- 97 Power Analysis
-
- 10 Study Administration
-
- 101 Cooperative Agreement Mechanism
- 102 IPFnet Steering Group
- 103 Data and Safety Monitoring Board
- 104 Recommendations on Interim Monitoring of Efficacy Safety and Futility
-
- 11 Investigator and Sponsor Obligations
-
- 111 Monitoring
- 112 Cost and Payment
- 113 Confidentiality and Health Insurance Portability and Accountability ActConsiderations
- 114 Informed Consent Procedures
- 115 Institutional Review Boards
-
- 12 Investigator Agreement
- 13 References
-

34
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Table 3 Schedule of Assessments
Procedure Screening Visit 0
Enrollment Visit 1
Week 15 Visit 2
Week 30Visit 3
Week 45 Visit 4
Week 60 Early
Withdrawal Visit 5
Final1
Visit (via phone)
Informed consent X
Medical history X
Inclusionexclusion criteria X
Serum pregnancy test (if applicable) X X X X X
Review of lung biopsy X
Arterial Blood Gas X X
6-Minute Walk Test
X
X X
Physical examination X X X
Vital signs with oximetry X X X X X X
Body height and weight X X X X X X
Complete Blood Count X X X
Chemistry panel X X X
Monitor Lab Values X X X
Urinalysis X Specimen repository substudy blood draw and urine collection (if consented)
X
X X X X
HRCT (if not completed within three months) X
Spirometry (pre- and post-bronchodilator) X
Spirometry (post-bronchodilator only) X X X X X
DLCO (post-bronchodilator only) X X X
Lung volumes (post-bronchodilator only) X
X
Evaluate for acute exacerbation X X X X X
Review Adverse Events X X X X X X
Review concomitant meds X X X X X X
Dispense subject diary X X X X
Review subject diary X X X X X
Dispense study agent X X X X
Gender Substudy questionnaire (female subjects only) X
EuroQol ICECAP UCSD SOBQ SGRQ SF-36 X X X
Abbreviations DLCO diffusing capacity of the lung for carbon monoxide QOL Quality of Life ICECAP Investigating Choice Experiments for Preferences of Older People UCSD SOBQ University of California Shortness of Breath Questionnaire SGRQ St Georgersquos Respiratory Questionnaire SF-36 Short Form 36 Health Survey
1Follow-up visit via phone will occur four weeks after final dose of study medication
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
45 Dose Justification
The general philosophy for determining dosing levels was to apply previously examined
treatment regimens With the focus of the study being to establish a standard of care for
mildmoderate IPF subjects the goal was to develop flexible yet standardized treatment rules that
allow for the temporary or permanent withholding of one or more components of treatment when
necessary Subjects developing laboratory abnormalities or symptoms that result in
discontinuation of one or more components of study treatment may continue on the other
components as long as there is no contraindication for this Complete follow-up is important for
the validity of any study As a strategy to maintain protocol adherence we are using a treatment
regimen that will detect potential side effects and prompt interventions proactively in the interest
of patient safety In addition subjects who permanently stop study medications during the course
of the study are encouraged to continue in the study completing all scheduled visits and tests
451 Rationale for N-acetylcysteine Dosing
To our knowledge there have been no IPF studies to correlate clinical outcome measures with
different dosages for NAC The dosage chosen is based on the IFIGENIA study However BAL
lung GSH levels from subjects with IPF have been augmented with the use of oral NAC at 600
mg 3 times per day In addition lung GSH levels have been associated with improved
PFTs212227 The dose chosen for this study was based on previous data including the IFIGENIA
study30
4511 Dosing of N-acetylcysteineplacebo
Dosing of NACPL will be 600 mg orally 3 times a day (1800 mgday)
4512 Reasons to Discontinue N-acetylcysteineplacebo
NACPL may be temporarily or permanently discontinued for the duration of the study for
gastrointestinal symptoms or dermatologic reactions
35
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Temporarily discontinue (hold) oral NACPL for subjects requiring inpatient admission for acute
exacerbation (AEx) or other conditions Resume NACPL after discharge
36
37
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
452 Dosage Algorithms
Dosage Adjustment Algorithm 1 NACPL Dose Modifications for Gastrointestinal Symptoms Nausea Vomiting Abdominal Discomfort Diarrhea
GI Symptoms determined by the PI to be clinically significant Nausea Vomiting Abdominal Discomfort Diarrhea
NACPL Temporarily dc (HOLD) x 3 Days
Monitor symptoms intervene as clinically indicated (eg fluid replacement antidiarrhea or antinausea medication)
Monitor or lab PRN
Are symptoms resolving after 3 days NO
Symptoms NOT resolving after 3 days of holding study medication Assessmentmanagement per clinical
discretion of investigator
Likely not study medication discuss resuming study medication with medical monitor when symptoms resolved
YES
Temporarily dc (HOLD) NACPL for 4 additional days (total hold 1 week) then NACPL Resume 600 MG TID
Did symptoms recur
YES
STOP NACPL for
duration of study
NO
NACPL No Change
38
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Dosage Adjustment Algorithm 2 NACPL Dose Modifications For Dermatologic Reactions
Dermatologic Reactions (Not Acneiform) ge Grade 2 Grading per Common Terminology Criteria for
Adverse Events V30 (httpctepcancergov) For example Grade 1 RASHDESQUAMATION Macular or papular eruption or erythema without associated symptoms Grade 2 RASHDESQUAMATION Macular or popular eruption or erythema with pruritus or other associated symptoms localized desquamation or other lesions covering lt50 of body surface area
NACPL Temporarily dc (HOLD) x 3 days
Are symptoms resolving after 3 days
NO Symptoms not resolving after 3 days of holding study medication Assessmentmanagement per clinical discretion of investigator Likely not study medication Discuss resuming study medication with medical monitor when symptoms
resolved YES
Temporarily dc (HOLD) NACPL for 4 additional days (total hold 1 week) then NACPL resume 600 MG TID
Did symptoms recur
YES
STOP NACPL for
duration of study
NO
NACPL No change
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
46 Contraindications Precautions and Side Effects of Study Medications
461 Contraindication
Contraindication to NAC is known hypersensitivity to it
462 Precautions
Concomitant administration of oral NAC and antibiotics has shown a slightly reduced absorption
of cephalexin and a slight increase in erythromycin serum levels NAC contains free sulfhydryl
groups There is no evidence that individuals sensitive to sulfa drugs are sensitive to NAC
The NAC preparation being administered in this study contains 20 mg of aspartame Because of
the phenylalanine component of aspartame individuals with phenylketonuria should avoid or
restrict aspartame intake to avoid increased blood levels of phenylalanine Because of this risk
labeling is required on all products containing aspartame
463 Side Effects
Side effects of NAC range from common to serious See Table 4
39
40
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Table 4 Side Effects of NAC
Undesirable Effects
System-organ class Uncommon
(gt11000 lt1100)
Rare
(gt110000 lt11000)
Very rare
(lt110000) Not known
Immune system disorders Hypersensitivity Anaphylactic shock
reaction
Nervous system disorders Headache
Ear and labyrinth disorders Tinnitus
Cardiac disorders Tachycardia
Vascular disorders Hemorrhage
Respiratory thoracic and
mediastinal disorders
Bronchospasm
Dyspnea
Gastrointestinal disorders
Vomiting diarrhea
stomatitis abdominal
pain nausea
Dyspepsia
Skin and subcutaneous tissue
disorders
Urticaria rash
angioedema itching
General disorders and
administration site conditions Pyrexia
Investigations Reduced arterial
pressure Face edema
In very rare cases the onset of severe skin reactions such as Stevens-Johnson syndrome and Lyell syndrome was reported to have a temporal relationship with N-acetylcysteine administration Although in most cases at least another suspect drug probably most involved in the genesis of the above mentioned mucocutaneous syndromes has been identified in case of mucocutaneous alterations it is appropriate to contact onersquos doctor and the administration of N-acetylcysteine should be immediately discontinued
Some studies confirmed a reduction of platelet aggregation during N-acetylcysteine administration The clinical significance of these findings has not been defined yet [Source Fluimucil Investigator Brochure]
47 Recruitment Procedures
Subjects recruited for this study will be established patients of the investigators or physician- or
self-referred to participating clinical centers in the IPFnet Each clinical center within IPFnet has
a well-developed infrastructure of local pulmonologists within the surrounding geographic area
These pulmonologists are kept informed of ongoing IPF clinical trials and regularly refer
subjects to studies conducted at IPFnet clinical centers
Additional steps will be taken to inform clinicians of the trials in progress within IPFnet
including presentations at faculty staff meetings at local hospitals medical grand rounds and
national conferences direct mail notification monthly faxes and advertisement of network trials
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
in pulmonary journals Clinical center patients previously diagnosed with IPF will be notified of
the trials by mail whenever possible
Recruitment of minorities and women will be monitored by the DCC and DSMB If necessary
additional recruitment efforts will be made at specific centers to ensure that the aggregate subject
sample contains appropriate representation of women and minorities
48 Study Procedures
The following procedures are detailed in the PANTHER-IPF MOOP accompanying this
protocol
1 PFT
2 ABG
3 HRCT scan of the chest (including imaging of pulmonary arteries)
4 CBC and serum chemistries
5 Pregnancy test
6 6MWTBorg Dyspnea Scale
7 QOL questionnaires (EuroQol HAD SF-36 SGRQ and ICE CAP)
8 UCSD SOBQ
9 Gender Substudy Questionnaire
All assessments of PFTs will be conducted by study personnel not directly involved in the
treatment of the subjects
481 Biological Specimen Management
4811 Biological Specimen Sample Management
Subjects at clinical centers participating in the specimen repository substudy who consent to
having blood drawn for research purposes and for the banking of blood blood components and
other biologic specimens (urine and BAL fluid) will have approximately 405 mL of blood
41
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
drawn 17 mL blood drawn for DNA and 20 mL of urine collected at enrollment visit Subjects
will have approximately 50 mL of blood drawn and 20 mL of urine collected at each 15-week
follow-up visit Blood specimens will be separated according to PANTHER-IPF MOOP
guidelines into the following components for banking in the repository serum plasma and
DNA Coding of all biologic specimens for the repository will be performed by study staff at the
clinical center The samples will be processed per PANTHER-IPF MOOP guidelines aliquoted
labeled with barcode labels and stored at -70degC at the clinical center and shipped to the central
repository
The only subject identifiers will be a sample ID number and subject initials This sample ID will
be linked in the IPFnet DCC clinical database to subject information No subject information will
be transferred to the biological-specimen database
The subjectrsquos samples may be used for approved sub-studies relating to human disease
including but not limited to IPF The studies for which an individualrsquos samples will be made
available will be determined by the subjectrsquos answers to questions on the biological-sample
informed consent form The subjects can choose to make their samples available for all options
or any combination Samples will be made available to researchers only with IPFnet Steering
Group approval until such time as the samples are made public through the NHLBI repository
49 Concomitant Medications
Concurrent treatment with FDA-approved therapy for IPF is allowed Colchicine may be used
for treatment of gout Temporary treatment with oral or IV corticosteroids for clinical worsening
or suspected AEx is permitted Nutritional supplements containing NAC are not allowed
410 Laboratory Testing
Clinical laboratory parameters will be assessed at screening and at the end of the study The
following tests will be performed at the two time points specified in the protocol chemistry (AG
ratio ALT [SGPT] AST [SGOT] albumin alkaline phosphatase amylase bilirubin-direct
42
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
bilirubin-indirect bilirubin-total BUN BUNcreatinine ratio calcium carbon dioxide
cholesterol-total chloride CPK-total creatinine GGT globulin glucose iron-total LDH
lipase magnesium phosphorus-inorganic potassium protein-total sodium TIBC triglycerides
uric acid) and hematology (red blood cell count WBC count hemoglobin hematocrit cell
indices differential platelet count)
411 Blinding of Study Drugs
Subjects and caregivers will be blinded to study treatment Every subject will receive NAC or
matching PLs at every study visit from the baseline visit to the week-45 visit No study agent
will be dispensed at the week-60 visit
43
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
5 Study Endpoints
51 Primary Study Endpoint
The primary endpoint will be the change in serial measurements of FVC over the study period
52 Secondary Study Endpoints
521 Time to Disease-progression
The time-to-death or a 10 decline in FVC will be defined as the time-to-disease progression
The 10 decline in FVC from enrollment must be confirmed on 2 consecutive visits no less than
6 weeks apart For subjects with 2 consecutive visits with a 10 decline in FVC the time-toshy
disease progression will be defined as the time interval between enrollment and the initial visit
with a 10 FVC decline For subjects who experience disease progression the study doctor will
determine whether or not the subject will remain in the study
522 Acute Exacerbations
The following 3 criteria will define AEx in subjects with acute worsening of their respiratory
conditions
1 Clinical (all of the following required)
A) Unexplained worsening of dyspnea or cough within 30 days triggering unscheduled
medical care (eg emergency room clinic study visit hospitalization)
B) No clinical suspicion or overt evidence of cardiac event pulmonary embolism or deep
venous thrombosis to explain acute worsening of dyspnea
C) No pneumothorax
44
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
2 RadiologicPhysiologic (A and B required)
A) New ground glass opacity or consolidation computed tomography (CT) scan OR new
alveolar opacities on chest x-ray
B) Decline of ge 5 in resting room air SpO2 from last recorded level OR decline of ge 8 mm
Hg in resting room air PaO2 from last recorded level
3 Microbiologic (all of the following required)
A) No clinical evidence for infection (ie absence of grossly purulent sputum fever gt 39degC
orally)
B) Lack of positive microbiological results (if done) from lower respiratory tract defined as
(1) Clinically significant bacterial growth on sputum or endotracheal aspirate cultures
(2) Quantitative culture by protected brush specimen ge 103 cfumL or BAL ge 104 cfumL
(3) The presence of specific pathogens on stains of any of the above
C) Lack of positive pathogen in blood cultures (if done)
Identification of Acute Exacerbations
All subjects will be educated about the importance of identifying AExs At the time of
enrollment subjects will be told about the possibility of developing acute symptomatic
worsening that might represent an AEx of IPF and instructed to contact their study clinical
center coordinator within 48 to 72 hours of the apparent event
All subjects will be contacted by phone monthly and questioned about any change in dyspnea or
cough and any interim clinic visits or hospitalizations Finally as part of the IPFnet outreach to
community referring physicians the importance of AExs will be emphasized When a subject is
identified who meets criterion 1A this will trigger the collection of additional clinical data to
evaluate a suspected AEx These data will be collected as part of standard clinical care (ie this
protocol does not require collection of all items) The additional items to be collected for
suspected AEx include
IPFnet AEx case report form (eCRF) (required)
45
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Chest x-ray CT scan withwithout pulmonary angiogram (reports should be faxed and
followed by the hard copiesdiscs)
Oxygen saturation (pulse oximetry)
ABG
Respiratory cultures (sputum endotracheal aspirate lavage)
Blood cultures
Clinichospital records related to the event
All potential cases of AEx will be reviewed by the clinical center PI first and a decision on
whether the case may represent an AEx will be made If AEx is suspected the case will be sent
to the IPFnet adjudication committee which will assign a final diagnosis (see Table 5) If there is
disagreement among members the majority opinion will be recorded
During episodes of suspected AEx as determined by the individual clinical center investigator
subjects will remain blinded and in the study
Table 5 Final Diagnoses in Evaluation of Suspected Acute Exacerbations
Definite acute exacerbation All criteria met no alternative etiology
Unclassifiable acute worsening
Insufficient data to evaluate all criteria no alternative etiology
Not acute exacerbation Alternative etiology identified that explains acute worsening
Management of the suspected AEx will be at the discretion of the treating physician Standard of
care generally involves evaluation for respiratory infection pulmonary embolism cardiac events
and pneumothorax and treatment with IV corticosteroids
Study drugs will be resumed at pre-suspected AEx doses after subjects clinically improve as
confirmed by the local PI All subjects should be seen at the clinical center within 2 to 4 weeks
of recovery for measurement of post-bronchodilator FVC (see Figure 4) Subjects unable to
return to the clinical center after suspected AEx due to medical frailty (eg continued
46
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
institutionalization progressive disability) will be categorized as failing to maintain FVC
response in secondary analyses
Suspected AEx (PI determined)
Hold study drug Treat AEx
(Attending physician determined)
Alive but unable to continue due to
medical frailty
Dead
Alive and able to continue
Site reviewvisit
Restart study drug
FVC within 2-4 weeks
Figure 4 Acute Exacerbation Flow Chart
523 Respiratory Infections
An upper respiratory infection will be defined as
Change in sputum discoloration
Increased cough of no more than 14 daysrsquo duration
A lower-respiratory infection (pneumonia) will be defined as new segmental or lobar airspace
opacities visualized by image studies (chest radiograph or HRCT) in addition to any of the
following
Positive pathogencultures in good sample of sputum or lower-airway secretions retrieved
by fiberoptic bronchoscope
Fever gt 39degC or gt 100degF
Leukocytosis gt 12000 (unexplained no increase in dose of corticosteroids)
47
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
524 Maintained FVC Response
Subjects with follow-up FVCpred measurements at or above their baseline FVCpred level
will be classified as having maintained FVC response Subjects with reduced FVCpred levels
or missing data for any reason including death or medical frailty will be classified as having not
maintained FVC response The FVCpred value is used because unadjusted FVC measurements
are expected to decline with age
48
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
6 Safety Evaluations and Procedures
61 Adverse Events
During a clinical trial the reporting of adverse experience information can lead to important
changes in the way a new treatment is developed as well as provide integral safety data
611 Definitions
An adverse event (AE) is any untoward medical occurrence in a subject or clinical investigation
subject who was administered a pharmaceutical product The AE does not necessarily have to
have a causal relationship with the drug administered An AE can be any unfavorable and
unintended sign (including an abnormal laboratory finding) symptom or disease temporarily
associated with the use of a medicinal product whether or not considered to be related to the
medicinal product Diseases signs symptoms or laboratory abnormalities already existing at
enrollment are not considered AEs unless they worsen (ie increase in intensity or frequency)
Surgical procedures themselves are not AEs they are therapeutic measures for conditions that
require surgery The condition for which the surgery is required may be an AE Surgical
procedures planned before randomization and the conditions necessitating the surgery are not
AEs
A serious adverse event is any untoward event that
Is fatal
Is life-threatening
Requires inpatient hospitalization or prolongation of existing hospitalization with the
following exceptions
o Preplanned (before the study) hospital admissions unless the hospitalization is
prolonged
o Planned admissions (as part of a study eg routine biopsies)
o Hospitalization lasting lt 24 hours
49
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
o Hospitalization for elective procedure
o Emergency room visits
Results in persistent or significant disability or incapacity
Is a congenital anomaly or birth defect
Important medical events that may not result in death be life-threatening or require
inpatient hospitalization may be considered serious adverse events (SAEs) when based
on appropriate medical judgment they may jeopardize the subject and may require
medical or surgical intervention to prevent one of the outcomes listed above
Life-threatening means that the subject was in the view of the investigator at immediate risk of
death from the AE as it occurred It does not include an AE that had it occurred in a more severe
form might have caused death
Persistent or significant disabilityincapacity means that the event resulted in permanent or
significant and substantial disruption of the subjectrsquos ability to carry out normal life functions
Causality
A reasonable possibility means the AE may have been caused byrelated to the study drug A
perceived or real lack of efficacy does not satisfy the definition of relatedness
612 Adverse Event (AE) Reporting
For the PANTHER-IPF trial all AEs (serious and nonserious) occurring from randomization
through final study visit (4 weeks after final dose of all study medication) will be recorded on the
AE page of the case report form (CRF)
6121 Serious Adverse Events (SAE) Reporting
For this trial all deaths and all SAEs which occur from randomization through final study visit
must be entered within the EDC system via the SAE eCRF page within 24 hours of the
investigative sitersquos knowledge of the event It is the responsibility of the clinical center
50
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
investigator to provide a causality assessment of the event for each study medications based upon
the information available at the time of the report It is understood that complete information
about the event may not be known at the time the initial report is submitted In the event the EDC
system is not accessible to the site at the time of event reporting investigative sites will complete
and forward a paper back-up SAE form to DCRI Safety Surveillance for processing
DCRI Safety Surveillance
Telephone 1-919-668-8624 or 1-866-668-7799 (toll free)
Fax 1-919-668-7138 or 1-866-668-7138 (toll free)
The investigator must complete and submit follow-up SAE information via the eCRF when
important new or follow-up information (eg final diagnosis outcome results of specific
investigations) becomes available Follow-up information should be submitted according to the
same process used for reporting the initial event as described above All SAEs will be followed
until resolution stabilization or 30 days after the subject has completed the final visit (4 weeks
after the final dose of study medication) whichever occurs first The investigator is responsible
for reporting SAEs to their institutional review board (IRB) per site specific IRB reporting
guidelines
6122 Regulatory Reporting
AEs that are serious study drug related and unexpected will be reported to the regulatory
authorities The DCRI Safety Surveillance medical monitor will perform a medical review of all
SAEs submitted and evaluate for ldquounexpectednessrdquo DCRI Safety Surveillance will prepare
MedWatch reports for those events identified as serious study drug related and unexpected as
determined by Safety Medical Monitor
DCRI Regulatory Services will submit all unexpected study drug-related SAEs as per 21 CFR
32 DCRI Safety Surveillance will provide a safety alert letter to the NHLBI DSMB and DCC
clinical operation (for distribution to sites) within 15 days of initial receipt of the information
51
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Investigators are responsible for promptly reporting these events to their reviewing IRBs
according to site specific IRB reporting guidelines
62 Clinical Medical Monitoring
There will be an unblinded physician at the IPFnet DCC serving as medical monitor The
medical monitor will be available to assist with questions about dosage adjustments of study
medications including discontinuation or resumption of medications
63 Unblinding Procedures
Unblinding of subjects or investigators to subject treatment is strongly discouraged For ongoing
clinical management all subjects should be presumed to be receiving ldquoactiverdquo study drug To
ensure the subjectrsquos safety the study treatment will be dose-adjusted based on laboratory test
results clinical findings and symptoms
The IPFnet DCC medical monitor and PANTHER-IPF co-chairs Drs Ganesh Raghu and
Fernando Martinez will be available to the study physicians to discuss study drug management
on a case-by-case basis Un-blinding will be considered ONLY when the knowledge of subject
treatment assignment is ABSOLUTELY ESSENTIAL for subject safety and after discussion of
the subjectrsquos case with the medical monitor and either Dr Raghu or Dr Martinez Unblinding of
study treatment should be minimized during the conduct of the trial In those cases where it is
felt to be medically necessary the DCC medical officer will communicate directly with the
managing physician to minimize unblinding of study personnel
52
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
7 Study Drug Procedures
At the baseline 15-week 30-week and 45-week study visits subjects will receive a supply of
study drug sufficient to last until the next visit at which study drug will be dispensed
53
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
8 Data Management
81 Hardware and Software Configuration
811 Hardware and Database Software
Data will be stored in an Oracle database system Oracle has advantages of processing efficiency
and smooth linkage with other software systems The application and database will be hosted on
Solaris Unix servers at the IPFnet DCC
812 Statistical Software
SAS will be used as the principal application for the management of analysis data files and
statistical computations S-Plus will be used to provide supplementary functions as needed
813 Access Control and Confidentiality Procedures
Access to databases will be controlled centrally by the IPFnet DCC through user passwords
linked to appropriate privileges This protects the data from unauthorized changes and
inadvertent loss or damage
814 Security
Database and Web servers will be secured by a firewall and through controlled physical access
Oracle has many security features to ensure that any staff member accessing the database has the
proper authority to perform the functions he or she requests of the system Within the secondary
SAS databases Unix group-access control maintains similar security The Sun workstation login
is secured by extensive user-password facilities under Unix
54
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
815 Back-up Procedures
Database back-up will be performed automatically every day and standard IPFnet DCC policies
and procedures will be applied to dictate tape rotation and retention practices
816 Virus Protection
All disk drives that provide network services and all user computers will be protected using
virus-scanning software Standard IPFnet DCC policies will be applied to update these protection
systems periodically through the study
82 Sources of Data
821 Design and Development
The IPFnet DCC will be responsible for development of the electronic case report forms
(eCRFs) development and validation of the clinical study database ensuring data integrity and
training clinical center staff on applicable data management procedures A web-based distributed
data entry model will be implemented This system will be developed to ensure that guidelines
and regulations surrounding the use of computerized systems used in clinical trials are upheld
The remainder of this section provides an overview of the data management plan associated with
this protocol
822 Data Collection Forms
The data collection process consists of direct data entry at the study clinical centers into the EDC
system(s) provided by the DCC A data collection worksheet will be provided to clinical centers
for recording data in the event the EDC system is unavailable Data entry of the eCRFs should
be completed according to the instructions provided and project specific training The
investigator is responsible for maintaining accurate complete and up-to-date records and for
ensuring the completion of the eCRFs for each research participant
55
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
823 Data Acquisition and Entry
Data entry into eCRFs shall be performed by authorized individuals Selected eCRFs may also
require the investigatorrsquos written signature or electronic signature as appropriate Electronic
CRFs will be monitored for completeness accuracy and attention to detail during the study
824 Data Center Responsibilities
The IPFnet DCC will 1) develop a data management plan and will conduct data management
activities 2) provide final eCRFs for the collection of all data required by the study 3) develop
data dictionaries for each eCRF that will comprehensively define each data element 4) conduct
ongoing data monitoring activities on study data 5) monitor any preliminary analysis data
cleanup activities and 6) rigorously monitor final study data clean up
825 Data Editing
Completed data will be entered into the IPFnet DCC automated data acquisition and
management system If incomplete or inaccurate data are found a data clarification request will
be generated and distributed to clinical centers for a response Clinical centers will resolve data
inconsistencies and errors and enter all corrections and changes into the IPFnet DCC automated
data acquisition and management system
826 Training
The training plan for clinical center staff includes provisions for training on assessments eCRF
completion guidelines data management procedures and the use of computerized systems
56
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
9 Study Design and Data Analysis
91 General Analytic Considerations
All primary analyses will be based on intent-to-treat (ITT) principles using all randomized
subjects Baseline factors across groups will be compared using mean (standard deviation) and
median (25th and 75th percentiles) summary measures Kaplan-Meier curves will be used to
display event rates Due to clinical interest in departures from both sides of the null hypothesis
all test statistics will be 2-sided
Reasonable caution needs to be taken when conducting multiple analyses on key clinical
subgroups For subgroup analyses a conservative significance level of 0001 will be used for all
interaction tests Thus subgroup comparisons will be considered exploratory unless the p-value
from the interaction test is smaller than 0001
92 Randomization Blinding and Reporting of Results
A permuted block-randomization scheme will be created with varying block sizes stratified by
clinical center Once a subject has completed the screening and baseline period and evaluation
for inclusionexclusion criteria the randomization process will begin Subjects will be
randomized to receive NAC or matching placebo with equal probability (11) via telephone
contact with a central interactive voice response system (IVRS) using a toll-free randomization
number On the day of randomization after the subject has successfully met all inclusion and
exclusion criteria the investigator or designee will call the central randomization number to
obtain the assigned kit randomization numbers for that subject At each subject visit the
investigator or designee will call the central randomization number to obtain the new kit
randomization numbers for resupply of the subject For resupply of the clinical center the IVRS
will monitor minimal volume of a kit type andor expiration date and will automatically notify
the pharmacy
57
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
The trial results will be reported according to guidelines specified in the CONSORT statement
A flow diagram describing screening recruitment randomization dropout and vital status will
be included in the primary manuscript AEs and efficacy data will be presented for all treatment
groups Adherence dropout and lost to follow-up will be carefully examined across all treatment
groups Analyses of safety will be based on data from all randomized subjects who received at
least one dose of study drug
93 Stratification
Subjects will be distributed to the two treatment arms in a 11 allocation ratio Stratification
blocks will be based on clinical centers
94 Specification of the Primary Analyses
A mixed model repeated measures (MMRM) analysis described in section 95 will be used to
compare differences in the slope of FVC measurements across the treatment groups Response
variables are values of the FVC measured at baseline and every 15 weeks until study completion
Variables in the model will include treatment time and time by treatment age sex race and
height Contrast estimates of differences in slopes of treatment over time (along with confidence
intervals) will be used to estimate the treatment effect The validity of this model in terms of
meeting modeling assumptions will be assessed via standard modeling diagnostics and goodness-
of-fit measures Based on the MMRM framework missing FVC data will not be imputed for the
primary analysis
95 Analysis of Longitudinal Endpoints
A common goal in clinical trials is to specify models that are easily implemented and
reproducible by independent data analysts On the other hand the models should have proper
statistical behavior in terms of low bias and high precision Many common approaches to
longitudinal data analysis including last observation carried forward (LOCF) imputation rely on
the missing completely at random (MCAR) assumption However the MCAR assumption is
58
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
unlikely to hold in many clinical trials because missing data are often related to disease
progression and prognosis A more reasonable assumption missing at random (MAR) specifies
that the complete data distribution can be modeled using only the observed data The likelihood-
based MMRM approach is valid under the more general MAR assumptions These models will
be applied to analyze the longitudinal data secondary endpoints
The advantages of MMRM analysis are that all important characteristics of the model can be preshy
specified standard software can be used to implement the models and results are based on ITT
principles43 In addition the MMRM approach offers superior control of Type I and Type II
errors compared with the LOCF approach
Response variables are values of the PFTs measured at enrollment and every 15 weeks until
study completion and 6MWT values measured at baseline week 30 and week 60 Covariates are
treatment time time by treatment and key baseline risk factors Contrasts (along with
confidence intervals) of treatment by time will be used to estimate the treatment effect
The correlation structure involves multiple pieces including measurement errors random
variation and interindividual variability For the longitudinal data analyses an unstructured
correlation matrix for within-subject errors will be assumed Other correlation structures
including compound symmetry will be examined as needed A careful examination of reasons
for study discontinuation will be conducted to assess the validity of MCAR Sensitivity analyses
will be used to examine the untestable assumption that the observed data violate the MAR
assumption The MMRM models will be implemented using PROC MIXED in SAS
96 Analysis of Binary Time-to-Event and Time-Lagged Endpoints
Regression modeling approaches using either the logistic regression model or Cox proportional
hazards regression model will be employed when appropriate The validity of these models will
be assessed via standard modeling diagnostics and goodness-of-fit measures Estimates of
cumulative frequencies for more general time-lagged responses will be calculated using the
partitioned version of the Bang-Tsiatis estimator44 The partitions will be set at 15-week intervals
59
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
to correspond with the data-collection process Covariate adjusted event rates will be calculated
using inverse probability-weighted regression estimates45
97 Power Analysis
971 Primary Analyses
Based on previously published IPF clinical trials the PL group is expected to experience a drop
in FVC of approximately 020 L over the study period (see Figure 1) The IPFnet Steering Group
determined a clinically important difference would be to preserve the majority of the decline
relative to PL over the study period In particular a treatment effect of 015 L was determined to
be a clinically meaningful difference Potential dropout is a key factor in the proposed study The
drop-out process assumed 5 lost to follow-up after every study visit Only 80 of subjects
were assumed to be followed for the entire study period All models assumed a compound
symmetry structure for the covariance matrix Power calculations were performed using a SAS
IML program for designing repeated measures studies46 Based on preliminary reviews of the
data from the University of Michigan the covariance matrix parameters were estimated at
approximately σ2 = 0757 (variance parameter) and ρ = 0936 (correlation parameter) To be
conservative the power calculations for the primary analysis were performed with parameter
setting of σ2 = 0810 (variance parameter) and ρ = 0925 (correlation parameter)
The power calculations assume a correction for imperfect compliance proposed by Lachin and
Foulkes to allow for 2 noncompliance for each of the treatment arms47 Thus the sample size
of 130 subjects per arm would be reduced to an adjusted sample size of 130(1-002-002)2 =
1198 or 120 subjects per arm
Under the assumed Type I error rate of 005 with a correlation parameter of 0925 and standard
deviation of 090 the difference of 015 L (or 00025 Lweek) shown in Table 6 would have
power of 93
60
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Table 6 Hypothetical Values of Mean FVC (L) Change from Baseline
Week 15 Week 30 Week 45 Week 60
NAC 00125 00250 00375 00500
Placebo 00500 01000 01500 02000
Difference 00375 00750 01125 01500
Abbreviations FVC forced vital capacity PL placebo
972 Power Analysis for Secondary Endpoints
Power calculations for secondary endpoint measurements are shown in Table 7 Standard
deviations are based on unpublished data provided by the University of Michigan The
calculations are based on a 2-sample t-test with Type I error rate set at 005 These calculations
are likely to be conservative because the statistical approach described in section 95 for
analyzing these endpoints will incorporate incomplete observations as well as intermediate data
points
Table 7 Detectable Differences in Treatment Means for Selected Endpoint Measurements
Secondary Endpoints Std Dev
of the Baseline Score
Detectable Difference for 80 Power
Std Dev of the Change Score
Difference Detectable for
80 Power
DLCOpred 166 58 91 32
6MWT Area Under the Desaturation Curve
219 76 175 61
6MWT Distance to Desaturation 224 78 315 110
6MWT Minutes Walked 210 073 205 071
Abbreviations Std Dev standard deviation DLCOpred diffusing capacity of the lung for carbon monoxide percent predicted 6MWT 6-minute walk test
61
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
10 Study Administration
101 Cooperative Agreement Mechanism
The administrative and funding mechanism used to undertake this project is a ldquocooperative
agreementrdquo (U01) which is an assistance mechanism Under the cooperative agreement the
NHLBI assists supports andor stimulates the project and is substantially involved with
investigators in conducting the study by facilitating performance of the effort in a ldquopartnerrdquo role
The NHLBI project scientist serves on the IPFnet Steering Group and he or another NHLBI
scientist may serve on other project committees when appropriate At the same time however
NHLBI does not assume a dominant role direction or prime responsibility for this research
program
As described below governance of the project is conducted through the IPFnet Steering Group
Principal investigators have lead responsibilities in all aspects of their trials and the project
including any modification of trial designs conduct of the trials quality control data analysis
and interpretation preparation of publications and collaboration with other investigators unless
otherwise provided for by the IPFnet Steering Group
PIs retain custody of and have primary rights to their center-specific and collaborative data
subject to government rights-of-access consistent with current Health amp Human Services (HHS)
Public Health Service (PHS) and National Institutes of Health policies The protocols and
governance policies call for the continual submission of data centrally to the IPFnet DCC for the
collaborative database which at a minimum will contain the key variables selected by the IPFnet
Steering Group for standardization across all clinical centers the submission of copies of the
collaborative datasets to each PI upon completion of the project procedures for data analysis
reporting and publication and procedures to protect and ensure the privacy of medical and
genetic data and records of individuals The NHLBI project scientist on behalf of the NHLBI
will have the same access privileges and responsibilities regarding the collaborative data as the
other members of the Steering Group
62
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
PIs are also encouraged to publish and to publicly release and disseminate results data and other
products of the project concordant with the project protocols and governance and the approved
plan for making data and materials available to the scientific community and to the NHLBI
However during the 3 years after the ending date of NHLBI project support unpublished data
unpublished results data sets not previously released and other study materials or products are
to be made available to any third party only with the approval of the IPFnet Steering Group
Upon completion of the project PIs are expected to put their intervention materials and
procedure manuals into the public domain andor make them available to other investigators
according to the approved plan for making data and materials available to the scientific
community and the NHLBI for the conduct of research at no charge other than the costs of
reproduction and distribution
The NHLBI reserves the right to terminate or curtail the project (or an individual award) in the
event of (a) failure to develop or implement mutually agreeable collaborative measurement
subject eligibility and data management sections of the protocols (b) substantial shortfall in
subject recruitment follow-up data reporting or quality control or other major breach of
protocol (c) substantive changes in the agreed-upon protocols with which NHLBI cannot
concur (d) reaching a major project outcome with persuasive statistical significance
substantially before schedule or (e) human subject ethical issues that may dictate a premature
termination
Any disagreement that may arise in scientificprogrammatic matters (within the scope of the
award) between award recipients and the NHLBI may be brought to arbitration An arbitration
panel will be composed of 3 membersmdash1 selected by the IPFnet Steering Group (with the
NHLBI member not voting) or by the individual PI in the event of an individual disagreement a
second selected by NHLBI and the third selected by the other 2 members This special
arbitration procedure in no way affects the PIrsquos right to appeal an adverse action that is otherwise
appealable in accordance with the PHS regulations at 42 CFR part 50 Subpart D and HHS
63
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
regulation at 45 CFR part 16 or the rights of the NHLBI under applicable statutes regulations
and terms of the award
102 IPFnet Steering Group
The IPFnet Steering Group is the main governing body of the project It is composed of the PIs
of the clinical centers the PI of the DCC and the NHLBI project scientist The clinical centers
the IPFnet DCC and the NHLBI each have 1 vote on the IPFnet Steering Group All decisions
are determined by majority vote
All major scientific decisions are determined by the IPFnet Steering Group It assumes overall
responsibility for the design and conduct of the trial It appoints (and disbands) committees and
subcommittees as the need arises designs approves and implements the study protocols
oversees the development of the MOOP monitors subject recruitment and treatment delivery
evaluates data collection and management oversees quality assurance procedures and
implements changes and enhancements to the study as required It also has primary responsibility
for facilitating the conduct of the trials and reporting the projectrsquos results
103 Data and Safety Monitoring Board
The NHLBI will establish a DSMB in accordance with established policies (see
httpwwwnhlbinihgovfundingpoliciesdsmb_insthtm) to ensure data quality and subject
safety and to provide independent advice to the NHLBI regarding progress and the
appropriateness of study continuation
104 Recommendations on Interim Monitoring of Efficacy Safety and Futility
First and foremost the role of the DSMB will be to review subject safety and trial conduct at
periodic points during the study The DSMB may require analyses of the primary endpoint
results for comparing the benefit and risks of treatment strategies The benefit of collecting
additional data on key secondary endpoints with extended follow-up and establishing a robust
64
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
evidence base for determining a standard of care will need to be carefully considered before
early termination of one or more treatment arms After careful consideration the IPFnet Steering
Group recommends conservative thresholds for the early examinations of the safety and efficacy
data
The DSMB will be expected to meet approximately every 6 months until trial completion to
review safety and toxicity data The DSMB may recommend stopping the study based on these
reviews Because the DSMB could stop the trial for safety concerns as well as for a large
efficacy benefit there could be multiple opportunities to reject the null hypothesis (no difference
in event rates between the PL and NAC groups) A Bonferroni approximation will be applied
during the one planned interim analysis for efficacy
Before locking the database a statistical analysis plan (SAP) will be developed to provide
complete details on the statistical analysis The SAP will include the specifics for how and when
the DSMB will be notified for AEs The IPFnet DCC will deliver to the DSMB all FDA-defined
AEs at 3-month intervals The IPFnet DCC will prepare narrative SAE reports in real time for
DSMB review including recommendations and analysis of similar events for each SAE
submitted to the FDA
65
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
11 Investigator and Sponsor Obligations
111 Monitoring
All monitoring activities for US clinical centers will be performed in accordance with DCRI
standard operating procedures Information regarding the types of visits will be outlined in the
PANTHER-IPF MOOP
112 Cost and Payment
There will be no cost to subjects enrolled in this trial Study-related procedures will be paid for
by the IPFnet
Subjects may be eligible for reimbursement for travel to the clinical center Details of payment
will be explained to each subject during the consent process
113 Confidentiality and Health Insurance Portability and Accountability Act
Considerations
Subject confidentiality will be protected throughout the study All subject data will be kept
strictly confidential and no subject-identifying information will be released to anyone outside
the project Confidentiality will be assured through several mechanisms First each subject will
be assigned an anonymous study ID which will then be used on all study forms Second any
study forms blood samples and paper records that contain subject information (eg address lists
phone lists) will be kept at the clinical centers in secured locked areas coded by number Once
blood is collected there will be no subject identifiers placed on blood samplesmdashonly the study
ID number and the date of sample collection Third access to all subject data and information
including laboratory specimens will be restricted to authorized personnel In the case of
computerized data this restricted access will be assured through user logon IDs and password
protection
66
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
At the IPFnet DCC only authorized personnel will have access to the data files containing study
data Security will be assured through user logon IDs passwords and appropriate access
privileges All study subjects will be identified only by their IPFnet ID numbers and no personal
identifying information such as name address or Social Security number will be entered into
the IPFnet DCC database Any subject-specific data reported to the IPFnet Steering Group will
be identified only by the IPFnet ID number
Finally subjects will not be identified by name in any reports or publications nor will the data
be presented in such a way that the identity of individual subjects can be inferred Analysis files
created for further study by the scientific community will have no subject identifiers These data
files will be created in accordance with the Ancillary Studies and Publication Policy of the
IPFnet
114 Informed Consent Procedures
All IPFnet subjects will provide written informed consent using procedures reviewed and
approved by each clinical centerrsquos IRB Informed consent will be undertaken by study personnel
in-person with the subject The subject has the option of declining further participation in the
study at that point No further study procedures will be conducted until the signed documents
have been provided to the IPFnet clinical center
115 Institutional Review Boards
Before initiating this study the protocol clinical center-specific informed consent forms Health
Insurance Portability and Accountability Act (HIPAA) forms recruitment materials and other
relevant information will be reviewed by a properly constituted IRB at each participating clinical
center A copy of the signed and dated IRB approval at each clinical center will be retrieved prior
to or during the site initiation visit and archived at the IPFnet DCC Any amendments to the
protocol other than simple administrative and typographical changes must be approved by each
IRB before they are implemented The clinical centers will seek annual renewals of their IRB
approvals in accordance with local procedures
67
__________________________________________ ________________
__________________________________________
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
12 Investigator Agreement
I have read the foregoing protocol PANTHER-IPF and agree that it contains all necessary
details for carrying out this study I will conduct the study as outlined herein and will complete
the study within the time designated
I will provide copies of the protocol and all pertinent information to all individuals responsible to
me who assist in the conduct of this study I will discuss this material with them to ensure they
are fully informed regarding the drug and the conduct of the study
I will fulfill all responsibilities for submitting pertinent information to the local IRB if
applicable that is responsible for this study
I further agree that NHLBI andor DCRI will have access to any source documents from which
eCRF information may have been generated
Signature of Principal Investigator Date
Name of Principal Investigator (printed or typed)
Protocol version date May 19 2009
Protocol Amendment 1 version date May 28 2010
Protocol Amendment 2 version date December 6 2011
68
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
13 References
1 Raghu G Brown KK Bradford WZ et al A placebo-controlled trial of interferon gamma-1b in patients with idiopathic pulmonary fibrosis N Engl J Med 2004350125-33 2 King TE Jr Safrin S Starko KM et al Analyses of efficacy end points in a controlled trial of interferon-gamma1b for idiopathic pulmonary fibrosis Chest 2005127171-7 3 Flaherty KR Thwaite EL Kazerooni EA et al Radiological versus histological diagnosis in UIP and NSIP survival implications Thorax 200358143-8 4 Wells AU Desai SR Rubens MB et al Idiopathic pulmonary fibrosis a composite physiologic index derived from disease extent observed by computed tomography Am J Respir Crit Care Med 2003167962-9 5 Raghu G Freudenberger TD Yang S et al High prevalence of abnormal acid gastroshyoesophageal reflux in idiopathic pulmonary fibrosis Eur Respir J 200627136-42 6 Kinnula VL Focus on antioxidant enzymes and antioxidant strategies in smoking related airway diseases Thorax 200560693-700 7 Coultas DB Zumwalt RE Black WC Sobonya RE The epidemiology of interstitial lung diseases Am J Respir Crit Care Med 1994150967-72 8 Raghu G Weycker D Edelsberg J Bradford WZ Oster G Incidence and prevalence of idiopathic pulmonary fibrosis Am J Respir Crit Care Med 2006174810-6 9 Olson AL Swigris JJ Lezotte DC Norris JM Wilson CG Brown KK Mortality from pulmonary fibrosis increased in the United States from 1992 to 2003 Am J Respir Crit Care Med 2007176277-84 10 Mannino DM Etzel RA Parrish RG Pulmonary fibrosis deaths in the United States 1979shy1991 An analysis of multiple-cause mortality data Am J Respir Crit Care Med 19961531548shy52 11 Hubbard R Johnston I Coultas DB Britton J Mortality rates from cryptogenic fibrosing alveolitis in seven countries Thorax 199651711-6 12 Johnston I Britton J Kinnear W Logan R Rising mortality from cryptogenic fibrosing alveolitis Bmj 19903011017-21 13 Raghu G Collard HR Egan JJ et al An official ATSERSJRSALAT statement idiopathic pulmonary fibrosis evidence-based guidelines for diagnosis and management Am J Respir Crit Care Med 2011183788-824 14 (USA) FDA FDA Public Health Advisory Interferon gamma-1b (marketed as Actimmune) In 2007 15 King TE Jr Pardo A Selman M Idiopathic pulmonary fibrosis Lancet 2011 16 Raghu G Brown KK Costabel U et al Treatment of idiopathic pulmonary fibrosis with etanercept an exploratory placebo-controlled trial Am J Respir Crit Care Med 2008178948shy55 17 Malouf MA Hopkins P Snell G Glanville AR An investigator-driven study of everolimus in surgical lung biopsy confirmed idiopathic pulmonary fibrosis Respirology 201116776-83 18 King TE Jr Behr J Brown KK et al BUILD-1 a randomized placebo-controlled trial of bosentan in idiopathic pulmonary fibrosis Am J Respir Crit Care Med 200817775-81 19 Richeldi L Costabel U Selman M et al Efficacy of a tyrosine kinase inhibitor in idiopathic pulmonary fibrosis N Engl J Med 20113651079-87
69
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
20 Borok Z Buhl R Grimes GJ et al Effect of glutathione aerosol on oxidant-antioxidant imbalance in idiopathic pulmonary fibrosis Lancet 1991338215-6 21 Meyer A Buhl R Magnussen H The effect of oral N-acetylcysteine on lung glutathione levels in idiopathic pulmonary fibrosis Eur Respir J 19947431-6 22 Behr J Maier K Degenkolb B Krombach F Vogelmeier C Antioxidative and clinical effects of high-dose N-acetylcysteine in fibrosing alveolitis Adjunctive therapy to maintenance immunosuppression Am J Respir Crit Care Med 19971561897-901 23 Cantin AM North SL Fells GA Hubbard RC Crystal RG Oxidant-mediated epithelial cell injury in idiopathic pulmonary fibrosis J Clin Invest 1987791665-73 24 Waghray M Cui Z Horowitz JC et al Hydrogen peroxide is a diffusible paracrine signal for the induction of epithelial cell death by activated myofibroblasts Faseb J 200519854-6 25 Larios JM Budhiraja R Fanburg BL Thannickal VJ Oxidative protein cross-linking reactions involving L-tyrosine in transforming growth factor-beta1-stimulated fibroblasts J Biol Chem 200127617437-41 26 Kinnula VL Fattman CL Tan RJ Oury TD Oxidative stress in pulmonary fibrosis a possible role for redox modulatory therapy Am J Respir Crit Care Med 2005172417-22 27 Meyer A Buhl R Kampf S Magnussen H Intravenous N-acetylcysteine and lung glutathione of patients with pulmonary fibrosis and normals Am J Respir Crit Care Med 19951521055-60 28 Behr J Degenkolb B Krombach F Vogelmeier C Intracellular glutathione and bronchoalveolar cells in fibrosing alveolitis effects of N-acetylcysteine Eur Respir J 200219906-11 29 Bando M Hosono T Mato N et al Long-term efficacy of inhaled N-acetylcysteine in patients with idiopathic pulmonary fibrosis Intern Med 2010492289-96 30 Demedts M Behr J Buhl R et al High-dose acetylcysteine in idiopathic pulmonary fibrosis N Engl J Med 20053532229-42 31 Toma TP Bhowmik A Rajakulasingam R Acetylcysteine in pulmonary fibrosis N Engl J Med 20063541086-9 author reply -9 32 Hunninghake GW Antioxidant therapy for idiopathic pulmonary fibrosis N Engl J Med 20053532285-7 33 Flaherty KR Mumford JA Murray S et al Prognostic implications of physiologic and radiographic changes in idiopathic interstitial pneumonia Am J Respir Crit Care Med 2003168543-8 34 Latsi PI du Bois RM Nicholson AG et al Fibrotic idiopathic interstitial pneumonia the prognostic value of longitudinal functional trends Am J Respir Crit Care Med 2003168531-7 35 Collard HR King TE Jr Bartelson BB Vourlekis JS Schwarz MI Brown KK Changes in clinical and physiologic variables predict survival in idiopathic pulmonary fibrosis Am J Respir Crit Care Med 2003168538-42 36 Jegal Y Kim DS Shim TS et al Physiology is a stronger predictor of survival than pathology in fibrotic interstitial pneumonia Am J Respir Crit Care Med 2005171639-44 37 Martinez FJ Safrin S Weycker D et al The clinical course of patients with idiopathic pulmonary fibrosis Ann Intern Med 2005142963-7 38 Hull JH Acetylcysteine in pulmonary fibrosis N Engl J Med 20063541089-91 author reply -91
70
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
39 Flaherty KR King TE Jr Raghu G et al Idiopathic interstitial pneumonia what is the effect of a multidisciplinary approach to diagnosis Am J Respir Crit Care Med 2004170904shy10 40 Raghu G Johnson WC Lockhart D Mageto Y Treatment of idiopathic pulmonary fibrosis with a new antifibrotic agent pirfenidone results of a prospective open-label Phase II study Am J Respir Crit Care Med 19991591061-9 41 Hunninghake GW Lynch DA Galvin JR et al Radiologic findings are strongly associated with a pathologic diagnosis of usual interstitial pneumonia Chest 20031241215-23 42 Lynch D Godwin J Safrin S et al High-resolution computed tomography in idiopathic pulmonary fibrosis diagnosis and prognosis Am J Respir Crit Care Med 2005172488-93 43 Mallinckrodt CH Watkin JG Molenberghs G Carroll RJ Choice of the primary analysis in longitudinal clinical trials Pharmaceutical Statistics 20043161-9 44 Bang H Tsiatis A Estimating medical costs with censored data Biometrika 200087329shy43 45 Lin DY Regression analysis of incomplete medical cost data Stat Med 2003221181-200 46 Rochon J Application of GEE procedures for sample size calculations in repeated measures experiments Stat Med 1998171643-58 47 Lachin JM Foulkes MA Evaluation of sample size and power for analyses of survival with allowance for nonuniform patient entry losses to follow-up noncompliance and stratification Biometrics 198642507-19
71
- PANTHER-IPFPREDNISONE AZATHIOPRINEAND N-ACETYLCYSTEINEA STUDY THAT EVALUATES RESPONSE INIDIOPATHIC PULMONARY FIBROSIS
-
- Protocol Summary
- Table of Contents
- List of Tables
- List of Figures
- List of Abbreviations
- 1 Summary
- 2 Hypotheses and Specific Aims
-
- 21 Null Hypothesis
- 22 Specific Aim 1
- 23 Specific Aim 2
- 24 Prespecified Subgroups of Interest
-
- 3 Background and Significance
-
- 31 Idiopathic Pulmonary Fibrosis is the Most Common Interstitial Lung Disease
- 32 Rationale for Placebo Control
- 33 Rationale for N-acetylcysteine
- 35 Rationale for N-acetylcysteine as a Stand-alone Therapy
- 36 Rationale for the Study Design and Primary Endpoint
- 37 Rationale for Blinding of Treatments
-
- 4 Methods
-
- 41 Inclusion Criteria
- 42 Diagnosis of IPF
- 43 Exclusion Criteria
- 44 Study Design and Study Visit
- 45 Dose Justification
- 46 Contraindications Precautions and Side Effects of Study Medications
- 47 Recruitment Procedures
- 48 Study Procedures
- 49 Concomitant Medications
- 410 Laboratory Testing
- 411 Blinding of Study Drugs
-
- 5 Study Endpoints
-
- 51 Primary Study Endpoint
- 52 Secondary Study Endpoints
-
- 6 Safety Evaluations and Procedures
-
- 61 Adverse Events
- 62 Clinical Medical Monitoring
- 63 Unblinding Procedures
-
- 7 Study Drug Procedures
- 8 Data Management
-
- 81 Hardware and Software Configuration
- 82 Sources of Data
-
- 9 Study Design and Data Analysis
-
- 91 General Analytic Considerations
- 92 Randomization Blinding and Reporting of Results
- 93 Stratification
- 94 Specification of the Primary Analyses
- 95 Analysis of Longitudinal Endpoints
- 96 Analysis of Binary Time-to-Event and Time-Lagged Endpoints
- 97 Power Analysis
-
- 10 Study Administration
-
- 101 Cooperative Agreement Mechanism
- 102 IPFnet Steering Group
- 103 Data and Safety Monitoring Board
- 104 Recommendations on Interim Monitoring of Efficacy Safety and Futility
-
- 11 Investigator and Sponsor Obligations
-
- 111 Monitoring
- 112 Cost and Payment
- 113 Confidentiality and Health Insurance Portability and Accountability ActConsiderations
- 114 Informed Consent Procedures
- 115 Institutional Review Boards
-
- 12 Investigator Agreement
- 13 References
-
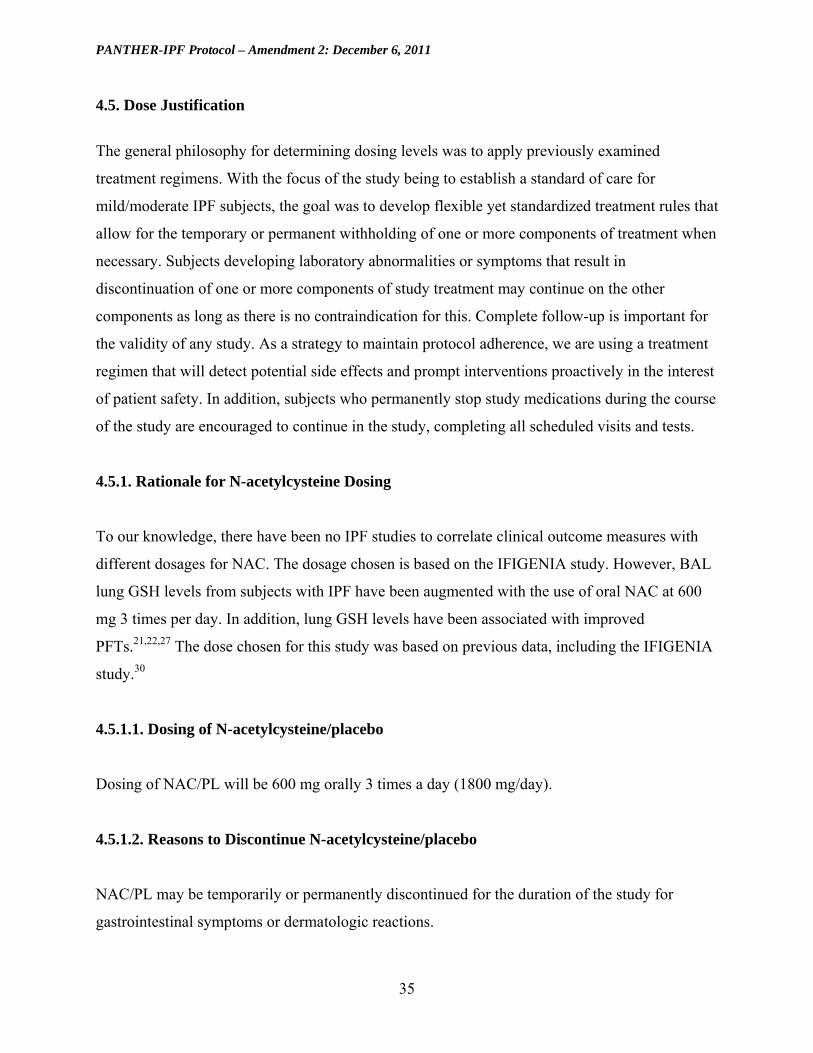
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
45 Dose Justification
The general philosophy for determining dosing levels was to apply previously examined
treatment regimens With the focus of the study being to establish a standard of care for
mildmoderate IPF subjects the goal was to develop flexible yet standardized treatment rules that
allow for the temporary or permanent withholding of one or more components of treatment when
necessary Subjects developing laboratory abnormalities or symptoms that result in
discontinuation of one or more components of study treatment may continue on the other
components as long as there is no contraindication for this Complete follow-up is important for
the validity of any study As a strategy to maintain protocol adherence we are using a treatment
regimen that will detect potential side effects and prompt interventions proactively in the interest
of patient safety In addition subjects who permanently stop study medications during the course
of the study are encouraged to continue in the study completing all scheduled visits and tests
451 Rationale for N-acetylcysteine Dosing
To our knowledge there have been no IPF studies to correlate clinical outcome measures with
different dosages for NAC The dosage chosen is based on the IFIGENIA study However BAL
lung GSH levels from subjects with IPF have been augmented with the use of oral NAC at 600
mg 3 times per day In addition lung GSH levels have been associated with improved
PFTs212227 The dose chosen for this study was based on previous data including the IFIGENIA
study30
4511 Dosing of N-acetylcysteineplacebo
Dosing of NACPL will be 600 mg orally 3 times a day (1800 mgday)
4512 Reasons to Discontinue N-acetylcysteineplacebo
NACPL may be temporarily or permanently discontinued for the duration of the study for
gastrointestinal symptoms or dermatologic reactions
35
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Temporarily discontinue (hold) oral NACPL for subjects requiring inpatient admission for acute
exacerbation (AEx) or other conditions Resume NACPL after discharge
36
37
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
452 Dosage Algorithms
Dosage Adjustment Algorithm 1 NACPL Dose Modifications for Gastrointestinal Symptoms Nausea Vomiting Abdominal Discomfort Diarrhea
GI Symptoms determined by the PI to be clinically significant Nausea Vomiting Abdominal Discomfort Diarrhea
NACPL Temporarily dc (HOLD) x 3 Days
Monitor symptoms intervene as clinically indicated (eg fluid replacement antidiarrhea or antinausea medication)
Monitor or lab PRN
Are symptoms resolving after 3 days NO
Symptoms NOT resolving after 3 days of holding study medication Assessmentmanagement per clinical
discretion of investigator
Likely not study medication discuss resuming study medication with medical monitor when symptoms resolved
YES
Temporarily dc (HOLD) NACPL for 4 additional days (total hold 1 week) then NACPL Resume 600 MG TID
Did symptoms recur
YES
STOP NACPL for
duration of study
NO
NACPL No Change
38
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Dosage Adjustment Algorithm 2 NACPL Dose Modifications For Dermatologic Reactions
Dermatologic Reactions (Not Acneiform) ge Grade 2 Grading per Common Terminology Criteria for
Adverse Events V30 (httpctepcancergov) For example Grade 1 RASHDESQUAMATION Macular or papular eruption or erythema without associated symptoms Grade 2 RASHDESQUAMATION Macular or popular eruption or erythema with pruritus or other associated symptoms localized desquamation or other lesions covering lt50 of body surface area
NACPL Temporarily dc (HOLD) x 3 days
Are symptoms resolving after 3 days
NO Symptoms not resolving after 3 days of holding study medication Assessmentmanagement per clinical discretion of investigator Likely not study medication Discuss resuming study medication with medical monitor when symptoms
resolved YES
Temporarily dc (HOLD) NACPL for 4 additional days (total hold 1 week) then NACPL resume 600 MG TID
Did symptoms recur
YES
STOP NACPL for
duration of study
NO
NACPL No change
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
46 Contraindications Precautions and Side Effects of Study Medications
461 Contraindication
Contraindication to NAC is known hypersensitivity to it
462 Precautions
Concomitant administration of oral NAC and antibiotics has shown a slightly reduced absorption
of cephalexin and a slight increase in erythromycin serum levels NAC contains free sulfhydryl
groups There is no evidence that individuals sensitive to sulfa drugs are sensitive to NAC
The NAC preparation being administered in this study contains 20 mg of aspartame Because of
the phenylalanine component of aspartame individuals with phenylketonuria should avoid or
restrict aspartame intake to avoid increased blood levels of phenylalanine Because of this risk
labeling is required on all products containing aspartame
463 Side Effects
Side effects of NAC range from common to serious See Table 4
39
40
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Table 4 Side Effects of NAC
Undesirable Effects
System-organ class Uncommon
(gt11000 lt1100)
Rare
(gt110000 lt11000)
Very rare
(lt110000) Not known
Immune system disorders Hypersensitivity Anaphylactic shock
reaction
Nervous system disorders Headache
Ear and labyrinth disorders Tinnitus
Cardiac disorders Tachycardia
Vascular disorders Hemorrhage
Respiratory thoracic and
mediastinal disorders
Bronchospasm
Dyspnea
Gastrointestinal disorders
Vomiting diarrhea
stomatitis abdominal
pain nausea
Dyspepsia
Skin and subcutaneous tissue
disorders
Urticaria rash
angioedema itching
General disorders and
administration site conditions Pyrexia
Investigations Reduced arterial
pressure Face edema
In very rare cases the onset of severe skin reactions such as Stevens-Johnson syndrome and Lyell syndrome was reported to have a temporal relationship with N-acetylcysteine administration Although in most cases at least another suspect drug probably most involved in the genesis of the above mentioned mucocutaneous syndromes has been identified in case of mucocutaneous alterations it is appropriate to contact onersquos doctor and the administration of N-acetylcysteine should be immediately discontinued
Some studies confirmed a reduction of platelet aggregation during N-acetylcysteine administration The clinical significance of these findings has not been defined yet [Source Fluimucil Investigator Brochure]
47 Recruitment Procedures
Subjects recruited for this study will be established patients of the investigators or physician- or
self-referred to participating clinical centers in the IPFnet Each clinical center within IPFnet has
a well-developed infrastructure of local pulmonologists within the surrounding geographic area
These pulmonologists are kept informed of ongoing IPF clinical trials and regularly refer
subjects to studies conducted at IPFnet clinical centers
Additional steps will be taken to inform clinicians of the trials in progress within IPFnet
including presentations at faculty staff meetings at local hospitals medical grand rounds and
national conferences direct mail notification monthly faxes and advertisement of network trials
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
in pulmonary journals Clinical center patients previously diagnosed with IPF will be notified of
the trials by mail whenever possible
Recruitment of minorities and women will be monitored by the DCC and DSMB If necessary
additional recruitment efforts will be made at specific centers to ensure that the aggregate subject
sample contains appropriate representation of women and minorities
48 Study Procedures
The following procedures are detailed in the PANTHER-IPF MOOP accompanying this
protocol
1 PFT
2 ABG
3 HRCT scan of the chest (including imaging of pulmonary arteries)
4 CBC and serum chemistries
5 Pregnancy test
6 6MWTBorg Dyspnea Scale
7 QOL questionnaires (EuroQol HAD SF-36 SGRQ and ICE CAP)
8 UCSD SOBQ
9 Gender Substudy Questionnaire
All assessments of PFTs will be conducted by study personnel not directly involved in the
treatment of the subjects
481 Biological Specimen Management
4811 Biological Specimen Sample Management
Subjects at clinical centers participating in the specimen repository substudy who consent to
having blood drawn for research purposes and for the banking of blood blood components and
other biologic specimens (urine and BAL fluid) will have approximately 405 mL of blood
41
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
drawn 17 mL blood drawn for DNA and 20 mL of urine collected at enrollment visit Subjects
will have approximately 50 mL of blood drawn and 20 mL of urine collected at each 15-week
follow-up visit Blood specimens will be separated according to PANTHER-IPF MOOP
guidelines into the following components for banking in the repository serum plasma and
DNA Coding of all biologic specimens for the repository will be performed by study staff at the
clinical center The samples will be processed per PANTHER-IPF MOOP guidelines aliquoted
labeled with barcode labels and stored at -70degC at the clinical center and shipped to the central
repository
The only subject identifiers will be a sample ID number and subject initials This sample ID will
be linked in the IPFnet DCC clinical database to subject information No subject information will
be transferred to the biological-specimen database
The subjectrsquos samples may be used for approved sub-studies relating to human disease
including but not limited to IPF The studies for which an individualrsquos samples will be made
available will be determined by the subjectrsquos answers to questions on the biological-sample
informed consent form The subjects can choose to make their samples available for all options
or any combination Samples will be made available to researchers only with IPFnet Steering
Group approval until such time as the samples are made public through the NHLBI repository
49 Concomitant Medications
Concurrent treatment with FDA-approved therapy for IPF is allowed Colchicine may be used
for treatment of gout Temporary treatment with oral or IV corticosteroids for clinical worsening
or suspected AEx is permitted Nutritional supplements containing NAC are not allowed
410 Laboratory Testing
Clinical laboratory parameters will be assessed at screening and at the end of the study The
following tests will be performed at the two time points specified in the protocol chemistry (AG
ratio ALT [SGPT] AST [SGOT] albumin alkaline phosphatase amylase bilirubin-direct
42
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
bilirubin-indirect bilirubin-total BUN BUNcreatinine ratio calcium carbon dioxide
cholesterol-total chloride CPK-total creatinine GGT globulin glucose iron-total LDH
lipase magnesium phosphorus-inorganic potassium protein-total sodium TIBC triglycerides
uric acid) and hematology (red blood cell count WBC count hemoglobin hematocrit cell
indices differential platelet count)
411 Blinding of Study Drugs
Subjects and caregivers will be blinded to study treatment Every subject will receive NAC or
matching PLs at every study visit from the baseline visit to the week-45 visit No study agent
will be dispensed at the week-60 visit
43
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
5 Study Endpoints
51 Primary Study Endpoint
The primary endpoint will be the change in serial measurements of FVC over the study period
52 Secondary Study Endpoints
521 Time to Disease-progression
The time-to-death or a 10 decline in FVC will be defined as the time-to-disease progression
The 10 decline in FVC from enrollment must be confirmed on 2 consecutive visits no less than
6 weeks apart For subjects with 2 consecutive visits with a 10 decline in FVC the time-toshy
disease progression will be defined as the time interval between enrollment and the initial visit
with a 10 FVC decline For subjects who experience disease progression the study doctor will
determine whether or not the subject will remain in the study
522 Acute Exacerbations
The following 3 criteria will define AEx in subjects with acute worsening of their respiratory
conditions
1 Clinical (all of the following required)
A) Unexplained worsening of dyspnea or cough within 30 days triggering unscheduled
medical care (eg emergency room clinic study visit hospitalization)
B) No clinical suspicion or overt evidence of cardiac event pulmonary embolism or deep
venous thrombosis to explain acute worsening of dyspnea
C) No pneumothorax
44
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
2 RadiologicPhysiologic (A and B required)
A) New ground glass opacity or consolidation computed tomography (CT) scan OR new
alveolar opacities on chest x-ray
B) Decline of ge 5 in resting room air SpO2 from last recorded level OR decline of ge 8 mm
Hg in resting room air PaO2 from last recorded level
3 Microbiologic (all of the following required)
A) No clinical evidence for infection (ie absence of grossly purulent sputum fever gt 39degC
orally)
B) Lack of positive microbiological results (if done) from lower respiratory tract defined as
(1) Clinically significant bacterial growth on sputum or endotracheal aspirate cultures
(2) Quantitative culture by protected brush specimen ge 103 cfumL or BAL ge 104 cfumL
(3) The presence of specific pathogens on stains of any of the above
C) Lack of positive pathogen in blood cultures (if done)
Identification of Acute Exacerbations
All subjects will be educated about the importance of identifying AExs At the time of
enrollment subjects will be told about the possibility of developing acute symptomatic
worsening that might represent an AEx of IPF and instructed to contact their study clinical
center coordinator within 48 to 72 hours of the apparent event
All subjects will be contacted by phone monthly and questioned about any change in dyspnea or
cough and any interim clinic visits or hospitalizations Finally as part of the IPFnet outreach to
community referring physicians the importance of AExs will be emphasized When a subject is
identified who meets criterion 1A this will trigger the collection of additional clinical data to
evaluate a suspected AEx These data will be collected as part of standard clinical care (ie this
protocol does not require collection of all items) The additional items to be collected for
suspected AEx include
IPFnet AEx case report form (eCRF) (required)
45
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Chest x-ray CT scan withwithout pulmonary angiogram (reports should be faxed and
followed by the hard copiesdiscs)
Oxygen saturation (pulse oximetry)
ABG
Respiratory cultures (sputum endotracheal aspirate lavage)
Blood cultures
Clinichospital records related to the event
All potential cases of AEx will be reviewed by the clinical center PI first and a decision on
whether the case may represent an AEx will be made If AEx is suspected the case will be sent
to the IPFnet adjudication committee which will assign a final diagnosis (see Table 5) If there is
disagreement among members the majority opinion will be recorded
During episodes of suspected AEx as determined by the individual clinical center investigator
subjects will remain blinded and in the study
Table 5 Final Diagnoses in Evaluation of Suspected Acute Exacerbations
Definite acute exacerbation All criteria met no alternative etiology
Unclassifiable acute worsening
Insufficient data to evaluate all criteria no alternative etiology
Not acute exacerbation Alternative etiology identified that explains acute worsening
Management of the suspected AEx will be at the discretion of the treating physician Standard of
care generally involves evaluation for respiratory infection pulmonary embolism cardiac events
and pneumothorax and treatment with IV corticosteroids
Study drugs will be resumed at pre-suspected AEx doses after subjects clinically improve as
confirmed by the local PI All subjects should be seen at the clinical center within 2 to 4 weeks
of recovery for measurement of post-bronchodilator FVC (see Figure 4) Subjects unable to
return to the clinical center after suspected AEx due to medical frailty (eg continued
46
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
institutionalization progressive disability) will be categorized as failing to maintain FVC
response in secondary analyses
Suspected AEx (PI determined)
Hold study drug Treat AEx
(Attending physician determined)
Alive but unable to continue due to
medical frailty
Dead
Alive and able to continue
Site reviewvisit
Restart study drug
FVC within 2-4 weeks
Figure 4 Acute Exacerbation Flow Chart
523 Respiratory Infections
An upper respiratory infection will be defined as
Change in sputum discoloration
Increased cough of no more than 14 daysrsquo duration
A lower-respiratory infection (pneumonia) will be defined as new segmental or lobar airspace
opacities visualized by image studies (chest radiograph or HRCT) in addition to any of the
following
Positive pathogencultures in good sample of sputum or lower-airway secretions retrieved
by fiberoptic bronchoscope
Fever gt 39degC or gt 100degF
Leukocytosis gt 12000 (unexplained no increase in dose of corticosteroids)
47
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
524 Maintained FVC Response
Subjects with follow-up FVCpred measurements at or above their baseline FVCpred level
will be classified as having maintained FVC response Subjects with reduced FVCpred levels
or missing data for any reason including death or medical frailty will be classified as having not
maintained FVC response The FVCpred value is used because unadjusted FVC measurements
are expected to decline with age
48
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
6 Safety Evaluations and Procedures
61 Adverse Events
During a clinical trial the reporting of adverse experience information can lead to important
changes in the way a new treatment is developed as well as provide integral safety data
611 Definitions
An adverse event (AE) is any untoward medical occurrence in a subject or clinical investigation
subject who was administered a pharmaceutical product The AE does not necessarily have to
have a causal relationship with the drug administered An AE can be any unfavorable and
unintended sign (including an abnormal laboratory finding) symptom or disease temporarily
associated with the use of a medicinal product whether or not considered to be related to the
medicinal product Diseases signs symptoms or laboratory abnormalities already existing at
enrollment are not considered AEs unless they worsen (ie increase in intensity or frequency)
Surgical procedures themselves are not AEs they are therapeutic measures for conditions that
require surgery The condition for which the surgery is required may be an AE Surgical
procedures planned before randomization and the conditions necessitating the surgery are not
AEs
A serious adverse event is any untoward event that
Is fatal
Is life-threatening
Requires inpatient hospitalization or prolongation of existing hospitalization with the
following exceptions
o Preplanned (before the study) hospital admissions unless the hospitalization is
prolonged
o Planned admissions (as part of a study eg routine biopsies)
o Hospitalization lasting lt 24 hours
49
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
o Hospitalization for elective procedure
o Emergency room visits
Results in persistent or significant disability or incapacity
Is a congenital anomaly or birth defect
Important medical events that may not result in death be life-threatening or require
inpatient hospitalization may be considered serious adverse events (SAEs) when based
on appropriate medical judgment they may jeopardize the subject and may require
medical or surgical intervention to prevent one of the outcomes listed above
Life-threatening means that the subject was in the view of the investigator at immediate risk of
death from the AE as it occurred It does not include an AE that had it occurred in a more severe
form might have caused death
Persistent or significant disabilityincapacity means that the event resulted in permanent or
significant and substantial disruption of the subjectrsquos ability to carry out normal life functions
Causality
A reasonable possibility means the AE may have been caused byrelated to the study drug A
perceived or real lack of efficacy does not satisfy the definition of relatedness
612 Adverse Event (AE) Reporting
For the PANTHER-IPF trial all AEs (serious and nonserious) occurring from randomization
through final study visit (4 weeks after final dose of all study medication) will be recorded on the
AE page of the case report form (CRF)
6121 Serious Adverse Events (SAE) Reporting
For this trial all deaths and all SAEs which occur from randomization through final study visit
must be entered within the EDC system via the SAE eCRF page within 24 hours of the
investigative sitersquos knowledge of the event It is the responsibility of the clinical center
50
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
investigator to provide a causality assessment of the event for each study medications based upon
the information available at the time of the report It is understood that complete information
about the event may not be known at the time the initial report is submitted In the event the EDC
system is not accessible to the site at the time of event reporting investigative sites will complete
and forward a paper back-up SAE form to DCRI Safety Surveillance for processing
DCRI Safety Surveillance
Telephone 1-919-668-8624 or 1-866-668-7799 (toll free)
Fax 1-919-668-7138 or 1-866-668-7138 (toll free)
The investigator must complete and submit follow-up SAE information via the eCRF when
important new or follow-up information (eg final diagnosis outcome results of specific
investigations) becomes available Follow-up information should be submitted according to the
same process used for reporting the initial event as described above All SAEs will be followed
until resolution stabilization or 30 days after the subject has completed the final visit (4 weeks
after the final dose of study medication) whichever occurs first The investigator is responsible
for reporting SAEs to their institutional review board (IRB) per site specific IRB reporting
guidelines
6122 Regulatory Reporting
AEs that are serious study drug related and unexpected will be reported to the regulatory
authorities The DCRI Safety Surveillance medical monitor will perform a medical review of all
SAEs submitted and evaluate for ldquounexpectednessrdquo DCRI Safety Surveillance will prepare
MedWatch reports for those events identified as serious study drug related and unexpected as
determined by Safety Medical Monitor
DCRI Regulatory Services will submit all unexpected study drug-related SAEs as per 21 CFR
32 DCRI Safety Surveillance will provide a safety alert letter to the NHLBI DSMB and DCC
clinical operation (for distribution to sites) within 15 days of initial receipt of the information
51
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Investigators are responsible for promptly reporting these events to their reviewing IRBs
according to site specific IRB reporting guidelines
62 Clinical Medical Monitoring
There will be an unblinded physician at the IPFnet DCC serving as medical monitor The
medical monitor will be available to assist with questions about dosage adjustments of study
medications including discontinuation or resumption of medications
63 Unblinding Procedures
Unblinding of subjects or investigators to subject treatment is strongly discouraged For ongoing
clinical management all subjects should be presumed to be receiving ldquoactiverdquo study drug To
ensure the subjectrsquos safety the study treatment will be dose-adjusted based on laboratory test
results clinical findings and symptoms
The IPFnet DCC medical monitor and PANTHER-IPF co-chairs Drs Ganesh Raghu and
Fernando Martinez will be available to the study physicians to discuss study drug management
on a case-by-case basis Un-blinding will be considered ONLY when the knowledge of subject
treatment assignment is ABSOLUTELY ESSENTIAL for subject safety and after discussion of
the subjectrsquos case with the medical monitor and either Dr Raghu or Dr Martinez Unblinding of
study treatment should be minimized during the conduct of the trial In those cases where it is
felt to be medically necessary the DCC medical officer will communicate directly with the
managing physician to minimize unblinding of study personnel
52
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
7 Study Drug Procedures
At the baseline 15-week 30-week and 45-week study visits subjects will receive a supply of
study drug sufficient to last until the next visit at which study drug will be dispensed
53
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
8 Data Management
81 Hardware and Software Configuration
811 Hardware and Database Software
Data will be stored in an Oracle database system Oracle has advantages of processing efficiency
and smooth linkage with other software systems The application and database will be hosted on
Solaris Unix servers at the IPFnet DCC
812 Statistical Software
SAS will be used as the principal application for the management of analysis data files and
statistical computations S-Plus will be used to provide supplementary functions as needed
813 Access Control and Confidentiality Procedures
Access to databases will be controlled centrally by the IPFnet DCC through user passwords
linked to appropriate privileges This protects the data from unauthorized changes and
inadvertent loss or damage
814 Security
Database and Web servers will be secured by a firewall and through controlled physical access
Oracle has many security features to ensure that any staff member accessing the database has the
proper authority to perform the functions he or she requests of the system Within the secondary
SAS databases Unix group-access control maintains similar security The Sun workstation login
is secured by extensive user-password facilities under Unix
54
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
815 Back-up Procedures
Database back-up will be performed automatically every day and standard IPFnet DCC policies
and procedures will be applied to dictate tape rotation and retention practices
816 Virus Protection
All disk drives that provide network services and all user computers will be protected using
virus-scanning software Standard IPFnet DCC policies will be applied to update these protection
systems periodically through the study
82 Sources of Data
821 Design and Development
The IPFnet DCC will be responsible for development of the electronic case report forms
(eCRFs) development and validation of the clinical study database ensuring data integrity and
training clinical center staff on applicable data management procedures A web-based distributed
data entry model will be implemented This system will be developed to ensure that guidelines
and regulations surrounding the use of computerized systems used in clinical trials are upheld
The remainder of this section provides an overview of the data management plan associated with
this protocol
822 Data Collection Forms
The data collection process consists of direct data entry at the study clinical centers into the EDC
system(s) provided by the DCC A data collection worksheet will be provided to clinical centers
for recording data in the event the EDC system is unavailable Data entry of the eCRFs should
be completed according to the instructions provided and project specific training The
investigator is responsible for maintaining accurate complete and up-to-date records and for
ensuring the completion of the eCRFs for each research participant
55
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
823 Data Acquisition and Entry
Data entry into eCRFs shall be performed by authorized individuals Selected eCRFs may also
require the investigatorrsquos written signature or electronic signature as appropriate Electronic
CRFs will be monitored for completeness accuracy and attention to detail during the study
824 Data Center Responsibilities
The IPFnet DCC will 1) develop a data management plan and will conduct data management
activities 2) provide final eCRFs for the collection of all data required by the study 3) develop
data dictionaries for each eCRF that will comprehensively define each data element 4) conduct
ongoing data monitoring activities on study data 5) monitor any preliminary analysis data
cleanup activities and 6) rigorously monitor final study data clean up
825 Data Editing
Completed data will be entered into the IPFnet DCC automated data acquisition and
management system If incomplete or inaccurate data are found a data clarification request will
be generated and distributed to clinical centers for a response Clinical centers will resolve data
inconsistencies and errors and enter all corrections and changes into the IPFnet DCC automated
data acquisition and management system
826 Training
The training plan for clinical center staff includes provisions for training on assessments eCRF
completion guidelines data management procedures and the use of computerized systems
56
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
9 Study Design and Data Analysis
91 General Analytic Considerations
All primary analyses will be based on intent-to-treat (ITT) principles using all randomized
subjects Baseline factors across groups will be compared using mean (standard deviation) and
median (25th and 75th percentiles) summary measures Kaplan-Meier curves will be used to
display event rates Due to clinical interest in departures from both sides of the null hypothesis
all test statistics will be 2-sided
Reasonable caution needs to be taken when conducting multiple analyses on key clinical
subgroups For subgroup analyses a conservative significance level of 0001 will be used for all
interaction tests Thus subgroup comparisons will be considered exploratory unless the p-value
from the interaction test is smaller than 0001
92 Randomization Blinding and Reporting of Results
A permuted block-randomization scheme will be created with varying block sizes stratified by
clinical center Once a subject has completed the screening and baseline period and evaluation
for inclusionexclusion criteria the randomization process will begin Subjects will be
randomized to receive NAC or matching placebo with equal probability (11) via telephone
contact with a central interactive voice response system (IVRS) using a toll-free randomization
number On the day of randomization after the subject has successfully met all inclusion and
exclusion criteria the investigator or designee will call the central randomization number to
obtain the assigned kit randomization numbers for that subject At each subject visit the
investigator or designee will call the central randomization number to obtain the new kit
randomization numbers for resupply of the subject For resupply of the clinical center the IVRS
will monitor minimal volume of a kit type andor expiration date and will automatically notify
the pharmacy
57
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
The trial results will be reported according to guidelines specified in the CONSORT statement
A flow diagram describing screening recruitment randomization dropout and vital status will
be included in the primary manuscript AEs and efficacy data will be presented for all treatment
groups Adherence dropout and lost to follow-up will be carefully examined across all treatment
groups Analyses of safety will be based on data from all randomized subjects who received at
least one dose of study drug
93 Stratification
Subjects will be distributed to the two treatment arms in a 11 allocation ratio Stratification
blocks will be based on clinical centers
94 Specification of the Primary Analyses
A mixed model repeated measures (MMRM) analysis described in section 95 will be used to
compare differences in the slope of FVC measurements across the treatment groups Response
variables are values of the FVC measured at baseline and every 15 weeks until study completion
Variables in the model will include treatment time and time by treatment age sex race and
height Contrast estimates of differences in slopes of treatment over time (along with confidence
intervals) will be used to estimate the treatment effect The validity of this model in terms of
meeting modeling assumptions will be assessed via standard modeling diagnostics and goodness-
of-fit measures Based on the MMRM framework missing FVC data will not be imputed for the
primary analysis
95 Analysis of Longitudinal Endpoints
A common goal in clinical trials is to specify models that are easily implemented and
reproducible by independent data analysts On the other hand the models should have proper
statistical behavior in terms of low bias and high precision Many common approaches to
longitudinal data analysis including last observation carried forward (LOCF) imputation rely on
the missing completely at random (MCAR) assumption However the MCAR assumption is
58
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
unlikely to hold in many clinical trials because missing data are often related to disease
progression and prognosis A more reasonable assumption missing at random (MAR) specifies
that the complete data distribution can be modeled using only the observed data The likelihood-
based MMRM approach is valid under the more general MAR assumptions These models will
be applied to analyze the longitudinal data secondary endpoints
The advantages of MMRM analysis are that all important characteristics of the model can be preshy
specified standard software can be used to implement the models and results are based on ITT
principles43 In addition the MMRM approach offers superior control of Type I and Type II
errors compared with the LOCF approach
Response variables are values of the PFTs measured at enrollment and every 15 weeks until
study completion and 6MWT values measured at baseline week 30 and week 60 Covariates are
treatment time time by treatment and key baseline risk factors Contrasts (along with
confidence intervals) of treatment by time will be used to estimate the treatment effect
The correlation structure involves multiple pieces including measurement errors random
variation and interindividual variability For the longitudinal data analyses an unstructured
correlation matrix for within-subject errors will be assumed Other correlation structures
including compound symmetry will be examined as needed A careful examination of reasons
for study discontinuation will be conducted to assess the validity of MCAR Sensitivity analyses
will be used to examine the untestable assumption that the observed data violate the MAR
assumption The MMRM models will be implemented using PROC MIXED in SAS
96 Analysis of Binary Time-to-Event and Time-Lagged Endpoints
Regression modeling approaches using either the logistic regression model or Cox proportional
hazards regression model will be employed when appropriate The validity of these models will
be assessed via standard modeling diagnostics and goodness-of-fit measures Estimates of
cumulative frequencies for more general time-lagged responses will be calculated using the
partitioned version of the Bang-Tsiatis estimator44 The partitions will be set at 15-week intervals
59
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
to correspond with the data-collection process Covariate adjusted event rates will be calculated
using inverse probability-weighted regression estimates45
97 Power Analysis
971 Primary Analyses
Based on previously published IPF clinical trials the PL group is expected to experience a drop
in FVC of approximately 020 L over the study period (see Figure 1) The IPFnet Steering Group
determined a clinically important difference would be to preserve the majority of the decline
relative to PL over the study period In particular a treatment effect of 015 L was determined to
be a clinically meaningful difference Potential dropout is a key factor in the proposed study The
drop-out process assumed 5 lost to follow-up after every study visit Only 80 of subjects
were assumed to be followed for the entire study period All models assumed a compound
symmetry structure for the covariance matrix Power calculations were performed using a SAS
IML program for designing repeated measures studies46 Based on preliminary reviews of the
data from the University of Michigan the covariance matrix parameters were estimated at
approximately σ2 = 0757 (variance parameter) and ρ = 0936 (correlation parameter) To be
conservative the power calculations for the primary analysis were performed with parameter
setting of σ2 = 0810 (variance parameter) and ρ = 0925 (correlation parameter)
The power calculations assume a correction for imperfect compliance proposed by Lachin and
Foulkes to allow for 2 noncompliance for each of the treatment arms47 Thus the sample size
of 130 subjects per arm would be reduced to an adjusted sample size of 130(1-002-002)2 =
1198 or 120 subjects per arm
Under the assumed Type I error rate of 005 with a correlation parameter of 0925 and standard
deviation of 090 the difference of 015 L (or 00025 Lweek) shown in Table 6 would have
power of 93
60
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Table 6 Hypothetical Values of Mean FVC (L) Change from Baseline
Week 15 Week 30 Week 45 Week 60
NAC 00125 00250 00375 00500
Placebo 00500 01000 01500 02000
Difference 00375 00750 01125 01500
Abbreviations FVC forced vital capacity PL placebo
972 Power Analysis for Secondary Endpoints
Power calculations for secondary endpoint measurements are shown in Table 7 Standard
deviations are based on unpublished data provided by the University of Michigan The
calculations are based on a 2-sample t-test with Type I error rate set at 005 These calculations
are likely to be conservative because the statistical approach described in section 95 for
analyzing these endpoints will incorporate incomplete observations as well as intermediate data
points
Table 7 Detectable Differences in Treatment Means for Selected Endpoint Measurements
Secondary Endpoints Std Dev
of the Baseline Score
Detectable Difference for 80 Power
Std Dev of the Change Score
Difference Detectable for
80 Power
DLCOpred 166 58 91 32
6MWT Area Under the Desaturation Curve
219 76 175 61
6MWT Distance to Desaturation 224 78 315 110
6MWT Minutes Walked 210 073 205 071
Abbreviations Std Dev standard deviation DLCOpred diffusing capacity of the lung for carbon monoxide percent predicted 6MWT 6-minute walk test
61
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
10 Study Administration
101 Cooperative Agreement Mechanism
The administrative and funding mechanism used to undertake this project is a ldquocooperative
agreementrdquo (U01) which is an assistance mechanism Under the cooperative agreement the
NHLBI assists supports andor stimulates the project and is substantially involved with
investigators in conducting the study by facilitating performance of the effort in a ldquopartnerrdquo role
The NHLBI project scientist serves on the IPFnet Steering Group and he or another NHLBI
scientist may serve on other project committees when appropriate At the same time however
NHLBI does not assume a dominant role direction or prime responsibility for this research
program
As described below governance of the project is conducted through the IPFnet Steering Group
Principal investigators have lead responsibilities in all aspects of their trials and the project
including any modification of trial designs conduct of the trials quality control data analysis
and interpretation preparation of publications and collaboration with other investigators unless
otherwise provided for by the IPFnet Steering Group
PIs retain custody of and have primary rights to their center-specific and collaborative data
subject to government rights-of-access consistent with current Health amp Human Services (HHS)
Public Health Service (PHS) and National Institutes of Health policies The protocols and
governance policies call for the continual submission of data centrally to the IPFnet DCC for the
collaborative database which at a minimum will contain the key variables selected by the IPFnet
Steering Group for standardization across all clinical centers the submission of copies of the
collaborative datasets to each PI upon completion of the project procedures for data analysis
reporting and publication and procedures to protect and ensure the privacy of medical and
genetic data and records of individuals The NHLBI project scientist on behalf of the NHLBI
will have the same access privileges and responsibilities regarding the collaborative data as the
other members of the Steering Group
62
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
PIs are also encouraged to publish and to publicly release and disseminate results data and other
products of the project concordant with the project protocols and governance and the approved
plan for making data and materials available to the scientific community and to the NHLBI
However during the 3 years after the ending date of NHLBI project support unpublished data
unpublished results data sets not previously released and other study materials or products are
to be made available to any third party only with the approval of the IPFnet Steering Group
Upon completion of the project PIs are expected to put their intervention materials and
procedure manuals into the public domain andor make them available to other investigators
according to the approved plan for making data and materials available to the scientific
community and the NHLBI for the conduct of research at no charge other than the costs of
reproduction and distribution
The NHLBI reserves the right to terminate or curtail the project (or an individual award) in the
event of (a) failure to develop or implement mutually agreeable collaborative measurement
subject eligibility and data management sections of the protocols (b) substantial shortfall in
subject recruitment follow-up data reporting or quality control or other major breach of
protocol (c) substantive changes in the agreed-upon protocols with which NHLBI cannot
concur (d) reaching a major project outcome with persuasive statistical significance
substantially before schedule or (e) human subject ethical issues that may dictate a premature
termination
Any disagreement that may arise in scientificprogrammatic matters (within the scope of the
award) between award recipients and the NHLBI may be brought to arbitration An arbitration
panel will be composed of 3 membersmdash1 selected by the IPFnet Steering Group (with the
NHLBI member not voting) or by the individual PI in the event of an individual disagreement a
second selected by NHLBI and the third selected by the other 2 members This special
arbitration procedure in no way affects the PIrsquos right to appeal an adverse action that is otherwise
appealable in accordance with the PHS regulations at 42 CFR part 50 Subpart D and HHS
63
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
regulation at 45 CFR part 16 or the rights of the NHLBI under applicable statutes regulations
and terms of the award
102 IPFnet Steering Group
The IPFnet Steering Group is the main governing body of the project It is composed of the PIs
of the clinical centers the PI of the DCC and the NHLBI project scientist The clinical centers
the IPFnet DCC and the NHLBI each have 1 vote on the IPFnet Steering Group All decisions
are determined by majority vote
All major scientific decisions are determined by the IPFnet Steering Group It assumes overall
responsibility for the design and conduct of the trial It appoints (and disbands) committees and
subcommittees as the need arises designs approves and implements the study protocols
oversees the development of the MOOP monitors subject recruitment and treatment delivery
evaluates data collection and management oversees quality assurance procedures and
implements changes and enhancements to the study as required It also has primary responsibility
for facilitating the conduct of the trials and reporting the projectrsquos results
103 Data and Safety Monitoring Board
The NHLBI will establish a DSMB in accordance with established policies (see
httpwwwnhlbinihgovfundingpoliciesdsmb_insthtm) to ensure data quality and subject
safety and to provide independent advice to the NHLBI regarding progress and the
appropriateness of study continuation
104 Recommendations on Interim Monitoring of Efficacy Safety and Futility
First and foremost the role of the DSMB will be to review subject safety and trial conduct at
periodic points during the study The DSMB may require analyses of the primary endpoint
results for comparing the benefit and risks of treatment strategies The benefit of collecting
additional data on key secondary endpoints with extended follow-up and establishing a robust
64
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
evidence base for determining a standard of care will need to be carefully considered before
early termination of one or more treatment arms After careful consideration the IPFnet Steering
Group recommends conservative thresholds for the early examinations of the safety and efficacy
data
The DSMB will be expected to meet approximately every 6 months until trial completion to
review safety and toxicity data The DSMB may recommend stopping the study based on these
reviews Because the DSMB could stop the trial for safety concerns as well as for a large
efficacy benefit there could be multiple opportunities to reject the null hypothesis (no difference
in event rates between the PL and NAC groups) A Bonferroni approximation will be applied
during the one planned interim analysis for efficacy
Before locking the database a statistical analysis plan (SAP) will be developed to provide
complete details on the statistical analysis The SAP will include the specifics for how and when
the DSMB will be notified for AEs The IPFnet DCC will deliver to the DSMB all FDA-defined
AEs at 3-month intervals The IPFnet DCC will prepare narrative SAE reports in real time for
DSMB review including recommendations and analysis of similar events for each SAE
submitted to the FDA
65
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
11 Investigator and Sponsor Obligations
111 Monitoring
All monitoring activities for US clinical centers will be performed in accordance with DCRI
standard operating procedures Information regarding the types of visits will be outlined in the
PANTHER-IPF MOOP
112 Cost and Payment
There will be no cost to subjects enrolled in this trial Study-related procedures will be paid for
by the IPFnet
Subjects may be eligible for reimbursement for travel to the clinical center Details of payment
will be explained to each subject during the consent process
113 Confidentiality and Health Insurance Portability and Accountability Act
Considerations
Subject confidentiality will be protected throughout the study All subject data will be kept
strictly confidential and no subject-identifying information will be released to anyone outside
the project Confidentiality will be assured through several mechanisms First each subject will
be assigned an anonymous study ID which will then be used on all study forms Second any
study forms blood samples and paper records that contain subject information (eg address lists
phone lists) will be kept at the clinical centers in secured locked areas coded by number Once
blood is collected there will be no subject identifiers placed on blood samplesmdashonly the study
ID number and the date of sample collection Third access to all subject data and information
including laboratory specimens will be restricted to authorized personnel In the case of
computerized data this restricted access will be assured through user logon IDs and password
protection
66
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
At the IPFnet DCC only authorized personnel will have access to the data files containing study
data Security will be assured through user logon IDs passwords and appropriate access
privileges All study subjects will be identified only by their IPFnet ID numbers and no personal
identifying information such as name address or Social Security number will be entered into
the IPFnet DCC database Any subject-specific data reported to the IPFnet Steering Group will
be identified only by the IPFnet ID number
Finally subjects will not be identified by name in any reports or publications nor will the data
be presented in such a way that the identity of individual subjects can be inferred Analysis files
created for further study by the scientific community will have no subject identifiers These data
files will be created in accordance with the Ancillary Studies and Publication Policy of the
IPFnet
114 Informed Consent Procedures
All IPFnet subjects will provide written informed consent using procedures reviewed and
approved by each clinical centerrsquos IRB Informed consent will be undertaken by study personnel
in-person with the subject The subject has the option of declining further participation in the
study at that point No further study procedures will be conducted until the signed documents
have been provided to the IPFnet clinical center
115 Institutional Review Boards
Before initiating this study the protocol clinical center-specific informed consent forms Health
Insurance Portability and Accountability Act (HIPAA) forms recruitment materials and other
relevant information will be reviewed by a properly constituted IRB at each participating clinical
center A copy of the signed and dated IRB approval at each clinical center will be retrieved prior
to or during the site initiation visit and archived at the IPFnet DCC Any amendments to the
protocol other than simple administrative and typographical changes must be approved by each
IRB before they are implemented The clinical centers will seek annual renewals of their IRB
approvals in accordance with local procedures
67
__________________________________________ ________________
__________________________________________
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
12 Investigator Agreement
I have read the foregoing protocol PANTHER-IPF and agree that it contains all necessary
details for carrying out this study I will conduct the study as outlined herein and will complete
the study within the time designated
I will provide copies of the protocol and all pertinent information to all individuals responsible to
me who assist in the conduct of this study I will discuss this material with them to ensure they
are fully informed regarding the drug and the conduct of the study
I will fulfill all responsibilities for submitting pertinent information to the local IRB if
applicable that is responsible for this study
I further agree that NHLBI andor DCRI will have access to any source documents from which
eCRF information may have been generated
Signature of Principal Investigator Date
Name of Principal Investigator (printed or typed)
Protocol version date May 19 2009
Protocol Amendment 1 version date May 28 2010
Protocol Amendment 2 version date December 6 2011
68
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
13 References
1 Raghu G Brown KK Bradford WZ et al A placebo-controlled trial of interferon gamma-1b in patients with idiopathic pulmonary fibrosis N Engl J Med 2004350125-33 2 King TE Jr Safrin S Starko KM et al Analyses of efficacy end points in a controlled trial of interferon-gamma1b for idiopathic pulmonary fibrosis Chest 2005127171-7 3 Flaherty KR Thwaite EL Kazerooni EA et al Radiological versus histological diagnosis in UIP and NSIP survival implications Thorax 200358143-8 4 Wells AU Desai SR Rubens MB et al Idiopathic pulmonary fibrosis a composite physiologic index derived from disease extent observed by computed tomography Am J Respir Crit Care Med 2003167962-9 5 Raghu G Freudenberger TD Yang S et al High prevalence of abnormal acid gastroshyoesophageal reflux in idiopathic pulmonary fibrosis Eur Respir J 200627136-42 6 Kinnula VL Focus on antioxidant enzymes and antioxidant strategies in smoking related airway diseases Thorax 200560693-700 7 Coultas DB Zumwalt RE Black WC Sobonya RE The epidemiology of interstitial lung diseases Am J Respir Crit Care Med 1994150967-72 8 Raghu G Weycker D Edelsberg J Bradford WZ Oster G Incidence and prevalence of idiopathic pulmonary fibrosis Am J Respir Crit Care Med 2006174810-6 9 Olson AL Swigris JJ Lezotte DC Norris JM Wilson CG Brown KK Mortality from pulmonary fibrosis increased in the United States from 1992 to 2003 Am J Respir Crit Care Med 2007176277-84 10 Mannino DM Etzel RA Parrish RG Pulmonary fibrosis deaths in the United States 1979shy1991 An analysis of multiple-cause mortality data Am J Respir Crit Care Med 19961531548shy52 11 Hubbard R Johnston I Coultas DB Britton J Mortality rates from cryptogenic fibrosing alveolitis in seven countries Thorax 199651711-6 12 Johnston I Britton J Kinnear W Logan R Rising mortality from cryptogenic fibrosing alveolitis Bmj 19903011017-21 13 Raghu G Collard HR Egan JJ et al An official ATSERSJRSALAT statement idiopathic pulmonary fibrosis evidence-based guidelines for diagnosis and management Am J Respir Crit Care Med 2011183788-824 14 (USA) FDA FDA Public Health Advisory Interferon gamma-1b (marketed as Actimmune) In 2007 15 King TE Jr Pardo A Selman M Idiopathic pulmonary fibrosis Lancet 2011 16 Raghu G Brown KK Costabel U et al Treatment of idiopathic pulmonary fibrosis with etanercept an exploratory placebo-controlled trial Am J Respir Crit Care Med 2008178948shy55 17 Malouf MA Hopkins P Snell G Glanville AR An investigator-driven study of everolimus in surgical lung biopsy confirmed idiopathic pulmonary fibrosis Respirology 201116776-83 18 King TE Jr Behr J Brown KK et al BUILD-1 a randomized placebo-controlled trial of bosentan in idiopathic pulmonary fibrosis Am J Respir Crit Care Med 200817775-81 19 Richeldi L Costabel U Selman M et al Efficacy of a tyrosine kinase inhibitor in idiopathic pulmonary fibrosis N Engl J Med 20113651079-87
69
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
20 Borok Z Buhl R Grimes GJ et al Effect of glutathione aerosol on oxidant-antioxidant imbalance in idiopathic pulmonary fibrosis Lancet 1991338215-6 21 Meyer A Buhl R Magnussen H The effect of oral N-acetylcysteine on lung glutathione levels in idiopathic pulmonary fibrosis Eur Respir J 19947431-6 22 Behr J Maier K Degenkolb B Krombach F Vogelmeier C Antioxidative and clinical effects of high-dose N-acetylcysteine in fibrosing alveolitis Adjunctive therapy to maintenance immunosuppression Am J Respir Crit Care Med 19971561897-901 23 Cantin AM North SL Fells GA Hubbard RC Crystal RG Oxidant-mediated epithelial cell injury in idiopathic pulmonary fibrosis J Clin Invest 1987791665-73 24 Waghray M Cui Z Horowitz JC et al Hydrogen peroxide is a diffusible paracrine signal for the induction of epithelial cell death by activated myofibroblasts Faseb J 200519854-6 25 Larios JM Budhiraja R Fanburg BL Thannickal VJ Oxidative protein cross-linking reactions involving L-tyrosine in transforming growth factor-beta1-stimulated fibroblasts J Biol Chem 200127617437-41 26 Kinnula VL Fattman CL Tan RJ Oury TD Oxidative stress in pulmonary fibrosis a possible role for redox modulatory therapy Am J Respir Crit Care Med 2005172417-22 27 Meyer A Buhl R Kampf S Magnussen H Intravenous N-acetylcysteine and lung glutathione of patients with pulmonary fibrosis and normals Am J Respir Crit Care Med 19951521055-60 28 Behr J Degenkolb B Krombach F Vogelmeier C Intracellular glutathione and bronchoalveolar cells in fibrosing alveolitis effects of N-acetylcysteine Eur Respir J 200219906-11 29 Bando M Hosono T Mato N et al Long-term efficacy of inhaled N-acetylcysteine in patients with idiopathic pulmonary fibrosis Intern Med 2010492289-96 30 Demedts M Behr J Buhl R et al High-dose acetylcysteine in idiopathic pulmonary fibrosis N Engl J Med 20053532229-42 31 Toma TP Bhowmik A Rajakulasingam R Acetylcysteine in pulmonary fibrosis N Engl J Med 20063541086-9 author reply -9 32 Hunninghake GW Antioxidant therapy for idiopathic pulmonary fibrosis N Engl J Med 20053532285-7 33 Flaherty KR Mumford JA Murray S et al Prognostic implications of physiologic and radiographic changes in idiopathic interstitial pneumonia Am J Respir Crit Care Med 2003168543-8 34 Latsi PI du Bois RM Nicholson AG et al Fibrotic idiopathic interstitial pneumonia the prognostic value of longitudinal functional trends Am J Respir Crit Care Med 2003168531-7 35 Collard HR King TE Jr Bartelson BB Vourlekis JS Schwarz MI Brown KK Changes in clinical and physiologic variables predict survival in idiopathic pulmonary fibrosis Am J Respir Crit Care Med 2003168538-42 36 Jegal Y Kim DS Shim TS et al Physiology is a stronger predictor of survival than pathology in fibrotic interstitial pneumonia Am J Respir Crit Care Med 2005171639-44 37 Martinez FJ Safrin S Weycker D et al The clinical course of patients with idiopathic pulmonary fibrosis Ann Intern Med 2005142963-7 38 Hull JH Acetylcysteine in pulmonary fibrosis N Engl J Med 20063541089-91 author reply -91
70
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
39 Flaherty KR King TE Jr Raghu G et al Idiopathic interstitial pneumonia what is the effect of a multidisciplinary approach to diagnosis Am J Respir Crit Care Med 2004170904shy10 40 Raghu G Johnson WC Lockhart D Mageto Y Treatment of idiopathic pulmonary fibrosis with a new antifibrotic agent pirfenidone results of a prospective open-label Phase II study Am J Respir Crit Care Med 19991591061-9 41 Hunninghake GW Lynch DA Galvin JR et al Radiologic findings are strongly associated with a pathologic diagnosis of usual interstitial pneumonia Chest 20031241215-23 42 Lynch D Godwin J Safrin S et al High-resolution computed tomography in idiopathic pulmonary fibrosis diagnosis and prognosis Am J Respir Crit Care Med 2005172488-93 43 Mallinckrodt CH Watkin JG Molenberghs G Carroll RJ Choice of the primary analysis in longitudinal clinical trials Pharmaceutical Statistics 20043161-9 44 Bang H Tsiatis A Estimating medical costs with censored data Biometrika 200087329shy43 45 Lin DY Regression analysis of incomplete medical cost data Stat Med 2003221181-200 46 Rochon J Application of GEE procedures for sample size calculations in repeated measures experiments Stat Med 1998171643-58 47 Lachin JM Foulkes MA Evaluation of sample size and power for analyses of survival with allowance for nonuniform patient entry losses to follow-up noncompliance and stratification Biometrics 198642507-19
71
- PANTHER-IPFPREDNISONE AZATHIOPRINEAND N-ACETYLCYSTEINEA STUDY THAT EVALUATES RESPONSE INIDIOPATHIC PULMONARY FIBROSIS
-
- Protocol Summary
- Table of Contents
- List of Tables
- List of Figures
- List of Abbreviations
- 1 Summary
- 2 Hypotheses and Specific Aims
-
- 21 Null Hypothesis
- 22 Specific Aim 1
- 23 Specific Aim 2
- 24 Prespecified Subgroups of Interest
-
- 3 Background and Significance
-
- 31 Idiopathic Pulmonary Fibrosis is the Most Common Interstitial Lung Disease
- 32 Rationale for Placebo Control
- 33 Rationale for N-acetylcysteine
- 35 Rationale for N-acetylcysteine as a Stand-alone Therapy
- 36 Rationale for the Study Design and Primary Endpoint
- 37 Rationale for Blinding of Treatments
-
- 4 Methods
-
- 41 Inclusion Criteria
- 42 Diagnosis of IPF
- 43 Exclusion Criteria
- 44 Study Design and Study Visit
- 45 Dose Justification
- 46 Contraindications Precautions and Side Effects of Study Medications
- 47 Recruitment Procedures
- 48 Study Procedures
- 49 Concomitant Medications
- 410 Laboratory Testing
- 411 Blinding of Study Drugs
-
- 5 Study Endpoints
-
- 51 Primary Study Endpoint
- 52 Secondary Study Endpoints
-
- 6 Safety Evaluations and Procedures
-
- 61 Adverse Events
- 62 Clinical Medical Monitoring
- 63 Unblinding Procedures
-
- 7 Study Drug Procedures
- 8 Data Management
-
- 81 Hardware and Software Configuration
- 82 Sources of Data
-
- 9 Study Design and Data Analysis
-
- 91 General Analytic Considerations
- 92 Randomization Blinding and Reporting of Results
- 93 Stratification
- 94 Specification of the Primary Analyses
- 95 Analysis of Longitudinal Endpoints
- 96 Analysis of Binary Time-to-Event and Time-Lagged Endpoints
- 97 Power Analysis
-
- 10 Study Administration
-
- 101 Cooperative Agreement Mechanism
- 102 IPFnet Steering Group
- 103 Data and Safety Monitoring Board
- 104 Recommendations on Interim Monitoring of Efficacy Safety and Futility
-
- 11 Investigator and Sponsor Obligations
-
- 111 Monitoring
- 112 Cost and Payment
- 113 Confidentiality and Health Insurance Portability and Accountability ActConsiderations
- 114 Informed Consent Procedures
- 115 Institutional Review Boards
-
- 12 Investigator Agreement
- 13 References
-

PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Temporarily discontinue (hold) oral NACPL for subjects requiring inpatient admission for acute
exacerbation (AEx) or other conditions Resume NACPL after discharge
36
37
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
452 Dosage Algorithms
Dosage Adjustment Algorithm 1 NACPL Dose Modifications for Gastrointestinal Symptoms Nausea Vomiting Abdominal Discomfort Diarrhea
GI Symptoms determined by the PI to be clinically significant Nausea Vomiting Abdominal Discomfort Diarrhea
NACPL Temporarily dc (HOLD) x 3 Days
Monitor symptoms intervene as clinically indicated (eg fluid replacement antidiarrhea or antinausea medication)
Monitor or lab PRN
Are symptoms resolving after 3 days NO
Symptoms NOT resolving after 3 days of holding study medication Assessmentmanagement per clinical
discretion of investigator
Likely not study medication discuss resuming study medication with medical monitor when symptoms resolved
YES
Temporarily dc (HOLD) NACPL for 4 additional days (total hold 1 week) then NACPL Resume 600 MG TID
Did symptoms recur
YES
STOP NACPL for
duration of study
NO
NACPL No Change
38
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Dosage Adjustment Algorithm 2 NACPL Dose Modifications For Dermatologic Reactions
Dermatologic Reactions (Not Acneiform) ge Grade 2 Grading per Common Terminology Criteria for
Adverse Events V30 (httpctepcancergov) For example Grade 1 RASHDESQUAMATION Macular or papular eruption or erythema without associated symptoms Grade 2 RASHDESQUAMATION Macular or popular eruption or erythema with pruritus or other associated symptoms localized desquamation or other lesions covering lt50 of body surface area
NACPL Temporarily dc (HOLD) x 3 days
Are symptoms resolving after 3 days
NO Symptoms not resolving after 3 days of holding study medication Assessmentmanagement per clinical discretion of investigator Likely not study medication Discuss resuming study medication with medical monitor when symptoms
resolved YES
Temporarily dc (HOLD) NACPL for 4 additional days (total hold 1 week) then NACPL resume 600 MG TID
Did symptoms recur
YES
STOP NACPL for
duration of study
NO
NACPL No change
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
46 Contraindications Precautions and Side Effects of Study Medications
461 Contraindication
Contraindication to NAC is known hypersensitivity to it
462 Precautions
Concomitant administration of oral NAC and antibiotics has shown a slightly reduced absorption
of cephalexin and a slight increase in erythromycin serum levels NAC contains free sulfhydryl
groups There is no evidence that individuals sensitive to sulfa drugs are sensitive to NAC
The NAC preparation being administered in this study contains 20 mg of aspartame Because of
the phenylalanine component of aspartame individuals with phenylketonuria should avoid or
restrict aspartame intake to avoid increased blood levels of phenylalanine Because of this risk
labeling is required on all products containing aspartame
463 Side Effects
Side effects of NAC range from common to serious See Table 4
39
40
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Table 4 Side Effects of NAC
Undesirable Effects
System-organ class Uncommon
(gt11000 lt1100)
Rare
(gt110000 lt11000)
Very rare
(lt110000) Not known
Immune system disorders Hypersensitivity Anaphylactic shock
reaction
Nervous system disorders Headache
Ear and labyrinth disorders Tinnitus
Cardiac disorders Tachycardia
Vascular disorders Hemorrhage
Respiratory thoracic and
mediastinal disorders
Bronchospasm
Dyspnea
Gastrointestinal disorders
Vomiting diarrhea
stomatitis abdominal
pain nausea
Dyspepsia
Skin and subcutaneous tissue
disorders
Urticaria rash
angioedema itching
General disorders and
administration site conditions Pyrexia
Investigations Reduced arterial
pressure Face edema
In very rare cases the onset of severe skin reactions such as Stevens-Johnson syndrome and Lyell syndrome was reported to have a temporal relationship with N-acetylcysteine administration Although in most cases at least another suspect drug probably most involved in the genesis of the above mentioned mucocutaneous syndromes has been identified in case of mucocutaneous alterations it is appropriate to contact onersquos doctor and the administration of N-acetylcysteine should be immediately discontinued
Some studies confirmed a reduction of platelet aggregation during N-acetylcysteine administration The clinical significance of these findings has not been defined yet [Source Fluimucil Investigator Brochure]
47 Recruitment Procedures
Subjects recruited for this study will be established patients of the investigators or physician- or
self-referred to participating clinical centers in the IPFnet Each clinical center within IPFnet has
a well-developed infrastructure of local pulmonologists within the surrounding geographic area
These pulmonologists are kept informed of ongoing IPF clinical trials and regularly refer
subjects to studies conducted at IPFnet clinical centers
Additional steps will be taken to inform clinicians of the trials in progress within IPFnet
including presentations at faculty staff meetings at local hospitals medical grand rounds and
national conferences direct mail notification monthly faxes and advertisement of network trials
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
in pulmonary journals Clinical center patients previously diagnosed with IPF will be notified of
the trials by mail whenever possible
Recruitment of minorities and women will be monitored by the DCC and DSMB If necessary
additional recruitment efforts will be made at specific centers to ensure that the aggregate subject
sample contains appropriate representation of women and minorities
48 Study Procedures
The following procedures are detailed in the PANTHER-IPF MOOP accompanying this
protocol
1 PFT
2 ABG
3 HRCT scan of the chest (including imaging of pulmonary arteries)
4 CBC and serum chemistries
5 Pregnancy test
6 6MWTBorg Dyspnea Scale
7 QOL questionnaires (EuroQol HAD SF-36 SGRQ and ICE CAP)
8 UCSD SOBQ
9 Gender Substudy Questionnaire
All assessments of PFTs will be conducted by study personnel not directly involved in the
treatment of the subjects
481 Biological Specimen Management
4811 Biological Specimen Sample Management
Subjects at clinical centers participating in the specimen repository substudy who consent to
having blood drawn for research purposes and for the banking of blood blood components and
other biologic specimens (urine and BAL fluid) will have approximately 405 mL of blood
41
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
drawn 17 mL blood drawn for DNA and 20 mL of urine collected at enrollment visit Subjects
will have approximately 50 mL of blood drawn and 20 mL of urine collected at each 15-week
follow-up visit Blood specimens will be separated according to PANTHER-IPF MOOP
guidelines into the following components for banking in the repository serum plasma and
DNA Coding of all biologic specimens for the repository will be performed by study staff at the
clinical center The samples will be processed per PANTHER-IPF MOOP guidelines aliquoted
labeled with barcode labels and stored at -70degC at the clinical center and shipped to the central
repository
The only subject identifiers will be a sample ID number and subject initials This sample ID will
be linked in the IPFnet DCC clinical database to subject information No subject information will
be transferred to the biological-specimen database
The subjectrsquos samples may be used for approved sub-studies relating to human disease
including but not limited to IPF The studies for which an individualrsquos samples will be made
available will be determined by the subjectrsquos answers to questions on the biological-sample
informed consent form The subjects can choose to make their samples available for all options
or any combination Samples will be made available to researchers only with IPFnet Steering
Group approval until such time as the samples are made public through the NHLBI repository
49 Concomitant Medications
Concurrent treatment with FDA-approved therapy for IPF is allowed Colchicine may be used
for treatment of gout Temporary treatment with oral or IV corticosteroids for clinical worsening
or suspected AEx is permitted Nutritional supplements containing NAC are not allowed
410 Laboratory Testing
Clinical laboratory parameters will be assessed at screening and at the end of the study The
following tests will be performed at the two time points specified in the protocol chemistry (AG
ratio ALT [SGPT] AST [SGOT] albumin alkaline phosphatase amylase bilirubin-direct
42
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
bilirubin-indirect bilirubin-total BUN BUNcreatinine ratio calcium carbon dioxide
cholesterol-total chloride CPK-total creatinine GGT globulin glucose iron-total LDH
lipase magnesium phosphorus-inorganic potassium protein-total sodium TIBC triglycerides
uric acid) and hematology (red blood cell count WBC count hemoglobin hematocrit cell
indices differential platelet count)
411 Blinding of Study Drugs
Subjects and caregivers will be blinded to study treatment Every subject will receive NAC or
matching PLs at every study visit from the baseline visit to the week-45 visit No study agent
will be dispensed at the week-60 visit
43
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
5 Study Endpoints
51 Primary Study Endpoint
The primary endpoint will be the change in serial measurements of FVC over the study period
52 Secondary Study Endpoints
521 Time to Disease-progression
The time-to-death or a 10 decline in FVC will be defined as the time-to-disease progression
The 10 decline in FVC from enrollment must be confirmed on 2 consecutive visits no less than
6 weeks apart For subjects with 2 consecutive visits with a 10 decline in FVC the time-toshy
disease progression will be defined as the time interval between enrollment and the initial visit
with a 10 FVC decline For subjects who experience disease progression the study doctor will
determine whether or not the subject will remain in the study
522 Acute Exacerbations
The following 3 criteria will define AEx in subjects with acute worsening of their respiratory
conditions
1 Clinical (all of the following required)
A) Unexplained worsening of dyspnea or cough within 30 days triggering unscheduled
medical care (eg emergency room clinic study visit hospitalization)
B) No clinical suspicion or overt evidence of cardiac event pulmonary embolism or deep
venous thrombosis to explain acute worsening of dyspnea
C) No pneumothorax
44
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
2 RadiologicPhysiologic (A and B required)
A) New ground glass opacity or consolidation computed tomography (CT) scan OR new
alveolar opacities on chest x-ray
B) Decline of ge 5 in resting room air SpO2 from last recorded level OR decline of ge 8 mm
Hg in resting room air PaO2 from last recorded level
3 Microbiologic (all of the following required)
A) No clinical evidence for infection (ie absence of grossly purulent sputum fever gt 39degC
orally)
B) Lack of positive microbiological results (if done) from lower respiratory tract defined as
(1) Clinically significant bacterial growth on sputum or endotracheal aspirate cultures
(2) Quantitative culture by protected brush specimen ge 103 cfumL or BAL ge 104 cfumL
(3) The presence of specific pathogens on stains of any of the above
C) Lack of positive pathogen in blood cultures (if done)
Identification of Acute Exacerbations
All subjects will be educated about the importance of identifying AExs At the time of
enrollment subjects will be told about the possibility of developing acute symptomatic
worsening that might represent an AEx of IPF and instructed to contact their study clinical
center coordinator within 48 to 72 hours of the apparent event
All subjects will be contacted by phone monthly and questioned about any change in dyspnea or
cough and any interim clinic visits or hospitalizations Finally as part of the IPFnet outreach to
community referring physicians the importance of AExs will be emphasized When a subject is
identified who meets criterion 1A this will trigger the collection of additional clinical data to
evaluate a suspected AEx These data will be collected as part of standard clinical care (ie this
protocol does not require collection of all items) The additional items to be collected for
suspected AEx include
IPFnet AEx case report form (eCRF) (required)
45
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Chest x-ray CT scan withwithout pulmonary angiogram (reports should be faxed and
followed by the hard copiesdiscs)
Oxygen saturation (pulse oximetry)
ABG
Respiratory cultures (sputum endotracheal aspirate lavage)
Blood cultures
Clinichospital records related to the event
All potential cases of AEx will be reviewed by the clinical center PI first and a decision on
whether the case may represent an AEx will be made If AEx is suspected the case will be sent
to the IPFnet adjudication committee which will assign a final diagnosis (see Table 5) If there is
disagreement among members the majority opinion will be recorded
During episodes of suspected AEx as determined by the individual clinical center investigator
subjects will remain blinded and in the study
Table 5 Final Diagnoses in Evaluation of Suspected Acute Exacerbations
Definite acute exacerbation All criteria met no alternative etiology
Unclassifiable acute worsening
Insufficient data to evaluate all criteria no alternative etiology
Not acute exacerbation Alternative etiology identified that explains acute worsening
Management of the suspected AEx will be at the discretion of the treating physician Standard of
care generally involves evaluation for respiratory infection pulmonary embolism cardiac events
and pneumothorax and treatment with IV corticosteroids
Study drugs will be resumed at pre-suspected AEx doses after subjects clinically improve as
confirmed by the local PI All subjects should be seen at the clinical center within 2 to 4 weeks
of recovery for measurement of post-bronchodilator FVC (see Figure 4) Subjects unable to
return to the clinical center after suspected AEx due to medical frailty (eg continued
46
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
institutionalization progressive disability) will be categorized as failing to maintain FVC
response in secondary analyses
Suspected AEx (PI determined)
Hold study drug Treat AEx
(Attending physician determined)
Alive but unable to continue due to
medical frailty
Dead
Alive and able to continue
Site reviewvisit
Restart study drug
FVC within 2-4 weeks
Figure 4 Acute Exacerbation Flow Chart
523 Respiratory Infections
An upper respiratory infection will be defined as
Change in sputum discoloration
Increased cough of no more than 14 daysrsquo duration
A lower-respiratory infection (pneumonia) will be defined as new segmental or lobar airspace
opacities visualized by image studies (chest radiograph or HRCT) in addition to any of the
following
Positive pathogencultures in good sample of sputum or lower-airway secretions retrieved
by fiberoptic bronchoscope
Fever gt 39degC or gt 100degF
Leukocytosis gt 12000 (unexplained no increase in dose of corticosteroids)
47
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
524 Maintained FVC Response
Subjects with follow-up FVCpred measurements at or above their baseline FVCpred level
will be classified as having maintained FVC response Subjects with reduced FVCpred levels
or missing data for any reason including death or medical frailty will be classified as having not
maintained FVC response The FVCpred value is used because unadjusted FVC measurements
are expected to decline with age
48
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
6 Safety Evaluations and Procedures
61 Adverse Events
During a clinical trial the reporting of adverse experience information can lead to important
changes in the way a new treatment is developed as well as provide integral safety data
611 Definitions
An adverse event (AE) is any untoward medical occurrence in a subject or clinical investigation
subject who was administered a pharmaceutical product The AE does not necessarily have to
have a causal relationship with the drug administered An AE can be any unfavorable and
unintended sign (including an abnormal laboratory finding) symptom or disease temporarily
associated with the use of a medicinal product whether or not considered to be related to the
medicinal product Diseases signs symptoms or laboratory abnormalities already existing at
enrollment are not considered AEs unless they worsen (ie increase in intensity or frequency)
Surgical procedures themselves are not AEs they are therapeutic measures for conditions that
require surgery The condition for which the surgery is required may be an AE Surgical
procedures planned before randomization and the conditions necessitating the surgery are not
AEs
A serious adverse event is any untoward event that
Is fatal
Is life-threatening
Requires inpatient hospitalization or prolongation of existing hospitalization with the
following exceptions
o Preplanned (before the study) hospital admissions unless the hospitalization is
prolonged
o Planned admissions (as part of a study eg routine biopsies)
o Hospitalization lasting lt 24 hours
49
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
o Hospitalization for elective procedure
o Emergency room visits
Results in persistent or significant disability or incapacity
Is a congenital anomaly or birth defect
Important medical events that may not result in death be life-threatening or require
inpatient hospitalization may be considered serious adverse events (SAEs) when based
on appropriate medical judgment they may jeopardize the subject and may require
medical or surgical intervention to prevent one of the outcomes listed above
Life-threatening means that the subject was in the view of the investigator at immediate risk of
death from the AE as it occurred It does not include an AE that had it occurred in a more severe
form might have caused death
Persistent or significant disabilityincapacity means that the event resulted in permanent or
significant and substantial disruption of the subjectrsquos ability to carry out normal life functions
Causality
A reasonable possibility means the AE may have been caused byrelated to the study drug A
perceived or real lack of efficacy does not satisfy the definition of relatedness
612 Adverse Event (AE) Reporting
For the PANTHER-IPF trial all AEs (serious and nonserious) occurring from randomization
through final study visit (4 weeks after final dose of all study medication) will be recorded on the
AE page of the case report form (CRF)
6121 Serious Adverse Events (SAE) Reporting
For this trial all deaths and all SAEs which occur from randomization through final study visit
must be entered within the EDC system via the SAE eCRF page within 24 hours of the
investigative sitersquos knowledge of the event It is the responsibility of the clinical center
50
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
investigator to provide a causality assessment of the event for each study medications based upon
the information available at the time of the report It is understood that complete information
about the event may not be known at the time the initial report is submitted In the event the EDC
system is not accessible to the site at the time of event reporting investigative sites will complete
and forward a paper back-up SAE form to DCRI Safety Surveillance for processing
DCRI Safety Surveillance
Telephone 1-919-668-8624 or 1-866-668-7799 (toll free)
Fax 1-919-668-7138 or 1-866-668-7138 (toll free)
The investigator must complete and submit follow-up SAE information via the eCRF when
important new or follow-up information (eg final diagnosis outcome results of specific
investigations) becomes available Follow-up information should be submitted according to the
same process used for reporting the initial event as described above All SAEs will be followed
until resolution stabilization or 30 days after the subject has completed the final visit (4 weeks
after the final dose of study medication) whichever occurs first The investigator is responsible
for reporting SAEs to their institutional review board (IRB) per site specific IRB reporting
guidelines
6122 Regulatory Reporting
AEs that are serious study drug related and unexpected will be reported to the regulatory
authorities The DCRI Safety Surveillance medical monitor will perform a medical review of all
SAEs submitted and evaluate for ldquounexpectednessrdquo DCRI Safety Surveillance will prepare
MedWatch reports for those events identified as serious study drug related and unexpected as
determined by Safety Medical Monitor
DCRI Regulatory Services will submit all unexpected study drug-related SAEs as per 21 CFR
32 DCRI Safety Surveillance will provide a safety alert letter to the NHLBI DSMB and DCC
clinical operation (for distribution to sites) within 15 days of initial receipt of the information
51
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Investigators are responsible for promptly reporting these events to their reviewing IRBs
according to site specific IRB reporting guidelines
62 Clinical Medical Monitoring
There will be an unblinded physician at the IPFnet DCC serving as medical monitor The
medical monitor will be available to assist with questions about dosage adjustments of study
medications including discontinuation or resumption of medications
63 Unblinding Procedures
Unblinding of subjects or investigators to subject treatment is strongly discouraged For ongoing
clinical management all subjects should be presumed to be receiving ldquoactiverdquo study drug To
ensure the subjectrsquos safety the study treatment will be dose-adjusted based on laboratory test
results clinical findings and symptoms
The IPFnet DCC medical monitor and PANTHER-IPF co-chairs Drs Ganesh Raghu and
Fernando Martinez will be available to the study physicians to discuss study drug management
on a case-by-case basis Un-blinding will be considered ONLY when the knowledge of subject
treatment assignment is ABSOLUTELY ESSENTIAL for subject safety and after discussion of
the subjectrsquos case with the medical monitor and either Dr Raghu or Dr Martinez Unblinding of
study treatment should be minimized during the conduct of the trial In those cases where it is
felt to be medically necessary the DCC medical officer will communicate directly with the
managing physician to minimize unblinding of study personnel
52
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
7 Study Drug Procedures
At the baseline 15-week 30-week and 45-week study visits subjects will receive a supply of
study drug sufficient to last until the next visit at which study drug will be dispensed
53
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
8 Data Management
81 Hardware and Software Configuration
811 Hardware and Database Software
Data will be stored in an Oracle database system Oracle has advantages of processing efficiency
and smooth linkage with other software systems The application and database will be hosted on
Solaris Unix servers at the IPFnet DCC
812 Statistical Software
SAS will be used as the principal application for the management of analysis data files and
statistical computations S-Plus will be used to provide supplementary functions as needed
813 Access Control and Confidentiality Procedures
Access to databases will be controlled centrally by the IPFnet DCC through user passwords
linked to appropriate privileges This protects the data from unauthorized changes and
inadvertent loss or damage
814 Security
Database and Web servers will be secured by a firewall and through controlled physical access
Oracle has many security features to ensure that any staff member accessing the database has the
proper authority to perform the functions he or she requests of the system Within the secondary
SAS databases Unix group-access control maintains similar security The Sun workstation login
is secured by extensive user-password facilities under Unix
54
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
815 Back-up Procedures
Database back-up will be performed automatically every day and standard IPFnet DCC policies
and procedures will be applied to dictate tape rotation and retention practices
816 Virus Protection
All disk drives that provide network services and all user computers will be protected using
virus-scanning software Standard IPFnet DCC policies will be applied to update these protection
systems periodically through the study
82 Sources of Data
821 Design and Development
The IPFnet DCC will be responsible for development of the electronic case report forms
(eCRFs) development and validation of the clinical study database ensuring data integrity and
training clinical center staff on applicable data management procedures A web-based distributed
data entry model will be implemented This system will be developed to ensure that guidelines
and regulations surrounding the use of computerized systems used in clinical trials are upheld
The remainder of this section provides an overview of the data management plan associated with
this protocol
822 Data Collection Forms
The data collection process consists of direct data entry at the study clinical centers into the EDC
system(s) provided by the DCC A data collection worksheet will be provided to clinical centers
for recording data in the event the EDC system is unavailable Data entry of the eCRFs should
be completed according to the instructions provided and project specific training The
investigator is responsible for maintaining accurate complete and up-to-date records and for
ensuring the completion of the eCRFs for each research participant
55
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
823 Data Acquisition and Entry
Data entry into eCRFs shall be performed by authorized individuals Selected eCRFs may also
require the investigatorrsquos written signature or electronic signature as appropriate Electronic
CRFs will be monitored for completeness accuracy and attention to detail during the study
824 Data Center Responsibilities
The IPFnet DCC will 1) develop a data management plan and will conduct data management
activities 2) provide final eCRFs for the collection of all data required by the study 3) develop
data dictionaries for each eCRF that will comprehensively define each data element 4) conduct
ongoing data monitoring activities on study data 5) monitor any preliminary analysis data
cleanup activities and 6) rigorously monitor final study data clean up
825 Data Editing
Completed data will be entered into the IPFnet DCC automated data acquisition and
management system If incomplete or inaccurate data are found a data clarification request will
be generated and distributed to clinical centers for a response Clinical centers will resolve data
inconsistencies and errors and enter all corrections and changes into the IPFnet DCC automated
data acquisition and management system
826 Training
The training plan for clinical center staff includes provisions for training on assessments eCRF
completion guidelines data management procedures and the use of computerized systems
56
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
9 Study Design and Data Analysis
91 General Analytic Considerations
All primary analyses will be based on intent-to-treat (ITT) principles using all randomized
subjects Baseline factors across groups will be compared using mean (standard deviation) and
median (25th and 75th percentiles) summary measures Kaplan-Meier curves will be used to
display event rates Due to clinical interest in departures from both sides of the null hypothesis
all test statistics will be 2-sided
Reasonable caution needs to be taken when conducting multiple analyses on key clinical
subgroups For subgroup analyses a conservative significance level of 0001 will be used for all
interaction tests Thus subgroup comparisons will be considered exploratory unless the p-value
from the interaction test is smaller than 0001
92 Randomization Blinding and Reporting of Results
A permuted block-randomization scheme will be created with varying block sizes stratified by
clinical center Once a subject has completed the screening and baseline period and evaluation
for inclusionexclusion criteria the randomization process will begin Subjects will be
randomized to receive NAC or matching placebo with equal probability (11) via telephone
contact with a central interactive voice response system (IVRS) using a toll-free randomization
number On the day of randomization after the subject has successfully met all inclusion and
exclusion criteria the investigator or designee will call the central randomization number to
obtain the assigned kit randomization numbers for that subject At each subject visit the
investigator or designee will call the central randomization number to obtain the new kit
randomization numbers for resupply of the subject For resupply of the clinical center the IVRS
will monitor minimal volume of a kit type andor expiration date and will automatically notify
the pharmacy
57
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
The trial results will be reported according to guidelines specified in the CONSORT statement
A flow diagram describing screening recruitment randomization dropout and vital status will
be included in the primary manuscript AEs and efficacy data will be presented for all treatment
groups Adherence dropout and lost to follow-up will be carefully examined across all treatment
groups Analyses of safety will be based on data from all randomized subjects who received at
least one dose of study drug
93 Stratification
Subjects will be distributed to the two treatment arms in a 11 allocation ratio Stratification
blocks will be based on clinical centers
94 Specification of the Primary Analyses
A mixed model repeated measures (MMRM) analysis described in section 95 will be used to
compare differences in the slope of FVC measurements across the treatment groups Response
variables are values of the FVC measured at baseline and every 15 weeks until study completion
Variables in the model will include treatment time and time by treatment age sex race and
height Contrast estimates of differences in slopes of treatment over time (along with confidence
intervals) will be used to estimate the treatment effect The validity of this model in terms of
meeting modeling assumptions will be assessed via standard modeling diagnostics and goodness-
of-fit measures Based on the MMRM framework missing FVC data will not be imputed for the
primary analysis
95 Analysis of Longitudinal Endpoints
A common goal in clinical trials is to specify models that are easily implemented and
reproducible by independent data analysts On the other hand the models should have proper
statistical behavior in terms of low bias and high precision Many common approaches to
longitudinal data analysis including last observation carried forward (LOCF) imputation rely on
the missing completely at random (MCAR) assumption However the MCAR assumption is
58
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
unlikely to hold in many clinical trials because missing data are often related to disease
progression and prognosis A more reasonable assumption missing at random (MAR) specifies
that the complete data distribution can be modeled using only the observed data The likelihood-
based MMRM approach is valid under the more general MAR assumptions These models will
be applied to analyze the longitudinal data secondary endpoints
The advantages of MMRM analysis are that all important characteristics of the model can be preshy
specified standard software can be used to implement the models and results are based on ITT
principles43 In addition the MMRM approach offers superior control of Type I and Type II
errors compared with the LOCF approach
Response variables are values of the PFTs measured at enrollment and every 15 weeks until
study completion and 6MWT values measured at baseline week 30 and week 60 Covariates are
treatment time time by treatment and key baseline risk factors Contrasts (along with
confidence intervals) of treatment by time will be used to estimate the treatment effect
The correlation structure involves multiple pieces including measurement errors random
variation and interindividual variability For the longitudinal data analyses an unstructured
correlation matrix for within-subject errors will be assumed Other correlation structures
including compound symmetry will be examined as needed A careful examination of reasons
for study discontinuation will be conducted to assess the validity of MCAR Sensitivity analyses
will be used to examine the untestable assumption that the observed data violate the MAR
assumption The MMRM models will be implemented using PROC MIXED in SAS
96 Analysis of Binary Time-to-Event and Time-Lagged Endpoints
Regression modeling approaches using either the logistic regression model or Cox proportional
hazards regression model will be employed when appropriate The validity of these models will
be assessed via standard modeling diagnostics and goodness-of-fit measures Estimates of
cumulative frequencies for more general time-lagged responses will be calculated using the
partitioned version of the Bang-Tsiatis estimator44 The partitions will be set at 15-week intervals
59
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
to correspond with the data-collection process Covariate adjusted event rates will be calculated
using inverse probability-weighted regression estimates45
97 Power Analysis
971 Primary Analyses
Based on previously published IPF clinical trials the PL group is expected to experience a drop
in FVC of approximately 020 L over the study period (see Figure 1) The IPFnet Steering Group
determined a clinically important difference would be to preserve the majority of the decline
relative to PL over the study period In particular a treatment effect of 015 L was determined to
be a clinically meaningful difference Potential dropout is a key factor in the proposed study The
drop-out process assumed 5 lost to follow-up after every study visit Only 80 of subjects
were assumed to be followed for the entire study period All models assumed a compound
symmetry structure for the covariance matrix Power calculations were performed using a SAS
IML program for designing repeated measures studies46 Based on preliminary reviews of the
data from the University of Michigan the covariance matrix parameters were estimated at
approximately σ2 = 0757 (variance parameter) and ρ = 0936 (correlation parameter) To be
conservative the power calculations for the primary analysis were performed with parameter
setting of σ2 = 0810 (variance parameter) and ρ = 0925 (correlation parameter)
The power calculations assume a correction for imperfect compliance proposed by Lachin and
Foulkes to allow for 2 noncompliance for each of the treatment arms47 Thus the sample size
of 130 subjects per arm would be reduced to an adjusted sample size of 130(1-002-002)2 =
1198 or 120 subjects per arm
Under the assumed Type I error rate of 005 with a correlation parameter of 0925 and standard
deviation of 090 the difference of 015 L (or 00025 Lweek) shown in Table 6 would have
power of 93
60
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Table 6 Hypothetical Values of Mean FVC (L) Change from Baseline
Week 15 Week 30 Week 45 Week 60
NAC 00125 00250 00375 00500
Placebo 00500 01000 01500 02000
Difference 00375 00750 01125 01500
Abbreviations FVC forced vital capacity PL placebo
972 Power Analysis for Secondary Endpoints
Power calculations for secondary endpoint measurements are shown in Table 7 Standard
deviations are based on unpublished data provided by the University of Michigan The
calculations are based on a 2-sample t-test with Type I error rate set at 005 These calculations
are likely to be conservative because the statistical approach described in section 95 for
analyzing these endpoints will incorporate incomplete observations as well as intermediate data
points
Table 7 Detectable Differences in Treatment Means for Selected Endpoint Measurements
Secondary Endpoints Std Dev
of the Baseline Score
Detectable Difference for 80 Power
Std Dev of the Change Score
Difference Detectable for
80 Power
DLCOpred 166 58 91 32
6MWT Area Under the Desaturation Curve
219 76 175 61
6MWT Distance to Desaturation 224 78 315 110
6MWT Minutes Walked 210 073 205 071
Abbreviations Std Dev standard deviation DLCOpred diffusing capacity of the lung for carbon monoxide percent predicted 6MWT 6-minute walk test
61
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
10 Study Administration
101 Cooperative Agreement Mechanism
The administrative and funding mechanism used to undertake this project is a ldquocooperative
agreementrdquo (U01) which is an assistance mechanism Under the cooperative agreement the
NHLBI assists supports andor stimulates the project and is substantially involved with
investigators in conducting the study by facilitating performance of the effort in a ldquopartnerrdquo role
The NHLBI project scientist serves on the IPFnet Steering Group and he or another NHLBI
scientist may serve on other project committees when appropriate At the same time however
NHLBI does not assume a dominant role direction or prime responsibility for this research
program
As described below governance of the project is conducted through the IPFnet Steering Group
Principal investigators have lead responsibilities in all aspects of their trials and the project
including any modification of trial designs conduct of the trials quality control data analysis
and interpretation preparation of publications and collaboration with other investigators unless
otherwise provided for by the IPFnet Steering Group
PIs retain custody of and have primary rights to their center-specific and collaborative data
subject to government rights-of-access consistent with current Health amp Human Services (HHS)
Public Health Service (PHS) and National Institutes of Health policies The protocols and
governance policies call for the continual submission of data centrally to the IPFnet DCC for the
collaborative database which at a minimum will contain the key variables selected by the IPFnet
Steering Group for standardization across all clinical centers the submission of copies of the
collaborative datasets to each PI upon completion of the project procedures for data analysis
reporting and publication and procedures to protect and ensure the privacy of medical and
genetic data and records of individuals The NHLBI project scientist on behalf of the NHLBI
will have the same access privileges and responsibilities regarding the collaborative data as the
other members of the Steering Group
62
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
PIs are also encouraged to publish and to publicly release and disseminate results data and other
products of the project concordant with the project protocols and governance and the approved
plan for making data and materials available to the scientific community and to the NHLBI
However during the 3 years after the ending date of NHLBI project support unpublished data
unpublished results data sets not previously released and other study materials or products are
to be made available to any third party only with the approval of the IPFnet Steering Group
Upon completion of the project PIs are expected to put their intervention materials and
procedure manuals into the public domain andor make them available to other investigators
according to the approved plan for making data and materials available to the scientific
community and the NHLBI for the conduct of research at no charge other than the costs of
reproduction and distribution
The NHLBI reserves the right to terminate or curtail the project (or an individual award) in the
event of (a) failure to develop or implement mutually agreeable collaborative measurement
subject eligibility and data management sections of the protocols (b) substantial shortfall in
subject recruitment follow-up data reporting or quality control or other major breach of
protocol (c) substantive changes in the agreed-upon protocols with which NHLBI cannot
concur (d) reaching a major project outcome with persuasive statistical significance
substantially before schedule or (e) human subject ethical issues that may dictate a premature
termination
Any disagreement that may arise in scientificprogrammatic matters (within the scope of the
award) between award recipients and the NHLBI may be brought to arbitration An arbitration
panel will be composed of 3 membersmdash1 selected by the IPFnet Steering Group (with the
NHLBI member not voting) or by the individual PI in the event of an individual disagreement a
second selected by NHLBI and the third selected by the other 2 members This special
arbitration procedure in no way affects the PIrsquos right to appeal an adverse action that is otherwise
appealable in accordance with the PHS regulations at 42 CFR part 50 Subpart D and HHS
63
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
regulation at 45 CFR part 16 or the rights of the NHLBI under applicable statutes regulations
and terms of the award
102 IPFnet Steering Group
The IPFnet Steering Group is the main governing body of the project It is composed of the PIs
of the clinical centers the PI of the DCC and the NHLBI project scientist The clinical centers
the IPFnet DCC and the NHLBI each have 1 vote on the IPFnet Steering Group All decisions
are determined by majority vote
All major scientific decisions are determined by the IPFnet Steering Group It assumes overall
responsibility for the design and conduct of the trial It appoints (and disbands) committees and
subcommittees as the need arises designs approves and implements the study protocols
oversees the development of the MOOP monitors subject recruitment and treatment delivery
evaluates data collection and management oversees quality assurance procedures and
implements changes and enhancements to the study as required It also has primary responsibility
for facilitating the conduct of the trials and reporting the projectrsquos results
103 Data and Safety Monitoring Board
The NHLBI will establish a DSMB in accordance with established policies (see
httpwwwnhlbinihgovfundingpoliciesdsmb_insthtm) to ensure data quality and subject
safety and to provide independent advice to the NHLBI regarding progress and the
appropriateness of study continuation
104 Recommendations on Interim Monitoring of Efficacy Safety and Futility
First and foremost the role of the DSMB will be to review subject safety and trial conduct at
periodic points during the study The DSMB may require analyses of the primary endpoint
results for comparing the benefit and risks of treatment strategies The benefit of collecting
additional data on key secondary endpoints with extended follow-up and establishing a robust
64
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
evidence base for determining a standard of care will need to be carefully considered before
early termination of one or more treatment arms After careful consideration the IPFnet Steering
Group recommends conservative thresholds for the early examinations of the safety and efficacy
data
The DSMB will be expected to meet approximately every 6 months until trial completion to
review safety and toxicity data The DSMB may recommend stopping the study based on these
reviews Because the DSMB could stop the trial for safety concerns as well as for a large
efficacy benefit there could be multiple opportunities to reject the null hypothesis (no difference
in event rates between the PL and NAC groups) A Bonferroni approximation will be applied
during the one planned interim analysis for efficacy
Before locking the database a statistical analysis plan (SAP) will be developed to provide
complete details on the statistical analysis The SAP will include the specifics for how and when
the DSMB will be notified for AEs The IPFnet DCC will deliver to the DSMB all FDA-defined
AEs at 3-month intervals The IPFnet DCC will prepare narrative SAE reports in real time for
DSMB review including recommendations and analysis of similar events for each SAE
submitted to the FDA
65
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
11 Investigator and Sponsor Obligations
111 Monitoring
All monitoring activities for US clinical centers will be performed in accordance with DCRI
standard operating procedures Information regarding the types of visits will be outlined in the
PANTHER-IPF MOOP
112 Cost and Payment
There will be no cost to subjects enrolled in this trial Study-related procedures will be paid for
by the IPFnet
Subjects may be eligible for reimbursement for travel to the clinical center Details of payment
will be explained to each subject during the consent process
113 Confidentiality and Health Insurance Portability and Accountability Act
Considerations
Subject confidentiality will be protected throughout the study All subject data will be kept
strictly confidential and no subject-identifying information will be released to anyone outside
the project Confidentiality will be assured through several mechanisms First each subject will
be assigned an anonymous study ID which will then be used on all study forms Second any
study forms blood samples and paper records that contain subject information (eg address lists
phone lists) will be kept at the clinical centers in secured locked areas coded by number Once
blood is collected there will be no subject identifiers placed on blood samplesmdashonly the study
ID number and the date of sample collection Third access to all subject data and information
including laboratory specimens will be restricted to authorized personnel In the case of
computerized data this restricted access will be assured through user logon IDs and password
protection
66
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
At the IPFnet DCC only authorized personnel will have access to the data files containing study
data Security will be assured through user logon IDs passwords and appropriate access
privileges All study subjects will be identified only by their IPFnet ID numbers and no personal
identifying information such as name address or Social Security number will be entered into
the IPFnet DCC database Any subject-specific data reported to the IPFnet Steering Group will
be identified only by the IPFnet ID number
Finally subjects will not be identified by name in any reports or publications nor will the data
be presented in such a way that the identity of individual subjects can be inferred Analysis files
created for further study by the scientific community will have no subject identifiers These data
files will be created in accordance with the Ancillary Studies and Publication Policy of the
IPFnet
114 Informed Consent Procedures
All IPFnet subjects will provide written informed consent using procedures reviewed and
approved by each clinical centerrsquos IRB Informed consent will be undertaken by study personnel
in-person with the subject The subject has the option of declining further participation in the
study at that point No further study procedures will be conducted until the signed documents
have been provided to the IPFnet clinical center
115 Institutional Review Boards
Before initiating this study the protocol clinical center-specific informed consent forms Health
Insurance Portability and Accountability Act (HIPAA) forms recruitment materials and other
relevant information will be reviewed by a properly constituted IRB at each participating clinical
center A copy of the signed and dated IRB approval at each clinical center will be retrieved prior
to or during the site initiation visit and archived at the IPFnet DCC Any amendments to the
protocol other than simple administrative and typographical changes must be approved by each
IRB before they are implemented The clinical centers will seek annual renewals of their IRB
approvals in accordance with local procedures
67
__________________________________________ ________________
__________________________________________
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
12 Investigator Agreement
I have read the foregoing protocol PANTHER-IPF and agree that it contains all necessary
details for carrying out this study I will conduct the study as outlined herein and will complete
the study within the time designated
I will provide copies of the protocol and all pertinent information to all individuals responsible to
me who assist in the conduct of this study I will discuss this material with them to ensure they
are fully informed regarding the drug and the conduct of the study
I will fulfill all responsibilities for submitting pertinent information to the local IRB if
applicable that is responsible for this study
I further agree that NHLBI andor DCRI will have access to any source documents from which
eCRF information may have been generated
Signature of Principal Investigator Date
Name of Principal Investigator (printed or typed)
Protocol version date May 19 2009
Protocol Amendment 1 version date May 28 2010
Protocol Amendment 2 version date December 6 2011
68
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
13 References
1 Raghu G Brown KK Bradford WZ et al A placebo-controlled trial of interferon gamma-1b in patients with idiopathic pulmonary fibrosis N Engl J Med 2004350125-33 2 King TE Jr Safrin S Starko KM et al Analyses of efficacy end points in a controlled trial of interferon-gamma1b for idiopathic pulmonary fibrosis Chest 2005127171-7 3 Flaherty KR Thwaite EL Kazerooni EA et al Radiological versus histological diagnosis in UIP and NSIP survival implications Thorax 200358143-8 4 Wells AU Desai SR Rubens MB et al Idiopathic pulmonary fibrosis a composite physiologic index derived from disease extent observed by computed tomography Am J Respir Crit Care Med 2003167962-9 5 Raghu G Freudenberger TD Yang S et al High prevalence of abnormal acid gastroshyoesophageal reflux in idiopathic pulmonary fibrosis Eur Respir J 200627136-42 6 Kinnula VL Focus on antioxidant enzymes and antioxidant strategies in smoking related airway diseases Thorax 200560693-700 7 Coultas DB Zumwalt RE Black WC Sobonya RE The epidemiology of interstitial lung diseases Am J Respir Crit Care Med 1994150967-72 8 Raghu G Weycker D Edelsberg J Bradford WZ Oster G Incidence and prevalence of idiopathic pulmonary fibrosis Am J Respir Crit Care Med 2006174810-6 9 Olson AL Swigris JJ Lezotte DC Norris JM Wilson CG Brown KK Mortality from pulmonary fibrosis increased in the United States from 1992 to 2003 Am J Respir Crit Care Med 2007176277-84 10 Mannino DM Etzel RA Parrish RG Pulmonary fibrosis deaths in the United States 1979shy1991 An analysis of multiple-cause mortality data Am J Respir Crit Care Med 19961531548shy52 11 Hubbard R Johnston I Coultas DB Britton J Mortality rates from cryptogenic fibrosing alveolitis in seven countries Thorax 199651711-6 12 Johnston I Britton J Kinnear W Logan R Rising mortality from cryptogenic fibrosing alveolitis Bmj 19903011017-21 13 Raghu G Collard HR Egan JJ et al An official ATSERSJRSALAT statement idiopathic pulmonary fibrosis evidence-based guidelines for diagnosis and management Am J Respir Crit Care Med 2011183788-824 14 (USA) FDA FDA Public Health Advisory Interferon gamma-1b (marketed as Actimmune) In 2007 15 King TE Jr Pardo A Selman M Idiopathic pulmonary fibrosis Lancet 2011 16 Raghu G Brown KK Costabel U et al Treatment of idiopathic pulmonary fibrosis with etanercept an exploratory placebo-controlled trial Am J Respir Crit Care Med 2008178948shy55 17 Malouf MA Hopkins P Snell G Glanville AR An investigator-driven study of everolimus in surgical lung biopsy confirmed idiopathic pulmonary fibrosis Respirology 201116776-83 18 King TE Jr Behr J Brown KK et al BUILD-1 a randomized placebo-controlled trial of bosentan in idiopathic pulmonary fibrosis Am J Respir Crit Care Med 200817775-81 19 Richeldi L Costabel U Selman M et al Efficacy of a tyrosine kinase inhibitor in idiopathic pulmonary fibrosis N Engl J Med 20113651079-87
69
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
20 Borok Z Buhl R Grimes GJ et al Effect of glutathione aerosol on oxidant-antioxidant imbalance in idiopathic pulmonary fibrosis Lancet 1991338215-6 21 Meyer A Buhl R Magnussen H The effect of oral N-acetylcysteine on lung glutathione levels in idiopathic pulmonary fibrosis Eur Respir J 19947431-6 22 Behr J Maier K Degenkolb B Krombach F Vogelmeier C Antioxidative and clinical effects of high-dose N-acetylcysteine in fibrosing alveolitis Adjunctive therapy to maintenance immunosuppression Am J Respir Crit Care Med 19971561897-901 23 Cantin AM North SL Fells GA Hubbard RC Crystal RG Oxidant-mediated epithelial cell injury in idiopathic pulmonary fibrosis J Clin Invest 1987791665-73 24 Waghray M Cui Z Horowitz JC et al Hydrogen peroxide is a diffusible paracrine signal for the induction of epithelial cell death by activated myofibroblasts Faseb J 200519854-6 25 Larios JM Budhiraja R Fanburg BL Thannickal VJ Oxidative protein cross-linking reactions involving L-tyrosine in transforming growth factor-beta1-stimulated fibroblasts J Biol Chem 200127617437-41 26 Kinnula VL Fattman CL Tan RJ Oury TD Oxidative stress in pulmonary fibrosis a possible role for redox modulatory therapy Am J Respir Crit Care Med 2005172417-22 27 Meyer A Buhl R Kampf S Magnussen H Intravenous N-acetylcysteine and lung glutathione of patients with pulmonary fibrosis and normals Am J Respir Crit Care Med 19951521055-60 28 Behr J Degenkolb B Krombach F Vogelmeier C Intracellular glutathione and bronchoalveolar cells in fibrosing alveolitis effects of N-acetylcysteine Eur Respir J 200219906-11 29 Bando M Hosono T Mato N et al Long-term efficacy of inhaled N-acetylcysteine in patients with idiopathic pulmonary fibrosis Intern Med 2010492289-96 30 Demedts M Behr J Buhl R et al High-dose acetylcysteine in idiopathic pulmonary fibrosis N Engl J Med 20053532229-42 31 Toma TP Bhowmik A Rajakulasingam R Acetylcysteine in pulmonary fibrosis N Engl J Med 20063541086-9 author reply -9 32 Hunninghake GW Antioxidant therapy for idiopathic pulmonary fibrosis N Engl J Med 20053532285-7 33 Flaherty KR Mumford JA Murray S et al Prognostic implications of physiologic and radiographic changes in idiopathic interstitial pneumonia Am J Respir Crit Care Med 2003168543-8 34 Latsi PI du Bois RM Nicholson AG et al Fibrotic idiopathic interstitial pneumonia the prognostic value of longitudinal functional trends Am J Respir Crit Care Med 2003168531-7 35 Collard HR King TE Jr Bartelson BB Vourlekis JS Schwarz MI Brown KK Changes in clinical and physiologic variables predict survival in idiopathic pulmonary fibrosis Am J Respir Crit Care Med 2003168538-42 36 Jegal Y Kim DS Shim TS et al Physiology is a stronger predictor of survival than pathology in fibrotic interstitial pneumonia Am J Respir Crit Care Med 2005171639-44 37 Martinez FJ Safrin S Weycker D et al The clinical course of patients with idiopathic pulmonary fibrosis Ann Intern Med 2005142963-7 38 Hull JH Acetylcysteine in pulmonary fibrosis N Engl J Med 20063541089-91 author reply -91
70
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
39 Flaherty KR King TE Jr Raghu G et al Idiopathic interstitial pneumonia what is the effect of a multidisciplinary approach to diagnosis Am J Respir Crit Care Med 2004170904shy10 40 Raghu G Johnson WC Lockhart D Mageto Y Treatment of idiopathic pulmonary fibrosis with a new antifibrotic agent pirfenidone results of a prospective open-label Phase II study Am J Respir Crit Care Med 19991591061-9 41 Hunninghake GW Lynch DA Galvin JR et al Radiologic findings are strongly associated with a pathologic diagnosis of usual interstitial pneumonia Chest 20031241215-23 42 Lynch D Godwin J Safrin S et al High-resolution computed tomography in idiopathic pulmonary fibrosis diagnosis and prognosis Am J Respir Crit Care Med 2005172488-93 43 Mallinckrodt CH Watkin JG Molenberghs G Carroll RJ Choice of the primary analysis in longitudinal clinical trials Pharmaceutical Statistics 20043161-9 44 Bang H Tsiatis A Estimating medical costs with censored data Biometrika 200087329shy43 45 Lin DY Regression analysis of incomplete medical cost data Stat Med 2003221181-200 46 Rochon J Application of GEE procedures for sample size calculations in repeated measures experiments Stat Med 1998171643-58 47 Lachin JM Foulkes MA Evaluation of sample size and power for analyses of survival with allowance for nonuniform patient entry losses to follow-up noncompliance and stratification Biometrics 198642507-19
71
- PANTHER-IPFPREDNISONE AZATHIOPRINEAND N-ACETYLCYSTEINEA STUDY THAT EVALUATES RESPONSE INIDIOPATHIC PULMONARY FIBROSIS
-
- Protocol Summary
- Table of Contents
- List of Tables
- List of Figures
- List of Abbreviations
- 1 Summary
- 2 Hypotheses and Specific Aims
-
- 21 Null Hypothesis
- 22 Specific Aim 1
- 23 Specific Aim 2
- 24 Prespecified Subgroups of Interest
-
- 3 Background and Significance
-
- 31 Idiopathic Pulmonary Fibrosis is the Most Common Interstitial Lung Disease
- 32 Rationale for Placebo Control
- 33 Rationale for N-acetylcysteine
- 35 Rationale for N-acetylcysteine as a Stand-alone Therapy
- 36 Rationale for the Study Design and Primary Endpoint
- 37 Rationale for Blinding of Treatments
-
- 4 Methods
-
- 41 Inclusion Criteria
- 42 Diagnosis of IPF
- 43 Exclusion Criteria
- 44 Study Design and Study Visit
- 45 Dose Justification
- 46 Contraindications Precautions and Side Effects of Study Medications
- 47 Recruitment Procedures
- 48 Study Procedures
- 49 Concomitant Medications
- 410 Laboratory Testing
- 411 Blinding of Study Drugs
-
- 5 Study Endpoints
-
- 51 Primary Study Endpoint
- 52 Secondary Study Endpoints
-
- 6 Safety Evaluations and Procedures
-
- 61 Adverse Events
- 62 Clinical Medical Monitoring
- 63 Unblinding Procedures
-
- 7 Study Drug Procedures
- 8 Data Management
-
- 81 Hardware and Software Configuration
- 82 Sources of Data
-
- 9 Study Design and Data Analysis
-
- 91 General Analytic Considerations
- 92 Randomization Blinding and Reporting of Results
- 93 Stratification
- 94 Specification of the Primary Analyses
- 95 Analysis of Longitudinal Endpoints
- 96 Analysis of Binary Time-to-Event and Time-Lagged Endpoints
- 97 Power Analysis
-
- 10 Study Administration
-
- 101 Cooperative Agreement Mechanism
- 102 IPFnet Steering Group
- 103 Data and Safety Monitoring Board
- 104 Recommendations on Interim Monitoring of Efficacy Safety and Futility
-
- 11 Investigator and Sponsor Obligations
-
- 111 Monitoring
- 112 Cost and Payment
- 113 Confidentiality and Health Insurance Portability and Accountability ActConsiderations
- 114 Informed Consent Procedures
- 115 Institutional Review Boards
-
- 12 Investigator Agreement
- 13 References
-

37
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
452 Dosage Algorithms
Dosage Adjustment Algorithm 1 NACPL Dose Modifications for Gastrointestinal Symptoms Nausea Vomiting Abdominal Discomfort Diarrhea
GI Symptoms determined by the PI to be clinically significant Nausea Vomiting Abdominal Discomfort Diarrhea
NACPL Temporarily dc (HOLD) x 3 Days
Monitor symptoms intervene as clinically indicated (eg fluid replacement antidiarrhea or antinausea medication)
Monitor or lab PRN
Are symptoms resolving after 3 days NO
Symptoms NOT resolving after 3 days of holding study medication Assessmentmanagement per clinical
discretion of investigator
Likely not study medication discuss resuming study medication with medical monitor when symptoms resolved
YES
Temporarily dc (HOLD) NACPL for 4 additional days (total hold 1 week) then NACPL Resume 600 MG TID
Did symptoms recur
YES
STOP NACPL for
duration of study
NO
NACPL No Change
38
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Dosage Adjustment Algorithm 2 NACPL Dose Modifications For Dermatologic Reactions
Dermatologic Reactions (Not Acneiform) ge Grade 2 Grading per Common Terminology Criteria for
Adverse Events V30 (httpctepcancergov) For example Grade 1 RASHDESQUAMATION Macular or papular eruption or erythema without associated symptoms Grade 2 RASHDESQUAMATION Macular or popular eruption or erythema with pruritus or other associated symptoms localized desquamation or other lesions covering lt50 of body surface area
NACPL Temporarily dc (HOLD) x 3 days
Are symptoms resolving after 3 days
NO Symptoms not resolving after 3 days of holding study medication Assessmentmanagement per clinical discretion of investigator Likely not study medication Discuss resuming study medication with medical monitor when symptoms
resolved YES
Temporarily dc (HOLD) NACPL for 4 additional days (total hold 1 week) then NACPL resume 600 MG TID
Did symptoms recur
YES
STOP NACPL for
duration of study
NO
NACPL No change
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
46 Contraindications Precautions and Side Effects of Study Medications
461 Contraindication
Contraindication to NAC is known hypersensitivity to it
462 Precautions
Concomitant administration of oral NAC and antibiotics has shown a slightly reduced absorption
of cephalexin and a slight increase in erythromycin serum levels NAC contains free sulfhydryl
groups There is no evidence that individuals sensitive to sulfa drugs are sensitive to NAC
The NAC preparation being administered in this study contains 20 mg of aspartame Because of
the phenylalanine component of aspartame individuals with phenylketonuria should avoid or
restrict aspartame intake to avoid increased blood levels of phenylalanine Because of this risk
labeling is required on all products containing aspartame
463 Side Effects
Side effects of NAC range from common to serious See Table 4
39
40
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Table 4 Side Effects of NAC
Undesirable Effects
System-organ class Uncommon
(gt11000 lt1100)
Rare
(gt110000 lt11000)
Very rare
(lt110000) Not known
Immune system disorders Hypersensitivity Anaphylactic shock
reaction
Nervous system disorders Headache
Ear and labyrinth disorders Tinnitus
Cardiac disorders Tachycardia
Vascular disorders Hemorrhage
Respiratory thoracic and
mediastinal disorders
Bronchospasm
Dyspnea
Gastrointestinal disorders
Vomiting diarrhea
stomatitis abdominal
pain nausea
Dyspepsia
Skin and subcutaneous tissue
disorders
Urticaria rash
angioedema itching
General disorders and
administration site conditions Pyrexia
Investigations Reduced arterial
pressure Face edema
In very rare cases the onset of severe skin reactions such as Stevens-Johnson syndrome and Lyell syndrome was reported to have a temporal relationship with N-acetylcysteine administration Although in most cases at least another suspect drug probably most involved in the genesis of the above mentioned mucocutaneous syndromes has been identified in case of mucocutaneous alterations it is appropriate to contact onersquos doctor and the administration of N-acetylcysteine should be immediately discontinued
Some studies confirmed a reduction of platelet aggregation during N-acetylcysteine administration The clinical significance of these findings has not been defined yet [Source Fluimucil Investigator Brochure]
47 Recruitment Procedures
Subjects recruited for this study will be established patients of the investigators or physician- or
self-referred to participating clinical centers in the IPFnet Each clinical center within IPFnet has
a well-developed infrastructure of local pulmonologists within the surrounding geographic area
These pulmonologists are kept informed of ongoing IPF clinical trials and regularly refer
subjects to studies conducted at IPFnet clinical centers
Additional steps will be taken to inform clinicians of the trials in progress within IPFnet
including presentations at faculty staff meetings at local hospitals medical grand rounds and
national conferences direct mail notification monthly faxes and advertisement of network trials
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
in pulmonary journals Clinical center patients previously diagnosed with IPF will be notified of
the trials by mail whenever possible
Recruitment of minorities and women will be monitored by the DCC and DSMB If necessary
additional recruitment efforts will be made at specific centers to ensure that the aggregate subject
sample contains appropriate representation of women and minorities
48 Study Procedures
The following procedures are detailed in the PANTHER-IPF MOOP accompanying this
protocol
1 PFT
2 ABG
3 HRCT scan of the chest (including imaging of pulmonary arteries)
4 CBC and serum chemistries
5 Pregnancy test
6 6MWTBorg Dyspnea Scale
7 QOL questionnaires (EuroQol HAD SF-36 SGRQ and ICE CAP)
8 UCSD SOBQ
9 Gender Substudy Questionnaire
All assessments of PFTs will be conducted by study personnel not directly involved in the
treatment of the subjects
481 Biological Specimen Management
4811 Biological Specimen Sample Management
Subjects at clinical centers participating in the specimen repository substudy who consent to
having blood drawn for research purposes and for the banking of blood blood components and
other biologic specimens (urine and BAL fluid) will have approximately 405 mL of blood
41
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
drawn 17 mL blood drawn for DNA and 20 mL of urine collected at enrollment visit Subjects
will have approximately 50 mL of blood drawn and 20 mL of urine collected at each 15-week
follow-up visit Blood specimens will be separated according to PANTHER-IPF MOOP
guidelines into the following components for banking in the repository serum plasma and
DNA Coding of all biologic specimens for the repository will be performed by study staff at the
clinical center The samples will be processed per PANTHER-IPF MOOP guidelines aliquoted
labeled with barcode labels and stored at -70degC at the clinical center and shipped to the central
repository
The only subject identifiers will be a sample ID number and subject initials This sample ID will
be linked in the IPFnet DCC clinical database to subject information No subject information will
be transferred to the biological-specimen database
The subjectrsquos samples may be used for approved sub-studies relating to human disease
including but not limited to IPF The studies for which an individualrsquos samples will be made
available will be determined by the subjectrsquos answers to questions on the biological-sample
informed consent form The subjects can choose to make their samples available for all options
or any combination Samples will be made available to researchers only with IPFnet Steering
Group approval until such time as the samples are made public through the NHLBI repository
49 Concomitant Medications
Concurrent treatment with FDA-approved therapy for IPF is allowed Colchicine may be used
for treatment of gout Temporary treatment with oral or IV corticosteroids for clinical worsening
or suspected AEx is permitted Nutritional supplements containing NAC are not allowed
410 Laboratory Testing
Clinical laboratory parameters will be assessed at screening and at the end of the study The
following tests will be performed at the two time points specified in the protocol chemistry (AG
ratio ALT [SGPT] AST [SGOT] albumin alkaline phosphatase amylase bilirubin-direct
42
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
bilirubin-indirect bilirubin-total BUN BUNcreatinine ratio calcium carbon dioxide
cholesterol-total chloride CPK-total creatinine GGT globulin glucose iron-total LDH
lipase magnesium phosphorus-inorganic potassium protein-total sodium TIBC triglycerides
uric acid) and hematology (red blood cell count WBC count hemoglobin hematocrit cell
indices differential platelet count)
411 Blinding of Study Drugs
Subjects and caregivers will be blinded to study treatment Every subject will receive NAC or
matching PLs at every study visit from the baseline visit to the week-45 visit No study agent
will be dispensed at the week-60 visit
43
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
5 Study Endpoints
51 Primary Study Endpoint
The primary endpoint will be the change in serial measurements of FVC over the study period
52 Secondary Study Endpoints
521 Time to Disease-progression
The time-to-death or a 10 decline in FVC will be defined as the time-to-disease progression
The 10 decline in FVC from enrollment must be confirmed on 2 consecutive visits no less than
6 weeks apart For subjects with 2 consecutive visits with a 10 decline in FVC the time-toshy
disease progression will be defined as the time interval between enrollment and the initial visit
with a 10 FVC decline For subjects who experience disease progression the study doctor will
determine whether or not the subject will remain in the study
522 Acute Exacerbations
The following 3 criteria will define AEx in subjects with acute worsening of their respiratory
conditions
1 Clinical (all of the following required)
A) Unexplained worsening of dyspnea or cough within 30 days triggering unscheduled
medical care (eg emergency room clinic study visit hospitalization)
B) No clinical suspicion or overt evidence of cardiac event pulmonary embolism or deep
venous thrombosis to explain acute worsening of dyspnea
C) No pneumothorax
44
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
2 RadiologicPhysiologic (A and B required)
A) New ground glass opacity or consolidation computed tomography (CT) scan OR new
alveolar opacities on chest x-ray
B) Decline of ge 5 in resting room air SpO2 from last recorded level OR decline of ge 8 mm
Hg in resting room air PaO2 from last recorded level
3 Microbiologic (all of the following required)
A) No clinical evidence for infection (ie absence of grossly purulent sputum fever gt 39degC
orally)
B) Lack of positive microbiological results (if done) from lower respiratory tract defined as
(1) Clinically significant bacterial growth on sputum or endotracheal aspirate cultures
(2) Quantitative culture by protected brush specimen ge 103 cfumL or BAL ge 104 cfumL
(3) The presence of specific pathogens on stains of any of the above
C) Lack of positive pathogen in blood cultures (if done)
Identification of Acute Exacerbations
All subjects will be educated about the importance of identifying AExs At the time of
enrollment subjects will be told about the possibility of developing acute symptomatic
worsening that might represent an AEx of IPF and instructed to contact their study clinical
center coordinator within 48 to 72 hours of the apparent event
All subjects will be contacted by phone monthly and questioned about any change in dyspnea or
cough and any interim clinic visits or hospitalizations Finally as part of the IPFnet outreach to
community referring physicians the importance of AExs will be emphasized When a subject is
identified who meets criterion 1A this will trigger the collection of additional clinical data to
evaluate a suspected AEx These data will be collected as part of standard clinical care (ie this
protocol does not require collection of all items) The additional items to be collected for
suspected AEx include
IPFnet AEx case report form (eCRF) (required)
45
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Chest x-ray CT scan withwithout pulmonary angiogram (reports should be faxed and
followed by the hard copiesdiscs)
Oxygen saturation (pulse oximetry)
ABG
Respiratory cultures (sputum endotracheal aspirate lavage)
Blood cultures
Clinichospital records related to the event
All potential cases of AEx will be reviewed by the clinical center PI first and a decision on
whether the case may represent an AEx will be made If AEx is suspected the case will be sent
to the IPFnet adjudication committee which will assign a final diagnosis (see Table 5) If there is
disagreement among members the majority opinion will be recorded
During episodes of suspected AEx as determined by the individual clinical center investigator
subjects will remain blinded and in the study
Table 5 Final Diagnoses in Evaluation of Suspected Acute Exacerbations
Definite acute exacerbation All criteria met no alternative etiology
Unclassifiable acute worsening
Insufficient data to evaluate all criteria no alternative etiology
Not acute exacerbation Alternative etiology identified that explains acute worsening
Management of the suspected AEx will be at the discretion of the treating physician Standard of
care generally involves evaluation for respiratory infection pulmonary embolism cardiac events
and pneumothorax and treatment with IV corticosteroids
Study drugs will be resumed at pre-suspected AEx doses after subjects clinically improve as
confirmed by the local PI All subjects should be seen at the clinical center within 2 to 4 weeks
of recovery for measurement of post-bronchodilator FVC (see Figure 4) Subjects unable to
return to the clinical center after suspected AEx due to medical frailty (eg continued
46
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
institutionalization progressive disability) will be categorized as failing to maintain FVC
response in secondary analyses
Suspected AEx (PI determined)
Hold study drug Treat AEx
(Attending physician determined)
Alive but unable to continue due to
medical frailty
Dead
Alive and able to continue
Site reviewvisit
Restart study drug
FVC within 2-4 weeks
Figure 4 Acute Exacerbation Flow Chart
523 Respiratory Infections
An upper respiratory infection will be defined as
Change in sputum discoloration
Increased cough of no more than 14 daysrsquo duration
A lower-respiratory infection (pneumonia) will be defined as new segmental or lobar airspace
opacities visualized by image studies (chest radiograph or HRCT) in addition to any of the
following
Positive pathogencultures in good sample of sputum or lower-airway secretions retrieved
by fiberoptic bronchoscope
Fever gt 39degC or gt 100degF
Leukocytosis gt 12000 (unexplained no increase in dose of corticosteroids)
47
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
524 Maintained FVC Response
Subjects with follow-up FVCpred measurements at or above their baseline FVCpred level
will be classified as having maintained FVC response Subjects with reduced FVCpred levels
or missing data for any reason including death or medical frailty will be classified as having not
maintained FVC response The FVCpred value is used because unadjusted FVC measurements
are expected to decline with age
48
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
6 Safety Evaluations and Procedures
61 Adverse Events
During a clinical trial the reporting of adverse experience information can lead to important
changes in the way a new treatment is developed as well as provide integral safety data
611 Definitions
An adverse event (AE) is any untoward medical occurrence in a subject or clinical investigation
subject who was administered a pharmaceutical product The AE does not necessarily have to
have a causal relationship with the drug administered An AE can be any unfavorable and
unintended sign (including an abnormal laboratory finding) symptom or disease temporarily
associated with the use of a medicinal product whether or not considered to be related to the
medicinal product Diseases signs symptoms or laboratory abnormalities already existing at
enrollment are not considered AEs unless they worsen (ie increase in intensity or frequency)
Surgical procedures themselves are not AEs they are therapeutic measures for conditions that
require surgery The condition for which the surgery is required may be an AE Surgical
procedures planned before randomization and the conditions necessitating the surgery are not
AEs
A serious adverse event is any untoward event that
Is fatal
Is life-threatening
Requires inpatient hospitalization or prolongation of existing hospitalization with the
following exceptions
o Preplanned (before the study) hospital admissions unless the hospitalization is
prolonged
o Planned admissions (as part of a study eg routine biopsies)
o Hospitalization lasting lt 24 hours
49
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
o Hospitalization for elective procedure
o Emergency room visits
Results in persistent or significant disability or incapacity
Is a congenital anomaly or birth defect
Important medical events that may not result in death be life-threatening or require
inpatient hospitalization may be considered serious adverse events (SAEs) when based
on appropriate medical judgment they may jeopardize the subject and may require
medical or surgical intervention to prevent one of the outcomes listed above
Life-threatening means that the subject was in the view of the investigator at immediate risk of
death from the AE as it occurred It does not include an AE that had it occurred in a more severe
form might have caused death
Persistent or significant disabilityincapacity means that the event resulted in permanent or
significant and substantial disruption of the subjectrsquos ability to carry out normal life functions
Causality
A reasonable possibility means the AE may have been caused byrelated to the study drug A
perceived or real lack of efficacy does not satisfy the definition of relatedness
612 Adverse Event (AE) Reporting
For the PANTHER-IPF trial all AEs (serious and nonserious) occurring from randomization
through final study visit (4 weeks after final dose of all study medication) will be recorded on the
AE page of the case report form (CRF)
6121 Serious Adverse Events (SAE) Reporting
For this trial all deaths and all SAEs which occur from randomization through final study visit
must be entered within the EDC system via the SAE eCRF page within 24 hours of the
investigative sitersquos knowledge of the event It is the responsibility of the clinical center
50
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
investigator to provide a causality assessment of the event for each study medications based upon
the information available at the time of the report It is understood that complete information
about the event may not be known at the time the initial report is submitted In the event the EDC
system is not accessible to the site at the time of event reporting investigative sites will complete
and forward a paper back-up SAE form to DCRI Safety Surveillance for processing
DCRI Safety Surveillance
Telephone 1-919-668-8624 or 1-866-668-7799 (toll free)
Fax 1-919-668-7138 or 1-866-668-7138 (toll free)
The investigator must complete and submit follow-up SAE information via the eCRF when
important new or follow-up information (eg final diagnosis outcome results of specific
investigations) becomes available Follow-up information should be submitted according to the
same process used for reporting the initial event as described above All SAEs will be followed
until resolution stabilization or 30 days after the subject has completed the final visit (4 weeks
after the final dose of study medication) whichever occurs first The investigator is responsible
for reporting SAEs to their institutional review board (IRB) per site specific IRB reporting
guidelines
6122 Regulatory Reporting
AEs that are serious study drug related and unexpected will be reported to the regulatory
authorities The DCRI Safety Surveillance medical monitor will perform a medical review of all
SAEs submitted and evaluate for ldquounexpectednessrdquo DCRI Safety Surveillance will prepare
MedWatch reports for those events identified as serious study drug related and unexpected as
determined by Safety Medical Monitor
DCRI Regulatory Services will submit all unexpected study drug-related SAEs as per 21 CFR
32 DCRI Safety Surveillance will provide a safety alert letter to the NHLBI DSMB and DCC
clinical operation (for distribution to sites) within 15 days of initial receipt of the information
51
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Investigators are responsible for promptly reporting these events to their reviewing IRBs
according to site specific IRB reporting guidelines
62 Clinical Medical Monitoring
There will be an unblinded physician at the IPFnet DCC serving as medical monitor The
medical monitor will be available to assist with questions about dosage adjustments of study
medications including discontinuation or resumption of medications
63 Unblinding Procedures
Unblinding of subjects or investigators to subject treatment is strongly discouraged For ongoing
clinical management all subjects should be presumed to be receiving ldquoactiverdquo study drug To
ensure the subjectrsquos safety the study treatment will be dose-adjusted based on laboratory test
results clinical findings and symptoms
The IPFnet DCC medical monitor and PANTHER-IPF co-chairs Drs Ganesh Raghu and
Fernando Martinez will be available to the study physicians to discuss study drug management
on a case-by-case basis Un-blinding will be considered ONLY when the knowledge of subject
treatment assignment is ABSOLUTELY ESSENTIAL for subject safety and after discussion of
the subjectrsquos case with the medical monitor and either Dr Raghu or Dr Martinez Unblinding of
study treatment should be minimized during the conduct of the trial In those cases where it is
felt to be medically necessary the DCC medical officer will communicate directly with the
managing physician to minimize unblinding of study personnel
52
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
7 Study Drug Procedures
At the baseline 15-week 30-week and 45-week study visits subjects will receive a supply of
study drug sufficient to last until the next visit at which study drug will be dispensed
53
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
8 Data Management
81 Hardware and Software Configuration
811 Hardware and Database Software
Data will be stored in an Oracle database system Oracle has advantages of processing efficiency
and smooth linkage with other software systems The application and database will be hosted on
Solaris Unix servers at the IPFnet DCC
812 Statistical Software
SAS will be used as the principal application for the management of analysis data files and
statistical computations S-Plus will be used to provide supplementary functions as needed
813 Access Control and Confidentiality Procedures
Access to databases will be controlled centrally by the IPFnet DCC through user passwords
linked to appropriate privileges This protects the data from unauthorized changes and
inadvertent loss or damage
814 Security
Database and Web servers will be secured by a firewall and through controlled physical access
Oracle has many security features to ensure that any staff member accessing the database has the
proper authority to perform the functions he or she requests of the system Within the secondary
SAS databases Unix group-access control maintains similar security The Sun workstation login
is secured by extensive user-password facilities under Unix
54
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
815 Back-up Procedures
Database back-up will be performed automatically every day and standard IPFnet DCC policies
and procedures will be applied to dictate tape rotation and retention practices
816 Virus Protection
All disk drives that provide network services and all user computers will be protected using
virus-scanning software Standard IPFnet DCC policies will be applied to update these protection
systems periodically through the study
82 Sources of Data
821 Design and Development
The IPFnet DCC will be responsible for development of the electronic case report forms
(eCRFs) development and validation of the clinical study database ensuring data integrity and
training clinical center staff on applicable data management procedures A web-based distributed
data entry model will be implemented This system will be developed to ensure that guidelines
and regulations surrounding the use of computerized systems used in clinical trials are upheld
The remainder of this section provides an overview of the data management plan associated with
this protocol
822 Data Collection Forms
The data collection process consists of direct data entry at the study clinical centers into the EDC
system(s) provided by the DCC A data collection worksheet will be provided to clinical centers
for recording data in the event the EDC system is unavailable Data entry of the eCRFs should
be completed according to the instructions provided and project specific training The
investigator is responsible for maintaining accurate complete and up-to-date records and for
ensuring the completion of the eCRFs for each research participant
55
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
823 Data Acquisition and Entry
Data entry into eCRFs shall be performed by authorized individuals Selected eCRFs may also
require the investigatorrsquos written signature or electronic signature as appropriate Electronic
CRFs will be monitored for completeness accuracy and attention to detail during the study
824 Data Center Responsibilities
The IPFnet DCC will 1) develop a data management plan and will conduct data management
activities 2) provide final eCRFs for the collection of all data required by the study 3) develop
data dictionaries for each eCRF that will comprehensively define each data element 4) conduct
ongoing data monitoring activities on study data 5) monitor any preliminary analysis data
cleanup activities and 6) rigorously monitor final study data clean up
825 Data Editing
Completed data will be entered into the IPFnet DCC automated data acquisition and
management system If incomplete or inaccurate data are found a data clarification request will
be generated and distributed to clinical centers for a response Clinical centers will resolve data
inconsistencies and errors and enter all corrections and changes into the IPFnet DCC automated
data acquisition and management system
826 Training
The training plan for clinical center staff includes provisions for training on assessments eCRF
completion guidelines data management procedures and the use of computerized systems
56
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
9 Study Design and Data Analysis
91 General Analytic Considerations
All primary analyses will be based on intent-to-treat (ITT) principles using all randomized
subjects Baseline factors across groups will be compared using mean (standard deviation) and
median (25th and 75th percentiles) summary measures Kaplan-Meier curves will be used to
display event rates Due to clinical interest in departures from both sides of the null hypothesis
all test statistics will be 2-sided
Reasonable caution needs to be taken when conducting multiple analyses on key clinical
subgroups For subgroup analyses a conservative significance level of 0001 will be used for all
interaction tests Thus subgroup comparisons will be considered exploratory unless the p-value
from the interaction test is smaller than 0001
92 Randomization Blinding and Reporting of Results
A permuted block-randomization scheme will be created with varying block sizes stratified by
clinical center Once a subject has completed the screening and baseline period and evaluation
for inclusionexclusion criteria the randomization process will begin Subjects will be
randomized to receive NAC or matching placebo with equal probability (11) via telephone
contact with a central interactive voice response system (IVRS) using a toll-free randomization
number On the day of randomization after the subject has successfully met all inclusion and
exclusion criteria the investigator or designee will call the central randomization number to
obtain the assigned kit randomization numbers for that subject At each subject visit the
investigator or designee will call the central randomization number to obtain the new kit
randomization numbers for resupply of the subject For resupply of the clinical center the IVRS
will monitor minimal volume of a kit type andor expiration date and will automatically notify
the pharmacy
57
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
The trial results will be reported according to guidelines specified in the CONSORT statement
A flow diagram describing screening recruitment randomization dropout and vital status will
be included in the primary manuscript AEs and efficacy data will be presented for all treatment
groups Adherence dropout and lost to follow-up will be carefully examined across all treatment
groups Analyses of safety will be based on data from all randomized subjects who received at
least one dose of study drug
93 Stratification
Subjects will be distributed to the two treatment arms in a 11 allocation ratio Stratification
blocks will be based on clinical centers
94 Specification of the Primary Analyses
A mixed model repeated measures (MMRM) analysis described in section 95 will be used to
compare differences in the slope of FVC measurements across the treatment groups Response
variables are values of the FVC measured at baseline and every 15 weeks until study completion
Variables in the model will include treatment time and time by treatment age sex race and
height Contrast estimates of differences in slopes of treatment over time (along with confidence
intervals) will be used to estimate the treatment effect The validity of this model in terms of
meeting modeling assumptions will be assessed via standard modeling diagnostics and goodness-
of-fit measures Based on the MMRM framework missing FVC data will not be imputed for the
primary analysis
95 Analysis of Longitudinal Endpoints
A common goal in clinical trials is to specify models that are easily implemented and
reproducible by independent data analysts On the other hand the models should have proper
statistical behavior in terms of low bias and high precision Many common approaches to
longitudinal data analysis including last observation carried forward (LOCF) imputation rely on
the missing completely at random (MCAR) assumption However the MCAR assumption is
58
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
unlikely to hold in many clinical trials because missing data are often related to disease
progression and prognosis A more reasonable assumption missing at random (MAR) specifies
that the complete data distribution can be modeled using only the observed data The likelihood-
based MMRM approach is valid under the more general MAR assumptions These models will
be applied to analyze the longitudinal data secondary endpoints
The advantages of MMRM analysis are that all important characteristics of the model can be preshy
specified standard software can be used to implement the models and results are based on ITT
principles43 In addition the MMRM approach offers superior control of Type I and Type II
errors compared with the LOCF approach
Response variables are values of the PFTs measured at enrollment and every 15 weeks until
study completion and 6MWT values measured at baseline week 30 and week 60 Covariates are
treatment time time by treatment and key baseline risk factors Contrasts (along with
confidence intervals) of treatment by time will be used to estimate the treatment effect
The correlation structure involves multiple pieces including measurement errors random
variation and interindividual variability For the longitudinal data analyses an unstructured
correlation matrix for within-subject errors will be assumed Other correlation structures
including compound symmetry will be examined as needed A careful examination of reasons
for study discontinuation will be conducted to assess the validity of MCAR Sensitivity analyses
will be used to examine the untestable assumption that the observed data violate the MAR
assumption The MMRM models will be implemented using PROC MIXED in SAS
96 Analysis of Binary Time-to-Event and Time-Lagged Endpoints
Regression modeling approaches using either the logistic regression model or Cox proportional
hazards regression model will be employed when appropriate The validity of these models will
be assessed via standard modeling diagnostics and goodness-of-fit measures Estimates of
cumulative frequencies for more general time-lagged responses will be calculated using the
partitioned version of the Bang-Tsiatis estimator44 The partitions will be set at 15-week intervals
59
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
to correspond with the data-collection process Covariate adjusted event rates will be calculated
using inverse probability-weighted regression estimates45
97 Power Analysis
971 Primary Analyses
Based on previously published IPF clinical trials the PL group is expected to experience a drop
in FVC of approximately 020 L over the study period (see Figure 1) The IPFnet Steering Group
determined a clinically important difference would be to preserve the majority of the decline
relative to PL over the study period In particular a treatment effect of 015 L was determined to
be a clinically meaningful difference Potential dropout is a key factor in the proposed study The
drop-out process assumed 5 lost to follow-up after every study visit Only 80 of subjects
were assumed to be followed for the entire study period All models assumed a compound
symmetry structure for the covariance matrix Power calculations were performed using a SAS
IML program for designing repeated measures studies46 Based on preliminary reviews of the
data from the University of Michigan the covariance matrix parameters were estimated at
approximately σ2 = 0757 (variance parameter) and ρ = 0936 (correlation parameter) To be
conservative the power calculations for the primary analysis were performed with parameter
setting of σ2 = 0810 (variance parameter) and ρ = 0925 (correlation parameter)
The power calculations assume a correction for imperfect compliance proposed by Lachin and
Foulkes to allow for 2 noncompliance for each of the treatment arms47 Thus the sample size
of 130 subjects per arm would be reduced to an adjusted sample size of 130(1-002-002)2 =
1198 or 120 subjects per arm
Under the assumed Type I error rate of 005 with a correlation parameter of 0925 and standard
deviation of 090 the difference of 015 L (or 00025 Lweek) shown in Table 6 would have
power of 93
60
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Table 6 Hypothetical Values of Mean FVC (L) Change from Baseline
Week 15 Week 30 Week 45 Week 60
NAC 00125 00250 00375 00500
Placebo 00500 01000 01500 02000
Difference 00375 00750 01125 01500
Abbreviations FVC forced vital capacity PL placebo
972 Power Analysis for Secondary Endpoints
Power calculations for secondary endpoint measurements are shown in Table 7 Standard
deviations are based on unpublished data provided by the University of Michigan The
calculations are based on a 2-sample t-test with Type I error rate set at 005 These calculations
are likely to be conservative because the statistical approach described in section 95 for
analyzing these endpoints will incorporate incomplete observations as well as intermediate data
points
Table 7 Detectable Differences in Treatment Means for Selected Endpoint Measurements
Secondary Endpoints Std Dev
of the Baseline Score
Detectable Difference for 80 Power
Std Dev of the Change Score
Difference Detectable for
80 Power
DLCOpred 166 58 91 32
6MWT Area Under the Desaturation Curve
219 76 175 61
6MWT Distance to Desaturation 224 78 315 110
6MWT Minutes Walked 210 073 205 071
Abbreviations Std Dev standard deviation DLCOpred diffusing capacity of the lung for carbon monoxide percent predicted 6MWT 6-minute walk test
61
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
10 Study Administration
101 Cooperative Agreement Mechanism
The administrative and funding mechanism used to undertake this project is a ldquocooperative
agreementrdquo (U01) which is an assistance mechanism Under the cooperative agreement the
NHLBI assists supports andor stimulates the project and is substantially involved with
investigators in conducting the study by facilitating performance of the effort in a ldquopartnerrdquo role
The NHLBI project scientist serves on the IPFnet Steering Group and he or another NHLBI
scientist may serve on other project committees when appropriate At the same time however
NHLBI does not assume a dominant role direction or prime responsibility for this research
program
As described below governance of the project is conducted through the IPFnet Steering Group
Principal investigators have lead responsibilities in all aspects of their trials and the project
including any modification of trial designs conduct of the trials quality control data analysis
and interpretation preparation of publications and collaboration with other investigators unless
otherwise provided for by the IPFnet Steering Group
PIs retain custody of and have primary rights to their center-specific and collaborative data
subject to government rights-of-access consistent with current Health amp Human Services (HHS)
Public Health Service (PHS) and National Institutes of Health policies The protocols and
governance policies call for the continual submission of data centrally to the IPFnet DCC for the
collaborative database which at a minimum will contain the key variables selected by the IPFnet
Steering Group for standardization across all clinical centers the submission of copies of the
collaborative datasets to each PI upon completion of the project procedures for data analysis
reporting and publication and procedures to protect and ensure the privacy of medical and
genetic data and records of individuals The NHLBI project scientist on behalf of the NHLBI
will have the same access privileges and responsibilities regarding the collaborative data as the
other members of the Steering Group
62
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
PIs are also encouraged to publish and to publicly release and disseminate results data and other
products of the project concordant with the project protocols and governance and the approved
plan for making data and materials available to the scientific community and to the NHLBI
However during the 3 years after the ending date of NHLBI project support unpublished data
unpublished results data sets not previously released and other study materials or products are
to be made available to any third party only with the approval of the IPFnet Steering Group
Upon completion of the project PIs are expected to put their intervention materials and
procedure manuals into the public domain andor make them available to other investigators
according to the approved plan for making data and materials available to the scientific
community and the NHLBI for the conduct of research at no charge other than the costs of
reproduction and distribution
The NHLBI reserves the right to terminate or curtail the project (or an individual award) in the
event of (a) failure to develop or implement mutually agreeable collaborative measurement
subject eligibility and data management sections of the protocols (b) substantial shortfall in
subject recruitment follow-up data reporting or quality control or other major breach of
protocol (c) substantive changes in the agreed-upon protocols with which NHLBI cannot
concur (d) reaching a major project outcome with persuasive statistical significance
substantially before schedule or (e) human subject ethical issues that may dictate a premature
termination
Any disagreement that may arise in scientificprogrammatic matters (within the scope of the
award) between award recipients and the NHLBI may be brought to arbitration An arbitration
panel will be composed of 3 membersmdash1 selected by the IPFnet Steering Group (with the
NHLBI member not voting) or by the individual PI in the event of an individual disagreement a
second selected by NHLBI and the third selected by the other 2 members This special
arbitration procedure in no way affects the PIrsquos right to appeal an adverse action that is otherwise
appealable in accordance with the PHS regulations at 42 CFR part 50 Subpart D and HHS
63
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
regulation at 45 CFR part 16 or the rights of the NHLBI under applicable statutes regulations
and terms of the award
102 IPFnet Steering Group
The IPFnet Steering Group is the main governing body of the project It is composed of the PIs
of the clinical centers the PI of the DCC and the NHLBI project scientist The clinical centers
the IPFnet DCC and the NHLBI each have 1 vote on the IPFnet Steering Group All decisions
are determined by majority vote
All major scientific decisions are determined by the IPFnet Steering Group It assumes overall
responsibility for the design and conduct of the trial It appoints (and disbands) committees and
subcommittees as the need arises designs approves and implements the study protocols
oversees the development of the MOOP monitors subject recruitment and treatment delivery
evaluates data collection and management oversees quality assurance procedures and
implements changes and enhancements to the study as required It also has primary responsibility
for facilitating the conduct of the trials and reporting the projectrsquos results
103 Data and Safety Monitoring Board
The NHLBI will establish a DSMB in accordance with established policies (see
httpwwwnhlbinihgovfundingpoliciesdsmb_insthtm) to ensure data quality and subject
safety and to provide independent advice to the NHLBI regarding progress and the
appropriateness of study continuation
104 Recommendations on Interim Monitoring of Efficacy Safety and Futility
First and foremost the role of the DSMB will be to review subject safety and trial conduct at
periodic points during the study The DSMB may require analyses of the primary endpoint
results for comparing the benefit and risks of treatment strategies The benefit of collecting
additional data on key secondary endpoints with extended follow-up and establishing a robust
64
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
evidence base for determining a standard of care will need to be carefully considered before
early termination of one or more treatment arms After careful consideration the IPFnet Steering
Group recommends conservative thresholds for the early examinations of the safety and efficacy
data
The DSMB will be expected to meet approximately every 6 months until trial completion to
review safety and toxicity data The DSMB may recommend stopping the study based on these
reviews Because the DSMB could stop the trial for safety concerns as well as for a large
efficacy benefit there could be multiple opportunities to reject the null hypothesis (no difference
in event rates between the PL and NAC groups) A Bonferroni approximation will be applied
during the one planned interim analysis for efficacy
Before locking the database a statistical analysis plan (SAP) will be developed to provide
complete details on the statistical analysis The SAP will include the specifics for how and when
the DSMB will be notified for AEs The IPFnet DCC will deliver to the DSMB all FDA-defined
AEs at 3-month intervals The IPFnet DCC will prepare narrative SAE reports in real time for
DSMB review including recommendations and analysis of similar events for each SAE
submitted to the FDA
65
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
11 Investigator and Sponsor Obligations
111 Monitoring
All monitoring activities for US clinical centers will be performed in accordance with DCRI
standard operating procedures Information regarding the types of visits will be outlined in the
PANTHER-IPF MOOP
112 Cost and Payment
There will be no cost to subjects enrolled in this trial Study-related procedures will be paid for
by the IPFnet
Subjects may be eligible for reimbursement for travel to the clinical center Details of payment
will be explained to each subject during the consent process
113 Confidentiality and Health Insurance Portability and Accountability Act
Considerations
Subject confidentiality will be protected throughout the study All subject data will be kept
strictly confidential and no subject-identifying information will be released to anyone outside
the project Confidentiality will be assured through several mechanisms First each subject will
be assigned an anonymous study ID which will then be used on all study forms Second any
study forms blood samples and paper records that contain subject information (eg address lists
phone lists) will be kept at the clinical centers in secured locked areas coded by number Once
blood is collected there will be no subject identifiers placed on blood samplesmdashonly the study
ID number and the date of sample collection Third access to all subject data and information
including laboratory specimens will be restricted to authorized personnel In the case of
computerized data this restricted access will be assured through user logon IDs and password
protection
66
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
At the IPFnet DCC only authorized personnel will have access to the data files containing study
data Security will be assured through user logon IDs passwords and appropriate access
privileges All study subjects will be identified only by their IPFnet ID numbers and no personal
identifying information such as name address or Social Security number will be entered into
the IPFnet DCC database Any subject-specific data reported to the IPFnet Steering Group will
be identified only by the IPFnet ID number
Finally subjects will not be identified by name in any reports or publications nor will the data
be presented in such a way that the identity of individual subjects can be inferred Analysis files
created for further study by the scientific community will have no subject identifiers These data
files will be created in accordance with the Ancillary Studies and Publication Policy of the
IPFnet
114 Informed Consent Procedures
All IPFnet subjects will provide written informed consent using procedures reviewed and
approved by each clinical centerrsquos IRB Informed consent will be undertaken by study personnel
in-person with the subject The subject has the option of declining further participation in the
study at that point No further study procedures will be conducted until the signed documents
have been provided to the IPFnet clinical center
115 Institutional Review Boards
Before initiating this study the protocol clinical center-specific informed consent forms Health
Insurance Portability and Accountability Act (HIPAA) forms recruitment materials and other
relevant information will be reviewed by a properly constituted IRB at each participating clinical
center A copy of the signed and dated IRB approval at each clinical center will be retrieved prior
to or during the site initiation visit and archived at the IPFnet DCC Any amendments to the
protocol other than simple administrative and typographical changes must be approved by each
IRB before they are implemented The clinical centers will seek annual renewals of their IRB
approvals in accordance with local procedures
67
__________________________________________ ________________
__________________________________________
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
12 Investigator Agreement
I have read the foregoing protocol PANTHER-IPF and agree that it contains all necessary
details for carrying out this study I will conduct the study as outlined herein and will complete
the study within the time designated
I will provide copies of the protocol and all pertinent information to all individuals responsible to
me who assist in the conduct of this study I will discuss this material with them to ensure they
are fully informed regarding the drug and the conduct of the study
I will fulfill all responsibilities for submitting pertinent information to the local IRB if
applicable that is responsible for this study
I further agree that NHLBI andor DCRI will have access to any source documents from which
eCRF information may have been generated
Signature of Principal Investigator Date
Name of Principal Investigator (printed or typed)
Protocol version date May 19 2009
Protocol Amendment 1 version date May 28 2010
Protocol Amendment 2 version date December 6 2011
68
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
13 References
1 Raghu G Brown KK Bradford WZ et al A placebo-controlled trial of interferon gamma-1b in patients with idiopathic pulmonary fibrosis N Engl J Med 2004350125-33 2 King TE Jr Safrin S Starko KM et al Analyses of efficacy end points in a controlled trial of interferon-gamma1b for idiopathic pulmonary fibrosis Chest 2005127171-7 3 Flaherty KR Thwaite EL Kazerooni EA et al Radiological versus histological diagnosis in UIP and NSIP survival implications Thorax 200358143-8 4 Wells AU Desai SR Rubens MB et al Idiopathic pulmonary fibrosis a composite physiologic index derived from disease extent observed by computed tomography Am J Respir Crit Care Med 2003167962-9 5 Raghu G Freudenberger TD Yang S et al High prevalence of abnormal acid gastroshyoesophageal reflux in idiopathic pulmonary fibrosis Eur Respir J 200627136-42 6 Kinnula VL Focus on antioxidant enzymes and antioxidant strategies in smoking related airway diseases Thorax 200560693-700 7 Coultas DB Zumwalt RE Black WC Sobonya RE The epidemiology of interstitial lung diseases Am J Respir Crit Care Med 1994150967-72 8 Raghu G Weycker D Edelsberg J Bradford WZ Oster G Incidence and prevalence of idiopathic pulmonary fibrosis Am J Respir Crit Care Med 2006174810-6 9 Olson AL Swigris JJ Lezotte DC Norris JM Wilson CG Brown KK Mortality from pulmonary fibrosis increased in the United States from 1992 to 2003 Am J Respir Crit Care Med 2007176277-84 10 Mannino DM Etzel RA Parrish RG Pulmonary fibrosis deaths in the United States 1979shy1991 An analysis of multiple-cause mortality data Am J Respir Crit Care Med 19961531548shy52 11 Hubbard R Johnston I Coultas DB Britton J Mortality rates from cryptogenic fibrosing alveolitis in seven countries Thorax 199651711-6 12 Johnston I Britton J Kinnear W Logan R Rising mortality from cryptogenic fibrosing alveolitis Bmj 19903011017-21 13 Raghu G Collard HR Egan JJ et al An official ATSERSJRSALAT statement idiopathic pulmonary fibrosis evidence-based guidelines for diagnosis and management Am J Respir Crit Care Med 2011183788-824 14 (USA) FDA FDA Public Health Advisory Interferon gamma-1b (marketed as Actimmune) In 2007 15 King TE Jr Pardo A Selman M Idiopathic pulmonary fibrosis Lancet 2011 16 Raghu G Brown KK Costabel U et al Treatment of idiopathic pulmonary fibrosis with etanercept an exploratory placebo-controlled trial Am J Respir Crit Care Med 2008178948shy55 17 Malouf MA Hopkins P Snell G Glanville AR An investigator-driven study of everolimus in surgical lung biopsy confirmed idiopathic pulmonary fibrosis Respirology 201116776-83 18 King TE Jr Behr J Brown KK et al BUILD-1 a randomized placebo-controlled trial of bosentan in idiopathic pulmonary fibrosis Am J Respir Crit Care Med 200817775-81 19 Richeldi L Costabel U Selman M et al Efficacy of a tyrosine kinase inhibitor in idiopathic pulmonary fibrosis N Engl J Med 20113651079-87
69
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
20 Borok Z Buhl R Grimes GJ et al Effect of glutathione aerosol on oxidant-antioxidant imbalance in idiopathic pulmonary fibrosis Lancet 1991338215-6 21 Meyer A Buhl R Magnussen H The effect of oral N-acetylcysteine on lung glutathione levels in idiopathic pulmonary fibrosis Eur Respir J 19947431-6 22 Behr J Maier K Degenkolb B Krombach F Vogelmeier C Antioxidative and clinical effects of high-dose N-acetylcysteine in fibrosing alveolitis Adjunctive therapy to maintenance immunosuppression Am J Respir Crit Care Med 19971561897-901 23 Cantin AM North SL Fells GA Hubbard RC Crystal RG Oxidant-mediated epithelial cell injury in idiopathic pulmonary fibrosis J Clin Invest 1987791665-73 24 Waghray M Cui Z Horowitz JC et al Hydrogen peroxide is a diffusible paracrine signal for the induction of epithelial cell death by activated myofibroblasts Faseb J 200519854-6 25 Larios JM Budhiraja R Fanburg BL Thannickal VJ Oxidative protein cross-linking reactions involving L-tyrosine in transforming growth factor-beta1-stimulated fibroblasts J Biol Chem 200127617437-41 26 Kinnula VL Fattman CL Tan RJ Oury TD Oxidative stress in pulmonary fibrosis a possible role for redox modulatory therapy Am J Respir Crit Care Med 2005172417-22 27 Meyer A Buhl R Kampf S Magnussen H Intravenous N-acetylcysteine and lung glutathione of patients with pulmonary fibrosis and normals Am J Respir Crit Care Med 19951521055-60 28 Behr J Degenkolb B Krombach F Vogelmeier C Intracellular glutathione and bronchoalveolar cells in fibrosing alveolitis effects of N-acetylcysteine Eur Respir J 200219906-11 29 Bando M Hosono T Mato N et al Long-term efficacy of inhaled N-acetylcysteine in patients with idiopathic pulmonary fibrosis Intern Med 2010492289-96 30 Demedts M Behr J Buhl R et al High-dose acetylcysteine in idiopathic pulmonary fibrosis N Engl J Med 20053532229-42 31 Toma TP Bhowmik A Rajakulasingam R Acetylcysteine in pulmonary fibrosis N Engl J Med 20063541086-9 author reply -9 32 Hunninghake GW Antioxidant therapy for idiopathic pulmonary fibrosis N Engl J Med 20053532285-7 33 Flaherty KR Mumford JA Murray S et al Prognostic implications of physiologic and radiographic changes in idiopathic interstitial pneumonia Am J Respir Crit Care Med 2003168543-8 34 Latsi PI du Bois RM Nicholson AG et al Fibrotic idiopathic interstitial pneumonia the prognostic value of longitudinal functional trends Am J Respir Crit Care Med 2003168531-7 35 Collard HR King TE Jr Bartelson BB Vourlekis JS Schwarz MI Brown KK Changes in clinical and physiologic variables predict survival in idiopathic pulmonary fibrosis Am J Respir Crit Care Med 2003168538-42 36 Jegal Y Kim DS Shim TS et al Physiology is a stronger predictor of survival than pathology in fibrotic interstitial pneumonia Am J Respir Crit Care Med 2005171639-44 37 Martinez FJ Safrin S Weycker D et al The clinical course of patients with idiopathic pulmonary fibrosis Ann Intern Med 2005142963-7 38 Hull JH Acetylcysteine in pulmonary fibrosis N Engl J Med 20063541089-91 author reply -91
70
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
39 Flaherty KR King TE Jr Raghu G et al Idiopathic interstitial pneumonia what is the effect of a multidisciplinary approach to diagnosis Am J Respir Crit Care Med 2004170904shy10 40 Raghu G Johnson WC Lockhart D Mageto Y Treatment of idiopathic pulmonary fibrosis with a new antifibrotic agent pirfenidone results of a prospective open-label Phase II study Am J Respir Crit Care Med 19991591061-9 41 Hunninghake GW Lynch DA Galvin JR et al Radiologic findings are strongly associated with a pathologic diagnosis of usual interstitial pneumonia Chest 20031241215-23 42 Lynch D Godwin J Safrin S et al High-resolution computed tomography in idiopathic pulmonary fibrosis diagnosis and prognosis Am J Respir Crit Care Med 2005172488-93 43 Mallinckrodt CH Watkin JG Molenberghs G Carroll RJ Choice of the primary analysis in longitudinal clinical trials Pharmaceutical Statistics 20043161-9 44 Bang H Tsiatis A Estimating medical costs with censored data Biometrika 200087329shy43 45 Lin DY Regression analysis of incomplete medical cost data Stat Med 2003221181-200 46 Rochon J Application of GEE procedures for sample size calculations in repeated measures experiments Stat Med 1998171643-58 47 Lachin JM Foulkes MA Evaluation of sample size and power for analyses of survival with allowance for nonuniform patient entry losses to follow-up noncompliance and stratification Biometrics 198642507-19
71
- PANTHER-IPFPREDNISONE AZATHIOPRINEAND N-ACETYLCYSTEINEA STUDY THAT EVALUATES RESPONSE INIDIOPATHIC PULMONARY FIBROSIS
-
- Protocol Summary
- Table of Contents
- List of Tables
- List of Figures
- List of Abbreviations
- 1 Summary
- 2 Hypotheses and Specific Aims
-
- 21 Null Hypothesis
- 22 Specific Aim 1
- 23 Specific Aim 2
- 24 Prespecified Subgroups of Interest
-
- 3 Background and Significance
-
- 31 Idiopathic Pulmonary Fibrosis is the Most Common Interstitial Lung Disease
- 32 Rationale for Placebo Control
- 33 Rationale for N-acetylcysteine
- 35 Rationale for N-acetylcysteine as a Stand-alone Therapy
- 36 Rationale for the Study Design and Primary Endpoint
- 37 Rationale for Blinding of Treatments
-
- 4 Methods
-
- 41 Inclusion Criteria
- 42 Diagnosis of IPF
- 43 Exclusion Criteria
- 44 Study Design and Study Visit
- 45 Dose Justification
- 46 Contraindications Precautions and Side Effects of Study Medications
- 47 Recruitment Procedures
- 48 Study Procedures
- 49 Concomitant Medications
- 410 Laboratory Testing
- 411 Blinding of Study Drugs
-
- 5 Study Endpoints
-
- 51 Primary Study Endpoint
- 52 Secondary Study Endpoints
-
- 6 Safety Evaluations and Procedures
-
- 61 Adverse Events
- 62 Clinical Medical Monitoring
- 63 Unblinding Procedures
-
- 7 Study Drug Procedures
- 8 Data Management
-
- 81 Hardware and Software Configuration
- 82 Sources of Data
-
- 9 Study Design and Data Analysis
-
- 91 General Analytic Considerations
- 92 Randomization Blinding and Reporting of Results
- 93 Stratification
- 94 Specification of the Primary Analyses
- 95 Analysis of Longitudinal Endpoints
- 96 Analysis of Binary Time-to-Event and Time-Lagged Endpoints
- 97 Power Analysis
-
- 10 Study Administration
-
- 101 Cooperative Agreement Mechanism
- 102 IPFnet Steering Group
- 103 Data and Safety Monitoring Board
- 104 Recommendations on Interim Monitoring of Efficacy Safety and Futility
-
- 11 Investigator and Sponsor Obligations
-
- 111 Monitoring
- 112 Cost and Payment
- 113 Confidentiality and Health Insurance Portability and Accountability ActConsiderations
- 114 Informed Consent Procedures
- 115 Institutional Review Boards
-
- 12 Investigator Agreement
- 13 References
-
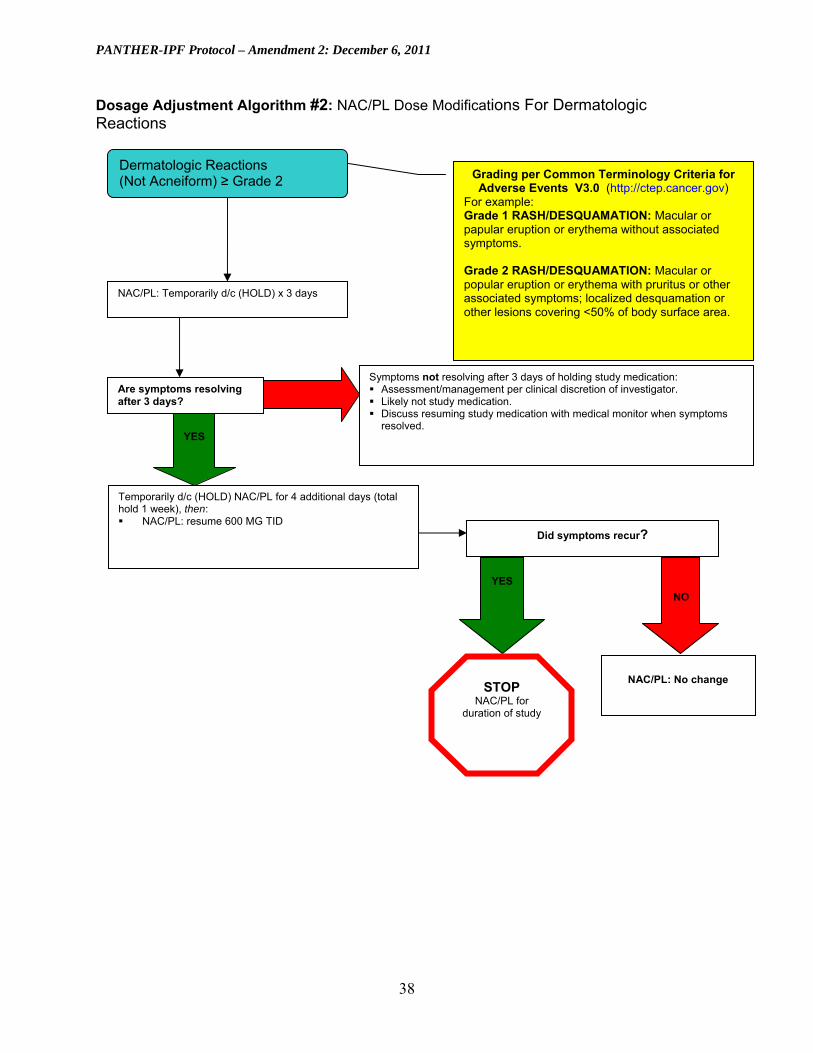
38
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Dosage Adjustment Algorithm 2 NACPL Dose Modifications For Dermatologic Reactions
Dermatologic Reactions (Not Acneiform) ge Grade 2 Grading per Common Terminology Criteria for
Adverse Events V30 (httpctepcancergov) For example Grade 1 RASHDESQUAMATION Macular or papular eruption or erythema without associated symptoms Grade 2 RASHDESQUAMATION Macular or popular eruption or erythema with pruritus or other associated symptoms localized desquamation or other lesions covering lt50 of body surface area
NACPL Temporarily dc (HOLD) x 3 days
Are symptoms resolving after 3 days
NO Symptoms not resolving after 3 days of holding study medication Assessmentmanagement per clinical discretion of investigator Likely not study medication Discuss resuming study medication with medical monitor when symptoms
resolved YES
Temporarily dc (HOLD) NACPL for 4 additional days (total hold 1 week) then NACPL resume 600 MG TID
Did symptoms recur
YES
STOP NACPL for
duration of study
NO
NACPL No change
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
46 Contraindications Precautions and Side Effects of Study Medications
461 Contraindication
Contraindication to NAC is known hypersensitivity to it
462 Precautions
Concomitant administration of oral NAC and antibiotics has shown a slightly reduced absorption
of cephalexin and a slight increase in erythromycin serum levels NAC contains free sulfhydryl
groups There is no evidence that individuals sensitive to sulfa drugs are sensitive to NAC
The NAC preparation being administered in this study contains 20 mg of aspartame Because of
the phenylalanine component of aspartame individuals with phenylketonuria should avoid or
restrict aspartame intake to avoid increased blood levels of phenylalanine Because of this risk
labeling is required on all products containing aspartame
463 Side Effects
Side effects of NAC range from common to serious See Table 4
39
40
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Table 4 Side Effects of NAC
Undesirable Effects
System-organ class Uncommon
(gt11000 lt1100)
Rare
(gt110000 lt11000)
Very rare
(lt110000) Not known
Immune system disorders Hypersensitivity Anaphylactic shock
reaction
Nervous system disorders Headache
Ear and labyrinth disorders Tinnitus
Cardiac disorders Tachycardia
Vascular disorders Hemorrhage
Respiratory thoracic and
mediastinal disorders
Bronchospasm
Dyspnea
Gastrointestinal disorders
Vomiting diarrhea
stomatitis abdominal
pain nausea
Dyspepsia
Skin and subcutaneous tissue
disorders
Urticaria rash
angioedema itching
General disorders and
administration site conditions Pyrexia
Investigations Reduced arterial
pressure Face edema
In very rare cases the onset of severe skin reactions such as Stevens-Johnson syndrome and Lyell syndrome was reported to have a temporal relationship with N-acetylcysteine administration Although in most cases at least another suspect drug probably most involved in the genesis of the above mentioned mucocutaneous syndromes has been identified in case of mucocutaneous alterations it is appropriate to contact onersquos doctor and the administration of N-acetylcysteine should be immediately discontinued
Some studies confirmed a reduction of platelet aggregation during N-acetylcysteine administration The clinical significance of these findings has not been defined yet [Source Fluimucil Investigator Brochure]
47 Recruitment Procedures
Subjects recruited for this study will be established patients of the investigators or physician- or
self-referred to participating clinical centers in the IPFnet Each clinical center within IPFnet has
a well-developed infrastructure of local pulmonologists within the surrounding geographic area
These pulmonologists are kept informed of ongoing IPF clinical trials and regularly refer
subjects to studies conducted at IPFnet clinical centers
Additional steps will be taken to inform clinicians of the trials in progress within IPFnet
including presentations at faculty staff meetings at local hospitals medical grand rounds and
national conferences direct mail notification monthly faxes and advertisement of network trials
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
in pulmonary journals Clinical center patients previously diagnosed with IPF will be notified of
the trials by mail whenever possible
Recruitment of minorities and women will be monitored by the DCC and DSMB If necessary
additional recruitment efforts will be made at specific centers to ensure that the aggregate subject
sample contains appropriate representation of women and minorities
48 Study Procedures
The following procedures are detailed in the PANTHER-IPF MOOP accompanying this
protocol
1 PFT
2 ABG
3 HRCT scan of the chest (including imaging of pulmonary arteries)
4 CBC and serum chemistries
5 Pregnancy test
6 6MWTBorg Dyspnea Scale
7 QOL questionnaires (EuroQol HAD SF-36 SGRQ and ICE CAP)
8 UCSD SOBQ
9 Gender Substudy Questionnaire
All assessments of PFTs will be conducted by study personnel not directly involved in the
treatment of the subjects
481 Biological Specimen Management
4811 Biological Specimen Sample Management
Subjects at clinical centers participating in the specimen repository substudy who consent to
having blood drawn for research purposes and for the banking of blood blood components and
other biologic specimens (urine and BAL fluid) will have approximately 405 mL of blood
41
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
drawn 17 mL blood drawn for DNA and 20 mL of urine collected at enrollment visit Subjects
will have approximately 50 mL of blood drawn and 20 mL of urine collected at each 15-week
follow-up visit Blood specimens will be separated according to PANTHER-IPF MOOP
guidelines into the following components for banking in the repository serum plasma and
DNA Coding of all biologic specimens for the repository will be performed by study staff at the
clinical center The samples will be processed per PANTHER-IPF MOOP guidelines aliquoted
labeled with barcode labels and stored at -70degC at the clinical center and shipped to the central
repository
The only subject identifiers will be a sample ID number and subject initials This sample ID will
be linked in the IPFnet DCC clinical database to subject information No subject information will
be transferred to the biological-specimen database
The subjectrsquos samples may be used for approved sub-studies relating to human disease
including but not limited to IPF The studies for which an individualrsquos samples will be made
available will be determined by the subjectrsquos answers to questions on the biological-sample
informed consent form The subjects can choose to make their samples available for all options
or any combination Samples will be made available to researchers only with IPFnet Steering
Group approval until such time as the samples are made public through the NHLBI repository
49 Concomitant Medications
Concurrent treatment with FDA-approved therapy for IPF is allowed Colchicine may be used
for treatment of gout Temporary treatment with oral or IV corticosteroids for clinical worsening
or suspected AEx is permitted Nutritional supplements containing NAC are not allowed
410 Laboratory Testing
Clinical laboratory parameters will be assessed at screening and at the end of the study The
following tests will be performed at the two time points specified in the protocol chemistry (AG
ratio ALT [SGPT] AST [SGOT] albumin alkaline phosphatase amylase bilirubin-direct
42
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
bilirubin-indirect bilirubin-total BUN BUNcreatinine ratio calcium carbon dioxide
cholesterol-total chloride CPK-total creatinine GGT globulin glucose iron-total LDH
lipase magnesium phosphorus-inorganic potassium protein-total sodium TIBC triglycerides
uric acid) and hematology (red blood cell count WBC count hemoglobin hematocrit cell
indices differential platelet count)
411 Blinding of Study Drugs
Subjects and caregivers will be blinded to study treatment Every subject will receive NAC or
matching PLs at every study visit from the baseline visit to the week-45 visit No study agent
will be dispensed at the week-60 visit
43
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
5 Study Endpoints
51 Primary Study Endpoint
The primary endpoint will be the change in serial measurements of FVC over the study period
52 Secondary Study Endpoints
521 Time to Disease-progression
The time-to-death or a 10 decline in FVC will be defined as the time-to-disease progression
The 10 decline in FVC from enrollment must be confirmed on 2 consecutive visits no less than
6 weeks apart For subjects with 2 consecutive visits with a 10 decline in FVC the time-toshy
disease progression will be defined as the time interval between enrollment and the initial visit
with a 10 FVC decline For subjects who experience disease progression the study doctor will
determine whether or not the subject will remain in the study
522 Acute Exacerbations
The following 3 criteria will define AEx in subjects with acute worsening of their respiratory
conditions
1 Clinical (all of the following required)
A) Unexplained worsening of dyspnea or cough within 30 days triggering unscheduled
medical care (eg emergency room clinic study visit hospitalization)
B) No clinical suspicion or overt evidence of cardiac event pulmonary embolism or deep
venous thrombosis to explain acute worsening of dyspnea
C) No pneumothorax
44
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
2 RadiologicPhysiologic (A and B required)
A) New ground glass opacity or consolidation computed tomography (CT) scan OR new
alveolar opacities on chest x-ray
B) Decline of ge 5 in resting room air SpO2 from last recorded level OR decline of ge 8 mm
Hg in resting room air PaO2 from last recorded level
3 Microbiologic (all of the following required)
A) No clinical evidence for infection (ie absence of grossly purulent sputum fever gt 39degC
orally)
B) Lack of positive microbiological results (if done) from lower respiratory tract defined as
(1) Clinically significant bacterial growth on sputum or endotracheal aspirate cultures
(2) Quantitative culture by protected brush specimen ge 103 cfumL or BAL ge 104 cfumL
(3) The presence of specific pathogens on stains of any of the above
C) Lack of positive pathogen in blood cultures (if done)
Identification of Acute Exacerbations
All subjects will be educated about the importance of identifying AExs At the time of
enrollment subjects will be told about the possibility of developing acute symptomatic
worsening that might represent an AEx of IPF and instructed to contact their study clinical
center coordinator within 48 to 72 hours of the apparent event
All subjects will be contacted by phone monthly and questioned about any change in dyspnea or
cough and any interim clinic visits or hospitalizations Finally as part of the IPFnet outreach to
community referring physicians the importance of AExs will be emphasized When a subject is
identified who meets criterion 1A this will trigger the collection of additional clinical data to
evaluate a suspected AEx These data will be collected as part of standard clinical care (ie this
protocol does not require collection of all items) The additional items to be collected for
suspected AEx include
IPFnet AEx case report form (eCRF) (required)
45
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Chest x-ray CT scan withwithout pulmonary angiogram (reports should be faxed and
followed by the hard copiesdiscs)
Oxygen saturation (pulse oximetry)
ABG
Respiratory cultures (sputum endotracheal aspirate lavage)
Blood cultures
Clinichospital records related to the event
All potential cases of AEx will be reviewed by the clinical center PI first and a decision on
whether the case may represent an AEx will be made If AEx is suspected the case will be sent
to the IPFnet adjudication committee which will assign a final diagnosis (see Table 5) If there is
disagreement among members the majority opinion will be recorded
During episodes of suspected AEx as determined by the individual clinical center investigator
subjects will remain blinded and in the study
Table 5 Final Diagnoses in Evaluation of Suspected Acute Exacerbations
Definite acute exacerbation All criteria met no alternative etiology
Unclassifiable acute worsening
Insufficient data to evaluate all criteria no alternative etiology
Not acute exacerbation Alternative etiology identified that explains acute worsening
Management of the suspected AEx will be at the discretion of the treating physician Standard of
care generally involves evaluation for respiratory infection pulmonary embolism cardiac events
and pneumothorax and treatment with IV corticosteroids
Study drugs will be resumed at pre-suspected AEx doses after subjects clinically improve as
confirmed by the local PI All subjects should be seen at the clinical center within 2 to 4 weeks
of recovery for measurement of post-bronchodilator FVC (see Figure 4) Subjects unable to
return to the clinical center after suspected AEx due to medical frailty (eg continued
46
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
institutionalization progressive disability) will be categorized as failing to maintain FVC
response in secondary analyses
Suspected AEx (PI determined)
Hold study drug Treat AEx
(Attending physician determined)
Alive but unable to continue due to
medical frailty
Dead
Alive and able to continue
Site reviewvisit
Restart study drug
FVC within 2-4 weeks
Figure 4 Acute Exacerbation Flow Chart
523 Respiratory Infections
An upper respiratory infection will be defined as
Change in sputum discoloration
Increased cough of no more than 14 daysrsquo duration
A lower-respiratory infection (pneumonia) will be defined as new segmental or lobar airspace
opacities visualized by image studies (chest radiograph or HRCT) in addition to any of the
following
Positive pathogencultures in good sample of sputum or lower-airway secretions retrieved
by fiberoptic bronchoscope
Fever gt 39degC or gt 100degF
Leukocytosis gt 12000 (unexplained no increase in dose of corticosteroids)
47
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
524 Maintained FVC Response
Subjects with follow-up FVCpred measurements at or above their baseline FVCpred level
will be classified as having maintained FVC response Subjects with reduced FVCpred levels
or missing data for any reason including death or medical frailty will be classified as having not
maintained FVC response The FVCpred value is used because unadjusted FVC measurements
are expected to decline with age
48
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
6 Safety Evaluations and Procedures
61 Adverse Events
During a clinical trial the reporting of adverse experience information can lead to important
changes in the way a new treatment is developed as well as provide integral safety data
611 Definitions
An adverse event (AE) is any untoward medical occurrence in a subject or clinical investigation
subject who was administered a pharmaceutical product The AE does not necessarily have to
have a causal relationship with the drug administered An AE can be any unfavorable and
unintended sign (including an abnormal laboratory finding) symptom or disease temporarily
associated with the use of a medicinal product whether or not considered to be related to the
medicinal product Diseases signs symptoms or laboratory abnormalities already existing at
enrollment are not considered AEs unless they worsen (ie increase in intensity or frequency)
Surgical procedures themselves are not AEs they are therapeutic measures for conditions that
require surgery The condition for which the surgery is required may be an AE Surgical
procedures planned before randomization and the conditions necessitating the surgery are not
AEs
A serious adverse event is any untoward event that
Is fatal
Is life-threatening
Requires inpatient hospitalization or prolongation of existing hospitalization with the
following exceptions
o Preplanned (before the study) hospital admissions unless the hospitalization is
prolonged
o Planned admissions (as part of a study eg routine biopsies)
o Hospitalization lasting lt 24 hours
49
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
o Hospitalization for elective procedure
o Emergency room visits
Results in persistent or significant disability or incapacity
Is a congenital anomaly or birth defect
Important medical events that may not result in death be life-threatening or require
inpatient hospitalization may be considered serious adverse events (SAEs) when based
on appropriate medical judgment they may jeopardize the subject and may require
medical or surgical intervention to prevent one of the outcomes listed above
Life-threatening means that the subject was in the view of the investigator at immediate risk of
death from the AE as it occurred It does not include an AE that had it occurred in a more severe
form might have caused death
Persistent or significant disabilityincapacity means that the event resulted in permanent or
significant and substantial disruption of the subjectrsquos ability to carry out normal life functions
Causality
A reasonable possibility means the AE may have been caused byrelated to the study drug A
perceived or real lack of efficacy does not satisfy the definition of relatedness
612 Adverse Event (AE) Reporting
For the PANTHER-IPF trial all AEs (serious and nonserious) occurring from randomization
through final study visit (4 weeks after final dose of all study medication) will be recorded on the
AE page of the case report form (CRF)
6121 Serious Adverse Events (SAE) Reporting
For this trial all deaths and all SAEs which occur from randomization through final study visit
must be entered within the EDC system via the SAE eCRF page within 24 hours of the
investigative sitersquos knowledge of the event It is the responsibility of the clinical center
50
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
investigator to provide a causality assessment of the event for each study medications based upon
the information available at the time of the report It is understood that complete information
about the event may not be known at the time the initial report is submitted In the event the EDC
system is not accessible to the site at the time of event reporting investigative sites will complete
and forward a paper back-up SAE form to DCRI Safety Surveillance for processing
DCRI Safety Surveillance
Telephone 1-919-668-8624 or 1-866-668-7799 (toll free)
Fax 1-919-668-7138 or 1-866-668-7138 (toll free)
The investigator must complete and submit follow-up SAE information via the eCRF when
important new or follow-up information (eg final diagnosis outcome results of specific
investigations) becomes available Follow-up information should be submitted according to the
same process used for reporting the initial event as described above All SAEs will be followed
until resolution stabilization or 30 days after the subject has completed the final visit (4 weeks
after the final dose of study medication) whichever occurs first The investigator is responsible
for reporting SAEs to their institutional review board (IRB) per site specific IRB reporting
guidelines
6122 Regulatory Reporting
AEs that are serious study drug related and unexpected will be reported to the regulatory
authorities The DCRI Safety Surveillance medical monitor will perform a medical review of all
SAEs submitted and evaluate for ldquounexpectednessrdquo DCRI Safety Surveillance will prepare
MedWatch reports for those events identified as serious study drug related and unexpected as
determined by Safety Medical Monitor
DCRI Regulatory Services will submit all unexpected study drug-related SAEs as per 21 CFR
32 DCRI Safety Surveillance will provide a safety alert letter to the NHLBI DSMB and DCC
clinical operation (for distribution to sites) within 15 days of initial receipt of the information
51
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Investigators are responsible for promptly reporting these events to their reviewing IRBs
according to site specific IRB reporting guidelines
62 Clinical Medical Monitoring
There will be an unblinded physician at the IPFnet DCC serving as medical monitor The
medical monitor will be available to assist with questions about dosage adjustments of study
medications including discontinuation or resumption of medications
63 Unblinding Procedures
Unblinding of subjects or investigators to subject treatment is strongly discouraged For ongoing
clinical management all subjects should be presumed to be receiving ldquoactiverdquo study drug To
ensure the subjectrsquos safety the study treatment will be dose-adjusted based on laboratory test
results clinical findings and symptoms
The IPFnet DCC medical monitor and PANTHER-IPF co-chairs Drs Ganesh Raghu and
Fernando Martinez will be available to the study physicians to discuss study drug management
on a case-by-case basis Un-blinding will be considered ONLY when the knowledge of subject
treatment assignment is ABSOLUTELY ESSENTIAL for subject safety and after discussion of
the subjectrsquos case with the medical monitor and either Dr Raghu or Dr Martinez Unblinding of
study treatment should be minimized during the conduct of the trial In those cases where it is
felt to be medically necessary the DCC medical officer will communicate directly with the
managing physician to minimize unblinding of study personnel
52
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
7 Study Drug Procedures
At the baseline 15-week 30-week and 45-week study visits subjects will receive a supply of
study drug sufficient to last until the next visit at which study drug will be dispensed
53
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
8 Data Management
81 Hardware and Software Configuration
811 Hardware and Database Software
Data will be stored in an Oracle database system Oracle has advantages of processing efficiency
and smooth linkage with other software systems The application and database will be hosted on
Solaris Unix servers at the IPFnet DCC
812 Statistical Software
SAS will be used as the principal application for the management of analysis data files and
statistical computations S-Plus will be used to provide supplementary functions as needed
813 Access Control and Confidentiality Procedures
Access to databases will be controlled centrally by the IPFnet DCC through user passwords
linked to appropriate privileges This protects the data from unauthorized changes and
inadvertent loss or damage
814 Security
Database and Web servers will be secured by a firewall and through controlled physical access
Oracle has many security features to ensure that any staff member accessing the database has the
proper authority to perform the functions he or she requests of the system Within the secondary
SAS databases Unix group-access control maintains similar security The Sun workstation login
is secured by extensive user-password facilities under Unix
54
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
815 Back-up Procedures
Database back-up will be performed automatically every day and standard IPFnet DCC policies
and procedures will be applied to dictate tape rotation and retention practices
816 Virus Protection
All disk drives that provide network services and all user computers will be protected using
virus-scanning software Standard IPFnet DCC policies will be applied to update these protection
systems periodically through the study
82 Sources of Data
821 Design and Development
The IPFnet DCC will be responsible for development of the electronic case report forms
(eCRFs) development and validation of the clinical study database ensuring data integrity and
training clinical center staff on applicable data management procedures A web-based distributed
data entry model will be implemented This system will be developed to ensure that guidelines
and regulations surrounding the use of computerized systems used in clinical trials are upheld
The remainder of this section provides an overview of the data management plan associated with
this protocol
822 Data Collection Forms
The data collection process consists of direct data entry at the study clinical centers into the EDC
system(s) provided by the DCC A data collection worksheet will be provided to clinical centers
for recording data in the event the EDC system is unavailable Data entry of the eCRFs should
be completed according to the instructions provided and project specific training The
investigator is responsible for maintaining accurate complete and up-to-date records and for
ensuring the completion of the eCRFs for each research participant
55
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
823 Data Acquisition and Entry
Data entry into eCRFs shall be performed by authorized individuals Selected eCRFs may also
require the investigatorrsquos written signature or electronic signature as appropriate Electronic
CRFs will be monitored for completeness accuracy and attention to detail during the study
824 Data Center Responsibilities
The IPFnet DCC will 1) develop a data management plan and will conduct data management
activities 2) provide final eCRFs for the collection of all data required by the study 3) develop
data dictionaries for each eCRF that will comprehensively define each data element 4) conduct
ongoing data monitoring activities on study data 5) monitor any preliminary analysis data
cleanup activities and 6) rigorously monitor final study data clean up
825 Data Editing
Completed data will be entered into the IPFnet DCC automated data acquisition and
management system If incomplete or inaccurate data are found a data clarification request will
be generated and distributed to clinical centers for a response Clinical centers will resolve data
inconsistencies and errors and enter all corrections and changes into the IPFnet DCC automated
data acquisition and management system
826 Training
The training plan for clinical center staff includes provisions for training on assessments eCRF
completion guidelines data management procedures and the use of computerized systems
56
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
9 Study Design and Data Analysis
91 General Analytic Considerations
All primary analyses will be based on intent-to-treat (ITT) principles using all randomized
subjects Baseline factors across groups will be compared using mean (standard deviation) and
median (25th and 75th percentiles) summary measures Kaplan-Meier curves will be used to
display event rates Due to clinical interest in departures from both sides of the null hypothesis
all test statistics will be 2-sided
Reasonable caution needs to be taken when conducting multiple analyses on key clinical
subgroups For subgroup analyses a conservative significance level of 0001 will be used for all
interaction tests Thus subgroup comparisons will be considered exploratory unless the p-value
from the interaction test is smaller than 0001
92 Randomization Blinding and Reporting of Results
A permuted block-randomization scheme will be created with varying block sizes stratified by
clinical center Once a subject has completed the screening and baseline period and evaluation
for inclusionexclusion criteria the randomization process will begin Subjects will be
randomized to receive NAC or matching placebo with equal probability (11) via telephone
contact with a central interactive voice response system (IVRS) using a toll-free randomization
number On the day of randomization after the subject has successfully met all inclusion and
exclusion criteria the investigator or designee will call the central randomization number to
obtain the assigned kit randomization numbers for that subject At each subject visit the
investigator or designee will call the central randomization number to obtain the new kit
randomization numbers for resupply of the subject For resupply of the clinical center the IVRS
will monitor minimal volume of a kit type andor expiration date and will automatically notify
the pharmacy
57
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
The trial results will be reported according to guidelines specified in the CONSORT statement
A flow diagram describing screening recruitment randomization dropout and vital status will
be included in the primary manuscript AEs and efficacy data will be presented for all treatment
groups Adherence dropout and lost to follow-up will be carefully examined across all treatment
groups Analyses of safety will be based on data from all randomized subjects who received at
least one dose of study drug
93 Stratification
Subjects will be distributed to the two treatment arms in a 11 allocation ratio Stratification
blocks will be based on clinical centers
94 Specification of the Primary Analyses
A mixed model repeated measures (MMRM) analysis described in section 95 will be used to
compare differences in the slope of FVC measurements across the treatment groups Response
variables are values of the FVC measured at baseline and every 15 weeks until study completion
Variables in the model will include treatment time and time by treatment age sex race and
height Contrast estimates of differences in slopes of treatment over time (along with confidence
intervals) will be used to estimate the treatment effect The validity of this model in terms of
meeting modeling assumptions will be assessed via standard modeling diagnostics and goodness-
of-fit measures Based on the MMRM framework missing FVC data will not be imputed for the
primary analysis
95 Analysis of Longitudinal Endpoints
A common goal in clinical trials is to specify models that are easily implemented and
reproducible by independent data analysts On the other hand the models should have proper
statistical behavior in terms of low bias and high precision Many common approaches to
longitudinal data analysis including last observation carried forward (LOCF) imputation rely on
the missing completely at random (MCAR) assumption However the MCAR assumption is
58
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
unlikely to hold in many clinical trials because missing data are often related to disease
progression and prognosis A more reasonable assumption missing at random (MAR) specifies
that the complete data distribution can be modeled using only the observed data The likelihood-
based MMRM approach is valid under the more general MAR assumptions These models will
be applied to analyze the longitudinal data secondary endpoints
The advantages of MMRM analysis are that all important characteristics of the model can be preshy
specified standard software can be used to implement the models and results are based on ITT
principles43 In addition the MMRM approach offers superior control of Type I and Type II
errors compared with the LOCF approach
Response variables are values of the PFTs measured at enrollment and every 15 weeks until
study completion and 6MWT values measured at baseline week 30 and week 60 Covariates are
treatment time time by treatment and key baseline risk factors Contrasts (along with
confidence intervals) of treatment by time will be used to estimate the treatment effect
The correlation structure involves multiple pieces including measurement errors random
variation and interindividual variability For the longitudinal data analyses an unstructured
correlation matrix for within-subject errors will be assumed Other correlation structures
including compound symmetry will be examined as needed A careful examination of reasons
for study discontinuation will be conducted to assess the validity of MCAR Sensitivity analyses
will be used to examine the untestable assumption that the observed data violate the MAR
assumption The MMRM models will be implemented using PROC MIXED in SAS
96 Analysis of Binary Time-to-Event and Time-Lagged Endpoints
Regression modeling approaches using either the logistic regression model or Cox proportional
hazards regression model will be employed when appropriate The validity of these models will
be assessed via standard modeling diagnostics and goodness-of-fit measures Estimates of
cumulative frequencies for more general time-lagged responses will be calculated using the
partitioned version of the Bang-Tsiatis estimator44 The partitions will be set at 15-week intervals
59
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
to correspond with the data-collection process Covariate adjusted event rates will be calculated
using inverse probability-weighted regression estimates45
97 Power Analysis
971 Primary Analyses
Based on previously published IPF clinical trials the PL group is expected to experience a drop
in FVC of approximately 020 L over the study period (see Figure 1) The IPFnet Steering Group
determined a clinically important difference would be to preserve the majority of the decline
relative to PL over the study period In particular a treatment effect of 015 L was determined to
be a clinically meaningful difference Potential dropout is a key factor in the proposed study The
drop-out process assumed 5 lost to follow-up after every study visit Only 80 of subjects
were assumed to be followed for the entire study period All models assumed a compound
symmetry structure for the covariance matrix Power calculations were performed using a SAS
IML program for designing repeated measures studies46 Based on preliminary reviews of the
data from the University of Michigan the covariance matrix parameters were estimated at
approximately σ2 = 0757 (variance parameter) and ρ = 0936 (correlation parameter) To be
conservative the power calculations for the primary analysis were performed with parameter
setting of σ2 = 0810 (variance parameter) and ρ = 0925 (correlation parameter)
The power calculations assume a correction for imperfect compliance proposed by Lachin and
Foulkes to allow for 2 noncompliance for each of the treatment arms47 Thus the sample size
of 130 subjects per arm would be reduced to an adjusted sample size of 130(1-002-002)2 =
1198 or 120 subjects per arm
Under the assumed Type I error rate of 005 with a correlation parameter of 0925 and standard
deviation of 090 the difference of 015 L (or 00025 Lweek) shown in Table 6 would have
power of 93
60
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Table 6 Hypothetical Values of Mean FVC (L) Change from Baseline
Week 15 Week 30 Week 45 Week 60
NAC 00125 00250 00375 00500
Placebo 00500 01000 01500 02000
Difference 00375 00750 01125 01500
Abbreviations FVC forced vital capacity PL placebo
972 Power Analysis for Secondary Endpoints
Power calculations for secondary endpoint measurements are shown in Table 7 Standard
deviations are based on unpublished data provided by the University of Michigan The
calculations are based on a 2-sample t-test with Type I error rate set at 005 These calculations
are likely to be conservative because the statistical approach described in section 95 for
analyzing these endpoints will incorporate incomplete observations as well as intermediate data
points
Table 7 Detectable Differences in Treatment Means for Selected Endpoint Measurements
Secondary Endpoints Std Dev
of the Baseline Score
Detectable Difference for 80 Power
Std Dev of the Change Score
Difference Detectable for
80 Power
DLCOpred 166 58 91 32
6MWT Area Under the Desaturation Curve
219 76 175 61
6MWT Distance to Desaturation 224 78 315 110
6MWT Minutes Walked 210 073 205 071
Abbreviations Std Dev standard deviation DLCOpred diffusing capacity of the lung for carbon monoxide percent predicted 6MWT 6-minute walk test
61
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
10 Study Administration
101 Cooperative Agreement Mechanism
The administrative and funding mechanism used to undertake this project is a ldquocooperative
agreementrdquo (U01) which is an assistance mechanism Under the cooperative agreement the
NHLBI assists supports andor stimulates the project and is substantially involved with
investigators in conducting the study by facilitating performance of the effort in a ldquopartnerrdquo role
The NHLBI project scientist serves on the IPFnet Steering Group and he or another NHLBI
scientist may serve on other project committees when appropriate At the same time however
NHLBI does not assume a dominant role direction or prime responsibility for this research
program
As described below governance of the project is conducted through the IPFnet Steering Group
Principal investigators have lead responsibilities in all aspects of their trials and the project
including any modification of trial designs conduct of the trials quality control data analysis
and interpretation preparation of publications and collaboration with other investigators unless
otherwise provided for by the IPFnet Steering Group
PIs retain custody of and have primary rights to their center-specific and collaborative data
subject to government rights-of-access consistent with current Health amp Human Services (HHS)
Public Health Service (PHS) and National Institutes of Health policies The protocols and
governance policies call for the continual submission of data centrally to the IPFnet DCC for the
collaborative database which at a minimum will contain the key variables selected by the IPFnet
Steering Group for standardization across all clinical centers the submission of copies of the
collaborative datasets to each PI upon completion of the project procedures for data analysis
reporting and publication and procedures to protect and ensure the privacy of medical and
genetic data and records of individuals The NHLBI project scientist on behalf of the NHLBI
will have the same access privileges and responsibilities regarding the collaborative data as the
other members of the Steering Group
62
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
PIs are also encouraged to publish and to publicly release and disseminate results data and other
products of the project concordant with the project protocols and governance and the approved
plan for making data and materials available to the scientific community and to the NHLBI
However during the 3 years after the ending date of NHLBI project support unpublished data
unpublished results data sets not previously released and other study materials or products are
to be made available to any third party only with the approval of the IPFnet Steering Group
Upon completion of the project PIs are expected to put their intervention materials and
procedure manuals into the public domain andor make them available to other investigators
according to the approved plan for making data and materials available to the scientific
community and the NHLBI for the conduct of research at no charge other than the costs of
reproduction and distribution
The NHLBI reserves the right to terminate or curtail the project (or an individual award) in the
event of (a) failure to develop or implement mutually agreeable collaborative measurement
subject eligibility and data management sections of the protocols (b) substantial shortfall in
subject recruitment follow-up data reporting or quality control or other major breach of
protocol (c) substantive changes in the agreed-upon protocols with which NHLBI cannot
concur (d) reaching a major project outcome with persuasive statistical significance
substantially before schedule or (e) human subject ethical issues that may dictate a premature
termination
Any disagreement that may arise in scientificprogrammatic matters (within the scope of the
award) between award recipients and the NHLBI may be brought to arbitration An arbitration
panel will be composed of 3 membersmdash1 selected by the IPFnet Steering Group (with the
NHLBI member not voting) or by the individual PI in the event of an individual disagreement a
second selected by NHLBI and the third selected by the other 2 members This special
arbitration procedure in no way affects the PIrsquos right to appeal an adverse action that is otherwise
appealable in accordance with the PHS regulations at 42 CFR part 50 Subpart D and HHS
63
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
regulation at 45 CFR part 16 or the rights of the NHLBI under applicable statutes regulations
and terms of the award
102 IPFnet Steering Group
The IPFnet Steering Group is the main governing body of the project It is composed of the PIs
of the clinical centers the PI of the DCC and the NHLBI project scientist The clinical centers
the IPFnet DCC and the NHLBI each have 1 vote on the IPFnet Steering Group All decisions
are determined by majority vote
All major scientific decisions are determined by the IPFnet Steering Group It assumes overall
responsibility for the design and conduct of the trial It appoints (and disbands) committees and
subcommittees as the need arises designs approves and implements the study protocols
oversees the development of the MOOP monitors subject recruitment and treatment delivery
evaluates data collection and management oversees quality assurance procedures and
implements changes and enhancements to the study as required It also has primary responsibility
for facilitating the conduct of the trials and reporting the projectrsquos results
103 Data and Safety Monitoring Board
The NHLBI will establish a DSMB in accordance with established policies (see
httpwwwnhlbinihgovfundingpoliciesdsmb_insthtm) to ensure data quality and subject
safety and to provide independent advice to the NHLBI regarding progress and the
appropriateness of study continuation
104 Recommendations on Interim Monitoring of Efficacy Safety and Futility
First and foremost the role of the DSMB will be to review subject safety and trial conduct at
periodic points during the study The DSMB may require analyses of the primary endpoint
results for comparing the benefit and risks of treatment strategies The benefit of collecting
additional data on key secondary endpoints with extended follow-up and establishing a robust
64
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
evidence base for determining a standard of care will need to be carefully considered before
early termination of one or more treatment arms After careful consideration the IPFnet Steering
Group recommends conservative thresholds for the early examinations of the safety and efficacy
data
The DSMB will be expected to meet approximately every 6 months until trial completion to
review safety and toxicity data The DSMB may recommend stopping the study based on these
reviews Because the DSMB could stop the trial for safety concerns as well as for a large
efficacy benefit there could be multiple opportunities to reject the null hypothesis (no difference
in event rates between the PL and NAC groups) A Bonferroni approximation will be applied
during the one planned interim analysis for efficacy
Before locking the database a statistical analysis plan (SAP) will be developed to provide
complete details on the statistical analysis The SAP will include the specifics for how and when
the DSMB will be notified for AEs The IPFnet DCC will deliver to the DSMB all FDA-defined
AEs at 3-month intervals The IPFnet DCC will prepare narrative SAE reports in real time for
DSMB review including recommendations and analysis of similar events for each SAE
submitted to the FDA
65
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
11 Investigator and Sponsor Obligations
111 Monitoring
All monitoring activities for US clinical centers will be performed in accordance with DCRI
standard operating procedures Information regarding the types of visits will be outlined in the
PANTHER-IPF MOOP
112 Cost and Payment
There will be no cost to subjects enrolled in this trial Study-related procedures will be paid for
by the IPFnet
Subjects may be eligible for reimbursement for travel to the clinical center Details of payment
will be explained to each subject during the consent process
113 Confidentiality and Health Insurance Portability and Accountability Act
Considerations
Subject confidentiality will be protected throughout the study All subject data will be kept
strictly confidential and no subject-identifying information will be released to anyone outside
the project Confidentiality will be assured through several mechanisms First each subject will
be assigned an anonymous study ID which will then be used on all study forms Second any
study forms blood samples and paper records that contain subject information (eg address lists
phone lists) will be kept at the clinical centers in secured locked areas coded by number Once
blood is collected there will be no subject identifiers placed on blood samplesmdashonly the study
ID number and the date of sample collection Third access to all subject data and information
including laboratory specimens will be restricted to authorized personnel In the case of
computerized data this restricted access will be assured through user logon IDs and password
protection
66
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
At the IPFnet DCC only authorized personnel will have access to the data files containing study
data Security will be assured through user logon IDs passwords and appropriate access
privileges All study subjects will be identified only by their IPFnet ID numbers and no personal
identifying information such as name address or Social Security number will be entered into
the IPFnet DCC database Any subject-specific data reported to the IPFnet Steering Group will
be identified only by the IPFnet ID number
Finally subjects will not be identified by name in any reports or publications nor will the data
be presented in such a way that the identity of individual subjects can be inferred Analysis files
created for further study by the scientific community will have no subject identifiers These data
files will be created in accordance with the Ancillary Studies and Publication Policy of the
IPFnet
114 Informed Consent Procedures
All IPFnet subjects will provide written informed consent using procedures reviewed and
approved by each clinical centerrsquos IRB Informed consent will be undertaken by study personnel
in-person with the subject The subject has the option of declining further participation in the
study at that point No further study procedures will be conducted until the signed documents
have been provided to the IPFnet clinical center
115 Institutional Review Boards
Before initiating this study the protocol clinical center-specific informed consent forms Health
Insurance Portability and Accountability Act (HIPAA) forms recruitment materials and other
relevant information will be reviewed by a properly constituted IRB at each participating clinical
center A copy of the signed and dated IRB approval at each clinical center will be retrieved prior
to or during the site initiation visit and archived at the IPFnet DCC Any amendments to the
protocol other than simple administrative and typographical changes must be approved by each
IRB before they are implemented The clinical centers will seek annual renewals of their IRB
approvals in accordance with local procedures
67
__________________________________________ ________________
__________________________________________
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
12 Investigator Agreement
I have read the foregoing protocol PANTHER-IPF and agree that it contains all necessary
details for carrying out this study I will conduct the study as outlined herein and will complete
the study within the time designated
I will provide copies of the protocol and all pertinent information to all individuals responsible to
me who assist in the conduct of this study I will discuss this material with them to ensure they
are fully informed regarding the drug and the conduct of the study
I will fulfill all responsibilities for submitting pertinent information to the local IRB if
applicable that is responsible for this study
I further agree that NHLBI andor DCRI will have access to any source documents from which
eCRF information may have been generated
Signature of Principal Investigator Date
Name of Principal Investigator (printed or typed)
Protocol version date May 19 2009
Protocol Amendment 1 version date May 28 2010
Protocol Amendment 2 version date December 6 2011
68
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
13 References
1 Raghu G Brown KK Bradford WZ et al A placebo-controlled trial of interferon gamma-1b in patients with idiopathic pulmonary fibrosis N Engl J Med 2004350125-33 2 King TE Jr Safrin S Starko KM et al Analyses of efficacy end points in a controlled trial of interferon-gamma1b for idiopathic pulmonary fibrosis Chest 2005127171-7 3 Flaherty KR Thwaite EL Kazerooni EA et al Radiological versus histological diagnosis in UIP and NSIP survival implications Thorax 200358143-8 4 Wells AU Desai SR Rubens MB et al Idiopathic pulmonary fibrosis a composite physiologic index derived from disease extent observed by computed tomography Am J Respir Crit Care Med 2003167962-9 5 Raghu G Freudenberger TD Yang S et al High prevalence of abnormal acid gastroshyoesophageal reflux in idiopathic pulmonary fibrosis Eur Respir J 200627136-42 6 Kinnula VL Focus on antioxidant enzymes and antioxidant strategies in smoking related airway diseases Thorax 200560693-700 7 Coultas DB Zumwalt RE Black WC Sobonya RE The epidemiology of interstitial lung diseases Am J Respir Crit Care Med 1994150967-72 8 Raghu G Weycker D Edelsberg J Bradford WZ Oster G Incidence and prevalence of idiopathic pulmonary fibrosis Am J Respir Crit Care Med 2006174810-6 9 Olson AL Swigris JJ Lezotte DC Norris JM Wilson CG Brown KK Mortality from pulmonary fibrosis increased in the United States from 1992 to 2003 Am J Respir Crit Care Med 2007176277-84 10 Mannino DM Etzel RA Parrish RG Pulmonary fibrosis deaths in the United States 1979shy1991 An analysis of multiple-cause mortality data Am J Respir Crit Care Med 19961531548shy52 11 Hubbard R Johnston I Coultas DB Britton J Mortality rates from cryptogenic fibrosing alveolitis in seven countries Thorax 199651711-6 12 Johnston I Britton J Kinnear W Logan R Rising mortality from cryptogenic fibrosing alveolitis Bmj 19903011017-21 13 Raghu G Collard HR Egan JJ et al An official ATSERSJRSALAT statement idiopathic pulmonary fibrosis evidence-based guidelines for diagnosis and management Am J Respir Crit Care Med 2011183788-824 14 (USA) FDA FDA Public Health Advisory Interferon gamma-1b (marketed as Actimmune) In 2007 15 King TE Jr Pardo A Selman M Idiopathic pulmonary fibrosis Lancet 2011 16 Raghu G Brown KK Costabel U et al Treatment of idiopathic pulmonary fibrosis with etanercept an exploratory placebo-controlled trial Am J Respir Crit Care Med 2008178948shy55 17 Malouf MA Hopkins P Snell G Glanville AR An investigator-driven study of everolimus in surgical lung biopsy confirmed idiopathic pulmonary fibrosis Respirology 201116776-83 18 King TE Jr Behr J Brown KK et al BUILD-1 a randomized placebo-controlled trial of bosentan in idiopathic pulmonary fibrosis Am J Respir Crit Care Med 200817775-81 19 Richeldi L Costabel U Selman M et al Efficacy of a tyrosine kinase inhibitor in idiopathic pulmonary fibrosis N Engl J Med 20113651079-87
69
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
20 Borok Z Buhl R Grimes GJ et al Effect of glutathione aerosol on oxidant-antioxidant imbalance in idiopathic pulmonary fibrosis Lancet 1991338215-6 21 Meyer A Buhl R Magnussen H The effect of oral N-acetylcysteine on lung glutathione levels in idiopathic pulmonary fibrosis Eur Respir J 19947431-6 22 Behr J Maier K Degenkolb B Krombach F Vogelmeier C Antioxidative and clinical effects of high-dose N-acetylcysteine in fibrosing alveolitis Adjunctive therapy to maintenance immunosuppression Am J Respir Crit Care Med 19971561897-901 23 Cantin AM North SL Fells GA Hubbard RC Crystal RG Oxidant-mediated epithelial cell injury in idiopathic pulmonary fibrosis J Clin Invest 1987791665-73 24 Waghray M Cui Z Horowitz JC et al Hydrogen peroxide is a diffusible paracrine signal for the induction of epithelial cell death by activated myofibroblasts Faseb J 200519854-6 25 Larios JM Budhiraja R Fanburg BL Thannickal VJ Oxidative protein cross-linking reactions involving L-tyrosine in transforming growth factor-beta1-stimulated fibroblasts J Biol Chem 200127617437-41 26 Kinnula VL Fattman CL Tan RJ Oury TD Oxidative stress in pulmonary fibrosis a possible role for redox modulatory therapy Am J Respir Crit Care Med 2005172417-22 27 Meyer A Buhl R Kampf S Magnussen H Intravenous N-acetylcysteine and lung glutathione of patients with pulmonary fibrosis and normals Am J Respir Crit Care Med 19951521055-60 28 Behr J Degenkolb B Krombach F Vogelmeier C Intracellular glutathione and bronchoalveolar cells in fibrosing alveolitis effects of N-acetylcysteine Eur Respir J 200219906-11 29 Bando M Hosono T Mato N et al Long-term efficacy of inhaled N-acetylcysteine in patients with idiopathic pulmonary fibrosis Intern Med 2010492289-96 30 Demedts M Behr J Buhl R et al High-dose acetylcysteine in idiopathic pulmonary fibrosis N Engl J Med 20053532229-42 31 Toma TP Bhowmik A Rajakulasingam R Acetylcysteine in pulmonary fibrosis N Engl J Med 20063541086-9 author reply -9 32 Hunninghake GW Antioxidant therapy for idiopathic pulmonary fibrosis N Engl J Med 20053532285-7 33 Flaherty KR Mumford JA Murray S et al Prognostic implications of physiologic and radiographic changes in idiopathic interstitial pneumonia Am J Respir Crit Care Med 2003168543-8 34 Latsi PI du Bois RM Nicholson AG et al Fibrotic idiopathic interstitial pneumonia the prognostic value of longitudinal functional trends Am J Respir Crit Care Med 2003168531-7 35 Collard HR King TE Jr Bartelson BB Vourlekis JS Schwarz MI Brown KK Changes in clinical and physiologic variables predict survival in idiopathic pulmonary fibrosis Am J Respir Crit Care Med 2003168538-42 36 Jegal Y Kim DS Shim TS et al Physiology is a stronger predictor of survival than pathology in fibrotic interstitial pneumonia Am J Respir Crit Care Med 2005171639-44 37 Martinez FJ Safrin S Weycker D et al The clinical course of patients with idiopathic pulmonary fibrosis Ann Intern Med 2005142963-7 38 Hull JH Acetylcysteine in pulmonary fibrosis N Engl J Med 20063541089-91 author reply -91
70
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
39 Flaherty KR King TE Jr Raghu G et al Idiopathic interstitial pneumonia what is the effect of a multidisciplinary approach to diagnosis Am J Respir Crit Care Med 2004170904shy10 40 Raghu G Johnson WC Lockhart D Mageto Y Treatment of idiopathic pulmonary fibrosis with a new antifibrotic agent pirfenidone results of a prospective open-label Phase II study Am J Respir Crit Care Med 19991591061-9 41 Hunninghake GW Lynch DA Galvin JR et al Radiologic findings are strongly associated with a pathologic diagnosis of usual interstitial pneumonia Chest 20031241215-23 42 Lynch D Godwin J Safrin S et al High-resolution computed tomography in idiopathic pulmonary fibrosis diagnosis and prognosis Am J Respir Crit Care Med 2005172488-93 43 Mallinckrodt CH Watkin JG Molenberghs G Carroll RJ Choice of the primary analysis in longitudinal clinical trials Pharmaceutical Statistics 20043161-9 44 Bang H Tsiatis A Estimating medical costs with censored data Biometrika 200087329shy43 45 Lin DY Regression analysis of incomplete medical cost data Stat Med 2003221181-200 46 Rochon J Application of GEE procedures for sample size calculations in repeated measures experiments Stat Med 1998171643-58 47 Lachin JM Foulkes MA Evaluation of sample size and power for analyses of survival with allowance for nonuniform patient entry losses to follow-up noncompliance and stratification Biometrics 198642507-19
71
- PANTHER-IPFPREDNISONE AZATHIOPRINEAND N-ACETYLCYSTEINEA STUDY THAT EVALUATES RESPONSE INIDIOPATHIC PULMONARY FIBROSIS
-
- Protocol Summary
- Table of Contents
- List of Tables
- List of Figures
- List of Abbreviations
- 1 Summary
- 2 Hypotheses and Specific Aims
-
- 21 Null Hypothesis
- 22 Specific Aim 1
- 23 Specific Aim 2
- 24 Prespecified Subgroups of Interest
-
- 3 Background and Significance
-
- 31 Idiopathic Pulmonary Fibrosis is the Most Common Interstitial Lung Disease
- 32 Rationale for Placebo Control
- 33 Rationale for N-acetylcysteine
- 35 Rationale for N-acetylcysteine as a Stand-alone Therapy
- 36 Rationale for the Study Design and Primary Endpoint
- 37 Rationale for Blinding of Treatments
-
- 4 Methods
-
- 41 Inclusion Criteria
- 42 Diagnosis of IPF
- 43 Exclusion Criteria
- 44 Study Design and Study Visit
- 45 Dose Justification
- 46 Contraindications Precautions and Side Effects of Study Medications
- 47 Recruitment Procedures
- 48 Study Procedures
- 49 Concomitant Medications
- 410 Laboratory Testing
- 411 Blinding of Study Drugs
-
- 5 Study Endpoints
-
- 51 Primary Study Endpoint
- 52 Secondary Study Endpoints
-
- 6 Safety Evaluations and Procedures
-
- 61 Adverse Events
- 62 Clinical Medical Monitoring
- 63 Unblinding Procedures
-
- 7 Study Drug Procedures
- 8 Data Management
-
- 81 Hardware and Software Configuration
- 82 Sources of Data
-
- 9 Study Design and Data Analysis
-
- 91 General Analytic Considerations
- 92 Randomization Blinding and Reporting of Results
- 93 Stratification
- 94 Specification of the Primary Analyses
- 95 Analysis of Longitudinal Endpoints
- 96 Analysis of Binary Time-to-Event and Time-Lagged Endpoints
- 97 Power Analysis
-
- 10 Study Administration
-
- 101 Cooperative Agreement Mechanism
- 102 IPFnet Steering Group
- 103 Data and Safety Monitoring Board
- 104 Recommendations on Interim Monitoring of Efficacy Safety and Futility
-
- 11 Investigator and Sponsor Obligations
-
- 111 Monitoring
- 112 Cost and Payment
- 113 Confidentiality and Health Insurance Portability and Accountability ActConsiderations
- 114 Informed Consent Procedures
- 115 Institutional Review Boards
-
- 12 Investigator Agreement
- 13 References
-

PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
46 Contraindications Precautions and Side Effects of Study Medications
461 Contraindication
Contraindication to NAC is known hypersensitivity to it
462 Precautions
Concomitant administration of oral NAC and antibiotics has shown a slightly reduced absorption
of cephalexin and a slight increase in erythromycin serum levels NAC contains free sulfhydryl
groups There is no evidence that individuals sensitive to sulfa drugs are sensitive to NAC
The NAC preparation being administered in this study contains 20 mg of aspartame Because of
the phenylalanine component of aspartame individuals with phenylketonuria should avoid or
restrict aspartame intake to avoid increased blood levels of phenylalanine Because of this risk
labeling is required on all products containing aspartame
463 Side Effects
Side effects of NAC range from common to serious See Table 4
39
40
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Table 4 Side Effects of NAC
Undesirable Effects
System-organ class Uncommon
(gt11000 lt1100)
Rare
(gt110000 lt11000)
Very rare
(lt110000) Not known
Immune system disorders Hypersensitivity Anaphylactic shock
reaction
Nervous system disorders Headache
Ear and labyrinth disorders Tinnitus
Cardiac disorders Tachycardia
Vascular disorders Hemorrhage
Respiratory thoracic and
mediastinal disorders
Bronchospasm
Dyspnea
Gastrointestinal disorders
Vomiting diarrhea
stomatitis abdominal
pain nausea
Dyspepsia
Skin and subcutaneous tissue
disorders
Urticaria rash
angioedema itching
General disorders and
administration site conditions Pyrexia
Investigations Reduced arterial
pressure Face edema
In very rare cases the onset of severe skin reactions such as Stevens-Johnson syndrome and Lyell syndrome was reported to have a temporal relationship with N-acetylcysteine administration Although in most cases at least another suspect drug probably most involved in the genesis of the above mentioned mucocutaneous syndromes has been identified in case of mucocutaneous alterations it is appropriate to contact onersquos doctor and the administration of N-acetylcysteine should be immediately discontinued
Some studies confirmed a reduction of platelet aggregation during N-acetylcysteine administration The clinical significance of these findings has not been defined yet [Source Fluimucil Investigator Brochure]
47 Recruitment Procedures
Subjects recruited for this study will be established patients of the investigators or physician- or
self-referred to participating clinical centers in the IPFnet Each clinical center within IPFnet has
a well-developed infrastructure of local pulmonologists within the surrounding geographic area
These pulmonologists are kept informed of ongoing IPF clinical trials and regularly refer
subjects to studies conducted at IPFnet clinical centers
Additional steps will be taken to inform clinicians of the trials in progress within IPFnet
including presentations at faculty staff meetings at local hospitals medical grand rounds and
national conferences direct mail notification monthly faxes and advertisement of network trials
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
in pulmonary journals Clinical center patients previously diagnosed with IPF will be notified of
the trials by mail whenever possible
Recruitment of minorities and women will be monitored by the DCC and DSMB If necessary
additional recruitment efforts will be made at specific centers to ensure that the aggregate subject
sample contains appropriate representation of women and minorities
48 Study Procedures
The following procedures are detailed in the PANTHER-IPF MOOP accompanying this
protocol
1 PFT
2 ABG
3 HRCT scan of the chest (including imaging of pulmonary arteries)
4 CBC and serum chemistries
5 Pregnancy test
6 6MWTBorg Dyspnea Scale
7 QOL questionnaires (EuroQol HAD SF-36 SGRQ and ICE CAP)
8 UCSD SOBQ
9 Gender Substudy Questionnaire
All assessments of PFTs will be conducted by study personnel not directly involved in the
treatment of the subjects
481 Biological Specimen Management
4811 Biological Specimen Sample Management
Subjects at clinical centers participating in the specimen repository substudy who consent to
having blood drawn for research purposes and for the banking of blood blood components and
other biologic specimens (urine and BAL fluid) will have approximately 405 mL of blood
41
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
drawn 17 mL blood drawn for DNA and 20 mL of urine collected at enrollment visit Subjects
will have approximately 50 mL of blood drawn and 20 mL of urine collected at each 15-week
follow-up visit Blood specimens will be separated according to PANTHER-IPF MOOP
guidelines into the following components for banking in the repository serum plasma and
DNA Coding of all biologic specimens for the repository will be performed by study staff at the
clinical center The samples will be processed per PANTHER-IPF MOOP guidelines aliquoted
labeled with barcode labels and stored at -70degC at the clinical center and shipped to the central
repository
The only subject identifiers will be a sample ID number and subject initials This sample ID will
be linked in the IPFnet DCC clinical database to subject information No subject information will
be transferred to the biological-specimen database
The subjectrsquos samples may be used for approved sub-studies relating to human disease
including but not limited to IPF The studies for which an individualrsquos samples will be made
available will be determined by the subjectrsquos answers to questions on the biological-sample
informed consent form The subjects can choose to make their samples available for all options
or any combination Samples will be made available to researchers only with IPFnet Steering
Group approval until such time as the samples are made public through the NHLBI repository
49 Concomitant Medications
Concurrent treatment with FDA-approved therapy for IPF is allowed Colchicine may be used
for treatment of gout Temporary treatment with oral or IV corticosteroids for clinical worsening
or suspected AEx is permitted Nutritional supplements containing NAC are not allowed
410 Laboratory Testing
Clinical laboratory parameters will be assessed at screening and at the end of the study The
following tests will be performed at the two time points specified in the protocol chemistry (AG
ratio ALT [SGPT] AST [SGOT] albumin alkaline phosphatase amylase bilirubin-direct
42
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
bilirubin-indirect bilirubin-total BUN BUNcreatinine ratio calcium carbon dioxide
cholesterol-total chloride CPK-total creatinine GGT globulin glucose iron-total LDH
lipase magnesium phosphorus-inorganic potassium protein-total sodium TIBC triglycerides
uric acid) and hematology (red blood cell count WBC count hemoglobin hematocrit cell
indices differential platelet count)
411 Blinding of Study Drugs
Subjects and caregivers will be blinded to study treatment Every subject will receive NAC or
matching PLs at every study visit from the baseline visit to the week-45 visit No study agent
will be dispensed at the week-60 visit
43
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
5 Study Endpoints
51 Primary Study Endpoint
The primary endpoint will be the change in serial measurements of FVC over the study period
52 Secondary Study Endpoints
521 Time to Disease-progression
The time-to-death or a 10 decline in FVC will be defined as the time-to-disease progression
The 10 decline in FVC from enrollment must be confirmed on 2 consecutive visits no less than
6 weeks apart For subjects with 2 consecutive visits with a 10 decline in FVC the time-toshy
disease progression will be defined as the time interval between enrollment and the initial visit
with a 10 FVC decline For subjects who experience disease progression the study doctor will
determine whether or not the subject will remain in the study
522 Acute Exacerbations
The following 3 criteria will define AEx in subjects with acute worsening of their respiratory
conditions
1 Clinical (all of the following required)
A) Unexplained worsening of dyspnea or cough within 30 days triggering unscheduled
medical care (eg emergency room clinic study visit hospitalization)
B) No clinical suspicion or overt evidence of cardiac event pulmonary embolism or deep
venous thrombosis to explain acute worsening of dyspnea
C) No pneumothorax
44
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
2 RadiologicPhysiologic (A and B required)
A) New ground glass opacity or consolidation computed tomography (CT) scan OR new
alveolar opacities on chest x-ray
B) Decline of ge 5 in resting room air SpO2 from last recorded level OR decline of ge 8 mm
Hg in resting room air PaO2 from last recorded level
3 Microbiologic (all of the following required)
A) No clinical evidence for infection (ie absence of grossly purulent sputum fever gt 39degC
orally)
B) Lack of positive microbiological results (if done) from lower respiratory tract defined as
(1) Clinically significant bacterial growth on sputum or endotracheal aspirate cultures
(2) Quantitative culture by protected brush specimen ge 103 cfumL or BAL ge 104 cfumL
(3) The presence of specific pathogens on stains of any of the above
C) Lack of positive pathogen in blood cultures (if done)
Identification of Acute Exacerbations
All subjects will be educated about the importance of identifying AExs At the time of
enrollment subjects will be told about the possibility of developing acute symptomatic
worsening that might represent an AEx of IPF and instructed to contact their study clinical
center coordinator within 48 to 72 hours of the apparent event
All subjects will be contacted by phone monthly and questioned about any change in dyspnea or
cough and any interim clinic visits or hospitalizations Finally as part of the IPFnet outreach to
community referring physicians the importance of AExs will be emphasized When a subject is
identified who meets criterion 1A this will trigger the collection of additional clinical data to
evaluate a suspected AEx These data will be collected as part of standard clinical care (ie this
protocol does not require collection of all items) The additional items to be collected for
suspected AEx include
IPFnet AEx case report form (eCRF) (required)
45
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Chest x-ray CT scan withwithout pulmonary angiogram (reports should be faxed and
followed by the hard copiesdiscs)
Oxygen saturation (pulse oximetry)
ABG
Respiratory cultures (sputum endotracheal aspirate lavage)
Blood cultures
Clinichospital records related to the event
All potential cases of AEx will be reviewed by the clinical center PI first and a decision on
whether the case may represent an AEx will be made If AEx is suspected the case will be sent
to the IPFnet adjudication committee which will assign a final diagnosis (see Table 5) If there is
disagreement among members the majority opinion will be recorded
During episodes of suspected AEx as determined by the individual clinical center investigator
subjects will remain blinded and in the study
Table 5 Final Diagnoses in Evaluation of Suspected Acute Exacerbations
Definite acute exacerbation All criteria met no alternative etiology
Unclassifiable acute worsening
Insufficient data to evaluate all criteria no alternative etiology
Not acute exacerbation Alternative etiology identified that explains acute worsening
Management of the suspected AEx will be at the discretion of the treating physician Standard of
care generally involves evaluation for respiratory infection pulmonary embolism cardiac events
and pneumothorax and treatment with IV corticosteroids
Study drugs will be resumed at pre-suspected AEx doses after subjects clinically improve as
confirmed by the local PI All subjects should be seen at the clinical center within 2 to 4 weeks
of recovery for measurement of post-bronchodilator FVC (see Figure 4) Subjects unable to
return to the clinical center after suspected AEx due to medical frailty (eg continued
46
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
institutionalization progressive disability) will be categorized as failing to maintain FVC
response in secondary analyses
Suspected AEx (PI determined)
Hold study drug Treat AEx
(Attending physician determined)
Alive but unable to continue due to
medical frailty
Dead
Alive and able to continue
Site reviewvisit
Restart study drug
FVC within 2-4 weeks
Figure 4 Acute Exacerbation Flow Chart
523 Respiratory Infections
An upper respiratory infection will be defined as
Change in sputum discoloration
Increased cough of no more than 14 daysrsquo duration
A lower-respiratory infection (pneumonia) will be defined as new segmental or lobar airspace
opacities visualized by image studies (chest radiograph or HRCT) in addition to any of the
following
Positive pathogencultures in good sample of sputum or lower-airway secretions retrieved
by fiberoptic bronchoscope
Fever gt 39degC or gt 100degF
Leukocytosis gt 12000 (unexplained no increase in dose of corticosteroids)
47
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
524 Maintained FVC Response
Subjects with follow-up FVCpred measurements at or above their baseline FVCpred level
will be classified as having maintained FVC response Subjects with reduced FVCpred levels
or missing data for any reason including death or medical frailty will be classified as having not
maintained FVC response The FVCpred value is used because unadjusted FVC measurements
are expected to decline with age
48
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
6 Safety Evaluations and Procedures
61 Adverse Events
During a clinical trial the reporting of adverse experience information can lead to important
changes in the way a new treatment is developed as well as provide integral safety data
611 Definitions
An adverse event (AE) is any untoward medical occurrence in a subject or clinical investigation
subject who was administered a pharmaceutical product The AE does not necessarily have to
have a causal relationship with the drug administered An AE can be any unfavorable and
unintended sign (including an abnormal laboratory finding) symptom or disease temporarily
associated with the use of a medicinal product whether or not considered to be related to the
medicinal product Diseases signs symptoms or laboratory abnormalities already existing at
enrollment are not considered AEs unless they worsen (ie increase in intensity or frequency)
Surgical procedures themselves are not AEs they are therapeutic measures for conditions that
require surgery The condition for which the surgery is required may be an AE Surgical
procedures planned before randomization and the conditions necessitating the surgery are not
AEs
A serious adverse event is any untoward event that
Is fatal
Is life-threatening
Requires inpatient hospitalization or prolongation of existing hospitalization with the
following exceptions
o Preplanned (before the study) hospital admissions unless the hospitalization is
prolonged
o Planned admissions (as part of a study eg routine biopsies)
o Hospitalization lasting lt 24 hours
49
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
o Hospitalization for elective procedure
o Emergency room visits
Results in persistent or significant disability or incapacity
Is a congenital anomaly or birth defect
Important medical events that may not result in death be life-threatening or require
inpatient hospitalization may be considered serious adverse events (SAEs) when based
on appropriate medical judgment they may jeopardize the subject and may require
medical or surgical intervention to prevent one of the outcomes listed above
Life-threatening means that the subject was in the view of the investigator at immediate risk of
death from the AE as it occurred It does not include an AE that had it occurred in a more severe
form might have caused death
Persistent or significant disabilityincapacity means that the event resulted in permanent or
significant and substantial disruption of the subjectrsquos ability to carry out normal life functions
Causality
A reasonable possibility means the AE may have been caused byrelated to the study drug A
perceived or real lack of efficacy does not satisfy the definition of relatedness
612 Adverse Event (AE) Reporting
For the PANTHER-IPF trial all AEs (serious and nonserious) occurring from randomization
through final study visit (4 weeks after final dose of all study medication) will be recorded on the
AE page of the case report form (CRF)
6121 Serious Adverse Events (SAE) Reporting
For this trial all deaths and all SAEs which occur from randomization through final study visit
must be entered within the EDC system via the SAE eCRF page within 24 hours of the
investigative sitersquos knowledge of the event It is the responsibility of the clinical center
50
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
investigator to provide a causality assessment of the event for each study medications based upon
the information available at the time of the report It is understood that complete information
about the event may not be known at the time the initial report is submitted In the event the EDC
system is not accessible to the site at the time of event reporting investigative sites will complete
and forward a paper back-up SAE form to DCRI Safety Surveillance for processing
DCRI Safety Surveillance
Telephone 1-919-668-8624 or 1-866-668-7799 (toll free)
Fax 1-919-668-7138 or 1-866-668-7138 (toll free)
The investigator must complete and submit follow-up SAE information via the eCRF when
important new or follow-up information (eg final diagnosis outcome results of specific
investigations) becomes available Follow-up information should be submitted according to the
same process used for reporting the initial event as described above All SAEs will be followed
until resolution stabilization or 30 days after the subject has completed the final visit (4 weeks
after the final dose of study medication) whichever occurs first The investigator is responsible
for reporting SAEs to their institutional review board (IRB) per site specific IRB reporting
guidelines
6122 Regulatory Reporting
AEs that are serious study drug related and unexpected will be reported to the regulatory
authorities The DCRI Safety Surveillance medical monitor will perform a medical review of all
SAEs submitted and evaluate for ldquounexpectednessrdquo DCRI Safety Surveillance will prepare
MedWatch reports for those events identified as serious study drug related and unexpected as
determined by Safety Medical Monitor
DCRI Regulatory Services will submit all unexpected study drug-related SAEs as per 21 CFR
32 DCRI Safety Surveillance will provide a safety alert letter to the NHLBI DSMB and DCC
clinical operation (for distribution to sites) within 15 days of initial receipt of the information
51
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Investigators are responsible for promptly reporting these events to their reviewing IRBs
according to site specific IRB reporting guidelines
62 Clinical Medical Monitoring
There will be an unblinded physician at the IPFnet DCC serving as medical monitor The
medical monitor will be available to assist with questions about dosage adjustments of study
medications including discontinuation or resumption of medications
63 Unblinding Procedures
Unblinding of subjects or investigators to subject treatment is strongly discouraged For ongoing
clinical management all subjects should be presumed to be receiving ldquoactiverdquo study drug To
ensure the subjectrsquos safety the study treatment will be dose-adjusted based on laboratory test
results clinical findings and symptoms
The IPFnet DCC medical monitor and PANTHER-IPF co-chairs Drs Ganesh Raghu and
Fernando Martinez will be available to the study physicians to discuss study drug management
on a case-by-case basis Un-blinding will be considered ONLY when the knowledge of subject
treatment assignment is ABSOLUTELY ESSENTIAL for subject safety and after discussion of
the subjectrsquos case with the medical monitor and either Dr Raghu or Dr Martinez Unblinding of
study treatment should be minimized during the conduct of the trial In those cases where it is
felt to be medically necessary the DCC medical officer will communicate directly with the
managing physician to minimize unblinding of study personnel
52
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
7 Study Drug Procedures
At the baseline 15-week 30-week and 45-week study visits subjects will receive a supply of
study drug sufficient to last until the next visit at which study drug will be dispensed
53
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
8 Data Management
81 Hardware and Software Configuration
811 Hardware and Database Software
Data will be stored in an Oracle database system Oracle has advantages of processing efficiency
and smooth linkage with other software systems The application and database will be hosted on
Solaris Unix servers at the IPFnet DCC
812 Statistical Software
SAS will be used as the principal application for the management of analysis data files and
statistical computations S-Plus will be used to provide supplementary functions as needed
813 Access Control and Confidentiality Procedures
Access to databases will be controlled centrally by the IPFnet DCC through user passwords
linked to appropriate privileges This protects the data from unauthorized changes and
inadvertent loss or damage
814 Security
Database and Web servers will be secured by a firewall and through controlled physical access
Oracle has many security features to ensure that any staff member accessing the database has the
proper authority to perform the functions he or she requests of the system Within the secondary
SAS databases Unix group-access control maintains similar security The Sun workstation login
is secured by extensive user-password facilities under Unix
54
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
815 Back-up Procedures
Database back-up will be performed automatically every day and standard IPFnet DCC policies
and procedures will be applied to dictate tape rotation and retention practices
816 Virus Protection
All disk drives that provide network services and all user computers will be protected using
virus-scanning software Standard IPFnet DCC policies will be applied to update these protection
systems periodically through the study
82 Sources of Data
821 Design and Development
The IPFnet DCC will be responsible for development of the electronic case report forms
(eCRFs) development and validation of the clinical study database ensuring data integrity and
training clinical center staff on applicable data management procedures A web-based distributed
data entry model will be implemented This system will be developed to ensure that guidelines
and regulations surrounding the use of computerized systems used in clinical trials are upheld
The remainder of this section provides an overview of the data management plan associated with
this protocol
822 Data Collection Forms
The data collection process consists of direct data entry at the study clinical centers into the EDC
system(s) provided by the DCC A data collection worksheet will be provided to clinical centers
for recording data in the event the EDC system is unavailable Data entry of the eCRFs should
be completed according to the instructions provided and project specific training The
investigator is responsible for maintaining accurate complete and up-to-date records and for
ensuring the completion of the eCRFs for each research participant
55
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
823 Data Acquisition and Entry
Data entry into eCRFs shall be performed by authorized individuals Selected eCRFs may also
require the investigatorrsquos written signature or electronic signature as appropriate Electronic
CRFs will be monitored for completeness accuracy and attention to detail during the study
824 Data Center Responsibilities
The IPFnet DCC will 1) develop a data management plan and will conduct data management
activities 2) provide final eCRFs for the collection of all data required by the study 3) develop
data dictionaries for each eCRF that will comprehensively define each data element 4) conduct
ongoing data monitoring activities on study data 5) monitor any preliminary analysis data
cleanup activities and 6) rigorously monitor final study data clean up
825 Data Editing
Completed data will be entered into the IPFnet DCC automated data acquisition and
management system If incomplete or inaccurate data are found a data clarification request will
be generated and distributed to clinical centers for a response Clinical centers will resolve data
inconsistencies and errors and enter all corrections and changes into the IPFnet DCC automated
data acquisition and management system
826 Training
The training plan for clinical center staff includes provisions for training on assessments eCRF
completion guidelines data management procedures and the use of computerized systems
56
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
9 Study Design and Data Analysis
91 General Analytic Considerations
All primary analyses will be based on intent-to-treat (ITT) principles using all randomized
subjects Baseline factors across groups will be compared using mean (standard deviation) and
median (25th and 75th percentiles) summary measures Kaplan-Meier curves will be used to
display event rates Due to clinical interest in departures from both sides of the null hypothesis
all test statistics will be 2-sided
Reasonable caution needs to be taken when conducting multiple analyses on key clinical
subgroups For subgroup analyses a conservative significance level of 0001 will be used for all
interaction tests Thus subgroup comparisons will be considered exploratory unless the p-value
from the interaction test is smaller than 0001
92 Randomization Blinding and Reporting of Results
A permuted block-randomization scheme will be created with varying block sizes stratified by
clinical center Once a subject has completed the screening and baseline period and evaluation
for inclusionexclusion criteria the randomization process will begin Subjects will be
randomized to receive NAC or matching placebo with equal probability (11) via telephone
contact with a central interactive voice response system (IVRS) using a toll-free randomization
number On the day of randomization after the subject has successfully met all inclusion and
exclusion criteria the investigator or designee will call the central randomization number to
obtain the assigned kit randomization numbers for that subject At each subject visit the
investigator or designee will call the central randomization number to obtain the new kit
randomization numbers for resupply of the subject For resupply of the clinical center the IVRS
will monitor minimal volume of a kit type andor expiration date and will automatically notify
the pharmacy
57
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
The trial results will be reported according to guidelines specified in the CONSORT statement
A flow diagram describing screening recruitment randomization dropout and vital status will
be included in the primary manuscript AEs and efficacy data will be presented for all treatment
groups Adherence dropout and lost to follow-up will be carefully examined across all treatment
groups Analyses of safety will be based on data from all randomized subjects who received at
least one dose of study drug
93 Stratification
Subjects will be distributed to the two treatment arms in a 11 allocation ratio Stratification
blocks will be based on clinical centers
94 Specification of the Primary Analyses
A mixed model repeated measures (MMRM) analysis described in section 95 will be used to
compare differences in the slope of FVC measurements across the treatment groups Response
variables are values of the FVC measured at baseline and every 15 weeks until study completion
Variables in the model will include treatment time and time by treatment age sex race and
height Contrast estimates of differences in slopes of treatment over time (along with confidence
intervals) will be used to estimate the treatment effect The validity of this model in terms of
meeting modeling assumptions will be assessed via standard modeling diagnostics and goodness-
of-fit measures Based on the MMRM framework missing FVC data will not be imputed for the
primary analysis
95 Analysis of Longitudinal Endpoints
A common goal in clinical trials is to specify models that are easily implemented and
reproducible by independent data analysts On the other hand the models should have proper
statistical behavior in terms of low bias and high precision Many common approaches to
longitudinal data analysis including last observation carried forward (LOCF) imputation rely on
the missing completely at random (MCAR) assumption However the MCAR assumption is
58
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
unlikely to hold in many clinical trials because missing data are often related to disease
progression and prognosis A more reasonable assumption missing at random (MAR) specifies
that the complete data distribution can be modeled using only the observed data The likelihood-
based MMRM approach is valid under the more general MAR assumptions These models will
be applied to analyze the longitudinal data secondary endpoints
The advantages of MMRM analysis are that all important characteristics of the model can be preshy
specified standard software can be used to implement the models and results are based on ITT
principles43 In addition the MMRM approach offers superior control of Type I and Type II
errors compared with the LOCF approach
Response variables are values of the PFTs measured at enrollment and every 15 weeks until
study completion and 6MWT values measured at baseline week 30 and week 60 Covariates are
treatment time time by treatment and key baseline risk factors Contrasts (along with
confidence intervals) of treatment by time will be used to estimate the treatment effect
The correlation structure involves multiple pieces including measurement errors random
variation and interindividual variability For the longitudinal data analyses an unstructured
correlation matrix for within-subject errors will be assumed Other correlation structures
including compound symmetry will be examined as needed A careful examination of reasons
for study discontinuation will be conducted to assess the validity of MCAR Sensitivity analyses
will be used to examine the untestable assumption that the observed data violate the MAR
assumption The MMRM models will be implemented using PROC MIXED in SAS
96 Analysis of Binary Time-to-Event and Time-Lagged Endpoints
Regression modeling approaches using either the logistic regression model or Cox proportional
hazards regression model will be employed when appropriate The validity of these models will
be assessed via standard modeling diagnostics and goodness-of-fit measures Estimates of
cumulative frequencies for more general time-lagged responses will be calculated using the
partitioned version of the Bang-Tsiatis estimator44 The partitions will be set at 15-week intervals
59
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
to correspond with the data-collection process Covariate adjusted event rates will be calculated
using inverse probability-weighted regression estimates45
97 Power Analysis
971 Primary Analyses
Based on previously published IPF clinical trials the PL group is expected to experience a drop
in FVC of approximately 020 L over the study period (see Figure 1) The IPFnet Steering Group
determined a clinically important difference would be to preserve the majority of the decline
relative to PL over the study period In particular a treatment effect of 015 L was determined to
be a clinically meaningful difference Potential dropout is a key factor in the proposed study The
drop-out process assumed 5 lost to follow-up after every study visit Only 80 of subjects
were assumed to be followed for the entire study period All models assumed a compound
symmetry structure for the covariance matrix Power calculations were performed using a SAS
IML program for designing repeated measures studies46 Based on preliminary reviews of the
data from the University of Michigan the covariance matrix parameters were estimated at
approximately σ2 = 0757 (variance parameter) and ρ = 0936 (correlation parameter) To be
conservative the power calculations for the primary analysis were performed with parameter
setting of σ2 = 0810 (variance parameter) and ρ = 0925 (correlation parameter)
The power calculations assume a correction for imperfect compliance proposed by Lachin and
Foulkes to allow for 2 noncompliance for each of the treatment arms47 Thus the sample size
of 130 subjects per arm would be reduced to an adjusted sample size of 130(1-002-002)2 =
1198 or 120 subjects per arm
Under the assumed Type I error rate of 005 with a correlation parameter of 0925 and standard
deviation of 090 the difference of 015 L (or 00025 Lweek) shown in Table 6 would have
power of 93
60
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Table 6 Hypothetical Values of Mean FVC (L) Change from Baseline
Week 15 Week 30 Week 45 Week 60
NAC 00125 00250 00375 00500
Placebo 00500 01000 01500 02000
Difference 00375 00750 01125 01500
Abbreviations FVC forced vital capacity PL placebo
972 Power Analysis for Secondary Endpoints
Power calculations for secondary endpoint measurements are shown in Table 7 Standard
deviations are based on unpublished data provided by the University of Michigan The
calculations are based on a 2-sample t-test with Type I error rate set at 005 These calculations
are likely to be conservative because the statistical approach described in section 95 for
analyzing these endpoints will incorporate incomplete observations as well as intermediate data
points
Table 7 Detectable Differences in Treatment Means for Selected Endpoint Measurements
Secondary Endpoints Std Dev
of the Baseline Score
Detectable Difference for 80 Power
Std Dev of the Change Score
Difference Detectable for
80 Power
DLCOpred 166 58 91 32
6MWT Area Under the Desaturation Curve
219 76 175 61
6MWT Distance to Desaturation 224 78 315 110
6MWT Minutes Walked 210 073 205 071
Abbreviations Std Dev standard deviation DLCOpred diffusing capacity of the lung for carbon monoxide percent predicted 6MWT 6-minute walk test
61
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
10 Study Administration
101 Cooperative Agreement Mechanism
The administrative and funding mechanism used to undertake this project is a ldquocooperative
agreementrdquo (U01) which is an assistance mechanism Under the cooperative agreement the
NHLBI assists supports andor stimulates the project and is substantially involved with
investigators in conducting the study by facilitating performance of the effort in a ldquopartnerrdquo role
The NHLBI project scientist serves on the IPFnet Steering Group and he or another NHLBI
scientist may serve on other project committees when appropriate At the same time however
NHLBI does not assume a dominant role direction or prime responsibility for this research
program
As described below governance of the project is conducted through the IPFnet Steering Group
Principal investigators have lead responsibilities in all aspects of their trials and the project
including any modification of trial designs conduct of the trials quality control data analysis
and interpretation preparation of publications and collaboration with other investigators unless
otherwise provided for by the IPFnet Steering Group
PIs retain custody of and have primary rights to their center-specific and collaborative data
subject to government rights-of-access consistent with current Health amp Human Services (HHS)
Public Health Service (PHS) and National Institutes of Health policies The protocols and
governance policies call for the continual submission of data centrally to the IPFnet DCC for the
collaborative database which at a minimum will contain the key variables selected by the IPFnet
Steering Group for standardization across all clinical centers the submission of copies of the
collaborative datasets to each PI upon completion of the project procedures for data analysis
reporting and publication and procedures to protect and ensure the privacy of medical and
genetic data and records of individuals The NHLBI project scientist on behalf of the NHLBI
will have the same access privileges and responsibilities regarding the collaborative data as the
other members of the Steering Group
62
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
PIs are also encouraged to publish and to publicly release and disseminate results data and other
products of the project concordant with the project protocols and governance and the approved
plan for making data and materials available to the scientific community and to the NHLBI
However during the 3 years after the ending date of NHLBI project support unpublished data
unpublished results data sets not previously released and other study materials or products are
to be made available to any third party only with the approval of the IPFnet Steering Group
Upon completion of the project PIs are expected to put their intervention materials and
procedure manuals into the public domain andor make them available to other investigators
according to the approved plan for making data and materials available to the scientific
community and the NHLBI for the conduct of research at no charge other than the costs of
reproduction and distribution
The NHLBI reserves the right to terminate or curtail the project (or an individual award) in the
event of (a) failure to develop or implement mutually agreeable collaborative measurement
subject eligibility and data management sections of the protocols (b) substantial shortfall in
subject recruitment follow-up data reporting or quality control or other major breach of
protocol (c) substantive changes in the agreed-upon protocols with which NHLBI cannot
concur (d) reaching a major project outcome with persuasive statistical significance
substantially before schedule or (e) human subject ethical issues that may dictate a premature
termination
Any disagreement that may arise in scientificprogrammatic matters (within the scope of the
award) between award recipients and the NHLBI may be brought to arbitration An arbitration
panel will be composed of 3 membersmdash1 selected by the IPFnet Steering Group (with the
NHLBI member not voting) or by the individual PI in the event of an individual disagreement a
second selected by NHLBI and the third selected by the other 2 members This special
arbitration procedure in no way affects the PIrsquos right to appeal an adverse action that is otherwise
appealable in accordance with the PHS regulations at 42 CFR part 50 Subpart D and HHS
63
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
regulation at 45 CFR part 16 or the rights of the NHLBI under applicable statutes regulations
and terms of the award
102 IPFnet Steering Group
The IPFnet Steering Group is the main governing body of the project It is composed of the PIs
of the clinical centers the PI of the DCC and the NHLBI project scientist The clinical centers
the IPFnet DCC and the NHLBI each have 1 vote on the IPFnet Steering Group All decisions
are determined by majority vote
All major scientific decisions are determined by the IPFnet Steering Group It assumes overall
responsibility for the design and conduct of the trial It appoints (and disbands) committees and
subcommittees as the need arises designs approves and implements the study protocols
oversees the development of the MOOP monitors subject recruitment and treatment delivery
evaluates data collection and management oversees quality assurance procedures and
implements changes and enhancements to the study as required It also has primary responsibility
for facilitating the conduct of the trials and reporting the projectrsquos results
103 Data and Safety Monitoring Board
The NHLBI will establish a DSMB in accordance with established policies (see
httpwwwnhlbinihgovfundingpoliciesdsmb_insthtm) to ensure data quality and subject
safety and to provide independent advice to the NHLBI regarding progress and the
appropriateness of study continuation
104 Recommendations on Interim Monitoring of Efficacy Safety and Futility
First and foremost the role of the DSMB will be to review subject safety and trial conduct at
periodic points during the study The DSMB may require analyses of the primary endpoint
results for comparing the benefit and risks of treatment strategies The benefit of collecting
additional data on key secondary endpoints with extended follow-up and establishing a robust
64
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
evidence base for determining a standard of care will need to be carefully considered before
early termination of one or more treatment arms After careful consideration the IPFnet Steering
Group recommends conservative thresholds for the early examinations of the safety and efficacy
data
The DSMB will be expected to meet approximately every 6 months until trial completion to
review safety and toxicity data The DSMB may recommend stopping the study based on these
reviews Because the DSMB could stop the trial for safety concerns as well as for a large
efficacy benefit there could be multiple opportunities to reject the null hypothesis (no difference
in event rates between the PL and NAC groups) A Bonferroni approximation will be applied
during the one planned interim analysis for efficacy
Before locking the database a statistical analysis plan (SAP) will be developed to provide
complete details on the statistical analysis The SAP will include the specifics for how and when
the DSMB will be notified for AEs The IPFnet DCC will deliver to the DSMB all FDA-defined
AEs at 3-month intervals The IPFnet DCC will prepare narrative SAE reports in real time for
DSMB review including recommendations and analysis of similar events for each SAE
submitted to the FDA
65
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
11 Investigator and Sponsor Obligations
111 Monitoring
All monitoring activities for US clinical centers will be performed in accordance with DCRI
standard operating procedures Information regarding the types of visits will be outlined in the
PANTHER-IPF MOOP
112 Cost and Payment
There will be no cost to subjects enrolled in this trial Study-related procedures will be paid for
by the IPFnet
Subjects may be eligible for reimbursement for travel to the clinical center Details of payment
will be explained to each subject during the consent process
113 Confidentiality and Health Insurance Portability and Accountability Act
Considerations
Subject confidentiality will be protected throughout the study All subject data will be kept
strictly confidential and no subject-identifying information will be released to anyone outside
the project Confidentiality will be assured through several mechanisms First each subject will
be assigned an anonymous study ID which will then be used on all study forms Second any
study forms blood samples and paper records that contain subject information (eg address lists
phone lists) will be kept at the clinical centers in secured locked areas coded by number Once
blood is collected there will be no subject identifiers placed on blood samplesmdashonly the study
ID number and the date of sample collection Third access to all subject data and information
including laboratory specimens will be restricted to authorized personnel In the case of
computerized data this restricted access will be assured through user logon IDs and password
protection
66
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
At the IPFnet DCC only authorized personnel will have access to the data files containing study
data Security will be assured through user logon IDs passwords and appropriate access
privileges All study subjects will be identified only by their IPFnet ID numbers and no personal
identifying information such as name address or Social Security number will be entered into
the IPFnet DCC database Any subject-specific data reported to the IPFnet Steering Group will
be identified only by the IPFnet ID number
Finally subjects will not be identified by name in any reports or publications nor will the data
be presented in such a way that the identity of individual subjects can be inferred Analysis files
created for further study by the scientific community will have no subject identifiers These data
files will be created in accordance with the Ancillary Studies and Publication Policy of the
IPFnet
114 Informed Consent Procedures
All IPFnet subjects will provide written informed consent using procedures reviewed and
approved by each clinical centerrsquos IRB Informed consent will be undertaken by study personnel
in-person with the subject The subject has the option of declining further participation in the
study at that point No further study procedures will be conducted until the signed documents
have been provided to the IPFnet clinical center
115 Institutional Review Boards
Before initiating this study the protocol clinical center-specific informed consent forms Health
Insurance Portability and Accountability Act (HIPAA) forms recruitment materials and other
relevant information will be reviewed by a properly constituted IRB at each participating clinical
center A copy of the signed and dated IRB approval at each clinical center will be retrieved prior
to or during the site initiation visit and archived at the IPFnet DCC Any amendments to the
protocol other than simple administrative and typographical changes must be approved by each
IRB before they are implemented The clinical centers will seek annual renewals of their IRB
approvals in accordance with local procedures
67
__________________________________________ ________________
__________________________________________
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
12 Investigator Agreement
I have read the foregoing protocol PANTHER-IPF and agree that it contains all necessary
details for carrying out this study I will conduct the study as outlined herein and will complete
the study within the time designated
I will provide copies of the protocol and all pertinent information to all individuals responsible to
me who assist in the conduct of this study I will discuss this material with them to ensure they
are fully informed regarding the drug and the conduct of the study
I will fulfill all responsibilities for submitting pertinent information to the local IRB if
applicable that is responsible for this study
I further agree that NHLBI andor DCRI will have access to any source documents from which
eCRF information may have been generated
Signature of Principal Investigator Date
Name of Principal Investigator (printed or typed)
Protocol version date May 19 2009
Protocol Amendment 1 version date May 28 2010
Protocol Amendment 2 version date December 6 2011
68
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
13 References
1 Raghu G Brown KK Bradford WZ et al A placebo-controlled trial of interferon gamma-1b in patients with idiopathic pulmonary fibrosis N Engl J Med 2004350125-33 2 King TE Jr Safrin S Starko KM et al Analyses of efficacy end points in a controlled trial of interferon-gamma1b for idiopathic pulmonary fibrosis Chest 2005127171-7 3 Flaherty KR Thwaite EL Kazerooni EA et al Radiological versus histological diagnosis in UIP and NSIP survival implications Thorax 200358143-8 4 Wells AU Desai SR Rubens MB et al Idiopathic pulmonary fibrosis a composite physiologic index derived from disease extent observed by computed tomography Am J Respir Crit Care Med 2003167962-9 5 Raghu G Freudenberger TD Yang S et al High prevalence of abnormal acid gastroshyoesophageal reflux in idiopathic pulmonary fibrosis Eur Respir J 200627136-42 6 Kinnula VL Focus on antioxidant enzymes and antioxidant strategies in smoking related airway diseases Thorax 200560693-700 7 Coultas DB Zumwalt RE Black WC Sobonya RE The epidemiology of interstitial lung diseases Am J Respir Crit Care Med 1994150967-72 8 Raghu G Weycker D Edelsberg J Bradford WZ Oster G Incidence and prevalence of idiopathic pulmonary fibrosis Am J Respir Crit Care Med 2006174810-6 9 Olson AL Swigris JJ Lezotte DC Norris JM Wilson CG Brown KK Mortality from pulmonary fibrosis increased in the United States from 1992 to 2003 Am J Respir Crit Care Med 2007176277-84 10 Mannino DM Etzel RA Parrish RG Pulmonary fibrosis deaths in the United States 1979shy1991 An analysis of multiple-cause mortality data Am J Respir Crit Care Med 19961531548shy52 11 Hubbard R Johnston I Coultas DB Britton J Mortality rates from cryptogenic fibrosing alveolitis in seven countries Thorax 199651711-6 12 Johnston I Britton J Kinnear W Logan R Rising mortality from cryptogenic fibrosing alveolitis Bmj 19903011017-21 13 Raghu G Collard HR Egan JJ et al An official ATSERSJRSALAT statement idiopathic pulmonary fibrosis evidence-based guidelines for diagnosis and management Am J Respir Crit Care Med 2011183788-824 14 (USA) FDA FDA Public Health Advisory Interferon gamma-1b (marketed as Actimmune) In 2007 15 King TE Jr Pardo A Selman M Idiopathic pulmonary fibrosis Lancet 2011 16 Raghu G Brown KK Costabel U et al Treatment of idiopathic pulmonary fibrosis with etanercept an exploratory placebo-controlled trial Am J Respir Crit Care Med 2008178948shy55 17 Malouf MA Hopkins P Snell G Glanville AR An investigator-driven study of everolimus in surgical lung biopsy confirmed idiopathic pulmonary fibrosis Respirology 201116776-83 18 King TE Jr Behr J Brown KK et al BUILD-1 a randomized placebo-controlled trial of bosentan in idiopathic pulmonary fibrosis Am J Respir Crit Care Med 200817775-81 19 Richeldi L Costabel U Selman M et al Efficacy of a tyrosine kinase inhibitor in idiopathic pulmonary fibrosis N Engl J Med 20113651079-87
69
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
20 Borok Z Buhl R Grimes GJ et al Effect of glutathione aerosol on oxidant-antioxidant imbalance in idiopathic pulmonary fibrosis Lancet 1991338215-6 21 Meyer A Buhl R Magnussen H The effect of oral N-acetylcysteine on lung glutathione levels in idiopathic pulmonary fibrosis Eur Respir J 19947431-6 22 Behr J Maier K Degenkolb B Krombach F Vogelmeier C Antioxidative and clinical effects of high-dose N-acetylcysteine in fibrosing alveolitis Adjunctive therapy to maintenance immunosuppression Am J Respir Crit Care Med 19971561897-901 23 Cantin AM North SL Fells GA Hubbard RC Crystal RG Oxidant-mediated epithelial cell injury in idiopathic pulmonary fibrosis J Clin Invest 1987791665-73 24 Waghray M Cui Z Horowitz JC et al Hydrogen peroxide is a diffusible paracrine signal for the induction of epithelial cell death by activated myofibroblasts Faseb J 200519854-6 25 Larios JM Budhiraja R Fanburg BL Thannickal VJ Oxidative protein cross-linking reactions involving L-tyrosine in transforming growth factor-beta1-stimulated fibroblasts J Biol Chem 200127617437-41 26 Kinnula VL Fattman CL Tan RJ Oury TD Oxidative stress in pulmonary fibrosis a possible role for redox modulatory therapy Am J Respir Crit Care Med 2005172417-22 27 Meyer A Buhl R Kampf S Magnussen H Intravenous N-acetylcysteine and lung glutathione of patients with pulmonary fibrosis and normals Am J Respir Crit Care Med 19951521055-60 28 Behr J Degenkolb B Krombach F Vogelmeier C Intracellular glutathione and bronchoalveolar cells in fibrosing alveolitis effects of N-acetylcysteine Eur Respir J 200219906-11 29 Bando M Hosono T Mato N et al Long-term efficacy of inhaled N-acetylcysteine in patients with idiopathic pulmonary fibrosis Intern Med 2010492289-96 30 Demedts M Behr J Buhl R et al High-dose acetylcysteine in idiopathic pulmonary fibrosis N Engl J Med 20053532229-42 31 Toma TP Bhowmik A Rajakulasingam R Acetylcysteine in pulmonary fibrosis N Engl J Med 20063541086-9 author reply -9 32 Hunninghake GW Antioxidant therapy for idiopathic pulmonary fibrosis N Engl J Med 20053532285-7 33 Flaherty KR Mumford JA Murray S et al Prognostic implications of physiologic and radiographic changes in idiopathic interstitial pneumonia Am J Respir Crit Care Med 2003168543-8 34 Latsi PI du Bois RM Nicholson AG et al Fibrotic idiopathic interstitial pneumonia the prognostic value of longitudinal functional trends Am J Respir Crit Care Med 2003168531-7 35 Collard HR King TE Jr Bartelson BB Vourlekis JS Schwarz MI Brown KK Changes in clinical and physiologic variables predict survival in idiopathic pulmonary fibrosis Am J Respir Crit Care Med 2003168538-42 36 Jegal Y Kim DS Shim TS et al Physiology is a stronger predictor of survival than pathology in fibrotic interstitial pneumonia Am J Respir Crit Care Med 2005171639-44 37 Martinez FJ Safrin S Weycker D et al The clinical course of patients with idiopathic pulmonary fibrosis Ann Intern Med 2005142963-7 38 Hull JH Acetylcysteine in pulmonary fibrosis N Engl J Med 20063541089-91 author reply -91
70
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
39 Flaherty KR King TE Jr Raghu G et al Idiopathic interstitial pneumonia what is the effect of a multidisciplinary approach to diagnosis Am J Respir Crit Care Med 2004170904shy10 40 Raghu G Johnson WC Lockhart D Mageto Y Treatment of idiopathic pulmonary fibrosis with a new antifibrotic agent pirfenidone results of a prospective open-label Phase II study Am J Respir Crit Care Med 19991591061-9 41 Hunninghake GW Lynch DA Galvin JR et al Radiologic findings are strongly associated with a pathologic diagnosis of usual interstitial pneumonia Chest 20031241215-23 42 Lynch D Godwin J Safrin S et al High-resolution computed tomography in idiopathic pulmonary fibrosis diagnosis and prognosis Am J Respir Crit Care Med 2005172488-93 43 Mallinckrodt CH Watkin JG Molenberghs G Carroll RJ Choice of the primary analysis in longitudinal clinical trials Pharmaceutical Statistics 20043161-9 44 Bang H Tsiatis A Estimating medical costs with censored data Biometrika 200087329shy43 45 Lin DY Regression analysis of incomplete medical cost data Stat Med 2003221181-200 46 Rochon J Application of GEE procedures for sample size calculations in repeated measures experiments Stat Med 1998171643-58 47 Lachin JM Foulkes MA Evaluation of sample size and power for analyses of survival with allowance for nonuniform patient entry losses to follow-up noncompliance and stratification Biometrics 198642507-19
71
- PANTHER-IPFPREDNISONE AZATHIOPRINEAND N-ACETYLCYSTEINEA STUDY THAT EVALUATES RESPONSE INIDIOPATHIC PULMONARY FIBROSIS
-
- Protocol Summary
- Table of Contents
- List of Tables
- List of Figures
- List of Abbreviations
- 1 Summary
- 2 Hypotheses and Specific Aims
-
- 21 Null Hypothesis
- 22 Specific Aim 1
- 23 Specific Aim 2
- 24 Prespecified Subgroups of Interest
-
- 3 Background and Significance
-
- 31 Idiopathic Pulmonary Fibrosis is the Most Common Interstitial Lung Disease
- 32 Rationale for Placebo Control
- 33 Rationale for N-acetylcysteine
- 35 Rationale for N-acetylcysteine as a Stand-alone Therapy
- 36 Rationale for the Study Design and Primary Endpoint
- 37 Rationale for Blinding of Treatments
-
- 4 Methods
-
- 41 Inclusion Criteria
- 42 Diagnosis of IPF
- 43 Exclusion Criteria
- 44 Study Design and Study Visit
- 45 Dose Justification
- 46 Contraindications Precautions and Side Effects of Study Medications
- 47 Recruitment Procedures
- 48 Study Procedures
- 49 Concomitant Medications
- 410 Laboratory Testing
- 411 Blinding of Study Drugs
-
- 5 Study Endpoints
-
- 51 Primary Study Endpoint
- 52 Secondary Study Endpoints
-
- 6 Safety Evaluations and Procedures
-
- 61 Adverse Events
- 62 Clinical Medical Monitoring
- 63 Unblinding Procedures
-
- 7 Study Drug Procedures
- 8 Data Management
-
- 81 Hardware and Software Configuration
- 82 Sources of Data
-
- 9 Study Design and Data Analysis
-
- 91 General Analytic Considerations
- 92 Randomization Blinding and Reporting of Results
- 93 Stratification
- 94 Specification of the Primary Analyses
- 95 Analysis of Longitudinal Endpoints
- 96 Analysis of Binary Time-to-Event and Time-Lagged Endpoints
- 97 Power Analysis
-
- 10 Study Administration
-
- 101 Cooperative Agreement Mechanism
- 102 IPFnet Steering Group
- 103 Data and Safety Monitoring Board
- 104 Recommendations on Interim Monitoring of Efficacy Safety and Futility
-
- 11 Investigator and Sponsor Obligations
-
- 111 Monitoring
- 112 Cost and Payment
- 113 Confidentiality and Health Insurance Portability and Accountability ActConsiderations
- 114 Informed Consent Procedures
- 115 Institutional Review Boards
-
- 12 Investigator Agreement
- 13 References
-
40
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Table 4 Side Effects of NAC
Undesirable Effects
System-organ class Uncommon
(gt11000 lt1100)
Rare
(gt110000 lt11000)
Very rare
(lt110000) Not known
Immune system disorders Hypersensitivity Anaphylactic shock
reaction
Nervous system disorders Headache
Ear and labyrinth disorders Tinnitus
Cardiac disorders Tachycardia
Vascular disorders Hemorrhage
Respiratory thoracic and
mediastinal disorders
Bronchospasm
Dyspnea
Gastrointestinal disorders
Vomiting diarrhea
stomatitis abdominal
pain nausea
Dyspepsia
Skin and subcutaneous tissue
disorders
Urticaria rash
angioedema itching
General disorders and
administration site conditions Pyrexia
Investigations Reduced arterial
pressure Face edema
In very rare cases the onset of severe skin reactions such as Stevens-Johnson syndrome and Lyell syndrome was reported to have a temporal relationship with N-acetylcysteine administration Although in most cases at least another suspect drug probably most involved in the genesis of the above mentioned mucocutaneous syndromes has been identified in case of mucocutaneous alterations it is appropriate to contact onersquos doctor and the administration of N-acetylcysteine should be immediately discontinued
Some studies confirmed a reduction of platelet aggregation during N-acetylcysteine administration The clinical significance of these findings has not been defined yet [Source Fluimucil Investigator Brochure]
47 Recruitment Procedures
Subjects recruited for this study will be established patients of the investigators or physician- or
self-referred to participating clinical centers in the IPFnet Each clinical center within IPFnet has
a well-developed infrastructure of local pulmonologists within the surrounding geographic area
These pulmonologists are kept informed of ongoing IPF clinical trials and regularly refer
subjects to studies conducted at IPFnet clinical centers
Additional steps will be taken to inform clinicians of the trials in progress within IPFnet
including presentations at faculty staff meetings at local hospitals medical grand rounds and
national conferences direct mail notification monthly faxes and advertisement of network trials
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
in pulmonary journals Clinical center patients previously diagnosed with IPF will be notified of
the trials by mail whenever possible
Recruitment of minorities and women will be monitored by the DCC and DSMB If necessary
additional recruitment efforts will be made at specific centers to ensure that the aggregate subject
sample contains appropriate representation of women and minorities
48 Study Procedures
The following procedures are detailed in the PANTHER-IPF MOOP accompanying this
protocol
1 PFT
2 ABG
3 HRCT scan of the chest (including imaging of pulmonary arteries)
4 CBC and serum chemistries
5 Pregnancy test
6 6MWTBorg Dyspnea Scale
7 QOL questionnaires (EuroQol HAD SF-36 SGRQ and ICE CAP)
8 UCSD SOBQ
9 Gender Substudy Questionnaire
All assessments of PFTs will be conducted by study personnel not directly involved in the
treatment of the subjects
481 Biological Specimen Management
4811 Biological Specimen Sample Management
Subjects at clinical centers participating in the specimen repository substudy who consent to
having blood drawn for research purposes and for the banking of blood blood components and
other biologic specimens (urine and BAL fluid) will have approximately 405 mL of blood
41
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
drawn 17 mL blood drawn for DNA and 20 mL of urine collected at enrollment visit Subjects
will have approximately 50 mL of blood drawn and 20 mL of urine collected at each 15-week
follow-up visit Blood specimens will be separated according to PANTHER-IPF MOOP
guidelines into the following components for banking in the repository serum plasma and
DNA Coding of all biologic specimens for the repository will be performed by study staff at the
clinical center The samples will be processed per PANTHER-IPF MOOP guidelines aliquoted
labeled with barcode labels and stored at -70degC at the clinical center and shipped to the central
repository
The only subject identifiers will be a sample ID number and subject initials This sample ID will
be linked in the IPFnet DCC clinical database to subject information No subject information will
be transferred to the biological-specimen database
The subjectrsquos samples may be used for approved sub-studies relating to human disease
including but not limited to IPF The studies for which an individualrsquos samples will be made
available will be determined by the subjectrsquos answers to questions on the biological-sample
informed consent form The subjects can choose to make their samples available for all options
or any combination Samples will be made available to researchers only with IPFnet Steering
Group approval until such time as the samples are made public through the NHLBI repository
49 Concomitant Medications
Concurrent treatment with FDA-approved therapy for IPF is allowed Colchicine may be used
for treatment of gout Temporary treatment with oral or IV corticosteroids for clinical worsening
or suspected AEx is permitted Nutritional supplements containing NAC are not allowed
410 Laboratory Testing
Clinical laboratory parameters will be assessed at screening and at the end of the study The
following tests will be performed at the two time points specified in the protocol chemistry (AG
ratio ALT [SGPT] AST [SGOT] albumin alkaline phosphatase amylase bilirubin-direct
42
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
bilirubin-indirect bilirubin-total BUN BUNcreatinine ratio calcium carbon dioxide
cholesterol-total chloride CPK-total creatinine GGT globulin glucose iron-total LDH
lipase magnesium phosphorus-inorganic potassium protein-total sodium TIBC triglycerides
uric acid) and hematology (red blood cell count WBC count hemoglobin hematocrit cell
indices differential platelet count)
411 Blinding of Study Drugs
Subjects and caregivers will be blinded to study treatment Every subject will receive NAC or
matching PLs at every study visit from the baseline visit to the week-45 visit No study agent
will be dispensed at the week-60 visit
43
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
5 Study Endpoints
51 Primary Study Endpoint
The primary endpoint will be the change in serial measurements of FVC over the study period
52 Secondary Study Endpoints
521 Time to Disease-progression
The time-to-death or a 10 decline in FVC will be defined as the time-to-disease progression
The 10 decline in FVC from enrollment must be confirmed on 2 consecutive visits no less than
6 weeks apart For subjects with 2 consecutive visits with a 10 decline in FVC the time-toshy
disease progression will be defined as the time interval between enrollment and the initial visit
with a 10 FVC decline For subjects who experience disease progression the study doctor will
determine whether or not the subject will remain in the study
522 Acute Exacerbations
The following 3 criteria will define AEx in subjects with acute worsening of their respiratory
conditions
1 Clinical (all of the following required)
A) Unexplained worsening of dyspnea or cough within 30 days triggering unscheduled
medical care (eg emergency room clinic study visit hospitalization)
B) No clinical suspicion or overt evidence of cardiac event pulmonary embolism or deep
venous thrombosis to explain acute worsening of dyspnea
C) No pneumothorax
44
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
2 RadiologicPhysiologic (A and B required)
A) New ground glass opacity or consolidation computed tomography (CT) scan OR new
alveolar opacities on chest x-ray
B) Decline of ge 5 in resting room air SpO2 from last recorded level OR decline of ge 8 mm
Hg in resting room air PaO2 from last recorded level
3 Microbiologic (all of the following required)
A) No clinical evidence for infection (ie absence of grossly purulent sputum fever gt 39degC
orally)
B) Lack of positive microbiological results (if done) from lower respiratory tract defined as
(1) Clinically significant bacterial growth on sputum or endotracheal aspirate cultures
(2) Quantitative culture by protected brush specimen ge 103 cfumL or BAL ge 104 cfumL
(3) The presence of specific pathogens on stains of any of the above
C) Lack of positive pathogen in blood cultures (if done)
Identification of Acute Exacerbations
All subjects will be educated about the importance of identifying AExs At the time of
enrollment subjects will be told about the possibility of developing acute symptomatic
worsening that might represent an AEx of IPF and instructed to contact their study clinical
center coordinator within 48 to 72 hours of the apparent event
All subjects will be contacted by phone monthly and questioned about any change in dyspnea or
cough and any interim clinic visits or hospitalizations Finally as part of the IPFnet outreach to
community referring physicians the importance of AExs will be emphasized When a subject is
identified who meets criterion 1A this will trigger the collection of additional clinical data to
evaluate a suspected AEx These data will be collected as part of standard clinical care (ie this
protocol does not require collection of all items) The additional items to be collected for
suspected AEx include
IPFnet AEx case report form (eCRF) (required)
45
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Chest x-ray CT scan withwithout pulmonary angiogram (reports should be faxed and
followed by the hard copiesdiscs)
Oxygen saturation (pulse oximetry)
ABG
Respiratory cultures (sputum endotracheal aspirate lavage)
Blood cultures
Clinichospital records related to the event
All potential cases of AEx will be reviewed by the clinical center PI first and a decision on
whether the case may represent an AEx will be made If AEx is suspected the case will be sent
to the IPFnet adjudication committee which will assign a final diagnosis (see Table 5) If there is
disagreement among members the majority opinion will be recorded
During episodes of suspected AEx as determined by the individual clinical center investigator
subjects will remain blinded and in the study
Table 5 Final Diagnoses in Evaluation of Suspected Acute Exacerbations
Definite acute exacerbation All criteria met no alternative etiology
Unclassifiable acute worsening
Insufficient data to evaluate all criteria no alternative etiology
Not acute exacerbation Alternative etiology identified that explains acute worsening
Management of the suspected AEx will be at the discretion of the treating physician Standard of
care generally involves evaluation for respiratory infection pulmonary embolism cardiac events
and pneumothorax and treatment with IV corticosteroids
Study drugs will be resumed at pre-suspected AEx doses after subjects clinically improve as
confirmed by the local PI All subjects should be seen at the clinical center within 2 to 4 weeks
of recovery for measurement of post-bronchodilator FVC (see Figure 4) Subjects unable to
return to the clinical center after suspected AEx due to medical frailty (eg continued
46
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
institutionalization progressive disability) will be categorized as failing to maintain FVC
response in secondary analyses
Suspected AEx (PI determined)
Hold study drug Treat AEx
(Attending physician determined)
Alive but unable to continue due to
medical frailty
Dead
Alive and able to continue
Site reviewvisit
Restart study drug
FVC within 2-4 weeks
Figure 4 Acute Exacerbation Flow Chart
523 Respiratory Infections
An upper respiratory infection will be defined as
Change in sputum discoloration
Increased cough of no more than 14 daysrsquo duration
A lower-respiratory infection (pneumonia) will be defined as new segmental or lobar airspace
opacities visualized by image studies (chest radiograph or HRCT) in addition to any of the
following
Positive pathogencultures in good sample of sputum or lower-airway secretions retrieved
by fiberoptic bronchoscope
Fever gt 39degC or gt 100degF
Leukocytosis gt 12000 (unexplained no increase in dose of corticosteroids)
47
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
524 Maintained FVC Response
Subjects with follow-up FVCpred measurements at or above their baseline FVCpred level
will be classified as having maintained FVC response Subjects with reduced FVCpred levels
or missing data for any reason including death or medical frailty will be classified as having not
maintained FVC response The FVCpred value is used because unadjusted FVC measurements
are expected to decline with age
48
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
6 Safety Evaluations and Procedures
61 Adverse Events
During a clinical trial the reporting of adverse experience information can lead to important
changes in the way a new treatment is developed as well as provide integral safety data
611 Definitions
An adverse event (AE) is any untoward medical occurrence in a subject or clinical investigation
subject who was administered a pharmaceutical product The AE does not necessarily have to
have a causal relationship with the drug administered An AE can be any unfavorable and
unintended sign (including an abnormal laboratory finding) symptom or disease temporarily
associated with the use of a medicinal product whether or not considered to be related to the
medicinal product Diseases signs symptoms or laboratory abnormalities already existing at
enrollment are not considered AEs unless they worsen (ie increase in intensity or frequency)
Surgical procedures themselves are not AEs they are therapeutic measures for conditions that
require surgery The condition for which the surgery is required may be an AE Surgical
procedures planned before randomization and the conditions necessitating the surgery are not
AEs
A serious adverse event is any untoward event that
Is fatal
Is life-threatening
Requires inpatient hospitalization or prolongation of existing hospitalization with the
following exceptions
o Preplanned (before the study) hospital admissions unless the hospitalization is
prolonged
o Planned admissions (as part of a study eg routine biopsies)
o Hospitalization lasting lt 24 hours
49
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
o Hospitalization for elective procedure
o Emergency room visits
Results in persistent or significant disability or incapacity
Is a congenital anomaly or birth defect
Important medical events that may not result in death be life-threatening or require
inpatient hospitalization may be considered serious adverse events (SAEs) when based
on appropriate medical judgment they may jeopardize the subject and may require
medical or surgical intervention to prevent one of the outcomes listed above
Life-threatening means that the subject was in the view of the investigator at immediate risk of
death from the AE as it occurred It does not include an AE that had it occurred in a more severe
form might have caused death
Persistent or significant disabilityincapacity means that the event resulted in permanent or
significant and substantial disruption of the subjectrsquos ability to carry out normal life functions
Causality
A reasonable possibility means the AE may have been caused byrelated to the study drug A
perceived or real lack of efficacy does not satisfy the definition of relatedness
612 Adverse Event (AE) Reporting
For the PANTHER-IPF trial all AEs (serious and nonserious) occurring from randomization
through final study visit (4 weeks after final dose of all study medication) will be recorded on the
AE page of the case report form (CRF)
6121 Serious Adverse Events (SAE) Reporting
For this trial all deaths and all SAEs which occur from randomization through final study visit
must be entered within the EDC system via the SAE eCRF page within 24 hours of the
investigative sitersquos knowledge of the event It is the responsibility of the clinical center
50
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
investigator to provide a causality assessment of the event for each study medications based upon
the information available at the time of the report It is understood that complete information
about the event may not be known at the time the initial report is submitted In the event the EDC
system is not accessible to the site at the time of event reporting investigative sites will complete
and forward a paper back-up SAE form to DCRI Safety Surveillance for processing
DCRI Safety Surveillance
Telephone 1-919-668-8624 or 1-866-668-7799 (toll free)
Fax 1-919-668-7138 or 1-866-668-7138 (toll free)
The investigator must complete and submit follow-up SAE information via the eCRF when
important new or follow-up information (eg final diagnosis outcome results of specific
investigations) becomes available Follow-up information should be submitted according to the
same process used for reporting the initial event as described above All SAEs will be followed
until resolution stabilization or 30 days after the subject has completed the final visit (4 weeks
after the final dose of study medication) whichever occurs first The investigator is responsible
for reporting SAEs to their institutional review board (IRB) per site specific IRB reporting
guidelines
6122 Regulatory Reporting
AEs that are serious study drug related and unexpected will be reported to the regulatory
authorities The DCRI Safety Surveillance medical monitor will perform a medical review of all
SAEs submitted and evaluate for ldquounexpectednessrdquo DCRI Safety Surveillance will prepare
MedWatch reports for those events identified as serious study drug related and unexpected as
determined by Safety Medical Monitor
DCRI Regulatory Services will submit all unexpected study drug-related SAEs as per 21 CFR
32 DCRI Safety Surveillance will provide a safety alert letter to the NHLBI DSMB and DCC
clinical operation (for distribution to sites) within 15 days of initial receipt of the information
51
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Investigators are responsible for promptly reporting these events to their reviewing IRBs
according to site specific IRB reporting guidelines
62 Clinical Medical Monitoring
There will be an unblinded physician at the IPFnet DCC serving as medical monitor The
medical monitor will be available to assist with questions about dosage adjustments of study
medications including discontinuation or resumption of medications
63 Unblinding Procedures
Unblinding of subjects or investigators to subject treatment is strongly discouraged For ongoing
clinical management all subjects should be presumed to be receiving ldquoactiverdquo study drug To
ensure the subjectrsquos safety the study treatment will be dose-adjusted based on laboratory test
results clinical findings and symptoms
The IPFnet DCC medical monitor and PANTHER-IPF co-chairs Drs Ganesh Raghu and
Fernando Martinez will be available to the study physicians to discuss study drug management
on a case-by-case basis Un-blinding will be considered ONLY when the knowledge of subject
treatment assignment is ABSOLUTELY ESSENTIAL for subject safety and after discussion of
the subjectrsquos case with the medical monitor and either Dr Raghu or Dr Martinez Unblinding of
study treatment should be minimized during the conduct of the trial In those cases where it is
felt to be medically necessary the DCC medical officer will communicate directly with the
managing physician to minimize unblinding of study personnel
52
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
7 Study Drug Procedures
At the baseline 15-week 30-week and 45-week study visits subjects will receive a supply of
study drug sufficient to last until the next visit at which study drug will be dispensed
53
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
8 Data Management
81 Hardware and Software Configuration
811 Hardware and Database Software
Data will be stored in an Oracle database system Oracle has advantages of processing efficiency
and smooth linkage with other software systems The application and database will be hosted on
Solaris Unix servers at the IPFnet DCC
812 Statistical Software
SAS will be used as the principal application for the management of analysis data files and
statistical computations S-Plus will be used to provide supplementary functions as needed
813 Access Control and Confidentiality Procedures
Access to databases will be controlled centrally by the IPFnet DCC through user passwords
linked to appropriate privileges This protects the data from unauthorized changes and
inadvertent loss or damage
814 Security
Database and Web servers will be secured by a firewall and through controlled physical access
Oracle has many security features to ensure that any staff member accessing the database has the
proper authority to perform the functions he or she requests of the system Within the secondary
SAS databases Unix group-access control maintains similar security The Sun workstation login
is secured by extensive user-password facilities under Unix
54
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
815 Back-up Procedures
Database back-up will be performed automatically every day and standard IPFnet DCC policies
and procedures will be applied to dictate tape rotation and retention practices
816 Virus Protection
All disk drives that provide network services and all user computers will be protected using
virus-scanning software Standard IPFnet DCC policies will be applied to update these protection
systems periodically through the study
82 Sources of Data
821 Design and Development
The IPFnet DCC will be responsible for development of the electronic case report forms
(eCRFs) development and validation of the clinical study database ensuring data integrity and
training clinical center staff on applicable data management procedures A web-based distributed
data entry model will be implemented This system will be developed to ensure that guidelines
and regulations surrounding the use of computerized systems used in clinical trials are upheld
The remainder of this section provides an overview of the data management plan associated with
this protocol
822 Data Collection Forms
The data collection process consists of direct data entry at the study clinical centers into the EDC
system(s) provided by the DCC A data collection worksheet will be provided to clinical centers
for recording data in the event the EDC system is unavailable Data entry of the eCRFs should
be completed according to the instructions provided and project specific training The
investigator is responsible for maintaining accurate complete and up-to-date records and for
ensuring the completion of the eCRFs for each research participant
55
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
823 Data Acquisition and Entry
Data entry into eCRFs shall be performed by authorized individuals Selected eCRFs may also
require the investigatorrsquos written signature or electronic signature as appropriate Electronic
CRFs will be monitored for completeness accuracy and attention to detail during the study
824 Data Center Responsibilities
The IPFnet DCC will 1) develop a data management plan and will conduct data management
activities 2) provide final eCRFs for the collection of all data required by the study 3) develop
data dictionaries for each eCRF that will comprehensively define each data element 4) conduct
ongoing data monitoring activities on study data 5) monitor any preliminary analysis data
cleanup activities and 6) rigorously monitor final study data clean up
825 Data Editing
Completed data will be entered into the IPFnet DCC automated data acquisition and
management system If incomplete or inaccurate data are found a data clarification request will
be generated and distributed to clinical centers for a response Clinical centers will resolve data
inconsistencies and errors and enter all corrections and changes into the IPFnet DCC automated
data acquisition and management system
826 Training
The training plan for clinical center staff includes provisions for training on assessments eCRF
completion guidelines data management procedures and the use of computerized systems
56
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
9 Study Design and Data Analysis
91 General Analytic Considerations
All primary analyses will be based on intent-to-treat (ITT) principles using all randomized
subjects Baseline factors across groups will be compared using mean (standard deviation) and
median (25th and 75th percentiles) summary measures Kaplan-Meier curves will be used to
display event rates Due to clinical interest in departures from both sides of the null hypothesis
all test statistics will be 2-sided
Reasonable caution needs to be taken when conducting multiple analyses on key clinical
subgroups For subgroup analyses a conservative significance level of 0001 will be used for all
interaction tests Thus subgroup comparisons will be considered exploratory unless the p-value
from the interaction test is smaller than 0001
92 Randomization Blinding and Reporting of Results
A permuted block-randomization scheme will be created with varying block sizes stratified by
clinical center Once a subject has completed the screening and baseline period and evaluation
for inclusionexclusion criteria the randomization process will begin Subjects will be
randomized to receive NAC or matching placebo with equal probability (11) via telephone
contact with a central interactive voice response system (IVRS) using a toll-free randomization
number On the day of randomization after the subject has successfully met all inclusion and
exclusion criteria the investigator or designee will call the central randomization number to
obtain the assigned kit randomization numbers for that subject At each subject visit the
investigator or designee will call the central randomization number to obtain the new kit
randomization numbers for resupply of the subject For resupply of the clinical center the IVRS
will monitor minimal volume of a kit type andor expiration date and will automatically notify
the pharmacy
57
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
The trial results will be reported according to guidelines specified in the CONSORT statement
A flow diagram describing screening recruitment randomization dropout and vital status will
be included in the primary manuscript AEs and efficacy data will be presented for all treatment
groups Adherence dropout and lost to follow-up will be carefully examined across all treatment
groups Analyses of safety will be based on data from all randomized subjects who received at
least one dose of study drug
93 Stratification
Subjects will be distributed to the two treatment arms in a 11 allocation ratio Stratification
blocks will be based on clinical centers
94 Specification of the Primary Analyses
A mixed model repeated measures (MMRM) analysis described in section 95 will be used to
compare differences in the slope of FVC measurements across the treatment groups Response
variables are values of the FVC measured at baseline and every 15 weeks until study completion
Variables in the model will include treatment time and time by treatment age sex race and
height Contrast estimates of differences in slopes of treatment over time (along with confidence
intervals) will be used to estimate the treatment effect The validity of this model in terms of
meeting modeling assumptions will be assessed via standard modeling diagnostics and goodness-
of-fit measures Based on the MMRM framework missing FVC data will not be imputed for the
primary analysis
95 Analysis of Longitudinal Endpoints
A common goal in clinical trials is to specify models that are easily implemented and
reproducible by independent data analysts On the other hand the models should have proper
statistical behavior in terms of low bias and high precision Many common approaches to
longitudinal data analysis including last observation carried forward (LOCF) imputation rely on
the missing completely at random (MCAR) assumption However the MCAR assumption is
58
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
unlikely to hold in many clinical trials because missing data are often related to disease
progression and prognosis A more reasonable assumption missing at random (MAR) specifies
that the complete data distribution can be modeled using only the observed data The likelihood-
based MMRM approach is valid under the more general MAR assumptions These models will
be applied to analyze the longitudinal data secondary endpoints
The advantages of MMRM analysis are that all important characteristics of the model can be preshy
specified standard software can be used to implement the models and results are based on ITT
principles43 In addition the MMRM approach offers superior control of Type I and Type II
errors compared with the LOCF approach
Response variables are values of the PFTs measured at enrollment and every 15 weeks until
study completion and 6MWT values measured at baseline week 30 and week 60 Covariates are
treatment time time by treatment and key baseline risk factors Contrasts (along with
confidence intervals) of treatment by time will be used to estimate the treatment effect
The correlation structure involves multiple pieces including measurement errors random
variation and interindividual variability For the longitudinal data analyses an unstructured
correlation matrix for within-subject errors will be assumed Other correlation structures
including compound symmetry will be examined as needed A careful examination of reasons
for study discontinuation will be conducted to assess the validity of MCAR Sensitivity analyses
will be used to examine the untestable assumption that the observed data violate the MAR
assumption The MMRM models will be implemented using PROC MIXED in SAS
96 Analysis of Binary Time-to-Event and Time-Lagged Endpoints
Regression modeling approaches using either the logistic regression model or Cox proportional
hazards regression model will be employed when appropriate The validity of these models will
be assessed via standard modeling diagnostics and goodness-of-fit measures Estimates of
cumulative frequencies for more general time-lagged responses will be calculated using the
partitioned version of the Bang-Tsiatis estimator44 The partitions will be set at 15-week intervals
59
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
to correspond with the data-collection process Covariate adjusted event rates will be calculated
using inverse probability-weighted regression estimates45
97 Power Analysis
971 Primary Analyses
Based on previously published IPF clinical trials the PL group is expected to experience a drop
in FVC of approximately 020 L over the study period (see Figure 1) The IPFnet Steering Group
determined a clinically important difference would be to preserve the majority of the decline
relative to PL over the study period In particular a treatment effect of 015 L was determined to
be a clinically meaningful difference Potential dropout is a key factor in the proposed study The
drop-out process assumed 5 lost to follow-up after every study visit Only 80 of subjects
were assumed to be followed for the entire study period All models assumed a compound
symmetry structure for the covariance matrix Power calculations were performed using a SAS
IML program for designing repeated measures studies46 Based on preliminary reviews of the
data from the University of Michigan the covariance matrix parameters were estimated at
approximately σ2 = 0757 (variance parameter) and ρ = 0936 (correlation parameter) To be
conservative the power calculations for the primary analysis were performed with parameter
setting of σ2 = 0810 (variance parameter) and ρ = 0925 (correlation parameter)
The power calculations assume a correction for imperfect compliance proposed by Lachin and
Foulkes to allow for 2 noncompliance for each of the treatment arms47 Thus the sample size
of 130 subjects per arm would be reduced to an adjusted sample size of 130(1-002-002)2 =
1198 or 120 subjects per arm
Under the assumed Type I error rate of 005 with a correlation parameter of 0925 and standard
deviation of 090 the difference of 015 L (or 00025 Lweek) shown in Table 6 would have
power of 93
60
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Table 6 Hypothetical Values of Mean FVC (L) Change from Baseline
Week 15 Week 30 Week 45 Week 60
NAC 00125 00250 00375 00500
Placebo 00500 01000 01500 02000
Difference 00375 00750 01125 01500
Abbreviations FVC forced vital capacity PL placebo
972 Power Analysis for Secondary Endpoints
Power calculations for secondary endpoint measurements are shown in Table 7 Standard
deviations are based on unpublished data provided by the University of Michigan The
calculations are based on a 2-sample t-test with Type I error rate set at 005 These calculations
are likely to be conservative because the statistical approach described in section 95 for
analyzing these endpoints will incorporate incomplete observations as well as intermediate data
points
Table 7 Detectable Differences in Treatment Means for Selected Endpoint Measurements
Secondary Endpoints Std Dev
of the Baseline Score
Detectable Difference for 80 Power
Std Dev of the Change Score
Difference Detectable for
80 Power
DLCOpred 166 58 91 32
6MWT Area Under the Desaturation Curve
219 76 175 61
6MWT Distance to Desaturation 224 78 315 110
6MWT Minutes Walked 210 073 205 071
Abbreviations Std Dev standard deviation DLCOpred diffusing capacity of the lung for carbon monoxide percent predicted 6MWT 6-minute walk test
61
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
10 Study Administration
101 Cooperative Agreement Mechanism
The administrative and funding mechanism used to undertake this project is a ldquocooperative
agreementrdquo (U01) which is an assistance mechanism Under the cooperative agreement the
NHLBI assists supports andor stimulates the project and is substantially involved with
investigators in conducting the study by facilitating performance of the effort in a ldquopartnerrdquo role
The NHLBI project scientist serves on the IPFnet Steering Group and he or another NHLBI
scientist may serve on other project committees when appropriate At the same time however
NHLBI does not assume a dominant role direction or prime responsibility for this research
program
As described below governance of the project is conducted through the IPFnet Steering Group
Principal investigators have lead responsibilities in all aspects of their trials and the project
including any modification of trial designs conduct of the trials quality control data analysis
and interpretation preparation of publications and collaboration with other investigators unless
otherwise provided for by the IPFnet Steering Group
PIs retain custody of and have primary rights to their center-specific and collaborative data
subject to government rights-of-access consistent with current Health amp Human Services (HHS)
Public Health Service (PHS) and National Institutes of Health policies The protocols and
governance policies call for the continual submission of data centrally to the IPFnet DCC for the
collaborative database which at a minimum will contain the key variables selected by the IPFnet
Steering Group for standardization across all clinical centers the submission of copies of the
collaborative datasets to each PI upon completion of the project procedures for data analysis
reporting and publication and procedures to protect and ensure the privacy of medical and
genetic data and records of individuals The NHLBI project scientist on behalf of the NHLBI
will have the same access privileges and responsibilities regarding the collaborative data as the
other members of the Steering Group
62
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
PIs are also encouraged to publish and to publicly release and disseminate results data and other
products of the project concordant with the project protocols and governance and the approved
plan for making data and materials available to the scientific community and to the NHLBI
However during the 3 years after the ending date of NHLBI project support unpublished data
unpublished results data sets not previously released and other study materials or products are
to be made available to any third party only with the approval of the IPFnet Steering Group
Upon completion of the project PIs are expected to put their intervention materials and
procedure manuals into the public domain andor make them available to other investigators
according to the approved plan for making data and materials available to the scientific
community and the NHLBI for the conduct of research at no charge other than the costs of
reproduction and distribution
The NHLBI reserves the right to terminate or curtail the project (or an individual award) in the
event of (a) failure to develop or implement mutually agreeable collaborative measurement
subject eligibility and data management sections of the protocols (b) substantial shortfall in
subject recruitment follow-up data reporting or quality control or other major breach of
protocol (c) substantive changes in the agreed-upon protocols with which NHLBI cannot
concur (d) reaching a major project outcome with persuasive statistical significance
substantially before schedule or (e) human subject ethical issues that may dictate a premature
termination
Any disagreement that may arise in scientificprogrammatic matters (within the scope of the
award) between award recipients and the NHLBI may be brought to arbitration An arbitration
panel will be composed of 3 membersmdash1 selected by the IPFnet Steering Group (with the
NHLBI member not voting) or by the individual PI in the event of an individual disagreement a
second selected by NHLBI and the third selected by the other 2 members This special
arbitration procedure in no way affects the PIrsquos right to appeal an adverse action that is otherwise
appealable in accordance with the PHS regulations at 42 CFR part 50 Subpart D and HHS
63
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
regulation at 45 CFR part 16 or the rights of the NHLBI under applicable statutes regulations
and terms of the award
102 IPFnet Steering Group
The IPFnet Steering Group is the main governing body of the project It is composed of the PIs
of the clinical centers the PI of the DCC and the NHLBI project scientist The clinical centers
the IPFnet DCC and the NHLBI each have 1 vote on the IPFnet Steering Group All decisions
are determined by majority vote
All major scientific decisions are determined by the IPFnet Steering Group It assumes overall
responsibility for the design and conduct of the trial It appoints (and disbands) committees and
subcommittees as the need arises designs approves and implements the study protocols
oversees the development of the MOOP monitors subject recruitment and treatment delivery
evaluates data collection and management oversees quality assurance procedures and
implements changes and enhancements to the study as required It also has primary responsibility
for facilitating the conduct of the trials and reporting the projectrsquos results
103 Data and Safety Monitoring Board
The NHLBI will establish a DSMB in accordance with established policies (see
httpwwwnhlbinihgovfundingpoliciesdsmb_insthtm) to ensure data quality and subject
safety and to provide independent advice to the NHLBI regarding progress and the
appropriateness of study continuation
104 Recommendations on Interim Monitoring of Efficacy Safety and Futility
First and foremost the role of the DSMB will be to review subject safety and trial conduct at
periodic points during the study The DSMB may require analyses of the primary endpoint
results for comparing the benefit and risks of treatment strategies The benefit of collecting
additional data on key secondary endpoints with extended follow-up and establishing a robust
64
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
evidence base for determining a standard of care will need to be carefully considered before
early termination of one or more treatment arms After careful consideration the IPFnet Steering
Group recommends conservative thresholds for the early examinations of the safety and efficacy
data
The DSMB will be expected to meet approximately every 6 months until trial completion to
review safety and toxicity data The DSMB may recommend stopping the study based on these
reviews Because the DSMB could stop the trial for safety concerns as well as for a large
efficacy benefit there could be multiple opportunities to reject the null hypothesis (no difference
in event rates between the PL and NAC groups) A Bonferroni approximation will be applied
during the one planned interim analysis for efficacy
Before locking the database a statistical analysis plan (SAP) will be developed to provide
complete details on the statistical analysis The SAP will include the specifics for how and when
the DSMB will be notified for AEs The IPFnet DCC will deliver to the DSMB all FDA-defined
AEs at 3-month intervals The IPFnet DCC will prepare narrative SAE reports in real time for
DSMB review including recommendations and analysis of similar events for each SAE
submitted to the FDA
65
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
11 Investigator and Sponsor Obligations
111 Monitoring
All monitoring activities for US clinical centers will be performed in accordance with DCRI
standard operating procedures Information regarding the types of visits will be outlined in the
PANTHER-IPF MOOP
112 Cost and Payment
There will be no cost to subjects enrolled in this trial Study-related procedures will be paid for
by the IPFnet
Subjects may be eligible for reimbursement for travel to the clinical center Details of payment
will be explained to each subject during the consent process
113 Confidentiality and Health Insurance Portability and Accountability Act
Considerations
Subject confidentiality will be protected throughout the study All subject data will be kept
strictly confidential and no subject-identifying information will be released to anyone outside
the project Confidentiality will be assured through several mechanisms First each subject will
be assigned an anonymous study ID which will then be used on all study forms Second any
study forms blood samples and paper records that contain subject information (eg address lists
phone lists) will be kept at the clinical centers in secured locked areas coded by number Once
blood is collected there will be no subject identifiers placed on blood samplesmdashonly the study
ID number and the date of sample collection Third access to all subject data and information
including laboratory specimens will be restricted to authorized personnel In the case of
computerized data this restricted access will be assured through user logon IDs and password
protection
66
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
At the IPFnet DCC only authorized personnel will have access to the data files containing study
data Security will be assured through user logon IDs passwords and appropriate access
privileges All study subjects will be identified only by their IPFnet ID numbers and no personal
identifying information such as name address or Social Security number will be entered into
the IPFnet DCC database Any subject-specific data reported to the IPFnet Steering Group will
be identified only by the IPFnet ID number
Finally subjects will not be identified by name in any reports or publications nor will the data
be presented in such a way that the identity of individual subjects can be inferred Analysis files
created for further study by the scientific community will have no subject identifiers These data
files will be created in accordance with the Ancillary Studies and Publication Policy of the
IPFnet
114 Informed Consent Procedures
All IPFnet subjects will provide written informed consent using procedures reviewed and
approved by each clinical centerrsquos IRB Informed consent will be undertaken by study personnel
in-person with the subject The subject has the option of declining further participation in the
study at that point No further study procedures will be conducted until the signed documents
have been provided to the IPFnet clinical center
115 Institutional Review Boards
Before initiating this study the protocol clinical center-specific informed consent forms Health
Insurance Portability and Accountability Act (HIPAA) forms recruitment materials and other
relevant information will be reviewed by a properly constituted IRB at each participating clinical
center A copy of the signed and dated IRB approval at each clinical center will be retrieved prior
to or during the site initiation visit and archived at the IPFnet DCC Any amendments to the
protocol other than simple administrative and typographical changes must be approved by each
IRB before they are implemented The clinical centers will seek annual renewals of their IRB
approvals in accordance with local procedures
67
__________________________________________ ________________
__________________________________________
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
12 Investigator Agreement
I have read the foregoing protocol PANTHER-IPF and agree that it contains all necessary
details for carrying out this study I will conduct the study as outlined herein and will complete
the study within the time designated
I will provide copies of the protocol and all pertinent information to all individuals responsible to
me who assist in the conduct of this study I will discuss this material with them to ensure they
are fully informed regarding the drug and the conduct of the study
I will fulfill all responsibilities for submitting pertinent information to the local IRB if
applicable that is responsible for this study
I further agree that NHLBI andor DCRI will have access to any source documents from which
eCRF information may have been generated
Signature of Principal Investigator Date
Name of Principal Investigator (printed or typed)
Protocol version date May 19 2009
Protocol Amendment 1 version date May 28 2010
Protocol Amendment 2 version date December 6 2011
68
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
13 References
1 Raghu G Brown KK Bradford WZ et al A placebo-controlled trial of interferon gamma-1b in patients with idiopathic pulmonary fibrosis N Engl J Med 2004350125-33 2 King TE Jr Safrin S Starko KM et al Analyses of efficacy end points in a controlled trial of interferon-gamma1b for idiopathic pulmonary fibrosis Chest 2005127171-7 3 Flaherty KR Thwaite EL Kazerooni EA et al Radiological versus histological diagnosis in UIP and NSIP survival implications Thorax 200358143-8 4 Wells AU Desai SR Rubens MB et al Idiopathic pulmonary fibrosis a composite physiologic index derived from disease extent observed by computed tomography Am J Respir Crit Care Med 2003167962-9 5 Raghu G Freudenberger TD Yang S et al High prevalence of abnormal acid gastroshyoesophageal reflux in idiopathic pulmonary fibrosis Eur Respir J 200627136-42 6 Kinnula VL Focus on antioxidant enzymes and antioxidant strategies in smoking related airway diseases Thorax 200560693-700 7 Coultas DB Zumwalt RE Black WC Sobonya RE The epidemiology of interstitial lung diseases Am J Respir Crit Care Med 1994150967-72 8 Raghu G Weycker D Edelsberg J Bradford WZ Oster G Incidence and prevalence of idiopathic pulmonary fibrosis Am J Respir Crit Care Med 2006174810-6 9 Olson AL Swigris JJ Lezotte DC Norris JM Wilson CG Brown KK Mortality from pulmonary fibrosis increased in the United States from 1992 to 2003 Am J Respir Crit Care Med 2007176277-84 10 Mannino DM Etzel RA Parrish RG Pulmonary fibrosis deaths in the United States 1979shy1991 An analysis of multiple-cause mortality data Am J Respir Crit Care Med 19961531548shy52 11 Hubbard R Johnston I Coultas DB Britton J Mortality rates from cryptogenic fibrosing alveolitis in seven countries Thorax 199651711-6 12 Johnston I Britton J Kinnear W Logan R Rising mortality from cryptogenic fibrosing alveolitis Bmj 19903011017-21 13 Raghu G Collard HR Egan JJ et al An official ATSERSJRSALAT statement idiopathic pulmonary fibrosis evidence-based guidelines for diagnosis and management Am J Respir Crit Care Med 2011183788-824 14 (USA) FDA FDA Public Health Advisory Interferon gamma-1b (marketed as Actimmune) In 2007 15 King TE Jr Pardo A Selman M Idiopathic pulmonary fibrosis Lancet 2011 16 Raghu G Brown KK Costabel U et al Treatment of idiopathic pulmonary fibrosis with etanercept an exploratory placebo-controlled trial Am J Respir Crit Care Med 2008178948shy55 17 Malouf MA Hopkins P Snell G Glanville AR An investigator-driven study of everolimus in surgical lung biopsy confirmed idiopathic pulmonary fibrosis Respirology 201116776-83 18 King TE Jr Behr J Brown KK et al BUILD-1 a randomized placebo-controlled trial of bosentan in idiopathic pulmonary fibrosis Am J Respir Crit Care Med 200817775-81 19 Richeldi L Costabel U Selman M et al Efficacy of a tyrosine kinase inhibitor in idiopathic pulmonary fibrosis N Engl J Med 20113651079-87
69
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
20 Borok Z Buhl R Grimes GJ et al Effect of glutathione aerosol on oxidant-antioxidant imbalance in idiopathic pulmonary fibrosis Lancet 1991338215-6 21 Meyer A Buhl R Magnussen H The effect of oral N-acetylcysteine on lung glutathione levels in idiopathic pulmonary fibrosis Eur Respir J 19947431-6 22 Behr J Maier K Degenkolb B Krombach F Vogelmeier C Antioxidative and clinical effects of high-dose N-acetylcysteine in fibrosing alveolitis Adjunctive therapy to maintenance immunosuppression Am J Respir Crit Care Med 19971561897-901 23 Cantin AM North SL Fells GA Hubbard RC Crystal RG Oxidant-mediated epithelial cell injury in idiopathic pulmonary fibrosis J Clin Invest 1987791665-73 24 Waghray M Cui Z Horowitz JC et al Hydrogen peroxide is a diffusible paracrine signal for the induction of epithelial cell death by activated myofibroblasts Faseb J 200519854-6 25 Larios JM Budhiraja R Fanburg BL Thannickal VJ Oxidative protein cross-linking reactions involving L-tyrosine in transforming growth factor-beta1-stimulated fibroblasts J Biol Chem 200127617437-41 26 Kinnula VL Fattman CL Tan RJ Oury TD Oxidative stress in pulmonary fibrosis a possible role for redox modulatory therapy Am J Respir Crit Care Med 2005172417-22 27 Meyer A Buhl R Kampf S Magnussen H Intravenous N-acetylcysteine and lung glutathione of patients with pulmonary fibrosis and normals Am J Respir Crit Care Med 19951521055-60 28 Behr J Degenkolb B Krombach F Vogelmeier C Intracellular glutathione and bronchoalveolar cells in fibrosing alveolitis effects of N-acetylcysteine Eur Respir J 200219906-11 29 Bando M Hosono T Mato N et al Long-term efficacy of inhaled N-acetylcysteine in patients with idiopathic pulmonary fibrosis Intern Med 2010492289-96 30 Demedts M Behr J Buhl R et al High-dose acetylcysteine in idiopathic pulmonary fibrosis N Engl J Med 20053532229-42 31 Toma TP Bhowmik A Rajakulasingam R Acetylcysteine in pulmonary fibrosis N Engl J Med 20063541086-9 author reply -9 32 Hunninghake GW Antioxidant therapy for idiopathic pulmonary fibrosis N Engl J Med 20053532285-7 33 Flaherty KR Mumford JA Murray S et al Prognostic implications of physiologic and radiographic changes in idiopathic interstitial pneumonia Am J Respir Crit Care Med 2003168543-8 34 Latsi PI du Bois RM Nicholson AG et al Fibrotic idiopathic interstitial pneumonia the prognostic value of longitudinal functional trends Am J Respir Crit Care Med 2003168531-7 35 Collard HR King TE Jr Bartelson BB Vourlekis JS Schwarz MI Brown KK Changes in clinical and physiologic variables predict survival in idiopathic pulmonary fibrosis Am J Respir Crit Care Med 2003168538-42 36 Jegal Y Kim DS Shim TS et al Physiology is a stronger predictor of survival than pathology in fibrotic interstitial pneumonia Am J Respir Crit Care Med 2005171639-44 37 Martinez FJ Safrin S Weycker D et al The clinical course of patients with idiopathic pulmonary fibrosis Ann Intern Med 2005142963-7 38 Hull JH Acetylcysteine in pulmonary fibrosis N Engl J Med 20063541089-91 author reply -91
70
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
39 Flaherty KR King TE Jr Raghu G et al Idiopathic interstitial pneumonia what is the effect of a multidisciplinary approach to diagnosis Am J Respir Crit Care Med 2004170904shy10 40 Raghu G Johnson WC Lockhart D Mageto Y Treatment of idiopathic pulmonary fibrosis with a new antifibrotic agent pirfenidone results of a prospective open-label Phase II study Am J Respir Crit Care Med 19991591061-9 41 Hunninghake GW Lynch DA Galvin JR et al Radiologic findings are strongly associated with a pathologic diagnosis of usual interstitial pneumonia Chest 20031241215-23 42 Lynch D Godwin J Safrin S et al High-resolution computed tomography in idiopathic pulmonary fibrosis diagnosis and prognosis Am J Respir Crit Care Med 2005172488-93 43 Mallinckrodt CH Watkin JG Molenberghs G Carroll RJ Choice of the primary analysis in longitudinal clinical trials Pharmaceutical Statistics 20043161-9 44 Bang H Tsiatis A Estimating medical costs with censored data Biometrika 200087329shy43 45 Lin DY Regression analysis of incomplete medical cost data Stat Med 2003221181-200 46 Rochon J Application of GEE procedures for sample size calculations in repeated measures experiments Stat Med 1998171643-58 47 Lachin JM Foulkes MA Evaluation of sample size and power for analyses of survival with allowance for nonuniform patient entry losses to follow-up noncompliance and stratification Biometrics 198642507-19
71
- PANTHER-IPFPREDNISONE AZATHIOPRINEAND N-ACETYLCYSTEINEA STUDY THAT EVALUATES RESPONSE INIDIOPATHIC PULMONARY FIBROSIS
-
- Protocol Summary
- Table of Contents
- List of Tables
- List of Figures
- List of Abbreviations
- 1 Summary
- 2 Hypotheses and Specific Aims
-
- 21 Null Hypothesis
- 22 Specific Aim 1
- 23 Specific Aim 2
- 24 Prespecified Subgroups of Interest
-
- 3 Background and Significance
-
- 31 Idiopathic Pulmonary Fibrosis is the Most Common Interstitial Lung Disease
- 32 Rationale for Placebo Control
- 33 Rationale for N-acetylcysteine
- 35 Rationale for N-acetylcysteine as a Stand-alone Therapy
- 36 Rationale for the Study Design and Primary Endpoint
- 37 Rationale for Blinding of Treatments
-
- 4 Methods
-
- 41 Inclusion Criteria
- 42 Diagnosis of IPF
- 43 Exclusion Criteria
- 44 Study Design and Study Visit
- 45 Dose Justification
- 46 Contraindications Precautions and Side Effects of Study Medications
- 47 Recruitment Procedures
- 48 Study Procedures
- 49 Concomitant Medications
- 410 Laboratory Testing
- 411 Blinding of Study Drugs
-
- 5 Study Endpoints
-
- 51 Primary Study Endpoint
- 52 Secondary Study Endpoints
-
- 6 Safety Evaluations and Procedures
-
- 61 Adverse Events
- 62 Clinical Medical Monitoring
- 63 Unblinding Procedures
-
- 7 Study Drug Procedures
- 8 Data Management
-
- 81 Hardware and Software Configuration
- 82 Sources of Data
-
- 9 Study Design and Data Analysis
-
- 91 General Analytic Considerations
- 92 Randomization Blinding and Reporting of Results
- 93 Stratification
- 94 Specification of the Primary Analyses
- 95 Analysis of Longitudinal Endpoints
- 96 Analysis of Binary Time-to-Event and Time-Lagged Endpoints
- 97 Power Analysis
-
- 10 Study Administration
-
- 101 Cooperative Agreement Mechanism
- 102 IPFnet Steering Group
- 103 Data and Safety Monitoring Board
- 104 Recommendations on Interim Monitoring of Efficacy Safety and Futility
-
- 11 Investigator and Sponsor Obligations
-
- 111 Monitoring
- 112 Cost and Payment
- 113 Confidentiality and Health Insurance Portability and Accountability ActConsiderations
- 114 Informed Consent Procedures
- 115 Institutional Review Boards
-
- 12 Investigator Agreement
- 13 References
-

PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
in pulmonary journals Clinical center patients previously diagnosed with IPF will be notified of
the trials by mail whenever possible
Recruitment of minorities and women will be monitored by the DCC and DSMB If necessary
additional recruitment efforts will be made at specific centers to ensure that the aggregate subject
sample contains appropriate representation of women and minorities
48 Study Procedures
The following procedures are detailed in the PANTHER-IPF MOOP accompanying this
protocol
1 PFT
2 ABG
3 HRCT scan of the chest (including imaging of pulmonary arteries)
4 CBC and serum chemistries
5 Pregnancy test
6 6MWTBorg Dyspnea Scale
7 QOL questionnaires (EuroQol HAD SF-36 SGRQ and ICE CAP)
8 UCSD SOBQ
9 Gender Substudy Questionnaire
All assessments of PFTs will be conducted by study personnel not directly involved in the
treatment of the subjects
481 Biological Specimen Management
4811 Biological Specimen Sample Management
Subjects at clinical centers participating in the specimen repository substudy who consent to
having blood drawn for research purposes and for the banking of blood blood components and
other biologic specimens (urine and BAL fluid) will have approximately 405 mL of blood
41
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
drawn 17 mL blood drawn for DNA and 20 mL of urine collected at enrollment visit Subjects
will have approximately 50 mL of blood drawn and 20 mL of urine collected at each 15-week
follow-up visit Blood specimens will be separated according to PANTHER-IPF MOOP
guidelines into the following components for banking in the repository serum plasma and
DNA Coding of all biologic specimens for the repository will be performed by study staff at the
clinical center The samples will be processed per PANTHER-IPF MOOP guidelines aliquoted
labeled with barcode labels and stored at -70degC at the clinical center and shipped to the central
repository
The only subject identifiers will be a sample ID number and subject initials This sample ID will
be linked in the IPFnet DCC clinical database to subject information No subject information will
be transferred to the biological-specimen database
The subjectrsquos samples may be used for approved sub-studies relating to human disease
including but not limited to IPF The studies for which an individualrsquos samples will be made
available will be determined by the subjectrsquos answers to questions on the biological-sample
informed consent form The subjects can choose to make their samples available for all options
or any combination Samples will be made available to researchers only with IPFnet Steering
Group approval until such time as the samples are made public through the NHLBI repository
49 Concomitant Medications
Concurrent treatment with FDA-approved therapy for IPF is allowed Colchicine may be used
for treatment of gout Temporary treatment with oral or IV corticosteroids for clinical worsening
or suspected AEx is permitted Nutritional supplements containing NAC are not allowed
410 Laboratory Testing
Clinical laboratory parameters will be assessed at screening and at the end of the study The
following tests will be performed at the two time points specified in the protocol chemistry (AG
ratio ALT [SGPT] AST [SGOT] albumin alkaline phosphatase amylase bilirubin-direct
42
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
bilirubin-indirect bilirubin-total BUN BUNcreatinine ratio calcium carbon dioxide
cholesterol-total chloride CPK-total creatinine GGT globulin glucose iron-total LDH
lipase magnesium phosphorus-inorganic potassium protein-total sodium TIBC triglycerides
uric acid) and hematology (red blood cell count WBC count hemoglobin hematocrit cell
indices differential platelet count)
411 Blinding of Study Drugs
Subjects and caregivers will be blinded to study treatment Every subject will receive NAC or
matching PLs at every study visit from the baseline visit to the week-45 visit No study agent
will be dispensed at the week-60 visit
43
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
5 Study Endpoints
51 Primary Study Endpoint
The primary endpoint will be the change in serial measurements of FVC over the study period
52 Secondary Study Endpoints
521 Time to Disease-progression
The time-to-death or a 10 decline in FVC will be defined as the time-to-disease progression
The 10 decline in FVC from enrollment must be confirmed on 2 consecutive visits no less than
6 weeks apart For subjects with 2 consecutive visits with a 10 decline in FVC the time-toshy
disease progression will be defined as the time interval between enrollment and the initial visit
with a 10 FVC decline For subjects who experience disease progression the study doctor will
determine whether or not the subject will remain in the study
522 Acute Exacerbations
The following 3 criteria will define AEx in subjects with acute worsening of their respiratory
conditions
1 Clinical (all of the following required)
A) Unexplained worsening of dyspnea or cough within 30 days triggering unscheduled
medical care (eg emergency room clinic study visit hospitalization)
B) No clinical suspicion or overt evidence of cardiac event pulmonary embolism or deep
venous thrombosis to explain acute worsening of dyspnea
C) No pneumothorax
44
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
2 RadiologicPhysiologic (A and B required)
A) New ground glass opacity or consolidation computed tomography (CT) scan OR new
alveolar opacities on chest x-ray
B) Decline of ge 5 in resting room air SpO2 from last recorded level OR decline of ge 8 mm
Hg in resting room air PaO2 from last recorded level
3 Microbiologic (all of the following required)
A) No clinical evidence for infection (ie absence of grossly purulent sputum fever gt 39degC
orally)
B) Lack of positive microbiological results (if done) from lower respiratory tract defined as
(1) Clinically significant bacterial growth on sputum or endotracheal aspirate cultures
(2) Quantitative culture by protected brush specimen ge 103 cfumL or BAL ge 104 cfumL
(3) The presence of specific pathogens on stains of any of the above
C) Lack of positive pathogen in blood cultures (if done)
Identification of Acute Exacerbations
All subjects will be educated about the importance of identifying AExs At the time of
enrollment subjects will be told about the possibility of developing acute symptomatic
worsening that might represent an AEx of IPF and instructed to contact their study clinical
center coordinator within 48 to 72 hours of the apparent event
All subjects will be contacted by phone monthly and questioned about any change in dyspnea or
cough and any interim clinic visits or hospitalizations Finally as part of the IPFnet outreach to
community referring physicians the importance of AExs will be emphasized When a subject is
identified who meets criterion 1A this will trigger the collection of additional clinical data to
evaluate a suspected AEx These data will be collected as part of standard clinical care (ie this
protocol does not require collection of all items) The additional items to be collected for
suspected AEx include
IPFnet AEx case report form (eCRF) (required)
45
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Chest x-ray CT scan withwithout pulmonary angiogram (reports should be faxed and
followed by the hard copiesdiscs)
Oxygen saturation (pulse oximetry)
ABG
Respiratory cultures (sputum endotracheal aspirate lavage)
Blood cultures
Clinichospital records related to the event
All potential cases of AEx will be reviewed by the clinical center PI first and a decision on
whether the case may represent an AEx will be made If AEx is suspected the case will be sent
to the IPFnet adjudication committee which will assign a final diagnosis (see Table 5) If there is
disagreement among members the majority opinion will be recorded
During episodes of suspected AEx as determined by the individual clinical center investigator
subjects will remain blinded and in the study
Table 5 Final Diagnoses in Evaluation of Suspected Acute Exacerbations
Definite acute exacerbation All criteria met no alternative etiology
Unclassifiable acute worsening
Insufficient data to evaluate all criteria no alternative etiology
Not acute exacerbation Alternative etiology identified that explains acute worsening
Management of the suspected AEx will be at the discretion of the treating physician Standard of
care generally involves evaluation for respiratory infection pulmonary embolism cardiac events
and pneumothorax and treatment with IV corticosteroids
Study drugs will be resumed at pre-suspected AEx doses after subjects clinically improve as
confirmed by the local PI All subjects should be seen at the clinical center within 2 to 4 weeks
of recovery for measurement of post-bronchodilator FVC (see Figure 4) Subjects unable to
return to the clinical center after suspected AEx due to medical frailty (eg continued
46
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
institutionalization progressive disability) will be categorized as failing to maintain FVC
response in secondary analyses
Suspected AEx (PI determined)
Hold study drug Treat AEx
(Attending physician determined)
Alive but unable to continue due to
medical frailty
Dead
Alive and able to continue
Site reviewvisit
Restart study drug
FVC within 2-4 weeks
Figure 4 Acute Exacerbation Flow Chart
523 Respiratory Infections
An upper respiratory infection will be defined as
Change in sputum discoloration
Increased cough of no more than 14 daysrsquo duration
A lower-respiratory infection (pneumonia) will be defined as new segmental or lobar airspace
opacities visualized by image studies (chest radiograph or HRCT) in addition to any of the
following
Positive pathogencultures in good sample of sputum or lower-airway secretions retrieved
by fiberoptic bronchoscope
Fever gt 39degC or gt 100degF
Leukocytosis gt 12000 (unexplained no increase in dose of corticosteroids)
47
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
524 Maintained FVC Response
Subjects with follow-up FVCpred measurements at or above their baseline FVCpred level
will be classified as having maintained FVC response Subjects with reduced FVCpred levels
or missing data for any reason including death or medical frailty will be classified as having not
maintained FVC response The FVCpred value is used because unadjusted FVC measurements
are expected to decline with age
48
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
6 Safety Evaluations and Procedures
61 Adverse Events
During a clinical trial the reporting of adverse experience information can lead to important
changes in the way a new treatment is developed as well as provide integral safety data
611 Definitions
An adverse event (AE) is any untoward medical occurrence in a subject or clinical investigation
subject who was administered a pharmaceutical product The AE does not necessarily have to
have a causal relationship with the drug administered An AE can be any unfavorable and
unintended sign (including an abnormal laboratory finding) symptom or disease temporarily
associated with the use of a medicinal product whether or not considered to be related to the
medicinal product Diseases signs symptoms or laboratory abnormalities already existing at
enrollment are not considered AEs unless they worsen (ie increase in intensity or frequency)
Surgical procedures themselves are not AEs they are therapeutic measures for conditions that
require surgery The condition for which the surgery is required may be an AE Surgical
procedures planned before randomization and the conditions necessitating the surgery are not
AEs
A serious adverse event is any untoward event that
Is fatal
Is life-threatening
Requires inpatient hospitalization or prolongation of existing hospitalization with the
following exceptions
o Preplanned (before the study) hospital admissions unless the hospitalization is
prolonged
o Planned admissions (as part of a study eg routine biopsies)
o Hospitalization lasting lt 24 hours
49
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
o Hospitalization for elective procedure
o Emergency room visits
Results in persistent or significant disability or incapacity
Is a congenital anomaly or birth defect
Important medical events that may not result in death be life-threatening or require
inpatient hospitalization may be considered serious adverse events (SAEs) when based
on appropriate medical judgment they may jeopardize the subject and may require
medical or surgical intervention to prevent one of the outcomes listed above
Life-threatening means that the subject was in the view of the investigator at immediate risk of
death from the AE as it occurred It does not include an AE that had it occurred in a more severe
form might have caused death
Persistent or significant disabilityincapacity means that the event resulted in permanent or
significant and substantial disruption of the subjectrsquos ability to carry out normal life functions
Causality
A reasonable possibility means the AE may have been caused byrelated to the study drug A
perceived or real lack of efficacy does not satisfy the definition of relatedness
612 Adverse Event (AE) Reporting
For the PANTHER-IPF trial all AEs (serious and nonserious) occurring from randomization
through final study visit (4 weeks after final dose of all study medication) will be recorded on the
AE page of the case report form (CRF)
6121 Serious Adverse Events (SAE) Reporting
For this trial all deaths and all SAEs which occur from randomization through final study visit
must be entered within the EDC system via the SAE eCRF page within 24 hours of the
investigative sitersquos knowledge of the event It is the responsibility of the clinical center
50
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
investigator to provide a causality assessment of the event for each study medications based upon
the information available at the time of the report It is understood that complete information
about the event may not be known at the time the initial report is submitted In the event the EDC
system is not accessible to the site at the time of event reporting investigative sites will complete
and forward a paper back-up SAE form to DCRI Safety Surveillance for processing
DCRI Safety Surveillance
Telephone 1-919-668-8624 or 1-866-668-7799 (toll free)
Fax 1-919-668-7138 or 1-866-668-7138 (toll free)
The investigator must complete and submit follow-up SAE information via the eCRF when
important new or follow-up information (eg final diagnosis outcome results of specific
investigations) becomes available Follow-up information should be submitted according to the
same process used for reporting the initial event as described above All SAEs will be followed
until resolution stabilization or 30 days after the subject has completed the final visit (4 weeks
after the final dose of study medication) whichever occurs first The investigator is responsible
for reporting SAEs to their institutional review board (IRB) per site specific IRB reporting
guidelines
6122 Regulatory Reporting
AEs that are serious study drug related and unexpected will be reported to the regulatory
authorities The DCRI Safety Surveillance medical monitor will perform a medical review of all
SAEs submitted and evaluate for ldquounexpectednessrdquo DCRI Safety Surveillance will prepare
MedWatch reports for those events identified as serious study drug related and unexpected as
determined by Safety Medical Monitor
DCRI Regulatory Services will submit all unexpected study drug-related SAEs as per 21 CFR
32 DCRI Safety Surveillance will provide a safety alert letter to the NHLBI DSMB and DCC
clinical operation (for distribution to sites) within 15 days of initial receipt of the information
51
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Investigators are responsible for promptly reporting these events to their reviewing IRBs
according to site specific IRB reporting guidelines
62 Clinical Medical Monitoring
There will be an unblinded physician at the IPFnet DCC serving as medical monitor The
medical monitor will be available to assist with questions about dosage adjustments of study
medications including discontinuation or resumption of medications
63 Unblinding Procedures
Unblinding of subjects or investigators to subject treatment is strongly discouraged For ongoing
clinical management all subjects should be presumed to be receiving ldquoactiverdquo study drug To
ensure the subjectrsquos safety the study treatment will be dose-adjusted based on laboratory test
results clinical findings and symptoms
The IPFnet DCC medical monitor and PANTHER-IPF co-chairs Drs Ganesh Raghu and
Fernando Martinez will be available to the study physicians to discuss study drug management
on a case-by-case basis Un-blinding will be considered ONLY when the knowledge of subject
treatment assignment is ABSOLUTELY ESSENTIAL for subject safety and after discussion of
the subjectrsquos case with the medical monitor and either Dr Raghu or Dr Martinez Unblinding of
study treatment should be minimized during the conduct of the trial In those cases where it is
felt to be medically necessary the DCC medical officer will communicate directly with the
managing physician to minimize unblinding of study personnel
52
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
7 Study Drug Procedures
At the baseline 15-week 30-week and 45-week study visits subjects will receive a supply of
study drug sufficient to last until the next visit at which study drug will be dispensed
53
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
8 Data Management
81 Hardware and Software Configuration
811 Hardware and Database Software
Data will be stored in an Oracle database system Oracle has advantages of processing efficiency
and smooth linkage with other software systems The application and database will be hosted on
Solaris Unix servers at the IPFnet DCC
812 Statistical Software
SAS will be used as the principal application for the management of analysis data files and
statistical computations S-Plus will be used to provide supplementary functions as needed
813 Access Control and Confidentiality Procedures
Access to databases will be controlled centrally by the IPFnet DCC through user passwords
linked to appropriate privileges This protects the data from unauthorized changes and
inadvertent loss or damage
814 Security
Database and Web servers will be secured by a firewall and through controlled physical access
Oracle has many security features to ensure that any staff member accessing the database has the
proper authority to perform the functions he or she requests of the system Within the secondary
SAS databases Unix group-access control maintains similar security The Sun workstation login
is secured by extensive user-password facilities under Unix
54
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
815 Back-up Procedures
Database back-up will be performed automatically every day and standard IPFnet DCC policies
and procedures will be applied to dictate tape rotation and retention practices
816 Virus Protection
All disk drives that provide network services and all user computers will be protected using
virus-scanning software Standard IPFnet DCC policies will be applied to update these protection
systems periodically through the study
82 Sources of Data
821 Design and Development
The IPFnet DCC will be responsible for development of the electronic case report forms
(eCRFs) development and validation of the clinical study database ensuring data integrity and
training clinical center staff on applicable data management procedures A web-based distributed
data entry model will be implemented This system will be developed to ensure that guidelines
and regulations surrounding the use of computerized systems used in clinical trials are upheld
The remainder of this section provides an overview of the data management plan associated with
this protocol
822 Data Collection Forms
The data collection process consists of direct data entry at the study clinical centers into the EDC
system(s) provided by the DCC A data collection worksheet will be provided to clinical centers
for recording data in the event the EDC system is unavailable Data entry of the eCRFs should
be completed according to the instructions provided and project specific training The
investigator is responsible for maintaining accurate complete and up-to-date records and for
ensuring the completion of the eCRFs for each research participant
55
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
823 Data Acquisition and Entry
Data entry into eCRFs shall be performed by authorized individuals Selected eCRFs may also
require the investigatorrsquos written signature or electronic signature as appropriate Electronic
CRFs will be monitored for completeness accuracy and attention to detail during the study
824 Data Center Responsibilities
The IPFnet DCC will 1) develop a data management plan and will conduct data management
activities 2) provide final eCRFs for the collection of all data required by the study 3) develop
data dictionaries for each eCRF that will comprehensively define each data element 4) conduct
ongoing data monitoring activities on study data 5) monitor any preliminary analysis data
cleanup activities and 6) rigorously monitor final study data clean up
825 Data Editing
Completed data will be entered into the IPFnet DCC automated data acquisition and
management system If incomplete or inaccurate data are found a data clarification request will
be generated and distributed to clinical centers for a response Clinical centers will resolve data
inconsistencies and errors and enter all corrections and changes into the IPFnet DCC automated
data acquisition and management system
826 Training
The training plan for clinical center staff includes provisions for training on assessments eCRF
completion guidelines data management procedures and the use of computerized systems
56
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
9 Study Design and Data Analysis
91 General Analytic Considerations
All primary analyses will be based on intent-to-treat (ITT) principles using all randomized
subjects Baseline factors across groups will be compared using mean (standard deviation) and
median (25th and 75th percentiles) summary measures Kaplan-Meier curves will be used to
display event rates Due to clinical interest in departures from both sides of the null hypothesis
all test statistics will be 2-sided
Reasonable caution needs to be taken when conducting multiple analyses on key clinical
subgroups For subgroup analyses a conservative significance level of 0001 will be used for all
interaction tests Thus subgroup comparisons will be considered exploratory unless the p-value
from the interaction test is smaller than 0001
92 Randomization Blinding and Reporting of Results
A permuted block-randomization scheme will be created with varying block sizes stratified by
clinical center Once a subject has completed the screening and baseline period and evaluation
for inclusionexclusion criteria the randomization process will begin Subjects will be
randomized to receive NAC or matching placebo with equal probability (11) via telephone
contact with a central interactive voice response system (IVRS) using a toll-free randomization
number On the day of randomization after the subject has successfully met all inclusion and
exclusion criteria the investigator or designee will call the central randomization number to
obtain the assigned kit randomization numbers for that subject At each subject visit the
investigator or designee will call the central randomization number to obtain the new kit
randomization numbers for resupply of the subject For resupply of the clinical center the IVRS
will monitor minimal volume of a kit type andor expiration date and will automatically notify
the pharmacy
57
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
The trial results will be reported according to guidelines specified in the CONSORT statement
A flow diagram describing screening recruitment randomization dropout and vital status will
be included in the primary manuscript AEs and efficacy data will be presented for all treatment
groups Adherence dropout and lost to follow-up will be carefully examined across all treatment
groups Analyses of safety will be based on data from all randomized subjects who received at
least one dose of study drug
93 Stratification
Subjects will be distributed to the two treatment arms in a 11 allocation ratio Stratification
blocks will be based on clinical centers
94 Specification of the Primary Analyses
A mixed model repeated measures (MMRM) analysis described in section 95 will be used to
compare differences in the slope of FVC measurements across the treatment groups Response
variables are values of the FVC measured at baseline and every 15 weeks until study completion
Variables in the model will include treatment time and time by treatment age sex race and
height Contrast estimates of differences in slopes of treatment over time (along with confidence
intervals) will be used to estimate the treatment effect The validity of this model in terms of
meeting modeling assumptions will be assessed via standard modeling diagnostics and goodness-
of-fit measures Based on the MMRM framework missing FVC data will not be imputed for the
primary analysis
95 Analysis of Longitudinal Endpoints
A common goal in clinical trials is to specify models that are easily implemented and
reproducible by independent data analysts On the other hand the models should have proper
statistical behavior in terms of low bias and high precision Many common approaches to
longitudinal data analysis including last observation carried forward (LOCF) imputation rely on
the missing completely at random (MCAR) assumption However the MCAR assumption is
58
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
unlikely to hold in many clinical trials because missing data are often related to disease
progression and prognosis A more reasonable assumption missing at random (MAR) specifies
that the complete data distribution can be modeled using only the observed data The likelihood-
based MMRM approach is valid under the more general MAR assumptions These models will
be applied to analyze the longitudinal data secondary endpoints
The advantages of MMRM analysis are that all important characteristics of the model can be preshy
specified standard software can be used to implement the models and results are based on ITT
principles43 In addition the MMRM approach offers superior control of Type I and Type II
errors compared with the LOCF approach
Response variables are values of the PFTs measured at enrollment and every 15 weeks until
study completion and 6MWT values measured at baseline week 30 and week 60 Covariates are
treatment time time by treatment and key baseline risk factors Contrasts (along with
confidence intervals) of treatment by time will be used to estimate the treatment effect
The correlation structure involves multiple pieces including measurement errors random
variation and interindividual variability For the longitudinal data analyses an unstructured
correlation matrix for within-subject errors will be assumed Other correlation structures
including compound symmetry will be examined as needed A careful examination of reasons
for study discontinuation will be conducted to assess the validity of MCAR Sensitivity analyses
will be used to examine the untestable assumption that the observed data violate the MAR
assumption The MMRM models will be implemented using PROC MIXED in SAS
96 Analysis of Binary Time-to-Event and Time-Lagged Endpoints
Regression modeling approaches using either the logistic regression model or Cox proportional
hazards regression model will be employed when appropriate The validity of these models will
be assessed via standard modeling diagnostics and goodness-of-fit measures Estimates of
cumulative frequencies for more general time-lagged responses will be calculated using the
partitioned version of the Bang-Tsiatis estimator44 The partitions will be set at 15-week intervals
59
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
to correspond with the data-collection process Covariate adjusted event rates will be calculated
using inverse probability-weighted regression estimates45
97 Power Analysis
971 Primary Analyses
Based on previously published IPF clinical trials the PL group is expected to experience a drop
in FVC of approximately 020 L over the study period (see Figure 1) The IPFnet Steering Group
determined a clinically important difference would be to preserve the majority of the decline
relative to PL over the study period In particular a treatment effect of 015 L was determined to
be a clinically meaningful difference Potential dropout is a key factor in the proposed study The
drop-out process assumed 5 lost to follow-up after every study visit Only 80 of subjects
were assumed to be followed for the entire study period All models assumed a compound
symmetry structure for the covariance matrix Power calculations were performed using a SAS
IML program for designing repeated measures studies46 Based on preliminary reviews of the
data from the University of Michigan the covariance matrix parameters were estimated at
approximately σ2 = 0757 (variance parameter) and ρ = 0936 (correlation parameter) To be
conservative the power calculations for the primary analysis were performed with parameter
setting of σ2 = 0810 (variance parameter) and ρ = 0925 (correlation parameter)
The power calculations assume a correction for imperfect compliance proposed by Lachin and
Foulkes to allow for 2 noncompliance for each of the treatment arms47 Thus the sample size
of 130 subjects per arm would be reduced to an adjusted sample size of 130(1-002-002)2 =
1198 or 120 subjects per arm
Under the assumed Type I error rate of 005 with a correlation parameter of 0925 and standard
deviation of 090 the difference of 015 L (or 00025 Lweek) shown in Table 6 would have
power of 93
60
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Table 6 Hypothetical Values of Mean FVC (L) Change from Baseline
Week 15 Week 30 Week 45 Week 60
NAC 00125 00250 00375 00500
Placebo 00500 01000 01500 02000
Difference 00375 00750 01125 01500
Abbreviations FVC forced vital capacity PL placebo
972 Power Analysis for Secondary Endpoints
Power calculations for secondary endpoint measurements are shown in Table 7 Standard
deviations are based on unpublished data provided by the University of Michigan The
calculations are based on a 2-sample t-test with Type I error rate set at 005 These calculations
are likely to be conservative because the statistical approach described in section 95 for
analyzing these endpoints will incorporate incomplete observations as well as intermediate data
points
Table 7 Detectable Differences in Treatment Means for Selected Endpoint Measurements
Secondary Endpoints Std Dev
of the Baseline Score
Detectable Difference for 80 Power
Std Dev of the Change Score
Difference Detectable for
80 Power
DLCOpred 166 58 91 32
6MWT Area Under the Desaturation Curve
219 76 175 61
6MWT Distance to Desaturation 224 78 315 110
6MWT Minutes Walked 210 073 205 071
Abbreviations Std Dev standard deviation DLCOpred diffusing capacity of the lung for carbon monoxide percent predicted 6MWT 6-minute walk test
61
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
10 Study Administration
101 Cooperative Agreement Mechanism
The administrative and funding mechanism used to undertake this project is a ldquocooperative
agreementrdquo (U01) which is an assistance mechanism Under the cooperative agreement the
NHLBI assists supports andor stimulates the project and is substantially involved with
investigators in conducting the study by facilitating performance of the effort in a ldquopartnerrdquo role
The NHLBI project scientist serves on the IPFnet Steering Group and he or another NHLBI
scientist may serve on other project committees when appropriate At the same time however
NHLBI does not assume a dominant role direction or prime responsibility for this research
program
As described below governance of the project is conducted through the IPFnet Steering Group
Principal investigators have lead responsibilities in all aspects of their trials and the project
including any modification of trial designs conduct of the trials quality control data analysis
and interpretation preparation of publications and collaboration with other investigators unless
otherwise provided for by the IPFnet Steering Group
PIs retain custody of and have primary rights to their center-specific and collaborative data
subject to government rights-of-access consistent with current Health amp Human Services (HHS)
Public Health Service (PHS) and National Institutes of Health policies The protocols and
governance policies call for the continual submission of data centrally to the IPFnet DCC for the
collaborative database which at a minimum will contain the key variables selected by the IPFnet
Steering Group for standardization across all clinical centers the submission of copies of the
collaborative datasets to each PI upon completion of the project procedures for data analysis
reporting and publication and procedures to protect and ensure the privacy of medical and
genetic data and records of individuals The NHLBI project scientist on behalf of the NHLBI
will have the same access privileges and responsibilities regarding the collaborative data as the
other members of the Steering Group
62
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
PIs are also encouraged to publish and to publicly release and disseminate results data and other
products of the project concordant with the project protocols and governance and the approved
plan for making data and materials available to the scientific community and to the NHLBI
However during the 3 years after the ending date of NHLBI project support unpublished data
unpublished results data sets not previously released and other study materials or products are
to be made available to any third party only with the approval of the IPFnet Steering Group
Upon completion of the project PIs are expected to put their intervention materials and
procedure manuals into the public domain andor make them available to other investigators
according to the approved plan for making data and materials available to the scientific
community and the NHLBI for the conduct of research at no charge other than the costs of
reproduction and distribution
The NHLBI reserves the right to terminate or curtail the project (or an individual award) in the
event of (a) failure to develop or implement mutually agreeable collaborative measurement
subject eligibility and data management sections of the protocols (b) substantial shortfall in
subject recruitment follow-up data reporting or quality control or other major breach of
protocol (c) substantive changes in the agreed-upon protocols with which NHLBI cannot
concur (d) reaching a major project outcome with persuasive statistical significance
substantially before schedule or (e) human subject ethical issues that may dictate a premature
termination
Any disagreement that may arise in scientificprogrammatic matters (within the scope of the
award) between award recipients and the NHLBI may be brought to arbitration An arbitration
panel will be composed of 3 membersmdash1 selected by the IPFnet Steering Group (with the
NHLBI member not voting) or by the individual PI in the event of an individual disagreement a
second selected by NHLBI and the third selected by the other 2 members This special
arbitration procedure in no way affects the PIrsquos right to appeal an adverse action that is otherwise
appealable in accordance with the PHS regulations at 42 CFR part 50 Subpart D and HHS
63
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
regulation at 45 CFR part 16 or the rights of the NHLBI under applicable statutes regulations
and terms of the award
102 IPFnet Steering Group
The IPFnet Steering Group is the main governing body of the project It is composed of the PIs
of the clinical centers the PI of the DCC and the NHLBI project scientist The clinical centers
the IPFnet DCC and the NHLBI each have 1 vote on the IPFnet Steering Group All decisions
are determined by majority vote
All major scientific decisions are determined by the IPFnet Steering Group It assumes overall
responsibility for the design and conduct of the trial It appoints (and disbands) committees and
subcommittees as the need arises designs approves and implements the study protocols
oversees the development of the MOOP monitors subject recruitment and treatment delivery
evaluates data collection and management oversees quality assurance procedures and
implements changes and enhancements to the study as required It also has primary responsibility
for facilitating the conduct of the trials and reporting the projectrsquos results
103 Data and Safety Monitoring Board
The NHLBI will establish a DSMB in accordance with established policies (see
httpwwwnhlbinihgovfundingpoliciesdsmb_insthtm) to ensure data quality and subject
safety and to provide independent advice to the NHLBI regarding progress and the
appropriateness of study continuation
104 Recommendations on Interim Monitoring of Efficacy Safety and Futility
First and foremost the role of the DSMB will be to review subject safety and trial conduct at
periodic points during the study The DSMB may require analyses of the primary endpoint
results for comparing the benefit and risks of treatment strategies The benefit of collecting
additional data on key secondary endpoints with extended follow-up and establishing a robust
64
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
evidence base for determining a standard of care will need to be carefully considered before
early termination of one or more treatment arms After careful consideration the IPFnet Steering
Group recommends conservative thresholds for the early examinations of the safety and efficacy
data
The DSMB will be expected to meet approximately every 6 months until trial completion to
review safety and toxicity data The DSMB may recommend stopping the study based on these
reviews Because the DSMB could stop the trial for safety concerns as well as for a large
efficacy benefit there could be multiple opportunities to reject the null hypothesis (no difference
in event rates between the PL and NAC groups) A Bonferroni approximation will be applied
during the one planned interim analysis for efficacy
Before locking the database a statistical analysis plan (SAP) will be developed to provide
complete details on the statistical analysis The SAP will include the specifics for how and when
the DSMB will be notified for AEs The IPFnet DCC will deliver to the DSMB all FDA-defined
AEs at 3-month intervals The IPFnet DCC will prepare narrative SAE reports in real time for
DSMB review including recommendations and analysis of similar events for each SAE
submitted to the FDA
65
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
11 Investigator and Sponsor Obligations
111 Monitoring
All monitoring activities for US clinical centers will be performed in accordance with DCRI
standard operating procedures Information regarding the types of visits will be outlined in the
PANTHER-IPF MOOP
112 Cost and Payment
There will be no cost to subjects enrolled in this trial Study-related procedures will be paid for
by the IPFnet
Subjects may be eligible for reimbursement for travel to the clinical center Details of payment
will be explained to each subject during the consent process
113 Confidentiality and Health Insurance Portability and Accountability Act
Considerations
Subject confidentiality will be protected throughout the study All subject data will be kept
strictly confidential and no subject-identifying information will be released to anyone outside
the project Confidentiality will be assured through several mechanisms First each subject will
be assigned an anonymous study ID which will then be used on all study forms Second any
study forms blood samples and paper records that contain subject information (eg address lists
phone lists) will be kept at the clinical centers in secured locked areas coded by number Once
blood is collected there will be no subject identifiers placed on blood samplesmdashonly the study
ID number and the date of sample collection Third access to all subject data and information
including laboratory specimens will be restricted to authorized personnel In the case of
computerized data this restricted access will be assured through user logon IDs and password
protection
66
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
At the IPFnet DCC only authorized personnel will have access to the data files containing study
data Security will be assured through user logon IDs passwords and appropriate access
privileges All study subjects will be identified only by their IPFnet ID numbers and no personal
identifying information such as name address or Social Security number will be entered into
the IPFnet DCC database Any subject-specific data reported to the IPFnet Steering Group will
be identified only by the IPFnet ID number
Finally subjects will not be identified by name in any reports or publications nor will the data
be presented in such a way that the identity of individual subjects can be inferred Analysis files
created for further study by the scientific community will have no subject identifiers These data
files will be created in accordance with the Ancillary Studies and Publication Policy of the
IPFnet
114 Informed Consent Procedures
All IPFnet subjects will provide written informed consent using procedures reviewed and
approved by each clinical centerrsquos IRB Informed consent will be undertaken by study personnel
in-person with the subject The subject has the option of declining further participation in the
study at that point No further study procedures will be conducted until the signed documents
have been provided to the IPFnet clinical center
115 Institutional Review Boards
Before initiating this study the protocol clinical center-specific informed consent forms Health
Insurance Portability and Accountability Act (HIPAA) forms recruitment materials and other
relevant information will be reviewed by a properly constituted IRB at each participating clinical
center A copy of the signed and dated IRB approval at each clinical center will be retrieved prior
to or during the site initiation visit and archived at the IPFnet DCC Any amendments to the
protocol other than simple administrative and typographical changes must be approved by each
IRB before they are implemented The clinical centers will seek annual renewals of their IRB
approvals in accordance with local procedures
67
__________________________________________ ________________
__________________________________________
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
12 Investigator Agreement
I have read the foregoing protocol PANTHER-IPF and agree that it contains all necessary
details for carrying out this study I will conduct the study as outlined herein and will complete
the study within the time designated
I will provide copies of the protocol and all pertinent information to all individuals responsible to
me who assist in the conduct of this study I will discuss this material with them to ensure they
are fully informed regarding the drug and the conduct of the study
I will fulfill all responsibilities for submitting pertinent information to the local IRB if
applicable that is responsible for this study
I further agree that NHLBI andor DCRI will have access to any source documents from which
eCRF information may have been generated
Signature of Principal Investigator Date
Name of Principal Investigator (printed or typed)
Protocol version date May 19 2009
Protocol Amendment 1 version date May 28 2010
Protocol Amendment 2 version date December 6 2011
68
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
13 References
1 Raghu G Brown KK Bradford WZ et al A placebo-controlled trial of interferon gamma-1b in patients with idiopathic pulmonary fibrosis N Engl J Med 2004350125-33 2 King TE Jr Safrin S Starko KM et al Analyses of efficacy end points in a controlled trial of interferon-gamma1b for idiopathic pulmonary fibrosis Chest 2005127171-7 3 Flaherty KR Thwaite EL Kazerooni EA et al Radiological versus histological diagnosis in UIP and NSIP survival implications Thorax 200358143-8 4 Wells AU Desai SR Rubens MB et al Idiopathic pulmonary fibrosis a composite physiologic index derived from disease extent observed by computed tomography Am J Respir Crit Care Med 2003167962-9 5 Raghu G Freudenberger TD Yang S et al High prevalence of abnormal acid gastroshyoesophageal reflux in idiopathic pulmonary fibrosis Eur Respir J 200627136-42 6 Kinnula VL Focus on antioxidant enzymes and antioxidant strategies in smoking related airway diseases Thorax 200560693-700 7 Coultas DB Zumwalt RE Black WC Sobonya RE The epidemiology of interstitial lung diseases Am J Respir Crit Care Med 1994150967-72 8 Raghu G Weycker D Edelsberg J Bradford WZ Oster G Incidence and prevalence of idiopathic pulmonary fibrosis Am J Respir Crit Care Med 2006174810-6 9 Olson AL Swigris JJ Lezotte DC Norris JM Wilson CG Brown KK Mortality from pulmonary fibrosis increased in the United States from 1992 to 2003 Am J Respir Crit Care Med 2007176277-84 10 Mannino DM Etzel RA Parrish RG Pulmonary fibrosis deaths in the United States 1979shy1991 An analysis of multiple-cause mortality data Am J Respir Crit Care Med 19961531548shy52 11 Hubbard R Johnston I Coultas DB Britton J Mortality rates from cryptogenic fibrosing alveolitis in seven countries Thorax 199651711-6 12 Johnston I Britton J Kinnear W Logan R Rising mortality from cryptogenic fibrosing alveolitis Bmj 19903011017-21 13 Raghu G Collard HR Egan JJ et al An official ATSERSJRSALAT statement idiopathic pulmonary fibrosis evidence-based guidelines for diagnosis and management Am J Respir Crit Care Med 2011183788-824 14 (USA) FDA FDA Public Health Advisory Interferon gamma-1b (marketed as Actimmune) In 2007 15 King TE Jr Pardo A Selman M Idiopathic pulmonary fibrosis Lancet 2011 16 Raghu G Brown KK Costabel U et al Treatment of idiopathic pulmonary fibrosis with etanercept an exploratory placebo-controlled trial Am J Respir Crit Care Med 2008178948shy55 17 Malouf MA Hopkins P Snell G Glanville AR An investigator-driven study of everolimus in surgical lung biopsy confirmed idiopathic pulmonary fibrosis Respirology 201116776-83 18 King TE Jr Behr J Brown KK et al BUILD-1 a randomized placebo-controlled trial of bosentan in idiopathic pulmonary fibrosis Am J Respir Crit Care Med 200817775-81 19 Richeldi L Costabel U Selman M et al Efficacy of a tyrosine kinase inhibitor in idiopathic pulmonary fibrosis N Engl J Med 20113651079-87
69
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
20 Borok Z Buhl R Grimes GJ et al Effect of glutathione aerosol on oxidant-antioxidant imbalance in idiopathic pulmonary fibrosis Lancet 1991338215-6 21 Meyer A Buhl R Magnussen H The effect of oral N-acetylcysteine on lung glutathione levels in idiopathic pulmonary fibrosis Eur Respir J 19947431-6 22 Behr J Maier K Degenkolb B Krombach F Vogelmeier C Antioxidative and clinical effects of high-dose N-acetylcysteine in fibrosing alveolitis Adjunctive therapy to maintenance immunosuppression Am J Respir Crit Care Med 19971561897-901 23 Cantin AM North SL Fells GA Hubbard RC Crystal RG Oxidant-mediated epithelial cell injury in idiopathic pulmonary fibrosis J Clin Invest 1987791665-73 24 Waghray M Cui Z Horowitz JC et al Hydrogen peroxide is a diffusible paracrine signal for the induction of epithelial cell death by activated myofibroblasts Faseb J 200519854-6 25 Larios JM Budhiraja R Fanburg BL Thannickal VJ Oxidative protein cross-linking reactions involving L-tyrosine in transforming growth factor-beta1-stimulated fibroblasts J Biol Chem 200127617437-41 26 Kinnula VL Fattman CL Tan RJ Oury TD Oxidative stress in pulmonary fibrosis a possible role for redox modulatory therapy Am J Respir Crit Care Med 2005172417-22 27 Meyer A Buhl R Kampf S Magnussen H Intravenous N-acetylcysteine and lung glutathione of patients with pulmonary fibrosis and normals Am J Respir Crit Care Med 19951521055-60 28 Behr J Degenkolb B Krombach F Vogelmeier C Intracellular glutathione and bronchoalveolar cells in fibrosing alveolitis effects of N-acetylcysteine Eur Respir J 200219906-11 29 Bando M Hosono T Mato N et al Long-term efficacy of inhaled N-acetylcysteine in patients with idiopathic pulmonary fibrosis Intern Med 2010492289-96 30 Demedts M Behr J Buhl R et al High-dose acetylcysteine in idiopathic pulmonary fibrosis N Engl J Med 20053532229-42 31 Toma TP Bhowmik A Rajakulasingam R Acetylcysteine in pulmonary fibrosis N Engl J Med 20063541086-9 author reply -9 32 Hunninghake GW Antioxidant therapy for idiopathic pulmonary fibrosis N Engl J Med 20053532285-7 33 Flaherty KR Mumford JA Murray S et al Prognostic implications of physiologic and radiographic changes in idiopathic interstitial pneumonia Am J Respir Crit Care Med 2003168543-8 34 Latsi PI du Bois RM Nicholson AG et al Fibrotic idiopathic interstitial pneumonia the prognostic value of longitudinal functional trends Am J Respir Crit Care Med 2003168531-7 35 Collard HR King TE Jr Bartelson BB Vourlekis JS Schwarz MI Brown KK Changes in clinical and physiologic variables predict survival in idiopathic pulmonary fibrosis Am J Respir Crit Care Med 2003168538-42 36 Jegal Y Kim DS Shim TS et al Physiology is a stronger predictor of survival than pathology in fibrotic interstitial pneumonia Am J Respir Crit Care Med 2005171639-44 37 Martinez FJ Safrin S Weycker D et al The clinical course of patients with idiopathic pulmonary fibrosis Ann Intern Med 2005142963-7 38 Hull JH Acetylcysteine in pulmonary fibrosis N Engl J Med 20063541089-91 author reply -91
70
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
39 Flaherty KR King TE Jr Raghu G et al Idiopathic interstitial pneumonia what is the effect of a multidisciplinary approach to diagnosis Am J Respir Crit Care Med 2004170904shy10 40 Raghu G Johnson WC Lockhart D Mageto Y Treatment of idiopathic pulmonary fibrosis with a new antifibrotic agent pirfenidone results of a prospective open-label Phase II study Am J Respir Crit Care Med 19991591061-9 41 Hunninghake GW Lynch DA Galvin JR et al Radiologic findings are strongly associated with a pathologic diagnosis of usual interstitial pneumonia Chest 20031241215-23 42 Lynch D Godwin J Safrin S et al High-resolution computed tomography in idiopathic pulmonary fibrosis diagnosis and prognosis Am J Respir Crit Care Med 2005172488-93 43 Mallinckrodt CH Watkin JG Molenberghs G Carroll RJ Choice of the primary analysis in longitudinal clinical trials Pharmaceutical Statistics 20043161-9 44 Bang H Tsiatis A Estimating medical costs with censored data Biometrika 200087329shy43 45 Lin DY Regression analysis of incomplete medical cost data Stat Med 2003221181-200 46 Rochon J Application of GEE procedures for sample size calculations in repeated measures experiments Stat Med 1998171643-58 47 Lachin JM Foulkes MA Evaluation of sample size and power for analyses of survival with allowance for nonuniform patient entry losses to follow-up noncompliance and stratification Biometrics 198642507-19
71
- PANTHER-IPFPREDNISONE AZATHIOPRINEAND N-ACETYLCYSTEINEA STUDY THAT EVALUATES RESPONSE INIDIOPATHIC PULMONARY FIBROSIS
-
- Protocol Summary
- Table of Contents
- List of Tables
- List of Figures
- List of Abbreviations
- 1 Summary
- 2 Hypotheses and Specific Aims
-
- 21 Null Hypothesis
- 22 Specific Aim 1
- 23 Specific Aim 2
- 24 Prespecified Subgroups of Interest
-
- 3 Background and Significance
-
- 31 Idiopathic Pulmonary Fibrosis is the Most Common Interstitial Lung Disease
- 32 Rationale for Placebo Control
- 33 Rationale for N-acetylcysteine
- 35 Rationale for N-acetylcysteine as a Stand-alone Therapy
- 36 Rationale for the Study Design and Primary Endpoint
- 37 Rationale for Blinding of Treatments
-
- 4 Methods
-
- 41 Inclusion Criteria
- 42 Diagnosis of IPF
- 43 Exclusion Criteria
- 44 Study Design and Study Visit
- 45 Dose Justification
- 46 Contraindications Precautions and Side Effects of Study Medications
- 47 Recruitment Procedures
- 48 Study Procedures
- 49 Concomitant Medications
- 410 Laboratory Testing
- 411 Blinding of Study Drugs
-
- 5 Study Endpoints
-
- 51 Primary Study Endpoint
- 52 Secondary Study Endpoints
-
- 6 Safety Evaluations and Procedures
-
- 61 Adverse Events
- 62 Clinical Medical Monitoring
- 63 Unblinding Procedures
-
- 7 Study Drug Procedures
- 8 Data Management
-
- 81 Hardware and Software Configuration
- 82 Sources of Data
-
- 9 Study Design and Data Analysis
-
- 91 General Analytic Considerations
- 92 Randomization Blinding and Reporting of Results
- 93 Stratification
- 94 Specification of the Primary Analyses
- 95 Analysis of Longitudinal Endpoints
- 96 Analysis of Binary Time-to-Event and Time-Lagged Endpoints
- 97 Power Analysis
-
- 10 Study Administration
-
- 101 Cooperative Agreement Mechanism
- 102 IPFnet Steering Group
- 103 Data and Safety Monitoring Board
- 104 Recommendations on Interim Monitoring of Efficacy Safety and Futility
-
- 11 Investigator and Sponsor Obligations
-
- 111 Monitoring
- 112 Cost and Payment
- 113 Confidentiality and Health Insurance Portability and Accountability ActConsiderations
- 114 Informed Consent Procedures
- 115 Institutional Review Boards
-
- 12 Investigator Agreement
- 13 References
-
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
drawn 17 mL blood drawn for DNA and 20 mL of urine collected at enrollment visit Subjects
will have approximately 50 mL of blood drawn and 20 mL of urine collected at each 15-week
follow-up visit Blood specimens will be separated according to PANTHER-IPF MOOP
guidelines into the following components for banking in the repository serum plasma and
DNA Coding of all biologic specimens for the repository will be performed by study staff at the
clinical center The samples will be processed per PANTHER-IPF MOOP guidelines aliquoted
labeled with barcode labels and stored at -70degC at the clinical center and shipped to the central
repository
The only subject identifiers will be a sample ID number and subject initials This sample ID will
be linked in the IPFnet DCC clinical database to subject information No subject information will
be transferred to the biological-specimen database
The subjectrsquos samples may be used for approved sub-studies relating to human disease
including but not limited to IPF The studies for which an individualrsquos samples will be made
available will be determined by the subjectrsquos answers to questions on the biological-sample
informed consent form The subjects can choose to make their samples available for all options
or any combination Samples will be made available to researchers only with IPFnet Steering
Group approval until such time as the samples are made public through the NHLBI repository
49 Concomitant Medications
Concurrent treatment with FDA-approved therapy for IPF is allowed Colchicine may be used
for treatment of gout Temporary treatment with oral or IV corticosteroids for clinical worsening
or suspected AEx is permitted Nutritional supplements containing NAC are not allowed
410 Laboratory Testing
Clinical laboratory parameters will be assessed at screening and at the end of the study The
following tests will be performed at the two time points specified in the protocol chemistry (AG
ratio ALT [SGPT] AST [SGOT] albumin alkaline phosphatase amylase bilirubin-direct
42
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
bilirubin-indirect bilirubin-total BUN BUNcreatinine ratio calcium carbon dioxide
cholesterol-total chloride CPK-total creatinine GGT globulin glucose iron-total LDH
lipase magnesium phosphorus-inorganic potassium protein-total sodium TIBC triglycerides
uric acid) and hematology (red blood cell count WBC count hemoglobin hematocrit cell
indices differential platelet count)
411 Blinding of Study Drugs
Subjects and caregivers will be blinded to study treatment Every subject will receive NAC or
matching PLs at every study visit from the baseline visit to the week-45 visit No study agent
will be dispensed at the week-60 visit
43
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
5 Study Endpoints
51 Primary Study Endpoint
The primary endpoint will be the change in serial measurements of FVC over the study period
52 Secondary Study Endpoints
521 Time to Disease-progression
The time-to-death or a 10 decline in FVC will be defined as the time-to-disease progression
The 10 decline in FVC from enrollment must be confirmed on 2 consecutive visits no less than
6 weeks apart For subjects with 2 consecutive visits with a 10 decline in FVC the time-toshy
disease progression will be defined as the time interval between enrollment and the initial visit
with a 10 FVC decline For subjects who experience disease progression the study doctor will
determine whether or not the subject will remain in the study
522 Acute Exacerbations
The following 3 criteria will define AEx in subjects with acute worsening of their respiratory
conditions
1 Clinical (all of the following required)
A) Unexplained worsening of dyspnea or cough within 30 days triggering unscheduled
medical care (eg emergency room clinic study visit hospitalization)
B) No clinical suspicion or overt evidence of cardiac event pulmonary embolism or deep
venous thrombosis to explain acute worsening of dyspnea
C) No pneumothorax
44
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
2 RadiologicPhysiologic (A and B required)
A) New ground glass opacity or consolidation computed tomography (CT) scan OR new
alveolar opacities on chest x-ray
B) Decline of ge 5 in resting room air SpO2 from last recorded level OR decline of ge 8 mm
Hg in resting room air PaO2 from last recorded level
3 Microbiologic (all of the following required)
A) No clinical evidence for infection (ie absence of grossly purulent sputum fever gt 39degC
orally)
B) Lack of positive microbiological results (if done) from lower respiratory tract defined as
(1) Clinically significant bacterial growth on sputum or endotracheal aspirate cultures
(2) Quantitative culture by protected brush specimen ge 103 cfumL or BAL ge 104 cfumL
(3) The presence of specific pathogens on stains of any of the above
C) Lack of positive pathogen in blood cultures (if done)
Identification of Acute Exacerbations
All subjects will be educated about the importance of identifying AExs At the time of
enrollment subjects will be told about the possibility of developing acute symptomatic
worsening that might represent an AEx of IPF and instructed to contact their study clinical
center coordinator within 48 to 72 hours of the apparent event
All subjects will be contacted by phone monthly and questioned about any change in dyspnea or
cough and any interim clinic visits or hospitalizations Finally as part of the IPFnet outreach to
community referring physicians the importance of AExs will be emphasized When a subject is
identified who meets criterion 1A this will trigger the collection of additional clinical data to
evaluate a suspected AEx These data will be collected as part of standard clinical care (ie this
protocol does not require collection of all items) The additional items to be collected for
suspected AEx include
IPFnet AEx case report form (eCRF) (required)
45
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Chest x-ray CT scan withwithout pulmonary angiogram (reports should be faxed and
followed by the hard copiesdiscs)
Oxygen saturation (pulse oximetry)
ABG
Respiratory cultures (sputum endotracheal aspirate lavage)
Blood cultures
Clinichospital records related to the event
All potential cases of AEx will be reviewed by the clinical center PI first and a decision on
whether the case may represent an AEx will be made If AEx is suspected the case will be sent
to the IPFnet adjudication committee which will assign a final diagnosis (see Table 5) If there is
disagreement among members the majority opinion will be recorded
During episodes of suspected AEx as determined by the individual clinical center investigator
subjects will remain blinded and in the study
Table 5 Final Diagnoses in Evaluation of Suspected Acute Exacerbations
Definite acute exacerbation All criteria met no alternative etiology
Unclassifiable acute worsening
Insufficient data to evaluate all criteria no alternative etiology
Not acute exacerbation Alternative etiology identified that explains acute worsening
Management of the suspected AEx will be at the discretion of the treating physician Standard of
care generally involves evaluation for respiratory infection pulmonary embolism cardiac events
and pneumothorax and treatment with IV corticosteroids
Study drugs will be resumed at pre-suspected AEx doses after subjects clinically improve as
confirmed by the local PI All subjects should be seen at the clinical center within 2 to 4 weeks
of recovery for measurement of post-bronchodilator FVC (see Figure 4) Subjects unable to
return to the clinical center after suspected AEx due to medical frailty (eg continued
46
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
institutionalization progressive disability) will be categorized as failing to maintain FVC
response in secondary analyses
Suspected AEx (PI determined)
Hold study drug Treat AEx
(Attending physician determined)
Alive but unable to continue due to
medical frailty
Dead
Alive and able to continue
Site reviewvisit
Restart study drug
FVC within 2-4 weeks
Figure 4 Acute Exacerbation Flow Chart
523 Respiratory Infections
An upper respiratory infection will be defined as
Change in sputum discoloration
Increased cough of no more than 14 daysrsquo duration
A lower-respiratory infection (pneumonia) will be defined as new segmental or lobar airspace
opacities visualized by image studies (chest radiograph or HRCT) in addition to any of the
following
Positive pathogencultures in good sample of sputum or lower-airway secretions retrieved
by fiberoptic bronchoscope
Fever gt 39degC or gt 100degF
Leukocytosis gt 12000 (unexplained no increase in dose of corticosteroids)
47
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
524 Maintained FVC Response
Subjects with follow-up FVCpred measurements at or above their baseline FVCpred level
will be classified as having maintained FVC response Subjects with reduced FVCpred levels
or missing data for any reason including death or medical frailty will be classified as having not
maintained FVC response The FVCpred value is used because unadjusted FVC measurements
are expected to decline with age
48
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
6 Safety Evaluations and Procedures
61 Adverse Events
During a clinical trial the reporting of adverse experience information can lead to important
changes in the way a new treatment is developed as well as provide integral safety data
611 Definitions
An adverse event (AE) is any untoward medical occurrence in a subject or clinical investigation
subject who was administered a pharmaceutical product The AE does not necessarily have to
have a causal relationship with the drug administered An AE can be any unfavorable and
unintended sign (including an abnormal laboratory finding) symptom or disease temporarily
associated with the use of a medicinal product whether or not considered to be related to the
medicinal product Diseases signs symptoms or laboratory abnormalities already existing at
enrollment are not considered AEs unless they worsen (ie increase in intensity or frequency)
Surgical procedures themselves are not AEs they are therapeutic measures for conditions that
require surgery The condition for which the surgery is required may be an AE Surgical
procedures planned before randomization and the conditions necessitating the surgery are not
AEs
A serious adverse event is any untoward event that
Is fatal
Is life-threatening
Requires inpatient hospitalization or prolongation of existing hospitalization with the
following exceptions
o Preplanned (before the study) hospital admissions unless the hospitalization is
prolonged
o Planned admissions (as part of a study eg routine biopsies)
o Hospitalization lasting lt 24 hours
49
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
o Hospitalization for elective procedure
o Emergency room visits
Results in persistent or significant disability or incapacity
Is a congenital anomaly or birth defect
Important medical events that may not result in death be life-threatening or require
inpatient hospitalization may be considered serious adverse events (SAEs) when based
on appropriate medical judgment they may jeopardize the subject and may require
medical or surgical intervention to prevent one of the outcomes listed above
Life-threatening means that the subject was in the view of the investigator at immediate risk of
death from the AE as it occurred It does not include an AE that had it occurred in a more severe
form might have caused death
Persistent or significant disabilityincapacity means that the event resulted in permanent or
significant and substantial disruption of the subjectrsquos ability to carry out normal life functions
Causality
A reasonable possibility means the AE may have been caused byrelated to the study drug A
perceived or real lack of efficacy does not satisfy the definition of relatedness
612 Adverse Event (AE) Reporting
For the PANTHER-IPF trial all AEs (serious and nonserious) occurring from randomization
through final study visit (4 weeks after final dose of all study medication) will be recorded on the
AE page of the case report form (CRF)
6121 Serious Adverse Events (SAE) Reporting
For this trial all deaths and all SAEs which occur from randomization through final study visit
must be entered within the EDC system via the SAE eCRF page within 24 hours of the
investigative sitersquos knowledge of the event It is the responsibility of the clinical center
50
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
investigator to provide a causality assessment of the event for each study medications based upon
the information available at the time of the report It is understood that complete information
about the event may not be known at the time the initial report is submitted In the event the EDC
system is not accessible to the site at the time of event reporting investigative sites will complete
and forward a paper back-up SAE form to DCRI Safety Surveillance for processing
DCRI Safety Surveillance
Telephone 1-919-668-8624 or 1-866-668-7799 (toll free)
Fax 1-919-668-7138 or 1-866-668-7138 (toll free)
The investigator must complete and submit follow-up SAE information via the eCRF when
important new or follow-up information (eg final diagnosis outcome results of specific
investigations) becomes available Follow-up information should be submitted according to the
same process used for reporting the initial event as described above All SAEs will be followed
until resolution stabilization or 30 days after the subject has completed the final visit (4 weeks
after the final dose of study medication) whichever occurs first The investigator is responsible
for reporting SAEs to their institutional review board (IRB) per site specific IRB reporting
guidelines
6122 Regulatory Reporting
AEs that are serious study drug related and unexpected will be reported to the regulatory
authorities The DCRI Safety Surveillance medical monitor will perform a medical review of all
SAEs submitted and evaluate for ldquounexpectednessrdquo DCRI Safety Surveillance will prepare
MedWatch reports for those events identified as serious study drug related and unexpected as
determined by Safety Medical Monitor
DCRI Regulatory Services will submit all unexpected study drug-related SAEs as per 21 CFR
32 DCRI Safety Surveillance will provide a safety alert letter to the NHLBI DSMB and DCC
clinical operation (for distribution to sites) within 15 days of initial receipt of the information
51
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Investigators are responsible for promptly reporting these events to their reviewing IRBs
according to site specific IRB reporting guidelines
62 Clinical Medical Monitoring
There will be an unblinded physician at the IPFnet DCC serving as medical monitor The
medical monitor will be available to assist with questions about dosage adjustments of study
medications including discontinuation or resumption of medications
63 Unblinding Procedures
Unblinding of subjects or investigators to subject treatment is strongly discouraged For ongoing
clinical management all subjects should be presumed to be receiving ldquoactiverdquo study drug To
ensure the subjectrsquos safety the study treatment will be dose-adjusted based on laboratory test
results clinical findings and symptoms
The IPFnet DCC medical monitor and PANTHER-IPF co-chairs Drs Ganesh Raghu and
Fernando Martinez will be available to the study physicians to discuss study drug management
on a case-by-case basis Un-blinding will be considered ONLY when the knowledge of subject
treatment assignment is ABSOLUTELY ESSENTIAL for subject safety and after discussion of
the subjectrsquos case with the medical monitor and either Dr Raghu or Dr Martinez Unblinding of
study treatment should be minimized during the conduct of the trial In those cases where it is
felt to be medically necessary the DCC medical officer will communicate directly with the
managing physician to minimize unblinding of study personnel
52
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
7 Study Drug Procedures
At the baseline 15-week 30-week and 45-week study visits subjects will receive a supply of
study drug sufficient to last until the next visit at which study drug will be dispensed
53
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
8 Data Management
81 Hardware and Software Configuration
811 Hardware and Database Software
Data will be stored in an Oracle database system Oracle has advantages of processing efficiency
and smooth linkage with other software systems The application and database will be hosted on
Solaris Unix servers at the IPFnet DCC
812 Statistical Software
SAS will be used as the principal application for the management of analysis data files and
statistical computations S-Plus will be used to provide supplementary functions as needed
813 Access Control and Confidentiality Procedures
Access to databases will be controlled centrally by the IPFnet DCC through user passwords
linked to appropriate privileges This protects the data from unauthorized changes and
inadvertent loss or damage
814 Security
Database and Web servers will be secured by a firewall and through controlled physical access
Oracle has many security features to ensure that any staff member accessing the database has the
proper authority to perform the functions he or she requests of the system Within the secondary
SAS databases Unix group-access control maintains similar security The Sun workstation login
is secured by extensive user-password facilities under Unix
54
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
815 Back-up Procedures
Database back-up will be performed automatically every day and standard IPFnet DCC policies
and procedures will be applied to dictate tape rotation and retention practices
816 Virus Protection
All disk drives that provide network services and all user computers will be protected using
virus-scanning software Standard IPFnet DCC policies will be applied to update these protection
systems periodically through the study
82 Sources of Data
821 Design and Development
The IPFnet DCC will be responsible for development of the electronic case report forms
(eCRFs) development and validation of the clinical study database ensuring data integrity and
training clinical center staff on applicable data management procedures A web-based distributed
data entry model will be implemented This system will be developed to ensure that guidelines
and regulations surrounding the use of computerized systems used in clinical trials are upheld
The remainder of this section provides an overview of the data management plan associated with
this protocol
822 Data Collection Forms
The data collection process consists of direct data entry at the study clinical centers into the EDC
system(s) provided by the DCC A data collection worksheet will be provided to clinical centers
for recording data in the event the EDC system is unavailable Data entry of the eCRFs should
be completed according to the instructions provided and project specific training The
investigator is responsible for maintaining accurate complete and up-to-date records and for
ensuring the completion of the eCRFs for each research participant
55
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
823 Data Acquisition and Entry
Data entry into eCRFs shall be performed by authorized individuals Selected eCRFs may also
require the investigatorrsquos written signature or electronic signature as appropriate Electronic
CRFs will be monitored for completeness accuracy and attention to detail during the study
824 Data Center Responsibilities
The IPFnet DCC will 1) develop a data management plan and will conduct data management
activities 2) provide final eCRFs for the collection of all data required by the study 3) develop
data dictionaries for each eCRF that will comprehensively define each data element 4) conduct
ongoing data monitoring activities on study data 5) monitor any preliminary analysis data
cleanup activities and 6) rigorously monitor final study data clean up
825 Data Editing
Completed data will be entered into the IPFnet DCC automated data acquisition and
management system If incomplete or inaccurate data are found a data clarification request will
be generated and distributed to clinical centers for a response Clinical centers will resolve data
inconsistencies and errors and enter all corrections and changes into the IPFnet DCC automated
data acquisition and management system
826 Training
The training plan for clinical center staff includes provisions for training on assessments eCRF
completion guidelines data management procedures and the use of computerized systems
56
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
9 Study Design and Data Analysis
91 General Analytic Considerations
All primary analyses will be based on intent-to-treat (ITT) principles using all randomized
subjects Baseline factors across groups will be compared using mean (standard deviation) and
median (25th and 75th percentiles) summary measures Kaplan-Meier curves will be used to
display event rates Due to clinical interest in departures from both sides of the null hypothesis
all test statistics will be 2-sided
Reasonable caution needs to be taken when conducting multiple analyses on key clinical
subgroups For subgroup analyses a conservative significance level of 0001 will be used for all
interaction tests Thus subgroup comparisons will be considered exploratory unless the p-value
from the interaction test is smaller than 0001
92 Randomization Blinding and Reporting of Results
A permuted block-randomization scheme will be created with varying block sizes stratified by
clinical center Once a subject has completed the screening and baseline period and evaluation
for inclusionexclusion criteria the randomization process will begin Subjects will be
randomized to receive NAC or matching placebo with equal probability (11) via telephone
contact with a central interactive voice response system (IVRS) using a toll-free randomization
number On the day of randomization after the subject has successfully met all inclusion and
exclusion criteria the investigator or designee will call the central randomization number to
obtain the assigned kit randomization numbers for that subject At each subject visit the
investigator or designee will call the central randomization number to obtain the new kit
randomization numbers for resupply of the subject For resupply of the clinical center the IVRS
will monitor minimal volume of a kit type andor expiration date and will automatically notify
the pharmacy
57
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
The trial results will be reported according to guidelines specified in the CONSORT statement
A flow diagram describing screening recruitment randomization dropout and vital status will
be included in the primary manuscript AEs and efficacy data will be presented for all treatment
groups Adherence dropout and lost to follow-up will be carefully examined across all treatment
groups Analyses of safety will be based on data from all randomized subjects who received at
least one dose of study drug
93 Stratification
Subjects will be distributed to the two treatment arms in a 11 allocation ratio Stratification
blocks will be based on clinical centers
94 Specification of the Primary Analyses
A mixed model repeated measures (MMRM) analysis described in section 95 will be used to
compare differences in the slope of FVC measurements across the treatment groups Response
variables are values of the FVC measured at baseline and every 15 weeks until study completion
Variables in the model will include treatment time and time by treatment age sex race and
height Contrast estimates of differences in slopes of treatment over time (along with confidence
intervals) will be used to estimate the treatment effect The validity of this model in terms of
meeting modeling assumptions will be assessed via standard modeling diagnostics and goodness-
of-fit measures Based on the MMRM framework missing FVC data will not be imputed for the
primary analysis
95 Analysis of Longitudinal Endpoints
A common goal in clinical trials is to specify models that are easily implemented and
reproducible by independent data analysts On the other hand the models should have proper
statistical behavior in terms of low bias and high precision Many common approaches to
longitudinal data analysis including last observation carried forward (LOCF) imputation rely on
the missing completely at random (MCAR) assumption However the MCAR assumption is
58
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
unlikely to hold in many clinical trials because missing data are often related to disease
progression and prognosis A more reasonable assumption missing at random (MAR) specifies
that the complete data distribution can be modeled using only the observed data The likelihood-
based MMRM approach is valid under the more general MAR assumptions These models will
be applied to analyze the longitudinal data secondary endpoints
The advantages of MMRM analysis are that all important characteristics of the model can be preshy
specified standard software can be used to implement the models and results are based on ITT
principles43 In addition the MMRM approach offers superior control of Type I and Type II
errors compared with the LOCF approach
Response variables are values of the PFTs measured at enrollment and every 15 weeks until
study completion and 6MWT values measured at baseline week 30 and week 60 Covariates are
treatment time time by treatment and key baseline risk factors Contrasts (along with
confidence intervals) of treatment by time will be used to estimate the treatment effect
The correlation structure involves multiple pieces including measurement errors random
variation and interindividual variability For the longitudinal data analyses an unstructured
correlation matrix for within-subject errors will be assumed Other correlation structures
including compound symmetry will be examined as needed A careful examination of reasons
for study discontinuation will be conducted to assess the validity of MCAR Sensitivity analyses
will be used to examine the untestable assumption that the observed data violate the MAR
assumption The MMRM models will be implemented using PROC MIXED in SAS
96 Analysis of Binary Time-to-Event and Time-Lagged Endpoints
Regression modeling approaches using either the logistic regression model or Cox proportional
hazards regression model will be employed when appropriate The validity of these models will
be assessed via standard modeling diagnostics and goodness-of-fit measures Estimates of
cumulative frequencies for more general time-lagged responses will be calculated using the
partitioned version of the Bang-Tsiatis estimator44 The partitions will be set at 15-week intervals
59
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
to correspond with the data-collection process Covariate adjusted event rates will be calculated
using inverse probability-weighted regression estimates45
97 Power Analysis
971 Primary Analyses
Based on previously published IPF clinical trials the PL group is expected to experience a drop
in FVC of approximately 020 L over the study period (see Figure 1) The IPFnet Steering Group
determined a clinically important difference would be to preserve the majority of the decline
relative to PL over the study period In particular a treatment effect of 015 L was determined to
be a clinically meaningful difference Potential dropout is a key factor in the proposed study The
drop-out process assumed 5 lost to follow-up after every study visit Only 80 of subjects
were assumed to be followed for the entire study period All models assumed a compound
symmetry structure for the covariance matrix Power calculations were performed using a SAS
IML program for designing repeated measures studies46 Based on preliminary reviews of the
data from the University of Michigan the covariance matrix parameters were estimated at
approximately σ2 = 0757 (variance parameter) and ρ = 0936 (correlation parameter) To be
conservative the power calculations for the primary analysis were performed with parameter
setting of σ2 = 0810 (variance parameter) and ρ = 0925 (correlation parameter)
The power calculations assume a correction for imperfect compliance proposed by Lachin and
Foulkes to allow for 2 noncompliance for each of the treatment arms47 Thus the sample size
of 130 subjects per arm would be reduced to an adjusted sample size of 130(1-002-002)2 =
1198 or 120 subjects per arm
Under the assumed Type I error rate of 005 with a correlation parameter of 0925 and standard
deviation of 090 the difference of 015 L (or 00025 Lweek) shown in Table 6 would have
power of 93
60
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Table 6 Hypothetical Values of Mean FVC (L) Change from Baseline
Week 15 Week 30 Week 45 Week 60
NAC 00125 00250 00375 00500
Placebo 00500 01000 01500 02000
Difference 00375 00750 01125 01500
Abbreviations FVC forced vital capacity PL placebo
972 Power Analysis for Secondary Endpoints
Power calculations for secondary endpoint measurements are shown in Table 7 Standard
deviations are based on unpublished data provided by the University of Michigan The
calculations are based on a 2-sample t-test with Type I error rate set at 005 These calculations
are likely to be conservative because the statistical approach described in section 95 for
analyzing these endpoints will incorporate incomplete observations as well as intermediate data
points
Table 7 Detectable Differences in Treatment Means for Selected Endpoint Measurements
Secondary Endpoints Std Dev
of the Baseline Score
Detectable Difference for 80 Power
Std Dev of the Change Score
Difference Detectable for
80 Power
DLCOpred 166 58 91 32
6MWT Area Under the Desaturation Curve
219 76 175 61
6MWT Distance to Desaturation 224 78 315 110
6MWT Minutes Walked 210 073 205 071
Abbreviations Std Dev standard deviation DLCOpred diffusing capacity of the lung for carbon monoxide percent predicted 6MWT 6-minute walk test
61
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
10 Study Administration
101 Cooperative Agreement Mechanism
The administrative and funding mechanism used to undertake this project is a ldquocooperative
agreementrdquo (U01) which is an assistance mechanism Under the cooperative agreement the
NHLBI assists supports andor stimulates the project and is substantially involved with
investigators in conducting the study by facilitating performance of the effort in a ldquopartnerrdquo role
The NHLBI project scientist serves on the IPFnet Steering Group and he or another NHLBI
scientist may serve on other project committees when appropriate At the same time however
NHLBI does not assume a dominant role direction or prime responsibility for this research
program
As described below governance of the project is conducted through the IPFnet Steering Group
Principal investigators have lead responsibilities in all aspects of their trials and the project
including any modification of trial designs conduct of the trials quality control data analysis
and interpretation preparation of publications and collaboration with other investigators unless
otherwise provided for by the IPFnet Steering Group
PIs retain custody of and have primary rights to their center-specific and collaborative data
subject to government rights-of-access consistent with current Health amp Human Services (HHS)
Public Health Service (PHS) and National Institutes of Health policies The protocols and
governance policies call for the continual submission of data centrally to the IPFnet DCC for the
collaborative database which at a minimum will contain the key variables selected by the IPFnet
Steering Group for standardization across all clinical centers the submission of copies of the
collaborative datasets to each PI upon completion of the project procedures for data analysis
reporting and publication and procedures to protect and ensure the privacy of medical and
genetic data and records of individuals The NHLBI project scientist on behalf of the NHLBI
will have the same access privileges and responsibilities regarding the collaborative data as the
other members of the Steering Group
62
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
PIs are also encouraged to publish and to publicly release and disseminate results data and other
products of the project concordant with the project protocols and governance and the approved
plan for making data and materials available to the scientific community and to the NHLBI
However during the 3 years after the ending date of NHLBI project support unpublished data
unpublished results data sets not previously released and other study materials or products are
to be made available to any third party only with the approval of the IPFnet Steering Group
Upon completion of the project PIs are expected to put their intervention materials and
procedure manuals into the public domain andor make them available to other investigators
according to the approved plan for making data and materials available to the scientific
community and the NHLBI for the conduct of research at no charge other than the costs of
reproduction and distribution
The NHLBI reserves the right to terminate or curtail the project (or an individual award) in the
event of (a) failure to develop or implement mutually agreeable collaborative measurement
subject eligibility and data management sections of the protocols (b) substantial shortfall in
subject recruitment follow-up data reporting or quality control or other major breach of
protocol (c) substantive changes in the agreed-upon protocols with which NHLBI cannot
concur (d) reaching a major project outcome with persuasive statistical significance
substantially before schedule or (e) human subject ethical issues that may dictate a premature
termination
Any disagreement that may arise in scientificprogrammatic matters (within the scope of the
award) between award recipients and the NHLBI may be brought to arbitration An arbitration
panel will be composed of 3 membersmdash1 selected by the IPFnet Steering Group (with the
NHLBI member not voting) or by the individual PI in the event of an individual disagreement a
second selected by NHLBI and the third selected by the other 2 members This special
arbitration procedure in no way affects the PIrsquos right to appeal an adverse action that is otherwise
appealable in accordance with the PHS regulations at 42 CFR part 50 Subpart D and HHS
63
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
regulation at 45 CFR part 16 or the rights of the NHLBI under applicable statutes regulations
and terms of the award
102 IPFnet Steering Group
The IPFnet Steering Group is the main governing body of the project It is composed of the PIs
of the clinical centers the PI of the DCC and the NHLBI project scientist The clinical centers
the IPFnet DCC and the NHLBI each have 1 vote on the IPFnet Steering Group All decisions
are determined by majority vote
All major scientific decisions are determined by the IPFnet Steering Group It assumes overall
responsibility for the design and conduct of the trial It appoints (and disbands) committees and
subcommittees as the need arises designs approves and implements the study protocols
oversees the development of the MOOP monitors subject recruitment and treatment delivery
evaluates data collection and management oversees quality assurance procedures and
implements changes and enhancements to the study as required It also has primary responsibility
for facilitating the conduct of the trials and reporting the projectrsquos results
103 Data and Safety Monitoring Board
The NHLBI will establish a DSMB in accordance with established policies (see
httpwwwnhlbinihgovfundingpoliciesdsmb_insthtm) to ensure data quality and subject
safety and to provide independent advice to the NHLBI regarding progress and the
appropriateness of study continuation
104 Recommendations on Interim Monitoring of Efficacy Safety and Futility
First and foremost the role of the DSMB will be to review subject safety and trial conduct at
periodic points during the study The DSMB may require analyses of the primary endpoint
results for comparing the benefit and risks of treatment strategies The benefit of collecting
additional data on key secondary endpoints with extended follow-up and establishing a robust
64
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
evidence base for determining a standard of care will need to be carefully considered before
early termination of one or more treatment arms After careful consideration the IPFnet Steering
Group recommends conservative thresholds for the early examinations of the safety and efficacy
data
The DSMB will be expected to meet approximately every 6 months until trial completion to
review safety and toxicity data The DSMB may recommend stopping the study based on these
reviews Because the DSMB could stop the trial for safety concerns as well as for a large
efficacy benefit there could be multiple opportunities to reject the null hypothesis (no difference
in event rates between the PL and NAC groups) A Bonferroni approximation will be applied
during the one planned interim analysis for efficacy
Before locking the database a statistical analysis plan (SAP) will be developed to provide
complete details on the statistical analysis The SAP will include the specifics for how and when
the DSMB will be notified for AEs The IPFnet DCC will deliver to the DSMB all FDA-defined
AEs at 3-month intervals The IPFnet DCC will prepare narrative SAE reports in real time for
DSMB review including recommendations and analysis of similar events for each SAE
submitted to the FDA
65
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
11 Investigator and Sponsor Obligations
111 Monitoring
All monitoring activities for US clinical centers will be performed in accordance with DCRI
standard operating procedures Information regarding the types of visits will be outlined in the
PANTHER-IPF MOOP
112 Cost and Payment
There will be no cost to subjects enrolled in this trial Study-related procedures will be paid for
by the IPFnet
Subjects may be eligible for reimbursement for travel to the clinical center Details of payment
will be explained to each subject during the consent process
113 Confidentiality and Health Insurance Portability and Accountability Act
Considerations
Subject confidentiality will be protected throughout the study All subject data will be kept
strictly confidential and no subject-identifying information will be released to anyone outside
the project Confidentiality will be assured through several mechanisms First each subject will
be assigned an anonymous study ID which will then be used on all study forms Second any
study forms blood samples and paper records that contain subject information (eg address lists
phone lists) will be kept at the clinical centers in secured locked areas coded by number Once
blood is collected there will be no subject identifiers placed on blood samplesmdashonly the study
ID number and the date of sample collection Third access to all subject data and information
including laboratory specimens will be restricted to authorized personnel In the case of
computerized data this restricted access will be assured through user logon IDs and password
protection
66
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
At the IPFnet DCC only authorized personnel will have access to the data files containing study
data Security will be assured through user logon IDs passwords and appropriate access
privileges All study subjects will be identified only by their IPFnet ID numbers and no personal
identifying information such as name address or Social Security number will be entered into
the IPFnet DCC database Any subject-specific data reported to the IPFnet Steering Group will
be identified only by the IPFnet ID number
Finally subjects will not be identified by name in any reports or publications nor will the data
be presented in such a way that the identity of individual subjects can be inferred Analysis files
created for further study by the scientific community will have no subject identifiers These data
files will be created in accordance with the Ancillary Studies and Publication Policy of the
IPFnet
114 Informed Consent Procedures
All IPFnet subjects will provide written informed consent using procedures reviewed and
approved by each clinical centerrsquos IRB Informed consent will be undertaken by study personnel
in-person with the subject The subject has the option of declining further participation in the
study at that point No further study procedures will be conducted until the signed documents
have been provided to the IPFnet clinical center
115 Institutional Review Boards
Before initiating this study the protocol clinical center-specific informed consent forms Health
Insurance Portability and Accountability Act (HIPAA) forms recruitment materials and other
relevant information will be reviewed by a properly constituted IRB at each participating clinical
center A copy of the signed and dated IRB approval at each clinical center will be retrieved prior
to or during the site initiation visit and archived at the IPFnet DCC Any amendments to the
protocol other than simple administrative and typographical changes must be approved by each
IRB before they are implemented The clinical centers will seek annual renewals of their IRB
approvals in accordance with local procedures
67
__________________________________________ ________________
__________________________________________
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
12 Investigator Agreement
I have read the foregoing protocol PANTHER-IPF and agree that it contains all necessary
details for carrying out this study I will conduct the study as outlined herein and will complete
the study within the time designated
I will provide copies of the protocol and all pertinent information to all individuals responsible to
me who assist in the conduct of this study I will discuss this material with them to ensure they
are fully informed regarding the drug and the conduct of the study
I will fulfill all responsibilities for submitting pertinent information to the local IRB if
applicable that is responsible for this study
I further agree that NHLBI andor DCRI will have access to any source documents from which
eCRF information may have been generated
Signature of Principal Investigator Date
Name of Principal Investigator (printed or typed)
Protocol version date May 19 2009
Protocol Amendment 1 version date May 28 2010
Protocol Amendment 2 version date December 6 2011
68
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
13 References
1 Raghu G Brown KK Bradford WZ et al A placebo-controlled trial of interferon gamma-1b in patients with idiopathic pulmonary fibrosis N Engl J Med 2004350125-33 2 King TE Jr Safrin S Starko KM et al Analyses of efficacy end points in a controlled trial of interferon-gamma1b for idiopathic pulmonary fibrosis Chest 2005127171-7 3 Flaherty KR Thwaite EL Kazerooni EA et al Radiological versus histological diagnosis in UIP and NSIP survival implications Thorax 200358143-8 4 Wells AU Desai SR Rubens MB et al Idiopathic pulmonary fibrosis a composite physiologic index derived from disease extent observed by computed tomography Am J Respir Crit Care Med 2003167962-9 5 Raghu G Freudenberger TD Yang S et al High prevalence of abnormal acid gastroshyoesophageal reflux in idiopathic pulmonary fibrosis Eur Respir J 200627136-42 6 Kinnula VL Focus on antioxidant enzymes and antioxidant strategies in smoking related airway diseases Thorax 200560693-700 7 Coultas DB Zumwalt RE Black WC Sobonya RE The epidemiology of interstitial lung diseases Am J Respir Crit Care Med 1994150967-72 8 Raghu G Weycker D Edelsberg J Bradford WZ Oster G Incidence and prevalence of idiopathic pulmonary fibrosis Am J Respir Crit Care Med 2006174810-6 9 Olson AL Swigris JJ Lezotte DC Norris JM Wilson CG Brown KK Mortality from pulmonary fibrosis increased in the United States from 1992 to 2003 Am J Respir Crit Care Med 2007176277-84 10 Mannino DM Etzel RA Parrish RG Pulmonary fibrosis deaths in the United States 1979shy1991 An analysis of multiple-cause mortality data Am J Respir Crit Care Med 19961531548shy52 11 Hubbard R Johnston I Coultas DB Britton J Mortality rates from cryptogenic fibrosing alveolitis in seven countries Thorax 199651711-6 12 Johnston I Britton J Kinnear W Logan R Rising mortality from cryptogenic fibrosing alveolitis Bmj 19903011017-21 13 Raghu G Collard HR Egan JJ et al An official ATSERSJRSALAT statement idiopathic pulmonary fibrosis evidence-based guidelines for diagnosis and management Am J Respir Crit Care Med 2011183788-824 14 (USA) FDA FDA Public Health Advisory Interferon gamma-1b (marketed as Actimmune) In 2007 15 King TE Jr Pardo A Selman M Idiopathic pulmonary fibrosis Lancet 2011 16 Raghu G Brown KK Costabel U et al Treatment of idiopathic pulmonary fibrosis with etanercept an exploratory placebo-controlled trial Am J Respir Crit Care Med 2008178948shy55 17 Malouf MA Hopkins P Snell G Glanville AR An investigator-driven study of everolimus in surgical lung biopsy confirmed idiopathic pulmonary fibrosis Respirology 201116776-83 18 King TE Jr Behr J Brown KK et al BUILD-1 a randomized placebo-controlled trial of bosentan in idiopathic pulmonary fibrosis Am J Respir Crit Care Med 200817775-81 19 Richeldi L Costabel U Selman M et al Efficacy of a tyrosine kinase inhibitor in idiopathic pulmonary fibrosis N Engl J Med 20113651079-87
69
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
20 Borok Z Buhl R Grimes GJ et al Effect of glutathione aerosol on oxidant-antioxidant imbalance in idiopathic pulmonary fibrosis Lancet 1991338215-6 21 Meyer A Buhl R Magnussen H The effect of oral N-acetylcysteine on lung glutathione levels in idiopathic pulmonary fibrosis Eur Respir J 19947431-6 22 Behr J Maier K Degenkolb B Krombach F Vogelmeier C Antioxidative and clinical effects of high-dose N-acetylcysteine in fibrosing alveolitis Adjunctive therapy to maintenance immunosuppression Am J Respir Crit Care Med 19971561897-901 23 Cantin AM North SL Fells GA Hubbard RC Crystal RG Oxidant-mediated epithelial cell injury in idiopathic pulmonary fibrosis J Clin Invest 1987791665-73 24 Waghray M Cui Z Horowitz JC et al Hydrogen peroxide is a diffusible paracrine signal for the induction of epithelial cell death by activated myofibroblasts Faseb J 200519854-6 25 Larios JM Budhiraja R Fanburg BL Thannickal VJ Oxidative protein cross-linking reactions involving L-tyrosine in transforming growth factor-beta1-stimulated fibroblasts J Biol Chem 200127617437-41 26 Kinnula VL Fattman CL Tan RJ Oury TD Oxidative stress in pulmonary fibrosis a possible role for redox modulatory therapy Am J Respir Crit Care Med 2005172417-22 27 Meyer A Buhl R Kampf S Magnussen H Intravenous N-acetylcysteine and lung glutathione of patients with pulmonary fibrosis and normals Am J Respir Crit Care Med 19951521055-60 28 Behr J Degenkolb B Krombach F Vogelmeier C Intracellular glutathione and bronchoalveolar cells in fibrosing alveolitis effects of N-acetylcysteine Eur Respir J 200219906-11 29 Bando M Hosono T Mato N et al Long-term efficacy of inhaled N-acetylcysteine in patients with idiopathic pulmonary fibrosis Intern Med 2010492289-96 30 Demedts M Behr J Buhl R et al High-dose acetylcysteine in idiopathic pulmonary fibrosis N Engl J Med 20053532229-42 31 Toma TP Bhowmik A Rajakulasingam R Acetylcysteine in pulmonary fibrosis N Engl J Med 20063541086-9 author reply -9 32 Hunninghake GW Antioxidant therapy for idiopathic pulmonary fibrosis N Engl J Med 20053532285-7 33 Flaherty KR Mumford JA Murray S et al Prognostic implications of physiologic and radiographic changes in idiopathic interstitial pneumonia Am J Respir Crit Care Med 2003168543-8 34 Latsi PI du Bois RM Nicholson AG et al Fibrotic idiopathic interstitial pneumonia the prognostic value of longitudinal functional trends Am J Respir Crit Care Med 2003168531-7 35 Collard HR King TE Jr Bartelson BB Vourlekis JS Schwarz MI Brown KK Changes in clinical and physiologic variables predict survival in idiopathic pulmonary fibrosis Am J Respir Crit Care Med 2003168538-42 36 Jegal Y Kim DS Shim TS et al Physiology is a stronger predictor of survival than pathology in fibrotic interstitial pneumonia Am J Respir Crit Care Med 2005171639-44 37 Martinez FJ Safrin S Weycker D et al The clinical course of patients with idiopathic pulmonary fibrosis Ann Intern Med 2005142963-7 38 Hull JH Acetylcysteine in pulmonary fibrosis N Engl J Med 20063541089-91 author reply -91
70
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
39 Flaherty KR King TE Jr Raghu G et al Idiopathic interstitial pneumonia what is the effect of a multidisciplinary approach to diagnosis Am J Respir Crit Care Med 2004170904shy10 40 Raghu G Johnson WC Lockhart D Mageto Y Treatment of idiopathic pulmonary fibrosis with a new antifibrotic agent pirfenidone results of a prospective open-label Phase II study Am J Respir Crit Care Med 19991591061-9 41 Hunninghake GW Lynch DA Galvin JR et al Radiologic findings are strongly associated with a pathologic diagnosis of usual interstitial pneumonia Chest 20031241215-23 42 Lynch D Godwin J Safrin S et al High-resolution computed tomography in idiopathic pulmonary fibrosis diagnosis and prognosis Am J Respir Crit Care Med 2005172488-93 43 Mallinckrodt CH Watkin JG Molenberghs G Carroll RJ Choice of the primary analysis in longitudinal clinical trials Pharmaceutical Statistics 20043161-9 44 Bang H Tsiatis A Estimating medical costs with censored data Biometrika 200087329shy43 45 Lin DY Regression analysis of incomplete medical cost data Stat Med 2003221181-200 46 Rochon J Application of GEE procedures for sample size calculations in repeated measures experiments Stat Med 1998171643-58 47 Lachin JM Foulkes MA Evaluation of sample size and power for analyses of survival with allowance for nonuniform patient entry losses to follow-up noncompliance and stratification Biometrics 198642507-19
71
- PANTHER-IPFPREDNISONE AZATHIOPRINEAND N-ACETYLCYSTEINEA STUDY THAT EVALUATES RESPONSE INIDIOPATHIC PULMONARY FIBROSIS
-
- Protocol Summary
- Table of Contents
- List of Tables
- List of Figures
- List of Abbreviations
- 1 Summary
- 2 Hypotheses and Specific Aims
-
- 21 Null Hypothesis
- 22 Specific Aim 1
- 23 Specific Aim 2
- 24 Prespecified Subgroups of Interest
-
- 3 Background and Significance
-
- 31 Idiopathic Pulmonary Fibrosis is the Most Common Interstitial Lung Disease
- 32 Rationale for Placebo Control
- 33 Rationale for N-acetylcysteine
- 35 Rationale for N-acetylcysteine as a Stand-alone Therapy
- 36 Rationale for the Study Design and Primary Endpoint
- 37 Rationale for Blinding of Treatments
-
- 4 Methods
-
- 41 Inclusion Criteria
- 42 Diagnosis of IPF
- 43 Exclusion Criteria
- 44 Study Design and Study Visit
- 45 Dose Justification
- 46 Contraindications Precautions and Side Effects of Study Medications
- 47 Recruitment Procedures
- 48 Study Procedures
- 49 Concomitant Medications
- 410 Laboratory Testing
- 411 Blinding of Study Drugs
-
- 5 Study Endpoints
-
- 51 Primary Study Endpoint
- 52 Secondary Study Endpoints
-
- 6 Safety Evaluations and Procedures
-
- 61 Adverse Events
- 62 Clinical Medical Monitoring
- 63 Unblinding Procedures
-
- 7 Study Drug Procedures
- 8 Data Management
-
- 81 Hardware and Software Configuration
- 82 Sources of Data
-
- 9 Study Design and Data Analysis
-
- 91 General Analytic Considerations
- 92 Randomization Blinding and Reporting of Results
- 93 Stratification
- 94 Specification of the Primary Analyses
- 95 Analysis of Longitudinal Endpoints
- 96 Analysis of Binary Time-to-Event and Time-Lagged Endpoints
- 97 Power Analysis
-
- 10 Study Administration
-
- 101 Cooperative Agreement Mechanism
- 102 IPFnet Steering Group
- 103 Data and Safety Monitoring Board
- 104 Recommendations on Interim Monitoring of Efficacy Safety and Futility
-
- 11 Investigator and Sponsor Obligations
-
- 111 Monitoring
- 112 Cost and Payment
- 113 Confidentiality and Health Insurance Portability and Accountability ActConsiderations
- 114 Informed Consent Procedures
- 115 Institutional Review Boards
-
- 12 Investigator Agreement
- 13 References
-
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
bilirubin-indirect bilirubin-total BUN BUNcreatinine ratio calcium carbon dioxide
cholesterol-total chloride CPK-total creatinine GGT globulin glucose iron-total LDH
lipase magnesium phosphorus-inorganic potassium protein-total sodium TIBC triglycerides
uric acid) and hematology (red blood cell count WBC count hemoglobin hematocrit cell
indices differential platelet count)
411 Blinding of Study Drugs
Subjects and caregivers will be blinded to study treatment Every subject will receive NAC or
matching PLs at every study visit from the baseline visit to the week-45 visit No study agent
will be dispensed at the week-60 visit
43
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
5 Study Endpoints
51 Primary Study Endpoint
The primary endpoint will be the change in serial measurements of FVC over the study period
52 Secondary Study Endpoints
521 Time to Disease-progression
The time-to-death or a 10 decline in FVC will be defined as the time-to-disease progression
The 10 decline in FVC from enrollment must be confirmed on 2 consecutive visits no less than
6 weeks apart For subjects with 2 consecutive visits with a 10 decline in FVC the time-toshy
disease progression will be defined as the time interval between enrollment and the initial visit
with a 10 FVC decline For subjects who experience disease progression the study doctor will
determine whether or not the subject will remain in the study
522 Acute Exacerbations
The following 3 criteria will define AEx in subjects with acute worsening of their respiratory
conditions
1 Clinical (all of the following required)
A) Unexplained worsening of dyspnea or cough within 30 days triggering unscheduled
medical care (eg emergency room clinic study visit hospitalization)
B) No clinical suspicion or overt evidence of cardiac event pulmonary embolism or deep
venous thrombosis to explain acute worsening of dyspnea
C) No pneumothorax
44
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
2 RadiologicPhysiologic (A and B required)
A) New ground glass opacity or consolidation computed tomography (CT) scan OR new
alveolar opacities on chest x-ray
B) Decline of ge 5 in resting room air SpO2 from last recorded level OR decline of ge 8 mm
Hg in resting room air PaO2 from last recorded level
3 Microbiologic (all of the following required)
A) No clinical evidence for infection (ie absence of grossly purulent sputum fever gt 39degC
orally)
B) Lack of positive microbiological results (if done) from lower respiratory tract defined as
(1) Clinically significant bacterial growth on sputum or endotracheal aspirate cultures
(2) Quantitative culture by protected brush specimen ge 103 cfumL or BAL ge 104 cfumL
(3) The presence of specific pathogens on stains of any of the above
C) Lack of positive pathogen in blood cultures (if done)
Identification of Acute Exacerbations
All subjects will be educated about the importance of identifying AExs At the time of
enrollment subjects will be told about the possibility of developing acute symptomatic
worsening that might represent an AEx of IPF and instructed to contact their study clinical
center coordinator within 48 to 72 hours of the apparent event
All subjects will be contacted by phone monthly and questioned about any change in dyspnea or
cough and any interim clinic visits or hospitalizations Finally as part of the IPFnet outreach to
community referring physicians the importance of AExs will be emphasized When a subject is
identified who meets criterion 1A this will trigger the collection of additional clinical data to
evaluate a suspected AEx These data will be collected as part of standard clinical care (ie this
protocol does not require collection of all items) The additional items to be collected for
suspected AEx include
IPFnet AEx case report form (eCRF) (required)
45
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Chest x-ray CT scan withwithout pulmonary angiogram (reports should be faxed and
followed by the hard copiesdiscs)
Oxygen saturation (pulse oximetry)
ABG
Respiratory cultures (sputum endotracheal aspirate lavage)
Blood cultures
Clinichospital records related to the event
All potential cases of AEx will be reviewed by the clinical center PI first and a decision on
whether the case may represent an AEx will be made If AEx is suspected the case will be sent
to the IPFnet adjudication committee which will assign a final diagnosis (see Table 5) If there is
disagreement among members the majority opinion will be recorded
During episodes of suspected AEx as determined by the individual clinical center investigator
subjects will remain blinded and in the study
Table 5 Final Diagnoses in Evaluation of Suspected Acute Exacerbations
Definite acute exacerbation All criteria met no alternative etiology
Unclassifiable acute worsening
Insufficient data to evaluate all criteria no alternative etiology
Not acute exacerbation Alternative etiology identified that explains acute worsening
Management of the suspected AEx will be at the discretion of the treating physician Standard of
care generally involves evaluation for respiratory infection pulmonary embolism cardiac events
and pneumothorax and treatment with IV corticosteroids
Study drugs will be resumed at pre-suspected AEx doses after subjects clinically improve as
confirmed by the local PI All subjects should be seen at the clinical center within 2 to 4 weeks
of recovery for measurement of post-bronchodilator FVC (see Figure 4) Subjects unable to
return to the clinical center after suspected AEx due to medical frailty (eg continued
46
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
institutionalization progressive disability) will be categorized as failing to maintain FVC
response in secondary analyses
Suspected AEx (PI determined)
Hold study drug Treat AEx
(Attending physician determined)
Alive but unable to continue due to
medical frailty
Dead
Alive and able to continue
Site reviewvisit
Restart study drug
FVC within 2-4 weeks
Figure 4 Acute Exacerbation Flow Chart
523 Respiratory Infections
An upper respiratory infection will be defined as
Change in sputum discoloration
Increased cough of no more than 14 daysrsquo duration
A lower-respiratory infection (pneumonia) will be defined as new segmental or lobar airspace
opacities visualized by image studies (chest radiograph or HRCT) in addition to any of the
following
Positive pathogencultures in good sample of sputum or lower-airway secretions retrieved
by fiberoptic bronchoscope
Fever gt 39degC or gt 100degF
Leukocytosis gt 12000 (unexplained no increase in dose of corticosteroids)
47
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
524 Maintained FVC Response
Subjects with follow-up FVCpred measurements at or above their baseline FVCpred level
will be classified as having maintained FVC response Subjects with reduced FVCpred levels
or missing data for any reason including death or medical frailty will be classified as having not
maintained FVC response The FVCpred value is used because unadjusted FVC measurements
are expected to decline with age
48
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
6 Safety Evaluations and Procedures
61 Adverse Events
During a clinical trial the reporting of adverse experience information can lead to important
changes in the way a new treatment is developed as well as provide integral safety data
611 Definitions
An adverse event (AE) is any untoward medical occurrence in a subject or clinical investigation
subject who was administered a pharmaceutical product The AE does not necessarily have to
have a causal relationship with the drug administered An AE can be any unfavorable and
unintended sign (including an abnormal laboratory finding) symptom or disease temporarily
associated with the use of a medicinal product whether or not considered to be related to the
medicinal product Diseases signs symptoms or laboratory abnormalities already existing at
enrollment are not considered AEs unless they worsen (ie increase in intensity or frequency)
Surgical procedures themselves are not AEs they are therapeutic measures for conditions that
require surgery The condition for which the surgery is required may be an AE Surgical
procedures planned before randomization and the conditions necessitating the surgery are not
AEs
A serious adverse event is any untoward event that
Is fatal
Is life-threatening
Requires inpatient hospitalization or prolongation of existing hospitalization with the
following exceptions
o Preplanned (before the study) hospital admissions unless the hospitalization is
prolonged
o Planned admissions (as part of a study eg routine biopsies)
o Hospitalization lasting lt 24 hours
49
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
o Hospitalization for elective procedure
o Emergency room visits
Results in persistent or significant disability or incapacity
Is a congenital anomaly or birth defect
Important medical events that may not result in death be life-threatening or require
inpatient hospitalization may be considered serious adverse events (SAEs) when based
on appropriate medical judgment they may jeopardize the subject and may require
medical or surgical intervention to prevent one of the outcomes listed above
Life-threatening means that the subject was in the view of the investigator at immediate risk of
death from the AE as it occurred It does not include an AE that had it occurred in a more severe
form might have caused death
Persistent or significant disabilityincapacity means that the event resulted in permanent or
significant and substantial disruption of the subjectrsquos ability to carry out normal life functions
Causality
A reasonable possibility means the AE may have been caused byrelated to the study drug A
perceived or real lack of efficacy does not satisfy the definition of relatedness
612 Adverse Event (AE) Reporting
For the PANTHER-IPF trial all AEs (serious and nonserious) occurring from randomization
through final study visit (4 weeks after final dose of all study medication) will be recorded on the
AE page of the case report form (CRF)
6121 Serious Adverse Events (SAE) Reporting
For this trial all deaths and all SAEs which occur from randomization through final study visit
must be entered within the EDC system via the SAE eCRF page within 24 hours of the
investigative sitersquos knowledge of the event It is the responsibility of the clinical center
50
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
investigator to provide a causality assessment of the event for each study medications based upon
the information available at the time of the report It is understood that complete information
about the event may not be known at the time the initial report is submitted In the event the EDC
system is not accessible to the site at the time of event reporting investigative sites will complete
and forward a paper back-up SAE form to DCRI Safety Surveillance for processing
DCRI Safety Surveillance
Telephone 1-919-668-8624 or 1-866-668-7799 (toll free)
Fax 1-919-668-7138 or 1-866-668-7138 (toll free)
The investigator must complete and submit follow-up SAE information via the eCRF when
important new or follow-up information (eg final diagnosis outcome results of specific
investigations) becomes available Follow-up information should be submitted according to the
same process used for reporting the initial event as described above All SAEs will be followed
until resolution stabilization or 30 days after the subject has completed the final visit (4 weeks
after the final dose of study medication) whichever occurs first The investigator is responsible
for reporting SAEs to their institutional review board (IRB) per site specific IRB reporting
guidelines
6122 Regulatory Reporting
AEs that are serious study drug related and unexpected will be reported to the regulatory
authorities The DCRI Safety Surveillance medical monitor will perform a medical review of all
SAEs submitted and evaluate for ldquounexpectednessrdquo DCRI Safety Surveillance will prepare
MedWatch reports for those events identified as serious study drug related and unexpected as
determined by Safety Medical Monitor
DCRI Regulatory Services will submit all unexpected study drug-related SAEs as per 21 CFR
32 DCRI Safety Surveillance will provide a safety alert letter to the NHLBI DSMB and DCC
clinical operation (for distribution to sites) within 15 days of initial receipt of the information
51
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Investigators are responsible for promptly reporting these events to their reviewing IRBs
according to site specific IRB reporting guidelines
62 Clinical Medical Monitoring
There will be an unblinded physician at the IPFnet DCC serving as medical monitor The
medical monitor will be available to assist with questions about dosage adjustments of study
medications including discontinuation or resumption of medications
63 Unblinding Procedures
Unblinding of subjects or investigators to subject treatment is strongly discouraged For ongoing
clinical management all subjects should be presumed to be receiving ldquoactiverdquo study drug To
ensure the subjectrsquos safety the study treatment will be dose-adjusted based on laboratory test
results clinical findings and symptoms
The IPFnet DCC medical monitor and PANTHER-IPF co-chairs Drs Ganesh Raghu and
Fernando Martinez will be available to the study physicians to discuss study drug management
on a case-by-case basis Un-blinding will be considered ONLY when the knowledge of subject
treatment assignment is ABSOLUTELY ESSENTIAL for subject safety and after discussion of
the subjectrsquos case with the medical monitor and either Dr Raghu or Dr Martinez Unblinding of
study treatment should be minimized during the conduct of the trial In those cases where it is
felt to be medically necessary the DCC medical officer will communicate directly with the
managing physician to minimize unblinding of study personnel
52
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
7 Study Drug Procedures
At the baseline 15-week 30-week and 45-week study visits subjects will receive a supply of
study drug sufficient to last until the next visit at which study drug will be dispensed
53
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
8 Data Management
81 Hardware and Software Configuration
811 Hardware and Database Software
Data will be stored in an Oracle database system Oracle has advantages of processing efficiency
and smooth linkage with other software systems The application and database will be hosted on
Solaris Unix servers at the IPFnet DCC
812 Statistical Software
SAS will be used as the principal application for the management of analysis data files and
statistical computations S-Plus will be used to provide supplementary functions as needed
813 Access Control and Confidentiality Procedures
Access to databases will be controlled centrally by the IPFnet DCC through user passwords
linked to appropriate privileges This protects the data from unauthorized changes and
inadvertent loss or damage
814 Security
Database and Web servers will be secured by a firewall and through controlled physical access
Oracle has many security features to ensure that any staff member accessing the database has the
proper authority to perform the functions he or she requests of the system Within the secondary
SAS databases Unix group-access control maintains similar security The Sun workstation login
is secured by extensive user-password facilities under Unix
54
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
815 Back-up Procedures
Database back-up will be performed automatically every day and standard IPFnet DCC policies
and procedures will be applied to dictate tape rotation and retention practices
816 Virus Protection
All disk drives that provide network services and all user computers will be protected using
virus-scanning software Standard IPFnet DCC policies will be applied to update these protection
systems periodically through the study
82 Sources of Data
821 Design and Development
The IPFnet DCC will be responsible for development of the electronic case report forms
(eCRFs) development and validation of the clinical study database ensuring data integrity and
training clinical center staff on applicable data management procedures A web-based distributed
data entry model will be implemented This system will be developed to ensure that guidelines
and regulations surrounding the use of computerized systems used in clinical trials are upheld
The remainder of this section provides an overview of the data management plan associated with
this protocol
822 Data Collection Forms
The data collection process consists of direct data entry at the study clinical centers into the EDC
system(s) provided by the DCC A data collection worksheet will be provided to clinical centers
for recording data in the event the EDC system is unavailable Data entry of the eCRFs should
be completed according to the instructions provided and project specific training The
investigator is responsible for maintaining accurate complete and up-to-date records and for
ensuring the completion of the eCRFs for each research participant
55
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
823 Data Acquisition and Entry
Data entry into eCRFs shall be performed by authorized individuals Selected eCRFs may also
require the investigatorrsquos written signature or electronic signature as appropriate Electronic
CRFs will be monitored for completeness accuracy and attention to detail during the study
824 Data Center Responsibilities
The IPFnet DCC will 1) develop a data management plan and will conduct data management
activities 2) provide final eCRFs for the collection of all data required by the study 3) develop
data dictionaries for each eCRF that will comprehensively define each data element 4) conduct
ongoing data monitoring activities on study data 5) monitor any preliminary analysis data
cleanup activities and 6) rigorously monitor final study data clean up
825 Data Editing
Completed data will be entered into the IPFnet DCC automated data acquisition and
management system If incomplete or inaccurate data are found a data clarification request will
be generated and distributed to clinical centers for a response Clinical centers will resolve data
inconsistencies and errors and enter all corrections and changes into the IPFnet DCC automated
data acquisition and management system
826 Training
The training plan for clinical center staff includes provisions for training on assessments eCRF
completion guidelines data management procedures and the use of computerized systems
56
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
9 Study Design and Data Analysis
91 General Analytic Considerations
All primary analyses will be based on intent-to-treat (ITT) principles using all randomized
subjects Baseline factors across groups will be compared using mean (standard deviation) and
median (25th and 75th percentiles) summary measures Kaplan-Meier curves will be used to
display event rates Due to clinical interest in departures from both sides of the null hypothesis
all test statistics will be 2-sided
Reasonable caution needs to be taken when conducting multiple analyses on key clinical
subgroups For subgroup analyses a conservative significance level of 0001 will be used for all
interaction tests Thus subgroup comparisons will be considered exploratory unless the p-value
from the interaction test is smaller than 0001
92 Randomization Blinding and Reporting of Results
A permuted block-randomization scheme will be created with varying block sizes stratified by
clinical center Once a subject has completed the screening and baseline period and evaluation
for inclusionexclusion criteria the randomization process will begin Subjects will be
randomized to receive NAC or matching placebo with equal probability (11) via telephone
contact with a central interactive voice response system (IVRS) using a toll-free randomization
number On the day of randomization after the subject has successfully met all inclusion and
exclusion criteria the investigator or designee will call the central randomization number to
obtain the assigned kit randomization numbers for that subject At each subject visit the
investigator or designee will call the central randomization number to obtain the new kit
randomization numbers for resupply of the subject For resupply of the clinical center the IVRS
will monitor minimal volume of a kit type andor expiration date and will automatically notify
the pharmacy
57
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
The trial results will be reported according to guidelines specified in the CONSORT statement
A flow diagram describing screening recruitment randomization dropout and vital status will
be included in the primary manuscript AEs and efficacy data will be presented for all treatment
groups Adherence dropout and lost to follow-up will be carefully examined across all treatment
groups Analyses of safety will be based on data from all randomized subjects who received at
least one dose of study drug
93 Stratification
Subjects will be distributed to the two treatment arms in a 11 allocation ratio Stratification
blocks will be based on clinical centers
94 Specification of the Primary Analyses
A mixed model repeated measures (MMRM) analysis described in section 95 will be used to
compare differences in the slope of FVC measurements across the treatment groups Response
variables are values of the FVC measured at baseline and every 15 weeks until study completion
Variables in the model will include treatment time and time by treatment age sex race and
height Contrast estimates of differences in slopes of treatment over time (along with confidence
intervals) will be used to estimate the treatment effect The validity of this model in terms of
meeting modeling assumptions will be assessed via standard modeling diagnostics and goodness-
of-fit measures Based on the MMRM framework missing FVC data will not be imputed for the
primary analysis
95 Analysis of Longitudinal Endpoints
A common goal in clinical trials is to specify models that are easily implemented and
reproducible by independent data analysts On the other hand the models should have proper
statistical behavior in terms of low bias and high precision Many common approaches to
longitudinal data analysis including last observation carried forward (LOCF) imputation rely on
the missing completely at random (MCAR) assumption However the MCAR assumption is
58
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
unlikely to hold in many clinical trials because missing data are often related to disease
progression and prognosis A more reasonable assumption missing at random (MAR) specifies
that the complete data distribution can be modeled using only the observed data The likelihood-
based MMRM approach is valid under the more general MAR assumptions These models will
be applied to analyze the longitudinal data secondary endpoints
The advantages of MMRM analysis are that all important characteristics of the model can be preshy
specified standard software can be used to implement the models and results are based on ITT
principles43 In addition the MMRM approach offers superior control of Type I and Type II
errors compared with the LOCF approach
Response variables are values of the PFTs measured at enrollment and every 15 weeks until
study completion and 6MWT values measured at baseline week 30 and week 60 Covariates are
treatment time time by treatment and key baseline risk factors Contrasts (along with
confidence intervals) of treatment by time will be used to estimate the treatment effect
The correlation structure involves multiple pieces including measurement errors random
variation and interindividual variability For the longitudinal data analyses an unstructured
correlation matrix for within-subject errors will be assumed Other correlation structures
including compound symmetry will be examined as needed A careful examination of reasons
for study discontinuation will be conducted to assess the validity of MCAR Sensitivity analyses
will be used to examine the untestable assumption that the observed data violate the MAR
assumption The MMRM models will be implemented using PROC MIXED in SAS
96 Analysis of Binary Time-to-Event and Time-Lagged Endpoints
Regression modeling approaches using either the logistic regression model or Cox proportional
hazards regression model will be employed when appropriate The validity of these models will
be assessed via standard modeling diagnostics and goodness-of-fit measures Estimates of
cumulative frequencies for more general time-lagged responses will be calculated using the
partitioned version of the Bang-Tsiatis estimator44 The partitions will be set at 15-week intervals
59
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
to correspond with the data-collection process Covariate adjusted event rates will be calculated
using inverse probability-weighted regression estimates45
97 Power Analysis
971 Primary Analyses
Based on previously published IPF clinical trials the PL group is expected to experience a drop
in FVC of approximately 020 L over the study period (see Figure 1) The IPFnet Steering Group
determined a clinically important difference would be to preserve the majority of the decline
relative to PL over the study period In particular a treatment effect of 015 L was determined to
be a clinically meaningful difference Potential dropout is a key factor in the proposed study The
drop-out process assumed 5 lost to follow-up after every study visit Only 80 of subjects
were assumed to be followed for the entire study period All models assumed a compound
symmetry structure for the covariance matrix Power calculations were performed using a SAS
IML program for designing repeated measures studies46 Based on preliminary reviews of the
data from the University of Michigan the covariance matrix parameters were estimated at
approximately σ2 = 0757 (variance parameter) and ρ = 0936 (correlation parameter) To be
conservative the power calculations for the primary analysis were performed with parameter
setting of σ2 = 0810 (variance parameter) and ρ = 0925 (correlation parameter)
The power calculations assume a correction for imperfect compliance proposed by Lachin and
Foulkes to allow for 2 noncompliance for each of the treatment arms47 Thus the sample size
of 130 subjects per arm would be reduced to an adjusted sample size of 130(1-002-002)2 =
1198 or 120 subjects per arm
Under the assumed Type I error rate of 005 with a correlation parameter of 0925 and standard
deviation of 090 the difference of 015 L (or 00025 Lweek) shown in Table 6 would have
power of 93
60
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Table 6 Hypothetical Values of Mean FVC (L) Change from Baseline
Week 15 Week 30 Week 45 Week 60
NAC 00125 00250 00375 00500
Placebo 00500 01000 01500 02000
Difference 00375 00750 01125 01500
Abbreviations FVC forced vital capacity PL placebo
972 Power Analysis for Secondary Endpoints
Power calculations for secondary endpoint measurements are shown in Table 7 Standard
deviations are based on unpublished data provided by the University of Michigan The
calculations are based on a 2-sample t-test with Type I error rate set at 005 These calculations
are likely to be conservative because the statistical approach described in section 95 for
analyzing these endpoints will incorporate incomplete observations as well as intermediate data
points
Table 7 Detectable Differences in Treatment Means for Selected Endpoint Measurements
Secondary Endpoints Std Dev
of the Baseline Score
Detectable Difference for 80 Power
Std Dev of the Change Score
Difference Detectable for
80 Power
DLCOpred 166 58 91 32
6MWT Area Under the Desaturation Curve
219 76 175 61
6MWT Distance to Desaturation 224 78 315 110
6MWT Minutes Walked 210 073 205 071
Abbreviations Std Dev standard deviation DLCOpred diffusing capacity of the lung for carbon monoxide percent predicted 6MWT 6-minute walk test
61
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
10 Study Administration
101 Cooperative Agreement Mechanism
The administrative and funding mechanism used to undertake this project is a ldquocooperative
agreementrdquo (U01) which is an assistance mechanism Under the cooperative agreement the
NHLBI assists supports andor stimulates the project and is substantially involved with
investigators in conducting the study by facilitating performance of the effort in a ldquopartnerrdquo role
The NHLBI project scientist serves on the IPFnet Steering Group and he or another NHLBI
scientist may serve on other project committees when appropriate At the same time however
NHLBI does not assume a dominant role direction or prime responsibility for this research
program
As described below governance of the project is conducted through the IPFnet Steering Group
Principal investigators have lead responsibilities in all aspects of their trials and the project
including any modification of trial designs conduct of the trials quality control data analysis
and interpretation preparation of publications and collaboration with other investigators unless
otherwise provided for by the IPFnet Steering Group
PIs retain custody of and have primary rights to their center-specific and collaborative data
subject to government rights-of-access consistent with current Health amp Human Services (HHS)
Public Health Service (PHS) and National Institutes of Health policies The protocols and
governance policies call for the continual submission of data centrally to the IPFnet DCC for the
collaborative database which at a minimum will contain the key variables selected by the IPFnet
Steering Group for standardization across all clinical centers the submission of copies of the
collaborative datasets to each PI upon completion of the project procedures for data analysis
reporting and publication and procedures to protect and ensure the privacy of medical and
genetic data and records of individuals The NHLBI project scientist on behalf of the NHLBI
will have the same access privileges and responsibilities regarding the collaborative data as the
other members of the Steering Group
62
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
PIs are also encouraged to publish and to publicly release and disseminate results data and other
products of the project concordant with the project protocols and governance and the approved
plan for making data and materials available to the scientific community and to the NHLBI
However during the 3 years after the ending date of NHLBI project support unpublished data
unpublished results data sets not previously released and other study materials or products are
to be made available to any third party only with the approval of the IPFnet Steering Group
Upon completion of the project PIs are expected to put their intervention materials and
procedure manuals into the public domain andor make them available to other investigators
according to the approved plan for making data and materials available to the scientific
community and the NHLBI for the conduct of research at no charge other than the costs of
reproduction and distribution
The NHLBI reserves the right to terminate or curtail the project (or an individual award) in the
event of (a) failure to develop or implement mutually agreeable collaborative measurement
subject eligibility and data management sections of the protocols (b) substantial shortfall in
subject recruitment follow-up data reporting or quality control or other major breach of
protocol (c) substantive changes in the agreed-upon protocols with which NHLBI cannot
concur (d) reaching a major project outcome with persuasive statistical significance
substantially before schedule or (e) human subject ethical issues that may dictate a premature
termination
Any disagreement that may arise in scientificprogrammatic matters (within the scope of the
award) between award recipients and the NHLBI may be brought to arbitration An arbitration
panel will be composed of 3 membersmdash1 selected by the IPFnet Steering Group (with the
NHLBI member not voting) or by the individual PI in the event of an individual disagreement a
second selected by NHLBI and the third selected by the other 2 members This special
arbitration procedure in no way affects the PIrsquos right to appeal an adverse action that is otherwise
appealable in accordance with the PHS regulations at 42 CFR part 50 Subpart D and HHS
63
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
regulation at 45 CFR part 16 or the rights of the NHLBI under applicable statutes regulations
and terms of the award
102 IPFnet Steering Group
The IPFnet Steering Group is the main governing body of the project It is composed of the PIs
of the clinical centers the PI of the DCC and the NHLBI project scientist The clinical centers
the IPFnet DCC and the NHLBI each have 1 vote on the IPFnet Steering Group All decisions
are determined by majority vote
All major scientific decisions are determined by the IPFnet Steering Group It assumes overall
responsibility for the design and conduct of the trial It appoints (and disbands) committees and
subcommittees as the need arises designs approves and implements the study protocols
oversees the development of the MOOP monitors subject recruitment and treatment delivery
evaluates data collection and management oversees quality assurance procedures and
implements changes and enhancements to the study as required It also has primary responsibility
for facilitating the conduct of the trials and reporting the projectrsquos results
103 Data and Safety Monitoring Board
The NHLBI will establish a DSMB in accordance with established policies (see
httpwwwnhlbinihgovfundingpoliciesdsmb_insthtm) to ensure data quality and subject
safety and to provide independent advice to the NHLBI regarding progress and the
appropriateness of study continuation
104 Recommendations on Interim Monitoring of Efficacy Safety and Futility
First and foremost the role of the DSMB will be to review subject safety and trial conduct at
periodic points during the study The DSMB may require analyses of the primary endpoint
results for comparing the benefit and risks of treatment strategies The benefit of collecting
additional data on key secondary endpoints with extended follow-up and establishing a robust
64
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
evidence base for determining a standard of care will need to be carefully considered before
early termination of one or more treatment arms After careful consideration the IPFnet Steering
Group recommends conservative thresholds for the early examinations of the safety and efficacy
data
The DSMB will be expected to meet approximately every 6 months until trial completion to
review safety and toxicity data The DSMB may recommend stopping the study based on these
reviews Because the DSMB could stop the trial for safety concerns as well as for a large
efficacy benefit there could be multiple opportunities to reject the null hypothesis (no difference
in event rates between the PL and NAC groups) A Bonferroni approximation will be applied
during the one planned interim analysis for efficacy
Before locking the database a statistical analysis plan (SAP) will be developed to provide
complete details on the statistical analysis The SAP will include the specifics for how and when
the DSMB will be notified for AEs The IPFnet DCC will deliver to the DSMB all FDA-defined
AEs at 3-month intervals The IPFnet DCC will prepare narrative SAE reports in real time for
DSMB review including recommendations and analysis of similar events for each SAE
submitted to the FDA
65
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
11 Investigator and Sponsor Obligations
111 Monitoring
All monitoring activities for US clinical centers will be performed in accordance with DCRI
standard operating procedures Information regarding the types of visits will be outlined in the
PANTHER-IPF MOOP
112 Cost and Payment
There will be no cost to subjects enrolled in this trial Study-related procedures will be paid for
by the IPFnet
Subjects may be eligible for reimbursement for travel to the clinical center Details of payment
will be explained to each subject during the consent process
113 Confidentiality and Health Insurance Portability and Accountability Act
Considerations
Subject confidentiality will be protected throughout the study All subject data will be kept
strictly confidential and no subject-identifying information will be released to anyone outside
the project Confidentiality will be assured through several mechanisms First each subject will
be assigned an anonymous study ID which will then be used on all study forms Second any
study forms blood samples and paper records that contain subject information (eg address lists
phone lists) will be kept at the clinical centers in secured locked areas coded by number Once
blood is collected there will be no subject identifiers placed on blood samplesmdashonly the study
ID number and the date of sample collection Third access to all subject data and information
including laboratory specimens will be restricted to authorized personnel In the case of
computerized data this restricted access will be assured through user logon IDs and password
protection
66
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
At the IPFnet DCC only authorized personnel will have access to the data files containing study
data Security will be assured through user logon IDs passwords and appropriate access
privileges All study subjects will be identified only by their IPFnet ID numbers and no personal
identifying information such as name address or Social Security number will be entered into
the IPFnet DCC database Any subject-specific data reported to the IPFnet Steering Group will
be identified only by the IPFnet ID number
Finally subjects will not be identified by name in any reports or publications nor will the data
be presented in such a way that the identity of individual subjects can be inferred Analysis files
created for further study by the scientific community will have no subject identifiers These data
files will be created in accordance with the Ancillary Studies and Publication Policy of the
IPFnet
114 Informed Consent Procedures
All IPFnet subjects will provide written informed consent using procedures reviewed and
approved by each clinical centerrsquos IRB Informed consent will be undertaken by study personnel
in-person with the subject The subject has the option of declining further participation in the
study at that point No further study procedures will be conducted until the signed documents
have been provided to the IPFnet clinical center
115 Institutional Review Boards
Before initiating this study the protocol clinical center-specific informed consent forms Health
Insurance Portability and Accountability Act (HIPAA) forms recruitment materials and other
relevant information will be reviewed by a properly constituted IRB at each participating clinical
center A copy of the signed and dated IRB approval at each clinical center will be retrieved prior
to or during the site initiation visit and archived at the IPFnet DCC Any amendments to the
protocol other than simple administrative and typographical changes must be approved by each
IRB before they are implemented The clinical centers will seek annual renewals of their IRB
approvals in accordance with local procedures
67
__________________________________________ ________________
__________________________________________
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
12 Investigator Agreement
I have read the foregoing protocol PANTHER-IPF and agree that it contains all necessary
details for carrying out this study I will conduct the study as outlined herein and will complete
the study within the time designated
I will provide copies of the protocol and all pertinent information to all individuals responsible to
me who assist in the conduct of this study I will discuss this material with them to ensure they
are fully informed regarding the drug and the conduct of the study
I will fulfill all responsibilities for submitting pertinent information to the local IRB if
applicable that is responsible for this study
I further agree that NHLBI andor DCRI will have access to any source documents from which
eCRF information may have been generated
Signature of Principal Investigator Date
Name of Principal Investigator (printed or typed)
Protocol version date May 19 2009
Protocol Amendment 1 version date May 28 2010
Protocol Amendment 2 version date December 6 2011
68
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
13 References
1 Raghu G Brown KK Bradford WZ et al A placebo-controlled trial of interferon gamma-1b in patients with idiopathic pulmonary fibrosis N Engl J Med 2004350125-33 2 King TE Jr Safrin S Starko KM et al Analyses of efficacy end points in a controlled trial of interferon-gamma1b for idiopathic pulmonary fibrosis Chest 2005127171-7 3 Flaherty KR Thwaite EL Kazerooni EA et al Radiological versus histological diagnosis in UIP and NSIP survival implications Thorax 200358143-8 4 Wells AU Desai SR Rubens MB et al Idiopathic pulmonary fibrosis a composite physiologic index derived from disease extent observed by computed tomography Am J Respir Crit Care Med 2003167962-9 5 Raghu G Freudenberger TD Yang S et al High prevalence of abnormal acid gastroshyoesophageal reflux in idiopathic pulmonary fibrosis Eur Respir J 200627136-42 6 Kinnula VL Focus on antioxidant enzymes and antioxidant strategies in smoking related airway diseases Thorax 200560693-700 7 Coultas DB Zumwalt RE Black WC Sobonya RE The epidemiology of interstitial lung diseases Am J Respir Crit Care Med 1994150967-72 8 Raghu G Weycker D Edelsberg J Bradford WZ Oster G Incidence and prevalence of idiopathic pulmonary fibrosis Am J Respir Crit Care Med 2006174810-6 9 Olson AL Swigris JJ Lezotte DC Norris JM Wilson CG Brown KK Mortality from pulmonary fibrosis increased in the United States from 1992 to 2003 Am J Respir Crit Care Med 2007176277-84 10 Mannino DM Etzel RA Parrish RG Pulmonary fibrosis deaths in the United States 1979shy1991 An analysis of multiple-cause mortality data Am J Respir Crit Care Med 19961531548shy52 11 Hubbard R Johnston I Coultas DB Britton J Mortality rates from cryptogenic fibrosing alveolitis in seven countries Thorax 199651711-6 12 Johnston I Britton J Kinnear W Logan R Rising mortality from cryptogenic fibrosing alveolitis Bmj 19903011017-21 13 Raghu G Collard HR Egan JJ et al An official ATSERSJRSALAT statement idiopathic pulmonary fibrosis evidence-based guidelines for diagnosis and management Am J Respir Crit Care Med 2011183788-824 14 (USA) FDA FDA Public Health Advisory Interferon gamma-1b (marketed as Actimmune) In 2007 15 King TE Jr Pardo A Selman M Idiopathic pulmonary fibrosis Lancet 2011 16 Raghu G Brown KK Costabel U et al Treatment of idiopathic pulmonary fibrosis with etanercept an exploratory placebo-controlled trial Am J Respir Crit Care Med 2008178948shy55 17 Malouf MA Hopkins P Snell G Glanville AR An investigator-driven study of everolimus in surgical lung biopsy confirmed idiopathic pulmonary fibrosis Respirology 201116776-83 18 King TE Jr Behr J Brown KK et al BUILD-1 a randomized placebo-controlled trial of bosentan in idiopathic pulmonary fibrosis Am J Respir Crit Care Med 200817775-81 19 Richeldi L Costabel U Selman M et al Efficacy of a tyrosine kinase inhibitor in idiopathic pulmonary fibrosis N Engl J Med 20113651079-87
69
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
20 Borok Z Buhl R Grimes GJ et al Effect of glutathione aerosol on oxidant-antioxidant imbalance in idiopathic pulmonary fibrosis Lancet 1991338215-6 21 Meyer A Buhl R Magnussen H The effect of oral N-acetylcysteine on lung glutathione levels in idiopathic pulmonary fibrosis Eur Respir J 19947431-6 22 Behr J Maier K Degenkolb B Krombach F Vogelmeier C Antioxidative and clinical effects of high-dose N-acetylcysteine in fibrosing alveolitis Adjunctive therapy to maintenance immunosuppression Am J Respir Crit Care Med 19971561897-901 23 Cantin AM North SL Fells GA Hubbard RC Crystal RG Oxidant-mediated epithelial cell injury in idiopathic pulmonary fibrosis J Clin Invest 1987791665-73 24 Waghray M Cui Z Horowitz JC et al Hydrogen peroxide is a diffusible paracrine signal for the induction of epithelial cell death by activated myofibroblasts Faseb J 200519854-6 25 Larios JM Budhiraja R Fanburg BL Thannickal VJ Oxidative protein cross-linking reactions involving L-tyrosine in transforming growth factor-beta1-stimulated fibroblasts J Biol Chem 200127617437-41 26 Kinnula VL Fattman CL Tan RJ Oury TD Oxidative stress in pulmonary fibrosis a possible role for redox modulatory therapy Am J Respir Crit Care Med 2005172417-22 27 Meyer A Buhl R Kampf S Magnussen H Intravenous N-acetylcysteine and lung glutathione of patients with pulmonary fibrosis and normals Am J Respir Crit Care Med 19951521055-60 28 Behr J Degenkolb B Krombach F Vogelmeier C Intracellular glutathione and bronchoalveolar cells in fibrosing alveolitis effects of N-acetylcysteine Eur Respir J 200219906-11 29 Bando M Hosono T Mato N et al Long-term efficacy of inhaled N-acetylcysteine in patients with idiopathic pulmonary fibrosis Intern Med 2010492289-96 30 Demedts M Behr J Buhl R et al High-dose acetylcysteine in idiopathic pulmonary fibrosis N Engl J Med 20053532229-42 31 Toma TP Bhowmik A Rajakulasingam R Acetylcysteine in pulmonary fibrosis N Engl J Med 20063541086-9 author reply -9 32 Hunninghake GW Antioxidant therapy for idiopathic pulmonary fibrosis N Engl J Med 20053532285-7 33 Flaherty KR Mumford JA Murray S et al Prognostic implications of physiologic and radiographic changes in idiopathic interstitial pneumonia Am J Respir Crit Care Med 2003168543-8 34 Latsi PI du Bois RM Nicholson AG et al Fibrotic idiopathic interstitial pneumonia the prognostic value of longitudinal functional trends Am J Respir Crit Care Med 2003168531-7 35 Collard HR King TE Jr Bartelson BB Vourlekis JS Schwarz MI Brown KK Changes in clinical and physiologic variables predict survival in idiopathic pulmonary fibrosis Am J Respir Crit Care Med 2003168538-42 36 Jegal Y Kim DS Shim TS et al Physiology is a stronger predictor of survival than pathology in fibrotic interstitial pneumonia Am J Respir Crit Care Med 2005171639-44 37 Martinez FJ Safrin S Weycker D et al The clinical course of patients with idiopathic pulmonary fibrosis Ann Intern Med 2005142963-7 38 Hull JH Acetylcysteine in pulmonary fibrosis N Engl J Med 20063541089-91 author reply -91
70
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
39 Flaherty KR King TE Jr Raghu G et al Idiopathic interstitial pneumonia what is the effect of a multidisciplinary approach to diagnosis Am J Respir Crit Care Med 2004170904shy10 40 Raghu G Johnson WC Lockhart D Mageto Y Treatment of idiopathic pulmonary fibrosis with a new antifibrotic agent pirfenidone results of a prospective open-label Phase II study Am J Respir Crit Care Med 19991591061-9 41 Hunninghake GW Lynch DA Galvin JR et al Radiologic findings are strongly associated with a pathologic diagnosis of usual interstitial pneumonia Chest 20031241215-23 42 Lynch D Godwin J Safrin S et al High-resolution computed tomography in idiopathic pulmonary fibrosis diagnosis and prognosis Am J Respir Crit Care Med 2005172488-93 43 Mallinckrodt CH Watkin JG Molenberghs G Carroll RJ Choice of the primary analysis in longitudinal clinical trials Pharmaceutical Statistics 20043161-9 44 Bang H Tsiatis A Estimating medical costs with censored data Biometrika 200087329shy43 45 Lin DY Regression analysis of incomplete medical cost data Stat Med 2003221181-200 46 Rochon J Application of GEE procedures for sample size calculations in repeated measures experiments Stat Med 1998171643-58 47 Lachin JM Foulkes MA Evaluation of sample size and power for analyses of survival with allowance for nonuniform patient entry losses to follow-up noncompliance and stratification Biometrics 198642507-19
71
- PANTHER-IPFPREDNISONE AZATHIOPRINEAND N-ACETYLCYSTEINEA STUDY THAT EVALUATES RESPONSE INIDIOPATHIC PULMONARY FIBROSIS
-
- Protocol Summary
- Table of Contents
- List of Tables
- List of Figures
- List of Abbreviations
- 1 Summary
- 2 Hypotheses and Specific Aims
-
- 21 Null Hypothesis
- 22 Specific Aim 1
- 23 Specific Aim 2
- 24 Prespecified Subgroups of Interest
-
- 3 Background and Significance
-
- 31 Idiopathic Pulmonary Fibrosis is the Most Common Interstitial Lung Disease
- 32 Rationale for Placebo Control
- 33 Rationale for N-acetylcysteine
- 35 Rationale for N-acetylcysteine as a Stand-alone Therapy
- 36 Rationale for the Study Design and Primary Endpoint
- 37 Rationale for Blinding of Treatments
-
- 4 Methods
-
- 41 Inclusion Criteria
- 42 Diagnosis of IPF
- 43 Exclusion Criteria
- 44 Study Design and Study Visit
- 45 Dose Justification
- 46 Contraindications Precautions and Side Effects of Study Medications
- 47 Recruitment Procedures
- 48 Study Procedures
- 49 Concomitant Medications
- 410 Laboratory Testing
- 411 Blinding of Study Drugs
-
- 5 Study Endpoints
-
- 51 Primary Study Endpoint
- 52 Secondary Study Endpoints
-
- 6 Safety Evaluations and Procedures
-
- 61 Adverse Events
- 62 Clinical Medical Monitoring
- 63 Unblinding Procedures
-
- 7 Study Drug Procedures
- 8 Data Management
-
- 81 Hardware and Software Configuration
- 82 Sources of Data
-
- 9 Study Design and Data Analysis
-
- 91 General Analytic Considerations
- 92 Randomization Blinding and Reporting of Results
- 93 Stratification
- 94 Specification of the Primary Analyses
- 95 Analysis of Longitudinal Endpoints
- 96 Analysis of Binary Time-to-Event and Time-Lagged Endpoints
- 97 Power Analysis
-
- 10 Study Administration
-
- 101 Cooperative Agreement Mechanism
- 102 IPFnet Steering Group
- 103 Data and Safety Monitoring Board
- 104 Recommendations on Interim Monitoring of Efficacy Safety and Futility
-
- 11 Investigator and Sponsor Obligations
-
- 111 Monitoring
- 112 Cost and Payment
- 113 Confidentiality and Health Insurance Portability and Accountability ActConsiderations
- 114 Informed Consent Procedures
- 115 Institutional Review Boards
-
- 12 Investigator Agreement
- 13 References
-

PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
5 Study Endpoints
51 Primary Study Endpoint
The primary endpoint will be the change in serial measurements of FVC over the study period
52 Secondary Study Endpoints
521 Time to Disease-progression
The time-to-death or a 10 decline in FVC will be defined as the time-to-disease progression
The 10 decline in FVC from enrollment must be confirmed on 2 consecutive visits no less than
6 weeks apart For subjects with 2 consecutive visits with a 10 decline in FVC the time-toshy
disease progression will be defined as the time interval between enrollment and the initial visit
with a 10 FVC decline For subjects who experience disease progression the study doctor will
determine whether or not the subject will remain in the study
522 Acute Exacerbations
The following 3 criteria will define AEx in subjects with acute worsening of their respiratory
conditions
1 Clinical (all of the following required)
A) Unexplained worsening of dyspnea or cough within 30 days triggering unscheduled
medical care (eg emergency room clinic study visit hospitalization)
B) No clinical suspicion or overt evidence of cardiac event pulmonary embolism or deep
venous thrombosis to explain acute worsening of dyspnea
C) No pneumothorax
44
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
2 RadiologicPhysiologic (A and B required)
A) New ground glass opacity or consolidation computed tomography (CT) scan OR new
alveolar opacities on chest x-ray
B) Decline of ge 5 in resting room air SpO2 from last recorded level OR decline of ge 8 mm
Hg in resting room air PaO2 from last recorded level
3 Microbiologic (all of the following required)
A) No clinical evidence for infection (ie absence of grossly purulent sputum fever gt 39degC
orally)
B) Lack of positive microbiological results (if done) from lower respiratory tract defined as
(1) Clinically significant bacterial growth on sputum or endotracheal aspirate cultures
(2) Quantitative culture by protected brush specimen ge 103 cfumL or BAL ge 104 cfumL
(3) The presence of specific pathogens on stains of any of the above
C) Lack of positive pathogen in blood cultures (if done)
Identification of Acute Exacerbations
All subjects will be educated about the importance of identifying AExs At the time of
enrollment subjects will be told about the possibility of developing acute symptomatic
worsening that might represent an AEx of IPF and instructed to contact their study clinical
center coordinator within 48 to 72 hours of the apparent event
All subjects will be contacted by phone monthly and questioned about any change in dyspnea or
cough and any interim clinic visits or hospitalizations Finally as part of the IPFnet outreach to
community referring physicians the importance of AExs will be emphasized When a subject is
identified who meets criterion 1A this will trigger the collection of additional clinical data to
evaluate a suspected AEx These data will be collected as part of standard clinical care (ie this
protocol does not require collection of all items) The additional items to be collected for
suspected AEx include
IPFnet AEx case report form (eCRF) (required)
45
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Chest x-ray CT scan withwithout pulmonary angiogram (reports should be faxed and
followed by the hard copiesdiscs)
Oxygen saturation (pulse oximetry)
ABG
Respiratory cultures (sputum endotracheal aspirate lavage)
Blood cultures
Clinichospital records related to the event
All potential cases of AEx will be reviewed by the clinical center PI first and a decision on
whether the case may represent an AEx will be made If AEx is suspected the case will be sent
to the IPFnet adjudication committee which will assign a final diagnosis (see Table 5) If there is
disagreement among members the majority opinion will be recorded
During episodes of suspected AEx as determined by the individual clinical center investigator
subjects will remain blinded and in the study
Table 5 Final Diagnoses in Evaluation of Suspected Acute Exacerbations
Definite acute exacerbation All criteria met no alternative etiology
Unclassifiable acute worsening
Insufficient data to evaluate all criteria no alternative etiology
Not acute exacerbation Alternative etiology identified that explains acute worsening
Management of the suspected AEx will be at the discretion of the treating physician Standard of
care generally involves evaluation for respiratory infection pulmonary embolism cardiac events
and pneumothorax and treatment with IV corticosteroids
Study drugs will be resumed at pre-suspected AEx doses after subjects clinically improve as
confirmed by the local PI All subjects should be seen at the clinical center within 2 to 4 weeks
of recovery for measurement of post-bronchodilator FVC (see Figure 4) Subjects unable to
return to the clinical center after suspected AEx due to medical frailty (eg continued
46
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
institutionalization progressive disability) will be categorized as failing to maintain FVC
response in secondary analyses
Suspected AEx (PI determined)
Hold study drug Treat AEx
(Attending physician determined)
Alive but unable to continue due to
medical frailty
Dead
Alive and able to continue
Site reviewvisit
Restart study drug
FVC within 2-4 weeks
Figure 4 Acute Exacerbation Flow Chart
523 Respiratory Infections
An upper respiratory infection will be defined as
Change in sputum discoloration
Increased cough of no more than 14 daysrsquo duration
A lower-respiratory infection (pneumonia) will be defined as new segmental or lobar airspace
opacities visualized by image studies (chest radiograph or HRCT) in addition to any of the
following
Positive pathogencultures in good sample of sputum or lower-airway secretions retrieved
by fiberoptic bronchoscope
Fever gt 39degC or gt 100degF
Leukocytosis gt 12000 (unexplained no increase in dose of corticosteroids)
47
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
524 Maintained FVC Response
Subjects with follow-up FVCpred measurements at or above their baseline FVCpred level
will be classified as having maintained FVC response Subjects with reduced FVCpred levels
or missing data for any reason including death or medical frailty will be classified as having not
maintained FVC response The FVCpred value is used because unadjusted FVC measurements
are expected to decline with age
48
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
6 Safety Evaluations and Procedures
61 Adverse Events
During a clinical trial the reporting of adverse experience information can lead to important
changes in the way a new treatment is developed as well as provide integral safety data
611 Definitions
An adverse event (AE) is any untoward medical occurrence in a subject or clinical investigation
subject who was administered a pharmaceutical product The AE does not necessarily have to
have a causal relationship with the drug administered An AE can be any unfavorable and
unintended sign (including an abnormal laboratory finding) symptom or disease temporarily
associated with the use of a medicinal product whether or not considered to be related to the
medicinal product Diseases signs symptoms or laboratory abnormalities already existing at
enrollment are not considered AEs unless they worsen (ie increase in intensity or frequency)
Surgical procedures themselves are not AEs they are therapeutic measures for conditions that
require surgery The condition for which the surgery is required may be an AE Surgical
procedures planned before randomization and the conditions necessitating the surgery are not
AEs
A serious adverse event is any untoward event that
Is fatal
Is life-threatening
Requires inpatient hospitalization or prolongation of existing hospitalization with the
following exceptions
o Preplanned (before the study) hospital admissions unless the hospitalization is
prolonged
o Planned admissions (as part of a study eg routine biopsies)
o Hospitalization lasting lt 24 hours
49
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
o Hospitalization for elective procedure
o Emergency room visits
Results in persistent or significant disability or incapacity
Is a congenital anomaly or birth defect
Important medical events that may not result in death be life-threatening or require
inpatient hospitalization may be considered serious adverse events (SAEs) when based
on appropriate medical judgment they may jeopardize the subject and may require
medical or surgical intervention to prevent one of the outcomes listed above
Life-threatening means that the subject was in the view of the investigator at immediate risk of
death from the AE as it occurred It does not include an AE that had it occurred in a more severe
form might have caused death
Persistent or significant disabilityincapacity means that the event resulted in permanent or
significant and substantial disruption of the subjectrsquos ability to carry out normal life functions
Causality
A reasonable possibility means the AE may have been caused byrelated to the study drug A
perceived or real lack of efficacy does not satisfy the definition of relatedness
612 Adverse Event (AE) Reporting
For the PANTHER-IPF trial all AEs (serious and nonserious) occurring from randomization
through final study visit (4 weeks after final dose of all study medication) will be recorded on the
AE page of the case report form (CRF)
6121 Serious Adverse Events (SAE) Reporting
For this trial all deaths and all SAEs which occur from randomization through final study visit
must be entered within the EDC system via the SAE eCRF page within 24 hours of the
investigative sitersquos knowledge of the event It is the responsibility of the clinical center
50
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
investigator to provide a causality assessment of the event for each study medications based upon
the information available at the time of the report It is understood that complete information
about the event may not be known at the time the initial report is submitted In the event the EDC
system is not accessible to the site at the time of event reporting investigative sites will complete
and forward a paper back-up SAE form to DCRI Safety Surveillance for processing
DCRI Safety Surveillance
Telephone 1-919-668-8624 or 1-866-668-7799 (toll free)
Fax 1-919-668-7138 or 1-866-668-7138 (toll free)
The investigator must complete and submit follow-up SAE information via the eCRF when
important new or follow-up information (eg final diagnosis outcome results of specific
investigations) becomes available Follow-up information should be submitted according to the
same process used for reporting the initial event as described above All SAEs will be followed
until resolution stabilization or 30 days after the subject has completed the final visit (4 weeks
after the final dose of study medication) whichever occurs first The investigator is responsible
for reporting SAEs to their institutional review board (IRB) per site specific IRB reporting
guidelines
6122 Regulatory Reporting
AEs that are serious study drug related and unexpected will be reported to the regulatory
authorities The DCRI Safety Surveillance medical monitor will perform a medical review of all
SAEs submitted and evaluate for ldquounexpectednessrdquo DCRI Safety Surveillance will prepare
MedWatch reports for those events identified as serious study drug related and unexpected as
determined by Safety Medical Monitor
DCRI Regulatory Services will submit all unexpected study drug-related SAEs as per 21 CFR
32 DCRI Safety Surveillance will provide a safety alert letter to the NHLBI DSMB and DCC
clinical operation (for distribution to sites) within 15 days of initial receipt of the information
51
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Investigators are responsible for promptly reporting these events to their reviewing IRBs
according to site specific IRB reporting guidelines
62 Clinical Medical Monitoring
There will be an unblinded physician at the IPFnet DCC serving as medical monitor The
medical monitor will be available to assist with questions about dosage adjustments of study
medications including discontinuation or resumption of medications
63 Unblinding Procedures
Unblinding of subjects or investigators to subject treatment is strongly discouraged For ongoing
clinical management all subjects should be presumed to be receiving ldquoactiverdquo study drug To
ensure the subjectrsquos safety the study treatment will be dose-adjusted based on laboratory test
results clinical findings and symptoms
The IPFnet DCC medical monitor and PANTHER-IPF co-chairs Drs Ganesh Raghu and
Fernando Martinez will be available to the study physicians to discuss study drug management
on a case-by-case basis Un-blinding will be considered ONLY when the knowledge of subject
treatment assignment is ABSOLUTELY ESSENTIAL for subject safety and after discussion of
the subjectrsquos case with the medical monitor and either Dr Raghu or Dr Martinez Unblinding of
study treatment should be minimized during the conduct of the trial In those cases where it is
felt to be medically necessary the DCC medical officer will communicate directly with the
managing physician to minimize unblinding of study personnel
52
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
7 Study Drug Procedures
At the baseline 15-week 30-week and 45-week study visits subjects will receive a supply of
study drug sufficient to last until the next visit at which study drug will be dispensed
53
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
8 Data Management
81 Hardware and Software Configuration
811 Hardware and Database Software
Data will be stored in an Oracle database system Oracle has advantages of processing efficiency
and smooth linkage with other software systems The application and database will be hosted on
Solaris Unix servers at the IPFnet DCC
812 Statistical Software
SAS will be used as the principal application for the management of analysis data files and
statistical computations S-Plus will be used to provide supplementary functions as needed
813 Access Control and Confidentiality Procedures
Access to databases will be controlled centrally by the IPFnet DCC through user passwords
linked to appropriate privileges This protects the data from unauthorized changes and
inadvertent loss or damage
814 Security
Database and Web servers will be secured by a firewall and through controlled physical access
Oracle has many security features to ensure that any staff member accessing the database has the
proper authority to perform the functions he or she requests of the system Within the secondary
SAS databases Unix group-access control maintains similar security The Sun workstation login
is secured by extensive user-password facilities under Unix
54
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
815 Back-up Procedures
Database back-up will be performed automatically every day and standard IPFnet DCC policies
and procedures will be applied to dictate tape rotation and retention practices
816 Virus Protection
All disk drives that provide network services and all user computers will be protected using
virus-scanning software Standard IPFnet DCC policies will be applied to update these protection
systems periodically through the study
82 Sources of Data
821 Design and Development
The IPFnet DCC will be responsible for development of the electronic case report forms
(eCRFs) development and validation of the clinical study database ensuring data integrity and
training clinical center staff on applicable data management procedures A web-based distributed
data entry model will be implemented This system will be developed to ensure that guidelines
and regulations surrounding the use of computerized systems used in clinical trials are upheld
The remainder of this section provides an overview of the data management plan associated with
this protocol
822 Data Collection Forms
The data collection process consists of direct data entry at the study clinical centers into the EDC
system(s) provided by the DCC A data collection worksheet will be provided to clinical centers
for recording data in the event the EDC system is unavailable Data entry of the eCRFs should
be completed according to the instructions provided and project specific training The
investigator is responsible for maintaining accurate complete and up-to-date records and for
ensuring the completion of the eCRFs for each research participant
55
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
823 Data Acquisition and Entry
Data entry into eCRFs shall be performed by authorized individuals Selected eCRFs may also
require the investigatorrsquos written signature or electronic signature as appropriate Electronic
CRFs will be monitored for completeness accuracy and attention to detail during the study
824 Data Center Responsibilities
The IPFnet DCC will 1) develop a data management plan and will conduct data management
activities 2) provide final eCRFs for the collection of all data required by the study 3) develop
data dictionaries for each eCRF that will comprehensively define each data element 4) conduct
ongoing data monitoring activities on study data 5) monitor any preliminary analysis data
cleanup activities and 6) rigorously monitor final study data clean up
825 Data Editing
Completed data will be entered into the IPFnet DCC automated data acquisition and
management system If incomplete or inaccurate data are found a data clarification request will
be generated and distributed to clinical centers for a response Clinical centers will resolve data
inconsistencies and errors and enter all corrections and changes into the IPFnet DCC automated
data acquisition and management system
826 Training
The training plan for clinical center staff includes provisions for training on assessments eCRF
completion guidelines data management procedures and the use of computerized systems
56
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
9 Study Design and Data Analysis
91 General Analytic Considerations
All primary analyses will be based on intent-to-treat (ITT) principles using all randomized
subjects Baseline factors across groups will be compared using mean (standard deviation) and
median (25th and 75th percentiles) summary measures Kaplan-Meier curves will be used to
display event rates Due to clinical interest in departures from both sides of the null hypothesis
all test statistics will be 2-sided
Reasonable caution needs to be taken when conducting multiple analyses on key clinical
subgroups For subgroup analyses a conservative significance level of 0001 will be used for all
interaction tests Thus subgroup comparisons will be considered exploratory unless the p-value
from the interaction test is smaller than 0001
92 Randomization Blinding and Reporting of Results
A permuted block-randomization scheme will be created with varying block sizes stratified by
clinical center Once a subject has completed the screening and baseline period and evaluation
for inclusionexclusion criteria the randomization process will begin Subjects will be
randomized to receive NAC or matching placebo with equal probability (11) via telephone
contact with a central interactive voice response system (IVRS) using a toll-free randomization
number On the day of randomization after the subject has successfully met all inclusion and
exclusion criteria the investigator or designee will call the central randomization number to
obtain the assigned kit randomization numbers for that subject At each subject visit the
investigator or designee will call the central randomization number to obtain the new kit
randomization numbers for resupply of the subject For resupply of the clinical center the IVRS
will monitor minimal volume of a kit type andor expiration date and will automatically notify
the pharmacy
57
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
The trial results will be reported according to guidelines specified in the CONSORT statement
A flow diagram describing screening recruitment randomization dropout and vital status will
be included in the primary manuscript AEs and efficacy data will be presented for all treatment
groups Adherence dropout and lost to follow-up will be carefully examined across all treatment
groups Analyses of safety will be based on data from all randomized subjects who received at
least one dose of study drug
93 Stratification
Subjects will be distributed to the two treatment arms in a 11 allocation ratio Stratification
blocks will be based on clinical centers
94 Specification of the Primary Analyses
A mixed model repeated measures (MMRM) analysis described in section 95 will be used to
compare differences in the slope of FVC measurements across the treatment groups Response
variables are values of the FVC measured at baseline and every 15 weeks until study completion
Variables in the model will include treatment time and time by treatment age sex race and
height Contrast estimates of differences in slopes of treatment over time (along with confidence
intervals) will be used to estimate the treatment effect The validity of this model in terms of
meeting modeling assumptions will be assessed via standard modeling diagnostics and goodness-
of-fit measures Based on the MMRM framework missing FVC data will not be imputed for the
primary analysis
95 Analysis of Longitudinal Endpoints
A common goal in clinical trials is to specify models that are easily implemented and
reproducible by independent data analysts On the other hand the models should have proper
statistical behavior in terms of low bias and high precision Many common approaches to
longitudinal data analysis including last observation carried forward (LOCF) imputation rely on
the missing completely at random (MCAR) assumption However the MCAR assumption is
58
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
unlikely to hold in many clinical trials because missing data are often related to disease
progression and prognosis A more reasonable assumption missing at random (MAR) specifies
that the complete data distribution can be modeled using only the observed data The likelihood-
based MMRM approach is valid under the more general MAR assumptions These models will
be applied to analyze the longitudinal data secondary endpoints
The advantages of MMRM analysis are that all important characteristics of the model can be preshy
specified standard software can be used to implement the models and results are based on ITT
principles43 In addition the MMRM approach offers superior control of Type I and Type II
errors compared with the LOCF approach
Response variables are values of the PFTs measured at enrollment and every 15 weeks until
study completion and 6MWT values measured at baseline week 30 and week 60 Covariates are
treatment time time by treatment and key baseline risk factors Contrasts (along with
confidence intervals) of treatment by time will be used to estimate the treatment effect
The correlation structure involves multiple pieces including measurement errors random
variation and interindividual variability For the longitudinal data analyses an unstructured
correlation matrix for within-subject errors will be assumed Other correlation structures
including compound symmetry will be examined as needed A careful examination of reasons
for study discontinuation will be conducted to assess the validity of MCAR Sensitivity analyses
will be used to examine the untestable assumption that the observed data violate the MAR
assumption The MMRM models will be implemented using PROC MIXED in SAS
96 Analysis of Binary Time-to-Event and Time-Lagged Endpoints
Regression modeling approaches using either the logistic regression model or Cox proportional
hazards regression model will be employed when appropriate The validity of these models will
be assessed via standard modeling diagnostics and goodness-of-fit measures Estimates of
cumulative frequencies for more general time-lagged responses will be calculated using the
partitioned version of the Bang-Tsiatis estimator44 The partitions will be set at 15-week intervals
59
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
to correspond with the data-collection process Covariate adjusted event rates will be calculated
using inverse probability-weighted regression estimates45
97 Power Analysis
971 Primary Analyses
Based on previously published IPF clinical trials the PL group is expected to experience a drop
in FVC of approximately 020 L over the study period (see Figure 1) The IPFnet Steering Group
determined a clinically important difference would be to preserve the majority of the decline
relative to PL over the study period In particular a treatment effect of 015 L was determined to
be a clinically meaningful difference Potential dropout is a key factor in the proposed study The
drop-out process assumed 5 lost to follow-up after every study visit Only 80 of subjects
were assumed to be followed for the entire study period All models assumed a compound
symmetry structure for the covariance matrix Power calculations were performed using a SAS
IML program for designing repeated measures studies46 Based on preliminary reviews of the
data from the University of Michigan the covariance matrix parameters were estimated at
approximately σ2 = 0757 (variance parameter) and ρ = 0936 (correlation parameter) To be
conservative the power calculations for the primary analysis were performed with parameter
setting of σ2 = 0810 (variance parameter) and ρ = 0925 (correlation parameter)
The power calculations assume a correction for imperfect compliance proposed by Lachin and
Foulkes to allow for 2 noncompliance for each of the treatment arms47 Thus the sample size
of 130 subjects per arm would be reduced to an adjusted sample size of 130(1-002-002)2 =
1198 or 120 subjects per arm
Under the assumed Type I error rate of 005 with a correlation parameter of 0925 and standard
deviation of 090 the difference of 015 L (or 00025 Lweek) shown in Table 6 would have
power of 93
60
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Table 6 Hypothetical Values of Mean FVC (L) Change from Baseline
Week 15 Week 30 Week 45 Week 60
NAC 00125 00250 00375 00500
Placebo 00500 01000 01500 02000
Difference 00375 00750 01125 01500
Abbreviations FVC forced vital capacity PL placebo
972 Power Analysis for Secondary Endpoints
Power calculations for secondary endpoint measurements are shown in Table 7 Standard
deviations are based on unpublished data provided by the University of Michigan The
calculations are based on a 2-sample t-test with Type I error rate set at 005 These calculations
are likely to be conservative because the statistical approach described in section 95 for
analyzing these endpoints will incorporate incomplete observations as well as intermediate data
points
Table 7 Detectable Differences in Treatment Means for Selected Endpoint Measurements
Secondary Endpoints Std Dev
of the Baseline Score
Detectable Difference for 80 Power
Std Dev of the Change Score
Difference Detectable for
80 Power
DLCOpred 166 58 91 32
6MWT Area Under the Desaturation Curve
219 76 175 61
6MWT Distance to Desaturation 224 78 315 110
6MWT Minutes Walked 210 073 205 071
Abbreviations Std Dev standard deviation DLCOpred diffusing capacity of the lung for carbon monoxide percent predicted 6MWT 6-minute walk test
61
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
10 Study Administration
101 Cooperative Agreement Mechanism
The administrative and funding mechanism used to undertake this project is a ldquocooperative
agreementrdquo (U01) which is an assistance mechanism Under the cooperative agreement the
NHLBI assists supports andor stimulates the project and is substantially involved with
investigators in conducting the study by facilitating performance of the effort in a ldquopartnerrdquo role
The NHLBI project scientist serves on the IPFnet Steering Group and he or another NHLBI
scientist may serve on other project committees when appropriate At the same time however
NHLBI does not assume a dominant role direction or prime responsibility for this research
program
As described below governance of the project is conducted through the IPFnet Steering Group
Principal investigators have lead responsibilities in all aspects of their trials and the project
including any modification of trial designs conduct of the trials quality control data analysis
and interpretation preparation of publications and collaboration with other investigators unless
otherwise provided for by the IPFnet Steering Group
PIs retain custody of and have primary rights to their center-specific and collaborative data
subject to government rights-of-access consistent with current Health amp Human Services (HHS)
Public Health Service (PHS) and National Institutes of Health policies The protocols and
governance policies call for the continual submission of data centrally to the IPFnet DCC for the
collaborative database which at a minimum will contain the key variables selected by the IPFnet
Steering Group for standardization across all clinical centers the submission of copies of the
collaborative datasets to each PI upon completion of the project procedures for data analysis
reporting and publication and procedures to protect and ensure the privacy of medical and
genetic data and records of individuals The NHLBI project scientist on behalf of the NHLBI
will have the same access privileges and responsibilities regarding the collaborative data as the
other members of the Steering Group
62
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
PIs are also encouraged to publish and to publicly release and disseminate results data and other
products of the project concordant with the project protocols and governance and the approved
plan for making data and materials available to the scientific community and to the NHLBI
However during the 3 years after the ending date of NHLBI project support unpublished data
unpublished results data sets not previously released and other study materials or products are
to be made available to any third party only with the approval of the IPFnet Steering Group
Upon completion of the project PIs are expected to put their intervention materials and
procedure manuals into the public domain andor make them available to other investigators
according to the approved plan for making data and materials available to the scientific
community and the NHLBI for the conduct of research at no charge other than the costs of
reproduction and distribution
The NHLBI reserves the right to terminate or curtail the project (or an individual award) in the
event of (a) failure to develop or implement mutually agreeable collaborative measurement
subject eligibility and data management sections of the protocols (b) substantial shortfall in
subject recruitment follow-up data reporting or quality control or other major breach of
protocol (c) substantive changes in the agreed-upon protocols with which NHLBI cannot
concur (d) reaching a major project outcome with persuasive statistical significance
substantially before schedule or (e) human subject ethical issues that may dictate a premature
termination
Any disagreement that may arise in scientificprogrammatic matters (within the scope of the
award) between award recipients and the NHLBI may be brought to arbitration An arbitration
panel will be composed of 3 membersmdash1 selected by the IPFnet Steering Group (with the
NHLBI member not voting) or by the individual PI in the event of an individual disagreement a
second selected by NHLBI and the third selected by the other 2 members This special
arbitration procedure in no way affects the PIrsquos right to appeal an adverse action that is otherwise
appealable in accordance with the PHS regulations at 42 CFR part 50 Subpart D and HHS
63
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
regulation at 45 CFR part 16 or the rights of the NHLBI under applicable statutes regulations
and terms of the award
102 IPFnet Steering Group
The IPFnet Steering Group is the main governing body of the project It is composed of the PIs
of the clinical centers the PI of the DCC and the NHLBI project scientist The clinical centers
the IPFnet DCC and the NHLBI each have 1 vote on the IPFnet Steering Group All decisions
are determined by majority vote
All major scientific decisions are determined by the IPFnet Steering Group It assumes overall
responsibility for the design and conduct of the trial It appoints (and disbands) committees and
subcommittees as the need arises designs approves and implements the study protocols
oversees the development of the MOOP monitors subject recruitment and treatment delivery
evaluates data collection and management oversees quality assurance procedures and
implements changes and enhancements to the study as required It also has primary responsibility
for facilitating the conduct of the trials and reporting the projectrsquos results
103 Data and Safety Monitoring Board
The NHLBI will establish a DSMB in accordance with established policies (see
httpwwwnhlbinihgovfundingpoliciesdsmb_insthtm) to ensure data quality and subject
safety and to provide independent advice to the NHLBI regarding progress and the
appropriateness of study continuation
104 Recommendations on Interim Monitoring of Efficacy Safety and Futility
First and foremost the role of the DSMB will be to review subject safety and trial conduct at
periodic points during the study The DSMB may require analyses of the primary endpoint
results for comparing the benefit and risks of treatment strategies The benefit of collecting
additional data on key secondary endpoints with extended follow-up and establishing a robust
64
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
evidence base for determining a standard of care will need to be carefully considered before
early termination of one or more treatment arms After careful consideration the IPFnet Steering
Group recommends conservative thresholds for the early examinations of the safety and efficacy
data
The DSMB will be expected to meet approximately every 6 months until trial completion to
review safety and toxicity data The DSMB may recommend stopping the study based on these
reviews Because the DSMB could stop the trial for safety concerns as well as for a large
efficacy benefit there could be multiple opportunities to reject the null hypothesis (no difference
in event rates between the PL and NAC groups) A Bonferroni approximation will be applied
during the one planned interim analysis for efficacy
Before locking the database a statistical analysis plan (SAP) will be developed to provide
complete details on the statistical analysis The SAP will include the specifics for how and when
the DSMB will be notified for AEs The IPFnet DCC will deliver to the DSMB all FDA-defined
AEs at 3-month intervals The IPFnet DCC will prepare narrative SAE reports in real time for
DSMB review including recommendations and analysis of similar events for each SAE
submitted to the FDA
65
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
11 Investigator and Sponsor Obligations
111 Monitoring
All monitoring activities for US clinical centers will be performed in accordance with DCRI
standard operating procedures Information regarding the types of visits will be outlined in the
PANTHER-IPF MOOP
112 Cost and Payment
There will be no cost to subjects enrolled in this trial Study-related procedures will be paid for
by the IPFnet
Subjects may be eligible for reimbursement for travel to the clinical center Details of payment
will be explained to each subject during the consent process
113 Confidentiality and Health Insurance Portability and Accountability Act
Considerations
Subject confidentiality will be protected throughout the study All subject data will be kept
strictly confidential and no subject-identifying information will be released to anyone outside
the project Confidentiality will be assured through several mechanisms First each subject will
be assigned an anonymous study ID which will then be used on all study forms Second any
study forms blood samples and paper records that contain subject information (eg address lists
phone lists) will be kept at the clinical centers in secured locked areas coded by number Once
blood is collected there will be no subject identifiers placed on blood samplesmdashonly the study
ID number and the date of sample collection Third access to all subject data and information
including laboratory specimens will be restricted to authorized personnel In the case of
computerized data this restricted access will be assured through user logon IDs and password
protection
66
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
At the IPFnet DCC only authorized personnel will have access to the data files containing study
data Security will be assured through user logon IDs passwords and appropriate access
privileges All study subjects will be identified only by their IPFnet ID numbers and no personal
identifying information such as name address or Social Security number will be entered into
the IPFnet DCC database Any subject-specific data reported to the IPFnet Steering Group will
be identified only by the IPFnet ID number
Finally subjects will not be identified by name in any reports or publications nor will the data
be presented in such a way that the identity of individual subjects can be inferred Analysis files
created for further study by the scientific community will have no subject identifiers These data
files will be created in accordance with the Ancillary Studies and Publication Policy of the
IPFnet
114 Informed Consent Procedures
All IPFnet subjects will provide written informed consent using procedures reviewed and
approved by each clinical centerrsquos IRB Informed consent will be undertaken by study personnel
in-person with the subject The subject has the option of declining further participation in the
study at that point No further study procedures will be conducted until the signed documents
have been provided to the IPFnet clinical center
115 Institutional Review Boards
Before initiating this study the protocol clinical center-specific informed consent forms Health
Insurance Portability and Accountability Act (HIPAA) forms recruitment materials and other
relevant information will be reviewed by a properly constituted IRB at each participating clinical
center A copy of the signed and dated IRB approval at each clinical center will be retrieved prior
to or during the site initiation visit and archived at the IPFnet DCC Any amendments to the
protocol other than simple administrative and typographical changes must be approved by each
IRB before they are implemented The clinical centers will seek annual renewals of their IRB
approvals in accordance with local procedures
67
__________________________________________ ________________
__________________________________________
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
12 Investigator Agreement
I have read the foregoing protocol PANTHER-IPF and agree that it contains all necessary
details for carrying out this study I will conduct the study as outlined herein and will complete
the study within the time designated
I will provide copies of the protocol and all pertinent information to all individuals responsible to
me who assist in the conduct of this study I will discuss this material with them to ensure they
are fully informed regarding the drug and the conduct of the study
I will fulfill all responsibilities for submitting pertinent information to the local IRB if
applicable that is responsible for this study
I further agree that NHLBI andor DCRI will have access to any source documents from which
eCRF information may have been generated
Signature of Principal Investigator Date
Name of Principal Investigator (printed or typed)
Protocol version date May 19 2009
Protocol Amendment 1 version date May 28 2010
Protocol Amendment 2 version date December 6 2011
68
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
13 References
1 Raghu G Brown KK Bradford WZ et al A placebo-controlled trial of interferon gamma-1b in patients with idiopathic pulmonary fibrosis N Engl J Med 2004350125-33 2 King TE Jr Safrin S Starko KM et al Analyses of efficacy end points in a controlled trial of interferon-gamma1b for idiopathic pulmonary fibrosis Chest 2005127171-7 3 Flaherty KR Thwaite EL Kazerooni EA et al Radiological versus histological diagnosis in UIP and NSIP survival implications Thorax 200358143-8 4 Wells AU Desai SR Rubens MB et al Idiopathic pulmonary fibrosis a composite physiologic index derived from disease extent observed by computed tomography Am J Respir Crit Care Med 2003167962-9 5 Raghu G Freudenberger TD Yang S et al High prevalence of abnormal acid gastroshyoesophageal reflux in idiopathic pulmonary fibrosis Eur Respir J 200627136-42 6 Kinnula VL Focus on antioxidant enzymes and antioxidant strategies in smoking related airway diseases Thorax 200560693-700 7 Coultas DB Zumwalt RE Black WC Sobonya RE The epidemiology of interstitial lung diseases Am J Respir Crit Care Med 1994150967-72 8 Raghu G Weycker D Edelsberg J Bradford WZ Oster G Incidence and prevalence of idiopathic pulmonary fibrosis Am J Respir Crit Care Med 2006174810-6 9 Olson AL Swigris JJ Lezotte DC Norris JM Wilson CG Brown KK Mortality from pulmonary fibrosis increased in the United States from 1992 to 2003 Am J Respir Crit Care Med 2007176277-84 10 Mannino DM Etzel RA Parrish RG Pulmonary fibrosis deaths in the United States 1979shy1991 An analysis of multiple-cause mortality data Am J Respir Crit Care Med 19961531548shy52 11 Hubbard R Johnston I Coultas DB Britton J Mortality rates from cryptogenic fibrosing alveolitis in seven countries Thorax 199651711-6 12 Johnston I Britton J Kinnear W Logan R Rising mortality from cryptogenic fibrosing alveolitis Bmj 19903011017-21 13 Raghu G Collard HR Egan JJ et al An official ATSERSJRSALAT statement idiopathic pulmonary fibrosis evidence-based guidelines for diagnosis and management Am J Respir Crit Care Med 2011183788-824 14 (USA) FDA FDA Public Health Advisory Interferon gamma-1b (marketed as Actimmune) In 2007 15 King TE Jr Pardo A Selman M Idiopathic pulmonary fibrosis Lancet 2011 16 Raghu G Brown KK Costabel U et al Treatment of idiopathic pulmonary fibrosis with etanercept an exploratory placebo-controlled trial Am J Respir Crit Care Med 2008178948shy55 17 Malouf MA Hopkins P Snell G Glanville AR An investigator-driven study of everolimus in surgical lung biopsy confirmed idiopathic pulmonary fibrosis Respirology 201116776-83 18 King TE Jr Behr J Brown KK et al BUILD-1 a randomized placebo-controlled trial of bosentan in idiopathic pulmonary fibrosis Am J Respir Crit Care Med 200817775-81 19 Richeldi L Costabel U Selman M et al Efficacy of a tyrosine kinase inhibitor in idiopathic pulmonary fibrosis N Engl J Med 20113651079-87
69
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
20 Borok Z Buhl R Grimes GJ et al Effect of glutathione aerosol on oxidant-antioxidant imbalance in idiopathic pulmonary fibrosis Lancet 1991338215-6 21 Meyer A Buhl R Magnussen H The effect of oral N-acetylcysteine on lung glutathione levels in idiopathic pulmonary fibrosis Eur Respir J 19947431-6 22 Behr J Maier K Degenkolb B Krombach F Vogelmeier C Antioxidative and clinical effects of high-dose N-acetylcysteine in fibrosing alveolitis Adjunctive therapy to maintenance immunosuppression Am J Respir Crit Care Med 19971561897-901 23 Cantin AM North SL Fells GA Hubbard RC Crystal RG Oxidant-mediated epithelial cell injury in idiopathic pulmonary fibrosis J Clin Invest 1987791665-73 24 Waghray M Cui Z Horowitz JC et al Hydrogen peroxide is a diffusible paracrine signal for the induction of epithelial cell death by activated myofibroblasts Faseb J 200519854-6 25 Larios JM Budhiraja R Fanburg BL Thannickal VJ Oxidative protein cross-linking reactions involving L-tyrosine in transforming growth factor-beta1-stimulated fibroblasts J Biol Chem 200127617437-41 26 Kinnula VL Fattman CL Tan RJ Oury TD Oxidative stress in pulmonary fibrosis a possible role for redox modulatory therapy Am J Respir Crit Care Med 2005172417-22 27 Meyer A Buhl R Kampf S Magnussen H Intravenous N-acetylcysteine and lung glutathione of patients with pulmonary fibrosis and normals Am J Respir Crit Care Med 19951521055-60 28 Behr J Degenkolb B Krombach F Vogelmeier C Intracellular glutathione and bronchoalveolar cells in fibrosing alveolitis effects of N-acetylcysteine Eur Respir J 200219906-11 29 Bando M Hosono T Mato N et al Long-term efficacy of inhaled N-acetylcysteine in patients with idiopathic pulmonary fibrosis Intern Med 2010492289-96 30 Demedts M Behr J Buhl R et al High-dose acetylcysteine in idiopathic pulmonary fibrosis N Engl J Med 20053532229-42 31 Toma TP Bhowmik A Rajakulasingam R Acetylcysteine in pulmonary fibrosis N Engl J Med 20063541086-9 author reply -9 32 Hunninghake GW Antioxidant therapy for idiopathic pulmonary fibrosis N Engl J Med 20053532285-7 33 Flaherty KR Mumford JA Murray S et al Prognostic implications of physiologic and radiographic changes in idiopathic interstitial pneumonia Am J Respir Crit Care Med 2003168543-8 34 Latsi PI du Bois RM Nicholson AG et al Fibrotic idiopathic interstitial pneumonia the prognostic value of longitudinal functional trends Am J Respir Crit Care Med 2003168531-7 35 Collard HR King TE Jr Bartelson BB Vourlekis JS Schwarz MI Brown KK Changes in clinical and physiologic variables predict survival in idiopathic pulmonary fibrosis Am J Respir Crit Care Med 2003168538-42 36 Jegal Y Kim DS Shim TS et al Physiology is a stronger predictor of survival than pathology in fibrotic interstitial pneumonia Am J Respir Crit Care Med 2005171639-44 37 Martinez FJ Safrin S Weycker D et al The clinical course of patients with idiopathic pulmonary fibrosis Ann Intern Med 2005142963-7 38 Hull JH Acetylcysteine in pulmonary fibrosis N Engl J Med 20063541089-91 author reply -91
70
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
39 Flaherty KR King TE Jr Raghu G et al Idiopathic interstitial pneumonia what is the effect of a multidisciplinary approach to diagnosis Am J Respir Crit Care Med 2004170904shy10 40 Raghu G Johnson WC Lockhart D Mageto Y Treatment of idiopathic pulmonary fibrosis with a new antifibrotic agent pirfenidone results of a prospective open-label Phase II study Am J Respir Crit Care Med 19991591061-9 41 Hunninghake GW Lynch DA Galvin JR et al Radiologic findings are strongly associated with a pathologic diagnosis of usual interstitial pneumonia Chest 20031241215-23 42 Lynch D Godwin J Safrin S et al High-resolution computed tomography in idiopathic pulmonary fibrosis diagnosis and prognosis Am J Respir Crit Care Med 2005172488-93 43 Mallinckrodt CH Watkin JG Molenberghs G Carroll RJ Choice of the primary analysis in longitudinal clinical trials Pharmaceutical Statistics 20043161-9 44 Bang H Tsiatis A Estimating medical costs with censored data Biometrika 200087329shy43 45 Lin DY Regression analysis of incomplete medical cost data Stat Med 2003221181-200 46 Rochon J Application of GEE procedures for sample size calculations in repeated measures experiments Stat Med 1998171643-58 47 Lachin JM Foulkes MA Evaluation of sample size and power for analyses of survival with allowance for nonuniform patient entry losses to follow-up noncompliance and stratification Biometrics 198642507-19
71
- PANTHER-IPFPREDNISONE AZATHIOPRINEAND N-ACETYLCYSTEINEA STUDY THAT EVALUATES RESPONSE INIDIOPATHIC PULMONARY FIBROSIS
-
- Protocol Summary
- Table of Contents
- List of Tables
- List of Figures
- List of Abbreviations
- 1 Summary
- 2 Hypotheses and Specific Aims
-
- 21 Null Hypothesis
- 22 Specific Aim 1
- 23 Specific Aim 2
- 24 Prespecified Subgroups of Interest
-
- 3 Background and Significance
-
- 31 Idiopathic Pulmonary Fibrosis is the Most Common Interstitial Lung Disease
- 32 Rationale for Placebo Control
- 33 Rationale for N-acetylcysteine
- 35 Rationale for N-acetylcysteine as a Stand-alone Therapy
- 36 Rationale for the Study Design and Primary Endpoint
- 37 Rationale for Blinding of Treatments
-
- 4 Methods
-
- 41 Inclusion Criteria
- 42 Diagnosis of IPF
- 43 Exclusion Criteria
- 44 Study Design and Study Visit
- 45 Dose Justification
- 46 Contraindications Precautions and Side Effects of Study Medications
- 47 Recruitment Procedures
- 48 Study Procedures
- 49 Concomitant Medications
- 410 Laboratory Testing
- 411 Blinding of Study Drugs
-
- 5 Study Endpoints
-
- 51 Primary Study Endpoint
- 52 Secondary Study Endpoints
-
- 6 Safety Evaluations and Procedures
-
- 61 Adverse Events
- 62 Clinical Medical Monitoring
- 63 Unblinding Procedures
-
- 7 Study Drug Procedures
- 8 Data Management
-
- 81 Hardware and Software Configuration
- 82 Sources of Data
-
- 9 Study Design and Data Analysis
-
- 91 General Analytic Considerations
- 92 Randomization Blinding and Reporting of Results
- 93 Stratification
- 94 Specification of the Primary Analyses
- 95 Analysis of Longitudinal Endpoints
- 96 Analysis of Binary Time-to-Event and Time-Lagged Endpoints
- 97 Power Analysis
-
- 10 Study Administration
-
- 101 Cooperative Agreement Mechanism
- 102 IPFnet Steering Group
- 103 Data and Safety Monitoring Board
- 104 Recommendations on Interim Monitoring of Efficacy Safety and Futility
-
- 11 Investigator and Sponsor Obligations
-
- 111 Monitoring
- 112 Cost and Payment
- 113 Confidentiality and Health Insurance Portability and Accountability ActConsiderations
- 114 Informed Consent Procedures
- 115 Institutional Review Boards
-
- 12 Investigator Agreement
- 13 References
-
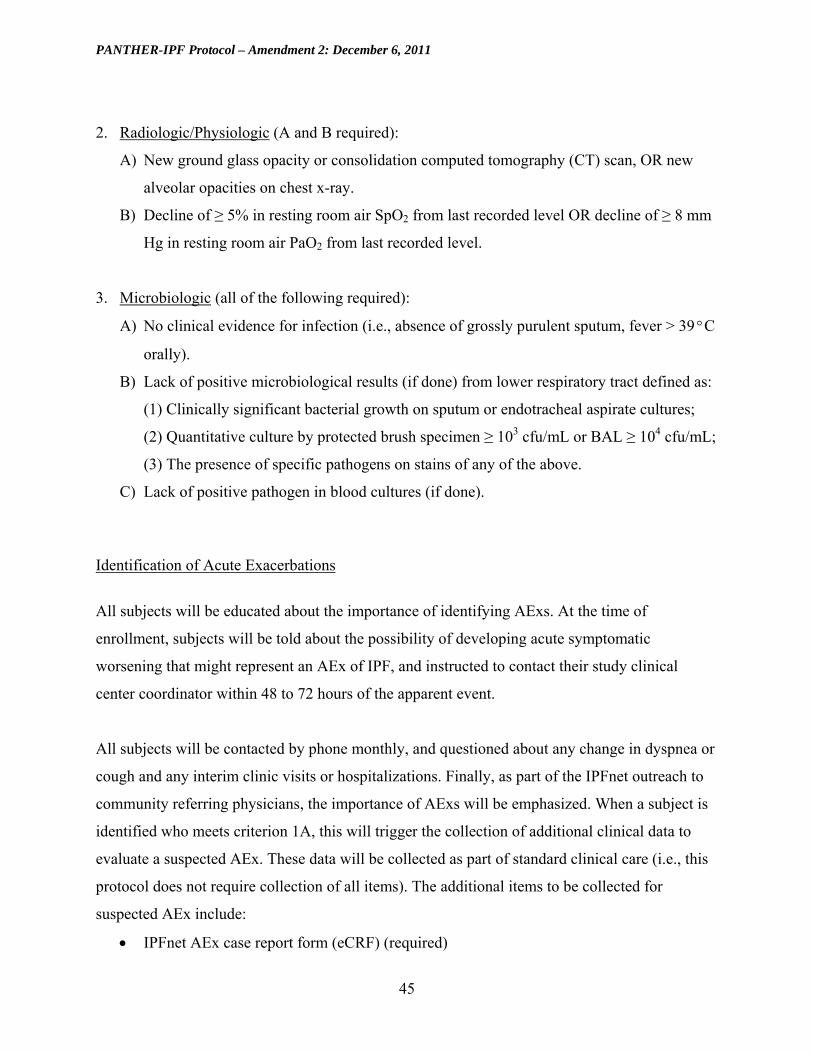
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
2 RadiologicPhysiologic (A and B required)
A) New ground glass opacity or consolidation computed tomography (CT) scan OR new
alveolar opacities on chest x-ray
B) Decline of ge 5 in resting room air SpO2 from last recorded level OR decline of ge 8 mm
Hg in resting room air PaO2 from last recorded level
3 Microbiologic (all of the following required)
A) No clinical evidence for infection (ie absence of grossly purulent sputum fever gt 39degC
orally)
B) Lack of positive microbiological results (if done) from lower respiratory tract defined as
(1) Clinically significant bacterial growth on sputum or endotracheal aspirate cultures
(2) Quantitative culture by protected brush specimen ge 103 cfumL or BAL ge 104 cfumL
(3) The presence of specific pathogens on stains of any of the above
C) Lack of positive pathogen in blood cultures (if done)
Identification of Acute Exacerbations
All subjects will be educated about the importance of identifying AExs At the time of
enrollment subjects will be told about the possibility of developing acute symptomatic
worsening that might represent an AEx of IPF and instructed to contact their study clinical
center coordinator within 48 to 72 hours of the apparent event
All subjects will be contacted by phone monthly and questioned about any change in dyspnea or
cough and any interim clinic visits or hospitalizations Finally as part of the IPFnet outreach to
community referring physicians the importance of AExs will be emphasized When a subject is
identified who meets criterion 1A this will trigger the collection of additional clinical data to
evaluate a suspected AEx These data will be collected as part of standard clinical care (ie this
protocol does not require collection of all items) The additional items to be collected for
suspected AEx include
IPFnet AEx case report form (eCRF) (required)
45
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Chest x-ray CT scan withwithout pulmonary angiogram (reports should be faxed and
followed by the hard copiesdiscs)
Oxygen saturation (pulse oximetry)
ABG
Respiratory cultures (sputum endotracheal aspirate lavage)
Blood cultures
Clinichospital records related to the event
All potential cases of AEx will be reviewed by the clinical center PI first and a decision on
whether the case may represent an AEx will be made If AEx is suspected the case will be sent
to the IPFnet adjudication committee which will assign a final diagnosis (see Table 5) If there is
disagreement among members the majority opinion will be recorded
During episodes of suspected AEx as determined by the individual clinical center investigator
subjects will remain blinded and in the study
Table 5 Final Diagnoses in Evaluation of Suspected Acute Exacerbations
Definite acute exacerbation All criteria met no alternative etiology
Unclassifiable acute worsening
Insufficient data to evaluate all criteria no alternative etiology
Not acute exacerbation Alternative etiology identified that explains acute worsening
Management of the suspected AEx will be at the discretion of the treating physician Standard of
care generally involves evaluation for respiratory infection pulmonary embolism cardiac events
and pneumothorax and treatment with IV corticosteroids
Study drugs will be resumed at pre-suspected AEx doses after subjects clinically improve as
confirmed by the local PI All subjects should be seen at the clinical center within 2 to 4 weeks
of recovery for measurement of post-bronchodilator FVC (see Figure 4) Subjects unable to
return to the clinical center after suspected AEx due to medical frailty (eg continued
46
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
institutionalization progressive disability) will be categorized as failing to maintain FVC
response in secondary analyses
Suspected AEx (PI determined)
Hold study drug Treat AEx
(Attending physician determined)
Alive but unable to continue due to
medical frailty
Dead
Alive and able to continue
Site reviewvisit
Restart study drug
FVC within 2-4 weeks
Figure 4 Acute Exacerbation Flow Chart
523 Respiratory Infections
An upper respiratory infection will be defined as
Change in sputum discoloration
Increased cough of no more than 14 daysrsquo duration
A lower-respiratory infection (pneumonia) will be defined as new segmental or lobar airspace
opacities visualized by image studies (chest radiograph or HRCT) in addition to any of the
following
Positive pathogencultures in good sample of sputum or lower-airway secretions retrieved
by fiberoptic bronchoscope
Fever gt 39degC or gt 100degF
Leukocytosis gt 12000 (unexplained no increase in dose of corticosteroids)
47
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
524 Maintained FVC Response
Subjects with follow-up FVCpred measurements at or above their baseline FVCpred level
will be classified as having maintained FVC response Subjects with reduced FVCpred levels
or missing data for any reason including death or medical frailty will be classified as having not
maintained FVC response The FVCpred value is used because unadjusted FVC measurements
are expected to decline with age
48
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
6 Safety Evaluations and Procedures
61 Adverse Events
During a clinical trial the reporting of adverse experience information can lead to important
changes in the way a new treatment is developed as well as provide integral safety data
611 Definitions
An adverse event (AE) is any untoward medical occurrence in a subject or clinical investigation
subject who was administered a pharmaceutical product The AE does not necessarily have to
have a causal relationship with the drug administered An AE can be any unfavorable and
unintended sign (including an abnormal laboratory finding) symptom or disease temporarily
associated with the use of a medicinal product whether or not considered to be related to the
medicinal product Diseases signs symptoms or laboratory abnormalities already existing at
enrollment are not considered AEs unless they worsen (ie increase in intensity or frequency)
Surgical procedures themselves are not AEs they are therapeutic measures for conditions that
require surgery The condition for which the surgery is required may be an AE Surgical
procedures planned before randomization and the conditions necessitating the surgery are not
AEs
A serious adverse event is any untoward event that
Is fatal
Is life-threatening
Requires inpatient hospitalization or prolongation of existing hospitalization with the
following exceptions
o Preplanned (before the study) hospital admissions unless the hospitalization is
prolonged
o Planned admissions (as part of a study eg routine biopsies)
o Hospitalization lasting lt 24 hours
49
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
o Hospitalization for elective procedure
o Emergency room visits
Results in persistent or significant disability or incapacity
Is a congenital anomaly or birth defect
Important medical events that may not result in death be life-threatening or require
inpatient hospitalization may be considered serious adverse events (SAEs) when based
on appropriate medical judgment they may jeopardize the subject and may require
medical or surgical intervention to prevent one of the outcomes listed above
Life-threatening means that the subject was in the view of the investigator at immediate risk of
death from the AE as it occurred It does not include an AE that had it occurred in a more severe
form might have caused death
Persistent or significant disabilityincapacity means that the event resulted in permanent or
significant and substantial disruption of the subjectrsquos ability to carry out normal life functions
Causality
A reasonable possibility means the AE may have been caused byrelated to the study drug A
perceived or real lack of efficacy does not satisfy the definition of relatedness
612 Adverse Event (AE) Reporting
For the PANTHER-IPF trial all AEs (serious and nonserious) occurring from randomization
through final study visit (4 weeks after final dose of all study medication) will be recorded on the
AE page of the case report form (CRF)
6121 Serious Adverse Events (SAE) Reporting
For this trial all deaths and all SAEs which occur from randomization through final study visit
must be entered within the EDC system via the SAE eCRF page within 24 hours of the
investigative sitersquos knowledge of the event It is the responsibility of the clinical center
50
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
investigator to provide a causality assessment of the event for each study medications based upon
the information available at the time of the report It is understood that complete information
about the event may not be known at the time the initial report is submitted In the event the EDC
system is not accessible to the site at the time of event reporting investigative sites will complete
and forward a paper back-up SAE form to DCRI Safety Surveillance for processing
DCRI Safety Surveillance
Telephone 1-919-668-8624 or 1-866-668-7799 (toll free)
Fax 1-919-668-7138 or 1-866-668-7138 (toll free)
The investigator must complete and submit follow-up SAE information via the eCRF when
important new or follow-up information (eg final diagnosis outcome results of specific
investigations) becomes available Follow-up information should be submitted according to the
same process used for reporting the initial event as described above All SAEs will be followed
until resolution stabilization or 30 days after the subject has completed the final visit (4 weeks
after the final dose of study medication) whichever occurs first The investigator is responsible
for reporting SAEs to their institutional review board (IRB) per site specific IRB reporting
guidelines
6122 Regulatory Reporting
AEs that are serious study drug related and unexpected will be reported to the regulatory
authorities The DCRI Safety Surveillance medical monitor will perform a medical review of all
SAEs submitted and evaluate for ldquounexpectednessrdquo DCRI Safety Surveillance will prepare
MedWatch reports for those events identified as serious study drug related and unexpected as
determined by Safety Medical Monitor
DCRI Regulatory Services will submit all unexpected study drug-related SAEs as per 21 CFR
32 DCRI Safety Surveillance will provide a safety alert letter to the NHLBI DSMB and DCC
clinical operation (for distribution to sites) within 15 days of initial receipt of the information
51
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Investigators are responsible for promptly reporting these events to their reviewing IRBs
according to site specific IRB reporting guidelines
62 Clinical Medical Monitoring
There will be an unblinded physician at the IPFnet DCC serving as medical monitor The
medical monitor will be available to assist with questions about dosage adjustments of study
medications including discontinuation or resumption of medications
63 Unblinding Procedures
Unblinding of subjects or investigators to subject treatment is strongly discouraged For ongoing
clinical management all subjects should be presumed to be receiving ldquoactiverdquo study drug To
ensure the subjectrsquos safety the study treatment will be dose-adjusted based on laboratory test
results clinical findings and symptoms
The IPFnet DCC medical monitor and PANTHER-IPF co-chairs Drs Ganesh Raghu and
Fernando Martinez will be available to the study physicians to discuss study drug management
on a case-by-case basis Un-blinding will be considered ONLY when the knowledge of subject
treatment assignment is ABSOLUTELY ESSENTIAL for subject safety and after discussion of
the subjectrsquos case with the medical monitor and either Dr Raghu or Dr Martinez Unblinding of
study treatment should be minimized during the conduct of the trial In those cases where it is
felt to be medically necessary the DCC medical officer will communicate directly with the
managing physician to minimize unblinding of study personnel
52
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
7 Study Drug Procedures
At the baseline 15-week 30-week and 45-week study visits subjects will receive a supply of
study drug sufficient to last until the next visit at which study drug will be dispensed
53
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
8 Data Management
81 Hardware and Software Configuration
811 Hardware and Database Software
Data will be stored in an Oracle database system Oracle has advantages of processing efficiency
and smooth linkage with other software systems The application and database will be hosted on
Solaris Unix servers at the IPFnet DCC
812 Statistical Software
SAS will be used as the principal application for the management of analysis data files and
statistical computations S-Plus will be used to provide supplementary functions as needed
813 Access Control and Confidentiality Procedures
Access to databases will be controlled centrally by the IPFnet DCC through user passwords
linked to appropriate privileges This protects the data from unauthorized changes and
inadvertent loss or damage
814 Security
Database and Web servers will be secured by a firewall and through controlled physical access
Oracle has many security features to ensure that any staff member accessing the database has the
proper authority to perform the functions he or she requests of the system Within the secondary
SAS databases Unix group-access control maintains similar security The Sun workstation login
is secured by extensive user-password facilities under Unix
54
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
815 Back-up Procedures
Database back-up will be performed automatically every day and standard IPFnet DCC policies
and procedures will be applied to dictate tape rotation and retention practices
816 Virus Protection
All disk drives that provide network services and all user computers will be protected using
virus-scanning software Standard IPFnet DCC policies will be applied to update these protection
systems periodically through the study
82 Sources of Data
821 Design and Development
The IPFnet DCC will be responsible for development of the electronic case report forms
(eCRFs) development and validation of the clinical study database ensuring data integrity and
training clinical center staff on applicable data management procedures A web-based distributed
data entry model will be implemented This system will be developed to ensure that guidelines
and regulations surrounding the use of computerized systems used in clinical trials are upheld
The remainder of this section provides an overview of the data management plan associated with
this protocol
822 Data Collection Forms
The data collection process consists of direct data entry at the study clinical centers into the EDC
system(s) provided by the DCC A data collection worksheet will be provided to clinical centers
for recording data in the event the EDC system is unavailable Data entry of the eCRFs should
be completed according to the instructions provided and project specific training The
investigator is responsible for maintaining accurate complete and up-to-date records and for
ensuring the completion of the eCRFs for each research participant
55
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
823 Data Acquisition and Entry
Data entry into eCRFs shall be performed by authorized individuals Selected eCRFs may also
require the investigatorrsquos written signature or electronic signature as appropriate Electronic
CRFs will be monitored for completeness accuracy and attention to detail during the study
824 Data Center Responsibilities
The IPFnet DCC will 1) develop a data management plan and will conduct data management
activities 2) provide final eCRFs for the collection of all data required by the study 3) develop
data dictionaries for each eCRF that will comprehensively define each data element 4) conduct
ongoing data monitoring activities on study data 5) monitor any preliminary analysis data
cleanup activities and 6) rigorously monitor final study data clean up
825 Data Editing
Completed data will be entered into the IPFnet DCC automated data acquisition and
management system If incomplete or inaccurate data are found a data clarification request will
be generated and distributed to clinical centers for a response Clinical centers will resolve data
inconsistencies and errors and enter all corrections and changes into the IPFnet DCC automated
data acquisition and management system
826 Training
The training plan for clinical center staff includes provisions for training on assessments eCRF
completion guidelines data management procedures and the use of computerized systems
56
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
9 Study Design and Data Analysis
91 General Analytic Considerations
All primary analyses will be based on intent-to-treat (ITT) principles using all randomized
subjects Baseline factors across groups will be compared using mean (standard deviation) and
median (25th and 75th percentiles) summary measures Kaplan-Meier curves will be used to
display event rates Due to clinical interest in departures from both sides of the null hypothesis
all test statistics will be 2-sided
Reasonable caution needs to be taken when conducting multiple analyses on key clinical
subgroups For subgroup analyses a conservative significance level of 0001 will be used for all
interaction tests Thus subgroup comparisons will be considered exploratory unless the p-value
from the interaction test is smaller than 0001
92 Randomization Blinding and Reporting of Results
A permuted block-randomization scheme will be created with varying block sizes stratified by
clinical center Once a subject has completed the screening and baseline period and evaluation
for inclusionexclusion criteria the randomization process will begin Subjects will be
randomized to receive NAC or matching placebo with equal probability (11) via telephone
contact with a central interactive voice response system (IVRS) using a toll-free randomization
number On the day of randomization after the subject has successfully met all inclusion and
exclusion criteria the investigator or designee will call the central randomization number to
obtain the assigned kit randomization numbers for that subject At each subject visit the
investigator or designee will call the central randomization number to obtain the new kit
randomization numbers for resupply of the subject For resupply of the clinical center the IVRS
will monitor minimal volume of a kit type andor expiration date and will automatically notify
the pharmacy
57
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
The trial results will be reported according to guidelines specified in the CONSORT statement
A flow diagram describing screening recruitment randomization dropout and vital status will
be included in the primary manuscript AEs and efficacy data will be presented for all treatment
groups Adherence dropout and lost to follow-up will be carefully examined across all treatment
groups Analyses of safety will be based on data from all randomized subjects who received at
least one dose of study drug
93 Stratification
Subjects will be distributed to the two treatment arms in a 11 allocation ratio Stratification
blocks will be based on clinical centers
94 Specification of the Primary Analyses
A mixed model repeated measures (MMRM) analysis described in section 95 will be used to
compare differences in the slope of FVC measurements across the treatment groups Response
variables are values of the FVC measured at baseline and every 15 weeks until study completion
Variables in the model will include treatment time and time by treatment age sex race and
height Contrast estimates of differences in slopes of treatment over time (along with confidence
intervals) will be used to estimate the treatment effect The validity of this model in terms of
meeting modeling assumptions will be assessed via standard modeling diagnostics and goodness-
of-fit measures Based on the MMRM framework missing FVC data will not be imputed for the
primary analysis
95 Analysis of Longitudinal Endpoints
A common goal in clinical trials is to specify models that are easily implemented and
reproducible by independent data analysts On the other hand the models should have proper
statistical behavior in terms of low bias and high precision Many common approaches to
longitudinal data analysis including last observation carried forward (LOCF) imputation rely on
the missing completely at random (MCAR) assumption However the MCAR assumption is
58
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
unlikely to hold in many clinical trials because missing data are often related to disease
progression and prognosis A more reasonable assumption missing at random (MAR) specifies
that the complete data distribution can be modeled using only the observed data The likelihood-
based MMRM approach is valid under the more general MAR assumptions These models will
be applied to analyze the longitudinal data secondary endpoints
The advantages of MMRM analysis are that all important characteristics of the model can be preshy
specified standard software can be used to implement the models and results are based on ITT
principles43 In addition the MMRM approach offers superior control of Type I and Type II
errors compared with the LOCF approach
Response variables are values of the PFTs measured at enrollment and every 15 weeks until
study completion and 6MWT values measured at baseline week 30 and week 60 Covariates are
treatment time time by treatment and key baseline risk factors Contrasts (along with
confidence intervals) of treatment by time will be used to estimate the treatment effect
The correlation structure involves multiple pieces including measurement errors random
variation and interindividual variability For the longitudinal data analyses an unstructured
correlation matrix for within-subject errors will be assumed Other correlation structures
including compound symmetry will be examined as needed A careful examination of reasons
for study discontinuation will be conducted to assess the validity of MCAR Sensitivity analyses
will be used to examine the untestable assumption that the observed data violate the MAR
assumption The MMRM models will be implemented using PROC MIXED in SAS
96 Analysis of Binary Time-to-Event and Time-Lagged Endpoints
Regression modeling approaches using either the logistic regression model or Cox proportional
hazards regression model will be employed when appropriate The validity of these models will
be assessed via standard modeling diagnostics and goodness-of-fit measures Estimates of
cumulative frequencies for more general time-lagged responses will be calculated using the
partitioned version of the Bang-Tsiatis estimator44 The partitions will be set at 15-week intervals
59
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
to correspond with the data-collection process Covariate adjusted event rates will be calculated
using inverse probability-weighted regression estimates45
97 Power Analysis
971 Primary Analyses
Based on previously published IPF clinical trials the PL group is expected to experience a drop
in FVC of approximately 020 L over the study period (see Figure 1) The IPFnet Steering Group
determined a clinically important difference would be to preserve the majority of the decline
relative to PL over the study period In particular a treatment effect of 015 L was determined to
be a clinically meaningful difference Potential dropout is a key factor in the proposed study The
drop-out process assumed 5 lost to follow-up after every study visit Only 80 of subjects
were assumed to be followed for the entire study period All models assumed a compound
symmetry structure for the covariance matrix Power calculations were performed using a SAS
IML program for designing repeated measures studies46 Based on preliminary reviews of the
data from the University of Michigan the covariance matrix parameters were estimated at
approximately σ2 = 0757 (variance parameter) and ρ = 0936 (correlation parameter) To be
conservative the power calculations for the primary analysis were performed with parameter
setting of σ2 = 0810 (variance parameter) and ρ = 0925 (correlation parameter)
The power calculations assume a correction for imperfect compliance proposed by Lachin and
Foulkes to allow for 2 noncompliance for each of the treatment arms47 Thus the sample size
of 130 subjects per arm would be reduced to an adjusted sample size of 130(1-002-002)2 =
1198 or 120 subjects per arm
Under the assumed Type I error rate of 005 with a correlation parameter of 0925 and standard
deviation of 090 the difference of 015 L (or 00025 Lweek) shown in Table 6 would have
power of 93
60
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Table 6 Hypothetical Values of Mean FVC (L) Change from Baseline
Week 15 Week 30 Week 45 Week 60
NAC 00125 00250 00375 00500
Placebo 00500 01000 01500 02000
Difference 00375 00750 01125 01500
Abbreviations FVC forced vital capacity PL placebo
972 Power Analysis for Secondary Endpoints
Power calculations for secondary endpoint measurements are shown in Table 7 Standard
deviations are based on unpublished data provided by the University of Michigan The
calculations are based on a 2-sample t-test with Type I error rate set at 005 These calculations
are likely to be conservative because the statistical approach described in section 95 for
analyzing these endpoints will incorporate incomplete observations as well as intermediate data
points
Table 7 Detectable Differences in Treatment Means for Selected Endpoint Measurements
Secondary Endpoints Std Dev
of the Baseline Score
Detectable Difference for 80 Power
Std Dev of the Change Score
Difference Detectable for
80 Power
DLCOpred 166 58 91 32
6MWT Area Under the Desaturation Curve
219 76 175 61
6MWT Distance to Desaturation 224 78 315 110
6MWT Minutes Walked 210 073 205 071
Abbreviations Std Dev standard deviation DLCOpred diffusing capacity of the lung for carbon monoxide percent predicted 6MWT 6-minute walk test
61
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
10 Study Administration
101 Cooperative Agreement Mechanism
The administrative and funding mechanism used to undertake this project is a ldquocooperative
agreementrdquo (U01) which is an assistance mechanism Under the cooperative agreement the
NHLBI assists supports andor stimulates the project and is substantially involved with
investigators in conducting the study by facilitating performance of the effort in a ldquopartnerrdquo role
The NHLBI project scientist serves on the IPFnet Steering Group and he or another NHLBI
scientist may serve on other project committees when appropriate At the same time however
NHLBI does not assume a dominant role direction or prime responsibility for this research
program
As described below governance of the project is conducted through the IPFnet Steering Group
Principal investigators have lead responsibilities in all aspects of their trials and the project
including any modification of trial designs conduct of the trials quality control data analysis
and interpretation preparation of publications and collaboration with other investigators unless
otherwise provided for by the IPFnet Steering Group
PIs retain custody of and have primary rights to their center-specific and collaborative data
subject to government rights-of-access consistent with current Health amp Human Services (HHS)
Public Health Service (PHS) and National Institutes of Health policies The protocols and
governance policies call for the continual submission of data centrally to the IPFnet DCC for the
collaborative database which at a minimum will contain the key variables selected by the IPFnet
Steering Group for standardization across all clinical centers the submission of copies of the
collaborative datasets to each PI upon completion of the project procedures for data analysis
reporting and publication and procedures to protect and ensure the privacy of medical and
genetic data and records of individuals The NHLBI project scientist on behalf of the NHLBI
will have the same access privileges and responsibilities regarding the collaborative data as the
other members of the Steering Group
62
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
PIs are also encouraged to publish and to publicly release and disseminate results data and other
products of the project concordant with the project protocols and governance and the approved
plan for making data and materials available to the scientific community and to the NHLBI
However during the 3 years after the ending date of NHLBI project support unpublished data
unpublished results data sets not previously released and other study materials or products are
to be made available to any third party only with the approval of the IPFnet Steering Group
Upon completion of the project PIs are expected to put their intervention materials and
procedure manuals into the public domain andor make them available to other investigators
according to the approved plan for making data and materials available to the scientific
community and the NHLBI for the conduct of research at no charge other than the costs of
reproduction and distribution
The NHLBI reserves the right to terminate or curtail the project (or an individual award) in the
event of (a) failure to develop or implement mutually agreeable collaborative measurement
subject eligibility and data management sections of the protocols (b) substantial shortfall in
subject recruitment follow-up data reporting or quality control or other major breach of
protocol (c) substantive changes in the agreed-upon protocols with which NHLBI cannot
concur (d) reaching a major project outcome with persuasive statistical significance
substantially before schedule or (e) human subject ethical issues that may dictate a premature
termination
Any disagreement that may arise in scientificprogrammatic matters (within the scope of the
award) between award recipients and the NHLBI may be brought to arbitration An arbitration
panel will be composed of 3 membersmdash1 selected by the IPFnet Steering Group (with the
NHLBI member not voting) or by the individual PI in the event of an individual disagreement a
second selected by NHLBI and the third selected by the other 2 members This special
arbitration procedure in no way affects the PIrsquos right to appeal an adverse action that is otherwise
appealable in accordance with the PHS regulations at 42 CFR part 50 Subpart D and HHS
63
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
regulation at 45 CFR part 16 or the rights of the NHLBI under applicable statutes regulations
and terms of the award
102 IPFnet Steering Group
The IPFnet Steering Group is the main governing body of the project It is composed of the PIs
of the clinical centers the PI of the DCC and the NHLBI project scientist The clinical centers
the IPFnet DCC and the NHLBI each have 1 vote on the IPFnet Steering Group All decisions
are determined by majority vote
All major scientific decisions are determined by the IPFnet Steering Group It assumes overall
responsibility for the design and conduct of the trial It appoints (and disbands) committees and
subcommittees as the need arises designs approves and implements the study protocols
oversees the development of the MOOP monitors subject recruitment and treatment delivery
evaluates data collection and management oversees quality assurance procedures and
implements changes and enhancements to the study as required It also has primary responsibility
for facilitating the conduct of the trials and reporting the projectrsquos results
103 Data and Safety Monitoring Board
The NHLBI will establish a DSMB in accordance with established policies (see
httpwwwnhlbinihgovfundingpoliciesdsmb_insthtm) to ensure data quality and subject
safety and to provide independent advice to the NHLBI regarding progress and the
appropriateness of study continuation
104 Recommendations on Interim Monitoring of Efficacy Safety and Futility
First and foremost the role of the DSMB will be to review subject safety and trial conduct at
periodic points during the study The DSMB may require analyses of the primary endpoint
results for comparing the benefit and risks of treatment strategies The benefit of collecting
additional data on key secondary endpoints with extended follow-up and establishing a robust
64
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
evidence base for determining a standard of care will need to be carefully considered before
early termination of one or more treatment arms After careful consideration the IPFnet Steering
Group recommends conservative thresholds for the early examinations of the safety and efficacy
data
The DSMB will be expected to meet approximately every 6 months until trial completion to
review safety and toxicity data The DSMB may recommend stopping the study based on these
reviews Because the DSMB could stop the trial for safety concerns as well as for a large
efficacy benefit there could be multiple opportunities to reject the null hypothesis (no difference
in event rates between the PL and NAC groups) A Bonferroni approximation will be applied
during the one planned interim analysis for efficacy
Before locking the database a statistical analysis plan (SAP) will be developed to provide
complete details on the statistical analysis The SAP will include the specifics for how and when
the DSMB will be notified for AEs The IPFnet DCC will deliver to the DSMB all FDA-defined
AEs at 3-month intervals The IPFnet DCC will prepare narrative SAE reports in real time for
DSMB review including recommendations and analysis of similar events for each SAE
submitted to the FDA
65
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
11 Investigator and Sponsor Obligations
111 Monitoring
All monitoring activities for US clinical centers will be performed in accordance with DCRI
standard operating procedures Information regarding the types of visits will be outlined in the
PANTHER-IPF MOOP
112 Cost and Payment
There will be no cost to subjects enrolled in this trial Study-related procedures will be paid for
by the IPFnet
Subjects may be eligible for reimbursement for travel to the clinical center Details of payment
will be explained to each subject during the consent process
113 Confidentiality and Health Insurance Portability and Accountability Act
Considerations
Subject confidentiality will be protected throughout the study All subject data will be kept
strictly confidential and no subject-identifying information will be released to anyone outside
the project Confidentiality will be assured through several mechanisms First each subject will
be assigned an anonymous study ID which will then be used on all study forms Second any
study forms blood samples and paper records that contain subject information (eg address lists
phone lists) will be kept at the clinical centers in secured locked areas coded by number Once
blood is collected there will be no subject identifiers placed on blood samplesmdashonly the study
ID number and the date of sample collection Third access to all subject data and information
including laboratory specimens will be restricted to authorized personnel In the case of
computerized data this restricted access will be assured through user logon IDs and password
protection
66
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
At the IPFnet DCC only authorized personnel will have access to the data files containing study
data Security will be assured through user logon IDs passwords and appropriate access
privileges All study subjects will be identified only by their IPFnet ID numbers and no personal
identifying information such as name address or Social Security number will be entered into
the IPFnet DCC database Any subject-specific data reported to the IPFnet Steering Group will
be identified only by the IPFnet ID number
Finally subjects will not be identified by name in any reports or publications nor will the data
be presented in such a way that the identity of individual subjects can be inferred Analysis files
created for further study by the scientific community will have no subject identifiers These data
files will be created in accordance with the Ancillary Studies and Publication Policy of the
IPFnet
114 Informed Consent Procedures
All IPFnet subjects will provide written informed consent using procedures reviewed and
approved by each clinical centerrsquos IRB Informed consent will be undertaken by study personnel
in-person with the subject The subject has the option of declining further participation in the
study at that point No further study procedures will be conducted until the signed documents
have been provided to the IPFnet clinical center
115 Institutional Review Boards
Before initiating this study the protocol clinical center-specific informed consent forms Health
Insurance Portability and Accountability Act (HIPAA) forms recruitment materials and other
relevant information will be reviewed by a properly constituted IRB at each participating clinical
center A copy of the signed and dated IRB approval at each clinical center will be retrieved prior
to or during the site initiation visit and archived at the IPFnet DCC Any amendments to the
protocol other than simple administrative and typographical changes must be approved by each
IRB before they are implemented The clinical centers will seek annual renewals of their IRB
approvals in accordance with local procedures
67
__________________________________________ ________________
__________________________________________
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
12 Investigator Agreement
I have read the foregoing protocol PANTHER-IPF and agree that it contains all necessary
details for carrying out this study I will conduct the study as outlined herein and will complete
the study within the time designated
I will provide copies of the protocol and all pertinent information to all individuals responsible to
me who assist in the conduct of this study I will discuss this material with them to ensure they
are fully informed regarding the drug and the conduct of the study
I will fulfill all responsibilities for submitting pertinent information to the local IRB if
applicable that is responsible for this study
I further agree that NHLBI andor DCRI will have access to any source documents from which
eCRF information may have been generated
Signature of Principal Investigator Date
Name of Principal Investigator (printed or typed)
Protocol version date May 19 2009
Protocol Amendment 1 version date May 28 2010
Protocol Amendment 2 version date December 6 2011
68
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
13 References
1 Raghu G Brown KK Bradford WZ et al A placebo-controlled trial of interferon gamma-1b in patients with idiopathic pulmonary fibrosis N Engl J Med 2004350125-33 2 King TE Jr Safrin S Starko KM et al Analyses of efficacy end points in a controlled trial of interferon-gamma1b for idiopathic pulmonary fibrosis Chest 2005127171-7 3 Flaherty KR Thwaite EL Kazerooni EA et al Radiological versus histological diagnosis in UIP and NSIP survival implications Thorax 200358143-8 4 Wells AU Desai SR Rubens MB et al Idiopathic pulmonary fibrosis a composite physiologic index derived from disease extent observed by computed tomography Am J Respir Crit Care Med 2003167962-9 5 Raghu G Freudenberger TD Yang S et al High prevalence of abnormal acid gastroshyoesophageal reflux in idiopathic pulmonary fibrosis Eur Respir J 200627136-42 6 Kinnula VL Focus on antioxidant enzymes and antioxidant strategies in smoking related airway diseases Thorax 200560693-700 7 Coultas DB Zumwalt RE Black WC Sobonya RE The epidemiology of interstitial lung diseases Am J Respir Crit Care Med 1994150967-72 8 Raghu G Weycker D Edelsberg J Bradford WZ Oster G Incidence and prevalence of idiopathic pulmonary fibrosis Am J Respir Crit Care Med 2006174810-6 9 Olson AL Swigris JJ Lezotte DC Norris JM Wilson CG Brown KK Mortality from pulmonary fibrosis increased in the United States from 1992 to 2003 Am J Respir Crit Care Med 2007176277-84 10 Mannino DM Etzel RA Parrish RG Pulmonary fibrosis deaths in the United States 1979shy1991 An analysis of multiple-cause mortality data Am J Respir Crit Care Med 19961531548shy52 11 Hubbard R Johnston I Coultas DB Britton J Mortality rates from cryptogenic fibrosing alveolitis in seven countries Thorax 199651711-6 12 Johnston I Britton J Kinnear W Logan R Rising mortality from cryptogenic fibrosing alveolitis Bmj 19903011017-21 13 Raghu G Collard HR Egan JJ et al An official ATSERSJRSALAT statement idiopathic pulmonary fibrosis evidence-based guidelines for diagnosis and management Am J Respir Crit Care Med 2011183788-824 14 (USA) FDA FDA Public Health Advisory Interferon gamma-1b (marketed as Actimmune) In 2007 15 King TE Jr Pardo A Selman M Idiopathic pulmonary fibrosis Lancet 2011 16 Raghu G Brown KK Costabel U et al Treatment of idiopathic pulmonary fibrosis with etanercept an exploratory placebo-controlled trial Am J Respir Crit Care Med 2008178948shy55 17 Malouf MA Hopkins P Snell G Glanville AR An investigator-driven study of everolimus in surgical lung biopsy confirmed idiopathic pulmonary fibrosis Respirology 201116776-83 18 King TE Jr Behr J Brown KK et al BUILD-1 a randomized placebo-controlled trial of bosentan in idiopathic pulmonary fibrosis Am J Respir Crit Care Med 200817775-81 19 Richeldi L Costabel U Selman M et al Efficacy of a tyrosine kinase inhibitor in idiopathic pulmonary fibrosis N Engl J Med 20113651079-87
69
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
20 Borok Z Buhl R Grimes GJ et al Effect of glutathione aerosol on oxidant-antioxidant imbalance in idiopathic pulmonary fibrosis Lancet 1991338215-6 21 Meyer A Buhl R Magnussen H The effect of oral N-acetylcysteine on lung glutathione levels in idiopathic pulmonary fibrosis Eur Respir J 19947431-6 22 Behr J Maier K Degenkolb B Krombach F Vogelmeier C Antioxidative and clinical effects of high-dose N-acetylcysteine in fibrosing alveolitis Adjunctive therapy to maintenance immunosuppression Am J Respir Crit Care Med 19971561897-901 23 Cantin AM North SL Fells GA Hubbard RC Crystal RG Oxidant-mediated epithelial cell injury in idiopathic pulmonary fibrosis J Clin Invest 1987791665-73 24 Waghray M Cui Z Horowitz JC et al Hydrogen peroxide is a diffusible paracrine signal for the induction of epithelial cell death by activated myofibroblasts Faseb J 200519854-6 25 Larios JM Budhiraja R Fanburg BL Thannickal VJ Oxidative protein cross-linking reactions involving L-tyrosine in transforming growth factor-beta1-stimulated fibroblasts J Biol Chem 200127617437-41 26 Kinnula VL Fattman CL Tan RJ Oury TD Oxidative stress in pulmonary fibrosis a possible role for redox modulatory therapy Am J Respir Crit Care Med 2005172417-22 27 Meyer A Buhl R Kampf S Magnussen H Intravenous N-acetylcysteine and lung glutathione of patients with pulmonary fibrosis and normals Am J Respir Crit Care Med 19951521055-60 28 Behr J Degenkolb B Krombach F Vogelmeier C Intracellular glutathione and bronchoalveolar cells in fibrosing alveolitis effects of N-acetylcysteine Eur Respir J 200219906-11 29 Bando M Hosono T Mato N et al Long-term efficacy of inhaled N-acetylcysteine in patients with idiopathic pulmonary fibrosis Intern Med 2010492289-96 30 Demedts M Behr J Buhl R et al High-dose acetylcysteine in idiopathic pulmonary fibrosis N Engl J Med 20053532229-42 31 Toma TP Bhowmik A Rajakulasingam R Acetylcysteine in pulmonary fibrosis N Engl J Med 20063541086-9 author reply -9 32 Hunninghake GW Antioxidant therapy for idiopathic pulmonary fibrosis N Engl J Med 20053532285-7 33 Flaherty KR Mumford JA Murray S et al Prognostic implications of physiologic and radiographic changes in idiopathic interstitial pneumonia Am J Respir Crit Care Med 2003168543-8 34 Latsi PI du Bois RM Nicholson AG et al Fibrotic idiopathic interstitial pneumonia the prognostic value of longitudinal functional trends Am J Respir Crit Care Med 2003168531-7 35 Collard HR King TE Jr Bartelson BB Vourlekis JS Schwarz MI Brown KK Changes in clinical and physiologic variables predict survival in idiopathic pulmonary fibrosis Am J Respir Crit Care Med 2003168538-42 36 Jegal Y Kim DS Shim TS et al Physiology is a stronger predictor of survival than pathology in fibrotic interstitial pneumonia Am J Respir Crit Care Med 2005171639-44 37 Martinez FJ Safrin S Weycker D et al The clinical course of patients with idiopathic pulmonary fibrosis Ann Intern Med 2005142963-7 38 Hull JH Acetylcysteine in pulmonary fibrosis N Engl J Med 20063541089-91 author reply -91
70
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
39 Flaherty KR King TE Jr Raghu G et al Idiopathic interstitial pneumonia what is the effect of a multidisciplinary approach to diagnosis Am J Respir Crit Care Med 2004170904shy10 40 Raghu G Johnson WC Lockhart D Mageto Y Treatment of idiopathic pulmonary fibrosis with a new antifibrotic agent pirfenidone results of a prospective open-label Phase II study Am J Respir Crit Care Med 19991591061-9 41 Hunninghake GW Lynch DA Galvin JR et al Radiologic findings are strongly associated with a pathologic diagnosis of usual interstitial pneumonia Chest 20031241215-23 42 Lynch D Godwin J Safrin S et al High-resolution computed tomography in idiopathic pulmonary fibrosis diagnosis and prognosis Am J Respir Crit Care Med 2005172488-93 43 Mallinckrodt CH Watkin JG Molenberghs G Carroll RJ Choice of the primary analysis in longitudinal clinical trials Pharmaceutical Statistics 20043161-9 44 Bang H Tsiatis A Estimating medical costs with censored data Biometrika 200087329shy43 45 Lin DY Regression analysis of incomplete medical cost data Stat Med 2003221181-200 46 Rochon J Application of GEE procedures for sample size calculations in repeated measures experiments Stat Med 1998171643-58 47 Lachin JM Foulkes MA Evaluation of sample size and power for analyses of survival with allowance for nonuniform patient entry losses to follow-up noncompliance and stratification Biometrics 198642507-19
71
- PANTHER-IPFPREDNISONE AZATHIOPRINEAND N-ACETYLCYSTEINEA STUDY THAT EVALUATES RESPONSE INIDIOPATHIC PULMONARY FIBROSIS
-
- Protocol Summary
- Table of Contents
- List of Tables
- List of Figures
- List of Abbreviations
- 1 Summary
- 2 Hypotheses and Specific Aims
-
- 21 Null Hypothesis
- 22 Specific Aim 1
- 23 Specific Aim 2
- 24 Prespecified Subgroups of Interest
-
- 3 Background and Significance
-
- 31 Idiopathic Pulmonary Fibrosis is the Most Common Interstitial Lung Disease
- 32 Rationale for Placebo Control
- 33 Rationale for N-acetylcysteine
- 35 Rationale for N-acetylcysteine as a Stand-alone Therapy
- 36 Rationale for the Study Design and Primary Endpoint
- 37 Rationale for Blinding of Treatments
-
- 4 Methods
-
- 41 Inclusion Criteria
- 42 Diagnosis of IPF
- 43 Exclusion Criteria
- 44 Study Design and Study Visit
- 45 Dose Justification
- 46 Contraindications Precautions and Side Effects of Study Medications
- 47 Recruitment Procedures
- 48 Study Procedures
- 49 Concomitant Medications
- 410 Laboratory Testing
- 411 Blinding of Study Drugs
-
- 5 Study Endpoints
-
- 51 Primary Study Endpoint
- 52 Secondary Study Endpoints
-
- 6 Safety Evaluations and Procedures
-
- 61 Adverse Events
- 62 Clinical Medical Monitoring
- 63 Unblinding Procedures
-
- 7 Study Drug Procedures
- 8 Data Management
-
- 81 Hardware and Software Configuration
- 82 Sources of Data
-
- 9 Study Design and Data Analysis
-
- 91 General Analytic Considerations
- 92 Randomization Blinding and Reporting of Results
- 93 Stratification
- 94 Specification of the Primary Analyses
- 95 Analysis of Longitudinal Endpoints
- 96 Analysis of Binary Time-to-Event and Time-Lagged Endpoints
- 97 Power Analysis
-
- 10 Study Administration
-
- 101 Cooperative Agreement Mechanism
- 102 IPFnet Steering Group
- 103 Data and Safety Monitoring Board
- 104 Recommendations on Interim Monitoring of Efficacy Safety and Futility
-
- 11 Investigator and Sponsor Obligations
-
- 111 Monitoring
- 112 Cost and Payment
- 113 Confidentiality and Health Insurance Portability and Accountability ActConsiderations
- 114 Informed Consent Procedures
- 115 Institutional Review Boards
-
- 12 Investigator Agreement
- 13 References
-
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Chest x-ray CT scan withwithout pulmonary angiogram (reports should be faxed and
followed by the hard copiesdiscs)
Oxygen saturation (pulse oximetry)
ABG
Respiratory cultures (sputum endotracheal aspirate lavage)
Blood cultures
Clinichospital records related to the event
All potential cases of AEx will be reviewed by the clinical center PI first and a decision on
whether the case may represent an AEx will be made If AEx is suspected the case will be sent
to the IPFnet adjudication committee which will assign a final diagnosis (see Table 5) If there is
disagreement among members the majority opinion will be recorded
During episodes of suspected AEx as determined by the individual clinical center investigator
subjects will remain blinded and in the study
Table 5 Final Diagnoses in Evaluation of Suspected Acute Exacerbations
Definite acute exacerbation All criteria met no alternative etiology
Unclassifiable acute worsening
Insufficient data to evaluate all criteria no alternative etiology
Not acute exacerbation Alternative etiology identified that explains acute worsening
Management of the suspected AEx will be at the discretion of the treating physician Standard of
care generally involves evaluation for respiratory infection pulmonary embolism cardiac events
and pneumothorax and treatment with IV corticosteroids
Study drugs will be resumed at pre-suspected AEx doses after subjects clinically improve as
confirmed by the local PI All subjects should be seen at the clinical center within 2 to 4 weeks
of recovery for measurement of post-bronchodilator FVC (see Figure 4) Subjects unable to
return to the clinical center after suspected AEx due to medical frailty (eg continued
46
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
institutionalization progressive disability) will be categorized as failing to maintain FVC
response in secondary analyses
Suspected AEx (PI determined)
Hold study drug Treat AEx
(Attending physician determined)
Alive but unable to continue due to
medical frailty
Dead
Alive and able to continue
Site reviewvisit
Restart study drug
FVC within 2-4 weeks
Figure 4 Acute Exacerbation Flow Chart
523 Respiratory Infections
An upper respiratory infection will be defined as
Change in sputum discoloration
Increased cough of no more than 14 daysrsquo duration
A lower-respiratory infection (pneumonia) will be defined as new segmental or lobar airspace
opacities visualized by image studies (chest radiograph or HRCT) in addition to any of the
following
Positive pathogencultures in good sample of sputum or lower-airway secretions retrieved
by fiberoptic bronchoscope
Fever gt 39degC or gt 100degF
Leukocytosis gt 12000 (unexplained no increase in dose of corticosteroids)
47
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
524 Maintained FVC Response
Subjects with follow-up FVCpred measurements at or above their baseline FVCpred level
will be classified as having maintained FVC response Subjects with reduced FVCpred levels
or missing data for any reason including death or medical frailty will be classified as having not
maintained FVC response The FVCpred value is used because unadjusted FVC measurements
are expected to decline with age
48
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
6 Safety Evaluations and Procedures
61 Adverse Events
During a clinical trial the reporting of adverse experience information can lead to important
changes in the way a new treatment is developed as well as provide integral safety data
611 Definitions
An adverse event (AE) is any untoward medical occurrence in a subject or clinical investigation
subject who was administered a pharmaceutical product The AE does not necessarily have to
have a causal relationship with the drug administered An AE can be any unfavorable and
unintended sign (including an abnormal laboratory finding) symptom or disease temporarily
associated with the use of a medicinal product whether or not considered to be related to the
medicinal product Diseases signs symptoms or laboratory abnormalities already existing at
enrollment are not considered AEs unless they worsen (ie increase in intensity or frequency)
Surgical procedures themselves are not AEs they are therapeutic measures for conditions that
require surgery The condition for which the surgery is required may be an AE Surgical
procedures planned before randomization and the conditions necessitating the surgery are not
AEs
A serious adverse event is any untoward event that
Is fatal
Is life-threatening
Requires inpatient hospitalization or prolongation of existing hospitalization with the
following exceptions
o Preplanned (before the study) hospital admissions unless the hospitalization is
prolonged
o Planned admissions (as part of a study eg routine biopsies)
o Hospitalization lasting lt 24 hours
49
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
o Hospitalization for elective procedure
o Emergency room visits
Results in persistent or significant disability or incapacity
Is a congenital anomaly or birth defect
Important medical events that may not result in death be life-threatening or require
inpatient hospitalization may be considered serious adverse events (SAEs) when based
on appropriate medical judgment they may jeopardize the subject and may require
medical or surgical intervention to prevent one of the outcomes listed above
Life-threatening means that the subject was in the view of the investigator at immediate risk of
death from the AE as it occurred It does not include an AE that had it occurred in a more severe
form might have caused death
Persistent or significant disabilityincapacity means that the event resulted in permanent or
significant and substantial disruption of the subjectrsquos ability to carry out normal life functions
Causality
A reasonable possibility means the AE may have been caused byrelated to the study drug A
perceived or real lack of efficacy does not satisfy the definition of relatedness
612 Adverse Event (AE) Reporting
For the PANTHER-IPF trial all AEs (serious and nonserious) occurring from randomization
through final study visit (4 weeks after final dose of all study medication) will be recorded on the
AE page of the case report form (CRF)
6121 Serious Adverse Events (SAE) Reporting
For this trial all deaths and all SAEs which occur from randomization through final study visit
must be entered within the EDC system via the SAE eCRF page within 24 hours of the
investigative sitersquos knowledge of the event It is the responsibility of the clinical center
50
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
investigator to provide a causality assessment of the event for each study medications based upon
the information available at the time of the report It is understood that complete information
about the event may not be known at the time the initial report is submitted In the event the EDC
system is not accessible to the site at the time of event reporting investigative sites will complete
and forward a paper back-up SAE form to DCRI Safety Surveillance for processing
DCRI Safety Surveillance
Telephone 1-919-668-8624 or 1-866-668-7799 (toll free)
Fax 1-919-668-7138 or 1-866-668-7138 (toll free)
The investigator must complete and submit follow-up SAE information via the eCRF when
important new or follow-up information (eg final diagnosis outcome results of specific
investigations) becomes available Follow-up information should be submitted according to the
same process used for reporting the initial event as described above All SAEs will be followed
until resolution stabilization or 30 days after the subject has completed the final visit (4 weeks
after the final dose of study medication) whichever occurs first The investigator is responsible
for reporting SAEs to their institutional review board (IRB) per site specific IRB reporting
guidelines
6122 Regulatory Reporting
AEs that are serious study drug related and unexpected will be reported to the regulatory
authorities The DCRI Safety Surveillance medical monitor will perform a medical review of all
SAEs submitted and evaluate for ldquounexpectednessrdquo DCRI Safety Surveillance will prepare
MedWatch reports for those events identified as serious study drug related and unexpected as
determined by Safety Medical Monitor
DCRI Regulatory Services will submit all unexpected study drug-related SAEs as per 21 CFR
32 DCRI Safety Surveillance will provide a safety alert letter to the NHLBI DSMB and DCC
clinical operation (for distribution to sites) within 15 days of initial receipt of the information
51
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Investigators are responsible for promptly reporting these events to their reviewing IRBs
according to site specific IRB reporting guidelines
62 Clinical Medical Monitoring
There will be an unblinded physician at the IPFnet DCC serving as medical monitor The
medical monitor will be available to assist with questions about dosage adjustments of study
medications including discontinuation or resumption of medications
63 Unblinding Procedures
Unblinding of subjects or investigators to subject treatment is strongly discouraged For ongoing
clinical management all subjects should be presumed to be receiving ldquoactiverdquo study drug To
ensure the subjectrsquos safety the study treatment will be dose-adjusted based on laboratory test
results clinical findings and symptoms
The IPFnet DCC medical monitor and PANTHER-IPF co-chairs Drs Ganesh Raghu and
Fernando Martinez will be available to the study physicians to discuss study drug management
on a case-by-case basis Un-blinding will be considered ONLY when the knowledge of subject
treatment assignment is ABSOLUTELY ESSENTIAL for subject safety and after discussion of
the subjectrsquos case with the medical monitor and either Dr Raghu or Dr Martinez Unblinding of
study treatment should be minimized during the conduct of the trial In those cases where it is
felt to be medically necessary the DCC medical officer will communicate directly with the
managing physician to minimize unblinding of study personnel
52
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
7 Study Drug Procedures
At the baseline 15-week 30-week and 45-week study visits subjects will receive a supply of
study drug sufficient to last until the next visit at which study drug will be dispensed
53
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
8 Data Management
81 Hardware and Software Configuration
811 Hardware and Database Software
Data will be stored in an Oracle database system Oracle has advantages of processing efficiency
and smooth linkage with other software systems The application and database will be hosted on
Solaris Unix servers at the IPFnet DCC
812 Statistical Software
SAS will be used as the principal application for the management of analysis data files and
statistical computations S-Plus will be used to provide supplementary functions as needed
813 Access Control and Confidentiality Procedures
Access to databases will be controlled centrally by the IPFnet DCC through user passwords
linked to appropriate privileges This protects the data from unauthorized changes and
inadvertent loss or damage
814 Security
Database and Web servers will be secured by a firewall and through controlled physical access
Oracle has many security features to ensure that any staff member accessing the database has the
proper authority to perform the functions he or she requests of the system Within the secondary
SAS databases Unix group-access control maintains similar security The Sun workstation login
is secured by extensive user-password facilities under Unix
54
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
815 Back-up Procedures
Database back-up will be performed automatically every day and standard IPFnet DCC policies
and procedures will be applied to dictate tape rotation and retention practices
816 Virus Protection
All disk drives that provide network services and all user computers will be protected using
virus-scanning software Standard IPFnet DCC policies will be applied to update these protection
systems periodically through the study
82 Sources of Data
821 Design and Development
The IPFnet DCC will be responsible for development of the electronic case report forms
(eCRFs) development and validation of the clinical study database ensuring data integrity and
training clinical center staff on applicable data management procedures A web-based distributed
data entry model will be implemented This system will be developed to ensure that guidelines
and regulations surrounding the use of computerized systems used in clinical trials are upheld
The remainder of this section provides an overview of the data management plan associated with
this protocol
822 Data Collection Forms
The data collection process consists of direct data entry at the study clinical centers into the EDC
system(s) provided by the DCC A data collection worksheet will be provided to clinical centers
for recording data in the event the EDC system is unavailable Data entry of the eCRFs should
be completed according to the instructions provided and project specific training The
investigator is responsible for maintaining accurate complete and up-to-date records and for
ensuring the completion of the eCRFs for each research participant
55
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
823 Data Acquisition and Entry
Data entry into eCRFs shall be performed by authorized individuals Selected eCRFs may also
require the investigatorrsquos written signature or electronic signature as appropriate Electronic
CRFs will be monitored for completeness accuracy and attention to detail during the study
824 Data Center Responsibilities
The IPFnet DCC will 1) develop a data management plan and will conduct data management
activities 2) provide final eCRFs for the collection of all data required by the study 3) develop
data dictionaries for each eCRF that will comprehensively define each data element 4) conduct
ongoing data monitoring activities on study data 5) monitor any preliminary analysis data
cleanup activities and 6) rigorously monitor final study data clean up
825 Data Editing
Completed data will be entered into the IPFnet DCC automated data acquisition and
management system If incomplete or inaccurate data are found a data clarification request will
be generated and distributed to clinical centers for a response Clinical centers will resolve data
inconsistencies and errors and enter all corrections and changes into the IPFnet DCC automated
data acquisition and management system
826 Training
The training plan for clinical center staff includes provisions for training on assessments eCRF
completion guidelines data management procedures and the use of computerized systems
56
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
9 Study Design and Data Analysis
91 General Analytic Considerations
All primary analyses will be based on intent-to-treat (ITT) principles using all randomized
subjects Baseline factors across groups will be compared using mean (standard deviation) and
median (25th and 75th percentiles) summary measures Kaplan-Meier curves will be used to
display event rates Due to clinical interest in departures from both sides of the null hypothesis
all test statistics will be 2-sided
Reasonable caution needs to be taken when conducting multiple analyses on key clinical
subgroups For subgroup analyses a conservative significance level of 0001 will be used for all
interaction tests Thus subgroup comparisons will be considered exploratory unless the p-value
from the interaction test is smaller than 0001
92 Randomization Blinding and Reporting of Results
A permuted block-randomization scheme will be created with varying block sizes stratified by
clinical center Once a subject has completed the screening and baseline period and evaluation
for inclusionexclusion criteria the randomization process will begin Subjects will be
randomized to receive NAC or matching placebo with equal probability (11) via telephone
contact with a central interactive voice response system (IVRS) using a toll-free randomization
number On the day of randomization after the subject has successfully met all inclusion and
exclusion criteria the investigator or designee will call the central randomization number to
obtain the assigned kit randomization numbers for that subject At each subject visit the
investigator or designee will call the central randomization number to obtain the new kit
randomization numbers for resupply of the subject For resupply of the clinical center the IVRS
will monitor minimal volume of a kit type andor expiration date and will automatically notify
the pharmacy
57
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
The trial results will be reported according to guidelines specified in the CONSORT statement
A flow diagram describing screening recruitment randomization dropout and vital status will
be included in the primary manuscript AEs and efficacy data will be presented for all treatment
groups Adherence dropout and lost to follow-up will be carefully examined across all treatment
groups Analyses of safety will be based on data from all randomized subjects who received at
least one dose of study drug
93 Stratification
Subjects will be distributed to the two treatment arms in a 11 allocation ratio Stratification
blocks will be based on clinical centers
94 Specification of the Primary Analyses
A mixed model repeated measures (MMRM) analysis described in section 95 will be used to
compare differences in the slope of FVC measurements across the treatment groups Response
variables are values of the FVC measured at baseline and every 15 weeks until study completion
Variables in the model will include treatment time and time by treatment age sex race and
height Contrast estimates of differences in slopes of treatment over time (along with confidence
intervals) will be used to estimate the treatment effect The validity of this model in terms of
meeting modeling assumptions will be assessed via standard modeling diagnostics and goodness-
of-fit measures Based on the MMRM framework missing FVC data will not be imputed for the
primary analysis
95 Analysis of Longitudinal Endpoints
A common goal in clinical trials is to specify models that are easily implemented and
reproducible by independent data analysts On the other hand the models should have proper
statistical behavior in terms of low bias and high precision Many common approaches to
longitudinal data analysis including last observation carried forward (LOCF) imputation rely on
the missing completely at random (MCAR) assumption However the MCAR assumption is
58
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
unlikely to hold in many clinical trials because missing data are often related to disease
progression and prognosis A more reasonable assumption missing at random (MAR) specifies
that the complete data distribution can be modeled using only the observed data The likelihood-
based MMRM approach is valid under the more general MAR assumptions These models will
be applied to analyze the longitudinal data secondary endpoints
The advantages of MMRM analysis are that all important characteristics of the model can be preshy
specified standard software can be used to implement the models and results are based on ITT
principles43 In addition the MMRM approach offers superior control of Type I and Type II
errors compared with the LOCF approach
Response variables are values of the PFTs measured at enrollment and every 15 weeks until
study completion and 6MWT values measured at baseline week 30 and week 60 Covariates are
treatment time time by treatment and key baseline risk factors Contrasts (along with
confidence intervals) of treatment by time will be used to estimate the treatment effect
The correlation structure involves multiple pieces including measurement errors random
variation and interindividual variability For the longitudinal data analyses an unstructured
correlation matrix for within-subject errors will be assumed Other correlation structures
including compound symmetry will be examined as needed A careful examination of reasons
for study discontinuation will be conducted to assess the validity of MCAR Sensitivity analyses
will be used to examine the untestable assumption that the observed data violate the MAR
assumption The MMRM models will be implemented using PROC MIXED in SAS
96 Analysis of Binary Time-to-Event and Time-Lagged Endpoints
Regression modeling approaches using either the logistic regression model or Cox proportional
hazards regression model will be employed when appropriate The validity of these models will
be assessed via standard modeling diagnostics and goodness-of-fit measures Estimates of
cumulative frequencies for more general time-lagged responses will be calculated using the
partitioned version of the Bang-Tsiatis estimator44 The partitions will be set at 15-week intervals
59
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
to correspond with the data-collection process Covariate adjusted event rates will be calculated
using inverse probability-weighted regression estimates45
97 Power Analysis
971 Primary Analyses
Based on previously published IPF clinical trials the PL group is expected to experience a drop
in FVC of approximately 020 L over the study period (see Figure 1) The IPFnet Steering Group
determined a clinically important difference would be to preserve the majority of the decline
relative to PL over the study period In particular a treatment effect of 015 L was determined to
be a clinically meaningful difference Potential dropout is a key factor in the proposed study The
drop-out process assumed 5 lost to follow-up after every study visit Only 80 of subjects
were assumed to be followed for the entire study period All models assumed a compound
symmetry structure for the covariance matrix Power calculations were performed using a SAS
IML program for designing repeated measures studies46 Based on preliminary reviews of the
data from the University of Michigan the covariance matrix parameters were estimated at
approximately σ2 = 0757 (variance parameter) and ρ = 0936 (correlation parameter) To be
conservative the power calculations for the primary analysis were performed with parameter
setting of σ2 = 0810 (variance parameter) and ρ = 0925 (correlation parameter)
The power calculations assume a correction for imperfect compliance proposed by Lachin and
Foulkes to allow for 2 noncompliance for each of the treatment arms47 Thus the sample size
of 130 subjects per arm would be reduced to an adjusted sample size of 130(1-002-002)2 =
1198 or 120 subjects per arm
Under the assumed Type I error rate of 005 with a correlation parameter of 0925 and standard
deviation of 090 the difference of 015 L (or 00025 Lweek) shown in Table 6 would have
power of 93
60
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Table 6 Hypothetical Values of Mean FVC (L) Change from Baseline
Week 15 Week 30 Week 45 Week 60
NAC 00125 00250 00375 00500
Placebo 00500 01000 01500 02000
Difference 00375 00750 01125 01500
Abbreviations FVC forced vital capacity PL placebo
972 Power Analysis for Secondary Endpoints
Power calculations for secondary endpoint measurements are shown in Table 7 Standard
deviations are based on unpublished data provided by the University of Michigan The
calculations are based on a 2-sample t-test with Type I error rate set at 005 These calculations
are likely to be conservative because the statistical approach described in section 95 for
analyzing these endpoints will incorporate incomplete observations as well as intermediate data
points
Table 7 Detectable Differences in Treatment Means for Selected Endpoint Measurements
Secondary Endpoints Std Dev
of the Baseline Score
Detectable Difference for 80 Power
Std Dev of the Change Score
Difference Detectable for
80 Power
DLCOpred 166 58 91 32
6MWT Area Under the Desaturation Curve
219 76 175 61
6MWT Distance to Desaturation 224 78 315 110
6MWT Minutes Walked 210 073 205 071
Abbreviations Std Dev standard deviation DLCOpred diffusing capacity of the lung for carbon monoxide percent predicted 6MWT 6-minute walk test
61
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
10 Study Administration
101 Cooperative Agreement Mechanism
The administrative and funding mechanism used to undertake this project is a ldquocooperative
agreementrdquo (U01) which is an assistance mechanism Under the cooperative agreement the
NHLBI assists supports andor stimulates the project and is substantially involved with
investigators in conducting the study by facilitating performance of the effort in a ldquopartnerrdquo role
The NHLBI project scientist serves on the IPFnet Steering Group and he or another NHLBI
scientist may serve on other project committees when appropriate At the same time however
NHLBI does not assume a dominant role direction or prime responsibility for this research
program
As described below governance of the project is conducted through the IPFnet Steering Group
Principal investigators have lead responsibilities in all aspects of their trials and the project
including any modification of trial designs conduct of the trials quality control data analysis
and interpretation preparation of publications and collaboration with other investigators unless
otherwise provided for by the IPFnet Steering Group
PIs retain custody of and have primary rights to their center-specific and collaborative data
subject to government rights-of-access consistent with current Health amp Human Services (HHS)
Public Health Service (PHS) and National Institutes of Health policies The protocols and
governance policies call for the continual submission of data centrally to the IPFnet DCC for the
collaborative database which at a minimum will contain the key variables selected by the IPFnet
Steering Group for standardization across all clinical centers the submission of copies of the
collaborative datasets to each PI upon completion of the project procedures for data analysis
reporting and publication and procedures to protect and ensure the privacy of medical and
genetic data and records of individuals The NHLBI project scientist on behalf of the NHLBI
will have the same access privileges and responsibilities regarding the collaborative data as the
other members of the Steering Group
62
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
PIs are also encouraged to publish and to publicly release and disseminate results data and other
products of the project concordant with the project protocols and governance and the approved
plan for making data and materials available to the scientific community and to the NHLBI
However during the 3 years after the ending date of NHLBI project support unpublished data
unpublished results data sets not previously released and other study materials or products are
to be made available to any third party only with the approval of the IPFnet Steering Group
Upon completion of the project PIs are expected to put their intervention materials and
procedure manuals into the public domain andor make them available to other investigators
according to the approved plan for making data and materials available to the scientific
community and the NHLBI for the conduct of research at no charge other than the costs of
reproduction and distribution
The NHLBI reserves the right to terminate or curtail the project (or an individual award) in the
event of (a) failure to develop or implement mutually agreeable collaborative measurement
subject eligibility and data management sections of the protocols (b) substantial shortfall in
subject recruitment follow-up data reporting or quality control or other major breach of
protocol (c) substantive changes in the agreed-upon protocols with which NHLBI cannot
concur (d) reaching a major project outcome with persuasive statistical significance
substantially before schedule or (e) human subject ethical issues that may dictate a premature
termination
Any disagreement that may arise in scientificprogrammatic matters (within the scope of the
award) between award recipients and the NHLBI may be brought to arbitration An arbitration
panel will be composed of 3 membersmdash1 selected by the IPFnet Steering Group (with the
NHLBI member not voting) or by the individual PI in the event of an individual disagreement a
second selected by NHLBI and the third selected by the other 2 members This special
arbitration procedure in no way affects the PIrsquos right to appeal an adverse action that is otherwise
appealable in accordance with the PHS regulations at 42 CFR part 50 Subpart D and HHS
63
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
regulation at 45 CFR part 16 or the rights of the NHLBI under applicable statutes regulations
and terms of the award
102 IPFnet Steering Group
The IPFnet Steering Group is the main governing body of the project It is composed of the PIs
of the clinical centers the PI of the DCC and the NHLBI project scientist The clinical centers
the IPFnet DCC and the NHLBI each have 1 vote on the IPFnet Steering Group All decisions
are determined by majority vote
All major scientific decisions are determined by the IPFnet Steering Group It assumes overall
responsibility for the design and conduct of the trial It appoints (and disbands) committees and
subcommittees as the need arises designs approves and implements the study protocols
oversees the development of the MOOP monitors subject recruitment and treatment delivery
evaluates data collection and management oversees quality assurance procedures and
implements changes and enhancements to the study as required It also has primary responsibility
for facilitating the conduct of the trials and reporting the projectrsquos results
103 Data and Safety Monitoring Board
The NHLBI will establish a DSMB in accordance with established policies (see
httpwwwnhlbinihgovfundingpoliciesdsmb_insthtm) to ensure data quality and subject
safety and to provide independent advice to the NHLBI regarding progress and the
appropriateness of study continuation
104 Recommendations on Interim Monitoring of Efficacy Safety and Futility
First and foremost the role of the DSMB will be to review subject safety and trial conduct at
periodic points during the study The DSMB may require analyses of the primary endpoint
results for comparing the benefit and risks of treatment strategies The benefit of collecting
additional data on key secondary endpoints with extended follow-up and establishing a robust
64
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
evidence base for determining a standard of care will need to be carefully considered before
early termination of one or more treatment arms After careful consideration the IPFnet Steering
Group recommends conservative thresholds for the early examinations of the safety and efficacy
data
The DSMB will be expected to meet approximately every 6 months until trial completion to
review safety and toxicity data The DSMB may recommend stopping the study based on these
reviews Because the DSMB could stop the trial for safety concerns as well as for a large
efficacy benefit there could be multiple opportunities to reject the null hypothesis (no difference
in event rates between the PL and NAC groups) A Bonferroni approximation will be applied
during the one planned interim analysis for efficacy
Before locking the database a statistical analysis plan (SAP) will be developed to provide
complete details on the statistical analysis The SAP will include the specifics for how and when
the DSMB will be notified for AEs The IPFnet DCC will deliver to the DSMB all FDA-defined
AEs at 3-month intervals The IPFnet DCC will prepare narrative SAE reports in real time for
DSMB review including recommendations and analysis of similar events for each SAE
submitted to the FDA
65
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
11 Investigator and Sponsor Obligations
111 Monitoring
All monitoring activities for US clinical centers will be performed in accordance with DCRI
standard operating procedures Information regarding the types of visits will be outlined in the
PANTHER-IPF MOOP
112 Cost and Payment
There will be no cost to subjects enrolled in this trial Study-related procedures will be paid for
by the IPFnet
Subjects may be eligible for reimbursement for travel to the clinical center Details of payment
will be explained to each subject during the consent process
113 Confidentiality and Health Insurance Portability and Accountability Act
Considerations
Subject confidentiality will be protected throughout the study All subject data will be kept
strictly confidential and no subject-identifying information will be released to anyone outside
the project Confidentiality will be assured through several mechanisms First each subject will
be assigned an anonymous study ID which will then be used on all study forms Second any
study forms blood samples and paper records that contain subject information (eg address lists
phone lists) will be kept at the clinical centers in secured locked areas coded by number Once
blood is collected there will be no subject identifiers placed on blood samplesmdashonly the study
ID number and the date of sample collection Third access to all subject data and information
including laboratory specimens will be restricted to authorized personnel In the case of
computerized data this restricted access will be assured through user logon IDs and password
protection
66
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
At the IPFnet DCC only authorized personnel will have access to the data files containing study
data Security will be assured through user logon IDs passwords and appropriate access
privileges All study subjects will be identified only by their IPFnet ID numbers and no personal
identifying information such as name address or Social Security number will be entered into
the IPFnet DCC database Any subject-specific data reported to the IPFnet Steering Group will
be identified only by the IPFnet ID number
Finally subjects will not be identified by name in any reports or publications nor will the data
be presented in such a way that the identity of individual subjects can be inferred Analysis files
created for further study by the scientific community will have no subject identifiers These data
files will be created in accordance with the Ancillary Studies and Publication Policy of the
IPFnet
114 Informed Consent Procedures
All IPFnet subjects will provide written informed consent using procedures reviewed and
approved by each clinical centerrsquos IRB Informed consent will be undertaken by study personnel
in-person with the subject The subject has the option of declining further participation in the
study at that point No further study procedures will be conducted until the signed documents
have been provided to the IPFnet clinical center
115 Institutional Review Boards
Before initiating this study the protocol clinical center-specific informed consent forms Health
Insurance Portability and Accountability Act (HIPAA) forms recruitment materials and other
relevant information will be reviewed by a properly constituted IRB at each participating clinical
center A copy of the signed and dated IRB approval at each clinical center will be retrieved prior
to or during the site initiation visit and archived at the IPFnet DCC Any amendments to the
protocol other than simple administrative and typographical changes must be approved by each
IRB before they are implemented The clinical centers will seek annual renewals of their IRB
approvals in accordance with local procedures
67
__________________________________________ ________________
__________________________________________
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
12 Investigator Agreement
I have read the foregoing protocol PANTHER-IPF and agree that it contains all necessary
details for carrying out this study I will conduct the study as outlined herein and will complete
the study within the time designated
I will provide copies of the protocol and all pertinent information to all individuals responsible to
me who assist in the conduct of this study I will discuss this material with them to ensure they
are fully informed regarding the drug and the conduct of the study
I will fulfill all responsibilities for submitting pertinent information to the local IRB if
applicable that is responsible for this study
I further agree that NHLBI andor DCRI will have access to any source documents from which
eCRF information may have been generated
Signature of Principal Investigator Date
Name of Principal Investigator (printed or typed)
Protocol version date May 19 2009
Protocol Amendment 1 version date May 28 2010
Protocol Amendment 2 version date December 6 2011
68
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
13 References
1 Raghu G Brown KK Bradford WZ et al A placebo-controlled trial of interferon gamma-1b in patients with idiopathic pulmonary fibrosis N Engl J Med 2004350125-33 2 King TE Jr Safrin S Starko KM et al Analyses of efficacy end points in a controlled trial of interferon-gamma1b for idiopathic pulmonary fibrosis Chest 2005127171-7 3 Flaherty KR Thwaite EL Kazerooni EA et al Radiological versus histological diagnosis in UIP and NSIP survival implications Thorax 200358143-8 4 Wells AU Desai SR Rubens MB et al Idiopathic pulmonary fibrosis a composite physiologic index derived from disease extent observed by computed tomography Am J Respir Crit Care Med 2003167962-9 5 Raghu G Freudenberger TD Yang S et al High prevalence of abnormal acid gastroshyoesophageal reflux in idiopathic pulmonary fibrosis Eur Respir J 200627136-42 6 Kinnula VL Focus on antioxidant enzymes and antioxidant strategies in smoking related airway diseases Thorax 200560693-700 7 Coultas DB Zumwalt RE Black WC Sobonya RE The epidemiology of interstitial lung diseases Am J Respir Crit Care Med 1994150967-72 8 Raghu G Weycker D Edelsberg J Bradford WZ Oster G Incidence and prevalence of idiopathic pulmonary fibrosis Am J Respir Crit Care Med 2006174810-6 9 Olson AL Swigris JJ Lezotte DC Norris JM Wilson CG Brown KK Mortality from pulmonary fibrosis increased in the United States from 1992 to 2003 Am J Respir Crit Care Med 2007176277-84 10 Mannino DM Etzel RA Parrish RG Pulmonary fibrosis deaths in the United States 1979shy1991 An analysis of multiple-cause mortality data Am J Respir Crit Care Med 19961531548shy52 11 Hubbard R Johnston I Coultas DB Britton J Mortality rates from cryptogenic fibrosing alveolitis in seven countries Thorax 199651711-6 12 Johnston I Britton J Kinnear W Logan R Rising mortality from cryptogenic fibrosing alveolitis Bmj 19903011017-21 13 Raghu G Collard HR Egan JJ et al An official ATSERSJRSALAT statement idiopathic pulmonary fibrosis evidence-based guidelines for diagnosis and management Am J Respir Crit Care Med 2011183788-824 14 (USA) FDA FDA Public Health Advisory Interferon gamma-1b (marketed as Actimmune) In 2007 15 King TE Jr Pardo A Selman M Idiopathic pulmonary fibrosis Lancet 2011 16 Raghu G Brown KK Costabel U et al Treatment of idiopathic pulmonary fibrosis with etanercept an exploratory placebo-controlled trial Am J Respir Crit Care Med 2008178948shy55 17 Malouf MA Hopkins P Snell G Glanville AR An investigator-driven study of everolimus in surgical lung biopsy confirmed idiopathic pulmonary fibrosis Respirology 201116776-83 18 King TE Jr Behr J Brown KK et al BUILD-1 a randomized placebo-controlled trial of bosentan in idiopathic pulmonary fibrosis Am J Respir Crit Care Med 200817775-81 19 Richeldi L Costabel U Selman M et al Efficacy of a tyrosine kinase inhibitor in idiopathic pulmonary fibrosis N Engl J Med 20113651079-87
69
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
20 Borok Z Buhl R Grimes GJ et al Effect of glutathione aerosol on oxidant-antioxidant imbalance in idiopathic pulmonary fibrosis Lancet 1991338215-6 21 Meyer A Buhl R Magnussen H The effect of oral N-acetylcysteine on lung glutathione levels in idiopathic pulmonary fibrosis Eur Respir J 19947431-6 22 Behr J Maier K Degenkolb B Krombach F Vogelmeier C Antioxidative and clinical effects of high-dose N-acetylcysteine in fibrosing alveolitis Adjunctive therapy to maintenance immunosuppression Am J Respir Crit Care Med 19971561897-901 23 Cantin AM North SL Fells GA Hubbard RC Crystal RG Oxidant-mediated epithelial cell injury in idiopathic pulmonary fibrosis J Clin Invest 1987791665-73 24 Waghray M Cui Z Horowitz JC et al Hydrogen peroxide is a diffusible paracrine signal for the induction of epithelial cell death by activated myofibroblasts Faseb J 200519854-6 25 Larios JM Budhiraja R Fanburg BL Thannickal VJ Oxidative protein cross-linking reactions involving L-tyrosine in transforming growth factor-beta1-stimulated fibroblasts J Biol Chem 200127617437-41 26 Kinnula VL Fattman CL Tan RJ Oury TD Oxidative stress in pulmonary fibrosis a possible role for redox modulatory therapy Am J Respir Crit Care Med 2005172417-22 27 Meyer A Buhl R Kampf S Magnussen H Intravenous N-acetylcysteine and lung glutathione of patients with pulmonary fibrosis and normals Am J Respir Crit Care Med 19951521055-60 28 Behr J Degenkolb B Krombach F Vogelmeier C Intracellular glutathione and bronchoalveolar cells in fibrosing alveolitis effects of N-acetylcysteine Eur Respir J 200219906-11 29 Bando M Hosono T Mato N et al Long-term efficacy of inhaled N-acetylcysteine in patients with idiopathic pulmonary fibrosis Intern Med 2010492289-96 30 Demedts M Behr J Buhl R et al High-dose acetylcysteine in idiopathic pulmonary fibrosis N Engl J Med 20053532229-42 31 Toma TP Bhowmik A Rajakulasingam R Acetylcysteine in pulmonary fibrosis N Engl J Med 20063541086-9 author reply -9 32 Hunninghake GW Antioxidant therapy for idiopathic pulmonary fibrosis N Engl J Med 20053532285-7 33 Flaherty KR Mumford JA Murray S et al Prognostic implications of physiologic and radiographic changes in idiopathic interstitial pneumonia Am J Respir Crit Care Med 2003168543-8 34 Latsi PI du Bois RM Nicholson AG et al Fibrotic idiopathic interstitial pneumonia the prognostic value of longitudinal functional trends Am J Respir Crit Care Med 2003168531-7 35 Collard HR King TE Jr Bartelson BB Vourlekis JS Schwarz MI Brown KK Changes in clinical and physiologic variables predict survival in idiopathic pulmonary fibrosis Am J Respir Crit Care Med 2003168538-42 36 Jegal Y Kim DS Shim TS et al Physiology is a stronger predictor of survival than pathology in fibrotic interstitial pneumonia Am J Respir Crit Care Med 2005171639-44 37 Martinez FJ Safrin S Weycker D et al The clinical course of patients with idiopathic pulmonary fibrosis Ann Intern Med 2005142963-7 38 Hull JH Acetylcysteine in pulmonary fibrosis N Engl J Med 20063541089-91 author reply -91
70
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
39 Flaherty KR King TE Jr Raghu G et al Idiopathic interstitial pneumonia what is the effect of a multidisciplinary approach to diagnosis Am J Respir Crit Care Med 2004170904shy10 40 Raghu G Johnson WC Lockhart D Mageto Y Treatment of idiopathic pulmonary fibrosis with a new antifibrotic agent pirfenidone results of a prospective open-label Phase II study Am J Respir Crit Care Med 19991591061-9 41 Hunninghake GW Lynch DA Galvin JR et al Radiologic findings are strongly associated with a pathologic diagnosis of usual interstitial pneumonia Chest 20031241215-23 42 Lynch D Godwin J Safrin S et al High-resolution computed tomography in idiopathic pulmonary fibrosis diagnosis and prognosis Am J Respir Crit Care Med 2005172488-93 43 Mallinckrodt CH Watkin JG Molenberghs G Carroll RJ Choice of the primary analysis in longitudinal clinical trials Pharmaceutical Statistics 20043161-9 44 Bang H Tsiatis A Estimating medical costs with censored data Biometrika 200087329shy43 45 Lin DY Regression analysis of incomplete medical cost data Stat Med 2003221181-200 46 Rochon J Application of GEE procedures for sample size calculations in repeated measures experiments Stat Med 1998171643-58 47 Lachin JM Foulkes MA Evaluation of sample size and power for analyses of survival with allowance for nonuniform patient entry losses to follow-up noncompliance and stratification Biometrics 198642507-19
71
- PANTHER-IPFPREDNISONE AZATHIOPRINEAND N-ACETYLCYSTEINEA STUDY THAT EVALUATES RESPONSE INIDIOPATHIC PULMONARY FIBROSIS
-
- Protocol Summary
- Table of Contents
- List of Tables
- List of Figures
- List of Abbreviations
- 1 Summary
- 2 Hypotheses and Specific Aims
-
- 21 Null Hypothesis
- 22 Specific Aim 1
- 23 Specific Aim 2
- 24 Prespecified Subgroups of Interest
-
- 3 Background and Significance
-
- 31 Idiopathic Pulmonary Fibrosis is the Most Common Interstitial Lung Disease
- 32 Rationale for Placebo Control
- 33 Rationale for N-acetylcysteine
- 35 Rationale for N-acetylcysteine as a Stand-alone Therapy
- 36 Rationale for the Study Design and Primary Endpoint
- 37 Rationale for Blinding of Treatments
-
- 4 Methods
-
- 41 Inclusion Criteria
- 42 Diagnosis of IPF
- 43 Exclusion Criteria
- 44 Study Design and Study Visit
- 45 Dose Justification
- 46 Contraindications Precautions and Side Effects of Study Medications
- 47 Recruitment Procedures
- 48 Study Procedures
- 49 Concomitant Medications
- 410 Laboratory Testing
- 411 Blinding of Study Drugs
-
- 5 Study Endpoints
-
- 51 Primary Study Endpoint
- 52 Secondary Study Endpoints
-
- 6 Safety Evaluations and Procedures
-
- 61 Adverse Events
- 62 Clinical Medical Monitoring
- 63 Unblinding Procedures
-
- 7 Study Drug Procedures
- 8 Data Management
-
- 81 Hardware and Software Configuration
- 82 Sources of Data
-
- 9 Study Design and Data Analysis
-
- 91 General Analytic Considerations
- 92 Randomization Blinding and Reporting of Results
- 93 Stratification
- 94 Specification of the Primary Analyses
- 95 Analysis of Longitudinal Endpoints
- 96 Analysis of Binary Time-to-Event and Time-Lagged Endpoints
- 97 Power Analysis
-
- 10 Study Administration
-
- 101 Cooperative Agreement Mechanism
- 102 IPFnet Steering Group
- 103 Data and Safety Monitoring Board
- 104 Recommendations on Interim Monitoring of Efficacy Safety and Futility
-
- 11 Investigator and Sponsor Obligations
-
- 111 Monitoring
- 112 Cost and Payment
- 113 Confidentiality and Health Insurance Portability and Accountability ActConsiderations
- 114 Informed Consent Procedures
- 115 Institutional Review Boards
-
- 12 Investigator Agreement
- 13 References
-
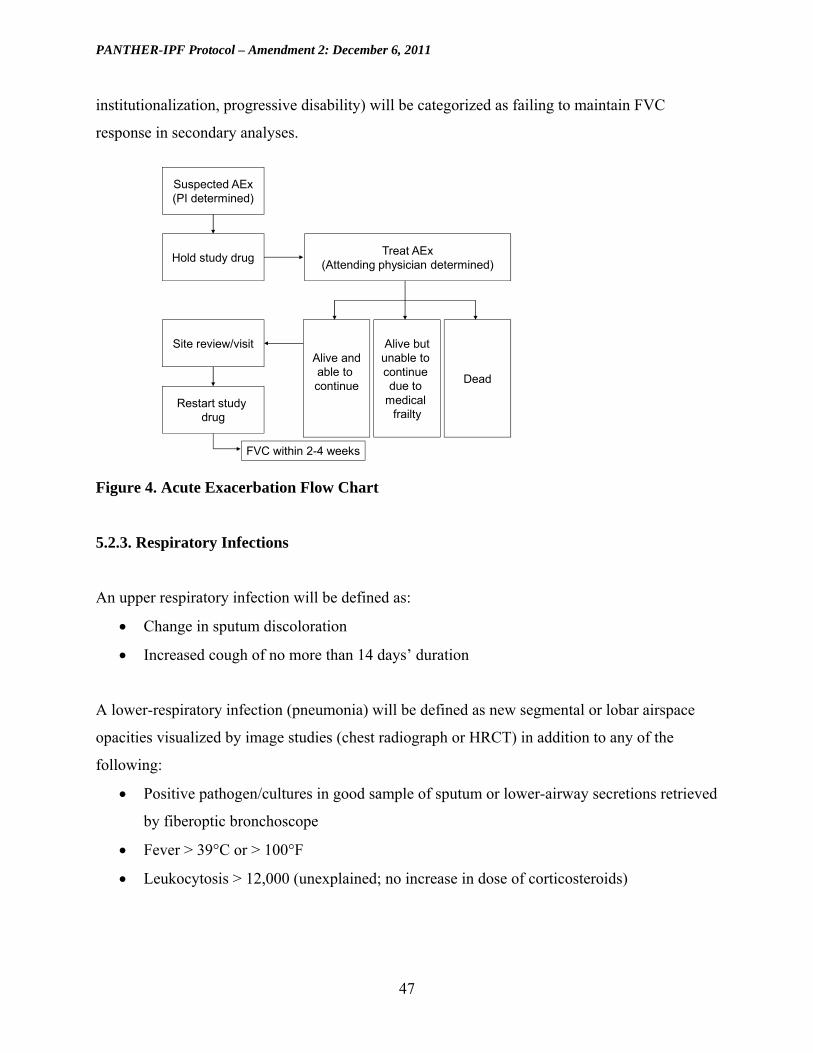
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
institutionalization progressive disability) will be categorized as failing to maintain FVC
response in secondary analyses
Suspected AEx (PI determined)
Hold study drug Treat AEx
(Attending physician determined)
Alive but unable to continue due to
medical frailty
Dead
Alive and able to continue
Site reviewvisit
Restart study drug
FVC within 2-4 weeks
Figure 4 Acute Exacerbation Flow Chart
523 Respiratory Infections
An upper respiratory infection will be defined as
Change in sputum discoloration
Increased cough of no more than 14 daysrsquo duration
A lower-respiratory infection (pneumonia) will be defined as new segmental or lobar airspace
opacities visualized by image studies (chest radiograph or HRCT) in addition to any of the
following
Positive pathogencultures in good sample of sputum or lower-airway secretions retrieved
by fiberoptic bronchoscope
Fever gt 39degC or gt 100degF
Leukocytosis gt 12000 (unexplained no increase in dose of corticosteroids)
47
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
524 Maintained FVC Response
Subjects with follow-up FVCpred measurements at or above their baseline FVCpred level
will be classified as having maintained FVC response Subjects with reduced FVCpred levels
or missing data for any reason including death or medical frailty will be classified as having not
maintained FVC response The FVCpred value is used because unadjusted FVC measurements
are expected to decline with age
48
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
6 Safety Evaluations and Procedures
61 Adverse Events
During a clinical trial the reporting of adverse experience information can lead to important
changes in the way a new treatment is developed as well as provide integral safety data
611 Definitions
An adverse event (AE) is any untoward medical occurrence in a subject or clinical investigation
subject who was administered a pharmaceutical product The AE does not necessarily have to
have a causal relationship with the drug administered An AE can be any unfavorable and
unintended sign (including an abnormal laboratory finding) symptom or disease temporarily
associated with the use of a medicinal product whether or not considered to be related to the
medicinal product Diseases signs symptoms or laboratory abnormalities already existing at
enrollment are not considered AEs unless they worsen (ie increase in intensity or frequency)
Surgical procedures themselves are not AEs they are therapeutic measures for conditions that
require surgery The condition for which the surgery is required may be an AE Surgical
procedures planned before randomization and the conditions necessitating the surgery are not
AEs
A serious adverse event is any untoward event that
Is fatal
Is life-threatening
Requires inpatient hospitalization or prolongation of existing hospitalization with the
following exceptions
o Preplanned (before the study) hospital admissions unless the hospitalization is
prolonged
o Planned admissions (as part of a study eg routine biopsies)
o Hospitalization lasting lt 24 hours
49
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
o Hospitalization for elective procedure
o Emergency room visits
Results in persistent or significant disability or incapacity
Is a congenital anomaly or birth defect
Important medical events that may not result in death be life-threatening or require
inpatient hospitalization may be considered serious adverse events (SAEs) when based
on appropriate medical judgment they may jeopardize the subject and may require
medical or surgical intervention to prevent one of the outcomes listed above
Life-threatening means that the subject was in the view of the investigator at immediate risk of
death from the AE as it occurred It does not include an AE that had it occurred in a more severe
form might have caused death
Persistent or significant disabilityincapacity means that the event resulted in permanent or
significant and substantial disruption of the subjectrsquos ability to carry out normal life functions
Causality
A reasonable possibility means the AE may have been caused byrelated to the study drug A
perceived or real lack of efficacy does not satisfy the definition of relatedness
612 Adverse Event (AE) Reporting
For the PANTHER-IPF trial all AEs (serious and nonserious) occurring from randomization
through final study visit (4 weeks after final dose of all study medication) will be recorded on the
AE page of the case report form (CRF)
6121 Serious Adverse Events (SAE) Reporting
For this trial all deaths and all SAEs which occur from randomization through final study visit
must be entered within the EDC system via the SAE eCRF page within 24 hours of the
investigative sitersquos knowledge of the event It is the responsibility of the clinical center
50
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
investigator to provide a causality assessment of the event for each study medications based upon
the information available at the time of the report It is understood that complete information
about the event may not be known at the time the initial report is submitted In the event the EDC
system is not accessible to the site at the time of event reporting investigative sites will complete
and forward a paper back-up SAE form to DCRI Safety Surveillance for processing
DCRI Safety Surveillance
Telephone 1-919-668-8624 or 1-866-668-7799 (toll free)
Fax 1-919-668-7138 or 1-866-668-7138 (toll free)
The investigator must complete and submit follow-up SAE information via the eCRF when
important new or follow-up information (eg final diagnosis outcome results of specific
investigations) becomes available Follow-up information should be submitted according to the
same process used for reporting the initial event as described above All SAEs will be followed
until resolution stabilization or 30 days after the subject has completed the final visit (4 weeks
after the final dose of study medication) whichever occurs first The investigator is responsible
for reporting SAEs to their institutional review board (IRB) per site specific IRB reporting
guidelines
6122 Regulatory Reporting
AEs that are serious study drug related and unexpected will be reported to the regulatory
authorities The DCRI Safety Surveillance medical monitor will perform a medical review of all
SAEs submitted and evaluate for ldquounexpectednessrdquo DCRI Safety Surveillance will prepare
MedWatch reports for those events identified as serious study drug related and unexpected as
determined by Safety Medical Monitor
DCRI Regulatory Services will submit all unexpected study drug-related SAEs as per 21 CFR
32 DCRI Safety Surveillance will provide a safety alert letter to the NHLBI DSMB and DCC
clinical operation (for distribution to sites) within 15 days of initial receipt of the information
51
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Investigators are responsible for promptly reporting these events to their reviewing IRBs
according to site specific IRB reporting guidelines
62 Clinical Medical Monitoring
There will be an unblinded physician at the IPFnet DCC serving as medical monitor The
medical monitor will be available to assist with questions about dosage adjustments of study
medications including discontinuation or resumption of medications
63 Unblinding Procedures
Unblinding of subjects or investigators to subject treatment is strongly discouraged For ongoing
clinical management all subjects should be presumed to be receiving ldquoactiverdquo study drug To
ensure the subjectrsquos safety the study treatment will be dose-adjusted based on laboratory test
results clinical findings and symptoms
The IPFnet DCC medical monitor and PANTHER-IPF co-chairs Drs Ganesh Raghu and
Fernando Martinez will be available to the study physicians to discuss study drug management
on a case-by-case basis Un-blinding will be considered ONLY when the knowledge of subject
treatment assignment is ABSOLUTELY ESSENTIAL for subject safety and after discussion of
the subjectrsquos case with the medical monitor and either Dr Raghu or Dr Martinez Unblinding of
study treatment should be minimized during the conduct of the trial In those cases where it is
felt to be medically necessary the DCC medical officer will communicate directly with the
managing physician to minimize unblinding of study personnel
52
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
7 Study Drug Procedures
At the baseline 15-week 30-week and 45-week study visits subjects will receive a supply of
study drug sufficient to last until the next visit at which study drug will be dispensed
53
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
8 Data Management
81 Hardware and Software Configuration
811 Hardware and Database Software
Data will be stored in an Oracle database system Oracle has advantages of processing efficiency
and smooth linkage with other software systems The application and database will be hosted on
Solaris Unix servers at the IPFnet DCC
812 Statistical Software
SAS will be used as the principal application for the management of analysis data files and
statistical computations S-Plus will be used to provide supplementary functions as needed
813 Access Control and Confidentiality Procedures
Access to databases will be controlled centrally by the IPFnet DCC through user passwords
linked to appropriate privileges This protects the data from unauthorized changes and
inadvertent loss or damage
814 Security
Database and Web servers will be secured by a firewall and through controlled physical access
Oracle has many security features to ensure that any staff member accessing the database has the
proper authority to perform the functions he or she requests of the system Within the secondary
SAS databases Unix group-access control maintains similar security The Sun workstation login
is secured by extensive user-password facilities under Unix
54
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
815 Back-up Procedures
Database back-up will be performed automatically every day and standard IPFnet DCC policies
and procedures will be applied to dictate tape rotation and retention practices
816 Virus Protection
All disk drives that provide network services and all user computers will be protected using
virus-scanning software Standard IPFnet DCC policies will be applied to update these protection
systems periodically through the study
82 Sources of Data
821 Design and Development
The IPFnet DCC will be responsible for development of the electronic case report forms
(eCRFs) development and validation of the clinical study database ensuring data integrity and
training clinical center staff on applicable data management procedures A web-based distributed
data entry model will be implemented This system will be developed to ensure that guidelines
and regulations surrounding the use of computerized systems used in clinical trials are upheld
The remainder of this section provides an overview of the data management plan associated with
this protocol
822 Data Collection Forms
The data collection process consists of direct data entry at the study clinical centers into the EDC
system(s) provided by the DCC A data collection worksheet will be provided to clinical centers
for recording data in the event the EDC system is unavailable Data entry of the eCRFs should
be completed according to the instructions provided and project specific training The
investigator is responsible for maintaining accurate complete and up-to-date records and for
ensuring the completion of the eCRFs for each research participant
55
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
823 Data Acquisition and Entry
Data entry into eCRFs shall be performed by authorized individuals Selected eCRFs may also
require the investigatorrsquos written signature or electronic signature as appropriate Electronic
CRFs will be monitored for completeness accuracy and attention to detail during the study
824 Data Center Responsibilities
The IPFnet DCC will 1) develop a data management plan and will conduct data management
activities 2) provide final eCRFs for the collection of all data required by the study 3) develop
data dictionaries for each eCRF that will comprehensively define each data element 4) conduct
ongoing data monitoring activities on study data 5) monitor any preliminary analysis data
cleanup activities and 6) rigorously monitor final study data clean up
825 Data Editing
Completed data will be entered into the IPFnet DCC automated data acquisition and
management system If incomplete or inaccurate data are found a data clarification request will
be generated and distributed to clinical centers for a response Clinical centers will resolve data
inconsistencies and errors and enter all corrections and changes into the IPFnet DCC automated
data acquisition and management system
826 Training
The training plan for clinical center staff includes provisions for training on assessments eCRF
completion guidelines data management procedures and the use of computerized systems
56
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
9 Study Design and Data Analysis
91 General Analytic Considerations
All primary analyses will be based on intent-to-treat (ITT) principles using all randomized
subjects Baseline factors across groups will be compared using mean (standard deviation) and
median (25th and 75th percentiles) summary measures Kaplan-Meier curves will be used to
display event rates Due to clinical interest in departures from both sides of the null hypothesis
all test statistics will be 2-sided
Reasonable caution needs to be taken when conducting multiple analyses on key clinical
subgroups For subgroup analyses a conservative significance level of 0001 will be used for all
interaction tests Thus subgroup comparisons will be considered exploratory unless the p-value
from the interaction test is smaller than 0001
92 Randomization Blinding and Reporting of Results
A permuted block-randomization scheme will be created with varying block sizes stratified by
clinical center Once a subject has completed the screening and baseline period and evaluation
for inclusionexclusion criteria the randomization process will begin Subjects will be
randomized to receive NAC or matching placebo with equal probability (11) via telephone
contact with a central interactive voice response system (IVRS) using a toll-free randomization
number On the day of randomization after the subject has successfully met all inclusion and
exclusion criteria the investigator or designee will call the central randomization number to
obtain the assigned kit randomization numbers for that subject At each subject visit the
investigator or designee will call the central randomization number to obtain the new kit
randomization numbers for resupply of the subject For resupply of the clinical center the IVRS
will monitor minimal volume of a kit type andor expiration date and will automatically notify
the pharmacy
57
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
The trial results will be reported according to guidelines specified in the CONSORT statement
A flow diagram describing screening recruitment randomization dropout and vital status will
be included in the primary manuscript AEs and efficacy data will be presented for all treatment
groups Adherence dropout and lost to follow-up will be carefully examined across all treatment
groups Analyses of safety will be based on data from all randomized subjects who received at
least one dose of study drug
93 Stratification
Subjects will be distributed to the two treatment arms in a 11 allocation ratio Stratification
blocks will be based on clinical centers
94 Specification of the Primary Analyses
A mixed model repeated measures (MMRM) analysis described in section 95 will be used to
compare differences in the slope of FVC measurements across the treatment groups Response
variables are values of the FVC measured at baseline and every 15 weeks until study completion
Variables in the model will include treatment time and time by treatment age sex race and
height Contrast estimates of differences in slopes of treatment over time (along with confidence
intervals) will be used to estimate the treatment effect The validity of this model in terms of
meeting modeling assumptions will be assessed via standard modeling diagnostics and goodness-
of-fit measures Based on the MMRM framework missing FVC data will not be imputed for the
primary analysis
95 Analysis of Longitudinal Endpoints
A common goal in clinical trials is to specify models that are easily implemented and
reproducible by independent data analysts On the other hand the models should have proper
statistical behavior in terms of low bias and high precision Many common approaches to
longitudinal data analysis including last observation carried forward (LOCF) imputation rely on
the missing completely at random (MCAR) assumption However the MCAR assumption is
58
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
unlikely to hold in many clinical trials because missing data are often related to disease
progression and prognosis A more reasonable assumption missing at random (MAR) specifies
that the complete data distribution can be modeled using only the observed data The likelihood-
based MMRM approach is valid under the more general MAR assumptions These models will
be applied to analyze the longitudinal data secondary endpoints
The advantages of MMRM analysis are that all important characteristics of the model can be preshy
specified standard software can be used to implement the models and results are based on ITT
principles43 In addition the MMRM approach offers superior control of Type I and Type II
errors compared with the LOCF approach
Response variables are values of the PFTs measured at enrollment and every 15 weeks until
study completion and 6MWT values measured at baseline week 30 and week 60 Covariates are
treatment time time by treatment and key baseline risk factors Contrasts (along with
confidence intervals) of treatment by time will be used to estimate the treatment effect
The correlation structure involves multiple pieces including measurement errors random
variation and interindividual variability For the longitudinal data analyses an unstructured
correlation matrix for within-subject errors will be assumed Other correlation structures
including compound symmetry will be examined as needed A careful examination of reasons
for study discontinuation will be conducted to assess the validity of MCAR Sensitivity analyses
will be used to examine the untestable assumption that the observed data violate the MAR
assumption The MMRM models will be implemented using PROC MIXED in SAS
96 Analysis of Binary Time-to-Event and Time-Lagged Endpoints
Regression modeling approaches using either the logistic regression model or Cox proportional
hazards regression model will be employed when appropriate The validity of these models will
be assessed via standard modeling diagnostics and goodness-of-fit measures Estimates of
cumulative frequencies for more general time-lagged responses will be calculated using the
partitioned version of the Bang-Tsiatis estimator44 The partitions will be set at 15-week intervals
59
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
to correspond with the data-collection process Covariate adjusted event rates will be calculated
using inverse probability-weighted regression estimates45
97 Power Analysis
971 Primary Analyses
Based on previously published IPF clinical trials the PL group is expected to experience a drop
in FVC of approximately 020 L over the study period (see Figure 1) The IPFnet Steering Group
determined a clinically important difference would be to preserve the majority of the decline
relative to PL over the study period In particular a treatment effect of 015 L was determined to
be a clinically meaningful difference Potential dropout is a key factor in the proposed study The
drop-out process assumed 5 lost to follow-up after every study visit Only 80 of subjects
were assumed to be followed for the entire study period All models assumed a compound
symmetry structure for the covariance matrix Power calculations were performed using a SAS
IML program for designing repeated measures studies46 Based on preliminary reviews of the
data from the University of Michigan the covariance matrix parameters were estimated at
approximately σ2 = 0757 (variance parameter) and ρ = 0936 (correlation parameter) To be
conservative the power calculations for the primary analysis were performed with parameter
setting of σ2 = 0810 (variance parameter) and ρ = 0925 (correlation parameter)
The power calculations assume a correction for imperfect compliance proposed by Lachin and
Foulkes to allow for 2 noncompliance for each of the treatment arms47 Thus the sample size
of 130 subjects per arm would be reduced to an adjusted sample size of 130(1-002-002)2 =
1198 or 120 subjects per arm
Under the assumed Type I error rate of 005 with a correlation parameter of 0925 and standard
deviation of 090 the difference of 015 L (or 00025 Lweek) shown in Table 6 would have
power of 93
60
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Table 6 Hypothetical Values of Mean FVC (L) Change from Baseline
Week 15 Week 30 Week 45 Week 60
NAC 00125 00250 00375 00500
Placebo 00500 01000 01500 02000
Difference 00375 00750 01125 01500
Abbreviations FVC forced vital capacity PL placebo
972 Power Analysis for Secondary Endpoints
Power calculations for secondary endpoint measurements are shown in Table 7 Standard
deviations are based on unpublished data provided by the University of Michigan The
calculations are based on a 2-sample t-test with Type I error rate set at 005 These calculations
are likely to be conservative because the statistical approach described in section 95 for
analyzing these endpoints will incorporate incomplete observations as well as intermediate data
points
Table 7 Detectable Differences in Treatment Means for Selected Endpoint Measurements
Secondary Endpoints Std Dev
of the Baseline Score
Detectable Difference for 80 Power
Std Dev of the Change Score
Difference Detectable for
80 Power
DLCOpred 166 58 91 32
6MWT Area Under the Desaturation Curve
219 76 175 61
6MWT Distance to Desaturation 224 78 315 110
6MWT Minutes Walked 210 073 205 071
Abbreviations Std Dev standard deviation DLCOpred diffusing capacity of the lung for carbon monoxide percent predicted 6MWT 6-minute walk test
61
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
10 Study Administration
101 Cooperative Agreement Mechanism
The administrative and funding mechanism used to undertake this project is a ldquocooperative
agreementrdquo (U01) which is an assistance mechanism Under the cooperative agreement the
NHLBI assists supports andor stimulates the project and is substantially involved with
investigators in conducting the study by facilitating performance of the effort in a ldquopartnerrdquo role
The NHLBI project scientist serves on the IPFnet Steering Group and he or another NHLBI
scientist may serve on other project committees when appropriate At the same time however
NHLBI does not assume a dominant role direction or prime responsibility for this research
program
As described below governance of the project is conducted through the IPFnet Steering Group
Principal investigators have lead responsibilities in all aspects of their trials and the project
including any modification of trial designs conduct of the trials quality control data analysis
and interpretation preparation of publications and collaboration with other investigators unless
otherwise provided for by the IPFnet Steering Group
PIs retain custody of and have primary rights to their center-specific and collaborative data
subject to government rights-of-access consistent with current Health amp Human Services (HHS)
Public Health Service (PHS) and National Institutes of Health policies The protocols and
governance policies call for the continual submission of data centrally to the IPFnet DCC for the
collaborative database which at a minimum will contain the key variables selected by the IPFnet
Steering Group for standardization across all clinical centers the submission of copies of the
collaborative datasets to each PI upon completion of the project procedures for data analysis
reporting and publication and procedures to protect and ensure the privacy of medical and
genetic data and records of individuals The NHLBI project scientist on behalf of the NHLBI
will have the same access privileges and responsibilities regarding the collaborative data as the
other members of the Steering Group
62
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
PIs are also encouraged to publish and to publicly release and disseminate results data and other
products of the project concordant with the project protocols and governance and the approved
plan for making data and materials available to the scientific community and to the NHLBI
However during the 3 years after the ending date of NHLBI project support unpublished data
unpublished results data sets not previously released and other study materials or products are
to be made available to any third party only with the approval of the IPFnet Steering Group
Upon completion of the project PIs are expected to put their intervention materials and
procedure manuals into the public domain andor make them available to other investigators
according to the approved plan for making data and materials available to the scientific
community and the NHLBI for the conduct of research at no charge other than the costs of
reproduction and distribution
The NHLBI reserves the right to terminate or curtail the project (or an individual award) in the
event of (a) failure to develop or implement mutually agreeable collaborative measurement
subject eligibility and data management sections of the protocols (b) substantial shortfall in
subject recruitment follow-up data reporting or quality control or other major breach of
protocol (c) substantive changes in the agreed-upon protocols with which NHLBI cannot
concur (d) reaching a major project outcome with persuasive statistical significance
substantially before schedule or (e) human subject ethical issues that may dictate a premature
termination
Any disagreement that may arise in scientificprogrammatic matters (within the scope of the
award) between award recipients and the NHLBI may be brought to arbitration An arbitration
panel will be composed of 3 membersmdash1 selected by the IPFnet Steering Group (with the
NHLBI member not voting) or by the individual PI in the event of an individual disagreement a
second selected by NHLBI and the third selected by the other 2 members This special
arbitration procedure in no way affects the PIrsquos right to appeal an adverse action that is otherwise
appealable in accordance with the PHS regulations at 42 CFR part 50 Subpart D and HHS
63
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
regulation at 45 CFR part 16 or the rights of the NHLBI under applicable statutes regulations
and terms of the award
102 IPFnet Steering Group
The IPFnet Steering Group is the main governing body of the project It is composed of the PIs
of the clinical centers the PI of the DCC and the NHLBI project scientist The clinical centers
the IPFnet DCC and the NHLBI each have 1 vote on the IPFnet Steering Group All decisions
are determined by majority vote
All major scientific decisions are determined by the IPFnet Steering Group It assumes overall
responsibility for the design and conduct of the trial It appoints (and disbands) committees and
subcommittees as the need arises designs approves and implements the study protocols
oversees the development of the MOOP monitors subject recruitment and treatment delivery
evaluates data collection and management oversees quality assurance procedures and
implements changes and enhancements to the study as required It also has primary responsibility
for facilitating the conduct of the trials and reporting the projectrsquos results
103 Data and Safety Monitoring Board
The NHLBI will establish a DSMB in accordance with established policies (see
httpwwwnhlbinihgovfundingpoliciesdsmb_insthtm) to ensure data quality and subject
safety and to provide independent advice to the NHLBI regarding progress and the
appropriateness of study continuation
104 Recommendations on Interim Monitoring of Efficacy Safety and Futility
First and foremost the role of the DSMB will be to review subject safety and trial conduct at
periodic points during the study The DSMB may require analyses of the primary endpoint
results for comparing the benefit and risks of treatment strategies The benefit of collecting
additional data on key secondary endpoints with extended follow-up and establishing a robust
64
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
evidence base for determining a standard of care will need to be carefully considered before
early termination of one or more treatment arms After careful consideration the IPFnet Steering
Group recommends conservative thresholds for the early examinations of the safety and efficacy
data
The DSMB will be expected to meet approximately every 6 months until trial completion to
review safety and toxicity data The DSMB may recommend stopping the study based on these
reviews Because the DSMB could stop the trial for safety concerns as well as for a large
efficacy benefit there could be multiple opportunities to reject the null hypothesis (no difference
in event rates between the PL and NAC groups) A Bonferroni approximation will be applied
during the one planned interim analysis for efficacy
Before locking the database a statistical analysis plan (SAP) will be developed to provide
complete details on the statistical analysis The SAP will include the specifics for how and when
the DSMB will be notified for AEs The IPFnet DCC will deliver to the DSMB all FDA-defined
AEs at 3-month intervals The IPFnet DCC will prepare narrative SAE reports in real time for
DSMB review including recommendations and analysis of similar events for each SAE
submitted to the FDA
65
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
11 Investigator and Sponsor Obligations
111 Monitoring
All monitoring activities for US clinical centers will be performed in accordance with DCRI
standard operating procedures Information regarding the types of visits will be outlined in the
PANTHER-IPF MOOP
112 Cost and Payment
There will be no cost to subjects enrolled in this trial Study-related procedures will be paid for
by the IPFnet
Subjects may be eligible for reimbursement for travel to the clinical center Details of payment
will be explained to each subject during the consent process
113 Confidentiality and Health Insurance Portability and Accountability Act
Considerations
Subject confidentiality will be protected throughout the study All subject data will be kept
strictly confidential and no subject-identifying information will be released to anyone outside
the project Confidentiality will be assured through several mechanisms First each subject will
be assigned an anonymous study ID which will then be used on all study forms Second any
study forms blood samples and paper records that contain subject information (eg address lists
phone lists) will be kept at the clinical centers in secured locked areas coded by number Once
blood is collected there will be no subject identifiers placed on blood samplesmdashonly the study
ID number and the date of sample collection Third access to all subject data and information
including laboratory specimens will be restricted to authorized personnel In the case of
computerized data this restricted access will be assured through user logon IDs and password
protection
66
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
At the IPFnet DCC only authorized personnel will have access to the data files containing study
data Security will be assured through user logon IDs passwords and appropriate access
privileges All study subjects will be identified only by their IPFnet ID numbers and no personal
identifying information such as name address or Social Security number will be entered into
the IPFnet DCC database Any subject-specific data reported to the IPFnet Steering Group will
be identified only by the IPFnet ID number
Finally subjects will not be identified by name in any reports or publications nor will the data
be presented in such a way that the identity of individual subjects can be inferred Analysis files
created for further study by the scientific community will have no subject identifiers These data
files will be created in accordance with the Ancillary Studies and Publication Policy of the
IPFnet
114 Informed Consent Procedures
All IPFnet subjects will provide written informed consent using procedures reviewed and
approved by each clinical centerrsquos IRB Informed consent will be undertaken by study personnel
in-person with the subject The subject has the option of declining further participation in the
study at that point No further study procedures will be conducted until the signed documents
have been provided to the IPFnet clinical center
115 Institutional Review Boards
Before initiating this study the protocol clinical center-specific informed consent forms Health
Insurance Portability and Accountability Act (HIPAA) forms recruitment materials and other
relevant information will be reviewed by a properly constituted IRB at each participating clinical
center A copy of the signed and dated IRB approval at each clinical center will be retrieved prior
to or during the site initiation visit and archived at the IPFnet DCC Any amendments to the
protocol other than simple administrative and typographical changes must be approved by each
IRB before they are implemented The clinical centers will seek annual renewals of their IRB
approvals in accordance with local procedures
67
__________________________________________ ________________
__________________________________________
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
12 Investigator Agreement
I have read the foregoing protocol PANTHER-IPF and agree that it contains all necessary
details for carrying out this study I will conduct the study as outlined herein and will complete
the study within the time designated
I will provide copies of the protocol and all pertinent information to all individuals responsible to
me who assist in the conduct of this study I will discuss this material with them to ensure they
are fully informed regarding the drug and the conduct of the study
I will fulfill all responsibilities for submitting pertinent information to the local IRB if
applicable that is responsible for this study
I further agree that NHLBI andor DCRI will have access to any source documents from which
eCRF information may have been generated
Signature of Principal Investigator Date
Name of Principal Investigator (printed or typed)
Protocol version date May 19 2009
Protocol Amendment 1 version date May 28 2010
Protocol Amendment 2 version date December 6 2011
68
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
13 References
1 Raghu G Brown KK Bradford WZ et al A placebo-controlled trial of interferon gamma-1b in patients with idiopathic pulmonary fibrosis N Engl J Med 2004350125-33 2 King TE Jr Safrin S Starko KM et al Analyses of efficacy end points in a controlled trial of interferon-gamma1b for idiopathic pulmonary fibrosis Chest 2005127171-7 3 Flaherty KR Thwaite EL Kazerooni EA et al Radiological versus histological diagnosis in UIP and NSIP survival implications Thorax 200358143-8 4 Wells AU Desai SR Rubens MB et al Idiopathic pulmonary fibrosis a composite physiologic index derived from disease extent observed by computed tomography Am J Respir Crit Care Med 2003167962-9 5 Raghu G Freudenberger TD Yang S et al High prevalence of abnormal acid gastroshyoesophageal reflux in idiopathic pulmonary fibrosis Eur Respir J 200627136-42 6 Kinnula VL Focus on antioxidant enzymes and antioxidant strategies in smoking related airway diseases Thorax 200560693-700 7 Coultas DB Zumwalt RE Black WC Sobonya RE The epidemiology of interstitial lung diseases Am J Respir Crit Care Med 1994150967-72 8 Raghu G Weycker D Edelsberg J Bradford WZ Oster G Incidence and prevalence of idiopathic pulmonary fibrosis Am J Respir Crit Care Med 2006174810-6 9 Olson AL Swigris JJ Lezotte DC Norris JM Wilson CG Brown KK Mortality from pulmonary fibrosis increased in the United States from 1992 to 2003 Am J Respir Crit Care Med 2007176277-84 10 Mannino DM Etzel RA Parrish RG Pulmonary fibrosis deaths in the United States 1979shy1991 An analysis of multiple-cause mortality data Am J Respir Crit Care Med 19961531548shy52 11 Hubbard R Johnston I Coultas DB Britton J Mortality rates from cryptogenic fibrosing alveolitis in seven countries Thorax 199651711-6 12 Johnston I Britton J Kinnear W Logan R Rising mortality from cryptogenic fibrosing alveolitis Bmj 19903011017-21 13 Raghu G Collard HR Egan JJ et al An official ATSERSJRSALAT statement idiopathic pulmonary fibrosis evidence-based guidelines for diagnosis and management Am J Respir Crit Care Med 2011183788-824 14 (USA) FDA FDA Public Health Advisory Interferon gamma-1b (marketed as Actimmune) In 2007 15 King TE Jr Pardo A Selman M Idiopathic pulmonary fibrosis Lancet 2011 16 Raghu G Brown KK Costabel U et al Treatment of idiopathic pulmonary fibrosis with etanercept an exploratory placebo-controlled trial Am J Respir Crit Care Med 2008178948shy55 17 Malouf MA Hopkins P Snell G Glanville AR An investigator-driven study of everolimus in surgical lung biopsy confirmed idiopathic pulmonary fibrosis Respirology 201116776-83 18 King TE Jr Behr J Brown KK et al BUILD-1 a randomized placebo-controlled trial of bosentan in idiopathic pulmonary fibrosis Am J Respir Crit Care Med 200817775-81 19 Richeldi L Costabel U Selman M et al Efficacy of a tyrosine kinase inhibitor in idiopathic pulmonary fibrosis N Engl J Med 20113651079-87
69
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
20 Borok Z Buhl R Grimes GJ et al Effect of glutathione aerosol on oxidant-antioxidant imbalance in idiopathic pulmonary fibrosis Lancet 1991338215-6 21 Meyer A Buhl R Magnussen H The effect of oral N-acetylcysteine on lung glutathione levels in idiopathic pulmonary fibrosis Eur Respir J 19947431-6 22 Behr J Maier K Degenkolb B Krombach F Vogelmeier C Antioxidative and clinical effects of high-dose N-acetylcysteine in fibrosing alveolitis Adjunctive therapy to maintenance immunosuppression Am J Respir Crit Care Med 19971561897-901 23 Cantin AM North SL Fells GA Hubbard RC Crystal RG Oxidant-mediated epithelial cell injury in idiopathic pulmonary fibrosis J Clin Invest 1987791665-73 24 Waghray M Cui Z Horowitz JC et al Hydrogen peroxide is a diffusible paracrine signal for the induction of epithelial cell death by activated myofibroblasts Faseb J 200519854-6 25 Larios JM Budhiraja R Fanburg BL Thannickal VJ Oxidative protein cross-linking reactions involving L-tyrosine in transforming growth factor-beta1-stimulated fibroblasts J Biol Chem 200127617437-41 26 Kinnula VL Fattman CL Tan RJ Oury TD Oxidative stress in pulmonary fibrosis a possible role for redox modulatory therapy Am J Respir Crit Care Med 2005172417-22 27 Meyer A Buhl R Kampf S Magnussen H Intravenous N-acetylcysteine and lung glutathione of patients with pulmonary fibrosis and normals Am J Respir Crit Care Med 19951521055-60 28 Behr J Degenkolb B Krombach F Vogelmeier C Intracellular glutathione and bronchoalveolar cells in fibrosing alveolitis effects of N-acetylcysteine Eur Respir J 200219906-11 29 Bando M Hosono T Mato N et al Long-term efficacy of inhaled N-acetylcysteine in patients with idiopathic pulmonary fibrosis Intern Med 2010492289-96 30 Demedts M Behr J Buhl R et al High-dose acetylcysteine in idiopathic pulmonary fibrosis N Engl J Med 20053532229-42 31 Toma TP Bhowmik A Rajakulasingam R Acetylcysteine in pulmonary fibrosis N Engl J Med 20063541086-9 author reply -9 32 Hunninghake GW Antioxidant therapy for idiopathic pulmonary fibrosis N Engl J Med 20053532285-7 33 Flaherty KR Mumford JA Murray S et al Prognostic implications of physiologic and radiographic changes in idiopathic interstitial pneumonia Am J Respir Crit Care Med 2003168543-8 34 Latsi PI du Bois RM Nicholson AG et al Fibrotic idiopathic interstitial pneumonia the prognostic value of longitudinal functional trends Am J Respir Crit Care Med 2003168531-7 35 Collard HR King TE Jr Bartelson BB Vourlekis JS Schwarz MI Brown KK Changes in clinical and physiologic variables predict survival in idiopathic pulmonary fibrosis Am J Respir Crit Care Med 2003168538-42 36 Jegal Y Kim DS Shim TS et al Physiology is a stronger predictor of survival than pathology in fibrotic interstitial pneumonia Am J Respir Crit Care Med 2005171639-44 37 Martinez FJ Safrin S Weycker D et al The clinical course of patients with idiopathic pulmonary fibrosis Ann Intern Med 2005142963-7 38 Hull JH Acetylcysteine in pulmonary fibrosis N Engl J Med 20063541089-91 author reply -91
70
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
39 Flaherty KR King TE Jr Raghu G et al Idiopathic interstitial pneumonia what is the effect of a multidisciplinary approach to diagnosis Am J Respir Crit Care Med 2004170904shy10 40 Raghu G Johnson WC Lockhart D Mageto Y Treatment of idiopathic pulmonary fibrosis with a new antifibrotic agent pirfenidone results of a prospective open-label Phase II study Am J Respir Crit Care Med 19991591061-9 41 Hunninghake GW Lynch DA Galvin JR et al Radiologic findings are strongly associated with a pathologic diagnosis of usual interstitial pneumonia Chest 20031241215-23 42 Lynch D Godwin J Safrin S et al High-resolution computed tomography in idiopathic pulmonary fibrosis diagnosis and prognosis Am J Respir Crit Care Med 2005172488-93 43 Mallinckrodt CH Watkin JG Molenberghs G Carroll RJ Choice of the primary analysis in longitudinal clinical trials Pharmaceutical Statistics 20043161-9 44 Bang H Tsiatis A Estimating medical costs with censored data Biometrika 200087329shy43 45 Lin DY Regression analysis of incomplete medical cost data Stat Med 2003221181-200 46 Rochon J Application of GEE procedures for sample size calculations in repeated measures experiments Stat Med 1998171643-58 47 Lachin JM Foulkes MA Evaluation of sample size and power for analyses of survival with allowance for nonuniform patient entry losses to follow-up noncompliance and stratification Biometrics 198642507-19
71
- PANTHER-IPFPREDNISONE AZATHIOPRINEAND N-ACETYLCYSTEINEA STUDY THAT EVALUATES RESPONSE INIDIOPATHIC PULMONARY FIBROSIS
-
- Protocol Summary
- Table of Contents
- List of Tables
- List of Figures
- List of Abbreviations
- 1 Summary
- 2 Hypotheses and Specific Aims
-
- 21 Null Hypothesis
- 22 Specific Aim 1
- 23 Specific Aim 2
- 24 Prespecified Subgroups of Interest
-
- 3 Background and Significance
-
- 31 Idiopathic Pulmonary Fibrosis is the Most Common Interstitial Lung Disease
- 32 Rationale for Placebo Control
- 33 Rationale for N-acetylcysteine
- 35 Rationale for N-acetylcysteine as a Stand-alone Therapy
- 36 Rationale for the Study Design and Primary Endpoint
- 37 Rationale for Blinding of Treatments
-
- 4 Methods
-
- 41 Inclusion Criteria
- 42 Diagnosis of IPF
- 43 Exclusion Criteria
- 44 Study Design and Study Visit
- 45 Dose Justification
- 46 Contraindications Precautions and Side Effects of Study Medications
- 47 Recruitment Procedures
- 48 Study Procedures
- 49 Concomitant Medications
- 410 Laboratory Testing
- 411 Blinding of Study Drugs
-
- 5 Study Endpoints
-
- 51 Primary Study Endpoint
- 52 Secondary Study Endpoints
-
- 6 Safety Evaluations and Procedures
-
- 61 Adverse Events
- 62 Clinical Medical Monitoring
- 63 Unblinding Procedures
-
- 7 Study Drug Procedures
- 8 Data Management
-
- 81 Hardware and Software Configuration
- 82 Sources of Data
-
- 9 Study Design and Data Analysis
-
- 91 General Analytic Considerations
- 92 Randomization Blinding and Reporting of Results
- 93 Stratification
- 94 Specification of the Primary Analyses
- 95 Analysis of Longitudinal Endpoints
- 96 Analysis of Binary Time-to-Event and Time-Lagged Endpoints
- 97 Power Analysis
-
- 10 Study Administration
-
- 101 Cooperative Agreement Mechanism
- 102 IPFnet Steering Group
- 103 Data and Safety Monitoring Board
- 104 Recommendations on Interim Monitoring of Efficacy Safety and Futility
-
- 11 Investigator and Sponsor Obligations
-
- 111 Monitoring
- 112 Cost and Payment
- 113 Confidentiality and Health Insurance Portability and Accountability ActConsiderations
- 114 Informed Consent Procedures
- 115 Institutional Review Boards
-
- 12 Investigator Agreement
- 13 References
-
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
524 Maintained FVC Response
Subjects with follow-up FVCpred measurements at or above their baseline FVCpred level
will be classified as having maintained FVC response Subjects with reduced FVCpred levels
or missing data for any reason including death or medical frailty will be classified as having not
maintained FVC response The FVCpred value is used because unadjusted FVC measurements
are expected to decline with age
48
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
6 Safety Evaluations and Procedures
61 Adverse Events
During a clinical trial the reporting of adverse experience information can lead to important
changes in the way a new treatment is developed as well as provide integral safety data
611 Definitions
An adverse event (AE) is any untoward medical occurrence in a subject or clinical investigation
subject who was administered a pharmaceutical product The AE does not necessarily have to
have a causal relationship with the drug administered An AE can be any unfavorable and
unintended sign (including an abnormal laboratory finding) symptom or disease temporarily
associated with the use of a medicinal product whether or not considered to be related to the
medicinal product Diseases signs symptoms or laboratory abnormalities already existing at
enrollment are not considered AEs unless they worsen (ie increase in intensity or frequency)
Surgical procedures themselves are not AEs they are therapeutic measures for conditions that
require surgery The condition for which the surgery is required may be an AE Surgical
procedures planned before randomization and the conditions necessitating the surgery are not
AEs
A serious adverse event is any untoward event that
Is fatal
Is life-threatening
Requires inpatient hospitalization or prolongation of existing hospitalization with the
following exceptions
o Preplanned (before the study) hospital admissions unless the hospitalization is
prolonged
o Planned admissions (as part of a study eg routine biopsies)
o Hospitalization lasting lt 24 hours
49
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
o Hospitalization for elective procedure
o Emergency room visits
Results in persistent or significant disability or incapacity
Is a congenital anomaly or birth defect
Important medical events that may not result in death be life-threatening or require
inpatient hospitalization may be considered serious adverse events (SAEs) when based
on appropriate medical judgment they may jeopardize the subject and may require
medical or surgical intervention to prevent one of the outcomes listed above
Life-threatening means that the subject was in the view of the investigator at immediate risk of
death from the AE as it occurred It does not include an AE that had it occurred in a more severe
form might have caused death
Persistent or significant disabilityincapacity means that the event resulted in permanent or
significant and substantial disruption of the subjectrsquos ability to carry out normal life functions
Causality
A reasonable possibility means the AE may have been caused byrelated to the study drug A
perceived or real lack of efficacy does not satisfy the definition of relatedness
612 Adverse Event (AE) Reporting
For the PANTHER-IPF trial all AEs (serious and nonserious) occurring from randomization
through final study visit (4 weeks after final dose of all study medication) will be recorded on the
AE page of the case report form (CRF)
6121 Serious Adverse Events (SAE) Reporting
For this trial all deaths and all SAEs which occur from randomization through final study visit
must be entered within the EDC system via the SAE eCRF page within 24 hours of the
investigative sitersquos knowledge of the event It is the responsibility of the clinical center
50
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
investigator to provide a causality assessment of the event for each study medications based upon
the information available at the time of the report It is understood that complete information
about the event may not be known at the time the initial report is submitted In the event the EDC
system is not accessible to the site at the time of event reporting investigative sites will complete
and forward a paper back-up SAE form to DCRI Safety Surveillance for processing
DCRI Safety Surveillance
Telephone 1-919-668-8624 or 1-866-668-7799 (toll free)
Fax 1-919-668-7138 or 1-866-668-7138 (toll free)
The investigator must complete and submit follow-up SAE information via the eCRF when
important new or follow-up information (eg final diagnosis outcome results of specific
investigations) becomes available Follow-up information should be submitted according to the
same process used for reporting the initial event as described above All SAEs will be followed
until resolution stabilization or 30 days after the subject has completed the final visit (4 weeks
after the final dose of study medication) whichever occurs first The investigator is responsible
for reporting SAEs to their institutional review board (IRB) per site specific IRB reporting
guidelines
6122 Regulatory Reporting
AEs that are serious study drug related and unexpected will be reported to the regulatory
authorities The DCRI Safety Surveillance medical monitor will perform a medical review of all
SAEs submitted and evaluate for ldquounexpectednessrdquo DCRI Safety Surveillance will prepare
MedWatch reports for those events identified as serious study drug related and unexpected as
determined by Safety Medical Monitor
DCRI Regulatory Services will submit all unexpected study drug-related SAEs as per 21 CFR
32 DCRI Safety Surveillance will provide a safety alert letter to the NHLBI DSMB and DCC
clinical operation (for distribution to sites) within 15 days of initial receipt of the information
51
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Investigators are responsible for promptly reporting these events to their reviewing IRBs
according to site specific IRB reporting guidelines
62 Clinical Medical Monitoring
There will be an unblinded physician at the IPFnet DCC serving as medical monitor The
medical monitor will be available to assist with questions about dosage adjustments of study
medications including discontinuation or resumption of medications
63 Unblinding Procedures
Unblinding of subjects or investigators to subject treatment is strongly discouraged For ongoing
clinical management all subjects should be presumed to be receiving ldquoactiverdquo study drug To
ensure the subjectrsquos safety the study treatment will be dose-adjusted based on laboratory test
results clinical findings and symptoms
The IPFnet DCC medical monitor and PANTHER-IPF co-chairs Drs Ganesh Raghu and
Fernando Martinez will be available to the study physicians to discuss study drug management
on a case-by-case basis Un-blinding will be considered ONLY when the knowledge of subject
treatment assignment is ABSOLUTELY ESSENTIAL for subject safety and after discussion of
the subjectrsquos case with the medical monitor and either Dr Raghu or Dr Martinez Unblinding of
study treatment should be minimized during the conduct of the trial In those cases where it is
felt to be medically necessary the DCC medical officer will communicate directly with the
managing physician to minimize unblinding of study personnel
52
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
7 Study Drug Procedures
At the baseline 15-week 30-week and 45-week study visits subjects will receive a supply of
study drug sufficient to last until the next visit at which study drug will be dispensed
53
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
8 Data Management
81 Hardware and Software Configuration
811 Hardware and Database Software
Data will be stored in an Oracle database system Oracle has advantages of processing efficiency
and smooth linkage with other software systems The application and database will be hosted on
Solaris Unix servers at the IPFnet DCC
812 Statistical Software
SAS will be used as the principal application for the management of analysis data files and
statistical computations S-Plus will be used to provide supplementary functions as needed
813 Access Control and Confidentiality Procedures
Access to databases will be controlled centrally by the IPFnet DCC through user passwords
linked to appropriate privileges This protects the data from unauthorized changes and
inadvertent loss or damage
814 Security
Database and Web servers will be secured by a firewall and through controlled physical access
Oracle has many security features to ensure that any staff member accessing the database has the
proper authority to perform the functions he or she requests of the system Within the secondary
SAS databases Unix group-access control maintains similar security The Sun workstation login
is secured by extensive user-password facilities under Unix
54
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
815 Back-up Procedures
Database back-up will be performed automatically every day and standard IPFnet DCC policies
and procedures will be applied to dictate tape rotation and retention practices
816 Virus Protection
All disk drives that provide network services and all user computers will be protected using
virus-scanning software Standard IPFnet DCC policies will be applied to update these protection
systems periodically through the study
82 Sources of Data
821 Design and Development
The IPFnet DCC will be responsible for development of the electronic case report forms
(eCRFs) development and validation of the clinical study database ensuring data integrity and
training clinical center staff on applicable data management procedures A web-based distributed
data entry model will be implemented This system will be developed to ensure that guidelines
and regulations surrounding the use of computerized systems used in clinical trials are upheld
The remainder of this section provides an overview of the data management plan associated with
this protocol
822 Data Collection Forms
The data collection process consists of direct data entry at the study clinical centers into the EDC
system(s) provided by the DCC A data collection worksheet will be provided to clinical centers
for recording data in the event the EDC system is unavailable Data entry of the eCRFs should
be completed according to the instructions provided and project specific training The
investigator is responsible for maintaining accurate complete and up-to-date records and for
ensuring the completion of the eCRFs for each research participant
55
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
823 Data Acquisition and Entry
Data entry into eCRFs shall be performed by authorized individuals Selected eCRFs may also
require the investigatorrsquos written signature or electronic signature as appropriate Electronic
CRFs will be monitored for completeness accuracy and attention to detail during the study
824 Data Center Responsibilities
The IPFnet DCC will 1) develop a data management plan and will conduct data management
activities 2) provide final eCRFs for the collection of all data required by the study 3) develop
data dictionaries for each eCRF that will comprehensively define each data element 4) conduct
ongoing data monitoring activities on study data 5) monitor any preliminary analysis data
cleanup activities and 6) rigorously monitor final study data clean up
825 Data Editing
Completed data will be entered into the IPFnet DCC automated data acquisition and
management system If incomplete or inaccurate data are found a data clarification request will
be generated and distributed to clinical centers for a response Clinical centers will resolve data
inconsistencies and errors and enter all corrections and changes into the IPFnet DCC automated
data acquisition and management system
826 Training
The training plan for clinical center staff includes provisions for training on assessments eCRF
completion guidelines data management procedures and the use of computerized systems
56
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
9 Study Design and Data Analysis
91 General Analytic Considerations
All primary analyses will be based on intent-to-treat (ITT) principles using all randomized
subjects Baseline factors across groups will be compared using mean (standard deviation) and
median (25th and 75th percentiles) summary measures Kaplan-Meier curves will be used to
display event rates Due to clinical interest in departures from both sides of the null hypothesis
all test statistics will be 2-sided
Reasonable caution needs to be taken when conducting multiple analyses on key clinical
subgroups For subgroup analyses a conservative significance level of 0001 will be used for all
interaction tests Thus subgroup comparisons will be considered exploratory unless the p-value
from the interaction test is smaller than 0001
92 Randomization Blinding and Reporting of Results
A permuted block-randomization scheme will be created with varying block sizes stratified by
clinical center Once a subject has completed the screening and baseline period and evaluation
for inclusionexclusion criteria the randomization process will begin Subjects will be
randomized to receive NAC or matching placebo with equal probability (11) via telephone
contact with a central interactive voice response system (IVRS) using a toll-free randomization
number On the day of randomization after the subject has successfully met all inclusion and
exclusion criteria the investigator or designee will call the central randomization number to
obtain the assigned kit randomization numbers for that subject At each subject visit the
investigator or designee will call the central randomization number to obtain the new kit
randomization numbers for resupply of the subject For resupply of the clinical center the IVRS
will monitor minimal volume of a kit type andor expiration date and will automatically notify
the pharmacy
57
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
The trial results will be reported according to guidelines specified in the CONSORT statement
A flow diagram describing screening recruitment randomization dropout and vital status will
be included in the primary manuscript AEs and efficacy data will be presented for all treatment
groups Adherence dropout and lost to follow-up will be carefully examined across all treatment
groups Analyses of safety will be based on data from all randomized subjects who received at
least one dose of study drug
93 Stratification
Subjects will be distributed to the two treatment arms in a 11 allocation ratio Stratification
blocks will be based on clinical centers
94 Specification of the Primary Analyses
A mixed model repeated measures (MMRM) analysis described in section 95 will be used to
compare differences in the slope of FVC measurements across the treatment groups Response
variables are values of the FVC measured at baseline and every 15 weeks until study completion
Variables in the model will include treatment time and time by treatment age sex race and
height Contrast estimates of differences in slopes of treatment over time (along with confidence
intervals) will be used to estimate the treatment effect The validity of this model in terms of
meeting modeling assumptions will be assessed via standard modeling diagnostics and goodness-
of-fit measures Based on the MMRM framework missing FVC data will not be imputed for the
primary analysis
95 Analysis of Longitudinal Endpoints
A common goal in clinical trials is to specify models that are easily implemented and
reproducible by independent data analysts On the other hand the models should have proper
statistical behavior in terms of low bias and high precision Many common approaches to
longitudinal data analysis including last observation carried forward (LOCF) imputation rely on
the missing completely at random (MCAR) assumption However the MCAR assumption is
58
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
unlikely to hold in many clinical trials because missing data are often related to disease
progression and prognosis A more reasonable assumption missing at random (MAR) specifies
that the complete data distribution can be modeled using only the observed data The likelihood-
based MMRM approach is valid under the more general MAR assumptions These models will
be applied to analyze the longitudinal data secondary endpoints
The advantages of MMRM analysis are that all important characteristics of the model can be preshy
specified standard software can be used to implement the models and results are based on ITT
principles43 In addition the MMRM approach offers superior control of Type I and Type II
errors compared with the LOCF approach
Response variables are values of the PFTs measured at enrollment and every 15 weeks until
study completion and 6MWT values measured at baseline week 30 and week 60 Covariates are
treatment time time by treatment and key baseline risk factors Contrasts (along with
confidence intervals) of treatment by time will be used to estimate the treatment effect
The correlation structure involves multiple pieces including measurement errors random
variation and interindividual variability For the longitudinal data analyses an unstructured
correlation matrix for within-subject errors will be assumed Other correlation structures
including compound symmetry will be examined as needed A careful examination of reasons
for study discontinuation will be conducted to assess the validity of MCAR Sensitivity analyses
will be used to examine the untestable assumption that the observed data violate the MAR
assumption The MMRM models will be implemented using PROC MIXED in SAS
96 Analysis of Binary Time-to-Event and Time-Lagged Endpoints
Regression modeling approaches using either the logistic regression model or Cox proportional
hazards regression model will be employed when appropriate The validity of these models will
be assessed via standard modeling diagnostics and goodness-of-fit measures Estimates of
cumulative frequencies for more general time-lagged responses will be calculated using the
partitioned version of the Bang-Tsiatis estimator44 The partitions will be set at 15-week intervals
59
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
to correspond with the data-collection process Covariate adjusted event rates will be calculated
using inverse probability-weighted regression estimates45
97 Power Analysis
971 Primary Analyses
Based on previously published IPF clinical trials the PL group is expected to experience a drop
in FVC of approximately 020 L over the study period (see Figure 1) The IPFnet Steering Group
determined a clinically important difference would be to preserve the majority of the decline
relative to PL over the study period In particular a treatment effect of 015 L was determined to
be a clinically meaningful difference Potential dropout is a key factor in the proposed study The
drop-out process assumed 5 lost to follow-up after every study visit Only 80 of subjects
were assumed to be followed for the entire study period All models assumed a compound
symmetry structure for the covariance matrix Power calculations were performed using a SAS
IML program for designing repeated measures studies46 Based on preliminary reviews of the
data from the University of Michigan the covariance matrix parameters were estimated at
approximately σ2 = 0757 (variance parameter) and ρ = 0936 (correlation parameter) To be
conservative the power calculations for the primary analysis were performed with parameter
setting of σ2 = 0810 (variance parameter) and ρ = 0925 (correlation parameter)
The power calculations assume a correction for imperfect compliance proposed by Lachin and
Foulkes to allow for 2 noncompliance for each of the treatment arms47 Thus the sample size
of 130 subjects per arm would be reduced to an adjusted sample size of 130(1-002-002)2 =
1198 or 120 subjects per arm
Under the assumed Type I error rate of 005 with a correlation parameter of 0925 and standard
deviation of 090 the difference of 015 L (or 00025 Lweek) shown in Table 6 would have
power of 93
60
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Table 6 Hypothetical Values of Mean FVC (L) Change from Baseline
Week 15 Week 30 Week 45 Week 60
NAC 00125 00250 00375 00500
Placebo 00500 01000 01500 02000
Difference 00375 00750 01125 01500
Abbreviations FVC forced vital capacity PL placebo
972 Power Analysis for Secondary Endpoints
Power calculations for secondary endpoint measurements are shown in Table 7 Standard
deviations are based on unpublished data provided by the University of Michigan The
calculations are based on a 2-sample t-test with Type I error rate set at 005 These calculations
are likely to be conservative because the statistical approach described in section 95 for
analyzing these endpoints will incorporate incomplete observations as well as intermediate data
points
Table 7 Detectable Differences in Treatment Means for Selected Endpoint Measurements
Secondary Endpoints Std Dev
of the Baseline Score
Detectable Difference for 80 Power
Std Dev of the Change Score
Difference Detectable for
80 Power
DLCOpred 166 58 91 32
6MWT Area Under the Desaturation Curve
219 76 175 61
6MWT Distance to Desaturation 224 78 315 110
6MWT Minutes Walked 210 073 205 071
Abbreviations Std Dev standard deviation DLCOpred diffusing capacity of the lung for carbon monoxide percent predicted 6MWT 6-minute walk test
61
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
10 Study Administration
101 Cooperative Agreement Mechanism
The administrative and funding mechanism used to undertake this project is a ldquocooperative
agreementrdquo (U01) which is an assistance mechanism Under the cooperative agreement the
NHLBI assists supports andor stimulates the project and is substantially involved with
investigators in conducting the study by facilitating performance of the effort in a ldquopartnerrdquo role
The NHLBI project scientist serves on the IPFnet Steering Group and he or another NHLBI
scientist may serve on other project committees when appropriate At the same time however
NHLBI does not assume a dominant role direction or prime responsibility for this research
program
As described below governance of the project is conducted through the IPFnet Steering Group
Principal investigators have lead responsibilities in all aspects of their trials and the project
including any modification of trial designs conduct of the trials quality control data analysis
and interpretation preparation of publications and collaboration with other investigators unless
otherwise provided for by the IPFnet Steering Group
PIs retain custody of and have primary rights to their center-specific and collaborative data
subject to government rights-of-access consistent with current Health amp Human Services (HHS)
Public Health Service (PHS) and National Institutes of Health policies The protocols and
governance policies call for the continual submission of data centrally to the IPFnet DCC for the
collaborative database which at a minimum will contain the key variables selected by the IPFnet
Steering Group for standardization across all clinical centers the submission of copies of the
collaborative datasets to each PI upon completion of the project procedures for data analysis
reporting and publication and procedures to protect and ensure the privacy of medical and
genetic data and records of individuals The NHLBI project scientist on behalf of the NHLBI
will have the same access privileges and responsibilities regarding the collaborative data as the
other members of the Steering Group
62
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
PIs are also encouraged to publish and to publicly release and disseminate results data and other
products of the project concordant with the project protocols and governance and the approved
plan for making data and materials available to the scientific community and to the NHLBI
However during the 3 years after the ending date of NHLBI project support unpublished data
unpublished results data sets not previously released and other study materials or products are
to be made available to any third party only with the approval of the IPFnet Steering Group
Upon completion of the project PIs are expected to put their intervention materials and
procedure manuals into the public domain andor make them available to other investigators
according to the approved plan for making data and materials available to the scientific
community and the NHLBI for the conduct of research at no charge other than the costs of
reproduction and distribution
The NHLBI reserves the right to terminate or curtail the project (or an individual award) in the
event of (a) failure to develop or implement mutually agreeable collaborative measurement
subject eligibility and data management sections of the protocols (b) substantial shortfall in
subject recruitment follow-up data reporting or quality control or other major breach of
protocol (c) substantive changes in the agreed-upon protocols with which NHLBI cannot
concur (d) reaching a major project outcome with persuasive statistical significance
substantially before schedule or (e) human subject ethical issues that may dictate a premature
termination
Any disagreement that may arise in scientificprogrammatic matters (within the scope of the
award) between award recipients and the NHLBI may be brought to arbitration An arbitration
panel will be composed of 3 membersmdash1 selected by the IPFnet Steering Group (with the
NHLBI member not voting) or by the individual PI in the event of an individual disagreement a
second selected by NHLBI and the third selected by the other 2 members This special
arbitration procedure in no way affects the PIrsquos right to appeal an adverse action that is otherwise
appealable in accordance with the PHS regulations at 42 CFR part 50 Subpart D and HHS
63
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
regulation at 45 CFR part 16 or the rights of the NHLBI under applicable statutes regulations
and terms of the award
102 IPFnet Steering Group
The IPFnet Steering Group is the main governing body of the project It is composed of the PIs
of the clinical centers the PI of the DCC and the NHLBI project scientist The clinical centers
the IPFnet DCC and the NHLBI each have 1 vote on the IPFnet Steering Group All decisions
are determined by majority vote
All major scientific decisions are determined by the IPFnet Steering Group It assumes overall
responsibility for the design and conduct of the trial It appoints (and disbands) committees and
subcommittees as the need arises designs approves and implements the study protocols
oversees the development of the MOOP monitors subject recruitment and treatment delivery
evaluates data collection and management oversees quality assurance procedures and
implements changes and enhancements to the study as required It also has primary responsibility
for facilitating the conduct of the trials and reporting the projectrsquos results
103 Data and Safety Monitoring Board
The NHLBI will establish a DSMB in accordance with established policies (see
httpwwwnhlbinihgovfundingpoliciesdsmb_insthtm) to ensure data quality and subject
safety and to provide independent advice to the NHLBI regarding progress and the
appropriateness of study continuation
104 Recommendations on Interim Monitoring of Efficacy Safety and Futility
First and foremost the role of the DSMB will be to review subject safety and trial conduct at
periodic points during the study The DSMB may require analyses of the primary endpoint
results for comparing the benefit and risks of treatment strategies The benefit of collecting
additional data on key secondary endpoints with extended follow-up and establishing a robust
64
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
evidence base for determining a standard of care will need to be carefully considered before
early termination of one or more treatment arms After careful consideration the IPFnet Steering
Group recommends conservative thresholds for the early examinations of the safety and efficacy
data
The DSMB will be expected to meet approximately every 6 months until trial completion to
review safety and toxicity data The DSMB may recommend stopping the study based on these
reviews Because the DSMB could stop the trial for safety concerns as well as for a large
efficacy benefit there could be multiple opportunities to reject the null hypothesis (no difference
in event rates between the PL and NAC groups) A Bonferroni approximation will be applied
during the one planned interim analysis for efficacy
Before locking the database a statistical analysis plan (SAP) will be developed to provide
complete details on the statistical analysis The SAP will include the specifics for how and when
the DSMB will be notified for AEs The IPFnet DCC will deliver to the DSMB all FDA-defined
AEs at 3-month intervals The IPFnet DCC will prepare narrative SAE reports in real time for
DSMB review including recommendations and analysis of similar events for each SAE
submitted to the FDA
65
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
11 Investigator and Sponsor Obligations
111 Monitoring
All monitoring activities for US clinical centers will be performed in accordance with DCRI
standard operating procedures Information regarding the types of visits will be outlined in the
PANTHER-IPF MOOP
112 Cost and Payment
There will be no cost to subjects enrolled in this trial Study-related procedures will be paid for
by the IPFnet
Subjects may be eligible for reimbursement for travel to the clinical center Details of payment
will be explained to each subject during the consent process
113 Confidentiality and Health Insurance Portability and Accountability Act
Considerations
Subject confidentiality will be protected throughout the study All subject data will be kept
strictly confidential and no subject-identifying information will be released to anyone outside
the project Confidentiality will be assured through several mechanisms First each subject will
be assigned an anonymous study ID which will then be used on all study forms Second any
study forms blood samples and paper records that contain subject information (eg address lists
phone lists) will be kept at the clinical centers in secured locked areas coded by number Once
blood is collected there will be no subject identifiers placed on blood samplesmdashonly the study
ID number and the date of sample collection Third access to all subject data and information
including laboratory specimens will be restricted to authorized personnel In the case of
computerized data this restricted access will be assured through user logon IDs and password
protection
66
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
At the IPFnet DCC only authorized personnel will have access to the data files containing study
data Security will be assured through user logon IDs passwords and appropriate access
privileges All study subjects will be identified only by their IPFnet ID numbers and no personal
identifying information such as name address or Social Security number will be entered into
the IPFnet DCC database Any subject-specific data reported to the IPFnet Steering Group will
be identified only by the IPFnet ID number
Finally subjects will not be identified by name in any reports or publications nor will the data
be presented in such a way that the identity of individual subjects can be inferred Analysis files
created for further study by the scientific community will have no subject identifiers These data
files will be created in accordance with the Ancillary Studies and Publication Policy of the
IPFnet
114 Informed Consent Procedures
All IPFnet subjects will provide written informed consent using procedures reviewed and
approved by each clinical centerrsquos IRB Informed consent will be undertaken by study personnel
in-person with the subject The subject has the option of declining further participation in the
study at that point No further study procedures will be conducted until the signed documents
have been provided to the IPFnet clinical center
115 Institutional Review Boards
Before initiating this study the protocol clinical center-specific informed consent forms Health
Insurance Portability and Accountability Act (HIPAA) forms recruitment materials and other
relevant information will be reviewed by a properly constituted IRB at each participating clinical
center A copy of the signed and dated IRB approval at each clinical center will be retrieved prior
to or during the site initiation visit and archived at the IPFnet DCC Any amendments to the
protocol other than simple administrative and typographical changes must be approved by each
IRB before they are implemented The clinical centers will seek annual renewals of their IRB
approvals in accordance with local procedures
67
__________________________________________ ________________
__________________________________________
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
12 Investigator Agreement
I have read the foregoing protocol PANTHER-IPF and agree that it contains all necessary
details for carrying out this study I will conduct the study as outlined herein and will complete
the study within the time designated
I will provide copies of the protocol and all pertinent information to all individuals responsible to
me who assist in the conduct of this study I will discuss this material with them to ensure they
are fully informed regarding the drug and the conduct of the study
I will fulfill all responsibilities for submitting pertinent information to the local IRB if
applicable that is responsible for this study
I further agree that NHLBI andor DCRI will have access to any source documents from which
eCRF information may have been generated
Signature of Principal Investigator Date
Name of Principal Investigator (printed or typed)
Protocol version date May 19 2009
Protocol Amendment 1 version date May 28 2010
Protocol Amendment 2 version date December 6 2011
68
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
13 References
1 Raghu G Brown KK Bradford WZ et al A placebo-controlled trial of interferon gamma-1b in patients with idiopathic pulmonary fibrosis N Engl J Med 2004350125-33 2 King TE Jr Safrin S Starko KM et al Analyses of efficacy end points in a controlled trial of interferon-gamma1b for idiopathic pulmonary fibrosis Chest 2005127171-7 3 Flaherty KR Thwaite EL Kazerooni EA et al Radiological versus histological diagnosis in UIP and NSIP survival implications Thorax 200358143-8 4 Wells AU Desai SR Rubens MB et al Idiopathic pulmonary fibrosis a composite physiologic index derived from disease extent observed by computed tomography Am J Respir Crit Care Med 2003167962-9 5 Raghu G Freudenberger TD Yang S et al High prevalence of abnormal acid gastroshyoesophageal reflux in idiopathic pulmonary fibrosis Eur Respir J 200627136-42 6 Kinnula VL Focus on antioxidant enzymes and antioxidant strategies in smoking related airway diseases Thorax 200560693-700 7 Coultas DB Zumwalt RE Black WC Sobonya RE The epidemiology of interstitial lung diseases Am J Respir Crit Care Med 1994150967-72 8 Raghu G Weycker D Edelsberg J Bradford WZ Oster G Incidence and prevalence of idiopathic pulmonary fibrosis Am J Respir Crit Care Med 2006174810-6 9 Olson AL Swigris JJ Lezotte DC Norris JM Wilson CG Brown KK Mortality from pulmonary fibrosis increased in the United States from 1992 to 2003 Am J Respir Crit Care Med 2007176277-84 10 Mannino DM Etzel RA Parrish RG Pulmonary fibrosis deaths in the United States 1979shy1991 An analysis of multiple-cause mortality data Am J Respir Crit Care Med 19961531548shy52 11 Hubbard R Johnston I Coultas DB Britton J Mortality rates from cryptogenic fibrosing alveolitis in seven countries Thorax 199651711-6 12 Johnston I Britton J Kinnear W Logan R Rising mortality from cryptogenic fibrosing alveolitis Bmj 19903011017-21 13 Raghu G Collard HR Egan JJ et al An official ATSERSJRSALAT statement idiopathic pulmonary fibrosis evidence-based guidelines for diagnosis and management Am J Respir Crit Care Med 2011183788-824 14 (USA) FDA FDA Public Health Advisory Interferon gamma-1b (marketed as Actimmune) In 2007 15 King TE Jr Pardo A Selman M Idiopathic pulmonary fibrosis Lancet 2011 16 Raghu G Brown KK Costabel U et al Treatment of idiopathic pulmonary fibrosis with etanercept an exploratory placebo-controlled trial Am J Respir Crit Care Med 2008178948shy55 17 Malouf MA Hopkins P Snell G Glanville AR An investigator-driven study of everolimus in surgical lung biopsy confirmed idiopathic pulmonary fibrosis Respirology 201116776-83 18 King TE Jr Behr J Brown KK et al BUILD-1 a randomized placebo-controlled trial of bosentan in idiopathic pulmonary fibrosis Am J Respir Crit Care Med 200817775-81 19 Richeldi L Costabel U Selman M et al Efficacy of a tyrosine kinase inhibitor in idiopathic pulmonary fibrosis N Engl J Med 20113651079-87
69
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
20 Borok Z Buhl R Grimes GJ et al Effect of glutathione aerosol on oxidant-antioxidant imbalance in idiopathic pulmonary fibrosis Lancet 1991338215-6 21 Meyer A Buhl R Magnussen H The effect of oral N-acetylcysteine on lung glutathione levels in idiopathic pulmonary fibrosis Eur Respir J 19947431-6 22 Behr J Maier K Degenkolb B Krombach F Vogelmeier C Antioxidative and clinical effects of high-dose N-acetylcysteine in fibrosing alveolitis Adjunctive therapy to maintenance immunosuppression Am J Respir Crit Care Med 19971561897-901 23 Cantin AM North SL Fells GA Hubbard RC Crystal RG Oxidant-mediated epithelial cell injury in idiopathic pulmonary fibrosis J Clin Invest 1987791665-73 24 Waghray M Cui Z Horowitz JC et al Hydrogen peroxide is a diffusible paracrine signal for the induction of epithelial cell death by activated myofibroblasts Faseb J 200519854-6 25 Larios JM Budhiraja R Fanburg BL Thannickal VJ Oxidative protein cross-linking reactions involving L-tyrosine in transforming growth factor-beta1-stimulated fibroblasts J Biol Chem 200127617437-41 26 Kinnula VL Fattman CL Tan RJ Oury TD Oxidative stress in pulmonary fibrosis a possible role for redox modulatory therapy Am J Respir Crit Care Med 2005172417-22 27 Meyer A Buhl R Kampf S Magnussen H Intravenous N-acetylcysteine and lung glutathione of patients with pulmonary fibrosis and normals Am J Respir Crit Care Med 19951521055-60 28 Behr J Degenkolb B Krombach F Vogelmeier C Intracellular glutathione and bronchoalveolar cells in fibrosing alveolitis effects of N-acetylcysteine Eur Respir J 200219906-11 29 Bando M Hosono T Mato N et al Long-term efficacy of inhaled N-acetylcysteine in patients with idiopathic pulmonary fibrosis Intern Med 2010492289-96 30 Demedts M Behr J Buhl R et al High-dose acetylcysteine in idiopathic pulmonary fibrosis N Engl J Med 20053532229-42 31 Toma TP Bhowmik A Rajakulasingam R Acetylcysteine in pulmonary fibrosis N Engl J Med 20063541086-9 author reply -9 32 Hunninghake GW Antioxidant therapy for idiopathic pulmonary fibrosis N Engl J Med 20053532285-7 33 Flaherty KR Mumford JA Murray S et al Prognostic implications of physiologic and radiographic changes in idiopathic interstitial pneumonia Am J Respir Crit Care Med 2003168543-8 34 Latsi PI du Bois RM Nicholson AG et al Fibrotic idiopathic interstitial pneumonia the prognostic value of longitudinal functional trends Am J Respir Crit Care Med 2003168531-7 35 Collard HR King TE Jr Bartelson BB Vourlekis JS Schwarz MI Brown KK Changes in clinical and physiologic variables predict survival in idiopathic pulmonary fibrosis Am J Respir Crit Care Med 2003168538-42 36 Jegal Y Kim DS Shim TS et al Physiology is a stronger predictor of survival than pathology in fibrotic interstitial pneumonia Am J Respir Crit Care Med 2005171639-44 37 Martinez FJ Safrin S Weycker D et al The clinical course of patients with idiopathic pulmonary fibrosis Ann Intern Med 2005142963-7 38 Hull JH Acetylcysteine in pulmonary fibrosis N Engl J Med 20063541089-91 author reply -91
70
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
39 Flaherty KR King TE Jr Raghu G et al Idiopathic interstitial pneumonia what is the effect of a multidisciplinary approach to diagnosis Am J Respir Crit Care Med 2004170904shy10 40 Raghu G Johnson WC Lockhart D Mageto Y Treatment of idiopathic pulmonary fibrosis with a new antifibrotic agent pirfenidone results of a prospective open-label Phase II study Am J Respir Crit Care Med 19991591061-9 41 Hunninghake GW Lynch DA Galvin JR et al Radiologic findings are strongly associated with a pathologic diagnosis of usual interstitial pneumonia Chest 20031241215-23 42 Lynch D Godwin J Safrin S et al High-resolution computed tomography in idiopathic pulmonary fibrosis diagnosis and prognosis Am J Respir Crit Care Med 2005172488-93 43 Mallinckrodt CH Watkin JG Molenberghs G Carroll RJ Choice of the primary analysis in longitudinal clinical trials Pharmaceutical Statistics 20043161-9 44 Bang H Tsiatis A Estimating medical costs with censored data Biometrika 200087329shy43 45 Lin DY Regression analysis of incomplete medical cost data Stat Med 2003221181-200 46 Rochon J Application of GEE procedures for sample size calculations in repeated measures experiments Stat Med 1998171643-58 47 Lachin JM Foulkes MA Evaluation of sample size and power for analyses of survival with allowance for nonuniform patient entry losses to follow-up noncompliance and stratification Biometrics 198642507-19
71
- PANTHER-IPFPREDNISONE AZATHIOPRINEAND N-ACETYLCYSTEINEA STUDY THAT EVALUATES RESPONSE INIDIOPATHIC PULMONARY FIBROSIS
-
- Protocol Summary
- Table of Contents
- List of Tables
- List of Figures
- List of Abbreviations
- 1 Summary
- 2 Hypotheses and Specific Aims
-
- 21 Null Hypothesis
- 22 Specific Aim 1
- 23 Specific Aim 2
- 24 Prespecified Subgroups of Interest
-
- 3 Background and Significance
-
- 31 Idiopathic Pulmonary Fibrosis is the Most Common Interstitial Lung Disease
- 32 Rationale for Placebo Control
- 33 Rationale for N-acetylcysteine
- 35 Rationale for N-acetylcysteine as a Stand-alone Therapy
- 36 Rationale for the Study Design and Primary Endpoint
- 37 Rationale for Blinding of Treatments
-
- 4 Methods
-
- 41 Inclusion Criteria
- 42 Diagnosis of IPF
- 43 Exclusion Criteria
- 44 Study Design and Study Visit
- 45 Dose Justification
- 46 Contraindications Precautions and Side Effects of Study Medications
- 47 Recruitment Procedures
- 48 Study Procedures
- 49 Concomitant Medications
- 410 Laboratory Testing
- 411 Blinding of Study Drugs
-
- 5 Study Endpoints
-
- 51 Primary Study Endpoint
- 52 Secondary Study Endpoints
-
- 6 Safety Evaluations and Procedures
-
- 61 Adverse Events
- 62 Clinical Medical Monitoring
- 63 Unblinding Procedures
-
- 7 Study Drug Procedures
- 8 Data Management
-
- 81 Hardware and Software Configuration
- 82 Sources of Data
-
- 9 Study Design and Data Analysis
-
- 91 General Analytic Considerations
- 92 Randomization Blinding and Reporting of Results
- 93 Stratification
- 94 Specification of the Primary Analyses
- 95 Analysis of Longitudinal Endpoints
- 96 Analysis of Binary Time-to-Event and Time-Lagged Endpoints
- 97 Power Analysis
-
- 10 Study Administration
-
- 101 Cooperative Agreement Mechanism
- 102 IPFnet Steering Group
- 103 Data and Safety Monitoring Board
- 104 Recommendations on Interim Monitoring of Efficacy Safety and Futility
-
- 11 Investigator and Sponsor Obligations
-
- 111 Monitoring
- 112 Cost and Payment
- 113 Confidentiality and Health Insurance Portability and Accountability ActConsiderations
- 114 Informed Consent Procedures
- 115 Institutional Review Boards
-
- 12 Investigator Agreement
- 13 References
-
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
6 Safety Evaluations and Procedures
61 Adverse Events
During a clinical trial the reporting of adverse experience information can lead to important
changes in the way a new treatment is developed as well as provide integral safety data
611 Definitions
An adverse event (AE) is any untoward medical occurrence in a subject or clinical investigation
subject who was administered a pharmaceutical product The AE does not necessarily have to
have a causal relationship with the drug administered An AE can be any unfavorable and
unintended sign (including an abnormal laboratory finding) symptom or disease temporarily
associated with the use of a medicinal product whether or not considered to be related to the
medicinal product Diseases signs symptoms or laboratory abnormalities already existing at
enrollment are not considered AEs unless they worsen (ie increase in intensity or frequency)
Surgical procedures themselves are not AEs they are therapeutic measures for conditions that
require surgery The condition for which the surgery is required may be an AE Surgical
procedures planned before randomization and the conditions necessitating the surgery are not
AEs
A serious adverse event is any untoward event that
Is fatal
Is life-threatening
Requires inpatient hospitalization or prolongation of existing hospitalization with the
following exceptions
o Preplanned (before the study) hospital admissions unless the hospitalization is
prolonged
o Planned admissions (as part of a study eg routine biopsies)
o Hospitalization lasting lt 24 hours
49
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
o Hospitalization for elective procedure
o Emergency room visits
Results in persistent or significant disability or incapacity
Is a congenital anomaly or birth defect
Important medical events that may not result in death be life-threatening or require
inpatient hospitalization may be considered serious adverse events (SAEs) when based
on appropriate medical judgment they may jeopardize the subject and may require
medical or surgical intervention to prevent one of the outcomes listed above
Life-threatening means that the subject was in the view of the investigator at immediate risk of
death from the AE as it occurred It does not include an AE that had it occurred in a more severe
form might have caused death
Persistent or significant disabilityincapacity means that the event resulted in permanent or
significant and substantial disruption of the subjectrsquos ability to carry out normal life functions
Causality
A reasonable possibility means the AE may have been caused byrelated to the study drug A
perceived or real lack of efficacy does not satisfy the definition of relatedness
612 Adverse Event (AE) Reporting
For the PANTHER-IPF trial all AEs (serious and nonserious) occurring from randomization
through final study visit (4 weeks after final dose of all study medication) will be recorded on the
AE page of the case report form (CRF)
6121 Serious Adverse Events (SAE) Reporting
For this trial all deaths and all SAEs which occur from randomization through final study visit
must be entered within the EDC system via the SAE eCRF page within 24 hours of the
investigative sitersquos knowledge of the event It is the responsibility of the clinical center
50
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
investigator to provide a causality assessment of the event for each study medications based upon
the information available at the time of the report It is understood that complete information
about the event may not be known at the time the initial report is submitted In the event the EDC
system is not accessible to the site at the time of event reporting investigative sites will complete
and forward a paper back-up SAE form to DCRI Safety Surveillance for processing
DCRI Safety Surveillance
Telephone 1-919-668-8624 or 1-866-668-7799 (toll free)
Fax 1-919-668-7138 or 1-866-668-7138 (toll free)
The investigator must complete and submit follow-up SAE information via the eCRF when
important new or follow-up information (eg final diagnosis outcome results of specific
investigations) becomes available Follow-up information should be submitted according to the
same process used for reporting the initial event as described above All SAEs will be followed
until resolution stabilization or 30 days after the subject has completed the final visit (4 weeks
after the final dose of study medication) whichever occurs first The investigator is responsible
for reporting SAEs to their institutional review board (IRB) per site specific IRB reporting
guidelines
6122 Regulatory Reporting
AEs that are serious study drug related and unexpected will be reported to the regulatory
authorities The DCRI Safety Surveillance medical monitor will perform a medical review of all
SAEs submitted and evaluate for ldquounexpectednessrdquo DCRI Safety Surveillance will prepare
MedWatch reports for those events identified as serious study drug related and unexpected as
determined by Safety Medical Monitor
DCRI Regulatory Services will submit all unexpected study drug-related SAEs as per 21 CFR
32 DCRI Safety Surveillance will provide a safety alert letter to the NHLBI DSMB and DCC
clinical operation (for distribution to sites) within 15 days of initial receipt of the information
51
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Investigators are responsible for promptly reporting these events to their reviewing IRBs
according to site specific IRB reporting guidelines
62 Clinical Medical Monitoring
There will be an unblinded physician at the IPFnet DCC serving as medical monitor The
medical monitor will be available to assist with questions about dosage adjustments of study
medications including discontinuation or resumption of medications
63 Unblinding Procedures
Unblinding of subjects or investigators to subject treatment is strongly discouraged For ongoing
clinical management all subjects should be presumed to be receiving ldquoactiverdquo study drug To
ensure the subjectrsquos safety the study treatment will be dose-adjusted based on laboratory test
results clinical findings and symptoms
The IPFnet DCC medical monitor and PANTHER-IPF co-chairs Drs Ganesh Raghu and
Fernando Martinez will be available to the study physicians to discuss study drug management
on a case-by-case basis Un-blinding will be considered ONLY when the knowledge of subject
treatment assignment is ABSOLUTELY ESSENTIAL for subject safety and after discussion of
the subjectrsquos case with the medical monitor and either Dr Raghu or Dr Martinez Unblinding of
study treatment should be minimized during the conduct of the trial In those cases where it is
felt to be medically necessary the DCC medical officer will communicate directly with the
managing physician to minimize unblinding of study personnel
52
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
7 Study Drug Procedures
At the baseline 15-week 30-week and 45-week study visits subjects will receive a supply of
study drug sufficient to last until the next visit at which study drug will be dispensed
53
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
8 Data Management
81 Hardware and Software Configuration
811 Hardware and Database Software
Data will be stored in an Oracle database system Oracle has advantages of processing efficiency
and smooth linkage with other software systems The application and database will be hosted on
Solaris Unix servers at the IPFnet DCC
812 Statistical Software
SAS will be used as the principal application for the management of analysis data files and
statistical computations S-Plus will be used to provide supplementary functions as needed
813 Access Control and Confidentiality Procedures
Access to databases will be controlled centrally by the IPFnet DCC through user passwords
linked to appropriate privileges This protects the data from unauthorized changes and
inadvertent loss or damage
814 Security
Database and Web servers will be secured by a firewall and through controlled physical access
Oracle has many security features to ensure that any staff member accessing the database has the
proper authority to perform the functions he or she requests of the system Within the secondary
SAS databases Unix group-access control maintains similar security The Sun workstation login
is secured by extensive user-password facilities under Unix
54
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
815 Back-up Procedures
Database back-up will be performed automatically every day and standard IPFnet DCC policies
and procedures will be applied to dictate tape rotation and retention practices
816 Virus Protection
All disk drives that provide network services and all user computers will be protected using
virus-scanning software Standard IPFnet DCC policies will be applied to update these protection
systems periodically through the study
82 Sources of Data
821 Design and Development
The IPFnet DCC will be responsible for development of the electronic case report forms
(eCRFs) development and validation of the clinical study database ensuring data integrity and
training clinical center staff on applicable data management procedures A web-based distributed
data entry model will be implemented This system will be developed to ensure that guidelines
and regulations surrounding the use of computerized systems used in clinical trials are upheld
The remainder of this section provides an overview of the data management plan associated with
this protocol
822 Data Collection Forms
The data collection process consists of direct data entry at the study clinical centers into the EDC
system(s) provided by the DCC A data collection worksheet will be provided to clinical centers
for recording data in the event the EDC system is unavailable Data entry of the eCRFs should
be completed according to the instructions provided and project specific training The
investigator is responsible for maintaining accurate complete and up-to-date records and for
ensuring the completion of the eCRFs for each research participant
55
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
823 Data Acquisition and Entry
Data entry into eCRFs shall be performed by authorized individuals Selected eCRFs may also
require the investigatorrsquos written signature or electronic signature as appropriate Electronic
CRFs will be monitored for completeness accuracy and attention to detail during the study
824 Data Center Responsibilities
The IPFnet DCC will 1) develop a data management plan and will conduct data management
activities 2) provide final eCRFs for the collection of all data required by the study 3) develop
data dictionaries for each eCRF that will comprehensively define each data element 4) conduct
ongoing data monitoring activities on study data 5) monitor any preliminary analysis data
cleanup activities and 6) rigorously monitor final study data clean up
825 Data Editing
Completed data will be entered into the IPFnet DCC automated data acquisition and
management system If incomplete or inaccurate data are found a data clarification request will
be generated and distributed to clinical centers for a response Clinical centers will resolve data
inconsistencies and errors and enter all corrections and changes into the IPFnet DCC automated
data acquisition and management system
826 Training
The training plan for clinical center staff includes provisions for training on assessments eCRF
completion guidelines data management procedures and the use of computerized systems
56
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
9 Study Design and Data Analysis
91 General Analytic Considerations
All primary analyses will be based on intent-to-treat (ITT) principles using all randomized
subjects Baseline factors across groups will be compared using mean (standard deviation) and
median (25th and 75th percentiles) summary measures Kaplan-Meier curves will be used to
display event rates Due to clinical interest in departures from both sides of the null hypothesis
all test statistics will be 2-sided
Reasonable caution needs to be taken when conducting multiple analyses on key clinical
subgroups For subgroup analyses a conservative significance level of 0001 will be used for all
interaction tests Thus subgroup comparisons will be considered exploratory unless the p-value
from the interaction test is smaller than 0001
92 Randomization Blinding and Reporting of Results
A permuted block-randomization scheme will be created with varying block sizes stratified by
clinical center Once a subject has completed the screening and baseline period and evaluation
for inclusionexclusion criteria the randomization process will begin Subjects will be
randomized to receive NAC or matching placebo with equal probability (11) via telephone
contact with a central interactive voice response system (IVRS) using a toll-free randomization
number On the day of randomization after the subject has successfully met all inclusion and
exclusion criteria the investigator or designee will call the central randomization number to
obtain the assigned kit randomization numbers for that subject At each subject visit the
investigator or designee will call the central randomization number to obtain the new kit
randomization numbers for resupply of the subject For resupply of the clinical center the IVRS
will monitor minimal volume of a kit type andor expiration date and will automatically notify
the pharmacy
57
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
The trial results will be reported according to guidelines specified in the CONSORT statement
A flow diagram describing screening recruitment randomization dropout and vital status will
be included in the primary manuscript AEs and efficacy data will be presented for all treatment
groups Adherence dropout and lost to follow-up will be carefully examined across all treatment
groups Analyses of safety will be based on data from all randomized subjects who received at
least one dose of study drug
93 Stratification
Subjects will be distributed to the two treatment arms in a 11 allocation ratio Stratification
blocks will be based on clinical centers
94 Specification of the Primary Analyses
A mixed model repeated measures (MMRM) analysis described in section 95 will be used to
compare differences in the slope of FVC measurements across the treatment groups Response
variables are values of the FVC measured at baseline and every 15 weeks until study completion
Variables in the model will include treatment time and time by treatment age sex race and
height Contrast estimates of differences in slopes of treatment over time (along with confidence
intervals) will be used to estimate the treatment effect The validity of this model in terms of
meeting modeling assumptions will be assessed via standard modeling diagnostics and goodness-
of-fit measures Based on the MMRM framework missing FVC data will not be imputed for the
primary analysis
95 Analysis of Longitudinal Endpoints
A common goal in clinical trials is to specify models that are easily implemented and
reproducible by independent data analysts On the other hand the models should have proper
statistical behavior in terms of low bias and high precision Many common approaches to
longitudinal data analysis including last observation carried forward (LOCF) imputation rely on
the missing completely at random (MCAR) assumption However the MCAR assumption is
58
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
unlikely to hold in many clinical trials because missing data are often related to disease
progression and prognosis A more reasonable assumption missing at random (MAR) specifies
that the complete data distribution can be modeled using only the observed data The likelihood-
based MMRM approach is valid under the more general MAR assumptions These models will
be applied to analyze the longitudinal data secondary endpoints
The advantages of MMRM analysis are that all important characteristics of the model can be preshy
specified standard software can be used to implement the models and results are based on ITT
principles43 In addition the MMRM approach offers superior control of Type I and Type II
errors compared with the LOCF approach
Response variables are values of the PFTs measured at enrollment and every 15 weeks until
study completion and 6MWT values measured at baseline week 30 and week 60 Covariates are
treatment time time by treatment and key baseline risk factors Contrasts (along with
confidence intervals) of treatment by time will be used to estimate the treatment effect
The correlation structure involves multiple pieces including measurement errors random
variation and interindividual variability For the longitudinal data analyses an unstructured
correlation matrix for within-subject errors will be assumed Other correlation structures
including compound symmetry will be examined as needed A careful examination of reasons
for study discontinuation will be conducted to assess the validity of MCAR Sensitivity analyses
will be used to examine the untestable assumption that the observed data violate the MAR
assumption The MMRM models will be implemented using PROC MIXED in SAS
96 Analysis of Binary Time-to-Event and Time-Lagged Endpoints
Regression modeling approaches using either the logistic regression model or Cox proportional
hazards regression model will be employed when appropriate The validity of these models will
be assessed via standard modeling diagnostics and goodness-of-fit measures Estimates of
cumulative frequencies for more general time-lagged responses will be calculated using the
partitioned version of the Bang-Tsiatis estimator44 The partitions will be set at 15-week intervals
59
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
to correspond with the data-collection process Covariate adjusted event rates will be calculated
using inverse probability-weighted regression estimates45
97 Power Analysis
971 Primary Analyses
Based on previously published IPF clinical trials the PL group is expected to experience a drop
in FVC of approximately 020 L over the study period (see Figure 1) The IPFnet Steering Group
determined a clinically important difference would be to preserve the majority of the decline
relative to PL over the study period In particular a treatment effect of 015 L was determined to
be a clinically meaningful difference Potential dropout is a key factor in the proposed study The
drop-out process assumed 5 lost to follow-up after every study visit Only 80 of subjects
were assumed to be followed for the entire study period All models assumed a compound
symmetry structure for the covariance matrix Power calculations were performed using a SAS
IML program for designing repeated measures studies46 Based on preliminary reviews of the
data from the University of Michigan the covariance matrix parameters were estimated at
approximately σ2 = 0757 (variance parameter) and ρ = 0936 (correlation parameter) To be
conservative the power calculations for the primary analysis were performed with parameter
setting of σ2 = 0810 (variance parameter) and ρ = 0925 (correlation parameter)
The power calculations assume a correction for imperfect compliance proposed by Lachin and
Foulkes to allow for 2 noncompliance for each of the treatment arms47 Thus the sample size
of 130 subjects per arm would be reduced to an adjusted sample size of 130(1-002-002)2 =
1198 or 120 subjects per arm
Under the assumed Type I error rate of 005 with a correlation parameter of 0925 and standard
deviation of 090 the difference of 015 L (or 00025 Lweek) shown in Table 6 would have
power of 93
60
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Table 6 Hypothetical Values of Mean FVC (L) Change from Baseline
Week 15 Week 30 Week 45 Week 60
NAC 00125 00250 00375 00500
Placebo 00500 01000 01500 02000
Difference 00375 00750 01125 01500
Abbreviations FVC forced vital capacity PL placebo
972 Power Analysis for Secondary Endpoints
Power calculations for secondary endpoint measurements are shown in Table 7 Standard
deviations are based on unpublished data provided by the University of Michigan The
calculations are based on a 2-sample t-test with Type I error rate set at 005 These calculations
are likely to be conservative because the statistical approach described in section 95 for
analyzing these endpoints will incorporate incomplete observations as well as intermediate data
points
Table 7 Detectable Differences in Treatment Means for Selected Endpoint Measurements
Secondary Endpoints Std Dev
of the Baseline Score
Detectable Difference for 80 Power
Std Dev of the Change Score
Difference Detectable for
80 Power
DLCOpred 166 58 91 32
6MWT Area Under the Desaturation Curve
219 76 175 61
6MWT Distance to Desaturation 224 78 315 110
6MWT Minutes Walked 210 073 205 071
Abbreviations Std Dev standard deviation DLCOpred diffusing capacity of the lung for carbon monoxide percent predicted 6MWT 6-minute walk test
61
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
10 Study Administration
101 Cooperative Agreement Mechanism
The administrative and funding mechanism used to undertake this project is a ldquocooperative
agreementrdquo (U01) which is an assistance mechanism Under the cooperative agreement the
NHLBI assists supports andor stimulates the project and is substantially involved with
investigators in conducting the study by facilitating performance of the effort in a ldquopartnerrdquo role
The NHLBI project scientist serves on the IPFnet Steering Group and he or another NHLBI
scientist may serve on other project committees when appropriate At the same time however
NHLBI does not assume a dominant role direction or prime responsibility for this research
program
As described below governance of the project is conducted through the IPFnet Steering Group
Principal investigators have lead responsibilities in all aspects of their trials and the project
including any modification of trial designs conduct of the trials quality control data analysis
and interpretation preparation of publications and collaboration with other investigators unless
otherwise provided for by the IPFnet Steering Group
PIs retain custody of and have primary rights to their center-specific and collaborative data
subject to government rights-of-access consistent with current Health amp Human Services (HHS)
Public Health Service (PHS) and National Institutes of Health policies The protocols and
governance policies call for the continual submission of data centrally to the IPFnet DCC for the
collaborative database which at a minimum will contain the key variables selected by the IPFnet
Steering Group for standardization across all clinical centers the submission of copies of the
collaborative datasets to each PI upon completion of the project procedures for data analysis
reporting and publication and procedures to protect and ensure the privacy of medical and
genetic data and records of individuals The NHLBI project scientist on behalf of the NHLBI
will have the same access privileges and responsibilities regarding the collaborative data as the
other members of the Steering Group
62
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
PIs are also encouraged to publish and to publicly release and disseminate results data and other
products of the project concordant with the project protocols and governance and the approved
plan for making data and materials available to the scientific community and to the NHLBI
However during the 3 years after the ending date of NHLBI project support unpublished data
unpublished results data sets not previously released and other study materials or products are
to be made available to any third party only with the approval of the IPFnet Steering Group
Upon completion of the project PIs are expected to put their intervention materials and
procedure manuals into the public domain andor make them available to other investigators
according to the approved plan for making data and materials available to the scientific
community and the NHLBI for the conduct of research at no charge other than the costs of
reproduction and distribution
The NHLBI reserves the right to terminate or curtail the project (or an individual award) in the
event of (a) failure to develop or implement mutually agreeable collaborative measurement
subject eligibility and data management sections of the protocols (b) substantial shortfall in
subject recruitment follow-up data reporting or quality control or other major breach of
protocol (c) substantive changes in the agreed-upon protocols with which NHLBI cannot
concur (d) reaching a major project outcome with persuasive statistical significance
substantially before schedule or (e) human subject ethical issues that may dictate a premature
termination
Any disagreement that may arise in scientificprogrammatic matters (within the scope of the
award) between award recipients and the NHLBI may be brought to arbitration An arbitration
panel will be composed of 3 membersmdash1 selected by the IPFnet Steering Group (with the
NHLBI member not voting) or by the individual PI in the event of an individual disagreement a
second selected by NHLBI and the third selected by the other 2 members This special
arbitration procedure in no way affects the PIrsquos right to appeal an adverse action that is otherwise
appealable in accordance with the PHS regulations at 42 CFR part 50 Subpart D and HHS
63
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
regulation at 45 CFR part 16 or the rights of the NHLBI under applicable statutes regulations
and terms of the award
102 IPFnet Steering Group
The IPFnet Steering Group is the main governing body of the project It is composed of the PIs
of the clinical centers the PI of the DCC and the NHLBI project scientist The clinical centers
the IPFnet DCC and the NHLBI each have 1 vote on the IPFnet Steering Group All decisions
are determined by majority vote
All major scientific decisions are determined by the IPFnet Steering Group It assumes overall
responsibility for the design and conduct of the trial It appoints (and disbands) committees and
subcommittees as the need arises designs approves and implements the study protocols
oversees the development of the MOOP monitors subject recruitment and treatment delivery
evaluates data collection and management oversees quality assurance procedures and
implements changes and enhancements to the study as required It also has primary responsibility
for facilitating the conduct of the trials and reporting the projectrsquos results
103 Data and Safety Monitoring Board
The NHLBI will establish a DSMB in accordance with established policies (see
httpwwwnhlbinihgovfundingpoliciesdsmb_insthtm) to ensure data quality and subject
safety and to provide independent advice to the NHLBI regarding progress and the
appropriateness of study continuation
104 Recommendations on Interim Monitoring of Efficacy Safety and Futility
First and foremost the role of the DSMB will be to review subject safety and trial conduct at
periodic points during the study The DSMB may require analyses of the primary endpoint
results for comparing the benefit and risks of treatment strategies The benefit of collecting
additional data on key secondary endpoints with extended follow-up and establishing a robust
64
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
evidence base for determining a standard of care will need to be carefully considered before
early termination of one or more treatment arms After careful consideration the IPFnet Steering
Group recommends conservative thresholds for the early examinations of the safety and efficacy
data
The DSMB will be expected to meet approximately every 6 months until trial completion to
review safety and toxicity data The DSMB may recommend stopping the study based on these
reviews Because the DSMB could stop the trial for safety concerns as well as for a large
efficacy benefit there could be multiple opportunities to reject the null hypothesis (no difference
in event rates between the PL and NAC groups) A Bonferroni approximation will be applied
during the one planned interim analysis for efficacy
Before locking the database a statistical analysis plan (SAP) will be developed to provide
complete details on the statistical analysis The SAP will include the specifics for how and when
the DSMB will be notified for AEs The IPFnet DCC will deliver to the DSMB all FDA-defined
AEs at 3-month intervals The IPFnet DCC will prepare narrative SAE reports in real time for
DSMB review including recommendations and analysis of similar events for each SAE
submitted to the FDA
65
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
11 Investigator and Sponsor Obligations
111 Monitoring
All monitoring activities for US clinical centers will be performed in accordance with DCRI
standard operating procedures Information regarding the types of visits will be outlined in the
PANTHER-IPF MOOP
112 Cost and Payment
There will be no cost to subjects enrolled in this trial Study-related procedures will be paid for
by the IPFnet
Subjects may be eligible for reimbursement for travel to the clinical center Details of payment
will be explained to each subject during the consent process
113 Confidentiality and Health Insurance Portability and Accountability Act
Considerations
Subject confidentiality will be protected throughout the study All subject data will be kept
strictly confidential and no subject-identifying information will be released to anyone outside
the project Confidentiality will be assured through several mechanisms First each subject will
be assigned an anonymous study ID which will then be used on all study forms Second any
study forms blood samples and paper records that contain subject information (eg address lists
phone lists) will be kept at the clinical centers in secured locked areas coded by number Once
blood is collected there will be no subject identifiers placed on blood samplesmdashonly the study
ID number and the date of sample collection Third access to all subject data and information
including laboratory specimens will be restricted to authorized personnel In the case of
computerized data this restricted access will be assured through user logon IDs and password
protection
66
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
At the IPFnet DCC only authorized personnel will have access to the data files containing study
data Security will be assured through user logon IDs passwords and appropriate access
privileges All study subjects will be identified only by their IPFnet ID numbers and no personal
identifying information such as name address or Social Security number will be entered into
the IPFnet DCC database Any subject-specific data reported to the IPFnet Steering Group will
be identified only by the IPFnet ID number
Finally subjects will not be identified by name in any reports or publications nor will the data
be presented in such a way that the identity of individual subjects can be inferred Analysis files
created for further study by the scientific community will have no subject identifiers These data
files will be created in accordance with the Ancillary Studies and Publication Policy of the
IPFnet
114 Informed Consent Procedures
All IPFnet subjects will provide written informed consent using procedures reviewed and
approved by each clinical centerrsquos IRB Informed consent will be undertaken by study personnel
in-person with the subject The subject has the option of declining further participation in the
study at that point No further study procedures will be conducted until the signed documents
have been provided to the IPFnet clinical center
115 Institutional Review Boards
Before initiating this study the protocol clinical center-specific informed consent forms Health
Insurance Portability and Accountability Act (HIPAA) forms recruitment materials and other
relevant information will be reviewed by a properly constituted IRB at each participating clinical
center A copy of the signed and dated IRB approval at each clinical center will be retrieved prior
to or during the site initiation visit and archived at the IPFnet DCC Any amendments to the
protocol other than simple administrative and typographical changes must be approved by each
IRB before they are implemented The clinical centers will seek annual renewals of their IRB
approvals in accordance with local procedures
67
__________________________________________ ________________
__________________________________________
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
12 Investigator Agreement
I have read the foregoing protocol PANTHER-IPF and agree that it contains all necessary
details for carrying out this study I will conduct the study as outlined herein and will complete
the study within the time designated
I will provide copies of the protocol and all pertinent information to all individuals responsible to
me who assist in the conduct of this study I will discuss this material with them to ensure they
are fully informed regarding the drug and the conduct of the study
I will fulfill all responsibilities for submitting pertinent information to the local IRB if
applicable that is responsible for this study
I further agree that NHLBI andor DCRI will have access to any source documents from which
eCRF information may have been generated
Signature of Principal Investigator Date
Name of Principal Investigator (printed or typed)
Protocol version date May 19 2009
Protocol Amendment 1 version date May 28 2010
Protocol Amendment 2 version date December 6 2011
68
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
13 References
1 Raghu G Brown KK Bradford WZ et al A placebo-controlled trial of interferon gamma-1b in patients with idiopathic pulmonary fibrosis N Engl J Med 2004350125-33 2 King TE Jr Safrin S Starko KM et al Analyses of efficacy end points in a controlled trial of interferon-gamma1b for idiopathic pulmonary fibrosis Chest 2005127171-7 3 Flaherty KR Thwaite EL Kazerooni EA et al Radiological versus histological diagnosis in UIP and NSIP survival implications Thorax 200358143-8 4 Wells AU Desai SR Rubens MB et al Idiopathic pulmonary fibrosis a composite physiologic index derived from disease extent observed by computed tomography Am J Respir Crit Care Med 2003167962-9 5 Raghu G Freudenberger TD Yang S et al High prevalence of abnormal acid gastroshyoesophageal reflux in idiopathic pulmonary fibrosis Eur Respir J 200627136-42 6 Kinnula VL Focus on antioxidant enzymes and antioxidant strategies in smoking related airway diseases Thorax 200560693-700 7 Coultas DB Zumwalt RE Black WC Sobonya RE The epidemiology of interstitial lung diseases Am J Respir Crit Care Med 1994150967-72 8 Raghu G Weycker D Edelsberg J Bradford WZ Oster G Incidence and prevalence of idiopathic pulmonary fibrosis Am J Respir Crit Care Med 2006174810-6 9 Olson AL Swigris JJ Lezotte DC Norris JM Wilson CG Brown KK Mortality from pulmonary fibrosis increased in the United States from 1992 to 2003 Am J Respir Crit Care Med 2007176277-84 10 Mannino DM Etzel RA Parrish RG Pulmonary fibrosis deaths in the United States 1979shy1991 An analysis of multiple-cause mortality data Am J Respir Crit Care Med 19961531548shy52 11 Hubbard R Johnston I Coultas DB Britton J Mortality rates from cryptogenic fibrosing alveolitis in seven countries Thorax 199651711-6 12 Johnston I Britton J Kinnear W Logan R Rising mortality from cryptogenic fibrosing alveolitis Bmj 19903011017-21 13 Raghu G Collard HR Egan JJ et al An official ATSERSJRSALAT statement idiopathic pulmonary fibrosis evidence-based guidelines for diagnosis and management Am J Respir Crit Care Med 2011183788-824 14 (USA) FDA FDA Public Health Advisory Interferon gamma-1b (marketed as Actimmune) In 2007 15 King TE Jr Pardo A Selman M Idiopathic pulmonary fibrosis Lancet 2011 16 Raghu G Brown KK Costabel U et al Treatment of idiopathic pulmonary fibrosis with etanercept an exploratory placebo-controlled trial Am J Respir Crit Care Med 2008178948shy55 17 Malouf MA Hopkins P Snell G Glanville AR An investigator-driven study of everolimus in surgical lung biopsy confirmed idiopathic pulmonary fibrosis Respirology 201116776-83 18 King TE Jr Behr J Brown KK et al BUILD-1 a randomized placebo-controlled trial of bosentan in idiopathic pulmonary fibrosis Am J Respir Crit Care Med 200817775-81 19 Richeldi L Costabel U Selman M et al Efficacy of a tyrosine kinase inhibitor in idiopathic pulmonary fibrosis N Engl J Med 20113651079-87
69
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
20 Borok Z Buhl R Grimes GJ et al Effect of glutathione aerosol on oxidant-antioxidant imbalance in idiopathic pulmonary fibrosis Lancet 1991338215-6 21 Meyer A Buhl R Magnussen H The effect of oral N-acetylcysteine on lung glutathione levels in idiopathic pulmonary fibrosis Eur Respir J 19947431-6 22 Behr J Maier K Degenkolb B Krombach F Vogelmeier C Antioxidative and clinical effects of high-dose N-acetylcysteine in fibrosing alveolitis Adjunctive therapy to maintenance immunosuppression Am J Respir Crit Care Med 19971561897-901 23 Cantin AM North SL Fells GA Hubbard RC Crystal RG Oxidant-mediated epithelial cell injury in idiopathic pulmonary fibrosis J Clin Invest 1987791665-73 24 Waghray M Cui Z Horowitz JC et al Hydrogen peroxide is a diffusible paracrine signal for the induction of epithelial cell death by activated myofibroblasts Faseb J 200519854-6 25 Larios JM Budhiraja R Fanburg BL Thannickal VJ Oxidative protein cross-linking reactions involving L-tyrosine in transforming growth factor-beta1-stimulated fibroblasts J Biol Chem 200127617437-41 26 Kinnula VL Fattman CL Tan RJ Oury TD Oxidative stress in pulmonary fibrosis a possible role for redox modulatory therapy Am J Respir Crit Care Med 2005172417-22 27 Meyer A Buhl R Kampf S Magnussen H Intravenous N-acetylcysteine and lung glutathione of patients with pulmonary fibrosis and normals Am J Respir Crit Care Med 19951521055-60 28 Behr J Degenkolb B Krombach F Vogelmeier C Intracellular glutathione and bronchoalveolar cells in fibrosing alveolitis effects of N-acetylcysteine Eur Respir J 200219906-11 29 Bando M Hosono T Mato N et al Long-term efficacy of inhaled N-acetylcysteine in patients with idiopathic pulmonary fibrosis Intern Med 2010492289-96 30 Demedts M Behr J Buhl R et al High-dose acetylcysteine in idiopathic pulmonary fibrosis N Engl J Med 20053532229-42 31 Toma TP Bhowmik A Rajakulasingam R Acetylcysteine in pulmonary fibrosis N Engl J Med 20063541086-9 author reply -9 32 Hunninghake GW Antioxidant therapy for idiopathic pulmonary fibrosis N Engl J Med 20053532285-7 33 Flaherty KR Mumford JA Murray S et al Prognostic implications of physiologic and radiographic changes in idiopathic interstitial pneumonia Am J Respir Crit Care Med 2003168543-8 34 Latsi PI du Bois RM Nicholson AG et al Fibrotic idiopathic interstitial pneumonia the prognostic value of longitudinal functional trends Am J Respir Crit Care Med 2003168531-7 35 Collard HR King TE Jr Bartelson BB Vourlekis JS Schwarz MI Brown KK Changes in clinical and physiologic variables predict survival in idiopathic pulmonary fibrosis Am J Respir Crit Care Med 2003168538-42 36 Jegal Y Kim DS Shim TS et al Physiology is a stronger predictor of survival than pathology in fibrotic interstitial pneumonia Am J Respir Crit Care Med 2005171639-44 37 Martinez FJ Safrin S Weycker D et al The clinical course of patients with idiopathic pulmonary fibrosis Ann Intern Med 2005142963-7 38 Hull JH Acetylcysteine in pulmonary fibrosis N Engl J Med 20063541089-91 author reply -91
70
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
39 Flaherty KR King TE Jr Raghu G et al Idiopathic interstitial pneumonia what is the effect of a multidisciplinary approach to diagnosis Am J Respir Crit Care Med 2004170904shy10 40 Raghu G Johnson WC Lockhart D Mageto Y Treatment of idiopathic pulmonary fibrosis with a new antifibrotic agent pirfenidone results of a prospective open-label Phase II study Am J Respir Crit Care Med 19991591061-9 41 Hunninghake GW Lynch DA Galvin JR et al Radiologic findings are strongly associated with a pathologic diagnosis of usual interstitial pneumonia Chest 20031241215-23 42 Lynch D Godwin J Safrin S et al High-resolution computed tomography in idiopathic pulmonary fibrosis diagnosis and prognosis Am J Respir Crit Care Med 2005172488-93 43 Mallinckrodt CH Watkin JG Molenberghs G Carroll RJ Choice of the primary analysis in longitudinal clinical trials Pharmaceutical Statistics 20043161-9 44 Bang H Tsiatis A Estimating medical costs with censored data Biometrika 200087329shy43 45 Lin DY Regression analysis of incomplete medical cost data Stat Med 2003221181-200 46 Rochon J Application of GEE procedures for sample size calculations in repeated measures experiments Stat Med 1998171643-58 47 Lachin JM Foulkes MA Evaluation of sample size and power for analyses of survival with allowance for nonuniform patient entry losses to follow-up noncompliance and stratification Biometrics 198642507-19
71
- PANTHER-IPFPREDNISONE AZATHIOPRINEAND N-ACETYLCYSTEINEA STUDY THAT EVALUATES RESPONSE INIDIOPATHIC PULMONARY FIBROSIS
-
- Protocol Summary
- Table of Contents
- List of Tables
- List of Figures
- List of Abbreviations
- 1 Summary
- 2 Hypotheses and Specific Aims
-
- 21 Null Hypothesis
- 22 Specific Aim 1
- 23 Specific Aim 2
- 24 Prespecified Subgroups of Interest
-
- 3 Background and Significance
-
- 31 Idiopathic Pulmonary Fibrosis is the Most Common Interstitial Lung Disease
- 32 Rationale for Placebo Control
- 33 Rationale for N-acetylcysteine
- 35 Rationale for N-acetylcysteine as a Stand-alone Therapy
- 36 Rationale for the Study Design and Primary Endpoint
- 37 Rationale for Blinding of Treatments
-
- 4 Methods
-
- 41 Inclusion Criteria
- 42 Diagnosis of IPF
- 43 Exclusion Criteria
- 44 Study Design and Study Visit
- 45 Dose Justification
- 46 Contraindications Precautions and Side Effects of Study Medications
- 47 Recruitment Procedures
- 48 Study Procedures
- 49 Concomitant Medications
- 410 Laboratory Testing
- 411 Blinding of Study Drugs
-
- 5 Study Endpoints
-
- 51 Primary Study Endpoint
- 52 Secondary Study Endpoints
-
- 6 Safety Evaluations and Procedures
-
- 61 Adverse Events
- 62 Clinical Medical Monitoring
- 63 Unblinding Procedures
-
- 7 Study Drug Procedures
- 8 Data Management
-
- 81 Hardware and Software Configuration
- 82 Sources of Data
-
- 9 Study Design and Data Analysis
-
- 91 General Analytic Considerations
- 92 Randomization Blinding and Reporting of Results
- 93 Stratification
- 94 Specification of the Primary Analyses
- 95 Analysis of Longitudinal Endpoints
- 96 Analysis of Binary Time-to-Event and Time-Lagged Endpoints
- 97 Power Analysis
-
- 10 Study Administration
-
- 101 Cooperative Agreement Mechanism
- 102 IPFnet Steering Group
- 103 Data and Safety Monitoring Board
- 104 Recommendations on Interim Monitoring of Efficacy Safety and Futility
-
- 11 Investigator and Sponsor Obligations
-
- 111 Monitoring
- 112 Cost and Payment
- 113 Confidentiality and Health Insurance Portability and Accountability ActConsiderations
- 114 Informed Consent Procedures
- 115 Institutional Review Boards
-
- 12 Investigator Agreement
- 13 References
-
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
o Hospitalization for elective procedure
o Emergency room visits
Results in persistent or significant disability or incapacity
Is a congenital anomaly or birth defect
Important medical events that may not result in death be life-threatening or require
inpatient hospitalization may be considered serious adverse events (SAEs) when based
on appropriate medical judgment they may jeopardize the subject and may require
medical or surgical intervention to prevent one of the outcomes listed above
Life-threatening means that the subject was in the view of the investigator at immediate risk of
death from the AE as it occurred It does not include an AE that had it occurred in a more severe
form might have caused death
Persistent or significant disabilityincapacity means that the event resulted in permanent or
significant and substantial disruption of the subjectrsquos ability to carry out normal life functions
Causality
A reasonable possibility means the AE may have been caused byrelated to the study drug A
perceived or real lack of efficacy does not satisfy the definition of relatedness
612 Adverse Event (AE) Reporting
For the PANTHER-IPF trial all AEs (serious and nonserious) occurring from randomization
through final study visit (4 weeks after final dose of all study medication) will be recorded on the
AE page of the case report form (CRF)
6121 Serious Adverse Events (SAE) Reporting
For this trial all deaths and all SAEs which occur from randomization through final study visit
must be entered within the EDC system via the SAE eCRF page within 24 hours of the
investigative sitersquos knowledge of the event It is the responsibility of the clinical center
50
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
investigator to provide a causality assessment of the event for each study medications based upon
the information available at the time of the report It is understood that complete information
about the event may not be known at the time the initial report is submitted In the event the EDC
system is not accessible to the site at the time of event reporting investigative sites will complete
and forward a paper back-up SAE form to DCRI Safety Surveillance for processing
DCRI Safety Surveillance
Telephone 1-919-668-8624 or 1-866-668-7799 (toll free)
Fax 1-919-668-7138 or 1-866-668-7138 (toll free)
The investigator must complete and submit follow-up SAE information via the eCRF when
important new or follow-up information (eg final diagnosis outcome results of specific
investigations) becomes available Follow-up information should be submitted according to the
same process used for reporting the initial event as described above All SAEs will be followed
until resolution stabilization or 30 days after the subject has completed the final visit (4 weeks
after the final dose of study medication) whichever occurs first The investigator is responsible
for reporting SAEs to their institutional review board (IRB) per site specific IRB reporting
guidelines
6122 Regulatory Reporting
AEs that are serious study drug related and unexpected will be reported to the regulatory
authorities The DCRI Safety Surveillance medical monitor will perform a medical review of all
SAEs submitted and evaluate for ldquounexpectednessrdquo DCRI Safety Surveillance will prepare
MedWatch reports for those events identified as serious study drug related and unexpected as
determined by Safety Medical Monitor
DCRI Regulatory Services will submit all unexpected study drug-related SAEs as per 21 CFR
32 DCRI Safety Surveillance will provide a safety alert letter to the NHLBI DSMB and DCC
clinical operation (for distribution to sites) within 15 days of initial receipt of the information
51
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Investigators are responsible for promptly reporting these events to their reviewing IRBs
according to site specific IRB reporting guidelines
62 Clinical Medical Monitoring
There will be an unblinded physician at the IPFnet DCC serving as medical monitor The
medical monitor will be available to assist with questions about dosage adjustments of study
medications including discontinuation or resumption of medications
63 Unblinding Procedures
Unblinding of subjects or investigators to subject treatment is strongly discouraged For ongoing
clinical management all subjects should be presumed to be receiving ldquoactiverdquo study drug To
ensure the subjectrsquos safety the study treatment will be dose-adjusted based on laboratory test
results clinical findings and symptoms
The IPFnet DCC medical monitor and PANTHER-IPF co-chairs Drs Ganesh Raghu and
Fernando Martinez will be available to the study physicians to discuss study drug management
on a case-by-case basis Un-blinding will be considered ONLY when the knowledge of subject
treatment assignment is ABSOLUTELY ESSENTIAL for subject safety and after discussion of
the subjectrsquos case with the medical monitor and either Dr Raghu or Dr Martinez Unblinding of
study treatment should be minimized during the conduct of the trial In those cases where it is
felt to be medically necessary the DCC medical officer will communicate directly with the
managing physician to minimize unblinding of study personnel
52
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
7 Study Drug Procedures
At the baseline 15-week 30-week and 45-week study visits subjects will receive a supply of
study drug sufficient to last until the next visit at which study drug will be dispensed
53
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
8 Data Management
81 Hardware and Software Configuration
811 Hardware and Database Software
Data will be stored in an Oracle database system Oracle has advantages of processing efficiency
and smooth linkage with other software systems The application and database will be hosted on
Solaris Unix servers at the IPFnet DCC
812 Statistical Software
SAS will be used as the principal application for the management of analysis data files and
statistical computations S-Plus will be used to provide supplementary functions as needed
813 Access Control and Confidentiality Procedures
Access to databases will be controlled centrally by the IPFnet DCC through user passwords
linked to appropriate privileges This protects the data from unauthorized changes and
inadvertent loss or damage
814 Security
Database and Web servers will be secured by a firewall and through controlled physical access
Oracle has many security features to ensure that any staff member accessing the database has the
proper authority to perform the functions he or she requests of the system Within the secondary
SAS databases Unix group-access control maintains similar security The Sun workstation login
is secured by extensive user-password facilities under Unix
54
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
815 Back-up Procedures
Database back-up will be performed automatically every day and standard IPFnet DCC policies
and procedures will be applied to dictate tape rotation and retention practices
816 Virus Protection
All disk drives that provide network services and all user computers will be protected using
virus-scanning software Standard IPFnet DCC policies will be applied to update these protection
systems periodically through the study
82 Sources of Data
821 Design and Development
The IPFnet DCC will be responsible for development of the electronic case report forms
(eCRFs) development and validation of the clinical study database ensuring data integrity and
training clinical center staff on applicable data management procedures A web-based distributed
data entry model will be implemented This system will be developed to ensure that guidelines
and regulations surrounding the use of computerized systems used in clinical trials are upheld
The remainder of this section provides an overview of the data management plan associated with
this protocol
822 Data Collection Forms
The data collection process consists of direct data entry at the study clinical centers into the EDC
system(s) provided by the DCC A data collection worksheet will be provided to clinical centers
for recording data in the event the EDC system is unavailable Data entry of the eCRFs should
be completed according to the instructions provided and project specific training The
investigator is responsible for maintaining accurate complete and up-to-date records and for
ensuring the completion of the eCRFs for each research participant
55
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
823 Data Acquisition and Entry
Data entry into eCRFs shall be performed by authorized individuals Selected eCRFs may also
require the investigatorrsquos written signature or electronic signature as appropriate Electronic
CRFs will be monitored for completeness accuracy and attention to detail during the study
824 Data Center Responsibilities
The IPFnet DCC will 1) develop a data management plan and will conduct data management
activities 2) provide final eCRFs for the collection of all data required by the study 3) develop
data dictionaries for each eCRF that will comprehensively define each data element 4) conduct
ongoing data monitoring activities on study data 5) monitor any preliminary analysis data
cleanup activities and 6) rigorously monitor final study data clean up
825 Data Editing
Completed data will be entered into the IPFnet DCC automated data acquisition and
management system If incomplete or inaccurate data are found a data clarification request will
be generated and distributed to clinical centers for a response Clinical centers will resolve data
inconsistencies and errors and enter all corrections and changes into the IPFnet DCC automated
data acquisition and management system
826 Training
The training plan for clinical center staff includes provisions for training on assessments eCRF
completion guidelines data management procedures and the use of computerized systems
56
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
9 Study Design and Data Analysis
91 General Analytic Considerations
All primary analyses will be based on intent-to-treat (ITT) principles using all randomized
subjects Baseline factors across groups will be compared using mean (standard deviation) and
median (25th and 75th percentiles) summary measures Kaplan-Meier curves will be used to
display event rates Due to clinical interest in departures from both sides of the null hypothesis
all test statistics will be 2-sided
Reasonable caution needs to be taken when conducting multiple analyses on key clinical
subgroups For subgroup analyses a conservative significance level of 0001 will be used for all
interaction tests Thus subgroup comparisons will be considered exploratory unless the p-value
from the interaction test is smaller than 0001
92 Randomization Blinding and Reporting of Results
A permuted block-randomization scheme will be created with varying block sizes stratified by
clinical center Once a subject has completed the screening and baseline period and evaluation
for inclusionexclusion criteria the randomization process will begin Subjects will be
randomized to receive NAC or matching placebo with equal probability (11) via telephone
contact with a central interactive voice response system (IVRS) using a toll-free randomization
number On the day of randomization after the subject has successfully met all inclusion and
exclusion criteria the investigator or designee will call the central randomization number to
obtain the assigned kit randomization numbers for that subject At each subject visit the
investigator or designee will call the central randomization number to obtain the new kit
randomization numbers for resupply of the subject For resupply of the clinical center the IVRS
will monitor minimal volume of a kit type andor expiration date and will automatically notify
the pharmacy
57
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
The trial results will be reported according to guidelines specified in the CONSORT statement
A flow diagram describing screening recruitment randomization dropout and vital status will
be included in the primary manuscript AEs and efficacy data will be presented for all treatment
groups Adherence dropout and lost to follow-up will be carefully examined across all treatment
groups Analyses of safety will be based on data from all randomized subjects who received at
least one dose of study drug
93 Stratification
Subjects will be distributed to the two treatment arms in a 11 allocation ratio Stratification
blocks will be based on clinical centers
94 Specification of the Primary Analyses
A mixed model repeated measures (MMRM) analysis described in section 95 will be used to
compare differences in the slope of FVC measurements across the treatment groups Response
variables are values of the FVC measured at baseline and every 15 weeks until study completion
Variables in the model will include treatment time and time by treatment age sex race and
height Contrast estimates of differences in slopes of treatment over time (along with confidence
intervals) will be used to estimate the treatment effect The validity of this model in terms of
meeting modeling assumptions will be assessed via standard modeling diagnostics and goodness-
of-fit measures Based on the MMRM framework missing FVC data will not be imputed for the
primary analysis
95 Analysis of Longitudinal Endpoints
A common goal in clinical trials is to specify models that are easily implemented and
reproducible by independent data analysts On the other hand the models should have proper
statistical behavior in terms of low bias and high precision Many common approaches to
longitudinal data analysis including last observation carried forward (LOCF) imputation rely on
the missing completely at random (MCAR) assumption However the MCAR assumption is
58
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
unlikely to hold in many clinical trials because missing data are often related to disease
progression and prognosis A more reasonable assumption missing at random (MAR) specifies
that the complete data distribution can be modeled using only the observed data The likelihood-
based MMRM approach is valid under the more general MAR assumptions These models will
be applied to analyze the longitudinal data secondary endpoints
The advantages of MMRM analysis are that all important characteristics of the model can be preshy
specified standard software can be used to implement the models and results are based on ITT
principles43 In addition the MMRM approach offers superior control of Type I and Type II
errors compared with the LOCF approach
Response variables are values of the PFTs measured at enrollment and every 15 weeks until
study completion and 6MWT values measured at baseline week 30 and week 60 Covariates are
treatment time time by treatment and key baseline risk factors Contrasts (along with
confidence intervals) of treatment by time will be used to estimate the treatment effect
The correlation structure involves multiple pieces including measurement errors random
variation and interindividual variability For the longitudinal data analyses an unstructured
correlation matrix for within-subject errors will be assumed Other correlation structures
including compound symmetry will be examined as needed A careful examination of reasons
for study discontinuation will be conducted to assess the validity of MCAR Sensitivity analyses
will be used to examine the untestable assumption that the observed data violate the MAR
assumption The MMRM models will be implemented using PROC MIXED in SAS
96 Analysis of Binary Time-to-Event and Time-Lagged Endpoints
Regression modeling approaches using either the logistic regression model or Cox proportional
hazards regression model will be employed when appropriate The validity of these models will
be assessed via standard modeling diagnostics and goodness-of-fit measures Estimates of
cumulative frequencies for more general time-lagged responses will be calculated using the
partitioned version of the Bang-Tsiatis estimator44 The partitions will be set at 15-week intervals
59
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
to correspond with the data-collection process Covariate adjusted event rates will be calculated
using inverse probability-weighted regression estimates45
97 Power Analysis
971 Primary Analyses
Based on previously published IPF clinical trials the PL group is expected to experience a drop
in FVC of approximately 020 L over the study period (see Figure 1) The IPFnet Steering Group
determined a clinically important difference would be to preserve the majority of the decline
relative to PL over the study period In particular a treatment effect of 015 L was determined to
be a clinically meaningful difference Potential dropout is a key factor in the proposed study The
drop-out process assumed 5 lost to follow-up after every study visit Only 80 of subjects
were assumed to be followed for the entire study period All models assumed a compound
symmetry structure for the covariance matrix Power calculations were performed using a SAS
IML program for designing repeated measures studies46 Based on preliminary reviews of the
data from the University of Michigan the covariance matrix parameters were estimated at
approximately σ2 = 0757 (variance parameter) and ρ = 0936 (correlation parameter) To be
conservative the power calculations for the primary analysis were performed with parameter
setting of σ2 = 0810 (variance parameter) and ρ = 0925 (correlation parameter)
The power calculations assume a correction for imperfect compliance proposed by Lachin and
Foulkes to allow for 2 noncompliance for each of the treatment arms47 Thus the sample size
of 130 subjects per arm would be reduced to an adjusted sample size of 130(1-002-002)2 =
1198 or 120 subjects per arm
Under the assumed Type I error rate of 005 with a correlation parameter of 0925 and standard
deviation of 090 the difference of 015 L (or 00025 Lweek) shown in Table 6 would have
power of 93
60
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Table 6 Hypothetical Values of Mean FVC (L) Change from Baseline
Week 15 Week 30 Week 45 Week 60
NAC 00125 00250 00375 00500
Placebo 00500 01000 01500 02000
Difference 00375 00750 01125 01500
Abbreviations FVC forced vital capacity PL placebo
972 Power Analysis for Secondary Endpoints
Power calculations for secondary endpoint measurements are shown in Table 7 Standard
deviations are based on unpublished data provided by the University of Michigan The
calculations are based on a 2-sample t-test with Type I error rate set at 005 These calculations
are likely to be conservative because the statistical approach described in section 95 for
analyzing these endpoints will incorporate incomplete observations as well as intermediate data
points
Table 7 Detectable Differences in Treatment Means for Selected Endpoint Measurements
Secondary Endpoints Std Dev
of the Baseline Score
Detectable Difference for 80 Power
Std Dev of the Change Score
Difference Detectable for
80 Power
DLCOpred 166 58 91 32
6MWT Area Under the Desaturation Curve
219 76 175 61
6MWT Distance to Desaturation 224 78 315 110
6MWT Minutes Walked 210 073 205 071
Abbreviations Std Dev standard deviation DLCOpred diffusing capacity of the lung for carbon monoxide percent predicted 6MWT 6-minute walk test
61
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
10 Study Administration
101 Cooperative Agreement Mechanism
The administrative and funding mechanism used to undertake this project is a ldquocooperative
agreementrdquo (U01) which is an assistance mechanism Under the cooperative agreement the
NHLBI assists supports andor stimulates the project and is substantially involved with
investigators in conducting the study by facilitating performance of the effort in a ldquopartnerrdquo role
The NHLBI project scientist serves on the IPFnet Steering Group and he or another NHLBI
scientist may serve on other project committees when appropriate At the same time however
NHLBI does not assume a dominant role direction or prime responsibility for this research
program
As described below governance of the project is conducted through the IPFnet Steering Group
Principal investigators have lead responsibilities in all aspects of their trials and the project
including any modification of trial designs conduct of the trials quality control data analysis
and interpretation preparation of publications and collaboration with other investigators unless
otherwise provided for by the IPFnet Steering Group
PIs retain custody of and have primary rights to their center-specific and collaborative data
subject to government rights-of-access consistent with current Health amp Human Services (HHS)
Public Health Service (PHS) and National Institutes of Health policies The protocols and
governance policies call for the continual submission of data centrally to the IPFnet DCC for the
collaborative database which at a minimum will contain the key variables selected by the IPFnet
Steering Group for standardization across all clinical centers the submission of copies of the
collaborative datasets to each PI upon completion of the project procedures for data analysis
reporting and publication and procedures to protect and ensure the privacy of medical and
genetic data and records of individuals The NHLBI project scientist on behalf of the NHLBI
will have the same access privileges and responsibilities regarding the collaborative data as the
other members of the Steering Group
62
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
PIs are also encouraged to publish and to publicly release and disseminate results data and other
products of the project concordant with the project protocols and governance and the approved
plan for making data and materials available to the scientific community and to the NHLBI
However during the 3 years after the ending date of NHLBI project support unpublished data
unpublished results data sets not previously released and other study materials or products are
to be made available to any third party only with the approval of the IPFnet Steering Group
Upon completion of the project PIs are expected to put their intervention materials and
procedure manuals into the public domain andor make them available to other investigators
according to the approved plan for making data and materials available to the scientific
community and the NHLBI for the conduct of research at no charge other than the costs of
reproduction and distribution
The NHLBI reserves the right to terminate or curtail the project (or an individual award) in the
event of (a) failure to develop or implement mutually agreeable collaborative measurement
subject eligibility and data management sections of the protocols (b) substantial shortfall in
subject recruitment follow-up data reporting or quality control or other major breach of
protocol (c) substantive changes in the agreed-upon protocols with which NHLBI cannot
concur (d) reaching a major project outcome with persuasive statistical significance
substantially before schedule or (e) human subject ethical issues that may dictate a premature
termination
Any disagreement that may arise in scientificprogrammatic matters (within the scope of the
award) between award recipients and the NHLBI may be brought to arbitration An arbitration
panel will be composed of 3 membersmdash1 selected by the IPFnet Steering Group (with the
NHLBI member not voting) or by the individual PI in the event of an individual disagreement a
second selected by NHLBI and the third selected by the other 2 members This special
arbitration procedure in no way affects the PIrsquos right to appeal an adverse action that is otherwise
appealable in accordance with the PHS regulations at 42 CFR part 50 Subpart D and HHS
63
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
regulation at 45 CFR part 16 or the rights of the NHLBI under applicable statutes regulations
and terms of the award
102 IPFnet Steering Group
The IPFnet Steering Group is the main governing body of the project It is composed of the PIs
of the clinical centers the PI of the DCC and the NHLBI project scientist The clinical centers
the IPFnet DCC and the NHLBI each have 1 vote on the IPFnet Steering Group All decisions
are determined by majority vote
All major scientific decisions are determined by the IPFnet Steering Group It assumes overall
responsibility for the design and conduct of the trial It appoints (and disbands) committees and
subcommittees as the need arises designs approves and implements the study protocols
oversees the development of the MOOP monitors subject recruitment and treatment delivery
evaluates data collection and management oversees quality assurance procedures and
implements changes and enhancements to the study as required It also has primary responsibility
for facilitating the conduct of the trials and reporting the projectrsquos results
103 Data and Safety Monitoring Board
The NHLBI will establish a DSMB in accordance with established policies (see
httpwwwnhlbinihgovfundingpoliciesdsmb_insthtm) to ensure data quality and subject
safety and to provide independent advice to the NHLBI regarding progress and the
appropriateness of study continuation
104 Recommendations on Interim Monitoring of Efficacy Safety and Futility
First and foremost the role of the DSMB will be to review subject safety and trial conduct at
periodic points during the study The DSMB may require analyses of the primary endpoint
results for comparing the benefit and risks of treatment strategies The benefit of collecting
additional data on key secondary endpoints with extended follow-up and establishing a robust
64
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
evidence base for determining a standard of care will need to be carefully considered before
early termination of one or more treatment arms After careful consideration the IPFnet Steering
Group recommends conservative thresholds for the early examinations of the safety and efficacy
data
The DSMB will be expected to meet approximately every 6 months until trial completion to
review safety and toxicity data The DSMB may recommend stopping the study based on these
reviews Because the DSMB could stop the trial for safety concerns as well as for a large
efficacy benefit there could be multiple opportunities to reject the null hypothesis (no difference
in event rates between the PL and NAC groups) A Bonferroni approximation will be applied
during the one planned interim analysis for efficacy
Before locking the database a statistical analysis plan (SAP) will be developed to provide
complete details on the statistical analysis The SAP will include the specifics for how and when
the DSMB will be notified for AEs The IPFnet DCC will deliver to the DSMB all FDA-defined
AEs at 3-month intervals The IPFnet DCC will prepare narrative SAE reports in real time for
DSMB review including recommendations and analysis of similar events for each SAE
submitted to the FDA
65
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
11 Investigator and Sponsor Obligations
111 Monitoring
All monitoring activities for US clinical centers will be performed in accordance with DCRI
standard operating procedures Information regarding the types of visits will be outlined in the
PANTHER-IPF MOOP
112 Cost and Payment
There will be no cost to subjects enrolled in this trial Study-related procedures will be paid for
by the IPFnet
Subjects may be eligible for reimbursement for travel to the clinical center Details of payment
will be explained to each subject during the consent process
113 Confidentiality and Health Insurance Portability and Accountability Act
Considerations
Subject confidentiality will be protected throughout the study All subject data will be kept
strictly confidential and no subject-identifying information will be released to anyone outside
the project Confidentiality will be assured through several mechanisms First each subject will
be assigned an anonymous study ID which will then be used on all study forms Second any
study forms blood samples and paper records that contain subject information (eg address lists
phone lists) will be kept at the clinical centers in secured locked areas coded by number Once
blood is collected there will be no subject identifiers placed on blood samplesmdashonly the study
ID number and the date of sample collection Third access to all subject data and information
including laboratory specimens will be restricted to authorized personnel In the case of
computerized data this restricted access will be assured through user logon IDs and password
protection
66
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
At the IPFnet DCC only authorized personnel will have access to the data files containing study
data Security will be assured through user logon IDs passwords and appropriate access
privileges All study subjects will be identified only by their IPFnet ID numbers and no personal
identifying information such as name address or Social Security number will be entered into
the IPFnet DCC database Any subject-specific data reported to the IPFnet Steering Group will
be identified only by the IPFnet ID number
Finally subjects will not be identified by name in any reports or publications nor will the data
be presented in such a way that the identity of individual subjects can be inferred Analysis files
created for further study by the scientific community will have no subject identifiers These data
files will be created in accordance with the Ancillary Studies and Publication Policy of the
IPFnet
114 Informed Consent Procedures
All IPFnet subjects will provide written informed consent using procedures reviewed and
approved by each clinical centerrsquos IRB Informed consent will be undertaken by study personnel
in-person with the subject The subject has the option of declining further participation in the
study at that point No further study procedures will be conducted until the signed documents
have been provided to the IPFnet clinical center
115 Institutional Review Boards
Before initiating this study the protocol clinical center-specific informed consent forms Health
Insurance Portability and Accountability Act (HIPAA) forms recruitment materials and other
relevant information will be reviewed by a properly constituted IRB at each participating clinical
center A copy of the signed and dated IRB approval at each clinical center will be retrieved prior
to or during the site initiation visit and archived at the IPFnet DCC Any amendments to the
protocol other than simple administrative and typographical changes must be approved by each
IRB before they are implemented The clinical centers will seek annual renewals of their IRB
approvals in accordance with local procedures
67
__________________________________________ ________________
__________________________________________
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
12 Investigator Agreement
I have read the foregoing protocol PANTHER-IPF and agree that it contains all necessary
details for carrying out this study I will conduct the study as outlined herein and will complete
the study within the time designated
I will provide copies of the protocol and all pertinent information to all individuals responsible to
me who assist in the conduct of this study I will discuss this material with them to ensure they
are fully informed regarding the drug and the conduct of the study
I will fulfill all responsibilities for submitting pertinent information to the local IRB if
applicable that is responsible for this study
I further agree that NHLBI andor DCRI will have access to any source documents from which
eCRF information may have been generated
Signature of Principal Investigator Date
Name of Principal Investigator (printed or typed)
Protocol version date May 19 2009
Protocol Amendment 1 version date May 28 2010
Protocol Amendment 2 version date December 6 2011
68
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
13 References
1 Raghu G Brown KK Bradford WZ et al A placebo-controlled trial of interferon gamma-1b in patients with idiopathic pulmonary fibrosis N Engl J Med 2004350125-33 2 King TE Jr Safrin S Starko KM et al Analyses of efficacy end points in a controlled trial of interferon-gamma1b for idiopathic pulmonary fibrosis Chest 2005127171-7 3 Flaherty KR Thwaite EL Kazerooni EA et al Radiological versus histological diagnosis in UIP and NSIP survival implications Thorax 200358143-8 4 Wells AU Desai SR Rubens MB et al Idiopathic pulmonary fibrosis a composite physiologic index derived from disease extent observed by computed tomography Am J Respir Crit Care Med 2003167962-9 5 Raghu G Freudenberger TD Yang S et al High prevalence of abnormal acid gastroshyoesophageal reflux in idiopathic pulmonary fibrosis Eur Respir J 200627136-42 6 Kinnula VL Focus on antioxidant enzymes and antioxidant strategies in smoking related airway diseases Thorax 200560693-700 7 Coultas DB Zumwalt RE Black WC Sobonya RE The epidemiology of interstitial lung diseases Am J Respir Crit Care Med 1994150967-72 8 Raghu G Weycker D Edelsberg J Bradford WZ Oster G Incidence and prevalence of idiopathic pulmonary fibrosis Am J Respir Crit Care Med 2006174810-6 9 Olson AL Swigris JJ Lezotte DC Norris JM Wilson CG Brown KK Mortality from pulmonary fibrosis increased in the United States from 1992 to 2003 Am J Respir Crit Care Med 2007176277-84 10 Mannino DM Etzel RA Parrish RG Pulmonary fibrosis deaths in the United States 1979shy1991 An analysis of multiple-cause mortality data Am J Respir Crit Care Med 19961531548shy52 11 Hubbard R Johnston I Coultas DB Britton J Mortality rates from cryptogenic fibrosing alveolitis in seven countries Thorax 199651711-6 12 Johnston I Britton J Kinnear W Logan R Rising mortality from cryptogenic fibrosing alveolitis Bmj 19903011017-21 13 Raghu G Collard HR Egan JJ et al An official ATSERSJRSALAT statement idiopathic pulmonary fibrosis evidence-based guidelines for diagnosis and management Am J Respir Crit Care Med 2011183788-824 14 (USA) FDA FDA Public Health Advisory Interferon gamma-1b (marketed as Actimmune) In 2007 15 King TE Jr Pardo A Selman M Idiopathic pulmonary fibrosis Lancet 2011 16 Raghu G Brown KK Costabel U et al Treatment of idiopathic pulmonary fibrosis with etanercept an exploratory placebo-controlled trial Am J Respir Crit Care Med 2008178948shy55 17 Malouf MA Hopkins P Snell G Glanville AR An investigator-driven study of everolimus in surgical lung biopsy confirmed idiopathic pulmonary fibrosis Respirology 201116776-83 18 King TE Jr Behr J Brown KK et al BUILD-1 a randomized placebo-controlled trial of bosentan in idiopathic pulmonary fibrosis Am J Respir Crit Care Med 200817775-81 19 Richeldi L Costabel U Selman M et al Efficacy of a tyrosine kinase inhibitor in idiopathic pulmonary fibrosis N Engl J Med 20113651079-87
69
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
20 Borok Z Buhl R Grimes GJ et al Effect of glutathione aerosol on oxidant-antioxidant imbalance in idiopathic pulmonary fibrosis Lancet 1991338215-6 21 Meyer A Buhl R Magnussen H The effect of oral N-acetylcysteine on lung glutathione levels in idiopathic pulmonary fibrosis Eur Respir J 19947431-6 22 Behr J Maier K Degenkolb B Krombach F Vogelmeier C Antioxidative and clinical effects of high-dose N-acetylcysteine in fibrosing alveolitis Adjunctive therapy to maintenance immunosuppression Am J Respir Crit Care Med 19971561897-901 23 Cantin AM North SL Fells GA Hubbard RC Crystal RG Oxidant-mediated epithelial cell injury in idiopathic pulmonary fibrosis J Clin Invest 1987791665-73 24 Waghray M Cui Z Horowitz JC et al Hydrogen peroxide is a diffusible paracrine signal for the induction of epithelial cell death by activated myofibroblasts Faseb J 200519854-6 25 Larios JM Budhiraja R Fanburg BL Thannickal VJ Oxidative protein cross-linking reactions involving L-tyrosine in transforming growth factor-beta1-stimulated fibroblasts J Biol Chem 200127617437-41 26 Kinnula VL Fattman CL Tan RJ Oury TD Oxidative stress in pulmonary fibrosis a possible role for redox modulatory therapy Am J Respir Crit Care Med 2005172417-22 27 Meyer A Buhl R Kampf S Magnussen H Intravenous N-acetylcysteine and lung glutathione of patients with pulmonary fibrosis and normals Am J Respir Crit Care Med 19951521055-60 28 Behr J Degenkolb B Krombach F Vogelmeier C Intracellular glutathione and bronchoalveolar cells in fibrosing alveolitis effects of N-acetylcysteine Eur Respir J 200219906-11 29 Bando M Hosono T Mato N et al Long-term efficacy of inhaled N-acetylcysteine in patients with idiopathic pulmonary fibrosis Intern Med 2010492289-96 30 Demedts M Behr J Buhl R et al High-dose acetylcysteine in idiopathic pulmonary fibrosis N Engl J Med 20053532229-42 31 Toma TP Bhowmik A Rajakulasingam R Acetylcysteine in pulmonary fibrosis N Engl J Med 20063541086-9 author reply -9 32 Hunninghake GW Antioxidant therapy for idiopathic pulmonary fibrosis N Engl J Med 20053532285-7 33 Flaherty KR Mumford JA Murray S et al Prognostic implications of physiologic and radiographic changes in idiopathic interstitial pneumonia Am J Respir Crit Care Med 2003168543-8 34 Latsi PI du Bois RM Nicholson AG et al Fibrotic idiopathic interstitial pneumonia the prognostic value of longitudinal functional trends Am J Respir Crit Care Med 2003168531-7 35 Collard HR King TE Jr Bartelson BB Vourlekis JS Schwarz MI Brown KK Changes in clinical and physiologic variables predict survival in idiopathic pulmonary fibrosis Am J Respir Crit Care Med 2003168538-42 36 Jegal Y Kim DS Shim TS et al Physiology is a stronger predictor of survival than pathology in fibrotic interstitial pneumonia Am J Respir Crit Care Med 2005171639-44 37 Martinez FJ Safrin S Weycker D et al The clinical course of patients with idiopathic pulmonary fibrosis Ann Intern Med 2005142963-7 38 Hull JH Acetylcysteine in pulmonary fibrosis N Engl J Med 20063541089-91 author reply -91
70
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
39 Flaherty KR King TE Jr Raghu G et al Idiopathic interstitial pneumonia what is the effect of a multidisciplinary approach to diagnosis Am J Respir Crit Care Med 2004170904shy10 40 Raghu G Johnson WC Lockhart D Mageto Y Treatment of idiopathic pulmonary fibrosis with a new antifibrotic agent pirfenidone results of a prospective open-label Phase II study Am J Respir Crit Care Med 19991591061-9 41 Hunninghake GW Lynch DA Galvin JR et al Radiologic findings are strongly associated with a pathologic diagnosis of usual interstitial pneumonia Chest 20031241215-23 42 Lynch D Godwin J Safrin S et al High-resolution computed tomography in idiopathic pulmonary fibrosis diagnosis and prognosis Am J Respir Crit Care Med 2005172488-93 43 Mallinckrodt CH Watkin JG Molenberghs G Carroll RJ Choice of the primary analysis in longitudinal clinical trials Pharmaceutical Statistics 20043161-9 44 Bang H Tsiatis A Estimating medical costs with censored data Biometrika 200087329shy43 45 Lin DY Regression analysis of incomplete medical cost data Stat Med 2003221181-200 46 Rochon J Application of GEE procedures for sample size calculations in repeated measures experiments Stat Med 1998171643-58 47 Lachin JM Foulkes MA Evaluation of sample size and power for analyses of survival with allowance for nonuniform patient entry losses to follow-up noncompliance and stratification Biometrics 198642507-19
71
- PANTHER-IPFPREDNISONE AZATHIOPRINEAND N-ACETYLCYSTEINEA STUDY THAT EVALUATES RESPONSE INIDIOPATHIC PULMONARY FIBROSIS
-
- Protocol Summary
- Table of Contents
- List of Tables
- List of Figures
- List of Abbreviations
- 1 Summary
- 2 Hypotheses and Specific Aims
-
- 21 Null Hypothesis
- 22 Specific Aim 1
- 23 Specific Aim 2
- 24 Prespecified Subgroups of Interest
-
- 3 Background and Significance
-
- 31 Idiopathic Pulmonary Fibrosis is the Most Common Interstitial Lung Disease
- 32 Rationale for Placebo Control
- 33 Rationale for N-acetylcysteine
- 35 Rationale for N-acetylcysteine as a Stand-alone Therapy
- 36 Rationale for the Study Design and Primary Endpoint
- 37 Rationale for Blinding of Treatments
-
- 4 Methods
-
- 41 Inclusion Criteria
- 42 Diagnosis of IPF
- 43 Exclusion Criteria
- 44 Study Design and Study Visit
- 45 Dose Justification
- 46 Contraindications Precautions and Side Effects of Study Medications
- 47 Recruitment Procedures
- 48 Study Procedures
- 49 Concomitant Medications
- 410 Laboratory Testing
- 411 Blinding of Study Drugs
-
- 5 Study Endpoints
-
- 51 Primary Study Endpoint
- 52 Secondary Study Endpoints
-
- 6 Safety Evaluations and Procedures
-
- 61 Adverse Events
- 62 Clinical Medical Monitoring
- 63 Unblinding Procedures
-
- 7 Study Drug Procedures
- 8 Data Management
-
- 81 Hardware and Software Configuration
- 82 Sources of Data
-
- 9 Study Design and Data Analysis
-
- 91 General Analytic Considerations
- 92 Randomization Blinding and Reporting of Results
- 93 Stratification
- 94 Specification of the Primary Analyses
- 95 Analysis of Longitudinal Endpoints
- 96 Analysis of Binary Time-to-Event and Time-Lagged Endpoints
- 97 Power Analysis
-
- 10 Study Administration
-
- 101 Cooperative Agreement Mechanism
- 102 IPFnet Steering Group
- 103 Data and Safety Monitoring Board
- 104 Recommendations on Interim Monitoring of Efficacy Safety and Futility
-
- 11 Investigator and Sponsor Obligations
-
- 111 Monitoring
- 112 Cost and Payment
- 113 Confidentiality and Health Insurance Portability and Accountability ActConsiderations
- 114 Informed Consent Procedures
- 115 Institutional Review Boards
-
- 12 Investigator Agreement
- 13 References
-
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
investigator to provide a causality assessment of the event for each study medications based upon
the information available at the time of the report It is understood that complete information
about the event may not be known at the time the initial report is submitted In the event the EDC
system is not accessible to the site at the time of event reporting investigative sites will complete
and forward a paper back-up SAE form to DCRI Safety Surveillance for processing
DCRI Safety Surveillance
Telephone 1-919-668-8624 or 1-866-668-7799 (toll free)
Fax 1-919-668-7138 or 1-866-668-7138 (toll free)
The investigator must complete and submit follow-up SAE information via the eCRF when
important new or follow-up information (eg final diagnosis outcome results of specific
investigations) becomes available Follow-up information should be submitted according to the
same process used for reporting the initial event as described above All SAEs will be followed
until resolution stabilization or 30 days after the subject has completed the final visit (4 weeks
after the final dose of study medication) whichever occurs first The investigator is responsible
for reporting SAEs to their institutional review board (IRB) per site specific IRB reporting
guidelines
6122 Regulatory Reporting
AEs that are serious study drug related and unexpected will be reported to the regulatory
authorities The DCRI Safety Surveillance medical monitor will perform a medical review of all
SAEs submitted and evaluate for ldquounexpectednessrdquo DCRI Safety Surveillance will prepare
MedWatch reports for those events identified as serious study drug related and unexpected as
determined by Safety Medical Monitor
DCRI Regulatory Services will submit all unexpected study drug-related SAEs as per 21 CFR
32 DCRI Safety Surveillance will provide a safety alert letter to the NHLBI DSMB and DCC
clinical operation (for distribution to sites) within 15 days of initial receipt of the information
51
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Investigators are responsible for promptly reporting these events to their reviewing IRBs
according to site specific IRB reporting guidelines
62 Clinical Medical Monitoring
There will be an unblinded physician at the IPFnet DCC serving as medical monitor The
medical monitor will be available to assist with questions about dosage adjustments of study
medications including discontinuation or resumption of medications
63 Unblinding Procedures
Unblinding of subjects or investigators to subject treatment is strongly discouraged For ongoing
clinical management all subjects should be presumed to be receiving ldquoactiverdquo study drug To
ensure the subjectrsquos safety the study treatment will be dose-adjusted based on laboratory test
results clinical findings and symptoms
The IPFnet DCC medical monitor and PANTHER-IPF co-chairs Drs Ganesh Raghu and
Fernando Martinez will be available to the study physicians to discuss study drug management
on a case-by-case basis Un-blinding will be considered ONLY when the knowledge of subject
treatment assignment is ABSOLUTELY ESSENTIAL for subject safety and after discussion of
the subjectrsquos case with the medical monitor and either Dr Raghu or Dr Martinez Unblinding of
study treatment should be minimized during the conduct of the trial In those cases where it is
felt to be medically necessary the DCC medical officer will communicate directly with the
managing physician to minimize unblinding of study personnel
52
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
7 Study Drug Procedures
At the baseline 15-week 30-week and 45-week study visits subjects will receive a supply of
study drug sufficient to last until the next visit at which study drug will be dispensed
53
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
8 Data Management
81 Hardware and Software Configuration
811 Hardware and Database Software
Data will be stored in an Oracle database system Oracle has advantages of processing efficiency
and smooth linkage with other software systems The application and database will be hosted on
Solaris Unix servers at the IPFnet DCC
812 Statistical Software
SAS will be used as the principal application for the management of analysis data files and
statistical computations S-Plus will be used to provide supplementary functions as needed
813 Access Control and Confidentiality Procedures
Access to databases will be controlled centrally by the IPFnet DCC through user passwords
linked to appropriate privileges This protects the data from unauthorized changes and
inadvertent loss or damage
814 Security
Database and Web servers will be secured by a firewall and through controlled physical access
Oracle has many security features to ensure that any staff member accessing the database has the
proper authority to perform the functions he or she requests of the system Within the secondary
SAS databases Unix group-access control maintains similar security The Sun workstation login
is secured by extensive user-password facilities under Unix
54
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
815 Back-up Procedures
Database back-up will be performed automatically every day and standard IPFnet DCC policies
and procedures will be applied to dictate tape rotation and retention practices
816 Virus Protection
All disk drives that provide network services and all user computers will be protected using
virus-scanning software Standard IPFnet DCC policies will be applied to update these protection
systems periodically through the study
82 Sources of Data
821 Design and Development
The IPFnet DCC will be responsible for development of the electronic case report forms
(eCRFs) development and validation of the clinical study database ensuring data integrity and
training clinical center staff on applicable data management procedures A web-based distributed
data entry model will be implemented This system will be developed to ensure that guidelines
and regulations surrounding the use of computerized systems used in clinical trials are upheld
The remainder of this section provides an overview of the data management plan associated with
this protocol
822 Data Collection Forms
The data collection process consists of direct data entry at the study clinical centers into the EDC
system(s) provided by the DCC A data collection worksheet will be provided to clinical centers
for recording data in the event the EDC system is unavailable Data entry of the eCRFs should
be completed according to the instructions provided and project specific training The
investigator is responsible for maintaining accurate complete and up-to-date records and for
ensuring the completion of the eCRFs for each research participant
55
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
823 Data Acquisition and Entry
Data entry into eCRFs shall be performed by authorized individuals Selected eCRFs may also
require the investigatorrsquos written signature or electronic signature as appropriate Electronic
CRFs will be monitored for completeness accuracy and attention to detail during the study
824 Data Center Responsibilities
The IPFnet DCC will 1) develop a data management plan and will conduct data management
activities 2) provide final eCRFs for the collection of all data required by the study 3) develop
data dictionaries for each eCRF that will comprehensively define each data element 4) conduct
ongoing data monitoring activities on study data 5) monitor any preliminary analysis data
cleanup activities and 6) rigorously monitor final study data clean up
825 Data Editing
Completed data will be entered into the IPFnet DCC automated data acquisition and
management system If incomplete or inaccurate data are found a data clarification request will
be generated and distributed to clinical centers for a response Clinical centers will resolve data
inconsistencies and errors and enter all corrections and changes into the IPFnet DCC automated
data acquisition and management system
826 Training
The training plan for clinical center staff includes provisions for training on assessments eCRF
completion guidelines data management procedures and the use of computerized systems
56
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
9 Study Design and Data Analysis
91 General Analytic Considerations
All primary analyses will be based on intent-to-treat (ITT) principles using all randomized
subjects Baseline factors across groups will be compared using mean (standard deviation) and
median (25th and 75th percentiles) summary measures Kaplan-Meier curves will be used to
display event rates Due to clinical interest in departures from both sides of the null hypothesis
all test statistics will be 2-sided
Reasonable caution needs to be taken when conducting multiple analyses on key clinical
subgroups For subgroup analyses a conservative significance level of 0001 will be used for all
interaction tests Thus subgroup comparisons will be considered exploratory unless the p-value
from the interaction test is smaller than 0001
92 Randomization Blinding and Reporting of Results
A permuted block-randomization scheme will be created with varying block sizes stratified by
clinical center Once a subject has completed the screening and baseline period and evaluation
for inclusionexclusion criteria the randomization process will begin Subjects will be
randomized to receive NAC or matching placebo with equal probability (11) via telephone
contact with a central interactive voice response system (IVRS) using a toll-free randomization
number On the day of randomization after the subject has successfully met all inclusion and
exclusion criteria the investigator or designee will call the central randomization number to
obtain the assigned kit randomization numbers for that subject At each subject visit the
investigator or designee will call the central randomization number to obtain the new kit
randomization numbers for resupply of the subject For resupply of the clinical center the IVRS
will monitor minimal volume of a kit type andor expiration date and will automatically notify
the pharmacy
57
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
The trial results will be reported according to guidelines specified in the CONSORT statement
A flow diagram describing screening recruitment randomization dropout and vital status will
be included in the primary manuscript AEs and efficacy data will be presented for all treatment
groups Adherence dropout and lost to follow-up will be carefully examined across all treatment
groups Analyses of safety will be based on data from all randomized subjects who received at
least one dose of study drug
93 Stratification
Subjects will be distributed to the two treatment arms in a 11 allocation ratio Stratification
blocks will be based on clinical centers
94 Specification of the Primary Analyses
A mixed model repeated measures (MMRM) analysis described in section 95 will be used to
compare differences in the slope of FVC measurements across the treatment groups Response
variables are values of the FVC measured at baseline and every 15 weeks until study completion
Variables in the model will include treatment time and time by treatment age sex race and
height Contrast estimates of differences in slopes of treatment over time (along with confidence
intervals) will be used to estimate the treatment effect The validity of this model in terms of
meeting modeling assumptions will be assessed via standard modeling diagnostics and goodness-
of-fit measures Based on the MMRM framework missing FVC data will not be imputed for the
primary analysis
95 Analysis of Longitudinal Endpoints
A common goal in clinical trials is to specify models that are easily implemented and
reproducible by independent data analysts On the other hand the models should have proper
statistical behavior in terms of low bias and high precision Many common approaches to
longitudinal data analysis including last observation carried forward (LOCF) imputation rely on
the missing completely at random (MCAR) assumption However the MCAR assumption is
58
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
unlikely to hold in many clinical trials because missing data are often related to disease
progression and prognosis A more reasonable assumption missing at random (MAR) specifies
that the complete data distribution can be modeled using only the observed data The likelihood-
based MMRM approach is valid under the more general MAR assumptions These models will
be applied to analyze the longitudinal data secondary endpoints
The advantages of MMRM analysis are that all important characteristics of the model can be preshy
specified standard software can be used to implement the models and results are based on ITT
principles43 In addition the MMRM approach offers superior control of Type I and Type II
errors compared with the LOCF approach
Response variables are values of the PFTs measured at enrollment and every 15 weeks until
study completion and 6MWT values measured at baseline week 30 and week 60 Covariates are
treatment time time by treatment and key baseline risk factors Contrasts (along with
confidence intervals) of treatment by time will be used to estimate the treatment effect
The correlation structure involves multiple pieces including measurement errors random
variation and interindividual variability For the longitudinal data analyses an unstructured
correlation matrix for within-subject errors will be assumed Other correlation structures
including compound symmetry will be examined as needed A careful examination of reasons
for study discontinuation will be conducted to assess the validity of MCAR Sensitivity analyses
will be used to examine the untestable assumption that the observed data violate the MAR
assumption The MMRM models will be implemented using PROC MIXED in SAS
96 Analysis of Binary Time-to-Event and Time-Lagged Endpoints
Regression modeling approaches using either the logistic regression model or Cox proportional
hazards regression model will be employed when appropriate The validity of these models will
be assessed via standard modeling diagnostics and goodness-of-fit measures Estimates of
cumulative frequencies for more general time-lagged responses will be calculated using the
partitioned version of the Bang-Tsiatis estimator44 The partitions will be set at 15-week intervals
59
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
to correspond with the data-collection process Covariate adjusted event rates will be calculated
using inverse probability-weighted regression estimates45
97 Power Analysis
971 Primary Analyses
Based on previously published IPF clinical trials the PL group is expected to experience a drop
in FVC of approximately 020 L over the study period (see Figure 1) The IPFnet Steering Group
determined a clinically important difference would be to preserve the majority of the decline
relative to PL over the study period In particular a treatment effect of 015 L was determined to
be a clinically meaningful difference Potential dropout is a key factor in the proposed study The
drop-out process assumed 5 lost to follow-up after every study visit Only 80 of subjects
were assumed to be followed for the entire study period All models assumed a compound
symmetry structure for the covariance matrix Power calculations were performed using a SAS
IML program for designing repeated measures studies46 Based on preliminary reviews of the
data from the University of Michigan the covariance matrix parameters were estimated at
approximately σ2 = 0757 (variance parameter) and ρ = 0936 (correlation parameter) To be
conservative the power calculations for the primary analysis were performed with parameter
setting of σ2 = 0810 (variance parameter) and ρ = 0925 (correlation parameter)
The power calculations assume a correction for imperfect compliance proposed by Lachin and
Foulkes to allow for 2 noncompliance for each of the treatment arms47 Thus the sample size
of 130 subjects per arm would be reduced to an adjusted sample size of 130(1-002-002)2 =
1198 or 120 subjects per arm
Under the assumed Type I error rate of 005 with a correlation parameter of 0925 and standard
deviation of 090 the difference of 015 L (or 00025 Lweek) shown in Table 6 would have
power of 93
60
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Table 6 Hypothetical Values of Mean FVC (L) Change from Baseline
Week 15 Week 30 Week 45 Week 60
NAC 00125 00250 00375 00500
Placebo 00500 01000 01500 02000
Difference 00375 00750 01125 01500
Abbreviations FVC forced vital capacity PL placebo
972 Power Analysis for Secondary Endpoints
Power calculations for secondary endpoint measurements are shown in Table 7 Standard
deviations are based on unpublished data provided by the University of Michigan The
calculations are based on a 2-sample t-test with Type I error rate set at 005 These calculations
are likely to be conservative because the statistical approach described in section 95 for
analyzing these endpoints will incorporate incomplete observations as well as intermediate data
points
Table 7 Detectable Differences in Treatment Means for Selected Endpoint Measurements
Secondary Endpoints Std Dev
of the Baseline Score
Detectable Difference for 80 Power
Std Dev of the Change Score
Difference Detectable for
80 Power
DLCOpred 166 58 91 32
6MWT Area Under the Desaturation Curve
219 76 175 61
6MWT Distance to Desaturation 224 78 315 110
6MWT Minutes Walked 210 073 205 071
Abbreviations Std Dev standard deviation DLCOpred diffusing capacity of the lung for carbon monoxide percent predicted 6MWT 6-minute walk test
61
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
10 Study Administration
101 Cooperative Agreement Mechanism
The administrative and funding mechanism used to undertake this project is a ldquocooperative
agreementrdquo (U01) which is an assistance mechanism Under the cooperative agreement the
NHLBI assists supports andor stimulates the project and is substantially involved with
investigators in conducting the study by facilitating performance of the effort in a ldquopartnerrdquo role
The NHLBI project scientist serves on the IPFnet Steering Group and he or another NHLBI
scientist may serve on other project committees when appropriate At the same time however
NHLBI does not assume a dominant role direction or prime responsibility for this research
program
As described below governance of the project is conducted through the IPFnet Steering Group
Principal investigators have lead responsibilities in all aspects of their trials and the project
including any modification of trial designs conduct of the trials quality control data analysis
and interpretation preparation of publications and collaboration with other investigators unless
otherwise provided for by the IPFnet Steering Group
PIs retain custody of and have primary rights to their center-specific and collaborative data
subject to government rights-of-access consistent with current Health amp Human Services (HHS)
Public Health Service (PHS) and National Institutes of Health policies The protocols and
governance policies call for the continual submission of data centrally to the IPFnet DCC for the
collaborative database which at a minimum will contain the key variables selected by the IPFnet
Steering Group for standardization across all clinical centers the submission of copies of the
collaborative datasets to each PI upon completion of the project procedures for data analysis
reporting and publication and procedures to protect and ensure the privacy of medical and
genetic data and records of individuals The NHLBI project scientist on behalf of the NHLBI
will have the same access privileges and responsibilities regarding the collaborative data as the
other members of the Steering Group
62
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
PIs are also encouraged to publish and to publicly release and disseminate results data and other
products of the project concordant with the project protocols and governance and the approved
plan for making data and materials available to the scientific community and to the NHLBI
However during the 3 years after the ending date of NHLBI project support unpublished data
unpublished results data sets not previously released and other study materials or products are
to be made available to any third party only with the approval of the IPFnet Steering Group
Upon completion of the project PIs are expected to put their intervention materials and
procedure manuals into the public domain andor make them available to other investigators
according to the approved plan for making data and materials available to the scientific
community and the NHLBI for the conduct of research at no charge other than the costs of
reproduction and distribution
The NHLBI reserves the right to terminate or curtail the project (or an individual award) in the
event of (a) failure to develop or implement mutually agreeable collaborative measurement
subject eligibility and data management sections of the protocols (b) substantial shortfall in
subject recruitment follow-up data reporting or quality control or other major breach of
protocol (c) substantive changes in the agreed-upon protocols with which NHLBI cannot
concur (d) reaching a major project outcome with persuasive statistical significance
substantially before schedule or (e) human subject ethical issues that may dictate a premature
termination
Any disagreement that may arise in scientificprogrammatic matters (within the scope of the
award) between award recipients and the NHLBI may be brought to arbitration An arbitration
panel will be composed of 3 membersmdash1 selected by the IPFnet Steering Group (with the
NHLBI member not voting) or by the individual PI in the event of an individual disagreement a
second selected by NHLBI and the third selected by the other 2 members This special
arbitration procedure in no way affects the PIrsquos right to appeal an adverse action that is otherwise
appealable in accordance with the PHS regulations at 42 CFR part 50 Subpart D and HHS
63
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
regulation at 45 CFR part 16 or the rights of the NHLBI under applicable statutes regulations
and terms of the award
102 IPFnet Steering Group
The IPFnet Steering Group is the main governing body of the project It is composed of the PIs
of the clinical centers the PI of the DCC and the NHLBI project scientist The clinical centers
the IPFnet DCC and the NHLBI each have 1 vote on the IPFnet Steering Group All decisions
are determined by majority vote
All major scientific decisions are determined by the IPFnet Steering Group It assumes overall
responsibility for the design and conduct of the trial It appoints (and disbands) committees and
subcommittees as the need arises designs approves and implements the study protocols
oversees the development of the MOOP monitors subject recruitment and treatment delivery
evaluates data collection and management oversees quality assurance procedures and
implements changes and enhancements to the study as required It also has primary responsibility
for facilitating the conduct of the trials and reporting the projectrsquos results
103 Data and Safety Monitoring Board
The NHLBI will establish a DSMB in accordance with established policies (see
httpwwwnhlbinihgovfundingpoliciesdsmb_insthtm) to ensure data quality and subject
safety and to provide independent advice to the NHLBI regarding progress and the
appropriateness of study continuation
104 Recommendations on Interim Monitoring of Efficacy Safety and Futility
First and foremost the role of the DSMB will be to review subject safety and trial conduct at
periodic points during the study The DSMB may require analyses of the primary endpoint
results for comparing the benefit and risks of treatment strategies The benefit of collecting
additional data on key secondary endpoints with extended follow-up and establishing a robust
64
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
evidence base for determining a standard of care will need to be carefully considered before
early termination of one or more treatment arms After careful consideration the IPFnet Steering
Group recommends conservative thresholds for the early examinations of the safety and efficacy
data
The DSMB will be expected to meet approximately every 6 months until trial completion to
review safety and toxicity data The DSMB may recommend stopping the study based on these
reviews Because the DSMB could stop the trial for safety concerns as well as for a large
efficacy benefit there could be multiple opportunities to reject the null hypothesis (no difference
in event rates between the PL and NAC groups) A Bonferroni approximation will be applied
during the one planned interim analysis for efficacy
Before locking the database a statistical analysis plan (SAP) will be developed to provide
complete details on the statistical analysis The SAP will include the specifics for how and when
the DSMB will be notified for AEs The IPFnet DCC will deliver to the DSMB all FDA-defined
AEs at 3-month intervals The IPFnet DCC will prepare narrative SAE reports in real time for
DSMB review including recommendations and analysis of similar events for each SAE
submitted to the FDA
65
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
11 Investigator and Sponsor Obligations
111 Monitoring
All monitoring activities for US clinical centers will be performed in accordance with DCRI
standard operating procedures Information regarding the types of visits will be outlined in the
PANTHER-IPF MOOP
112 Cost and Payment
There will be no cost to subjects enrolled in this trial Study-related procedures will be paid for
by the IPFnet
Subjects may be eligible for reimbursement for travel to the clinical center Details of payment
will be explained to each subject during the consent process
113 Confidentiality and Health Insurance Portability and Accountability Act
Considerations
Subject confidentiality will be protected throughout the study All subject data will be kept
strictly confidential and no subject-identifying information will be released to anyone outside
the project Confidentiality will be assured through several mechanisms First each subject will
be assigned an anonymous study ID which will then be used on all study forms Second any
study forms blood samples and paper records that contain subject information (eg address lists
phone lists) will be kept at the clinical centers in secured locked areas coded by number Once
blood is collected there will be no subject identifiers placed on blood samplesmdashonly the study
ID number and the date of sample collection Third access to all subject data and information
including laboratory specimens will be restricted to authorized personnel In the case of
computerized data this restricted access will be assured through user logon IDs and password
protection
66
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
At the IPFnet DCC only authorized personnel will have access to the data files containing study
data Security will be assured through user logon IDs passwords and appropriate access
privileges All study subjects will be identified only by their IPFnet ID numbers and no personal
identifying information such as name address or Social Security number will be entered into
the IPFnet DCC database Any subject-specific data reported to the IPFnet Steering Group will
be identified only by the IPFnet ID number
Finally subjects will not be identified by name in any reports or publications nor will the data
be presented in such a way that the identity of individual subjects can be inferred Analysis files
created for further study by the scientific community will have no subject identifiers These data
files will be created in accordance with the Ancillary Studies and Publication Policy of the
IPFnet
114 Informed Consent Procedures
All IPFnet subjects will provide written informed consent using procedures reviewed and
approved by each clinical centerrsquos IRB Informed consent will be undertaken by study personnel
in-person with the subject The subject has the option of declining further participation in the
study at that point No further study procedures will be conducted until the signed documents
have been provided to the IPFnet clinical center
115 Institutional Review Boards
Before initiating this study the protocol clinical center-specific informed consent forms Health
Insurance Portability and Accountability Act (HIPAA) forms recruitment materials and other
relevant information will be reviewed by a properly constituted IRB at each participating clinical
center A copy of the signed and dated IRB approval at each clinical center will be retrieved prior
to or during the site initiation visit and archived at the IPFnet DCC Any amendments to the
protocol other than simple administrative and typographical changes must be approved by each
IRB before they are implemented The clinical centers will seek annual renewals of their IRB
approvals in accordance with local procedures
67
__________________________________________ ________________
__________________________________________
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
12 Investigator Agreement
I have read the foregoing protocol PANTHER-IPF and agree that it contains all necessary
details for carrying out this study I will conduct the study as outlined herein and will complete
the study within the time designated
I will provide copies of the protocol and all pertinent information to all individuals responsible to
me who assist in the conduct of this study I will discuss this material with them to ensure they
are fully informed regarding the drug and the conduct of the study
I will fulfill all responsibilities for submitting pertinent information to the local IRB if
applicable that is responsible for this study
I further agree that NHLBI andor DCRI will have access to any source documents from which
eCRF information may have been generated
Signature of Principal Investigator Date
Name of Principal Investigator (printed or typed)
Protocol version date May 19 2009
Protocol Amendment 1 version date May 28 2010
Protocol Amendment 2 version date December 6 2011
68
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
13 References
1 Raghu G Brown KK Bradford WZ et al A placebo-controlled trial of interferon gamma-1b in patients with idiopathic pulmonary fibrosis N Engl J Med 2004350125-33 2 King TE Jr Safrin S Starko KM et al Analyses of efficacy end points in a controlled trial of interferon-gamma1b for idiopathic pulmonary fibrosis Chest 2005127171-7 3 Flaherty KR Thwaite EL Kazerooni EA et al Radiological versus histological diagnosis in UIP and NSIP survival implications Thorax 200358143-8 4 Wells AU Desai SR Rubens MB et al Idiopathic pulmonary fibrosis a composite physiologic index derived from disease extent observed by computed tomography Am J Respir Crit Care Med 2003167962-9 5 Raghu G Freudenberger TD Yang S et al High prevalence of abnormal acid gastroshyoesophageal reflux in idiopathic pulmonary fibrosis Eur Respir J 200627136-42 6 Kinnula VL Focus on antioxidant enzymes and antioxidant strategies in smoking related airway diseases Thorax 200560693-700 7 Coultas DB Zumwalt RE Black WC Sobonya RE The epidemiology of interstitial lung diseases Am J Respir Crit Care Med 1994150967-72 8 Raghu G Weycker D Edelsberg J Bradford WZ Oster G Incidence and prevalence of idiopathic pulmonary fibrosis Am J Respir Crit Care Med 2006174810-6 9 Olson AL Swigris JJ Lezotte DC Norris JM Wilson CG Brown KK Mortality from pulmonary fibrosis increased in the United States from 1992 to 2003 Am J Respir Crit Care Med 2007176277-84 10 Mannino DM Etzel RA Parrish RG Pulmonary fibrosis deaths in the United States 1979shy1991 An analysis of multiple-cause mortality data Am J Respir Crit Care Med 19961531548shy52 11 Hubbard R Johnston I Coultas DB Britton J Mortality rates from cryptogenic fibrosing alveolitis in seven countries Thorax 199651711-6 12 Johnston I Britton J Kinnear W Logan R Rising mortality from cryptogenic fibrosing alveolitis Bmj 19903011017-21 13 Raghu G Collard HR Egan JJ et al An official ATSERSJRSALAT statement idiopathic pulmonary fibrosis evidence-based guidelines for diagnosis and management Am J Respir Crit Care Med 2011183788-824 14 (USA) FDA FDA Public Health Advisory Interferon gamma-1b (marketed as Actimmune) In 2007 15 King TE Jr Pardo A Selman M Idiopathic pulmonary fibrosis Lancet 2011 16 Raghu G Brown KK Costabel U et al Treatment of idiopathic pulmonary fibrosis with etanercept an exploratory placebo-controlled trial Am J Respir Crit Care Med 2008178948shy55 17 Malouf MA Hopkins P Snell G Glanville AR An investigator-driven study of everolimus in surgical lung biopsy confirmed idiopathic pulmonary fibrosis Respirology 201116776-83 18 King TE Jr Behr J Brown KK et al BUILD-1 a randomized placebo-controlled trial of bosentan in idiopathic pulmonary fibrosis Am J Respir Crit Care Med 200817775-81 19 Richeldi L Costabel U Selman M et al Efficacy of a tyrosine kinase inhibitor in idiopathic pulmonary fibrosis N Engl J Med 20113651079-87
69
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
20 Borok Z Buhl R Grimes GJ et al Effect of glutathione aerosol on oxidant-antioxidant imbalance in idiopathic pulmonary fibrosis Lancet 1991338215-6 21 Meyer A Buhl R Magnussen H The effect of oral N-acetylcysteine on lung glutathione levels in idiopathic pulmonary fibrosis Eur Respir J 19947431-6 22 Behr J Maier K Degenkolb B Krombach F Vogelmeier C Antioxidative and clinical effects of high-dose N-acetylcysteine in fibrosing alveolitis Adjunctive therapy to maintenance immunosuppression Am J Respir Crit Care Med 19971561897-901 23 Cantin AM North SL Fells GA Hubbard RC Crystal RG Oxidant-mediated epithelial cell injury in idiopathic pulmonary fibrosis J Clin Invest 1987791665-73 24 Waghray M Cui Z Horowitz JC et al Hydrogen peroxide is a diffusible paracrine signal for the induction of epithelial cell death by activated myofibroblasts Faseb J 200519854-6 25 Larios JM Budhiraja R Fanburg BL Thannickal VJ Oxidative protein cross-linking reactions involving L-tyrosine in transforming growth factor-beta1-stimulated fibroblasts J Biol Chem 200127617437-41 26 Kinnula VL Fattman CL Tan RJ Oury TD Oxidative stress in pulmonary fibrosis a possible role for redox modulatory therapy Am J Respir Crit Care Med 2005172417-22 27 Meyer A Buhl R Kampf S Magnussen H Intravenous N-acetylcysteine and lung glutathione of patients with pulmonary fibrosis and normals Am J Respir Crit Care Med 19951521055-60 28 Behr J Degenkolb B Krombach F Vogelmeier C Intracellular glutathione and bronchoalveolar cells in fibrosing alveolitis effects of N-acetylcysteine Eur Respir J 200219906-11 29 Bando M Hosono T Mato N et al Long-term efficacy of inhaled N-acetylcysteine in patients with idiopathic pulmonary fibrosis Intern Med 2010492289-96 30 Demedts M Behr J Buhl R et al High-dose acetylcysteine in idiopathic pulmonary fibrosis N Engl J Med 20053532229-42 31 Toma TP Bhowmik A Rajakulasingam R Acetylcysteine in pulmonary fibrosis N Engl J Med 20063541086-9 author reply -9 32 Hunninghake GW Antioxidant therapy for idiopathic pulmonary fibrosis N Engl J Med 20053532285-7 33 Flaherty KR Mumford JA Murray S et al Prognostic implications of physiologic and radiographic changes in idiopathic interstitial pneumonia Am J Respir Crit Care Med 2003168543-8 34 Latsi PI du Bois RM Nicholson AG et al Fibrotic idiopathic interstitial pneumonia the prognostic value of longitudinal functional trends Am J Respir Crit Care Med 2003168531-7 35 Collard HR King TE Jr Bartelson BB Vourlekis JS Schwarz MI Brown KK Changes in clinical and physiologic variables predict survival in idiopathic pulmonary fibrosis Am J Respir Crit Care Med 2003168538-42 36 Jegal Y Kim DS Shim TS et al Physiology is a stronger predictor of survival than pathology in fibrotic interstitial pneumonia Am J Respir Crit Care Med 2005171639-44 37 Martinez FJ Safrin S Weycker D et al The clinical course of patients with idiopathic pulmonary fibrosis Ann Intern Med 2005142963-7 38 Hull JH Acetylcysteine in pulmonary fibrosis N Engl J Med 20063541089-91 author reply -91
70
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
39 Flaherty KR King TE Jr Raghu G et al Idiopathic interstitial pneumonia what is the effect of a multidisciplinary approach to diagnosis Am J Respir Crit Care Med 2004170904shy10 40 Raghu G Johnson WC Lockhart D Mageto Y Treatment of idiopathic pulmonary fibrosis with a new antifibrotic agent pirfenidone results of a prospective open-label Phase II study Am J Respir Crit Care Med 19991591061-9 41 Hunninghake GW Lynch DA Galvin JR et al Radiologic findings are strongly associated with a pathologic diagnosis of usual interstitial pneumonia Chest 20031241215-23 42 Lynch D Godwin J Safrin S et al High-resolution computed tomography in idiopathic pulmonary fibrosis diagnosis and prognosis Am J Respir Crit Care Med 2005172488-93 43 Mallinckrodt CH Watkin JG Molenberghs G Carroll RJ Choice of the primary analysis in longitudinal clinical trials Pharmaceutical Statistics 20043161-9 44 Bang H Tsiatis A Estimating medical costs with censored data Biometrika 200087329shy43 45 Lin DY Regression analysis of incomplete medical cost data Stat Med 2003221181-200 46 Rochon J Application of GEE procedures for sample size calculations in repeated measures experiments Stat Med 1998171643-58 47 Lachin JM Foulkes MA Evaluation of sample size and power for analyses of survival with allowance for nonuniform patient entry losses to follow-up noncompliance and stratification Biometrics 198642507-19
71
- PANTHER-IPFPREDNISONE AZATHIOPRINEAND N-ACETYLCYSTEINEA STUDY THAT EVALUATES RESPONSE INIDIOPATHIC PULMONARY FIBROSIS
-
- Protocol Summary
- Table of Contents
- List of Tables
- List of Figures
- List of Abbreviations
- 1 Summary
- 2 Hypotheses and Specific Aims
-
- 21 Null Hypothesis
- 22 Specific Aim 1
- 23 Specific Aim 2
- 24 Prespecified Subgroups of Interest
-
- 3 Background and Significance
-
- 31 Idiopathic Pulmonary Fibrosis is the Most Common Interstitial Lung Disease
- 32 Rationale for Placebo Control
- 33 Rationale for N-acetylcysteine
- 35 Rationale for N-acetylcysteine as a Stand-alone Therapy
- 36 Rationale for the Study Design and Primary Endpoint
- 37 Rationale for Blinding of Treatments
-
- 4 Methods
-
- 41 Inclusion Criteria
- 42 Diagnosis of IPF
- 43 Exclusion Criteria
- 44 Study Design and Study Visit
- 45 Dose Justification
- 46 Contraindications Precautions and Side Effects of Study Medications
- 47 Recruitment Procedures
- 48 Study Procedures
- 49 Concomitant Medications
- 410 Laboratory Testing
- 411 Blinding of Study Drugs
-
- 5 Study Endpoints
-
- 51 Primary Study Endpoint
- 52 Secondary Study Endpoints
-
- 6 Safety Evaluations and Procedures
-
- 61 Adverse Events
- 62 Clinical Medical Monitoring
- 63 Unblinding Procedures
-
- 7 Study Drug Procedures
- 8 Data Management
-
- 81 Hardware and Software Configuration
- 82 Sources of Data
-
- 9 Study Design and Data Analysis
-
- 91 General Analytic Considerations
- 92 Randomization Blinding and Reporting of Results
- 93 Stratification
- 94 Specification of the Primary Analyses
- 95 Analysis of Longitudinal Endpoints
- 96 Analysis of Binary Time-to-Event and Time-Lagged Endpoints
- 97 Power Analysis
-
- 10 Study Administration
-
- 101 Cooperative Agreement Mechanism
- 102 IPFnet Steering Group
- 103 Data and Safety Monitoring Board
- 104 Recommendations on Interim Monitoring of Efficacy Safety and Futility
-
- 11 Investigator and Sponsor Obligations
-
- 111 Monitoring
- 112 Cost and Payment
- 113 Confidentiality and Health Insurance Portability and Accountability ActConsiderations
- 114 Informed Consent Procedures
- 115 Institutional Review Boards
-
- 12 Investigator Agreement
- 13 References
-

PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Investigators are responsible for promptly reporting these events to their reviewing IRBs
according to site specific IRB reporting guidelines
62 Clinical Medical Monitoring
There will be an unblinded physician at the IPFnet DCC serving as medical monitor The
medical monitor will be available to assist with questions about dosage adjustments of study
medications including discontinuation or resumption of medications
63 Unblinding Procedures
Unblinding of subjects or investigators to subject treatment is strongly discouraged For ongoing
clinical management all subjects should be presumed to be receiving ldquoactiverdquo study drug To
ensure the subjectrsquos safety the study treatment will be dose-adjusted based on laboratory test
results clinical findings and symptoms
The IPFnet DCC medical monitor and PANTHER-IPF co-chairs Drs Ganesh Raghu and
Fernando Martinez will be available to the study physicians to discuss study drug management
on a case-by-case basis Un-blinding will be considered ONLY when the knowledge of subject
treatment assignment is ABSOLUTELY ESSENTIAL for subject safety and after discussion of
the subjectrsquos case with the medical monitor and either Dr Raghu or Dr Martinez Unblinding of
study treatment should be minimized during the conduct of the trial In those cases where it is
felt to be medically necessary the DCC medical officer will communicate directly with the
managing physician to minimize unblinding of study personnel
52
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
7 Study Drug Procedures
At the baseline 15-week 30-week and 45-week study visits subjects will receive a supply of
study drug sufficient to last until the next visit at which study drug will be dispensed
53
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
8 Data Management
81 Hardware and Software Configuration
811 Hardware and Database Software
Data will be stored in an Oracle database system Oracle has advantages of processing efficiency
and smooth linkage with other software systems The application and database will be hosted on
Solaris Unix servers at the IPFnet DCC
812 Statistical Software
SAS will be used as the principal application for the management of analysis data files and
statistical computations S-Plus will be used to provide supplementary functions as needed
813 Access Control and Confidentiality Procedures
Access to databases will be controlled centrally by the IPFnet DCC through user passwords
linked to appropriate privileges This protects the data from unauthorized changes and
inadvertent loss or damage
814 Security
Database and Web servers will be secured by a firewall and through controlled physical access
Oracle has many security features to ensure that any staff member accessing the database has the
proper authority to perform the functions he or she requests of the system Within the secondary
SAS databases Unix group-access control maintains similar security The Sun workstation login
is secured by extensive user-password facilities under Unix
54
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
815 Back-up Procedures
Database back-up will be performed automatically every day and standard IPFnet DCC policies
and procedures will be applied to dictate tape rotation and retention practices
816 Virus Protection
All disk drives that provide network services and all user computers will be protected using
virus-scanning software Standard IPFnet DCC policies will be applied to update these protection
systems periodically through the study
82 Sources of Data
821 Design and Development
The IPFnet DCC will be responsible for development of the electronic case report forms
(eCRFs) development and validation of the clinical study database ensuring data integrity and
training clinical center staff on applicable data management procedures A web-based distributed
data entry model will be implemented This system will be developed to ensure that guidelines
and regulations surrounding the use of computerized systems used in clinical trials are upheld
The remainder of this section provides an overview of the data management plan associated with
this protocol
822 Data Collection Forms
The data collection process consists of direct data entry at the study clinical centers into the EDC
system(s) provided by the DCC A data collection worksheet will be provided to clinical centers
for recording data in the event the EDC system is unavailable Data entry of the eCRFs should
be completed according to the instructions provided and project specific training The
investigator is responsible for maintaining accurate complete and up-to-date records and for
ensuring the completion of the eCRFs for each research participant
55
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
823 Data Acquisition and Entry
Data entry into eCRFs shall be performed by authorized individuals Selected eCRFs may also
require the investigatorrsquos written signature or electronic signature as appropriate Electronic
CRFs will be monitored for completeness accuracy and attention to detail during the study
824 Data Center Responsibilities
The IPFnet DCC will 1) develop a data management plan and will conduct data management
activities 2) provide final eCRFs for the collection of all data required by the study 3) develop
data dictionaries for each eCRF that will comprehensively define each data element 4) conduct
ongoing data monitoring activities on study data 5) monitor any preliminary analysis data
cleanup activities and 6) rigorously monitor final study data clean up
825 Data Editing
Completed data will be entered into the IPFnet DCC automated data acquisition and
management system If incomplete or inaccurate data are found a data clarification request will
be generated and distributed to clinical centers for a response Clinical centers will resolve data
inconsistencies and errors and enter all corrections and changes into the IPFnet DCC automated
data acquisition and management system
826 Training
The training plan for clinical center staff includes provisions for training on assessments eCRF
completion guidelines data management procedures and the use of computerized systems
56
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
9 Study Design and Data Analysis
91 General Analytic Considerations
All primary analyses will be based on intent-to-treat (ITT) principles using all randomized
subjects Baseline factors across groups will be compared using mean (standard deviation) and
median (25th and 75th percentiles) summary measures Kaplan-Meier curves will be used to
display event rates Due to clinical interest in departures from both sides of the null hypothesis
all test statistics will be 2-sided
Reasonable caution needs to be taken when conducting multiple analyses on key clinical
subgroups For subgroup analyses a conservative significance level of 0001 will be used for all
interaction tests Thus subgroup comparisons will be considered exploratory unless the p-value
from the interaction test is smaller than 0001
92 Randomization Blinding and Reporting of Results
A permuted block-randomization scheme will be created with varying block sizes stratified by
clinical center Once a subject has completed the screening and baseline period and evaluation
for inclusionexclusion criteria the randomization process will begin Subjects will be
randomized to receive NAC or matching placebo with equal probability (11) via telephone
contact with a central interactive voice response system (IVRS) using a toll-free randomization
number On the day of randomization after the subject has successfully met all inclusion and
exclusion criteria the investigator or designee will call the central randomization number to
obtain the assigned kit randomization numbers for that subject At each subject visit the
investigator or designee will call the central randomization number to obtain the new kit
randomization numbers for resupply of the subject For resupply of the clinical center the IVRS
will monitor minimal volume of a kit type andor expiration date and will automatically notify
the pharmacy
57
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
The trial results will be reported according to guidelines specified in the CONSORT statement
A flow diagram describing screening recruitment randomization dropout and vital status will
be included in the primary manuscript AEs and efficacy data will be presented for all treatment
groups Adherence dropout and lost to follow-up will be carefully examined across all treatment
groups Analyses of safety will be based on data from all randomized subjects who received at
least one dose of study drug
93 Stratification
Subjects will be distributed to the two treatment arms in a 11 allocation ratio Stratification
blocks will be based on clinical centers
94 Specification of the Primary Analyses
A mixed model repeated measures (MMRM) analysis described in section 95 will be used to
compare differences in the slope of FVC measurements across the treatment groups Response
variables are values of the FVC measured at baseline and every 15 weeks until study completion
Variables in the model will include treatment time and time by treatment age sex race and
height Contrast estimates of differences in slopes of treatment over time (along with confidence
intervals) will be used to estimate the treatment effect The validity of this model in terms of
meeting modeling assumptions will be assessed via standard modeling diagnostics and goodness-
of-fit measures Based on the MMRM framework missing FVC data will not be imputed for the
primary analysis
95 Analysis of Longitudinal Endpoints
A common goal in clinical trials is to specify models that are easily implemented and
reproducible by independent data analysts On the other hand the models should have proper
statistical behavior in terms of low bias and high precision Many common approaches to
longitudinal data analysis including last observation carried forward (LOCF) imputation rely on
the missing completely at random (MCAR) assumption However the MCAR assumption is
58
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
unlikely to hold in many clinical trials because missing data are often related to disease
progression and prognosis A more reasonable assumption missing at random (MAR) specifies
that the complete data distribution can be modeled using only the observed data The likelihood-
based MMRM approach is valid under the more general MAR assumptions These models will
be applied to analyze the longitudinal data secondary endpoints
The advantages of MMRM analysis are that all important characteristics of the model can be preshy
specified standard software can be used to implement the models and results are based on ITT
principles43 In addition the MMRM approach offers superior control of Type I and Type II
errors compared with the LOCF approach
Response variables are values of the PFTs measured at enrollment and every 15 weeks until
study completion and 6MWT values measured at baseline week 30 and week 60 Covariates are
treatment time time by treatment and key baseline risk factors Contrasts (along with
confidence intervals) of treatment by time will be used to estimate the treatment effect
The correlation structure involves multiple pieces including measurement errors random
variation and interindividual variability For the longitudinal data analyses an unstructured
correlation matrix for within-subject errors will be assumed Other correlation structures
including compound symmetry will be examined as needed A careful examination of reasons
for study discontinuation will be conducted to assess the validity of MCAR Sensitivity analyses
will be used to examine the untestable assumption that the observed data violate the MAR
assumption The MMRM models will be implemented using PROC MIXED in SAS
96 Analysis of Binary Time-to-Event and Time-Lagged Endpoints
Regression modeling approaches using either the logistic regression model or Cox proportional
hazards regression model will be employed when appropriate The validity of these models will
be assessed via standard modeling diagnostics and goodness-of-fit measures Estimates of
cumulative frequencies for more general time-lagged responses will be calculated using the
partitioned version of the Bang-Tsiatis estimator44 The partitions will be set at 15-week intervals
59
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
to correspond with the data-collection process Covariate adjusted event rates will be calculated
using inverse probability-weighted regression estimates45
97 Power Analysis
971 Primary Analyses
Based on previously published IPF clinical trials the PL group is expected to experience a drop
in FVC of approximately 020 L over the study period (see Figure 1) The IPFnet Steering Group
determined a clinically important difference would be to preserve the majority of the decline
relative to PL over the study period In particular a treatment effect of 015 L was determined to
be a clinically meaningful difference Potential dropout is a key factor in the proposed study The
drop-out process assumed 5 lost to follow-up after every study visit Only 80 of subjects
were assumed to be followed for the entire study period All models assumed a compound
symmetry structure for the covariance matrix Power calculations were performed using a SAS
IML program for designing repeated measures studies46 Based on preliminary reviews of the
data from the University of Michigan the covariance matrix parameters were estimated at
approximately σ2 = 0757 (variance parameter) and ρ = 0936 (correlation parameter) To be
conservative the power calculations for the primary analysis were performed with parameter
setting of σ2 = 0810 (variance parameter) and ρ = 0925 (correlation parameter)
The power calculations assume a correction for imperfect compliance proposed by Lachin and
Foulkes to allow for 2 noncompliance for each of the treatment arms47 Thus the sample size
of 130 subjects per arm would be reduced to an adjusted sample size of 130(1-002-002)2 =
1198 or 120 subjects per arm
Under the assumed Type I error rate of 005 with a correlation parameter of 0925 and standard
deviation of 090 the difference of 015 L (or 00025 Lweek) shown in Table 6 would have
power of 93
60
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Table 6 Hypothetical Values of Mean FVC (L) Change from Baseline
Week 15 Week 30 Week 45 Week 60
NAC 00125 00250 00375 00500
Placebo 00500 01000 01500 02000
Difference 00375 00750 01125 01500
Abbreviations FVC forced vital capacity PL placebo
972 Power Analysis for Secondary Endpoints
Power calculations for secondary endpoint measurements are shown in Table 7 Standard
deviations are based on unpublished data provided by the University of Michigan The
calculations are based on a 2-sample t-test with Type I error rate set at 005 These calculations
are likely to be conservative because the statistical approach described in section 95 for
analyzing these endpoints will incorporate incomplete observations as well as intermediate data
points
Table 7 Detectable Differences in Treatment Means for Selected Endpoint Measurements
Secondary Endpoints Std Dev
of the Baseline Score
Detectable Difference for 80 Power
Std Dev of the Change Score
Difference Detectable for
80 Power
DLCOpred 166 58 91 32
6MWT Area Under the Desaturation Curve
219 76 175 61
6MWT Distance to Desaturation 224 78 315 110
6MWT Minutes Walked 210 073 205 071
Abbreviations Std Dev standard deviation DLCOpred diffusing capacity of the lung for carbon monoxide percent predicted 6MWT 6-minute walk test
61
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
10 Study Administration
101 Cooperative Agreement Mechanism
The administrative and funding mechanism used to undertake this project is a ldquocooperative
agreementrdquo (U01) which is an assistance mechanism Under the cooperative agreement the
NHLBI assists supports andor stimulates the project and is substantially involved with
investigators in conducting the study by facilitating performance of the effort in a ldquopartnerrdquo role
The NHLBI project scientist serves on the IPFnet Steering Group and he or another NHLBI
scientist may serve on other project committees when appropriate At the same time however
NHLBI does not assume a dominant role direction or prime responsibility for this research
program
As described below governance of the project is conducted through the IPFnet Steering Group
Principal investigators have lead responsibilities in all aspects of their trials and the project
including any modification of trial designs conduct of the trials quality control data analysis
and interpretation preparation of publications and collaboration with other investigators unless
otherwise provided for by the IPFnet Steering Group
PIs retain custody of and have primary rights to their center-specific and collaborative data
subject to government rights-of-access consistent with current Health amp Human Services (HHS)
Public Health Service (PHS) and National Institutes of Health policies The protocols and
governance policies call for the continual submission of data centrally to the IPFnet DCC for the
collaborative database which at a minimum will contain the key variables selected by the IPFnet
Steering Group for standardization across all clinical centers the submission of copies of the
collaborative datasets to each PI upon completion of the project procedures for data analysis
reporting and publication and procedures to protect and ensure the privacy of medical and
genetic data and records of individuals The NHLBI project scientist on behalf of the NHLBI
will have the same access privileges and responsibilities regarding the collaborative data as the
other members of the Steering Group
62
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
PIs are also encouraged to publish and to publicly release and disseminate results data and other
products of the project concordant with the project protocols and governance and the approved
plan for making data and materials available to the scientific community and to the NHLBI
However during the 3 years after the ending date of NHLBI project support unpublished data
unpublished results data sets not previously released and other study materials or products are
to be made available to any third party only with the approval of the IPFnet Steering Group
Upon completion of the project PIs are expected to put their intervention materials and
procedure manuals into the public domain andor make them available to other investigators
according to the approved plan for making data and materials available to the scientific
community and the NHLBI for the conduct of research at no charge other than the costs of
reproduction and distribution
The NHLBI reserves the right to terminate or curtail the project (or an individual award) in the
event of (a) failure to develop or implement mutually agreeable collaborative measurement
subject eligibility and data management sections of the protocols (b) substantial shortfall in
subject recruitment follow-up data reporting or quality control or other major breach of
protocol (c) substantive changes in the agreed-upon protocols with which NHLBI cannot
concur (d) reaching a major project outcome with persuasive statistical significance
substantially before schedule or (e) human subject ethical issues that may dictate a premature
termination
Any disagreement that may arise in scientificprogrammatic matters (within the scope of the
award) between award recipients and the NHLBI may be brought to arbitration An arbitration
panel will be composed of 3 membersmdash1 selected by the IPFnet Steering Group (with the
NHLBI member not voting) or by the individual PI in the event of an individual disagreement a
second selected by NHLBI and the third selected by the other 2 members This special
arbitration procedure in no way affects the PIrsquos right to appeal an adverse action that is otherwise
appealable in accordance with the PHS regulations at 42 CFR part 50 Subpart D and HHS
63
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
regulation at 45 CFR part 16 or the rights of the NHLBI under applicable statutes regulations
and terms of the award
102 IPFnet Steering Group
The IPFnet Steering Group is the main governing body of the project It is composed of the PIs
of the clinical centers the PI of the DCC and the NHLBI project scientist The clinical centers
the IPFnet DCC and the NHLBI each have 1 vote on the IPFnet Steering Group All decisions
are determined by majority vote
All major scientific decisions are determined by the IPFnet Steering Group It assumes overall
responsibility for the design and conduct of the trial It appoints (and disbands) committees and
subcommittees as the need arises designs approves and implements the study protocols
oversees the development of the MOOP monitors subject recruitment and treatment delivery
evaluates data collection and management oversees quality assurance procedures and
implements changes and enhancements to the study as required It also has primary responsibility
for facilitating the conduct of the trials and reporting the projectrsquos results
103 Data and Safety Monitoring Board
The NHLBI will establish a DSMB in accordance with established policies (see
httpwwwnhlbinihgovfundingpoliciesdsmb_insthtm) to ensure data quality and subject
safety and to provide independent advice to the NHLBI regarding progress and the
appropriateness of study continuation
104 Recommendations on Interim Monitoring of Efficacy Safety and Futility
First and foremost the role of the DSMB will be to review subject safety and trial conduct at
periodic points during the study The DSMB may require analyses of the primary endpoint
results for comparing the benefit and risks of treatment strategies The benefit of collecting
additional data on key secondary endpoints with extended follow-up and establishing a robust
64
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
evidence base for determining a standard of care will need to be carefully considered before
early termination of one or more treatment arms After careful consideration the IPFnet Steering
Group recommends conservative thresholds for the early examinations of the safety and efficacy
data
The DSMB will be expected to meet approximately every 6 months until trial completion to
review safety and toxicity data The DSMB may recommend stopping the study based on these
reviews Because the DSMB could stop the trial for safety concerns as well as for a large
efficacy benefit there could be multiple opportunities to reject the null hypothesis (no difference
in event rates between the PL and NAC groups) A Bonferroni approximation will be applied
during the one planned interim analysis for efficacy
Before locking the database a statistical analysis plan (SAP) will be developed to provide
complete details on the statistical analysis The SAP will include the specifics for how and when
the DSMB will be notified for AEs The IPFnet DCC will deliver to the DSMB all FDA-defined
AEs at 3-month intervals The IPFnet DCC will prepare narrative SAE reports in real time for
DSMB review including recommendations and analysis of similar events for each SAE
submitted to the FDA
65
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
11 Investigator and Sponsor Obligations
111 Monitoring
All monitoring activities for US clinical centers will be performed in accordance with DCRI
standard operating procedures Information regarding the types of visits will be outlined in the
PANTHER-IPF MOOP
112 Cost and Payment
There will be no cost to subjects enrolled in this trial Study-related procedures will be paid for
by the IPFnet
Subjects may be eligible for reimbursement for travel to the clinical center Details of payment
will be explained to each subject during the consent process
113 Confidentiality and Health Insurance Portability and Accountability Act
Considerations
Subject confidentiality will be protected throughout the study All subject data will be kept
strictly confidential and no subject-identifying information will be released to anyone outside
the project Confidentiality will be assured through several mechanisms First each subject will
be assigned an anonymous study ID which will then be used on all study forms Second any
study forms blood samples and paper records that contain subject information (eg address lists
phone lists) will be kept at the clinical centers in secured locked areas coded by number Once
blood is collected there will be no subject identifiers placed on blood samplesmdashonly the study
ID number and the date of sample collection Third access to all subject data and information
including laboratory specimens will be restricted to authorized personnel In the case of
computerized data this restricted access will be assured through user logon IDs and password
protection
66
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
At the IPFnet DCC only authorized personnel will have access to the data files containing study
data Security will be assured through user logon IDs passwords and appropriate access
privileges All study subjects will be identified only by their IPFnet ID numbers and no personal
identifying information such as name address or Social Security number will be entered into
the IPFnet DCC database Any subject-specific data reported to the IPFnet Steering Group will
be identified only by the IPFnet ID number
Finally subjects will not be identified by name in any reports or publications nor will the data
be presented in such a way that the identity of individual subjects can be inferred Analysis files
created for further study by the scientific community will have no subject identifiers These data
files will be created in accordance with the Ancillary Studies and Publication Policy of the
IPFnet
114 Informed Consent Procedures
All IPFnet subjects will provide written informed consent using procedures reviewed and
approved by each clinical centerrsquos IRB Informed consent will be undertaken by study personnel
in-person with the subject The subject has the option of declining further participation in the
study at that point No further study procedures will be conducted until the signed documents
have been provided to the IPFnet clinical center
115 Institutional Review Boards
Before initiating this study the protocol clinical center-specific informed consent forms Health
Insurance Portability and Accountability Act (HIPAA) forms recruitment materials and other
relevant information will be reviewed by a properly constituted IRB at each participating clinical
center A copy of the signed and dated IRB approval at each clinical center will be retrieved prior
to or during the site initiation visit and archived at the IPFnet DCC Any amendments to the
protocol other than simple administrative and typographical changes must be approved by each
IRB before they are implemented The clinical centers will seek annual renewals of their IRB
approvals in accordance with local procedures
67
__________________________________________ ________________
__________________________________________
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
12 Investigator Agreement
I have read the foregoing protocol PANTHER-IPF and agree that it contains all necessary
details for carrying out this study I will conduct the study as outlined herein and will complete
the study within the time designated
I will provide copies of the protocol and all pertinent information to all individuals responsible to
me who assist in the conduct of this study I will discuss this material with them to ensure they
are fully informed regarding the drug and the conduct of the study
I will fulfill all responsibilities for submitting pertinent information to the local IRB if
applicable that is responsible for this study
I further agree that NHLBI andor DCRI will have access to any source documents from which
eCRF information may have been generated
Signature of Principal Investigator Date
Name of Principal Investigator (printed or typed)
Protocol version date May 19 2009
Protocol Amendment 1 version date May 28 2010
Protocol Amendment 2 version date December 6 2011
68
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
13 References
1 Raghu G Brown KK Bradford WZ et al A placebo-controlled trial of interferon gamma-1b in patients with idiopathic pulmonary fibrosis N Engl J Med 2004350125-33 2 King TE Jr Safrin S Starko KM et al Analyses of efficacy end points in a controlled trial of interferon-gamma1b for idiopathic pulmonary fibrosis Chest 2005127171-7 3 Flaherty KR Thwaite EL Kazerooni EA et al Radiological versus histological diagnosis in UIP and NSIP survival implications Thorax 200358143-8 4 Wells AU Desai SR Rubens MB et al Idiopathic pulmonary fibrosis a composite physiologic index derived from disease extent observed by computed tomography Am J Respir Crit Care Med 2003167962-9 5 Raghu G Freudenberger TD Yang S et al High prevalence of abnormal acid gastroshyoesophageal reflux in idiopathic pulmonary fibrosis Eur Respir J 200627136-42 6 Kinnula VL Focus on antioxidant enzymes and antioxidant strategies in smoking related airway diseases Thorax 200560693-700 7 Coultas DB Zumwalt RE Black WC Sobonya RE The epidemiology of interstitial lung diseases Am J Respir Crit Care Med 1994150967-72 8 Raghu G Weycker D Edelsberg J Bradford WZ Oster G Incidence and prevalence of idiopathic pulmonary fibrosis Am J Respir Crit Care Med 2006174810-6 9 Olson AL Swigris JJ Lezotte DC Norris JM Wilson CG Brown KK Mortality from pulmonary fibrosis increased in the United States from 1992 to 2003 Am J Respir Crit Care Med 2007176277-84 10 Mannino DM Etzel RA Parrish RG Pulmonary fibrosis deaths in the United States 1979shy1991 An analysis of multiple-cause mortality data Am J Respir Crit Care Med 19961531548shy52 11 Hubbard R Johnston I Coultas DB Britton J Mortality rates from cryptogenic fibrosing alveolitis in seven countries Thorax 199651711-6 12 Johnston I Britton J Kinnear W Logan R Rising mortality from cryptogenic fibrosing alveolitis Bmj 19903011017-21 13 Raghu G Collard HR Egan JJ et al An official ATSERSJRSALAT statement idiopathic pulmonary fibrosis evidence-based guidelines for diagnosis and management Am J Respir Crit Care Med 2011183788-824 14 (USA) FDA FDA Public Health Advisory Interferon gamma-1b (marketed as Actimmune) In 2007 15 King TE Jr Pardo A Selman M Idiopathic pulmonary fibrosis Lancet 2011 16 Raghu G Brown KK Costabel U et al Treatment of idiopathic pulmonary fibrosis with etanercept an exploratory placebo-controlled trial Am J Respir Crit Care Med 2008178948shy55 17 Malouf MA Hopkins P Snell G Glanville AR An investigator-driven study of everolimus in surgical lung biopsy confirmed idiopathic pulmonary fibrosis Respirology 201116776-83 18 King TE Jr Behr J Brown KK et al BUILD-1 a randomized placebo-controlled trial of bosentan in idiopathic pulmonary fibrosis Am J Respir Crit Care Med 200817775-81 19 Richeldi L Costabel U Selman M et al Efficacy of a tyrosine kinase inhibitor in idiopathic pulmonary fibrosis N Engl J Med 20113651079-87
69
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
20 Borok Z Buhl R Grimes GJ et al Effect of glutathione aerosol on oxidant-antioxidant imbalance in idiopathic pulmonary fibrosis Lancet 1991338215-6 21 Meyer A Buhl R Magnussen H The effect of oral N-acetylcysteine on lung glutathione levels in idiopathic pulmonary fibrosis Eur Respir J 19947431-6 22 Behr J Maier K Degenkolb B Krombach F Vogelmeier C Antioxidative and clinical effects of high-dose N-acetylcysteine in fibrosing alveolitis Adjunctive therapy to maintenance immunosuppression Am J Respir Crit Care Med 19971561897-901 23 Cantin AM North SL Fells GA Hubbard RC Crystal RG Oxidant-mediated epithelial cell injury in idiopathic pulmonary fibrosis J Clin Invest 1987791665-73 24 Waghray M Cui Z Horowitz JC et al Hydrogen peroxide is a diffusible paracrine signal for the induction of epithelial cell death by activated myofibroblasts Faseb J 200519854-6 25 Larios JM Budhiraja R Fanburg BL Thannickal VJ Oxidative protein cross-linking reactions involving L-tyrosine in transforming growth factor-beta1-stimulated fibroblasts J Biol Chem 200127617437-41 26 Kinnula VL Fattman CL Tan RJ Oury TD Oxidative stress in pulmonary fibrosis a possible role for redox modulatory therapy Am J Respir Crit Care Med 2005172417-22 27 Meyer A Buhl R Kampf S Magnussen H Intravenous N-acetylcysteine and lung glutathione of patients with pulmonary fibrosis and normals Am J Respir Crit Care Med 19951521055-60 28 Behr J Degenkolb B Krombach F Vogelmeier C Intracellular glutathione and bronchoalveolar cells in fibrosing alveolitis effects of N-acetylcysteine Eur Respir J 200219906-11 29 Bando M Hosono T Mato N et al Long-term efficacy of inhaled N-acetylcysteine in patients with idiopathic pulmonary fibrosis Intern Med 2010492289-96 30 Demedts M Behr J Buhl R et al High-dose acetylcysteine in idiopathic pulmonary fibrosis N Engl J Med 20053532229-42 31 Toma TP Bhowmik A Rajakulasingam R Acetylcysteine in pulmonary fibrosis N Engl J Med 20063541086-9 author reply -9 32 Hunninghake GW Antioxidant therapy for idiopathic pulmonary fibrosis N Engl J Med 20053532285-7 33 Flaherty KR Mumford JA Murray S et al Prognostic implications of physiologic and radiographic changes in idiopathic interstitial pneumonia Am J Respir Crit Care Med 2003168543-8 34 Latsi PI du Bois RM Nicholson AG et al Fibrotic idiopathic interstitial pneumonia the prognostic value of longitudinal functional trends Am J Respir Crit Care Med 2003168531-7 35 Collard HR King TE Jr Bartelson BB Vourlekis JS Schwarz MI Brown KK Changes in clinical and physiologic variables predict survival in idiopathic pulmonary fibrosis Am J Respir Crit Care Med 2003168538-42 36 Jegal Y Kim DS Shim TS et al Physiology is a stronger predictor of survival than pathology in fibrotic interstitial pneumonia Am J Respir Crit Care Med 2005171639-44 37 Martinez FJ Safrin S Weycker D et al The clinical course of patients with idiopathic pulmonary fibrosis Ann Intern Med 2005142963-7 38 Hull JH Acetylcysteine in pulmonary fibrosis N Engl J Med 20063541089-91 author reply -91
70
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
39 Flaherty KR King TE Jr Raghu G et al Idiopathic interstitial pneumonia what is the effect of a multidisciplinary approach to diagnosis Am J Respir Crit Care Med 2004170904shy10 40 Raghu G Johnson WC Lockhart D Mageto Y Treatment of idiopathic pulmonary fibrosis with a new antifibrotic agent pirfenidone results of a prospective open-label Phase II study Am J Respir Crit Care Med 19991591061-9 41 Hunninghake GW Lynch DA Galvin JR et al Radiologic findings are strongly associated with a pathologic diagnosis of usual interstitial pneumonia Chest 20031241215-23 42 Lynch D Godwin J Safrin S et al High-resolution computed tomography in idiopathic pulmonary fibrosis diagnosis and prognosis Am J Respir Crit Care Med 2005172488-93 43 Mallinckrodt CH Watkin JG Molenberghs G Carroll RJ Choice of the primary analysis in longitudinal clinical trials Pharmaceutical Statistics 20043161-9 44 Bang H Tsiatis A Estimating medical costs with censored data Biometrika 200087329shy43 45 Lin DY Regression analysis of incomplete medical cost data Stat Med 2003221181-200 46 Rochon J Application of GEE procedures for sample size calculations in repeated measures experiments Stat Med 1998171643-58 47 Lachin JM Foulkes MA Evaluation of sample size and power for analyses of survival with allowance for nonuniform patient entry losses to follow-up noncompliance and stratification Biometrics 198642507-19
71
- PANTHER-IPFPREDNISONE AZATHIOPRINEAND N-ACETYLCYSTEINEA STUDY THAT EVALUATES RESPONSE INIDIOPATHIC PULMONARY FIBROSIS
-
- Protocol Summary
- Table of Contents
- List of Tables
- List of Figures
- List of Abbreviations
- 1 Summary
- 2 Hypotheses and Specific Aims
-
- 21 Null Hypothesis
- 22 Specific Aim 1
- 23 Specific Aim 2
- 24 Prespecified Subgroups of Interest
-
- 3 Background and Significance
-
- 31 Idiopathic Pulmonary Fibrosis is the Most Common Interstitial Lung Disease
- 32 Rationale for Placebo Control
- 33 Rationale for N-acetylcysteine
- 35 Rationale for N-acetylcysteine as a Stand-alone Therapy
- 36 Rationale for the Study Design and Primary Endpoint
- 37 Rationale for Blinding of Treatments
-
- 4 Methods
-
- 41 Inclusion Criteria
- 42 Diagnosis of IPF
- 43 Exclusion Criteria
- 44 Study Design and Study Visit
- 45 Dose Justification
- 46 Contraindications Precautions and Side Effects of Study Medications
- 47 Recruitment Procedures
- 48 Study Procedures
- 49 Concomitant Medications
- 410 Laboratory Testing
- 411 Blinding of Study Drugs
-
- 5 Study Endpoints
-
- 51 Primary Study Endpoint
- 52 Secondary Study Endpoints
-
- 6 Safety Evaluations and Procedures
-
- 61 Adverse Events
- 62 Clinical Medical Monitoring
- 63 Unblinding Procedures
-
- 7 Study Drug Procedures
- 8 Data Management
-
- 81 Hardware and Software Configuration
- 82 Sources of Data
-
- 9 Study Design and Data Analysis
-
- 91 General Analytic Considerations
- 92 Randomization Blinding and Reporting of Results
- 93 Stratification
- 94 Specification of the Primary Analyses
- 95 Analysis of Longitudinal Endpoints
- 96 Analysis of Binary Time-to-Event and Time-Lagged Endpoints
- 97 Power Analysis
-
- 10 Study Administration
-
- 101 Cooperative Agreement Mechanism
- 102 IPFnet Steering Group
- 103 Data and Safety Monitoring Board
- 104 Recommendations on Interim Monitoring of Efficacy Safety and Futility
-
- 11 Investigator and Sponsor Obligations
-
- 111 Monitoring
- 112 Cost and Payment
- 113 Confidentiality and Health Insurance Portability and Accountability ActConsiderations
- 114 Informed Consent Procedures
- 115 Institutional Review Boards
-
- 12 Investigator Agreement
- 13 References
-

PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
7 Study Drug Procedures
At the baseline 15-week 30-week and 45-week study visits subjects will receive a supply of
study drug sufficient to last until the next visit at which study drug will be dispensed
53
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
8 Data Management
81 Hardware and Software Configuration
811 Hardware and Database Software
Data will be stored in an Oracle database system Oracle has advantages of processing efficiency
and smooth linkage with other software systems The application and database will be hosted on
Solaris Unix servers at the IPFnet DCC
812 Statistical Software
SAS will be used as the principal application for the management of analysis data files and
statistical computations S-Plus will be used to provide supplementary functions as needed
813 Access Control and Confidentiality Procedures
Access to databases will be controlled centrally by the IPFnet DCC through user passwords
linked to appropriate privileges This protects the data from unauthorized changes and
inadvertent loss or damage
814 Security
Database and Web servers will be secured by a firewall and through controlled physical access
Oracle has many security features to ensure that any staff member accessing the database has the
proper authority to perform the functions he or she requests of the system Within the secondary
SAS databases Unix group-access control maintains similar security The Sun workstation login
is secured by extensive user-password facilities under Unix
54
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
815 Back-up Procedures
Database back-up will be performed automatically every day and standard IPFnet DCC policies
and procedures will be applied to dictate tape rotation and retention practices
816 Virus Protection
All disk drives that provide network services and all user computers will be protected using
virus-scanning software Standard IPFnet DCC policies will be applied to update these protection
systems periodically through the study
82 Sources of Data
821 Design and Development
The IPFnet DCC will be responsible for development of the electronic case report forms
(eCRFs) development and validation of the clinical study database ensuring data integrity and
training clinical center staff on applicable data management procedures A web-based distributed
data entry model will be implemented This system will be developed to ensure that guidelines
and regulations surrounding the use of computerized systems used in clinical trials are upheld
The remainder of this section provides an overview of the data management plan associated with
this protocol
822 Data Collection Forms
The data collection process consists of direct data entry at the study clinical centers into the EDC
system(s) provided by the DCC A data collection worksheet will be provided to clinical centers
for recording data in the event the EDC system is unavailable Data entry of the eCRFs should
be completed according to the instructions provided and project specific training The
investigator is responsible for maintaining accurate complete and up-to-date records and for
ensuring the completion of the eCRFs for each research participant
55
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
823 Data Acquisition and Entry
Data entry into eCRFs shall be performed by authorized individuals Selected eCRFs may also
require the investigatorrsquos written signature or electronic signature as appropriate Electronic
CRFs will be monitored for completeness accuracy and attention to detail during the study
824 Data Center Responsibilities
The IPFnet DCC will 1) develop a data management plan and will conduct data management
activities 2) provide final eCRFs for the collection of all data required by the study 3) develop
data dictionaries for each eCRF that will comprehensively define each data element 4) conduct
ongoing data monitoring activities on study data 5) monitor any preliminary analysis data
cleanup activities and 6) rigorously monitor final study data clean up
825 Data Editing
Completed data will be entered into the IPFnet DCC automated data acquisition and
management system If incomplete or inaccurate data are found a data clarification request will
be generated and distributed to clinical centers for a response Clinical centers will resolve data
inconsistencies and errors and enter all corrections and changes into the IPFnet DCC automated
data acquisition and management system
826 Training
The training plan for clinical center staff includes provisions for training on assessments eCRF
completion guidelines data management procedures and the use of computerized systems
56
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
9 Study Design and Data Analysis
91 General Analytic Considerations
All primary analyses will be based on intent-to-treat (ITT) principles using all randomized
subjects Baseline factors across groups will be compared using mean (standard deviation) and
median (25th and 75th percentiles) summary measures Kaplan-Meier curves will be used to
display event rates Due to clinical interest in departures from both sides of the null hypothesis
all test statistics will be 2-sided
Reasonable caution needs to be taken when conducting multiple analyses on key clinical
subgroups For subgroup analyses a conservative significance level of 0001 will be used for all
interaction tests Thus subgroup comparisons will be considered exploratory unless the p-value
from the interaction test is smaller than 0001
92 Randomization Blinding and Reporting of Results
A permuted block-randomization scheme will be created with varying block sizes stratified by
clinical center Once a subject has completed the screening and baseline period and evaluation
for inclusionexclusion criteria the randomization process will begin Subjects will be
randomized to receive NAC or matching placebo with equal probability (11) via telephone
contact with a central interactive voice response system (IVRS) using a toll-free randomization
number On the day of randomization after the subject has successfully met all inclusion and
exclusion criteria the investigator or designee will call the central randomization number to
obtain the assigned kit randomization numbers for that subject At each subject visit the
investigator or designee will call the central randomization number to obtain the new kit
randomization numbers for resupply of the subject For resupply of the clinical center the IVRS
will monitor minimal volume of a kit type andor expiration date and will automatically notify
the pharmacy
57
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
The trial results will be reported according to guidelines specified in the CONSORT statement
A flow diagram describing screening recruitment randomization dropout and vital status will
be included in the primary manuscript AEs and efficacy data will be presented for all treatment
groups Adherence dropout and lost to follow-up will be carefully examined across all treatment
groups Analyses of safety will be based on data from all randomized subjects who received at
least one dose of study drug
93 Stratification
Subjects will be distributed to the two treatment arms in a 11 allocation ratio Stratification
blocks will be based on clinical centers
94 Specification of the Primary Analyses
A mixed model repeated measures (MMRM) analysis described in section 95 will be used to
compare differences in the slope of FVC measurements across the treatment groups Response
variables are values of the FVC measured at baseline and every 15 weeks until study completion
Variables in the model will include treatment time and time by treatment age sex race and
height Contrast estimates of differences in slopes of treatment over time (along with confidence
intervals) will be used to estimate the treatment effect The validity of this model in terms of
meeting modeling assumptions will be assessed via standard modeling diagnostics and goodness-
of-fit measures Based on the MMRM framework missing FVC data will not be imputed for the
primary analysis
95 Analysis of Longitudinal Endpoints
A common goal in clinical trials is to specify models that are easily implemented and
reproducible by independent data analysts On the other hand the models should have proper
statistical behavior in terms of low bias and high precision Many common approaches to
longitudinal data analysis including last observation carried forward (LOCF) imputation rely on
the missing completely at random (MCAR) assumption However the MCAR assumption is
58
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
unlikely to hold in many clinical trials because missing data are often related to disease
progression and prognosis A more reasonable assumption missing at random (MAR) specifies
that the complete data distribution can be modeled using only the observed data The likelihood-
based MMRM approach is valid under the more general MAR assumptions These models will
be applied to analyze the longitudinal data secondary endpoints
The advantages of MMRM analysis are that all important characteristics of the model can be preshy
specified standard software can be used to implement the models and results are based on ITT
principles43 In addition the MMRM approach offers superior control of Type I and Type II
errors compared with the LOCF approach
Response variables are values of the PFTs measured at enrollment and every 15 weeks until
study completion and 6MWT values measured at baseline week 30 and week 60 Covariates are
treatment time time by treatment and key baseline risk factors Contrasts (along with
confidence intervals) of treatment by time will be used to estimate the treatment effect
The correlation structure involves multiple pieces including measurement errors random
variation and interindividual variability For the longitudinal data analyses an unstructured
correlation matrix for within-subject errors will be assumed Other correlation structures
including compound symmetry will be examined as needed A careful examination of reasons
for study discontinuation will be conducted to assess the validity of MCAR Sensitivity analyses
will be used to examine the untestable assumption that the observed data violate the MAR
assumption The MMRM models will be implemented using PROC MIXED in SAS
96 Analysis of Binary Time-to-Event and Time-Lagged Endpoints
Regression modeling approaches using either the logistic regression model or Cox proportional
hazards regression model will be employed when appropriate The validity of these models will
be assessed via standard modeling diagnostics and goodness-of-fit measures Estimates of
cumulative frequencies for more general time-lagged responses will be calculated using the
partitioned version of the Bang-Tsiatis estimator44 The partitions will be set at 15-week intervals
59
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
to correspond with the data-collection process Covariate adjusted event rates will be calculated
using inverse probability-weighted regression estimates45
97 Power Analysis
971 Primary Analyses
Based on previously published IPF clinical trials the PL group is expected to experience a drop
in FVC of approximately 020 L over the study period (see Figure 1) The IPFnet Steering Group
determined a clinically important difference would be to preserve the majority of the decline
relative to PL over the study period In particular a treatment effect of 015 L was determined to
be a clinically meaningful difference Potential dropout is a key factor in the proposed study The
drop-out process assumed 5 lost to follow-up after every study visit Only 80 of subjects
were assumed to be followed for the entire study period All models assumed a compound
symmetry structure for the covariance matrix Power calculations were performed using a SAS
IML program for designing repeated measures studies46 Based on preliminary reviews of the
data from the University of Michigan the covariance matrix parameters were estimated at
approximately σ2 = 0757 (variance parameter) and ρ = 0936 (correlation parameter) To be
conservative the power calculations for the primary analysis were performed with parameter
setting of σ2 = 0810 (variance parameter) and ρ = 0925 (correlation parameter)
The power calculations assume a correction for imperfect compliance proposed by Lachin and
Foulkes to allow for 2 noncompliance for each of the treatment arms47 Thus the sample size
of 130 subjects per arm would be reduced to an adjusted sample size of 130(1-002-002)2 =
1198 or 120 subjects per arm
Under the assumed Type I error rate of 005 with a correlation parameter of 0925 and standard
deviation of 090 the difference of 015 L (or 00025 Lweek) shown in Table 6 would have
power of 93
60
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Table 6 Hypothetical Values of Mean FVC (L) Change from Baseline
Week 15 Week 30 Week 45 Week 60
NAC 00125 00250 00375 00500
Placebo 00500 01000 01500 02000
Difference 00375 00750 01125 01500
Abbreviations FVC forced vital capacity PL placebo
972 Power Analysis for Secondary Endpoints
Power calculations for secondary endpoint measurements are shown in Table 7 Standard
deviations are based on unpublished data provided by the University of Michigan The
calculations are based on a 2-sample t-test with Type I error rate set at 005 These calculations
are likely to be conservative because the statistical approach described in section 95 for
analyzing these endpoints will incorporate incomplete observations as well as intermediate data
points
Table 7 Detectable Differences in Treatment Means for Selected Endpoint Measurements
Secondary Endpoints Std Dev
of the Baseline Score
Detectable Difference for 80 Power
Std Dev of the Change Score
Difference Detectable for
80 Power
DLCOpred 166 58 91 32
6MWT Area Under the Desaturation Curve
219 76 175 61
6MWT Distance to Desaturation 224 78 315 110
6MWT Minutes Walked 210 073 205 071
Abbreviations Std Dev standard deviation DLCOpred diffusing capacity of the lung for carbon monoxide percent predicted 6MWT 6-minute walk test
61
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
10 Study Administration
101 Cooperative Agreement Mechanism
The administrative and funding mechanism used to undertake this project is a ldquocooperative
agreementrdquo (U01) which is an assistance mechanism Under the cooperative agreement the
NHLBI assists supports andor stimulates the project and is substantially involved with
investigators in conducting the study by facilitating performance of the effort in a ldquopartnerrdquo role
The NHLBI project scientist serves on the IPFnet Steering Group and he or another NHLBI
scientist may serve on other project committees when appropriate At the same time however
NHLBI does not assume a dominant role direction or prime responsibility for this research
program
As described below governance of the project is conducted through the IPFnet Steering Group
Principal investigators have lead responsibilities in all aspects of their trials and the project
including any modification of trial designs conduct of the trials quality control data analysis
and interpretation preparation of publications and collaboration with other investigators unless
otherwise provided for by the IPFnet Steering Group
PIs retain custody of and have primary rights to their center-specific and collaborative data
subject to government rights-of-access consistent with current Health amp Human Services (HHS)
Public Health Service (PHS) and National Institutes of Health policies The protocols and
governance policies call for the continual submission of data centrally to the IPFnet DCC for the
collaborative database which at a minimum will contain the key variables selected by the IPFnet
Steering Group for standardization across all clinical centers the submission of copies of the
collaborative datasets to each PI upon completion of the project procedures for data analysis
reporting and publication and procedures to protect and ensure the privacy of medical and
genetic data and records of individuals The NHLBI project scientist on behalf of the NHLBI
will have the same access privileges and responsibilities regarding the collaborative data as the
other members of the Steering Group
62
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
PIs are also encouraged to publish and to publicly release and disseminate results data and other
products of the project concordant with the project protocols and governance and the approved
plan for making data and materials available to the scientific community and to the NHLBI
However during the 3 years after the ending date of NHLBI project support unpublished data
unpublished results data sets not previously released and other study materials or products are
to be made available to any third party only with the approval of the IPFnet Steering Group
Upon completion of the project PIs are expected to put their intervention materials and
procedure manuals into the public domain andor make them available to other investigators
according to the approved plan for making data and materials available to the scientific
community and the NHLBI for the conduct of research at no charge other than the costs of
reproduction and distribution
The NHLBI reserves the right to terminate or curtail the project (or an individual award) in the
event of (a) failure to develop or implement mutually agreeable collaborative measurement
subject eligibility and data management sections of the protocols (b) substantial shortfall in
subject recruitment follow-up data reporting or quality control or other major breach of
protocol (c) substantive changes in the agreed-upon protocols with which NHLBI cannot
concur (d) reaching a major project outcome with persuasive statistical significance
substantially before schedule or (e) human subject ethical issues that may dictate a premature
termination
Any disagreement that may arise in scientificprogrammatic matters (within the scope of the
award) between award recipients and the NHLBI may be brought to arbitration An arbitration
panel will be composed of 3 membersmdash1 selected by the IPFnet Steering Group (with the
NHLBI member not voting) or by the individual PI in the event of an individual disagreement a
second selected by NHLBI and the third selected by the other 2 members This special
arbitration procedure in no way affects the PIrsquos right to appeal an adverse action that is otherwise
appealable in accordance with the PHS regulations at 42 CFR part 50 Subpart D and HHS
63
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
regulation at 45 CFR part 16 or the rights of the NHLBI under applicable statutes regulations
and terms of the award
102 IPFnet Steering Group
The IPFnet Steering Group is the main governing body of the project It is composed of the PIs
of the clinical centers the PI of the DCC and the NHLBI project scientist The clinical centers
the IPFnet DCC and the NHLBI each have 1 vote on the IPFnet Steering Group All decisions
are determined by majority vote
All major scientific decisions are determined by the IPFnet Steering Group It assumes overall
responsibility for the design and conduct of the trial It appoints (and disbands) committees and
subcommittees as the need arises designs approves and implements the study protocols
oversees the development of the MOOP monitors subject recruitment and treatment delivery
evaluates data collection and management oversees quality assurance procedures and
implements changes and enhancements to the study as required It also has primary responsibility
for facilitating the conduct of the trials and reporting the projectrsquos results
103 Data and Safety Monitoring Board
The NHLBI will establish a DSMB in accordance with established policies (see
httpwwwnhlbinihgovfundingpoliciesdsmb_insthtm) to ensure data quality and subject
safety and to provide independent advice to the NHLBI regarding progress and the
appropriateness of study continuation
104 Recommendations on Interim Monitoring of Efficacy Safety and Futility
First and foremost the role of the DSMB will be to review subject safety and trial conduct at
periodic points during the study The DSMB may require analyses of the primary endpoint
results for comparing the benefit and risks of treatment strategies The benefit of collecting
additional data on key secondary endpoints with extended follow-up and establishing a robust
64
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
evidence base for determining a standard of care will need to be carefully considered before
early termination of one or more treatment arms After careful consideration the IPFnet Steering
Group recommends conservative thresholds for the early examinations of the safety and efficacy
data
The DSMB will be expected to meet approximately every 6 months until trial completion to
review safety and toxicity data The DSMB may recommend stopping the study based on these
reviews Because the DSMB could stop the trial for safety concerns as well as for a large
efficacy benefit there could be multiple opportunities to reject the null hypothesis (no difference
in event rates between the PL and NAC groups) A Bonferroni approximation will be applied
during the one planned interim analysis for efficacy
Before locking the database a statistical analysis plan (SAP) will be developed to provide
complete details on the statistical analysis The SAP will include the specifics for how and when
the DSMB will be notified for AEs The IPFnet DCC will deliver to the DSMB all FDA-defined
AEs at 3-month intervals The IPFnet DCC will prepare narrative SAE reports in real time for
DSMB review including recommendations and analysis of similar events for each SAE
submitted to the FDA
65
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
11 Investigator and Sponsor Obligations
111 Monitoring
All monitoring activities for US clinical centers will be performed in accordance with DCRI
standard operating procedures Information regarding the types of visits will be outlined in the
PANTHER-IPF MOOP
112 Cost and Payment
There will be no cost to subjects enrolled in this trial Study-related procedures will be paid for
by the IPFnet
Subjects may be eligible for reimbursement for travel to the clinical center Details of payment
will be explained to each subject during the consent process
113 Confidentiality and Health Insurance Portability and Accountability Act
Considerations
Subject confidentiality will be protected throughout the study All subject data will be kept
strictly confidential and no subject-identifying information will be released to anyone outside
the project Confidentiality will be assured through several mechanisms First each subject will
be assigned an anonymous study ID which will then be used on all study forms Second any
study forms blood samples and paper records that contain subject information (eg address lists
phone lists) will be kept at the clinical centers in secured locked areas coded by number Once
blood is collected there will be no subject identifiers placed on blood samplesmdashonly the study
ID number and the date of sample collection Third access to all subject data and information
including laboratory specimens will be restricted to authorized personnel In the case of
computerized data this restricted access will be assured through user logon IDs and password
protection
66
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
At the IPFnet DCC only authorized personnel will have access to the data files containing study
data Security will be assured through user logon IDs passwords and appropriate access
privileges All study subjects will be identified only by their IPFnet ID numbers and no personal
identifying information such as name address or Social Security number will be entered into
the IPFnet DCC database Any subject-specific data reported to the IPFnet Steering Group will
be identified only by the IPFnet ID number
Finally subjects will not be identified by name in any reports or publications nor will the data
be presented in such a way that the identity of individual subjects can be inferred Analysis files
created for further study by the scientific community will have no subject identifiers These data
files will be created in accordance with the Ancillary Studies and Publication Policy of the
IPFnet
114 Informed Consent Procedures
All IPFnet subjects will provide written informed consent using procedures reviewed and
approved by each clinical centerrsquos IRB Informed consent will be undertaken by study personnel
in-person with the subject The subject has the option of declining further participation in the
study at that point No further study procedures will be conducted until the signed documents
have been provided to the IPFnet clinical center
115 Institutional Review Boards
Before initiating this study the protocol clinical center-specific informed consent forms Health
Insurance Portability and Accountability Act (HIPAA) forms recruitment materials and other
relevant information will be reviewed by a properly constituted IRB at each participating clinical
center A copy of the signed and dated IRB approval at each clinical center will be retrieved prior
to or during the site initiation visit and archived at the IPFnet DCC Any amendments to the
protocol other than simple administrative and typographical changes must be approved by each
IRB before they are implemented The clinical centers will seek annual renewals of their IRB
approvals in accordance with local procedures
67
__________________________________________ ________________
__________________________________________
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
12 Investigator Agreement
I have read the foregoing protocol PANTHER-IPF and agree that it contains all necessary
details for carrying out this study I will conduct the study as outlined herein and will complete
the study within the time designated
I will provide copies of the protocol and all pertinent information to all individuals responsible to
me who assist in the conduct of this study I will discuss this material with them to ensure they
are fully informed regarding the drug and the conduct of the study
I will fulfill all responsibilities for submitting pertinent information to the local IRB if
applicable that is responsible for this study
I further agree that NHLBI andor DCRI will have access to any source documents from which
eCRF information may have been generated
Signature of Principal Investigator Date
Name of Principal Investigator (printed or typed)
Protocol version date May 19 2009
Protocol Amendment 1 version date May 28 2010
Protocol Amendment 2 version date December 6 2011
68
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
13 References
1 Raghu G Brown KK Bradford WZ et al A placebo-controlled trial of interferon gamma-1b in patients with idiopathic pulmonary fibrosis N Engl J Med 2004350125-33 2 King TE Jr Safrin S Starko KM et al Analyses of efficacy end points in a controlled trial of interferon-gamma1b for idiopathic pulmonary fibrosis Chest 2005127171-7 3 Flaherty KR Thwaite EL Kazerooni EA et al Radiological versus histological diagnosis in UIP and NSIP survival implications Thorax 200358143-8 4 Wells AU Desai SR Rubens MB et al Idiopathic pulmonary fibrosis a composite physiologic index derived from disease extent observed by computed tomography Am J Respir Crit Care Med 2003167962-9 5 Raghu G Freudenberger TD Yang S et al High prevalence of abnormal acid gastroshyoesophageal reflux in idiopathic pulmonary fibrosis Eur Respir J 200627136-42 6 Kinnula VL Focus on antioxidant enzymes and antioxidant strategies in smoking related airway diseases Thorax 200560693-700 7 Coultas DB Zumwalt RE Black WC Sobonya RE The epidemiology of interstitial lung diseases Am J Respir Crit Care Med 1994150967-72 8 Raghu G Weycker D Edelsberg J Bradford WZ Oster G Incidence and prevalence of idiopathic pulmonary fibrosis Am J Respir Crit Care Med 2006174810-6 9 Olson AL Swigris JJ Lezotte DC Norris JM Wilson CG Brown KK Mortality from pulmonary fibrosis increased in the United States from 1992 to 2003 Am J Respir Crit Care Med 2007176277-84 10 Mannino DM Etzel RA Parrish RG Pulmonary fibrosis deaths in the United States 1979shy1991 An analysis of multiple-cause mortality data Am J Respir Crit Care Med 19961531548shy52 11 Hubbard R Johnston I Coultas DB Britton J Mortality rates from cryptogenic fibrosing alveolitis in seven countries Thorax 199651711-6 12 Johnston I Britton J Kinnear W Logan R Rising mortality from cryptogenic fibrosing alveolitis Bmj 19903011017-21 13 Raghu G Collard HR Egan JJ et al An official ATSERSJRSALAT statement idiopathic pulmonary fibrosis evidence-based guidelines for diagnosis and management Am J Respir Crit Care Med 2011183788-824 14 (USA) FDA FDA Public Health Advisory Interferon gamma-1b (marketed as Actimmune) In 2007 15 King TE Jr Pardo A Selman M Idiopathic pulmonary fibrosis Lancet 2011 16 Raghu G Brown KK Costabel U et al Treatment of idiopathic pulmonary fibrosis with etanercept an exploratory placebo-controlled trial Am J Respir Crit Care Med 2008178948shy55 17 Malouf MA Hopkins P Snell G Glanville AR An investigator-driven study of everolimus in surgical lung biopsy confirmed idiopathic pulmonary fibrosis Respirology 201116776-83 18 King TE Jr Behr J Brown KK et al BUILD-1 a randomized placebo-controlled trial of bosentan in idiopathic pulmonary fibrosis Am J Respir Crit Care Med 200817775-81 19 Richeldi L Costabel U Selman M et al Efficacy of a tyrosine kinase inhibitor in idiopathic pulmonary fibrosis N Engl J Med 20113651079-87
69
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
20 Borok Z Buhl R Grimes GJ et al Effect of glutathione aerosol on oxidant-antioxidant imbalance in idiopathic pulmonary fibrosis Lancet 1991338215-6 21 Meyer A Buhl R Magnussen H The effect of oral N-acetylcysteine on lung glutathione levels in idiopathic pulmonary fibrosis Eur Respir J 19947431-6 22 Behr J Maier K Degenkolb B Krombach F Vogelmeier C Antioxidative and clinical effects of high-dose N-acetylcysteine in fibrosing alveolitis Adjunctive therapy to maintenance immunosuppression Am J Respir Crit Care Med 19971561897-901 23 Cantin AM North SL Fells GA Hubbard RC Crystal RG Oxidant-mediated epithelial cell injury in idiopathic pulmonary fibrosis J Clin Invest 1987791665-73 24 Waghray M Cui Z Horowitz JC et al Hydrogen peroxide is a diffusible paracrine signal for the induction of epithelial cell death by activated myofibroblasts Faseb J 200519854-6 25 Larios JM Budhiraja R Fanburg BL Thannickal VJ Oxidative protein cross-linking reactions involving L-tyrosine in transforming growth factor-beta1-stimulated fibroblasts J Biol Chem 200127617437-41 26 Kinnula VL Fattman CL Tan RJ Oury TD Oxidative stress in pulmonary fibrosis a possible role for redox modulatory therapy Am J Respir Crit Care Med 2005172417-22 27 Meyer A Buhl R Kampf S Magnussen H Intravenous N-acetylcysteine and lung glutathione of patients with pulmonary fibrosis and normals Am J Respir Crit Care Med 19951521055-60 28 Behr J Degenkolb B Krombach F Vogelmeier C Intracellular glutathione and bronchoalveolar cells in fibrosing alveolitis effects of N-acetylcysteine Eur Respir J 200219906-11 29 Bando M Hosono T Mato N et al Long-term efficacy of inhaled N-acetylcysteine in patients with idiopathic pulmonary fibrosis Intern Med 2010492289-96 30 Demedts M Behr J Buhl R et al High-dose acetylcysteine in idiopathic pulmonary fibrosis N Engl J Med 20053532229-42 31 Toma TP Bhowmik A Rajakulasingam R Acetylcysteine in pulmonary fibrosis N Engl J Med 20063541086-9 author reply -9 32 Hunninghake GW Antioxidant therapy for idiopathic pulmonary fibrosis N Engl J Med 20053532285-7 33 Flaherty KR Mumford JA Murray S et al Prognostic implications of physiologic and radiographic changes in idiopathic interstitial pneumonia Am J Respir Crit Care Med 2003168543-8 34 Latsi PI du Bois RM Nicholson AG et al Fibrotic idiopathic interstitial pneumonia the prognostic value of longitudinal functional trends Am J Respir Crit Care Med 2003168531-7 35 Collard HR King TE Jr Bartelson BB Vourlekis JS Schwarz MI Brown KK Changes in clinical and physiologic variables predict survival in idiopathic pulmonary fibrosis Am J Respir Crit Care Med 2003168538-42 36 Jegal Y Kim DS Shim TS et al Physiology is a stronger predictor of survival than pathology in fibrotic interstitial pneumonia Am J Respir Crit Care Med 2005171639-44 37 Martinez FJ Safrin S Weycker D et al The clinical course of patients with idiopathic pulmonary fibrosis Ann Intern Med 2005142963-7 38 Hull JH Acetylcysteine in pulmonary fibrosis N Engl J Med 20063541089-91 author reply -91
70
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
39 Flaherty KR King TE Jr Raghu G et al Idiopathic interstitial pneumonia what is the effect of a multidisciplinary approach to diagnosis Am J Respir Crit Care Med 2004170904shy10 40 Raghu G Johnson WC Lockhart D Mageto Y Treatment of idiopathic pulmonary fibrosis with a new antifibrotic agent pirfenidone results of a prospective open-label Phase II study Am J Respir Crit Care Med 19991591061-9 41 Hunninghake GW Lynch DA Galvin JR et al Radiologic findings are strongly associated with a pathologic diagnosis of usual interstitial pneumonia Chest 20031241215-23 42 Lynch D Godwin J Safrin S et al High-resolution computed tomography in idiopathic pulmonary fibrosis diagnosis and prognosis Am J Respir Crit Care Med 2005172488-93 43 Mallinckrodt CH Watkin JG Molenberghs G Carroll RJ Choice of the primary analysis in longitudinal clinical trials Pharmaceutical Statistics 20043161-9 44 Bang H Tsiatis A Estimating medical costs with censored data Biometrika 200087329shy43 45 Lin DY Regression analysis of incomplete medical cost data Stat Med 2003221181-200 46 Rochon J Application of GEE procedures for sample size calculations in repeated measures experiments Stat Med 1998171643-58 47 Lachin JM Foulkes MA Evaluation of sample size and power for analyses of survival with allowance for nonuniform patient entry losses to follow-up noncompliance and stratification Biometrics 198642507-19
71
- PANTHER-IPFPREDNISONE AZATHIOPRINEAND N-ACETYLCYSTEINEA STUDY THAT EVALUATES RESPONSE INIDIOPATHIC PULMONARY FIBROSIS
-
- Protocol Summary
- Table of Contents
- List of Tables
- List of Figures
- List of Abbreviations
- 1 Summary
- 2 Hypotheses and Specific Aims
-
- 21 Null Hypothesis
- 22 Specific Aim 1
- 23 Specific Aim 2
- 24 Prespecified Subgroups of Interest
-
- 3 Background and Significance
-
- 31 Idiopathic Pulmonary Fibrosis is the Most Common Interstitial Lung Disease
- 32 Rationale for Placebo Control
- 33 Rationale for N-acetylcysteine
- 35 Rationale for N-acetylcysteine as a Stand-alone Therapy
- 36 Rationale for the Study Design and Primary Endpoint
- 37 Rationale for Blinding of Treatments
-
- 4 Methods
-
- 41 Inclusion Criteria
- 42 Diagnosis of IPF
- 43 Exclusion Criteria
- 44 Study Design and Study Visit
- 45 Dose Justification
- 46 Contraindications Precautions and Side Effects of Study Medications
- 47 Recruitment Procedures
- 48 Study Procedures
- 49 Concomitant Medications
- 410 Laboratory Testing
- 411 Blinding of Study Drugs
-
- 5 Study Endpoints
-
- 51 Primary Study Endpoint
- 52 Secondary Study Endpoints
-
- 6 Safety Evaluations and Procedures
-
- 61 Adverse Events
- 62 Clinical Medical Monitoring
- 63 Unblinding Procedures
-
- 7 Study Drug Procedures
- 8 Data Management
-
- 81 Hardware and Software Configuration
- 82 Sources of Data
-
- 9 Study Design and Data Analysis
-
- 91 General Analytic Considerations
- 92 Randomization Blinding and Reporting of Results
- 93 Stratification
- 94 Specification of the Primary Analyses
- 95 Analysis of Longitudinal Endpoints
- 96 Analysis of Binary Time-to-Event and Time-Lagged Endpoints
- 97 Power Analysis
-
- 10 Study Administration
-
- 101 Cooperative Agreement Mechanism
- 102 IPFnet Steering Group
- 103 Data and Safety Monitoring Board
- 104 Recommendations on Interim Monitoring of Efficacy Safety and Futility
-
- 11 Investigator and Sponsor Obligations
-
- 111 Monitoring
- 112 Cost and Payment
- 113 Confidentiality and Health Insurance Portability and Accountability ActConsiderations
- 114 Informed Consent Procedures
- 115 Institutional Review Boards
-
- 12 Investigator Agreement
- 13 References
-

PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
8 Data Management
81 Hardware and Software Configuration
811 Hardware and Database Software
Data will be stored in an Oracle database system Oracle has advantages of processing efficiency
and smooth linkage with other software systems The application and database will be hosted on
Solaris Unix servers at the IPFnet DCC
812 Statistical Software
SAS will be used as the principal application for the management of analysis data files and
statistical computations S-Plus will be used to provide supplementary functions as needed
813 Access Control and Confidentiality Procedures
Access to databases will be controlled centrally by the IPFnet DCC through user passwords
linked to appropriate privileges This protects the data from unauthorized changes and
inadvertent loss or damage
814 Security
Database and Web servers will be secured by a firewall and through controlled physical access
Oracle has many security features to ensure that any staff member accessing the database has the
proper authority to perform the functions he or she requests of the system Within the secondary
SAS databases Unix group-access control maintains similar security The Sun workstation login
is secured by extensive user-password facilities under Unix
54
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
815 Back-up Procedures
Database back-up will be performed automatically every day and standard IPFnet DCC policies
and procedures will be applied to dictate tape rotation and retention practices
816 Virus Protection
All disk drives that provide network services and all user computers will be protected using
virus-scanning software Standard IPFnet DCC policies will be applied to update these protection
systems periodically through the study
82 Sources of Data
821 Design and Development
The IPFnet DCC will be responsible for development of the electronic case report forms
(eCRFs) development and validation of the clinical study database ensuring data integrity and
training clinical center staff on applicable data management procedures A web-based distributed
data entry model will be implemented This system will be developed to ensure that guidelines
and regulations surrounding the use of computerized systems used in clinical trials are upheld
The remainder of this section provides an overview of the data management plan associated with
this protocol
822 Data Collection Forms
The data collection process consists of direct data entry at the study clinical centers into the EDC
system(s) provided by the DCC A data collection worksheet will be provided to clinical centers
for recording data in the event the EDC system is unavailable Data entry of the eCRFs should
be completed according to the instructions provided and project specific training The
investigator is responsible for maintaining accurate complete and up-to-date records and for
ensuring the completion of the eCRFs for each research participant
55
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
823 Data Acquisition and Entry
Data entry into eCRFs shall be performed by authorized individuals Selected eCRFs may also
require the investigatorrsquos written signature or electronic signature as appropriate Electronic
CRFs will be monitored for completeness accuracy and attention to detail during the study
824 Data Center Responsibilities
The IPFnet DCC will 1) develop a data management plan and will conduct data management
activities 2) provide final eCRFs for the collection of all data required by the study 3) develop
data dictionaries for each eCRF that will comprehensively define each data element 4) conduct
ongoing data monitoring activities on study data 5) monitor any preliminary analysis data
cleanup activities and 6) rigorously monitor final study data clean up
825 Data Editing
Completed data will be entered into the IPFnet DCC automated data acquisition and
management system If incomplete or inaccurate data are found a data clarification request will
be generated and distributed to clinical centers for a response Clinical centers will resolve data
inconsistencies and errors and enter all corrections and changes into the IPFnet DCC automated
data acquisition and management system
826 Training
The training plan for clinical center staff includes provisions for training on assessments eCRF
completion guidelines data management procedures and the use of computerized systems
56
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
9 Study Design and Data Analysis
91 General Analytic Considerations
All primary analyses will be based on intent-to-treat (ITT) principles using all randomized
subjects Baseline factors across groups will be compared using mean (standard deviation) and
median (25th and 75th percentiles) summary measures Kaplan-Meier curves will be used to
display event rates Due to clinical interest in departures from both sides of the null hypothesis
all test statistics will be 2-sided
Reasonable caution needs to be taken when conducting multiple analyses on key clinical
subgroups For subgroup analyses a conservative significance level of 0001 will be used for all
interaction tests Thus subgroup comparisons will be considered exploratory unless the p-value
from the interaction test is smaller than 0001
92 Randomization Blinding and Reporting of Results
A permuted block-randomization scheme will be created with varying block sizes stratified by
clinical center Once a subject has completed the screening and baseline period and evaluation
for inclusionexclusion criteria the randomization process will begin Subjects will be
randomized to receive NAC or matching placebo with equal probability (11) via telephone
contact with a central interactive voice response system (IVRS) using a toll-free randomization
number On the day of randomization after the subject has successfully met all inclusion and
exclusion criteria the investigator or designee will call the central randomization number to
obtain the assigned kit randomization numbers for that subject At each subject visit the
investigator or designee will call the central randomization number to obtain the new kit
randomization numbers for resupply of the subject For resupply of the clinical center the IVRS
will monitor minimal volume of a kit type andor expiration date and will automatically notify
the pharmacy
57
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
The trial results will be reported according to guidelines specified in the CONSORT statement
A flow diagram describing screening recruitment randomization dropout and vital status will
be included in the primary manuscript AEs and efficacy data will be presented for all treatment
groups Adherence dropout and lost to follow-up will be carefully examined across all treatment
groups Analyses of safety will be based on data from all randomized subjects who received at
least one dose of study drug
93 Stratification
Subjects will be distributed to the two treatment arms in a 11 allocation ratio Stratification
blocks will be based on clinical centers
94 Specification of the Primary Analyses
A mixed model repeated measures (MMRM) analysis described in section 95 will be used to
compare differences in the slope of FVC measurements across the treatment groups Response
variables are values of the FVC measured at baseline and every 15 weeks until study completion
Variables in the model will include treatment time and time by treatment age sex race and
height Contrast estimates of differences in slopes of treatment over time (along with confidence
intervals) will be used to estimate the treatment effect The validity of this model in terms of
meeting modeling assumptions will be assessed via standard modeling diagnostics and goodness-
of-fit measures Based on the MMRM framework missing FVC data will not be imputed for the
primary analysis
95 Analysis of Longitudinal Endpoints
A common goal in clinical trials is to specify models that are easily implemented and
reproducible by independent data analysts On the other hand the models should have proper
statistical behavior in terms of low bias and high precision Many common approaches to
longitudinal data analysis including last observation carried forward (LOCF) imputation rely on
the missing completely at random (MCAR) assumption However the MCAR assumption is
58
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
unlikely to hold in many clinical trials because missing data are often related to disease
progression and prognosis A more reasonable assumption missing at random (MAR) specifies
that the complete data distribution can be modeled using only the observed data The likelihood-
based MMRM approach is valid under the more general MAR assumptions These models will
be applied to analyze the longitudinal data secondary endpoints
The advantages of MMRM analysis are that all important characteristics of the model can be preshy
specified standard software can be used to implement the models and results are based on ITT
principles43 In addition the MMRM approach offers superior control of Type I and Type II
errors compared with the LOCF approach
Response variables are values of the PFTs measured at enrollment and every 15 weeks until
study completion and 6MWT values measured at baseline week 30 and week 60 Covariates are
treatment time time by treatment and key baseline risk factors Contrasts (along with
confidence intervals) of treatment by time will be used to estimate the treatment effect
The correlation structure involves multiple pieces including measurement errors random
variation and interindividual variability For the longitudinal data analyses an unstructured
correlation matrix for within-subject errors will be assumed Other correlation structures
including compound symmetry will be examined as needed A careful examination of reasons
for study discontinuation will be conducted to assess the validity of MCAR Sensitivity analyses
will be used to examine the untestable assumption that the observed data violate the MAR
assumption The MMRM models will be implemented using PROC MIXED in SAS
96 Analysis of Binary Time-to-Event and Time-Lagged Endpoints
Regression modeling approaches using either the logistic regression model or Cox proportional
hazards regression model will be employed when appropriate The validity of these models will
be assessed via standard modeling diagnostics and goodness-of-fit measures Estimates of
cumulative frequencies for more general time-lagged responses will be calculated using the
partitioned version of the Bang-Tsiatis estimator44 The partitions will be set at 15-week intervals
59
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
to correspond with the data-collection process Covariate adjusted event rates will be calculated
using inverse probability-weighted regression estimates45
97 Power Analysis
971 Primary Analyses
Based on previously published IPF clinical trials the PL group is expected to experience a drop
in FVC of approximately 020 L over the study period (see Figure 1) The IPFnet Steering Group
determined a clinically important difference would be to preserve the majority of the decline
relative to PL over the study period In particular a treatment effect of 015 L was determined to
be a clinically meaningful difference Potential dropout is a key factor in the proposed study The
drop-out process assumed 5 lost to follow-up after every study visit Only 80 of subjects
were assumed to be followed for the entire study period All models assumed a compound
symmetry structure for the covariance matrix Power calculations were performed using a SAS
IML program for designing repeated measures studies46 Based on preliminary reviews of the
data from the University of Michigan the covariance matrix parameters were estimated at
approximately σ2 = 0757 (variance parameter) and ρ = 0936 (correlation parameter) To be
conservative the power calculations for the primary analysis were performed with parameter
setting of σ2 = 0810 (variance parameter) and ρ = 0925 (correlation parameter)
The power calculations assume a correction for imperfect compliance proposed by Lachin and
Foulkes to allow for 2 noncompliance for each of the treatment arms47 Thus the sample size
of 130 subjects per arm would be reduced to an adjusted sample size of 130(1-002-002)2 =
1198 or 120 subjects per arm
Under the assumed Type I error rate of 005 with a correlation parameter of 0925 and standard
deviation of 090 the difference of 015 L (or 00025 Lweek) shown in Table 6 would have
power of 93
60
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Table 6 Hypothetical Values of Mean FVC (L) Change from Baseline
Week 15 Week 30 Week 45 Week 60
NAC 00125 00250 00375 00500
Placebo 00500 01000 01500 02000
Difference 00375 00750 01125 01500
Abbreviations FVC forced vital capacity PL placebo
972 Power Analysis for Secondary Endpoints
Power calculations for secondary endpoint measurements are shown in Table 7 Standard
deviations are based on unpublished data provided by the University of Michigan The
calculations are based on a 2-sample t-test with Type I error rate set at 005 These calculations
are likely to be conservative because the statistical approach described in section 95 for
analyzing these endpoints will incorporate incomplete observations as well as intermediate data
points
Table 7 Detectable Differences in Treatment Means for Selected Endpoint Measurements
Secondary Endpoints Std Dev
of the Baseline Score
Detectable Difference for 80 Power
Std Dev of the Change Score
Difference Detectable for
80 Power
DLCOpred 166 58 91 32
6MWT Area Under the Desaturation Curve
219 76 175 61
6MWT Distance to Desaturation 224 78 315 110
6MWT Minutes Walked 210 073 205 071
Abbreviations Std Dev standard deviation DLCOpred diffusing capacity of the lung for carbon monoxide percent predicted 6MWT 6-minute walk test
61
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
10 Study Administration
101 Cooperative Agreement Mechanism
The administrative and funding mechanism used to undertake this project is a ldquocooperative
agreementrdquo (U01) which is an assistance mechanism Under the cooperative agreement the
NHLBI assists supports andor stimulates the project and is substantially involved with
investigators in conducting the study by facilitating performance of the effort in a ldquopartnerrdquo role
The NHLBI project scientist serves on the IPFnet Steering Group and he or another NHLBI
scientist may serve on other project committees when appropriate At the same time however
NHLBI does not assume a dominant role direction or prime responsibility for this research
program
As described below governance of the project is conducted through the IPFnet Steering Group
Principal investigators have lead responsibilities in all aspects of their trials and the project
including any modification of trial designs conduct of the trials quality control data analysis
and interpretation preparation of publications and collaboration with other investigators unless
otherwise provided for by the IPFnet Steering Group
PIs retain custody of and have primary rights to their center-specific and collaborative data
subject to government rights-of-access consistent with current Health amp Human Services (HHS)
Public Health Service (PHS) and National Institutes of Health policies The protocols and
governance policies call for the continual submission of data centrally to the IPFnet DCC for the
collaborative database which at a minimum will contain the key variables selected by the IPFnet
Steering Group for standardization across all clinical centers the submission of copies of the
collaborative datasets to each PI upon completion of the project procedures for data analysis
reporting and publication and procedures to protect and ensure the privacy of medical and
genetic data and records of individuals The NHLBI project scientist on behalf of the NHLBI
will have the same access privileges and responsibilities regarding the collaborative data as the
other members of the Steering Group
62
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
PIs are also encouraged to publish and to publicly release and disseminate results data and other
products of the project concordant with the project protocols and governance and the approved
plan for making data and materials available to the scientific community and to the NHLBI
However during the 3 years after the ending date of NHLBI project support unpublished data
unpublished results data sets not previously released and other study materials or products are
to be made available to any third party only with the approval of the IPFnet Steering Group
Upon completion of the project PIs are expected to put their intervention materials and
procedure manuals into the public domain andor make them available to other investigators
according to the approved plan for making data and materials available to the scientific
community and the NHLBI for the conduct of research at no charge other than the costs of
reproduction and distribution
The NHLBI reserves the right to terminate or curtail the project (or an individual award) in the
event of (a) failure to develop or implement mutually agreeable collaborative measurement
subject eligibility and data management sections of the protocols (b) substantial shortfall in
subject recruitment follow-up data reporting or quality control or other major breach of
protocol (c) substantive changes in the agreed-upon protocols with which NHLBI cannot
concur (d) reaching a major project outcome with persuasive statistical significance
substantially before schedule or (e) human subject ethical issues that may dictate a premature
termination
Any disagreement that may arise in scientificprogrammatic matters (within the scope of the
award) between award recipients and the NHLBI may be brought to arbitration An arbitration
panel will be composed of 3 membersmdash1 selected by the IPFnet Steering Group (with the
NHLBI member not voting) or by the individual PI in the event of an individual disagreement a
second selected by NHLBI and the third selected by the other 2 members This special
arbitration procedure in no way affects the PIrsquos right to appeal an adverse action that is otherwise
appealable in accordance with the PHS regulations at 42 CFR part 50 Subpart D and HHS
63
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
regulation at 45 CFR part 16 or the rights of the NHLBI under applicable statutes regulations
and terms of the award
102 IPFnet Steering Group
The IPFnet Steering Group is the main governing body of the project It is composed of the PIs
of the clinical centers the PI of the DCC and the NHLBI project scientist The clinical centers
the IPFnet DCC and the NHLBI each have 1 vote on the IPFnet Steering Group All decisions
are determined by majority vote
All major scientific decisions are determined by the IPFnet Steering Group It assumes overall
responsibility for the design and conduct of the trial It appoints (and disbands) committees and
subcommittees as the need arises designs approves and implements the study protocols
oversees the development of the MOOP monitors subject recruitment and treatment delivery
evaluates data collection and management oversees quality assurance procedures and
implements changes and enhancements to the study as required It also has primary responsibility
for facilitating the conduct of the trials and reporting the projectrsquos results
103 Data and Safety Monitoring Board
The NHLBI will establish a DSMB in accordance with established policies (see
httpwwwnhlbinihgovfundingpoliciesdsmb_insthtm) to ensure data quality and subject
safety and to provide independent advice to the NHLBI regarding progress and the
appropriateness of study continuation
104 Recommendations on Interim Monitoring of Efficacy Safety and Futility
First and foremost the role of the DSMB will be to review subject safety and trial conduct at
periodic points during the study The DSMB may require analyses of the primary endpoint
results for comparing the benefit and risks of treatment strategies The benefit of collecting
additional data on key secondary endpoints with extended follow-up and establishing a robust
64
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
evidence base for determining a standard of care will need to be carefully considered before
early termination of one or more treatment arms After careful consideration the IPFnet Steering
Group recommends conservative thresholds for the early examinations of the safety and efficacy
data
The DSMB will be expected to meet approximately every 6 months until trial completion to
review safety and toxicity data The DSMB may recommend stopping the study based on these
reviews Because the DSMB could stop the trial for safety concerns as well as for a large
efficacy benefit there could be multiple opportunities to reject the null hypothesis (no difference
in event rates between the PL and NAC groups) A Bonferroni approximation will be applied
during the one planned interim analysis for efficacy
Before locking the database a statistical analysis plan (SAP) will be developed to provide
complete details on the statistical analysis The SAP will include the specifics for how and when
the DSMB will be notified for AEs The IPFnet DCC will deliver to the DSMB all FDA-defined
AEs at 3-month intervals The IPFnet DCC will prepare narrative SAE reports in real time for
DSMB review including recommendations and analysis of similar events for each SAE
submitted to the FDA
65
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
11 Investigator and Sponsor Obligations
111 Monitoring
All monitoring activities for US clinical centers will be performed in accordance with DCRI
standard operating procedures Information regarding the types of visits will be outlined in the
PANTHER-IPF MOOP
112 Cost and Payment
There will be no cost to subjects enrolled in this trial Study-related procedures will be paid for
by the IPFnet
Subjects may be eligible for reimbursement for travel to the clinical center Details of payment
will be explained to each subject during the consent process
113 Confidentiality and Health Insurance Portability and Accountability Act
Considerations
Subject confidentiality will be protected throughout the study All subject data will be kept
strictly confidential and no subject-identifying information will be released to anyone outside
the project Confidentiality will be assured through several mechanisms First each subject will
be assigned an anonymous study ID which will then be used on all study forms Second any
study forms blood samples and paper records that contain subject information (eg address lists
phone lists) will be kept at the clinical centers in secured locked areas coded by number Once
blood is collected there will be no subject identifiers placed on blood samplesmdashonly the study
ID number and the date of sample collection Third access to all subject data and information
including laboratory specimens will be restricted to authorized personnel In the case of
computerized data this restricted access will be assured through user logon IDs and password
protection
66
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
At the IPFnet DCC only authorized personnel will have access to the data files containing study
data Security will be assured through user logon IDs passwords and appropriate access
privileges All study subjects will be identified only by their IPFnet ID numbers and no personal
identifying information such as name address or Social Security number will be entered into
the IPFnet DCC database Any subject-specific data reported to the IPFnet Steering Group will
be identified only by the IPFnet ID number
Finally subjects will not be identified by name in any reports or publications nor will the data
be presented in such a way that the identity of individual subjects can be inferred Analysis files
created for further study by the scientific community will have no subject identifiers These data
files will be created in accordance with the Ancillary Studies and Publication Policy of the
IPFnet
114 Informed Consent Procedures
All IPFnet subjects will provide written informed consent using procedures reviewed and
approved by each clinical centerrsquos IRB Informed consent will be undertaken by study personnel
in-person with the subject The subject has the option of declining further participation in the
study at that point No further study procedures will be conducted until the signed documents
have been provided to the IPFnet clinical center
115 Institutional Review Boards
Before initiating this study the protocol clinical center-specific informed consent forms Health
Insurance Portability and Accountability Act (HIPAA) forms recruitment materials and other
relevant information will be reviewed by a properly constituted IRB at each participating clinical
center A copy of the signed and dated IRB approval at each clinical center will be retrieved prior
to or during the site initiation visit and archived at the IPFnet DCC Any amendments to the
protocol other than simple administrative and typographical changes must be approved by each
IRB before they are implemented The clinical centers will seek annual renewals of their IRB
approvals in accordance with local procedures
67
__________________________________________ ________________
__________________________________________
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
12 Investigator Agreement
I have read the foregoing protocol PANTHER-IPF and agree that it contains all necessary
details for carrying out this study I will conduct the study as outlined herein and will complete
the study within the time designated
I will provide copies of the protocol and all pertinent information to all individuals responsible to
me who assist in the conduct of this study I will discuss this material with them to ensure they
are fully informed regarding the drug and the conduct of the study
I will fulfill all responsibilities for submitting pertinent information to the local IRB if
applicable that is responsible for this study
I further agree that NHLBI andor DCRI will have access to any source documents from which
eCRF information may have been generated
Signature of Principal Investigator Date
Name of Principal Investigator (printed or typed)
Protocol version date May 19 2009
Protocol Amendment 1 version date May 28 2010
Protocol Amendment 2 version date December 6 2011
68
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
13 References
1 Raghu G Brown KK Bradford WZ et al A placebo-controlled trial of interferon gamma-1b in patients with idiopathic pulmonary fibrosis N Engl J Med 2004350125-33 2 King TE Jr Safrin S Starko KM et al Analyses of efficacy end points in a controlled trial of interferon-gamma1b for idiopathic pulmonary fibrosis Chest 2005127171-7 3 Flaherty KR Thwaite EL Kazerooni EA et al Radiological versus histological diagnosis in UIP and NSIP survival implications Thorax 200358143-8 4 Wells AU Desai SR Rubens MB et al Idiopathic pulmonary fibrosis a composite physiologic index derived from disease extent observed by computed tomography Am J Respir Crit Care Med 2003167962-9 5 Raghu G Freudenberger TD Yang S et al High prevalence of abnormal acid gastroshyoesophageal reflux in idiopathic pulmonary fibrosis Eur Respir J 200627136-42 6 Kinnula VL Focus on antioxidant enzymes and antioxidant strategies in smoking related airway diseases Thorax 200560693-700 7 Coultas DB Zumwalt RE Black WC Sobonya RE The epidemiology of interstitial lung diseases Am J Respir Crit Care Med 1994150967-72 8 Raghu G Weycker D Edelsberg J Bradford WZ Oster G Incidence and prevalence of idiopathic pulmonary fibrosis Am J Respir Crit Care Med 2006174810-6 9 Olson AL Swigris JJ Lezotte DC Norris JM Wilson CG Brown KK Mortality from pulmonary fibrosis increased in the United States from 1992 to 2003 Am J Respir Crit Care Med 2007176277-84 10 Mannino DM Etzel RA Parrish RG Pulmonary fibrosis deaths in the United States 1979shy1991 An analysis of multiple-cause mortality data Am J Respir Crit Care Med 19961531548shy52 11 Hubbard R Johnston I Coultas DB Britton J Mortality rates from cryptogenic fibrosing alveolitis in seven countries Thorax 199651711-6 12 Johnston I Britton J Kinnear W Logan R Rising mortality from cryptogenic fibrosing alveolitis Bmj 19903011017-21 13 Raghu G Collard HR Egan JJ et al An official ATSERSJRSALAT statement idiopathic pulmonary fibrosis evidence-based guidelines for diagnosis and management Am J Respir Crit Care Med 2011183788-824 14 (USA) FDA FDA Public Health Advisory Interferon gamma-1b (marketed as Actimmune) In 2007 15 King TE Jr Pardo A Selman M Idiopathic pulmonary fibrosis Lancet 2011 16 Raghu G Brown KK Costabel U et al Treatment of idiopathic pulmonary fibrosis with etanercept an exploratory placebo-controlled trial Am J Respir Crit Care Med 2008178948shy55 17 Malouf MA Hopkins P Snell G Glanville AR An investigator-driven study of everolimus in surgical lung biopsy confirmed idiopathic pulmonary fibrosis Respirology 201116776-83 18 King TE Jr Behr J Brown KK et al BUILD-1 a randomized placebo-controlled trial of bosentan in idiopathic pulmonary fibrosis Am J Respir Crit Care Med 200817775-81 19 Richeldi L Costabel U Selman M et al Efficacy of a tyrosine kinase inhibitor in idiopathic pulmonary fibrosis N Engl J Med 20113651079-87
69
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
20 Borok Z Buhl R Grimes GJ et al Effect of glutathione aerosol on oxidant-antioxidant imbalance in idiopathic pulmonary fibrosis Lancet 1991338215-6 21 Meyer A Buhl R Magnussen H The effect of oral N-acetylcysteine on lung glutathione levels in idiopathic pulmonary fibrosis Eur Respir J 19947431-6 22 Behr J Maier K Degenkolb B Krombach F Vogelmeier C Antioxidative and clinical effects of high-dose N-acetylcysteine in fibrosing alveolitis Adjunctive therapy to maintenance immunosuppression Am J Respir Crit Care Med 19971561897-901 23 Cantin AM North SL Fells GA Hubbard RC Crystal RG Oxidant-mediated epithelial cell injury in idiopathic pulmonary fibrosis J Clin Invest 1987791665-73 24 Waghray M Cui Z Horowitz JC et al Hydrogen peroxide is a diffusible paracrine signal for the induction of epithelial cell death by activated myofibroblasts Faseb J 200519854-6 25 Larios JM Budhiraja R Fanburg BL Thannickal VJ Oxidative protein cross-linking reactions involving L-tyrosine in transforming growth factor-beta1-stimulated fibroblasts J Biol Chem 200127617437-41 26 Kinnula VL Fattman CL Tan RJ Oury TD Oxidative stress in pulmonary fibrosis a possible role for redox modulatory therapy Am J Respir Crit Care Med 2005172417-22 27 Meyer A Buhl R Kampf S Magnussen H Intravenous N-acetylcysteine and lung glutathione of patients with pulmonary fibrosis and normals Am J Respir Crit Care Med 19951521055-60 28 Behr J Degenkolb B Krombach F Vogelmeier C Intracellular glutathione and bronchoalveolar cells in fibrosing alveolitis effects of N-acetylcysteine Eur Respir J 200219906-11 29 Bando M Hosono T Mato N et al Long-term efficacy of inhaled N-acetylcysteine in patients with idiopathic pulmonary fibrosis Intern Med 2010492289-96 30 Demedts M Behr J Buhl R et al High-dose acetylcysteine in idiopathic pulmonary fibrosis N Engl J Med 20053532229-42 31 Toma TP Bhowmik A Rajakulasingam R Acetylcysteine in pulmonary fibrosis N Engl J Med 20063541086-9 author reply -9 32 Hunninghake GW Antioxidant therapy for idiopathic pulmonary fibrosis N Engl J Med 20053532285-7 33 Flaherty KR Mumford JA Murray S et al Prognostic implications of physiologic and radiographic changes in idiopathic interstitial pneumonia Am J Respir Crit Care Med 2003168543-8 34 Latsi PI du Bois RM Nicholson AG et al Fibrotic idiopathic interstitial pneumonia the prognostic value of longitudinal functional trends Am J Respir Crit Care Med 2003168531-7 35 Collard HR King TE Jr Bartelson BB Vourlekis JS Schwarz MI Brown KK Changes in clinical and physiologic variables predict survival in idiopathic pulmonary fibrosis Am J Respir Crit Care Med 2003168538-42 36 Jegal Y Kim DS Shim TS et al Physiology is a stronger predictor of survival than pathology in fibrotic interstitial pneumonia Am J Respir Crit Care Med 2005171639-44 37 Martinez FJ Safrin S Weycker D et al The clinical course of patients with idiopathic pulmonary fibrosis Ann Intern Med 2005142963-7 38 Hull JH Acetylcysteine in pulmonary fibrosis N Engl J Med 20063541089-91 author reply -91
70
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
39 Flaherty KR King TE Jr Raghu G et al Idiopathic interstitial pneumonia what is the effect of a multidisciplinary approach to diagnosis Am J Respir Crit Care Med 2004170904shy10 40 Raghu G Johnson WC Lockhart D Mageto Y Treatment of idiopathic pulmonary fibrosis with a new antifibrotic agent pirfenidone results of a prospective open-label Phase II study Am J Respir Crit Care Med 19991591061-9 41 Hunninghake GW Lynch DA Galvin JR et al Radiologic findings are strongly associated with a pathologic diagnosis of usual interstitial pneumonia Chest 20031241215-23 42 Lynch D Godwin J Safrin S et al High-resolution computed tomography in idiopathic pulmonary fibrosis diagnosis and prognosis Am J Respir Crit Care Med 2005172488-93 43 Mallinckrodt CH Watkin JG Molenberghs G Carroll RJ Choice of the primary analysis in longitudinal clinical trials Pharmaceutical Statistics 20043161-9 44 Bang H Tsiatis A Estimating medical costs with censored data Biometrika 200087329shy43 45 Lin DY Regression analysis of incomplete medical cost data Stat Med 2003221181-200 46 Rochon J Application of GEE procedures for sample size calculations in repeated measures experiments Stat Med 1998171643-58 47 Lachin JM Foulkes MA Evaluation of sample size and power for analyses of survival with allowance for nonuniform patient entry losses to follow-up noncompliance and stratification Biometrics 198642507-19
71
- PANTHER-IPFPREDNISONE AZATHIOPRINEAND N-ACETYLCYSTEINEA STUDY THAT EVALUATES RESPONSE INIDIOPATHIC PULMONARY FIBROSIS
-
- Protocol Summary
- Table of Contents
- List of Tables
- List of Figures
- List of Abbreviations
- 1 Summary
- 2 Hypotheses and Specific Aims
-
- 21 Null Hypothesis
- 22 Specific Aim 1
- 23 Specific Aim 2
- 24 Prespecified Subgroups of Interest
-
- 3 Background and Significance
-
- 31 Idiopathic Pulmonary Fibrosis is the Most Common Interstitial Lung Disease
- 32 Rationale for Placebo Control
- 33 Rationale for N-acetylcysteine
- 35 Rationale for N-acetylcysteine as a Stand-alone Therapy
- 36 Rationale for the Study Design and Primary Endpoint
- 37 Rationale for Blinding of Treatments
-
- 4 Methods
-
- 41 Inclusion Criteria
- 42 Diagnosis of IPF
- 43 Exclusion Criteria
- 44 Study Design and Study Visit
- 45 Dose Justification
- 46 Contraindications Precautions and Side Effects of Study Medications
- 47 Recruitment Procedures
- 48 Study Procedures
- 49 Concomitant Medications
- 410 Laboratory Testing
- 411 Blinding of Study Drugs
-
- 5 Study Endpoints
-
- 51 Primary Study Endpoint
- 52 Secondary Study Endpoints
-
- 6 Safety Evaluations and Procedures
-
- 61 Adverse Events
- 62 Clinical Medical Monitoring
- 63 Unblinding Procedures
-
- 7 Study Drug Procedures
- 8 Data Management
-
- 81 Hardware and Software Configuration
- 82 Sources of Data
-
- 9 Study Design and Data Analysis
-
- 91 General Analytic Considerations
- 92 Randomization Blinding and Reporting of Results
- 93 Stratification
- 94 Specification of the Primary Analyses
- 95 Analysis of Longitudinal Endpoints
- 96 Analysis of Binary Time-to-Event and Time-Lagged Endpoints
- 97 Power Analysis
-
- 10 Study Administration
-
- 101 Cooperative Agreement Mechanism
- 102 IPFnet Steering Group
- 103 Data and Safety Monitoring Board
- 104 Recommendations on Interim Monitoring of Efficacy Safety and Futility
-
- 11 Investigator and Sponsor Obligations
-
- 111 Monitoring
- 112 Cost and Payment
- 113 Confidentiality and Health Insurance Portability and Accountability ActConsiderations
- 114 Informed Consent Procedures
- 115 Institutional Review Boards
-
- 12 Investigator Agreement
- 13 References
-

PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
815 Back-up Procedures
Database back-up will be performed automatically every day and standard IPFnet DCC policies
and procedures will be applied to dictate tape rotation and retention practices
816 Virus Protection
All disk drives that provide network services and all user computers will be protected using
virus-scanning software Standard IPFnet DCC policies will be applied to update these protection
systems periodically through the study
82 Sources of Data
821 Design and Development
The IPFnet DCC will be responsible for development of the electronic case report forms
(eCRFs) development and validation of the clinical study database ensuring data integrity and
training clinical center staff on applicable data management procedures A web-based distributed
data entry model will be implemented This system will be developed to ensure that guidelines
and regulations surrounding the use of computerized systems used in clinical trials are upheld
The remainder of this section provides an overview of the data management plan associated with
this protocol
822 Data Collection Forms
The data collection process consists of direct data entry at the study clinical centers into the EDC
system(s) provided by the DCC A data collection worksheet will be provided to clinical centers
for recording data in the event the EDC system is unavailable Data entry of the eCRFs should
be completed according to the instructions provided and project specific training The
investigator is responsible for maintaining accurate complete and up-to-date records and for
ensuring the completion of the eCRFs for each research participant
55
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
823 Data Acquisition and Entry
Data entry into eCRFs shall be performed by authorized individuals Selected eCRFs may also
require the investigatorrsquos written signature or electronic signature as appropriate Electronic
CRFs will be monitored for completeness accuracy and attention to detail during the study
824 Data Center Responsibilities
The IPFnet DCC will 1) develop a data management plan and will conduct data management
activities 2) provide final eCRFs for the collection of all data required by the study 3) develop
data dictionaries for each eCRF that will comprehensively define each data element 4) conduct
ongoing data monitoring activities on study data 5) monitor any preliminary analysis data
cleanup activities and 6) rigorously monitor final study data clean up
825 Data Editing
Completed data will be entered into the IPFnet DCC automated data acquisition and
management system If incomplete or inaccurate data are found a data clarification request will
be generated and distributed to clinical centers for a response Clinical centers will resolve data
inconsistencies and errors and enter all corrections and changes into the IPFnet DCC automated
data acquisition and management system
826 Training
The training plan for clinical center staff includes provisions for training on assessments eCRF
completion guidelines data management procedures and the use of computerized systems
56
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
9 Study Design and Data Analysis
91 General Analytic Considerations
All primary analyses will be based on intent-to-treat (ITT) principles using all randomized
subjects Baseline factors across groups will be compared using mean (standard deviation) and
median (25th and 75th percentiles) summary measures Kaplan-Meier curves will be used to
display event rates Due to clinical interest in departures from both sides of the null hypothesis
all test statistics will be 2-sided
Reasonable caution needs to be taken when conducting multiple analyses on key clinical
subgroups For subgroup analyses a conservative significance level of 0001 will be used for all
interaction tests Thus subgroup comparisons will be considered exploratory unless the p-value
from the interaction test is smaller than 0001
92 Randomization Blinding and Reporting of Results
A permuted block-randomization scheme will be created with varying block sizes stratified by
clinical center Once a subject has completed the screening and baseline period and evaluation
for inclusionexclusion criteria the randomization process will begin Subjects will be
randomized to receive NAC or matching placebo with equal probability (11) via telephone
contact with a central interactive voice response system (IVRS) using a toll-free randomization
number On the day of randomization after the subject has successfully met all inclusion and
exclusion criteria the investigator or designee will call the central randomization number to
obtain the assigned kit randomization numbers for that subject At each subject visit the
investigator or designee will call the central randomization number to obtain the new kit
randomization numbers for resupply of the subject For resupply of the clinical center the IVRS
will monitor minimal volume of a kit type andor expiration date and will automatically notify
the pharmacy
57
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
The trial results will be reported according to guidelines specified in the CONSORT statement
A flow diagram describing screening recruitment randomization dropout and vital status will
be included in the primary manuscript AEs and efficacy data will be presented for all treatment
groups Adherence dropout and lost to follow-up will be carefully examined across all treatment
groups Analyses of safety will be based on data from all randomized subjects who received at
least one dose of study drug
93 Stratification
Subjects will be distributed to the two treatment arms in a 11 allocation ratio Stratification
blocks will be based on clinical centers
94 Specification of the Primary Analyses
A mixed model repeated measures (MMRM) analysis described in section 95 will be used to
compare differences in the slope of FVC measurements across the treatment groups Response
variables are values of the FVC measured at baseline and every 15 weeks until study completion
Variables in the model will include treatment time and time by treatment age sex race and
height Contrast estimates of differences in slopes of treatment over time (along with confidence
intervals) will be used to estimate the treatment effect The validity of this model in terms of
meeting modeling assumptions will be assessed via standard modeling diagnostics and goodness-
of-fit measures Based on the MMRM framework missing FVC data will not be imputed for the
primary analysis
95 Analysis of Longitudinal Endpoints
A common goal in clinical trials is to specify models that are easily implemented and
reproducible by independent data analysts On the other hand the models should have proper
statistical behavior in terms of low bias and high precision Many common approaches to
longitudinal data analysis including last observation carried forward (LOCF) imputation rely on
the missing completely at random (MCAR) assumption However the MCAR assumption is
58
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
unlikely to hold in many clinical trials because missing data are often related to disease
progression and prognosis A more reasonable assumption missing at random (MAR) specifies
that the complete data distribution can be modeled using only the observed data The likelihood-
based MMRM approach is valid under the more general MAR assumptions These models will
be applied to analyze the longitudinal data secondary endpoints
The advantages of MMRM analysis are that all important characteristics of the model can be preshy
specified standard software can be used to implement the models and results are based on ITT
principles43 In addition the MMRM approach offers superior control of Type I and Type II
errors compared with the LOCF approach
Response variables are values of the PFTs measured at enrollment and every 15 weeks until
study completion and 6MWT values measured at baseline week 30 and week 60 Covariates are
treatment time time by treatment and key baseline risk factors Contrasts (along with
confidence intervals) of treatment by time will be used to estimate the treatment effect
The correlation structure involves multiple pieces including measurement errors random
variation and interindividual variability For the longitudinal data analyses an unstructured
correlation matrix for within-subject errors will be assumed Other correlation structures
including compound symmetry will be examined as needed A careful examination of reasons
for study discontinuation will be conducted to assess the validity of MCAR Sensitivity analyses
will be used to examine the untestable assumption that the observed data violate the MAR
assumption The MMRM models will be implemented using PROC MIXED in SAS
96 Analysis of Binary Time-to-Event and Time-Lagged Endpoints
Regression modeling approaches using either the logistic regression model or Cox proportional
hazards regression model will be employed when appropriate The validity of these models will
be assessed via standard modeling diagnostics and goodness-of-fit measures Estimates of
cumulative frequencies for more general time-lagged responses will be calculated using the
partitioned version of the Bang-Tsiatis estimator44 The partitions will be set at 15-week intervals
59
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
to correspond with the data-collection process Covariate adjusted event rates will be calculated
using inverse probability-weighted regression estimates45
97 Power Analysis
971 Primary Analyses
Based on previously published IPF clinical trials the PL group is expected to experience a drop
in FVC of approximately 020 L over the study period (see Figure 1) The IPFnet Steering Group
determined a clinically important difference would be to preserve the majority of the decline
relative to PL over the study period In particular a treatment effect of 015 L was determined to
be a clinically meaningful difference Potential dropout is a key factor in the proposed study The
drop-out process assumed 5 lost to follow-up after every study visit Only 80 of subjects
were assumed to be followed for the entire study period All models assumed a compound
symmetry structure for the covariance matrix Power calculations were performed using a SAS
IML program for designing repeated measures studies46 Based on preliminary reviews of the
data from the University of Michigan the covariance matrix parameters were estimated at
approximately σ2 = 0757 (variance parameter) and ρ = 0936 (correlation parameter) To be
conservative the power calculations for the primary analysis were performed with parameter
setting of σ2 = 0810 (variance parameter) and ρ = 0925 (correlation parameter)
The power calculations assume a correction for imperfect compliance proposed by Lachin and
Foulkes to allow for 2 noncompliance for each of the treatment arms47 Thus the sample size
of 130 subjects per arm would be reduced to an adjusted sample size of 130(1-002-002)2 =
1198 or 120 subjects per arm
Under the assumed Type I error rate of 005 with a correlation parameter of 0925 and standard
deviation of 090 the difference of 015 L (or 00025 Lweek) shown in Table 6 would have
power of 93
60
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Table 6 Hypothetical Values of Mean FVC (L) Change from Baseline
Week 15 Week 30 Week 45 Week 60
NAC 00125 00250 00375 00500
Placebo 00500 01000 01500 02000
Difference 00375 00750 01125 01500
Abbreviations FVC forced vital capacity PL placebo
972 Power Analysis for Secondary Endpoints
Power calculations for secondary endpoint measurements are shown in Table 7 Standard
deviations are based on unpublished data provided by the University of Michigan The
calculations are based on a 2-sample t-test with Type I error rate set at 005 These calculations
are likely to be conservative because the statistical approach described in section 95 for
analyzing these endpoints will incorporate incomplete observations as well as intermediate data
points
Table 7 Detectable Differences in Treatment Means for Selected Endpoint Measurements
Secondary Endpoints Std Dev
of the Baseline Score
Detectable Difference for 80 Power
Std Dev of the Change Score
Difference Detectable for
80 Power
DLCOpred 166 58 91 32
6MWT Area Under the Desaturation Curve
219 76 175 61
6MWT Distance to Desaturation 224 78 315 110
6MWT Minutes Walked 210 073 205 071
Abbreviations Std Dev standard deviation DLCOpred diffusing capacity of the lung for carbon monoxide percent predicted 6MWT 6-minute walk test
61
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
10 Study Administration
101 Cooperative Agreement Mechanism
The administrative and funding mechanism used to undertake this project is a ldquocooperative
agreementrdquo (U01) which is an assistance mechanism Under the cooperative agreement the
NHLBI assists supports andor stimulates the project and is substantially involved with
investigators in conducting the study by facilitating performance of the effort in a ldquopartnerrdquo role
The NHLBI project scientist serves on the IPFnet Steering Group and he or another NHLBI
scientist may serve on other project committees when appropriate At the same time however
NHLBI does not assume a dominant role direction or prime responsibility for this research
program
As described below governance of the project is conducted through the IPFnet Steering Group
Principal investigators have lead responsibilities in all aspects of their trials and the project
including any modification of trial designs conduct of the trials quality control data analysis
and interpretation preparation of publications and collaboration with other investigators unless
otherwise provided for by the IPFnet Steering Group
PIs retain custody of and have primary rights to their center-specific and collaborative data
subject to government rights-of-access consistent with current Health amp Human Services (HHS)
Public Health Service (PHS) and National Institutes of Health policies The protocols and
governance policies call for the continual submission of data centrally to the IPFnet DCC for the
collaborative database which at a minimum will contain the key variables selected by the IPFnet
Steering Group for standardization across all clinical centers the submission of copies of the
collaborative datasets to each PI upon completion of the project procedures for data analysis
reporting and publication and procedures to protect and ensure the privacy of medical and
genetic data and records of individuals The NHLBI project scientist on behalf of the NHLBI
will have the same access privileges and responsibilities regarding the collaborative data as the
other members of the Steering Group
62
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
PIs are also encouraged to publish and to publicly release and disseminate results data and other
products of the project concordant with the project protocols and governance and the approved
plan for making data and materials available to the scientific community and to the NHLBI
However during the 3 years after the ending date of NHLBI project support unpublished data
unpublished results data sets not previously released and other study materials or products are
to be made available to any third party only with the approval of the IPFnet Steering Group
Upon completion of the project PIs are expected to put their intervention materials and
procedure manuals into the public domain andor make them available to other investigators
according to the approved plan for making data and materials available to the scientific
community and the NHLBI for the conduct of research at no charge other than the costs of
reproduction and distribution
The NHLBI reserves the right to terminate or curtail the project (or an individual award) in the
event of (a) failure to develop or implement mutually agreeable collaborative measurement
subject eligibility and data management sections of the protocols (b) substantial shortfall in
subject recruitment follow-up data reporting or quality control or other major breach of
protocol (c) substantive changes in the agreed-upon protocols with which NHLBI cannot
concur (d) reaching a major project outcome with persuasive statistical significance
substantially before schedule or (e) human subject ethical issues that may dictate a premature
termination
Any disagreement that may arise in scientificprogrammatic matters (within the scope of the
award) between award recipients and the NHLBI may be brought to arbitration An arbitration
panel will be composed of 3 membersmdash1 selected by the IPFnet Steering Group (with the
NHLBI member not voting) or by the individual PI in the event of an individual disagreement a
second selected by NHLBI and the third selected by the other 2 members This special
arbitration procedure in no way affects the PIrsquos right to appeal an adverse action that is otherwise
appealable in accordance with the PHS regulations at 42 CFR part 50 Subpart D and HHS
63
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
regulation at 45 CFR part 16 or the rights of the NHLBI under applicable statutes regulations
and terms of the award
102 IPFnet Steering Group
The IPFnet Steering Group is the main governing body of the project It is composed of the PIs
of the clinical centers the PI of the DCC and the NHLBI project scientist The clinical centers
the IPFnet DCC and the NHLBI each have 1 vote on the IPFnet Steering Group All decisions
are determined by majority vote
All major scientific decisions are determined by the IPFnet Steering Group It assumes overall
responsibility for the design and conduct of the trial It appoints (and disbands) committees and
subcommittees as the need arises designs approves and implements the study protocols
oversees the development of the MOOP monitors subject recruitment and treatment delivery
evaluates data collection and management oversees quality assurance procedures and
implements changes and enhancements to the study as required It also has primary responsibility
for facilitating the conduct of the trials and reporting the projectrsquos results
103 Data and Safety Monitoring Board
The NHLBI will establish a DSMB in accordance with established policies (see
httpwwwnhlbinihgovfundingpoliciesdsmb_insthtm) to ensure data quality and subject
safety and to provide independent advice to the NHLBI regarding progress and the
appropriateness of study continuation
104 Recommendations on Interim Monitoring of Efficacy Safety and Futility
First and foremost the role of the DSMB will be to review subject safety and trial conduct at
periodic points during the study The DSMB may require analyses of the primary endpoint
results for comparing the benefit and risks of treatment strategies The benefit of collecting
additional data on key secondary endpoints with extended follow-up and establishing a robust
64
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
evidence base for determining a standard of care will need to be carefully considered before
early termination of one or more treatment arms After careful consideration the IPFnet Steering
Group recommends conservative thresholds for the early examinations of the safety and efficacy
data
The DSMB will be expected to meet approximately every 6 months until trial completion to
review safety and toxicity data The DSMB may recommend stopping the study based on these
reviews Because the DSMB could stop the trial for safety concerns as well as for a large
efficacy benefit there could be multiple opportunities to reject the null hypothesis (no difference
in event rates between the PL and NAC groups) A Bonferroni approximation will be applied
during the one planned interim analysis for efficacy
Before locking the database a statistical analysis plan (SAP) will be developed to provide
complete details on the statistical analysis The SAP will include the specifics for how and when
the DSMB will be notified for AEs The IPFnet DCC will deliver to the DSMB all FDA-defined
AEs at 3-month intervals The IPFnet DCC will prepare narrative SAE reports in real time for
DSMB review including recommendations and analysis of similar events for each SAE
submitted to the FDA
65
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
11 Investigator and Sponsor Obligations
111 Monitoring
All monitoring activities for US clinical centers will be performed in accordance with DCRI
standard operating procedures Information regarding the types of visits will be outlined in the
PANTHER-IPF MOOP
112 Cost and Payment
There will be no cost to subjects enrolled in this trial Study-related procedures will be paid for
by the IPFnet
Subjects may be eligible for reimbursement for travel to the clinical center Details of payment
will be explained to each subject during the consent process
113 Confidentiality and Health Insurance Portability and Accountability Act
Considerations
Subject confidentiality will be protected throughout the study All subject data will be kept
strictly confidential and no subject-identifying information will be released to anyone outside
the project Confidentiality will be assured through several mechanisms First each subject will
be assigned an anonymous study ID which will then be used on all study forms Second any
study forms blood samples and paper records that contain subject information (eg address lists
phone lists) will be kept at the clinical centers in secured locked areas coded by number Once
blood is collected there will be no subject identifiers placed on blood samplesmdashonly the study
ID number and the date of sample collection Third access to all subject data and information
including laboratory specimens will be restricted to authorized personnel In the case of
computerized data this restricted access will be assured through user logon IDs and password
protection
66
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
At the IPFnet DCC only authorized personnel will have access to the data files containing study
data Security will be assured through user logon IDs passwords and appropriate access
privileges All study subjects will be identified only by their IPFnet ID numbers and no personal
identifying information such as name address or Social Security number will be entered into
the IPFnet DCC database Any subject-specific data reported to the IPFnet Steering Group will
be identified only by the IPFnet ID number
Finally subjects will not be identified by name in any reports or publications nor will the data
be presented in such a way that the identity of individual subjects can be inferred Analysis files
created for further study by the scientific community will have no subject identifiers These data
files will be created in accordance with the Ancillary Studies and Publication Policy of the
IPFnet
114 Informed Consent Procedures
All IPFnet subjects will provide written informed consent using procedures reviewed and
approved by each clinical centerrsquos IRB Informed consent will be undertaken by study personnel
in-person with the subject The subject has the option of declining further participation in the
study at that point No further study procedures will be conducted until the signed documents
have been provided to the IPFnet clinical center
115 Institutional Review Boards
Before initiating this study the protocol clinical center-specific informed consent forms Health
Insurance Portability and Accountability Act (HIPAA) forms recruitment materials and other
relevant information will be reviewed by a properly constituted IRB at each participating clinical
center A copy of the signed and dated IRB approval at each clinical center will be retrieved prior
to or during the site initiation visit and archived at the IPFnet DCC Any amendments to the
protocol other than simple administrative and typographical changes must be approved by each
IRB before they are implemented The clinical centers will seek annual renewals of their IRB
approvals in accordance with local procedures
67
__________________________________________ ________________
__________________________________________
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
12 Investigator Agreement
I have read the foregoing protocol PANTHER-IPF and agree that it contains all necessary
details for carrying out this study I will conduct the study as outlined herein and will complete
the study within the time designated
I will provide copies of the protocol and all pertinent information to all individuals responsible to
me who assist in the conduct of this study I will discuss this material with them to ensure they
are fully informed regarding the drug and the conduct of the study
I will fulfill all responsibilities for submitting pertinent information to the local IRB if
applicable that is responsible for this study
I further agree that NHLBI andor DCRI will have access to any source documents from which
eCRF information may have been generated
Signature of Principal Investigator Date
Name of Principal Investigator (printed or typed)
Protocol version date May 19 2009
Protocol Amendment 1 version date May 28 2010
Protocol Amendment 2 version date December 6 2011
68
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
13 References
1 Raghu G Brown KK Bradford WZ et al A placebo-controlled trial of interferon gamma-1b in patients with idiopathic pulmonary fibrosis N Engl J Med 2004350125-33 2 King TE Jr Safrin S Starko KM et al Analyses of efficacy end points in a controlled trial of interferon-gamma1b for idiopathic pulmonary fibrosis Chest 2005127171-7 3 Flaherty KR Thwaite EL Kazerooni EA et al Radiological versus histological diagnosis in UIP and NSIP survival implications Thorax 200358143-8 4 Wells AU Desai SR Rubens MB et al Idiopathic pulmonary fibrosis a composite physiologic index derived from disease extent observed by computed tomography Am J Respir Crit Care Med 2003167962-9 5 Raghu G Freudenberger TD Yang S et al High prevalence of abnormal acid gastroshyoesophageal reflux in idiopathic pulmonary fibrosis Eur Respir J 200627136-42 6 Kinnula VL Focus on antioxidant enzymes and antioxidant strategies in smoking related airway diseases Thorax 200560693-700 7 Coultas DB Zumwalt RE Black WC Sobonya RE The epidemiology of interstitial lung diseases Am J Respir Crit Care Med 1994150967-72 8 Raghu G Weycker D Edelsberg J Bradford WZ Oster G Incidence and prevalence of idiopathic pulmonary fibrosis Am J Respir Crit Care Med 2006174810-6 9 Olson AL Swigris JJ Lezotte DC Norris JM Wilson CG Brown KK Mortality from pulmonary fibrosis increased in the United States from 1992 to 2003 Am J Respir Crit Care Med 2007176277-84 10 Mannino DM Etzel RA Parrish RG Pulmonary fibrosis deaths in the United States 1979shy1991 An analysis of multiple-cause mortality data Am J Respir Crit Care Med 19961531548shy52 11 Hubbard R Johnston I Coultas DB Britton J Mortality rates from cryptogenic fibrosing alveolitis in seven countries Thorax 199651711-6 12 Johnston I Britton J Kinnear W Logan R Rising mortality from cryptogenic fibrosing alveolitis Bmj 19903011017-21 13 Raghu G Collard HR Egan JJ et al An official ATSERSJRSALAT statement idiopathic pulmonary fibrosis evidence-based guidelines for diagnosis and management Am J Respir Crit Care Med 2011183788-824 14 (USA) FDA FDA Public Health Advisory Interferon gamma-1b (marketed as Actimmune) In 2007 15 King TE Jr Pardo A Selman M Idiopathic pulmonary fibrosis Lancet 2011 16 Raghu G Brown KK Costabel U et al Treatment of idiopathic pulmonary fibrosis with etanercept an exploratory placebo-controlled trial Am J Respir Crit Care Med 2008178948shy55 17 Malouf MA Hopkins P Snell G Glanville AR An investigator-driven study of everolimus in surgical lung biopsy confirmed idiopathic pulmonary fibrosis Respirology 201116776-83 18 King TE Jr Behr J Brown KK et al BUILD-1 a randomized placebo-controlled trial of bosentan in idiopathic pulmonary fibrosis Am J Respir Crit Care Med 200817775-81 19 Richeldi L Costabel U Selman M et al Efficacy of a tyrosine kinase inhibitor in idiopathic pulmonary fibrosis N Engl J Med 20113651079-87
69
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
20 Borok Z Buhl R Grimes GJ et al Effect of glutathione aerosol on oxidant-antioxidant imbalance in idiopathic pulmonary fibrosis Lancet 1991338215-6 21 Meyer A Buhl R Magnussen H The effect of oral N-acetylcysteine on lung glutathione levels in idiopathic pulmonary fibrosis Eur Respir J 19947431-6 22 Behr J Maier K Degenkolb B Krombach F Vogelmeier C Antioxidative and clinical effects of high-dose N-acetylcysteine in fibrosing alveolitis Adjunctive therapy to maintenance immunosuppression Am J Respir Crit Care Med 19971561897-901 23 Cantin AM North SL Fells GA Hubbard RC Crystal RG Oxidant-mediated epithelial cell injury in idiopathic pulmonary fibrosis J Clin Invest 1987791665-73 24 Waghray M Cui Z Horowitz JC et al Hydrogen peroxide is a diffusible paracrine signal for the induction of epithelial cell death by activated myofibroblasts Faseb J 200519854-6 25 Larios JM Budhiraja R Fanburg BL Thannickal VJ Oxidative protein cross-linking reactions involving L-tyrosine in transforming growth factor-beta1-stimulated fibroblasts J Biol Chem 200127617437-41 26 Kinnula VL Fattman CL Tan RJ Oury TD Oxidative stress in pulmonary fibrosis a possible role for redox modulatory therapy Am J Respir Crit Care Med 2005172417-22 27 Meyer A Buhl R Kampf S Magnussen H Intravenous N-acetylcysteine and lung glutathione of patients with pulmonary fibrosis and normals Am J Respir Crit Care Med 19951521055-60 28 Behr J Degenkolb B Krombach F Vogelmeier C Intracellular glutathione and bronchoalveolar cells in fibrosing alveolitis effects of N-acetylcysteine Eur Respir J 200219906-11 29 Bando M Hosono T Mato N et al Long-term efficacy of inhaled N-acetylcysteine in patients with idiopathic pulmonary fibrosis Intern Med 2010492289-96 30 Demedts M Behr J Buhl R et al High-dose acetylcysteine in idiopathic pulmonary fibrosis N Engl J Med 20053532229-42 31 Toma TP Bhowmik A Rajakulasingam R Acetylcysteine in pulmonary fibrosis N Engl J Med 20063541086-9 author reply -9 32 Hunninghake GW Antioxidant therapy for idiopathic pulmonary fibrosis N Engl J Med 20053532285-7 33 Flaherty KR Mumford JA Murray S et al Prognostic implications of physiologic and radiographic changes in idiopathic interstitial pneumonia Am J Respir Crit Care Med 2003168543-8 34 Latsi PI du Bois RM Nicholson AG et al Fibrotic idiopathic interstitial pneumonia the prognostic value of longitudinal functional trends Am J Respir Crit Care Med 2003168531-7 35 Collard HR King TE Jr Bartelson BB Vourlekis JS Schwarz MI Brown KK Changes in clinical and physiologic variables predict survival in idiopathic pulmonary fibrosis Am J Respir Crit Care Med 2003168538-42 36 Jegal Y Kim DS Shim TS et al Physiology is a stronger predictor of survival than pathology in fibrotic interstitial pneumonia Am J Respir Crit Care Med 2005171639-44 37 Martinez FJ Safrin S Weycker D et al The clinical course of patients with idiopathic pulmonary fibrosis Ann Intern Med 2005142963-7 38 Hull JH Acetylcysteine in pulmonary fibrosis N Engl J Med 20063541089-91 author reply -91
70
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
39 Flaherty KR King TE Jr Raghu G et al Idiopathic interstitial pneumonia what is the effect of a multidisciplinary approach to diagnosis Am J Respir Crit Care Med 2004170904shy10 40 Raghu G Johnson WC Lockhart D Mageto Y Treatment of idiopathic pulmonary fibrosis with a new antifibrotic agent pirfenidone results of a prospective open-label Phase II study Am J Respir Crit Care Med 19991591061-9 41 Hunninghake GW Lynch DA Galvin JR et al Radiologic findings are strongly associated with a pathologic diagnosis of usual interstitial pneumonia Chest 20031241215-23 42 Lynch D Godwin J Safrin S et al High-resolution computed tomography in idiopathic pulmonary fibrosis diagnosis and prognosis Am J Respir Crit Care Med 2005172488-93 43 Mallinckrodt CH Watkin JG Molenberghs G Carroll RJ Choice of the primary analysis in longitudinal clinical trials Pharmaceutical Statistics 20043161-9 44 Bang H Tsiatis A Estimating medical costs with censored data Biometrika 200087329shy43 45 Lin DY Regression analysis of incomplete medical cost data Stat Med 2003221181-200 46 Rochon J Application of GEE procedures for sample size calculations in repeated measures experiments Stat Med 1998171643-58 47 Lachin JM Foulkes MA Evaluation of sample size and power for analyses of survival with allowance for nonuniform patient entry losses to follow-up noncompliance and stratification Biometrics 198642507-19
71
- PANTHER-IPFPREDNISONE AZATHIOPRINEAND N-ACETYLCYSTEINEA STUDY THAT EVALUATES RESPONSE INIDIOPATHIC PULMONARY FIBROSIS
-
- Protocol Summary
- Table of Contents
- List of Tables
- List of Figures
- List of Abbreviations
- 1 Summary
- 2 Hypotheses and Specific Aims
-
- 21 Null Hypothesis
- 22 Specific Aim 1
- 23 Specific Aim 2
- 24 Prespecified Subgroups of Interest
-
- 3 Background and Significance
-
- 31 Idiopathic Pulmonary Fibrosis is the Most Common Interstitial Lung Disease
- 32 Rationale for Placebo Control
- 33 Rationale for N-acetylcysteine
- 35 Rationale for N-acetylcysteine as a Stand-alone Therapy
- 36 Rationale for the Study Design and Primary Endpoint
- 37 Rationale for Blinding of Treatments
-
- 4 Methods
-
- 41 Inclusion Criteria
- 42 Diagnosis of IPF
- 43 Exclusion Criteria
- 44 Study Design and Study Visit
- 45 Dose Justification
- 46 Contraindications Precautions and Side Effects of Study Medications
- 47 Recruitment Procedures
- 48 Study Procedures
- 49 Concomitant Medications
- 410 Laboratory Testing
- 411 Blinding of Study Drugs
-
- 5 Study Endpoints
-
- 51 Primary Study Endpoint
- 52 Secondary Study Endpoints
-
- 6 Safety Evaluations and Procedures
-
- 61 Adverse Events
- 62 Clinical Medical Monitoring
- 63 Unblinding Procedures
-
- 7 Study Drug Procedures
- 8 Data Management
-
- 81 Hardware and Software Configuration
- 82 Sources of Data
-
- 9 Study Design and Data Analysis
-
- 91 General Analytic Considerations
- 92 Randomization Blinding and Reporting of Results
- 93 Stratification
- 94 Specification of the Primary Analyses
- 95 Analysis of Longitudinal Endpoints
- 96 Analysis of Binary Time-to-Event and Time-Lagged Endpoints
- 97 Power Analysis
-
- 10 Study Administration
-
- 101 Cooperative Agreement Mechanism
- 102 IPFnet Steering Group
- 103 Data and Safety Monitoring Board
- 104 Recommendations on Interim Monitoring of Efficacy Safety and Futility
-
- 11 Investigator and Sponsor Obligations
-
- 111 Monitoring
- 112 Cost and Payment
- 113 Confidentiality and Health Insurance Portability and Accountability ActConsiderations
- 114 Informed Consent Procedures
- 115 Institutional Review Boards
-
- 12 Investigator Agreement
- 13 References
-
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
823 Data Acquisition and Entry
Data entry into eCRFs shall be performed by authorized individuals Selected eCRFs may also
require the investigatorrsquos written signature or electronic signature as appropriate Electronic
CRFs will be monitored for completeness accuracy and attention to detail during the study
824 Data Center Responsibilities
The IPFnet DCC will 1) develop a data management plan and will conduct data management
activities 2) provide final eCRFs for the collection of all data required by the study 3) develop
data dictionaries for each eCRF that will comprehensively define each data element 4) conduct
ongoing data monitoring activities on study data 5) monitor any preliminary analysis data
cleanup activities and 6) rigorously monitor final study data clean up
825 Data Editing
Completed data will be entered into the IPFnet DCC automated data acquisition and
management system If incomplete or inaccurate data are found a data clarification request will
be generated and distributed to clinical centers for a response Clinical centers will resolve data
inconsistencies and errors and enter all corrections and changes into the IPFnet DCC automated
data acquisition and management system
826 Training
The training plan for clinical center staff includes provisions for training on assessments eCRF
completion guidelines data management procedures and the use of computerized systems
56
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
9 Study Design and Data Analysis
91 General Analytic Considerations
All primary analyses will be based on intent-to-treat (ITT) principles using all randomized
subjects Baseline factors across groups will be compared using mean (standard deviation) and
median (25th and 75th percentiles) summary measures Kaplan-Meier curves will be used to
display event rates Due to clinical interest in departures from both sides of the null hypothesis
all test statistics will be 2-sided
Reasonable caution needs to be taken when conducting multiple analyses on key clinical
subgroups For subgroup analyses a conservative significance level of 0001 will be used for all
interaction tests Thus subgroup comparisons will be considered exploratory unless the p-value
from the interaction test is smaller than 0001
92 Randomization Blinding and Reporting of Results
A permuted block-randomization scheme will be created with varying block sizes stratified by
clinical center Once a subject has completed the screening and baseline period and evaluation
for inclusionexclusion criteria the randomization process will begin Subjects will be
randomized to receive NAC or matching placebo with equal probability (11) via telephone
contact with a central interactive voice response system (IVRS) using a toll-free randomization
number On the day of randomization after the subject has successfully met all inclusion and
exclusion criteria the investigator or designee will call the central randomization number to
obtain the assigned kit randomization numbers for that subject At each subject visit the
investigator or designee will call the central randomization number to obtain the new kit
randomization numbers for resupply of the subject For resupply of the clinical center the IVRS
will monitor minimal volume of a kit type andor expiration date and will automatically notify
the pharmacy
57
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
The trial results will be reported according to guidelines specified in the CONSORT statement
A flow diagram describing screening recruitment randomization dropout and vital status will
be included in the primary manuscript AEs and efficacy data will be presented for all treatment
groups Adherence dropout and lost to follow-up will be carefully examined across all treatment
groups Analyses of safety will be based on data from all randomized subjects who received at
least one dose of study drug
93 Stratification
Subjects will be distributed to the two treatment arms in a 11 allocation ratio Stratification
blocks will be based on clinical centers
94 Specification of the Primary Analyses
A mixed model repeated measures (MMRM) analysis described in section 95 will be used to
compare differences in the slope of FVC measurements across the treatment groups Response
variables are values of the FVC measured at baseline and every 15 weeks until study completion
Variables in the model will include treatment time and time by treatment age sex race and
height Contrast estimates of differences in slopes of treatment over time (along with confidence
intervals) will be used to estimate the treatment effect The validity of this model in terms of
meeting modeling assumptions will be assessed via standard modeling diagnostics and goodness-
of-fit measures Based on the MMRM framework missing FVC data will not be imputed for the
primary analysis
95 Analysis of Longitudinal Endpoints
A common goal in clinical trials is to specify models that are easily implemented and
reproducible by independent data analysts On the other hand the models should have proper
statistical behavior in terms of low bias and high precision Many common approaches to
longitudinal data analysis including last observation carried forward (LOCF) imputation rely on
the missing completely at random (MCAR) assumption However the MCAR assumption is
58
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
unlikely to hold in many clinical trials because missing data are often related to disease
progression and prognosis A more reasonable assumption missing at random (MAR) specifies
that the complete data distribution can be modeled using only the observed data The likelihood-
based MMRM approach is valid under the more general MAR assumptions These models will
be applied to analyze the longitudinal data secondary endpoints
The advantages of MMRM analysis are that all important characteristics of the model can be preshy
specified standard software can be used to implement the models and results are based on ITT
principles43 In addition the MMRM approach offers superior control of Type I and Type II
errors compared with the LOCF approach
Response variables are values of the PFTs measured at enrollment and every 15 weeks until
study completion and 6MWT values measured at baseline week 30 and week 60 Covariates are
treatment time time by treatment and key baseline risk factors Contrasts (along with
confidence intervals) of treatment by time will be used to estimate the treatment effect
The correlation structure involves multiple pieces including measurement errors random
variation and interindividual variability For the longitudinal data analyses an unstructured
correlation matrix for within-subject errors will be assumed Other correlation structures
including compound symmetry will be examined as needed A careful examination of reasons
for study discontinuation will be conducted to assess the validity of MCAR Sensitivity analyses
will be used to examine the untestable assumption that the observed data violate the MAR
assumption The MMRM models will be implemented using PROC MIXED in SAS
96 Analysis of Binary Time-to-Event and Time-Lagged Endpoints
Regression modeling approaches using either the logistic regression model or Cox proportional
hazards regression model will be employed when appropriate The validity of these models will
be assessed via standard modeling diagnostics and goodness-of-fit measures Estimates of
cumulative frequencies for more general time-lagged responses will be calculated using the
partitioned version of the Bang-Tsiatis estimator44 The partitions will be set at 15-week intervals
59
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
to correspond with the data-collection process Covariate adjusted event rates will be calculated
using inverse probability-weighted regression estimates45
97 Power Analysis
971 Primary Analyses
Based on previously published IPF clinical trials the PL group is expected to experience a drop
in FVC of approximately 020 L over the study period (see Figure 1) The IPFnet Steering Group
determined a clinically important difference would be to preserve the majority of the decline
relative to PL over the study period In particular a treatment effect of 015 L was determined to
be a clinically meaningful difference Potential dropout is a key factor in the proposed study The
drop-out process assumed 5 lost to follow-up after every study visit Only 80 of subjects
were assumed to be followed for the entire study period All models assumed a compound
symmetry structure for the covariance matrix Power calculations were performed using a SAS
IML program for designing repeated measures studies46 Based on preliminary reviews of the
data from the University of Michigan the covariance matrix parameters were estimated at
approximately σ2 = 0757 (variance parameter) and ρ = 0936 (correlation parameter) To be
conservative the power calculations for the primary analysis were performed with parameter
setting of σ2 = 0810 (variance parameter) and ρ = 0925 (correlation parameter)
The power calculations assume a correction for imperfect compliance proposed by Lachin and
Foulkes to allow for 2 noncompliance for each of the treatment arms47 Thus the sample size
of 130 subjects per arm would be reduced to an adjusted sample size of 130(1-002-002)2 =
1198 or 120 subjects per arm
Under the assumed Type I error rate of 005 with a correlation parameter of 0925 and standard
deviation of 090 the difference of 015 L (or 00025 Lweek) shown in Table 6 would have
power of 93
60
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Table 6 Hypothetical Values of Mean FVC (L) Change from Baseline
Week 15 Week 30 Week 45 Week 60
NAC 00125 00250 00375 00500
Placebo 00500 01000 01500 02000
Difference 00375 00750 01125 01500
Abbreviations FVC forced vital capacity PL placebo
972 Power Analysis for Secondary Endpoints
Power calculations for secondary endpoint measurements are shown in Table 7 Standard
deviations are based on unpublished data provided by the University of Michigan The
calculations are based on a 2-sample t-test with Type I error rate set at 005 These calculations
are likely to be conservative because the statistical approach described in section 95 for
analyzing these endpoints will incorporate incomplete observations as well as intermediate data
points
Table 7 Detectable Differences in Treatment Means for Selected Endpoint Measurements
Secondary Endpoints Std Dev
of the Baseline Score
Detectable Difference for 80 Power
Std Dev of the Change Score
Difference Detectable for
80 Power
DLCOpred 166 58 91 32
6MWT Area Under the Desaturation Curve
219 76 175 61
6MWT Distance to Desaturation 224 78 315 110
6MWT Minutes Walked 210 073 205 071
Abbreviations Std Dev standard deviation DLCOpred diffusing capacity of the lung for carbon monoxide percent predicted 6MWT 6-minute walk test
61
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
10 Study Administration
101 Cooperative Agreement Mechanism
The administrative and funding mechanism used to undertake this project is a ldquocooperative
agreementrdquo (U01) which is an assistance mechanism Under the cooperative agreement the
NHLBI assists supports andor stimulates the project and is substantially involved with
investigators in conducting the study by facilitating performance of the effort in a ldquopartnerrdquo role
The NHLBI project scientist serves on the IPFnet Steering Group and he or another NHLBI
scientist may serve on other project committees when appropriate At the same time however
NHLBI does not assume a dominant role direction or prime responsibility for this research
program
As described below governance of the project is conducted through the IPFnet Steering Group
Principal investigators have lead responsibilities in all aspects of their trials and the project
including any modification of trial designs conduct of the trials quality control data analysis
and interpretation preparation of publications and collaboration with other investigators unless
otherwise provided for by the IPFnet Steering Group
PIs retain custody of and have primary rights to their center-specific and collaborative data
subject to government rights-of-access consistent with current Health amp Human Services (HHS)
Public Health Service (PHS) and National Institutes of Health policies The protocols and
governance policies call for the continual submission of data centrally to the IPFnet DCC for the
collaborative database which at a minimum will contain the key variables selected by the IPFnet
Steering Group for standardization across all clinical centers the submission of copies of the
collaborative datasets to each PI upon completion of the project procedures for data analysis
reporting and publication and procedures to protect and ensure the privacy of medical and
genetic data and records of individuals The NHLBI project scientist on behalf of the NHLBI
will have the same access privileges and responsibilities regarding the collaborative data as the
other members of the Steering Group
62
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
PIs are also encouraged to publish and to publicly release and disseminate results data and other
products of the project concordant with the project protocols and governance and the approved
plan for making data and materials available to the scientific community and to the NHLBI
However during the 3 years after the ending date of NHLBI project support unpublished data
unpublished results data sets not previously released and other study materials or products are
to be made available to any third party only with the approval of the IPFnet Steering Group
Upon completion of the project PIs are expected to put their intervention materials and
procedure manuals into the public domain andor make them available to other investigators
according to the approved plan for making data and materials available to the scientific
community and the NHLBI for the conduct of research at no charge other than the costs of
reproduction and distribution
The NHLBI reserves the right to terminate or curtail the project (or an individual award) in the
event of (a) failure to develop or implement mutually agreeable collaborative measurement
subject eligibility and data management sections of the protocols (b) substantial shortfall in
subject recruitment follow-up data reporting or quality control or other major breach of
protocol (c) substantive changes in the agreed-upon protocols with which NHLBI cannot
concur (d) reaching a major project outcome with persuasive statistical significance
substantially before schedule or (e) human subject ethical issues that may dictate a premature
termination
Any disagreement that may arise in scientificprogrammatic matters (within the scope of the
award) between award recipients and the NHLBI may be brought to arbitration An arbitration
panel will be composed of 3 membersmdash1 selected by the IPFnet Steering Group (with the
NHLBI member not voting) or by the individual PI in the event of an individual disagreement a
second selected by NHLBI and the third selected by the other 2 members This special
arbitration procedure in no way affects the PIrsquos right to appeal an adverse action that is otherwise
appealable in accordance with the PHS regulations at 42 CFR part 50 Subpart D and HHS
63
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
regulation at 45 CFR part 16 or the rights of the NHLBI under applicable statutes regulations
and terms of the award
102 IPFnet Steering Group
The IPFnet Steering Group is the main governing body of the project It is composed of the PIs
of the clinical centers the PI of the DCC and the NHLBI project scientist The clinical centers
the IPFnet DCC and the NHLBI each have 1 vote on the IPFnet Steering Group All decisions
are determined by majority vote
All major scientific decisions are determined by the IPFnet Steering Group It assumes overall
responsibility for the design and conduct of the trial It appoints (and disbands) committees and
subcommittees as the need arises designs approves and implements the study protocols
oversees the development of the MOOP monitors subject recruitment and treatment delivery
evaluates data collection and management oversees quality assurance procedures and
implements changes and enhancements to the study as required It also has primary responsibility
for facilitating the conduct of the trials and reporting the projectrsquos results
103 Data and Safety Monitoring Board
The NHLBI will establish a DSMB in accordance with established policies (see
httpwwwnhlbinihgovfundingpoliciesdsmb_insthtm) to ensure data quality and subject
safety and to provide independent advice to the NHLBI regarding progress and the
appropriateness of study continuation
104 Recommendations on Interim Monitoring of Efficacy Safety and Futility
First and foremost the role of the DSMB will be to review subject safety and trial conduct at
periodic points during the study The DSMB may require analyses of the primary endpoint
results for comparing the benefit and risks of treatment strategies The benefit of collecting
additional data on key secondary endpoints with extended follow-up and establishing a robust
64
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
evidence base for determining a standard of care will need to be carefully considered before
early termination of one or more treatment arms After careful consideration the IPFnet Steering
Group recommends conservative thresholds for the early examinations of the safety and efficacy
data
The DSMB will be expected to meet approximately every 6 months until trial completion to
review safety and toxicity data The DSMB may recommend stopping the study based on these
reviews Because the DSMB could stop the trial for safety concerns as well as for a large
efficacy benefit there could be multiple opportunities to reject the null hypothesis (no difference
in event rates between the PL and NAC groups) A Bonferroni approximation will be applied
during the one planned interim analysis for efficacy
Before locking the database a statistical analysis plan (SAP) will be developed to provide
complete details on the statistical analysis The SAP will include the specifics for how and when
the DSMB will be notified for AEs The IPFnet DCC will deliver to the DSMB all FDA-defined
AEs at 3-month intervals The IPFnet DCC will prepare narrative SAE reports in real time for
DSMB review including recommendations and analysis of similar events for each SAE
submitted to the FDA
65
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
11 Investigator and Sponsor Obligations
111 Monitoring
All monitoring activities for US clinical centers will be performed in accordance with DCRI
standard operating procedures Information regarding the types of visits will be outlined in the
PANTHER-IPF MOOP
112 Cost and Payment
There will be no cost to subjects enrolled in this trial Study-related procedures will be paid for
by the IPFnet
Subjects may be eligible for reimbursement for travel to the clinical center Details of payment
will be explained to each subject during the consent process
113 Confidentiality and Health Insurance Portability and Accountability Act
Considerations
Subject confidentiality will be protected throughout the study All subject data will be kept
strictly confidential and no subject-identifying information will be released to anyone outside
the project Confidentiality will be assured through several mechanisms First each subject will
be assigned an anonymous study ID which will then be used on all study forms Second any
study forms blood samples and paper records that contain subject information (eg address lists
phone lists) will be kept at the clinical centers in secured locked areas coded by number Once
blood is collected there will be no subject identifiers placed on blood samplesmdashonly the study
ID number and the date of sample collection Third access to all subject data and information
including laboratory specimens will be restricted to authorized personnel In the case of
computerized data this restricted access will be assured through user logon IDs and password
protection
66
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
At the IPFnet DCC only authorized personnel will have access to the data files containing study
data Security will be assured through user logon IDs passwords and appropriate access
privileges All study subjects will be identified only by their IPFnet ID numbers and no personal
identifying information such as name address or Social Security number will be entered into
the IPFnet DCC database Any subject-specific data reported to the IPFnet Steering Group will
be identified only by the IPFnet ID number
Finally subjects will not be identified by name in any reports or publications nor will the data
be presented in such a way that the identity of individual subjects can be inferred Analysis files
created for further study by the scientific community will have no subject identifiers These data
files will be created in accordance with the Ancillary Studies and Publication Policy of the
IPFnet
114 Informed Consent Procedures
All IPFnet subjects will provide written informed consent using procedures reviewed and
approved by each clinical centerrsquos IRB Informed consent will be undertaken by study personnel
in-person with the subject The subject has the option of declining further participation in the
study at that point No further study procedures will be conducted until the signed documents
have been provided to the IPFnet clinical center
115 Institutional Review Boards
Before initiating this study the protocol clinical center-specific informed consent forms Health
Insurance Portability and Accountability Act (HIPAA) forms recruitment materials and other
relevant information will be reviewed by a properly constituted IRB at each participating clinical
center A copy of the signed and dated IRB approval at each clinical center will be retrieved prior
to or during the site initiation visit and archived at the IPFnet DCC Any amendments to the
protocol other than simple administrative and typographical changes must be approved by each
IRB before they are implemented The clinical centers will seek annual renewals of their IRB
approvals in accordance with local procedures
67
__________________________________________ ________________
__________________________________________
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
12 Investigator Agreement
I have read the foregoing protocol PANTHER-IPF and agree that it contains all necessary
details for carrying out this study I will conduct the study as outlined herein and will complete
the study within the time designated
I will provide copies of the protocol and all pertinent information to all individuals responsible to
me who assist in the conduct of this study I will discuss this material with them to ensure they
are fully informed regarding the drug and the conduct of the study
I will fulfill all responsibilities for submitting pertinent information to the local IRB if
applicable that is responsible for this study
I further agree that NHLBI andor DCRI will have access to any source documents from which
eCRF information may have been generated
Signature of Principal Investigator Date
Name of Principal Investigator (printed or typed)
Protocol version date May 19 2009
Protocol Amendment 1 version date May 28 2010
Protocol Amendment 2 version date December 6 2011
68
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
13 References
1 Raghu G Brown KK Bradford WZ et al A placebo-controlled trial of interferon gamma-1b in patients with idiopathic pulmonary fibrosis N Engl J Med 2004350125-33 2 King TE Jr Safrin S Starko KM et al Analyses of efficacy end points in a controlled trial of interferon-gamma1b for idiopathic pulmonary fibrosis Chest 2005127171-7 3 Flaherty KR Thwaite EL Kazerooni EA et al Radiological versus histological diagnosis in UIP and NSIP survival implications Thorax 200358143-8 4 Wells AU Desai SR Rubens MB et al Idiopathic pulmonary fibrosis a composite physiologic index derived from disease extent observed by computed tomography Am J Respir Crit Care Med 2003167962-9 5 Raghu G Freudenberger TD Yang S et al High prevalence of abnormal acid gastroshyoesophageal reflux in idiopathic pulmonary fibrosis Eur Respir J 200627136-42 6 Kinnula VL Focus on antioxidant enzymes and antioxidant strategies in smoking related airway diseases Thorax 200560693-700 7 Coultas DB Zumwalt RE Black WC Sobonya RE The epidemiology of interstitial lung diseases Am J Respir Crit Care Med 1994150967-72 8 Raghu G Weycker D Edelsberg J Bradford WZ Oster G Incidence and prevalence of idiopathic pulmonary fibrosis Am J Respir Crit Care Med 2006174810-6 9 Olson AL Swigris JJ Lezotte DC Norris JM Wilson CG Brown KK Mortality from pulmonary fibrosis increased in the United States from 1992 to 2003 Am J Respir Crit Care Med 2007176277-84 10 Mannino DM Etzel RA Parrish RG Pulmonary fibrosis deaths in the United States 1979shy1991 An analysis of multiple-cause mortality data Am J Respir Crit Care Med 19961531548shy52 11 Hubbard R Johnston I Coultas DB Britton J Mortality rates from cryptogenic fibrosing alveolitis in seven countries Thorax 199651711-6 12 Johnston I Britton J Kinnear W Logan R Rising mortality from cryptogenic fibrosing alveolitis Bmj 19903011017-21 13 Raghu G Collard HR Egan JJ et al An official ATSERSJRSALAT statement idiopathic pulmonary fibrosis evidence-based guidelines for diagnosis and management Am J Respir Crit Care Med 2011183788-824 14 (USA) FDA FDA Public Health Advisory Interferon gamma-1b (marketed as Actimmune) In 2007 15 King TE Jr Pardo A Selman M Idiopathic pulmonary fibrosis Lancet 2011 16 Raghu G Brown KK Costabel U et al Treatment of idiopathic pulmonary fibrosis with etanercept an exploratory placebo-controlled trial Am J Respir Crit Care Med 2008178948shy55 17 Malouf MA Hopkins P Snell G Glanville AR An investigator-driven study of everolimus in surgical lung biopsy confirmed idiopathic pulmonary fibrosis Respirology 201116776-83 18 King TE Jr Behr J Brown KK et al BUILD-1 a randomized placebo-controlled trial of bosentan in idiopathic pulmonary fibrosis Am J Respir Crit Care Med 200817775-81 19 Richeldi L Costabel U Selman M et al Efficacy of a tyrosine kinase inhibitor in idiopathic pulmonary fibrosis N Engl J Med 20113651079-87
69
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
20 Borok Z Buhl R Grimes GJ et al Effect of glutathione aerosol on oxidant-antioxidant imbalance in idiopathic pulmonary fibrosis Lancet 1991338215-6 21 Meyer A Buhl R Magnussen H The effect of oral N-acetylcysteine on lung glutathione levels in idiopathic pulmonary fibrosis Eur Respir J 19947431-6 22 Behr J Maier K Degenkolb B Krombach F Vogelmeier C Antioxidative and clinical effects of high-dose N-acetylcysteine in fibrosing alveolitis Adjunctive therapy to maintenance immunosuppression Am J Respir Crit Care Med 19971561897-901 23 Cantin AM North SL Fells GA Hubbard RC Crystal RG Oxidant-mediated epithelial cell injury in idiopathic pulmonary fibrosis J Clin Invest 1987791665-73 24 Waghray M Cui Z Horowitz JC et al Hydrogen peroxide is a diffusible paracrine signal for the induction of epithelial cell death by activated myofibroblasts Faseb J 200519854-6 25 Larios JM Budhiraja R Fanburg BL Thannickal VJ Oxidative protein cross-linking reactions involving L-tyrosine in transforming growth factor-beta1-stimulated fibroblasts J Biol Chem 200127617437-41 26 Kinnula VL Fattman CL Tan RJ Oury TD Oxidative stress in pulmonary fibrosis a possible role for redox modulatory therapy Am J Respir Crit Care Med 2005172417-22 27 Meyer A Buhl R Kampf S Magnussen H Intravenous N-acetylcysteine and lung glutathione of patients with pulmonary fibrosis and normals Am J Respir Crit Care Med 19951521055-60 28 Behr J Degenkolb B Krombach F Vogelmeier C Intracellular glutathione and bronchoalveolar cells in fibrosing alveolitis effects of N-acetylcysteine Eur Respir J 200219906-11 29 Bando M Hosono T Mato N et al Long-term efficacy of inhaled N-acetylcysteine in patients with idiopathic pulmonary fibrosis Intern Med 2010492289-96 30 Demedts M Behr J Buhl R et al High-dose acetylcysteine in idiopathic pulmonary fibrosis N Engl J Med 20053532229-42 31 Toma TP Bhowmik A Rajakulasingam R Acetylcysteine in pulmonary fibrosis N Engl J Med 20063541086-9 author reply -9 32 Hunninghake GW Antioxidant therapy for idiopathic pulmonary fibrosis N Engl J Med 20053532285-7 33 Flaherty KR Mumford JA Murray S et al Prognostic implications of physiologic and radiographic changes in idiopathic interstitial pneumonia Am J Respir Crit Care Med 2003168543-8 34 Latsi PI du Bois RM Nicholson AG et al Fibrotic idiopathic interstitial pneumonia the prognostic value of longitudinal functional trends Am J Respir Crit Care Med 2003168531-7 35 Collard HR King TE Jr Bartelson BB Vourlekis JS Schwarz MI Brown KK Changes in clinical and physiologic variables predict survival in idiopathic pulmonary fibrosis Am J Respir Crit Care Med 2003168538-42 36 Jegal Y Kim DS Shim TS et al Physiology is a stronger predictor of survival than pathology in fibrotic interstitial pneumonia Am J Respir Crit Care Med 2005171639-44 37 Martinez FJ Safrin S Weycker D et al The clinical course of patients with idiopathic pulmonary fibrosis Ann Intern Med 2005142963-7 38 Hull JH Acetylcysteine in pulmonary fibrosis N Engl J Med 20063541089-91 author reply -91
70
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
39 Flaherty KR King TE Jr Raghu G et al Idiopathic interstitial pneumonia what is the effect of a multidisciplinary approach to diagnosis Am J Respir Crit Care Med 2004170904shy10 40 Raghu G Johnson WC Lockhart D Mageto Y Treatment of idiopathic pulmonary fibrosis with a new antifibrotic agent pirfenidone results of a prospective open-label Phase II study Am J Respir Crit Care Med 19991591061-9 41 Hunninghake GW Lynch DA Galvin JR et al Radiologic findings are strongly associated with a pathologic diagnosis of usual interstitial pneumonia Chest 20031241215-23 42 Lynch D Godwin J Safrin S et al High-resolution computed tomography in idiopathic pulmonary fibrosis diagnosis and prognosis Am J Respir Crit Care Med 2005172488-93 43 Mallinckrodt CH Watkin JG Molenberghs G Carroll RJ Choice of the primary analysis in longitudinal clinical trials Pharmaceutical Statistics 20043161-9 44 Bang H Tsiatis A Estimating medical costs with censored data Biometrika 200087329shy43 45 Lin DY Regression analysis of incomplete medical cost data Stat Med 2003221181-200 46 Rochon J Application of GEE procedures for sample size calculations in repeated measures experiments Stat Med 1998171643-58 47 Lachin JM Foulkes MA Evaluation of sample size and power for analyses of survival with allowance for nonuniform patient entry losses to follow-up noncompliance and stratification Biometrics 198642507-19
71
- PANTHER-IPFPREDNISONE AZATHIOPRINEAND N-ACETYLCYSTEINEA STUDY THAT EVALUATES RESPONSE INIDIOPATHIC PULMONARY FIBROSIS
-
- Protocol Summary
- Table of Contents
- List of Tables
- List of Figures
- List of Abbreviations
- 1 Summary
- 2 Hypotheses and Specific Aims
-
- 21 Null Hypothesis
- 22 Specific Aim 1
- 23 Specific Aim 2
- 24 Prespecified Subgroups of Interest
-
- 3 Background and Significance
-
- 31 Idiopathic Pulmonary Fibrosis is the Most Common Interstitial Lung Disease
- 32 Rationale for Placebo Control
- 33 Rationale for N-acetylcysteine
- 35 Rationale for N-acetylcysteine as a Stand-alone Therapy
- 36 Rationale for the Study Design and Primary Endpoint
- 37 Rationale for Blinding of Treatments
-
- 4 Methods
-
- 41 Inclusion Criteria
- 42 Diagnosis of IPF
- 43 Exclusion Criteria
- 44 Study Design and Study Visit
- 45 Dose Justification
- 46 Contraindications Precautions and Side Effects of Study Medications
- 47 Recruitment Procedures
- 48 Study Procedures
- 49 Concomitant Medications
- 410 Laboratory Testing
- 411 Blinding of Study Drugs
-
- 5 Study Endpoints
-
- 51 Primary Study Endpoint
- 52 Secondary Study Endpoints
-
- 6 Safety Evaluations and Procedures
-
- 61 Adverse Events
- 62 Clinical Medical Monitoring
- 63 Unblinding Procedures
-
- 7 Study Drug Procedures
- 8 Data Management
-
- 81 Hardware and Software Configuration
- 82 Sources of Data
-
- 9 Study Design and Data Analysis
-
- 91 General Analytic Considerations
- 92 Randomization Blinding and Reporting of Results
- 93 Stratification
- 94 Specification of the Primary Analyses
- 95 Analysis of Longitudinal Endpoints
- 96 Analysis of Binary Time-to-Event and Time-Lagged Endpoints
- 97 Power Analysis
-
- 10 Study Administration
-
- 101 Cooperative Agreement Mechanism
- 102 IPFnet Steering Group
- 103 Data and Safety Monitoring Board
- 104 Recommendations on Interim Monitoring of Efficacy Safety and Futility
-
- 11 Investigator and Sponsor Obligations
-
- 111 Monitoring
- 112 Cost and Payment
- 113 Confidentiality and Health Insurance Portability and Accountability ActConsiderations
- 114 Informed Consent Procedures
- 115 Institutional Review Boards
-
- 12 Investigator Agreement
- 13 References
-

PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
9 Study Design and Data Analysis
91 General Analytic Considerations
All primary analyses will be based on intent-to-treat (ITT) principles using all randomized
subjects Baseline factors across groups will be compared using mean (standard deviation) and
median (25th and 75th percentiles) summary measures Kaplan-Meier curves will be used to
display event rates Due to clinical interest in departures from both sides of the null hypothesis
all test statistics will be 2-sided
Reasonable caution needs to be taken when conducting multiple analyses on key clinical
subgroups For subgroup analyses a conservative significance level of 0001 will be used for all
interaction tests Thus subgroup comparisons will be considered exploratory unless the p-value
from the interaction test is smaller than 0001
92 Randomization Blinding and Reporting of Results
A permuted block-randomization scheme will be created with varying block sizes stratified by
clinical center Once a subject has completed the screening and baseline period and evaluation
for inclusionexclusion criteria the randomization process will begin Subjects will be
randomized to receive NAC or matching placebo with equal probability (11) via telephone
contact with a central interactive voice response system (IVRS) using a toll-free randomization
number On the day of randomization after the subject has successfully met all inclusion and
exclusion criteria the investigator or designee will call the central randomization number to
obtain the assigned kit randomization numbers for that subject At each subject visit the
investigator or designee will call the central randomization number to obtain the new kit
randomization numbers for resupply of the subject For resupply of the clinical center the IVRS
will monitor minimal volume of a kit type andor expiration date and will automatically notify
the pharmacy
57
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
The trial results will be reported according to guidelines specified in the CONSORT statement
A flow diagram describing screening recruitment randomization dropout and vital status will
be included in the primary manuscript AEs and efficacy data will be presented for all treatment
groups Adherence dropout and lost to follow-up will be carefully examined across all treatment
groups Analyses of safety will be based on data from all randomized subjects who received at
least one dose of study drug
93 Stratification
Subjects will be distributed to the two treatment arms in a 11 allocation ratio Stratification
blocks will be based on clinical centers
94 Specification of the Primary Analyses
A mixed model repeated measures (MMRM) analysis described in section 95 will be used to
compare differences in the slope of FVC measurements across the treatment groups Response
variables are values of the FVC measured at baseline and every 15 weeks until study completion
Variables in the model will include treatment time and time by treatment age sex race and
height Contrast estimates of differences in slopes of treatment over time (along with confidence
intervals) will be used to estimate the treatment effect The validity of this model in terms of
meeting modeling assumptions will be assessed via standard modeling diagnostics and goodness-
of-fit measures Based on the MMRM framework missing FVC data will not be imputed for the
primary analysis
95 Analysis of Longitudinal Endpoints
A common goal in clinical trials is to specify models that are easily implemented and
reproducible by independent data analysts On the other hand the models should have proper
statistical behavior in terms of low bias and high precision Many common approaches to
longitudinal data analysis including last observation carried forward (LOCF) imputation rely on
the missing completely at random (MCAR) assumption However the MCAR assumption is
58
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
unlikely to hold in many clinical trials because missing data are often related to disease
progression and prognosis A more reasonable assumption missing at random (MAR) specifies
that the complete data distribution can be modeled using only the observed data The likelihood-
based MMRM approach is valid under the more general MAR assumptions These models will
be applied to analyze the longitudinal data secondary endpoints
The advantages of MMRM analysis are that all important characteristics of the model can be preshy
specified standard software can be used to implement the models and results are based on ITT
principles43 In addition the MMRM approach offers superior control of Type I and Type II
errors compared with the LOCF approach
Response variables are values of the PFTs measured at enrollment and every 15 weeks until
study completion and 6MWT values measured at baseline week 30 and week 60 Covariates are
treatment time time by treatment and key baseline risk factors Contrasts (along with
confidence intervals) of treatment by time will be used to estimate the treatment effect
The correlation structure involves multiple pieces including measurement errors random
variation and interindividual variability For the longitudinal data analyses an unstructured
correlation matrix for within-subject errors will be assumed Other correlation structures
including compound symmetry will be examined as needed A careful examination of reasons
for study discontinuation will be conducted to assess the validity of MCAR Sensitivity analyses
will be used to examine the untestable assumption that the observed data violate the MAR
assumption The MMRM models will be implemented using PROC MIXED in SAS
96 Analysis of Binary Time-to-Event and Time-Lagged Endpoints
Regression modeling approaches using either the logistic regression model or Cox proportional
hazards regression model will be employed when appropriate The validity of these models will
be assessed via standard modeling diagnostics and goodness-of-fit measures Estimates of
cumulative frequencies for more general time-lagged responses will be calculated using the
partitioned version of the Bang-Tsiatis estimator44 The partitions will be set at 15-week intervals
59
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
to correspond with the data-collection process Covariate adjusted event rates will be calculated
using inverse probability-weighted regression estimates45
97 Power Analysis
971 Primary Analyses
Based on previously published IPF clinical trials the PL group is expected to experience a drop
in FVC of approximately 020 L over the study period (see Figure 1) The IPFnet Steering Group
determined a clinically important difference would be to preserve the majority of the decline
relative to PL over the study period In particular a treatment effect of 015 L was determined to
be a clinically meaningful difference Potential dropout is a key factor in the proposed study The
drop-out process assumed 5 lost to follow-up after every study visit Only 80 of subjects
were assumed to be followed for the entire study period All models assumed a compound
symmetry structure for the covariance matrix Power calculations were performed using a SAS
IML program for designing repeated measures studies46 Based on preliminary reviews of the
data from the University of Michigan the covariance matrix parameters were estimated at
approximately σ2 = 0757 (variance parameter) and ρ = 0936 (correlation parameter) To be
conservative the power calculations for the primary analysis were performed with parameter
setting of σ2 = 0810 (variance parameter) and ρ = 0925 (correlation parameter)
The power calculations assume a correction for imperfect compliance proposed by Lachin and
Foulkes to allow for 2 noncompliance for each of the treatment arms47 Thus the sample size
of 130 subjects per arm would be reduced to an adjusted sample size of 130(1-002-002)2 =
1198 or 120 subjects per arm
Under the assumed Type I error rate of 005 with a correlation parameter of 0925 and standard
deviation of 090 the difference of 015 L (or 00025 Lweek) shown in Table 6 would have
power of 93
60
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Table 6 Hypothetical Values of Mean FVC (L) Change from Baseline
Week 15 Week 30 Week 45 Week 60
NAC 00125 00250 00375 00500
Placebo 00500 01000 01500 02000
Difference 00375 00750 01125 01500
Abbreviations FVC forced vital capacity PL placebo
972 Power Analysis for Secondary Endpoints
Power calculations for secondary endpoint measurements are shown in Table 7 Standard
deviations are based on unpublished data provided by the University of Michigan The
calculations are based on a 2-sample t-test with Type I error rate set at 005 These calculations
are likely to be conservative because the statistical approach described in section 95 for
analyzing these endpoints will incorporate incomplete observations as well as intermediate data
points
Table 7 Detectable Differences in Treatment Means for Selected Endpoint Measurements
Secondary Endpoints Std Dev
of the Baseline Score
Detectable Difference for 80 Power
Std Dev of the Change Score
Difference Detectable for
80 Power
DLCOpred 166 58 91 32
6MWT Area Under the Desaturation Curve
219 76 175 61
6MWT Distance to Desaturation 224 78 315 110
6MWT Minutes Walked 210 073 205 071
Abbreviations Std Dev standard deviation DLCOpred diffusing capacity of the lung for carbon monoxide percent predicted 6MWT 6-minute walk test
61
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
10 Study Administration
101 Cooperative Agreement Mechanism
The administrative and funding mechanism used to undertake this project is a ldquocooperative
agreementrdquo (U01) which is an assistance mechanism Under the cooperative agreement the
NHLBI assists supports andor stimulates the project and is substantially involved with
investigators in conducting the study by facilitating performance of the effort in a ldquopartnerrdquo role
The NHLBI project scientist serves on the IPFnet Steering Group and he or another NHLBI
scientist may serve on other project committees when appropriate At the same time however
NHLBI does not assume a dominant role direction or prime responsibility for this research
program
As described below governance of the project is conducted through the IPFnet Steering Group
Principal investigators have lead responsibilities in all aspects of their trials and the project
including any modification of trial designs conduct of the trials quality control data analysis
and interpretation preparation of publications and collaboration with other investigators unless
otherwise provided for by the IPFnet Steering Group
PIs retain custody of and have primary rights to their center-specific and collaborative data
subject to government rights-of-access consistent with current Health amp Human Services (HHS)
Public Health Service (PHS) and National Institutes of Health policies The protocols and
governance policies call for the continual submission of data centrally to the IPFnet DCC for the
collaborative database which at a minimum will contain the key variables selected by the IPFnet
Steering Group for standardization across all clinical centers the submission of copies of the
collaborative datasets to each PI upon completion of the project procedures for data analysis
reporting and publication and procedures to protect and ensure the privacy of medical and
genetic data and records of individuals The NHLBI project scientist on behalf of the NHLBI
will have the same access privileges and responsibilities regarding the collaborative data as the
other members of the Steering Group
62
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
PIs are also encouraged to publish and to publicly release and disseminate results data and other
products of the project concordant with the project protocols and governance and the approved
plan for making data and materials available to the scientific community and to the NHLBI
However during the 3 years after the ending date of NHLBI project support unpublished data
unpublished results data sets not previously released and other study materials or products are
to be made available to any third party only with the approval of the IPFnet Steering Group
Upon completion of the project PIs are expected to put their intervention materials and
procedure manuals into the public domain andor make them available to other investigators
according to the approved plan for making data and materials available to the scientific
community and the NHLBI for the conduct of research at no charge other than the costs of
reproduction and distribution
The NHLBI reserves the right to terminate or curtail the project (or an individual award) in the
event of (a) failure to develop or implement mutually agreeable collaborative measurement
subject eligibility and data management sections of the protocols (b) substantial shortfall in
subject recruitment follow-up data reporting or quality control or other major breach of
protocol (c) substantive changes in the agreed-upon protocols with which NHLBI cannot
concur (d) reaching a major project outcome with persuasive statistical significance
substantially before schedule or (e) human subject ethical issues that may dictate a premature
termination
Any disagreement that may arise in scientificprogrammatic matters (within the scope of the
award) between award recipients and the NHLBI may be brought to arbitration An arbitration
panel will be composed of 3 membersmdash1 selected by the IPFnet Steering Group (with the
NHLBI member not voting) or by the individual PI in the event of an individual disagreement a
second selected by NHLBI and the third selected by the other 2 members This special
arbitration procedure in no way affects the PIrsquos right to appeal an adverse action that is otherwise
appealable in accordance with the PHS regulations at 42 CFR part 50 Subpart D and HHS
63
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
regulation at 45 CFR part 16 or the rights of the NHLBI under applicable statutes regulations
and terms of the award
102 IPFnet Steering Group
The IPFnet Steering Group is the main governing body of the project It is composed of the PIs
of the clinical centers the PI of the DCC and the NHLBI project scientist The clinical centers
the IPFnet DCC and the NHLBI each have 1 vote on the IPFnet Steering Group All decisions
are determined by majority vote
All major scientific decisions are determined by the IPFnet Steering Group It assumes overall
responsibility for the design and conduct of the trial It appoints (and disbands) committees and
subcommittees as the need arises designs approves and implements the study protocols
oversees the development of the MOOP monitors subject recruitment and treatment delivery
evaluates data collection and management oversees quality assurance procedures and
implements changes and enhancements to the study as required It also has primary responsibility
for facilitating the conduct of the trials and reporting the projectrsquos results
103 Data and Safety Monitoring Board
The NHLBI will establish a DSMB in accordance with established policies (see
httpwwwnhlbinihgovfundingpoliciesdsmb_insthtm) to ensure data quality and subject
safety and to provide independent advice to the NHLBI regarding progress and the
appropriateness of study continuation
104 Recommendations on Interim Monitoring of Efficacy Safety and Futility
First and foremost the role of the DSMB will be to review subject safety and trial conduct at
periodic points during the study The DSMB may require analyses of the primary endpoint
results for comparing the benefit and risks of treatment strategies The benefit of collecting
additional data on key secondary endpoints with extended follow-up and establishing a robust
64
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
evidence base for determining a standard of care will need to be carefully considered before
early termination of one or more treatment arms After careful consideration the IPFnet Steering
Group recommends conservative thresholds for the early examinations of the safety and efficacy
data
The DSMB will be expected to meet approximately every 6 months until trial completion to
review safety and toxicity data The DSMB may recommend stopping the study based on these
reviews Because the DSMB could stop the trial for safety concerns as well as for a large
efficacy benefit there could be multiple opportunities to reject the null hypothesis (no difference
in event rates between the PL and NAC groups) A Bonferroni approximation will be applied
during the one planned interim analysis for efficacy
Before locking the database a statistical analysis plan (SAP) will be developed to provide
complete details on the statistical analysis The SAP will include the specifics for how and when
the DSMB will be notified for AEs The IPFnet DCC will deliver to the DSMB all FDA-defined
AEs at 3-month intervals The IPFnet DCC will prepare narrative SAE reports in real time for
DSMB review including recommendations and analysis of similar events for each SAE
submitted to the FDA
65
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
11 Investigator and Sponsor Obligations
111 Monitoring
All monitoring activities for US clinical centers will be performed in accordance with DCRI
standard operating procedures Information regarding the types of visits will be outlined in the
PANTHER-IPF MOOP
112 Cost and Payment
There will be no cost to subjects enrolled in this trial Study-related procedures will be paid for
by the IPFnet
Subjects may be eligible for reimbursement for travel to the clinical center Details of payment
will be explained to each subject during the consent process
113 Confidentiality and Health Insurance Portability and Accountability Act
Considerations
Subject confidentiality will be protected throughout the study All subject data will be kept
strictly confidential and no subject-identifying information will be released to anyone outside
the project Confidentiality will be assured through several mechanisms First each subject will
be assigned an anonymous study ID which will then be used on all study forms Second any
study forms blood samples and paper records that contain subject information (eg address lists
phone lists) will be kept at the clinical centers in secured locked areas coded by number Once
blood is collected there will be no subject identifiers placed on blood samplesmdashonly the study
ID number and the date of sample collection Third access to all subject data and information
including laboratory specimens will be restricted to authorized personnel In the case of
computerized data this restricted access will be assured through user logon IDs and password
protection
66
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
At the IPFnet DCC only authorized personnel will have access to the data files containing study
data Security will be assured through user logon IDs passwords and appropriate access
privileges All study subjects will be identified only by their IPFnet ID numbers and no personal
identifying information such as name address or Social Security number will be entered into
the IPFnet DCC database Any subject-specific data reported to the IPFnet Steering Group will
be identified only by the IPFnet ID number
Finally subjects will not be identified by name in any reports or publications nor will the data
be presented in such a way that the identity of individual subjects can be inferred Analysis files
created for further study by the scientific community will have no subject identifiers These data
files will be created in accordance with the Ancillary Studies and Publication Policy of the
IPFnet
114 Informed Consent Procedures
All IPFnet subjects will provide written informed consent using procedures reviewed and
approved by each clinical centerrsquos IRB Informed consent will be undertaken by study personnel
in-person with the subject The subject has the option of declining further participation in the
study at that point No further study procedures will be conducted until the signed documents
have been provided to the IPFnet clinical center
115 Institutional Review Boards
Before initiating this study the protocol clinical center-specific informed consent forms Health
Insurance Portability and Accountability Act (HIPAA) forms recruitment materials and other
relevant information will be reviewed by a properly constituted IRB at each participating clinical
center A copy of the signed and dated IRB approval at each clinical center will be retrieved prior
to or during the site initiation visit and archived at the IPFnet DCC Any amendments to the
protocol other than simple administrative and typographical changes must be approved by each
IRB before they are implemented The clinical centers will seek annual renewals of their IRB
approvals in accordance with local procedures
67
__________________________________________ ________________
__________________________________________
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
12 Investigator Agreement
I have read the foregoing protocol PANTHER-IPF and agree that it contains all necessary
details for carrying out this study I will conduct the study as outlined herein and will complete
the study within the time designated
I will provide copies of the protocol and all pertinent information to all individuals responsible to
me who assist in the conduct of this study I will discuss this material with them to ensure they
are fully informed regarding the drug and the conduct of the study
I will fulfill all responsibilities for submitting pertinent information to the local IRB if
applicable that is responsible for this study
I further agree that NHLBI andor DCRI will have access to any source documents from which
eCRF information may have been generated
Signature of Principal Investigator Date
Name of Principal Investigator (printed or typed)
Protocol version date May 19 2009
Protocol Amendment 1 version date May 28 2010
Protocol Amendment 2 version date December 6 2011
68
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
13 References
1 Raghu G Brown KK Bradford WZ et al A placebo-controlled trial of interferon gamma-1b in patients with idiopathic pulmonary fibrosis N Engl J Med 2004350125-33 2 King TE Jr Safrin S Starko KM et al Analyses of efficacy end points in a controlled trial of interferon-gamma1b for idiopathic pulmonary fibrosis Chest 2005127171-7 3 Flaherty KR Thwaite EL Kazerooni EA et al Radiological versus histological diagnosis in UIP and NSIP survival implications Thorax 200358143-8 4 Wells AU Desai SR Rubens MB et al Idiopathic pulmonary fibrosis a composite physiologic index derived from disease extent observed by computed tomography Am J Respir Crit Care Med 2003167962-9 5 Raghu G Freudenberger TD Yang S et al High prevalence of abnormal acid gastroshyoesophageal reflux in idiopathic pulmonary fibrosis Eur Respir J 200627136-42 6 Kinnula VL Focus on antioxidant enzymes and antioxidant strategies in smoking related airway diseases Thorax 200560693-700 7 Coultas DB Zumwalt RE Black WC Sobonya RE The epidemiology of interstitial lung diseases Am J Respir Crit Care Med 1994150967-72 8 Raghu G Weycker D Edelsberg J Bradford WZ Oster G Incidence and prevalence of idiopathic pulmonary fibrosis Am J Respir Crit Care Med 2006174810-6 9 Olson AL Swigris JJ Lezotte DC Norris JM Wilson CG Brown KK Mortality from pulmonary fibrosis increased in the United States from 1992 to 2003 Am J Respir Crit Care Med 2007176277-84 10 Mannino DM Etzel RA Parrish RG Pulmonary fibrosis deaths in the United States 1979shy1991 An analysis of multiple-cause mortality data Am J Respir Crit Care Med 19961531548shy52 11 Hubbard R Johnston I Coultas DB Britton J Mortality rates from cryptogenic fibrosing alveolitis in seven countries Thorax 199651711-6 12 Johnston I Britton J Kinnear W Logan R Rising mortality from cryptogenic fibrosing alveolitis Bmj 19903011017-21 13 Raghu G Collard HR Egan JJ et al An official ATSERSJRSALAT statement idiopathic pulmonary fibrosis evidence-based guidelines for diagnosis and management Am J Respir Crit Care Med 2011183788-824 14 (USA) FDA FDA Public Health Advisory Interferon gamma-1b (marketed as Actimmune) In 2007 15 King TE Jr Pardo A Selman M Idiopathic pulmonary fibrosis Lancet 2011 16 Raghu G Brown KK Costabel U et al Treatment of idiopathic pulmonary fibrosis with etanercept an exploratory placebo-controlled trial Am J Respir Crit Care Med 2008178948shy55 17 Malouf MA Hopkins P Snell G Glanville AR An investigator-driven study of everolimus in surgical lung biopsy confirmed idiopathic pulmonary fibrosis Respirology 201116776-83 18 King TE Jr Behr J Brown KK et al BUILD-1 a randomized placebo-controlled trial of bosentan in idiopathic pulmonary fibrosis Am J Respir Crit Care Med 200817775-81 19 Richeldi L Costabel U Selman M et al Efficacy of a tyrosine kinase inhibitor in idiopathic pulmonary fibrosis N Engl J Med 20113651079-87
69
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
20 Borok Z Buhl R Grimes GJ et al Effect of glutathione aerosol on oxidant-antioxidant imbalance in idiopathic pulmonary fibrosis Lancet 1991338215-6 21 Meyer A Buhl R Magnussen H The effect of oral N-acetylcysteine on lung glutathione levels in idiopathic pulmonary fibrosis Eur Respir J 19947431-6 22 Behr J Maier K Degenkolb B Krombach F Vogelmeier C Antioxidative and clinical effects of high-dose N-acetylcysteine in fibrosing alveolitis Adjunctive therapy to maintenance immunosuppression Am J Respir Crit Care Med 19971561897-901 23 Cantin AM North SL Fells GA Hubbard RC Crystal RG Oxidant-mediated epithelial cell injury in idiopathic pulmonary fibrosis J Clin Invest 1987791665-73 24 Waghray M Cui Z Horowitz JC et al Hydrogen peroxide is a diffusible paracrine signal for the induction of epithelial cell death by activated myofibroblasts Faseb J 200519854-6 25 Larios JM Budhiraja R Fanburg BL Thannickal VJ Oxidative protein cross-linking reactions involving L-tyrosine in transforming growth factor-beta1-stimulated fibroblasts J Biol Chem 200127617437-41 26 Kinnula VL Fattman CL Tan RJ Oury TD Oxidative stress in pulmonary fibrosis a possible role for redox modulatory therapy Am J Respir Crit Care Med 2005172417-22 27 Meyer A Buhl R Kampf S Magnussen H Intravenous N-acetylcysteine and lung glutathione of patients with pulmonary fibrosis and normals Am J Respir Crit Care Med 19951521055-60 28 Behr J Degenkolb B Krombach F Vogelmeier C Intracellular glutathione and bronchoalveolar cells in fibrosing alveolitis effects of N-acetylcysteine Eur Respir J 200219906-11 29 Bando M Hosono T Mato N et al Long-term efficacy of inhaled N-acetylcysteine in patients with idiopathic pulmonary fibrosis Intern Med 2010492289-96 30 Demedts M Behr J Buhl R et al High-dose acetylcysteine in idiopathic pulmonary fibrosis N Engl J Med 20053532229-42 31 Toma TP Bhowmik A Rajakulasingam R Acetylcysteine in pulmonary fibrosis N Engl J Med 20063541086-9 author reply -9 32 Hunninghake GW Antioxidant therapy for idiopathic pulmonary fibrosis N Engl J Med 20053532285-7 33 Flaherty KR Mumford JA Murray S et al Prognostic implications of physiologic and radiographic changes in idiopathic interstitial pneumonia Am J Respir Crit Care Med 2003168543-8 34 Latsi PI du Bois RM Nicholson AG et al Fibrotic idiopathic interstitial pneumonia the prognostic value of longitudinal functional trends Am J Respir Crit Care Med 2003168531-7 35 Collard HR King TE Jr Bartelson BB Vourlekis JS Schwarz MI Brown KK Changes in clinical and physiologic variables predict survival in idiopathic pulmonary fibrosis Am J Respir Crit Care Med 2003168538-42 36 Jegal Y Kim DS Shim TS et al Physiology is a stronger predictor of survival than pathology in fibrotic interstitial pneumonia Am J Respir Crit Care Med 2005171639-44 37 Martinez FJ Safrin S Weycker D et al The clinical course of patients with idiopathic pulmonary fibrosis Ann Intern Med 2005142963-7 38 Hull JH Acetylcysteine in pulmonary fibrosis N Engl J Med 20063541089-91 author reply -91
70
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
39 Flaherty KR King TE Jr Raghu G et al Idiopathic interstitial pneumonia what is the effect of a multidisciplinary approach to diagnosis Am J Respir Crit Care Med 2004170904shy10 40 Raghu G Johnson WC Lockhart D Mageto Y Treatment of idiopathic pulmonary fibrosis with a new antifibrotic agent pirfenidone results of a prospective open-label Phase II study Am J Respir Crit Care Med 19991591061-9 41 Hunninghake GW Lynch DA Galvin JR et al Radiologic findings are strongly associated with a pathologic diagnosis of usual interstitial pneumonia Chest 20031241215-23 42 Lynch D Godwin J Safrin S et al High-resolution computed tomography in idiopathic pulmonary fibrosis diagnosis and prognosis Am J Respir Crit Care Med 2005172488-93 43 Mallinckrodt CH Watkin JG Molenberghs G Carroll RJ Choice of the primary analysis in longitudinal clinical trials Pharmaceutical Statistics 20043161-9 44 Bang H Tsiatis A Estimating medical costs with censored data Biometrika 200087329shy43 45 Lin DY Regression analysis of incomplete medical cost data Stat Med 2003221181-200 46 Rochon J Application of GEE procedures for sample size calculations in repeated measures experiments Stat Med 1998171643-58 47 Lachin JM Foulkes MA Evaluation of sample size and power for analyses of survival with allowance for nonuniform patient entry losses to follow-up noncompliance and stratification Biometrics 198642507-19
71
- PANTHER-IPFPREDNISONE AZATHIOPRINEAND N-ACETYLCYSTEINEA STUDY THAT EVALUATES RESPONSE INIDIOPATHIC PULMONARY FIBROSIS
-
- Protocol Summary
- Table of Contents
- List of Tables
- List of Figures
- List of Abbreviations
- 1 Summary
- 2 Hypotheses and Specific Aims
-
- 21 Null Hypothesis
- 22 Specific Aim 1
- 23 Specific Aim 2
- 24 Prespecified Subgroups of Interest
-
- 3 Background and Significance
-
- 31 Idiopathic Pulmonary Fibrosis is the Most Common Interstitial Lung Disease
- 32 Rationale for Placebo Control
- 33 Rationale for N-acetylcysteine
- 35 Rationale for N-acetylcysteine as a Stand-alone Therapy
- 36 Rationale for the Study Design and Primary Endpoint
- 37 Rationale for Blinding of Treatments
-
- 4 Methods
-
- 41 Inclusion Criteria
- 42 Diagnosis of IPF
- 43 Exclusion Criteria
- 44 Study Design and Study Visit
- 45 Dose Justification
- 46 Contraindications Precautions and Side Effects of Study Medications
- 47 Recruitment Procedures
- 48 Study Procedures
- 49 Concomitant Medications
- 410 Laboratory Testing
- 411 Blinding of Study Drugs
-
- 5 Study Endpoints
-
- 51 Primary Study Endpoint
- 52 Secondary Study Endpoints
-
- 6 Safety Evaluations and Procedures
-
- 61 Adverse Events
- 62 Clinical Medical Monitoring
- 63 Unblinding Procedures
-
- 7 Study Drug Procedures
- 8 Data Management
-
- 81 Hardware and Software Configuration
- 82 Sources of Data
-
- 9 Study Design and Data Analysis
-
- 91 General Analytic Considerations
- 92 Randomization Blinding and Reporting of Results
- 93 Stratification
- 94 Specification of the Primary Analyses
- 95 Analysis of Longitudinal Endpoints
- 96 Analysis of Binary Time-to-Event and Time-Lagged Endpoints
- 97 Power Analysis
-
- 10 Study Administration
-
- 101 Cooperative Agreement Mechanism
- 102 IPFnet Steering Group
- 103 Data and Safety Monitoring Board
- 104 Recommendations on Interim Monitoring of Efficacy Safety and Futility
-
- 11 Investigator and Sponsor Obligations
-
- 111 Monitoring
- 112 Cost and Payment
- 113 Confidentiality and Health Insurance Portability and Accountability ActConsiderations
- 114 Informed Consent Procedures
- 115 Institutional Review Boards
-
- 12 Investigator Agreement
- 13 References
-

PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
The trial results will be reported according to guidelines specified in the CONSORT statement
A flow diagram describing screening recruitment randomization dropout and vital status will
be included in the primary manuscript AEs and efficacy data will be presented for all treatment
groups Adherence dropout and lost to follow-up will be carefully examined across all treatment
groups Analyses of safety will be based on data from all randomized subjects who received at
least one dose of study drug
93 Stratification
Subjects will be distributed to the two treatment arms in a 11 allocation ratio Stratification
blocks will be based on clinical centers
94 Specification of the Primary Analyses
A mixed model repeated measures (MMRM) analysis described in section 95 will be used to
compare differences in the slope of FVC measurements across the treatment groups Response
variables are values of the FVC measured at baseline and every 15 weeks until study completion
Variables in the model will include treatment time and time by treatment age sex race and
height Contrast estimates of differences in slopes of treatment over time (along with confidence
intervals) will be used to estimate the treatment effect The validity of this model in terms of
meeting modeling assumptions will be assessed via standard modeling diagnostics and goodness-
of-fit measures Based on the MMRM framework missing FVC data will not be imputed for the
primary analysis
95 Analysis of Longitudinal Endpoints
A common goal in clinical trials is to specify models that are easily implemented and
reproducible by independent data analysts On the other hand the models should have proper
statistical behavior in terms of low bias and high precision Many common approaches to
longitudinal data analysis including last observation carried forward (LOCF) imputation rely on
the missing completely at random (MCAR) assumption However the MCAR assumption is
58
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
unlikely to hold in many clinical trials because missing data are often related to disease
progression and prognosis A more reasonable assumption missing at random (MAR) specifies
that the complete data distribution can be modeled using only the observed data The likelihood-
based MMRM approach is valid under the more general MAR assumptions These models will
be applied to analyze the longitudinal data secondary endpoints
The advantages of MMRM analysis are that all important characteristics of the model can be preshy
specified standard software can be used to implement the models and results are based on ITT
principles43 In addition the MMRM approach offers superior control of Type I and Type II
errors compared with the LOCF approach
Response variables are values of the PFTs measured at enrollment and every 15 weeks until
study completion and 6MWT values measured at baseline week 30 and week 60 Covariates are
treatment time time by treatment and key baseline risk factors Contrasts (along with
confidence intervals) of treatment by time will be used to estimate the treatment effect
The correlation structure involves multiple pieces including measurement errors random
variation and interindividual variability For the longitudinal data analyses an unstructured
correlation matrix for within-subject errors will be assumed Other correlation structures
including compound symmetry will be examined as needed A careful examination of reasons
for study discontinuation will be conducted to assess the validity of MCAR Sensitivity analyses
will be used to examine the untestable assumption that the observed data violate the MAR
assumption The MMRM models will be implemented using PROC MIXED in SAS
96 Analysis of Binary Time-to-Event and Time-Lagged Endpoints
Regression modeling approaches using either the logistic regression model or Cox proportional
hazards regression model will be employed when appropriate The validity of these models will
be assessed via standard modeling diagnostics and goodness-of-fit measures Estimates of
cumulative frequencies for more general time-lagged responses will be calculated using the
partitioned version of the Bang-Tsiatis estimator44 The partitions will be set at 15-week intervals
59
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
to correspond with the data-collection process Covariate adjusted event rates will be calculated
using inverse probability-weighted regression estimates45
97 Power Analysis
971 Primary Analyses
Based on previously published IPF clinical trials the PL group is expected to experience a drop
in FVC of approximately 020 L over the study period (see Figure 1) The IPFnet Steering Group
determined a clinically important difference would be to preserve the majority of the decline
relative to PL over the study period In particular a treatment effect of 015 L was determined to
be a clinically meaningful difference Potential dropout is a key factor in the proposed study The
drop-out process assumed 5 lost to follow-up after every study visit Only 80 of subjects
were assumed to be followed for the entire study period All models assumed a compound
symmetry structure for the covariance matrix Power calculations were performed using a SAS
IML program for designing repeated measures studies46 Based on preliminary reviews of the
data from the University of Michigan the covariance matrix parameters were estimated at
approximately σ2 = 0757 (variance parameter) and ρ = 0936 (correlation parameter) To be
conservative the power calculations for the primary analysis were performed with parameter
setting of σ2 = 0810 (variance parameter) and ρ = 0925 (correlation parameter)
The power calculations assume a correction for imperfect compliance proposed by Lachin and
Foulkes to allow for 2 noncompliance for each of the treatment arms47 Thus the sample size
of 130 subjects per arm would be reduced to an adjusted sample size of 130(1-002-002)2 =
1198 or 120 subjects per arm
Under the assumed Type I error rate of 005 with a correlation parameter of 0925 and standard
deviation of 090 the difference of 015 L (or 00025 Lweek) shown in Table 6 would have
power of 93
60
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Table 6 Hypothetical Values of Mean FVC (L) Change from Baseline
Week 15 Week 30 Week 45 Week 60
NAC 00125 00250 00375 00500
Placebo 00500 01000 01500 02000
Difference 00375 00750 01125 01500
Abbreviations FVC forced vital capacity PL placebo
972 Power Analysis for Secondary Endpoints
Power calculations for secondary endpoint measurements are shown in Table 7 Standard
deviations are based on unpublished data provided by the University of Michigan The
calculations are based on a 2-sample t-test with Type I error rate set at 005 These calculations
are likely to be conservative because the statistical approach described in section 95 for
analyzing these endpoints will incorporate incomplete observations as well as intermediate data
points
Table 7 Detectable Differences in Treatment Means for Selected Endpoint Measurements
Secondary Endpoints Std Dev
of the Baseline Score
Detectable Difference for 80 Power
Std Dev of the Change Score
Difference Detectable for
80 Power
DLCOpred 166 58 91 32
6MWT Area Under the Desaturation Curve
219 76 175 61
6MWT Distance to Desaturation 224 78 315 110
6MWT Minutes Walked 210 073 205 071
Abbreviations Std Dev standard deviation DLCOpred diffusing capacity of the lung for carbon monoxide percent predicted 6MWT 6-minute walk test
61
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
10 Study Administration
101 Cooperative Agreement Mechanism
The administrative and funding mechanism used to undertake this project is a ldquocooperative
agreementrdquo (U01) which is an assistance mechanism Under the cooperative agreement the
NHLBI assists supports andor stimulates the project and is substantially involved with
investigators in conducting the study by facilitating performance of the effort in a ldquopartnerrdquo role
The NHLBI project scientist serves on the IPFnet Steering Group and he or another NHLBI
scientist may serve on other project committees when appropriate At the same time however
NHLBI does not assume a dominant role direction or prime responsibility for this research
program
As described below governance of the project is conducted through the IPFnet Steering Group
Principal investigators have lead responsibilities in all aspects of their trials and the project
including any modification of trial designs conduct of the trials quality control data analysis
and interpretation preparation of publications and collaboration with other investigators unless
otherwise provided for by the IPFnet Steering Group
PIs retain custody of and have primary rights to their center-specific and collaborative data
subject to government rights-of-access consistent with current Health amp Human Services (HHS)
Public Health Service (PHS) and National Institutes of Health policies The protocols and
governance policies call for the continual submission of data centrally to the IPFnet DCC for the
collaborative database which at a minimum will contain the key variables selected by the IPFnet
Steering Group for standardization across all clinical centers the submission of copies of the
collaborative datasets to each PI upon completion of the project procedures for data analysis
reporting and publication and procedures to protect and ensure the privacy of medical and
genetic data and records of individuals The NHLBI project scientist on behalf of the NHLBI
will have the same access privileges and responsibilities regarding the collaborative data as the
other members of the Steering Group
62
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
PIs are also encouraged to publish and to publicly release and disseminate results data and other
products of the project concordant with the project protocols and governance and the approved
plan for making data and materials available to the scientific community and to the NHLBI
However during the 3 years after the ending date of NHLBI project support unpublished data
unpublished results data sets not previously released and other study materials or products are
to be made available to any third party only with the approval of the IPFnet Steering Group
Upon completion of the project PIs are expected to put their intervention materials and
procedure manuals into the public domain andor make them available to other investigators
according to the approved plan for making data and materials available to the scientific
community and the NHLBI for the conduct of research at no charge other than the costs of
reproduction and distribution
The NHLBI reserves the right to terminate or curtail the project (or an individual award) in the
event of (a) failure to develop or implement mutually agreeable collaborative measurement
subject eligibility and data management sections of the protocols (b) substantial shortfall in
subject recruitment follow-up data reporting or quality control or other major breach of
protocol (c) substantive changes in the agreed-upon protocols with which NHLBI cannot
concur (d) reaching a major project outcome with persuasive statistical significance
substantially before schedule or (e) human subject ethical issues that may dictate a premature
termination
Any disagreement that may arise in scientificprogrammatic matters (within the scope of the
award) between award recipients and the NHLBI may be brought to arbitration An arbitration
panel will be composed of 3 membersmdash1 selected by the IPFnet Steering Group (with the
NHLBI member not voting) or by the individual PI in the event of an individual disagreement a
second selected by NHLBI and the third selected by the other 2 members This special
arbitration procedure in no way affects the PIrsquos right to appeal an adverse action that is otherwise
appealable in accordance with the PHS regulations at 42 CFR part 50 Subpart D and HHS
63
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
regulation at 45 CFR part 16 or the rights of the NHLBI under applicable statutes regulations
and terms of the award
102 IPFnet Steering Group
The IPFnet Steering Group is the main governing body of the project It is composed of the PIs
of the clinical centers the PI of the DCC and the NHLBI project scientist The clinical centers
the IPFnet DCC and the NHLBI each have 1 vote on the IPFnet Steering Group All decisions
are determined by majority vote
All major scientific decisions are determined by the IPFnet Steering Group It assumes overall
responsibility for the design and conduct of the trial It appoints (and disbands) committees and
subcommittees as the need arises designs approves and implements the study protocols
oversees the development of the MOOP monitors subject recruitment and treatment delivery
evaluates data collection and management oversees quality assurance procedures and
implements changes and enhancements to the study as required It also has primary responsibility
for facilitating the conduct of the trials and reporting the projectrsquos results
103 Data and Safety Monitoring Board
The NHLBI will establish a DSMB in accordance with established policies (see
httpwwwnhlbinihgovfundingpoliciesdsmb_insthtm) to ensure data quality and subject
safety and to provide independent advice to the NHLBI regarding progress and the
appropriateness of study continuation
104 Recommendations on Interim Monitoring of Efficacy Safety and Futility
First and foremost the role of the DSMB will be to review subject safety and trial conduct at
periodic points during the study The DSMB may require analyses of the primary endpoint
results for comparing the benefit and risks of treatment strategies The benefit of collecting
additional data on key secondary endpoints with extended follow-up and establishing a robust
64
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
evidence base for determining a standard of care will need to be carefully considered before
early termination of one or more treatment arms After careful consideration the IPFnet Steering
Group recommends conservative thresholds for the early examinations of the safety and efficacy
data
The DSMB will be expected to meet approximately every 6 months until trial completion to
review safety and toxicity data The DSMB may recommend stopping the study based on these
reviews Because the DSMB could stop the trial for safety concerns as well as for a large
efficacy benefit there could be multiple opportunities to reject the null hypothesis (no difference
in event rates between the PL and NAC groups) A Bonferroni approximation will be applied
during the one planned interim analysis for efficacy
Before locking the database a statistical analysis plan (SAP) will be developed to provide
complete details on the statistical analysis The SAP will include the specifics for how and when
the DSMB will be notified for AEs The IPFnet DCC will deliver to the DSMB all FDA-defined
AEs at 3-month intervals The IPFnet DCC will prepare narrative SAE reports in real time for
DSMB review including recommendations and analysis of similar events for each SAE
submitted to the FDA
65
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
11 Investigator and Sponsor Obligations
111 Monitoring
All monitoring activities for US clinical centers will be performed in accordance with DCRI
standard operating procedures Information regarding the types of visits will be outlined in the
PANTHER-IPF MOOP
112 Cost and Payment
There will be no cost to subjects enrolled in this trial Study-related procedures will be paid for
by the IPFnet
Subjects may be eligible for reimbursement for travel to the clinical center Details of payment
will be explained to each subject during the consent process
113 Confidentiality and Health Insurance Portability and Accountability Act
Considerations
Subject confidentiality will be protected throughout the study All subject data will be kept
strictly confidential and no subject-identifying information will be released to anyone outside
the project Confidentiality will be assured through several mechanisms First each subject will
be assigned an anonymous study ID which will then be used on all study forms Second any
study forms blood samples and paper records that contain subject information (eg address lists
phone lists) will be kept at the clinical centers in secured locked areas coded by number Once
blood is collected there will be no subject identifiers placed on blood samplesmdashonly the study
ID number and the date of sample collection Third access to all subject data and information
including laboratory specimens will be restricted to authorized personnel In the case of
computerized data this restricted access will be assured through user logon IDs and password
protection
66
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
At the IPFnet DCC only authorized personnel will have access to the data files containing study
data Security will be assured through user logon IDs passwords and appropriate access
privileges All study subjects will be identified only by their IPFnet ID numbers and no personal
identifying information such as name address or Social Security number will be entered into
the IPFnet DCC database Any subject-specific data reported to the IPFnet Steering Group will
be identified only by the IPFnet ID number
Finally subjects will not be identified by name in any reports or publications nor will the data
be presented in such a way that the identity of individual subjects can be inferred Analysis files
created for further study by the scientific community will have no subject identifiers These data
files will be created in accordance with the Ancillary Studies and Publication Policy of the
IPFnet
114 Informed Consent Procedures
All IPFnet subjects will provide written informed consent using procedures reviewed and
approved by each clinical centerrsquos IRB Informed consent will be undertaken by study personnel
in-person with the subject The subject has the option of declining further participation in the
study at that point No further study procedures will be conducted until the signed documents
have been provided to the IPFnet clinical center
115 Institutional Review Boards
Before initiating this study the protocol clinical center-specific informed consent forms Health
Insurance Portability and Accountability Act (HIPAA) forms recruitment materials and other
relevant information will be reviewed by a properly constituted IRB at each participating clinical
center A copy of the signed and dated IRB approval at each clinical center will be retrieved prior
to or during the site initiation visit and archived at the IPFnet DCC Any amendments to the
protocol other than simple administrative and typographical changes must be approved by each
IRB before they are implemented The clinical centers will seek annual renewals of their IRB
approvals in accordance with local procedures
67
__________________________________________ ________________
__________________________________________
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
12 Investigator Agreement
I have read the foregoing protocol PANTHER-IPF and agree that it contains all necessary
details for carrying out this study I will conduct the study as outlined herein and will complete
the study within the time designated
I will provide copies of the protocol and all pertinent information to all individuals responsible to
me who assist in the conduct of this study I will discuss this material with them to ensure they
are fully informed regarding the drug and the conduct of the study
I will fulfill all responsibilities for submitting pertinent information to the local IRB if
applicable that is responsible for this study
I further agree that NHLBI andor DCRI will have access to any source documents from which
eCRF information may have been generated
Signature of Principal Investigator Date
Name of Principal Investigator (printed or typed)
Protocol version date May 19 2009
Protocol Amendment 1 version date May 28 2010
Protocol Amendment 2 version date December 6 2011
68
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
13 References
1 Raghu G Brown KK Bradford WZ et al A placebo-controlled trial of interferon gamma-1b in patients with idiopathic pulmonary fibrosis N Engl J Med 2004350125-33 2 King TE Jr Safrin S Starko KM et al Analyses of efficacy end points in a controlled trial of interferon-gamma1b for idiopathic pulmonary fibrosis Chest 2005127171-7 3 Flaherty KR Thwaite EL Kazerooni EA et al Radiological versus histological diagnosis in UIP and NSIP survival implications Thorax 200358143-8 4 Wells AU Desai SR Rubens MB et al Idiopathic pulmonary fibrosis a composite physiologic index derived from disease extent observed by computed tomography Am J Respir Crit Care Med 2003167962-9 5 Raghu G Freudenberger TD Yang S et al High prevalence of abnormal acid gastroshyoesophageal reflux in idiopathic pulmonary fibrosis Eur Respir J 200627136-42 6 Kinnula VL Focus on antioxidant enzymes and antioxidant strategies in smoking related airway diseases Thorax 200560693-700 7 Coultas DB Zumwalt RE Black WC Sobonya RE The epidemiology of interstitial lung diseases Am J Respir Crit Care Med 1994150967-72 8 Raghu G Weycker D Edelsberg J Bradford WZ Oster G Incidence and prevalence of idiopathic pulmonary fibrosis Am J Respir Crit Care Med 2006174810-6 9 Olson AL Swigris JJ Lezotte DC Norris JM Wilson CG Brown KK Mortality from pulmonary fibrosis increased in the United States from 1992 to 2003 Am J Respir Crit Care Med 2007176277-84 10 Mannino DM Etzel RA Parrish RG Pulmonary fibrosis deaths in the United States 1979shy1991 An analysis of multiple-cause mortality data Am J Respir Crit Care Med 19961531548shy52 11 Hubbard R Johnston I Coultas DB Britton J Mortality rates from cryptogenic fibrosing alveolitis in seven countries Thorax 199651711-6 12 Johnston I Britton J Kinnear W Logan R Rising mortality from cryptogenic fibrosing alveolitis Bmj 19903011017-21 13 Raghu G Collard HR Egan JJ et al An official ATSERSJRSALAT statement idiopathic pulmonary fibrosis evidence-based guidelines for diagnosis and management Am J Respir Crit Care Med 2011183788-824 14 (USA) FDA FDA Public Health Advisory Interferon gamma-1b (marketed as Actimmune) In 2007 15 King TE Jr Pardo A Selman M Idiopathic pulmonary fibrosis Lancet 2011 16 Raghu G Brown KK Costabel U et al Treatment of idiopathic pulmonary fibrosis with etanercept an exploratory placebo-controlled trial Am J Respir Crit Care Med 2008178948shy55 17 Malouf MA Hopkins P Snell G Glanville AR An investigator-driven study of everolimus in surgical lung biopsy confirmed idiopathic pulmonary fibrosis Respirology 201116776-83 18 King TE Jr Behr J Brown KK et al BUILD-1 a randomized placebo-controlled trial of bosentan in idiopathic pulmonary fibrosis Am J Respir Crit Care Med 200817775-81 19 Richeldi L Costabel U Selman M et al Efficacy of a tyrosine kinase inhibitor in idiopathic pulmonary fibrosis N Engl J Med 20113651079-87
69
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
20 Borok Z Buhl R Grimes GJ et al Effect of glutathione aerosol on oxidant-antioxidant imbalance in idiopathic pulmonary fibrosis Lancet 1991338215-6 21 Meyer A Buhl R Magnussen H The effect of oral N-acetylcysteine on lung glutathione levels in idiopathic pulmonary fibrosis Eur Respir J 19947431-6 22 Behr J Maier K Degenkolb B Krombach F Vogelmeier C Antioxidative and clinical effects of high-dose N-acetylcysteine in fibrosing alveolitis Adjunctive therapy to maintenance immunosuppression Am J Respir Crit Care Med 19971561897-901 23 Cantin AM North SL Fells GA Hubbard RC Crystal RG Oxidant-mediated epithelial cell injury in idiopathic pulmonary fibrosis J Clin Invest 1987791665-73 24 Waghray M Cui Z Horowitz JC et al Hydrogen peroxide is a diffusible paracrine signal for the induction of epithelial cell death by activated myofibroblasts Faseb J 200519854-6 25 Larios JM Budhiraja R Fanburg BL Thannickal VJ Oxidative protein cross-linking reactions involving L-tyrosine in transforming growth factor-beta1-stimulated fibroblasts J Biol Chem 200127617437-41 26 Kinnula VL Fattman CL Tan RJ Oury TD Oxidative stress in pulmonary fibrosis a possible role for redox modulatory therapy Am J Respir Crit Care Med 2005172417-22 27 Meyer A Buhl R Kampf S Magnussen H Intravenous N-acetylcysteine and lung glutathione of patients with pulmonary fibrosis and normals Am J Respir Crit Care Med 19951521055-60 28 Behr J Degenkolb B Krombach F Vogelmeier C Intracellular glutathione and bronchoalveolar cells in fibrosing alveolitis effects of N-acetylcysteine Eur Respir J 200219906-11 29 Bando M Hosono T Mato N et al Long-term efficacy of inhaled N-acetylcysteine in patients with idiopathic pulmonary fibrosis Intern Med 2010492289-96 30 Demedts M Behr J Buhl R et al High-dose acetylcysteine in idiopathic pulmonary fibrosis N Engl J Med 20053532229-42 31 Toma TP Bhowmik A Rajakulasingam R Acetylcysteine in pulmonary fibrosis N Engl J Med 20063541086-9 author reply -9 32 Hunninghake GW Antioxidant therapy for idiopathic pulmonary fibrosis N Engl J Med 20053532285-7 33 Flaherty KR Mumford JA Murray S et al Prognostic implications of physiologic and radiographic changes in idiopathic interstitial pneumonia Am J Respir Crit Care Med 2003168543-8 34 Latsi PI du Bois RM Nicholson AG et al Fibrotic idiopathic interstitial pneumonia the prognostic value of longitudinal functional trends Am J Respir Crit Care Med 2003168531-7 35 Collard HR King TE Jr Bartelson BB Vourlekis JS Schwarz MI Brown KK Changes in clinical and physiologic variables predict survival in idiopathic pulmonary fibrosis Am J Respir Crit Care Med 2003168538-42 36 Jegal Y Kim DS Shim TS et al Physiology is a stronger predictor of survival than pathology in fibrotic interstitial pneumonia Am J Respir Crit Care Med 2005171639-44 37 Martinez FJ Safrin S Weycker D et al The clinical course of patients with idiopathic pulmonary fibrosis Ann Intern Med 2005142963-7 38 Hull JH Acetylcysteine in pulmonary fibrosis N Engl J Med 20063541089-91 author reply -91
70
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
39 Flaherty KR King TE Jr Raghu G et al Idiopathic interstitial pneumonia what is the effect of a multidisciplinary approach to diagnosis Am J Respir Crit Care Med 2004170904shy10 40 Raghu G Johnson WC Lockhart D Mageto Y Treatment of idiopathic pulmonary fibrosis with a new antifibrotic agent pirfenidone results of a prospective open-label Phase II study Am J Respir Crit Care Med 19991591061-9 41 Hunninghake GW Lynch DA Galvin JR et al Radiologic findings are strongly associated with a pathologic diagnosis of usual interstitial pneumonia Chest 20031241215-23 42 Lynch D Godwin J Safrin S et al High-resolution computed tomography in idiopathic pulmonary fibrosis diagnosis and prognosis Am J Respir Crit Care Med 2005172488-93 43 Mallinckrodt CH Watkin JG Molenberghs G Carroll RJ Choice of the primary analysis in longitudinal clinical trials Pharmaceutical Statistics 20043161-9 44 Bang H Tsiatis A Estimating medical costs with censored data Biometrika 200087329shy43 45 Lin DY Regression analysis of incomplete medical cost data Stat Med 2003221181-200 46 Rochon J Application of GEE procedures for sample size calculations in repeated measures experiments Stat Med 1998171643-58 47 Lachin JM Foulkes MA Evaluation of sample size and power for analyses of survival with allowance for nonuniform patient entry losses to follow-up noncompliance and stratification Biometrics 198642507-19
71
- PANTHER-IPFPREDNISONE AZATHIOPRINEAND N-ACETYLCYSTEINEA STUDY THAT EVALUATES RESPONSE INIDIOPATHIC PULMONARY FIBROSIS
-
- Protocol Summary
- Table of Contents
- List of Tables
- List of Figures
- List of Abbreviations
- 1 Summary
- 2 Hypotheses and Specific Aims
-
- 21 Null Hypothesis
- 22 Specific Aim 1
- 23 Specific Aim 2
- 24 Prespecified Subgroups of Interest
-
- 3 Background and Significance
-
- 31 Idiopathic Pulmonary Fibrosis is the Most Common Interstitial Lung Disease
- 32 Rationale for Placebo Control
- 33 Rationale for N-acetylcysteine
- 35 Rationale for N-acetylcysteine as a Stand-alone Therapy
- 36 Rationale for the Study Design and Primary Endpoint
- 37 Rationale for Blinding of Treatments
-
- 4 Methods
-
- 41 Inclusion Criteria
- 42 Diagnosis of IPF
- 43 Exclusion Criteria
- 44 Study Design and Study Visit
- 45 Dose Justification
- 46 Contraindications Precautions and Side Effects of Study Medications
- 47 Recruitment Procedures
- 48 Study Procedures
- 49 Concomitant Medications
- 410 Laboratory Testing
- 411 Blinding of Study Drugs
-
- 5 Study Endpoints
-
- 51 Primary Study Endpoint
- 52 Secondary Study Endpoints
-
- 6 Safety Evaluations and Procedures
-
- 61 Adverse Events
- 62 Clinical Medical Monitoring
- 63 Unblinding Procedures
-
- 7 Study Drug Procedures
- 8 Data Management
-
- 81 Hardware and Software Configuration
- 82 Sources of Data
-
- 9 Study Design and Data Analysis
-
- 91 General Analytic Considerations
- 92 Randomization Blinding and Reporting of Results
- 93 Stratification
- 94 Specification of the Primary Analyses
- 95 Analysis of Longitudinal Endpoints
- 96 Analysis of Binary Time-to-Event and Time-Lagged Endpoints
- 97 Power Analysis
-
- 10 Study Administration
-
- 101 Cooperative Agreement Mechanism
- 102 IPFnet Steering Group
- 103 Data and Safety Monitoring Board
- 104 Recommendations on Interim Monitoring of Efficacy Safety and Futility
-
- 11 Investigator and Sponsor Obligations
-
- 111 Monitoring
- 112 Cost and Payment
- 113 Confidentiality and Health Insurance Portability and Accountability ActConsiderations
- 114 Informed Consent Procedures
- 115 Institutional Review Boards
-
- 12 Investigator Agreement
- 13 References
-
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
unlikely to hold in many clinical trials because missing data are often related to disease
progression and prognosis A more reasonable assumption missing at random (MAR) specifies
that the complete data distribution can be modeled using only the observed data The likelihood-
based MMRM approach is valid under the more general MAR assumptions These models will
be applied to analyze the longitudinal data secondary endpoints
The advantages of MMRM analysis are that all important characteristics of the model can be preshy
specified standard software can be used to implement the models and results are based on ITT
principles43 In addition the MMRM approach offers superior control of Type I and Type II
errors compared with the LOCF approach
Response variables are values of the PFTs measured at enrollment and every 15 weeks until
study completion and 6MWT values measured at baseline week 30 and week 60 Covariates are
treatment time time by treatment and key baseline risk factors Contrasts (along with
confidence intervals) of treatment by time will be used to estimate the treatment effect
The correlation structure involves multiple pieces including measurement errors random
variation and interindividual variability For the longitudinal data analyses an unstructured
correlation matrix for within-subject errors will be assumed Other correlation structures
including compound symmetry will be examined as needed A careful examination of reasons
for study discontinuation will be conducted to assess the validity of MCAR Sensitivity analyses
will be used to examine the untestable assumption that the observed data violate the MAR
assumption The MMRM models will be implemented using PROC MIXED in SAS
96 Analysis of Binary Time-to-Event and Time-Lagged Endpoints
Regression modeling approaches using either the logistic regression model or Cox proportional
hazards regression model will be employed when appropriate The validity of these models will
be assessed via standard modeling diagnostics and goodness-of-fit measures Estimates of
cumulative frequencies for more general time-lagged responses will be calculated using the
partitioned version of the Bang-Tsiatis estimator44 The partitions will be set at 15-week intervals
59
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
to correspond with the data-collection process Covariate adjusted event rates will be calculated
using inverse probability-weighted regression estimates45
97 Power Analysis
971 Primary Analyses
Based on previously published IPF clinical trials the PL group is expected to experience a drop
in FVC of approximately 020 L over the study period (see Figure 1) The IPFnet Steering Group
determined a clinically important difference would be to preserve the majority of the decline
relative to PL over the study period In particular a treatment effect of 015 L was determined to
be a clinically meaningful difference Potential dropout is a key factor in the proposed study The
drop-out process assumed 5 lost to follow-up after every study visit Only 80 of subjects
were assumed to be followed for the entire study period All models assumed a compound
symmetry structure for the covariance matrix Power calculations were performed using a SAS
IML program for designing repeated measures studies46 Based on preliminary reviews of the
data from the University of Michigan the covariance matrix parameters were estimated at
approximately σ2 = 0757 (variance parameter) and ρ = 0936 (correlation parameter) To be
conservative the power calculations for the primary analysis were performed with parameter
setting of σ2 = 0810 (variance parameter) and ρ = 0925 (correlation parameter)
The power calculations assume a correction for imperfect compliance proposed by Lachin and
Foulkes to allow for 2 noncompliance for each of the treatment arms47 Thus the sample size
of 130 subjects per arm would be reduced to an adjusted sample size of 130(1-002-002)2 =
1198 or 120 subjects per arm
Under the assumed Type I error rate of 005 with a correlation parameter of 0925 and standard
deviation of 090 the difference of 015 L (or 00025 Lweek) shown in Table 6 would have
power of 93
60
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Table 6 Hypothetical Values of Mean FVC (L) Change from Baseline
Week 15 Week 30 Week 45 Week 60
NAC 00125 00250 00375 00500
Placebo 00500 01000 01500 02000
Difference 00375 00750 01125 01500
Abbreviations FVC forced vital capacity PL placebo
972 Power Analysis for Secondary Endpoints
Power calculations for secondary endpoint measurements are shown in Table 7 Standard
deviations are based on unpublished data provided by the University of Michigan The
calculations are based on a 2-sample t-test with Type I error rate set at 005 These calculations
are likely to be conservative because the statistical approach described in section 95 for
analyzing these endpoints will incorporate incomplete observations as well as intermediate data
points
Table 7 Detectable Differences in Treatment Means for Selected Endpoint Measurements
Secondary Endpoints Std Dev
of the Baseline Score
Detectable Difference for 80 Power
Std Dev of the Change Score
Difference Detectable for
80 Power
DLCOpred 166 58 91 32
6MWT Area Under the Desaturation Curve
219 76 175 61
6MWT Distance to Desaturation 224 78 315 110
6MWT Minutes Walked 210 073 205 071
Abbreviations Std Dev standard deviation DLCOpred diffusing capacity of the lung for carbon monoxide percent predicted 6MWT 6-minute walk test
61
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
10 Study Administration
101 Cooperative Agreement Mechanism
The administrative and funding mechanism used to undertake this project is a ldquocooperative
agreementrdquo (U01) which is an assistance mechanism Under the cooperative agreement the
NHLBI assists supports andor stimulates the project and is substantially involved with
investigators in conducting the study by facilitating performance of the effort in a ldquopartnerrdquo role
The NHLBI project scientist serves on the IPFnet Steering Group and he or another NHLBI
scientist may serve on other project committees when appropriate At the same time however
NHLBI does not assume a dominant role direction or prime responsibility for this research
program
As described below governance of the project is conducted through the IPFnet Steering Group
Principal investigators have lead responsibilities in all aspects of their trials and the project
including any modification of trial designs conduct of the trials quality control data analysis
and interpretation preparation of publications and collaboration with other investigators unless
otherwise provided for by the IPFnet Steering Group
PIs retain custody of and have primary rights to their center-specific and collaborative data
subject to government rights-of-access consistent with current Health amp Human Services (HHS)
Public Health Service (PHS) and National Institutes of Health policies The protocols and
governance policies call for the continual submission of data centrally to the IPFnet DCC for the
collaborative database which at a minimum will contain the key variables selected by the IPFnet
Steering Group for standardization across all clinical centers the submission of copies of the
collaborative datasets to each PI upon completion of the project procedures for data analysis
reporting and publication and procedures to protect and ensure the privacy of medical and
genetic data and records of individuals The NHLBI project scientist on behalf of the NHLBI
will have the same access privileges and responsibilities regarding the collaborative data as the
other members of the Steering Group
62
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
PIs are also encouraged to publish and to publicly release and disseminate results data and other
products of the project concordant with the project protocols and governance and the approved
plan for making data and materials available to the scientific community and to the NHLBI
However during the 3 years after the ending date of NHLBI project support unpublished data
unpublished results data sets not previously released and other study materials or products are
to be made available to any third party only with the approval of the IPFnet Steering Group
Upon completion of the project PIs are expected to put their intervention materials and
procedure manuals into the public domain andor make them available to other investigators
according to the approved plan for making data and materials available to the scientific
community and the NHLBI for the conduct of research at no charge other than the costs of
reproduction and distribution
The NHLBI reserves the right to terminate or curtail the project (or an individual award) in the
event of (a) failure to develop or implement mutually agreeable collaborative measurement
subject eligibility and data management sections of the protocols (b) substantial shortfall in
subject recruitment follow-up data reporting or quality control or other major breach of
protocol (c) substantive changes in the agreed-upon protocols with which NHLBI cannot
concur (d) reaching a major project outcome with persuasive statistical significance
substantially before schedule or (e) human subject ethical issues that may dictate a premature
termination
Any disagreement that may arise in scientificprogrammatic matters (within the scope of the
award) between award recipients and the NHLBI may be brought to arbitration An arbitration
panel will be composed of 3 membersmdash1 selected by the IPFnet Steering Group (with the
NHLBI member not voting) or by the individual PI in the event of an individual disagreement a
second selected by NHLBI and the third selected by the other 2 members This special
arbitration procedure in no way affects the PIrsquos right to appeal an adverse action that is otherwise
appealable in accordance with the PHS regulations at 42 CFR part 50 Subpart D and HHS
63
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
regulation at 45 CFR part 16 or the rights of the NHLBI under applicable statutes regulations
and terms of the award
102 IPFnet Steering Group
The IPFnet Steering Group is the main governing body of the project It is composed of the PIs
of the clinical centers the PI of the DCC and the NHLBI project scientist The clinical centers
the IPFnet DCC and the NHLBI each have 1 vote on the IPFnet Steering Group All decisions
are determined by majority vote
All major scientific decisions are determined by the IPFnet Steering Group It assumes overall
responsibility for the design and conduct of the trial It appoints (and disbands) committees and
subcommittees as the need arises designs approves and implements the study protocols
oversees the development of the MOOP monitors subject recruitment and treatment delivery
evaluates data collection and management oversees quality assurance procedures and
implements changes and enhancements to the study as required It also has primary responsibility
for facilitating the conduct of the trials and reporting the projectrsquos results
103 Data and Safety Monitoring Board
The NHLBI will establish a DSMB in accordance with established policies (see
httpwwwnhlbinihgovfundingpoliciesdsmb_insthtm) to ensure data quality and subject
safety and to provide independent advice to the NHLBI regarding progress and the
appropriateness of study continuation
104 Recommendations on Interim Monitoring of Efficacy Safety and Futility
First and foremost the role of the DSMB will be to review subject safety and trial conduct at
periodic points during the study The DSMB may require analyses of the primary endpoint
results for comparing the benefit and risks of treatment strategies The benefit of collecting
additional data on key secondary endpoints with extended follow-up and establishing a robust
64
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
evidence base for determining a standard of care will need to be carefully considered before
early termination of one or more treatment arms After careful consideration the IPFnet Steering
Group recommends conservative thresholds for the early examinations of the safety and efficacy
data
The DSMB will be expected to meet approximately every 6 months until trial completion to
review safety and toxicity data The DSMB may recommend stopping the study based on these
reviews Because the DSMB could stop the trial for safety concerns as well as for a large
efficacy benefit there could be multiple opportunities to reject the null hypothesis (no difference
in event rates between the PL and NAC groups) A Bonferroni approximation will be applied
during the one planned interim analysis for efficacy
Before locking the database a statistical analysis plan (SAP) will be developed to provide
complete details on the statistical analysis The SAP will include the specifics for how and when
the DSMB will be notified for AEs The IPFnet DCC will deliver to the DSMB all FDA-defined
AEs at 3-month intervals The IPFnet DCC will prepare narrative SAE reports in real time for
DSMB review including recommendations and analysis of similar events for each SAE
submitted to the FDA
65
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
11 Investigator and Sponsor Obligations
111 Monitoring
All monitoring activities for US clinical centers will be performed in accordance with DCRI
standard operating procedures Information regarding the types of visits will be outlined in the
PANTHER-IPF MOOP
112 Cost and Payment
There will be no cost to subjects enrolled in this trial Study-related procedures will be paid for
by the IPFnet
Subjects may be eligible for reimbursement for travel to the clinical center Details of payment
will be explained to each subject during the consent process
113 Confidentiality and Health Insurance Portability and Accountability Act
Considerations
Subject confidentiality will be protected throughout the study All subject data will be kept
strictly confidential and no subject-identifying information will be released to anyone outside
the project Confidentiality will be assured through several mechanisms First each subject will
be assigned an anonymous study ID which will then be used on all study forms Second any
study forms blood samples and paper records that contain subject information (eg address lists
phone lists) will be kept at the clinical centers in secured locked areas coded by number Once
blood is collected there will be no subject identifiers placed on blood samplesmdashonly the study
ID number and the date of sample collection Third access to all subject data and information
including laboratory specimens will be restricted to authorized personnel In the case of
computerized data this restricted access will be assured through user logon IDs and password
protection
66
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
At the IPFnet DCC only authorized personnel will have access to the data files containing study
data Security will be assured through user logon IDs passwords and appropriate access
privileges All study subjects will be identified only by their IPFnet ID numbers and no personal
identifying information such as name address or Social Security number will be entered into
the IPFnet DCC database Any subject-specific data reported to the IPFnet Steering Group will
be identified only by the IPFnet ID number
Finally subjects will not be identified by name in any reports or publications nor will the data
be presented in such a way that the identity of individual subjects can be inferred Analysis files
created for further study by the scientific community will have no subject identifiers These data
files will be created in accordance with the Ancillary Studies and Publication Policy of the
IPFnet
114 Informed Consent Procedures
All IPFnet subjects will provide written informed consent using procedures reviewed and
approved by each clinical centerrsquos IRB Informed consent will be undertaken by study personnel
in-person with the subject The subject has the option of declining further participation in the
study at that point No further study procedures will be conducted until the signed documents
have been provided to the IPFnet clinical center
115 Institutional Review Boards
Before initiating this study the protocol clinical center-specific informed consent forms Health
Insurance Portability and Accountability Act (HIPAA) forms recruitment materials and other
relevant information will be reviewed by a properly constituted IRB at each participating clinical
center A copy of the signed and dated IRB approval at each clinical center will be retrieved prior
to or during the site initiation visit and archived at the IPFnet DCC Any amendments to the
protocol other than simple administrative and typographical changes must be approved by each
IRB before they are implemented The clinical centers will seek annual renewals of their IRB
approvals in accordance with local procedures
67
__________________________________________ ________________
__________________________________________
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
12 Investigator Agreement
I have read the foregoing protocol PANTHER-IPF and agree that it contains all necessary
details for carrying out this study I will conduct the study as outlined herein and will complete
the study within the time designated
I will provide copies of the protocol and all pertinent information to all individuals responsible to
me who assist in the conduct of this study I will discuss this material with them to ensure they
are fully informed regarding the drug and the conduct of the study
I will fulfill all responsibilities for submitting pertinent information to the local IRB if
applicable that is responsible for this study
I further agree that NHLBI andor DCRI will have access to any source documents from which
eCRF information may have been generated
Signature of Principal Investigator Date
Name of Principal Investigator (printed or typed)
Protocol version date May 19 2009
Protocol Amendment 1 version date May 28 2010
Protocol Amendment 2 version date December 6 2011
68
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
13 References
1 Raghu G Brown KK Bradford WZ et al A placebo-controlled trial of interferon gamma-1b in patients with idiopathic pulmonary fibrosis N Engl J Med 2004350125-33 2 King TE Jr Safrin S Starko KM et al Analyses of efficacy end points in a controlled trial of interferon-gamma1b for idiopathic pulmonary fibrosis Chest 2005127171-7 3 Flaherty KR Thwaite EL Kazerooni EA et al Radiological versus histological diagnosis in UIP and NSIP survival implications Thorax 200358143-8 4 Wells AU Desai SR Rubens MB et al Idiopathic pulmonary fibrosis a composite physiologic index derived from disease extent observed by computed tomography Am J Respir Crit Care Med 2003167962-9 5 Raghu G Freudenberger TD Yang S et al High prevalence of abnormal acid gastroshyoesophageal reflux in idiopathic pulmonary fibrosis Eur Respir J 200627136-42 6 Kinnula VL Focus on antioxidant enzymes and antioxidant strategies in smoking related airway diseases Thorax 200560693-700 7 Coultas DB Zumwalt RE Black WC Sobonya RE The epidemiology of interstitial lung diseases Am J Respir Crit Care Med 1994150967-72 8 Raghu G Weycker D Edelsberg J Bradford WZ Oster G Incidence and prevalence of idiopathic pulmonary fibrosis Am J Respir Crit Care Med 2006174810-6 9 Olson AL Swigris JJ Lezotte DC Norris JM Wilson CG Brown KK Mortality from pulmonary fibrosis increased in the United States from 1992 to 2003 Am J Respir Crit Care Med 2007176277-84 10 Mannino DM Etzel RA Parrish RG Pulmonary fibrosis deaths in the United States 1979shy1991 An analysis of multiple-cause mortality data Am J Respir Crit Care Med 19961531548shy52 11 Hubbard R Johnston I Coultas DB Britton J Mortality rates from cryptogenic fibrosing alveolitis in seven countries Thorax 199651711-6 12 Johnston I Britton J Kinnear W Logan R Rising mortality from cryptogenic fibrosing alveolitis Bmj 19903011017-21 13 Raghu G Collard HR Egan JJ et al An official ATSERSJRSALAT statement idiopathic pulmonary fibrosis evidence-based guidelines for diagnosis and management Am J Respir Crit Care Med 2011183788-824 14 (USA) FDA FDA Public Health Advisory Interferon gamma-1b (marketed as Actimmune) In 2007 15 King TE Jr Pardo A Selman M Idiopathic pulmonary fibrosis Lancet 2011 16 Raghu G Brown KK Costabel U et al Treatment of idiopathic pulmonary fibrosis with etanercept an exploratory placebo-controlled trial Am J Respir Crit Care Med 2008178948shy55 17 Malouf MA Hopkins P Snell G Glanville AR An investigator-driven study of everolimus in surgical lung biopsy confirmed idiopathic pulmonary fibrosis Respirology 201116776-83 18 King TE Jr Behr J Brown KK et al BUILD-1 a randomized placebo-controlled trial of bosentan in idiopathic pulmonary fibrosis Am J Respir Crit Care Med 200817775-81 19 Richeldi L Costabel U Selman M et al Efficacy of a tyrosine kinase inhibitor in idiopathic pulmonary fibrosis N Engl J Med 20113651079-87
69
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
20 Borok Z Buhl R Grimes GJ et al Effect of glutathione aerosol on oxidant-antioxidant imbalance in idiopathic pulmonary fibrosis Lancet 1991338215-6 21 Meyer A Buhl R Magnussen H The effect of oral N-acetylcysteine on lung glutathione levels in idiopathic pulmonary fibrosis Eur Respir J 19947431-6 22 Behr J Maier K Degenkolb B Krombach F Vogelmeier C Antioxidative and clinical effects of high-dose N-acetylcysteine in fibrosing alveolitis Adjunctive therapy to maintenance immunosuppression Am J Respir Crit Care Med 19971561897-901 23 Cantin AM North SL Fells GA Hubbard RC Crystal RG Oxidant-mediated epithelial cell injury in idiopathic pulmonary fibrosis J Clin Invest 1987791665-73 24 Waghray M Cui Z Horowitz JC et al Hydrogen peroxide is a diffusible paracrine signal for the induction of epithelial cell death by activated myofibroblasts Faseb J 200519854-6 25 Larios JM Budhiraja R Fanburg BL Thannickal VJ Oxidative protein cross-linking reactions involving L-tyrosine in transforming growth factor-beta1-stimulated fibroblasts J Biol Chem 200127617437-41 26 Kinnula VL Fattman CL Tan RJ Oury TD Oxidative stress in pulmonary fibrosis a possible role for redox modulatory therapy Am J Respir Crit Care Med 2005172417-22 27 Meyer A Buhl R Kampf S Magnussen H Intravenous N-acetylcysteine and lung glutathione of patients with pulmonary fibrosis and normals Am J Respir Crit Care Med 19951521055-60 28 Behr J Degenkolb B Krombach F Vogelmeier C Intracellular glutathione and bronchoalveolar cells in fibrosing alveolitis effects of N-acetylcysteine Eur Respir J 200219906-11 29 Bando M Hosono T Mato N et al Long-term efficacy of inhaled N-acetylcysteine in patients with idiopathic pulmonary fibrosis Intern Med 2010492289-96 30 Demedts M Behr J Buhl R et al High-dose acetylcysteine in idiopathic pulmonary fibrosis N Engl J Med 20053532229-42 31 Toma TP Bhowmik A Rajakulasingam R Acetylcysteine in pulmonary fibrosis N Engl J Med 20063541086-9 author reply -9 32 Hunninghake GW Antioxidant therapy for idiopathic pulmonary fibrosis N Engl J Med 20053532285-7 33 Flaherty KR Mumford JA Murray S et al Prognostic implications of physiologic and radiographic changes in idiopathic interstitial pneumonia Am J Respir Crit Care Med 2003168543-8 34 Latsi PI du Bois RM Nicholson AG et al Fibrotic idiopathic interstitial pneumonia the prognostic value of longitudinal functional trends Am J Respir Crit Care Med 2003168531-7 35 Collard HR King TE Jr Bartelson BB Vourlekis JS Schwarz MI Brown KK Changes in clinical and physiologic variables predict survival in idiopathic pulmonary fibrosis Am J Respir Crit Care Med 2003168538-42 36 Jegal Y Kim DS Shim TS et al Physiology is a stronger predictor of survival than pathology in fibrotic interstitial pneumonia Am J Respir Crit Care Med 2005171639-44 37 Martinez FJ Safrin S Weycker D et al The clinical course of patients with idiopathic pulmonary fibrosis Ann Intern Med 2005142963-7 38 Hull JH Acetylcysteine in pulmonary fibrosis N Engl J Med 20063541089-91 author reply -91
70
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
39 Flaherty KR King TE Jr Raghu G et al Idiopathic interstitial pneumonia what is the effect of a multidisciplinary approach to diagnosis Am J Respir Crit Care Med 2004170904shy10 40 Raghu G Johnson WC Lockhart D Mageto Y Treatment of idiopathic pulmonary fibrosis with a new antifibrotic agent pirfenidone results of a prospective open-label Phase II study Am J Respir Crit Care Med 19991591061-9 41 Hunninghake GW Lynch DA Galvin JR et al Radiologic findings are strongly associated with a pathologic diagnosis of usual interstitial pneumonia Chest 20031241215-23 42 Lynch D Godwin J Safrin S et al High-resolution computed tomography in idiopathic pulmonary fibrosis diagnosis and prognosis Am J Respir Crit Care Med 2005172488-93 43 Mallinckrodt CH Watkin JG Molenberghs G Carroll RJ Choice of the primary analysis in longitudinal clinical trials Pharmaceutical Statistics 20043161-9 44 Bang H Tsiatis A Estimating medical costs with censored data Biometrika 200087329shy43 45 Lin DY Regression analysis of incomplete medical cost data Stat Med 2003221181-200 46 Rochon J Application of GEE procedures for sample size calculations in repeated measures experiments Stat Med 1998171643-58 47 Lachin JM Foulkes MA Evaluation of sample size and power for analyses of survival with allowance for nonuniform patient entry losses to follow-up noncompliance and stratification Biometrics 198642507-19
71
- PANTHER-IPFPREDNISONE AZATHIOPRINEAND N-ACETYLCYSTEINEA STUDY THAT EVALUATES RESPONSE INIDIOPATHIC PULMONARY FIBROSIS
-
- Protocol Summary
- Table of Contents
- List of Tables
- List of Figures
- List of Abbreviations
- 1 Summary
- 2 Hypotheses and Specific Aims
-
- 21 Null Hypothesis
- 22 Specific Aim 1
- 23 Specific Aim 2
- 24 Prespecified Subgroups of Interest
-
- 3 Background and Significance
-
- 31 Idiopathic Pulmonary Fibrosis is the Most Common Interstitial Lung Disease
- 32 Rationale for Placebo Control
- 33 Rationale for N-acetylcysteine
- 35 Rationale for N-acetylcysteine as a Stand-alone Therapy
- 36 Rationale for the Study Design and Primary Endpoint
- 37 Rationale for Blinding of Treatments
-
- 4 Methods
-
- 41 Inclusion Criteria
- 42 Diagnosis of IPF
- 43 Exclusion Criteria
- 44 Study Design and Study Visit
- 45 Dose Justification
- 46 Contraindications Precautions and Side Effects of Study Medications
- 47 Recruitment Procedures
- 48 Study Procedures
- 49 Concomitant Medications
- 410 Laboratory Testing
- 411 Blinding of Study Drugs
-
- 5 Study Endpoints
-
- 51 Primary Study Endpoint
- 52 Secondary Study Endpoints
-
- 6 Safety Evaluations and Procedures
-
- 61 Adverse Events
- 62 Clinical Medical Monitoring
- 63 Unblinding Procedures
-
- 7 Study Drug Procedures
- 8 Data Management
-
- 81 Hardware and Software Configuration
- 82 Sources of Data
-
- 9 Study Design and Data Analysis
-
- 91 General Analytic Considerations
- 92 Randomization Blinding and Reporting of Results
- 93 Stratification
- 94 Specification of the Primary Analyses
- 95 Analysis of Longitudinal Endpoints
- 96 Analysis of Binary Time-to-Event and Time-Lagged Endpoints
- 97 Power Analysis
-
- 10 Study Administration
-
- 101 Cooperative Agreement Mechanism
- 102 IPFnet Steering Group
- 103 Data and Safety Monitoring Board
- 104 Recommendations on Interim Monitoring of Efficacy Safety and Futility
-
- 11 Investigator and Sponsor Obligations
-
- 111 Monitoring
- 112 Cost and Payment
- 113 Confidentiality and Health Insurance Portability and Accountability ActConsiderations
- 114 Informed Consent Procedures
- 115 Institutional Review Boards
-
- 12 Investigator Agreement
- 13 References
-

PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
to correspond with the data-collection process Covariate adjusted event rates will be calculated
using inverse probability-weighted regression estimates45
97 Power Analysis
971 Primary Analyses
Based on previously published IPF clinical trials the PL group is expected to experience a drop
in FVC of approximately 020 L over the study period (see Figure 1) The IPFnet Steering Group
determined a clinically important difference would be to preserve the majority of the decline
relative to PL over the study period In particular a treatment effect of 015 L was determined to
be a clinically meaningful difference Potential dropout is a key factor in the proposed study The
drop-out process assumed 5 lost to follow-up after every study visit Only 80 of subjects
were assumed to be followed for the entire study period All models assumed a compound
symmetry structure for the covariance matrix Power calculations were performed using a SAS
IML program for designing repeated measures studies46 Based on preliminary reviews of the
data from the University of Michigan the covariance matrix parameters were estimated at
approximately σ2 = 0757 (variance parameter) and ρ = 0936 (correlation parameter) To be
conservative the power calculations for the primary analysis were performed with parameter
setting of σ2 = 0810 (variance parameter) and ρ = 0925 (correlation parameter)
The power calculations assume a correction for imperfect compliance proposed by Lachin and
Foulkes to allow for 2 noncompliance for each of the treatment arms47 Thus the sample size
of 130 subjects per arm would be reduced to an adjusted sample size of 130(1-002-002)2 =
1198 or 120 subjects per arm
Under the assumed Type I error rate of 005 with a correlation parameter of 0925 and standard
deviation of 090 the difference of 015 L (or 00025 Lweek) shown in Table 6 would have
power of 93
60
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Table 6 Hypothetical Values of Mean FVC (L) Change from Baseline
Week 15 Week 30 Week 45 Week 60
NAC 00125 00250 00375 00500
Placebo 00500 01000 01500 02000
Difference 00375 00750 01125 01500
Abbreviations FVC forced vital capacity PL placebo
972 Power Analysis for Secondary Endpoints
Power calculations for secondary endpoint measurements are shown in Table 7 Standard
deviations are based on unpublished data provided by the University of Michigan The
calculations are based on a 2-sample t-test with Type I error rate set at 005 These calculations
are likely to be conservative because the statistical approach described in section 95 for
analyzing these endpoints will incorporate incomplete observations as well as intermediate data
points
Table 7 Detectable Differences in Treatment Means for Selected Endpoint Measurements
Secondary Endpoints Std Dev
of the Baseline Score
Detectable Difference for 80 Power
Std Dev of the Change Score
Difference Detectable for
80 Power
DLCOpred 166 58 91 32
6MWT Area Under the Desaturation Curve
219 76 175 61
6MWT Distance to Desaturation 224 78 315 110
6MWT Minutes Walked 210 073 205 071
Abbreviations Std Dev standard deviation DLCOpred diffusing capacity of the lung for carbon monoxide percent predicted 6MWT 6-minute walk test
61
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
10 Study Administration
101 Cooperative Agreement Mechanism
The administrative and funding mechanism used to undertake this project is a ldquocooperative
agreementrdquo (U01) which is an assistance mechanism Under the cooperative agreement the
NHLBI assists supports andor stimulates the project and is substantially involved with
investigators in conducting the study by facilitating performance of the effort in a ldquopartnerrdquo role
The NHLBI project scientist serves on the IPFnet Steering Group and he or another NHLBI
scientist may serve on other project committees when appropriate At the same time however
NHLBI does not assume a dominant role direction or prime responsibility for this research
program
As described below governance of the project is conducted through the IPFnet Steering Group
Principal investigators have lead responsibilities in all aspects of their trials and the project
including any modification of trial designs conduct of the trials quality control data analysis
and interpretation preparation of publications and collaboration with other investigators unless
otherwise provided for by the IPFnet Steering Group
PIs retain custody of and have primary rights to their center-specific and collaborative data
subject to government rights-of-access consistent with current Health amp Human Services (HHS)
Public Health Service (PHS) and National Institutes of Health policies The protocols and
governance policies call for the continual submission of data centrally to the IPFnet DCC for the
collaborative database which at a minimum will contain the key variables selected by the IPFnet
Steering Group for standardization across all clinical centers the submission of copies of the
collaborative datasets to each PI upon completion of the project procedures for data analysis
reporting and publication and procedures to protect and ensure the privacy of medical and
genetic data and records of individuals The NHLBI project scientist on behalf of the NHLBI
will have the same access privileges and responsibilities regarding the collaborative data as the
other members of the Steering Group
62
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
PIs are also encouraged to publish and to publicly release and disseminate results data and other
products of the project concordant with the project protocols and governance and the approved
plan for making data and materials available to the scientific community and to the NHLBI
However during the 3 years after the ending date of NHLBI project support unpublished data
unpublished results data sets not previously released and other study materials or products are
to be made available to any third party only with the approval of the IPFnet Steering Group
Upon completion of the project PIs are expected to put their intervention materials and
procedure manuals into the public domain andor make them available to other investigators
according to the approved plan for making data and materials available to the scientific
community and the NHLBI for the conduct of research at no charge other than the costs of
reproduction and distribution
The NHLBI reserves the right to terminate or curtail the project (or an individual award) in the
event of (a) failure to develop or implement mutually agreeable collaborative measurement
subject eligibility and data management sections of the protocols (b) substantial shortfall in
subject recruitment follow-up data reporting or quality control or other major breach of
protocol (c) substantive changes in the agreed-upon protocols with which NHLBI cannot
concur (d) reaching a major project outcome with persuasive statistical significance
substantially before schedule or (e) human subject ethical issues that may dictate a premature
termination
Any disagreement that may arise in scientificprogrammatic matters (within the scope of the
award) between award recipients and the NHLBI may be brought to arbitration An arbitration
panel will be composed of 3 membersmdash1 selected by the IPFnet Steering Group (with the
NHLBI member not voting) or by the individual PI in the event of an individual disagreement a
second selected by NHLBI and the third selected by the other 2 members This special
arbitration procedure in no way affects the PIrsquos right to appeal an adverse action that is otherwise
appealable in accordance with the PHS regulations at 42 CFR part 50 Subpart D and HHS
63
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
regulation at 45 CFR part 16 or the rights of the NHLBI under applicable statutes regulations
and terms of the award
102 IPFnet Steering Group
The IPFnet Steering Group is the main governing body of the project It is composed of the PIs
of the clinical centers the PI of the DCC and the NHLBI project scientist The clinical centers
the IPFnet DCC and the NHLBI each have 1 vote on the IPFnet Steering Group All decisions
are determined by majority vote
All major scientific decisions are determined by the IPFnet Steering Group It assumes overall
responsibility for the design and conduct of the trial It appoints (and disbands) committees and
subcommittees as the need arises designs approves and implements the study protocols
oversees the development of the MOOP monitors subject recruitment and treatment delivery
evaluates data collection and management oversees quality assurance procedures and
implements changes and enhancements to the study as required It also has primary responsibility
for facilitating the conduct of the trials and reporting the projectrsquos results
103 Data and Safety Monitoring Board
The NHLBI will establish a DSMB in accordance with established policies (see
httpwwwnhlbinihgovfundingpoliciesdsmb_insthtm) to ensure data quality and subject
safety and to provide independent advice to the NHLBI regarding progress and the
appropriateness of study continuation
104 Recommendations on Interim Monitoring of Efficacy Safety and Futility
First and foremost the role of the DSMB will be to review subject safety and trial conduct at
periodic points during the study The DSMB may require analyses of the primary endpoint
results for comparing the benefit and risks of treatment strategies The benefit of collecting
additional data on key secondary endpoints with extended follow-up and establishing a robust
64
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
evidence base for determining a standard of care will need to be carefully considered before
early termination of one or more treatment arms After careful consideration the IPFnet Steering
Group recommends conservative thresholds for the early examinations of the safety and efficacy
data
The DSMB will be expected to meet approximately every 6 months until trial completion to
review safety and toxicity data The DSMB may recommend stopping the study based on these
reviews Because the DSMB could stop the trial for safety concerns as well as for a large
efficacy benefit there could be multiple opportunities to reject the null hypothesis (no difference
in event rates between the PL and NAC groups) A Bonferroni approximation will be applied
during the one planned interim analysis for efficacy
Before locking the database a statistical analysis plan (SAP) will be developed to provide
complete details on the statistical analysis The SAP will include the specifics for how and when
the DSMB will be notified for AEs The IPFnet DCC will deliver to the DSMB all FDA-defined
AEs at 3-month intervals The IPFnet DCC will prepare narrative SAE reports in real time for
DSMB review including recommendations and analysis of similar events for each SAE
submitted to the FDA
65
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
11 Investigator and Sponsor Obligations
111 Monitoring
All monitoring activities for US clinical centers will be performed in accordance with DCRI
standard operating procedures Information regarding the types of visits will be outlined in the
PANTHER-IPF MOOP
112 Cost and Payment
There will be no cost to subjects enrolled in this trial Study-related procedures will be paid for
by the IPFnet
Subjects may be eligible for reimbursement for travel to the clinical center Details of payment
will be explained to each subject during the consent process
113 Confidentiality and Health Insurance Portability and Accountability Act
Considerations
Subject confidentiality will be protected throughout the study All subject data will be kept
strictly confidential and no subject-identifying information will be released to anyone outside
the project Confidentiality will be assured through several mechanisms First each subject will
be assigned an anonymous study ID which will then be used on all study forms Second any
study forms blood samples and paper records that contain subject information (eg address lists
phone lists) will be kept at the clinical centers in secured locked areas coded by number Once
blood is collected there will be no subject identifiers placed on blood samplesmdashonly the study
ID number and the date of sample collection Third access to all subject data and information
including laboratory specimens will be restricted to authorized personnel In the case of
computerized data this restricted access will be assured through user logon IDs and password
protection
66
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
At the IPFnet DCC only authorized personnel will have access to the data files containing study
data Security will be assured through user logon IDs passwords and appropriate access
privileges All study subjects will be identified only by their IPFnet ID numbers and no personal
identifying information such as name address or Social Security number will be entered into
the IPFnet DCC database Any subject-specific data reported to the IPFnet Steering Group will
be identified only by the IPFnet ID number
Finally subjects will not be identified by name in any reports or publications nor will the data
be presented in such a way that the identity of individual subjects can be inferred Analysis files
created for further study by the scientific community will have no subject identifiers These data
files will be created in accordance with the Ancillary Studies and Publication Policy of the
IPFnet
114 Informed Consent Procedures
All IPFnet subjects will provide written informed consent using procedures reviewed and
approved by each clinical centerrsquos IRB Informed consent will be undertaken by study personnel
in-person with the subject The subject has the option of declining further participation in the
study at that point No further study procedures will be conducted until the signed documents
have been provided to the IPFnet clinical center
115 Institutional Review Boards
Before initiating this study the protocol clinical center-specific informed consent forms Health
Insurance Portability and Accountability Act (HIPAA) forms recruitment materials and other
relevant information will be reviewed by a properly constituted IRB at each participating clinical
center A copy of the signed and dated IRB approval at each clinical center will be retrieved prior
to or during the site initiation visit and archived at the IPFnet DCC Any amendments to the
protocol other than simple administrative and typographical changes must be approved by each
IRB before they are implemented The clinical centers will seek annual renewals of their IRB
approvals in accordance with local procedures
67
__________________________________________ ________________
__________________________________________
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
12 Investigator Agreement
I have read the foregoing protocol PANTHER-IPF and agree that it contains all necessary
details for carrying out this study I will conduct the study as outlined herein and will complete
the study within the time designated
I will provide copies of the protocol and all pertinent information to all individuals responsible to
me who assist in the conduct of this study I will discuss this material with them to ensure they
are fully informed regarding the drug and the conduct of the study
I will fulfill all responsibilities for submitting pertinent information to the local IRB if
applicable that is responsible for this study
I further agree that NHLBI andor DCRI will have access to any source documents from which
eCRF information may have been generated
Signature of Principal Investigator Date
Name of Principal Investigator (printed or typed)
Protocol version date May 19 2009
Protocol Amendment 1 version date May 28 2010
Protocol Amendment 2 version date December 6 2011
68
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
13 References
1 Raghu G Brown KK Bradford WZ et al A placebo-controlled trial of interferon gamma-1b in patients with idiopathic pulmonary fibrosis N Engl J Med 2004350125-33 2 King TE Jr Safrin S Starko KM et al Analyses of efficacy end points in a controlled trial of interferon-gamma1b for idiopathic pulmonary fibrosis Chest 2005127171-7 3 Flaherty KR Thwaite EL Kazerooni EA et al Radiological versus histological diagnosis in UIP and NSIP survival implications Thorax 200358143-8 4 Wells AU Desai SR Rubens MB et al Idiopathic pulmonary fibrosis a composite physiologic index derived from disease extent observed by computed tomography Am J Respir Crit Care Med 2003167962-9 5 Raghu G Freudenberger TD Yang S et al High prevalence of abnormal acid gastroshyoesophageal reflux in idiopathic pulmonary fibrosis Eur Respir J 200627136-42 6 Kinnula VL Focus on antioxidant enzymes and antioxidant strategies in smoking related airway diseases Thorax 200560693-700 7 Coultas DB Zumwalt RE Black WC Sobonya RE The epidemiology of interstitial lung diseases Am J Respir Crit Care Med 1994150967-72 8 Raghu G Weycker D Edelsberg J Bradford WZ Oster G Incidence and prevalence of idiopathic pulmonary fibrosis Am J Respir Crit Care Med 2006174810-6 9 Olson AL Swigris JJ Lezotte DC Norris JM Wilson CG Brown KK Mortality from pulmonary fibrosis increased in the United States from 1992 to 2003 Am J Respir Crit Care Med 2007176277-84 10 Mannino DM Etzel RA Parrish RG Pulmonary fibrosis deaths in the United States 1979shy1991 An analysis of multiple-cause mortality data Am J Respir Crit Care Med 19961531548shy52 11 Hubbard R Johnston I Coultas DB Britton J Mortality rates from cryptogenic fibrosing alveolitis in seven countries Thorax 199651711-6 12 Johnston I Britton J Kinnear W Logan R Rising mortality from cryptogenic fibrosing alveolitis Bmj 19903011017-21 13 Raghu G Collard HR Egan JJ et al An official ATSERSJRSALAT statement idiopathic pulmonary fibrosis evidence-based guidelines for diagnosis and management Am J Respir Crit Care Med 2011183788-824 14 (USA) FDA FDA Public Health Advisory Interferon gamma-1b (marketed as Actimmune) In 2007 15 King TE Jr Pardo A Selman M Idiopathic pulmonary fibrosis Lancet 2011 16 Raghu G Brown KK Costabel U et al Treatment of idiopathic pulmonary fibrosis with etanercept an exploratory placebo-controlled trial Am J Respir Crit Care Med 2008178948shy55 17 Malouf MA Hopkins P Snell G Glanville AR An investigator-driven study of everolimus in surgical lung biopsy confirmed idiopathic pulmonary fibrosis Respirology 201116776-83 18 King TE Jr Behr J Brown KK et al BUILD-1 a randomized placebo-controlled trial of bosentan in idiopathic pulmonary fibrosis Am J Respir Crit Care Med 200817775-81 19 Richeldi L Costabel U Selman M et al Efficacy of a tyrosine kinase inhibitor in idiopathic pulmonary fibrosis N Engl J Med 20113651079-87
69
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
20 Borok Z Buhl R Grimes GJ et al Effect of glutathione aerosol on oxidant-antioxidant imbalance in idiopathic pulmonary fibrosis Lancet 1991338215-6 21 Meyer A Buhl R Magnussen H The effect of oral N-acetylcysteine on lung glutathione levels in idiopathic pulmonary fibrosis Eur Respir J 19947431-6 22 Behr J Maier K Degenkolb B Krombach F Vogelmeier C Antioxidative and clinical effects of high-dose N-acetylcysteine in fibrosing alveolitis Adjunctive therapy to maintenance immunosuppression Am J Respir Crit Care Med 19971561897-901 23 Cantin AM North SL Fells GA Hubbard RC Crystal RG Oxidant-mediated epithelial cell injury in idiopathic pulmonary fibrosis J Clin Invest 1987791665-73 24 Waghray M Cui Z Horowitz JC et al Hydrogen peroxide is a diffusible paracrine signal for the induction of epithelial cell death by activated myofibroblasts Faseb J 200519854-6 25 Larios JM Budhiraja R Fanburg BL Thannickal VJ Oxidative protein cross-linking reactions involving L-tyrosine in transforming growth factor-beta1-stimulated fibroblasts J Biol Chem 200127617437-41 26 Kinnula VL Fattman CL Tan RJ Oury TD Oxidative stress in pulmonary fibrosis a possible role for redox modulatory therapy Am J Respir Crit Care Med 2005172417-22 27 Meyer A Buhl R Kampf S Magnussen H Intravenous N-acetylcysteine and lung glutathione of patients with pulmonary fibrosis and normals Am J Respir Crit Care Med 19951521055-60 28 Behr J Degenkolb B Krombach F Vogelmeier C Intracellular glutathione and bronchoalveolar cells in fibrosing alveolitis effects of N-acetylcysteine Eur Respir J 200219906-11 29 Bando M Hosono T Mato N et al Long-term efficacy of inhaled N-acetylcysteine in patients with idiopathic pulmonary fibrosis Intern Med 2010492289-96 30 Demedts M Behr J Buhl R et al High-dose acetylcysteine in idiopathic pulmonary fibrosis N Engl J Med 20053532229-42 31 Toma TP Bhowmik A Rajakulasingam R Acetylcysteine in pulmonary fibrosis N Engl J Med 20063541086-9 author reply -9 32 Hunninghake GW Antioxidant therapy for idiopathic pulmonary fibrosis N Engl J Med 20053532285-7 33 Flaherty KR Mumford JA Murray S et al Prognostic implications of physiologic and radiographic changes in idiopathic interstitial pneumonia Am J Respir Crit Care Med 2003168543-8 34 Latsi PI du Bois RM Nicholson AG et al Fibrotic idiopathic interstitial pneumonia the prognostic value of longitudinal functional trends Am J Respir Crit Care Med 2003168531-7 35 Collard HR King TE Jr Bartelson BB Vourlekis JS Schwarz MI Brown KK Changes in clinical and physiologic variables predict survival in idiopathic pulmonary fibrosis Am J Respir Crit Care Med 2003168538-42 36 Jegal Y Kim DS Shim TS et al Physiology is a stronger predictor of survival than pathology in fibrotic interstitial pneumonia Am J Respir Crit Care Med 2005171639-44 37 Martinez FJ Safrin S Weycker D et al The clinical course of patients with idiopathic pulmonary fibrosis Ann Intern Med 2005142963-7 38 Hull JH Acetylcysteine in pulmonary fibrosis N Engl J Med 20063541089-91 author reply -91
70
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
39 Flaherty KR King TE Jr Raghu G et al Idiopathic interstitial pneumonia what is the effect of a multidisciplinary approach to diagnosis Am J Respir Crit Care Med 2004170904shy10 40 Raghu G Johnson WC Lockhart D Mageto Y Treatment of idiopathic pulmonary fibrosis with a new antifibrotic agent pirfenidone results of a prospective open-label Phase II study Am J Respir Crit Care Med 19991591061-9 41 Hunninghake GW Lynch DA Galvin JR et al Radiologic findings are strongly associated with a pathologic diagnosis of usual interstitial pneumonia Chest 20031241215-23 42 Lynch D Godwin J Safrin S et al High-resolution computed tomography in idiopathic pulmonary fibrosis diagnosis and prognosis Am J Respir Crit Care Med 2005172488-93 43 Mallinckrodt CH Watkin JG Molenberghs G Carroll RJ Choice of the primary analysis in longitudinal clinical trials Pharmaceutical Statistics 20043161-9 44 Bang H Tsiatis A Estimating medical costs with censored data Biometrika 200087329shy43 45 Lin DY Regression analysis of incomplete medical cost data Stat Med 2003221181-200 46 Rochon J Application of GEE procedures for sample size calculations in repeated measures experiments Stat Med 1998171643-58 47 Lachin JM Foulkes MA Evaluation of sample size and power for analyses of survival with allowance for nonuniform patient entry losses to follow-up noncompliance and stratification Biometrics 198642507-19
71
- PANTHER-IPFPREDNISONE AZATHIOPRINEAND N-ACETYLCYSTEINEA STUDY THAT EVALUATES RESPONSE INIDIOPATHIC PULMONARY FIBROSIS
-
- Protocol Summary
- Table of Contents
- List of Tables
- List of Figures
- List of Abbreviations
- 1 Summary
- 2 Hypotheses and Specific Aims
-
- 21 Null Hypothesis
- 22 Specific Aim 1
- 23 Specific Aim 2
- 24 Prespecified Subgroups of Interest
-
- 3 Background and Significance
-
- 31 Idiopathic Pulmonary Fibrosis is the Most Common Interstitial Lung Disease
- 32 Rationale for Placebo Control
- 33 Rationale for N-acetylcysteine
- 35 Rationale for N-acetylcysteine as a Stand-alone Therapy
- 36 Rationale for the Study Design and Primary Endpoint
- 37 Rationale for Blinding of Treatments
-
- 4 Methods
-
- 41 Inclusion Criteria
- 42 Diagnosis of IPF
- 43 Exclusion Criteria
- 44 Study Design and Study Visit
- 45 Dose Justification
- 46 Contraindications Precautions and Side Effects of Study Medications
- 47 Recruitment Procedures
- 48 Study Procedures
- 49 Concomitant Medications
- 410 Laboratory Testing
- 411 Blinding of Study Drugs
-
- 5 Study Endpoints
-
- 51 Primary Study Endpoint
- 52 Secondary Study Endpoints
-
- 6 Safety Evaluations and Procedures
-
- 61 Adverse Events
- 62 Clinical Medical Monitoring
- 63 Unblinding Procedures
-
- 7 Study Drug Procedures
- 8 Data Management
-
- 81 Hardware and Software Configuration
- 82 Sources of Data
-
- 9 Study Design and Data Analysis
-
- 91 General Analytic Considerations
- 92 Randomization Blinding and Reporting of Results
- 93 Stratification
- 94 Specification of the Primary Analyses
- 95 Analysis of Longitudinal Endpoints
- 96 Analysis of Binary Time-to-Event and Time-Lagged Endpoints
- 97 Power Analysis
-
- 10 Study Administration
-
- 101 Cooperative Agreement Mechanism
- 102 IPFnet Steering Group
- 103 Data and Safety Monitoring Board
- 104 Recommendations on Interim Monitoring of Efficacy Safety and Futility
-
- 11 Investigator and Sponsor Obligations
-
- 111 Monitoring
- 112 Cost and Payment
- 113 Confidentiality and Health Insurance Portability and Accountability ActConsiderations
- 114 Informed Consent Procedures
- 115 Institutional Review Boards
-
- 12 Investigator Agreement
- 13 References
-
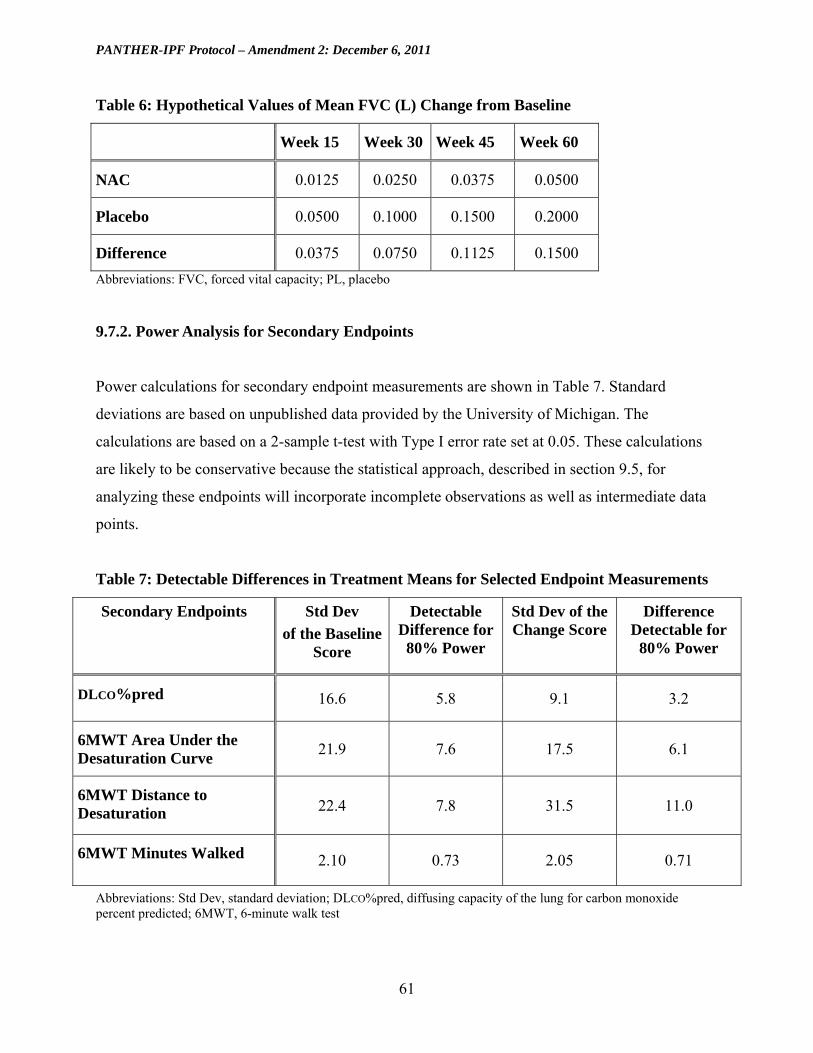
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
Table 6 Hypothetical Values of Mean FVC (L) Change from Baseline
Week 15 Week 30 Week 45 Week 60
NAC 00125 00250 00375 00500
Placebo 00500 01000 01500 02000
Difference 00375 00750 01125 01500
Abbreviations FVC forced vital capacity PL placebo
972 Power Analysis for Secondary Endpoints
Power calculations for secondary endpoint measurements are shown in Table 7 Standard
deviations are based on unpublished data provided by the University of Michigan The
calculations are based on a 2-sample t-test with Type I error rate set at 005 These calculations
are likely to be conservative because the statistical approach described in section 95 for
analyzing these endpoints will incorporate incomplete observations as well as intermediate data
points
Table 7 Detectable Differences in Treatment Means for Selected Endpoint Measurements
Secondary Endpoints Std Dev
of the Baseline Score
Detectable Difference for 80 Power
Std Dev of the Change Score
Difference Detectable for
80 Power
DLCOpred 166 58 91 32
6MWT Area Under the Desaturation Curve
219 76 175 61
6MWT Distance to Desaturation 224 78 315 110
6MWT Minutes Walked 210 073 205 071
Abbreviations Std Dev standard deviation DLCOpred diffusing capacity of the lung for carbon monoxide percent predicted 6MWT 6-minute walk test
61
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
10 Study Administration
101 Cooperative Agreement Mechanism
The administrative and funding mechanism used to undertake this project is a ldquocooperative
agreementrdquo (U01) which is an assistance mechanism Under the cooperative agreement the
NHLBI assists supports andor stimulates the project and is substantially involved with
investigators in conducting the study by facilitating performance of the effort in a ldquopartnerrdquo role
The NHLBI project scientist serves on the IPFnet Steering Group and he or another NHLBI
scientist may serve on other project committees when appropriate At the same time however
NHLBI does not assume a dominant role direction or prime responsibility for this research
program
As described below governance of the project is conducted through the IPFnet Steering Group
Principal investigators have lead responsibilities in all aspects of their trials and the project
including any modification of trial designs conduct of the trials quality control data analysis
and interpretation preparation of publications and collaboration with other investigators unless
otherwise provided for by the IPFnet Steering Group
PIs retain custody of and have primary rights to their center-specific and collaborative data
subject to government rights-of-access consistent with current Health amp Human Services (HHS)
Public Health Service (PHS) and National Institutes of Health policies The protocols and
governance policies call for the continual submission of data centrally to the IPFnet DCC for the
collaborative database which at a minimum will contain the key variables selected by the IPFnet
Steering Group for standardization across all clinical centers the submission of copies of the
collaborative datasets to each PI upon completion of the project procedures for data analysis
reporting and publication and procedures to protect and ensure the privacy of medical and
genetic data and records of individuals The NHLBI project scientist on behalf of the NHLBI
will have the same access privileges and responsibilities regarding the collaborative data as the
other members of the Steering Group
62
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
PIs are also encouraged to publish and to publicly release and disseminate results data and other
products of the project concordant with the project protocols and governance and the approved
plan for making data and materials available to the scientific community and to the NHLBI
However during the 3 years after the ending date of NHLBI project support unpublished data
unpublished results data sets not previously released and other study materials or products are
to be made available to any third party only with the approval of the IPFnet Steering Group
Upon completion of the project PIs are expected to put their intervention materials and
procedure manuals into the public domain andor make them available to other investigators
according to the approved plan for making data and materials available to the scientific
community and the NHLBI for the conduct of research at no charge other than the costs of
reproduction and distribution
The NHLBI reserves the right to terminate or curtail the project (or an individual award) in the
event of (a) failure to develop or implement mutually agreeable collaborative measurement
subject eligibility and data management sections of the protocols (b) substantial shortfall in
subject recruitment follow-up data reporting or quality control or other major breach of
protocol (c) substantive changes in the agreed-upon protocols with which NHLBI cannot
concur (d) reaching a major project outcome with persuasive statistical significance
substantially before schedule or (e) human subject ethical issues that may dictate a premature
termination
Any disagreement that may arise in scientificprogrammatic matters (within the scope of the
award) between award recipients and the NHLBI may be brought to arbitration An arbitration
panel will be composed of 3 membersmdash1 selected by the IPFnet Steering Group (with the
NHLBI member not voting) or by the individual PI in the event of an individual disagreement a
second selected by NHLBI and the third selected by the other 2 members This special
arbitration procedure in no way affects the PIrsquos right to appeal an adverse action that is otherwise
appealable in accordance with the PHS regulations at 42 CFR part 50 Subpart D and HHS
63
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
regulation at 45 CFR part 16 or the rights of the NHLBI under applicable statutes regulations
and terms of the award
102 IPFnet Steering Group
The IPFnet Steering Group is the main governing body of the project It is composed of the PIs
of the clinical centers the PI of the DCC and the NHLBI project scientist The clinical centers
the IPFnet DCC and the NHLBI each have 1 vote on the IPFnet Steering Group All decisions
are determined by majority vote
All major scientific decisions are determined by the IPFnet Steering Group It assumes overall
responsibility for the design and conduct of the trial It appoints (and disbands) committees and
subcommittees as the need arises designs approves and implements the study protocols
oversees the development of the MOOP monitors subject recruitment and treatment delivery
evaluates data collection and management oversees quality assurance procedures and
implements changes and enhancements to the study as required It also has primary responsibility
for facilitating the conduct of the trials and reporting the projectrsquos results
103 Data and Safety Monitoring Board
The NHLBI will establish a DSMB in accordance with established policies (see
httpwwwnhlbinihgovfundingpoliciesdsmb_insthtm) to ensure data quality and subject
safety and to provide independent advice to the NHLBI regarding progress and the
appropriateness of study continuation
104 Recommendations on Interim Monitoring of Efficacy Safety and Futility
First and foremost the role of the DSMB will be to review subject safety and trial conduct at
periodic points during the study The DSMB may require analyses of the primary endpoint
results for comparing the benefit and risks of treatment strategies The benefit of collecting
additional data on key secondary endpoints with extended follow-up and establishing a robust
64
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
evidence base for determining a standard of care will need to be carefully considered before
early termination of one or more treatment arms After careful consideration the IPFnet Steering
Group recommends conservative thresholds for the early examinations of the safety and efficacy
data
The DSMB will be expected to meet approximately every 6 months until trial completion to
review safety and toxicity data The DSMB may recommend stopping the study based on these
reviews Because the DSMB could stop the trial for safety concerns as well as for a large
efficacy benefit there could be multiple opportunities to reject the null hypothesis (no difference
in event rates between the PL and NAC groups) A Bonferroni approximation will be applied
during the one planned interim analysis for efficacy
Before locking the database a statistical analysis plan (SAP) will be developed to provide
complete details on the statistical analysis The SAP will include the specifics for how and when
the DSMB will be notified for AEs The IPFnet DCC will deliver to the DSMB all FDA-defined
AEs at 3-month intervals The IPFnet DCC will prepare narrative SAE reports in real time for
DSMB review including recommendations and analysis of similar events for each SAE
submitted to the FDA
65
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
11 Investigator and Sponsor Obligations
111 Monitoring
All monitoring activities for US clinical centers will be performed in accordance with DCRI
standard operating procedures Information regarding the types of visits will be outlined in the
PANTHER-IPF MOOP
112 Cost and Payment
There will be no cost to subjects enrolled in this trial Study-related procedures will be paid for
by the IPFnet
Subjects may be eligible for reimbursement for travel to the clinical center Details of payment
will be explained to each subject during the consent process
113 Confidentiality and Health Insurance Portability and Accountability Act
Considerations
Subject confidentiality will be protected throughout the study All subject data will be kept
strictly confidential and no subject-identifying information will be released to anyone outside
the project Confidentiality will be assured through several mechanisms First each subject will
be assigned an anonymous study ID which will then be used on all study forms Second any
study forms blood samples and paper records that contain subject information (eg address lists
phone lists) will be kept at the clinical centers in secured locked areas coded by number Once
blood is collected there will be no subject identifiers placed on blood samplesmdashonly the study
ID number and the date of sample collection Third access to all subject data and information
including laboratory specimens will be restricted to authorized personnel In the case of
computerized data this restricted access will be assured through user logon IDs and password
protection
66
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
At the IPFnet DCC only authorized personnel will have access to the data files containing study
data Security will be assured through user logon IDs passwords and appropriate access
privileges All study subjects will be identified only by their IPFnet ID numbers and no personal
identifying information such as name address or Social Security number will be entered into
the IPFnet DCC database Any subject-specific data reported to the IPFnet Steering Group will
be identified only by the IPFnet ID number
Finally subjects will not be identified by name in any reports or publications nor will the data
be presented in such a way that the identity of individual subjects can be inferred Analysis files
created for further study by the scientific community will have no subject identifiers These data
files will be created in accordance with the Ancillary Studies and Publication Policy of the
IPFnet
114 Informed Consent Procedures
All IPFnet subjects will provide written informed consent using procedures reviewed and
approved by each clinical centerrsquos IRB Informed consent will be undertaken by study personnel
in-person with the subject The subject has the option of declining further participation in the
study at that point No further study procedures will be conducted until the signed documents
have been provided to the IPFnet clinical center
115 Institutional Review Boards
Before initiating this study the protocol clinical center-specific informed consent forms Health
Insurance Portability and Accountability Act (HIPAA) forms recruitment materials and other
relevant information will be reviewed by a properly constituted IRB at each participating clinical
center A copy of the signed and dated IRB approval at each clinical center will be retrieved prior
to or during the site initiation visit and archived at the IPFnet DCC Any amendments to the
protocol other than simple administrative and typographical changes must be approved by each
IRB before they are implemented The clinical centers will seek annual renewals of their IRB
approvals in accordance with local procedures
67
__________________________________________ ________________
__________________________________________
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
12 Investigator Agreement
I have read the foregoing protocol PANTHER-IPF and agree that it contains all necessary
details for carrying out this study I will conduct the study as outlined herein and will complete
the study within the time designated
I will provide copies of the protocol and all pertinent information to all individuals responsible to
me who assist in the conduct of this study I will discuss this material with them to ensure they
are fully informed regarding the drug and the conduct of the study
I will fulfill all responsibilities for submitting pertinent information to the local IRB if
applicable that is responsible for this study
I further agree that NHLBI andor DCRI will have access to any source documents from which
eCRF information may have been generated
Signature of Principal Investigator Date
Name of Principal Investigator (printed or typed)
Protocol version date May 19 2009
Protocol Amendment 1 version date May 28 2010
Protocol Amendment 2 version date December 6 2011
68
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
13 References
1 Raghu G Brown KK Bradford WZ et al A placebo-controlled trial of interferon gamma-1b in patients with idiopathic pulmonary fibrosis N Engl J Med 2004350125-33 2 King TE Jr Safrin S Starko KM et al Analyses of efficacy end points in a controlled trial of interferon-gamma1b for idiopathic pulmonary fibrosis Chest 2005127171-7 3 Flaherty KR Thwaite EL Kazerooni EA et al Radiological versus histological diagnosis in UIP and NSIP survival implications Thorax 200358143-8 4 Wells AU Desai SR Rubens MB et al Idiopathic pulmonary fibrosis a composite physiologic index derived from disease extent observed by computed tomography Am J Respir Crit Care Med 2003167962-9 5 Raghu G Freudenberger TD Yang S et al High prevalence of abnormal acid gastroshyoesophageal reflux in idiopathic pulmonary fibrosis Eur Respir J 200627136-42 6 Kinnula VL Focus on antioxidant enzymes and antioxidant strategies in smoking related airway diseases Thorax 200560693-700 7 Coultas DB Zumwalt RE Black WC Sobonya RE The epidemiology of interstitial lung diseases Am J Respir Crit Care Med 1994150967-72 8 Raghu G Weycker D Edelsberg J Bradford WZ Oster G Incidence and prevalence of idiopathic pulmonary fibrosis Am J Respir Crit Care Med 2006174810-6 9 Olson AL Swigris JJ Lezotte DC Norris JM Wilson CG Brown KK Mortality from pulmonary fibrosis increased in the United States from 1992 to 2003 Am J Respir Crit Care Med 2007176277-84 10 Mannino DM Etzel RA Parrish RG Pulmonary fibrosis deaths in the United States 1979shy1991 An analysis of multiple-cause mortality data Am J Respir Crit Care Med 19961531548shy52 11 Hubbard R Johnston I Coultas DB Britton J Mortality rates from cryptogenic fibrosing alveolitis in seven countries Thorax 199651711-6 12 Johnston I Britton J Kinnear W Logan R Rising mortality from cryptogenic fibrosing alveolitis Bmj 19903011017-21 13 Raghu G Collard HR Egan JJ et al An official ATSERSJRSALAT statement idiopathic pulmonary fibrosis evidence-based guidelines for diagnosis and management Am J Respir Crit Care Med 2011183788-824 14 (USA) FDA FDA Public Health Advisory Interferon gamma-1b (marketed as Actimmune) In 2007 15 King TE Jr Pardo A Selman M Idiopathic pulmonary fibrosis Lancet 2011 16 Raghu G Brown KK Costabel U et al Treatment of idiopathic pulmonary fibrosis with etanercept an exploratory placebo-controlled trial Am J Respir Crit Care Med 2008178948shy55 17 Malouf MA Hopkins P Snell G Glanville AR An investigator-driven study of everolimus in surgical lung biopsy confirmed idiopathic pulmonary fibrosis Respirology 201116776-83 18 King TE Jr Behr J Brown KK et al BUILD-1 a randomized placebo-controlled trial of bosentan in idiopathic pulmonary fibrosis Am J Respir Crit Care Med 200817775-81 19 Richeldi L Costabel U Selman M et al Efficacy of a tyrosine kinase inhibitor in idiopathic pulmonary fibrosis N Engl J Med 20113651079-87
69
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
20 Borok Z Buhl R Grimes GJ et al Effect of glutathione aerosol on oxidant-antioxidant imbalance in idiopathic pulmonary fibrosis Lancet 1991338215-6 21 Meyer A Buhl R Magnussen H The effect of oral N-acetylcysteine on lung glutathione levels in idiopathic pulmonary fibrosis Eur Respir J 19947431-6 22 Behr J Maier K Degenkolb B Krombach F Vogelmeier C Antioxidative and clinical effects of high-dose N-acetylcysteine in fibrosing alveolitis Adjunctive therapy to maintenance immunosuppression Am J Respir Crit Care Med 19971561897-901 23 Cantin AM North SL Fells GA Hubbard RC Crystal RG Oxidant-mediated epithelial cell injury in idiopathic pulmonary fibrosis J Clin Invest 1987791665-73 24 Waghray M Cui Z Horowitz JC et al Hydrogen peroxide is a diffusible paracrine signal for the induction of epithelial cell death by activated myofibroblasts Faseb J 200519854-6 25 Larios JM Budhiraja R Fanburg BL Thannickal VJ Oxidative protein cross-linking reactions involving L-tyrosine in transforming growth factor-beta1-stimulated fibroblasts J Biol Chem 200127617437-41 26 Kinnula VL Fattman CL Tan RJ Oury TD Oxidative stress in pulmonary fibrosis a possible role for redox modulatory therapy Am J Respir Crit Care Med 2005172417-22 27 Meyer A Buhl R Kampf S Magnussen H Intravenous N-acetylcysteine and lung glutathione of patients with pulmonary fibrosis and normals Am J Respir Crit Care Med 19951521055-60 28 Behr J Degenkolb B Krombach F Vogelmeier C Intracellular glutathione and bronchoalveolar cells in fibrosing alveolitis effects of N-acetylcysteine Eur Respir J 200219906-11 29 Bando M Hosono T Mato N et al Long-term efficacy of inhaled N-acetylcysteine in patients with idiopathic pulmonary fibrosis Intern Med 2010492289-96 30 Demedts M Behr J Buhl R et al High-dose acetylcysteine in idiopathic pulmonary fibrosis N Engl J Med 20053532229-42 31 Toma TP Bhowmik A Rajakulasingam R Acetylcysteine in pulmonary fibrosis N Engl J Med 20063541086-9 author reply -9 32 Hunninghake GW Antioxidant therapy for idiopathic pulmonary fibrosis N Engl J Med 20053532285-7 33 Flaherty KR Mumford JA Murray S et al Prognostic implications of physiologic and radiographic changes in idiopathic interstitial pneumonia Am J Respir Crit Care Med 2003168543-8 34 Latsi PI du Bois RM Nicholson AG et al Fibrotic idiopathic interstitial pneumonia the prognostic value of longitudinal functional trends Am J Respir Crit Care Med 2003168531-7 35 Collard HR King TE Jr Bartelson BB Vourlekis JS Schwarz MI Brown KK Changes in clinical and physiologic variables predict survival in idiopathic pulmonary fibrosis Am J Respir Crit Care Med 2003168538-42 36 Jegal Y Kim DS Shim TS et al Physiology is a stronger predictor of survival than pathology in fibrotic interstitial pneumonia Am J Respir Crit Care Med 2005171639-44 37 Martinez FJ Safrin S Weycker D et al The clinical course of patients with idiopathic pulmonary fibrosis Ann Intern Med 2005142963-7 38 Hull JH Acetylcysteine in pulmonary fibrosis N Engl J Med 20063541089-91 author reply -91
70
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
39 Flaherty KR King TE Jr Raghu G et al Idiopathic interstitial pneumonia what is the effect of a multidisciplinary approach to diagnosis Am J Respir Crit Care Med 2004170904shy10 40 Raghu G Johnson WC Lockhart D Mageto Y Treatment of idiopathic pulmonary fibrosis with a new antifibrotic agent pirfenidone results of a prospective open-label Phase II study Am J Respir Crit Care Med 19991591061-9 41 Hunninghake GW Lynch DA Galvin JR et al Radiologic findings are strongly associated with a pathologic diagnosis of usual interstitial pneumonia Chest 20031241215-23 42 Lynch D Godwin J Safrin S et al High-resolution computed tomography in idiopathic pulmonary fibrosis diagnosis and prognosis Am J Respir Crit Care Med 2005172488-93 43 Mallinckrodt CH Watkin JG Molenberghs G Carroll RJ Choice of the primary analysis in longitudinal clinical trials Pharmaceutical Statistics 20043161-9 44 Bang H Tsiatis A Estimating medical costs with censored data Biometrika 200087329shy43 45 Lin DY Regression analysis of incomplete medical cost data Stat Med 2003221181-200 46 Rochon J Application of GEE procedures for sample size calculations in repeated measures experiments Stat Med 1998171643-58 47 Lachin JM Foulkes MA Evaluation of sample size and power for analyses of survival with allowance for nonuniform patient entry losses to follow-up noncompliance and stratification Biometrics 198642507-19
71
- PANTHER-IPFPREDNISONE AZATHIOPRINEAND N-ACETYLCYSTEINEA STUDY THAT EVALUATES RESPONSE INIDIOPATHIC PULMONARY FIBROSIS
-
- Protocol Summary
- Table of Contents
- List of Tables
- List of Figures
- List of Abbreviations
- 1 Summary
- 2 Hypotheses and Specific Aims
-
- 21 Null Hypothesis
- 22 Specific Aim 1
- 23 Specific Aim 2
- 24 Prespecified Subgroups of Interest
-
- 3 Background and Significance
-
- 31 Idiopathic Pulmonary Fibrosis is the Most Common Interstitial Lung Disease
- 32 Rationale for Placebo Control
- 33 Rationale for N-acetylcysteine
- 35 Rationale for N-acetylcysteine as a Stand-alone Therapy
- 36 Rationale for the Study Design and Primary Endpoint
- 37 Rationale for Blinding of Treatments
-
- 4 Methods
-
- 41 Inclusion Criteria
- 42 Diagnosis of IPF
- 43 Exclusion Criteria
- 44 Study Design and Study Visit
- 45 Dose Justification
- 46 Contraindications Precautions and Side Effects of Study Medications
- 47 Recruitment Procedures
- 48 Study Procedures
- 49 Concomitant Medications
- 410 Laboratory Testing
- 411 Blinding of Study Drugs
-
- 5 Study Endpoints
-
- 51 Primary Study Endpoint
- 52 Secondary Study Endpoints
-
- 6 Safety Evaluations and Procedures
-
- 61 Adverse Events
- 62 Clinical Medical Monitoring
- 63 Unblinding Procedures
-
- 7 Study Drug Procedures
- 8 Data Management
-
- 81 Hardware and Software Configuration
- 82 Sources of Data
-
- 9 Study Design and Data Analysis
-
- 91 General Analytic Considerations
- 92 Randomization Blinding and Reporting of Results
- 93 Stratification
- 94 Specification of the Primary Analyses
- 95 Analysis of Longitudinal Endpoints
- 96 Analysis of Binary Time-to-Event and Time-Lagged Endpoints
- 97 Power Analysis
-
- 10 Study Administration
-
- 101 Cooperative Agreement Mechanism
- 102 IPFnet Steering Group
- 103 Data and Safety Monitoring Board
- 104 Recommendations on Interim Monitoring of Efficacy Safety and Futility
-
- 11 Investigator and Sponsor Obligations
-
- 111 Monitoring
- 112 Cost and Payment
- 113 Confidentiality and Health Insurance Portability and Accountability ActConsiderations
- 114 Informed Consent Procedures
- 115 Institutional Review Boards
-
- 12 Investigator Agreement
- 13 References
-
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
10 Study Administration
101 Cooperative Agreement Mechanism
The administrative and funding mechanism used to undertake this project is a ldquocooperative
agreementrdquo (U01) which is an assistance mechanism Under the cooperative agreement the
NHLBI assists supports andor stimulates the project and is substantially involved with
investigators in conducting the study by facilitating performance of the effort in a ldquopartnerrdquo role
The NHLBI project scientist serves on the IPFnet Steering Group and he or another NHLBI
scientist may serve on other project committees when appropriate At the same time however
NHLBI does not assume a dominant role direction or prime responsibility for this research
program
As described below governance of the project is conducted through the IPFnet Steering Group
Principal investigators have lead responsibilities in all aspects of their trials and the project
including any modification of trial designs conduct of the trials quality control data analysis
and interpretation preparation of publications and collaboration with other investigators unless
otherwise provided for by the IPFnet Steering Group
PIs retain custody of and have primary rights to their center-specific and collaborative data
subject to government rights-of-access consistent with current Health amp Human Services (HHS)
Public Health Service (PHS) and National Institutes of Health policies The protocols and
governance policies call for the continual submission of data centrally to the IPFnet DCC for the
collaborative database which at a minimum will contain the key variables selected by the IPFnet
Steering Group for standardization across all clinical centers the submission of copies of the
collaborative datasets to each PI upon completion of the project procedures for data analysis
reporting and publication and procedures to protect and ensure the privacy of medical and
genetic data and records of individuals The NHLBI project scientist on behalf of the NHLBI
will have the same access privileges and responsibilities regarding the collaborative data as the
other members of the Steering Group
62
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
PIs are also encouraged to publish and to publicly release and disseminate results data and other
products of the project concordant with the project protocols and governance and the approved
plan for making data and materials available to the scientific community and to the NHLBI
However during the 3 years after the ending date of NHLBI project support unpublished data
unpublished results data sets not previously released and other study materials or products are
to be made available to any third party only with the approval of the IPFnet Steering Group
Upon completion of the project PIs are expected to put their intervention materials and
procedure manuals into the public domain andor make them available to other investigators
according to the approved plan for making data and materials available to the scientific
community and the NHLBI for the conduct of research at no charge other than the costs of
reproduction and distribution
The NHLBI reserves the right to terminate or curtail the project (or an individual award) in the
event of (a) failure to develop or implement mutually agreeable collaborative measurement
subject eligibility and data management sections of the protocols (b) substantial shortfall in
subject recruitment follow-up data reporting or quality control or other major breach of
protocol (c) substantive changes in the agreed-upon protocols with which NHLBI cannot
concur (d) reaching a major project outcome with persuasive statistical significance
substantially before schedule or (e) human subject ethical issues that may dictate a premature
termination
Any disagreement that may arise in scientificprogrammatic matters (within the scope of the
award) between award recipients and the NHLBI may be brought to arbitration An arbitration
panel will be composed of 3 membersmdash1 selected by the IPFnet Steering Group (with the
NHLBI member not voting) or by the individual PI in the event of an individual disagreement a
second selected by NHLBI and the third selected by the other 2 members This special
arbitration procedure in no way affects the PIrsquos right to appeal an adverse action that is otherwise
appealable in accordance with the PHS regulations at 42 CFR part 50 Subpart D and HHS
63
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
regulation at 45 CFR part 16 or the rights of the NHLBI under applicable statutes regulations
and terms of the award
102 IPFnet Steering Group
The IPFnet Steering Group is the main governing body of the project It is composed of the PIs
of the clinical centers the PI of the DCC and the NHLBI project scientist The clinical centers
the IPFnet DCC and the NHLBI each have 1 vote on the IPFnet Steering Group All decisions
are determined by majority vote
All major scientific decisions are determined by the IPFnet Steering Group It assumes overall
responsibility for the design and conduct of the trial It appoints (and disbands) committees and
subcommittees as the need arises designs approves and implements the study protocols
oversees the development of the MOOP monitors subject recruitment and treatment delivery
evaluates data collection and management oversees quality assurance procedures and
implements changes and enhancements to the study as required It also has primary responsibility
for facilitating the conduct of the trials and reporting the projectrsquos results
103 Data and Safety Monitoring Board
The NHLBI will establish a DSMB in accordance with established policies (see
httpwwwnhlbinihgovfundingpoliciesdsmb_insthtm) to ensure data quality and subject
safety and to provide independent advice to the NHLBI regarding progress and the
appropriateness of study continuation
104 Recommendations on Interim Monitoring of Efficacy Safety and Futility
First and foremost the role of the DSMB will be to review subject safety and trial conduct at
periodic points during the study The DSMB may require analyses of the primary endpoint
results for comparing the benefit and risks of treatment strategies The benefit of collecting
additional data on key secondary endpoints with extended follow-up and establishing a robust
64
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
evidence base for determining a standard of care will need to be carefully considered before
early termination of one or more treatment arms After careful consideration the IPFnet Steering
Group recommends conservative thresholds for the early examinations of the safety and efficacy
data
The DSMB will be expected to meet approximately every 6 months until trial completion to
review safety and toxicity data The DSMB may recommend stopping the study based on these
reviews Because the DSMB could stop the trial for safety concerns as well as for a large
efficacy benefit there could be multiple opportunities to reject the null hypothesis (no difference
in event rates between the PL and NAC groups) A Bonferroni approximation will be applied
during the one planned interim analysis for efficacy
Before locking the database a statistical analysis plan (SAP) will be developed to provide
complete details on the statistical analysis The SAP will include the specifics for how and when
the DSMB will be notified for AEs The IPFnet DCC will deliver to the DSMB all FDA-defined
AEs at 3-month intervals The IPFnet DCC will prepare narrative SAE reports in real time for
DSMB review including recommendations and analysis of similar events for each SAE
submitted to the FDA
65
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
11 Investigator and Sponsor Obligations
111 Monitoring
All monitoring activities for US clinical centers will be performed in accordance with DCRI
standard operating procedures Information regarding the types of visits will be outlined in the
PANTHER-IPF MOOP
112 Cost and Payment
There will be no cost to subjects enrolled in this trial Study-related procedures will be paid for
by the IPFnet
Subjects may be eligible for reimbursement for travel to the clinical center Details of payment
will be explained to each subject during the consent process
113 Confidentiality and Health Insurance Portability and Accountability Act
Considerations
Subject confidentiality will be protected throughout the study All subject data will be kept
strictly confidential and no subject-identifying information will be released to anyone outside
the project Confidentiality will be assured through several mechanisms First each subject will
be assigned an anonymous study ID which will then be used on all study forms Second any
study forms blood samples and paper records that contain subject information (eg address lists
phone lists) will be kept at the clinical centers in secured locked areas coded by number Once
blood is collected there will be no subject identifiers placed on blood samplesmdashonly the study
ID number and the date of sample collection Third access to all subject data and information
including laboratory specimens will be restricted to authorized personnel In the case of
computerized data this restricted access will be assured through user logon IDs and password
protection
66
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
At the IPFnet DCC only authorized personnel will have access to the data files containing study
data Security will be assured through user logon IDs passwords and appropriate access
privileges All study subjects will be identified only by their IPFnet ID numbers and no personal
identifying information such as name address or Social Security number will be entered into
the IPFnet DCC database Any subject-specific data reported to the IPFnet Steering Group will
be identified only by the IPFnet ID number
Finally subjects will not be identified by name in any reports or publications nor will the data
be presented in such a way that the identity of individual subjects can be inferred Analysis files
created for further study by the scientific community will have no subject identifiers These data
files will be created in accordance with the Ancillary Studies and Publication Policy of the
IPFnet
114 Informed Consent Procedures
All IPFnet subjects will provide written informed consent using procedures reviewed and
approved by each clinical centerrsquos IRB Informed consent will be undertaken by study personnel
in-person with the subject The subject has the option of declining further participation in the
study at that point No further study procedures will be conducted until the signed documents
have been provided to the IPFnet clinical center
115 Institutional Review Boards
Before initiating this study the protocol clinical center-specific informed consent forms Health
Insurance Portability and Accountability Act (HIPAA) forms recruitment materials and other
relevant information will be reviewed by a properly constituted IRB at each participating clinical
center A copy of the signed and dated IRB approval at each clinical center will be retrieved prior
to or during the site initiation visit and archived at the IPFnet DCC Any amendments to the
protocol other than simple administrative and typographical changes must be approved by each
IRB before they are implemented The clinical centers will seek annual renewals of their IRB
approvals in accordance with local procedures
67
__________________________________________ ________________
__________________________________________
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
12 Investigator Agreement
I have read the foregoing protocol PANTHER-IPF and agree that it contains all necessary
details for carrying out this study I will conduct the study as outlined herein and will complete
the study within the time designated
I will provide copies of the protocol and all pertinent information to all individuals responsible to
me who assist in the conduct of this study I will discuss this material with them to ensure they
are fully informed regarding the drug and the conduct of the study
I will fulfill all responsibilities for submitting pertinent information to the local IRB if
applicable that is responsible for this study
I further agree that NHLBI andor DCRI will have access to any source documents from which
eCRF information may have been generated
Signature of Principal Investigator Date
Name of Principal Investigator (printed or typed)
Protocol version date May 19 2009
Protocol Amendment 1 version date May 28 2010
Protocol Amendment 2 version date December 6 2011
68
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
13 References
1 Raghu G Brown KK Bradford WZ et al A placebo-controlled trial of interferon gamma-1b in patients with idiopathic pulmonary fibrosis N Engl J Med 2004350125-33 2 King TE Jr Safrin S Starko KM et al Analyses of efficacy end points in a controlled trial of interferon-gamma1b for idiopathic pulmonary fibrosis Chest 2005127171-7 3 Flaherty KR Thwaite EL Kazerooni EA et al Radiological versus histological diagnosis in UIP and NSIP survival implications Thorax 200358143-8 4 Wells AU Desai SR Rubens MB et al Idiopathic pulmonary fibrosis a composite physiologic index derived from disease extent observed by computed tomography Am J Respir Crit Care Med 2003167962-9 5 Raghu G Freudenberger TD Yang S et al High prevalence of abnormal acid gastroshyoesophageal reflux in idiopathic pulmonary fibrosis Eur Respir J 200627136-42 6 Kinnula VL Focus on antioxidant enzymes and antioxidant strategies in smoking related airway diseases Thorax 200560693-700 7 Coultas DB Zumwalt RE Black WC Sobonya RE The epidemiology of interstitial lung diseases Am J Respir Crit Care Med 1994150967-72 8 Raghu G Weycker D Edelsberg J Bradford WZ Oster G Incidence and prevalence of idiopathic pulmonary fibrosis Am J Respir Crit Care Med 2006174810-6 9 Olson AL Swigris JJ Lezotte DC Norris JM Wilson CG Brown KK Mortality from pulmonary fibrosis increased in the United States from 1992 to 2003 Am J Respir Crit Care Med 2007176277-84 10 Mannino DM Etzel RA Parrish RG Pulmonary fibrosis deaths in the United States 1979shy1991 An analysis of multiple-cause mortality data Am J Respir Crit Care Med 19961531548shy52 11 Hubbard R Johnston I Coultas DB Britton J Mortality rates from cryptogenic fibrosing alveolitis in seven countries Thorax 199651711-6 12 Johnston I Britton J Kinnear W Logan R Rising mortality from cryptogenic fibrosing alveolitis Bmj 19903011017-21 13 Raghu G Collard HR Egan JJ et al An official ATSERSJRSALAT statement idiopathic pulmonary fibrosis evidence-based guidelines for diagnosis and management Am J Respir Crit Care Med 2011183788-824 14 (USA) FDA FDA Public Health Advisory Interferon gamma-1b (marketed as Actimmune) In 2007 15 King TE Jr Pardo A Selman M Idiopathic pulmonary fibrosis Lancet 2011 16 Raghu G Brown KK Costabel U et al Treatment of idiopathic pulmonary fibrosis with etanercept an exploratory placebo-controlled trial Am J Respir Crit Care Med 2008178948shy55 17 Malouf MA Hopkins P Snell G Glanville AR An investigator-driven study of everolimus in surgical lung biopsy confirmed idiopathic pulmonary fibrosis Respirology 201116776-83 18 King TE Jr Behr J Brown KK et al BUILD-1 a randomized placebo-controlled trial of bosentan in idiopathic pulmonary fibrosis Am J Respir Crit Care Med 200817775-81 19 Richeldi L Costabel U Selman M et al Efficacy of a tyrosine kinase inhibitor in idiopathic pulmonary fibrosis N Engl J Med 20113651079-87
69
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
20 Borok Z Buhl R Grimes GJ et al Effect of glutathione aerosol on oxidant-antioxidant imbalance in idiopathic pulmonary fibrosis Lancet 1991338215-6 21 Meyer A Buhl R Magnussen H The effect of oral N-acetylcysteine on lung glutathione levels in idiopathic pulmonary fibrosis Eur Respir J 19947431-6 22 Behr J Maier K Degenkolb B Krombach F Vogelmeier C Antioxidative and clinical effects of high-dose N-acetylcysteine in fibrosing alveolitis Adjunctive therapy to maintenance immunosuppression Am J Respir Crit Care Med 19971561897-901 23 Cantin AM North SL Fells GA Hubbard RC Crystal RG Oxidant-mediated epithelial cell injury in idiopathic pulmonary fibrosis J Clin Invest 1987791665-73 24 Waghray M Cui Z Horowitz JC et al Hydrogen peroxide is a diffusible paracrine signal for the induction of epithelial cell death by activated myofibroblasts Faseb J 200519854-6 25 Larios JM Budhiraja R Fanburg BL Thannickal VJ Oxidative protein cross-linking reactions involving L-tyrosine in transforming growth factor-beta1-stimulated fibroblasts J Biol Chem 200127617437-41 26 Kinnula VL Fattman CL Tan RJ Oury TD Oxidative stress in pulmonary fibrosis a possible role for redox modulatory therapy Am J Respir Crit Care Med 2005172417-22 27 Meyer A Buhl R Kampf S Magnussen H Intravenous N-acetylcysteine and lung glutathione of patients with pulmonary fibrosis and normals Am J Respir Crit Care Med 19951521055-60 28 Behr J Degenkolb B Krombach F Vogelmeier C Intracellular glutathione and bronchoalveolar cells in fibrosing alveolitis effects of N-acetylcysteine Eur Respir J 200219906-11 29 Bando M Hosono T Mato N et al Long-term efficacy of inhaled N-acetylcysteine in patients with idiopathic pulmonary fibrosis Intern Med 2010492289-96 30 Demedts M Behr J Buhl R et al High-dose acetylcysteine in idiopathic pulmonary fibrosis N Engl J Med 20053532229-42 31 Toma TP Bhowmik A Rajakulasingam R Acetylcysteine in pulmonary fibrosis N Engl J Med 20063541086-9 author reply -9 32 Hunninghake GW Antioxidant therapy for idiopathic pulmonary fibrosis N Engl J Med 20053532285-7 33 Flaherty KR Mumford JA Murray S et al Prognostic implications of physiologic and radiographic changes in idiopathic interstitial pneumonia Am J Respir Crit Care Med 2003168543-8 34 Latsi PI du Bois RM Nicholson AG et al Fibrotic idiopathic interstitial pneumonia the prognostic value of longitudinal functional trends Am J Respir Crit Care Med 2003168531-7 35 Collard HR King TE Jr Bartelson BB Vourlekis JS Schwarz MI Brown KK Changes in clinical and physiologic variables predict survival in idiopathic pulmonary fibrosis Am J Respir Crit Care Med 2003168538-42 36 Jegal Y Kim DS Shim TS et al Physiology is a stronger predictor of survival than pathology in fibrotic interstitial pneumonia Am J Respir Crit Care Med 2005171639-44 37 Martinez FJ Safrin S Weycker D et al The clinical course of patients with idiopathic pulmonary fibrosis Ann Intern Med 2005142963-7 38 Hull JH Acetylcysteine in pulmonary fibrosis N Engl J Med 20063541089-91 author reply -91
70
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
39 Flaherty KR King TE Jr Raghu G et al Idiopathic interstitial pneumonia what is the effect of a multidisciplinary approach to diagnosis Am J Respir Crit Care Med 2004170904shy10 40 Raghu G Johnson WC Lockhart D Mageto Y Treatment of idiopathic pulmonary fibrosis with a new antifibrotic agent pirfenidone results of a prospective open-label Phase II study Am J Respir Crit Care Med 19991591061-9 41 Hunninghake GW Lynch DA Galvin JR et al Radiologic findings are strongly associated with a pathologic diagnosis of usual interstitial pneumonia Chest 20031241215-23 42 Lynch D Godwin J Safrin S et al High-resolution computed tomography in idiopathic pulmonary fibrosis diagnosis and prognosis Am J Respir Crit Care Med 2005172488-93 43 Mallinckrodt CH Watkin JG Molenberghs G Carroll RJ Choice of the primary analysis in longitudinal clinical trials Pharmaceutical Statistics 20043161-9 44 Bang H Tsiatis A Estimating medical costs with censored data Biometrika 200087329shy43 45 Lin DY Regression analysis of incomplete medical cost data Stat Med 2003221181-200 46 Rochon J Application of GEE procedures for sample size calculations in repeated measures experiments Stat Med 1998171643-58 47 Lachin JM Foulkes MA Evaluation of sample size and power for analyses of survival with allowance for nonuniform patient entry losses to follow-up noncompliance and stratification Biometrics 198642507-19
71
- PANTHER-IPFPREDNISONE AZATHIOPRINEAND N-ACETYLCYSTEINEA STUDY THAT EVALUATES RESPONSE INIDIOPATHIC PULMONARY FIBROSIS
-
- Protocol Summary
- Table of Contents
- List of Tables
- List of Figures
- List of Abbreviations
- 1 Summary
- 2 Hypotheses and Specific Aims
-
- 21 Null Hypothesis
- 22 Specific Aim 1
- 23 Specific Aim 2
- 24 Prespecified Subgroups of Interest
-
- 3 Background and Significance
-
- 31 Idiopathic Pulmonary Fibrosis is the Most Common Interstitial Lung Disease
- 32 Rationale for Placebo Control
- 33 Rationale for N-acetylcysteine
- 35 Rationale for N-acetylcysteine as a Stand-alone Therapy
- 36 Rationale for the Study Design and Primary Endpoint
- 37 Rationale for Blinding of Treatments
-
- 4 Methods
-
- 41 Inclusion Criteria
- 42 Diagnosis of IPF
- 43 Exclusion Criteria
- 44 Study Design and Study Visit
- 45 Dose Justification
- 46 Contraindications Precautions and Side Effects of Study Medications
- 47 Recruitment Procedures
- 48 Study Procedures
- 49 Concomitant Medications
- 410 Laboratory Testing
- 411 Blinding of Study Drugs
-
- 5 Study Endpoints
-
- 51 Primary Study Endpoint
- 52 Secondary Study Endpoints
-
- 6 Safety Evaluations and Procedures
-
- 61 Adverse Events
- 62 Clinical Medical Monitoring
- 63 Unblinding Procedures
-
- 7 Study Drug Procedures
- 8 Data Management
-
- 81 Hardware and Software Configuration
- 82 Sources of Data
-
- 9 Study Design and Data Analysis
-
- 91 General Analytic Considerations
- 92 Randomization Blinding and Reporting of Results
- 93 Stratification
- 94 Specification of the Primary Analyses
- 95 Analysis of Longitudinal Endpoints
- 96 Analysis of Binary Time-to-Event and Time-Lagged Endpoints
- 97 Power Analysis
-
- 10 Study Administration
-
- 101 Cooperative Agreement Mechanism
- 102 IPFnet Steering Group
- 103 Data and Safety Monitoring Board
- 104 Recommendations on Interim Monitoring of Efficacy Safety and Futility
-
- 11 Investigator and Sponsor Obligations
-
- 111 Monitoring
- 112 Cost and Payment
- 113 Confidentiality and Health Insurance Portability and Accountability ActConsiderations
- 114 Informed Consent Procedures
- 115 Institutional Review Boards
-
- 12 Investigator Agreement
- 13 References
-

PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
PIs are also encouraged to publish and to publicly release and disseminate results data and other
products of the project concordant with the project protocols and governance and the approved
plan for making data and materials available to the scientific community and to the NHLBI
However during the 3 years after the ending date of NHLBI project support unpublished data
unpublished results data sets not previously released and other study materials or products are
to be made available to any third party only with the approval of the IPFnet Steering Group
Upon completion of the project PIs are expected to put their intervention materials and
procedure manuals into the public domain andor make them available to other investigators
according to the approved plan for making data and materials available to the scientific
community and the NHLBI for the conduct of research at no charge other than the costs of
reproduction and distribution
The NHLBI reserves the right to terminate or curtail the project (or an individual award) in the
event of (a) failure to develop or implement mutually agreeable collaborative measurement
subject eligibility and data management sections of the protocols (b) substantial shortfall in
subject recruitment follow-up data reporting or quality control or other major breach of
protocol (c) substantive changes in the agreed-upon protocols with which NHLBI cannot
concur (d) reaching a major project outcome with persuasive statistical significance
substantially before schedule or (e) human subject ethical issues that may dictate a premature
termination
Any disagreement that may arise in scientificprogrammatic matters (within the scope of the
award) between award recipients and the NHLBI may be brought to arbitration An arbitration
panel will be composed of 3 membersmdash1 selected by the IPFnet Steering Group (with the
NHLBI member not voting) or by the individual PI in the event of an individual disagreement a
second selected by NHLBI and the third selected by the other 2 members This special
arbitration procedure in no way affects the PIrsquos right to appeal an adverse action that is otherwise
appealable in accordance with the PHS regulations at 42 CFR part 50 Subpart D and HHS
63
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
regulation at 45 CFR part 16 or the rights of the NHLBI under applicable statutes regulations
and terms of the award
102 IPFnet Steering Group
The IPFnet Steering Group is the main governing body of the project It is composed of the PIs
of the clinical centers the PI of the DCC and the NHLBI project scientist The clinical centers
the IPFnet DCC and the NHLBI each have 1 vote on the IPFnet Steering Group All decisions
are determined by majority vote
All major scientific decisions are determined by the IPFnet Steering Group It assumes overall
responsibility for the design and conduct of the trial It appoints (and disbands) committees and
subcommittees as the need arises designs approves and implements the study protocols
oversees the development of the MOOP monitors subject recruitment and treatment delivery
evaluates data collection and management oversees quality assurance procedures and
implements changes and enhancements to the study as required It also has primary responsibility
for facilitating the conduct of the trials and reporting the projectrsquos results
103 Data and Safety Monitoring Board
The NHLBI will establish a DSMB in accordance with established policies (see
httpwwwnhlbinihgovfundingpoliciesdsmb_insthtm) to ensure data quality and subject
safety and to provide independent advice to the NHLBI regarding progress and the
appropriateness of study continuation
104 Recommendations on Interim Monitoring of Efficacy Safety and Futility
First and foremost the role of the DSMB will be to review subject safety and trial conduct at
periodic points during the study The DSMB may require analyses of the primary endpoint
results for comparing the benefit and risks of treatment strategies The benefit of collecting
additional data on key secondary endpoints with extended follow-up and establishing a robust
64
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
evidence base for determining a standard of care will need to be carefully considered before
early termination of one or more treatment arms After careful consideration the IPFnet Steering
Group recommends conservative thresholds for the early examinations of the safety and efficacy
data
The DSMB will be expected to meet approximately every 6 months until trial completion to
review safety and toxicity data The DSMB may recommend stopping the study based on these
reviews Because the DSMB could stop the trial for safety concerns as well as for a large
efficacy benefit there could be multiple opportunities to reject the null hypothesis (no difference
in event rates between the PL and NAC groups) A Bonferroni approximation will be applied
during the one planned interim analysis for efficacy
Before locking the database a statistical analysis plan (SAP) will be developed to provide
complete details on the statistical analysis The SAP will include the specifics for how and when
the DSMB will be notified for AEs The IPFnet DCC will deliver to the DSMB all FDA-defined
AEs at 3-month intervals The IPFnet DCC will prepare narrative SAE reports in real time for
DSMB review including recommendations and analysis of similar events for each SAE
submitted to the FDA
65
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
11 Investigator and Sponsor Obligations
111 Monitoring
All monitoring activities for US clinical centers will be performed in accordance with DCRI
standard operating procedures Information regarding the types of visits will be outlined in the
PANTHER-IPF MOOP
112 Cost and Payment
There will be no cost to subjects enrolled in this trial Study-related procedures will be paid for
by the IPFnet
Subjects may be eligible for reimbursement for travel to the clinical center Details of payment
will be explained to each subject during the consent process
113 Confidentiality and Health Insurance Portability and Accountability Act
Considerations
Subject confidentiality will be protected throughout the study All subject data will be kept
strictly confidential and no subject-identifying information will be released to anyone outside
the project Confidentiality will be assured through several mechanisms First each subject will
be assigned an anonymous study ID which will then be used on all study forms Second any
study forms blood samples and paper records that contain subject information (eg address lists
phone lists) will be kept at the clinical centers in secured locked areas coded by number Once
blood is collected there will be no subject identifiers placed on blood samplesmdashonly the study
ID number and the date of sample collection Third access to all subject data and information
including laboratory specimens will be restricted to authorized personnel In the case of
computerized data this restricted access will be assured through user logon IDs and password
protection
66
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
At the IPFnet DCC only authorized personnel will have access to the data files containing study
data Security will be assured through user logon IDs passwords and appropriate access
privileges All study subjects will be identified only by their IPFnet ID numbers and no personal
identifying information such as name address or Social Security number will be entered into
the IPFnet DCC database Any subject-specific data reported to the IPFnet Steering Group will
be identified only by the IPFnet ID number
Finally subjects will not be identified by name in any reports or publications nor will the data
be presented in such a way that the identity of individual subjects can be inferred Analysis files
created for further study by the scientific community will have no subject identifiers These data
files will be created in accordance with the Ancillary Studies and Publication Policy of the
IPFnet
114 Informed Consent Procedures
All IPFnet subjects will provide written informed consent using procedures reviewed and
approved by each clinical centerrsquos IRB Informed consent will be undertaken by study personnel
in-person with the subject The subject has the option of declining further participation in the
study at that point No further study procedures will be conducted until the signed documents
have been provided to the IPFnet clinical center
115 Institutional Review Boards
Before initiating this study the protocol clinical center-specific informed consent forms Health
Insurance Portability and Accountability Act (HIPAA) forms recruitment materials and other
relevant information will be reviewed by a properly constituted IRB at each participating clinical
center A copy of the signed and dated IRB approval at each clinical center will be retrieved prior
to or during the site initiation visit and archived at the IPFnet DCC Any amendments to the
protocol other than simple administrative and typographical changes must be approved by each
IRB before they are implemented The clinical centers will seek annual renewals of their IRB
approvals in accordance with local procedures
67
__________________________________________ ________________
__________________________________________
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
12 Investigator Agreement
I have read the foregoing protocol PANTHER-IPF and agree that it contains all necessary
details for carrying out this study I will conduct the study as outlined herein and will complete
the study within the time designated
I will provide copies of the protocol and all pertinent information to all individuals responsible to
me who assist in the conduct of this study I will discuss this material with them to ensure they
are fully informed regarding the drug and the conduct of the study
I will fulfill all responsibilities for submitting pertinent information to the local IRB if
applicable that is responsible for this study
I further agree that NHLBI andor DCRI will have access to any source documents from which
eCRF information may have been generated
Signature of Principal Investigator Date
Name of Principal Investigator (printed or typed)
Protocol version date May 19 2009
Protocol Amendment 1 version date May 28 2010
Protocol Amendment 2 version date December 6 2011
68
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
13 References
1 Raghu G Brown KK Bradford WZ et al A placebo-controlled trial of interferon gamma-1b in patients with idiopathic pulmonary fibrosis N Engl J Med 2004350125-33 2 King TE Jr Safrin S Starko KM et al Analyses of efficacy end points in a controlled trial of interferon-gamma1b for idiopathic pulmonary fibrosis Chest 2005127171-7 3 Flaherty KR Thwaite EL Kazerooni EA et al Radiological versus histological diagnosis in UIP and NSIP survival implications Thorax 200358143-8 4 Wells AU Desai SR Rubens MB et al Idiopathic pulmonary fibrosis a composite physiologic index derived from disease extent observed by computed tomography Am J Respir Crit Care Med 2003167962-9 5 Raghu G Freudenberger TD Yang S et al High prevalence of abnormal acid gastroshyoesophageal reflux in idiopathic pulmonary fibrosis Eur Respir J 200627136-42 6 Kinnula VL Focus on antioxidant enzymes and antioxidant strategies in smoking related airway diseases Thorax 200560693-700 7 Coultas DB Zumwalt RE Black WC Sobonya RE The epidemiology of interstitial lung diseases Am J Respir Crit Care Med 1994150967-72 8 Raghu G Weycker D Edelsberg J Bradford WZ Oster G Incidence and prevalence of idiopathic pulmonary fibrosis Am J Respir Crit Care Med 2006174810-6 9 Olson AL Swigris JJ Lezotte DC Norris JM Wilson CG Brown KK Mortality from pulmonary fibrosis increased in the United States from 1992 to 2003 Am J Respir Crit Care Med 2007176277-84 10 Mannino DM Etzel RA Parrish RG Pulmonary fibrosis deaths in the United States 1979shy1991 An analysis of multiple-cause mortality data Am J Respir Crit Care Med 19961531548shy52 11 Hubbard R Johnston I Coultas DB Britton J Mortality rates from cryptogenic fibrosing alveolitis in seven countries Thorax 199651711-6 12 Johnston I Britton J Kinnear W Logan R Rising mortality from cryptogenic fibrosing alveolitis Bmj 19903011017-21 13 Raghu G Collard HR Egan JJ et al An official ATSERSJRSALAT statement idiopathic pulmonary fibrosis evidence-based guidelines for diagnosis and management Am J Respir Crit Care Med 2011183788-824 14 (USA) FDA FDA Public Health Advisory Interferon gamma-1b (marketed as Actimmune) In 2007 15 King TE Jr Pardo A Selman M Idiopathic pulmonary fibrosis Lancet 2011 16 Raghu G Brown KK Costabel U et al Treatment of idiopathic pulmonary fibrosis with etanercept an exploratory placebo-controlled trial Am J Respir Crit Care Med 2008178948shy55 17 Malouf MA Hopkins P Snell G Glanville AR An investigator-driven study of everolimus in surgical lung biopsy confirmed idiopathic pulmonary fibrosis Respirology 201116776-83 18 King TE Jr Behr J Brown KK et al BUILD-1 a randomized placebo-controlled trial of bosentan in idiopathic pulmonary fibrosis Am J Respir Crit Care Med 200817775-81 19 Richeldi L Costabel U Selman M et al Efficacy of a tyrosine kinase inhibitor in idiopathic pulmonary fibrosis N Engl J Med 20113651079-87
69
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
20 Borok Z Buhl R Grimes GJ et al Effect of glutathione aerosol on oxidant-antioxidant imbalance in idiopathic pulmonary fibrosis Lancet 1991338215-6 21 Meyer A Buhl R Magnussen H The effect of oral N-acetylcysteine on lung glutathione levels in idiopathic pulmonary fibrosis Eur Respir J 19947431-6 22 Behr J Maier K Degenkolb B Krombach F Vogelmeier C Antioxidative and clinical effects of high-dose N-acetylcysteine in fibrosing alveolitis Adjunctive therapy to maintenance immunosuppression Am J Respir Crit Care Med 19971561897-901 23 Cantin AM North SL Fells GA Hubbard RC Crystal RG Oxidant-mediated epithelial cell injury in idiopathic pulmonary fibrosis J Clin Invest 1987791665-73 24 Waghray M Cui Z Horowitz JC et al Hydrogen peroxide is a diffusible paracrine signal for the induction of epithelial cell death by activated myofibroblasts Faseb J 200519854-6 25 Larios JM Budhiraja R Fanburg BL Thannickal VJ Oxidative protein cross-linking reactions involving L-tyrosine in transforming growth factor-beta1-stimulated fibroblasts J Biol Chem 200127617437-41 26 Kinnula VL Fattman CL Tan RJ Oury TD Oxidative stress in pulmonary fibrosis a possible role for redox modulatory therapy Am J Respir Crit Care Med 2005172417-22 27 Meyer A Buhl R Kampf S Magnussen H Intravenous N-acetylcysteine and lung glutathione of patients with pulmonary fibrosis and normals Am J Respir Crit Care Med 19951521055-60 28 Behr J Degenkolb B Krombach F Vogelmeier C Intracellular glutathione and bronchoalveolar cells in fibrosing alveolitis effects of N-acetylcysteine Eur Respir J 200219906-11 29 Bando M Hosono T Mato N et al Long-term efficacy of inhaled N-acetylcysteine in patients with idiopathic pulmonary fibrosis Intern Med 2010492289-96 30 Demedts M Behr J Buhl R et al High-dose acetylcysteine in idiopathic pulmonary fibrosis N Engl J Med 20053532229-42 31 Toma TP Bhowmik A Rajakulasingam R Acetylcysteine in pulmonary fibrosis N Engl J Med 20063541086-9 author reply -9 32 Hunninghake GW Antioxidant therapy for idiopathic pulmonary fibrosis N Engl J Med 20053532285-7 33 Flaherty KR Mumford JA Murray S et al Prognostic implications of physiologic and radiographic changes in idiopathic interstitial pneumonia Am J Respir Crit Care Med 2003168543-8 34 Latsi PI du Bois RM Nicholson AG et al Fibrotic idiopathic interstitial pneumonia the prognostic value of longitudinal functional trends Am J Respir Crit Care Med 2003168531-7 35 Collard HR King TE Jr Bartelson BB Vourlekis JS Schwarz MI Brown KK Changes in clinical and physiologic variables predict survival in idiopathic pulmonary fibrosis Am J Respir Crit Care Med 2003168538-42 36 Jegal Y Kim DS Shim TS et al Physiology is a stronger predictor of survival than pathology in fibrotic interstitial pneumonia Am J Respir Crit Care Med 2005171639-44 37 Martinez FJ Safrin S Weycker D et al The clinical course of patients with idiopathic pulmonary fibrosis Ann Intern Med 2005142963-7 38 Hull JH Acetylcysteine in pulmonary fibrosis N Engl J Med 20063541089-91 author reply -91
70
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
39 Flaherty KR King TE Jr Raghu G et al Idiopathic interstitial pneumonia what is the effect of a multidisciplinary approach to diagnosis Am J Respir Crit Care Med 2004170904shy10 40 Raghu G Johnson WC Lockhart D Mageto Y Treatment of idiopathic pulmonary fibrosis with a new antifibrotic agent pirfenidone results of a prospective open-label Phase II study Am J Respir Crit Care Med 19991591061-9 41 Hunninghake GW Lynch DA Galvin JR et al Radiologic findings are strongly associated with a pathologic diagnosis of usual interstitial pneumonia Chest 20031241215-23 42 Lynch D Godwin J Safrin S et al High-resolution computed tomography in idiopathic pulmonary fibrosis diagnosis and prognosis Am J Respir Crit Care Med 2005172488-93 43 Mallinckrodt CH Watkin JG Molenberghs G Carroll RJ Choice of the primary analysis in longitudinal clinical trials Pharmaceutical Statistics 20043161-9 44 Bang H Tsiatis A Estimating medical costs with censored data Biometrika 200087329shy43 45 Lin DY Regression analysis of incomplete medical cost data Stat Med 2003221181-200 46 Rochon J Application of GEE procedures for sample size calculations in repeated measures experiments Stat Med 1998171643-58 47 Lachin JM Foulkes MA Evaluation of sample size and power for analyses of survival with allowance for nonuniform patient entry losses to follow-up noncompliance and stratification Biometrics 198642507-19
71
- PANTHER-IPFPREDNISONE AZATHIOPRINEAND N-ACETYLCYSTEINEA STUDY THAT EVALUATES RESPONSE INIDIOPATHIC PULMONARY FIBROSIS
-
- Protocol Summary
- Table of Contents
- List of Tables
- List of Figures
- List of Abbreviations
- 1 Summary
- 2 Hypotheses and Specific Aims
-
- 21 Null Hypothesis
- 22 Specific Aim 1
- 23 Specific Aim 2
- 24 Prespecified Subgroups of Interest
-
- 3 Background and Significance
-
- 31 Idiopathic Pulmonary Fibrosis is the Most Common Interstitial Lung Disease
- 32 Rationale for Placebo Control
- 33 Rationale for N-acetylcysteine
- 35 Rationale for N-acetylcysteine as a Stand-alone Therapy
- 36 Rationale for the Study Design and Primary Endpoint
- 37 Rationale for Blinding of Treatments
-
- 4 Methods
-
- 41 Inclusion Criteria
- 42 Diagnosis of IPF
- 43 Exclusion Criteria
- 44 Study Design and Study Visit
- 45 Dose Justification
- 46 Contraindications Precautions and Side Effects of Study Medications
- 47 Recruitment Procedures
- 48 Study Procedures
- 49 Concomitant Medications
- 410 Laboratory Testing
- 411 Blinding of Study Drugs
-
- 5 Study Endpoints
-
- 51 Primary Study Endpoint
- 52 Secondary Study Endpoints
-
- 6 Safety Evaluations and Procedures
-
- 61 Adverse Events
- 62 Clinical Medical Monitoring
- 63 Unblinding Procedures
-
- 7 Study Drug Procedures
- 8 Data Management
-
- 81 Hardware and Software Configuration
- 82 Sources of Data
-
- 9 Study Design and Data Analysis
-
- 91 General Analytic Considerations
- 92 Randomization Blinding and Reporting of Results
- 93 Stratification
- 94 Specification of the Primary Analyses
- 95 Analysis of Longitudinal Endpoints
- 96 Analysis of Binary Time-to-Event and Time-Lagged Endpoints
- 97 Power Analysis
-
- 10 Study Administration
-
- 101 Cooperative Agreement Mechanism
- 102 IPFnet Steering Group
- 103 Data and Safety Monitoring Board
- 104 Recommendations on Interim Monitoring of Efficacy Safety and Futility
-
- 11 Investigator and Sponsor Obligations
-
- 111 Monitoring
- 112 Cost and Payment
- 113 Confidentiality and Health Insurance Portability and Accountability ActConsiderations
- 114 Informed Consent Procedures
- 115 Institutional Review Boards
-
- 12 Investigator Agreement
- 13 References
-

PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
regulation at 45 CFR part 16 or the rights of the NHLBI under applicable statutes regulations
and terms of the award
102 IPFnet Steering Group
The IPFnet Steering Group is the main governing body of the project It is composed of the PIs
of the clinical centers the PI of the DCC and the NHLBI project scientist The clinical centers
the IPFnet DCC and the NHLBI each have 1 vote on the IPFnet Steering Group All decisions
are determined by majority vote
All major scientific decisions are determined by the IPFnet Steering Group It assumes overall
responsibility for the design and conduct of the trial It appoints (and disbands) committees and
subcommittees as the need arises designs approves and implements the study protocols
oversees the development of the MOOP monitors subject recruitment and treatment delivery
evaluates data collection and management oversees quality assurance procedures and
implements changes and enhancements to the study as required It also has primary responsibility
for facilitating the conduct of the trials and reporting the projectrsquos results
103 Data and Safety Monitoring Board
The NHLBI will establish a DSMB in accordance with established policies (see
httpwwwnhlbinihgovfundingpoliciesdsmb_insthtm) to ensure data quality and subject
safety and to provide independent advice to the NHLBI regarding progress and the
appropriateness of study continuation
104 Recommendations on Interim Monitoring of Efficacy Safety and Futility
First and foremost the role of the DSMB will be to review subject safety and trial conduct at
periodic points during the study The DSMB may require analyses of the primary endpoint
results for comparing the benefit and risks of treatment strategies The benefit of collecting
additional data on key secondary endpoints with extended follow-up and establishing a robust
64
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
evidence base for determining a standard of care will need to be carefully considered before
early termination of one or more treatment arms After careful consideration the IPFnet Steering
Group recommends conservative thresholds for the early examinations of the safety and efficacy
data
The DSMB will be expected to meet approximately every 6 months until trial completion to
review safety and toxicity data The DSMB may recommend stopping the study based on these
reviews Because the DSMB could stop the trial for safety concerns as well as for a large
efficacy benefit there could be multiple opportunities to reject the null hypothesis (no difference
in event rates between the PL and NAC groups) A Bonferroni approximation will be applied
during the one planned interim analysis for efficacy
Before locking the database a statistical analysis plan (SAP) will be developed to provide
complete details on the statistical analysis The SAP will include the specifics for how and when
the DSMB will be notified for AEs The IPFnet DCC will deliver to the DSMB all FDA-defined
AEs at 3-month intervals The IPFnet DCC will prepare narrative SAE reports in real time for
DSMB review including recommendations and analysis of similar events for each SAE
submitted to the FDA
65
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
11 Investigator and Sponsor Obligations
111 Monitoring
All monitoring activities for US clinical centers will be performed in accordance with DCRI
standard operating procedures Information regarding the types of visits will be outlined in the
PANTHER-IPF MOOP
112 Cost and Payment
There will be no cost to subjects enrolled in this trial Study-related procedures will be paid for
by the IPFnet
Subjects may be eligible for reimbursement for travel to the clinical center Details of payment
will be explained to each subject during the consent process
113 Confidentiality and Health Insurance Portability and Accountability Act
Considerations
Subject confidentiality will be protected throughout the study All subject data will be kept
strictly confidential and no subject-identifying information will be released to anyone outside
the project Confidentiality will be assured through several mechanisms First each subject will
be assigned an anonymous study ID which will then be used on all study forms Second any
study forms blood samples and paper records that contain subject information (eg address lists
phone lists) will be kept at the clinical centers in secured locked areas coded by number Once
blood is collected there will be no subject identifiers placed on blood samplesmdashonly the study
ID number and the date of sample collection Third access to all subject data and information
including laboratory specimens will be restricted to authorized personnel In the case of
computerized data this restricted access will be assured through user logon IDs and password
protection
66
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
At the IPFnet DCC only authorized personnel will have access to the data files containing study
data Security will be assured through user logon IDs passwords and appropriate access
privileges All study subjects will be identified only by their IPFnet ID numbers and no personal
identifying information such as name address or Social Security number will be entered into
the IPFnet DCC database Any subject-specific data reported to the IPFnet Steering Group will
be identified only by the IPFnet ID number
Finally subjects will not be identified by name in any reports or publications nor will the data
be presented in such a way that the identity of individual subjects can be inferred Analysis files
created for further study by the scientific community will have no subject identifiers These data
files will be created in accordance with the Ancillary Studies and Publication Policy of the
IPFnet
114 Informed Consent Procedures
All IPFnet subjects will provide written informed consent using procedures reviewed and
approved by each clinical centerrsquos IRB Informed consent will be undertaken by study personnel
in-person with the subject The subject has the option of declining further participation in the
study at that point No further study procedures will be conducted until the signed documents
have been provided to the IPFnet clinical center
115 Institutional Review Boards
Before initiating this study the protocol clinical center-specific informed consent forms Health
Insurance Portability and Accountability Act (HIPAA) forms recruitment materials and other
relevant information will be reviewed by a properly constituted IRB at each participating clinical
center A copy of the signed and dated IRB approval at each clinical center will be retrieved prior
to or during the site initiation visit and archived at the IPFnet DCC Any amendments to the
protocol other than simple administrative and typographical changes must be approved by each
IRB before they are implemented The clinical centers will seek annual renewals of their IRB
approvals in accordance with local procedures
67
__________________________________________ ________________
__________________________________________
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
12 Investigator Agreement
I have read the foregoing protocol PANTHER-IPF and agree that it contains all necessary
details for carrying out this study I will conduct the study as outlined herein and will complete
the study within the time designated
I will provide copies of the protocol and all pertinent information to all individuals responsible to
me who assist in the conduct of this study I will discuss this material with them to ensure they
are fully informed regarding the drug and the conduct of the study
I will fulfill all responsibilities for submitting pertinent information to the local IRB if
applicable that is responsible for this study
I further agree that NHLBI andor DCRI will have access to any source documents from which
eCRF information may have been generated
Signature of Principal Investigator Date
Name of Principal Investigator (printed or typed)
Protocol version date May 19 2009
Protocol Amendment 1 version date May 28 2010
Protocol Amendment 2 version date December 6 2011
68
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
13 References
1 Raghu G Brown KK Bradford WZ et al A placebo-controlled trial of interferon gamma-1b in patients with idiopathic pulmonary fibrosis N Engl J Med 2004350125-33 2 King TE Jr Safrin S Starko KM et al Analyses of efficacy end points in a controlled trial of interferon-gamma1b for idiopathic pulmonary fibrosis Chest 2005127171-7 3 Flaherty KR Thwaite EL Kazerooni EA et al Radiological versus histological diagnosis in UIP and NSIP survival implications Thorax 200358143-8 4 Wells AU Desai SR Rubens MB et al Idiopathic pulmonary fibrosis a composite physiologic index derived from disease extent observed by computed tomography Am J Respir Crit Care Med 2003167962-9 5 Raghu G Freudenberger TD Yang S et al High prevalence of abnormal acid gastroshyoesophageal reflux in idiopathic pulmonary fibrosis Eur Respir J 200627136-42 6 Kinnula VL Focus on antioxidant enzymes and antioxidant strategies in smoking related airway diseases Thorax 200560693-700 7 Coultas DB Zumwalt RE Black WC Sobonya RE The epidemiology of interstitial lung diseases Am J Respir Crit Care Med 1994150967-72 8 Raghu G Weycker D Edelsberg J Bradford WZ Oster G Incidence and prevalence of idiopathic pulmonary fibrosis Am J Respir Crit Care Med 2006174810-6 9 Olson AL Swigris JJ Lezotte DC Norris JM Wilson CG Brown KK Mortality from pulmonary fibrosis increased in the United States from 1992 to 2003 Am J Respir Crit Care Med 2007176277-84 10 Mannino DM Etzel RA Parrish RG Pulmonary fibrosis deaths in the United States 1979shy1991 An analysis of multiple-cause mortality data Am J Respir Crit Care Med 19961531548shy52 11 Hubbard R Johnston I Coultas DB Britton J Mortality rates from cryptogenic fibrosing alveolitis in seven countries Thorax 199651711-6 12 Johnston I Britton J Kinnear W Logan R Rising mortality from cryptogenic fibrosing alveolitis Bmj 19903011017-21 13 Raghu G Collard HR Egan JJ et al An official ATSERSJRSALAT statement idiopathic pulmonary fibrosis evidence-based guidelines for diagnosis and management Am J Respir Crit Care Med 2011183788-824 14 (USA) FDA FDA Public Health Advisory Interferon gamma-1b (marketed as Actimmune) In 2007 15 King TE Jr Pardo A Selman M Idiopathic pulmonary fibrosis Lancet 2011 16 Raghu G Brown KK Costabel U et al Treatment of idiopathic pulmonary fibrosis with etanercept an exploratory placebo-controlled trial Am J Respir Crit Care Med 2008178948shy55 17 Malouf MA Hopkins P Snell G Glanville AR An investigator-driven study of everolimus in surgical lung biopsy confirmed idiopathic pulmonary fibrosis Respirology 201116776-83 18 King TE Jr Behr J Brown KK et al BUILD-1 a randomized placebo-controlled trial of bosentan in idiopathic pulmonary fibrosis Am J Respir Crit Care Med 200817775-81 19 Richeldi L Costabel U Selman M et al Efficacy of a tyrosine kinase inhibitor in idiopathic pulmonary fibrosis N Engl J Med 20113651079-87
69
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
20 Borok Z Buhl R Grimes GJ et al Effect of glutathione aerosol on oxidant-antioxidant imbalance in idiopathic pulmonary fibrosis Lancet 1991338215-6 21 Meyer A Buhl R Magnussen H The effect of oral N-acetylcysteine on lung glutathione levels in idiopathic pulmonary fibrosis Eur Respir J 19947431-6 22 Behr J Maier K Degenkolb B Krombach F Vogelmeier C Antioxidative and clinical effects of high-dose N-acetylcysteine in fibrosing alveolitis Adjunctive therapy to maintenance immunosuppression Am J Respir Crit Care Med 19971561897-901 23 Cantin AM North SL Fells GA Hubbard RC Crystal RG Oxidant-mediated epithelial cell injury in idiopathic pulmonary fibrosis J Clin Invest 1987791665-73 24 Waghray M Cui Z Horowitz JC et al Hydrogen peroxide is a diffusible paracrine signal for the induction of epithelial cell death by activated myofibroblasts Faseb J 200519854-6 25 Larios JM Budhiraja R Fanburg BL Thannickal VJ Oxidative protein cross-linking reactions involving L-tyrosine in transforming growth factor-beta1-stimulated fibroblasts J Biol Chem 200127617437-41 26 Kinnula VL Fattman CL Tan RJ Oury TD Oxidative stress in pulmonary fibrosis a possible role for redox modulatory therapy Am J Respir Crit Care Med 2005172417-22 27 Meyer A Buhl R Kampf S Magnussen H Intravenous N-acetylcysteine and lung glutathione of patients with pulmonary fibrosis and normals Am J Respir Crit Care Med 19951521055-60 28 Behr J Degenkolb B Krombach F Vogelmeier C Intracellular glutathione and bronchoalveolar cells in fibrosing alveolitis effects of N-acetylcysteine Eur Respir J 200219906-11 29 Bando M Hosono T Mato N et al Long-term efficacy of inhaled N-acetylcysteine in patients with idiopathic pulmonary fibrosis Intern Med 2010492289-96 30 Demedts M Behr J Buhl R et al High-dose acetylcysteine in idiopathic pulmonary fibrosis N Engl J Med 20053532229-42 31 Toma TP Bhowmik A Rajakulasingam R Acetylcysteine in pulmonary fibrosis N Engl J Med 20063541086-9 author reply -9 32 Hunninghake GW Antioxidant therapy for idiopathic pulmonary fibrosis N Engl J Med 20053532285-7 33 Flaherty KR Mumford JA Murray S et al Prognostic implications of physiologic and radiographic changes in idiopathic interstitial pneumonia Am J Respir Crit Care Med 2003168543-8 34 Latsi PI du Bois RM Nicholson AG et al Fibrotic idiopathic interstitial pneumonia the prognostic value of longitudinal functional trends Am J Respir Crit Care Med 2003168531-7 35 Collard HR King TE Jr Bartelson BB Vourlekis JS Schwarz MI Brown KK Changes in clinical and physiologic variables predict survival in idiopathic pulmonary fibrosis Am J Respir Crit Care Med 2003168538-42 36 Jegal Y Kim DS Shim TS et al Physiology is a stronger predictor of survival than pathology in fibrotic interstitial pneumonia Am J Respir Crit Care Med 2005171639-44 37 Martinez FJ Safrin S Weycker D et al The clinical course of patients with idiopathic pulmonary fibrosis Ann Intern Med 2005142963-7 38 Hull JH Acetylcysteine in pulmonary fibrosis N Engl J Med 20063541089-91 author reply -91
70
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
39 Flaherty KR King TE Jr Raghu G et al Idiopathic interstitial pneumonia what is the effect of a multidisciplinary approach to diagnosis Am J Respir Crit Care Med 2004170904shy10 40 Raghu G Johnson WC Lockhart D Mageto Y Treatment of idiopathic pulmonary fibrosis with a new antifibrotic agent pirfenidone results of a prospective open-label Phase II study Am J Respir Crit Care Med 19991591061-9 41 Hunninghake GW Lynch DA Galvin JR et al Radiologic findings are strongly associated with a pathologic diagnosis of usual interstitial pneumonia Chest 20031241215-23 42 Lynch D Godwin J Safrin S et al High-resolution computed tomography in idiopathic pulmonary fibrosis diagnosis and prognosis Am J Respir Crit Care Med 2005172488-93 43 Mallinckrodt CH Watkin JG Molenberghs G Carroll RJ Choice of the primary analysis in longitudinal clinical trials Pharmaceutical Statistics 20043161-9 44 Bang H Tsiatis A Estimating medical costs with censored data Biometrika 200087329shy43 45 Lin DY Regression analysis of incomplete medical cost data Stat Med 2003221181-200 46 Rochon J Application of GEE procedures for sample size calculations in repeated measures experiments Stat Med 1998171643-58 47 Lachin JM Foulkes MA Evaluation of sample size and power for analyses of survival with allowance for nonuniform patient entry losses to follow-up noncompliance and stratification Biometrics 198642507-19
71
- PANTHER-IPFPREDNISONE AZATHIOPRINEAND N-ACETYLCYSTEINEA STUDY THAT EVALUATES RESPONSE INIDIOPATHIC PULMONARY FIBROSIS
-
- Protocol Summary
- Table of Contents
- List of Tables
- List of Figures
- List of Abbreviations
- 1 Summary
- 2 Hypotheses and Specific Aims
-
- 21 Null Hypothesis
- 22 Specific Aim 1
- 23 Specific Aim 2
- 24 Prespecified Subgroups of Interest
-
- 3 Background and Significance
-
- 31 Idiopathic Pulmonary Fibrosis is the Most Common Interstitial Lung Disease
- 32 Rationale for Placebo Control
- 33 Rationale for N-acetylcysteine
- 35 Rationale for N-acetylcysteine as a Stand-alone Therapy
- 36 Rationale for the Study Design and Primary Endpoint
- 37 Rationale for Blinding of Treatments
-
- 4 Methods
-
- 41 Inclusion Criteria
- 42 Diagnosis of IPF
- 43 Exclusion Criteria
- 44 Study Design and Study Visit
- 45 Dose Justification
- 46 Contraindications Precautions and Side Effects of Study Medications
- 47 Recruitment Procedures
- 48 Study Procedures
- 49 Concomitant Medications
- 410 Laboratory Testing
- 411 Blinding of Study Drugs
-
- 5 Study Endpoints
-
- 51 Primary Study Endpoint
- 52 Secondary Study Endpoints
-
- 6 Safety Evaluations and Procedures
-
- 61 Adverse Events
- 62 Clinical Medical Monitoring
- 63 Unblinding Procedures
-
- 7 Study Drug Procedures
- 8 Data Management
-
- 81 Hardware and Software Configuration
- 82 Sources of Data
-
- 9 Study Design and Data Analysis
-
- 91 General Analytic Considerations
- 92 Randomization Blinding and Reporting of Results
- 93 Stratification
- 94 Specification of the Primary Analyses
- 95 Analysis of Longitudinal Endpoints
- 96 Analysis of Binary Time-to-Event and Time-Lagged Endpoints
- 97 Power Analysis
-
- 10 Study Administration
-
- 101 Cooperative Agreement Mechanism
- 102 IPFnet Steering Group
- 103 Data and Safety Monitoring Board
- 104 Recommendations on Interim Monitoring of Efficacy Safety and Futility
-
- 11 Investigator and Sponsor Obligations
-
- 111 Monitoring
- 112 Cost and Payment
- 113 Confidentiality and Health Insurance Portability and Accountability ActConsiderations
- 114 Informed Consent Procedures
- 115 Institutional Review Boards
-
- 12 Investigator Agreement
- 13 References
-

PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
evidence base for determining a standard of care will need to be carefully considered before
early termination of one or more treatment arms After careful consideration the IPFnet Steering
Group recommends conservative thresholds for the early examinations of the safety and efficacy
data
The DSMB will be expected to meet approximately every 6 months until trial completion to
review safety and toxicity data The DSMB may recommend stopping the study based on these
reviews Because the DSMB could stop the trial for safety concerns as well as for a large
efficacy benefit there could be multiple opportunities to reject the null hypothesis (no difference
in event rates between the PL and NAC groups) A Bonferroni approximation will be applied
during the one planned interim analysis for efficacy
Before locking the database a statistical analysis plan (SAP) will be developed to provide
complete details on the statistical analysis The SAP will include the specifics for how and when
the DSMB will be notified for AEs The IPFnet DCC will deliver to the DSMB all FDA-defined
AEs at 3-month intervals The IPFnet DCC will prepare narrative SAE reports in real time for
DSMB review including recommendations and analysis of similar events for each SAE
submitted to the FDA
65
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
11 Investigator and Sponsor Obligations
111 Monitoring
All monitoring activities for US clinical centers will be performed in accordance with DCRI
standard operating procedures Information regarding the types of visits will be outlined in the
PANTHER-IPF MOOP
112 Cost and Payment
There will be no cost to subjects enrolled in this trial Study-related procedures will be paid for
by the IPFnet
Subjects may be eligible for reimbursement for travel to the clinical center Details of payment
will be explained to each subject during the consent process
113 Confidentiality and Health Insurance Portability and Accountability Act
Considerations
Subject confidentiality will be protected throughout the study All subject data will be kept
strictly confidential and no subject-identifying information will be released to anyone outside
the project Confidentiality will be assured through several mechanisms First each subject will
be assigned an anonymous study ID which will then be used on all study forms Second any
study forms blood samples and paper records that contain subject information (eg address lists
phone lists) will be kept at the clinical centers in secured locked areas coded by number Once
blood is collected there will be no subject identifiers placed on blood samplesmdashonly the study
ID number and the date of sample collection Third access to all subject data and information
including laboratory specimens will be restricted to authorized personnel In the case of
computerized data this restricted access will be assured through user logon IDs and password
protection
66
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
At the IPFnet DCC only authorized personnel will have access to the data files containing study
data Security will be assured through user logon IDs passwords and appropriate access
privileges All study subjects will be identified only by their IPFnet ID numbers and no personal
identifying information such as name address or Social Security number will be entered into
the IPFnet DCC database Any subject-specific data reported to the IPFnet Steering Group will
be identified only by the IPFnet ID number
Finally subjects will not be identified by name in any reports or publications nor will the data
be presented in such a way that the identity of individual subjects can be inferred Analysis files
created for further study by the scientific community will have no subject identifiers These data
files will be created in accordance with the Ancillary Studies and Publication Policy of the
IPFnet
114 Informed Consent Procedures
All IPFnet subjects will provide written informed consent using procedures reviewed and
approved by each clinical centerrsquos IRB Informed consent will be undertaken by study personnel
in-person with the subject The subject has the option of declining further participation in the
study at that point No further study procedures will be conducted until the signed documents
have been provided to the IPFnet clinical center
115 Institutional Review Boards
Before initiating this study the protocol clinical center-specific informed consent forms Health
Insurance Portability and Accountability Act (HIPAA) forms recruitment materials and other
relevant information will be reviewed by a properly constituted IRB at each participating clinical
center A copy of the signed and dated IRB approval at each clinical center will be retrieved prior
to or during the site initiation visit and archived at the IPFnet DCC Any amendments to the
protocol other than simple administrative and typographical changes must be approved by each
IRB before they are implemented The clinical centers will seek annual renewals of their IRB
approvals in accordance with local procedures
67
__________________________________________ ________________
__________________________________________
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
12 Investigator Agreement
I have read the foregoing protocol PANTHER-IPF and agree that it contains all necessary
details for carrying out this study I will conduct the study as outlined herein and will complete
the study within the time designated
I will provide copies of the protocol and all pertinent information to all individuals responsible to
me who assist in the conduct of this study I will discuss this material with them to ensure they
are fully informed regarding the drug and the conduct of the study
I will fulfill all responsibilities for submitting pertinent information to the local IRB if
applicable that is responsible for this study
I further agree that NHLBI andor DCRI will have access to any source documents from which
eCRF information may have been generated
Signature of Principal Investigator Date
Name of Principal Investigator (printed or typed)
Protocol version date May 19 2009
Protocol Amendment 1 version date May 28 2010
Protocol Amendment 2 version date December 6 2011
68
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
13 References
1 Raghu G Brown KK Bradford WZ et al A placebo-controlled trial of interferon gamma-1b in patients with idiopathic pulmonary fibrosis N Engl J Med 2004350125-33 2 King TE Jr Safrin S Starko KM et al Analyses of efficacy end points in a controlled trial of interferon-gamma1b for idiopathic pulmonary fibrosis Chest 2005127171-7 3 Flaherty KR Thwaite EL Kazerooni EA et al Radiological versus histological diagnosis in UIP and NSIP survival implications Thorax 200358143-8 4 Wells AU Desai SR Rubens MB et al Idiopathic pulmonary fibrosis a composite physiologic index derived from disease extent observed by computed tomography Am J Respir Crit Care Med 2003167962-9 5 Raghu G Freudenberger TD Yang S et al High prevalence of abnormal acid gastroshyoesophageal reflux in idiopathic pulmonary fibrosis Eur Respir J 200627136-42 6 Kinnula VL Focus on antioxidant enzymes and antioxidant strategies in smoking related airway diseases Thorax 200560693-700 7 Coultas DB Zumwalt RE Black WC Sobonya RE The epidemiology of interstitial lung diseases Am J Respir Crit Care Med 1994150967-72 8 Raghu G Weycker D Edelsberg J Bradford WZ Oster G Incidence and prevalence of idiopathic pulmonary fibrosis Am J Respir Crit Care Med 2006174810-6 9 Olson AL Swigris JJ Lezotte DC Norris JM Wilson CG Brown KK Mortality from pulmonary fibrosis increased in the United States from 1992 to 2003 Am J Respir Crit Care Med 2007176277-84 10 Mannino DM Etzel RA Parrish RG Pulmonary fibrosis deaths in the United States 1979shy1991 An analysis of multiple-cause mortality data Am J Respir Crit Care Med 19961531548shy52 11 Hubbard R Johnston I Coultas DB Britton J Mortality rates from cryptogenic fibrosing alveolitis in seven countries Thorax 199651711-6 12 Johnston I Britton J Kinnear W Logan R Rising mortality from cryptogenic fibrosing alveolitis Bmj 19903011017-21 13 Raghu G Collard HR Egan JJ et al An official ATSERSJRSALAT statement idiopathic pulmonary fibrosis evidence-based guidelines for diagnosis and management Am J Respir Crit Care Med 2011183788-824 14 (USA) FDA FDA Public Health Advisory Interferon gamma-1b (marketed as Actimmune) In 2007 15 King TE Jr Pardo A Selman M Idiopathic pulmonary fibrosis Lancet 2011 16 Raghu G Brown KK Costabel U et al Treatment of idiopathic pulmonary fibrosis with etanercept an exploratory placebo-controlled trial Am J Respir Crit Care Med 2008178948shy55 17 Malouf MA Hopkins P Snell G Glanville AR An investigator-driven study of everolimus in surgical lung biopsy confirmed idiopathic pulmonary fibrosis Respirology 201116776-83 18 King TE Jr Behr J Brown KK et al BUILD-1 a randomized placebo-controlled trial of bosentan in idiopathic pulmonary fibrosis Am J Respir Crit Care Med 200817775-81 19 Richeldi L Costabel U Selman M et al Efficacy of a tyrosine kinase inhibitor in idiopathic pulmonary fibrosis N Engl J Med 20113651079-87
69
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
20 Borok Z Buhl R Grimes GJ et al Effect of glutathione aerosol on oxidant-antioxidant imbalance in idiopathic pulmonary fibrosis Lancet 1991338215-6 21 Meyer A Buhl R Magnussen H The effect of oral N-acetylcysteine on lung glutathione levels in idiopathic pulmonary fibrosis Eur Respir J 19947431-6 22 Behr J Maier K Degenkolb B Krombach F Vogelmeier C Antioxidative and clinical effects of high-dose N-acetylcysteine in fibrosing alveolitis Adjunctive therapy to maintenance immunosuppression Am J Respir Crit Care Med 19971561897-901 23 Cantin AM North SL Fells GA Hubbard RC Crystal RG Oxidant-mediated epithelial cell injury in idiopathic pulmonary fibrosis J Clin Invest 1987791665-73 24 Waghray M Cui Z Horowitz JC et al Hydrogen peroxide is a diffusible paracrine signal for the induction of epithelial cell death by activated myofibroblasts Faseb J 200519854-6 25 Larios JM Budhiraja R Fanburg BL Thannickal VJ Oxidative protein cross-linking reactions involving L-tyrosine in transforming growth factor-beta1-stimulated fibroblasts J Biol Chem 200127617437-41 26 Kinnula VL Fattman CL Tan RJ Oury TD Oxidative stress in pulmonary fibrosis a possible role for redox modulatory therapy Am J Respir Crit Care Med 2005172417-22 27 Meyer A Buhl R Kampf S Magnussen H Intravenous N-acetylcysteine and lung glutathione of patients with pulmonary fibrosis and normals Am J Respir Crit Care Med 19951521055-60 28 Behr J Degenkolb B Krombach F Vogelmeier C Intracellular glutathione and bronchoalveolar cells in fibrosing alveolitis effects of N-acetylcysteine Eur Respir J 200219906-11 29 Bando M Hosono T Mato N et al Long-term efficacy of inhaled N-acetylcysteine in patients with idiopathic pulmonary fibrosis Intern Med 2010492289-96 30 Demedts M Behr J Buhl R et al High-dose acetylcysteine in idiopathic pulmonary fibrosis N Engl J Med 20053532229-42 31 Toma TP Bhowmik A Rajakulasingam R Acetylcysteine in pulmonary fibrosis N Engl J Med 20063541086-9 author reply -9 32 Hunninghake GW Antioxidant therapy for idiopathic pulmonary fibrosis N Engl J Med 20053532285-7 33 Flaherty KR Mumford JA Murray S et al Prognostic implications of physiologic and radiographic changes in idiopathic interstitial pneumonia Am J Respir Crit Care Med 2003168543-8 34 Latsi PI du Bois RM Nicholson AG et al Fibrotic idiopathic interstitial pneumonia the prognostic value of longitudinal functional trends Am J Respir Crit Care Med 2003168531-7 35 Collard HR King TE Jr Bartelson BB Vourlekis JS Schwarz MI Brown KK Changes in clinical and physiologic variables predict survival in idiopathic pulmonary fibrosis Am J Respir Crit Care Med 2003168538-42 36 Jegal Y Kim DS Shim TS et al Physiology is a stronger predictor of survival than pathology in fibrotic interstitial pneumonia Am J Respir Crit Care Med 2005171639-44 37 Martinez FJ Safrin S Weycker D et al The clinical course of patients with idiopathic pulmonary fibrosis Ann Intern Med 2005142963-7 38 Hull JH Acetylcysteine in pulmonary fibrosis N Engl J Med 20063541089-91 author reply -91
70
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
39 Flaherty KR King TE Jr Raghu G et al Idiopathic interstitial pneumonia what is the effect of a multidisciplinary approach to diagnosis Am J Respir Crit Care Med 2004170904shy10 40 Raghu G Johnson WC Lockhart D Mageto Y Treatment of idiopathic pulmonary fibrosis with a new antifibrotic agent pirfenidone results of a prospective open-label Phase II study Am J Respir Crit Care Med 19991591061-9 41 Hunninghake GW Lynch DA Galvin JR et al Radiologic findings are strongly associated with a pathologic diagnosis of usual interstitial pneumonia Chest 20031241215-23 42 Lynch D Godwin J Safrin S et al High-resolution computed tomography in idiopathic pulmonary fibrosis diagnosis and prognosis Am J Respir Crit Care Med 2005172488-93 43 Mallinckrodt CH Watkin JG Molenberghs G Carroll RJ Choice of the primary analysis in longitudinal clinical trials Pharmaceutical Statistics 20043161-9 44 Bang H Tsiatis A Estimating medical costs with censored data Biometrika 200087329shy43 45 Lin DY Regression analysis of incomplete medical cost data Stat Med 2003221181-200 46 Rochon J Application of GEE procedures for sample size calculations in repeated measures experiments Stat Med 1998171643-58 47 Lachin JM Foulkes MA Evaluation of sample size and power for analyses of survival with allowance for nonuniform patient entry losses to follow-up noncompliance and stratification Biometrics 198642507-19
71
- PANTHER-IPFPREDNISONE AZATHIOPRINEAND N-ACETYLCYSTEINEA STUDY THAT EVALUATES RESPONSE INIDIOPATHIC PULMONARY FIBROSIS
-
- Protocol Summary
- Table of Contents
- List of Tables
- List of Figures
- List of Abbreviations
- 1 Summary
- 2 Hypotheses and Specific Aims
-
- 21 Null Hypothesis
- 22 Specific Aim 1
- 23 Specific Aim 2
- 24 Prespecified Subgroups of Interest
-
- 3 Background and Significance
-
- 31 Idiopathic Pulmonary Fibrosis is the Most Common Interstitial Lung Disease
- 32 Rationale for Placebo Control
- 33 Rationale for N-acetylcysteine
- 35 Rationale for N-acetylcysteine as a Stand-alone Therapy
- 36 Rationale for the Study Design and Primary Endpoint
- 37 Rationale for Blinding of Treatments
-
- 4 Methods
-
- 41 Inclusion Criteria
- 42 Diagnosis of IPF
- 43 Exclusion Criteria
- 44 Study Design and Study Visit
- 45 Dose Justification
- 46 Contraindications Precautions and Side Effects of Study Medications
- 47 Recruitment Procedures
- 48 Study Procedures
- 49 Concomitant Medications
- 410 Laboratory Testing
- 411 Blinding of Study Drugs
-
- 5 Study Endpoints
-
- 51 Primary Study Endpoint
- 52 Secondary Study Endpoints
-
- 6 Safety Evaluations and Procedures
-
- 61 Adverse Events
- 62 Clinical Medical Monitoring
- 63 Unblinding Procedures
-
- 7 Study Drug Procedures
- 8 Data Management
-
- 81 Hardware and Software Configuration
- 82 Sources of Data
-
- 9 Study Design and Data Analysis
-
- 91 General Analytic Considerations
- 92 Randomization Blinding and Reporting of Results
- 93 Stratification
- 94 Specification of the Primary Analyses
- 95 Analysis of Longitudinal Endpoints
- 96 Analysis of Binary Time-to-Event and Time-Lagged Endpoints
- 97 Power Analysis
-
- 10 Study Administration
-
- 101 Cooperative Agreement Mechanism
- 102 IPFnet Steering Group
- 103 Data and Safety Monitoring Board
- 104 Recommendations on Interim Monitoring of Efficacy Safety and Futility
-
- 11 Investigator and Sponsor Obligations
-
- 111 Monitoring
- 112 Cost and Payment
- 113 Confidentiality and Health Insurance Portability and Accountability ActConsiderations
- 114 Informed Consent Procedures
- 115 Institutional Review Boards
-
- 12 Investigator Agreement
- 13 References
-

PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
11 Investigator and Sponsor Obligations
111 Monitoring
All monitoring activities for US clinical centers will be performed in accordance with DCRI
standard operating procedures Information regarding the types of visits will be outlined in the
PANTHER-IPF MOOP
112 Cost and Payment
There will be no cost to subjects enrolled in this trial Study-related procedures will be paid for
by the IPFnet
Subjects may be eligible for reimbursement for travel to the clinical center Details of payment
will be explained to each subject during the consent process
113 Confidentiality and Health Insurance Portability and Accountability Act
Considerations
Subject confidentiality will be protected throughout the study All subject data will be kept
strictly confidential and no subject-identifying information will be released to anyone outside
the project Confidentiality will be assured through several mechanisms First each subject will
be assigned an anonymous study ID which will then be used on all study forms Second any
study forms blood samples and paper records that contain subject information (eg address lists
phone lists) will be kept at the clinical centers in secured locked areas coded by number Once
blood is collected there will be no subject identifiers placed on blood samplesmdashonly the study
ID number and the date of sample collection Third access to all subject data and information
including laboratory specimens will be restricted to authorized personnel In the case of
computerized data this restricted access will be assured through user logon IDs and password
protection
66
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
At the IPFnet DCC only authorized personnel will have access to the data files containing study
data Security will be assured through user logon IDs passwords and appropriate access
privileges All study subjects will be identified only by their IPFnet ID numbers and no personal
identifying information such as name address or Social Security number will be entered into
the IPFnet DCC database Any subject-specific data reported to the IPFnet Steering Group will
be identified only by the IPFnet ID number
Finally subjects will not be identified by name in any reports or publications nor will the data
be presented in such a way that the identity of individual subjects can be inferred Analysis files
created for further study by the scientific community will have no subject identifiers These data
files will be created in accordance with the Ancillary Studies and Publication Policy of the
IPFnet
114 Informed Consent Procedures
All IPFnet subjects will provide written informed consent using procedures reviewed and
approved by each clinical centerrsquos IRB Informed consent will be undertaken by study personnel
in-person with the subject The subject has the option of declining further participation in the
study at that point No further study procedures will be conducted until the signed documents
have been provided to the IPFnet clinical center
115 Institutional Review Boards
Before initiating this study the protocol clinical center-specific informed consent forms Health
Insurance Portability and Accountability Act (HIPAA) forms recruitment materials and other
relevant information will be reviewed by a properly constituted IRB at each participating clinical
center A copy of the signed and dated IRB approval at each clinical center will be retrieved prior
to or during the site initiation visit and archived at the IPFnet DCC Any amendments to the
protocol other than simple administrative and typographical changes must be approved by each
IRB before they are implemented The clinical centers will seek annual renewals of their IRB
approvals in accordance with local procedures
67
__________________________________________ ________________
__________________________________________
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
12 Investigator Agreement
I have read the foregoing protocol PANTHER-IPF and agree that it contains all necessary
details for carrying out this study I will conduct the study as outlined herein and will complete
the study within the time designated
I will provide copies of the protocol and all pertinent information to all individuals responsible to
me who assist in the conduct of this study I will discuss this material with them to ensure they
are fully informed regarding the drug and the conduct of the study
I will fulfill all responsibilities for submitting pertinent information to the local IRB if
applicable that is responsible for this study
I further agree that NHLBI andor DCRI will have access to any source documents from which
eCRF information may have been generated
Signature of Principal Investigator Date
Name of Principal Investigator (printed or typed)
Protocol version date May 19 2009
Protocol Amendment 1 version date May 28 2010
Protocol Amendment 2 version date December 6 2011
68
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
13 References
1 Raghu G Brown KK Bradford WZ et al A placebo-controlled trial of interferon gamma-1b in patients with idiopathic pulmonary fibrosis N Engl J Med 2004350125-33 2 King TE Jr Safrin S Starko KM et al Analyses of efficacy end points in a controlled trial of interferon-gamma1b for idiopathic pulmonary fibrosis Chest 2005127171-7 3 Flaherty KR Thwaite EL Kazerooni EA et al Radiological versus histological diagnosis in UIP and NSIP survival implications Thorax 200358143-8 4 Wells AU Desai SR Rubens MB et al Idiopathic pulmonary fibrosis a composite physiologic index derived from disease extent observed by computed tomography Am J Respir Crit Care Med 2003167962-9 5 Raghu G Freudenberger TD Yang S et al High prevalence of abnormal acid gastroshyoesophageal reflux in idiopathic pulmonary fibrosis Eur Respir J 200627136-42 6 Kinnula VL Focus on antioxidant enzymes and antioxidant strategies in smoking related airway diseases Thorax 200560693-700 7 Coultas DB Zumwalt RE Black WC Sobonya RE The epidemiology of interstitial lung diseases Am J Respir Crit Care Med 1994150967-72 8 Raghu G Weycker D Edelsberg J Bradford WZ Oster G Incidence and prevalence of idiopathic pulmonary fibrosis Am J Respir Crit Care Med 2006174810-6 9 Olson AL Swigris JJ Lezotte DC Norris JM Wilson CG Brown KK Mortality from pulmonary fibrosis increased in the United States from 1992 to 2003 Am J Respir Crit Care Med 2007176277-84 10 Mannino DM Etzel RA Parrish RG Pulmonary fibrosis deaths in the United States 1979shy1991 An analysis of multiple-cause mortality data Am J Respir Crit Care Med 19961531548shy52 11 Hubbard R Johnston I Coultas DB Britton J Mortality rates from cryptogenic fibrosing alveolitis in seven countries Thorax 199651711-6 12 Johnston I Britton J Kinnear W Logan R Rising mortality from cryptogenic fibrosing alveolitis Bmj 19903011017-21 13 Raghu G Collard HR Egan JJ et al An official ATSERSJRSALAT statement idiopathic pulmonary fibrosis evidence-based guidelines for diagnosis and management Am J Respir Crit Care Med 2011183788-824 14 (USA) FDA FDA Public Health Advisory Interferon gamma-1b (marketed as Actimmune) In 2007 15 King TE Jr Pardo A Selman M Idiopathic pulmonary fibrosis Lancet 2011 16 Raghu G Brown KK Costabel U et al Treatment of idiopathic pulmonary fibrosis with etanercept an exploratory placebo-controlled trial Am J Respir Crit Care Med 2008178948shy55 17 Malouf MA Hopkins P Snell G Glanville AR An investigator-driven study of everolimus in surgical lung biopsy confirmed idiopathic pulmonary fibrosis Respirology 201116776-83 18 King TE Jr Behr J Brown KK et al BUILD-1 a randomized placebo-controlled trial of bosentan in idiopathic pulmonary fibrosis Am J Respir Crit Care Med 200817775-81 19 Richeldi L Costabel U Selman M et al Efficacy of a tyrosine kinase inhibitor in idiopathic pulmonary fibrosis N Engl J Med 20113651079-87
69
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
20 Borok Z Buhl R Grimes GJ et al Effect of glutathione aerosol on oxidant-antioxidant imbalance in idiopathic pulmonary fibrosis Lancet 1991338215-6 21 Meyer A Buhl R Magnussen H The effect of oral N-acetylcysteine on lung glutathione levels in idiopathic pulmonary fibrosis Eur Respir J 19947431-6 22 Behr J Maier K Degenkolb B Krombach F Vogelmeier C Antioxidative and clinical effects of high-dose N-acetylcysteine in fibrosing alveolitis Adjunctive therapy to maintenance immunosuppression Am J Respir Crit Care Med 19971561897-901 23 Cantin AM North SL Fells GA Hubbard RC Crystal RG Oxidant-mediated epithelial cell injury in idiopathic pulmonary fibrosis J Clin Invest 1987791665-73 24 Waghray M Cui Z Horowitz JC et al Hydrogen peroxide is a diffusible paracrine signal for the induction of epithelial cell death by activated myofibroblasts Faseb J 200519854-6 25 Larios JM Budhiraja R Fanburg BL Thannickal VJ Oxidative protein cross-linking reactions involving L-tyrosine in transforming growth factor-beta1-stimulated fibroblasts J Biol Chem 200127617437-41 26 Kinnula VL Fattman CL Tan RJ Oury TD Oxidative stress in pulmonary fibrosis a possible role for redox modulatory therapy Am J Respir Crit Care Med 2005172417-22 27 Meyer A Buhl R Kampf S Magnussen H Intravenous N-acetylcysteine and lung glutathione of patients with pulmonary fibrosis and normals Am J Respir Crit Care Med 19951521055-60 28 Behr J Degenkolb B Krombach F Vogelmeier C Intracellular glutathione and bronchoalveolar cells in fibrosing alveolitis effects of N-acetylcysteine Eur Respir J 200219906-11 29 Bando M Hosono T Mato N et al Long-term efficacy of inhaled N-acetylcysteine in patients with idiopathic pulmonary fibrosis Intern Med 2010492289-96 30 Demedts M Behr J Buhl R et al High-dose acetylcysteine in idiopathic pulmonary fibrosis N Engl J Med 20053532229-42 31 Toma TP Bhowmik A Rajakulasingam R Acetylcysteine in pulmonary fibrosis N Engl J Med 20063541086-9 author reply -9 32 Hunninghake GW Antioxidant therapy for idiopathic pulmonary fibrosis N Engl J Med 20053532285-7 33 Flaherty KR Mumford JA Murray S et al Prognostic implications of physiologic and radiographic changes in idiopathic interstitial pneumonia Am J Respir Crit Care Med 2003168543-8 34 Latsi PI du Bois RM Nicholson AG et al Fibrotic idiopathic interstitial pneumonia the prognostic value of longitudinal functional trends Am J Respir Crit Care Med 2003168531-7 35 Collard HR King TE Jr Bartelson BB Vourlekis JS Schwarz MI Brown KK Changes in clinical and physiologic variables predict survival in idiopathic pulmonary fibrosis Am J Respir Crit Care Med 2003168538-42 36 Jegal Y Kim DS Shim TS et al Physiology is a stronger predictor of survival than pathology in fibrotic interstitial pneumonia Am J Respir Crit Care Med 2005171639-44 37 Martinez FJ Safrin S Weycker D et al The clinical course of patients with idiopathic pulmonary fibrosis Ann Intern Med 2005142963-7 38 Hull JH Acetylcysteine in pulmonary fibrosis N Engl J Med 20063541089-91 author reply -91
70
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
39 Flaherty KR King TE Jr Raghu G et al Idiopathic interstitial pneumonia what is the effect of a multidisciplinary approach to diagnosis Am J Respir Crit Care Med 2004170904shy10 40 Raghu G Johnson WC Lockhart D Mageto Y Treatment of idiopathic pulmonary fibrosis with a new antifibrotic agent pirfenidone results of a prospective open-label Phase II study Am J Respir Crit Care Med 19991591061-9 41 Hunninghake GW Lynch DA Galvin JR et al Radiologic findings are strongly associated with a pathologic diagnosis of usual interstitial pneumonia Chest 20031241215-23 42 Lynch D Godwin J Safrin S et al High-resolution computed tomography in idiopathic pulmonary fibrosis diagnosis and prognosis Am J Respir Crit Care Med 2005172488-93 43 Mallinckrodt CH Watkin JG Molenberghs G Carroll RJ Choice of the primary analysis in longitudinal clinical trials Pharmaceutical Statistics 20043161-9 44 Bang H Tsiatis A Estimating medical costs with censored data Biometrika 200087329shy43 45 Lin DY Regression analysis of incomplete medical cost data Stat Med 2003221181-200 46 Rochon J Application of GEE procedures for sample size calculations in repeated measures experiments Stat Med 1998171643-58 47 Lachin JM Foulkes MA Evaluation of sample size and power for analyses of survival with allowance for nonuniform patient entry losses to follow-up noncompliance and stratification Biometrics 198642507-19
71
- PANTHER-IPFPREDNISONE AZATHIOPRINEAND N-ACETYLCYSTEINEA STUDY THAT EVALUATES RESPONSE INIDIOPATHIC PULMONARY FIBROSIS
-
- Protocol Summary
- Table of Contents
- List of Tables
- List of Figures
- List of Abbreviations
- 1 Summary
- 2 Hypotheses and Specific Aims
-
- 21 Null Hypothesis
- 22 Specific Aim 1
- 23 Specific Aim 2
- 24 Prespecified Subgroups of Interest
-
- 3 Background and Significance
-
- 31 Idiopathic Pulmonary Fibrosis is the Most Common Interstitial Lung Disease
- 32 Rationale for Placebo Control
- 33 Rationale for N-acetylcysteine
- 35 Rationale for N-acetylcysteine as a Stand-alone Therapy
- 36 Rationale for the Study Design and Primary Endpoint
- 37 Rationale for Blinding of Treatments
-
- 4 Methods
-
- 41 Inclusion Criteria
- 42 Diagnosis of IPF
- 43 Exclusion Criteria
- 44 Study Design and Study Visit
- 45 Dose Justification
- 46 Contraindications Precautions and Side Effects of Study Medications
- 47 Recruitment Procedures
- 48 Study Procedures
- 49 Concomitant Medications
- 410 Laboratory Testing
- 411 Blinding of Study Drugs
-
- 5 Study Endpoints
-
- 51 Primary Study Endpoint
- 52 Secondary Study Endpoints
-
- 6 Safety Evaluations and Procedures
-
- 61 Adverse Events
- 62 Clinical Medical Monitoring
- 63 Unblinding Procedures
-
- 7 Study Drug Procedures
- 8 Data Management
-
- 81 Hardware and Software Configuration
- 82 Sources of Data
-
- 9 Study Design and Data Analysis
-
- 91 General Analytic Considerations
- 92 Randomization Blinding and Reporting of Results
- 93 Stratification
- 94 Specification of the Primary Analyses
- 95 Analysis of Longitudinal Endpoints
- 96 Analysis of Binary Time-to-Event and Time-Lagged Endpoints
- 97 Power Analysis
-
- 10 Study Administration
-
- 101 Cooperative Agreement Mechanism
- 102 IPFnet Steering Group
- 103 Data and Safety Monitoring Board
- 104 Recommendations on Interim Monitoring of Efficacy Safety and Futility
-
- 11 Investigator and Sponsor Obligations
-
- 111 Monitoring
- 112 Cost and Payment
- 113 Confidentiality and Health Insurance Portability and Accountability ActConsiderations
- 114 Informed Consent Procedures
- 115 Institutional Review Boards
-
- 12 Investigator Agreement
- 13 References
-
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
At the IPFnet DCC only authorized personnel will have access to the data files containing study
data Security will be assured through user logon IDs passwords and appropriate access
privileges All study subjects will be identified only by their IPFnet ID numbers and no personal
identifying information such as name address or Social Security number will be entered into
the IPFnet DCC database Any subject-specific data reported to the IPFnet Steering Group will
be identified only by the IPFnet ID number
Finally subjects will not be identified by name in any reports or publications nor will the data
be presented in such a way that the identity of individual subjects can be inferred Analysis files
created for further study by the scientific community will have no subject identifiers These data
files will be created in accordance with the Ancillary Studies and Publication Policy of the
IPFnet
114 Informed Consent Procedures
All IPFnet subjects will provide written informed consent using procedures reviewed and
approved by each clinical centerrsquos IRB Informed consent will be undertaken by study personnel
in-person with the subject The subject has the option of declining further participation in the
study at that point No further study procedures will be conducted until the signed documents
have been provided to the IPFnet clinical center
115 Institutional Review Boards
Before initiating this study the protocol clinical center-specific informed consent forms Health
Insurance Portability and Accountability Act (HIPAA) forms recruitment materials and other
relevant information will be reviewed by a properly constituted IRB at each participating clinical
center A copy of the signed and dated IRB approval at each clinical center will be retrieved prior
to or during the site initiation visit and archived at the IPFnet DCC Any amendments to the
protocol other than simple administrative and typographical changes must be approved by each
IRB before they are implemented The clinical centers will seek annual renewals of their IRB
approvals in accordance with local procedures
67
__________________________________________ ________________
__________________________________________
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
12 Investigator Agreement
I have read the foregoing protocol PANTHER-IPF and agree that it contains all necessary
details for carrying out this study I will conduct the study as outlined herein and will complete
the study within the time designated
I will provide copies of the protocol and all pertinent information to all individuals responsible to
me who assist in the conduct of this study I will discuss this material with them to ensure they
are fully informed regarding the drug and the conduct of the study
I will fulfill all responsibilities for submitting pertinent information to the local IRB if
applicable that is responsible for this study
I further agree that NHLBI andor DCRI will have access to any source documents from which
eCRF information may have been generated
Signature of Principal Investigator Date
Name of Principal Investigator (printed or typed)
Protocol version date May 19 2009
Protocol Amendment 1 version date May 28 2010
Protocol Amendment 2 version date December 6 2011
68
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
13 References
1 Raghu G Brown KK Bradford WZ et al A placebo-controlled trial of interferon gamma-1b in patients with idiopathic pulmonary fibrosis N Engl J Med 2004350125-33 2 King TE Jr Safrin S Starko KM et al Analyses of efficacy end points in a controlled trial of interferon-gamma1b for idiopathic pulmonary fibrosis Chest 2005127171-7 3 Flaherty KR Thwaite EL Kazerooni EA et al Radiological versus histological diagnosis in UIP and NSIP survival implications Thorax 200358143-8 4 Wells AU Desai SR Rubens MB et al Idiopathic pulmonary fibrosis a composite physiologic index derived from disease extent observed by computed tomography Am J Respir Crit Care Med 2003167962-9 5 Raghu G Freudenberger TD Yang S et al High prevalence of abnormal acid gastroshyoesophageal reflux in idiopathic pulmonary fibrosis Eur Respir J 200627136-42 6 Kinnula VL Focus on antioxidant enzymes and antioxidant strategies in smoking related airway diseases Thorax 200560693-700 7 Coultas DB Zumwalt RE Black WC Sobonya RE The epidemiology of interstitial lung diseases Am J Respir Crit Care Med 1994150967-72 8 Raghu G Weycker D Edelsberg J Bradford WZ Oster G Incidence and prevalence of idiopathic pulmonary fibrosis Am J Respir Crit Care Med 2006174810-6 9 Olson AL Swigris JJ Lezotte DC Norris JM Wilson CG Brown KK Mortality from pulmonary fibrosis increased in the United States from 1992 to 2003 Am J Respir Crit Care Med 2007176277-84 10 Mannino DM Etzel RA Parrish RG Pulmonary fibrosis deaths in the United States 1979shy1991 An analysis of multiple-cause mortality data Am J Respir Crit Care Med 19961531548shy52 11 Hubbard R Johnston I Coultas DB Britton J Mortality rates from cryptogenic fibrosing alveolitis in seven countries Thorax 199651711-6 12 Johnston I Britton J Kinnear W Logan R Rising mortality from cryptogenic fibrosing alveolitis Bmj 19903011017-21 13 Raghu G Collard HR Egan JJ et al An official ATSERSJRSALAT statement idiopathic pulmonary fibrosis evidence-based guidelines for diagnosis and management Am J Respir Crit Care Med 2011183788-824 14 (USA) FDA FDA Public Health Advisory Interferon gamma-1b (marketed as Actimmune) In 2007 15 King TE Jr Pardo A Selman M Idiopathic pulmonary fibrosis Lancet 2011 16 Raghu G Brown KK Costabel U et al Treatment of idiopathic pulmonary fibrosis with etanercept an exploratory placebo-controlled trial Am J Respir Crit Care Med 2008178948shy55 17 Malouf MA Hopkins P Snell G Glanville AR An investigator-driven study of everolimus in surgical lung biopsy confirmed idiopathic pulmonary fibrosis Respirology 201116776-83 18 King TE Jr Behr J Brown KK et al BUILD-1 a randomized placebo-controlled trial of bosentan in idiopathic pulmonary fibrosis Am J Respir Crit Care Med 200817775-81 19 Richeldi L Costabel U Selman M et al Efficacy of a tyrosine kinase inhibitor in idiopathic pulmonary fibrosis N Engl J Med 20113651079-87
69
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
20 Borok Z Buhl R Grimes GJ et al Effect of glutathione aerosol on oxidant-antioxidant imbalance in idiopathic pulmonary fibrosis Lancet 1991338215-6 21 Meyer A Buhl R Magnussen H The effect of oral N-acetylcysteine on lung glutathione levels in idiopathic pulmonary fibrosis Eur Respir J 19947431-6 22 Behr J Maier K Degenkolb B Krombach F Vogelmeier C Antioxidative and clinical effects of high-dose N-acetylcysteine in fibrosing alveolitis Adjunctive therapy to maintenance immunosuppression Am J Respir Crit Care Med 19971561897-901 23 Cantin AM North SL Fells GA Hubbard RC Crystal RG Oxidant-mediated epithelial cell injury in idiopathic pulmonary fibrosis J Clin Invest 1987791665-73 24 Waghray M Cui Z Horowitz JC et al Hydrogen peroxide is a diffusible paracrine signal for the induction of epithelial cell death by activated myofibroblasts Faseb J 200519854-6 25 Larios JM Budhiraja R Fanburg BL Thannickal VJ Oxidative protein cross-linking reactions involving L-tyrosine in transforming growth factor-beta1-stimulated fibroblasts J Biol Chem 200127617437-41 26 Kinnula VL Fattman CL Tan RJ Oury TD Oxidative stress in pulmonary fibrosis a possible role for redox modulatory therapy Am J Respir Crit Care Med 2005172417-22 27 Meyer A Buhl R Kampf S Magnussen H Intravenous N-acetylcysteine and lung glutathione of patients with pulmonary fibrosis and normals Am J Respir Crit Care Med 19951521055-60 28 Behr J Degenkolb B Krombach F Vogelmeier C Intracellular glutathione and bronchoalveolar cells in fibrosing alveolitis effects of N-acetylcysteine Eur Respir J 200219906-11 29 Bando M Hosono T Mato N et al Long-term efficacy of inhaled N-acetylcysteine in patients with idiopathic pulmonary fibrosis Intern Med 2010492289-96 30 Demedts M Behr J Buhl R et al High-dose acetylcysteine in idiopathic pulmonary fibrosis N Engl J Med 20053532229-42 31 Toma TP Bhowmik A Rajakulasingam R Acetylcysteine in pulmonary fibrosis N Engl J Med 20063541086-9 author reply -9 32 Hunninghake GW Antioxidant therapy for idiopathic pulmonary fibrosis N Engl J Med 20053532285-7 33 Flaherty KR Mumford JA Murray S et al Prognostic implications of physiologic and radiographic changes in idiopathic interstitial pneumonia Am J Respir Crit Care Med 2003168543-8 34 Latsi PI du Bois RM Nicholson AG et al Fibrotic idiopathic interstitial pneumonia the prognostic value of longitudinal functional trends Am J Respir Crit Care Med 2003168531-7 35 Collard HR King TE Jr Bartelson BB Vourlekis JS Schwarz MI Brown KK Changes in clinical and physiologic variables predict survival in idiopathic pulmonary fibrosis Am J Respir Crit Care Med 2003168538-42 36 Jegal Y Kim DS Shim TS et al Physiology is a stronger predictor of survival than pathology in fibrotic interstitial pneumonia Am J Respir Crit Care Med 2005171639-44 37 Martinez FJ Safrin S Weycker D et al The clinical course of patients with idiopathic pulmonary fibrosis Ann Intern Med 2005142963-7 38 Hull JH Acetylcysteine in pulmonary fibrosis N Engl J Med 20063541089-91 author reply -91
70
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
39 Flaherty KR King TE Jr Raghu G et al Idiopathic interstitial pneumonia what is the effect of a multidisciplinary approach to diagnosis Am J Respir Crit Care Med 2004170904shy10 40 Raghu G Johnson WC Lockhart D Mageto Y Treatment of idiopathic pulmonary fibrosis with a new antifibrotic agent pirfenidone results of a prospective open-label Phase II study Am J Respir Crit Care Med 19991591061-9 41 Hunninghake GW Lynch DA Galvin JR et al Radiologic findings are strongly associated with a pathologic diagnosis of usual interstitial pneumonia Chest 20031241215-23 42 Lynch D Godwin J Safrin S et al High-resolution computed tomography in idiopathic pulmonary fibrosis diagnosis and prognosis Am J Respir Crit Care Med 2005172488-93 43 Mallinckrodt CH Watkin JG Molenberghs G Carroll RJ Choice of the primary analysis in longitudinal clinical trials Pharmaceutical Statistics 20043161-9 44 Bang H Tsiatis A Estimating medical costs with censored data Biometrika 200087329shy43 45 Lin DY Regression analysis of incomplete medical cost data Stat Med 2003221181-200 46 Rochon J Application of GEE procedures for sample size calculations in repeated measures experiments Stat Med 1998171643-58 47 Lachin JM Foulkes MA Evaluation of sample size and power for analyses of survival with allowance for nonuniform patient entry losses to follow-up noncompliance and stratification Biometrics 198642507-19
71
- PANTHER-IPFPREDNISONE AZATHIOPRINEAND N-ACETYLCYSTEINEA STUDY THAT EVALUATES RESPONSE INIDIOPATHIC PULMONARY FIBROSIS
-
- Protocol Summary
- Table of Contents
- List of Tables
- List of Figures
- List of Abbreviations
- 1 Summary
- 2 Hypotheses and Specific Aims
-
- 21 Null Hypothesis
- 22 Specific Aim 1
- 23 Specific Aim 2
- 24 Prespecified Subgroups of Interest
-
- 3 Background and Significance
-
- 31 Idiopathic Pulmonary Fibrosis is the Most Common Interstitial Lung Disease
- 32 Rationale for Placebo Control
- 33 Rationale for N-acetylcysteine
- 35 Rationale for N-acetylcysteine as a Stand-alone Therapy
- 36 Rationale for the Study Design and Primary Endpoint
- 37 Rationale for Blinding of Treatments
-
- 4 Methods
-
- 41 Inclusion Criteria
- 42 Diagnosis of IPF
- 43 Exclusion Criteria
- 44 Study Design and Study Visit
- 45 Dose Justification
- 46 Contraindications Precautions and Side Effects of Study Medications
- 47 Recruitment Procedures
- 48 Study Procedures
- 49 Concomitant Medications
- 410 Laboratory Testing
- 411 Blinding of Study Drugs
-
- 5 Study Endpoints
-
- 51 Primary Study Endpoint
- 52 Secondary Study Endpoints
-
- 6 Safety Evaluations and Procedures
-
- 61 Adverse Events
- 62 Clinical Medical Monitoring
- 63 Unblinding Procedures
-
- 7 Study Drug Procedures
- 8 Data Management
-
- 81 Hardware and Software Configuration
- 82 Sources of Data
-
- 9 Study Design and Data Analysis
-
- 91 General Analytic Considerations
- 92 Randomization Blinding and Reporting of Results
- 93 Stratification
- 94 Specification of the Primary Analyses
- 95 Analysis of Longitudinal Endpoints
- 96 Analysis of Binary Time-to-Event and Time-Lagged Endpoints
- 97 Power Analysis
-
- 10 Study Administration
-
- 101 Cooperative Agreement Mechanism
- 102 IPFnet Steering Group
- 103 Data and Safety Monitoring Board
- 104 Recommendations on Interim Monitoring of Efficacy Safety and Futility
-
- 11 Investigator and Sponsor Obligations
-
- 111 Monitoring
- 112 Cost and Payment
- 113 Confidentiality and Health Insurance Portability and Accountability ActConsiderations
- 114 Informed Consent Procedures
- 115 Institutional Review Boards
-
- 12 Investigator Agreement
- 13 References
-

__________________________________________ ________________
__________________________________________
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
12 Investigator Agreement
I have read the foregoing protocol PANTHER-IPF and agree that it contains all necessary
details for carrying out this study I will conduct the study as outlined herein and will complete
the study within the time designated
I will provide copies of the protocol and all pertinent information to all individuals responsible to
me who assist in the conduct of this study I will discuss this material with them to ensure they
are fully informed regarding the drug and the conduct of the study
I will fulfill all responsibilities for submitting pertinent information to the local IRB if
applicable that is responsible for this study
I further agree that NHLBI andor DCRI will have access to any source documents from which
eCRF information may have been generated
Signature of Principal Investigator Date
Name of Principal Investigator (printed or typed)
Protocol version date May 19 2009
Protocol Amendment 1 version date May 28 2010
Protocol Amendment 2 version date December 6 2011
68
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
13 References
1 Raghu G Brown KK Bradford WZ et al A placebo-controlled trial of interferon gamma-1b in patients with idiopathic pulmonary fibrosis N Engl J Med 2004350125-33 2 King TE Jr Safrin S Starko KM et al Analyses of efficacy end points in a controlled trial of interferon-gamma1b for idiopathic pulmonary fibrosis Chest 2005127171-7 3 Flaherty KR Thwaite EL Kazerooni EA et al Radiological versus histological diagnosis in UIP and NSIP survival implications Thorax 200358143-8 4 Wells AU Desai SR Rubens MB et al Idiopathic pulmonary fibrosis a composite physiologic index derived from disease extent observed by computed tomography Am J Respir Crit Care Med 2003167962-9 5 Raghu G Freudenberger TD Yang S et al High prevalence of abnormal acid gastroshyoesophageal reflux in idiopathic pulmonary fibrosis Eur Respir J 200627136-42 6 Kinnula VL Focus on antioxidant enzymes and antioxidant strategies in smoking related airway diseases Thorax 200560693-700 7 Coultas DB Zumwalt RE Black WC Sobonya RE The epidemiology of interstitial lung diseases Am J Respir Crit Care Med 1994150967-72 8 Raghu G Weycker D Edelsberg J Bradford WZ Oster G Incidence and prevalence of idiopathic pulmonary fibrosis Am J Respir Crit Care Med 2006174810-6 9 Olson AL Swigris JJ Lezotte DC Norris JM Wilson CG Brown KK Mortality from pulmonary fibrosis increased in the United States from 1992 to 2003 Am J Respir Crit Care Med 2007176277-84 10 Mannino DM Etzel RA Parrish RG Pulmonary fibrosis deaths in the United States 1979shy1991 An analysis of multiple-cause mortality data Am J Respir Crit Care Med 19961531548shy52 11 Hubbard R Johnston I Coultas DB Britton J Mortality rates from cryptogenic fibrosing alveolitis in seven countries Thorax 199651711-6 12 Johnston I Britton J Kinnear W Logan R Rising mortality from cryptogenic fibrosing alveolitis Bmj 19903011017-21 13 Raghu G Collard HR Egan JJ et al An official ATSERSJRSALAT statement idiopathic pulmonary fibrosis evidence-based guidelines for diagnosis and management Am J Respir Crit Care Med 2011183788-824 14 (USA) FDA FDA Public Health Advisory Interferon gamma-1b (marketed as Actimmune) In 2007 15 King TE Jr Pardo A Selman M Idiopathic pulmonary fibrosis Lancet 2011 16 Raghu G Brown KK Costabel U et al Treatment of idiopathic pulmonary fibrosis with etanercept an exploratory placebo-controlled trial Am J Respir Crit Care Med 2008178948shy55 17 Malouf MA Hopkins P Snell G Glanville AR An investigator-driven study of everolimus in surgical lung biopsy confirmed idiopathic pulmonary fibrosis Respirology 201116776-83 18 King TE Jr Behr J Brown KK et al BUILD-1 a randomized placebo-controlled trial of bosentan in idiopathic pulmonary fibrosis Am J Respir Crit Care Med 200817775-81 19 Richeldi L Costabel U Selman M et al Efficacy of a tyrosine kinase inhibitor in idiopathic pulmonary fibrosis N Engl J Med 20113651079-87
69
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
20 Borok Z Buhl R Grimes GJ et al Effect of glutathione aerosol on oxidant-antioxidant imbalance in idiopathic pulmonary fibrosis Lancet 1991338215-6 21 Meyer A Buhl R Magnussen H The effect of oral N-acetylcysteine on lung glutathione levels in idiopathic pulmonary fibrosis Eur Respir J 19947431-6 22 Behr J Maier K Degenkolb B Krombach F Vogelmeier C Antioxidative and clinical effects of high-dose N-acetylcysteine in fibrosing alveolitis Adjunctive therapy to maintenance immunosuppression Am J Respir Crit Care Med 19971561897-901 23 Cantin AM North SL Fells GA Hubbard RC Crystal RG Oxidant-mediated epithelial cell injury in idiopathic pulmonary fibrosis J Clin Invest 1987791665-73 24 Waghray M Cui Z Horowitz JC et al Hydrogen peroxide is a diffusible paracrine signal for the induction of epithelial cell death by activated myofibroblasts Faseb J 200519854-6 25 Larios JM Budhiraja R Fanburg BL Thannickal VJ Oxidative protein cross-linking reactions involving L-tyrosine in transforming growth factor-beta1-stimulated fibroblasts J Biol Chem 200127617437-41 26 Kinnula VL Fattman CL Tan RJ Oury TD Oxidative stress in pulmonary fibrosis a possible role for redox modulatory therapy Am J Respir Crit Care Med 2005172417-22 27 Meyer A Buhl R Kampf S Magnussen H Intravenous N-acetylcysteine and lung glutathione of patients with pulmonary fibrosis and normals Am J Respir Crit Care Med 19951521055-60 28 Behr J Degenkolb B Krombach F Vogelmeier C Intracellular glutathione and bronchoalveolar cells in fibrosing alveolitis effects of N-acetylcysteine Eur Respir J 200219906-11 29 Bando M Hosono T Mato N et al Long-term efficacy of inhaled N-acetylcysteine in patients with idiopathic pulmonary fibrosis Intern Med 2010492289-96 30 Demedts M Behr J Buhl R et al High-dose acetylcysteine in idiopathic pulmonary fibrosis N Engl J Med 20053532229-42 31 Toma TP Bhowmik A Rajakulasingam R Acetylcysteine in pulmonary fibrosis N Engl J Med 20063541086-9 author reply -9 32 Hunninghake GW Antioxidant therapy for idiopathic pulmonary fibrosis N Engl J Med 20053532285-7 33 Flaherty KR Mumford JA Murray S et al Prognostic implications of physiologic and radiographic changes in idiopathic interstitial pneumonia Am J Respir Crit Care Med 2003168543-8 34 Latsi PI du Bois RM Nicholson AG et al Fibrotic idiopathic interstitial pneumonia the prognostic value of longitudinal functional trends Am J Respir Crit Care Med 2003168531-7 35 Collard HR King TE Jr Bartelson BB Vourlekis JS Schwarz MI Brown KK Changes in clinical and physiologic variables predict survival in idiopathic pulmonary fibrosis Am J Respir Crit Care Med 2003168538-42 36 Jegal Y Kim DS Shim TS et al Physiology is a stronger predictor of survival than pathology in fibrotic interstitial pneumonia Am J Respir Crit Care Med 2005171639-44 37 Martinez FJ Safrin S Weycker D et al The clinical course of patients with idiopathic pulmonary fibrosis Ann Intern Med 2005142963-7 38 Hull JH Acetylcysteine in pulmonary fibrosis N Engl J Med 20063541089-91 author reply -91
70
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
39 Flaherty KR King TE Jr Raghu G et al Idiopathic interstitial pneumonia what is the effect of a multidisciplinary approach to diagnosis Am J Respir Crit Care Med 2004170904shy10 40 Raghu G Johnson WC Lockhart D Mageto Y Treatment of idiopathic pulmonary fibrosis with a new antifibrotic agent pirfenidone results of a prospective open-label Phase II study Am J Respir Crit Care Med 19991591061-9 41 Hunninghake GW Lynch DA Galvin JR et al Radiologic findings are strongly associated with a pathologic diagnosis of usual interstitial pneumonia Chest 20031241215-23 42 Lynch D Godwin J Safrin S et al High-resolution computed tomography in idiopathic pulmonary fibrosis diagnosis and prognosis Am J Respir Crit Care Med 2005172488-93 43 Mallinckrodt CH Watkin JG Molenberghs G Carroll RJ Choice of the primary analysis in longitudinal clinical trials Pharmaceutical Statistics 20043161-9 44 Bang H Tsiatis A Estimating medical costs with censored data Biometrika 200087329shy43 45 Lin DY Regression analysis of incomplete medical cost data Stat Med 2003221181-200 46 Rochon J Application of GEE procedures for sample size calculations in repeated measures experiments Stat Med 1998171643-58 47 Lachin JM Foulkes MA Evaluation of sample size and power for analyses of survival with allowance for nonuniform patient entry losses to follow-up noncompliance and stratification Biometrics 198642507-19
71
- PANTHER-IPFPREDNISONE AZATHIOPRINEAND N-ACETYLCYSTEINEA STUDY THAT EVALUATES RESPONSE INIDIOPATHIC PULMONARY FIBROSIS
-
- Protocol Summary
- Table of Contents
- List of Tables
- List of Figures
- List of Abbreviations
- 1 Summary
- 2 Hypotheses and Specific Aims
-
- 21 Null Hypothesis
- 22 Specific Aim 1
- 23 Specific Aim 2
- 24 Prespecified Subgroups of Interest
-
- 3 Background and Significance
-
- 31 Idiopathic Pulmonary Fibrosis is the Most Common Interstitial Lung Disease
- 32 Rationale for Placebo Control
- 33 Rationale for N-acetylcysteine
- 35 Rationale for N-acetylcysteine as a Stand-alone Therapy
- 36 Rationale for the Study Design and Primary Endpoint
- 37 Rationale for Blinding of Treatments
-
- 4 Methods
-
- 41 Inclusion Criteria
- 42 Diagnosis of IPF
- 43 Exclusion Criteria
- 44 Study Design and Study Visit
- 45 Dose Justification
- 46 Contraindications Precautions and Side Effects of Study Medications
- 47 Recruitment Procedures
- 48 Study Procedures
- 49 Concomitant Medications
- 410 Laboratory Testing
- 411 Blinding of Study Drugs
-
- 5 Study Endpoints
-
- 51 Primary Study Endpoint
- 52 Secondary Study Endpoints
-
- 6 Safety Evaluations and Procedures
-
- 61 Adverse Events
- 62 Clinical Medical Monitoring
- 63 Unblinding Procedures
-
- 7 Study Drug Procedures
- 8 Data Management
-
- 81 Hardware and Software Configuration
- 82 Sources of Data
-
- 9 Study Design and Data Analysis
-
- 91 General Analytic Considerations
- 92 Randomization Blinding and Reporting of Results
- 93 Stratification
- 94 Specification of the Primary Analyses
- 95 Analysis of Longitudinal Endpoints
- 96 Analysis of Binary Time-to-Event and Time-Lagged Endpoints
- 97 Power Analysis
-
- 10 Study Administration
-
- 101 Cooperative Agreement Mechanism
- 102 IPFnet Steering Group
- 103 Data and Safety Monitoring Board
- 104 Recommendations on Interim Monitoring of Efficacy Safety and Futility
-
- 11 Investigator and Sponsor Obligations
-
- 111 Monitoring
- 112 Cost and Payment
- 113 Confidentiality and Health Insurance Portability and Accountability ActConsiderations
- 114 Informed Consent Procedures
- 115 Institutional Review Boards
-
- 12 Investigator Agreement
- 13 References
-

PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
13 References
1 Raghu G Brown KK Bradford WZ et al A placebo-controlled trial of interferon gamma-1b in patients with idiopathic pulmonary fibrosis N Engl J Med 2004350125-33 2 King TE Jr Safrin S Starko KM et al Analyses of efficacy end points in a controlled trial of interferon-gamma1b for idiopathic pulmonary fibrosis Chest 2005127171-7 3 Flaherty KR Thwaite EL Kazerooni EA et al Radiological versus histological diagnosis in UIP and NSIP survival implications Thorax 200358143-8 4 Wells AU Desai SR Rubens MB et al Idiopathic pulmonary fibrosis a composite physiologic index derived from disease extent observed by computed tomography Am J Respir Crit Care Med 2003167962-9 5 Raghu G Freudenberger TD Yang S et al High prevalence of abnormal acid gastroshyoesophageal reflux in idiopathic pulmonary fibrosis Eur Respir J 200627136-42 6 Kinnula VL Focus on antioxidant enzymes and antioxidant strategies in smoking related airway diseases Thorax 200560693-700 7 Coultas DB Zumwalt RE Black WC Sobonya RE The epidemiology of interstitial lung diseases Am J Respir Crit Care Med 1994150967-72 8 Raghu G Weycker D Edelsberg J Bradford WZ Oster G Incidence and prevalence of idiopathic pulmonary fibrosis Am J Respir Crit Care Med 2006174810-6 9 Olson AL Swigris JJ Lezotte DC Norris JM Wilson CG Brown KK Mortality from pulmonary fibrosis increased in the United States from 1992 to 2003 Am J Respir Crit Care Med 2007176277-84 10 Mannino DM Etzel RA Parrish RG Pulmonary fibrosis deaths in the United States 1979shy1991 An analysis of multiple-cause mortality data Am J Respir Crit Care Med 19961531548shy52 11 Hubbard R Johnston I Coultas DB Britton J Mortality rates from cryptogenic fibrosing alveolitis in seven countries Thorax 199651711-6 12 Johnston I Britton J Kinnear W Logan R Rising mortality from cryptogenic fibrosing alveolitis Bmj 19903011017-21 13 Raghu G Collard HR Egan JJ et al An official ATSERSJRSALAT statement idiopathic pulmonary fibrosis evidence-based guidelines for diagnosis and management Am J Respir Crit Care Med 2011183788-824 14 (USA) FDA FDA Public Health Advisory Interferon gamma-1b (marketed as Actimmune) In 2007 15 King TE Jr Pardo A Selman M Idiopathic pulmonary fibrosis Lancet 2011 16 Raghu G Brown KK Costabel U et al Treatment of idiopathic pulmonary fibrosis with etanercept an exploratory placebo-controlled trial Am J Respir Crit Care Med 2008178948shy55 17 Malouf MA Hopkins P Snell G Glanville AR An investigator-driven study of everolimus in surgical lung biopsy confirmed idiopathic pulmonary fibrosis Respirology 201116776-83 18 King TE Jr Behr J Brown KK et al BUILD-1 a randomized placebo-controlled trial of bosentan in idiopathic pulmonary fibrosis Am J Respir Crit Care Med 200817775-81 19 Richeldi L Costabel U Selman M et al Efficacy of a tyrosine kinase inhibitor in idiopathic pulmonary fibrosis N Engl J Med 20113651079-87
69
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
20 Borok Z Buhl R Grimes GJ et al Effect of glutathione aerosol on oxidant-antioxidant imbalance in idiopathic pulmonary fibrosis Lancet 1991338215-6 21 Meyer A Buhl R Magnussen H The effect of oral N-acetylcysteine on lung glutathione levels in idiopathic pulmonary fibrosis Eur Respir J 19947431-6 22 Behr J Maier K Degenkolb B Krombach F Vogelmeier C Antioxidative and clinical effects of high-dose N-acetylcysteine in fibrosing alveolitis Adjunctive therapy to maintenance immunosuppression Am J Respir Crit Care Med 19971561897-901 23 Cantin AM North SL Fells GA Hubbard RC Crystal RG Oxidant-mediated epithelial cell injury in idiopathic pulmonary fibrosis J Clin Invest 1987791665-73 24 Waghray M Cui Z Horowitz JC et al Hydrogen peroxide is a diffusible paracrine signal for the induction of epithelial cell death by activated myofibroblasts Faseb J 200519854-6 25 Larios JM Budhiraja R Fanburg BL Thannickal VJ Oxidative protein cross-linking reactions involving L-tyrosine in transforming growth factor-beta1-stimulated fibroblasts J Biol Chem 200127617437-41 26 Kinnula VL Fattman CL Tan RJ Oury TD Oxidative stress in pulmonary fibrosis a possible role for redox modulatory therapy Am J Respir Crit Care Med 2005172417-22 27 Meyer A Buhl R Kampf S Magnussen H Intravenous N-acetylcysteine and lung glutathione of patients with pulmonary fibrosis and normals Am J Respir Crit Care Med 19951521055-60 28 Behr J Degenkolb B Krombach F Vogelmeier C Intracellular glutathione and bronchoalveolar cells in fibrosing alveolitis effects of N-acetylcysteine Eur Respir J 200219906-11 29 Bando M Hosono T Mato N et al Long-term efficacy of inhaled N-acetylcysteine in patients with idiopathic pulmonary fibrosis Intern Med 2010492289-96 30 Demedts M Behr J Buhl R et al High-dose acetylcysteine in idiopathic pulmonary fibrosis N Engl J Med 20053532229-42 31 Toma TP Bhowmik A Rajakulasingam R Acetylcysteine in pulmonary fibrosis N Engl J Med 20063541086-9 author reply -9 32 Hunninghake GW Antioxidant therapy for idiopathic pulmonary fibrosis N Engl J Med 20053532285-7 33 Flaherty KR Mumford JA Murray S et al Prognostic implications of physiologic and radiographic changes in idiopathic interstitial pneumonia Am J Respir Crit Care Med 2003168543-8 34 Latsi PI du Bois RM Nicholson AG et al Fibrotic idiopathic interstitial pneumonia the prognostic value of longitudinal functional trends Am J Respir Crit Care Med 2003168531-7 35 Collard HR King TE Jr Bartelson BB Vourlekis JS Schwarz MI Brown KK Changes in clinical and physiologic variables predict survival in idiopathic pulmonary fibrosis Am J Respir Crit Care Med 2003168538-42 36 Jegal Y Kim DS Shim TS et al Physiology is a stronger predictor of survival than pathology in fibrotic interstitial pneumonia Am J Respir Crit Care Med 2005171639-44 37 Martinez FJ Safrin S Weycker D et al The clinical course of patients with idiopathic pulmonary fibrosis Ann Intern Med 2005142963-7 38 Hull JH Acetylcysteine in pulmonary fibrosis N Engl J Med 20063541089-91 author reply -91
70
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
39 Flaherty KR King TE Jr Raghu G et al Idiopathic interstitial pneumonia what is the effect of a multidisciplinary approach to diagnosis Am J Respir Crit Care Med 2004170904shy10 40 Raghu G Johnson WC Lockhart D Mageto Y Treatment of idiopathic pulmonary fibrosis with a new antifibrotic agent pirfenidone results of a prospective open-label Phase II study Am J Respir Crit Care Med 19991591061-9 41 Hunninghake GW Lynch DA Galvin JR et al Radiologic findings are strongly associated with a pathologic diagnosis of usual interstitial pneumonia Chest 20031241215-23 42 Lynch D Godwin J Safrin S et al High-resolution computed tomography in idiopathic pulmonary fibrosis diagnosis and prognosis Am J Respir Crit Care Med 2005172488-93 43 Mallinckrodt CH Watkin JG Molenberghs G Carroll RJ Choice of the primary analysis in longitudinal clinical trials Pharmaceutical Statistics 20043161-9 44 Bang H Tsiatis A Estimating medical costs with censored data Biometrika 200087329shy43 45 Lin DY Regression analysis of incomplete medical cost data Stat Med 2003221181-200 46 Rochon J Application of GEE procedures for sample size calculations in repeated measures experiments Stat Med 1998171643-58 47 Lachin JM Foulkes MA Evaluation of sample size and power for analyses of survival with allowance for nonuniform patient entry losses to follow-up noncompliance and stratification Biometrics 198642507-19
71
- PANTHER-IPFPREDNISONE AZATHIOPRINEAND N-ACETYLCYSTEINEA STUDY THAT EVALUATES RESPONSE INIDIOPATHIC PULMONARY FIBROSIS
-
- Protocol Summary
- Table of Contents
- List of Tables
- List of Figures
- List of Abbreviations
- 1 Summary
- 2 Hypotheses and Specific Aims
-
- 21 Null Hypothesis
- 22 Specific Aim 1
- 23 Specific Aim 2
- 24 Prespecified Subgroups of Interest
-
- 3 Background and Significance
-
- 31 Idiopathic Pulmonary Fibrosis is the Most Common Interstitial Lung Disease
- 32 Rationale for Placebo Control
- 33 Rationale for N-acetylcysteine
- 35 Rationale for N-acetylcysteine as a Stand-alone Therapy
- 36 Rationale for the Study Design and Primary Endpoint
- 37 Rationale for Blinding of Treatments
-
- 4 Methods
-
- 41 Inclusion Criteria
- 42 Diagnosis of IPF
- 43 Exclusion Criteria
- 44 Study Design and Study Visit
- 45 Dose Justification
- 46 Contraindications Precautions and Side Effects of Study Medications
- 47 Recruitment Procedures
- 48 Study Procedures
- 49 Concomitant Medications
- 410 Laboratory Testing
- 411 Blinding of Study Drugs
-
- 5 Study Endpoints
-
- 51 Primary Study Endpoint
- 52 Secondary Study Endpoints
-
- 6 Safety Evaluations and Procedures
-
- 61 Adverse Events
- 62 Clinical Medical Monitoring
- 63 Unblinding Procedures
-
- 7 Study Drug Procedures
- 8 Data Management
-
- 81 Hardware and Software Configuration
- 82 Sources of Data
-
- 9 Study Design and Data Analysis
-
- 91 General Analytic Considerations
- 92 Randomization Blinding and Reporting of Results
- 93 Stratification
- 94 Specification of the Primary Analyses
- 95 Analysis of Longitudinal Endpoints
- 96 Analysis of Binary Time-to-Event and Time-Lagged Endpoints
- 97 Power Analysis
-
- 10 Study Administration
-
- 101 Cooperative Agreement Mechanism
- 102 IPFnet Steering Group
- 103 Data and Safety Monitoring Board
- 104 Recommendations on Interim Monitoring of Efficacy Safety and Futility
-
- 11 Investigator and Sponsor Obligations
-
- 111 Monitoring
- 112 Cost and Payment
- 113 Confidentiality and Health Insurance Portability and Accountability ActConsiderations
- 114 Informed Consent Procedures
- 115 Institutional Review Boards
-
- 12 Investigator Agreement
- 13 References
-

PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
20 Borok Z Buhl R Grimes GJ et al Effect of glutathione aerosol on oxidant-antioxidant imbalance in idiopathic pulmonary fibrosis Lancet 1991338215-6 21 Meyer A Buhl R Magnussen H The effect of oral N-acetylcysteine on lung glutathione levels in idiopathic pulmonary fibrosis Eur Respir J 19947431-6 22 Behr J Maier K Degenkolb B Krombach F Vogelmeier C Antioxidative and clinical effects of high-dose N-acetylcysteine in fibrosing alveolitis Adjunctive therapy to maintenance immunosuppression Am J Respir Crit Care Med 19971561897-901 23 Cantin AM North SL Fells GA Hubbard RC Crystal RG Oxidant-mediated epithelial cell injury in idiopathic pulmonary fibrosis J Clin Invest 1987791665-73 24 Waghray M Cui Z Horowitz JC et al Hydrogen peroxide is a diffusible paracrine signal for the induction of epithelial cell death by activated myofibroblasts Faseb J 200519854-6 25 Larios JM Budhiraja R Fanburg BL Thannickal VJ Oxidative protein cross-linking reactions involving L-tyrosine in transforming growth factor-beta1-stimulated fibroblasts J Biol Chem 200127617437-41 26 Kinnula VL Fattman CL Tan RJ Oury TD Oxidative stress in pulmonary fibrosis a possible role for redox modulatory therapy Am J Respir Crit Care Med 2005172417-22 27 Meyer A Buhl R Kampf S Magnussen H Intravenous N-acetylcysteine and lung glutathione of patients with pulmonary fibrosis and normals Am J Respir Crit Care Med 19951521055-60 28 Behr J Degenkolb B Krombach F Vogelmeier C Intracellular glutathione and bronchoalveolar cells in fibrosing alveolitis effects of N-acetylcysteine Eur Respir J 200219906-11 29 Bando M Hosono T Mato N et al Long-term efficacy of inhaled N-acetylcysteine in patients with idiopathic pulmonary fibrosis Intern Med 2010492289-96 30 Demedts M Behr J Buhl R et al High-dose acetylcysteine in idiopathic pulmonary fibrosis N Engl J Med 20053532229-42 31 Toma TP Bhowmik A Rajakulasingam R Acetylcysteine in pulmonary fibrosis N Engl J Med 20063541086-9 author reply -9 32 Hunninghake GW Antioxidant therapy for idiopathic pulmonary fibrosis N Engl J Med 20053532285-7 33 Flaherty KR Mumford JA Murray S et al Prognostic implications of physiologic and radiographic changes in idiopathic interstitial pneumonia Am J Respir Crit Care Med 2003168543-8 34 Latsi PI du Bois RM Nicholson AG et al Fibrotic idiopathic interstitial pneumonia the prognostic value of longitudinal functional trends Am J Respir Crit Care Med 2003168531-7 35 Collard HR King TE Jr Bartelson BB Vourlekis JS Schwarz MI Brown KK Changes in clinical and physiologic variables predict survival in idiopathic pulmonary fibrosis Am J Respir Crit Care Med 2003168538-42 36 Jegal Y Kim DS Shim TS et al Physiology is a stronger predictor of survival than pathology in fibrotic interstitial pneumonia Am J Respir Crit Care Med 2005171639-44 37 Martinez FJ Safrin S Weycker D et al The clinical course of patients with idiopathic pulmonary fibrosis Ann Intern Med 2005142963-7 38 Hull JH Acetylcysteine in pulmonary fibrosis N Engl J Med 20063541089-91 author reply -91
70
PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
39 Flaherty KR King TE Jr Raghu G et al Idiopathic interstitial pneumonia what is the effect of a multidisciplinary approach to diagnosis Am J Respir Crit Care Med 2004170904shy10 40 Raghu G Johnson WC Lockhart D Mageto Y Treatment of idiopathic pulmonary fibrosis with a new antifibrotic agent pirfenidone results of a prospective open-label Phase II study Am J Respir Crit Care Med 19991591061-9 41 Hunninghake GW Lynch DA Galvin JR et al Radiologic findings are strongly associated with a pathologic diagnosis of usual interstitial pneumonia Chest 20031241215-23 42 Lynch D Godwin J Safrin S et al High-resolution computed tomography in idiopathic pulmonary fibrosis diagnosis and prognosis Am J Respir Crit Care Med 2005172488-93 43 Mallinckrodt CH Watkin JG Molenberghs G Carroll RJ Choice of the primary analysis in longitudinal clinical trials Pharmaceutical Statistics 20043161-9 44 Bang H Tsiatis A Estimating medical costs with censored data Biometrika 200087329shy43 45 Lin DY Regression analysis of incomplete medical cost data Stat Med 2003221181-200 46 Rochon J Application of GEE procedures for sample size calculations in repeated measures experiments Stat Med 1998171643-58 47 Lachin JM Foulkes MA Evaluation of sample size and power for analyses of survival with allowance for nonuniform patient entry losses to follow-up noncompliance and stratification Biometrics 198642507-19
71
- PANTHER-IPFPREDNISONE AZATHIOPRINEAND N-ACETYLCYSTEINEA STUDY THAT EVALUATES RESPONSE INIDIOPATHIC PULMONARY FIBROSIS
-
- Protocol Summary
- Table of Contents
- List of Tables
- List of Figures
- List of Abbreviations
- 1 Summary
- 2 Hypotheses and Specific Aims
-
- 21 Null Hypothesis
- 22 Specific Aim 1
- 23 Specific Aim 2
- 24 Prespecified Subgroups of Interest
-
- 3 Background and Significance
-
- 31 Idiopathic Pulmonary Fibrosis is the Most Common Interstitial Lung Disease
- 32 Rationale for Placebo Control
- 33 Rationale for N-acetylcysteine
- 35 Rationale for N-acetylcysteine as a Stand-alone Therapy
- 36 Rationale for the Study Design and Primary Endpoint
- 37 Rationale for Blinding of Treatments
-
- 4 Methods
-
- 41 Inclusion Criteria
- 42 Diagnosis of IPF
- 43 Exclusion Criteria
- 44 Study Design and Study Visit
- 45 Dose Justification
- 46 Contraindications Precautions and Side Effects of Study Medications
- 47 Recruitment Procedures
- 48 Study Procedures
- 49 Concomitant Medications
- 410 Laboratory Testing
- 411 Blinding of Study Drugs
-
- 5 Study Endpoints
-
- 51 Primary Study Endpoint
- 52 Secondary Study Endpoints
-
- 6 Safety Evaluations and Procedures
-
- 61 Adverse Events
- 62 Clinical Medical Monitoring
- 63 Unblinding Procedures
-
- 7 Study Drug Procedures
- 8 Data Management
-
- 81 Hardware and Software Configuration
- 82 Sources of Data
-
- 9 Study Design and Data Analysis
-
- 91 General Analytic Considerations
- 92 Randomization Blinding and Reporting of Results
- 93 Stratification
- 94 Specification of the Primary Analyses
- 95 Analysis of Longitudinal Endpoints
- 96 Analysis of Binary Time-to-Event and Time-Lagged Endpoints
- 97 Power Analysis
-
- 10 Study Administration
-
- 101 Cooperative Agreement Mechanism
- 102 IPFnet Steering Group
- 103 Data and Safety Monitoring Board
- 104 Recommendations on Interim Monitoring of Efficacy Safety and Futility
-
- 11 Investigator and Sponsor Obligations
-
- 111 Monitoring
- 112 Cost and Payment
- 113 Confidentiality and Health Insurance Portability and Accountability ActConsiderations
- 114 Informed Consent Procedures
- 115 Institutional Review Boards
-
- 12 Investigator Agreement
- 13 References
-

PANTHER-IPF Protocol ndash Amendment 2 December 6 2011
39 Flaherty KR King TE Jr Raghu G et al Idiopathic interstitial pneumonia what is the effect of a multidisciplinary approach to diagnosis Am J Respir Crit Care Med 2004170904shy10 40 Raghu G Johnson WC Lockhart D Mageto Y Treatment of idiopathic pulmonary fibrosis with a new antifibrotic agent pirfenidone results of a prospective open-label Phase II study Am J Respir Crit Care Med 19991591061-9 41 Hunninghake GW Lynch DA Galvin JR et al Radiologic findings are strongly associated with a pathologic diagnosis of usual interstitial pneumonia Chest 20031241215-23 42 Lynch D Godwin J Safrin S et al High-resolution computed tomography in idiopathic pulmonary fibrosis diagnosis and prognosis Am J Respir Crit Care Med 2005172488-93 43 Mallinckrodt CH Watkin JG Molenberghs G Carroll RJ Choice of the primary analysis in longitudinal clinical trials Pharmaceutical Statistics 20043161-9 44 Bang H Tsiatis A Estimating medical costs with censored data Biometrika 200087329shy43 45 Lin DY Regression analysis of incomplete medical cost data Stat Med 2003221181-200 46 Rochon J Application of GEE procedures for sample size calculations in repeated measures experiments Stat Med 1998171643-58 47 Lachin JM Foulkes MA Evaluation of sample size and power for analyses of survival with allowance for nonuniform patient entry losses to follow-up noncompliance and stratification Biometrics 198642507-19
71
- PANTHER-IPFPREDNISONE AZATHIOPRINEAND N-ACETYLCYSTEINEA STUDY THAT EVALUATES RESPONSE INIDIOPATHIC PULMONARY FIBROSIS
-
- Protocol Summary
- Table of Contents
- List of Tables
- List of Figures
- List of Abbreviations
- 1 Summary
- 2 Hypotheses and Specific Aims
-
- 21 Null Hypothesis
- 22 Specific Aim 1
- 23 Specific Aim 2
- 24 Prespecified Subgroups of Interest
-
- 3 Background and Significance
-
- 31 Idiopathic Pulmonary Fibrosis is the Most Common Interstitial Lung Disease
- 32 Rationale for Placebo Control
- 33 Rationale for N-acetylcysteine
- 35 Rationale for N-acetylcysteine as a Stand-alone Therapy
- 36 Rationale for the Study Design and Primary Endpoint
- 37 Rationale for Blinding of Treatments
-
- 4 Methods
-
- 41 Inclusion Criteria
- 42 Diagnosis of IPF
- 43 Exclusion Criteria
- 44 Study Design and Study Visit
- 45 Dose Justification
- 46 Contraindications Precautions and Side Effects of Study Medications
- 47 Recruitment Procedures
- 48 Study Procedures
- 49 Concomitant Medications
- 410 Laboratory Testing
- 411 Blinding of Study Drugs
-
- 5 Study Endpoints
-
- 51 Primary Study Endpoint
- 52 Secondary Study Endpoints
-
- 6 Safety Evaluations and Procedures
-
- 61 Adverse Events
- 62 Clinical Medical Monitoring
- 63 Unblinding Procedures
-
- 7 Study Drug Procedures
- 8 Data Management
-
- 81 Hardware and Software Configuration
- 82 Sources of Data
-
- 9 Study Design and Data Analysis
-
- 91 General Analytic Considerations
- 92 Randomization Blinding and Reporting of Results
- 93 Stratification
- 94 Specification of the Primary Analyses
- 95 Analysis of Longitudinal Endpoints
- 96 Analysis of Binary Time-to-Event and Time-Lagged Endpoints
- 97 Power Analysis
-
- 10 Study Administration
-
- 101 Cooperative Agreement Mechanism
- 102 IPFnet Steering Group
- 103 Data and Safety Monitoring Board
- 104 Recommendations on Interim Monitoring of Efficacy Safety and Futility
-
- 11 Investigator and Sponsor Obligations
-
- 111 Monitoring
- 112 Cost and Payment
- 113 Confidentiality and Health Insurance Portability and Accountability ActConsiderations
- 114 Informed Consent Procedures
- 115 Institutional Review Boards
-
- 12 Investigator Agreement
- 13 References
-
Related Documents











