6/22/2011 1 พงศ์ภารดี เจาฑะเกษตริน หัวหน้าสาขาการบาบัดความปวด ภาควิชาวิสัญญีวิทยา คณะแพทย์ศาสตร์ศิริราชพยาบาล Palliative care ไม่ใช่ เพียงแค่ให้ยาแก้ปวดแก่ผู้ป่วย!! - การตรวจร่างกาย / Clinical examination ถือว่า เป็นสิ ่งสาคัญที ่สุดเมื ่อ เทียบกับกิจกรรมอื ่นๆ ที ่ให้เพื ่อการบาบัดรักษาผู ้ป่ วย - - รวมทั้ง palliative and terminal care - รวมทั้ง การบาบัดอาการปวด และอาการอื ่นๆ - ปัจจัยทางสังคม , สุขภาพจิต และ spiritual จะมีบทบาทสาคัญมากขึ้น เรื ่อยๆ ตามการเปลี ่ยนแปลง : Curative therapy Palliative therapy Palliative/terminal care Pain Fatigue/Asthenia Constipation Dyspnea Nausea Vomiting Delirium Depression/suffering 80 - 90% 75 - 90% 70% 60% 50 - 60% 30% 30 - 90% 40 - 60% palliative care Oncological patients 100 % 0 curative therapy Diagnosis Death 30% 60% PAIN PREVALENCE 80 to 90% Pain Treatment ไม่มีทางรักษาให้หายขาด = รักษาไม่ได้ การรักษาอาการ ก็ต้องรักษาตามสาเหตุ ยิ ่งเมื ่อผู ้ป ่วยเข้าสู่ระยะสุดท้าย การปรึกษาหารือภายใน ทีมผู้รักษา หรือกับผู้มีส่วนร่วมอื ่นๆ โดยเฉพาะ ครอบครัว ก็ยิ ่งทวีความสาคัญมากขึ ้นตามลาดับ

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

6/22/2011
1
พงศภารด เจาฑะเกษตรน
หวหนาสาขาการบ าบดความปวด
ภาควชาวสญญวทยา คณะแพทยศาสตรศรราชพยาบาล
Palliative care ไมใช เพยงแคใหยาแกปวดแกผปวย!! - การตรวจรางกาย / Clinical examination ถอวา เปนสงส าคญทสดเมอ
เทยบกบกจกรรมอนๆ ทใหเพอการบ าบดรกษาผปวย - - รวมทง palliative and terminal care - รวมทง การบ าบดอาการปวด และอาการอนๆ
- ปจจยทางสงคม , สขภาพจต และ spiritual จะมบทบาทส าคญมากขน
เรอยๆ ตามการเปลยนแปลง :
Curative therapy
Palliative therapy
Palliative/terminal care
Pain
Fatigue/Asthenia
Constipation
Dyspnea
Nausea
Vomiting
Delirium
Depression/suffering
80 - 90%
75 - 90%
70%
60%
50 - 60%
30%
30 - 90%
40 - 60% palliative care
On
colo
gic
al p
atie
nts
100 %
0
curative therapy
Diagnosis Death
30%
60%
PAIN PREVALENCE
80 to 90%
Pain Treatment
ไมมทางรกษาใหหายขาด = รกษาไมได
การรกษาอาการ กตองรกษาตามสาเหต
ยงเมอผปวยเขาสระยะสดทาย การปรกษาหารอภายใน
ทมผรกษา หรอกบผมสวนรวมอนๆ โดยเฉพาะ
ครอบครว กยงทวความส าคญมากขนตามล าดบ
6/22/2011
2
ผใหการดแลคอผทบอกไดดทสดวาผปวยมความปวด
ผปวยทปวดจะตองมอาการแสดงทชดเจน เชน รองครวญ
คราง มสญญาณชพผดปกต หรอ กนไมได
ความปวดเปนสวนหนงของภาวะสงวย
การใชยา โอปออยด จะท าใหผปวยตดยา
ควรเกบมอรฟนและยาโอปออยดชนดแรง ไวใชในผปวย
ระยะสดทายเทานน
มอรฟนและโอปออยดอนๆ สามารถท าใหเกดการกด
หายใจ จนถงตายได
ยาแกปวดควรใหแก ผปวยทมอาการปวดเทานน
ความกงวลใจมกจะท าใหปวดมากขน
เบออาหาร น าหนกลด
นอนไมหลบ
ไมอยากพดคย หรอมสงคมกบผอน
เศรา , กงวลใจ, หรอ ซมเศรา
เกดความกดดนทางกาย และทางการพดจา , ไมแนนอน , มพฤตกรรมเปลยนแปลงและ ตอตานการดแล
เดนไมคลอง หรอ ไมอยากเลอนไหว และ ตดเตยง
มแผลตามผวหนง
ปสสาวะล าบาก
มความเสยงตอการ ใชสารเสพตด
ลดความสามารถในการท ากจกรรมท วไป
ความตานทานโรคลดลง
ผปวยทเสยงตอการไดรบการรกษาไมเพยงพอ
ชนกลมนอย / ผอพยพ / ผมปญหาในการสอสาร
ผหญง
ผสงอาย > 70 ป
Vuorinen E. Clin J Pain 1993; 9:272-8. Cleeland CS, et al New Engl J Med 1994;330:592-6. Brescia J
¼ ของผปวยพบเมอเรมวนจฉย
2/3 ของผปวยพบระหวางท รบการรกษามะเรง
¾ ของผปวยพบในระยะทโรคลกลาม
6/22/2011
3
14
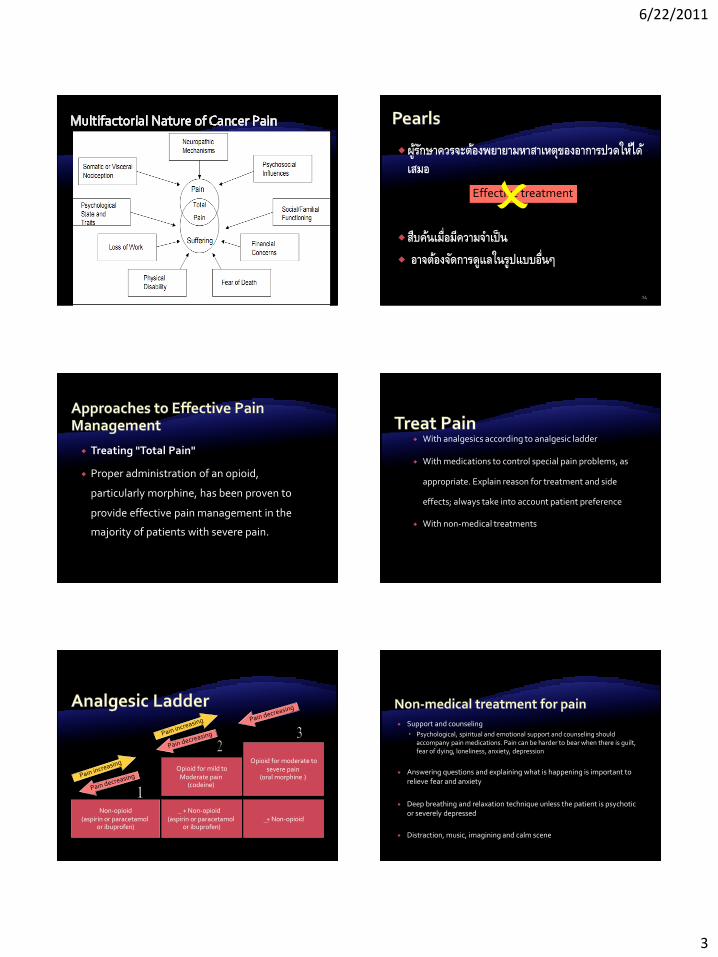
ผรกษาควรจะตองพยายามหาสาเหตของอาการปวดใหได
เสมอ
สบคนเมอมความจ าเปน
อาจตองจดการดแลในรปแบบอนๆ
Effective treatment
Treating "Total Pain"
Proper administration of an opioid,
particularly morphine, has been proven to
provide effective pain management in the
majority of patients with severe pain.
With analgesics according to analgesic ladder
With medications to control special pain problems, as
appropriate. Explain reason for treatment and side
effects; always take into account patient preference
With non-medical treatments
Non-opioid (aspirin or paracetamol
or ibuprofen)
+ Non-opioid (aspirin or paracetamol
or ibuprofen)
Opioid for mild to Moderate pain
(codeine)
+ Non-opioid
Opioid for moderate to severe pain
(oral morphine )
Support and counseling
Psychological, spiritual and emotional support and counseling should accompany pain medications. Pain can be harder to bear when there is guilt, fear of dying, loneliness, anxiety, depression
Answering questions and explaining what is happening is important to relieve fear and anxiety
Deep breathing and relaxation technique unless the patient is psychotic or severely depressed
Distraction, music, imagining and calm scene

6/22/2011
4
By mouth ( rectal is an alternative –avoid IM)
By clock
Give pain killers at fixed time interval ( by clock or radio or sun)
Start with small dose, then titrate dose against patient’s pain, until the
patient is comfortable
Next dose should happen before effect of previous dose wears off.
For breakthrough pain, give an extra “ rescue” dose same dosing of the
4- hourly dose) in addition to the regular schedule.
By the individual
20
• Tumor: 77-80% Bone pain
Compression of spinal cord/other structures
Neural damage
Obstruction hollow organs
Paraneoplastic pain syndromes
• Cancer treatment: 15-25 %
Surgical (amputation; thoracotomy; mastectomy)
Chemotherapy (neuropathy, inflammation)
Radiotherapy (plexopathy, myelopathy, inflammation)
Paraneoplastic pain syndromes
• Non-cancer related pain: 3-5 %
• Pain of unknown origin
21
• Temporal relationship Acute pain
Chronic pain
Incident pain/break through pain
• Physiopathological mechanism Nociceptive pain
• Somatic pain
Deep
Superficial
• Visceral pain
Neuropathic pain
22 Baron R, Binder A. 2004 Orthopade 2004; 33: 568-75.
Tissue/ organs
C Fibre
C Fibre
A Fibre
Nociceptive component: Sprouting from C-Fibres into the disc
Neuropathic component I: Damage to a branch of the C Fibre due to compression and inflammatory mediators
Neuropathic component II: Compression of nerve root
Neuropathic component III: Damage to nerve root by inflammatory mediators
Central sensitisation
Tumor growth
“อาการแนนทองตรงน นาจะเกดจากตบโต” “การเจบแขนและชา นาจะเกดจากเสนประสาทแขนถกตอมน าเหลองกดทบ” ฯลฯ
“การรกษาทนาจะดทสดส าหรบคณในขณะน
คอ การใชยาระงบปวด” ยงมการรกษาอนอกเชน การฉายรงส ....ทนาจะไดผล ฯลฯ

6/22/2011
5
Acute Pain
Follows injury...resolves
Objective physical signs—COMMON
Chronic Pain--cancer, term. illness
Objective signs RARE
Patient may not “look” like he/she is in pain
Acute Pain
Nociceptive
Neuropathic
Mixed
Chronic Pain
Nociceptive
Neuropathic
Mixed
PAIN
Persistent Pain (Back ground)
Breakthrough Pain
1. Which cancer patients need strong opioids ?
2. How do we administer strong opioids?
3. Opioids and the myths…
4. Which strong opioids do we have to use?
Step 1:
non opioid + adjuvant
Step 2:
“weak” opioid + step 1 meds
Step 3:
“strong” opioid + step 1 meds
Non-opioid ± Adjuvant
Weak opioid ± Non-opioid ± Adjuvant
Strong opioid ± Non-opioid
± Adjuvant
By the ladder
By the clock
By the mouth
By individual
To cure sometimes To relief often To comfort always
28
Mild Moderate Severe
1. Assess pain severity
Place a cross X along the line to indicate how strong your
pain is at the present time
No pain|______________________________|Worst possible pain
No pain|______________________________|Complete pain relief
Relief 0 100
No sleep|_____________________________|Best sleep ever
Lowest 0 100 Best feeling ever
feeling
Note: Lines must be exactly 100 mm long
A detailed history.
A physical examination.
A psychosocial assessment.
A diagnostic evaluation.
Assess patient for pain
JCAHO recognize the right of patients to appropriate assessment and management of pain
ความปวดมหลายมต
ความปวด และอาการอนๆอาจเปลยนแปลงอยางรวดเรว
โดยเฉพาะ ผทโรคลกลาม
ประเมนผปวยทกราย และตองเชอ ผปวย
ใหความเชอมนวา ความปวดสวนใหญนนสามารถบรรเทาได

6/22/2011
6
Step 1: ประเมนวาอาการปวดเกดจากการกระจายของกอนทม วธการรกษา หรอ ไมเกยวของกบสาเหตดงกลาว
Step 2: วด ความรนแรงของอาการปวด และอาการอนๆ .
Step 3: ประเมนมตอนๆ ทอาจเปนสาเหตและการแสดงออกของอาการปวดไดในรายนนๆ.
Step 4: รวาอะไรเปนปจจยทอาจท าใหการรกษาไมไดผล.
ประวตความเจบปวยและการรกษาโรค
อาการทางกาย
อาการทางจตใจ
อ านาจในการตดสนใจ
ความสามารถในการใหขอมล แกแพทย
สงคม และสถานการณ
ความตองการทางจตวญญาณ
ความตองการท วไป
ความพรอมในการเผชญความตาย
PHYSICAL Other symptoms
Undesirable effects of Rx
Insomnia & chronic fatigue
PSYCHOLOGICAL Anger at delay in Dx
Anger at therapeutic failure
Disfigurement
Fears of pain and/ or death
Feelings of helplessness
SPIRITUAL Why has this happened to me?
Why does God allow me to suffer like this?
What’s the point of it all
Is there any meaning or purpose in life?
Can I be forgiven for past wrongdoing?
SOCIAL Worry about family & financial
Loss of job prestige & income
Loss of social position
Loss of role in family
Feelings of abandonment and isolation
soma
Spiritual
Social Psyche
Male
Female
Deceased
Ill person
Married or permanent relationship
Transitory relationship
Separation
Divorce
Miscarriage
Twins
Give only one drug from the opioid and non-opioid group at a time:* * exception : if no codeine, aspirin q 4 hours can be combined with Paracetamol q 4 hrs –overlap so one is given every 2 hrs.
แบงเปาหมายออกเปนล าดบขน
STEPWISE GOALS FOR PAIN CONTROL
ไมปวดเลยตอนกลางคน Pain free at night
ไมปวดเลยเวลาพกผอน Pain free at rest
ไมปวดเลยเวลาเคลอนไหว Pain free on movement
6/22/2011
7
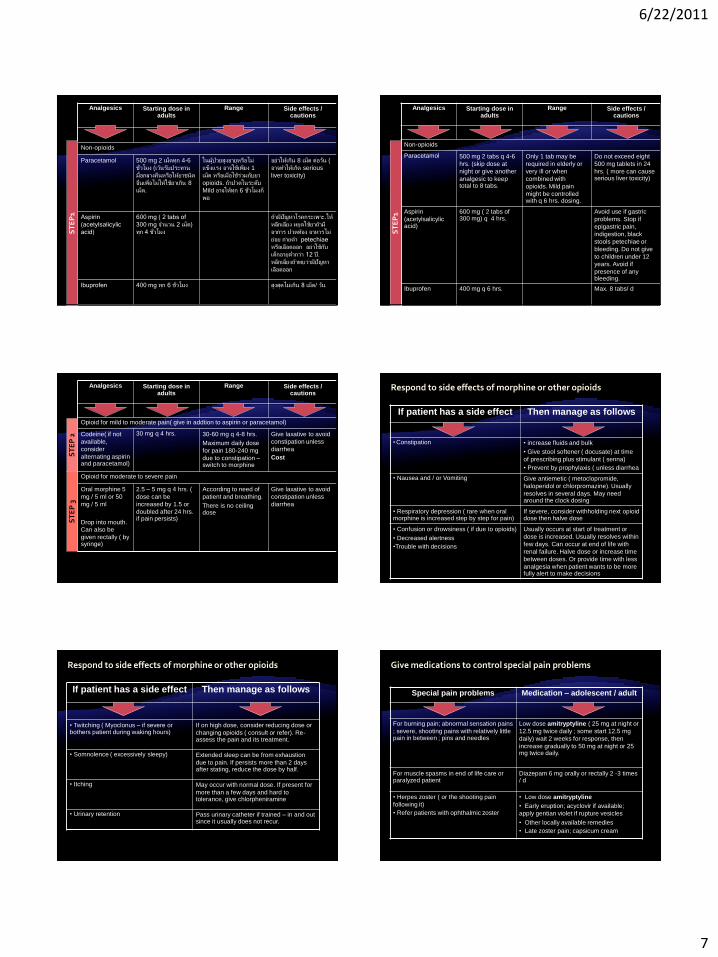
Analgesics Starting dose in adults
Range Side effects / cautions
Non-opioids
Paracetamol 500 mg 2 เมดทก 4-6
ชวโมง (เวนรบประทาน
มอกลางคนหรอใหยาชนด
อนเพอไมใหใชยาเกน 8
เมด.
ในผปวยสงอายหรอไม
แขงแรง อาจใชเพยง 1
เมด หรอเมอใชรวมกบยา
opioids. ถาปวดในระดบ
Mild อาจใหทก 6 ชวโมงก
พอ
อยาใหเกน 8 เมด ตอวน (
อาจท าใหเกด serious
liver toxicity)
Aspirin
(acetylsalicylic
acid)
600 mg ( 2 tabs of
300 mg จ านวน 2 เมด)
ทก 4 ชวโมง
ถามปญหาโรคกระเพาะ.ให
หลกเลยง หยดใชยาถาม
อาการ ปวดทอง อาหารไม
ยอย ถายด า petechiae
หรอเลอดออก อยาใชกบ
เดกอายต ากวา 12 ป.
หลกเลยงถาพบวามปญหา
เลอดออก
Ibuprofen 400 mg ทก 6 ชวโมง สงสดไมเกน 8 เมด/ วน
ST
EP
1
Analgesics Starting dose in adults
Range Side effects / cautions
Non-opioids
Paracetamol 500 mg 2 tabs q 4-6
hrs. (skip dose at
night or give another
analgesic to keep total to 8 tabs.
Only 1 tab may be
required in elderly or
very ill or when
combined with
opioids. Mild pain
might be controlled with q 6 hrs. dosing.
Do not exceed eight
500 mg tablets in 24
hrs. ( more can cause serious liver toxicity)
Aspirin
(acetylsalicylic acid)
600 mg ( 2 tabs of 300 mg) q 4 hrs.
Avoid use if gastric
problems. Stop if
epigastric pain,
indigestion, black
stools petechiae or
bleeding. Do not give
to children under 12
years. Avoid if
presence of any bleeding.
Ibuprofen 400 mg q 6 hrs. Max. 8 tabs/ d
ST
EP
1 Analgesics Starting dose in
adults Range Side effects /
cautions
Opioid for mild to moderate pain( give in addtion to aspirin or paracetamol)
Codeine( if not
available,
consider
alternating aspirin and paracetamol)
30 mg q 4 hrs. 30-60 mg q 4-8 hrs.
Maximum daily dose
for pain 180-240 mg
due to constipation – switch to morphine
Give laxative to avoid
constipation unless
diarrhea
Cost
Opioid for moderate to severe pain
Oral morphine 5
mg / 5 ml or 50
mg / 5 ml
Drop into mouth.
Can also be
given rectally ( by syringe)
2.5 – 5 mg q 4 hrs. (
dose can be
increased by 1.5 or
doubled after 24 hrs. if pain persists)
According to need of
patient and breathing.
There is no ceiling dose
Give laxative to avoid
constipation unless
diarrhea
ST
EP
2
ST
EP
3
If patient has a side effect Then manage as follows
• Constipation • increase fluids and bulk
• Give stool softener ( docusate) at time
of prescribing plus stimulant ( senna)
• Prevent by prophylaxis ( unless diarrhea
• Nausea and / or Vomiting Give antiemetic ( metoclopromide,
haloperidol or chlorpromazine). Usually
resolves in several days. May need around the clock dosing
• Respiratory depression ( rare when oral morphine is increased step by step for pain)
If severe, consider withholding next opioid dose then halve dose
• Confusion or drowsiness ( if due to opioids)
• Decreased alertness
•Trouble with decisions
Usually occurs at start of treatment or
dose is increased. Usually resolves within
few days. Can occur at end of life with
renal failure. Halve dose or increase time
between doses. Or provide time with less
analgesia when patient wants to be more fully alert to make decisions
Respond to side effects of morphine or other opioids
If patient has a side effect Then manage as follows
• Twitching ( Myoclonus – if severe or bothers patient during waking hours)
If on high dose, consider reducing dose or
changing opioids ( consult or refer). Re-assess the pain and its treatment.
• Somnolence ( excessively sleepy) Extended sleep can be from exhaustion
due to pain. If persists more than 2 days after stating, reduce the dose by half.
• Itching May occur with normal dose. If present for
more than a few days and hard to tolerance, give chlorpheniramine
• Urinary retention Pass urinary catheter if trained – in and out since it usually does not recur.
Respond to side effects of morphine or other opioids
Special pain problems Medication – adolescent / adult
For burning pain; abnormal sensation pains
; severe, shooting pains with relatively little pain in between ; pins and needles
Low dose amitryptyline ( 25 mg at night or
12.5 mg twice daily ; some start 12.5 mg
daily) wait 2 weeks for response, then
increase gradually to 50 mg at night or 25 mg twice daily.
For muscle spasms in end of life care or paralyzed patient
Diazepam 6 mg orally or rectally 2 -3 times / d
• Herpes zoster ( or the shooting pain
following it)
• Refer patients with ophthalmic zoster
• Low dose amitryptyline
• Early eruption; acyclovir if available;
apply gentian violet if rupture vesicles
• Other locally available remedies
• Late zoster pain; capsicum cream
Give medications to control special pain problems

6/22/2011
8
Special pain problems Medication – adolescent / adult
Gastrointestinal pain from colic only after
exclusion of intestinal obstruction
( vomiting, no stool and gas passing, visible bowel movements.)
Codeine 30 mg q 4 hrs. or hyoscine (
Buscopan®) 10 mg x3 daily ( can increased up to 40 mgs x3 daily.
Bone pain or renal colic or dysmenorrhea Ibuprofen ( or other NSAIDs)
If pain from
• swelling around tumor
• Severe esophagus ulceration and can not
swallow
• Nerve or spinal cord compression
• Persistent severe headache ( likely from increased ICP
•When giving end of life care and referral
not desired, see instruction for careful steroids use under clinical supervision.
Give medications to control special pain problems
สอนใหผปวยและญาต ชวยตวเองท
บานได เมอมอาการ
ใหยาแกปวดและยาอนๆตามความจ า
เปน
นกถงวธการอนทอาจชวยลดอาการ
ปวดได
ใหความรและขอมลทผปวยตองการ
ทราบ และทควรจะทราบ
สอนครอบครวของผปวยใหใช
oral morphine แนะน าการใชยาอยางถกตอง รกษาอาการขางเคยง ถาอาการปวด
มากขน : เพมขนาดยา ดขน: ใหลดขนาดยาลงครงหนง
อยาหยดยามอรฟนทนท
อธบายความถ และเหตผลทตองไดรบยา ตามเวลาอยางตอเนอง
ไมตองรอใหปวดมากจงจะกนยา ยาทจะใหในชวงตอไป ควรจะใหกอนท
ยาทไดรบในชวงแรกจะหมดฤทธ – โดยมา ทก 4 ชวโมง
เปาหมายของการรกษาคอ
ไมมอาการปวดอก
ผปวยควรครองสต รสกตวไดดพอประมาณ
เทยาน ามอรฟนลงในถวย ใช syringe ดดยาน า ในขนาดทตองการ
คอยๆ หยดยา จาก syringe เขาปากคนไข อยาใชเขม เทยาน ามอรฟนกลบเขาไปในขวด ใหยาสม าเสมอทก 4 ชวโมง และใหยาน า 2 เทาในมอกอนนอน
ใหยาเพมอกไดถามอาการปวด กอนทจะถงมอตอไป อยาหยดใหมอรฟน อยางกระทนหน

6/22/2011
9
ใชวธอนๆรวมกบยาแกปวด ถาผปวยเหน
ดวย และถาพบวาไดผล
ประคบประคองอารมย ความรสก
Emotional support
ใชวธทางกายภาพ
สมผส ( ลบไล , นวด , เขยา , ส น )
ความเยน หรอ ความรอน
หายใจลกๆ
ใชวธอนๆรวมกบยาแกปวด ถาผปวยเหนดวย
และถาพบวาไดผล ใชวธรบร เบยงเบนความสนใจ เสยงเพลง จนตนาการวารสกสบาย
สวดมนต ( respect patient’s
practice) การปฏบตพนบานทชวยเหลอได และไมเปนอนตราย
– ตองรวามวธอะไรบางทชมชนใชอยแลว
คลนไส – มกจะหายภายใน 2-3 วน หลงการใชมอรฟน และไมกลบมามอาการอก.
ทองผก
ปากแหง – วธแกใหจบน า
งวงซม – มกจะหายภายใน 2-3 วน หลงการใชมอรฟน; ถาอาการยงมอย หรอ ไมดขน ใหลดขนาดยาลงครงหนง และหาคนชวย
Each point represents at least ≥ 20 patients
0
50
100
150
200
250
Basis M1 M2 M3 M4 M5 M6 Eindp
Mea
n T
TS
-fen
tany
l dos
is
(µg/
h.+
/- S
D)
Lung Prostate Breast Gastro-intestinal
Which cancer patients need strong opioids?
65
~200mg/d oral morphine
~600mg/d oral morphine
Each point represents ≥ patients
0
50
100
150
200
250
Basis M2 M4 M6 Eindp
Mea
n T
TS
-fen
tany
l dos
e (µ
g/h.
+/-S
D)
Totaal 60-69 y. 70-79 y. ≥80 y.
453
412
209 162 116
101
65 452
Mean dose TTS-fentanyl in function of age
~200mg/d oral morphine
~600mg/d oral morphine
1 - Identify the pain
Acute - chronic
Nociceptive – neuropathic
Pain syndrome
- Measure pain (NRS-VAS)
2 – Explain pain to patient /family/caregivers
4 How do we administer strong opioids?
6/22/2011
10
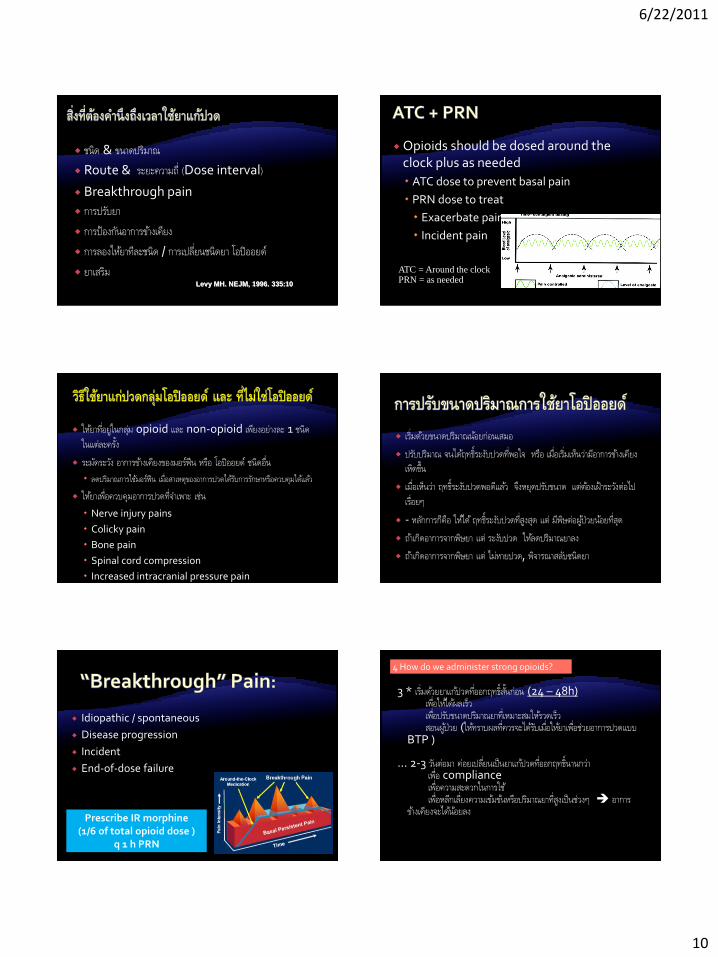
ชนด & ขนาดปรมาณ
Route & ระยะความถ (Dose interval)
Breakthrough pain
การปรบยา
การปองกนอาการขางเคยง
การลองใหยาทละชนด / การเปลยนชนดยา โอปออยด
ยาเสรม Levy MH. NEJM, 1996. 335:10
Opioids should be dosed around the clock plus as needed
ATC dose to prevent basal pain
PRN dose to treat
Exacerbate pain
Incident pain
ATC = Around the clock PRN = as needed
ใหยาทอยในกลม opioid และ non-opioid เพยงอยางละ 1 ชนด ในแตละคร ง
ระมดระวง อาการขางเคยงของมอรฟน หรอ โอปออยด ชนดอน
ลดปรมาณการใชมอรฟน เมอสาเหตของอาการปวดไดรบการรกษาหรอควบคมไดแลว
ใหยาเพอควบคมอาการปวดทจ าเพาะ เชน
Nerve injury pains
Colicky pain
Bone pain
Spinal cord compression
Increased intracranial pressure pain
เรมดวยขนาดปรมาณนอยกอนเสมอ
ปรบปรมาณ จนไดฤทธระงบปวดทพอใจ หรอ เมอเรมเหนวามอาการขางเคยงเหดขน
เมอเหนวา ฤทธระงบปวดพอดแลว จงหยดปรบขนาด แตตองเฝาระวงตอไป
เรอยๆ
- หลกการกคอ ใหได ฤทธระงบปวดทสงสด แต มพษตอผปวยนอยทสด
ถาเกดอาการจากพษยา แต ระงบปวด ใหลดปรมาณยาลง
ถาเกดอาการจากพษยา แต ไมหายปวด, พจารณาสลบชนดยา
Idiopathic / spontaneous
Disease progression
Incident
End-of-dose failure
Prescribe IR morphine (1/6 of total opioid dose )
q 1 h PRN
3 * เรมดวยยาแกปวดทออกฤทธส นกอน (24 – 48h) เพอใหไดผลเรว เพอปรบขนาดปรมาณยาทเหมาะสมใหรวดเรว สอนผปวย (ใหทราบผลทควรจะไดรบเมอใหยาเพอชวยอาการปวดแบบ
BTP ) … 2-3 วนตอมา คอยเปลยนเปนยาแกปวดทออกฤทธนานกวา เพอ compliance เพอความสะดวกในการใช เพอหลกเลยงความเขมขนหรอปรมาณยาทสงเปนชวงๆ อาการ
ขางเคยงจะไดนอยลง
4 How do we administer strong opioids?

6/22/2011
11
* เรมใหยาแกปวดทออกฤทธนาน ถาไมมปญหาปวดรนแรง แตเรอรง …ใหยาแกปวด โอปออยดทออกฤทธสน เพอชวยบรรเทาอาการปวดแบบ
breakthrough pain ใหปรมาณ - 1/12 ของขนาดทใช ถาการบรรเทาปวด VAS นอยกวา ≤
5 ใหปรมาณ- 1/6 ของขนาดทใช หากบรรเทาอาการปวดไดไมคอยดเทาไหร VAS >5
…ประเมน และเปลยน ปรมาณยาแกปวดทใชเพอลดอาการ BTP มาเปนปรมาณยาทใหแบบตอเนอง
ถาตองใหยาแกปวดเพอลดอาการปวด breakthrough มากกวา ≥3 ครง / วน
4 How do we administer strong opioids?
Regular ATC opioid administration with adequate breakthrough dosing and adjuvants as required
Route Selection
Use least invasive route possible
Consider patient convenience and compliance
4 Side effects management
laxatives always
anti-emetics as needed
(confusion-somnolence)
5 Use co analgesics if needed
Corticosteroids
Antidepressants-Anticonvulsants
Constipation
Nausea/vomiting
Urinary retention
Itch/rash
Dry mouth
Respiratory depression
Drug interactions
Common Less frequent
Rare
Constipation Urinary retention Allergy
Nausea Pruritis Respiratory depression
Sedation Severe myoclonus
Dry mouth confusion
Psychotomimetic effects
Sedation
Patience
Stimulants Methylphenidate
Nausea
Patience
Anti-emetic
Constipation
No patience
Stool softener and cathartic: Senna
lactulose

6/22/2011
12
6. A given analgesic drug “does not work”:
most frequent reasons:
inadequate titration (dose x 3 by our PST)
less than optimal management of side effects
resistant pain to this drug
Compliance
Absorption
Adjuvant Rx, drug and non-drug
Increase the dose
Change route of administration
Change the drug, i.e. opioid switch
Address psychosocial problems
Specific therapies Radiotherapy, chemotherapy,surgery
Co-analgesics Drugs, nerve blocks, TENS, relaxation, acupuncture
Morphine Fentanyl
Methadone Hydromorphone
Oxycodone
Severe pain
APAP + codeine APAP + hydrocodone
APAP + tramal APAP + oxycodone
Aspirin Acetaminophen
NSAIDs
Moderate pain
Mild pain
Non-steroidal anti-inflammatory drugs
Corticosteroids
Anti-convulsants
Anti-depressants
Anti-spasmodics
Anxiolytics
Oral local anaesthetic agents
NMDA receptor antagonists
Effective in mild to moderate Pain
Especially good for pain of bone metastasis
Ceiling effect
GI and renal toxicity
Opioid sparing
Surgery
Radiotherapy
Interventional radiology
Physiotherapy
Occupational therapy
Massage / Lymphatic drainage
6/22/2011
13
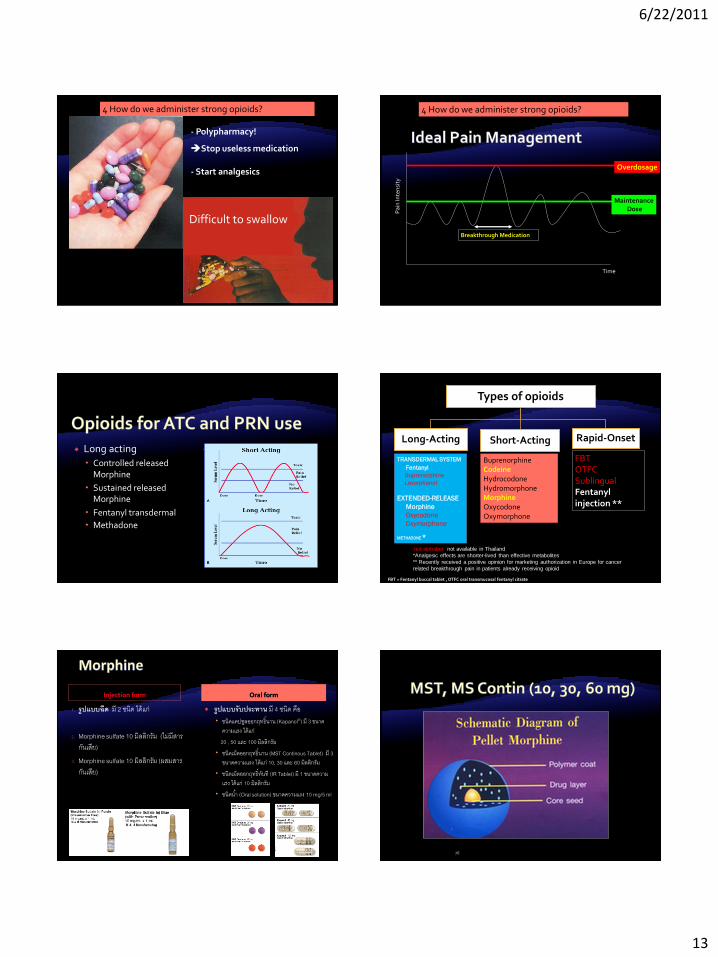
- Polypharmacy!
Stop useless medication
- Start analgesics
Difficult to swallow
4 How do we administer strong opioids?
Pai
n In
ten
sity
Time
Maintenance Dose
Overdosage
Breakthrough Medication
4 How do we administer strong opioids?
Long acting
Controlled released Morphine
Sustained released Morphine
Fentanyl transdermal
Methadone
Short acting
Morphine syrup
Transmucosal fentanyl
Types of opioids
Long-Acting Short-Acting Rapid-Onset
TRANSDERMAL SYSTEM
Fentanyl
Buprenorphine
Levorphanol
EXTENDED-RELEASE
Morphine
Oxycodone
Oxymorphone
METHADONE *
Buprenorphine Codeine Hydrocodone Hydromorphone Morphine Oxycodone Oxymorphone
FBT OTFC Sublingual Fentanyl injection **
red alphabet not available in Thailand
*Analgesic effects are shorter-lived than effective metabolites
** Recently received a positive opinion for marketing authorization in Europe for cancer
related breakthrough pain in patients already receiving opioid
FBT = Fentanyl buccal tablet , OTFC oral transmucosal fentanyl citrate
Injection form
1. รปแบบฉด ม 2 ชนด ไดแก
2. Morphine sulfate 10 มลลกรม (ไมมสารกนเสย)
3. Morphine sulfate 10 มลลกรม (ผสมสารกนเสย)
Oral form
รปแบบรบประทาน ม 4 ชนด คอ ชนดแคปซลออกฤทธนาน (Kapanol®) ม 3 ขนาด
ความแรง ไดแก 20 , 50 และ 100 มลลกรม
ชนดเมดออกฤทธนาน (MST Continous Tablet) ม 3 ขนาดความแรง ไดแก 10, 30 และ 60 มลลกรม
ชนดเมดออกฤทธทนท (IR Tablet) ม 1 ขนาดความแรง ไดแก 10 มลลกรม
ชนดน า (Oral solution) ขนาดความแรง 10 mg/5 ml
78

6/22/2011
14
Injection form
25 µg/ml
1.2 ml ampule Fentanyl
citrate 2.10 ml ampule Fentanyl citrate
Transdermal form
1. Fentanyl TTS 12 mcg/hour *
2. Fentanyl TTS 25 mcg/hour
3. Fentanyl TTS 50 mcg/hour
FENTANYL
80
Only Injection form is available
Pethidine HCL 50 mg/ml (1 ml) ampule
Not recommend for any type of pain control
Pethidine (Meperidine) Poor oral absorption
Norpethidine is a toxic metabolite
Longer half life than pethidine (6 hours)
Accumulates with repeated dosing – normal kidneys
Severe accumulation with kidney failure
- No analgesia
Myoclonus (twitches) and seizures
Philippines, Indonesia, Thailand
1. Methadone HCL 5 mg/tab
2. Methadone HCL Oral Solution 10 mg/ml (For medical institutes of treating addicts)
Only Oral Form is available Preperation
1. Single formula
Codeine PO4 15 mg
Codeine PO4 30 mg
N 2
N 3 2. Anti-tussive , Analgesic As ingredients in medicinal formula

6/22/2011
15
85
Tablets
Liquid suspensions Liquid solutions Sprinkling on solid foods
Wide variety of formulations of opioid analgesics increases their clinical utility
Oral opioid of choice
Low oral bioavailability (20 – 30%)
Familiarity, availability and cost
Titrate to analgesia OR toxicity
Constipation
COMPREHENSIVE CANCER PAIN MANAGEMENT
Disease progression
Development of tolerance
Appearance of intractable side effects
Effects of morphine metabolites
Individual factors
metabolite may be responsible for the increase in
neuroexcitatory symptoms.
Symptoms (neurologic and psychological)
Sedation most common considered the "tip of the iceberg" leading toward delirium and
obtundation.
Hallucinations Myoclonus Seizures cognitive dysfunction
Neuropsychiatric syndrome
Cognitive dysfunction
Delirium
Hallucinations
Myoclonus/seizures
Hyperalgesia/allodynia
6/22/2011
16
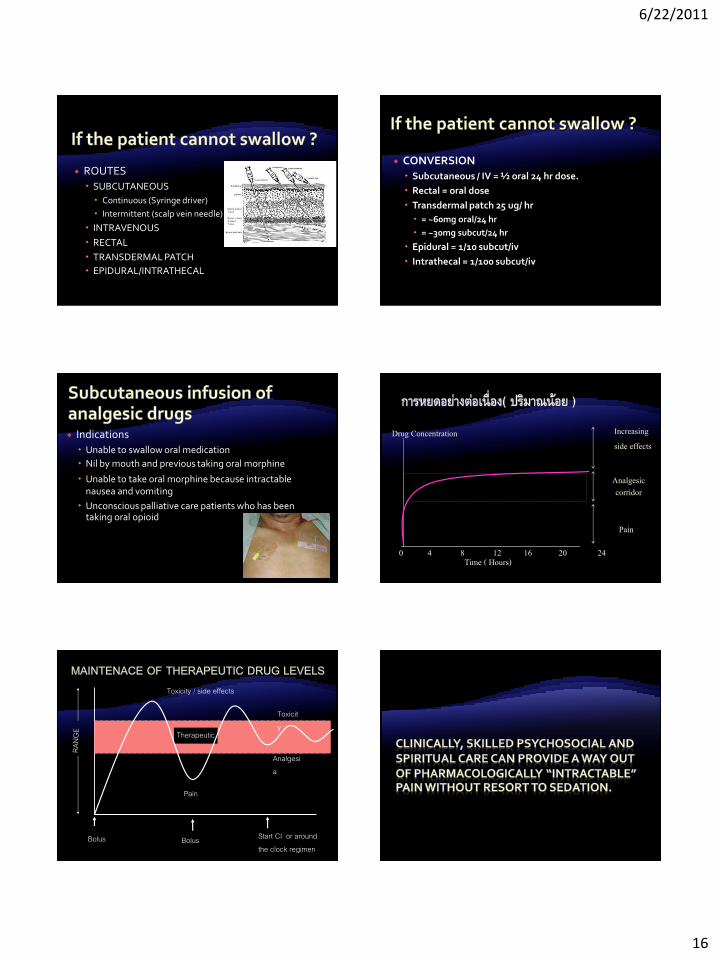
ROUTES
SUBCUTANEOUS
Continuous (Syringe driver)
Intermittent (scalp vein needle)
INTRAVENOUS
RECTAL
TRANSDERMAL PATCH
EPIDURAL/INTRATHECAL
CONVERSION
Subcutaneous / IV = ½ oral 24 hr dose.
Rectal = oral dose
Transdermal patch 25 ug/ hr
= ~60mg oral/24 hr
= ~30mg subcut/24 hr
Epidural = 1/10 subcut/iv
Intrathecal = 1/100 subcut/iv
Indications
Unable to swallow oral medication
Nil by mouth and previous taking oral morphine
Unable to take oral morphine because intractable nausea and vomiting
Unconscious palliative care patients who has been taking oral opioid
0 4 8 12 16 20 24
Drug Concentration Increasing side effects
Analgesic corridor
Pain
Time ( Hours)
Bolus Bolus
Toxicity / side effects
Pain
Toxicity
Therapeutic
Analgesia
Start CI or around the clock regimen
6/22/2011
17
52 % received insignificant amounts of sedatives or none at all
13 % received sedatives for 7 days or more
27 % commenced sedatives only in the last 48 hours of life.
St.Christopher hospise,Dr.Nigel Sykes
3 – 52 % ของผปวยฝร งตองการความชวยเหลอใหหลบและหมดความรสกดวยเหตผลทแตกตางกน
มการเสยโลหต 0.8 %
กระสบกระสาย 1.8 %
มอาการปวด 1.8 %
มอาการคลนไสอาเจยน 2.3 %
มอาการหายใจล าบาก 6.5 %
มอาการสบสน 15.2 %
(Fainsinger et.al, 2000)
Sedation should not be intended as a terminal event
All other options should have been explored first
The level of sedation is only that required to relieve distress
Sedation is achieved with sedatives, not opioid
Uncontrolled pain and other symptoms
Drugs
Metabolic
Infections
Constipation
Cerebral causes
Postictal
Anxiety
Withdrawal
การรกษาแบบประคบประคอง การชวยใหหลบดวยยา
Benzodiazepines Midazolam 5-20 mg ทก 4 ชวโมง เขาชน ใตผวหนง หรอ หยดตอเนองทาง syringe driver
Neuroleptics Haloperidol 0.5-3 mg ทก 4-6 hr เขาชน ใตผวหนง
Barbiturates

6/22/2011
18
52 % ของผปวย ไดรบเพยงเลกนอย หรอ ไมไดรบเลย
13 % ของผปวยไดรบการชวยเหลอใหหลบเปนเวลา 7 วนถงมากกวา
27 % ตองการการชวยเหลอใหหลบในชวง 48 ช วโมงกอนทจะเสยชวต.
St.Christopher hospise,Dr.Nigel Sykes
Related Documents











