(opvright I 992 h i/ti Journal of Biiii ig,ii! Joint Ssrgerv. Iili-i’rtiiirI1i.il 1042 THE JOURNAL OF BONE AND JOINT SURGERY Pantalar and Tibiotalocalcaneal Arthrodesis for Post-Traumatic Osteoarthrosis of the Ankle and Hindfoot* BY JOHN A. PAPA. M.D.t. AND MARK S. MYERSON. MDI. BALTIMORE. MARYLAND In vc’stigatioll J)t’rforlne(l at Union Me,norial Hospital, Tile Johns Hopkins Universit% Baltintore ABSTRACT: Twenty-one patients had a unilateral extended arthrodesis of the ankle and hindfoot (a tib- iotalocalcaneal procedure in thirteen patients and a pantalar procedure in eight) for post-traumatic os- teoarthrosis or deformity, or both. The operation was performed through a transfibular extended lateral ap- proach, and autogenous bone graft and rigid internal fixation was used. A final alignment of 0 to S degrees of valgus, 0 to S degrees ofcalcaneus, and external rotation equal to that of the contralateral side was sought. Subjective and objective evaluation, including a per- sonal interview, physical examination, and radiographic and dynamic pedobarographic analysis, was performed at a mean interval of thirty-two months (range, twenty- four to fifty-four months) after the operation. A solid fusion was achieved in eighteen (86 per cent) of the twenty-one patients. There were five malunions (24 per cent) and two superficial wound problems (10 per cent). Ofthe seventeen patients who were not retired from work, eleven returned to work: nine to an occupation that involved standing and two to a sedentary occupa- lion. Although seventeen (81 per cent) of the twenty- one patients reported that they were much improved, twenty (95 per cent) had some pain, and most benefited from modifications in shoe-wear. Patients who had had a tibiotalocalcaneal arthrodesis were more mobile and functioned at a higher level than those who had had a pantalar arthrodesis. Extended arthrodesis of the ankle and hindfoot is a complex, technically demanding procedure, and should be regarded as a salvage operation capable of producing a satisfactory result and usually providing a reasonable alternative to amputation. Patients who have post-traumatic osteoanthnosis in- volving both the ankle and the subtalar joints pose a difficult therapeutic challenge. In addition to debilitat- ing pain. these patients frequently have diffuse stiffness of the forefoot, midfoot. hindfoot, and ankle second- *No benefits in any form have been received or will be received from a commercial party related directly or indirectly to the subject of this article. No funds were received in support of this study. tMatthews Orthopaedic Clinic. 1315 South Orange Avenue, Or- lando, Florida 32856. IFoot and Ankle Center, Union Memorial Hospital. 201 East Uni- versity Parkway. Baltimore, Maryland 21218. any to associated injuries, prolonged immobilization, and previous operations. Operative tneatment is limited to extended arthnodesis or to Syme or below-the-knee am- putation. The anticipated outcome after amputation is well known27’”’3’7’525. After a post-traumatic Syme on below-the-knee amputation, patients can be expected to walk rather well, with only a minimum increase in expen- diture of energy compared with normal individuals”326. In addition, the pain that is often perceived as coming from the amputated part is, in most patients, eliminated. However, patients who have had a Syme on below-the- knee amputation need a prosthesis for walking, with the exception of limited distances for patients who have had a Syme amputation. The expected functional results in patients who have had an extended arthrodesis are not well established. Most of the previous reports of pantalar arthrodesis have dealt primarily with treatment of deformities of the paralytic lower extnemity’3469’2”2427. Debate continues concerning the merits of a one-stage procedure’3’2’624 compared with a two-stage procedure”2’22, different op- enative approaches (anterolateral”, lateral2’25, or poste- non2524), type of fixation (external23 or internal6’4), and need for bone-grafting. We performed this retrospective study of our experience with extended arthrodesis of the ankle and hindfoot to determine the associated morbid- ity and the expected functional nesults and limitations. Materials and Methods Between 1986 and 1989, twenty-one patients (four- teen men and seven women) had a unilateral extended anthrodesis of the ankle and hindfoot (a tibiotalocal- caneal procedure in thirteen patients and a pantalan procedure in eight) performed by the senior one of us (M. S. M.). The term pantalar is used if the tibiotalan, talocalcaneal, talonavicular, and calcaneocuboid joints are included in the arthrodesis. The average age of the patients at the time of the operation was forty-five years (range, twenty-one to sixty-eight years). The operation was done on the right foot in ten patients and on the left in eleven. All of the operations were done as salvage proce- dures for the treatment of painful, disabling osteoar- throsis on deformity. or both, involving both the ankle and subtalar joints. An operation was done only after failure of non-operative management. which generally

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

(opvright I 992 h� i�/ti� Journal of Biiii ig,ii! Joint Ss�rgerv. Iili-i’rtiiir�I1i.il
1042 THE JOURNAL OF BONE AND JOINT SURGERY
Pantalar and Tibiotalocalcaneal Arthrodesis
for Post-Traumatic Osteoarthrosis of the Ankle and Hindfoot*BY JOHN A. PAPA. M.D.t. AND MARK S. MYERSON. MDI. BALTIMORE. MARYLAND
In vc’stigatioll J)t’rforlne(l at Union Me,norial Hospital, Tile Johns Hopkins Universit%� Baltintore
ABSTRACT: Twenty-one patients had a unilateral
extended arthrodesis of the ankle and hindfoot (a tib-
iotalocalcaneal procedure in thirteen patients and a
pantalar procedure in eight) for post-traumatic os-
teoarthrosis or deformity, or both. The operation was
performed through a transfibular extended lateral ap-
proach, and autogenous bone graft and rigid internal
fixation was used. A final alignment of 0 to S degrees of
valgus, 0 to S degrees ofcalcaneus, and external rotation
equal to that of the contralateral side was sought.
Subjective and objective evaluation, including a per-
sonal interview, physical examination, and radiographic
and dynamic pedobarographic analysis, was performed
at a mean interval of thirty-two months (range, twenty-
four to fifty-four months) after the operation. A solid
fusion was achieved in eighteen (86 per cent) of the
twenty-one patients. There were five malunions (24 per
cent) and two superficial wound problems (10 per cent).
Ofthe seventeen patients who were not retired from
work, eleven returned to work: nine to an occupation
that involved standing and two to a sedentary occupa-
lion. Although seventeen (81 per cent) of the twenty-
one patients reported that they were much improved,
twenty (95 per cent) had some pain, and most benefited
from modifications in shoe-wear. Patients who had had
a tibiotalocalcaneal arthrodesis were more mobile and
functioned at a higher level than those who had had apantalar arthrodesis.
Extended arthrodesis of the ankle and hindfoot is a
complex, technically demanding procedure, and should
be regarded as a salvage operation capable of producing
a satisfactory result and usually providing a reasonable
alternative to amputation.
Patients who have post-traumatic osteoanthnosis in-
volving both the ankle and the subtalar joints pose a
difficult therapeutic challenge. In addition to debilitat-
ing pain. these patients frequently have diffuse stiffness
of the forefoot, midfoot. hindfoot, and ankle second-
*No benefits in any form have been received or will be received
from a commercial party related directly or indirectly to the subject ofthis article. No funds were received in support of this study.
tMatthews Orthopaedic Clinic. 1315 South Orange Avenue, Or-
lando, Florida 32856.
IFoot and Ankle Center, Union Memorial Hospital. 201 East Uni-versity Parkway. Baltimore, Maryland 21218.
any to associated injuries, prolonged immobilization, and
previous operations. Operative tneatment is limited to
extended arthnodesis or to Syme or below-the-knee am-
putation. The anticipated outcome after amputation is
well known27’”’3’7’525. After a post-traumatic Syme on
below-the-knee amputation, patients can be expected to
walk rather well, with only a minimum increase in expen-
diture of energy compared with normal individuals”326.
In addition, the pain that is often perceived as coming
from the amputated part is, in most patients, eliminated.
However, patients who have had a Syme on below-the-
knee amputation need a prosthesis for walking, with the
exception of limited distances for patients who have had
a Syme amputation.
The expected functional results in patients who have
had an extended arthrodesis are not well established.
Most of the previous reports of pantalar arthrodesis
have dealt primarily with treatment of deformities of the
paralytic lower extnemity’3469’2”�24�27. Debate continues
concerning the merits of a one-stage procedure’3’2’624
compared with a two-stage procedure”2’22, different op-
enative approaches (anterolateral”, lateral2’25, or poste-
non2524), type of fixation (external23 or internal6’4), and
need for bone-grafting. We performed this retrospective
study of our experience with extended arthrodesis of the
ankle and hindfoot to determine the associated morbid-
ity and the expected functional nesults and limitations.
Materials and Methods
Between 1986 and 1989, twenty-one patients (four-
teen men and seven women) had a unilateral extended
anthrodesis of the ankle and hindfoot (a tibiotalocal-
caneal procedure in thirteen patients and a pantalan
procedure in eight) performed by the senior one of us
(M. S. M.). The term pantalar is used if the tibiotalan,
talocalcaneal, talonavicular, and calcaneocuboid joints
are included in the arthrodesis. The average age of the
patients at the time of the operation was forty-five years
(range, twenty-one to sixty-eight years). The operation
was done on the right foot in ten patients and on the left
in eleven.
All of the operations were done as salvage proce-
dures for the treatment of painful, disabling osteoar-
throsis on deformity. or both, involving both the ankle
and subtalar joints. An operation was done only after
failure of non-operative management. which generally
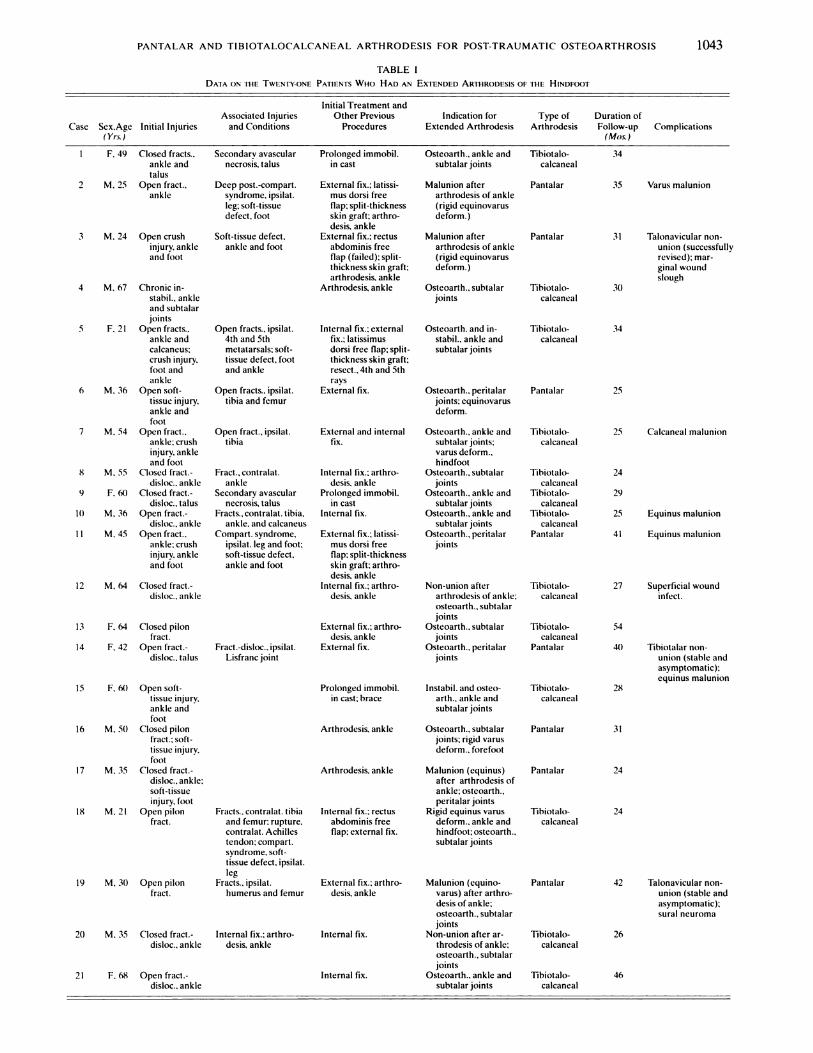
F. 49 Closed fracts., Secondary avascularankle and necrosis, talus
DATA ON THE TWENTY.ONE PATIENTS WHo HAD AN EXTENDED ARmR0DEsI5 OF THE HINDFOOT
Initial Treatment andAssociated Injuries Other Previous Indication for Type of Duration of
Case Sex.Age Initial Injuries and Conditions Procedures Extended Arthrodesis Arthrodesis Follow-up Complications(Yr.s.) (Mos.)
Prolonged immobil. Osteoarth., ankle and tibiotalo-in cast subtalar joints calcaneal
External fix.: latissi- Malunion after Pantalar
mus dorsi free arthrodesis of ankleflap: split-thickness (rigid equinovarusskin graft; arthro- deform.)
desis, ankleExternal fix.: rectus Malunion after Pantalar
abdominis free arthrodesis of ankleflap (failed): split- (rigid equinovarusthickness skin graft: deform.)
arthrodesis. ankle4 M. 67 Chronic in- Arthrodesis, ankle
stahil., ankle
and subtalarjoints
5 F. 21 Open fracts.. Open fracts., ipsilat. Internal fix.: external Osteoarth. and in- Tihiotalo-
ankle and 4th and 5th fix.: latissimus stabil.. ankle and calcanealcalcaneus: metatarsals: soft- dorsi free flap: split- subtalar jointscrush injury. tissue defect, foot thickness skin graft:foot and and ankle resect.. 4th and 5th
ankle raysft M. 36 Open soft- Open fracts.. ipsilat. External fix. Osteoarth., peritalar Pantalar
tissue injury, tibia and femur joints: equinovarus
ankle and deform.foot
7 M. 54 Open fract.. Open fract., ipsilat. External and internal Osteoarth., ankle and Tihiotalo-ankle; crush tibia fix. subtalar joints: calcanealinjury. ankle varus deform..and foot hindfoot
8 M. 55 Closed fract.- Fract., contralat. Internal fix.: arthro- Osteoarth., subtalar Tihiotalo-disloc.. ankle ankle desis, ankle joints calcaneal
9 F. 6() Closed fract.- Secondary avascular Prolonged immobil. Osteoarth., ankle and Tibiotalo-
disloc.. talus necrosis, talus in cast subtalar joints calcaneal10 M. 36 Open fract.- Fracts.. contralat. tibia, Internal fix. Osteoarth.. ankle and Tihiotalo-
disloc., ankle ankle. and calcaneus subtalar joints calcaneal
I I M. 45 Open fract.. Compart. syndrome. External fix.; latissi- Osteoarth., peritalar Pantalarankle: crush ipsilat. leg and foot: mus dorsi free jointsinjury. ankle soft-tissue defect, flap: split-thicknessand foot ankle and foot skin graft: arthro-
desis, ankle12 M. 64 Closed fract.- Internal fix.; arthro-
disloc.. ankle desis. ankle
35 Varus malunion
31 Talonavicular non-
union (successfullyrevised); mar-ginal woundslough
30
34
25
25 Calcaneal malunion
24
29
25 Equinus malunion
41 Equinus malunion
Tihiotalo-
calcaneal
54
‘U) Tibiotalar non.
union (stable andasymptomatic):
equinus malunion28
31
24
24
42 Talonavicular non-union (stable andasymptomatic):sural neuroma
2620 M. 35 Closed fract.- Internal fix.: arthro-disloc.. ankle desis, ankle
Internal fix.
Internal fix. 46
PANTALAR AND TIBIOTALOCALCANEAL ARTHRODESIS FOR POST-TRAUMATIC OSTEOARTHROSIS
TABLE I
1043
talus2 M. 25 Open fract..
ankle
3 M. 24 Open crushinjury. ankleand foot
13 F. 64 Closed pilonfract.
14 F. 42 Open fract.-disloc.. talus
15 F. 6() Open soft-
tissue injury.ankle and
foot16 M. 50 Closed pilon
fract.: soft-tissue injury,
foot
17 M. 35 Closed fract.-disloc., ankle:soft-tissueinjury. foot
18 M.2I Openpilon
fract.
19 M. 30 Open pilonfract.
21 F. 68 Open fract.-disloc.. ankle
Deep post.-compart.syndrome. ipsilat.leg; soft-tissue
defect, foot
Soft-tissue defect.
ankle and foot
External fix.: arthro-desis, ankle
Fract.-disloc.. ipsilat. External fix.Lisfranc joint
Prolonged immobil.in cast: brace
Arthrodesis, ankle
Arthrodesis, ankle
Fracts.. contralat. tibia Internal fix.: rectusand femur: rupture. abdominis freecontralat. Achilles flap: external fix.tendon: compart.syndrome. soft-tissue defect. ipsilat.leg
Fracts., ipsilat. External fix.: arthro-humerus and femur desis, ankle
Osteoarth., subtalar Tihiotalo-joints calcaneal
Non-union after Tihiotalo-arthrodesis of ankle: calcanealosteoarth., subtalarjoints
Osteoarth.. subtalar Tibiotalo-joints calcaneal
Osteoarth.. peritalar Pantalarjoints
Instabil. and osteo-
arth., ankle andsubtalar joints
Osteoarth.. subtalar Pantalarjoints: rigid varusdeform., forefoot
Malunion (equinus) Pantalar
after arthrodesis ofankle; osteoarih..pentalar joints
Rigid equinus varus tibiotalo-deform., ankle and calcanealhindfoot; osteoarth.,subtalar joints
Malunion (equino- Pantalarvarus) after arthro-desis of ankle;osteoarth., subtalarjoints
Non-union afterar- Tihiotalo-throdesis of ankle: calcanealosteoarth., subtalarjoints
Osteoarth.. ankle and Tibiotalo-subtalar joints calcaneal
34
27 Superficial woundinfect.
I
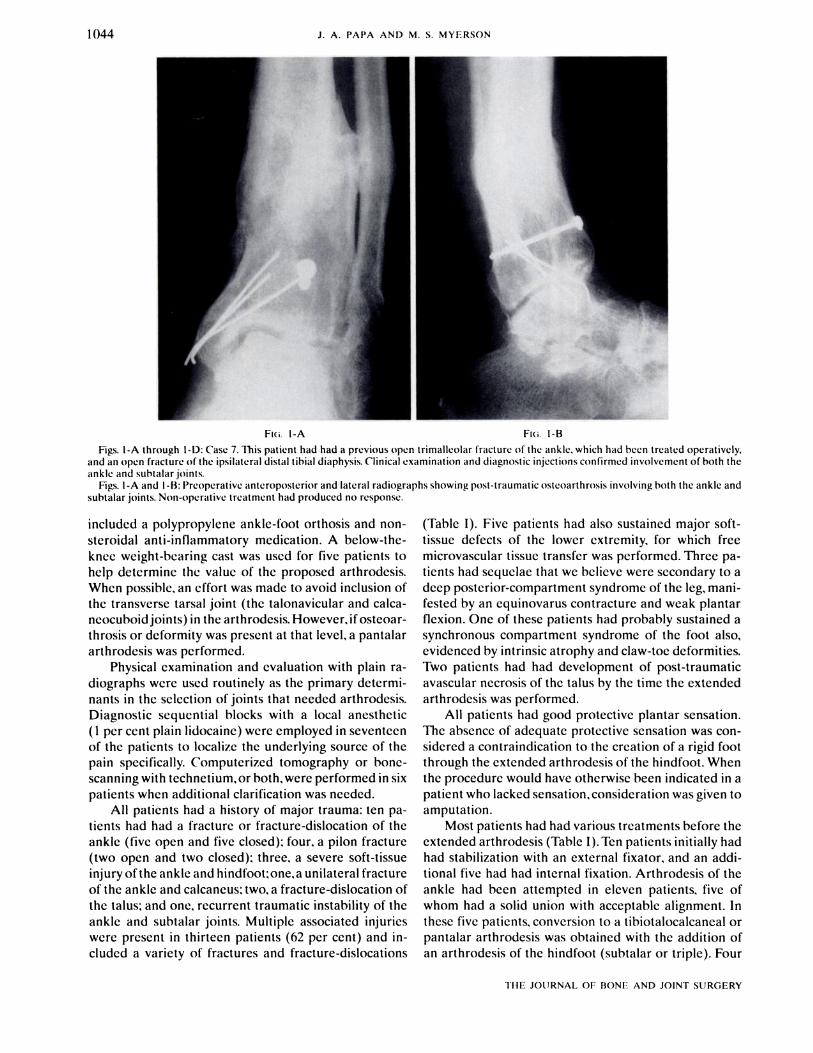
FI;. I-A Fui. 1-B
Figs. I-A through l-D: Case 7. This patient had had a previous O�Cfl trimalleolar fracture of the ankle. which had been treated operatively,
and an open fracture of the ipsilateral distal tihial diaphysis. Clinical examination and diagnostic injections confirmed involvement of both theankle and subtalar joints.
Figs. I-A and 1-B: Preoperative anteroposterior and lateral radiographs showing post-traumatic osteoarthrosis involving both the ankle and
subtalar joints. Non-operative treatment had produced no response.
1044 J. A. PAPA AND M. 5. MYERSON
TIlE JOURNAL OF BONE AND JOINT SURGERY
included a polypropylene ankle-foot orthosis and non-
steroidal anti-inflammatory medication. A below-the-
knee weight-bearing cast was used for five patients to
help determine the value of the proposed arthrodesis.
When possible, an effort was made to avoid inclusion of
the transverse tarsal joint (the talonavicular and calca-
neocuhoidjoints) in the arthrodesis. However. if osteoar-
throsis or deformity was present at that level, a pantalar
arthrodesis was performed.
Physical examination and evaluation with plain ra-
diognaphs were used routinely as the primary determi-
nants in the selection of joints that needed anthrodesis.
Diagnostic sequential blocks with a local anesthetic
( 1 per cent plain lidocaine) were employed in seventeen
of the patients to localize the underlying source of the
pain specifically. Computerized tomography or hone-
scanning with technetium. or both. were performed in six
patients when additional clarification was needed.
All patients had a history of major trauma: ten pa-
tients had had a fracture on fracture-dislocation of the
ankle (five open and five closed): four. a pilon fracture
(two open and two closed): three. a severe soft-tissue
injury ofthe ankle and hindfoot;one,a unilateral fracture
of the ankle and calcaneus: two. a fracture-dislocation of
the talus: and one, recurrent traumatic instability of the
ankle and subtalar joints. Multiple associated injuries
were present in thirteen patients (62 per cent) and in-
cluded a variety of fractures and fracture-dislocations
(Table I). Five patients had also sustained major soft-
tissue defects of the lower extremity. for which free
microvascular tissue transfer was performed. Three pa-
tients had sequelae that we believe were secondary to a
deep posterior-compartment syndrome of the leg, mani-
fested by an equinovarus contracture and weak plantar
flexion. One of these patients had probably sustained a
synchronous compartment syndrome of the foot also,
evidenced by intrinsic atrophy and claw-toe deformities.
Two patients had had development of post-traumatic
avascular necrosis of the talus by the time the extended
anthrodesis was performed.
All patients had good protective plantan sensation.
The absence of adequate protective sensation was con-
sidered a contraindication to the creation of a rigid foot
through the extended arthrodesis of the hindfoot. When
the procedure would have otherwise been indicated in a
patient who lacked sensation. consideration was given to
amputation.
Most patients had had various treatments before the
extended anthrodesis (Table I).Ten patients initially had
had stabilization with an external fixator. and an addi-
tional five had had internal fixation. Arthnodesis of the
ankle had been attempted in eleven patients, five of
whom had a solid union with acceptable alignment. In
these five patients, conversion to a tibiotalocalcaneal on
pantalar arthrodesis was obtained with the addition of
an arthrodesis of the hindfoot (subtalan or triple). Four
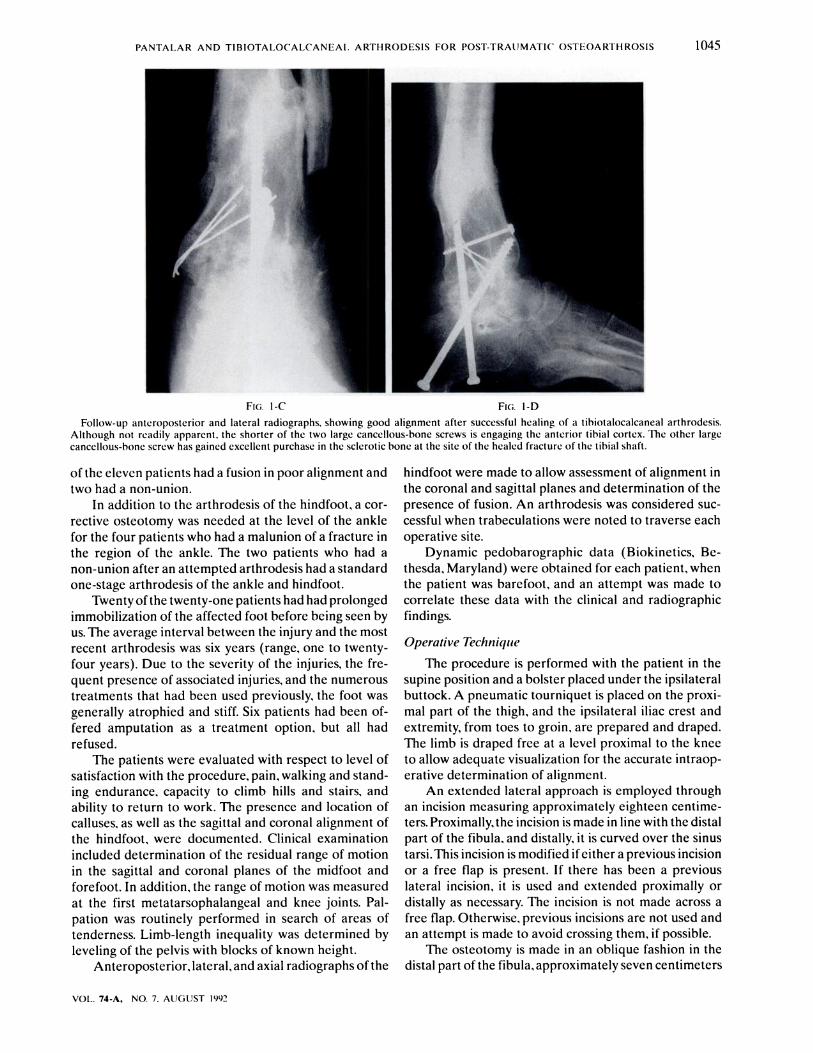
FIG. I-C Fl;. 1-D
Follow-up anteroposterior and lateral radiographs, showing good alignment after successful healing of a tihiotalocalcaneal arthrodesis.
Although not readily apparent. the shorter of the two large cancellous-bone screws is engaging the anterior tihial cortex. The other large
cancellous-bone screw has gained excellent purchase in the sclerotic hone at the site of the healed fracture of the tihial shaft.
PANTALAR AND TIBIOTALOCALCANEA1. ARTHRODESIS FOR POST-TRAUMATIC OSTEOARTHROSIS 1045
VOL. 74-A, NO. 7. AUGUST 1992
of the eleven patients had a fusion in poor alignment and
two had a non-union.
In addition to the arthrodesis of the hindfoot, a con-
rective osteotomy was needed at the level of the ankle
for the four patients who had a malunion of a fracture in
the region of the ankle. The two patients who had a
non-union after an attempted arthrodesis had a standard
one-stage anthrodesis of the ankle and hindfoot.
Twenty of the twenty-one patients had had prolonged
immobilization of the affected foot before being seen by
us. The average interval between the injury and the most
recent anthrodesis was six years (range, one to twenty-
four years). Due to the severity of the injuries, the fre-
quent presence of associated injuries, and the numerous
treatments that had been used previously, the foot was
generally atrophied and stiff. Six patients had been of-
fered amputation as a treatment option. but all had
refused.
The patients were evaluated with respect to level of
satisfaction with the procedure, pain. walking and stand-
ing endurance, capacity to climb hills and stairs. and
ability to return to work. The presence and location of
calluses, as well as the sagittal and coronal alignment of
the hindfoot, were documented. Clinical examination
included determination of the residual range of motion
in the sagittal and coronal planes of the midfoot and
forefoot. In addition, the range of motion was measured
at the first metatarsophalangeal and knee joints. Pal-
pation was routinely performed in search of areas of
tenderness. Limb-length inequality was determined by
leveling of the pelvis with blocks of known height.
Anteropostenior. lateral, and axial radiographs of the
hindfoot were made to allow assessment of alignment in
the coronal and sagittal planes and determination of the
presence of fusion. An arthnodesis was considered sue-
cessful when tnabeculations were noted to traverse each
operative site.
Dynamic pedobanognaphic data (Biokinetics, Be-
thesda, Maryland) were obtained for each patient, when
the patient was barefoot, and an attempt was made to
correlate these data with the clinical and radiographic
findings.
Operative Technique
The procedure is performed with the patient in the
supine position and a bolster placed under the ipsilateral
buttock. A pneumatic tourniquet is placed on the proxi-
mal part of the thigh. and the ipsilateral iliac crest and
extremity, from toes to groin, are prepared and draped.
The limb is draped free at a level proximal to the knee
to allow adequate visualization for the accurate intnaop-
erative determination of alignment.
An extended lateral approach is employed through
an incision measuring approximately eighteen centime-
tens. Proximally.the incision is made in line with the distal
part of the fibula, and distally. it is curved over the sinus
tansi.This incision is modified ifeithen a previous incision
or a free flap is present. If there has been a previous
lateral incision, it is used and extended proximally or
distally as necessary. The incision is not made across a
free flap. Otherwise, previous incisions are not used and
an attempt is made to avoid crossing them, if possible.
The osteotomy is made in an oblique fashion in the
distal pant of the fibula, approximately seven centimeters

1046 J. A. PAPA AND M. S. MYERSON
TIlE JOURNAL OF BONE AND JOINT SURGERY
proximal to its tip. with an oscillating saw. That portion
of the fibula is then removed. A second incision is made
anteromedially. directly over the medial malleolus for a
tibiotalocalcaneal arthnodesis and slightly anterior to the
medial malleolus, with extension distally over the dorsal
aspect of the talonavicular joint, for a pantalan arthno-
desis. The medial malleolus is removed after osteotomy
is performed obliquely with a chisel. The tibiotalan antic-
ular surfaces are removed with an oscillating saw held
perpendicular to the long axis of the tibia, with cane being
taken to preserve as much bone stock as possible. Sharp
chisels are used to remove all articulan cartilage from the
subtalar joints and, when appropriate, from the tab-
naviculan and calcaneocuboid joints.
Because most patients who have this type of salvage
procedure have underlying deformities of the foot, an in
situ arthrodesis is rarely performed. Therefore, wedges
are removed, as necessary, to allow connection of deform-
ities in an effort to obtain a plantigrade foot. An equino-
varus deformity is corrected with a dorsolatenal biplane
wedge resection. preferably from the apex of the defon-
mity. which is typically at the level of the subtalar joint.
Final alignment of the hindfoot in 0 to 5 degrees of valgus,
0 to 5 degrees of calcaneus, external rotation equal to that
of the contralateral side, and one-half to one centimeter
of posterior translation of the talus under the tibia is
sought. The effects of wedge resection of the hindfoot on
the positions of the midfoot and forefoot are closely
monitored. In the absence of a supple midfoot and fore-
foot, correction of deformities of the hindfoot frequently
necessitates rotational correction and arthnodesis at the
level of the transverse tarsal joint.
Initial fixation is obtained with 2.0-millimeter guide-
pins. and the position is checked with intraoperative
radiographs to verify the alignment and placement of the
wires. An autogenous graft composed ofcancellous bone
always is packed into available spaces before final in-
ternal fixation is achieved with 7.0-millimeter, partially
threaded, cannulated cancelbous-bone screws (Synthes
USA. Monument, Colorado). Adequate cancellous bone
is usually obtained from the removed malleoli. Occasion-
ally. the malleoli do not provide sufficient cancelbous
bone for the graft. and in such instances, additional can-
cellous bone is obtained from the anterior iliac crest.
Two screws are inserted through separate stab mci-
sions in the skin and directed from posterior and distal
to anterior and proximal, passing through the calcaneus
and the body of the talus and into the distal part of the
tibia. An attempt is made to gain purchase, with at least
one screw, on the anterior tibial cortex. An additional
screw is occasionally placed from the distal pant of the
tibia into the calcaneus (Figs. 1-A through 1-D). Excel-
lent compression usually is obtained across the operative
sites in both the ankle and subtalar joints. A pantalar
arthrodesis also includes fixation of the operative sites in
the talonavicubar and calcaneocuboid joints with screws
or power staples.
The wounds are then closed in layers oven suction
drains, and a bulky dressing, reinforced with posterior
and u-shaped plaster splints, is applied. The drains are
removed at twenty-four to forty-eight hours. The patient
is usually discharged from the hospital by the third or
fourth postoperative day.
At ten to fourteen days postoperatively, the beg is
placed in a non-weight-bearing below-the-knee fiber-
glass cast. Six weeks postoperatively. weight-beaning is
begun in a below-the-knee weight-beaning cast. Changes
of the cast, clinical evaluation, and radiographic exami-
nation are performed at approximately three to four-
week intervals until union. The patient is then allowed to
walk as tolerated, wearing a shoe with a cushioned heel
and rocker sole. A shoe-lift is used to compensate for
leg-length inequality. The lift is selectedso that the side
that was operated on will remain approximately 0.5 cen-
timeter shorter than the contralateral side.
Results
The twenty-one patients were followed for an aver-
age of thirty-two months (range, twenty-four to fifty-four
months) after the operation. Seventeen patients (81 pen
cent) reported that they were much improved after the
operation. Twenty patients (95 pen cent) noted some pain
with walking; this varied in severity and threshold. Re-
sidual pain was generally described as mild, intermittent,
and not incapacitating. Of the twenty patients who had
pain, six (30 per cent) did not use any medication for it.
Eleven patients (55 pen cent) took non-narcotic analge-
sic medication occasionally and rarely or never had pain
at rest. Two patients (10 per cent) reported daily use of
a short-acting non-steroidal anti-inflammatory medica-
tion. One patient used a narcotic analgesic persistently,
although intermittently.
The patients’ standing endurance at the most recent
follow-up averaged three hours (range, one-half hour to
eight hours), and the mean walking endurance was nine-
teen blocks (range. three to forty-five blocks), compared
with the preoperative values of fifteen minutes (maxi-
mum, one hour) and one and one-half blocks (range,
one-half to three blocks). All patients reported some
difficulty on uneven ground or when ascending or de-
scending a hill. Most patients compensated for the lost
motion with external rotation of the limb to negotiate
inclines. Two patients reported going up and down hills
in a sideways fashion.
No patient used a cane, crutches, or a walker because
of the foot. One patient, who was seventy-two years old
at the latest follow-up. had unrelated low-back pain and
stated that she often used a cane to minimize the risk of
falling. All but two patients had some difficulty with
climbing and descending stairs; eighteen used a banister
if one was available, and ten negotiated one step at a time.
No patient could run effectively.
In general, the patients were found to benefit subjec-
tively from modifications in shoe-wean. Optimum results

PANTALAR AND TIBIOTALOCALCANEAL ARTHRODESIS FOR POST-TRAtJMATIC OSTEOARTHROSIS 1047
VOL. 74-A, NO. 7. AUGUST 1992
were noted with a combination of a cushioned heel, a
tapered rocker-sole, and an appropriate heel-and-sole
lift. In addition, soft, accommodating onthotic inserts
were helpful for several patients who had well localized
problems of the forefoot.
At the latest follow-up examination, all patients had
an excellent range of motion of the ipsilateral knee
(average flexion, 132 degrees and average extension.
0 degree) without recurvatum, except for one patient
who had sustained severe intra-articular trauma to the
ipsilateral knee at the time of the original injury. This
knee lacked 13 degrees of full extension and flexed
to only 70 degrees. Motion of the metatarsophalangeal
joint of the ipsilateral great toe was frequently noted
to be limited, with mean dorsiflexion of only 34 degrees
(range, 20 to 76 degrees). The remaining motion of the
mid-tarsal joints (joints between the metatarsophalan-
geal and transverse tarsal joints) and of the transverse
tarsal joint (if fusion had not occurred) of the involved
foot averaged 1 1 degrees in the sagittal plane (range, 5 to
25 degrees) and 5 degrees in the coronal plane (range,
0 to 12 degrees).
No clinically notable rotational malunions were seen.
Each involved foot was found to be in external rotation,
within 5 degrees of the angle on the contralatenal side.
Alignment in the sagittal plane was best determined
nadiographically; the mean alignment, as measured by
the angle subtended by the long axis of the tibia and
the plantar plane of support of the foot during weight-
bearing, was 1 degree of calcaneus (range, 6 degrees of
equinus to 8 degrees of calcaneus). Alignment in the
coronal plane was measured clinically; the mean align-
ment was 1 degree of valgus (range, 5 degrees of vanus to
5 degrees of valgus).
The mean amount of shortening of the ipsilateral leg
was 1.5 centimeters (range, 1.0 to 2.5 centimeters).
A solid union was noted clinically and radiognaphi-
cally at a mean of fourteen weeks (range, eight to twenty-
four weeks) postoperatively in eighteen (86 per cent) of
the twenty-one patients. There were three non-unions,
two involving the tabonaviculan articulation and the
other, the tibiotalar joint. Failure occurred, therefore,
in only S per cent of the fifty-eight fusion sites. Neither
of the two patients who had avascular necrosis of the
talus had a non-union. One of the patients who had a
tabonaviculan non-union was symptomatic, and a success-
ful revision operation was performed with an autoge-
nous bone graft from the iliac crest. This patient had
sustained a crush injury to the foot, with loss of skin, and
the dorsomedial portion of the midfoot was relatively
avascular. The remaining two patients who had a non-
union were clinically stable and asymptomatic with ne-
spect to those sites.
Ten mild. asymptomatic plantar calluses were noted
in seven of the patients. The calluses were under the
interphalangeal joint of the great toe in three patients;
under the first, second, and third metatarsal heads in
two patients each: and under the second metatarsal head
in one.
Return to work was achieved by eleven of the seven-
teen patients who had not yet retired. Of these seventeen
patients. five were involved in Workers’ Compensation
cases and one, in ongoing litigation; only one of those six
had returned to work. Of the eleven patients who were
not involved in litigation or a Workers’ Compensation
case, only one did not return to work. That patient had
remained out of work due to an ongoing problem with
the ipsilateral knee,which was treated operatively twelve
months after the pantalar anthrodesis. He was receiving
therapy for the knee at the latest follow-up and was
expected to return to work within three months.
The pedobarographic investigation confirmed clini-
cal impressions derived from the evaluation of alignment
of the hindfoot, the flexibility of the midfoot. and the
range of motion of the metatarsophalangeal joint of the
great toe.
One patient, who was noted, clinically and radio-
graphically. to have 5 degrees of varus of the hindfoot
with a fused but incompletely pronated transtarsal joint,
was found to have increased pressure of prolonged du-
ration under the fifth metatarsal head. Five patients who
had a markedly restricted range of motion (30 degrees
or less) of the metatarsophalangeal joint of the great toe
had abnormally high pressures in the region of the distal
pant of the great toe. This finding was accentuated in
the subset of patients who also had a limited range of
motion ofthe mid-tarsaljoint in the sagittal plane. All ten
sites that had plantan calluses had corresponding evi-
dence of prolonged increases in local pressure. recorded
pedobanognaphically.
Complications
There was one superficial wound infection hut no
deep wound infections (Table I). One patient had a
minor wound slough, which healed after d#{233}hnidement in
the office. Non-union occurred in three patients, at one
site each (two. at the talonavicular joint and one. at the
ankle). Three patients had a malunion in 2 to 4 degrees
ofequinus:one patient,in 8 degrees ofcalcaneus:and one
patient, in 5 degrees of varus. In one patient. a sural
neuroma developed; this was excised, and the stump of
the nerve was transposed into the peroneus brevis mus-
dc. Calluses were frequently associated with malunion,
but no patient had a plantar ulcer. We attribute the lack
of ulceration largely to the fact that all patients had
normal plantan sensation.
Discussion
Staging of pantalar arthrodesis has been advocated
by numerous authors who have believed that a one-stage
procedure is associated with an increased prevalence
of avascular necrosis, malunion, non-union, and wound
problems’52’22. Avascular necrosis has been reported in
close association with arthnodesis of the hindfoof’�2.

1048 j. A. PAPA AND M. S. MYERSON
THE JOURNAL OF BONE AND JOINT SURGERY
This complication. however. was not found in our pa-
tients. and probably it is relevant clinically only when
techniques associated with the temporary removal of the
talus are employed, such as that originally described by
Lorthioir.
Non-union is a frequent complication of extended
arthrodesis of the hindfoot. with reported pnevalences of
0 to 28 per cent (mean. 15 per cent)�4’’5272t7.The ankle
has been the most frequently reported site of pseudar-
thnosis,folbowed by the talonavicularjoint. In the current
series. three patients (14 per cent) had a non-union: one.
at the ankle.and the other two,at the tabonaviculan joint.
If the total number of sites of attempted arthnodesis
is considered. failure of healing was noted in only three
(5 per cent) of fifty-eight sites. It has been our impression
that. when using lag-screw fixation. superior purchase
with increased compression is achieved by crossing both
the talocalcanealjoint and the tibiotalar joint. compared
with crossing either joint alone. This is particularly cvi-
dent when one or both of the two screws engages the
anterior tihial cortex.
Theonetically. the prevalence of wound problems,
including infection. would be expected to he higher with
the more extensive single-stage arthrodesis than with
the two-stage procedure. This might be anticipated if
there was marked deformity that needed correction. In
the current series. there was one superficial and no deep
wound infection. The superficial infection responded
rapidly to standard measures. including local care of the
wound and a short course of a broad-spectrum antibiotic.
One minor wound slough was noted at the postero-
inferior aspect of the incision: it resolved readily with
routine care of the wound. This I 0 per cent prevalence of
local wound problems compares favorably with the rates
reported previously for extensive on isolated arthrodesis
of the hindfoot’�’222�.
The technical demands of a single-stage pantalar or
tibiotalocalcaneal arthnodesis are great. Unlike an iso-
lated anthrodesis of the ankle or hindfoot. after which
motion of either the subtalar joints on the ankle is possi-
ble. an extended anthrodesis eliminates all local compen-
satory motion except minimum residual motion in the
midfoot and forefoot. Therefore, when performing these
extensive procedures. the need to obtain precise final
alignment in multiple planes is critical.
Despite meticulous attention to detail. there were
five malunions (four in the sagittal plane and one in the
coronal plane) in this series. Three patients had fusion in
mild equinus ranging from 2 to 4 degrees. Although.
subjectively. these three patients did not differ markedly
from the other eighteen patients at the latest follow-up.
none had yet returned to work. and two of the three had
greatly increased peak pressures ofthe forefoot on pedo-
barographic analysis. Because dynamic gait analysis was
not performed as part of this study. and no gross devia-
tion in observable gait was noted in these three patients.
no specific data regarding subtle alterations in gait can
be provided. We believe that an equinus position will
lead to increased loading of the forefoot and, possibly, to
metatarsalgia. In addition, equinus may be associated
with an awkward gait and the possible development of
genu recurvatum. Therefore. we think that no attempt
should be made to compensate for leg-length inequality
by placement of the foot in an equinus position: rather, a
shoe-lift should be employed for this purpose. One pa-
tient had fusion in 8 degrees of calcaneus but did not
complain of pain in the heel. On the basis of this series,
as much as 8 degrees of mild calcaneus is well tolerated.
without the development of pain in the heel.
Malunion in the coronal plane was observed in one
patient who had had a pantalar arthrodesis and in whom
the hindfoot was fused in 5 degrees of varus. Pronation
at the site of the transverse tarsal arthrodesis provided
partial compensation: the patient returned to demanding
work in a warehouse and was quite satisfied with the
result of the operation. He did, however. have formation
of a mild callus under the fifth metatarsal head, as well
as pedobarographic evidence of increased pressures in
the lateral part of the forefoot. Therefore. when a true
pantalar arthrodesis is performed, care must be taken to
position the midfoot and forefoot appropriately in the
coronal plane. in order to obtain a plantigrade foot. This
is particularly true for patients who have minimum mo-
tion of the forefoot and little ability to compensate for
the fusion of the hindfoot during toe-off.
No rotational malunions were observed in this series.
We believe that avoidance of internal rotation combined
with mild posterior subluxation of the talus on the tibia
will enhance gait by minimizing the length of the rela-
tively rigid appendage. which must be stepped oven.
When indicated, it appears that the transverse tarsal
joint should be spared arthrodesis. Patients who had had
a tihiotabocalcaneal arthnodesis maintained greater aver-
age motion in the sagittal and coronal planes than those
who had had a pantalar arthrodesis (13 and 6 degrees,
compared with 7 and 3 degrees). These differences were
significant when they were analyzed with an unpaired
Student t test (p < 0.008 and p < 0.025). The over-all
degree of motion at the latest follow-up, however, was
less than half of what would be expected in normal feet
that had had a similar procedure, according to labo-
ratory data reported by Gellman et a!. These findings
are. nonetheless, not surprising. considering that most
of our patients had sustained severe injuries and many
had had multiple operations and prolonged immobili-
zation. Even if it is minimum, residual range of motion
does provide some functional compensatory ability and,
therefore, should be preserved if it is not painful. No
severe degenerative changes were noted in the thirteen
patients who had had preservation of the transverse
tarsal joint (a tibiotalocalcaneal arthrodesis), at an aver-
age follow-up of thirty-two months (range. twenty-four
to fifty-four months).
All but one of the patients in this study reported

PANTALAR AND TIBIOTALOCALCANEAL ARTHRODESIS FOR POST.TRAt MATIC OSTEOARTII ROSIS 1049
VOL. 74-A, NO. 7. AtJGtJST 1992
some persistent pain in the affected foot at the most
recent follow-up. Residual pain was generally described
as mild, intermittent, and not incapacitating. Although
most patients were very satisfied with the result of the
operation and had marked improvement in the oven-all
level of function, the effects of the initial trauma, pre-
vious operations. and prolonged immobilization proba-
bly were responsible for the persistent symptoms.
In summary, although extended arthnodesis of the
ankle and hindfoot in patients who have post-traumatic
osteoarthrosis usually provides an effective alternative
to amputation. it should be regarded as a salvage proce-
dune. It is a complex. technically demanding operation in
which attainment of precise final alignment is critical.
The described single-stage technique. employing a trans-
fibular extended lateral approach with an autogenous
bone graft and rigid internal fixation. provided satis-
factory results. with most of the patients who had not
yet retired being able to return to work. The decision
between extended arthrodesis or amputation must he
guided. in part. by the wishes of the individual patient
and the philosophy of the treating physician. It is hoped
that the results reported here will help with this often-
difficult decision.
References
1. Ansart, M. B.: Pan-arthrodesis for paralytic flail foot.J. Bone andJoint Surg.. 33-B(4): 503-507. 1951.
2. Baker, G. C. W., and Stableforth, P. G.: Syme’s amputation. A review of sixty-seven cases. J. Bone andJouit Siirg.. 5l-B(3): 482-487. 1969.
3. Barrett, C. R.; Meyer, L. C.; Bray, E. W., Ill; Taylor, R. G.,Jr.; and Koib, F. J.: Pantalar arthrodesis: a long-term follow-up. hotu,ulflnkle,
1:279-283, 1981.
4. Bingold, A. C.: Ankle and subtalar fusion by a transarticular graft. J. Bone and Joint Siirg., 38-B(4): 862-870. 1956.
5. Blair, H. C.: Comminuted fractures and fracture dislocations of the body of the astragalus. Operative treatment. Am. J. Siirg.. 59: 37-
43. 1943.
6. Danan, J. P., and Tomeno, B.: Panarthrod#{232}se de l’arri#{232}re-pied. Technique. tolerance Ct r#{235}sultats lointains de Ia triple arthrod�sc. Rev. hir.
orthop., 65: 433-439, 1979.
7. Fleurant, F W., and Alexander,Justin: Below knee amputation and rehabilitation of amputees. Surg.. Gvnee. ullil ()hstet.. 151: 41-44. 1980.
8. Cellman, Harris; Lenihan, Michael; Halikis, Nick; Botte, M. J.; Giordani, Mauro; and Perry, Jacquelin: Selective tarsal arthrodesis: an in
vitro analysis of the effect on foot motion. Foot and Ankle. 8: 127-133. 1987.
9. Hamsa, W. R.: Panastragaloid arthrodesis. A study of end results in eighty-five cases. J. Bone (111(1 Joint .ciug.. 18: 732-736. July 1936.
10. Hornby, Roger,and Harris,W.R.:Syme’samputation.Follow-upstudyofweight-hearing in sixty-eight patients.J. Bone and Joint Surg..
57-A: 346-349, April 1975.
I I . Huang, C.-T.; Jackson, J. R.; Moore, N. B.; Fine, P. R.; Kuhlemeier, K. V.; Traugh, C. H.; and Saunders. P. T.: Amputation: energy cost of
ambulation. Arch. Phvs. Med. and Re/iab., 60: 18-24, 1979.
12. Hunt, W. S., Jr., and Thompson, H. A.: Pantalar arthrodesis. A one-stage operation. J. Bone and Joint Siug.. 36-A: 349-361). April 1954.
13. Kegel, Bernice; Carpenter, M. L.; and Burgess, E. M.: Functional capabilities of lower extremity amputees. Arc/i. P/n’s. Med. and Re/lab.
59: 109-120, 1978.
14. Kivilaakso, R.; Langenski#{246}ld, A.; and Sal#{233}nius, P.: Results of talocruralarthrodesis and pantalar arthrodesis of the ankle joint in post-
traumatic conditions labstracti. Acta Orthop. Scandinavica, 36: 339-340, 1965.
15. Liebolt, F. L.: Pantalar arthrodesis in poliomyelitis. Surgery, 6: 31-34, 1939.16. Lorthioir,J.: Huit cas d’arthrod#{232}se du pied avec extirpation temporaire de Uastragale.J. c/iir. unit. -- Soc. BeIge c/hr.. II: 18-1-187. 191 1.
17. McElwain, J. P.; Hunter, G. A.; and English, E.: Syme’s amputation in adults: a long-term review. Canadian J. Surg.. 28: 203-205. 1985.
18. Malone,J. M.; Moore,Wesley; Leal,J. M.;and Childers,S.J.: Rehabilitation forlower extremity amputation. Arc/i. Surg.. I 16: 93-98. 1981.
19. Marek, F. M., and Schein, A. J.: Aseptic necrosis of the astragalus following arthrodesing procedures of the tarsus. J. Born’ an(/Joint Surg..
27: 587-594. Oct. 1945.
20. Mazur, J. M.; Schwartz, Evan; and Simon, S. R.: Ankle arthrodesis. Long-term follow-up with gait analysis. J. Bone (111(1 Joint .curg.. 61 -A:
964-975, Oct. 1979.
21 . Ouzounian, T. J., and Kleiger, Barnard: Arthrodesis in the foot and ankle. In Disorders of the Foot and Ankle. Medical and Surgical
Management, edited by M. H. Jahss. Ed. 2, vol. 3. pp. 2614-2646. Philadelphia. W. B. Saunders. 1991.
22. Patterson, R. L., Jr.; Parrish, F. F.; and Hathaway, E. N.: Stabilizing operations of the foot. A study of the indications. techniques used. and
end results. J. Bone andJoint Stag., 32-A: 1-26, Jan. 1950.23. Russotti, 6. M.; Johnson, K. A.; and Cass, J. R.: Tihiotalocalcaneal arthrodesis for arthritis and deformity of the hind part of the foot.
J. Bone alidioilit Surg., 70-A: 1304-1307. Oct. 1988.
24. Staples, 0. 5.: Posterior arthrodesis of the ankle and subtalar joints. I Bone andJoint Surg., 38-A: 50-58. Jan. 1956.
25. Steindler, Arthur The treatment of the flail ankle; pan-astragaloid arthrodesis. J. Bone and Joint Surg., 5: 284-293. April 1923.
26. Waters, R. L.; Perry, Jacquelin; Antonelli, Daniel; and Hislop, Helen: Energy cost of walking of amputees: the influence of le�el of
amputation. J. Bone and Joint Surg., 58-A: 42-46, Jan. 1976.
27. Waugh, T. R.; Wagner, Jay; and Stinchileld, F. E.: An evaluation of pantalar arthrodesis. A follow-up study of one hundred atid sixteen
operations.J. Bone andfoint Surg., 47-A: 1315-1321,Oct. 1965.
Related Documents











