UROLOGIC NURSING / May-June 2009 / Volume 29 Number 3 177 Overactive bl a dder affects 16% of the adult population. This retro - spective analysis evaluated the application of percutaneous tibial nerve stimulation (PTNS), a minimally invasive neuromodulation ther - apy, in a population of patients who failed to achieve adequate con - trol of symptoms of urinary urgency, u r i n a ry frequency, and urinary incontinence with conservative treatments. A course of 12 PTNS ses - sions was prescribed and administered in the context of an inde - pendent community-based, nurse practitioner-led continence prac - t i c e.The results of this analysis indicated that patients treated with PTNS therapy experienced statistically significant decreases in both day and night voids, and in episodes of urge incontinence.This study confirmed the results of previous studies indicating that PTNS thera - py is a safe and effective treatment that can be successfully incorpo - rated in a community-based setting. © 2009 Society of Urologic Nurses and Associates Urologic Nursing, pp. 177-185. Key Words: Overactive bladder, u r i n a ryurge n cy, u r i n a ry frequency, urge incontinence, percutaneous tibial n e rve stimulation, incontinence. A pproximately 16% of the adult population in the United States has symptoms of urinary urgency, urinary frequency, and u rge incontinence (Stewart et al., 2003). These symptoms can have a significant impact on quality of life leading to disruptions in work routines and activities of daily living, social isolation, and loss of sleep. Additionally, these symptoms are associated with medical co-morbidities, includ- ing skin and urinary tract infec- tions, as well as falls and frac- tures (Brown, 2002). However, only 40% of those with symptoms seek treatment (Kinchen et al., 2003). For those seeking treatment, typical first- line therapy encompasses con- servative measures, including fluid and food restrictions, blad- der retraining, pelvic floor mus- cle therapy, and the use of pro- Percutaneous Tibial Nerve Stimulation For the Treatment of Urinary Frequency, Urinary Urgency, and Urge Incontinence: Results from a Community-Based Clinic Leslie Saltzstein Wooldridge Leslie Saltzstein Wooldridge, MSN, RNCS, GNP, F-AGS, BCIA-PMBD , is Director, the Bladder Control Clinic, Mercy Health Partners at the Lakes, Muskegon, MI. Acknowledgment: The author would like to thank Harriet Guthertz, medical writer at Medical Marketing and Communications, St. Paul, MN, for assistance in preparing the manu s c ript, and Teresa Yurik, MS, The Integra Group, Brooklyn Park, MN, for assis - tance in performing the statistical analysis. tective briefs or pads, possibly in combination with pharmacother- apy. Available medications for the treatment of bladder-related com- plaints include antimuscarinics, anticholinergics, and occasional- ly, a tricyclic antidepressant. Antimuscarinic and anticholiner- gic drugs decrease overactive d e t russor contractions by inhibit- ing the binding of acetylcholine at muscarinic receptors on detru- sor smooth muscle cells. Tricyclic a n t i d e p ressants facilitate urine storage by decreasing bladder contractility and by incre a s i n g outlet resistance. Despite advances in drug ther- apy, there is a significant dro p o u t rate for drug therapy. In a study of over 23,000 patients with symp- toms of overactive bladder (OAB), a p p roximately 60% of patients had stopped drug therapy within 90 days, and over 80% stopped b e f o re one year (Perfetto, Prasan, & Jumadilova, 2005). Patients may be refractory to medications, or the use of medications may be contraindicated for patients with OAB who have concurrent med- ical conditions, such as narro w - angle glaucoma, slow gastric emptying, and urinary retention.

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
UROLOGIC NURSING / May-June 2009 / Volume 29 Number 3 177
Overactive bl a dder affects 16% of the adult population. This retro -spective analysis evaluated the application of percutaneous tibialn e rve stimulation (PTNS), a minimally invasive neuromodulation ther -a py, in a population of patients who failed to ach i eve adequate con -t rol of symptoms of urinary urge n cy, u r i n a ry frequency, and urinaryincontinence with conservative treatments. A course of 12 PTNS ses -sions was prescribed and administered in the context of an inde -pendent commu n i t y - b a s e d , nu rse practitioner-led continence prac -t i c e.The results of this analysis indicated that patients treated withPTNS therapy experienced statistically significant decreases in bothd ay and night vo i d s , and in episodes of urge incontinence.This studyconfirmed the results of previous studies indicating that PTNS thera -py is a safe and effective treatment that can be successfully incorpo -rated in a community-based setting.
© 2009 Society of Urologic Nurses and AssociatesU rologic Nurs i n g , p p . 1 7 7 - 1 8 5 .
Key Wo rd s : Overactive bl a dd e r, u r i n a ry urge n cy, u r i n a ry f r e q u e n cy, u rge incontinence, p e rcutaneous tibialn e rve stimu l a t i o n , i n c o n t i n e n c e.
Ap p roximately 16% ofthe adult population inthe United States hassymptoms of urinary
u rg e n c y, urinary fre q u e n c y, andu rge incontinence (Stewart et al.,2003). These symptoms can havea significant impact on quality oflife leading to disruptions inwork routines and activities ofdaily living, social isolation, andloss of sleep. Additionally, thesesymptoms are associated withmedical co-morbidities, includ-ing skin and urinary tract infec-tions, as well as falls and frac-t u res (Brown, 2002).
H o w e v e r, only 40% of thosewith symptoms seek tre a t m e n t(Kinchen et al., 2003). For thoseseeking treatment, typical first-line therapy encompasses con-s e rvative measures, includingfluid and food restrictions, blad-der retraining, pelvic floor mus-cle therapy, and the use of pro-
P e rcutaneous Tibial Nerve StimulationFor the Treatment of UrinaryF re q u e n c y, Urinary Urg e n c y, and U rge Incontinence: Results from aCommunity-Based ClinicLeslie Saltzstein Wo o l d r i d g e
Leslie Saltzstein Wo o l d r i d ge, M S N ,R N C S , G N P, F - AG S , B C I A - P M B D, isD i r e c t o r, the Bladder Control Clinic, MercyHealth Pa rtners at the Lake s, Muske g o n ,M I .
A ck n ow l e d g m e n t : The author would like tothank Harriet Guthertz, medical writer atMedical Marketing and Commu n i c a t i o n s,S t . Paul, MN, for assistance in preparing them a nu s c ript, and Teresa Yu rik, MS, T h eI n t e gra Group, Brooklyn Pa rk, MN, for assis -tance in perfo rming the statistical analysis.
tective briefs or pads, possibly incombination with pharm a c o t h e r-a p y. Available medications for thet reatment of bladder- related com-plaints include antimuscarinics,a n t i c h o l i n e rgics, and occasional-l y, a tricyclic antidepre s s a n t .Antimuscarinic and anticholiner-gic drugs decrease overactived e t russor contractions by inhibit-ing the binding of acetylcholineat muscarinic receptors on detru-sor smooth muscle cells. Tr i c y c l i ca n t i d e p ressants facilitate urinestorage by decreasing bladdercontractility and by incre a s i n goutlet re s i s t a n c e .
Despite advances in drug ther-a p y, there is a significant dro p o u trate for drug therapy. In a study ofover 23,000 patients with symp-toms of overactive bladder (OAB),a p p roximately 60% of patientshad stopped drug therapy within90 days, and over 80% stoppedb e f o re one year (Perfetto, Prasan,& Jumadilova, 2005). Patientsmay be re f r a c t o ry to medications,or the use of medications may becontraindicated for patients withOAB who have concurrent med-ical conditions, such as narro w -angle glaucoma, slow gastricemptying, and urinary re t e n t i o n .

178 UROLOGIC NURSING / May-June 2009 / Volume 29 Number 3
The efficacy of drugs is limitedby compliance issues due tointolerable side effects or bypatients who do not wish to con-tinue chronic, systemic dru gt h e r a p y. Neuromodulation in thef o rm of percutaneous tibial nerv estimulation (PTNS) is an attrac-tive option for these patients.
PTNS is a minimally invasive,o ffice-based therapy that canmeet the needs of patients whowant an effective altern a t i v et reatment for symptoms of uri-n a ry urg e n c y, urinary fre q u e n c y,and urge incontinence in which as u rgical intervention is not indi-cated or in those who do notwish to pursue a surgical inter-vention (Govier, Litwiller, Nitti,K re d e r, & Rosenblatt, 2001).PTNS therapy provides healthc a re practitioners with an addi-tional tool in the therapeutica rmamentarium for OAB. De-monstrated as a safe, eff e c t i v e ,and well-tolerated treatment forsymptoms of urinary fre q u e n c y,u r i n a ry urg e n c y, and urge incon-tinence (Govier et al., 2001),PTNS can be delivered in ano ffice-based setting by a trained
clinician under a physician’sd i re c t i o n .
O v e rview of PTNS Therapy
PTNS is a non-drug, non-sur-gical therapy involving the use ofelectrical stimulation to modu-late bladder function. Stim-ulation of the posterior tibialn e rves for the treatment of urg eincontinence was first re p o rt e din 1983 (McGuire, Zhang,H o rwinski, & Lytton, 1983), andthe technology was commerc i a l-ized in the 1990s. Although theexact mechanism of action isunknown, neuromodulation foru r i n a ry dysfunction is based onthe premise that nerves in thesacral plexus regulate bladderfunction and can change bladdera c t i v i t y. The posterior tibialn e rve is a mixed sensory andmotor nerve containing fibersthat originate from L4 to S3( C o o p e r b e rg & Stoller, 2005).During PTNS therapy, impulsesf rom the tibial nerve travel to thesacral nerve plexus, there b ymodulating signals to the bladder(see Figure 1). It is important to
note that the efficacy of PTNStherapy in patients with diabeticn e u ropathy is unknown.
The current generation PTNSsystem, the Urg e n t® PC Neuro-modulation System, UPC-200,(Uroplasty, Inc., Minnetonka,MN) (see Figure 2), has been avail-able since 2006. With the Urg e n t®
PC system, PTNS therapy can bed e l i v e red easily and convenientlyin an office setting by a midlevelp rovider or RN under a physi-c i a n ’s direction. To deliver thera-p y, the patient is placed in a com-
I n t ro d u c t i o n
U ri n a ry urgency, frequency, andurge incontinence are common con-ditions that can severely impact ap a t i e n t ’s quality of life and also resultin medical co-morbidities. M a nypatients do not achieve optimu msymptom management with commonfirst-line treatments, including pelvicfloor muscle thera py, bladder retra i n-ing, and pharm a c o t h e ra py. Pe r c u-taneous tibial nerve stimu l a t i o n(PTNS) is a minimally inva s i ve per-cutaneous neuromodulation thera pythat can be used to treat selectpatients with symptoms of uri n a ryu r g e n c y, uri n a ry frequency, and urgei n c o n t i n e n c e.
O b j e c t i v e
The purpose of this study was todocument the efficacy of a course of12 PTNS thera py sessions for thetreatment of uri n a ry urgency, uri n a ryf r e q u e n c y, and urge incontinence ina community-based, nurse pra c t i-tioner-led continence pra c t i c e.
M e t h o d s
Fifty-three patients presentingwith documented urgency, frequen-c y, and urge incontinence who fa i l e dto obtain adequate symptom reliefwith diet modification, Kegel exe r c i s-e s, biofe e d b a ck, or drug thera pywere treated with 12, 30-minu t ePTNS sessions perfo rmed approx i-mately one week apart .
R e s u l t s
The 53 patients included in this ret-r o s p e c t i ve analysis ex p e rienced astatistically significant mean decreasein day and night voids and episodes ofurge incontinence when compared tob a s e l i n e. PTNS thera py was part i c u-l a rly effe c t i ve in reducing or curi n gincontinence episodes.There were nosignificant side effects or adve r s eeve n t s.
C o n cl u s i o n
PTNS was shown to be a safeand effe c t i ve treatment for symptomsof uri n a ry urgency, uri n a ry frequency,and urge incontinence in this gr o u p.
L evel of Evidence – V I( M e l nyk & Fineout-Overholt, 2005)
Figure 1.The posterior tibial nerve is
t a rgeted for stimulation duringPTNS therapy. F rom the tibialn e rv e, the impulse travels to
the sacral nerve plexus whichregulates bl a dder and pelvic
floor function.
S o u rc e : C o py right Uroplasty, Inc.R e p rinted with perm i s s i o n .

UROLOGIC NURSING / May-June 2009 / Volume 29 Number 3 179
f o rtable seated position, and a 34-gauge needle electrode is insert e dnear but not directly on the tibialn e rve (approximately three finger-b readths [5 cm] cephalad to themedial malleolus and appro x i-mately 1 fingerbreadth [2 cm] pos-terior to the tibia) (see Figure 3).The needle electrode is placed ina position creating a 60-degre eangle between the electrode andthe ankle, while advancing it in apath that is parallel to the tibialn e rv e .
When appropriately posi-tioned, approximately 2 cm of theneedle electrode will be insert e din the leg (see Figure 4). A customlead wire is then connected to theUrgent® PC stimulator, and ag rounding surface electrode isplaced near the medial aspect ofthe calcaneous on the same leg asthe needle insertion (see Figure 5).The lead is connected to the nee-dle electrode using an integratedclip. The stimulator is then usedto verify the correct electro d eposition by slowly increasing thecurrent and observing thep a t i e n t ’s foot for toe flex or fan,extension of the entire foot, orstimulation of the heel and/orfoot, as an indicator for successfulplacement. After proper electro d eposition has been verified, stimu-lation is started at the observ e dlevel of response if tolerable, or
Figure 2.The Urgent PC® system used toadminister percutaneous tibial
n e rve stimulation (PTNS) t h e r a py consists of a hand-heldexternal pulse ge n e r a t o r, a lead
w i r e, a needle electro d e,and a surface electro d e.
S o u rc e : C o py right Uroplasty, Inc.R e p rinted with perm i s s i o n .
Figure 3.PTNS therapy can be administered in an office setting with the
patient seated comfo rt a bly. The area near but not directly on theposterior tibial nerve is targeted for stimulation during PTNS t h e r a py. The target can be identified as approx i m a t e ly three f i n gerbreadths (5 cm) cephalad to the medial malleolus and a p p rox i m a t e ly 1 fingerbreadth (2 cm) posterior to the tibia.
S o u rc e : C o py right Uroplasty, Inc. R e p rinted with perm i s s i o n .
Figure 4.Maintain a 60-degree angle with the needle electrode while
a dvancing it in a path that is parallel to the tibia.
S o u rc e : C o py right Uroplasty, Inc. R e p rinted with perm i s s i o n .
Needle electrode at 60° angle nearthe tibial nerve
Figure 5.A surface electrode is placed near the medial aspect of the calcaneous on the same leg as needle electrode insert i o n .
S o u rc e : C o py right Uroplasty, Inc. R e p rinted with perm i s s i o n .
Tibial nerve
180 UROLOGIC NURSING / May-June 2009 / Volume 29 Number 3
the current setting is reduced byone increment for patient comfort .C u rrent is adjustable from 0.15mA to 9 mA. Therapy is thendelivered continuously for 30minutes. PTNS therapy is welltolerated, and has been describedas producing a sensation of tap-ping, tingling, or vibration.
The recommended initialcourse of PTNS therapy forsymptoms of urinary fre q u e n c y,u r i n a ry urg e n c y, and urge incon-tinence consists of a series of 12individual treatments, eacha p p roximately one week apart .This protocol was described byGovier et al. (2001) and was usedas the basis for United StatesFood and Drug Administration(FDA) approval of the therapy. Itmay also be possible to titratedosages of OAB drugs downwardduring the initial course of PTNSt h e r a p y. To maintain therapeutice ffect after the initial 12 tre a t-ments, the interval between fol-low-up sessions is individual-ized according to the patient’sresponse. In this practice, follow-up session frequency has rangedf rom two weeks to severalmonths. Because the treatment isminimally invasive, completelyreversible, and can be stopped atany time, it does not preclude theuse of other therapeutic options,including new drugs and/ord e v i c e s .
No significant pro d u c t - re l a t e dadverse events or side effects havebeen associated with the therapy.H o w e v e r, it should be noted thatPTNS therapy is contraindicatedin patients who have the follow-ing history or conditions( U ro p l a s t y, Inc., 2006):• Patients with pacemakers or
implantable defibrillators.• Patients prone to excessive
b l e e d i n g .• Patients with nerve damage
that could impact either per-cutaneous tibial nerve orpelvic floor function.
• Patients who are pregnant orplanning to become pre g n a n twhile using this pro d u c t .
A d d i t i o n a l l y, the product isnot intended for intracardiac ortransthoracic use. Concurre n tuse of medical monitoring equip-
ment during stimulation is notrecommended. The device is notsuitable for use in the presence ofa flammable anesthetic mixturewith air or with oxygen orn i t rous oxide.
PTNS therapy is an option forpatients with symptoms of uri-n a ry fre q u e n c y, urinary urg e n c y,and urge incontinence who arere f r a c t o ry to drug therapy or whoexperience intolerable side eff e c t sof drug therapy. It also provides atherapy option for patients whodo not wish to pursue more inva-sive pro c e d u res, including b o t u -l i n u m toxin type A injections( B o t o x®), implantable neuro m o d-ulation therapy, or surg e ry.
Review of the Literature
A c c o rding to data on file atU ro p l a s t y, Inc., PTNS therapyhas been the subject of appro x i-mately 60 papers in the medicall i t e r a t u re worldwide. Ap rospective, multicenter FDAinvestigational device exemp-tion study utilizing PTNS onpatients with symptoms of OABwho had failed medical therapy,Kegel exercise, biofeedback,and pelvic floor stimulatorse n rolled 53 patients and had amean follow up of 12 months(Govier et al., 2001). Of the 47patients who completed the 12-week study, 71% achieved 25%or more reduction in mean day-time voids and/or nighttimevoiding fre q u e n c y. On average,patients noticed a 25% re d u c-tion in mean daytime fre q u e n c y,a 21% reduction in mean night-time fre q u e n c y, and a 35%reduction in urge incontinenceepisodes, with a mean follow upof 12 weeks (Govier et al., 2001).
Another prospective studyfollowed 90 patients with OAB.Of these, 56% achieved 50% orm o re reduction in the numberof leakage episodes per 24 hours( Vandoninck et al., 2003).
One randomized study com-pared PTNS therapy (12 weeklysessions, 30 minutes each) withtolterodine therapy (2 mg, BID)in 31 women with symptoms ofu rge and urge incontinence.This study found no statistically
significant diff e rence betweenthe two groups in terms of themajor endpoints of micturitionsin 24 hours and the patient’squality of life, and the minorendpoints of incontinenceepisodes in 24 hours and sideeffects of the therapy after 12months of follow up (Preyer etal., 2007). However, the PTNSgroup experienced a significant-ly lower rate of side effects –3.4% in the PTNS group versus20.7% in the tolterodine group.This led the authors to concludethat PTNS is particularly advan-tageous given the number ofcomorbidities and high dru gload in their study population.
In a recent prospective, mul-ticenter study, 100 patients (94female) with OAB at 11 U.S.centers were randomized 1:1 toeither 12 weekly treatments ofPTNS therapy or tolterodine tar-tarate extended release 4mg/day for 12 weeks (a fewpatients were reduced to 2mg/day based on tolerability)(Peters et al., 2008). This studywas powered to show a non-inferiority margin of 20%. Thismeans that the mean re d u c t i o nin the number of voids per 24hours in the PTNS arm of thestudy was no more than 20%lower than the mean re d u c t i o nin the number of voids per 24hours in the tolterodine arm .Based on an analysis of 41patients in the PTNS group and43 patients in the toltero d i n eg roup, both treatments werewell tolerated and resulted insimilar improvements in voidsper day, voids at night, and urg eincontinence as measured by a2-day voiding diary. Quality-of-life scores showed a statisticallysignificant improvement fro mbaseline for both groups. Thecomparable efficacy betweenboth treatment groups led theauthors to conclude that PTNSmay be considered a first-linetherapy for OAB.
It is important to note that therelatively small sample sizes inthese studies are typical ofdevice studies, which usuallyhave smaller sample sizes thand rug studies.
UROLOGIC NURSING / May-June 2009 / Volume 29 Number 3 181
Experience at a Community-BasedUrology Practice
P u r p o s eThe purpose of this study was
to re p o rt an initial experience inan independent, community-based, nurse practitioner- l e dcontinence practice in an eff o rtto gain further knowledge aboutthis novel therapy. Researc h e r shope this information may bevaluable to other health carepractitioners interested in incor-porating this therapy into theirtherapeutic armamentarium forbladder dysfunction. This studyinvolved a re t rospective chartreview to describe the patientpopulation, the change in base-line symptoms after a course of12 PTNS therapy sessions, andthe place of PTNS in the continu-um of care for patients suff e r i n gwith the chronic condition ofoveractive bladder syndro m e .
M e t h o d sF rom May 2006 through April
2008, 53 patients (52 female), allCaucasian, with chronic OABsymptoms were re f e rred to acommunity-based, nurse practi-t i o n e r-led continence practice.Complete medical, surg i c a l ,medication, and social historiesw e re completed for all patients.All physical and genitourinaryexaminations were perf o rmed bythe same nurse practitioner spe-cializing in continence manage-ment, and each patient complet-ed a 3-day voiding diary. Patientswith urg e n c y, fre q u e n c y, andu rge incontinence documentedon the 3-day voiding diary, whofailed to achieve symptom re l i e fwith treatments, such as dietmodification, Kegel exerc i s e s ,biofeedback, or behavioral ormedical therapy, were off e re dPTNS therapy.
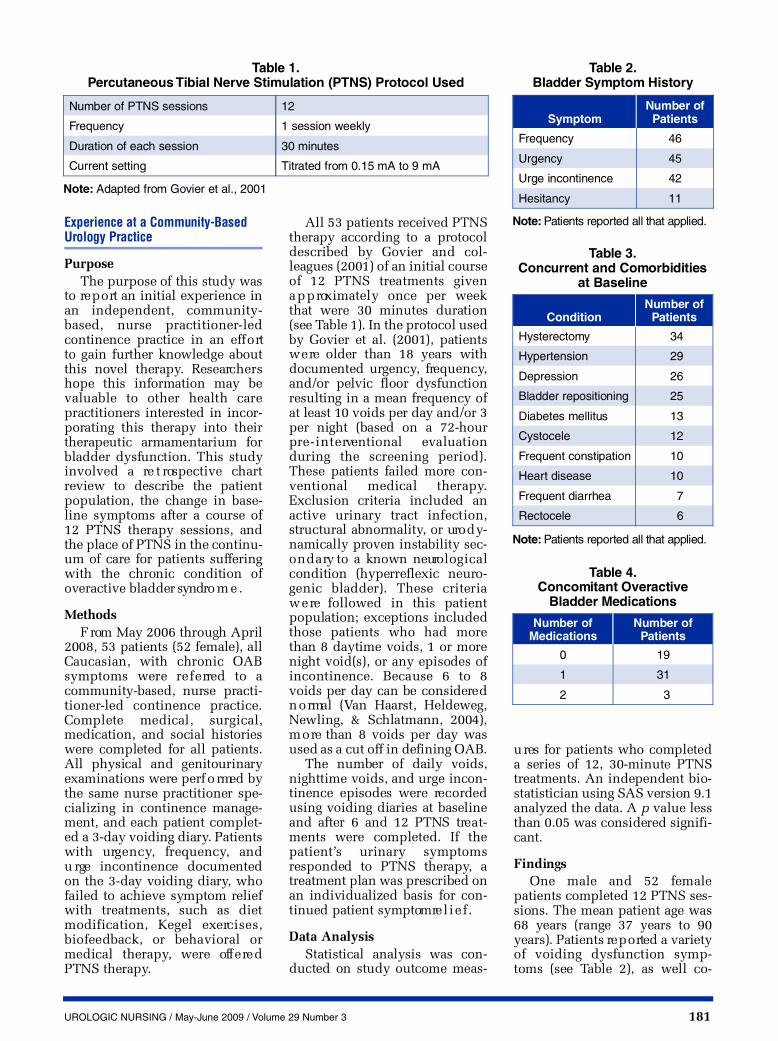
All 53 patients received PTNStherapy according to a pro t o c o ldescribed by Govier and col-leagues (2001) of an initial courseof 12 PTNS treatments givena p p roximately once per weekthat were 30 minutes duration(see Table 1). In the protocol usedby Govier et al. (2001), patientsw e re older than 18 years withdocumented urg e n c y, fre q u e n c y,and/or pelvic floor dysfunctionresulting in a mean frequency ofat least 10 voids per day and/or 3per night (based on a 72-hourp re - i n t e rventional evaluationduring the screening period).These patients failed more con-ventional medical therapy.Exclusion criteria included anactive urinary tract infection,s t ructural abnorm a l i t y, or uro d y-namically proven instability sec-o n d a ry to a known neuro l o g i c a lcondition (hyperreflexic neuro-genic bladder). These criteriaw e re followed in this patientpopulation; exceptions includedthose patients who had morethan 8 daytime voids, 1 or morenight void(s), or any episodes ofincontinence. Because 6 to 8voids per day can be considere dn o rmal (Van Haarst, Heldeweg,Newling, & Schlatmann, 2004),m o re than 8 voids per day wasused as a cut off in defining OAB.
The number of daily voids,nighttime voids, and urge incon-tinence episodes were re c o rd e dusing voiding diaries at baselineand after 6 and 12 PTNS tre a t-ments were completed. If thep a t i e n t ’s urinary symptomsresponded to PTNS therapy, at reatment plan was prescribed onan individualized basis for con-tinued patient symptom re l i e f .
Data AnalysisStatistical analysis was con-
ducted on study outcome meas-
u res for patients who completeda series of 12, 30-minute PTNSt reatments. An independent bio-statistician using SAS version 9.1analyzed the data. A p value lessthan 0.05 was considered signifi-c a n t .
Findings One male and 52 female
patients completed 12 PTNS ses-sions. The mean patient age was68 years (range 37 years to 90years). Patients re p o rted a varietyof voiding dysfunction symp-toms (see Table 2), as well co-
N o t e : Adapted from Govier et al., 2001
Ta ble 1.Pe rcutaneous Tibial Nerve Stimulation (PTNS) Protocol Used
Number of PTNS sessions 1 2
Fr e q u e n c y 1 session we e k l y
D u ration of each session 30 minu t e s
Current setting T i t rated from 0.15 mA to 9 mA
N o t e : Patients reported all that applied.
Ta ble 2.B l a dder Symptom History
S y m p t o mNumber of
Pa t i e n t s
Fr e q u e n c y 4 6
U r g e n c y 4 5
Urge incontinence 4 2
H e s i t a n c y 1 1
N o t e : Patients reported all that applied.
Ta ble 3.Concurrent and Comorbidities
at Baseline
C o n d i t i o nNumber of
Pa t i e n t s
H y s t e r e c t o my 3 4
H y p e rt e n s i o n 2 9
D e p r e s s i o n 2 6
Bladder repositioning 2 5
Diabetes mellitus 1 3
C y s t o c e l e 1 2
Frequent constipation 1 0
H e a rt disease 1 0
Frequent diarrhea 7
R e c t o c e l e 6
Ta ble 4.Concomitant Overactive
B l a dder Medications
Number ofM e d i c a t i o n s
Number ofPa t i e n t s
0 1 9
1 3 1
2 3

182 UROLOGIC NURSING / May-June 2009 / Volume 29 Number 3
morbidities and concomitantconditions (see Table 3). At base-line, 34 of the patients were on atleast one OAB medication (seeTable 4).
All patients experienced atleast one abnormal symptom ofan overactive bladder at baselinedefined as more than 8 daytimevoids (n = 33), 1 or more nightvoids (n = 50), or any episodes ofincontinence (n = 42). Tw e l v ePTNS treatments with theU rg e n t® P C system resulted in astatistically significant decre a s ewith each of these symptomsf rom baseline to 12 weeks.
For the 33 patients with ana b n o rmal number of daytimevoids, mean daytime voidsd e c reased significantly from anaverage of 13.8 at baseline to 7.9after 12 treatments (p < 0.0001)(see Figure 6). Patients experi-enced a statistically significantaverage decrease in daytimevoids of 27.9% from baseline (p <0 . 0 0 0 1 ) .
S i m i l a r l y, the mean voids pernight decreased from an averageof 3.1 at baseline to 1.2 after 12t reatments (p < 0.001) (see Figure7). Patients experienced an aver-age 63.5% decrease in nighttimevoids from baseline (p < 0.0001).A total of 82% (41 of 50) patientswith 1 or more night voids atbaseline showed some impro v e-ment in night voids.
Of importance to patients whore p o rt that incontinence is themost distressing and sociallylimiting aspect of their urinarydysfunction, treatment with
Figure 6.Mean Voids per Day at Baseline and
after 12 PTNS Tr e a t m e n t s
1 5
1 0
5
0Tr e a t m e n t s
Baseline
After 12 PTNSTreatments
1 3 . 8
7 . 9
Figure 8.Mean Urge Incontinence Episodes at
Baseline and after 6 and 12 PTNS Tr e a t m e n t s
1 5
1 0
5
0Tr e a t m e n t s
Baseline
After 6 PTNSTreatments
After 12 PTNSTreatments
4 . 9
1 . 2 0 . 7
Figure 7.Mean Voids per Night at Baseline and
after 12 PTNS Tr e a t m e n t s
1 5
1 0
5
0Tr e a t m e n t s
Baseline
After 12 PTNSTreatments
3 . 1
1 . 2
PTNS therapy was part i c u l a r l ye ffective in reducing or curingu rge incontinence episodes. Atotal of 42 patients re p o rted urg eincontinence at baseline with anaverage of 4.9 incontinenceepisodes daily (see Figure 8).After only 6 PTNS treatments, theaverage number of incontinenceepisodes for patients who re p o rt-ed incontinence episodes at base-line decreased dramatically to 1.2episodes (p < 0.0001), withpatients experiencing an average69.4% decrease to their numberof incontinence episodes. After12 PTNS treatments, the numberof incontinence episodes im-p roved further to a total averageof 0.7 daily episodes (p < 0.0001).T h i rty-seven of the 42 patientsre p o rting incontinence at baseline(88%) improved with 59.5% (25of 42) patients cured (such asreporting no incontinenceepisodes during the period of
review for the study). A total of88.1% (37 of 42) patients experi-enced some improvement to theiru rge incontinence, with patientsre p o rting a substantial 79.3%average decrease to their inconti-nence episodes (p < 0.0001).
The efficacy of PTNS therapyin patients concurrently takingOAB medications was also ana-lyzed. Since 31 of the 34 patientson OAB medications were takingonly one OAB medication, dataw e re analyzed in terms ofwhether a patient was taking anOAB medication and re c e i v i n gPTNS therapy or whether thepatient received PTNS therapyalone. This analysis showed thatPTNS therapy is highly eff e c t i v ere g a rdless of whether patients aretaking OAB medications at base-line (see F i g u res 9-11). For exam-ple, mean daytime voidsd e c reased from an average of 10.6at baseline to 7.4 after 12 PTNS

UROLOGIC NURSING / May-June 2009 / Volume 29 Number 3 183
t reatments (p = 0.0007) forpatients on medication at base-line (n = 34) compared to an aver-age decrease from 12.3 at base-line to 7.8 after 12 PTNS tre a t-ments (p = 0.0004) for patientswho were not taking OAB med-ications at baseline (n = 19) (seeF i g u re 9). Similar results wereobtained in an analysis of nightvoids (see Figure 10) and urg eincontinence episodes (seeF i g u re 11).
F i n a l l y, there were no compli-cations or adverse events withPTNS, and patients were quitepleased with the treatment pro-cess and outcomes. They viewedPTNS as a safe and effective wayof controlling their bladdersymptoms and re p o rted theylooked forw a rd to the 30-minute
t reatment sessions as a time forrest, relaxation, reading, or medi-t a t i o n .
D i s c u s s i o nDeveloping an effective tre a t-
ment plan for symptoms of uri-n a ry fre q u e n c y, urinary urg e n c y,and urge incontinence can some-times involve the trial of severaltherapy modalities, starting withc o n s e rvative measures, such aspelvic floor exercises, and behav-ioral therapies and medications.H o w e v e r, for a significant numberof patients, these measures maynot result in satisfactory symptomrelief. They may experience intol-erable side effects from the pre-scribed medications or have com-pliance issues, or their symptomsmay be re f r a c t o ry to these first-
line measures. The question ofhow to proceed can be challeng-ing. Patients may be unwilling tot ry additional medications, but atthe same time, may not be re a d yfor a surgically implanted deviceor surgical re c o n s t ruction. PTNStherapy is an option for thesepatients and can be used con-comitantly with behavioral thera-pies and pharm a c o t h e r a p y. Con-sidering the social embarr a s s m e n tassociated with incontinence, thereduction in urge incontinenceseen in this study likely re s u l t e din a significant positive impact onthe patient’s quality of life.
In this re t rospective re v i e w,PTNS was shown to be eff e c t i v eeither with or without concurre n tOAB medications. There were nosignificant diff e rences betweenthe groups of patients defined bymedication use at baseline int e rms of mean change in daytimevoids, nighttime voids, and urg eincontinence episodes. PTNStherapy was found to reduce orc u re incontinence episodes in amajority of patients re p o rting urg eincontinence at baseline for theduration of the study. Fre q u e n c yand nocturia in patients re p o rt i n gnighttime voids at baseline werealso improved. The therapy isminimally invasive and can beadministered by appropriatelytrained practitioners in an off i c esetting. The therapy has not beenassociated with any significantside effects or adverse events, andits use does not preclude the use
Figure 9.Av e r age Decrease in Daytime Voids
by Medication Status
1 5
1 0
5
0No OAB Medications
at Baselinen = 1 9
OAB Medicationsat Baseline
n = 3 4
Baseline
After 12 PTNSTreatments
1 2 . 3
7 . 8
1 0 . 6
7 . 4
Figure 10.Av e r age Decrease in Nighttime Voids
by Medication Status
1 5
1 0
5
0No OAB Medications
at Baselinen = 1 9
OAB Medicationsat Baseline
n = 3 4
Baseline
After 12 PTNSTreatments
2 . 5
0 . 9
3 . 2
1 . 4
Figure 11.Av e r age Decrease in Urge Incontinence
Episodes by Medication Status
1 5
1 0
5
0No OAB Medications
at Baselinen = 1 9
OAB Medicationsat Baseline
n = 3 4
Baseline
After 12 PTNSTreatments
3 . 5
0 . 2
4 . 1
0 . 8

184 UROLOGIC NURSING / May-June 2009 / Volume 29 Number 3
of other therapies, including moreinvasive options in the future .This experience with PTNS thera-py confirms previously publishedresults demonstrating a signifi-cant reduction in mean voids dur-ing the day and night, as well as ina reduction in urge incontinenceepisodes.
A number of factors are neces-s a ry to successfully incorporatethe therapy into the continuum ofc a re, including patient selection,patient education, practitionertechnique, and documentation. Athorough medical history andphysical examination are neces-s a ry prior to prescribing PTNS.E v e ry eff o rt should be made tod e t e rmine if there is a re v e r s i b l ecause of urinary urg e n c y, urinaryf re q u e n c y, and urge incontinence.The pathophysiology of bladderoutlet obstruction, bladderinflammation, overactivity, dener-vation, spinal cord injury, or agingshould be considered as the etiol-ogy of these symptoms.
Reversible causes of OAB mayinclude constipation, urinary tractinfection, atrophic vaginitis,ingestion of irritative food or flu-ids, or the consequences of chro n-ic disease. All patients in thisstudy were evaluated andassessed with these factors inmind. Bladder diaries are anessential and detailed re c o rd of ap a t i e n t ’s response to medicationsincluding efficacy and toleration.In case of questions in diff e re n t i a-tion of stress and urge inconti-nence during the diagnosticworkup, urodynamic testing maybe useful; however, this was notthe case for any patients includedin this retrospective analysis.S i m i l a r l y, cystoscopy can be auseful tool for the diagnosis ofintractable urgency or assessmentof other findings indicating fur-ther investigation. Again, this wasnot perf o rmed in the patients dis-cussed in this art i c l e .
Prior to prescribing PTNS ther-a p y, the entire treatment re g i m e nshould be reviewed with thepatient. This includes settingexpectations re g a rding what hap-pens during a PTNS therapy ses-sion, the length of a session, thenumber of weekly sessions
re q u i red, and the potential needfor follow-up sessions. Thepatient must also realize the needfor continued commitment tobehavioral treatments and theongoing titration of medications.
As part of this author’s prac-tice, continued pelvic floor educa-tion measures, including Kegele x e rcises, bladder retraining, andhabit training, have been impor-tant. Urge reduction measure s ,including fluid management andthe avoidance of bladder irr i t a n t s ,w e re also continued.
After starting PTNS therapy, at reatment log should be start e d ,and the results should be docu-mented carefully to include aquality-of-life survey and voidingdiaries at baseline, and after tre a t-ment 6 and 12. The OAB-q, ver-sion 1, 2004 survey (Coyne,Matza, & Thompson, 2005) wasused to document quality of life inthis study. Similarly, a therapycontinuance plan should bedeveloped if needed and theresults documented. These re-c o rds prove valuable for use dur-ing ongoing patient education andb i l l i n g .
L i m i t a t i o n s
This study was limited by thefact that it was a re t ro s p e c t i v eanalysis. Although both men andwomen are affected equally byOAB, the overwhelming majorityof patients undergoing PTNS ther-apy in this author’s practice arefemale. Because descriptive statis-tics were used to analyze data inaddition to the resultant small nsizes, meaningful subgroup analy-sis that might provide furt h e rinsight into which patients couldbenefit most from PTNS therapywas not perf o rm e d .
Additional limitations includ-ed that a standardized tool wasnot used to capture quality-of-lifedata and that these results cannotbe generalized to the larger popu-lation of patients with OAB. Thelack of an accepted, standard i z e dp rotocol for treatment with PTNSalso makes the comparison of out-comes among studies using thisp roduct diff i c u l t .
Implications for Nursing Practice
PTNS is a successful altern a-tive for the treatment of urinaryu rg e n c y, urinary fre q u e n c y, andu rge incontinence when medica-tions and other behavior interv e n-tions do not provide the desire dlevel of bladder control. PTNStherapy can be used independent-ly or in conjunction with medica-tions to achieve normal voidingp a t t e rns and reduce urg e n c y. Thetime allotted for each PTNS thera-py session also provides anadvanced practice nurse with theo p p o rtunity to re i n f o rce behav-ioral interventions critical forachieving long-term bladder con-t ro l .
C o n c l u s i o n s
Results of previously pub-lished clinical studies and thoseobtained in the 53 patients tre a t e dwith PTNS in this re t ro s p e c t i v estudy in an independent commu-nity-based, nurse practitioner- l e dcontinence practice indicate thatPTNS significantly decreasedsymptoms of urinary fre q u e n c yand urinary urg e n c y. It was part i c-ularly effective in reducing or cur-ing urge incontinence, which isperhaps the most distressingaspect of urinary dysfunction forpatients. Patients have been satis-fied with the results and pleasedwith the availability of this tre a t-ment alternative. In summary,PTNS therapy can be successfullyincorporated into the therapy con-tinuum in a community-basedsetting.
R e f e rences B rown, J.S. (2002). Epidemiology and
changing demographics of overactivebladder: A focus on the post-menopausal woman. Geriatrics,5 7(Suppl.1), 6-12.
C o o p e r b e rg, M.R., & Stoller, M.L. (2005).P e rcutaneous neuromodulation. T h eU rologic Clinics of North America,3 2, 71-78.
Coyne, K.S., Matza, L.S., & Thompson, C.L.(2005). The responsiveness of theOveractive Bladder Questionnaire(OAB-q). Quality of Life Researc h , 1 4,8 4 9 - 8 5 5 .
G o v i e r, F.E., Litwiller, S., Nitti, V., Kre d e r,K.J., Jr., & Rosenblatt, P. (2001).P e rcutaneous aff e rent neuro m o d u l a-tion for the re f r a c t o ry overactive blad-der: Results of a multicenter study.J o u rnal of Uro l o g y, 165, 1193-1198.

UROLOGIC NURSING / May-June 2009 / Volume 29 Number 3 185
Kinchen, K.S., Burgio, K., Diokno, A.C.,Fultz, N.H., Bump, R., & Obenchain,R. (2003). Factors associated withw o m e n ’s decisions to seek tre a t m e n tfor urinary incontinence. J o u rnal ofWo m e n ’s Health, 12, 687-698.
M c G u i re, E.J., Zhang, S.C., Horw i n s k i ,E.R., & Lytton, B. (1983). Tre a t m e n tof motor and sensory detrusor insta-bility by electrical stimulation.J o u rnal of Uro l o g y, 129, 78-79.
Melnyk, B.M., & Fineout-Overholt, E.( 2 0 0 5 ) . Evidence-based practice innursing & healthcare: A guide to bestpractice. Philadelphia: Lippincott,Williams & Wilkins.
P e rfetto, E.M., Prasan, S., & Jumadilova,Z. (2005). Treatment of overactivebladder: A model comparing extend-ed release formulations of toltero-dine and oxybutynin. The AmericanJ o u rnal of Managed Care, 11, S150-1 5 7 .
Peters, K.M., Leong, F.C., Shobeiri, S.A.,MacDiarmid, S.A., Rovner, E.E.,Wooldridge, L.S., et al. (2008). A ran -domized multicenter study compar -ing percutaneous tibial nerve stimu -lation with pharmaceutical therapyfor the treatment of overactive blad -der . Abstract. Presented at theAmerican Urological Associationmeeting, May 21, 2008, Orlando, FL.
P re y e r, O., Gabriel, B., Mailath-Pokony, M.,D o e rf l e r, D., Laml, T., Umek, W., et al.(2007). Peripheral tibial neuro s t i m u l a-tion (PTNS) versus To l t e rodine in thet reatment of women with urge urinaryincontinence and urge symptoms.I n t e rnational Urogynecology Journ a l .Retrieved April 10, 2009, fro mh t t p : / / w w w. u ro p l a s t y. c o m /i n d e x .c f m / g o / P h y s i c i a n s . U P C d a t a / d a t a / 0 2
S t e w a rt, W. F., Rooyen, J.B.V., Cundiff ,G . W., Abrams, P., Herzog, A.R.,C o re y, R., et al. (2003). Pre v a l e n c eand burden of overactive bladder inthe United States. World Journal ofU ro l o g y, 20, 327-336.
U ro p l a s t y, Inc. (2006). U rg e n t® P CN e u romodulation System. Instru c -tions for use. Minnetonka, MN.Retrieved April 10, 2009, fro mh t t p : / / w w w. u ro p l a s t y. c o m / v i e w / f i l e s /f c k / p d f / 0 5 2 0 0 4 4 . p d f
Vandoninck, V., Van Balken, M.R., FinazziAgrò, E., Petta, F., Micali, F.,Heesakkers, J.P., et al. (2003).P e rcutaneous tibial nerve stimulationin the treatment of overactive blad-der: Urodynamic data. N e u ro u ro l o g yand Urodynamics, 22, 227-232.
Van Haarst, E.P., Heldeweg, E.A.,Newling, D.W., & Schlatmann, T. J .(2004). The 24-h fre q u e n c y - v o l u m ec h a rt in adults re p o rting no voidingcomplaints: Defining re f e rence val-ues and analysing variables. B J UI n t e rnational, 93, 1257-1261.
Related Documents











