Palliative care Ammar Tarik SpR Diabetes and Endocrinology

Palliative care
Jan 04, 2016
Palliative care. Ammar Tarik SpR Diabetes and Endocrinology. Introduction There are currently over 2.3 million people with diabetes in the UK and there are more than half a million people with diabetes who have the condition and don’t know it. 85-90% of Diabetic patients are Type 2 - PowerPoint PPT Presentation
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Palliative care
Ammar Tarik
SpR Diabetes and Endocrinology

• Introduction• There are currently over 2.3 million people with
diabetes in the UK and there are more than half a million people with diabetes who have the condition and don’t know it.
• 85-90% of Diabetic patients are Type 2• The body resisting the action of the insulin or the
pancreas fails at later stages to produce insulin• 10 to 20% of acute trust beds occupied by a
patient with diabetes

Symptoms of DM
• Increased thirst • Polyuria• Tiredness• Blurred vision• Unexplained weight loss• Genital itching or regular episodes of thrush • Feeling generally unwell/poor concentration• Nocturia / incontinence in the elderly• Asymptomatic (( routine check up))

• To make a diagnosis of diabetes patients must have:
• Symptoms plus one abnormal blood test i.e. FPG≥ 7.0 mmol/L or random ≥ 11mmol/L
• Asymptomatic patient requires 2 abnormal blood tests on separate occasions i.e. a FPG ≥ 7.0 mmol/L on two occasions OR a random plasma glucose ≥11 mmol/L on two occasions OR one of each

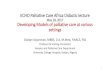
Incretins and glycaemic control7,8
Adapted from 7. Drucker DJ. Cell Metab. 2006;3:153–165. 8. Miller S, St Onge EL. Ann Pharmacother 2006;40:1336-1343.
Active GLP-1 and
GIP
Release of incretin gut hormones
Pancreas
Bloodglucose control
GI tract
Glucagon from alpha cells
(GLP-1)Glucose
dependent
Alpha cells
Increased insulin and decreasedglucagon reduce hepatic glucose output
Glucose dependent Insulin
from beta cells(GLP-1 and GIP)
Beta cells
Insulinincreases peripheral glucose uptake
Ingestion of food
DPP-4enzyme rapidly
degrades
incretins


• GLP-1 mimetic (Exenatide)• HbA1c > 7.5 and their BMI >35kg/m2• Reduce appetite, slow gastric emptying
weight reduction • BD, sc injection• Does not cause hypoglycaemia • Nausea, Pancreatitis • Liraglutide, Exenatide LAR

• DPP-4 Inhibitor: Sitagliptin/ Vildagliptin• Once daily • Minor risk of Hypoglycaemia• No GI side effect• Weight neutral• Oral dosing• Approved for monotherapy , or use with
metformin or sulphonylurea

• http://www.nice.org.uk/nicemedia/live/12165/44322/44322.pdf



• Premixed combinations of short and intermediate acting analogues
• 3 different combinations• (25, 30, 50)• Onset 10 - 20 minutes• Peak 1 - 4 hours• Duration of action up to 24 hours
• Long acting ( Basal Insulin) provides gentle continuous supply of insulin even during sleep
• Onset 4h, Peak 6-18, Duration said to be 24hr acting ( 18-20 more likely)
• e.g. Glargin (Lantus), Levemir (Detemir)

• - Four injections (Basal Bolus)
• Basal ( background) • • Bolus , three times
before each meal, quick response to reduce blood sugar after once , before bed, slowly absorbed over 24hour period each meal
• Flexible ( vary doses with meal)/exercise , less problems with hypos and weight gain
Basal insulin(Lantus)

• A patient with a background of Ca lung and type 2 diabetes who is usually on Humalog mix 25 60 units BD and Metformin 500 mg BD is admitted with sepsis.blood glucose levels in the first 24 hours are 16.7, 21.1 and 18.8. A suitable strategy to treat the raised blood glucose levels in this patient is
• A. Intravenous insulin infusion• B. Increase in their usual insulin dose• C. 4 units of Actrapid immediately• D. Increase in the dose of Metformin

• Short acting insulin is not a sufficient strategy• - Do not use IV insulin to “stabilise” glucose control, only
in special circumstances.• Start making the insulin dose adjustment
( increase it by 10-20%)
• Do not react to one off high/low sugar readings • Consider what might have caused the problem• Look for trends and adjust insulin prior to problem time

Steroids induced Hyperglycaemia
• new onset hyperglycaemia or worsening pre-existing Diabetic control, may cause DKA or HHS.
• duration of the treatment, dose of steroids• Glucocorticoid-induced diabetes improves with reduction in the dose
of glucocorticoid and, over many months, it may fully reverse when the medication is stopped
• To start with we need a potent and quick acting antidiabetic agents e.g. Sulphanylurea
• Basal insulin Humilin I or Glargine• OR• If they are already diabetic • Hyperglycaemia associated with steroids usual occurs acutely
which requires proactive measures, often insulin. Or further early adjustment of insulin

Insulin Pump• Accurate, continuous, controlled
delivery of Insulin in Pulses.( Regulated by the patient)
• Type 1 only, multiple injections failed
• Patients were carefully trying to keep blood sugar to the recommended level
• Without having disabling hypos (repeated and unpredicted)
• Trained specialist team
Related Documents