OXYGEN THERAPY: OXYGEN THERAPY: PRINCIPLES & PRINCIPLES & PRACTICE PRACTICE Dr.NARASIMHA REDDY Dr.NARASIMHA REDDY PROFFESSOR &H.O.D PROFFESSOR &H.O.D DEPT.OF ANESTHESIOLOGY DEPT.OF ANESTHESIOLOGY

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
OXYGEN THERAPY: OXYGEN THERAPY: PRINCIPLES & PRINCIPLES &
PRACTICEPRACTICE
Dr.NARASIMHA REDDYDr.NARASIMHA REDDY
PROFFESSOR &H.O.DPROFFESSOR &H.O.D
DEPT.OF ANESTHESIOLOGYDEPT.OF ANESTHESIOLOGY

Oxygen is also like a drug.Oxygen is also like a drug. It must be used meticulously & It must be used meticulously &
deligently.deligently. If abused it can cause complications.If abused it can cause complications.
FEW IMPORTANT FEW IMPORTANT QUESTIONSQUESTIONS::
1.What are the indications for O2?1.What are the indications for O2?
2.How to administer optimally?2.How to administer optimally?
3.What are the hazards?3.What are the hazards?
Enrichment of inspired gases with Enrichment of inspired gases with O2 .O2 .
The major reason for O2 therapy is The major reason for O2 therapy is hypoxia.hypoxia.
Hypoxia is defiency of O2 at tissue Hypoxia is defiency of O2 at tissue levels.levels.
Hypoxemia refers to reduced O2 Hypoxemia refers to reduced O2 tension in arterial blood.tension in arterial blood.

TYPES OF HYPOXIATYPES OF HYPOXIA
1.HYPOXIC HYPOXIA1.HYPOXIC HYPOXIA::
- Dec. in O2 saturation of Hb like Dec. in O2 saturation of Hb like alveolar hypoventilation& low FiO2.alveolar hypoventilation& low FiO2.
- O2 therapy fruitful results.O2 therapy fruitful results.
2.STAGNANT HYPOXIA2.STAGNANT HYPOXIA::
- Due to low cardiac output states & Due to low cardiac output states & vascular occlusion.vascular occlusion.
- O2 therapy helps to less extent.O2 therapy helps to less extent.
3.ANEMIC HYPOXIA3.ANEMIC HYPOXIA::
- O2 carrying capacity is reduced like O2 carrying capacity is reduced like anemia,hemodilution,CO poisoning.anemia,hemodilution,CO poisoning.
- O2 therapy useful to some extent.O2 therapy useful to some extent.

4.HISTOTOXIC HYPOXIA4.HISTOTOXIC HYPOXIA::
- Due to cyanide poisoning.Due to cyanide poisoning.- Cells cannot utilise O2.Cells cannot utilise O2.- O2 therapy least likely useful.O2 therapy least likely useful.
INDICATIONS FOR O2 INDICATIONS FOR O2 THERAPYTHERAPY
1.Hypoxia 1.Hypoxia – when PaO2 comes down to – when PaO2 comes down to 60mmhg.60mmhg.
2.Normoxic hypoxia2.Normoxic hypoxia – like low cardiac – like low cardiac output output states,M.I,anemia,hemodilution,CO states,M.I,anemia,hemodilution,CO poisoning,acute hypermetabolic states.poisoning,acute hypermetabolic states.
3.Trapped gases3.Trapped gases – like obstruction,pneumo – like obstruction,pneumo encephalus.encephalus.
4.Special situations4.Special situations – like anesthesia. – like anesthesia.
GUIDELINES FOR O2 GUIDELINES FOR O2 THERAPYTHERAPY
1.To alleviate hypoxemia.1.To alleviate hypoxemia.
2.To alleviate endorgan dysfunction 2.To alleviate endorgan dysfunction due to hypoxia.due to hypoxia.
3.To avoid deleterious effects of O3 3.To avoid deleterious effects of O3 therapy.therapy.

O2 DELIVERY SYSTEMSO2 DELIVERY SYSTEMS::
1.Low flow or variable performance 1.Low flow or variable performance systems.systems.
2.High flow fixed performance 2.High flow fixed performance systems.systems.

LOW FLOW SYSTEMSLOW FLOW SYSTEMS::
1.Nasal catheters1.Nasal catheters..- 8-14 G ,passed through into 8-14 G ,passed through into
oropharynx.oropharynx.
- Reservoir of O2 builds up in Reservoir of O2 builds up in pharynx.pharynx.

2.Nasal prongs2.Nasal prongs::
- The prongs protrude 1cm into nares.The prongs protrude 1cm into nares.- Well tolerated.Well tolerated.- Less interference in day to day Less interference in day to day
activities.activities.- Useless in mouth breathers.Useless in mouth breathers.- No reservoir system.No reservoir system.- FiO2 unpredictable.FiO2 unpredictable.

3.Simple O2 masks3.Simple O2 masks::- Covers the nose & mouth.Covers the nose & mouth.- 4-6 lits/min.4-6 lits/min.- 0.4 -0.6 FiO20.4 -0.6 FiO2- Feeling of suffocation.Feeling of suffocation.- Interference with daily activities.Interference with daily activities.- FiO2 unpredictable.FiO2 unpredictable.- Displacement at nights.Displacement at nights.

4.Mask with reservoir bags4.Mask with reservoir bags::
-Polymask with 2 chambers.-Polymask with 2 chambers.
-High FiOP2 with 5-6 lits of O2.-High FiOP2 with 5-6 lits of O2.
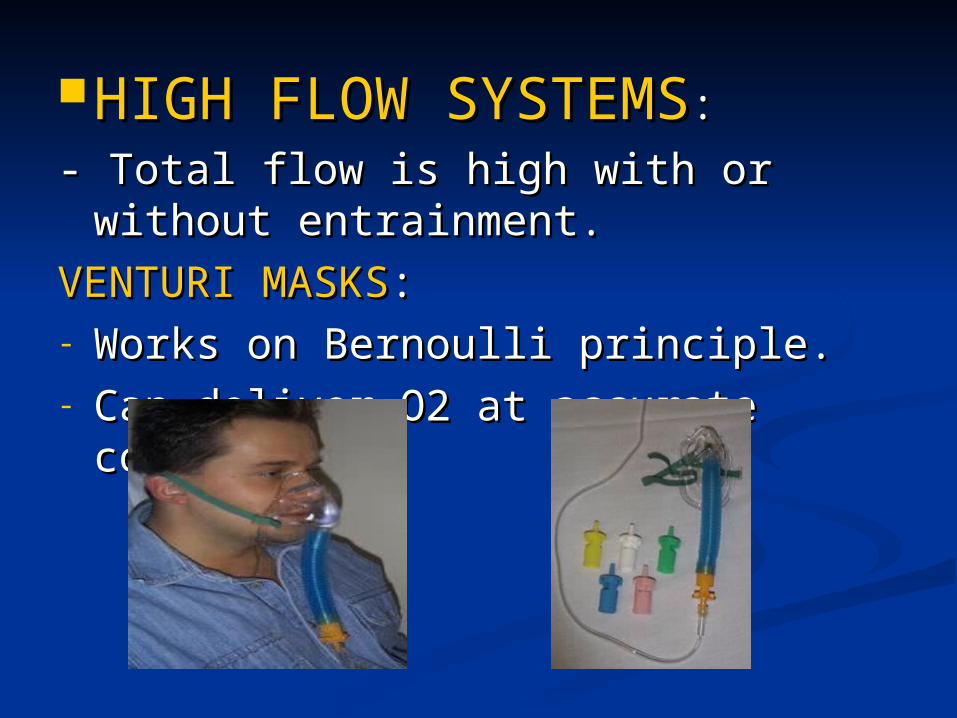
HIGH FLOW SYSTEMSHIGH FLOW SYSTEMS::
- Total flow is high with or without - Total flow is high with or without entrainment.entrainment.
VENTURI MASKSVENTURI MASKS::- Works on Bernoulli principle.Works on Bernoulli principle.- Can deliver O2 at accurate concs.Can deliver O2 at accurate concs.

O2 hoodO2 hood::- Used in bed bound infants not Used in bed bound infants not
intubated.intubated.- Made of plexi glass.Made of plexi glass.- Humidified O2 3 times M.V.Humidified O2 3 times M.V.

O2 tentO2 tent::- Used in pediatric practise.Used in pediatric practise.- 10-12 lits/min.10-12 lits/min.- Fire accidents.Fire accidents.
CYLLINDERS:CYLLINDERS:

HOME O2 CONCENTRATORHOME O2 CONCENTRATOR

JET VENTILATIONJET VENTILATION::- High frequency oscillation.High frequency oscillation.

HAZARDS OF O2 HAZARDS OF O2 THERAPYTHERAPY
1.Drying of mucous membrane.1.Drying of mucous membrane.
2.Depression of ventilation in COPD.2.Depression of ventilation in COPD.
3.Reversal of compensatory hypoxic 3.Reversal of compensatory hypoxic vasoconstriction.vasoconstriction.
4.Atelectasis due to absorption 4.Atelectasis due to absorption collapse.collapse.
5.O2 toxicity.5.O2 toxicity.
OXYGEN TOXICITYOXYGEN TOXICITY
1.Pulmonary oxygen toxicity 1.Pulmonary oxygen toxicity (Lorrain-Smith effect):(Lorrain-Smith effect):
- 100%O2 given for 12 hours or more.100%O2 given for 12 hours or more.- 80% O2 for more than 24hrs.80% O2 for more than 24hrs.- 60%O2 more than 36hrs.60%O2 more than 36hrs.
- SymptomsSymptoms: substernal pain,irresistable : substernal pain,irresistable cough,dyspnoea,V.C dec.,compliance cough,dyspnoea,V.C dec.,compliance dec.,pulmonary interstitial edema leading dec.,pulmonary interstitial edema leading to fibrosis.to fibrosis.

2.Retrolental fibroplasia2.Retrolental fibroplasia : :
- Occurs when PaO2 more than 80mmhg Occurs when PaO2 more than 80mmhg for more than 3 hrs in new born.for more than 3 hrs in new born.
- Very premature babies are more Very premature babies are more susceptible.susceptible.
- O2 saturation must be around 90-92 %.O2 saturation must be around 90-92 %.

3.C.N.S O2 toxicity (Paul-Bert 3.C.N.S O2 toxicity (Paul-Bert effecteffect):):
- O2 is given in hyperbaric chambers.O2 is given in hyperbaric chambers.

Related Documents