Pain Management in Geriatrics Min H. Huang, PT, PhD, NCS 1

Pain Management in Geriatrics Min H. Huang, PT, PhD, NCS 1.
Dec 26, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Pain Management in Geriatrics
Min H. Huang, PT, PhD, NCS
1

Learning Objectives
• Discuss the challenges and consideration for pain management in geriatric clients.
• Apply physical therapy interventions to address pain in geriatric clients.

Reading Assignments
• Guccione 2012, Chapter 21
Definition of Pain
• Pain (IASP Task Force, 1994)―Unpleasant sensory and emotional
experience
―Subjective
• Pain signals are sent to many areas in the brain that process the perception, memory/cognitive, affective/emotional, and behavioral perspectives of pain.

Pop Quiz
• Identify and compare the following terms―Transient pain
―Acute pain
―Breakthrough pain
―Chronic pain due to cancer
―Chronic pain due to non-malignant
―Persistent pain
Pain management in geriatrics
• Prevalence of pain in community dwelling older adults: 25% to 49%
• Older adults have longer pain duration and more pain sites than working-age adults.
• Challenges of pain management in geriatrics―Underreported and undertreated―Medication adherence and adverse effects―Impact of pain on function and mobility―Comorbidity: physical, mental, cognitive―Associated with socioeconomic factors
6

Consideration in the examination of pain in geriatrics
• Standard exam procedures may have to be modified, e.g. patients with congestive heart failure and COPD cannot lie flat in supine or prone during exam
• May require more time to evaluate
• May fatigue in long sessions
• May have difficulty answering abstract questions or questions that are designed for working adults
7
Persistent pain in older adults
• The American Geriatrics Society (AGS) Panel defined persistent pain as “prolonged period of time that may or may not be associated with a recognizable disease process.’’
• Etzioni 2007: “Pain of a duration or intensity that adversely affects the function or well-being of the patient, attributable to ANY etiology.”
• Chronic pain defined by the American Society of Anesthesiologists Task Force on Pain Management does NOT include cancer pain.
Screening for persistent pain in vulnerable elders (Etzioni 2007. JAGS. 55. S403-S408)
• Vulnerable Elders defined in RAND’s ACOVE project― Persons 65 + years who are at high risk for
death or functional decline
― Self-rated functional status as the predictor of death and functional decline
• IF a vulnerable elder presents for an initial evaluation, THEN a quantitative and qualitative assessment for persistent pain should be documented

Screening for persistent pain in vulnerable elders (Etzioni 2007. JAGS. 55. S403-S408
• The prevalence of inadequately treated persistent pain is high
• In community living older adults experiencing daily pain, ~ 25% received analgesia.
• Risk factors for failing to receive analgesia in patients with cancer (Centers for Medicare and Medicaid Services data, n=13,625)
―Aged 85 and older―Cognitive dysfunction―Minority ethnicity―Receiving 11 or more medications
Screening for persistent pain in vulnerable elders (Etzioni 2007. JAGS. 55. S403-S408
• If cognitively impaired, a standardized pain scale, behavioral assessment or proxy report of pain should be used.
• ALL vulnerable elderly should be screened for persistent pain annually.
• BECAUSE pain is common and underdiagnosed in older patients, and routine assessment will result in better detection and treatment and less pain.

Pop Quiz: Screening for persistent pain in vulnerable elders
• ALL adults aged 65+ years and older are considered as “vulnerable elders”True/False
• What is the frequency of screening for persistent pain in vulnerable elders?a. Twice an year
b. Once an year
• It is impossible to assess persistent pain in vulnerable elders with cognitive impairmentsTrue/False: use FACES to rate pain

Pop Quiz: pain intensity scale
• Compare the clinical utility of the following pain intensity scales―Visual analog scale (VAS)
―Verbal description scale
―Numerical Verbal rating scale: BEST
―Faces pain scale revised
―Iowa pain thermometer
Your choice and why?

Standardized assessment tool: Geriatric Pain Measure
• 24-item multidimensional questionnaire that measure pain among older adults with multiple medical problems (see form and article on Blackboard)
• Based on the relationship of pain to function in older adults.
• Identifies dimensions of pain including intensity, affect, and functional limitations
• Good Validity with comparison to McGill Pain Questionnaire (Ferrell 2000. JAGS. 48(12): 1169-73)

Pop Quiz: Consideration in plan of care
• Passive treatment modalities focused solely on temporarily decreasing pain symptoms, such as heat, cryotherapy, TENS, should be used sparingly and as a means to allow patients to participate in subsequent active treatment aimed at positively affecting functional abilities.
True/False

Ultrasound
• Evidence of use in shoulder tendinitis• OA in knee (Cochrane Review 2010 (Rutjes, 2010)
―Pulsed or continuous―Improvement in pain measured by VAS by 1.2cm
on 10 cm scale (95% CI)―Improvement in function by WOMAC disability
scale―No adverse events―Problems in studies’ methodology (low quality)
• Lack of evidence for pain in neck, hip, knee

Pop Quiz: Thermal agents
• When physical agents were applied prior to exercise, older women with knee OA generated greater force during isokinetic exercise.
True/False. Why? –Studies show an increase in muscle performance –either due to pain relief or comforting
• Use of thermal agents (heat or cool) is a commonly used home remedy for older adults, even among minority.
True/False

Manual therapy
• Spinal manipulation for low back pain ―2011 National Guideline Clearinghouse (NGC-
9259) indicate NO or INSUFFICIENT evidence ―2007 American Pain Society's clinical practice
guidelines indicate GOOD evidence―2004 Cochran review supports the use for
headache
• Manipulative therapy + exercises―Level B (fair) evidence for knee osteoarthritis―Level C (limited) evidence for hip osteoarthritis―Cochran review supports the use for neck pain
TENS
• 2009 Cochrane review― Compared TENS with sham treatment for knee
OA
― 11 Used TENS, 4 Interferential, 1 TENS and IFC, and 2 pulsed electrostimulation
― Change of 0.2 cm on 10 cm VAS (SMD was -.07 cm)
― Could NOT determine if TENS helped with function or pain relief

Pop Quiz: TENS parameters
• Describe the key parameters of TENS for management of postoperative pain―Review Table 21-1 on page 407 in your
textbook
―Frequency: 100hz
―Intensity: highest to tolerance
―Duration/; 30min to 24hrs
―What were the conditions of patients listed in this table? CABG, postthoracotomy, cardiac suergery, TKA, abdominal surgery

Guided imagery
• An alternative medicine technique
• A powerful psychological strategy
• Focus on relaxation, mind and body harmony
• Aid clients to use mental imagery to help with health problems, e.g. imagining the busy, focused buzz of thousands of loyal immune cells
www.med.umich.edu/cancer/support/guided_imagery.shtml

Guided imagery in patients with fibromyalgia (Verkaik, 2013. RCT, n=65)
• Daily imagery for 4 weeks―Example of the instruction “now imagine that you
leave all the pain you experience at the beach post.”
• Visual Analogue Scale for pain
• Fibromyalgia Impact Questionnaire for functional status
• Chronic Pain Self-Efficacy Scale for self-efficacy
• NO effects could be established
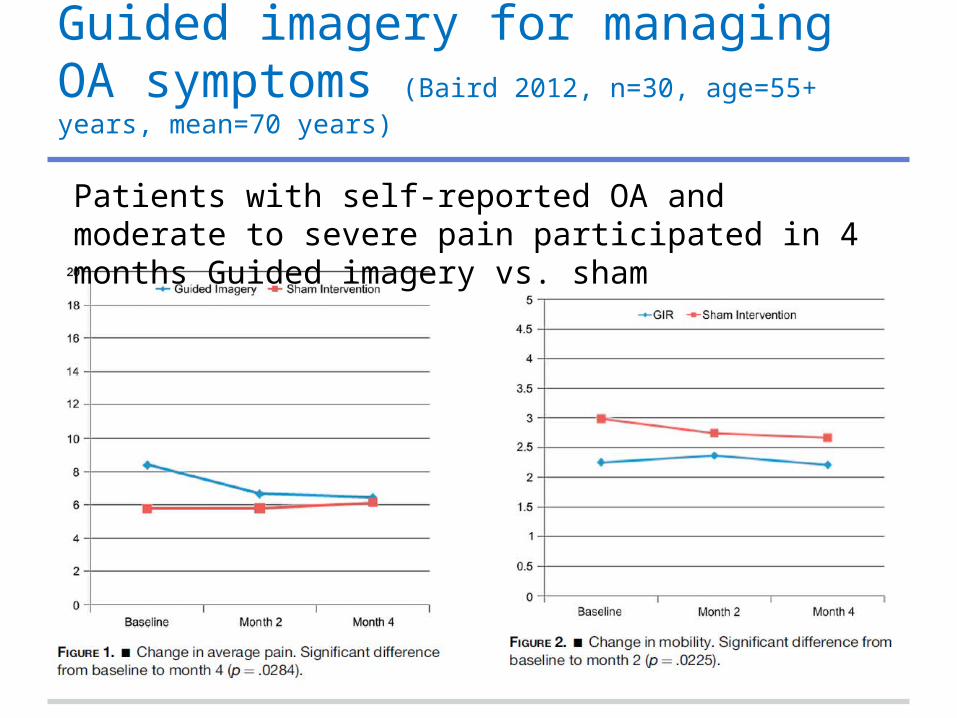
Guided imagery for managing OA symptoms (Baird 2012, n=30, age=55+ years, mean=70 years)
Patients with self-reported OA and moderate to severe pain participated in 4 months Guided imagery vs. sham

Using real-time functional MRI as biofeedback to control pain
• Real-time fMRI feedback is a potential tool for pain modulation that directly targets the brain to restore pain regulatory function
• After training, patients with chronic pain improved their ability to control anterior cingulate cortex activation and consequently, ability to modulate the pain
• Stanford’s lab: Human Body - Pushing The Limits http://paincenter.stanford.edu/press/ video_discovery.html

Cognitive behavioral therapy (CBT)
• Standard treatment for chronic pain patients who have to deal with psychological distress and disabilities

Cognitive behavioral therapy (CBT)
• Teach patients specific cognitive and behavioral skills to better manage pain
• Inform patients regarding the effects that specific cognitions (thoughts, beliefs, attitudes), emotions (fear of pain), and behaviors (activity avoidance due to fear of pain) can have on pain
• Emphasize the primary role that patients can play in controlling their own pain as well as adaptations to pain

Use of cognitive behavioral therapy by PTs nationwide (Beissner 2009. PTJ. 89(5): 456–469)
• CBT techniques: pacing (81%), pleasurable activity scheduling (30%)
• Non-CBT interventions: exercises focusing on joint stability (94%) and mobility (94%), strengthening and stretching (91%).
• Barriers to use of CBT: lack of knowledge of and skill in the techniques, reimbursement concerns, and time constraints.
http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2716379/

Acceptance and commitment therapy (ACT)
• Attempts to change certain aversive internal experiences (e.g. chronic pain) are likely to be futile and may result in increased distress
• Awareness and non-judgmental acceptance of all experiences, both negative and positive
• Identify valued life directions and appropriate action toward goals that support those values
• The objective is to improve function and decrease interference of pain

RCT comparing CBT and ACT (Wetherell 2011. PAIN 152 (2011) 2098–2107)
• Individuals with chronic, non-malignant pain for at least 6 months (N = 114) received 8 weeks of CBT or ACT
• All participants improved on pain interference, depression, pain-related anxiety
• NO significant group differences in improvement on any outcome variables
• ACT participants reported significantly higher satisfaction than did CBT participants
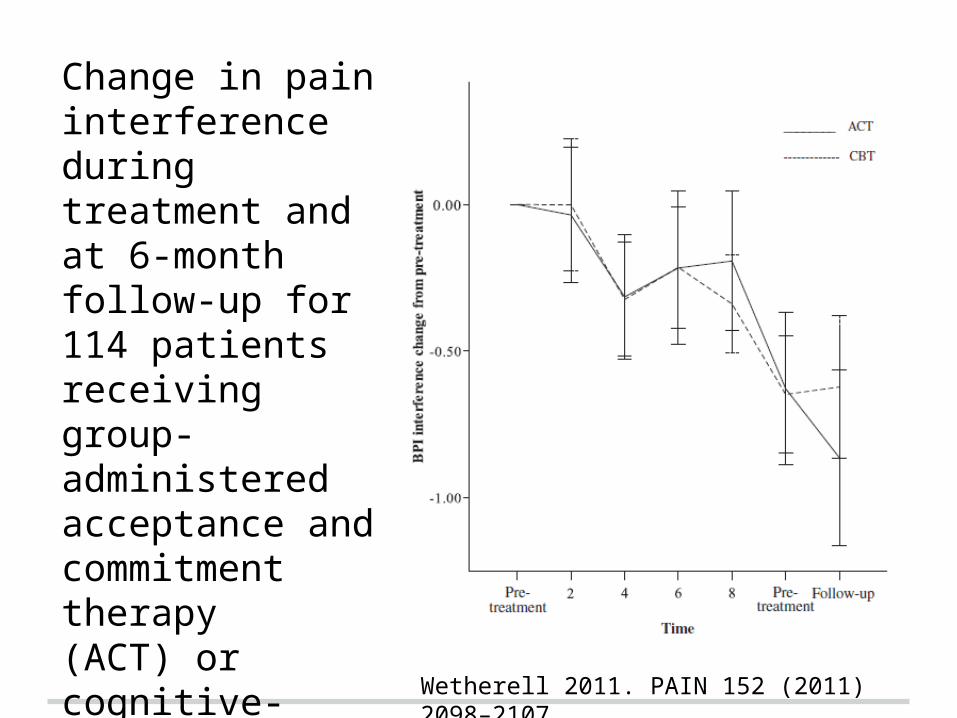
Change in pain interference during treatment and at 6-month follow-up for114 patients receiving group-administered acceptance and commitment therapy(ACT) or cognitive-behavioral therapy (CBT) for chronic pain.
Wetherell 2011. PAIN 152 (2011) 2098–2107
Related Documents











