Painful Diabetic Neuropathy is More than Pain Alone: Examining the Role of Anxiety and Depression as Mediators and Complicators Rakesh Jain & Shailesh Jain & Charles L. Raison & Vladimir Maletic Published online: 25 May 2011 # Springer Science+Business Media, LLC 2011 Abstract A wealth of information exists regarding the plight of patients suffering with diabetic peripheral neuro- pathic pain (DPNP). Although physical pain is certainly a primary challenge in the management of this condition, disorders associated with emotional pain—especially de- pression and anxiety—also greatly complicate the clini- cian’s efforts to attain optimal outcomes for DPNP patients. This article reviews the high rate of comorbidity between DPNP and depression/anxiety with a focus on why this pattern of comorbidity exists and what can be done about it. To accomplish this, the many physiologic similarities between neuropathic pain and depression/anxiety are reviewed as a basis for better understanding how, and why, optimal treatment strategies use behavioral and pharmacologic modalities known to improve both physical pain and symptoms of depression and anxiety. We conclude by highlighting that screening, diagnosing, and optimally treating comorbid depression/anxiety not only improves quality of life, these but also positively impacts DPNP pain. Keywords Diabetes mellitus . Diabetic peripheral neuropathic pain (DPNP) . Major depression . Depressive symptoms . Anxiety . Prevalence . Inflammation . Peripheral nerves . Central sensitization . Kindling . Serotonin reuptake inhibitors . Serotonin-norepinephrine reuptake inhibitors . Duloxetine . Pregabalin . α-2-δ ligands . Tricyclic antidepressants . Psychotherapy, Cognitive behavior l therapy . Screening instruments Introduction In the past few months, the appearance of articles with a title such as “Diabetes and depression – a risky combina- tion” [1] have alerted clinicians to the nefarious relation- ship that exists between psychiatric illnesses and diabetes. Depression/anxiety and diabetes will surely rank among the defining epidemics of the 21st century, given the current explosion in the prevalence rates of both conditions in both the developed and developing worlds. A collision between such highly prevalent disorders is to be expected; yet it R. Jain Department of Psychiatry, Texas Tech Health Sciences Center Medical School at Permian Basin, Midland, TX, USA S. Jain Department of Psychiatry, Texas Tech Health Sciences Center Medical School at Permian Basin, 301 North N. Street, Midland, TX 79701, USA e-mail: [email protected] C. L. Raison Department of Psychiatry and Behavioral Sciences, Emory University School of Medicine, 1365B Clifton Road, Room 51003, Atlanta, GA 30322, USA e-mail: [email protected] V. Maletic Department of Neuropsychiatry and Behavioral Sciences, University of South Carolina School of Medicine, Columbia, SC, USA e-mail: [email protected] R. Jain (*) 129 Circle Way, Suite 110, Lake Jackson, TX 77566, USA e-mail: [email protected] Present Address: V. Maletic 38 Parkway Commons Way, Greer, SC 29650, USA Curr Diab Rep (2011) 11:275–284 DOI 10.1007/s11892-011-0202-2

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Painful Diabetic Neuropathy is More than Pain Alone:Examining the Role of Anxiety and Depression as Mediatorsand Complicators
Rakesh Jain & Shailesh Jain & Charles L. Raison &
Vladimir Maletic
Published online: 25 May 2011# Springer Science+Business Media, LLC 2011
Abstract A wealth of information exists regarding theplight of patients suffering with diabetic peripheral neuro-pathic pain (DPNP). Although physical pain is certainly aprimary challenge in the management of this condition,disorders associated with emotional pain—especially de-pression and anxiety—also greatly complicate the clini-
cian’s efforts to attain optimal outcomes for DPNP patients.This article reviews the high rate of comorbidity betweenDPNP and depression/anxiety with a focus on why thispattern of comorbidity exists and what can be done about it.To accomplish this, the many physiologic similaritiesbetween neuropathic pain and depression/anxiety arereviewed as a basis for better understanding how, andwhy, optimal treatment strategies use behavioral andpharmacologic modalities known to improve both physicalpain and symptoms of depression and anxiety. We concludeby highlighting that screening, diagnosing, and optimallytreating comorbid depression/anxiety not only improvesquality of life, these but also positively impacts DPNP pain.
Keywords Diabetes mellitus . Diabetic peripheralneuropathic pain (DPNP) .Major depression . Depressivesymptoms . Anxiety . Prevalence . Inflammation . Peripheralnerves . Central sensitization . Kindling . Serotonin reuptakeinhibitors . Serotonin-norepinephrine reuptake inhibitors .
Duloxetine . Pregabalin .α-2-δ ligands . Tricyclicantidepressants . Psychotherapy, Cognitive behaviorl therapy . Screening instruments
Introduction
In the past few months, the appearance of articles with atitle such as “Diabetes and depression – a risky combina-tion” [1] have alerted clinicians to the nefarious relation-ship that exists between psychiatric illnesses and diabetes.Depression/anxiety and diabetes will surely rank among thedefining epidemics of the 21st century, given the currentexplosion in the prevalence rates of both conditions in boththe developed and developing worlds. A collision betweensuch highly prevalent disorders is to be expected; yet it
R. JainDepartment of Psychiatry, Texas Tech Health Sciences CenterMedical School at Permian Basin,Midland, TX, USA
S. JainDepartment of Psychiatry, Texas Tech Health Sciences CenterMedical School at Permian Basin,301 North N. Street,Midland, TX 79701, USAe-mail: [email protected]
C. L. RaisonDepartment of Psychiatry and Behavioral Sciences, EmoryUniversity School of Medicine,1365B Clifton Road, Room 51003,Atlanta, GA 30322, USAe-mail: [email protected]
V. MaleticDepartment of Neuropsychiatry and Behavioral Sciences,University of South Carolina School of Medicine,Columbia, SC, USAe-mail: [email protected]
R. Jain (*)129 Circle Way, Suite 110,Lake Jackson, TX 77566, USAe-mail: [email protected]
Present Address:V. Maletic38 Parkway Commons Way,Greer, SC 29650, USA
Curr Diab Rep (2011) 11:275–284DOI 10.1007/s11892-011-0202-2

appears that these disorders associate in ways that transcendmere coincidence, and that, in fact, there are numerousbiological reasons why diabetes and depression/anxietyincrease each other’s prevalence, and compound theimpairment associated with each disorder. For example,diabetic peripheral neuropathic pain (DPNP) is a commoncomplication of diabetes. Interestingly, pain is also afrequent symptom of both depressive and anxiety disorders.Emerging data demonstrate that in patients with DPNP, thepresence of depression/anxiety worsens pain and negativelyimpacts treatment. In fact, the more pain perceived by apatient as a result of DPNP, the poorer will be his or hermental health [2•]. In other words, depression and anxietyare more than just emotional disorders, and DPNP is morethan just a pain condition. In patients with DPNP,depression and anxiety commonly coexist and act asmediators and complicators of eventual outcomes. Fortu-nately, optimized treatment of depression/anxiety canpositively impact both the pain and functioning of patientsafflicted with DPNP.
How Common is the Overlap Between Diabetesand Depression/Anxiety?
It is important to realize that psychiatric illnesses arecommon in our society in general, and in clinicalpopulations in particular, with prevalence rates that appearto be increasing with the passage of time. A large US-basedsurvey put the lifetime prevalence of major depression at12.7% and any anxiety disorder at 19.2% [3]. More recentprevalence data from epidemiologic surveys unfortunatelyshow that mental illnesses continue to have an upwardtrajectory. Moreover, the World Health Organization hasestimated depression to be one of the world’s leadingdisabling conditions [4].
As with depression and anxiety, prevalence rates ofdiabetes and its complications have increased explosively inthe last half century [5, 6]. Because of this, it should comeas no surprise that clinicians see these conditions repeated-ly, and see them intertwined more often than not. A recentsurvey of US adults found the overall age-adjustedprevalence of anxiety to be 10.9% in people withoutdiabetes compared to 19.5% in those with diabetes. Evenafter adjusting for educational level, marital status, em-ployment status, current smoking, leisure time, physicalactivity, and body mass index, people with diabetes had a20% higher prevalence of a lifetime diagnosis of anxiety[7•]. Depression has often received the lion’s share ofattention from clinicians, but anxiety disorders are verycommon in the context of diabetes. In fact, in one recentstudy anxiety disorders were actually found to be moreprevalent than depression in diabetes, with 32% of patients
meeting the threshold for anxiety disorder and 22.4% fordepression [8]. This replicates findings from a previousstudy that also found anxiety disorders to be at least asfrequent, if not more so, than depressive disorders in DPNPpatients [9.]
As with anxiety, there is considerable overlap betweenDPNP and depression. In 2001, a meta-analysis of extantliterature (27 studies, 5374 patients) that examined therelationship between depression and DPNP found asignificant and positive relationship between the twoconditions (effect size=0.25). Of concern, depression wasassociated with a number of diabetic complications,including retinopathy, nephropathy, macrovascular compli-cations, sexual dysfunction, and neuropathy [10]. Studiesconducted in the past decade have replicated these findingsof high prevalence of depression in patients with diabetes[9, 11, 12]. Moreover, the complex relationship betweendiabetes and anxiety/depression is not just observed here inthe United States, but also in other parts of the world [13].A recent study from the United Arab Emirates found highrates of mental distress in diabetic patients and found thatperipheral neuropathy was a correlate of poorer mentalhealth [14]. A recent study from India found a similarrelationship between depression and neuropathy in individ-uals suffering from diabetes, with depression increasing theodds of neuropathy with an odds ratio of 1.94 [15].
What Impact Does this Overlap Have on the Livesof Patients?
One word summarizes the impact of depression and anxietyon outcomes in diabetic patients: significant. The presenceof anxiety and/or depression leads to poorer outcomes formicro- and macrovascular complications of diabetes, withpain and physical mobility being added complications [11].An additional complication of having depression and/oranxiety is that diabetic patients with these comorbidities areless compliant with self-monitoring, keep fewer appoint-ments with primary care clinicians, exercise less, and havelower dietary adherence [16, 17]. Cardiovascular riskfactors are clearly elevated in patients with diabetes whoalso screen positive for depression [18]. Additionally,depressed diabetic patients are at increased risk formetabolic syndrome, higher waist circumference, andincreased triglycerides—all factors known to worsen out-comes for depression [19]. As stated above, neuropathyalso appears to occur at elevated rates when depressioncomplicates diabetes [20]. Anxiety does not appear to takea backseat to depression in its ability to produce pooreroutcomes when it is comorbid with diabetes. Patients withdiabetes and anxiety were found to have poorer glycemiccontrol and less frequent blood glucose monitoring [21].
276 Curr Diab Rep (2011) 11:275–284

And finally, neuropathy has been found to be independentlyassociated with depression in diabetic patients [13].
The impact of comorbid depression/anxiety in patientswith diabetes is also financial [22]. A recent study ofMedicare-insured patients with diabetic neuropathy anddepression and/or anxiety found an increase of $9235 intotal health care costs compared with patients who only haddiabetes. Commercially insured patients with depressionand/or anxiety comorbid with diabetes also cost more thanpatients with diabetes alone, with a cost differential of$10,389 [23]. Although cross-sectional studies have shownfor some time that having depression and/or anxietynegatively impacts outcomes for diabetic patients, we nowhave high-quality prospective data demonstrating thatcomplications of diabetes are significantly and negativelyimpacted by comorbid depression [24]. Moreover, theimpact of comorbid depression on diabetes is felt not juston individual complications of diabetes, but on generalquality of life [25]. Finally, just as anxiety/depressionnegatively impact diabetic complications, it is equallyimportant to keep in mind that the reverse is also true:diabetic complications can powerfully increase depression/anxiety with all their attendant disabilities. Nowhere is thisseen more clearly than in data showing that the degree ofpain experienced by DPNP patients directly impacts theirfunctioning and that increasing levels of pain are alsolinked to increases in depressive and anxiety symptoms [9].
Does Emotional Stress Cause Diabetes (and Thereforeits Complications)?
This is a provocative question, no doubt. And the answer iseven more provocative, in that there is growing evidencefrom a number of well-designed, prospective epidemiologictrials that emotional stress (and depression and anxiety areconditions associated with significant emotional stress) mayincrease an individual’s chances of developing diabetes[26••]. Furthermore, there are recent data suggesting abidirectional relationship between depression and diabetes,such that no matter which condition develops first, it setsthe stage for the arrival of the other disorder [27•, 28, 29].A natural question that’s raised at this point is, why? Whyis there a potential bidirectional relationship betweendiabetes and depression and/or anxiety? We will explorethe potential links and offer explanations in the neurobiol-ogy section that follows.
Shared Neurobiology of DPNP and Depression/Anxiety
DPNP occurs in context of both type 1 and type 2 diabetes[30]. Numerous abnormalities associated with diabetes
likely contribute to its occurrence [30]. DPNP initiallytakes on a “glove and stocking distribution” that eventuallyprogresses from toes and feet upward to involve increas-ingly large areas of the body. It is important at this junctureto emphasize that etiologic factors that initiate peripheralnerve damage do not necessarily overlap with the ones thatare responsible for the key feature of DPNP, such as centralsensitization caused by maladaptive neuroplastic changes[31].
Both peripheral and central sensitization play importantroles in producing the signs and symptoms of DPNP.Unfortunately, there are very few human studies character-izing biomarkers for DPNP, especially ones that mightdifferentiate painful- from non-painful diabetic neuropathy.Therefore, preclinical studies are our main source ofinformation about the pathophysiology of peripheral sensi-tization in the context of DPNP [31]. One of thesepreclinical studies has recently found a greater increase ininflammatory and endothelial dysfunction markers inpainful- relative to non-painful diabetic neuropathy [32•].Emerging evidence suggests that peripheral nociceptiveneural tissue damage may be caused by a sustained localinflammatory response. This response promotes the devel-opment of an “inflammatory soup” that surrounds nocicep-tive nerve endings [31, 33, 34, 35•]. Many of the moleculesin this “inflammatory soup” bind to G-protein-coupledreceptors on nerve cells and induce protein kinases. Theensuing cascade of intracellular events leads to increasedproduction and membrane insertion of ion channels andreceptors that alter the signaling characteristics of nocicep-tive neurons. This causes the activation threshold for painneurons to be substantially reduced, inducing them to firemore easily. This spontaneous and ectopic firing of theperipheral nociceptive fibers is the hallmark of peripheralsensitization [31, 33, 34, 35•]. These facilitated andamplified pain signals are subsequently propagated todorsal root ganglia, and eventually to dorsal horn neuronsand from there to the brain.
There is very little preclinical evidence differentiatingthe pathophysiology of DPNP at the central nervous system(CNS) level from non-painful diabetic neuropathy, or fromother forms of neuropathic pain [31, 32•]. In fact, centralsensitization is a pathophysiologic mechanism shared bychronic neuropathic, inflammatory, and dysfunctional pain[31].
Allodynia and secondary hypersensitivity, which arecharacteristic features of central sensitization, appear to bemediated by synaptic strengthening and neuroplasticchanges at multiple CNS levels [31]. At the level of dorsalhorn of the spinal cord, pathologically sensitized C-fiberand A-δ fiber inputs lead to significant synaptic changes indorsal horn neurons [36]. The combination of excessiveincoming pain signals conveyed by glutamate binding to N-
Curr Diab Rep (2011) 11:275–284 277

methyl-D-aspartate (NMDA) receptors, substance P, neuro-trophic factors, and inflammatory mediators (includingcytokines, chemokines, and prostaglandins) alters thedelicate signaling balance that typically exists between,astroglia, microglia, γ-aminobutyric acid interneurons, anddorsal horn neurons [34, 35•, [36–39]. These signalingalterations promote second-order changes in postsynapticdorsal horn neurons that are manifested by alterations in thedensity, activity and membrane insertion of NMDAreceptors, enhanced synthesis of ion channels, and struc-tural proteins [34, 35•, 36, 38–40]. The cumulative effect ofthese alterations translates into long-term potentiation,which is the most important neurobiological substrate ofcentral sensitization [35•, 39].
Current scientific evidence emphasizes central sensitiza-tion as a fundamental feature of all forms of neuropathicpain [31, 41, 42]. Interestingly, conditions such as depres-sion/anxiety, which are characterized by emotional pain,may also be driven by physiologic processes similar tocentral sensitization. For example, major depression iswidely considered to be associated with a “kindling”phenomenon. In the context of depression, kindling impliesthat each episode of depression makes subsequent depres-sive episodes more likely and less dependent upon anexternal impetus such as stress or sickness [43]. Robert Post[44]—who initially introduced kindling as an explanatoryconstruct to account for the tendency of mood disorders toworsen over time—has recently proposed that kindling andsensitization may have similar neurobiological underpin-nings, such as neuroplastic changes and alterations in geneexpression. In the same vein, other authors have gone so faras to suggest “neurosensitization” as a common etiology forchronic pain, depression, and anxiety disorders [45].
In addition to peripheral and central sensitization,neuropathic pain is also characterized by altered limbicand cortical function and structure [41, 46, 47]. The braincircuitry involved in pain modulation (often referred to as“the pain matrix”) shares elements with brain networksresponsible for the modulation of mood and the stressresponse [48–54].
Neuroimaging studies of neuropathic pain are not nearlyas numerous as those focusing on major depression.Nevertheless, functional MRI (fMRI) studies of neuropathicpain have implicated the same brain areas known to befunctionally abnormal in chronic non-neuropathic pain,such as prefrontal cortex, thalamus, insula, and anteriorcingulate cortex (ACC) [47, 52]. Apkarian et al. [55]conducted volumetric MRI to assess gray matter changes ina group of chronic back pain (CBP) sufferers, the majorityof whom experienced pain of neuropathic origin. Theseinvestigators found significantly reduced gray mattervolume in dorsolateral prefrontal cortex (DLPFC) andthalamus of CBP patients relative to controls. Furthermore,
decreased gray matter density in DLPFC correlated withpain intensity, duration, and negative emotional character-istics in this population. Additionally, the magnitude ofgray matter reduction in CBP patients was equivalent to 10to 20 years of normal aging. Considering the well-established role of DLPFC in top-down regulation of limbicand paralimbic prefrontal areas [35•], it is conceivable thatmorphologic changes in DLPFC may contribute to thecompromised emotional and pain modulation apparent inmany neuropathic pain patients [55].
In another recent study, a group of diabetic patients wascompared with healthy controls using magnetic resonancespectroscopy [56]. Diabetic subjects had decreased brain N-acetyl aspartate (NAA) levels relative to the control group.Moreover, diabetic subjects suffering from pain had agreater reduction of NAA in thalamus than subjects whohad diabetes but no pain [56]. These findings suggest thatdiabetes on its own maybe associated with metabolicchanges in DLPFC [35•, 56]. Additionally, significantreduction in thalamic NAA in diabetic subjects sufferingfrom pain compared with ones who are pain free may implygreater functional disturbances in these patients that resultin altered perception and pain amplification [56•].
Another group of investigators used fMRI to studyfunctional connectivity between brain areas in patientssuffering from DPNP [57]. Activity in several cortical areasincluding the fusiform gyrus, left inferior temporal gyrus,and dorsal ACC negatively correlated with pain, whereasactivity in DLPFC, both insulae, and thalamus showed apositive association with the experience of pain. This wasthe first functional study to characterize aberrant defaultmode functional connectivity in the context of spontaneousdiabetic neuropathic pain. In a subsequent study the samegroup found disruption in thalamocortical processing inpatients suffering from DPNP relative to healthy controls[58]. Given the multiple overlaps observed betweendepression and neuropathic pain it is not surprising thatsimilar functional and structural changes in amygdala andhippocampus have been described in major depressivedisorder and neuropathic pain [59–62].
Altered function of these limbic-cortical circuits isbelieved to lead to disruptions in neuroendocrine, auto-nomic, and immune regulation that may further contributeto the initiation and/or worsening of mood and painsymptoms [41, 46, 53, 63]. Emerging evidence suggeststhat a combination of excessive sympathetic activity andelevated proinflammatory cytokine production and releaselikely plays a role in the etiology of both depression andneuropathic pain [35•, 64]. Furthermore, major depressionand neuropathic pain are both associated with disturbedneuron-glia relationships, alterations in glutamatergic andintracellular signaling cascades, and neurotrophic traffick-ing [34, 65–69].
278 Curr Diab Rep (2011) 11:275–284
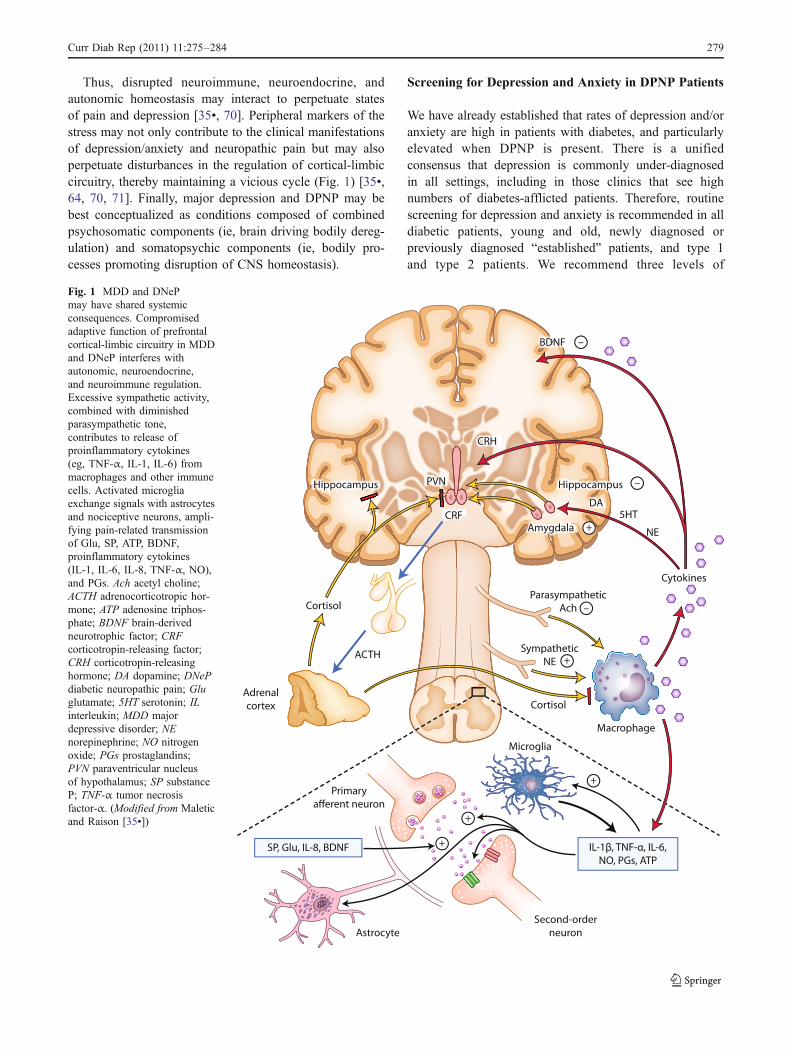
Thus, disrupted neuroimmune, neuroendocrine, andautonomic homeostasis may interact to perpetuate statesof pain and depression [35•, 70]. Peripheral markers of thestress may not only contribute to the clinical manifestationsof depression/anxiety and neuropathic pain but may alsoperpetuate disturbances in the regulation of cortical-limbiccircuitry, thereby maintaining a vicious cycle (Fig. 1) [35•,64, 70, 71]. Finally, major depression and DPNP may bebest conceptualized as conditions composed of combinedpsychosomatic components (ie, brain driving bodily dereg-ulation) and somatopsychic components (ie, bodily pro-cesses promoting disruption of CNS homeostasis).
Screening for Depression and Anxiety in DPNP Patients
We have already established that rates of depression and/oranxiety are high in patients with diabetes, and particularlyelevated when DPNP is present. There is a unifiedconsensus that depression is commonly under-diagnosedin all settings, including in those clinics that see highnumbers of diabetes-afflicted patients. Therefore, routinescreening for depression and anxiety is recommended in alldiabetic patients, young and old, newly diagnosed orpreviously diagnosed “established” patients, and type 1and type 2 patients. We recommend three levels of
Fig. 1 MDD and DNePmay have shared systemicconsequences. Compromisedadaptive function of prefrontalcortical-limbic circuitry in MDDand DNeP interferes withautonomic, neuroendocrine,and neuroimmune regulation.Excessive sympathetic activity,combined with diminishedparasympathetic tone,contributes to release ofproinflammatory cytokines(eg, TNF-α, IL-1, IL-6) frommacrophages and other immunecells. Activated microgliaexchange signals with astrocytesand nociceptive neurons, ampli-fying pain-related transmissionof Glu, SP, ATP, BDNF,proinflammatory cytokines(IL-1, IL-6, IL-8, TNF-α, NO),and PGs. Ach acetyl choline;ACTH adrenocorticotropic hor-mone; ATP adenosine triphos-phate; BDNF brain-derivedneurotrophic factor; CRFcorticotropin-releasing factor;CRH corticotropin-releasinghormone; DA dopamine; DNePdiabetic neuropathic pain; Gluglutamate; 5HT serotonin; ILinterleukin; MDD majordepressive disorder; NEnorepinephrine; NO nitrogenoxide; PGs prostaglandins;PVN paraventricular nucleusof hypothalamus; SP substanceP; TNF-α tumor necrosisfactor-α. (Modified from Maleticand Raison [35•])
Curr Diab Rep (2011) 11:275–284 279

screening. Step 1 is asking the patient directly about thepresence of symptoms of depression and anxiety (Table 1).Step 2 is to collect collateral information from spouse,family, friends, previous and other health care providers.This can be very valuable. Step 3 is to use screening toolsthat can help detect depression and anxiety.
To screen for depression we would like to recommend aspecific tool that has been studied in diabetic patients, thePHQ-9 (Physical Health Questionnaire-9) [72]. It hasdemonstrated good psychometric properties in diabeticpatients [73]. Another instrument we find useful is theHADS (Hospital Anxiety and Depression Scale), which hasalso been used for screening purposes in studies of diabeticpatients [74, 75]. A specific questionnaire for generalizedanxiety disorder is GAD-7 (Generalized Anxiety Disorder-7) [76, 77]. A few words of caution: these instruments arenot diagnostic; their main purpose is to screen (and to useas a measurement tool for response assessment aftertreatment has been initiated). Therefore, the clinicianshould not assume that elevated scores on PHQ-9, GAD-7, or HADS automatically suggest a psychiatric diagnosis,as some symptoms of diabetes can mimic the symptoms ofanxiety or depression on these scales [78•]. Despite thesepotential weaknesses, scales such as the ones we recom-mend are highly useful, and we strongly recommend thatdiabetologists develop familiarity with them and use themon a regular basis. For further details on these threescreening instruments, please refer to Table 2.
Treatment Options
An integrated treatment approach to treating patients withDPNP and depression/anxiety is recommended, with thetreatment team including (depending on the individualpatient’s needs) a diabetic medicine specialist, primary careclinician, psychiatrist, psychologist, social worker, diabeticeducation specialist, and dietician. The focus should be on
addressing the following needs: improved control overmood and anxiety disorders, better glycemic control, bettercompliance with medications, appointments, exercise, anddiet. One advantage of an integrated team approach is that ittends to promote an equal focus being placed on biological,environmental/social, and psychological issues [79–83].
Nonpharmacologic treatments are important componentsin the treatment of patents with DPNP and anxiety/depression. Convincing data demonstrate that cognitivebehavioral therapy (CBT) is helpful either by itself or whencombined with psychotropic medications in reducingsymptoms of depression and anxiety. More recent datasuggest that both motivational enhancement therapy andCBT can help improve suboptimal glycemic levels, sug-gesting that psychotherapeutic approaches may be benefi-cial not just for emotional issues, but may actually helpactual core disease processes [84•, 85]. Given thesefindings, we feel the level of evidence supporting CBT’seffectiveness in treating depression and anxiety is highenough that offering CBT to DPNP patients with depres-sion and/or anxiety is appropriate. The fact that CBT hasdemonstrated helpfulness in improving glycemic control isan added benefit.
Pharmacologic therapies are often needed and indicatedfor patients with DPNP who also have depression and/oranxiety [86, 87]. We recommend against the routine use ofselective serotonin reuptake inhibitors (SSRIs) as first-lineagents in this patient population and strongly advise againstthe routine use of benzodiazepines. Our recommendation ofnot generally using SSRIs as first-line agents is based on alarge dataset showing that these agents are not particularlyeffective in patients with comorbid pain and depression[88]. Our strong opposition to benzodiazepine for routineuse as an anxiolytic or sedative is based on several factors,including their potential for addiction, gait disturbance withattendant increased fall risk, and memory impairment.These agents are also known to increase the risk foraccidents [89, 90]. DPNP patients are typically ill-suited to
Symptoms of major depression Symptoms of generalized anxiety disorder
Sad mood Excessive anxiety/tension
Irritable mood Difficulty controlling the worry
Anhedonia (loss of pleasure) Restlessness
Sleep disturbances Fatigue
Appetite disturbances Concentration/mind going blank
Psychomotor changes Irritability
Helplessness/hopelessness Muscle tension
Concentration/memory difficulties Sleep disturbances
Fatigue/energy difficulties
Suicidal thoughts
Table 1 DSM-IV symptomsof major depression andgeneralized anxiety disorder
In addition to a certain numberof symptoms, impairment andduration criteria must also bemet before a DSM-IV diagnosisis made.
(Adapted from Diagnostic andStatistical Manual of MentalDisorders (DSM-IV) [103].)
280 Curr Diab Rep (2011) 11:275–284

face these challenges and thus we recommend against theroutine use of benzodiazepines. We also recommendagainst the use of tricyclic antidepressants (TCAs) as first-line agents in these patients. Our primary rationale for thisrecommendation is that the side-effect burden of TCAs is acause of concern in many DPNP patients. These olderantidepressants are best reserved for use as second- or third-line pharmacologic interventions. When these agents areused it is extremely important that this be done cautiouslywith close monitoring.
We recommend two classes of medications as first-lineagents for patients with comorbid DPNP and depression/anxiety: serotonin norepinephrine reuptake inhibitors(SNRIs; for comorbid DPNP and depression) and α-2-δligand medications. SNRIs modulate both serotonin andnorepinephrine and one of them, duloxetine, has sepa-rately demonstrated effectiveness in major depression,GAD, and DPNP, and has an approved indication foreach of these disorders from the US Food and DrugAdministration (FDA) [91–93]. Other SNRIs, such asvenlafaxine, desvenlafaxine, and milnacipran are mostlikely effective too, but the evidence base for theireffectiveness in patients with all these conditions at onceis limited [94–97].
A-2-δ ligands induce their therapeutic effects bymodulating calcium influx into neurons [98]. Twomedications from this class are available for use: gaba-pentin and pregabalin. Particularly with pregabalin, thereis established evidence in the literature of its effectivenesswith DPNP [99] and GAD [100]. However, it is importantto note that pregabalin has FDA approval for DPNP, butnot GAD.
We would like to point out a significant shortcoming ofthe treatment literature in the area of DPNP comorbid withdepression/anxiety. Although there are studies showingeffectiveness of various agents in individual conditions(DPNP, anxiety disorders, depression), there is hardly anyhigh-quality evidence for how these medications performwhen a patient is comorbid for all these disorders, as sofrequently happens in clinical practice. As a result, we areforced to extrapolate our recommendations for thesecomorbid patients from data from individual disease states.We are hopeful that in time high-quality pharmacologicstudies will be conducted in patients with two, or even threecoexisting disorders.
Clinical Recommendations
Based on data and experience, we feel that depression andanxiety disorders exist frequently in diabetic patients withDPNP. However, although challenging, the presence ofdiabetes along with depression should not be a barrier togood treatment outcomes for depression [101]. The pain ofDPNP appears to be worsened and the impairmentmagnified when depression and/or anxiety coexists. As adiabetologist, we are certain your goal is to improve yourpatient’s functioning as well as reduce suffering from allcauses. We suggest, again based on data, that depressionand anxiety disorders are both mediators and complicatorsof outcomes for your DPNP patients. There are complex,but increasingly better understood neurobiological reasonsfor this fact. We suggest routine screening for depressionand anxiety in your DPNP patients. We recommend
Table 2 Recommended screening tools for depression and anxiety
Nameof scale
Used to assess Patient orclinician rated
Scoring Availability
GAD-7 -Generalized anxietydisorder
Patient rated GAD-7 total score for the seven items rangesfrom 0 to 21. Scores of 5, 10, and 15 representcut-points for mild, moderate, and severeanxiety, respectively.
Public domain: http://www.phqscreeners.com/overview.aspx?Screener=03_GAD-7
When screening for anxiety disorders,a recommended cut-point for furtherevaluation is a score of 10 or greater
PHQ-9 -Screening for depression Patient rated Total score ranges from 0 to 27. Scores of 5,10, 15, and 20 represent cut-points for mild,moderate, moderately severe. and severedepression, respectively
Public domain: http://www.phqscreeners.com/overview.aspx?Screener=02_PHQ-9
-Sensitive to detect changein symptom severity inresponse to intervention
HADS Detects states of anxietyand depression
Patient rated Anxiety and depression. Copyrighted. Requires user feefor all users: http://shop.gl-assessment.co.uk/home.php?cat=417
None (0–7), borderline cases (8–10),definite cases (11 and above)
GAD-7 Generalized Anxiety Disorder-7; HADS Hospital Anxiety and Depression Scale; PHQ-9 Physical Health Questionnaire-9.
Curr Diab Rep (2011) 11:275–284 281

increasing familiarity with screening tools such as HADS,PHQ-9, and GAD-7, and to use them routinely in yourpractice. They are quick, efficient, and reliable. If either orboth disorders are detected, we suggest patient education,patient and family alliance building, and the offering of ajudicious treatment plan that may include nonpharmacologicand/or pharmacologic options. Long-term, measurement-based care is recommended for DPNP patients who are alsoafflicted with depression and/or anxiety disorders. Finally, werecommend the institution of more widespread disseminationof this information through continuing medical educationprograms and other relevant means [102].
Conclusions
The past few years have produced a wealth of informa-tion and understanding regarding the plight of DPNPpatients. Pain is clearly a major challenge and itsmanagement is a goal of treatment. In this article wehave also attempted to alert you to the fact thatdepression and anxiety are also common in these patientsand that these conditions complicate matters and impairoutcomes. Numerous neurobiological threads tie diabetes,pain, depression, and anxiety together—these threadsinclude the neuroendocrine system, autonomic system,and the inflammatory cytokine system, and a host ofother, interrelated physiologic pathways in brain andbody. Screening, diagnosing, and finally optimally treat-ing the depression and anxiety not only improves apatient’s quality of life, but these interventions alsoappear to impact the pain of DPNP patents.
Disclosure Conflicts of interest: R. Jain: is on the advisory boardsand speakers panels for Eli Lilly, Pfizer, Forest Pharmaceuticals, andTakeda Pharmaceutical Co.; S. Jain: none; C.L. Raison: none; V.Maletic: is on the advisory boards and speakers panels for Eli Lilly,Pfizer, Forest Pharmaceuticals, and Takeda Pharmaceutical Co.
References
Papers of particular interest, published recently, have beenhighlighted as:• Of importance•• Of major importance
1. Daly M. Diabetes and depression–a risky combination. Nurs NZ. 2010;16(2):14–5.
2. • Bair MJ et al. Prevalence of pain and association with qualityof life, depression and glycaemic control in patients withdiabetes. Diabet Med. 2010; 27(5):578–84. This article demon-strates the significant association between diabetes and pain.
3. Kessler RC, McGonagle KA, Zhao S, Nelson CB. Lifetime and12 month prevalence of DSM-III-R psychiatric disorders in theUnited States. Arch Gen Psychiatry. 1994;51:8–19.
4. Michaud CM, Murray CJ, Bloom BR. Burden of disease -implications for future research. JAMA. 2001;285(5):535–9.
5. Vehik K, Dabelea D. The changing epidemiology of type 1diabetes: why is it going through the roof? Diabetes Metab ResRev. 2010.
6. Farag YM, Gaballa MR. Diabesity: an overview of a risingepidemic. Nephrol Dial Transplant. 2011;26(1):28–35.
7. • Li C et al. Diabetes and anxiety in US adults: findings from the2006 behavioral risk factor surveillance system. Diabet Med.2008; 25(7):878–81. This article articulates the issue of anxietydisorders in adults with diabetes.
8. Collins MM, Corcoran P, Perry IJ. Anxiety and depressionsymptoms in patients with diabetes. Diabet Med. 2009;26(2):153–61.
9. Gore M, Brandenburg N, Dukes E, Hoffman DL, Tai KS, StaceyB. Pain severity in diabetic peripheral neuropathy is associatedwith patient functioning, symptom levels of anxiety anddepression, and sleep. J Pain Symptom Manage. 2005;30(4):374–85.
10. de Groot M, Anderson R, Freedland KE, Clouse RE, LustmanPJ. Association of depressive and diabetic complications: a meta-analysis. Psychosom Med. 2001;63(4):619–30.
11. Waitzfelder B et al. Correlates of depression among people withdiabetes: The Translating Research Into Action for Diabetes(TRIAD) study. Prim Care Diabetes. 2010;4(4):215–22.
12. Pouwer F et al. Prevalence of comorbid depression is high in out-patients with Type 1 or Type 2 diabetes mellitus. Results from threeout-patient clinics in the Netherlands. Diabet Med. 2010;27(2):217–24.
13. Yoshida S et al. Neuropathy is associated with depressionindependently of health-related quality of life in Japanesepatients with diabetes. Psychiatry Clin Neurosci. 2009;63(1):65–72.
14. Sulaiman N, Handam A, Tamim H, Mahmood DA, Young D,The prevalence and coorelates of depression and anxiety in asampe of diabetic patients in Sharjah, United Arab Emirates.BMC Fam Pract. 2010; 11.
15. Raval A, Dhanaraj E, Bhansali A, Grover S, Tiwari P.Prevalence and determinants of depression in type 2 diabetespatients in a tertiary care centre. Indian J Med Res.2010;132:195–200.
16. Wagner JA, Tennen H, Osborn CY. Lifetime depression anddiabetes self-management in women with Type 2 diabetes: acase-control study. Diabet Med. 2010;27(6):713–7.
17. Katon WJ et al. The relationship between changes in depressionsymptoms and changes in health risk behaviors in patients withdiabetes. Int J Geriatr Psychiatry. 2010;25(5):466–75.
18. Rubin RR et al. Cardiovascular disease risk factors, depressionsymptoms and antidepressant medicine use in the Look AHEAD(Action for Health in Diabetes) clinical trial of weight loss indiabetes. Diabetologia. 2010;53(8):1581–9.
19. Ahola AJ et al. Depression is associated with the metabolicsyndrome among patients with type 1 diabetes. Ann Med.2010;42(7):495–501.
20. Raval A et al. Prevalence & determinants of depression in type 2diabetes patients in a tertiary care centre. Indian J Med Res.2010;132:195–200.
21. Herzer M, Hood KK. Anxiety symptoms in adolescents withtype 1 diabetes: association with blood glucose monitoring andglycemic control. J Pediatr Psychol. 2010;35(4):415–25.
22. Le TK, Able SL, Lage MJ. Resource use among patients withdiabetes, diabetic neuropathy, or diabetes with depression. CostEff Resour Alloc. 2006;4:18.
282 Curr Diab Rep (2011) 11:275–284

23. Boulanger L, Zhao Y, Bao Y, Russell MW. A retrospective studyon the impact of comorbid depression or anxiety on healthcareresource use and costs among diabetic neuropathy patients. BMCHealth serv Res. 2009; 9(111).
24. Lin EH et al. Depression and advanced complications ofdiabetes: a prospective cohort study. Diabetes Care. 2010;33(2):264–9.
25. Ali S et al. The association between depression and health-related quality of life in people with type 2 diabetes: a systematicliterature review. Diabetes Metab Res Rev. 2010;26(2):75–89.
26. •• Pouwer F, Kupper N, Adriaanse MC. Does emotional stresscause type 2 diabetes mellitus? A review from the EuropeanDepression in Diabetes (EDID) Research Consortium. DiscovMed. 2010; 9(45):112–8. This thought-provoking article asks animportant question: does stress act as a catalyst for thedevelopment of type 2 diabetes (and presumably its complica-tions) in a prospective fashion?
27. • Pan A et al. Bidirectional association between depression andtype 2 diabetes mellitus in women. Arch Intern Med. 2010; 170(21):1884–91. This article offers a well-reasoned look at thedata on the bi-irectional nature of diabetes and depression.
28. Atlantis E et al. Diabetes incidence associated with depressionand antidepressants in the Melbourne Longitudinal Studies onHealthy Ageing (MELSHA). Int J Geriatr Psychiatry. 2010;25(7):688–96.
29. Nouwen A et al. Type 2 diabetes mellitus as a risk factor for theonset of depression: a systematic review and meta-analysis.Diabetologia. 2010;53(12):2480–6.
30. Vinik AI et al. Diabetic neuropathy in older adults. Clin GeriatrMed. 2008;24(3):407–35. v.
31. Costigan M, Scholz J, Woolf CJ. Neuropathic pain: a maladap-tive response of the nervous system to damage. Annual Reviewof Neuroscience. 2009;32(1):1–32.
32. • Doupis J et al. Microvascular reactivity and inflammatorycytokines in painful and painless peripheral diabetic neuropathy.J Clin Endocrinol Metab. 2009; 94(6):2157–63. This is anexcellent review of the issue of inflammatory cytokines in DPNP.
33. Scholz J, Woolf CJ. Can we conquer pain? Nat Neurosci. 2002;5(Suppl):1062–7.
34. Scholz J, Woolf CJ. The neuropathic pain triad: neurons,immune cells and glia. Nat Neurosci. 2007;10(11):1361–8.
35. • Maletic V, Raison CL. Neurobiology of depression, fibromy-algia and neuropathic pain. Front Biosci. 2009; 14:5291–338.This article offers a comprehensive review of the sharedneurobiology of pain and depression.
36. Baron R. Mechanisms of disease: neuropathic pain–a clinicalperspective. Nat Clin Pract Neurol. 2006;2(2):95–106.
37. Marx J. Pain research. Prolonging the agony. Science. 2004;305(5682):326–9.
38. Moalem G, Tracey DJ. Immune and inflammatory mechanismsin neuropathic pain. Brain Res Rev. 2006;51(2):240–64.
39. Ji RR et al. Central sensitization and LTP: do pain and memoryshare similar mechanisms? Trends Neurosci. 2003;26(12):696–705.
40. Ren K, Dubner R. Neuron-glia crosstalk gets serious: role in painhypersensitivity. Curr Opin Anaesthesiol. 2008;21(5):570–9.
41. Yunus MB. Role of central sensitization in symptoms beyondmuscle pain, and the evaluation of a patient with widespreadpain. Best Pract Res Clin Rheumatol. 2007;21(3):481–97.
42. Woolf CJ, Mannion RJ. Neuropathic pain: aetiology, symp-toms, mechanisms, and management. Lancet. 1999;353(9168):1959–64.
43. Kendler KS, Thornton LM, Gardner CO. Stressful life eventsand previous episodes in the etiology of major depression inwomen: an evaluation of the “kindling” hypothesis. Am JPsychiatry. 2000;157(8):1243–51.
44. Post RM. Kindling and sensitization as models for affectiveepisode recurrence, cyclicity, and tolerance phenomena. Neuro-sci Biobehav Rev. 2007;31(6):858–73.
45. Miller L. Neurosensitization: A model for persistent disability inchronic pain, depression, and posttraumatic stress disorderfollowing injury. NeuroRehabilitation. 2000;14(1):25–32.
46. Dadabhoy D et al. Biology and therapy of fibromyalgia.Evidence-based biomarkers for fibromyalgia syndrome. ArthritisRes Ther. 2008;10(4):211.
47. Tracey I, Mantyh PW. The cerebral signature for pain perceptionand its modulation. Neuron. 2007;55(3):377–91.
48. Blackburn-Munro G, Blackburn-Munro RE. Chronic pain,chronic stress and depression: coincidence or consequence? JNeuroendocrinol. 2001;13(12):1009–23.
49. Schweinhardt P et al. Investigation into the neural correlates ofemotional augmentation of clinical pain. Neuroimage. 2008;40(2):759–66.
50. Borsook D et al. Neuroimaging revolutionizes therapeuticapproaches to chronic pain. Mol Pain. 2007;3:25.
51. Zhuo M. Cortical excitation and chronic pain. Trends Neurosci.2008;31(4):199–207.
52. Apkarian AVet al. Human brain mechanisms of pain perception andregulation in health and disease. Eur J Pain. 2005;9(4):463–84.
53. Raison CL, Capuron L, Miller AH. Cytokines sing the blues:inflammation and the pathogenesis of depression. TrendsImmunol. 2006;27(1):24–31.
54. Neugebauer V et al. The amygdala and persistent pain.Neuroscientist. 2004;10(3):221–34.
55. Apkarian AV et al. Chronic back pain is associated withdecreased prefrontal and thalamic gray matter density. J Neuro-sci. 2004;24(46):10410–5.
56. Sorensen L et al. Differences in metabolites in pain-processingbrain regions in patients with diabetes and painful neuropathy.Diabetes Care. 2008;31(5):980–1.
57. Cauda F et al. Altered resting state in diabetic neuropathic pain.PLoS ONE. 2009;4(2):e4542.
58. Cauda F et al. Low-frequency BOLD fluctuations demonstratealtered thalamocortical connectivity in diabetic neuropathic pain.BMC Neurosci. 2009;10:138.
59. Frodl T et al. Effect of hippocampal and amygdala volumes onclinical outcomes in major depression: a 3-year prospectivemagnetic resonance imaging study. J Psychiatry Neurosci.2008;33(5):423–30.
60. Matthews SC et al. Decreased functional coupling of theamygdala and supragenual cingulate is related to increaseddepression in unmedicated individuals with current majordepressive disorder. J Affect Disord. 2008;111(1):13–20.
61. Baliki MN et al. Chronic pain and the emotional brain: specificbrain activity associated with spontaneous fluctuations ofintensity of chronic back pain. J Neurosci. 2006;26(47):12165–73.
62. Goncalves L et al. Neuropathic pain is associated withdepressive behaviour and induces neuroplasticity in the amyg-dala of the rat. Exp Neurol. 2008;213(1):48–56.
63. Tsigos C, Chrousos GP. Hypothalamic-pituitary-adrenal axis,neuroendocrine factors and stress. J Psychosom Res. 2002;53(4):865–71.
64. Strouse TB. The relationship between cytokines and pain/depression: a review and current status. Curr Pain HeadacheRep. 2007;11(2):98–103.
65. Rajkowska G, Miguel-Hidalgo JJ. Gliogenesis and glial pathol-ogy in depression. CNS Neurol Disord Drug Targets. 2007;6(3):219–33.
66. Pav M et al. Neurobiological aspects of depressive disorder andantidepressant treatment: role of glia. Physiol Res. 2008;57(2):151–64.
Curr Diab Rep (2011) 11:275–284 283

67. McNally L, Bhagwagar Z, Hannestad J. Inflammation, gluta-mate, and glia in depression: a literature review. CNS Spectr.2008;13(6):501–10.
68. Tsuda M, Inoue K, Salter MW. Neuropathic pain and spinalmicroglia: a big problem from molecules in “small” glia. TrendsNeurosci. 2005;28(2):101–7.
69. Zieglgansberger W, Berthele A, Tolle TR. Understandingneuropathic pain. CNS Spectr. 2005;10(4):298–308.
70. Chapman CR, Tuckett RP, Song CW. Pain and stress in asystems perspective: reciprocal neural, endocrine, and immuneinteractions. J Pain. 2008;9(2):122–45.
71. Wieseler-Frank J, Maier SF, Watkins LR. Immune-to-braincommunication dynamically modulates pain: physiological andpathological consequences. Brain Behav Immun. 2005;19(2):104–11.
72. Acee AM. Detecting and managing depression in type IIdiabetes: PHQ-9 is the answer! Medsurg Nurs. 2010;19(1):32–8.
73. van Steenbergen-Weijenburg KM et al. Validation of the PHQ-9 asa screening instrument for depression in diabetes patients inspecialized outpatient clinics. BMC Health Serv Res. 2010;10:235.
74. Brennan C et al. The hospital anxiety and depression scale: adiagnostic meta-analysis of case-finding ability. J PsychosomRes. 2010;69(4):371–8.
75. Lloyd CE, Dyer PH, Barnett AH. Prevalence of symptoms ofdepression and anxiety in a diabetes clinic population. DiabetMed. 2000;17(3):198–202.
76. Spitzer RL et al. A brief measure for assessing generalizedanxiety disorder: the GAD-7. Arch Intern Med. 2006;166(10):1092–7.
77. Lowe B et al. Validation and standardization of the GeneralizedAnxiety Disorder Screener (GAD-7) in the general population.Med Care. 2008;46(3):266–74.
78. • Reddy P et al. Identification of depression in diabetes: theefficacy of PHQ-9 and HADS-D. Br J Gen Pract. 2010; 60(575):239–45. This article offers a fair balanced review of thebenefits and potential pitfalls of using PHQ-9 and HADS-D inDPNP patients.
79. Gonzalez JS, Esbitt SA. Depression and treatment nonadherencein type 2 diabetes: assessment issues and an integrative treatmentapproach. Epidemiol Psichiatr Soc. 2010;19(2):110–5.
80. Fortmann AL et al. Support for disease management, depression,self-care, and clinical indicators among Hispanics with type 2diabetes in San Diego County, United States of America. RevPanam Salud Publica. 2010;28(3):230–4.
81. Echeverry D et al. Effect of pharmacological treatment ofdepression on A1C and quality of life in low-income Hispanicsand African Americans with diabetes: a randomized, double-blind,placebo-controlled trial. Diabetes Care. 2009;32(12):2156–60.
82. Bogner HR, de Vries HF. Integrating type 2 diabetes mellitus anddepression treatment among African Americans: a randomizedcontrolled pilot trial. Diabetes Educ. 2010;36(2):284–92.
83. Ell K et al. Collaborative care management of major depressionamong low-income, predominantly Hispanic subjects withdiabetes: a randomized controlled trial. Diabetes Care. 2010;33(4):706–13.
84. • Ismail K et al. A randomised controlled trial of cognitivebehaviour therapy and motivational interviewing for people withType 1 diabetes mellitus with persistent sub-optimal glycaemiccontrol: a Diabetes and Psychological Therapies (ADaPT) study.
Health Technol Assess. 2010; 14(22):1–101, iii-iv. This articledemosntates the importnace of nonpharmacologic interventionsin diabetes.
85. van Bastelaar K et al. Development and reach of a web-basedcognitive behavioural therapy programme to reduce symptoms ofdepression and diabetes-specific distress. Patient Educ Couns.2010.
86. Kuritzky L. Managing diabetic peripheral neuropathic pain inprimary care. J Fam Pract. 2010;59(5 Suppl):S15–22.
87. Tesfaye S. Advances in the management of diabetic peripheralneuropathy. Curr Opin Support Palliat Care. 2009;3(2):136–43.
88. Greist JH et al. Depression and pain. J Clin Psychiatry. 2008;69(12):1970–8.
89. Smink BE, Egberts ACG, Lusthof KJ. The relationship betweenbenzodiazepine use and traffic accident: a systematic litreaturereview. CNS Drugs. 2010;24(8):639–53.
90. Uzun S et al. Side effects of treatment with benzodiazepines.Psychiatr Danub. 2010;22(1):90–3.
91. Skljarevski V et al. Evaluating the maintenance of effect ofduloxetine in patients with diabetic peripheral neuropathic pain.Diabetes Metab Res Rev. 2009;25(7):623–31.
92. Rynn M et al. Efficacy and safety of duloxetine in the treatmentof generalized anxiety disorder: a flexible-dose, progressive-titration, placebo-controlled trial. Depress Anxiety. 2008;25(3):182–9.
93. Kornstein SG et al. A randomized, double-blind study ofincreasing or maintaining duloxetine dose in patients withoutremission of major depressive disorder after initial duloxetinetherapy. J Clin Psychiatry. 2008;69(9):1383–92.
94. Abrahamian H et al. Diabetes mellitus and co-morbid depres-sion: treatment with milnacipran results in significant improve-ment of both diseases (results from the Austrian MDDM studygroup). Neuropsychiatr Dis Treat. 2009;5:261–6.
95. Lieberman DZ, Massey SH. Desvenlafaxine in major depressivedisorder: an evidence-based review of its place in therapy. CoreEvid. 2010;4:67–82.
96. Pae CU et al. Milnacipran: beyond a role of antidepressant. ClinNeuropharmacol. 2009;32(6):355–63.
97. Golden RN, Nicholas L. Antidepressant efficacy of venlafaxine.Depress Anxiety. 2000;12 Suppl 1:45–9.
98. Di Guilmi MN et al. Pregabalin modulation of neurotransmitterrelease is mediated by change in intrinsic activation/inactivationproperties of CaV2.1 calcium channels. J Pharmacol Exp Ther.2010.
99. Satosh J, Yagihashi S, Baba M, Suzuki M. Efficacy and safety ofpregabalin for treating neuropathic pain associated with diabeticperipheral neuropathy: a 14 week, randomized, double blind,placebo-controlled trial. Diabet Med. 2011;28(1):109–16.
100. Montgomery SA, Herman BK, Schweizer E. The efficacy ofpregabalin and benzodiazepines in generalized anxiety disorderpresenting with high levels of insomnia. Int Clin Psychophar-macology. 2009;24(4):214–22.
101. Bryan C et al. The impact of diabetes on depression treatmentoutcomes. Gen Hosp Psychiatry. 2010;32(1):33–41.
102. Osborn CY, Kozak C, Wagner J. Theory in practice: helpingproviders address depression in diabetes care. J Contin EducHealth Prof. 2010;30(3):172–9.
103. Diagnostic and Statistical Manual of Mental Disorders (DSM-IV). Arlington, VA: APA Press; 2000.
284 Curr Diab Rep (2011) 11:275–284
Related Documents











