Pain – Anatomy and Pain – Anatomy and Physiology Physiology

Pain
Dec 01, 2014
anatomy and physiology of pain
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Pain – Anatomy and Pain – Anatomy and PhysiologyPhysiology

DefinitionDefinition
An unpleasant sensory and emotional experience... An unpleasant sensory and emotional experience...
...caused by actual or potential tissue injury,...caused by actual or potential tissue injury, ...or described in terms of such injury....or described in terms of such injury.
International Association for the Study of Pain

Sources of PainSources of Pain
NociceptiveNociceptive: pain that is usually transmitted : pain that is usually transmitted after normal processing of noxious stimuli after normal processing of noxious stimuli
NeuropathicNeuropathic: results from injury or abnormal : results from injury or abnormal functioning of peripheral nerves or CNS functioning of peripheral nerves or CNS
PsychogenicPsychogenic: unknown physical cause : unknown physical cause

Classification of Pain Classification of Pain NociceptionNociception
Proportionate to the stimulation of the Proportionate to the stimulation of the nociceptornociceptor
When acuteWhen acutePhysiologic painPhysiologic painServes a protective functionServes a protective functionNormal painNormal pain
Pathologic when chronicPathologic when chronic

Describe the different types of pain Describe the different types of pain sensationsensation
bright,bright, sharp,sharp, stabbing types of painstabbing types of paindull, dull, throbbing,throbbing,aching types.aching types.

Where Does Pain Come From?Where Does Pain Come From?
Cutaneous PainCutaneous Pain – sharp, bright, burning; can – sharp, bright, burning; can have a fast or slow onsethave a fast or slow onset
Deep Somatic PainDeep Somatic Pain – stems from tendons, – stems from tendons, muscles, joints, periosteum, & b. vesselsmuscles, joints, periosteum, & b. vessels
Visceral PainVisceral Pain – originates from internal – originates from internal organs; diffused @ 1organs; diffused @ 1stst & later may be & later may be localized (i.e. appendicitis)localized (i.e. appendicitis)
Psychogenic PainPsychogenic Pain – individual feels pain but – individual feels pain but cause is emotional rather than physicalcause is emotional rather than physical

Neuropathic PainNeuropathic Pain
Sustained by aberrant processes in Sustained by aberrant processes in PNS or CNSPNS or CNS
Disproportionate to the stimulation of Disproportionate to the stimulation of nociceptornociceptor
Serves no protective functionServes no protective functionPathologic painPathologic pain

PHYSIOLOGY OF PAIN
SOURCES
Chemical/Thermal
Injury, Inflammation Heat, Cold
PAIN RECEPTORS
(Nociceptors)
DISCHARGE IMPULSES
Electrical Activity to spinal cord and onto the Brain
BRAIN = Electrical activity becomes the experience of
PAIN

Sensory ReceptorsSensory Receptors MechanoreceptorsMechanoreceptors – touch, light or deep – touch, light or deep
pressurepressure Meissner’s corpuscles (light touch), Pacinian Meissner’s corpuscles (light touch), Pacinian
corpuscles (deep pressure), Merkel’s corpuscles corpuscles (deep pressure), Merkel’s corpuscles (deep pressure)(deep pressure)
ThermoreceptorsThermoreceptors - heat, cold - heat, cold Krause’s end bulbs (Krause’s end bulbs ( temp & touch), Ruffini temp & touch), Ruffini
corpuscles (in the skin) – touch, tension, heat; (in corpuscles (in the skin) – touch, tension, heat; (in joint capsules & ligaments – change of position)joint capsules & ligaments – change of position)
Proprioceptors Proprioceptors – change in length or tension– change in length or tension Muscle SpindlesMuscle Spindles
NociceptorsNociceptors – painful stimuli – painful stimuli mechanosensitivemechanosensitive chemosensitivechemosensitive

Nerve EndingsNerve Endings
““A nerve ending is the termination of a A nerve ending is the termination of a nerve fiber in a peripheral structure.” nerve fiber in a peripheral structure.”
Nerve endings may be sensory Nerve endings may be sensory (receptor) or motor (effector).(receptor) or motor (effector).
Nerve endings may be: Nerve endings may be: Respond to phasic activity - produce an Respond to phasic activity - produce an
impulse when the stimulus is impulse when the stimulus is or or ,,))
Superficial – Merkel’s corpuscles/disks, Superficial – Merkel’s corpuscles/disks, Meissner’s corpusclesMeissner’s corpuscles
Deep – Pacinian corpuscles, Deep – Pacinian corpuscles,

Nerve EndingsNerve Endings Merkel’s corpuscles/disks - Merkel’s corpuscles/disks -
Sensitive to touch & vibrationSensitive to touch & vibration Slow adaptingSlow adapting Superficial location Superficial location Most sensitiveMost sensitive
Meissner’s corpuscles – Meissner’s corpuscles – Sensitive to light touch & vibrationsSensitive to light touch & vibrations Rapid adaptingRapid adapting Superficial locationSuperficial location
Pacinian corpuscles -Pacinian corpuscles - Sensitive to deep pressure & Sensitive to deep pressure &
vibrationsvibrations Rapid adaptingRapid adapting Deep subcutaneous tissue locationDeep subcutaneous tissue location
Krause’s end bulbs – Krause’s end bulbs – Thermoreceptor Thermoreceptor
Ruffini Ruffini corpuscles/endingscorpuscles/endings ThermoreceptorThermoreceptor Sensitive to touch & Sensitive to touch &
tensiontension Slow adaptingSlow adapting
Free nerve endings -Free nerve endings - Afferent Afferent Detects pain, touch, Detects pain, touch,
temperature, mechanical temperature, mechanical stimulistimuli

The skin receptors The skin receptors (transducers)(transducers)
a) Merkel b) Meissner
c) Ruffini d) Pacinian

NociceptorsNociceptors Sensitive to repeated or prolonged stimulationSensitive to repeated or prolonged stimulation Mechanosensitive – excited by stress & tissue damageMechanosensitive – excited by stress & tissue damage Chemosensitive – excited by the release of chemical Chemosensitive – excited by the release of chemical
mediatorsmediators Bradykinin, Histamine, Prostaglandins, Arachadonic AcidBradykinin, Histamine, Prostaglandins, Arachadonic Acid
Primary Hyperalgesia – due to injuryPrimary Hyperalgesia – due to injury Secondary Hyperalgesia – due to spreading of chemical Secondary Hyperalgesia – due to spreading of chemical
mediatorsmediators


Noxiousstimulus
Transduction Conduction Transmission
primary sensory neuron central neuron
Modulation
NociceptionNociception
“Ouch” Pain

Nociceptor ActivatorsNociceptor Activators
Heat
H+
VR1
ASIC TRPV3
Bradykinin
B1/B2 DRASIC/mDEG
Mechanical
generator potential
action potentials
Nociception – TransductionNociception – TransductionNociception – TransductionNociception – Transduction
Cold
CRM1
COX-2 Insensitive



Injury responseInjury response



Pain nerve fibers – fast pain and Pain nerve fibers – fast pain and slow painslow pain
From the pain receptors, the pain stimulus From the pain receptors, the pain stimulus is transmitted through peripheral nerves to is transmitted through peripheral nerves to the spinal cord and from there to the brain. the spinal cord and from there to the brain. This happens through two different types This happens through two different types of nerves fibers: of nerves fibers:
A-delta "fast pain” andA-delta "fast pain” andC-fibers “slow pain” nerve fibers. C-fibers “slow pain” nerve fibers.

What is “fast pain” and “slow What is “fast pain” and “slow pain”?pain”?
A pain stimulus, e.g. if you cut yourself, A pain stimulus, e.g. if you cut yourself, consists of two sensations.consists of two sensations.
first “fast pain” sensation-is experienced as first “fast pain” sensation-is experienced as sharp, bright and localized pain followed by sharp, bright and localized pain followed by
““slow pain”, more a dull, burning and slow pain”, more a dull, burning and diffused. diffused.
So,pain occurs after a short time, and So,pain occurs after a short time, and lasts a few days or weeks,lasts a few days or weeks,Chronic pain-if inappropriately processed by Chronic pain-if inappropriately processed by
the body, it can last several monthsthe body, it can last several months

Fast painFast pain
Relatively thick size nerve fibers allow the Relatively thick size nerve fibers allow the pain stimulus to be transferred very fast (at pain stimulus to be transferred very fast (at a speed of five to 30 meter/second), hence a speed of five to 30 meter/second), hence the namethe name
Due to activity of A delta fibers Due to activity of A delta fibers This is all to make the body withdraw This is all to make the body withdraw
immediately from the painful and harmful immediately from the painful and harmful stimulus, in order to avoid further damage. stimulus, in order to avoid further damage.

Slow PainSlow Painstarts immediately after the fast painstarts immediately after the fast pain is transmitted by very thin nerve fibers, is transmitted by very thin nerve fibers,
called C-nerve fibers (their diameter is called C-nerve fibers (their diameter is between 0.2 to 1 thousandth of a between 0.2 to 1 thousandth of a millimeter).millimeter).
pain impulse can only be transmitted pain impulse can only be transmitted slowly to the brain, at a speed of less than slowly to the brain, at a speed of less than 2 meters per second. 2 meters per second.
Body response -immobilization (guarding, Body response -immobilization (guarding, spasm or rigidity), so that healing can take spasm or rigidity), so that healing can take place. place.


Types of NervesTypes of Nerves
Afferent (Ascending) – transmit impulses Afferent (Ascending) – transmit impulses from the periphery to the brainfrom the periphery to the brainFirst Order neuronFirst Order neuronSecond Order neuronSecond Order neuronThird Order neuronThird Order neuron
Efferent (Descending) – transmit impulses Efferent (Descending) – transmit impulses from the brain to the peripheryfrom the brain to the periphery


First Order NeuronsFirst Order Neurons Stimulated by sensory receptorsStimulated by sensory receptors End in the dorsal horn of the spinal cordEnd in the dorsal horn of the spinal cord TypesTypes
A-alpha – non-pain impulsesA-alpha – non-pain impulses A-beta – non-pain impulsesA-beta – non-pain impulses
Large, myelinatedLarge, myelinated Low threshold mechanoreceptor; respond to light touch & Low threshold mechanoreceptor; respond to light touch &
low-intensity mechanical infolow-intensity mechanical info A-delta – A-delta – pain impulsespain impulses due to mechanical pressure due to mechanical pressure
Large diameter, thinly myelinatedLarge diameter, thinly myelinated Short duration, sharp, fast, bright, localized sensation Short duration, sharp, fast, bright, localized sensation
(prickling, stinging, burning)(prickling, stinging, burning) C – C – pain impulsespain impulses due to chemicals or mechanical due to chemicals or mechanical
Small diameter, unmyelinatedSmall diameter, unmyelinated Delayed onset, diffuse nagging sensation (aching, Delayed onset, diffuse nagging sensation (aching,
throbbing)throbbing)

Second Order NeuronsSecond Order Neurons
Receive impulses from the FON in the dorsal Receive impulses from the FON in the dorsal hornhorn Lamina II, Substantia Gelatinosa (SG) - Lamina II, Substantia Gelatinosa (SG) -
determines the input sent to Tdetermines the input sent to Transmissionransmission cells cells from peripheral nervefrom peripheral nerve
Travel along the spinothalmic tract Travel along the spinothalmic tract Pass through Reticular FormationPass through Reticular Formation
TypesTypes Wide range specificWide range specific
Receive impulses from A-beta, A-delta, & CReceive impulses from A-beta, A-delta, & C Nociceptive specificNociceptive specific
Receive impulses from A-delta & CReceive impulses from A-delta & C Ends in thalamusEnds in thalamus

Third Order NeuronsThird Order Neurons
Begins in thalamusBegins in thalamusEnds in specific brain centers (cerebral Ends in specific brain centers (cerebral
cortex)cortex)Perceive location, quality, intensityPerceive location, quality, intensityAllows to feel pain, integrate past experiences Allows to feel pain, integrate past experiences
& emotions and determine reaction to & emotions and determine reaction to stimulusstimulus

Brain mappingBrain mapping

NeurotransmittersNeurotransmitters Chemical substances that allow nerve impulses to move Chemical substances that allow nerve impulses to move
from one neuron to anotherfrom one neuron to another Found in synapsesFound in synapses
Substance P - thought to be responsible for the transmission of Substance P - thought to be responsible for the transmission of pain-producing impulsespain-producing impulses
Acetylcholine – responsible for transmitting motor nerve Acetylcholine – responsible for transmitting motor nerve impulsesimpulses
Enkephalins – reduces pain perception by bonding to pain Enkephalins – reduces pain perception by bonding to pain receptor sitesreceptor sites
Norepinephrine – causes vasoconstriction Norepinephrine – causes vasoconstriction 2 types of chemical neurotransmitters that mediate pain2 types of chemical neurotransmitters that mediate pain
Endorphins - Endorphins - morphine-like neurohormone; thought to morphine-like neurohormone; thought to pain threshold by pain threshold by binding to receptor sitesbinding to receptor sites
Serotonin - Serotonin - substance that causes local vasodilation & substance that causes local vasodilation & permeability of permeability of capillariescapillaries
Both are generated by noxious stimuli, which activate the inhibition Both are generated by noxious stimuli, which activate the inhibition of pain transmissionof pain transmission
Can be either excitatory or inhibitoryCan be either excitatory or inhibitory

Pain Control TheoriesPain Control TheoriesGate Control TheoryGate Control TheoryCentral Biasing TheoryCentral Biasing TheoryEndogenous Opiates TheoryEndogenous Opiates Theory

Endogenous Opiates TheoryEndogenous Opiates Theory
Least understood of all the theoriesLeast understood of all the theoriesStimulation of A-delta & C fibers causes Stimulation of A-delta & C fibers causes
release of B-endorphinsrelease of B-endorphinsMechanism of action – similar to Mechanism of action – similar to
enkephalins to block ascending nerve enkephalins to block ascending nerve impulsesimpulses
Examples: TENS (low freq. & long Examples: TENS (low freq. & long pulse duration)pulse duration)

Descending NeuronsDescending Neurons
Descending Pain Modulation Descending Pain Modulation (Descending Pain Control Mechanism)(Descending Pain Control Mechanism)
Transmit impulses from the brain Transmit impulses from the brain (corticospinal tract in the cortex) to the (corticospinal tract in the cortex) to the spinal cord (lamina)spinal cord (lamina) release enkephalinsrelease enkephalins release serotoninrelease serotonin

Natural Opioids-EndorphinsNatural Opioids-Endorphins
released from their storage areas in the released from their storage areas in the brain when a pain impulse reaches the brain when a pain impulse reaches the brain,brain,
bind to receptors in the pain pathway to bind to receptors in the pain pathway to block transmission and perception of pain.block transmission and perception of pain.

Central Biasing TheoryCentral Biasing Theory
Descending neurons are manipulated by: Descending neurons are manipulated by: stimulation of A-delta & C neurons, stimulation of A-delta & C neurons, cognitive processes, anxiety, depression, cognitive processes, anxiety, depression, previous experiences, expectationsprevious experiences, expectations
Mediates release of enkephalins and Mediates release of enkephalins and serotonin serotonin

Gate Control TheoryGate Control Theory
Gate - located in the dorsal horn of the spinal cordGate - located in the dorsal horn of the spinal cord Smaller, slower n. carry pain impulsesSmaller, slower n. carry pain impulses Larger, faster n. fibers carry other sensationsLarger, faster n. fibers carry other sensations Impulses from faster fibers arriving @ gate 1Impulses from faster fibers arriving @ gate 1stst inhibit pain inhibit pain
impulses impulses (acupuncture/pressure, cold, heat, chem. skin irritation).(acupuncture/pressure, cold, heat, chem. skin irritation).
Brain
Pain
Heat, Cold, Mechanical
Gate (T cells/ SG)

Gate Control TheoryGate Control TheoryMelzack and Wall 1965.Melzack and Wall 1965.
Physiological and psychological Physiological and psychological interactionsinteractions
Suggested spinal gates in the dorsal horn Suggested spinal gates in the dorsal horn at each segment of the spinal cordat each segment of the spinal cord
Competition at each gate for heat, touch or Competition at each gate for heat, touch or pain to be transmitted at each pointpain to be transmitted at each point






Pain-Inhibitory and Pain-Facilitatory Pain-Inhibitory and Pain-Facilitatory Mechanisms Within the Dorsal HornMechanisms Within the Dorsal Horn
A-DELTAA-BETA C
Neuronal circuitryNeuronal circuitrywithin the dorsal horn.within the dorsal horn.Primary afferent neuronPrimary afferent neuronaxons synapse onto axons synapse onto spinothalamic neurons spinothalamic neurons and onto inhibitory and and onto inhibitory and excitatory neurons.excitatory neurons.
TO BRAIN
+ +
+_ _+
0
STTSTTNEURONNEURON
STTSTTNEURONNEURON

Mechanisms of Pathophysiologic Pain: Mechanisms of Pathophysiologic Pain: Central Sensitization ProcessesCentral Sensitization Processes
Repeated impulse activity in C nociceptive Repeated impulse activity in C nociceptive neurons produces sensitization of neurons produces sensitization of neurons over timeneurons over time
Causes hyperalgesia, allodynia, and Causes hyperalgesia, allodynia, and spontaneous painspontaneous pain

Origin of PainOrigin of Pain
Physical cause — cause of pain can be Physical cause — cause of pain can be identifiedidentified
Psychogenic — cause of pain cannot be Psychogenic — cause of pain cannot be identifiedidentified
Referred — pain is perceived in an area Referred — pain is perceived in an area distant from its point of origindistant from its point of origin

What is Referred Pain?What is Referred Pain?
Occurs away from pain siteOccurs away from pain site
Examples: McBurney’s pointExamples: McBurney’s point


Phantom limbPhantom limb

Phantom LimbPhantom Limb

Pain thresholdPain threshold
Is the lowest intensity of stimulus that Is the lowest intensity of stimulus that causes the subject to recognize pain causes the subject to recognize pain

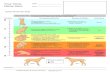
Pain Assessment ToolsPain Assessment Tools

Pain Assessment ToolsPain Assessment Tools

Common Responses to PainCommon Responses to Pain
Physiologic: ↑BP, ↑HR,↑RR, pupil dilation, Physiologic: ↑BP, ↑HR,↑RR, pupil dilation, muscle tension and tension rigidity, pallor, muscle tension and tension rigidity, pallor, ↑adrenaline level, ↑blood glucose ↑adrenaline level, ↑blood glucose
Behavioral: grimacing, moaning, crying, Behavioral: grimacing, moaning, crying, restlessnessrestlessness


Common Responses to PainCommon Responses to Pain
Affective: exaggerated weeping, Affective: exaggerated weeping, withdrawal, anxiety, depression, fear, withdrawal, anxiety, depression, fear, anger, anorexia, fatigue, hopelessness, anger, anorexia, fatigue, hopelessness, powerlessness.powerlessness.

The 4 components of painThe 4 components of pain
Sensory / PhysicalSensory / Physical Action in pain nerves (actually just sensory nerves)Action in pain nerves (actually just sensory nerves) NB: Activity in pain nerves ≠ painNB: Activity in pain nerves ≠ pain
BeliefsBeliefs Knowledge, expectations, fears, and Knowledge, expectations, fears, and attributionsattributions
BehaviouralBehavioural The effect of pain on behaviour, physical and emotionalThe effect of pain on behaviour, physical and emotional coping strategiescoping strategies
EmotionsEmotions The effect of the other three on mood and mood on the The effect of the other three on mood and mood on the
other threeother three


Cortical pain processingCortical pain processing
Sensory aspects of pain seem to be processed in the Sensory aspects of pain seem to be processed in the Somatosensory cortex.Somatosensory cortex.
Emotional distress associated with pain seems to be Emotional distress associated with pain seems to be processed in the Anterior Cingulate Cortex (ACC).processed in the Anterior Cingulate Cortex (ACC).

Factors Affecting Pain Factors Affecting Pain ExperienceExperience
CultureCultureEthnic variablesEthnic variablesFamily, gender, and age variablesFamily, gender, and age variablesReligious beliefsReligious beliefsEnvironment and support peopleEnvironment and support peopleAnxiety and other stressorsAnxiety and other stressorsPast pain experiencePast pain experience

Manipulating Pain Experience Manipulating Pain Experience FactorsFactors
Remove or alter cause of painRemove or alter cause of pain
Alter factors affecting pain toleranceAlter factors affecting pain tolerance
Initiate nonpharmacologic relief measuresInitiate nonpharmacologic relief measures

Nonpharmacologic Pain Relief Nonpharmacologic Pain Relief MeasuresMeasures
DistractionDistractionHumorHumorMusicMusic ImageryImageryRelaxationRelaxationAcupuncture Acupuncture HypnosisHypnosisTherapeutic touchTherapeutic touch

RelaxationRelaxation

AcupunctureAcupuncture

HypnosisHypnosis

Therapeutic touchTherapeutic touch

Pharmacologic Pain Relief Pharmacologic Pain Relief MeasuresMeasures
Analgesic administrationAnalgesic administration
Nonopiod analgesics e.g. NSAIDsNonopiod analgesics e.g. NSAIDs
Opioids or narcotic analgesicsOpioids or narcotic analgesics
Adjuvant drugs e.g. anticonvulsants, Adjuvant drugs e.g. anticonvulsants, antidepressants, .. antidepressants, ..

Additional Methods for Administering Additional Methods for Administering AnalgesicsAnalgesics
Patient controlled analgesiaPatient controlled analgesia
Epidural analgesiaEpidural analgesia
Local anesthesiaLocal anesthesia

Local anesthesiaLocal anesthesia

Spinal Anesthesia

EPIDURAL CATHETEREPIDURAL CATHETER


TENS



PREEMPTIVE ANALGESIAPREEMPTIVE ANALGESIAIf the body doesn’t sense the pain during If the body doesn’t sense the pain during
the procedure, the pain will be easier to the procedure, the pain will be easier to deal with post-operativelydeal with post-operatively
A patient in surgical anesthesia is not aware of A patient in surgical anesthesia is not aware of pain, but the body is still respondingpain, but the body is still responding sensitizes the nervous systemsensitizes the nervous system

CAPSAICINCAPSAICIN
Hot peppersHot peppersExcites then fatigues Excites then fatigues
nerve transmissionnerve transmissionlocal local analgesiaanalgesia
Also get endorphin Also get endorphin releaserelease

ST. JOHNSWORTST. JOHNSWORT
Arthritic painArthritic painHypericinHypericin
Stimulates neural Stimulates neural inhibitory inhibitory pathwayspathways analgesiaanalgesia
Related Documents