Review Oxidative stress and antioxidant therapy in cystic fibrosis ☆ , ☆☆ Francesco Galli a, ⁎, Andrea Battistoni b , Roberto Gambari c , Alfonso Pompella d , Alessandra Bragonzi e , Francesca Pilolli a , Luigi Iuliano f , Marta Piroddi a , Maria Cristina Dechecchi g , Giulio Cabrini g a Department of Internal Medicine, Laboratory of Clinical Biochemistry and Nutrition, University of Perugia, Italy b Department of Biology, University of Rome Tor Vergata, Italy c Department of Biochemistry and Molecular Biology, University of Ferrara, Italy d Dept. of Experimental Pathology & BMIE University of Pisa Medical School, Pisa, Italy e Infections and cystic fibrosis unit, San Raffaele Scientific Institute, Milan, Italy f Department of Medico-Surgical Sciences and Biotechnology, Vascular Biology & Mass Spectrometry Lab, Sapienza University of Rome, Italy g Laboratory of Molecular Pathology, Department of Pathology and Diagnostics, University Hospital of Verona, Italy abstract article info Article history: Received 20 October 2011 Received in revised form 16 December 2011 Accepted 17 December 2011 Available online 28 December 2011 Keywords: Cystic fibrosis Antioxidant Oxidative stress Reactive oxygen species Inflammation Glutathione Cystic fibrosis is a lethal autosomal recessive condition caused by a defect of the transmembrane conductance regulator gene that has a key role in cell homeostasis. A dysfunctional cystic fibrosis transmembrane conduc- tance regulator impairs the efflux of cell anions such as chloride and bicarbonate, and also that of other solutes such as reduced glutathione. This defect produces an increased viscosity of secretions together with other met- abolic defects of epithelia that ultimately promote the obstruction and fibrosis of organs. Recurrent pulmonary infections and respiratory dysfunction are main clinical consequences of these pathogenetic events, followed by pancreatic and liver insufficiency, diabetes, protein-energy malnutrition, etc. This complex comorbidity is asso- ciated with the extensive injury of different biomolecular targets by reactive oxygen species, which is the bio- chemical hallmark of oxidative stress. These biological lesions are particularly pronounced in the lung, in which the extent of oxidative markers parallels that of inflammatory markers between chronic events and acute exac- erbations along the progression of the disease. Herein, an abnormal flux of reactive oxygen species is present by the sustained activation of neutrophils and other cystic fibrosis-derived defects in the homeostatic processes of pulmonary epithelia and lining fluids. A sub-optimal antioxidant protection is believed to represent a main con- tributor to oxidative stress and to the poor control of immuno-inflammatory pathways in these patients. Ob- served defects include an impaired reduced glutathione metabolism and lowered intake and absorption of fat-soluble antioxidants (vitamin E, carotenoids, coenzyme Q-10, some polyunsaturated fatty acids, etc.) and oligoelements (such as Se, Cu and Zn) that are involved in reactive oxygen species detoxification by means of enzymatic defenses. Oral supplements and aerosolized formulations of thiols have been used in the antioxidant therapy of this inherited disease with the main aim of reducing the extent of oxidative lesions and the rate of lung deterioration. Despite positive effects on laboratory end points, poor evidence was obtained on the side of clinical outcome so far. These aspects examined in this critical review of the literature clearly suggest that fur- ther and more rigorous trials are needed together with new generations of pharmacological tools to a more ef- fective antioxidant and anti-inflammatory therapy of cystic fibrosis patients. This article is part of a Special Issue entitled: Antioxidants and Antioxidant Treatment in Disease. © 2012 Elsevier B.V. All rights reserved. 1. Introduction Cystic fibrosis (CF) is a lethal autosomal recessive disorder caused by a single gene defect. This was identified in 1989 to map on the chromosome 7 and to correspond to the gene coding for the trans- membrane conductance regulator (CFTR) that is mainly expressed in the apical membrane of epithelial cells that line mucous mem- branes and submucosal glands [1]. Several mutations have been identified to cause this gene defect with the Phe508del, or ΔF508, as one of the most common mutations in Caucasians. The prevalence at birth varies in the different regions according with ethnic back- ground, from roughly 1 in 3000 white Americans and northern Biochimica et Biophysica Acta 1822 (2012) 690–713 ☆ This article is part of a Special Issue entitled: Antioxidants and Antioxidant Treatment in Disease. ☆☆ For the “Working Group on Inflammation in Cystic Fibrosis” of the Italian Society for Cystic Fibrosis and the Italian Cystic Fibrosis Research Foundation. ⁎ Corresponding author. E-mail addresses: [email protected] (F. Galli), [email protected] (A. Battistoni), [email protected] (R. Gambari), [email protected] (A. Pompella), [email protected] (A. Bragonzi), [email protected] (F. Pilolli), [email protected] (L. Iuliano), [email protected] (M. Piroddi), [email protected] (M.C. Dechecchi), [email protected] (G. Cabrini). 0925-4439/$ – see front matter © 2012 Elsevier B.V. All rights reserved. doi:10.1016/j.bbadis.2011.12.012 Contents lists available at SciVerse ScienceDirect Biochimica et Biophysica Acta journal homepage: www.elsevier.com/locate/bbadis

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Biochimica et Biophysica Acta 1822 (2012) 690ndash713
Contents lists available at SciVerse ScienceDirect
Biochimica et Biophysica Acta
j ourna l homepage wwwe lsev ie r com locate bbad is
Review
Oxidative stress and antioxidant therapy in cystic fibrosis
Francesco Galli a Andrea Battistoni b Roberto Gambari c Alfonso Pompella d Alessandra Bragonzi eFrancesca Pilolli a Luigi Iuliano f Marta Piroddi a Maria Cristina Dechecchi g Giulio Cabrini g
a Department of Internal Medicine Laboratory of Clinical Biochemistry and Nutrition University of Perugia Italyb Department of Biology University of Rome Tor Vergata Italyc Department of Biochemistry and Molecular Biology University of Ferrara Italyd Dept of Experimental Pathology amp BMIE University of Pisa Medical School Pisa Italye Infections and cystic fibrosis unit San Raffaele Scientific Institute Milan Italyf Department of Medico-Surgical Sciences and Biotechnology Vascular Biology amp Mass Spectrometry Lab Sapienza University of Rome Italyg Laboratory of Molecular Pathology Department of Pathology and Diagnostics University Hospital of Verona Italy
This article is part of a Special Issue entitled Antio For the ldquoWorking Group on Inflammation in Cystic
Corresponding authorE-mail addresses fgalliunipgit (F Galli) andreab
bragonzialessandrahsrit (A Bragonzi) francescapilhcristinadechecchiospedaleuniveronait (MC Dechecch
0925-4439$ ndash see front matter copy 2012 Elsevier BV Aldoi101016jbbadis201112012
a b s t r a c t
a r t i c l e i n f o
Article historyReceived 20 October 2011Received in revised form 16 December 2011Accepted 17 December 2011Available online 28 December 2011
KeywordsCystic fibrosisAntioxidantOxidative stressReactive oxygen speciesInflammationGlutathione
Cystic fibrosis is a lethal autosomal recessive condition caused by a defect of the transmembrane conductanceregulator gene that has a key role in cell homeostasis A dysfunctional cystic fibrosis transmembrane conduc-tance regulator impairs the efflux of cell anions such as chloride and bicarbonate and also that of other solutessuch as reduced glutathione This defect produces an increased viscosity of secretions together with other met-abolic defects of epithelia that ultimately promote the obstruction and fibrosis of organs Recurrent pulmonaryinfections and respiratory dysfunction are main clinical consequences of these pathogenetic events followed bypancreatic and liver insufficiency diabetes protein-energy malnutrition etc This complex comorbidity is asso-ciated with the extensive injury of different biomolecular targets by reactive oxygen species which is the bio-chemical hallmark of oxidative stress These biological lesions are particularly pronounced in the lung in whichthe extent of oxidative markers parallels that of inflammatory markers between chronic events and acute exac-erbations along the progression of the disease Herein an abnormal flux of reactive oxygen species is present bythe sustained activation of neutrophils and other cystic fibrosis-derived defects in the homeostatic processes ofpulmonary epithelia and lining fluids A sub-optimal antioxidant protection is believed to represent a main con-tributor to oxidative stress and to the poor control of immuno-inflammatory pathways in these patients Ob-served defects include an impaired reduced glutathione metabolism and lowered intake and absorption offat-soluble antioxidants (vitamin E carotenoids coenzyme Q-10 some polyunsaturated fatty acids etc) andoligoelements (such as Se Cu and Zn) that are involved in reactive oxygen species detoxification by means ofenzymatic defenses Oral supplements and aerosolized formulations of thiols have been used in the antioxidanttherapy of this inherited disease with the main aim of reducing the extent of oxidative lesions and the rate oflung deterioration Despite positive effects on laboratory end points poor evidence was obtained on the sideof clinical outcome so far These aspects examined in this critical review of the literature clearly suggest that fur-ther and more rigorous trials are needed together with new generations of pharmacological tools to a more ef-fective antioxidant and anti-inflammatory therapy of cystic fibrosis patients This article is part of a Special Issueentitled Antioxidants and Antioxidant Treatment in Disease
copy 2012 Elsevier BV All rights reserved
1 Introduction
Cystic fibrosis (CF) is a lethal autosomal recessive disorder causedby a single gene defect This was identified in 1989 to map on thechromosome 7 and to correspond to the gene coding for the trans-membrane conductance regulator (CFTR) that is mainly expressed
xidants and Antioxidant TreatmentFibrosisrdquo of the Italian Society for C
attistoniuniroma2it (A Battistoniotmailcom (F Pilolli) iulianoluigii) giuliocabriniunivrit (G Cabrin
l rights reserved
in the apical membrane of epithelial cells that line mucous mem-branes and submucosal glands [1] Several mutations have beenidentified to cause this gene defect with the Phe508del or ΔF508as one of the most common mutations in Caucasians The prevalenceat birth varies in the different regions according with ethnic back-ground from roughly 1 in 3000 white Americans and northern
in Diseaseystic Fibrosis and the Italian Cystic Fibrosis Research Foundation
) gamunifeit (R Gambari) alfonsopompellamedunipiit (A Pompella)gmailcom (L Iuliano) mpiroddi76yahooit (M Piroddi)i)
691F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
Europeans to 1 in 350000 in Japan Mutations are grouped in 6 clas-ses based on the type of defect caused on CFTR protein metabolismand function Several physiological processes affected by these muta-tions are related to the role of CFTR as anion channel This mainlyregulates chloride efflux but other and larger anions such as reducedglutathione cross the plasmalemma throughout this transmembraneprotein widely expressed in diverse epithelial tissues Other iontransport systems are under its influence such as bicarbonateanion and sodium channels so that a defective CFTR can impairseveral processes such as cell volume and pH regulation transepithe-lial transport membrane conductance and the GSH-related antioxi-dant and detoxification activity in the extracellular milieu [23]CFTR dysfunction is associated with an altered fluid and electrolytecomposition of secretions their increased viscosity and progressiveobstruction and fibrosis of organs [4] The severity of these CF symp-toms varies independently of the type and number of mutationsdiagnosed suggesting that CFTR gene and its mutations interactwith other genes at the transcriptional and post-translational levelto influence a wide series of physiological processes Lung pancreasand liver are severely affected by these events and recurrent infec-tions of the airways together with pancreatic insufficiency and diabe-tes are most common conditions secondary to CF [1]
The presence of a defective CFTR appears to produce a redox im-balance in epithelial cells and extracellular fluids and to cause an ab-normal generation of reactive oxygen species (ROS) A constitutivedefect of GSHmetabolism together with a lowered intake and absorp-tion of fat-soluble antioxidant vitamins (vitamin E and carotenoids)could contribute to a defective antioxidant protection which is be-lieved to exacerbate oxidative stress indices along with the progres-sion of clinical status [5ndash7] The development of inflammatory anddegenerative lesions in target tissues such as lung pancreas andliver further exacerbate the shift from normal to abnormal flux ofROS in several organs thereby leading to develop systemic oxidativestress This is a chronic-degenerative trait common to other andsevere inflammatory diseases such as chronic kidney disease andsome auto-immune syndromes (reviewed in [89]) which may
Fig 1 Oxidative unbalance in conductive airways of patients affected by cystic fibrosis airwreactive oxygen species (ROS) 2 lowered levels of glutathione (GSH) and 3 reduced nitric oof both neutrophils and bronchial epithelial cells contributes to the progressive lung tissuecharacterized by the release of chemokines and cytokines (eg IL-8 and IL-6 respectively) NIL interleukin
conspire with further mechanisms to worsen the prognosis of thisinherited disorder (recently reviewed in [10])
In view of these aspects the CF patient is assumed to have a higherantioxidant demand This has provided the rationale for the systematicinvestigation of antioxidant levels in blood and targeted tissues of CFpatients mainly the epithelium and lining fluids of the airways andto plan for antioxidant interventions that might rescue specific defectsof these patients These also include the use of anti-inflammatoryagents and nutritional formulations which can produce an ldquoantioxi-dant effectrdquo ie the lowering of oxidative stress indices as a result oftheir direct or indirect action Despite a number of promising in vitroand pre-clinical observations antioxidants used as oral supplementsor directly administered in the CF airways have failed to provide con-vincing evidence at the clinical level Future efforts are required to iden-tify more advanced agents and therapeutic strategies thatmay enhancesecondary prevention and chemotherapy of airway inflammation andoxidative stress in CF patients Advances in the approaches capable ofimproving nutritional status and antimicrobial therapy are of mainrelevance to further ameliorate quality of life and survival rates in CF
These aspects will be discussed in this manuscript with the aim ofproviding an updated review of the literature as well as of strategiesand future directions of antioxidant therapies in CF patients
2 Inflammatory pathways and oxidative stress in CF
21 Progressive inflammatory damage in CF lungs and the contributionof oxidants
Evidence supporting the occurrence of oxidative stress in CF is bynow established and extensive [610ndash12] As introduced above CF-related defects of the pulmonary epithelium and a sustained PMNactivation by recurrent infections create the conditions for an abnor-mal flux of reactive oxygen species (ROS) in the CF lung (Fig 1) be-tween events of acute and chronic inflammation Abnormalities ofmarkers of ROS activity and inflammation are most evident duringacute respiratory exacerbations and show improvement with the
ay surface liquid (ASL) in CF bronchi is characterized by 1 increased concentration ofxide (NO) The net increase of pro-oxidative species in ASL as a result of derangementsdamage and to the amplification of the inflammatory response in CF airways This is
OX NADPH oxidase MPO mieloperoxidase DUOX dual oxidase LPO lactoperoxidase
692 F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
intensive treatment of the infection [13ndash15] The fact that relapses orsuccessful therapy of infection do not normalize these markers dem-onstrates the presence of a chronic inflammatory syndrome that isintrinsic to the CF defect In this context ROS may lose their physio-logical role in the killing of pathogens to turn into toxic effectors re-sponsible for the damage of the pulmonary epithelium as well as ofother components of the lung parenchyma and lining fluids Impor-tantly ROS can modify the thiol homeostasis of extracellular fluidsand epithelia [16] and promote the activation of MAPK signalingpathways [17] which regulate both the NFkβ-dependent and-independent transcription of pro-inflammatory genes and other mo-lecular effects associated with the immuno-inflammatory imbalanceobserved in the CF lung
Hallmark of the chronic inflammatory lung disease in CF is therelease of chemokines mainly interleukin (IL)-8 [1819] leading tothe neutrophil recruitment in the bronchial lumen (see [20] for areview) Whether CF lung inflammation arises independently andbefore bacterial infection remains to be fully established althoughIL-8 and pro-inflammatory cytokines have been found in bronchoal-veolar lavage fluids of CF infants even before the onset of an overtbacterial infection [21] Although directed against infective agentsthe chronic inflammation in CF lungs is largely recognized as mainlyresponsible for the progressive tissue damage leading to respiratoryinsufficiency Dissection of the pathophysiology of CF chronic lunginflammation should take into account the bronchial epithelial cellsexpressing the mutated CFTR protein the polymorphonuclear neu-trophils recruited into the bronchial lumens and the bacterial infec-tion itself with special regards to Pseudomonas aeruginosa the mostcommon gram negative microorganism which colonizes CF airways[22] Thus novel anti-inflammatory therapies against the progressivedamage of the CF respiratory tissue should be mainly aimed i) to re-duce the excessive recruitment of neutrophils by intervening on thetransmembrane signaling pivoting the excessive expression of IL-8 [23ndash26] ii) to inactivate proteases released by the neutrophils con-tinuously activated by bacterial products [27] and iii) to circumventthe effect of the unbalanced production of oxidants deriving fromboth phagocytes and bronchial epithelial cells [2228ndash30] Identifica-tion of oxidants produced in the CF airway tract is of high importancein order to identify novel molecular targets for specific pharmacolog-ical intervention
22 Respiratory epithelial cells and neutrophils as sources of oxidants inthe CF lung
It is largely accepted that neutrophils migrating inside the CFbronchial lumina release large amounts of reactive oxygen species(ROS) including the superoxide anion (O2
minusbull) hydrogen peroxide(H2O2) and the hydroxyl free radical (OH) mainly by the activationof the NADPH oxidase (NOX) To such exaggerated ROS productioncontribute both the continuous interaction of neutrophils with bacte-ria and bacterial degradation products and the inability to engulf bac-teria in biofilms leading to a condition of ldquofrustrated phagocytosisrdquoNeutrophils are therefore recognized as a major source of ROS inthe airway surface liquid (ASL) of young children with CF [1431]However bronchial ciliated and alveolar type II epithelial cells bythemselves are able to produce significant amounts of ROS throughthe two isoforms of NADPH oxidase expressed in the apical membraneof these epithelial cells namely DUOX1 and DUOX2 [32] A major pro-posed function of DUOXs is to support lactoperoxidase (LPO) which isin turn released by goblet and submucosal gland airway cells to gen-erate bactericidal hypothiocyanite (OSCNminus) starting from thiocyanate(SCNminus) and H2O2 Thus the DUOXLPO coupled system of the respira-tory epithelial cells parallels the NOXmieloperoxidase (MPO) systemof phagocytes in releasing and processing oxidants in the ASL Whilethe NOXMPO system of phagocytes is mainly activated in theinfection-induced respiratory burst the release of ROS from epithelia
is continuous and even independent of the presence of overt bacterialinfection [33] Interestingly it was proposed that the efficiency of theDUOXLPO defense system is dependent on the ion transport functionof the CFTR Clminus channel which could also intervene both in the con-ductive secretion of SCNminus (for LPO function) and of HCO3
minus (for pHadjustment) into the ASL [34] However more recent ex vivo observa-tions while confirming a positive role of DUOXLPO system in produc-ing OSCNminus as a general defense mechanism of the airways do notdirectly relate SCNminus concentrations in ASL with CFTR function [35]The LPO-mediated scavenging of H2O2 has suggested a role of SCNminus
as physiological antioxidant of ASL [36] which may be defective inCF Besides this role of LPO and SCNminus an abnormal flux of H2O2 inthe CF airways may also depend on other factors that are associatedwith an alteredmetabolism of ROS For instance lowered levels of Lac-toferrin (LF) have been described in CF secretions [37] This iron-chelating homologue of transferrin contained in the granules of neu-trophils is also secreted by several mucosal tissues in biological fluidsto contribute antimicrobial effects by a variety of mechanisms includ-ing the chelating activity of iron as Fenton chemistry catalyst [38]
As regards the progression of CF lung disease in the early phasesbefore the onset of chronic bacterial colonization epithelial DUOXcontinuously releases H2O2 thus being a predominant source inrespect to the NADPH oxidase from phagocytes The latter is mainlyactive when the respiratory burst is ldquotriggered on demandrdquo by infec-tious components On the other side in advanced phases of chronicinfection of CF lungs neutrophil-derived ROS are predominant [32]due to neutrophil activation as well as to the decreasing number ofH2O2-producing ciliated cells which are reduced by extensive apo-ptosis and tissue remodeling A further reduction of epithelial DUOXactivity has been observed as a result of infection with P aeruginosain conductive airways P aeruginosa-derived toxin pyocyanin in factinhibits DUOX-dependent H2O2 production by consuming intracellu-lar NADPH which represents an interesting adaptive mechanism todownregulate innate anti-bacterial defenses [39]
23 Redox disturbances of CF airways the role of GSH NO and H2O2
Intracellular impairment of redox balance between oxidants andanti-oxidants has been proposed to occur in CF bronchial epithelialcells although a significant difference in respect to normal CFTR-expressing cells is still controversial and debated [40] Three majorissues have been investigated concerning the intracellular redox bal-ance in CF bronchial cells namely i) a defect in GSH homeostasis[4142] ii) an alteration of nitric oxide (NO) metabolism and iii) animbalance of intracellular H2O2 production
As far as GSH is concerned the defective CFTR channel functionhas been proposed to lead to a lowered cell content of this tripeptidewhich is crucial to control the flux of H2O2 in both the CF bronchialepithelial cells and lining fluids This aspect ndash discussed in detailbelow in this review ndash is associated with characteristic defects ofGSH-related enzymes and may represent a key underlying factor inthe oxidative stress of CF airways
Altered NO concentration has been found in chronic respiratorydiseases such as bronchial asthma and chronic obstructive pulmonarydisease [43] and reduced NO concentrations have been observed inthe bronchial airways of patients affected by CF which directly corre-lated with worsening of lung function [44] Thus NO concentration inCF lung exhalate has been subsequently tested as a possible marker ofpulmonary exacerbations andor the inflammatoryinfective statusand its fluctuations over time [4546]
This opened the way to further analysis of the mechanisms of thisderangement and it has been proposed that an excessive productionof asymmetric dimethylarginine an inhibitor of endogenous NOSynthase (NOS) could be involved in the reduced concentrationof NO in CF airways [47ndash49] Possible corrective therapies such asthe inhalation of L-arginine have provided preliminary evidence of
693F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
correction of the defective NO concentration and improvement oflung function in CF patients [49ndash51]
Although exhaled NO is decreased in CF increased immunohisto-chemical staining for nitrotyrosine was demonstrated in lung tissuesfrom CF patients [52] Therefore a decreased production or accelerat-ed metabolism of NO could be present in association with an abnor-mal reactivity of this radical and its derived species (NOx) towardbiomolecular components of the CF airways Peroxynitrite is one ofthe most relevant mediators of the biological activity of NO withtoxic properties and damaging activity on several biomolecules [53]
A third emerging issue takes into consideration the expressionof different enzymatic systems affecting the redox balance in CF bron-chial epithelial cells For instance intracellular concentration of H2O2
has been found abnormally elevated in both immortalized bronchialand primary nasal epithelial cells derived from CF patients bothin the presence and the absence of proinflammatory cytokines [54]This has been accompanied by a marked decrease of expressionof proteins regulating H2O2 levels such as thioredoxin 1 (TRX-1)glutathione-S-transferase pi (GST-pi) peroxyredoxin (PRDX) 6TRX-dependent peroxide reductase (PRDX-1) catalase and con-versely a significant increase of Mn superoxide dismutase (SOD2)[54] Interestingly to link these modifications with CF specific charac-teristics dysfunctional CFTR channel was found associated withreduced activity of the transcription factor Nrf-2 (nuclear factor-erythroid 2 p45 subunit-related factor 2) which could at least inpart explain the differential expression of the enzymatic systemsresulting in the elevated intracellular steady-state concentration ofH2O2 found in CF nasal and bronchial epithelial cells [54] In synthesisthe ASL of CF patients during advanced stages of the lung disease con-tains elevated concentrations of ROS mainly derived from neutro-phils migrated into the airway lumen and a reduced concentrationof NO which can strongly contribute to respiratory tissue injurytogether with the proteases released by the activated neutrophilsThe homeostatic role of the GSH-related defenses appears constitu-tively impaired by the dysfunctional CFTR thus increasing suscepti-bility to develop oxidative stress and lung tissue degeneration(Fig 1) as described in detail in the sections below
24 Conductive airway epithelium as target of ROS
Oxidants can target different biomolecules to damage epithelialcells and extracellular fluids of the airways Lipid peroxidationand post-translational modifications of proteins on both cell mem-branes and extracellular targets are common biomarkers of thisdamage which can occur by the direct reaction between ROS and bio-molecules or through the formation of second-generation reactivebyproducts [955] All levels of this interaction between ROS and bio-logical components can produce toxic and bioactive intermediatesOxidants are known to activate secondmessengers through phospho-lipases A2 C and D and to induce the production of cytokines andmucins a series of molecular events that contribute to progressiveobstructive disease and reduction of lung function [56] Besides thedirect oxidative damage to cellular structures of the bronchial epithe-lial cells the excessive concentration of oxidants in CF both in the ASLlining the apical membranes and inside the bronchial cells has beenstudied in respect to the regulation of the inflammatory response
ROS are often considered a sort of secondmessengers in activatingthe Nuclear Factor (NF)-κB which is in turn involved in the activationof transcription of several proinflammatory cytokines and chemo-kines [57] For instance it has been shown that H2O2 partly controlsNF-κB activation by IL-1beta by facilitating the activation of NIKand subsequent phosphorylation of IKKβ [58] In this respect a directlink has been proposed between the excessive production of intracel-lular H2O2 and the elevated expression of IL-6 and IL-8 the mostabundant pro-inflammatory cytokine and neutrophilic chemokinefound in CF airways [54] which has been further confirmed [59]
Moreover oxidants could be synergic in the induction of mucins aspromoted by neutrophil elastase which further impairs ASL fluidityin CF [60] Finally bacterial infection with P aeruginosa strains releas-ing the toxin pyocyanin (PCN) has been shown to reduce ion trans-port through the CFTR channel thus potentially counteracting thetherapeutic effects of correctors and potentiators of mutated CFTRprotein [6162] In summary excessive oxidants in CF conductive air-ways have different negative effects in the amplification of the al-ready excessive lung inflammation and secretion of mucin togetherwith a direct deleterious effect on CFTR channel function
25 Oxidative stress and surfactant
Oxidative stress and inflammation in cystic fibrosis can affect sur-factant biophysical activity thus leading to early alterations of lungfunction in patients with CF [63] Altered phospholipid-to-protein ra-tios and phospholipid subclasses a modified fatty acid profiles anddecreased association of proteins such as SP-A with lipid componentsof isolated surfactant indicate that components of this fluid are con-siderably altered and dysfunctional in lower respiratory tract secre-tions of CF patients [64]
Oxidative damage of surfactant may involve both lipid and proteincomponents Alteration of lipid components can in turn generatetoxic lipid species with cytotoxic activity towards nearby epithelialcells [65] Altered protein components have been shown in cysticfibrosis [66] Notably surfactant protein D which is an important in-nate host defense molecule becomes unable to agglutinate bacteriawhen it is modified by oxidation which facilitates pathogen coloniza-tion in the lung [67] In a cross-sectional analysis of CF patients withmild lung disease reduced surfactant activity was correlated to in-creased neutrophilic airway inflammation but not to lung function[68] So far longitudinal measurements of surfactant function in CFpatients are lacking and it remains unclear how these alterationsrelate to progression of airway inflammation as well as to the rateof decline of pulmonary function [69]
26 Laboratory indices of oxidative stress in CF
Appropriate biochemical and clinical tools are of importance forthe monitoring of antioxidant therapies in CF and a crucial aspect isthe selection of proper biomarkers and protocols to assess biologicalpathways of oxidation
Pancreatic insufficiency and a diminished bile acid pool cause mal-absorption of important essential nutrients and other dietary compo-nents in CF Of particular significance is the malabsorption of fat-soluble antioxidants such as carotenoids tocopherols and coenzymeQ-10 (CoQ-10) which act as chain breakers in the peroxidation reac-tions of polyunsaturated lipids Accordingly lipid peroxidation is oneof the main signs encountered in the CF plasma buccal mucosal cellsbreath condensate and BALF as measured by the non-enzymaticoxidation product of arachidonic acid 8-iso prostaglandin F2α[570ndash73] Elevations of this and other eicosanoids in human bodyfluids and tissues have been found in a diverse array of human disor-ders including atherosclerosis diabetes obesity cigarette smokingneurodegenerative diseases and many others [74] Further treat-ments for some of these conditions including antioxidant supple-mentation have been shown to decrease the levels of this class ofbiomarkers In CF patients respiratory exacerbations increase plasmalevels of 8-iso-F2α [70] the levels of which in the breath condensatenegatively correlate with respiratory function data [71] At the sametime successful in vivo antioxidant therapy by GSH inhalation hasbeen shown to decreased PGE levels in BALF in association withchanges in the number and activity of leukocyte subpopulations re-sponsible for lung inflammation [73]
Oxysterols a biomarker of cholesterol oxidation were found toincrease in CF plasma as a further proof of the abnormal lipid
694 F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
metabolism and increased susceptibility to oxidation of lipoproteinlipids in CF patients [7] Importantly an increased oxidative burdenof lung and blood lipids may produce bioactive lipid products thatfurther sustain CF symptoms Besides to 8-iso-F2α and other ana-logues with some bioactivity [74] arachidonic acid oxidation maycontribute to persistent platelet activation and pulmonary dysfunc-tion in CF via generation of bioactive isoeicosanoids [75] which pro-vides sufficient rationale for a prevention therapy with fat solubleantioxidants such as vitamin E Evidence has recently accumulatedon the systemic effects of oxysterols on various tissues and organs[76] The role of this lipid oxidation product alone or in combinationwith other factors could be further investigated in the context ofmechanisms and clinical progression of multi-organ failure of CFpatients
The impaired pancreatic and liver functions of CF patients repre-sent the underlying factor for a defective lipoprotein metabolismand hypocholesterolemia which exponentially increase the burdenof damage by cholesterol and other lipids due to reduced blood trans-port of fat-soluble antioxidants with nascent VLDL particles Besidesoxysterol accumulation plasma fatty acid composition is also affected[7] and an increased ratio between unsaturated and saturated fattyacid species may contribute to lower cellular antioxidant defenses
Altogether these findings suggest that lipid oxidation biomarkerscan provide a reliable measure of systemic and lung-specific oxidativestress in CF
Markers of protein damage are also detectable in the airways ofchildren with CF and their levels are observed to parallel the extentof neutrophilic markers and lung dysfunction [143166] Bronchoal-veolar lavage proteins undergo halogenation of Tyr residues aradical-mediated process presumably depending on MPO enzyme ac-tivity and assessed through the analysis of 3-chlorotyrosine and 3-bromotyrosine Thiocyanate and protein carbonyls are also useful bio-markers to assess the inflammation-related injury of BALF proteins inCF [1431]
3 Antioxidants in CF
31 Glutathione and its related defense system
311 Defects in GSH homeostasisOther studies have pointed to alterations in the levels of extracel-
lular antioxidants in respiratory tract lining fluids [3] In particularthe analyses of broncheoalveolar lavages (BAL) have revealed thepresence of decreased levels of GSH in the alveolar epithelial liningfluid of CF patients The normal level of extracellular GSH in thelung is 140 times that present in blood plasma and the lung is a netimporter of circulating GSH [77] As a result GSH concentration inELF is close to 400 μM whereas significantly reduced GSH levels arepresent in adult CF patients [41] Low levels of GSH have been ob-served in plasma and blood neutrophils [4178] suggesting systemicGSH dyshomeostasis in CF Moreover some studies have shown thatat the cellular level the CFTR mutation causes mitochondrial deple-tion of GSH [7980] The consequences of this defect are still difficultto be understood due to our poor knowledge about the exact func-tions of GSH in the lung but there are reasons to believe that thedecrease of GSH in the ASL contributes to lung infection and inflam-mation [4281] At the same time it must be underlined that a recentstudy has shown that the GSH content in sputum samples is higher inCF patients than in healthy people indicating that GSH deficiency inCF is restricted to the lower respiratory tract [82] Several hypotheseshave been proposed to explain such a local increase in GSH includingthe possibility that it may derive from apoptotic neutrophils The re-lease of high levels of GSH may be part of a compensatory mechanismaimed at controlling disulfide bonds-mediated aggregation of mucinsSecretions of the upper respiratory tract contain abundant levels ofthese glycosylated and cysteine-rich proteins likely playing a role in
the airway antioxidant defense Indeed these proteins are potent invitro ROS scavenges [83] and their synthesis is upregulated upon ox-idative stress via epidermal growth factor receptor (EGFR) transacti-vation [84]
GSH a major component of cellular antioxidant defenses exerts im-portant functions related to its electron-donating capacity includingprotection from the damaging effects of ROS and regulation of a pletho-ra of cellular events such as gene expression proliferation and differen-tiation apoptosis and immune response [85] GSH is synthesized by twosequential ATP-dependent reactions catalyzed by γ-glutamylcysteinesynthetase (recently renamed glutamate-cysteine ligase) andGSH syn-thetase The reaction catalyzed by γ-glutamylcysteine synthetase iethe formation of γ-glutamylcysteine from glutamate and cysteine isthe rate-limiting step in GSH synthesis and is feedback regulated byGSH itself In fact this enzyme represents an interesting case of redox-regulation of catalytic activity that is mediated by the reversible forma-tion of disulfide bonds [86] Oxidizing conditions causing GSH depletionpromote the formation of a disulfide bondbetween the catalytic and theregulatory subunits of the enzyme leading to a conformational changewhich favors the binding of glutamate In contrast physiological levelsof GSH reduce this disulfide bond thus explaining GSH feedbackinhibition
Either in intracellular or extracellular compartments GSH is pre-dominantly found in the reduced form although small amounts ofthe oxidized disulfide forms (GSSG or GSSR where a GSH moleculeis linked to a free or a protein thiol) can always be detected GSSG isproduced by the catalysis of glutathione peroxidase during thedetoxification from hydrogen peroxide and other peroxides or bythe direct reactions of GSH with electrophilic compounds such asradical species Despite the bulk of GSH synthesis occurring in thecytoplasm GSH is distributed in intracellular organelles includingthe endoplasmic reticulum mitochondria and nucleus Under physio-logical conditions the GSH to GSSG ratio in these compartments ishigh frequently gt1001 but this may change under conditions of ox-idative stress [87] A major exception is represented by the endoplas-mic reticulum where GSSG is present at much higher levels to favordisulfide bond formation [88] Interestingly the compartmentaliza-tion of GSH in separate pools within organelles allows localized alter-ations in the balance between GSH and GSSG that may haveconsiderable functional and pathological significance [89] Thiscould be particularly important in CF in view of the above mentionedstudies showing that cultured CF cells have an apparent normal GSHGSSG content but are characterized by a marked decrease in mito-chondrial GSH in association to elevated mitochondrial ROS [7980]
Different roles of high levels of GSH in the ELF may be hypothe-sized including a) preventing inflammation and tissue damage byscavenging the ROS spontaneously generated in this highly oxidizingenvironment actively produced by neutrophils during inflammationor originating from lipid peroxidation b) regulating the redox statusof membrane proteins involved in the transduction of signals leadingto changes in the expression of genes involved in the immune re-sponse c) controlling mucus viscosity by breaking disulphide bondsd) modulating the response to bacterial infections This last possibili-ty is suggested by the observation that GSH significantly increasesin the ASL of wild type mice following P aeruginosa infection where-as this response is not observed in CFTR mutant mice [90] Interest-ingly some authors have suggested the ability of GSH to control Paeruginosa growth and resistance to antibiotics although these stud-ies should be considered with some cautions due to the likely use ofunbuffered GSH [91]
Although the decreased levels of GSH in ELF could be due to in-creased consumption during inflammation-related oxidative stress[4192] GSH deficiency in CF ELF likely derives from CFTR channeldysfunction In fact comparable alterations in GSH extracellular con-tent characterize the lung of CFTR knockout mice [93] indicating thatthis defect is correlated to mutations in CFTR
695F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
In particular ELF and lung tissue from CFTR knockout (Cftr KOB6129P2-Cftrtm1Unc) and wild-type mice were compared for GSHcontent and the activities of glutathione-related enzymes [93] Inthe ELF the concentration of GSH was significantly decreased in theCftr KO mice compared to WT whereas tissue concentrations ofGSH were similar [92] In the Cftr KO lung the activities of glutathionereductase and glutathione peroxidase were increased whereas theactivity of γ-glutamyltransferase was unchanged Two indicators ofoxidative stress thiobarbituric acid reactive substances (TBARS) and8-hydroxy-2-deoxyguanosine (8-OHdG) were also increased in theCftr KO lung tissue [90] These data support the hypothesis that a mu-tation in the CFTR gene can affect the antioxidant defenses in the lungand may contribute to the exaggerated inflammatory response ob-served in CF Thereby CFTR could be considered as an importantactor of ELF antioxidant homeostasis and thus an intrinsic cause ofoxidative imbalance in CF airways of human patients as well as CftrKO mice
Moreover CFTR belongs to the MRPABC family of proteins whichincludes several GSH transporters and some in vitro studies have in-dicated that CFTR may mediate GSH export across membranes[2394] Despite these evidences there is still debate about the phys-iological implication of CFTR in GSH transport outside the cells asother studies have raised the possibility that CFTR may not actuallyconduct GSH but regulate its transport indirectly through chloridetransport [85]
312 In vitro studies suggesting a protective role of GSH in CF modelsystems
Possible protective roles of extracellular GSH in the CF lung havebeen long proposed and recent in vitro studies have provided furtherand more robust support to this clue For example it has been sug-gested that GSH may control the levels of chlorinated compoundsformed by the activity of myeloperoxidase a neutrophil-releasedprotein abundantly present in CF patients secretions [9596] and pre-vent NK-κB activation [96] Other studies have suggested that CFTRmutant cells produce higher levels of proinflammatory cytokines inresponse to P aeruginosa diffusible material with respect to wildtype cells through a mechanism involving the activation of NADPHoxidase This effect may be significantly reversed by the addition ofextracellular GSH [97]
GSH could also play an important role in protecting the lung epi-thelia from the toxic effects of pyocyanin (PCN) a redox-active exo-toxin released by P aeruginosa which is supposed to cause a varietyof deleterious effects on the airway physiology [98] PCN levels ashigh as 130 μM have been measured in pulmonary secretions of pa-tients with CF and individuals with chronic bronchiectasis [99] Atconcentrations within the range measured in the sputum from CF pa-tients PCN induces a drastic reduction of intracellular GSH [100101]promotes death of cultured cells [100] and causes pathophysiologicalalterations in the lung of wild type mice that are consistent with thechanges observed in CF patients [102] PCN toxicity likely derivesfrom its ability to accept electrons from cellular reductants and thenreact with oxygen to generate superoxide and other ROS [103] There-fore GSH deficiency is explained either by the reaction of GSH withsuch oxidants or through the direct reaction of PCN with GSH thatleads to the formation of a PCN radical [103] However the electrontransfer from GSH to PCN does not occur at neutral pH and recent ob-servations suggest that extracellular GSH provides significant protec-tion against the toxic effects of PCN [104] Moreover GSH can reactwith PCN to form a stable adduct which is likely redox inactive[105] Although the relationships between extracellular GSH andPCN are still contradictory it is worth mentioning that extracellularGSH increases to millimolar levels in the ELF of wild type miceinfected with P aeruginosa indicating that GSH may be useful to re-sist to bacterial colonization [90] Interestingly in vitro studies have
revealed that extracellular GSH inhibits the ability of Burkholderiacenocepacia to enter epithelial respiratory cells and reduces bacterialinduced expression of proinflammatory cytokines (DOrazio Pacelloand Battistoni 2011 unpublished results)
32 GSH-based antioxidant therapies
321 Preclinical studies in animal models of CFMice genetically modified for the Cftr gene along with acute and
chronic infection induced by CF-related pathogens are a key asset inCF research Although much has been learned through these CFmousemodels limitations in the ability of this species to recapitulatespontaneous lung disease and several other organ abnormalitiesseen in CF humans including few airway mucous glands have creat-ed a need for additional species on which to study CF [106] To thisend pig and ferret CF models have been generated and are currentlybeing characterized [107108] These new larger animal models havephenotypes that appear to closely resemble human CF disease seenin newborns and efforts to characterize their adult phenotypes areongoing However mice have been the dominant species by whichto study CF disease processes in vivo and develop therapies for thepast two decades including GSH-based antioxidant treatment
Despite limitations and significant species differences betweenmice and humans these models proved to be useful tools to mimicthe initial and progressive bronchopulmonary infection typical of CFpatients [109] In particular the model of chronic infection whichchallenge bacterial cells with agar as an immobilizing agent hasbeen extensively characterized and induce the long-term persistenceof the bacterial infection and lung pathology including airway inflam-mation [110111] Lung pathology associatedwith chronic experimen-tal infection resembled some aspects of the advanced chronicpulmonary disease at autopsy in CF patients [112ndash114] Both naturallyoccurring and experimental infections frequently manifest broncho-pneumonia bronchiectasis mucus plugging epithelial metaplasiafibrosis and alveolar exudates with inflammatory cells Lymphoidhyperplasia which was prominent in the infected animals was alsoa common finding in the lungs of CF patients In addition significantdifferences with regard to weight loss BAL neutrophil counts andcytokine concentrations have been detected Infected mice had arapid though transient rise in absolute neutrophil counts TNF-α IL-1β IL-6 MIP-2 and KC in bronchoalveolar lavage (BAL) [110115] Inaddition the generation of CF mice has allowed the possibility of invivo testing of novel therapies before entering in clinical trial Theseinclude the pre-clinical evaluation of antibiotics and biotechnologicaldrugs as well as of natural and synthetic anti-inflammatory agentsthat reduce the excessive recruitment of neutrophils and the progres-sive damage of the respiratory tissue by the unbalanced production ofoxidants
Regarding antioxidants GSH and its pro-drug N-acetylcysteine(NAC) remain the so far most investigated antioxidant agents in CFand several strategies have been proposed to improve systemic andlung GSH status of CF patients based on pre-clinical studies includingthe administration of nebulized GSH by inhalation or the oral supple-mentation of GSH or NAC Oral GSH administration can raise serumand lung tissue GSH levels in rodents [116117] In these studiesGSH was administered to animals dissolved in saline or PBS Thepharmacokinetic profile of an oral bolus dose of GSH (300 mgkg)was determined in mice in other studies [118] Plasma ELF BALcells and lung tissue were analyzed for GSH content There was arapid elevation in the GSH levels that peaked at 30 min in the plasmaand 60 min in the lung ELF and BAL cells after oral GSH dosing OralGSH treatment produced a selective increase in the reduced and ac-tive form of GSH in all lung compartments examined Oral GSSG treat-ment (300 mgkg) resulted in a smaller increase of GSH levels Toevaluate the role of CFTR in this process Cftr KO mice and gut-
Table 1Intervention trials on antioxidant therapy in CF patients found at ClinicalTrialsgov databasea
Rank Title PI Location Recruitment Interventions Age groups Phasesnumberenrolled
Study designsb Outcome measures Start andcompletion date
NCT ID
1 Efficacy and safety studyof inhaled GSH in CFpatients
GrieseM
Germany Completed Drugbull reduced GSH sodium salt
C|A|S II138
1 R|E2 Safetyeff3 PA4 DB (Sub Inv)5 Treatment
bull Differences between inhaled GSHand inhaled normal saline withrespect to the area under the curveof FEV1 predicted within the periodfrom baseline to week 24
bull Treatment changes with respect tothe variablesspirometry peak flowquality-of-life weightheightpercentage of neutrophilsothercell types (induced sputum) inducedsputum levels of GSHinflammatorymediators pulmonary exacerbation
Jul-07May-10
00506688
bull 09 saline (control)
2 A phase I study of inhaledsodium pyruvate for thetreatment of CF
BillingsMCE
United States Terminated Drugbull Inhaled sodium pyruvate
A|S I70
1 R|E2 Safetyeff3 PA4 DB5 Treatment
bull Assessment of safety of inhaled sodiumpyruvate in Subs with CF Subs will beevaluated for the presence of symptomsand safety laboratory measurements
bull Determination of improvement inlungs of CF Subs as determined bymeasurement of FEV1 and measurementof inflammatory markers ininduced sputum
Feb-06na
00332215
3 Inhaled GSH versusplacebo in CF
MarsicoS
Italy Recruiting Drugbull Inhaled reduced GSHbull Physiological solution
C|A III150
1 R|E2 Eff3 PA4 SB (Sub)5 Treatment
bull FEV1bull Small airway function exercise capacityBMI dyspnoea cough quality of lifepulmonary exacerbations markers ofoxidative stress (H2O2)in serum and inEBC epithelial inflammatory markerson BNEC
Jun-10Dec-12
01450267
4 Safety and efficacy ofan antioxidant-richmultivitaminsupplement in CF
SagelSD
United States Completed Dietary supplementbull AquADEKs
C|A IIndashII17
1 NR|E2 Safetyeff3 SGA4 OL5 Treatment
bull Plasma levels of β-carotenebull Plasma levels of coenzyme Q-10retinol (Vitamin A) 25-hydroxy vitaminD α- and γ-tocopherols (Vitamin E)PIVKA-II
Aug-07Nov-09
01018303
5 Efficacy and safety ofepigallocatechin gallate(EGCG)tocotrienol in18 patients with splicing-mutation-mediated CF
KeremE
Israel Not yetrecruiting
Dietary supplementbull EGCGbull Tocotrienolbull EGCG+tocotrienol
A|S na18
2 Safetyeff3 CA4 OL5 Treatment
bull Changes in nasal chloride secretion asassessed by TEPD with assessment ofmean changes in TEPD by drug comparedto baseline and the proportion of patientswith a chloride secretion response bydrug compared to baseline
bull Pulmonary function testing FEV1FVC MEF25-75
Sep-09Jun-11
00889434
6 The effect of inhaledNAC compared tonormal saline onsputum rheology andlung function
VanDaele S
Belgium Terminated Drugbull Acetyl-Cysbull Normal saline
C|A IV19
1 NR|E2 Eff3 CA4 OL5 Treatment
bull Changes in visco-elasticity andlung function
Jan-10Dec-10
00996424
696FG
allietal
Biochimica
etBiophysica
Acta
1822(2012)
690ndash713
7 Safety of orallyadministeredcurcuminoids in adultsubjects with CF
Goss C United States Completed Drugbull Standardized turmericroot extract
A I11
1 NR|E2 Safetyeff3 SGA4 OL5 Treatment
bull Safety and tolerability of 14 days oftreatment with orally administeredcurcuminoids as assessed by adverseevents laboratory parameters andspirometry
bull Pharmacokinetics of repeated dosesof orally administered curcuminoidschange in NPD measurementschange in sweat chloride measurements
Apr-05Jan-06
00219882
8 Nasal potential studiesutilizing CF transmembraneregulator (CFTR) modulators
Rowe S United States Recruiting Other quercetin C|A II46
2 Eff3 SGA4 OL5 BS
bull NPD(NPD) Biomarkerbull Residual CFTR activity
Mar-10Nov-11
01348204
9 Safety and tolerability ofinhaled nitric oxide inpatients with CF
Sagel S United States Completed Drugbull Nitric oxide for inhalationbull Nitrogen
C|A|S IIndashII18
1 R|E2 Saf3 PA4 DB (Sub Care Inv OA)5 Treatment
bull Safety and tolerability of drugassessed by change in methemoglobinlevels oxygensaturation FEV1
bull Assess the difference in sputumbacterial density before and afterNO inhalation and the differencein lower airway inflammatorymeasures before and after NO inhalation
Jul-04Dec-08
00570349
10 NAC Phase IIB a multi-center phase IIBrandomized placebo-controlled DB study ofthe effects of NAC onredox changes and lunginflammation in CF patients
ConradC
United States Completed Drugbull NAC
C|A|S II80
1 R|E2 Eff3 SGA4 DB (Sub Care Inv OA)5 Treatment
bull Change in the logarithm of the levelof human neutrophil elastase(HNE) activity measured in sputum
bull Change in concentration of IL-8measured in sputum and plasmaconcentration of GSH measured inwhole blood the neutrophil countmeasured in sputum
Nov-08Feb-11
00809094
11 Glutamine supplementationin CF
na United States Not yetrecruiting
Dietary supplementbull Glutaminebull L-alanine
A|S II40
1 R3 PA4 DB (Sub Care Inv OA)5 Prev
bull Percent increase in plasma glutamineand GSH redox levels measured atweeks 0 4 8 and 12
Feb-10Feb-11
01051999
12 Effect of sulforaphane inbroccoli sprouts onNrf2 activation
ChmielJF
United States Active notrecruiting
Dietary supplementbull Broccoli sprouts
A na15
3 SGA4 OL5 BS
bull Nrf2 activation in NECbull Measures of lipid peroxidation in NECGSH from blood lymphocytesoxidative stress in urineneutrophil migration into thegingival crevices
Apr-11Sep-11
01315665
AbbreviationsA=adult BC=breath condensate BNEC=brushed nasal epithelial cells BS=basic science C=child CA=crossover assignment Care=caregiver CF=cystic fibrosis DB=double blind EBC=exhaled breath condensate Eff=efficacystudy FEV1=forced expiratory volume in 1 s FVC=forced vital capacity GSH=glutathione Inv=investigator MEF25ndash75=maximal expiratory flow 25ndash75 na=not available NAC=N-acetylcysteine NEC=nasal epithelial cellsNLF=nasal lavage fluid NPD=nasal potential difference NR|E=non-randomized|endpoint OA=outcomes assessor OL=open label PA=parallel assignment PI=principal investigator Prev=prevention R|E=randomized|endpoint S=senior Saf=safety study SB=single blind SGA=single group assignment Sub=subject
a Search was done matching the terms ldquoantioxidant therapyrdquo or ldquoGlutathionerdquo with ldquoCystic Fibrosisrdquob 1 Allocation 2 Classification 3 Intervention model 4 Masking 5 Primary purpose
697FG
allietal
Biochimica
etBiophysica
Acta
1822(2012)
690ndash713
698 F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
corrected Cftr KO-transgenic mice were given an oral bolus dose ofGSH (300 mgkg) and compared with WT mice for changes in GSHlevels in plasma lung ELF and BAL cells There was a twofold in-crease in plasma a twofold increase in lung a fivefold increase inELF and a threefold increase in BAL cell GSH levels at 60 min in WTmice however GSH levels only increased by 40 in the plasma 60in the lung 50 in the ELF and twofold in the BAL cells within thegut-corrected Cftr KO-Tg mice No change in GSH levels was observedin the uncorrected Cftr KO mice These studies suggest that oral GSHadministration can increase plasma and lung compartment GSHlevels in WT mice and to a lesser extent in gut-corrected Cftr KO-Tganimals It also suggests that oral GSH treatment can boost BAL cellGSH levels However since this study failed to show significant in-creases in serum and lung compartment GSH levels in uncorrectedCftr KO mice it is questionable whether oral GSH administration toCF patients with intestinal malabsorption would benefit from thistherapy It was also shown that GSH is rapidly distributed to theserum and lung compartments Kariya et al [118] speculate thatother transporter(s) besides CFTR are responsible of the transport ofGSH and probably of other dietary molecules to the lung whichmay be responsible for dietary deficiencies observed in various lungdiseases
Another strategy is represented by the oral supplementation ofhigh doses of NAC a well known cysteine donor for the synthesis ofglutathione NAC is considered a safe molecule which has beenused successfully to treat GSH deficiency in a wide range of diseases[119] As CF mice display defects in GSH export in the ELF comparableto those of patients they could provide a useful tool to assess the ef-fects of NAC administration on the GSH status However only limitedstudies exploring the effects of NAC on CF animal models have beenso far carried out The effects of NAC have been tested on mucus accu-mulation bacterial load transit and inflammation in the CF mousesmall intestine showing that NAC may reduce intestinal mucus accu-mulation bacterial overgrowth in the gut [120]
Moreover NAC has been reported to restore the accumulationof unwantedmisfolded proteins in aggregates that are associated withthe CF airway phenotype as a cause of lung inflammation [121] Themechanism of this NAC-derived effect seems to involve the restorationof beclin 1 expression and activity in the autophagy pathway of theendoplasmic reticulum that was investigated in vivo using Scnn1b-transgenic and Cftr(F508del) homozygous mice The restoration ofthis pathway also produced a rescued trafficking of CFTR (F508del) tothe cell surface of CF cells obtained from human CF nasal biopsies
Given the defective GSH metabolism of CF reviewed in the previ-ous sections and in [122] and the reduced response to GSH therapyin CF mice [93] some Authors have investigated the influence of bac-terial infections on lung oxidative stress The effects of P aeruginosainfection on ELF and lung tissue antioxidants and the oxidation ofDNA and lipids were investigated in mice challenged with bacterialcells [90] CFTR-KO (B6129P2-Cftrtm1Unc) and WT mice were chal-lenged intratracheally with a clinical isolate of mucoid P aeruginosaembedded in agar beads and on the third day of infection BALF andlung tissue were obtained and analyzed for cytokines antioxidantsand enzyme activities [90] P aeruginosa lung infection increasedlevels of inflammatory cytokines and neutrophils in the ELF This cor-responded with a marked increase in GSH and in urate levels in theELF of P aeruginosa-infected WT mice A twofold increase in uratelevels was also observed among lung tissue antioxidants of Paeruginosa-infected WT mice There were no changes in markers oflung oxidative stress associated with the P aeruginosa lung infectionIn contrast to WT mice the CFTR-KO mice lacked a significant in-crease in ELF GSH when challenged with P aeruginosa and this corre-lated with a decrease in the ratio of reduced to oxidized GSH in theELF a marker of oxidative stress These data would suggest that thelung adapts to infectious agents with elevated ELF GSH and urateTherefore individuals with lung diseases associated with altered
antioxidant transport such as CF might lack the ability to adapt tothe infection which may lead to a more severe inflammatoryresponse
322 Clinical trials on GSHThe discovery of the defect in GSH export has suggested that ther-
apies able to restore or increase GSH levels in the ASL could counteractthe inflammation and oxidative stress conditions typical of CF pa-tients In an attempt to strengthen extracellular defenses againstROS some pilot studies have analyzed the effect of GSH inhalation orthat of oral GSH prodrug N-acetylcysteine (NAC) All these treatmentswere well tolerated by the CF patients and most authors were able tomeasure increased ELF concentrations of GSH in association withsome positive clinical outcomes [4041737896122ndash128] Althoughpotentially promising these findings need stronger clinical evidencein that the majority of these were obtained on very limited numberof patients investigated in non-randomized controlled trials This ishighlighted in a recently published meta-analysis [129] that providesalso a thoroughly analysis of the literature on this aspect of the antiox-idant and anti-inflammatory therapy of CF Among the American CFfoundation sponsored trials two phase II trials on inhaled GSH andoral NAC are in progress in US and Germany (ClinicalTrialsgov Iden-tifier NCT00506688 and NCT00809094 respectively Table 1) andsafety and tolerability of aerosolized glutathione is also matter ofinvestigation by another (not registered) US trial (more informationon this can be found in [130]) Nevertheless the diffusion among CFpatients of NAC preparations for inhalation (Mucomystreg) has in-creased in recent years
γ-Glutamylcysteine ethyl ester (GCEE) is another potentially inter-esting GSH pro-drug which has proved some efficacy in the ameliora-tion of oxidative stress eg in experimental myocardial infarction[131] and central nervous system conditions (see eg [132]) HoweverGCEE has not been investigated in CF yet
33 Limits and potential problems associated to thiol-based therapies
Although the above cited clinical trials may be considered promis-ing attempts to improve the antioxidant levels in the ELF the actualcapacity of these treatments to produce positive clinical effects mustbe considered with caution For example indices of oxidative damagewere found to be unaffected by aerosolized GSH treatment [122]Some in vitro studies have suggested that the reaction of GSH withPCN could produce hydrogen peroxide with potential exacerbationof oxidative damage [101] The exact mechanisms of PCN toxicityand the reaction of this toxin with GSH must be better understoodin order to evaluate the safety of GSH administration to patients col-onized by P aeruginosa
Inhalation of GSH ensures its direct delivery in the airways butsince GSH can rapidly convert to its oxidized form GSSG frequentGSH inhalations are required to maintain a high GSHGSSG As a con-sequence of this limit four separate inhalations have been used inthe study carried out by Bishop et al [123] Unless justified by clearclinical improvements these repeated treatments may represent aburden for patients already undergoing complex therapies Moreoverrepeated inhalations of GSH increase the levels of GSSG in ELF[133134] In the absence of effective homeostatic mechanisms ensur-ing the fast recycling of GSSG to GSH this might produce unwantedeffects and even the exacerbation of CF symptoms being GSSG re-sponsible of the S-glutathiolation and functional inhibition of CFTR[124]
In principle the oral administration of GSH could be considered asafe strategy to prevent GSSG accumulation but this strategy is likelynot feasible due to the substantial inability of this water-soluble mol-ecule to cross biological membranes Moreover a study carried out inmice has established that GSH absorption in the gastrointestinal tractif any is mediated by CFTR itself thus excluding the possibility to
699F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
improve circulating levels of GSH in CF patients through the dietarysupplementation of the antioxidant [127] The limited absorption ofGSH could be overcome by GSH-esters as in vitro studies haveshown that this form of GSH may be specifically useful to rescue mi-tochondrial defects in cystic fibrosis models [80] Safety of these GSHderivatives in humans has been poorly investigated
Two independent studies have shown that the treatment of CF pa-tients with high doses of NAC increases extracellular GSH in sputum[78125] but contrasting results have been reported concerning theeffects of NAC on the concentrations of blood GSH and on the levelsof IL-8 and other markers of inflammation NAC treatments may beuseful to modulate the GSH content in cells but it should be remindedthat an enhanced cysteine supply cannot lead to an increase of GSHabove physiological levels due to the feedback inhibition mechanismof γ-glutamylcysteine synthetase described in the Section 311
331 Gamma-glutamyltransferase and GSH therapySo far none of the studies mentioned above has taken into account
the fact that GSH is degraded by GGT enzyme activity GGT concentra-tions are known to increase several fold in ELF of CF patients even ifthe mechanisms for this effect were not determined [135] and thisphenomenon parallels the above described decrease of GSH levels inELF Preliminary data suggest that a major source of increased ELFGGT is represented by activated neutrophils accumulating in diseasedairways (Corti and Pompella 2011 unpublished observation) Re-gardless of its origin it is likely that increased GGT in ELF would de-grade locally administered GSH to variable extents which couldcontribute to the so far inconclusive results of therapies based onaerosolized GSH Besides its role in GSH catabolism GGT has beenshown to mediate protein S-thiolation [136] suggesting that GSH ad-ministration in the presence of active GGT enzyme might alter CFTRglutathiolation status and function in a potentially unfavorable wayOn the other hand a potential role of GGT in favoring bronchial up-take of antioxidant vitamin C has also been suggested [137]
These controversial findings may add further issues to the ques-tion of whether the therapy of lung oxidative stress by aerosolizedGSH could be safe in all the CF patients regardless of specific strate-gies that would ascertain the extent of lung inflammation Thesestrategies should include the assay of GGT levels in ELF In principleonce an adverse role of ELF GGT in GSH therapies will be confirmedthe association of GGT inhibitors in the GSH formulations for inhala-tion could represent a promising pharmacological strategy
34 Malnutrition as a possible cause of defective thiol-dependentantioxidant protection
Successful nutritional interventions strongly impact on the clinicaloutcome of CF patients [138ndash140] Malnutrition by pancreatic insuffi-ciency and other CF-related factors influence the susceptibility to de-velop recurrent infections and severe inflammatory lesions of thelung tissue If the onset of a defective (sub-optimal) antioxidant sta-tus may represent an underlying component in the clinical effects ofmalnutrition remains a matter of investigation Clinicians have topay particular care to avoid these disturbances and successful proto-cols of nutritional intervention in CF have been developed whichare essentially aimed to avoid the onset of protein-energy malnutri-tion (PEM) [141] Despite this the risk of developing such an unto-ward complication in CF infants and children remains high assuggested by the prevalence data registered in some areas Actuallya prevalence of PEM between 5 and 14 in Moldavian infants was re-cently reported [142] and PEM is associated with poor outcome andparticularly with the risk of developing edema and anemia
Besides lowered intake and absorption of micronutrient antioxi-dants discussed in the other sections malabsorption of dietary proteinand excess fecal amino acid losses result in hypoproteinemiahypoalbu-minemia as key biochemical signs of PEM Hypoalbuminemia is
considered to be linked with a causendasheffect relationship with oxidativestress and is proposed to influence morbidity and mortality in condi-tions associated with chronic inflammation and severe oxidative stress[143144] The human serum albumin (HAS) molecule contains only areactive thiol group eg the Cys 34 the importance of which as an anti-oxidant defense system in blood and for the entire organism is welldocumented [145] This is the second main thiol (and the main proteinthiol) in the circulation (approx 2 mmol in the adult organism assum-ing 5 l of total blood volume anHt of 40 and [HAS] of 45 gl of plasma)being the RBCGSH thefirst thiol in blood (near to 5 mmol assuming thesame parameters of above and an average concentration of GSH inpacked RBC of 25 mM) [146147] The antioxidant role of HSA is notonly a consequence of the relative abundance of its Cys thiol A specificcapability of acting as a sacrificial target for a series of electrophils andmost biologically relevant ROS ie hydrogen peroxide and peroxyni-trite has been demonstrated in a series of studies [145148149] Li-gand binding activity can contribute to promote antioxidant effectsby the HSA molecule [145] Transitions metals particularly copperand also iron in the case of iron-overload diseases bind to HSA Inthis way these are less available to promote the Fenton chemistryand hydroxyl radicals eventually released from this oxidative reactionare mostly directed to the HAS protein sparing more important tar-gets A free radical-trapping activity of HSA has been also demonstratedand this was proposed to be directed toward both hydrophilic and fat-soluble species This activity may result from the interaction withother antioxidants such as α-tocopherol [150] and may influence theantioxidant activity of food-derived phenolic antioxidants [151]
However Cys 34 is considered the main contributor to the antiox-idant function of HAS which plays its role in the antioxidant homeo-stasis of blood thanks to a complex series of interactions with themetabolism and antioxidant function of the pool of free thiols in plas-ma and in the circulating RBC with the latter playing a significantcontribution to the extracellular pool of GSH [146] and to the dynam-ics of inter-organ GSHmetabolism in cooperation with liver and othertissues [147] Immuno-inflammatory cells and the lung tissue areamong the main terminals of this metabolism The RBC contain theentire machinery to synthesize GSH to restore its redox (by enzymat-ic reduction of the oxidized form) and to use this as cofactor of Se-GPx and GSH-S-transferase enzymatic activities that are responsibleof the detoxification of hydroperoxides and alkylating agents thatmay form in or enter the RBC cytosol [147] In this sense the RBC rep-resents a circulating reservoir of GSH that in addition to maintainingthe redox and respiratory function of Hb participates to systemic pro-tection of xenobiotics of endogenous and exogenous origin In consid-eration of these aspects the combination of hypoalbuminemia andanemia may exponentially increase the risk of developing oxidativestress in CF patients as it is supposed to occur in other oxidative stressconditions such as chronic kidney disease [55143152] Additionalclinical investigation should verify the hypothesis that hypoalbumi-nemia together with a defective uptake and metabolism of sulfur-containing amino acids and CF-specific defects of the GSH metabo-lism may represent a causal risk factor for an impaired antioxidantdefense and systemic oxidative stress in CF patients
35 Fat-soluble antioxidants
Pancreatic insufficiency and a diminished bile acid pool cause mal-absorption of important essential nutrients and other dietary compo-nents in CF Of particular significance is the malabsorption of fat-soluble antioxidants such as tocopherols carotenoids and coenzymeQ-10 (Co-Q10) and that of essential fatty acids (EFA)
351 Vitamin EVitamin E therapy in CF has been proposed in several decades of
research as a useful approach to overcome both the lower absorptionof this fat-soluble micronutrient and the increased antioxidant
700 F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
demand by the abnormal generation of ROS in CF tissues (see for in-stance the recommendations by the Cystic Fibrosis Foundation Con-sensus Conference on nutrition [153])
The first report of a vitamin E deficiency in CF appeared in literaturein 1951 by Filer et al [154] In this study the absorption of the mainform of this vitamin eg α-tocopherol and its ester derivatives was in-vestigated in several subsets of infants and children Thanks to a simplebioavailability (or tolerance) test these authors observed that ldquoin-fantshellip diagnosed as fibrocystic disease of the pancreas diarrhea andcirrhosis were characterized by a poor response to the test ie the tol-erance curve was lowrdquo However abnormalities were also observed inother subgroups of infants with a variety of disorders not associatedwith fat or fat-soluble vitamin intolerance such as sprue celiac syn-drome and lupus erythematosus which suggests the general observa-tion that malnutrition and inflammatory and degenerative diseases ofthe GI tract may lead to absorb tocopherols poorly At the same timethese authors reported that ldquoMetabolic disorders with associated hy-percholesterolemia were observed to give abnormally high values forthe area under the curverdquo and that patients responding poorly to to-copherol absorption test did also in vitamin A absorption tests
The finding of lowered (lipid uncorrected) levels of vitamin E wasconfirmed in other studies in which this relative deficiency was foundto occur irrespective of pancreatic comorbidity and in associationwith lowered levels of other liposoluble vitamins such as vitamin Aand D [155] regardless of their different liver metabolism and tissuedelivery mechanisms [156157]
Plasma buccal mucosal cells (BMCs) and breath condensate α-tocopherol decreased significantly with age in association with a de-creased respiratory function [5] This was accompanied by loweredlevels of other antioxidants such as vitamin C and increased oxidativestress markers of different origin such as protein carbonyls thiobarbi-turic acid-reactive substances and F2-IsoPs
Clinical symptoms of vitamin E deficiency in CF have not beenconclusively investigated Dolan et al [158] described that anemiaof CF patients is related to vitamin E deficiency and increasedperoxide-induced hemolysis of RBC Other authors however ob-served an increased susceptibility to peroxide-induced hemolysisalso in the presence of normal levels of vitamin E [159] Peters andKelly [160] observed that RBC vitamin E concentrations were belowthe normal range in almost all unsupplemented patients and roseinto the normal range with a 1-year supplement of 100 mg per daybut not 15 mg per day Since RBC vitamin E concentration has beenshown to correlate well with tissue concentrations of the vitamin inanimals tissue levels of vitamin E are expected to be lower than nor-mal in CF patients
Bioavailability of fat-soluble vitamin is limited in CF Vitamin Edeficiency of CF is also associated with hypocholesterolemia [7] Asa consequence the relative deficiency of this vitamin is compensatedwhen the absolute levels are normalized for cholesterol levels andthis suggests a poor transferring of this vitamin in the circulation bya defective lipid and lipoprotein metabolism Pancreatic insufficiencyand the consequent lipid malnutrition cannot completely explain thisdefect and other possibly CF-specific dysfunctions could play a roleLiver metabolism and specific plasma transport systems of this vita-min need further elucidation in CF
As a consequence of these aspects it is not presently clear whichform and level of supplementation of this vitamin is most appropriateto treat these patients Usingα-tocopherol as a vitamin E supplementPeters et al [160] reported that 100 mg per day are required to nor-malize RBC concentrations Other authors described unsuccessfulsupplementation protocols with higher doses and this has led to de-velop formulations with higher bioavailability in order to achieve bet-ter compliance to oral supplementation (see below and the literaturereviewed in [161ndash163])
Besides absorption and tissue delivery issues specificity of actionis another critical item of antioxidant therapy with fat-soluble agents
in CF As further addressed below this aspect could be themain limit toa successful use of natural forms of vitamin E in the clinical manage-ment of CF inflammation even if a local lung-targeted therapy wouldbe developed according with so far proposed pre-clinical models ofaerosolized vitamin E [164165]
Current pharmacological research is aimed to develop synthetic formsof this and other fat-soluble antioxidants with better radical scavengingproperties at the lipidndashwater interface Type of ROS target and the sitesof action greatly influence the chances of a fat-soluble antioxidant of alle-viating oxidative stress in the airways as well as in other organs such asliver and pancreas These aspects dealing with specificity of action[163166167] have stimulated the search of novel vitamin E-derived an-tioxidants that may help to scavenge radicals at the lipidndashwater interfaceof the epithelial cell membrane and surfactant Amine derivativesof tocopherols and tocotrienols have been recently demonstrated toshow higher antioxidant and free radical scavenging activity than α-tocopherol [168] Further in vitro pharmacological analysis has includedtoxicity evaluations and the detailed investigation of scavenging of azo-and phenolic radicals with different degrees of hydrophobicity and theinhibitory activity on IL-8 gene expression and phospholipase activityin CF cells Comparative evaluation with other synthetic derivativessuch asα-tocopheryl succinate and natural forms of vitamin E suggestedthat these amine derivatives are promising antioxidant and anti-inflammatory agents [Galli F and Pilolli F unpublished observation]deserving further pre-clinical investigation in CF model systems
Anti-inflammatory effects of natural and synthetic analogues of vi-tamin E are also an intriguing pharmacological opportunity currentlyunder investigation by several laboratories [169170]
Recently vitamin E supplementation has been at the center of adispute regarding its safety when used at high dosages in certainpopulations of patients An extensive and speculative debate originat-ed on this subject after a meta-analysis study byMiller et al [171] thatexamined the largest secondary prevention trials on vitamin E trials incardiovascular patients finding a significantly increased mortality riskfor all the causes (about 4 1ndash8 in the 95 interval of confidence)when the patients were treated with doses gt400 IUdie (that areequivalent to 400 mgdie of the synthetic form allrac-α-tocopheroland to 185 mgdie of the natural form RRR-α-tocopherol) This debateresulted in a careful examination of this meta-analysis study by severalother authors and in further revisions of the literature on vitamin E tox-icity in humans [see the literature recently reviewed in [163172ndash174]]that clearly demonstrated the poor consistency of the conclusionsraisedwithMillersmeta-analysis study and the paucity of the concernsthat derived from that These conclusions have been verified in the re-cent international symposium on vitamin E of the Society for Free Rad-ical Research Europe branch of Rome 2009 [173175] Vitamin E used assupplement for humans in all its forms (eg α-tocopherol and othertocopherols and tocotrienols) is safe in abroad range of intakes[172176] The tolerable upper intake level (UL) and the AcceptableDaily Intake (ADI) established by the Joint FAOWHOExpert Committeeon Food Additives for the natural form of vitamin E as α-tocopherolequivalents are of 300 mgdie and 015ndash20 mgkg body weightdierespectively [172177]
352 CarotenoidsLevels of plasma carotenoids such as β-carotene β-cryptoxanthin
and total lycopene are significantly lowered in CF patients and thiswas associated with higher susceptibility to lipid peroxidation[5178ndash180] Rust et al [178] demonstrated that the long-term oralsupplementation with 50 mg β-caroteneday (ie 1 mg β-carotenekg BWday) restored the levels of this carotenoid while sub-optimalsupplementation was observed at doses of 10 mg β-caroteneday orlower thus confirming the need of high doses of this fat-soluble factorto overcome the limited absorption and thus to achieve plasma con-centrations of healthy control subjects Successful high-dose treat-ments appear to lower oxidative stress markers such as TBA-MDA
701F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
complexes and to correct total antioxidant capacity of plasma Inanother study β-carotene supplementation was observed to de-creased lipid peroxide formation as quantitated by malondialdehydeconcentrations in plasma (TBAHPLC method) and to enhance the re-sistance to copper(II) ion-induced oxidation of low density lipopro-teins [180]
At the same time toxicity issues have been raised for human sup-plementation with carotenoid formulations and particularly of water-miscible formulations of preformed vitamin A that is regularly sup-plemented to CF patients which may increase serum retinol andpossible risk of CF-associated liver and bone complications (reviewedin [161181]) However β-carotene supplementation seems to be safesince this does not affect plasma concentrations of other carotenoidsand retinol as well as of other fat-soluble vitamins as α- and γ-tocopherol [178] Recent studies designed to test the clinical efficacyof a CF tailored multivitamin formulation (commercial name AquA-DEKsreg) also tested the safety of this type of formulation and demon-strated that this does not increase vitamin A above the normal levelsobserved in healthy controls [162182183] The normalization of β-carotene levels obtained in these studies was associated only withminor improvements on respiratory and growth parameters whilethe levels of urinary F2-IsoPs used as index of lipid peroxidationwere not affected [162] The surrogate marker of lipid peroxidationMDA was affected together with some selected antioxidant parame-ters (RBC thiols and superoxide dismutase) in another study inwhich this multivitamin formulation was preliminarily evaluated incomparison with standard formulations of vitamin E and A [182]
353 Coenzyme Q-10Coenzyme Q-10 (Q10) is a well-known electron transporter in the
mitochondrial respiratory chain with fundamental role in cellularbioenergetics and scavenging of radical species [184] This lipophilicsubstance is present in the circulation at low levels (serum concentra-tionsle2 μM) mainly as ubiquinol-10 eg the reduced form with anapproximate ratio of 955 with the oxidized form ubiquinone-10[185186] A mechanism for a preferential distribution and accumula-tion in mitochondria has been suggested for both the reduced and ox-idized forms of CoQ10 that are taken up by the cells in a time- andconcentration-dependent Subcellular localization and trafficking ofexogenous Q10 are similar to those of the endogenous form butwere different from that of α-tocopherol that is related with lipidcomposition particularly in the mitochondrial and microsomal frac-tions [184] Ubiquinol-10 readily oxidizes ex vivo by the reactionwith other lipophilic antioxidants such as α-tocopherol and butylatedhydroxytoluene [185] Therefore a higher reduction potential thanother physiological fat-soluble antioxidants such as vitamin E and aselective metabolism and cellular trafficking show peculiar role forthe cell CoQ which may also represent an important lipophilic antiox-idant in cells and body fluids
Human cells synthesize this coenzyme through the cholesterol bio-synthesis pathway so thatmore than two thirds of the tissue levels ap-pear to have an endogenous origin dietary sources provide acontribution to Co-Q10 levels of blood and all solid tissues that variesdepending on the dose applied and type of dietary source [187] How-ever in the case of oral supplements it has to be considered that hy-drophobicity and large molecular weight of this coenzyme influenceits absorption that ultimately is slow and limited [186187] Likewiseto vitamin E pharmacokinetics [188189] Co-Q10 showed T(max) ofaround 6 h that coincides with that of dietary lipids Elimination isclose to that of the more retained form of vitamin E in human bodyeg α-tocopherol with a half-life of about 33 h which suggests poorhepatic metabolism However commercially available formulationsare reported to be safe even at high doses and solubilized formulationsshow enhanced bioavailability In healthy subjects plasma Q10 re-sponse to oral ingestion show saturation profiles with a plateau at a
dose of 2400 mg and the higher plasma concentrations were foundto facilitate uptake by peripheral tissues and also the brain [186187]
Laguna et al [190] recently investigated total serum levels ofcoenzyme Q-10 in a wide population of CF children (n=381) and esti-mated their association with clinical outcome Near to 50 of these CFpatients were deficient of Co-Q10 and this defect was significantlymore prevalent in patients with pancreatic insufficiency and signifi-cantly associated with P aeruginosa colonization in infants (under24 months of age) Importantly low Co-Q10 levels correlated to otherlipid markers of a poor nutritional status such as total lipids and alsothe other fat-soluble antioxidants β-carotene and α-tocopherolwhich confirms the presence of a common defect in the absorptionand metabolic pathways of this coenzyme with dietary lipids
The deficit of Co-Q10 may contribute to the impaired energy func-tion of mitochondria of CF tissues and this may exacerbate CF-linkedinflammation infection and cellular stress response of the lung A sys-tematic analysis of molecular lesions in CF bronchial tissue has beenrecently carried out by proteomic approach [191] Comparative eval-uation of protein expressional pattern in CF and healthy controltissues has revealed aberrant levels of some mitochondrial andenergy-related proteins in CF specimens that included the ubiqui-nolndashcytochrome c reductase complex core protein I and one form ofnidogen a pseudogene of aconitase 2 These changes in CF may reflectmolecular changes which could be associated with an altered mito-chondrial homeostasis and Co-Q10 redox
Multivitamin supplements with high bioavailability containingCo-Q10 have demonstrated to correct the deficit of this antioxidantand were preliminarily observed to improve airway inflammationmarkers in CF patients [183] However further clinical investigationfailed to demonstrate that such an improved biochemical profile isassociated with significant improvements in weight percentile andpulmonary function [162]
354 Fatty acidsA key pathophysiological role in sustaining inflammation in CF has
been attributed to the abnormal polyunsaturated fatty acid (FA) pat-tern Abnormalities in FA profiling are potentially linked to CFTRmutation-driven alterations in the absorption andor metabolism ofdietary lipids [192193] and to the consumption of high oxidizableFA involved in the free radical-mediated lipid peroxidation [7]Among those alterations dysregulation of the docosahexaenoic acidand arachidonic acid balance has been extensively studied with re-portedly significant reduction of DHA in CF and a parallel increasein the levels of AA and inflammatory indices [193ndash195] Actually AAis the progenitor of both enzymatic- and free radical-derived inflam-matory mediators including leukotrienes prostaglandins and iso-prostanes On the other hand n-3 PUFA (eicosapentaenoic acid anddocosahexaenoic acid) are involved in the generation of potent medi-ators namely resolvins and protectins which are able to resolveexudates and to act as organ protective and antifibrotic Secondarilyto their anti-inflammatory action n-3 FA may also produce anantioxidant-like response (eg a reduced demand of antioxidants toachieve an optimal control of oxidative pathways) As a consequencen-3 PUFA have been suggested and widely used as supplements in CFpatients usually under the form of fish oil [196ndash198] It is worth ofnote however that defective levels of DHA in CF patients was notconfirmed in recent studies [7] It was also shown that patients onDHA supplements did not have increased plasma n-3 FA concentra-tions but showed more severe oxidative stress compared to theunsupplemented patients [7] This observation of an increased riskof oxidative stress in CF subjects receiving n-3 fatty acids supple-ments has also been described by other authors [199]
Studies reporting increased AA levels in CF patients have beencontradicted by others [7200201] thus contributing to weakeningthe pathophysiological role of the altered DHAndashAA balance as turnpoint of an upregulated inflammatory status in CF In this context a
702 F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
recent Cochrane meta-analysis on n-3 supplementation in CF patients[202] highlighted the lack of evidence for a significant correction ofthe assessed clinical end points (mainly respiratory symptoms)even when inflammatory indices and other laboratory end pointswere met Taken together these data suggest that there is insufficientevidence to draw firm conclusions or recommend routine use of n-3supplements in CF Notwithstanding it is common belief that n-3supplements provide some benefits for people with CF with relativelyfew adverse effects and thus their use is not discouraged
Further alterations in fatty acid metabolism have been highlight-ed including the consistent findings of an increase in circulatinglevels of saturated and monounsaturated fatty acids [7203204]Decreased levels of essential FA (EFA) ie the FA that have to be in-troduced with the diet correlates with the severity of respiratoryinsufficiency and the same clinical correlation was observed with al-tered proportions of FA species converted by the activity of desatur-ase enzymes (reviewed in [204]) The close relationship betweencertain fatty acids and oxidative stress including the negative correla-tion of C240 and linoleic acid with oxysterol levels point to the needof intensive investigation in CF patients of previously neglected lipidspecies that are emerging candidates in the control of metabolismQuantitative lipidomic analyses have lead to identify C161n7 palmi-toleate as a ldquoprotectiverdquo adipose-derived lipid hormone that stronglystimulates insulin activity in muscle and liver also suppressing in-flammatory cytokine output from mice fat cells [205] Specific meta-bolic activities have been also demonstrated by medium chainsaturated fatty acids caprylic acid (C80) capric acid (C100) and lau-ric acid (C120) Capric acid acts as a direct ligand of PPARγ using abinding pocket different from the binding pocket of thiazolidinedioneor long chain fatty acids [206] Additional activities of medium chainfatty acids which are ligands of free fatty acids receptors detectedin the immune cells the gastrointestinal tract and adipocytes maycontribute to metabolic homeostasis and inflammatory responses[207] These data underscore the importance of a lipid-mediated ldquoen-docrine networkrdquo demonstrating how specific alteration of one orfew serum lipids would be per se sufficient to influence metabolic ho-meostasis Given the relevance of this emerging information and thealteration of lipid metabolism and inflammatory status in CF fattyacid lipidomics need to be deeply investigated in CF
Again these studies have obvious nutritional implications Satu-rated fatty acids with chain lengths higher than C18 are poorlyabsorbed partly because they form insoluble calcium salts [208]Medium chain saturated fatty acids are well known for being highlyabsorbed through the intestine providing rapid delivery of energyvia oxidation of the more hydrophilic short chains and have beensuggested to provide proper nourishment in patients with CF [209]Recent studies have shown that consumption of a high-fat diet richin medium chain fatty acids as opposed to long chain fatty acidsdoes not lead to ectopic fat accumulation in skeletal muscle andliver of both rats and mice [210] In light of the close association be-tween nutritional status inflammation and life expectancy in CF pa-tients the manipulation of dietary lipids in these patients must befurther explored as a possible strategy to provide adequate nutritionand better management of oxidative stress
36 Hydrosoluble antioxidants oligoelements and enzymatic antioxidants
361 Vitamin CVitamin C status in CF patients has been poorly investigated Early
studies suggested a defective vitamin C status that was refractory tooral supplementation [211] Other and more recent studies showednormal or slightly decreased levels of vitamin C in CF patients as com-pared to healthy controls but age- and disease-related decline of thiswater-soluble antioxidant was reported in these patients [5212]In the study of Winklhofer-Roob et al [212] on mid-European CFpatients vitamin C concentrations decreased with age with an
estimated rate of 5 μmollyr and vitamin C concentrationsb40 μ-moll were associated with highest indexes of inflammation whichis consistent with the hypothesis that optimal levels of vitamin Cmay influence immuno-inflammatory activity of alveolar macro-phages and neutrophils Other few studies have examined the effectof supplements containing vitamin C on CF inflammation and oxida-tive stress since the levels of this vitamin do not significantly improvewith supplementation (reviewed in [213]) This highlights the com-mon fate that this hydrosoluble vitamin shares with several fat-soluble counterparts in the ldquomicronutrient paradoxrdquo of CF patients inwhich the need for a correction of their status along the progressionof the disease is frustrated by the poor efficacy of oral supplementa-tion protocols Formulations and appropriate supplementation proto-cols that may produce a better correction of vitamin C status of CFpatients are awaited for further clinical evaluation
362 Selenium and selenium-dependent peroxidasesSelenium is a trace element with marked electrophilicity [214]
that once converted to the organic form of Se-Cys can be introducedin protein structures to play its important role in H2O2 metabolismand signaling [215] As catalytic center of the enzyme GSH-peroxidase (SeGSH-Px) Se plays a crucial role to protect polyunsatu-rated lipids of plasma membrane and circulating lipoproteins formperoxidative insults With other Se-proteins such as the high molecu-lar weight thioredoxin reductases this oligoelement participates tothe control of protein thiol-disulfide oxidoreduction and glutathiony-lation which regulate signaling pathways of crucial importance in theregulation of immunity and inflammation [16] but also the function-ing of other redox-sensitive proteins such as the same CFTR [124]
The activity of SeGSH-Px in blood is considered a functional as-sessment of selenium status even if this assumption has some limita-tions related with the saturation profile that the Se stores show atincreasing doses of Se administration Investigations of the seleniumstatus in CF patients have produced conflicting findings which maydepend on differences in dietary intake ethnicity and environmentalfactors in the diverse patient populations (reviewed in [216217]) CFchildren have been reported to have lowered blood selenium and RBCSeGSH-Px activity [218219] normal plasma selenium and loweredRBC SeGSH-Px [220] and even normal levels of both these two param-eters [221] The supplementation with selenium in combination withother antioxidants was observed to increase the concentrations ofblood selenium that likewise β-carotene and fatty acid were posi-tively correlated with improved lung function [6]
Foucaud et al [218] observed that a defective selenium statuswas associated with lowered levels of other antioxidants that contrib-ute to the anti-peroxidative activity of this microelement such asvitamin E (reviewed in [222]) and the severity of this deficiencywas lower in children with pancreatic enzyme replacement and vita-min E supplementation
Treatments to substitute for exocrine pancreatic insufficiency bypancreatic enzymes from animal sources such as porcine pancreashave been confirmed to be a source of Se [220] These affects RBCSeGSH-Px activity and plasma selenium concentrations which hasto be taken into account when selenium supplements are given toCF patients
Selenium has been used to develop a series of organoseleniumcompounds that may open the way to new therapeutic opportunitiesin CF (see Section 392) These include GPX mimetic drugs and phaseII enzyme inducers which may provide higher antioxidant activity ofASL and cellular protection effects in the airways
363 Zinc and copperZinc and copper (Zn and Cu respectively) are present in many
proteins so that a deficiency of these trace metals could have pleiotro-pic effects in humans As regards antioxidant systems these two oli-goelements contribute an important role being cofactors of two
703F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
isoforms of the superoxide dismutase enzymes eg the extracellularform eg the EC-SOD or Sod 3 and the CundashZn-SOD or Sod 1 that isfound in several tissues and cells [223] The EC-SOD exerts its antiox-idant role also in the lining fluids of the airways [224]
The notion that CF patients have defective concentrations of bloodZn and Cu is controversial As far as Cu status is concerned few datahave been produced and are available in the literature suggestingthe notion that CF patients develop a moderate copper deficiency[225226] That was essentially demonstrated on the bases of a defec-tive activity of Cu-related proteins such as plasma ceruloplasmindiamine oxidase and RBC SOD This defect seems to be refractory toCu and Zn supplementation (see below)
More advanced studies have been carried out in the case of Zn sta-tus in CF Low plasma zinc concentrations were reported in approxi-mately 30 of young infants with CF identified by newbornscreening [227] and an impaired zinc homeostasis in CF patientswas described by Easley et al [228] This is characterized by poor con-servation of the endogenous pool with fecal loss and impaired frac-tional absorption of zinc which are the consequences of pancreaticinsufficiency and persisting steatorrhea These studies suggestedthat in the clinical management of CF patients these defects can beat least in part corrected by exocrine pancreatic enzyme replacement
A series of studies by Van Biervliet et al [229230] demonstratedin a Dutch population of CF infants and children that serum Zn variesin an age-dependent manner but remained unchanged with respectto healthy control levels In CF patients no difference in serum Zn con-centration between pancreatic-sufficient or pancreatic-insufficientpatients was observed and no correlation was found with the nutri-tional status or height z-score Importantly in these studies a signifi-cant correlation of serum Zn was observed with the fat solublevitamins A and E thus confirming the relationship between the ab-normalities of lipid and Zn metabolism in CF This suggests that co-supplementation of Zn and fat-soluble vitamins should be advisedin the presence of pancreatic insufficiency and persisting steatorrhea
Neve et al [219] in a study aimed to assess plasma and erythrocytezinc copper and selenium in CF children showed that mean plasmazinc and copper levels were not different from those in age-matched controls which confirms the observations by Van Biervlietet al described above However plasma zinc concentrations de-creased in patients with moderate-to-severe growth retardation andwith severe pulmonary disease but very low zinc levels occur sporad-ically Erythrocyte zinc and copper levels were significantly higherthan normal while RBC selenium was lower than in age-matchedcontrols These trace element concentrations in erythrocytes werediscussed in relation to the activities of the CuZn-SOD and the Se-enzyme GPx This observation suggests a compensatory upregulationof the erythrocyte CuZn-SOD by the exposure of erythroid precursorsto ROS andor other CF-related stressors
Best et al [225] also studied RBC SOD activity using this as a bio-logical sensor of Cu status in CF patients A lowered activity of thisenzyme was reported in CF together with that of the other Cu-dependent enzyme plasma diamine oxidase while plasma ceruplas-min showed normal activity Degradation rates of copper proteinsare known to be accelerated in conditions of copper deficiencywhich could explain the finding at least in part Anyway when Cuand Zn were supplemented to CF patients either separate or incombination (6 weeks of 3 mg copperd as copper-glycinate and30 mg zincd as zinc-glycinate) any of the copper enzyme activitieswas affected Therefore the moderate copper deficiency of CF patientsappears to be refractory to the intervention by increased copper andor zinc intake
Erythrocyte CuZn-SOD and the plasma levels of Cu and Zn werealso measured in the study of Wood et al [6] in which Australian CFpatients (agegt5 years) were treated with a high-dose antioxidantmultivitamin formulation containing 200 mg vitamin E (as RRR-α-tocopherol) 300 mg vitamin C (as sodium ascorbate) 25 mg β-
carotene (all-trans isomer) 90 μg Se (as selenomethionine) and500 μg vitamin A (as retinyl palmitate) in oil Plasma oligoelementsand particularly Zn were in the normal range at baseline (as com-pared with the data reported in [229230]) and were not affected bythis multivitamin supplement The same was found for the activityof RBC SOD and for plasma 8-iso-PGF2α as surrogate biomarker oflipid peroxidation
In a recent non-randomized small population (n=21) casendashcon-trol study in CF children Zn supplementation was proven to producepositive clinical effects in Zn-deficient patients [196] The supplemen-tation with 5 mgkg Zn sulfateday (maximum 150 mg) significantlydecreased the number of infections and increased the forced expira-tory volume in 1 s energy intake and growth parameters also im-proved These parameters were unaffected in untreated patientsexcept that in the case of the pulmonary function that decreased sig-nificantly These clinical observations on Zn supplementation need tobe confirmed in prospective double-blind randomized control trial
37 Appropriateness and targeting of antioxidant therapies in CF
The choice of the appropriate antioxidant and dose to correct a cer-tain biomarker and its associated biochemical lesion is another impor-tant point that appears to have disregarded in many clinical studiesFor instance unlike vitamin E vitamin C supplementation does notalter F2-IsoPs levels in humans (reviewed in [74]) This appears tobe true also in the antioxidant therapy of CF in which vitamin C(300 mgday) was administered together with other antioxidantsthat included a dose of vitamin E of 200 mgday without any signifi-cant effect on the surrogate biomarker of lipid peroxidation F2-IsoPs[6] When carotenoids are used as supplements to prevent the damag-ing action of ROS in the CF airways it is noteworthy that these are notparticularly good quenchers of peroxyl radicals relative to phenolicsand other antioxidants but are exceptional in quenching singlet oxy-gen at which most other phenolics and antioxidants are relativelyineffective Singlet oxygen is not a radical and does not react via radi-cal mechanisms but reacts mostly by the addition to double bondsforming endoperoxides that can be reduced to alkoxyl radicals that ini-tiate radical chain reactions typical of the peroxidative damage of PUFA[38] In this case the analysis of F2-IsoPs lipid peroxide formation andtransition metal-induced oxidizability of lipoproteins [162180] are allappropriate to evaluate the effect of carotenoids in preventing lipidperoxidation
As far as the dose is concerned clinical pharmacology of vitamin Eas an antioxidant was recently investigated by means of the effect onF2-IsoPs production and doses of α-tocopherol of 1600 IUday orgreater were found to be required to statistically affect plasma F2-IsoPs levels in hypercholeterolemic subjects [176] Several vitamin Esupplementation studies in CF patients have been performed withdoses of lower than 300 IUday regardless of the lowered absorptionby pancreatic and liver defects and the regular supplementationwith these doses does not appear to correct lipid oxidation markersin CF [7]
In the clinical practice and planning trials it has to be taken intoconsideration that in spite of substantial evidence supporting ahigher antioxidant demand in CF interventions with several antioxi-dant formulations produce poor responsiveness particularly in thecase of fat-soluble antioxidants which are poorly absorbed [6162]
Since many oxidants and antioxidants are present in tissuesand biological fluids and these have different chemical and physicalcharacteristics the possibility to produce a successful therapy witha single antioxidant molecule is too far to be realistic Moreover an-tioxidants act by multiple mechanisms in a single system or by adifferent single mechanism depending on the reaction systemresponding in a different manner to different radical or oxidantsources Because multiple reaction characteristics and mechanismsas well as different phase localizations are usually involved no single
704 F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
therapeutic approach will effectively prevent damage by multipleROS sources The defect of physiological antioxidants may also interferewith antioxidant therapies that are based on one or few exogenousantioxidants
Moreover several antioxidant vitamins such as vitamin E and ca-rotenoids have multiple natural forms with different bioavailabilitymetabolism and bioactivity [157167231] As far as the case of vita-min E supplementation concerns α-tocopherol was used as uniquevitamer in the large majority of supplementation trials so far per-formed and is the form used in the nutritional management of CFpatients Moreover several supplements contain the synthetic (or ra-cemic) form of this vitamin that has lower bioavailability than thenatural form Other forms present in nature and abundantly con-tained in vegetables such as tocotrienols and the less methylatedforms of tocopherol are not represented in many of the supplementformulations so far available in clinical centers and the supplementa-tion with α-tocopherol also limits their bioavailability These formsshow markedly higher susceptibility to hepatic metabolism and bili-ary excretion with respect to α-tocopherol eg the most representedform in blood and solid tissues and if co-supplemented these areeasily displaced during liver uptake and excreted with bile bymeans of competition with the same α-tocopherol Notwithstandingthese minor forms have been proposed to play important physiolog-ical roles showing molecular characteristics transcriptional effectsand antioxidant activities that clearly differentiate them in subfam-ilies with distinct biological functions Some of these such as α-tocopherol eg the second vitamin E form as relative abundance inblood and its carboxyethyl-hydroxychroman metabolite [189] ap-pear to have health-related anti-inflammatory effects which are par-ticularly relevant in lung protection [232233] This has suggestedthat such a group of ldquonon-α-tocopherolrdquo forms may represent anoth-er family of vitamins within the family of vitamin E with an impor-tant but often missed contribution to the proposed health effects ofthis vitamin [163]
These aspects may thus limit the possibility to provide CF patientsof optimal levels of this vitamin in all its components even if they areregularly treated with a vitamin E supplement eg withα-tocopherol
Targeted antioxidant therapy with formulations with higher bio-availability and bioactivity has been anticipated in CF New antioxi-dant formulations have been proposed to overcome main limits ofantioxidant therapies so far proposed for these patients Water-miscible α-tocopheryl acetate containing polysorbate propylene gly-col or polyethylene glycol as emulsifiers form micellar structureswere suggested to providing greater bioavailability than the fat-soluble counterparts These were commercialized with the brandnames of E-viminreg Cremophorreg EL and Aquasolreg E but despitethe original positive expectation [234235] some studies failed to ob-serve a higher response in vitamin E levels when these were com-pared with fat-soluble formulations [236237]
In a pilot study by Papas et al [183] a micellar formulation of fat-soluble nutrients and antioxidants was found to improve plasmalevels of β-carotene γ-tocopherol and CoQ(10) reducing at thesame time some inflammatory markers in induced sputum eg mye-loperoxidase and to a lower extent PMN elastase and total cell countswhile lung function and sputum bacterial counts were unaffectedThe same group recently confirmed the possibility to increase the ab-sorption of fat-soluble micronutrients using formulations with higherbioavailability specifically designed for malabsorbing patients such asCF patients that include also vitamin K and commercialized with thebrand name of AquADEKsreg [162] Despite improved vitamin and mi-cronutrient levels in this non-randomized open-label study AquA-DEKsreg produced only modest improvements in weight percentileand pulmonary function Another recent pilot observation [182] hassuggested the beneficial effect of this formulation on antioxidant andoxidative stress parameters of this oral supplement that surely deservesmore clinical investigation by larger randomized controlled trials
Recent multivitaminic formulations have been designed to containalso the minor forms of vitamin E and specifically γ-tocopherol [238]the expected superiority of which with respect to formulations con-taining only α-tocopherol needs to be verified As discussed abovein the section dedicated to vitamin E further advancements in thetherapy of CF inflammation and oxidative stress could be based onsynthetic forms and natural metabolites of this vitamin that havebeen recently identified to possess higher antioxidant and also anti-inflammatory activity than α-tocopherol (reviewed in [163168])
Pre-clinical investigation of these and other fat-soluble agents iscurrently addressed to develop formulations and administration pro-tocols that may increase the therapeutic efficacy in the airways In theantioxidant therapy of lung dysfunction in CF local administrationprotocols may overcome the limits of oral and systemic administra-tion protocols increasing bioavailability and providing targetedapproach to inflammation and oxidative stress Aerosolization of vita-min E and other fat-soluble micronutrients is possible and may allowdirect administration in the airways to prevent toxicity of smokewhich is closely associated with inflammation and oxidative stress[164165] To our knowledge this as well as other strategies of localadministration such as instillation of solutions such as surfactant-like solutions enriched of vitamin E have not been previously inves-tigated in CF patients and other CF model systems
On the contrary inhalation is an administration route widelyadopted in the case of GSH and NAC therapy described above Inthis context Cys formulations alternative to NAC have been proposedfor use as antioxidant and anti-inflammatory agent for inhalationNacystelyn is a lysine adduct of NAC that thanks to a higher proton-ation equilibrium shows increased water solubility and thus betterbioavailability Nacystelyn has been described to influence IL-8 gener-ation and the inflammatory signaling of bronchial epithelial cells[239] and preliminary clinical evaluation has demonstrated the safetyof this drug [240] Further clinical trials aimed to assess the effect onlung symptomatology of CF patients are needed Direct administra-tion in the airways could also be adopted for micronutrient vitaminswith poor absorption and bioavailability due to GI defects
38 Clinical impact of antioxidant therapy in CF
Huge in vitro and pre-clinical evidence has provided the rationaleto support clinical investigation of antioxidant strategies in CF Theseshould aim to restore the oxidantndashantioxidant balance of CF airwaychallenged by chronic infection and inflammatory cell activation
Some observational trials have confirmed that antioxidants usedas either supplements to the diet or drugs for lung administrationby aerosolized formulations may help in relieving progressive lungdamage and other adverse clinical events of CF such as poor growthSo far few studies have examined with sufficient methodologicalrigor the clinical efficacy of antioxidant therapy in CF This was alsoconcluded in a previous review of the literature by Cantin et al [12]that was published in the beginning of 2006 and is confirmed alsoin a recent analysis of clinical trials on antioxidant therapy in CF pa-tients [213] that examined the literature until September 2010using as sources the databases of the Cochrane CF and Genetic Disor-ders Group CF Trials Register PubMed CINAHL and AMED Useful in-formation was retrieved from just four randomized controlled trialsand one quasi-randomized controlled trial on vitamin C vitamin Eβ-carotene and selenium used as supplements administered aloneor in combination Post-hoc data analysis that was possible only inthree studies on a total of 87 CF patients showed the absence ofany significant improvement in lung function that was selected as pri-mary outcome together with quality of life that improved in one trialSecondary outcomes concerning laboratory indices of oxidative stressand antioxidant status showed several improvements These includedan increase of RBC SeGPx by selenium supplementation done as
705F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
individual or combined supplementation and increased levels of allplasma antioxidants except vitamin C that were observed in all thetrials
The message from these studies to pediatricians and nutritionistswithin the clinical staff of CF centers is that in the absence of solid ev-idence regarding the clinical effectiveness of oral formulations of an-tioxidant supplements in CF (including PUFA) their use as a routineclinical practice should be considered with caution keeping clear inmind that this should represent just a complement of one of themost critical interventions in the life-long clinical management pro-gram of CF patients eg providing an adequate nutriture [140] Inthis context compensating energy and protein malnutrition has toremain the first goal of nutritional management programs Providinghigher intakes of antioxidant micronutrients with food naturally-enriched (or functionalized) of micronutrient antioxidants shouldbe preferred in order to have the higher combination of positive nu-tritional factors that are lost during refinement procedures and over-all industrial processing of dietary supplements
Measures of good practice in clinical management of micro-malnutrition in CF patients would include the support of specializedpersonnel and laboratories The centers should have the possibilityto ascertain with appropriate nutritional and laboratory tests whatthe level of deficiency is for the different micronutrients that each pa-tient may suffer from during a dietary program Monitoring dietaryintakes and blood levels of micronutrients is not sufficient to set apersonalized nutritional intervention with supplements or functionalfoods Sub-optimal intakes and the compliance to nutritional inter-ventions should be verified by means of selected biochemical andclinical criteria Unluckily the latter are still not well established forsome micronutrients such as the fat-soluble vitamins E (reviewed in[163173241]) and K [242243] and also for trace elements such asSe [244] For many of the antioxidants used as supplements inhumans we still do not know exactly several of the biological effectsthat these may provide when introduced in a healthy body and weknow less what these can do in disease These aspects hardly impacton the concept of optimal levels of intake that should be identified foreach micronutrient on an individual basis According with the aspectsdiscussed in the previous sections optimal levels of intake for antiox-idant micronutrients are different in CF patients and healthy subjectsand vary with age and several individual factors
Lung administration of antioxidants by means of aerosolized for-mulations so far used for GSH therapy (see above) is a promisingfield of clinical investigation in CF Toxicity issues are currently themain concern and the subject of clinical evaluation by several groups(described above)
Information on future directions of antioxidant therapy in CF canbe inferred by the analysis of pending or recently completed clinicaltrials that have been searched (December 2011) at ClinicalTrialsgovdatabase matching the terms ldquoantioxidant therapyrdquo or ldquoglutathionerdquowith ldquocystic fibrosisrdquo Fifteen trials were retrieved and those directlyrelated to antioxidant therapy (n=12) are presented in Table 1 andinclude efficacy and safety studies of inhaled drugs as GSH sodiumpyruvate NAC and NO and the dietary supplements AquADEKsregan antioxidant-rich multivitamin supplement epigallocatechin gal-late (EGCG)tocotrienol curcuminoids the amino acid glutaminesulforaphane in broccoli sprouts One trial is investigating the flavo-noid quercetin as CFTR modulator
39 Emerging antioxidant and anti-inflammatory approaches in CF
Mediterranean foods such as olive oil and red wine or severalplant extracts such as herbal tea or grape seed extracts contain aseries of natural compounds with important antioxidant and NOscavenging activity that have been widely investigated for the pre-vention of oxidative stress-related diseases [38245] These havebeen long investigated as template molecules to develop antioxidant
and anti-inflammatory drugs Between the multitudes of natural sub-stances most investigated ones include for instance tyrosol hydroxy-tyrosol gallic and caffeic acids belonging to the family of phenolswhile resveratrol of the stilbenes family epicatechin kaempferoland cianidin are examples of flavonoids examples of fat-soluble phe-nolics are those of the family of tocols (vitamin E) and carotenoids Allthese compounds show different metabolisms and signaling effects[246] Antioxidant and cell protection mechanisms are associatedwith different and sometimes concurrent processes as H-atom trans-fer and electron donation radical trapping and chelation of transitionmetals that can be easily investigated at the chemical level [247] Be-sides these direct antioxidant effects metabolic responses and signal-ing effects of natural compounds are also important to producesecond-generation responses that modify the level of antioxidantprotection and the potential for ROS detoxification in cells and bodyfluids These derive from the transcriptional regulation of antioxidantand pro-oxidant genes that coexist with the modulation of cytokinesecretion and inflammatory enzyme activities
Some of these natural plant-derived antioxidants may provide fur-ther pharmacological activities of possible relevance in CF This is thecase for instance of the plant flavonoids genistein apigenin kaemp-ferol quercetin and hesperidin [248ndash251] that fall in the pharmaco-logical category of ldquopotentiatorsrdquo [252] in that these activate at leastto a certain extent CTFR-mediated Cl currents in normal and CF airwayepithelium investigated either in vitro or in vivo in humans and ani-mal models Actually as prototypal flavonoid-derived potentiatorthe tyrosine kinase inhibitor genistein potentiates the gating of wild-type as well as ΔF508 CFTR and G551D CFTR [253] but at higherdoses it inhibits CFTR gating which make this an unlikely clinical can-didate Similar potentiation effects have been reported for the antiox-idant curcumin [250] that shows an additive effect with respect togenistein-induced potentiation Besides CFTR potentiation whichdoes not appear to have a direct influence on GSH and nutrient trans-port in the lung tissue all these natural substances have been usedalone or in combination with other agents as in vivo enhancers oflung antioxidant protection [246254255] In the case of quercetinthiol-reactive phenolic [256] bronchodilation and anti-inflammatoryeffects by a restoration of the Th1Th2 balance have been reportedin inflammatory syndromes of the lung [255257ndash259] but theseeffects have not been explored in CF Pyocyanin toxicity (see abovein the Section 2) could represent an issue for the use of quercetinand other catechols in infectious diseases of the lung [260]
Other natural antioxidants of potential interest in CF therapy in-clude terpenoids [261] such as terpinen-4-ol a major constituentof tea tree oil that is being investigated in the therapy of anti-biotic resistant organisms specifically against methicillin-resistantStaphylococcus aureus (MRSA) [262] a problem in CF [263] Otherthan being lipophilic antioxidants terpenes can prevent oxidativestress of the CF lung secondarily to the antibiotic effect thereby pro-moting a better control of immuno-inflammatory pathways and lungantioxidants
391 Targeting NF-κB with natural compounds resveratrol and plantextracts
Natural compounds were long known to be useful in designinganti-inflammatory drugs and some of these could find an applicationin the control of the transcription factor kappa-B (NF-κB) that maylead to develop advanced pharmacological tools to control inflamma-tion and to produce higher antioxidant protection to CF airwaysInhibitors targeting NF-κB including transcription factors decoymolecules (TFD) are potent down-regulators of gene expressionand release of IL-8 in CF cells infected with P aeruginosa [264265]
Resveratrol (354prime-trihydroxystilbene ldquoErdquo form) is one of the mostinvestigated natural antioxidant with proposed activity as NF-κBinhibitor This is a phytoalexin present in large quantity in red winepreferentially in the skin of grapes being its concentration
706 F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
50ndash100 μgmg of fresh skin and 13ndash3 mgl of red wine [266]Furthermore resveratrol is a constituent of lsquoDarakchasavarsquo (13ndash6 mgl) an ayurvedic medicine from India [267] The antioxidant activity ofresveratrol has been reported in several papers and occurs also in lungtissues suggesting that resveratrol has potential as a therapeuticagent in respiratory disease [268ndash270] Resveratrol can be consideredone of the most interesting molecules from the natural worldexhibiting strong antioxidant activity that at the same time is able toexert anti inflammatory activity through alteration of NF-κB functionsand efficient inhibition of pro-inflammatory genes [271272] As far asthe effects on CF model systems are concerned Cabrini et al [26]reported the effects of resveratrol on P aeruginosa infected CF IB3-1cells The results obtained demonstrate that resveratrol exhibits minoreffects of IB3-1 cell growth and important inhibitory effects on accumu-lation of IL-8 and GRO-α mRNA while minor effects on IL-6 gene ex-pression were observed These data support recently publishedobservations suggesting inhibitory effects of resveratrol in infection-mediated inflammatory processes [273] Interestingly resveratrol hasbeen reported as a potent inhibitor of NF-κB activity and a promisinganti-inflammatory agent [272274] also in combinationwith othermol-ecules [274275] However in vivo translation of this pre-clinical on res-veratrol is hard to be foreseen This natural compound displays poorbioavailability [276] and further characterization of resveratrol pharma-cokinetics is troublesome since it is hardly measurable in vivo [277]Furthermore the regulation of inflammatory responses by resveratrolhas been suggested to be far more complex than simple direct suppres-sion of NF-κB activity Actually some aspects of the immune responsecould be enhanced by this natural substance which may lead tohypothesize broad negative feedback events on immuno-inflammatorypathways [278] In any case and with these cautions in mind the pub-lished observations on cellular model systems support the concept thatresveratrol and resveratrol-containing formulations deserve further con-sideration to determine their possible therapeutic values in CF
Other inhibitors can be identified from systematic studies of naturalproducts and their ability to interfere with NF-κB activity [279ndash281]Recent studies have demonstrated that the whole extract of Aeglemarmelos (Rutaceae) has strong inhibitory effect on the P aeruginosa-dependent IL-8 induction in human CF-derived bronchial IB3-1 cellswithout affecting cell proliferation [280] Molecular analysis of compo-nents contained in A marmelos extracts revealed that three major com-pounds namely 56-dimethoxy-1-indanone 2-hydroxy-cinnamic acidand 5-methoxy psoralen (5-MOP) reproduce the inhibitory effect ob-servedwith thewhole extract [280] A further example has been recent-ly published using extracts from bergamot (Citrus bergamia Risso) Inthis study the extracts were characterized and the main detected con-stituents were assayed for their biological activity [281] The resultsobtained demonstrated that the extracts from bergamot epicarps con-tain components displaying an inhibitory activity on IL-8 Particularlythe most active molecules were bergapten and citropten These effectshave been confirmed by analyzing mRNA levels and protein release inthe CF cellularmodels IB3-1 and CuFi-1 inducedwith TNF-α or exposedto P aeruginosa
A parallel strategy linking NF-κB inhibition and down-regulationof NF-κB-dependent functions is described in recently publishedstudies based on a structured-based virtual screening (VS) of differ-ently substituted furocoumarins and analogues against NF-κB withthe objective of selecting molecules able to inhibit the binding ofthis transcription factor to DNA [282283] Novel compounds wereidentified with this strategy as potent inhibitors of NF-κB dependentbiological functions to be proposed for the control lung inflammationoccurring in patients affected by CF [282ndash284]
392 Scavengers and regulators of H2O2 and NO
3921 Lactoferrin and OSCNmacr The impaired DUOXLPO system of CFpatients could be the target of therapeutic strategies that may
produce concomitant antimicrobial and antioxidant effects This sys-tem described above in Section 22 represents an important compo-nent of innate immunity with a role in bactericidal defense andregulation of H2O2 metabolism of airways [32] CF patients have alsoreported to show lowered LF levels in the ASL [37] that togetherwith a CFTR-dependent defective efflux of SCNmacr and LPO [36] may cre-ate the environment for a sustained flux of H2O2 and for the genera-tion of highly reactive Fenton species [1138] An ideal therapeuticintervention should restore the LPO-dependent generation of bacteri-cidal OSCNmacr from DUOX-derived H2O2 and SCNmacr in the ASL to controlat the same time the microbial biofilm and the flux of H2O2 into theASL An approach close to this therapeutic mechanism was recentlyproposed for the drug Meveolreg This is a complex of LF and OSCNmacrwith proposed in vivo antimicrobial activity [285] to be evaluatedin clinical trials for the aerosol treatment of lung infections in CFpatients The role for this drug in the control of H2O2 levels of ASLremains to be investigated
3922 Organoselenium compounds Organoselenium compoundshave been proposed as therapeutic agents useful in the antioxidanttherapy of inflammatory conditions These include GPX mimetic mol-ecules such as Ebselenreg (2-phenyl-12-benzisoselenazol-3(2H)-one)or other and more recently developed molecules that are still inpre-clinical steps of evaluation [286] Selectively and specificity of ac-tion are main issues in the therapeutic mechanism of this candidateantioxidant drug that thanks to the electrophilic properties of Se[214] reacts with thiols to reduce H2O2 and other species MoreoverEbselenreg has been described to act as potent non-competitive inhib-itor of extracellular nucleoside diphosphokinase (NDPK) having neg-ligible effect on ecto-ATPase and adenyl kinase activities which areother players of the metabolism of extracellular nucleotides [287]This enzyme together with other nucleoside di- and triphosphatescontributes to regulate several components of the mucociliary clear-ance process (MCC) that protects the lung against infections via acti-vation of epithelial purinergic receptors The inhibition of NDPK bythis GPX-mimetic drug may also impact on the energy status of endo-thelial cells [287] This aspect could be further investigated as a cellu-lar protection mechanism in the pulmonary epithelium of CF patientsbeing the control of cell energy of fundamental importance to preventthe activation of death pathways [288]
Further therapeutic mechanisms for these Se-derived drugs mayderive from the marked activity as inducers of phase II enzymessuch as quinone reductase (QR) and glutathione-S-transferase (GST)[289] This induction response also observed with other electrophilsand redox-active molecules such as natural phenolic antioxidantscould produce higher cellular protection by the acquisition of anincreased capability to detoxify endobiotics generated during oxida-tive stress and inflammation [246]
3923 Melatonin and GSNO as NOx regulators Increased markers ofNO-derived biological damage are present in the CF lung suggestingthe abnormal reactivity of NOx in the inflamed lung of CF patients[52] However an impaired metabolism and biological function ofNO in CF airways (see Section 23) suggests a cautious approach tothe use of agents that may influence the levels and chemical behaviorof NO-derived species (NOx) with possible impact on the physiologi-cal roles of NO in vasodilatation innate immunity and H2O2 metabo-lism of the respiratory tract [290291] NO donors also appear toinfluence CFTR function of alveolar epithelium and gland serouscells [292293]
Main physiological role of the pineal gland hormone melatonin isthe synchronization of circadian rhythms including the sleepndashwakecycle but several other functions dealing with immunomodulatoryantioxidant and cellular protection effects have been identified[294] Melatonin receptor stimulation may also influence cyclic AMPsignaling and the regulation of CFTR ion channel [295296]
707F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
A recent randomized double-blind placebo-controlled study hasexamined the effects of short term melatonin administration (3 mgfor 3 weeks) on sleep and oxidative stress markers in CF [297]According with the expected pharmacological effect of this hormonalsubstance the treatment was successful in improving sleep indicesAt the same time nitrite levels determined in exhaled breath conden-sate (EBC) were reduced to suggest a better control of NOmetabolismof CF airways (discussed above in Section 23) but these effects how-ever were not associated with a significant correction of isoprostaneas lipid peroxidation marker measured in EBC Increasing dosages ofmelatonin could be investigated for the pharmacological treatmentof oxidative stress and immune dysfunction of CF patients due tothe absence of adverse effects of this hormonal substance in humans
The S-nitrosation reaction of thiols is another interesting aspect ofNO pharmacology [53] that may find an application in the therapy oflung complications of CF This has been the case for instance of theS-nitrosothiol GSNO that has been used safely in human trials[298299] This endogenous nitrosothiol with proposed regulatory ef-fect on the CFTR of lung epithelia [292293] is well tolerated in pa-tients with CF when administered by aerosolization and mayproduce better oxygenation [299] thereby suggesting that therapyaimed at restoring endogenous GSNO levels in the CF airway maymerit further clinical evaluation Since the administered GSNO de-composes as shown by the increased levels of expired NO in CF pa-tients under treatment with this nitrosothiol [299] furtherinvestigation should be addressed to ascertain whether GSNO thera-py may merely correspond to a GSH therapy
NO dependent effects on CFTR function should be considered toevaluate mechanism of action and specificity of antioxidant therapiesthat target NO metabolism and function in the CF airways
4 Conclusions and future perspectives
The presence of clinical and biochemical symptoms of inflammationand oxidative stress implies that CF patients have a higher demand ofantioxidant protection The combination of the dysfunctional CFTRwith a lowered intake and absorption of dietary antioxidants producesub-optimal levels of protection from both enzymatic and non-enzymatic defense systems The former could be associated with a de-fective glutathionemetabolism and lowered intake of sulfur-containingamino acids and oligoelements such as zinc and possibly seleniumwhile fat-soluble antioxidant vitamins such as vitamin E and caroten-oids and the water-soluble vitamin C are lowered than in healthy sub-jects due to malabsorption and possibly higher consumption
The increased antioxidant demand in CF patients should be evenhigher in the presence of complications of the lung pancreas andliver Lung comorbidity is particularly important in this contextbeing associated with recurrent infections which results in the alter-nation of inflammatory exacerbates and chronic inflammation Thesesustain the flux of ROS in the airways and promote the formation ofsecond-generation byproducts by the damage of biomolecules suchas PUFA and proteins which may diffuse also at the systemic level tofurther promote adverse biological responses and toxic reactions Pan-creatic insufficiency causes malnutrition and may lead to develop en-docrine and metabolic defects associated with diabetes of CF Theseevents can be further aggravated by the concomitance of liver dys-function and a poor nutritional status Malnutrition is strongly associ-ated with poor prognosis as assessed by pulmonary function andsurvival data [138ndash140] The more aggressive nutritional interven-tions seem to produce better clinical outcomes in these patients andthe possibility of achieving higher antioxidant protection in well-nourished patients by dietary factors could be a key aspect to explainsuch a clinical advantage The assumption that food-derived compo-nentsmay help to prevent the damaging effects of oxidative stress im-proving the antioxidant defenses deserves further investigation at theclinical level This together with the investigation of appropriate
laboratory biomarkers could provide critical information to establishintervention criteria for an early nutritional management of newly di-agnosed patients [5] It is expected that a timely secondary preventionstrategy could influence the progression of CF symptoms thusaffecting with a self-feeding mechanism the same extent of malnutri-tion and oxidative stress along the life of CF patients Since severalfactors contribute to impair the nutritional status of CF patients(such as pancreatic insufficiency chronic malabsorption recurrentsinopulmonary infections and progressive lung disease chronic in-flammation increased energy expenditure suboptimal intake multi-therapy) careful monitoring of the antioxidant status should berecommended According with international guidelines fat-solublevitamin supplementation is of utmost importance in daily practice to-gether with energy intake requirements and pancreatic enzyme-replacement therapy Among these vitamin E β-carotene and ω-3FA have observed to alleviate selected biochemical signs of oxidativestress as measured for instance with well established laboratory indi-ces of lipid peroxidation and in some studies these effects werepreliminarily associated with positive clinical outcomes Notwith-standing randomizedndashcontrolled clinical trials on antioxidant supple-ments (including ω-3 FA) so far carried out in CF have failed toconclusively demonstrate significant beneficial effects on respiratorysymptoms and on the consequent impact that these have on the qual-ity of life of these patients (reviewed in [202213]) whichmay provideno support for the use of these supplements in CF An absence of effi-cacy in prevention studies on antioxidant supplements has also beenobserved in other and possibly less severe oxidative stress-relatedconditions particularly in the secondary prevention of cardiovasculardisease and some forms of cancer by vitamin E and other antioxidantssuch as vitamin C selenium and β-carotene (reviewed in [163]) Dif-ferent biases however have been identified in randomize large clini-cal trials that may account for these disappointing findings Theseinclude patient selection criteria (early interventions and primaryprevention could have more chances of success than secondaryprevention) duration and doses of the treatment use of wrong anti-oxidant formulations and administration protocols absence of verifi-cations of the biological compliance to the treatment etc The samebiases apply for the few trials carried out in CF patients Thus the ap-propriateness and efficacy of nutritional interventions with naturalfood-derived or synthetic antioxidants should be verifiedwith respectto the biological pathways of oxidative stress and clinical variablesthat are identified as end-points Profiles of blood and tissue antioxi-dants as well as of reliable surrogate markers of oxidative stresshave to be selected and determined in highly specialized laboratorieswith a well-established experience on these analyses
Well-timed (early) interventions with appropriate antioxidantformulationsprotocols need to be proposed for the next generationof trials and the development of novel CF-tailored antioxidant andanti-inflammatory agents should be promoted
As a consequence of these considerations more clinical investiga-tion is awaited to identify future successful approaches to the antiox-idant therapy as a measure to further enhance quality of life and theoverall clinical outcome of CF patients
Acknowledgments
We are indebted with the Italian Cystic Fibrosis Research Founda-tion for the support that it provided with its grant program to the re-search activity of the authors of this paper This is a scientific initiativeof the ldquoWorking Group on Inflammation in Cystic Fibrosisrdquo (BragonziA Bravo E Cabrini G Conese M Cuzzocrea S Dechecchi MC De Ales-sandri A Evangelista V Galli F Gambari R Lambiase A Lucidi VManca A Melotti P Minicucci L Motta A Pietraforte D Pompella AQuattrucci S Rizzo R Romano M Sorio C Tesse R) of the Italian Soci-ety for Cystic Fibrosis A particular thank goes to the Prof GianniMastella for the critical revision of the manuscript and for the
708 F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
stimulating research environment that he has contributed to createwithin the Italian Cystic Fibrosis Research Foundation
References
[1] BP OSullivan SD Freedman Cystic fibrosis Lancet 373 (2009) 1891ndash1904[2] P Linsdell JW Hanrahan Glutathione permeability of CFTR Am J Physiol 275
(1998) C323ndashC326[3] L Gao KJ Kim JR Yankaskas HJ Forman Abnormal glutathione transport in
cystic fibrosis airway epithelia Am J Physiol 277 (1999) L113ndashL118[4] RK Rowntree A Harris The phenotypic consequences of CFTR mutations Ann
Hum Genet 67 (2003) 471ndash485[5] EI Back C Frindt D Nohr J Frank R Ziebach M Stern M Ranke HK Biesalski
Antioxidant deficiency in cystic fibrosis when is the right time to take actionAm J Clin Nutr 80 (2004) 374ndash384
[6] LG Wood DA Fitzgerald AK Lee ML Garg Improved antioxidant and fattyacid status of patients with cystic fibrosis after antioxidant supplementation islinked to improved lung function Am J Clin Nutr 77 (2003) 150ndash159
[7] L Iuliano R Monticolo G Straface S Zullo F Galli M Boaz S Quattrucci Asso-ciation of cholesterol oxidation and abnormalities in fatty acid metabolism incystic fibrosis Am J Clin Nutr 90 (2009) 477ndash484
[8] C Libetta V Sepe P Esposito F Galli A Dal Canton Oxidative stress and inflam-mation implications in uremia and hemodialysis Clin Biochem 44 (2011)1189ndash1198
[9] G Bartosz Reactive oxygen species destroyers or messengers Biochem Phar-macol 77 (2009) 1303ndash1315
[10] T Ntimbane B Comte G Mailhot Y Berthiaume V Poitout M Prentki RRabasa-Lhoret E Levy Cystic fibrosis-related diabetes from CFTR dysfunctionto oxidative stress Clin Biochem 30 (2009) 153ndash177
[11] A van der Vliet JP Eiserich GP Marelich B Halliwell CE Cross Oxidativestress in cystic fibrosis does it occur and does it matter Adv Pharmacol 38(1997) 491ndash513
[12] AM Cantin TB White CE Cross HJ Forman RJ Sokol D Borowitz Antioxi-dants in cystic fibrosis Conclusions from the CF antioxidant workshop Bethes-da Maryland Free Radic Biol Med 42 (2007) 15ndash31
[13] LT McGrath P Mallon L Dowey B Silke E McClean M McDonnell A DevineS Copeland S Elborn Oxidative stress during acute respiratory exacerbations incystic fibrosis Thorax 54 (1999) 518ndash523
[14] E Thomson S Brennan R Senthilmohan CL Gangell AL Chapman PD SlyAJ Kettle E Balding LJ Berry JB Carlin R Carzino N de Klerk T Douglas CFoo LW Garratt GL Hall J Harrison A Kicic IA Laing KM Logie J MassieLS Mott C Murray F Parsons N Pillarisetti SR Poreddy SC RanganathanCF Robertson R Robins-Browne PJ Robinson B Skoric SM Stick ENSutanto E Williamson Identifying peroxidases and their oxidants in the earlypathology of cystic fibrosis Free Radic Biol Med 49 (2010) 1354ndash1360
[15] SP Range C Dunster AJ Knox FJ Kelly Treatment of pulmonary exacerba-tions of cystic fibrosis leads to improved antioxidant status Eur Respir J 13(1999) 560ndash564
[16] L Coppo P Ghezzi Thiol regulation of pro-inflammatory cytokines and innateimmunity protein S-thiolation as a novel molecular mechanism Biochem SocTrans 39 (2011) 1268ndash1272
[17] C Verhaeghe C Remouchamps B Hennuy A Vanderplasschen A Chariot SPTabruyn C Oury V Bours Role of IKK and ERK pathways in intrinsic inflamma-tion of cystic fibrosis airways Biochem Pharmacol 73 (2007) 1982ndash1994
[18] TL Bonfield JR Panuska MW Konstan KA Hilliard JB Hilliard H Ghnaim MBerger Inflammatory cytokines in cystic fibrosis lungs Am J Respir Crit CareMed 152 (1995) 2111ndash2118
[19] TL Noah HR Black PW Cheng RE Wood MW Leigh Nasal and bronchoal-veolar lavage fluid cytokines in early cystic fibrosis J Infect Dis 175 (1997)638ndash647
[20] MJ Welsh BW Ramsey FJ Accurso GR Cutting Cystic Fibrosis McGraw-HillNew York 2001
[21] TZ Khan JS Wagener T Bost J Martinez FJ Accurso DW Riches Early pul-monary inflammation in infants with cystic fibrosis Am J Respir Crit CareMed 151 (1995) 1075ndash1082
[22] FA Ratjen Cystic fibrosis pathogenesis and future treatment strategies RespirCare 54 (2009) 595ndash605
[23] J Jacquot O Tabary P Le Rouzic A Clement Airway epithelial cell inflamma-tory signalling in cystic fibrosis Int J Biochem Cell Biol 40 (2008)1703ndash1715
[24] CM Greene P Branagan NG McElvaney Toll-like receptors as therapeutic tar-gets in cystic fibrosis Expert Opin Ther Targets 12 (2008) 1481ndash1495
[25] M Rottner JM Freyssinet MC Martinez Mechanisms of the noxious inflam-matory cycle in cystic fibrosis Respir Res 10 (2009) 23
[26] G Cabrini V Bezzerri I Mancini E Nicolis MC Dechecchi A Tamanini ILampronti L Piccagli N Bianchi M Borgatti R Gambari Targeting transcrip-tion factor activity as a strategy to inhibit pro-inflammatory genes involved incystic fibrosis decoy oligonucleotides and low-molecular weight compoundsCurr Med Chem 17 (2010) 4392ndash4404
[27] CM Greene NG McElvaney Proteases and antiproteases in chronic neutrophiliclungdiseasemdash relevance to drug discovery Br J Pharmacol 158 (2009) 1048ndash1058
[28] AM Cantin Potential for antioxidant therapy of cystic fibrosis Curr Opin PulmMed 10 (2004) 531ndash536
[29] JF Chmiel MW Konstan Inflammation and anti-inflammatory therapies forcystic fibrosis Clin Chest Med 28 (2007) 331ndash346
[30] DP Nichols MW Konstan JF Chmiel Anti-inflammatory therapies for cys-tic fibrosis-related lung disease Clin Rev Allergy Immunol 35 (2008)135ndash153
[31] AJ Kettle T Chan I Osberg R Senthilmohan AL Chapman TJ Mocatta JSWagener Myeloperoxidase and protein oxidation in the airways of youngchildren with cystic fibrosis Am J Respir Crit Care Med 170 (2004)1317ndash1323
[32] H Fischer Mechanisms and function of DUOX in epithelia of the lung AntioxidRedox Signal 11 (2009) 2453ndash2465
[33] B Rada TL Leto Oxidative innate immune defenses by NoxDuox familyNADPH oxidases Contrib Microbiol 15 (2008) 164ndash187
[34] P Moskwa D Lorentzen KJ Excoffon J Zabner PB McCray Jr WM NauseefC Dupuy B Banfi A novel host defense system of airways is defective in cysticfibrosis Am J Respir Crit Care Med 175 (2007) 174ndash183
[35] D Lorentzen L Durairaj AA Pezzulo Y Nakano J Launspach DA Stoltz GZamba PB McCray Jr J Zabner MJ Welsh WM Nauseef B Banfi Concentra-tion of the antibacterial precursor thiocyanate in cystic fibrosis airway secre-tions Free Radic Biol Med 50 (2011) 1144ndash1150
[36] Y Xu S Szep Z Lu The antioxidant role of thiocyanate in the pathogenesis ofcystic fibrosis and other inflammation-related diseases Proc Natl Acad Sci US A 106 (2009) 20515ndash20519
[37] MP Rogan CC Taggart CM Greene PG Murphy SJ ONeill NG McElvaneyLoss of microbicidal activity and increased formation of biofilm due to decreasedlactoferrin activity in patients with cystic fibrosis J Infect Dis 190 (2004)1245ndash1253
[38] B Halliwell JM Guttridge Free Radicals in Biology and Medicine Fourth editionOxford University Press New York 2007
[39] B Rada K Lekstrom S Damian C Dupuy TL Leto The Pseudomonastoxin pyocyanin inhibits the dual oxidase-based antimicrobial system as itimposes oxidative stress on airway epithelial cells J Immunol 181 (2008)4883ndash4893
[40] C Schwarzer B Illek JH Suh SJ Remington H Fischer TE Machen Organelleredox of CF and CFTR-corrected airway epithelia Free Radic Biol Med 43(2007) 300ndash316
[41] JH Roum R Buhl NG McElvaney Z Borok RG Crystal Systemic deficiency ofglutathione in cystic fibrosis J Appl Physiol 75 (1993) 2419ndash2424
[42] VM Hudson Rethinking cystic fibrosis pathology the critical role of abnormalreduced glutathione (GSH) transport caused by CFTR mutation Free RadicBiol Med 30 (2001) 1440ndash1461
[43] PJ Barnes RA Dweik AF Gelb PG Gibson SC George H Grasemann IDPavord F Ratjen PE Silkoff DR Taylor N Zamel Exhaled nitric oxide in pul-monary diseases a comprehensive review Chest 138 (2010) 682ndash692
[44] H Grasemann E Michler M Wallot F Ratjen Decreased concentration of ex-haled nitric oxide (NO) in patients with cystic fibrosis Pediatr Pulmonol 24(1997) 173ndash177
[45] H Grasemann F Ratjen Cystic fibrosis lung disease the role of nitric oxidePediatr Pulmonol 28 (1999) 442ndash448
[46] B Gaston F Ratjen JW Vaughan NR Malhotra RG Canady AH Snyder JFHunt S Gaertig JB Goldberg Nitrogen redox balance in the cystic fibrosis air-way effects of antipseudomonal therapy Am J Respir Crit Care Med 165(2002) 387ndash390
[47] H Grasemann I Ioannidis RP Tomkiewicz H de Groot BK Rubin F RatjenNitric oxide metabolites in cystic fibrosis lung disease Arch Dis Child 78(1998) 49ndash53
[48] H Grasemann R Schwiertz S Matthiesen K Racke F Ratjen Increased argi-nase activity in cystic fibrosis airways Am J Respir Crit Care Med 172(2005) 1523ndash1528
[49] H Grasemann S Al-Saleh JA Scott D Shehnaz A Mehl R Amin M Rafii PPencharz J Belik F Ratjen Asymmetric dimethylarginine contributes to airwaynitric oxide deficiency in patients with cystic fibrosis Am J Respir Crit CareMed 183 (2011) 1363ndash1368
[50] H Grasemann F Kurtz F Ratjen Inhaled L-arginine improves exhaled nitricoxide and pulmonary function in patients with cystic fibrosis Am J RespirCrit Care Med 174 (2006) 208ndash212
[51] H Grasemann F Ratjen Emerging therapies for cystic fibrosis lung disease Ex-pert Opin Emerg Drugs 15 (2010) 653ndash659
[52] BM Morrissey K Schilling JV Weil PE Silkoff DM Rodman Nitric oxide andprotein nitration in the cystic fibrosis airway Arch Biochem Biophys 406(2002) 33ndash39
[53] R Radi Nitric oxide oxidants and protein tyrosine nitration Proc Natl AcadSci U S A 101 (2004) 4003ndash4008
[54] J Chen M Kinter S Shank C Cotton TJ Kelley AG Ziady Dysfunction of Nrf-2in CF epithelia leads to excess intracellular H2O2 and inflammatory cytokineproduction PLoS One 3 (2008) e3367
[55] F Galli M Piroddi C Annetti C Aisa E Floridi A Floridi Oxidative stress andreactive oxygen species Contrib Nephrol 149 (2005) 240ndash260
[56] DT Wright LA Cohn H Li B Fischer CM Li KB Adler Interactions of oxygenradicals with airway epithelium Environ Health Perspect 102 (Suppl 10)(1994) 85ndash90
[57] I Rahman SR Yang SK Biswas Current concepts of redox signaling in thelungs Antioxid Redox Signal 8 (2006) 681ndash689
[58] Q Li JF Engelhardt Interleukin-1beta induction of NFκB is partially regulatedby H2O2-mediated activation of NFκB-inducing kinase J Biol Chem 281(2006) 1495ndash1505
709F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
[59] E Boncoeur VS Criq E Bonvin T Roque A Henrion-Caude DC Gruenert AClement J Jacquot O Tabary Oxidative stress induces extracellular signal-regulated kinase 12 mitogen-activated protein kinase in cystic fibrosis lung ep-ithelial cells potential mechanism for excessive IL-8 expression Int J BiochemCell Biol 40 (2008) 432ndash446
[60] B Fischer J Voynow Neutrophil elastase induces MUC5AC messenger RNA ex-pression by an oxidant-dependent mechanism Chest 117 (2000) 317Sndash320S
[61] B Rada P Gardina TG Myers TL Leto Reactive oxygen species mediate in-flammatory cytokine release and EGFR-dependent mucin secretion in airwayepithelial cells exposed to Pseudomonas pyocyanin Mucosal Immunol 4(2011) 158ndash171
[62] C Schwarzer H Fischer EJ Kim KJ Barber AD Mills MJ Kurth DC GruenertJH Suh TE Machen B Illek Oxidative stress caused by pyocyanin impairs CFTRClminus transport in human bronchial epithelial cells Free Radic Biol Med 45(2008) 1653ndash1662
[63] J Hull M South P Phelan K Grimwood Surfactant composition in infants andyoung children with cystic fibrosis Am J Respir Crit Care Med 156 (1997)161ndash165
[64] KC Meyer A Sharma R Brown M Weatherly FR Moya J Lewandoski JJZimmerman Function and composition of pulmonary surfactant andsurfactant-derived fatty acid profiles are altered in young adults with cystic fi-brosis Chest 118 (2000) 164ndash174
[65] MK Pulfer RC Murphy Formation of biologically active oxysterols during ozo-nolysis of cholesterol present in lung surfactant J Biol Chem 279 (2004)26331ndash26338
[66] V Starosta E Rietschel K Paul U Baumann M Griese Oxidative changes ofbronchoalveolar proteins in cystic fibrosis Chest 129 (2006) 431ndash437
[67] V Starosta M Griese Oxidative damage to surfactant protein D in pulmonarydiseases Free Radic Res 40 (2006) 419ndash425
[68] M Griese R Essl R Schmidt E Rietschel F Ratjen M Ballmann K Paul Pulmo-nary surfactant lung function and endobronchial inflammation in cystic fibro-sis Am J Respir Crit Care Med 170 (2004) 1000ndash1005
[69] M Griese R Essl R Schmidt M Ballmann K Paul E Rietschel F Ratjen Se-quential analysis of surfactant lung function and inflammation in cystic fibrosispatients Respir Res 6 (2005) 133
[70] LG Wood DA Fitzgerald PG Gibson DM Cooper ML Garg Increased plasmafatty acid concentrations after respiratory exacerbations are associated with el-evated oxidative stress in cystic fibrosis patients Am J Clin Nutr 75 (2002)668ndash675
[71] P Montuschi SA Kharitonov G Ciabattoni M Corradi L van Rensen DM Ged-des ME Hodson PJ Barnes Exhaled 8-isoprostane as a new non-invasive bio-marker of oxidative stress in cystic fibrosis Thorax 55 (2000) 205ndash209
[72] CE Collins P Quaggiotto L Wood EV OLoughlin RL Henry ML Garg Elevat-ed plasma levels of F2 alpha isoprostane in cystic fibrosis Lipids 34 (1999)551ndash556
[73] D Hartl V Starosta K Maier I Beck-Speier C Rebhan BF Becker P Latzin RFischer F Ratjen RM Huber E Rietschel S Krauss-Etschmann M Griese In-haled glutathione decreases PGE2 and increases lymphocytes in cystic fibrosislungs Free Radic Biol Med 39 (2005) 463ndash472
[74] GL Milne H Yin JD Morrow Human biochemistry of the isoprostane pathwayJ Biol Chem 283 (2008) 15533ndash15537
[75] G Ciabattoni G Davi M Collura L Iapichino F Pardo A Ganci R Romagnoli JMaclouf C Patrono In vivo lipid peroxidation and platelet activation in cystic fi-brosis Am J Respir Crit Care Med 162 (2000) 1195ndash1201
[76] C Garenc P Julien E Levy Oxysterols in biological systems the gastrointestinaltract liver vascular wall and central nervous system Free Radic Res 44 (2011)47ndash73
[77] AM Cantin SL North RC Hubbard RG Crystal Normal alveolar epithelial lin-ing fluid contains high levels of glutathione J Appl Physiol 63 (1987) 152ndash157
[78] R Tirouvanziam CK Conrad T Bottiglieri LA Herzenberg RB Moss High-dose oral N-acetylcysteine a glutathione prodrug modulates inflammation incystic fibrosis Proc Natl Acad Sci U S A 103 (2006) 4628ndash4633
[79] LW Velsor C Kariya R Kachadourian BJ Day Mitochondrial oxidative stressin the lungs of cystic fibrosis transmembrane conductance regulator proteinmutant mice Am J Respir Cell Mol Biol 35 (2006) 579ndash586
[80] M Kelly-Aubert S Trudel J Fritsch T Nguyen-Khoa M Baudouin-Legros SMoriceau L Jeanson F Djouadi C Matar M Conti M Ollero F Brouillard AEdelman GSH monoethyl ester rescues mitochondrial defects in cystic fibrosismodels Hum Mol Genet 20 (2011) 2745ndash2759
[81] P Ghezzi Role of glutathione in immunity and inflammation in the lung Int JGen Med 4 (2011) 105ndash113
[82] N Dauletbaev K Viel R Buhl TO Wagner J Bargon Glutathione and glutathi-one peroxidase in sputum samples of adult patients with cystic fibrosis J CystFibros 3 (2004) 119ndash124
[83] CE Cross A van der Vliet CA ONeill S Louie B Halliwell Oxidants antioxi-dants and respiratory tract lining fluids Environ Health Perspect 102 (Suppl10) (1994) 185ndash191
[84] K Takeyama K Dabbagh J Jeong Shim T Dao-Pick IF Ueki JA Nadel Oxida-tive stress causes mucin synthesis via transactivation of epidermal growth factorreceptor role of neutrophils J Immunol 164 (2000) 1546ndash1552
[85] N Ballatori SM Krance S Notenboom S Shi K Tieu CL Hammond Glutathi-one dysregulation and the etiology and progression of human diseases BiolChem 390 (2009) 191ndash214
[86] SR Soltaninassab KR Sekhar MJ Meredith ML Freeman Multi-faceted regu-lation of gamma-glutamylcysteine synthetase J Cell Physiol 182 (2000)163ndash170
[87] HR Lopez-Mirabal JR Winther Redox characteristics of the eukaryotic cytosolBiochim Biophys Acta 1783 (2008) 629ndash640
[88] C Hwang AJ Sinskey HF Lodish Oxidized redox state of glutathione in the en-doplasmic reticulum Science 257 (1992) 1496ndash1502
[89] M Murphy Mitochondrial thiols in antioxidant protection and redox signallingdistinct roles for glutathionylation and other thiol modifications AntioxidRedox Signal (2011) ahead of print doi101089ars20114289
[90] BJ Day AM van Heeckeren E Min LW Velsor Role for cystic fibrosis trans-membrane conductance regulator protein in a glutathione response to bronch-opulmonary Pseudomonas infection Infect Immun 72 (2004) 2045ndash2051
[91] Y Zhang K Duan Glutathione exhibits antibacterial activity and increases tetra-cycline efficacy against Pseudomonas aeruginosa Sci China C Life Sci 52 (2009)501ndash505
[92] VM Hudson New insights into the pathogenesis of cystic fibrosis pivotal roleof glutathione system dysfunction and implications for therapy Treat RespirMed 3 (2004) 353ndash363
[93] LW Velsor A van Heeckeren BJ Day Antioxidant imbalance in the lungs ofcystic fibrosis transmembrane conductance regulator protein mutant miceAm J Physiol Lung Cell Mol Physiol 281 (2001) L31ndashL38
[94] I Kogan M Ramjeesingh C Li JF Kidd Y Wang EM Leslie SP Cole CE BearCFTR directly mediates nucleotide-regulated glutathione flux EMBO J 22(2003) 1981ndash1989
[95] NS Gould S Gauthier CT Kariya E Min J Huang DJ Brian Hypertonic salineincreases lung epithelial lining fluid glutathione and thiocyanate two protectiveCFTR-dependent thiols against oxidative injury Respir Res 11 (2010) 119
[96] VT Vasu SJ de Cruz JS Houghton KA Hayakawa BM Morrissey CE CrossJP Eiserich Evaluation of thiol-based antioxidant therapeutics in cystic fibrosissputum focus on myeloperoxidase Free Radic Res 45 (2011) 165ndash176
[97] L Roussel G Martel J Berube S Rousseau P aeruginosa drives CXCL8 synthesisvia redundant toll-like receptors and NADPH oxidase in CFTRF508 airway epi-thelial cells J Cyst Fibros 10 (2011) 107ndash113
[98] GW Lau DJ Hassett H Ran F Kong The role of pyocyanin in Pseudomonas aer-uginosa infection Trends Mol Med 10 (2004) 599ndash606
[99] R Wilson DA Sykes D Watson A Rutman GW Taylor PJ Cole Measurementof Pseudomonas aeruginosa phenazine pigments in sputum and assessment oftheir contribution to sputum sol toxicity for respiratory epithelium InfectImmun 56 (1988) 2515ndash2517
[100] M Muller Pyocyanin induces oxidative stress in human endothelial cells andmodulates the glutathione redox cycle Free Radic Biol Med 33 (2002)1527ndash1533
[101] YQ OMalley KJ Reszka BE Britigan Direct oxidation of 2prime7prime-dichlorodihy-drofluorescein by pyocyanin and other redox-active compounds independentof reactive oxygen species production Free Radic Biol Med 36 (2004)90ndash100
[102] CC Caldwell Y Chen HS Goetzmann Y Hao MT Borchers DJ Hassett LRYoung D Mavrodi L Thomashow GW Lau Pseudomonas aeruginosa exotoxinpyocyanin causes cystic fibrosis airway pathogenesis Am J Pathol 175 (2009)2473ndash2488
[103] YQ OMalley KJ Reszka DR Spitz GM Denning BE Britigan Pseudomonasaeruginosa pyocyanin directly oxidizes glutathione and decreases its levels inairway epithelial cells Am J Physiol Lung Cell Mol Physiol 287 (2004)L94ndashL103
[104] M Muller Glutathione modulates the toxicity of but is not a biologically rele-vant reductant for the Pseudomonas aeruginosa redox toxin pyocyanin FreeRadic Biol Med 50 (2011) 971ndash977
[105] R Cheluvappa R Shimmon M Dawson SN Hilmer DG Le Couteur Reactionsof Pseudomonas aeruginosa pyocyanin with reduced glutathione Acta BiochimPol 55 (2008) 571ndash580
[106] JH Widdicombe Transgenic animals may help resolve a sticky situation in cys-tic fibrosis J Clin Invest 120 (2010) 3093ndash3096
[107] X Sun H Sui JT Fisher Z Yan X Liu HJ Cho NS Joo Y Zhang W Zhou Y YiJM Kinyon DC Lei-Butters MA Griffin P Naumann M Luo J Ascher KWang T Frana JJ Wine DK Meyerholz JF Engelhardt Disease phenotype ofa ferret CFTR-knockout model of cystic fibrosis J Clin Invest 120 (2010)3149ndash3160
[108] NS Joo HJ Cho M Khansaheb JJ Wine Hyposecretion of fluid from trachealsubmucosal glands of CFTR-deficient pigs J Clin Invest 120 (2010) 3161ndash3166
[109] A Bragonzi Murine models of acute and chronic lung infection with cystic fibro-sis pathogens IJMM 300 (2010) 584ndash593
[110] AM van Heeckeren MD Schluchter Murine models of chronic Pseudomonasaeruginosa lung infection Lab Anim 36 (2002) 291ndash312
[111] A Bragonzi D Worlitzsch GB Pier P Timpert M Ulrich M Hentzer JB Ander-sen M Givskov M Conese G Doring Nonmucoid Pseudomonas aeruginosa ex-presses alginate in the lungs of patients with cystic fibrosis and in a mousemodel J Infect Dis 192 (2005) 410ndash419
[112] GS CW Bedrossian DB Singer JJ Hansen HS Rosenberg The lung in cysticfibrosis A quantitative study including prevalence of pathologic findingsamong different age groups Hum Pathol 7 (1976) 195ndash204
[113] WD HA Cash B McCullough WG Johanson Jr JA Bass A rat model of chron-ic respiratory infection with Pseudomonas aeruginosa Am Rev Respir Dis 119(1979) 453ndash459
[114] EM JR Starke C Langston CJ Baker A mouse model of chronic pulmonary in-fection with Pseudomonas aeruginosa and Pseudomonas cepacia Pediatr Res 22(1987) 698ndash702
[115] TJ AM van Heeckeren RW Walenga MW Konstan PB Davis B ErokwuMA Haxhiu TW Ferkol Effect of Pseudomonas infection on weight loss lung
710 F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
mechanics and cytokines in mice Am J Respir Crit Care Med 161 (2000)271ndash279
[116] T Aw G Wierzbicka DP Jones Oral glutathione increases tissue glutathione invivo Chem Biol Interact 80 (1991) 89ndash97
[117] F Favilli P Marraccini T Iantomasi MT Vincenzini Effect of orally adminis-tered glutathione on glutathione levels in some organs of rats role of specifictransporters Br J Nutr 78 (1997) 293ndash300
[118] C Kariya H Leitner E Min C van Heeckeren A van Heeckeren BJ Day A rolefor CFTR in the elevation of glutathione levels in the lung by oral glutathione ad-ministration Am J Physiol Lung Cell Mol Physiol 292 (2007) L1590ndashL1597
[119] K Atkuri JJ Mantovani LA Herzenberg LA Herzenberg N-Acetylcysteinemdashasafe antidote for cysteineglutathione deficiency Curr Opin Pharmacol 7(2007) 355ndash359
[120] R De Lisle E Roach K Jansson Effects of laxative and N-acetylcysteine onmucus accumulation bacterial load transit and inflammation in the cystic fi-brosis mouse small intestine Am J Physiol Gastrointest Liver Physiol 293(2007) G577ndashG584
[121] A Luciani VR Villella S Esposito N Brunetti-Pierri D Medina C Settembre MGavina L Pulze I Giardino M Pettoello-Mantovani M DApolito S Guido EMasliah B Spencer S Quaratino V Raia A Ballabio L Maiuri Defective CFTRinduces aggresome formation and lung inflammation in cystic fibrosis throughROS-mediated autophagy inhibition Nat Cell Biol 12 863ndash875
[122] M Griese J Ramakers A Krasselt V Starosta S Van Koningsbruggen R FischerF Ratjen B Mullinger RM Huber K Maier E Rietschel G Scheuch Improve-ment of alveolar glutathione and lung function but not oxidative state in cysticfibrosis Am J Respir Crit Care Med 169 (2004) 822ndash828
[123] C Bishop VM Hudson SC Hilton C Wilde A pilot study of the effect of inhaledbuffered reduced glutathione on the clinical status of patients with cystic fibro-sis Chest 127 (2005) 308ndash317
[124] WWang C Oliva G Li A Holmgren CH Lillig KL Kirk Reversible silencing of CFTRchloride channels by glutathionylation J Gen Physiol 125 (2005) 127ndash141
[125] N Dauletbaev P Fischer B Aulbach J Gross W Kusche U Thyroff-FriesingerTO Wagner J Bargon A phase II study on safety and efficacy of high-dose N-acetylcysteine in patients with cystic fibrosis Eur J Med Res 14 (2009)352ndash358
[126] R Tirouvanziam Y Gernez CK Conrad RB Moss I Schrijver CE Dunn ZADavies LA Herzenberg Profound functional and signaling changes in viable in-flammatory neutrophils homing to cystic fibrosis airways Proc Natl Acad SciU S A 105 (2008) 4335ndash4339
[127] JH Roum Z Borok NG McElvaney GJ Grimes AD Bokser R Buhl RG Crys-tal Glutathione aerosol suppresses lung epithelial surface inflammatory cell-derived oxidants in cystic fibrosis J Appl Physiol 87 (1999) 438ndash443
[128] A Visca CT Bishop SC Hilton VM Hudson Improvement in clinical markersin CF patients using a reduced glutathione regimen an uncontrolled observa-tional study J Cyst Fibros 7 (2008) 433ndash436
[129] EF Nash A Stephenson F Ratjen E Tullis Nebulized and oral thiol derivativesfor pulmonary disease in cystic fibrosis Cochrane Database Syst Rev (2009)CD007168
[130] AC foundation Drug Development Pipeline 2011[131] S Hoshida T Kuzuya N Yamashita M Nishida S Kitahara M Hori T
Kamada M Tada Gamma-glutamylcysteine ethyl ester for myocardial protec-tion in dogs during ischemia and reperfusion J Am Coll Cardiol 24 (1994)1391ndash1397
[132] J Lok W Leung S Zhao S Pallast K van Leyen S Guo X Wang A Yalcin EHLo Gamma-glutamylcysteine ethyl ester protects cerebral endothelial cells dur-ing injury and decreases bloodndashbrain barrier permeability after experimentalbrain trauma J Neurochem 118 (2011) 248ndash255
[133] Z Borok R Buhl GJ Grimes AD Bokser RC Hubbard KJ Holroyd JH RoumDB Czerski AM Cantin RG Crystal Effect of glutathione aerosol on oxidantndashantioxidant imbalance in idiopathic pulmonary fibrosis Lancet 338 (1991)215ndash216
[134] KJ Holroyd R Buhl Z Borok JH Roum AD Bokser GJ Grimes D Czerski AMCantin RG Crystal Correction of glutathione deficiency in the lower respiratorytract of HIV seropositive individuals by glutathione aerosol treatment Thorax 48(1993) 985ndash989
[135] J Hull P Vervaart K Grimwood P Phelan Pulmonary oxidative stress responsein young children with cystic fibrosis Thorax 52 (1997) 557ndash560
[136] A Corti A Paolicchi M Franzini S Dominici AF Casini A Pompella The S-thiolating activity of membrane gamma-glutamyltransferase formation ofcysteinyl-glycine mixed disulfides with cellular proteins and in the cell microen-vironment Antioxid Redox Signal 7 (2005) 911ndash918
[137] A Corti M Franzini AF Casini A Paolicchi A Pompella Vitamin C supply tobronchial epithelial cells linked to glutathione availability in elfmdasha role for se-creted gamma-glutamyltransferase J Cyst Fibros 7 (2008) 174ndash178
[138] A Munck Nutritional considerations in patients with cystic fibrosis Expert RevRespir Med 4 (2010) 47ndash56
[139] JL Matel CE Milla Nutrition in cystic fibrosis Semin Respir Crit Care Med 30(2009) 579ndash586
[140] D Salvatore R Buzzetti E Baldo MP Forneris V Lucidi D Manunza IMarinelli B Messore AS Neri V Raia ML Furnari G Mastella An overviewof international literature from cystic fibrosis registries 2 Neonatal screeningand nutritiongrowth J Cyst Fibros 9 (2010) 75ndash83
[141] KF Joosten JM Hulst Malnutrition in pediatric hospital patients current is-sues Nutrition 27 (2011) 133ndash137
[142] S Fustik T Jacovska L Spirevska S Koceva Protein-energy malnutrition as thefirst manifestation of cystic fibrosis in infancy Pediatr Int 51 (2009) 678ndash683
[143] J Himmelfarb E McMonagle Albumin is the major plasma protein target of ox-idant stress in uremia Kidney Int 60 (2001) 358ndash363
[144] P Stenvinkel JJ Carrero J Axelsson B Lindholm O Heimburger Z MassyEmerging biomarkers for evaluating cardiovascular risk in the chronic kidneydisease patient how do new pieces fit into the uremic puzzle Clin J Am SocNephrol 3 (2008) 505ndash521
[145] M Roche P Rondeau NR Singh E Tarnus E Bourdon The antioxidant proper-ties of serum albumin FEBS Lett 582 (2008) 1783ndash1787
[146] D Giustarini A Milzani I Dalle-Donne R Rossi Red blood cells as a physiolog-ical source of glutathione for extracellular fluids Blood Cells Mol Dis 40 (2008)174ndash179
[147] A Meister ME Anderson Glutathione Annu Rev Biochem 52 (1983) 711ndash760[148] B Alvarez S Carballal L Turell R Radi Formation and reactions of sulfenic acid
in human serum albumin Methods Enzymol 473 (2010) 117ndash136[149] S Carballal B Alvarez L Turell H Botti BA Freeman R Radi Sulfenic acid in
human serum albumin Amino Acids 32 (2007) 543ndash551[150] LR Barclay AM Bailey D Kong The antioxidant activity of alpha-tocopherol-
bovine serum albumin complex in micellar and liposome autoxidations J BiolChem 260 (1985) 15809ndash15814
[151] T Ishii T Ichikawa K Minoda K Kusaka S Ito Y Suzuki M Akagawa K Mochi-zuki T Goda T Nakayama Human serum albumin as an antioxidant in the ox-idation of (minus)-epigallocatechin gallate participation of reversible covalentbinding for interaction and stabilization Biosci Biotechnol Biochem 75(2011) 100ndash106
[152] F Galli S Rovidati S Benedetti U Buoncristiani C Covarelli A Floridi F Canes-trari Overexpression of erythrocyte glutathione S-transferase in uremia and di-alysis Clin Chem 45 (1999) 1781ndash1788
[153] D Borowitz RD Baker V Stallings Consensus report on nutrition for pediat-ric patients with cystic fibrosis J Pediatr Gastroenterol Nutr 35 (2002)246ndash259
[154] LJ Filer Jr SW Wright MP Manning KE Mason Absorption of alpha-tocopherol and tocopherylesters by premature and full term infants and chil-dren in health and disease Pediatrics 8 (1951) 328ndash339
[155] L Lancellotti C DOrazio G Mastella G Mazzi U Lippi Deficiency of vitamins Eand A in cystic fibrosis is independent of pancreatic function and current en-zyme and vitamin supplementation Eur J Pediatr 155 (1996) 281ndash285
[156] MN Sathe AS Patel Update in pediatrics focus on fat-soluble vitamins NutrClin Pract 25 (2010) 340ndash346
[157] MG Traber The ABCs of vitamin E and beta-carotene absorption Am J ClinNutr 80 (2004) 3ndash4
[158] TF Dolan Jr Hemolytic anemia and edema as the initial signs in infants withcystic fibrosis Consider this diagnosis even in absence of pulmonary symptomsClin Pediatr 15 (1976) 597ndash600
[159] DR James M Alfaham MC Goodchild Increased susceptibility to peroxide-induced haemolysis with normal vitamin E concentrations in cystic fibrosisClin Chim Acta 204 (1991) 279ndash290
[160] SA Peters FJ Kelly Vitamin E supplementation in cystic fibrosis J Pediatr Gas-troenterol Nutr 22 (1996) 341ndash345
[161] A Maqbool VA Stallings Update on fat-soluble vitamins in cystic fibrosis CurrOpin Pulm Med 14 (2008) 574ndash581
[162] SD Sagel MK Sontag MM Anthony P Emmett KA Papas Effect of anantioxidant-rich multivitamin supplement in cystic fibrosis J Cyst Fibros 10(2011) 31ndash36
[163] F Galli A Azzi Present trends in vitamin E research Biofactors 36 (2010)33ndash42
[164] A Hamahata P Enkhbaatar ER Kraft M Lange SW Leonard MG Traber RACox FC Schmalstieg HK Hawkins EB Whorton EM Horvath C Szabo LDTraber DN Herndon DL Traber Gamma-tocopherol nebulization by a lipidaerosolization device improves pulmonary function in sheep with burn andsmoke inhalation injury Free Radic Biol Med 45 (2008) 425ndash433
[165] JP Anais N Razzouq M Carvalho C Fernandez A Astier M Paul A AstierH Fessi AM Lorino Development of alpha-tocopherol acetate nanoparti-cles influence of preparative processes Drug Dev Ind Pharm 35 (2009)216ndash223
[166] JM Zingg Molecular and cellular activities of vitamin E analogues Mini RevMed Chem 7 (2007) 543ndash558
[167] V Viola F Pilolli M Piroddi E Pierpaoli F Orlando M Provinciali M Betti FMazzini F Galli Why tocotrienols work better insights into the in vitro anti-cancer mechanism of vitamin E Genes Nutr 7 (2011) 29ndash41
[168] F Galli F Mazzini L Bamonti L Gille S Bohmdorfer M Piroddi T Netscher FJKelly T Rosenau Tocotrienamines and tocopheramines reactions with radicalsand metal ions Bioorg Med Chem 19 (2011) 6483ndash6491
[169] A Kuhad K Chopra Attenuation of diabetic nephropathy by tocotrienol in-volvement of NFκB signaling pathway Life Sci 84 (2009) 296ndash301
[170] Q Jiang X Yin MA Lill ML Danielson H Freiser J Huang Long-chain carbox-ychromanols metabolites of vitamin E are potent inhibitors of cyclooxygenasesProc Natl Acad Sci U S A 105 (2008) 20464ndash20469
[171] ER Miller III R Pastor-Barriuso D Dalal RA Riemersma LJ Appel E GuallarMeta-analysis high-dosage vitamin E supplementation may increase all-causemortality Ann Intern Med 142 (2005) 37ndash46
[172] JN Hathcock A Azzi J Blumberg T Bray A Dickinson B Frei I Jialal CSJohnston FJ Kelly K Kraemer L Packer S Parthasarathy H Sies MG TraberVitamins E and C are safe across a broad range of intakes Am J Clin Nutr 81(2005) 736ndash745
[173] R Brigelius-Flohe F Galli Vitamin E a vitamin still awaiting the detection of itsbiological function Mol Nutr Food Res 54 (2010) 583ndash587
711F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
[174] MG Traber B Frei JS Beckman Vitamin E revisited do new data validate ben-efits for chronic disease prevention Curr Opin Lipidol 19 (2008) 30ndash38
[175] F Galli Meeting report Vitamin E Satellite Symposium (VESS) associated to theAnnual Meeting of the SFRR-Europe Rome 26 August 2009 Free Radic Res 43(2009) 1256ndash1257
[176] LJ Roberts II JA Oates MF Linton S Fazio BP Meador MD Gross Y Shyr JDMorrow The relationship between dose of vitamin E and suppression of oxida-tive stress in humans Free Radic Biol Med 43 (2007) 1388ndash1393
[177] EFSA- EFSA Scientific Opinion of the Panel on Food Additives FlavouringsProcessing Aids and Materials in Contact with Food on a request from the Com-mission on mixed tocopherols tocotrienol tocopherol and tocotrienols assources for vitamin E in EFSA- EFSA (Ed) vol 640 The EFSA Journal2008 pp 1ndash34
[178] P Rust I Eichler S Renner I Elmadfa Long-term oral beta-carotene supple-mentation in patients with cystic fibrosis mdash effects on antioxidative status andpulmonary function Ann Nutr Metab 44 (2000) 30ndash37
[179] G Lepage J Champagne N Ronco A Lamarre I Osberg RJ Sokol CC Roy Sup-plementation with carotenoids corrects increased lipid peroxidation in childrenwith cystic fibrosis Am J Clin Nutr 64 (1996) 87ndash93
[180] BM Winklhofer-Roob H Puhl G Khoschsorur MA vant Hof H EsterbauerDH Shmerling Enhanced resistance to oxidation of low density lipoproteinsand decreased lipid peroxide formation during beta-carotene supplementationin cystic fibrosis Free Radic Biol Med 18 (1995) 849ndash859
[181] RC Graham-Maar JI Schall N Stettler BS Zemel VA Stallings Elevated vita-min A intake and serum retinol in preadolescent children with cystic fibrosisAm J Clin Nutr 84 (2006) 174ndash182
[182] I Sadowska-Woda M Rachel J Pazdan E Bieszczad-Bedrejczuk K PawliszakNutritional supplement attenuates selected oxidative stress markers in pediatricpatients with cystic fibrosis Nutr Res (New York NY) 31 (2011) 509ndash518
[183] KA Papas MK Sontag C Pardee RJ Sokol SD Sagel FJ Accurso JS WagenerA pilot study on the safety and efficacy of a novel antioxidant rich formulation inpatients with cystic fibrosis J Cyst Fibros 7 (2008) 60ndash67
[184] Y Saito A Fukuhara K Nishio M Hayakawa Y Ogawa H Sakamoto K Fujii YYoshida E Niki Characterization of cellular uptake and distribution of coen-zyme Q10 and vitamin E in PC12 cells J Nutr Biochem 20 (2009) 350ndash357
[185] AA Franke CM Morrison JL Bakke LJ Custer X Li RV Cooney CoenzymeQ10 in human blood native levels and determinants of oxidation during proces-sing and storage Free Radic Biol Med 48 (2010) 1610ndash1617
[186] HN Bhagavan RK Chopra Plasma coenzyme Q10 response to oral ingestion ofcoenzyme Q10 formulations Mitochondrion 7 (2007) S78ndashS88 (Suppl)
[187] HN Bhagavan RK Chopra Coenzyme Q10 absorption tissue uptake metabo-lism and pharmacokinetics Free Radic Res 40 (2006) 445ndash453
[188] F Galli R Lee C Dunster FJ Kelly Gas chromatography mass spectrometryanalysis of carboxyethyl-hydroxychroman metabolites of alpha- and gamma-tocopherol in human plasma Free Radic Biol Med 32 (2002) 333ndash340
[189] F Galli R Lee J Atkinson A Floridi FJ Kelly Gamma-tocopherol biokineticsand transformation in humans Free Radic Res 37 (2003) 1225ndash1233
[190] TA Laguna MK Sontag I Osberg JS Wagener FJ Accurso RJ Sokol De-creased total serum coenzyme-Q10 concentrations a longitudinal study in chil-dren with cystic fibrosis J Pediatr 153 (2008) 402ndash407
[191] T Frischer JK Myung G Maurer I Eichler Z Szepfalusi G Lubec Possible dys-regulation of chaperon and metabolic proteins in cystic fibrosis bronchial tissueProteomics 6 (2006) 3381ndash3388
[192] C Andersson MM Zaman AB Jones SD Freedman Alterations in immune re-sponse and PPARLXR regulation in cystic fibrosis macrophages J Cyst Fibros 7(2008) 68ndash78
[193] SD Freedman PG Blanco MM Zaman JC Shea M Ollero IK Hopper DAWeed A Gelrud MM Regan M Laposata JG Alvarez BP OSullivan Associa-tion of cystic fibrosis with abnormalities in fatty acid metabolism N Engl JMed 350 (2004) 560ndash569
[194] S Van Biervliet G Vanbillemont JP Van Biervliet D Declercq E Robberecht AChristophe Relation between fatty acid composition and clinical status or geno-type in cystic fibrosis patients Ann Nutr Metab 51 (2007) 541ndash549
[195] SD Freedman MH Katz EM Parker M Laposata MY Urman JG AlvarezA membrane lipid imbalance plays a role in the phenotypic expression ofcystic fibrosis in cftr(minusminus) mice Proc Natl Acad Sci U S A 96 (1999)13995ndash14000
[196] S Van Biervliet S Vande Velde JP Van Biervliet E Robberecht The effect ofzinc supplements in cystic fibrosis patients Ann Nutr Metab 52 (2008)152ndash156
[197] WR Henderson Jr SJ Astley MM McCready P Kushmerick S Casey JWBecker BW Ramsey Oral absorption of omega-3 fatty acids in patients withcystic fibrosis who have pancreatic insufficiency and in healthy control subjectsJ Pediatr 124 (1994) 400ndash408
[198] I Durieu E Vericel D Guichardant H Roth JP Steghens J Drai RN JosserandE Fontaine M Lagarde G Bellon Fatty acids platelets and oxidative markersfollowing intravenous n-3 fatty acids administration in cystic fibrosis an openpilot observational study J Cyst Fibros 6 (2007) 320ndash326
[199] LG Wood DA Fitzgerald ML Garg Hypothesis vitamin E complements poly-unsaturated fatty acids in essential fatty acid deficiency in cystic fibrosis J AmColl Nutr 22 (2003) 253ndash257
[200] JD Lloyd-Still SB Johnson RT Holman Essential fatty acid status in cystic fi-brosis and the effects of safflower oil supplementation Am J Clin Nutr 34(1981) 1ndash7
[201] A Maqbool JI Schall JF Garcia-Espana BS Zemel B Strandvik VAStallings Serum linoleic acid status as a clinical indicator of essential fatty
acid status in children with cystic fibrosis J Pediatr Gastroenterol Nutr 47(2008) 635ndash644
[202] C Oliver N Jahnke Omega-3 fatty acids for cystic fibrosis Cochrane DatabaseSyst Rev (2011) CD002201
[203] B Strandvik E Gronowitz F Enlund T Martinsson J Wahlstrom Essential fattyacid deficiency in relation to genotype in patients with cystic fibrosis J Pediatr139 (2001) 650ndash655
[204] P Rise S Volpi C Colombo RF Padoan C DOrazio S Ghezzi PMelotti V BennatoC Agostoni BM Assael C Galli Whole blood fatty acid analysis with micromethodin cystic fibrosis and pulmonary disease J Cyst Fibros 9 (2010) 228ndash233
[205] H Cao K Gerhold JR Mayers MM Wiest SM Watkins GS Hotamisligil Iden-tification of a lipokine a lipid hormone linking adipose tissue to systemic me-tabolism Cell 134 (2008) 933ndash944
[206] RR Malapaka SK Khoo J Zhang JH Choi XE Zhou Y Xu Y Gong J Li ELYong MJ Chalmers L Chang JH Resau PR Griffin YE Chen HE Xu Iden-tification and mechanism of a ten carbon fatty acid as a modulating ligand ofperoxisome proliferator activated receptors J Biol Chem 287 (2012)183ndash195
[207] T Hara A Hirasawa A Ichimura I Kimura G Tsujimoto Free fatty acid recep-tors FFAR1 and GPR120 as novel therapeutic targets for metabolic disorders JPharm Sci 100 (2011) 3594ndash3601
[208] R Gupta P Rathi S Bradoo Lipase mediated upgradation of dietary fats andoils Crit Rev Food Sci Nutr 43 (2003) 635ndash644
[209] BH Jennings CC Akoh Lipase-catalyzed modification of rice bran oil to incor-porate capric acid J Agric Food Chem 48 (2000) 4439ndash4443
[210] J Hoeks M Mensink MK Hesselink K Ekroos P Schrauwen Long- andMedium-Chain Fatty Acids Induce Insulin Resistance to a Similar Extent inHumans Despite Marked Differences in Muscle Fat Accumulation J Clin Endo-crinol Metab 97 (2012) 208ndash216
[211] PJ Congden G Bruce MM Rothburn PC Clarke JM Littlewood J KelleherMS Losowsky Vitamin status in treated patients with cystic fibrosis ArchDis Child 56 (1981) 708ndash714
[212] BM Winklhofer-Roob H Ellemunter M Fruhwirth SE Schlegel-Haueter GKhoschsorur MA vant Hof DH Shmerling Plasma vitamin C concentrationsin patients with cystic fibrosis evidence of associations with lung inflammationAm J Clin Nutr 65 (1997) 1858ndash1866
[213] L Shamseer D Adams N Brown JA Johnson S Vohra Antioxidant micronutri-ents for lung disease in cystic fibrosis Cochrane Database Syst Rev (2010)CD007020
[214] C Santi S Santoro Electrophilic Selenium First edition Wiley-VCH VerlagGmbH amp Co KGaA 2012
[215] L Flohe S Toppo G Cozza F Ursini A comparison of thiol peroxidase mecha-nisms Antioxid Redox Signal 15 (2010) 763ndash780
[216] L Flohe JR Andreesen R Brigelius-Flohe M Maiorino F Ursini Selenium theelement of the moon in life on earth IUBMB Life 49 (2000) 411ndash420
[217] V Valdiglesias E Pasaro J Mendez B Laffon In vitro evaluation of seleniumgenotoxic cytotoxic and protective effects a review Arch Toxicol 84(2010) 337ndash351
[218] P Foucaud P Therond M Marchand F Brion JF Demelier J Navarro Seleniumand vitamin E in mucoviscidosis Arch Fr Pediatr 45 (1988) 383ndash386
[219] J Neve R Van Geffel M Hanocq L Molle Plasma and erythrocyte zinc copperand selenium in cystic fibrosis Acta Paediatr Scand 72 (1983) 437ndash440
[220] BM Winklhofer-Roob B Tiran PE Tuchschmid MA vant Hof DH ShmerlingEffects of pancreatic enzyme preparations on erythrocyte glutathione peroxi-dase activities and plasma selenium concentrations in cystic fibrosis FreeRadic Biol Med 25 (1998) 242ndash249
[221] JD Lloyd-Still HE Ganther Selenium and glutathione peroxidase levels in cys-tic fibrosis Pediatrics 65 (1980) 1010ndash1012
[222] D Tsavachidou TJ McDonnell S Wen X Wang F Vakar-Lopez LL Pisters CAPettaway CG Wood KA Do PF Thall C Stephens E Efstathiou R Taylor DGMenter P Troncoso SM Lippman CJ Logothetis J Kim Selenium and vitaminE cell type- and intervention-specific tissue effects in prostate cancer J NatlCancer Inst 101 (2009) 306ndash320
[223] IN Zelko TJ Mariani RJ Folz Superoxide dismutase multigene family acomparison of the CuZn-SOD (SOD1) Mn-SOD (SOD2) and EC-SOD (SOD3)gene structures evolution and expression Free Radic Biol Med 33 (2002)337ndash349
[224] RP Bowler JD Crapo Oxidative stress in airways is there a role for extracellu-lar superoxide dismutase Am J Respir Crit Care Med 166 (2002) S38ndashS43
[225] K Best K McCoy S Gemma RA Disilvestro Copper enzyme activities in cysticfibrosis before and after copper supplementation plus or minus zinc Metabo-lism 53 (2004) 37ndash41
[226] SS Percival GP Kauwell E Bowser M Wagner Altered copper status in adultmen with cystic fibrosis J Am Coll Nutr 18 (1999) 614ndash619
[227] NF Krebs JE Westcott TD Arnold BM Kluger FJ Accurso LV Miller KMHambidge Abnormalities in zinc homeostasis in young infants with cystic fibro-sis Pediatr Res 48 (2000) 256ndash261
[228] D Easley N Krebs M Jefferson L Miller J Erskine F Accurso KM HambidgeEffect of pancreatic enzymes on zinc absorption in cystic fibrosis J Pediatr Gas-troenterol Nutr 26 (1998) 136ndash139
[229] S Van Biervliet JP Van Biervliet E Robberecht Serum zinc in patients with cys-tic fibrosis at diagnosis and after one year of therapy Biol Trace Elem Res 112(2006) 205ndash211
[230] S Van Biervliet JP Van Biervliet S Vande Velde E Robberecht Serum zinc con-centrations in cystic fibrosis patients aged above 4 years a cross-sectional eval-uation Biol Trace Elem Res 119 (2007) 19ndash26
712 F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
[231] F Galli M Cristina Polidori W Stahl P Mecocci FJ Kelly Vitamin E biotransfor-mation in humans Vitam Horm 76 (2007) 263ndash280
[232] J Wiser NE Alexis Q Jiang W Wu C Robinette R Roubey DB Peden In vivogamma-tocopherol supplementation decreases systemic oxidative stress andcytokine responses of human monocytes in normal and asthmatic subjectsFree Radic Biol Med 45 (2008) 40ndash49
[233] JG Wagner Q Jiang JR Harkema B Illek DD Patel BN Ames DB PedenOzone enhancement of lower airway allergic inflammation is prevented bygamma-tocopherol Free Radic Biol Med 43 (2007) 1176ndash1188
[234] JT Harries DP Muller Absorption of different doses of fat soluble and watermiscible preparations of vitamin E in children with cystic fibrosis Arch DisChild 46 (1971) 341ndash344
[235] EI Back C Frindt E Ocenaskova D Nohr M Stern HK Biesalski Can changesin hydrophobicity increase the bioavailability of alpha-tocopherol Eur J Nutr45 (2006) 1ndash6
[236] SZ Nasr MH OLeary C Hillermeier Correction of vitamin E deficiency withfat-soluble versus water-miscible preparations of vitamin E in patients with cys-tic fibrosis J Pediatr 122 (1993) 810ndash812
[237] S Soltani-Frisk E Gronowitz H Andersson B Strandvik Water-miscibletocopherol is not superior to fat-soluble preparation for vitamin E absorptionin cystic fibrosis Acta Paediatr 90 (2001) 1112ndash1115
[238] K Papas J Kalbfleisch R Mohon Bioavailability of a novel water-soluble vi-tamin E formulation in malabsorbing patients Dig Dis Sci 52 (2007)347ndash352
[239] F Antonicelli M Parmentier EM Drost N Hirani I Rahman K Donaldson WMacNee Nacystelyn inhibits oxidant-mediated interleukin-8 expression andNF-kappaB nuclear binding in alveolar epithelial cells Free Radic Biol Med 32(2002) 492ndash502
[240] EM App D Baran I Dab A Malfroot M Coffiner F Vanderbist M King Dose-finding and 24-h monitoring for efficacy and safety of aerosolized Nacystelyn incystic fibrosis Eur Respir J 19 (2002) 294ndash302
[241] MG Traber How much vitamin E hellip Just enough Am J Clin Nutr 84 (2006)959ndash960
[242] JC McCann BN Ames Vitamin K an example of triage theory is micronu-trient inadequacy linked to diseases of aging Am J Clin Nutr 90 (2009)889ndash907
[243] M Fusaro G Crepaldi S Maggi F Galli A DAngelo L Calo S Giannini DMiozzo M Gallieni Vitamin K bone fractures and vascular calcifications inchronic kidney disease an important but poorly studied relationship J Endocri-nol Invest 34 (2010) 317ndash323
[244] JC McCann BN Ames Adaptive dysfunction of selenoproteins from the per-spective of the triage theory why modest selenium deficiency may increaserisk of diseases of aging FASEB J 25 (2011) 1793ndash1814
[245] R Apak K Guclu M Ozyurek B Bektas Oglu M Bener Cupric ion reducing an-tioxidant capacity assay for food antioxidants vitamins polyphenolics and fla-vonoids in food extracts Methods Mol Biol 477 (2008) 163ndash193
[246] F Galli Interactions of polyphenolic compounds with drug disposition and me-tabolism Curr Drug Metab 8 (2007) 830ndash838
[247] RL Prior X Wu K Schaich Standardized methods for the determination of an-tioxidant capacity and phenolics in foods and dietary supplements J Agric FoodChem 53 (2005) 4290ndash4302
[248] C Azbell S Zhang D Skinner J Fortenberry EJ Sorscher BA WoodworthHesperidin stimulates cystic fibrosis transmembrane conductance regulator-mediated chloride secretion and ciliary beat frequency in sinonasal epitheliumOtolaryngol Head Neck Surg 143 (2010) 397ndash404
[249] G Wegrzyn J Jakobkiewicz-Banecka M Gabig-Ciminska E Piotrowska M Nar-ajczyk A Kloska M Malinowska D Dziedzic I Golebiewska M Moskot AWegrzyn Genistein a natural isoflavone with a potential for treatment of ge-netic diseases Biochem Soc Trans 38 (2010) 695ndash701
[250] YC Yu H Miki Y Nakamura A Hanyuda Y Matsuzaki Y Abe M Yasui K Ta-naka TC Hwang SG Bompadre Y Sohma Curcumin and genistein additivelypotentiate G551D-CFTR J Cyst Fibros 10 (2011) 243ndash252
[251] B Illek H Fischer Flavonoids stimulate Cl conductance of human airway epithe-lium in vitro and in vivo Am J Physiol 275 (1998) L902ndashL910
[252] JL Kreindler Cystic fibrosis exploiting its genetic basis in the hunt for newtherapies Pharmacol Ther 125 (2010) 219ndash229
[253] B Illek L Zhang NC Lewis RB Moss JY Dong H Fischer Defective function ofthe cystic fibrosis-causing missense mutation G551D is recovered by genisteinAm J Physiol 277 (1999) C833ndashC839
[254] P Anandakumar S Kamaraj S Jagan G Ramakrishnan R Vinodhkumar TDevaki Capsaicin modulates pulmonary antioxidant defense system during ben-zo(a)pyrene-induced lung cancer in Swiss albinomice Phytother Res 22 (2008)529ndash533
[255] I Rahman Antioxidant therapeutic advances in COPD Ther Adv Respir Dis 2(2008) 351ndash374
[256] AW Boots H Li RP Schins R Duffin JW Heemskerk A Bast GR Haenen Thequercetin paradox Toxicol Appl Pharmacol 222 (2007) 89ndash96
[257] M Joskova S Franova V Sadlonova Acute bronchodilator effect of quercetin inexperimental allergic asthma Bratisl Lek Listy 112 (2011) 9ndash12
[258] HJ Park CM Lee ID Jung JS Lee YI Jeong JH Chang SH Chun MJ Kim IWChoi SC Ahn YK Shin SR Yeom YM Park Quercetin regulates Th1Th2 balancein a murine model of asthma Int Immunopharmacol 9 (2009) 261ndash267
[259] AP Rogerio A Kanashiro C Fontanari EV da Silva YM Lucisano-ValimEG Soares LH Faccioli Anti-inflammatory activity of quercetin and iso-quercitrin in experimental murine allergic asthma Inflamm Res 56 (2007)402ndash408
[260] M Muller Polyphenol cytotoxicity induced by the bacterial toxin pyocyaninrole of NQO1 Free Radic Biol Med 47 (2009) 84ndash91
[261] J Grassmann Terpenoids as plant antioxidants Vitam Horm 72 (2005)505ndash535
[262] P Allen Tea tree oil the science behind the antimicrobial hype Lancet 358(2001) 1245
[263] EC Dasenbrook W Checkley CA Merlo MW Konstan N Lechtzin MP BoyleAssociation between respiratory tract methicillin-resistant Staphylococcus aure-us and survival in cystic fibrosis JAMA 303 (2010) 2386ndash2392
[264] V Bezzerri M Borgatti E Nicolis I Lampronti MC Dechecchi I Mancini PRizzotti R Gambari G Cabrini Transcription factor oligodeoxynucleotides toNF-kappaB inhibit transcription of IL-8 in bronchial cells Am J Respir CellMol Biol 39 (2008) 86ndash96
[265] R Gambari M Borgatti V Bezzerri E Nicolis I Lampronti MC Dechecchi IMancini A Tamanini G Cabrini Decoy oligodeoxyribonucleotides and peptidenucleic acids-DNA chimeras targeting nuclear factor kappa-B inhibition of IL-8 gene expression in cystic fibrosis cells infected with Pseudomonas aeruginosaBiochem Pharmacol 80 (2010) 1887ndash1894
[266] M Adrian P Jeandet AC Douillet-Breuil L Tesson R Bessis Stilbene content ofmature Vitis vinifera berries in response to UV-C elicitation J Agric Food Chem48 (2000) 6103ndash6105
[267] B Paul I Masih J Deopujari C Charpentier Occurrence of resveratrol and pter-ostilbene in age-old darakchasava an ayurvedic medicine from India J Ethno-pharmacol 68 (1999) 71ndash76
[268] I Rahman Antioxidant therapies in COPD Int J Chron Obstruct Pulmon Dis 1(2006) 15ndash29
[269] M Lee S Kim OK Kwon SR Oh HK Lee K Ahn Anti-inflammatory and anti-asthmatic effects of resveratrol a polyphenolic stilbene in a mouse model ofallergic asthma Int Immunopharmacol 9 (2009) 418ndash424
[270] LG Wood PA Wark ML Garg Antioxidant and anti-inflammatory effectsof resveratrol in airway disease Antioxid Redox Signal 13 (2010)1535ndash1548
[271] KV Kiselev Perspectives for production and application of resveratrol ApplMicrobiol Biotechnol 90 (2011) 417ndash425
[272] M Shakibaei C Buhrmann A Mobasheri Resveratrol-mediated SIRT-1 interac-tions with p300 modulate receptor activator of NF-kappaB ligand (RANKL) acti-vation of NF-kappaB signaling and inhibit osteoclastogenesis in bone-derivedcells J Biol Chem 286 (2011) 11492ndash11505
[273] SF Zaidi K Ahmed T Yamamoto T Kondo K Usmanghani M Kadowaki TSugiyama Effect of resveratrol on Helicobacter pylori-induced interleukin-8 secre-tion reactive oxygen species generation and morphological changes in human gas-tric epithelial cells Biol Pharm Bull 32 (2009) 1931ndash1935
[274] JK Kundu YK Shin YJ Surh Resveratrol modulates phorbol ester-inducedpro-inflammatory signal transduction pathways in mouse skin in vivo NF-kappaB and AP-1 as prime targets Biochem Pharmacol 72 (2006)1506ndash1515
[275] NH Nam Naturally occurring NF-kappaB inhibitors Mini Rev Med Chem 6(2006) 945ndash951
[276] JM Smoliga JA Baur HA Hausenblas Resveratrol and healthmdasha comprehen-sive review of human clinical trials Mol Nutr Food Res 55 (2011) 1129ndash1141
[277] ME Juan M Maijo JM Planas Quantification of trans-resveratrol and itsmetabolites in rat plasma and tissues by HPLC J Pharm Biomed Anal 51(2010) 391ndash398
[278] JA Baur DA Sinclair Therapeutic potential of resveratrol the in vivo evidenceNat Rev 5 (2006) 493ndash506
[279] E Nicolis I Lampronti MC Dechecchi M Borgatti A Tamanini N Bianchi VBezzerri I Mancini MG Giri P Rizzotti R Gambari G Cabrini Pyrogallol anactive compound from the medicinal plant Emblica officinalis regulates expres-sion of pro-inflammatory genes in bronchial epithelial cells Int Immunophar-macol 8 (2008) 1672ndash1680
[280] E Nicolis I Lampronti MC Dechecchi M Borgatti A Tamanini V Bezzerri NBianchi M Mazzon I Mancini MG Giri P Rizzotti R Gambari G CabriniModulation of expression of IL-8 gene in bronchial epithelial cells by 5-methoxypsoralen Int Immunopharmacol 9 (2009) 1411ndash1422
[281] M Borgatti I Mancini N Bianchi A Guerrini I Lampronti D Rossi G SacchettiR Gambari Bergamot (Citrus bergamia Risso) fruit extracts and identified com-ponents alter expression of interleukin 8 gene in cystic fibrosis bronchial epithe-lial cell lines BMC Biochem 12 (2011) 15
[282] L Piccagli E Fabbri M Borgatti N Bianchi V Bezzerri I Mancini E Nicolis CMDechecchi I Lampronti G Cabrini R Gambari Virtual screening against p50NF-kappaB transcription factor for the identification of inhibitors of the NF-kappaB-DNA interaction and expression of NF-kappaB upregulated genesChemMedChem 4 (2009) 2024ndash2033
[283] L Piccagli M Borgatti E Nicolis N Bianchi I Mancini I Lampronti D VevaldiF DallAcqua G Cabrini R Gambari Virtual screening against nuclear factorkappaB (NF-kappaB) of a focus library identification of bioactive furocoumarinderivatives inhibiting NF-kappaB dependent biological functions involved incystic fibrosis Bioorg Med Chem 18 (2010) 8341ndash8349
[284] M Borgatti A Chilin L Piccagli I Lampronti N Bianchi I Mancini G Mar-zaro Da Francesco A Guiotto R Gambari Development of a novel furocou-marin derivative inhibiting NF-kappaB dependent biological functionsdesign synthesis and biological effects Eur J Med Chem 46 (2011)4870ndash4877
[285] E Georgy S Le Guellec L Vecellio E Fichant P Stordeur P Bordeau JP PerraudinFeasibility study of OSCN- and lactoferrin (Meveol) nebulization for cysticfibrosis JCyst Fibros 10 (2011) S18
713F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
[286] C Tidei M Piroddi F Galli C Santi Oxidation of thiols promoted by PhSeZnClTetrahedron Lett 53 (2012) 232ndash234
[287] L Semianrio-Vidal C van Hesuden G Mugesh ER Lazarowski Ebselen is a po-tent non-competitive inhibitor of extracellular nucleoside diphosphokinasePurinergic Signal 6 (2010) 383ndash391
[288] C ColussiMC Albertini S Coppola S Rovidati F Galli L Ghibelli H2O2-inducedblockof glycolysis as an active ADP-ribosylation reaction protecting cells from apoptosisFASEB J 14 (2000) 2266ndash2276
[289] H Xiao KL Parkin Induction of phase II enzyme activity by various seleniumcompounds Nutr Cancer 55 (2006) 210ndash223
[290] G Peluffo R Radi Biochemistry of protein tyrosine nitration in cardiovascularpathology Cardiovasc Res 75 (2007) 291ndash302
[291] B Alvarez R Radi Peroxynitrite reactivity with amino acids and proteinsAmino Acids 25 (2003) 295ndash311
[292] B Kamosinska MW Radomski M Duszyk A Radomski SF Man Nitric oxideactivates chloride currents in human lung epithelial cells Am J Physiol 272(1997) L1098ndashL1104
[293] L Chen RP Patel X Teng CA Bosworth JR Lancaster Jr S Matalon Mecha-nisms of cystic fibrosis transmembrane conductance regulator activation by S-nitrosoglutathione J Biol Chem 281 (2006) 9190ndash9199
[294] F Luchetti B CanonicoM BettiM Arcangeletti F PilolliM Piroddi L Canesi S PapaF Galli Melatonin signaling and cell protection function FASEB J 24 (2010)3603ndash3624
[295] MW Bengtsson G Jedstedt G Flemstrom Duodenal bicarbonate secretion inrats stimulation by intra-arterial and luminal guanylin and uroguanylin ActaPhysiol (Oxf) 191 (2007) 309ndash317
[296] CS Nelson JL Marino CN Allen Melatonin receptor potentiation of cyclic AMP andthe cystic fibrosis transmembrane conductance regulator ion channel J Pineal Res 26(1999) 113ndash121
[297] C de Castro-Silva VM de Bruin GM Cunha DM Nunes CAMedeiros PF de BruinMelatonin improves sleep and reduces nitrite in the exhaled breath condensate incystic fibrosismdasha randomized double-blind placebo-controlled study J Pineal Res48 (2010) 65ndash71
[298] I Hornyak E Pankotai L Kiss Z Lacza Current developments in the the-rapeutic potential of S-nitrosoglutathione an endogenous NO-donor mole-cule Curr Pharm Biotechnol (2011) Jan 11 [Epub ahead of print] - PMID21235457
[299] AH Snyder ME McPherson JF Hunt M Johnson JS Stamler B Gaston Acuteeffects of aerosolized S-nitrosoglutathione in cystic fibrosis Am J Respir CritCare Med 165 (2002) 922ndash926
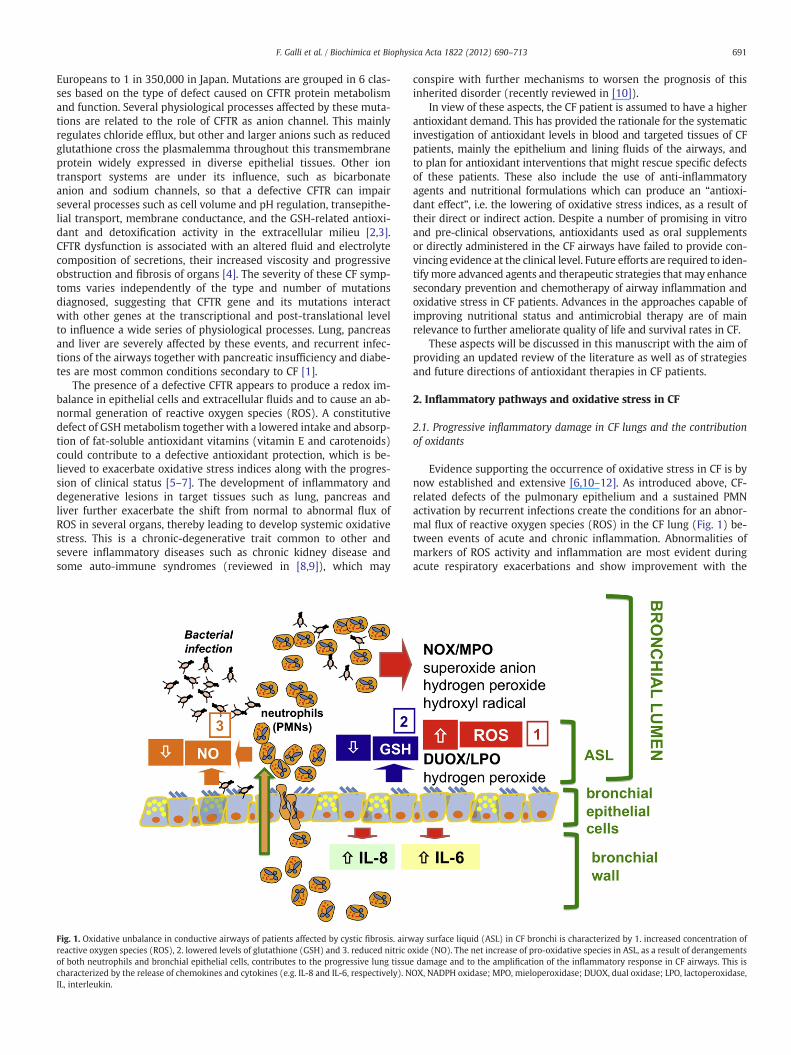
691F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
Europeans to 1 in 350000 in Japan Mutations are grouped in 6 clas-ses based on the type of defect caused on CFTR protein metabolismand function Several physiological processes affected by these muta-tions are related to the role of CFTR as anion channel This mainlyregulates chloride efflux but other and larger anions such as reducedglutathione cross the plasmalemma throughout this transmembraneprotein widely expressed in diverse epithelial tissues Other iontransport systems are under its influence such as bicarbonateanion and sodium channels so that a defective CFTR can impairseveral processes such as cell volume and pH regulation transepithe-lial transport membrane conductance and the GSH-related antioxi-dant and detoxification activity in the extracellular milieu [23]CFTR dysfunction is associated with an altered fluid and electrolytecomposition of secretions their increased viscosity and progressiveobstruction and fibrosis of organs [4] The severity of these CF symp-toms varies independently of the type and number of mutationsdiagnosed suggesting that CFTR gene and its mutations interactwith other genes at the transcriptional and post-translational levelto influence a wide series of physiological processes Lung pancreasand liver are severely affected by these events and recurrent infec-tions of the airways together with pancreatic insufficiency and diabe-tes are most common conditions secondary to CF [1]
The presence of a defective CFTR appears to produce a redox im-balance in epithelial cells and extracellular fluids and to cause an ab-normal generation of reactive oxygen species (ROS) A constitutivedefect of GSHmetabolism together with a lowered intake and absorp-tion of fat-soluble antioxidant vitamins (vitamin E and carotenoids)could contribute to a defective antioxidant protection which is be-lieved to exacerbate oxidative stress indices along with the progres-sion of clinical status [5ndash7] The development of inflammatory anddegenerative lesions in target tissues such as lung pancreas andliver further exacerbate the shift from normal to abnormal flux ofROS in several organs thereby leading to develop systemic oxidativestress This is a chronic-degenerative trait common to other andsevere inflammatory diseases such as chronic kidney disease andsome auto-immune syndromes (reviewed in [89]) which may
Fig 1 Oxidative unbalance in conductive airways of patients affected by cystic fibrosis airwreactive oxygen species (ROS) 2 lowered levels of glutathione (GSH) and 3 reduced nitric oof both neutrophils and bronchial epithelial cells contributes to the progressive lung tissuecharacterized by the release of chemokines and cytokines (eg IL-8 and IL-6 respectively) NIL interleukin
conspire with further mechanisms to worsen the prognosis of thisinherited disorder (recently reviewed in [10])
In view of these aspects the CF patient is assumed to have a higherantioxidant demand This has provided the rationale for the systematicinvestigation of antioxidant levels in blood and targeted tissues of CFpatients mainly the epithelium and lining fluids of the airways andto plan for antioxidant interventions that might rescue specific defectsof these patients These also include the use of anti-inflammatoryagents and nutritional formulations which can produce an ldquoantioxi-dant effectrdquo ie the lowering of oxidative stress indices as a result oftheir direct or indirect action Despite a number of promising in vitroand pre-clinical observations antioxidants used as oral supplementsor directly administered in the CF airways have failed to provide con-vincing evidence at the clinical level Future efforts are required to iden-tify more advanced agents and therapeutic strategies thatmay enhancesecondary prevention and chemotherapy of airway inflammation andoxidative stress in CF patients Advances in the approaches capable ofimproving nutritional status and antimicrobial therapy are of mainrelevance to further ameliorate quality of life and survival rates in CF
These aspects will be discussed in this manuscript with the aim ofproviding an updated review of the literature as well as of strategiesand future directions of antioxidant therapies in CF patients
2 Inflammatory pathways and oxidative stress in CF
21 Progressive inflammatory damage in CF lungs and the contributionof oxidants
Evidence supporting the occurrence of oxidative stress in CF is bynow established and extensive [610ndash12] As introduced above CF-related defects of the pulmonary epithelium and a sustained PMNactivation by recurrent infections create the conditions for an abnor-mal flux of reactive oxygen species (ROS) in the CF lung (Fig 1) be-tween events of acute and chronic inflammation Abnormalities ofmarkers of ROS activity and inflammation are most evident duringacute respiratory exacerbations and show improvement with the
ay surface liquid (ASL) in CF bronchi is characterized by 1 increased concentration ofxide (NO) The net increase of pro-oxidative species in ASL as a result of derangementsdamage and to the amplification of the inflammatory response in CF airways This is
OX NADPH oxidase MPO mieloperoxidase DUOX dual oxidase LPO lactoperoxidase
692 F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
intensive treatment of the infection [13ndash15] The fact that relapses orsuccessful therapy of infection do not normalize these markers dem-onstrates the presence of a chronic inflammatory syndrome that isintrinsic to the CF defect In this context ROS may lose their physio-logical role in the killing of pathogens to turn into toxic effectors re-sponsible for the damage of the pulmonary epithelium as well as ofother components of the lung parenchyma and lining fluids Impor-tantly ROS can modify the thiol homeostasis of extracellular fluidsand epithelia [16] and promote the activation of MAPK signalingpathways [17] which regulate both the NFkβ-dependent and-independent transcription of pro-inflammatory genes and other mo-lecular effects associated with the immuno-inflammatory imbalanceobserved in the CF lung
Hallmark of the chronic inflammatory lung disease in CF is therelease of chemokines mainly interleukin (IL)-8 [1819] leading tothe neutrophil recruitment in the bronchial lumen (see [20] for areview) Whether CF lung inflammation arises independently andbefore bacterial infection remains to be fully established althoughIL-8 and pro-inflammatory cytokines have been found in bronchoal-veolar lavage fluids of CF infants even before the onset of an overtbacterial infection [21] Although directed against infective agentsthe chronic inflammation in CF lungs is largely recognized as mainlyresponsible for the progressive tissue damage leading to respiratoryinsufficiency Dissection of the pathophysiology of CF chronic lunginflammation should take into account the bronchial epithelial cellsexpressing the mutated CFTR protein the polymorphonuclear neu-trophils recruited into the bronchial lumens and the bacterial infec-tion itself with special regards to Pseudomonas aeruginosa the mostcommon gram negative microorganism which colonizes CF airways[22] Thus novel anti-inflammatory therapies against the progressivedamage of the CF respiratory tissue should be mainly aimed i) to re-duce the excessive recruitment of neutrophils by intervening on thetransmembrane signaling pivoting the excessive expression of IL-8 [23ndash26] ii) to inactivate proteases released by the neutrophils con-tinuously activated by bacterial products [27] and iii) to circumventthe effect of the unbalanced production of oxidants deriving fromboth phagocytes and bronchial epithelial cells [2228ndash30] Identifica-tion of oxidants produced in the CF airway tract is of high importancein order to identify novel molecular targets for specific pharmacolog-ical intervention
22 Respiratory epithelial cells and neutrophils as sources of oxidants inthe CF lung
It is largely accepted that neutrophils migrating inside the CFbronchial lumina release large amounts of reactive oxygen species(ROS) including the superoxide anion (O2
minusbull) hydrogen peroxide(H2O2) and the hydroxyl free radical (OH) mainly by the activationof the NADPH oxidase (NOX) To such exaggerated ROS productioncontribute both the continuous interaction of neutrophils with bacte-ria and bacterial degradation products and the inability to engulf bac-teria in biofilms leading to a condition of ldquofrustrated phagocytosisrdquoNeutrophils are therefore recognized as a major source of ROS inthe airway surface liquid (ASL) of young children with CF [1431]However bronchial ciliated and alveolar type II epithelial cells bythemselves are able to produce significant amounts of ROS throughthe two isoforms of NADPH oxidase expressed in the apical membraneof these epithelial cells namely DUOX1 and DUOX2 [32] A major pro-posed function of DUOXs is to support lactoperoxidase (LPO) which isin turn released by goblet and submucosal gland airway cells to gen-erate bactericidal hypothiocyanite (OSCNminus) starting from thiocyanate(SCNminus) and H2O2 Thus the DUOXLPO coupled system of the respira-tory epithelial cells parallels the NOXmieloperoxidase (MPO) systemof phagocytes in releasing and processing oxidants in the ASL Whilethe NOXMPO system of phagocytes is mainly activated in theinfection-induced respiratory burst the release of ROS from epithelia
is continuous and even independent of the presence of overt bacterialinfection [33] Interestingly it was proposed that the efficiency of theDUOXLPO defense system is dependent on the ion transport functionof the CFTR Clminus channel which could also intervene both in the con-ductive secretion of SCNminus (for LPO function) and of HCO3
minus (for pHadjustment) into the ASL [34] However more recent ex vivo observa-tions while confirming a positive role of DUOXLPO system in produc-ing OSCNminus as a general defense mechanism of the airways do notdirectly relate SCNminus concentrations in ASL with CFTR function [35]The LPO-mediated scavenging of H2O2 has suggested a role of SCNminus
as physiological antioxidant of ASL [36] which may be defective inCF Besides this role of LPO and SCNminus an abnormal flux of H2O2 inthe CF airways may also depend on other factors that are associatedwith an alteredmetabolism of ROS For instance lowered levels of Lac-toferrin (LF) have been described in CF secretions [37] This iron-chelating homologue of transferrin contained in the granules of neu-trophils is also secreted by several mucosal tissues in biological fluidsto contribute antimicrobial effects by a variety of mechanisms includ-ing the chelating activity of iron as Fenton chemistry catalyst [38]
As regards the progression of CF lung disease in the early phasesbefore the onset of chronic bacterial colonization epithelial DUOXcontinuously releases H2O2 thus being a predominant source inrespect to the NADPH oxidase from phagocytes The latter is mainlyactive when the respiratory burst is ldquotriggered on demandrdquo by infec-tious components On the other side in advanced phases of chronicinfection of CF lungs neutrophil-derived ROS are predominant [32]due to neutrophil activation as well as to the decreasing number ofH2O2-producing ciliated cells which are reduced by extensive apo-ptosis and tissue remodeling A further reduction of epithelial DUOXactivity has been observed as a result of infection with P aeruginosain conductive airways P aeruginosa-derived toxin pyocyanin in factinhibits DUOX-dependent H2O2 production by consuming intracellu-lar NADPH which represents an interesting adaptive mechanism todownregulate innate anti-bacterial defenses [39]
23 Redox disturbances of CF airways the role of GSH NO and H2O2
Intracellular impairment of redox balance between oxidants andanti-oxidants has been proposed to occur in CF bronchial epithelialcells although a significant difference in respect to normal CFTR-expressing cells is still controversial and debated [40] Three majorissues have been investigated concerning the intracellular redox bal-ance in CF bronchial cells namely i) a defect in GSH homeostasis[4142] ii) an alteration of nitric oxide (NO) metabolism and iii) animbalance of intracellular H2O2 production
As far as GSH is concerned the defective CFTR channel functionhas been proposed to lead to a lowered cell content of this tripeptidewhich is crucial to control the flux of H2O2 in both the CF bronchialepithelial cells and lining fluids This aspect ndash discussed in detailbelow in this review ndash is associated with characteristic defects ofGSH-related enzymes and may represent a key underlying factor inthe oxidative stress of CF airways
Altered NO concentration has been found in chronic respiratorydiseases such as bronchial asthma and chronic obstructive pulmonarydisease [43] and reduced NO concentrations have been observed inthe bronchial airways of patients affected by CF which directly corre-lated with worsening of lung function [44] Thus NO concentration inCF lung exhalate has been subsequently tested as a possible marker ofpulmonary exacerbations andor the inflammatoryinfective statusand its fluctuations over time [4546]
This opened the way to further analysis of the mechanisms of thisderangement and it has been proposed that an excessive productionof asymmetric dimethylarginine an inhibitor of endogenous NOSynthase (NOS) could be involved in the reduced concentrationof NO in CF airways [47ndash49] Possible corrective therapies such asthe inhalation of L-arginine have provided preliminary evidence of
693F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
correction of the defective NO concentration and improvement oflung function in CF patients [49ndash51]
Although exhaled NO is decreased in CF increased immunohisto-chemical staining for nitrotyrosine was demonstrated in lung tissuesfrom CF patients [52] Therefore a decreased production or accelerat-ed metabolism of NO could be present in association with an abnor-mal reactivity of this radical and its derived species (NOx) towardbiomolecular components of the CF airways Peroxynitrite is one ofthe most relevant mediators of the biological activity of NO withtoxic properties and damaging activity on several biomolecules [53]
A third emerging issue takes into consideration the expressionof different enzymatic systems affecting the redox balance in CF bron-chial epithelial cells For instance intracellular concentration of H2O2
has been found abnormally elevated in both immortalized bronchialand primary nasal epithelial cells derived from CF patients bothin the presence and the absence of proinflammatory cytokines [54]This has been accompanied by a marked decrease of expressionof proteins regulating H2O2 levels such as thioredoxin 1 (TRX-1)glutathione-S-transferase pi (GST-pi) peroxyredoxin (PRDX) 6TRX-dependent peroxide reductase (PRDX-1) catalase and con-versely a significant increase of Mn superoxide dismutase (SOD2)[54] Interestingly to link these modifications with CF specific charac-teristics dysfunctional CFTR channel was found associated withreduced activity of the transcription factor Nrf-2 (nuclear factor-erythroid 2 p45 subunit-related factor 2) which could at least inpart explain the differential expression of the enzymatic systemsresulting in the elevated intracellular steady-state concentration ofH2O2 found in CF nasal and bronchial epithelial cells [54] In synthesisthe ASL of CF patients during advanced stages of the lung disease con-tains elevated concentrations of ROS mainly derived from neutro-phils migrated into the airway lumen and a reduced concentrationof NO which can strongly contribute to respiratory tissue injurytogether with the proteases released by the activated neutrophilsThe homeostatic role of the GSH-related defenses appears constitu-tively impaired by the dysfunctional CFTR thus increasing suscepti-bility to develop oxidative stress and lung tissue degeneration(Fig 1) as described in detail in the sections below
24 Conductive airway epithelium as target of ROS
Oxidants can target different biomolecules to damage epithelialcells and extracellular fluids of the airways Lipid peroxidationand post-translational modifications of proteins on both cell mem-branes and extracellular targets are common biomarkers of thisdamage which can occur by the direct reaction between ROS and bio-molecules or through the formation of second-generation reactivebyproducts [955] All levels of this interaction between ROS and bio-logical components can produce toxic and bioactive intermediatesOxidants are known to activate secondmessengers through phospho-lipases A2 C and D and to induce the production of cytokines andmucins a series of molecular events that contribute to progressiveobstructive disease and reduction of lung function [56] Besides thedirect oxidative damage to cellular structures of the bronchial epithe-lial cells the excessive concentration of oxidants in CF both in the ASLlining the apical membranes and inside the bronchial cells has beenstudied in respect to the regulation of the inflammatory response
ROS are often considered a sort of secondmessengers in activatingthe Nuclear Factor (NF)-κB which is in turn involved in the activationof transcription of several proinflammatory cytokines and chemo-kines [57] For instance it has been shown that H2O2 partly controlsNF-κB activation by IL-1beta by facilitating the activation of NIKand subsequent phosphorylation of IKKβ [58] In this respect a directlink has been proposed between the excessive production of intracel-lular H2O2 and the elevated expression of IL-6 and IL-8 the mostabundant pro-inflammatory cytokine and neutrophilic chemokinefound in CF airways [54] which has been further confirmed [59]
Moreover oxidants could be synergic in the induction of mucins aspromoted by neutrophil elastase which further impairs ASL fluidityin CF [60] Finally bacterial infection with P aeruginosa strains releas-ing the toxin pyocyanin (PCN) has been shown to reduce ion trans-port through the CFTR channel thus potentially counteracting thetherapeutic effects of correctors and potentiators of mutated CFTRprotein [6162] In summary excessive oxidants in CF conductive air-ways have different negative effects in the amplification of the al-ready excessive lung inflammation and secretion of mucin togetherwith a direct deleterious effect on CFTR channel function
25 Oxidative stress and surfactant
Oxidative stress and inflammation in cystic fibrosis can affect sur-factant biophysical activity thus leading to early alterations of lungfunction in patients with CF [63] Altered phospholipid-to-protein ra-tios and phospholipid subclasses a modified fatty acid profiles anddecreased association of proteins such as SP-A with lipid componentsof isolated surfactant indicate that components of this fluid are con-siderably altered and dysfunctional in lower respiratory tract secre-tions of CF patients [64]
Oxidative damage of surfactant may involve both lipid and proteincomponents Alteration of lipid components can in turn generatetoxic lipid species with cytotoxic activity towards nearby epithelialcells [65] Altered protein components have been shown in cysticfibrosis [66] Notably surfactant protein D which is an important in-nate host defense molecule becomes unable to agglutinate bacteriawhen it is modified by oxidation which facilitates pathogen coloniza-tion in the lung [67] In a cross-sectional analysis of CF patients withmild lung disease reduced surfactant activity was correlated to in-creased neutrophilic airway inflammation but not to lung function[68] So far longitudinal measurements of surfactant function in CFpatients are lacking and it remains unclear how these alterationsrelate to progression of airway inflammation as well as to the rateof decline of pulmonary function [69]
26 Laboratory indices of oxidative stress in CF
Appropriate biochemical and clinical tools are of importance forthe monitoring of antioxidant therapies in CF and a crucial aspect isthe selection of proper biomarkers and protocols to assess biologicalpathways of oxidation
Pancreatic insufficiency and a diminished bile acid pool cause mal-absorption of important essential nutrients and other dietary compo-nents in CF Of particular significance is the malabsorption of fat-soluble antioxidants such as carotenoids tocopherols and coenzymeQ-10 (CoQ-10) which act as chain breakers in the peroxidation reac-tions of polyunsaturated lipids Accordingly lipid peroxidation is oneof the main signs encountered in the CF plasma buccal mucosal cellsbreath condensate and BALF as measured by the non-enzymaticoxidation product of arachidonic acid 8-iso prostaglandin F2α[570ndash73] Elevations of this and other eicosanoids in human bodyfluids and tissues have been found in a diverse array of human disor-ders including atherosclerosis diabetes obesity cigarette smokingneurodegenerative diseases and many others [74] Further treat-ments for some of these conditions including antioxidant supple-mentation have been shown to decrease the levels of this class ofbiomarkers In CF patients respiratory exacerbations increase plasmalevels of 8-iso-F2α [70] the levels of which in the breath condensatenegatively correlate with respiratory function data [71] At the sametime successful in vivo antioxidant therapy by GSH inhalation hasbeen shown to decreased PGE levels in BALF in association withchanges in the number and activity of leukocyte subpopulations re-sponsible for lung inflammation [73]
Oxysterols a biomarker of cholesterol oxidation were found toincrease in CF plasma as a further proof of the abnormal lipid
694 F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
metabolism and increased susceptibility to oxidation of lipoproteinlipids in CF patients [7] Importantly an increased oxidative burdenof lung and blood lipids may produce bioactive lipid products thatfurther sustain CF symptoms Besides to 8-iso-F2α and other ana-logues with some bioactivity [74] arachidonic acid oxidation maycontribute to persistent platelet activation and pulmonary dysfunc-tion in CF via generation of bioactive isoeicosanoids [75] which pro-vides sufficient rationale for a prevention therapy with fat solubleantioxidants such as vitamin E Evidence has recently accumulatedon the systemic effects of oxysterols on various tissues and organs[76] The role of this lipid oxidation product alone or in combinationwith other factors could be further investigated in the context ofmechanisms and clinical progression of multi-organ failure of CFpatients
The impaired pancreatic and liver functions of CF patients repre-sent the underlying factor for a defective lipoprotein metabolismand hypocholesterolemia which exponentially increase the burdenof damage by cholesterol and other lipids due to reduced blood trans-port of fat-soluble antioxidants with nascent VLDL particles Besidesoxysterol accumulation plasma fatty acid composition is also affected[7] and an increased ratio between unsaturated and saturated fattyacid species may contribute to lower cellular antioxidant defenses
Altogether these findings suggest that lipid oxidation biomarkerscan provide a reliable measure of systemic and lung-specific oxidativestress in CF
Markers of protein damage are also detectable in the airways ofchildren with CF and their levels are observed to parallel the extentof neutrophilic markers and lung dysfunction [143166] Bronchoal-veolar lavage proteins undergo halogenation of Tyr residues aradical-mediated process presumably depending on MPO enzyme ac-tivity and assessed through the analysis of 3-chlorotyrosine and 3-bromotyrosine Thiocyanate and protein carbonyls are also useful bio-markers to assess the inflammation-related injury of BALF proteins inCF [1431]
3 Antioxidants in CF
31 Glutathione and its related defense system
311 Defects in GSH homeostasisOther studies have pointed to alterations in the levels of extracel-
lular antioxidants in respiratory tract lining fluids [3] In particularthe analyses of broncheoalveolar lavages (BAL) have revealed thepresence of decreased levels of GSH in the alveolar epithelial liningfluid of CF patients The normal level of extracellular GSH in thelung is 140 times that present in blood plasma and the lung is a netimporter of circulating GSH [77] As a result GSH concentration inELF is close to 400 μM whereas significantly reduced GSH levels arepresent in adult CF patients [41] Low levels of GSH have been ob-served in plasma and blood neutrophils [4178] suggesting systemicGSH dyshomeostasis in CF Moreover some studies have shown thatat the cellular level the CFTR mutation causes mitochondrial deple-tion of GSH [7980] The consequences of this defect are still difficultto be understood due to our poor knowledge about the exact func-tions of GSH in the lung but there are reasons to believe that thedecrease of GSH in the ASL contributes to lung infection and inflam-mation [4281] At the same time it must be underlined that a recentstudy has shown that the GSH content in sputum samples is higher inCF patients than in healthy people indicating that GSH deficiency inCF is restricted to the lower respiratory tract [82] Several hypotheseshave been proposed to explain such a local increase in GSH includingthe possibility that it may derive from apoptotic neutrophils The re-lease of high levels of GSH may be part of a compensatory mechanismaimed at controlling disulfide bonds-mediated aggregation of mucinsSecretions of the upper respiratory tract contain abundant levels ofthese glycosylated and cysteine-rich proteins likely playing a role in
the airway antioxidant defense Indeed these proteins are potent invitro ROS scavenges [83] and their synthesis is upregulated upon ox-idative stress via epidermal growth factor receptor (EGFR) transacti-vation [84]
GSH a major component of cellular antioxidant defenses exerts im-portant functions related to its electron-donating capacity includingprotection from the damaging effects of ROS and regulation of a pletho-ra of cellular events such as gene expression proliferation and differen-tiation apoptosis and immune response [85] GSH is synthesized by twosequential ATP-dependent reactions catalyzed by γ-glutamylcysteinesynthetase (recently renamed glutamate-cysteine ligase) andGSH syn-thetase The reaction catalyzed by γ-glutamylcysteine synthetase iethe formation of γ-glutamylcysteine from glutamate and cysteine isthe rate-limiting step in GSH synthesis and is feedback regulated byGSH itself In fact this enzyme represents an interesting case of redox-regulation of catalytic activity that is mediated by the reversible forma-tion of disulfide bonds [86] Oxidizing conditions causing GSH depletionpromote the formation of a disulfide bondbetween the catalytic and theregulatory subunits of the enzyme leading to a conformational changewhich favors the binding of glutamate In contrast physiological levelsof GSH reduce this disulfide bond thus explaining GSH feedbackinhibition
Either in intracellular or extracellular compartments GSH is pre-dominantly found in the reduced form although small amounts ofthe oxidized disulfide forms (GSSG or GSSR where a GSH moleculeis linked to a free or a protein thiol) can always be detected GSSG isproduced by the catalysis of glutathione peroxidase during thedetoxification from hydrogen peroxide and other peroxides or bythe direct reactions of GSH with electrophilic compounds such asradical species Despite the bulk of GSH synthesis occurring in thecytoplasm GSH is distributed in intracellular organelles includingthe endoplasmic reticulum mitochondria and nucleus Under physio-logical conditions the GSH to GSSG ratio in these compartments ishigh frequently gt1001 but this may change under conditions of ox-idative stress [87] A major exception is represented by the endoplas-mic reticulum where GSSG is present at much higher levels to favordisulfide bond formation [88] Interestingly the compartmentaliza-tion of GSH in separate pools within organelles allows localized alter-ations in the balance between GSH and GSSG that may haveconsiderable functional and pathological significance [89] Thiscould be particularly important in CF in view of the above mentionedstudies showing that cultured CF cells have an apparent normal GSHGSSG content but are characterized by a marked decrease in mito-chondrial GSH in association to elevated mitochondrial ROS [7980]
Different roles of high levels of GSH in the ELF may be hypothe-sized including a) preventing inflammation and tissue damage byscavenging the ROS spontaneously generated in this highly oxidizingenvironment actively produced by neutrophils during inflammationor originating from lipid peroxidation b) regulating the redox statusof membrane proteins involved in the transduction of signals leadingto changes in the expression of genes involved in the immune re-sponse c) controlling mucus viscosity by breaking disulphide bondsd) modulating the response to bacterial infections This last possibili-ty is suggested by the observation that GSH significantly increasesin the ASL of wild type mice following P aeruginosa infection where-as this response is not observed in CFTR mutant mice [90] Interest-ingly some authors have suggested the ability of GSH to control Paeruginosa growth and resistance to antibiotics although these stud-ies should be considered with some cautions due to the likely use ofunbuffered GSH [91]
Although the decreased levels of GSH in ELF could be due to in-creased consumption during inflammation-related oxidative stress[4192] GSH deficiency in CF ELF likely derives from CFTR channeldysfunction In fact comparable alterations in GSH extracellular con-tent characterize the lung of CFTR knockout mice [93] indicating thatthis defect is correlated to mutations in CFTR
695F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
In particular ELF and lung tissue from CFTR knockout (Cftr KOB6129P2-Cftrtm1Unc) and wild-type mice were compared for GSHcontent and the activities of glutathione-related enzymes [93] Inthe ELF the concentration of GSH was significantly decreased in theCftr KO mice compared to WT whereas tissue concentrations ofGSH were similar [92] In the Cftr KO lung the activities of glutathionereductase and glutathione peroxidase were increased whereas theactivity of γ-glutamyltransferase was unchanged Two indicators ofoxidative stress thiobarbituric acid reactive substances (TBARS) and8-hydroxy-2-deoxyguanosine (8-OHdG) were also increased in theCftr KO lung tissue [90] These data support the hypothesis that a mu-tation in the CFTR gene can affect the antioxidant defenses in the lungand may contribute to the exaggerated inflammatory response ob-served in CF Thereby CFTR could be considered as an importantactor of ELF antioxidant homeostasis and thus an intrinsic cause ofoxidative imbalance in CF airways of human patients as well as CftrKO mice
Moreover CFTR belongs to the MRPABC family of proteins whichincludes several GSH transporters and some in vitro studies have in-dicated that CFTR may mediate GSH export across membranes[2394] Despite these evidences there is still debate about the phys-iological implication of CFTR in GSH transport outside the cells asother studies have raised the possibility that CFTR may not actuallyconduct GSH but regulate its transport indirectly through chloridetransport [85]
312 In vitro studies suggesting a protective role of GSH in CF modelsystems
Possible protective roles of extracellular GSH in the CF lung havebeen long proposed and recent in vitro studies have provided furtherand more robust support to this clue For example it has been sug-gested that GSH may control the levels of chlorinated compoundsformed by the activity of myeloperoxidase a neutrophil-releasedprotein abundantly present in CF patients secretions [9596] and pre-vent NK-κB activation [96] Other studies have suggested that CFTRmutant cells produce higher levels of proinflammatory cytokines inresponse to P aeruginosa diffusible material with respect to wildtype cells through a mechanism involving the activation of NADPHoxidase This effect may be significantly reversed by the addition ofextracellular GSH [97]
GSH could also play an important role in protecting the lung epi-thelia from the toxic effects of pyocyanin (PCN) a redox-active exo-toxin released by P aeruginosa which is supposed to cause a varietyof deleterious effects on the airway physiology [98] PCN levels ashigh as 130 μM have been measured in pulmonary secretions of pa-tients with CF and individuals with chronic bronchiectasis [99] Atconcentrations within the range measured in the sputum from CF pa-tients PCN induces a drastic reduction of intracellular GSH [100101]promotes death of cultured cells [100] and causes pathophysiologicalalterations in the lung of wild type mice that are consistent with thechanges observed in CF patients [102] PCN toxicity likely derivesfrom its ability to accept electrons from cellular reductants and thenreact with oxygen to generate superoxide and other ROS [103] There-fore GSH deficiency is explained either by the reaction of GSH withsuch oxidants or through the direct reaction of PCN with GSH thatleads to the formation of a PCN radical [103] However the electrontransfer from GSH to PCN does not occur at neutral pH and recent ob-servations suggest that extracellular GSH provides significant protec-tion against the toxic effects of PCN [104] Moreover GSH can reactwith PCN to form a stable adduct which is likely redox inactive[105] Although the relationships between extracellular GSH andPCN are still contradictory it is worth mentioning that extracellularGSH increases to millimolar levels in the ELF of wild type miceinfected with P aeruginosa indicating that GSH may be useful to re-sist to bacterial colonization [90] Interestingly in vitro studies have
revealed that extracellular GSH inhibits the ability of Burkholderiacenocepacia to enter epithelial respiratory cells and reduces bacterialinduced expression of proinflammatory cytokines (DOrazio Pacelloand Battistoni 2011 unpublished results)
32 GSH-based antioxidant therapies
321 Preclinical studies in animal models of CFMice genetically modified for the Cftr gene along with acute and
chronic infection induced by CF-related pathogens are a key asset inCF research Although much has been learned through these CFmousemodels limitations in the ability of this species to recapitulatespontaneous lung disease and several other organ abnormalitiesseen in CF humans including few airway mucous glands have creat-ed a need for additional species on which to study CF [106] To thisend pig and ferret CF models have been generated and are currentlybeing characterized [107108] These new larger animal models havephenotypes that appear to closely resemble human CF disease seenin newborns and efforts to characterize their adult phenotypes areongoing However mice have been the dominant species by whichto study CF disease processes in vivo and develop therapies for thepast two decades including GSH-based antioxidant treatment
Despite limitations and significant species differences betweenmice and humans these models proved to be useful tools to mimicthe initial and progressive bronchopulmonary infection typical of CFpatients [109] In particular the model of chronic infection whichchallenge bacterial cells with agar as an immobilizing agent hasbeen extensively characterized and induce the long-term persistenceof the bacterial infection and lung pathology including airway inflam-mation [110111] Lung pathology associatedwith chronic experimen-tal infection resembled some aspects of the advanced chronicpulmonary disease at autopsy in CF patients [112ndash114] Both naturallyoccurring and experimental infections frequently manifest broncho-pneumonia bronchiectasis mucus plugging epithelial metaplasiafibrosis and alveolar exudates with inflammatory cells Lymphoidhyperplasia which was prominent in the infected animals was alsoa common finding in the lungs of CF patients In addition significantdifferences with regard to weight loss BAL neutrophil counts andcytokine concentrations have been detected Infected mice had arapid though transient rise in absolute neutrophil counts TNF-α IL-1β IL-6 MIP-2 and KC in bronchoalveolar lavage (BAL) [110115] Inaddition the generation of CF mice has allowed the possibility of invivo testing of novel therapies before entering in clinical trial Theseinclude the pre-clinical evaluation of antibiotics and biotechnologicaldrugs as well as of natural and synthetic anti-inflammatory agentsthat reduce the excessive recruitment of neutrophils and the progres-sive damage of the respiratory tissue by the unbalanced production ofoxidants
Regarding antioxidants GSH and its pro-drug N-acetylcysteine(NAC) remain the so far most investigated antioxidant agents in CFand several strategies have been proposed to improve systemic andlung GSH status of CF patients based on pre-clinical studies includingthe administration of nebulized GSH by inhalation or the oral supple-mentation of GSH or NAC Oral GSH administration can raise serumand lung tissue GSH levels in rodents [116117] In these studiesGSH was administered to animals dissolved in saline or PBS Thepharmacokinetic profile of an oral bolus dose of GSH (300 mgkg)was determined in mice in other studies [118] Plasma ELF BALcells and lung tissue were analyzed for GSH content There was arapid elevation in the GSH levels that peaked at 30 min in the plasmaand 60 min in the lung ELF and BAL cells after oral GSH dosing OralGSH treatment produced a selective increase in the reduced and ac-tive form of GSH in all lung compartments examined Oral GSSG treat-ment (300 mgkg) resulted in a smaller increase of GSH levels Toevaluate the role of CFTR in this process Cftr KO mice and gut-
Table 1Intervention trials on antioxidant therapy in CF patients found at ClinicalTrialsgov databasea
Rank Title PI Location Recruitment Interventions Age groups Phasesnumberenrolled
Study designsb Outcome measures Start andcompletion date
NCT ID
1 Efficacy and safety studyof inhaled GSH in CFpatients
GrieseM
Germany Completed Drugbull reduced GSH sodium salt
C|A|S II138
1 R|E2 Safetyeff3 PA4 DB (Sub Inv)5 Treatment
bull Differences between inhaled GSHand inhaled normal saline withrespect to the area under the curveof FEV1 predicted within the periodfrom baseline to week 24
bull Treatment changes with respect tothe variablesspirometry peak flowquality-of-life weightheightpercentage of neutrophilsothercell types (induced sputum) inducedsputum levels of GSHinflammatorymediators pulmonary exacerbation
Jul-07May-10
00506688
bull 09 saline (control)
2 A phase I study of inhaledsodium pyruvate for thetreatment of CF
BillingsMCE
United States Terminated Drugbull Inhaled sodium pyruvate
A|S I70
1 R|E2 Safetyeff3 PA4 DB5 Treatment
bull Assessment of safety of inhaled sodiumpyruvate in Subs with CF Subs will beevaluated for the presence of symptomsand safety laboratory measurements
bull Determination of improvement inlungs of CF Subs as determined bymeasurement of FEV1 and measurementof inflammatory markers ininduced sputum
Feb-06na
00332215
3 Inhaled GSH versusplacebo in CF
MarsicoS
Italy Recruiting Drugbull Inhaled reduced GSHbull Physiological solution
C|A III150
1 R|E2 Eff3 PA4 SB (Sub)5 Treatment
bull FEV1bull Small airway function exercise capacityBMI dyspnoea cough quality of lifepulmonary exacerbations markers ofoxidative stress (H2O2)in serum and inEBC epithelial inflammatory markerson BNEC
Jun-10Dec-12
01450267
4 Safety and efficacy ofan antioxidant-richmultivitaminsupplement in CF
SagelSD
United States Completed Dietary supplementbull AquADEKs
C|A IIndashII17
1 NR|E2 Safetyeff3 SGA4 OL5 Treatment
bull Plasma levels of β-carotenebull Plasma levels of coenzyme Q-10retinol (Vitamin A) 25-hydroxy vitaminD α- and γ-tocopherols (Vitamin E)PIVKA-II
Aug-07Nov-09
01018303
5 Efficacy and safety ofepigallocatechin gallate(EGCG)tocotrienol in18 patients with splicing-mutation-mediated CF
KeremE
Israel Not yetrecruiting
Dietary supplementbull EGCGbull Tocotrienolbull EGCG+tocotrienol
A|S na18
2 Safetyeff3 CA4 OL5 Treatment
bull Changes in nasal chloride secretion asassessed by TEPD with assessment ofmean changes in TEPD by drug comparedto baseline and the proportion of patientswith a chloride secretion response bydrug compared to baseline
bull Pulmonary function testing FEV1FVC MEF25-75
Sep-09Jun-11
00889434
6 The effect of inhaledNAC compared tonormal saline onsputum rheology andlung function
VanDaele S
Belgium Terminated Drugbull Acetyl-Cysbull Normal saline
C|A IV19
1 NR|E2 Eff3 CA4 OL5 Treatment
bull Changes in visco-elasticity andlung function
Jan-10Dec-10
00996424
696FG
allietal
Biochimica
etBiophysica
Acta
1822(2012)
690ndash713
7 Safety of orallyadministeredcurcuminoids in adultsubjects with CF
Goss C United States Completed Drugbull Standardized turmericroot extract
A I11
1 NR|E2 Safetyeff3 SGA4 OL5 Treatment
bull Safety and tolerability of 14 days oftreatment with orally administeredcurcuminoids as assessed by adverseevents laboratory parameters andspirometry
bull Pharmacokinetics of repeated dosesof orally administered curcuminoidschange in NPD measurementschange in sweat chloride measurements
Apr-05Jan-06
00219882
8 Nasal potential studiesutilizing CF transmembraneregulator (CFTR) modulators
Rowe S United States Recruiting Other quercetin C|A II46
2 Eff3 SGA4 OL5 BS
bull NPD(NPD) Biomarkerbull Residual CFTR activity
Mar-10Nov-11
01348204
9 Safety and tolerability ofinhaled nitric oxide inpatients with CF
Sagel S United States Completed Drugbull Nitric oxide for inhalationbull Nitrogen
C|A|S IIndashII18
1 R|E2 Saf3 PA4 DB (Sub Care Inv OA)5 Treatment
bull Safety and tolerability of drugassessed by change in methemoglobinlevels oxygensaturation FEV1
bull Assess the difference in sputumbacterial density before and afterNO inhalation and the differencein lower airway inflammatorymeasures before and after NO inhalation
Jul-04Dec-08
00570349
10 NAC Phase IIB a multi-center phase IIBrandomized placebo-controlled DB study ofthe effects of NAC onredox changes and lunginflammation in CF patients
ConradC
United States Completed Drugbull NAC
C|A|S II80
1 R|E2 Eff3 SGA4 DB (Sub Care Inv OA)5 Treatment
bull Change in the logarithm of the levelof human neutrophil elastase(HNE) activity measured in sputum
bull Change in concentration of IL-8measured in sputum and plasmaconcentration of GSH measured inwhole blood the neutrophil countmeasured in sputum
Nov-08Feb-11
00809094
11 Glutamine supplementationin CF
na United States Not yetrecruiting
Dietary supplementbull Glutaminebull L-alanine
A|S II40
1 R3 PA4 DB (Sub Care Inv OA)5 Prev
bull Percent increase in plasma glutamineand GSH redox levels measured atweeks 0 4 8 and 12
Feb-10Feb-11
01051999
12 Effect of sulforaphane inbroccoli sprouts onNrf2 activation
ChmielJF
United States Active notrecruiting
Dietary supplementbull Broccoli sprouts
A na15
3 SGA4 OL5 BS
bull Nrf2 activation in NECbull Measures of lipid peroxidation in NECGSH from blood lymphocytesoxidative stress in urineneutrophil migration into thegingival crevices
Apr-11Sep-11
01315665
AbbreviationsA=adult BC=breath condensate BNEC=brushed nasal epithelial cells BS=basic science C=child CA=crossover assignment Care=caregiver CF=cystic fibrosis DB=double blind EBC=exhaled breath condensate Eff=efficacystudy FEV1=forced expiratory volume in 1 s FVC=forced vital capacity GSH=glutathione Inv=investigator MEF25ndash75=maximal expiratory flow 25ndash75 na=not available NAC=N-acetylcysteine NEC=nasal epithelial cellsNLF=nasal lavage fluid NPD=nasal potential difference NR|E=non-randomized|endpoint OA=outcomes assessor OL=open label PA=parallel assignment PI=principal investigator Prev=prevention R|E=randomized|endpoint S=senior Saf=safety study SB=single blind SGA=single group assignment Sub=subject
a Search was done matching the terms ldquoantioxidant therapyrdquo or ldquoGlutathionerdquo with ldquoCystic Fibrosisrdquob 1 Allocation 2 Classification 3 Intervention model 4 Masking 5 Primary purpose
697FG
allietal
Biochimica
etBiophysica
Acta
1822(2012)
690ndash713
698 F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
corrected Cftr KO-transgenic mice were given an oral bolus dose ofGSH (300 mgkg) and compared with WT mice for changes in GSHlevels in plasma lung ELF and BAL cells There was a twofold in-crease in plasma a twofold increase in lung a fivefold increase inELF and a threefold increase in BAL cell GSH levels at 60 min in WTmice however GSH levels only increased by 40 in the plasma 60in the lung 50 in the ELF and twofold in the BAL cells within thegut-corrected Cftr KO-Tg mice No change in GSH levels was observedin the uncorrected Cftr KO mice These studies suggest that oral GSHadministration can increase plasma and lung compartment GSHlevels in WT mice and to a lesser extent in gut-corrected Cftr KO-Tganimals It also suggests that oral GSH treatment can boost BAL cellGSH levels However since this study failed to show significant in-creases in serum and lung compartment GSH levels in uncorrectedCftr KO mice it is questionable whether oral GSH administration toCF patients with intestinal malabsorption would benefit from thistherapy It was also shown that GSH is rapidly distributed to theserum and lung compartments Kariya et al [118] speculate thatother transporter(s) besides CFTR are responsible of the transport ofGSH and probably of other dietary molecules to the lung whichmay be responsible for dietary deficiencies observed in various lungdiseases
Another strategy is represented by the oral supplementation ofhigh doses of NAC a well known cysteine donor for the synthesis ofglutathione NAC is considered a safe molecule which has beenused successfully to treat GSH deficiency in a wide range of diseases[119] As CF mice display defects in GSH export in the ELF comparableto those of patients they could provide a useful tool to assess the ef-fects of NAC administration on the GSH status However only limitedstudies exploring the effects of NAC on CF animal models have beenso far carried out The effects of NAC have been tested on mucus accu-mulation bacterial load transit and inflammation in the CF mousesmall intestine showing that NAC may reduce intestinal mucus accu-mulation bacterial overgrowth in the gut [120]
Moreover NAC has been reported to restore the accumulationof unwantedmisfolded proteins in aggregates that are associated withthe CF airway phenotype as a cause of lung inflammation [121] Themechanism of this NAC-derived effect seems to involve the restorationof beclin 1 expression and activity in the autophagy pathway of theendoplasmic reticulum that was investigated in vivo using Scnn1b-transgenic and Cftr(F508del) homozygous mice The restoration ofthis pathway also produced a rescued trafficking of CFTR (F508del) tothe cell surface of CF cells obtained from human CF nasal biopsies
Given the defective GSH metabolism of CF reviewed in the previ-ous sections and in [122] and the reduced response to GSH therapyin CF mice [93] some Authors have investigated the influence of bac-terial infections on lung oxidative stress The effects of P aeruginosainfection on ELF and lung tissue antioxidants and the oxidation ofDNA and lipids were investigated in mice challenged with bacterialcells [90] CFTR-KO (B6129P2-Cftrtm1Unc) and WT mice were chal-lenged intratracheally with a clinical isolate of mucoid P aeruginosaembedded in agar beads and on the third day of infection BALF andlung tissue were obtained and analyzed for cytokines antioxidantsand enzyme activities [90] P aeruginosa lung infection increasedlevels of inflammatory cytokines and neutrophils in the ELF This cor-responded with a marked increase in GSH and in urate levels in theELF of P aeruginosa-infected WT mice A twofold increase in uratelevels was also observed among lung tissue antioxidants of Paeruginosa-infected WT mice There were no changes in markers oflung oxidative stress associated with the P aeruginosa lung infectionIn contrast to WT mice the CFTR-KO mice lacked a significant in-crease in ELF GSH when challenged with P aeruginosa and this corre-lated with a decrease in the ratio of reduced to oxidized GSH in theELF a marker of oxidative stress These data would suggest that thelung adapts to infectious agents with elevated ELF GSH and urateTherefore individuals with lung diseases associated with altered
antioxidant transport such as CF might lack the ability to adapt tothe infection which may lead to a more severe inflammatoryresponse
322 Clinical trials on GSHThe discovery of the defect in GSH export has suggested that ther-
apies able to restore or increase GSH levels in the ASL could counteractthe inflammation and oxidative stress conditions typical of CF pa-tients In an attempt to strengthen extracellular defenses againstROS some pilot studies have analyzed the effect of GSH inhalation orthat of oral GSH prodrug N-acetylcysteine (NAC) All these treatmentswere well tolerated by the CF patients and most authors were able tomeasure increased ELF concentrations of GSH in association withsome positive clinical outcomes [4041737896122ndash128] Althoughpotentially promising these findings need stronger clinical evidencein that the majority of these were obtained on very limited numberof patients investigated in non-randomized controlled trials This ishighlighted in a recently published meta-analysis [129] that providesalso a thoroughly analysis of the literature on this aspect of the antiox-idant and anti-inflammatory therapy of CF Among the American CFfoundation sponsored trials two phase II trials on inhaled GSH andoral NAC are in progress in US and Germany (ClinicalTrialsgov Iden-tifier NCT00506688 and NCT00809094 respectively Table 1) andsafety and tolerability of aerosolized glutathione is also matter ofinvestigation by another (not registered) US trial (more informationon this can be found in [130]) Nevertheless the diffusion among CFpatients of NAC preparations for inhalation (Mucomystreg) has in-creased in recent years
γ-Glutamylcysteine ethyl ester (GCEE) is another potentially inter-esting GSH pro-drug which has proved some efficacy in the ameliora-tion of oxidative stress eg in experimental myocardial infarction[131] and central nervous system conditions (see eg [132]) HoweverGCEE has not been investigated in CF yet
33 Limits and potential problems associated to thiol-based therapies
Although the above cited clinical trials may be considered promis-ing attempts to improve the antioxidant levels in the ELF the actualcapacity of these treatments to produce positive clinical effects mustbe considered with caution For example indices of oxidative damagewere found to be unaffected by aerosolized GSH treatment [122]Some in vitro studies have suggested that the reaction of GSH withPCN could produce hydrogen peroxide with potential exacerbationof oxidative damage [101] The exact mechanisms of PCN toxicityand the reaction of this toxin with GSH must be better understoodin order to evaluate the safety of GSH administration to patients col-onized by P aeruginosa
Inhalation of GSH ensures its direct delivery in the airways butsince GSH can rapidly convert to its oxidized form GSSG frequentGSH inhalations are required to maintain a high GSHGSSG As a con-sequence of this limit four separate inhalations have been used inthe study carried out by Bishop et al [123] Unless justified by clearclinical improvements these repeated treatments may represent aburden for patients already undergoing complex therapies Moreoverrepeated inhalations of GSH increase the levels of GSSG in ELF[133134] In the absence of effective homeostatic mechanisms ensur-ing the fast recycling of GSSG to GSH this might produce unwantedeffects and even the exacerbation of CF symptoms being GSSG re-sponsible of the S-glutathiolation and functional inhibition of CFTR[124]
In principle the oral administration of GSH could be considered asafe strategy to prevent GSSG accumulation but this strategy is likelynot feasible due to the substantial inability of this water-soluble mol-ecule to cross biological membranes Moreover a study carried out inmice has established that GSH absorption in the gastrointestinal tractif any is mediated by CFTR itself thus excluding the possibility to
699F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
improve circulating levels of GSH in CF patients through the dietarysupplementation of the antioxidant [127] The limited absorption ofGSH could be overcome by GSH-esters as in vitro studies haveshown that this form of GSH may be specifically useful to rescue mi-tochondrial defects in cystic fibrosis models [80] Safety of these GSHderivatives in humans has been poorly investigated
Two independent studies have shown that the treatment of CF pa-tients with high doses of NAC increases extracellular GSH in sputum[78125] but contrasting results have been reported concerning theeffects of NAC on the concentrations of blood GSH and on the levelsof IL-8 and other markers of inflammation NAC treatments may beuseful to modulate the GSH content in cells but it should be remindedthat an enhanced cysteine supply cannot lead to an increase of GSHabove physiological levels due to the feedback inhibition mechanismof γ-glutamylcysteine synthetase described in the Section 311
331 Gamma-glutamyltransferase and GSH therapySo far none of the studies mentioned above has taken into account
the fact that GSH is degraded by GGT enzyme activity GGT concentra-tions are known to increase several fold in ELF of CF patients even ifthe mechanisms for this effect were not determined [135] and thisphenomenon parallels the above described decrease of GSH levels inELF Preliminary data suggest that a major source of increased ELFGGT is represented by activated neutrophils accumulating in diseasedairways (Corti and Pompella 2011 unpublished observation) Re-gardless of its origin it is likely that increased GGT in ELF would de-grade locally administered GSH to variable extents which couldcontribute to the so far inconclusive results of therapies based onaerosolized GSH Besides its role in GSH catabolism GGT has beenshown to mediate protein S-thiolation [136] suggesting that GSH ad-ministration in the presence of active GGT enzyme might alter CFTRglutathiolation status and function in a potentially unfavorable wayOn the other hand a potential role of GGT in favoring bronchial up-take of antioxidant vitamin C has also been suggested [137]
These controversial findings may add further issues to the ques-tion of whether the therapy of lung oxidative stress by aerosolizedGSH could be safe in all the CF patients regardless of specific strate-gies that would ascertain the extent of lung inflammation Thesestrategies should include the assay of GGT levels in ELF In principleonce an adverse role of ELF GGT in GSH therapies will be confirmedthe association of GGT inhibitors in the GSH formulations for inhala-tion could represent a promising pharmacological strategy
34 Malnutrition as a possible cause of defective thiol-dependentantioxidant protection
Successful nutritional interventions strongly impact on the clinicaloutcome of CF patients [138ndash140] Malnutrition by pancreatic insuffi-ciency and other CF-related factors influence the susceptibility to de-velop recurrent infections and severe inflammatory lesions of thelung tissue If the onset of a defective (sub-optimal) antioxidant sta-tus may represent an underlying component in the clinical effects ofmalnutrition remains a matter of investigation Clinicians have topay particular care to avoid these disturbances and successful proto-cols of nutritional intervention in CF have been developed whichare essentially aimed to avoid the onset of protein-energy malnutri-tion (PEM) [141] Despite this the risk of developing such an unto-ward complication in CF infants and children remains high assuggested by the prevalence data registered in some areas Actuallya prevalence of PEM between 5 and 14 in Moldavian infants was re-cently reported [142] and PEM is associated with poor outcome andparticularly with the risk of developing edema and anemia
Besides lowered intake and absorption of micronutrient antioxi-dants discussed in the other sections malabsorption of dietary proteinand excess fecal amino acid losses result in hypoproteinemiahypoalbu-minemia as key biochemical signs of PEM Hypoalbuminemia is
considered to be linked with a causendasheffect relationship with oxidativestress and is proposed to influence morbidity and mortality in condi-tions associated with chronic inflammation and severe oxidative stress[143144] The human serum albumin (HAS) molecule contains only areactive thiol group eg the Cys 34 the importance of which as an anti-oxidant defense system in blood and for the entire organism is welldocumented [145] This is the second main thiol (and the main proteinthiol) in the circulation (approx 2 mmol in the adult organism assum-ing 5 l of total blood volume anHt of 40 and [HAS] of 45 gl of plasma)being the RBCGSH thefirst thiol in blood (near to 5 mmol assuming thesame parameters of above and an average concentration of GSH inpacked RBC of 25 mM) [146147] The antioxidant role of HSA is notonly a consequence of the relative abundance of its Cys thiol A specificcapability of acting as a sacrificial target for a series of electrophils andmost biologically relevant ROS ie hydrogen peroxide and peroxyni-trite has been demonstrated in a series of studies [145148149] Li-gand binding activity can contribute to promote antioxidant effectsby the HSA molecule [145] Transitions metals particularly copperand also iron in the case of iron-overload diseases bind to HSA Inthis way these are less available to promote the Fenton chemistryand hydroxyl radicals eventually released from this oxidative reactionare mostly directed to the HAS protein sparing more important tar-gets A free radical-trapping activity of HSA has been also demonstratedand this was proposed to be directed toward both hydrophilic and fat-soluble species This activity may result from the interaction withother antioxidants such as α-tocopherol [150] and may influence theantioxidant activity of food-derived phenolic antioxidants [151]
However Cys 34 is considered the main contributor to the antiox-idant function of HAS which plays its role in the antioxidant homeo-stasis of blood thanks to a complex series of interactions with themetabolism and antioxidant function of the pool of free thiols in plas-ma and in the circulating RBC with the latter playing a significantcontribution to the extracellular pool of GSH [146] and to the dynam-ics of inter-organ GSHmetabolism in cooperation with liver and othertissues [147] Immuno-inflammatory cells and the lung tissue areamong the main terminals of this metabolism The RBC contain theentire machinery to synthesize GSH to restore its redox (by enzymat-ic reduction of the oxidized form) and to use this as cofactor of Se-GPx and GSH-S-transferase enzymatic activities that are responsibleof the detoxification of hydroperoxides and alkylating agents thatmay form in or enter the RBC cytosol [147] In this sense the RBC rep-resents a circulating reservoir of GSH that in addition to maintainingthe redox and respiratory function of Hb participates to systemic pro-tection of xenobiotics of endogenous and exogenous origin In consid-eration of these aspects the combination of hypoalbuminemia andanemia may exponentially increase the risk of developing oxidativestress in CF patients as it is supposed to occur in other oxidative stressconditions such as chronic kidney disease [55143152] Additionalclinical investigation should verify the hypothesis that hypoalbumi-nemia together with a defective uptake and metabolism of sulfur-containing amino acids and CF-specific defects of the GSH metabo-lism may represent a causal risk factor for an impaired antioxidantdefense and systemic oxidative stress in CF patients
35 Fat-soluble antioxidants
Pancreatic insufficiency and a diminished bile acid pool cause mal-absorption of important essential nutrients and other dietary compo-nents in CF Of particular significance is the malabsorption of fat-soluble antioxidants such as tocopherols carotenoids and coenzymeQ-10 (Co-Q10) and that of essential fatty acids (EFA)
351 Vitamin EVitamin E therapy in CF has been proposed in several decades of
research as a useful approach to overcome both the lower absorptionof this fat-soluble micronutrient and the increased antioxidant
700 F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
demand by the abnormal generation of ROS in CF tissues (see for in-stance the recommendations by the Cystic Fibrosis Foundation Con-sensus Conference on nutrition [153])
The first report of a vitamin E deficiency in CF appeared in literaturein 1951 by Filer et al [154] In this study the absorption of the mainform of this vitamin eg α-tocopherol and its ester derivatives was in-vestigated in several subsets of infants and children Thanks to a simplebioavailability (or tolerance) test these authors observed that ldquoin-fantshellip diagnosed as fibrocystic disease of the pancreas diarrhea andcirrhosis were characterized by a poor response to the test ie the tol-erance curve was lowrdquo However abnormalities were also observed inother subgroups of infants with a variety of disorders not associatedwith fat or fat-soluble vitamin intolerance such as sprue celiac syn-drome and lupus erythematosus which suggests the general observa-tion that malnutrition and inflammatory and degenerative diseases ofthe GI tract may lead to absorb tocopherols poorly At the same timethese authors reported that ldquoMetabolic disorders with associated hy-percholesterolemia were observed to give abnormally high values forthe area under the curverdquo and that patients responding poorly to to-copherol absorption test did also in vitamin A absorption tests
The finding of lowered (lipid uncorrected) levels of vitamin E wasconfirmed in other studies in which this relative deficiency was foundto occur irrespective of pancreatic comorbidity and in associationwith lowered levels of other liposoluble vitamins such as vitamin Aand D [155] regardless of their different liver metabolism and tissuedelivery mechanisms [156157]
Plasma buccal mucosal cells (BMCs) and breath condensate α-tocopherol decreased significantly with age in association with a de-creased respiratory function [5] This was accompanied by loweredlevels of other antioxidants such as vitamin C and increased oxidativestress markers of different origin such as protein carbonyls thiobarbi-turic acid-reactive substances and F2-IsoPs
Clinical symptoms of vitamin E deficiency in CF have not beenconclusively investigated Dolan et al [158] described that anemiaof CF patients is related to vitamin E deficiency and increasedperoxide-induced hemolysis of RBC Other authors however ob-served an increased susceptibility to peroxide-induced hemolysisalso in the presence of normal levels of vitamin E [159] Peters andKelly [160] observed that RBC vitamin E concentrations were belowthe normal range in almost all unsupplemented patients and roseinto the normal range with a 1-year supplement of 100 mg per daybut not 15 mg per day Since RBC vitamin E concentration has beenshown to correlate well with tissue concentrations of the vitamin inanimals tissue levels of vitamin E are expected to be lower than nor-mal in CF patients
Bioavailability of fat-soluble vitamin is limited in CF Vitamin Edeficiency of CF is also associated with hypocholesterolemia [7] Asa consequence the relative deficiency of this vitamin is compensatedwhen the absolute levels are normalized for cholesterol levels andthis suggests a poor transferring of this vitamin in the circulation bya defective lipid and lipoprotein metabolism Pancreatic insufficiencyand the consequent lipid malnutrition cannot completely explain thisdefect and other possibly CF-specific dysfunctions could play a roleLiver metabolism and specific plasma transport systems of this vita-min need further elucidation in CF
As a consequence of these aspects it is not presently clear whichform and level of supplementation of this vitamin is most appropriateto treat these patients Usingα-tocopherol as a vitamin E supplementPeters et al [160] reported that 100 mg per day are required to nor-malize RBC concentrations Other authors described unsuccessfulsupplementation protocols with higher doses and this has led to de-velop formulations with higher bioavailability in order to achieve bet-ter compliance to oral supplementation (see below and the literaturereviewed in [161ndash163])
Besides absorption and tissue delivery issues specificity of actionis another critical item of antioxidant therapy with fat-soluble agents
in CF As further addressed below this aspect could be themain limit toa successful use of natural forms of vitamin E in the clinical manage-ment of CF inflammation even if a local lung-targeted therapy wouldbe developed according with so far proposed pre-clinical models ofaerosolized vitamin E [164165]
Current pharmacological research is aimed to develop synthetic formsof this and other fat-soluble antioxidants with better radical scavengingproperties at the lipidndashwater interface Type of ROS target and the sitesof action greatly influence the chances of a fat-soluble antioxidant of alle-viating oxidative stress in the airways as well as in other organs such asliver and pancreas These aspects dealing with specificity of action[163166167] have stimulated the search of novel vitamin E-derived an-tioxidants that may help to scavenge radicals at the lipidndashwater interfaceof the epithelial cell membrane and surfactant Amine derivativesof tocopherols and tocotrienols have been recently demonstrated toshow higher antioxidant and free radical scavenging activity than α-tocopherol [168] Further in vitro pharmacological analysis has includedtoxicity evaluations and the detailed investigation of scavenging of azo-and phenolic radicals with different degrees of hydrophobicity and theinhibitory activity on IL-8 gene expression and phospholipase activityin CF cells Comparative evaluation with other synthetic derivativessuch asα-tocopheryl succinate and natural forms of vitamin E suggestedthat these amine derivatives are promising antioxidant and anti-inflammatory agents [Galli F and Pilolli F unpublished observation]deserving further pre-clinical investigation in CF model systems
Anti-inflammatory effects of natural and synthetic analogues of vi-tamin E are also an intriguing pharmacological opportunity currentlyunder investigation by several laboratories [169170]
Recently vitamin E supplementation has been at the center of adispute regarding its safety when used at high dosages in certainpopulations of patients An extensive and speculative debate originat-ed on this subject after a meta-analysis study byMiller et al [171] thatexamined the largest secondary prevention trials on vitamin E trials incardiovascular patients finding a significantly increased mortality riskfor all the causes (about 4 1ndash8 in the 95 interval of confidence)when the patients were treated with doses gt400 IUdie (that areequivalent to 400 mgdie of the synthetic form allrac-α-tocopheroland to 185 mgdie of the natural form RRR-α-tocopherol) This debateresulted in a careful examination of this meta-analysis study by severalother authors and in further revisions of the literature on vitamin E tox-icity in humans [see the literature recently reviewed in [163172ndash174]]that clearly demonstrated the poor consistency of the conclusionsraisedwithMillersmeta-analysis study and the paucity of the concernsthat derived from that These conclusions have been verified in the re-cent international symposium on vitamin E of the Society for Free Rad-ical Research Europe branch of Rome 2009 [173175] Vitamin E used assupplement for humans in all its forms (eg α-tocopherol and othertocopherols and tocotrienols) is safe in abroad range of intakes[172176] The tolerable upper intake level (UL) and the AcceptableDaily Intake (ADI) established by the Joint FAOWHOExpert Committeeon Food Additives for the natural form of vitamin E as α-tocopherolequivalents are of 300 mgdie and 015ndash20 mgkg body weightdierespectively [172177]
352 CarotenoidsLevels of plasma carotenoids such as β-carotene β-cryptoxanthin
and total lycopene are significantly lowered in CF patients and thiswas associated with higher susceptibility to lipid peroxidation[5178ndash180] Rust et al [178] demonstrated that the long-term oralsupplementation with 50 mg β-caroteneday (ie 1 mg β-carotenekg BWday) restored the levels of this carotenoid while sub-optimalsupplementation was observed at doses of 10 mg β-caroteneday orlower thus confirming the need of high doses of this fat-soluble factorto overcome the limited absorption and thus to achieve plasma con-centrations of healthy control subjects Successful high-dose treat-ments appear to lower oxidative stress markers such as TBA-MDA
701F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
complexes and to correct total antioxidant capacity of plasma Inanother study β-carotene supplementation was observed to de-creased lipid peroxide formation as quantitated by malondialdehydeconcentrations in plasma (TBAHPLC method) and to enhance the re-sistance to copper(II) ion-induced oxidation of low density lipopro-teins [180]
At the same time toxicity issues have been raised for human sup-plementation with carotenoid formulations and particularly of water-miscible formulations of preformed vitamin A that is regularly sup-plemented to CF patients which may increase serum retinol andpossible risk of CF-associated liver and bone complications (reviewedin [161181]) However β-carotene supplementation seems to be safesince this does not affect plasma concentrations of other carotenoidsand retinol as well as of other fat-soluble vitamins as α- and γ-tocopherol [178] Recent studies designed to test the clinical efficacyof a CF tailored multivitamin formulation (commercial name AquA-DEKsreg) also tested the safety of this type of formulation and demon-strated that this does not increase vitamin A above the normal levelsobserved in healthy controls [162182183] The normalization of β-carotene levels obtained in these studies was associated only withminor improvements on respiratory and growth parameters whilethe levels of urinary F2-IsoPs used as index of lipid peroxidationwere not affected [162] The surrogate marker of lipid peroxidationMDA was affected together with some selected antioxidant parame-ters (RBC thiols and superoxide dismutase) in another study inwhich this multivitamin formulation was preliminarily evaluated incomparison with standard formulations of vitamin E and A [182]
353 Coenzyme Q-10Coenzyme Q-10 (Q10) is a well-known electron transporter in the
mitochondrial respiratory chain with fundamental role in cellularbioenergetics and scavenging of radical species [184] This lipophilicsubstance is present in the circulation at low levels (serum concentra-tionsle2 μM) mainly as ubiquinol-10 eg the reduced form with anapproximate ratio of 955 with the oxidized form ubiquinone-10[185186] A mechanism for a preferential distribution and accumula-tion in mitochondria has been suggested for both the reduced and ox-idized forms of CoQ10 that are taken up by the cells in a time- andconcentration-dependent Subcellular localization and trafficking ofexogenous Q10 are similar to those of the endogenous form butwere different from that of α-tocopherol that is related with lipidcomposition particularly in the mitochondrial and microsomal frac-tions [184] Ubiquinol-10 readily oxidizes ex vivo by the reactionwith other lipophilic antioxidants such as α-tocopherol and butylatedhydroxytoluene [185] Therefore a higher reduction potential thanother physiological fat-soluble antioxidants such as vitamin E and aselective metabolism and cellular trafficking show peculiar role forthe cell CoQ which may also represent an important lipophilic antiox-idant in cells and body fluids
Human cells synthesize this coenzyme through the cholesterol bio-synthesis pathway so thatmore than two thirds of the tissue levels ap-pear to have an endogenous origin dietary sources provide acontribution to Co-Q10 levels of blood and all solid tissues that variesdepending on the dose applied and type of dietary source [187] How-ever in the case of oral supplements it has to be considered that hy-drophobicity and large molecular weight of this coenzyme influenceits absorption that ultimately is slow and limited [186187] Likewiseto vitamin E pharmacokinetics [188189] Co-Q10 showed T(max) ofaround 6 h that coincides with that of dietary lipids Elimination isclose to that of the more retained form of vitamin E in human bodyeg α-tocopherol with a half-life of about 33 h which suggests poorhepatic metabolism However commercially available formulationsare reported to be safe even at high doses and solubilized formulationsshow enhanced bioavailability In healthy subjects plasma Q10 re-sponse to oral ingestion show saturation profiles with a plateau at a
dose of 2400 mg and the higher plasma concentrations were foundto facilitate uptake by peripheral tissues and also the brain [186187]
Laguna et al [190] recently investigated total serum levels ofcoenzyme Q-10 in a wide population of CF children (n=381) and esti-mated their association with clinical outcome Near to 50 of these CFpatients were deficient of Co-Q10 and this defect was significantlymore prevalent in patients with pancreatic insufficiency and signifi-cantly associated with P aeruginosa colonization in infants (under24 months of age) Importantly low Co-Q10 levels correlated to otherlipid markers of a poor nutritional status such as total lipids and alsothe other fat-soluble antioxidants β-carotene and α-tocopherolwhich confirms the presence of a common defect in the absorptionand metabolic pathways of this coenzyme with dietary lipids
The deficit of Co-Q10 may contribute to the impaired energy func-tion of mitochondria of CF tissues and this may exacerbate CF-linkedinflammation infection and cellular stress response of the lung A sys-tematic analysis of molecular lesions in CF bronchial tissue has beenrecently carried out by proteomic approach [191] Comparative eval-uation of protein expressional pattern in CF and healthy controltissues has revealed aberrant levels of some mitochondrial andenergy-related proteins in CF specimens that included the ubiqui-nolndashcytochrome c reductase complex core protein I and one form ofnidogen a pseudogene of aconitase 2 These changes in CF may reflectmolecular changes which could be associated with an altered mito-chondrial homeostasis and Co-Q10 redox
Multivitamin supplements with high bioavailability containingCo-Q10 have demonstrated to correct the deficit of this antioxidantand were preliminarily observed to improve airway inflammationmarkers in CF patients [183] However further clinical investigationfailed to demonstrate that such an improved biochemical profile isassociated with significant improvements in weight percentile andpulmonary function [162]
354 Fatty acidsA key pathophysiological role in sustaining inflammation in CF has
been attributed to the abnormal polyunsaturated fatty acid (FA) pat-tern Abnormalities in FA profiling are potentially linked to CFTRmutation-driven alterations in the absorption andor metabolism ofdietary lipids [192193] and to the consumption of high oxidizableFA involved in the free radical-mediated lipid peroxidation [7]Among those alterations dysregulation of the docosahexaenoic acidand arachidonic acid balance has been extensively studied with re-portedly significant reduction of DHA in CF and a parallel increasein the levels of AA and inflammatory indices [193ndash195] Actually AAis the progenitor of both enzymatic- and free radical-derived inflam-matory mediators including leukotrienes prostaglandins and iso-prostanes On the other hand n-3 PUFA (eicosapentaenoic acid anddocosahexaenoic acid) are involved in the generation of potent medi-ators namely resolvins and protectins which are able to resolveexudates and to act as organ protective and antifibrotic Secondarilyto their anti-inflammatory action n-3 FA may also produce anantioxidant-like response (eg a reduced demand of antioxidants toachieve an optimal control of oxidative pathways) As a consequencen-3 PUFA have been suggested and widely used as supplements in CFpatients usually under the form of fish oil [196ndash198] It is worth ofnote however that defective levels of DHA in CF patients was notconfirmed in recent studies [7] It was also shown that patients onDHA supplements did not have increased plasma n-3 FA concentra-tions but showed more severe oxidative stress compared to theunsupplemented patients [7] This observation of an increased riskof oxidative stress in CF subjects receiving n-3 fatty acids supple-ments has also been described by other authors [199]
Studies reporting increased AA levels in CF patients have beencontradicted by others [7200201] thus contributing to weakeningthe pathophysiological role of the altered DHAndashAA balance as turnpoint of an upregulated inflammatory status in CF In this context a
702 F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
recent Cochrane meta-analysis on n-3 supplementation in CF patients[202] highlighted the lack of evidence for a significant correction ofthe assessed clinical end points (mainly respiratory symptoms)even when inflammatory indices and other laboratory end pointswere met Taken together these data suggest that there is insufficientevidence to draw firm conclusions or recommend routine use of n-3supplements in CF Notwithstanding it is common belief that n-3supplements provide some benefits for people with CF with relativelyfew adverse effects and thus their use is not discouraged
Further alterations in fatty acid metabolism have been highlight-ed including the consistent findings of an increase in circulatinglevels of saturated and monounsaturated fatty acids [7203204]Decreased levels of essential FA (EFA) ie the FA that have to be in-troduced with the diet correlates with the severity of respiratoryinsufficiency and the same clinical correlation was observed with al-tered proportions of FA species converted by the activity of desatur-ase enzymes (reviewed in [204]) The close relationship betweencertain fatty acids and oxidative stress including the negative correla-tion of C240 and linoleic acid with oxysterol levels point to the needof intensive investigation in CF patients of previously neglected lipidspecies that are emerging candidates in the control of metabolismQuantitative lipidomic analyses have lead to identify C161n7 palmi-toleate as a ldquoprotectiverdquo adipose-derived lipid hormone that stronglystimulates insulin activity in muscle and liver also suppressing in-flammatory cytokine output from mice fat cells [205] Specific meta-bolic activities have been also demonstrated by medium chainsaturated fatty acids caprylic acid (C80) capric acid (C100) and lau-ric acid (C120) Capric acid acts as a direct ligand of PPARγ using abinding pocket different from the binding pocket of thiazolidinedioneor long chain fatty acids [206] Additional activities of medium chainfatty acids which are ligands of free fatty acids receptors detectedin the immune cells the gastrointestinal tract and adipocytes maycontribute to metabolic homeostasis and inflammatory responses[207] These data underscore the importance of a lipid-mediated ldquoen-docrine networkrdquo demonstrating how specific alteration of one orfew serum lipids would be per se sufficient to influence metabolic ho-meostasis Given the relevance of this emerging information and thealteration of lipid metabolism and inflammatory status in CF fattyacid lipidomics need to be deeply investigated in CF
Again these studies have obvious nutritional implications Satu-rated fatty acids with chain lengths higher than C18 are poorlyabsorbed partly because they form insoluble calcium salts [208]Medium chain saturated fatty acids are well known for being highlyabsorbed through the intestine providing rapid delivery of energyvia oxidation of the more hydrophilic short chains and have beensuggested to provide proper nourishment in patients with CF [209]Recent studies have shown that consumption of a high-fat diet richin medium chain fatty acids as opposed to long chain fatty acidsdoes not lead to ectopic fat accumulation in skeletal muscle andliver of both rats and mice [210] In light of the close association be-tween nutritional status inflammation and life expectancy in CF pa-tients the manipulation of dietary lipids in these patients must befurther explored as a possible strategy to provide adequate nutritionand better management of oxidative stress
36 Hydrosoluble antioxidants oligoelements and enzymatic antioxidants
361 Vitamin CVitamin C status in CF patients has been poorly investigated Early
studies suggested a defective vitamin C status that was refractory tooral supplementation [211] Other and more recent studies showednormal or slightly decreased levels of vitamin C in CF patients as com-pared to healthy controls but age- and disease-related decline of thiswater-soluble antioxidant was reported in these patients [5212]In the study of Winklhofer-Roob et al [212] on mid-European CFpatients vitamin C concentrations decreased with age with an
estimated rate of 5 μmollyr and vitamin C concentrationsb40 μ-moll were associated with highest indexes of inflammation whichis consistent with the hypothesis that optimal levels of vitamin Cmay influence immuno-inflammatory activity of alveolar macro-phages and neutrophils Other few studies have examined the effectof supplements containing vitamin C on CF inflammation and oxida-tive stress since the levels of this vitamin do not significantly improvewith supplementation (reviewed in [213]) This highlights the com-mon fate that this hydrosoluble vitamin shares with several fat-soluble counterparts in the ldquomicronutrient paradoxrdquo of CF patients inwhich the need for a correction of their status along the progressionof the disease is frustrated by the poor efficacy of oral supplementa-tion protocols Formulations and appropriate supplementation proto-cols that may produce a better correction of vitamin C status of CFpatients are awaited for further clinical evaluation
362 Selenium and selenium-dependent peroxidasesSelenium is a trace element with marked electrophilicity [214]
that once converted to the organic form of Se-Cys can be introducedin protein structures to play its important role in H2O2 metabolismand signaling [215] As catalytic center of the enzyme GSH-peroxidase (SeGSH-Px) Se plays a crucial role to protect polyunsatu-rated lipids of plasma membrane and circulating lipoproteins formperoxidative insults With other Se-proteins such as the high molecu-lar weight thioredoxin reductases this oligoelement participates tothe control of protein thiol-disulfide oxidoreduction and glutathiony-lation which regulate signaling pathways of crucial importance in theregulation of immunity and inflammation [16] but also the function-ing of other redox-sensitive proteins such as the same CFTR [124]
The activity of SeGSH-Px in blood is considered a functional as-sessment of selenium status even if this assumption has some limita-tions related with the saturation profile that the Se stores show atincreasing doses of Se administration Investigations of the seleniumstatus in CF patients have produced conflicting findings which maydepend on differences in dietary intake ethnicity and environmentalfactors in the diverse patient populations (reviewed in [216217]) CFchildren have been reported to have lowered blood selenium and RBCSeGSH-Px activity [218219] normal plasma selenium and loweredRBC SeGSH-Px [220] and even normal levels of both these two param-eters [221] The supplementation with selenium in combination withother antioxidants was observed to increase the concentrations ofblood selenium that likewise β-carotene and fatty acid were posi-tively correlated with improved lung function [6]
Foucaud et al [218] observed that a defective selenium statuswas associated with lowered levels of other antioxidants that contrib-ute to the anti-peroxidative activity of this microelement such asvitamin E (reviewed in [222]) and the severity of this deficiencywas lower in children with pancreatic enzyme replacement and vita-min E supplementation
Treatments to substitute for exocrine pancreatic insufficiency bypancreatic enzymes from animal sources such as porcine pancreashave been confirmed to be a source of Se [220] These affects RBCSeGSH-Px activity and plasma selenium concentrations which hasto be taken into account when selenium supplements are given toCF patients
Selenium has been used to develop a series of organoseleniumcompounds that may open the way to new therapeutic opportunitiesin CF (see Section 392) These include GPX mimetic drugs and phaseII enzyme inducers which may provide higher antioxidant activity ofASL and cellular protection effects in the airways
363 Zinc and copperZinc and copper (Zn and Cu respectively) are present in many
proteins so that a deficiency of these trace metals could have pleiotro-pic effects in humans As regards antioxidant systems these two oli-goelements contribute an important role being cofactors of two
703F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
isoforms of the superoxide dismutase enzymes eg the extracellularform eg the EC-SOD or Sod 3 and the CundashZn-SOD or Sod 1 that isfound in several tissues and cells [223] The EC-SOD exerts its antiox-idant role also in the lining fluids of the airways [224]
The notion that CF patients have defective concentrations of bloodZn and Cu is controversial As far as Cu status is concerned few datahave been produced and are available in the literature suggestingthe notion that CF patients develop a moderate copper deficiency[225226] That was essentially demonstrated on the bases of a defec-tive activity of Cu-related proteins such as plasma ceruloplasmindiamine oxidase and RBC SOD This defect seems to be refractory toCu and Zn supplementation (see below)
More advanced studies have been carried out in the case of Zn sta-tus in CF Low plasma zinc concentrations were reported in approxi-mately 30 of young infants with CF identified by newbornscreening [227] and an impaired zinc homeostasis in CF patientswas described by Easley et al [228] This is characterized by poor con-servation of the endogenous pool with fecal loss and impaired frac-tional absorption of zinc which are the consequences of pancreaticinsufficiency and persisting steatorrhea These studies suggestedthat in the clinical management of CF patients these defects can beat least in part corrected by exocrine pancreatic enzyme replacement
A series of studies by Van Biervliet et al [229230] demonstratedin a Dutch population of CF infants and children that serum Zn variesin an age-dependent manner but remained unchanged with respectto healthy control levels In CF patients no difference in serum Zn con-centration between pancreatic-sufficient or pancreatic-insufficientpatients was observed and no correlation was found with the nutri-tional status or height z-score Importantly in these studies a signifi-cant correlation of serum Zn was observed with the fat solublevitamins A and E thus confirming the relationship between the ab-normalities of lipid and Zn metabolism in CF This suggests that co-supplementation of Zn and fat-soluble vitamins should be advisedin the presence of pancreatic insufficiency and persisting steatorrhea
Neve et al [219] in a study aimed to assess plasma and erythrocytezinc copper and selenium in CF children showed that mean plasmazinc and copper levels were not different from those in age-matched controls which confirms the observations by Van Biervlietet al described above However plasma zinc concentrations de-creased in patients with moderate-to-severe growth retardation andwith severe pulmonary disease but very low zinc levels occur sporad-ically Erythrocyte zinc and copper levels were significantly higherthan normal while RBC selenium was lower than in age-matchedcontrols These trace element concentrations in erythrocytes werediscussed in relation to the activities of the CuZn-SOD and the Se-enzyme GPx This observation suggests a compensatory upregulationof the erythrocyte CuZn-SOD by the exposure of erythroid precursorsto ROS andor other CF-related stressors
Best et al [225] also studied RBC SOD activity using this as a bio-logical sensor of Cu status in CF patients A lowered activity of thisenzyme was reported in CF together with that of the other Cu-dependent enzyme plasma diamine oxidase while plasma ceruplas-min showed normal activity Degradation rates of copper proteinsare known to be accelerated in conditions of copper deficiencywhich could explain the finding at least in part Anyway when Cuand Zn were supplemented to CF patients either separate or incombination (6 weeks of 3 mg copperd as copper-glycinate and30 mg zincd as zinc-glycinate) any of the copper enzyme activitieswas affected Therefore the moderate copper deficiency of CF patientsappears to be refractory to the intervention by increased copper andor zinc intake
Erythrocyte CuZn-SOD and the plasma levels of Cu and Zn werealso measured in the study of Wood et al [6] in which Australian CFpatients (agegt5 years) were treated with a high-dose antioxidantmultivitamin formulation containing 200 mg vitamin E (as RRR-α-tocopherol) 300 mg vitamin C (as sodium ascorbate) 25 mg β-
carotene (all-trans isomer) 90 μg Se (as selenomethionine) and500 μg vitamin A (as retinyl palmitate) in oil Plasma oligoelementsand particularly Zn were in the normal range at baseline (as com-pared with the data reported in [229230]) and were not affected bythis multivitamin supplement The same was found for the activityof RBC SOD and for plasma 8-iso-PGF2α as surrogate biomarker oflipid peroxidation
In a recent non-randomized small population (n=21) casendashcon-trol study in CF children Zn supplementation was proven to producepositive clinical effects in Zn-deficient patients [196] The supplemen-tation with 5 mgkg Zn sulfateday (maximum 150 mg) significantlydecreased the number of infections and increased the forced expira-tory volume in 1 s energy intake and growth parameters also im-proved These parameters were unaffected in untreated patientsexcept that in the case of the pulmonary function that decreased sig-nificantly These clinical observations on Zn supplementation need tobe confirmed in prospective double-blind randomized control trial
37 Appropriateness and targeting of antioxidant therapies in CF
The choice of the appropriate antioxidant and dose to correct a cer-tain biomarker and its associated biochemical lesion is another impor-tant point that appears to have disregarded in many clinical studiesFor instance unlike vitamin E vitamin C supplementation does notalter F2-IsoPs levels in humans (reviewed in [74]) This appears tobe true also in the antioxidant therapy of CF in which vitamin C(300 mgday) was administered together with other antioxidantsthat included a dose of vitamin E of 200 mgday without any signifi-cant effect on the surrogate biomarker of lipid peroxidation F2-IsoPs[6] When carotenoids are used as supplements to prevent the damag-ing action of ROS in the CF airways it is noteworthy that these are notparticularly good quenchers of peroxyl radicals relative to phenolicsand other antioxidants but are exceptional in quenching singlet oxy-gen at which most other phenolics and antioxidants are relativelyineffective Singlet oxygen is not a radical and does not react via radi-cal mechanisms but reacts mostly by the addition to double bondsforming endoperoxides that can be reduced to alkoxyl radicals that ini-tiate radical chain reactions typical of the peroxidative damage of PUFA[38] In this case the analysis of F2-IsoPs lipid peroxide formation andtransition metal-induced oxidizability of lipoproteins [162180] are allappropriate to evaluate the effect of carotenoids in preventing lipidperoxidation
As far as the dose is concerned clinical pharmacology of vitamin Eas an antioxidant was recently investigated by means of the effect onF2-IsoPs production and doses of α-tocopherol of 1600 IUday orgreater were found to be required to statistically affect plasma F2-IsoPs levels in hypercholeterolemic subjects [176] Several vitamin Esupplementation studies in CF patients have been performed withdoses of lower than 300 IUday regardless of the lowered absorptionby pancreatic and liver defects and the regular supplementationwith these doses does not appear to correct lipid oxidation markersin CF [7]
In the clinical practice and planning trials it has to be taken intoconsideration that in spite of substantial evidence supporting ahigher antioxidant demand in CF interventions with several antioxi-dant formulations produce poor responsiveness particularly in thecase of fat-soluble antioxidants which are poorly absorbed [6162]
Since many oxidants and antioxidants are present in tissuesand biological fluids and these have different chemical and physicalcharacteristics the possibility to produce a successful therapy witha single antioxidant molecule is too far to be realistic Moreover an-tioxidants act by multiple mechanisms in a single system or by adifferent single mechanism depending on the reaction systemresponding in a different manner to different radical or oxidantsources Because multiple reaction characteristics and mechanismsas well as different phase localizations are usually involved no single
704 F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
therapeutic approach will effectively prevent damage by multipleROS sources The defect of physiological antioxidants may also interferewith antioxidant therapies that are based on one or few exogenousantioxidants
Moreover several antioxidant vitamins such as vitamin E and ca-rotenoids have multiple natural forms with different bioavailabilitymetabolism and bioactivity [157167231] As far as the case of vita-min E supplementation concerns α-tocopherol was used as uniquevitamer in the large majority of supplementation trials so far per-formed and is the form used in the nutritional management of CFpatients Moreover several supplements contain the synthetic (or ra-cemic) form of this vitamin that has lower bioavailability than thenatural form Other forms present in nature and abundantly con-tained in vegetables such as tocotrienols and the less methylatedforms of tocopherol are not represented in many of the supplementformulations so far available in clinical centers and the supplementa-tion with α-tocopherol also limits their bioavailability These formsshow markedly higher susceptibility to hepatic metabolism and bili-ary excretion with respect to α-tocopherol eg the most representedform in blood and solid tissues and if co-supplemented these areeasily displaced during liver uptake and excreted with bile bymeans of competition with the same α-tocopherol Notwithstandingthese minor forms have been proposed to play important physiolog-ical roles showing molecular characteristics transcriptional effectsand antioxidant activities that clearly differentiate them in subfam-ilies with distinct biological functions Some of these such as α-tocopherol eg the second vitamin E form as relative abundance inblood and its carboxyethyl-hydroxychroman metabolite [189] ap-pear to have health-related anti-inflammatory effects which are par-ticularly relevant in lung protection [232233] This has suggestedthat such a group of ldquonon-α-tocopherolrdquo forms may represent anoth-er family of vitamins within the family of vitamin E with an impor-tant but often missed contribution to the proposed health effects ofthis vitamin [163]
These aspects may thus limit the possibility to provide CF patientsof optimal levels of this vitamin in all its components even if they areregularly treated with a vitamin E supplement eg withα-tocopherol
Targeted antioxidant therapy with formulations with higher bio-availability and bioactivity has been anticipated in CF New antioxi-dant formulations have been proposed to overcome main limits ofantioxidant therapies so far proposed for these patients Water-miscible α-tocopheryl acetate containing polysorbate propylene gly-col or polyethylene glycol as emulsifiers form micellar structureswere suggested to providing greater bioavailability than the fat-soluble counterparts These were commercialized with the brandnames of E-viminreg Cremophorreg EL and Aquasolreg E but despitethe original positive expectation [234235] some studies failed to ob-serve a higher response in vitamin E levels when these were com-pared with fat-soluble formulations [236237]
In a pilot study by Papas et al [183] a micellar formulation of fat-soluble nutrients and antioxidants was found to improve plasmalevels of β-carotene γ-tocopherol and CoQ(10) reducing at thesame time some inflammatory markers in induced sputum eg mye-loperoxidase and to a lower extent PMN elastase and total cell countswhile lung function and sputum bacterial counts were unaffectedThe same group recently confirmed the possibility to increase the ab-sorption of fat-soluble micronutrients using formulations with higherbioavailability specifically designed for malabsorbing patients such asCF patients that include also vitamin K and commercialized with thebrand name of AquADEKsreg [162] Despite improved vitamin and mi-cronutrient levels in this non-randomized open-label study AquA-DEKsreg produced only modest improvements in weight percentileand pulmonary function Another recent pilot observation [182] hassuggested the beneficial effect of this formulation on antioxidant andoxidative stress parameters of this oral supplement that surely deservesmore clinical investigation by larger randomized controlled trials
Recent multivitaminic formulations have been designed to containalso the minor forms of vitamin E and specifically γ-tocopherol [238]the expected superiority of which with respect to formulations con-taining only α-tocopherol needs to be verified As discussed abovein the section dedicated to vitamin E further advancements in thetherapy of CF inflammation and oxidative stress could be based onsynthetic forms and natural metabolites of this vitamin that havebeen recently identified to possess higher antioxidant and also anti-inflammatory activity than α-tocopherol (reviewed in [163168])
Pre-clinical investigation of these and other fat-soluble agents iscurrently addressed to develop formulations and administration pro-tocols that may increase the therapeutic efficacy in the airways In theantioxidant therapy of lung dysfunction in CF local administrationprotocols may overcome the limits of oral and systemic administra-tion protocols increasing bioavailability and providing targetedapproach to inflammation and oxidative stress Aerosolization of vita-min E and other fat-soluble micronutrients is possible and may allowdirect administration in the airways to prevent toxicity of smokewhich is closely associated with inflammation and oxidative stress[164165] To our knowledge this as well as other strategies of localadministration such as instillation of solutions such as surfactant-like solutions enriched of vitamin E have not been previously inves-tigated in CF patients and other CF model systems
On the contrary inhalation is an administration route widelyadopted in the case of GSH and NAC therapy described above Inthis context Cys formulations alternative to NAC have been proposedfor use as antioxidant and anti-inflammatory agent for inhalationNacystelyn is a lysine adduct of NAC that thanks to a higher proton-ation equilibrium shows increased water solubility and thus betterbioavailability Nacystelyn has been described to influence IL-8 gener-ation and the inflammatory signaling of bronchial epithelial cells[239] and preliminary clinical evaluation has demonstrated the safetyof this drug [240] Further clinical trials aimed to assess the effect onlung symptomatology of CF patients are needed Direct administra-tion in the airways could also be adopted for micronutrient vitaminswith poor absorption and bioavailability due to GI defects
38 Clinical impact of antioxidant therapy in CF
Huge in vitro and pre-clinical evidence has provided the rationaleto support clinical investigation of antioxidant strategies in CF Theseshould aim to restore the oxidantndashantioxidant balance of CF airwaychallenged by chronic infection and inflammatory cell activation
Some observational trials have confirmed that antioxidants usedas either supplements to the diet or drugs for lung administrationby aerosolized formulations may help in relieving progressive lungdamage and other adverse clinical events of CF such as poor growthSo far few studies have examined with sufficient methodologicalrigor the clinical efficacy of antioxidant therapy in CF This was alsoconcluded in a previous review of the literature by Cantin et al [12]that was published in the beginning of 2006 and is confirmed alsoin a recent analysis of clinical trials on antioxidant therapy in CF pa-tients [213] that examined the literature until September 2010using as sources the databases of the Cochrane CF and Genetic Disor-ders Group CF Trials Register PubMed CINAHL and AMED Useful in-formation was retrieved from just four randomized controlled trialsand one quasi-randomized controlled trial on vitamin C vitamin Eβ-carotene and selenium used as supplements administered aloneor in combination Post-hoc data analysis that was possible only inthree studies on a total of 87 CF patients showed the absence ofany significant improvement in lung function that was selected as pri-mary outcome together with quality of life that improved in one trialSecondary outcomes concerning laboratory indices of oxidative stressand antioxidant status showed several improvements These includedan increase of RBC SeGPx by selenium supplementation done as
705F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
individual or combined supplementation and increased levels of allplasma antioxidants except vitamin C that were observed in all thetrials
The message from these studies to pediatricians and nutritionistswithin the clinical staff of CF centers is that in the absence of solid ev-idence regarding the clinical effectiveness of oral formulations of an-tioxidant supplements in CF (including PUFA) their use as a routineclinical practice should be considered with caution keeping clear inmind that this should represent just a complement of one of themost critical interventions in the life-long clinical management pro-gram of CF patients eg providing an adequate nutriture [140] Inthis context compensating energy and protein malnutrition has toremain the first goal of nutritional management programs Providinghigher intakes of antioxidant micronutrients with food naturally-enriched (or functionalized) of micronutrient antioxidants shouldbe preferred in order to have the higher combination of positive nu-tritional factors that are lost during refinement procedures and over-all industrial processing of dietary supplements
Measures of good practice in clinical management of micro-malnutrition in CF patients would include the support of specializedpersonnel and laboratories The centers should have the possibilityto ascertain with appropriate nutritional and laboratory tests whatthe level of deficiency is for the different micronutrients that each pa-tient may suffer from during a dietary program Monitoring dietaryintakes and blood levels of micronutrients is not sufficient to set apersonalized nutritional intervention with supplements or functionalfoods Sub-optimal intakes and the compliance to nutritional inter-ventions should be verified by means of selected biochemical andclinical criteria Unluckily the latter are still not well established forsome micronutrients such as the fat-soluble vitamins E (reviewed in[163173241]) and K [242243] and also for trace elements such asSe [244] For many of the antioxidants used as supplements inhumans we still do not know exactly several of the biological effectsthat these may provide when introduced in a healthy body and weknow less what these can do in disease These aspects hardly impacton the concept of optimal levels of intake that should be identified foreach micronutrient on an individual basis According with the aspectsdiscussed in the previous sections optimal levels of intake for antiox-idant micronutrients are different in CF patients and healthy subjectsand vary with age and several individual factors
Lung administration of antioxidants by means of aerosolized for-mulations so far used for GSH therapy (see above) is a promisingfield of clinical investigation in CF Toxicity issues are currently themain concern and the subject of clinical evaluation by several groups(described above)
Information on future directions of antioxidant therapy in CF canbe inferred by the analysis of pending or recently completed clinicaltrials that have been searched (December 2011) at ClinicalTrialsgovdatabase matching the terms ldquoantioxidant therapyrdquo or ldquoglutathionerdquowith ldquocystic fibrosisrdquo Fifteen trials were retrieved and those directlyrelated to antioxidant therapy (n=12) are presented in Table 1 andinclude efficacy and safety studies of inhaled drugs as GSH sodiumpyruvate NAC and NO and the dietary supplements AquADEKsregan antioxidant-rich multivitamin supplement epigallocatechin gal-late (EGCG)tocotrienol curcuminoids the amino acid glutaminesulforaphane in broccoli sprouts One trial is investigating the flavo-noid quercetin as CFTR modulator
39 Emerging antioxidant and anti-inflammatory approaches in CF
Mediterranean foods such as olive oil and red wine or severalplant extracts such as herbal tea or grape seed extracts contain aseries of natural compounds with important antioxidant and NOscavenging activity that have been widely investigated for the pre-vention of oxidative stress-related diseases [38245] These havebeen long investigated as template molecules to develop antioxidant
and anti-inflammatory drugs Between the multitudes of natural sub-stances most investigated ones include for instance tyrosol hydroxy-tyrosol gallic and caffeic acids belonging to the family of phenolswhile resveratrol of the stilbenes family epicatechin kaempferoland cianidin are examples of flavonoids examples of fat-soluble phe-nolics are those of the family of tocols (vitamin E) and carotenoids Allthese compounds show different metabolisms and signaling effects[246] Antioxidant and cell protection mechanisms are associatedwith different and sometimes concurrent processes as H-atom trans-fer and electron donation radical trapping and chelation of transitionmetals that can be easily investigated at the chemical level [247] Be-sides these direct antioxidant effects metabolic responses and signal-ing effects of natural compounds are also important to producesecond-generation responses that modify the level of antioxidantprotection and the potential for ROS detoxification in cells and bodyfluids These derive from the transcriptional regulation of antioxidantand pro-oxidant genes that coexist with the modulation of cytokinesecretion and inflammatory enzyme activities
Some of these natural plant-derived antioxidants may provide fur-ther pharmacological activities of possible relevance in CF This is thecase for instance of the plant flavonoids genistein apigenin kaemp-ferol quercetin and hesperidin [248ndash251] that fall in the pharmaco-logical category of ldquopotentiatorsrdquo [252] in that these activate at leastto a certain extent CTFR-mediated Cl currents in normal and CF airwayepithelium investigated either in vitro or in vivo in humans and ani-mal models Actually as prototypal flavonoid-derived potentiatorthe tyrosine kinase inhibitor genistein potentiates the gating of wild-type as well as ΔF508 CFTR and G551D CFTR [253] but at higherdoses it inhibits CFTR gating which make this an unlikely clinical can-didate Similar potentiation effects have been reported for the antiox-idant curcumin [250] that shows an additive effect with respect togenistein-induced potentiation Besides CFTR potentiation whichdoes not appear to have a direct influence on GSH and nutrient trans-port in the lung tissue all these natural substances have been usedalone or in combination with other agents as in vivo enhancers oflung antioxidant protection [246254255] In the case of quercetinthiol-reactive phenolic [256] bronchodilation and anti-inflammatoryeffects by a restoration of the Th1Th2 balance have been reportedin inflammatory syndromes of the lung [255257ndash259] but theseeffects have not been explored in CF Pyocyanin toxicity (see abovein the Section 2) could represent an issue for the use of quercetinand other catechols in infectious diseases of the lung [260]
Other natural antioxidants of potential interest in CF therapy in-clude terpenoids [261] such as terpinen-4-ol a major constituentof tea tree oil that is being investigated in the therapy of anti-biotic resistant organisms specifically against methicillin-resistantStaphylococcus aureus (MRSA) [262] a problem in CF [263] Otherthan being lipophilic antioxidants terpenes can prevent oxidativestress of the CF lung secondarily to the antibiotic effect thereby pro-moting a better control of immuno-inflammatory pathways and lungantioxidants
391 Targeting NF-κB with natural compounds resveratrol and plantextracts
Natural compounds were long known to be useful in designinganti-inflammatory drugs and some of these could find an applicationin the control of the transcription factor kappa-B (NF-κB) that maylead to develop advanced pharmacological tools to control inflamma-tion and to produce higher antioxidant protection to CF airwaysInhibitors targeting NF-κB including transcription factors decoymolecules (TFD) are potent down-regulators of gene expressionand release of IL-8 in CF cells infected with P aeruginosa [264265]
Resveratrol (354prime-trihydroxystilbene ldquoErdquo form) is one of the mostinvestigated natural antioxidant with proposed activity as NF-κBinhibitor This is a phytoalexin present in large quantity in red winepreferentially in the skin of grapes being its concentration
706 F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
50ndash100 μgmg of fresh skin and 13ndash3 mgl of red wine [266]Furthermore resveratrol is a constituent of lsquoDarakchasavarsquo (13ndash6 mgl) an ayurvedic medicine from India [267] The antioxidant activity ofresveratrol has been reported in several papers and occurs also in lungtissues suggesting that resveratrol has potential as a therapeuticagent in respiratory disease [268ndash270] Resveratrol can be consideredone of the most interesting molecules from the natural worldexhibiting strong antioxidant activity that at the same time is able toexert anti inflammatory activity through alteration of NF-κB functionsand efficient inhibition of pro-inflammatory genes [271272] As far asthe effects on CF model systems are concerned Cabrini et al [26]reported the effects of resveratrol on P aeruginosa infected CF IB3-1cells The results obtained demonstrate that resveratrol exhibits minoreffects of IB3-1 cell growth and important inhibitory effects on accumu-lation of IL-8 and GRO-α mRNA while minor effects on IL-6 gene ex-pression were observed These data support recently publishedobservations suggesting inhibitory effects of resveratrol in infection-mediated inflammatory processes [273] Interestingly resveratrol hasbeen reported as a potent inhibitor of NF-κB activity and a promisinganti-inflammatory agent [272274] also in combinationwith othermol-ecules [274275] However in vivo translation of this pre-clinical on res-veratrol is hard to be foreseen This natural compound displays poorbioavailability [276] and further characterization of resveratrol pharma-cokinetics is troublesome since it is hardly measurable in vivo [277]Furthermore the regulation of inflammatory responses by resveratrolhas been suggested to be far more complex than simple direct suppres-sion of NF-κB activity Actually some aspects of the immune responsecould be enhanced by this natural substance which may lead tohypothesize broad negative feedback events on immuno-inflammatorypathways [278] In any case and with these cautions in mind the pub-lished observations on cellular model systems support the concept thatresveratrol and resveratrol-containing formulations deserve further con-sideration to determine their possible therapeutic values in CF
Other inhibitors can be identified from systematic studies of naturalproducts and their ability to interfere with NF-κB activity [279ndash281]Recent studies have demonstrated that the whole extract of Aeglemarmelos (Rutaceae) has strong inhibitory effect on the P aeruginosa-dependent IL-8 induction in human CF-derived bronchial IB3-1 cellswithout affecting cell proliferation [280] Molecular analysis of compo-nents contained in A marmelos extracts revealed that three major com-pounds namely 56-dimethoxy-1-indanone 2-hydroxy-cinnamic acidand 5-methoxy psoralen (5-MOP) reproduce the inhibitory effect ob-servedwith thewhole extract [280] A further example has been recent-ly published using extracts from bergamot (Citrus bergamia Risso) Inthis study the extracts were characterized and the main detected con-stituents were assayed for their biological activity [281] The resultsobtained demonstrated that the extracts from bergamot epicarps con-tain components displaying an inhibitory activity on IL-8 Particularlythe most active molecules were bergapten and citropten These effectshave been confirmed by analyzing mRNA levels and protein release inthe CF cellularmodels IB3-1 and CuFi-1 inducedwith TNF-α or exposedto P aeruginosa
A parallel strategy linking NF-κB inhibition and down-regulationof NF-κB-dependent functions is described in recently publishedstudies based on a structured-based virtual screening (VS) of differ-ently substituted furocoumarins and analogues against NF-κB withthe objective of selecting molecules able to inhibit the binding ofthis transcription factor to DNA [282283] Novel compounds wereidentified with this strategy as potent inhibitors of NF-κB dependentbiological functions to be proposed for the control lung inflammationoccurring in patients affected by CF [282ndash284]
392 Scavengers and regulators of H2O2 and NO
3921 Lactoferrin and OSCNmacr The impaired DUOXLPO system of CFpatients could be the target of therapeutic strategies that may
produce concomitant antimicrobial and antioxidant effects This sys-tem described above in Section 22 represents an important compo-nent of innate immunity with a role in bactericidal defense andregulation of H2O2 metabolism of airways [32] CF patients have alsoreported to show lowered LF levels in the ASL [37] that togetherwith a CFTR-dependent defective efflux of SCNmacr and LPO [36] may cre-ate the environment for a sustained flux of H2O2 and for the genera-tion of highly reactive Fenton species [1138] An ideal therapeuticintervention should restore the LPO-dependent generation of bacteri-cidal OSCNmacr from DUOX-derived H2O2 and SCNmacr in the ASL to controlat the same time the microbial biofilm and the flux of H2O2 into theASL An approach close to this therapeutic mechanism was recentlyproposed for the drug Meveolreg This is a complex of LF and OSCNmacrwith proposed in vivo antimicrobial activity [285] to be evaluatedin clinical trials for the aerosol treatment of lung infections in CFpatients The role for this drug in the control of H2O2 levels of ASLremains to be investigated
3922 Organoselenium compounds Organoselenium compoundshave been proposed as therapeutic agents useful in the antioxidanttherapy of inflammatory conditions These include GPX mimetic mol-ecules such as Ebselenreg (2-phenyl-12-benzisoselenazol-3(2H)-one)or other and more recently developed molecules that are still inpre-clinical steps of evaluation [286] Selectively and specificity of ac-tion are main issues in the therapeutic mechanism of this candidateantioxidant drug that thanks to the electrophilic properties of Se[214] reacts with thiols to reduce H2O2 and other species MoreoverEbselenreg has been described to act as potent non-competitive inhib-itor of extracellular nucleoside diphosphokinase (NDPK) having neg-ligible effect on ecto-ATPase and adenyl kinase activities which areother players of the metabolism of extracellular nucleotides [287]This enzyme together with other nucleoside di- and triphosphatescontributes to regulate several components of the mucociliary clear-ance process (MCC) that protects the lung against infections via acti-vation of epithelial purinergic receptors The inhibition of NDPK bythis GPX-mimetic drug may also impact on the energy status of endo-thelial cells [287] This aspect could be further investigated as a cellu-lar protection mechanism in the pulmonary epithelium of CF patientsbeing the control of cell energy of fundamental importance to preventthe activation of death pathways [288]
Further therapeutic mechanisms for these Se-derived drugs mayderive from the marked activity as inducers of phase II enzymessuch as quinone reductase (QR) and glutathione-S-transferase (GST)[289] This induction response also observed with other electrophilsand redox-active molecules such as natural phenolic antioxidantscould produce higher cellular protection by the acquisition of anincreased capability to detoxify endobiotics generated during oxida-tive stress and inflammation [246]
3923 Melatonin and GSNO as NOx regulators Increased markers ofNO-derived biological damage are present in the CF lung suggestingthe abnormal reactivity of NOx in the inflamed lung of CF patients[52] However an impaired metabolism and biological function ofNO in CF airways (see Section 23) suggests a cautious approach tothe use of agents that may influence the levels and chemical behaviorof NO-derived species (NOx) with possible impact on the physiologi-cal roles of NO in vasodilatation innate immunity and H2O2 metabo-lism of the respiratory tract [290291] NO donors also appear toinfluence CFTR function of alveolar epithelium and gland serouscells [292293]
Main physiological role of the pineal gland hormone melatonin isthe synchronization of circadian rhythms including the sleepndashwakecycle but several other functions dealing with immunomodulatoryantioxidant and cellular protection effects have been identified[294] Melatonin receptor stimulation may also influence cyclic AMPsignaling and the regulation of CFTR ion channel [295296]
707F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
A recent randomized double-blind placebo-controlled study hasexamined the effects of short term melatonin administration (3 mgfor 3 weeks) on sleep and oxidative stress markers in CF [297]According with the expected pharmacological effect of this hormonalsubstance the treatment was successful in improving sleep indicesAt the same time nitrite levels determined in exhaled breath conden-sate (EBC) were reduced to suggest a better control of NOmetabolismof CF airways (discussed above in Section 23) but these effects how-ever were not associated with a significant correction of isoprostaneas lipid peroxidation marker measured in EBC Increasing dosages ofmelatonin could be investigated for the pharmacological treatmentof oxidative stress and immune dysfunction of CF patients due tothe absence of adverse effects of this hormonal substance in humans
The S-nitrosation reaction of thiols is another interesting aspect ofNO pharmacology [53] that may find an application in the therapy oflung complications of CF This has been the case for instance of theS-nitrosothiol GSNO that has been used safely in human trials[298299] This endogenous nitrosothiol with proposed regulatory ef-fect on the CFTR of lung epithelia [292293] is well tolerated in pa-tients with CF when administered by aerosolization and mayproduce better oxygenation [299] thereby suggesting that therapyaimed at restoring endogenous GSNO levels in the CF airway maymerit further clinical evaluation Since the administered GSNO de-composes as shown by the increased levels of expired NO in CF pa-tients under treatment with this nitrosothiol [299] furtherinvestigation should be addressed to ascertain whether GSNO thera-py may merely correspond to a GSH therapy
NO dependent effects on CFTR function should be considered toevaluate mechanism of action and specificity of antioxidant therapiesthat target NO metabolism and function in the CF airways
4 Conclusions and future perspectives
The presence of clinical and biochemical symptoms of inflammationand oxidative stress implies that CF patients have a higher demand ofantioxidant protection The combination of the dysfunctional CFTRwith a lowered intake and absorption of dietary antioxidants producesub-optimal levels of protection from both enzymatic and non-enzymatic defense systems The former could be associated with a de-fective glutathionemetabolism and lowered intake of sulfur-containingamino acids and oligoelements such as zinc and possibly seleniumwhile fat-soluble antioxidant vitamins such as vitamin E and caroten-oids and the water-soluble vitamin C are lowered than in healthy sub-jects due to malabsorption and possibly higher consumption
The increased antioxidant demand in CF patients should be evenhigher in the presence of complications of the lung pancreas andliver Lung comorbidity is particularly important in this contextbeing associated with recurrent infections which results in the alter-nation of inflammatory exacerbates and chronic inflammation Thesesustain the flux of ROS in the airways and promote the formation ofsecond-generation byproducts by the damage of biomolecules suchas PUFA and proteins which may diffuse also at the systemic level tofurther promote adverse biological responses and toxic reactions Pan-creatic insufficiency causes malnutrition and may lead to develop en-docrine and metabolic defects associated with diabetes of CF Theseevents can be further aggravated by the concomitance of liver dys-function and a poor nutritional status Malnutrition is strongly associ-ated with poor prognosis as assessed by pulmonary function andsurvival data [138ndash140] The more aggressive nutritional interven-tions seem to produce better clinical outcomes in these patients andthe possibility of achieving higher antioxidant protection in well-nourished patients by dietary factors could be a key aspect to explainsuch a clinical advantage The assumption that food-derived compo-nentsmay help to prevent the damaging effects of oxidative stress im-proving the antioxidant defenses deserves further investigation at theclinical level This together with the investigation of appropriate
laboratory biomarkers could provide critical information to establishintervention criteria for an early nutritional management of newly di-agnosed patients [5] It is expected that a timely secondary preventionstrategy could influence the progression of CF symptoms thusaffecting with a self-feeding mechanism the same extent of malnutri-tion and oxidative stress along the life of CF patients Since severalfactors contribute to impair the nutritional status of CF patients(such as pancreatic insufficiency chronic malabsorption recurrentsinopulmonary infections and progressive lung disease chronic in-flammation increased energy expenditure suboptimal intake multi-therapy) careful monitoring of the antioxidant status should berecommended According with international guidelines fat-solublevitamin supplementation is of utmost importance in daily practice to-gether with energy intake requirements and pancreatic enzyme-replacement therapy Among these vitamin E β-carotene and ω-3FA have observed to alleviate selected biochemical signs of oxidativestress as measured for instance with well established laboratory indi-ces of lipid peroxidation and in some studies these effects werepreliminarily associated with positive clinical outcomes Notwith-standing randomizedndashcontrolled clinical trials on antioxidant supple-ments (including ω-3 FA) so far carried out in CF have failed toconclusively demonstrate significant beneficial effects on respiratorysymptoms and on the consequent impact that these have on the qual-ity of life of these patients (reviewed in [202213]) whichmay provideno support for the use of these supplements in CF An absence of effi-cacy in prevention studies on antioxidant supplements has also beenobserved in other and possibly less severe oxidative stress-relatedconditions particularly in the secondary prevention of cardiovasculardisease and some forms of cancer by vitamin E and other antioxidantssuch as vitamin C selenium and β-carotene (reviewed in [163]) Dif-ferent biases however have been identified in randomize large clini-cal trials that may account for these disappointing findings Theseinclude patient selection criteria (early interventions and primaryprevention could have more chances of success than secondaryprevention) duration and doses of the treatment use of wrong anti-oxidant formulations and administration protocols absence of verifi-cations of the biological compliance to the treatment etc The samebiases apply for the few trials carried out in CF patients Thus the ap-propriateness and efficacy of nutritional interventions with naturalfood-derived or synthetic antioxidants should be verifiedwith respectto the biological pathways of oxidative stress and clinical variablesthat are identified as end-points Profiles of blood and tissue antioxi-dants as well as of reliable surrogate markers of oxidative stresshave to be selected and determined in highly specialized laboratorieswith a well-established experience on these analyses
Well-timed (early) interventions with appropriate antioxidantformulationsprotocols need to be proposed for the next generationof trials and the development of novel CF-tailored antioxidant andanti-inflammatory agents should be promoted
As a consequence of these considerations more clinical investiga-tion is awaited to identify future successful approaches to the antiox-idant therapy as a measure to further enhance quality of life and theoverall clinical outcome of CF patients
Acknowledgments
We are indebted with the Italian Cystic Fibrosis Research Founda-tion for the support that it provided with its grant program to the re-search activity of the authors of this paper This is a scientific initiativeof the ldquoWorking Group on Inflammation in Cystic Fibrosisrdquo (BragonziA Bravo E Cabrini G Conese M Cuzzocrea S Dechecchi MC De Ales-sandri A Evangelista V Galli F Gambari R Lambiase A Lucidi VManca A Melotti P Minicucci L Motta A Pietraforte D Pompella AQuattrucci S Rizzo R Romano M Sorio C Tesse R) of the Italian Soci-ety for Cystic Fibrosis A particular thank goes to the Prof GianniMastella for the critical revision of the manuscript and for the
708 F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
stimulating research environment that he has contributed to createwithin the Italian Cystic Fibrosis Research Foundation
References
[1] BP OSullivan SD Freedman Cystic fibrosis Lancet 373 (2009) 1891ndash1904[2] P Linsdell JW Hanrahan Glutathione permeability of CFTR Am J Physiol 275
(1998) C323ndashC326[3] L Gao KJ Kim JR Yankaskas HJ Forman Abnormal glutathione transport in
cystic fibrosis airway epithelia Am J Physiol 277 (1999) L113ndashL118[4] RK Rowntree A Harris The phenotypic consequences of CFTR mutations Ann
Hum Genet 67 (2003) 471ndash485[5] EI Back C Frindt D Nohr J Frank R Ziebach M Stern M Ranke HK Biesalski
Antioxidant deficiency in cystic fibrosis when is the right time to take actionAm J Clin Nutr 80 (2004) 374ndash384
[6] LG Wood DA Fitzgerald AK Lee ML Garg Improved antioxidant and fattyacid status of patients with cystic fibrosis after antioxidant supplementation islinked to improved lung function Am J Clin Nutr 77 (2003) 150ndash159
[7] L Iuliano R Monticolo G Straface S Zullo F Galli M Boaz S Quattrucci Asso-ciation of cholesterol oxidation and abnormalities in fatty acid metabolism incystic fibrosis Am J Clin Nutr 90 (2009) 477ndash484
[8] C Libetta V Sepe P Esposito F Galli A Dal Canton Oxidative stress and inflam-mation implications in uremia and hemodialysis Clin Biochem 44 (2011)1189ndash1198
[9] G Bartosz Reactive oxygen species destroyers or messengers Biochem Phar-macol 77 (2009) 1303ndash1315
[10] T Ntimbane B Comte G Mailhot Y Berthiaume V Poitout M Prentki RRabasa-Lhoret E Levy Cystic fibrosis-related diabetes from CFTR dysfunctionto oxidative stress Clin Biochem 30 (2009) 153ndash177
[11] A van der Vliet JP Eiserich GP Marelich B Halliwell CE Cross Oxidativestress in cystic fibrosis does it occur and does it matter Adv Pharmacol 38(1997) 491ndash513
[12] AM Cantin TB White CE Cross HJ Forman RJ Sokol D Borowitz Antioxi-dants in cystic fibrosis Conclusions from the CF antioxidant workshop Bethes-da Maryland Free Radic Biol Med 42 (2007) 15ndash31
[13] LT McGrath P Mallon L Dowey B Silke E McClean M McDonnell A DevineS Copeland S Elborn Oxidative stress during acute respiratory exacerbations incystic fibrosis Thorax 54 (1999) 518ndash523
[14] E Thomson S Brennan R Senthilmohan CL Gangell AL Chapman PD SlyAJ Kettle E Balding LJ Berry JB Carlin R Carzino N de Klerk T Douglas CFoo LW Garratt GL Hall J Harrison A Kicic IA Laing KM Logie J MassieLS Mott C Murray F Parsons N Pillarisetti SR Poreddy SC RanganathanCF Robertson R Robins-Browne PJ Robinson B Skoric SM Stick ENSutanto E Williamson Identifying peroxidases and their oxidants in the earlypathology of cystic fibrosis Free Radic Biol Med 49 (2010) 1354ndash1360
[15] SP Range C Dunster AJ Knox FJ Kelly Treatment of pulmonary exacerba-tions of cystic fibrosis leads to improved antioxidant status Eur Respir J 13(1999) 560ndash564
[16] L Coppo P Ghezzi Thiol regulation of pro-inflammatory cytokines and innateimmunity protein S-thiolation as a novel molecular mechanism Biochem SocTrans 39 (2011) 1268ndash1272
[17] C Verhaeghe C Remouchamps B Hennuy A Vanderplasschen A Chariot SPTabruyn C Oury V Bours Role of IKK and ERK pathways in intrinsic inflamma-tion of cystic fibrosis airways Biochem Pharmacol 73 (2007) 1982ndash1994
[18] TL Bonfield JR Panuska MW Konstan KA Hilliard JB Hilliard H Ghnaim MBerger Inflammatory cytokines in cystic fibrosis lungs Am J Respir Crit CareMed 152 (1995) 2111ndash2118
[19] TL Noah HR Black PW Cheng RE Wood MW Leigh Nasal and bronchoal-veolar lavage fluid cytokines in early cystic fibrosis J Infect Dis 175 (1997)638ndash647
[20] MJ Welsh BW Ramsey FJ Accurso GR Cutting Cystic Fibrosis McGraw-HillNew York 2001
[21] TZ Khan JS Wagener T Bost J Martinez FJ Accurso DW Riches Early pul-monary inflammation in infants with cystic fibrosis Am J Respir Crit CareMed 151 (1995) 1075ndash1082
[22] FA Ratjen Cystic fibrosis pathogenesis and future treatment strategies RespirCare 54 (2009) 595ndash605
[23] J Jacquot O Tabary P Le Rouzic A Clement Airway epithelial cell inflamma-tory signalling in cystic fibrosis Int J Biochem Cell Biol 40 (2008)1703ndash1715
[24] CM Greene P Branagan NG McElvaney Toll-like receptors as therapeutic tar-gets in cystic fibrosis Expert Opin Ther Targets 12 (2008) 1481ndash1495
[25] M Rottner JM Freyssinet MC Martinez Mechanisms of the noxious inflam-matory cycle in cystic fibrosis Respir Res 10 (2009) 23
[26] G Cabrini V Bezzerri I Mancini E Nicolis MC Dechecchi A Tamanini ILampronti L Piccagli N Bianchi M Borgatti R Gambari Targeting transcrip-tion factor activity as a strategy to inhibit pro-inflammatory genes involved incystic fibrosis decoy oligonucleotides and low-molecular weight compoundsCurr Med Chem 17 (2010) 4392ndash4404
[27] CM Greene NG McElvaney Proteases and antiproteases in chronic neutrophiliclungdiseasemdash relevance to drug discovery Br J Pharmacol 158 (2009) 1048ndash1058
[28] AM Cantin Potential for antioxidant therapy of cystic fibrosis Curr Opin PulmMed 10 (2004) 531ndash536
[29] JF Chmiel MW Konstan Inflammation and anti-inflammatory therapies forcystic fibrosis Clin Chest Med 28 (2007) 331ndash346
[30] DP Nichols MW Konstan JF Chmiel Anti-inflammatory therapies for cys-tic fibrosis-related lung disease Clin Rev Allergy Immunol 35 (2008)135ndash153
[31] AJ Kettle T Chan I Osberg R Senthilmohan AL Chapman TJ Mocatta JSWagener Myeloperoxidase and protein oxidation in the airways of youngchildren with cystic fibrosis Am J Respir Crit Care Med 170 (2004)1317ndash1323
[32] H Fischer Mechanisms and function of DUOX in epithelia of the lung AntioxidRedox Signal 11 (2009) 2453ndash2465
[33] B Rada TL Leto Oxidative innate immune defenses by NoxDuox familyNADPH oxidases Contrib Microbiol 15 (2008) 164ndash187
[34] P Moskwa D Lorentzen KJ Excoffon J Zabner PB McCray Jr WM NauseefC Dupuy B Banfi A novel host defense system of airways is defective in cysticfibrosis Am J Respir Crit Care Med 175 (2007) 174ndash183
[35] D Lorentzen L Durairaj AA Pezzulo Y Nakano J Launspach DA Stoltz GZamba PB McCray Jr J Zabner MJ Welsh WM Nauseef B Banfi Concentra-tion of the antibacterial precursor thiocyanate in cystic fibrosis airway secre-tions Free Radic Biol Med 50 (2011) 1144ndash1150
[36] Y Xu S Szep Z Lu The antioxidant role of thiocyanate in the pathogenesis ofcystic fibrosis and other inflammation-related diseases Proc Natl Acad Sci US A 106 (2009) 20515ndash20519
[37] MP Rogan CC Taggart CM Greene PG Murphy SJ ONeill NG McElvaneyLoss of microbicidal activity and increased formation of biofilm due to decreasedlactoferrin activity in patients with cystic fibrosis J Infect Dis 190 (2004)1245ndash1253
[38] B Halliwell JM Guttridge Free Radicals in Biology and Medicine Fourth editionOxford University Press New York 2007
[39] B Rada K Lekstrom S Damian C Dupuy TL Leto The Pseudomonastoxin pyocyanin inhibits the dual oxidase-based antimicrobial system as itimposes oxidative stress on airway epithelial cells J Immunol 181 (2008)4883ndash4893
[40] C Schwarzer B Illek JH Suh SJ Remington H Fischer TE Machen Organelleredox of CF and CFTR-corrected airway epithelia Free Radic Biol Med 43(2007) 300ndash316
[41] JH Roum R Buhl NG McElvaney Z Borok RG Crystal Systemic deficiency ofglutathione in cystic fibrosis J Appl Physiol 75 (1993) 2419ndash2424
[42] VM Hudson Rethinking cystic fibrosis pathology the critical role of abnormalreduced glutathione (GSH) transport caused by CFTR mutation Free RadicBiol Med 30 (2001) 1440ndash1461
[43] PJ Barnes RA Dweik AF Gelb PG Gibson SC George H Grasemann IDPavord F Ratjen PE Silkoff DR Taylor N Zamel Exhaled nitric oxide in pul-monary diseases a comprehensive review Chest 138 (2010) 682ndash692
[44] H Grasemann E Michler M Wallot F Ratjen Decreased concentration of ex-haled nitric oxide (NO) in patients with cystic fibrosis Pediatr Pulmonol 24(1997) 173ndash177
[45] H Grasemann F Ratjen Cystic fibrosis lung disease the role of nitric oxidePediatr Pulmonol 28 (1999) 442ndash448
[46] B Gaston F Ratjen JW Vaughan NR Malhotra RG Canady AH Snyder JFHunt S Gaertig JB Goldberg Nitrogen redox balance in the cystic fibrosis air-way effects of antipseudomonal therapy Am J Respir Crit Care Med 165(2002) 387ndash390
[47] H Grasemann I Ioannidis RP Tomkiewicz H de Groot BK Rubin F RatjenNitric oxide metabolites in cystic fibrosis lung disease Arch Dis Child 78(1998) 49ndash53
[48] H Grasemann R Schwiertz S Matthiesen K Racke F Ratjen Increased argi-nase activity in cystic fibrosis airways Am J Respir Crit Care Med 172(2005) 1523ndash1528
[49] H Grasemann S Al-Saleh JA Scott D Shehnaz A Mehl R Amin M Rafii PPencharz J Belik F Ratjen Asymmetric dimethylarginine contributes to airwaynitric oxide deficiency in patients with cystic fibrosis Am J Respir Crit CareMed 183 (2011) 1363ndash1368
[50] H Grasemann F Kurtz F Ratjen Inhaled L-arginine improves exhaled nitricoxide and pulmonary function in patients with cystic fibrosis Am J RespirCrit Care Med 174 (2006) 208ndash212
[51] H Grasemann F Ratjen Emerging therapies for cystic fibrosis lung disease Ex-pert Opin Emerg Drugs 15 (2010) 653ndash659
[52] BM Morrissey K Schilling JV Weil PE Silkoff DM Rodman Nitric oxide andprotein nitration in the cystic fibrosis airway Arch Biochem Biophys 406(2002) 33ndash39
[53] R Radi Nitric oxide oxidants and protein tyrosine nitration Proc Natl AcadSci U S A 101 (2004) 4003ndash4008
[54] J Chen M Kinter S Shank C Cotton TJ Kelley AG Ziady Dysfunction of Nrf-2in CF epithelia leads to excess intracellular H2O2 and inflammatory cytokineproduction PLoS One 3 (2008) e3367
[55] F Galli M Piroddi C Annetti C Aisa E Floridi A Floridi Oxidative stress andreactive oxygen species Contrib Nephrol 149 (2005) 240ndash260
[56] DT Wright LA Cohn H Li B Fischer CM Li KB Adler Interactions of oxygenradicals with airway epithelium Environ Health Perspect 102 (Suppl 10)(1994) 85ndash90
[57] I Rahman SR Yang SK Biswas Current concepts of redox signaling in thelungs Antioxid Redox Signal 8 (2006) 681ndash689
[58] Q Li JF Engelhardt Interleukin-1beta induction of NFκB is partially regulatedby H2O2-mediated activation of NFκB-inducing kinase J Biol Chem 281(2006) 1495ndash1505
709F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
[59] E Boncoeur VS Criq E Bonvin T Roque A Henrion-Caude DC Gruenert AClement J Jacquot O Tabary Oxidative stress induces extracellular signal-regulated kinase 12 mitogen-activated protein kinase in cystic fibrosis lung ep-ithelial cells potential mechanism for excessive IL-8 expression Int J BiochemCell Biol 40 (2008) 432ndash446
[60] B Fischer J Voynow Neutrophil elastase induces MUC5AC messenger RNA ex-pression by an oxidant-dependent mechanism Chest 117 (2000) 317Sndash320S
[61] B Rada P Gardina TG Myers TL Leto Reactive oxygen species mediate in-flammatory cytokine release and EGFR-dependent mucin secretion in airwayepithelial cells exposed to Pseudomonas pyocyanin Mucosal Immunol 4(2011) 158ndash171
[62] C Schwarzer H Fischer EJ Kim KJ Barber AD Mills MJ Kurth DC GruenertJH Suh TE Machen B Illek Oxidative stress caused by pyocyanin impairs CFTRClminus transport in human bronchial epithelial cells Free Radic Biol Med 45(2008) 1653ndash1662
[63] J Hull M South P Phelan K Grimwood Surfactant composition in infants andyoung children with cystic fibrosis Am J Respir Crit Care Med 156 (1997)161ndash165
[64] KC Meyer A Sharma R Brown M Weatherly FR Moya J Lewandoski JJZimmerman Function and composition of pulmonary surfactant andsurfactant-derived fatty acid profiles are altered in young adults with cystic fi-brosis Chest 118 (2000) 164ndash174
[65] MK Pulfer RC Murphy Formation of biologically active oxysterols during ozo-nolysis of cholesterol present in lung surfactant J Biol Chem 279 (2004)26331ndash26338
[66] V Starosta E Rietschel K Paul U Baumann M Griese Oxidative changes ofbronchoalveolar proteins in cystic fibrosis Chest 129 (2006) 431ndash437
[67] V Starosta M Griese Oxidative damage to surfactant protein D in pulmonarydiseases Free Radic Res 40 (2006) 419ndash425
[68] M Griese R Essl R Schmidt E Rietschel F Ratjen M Ballmann K Paul Pulmo-nary surfactant lung function and endobronchial inflammation in cystic fibro-sis Am J Respir Crit Care Med 170 (2004) 1000ndash1005
[69] M Griese R Essl R Schmidt M Ballmann K Paul E Rietschel F Ratjen Se-quential analysis of surfactant lung function and inflammation in cystic fibrosispatients Respir Res 6 (2005) 133
[70] LG Wood DA Fitzgerald PG Gibson DM Cooper ML Garg Increased plasmafatty acid concentrations after respiratory exacerbations are associated with el-evated oxidative stress in cystic fibrosis patients Am J Clin Nutr 75 (2002)668ndash675
[71] P Montuschi SA Kharitonov G Ciabattoni M Corradi L van Rensen DM Ged-des ME Hodson PJ Barnes Exhaled 8-isoprostane as a new non-invasive bio-marker of oxidative stress in cystic fibrosis Thorax 55 (2000) 205ndash209
[72] CE Collins P Quaggiotto L Wood EV OLoughlin RL Henry ML Garg Elevat-ed plasma levels of F2 alpha isoprostane in cystic fibrosis Lipids 34 (1999)551ndash556
[73] D Hartl V Starosta K Maier I Beck-Speier C Rebhan BF Becker P Latzin RFischer F Ratjen RM Huber E Rietschel S Krauss-Etschmann M Griese In-haled glutathione decreases PGE2 and increases lymphocytes in cystic fibrosislungs Free Radic Biol Med 39 (2005) 463ndash472
[74] GL Milne H Yin JD Morrow Human biochemistry of the isoprostane pathwayJ Biol Chem 283 (2008) 15533ndash15537
[75] G Ciabattoni G Davi M Collura L Iapichino F Pardo A Ganci R Romagnoli JMaclouf C Patrono In vivo lipid peroxidation and platelet activation in cystic fi-brosis Am J Respir Crit Care Med 162 (2000) 1195ndash1201
[76] C Garenc P Julien E Levy Oxysterols in biological systems the gastrointestinaltract liver vascular wall and central nervous system Free Radic Res 44 (2011)47ndash73
[77] AM Cantin SL North RC Hubbard RG Crystal Normal alveolar epithelial lin-ing fluid contains high levels of glutathione J Appl Physiol 63 (1987) 152ndash157
[78] R Tirouvanziam CK Conrad T Bottiglieri LA Herzenberg RB Moss High-dose oral N-acetylcysteine a glutathione prodrug modulates inflammation incystic fibrosis Proc Natl Acad Sci U S A 103 (2006) 4628ndash4633
[79] LW Velsor C Kariya R Kachadourian BJ Day Mitochondrial oxidative stressin the lungs of cystic fibrosis transmembrane conductance regulator proteinmutant mice Am J Respir Cell Mol Biol 35 (2006) 579ndash586
[80] M Kelly-Aubert S Trudel J Fritsch T Nguyen-Khoa M Baudouin-Legros SMoriceau L Jeanson F Djouadi C Matar M Conti M Ollero F Brouillard AEdelman GSH monoethyl ester rescues mitochondrial defects in cystic fibrosismodels Hum Mol Genet 20 (2011) 2745ndash2759
[81] P Ghezzi Role of glutathione in immunity and inflammation in the lung Int JGen Med 4 (2011) 105ndash113
[82] N Dauletbaev K Viel R Buhl TO Wagner J Bargon Glutathione and glutathi-one peroxidase in sputum samples of adult patients with cystic fibrosis J CystFibros 3 (2004) 119ndash124
[83] CE Cross A van der Vliet CA ONeill S Louie B Halliwell Oxidants antioxi-dants and respiratory tract lining fluids Environ Health Perspect 102 (Suppl10) (1994) 185ndash191
[84] K Takeyama K Dabbagh J Jeong Shim T Dao-Pick IF Ueki JA Nadel Oxida-tive stress causes mucin synthesis via transactivation of epidermal growth factorreceptor role of neutrophils J Immunol 164 (2000) 1546ndash1552
[85] N Ballatori SM Krance S Notenboom S Shi K Tieu CL Hammond Glutathi-one dysregulation and the etiology and progression of human diseases BiolChem 390 (2009) 191ndash214
[86] SR Soltaninassab KR Sekhar MJ Meredith ML Freeman Multi-faceted regu-lation of gamma-glutamylcysteine synthetase J Cell Physiol 182 (2000)163ndash170
[87] HR Lopez-Mirabal JR Winther Redox characteristics of the eukaryotic cytosolBiochim Biophys Acta 1783 (2008) 629ndash640
[88] C Hwang AJ Sinskey HF Lodish Oxidized redox state of glutathione in the en-doplasmic reticulum Science 257 (1992) 1496ndash1502
[89] M Murphy Mitochondrial thiols in antioxidant protection and redox signallingdistinct roles for glutathionylation and other thiol modifications AntioxidRedox Signal (2011) ahead of print doi101089ars20114289
[90] BJ Day AM van Heeckeren E Min LW Velsor Role for cystic fibrosis trans-membrane conductance regulator protein in a glutathione response to bronch-opulmonary Pseudomonas infection Infect Immun 72 (2004) 2045ndash2051
[91] Y Zhang K Duan Glutathione exhibits antibacterial activity and increases tetra-cycline efficacy against Pseudomonas aeruginosa Sci China C Life Sci 52 (2009)501ndash505
[92] VM Hudson New insights into the pathogenesis of cystic fibrosis pivotal roleof glutathione system dysfunction and implications for therapy Treat RespirMed 3 (2004) 353ndash363
[93] LW Velsor A van Heeckeren BJ Day Antioxidant imbalance in the lungs ofcystic fibrosis transmembrane conductance regulator protein mutant miceAm J Physiol Lung Cell Mol Physiol 281 (2001) L31ndashL38
[94] I Kogan M Ramjeesingh C Li JF Kidd Y Wang EM Leslie SP Cole CE BearCFTR directly mediates nucleotide-regulated glutathione flux EMBO J 22(2003) 1981ndash1989
[95] NS Gould S Gauthier CT Kariya E Min J Huang DJ Brian Hypertonic salineincreases lung epithelial lining fluid glutathione and thiocyanate two protectiveCFTR-dependent thiols against oxidative injury Respir Res 11 (2010) 119
[96] VT Vasu SJ de Cruz JS Houghton KA Hayakawa BM Morrissey CE CrossJP Eiserich Evaluation of thiol-based antioxidant therapeutics in cystic fibrosissputum focus on myeloperoxidase Free Radic Res 45 (2011) 165ndash176
[97] L Roussel G Martel J Berube S Rousseau P aeruginosa drives CXCL8 synthesisvia redundant toll-like receptors and NADPH oxidase in CFTRF508 airway epi-thelial cells J Cyst Fibros 10 (2011) 107ndash113
[98] GW Lau DJ Hassett H Ran F Kong The role of pyocyanin in Pseudomonas aer-uginosa infection Trends Mol Med 10 (2004) 599ndash606
[99] R Wilson DA Sykes D Watson A Rutman GW Taylor PJ Cole Measurementof Pseudomonas aeruginosa phenazine pigments in sputum and assessment oftheir contribution to sputum sol toxicity for respiratory epithelium InfectImmun 56 (1988) 2515ndash2517
[100] M Muller Pyocyanin induces oxidative stress in human endothelial cells andmodulates the glutathione redox cycle Free Radic Biol Med 33 (2002)1527ndash1533
[101] YQ OMalley KJ Reszka BE Britigan Direct oxidation of 2prime7prime-dichlorodihy-drofluorescein by pyocyanin and other redox-active compounds independentof reactive oxygen species production Free Radic Biol Med 36 (2004)90ndash100
[102] CC Caldwell Y Chen HS Goetzmann Y Hao MT Borchers DJ Hassett LRYoung D Mavrodi L Thomashow GW Lau Pseudomonas aeruginosa exotoxinpyocyanin causes cystic fibrosis airway pathogenesis Am J Pathol 175 (2009)2473ndash2488
[103] YQ OMalley KJ Reszka DR Spitz GM Denning BE Britigan Pseudomonasaeruginosa pyocyanin directly oxidizes glutathione and decreases its levels inairway epithelial cells Am J Physiol Lung Cell Mol Physiol 287 (2004)L94ndashL103
[104] M Muller Glutathione modulates the toxicity of but is not a biologically rele-vant reductant for the Pseudomonas aeruginosa redox toxin pyocyanin FreeRadic Biol Med 50 (2011) 971ndash977
[105] R Cheluvappa R Shimmon M Dawson SN Hilmer DG Le Couteur Reactionsof Pseudomonas aeruginosa pyocyanin with reduced glutathione Acta BiochimPol 55 (2008) 571ndash580
[106] JH Widdicombe Transgenic animals may help resolve a sticky situation in cys-tic fibrosis J Clin Invest 120 (2010) 3093ndash3096
[107] X Sun H Sui JT Fisher Z Yan X Liu HJ Cho NS Joo Y Zhang W Zhou Y YiJM Kinyon DC Lei-Butters MA Griffin P Naumann M Luo J Ascher KWang T Frana JJ Wine DK Meyerholz JF Engelhardt Disease phenotype ofa ferret CFTR-knockout model of cystic fibrosis J Clin Invest 120 (2010)3149ndash3160
[108] NS Joo HJ Cho M Khansaheb JJ Wine Hyposecretion of fluid from trachealsubmucosal glands of CFTR-deficient pigs J Clin Invest 120 (2010) 3161ndash3166
[109] A Bragonzi Murine models of acute and chronic lung infection with cystic fibro-sis pathogens IJMM 300 (2010) 584ndash593
[110] AM van Heeckeren MD Schluchter Murine models of chronic Pseudomonasaeruginosa lung infection Lab Anim 36 (2002) 291ndash312
[111] A Bragonzi D Worlitzsch GB Pier P Timpert M Ulrich M Hentzer JB Ander-sen M Givskov M Conese G Doring Nonmucoid Pseudomonas aeruginosa ex-presses alginate in the lungs of patients with cystic fibrosis and in a mousemodel J Infect Dis 192 (2005) 410ndash419
[112] GS CW Bedrossian DB Singer JJ Hansen HS Rosenberg The lung in cysticfibrosis A quantitative study including prevalence of pathologic findingsamong different age groups Hum Pathol 7 (1976) 195ndash204
[113] WD HA Cash B McCullough WG Johanson Jr JA Bass A rat model of chron-ic respiratory infection with Pseudomonas aeruginosa Am Rev Respir Dis 119(1979) 453ndash459
[114] EM JR Starke C Langston CJ Baker A mouse model of chronic pulmonary in-fection with Pseudomonas aeruginosa and Pseudomonas cepacia Pediatr Res 22(1987) 698ndash702
[115] TJ AM van Heeckeren RW Walenga MW Konstan PB Davis B ErokwuMA Haxhiu TW Ferkol Effect of Pseudomonas infection on weight loss lung
710 F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
mechanics and cytokines in mice Am J Respir Crit Care Med 161 (2000)271ndash279
[116] T Aw G Wierzbicka DP Jones Oral glutathione increases tissue glutathione invivo Chem Biol Interact 80 (1991) 89ndash97
[117] F Favilli P Marraccini T Iantomasi MT Vincenzini Effect of orally adminis-tered glutathione on glutathione levels in some organs of rats role of specifictransporters Br J Nutr 78 (1997) 293ndash300
[118] C Kariya H Leitner E Min C van Heeckeren A van Heeckeren BJ Day A rolefor CFTR in the elevation of glutathione levels in the lung by oral glutathione ad-ministration Am J Physiol Lung Cell Mol Physiol 292 (2007) L1590ndashL1597
[119] K Atkuri JJ Mantovani LA Herzenberg LA Herzenberg N-Acetylcysteinemdashasafe antidote for cysteineglutathione deficiency Curr Opin Pharmacol 7(2007) 355ndash359
[120] R De Lisle E Roach K Jansson Effects of laxative and N-acetylcysteine onmucus accumulation bacterial load transit and inflammation in the cystic fi-brosis mouse small intestine Am J Physiol Gastrointest Liver Physiol 293(2007) G577ndashG584
[121] A Luciani VR Villella S Esposito N Brunetti-Pierri D Medina C Settembre MGavina L Pulze I Giardino M Pettoello-Mantovani M DApolito S Guido EMasliah B Spencer S Quaratino V Raia A Ballabio L Maiuri Defective CFTRinduces aggresome formation and lung inflammation in cystic fibrosis throughROS-mediated autophagy inhibition Nat Cell Biol 12 863ndash875
[122] M Griese J Ramakers A Krasselt V Starosta S Van Koningsbruggen R FischerF Ratjen B Mullinger RM Huber K Maier E Rietschel G Scheuch Improve-ment of alveolar glutathione and lung function but not oxidative state in cysticfibrosis Am J Respir Crit Care Med 169 (2004) 822ndash828
[123] C Bishop VM Hudson SC Hilton C Wilde A pilot study of the effect of inhaledbuffered reduced glutathione on the clinical status of patients with cystic fibro-sis Chest 127 (2005) 308ndash317
[124] WWang C Oliva G Li A Holmgren CH Lillig KL Kirk Reversible silencing of CFTRchloride channels by glutathionylation J Gen Physiol 125 (2005) 127ndash141
[125] N Dauletbaev P Fischer B Aulbach J Gross W Kusche U Thyroff-FriesingerTO Wagner J Bargon A phase II study on safety and efficacy of high-dose N-acetylcysteine in patients with cystic fibrosis Eur J Med Res 14 (2009)352ndash358
[126] R Tirouvanziam Y Gernez CK Conrad RB Moss I Schrijver CE Dunn ZADavies LA Herzenberg Profound functional and signaling changes in viable in-flammatory neutrophils homing to cystic fibrosis airways Proc Natl Acad SciU S A 105 (2008) 4335ndash4339
[127] JH Roum Z Borok NG McElvaney GJ Grimes AD Bokser R Buhl RG Crys-tal Glutathione aerosol suppresses lung epithelial surface inflammatory cell-derived oxidants in cystic fibrosis J Appl Physiol 87 (1999) 438ndash443
[128] A Visca CT Bishop SC Hilton VM Hudson Improvement in clinical markersin CF patients using a reduced glutathione regimen an uncontrolled observa-tional study J Cyst Fibros 7 (2008) 433ndash436
[129] EF Nash A Stephenson F Ratjen E Tullis Nebulized and oral thiol derivativesfor pulmonary disease in cystic fibrosis Cochrane Database Syst Rev (2009)CD007168
[130] AC foundation Drug Development Pipeline 2011[131] S Hoshida T Kuzuya N Yamashita M Nishida S Kitahara M Hori T
Kamada M Tada Gamma-glutamylcysteine ethyl ester for myocardial protec-tion in dogs during ischemia and reperfusion J Am Coll Cardiol 24 (1994)1391ndash1397
[132] J Lok W Leung S Zhao S Pallast K van Leyen S Guo X Wang A Yalcin EHLo Gamma-glutamylcysteine ethyl ester protects cerebral endothelial cells dur-ing injury and decreases bloodndashbrain barrier permeability after experimentalbrain trauma J Neurochem 118 (2011) 248ndash255
[133] Z Borok R Buhl GJ Grimes AD Bokser RC Hubbard KJ Holroyd JH RoumDB Czerski AM Cantin RG Crystal Effect of glutathione aerosol on oxidantndashantioxidant imbalance in idiopathic pulmonary fibrosis Lancet 338 (1991)215ndash216
[134] KJ Holroyd R Buhl Z Borok JH Roum AD Bokser GJ Grimes D Czerski AMCantin RG Crystal Correction of glutathione deficiency in the lower respiratorytract of HIV seropositive individuals by glutathione aerosol treatment Thorax 48(1993) 985ndash989
[135] J Hull P Vervaart K Grimwood P Phelan Pulmonary oxidative stress responsein young children with cystic fibrosis Thorax 52 (1997) 557ndash560
[136] A Corti A Paolicchi M Franzini S Dominici AF Casini A Pompella The S-thiolating activity of membrane gamma-glutamyltransferase formation ofcysteinyl-glycine mixed disulfides with cellular proteins and in the cell microen-vironment Antioxid Redox Signal 7 (2005) 911ndash918
[137] A Corti M Franzini AF Casini A Paolicchi A Pompella Vitamin C supply tobronchial epithelial cells linked to glutathione availability in elfmdasha role for se-creted gamma-glutamyltransferase J Cyst Fibros 7 (2008) 174ndash178
[138] A Munck Nutritional considerations in patients with cystic fibrosis Expert RevRespir Med 4 (2010) 47ndash56
[139] JL Matel CE Milla Nutrition in cystic fibrosis Semin Respir Crit Care Med 30(2009) 579ndash586
[140] D Salvatore R Buzzetti E Baldo MP Forneris V Lucidi D Manunza IMarinelli B Messore AS Neri V Raia ML Furnari G Mastella An overviewof international literature from cystic fibrosis registries 2 Neonatal screeningand nutritiongrowth J Cyst Fibros 9 (2010) 75ndash83
[141] KF Joosten JM Hulst Malnutrition in pediatric hospital patients current is-sues Nutrition 27 (2011) 133ndash137
[142] S Fustik T Jacovska L Spirevska S Koceva Protein-energy malnutrition as thefirst manifestation of cystic fibrosis in infancy Pediatr Int 51 (2009) 678ndash683
[143] J Himmelfarb E McMonagle Albumin is the major plasma protein target of ox-idant stress in uremia Kidney Int 60 (2001) 358ndash363
[144] P Stenvinkel JJ Carrero J Axelsson B Lindholm O Heimburger Z MassyEmerging biomarkers for evaluating cardiovascular risk in the chronic kidneydisease patient how do new pieces fit into the uremic puzzle Clin J Am SocNephrol 3 (2008) 505ndash521
[145] M Roche P Rondeau NR Singh E Tarnus E Bourdon The antioxidant proper-ties of serum albumin FEBS Lett 582 (2008) 1783ndash1787
[146] D Giustarini A Milzani I Dalle-Donne R Rossi Red blood cells as a physiolog-ical source of glutathione for extracellular fluids Blood Cells Mol Dis 40 (2008)174ndash179
[147] A Meister ME Anderson Glutathione Annu Rev Biochem 52 (1983) 711ndash760[148] B Alvarez S Carballal L Turell R Radi Formation and reactions of sulfenic acid
in human serum albumin Methods Enzymol 473 (2010) 117ndash136[149] S Carballal B Alvarez L Turell H Botti BA Freeman R Radi Sulfenic acid in
human serum albumin Amino Acids 32 (2007) 543ndash551[150] LR Barclay AM Bailey D Kong The antioxidant activity of alpha-tocopherol-
bovine serum albumin complex in micellar and liposome autoxidations J BiolChem 260 (1985) 15809ndash15814
[151] T Ishii T Ichikawa K Minoda K Kusaka S Ito Y Suzuki M Akagawa K Mochi-zuki T Goda T Nakayama Human serum albumin as an antioxidant in the ox-idation of (minus)-epigallocatechin gallate participation of reversible covalentbinding for interaction and stabilization Biosci Biotechnol Biochem 75(2011) 100ndash106
[152] F Galli S Rovidati S Benedetti U Buoncristiani C Covarelli A Floridi F Canes-trari Overexpression of erythrocyte glutathione S-transferase in uremia and di-alysis Clin Chem 45 (1999) 1781ndash1788
[153] D Borowitz RD Baker V Stallings Consensus report on nutrition for pediat-ric patients with cystic fibrosis J Pediatr Gastroenterol Nutr 35 (2002)246ndash259
[154] LJ Filer Jr SW Wright MP Manning KE Mason Absorption of alpha-tocopherol and tocopherylesters by premature and full term infants and chil-dren in health and disease Pediatrics 8 (1951) 328ndash339
[155] L Lancellotti C DOrazio G Mastella G Mazzi U Lippi Deficiency of vitamins Eand A in cystic fibrosis is independent of pancreatic function and current en-zyme and vitamin supplementation Eur J Pediatr 155 (1996) 281ndash285
[156] MN Sathe AS Patel Update in pediatrics focus on fat-soluble vitamins NutrClin Pract 25 (2010) 340ndash346
[157] MG Traber The ABCs of vitamin E and beta-carotene absorption Am J ClinNutr 80 (2004) 3ndash4
[158] TF Dolan Jr Hemolytic anemia and edema as the initial signs in infants withcystic fibrosis Consider this diagnosis even in absence of pulmonary symptomsClin Pediatr 15 (1976) 597ndash600
[159] DR James M Alfaham MC Goodchild Increased susceptibility to peroxide-induced haemolysis with normal vitamin E concentrations in cystic fibrosisClin Chim Acta 204 (1991) 279ndash290
[160] SA Peters FJ Kelly Vitamin E supplementation in cystic fibrosis J Pediatr Gas-troenterol Nutr 22 (1996) 341ndash345
[161] A Maqbool VA Stallings Update on fat-soluble vitamins in cystic fibrosis CurrOpin Pulm Med 14 (2008) 574ndash581
[162] SD Sagel MK Sontag MM Anthony P Emmett KA Papas Effect of anantioxidant-rich multivitamin supplement in cystic fibrosis J Cyst Fibros 10(2011) 31ndash36
[163] F Galli A Azzi Present trends in vitamin E research Biofactors 36 (2010)33ndash42
[164] A Hamahata P Enkhbaatar ER Kraft M Lange SW Leonard MG Traber RACox FC Schmalstieg HK Hawkins EB Whorton EM Horvath C Szabo LDTraber DN Herndon DL Traber Gamma-tocopherol nebulization by a lipidaerosolization device improves pulmonary function in sheep with burn andsmoke inhalation injury Free Radic Biol Med 45 (2008) 425ndash433
[165] JP Anais N Razzouq M Carvalho C Fernandez A Astier M Paul A AstierH Fessi AM Lorino Development of alpha-tocopherol acetate nanoparti-cles influence of preparative processes Drug Dev Ind Pharm 35 (2009)216ndash223
[166] JM Zingg Molecular and cellular activities of vitamin E analogues Mini RevMed Chem 7 (2007) 543ndash558
[167] V Viola F Pilolli M Piroddi E Pierpaoli F Orlando M Provinciali M Betti FMazzini F Galli Why tocotrienols work better insights into the in vitro anti-cancer mechanism of vitamin E Genes Nutr 7 (2011) 29ndash41
[168] F Galli F Mazzini L Bamonti L Gille S Bohmdorfer M Piroddi T Netscher FJKelly T Rosenau Tocotrienamines and tocopheramines reactions with radicalsand metal ions Bioorg Med Chem 19 (2011) 6483ndash6491
[169] A Kuhad K Chopra Attenuation of diabetic nephropathy by tocotrienol in-volvement of NFκB signaling pathway Life Sci 84 (2009) 296ndash301
[170] Q Jiang X Yin MA Lill ML Danielson H Freiser J Huang Long-chain carbox-ychromanols metabolites of vitamin E are potent inhibitors of cyclooxygenasesProc Natl Acad Sci U S A 105 (2008) 20464ndash20469
[171] ER Miller III R Pastor-Barriuso D Dalal RA Riemersma LJ Appel E GuallarMeta-analysis high-dosage vitamin E supplementation may increase all-causemortality Ann Intern Med 142 (2005) 37ndash46
[172] JN Hathcock A Azzi J Blumberg T Bray A Dickinson B Frei I Jialal CSJohnston FJ Kelly K Kraemer L Packer S Parthasarathy H Sies MG TraberVitamins E and C are safe across a broad range of intakes Am J Clin Nutr 81(2005) 736ndash745
[173] R Brigelius-Flohe F Galli Vitamin E a vitamin still awaiting the detection of itsbiological function Mol Nutr Food Res 54 (2010) 583ndash587
711F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
[174] MG Traber B Frei JS Beckman Vitamin E revisited do new data validate ben-efits for chronic disease prevention Curr Opin Lipidol 19 (2008) 30ndash38
[175] F Galli Meeting report Vitamin E Satellite Symposium (VESS) associated to theAnnual Meeting of the SFRR-Europe Rome 26 August 2009 Free Radic Res 43(2009) 1256ndash1257
[176] LJ Roberts II JA Oates MF Linton S Fazio BP Meador MD Gross Y Shyr JDMorrow The relationship between dose of vitamin E and suppression of oxida-tive stress in humans Free Radic Biol Med 43 (2007) 1388ndash1393
[177] EFSA- EFSA Scientific Opinion of the Panel on Food Additives FlavouringsProcessing Aids and Materials in Contact with Food on a request from the Com-mission on mixed tocopherols tocotrienol tocopherol and tocotrienols assources for vitamin E in EFSA- EFSA (Ed) vol 640 The EFSA Journal2008 pp 1ndash34
[178] P Rust I Eichler S Renner I Elmadfa Long-term oral beta-carotene supple-mentation in patients with cystic fibrosis mdash effects on antioxidative status andpulmonary function Ann Nutr Metab 44 (2000) 30ndash37
[179] G Lepage J Champagne N Ronco A Lamarre I Osberg RJ Sokol CC Roy Sup-plementation with carotenoids corrects increased lipid peroxidation in childrenwith cystic fibrosis Am J Clin Nutr 64 (1996) 87ndash93
[180] BM Winklhofer-Roob H Puhl G Khoschsorur MA vant Hof H EsterbauerDH Shmerling Enhanced resistance to oxidation of low density lipoproteinsand decreased lipid peroxide formation during beta-carotene supplementationin cystic fibrosis Free Radic Biol Med 18 (1995) 849ndash859
[181] RC Graham-Maar JI Schall N Stettler BS Zemel VA Stallings Elevated vita-min A intake and serum retinol in preadolescent children with cystic fibrosisAm J Clin Nutr 84 (2006) 174ndash182
[182] I Sadowska-Woda M Rachel J Pazdan E Bieszczad-Bedrejczuk K PawliszakNutritional supplement attenuates selected oxidative stress markers in pediatricpatients with cystic fibrosis Nutr Res (New York NY) 31 (2011) 509ndash518
[183] KA Papas MK Sontag C Pardee RJ Sokol SD Sagel FJ Accurso JS WagenerA pilot study on the safety and efficacy of a novel antioxidant rich formulation inpatients with cystic fibrosis J Cyst Fibros 7 (2008) 60ndash67
[184] Y Saito A Fukuhara K Nishio M Hayakawa Y Ogawa H Sakamoto K Fujii YYoshida E Niki Characterization of cellular uptake and distribution of coen-zyme Q10 and vitamin E in PC12 cells J Nutr Biochem 20 (2009) 350ndash357
[185] AA Franke CM Morrison JL Bakke LJ Custer X Li RV Cooney CoenzymeQ10 in human blood native levels and determinants of oxidation during proces-sing and storage Free Radic Biol Med 48 (2010) 1610ndash1617
[186] HN Bhagavan RK Chopra Plasma coenzyme Q10 response to oral ingestion ofcoenzyme Q10 formulations Mitochondrion 7 (2007) S78ndashS88 (Suppl)
[187] HN Bhagavan RK Chopra Coenzyme Q10 absorption tissue uptake metabo-lism and pharmacokinetics Free Radic Res 40 (2006) 445ndash453
[188] F Galli R Lee C Dunster FJ Kelly Gas chromatography mass spectrometryanalysis of carboxyethyl-hydroxychroman metabolites of alpha- and gamma-tocopherol in human plasma Free Radic Biol Med 32 (2002) 333ndash340
[189] F Galli R Lee J Atkinson A Floridi FJ Kelly Gamma-tocopherol biokineticsand transformation in humans Free Radic Res 37 (2003) 1225ndash1233
[190] TA Laguna MK Sontag I Osberg JS Wagener FJ Accurso RJ Sokol De-creased total serum coenzyme-Q10 concentrations a longitudinal study in chil-dren with cystic fibrosis J Pediatr 153 (2008) 402ndash407
[191] T Frischer JK Myung G Maurer I Eichler Z Szepfalusi G Lubec Possible dys-regulation of chaperon and metabolic proteins in cystic fibrosis bronchial tissueProteomics 6 (2006) 3381ndash3388
[192] C Andersson MM Zaman AB Jones SD Freedman Alterations in immune re-sponse and PPARLXR regulation in cystic fibrosis macrophages J Cyst Fibros 7(2008) 68ndash78
[193] SD Freedman PG Blanco MM Zaman JC Shea M Ollero IK Hopper DAWeed A Gelrud MM Regan M Laposata JG Alvarez BP OSullivan Associa-tion of cystic fibrosis with abnormalities in fatty acid metabolism N Engl JMed 350 (2004) 560ndash569
[194] S Van Biervliet G Vanbillemont JP Van Biervliet D Declercq E Robberecht AChristophe Relation between fatty acid composition and clinical status or geno-type in cystic fibrosis patients Ann Nutr Metab 51 (2007) 541ndash549
[195] SD Freedman MH Katz EM Parker M Laposata MY Urman JG AlvarezA membrane lipid imbalance plays a role in the phenotypic expression ofcystic fibrosis in cftr(minusminus) mice Proc Natl Acad Sci U S A 96 (1999)13995ndash14000
[196] S Van Biervliet S Vande Velde JP Van Biervliet E Robberecht The effect ofzinc supplements in cystic fibrosis patients Ann Nutr Metab 52 (2008)152ndash156
[197] WR Henderson Jr SJ Astley MM McCready P Kushmerick S Casey JWBecker BW Ramsey Oral absorption of omega-3 fatty acids in patients withcystic fibrosis who have pancreatic insufficiency and in healthy control subjectsJ Pediatr 124 (1994) 400ndash408
[198] I Durieu E Vericel D Guichardant H Roth JP Steghens J Drai RN JosserandE Fontaine M Lagarde G Bellon Fatty acids platelets and oxidative markersfollowing intravenous n-3 fatty acids administration in cystic fibrosis an openpilot observational study J Cyst Fibros 6 (2007) 320ndash326
[199] LG Wood DA Fitzgerald ML Garg Hypothesis vitamin E complements poly-unsaturated fatty acids in essential fatty acid deficiency in cystic fibrosis J AmColl Nutr 22 (2003) 253ndash257
[200] JD Lloyd-Still SB Johnson RT Holman Essential fatty acid status in cystic fi-brosis and the effects of safflower oil supplementation Am J Clin Nutr 34(1981) 1ndash7
[201] A Maqbool JI Schall JF Garcia-Espana BS Zemel B Strandvik VAStallings Serum linoleic acid status as a clinical indicator of essential fatty
acid status in children with cystic fibrosis J Pediatr Gastroenterol Nutr 47(2008) 635ndash644
[202] C Oliver N Jahnke Omega-3 fatty acids for cystic fibrosis Cochrane DatabaseSyst Rev (2011) CD002201
[203] B Strandvik E Gronowitz F Enlund T Martinsson J Wahlstrom Essential fattyacid deficiency in relation to genotype in patients with cystic fibrosis J Pediatr139 (2001) 650ndash655
[204] P Rise S Volpi C Colombo RF Padoan C DOrazio S Ghezzi PMelotti V BennatoC Agostoni BM Assael C Galli Whole blood fatty acid analysis with micromethodin cystic fibrosis and pulmonary disease J Cyst Fibros 9 (2010) 228ndash233
[205] H Cao K Gerhold JR Mayers MM Wiest SM Watkins GS Hotamisligil Iden-tification of a lipokine a lipid hormone linking adipose tissue to systemic me-tabolism Cell 134 (2008) 933ndash944
[206] RR Malapaka SK Khoo J Zhang JH Choi XE Zhou Y Xu Y Gong J Li ELYong MJ Chalmers L Chang JH Resau PR Griffin YE Chen HE Xu Iden-tification and mechanism of a ten carbon fatty acid as a modulating ligand ofperoxisome proliferator activated receptors J Biol Chem 287 (2012)183ndash195
[207] T Hara A Hirasawa A Ichimura I Kimura G Tsujimoto Free fatty acid recep-tors FFAR1 and GPR120 as novel therapeutic targets for metabolic disorders JPharm Sci 100 (2011) 3594ndash3601
[208] R Gupta P Rathi S Bradoo Lipase mediated upgradation of dietary fats andoils Crit Rev Food Sci Nutr 43 (2003) 635ndash644
[209] BH Jennings CC Akoh Lipase-catalyzed modification of rice bran oil to incor-porate capric acid J Agric Food Chem 48 (2000) 4439ndash4443
[210] J Hoeks M Mensink MK Hesselink K Ekroos P Schrauwen Long- andMedium-Chain Fatty Acids Induce Insulin Resistance to a Similar Extent inHumans Despite Marked Differences in Muscle Fat Accumulation J Clin Endo-crinol Metab 97 (2012) 208ndash216
[211] PJ Congden G Bruce MM Rothburn PC Clarke JM Littlewood J KelleherMS Losowsky Vitamin status in treated patients with cystic fibrosis ArchDis Child 56 (1981) 708ndash714
[212] BM Winklhofer-Roob H Ellemunter M Fruhwirth SE Schlegel-Haueter GKhoschsorur MA vant Hof DH Shmerling Plasma vitamin C concentrationsin patients with cystic fibrosis evidence of associations with lung inflammationAm J Clin Nutr 65 (1997) 1858ndash1866
[213] L Shamseer D Adams N Brown JA Johnson S Vohra Antioxidant micronutri-ents for lung disease in cystic fibrosis Cochrane Database Syst Rev (2010)CD007020
[214] C Santi S Santoro Electrophilic Selenium First edition Wiley-VCH VerlagGmbH amp Co KGaA 2012
[215] L Flohe S Toppo G Cozza F Ursini A comparison of thiol peroxidase mecha-nisms Antioxid Redox Signal 15 (2010) 763ndash780
[216] L Flohe JR Andreesen R Brigelius-Flohe M Maiorino F Ursini Selenium theelement of the moon in life on earth IUBMB Life 49 (2000) 411ndash420
[217] V Valdiglesias E Pasaro J Mendez B Laffon In vitro evaluation of seleniumgenotoxic cytotoxic and protective effects a review Arch Toxicol 84(2010) 337ndash351
[218] P Foucaud P Therond M Marchand F Brion JF Demelier J Navarro Seleniumand vitamin E in mucoviscidosis Arch Fr Pediatr 45 (1988) 383ndash386
[219] J Neve R Van Geffel M Hanocq L Molle Plasma and erythrocyte zinc copperand selenium in cystic fibrosis Acta Paediatr Scand 72 (1983) 437ndash440
[220] BM Winklhofer-Roob B Tiran PE Tuchschmid MA vant Hof DH ShmerlingEffects of pancreatic enzyme preparations on erythrocyte glutathione peroxi-dase activities and plasma selenium concentrations in cystic fibrosis FreeRadic Biol Med 25 (1998) 242ndash249
[221] JD Lloyd-Still HE Ganther Selenium and glutathione peroxidase levels in cys-tic fibrosis Pediatrics 65 (1980) 1010ndash1012
[222] D Tsavachidou TJ McDonnell S Wen X Wang F Vakar-Lopez LL Pisters CAPettaway CG Wood KA Do PF Thall C Stephens E Efstathiou R Taylor DGMenter P Troncoso SM Lippman CJ Logothetis J Kim Selenium and vitaminE cell type- and intervention-specific tissue effects in prostate cancer J NatlCancer Inst 101 (2009) 306ndash320
[223] IN Zelko TJ Mariani RJ Folz Superoxide dismutase multigene family acomparison of the CuZn-SOD (SOD1) Mn-SOD (SOD2) and EC-SOD (SOD3)gene structures evolution and expression Free Radic Biol Med 33 (2002)337ndash349
[224] RP Bowler JD Crapo Oxidative stress in airways is there a role for extracellu-lar superoxide dismutase Am J Respir Crit Care Med 166 (2002) S38ndashS43
[225] K Best K McCoy S Gemma RA Disilvestro Copper enzyme activities in cysticfibrosis before and after copper supplementation plus or minus zinc Metabo-lism 53 (2004) 37ndash41
[226] SS Percival GP Kauwell E Bowser M Wagner Altered copper status in adultmen with cystic fibrosis J Am Coll Nutr 18 (1999) 614ndash619
[227] NF Krebs JE Westcott TD Arnold BM Kluger FJ Accurso LV Miller KMHambidge Abnormalities in zinc homeostasis in young infants with cystic fibro-sis Pediatr Res 48 (2000) 256ndash261
[228] D Easley N Krebs M Jefferson L Miller J Erskine F Accurso KM HambidgeEffect of pancreatic enzymes on zinc absorption in cystic fibrosis J Pediatr Gas-troenterol Nutr 26 (1998) 136ndash139
[229] S Van Biervliet JP Van Biervliet E Robberecht Serum zinc in patients with cys-tic fibrosis at diagnosis and after one year of therapy Biol Trace Elem Res 112(2006) 205ndash211
[230] S Van Biervliet JP Van Biervliet S Vande Velde E Robberecht Serum zinc con-centrations in cystic fibrosis patients aged above 4 years a cross-sectional eval-uation Biol Trace Elem Res 119 (2007) 19ndash26
712 F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
[231] F Galli M Cristina Polidori W Stahl P Mecocci FJ Kelly Vitamin E biotransfor-mation in humans Vitam Horm 76 (2007) 263ndash280
[232] J Wiser NE Alexis Q Jiang W Wu C Robinette R Roubey DB Peden In vivogamma-tocopherol supplementation decreases systemic oxidative stress andcytokine responses of human monocytes in normal and asthmatic subjectsFree Radic Biol Med 45 (2008) 40ndash49
[233] JG Wagner Q Jiang JR Harkema B Illek DD Patel BN Ames DB PedenOzone enhancement of lower airway allergic inflammation is prevented bygamma-tocopherol Free Radic Biol Med 43 (2007) 1176ndash1188
[234] JT Harries DP Muller Absorption of different doses of fat soluble and watermiscible preparations of vitamin E in children with cystic fibrosis Arch DisChild 46 (1971) 341ndash344
[235] EI Back C Frindt E Ocenaskova D Nohr M Stern HK Biesalski Can changesin hydrophobicity increase the bioavailability of alpha-tocopherol Eur J Nutr45 (2006) 1ndash6
[236] SZ Nasr MH OLeary C Hillermeier Correction of vitamin E deficiency withfat-soluble versus water-miscible preparations of vitamin E in patients with cys-tic fibrosis J Pediatr 122 (1993) 810ndash812
[237] S Soltani-Frisk E Gronowitz H Andersson B Strandvik Water-miscibletocopherol is not superior to fat-soluble preparation for vitamin E absorptionin cystic fibrosis Acta Paediatr 90 (2001) 1112ndash1115
[238] K Papas J Kalbfleisch R Mohon Bioavailability of a novel water-soluble vi-tamin E formulation in malabsorbing patients Dig Dis Sci 52 (2007)347ndash352
[239] F Antonicelli M Parmentier EM Drost N Hirani I Rahman K Donaldson WMacNee Nacystelyn inhibits oxidant-mediated interleukin-8 expression andNF-kappaB nuclear binding in alveolar epithelial cells Free Radic Biol Med 32(2002) 492ndash502
[240] EM App D Baran I Dab A Malfroot M Coffiner F Vanderbist M King Dose-finding and 24-h monitoring for efficacy and safety of aerosolized Nacystelyn incystic fibrosis Eur Respir J 19 (2002) 294ndash302
[241] MG Traber How much vitamin E hellip Just enough Am J Clin Nutr 84 (2006)959ndash960
[242] JC McCann BN Ames Vitamin K an example of triage theory is micronu-trient inadequacy linked to diseases of aging Am J Clin Nutr 90 (2009)889ndash907
[243] M Fusaro G Crepaldi S Maggi F Galli A DAngelo L Calo S Giannini DMiozzo M Gallieni Vitamin K bone fractures and vascular calcifications inchronic kidney disease an important but poorly studied relationship J Endocri-nol Invest 34 (2010) 317ndash323
[244] JC McCann BN Ames Adaptive dysfunction of selenoproteins from the per-spective of the triage theory why modest selenium deficiency may increaserisk of diseases of aging FASEB J 25 (2011) 1793ndash1814
[245] R Apak K Guclu M Ozyurek B Bektas Oglu M Bener Cupric ion reducing an-tioxidant capacity assay for food antioxidants vitamins polyphenolics and fla-vonoids in food extracts Methods Mol Biol 477 (2008) 163ndash193
[246] F Galli Interactions of polyphenolic compounds with drug disposition and me-tabolism Curr Drug Metab 8 (2007) 830ndash838
[247] RL Prior X Wu K Schaich Standardized methods for the determination of an-tioxidant capacity and phenolics in foods and dietary supplements J Agric FoodChem 53 (2005) 4290ndash4302
[248] C Azbell S Zhang D Skinner J Fortenberry EJ Sorscher BA WoodworthHesperidin stimulates cystic fibrosis transmembrane conductance regulator-mediated chloride secretion and ciliary beat frequency in sinonasal epitheliumOtolaryngol Head Neck Surg 143 (2010) 397ndash404
[249] G Wegrzyn J Jakobkiewicz-Banecka M Gabig-Ciminska E Piotrowska M Nar-ajczyk A Kloska M Malinowska D Dziedzic I Golebiewska M Moskot AWegrzyn Genistein a natural isoflavone with a potential for treatment of ge-netic diseases Biochem Soc Trans 38 (2010) 695ndash701
[250] YC Yu H Miki Y Nakamura A Hanyuda Y Matsuzaki Y Abe M Yasui K Ta-naka TC Hwang SG Bompadre Y Sohma Curcumin and genistein additivelypotentiate G551D-CFTR J Cyst Fibros 10 (2011) 243ndash252
[251] B Illek H Fischer Flavonoids stimulate Cl conductance of human airway epithe-lium in vitro and in vivo Am J Physiol 275 (1998) L902ndashL910
[252] JL Kreindler Cystic fibrosis exploiting its genetic basis in the hunt for newtherapies Pharmacol Ther 125 (2010) 219ndash229
[253] B Illek L Zhang NC Lewis RB Moss JY Dong H Fischer Defective function ofthe cystic fibrosis-causing missense mutation G551D is recovered by genisteinAm J Physiol 277 (1999) C833ndashC839
[254] P Anandakumar S Kamaraj S Jagan G Ramakrishnan R Vinodhkumar TDevaki Capsaicin modulates pulmonary antioxidant defense system during ben-zo(a)pyrene-induced lung cancer in Swiss albinomice Phytother Res 22 (2008)529ndash533
[255] I Rahman Antioxidant therapeutic advances in COPD Ther Adv Respir Dis 2(2008) 351ndash374
[256] AW Boots H Li RP Schins R Duffin JW Heemskerk A Bast GR Haenen Thequercetin paradox Toxicol Appl Pharmacol 222 (2007) 89ndash96
[257] M Joskova S Franova V Sadlonova Acute bronchodilator effect of quercetin inexperimental allergic asthma Bratisl Lek Listy 112 (2011) 9ndash12
[258] HJ Park CM Lee ID Jung JS Lee YI Jeong JH Chang SH Chun MJ Kim IWChoi SC Ahn YK Shin SR Yeom YM Park Quercetin regulates Th1Th2 balancein a murine model of asthma Int Immunopharmacol 9 (2009) 261ndash267
[259] AP Rogerio A Kanashiro C Fontanari EV da Silva YM Lucisano-ValimEG Soares LH Faccioli Anti-inflammatory activity of quercetin and iso-quercitrin in experimental murine allergic asthma Inflamm Res 56 (2007)402ndash408
[260] M Muller Polyphenol cytotoxicity induced by the bacterial toxin pyocyaninrole of NQO1 Free Radic Biol Med 47 (2009) 84ndash91
[261] J Grassmann Terpenoids as plant antioxidants Vitam Horm 72 (2005)505ndash535
[262] P Allen Tea tree oil the science behind the antimicrobial hype Lancet 358(2001) 1245
[263] EC Dasenbrook W Checkley CA Merlo MW Konstan N Lechtzin MP BoyleAssociation between respiratory tract methicillin-resistant Staphylococcus aure-us and survival in cystic fibrosis JAMA 303 (2010) 2386ndash2392
[264] V Bezzerri M Borgatti E Nicolis I Lampronti MC Dechecchi I Mancini PRizzotti R Gambari G Cabrini Transcription factor oligodeoxynucleotides toNF-kappaB inhibit transcription of IL-8 in bronchial cells Am J Respir CellMol Biol 39 (2008) 86ndash96
[265] R Gambari M Borgatti V Bezzerri E Nicolis I Lampronti MC Dechecchi IMancini A Tamanini G Cabrini Decoy oligodeoxyribonucleotides and peptidenucleic acids-DNA chimeras targeting nuclear factor kappa-B inhibition of IL-8 gene expression in cystic fibrosis cells infected with Pseudomonas aeruginosaBiochem Pharmacol 80 (2010) 1887ndash1894
[266] M Adrian P Jeandet AC Douillet-Breuil L Tesson R Bessis Stilbene content ofmature Vitis vinifera berries in response to UV-C elicitation J Agric Food Chem48 (2000) 6103ndash6105
[267] B Paul I Masih J Deopujari C Charpentier Occurrence of resveratrol and pter-ostilbene in age-old darakchasava an ayurvedic medicine from India J Ethno-pharmacol 68 (1999) 71ndash76
[268] I Rahman Antioxidant therapies in COPD Int J Chron Obstruct Pulmon Dis 1(2006) 15ndash29
[269] M Lee S Kim OK Kwon SR Oh HK Lee K Ahn Anti-inflammatory and anti-asthmatic effects of resveratrol a polyphenolic stilbene in a mouse model ofallergic asthma Int Immunopharmacol 9 (2009) 418ndash424
[270] LG Wood PA Wark ML Garg Antioxidant and anti-inflammatory effectsof resveratrol in airway disease Antioxid Redox Signal 13 (2010)1535ndash1548
[271] KV Kiselev Perspectives for production and application of resveratrol ApplMicrobiol Biotechnol 90 (2011) 417ndash425
[272] M Shakibaei C Buhrmann A Mobasheri Resveratrol-mediated SIRT-1 interac-tions with p300 modulate receptor activator of NF-kappaB ligand (RANKL) acti-vation of NF-kappaB signaling and inhibit osteoclastogenesis in bone-derivedcells J Biol Chem 286 (2011) 11492ndash11505
[273] SF Zaidi K Ahmed T Yamamoto T Kondo K Usmanghani M Kadowaki TSugiyama Effect of resveratrol on Helicobacter pylori-induced interleukin-8 secre-tion reactive oxygen species generation and morphological changes in human gas-tric epithelial cells Biol Pharm Bull 32 (2009) 1931ndash1935
[274] JK Kundu YK Shin YJ Surh Resveratrol modulates phorbol ester-inducedpro-inflammatory signal transduction pathways in mouse skin in vivo NF-kappaB and AP-1 as prime targets Biochem Pharmacol 72 (2006)1506ndash1515
[275] NH Nam Naturally occurring NF-kappaB inhibitors Mini Rev Med Chem 6(2006) 945ndash951
[276] JM Smoliga JA Baur HA Hausenblas Resveratrol and healthmdasha comprehen-sive review of human clinical trials Mol Nutr Food Res 55 (2011) 1129ndash1141
[277] ME Juan M Maijo JM Planas Quantification of trans-resveratrol and itsmetabolites in rat plasma and tissues by HPLC J Pharm Biomed Anal 51(2010) 391ndash398
[278] JA Baur DA Sinclair Therapeutic potential of resveratrol the in vivo evidenceNat Rev 5 (2006) 493ndash506
[279] E Nicolis I Lampronti MC Dechecchi M Borgatti A Tamanini N Bianchi VBezzerri I Mancini MG Giri P Rizzotti R Gambari G Cabrini Pyrogallol anactive compound from the medicinal plant Emblica officinalis regulates expres-sion of pro-inflammatory genes in bronchial epithelial cells Int Immunophar-macol 8 (2008) 1672ndash1680
[280] E Nicolis I Lampronti MC Dechecchi M Borgatti A Tamanini V Bezzerri NBianchi M Mazzon I Mancini MG Giri P Rizzotti R Gambari G CabriniModulation of expression of IL-8 gene in bronchial epithelial cells by 5-methoxypsoralen Int Immunopharmacol 9 (2009) 1411ndash1422
[281] M Borgatti I Mancini N Bianchi A Guerrini I Lampronti D Rossi G SacchettiR Gambari Bergamot (Citrus bergamia Risso) fruit extracts and identified com-ponents alter expression of interleukin 8 gene in cystic fibrosis bronchial epithe-lial cell lines BMC Biochem 12 (2011) 15
[282] L Piccagli E Fabbri M Borgatti N Bianchi V Bezzerri I Mancini E Nicolis CMDechecchi I Lampronti G Cabrini R Gambari Virtual screening against p50NF-kappaB transcription factor for the identification of inhibitors of the NF-kappaB-DNA interaction and expression of NF-kappaB upregulated genesChemMedChem 4 (2009) 2024ndash2033
[283] L Piccagli M Borgatti E Nicolis N Bianchi I Mancini I Lampronti D VevaldiF DallAcqua G Cabrini R Gambari Virtual screening against nuclear factorkappaB (NF-kappaB) of a focus library identification of bioactive furocoumarinderivatives inhibiting NF-kappaB dependent biological functions involved incystic fibrosis Bioorg Med Chem 18 (2010) 8341ndash8349
[284] M Borgatti A Chilin L Piccagli I Lampronti N Bianchi I Mancini G Mar-zaro Da Francesco A Guiotto R Gambari Development of a novel furocou-marin derivative inhibiting NF-kappaB dependent biological functionsdesign synthesis and biological effects Eur J Med Chem 46 (2011)4870ndash4877
[285] E Georgy S Le Guellec L Vecellio E Fichant P Stordeur P Bordeau JP PerraudinFeasibility study of OSCN- and lactoferrin (Meveol) nebulization for cysticfibrosis JCyst Fibros 10 (2011) S18
713F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
[286] C Tidei M Piroddi F Galli C Santi Oxidation of thiols promoted by PhSeZnClTetrahedron Lett 53 (2012) 232ndash234
[287] L Semianrio-Vidal C van Hesuden G Mugesh ER Lazarowski Ebselen is a po-tent non-competitive inhibitor of extracellular nucleoside diphosphokinasePurinergic Signal 6 (2010) 383ndash391
[288] C ColussiMC Albertini S Coppola S Rovidati F Galli L Ghibelli H2O2-inducedblockof glycolysis as an active ADP-ribosylation reaction protecting cells from apoptosisFASEB J 14 (2000) 2266ndash2276
[289] H Xiao KL Parkin Induction of phase II enzyme activity by various seleniumcompounds Nutr Cancer 55 (2006) 210ndash223
[290] G Peluffo R Radi Biochemistry of protein tyrosine nitration in cardiovascularpathology Cardiovasc Res 75 (2007) 291ndash302
[291] B Alvarez R Radi Peroxynitrite reactivity with amino acids and proteinsAmino Acids 25 (2003) 295ndash311
[292] B Kamosinska MW Radomski M Duszyk A Radomski SF Man Nitric oxideactivates chloride currents in human lung epithelial cells Am J Physiol 272(1997) L1098ndashL1104
[293] L Chen RP Patel X Teng CA Bosworth JR Lancaster Jr S Matalon Mecha-nisms of cystic fibrosis transmembrane conductance regulator activation by S-nitrosoglutathione J Biol Chem 281 (2006) 9190ndash9199
[294] F Luchetti B CanonicoM BettiM Arcangeletti F PilolliM Piroddi L Canesi S PapaF Galli Melatonin signaling and cell protection function FASEB J 24 (2010)3603ndash3624
[295] MW Bengtsson G Jedstedt G Flemstrom Duodenal bicarbonate secretion inrats stimulation by intra-arterial and luminal guanylin and uroguanylin ActaPhysiol (Oxf) 191 (2007) 309ndash317
[296] CS Nelson JL Marino CN Allen Melatonin receptor potentiation of cyclic AMP andthe cystic fibrosis transmembrane conductance regulator ion channel J Pineal Res 26(1999) 113ndash121
[297] C de Castro-Silva VM de Bruin GM Cunha DM Nunes CAMedeiros PF de BruinMelatonin improves sleep and reduces nitrite in the exhaled breath condensate incystic fibrosismdasha randomized double-blind placebo-controlled study J Pineal Res48 (2010) 65ndash71
[298] I Hornyak E Pankotai L Kiss Z Lacza Current developments in the the-rapeutic potential of S-nitrosoglutathione an endogenous NO-donor mole-cule Curr Pharm Biotechnol (2011) Jan 11 [Epub ahead of print] - PMID21235457
[299] AH Snyder ME McPherson JF Hunt M Johnson JS Stamler B Gaston Acuteeffects of aerosolized S-nitrosoglutathione in cystic fibrosis Am J Respir CritCare Med 165 (2002) 922ndash926

692 F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
intensive treatment of the infection [13ndash15] The fact that relapses orsuccessful therapy of infection do not normalize these markers dem-onstrates the presence of a chronic inflammatory syndrome that isintrinsic to the CF defect In this context ROS may lose their physio-logical role in the killing of pathogens to turn into toxic effectors re-sponsible for the damage of the pulmonary epithelium as well as ofother components of the lung parenchyma and lining fluids Impor-tantly ROS can modify the thiol homeostasis of extracellular fluidsand epithelia [16] and promote the activation of MAPK signalingpathways [17] which regulate both the NFkβ-dependent and-independent transcription of pro-inflammatory genes and other mo-lecular effects associated with the immuno-inflammatory imbalanceobserved in the CF lung
Hallmark of the chronic inflammatory lung disease in CF is therelease of chemokines mainly interleukin (IL)-8 [1819] leading tothe neutrophil recruitment in the bronchial lumen (see [20] for areview) Whether CF lung inflammation arises independently andbefore bacterial infection remains to be fully established althoughIL-8 and pro-inflammatory cytokines have been found in bronchoal-veolar lavage fluids of CF infants even before the onset of an overtbacterial infection [21] Although directed against infective agentsthe chronic inflammation in CF lungs is largely recognized as mainlyresponsible for the progressive tissue damage leading to respiratoryinsufficiency Dissection of the pathophysiology of CF chronic lunginflammation should take into account the bronchial epithelial cellsexpressing the mutated CFTR protein the polymorphonuclear neu-trophils recruited into the bronchial lumens and the bacterial infec-tion itself with special regards to Pseudomonas aeruginosa the mostcommon gram negative microorganism which colonizes CF airways[22] Thus novel anti-inflammatory therapies against the progressivedamage of the CF respiratory tissue should be mainly aimed i) to re-duce the excessive recruitment of neutrophils by intervening on thetransmembrane signaling pivoting the excessive expression of IL-8 [23ndash26] ii) to inactivate proteases released by the neutrophils con-tinuously activated by bacterial products [27] and iii) to circumventthe effect of the unbalanced production of oxidants deriving fromboth phagocytes and bronchial epithelial cells [2228ndash30] Identifica-tion of oxidants produced in the CF airway tract is of high importancein order to identify novel molecular targets for specific pharmacolog-ical intervention
22 Respiratory epithelial cells and neutrophils as sources of oxidants inthe CF lung
It is largely accepted that neutrophils migrating inside the CFbronchial lumina release large amounts of reactive oxygen species(ROS) including the superoxide anion (O2
minusbull) hydrogen peroxide(H2O2) and the hydroxyl free radical (OH) mainly by the activationof the NADPH oxidase (NOX) To such exaggerated ROS productioncontribute both the continuous interaction of neutrophils with bacte-ria and bacterial degradation products and the inability to engulf bac-teria in biofilms leading to a condition of ldquofrustrated phagocytosisrdquoNeutrophils are therefore recognized as a major source of ROS inthe airway surface liquid (ASL) of young children with CF [1431]However bronchial ciliated and alveolar type II epithelial cells bythemselves are able to produce significant amounts of ROS throughthe two isoforms of NADPH oxidase expressed in the apical membraneof these epithelial cells namely DUOX1 and DUOX2 [32] A major pro-posed function of DUOXs is to support lactoperoxidase (LPO) which isin turn released by goblet and submucosal gland airway cells to gen-erate bactericidal hypothiocyanite (OSCNminus) starting from thiocyanate(SCNminus) and H2O2 Thus the DUOXLPO coupled system of the respira-tory epithelial cells parallels the NOXmieloperoxidase (MPO) systemof phagocytes in releasing and processing oxidants in the ASL Whilethe NOXMPO system of phagocytes is mainly activated in theinfection-induced respiratory burst the release of ROS from epithelia
is continuous and even independent of the presence of overt bacterialinfection [33] Interestingly it was proposed that the efficiency of theDUOXLPO defense system is dependent on the ion transport functionof the CFTR Clminus channel which could also intervene both in the con-ductive secretion of SCNminus (for LPO function) and of HCO3
minus (for pHadjustment) into the ASL [34] However more recent ex vivo observa-tions while confirming a positive role of DUOXLPO system in produc-ing OSCNminus as a general defense mechanism of the airways do notdirectly relate SCNminus concentrations in ASL with CFTR function [35]The LPO-mediated scavenging of H2O2 has suggested a role of SCNminus
as physiological antioxidant of ASL [36] which may be defective inCF Besides this role of LPO and SCNminus an abnormal flux of H2O2 inthe CF airways may also depend on other factors that are associatedwith an alteredmetabolism of ROS For instance lowered levels of Lac-toferrin (LF) have been described in CF secretions [37] This iron-chelating homologue of transferrin contained in the granules of neu-trophils is also secreted by several mucosal tissues in biological fluidsto contribute antimicrobial effects by a variety of mechanisms includ-ing the chelating activity of iron as Fenton chemistry catalyst [38]
As regards the progression of CF lung disease in the early phasesbefore the onset of chronic bacterial colonization epithelial DUOXcontinuously releases H2O2 thus being a predominant source inrespect to the NADPH oxidase from phagocytes The latter is mainlyactive when the respiratory burst is ldquotriggered on demandrdquo by infec-tious components On the other side in advanced phases of chronicinfection of CF lungs neutrophil-derived ROS are predominant [32]due to neutrophil activation as well as to the decreasing number ofH2O2-producing ciliated cells which are reduced by extensive apo-ptosis and tissue remodeling A further reduction of epithelial DUOXactivity has been observed as a result of infection with P aeruginosain conductive airways P aeruginosa-derived toxin pyocyanin in factinhibits DUOX-dependent H2O2 production by consuming intracellu-lar NADPH which represents an interesting adaptive mechanism todownregulate innate anti-bacterial defenses [39]
23 Redox disturbances of CF airways the role of GSH NO and H2O2
Intracellular impairment of redox balance between oxidants andanti-oxidants has been proposed to occur in CF bronchial epithelialcells although a significant difference in respect to normal CFTR-expressing cells is still controversial and debated [40] Three majorissues have been investigated concerning the intracellular redox bal-ance in CF bronchial cells namely i) a defect in GSH homeostasis[4142] ii) an alteration of nitric oxide (NO) metabolism and iii) animbalance of intracellular H2O2 production
As far as GSH is concerned the defective CFTR channel functionhas been proposed to lead to a lowered cell content of this tripeptidewhich is crucial to control the flux of H2O2 in both the CF bronchialepithelial cells and lining fluids This aspect ndash discussed in detailbelow in this review ndash is associated with characteristic defects ofGSH-related enzymes and may represent a key underlying factor inthe oxidative stress of CF airways
Altered NO concentration has been found in chronic respiratorydiseases such as bronchial asthma and chronic obstructive pulmonarydisease [43] and reduced NO concentrations have been observed inthe bronchial airways of patients affected by CF which directly corre-lated with worsening of lung function [44] Thus NO concentration inCF lung exhalate has been subsequently tested as a possible marker ofpulmonary exacerbations andor the inflammatoryinfective statusand its fluctuations over time [4546]
This opened the way to further analysis of the mechanisms of thisderangement and it has been proposed that an excessive productionof asymmetric dimethylarginine an inhibitor of endogenous NOSynthase (NOS) could be involved in the reduced concentrationof NO in CF airways [47ndash49] Possible corrective therapies such asthe inhalation of L-arginine have provided preliminary evidence of
693F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
correction of the defective NO concentration and improvement oflung function in CF patients [49ndash51]
Although exhaled NO is decreased in CF increased immunohisto-chemical staining for nitrotyrosine was demonstrated in lung tissuesfrom CF patients [52] Therefore a decreased production or accelerat-ed metabolism of NO could be present in association with an abnor-mal reactivity of this radical and its derived species (NOx) towardbiomolecular components of the CF airways Peroxynitrite is one ofthe most relevant mediators of the biological activity of NO withtoxic properties and damaging activity on several biomolecules [53]
A third emerging issue takes into consideration the expressionof different enzymatic systems affecting the redox balance in CF bron-chial epithelial cells For instance intracellular concentration of H2O2
has been found abnormally elevated in both immortalized bronchialand primary nasal epithelial cells derived from CF patients bothin the presence and the absence of proinflammatory cytokines [54]This has been accompanied by a marked decrease of expressionof proteins regulating H2O2 levels such as thioredoxin 1 (TRX-1)glutathione-S-transferase pi (GST-pi) peroxyredoxin (PRDX) 6TRX-dependent peroxide reductase (PRDX-1) catalase and con-versely a significant increase of Mn superoxide dismutase (SOD2)[54] Interestingly to link these modifications with CF specific charac-teristics dysfunctional CFTR channel was found associated withreduced activity of the transcription factor Nrf-2 (nuclear factor-erythroid 2 p45 subunit-related factor 2) which could at least inpart explain the differential expression of the enzymatic systemsresulting in the elevated intracellular steady-state concentration ofH2O2 found in CF nasal and bronchial epithelial cells [54] In synthesisthe ASL of CF patients during advanced stages of the lung disease con-tains elevated concentrations of ROS mainly derived from neutro-phils migrated into the airway lumen and a reduced concentrationof NO which can strongly contribute to respiratory tissue injurytogether with the proteases released by the activated neutrophilsThe homeostatic role of the GSH-related defenses appears constitu-tively impaired by the dysfunctional CFTR thus increasing suscepti-bility to develop oxidative stress and lung tissue degeneration(Fig 1) as described in detail in the sections below
24 Conductive airway epithelium as target of ROS
Oxidants can target different biomolecules to damage epithelialcells and extracellular fluids of the airways Lipid peroxidationand post-translational modifications of proteins on both cell mem-branes and extracellular targets are common biomarkers of thisdamage which can occur by the direct reaction between ROS and bio-molecules or through the formation of second-generation reactivebyproducts [955] All levels of this interaction between ROS and bio-logical components can produce toxic and bioactive intermediatesOxidants are known to activate secondmessengers through phospho-lipases A2 C and D and to induce the production of cytokines andmucins a series of molecular events that contribute to progressiveobstructive disease and reduction of lung function [56] Besides thedirect oxidative damage to cellular structures of the bronchial epithe-lial cells the excessive concentration of oxidants in CF both in the ASLlining the apical membranes and inside the bronchial cells has beenstudied in respect to the regulation of the inflammatory response
ROS are often considered a sort of secondmessengers in activatingthe Nuclear Factor (NF)-κB which is in turn involved in the activationof transcription of several proinflammatory cytokines and chemo-kines [57] For instance it has been shown that H2O2 partly controlsNF-κB activation by IL-1beta by facilitating the activation of NIKand subsequent phosphorylation of IKKβ [58] In this respect a directlink has been proposed between the excessive production of intracel-lular H2O2 and the elevated expression of IL-6 and IL-8 the mostabundant pro-inflammatory cytokine and neutrophilic chemokinefound in CF airways [54] which has been further confirmed [59]
Moreover oxidants could be synergic in the induction of mucins aspromoted by neutrophil elastase which further impairs ASL fluidityin CF [60] Finally bacterial infection with P aeruginosa strains releas-ing the toxin pyocyanin (PCN) has been shown to reduce ion trans-port through the CFTR channel thus potentially counteracting thetherapeutic effects of correctors and potentiators of mutated CFTRprotein [6162] In summary excessive oxidants in CF conductive air-ways have different negative effects in the amplification of the al-ready excessive lung inflammation and secretion of mucin togetherwith a direct deleterious effect on CFTR channel function
25 Oxidative stress and surfactant
Oxidative stress and inflammation in cystic fibrosis can affect sur-factant biophysical activity thus leading to early alterations of lungfunction in patients with CF [63] Altered phospholipid-to-protein ra-tios and phospholipid subclasses a modified fatty acid profiles anddecreased association of proteins such as SP-A with lipid componentsof isolated surfactant indicate that components of this fluid are con-siderably altered and dysfunctional in lower respiratory tract secre-tions of CF patients [64]
Oxidative damage of surfactant may involve both lipid and proteincomponents Alteration of lipid components can in turn generatetoxic lipid species with cytotoxic activity towards nearby epithelialcells [65] Altered protein components have been shown in cysticfibrosis [66] Notably surfactant protein D which is an important in-nate host defense molecule becomes unable to agglutinate bacteriawhen it is modified by oxidation which facilitates pathogen coloniza-tion in the lung [67] In a cross-sectional analysis of CF patients withmild lung disease reduced surfactant activity was correlated to in-creased neutrophilic airway inflammation but not to lung function[68] So far longitudinal measurements of surfactant function in CFpatients are lacking and it remains unclear how these alterationsrelate to progression of airway inflammation as well as to the rateof decline of pulmonary function [69]
26 Laboratory indices of oxidative stress in CF
Appropriate biochemical and clinical tools are of importance forthe monitoring of antioxidant therapies in CF and a crucial aspect isthe selection of proper biomarkers and protocols to assess biologicalpathways of oxidation
Pancreatic insufficiency and a diminished bile acid pool cause mal-absorption of important essential nutrients and other dietary compo-nents in CF Of particular significance is the malabsorption of fat-soluble antioxidants such as carotenoids tocopherols and coenzymeQ-10 (CoQ-10) which act as chain breakers in the peroxidation reac-tions of polyunsaturated lipids Accordingly lipid peroxidation is oneof the main signs encountered in the CF plasma buccal mucosal cellsbreath condensate and BALF as measured by the non-enzymaticoxidation product of arachidonic acid 8-iso prostaglandin F2α[570ndash73] Elevations of this and other eicosanoids in human bodyfluids and tissues have been found in a diverse array of human disor-ders including atherosclerosis diabetes obesity cigarette smokingneurodegenerative diseases and many others [74] Further treat-ments for some of these conditions including antioxidant supple-mentation have been shown to decrease the levels of this class ofbiomarkers In CF patients respiratory exacerbations increase plasmalevels of 8-iso-F2α [70] the levels of which in the breath condensatenegatively correlate with respiratory function data [71] At the sametime successful in vivo antioxidant therapy by GSH inhalation hasbeen shown to decreased PGE levels in BALF in association withchanges in the number and activity of leukocyte subpopulations re-sponsible for lung inflammation [73]
Oxysterols a biomarker of cholesterol oxidation were found toincrease in CF plasma as a further proof of the abnormal lipid
694 F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
metabolism and increased susceptibility to oxidation of lipoproteinlipids in CF patients [7] Importantly an increased oxidative burdenof lung and blood lipids may produce bioactive lipid products thatfurther sustain CF symptoms Besides to 8-iso-F2α and other ana-logues with some bioactivity [74] arachidonic acid oxidation maycontribute to persistent platelet activation and pulmonary dysfunc-tion in CF via generation of bioactive isoeicosanoids [75] which pro-vides sufficient rationale for a prevention therapy with fat solubleantioxidants such as vitamin E Evidence has recently accumulatedon the systemic effects of oxysterols on various tissues and organs[76] The role of this lipid oxidation product alone or in combinationwith other factors could be further investigated in the context ofmechanisms and clinical progression of multi-organ failure of CFpatients
The impaired pancreatic and liver functions of CF patients repre-sent the underlying factor for a defective lipoprotein metabolismand hypocholesterolemia which exponentially increase the burdenof damage by cholesterol and other lipids due to reduced blood trans-port of fat-soluble antioxidants with nascent VLDL particles Besidesoxysterol accumulation plasma fatty acid composition is also affected[7] and an increased ratio between unsaturated and saturated fattyacid species may contribute to lower cellular antioxidant defenses
Altogether these findings suggest that lipid oxidation biomarkerscan provide a reliable measure of systemic and lung-specific oxidativestress in CF
Markers of protein damage are also detectable in the airways ofchildren with CF and their levels are observed to parallel the extentof neutrophilic markers and lung dysfunction [143166] Bronchoal-veolar lavage proteins undergo halogenation of Tyr residues aradical-mediated process presumably depending on MPO enzyme ac-tivity and assessed through the analysis of 3-chlorotyrosine and 3-bromotyrosine Thiocyanate and protein carbonyls are also useful bio-markers to assess the inflammation-related injury of BALF proteins inCF [1431]
3 Antioxidants in CF
31 Glutathione and its related defense system
311 Defects in GSH homeostasisOther studies have pointed to alterations in the levels of extracel-
lular antioxidants in respiratory tract lining fluids [3] In particularthe analyses of broncheoalveolar lavages (BAL) have revealed thepresence of decreased levels of GSH in the alveolar epithelial liningfluid of CF patients The normal level of extracellular GSH in thelung is 140 times that present in blood plasma and the lung is a netimporter of circulating GSH [77] As a result GSH concentration inELF is close to 400 μM whereas significantly reduced GSH levels arepresent in adult CF patients [41] Low levels of GSH have been ob-served in plasma and blood neutrophils [4178] suggesting systemicGSH dyshomeostasis in CF Moreover some studies have shown thatat the cellular level the CFTR mutation causes mitochondrial deple-tion of GSH [7980] The consequences of this defect are still difficultto be understood due to our poor knowledge about the exact func-tions of GSH in the lung but there are reasons to believe that thedecrease of GSH in the ASL contributes to lung infection and inflam-mation [4281] At the same time it must be underlined that a recentstudy has shown that the GSH content in sputum samples is higher inCF patients than in healthy people indicating that GSH deficiency inCF is restricted to the lower respiratory tract [82] Several hypotheseshave been proposed to explain such a local increase in GSH includingthe possibility that it may derive from apoptotic neutrophils The re-lease of high levels of GSH may be part of a compensatory mechanismaimed at controlling disulfide bonds-mediated aggregation of mucinsSecretions of the upper respiratory tract contain abundant levels ofthese glycosylated and cysteine-rich proteins likely playing a role in
the airway antioxidant defense Indeed these proteins are potent invitro ROS scavenges [83] and their synthesis is upregulated upon ox-idative stress via epidermal growth factor receptor (EGFR) transacti-vation [84]
GSH a major component of cellular antioxidant defenses exerts im-portant functions related to its electron-donating capacity includingprotection from the damaging effects of ROS and regulation of a pletho-ra of cellular events such as gene expression proliferation and differen-tiation apoptosis and immune response [85] GSH is synthesized by twosequential ATP-dependent reactions catalyzed by γ-glutamylcysteinesynthetase (recently renamed glutamate-cysteine ligase) andGSH syn-thetase The reaction catalyzed by γ-glutamylcysteine synthetase iethe formation of γ-glutamylcysteine from glutamate and cysteine isthe rate-limiting step in GSH synthesis and is feedback regulated byGSH itself In fact this enzyme represents an interesting case of redox-regulation of catalytic activity that is mediated by the reversible forma-tion of disulfide bonds [86] Oxidizing conditions causing GSH depletionpromote the formation of a disulfide bondbetween the catalytic and theregulatory subunits of the enzyme leading to a conformational changewhich favors the binding of glutamate In contrast physiological levelsof GSH reduce this disulfide bond thus explaining GSH feedbackinhibition
Either in intracellular or extracellular compartments GSH is pre-dominantly found in the reduced form although small amounts ofthe oxidized disulfide forms (GSSG or GSSR where a GSH moleculeis linked to a free or a protein thiol) can always be detected GSSG isproduced by the catalysis of glutathione peroxidase during thedetoxification from hydrogen peroxide and other peroxides or bythe direct reactions of GSH with electrophilic compounds such asradical species Despite the bulk of GSH synthesis occurring in thecytoplasm GSH is distributed in intracellular organelles includingthe endoplasmic reticulum mitochondria and nucleus Under physio-logical conditions the GSH to GSSG ratio in these compartments ishigh frequently gt1001 but this may change under conditions of ox-idative stress [87] A major exception is represented by the endoplas-mic reticulum where GSSG is present at much higher levels to favordisulfide bond formation [88] Interestingly the compartmentaliza-tion of GSH in separate pools within organelles allows localized alter-ations in the balance between GSH and GSSG that may haveconsiderable functional and pathological significance [89] Thiscould be particularly important in CF in view of the above mentionedstudies showing that cultured CF cells have an apparent normal GSHGSSG content but are characterized by a marked decrease in mito-chondrial GSH in association to elevated mitochondrial ROS [7980]
Different roles of high levels of GSH in the ELF may be hypothe-sized including a) preventing inflammation and tissue damage byscavenging the ROS spontaneously generated in this highly oxidizingenvironment actively produced by neutrophils during inflammationor originating from lipid peroxidation b) regulating the redox statusof membrane proteins involved in the transduction of signals leadingto changes in the expression of genes involved in the immune re-sponse c) controlling mucus viscosity by breaking disulphide bondsd) modulating the response to bacterial infections This last possibili-ty is suggested by the observation that GSH significantly increasesin the ASL of wild type mice following P aeruginosa infection where-as this response is not observed in CFTR mutant mice [90] Interest-ingly some authors have suggested the ability of GSH to control Paeruginosa growth and resistance to antibiotics although these stud-ies should be considered with some cautions due to the likely use ofunbuffered GSH [91]
Although the decreased levels of GSH in ELF could be due to in-creased consumption during inflammation-related oxidative stress[4192] GSH deficiency in CF ELF likely derives from CFTR channeldysfunction In fact comparable alterations in GSH extracellular con-tent characterize the lung of CFTR knockout mice [93] indicating thatthis defect is correlated to mutations in CFTR
695F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
In particular ELF and lung tissue from CFTR knockout (Cftr KOB6129P2-Cftrtm1Unc) and wild-type mice were compared for GSHcontent and the activities of glutathione-related enzymes [93] Inthe ELF the concentration of GSH was significantly decreased in theCftr KO mice compared to WT whereas tissue concentrations ofGSH were similar [92] In the Cftr KO lung the activities of glutathionereductase and glutathione peroxidase were increased whereas theactivity of γ-glutamyltransferase was unchanged Two indicators ofoxidative stress thiobarbituric acid reactive substances (TBARS) and8-hydroxy-2-deoxyguanosine (8-OHdG) were also increased in theCftr KO lung tissue [90] These data support the hypothesis that a mu-tation in the CFTR gene can affect the antioxidant defenses in the lungand may contribute to the exaggerated inflammatory response ob-served in CF Thereby CFTR could be considered as an importantactor of ELF antioxidant homeostasis and thus an intrinsic cause ofoxidative imbalance in CF airways of human patients as well as CftrKO mice
Moreover CFTR belongs to the MRPABC family of proteins whichincludes several GSH transporters and some in vitro studies have in-dicated that CFTR may mediate GSH export across membranes[2394] Despite these evidences there is still debate about the phys-iological implication of CFTR in GSH transport outside the cells asother studies have raised the possibility that CFTR may not actuallyconduct GSH but regulate its transport indirectly through chloridetransport [85]
312 In vitro studies suggesting a protective role of GSH in CF modelsystems
Possible protective roles of extracellular GSH in the CF lung havebeen long proposed and recent in vitro studies have provided furtherand more robust support to this clue For example it has been sug-gested that GSH may control the levels of chlorinated compoundsformed by the activity of myeloperoxidase a neutrophil-releasedprotein abundantly present in CF patients secretions [9596] and pre-vent NK-κB activation [96] Other studies have suggested that CFTRmutant cells produce higher levels of proinflammatory cytokines inresponse to P aeruginosa diffusible material with respect to wildtype cells through a mechanism involving the activation of NADPHoxidase This effect may be significantly reversed by the addition ofextracellular GSH [97]
GSH could also play an important role in protecting the lung epi-thelia from the toxic effects of pyocyanin (PCN) a redox-active exo-toxin released by P aeruginosa which is supposed to cause a varietyof deleterious effects on the airway physiology [98] PCN levels ashigh as 130 μM have been measured in pulmonary secretions of pa-tients with CF and individuals with chronic bronchiectasis [99] Atconcentrations within the range measured in the sputum from CF pa-tients PCN induces a drastic reduction of intracellular GSH [100101]promotes death of cultured cells [100] and causes pathophysiologicalalterations in the lung of wild type mice that are consistent with thechanges observed in CF patients [102] PCN toxicity likely derivesfrom its ability to accept electrons from cellular reductants and thenreact with oxygen to generate superoxide and other ROS [103] There-fore GSH deficiency is explained either by the reaction of GSH withsuch oxidants or through the direct reaction of PCN with GSH thatleads to the formation of a PCN radical [103] However the electrontransfer from GSH to PCN does not occur at neutral pH and recent ob-servations suggest that extracellular GSH provides significant protec-tion against the toxic effects of PCN [104] Moreover GSH can reactwith PCN to form a stable adduct which is likely redox inactive[105] Although the relationships between extracellular GSH andPCN are still contradictory it is worth mentioning that extracellularGSH increases to millimolar levels in the ELF of wild type miceinfected with P aeruginosa indicating that GSH may be useful to re-sist to bacterial colonization [90] Interestingly in vitro studies have
revealed that extracellular GSH inhibits the ability of Burkholderiacenocepacia to enter epithelial respiratory cells and reduces bacterialinduced expression of proinflammatory cytokines (DOrazio Pacelloand Battistoni 2011 unpublished results)
32 GSH-based antioxidant therapies
321 Preclinical studies in animal models of CFMice genetically modified for the Cftr gene along with acute and
chronic infection induced by CF-related pathogens are a key asset inCF research Although much has been learned through these CFmousemodels limitations in the ability of this species to recapitulatespontaneous lung disease and several other organ abnormalitiesseen in CF humans including few airway mucous glands have creat-ed a need for additional species on which to study CF [106] To thisend pig and ferret CF models have been generated and are currentlybeing characterized [107108] These new larger animal models havephenotypes that appear to closely resemble human CF disease seenin newborns and efforts to characterize their adult phenotypes areongoing However mice have been the dominant species by whichto study CF disease processes in vivo and develop therapies for thepast two decades including GSH-based antioxidant treatment
Despite limitations and significant species differences betweenmice and humans these models proved to be useful tools to mimicthe initial and progressive bronchopulmonary infection typical of CFpatients [109] In particular the model of chronic infection whichchallenge bacterial cells with agar as an immobilizing agent hasbeen extensively characterized and induce the long-term persistenceof the bacterial infection and lung pathology including airway inflam-mation [110111] Lung pathology associatedwith chronic experimen-tal infection resembled some aspects of the advanced chronicpulmonary disease at autopsy in CF patients [112ndash114] Both naturallyoccurring and experimental infections frequently manifest broncho-pneumonia bronchiectasis mucus plugging epithelial metaplasiafibrosis and alveolar exudates with inflammatory cells Lymphoidhyperplasia which was prominent in the infected animals was alsoa common finding in the lungs of CF patients In addition significantdifferences with regard to weight loss BAL neutrophil counts andcytokine concentrations have been detected Infected mice had arapid though transient rise in absolute neutrophil counts TNF-α IL-1β IL-6 MIP-2 and KC in bronchoalveolar lavage (BAL) [110115] Inaddition the generation of CF mice has allowed the possibility of invivo testing of novel therapies before entering in clinical trial Theseinclude the pre-clinical evaluation of antibiotics and biotechnologicaldrugs as well as of natural and synthetic anti-inflammatory agentsthat reduce the excessive recruitment of neutrophils and the progres-sive damage of the respiratory tissue by the unbalanced production ofoxidants
Regarding antioxidants GSH and its pro-drug N-acetylcysteine(NAC) remain the so far most investigated antioxidant agents in CFand several strategies have been proposed to improve systemic andlung GSH status of CF patients based on pre-clinical studies includingthe administration of nebulized GSH by inhalation or the oral supple-mentation of GSH or NAC Oral GSH administration can raise serumand lung tissue GSH levels in rodents [116117] In these studiesGSH was administered to animals dissolved in saline or PBS Thepharmacokinetic profile of an oral bolus dose of GSH (300 mgkg)was determined in mice in other studies [118] Plasma ELF BALcells and lung tissue were analyzed for GSH content There was arapid elevation in the GSH levels that peaked at 30 min in the plasmaand 60 min in the lung ELF and BAL cells after oral GSH dosing OralGSH treatment produced a selective increase in the reduced and ac-tive form of GSH in all lung compartments examined Oral GSSG treat-ment (300 mgkg) resulted in a smaller increase of GSH levels Toevaluate the role of CFTR in this process Cftr KO mice and gut-
Table 1Intervention trials on antioxidant therapy in CF patients found at ClinicalTrialsgov databasea
Rank Title PI Location Recruitment Interventions Age groups Phasesnumberenrolled
Study designsb Outcome measures Start andcompletion date
NCT ID
1 Efficacy and safety studyof inhaled GSH in CFpatients
GrieseM
Germany Completed Drugbull reduced GSH sodium salt
C|A|S II138
1 R|E2 Safetyeff3 PA4 DB (Sub Inv)5 Treatment
bull Differences between inhaled GSHand inhaled normal saline withrespect to the area under the curveof FEV1 predicted within the periodfrom baseline to week 24
bull Treatment changes with respect tothe variablesspirometry peak flowquality-of-life weightheightpercentage of neutrophilsothercell types (induced sputum) inducedsputum levels of GSHinflammatorymediators pulmonary exacerbation
Jul-07May-10
00506688
bull 09 saline (control)
2 A phase I study of inhaledsodium pyruvate for thetreatment of CF
BillingsMCE
United States Terminated Drugbull Inhaled sodium pyruvate
A|S I70
1 R|E2 Safetyeff3 PA4 DB5 Treatment
bull Assessment of safety of inhaled sodiumpyruvate in Subs with CF Subs will beevaluated for the presence of symptomsand safety laboratory measurements
bull Determination of improvement inlungs of CF Subs as determined bymeasurement of FEV1 and measurementof inflammatory markers ininduced sputum
Feb-06na
00332215
3 Inhaled GSH versusplacebo in CF
MarsicoS
Italy Recruiting Drugbull Inhaled reduced GSHbull Physiological solution
C|A III150
1 R|E2 Eff3 PA4 SB (Sub)5 Treatment
bull FEV1bull Small airway function exercise capacityBMI dyspnoea cough quality of lifepulmonary exacerbations markers ofoxidative stress (H2O2)in serum and inEBC epithelial inflammatory markerson BNEC
Jun-10Dec-12
01450267
4 Safety and efficacy ofan antioxidant-richmultivitaminsupplement in CF
SagelSD
United States Completed Dietary supplementbull AquADEKs
C|A IIndashII17
1 NR|E2 Safetyeff3 SGA4 OL5 Treatment
bull Plasma levels of β-carotenebull Plasma levels of coenzyme Q-10retinol (Vitamin A) 25-hydroxy vitaminD α- and γ-tocopherols (Vitamin E)PIVKA-II
Aug-07Nov-09
01018303
5 Efficacy and safety ofepigallocatechin gallate(EGCG)tocotrienol in18 patients with splicing-mutation-mediated CF
KeremE
Israel Not yetrecruiting
Dietary supplementbull EGCGbull Tocotrienolbull EGCG+tocotrienol
A|S na18
2 Safetyeff3 CA4 OL5 Treatment
bull Changes in nasal chloride secretion asassessed by TEPD with assessment ofmean changes in TEPD by drug comparedto baseline and the proportion of patientswith a chloride secretion response bydrug compared to baseline
bull Pulmonary function testing FEV1FVC MEF25-75
Sep-09Jun-11
00889434
6 The effect of inhaledNAC compared tonormal saline onsputum rheology andlung function
VanDaele S
Belgium Terminated Drugbull Acetyl-Cysbull Normal saline
C|A IV19
1 NR|E2 Eff3 CA4 OL5 Treatment
bull Changes in visco-elasticity andlung function
Jan-10Dec-10
00996424
696FG
allietal
Biochimica
etBiophysica
Acta
1822(2012)
690ndash713
7 Safety of orallyadministeredcurcuminoids in adultsubjects with CF
Goss C United States Completed Drugbull Standardized turmericroot extract
A I11
1 NR|E2 Safetyeff3 SGA4 OL5 Treatment
bull Safety and tolerability of 14 days oftreatment with orally administeredcurcuminoids as assessed by adverseevents laboratory parameters andspirometry
bull Pharmacokinetics of repeated dosesof orally administered curcuminoidschange in NPD measurementschange in sweat chloride measurements
Apr-05Jan-06
00219882
8 Nasal potential studiesutilizing CF transmembraneregulator (CFTR) modulators
Rowe S United States Recruiting Other quercetin C|A II46
2 Eff3 SGA4 OL5 BS
bull NPD(NPD) Biomarkerbull Residual CFTR activity
Mar-10Nov-11
01348204
9 Safety and tolerability ofinhaled nitric oxide inpatients with CF
Sagel S United States Completed Drugbull Nitric oxide for inhalationbull Nitrogen
C|A|S IIndashII18
1 R|E2 Saf3 PA4 DB (Sub Care Inv OA)5 Treatment
bull Safety and tolerability of drugassessed by change in methemoglobinlevels oxygensaturation FEV1
bull Assess the difference in sputumbacterial density before and afterNO inhalation and the differencein lower airway inflammatorymeasures before and after NO inhalation
Jul-04Dec-08
00570349
10 NAC Phase IIB a multi-center phase IIBrandomized placebo-controlled DB study ofthe effects of NAC onredox changes and lunginflammation in CF patients
ConradC
United States Completed Drugbull NAC
C|A|S II80
1 R|E2 Eff3 SGA4 DB (Sub Care Inv OA)5 Treatment
bull Change in the logarithm of the levelof human neutrophil elastase(HNE) activity measured in sputum
bull Change in concentration of IL-8measured in sputum and plasmaconcentration of GSH measured inwhole blood the neutrophil countmeasured in sputum
Nov-08Feb-11
00809094
11 Glutamine supplementationin CF
na United States Not yetrecruiting
Dietary supplementbull Glutaminebull L-alanine
A|S II40
1 R3 PA4 DB (Sub Care Inv OA)5 Prev
bull Percent increase in plasma glutamineand GSH redox levels measured atweeks 0 4 8 and 12
Feb-10Feb-11
01051999
12 Effect of sulforaphane inbroccoli sprouts onNrf2 activation
ChmielJF
United States Active notrecruiting
Dietary supplementbull Broccoli sprouts
A na15
3 SGA4 OL5 BS
bull Nrf2 activation in NECbull Measures of lipid peroxidation in NECGSH from blood lymphocytesoxidative stress in urineneutrophil migration into thegingival crevices
Apr-11Sep-11
01315665
AbbreviationsA=adult BC=breath condensate BNEC=brushed nasal epithelial cells BS=basic science C=child CA=crossover assignment Care=caregiver CF=cystic fibrosis DB=double blind EBC=exhaled breath condensate Eff=efficacystudy FEV1=forced expiratory volume in 1 s FVC=forced vital capacity GSH=glutathione Inv=investigator MEF25ndash75=maximal expiratory flow 25ndash75 na=not available NAC=N-acetylcysteine NEC=nasal epithelial cellsNLF=nasal lavage fluid NPD=nasal potential difference NR|E=non-randomized|endpoint OA=outcomes assessor OL=open label PA=parallel assignment PI=principal investigator Prev=prevention R|E=randomized|endpoint S=senior Saf=safety study SB=single blind SGA=single group assignment Sub=subject
a Search was done matching the terms ldquoantioxidant therapyrdquo or ldquoGlutathionerdquo with ldquoCystic Fibrosisrdquob 1 Allocation 2 Classification 3 Intervention model 4 Masking 5 Primary purpose
697FG
allietal
Biochimica
etBiophysica
Acta
1822(2012)
690ndash713
698 F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
corrected Cftr KO-transgenic mice were given an oral bolus dose ofGSH (300 mgkg) and compared with WT mice for changes in GSHlevels in plasma lung ELF and BAL cells There was a twofold in-crease in plasma a twofold increase in lung a fivefold increase inELF and a threefold increase in BAL cell GSH levels at 60 min in WTmice however GSH levels only increased by 40 in the plasma 60in the lung 50 in the ELF and twofold in the BAL cells within thegut-corrected Cftr KO-Tg mice No change in GSH levels was observedin the uncorrected Cftr KO mice These studies suggest that oral GSHadministration can increase plasma and lung compartment GSHlevels in WT mice and to a lesser extent in gut-corrected Cftr KO-Tganimals It also suggests that oral GSH treatment can boost BAL cellGSH levels However since this study failed to show significant in-creases in serum and lung compartment GSH levels in uncorrectedCftr KO mice it is questionable whether oral GSH administration toCF patients with intestinal malabsorption would benefit from thistherapy It was also shown that GSH is rapidly distributed to theserum and lung compartments Kariya et al [118] speculate thatother transporter(s) besides CFTR are responsible of the transport ofGSH and probably of other dietary molecules to the lung whichmay be responsible for dietary deficiencies observed in various lungdiseases
Another strategy is represented by the oral supplementation ofhigh doses of NAC a well known cysteine donor for the synthesis ofglutathione NAC is considered a safe molecule which has beenused successfully to treat GSH deficiency in a wide range of diseases[119] As CF mice display defects in GSH export in the ELF comparableto those of patients they could provide a useful tool to assess the ef-fects of NAC administration on the GSH status However only limitedstudies exploring the effects of NAC on CF animal models have beenso far carried out The effects of NAC have been tested on mucus accu-mulation bacterial load transit and inflammation in the CF mousesmall intestine showing that NAC may reduce intestinal mucus accu-mulation bacterial overgrowth in the gut [120]
Moreover NAC has been reported to restore the accumulationof unwantedmisfolded proteins in aggregates that are associated withthe CF airway phenotype as a cause of lung inflammation [121] Themechanism of this NAC-derived effect seems to involve the restorationof beclin 1 expression and activity in the autophagy pathway of theendoplasmic reticulum that was investigated in vivo using Scnn1b-transgenic and Cftr(F508del) homozygous mice The restoration ofthis pathway also produced a rescued trafficking of CFTR (F508del) tothe cell surface of CF cells obtained from human CF nasal biopsies
Given the defective GSH metabolism of CF reviewed in the previ-ous sections and in [122] and the reduced response to GSH therapyin CF mice [93] some Authors have investigated the influence of bac-terial infections on lung oxidative stress The effects of P aeruginosainfection on ELF and lung tissue antioxidants and the oxidation ofDNA and lipids were investigated in mice challenged with bacterialcells [90] CFTR-KO (B6129P2-Cftrtm1Unc) and WT mice were chal-lenged intratracheally with a clinical isolate of mucoid P aeruginosaembedded in agar beads and on the third day of infection BALF andlung tissue were obtained and analyzed for cytokines antioxidantsand enzyme activities [90] P aeruginosa lung infection increasedlevels of inflammatory cytokines and neutrophils in the ELF This cor-responded with a marked increase in GSH and in urate levels in theELF of P aeruginosa-infected WT mice A twofold increase in uratelevels was also observed among lung tissue antioxidants of Paeruginosa-infected WT mice There were no changes in markers oflung oxidative stress associated with the P aeruginosa lung infectionIn contrast to WT mice the CFTR-KO mice lacked a significant in-crease in ELF GSH when challenged with P aeruginosa and this corre-lated with a decrease in the ratio of reduced to oxidized GSH in theELF a marker of oxidative stress These data would suggest that thelung adapts to infectious agents with elevated ELF GSH and urateTherefore individuals with lung diseases associated with altered
antioxidant transport such as CF might lack the ability to adapt tothe infection which may lead to a more severe inflammatoryresponse
322 Clinical trials on GSHThe discovery of the defect in GSH export has suggested that ther-
apies able to restore or increase GSH levels in the ASL could counteractthe inflammation and oxidative stress conditions typical of CF pa-tients In an attempt to strengthen extracellular defenses againstROS some pilot studies have analyzed the effect of GSH inhalation orthat of oral GSH prodrug N-acetylcysteine (NAC) All these treatmentswere well tolerated by the CF patients and most authors were able tomeasure increased ELF concentrations of GSH in association withsome positive clinical outcomes [4041737896122ndash128] Althoughpotentially promising these findings need stronger clinical evidencein that the majority of these were obtained on very limited numberof patients investigated in non-randomized controlled trials This ishighlighted in a recently published meta-analysis [129] that providesalso a thoroughly analysis of the literature on this aspect of the antiox-idant and anti-inflammatory therapy of CF Among the American CFfoundation sponsored trials two phase II trials on inhaled GSH andoral NAC are in progress in US and Germany (ClinicalTrialsgov Iden-tifier NCT00506688 and NCT00809094 respectively Table 1) andsafety and tolerability of aerosolized glutathione is also matter ofinvestigation by another (not registered) US trial (more informationon this can be found in [130]) Nevertheless the diffusion among CFpatients of NAC preparations for inhalation (Mucomystreg) has in-creased in recent years
γ-Glutamylcysteine ethyl ester (GCEE) is another potentially inter-esting GSH pro-drug which has proved some efficacy in the ameliora-tion of oxidative stress eg in experimental myocardial infarction[131] and central nervous system conditions (see eg [132]) HoweverGCEE has not been investigated in CF yet
33 Limits and potential problems associated to thiol-based therapies
Although the above cited clinical trials may be considered promis-ing attempts to improve the antioxidant levels in the ELF the actualcapacity of these treatments to produce positive clinical effects mustbe considered with caution For example indices of oxidative damagewere found to be unaffected by aerosolized GSH treatment [122]Some in vitro studies have suggested that the reaction of GSH withPCN could produce hydrogen peroxide with potential exacerbationof oxidative damage [101] The exact mechanisms of PCN toxicityand the reaction of this toxin with GSH must be better understoodin order to evaluate the safety of GSH administration to patients col-onized by P aeruginosa
Inhalation of GSH ensures its direct delivery in the airways butsince GSH can rapidly convert to its oxidized form GSSG frequentGSH inhalations are required to maintain a high GSHGSSG As a con-sequence of this limit four separate inhalations have been used inthe study carried out by Bishop et al [123] Unless justified by clearclinical improvements these repeated treatments may represent aburden for patients already undergoing complex therapies Moreoverrepeated inhalations of GSH increase the levels of GSSG in ELF[133134] In the absence of effective homeostatic mechanisms ensur-ing the fast recycling of GSSG to GSH this might produce unwantedeffects and even the exacerbation of CF symptoms being GSSG re-sponsible of the S-glutathiolation and functional inhibition of CFTR[124]
In principle the oral administration of GSH could be considered asafe strategy to prevent GSSG accumulation but this strategy is likelynot feasible due to the substantial inability of this water-soluble mol-ecule to cross biological membranes Moreover a study carried out inmice has established that GSH absorption in the gastrointestinal tractif any is mediated by CFTR itself thus excluding the possibility to
699F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
improve circulating levels of GSH in CF patients through the dietarysupplementation of the antioxidant [127] The limited absorption ofGSH could be overcome by GSH-esters as in vitro studies haveshown that this form of GSH may be specifically useful to rescue mi-tochondrial defects in cystic fibrosis models [80] Safety of these GSHderivatives in humans has been poorly investigated
Two independent studies have shown that the treatment of CF pa-tients with high doses of NAC increases extracellular GSH in sputum[78125] but contrasting results have been reported concerning theeffects of NAC on the concentrations of blood GSH and on the levelsof IL-8 and other markers of inflammation NAC treatments may beuseful to modulate the GSH content in cells but it should be remindedthat an enhanced cysteine supply cannot lead to an increase of GSHabove physiological levels due to the feedback inhibition mechanismof γ-glutamylcysteine synthetase described in the Section 311
331 Gamma-glutamyltransferase and GSH therapySo far none of the studies mentioned above has taken into account
the fact that GSH is degraded by GGT enzyme activity GGT concentra-tions are known to increase several fold in ELF of CF patients even ifthe mechanisms for this effect were not determined [135] and thisphenomenon parallels the above described decrease of GSH levels inELF Preliminary data suggest that a major source of increased ELFGGT is represented by activated neutrophils accumulating in diseasedairways (Corti and Pompella 2011 unpublished observation) Re-gardless of its origin it is likely that increased GGT in ELF would de-grade locally administered GSH to variable extents which couldcontribute to the so far inconclusive results of therapies based onaerosolized GSH Besides its role in GSH catabolism GGT has beenshown to mediate protein S-thiolation [136] suggesting that GSH ad-ministration in the presence of active GGT enzyme might alter CFTRglutathiolation status and function in a potentially unfavorable wayOn the other hand a potential role of GGT in favoring bronchial up-take of antioxidant vitamin C has also been suggested [137]
These controversial findings may add further issues to the ques-tion of whether the therapy of lung oxidative stress by aerosolizedGSH could be safe in all the CF patients regardless of specific strate-gies that would ascertain the extent of lung inflammation Thesestrategies should include the assay of GGT levels in ELF In principleonce an adverse role of ELF GGT in GSH therapies will be confirmedthe association of GGT inhibitors in the GSH formulations for inhala-tion could represent a promising pharmacological strategy
34 Malnutrition as a possible cause of defective thiol-dependentantioxidant protection
Successful nutritional interventions strongly impact on the clinicaloutcome of CF patients [138ndash140] Malnutrition by pancreatic insuffi-ciency and other CF-related factors influence the susceptibility to de-velop recurrent infections and severe inflammatory lesions of thelung tissue If the onset of a defective (sub-optimal) antioxidant sta-tus may represent an underlying component in the clinical effects ofmalnutrition remains a matter of investigation Clinicians have topay particular care to avoid these disturbances and successful proto-cols of nutritional intervention in CF have been developed whichare essentially aimed to avoid the onset of protein-energy malnutri-tion (PEM) [141] Despite this the risk of developing such an unto-ward complication in CF infants and children remains high assuggested by the prevalence data registered in some areas Actuallya prevalence of PEM between 5 and 14 in Moldavian infants was re-cently reported [142] and PEM is associated with poor outcome andparticularly with the risk of developing edema and anemia
Besides lowered intake and absorption of micronutrient antioxi-dants discussed in the other sections malabsorption of dietary proteinand excess fecal amino acid losses result in hypoproteinemiahypoalbu-minemia as key biochemical signs of PEM Hypoalbuminemia is
considered to be linked with a causendasheffect relationship with oxidativestress and is proposed to influence morbidity and mortality in condi-tions associated with chronic inflammation and severe oxidative stress[143144] The human serum albumin (HAS) molecule contains only areactive thiol group eg the Cys 34 the importance of which as an anti-oxidant defense system in blood and for the entire organism is welldocumented [145] This is the second main thiol (and the main proteinthiol) in the circulation (approx 2 mmol in the adult organism assum-ing 5 l of total blood volume anHt of 40 and [HAS] of 45 gl of plasma)being the RBCGSH thefirst thiol in blood (near to 5 mmol assuming thesame parameters of above and an average concentration of GSH inpacked RBC of 25 mM) [146147] The antioxidant role of HSA is notonly a consequence of the relative abundance of its Cys thiol A specificcapability of acting as a sacrificial target for a series of electrophils andmost biologically relevant ROS ie hydrogen peroxide and peroxyni-trite has been demonstrated in a series of studies [145148149] Li-gand binding activity can contribute to promote antioxidant effectsby the HSA molecule [145] Transitions metals particularly copperand also iron in the case of iron-overload diseases bind to HSA Inthis way these are less available to promote the Fenton chemistryand hydroxyl radicals eventually released from this oxidative reactionare mostly directed to the HAS protein sparing more important tar-gets A free radical-trapping activity of HSA has been also demonstratedand this was proposed to be directed toward both hydrophilic and fat-soluble species This activity may result from the interaction withother antioxidants such as α-tocopherol [150] and may influence theantioxidant activity of food-derived phenolic antioxidants [151]
However Cys 34 is considered the main contributor to the antiox-idant function of HAS which plays its role in the antioxidant homeo-stasis of blood thanks to a complex series of interactions with themetabolism and antioxidant function of the pool of free thiols in plas-ma and in the circulating RBC with the latter playing a significantcontribution to the extracellular pool of GSH [146] and to the dynam-ics of inter-organ GSHmetabolism in cooperation with liver and othertissues [147] Immuno-inflammatory cells and the lung tissue areamong the main terminals of this metabolism The RBC contain theentire machinery to synthesize GSH to restore its redox (by enzymat-ic reduction of the oxidized form) and to use this as cofactor of Se-GPx and GSH-S-transferase enzymatic activities that are responsibleof the detoxification of hydroperoxides and alkylating agents thatmay form in or enter the RBC cytosol [147] In this sense the RBC rep-resents a circulating reservoir of GSH that in addition to maintainingthe redox and respiratory function of Hb participates to systemic pro-tection of xenobiotics of endogenous and exogenous origin In consid-eration of these aspects the combination of hypoalbuminemia andanemia may exponentially increase the risk of developing oxidativestress in CF patients as it is supposed to occur in other oxidative stressconditions such as chronic kidney disease [55143152] Additionalclinical investigation should verify the hypothesis that hypoalbumi-nemia together with a defective uptake and metabolism of sulfur-containing amino acids and CF-specific defects of the GSH metabo-lism may represent a causal risk factor for an impaired antioxidantdefense and systemic oxidative stress in CF patients
35 Fat-soluble antioxidants
Pancreatic insufficiency and a diminished bile acid pool cause mal-absorption of important essential nutrients and other dietary compo-nents in CF Of particular significance is the malabsorption of fat-soluble antioxidants such as tocopherols carotenoids and coenzymeQ-10 (Co-Q10) and that of essential fatty acids (EFA)
351 Vitamin EVitamin E therapy in CF has been proposed in several decades of
research as a useful approach to overcome both the lower absorptionof this fat-soluble micronutrient and the increased antioxidant
700 F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
demand by the abnormal generation of ROS in CF tissues (see for in-stance the recommendations by the Cystic Fibrosis Foundation Con-sensus Conference on nutrition [153])
The first report of a vitamin E deficiency in CF appeared in literaturein 1951 by Filer et al [154] In this study the absorption of the mainform of this vitamin eg α-tocopherol and its ester derivatives was in-vestigated in several subsets of infants and children Thanks to a simplebioavailability (or tolerance) test these authors observed that ldquoin-fantshellip diagnosed as fibrocystic disease of the pancreas diarrhea andcirrhosis were characterized by a poor response to the test ie the tol-erance curve was lowrdquo However abnormalities were also observed inother subgroups of infants with a variety of disorders not associatedwith fat or fat-soluble vitamin intolerance such as sprue celiac syn-drome and lupus erythematosus which suggests the general observa-tion that malnutrition and inflammatory and degenerative diseases ofthe GI tract may lead to absorb tocopherols poorly At the same timethese authors reported that ldquoMetabolic disorders with associated hy-percholesterolemia were observed to give abnormally high values forthe area under the curverdquo and that patients responding poorly to to-copherol absorption test did also in vitamin A absorption tests
The finding of lowered (lipid uncorrected) levels of vitamin E wasconfirmed in other studies in which this relative deficiency was foundto occur irrespective of pancreatic comorbidity and in associationwith lowered levels of other liposoluble vitamins such as vitamin Aand D [155] regardless of their different liver metabolism and tissuedelivery mechanisms [156157]
Plasma buccal mucosal cells (BMCs) and breath condensate α-tocopherol decreased significantly with age in association with a de-creased respiratory function [5] This was accompanied by loweredlevels of other antioxidants such as vitamin C and increased oxidativestress markers of different origin such as protein carbonyls thiobarbi-turic acid-reactive substances and F2-IsoPs
Clinical symptoms of vitamin E deficiency in CF have not beenconclusively investigated Dolan et al [158] described that anemiaof CF patients is related to vitamin E deficiency and increasedperoxide-induced hemolysis of RBC Other authors however ob-served an increased susceptibility to peroxide-induced hemolysisalso in the presence of normal levels of vitamin E [159] Peters andKelly [160] observed that RBC vitamin E concentrations were belowthe normal range in almost all unsupplemented patients and roseinto the normal range with a 1-year supplement of 100 mg per daybut not 15 mg per day Since RBC vitamin E concentration has beenshown to correlate well with tissue concentrations of the vitamin inanimals tissue levels of vitamin E are expected to be lower than nor-mal in CF patients
Bioavailability of fat-soluble vitamin is limited in CF Vitamin Edeficiency of CF is also associated with hypocholesterolemia [7] Asa consequence the relative deficiency of this vitamin is compensatedwhen the absolute levels are normalized for cholesterol levels andthis suggests a poor transferring of this vitamin in the circulation bya defective lipid and lipoprotein metabolism Pancreatic insufficiencyand the consequent lipid malnutrition cannot completely explain thisdefect and other possibly CF-specific dysfunctions could play a roleLiver metabolism and specific plasma transport systems of this vita-min need further elucidation in CF
As a consequence of these aspects it is not presently clear whichform and level of supplementation of this vitamin is most appropriateto treat these patients Usingα-tocopherol as a vitamin E supplementPeters et al [160] reported that 100 mg per day are required to nor-malize RBC concentrations Other authors described unsuccessfulsupplementation protocols with higher doses and this has led to de-velop formulations with higher bioavailability in order to achieve bet-ter compliance to oral supplementation (see below and the literaturereviewed in [161ndash163])
Besides absorption and tissue delivery issues specificity of actionis another critical item of antioxidant therapy with fat-soluble agents
in CF As further addressed below this aspect could be themain limit toa successful use of natural forms of vitamin E in the clinical manage-ment of CF inflammation even if a local lung-targeted therapy wouldbe developed according with so far proposed pre-clinical models ofaerosolized vitamin E [164165]
Current pharmacological research is aimed to develop synthetic formsof this and other fat-soluble antioxidants with better radical scavengingproperties at the lipidndashwater interface Type of ROS target and the sitesof action greatly influence the chances of a fat-soluble antioxidant of alle-viating oxidative stress in the airways as well as in other organs such asliver and pancreas These aspects dealing with specificity of action[163166167] have stimulated the search of novel vitamin E-derived an-tioxidants that may help to scavenge radicals at the lipidndashwater interfaceof the epithelial cell membrane and surfactant Amine derivativesof tocopherols and tocotrienols have been recently demonstrated toshow higher antioxidant and free radical scavenging activity than α-tocopherol [168] Further in vitro pharmacological analysis has includedtoxicity evaluations and the detailed investigation of scavenging of azo-and phenolic radicals with different degrees of hydrophobicity and theinhibitory activity on IL-8 gene expression and phospholipase activityin CF cells Comparative evaluation with other synthetic derivativessuch asα-tocopheryl succinate and natural forms of vitamin E suggestedthat these amine derivatives are promising antioxidant and anti-inflammatory agents [Galli F and Pilolli F unpublished observation]deserving further pre-clinical investigation in CF model systems
Anti-inflammatory effects of natural and synthetic analogues of vi-tamin E are also an intriguing pharmacological opportunity currentlyunder investigation by several laboratories [169170]
Recently vitamin E supplementation has been at the center of adispute regarding its safety when used at high dosages in certainpopulations of patients An extensive and speculative debate originat-ed on this subject after a meta-analysis study byMiller et al [171] thatexamined the largest secondary prevention trials on vitamin E trials incardiovascular patients finding a significantly increased mortality riskfor all the causes (about 4 1ndash8 in the 95 interval of confidence)when the patients were treated with doses gt400 IUdie (that areequivalent to 400 mgdie of the synthetic form allrac-α-tocopheroland to 185 mgdie of the natural form RRR-α-tocopherol) This debateresulted in a careful examination of this meta-analysis study by severalother authors and in further revisions of the literature on vitamin E tox-icity in humans [see the literature recently reviewed in [163172ndash174]]that clearly demonstrated the poor consistency of the conclusionsraisedwithMillersmeta-analysis study and the paucity of the concernsthat derived from that These conclusions have been verified in the re-cent international symposium on vitamin E of the Society for Free Rad-ical Research Europe branch of Rome 2009 [173175] Vitamin E used assupplement for humans in all its forms (eg α-tocopherol and othertocopherols and tocotrienols) is safe in abroad range of intakes[172176] The tolerable upper intake level (UL) and the AcceptableDaily Intake (ADI) established by the Joint FAOWHOExpert Committeeon Food Additives for the natural form of vitamin E as α-tocopherolequivalents are of 300 mgdie and 015ndash20 mgkg body weightdierespectively [172177]
352 CarotenoidsLevels of plasma carotenoids such as β-carotene β-cryptoxanthin
and total lycopene are significantly lowered in CF patients and thiswas associated with higher susceptibility to lipid peroxidation[5178ndash180] Rust et al [178] demonstrated that the long-term oralsupplementation with 50 mg β-caroteneday (ie 1 mg β-carotenekg BWday) restored the levels of this carotenoid while sub-optimalsupplementation was observed at doses of 10 mg β-caroteneday orlower thus confirming the need of high doses of this fat-soluble factorto overcome the limited absorption and thus to achieve plasma con-centrations of healthy control subjects Successful high-dose treat-ments appear to lower oxidative stress markers such as TBA-MDA
701F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
complexes and to correct total antioxidant capacity of plasma Inanother study β-carotene supplementation was observed to de-creased lipid peroxide formation as quantitated by malondialdehydeconcentrations in plasma (TBAHPLC method) and to enhance the re-sistance to copper(II) ion-induced oxidation of low density lipopro-teins [180]
At the same time toxicity issues have been raised for human sup-plementation with carotenoid formulations and particularly of water-miscible formulations of preformed vitamin A that is regularly sup-plemented to CF patients which may increase serum retinol andpossible risk of CF-associated liver and bone complications (reviewedin [161181]) However β-carotene supplementation seems to be safesince this does not affect plasma concentrations of other carotenoidsand retinol as well as of other fat-soluble vitamins as α- and γ-tocopherol [178] Recent studies designed to test the clinical efficacyof a CF tailored multivitamin formulation (commercial name AquA-DEKsreg) also tested the safety of this type of formulation and demon-strated that this does not increase vitamin A above the normal levelsobserved in healthy controls [162182183] The normalization of β-carotene levels obtained in these studies was associated only withminor improvements on respiratory and growth parameters whilethe levels of urinary F2-IsoPs used as index of lipid peroxidationwere not affected [162] The surrogate marker of lipid peroxidationMDA was affected together with some selected antioxidant parame-ters (RBC thiols and superoxide dismutase) in another study inwhich this multivitamin formulation was preliminarily evaluated incomparison with standard formulations of vitamin E and A [182]
353 Coenzyme Q-10Coenzyme Q-10 (Q10) is a well-known electron transporter in the
mitochondrial respiratory chain with fundamental role in cellularbioenergetics and scavenging of radical species [184] This lipophilicsubstance is present in the circulation at low levels (serum concentra-tionsle2 μM) mainly as ubiquinol-10 eg the reduced form with anapproximate ratio of 955 with the oxidized form ubiquinone-10[185186] A mechanism for a preferential distribution and accumula-tion in mitochondria has been suggested for both the reduced and ox-idized forms of CoQ10 that are taken up by the cells in a time- andconcentration-dependent Subcellular localization and trafficking ofexogenous Q10 are similar to those of the endogenous form butwere different from that of α-tocopherol that is related with lipidcomposition particularly in the mitochondrial and microsomal frac-tions [184] Ubiquinol-10 readily oxidizes ex vivo by the reactionwith other lipophilic antioxidants such as α-tocopherol and butylatedhydroxytoluene [185] Therefore a higher reduction potential thanother physiological fat-soluble antioxidants such as vitamin E and aselective metabolism and cellular trafficking show peculiar role forthe cell CoQ which may also represent an important lipophilic antiox-idant in cells and body fluids
Human cells synthesize this coenzyme through the cholesterol bio-synthesis pathway so thatmore than two thirds of the tissue levels ap-pear to have an endogenous origin dietary sources provide acontribution to Co-Q10 levels of blood and all solid tissues that variesdepending on the dose applied and type of dietary source [187] How-ever in the case of oral supplements it has to be considered that hy-drophobicity and large molecular weight of this coenzyme influenceits absorption that ultimately is slow and limited [186187] Likewiseto vitamin E pharmacokinetics [188189] Co-Q10 showed T(max) ofaround 6 h that coincides with that of dietary lipids Elimination isclose to that of the more retained form of vitamin E in human bodyeg α-tocopherol with a half-life of about 33 h which suggests poorhepatic metabolism However commercially available formulationsare reported to be safe even at high doses and solubilized formulationsshow enhanced bioavailability In healthy subjects plasma Q10 re-sponse to oral ingestion show saturation profiles with a plateau at a
dose of 2400 mg and the higher plasma concentrations were foundto facilitate uptake by peripheral tissues and also the brain [186187]
Laguna et al [190] recently investigated total serum levels ofcoenzyme Q-10 in a wide population of CF children (n=381) and esti-mated their association with clinical outcome Near to 50 of these CFpatients were deficient of Co-Q10 and this defect was significantlymore prevalent in patients with pancreatic insufficiency and signifi-cantly associated with P aeruginosa colonization in infants (under24 months of age) Importantly low Co-Q10 levels correlated to otherlipid markers of a poor nutritional status such as total lipids and alsothe other fat-soluble antioxidants β-carotene and α-tocopherolwhich confirms the presence of a common defect in the absorptionand metabolic pathways of this coenzyme with dietary lipids
The deficit of Co-Q10 may contribute to the impaired energy func-tion of mitochondria of CF tissues and this may exacerbate CF-linkedinflammation infection and cellular stress response of the lung A sys-tematic analysis of molecular lesions in CF bronchial tissue has beenrecently carried out by proteomic approach [191] Comparative eval-uation of protein expressional pattern in CF and healthy controltissues has revealed aberrant levels of some mitochondrial andenergy-related proteins in CF specimens that included the ubiqui-nolndashcytochrome c reductase complex core protein I and one form ofnidogen a pseudogene of aconitase 2 These changes in CF may reflectmolecular changes which could be associated with an altered mito-chondrial homeostasis and Co-Q10 redox
Multivitamin supplements with high bioavailability containingCo-Q10 have demonstrated to correct the deficit of this antioxidantand were preliminarily observed to improve airway inflammationmarkers in CF patients [183] However further clinical investigationfailed to demonstrate that such an improved biochemical profile isassociated with significant improvements in weight percentile andpulmonary function [162]
354 Fatty acidsA key pathophysiological role in sustaining inflammation in CF has
been attributed to the abnormal polyunsaturated fatty acid (FA) pat-tern Abnormalities in FA profiling are potentially linked to CFTRmutation-driven alterations in the absorption andor metabolism ofdietary lipids [192193] and to the consumption of high oxidizableFA involved in the free radical-mediated lipid peroxidation [7]Among those alterations dysregulation of the docosahexaenoic acidand arachidonic acid balance has been extensively studied with re-portedly significant reduction of DHA in CF and a parallel increasein the levels of AA and inflammatory indices [193ndash195] Actually AAis the progenitor of both enzymatic- and free radical-derived inflam-matory mediators including leukotrienes prostaglandins and iso-prostanes On the other hand n-3 PUFA (eicosapentaenoic acid anddocosahexaenoic acid) are involved in the generation of potent medi-ators namely resolvins and protectins which are able to resolveexudates and to act as organ protective and antifibrotic Secondarilyto their anti-inflammatory action n-3 FA may also produce anantioxidant-like response (eg a reduced demand of antioxidants toachieve an optimal control of oxidative pathways) As a consequencen-3 PUFA have been suggested and widely used as supplements in CFpatients usually under the form of fish oil [196ndash198] It is worth ofnote however that defective levels of DHA in CF patients was notconfirmed in recent studies [7] It was also shown that patients onDHA supplements did not have increased plasma n-3 FA concentra-tions but showed more severe oxidative stress compared to theunsupplemented patients [7] This observation of an increased riskof oxidative stress in CF subjects receiving n-3 fatty acids supple-ments has also been described by other authors [199]
Studies reporting increased AA levels in CF patients have beencontradicted by others [7200201] thus contributing to weakeningthe pathophysiological role of the altered DHAndashAA balance as turnpoint of an upregulated inflammatory status in CF In this context a
702 F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
recent Cochrane meta-analysis on n-3 supplementation in CF patients[202] highlighted the lack of evidence for a significant correction ofthe assessed clinical end points (mainly respiratory symptoms)even when inflammatory indices and other laboratory end pointswere met Taken together these data suggest that there is insufficientevidence to draw firm conclusions or recommend routine use of n-3supplements in CF Notwithstanding it is common belief that n-3supplements provide some benefits for people with CF with relativelyfew adverse effects and thus their use is not discouraged
Further alterations in fatty acid metabolism have been highlight-ed including the consistent findings of an increase in circulatinglevels of saturated and monounsaturated fatty acids [7203204]Decreased levels of essential FA (EFA) ie the FA that have to be in-troduced with the diet correlates with the severity of respiratoryinsufficiency and the same clinical correlation was observed with al-tered proportions of FA species converted by the activity of desatur-ase enzymes (reviewed in [204]) The close relationship betweencertain fatty acids and oxidative stress including the negative correla-tion of C240 and linoleic acid with oxysterol levels point to the needof intensive investigation in CF patients of previously neglected lipidspecies that are emerging candidates in the control of metabolismQuantitative lipidomic analyses have lead to identify C161n7 palmi-toleate as a ldquoprotectiverdquo adipose-derived lipid hormone that stronglystimulates insulin activity in muscle and liver also suppressing in-flammatory cytokine output from mice fat cells [205] Specific meta-bolic activities have been also demonstrated by medium chainsaturated fatty acids caprylic acid (C80) capric acid (C100) and lau-ric acid (C120) Capric acid acts as a direct ligand of PPARγ using abinding pocket different from the binding pocket of thiazolidinedioneor long chain fatty acids [206] Additional activities of medium chainfatty acids which are ligands of free fatty acids receptors detectedin the immune cells the gastrointestinal tract and adipocytes maycontribute to metabolic homeostasis and inflammatory responses[207] These data underscore the importance of a lipid-mediated ldquoen-docrine networkrdquo demonstrating how specific alteration of one orfew serum lipids would be per se sufficient to influence metabolic ho-meostasis Given the relevance of this emerging information and thealteration of lipid metabolism and inflammatory status in CF fattyacid lipidomics need to be deeply investigated in CF
Again these studies have obvious nutritional implications Satu-rated fatty acids with chain lengths higher than C18 are poorlyabsorbed partly because they form insoluble calcium salts [208]Medium chain saturated fatty acids are well known for being highlyabsorbed through the intestine providing rapid delivery of energyvia oxidation of the more hydrophilic short chains and have beensuggested to provide proper nourishment in patients with CF [209]Recent studies have shown that consumption of a high-fat diet richin medium chain fatty acids as opposed to long chain fatty acidsdoes not lead to ectopic fat accumulation in skeletal muscle andliver of both rats and mice [210] In light of the close association be-tween nutritional status inflammation and life expectancy in CF pa-tients the manipulation of dietary lipids in these patients must befurther explored as a possible strategy to provide adequate nutritionand better management of oxidative stress
36 Hydrosoluble antioxidants oligoelements and enzymatic antioxidants
361 Vitamin CVitamin C status in CF patients has been poorly investigated Early
studies suggested a defective vitamin C status that was refractory tooral supplementation [211] Other and more recent studies showednormal or slightly decreased levels of vitamin C in CF patients as com-pared to healthy controls but age- and disease-related decline of thiswater-soluble antioxidant was reported in these patients [5212]In the study of Winklhofer-Roob et al [212] on mid-European CFpatients vitamin C concentrations decreased with age with an
estimated rate of 5 μmollyr and vitamin C concentrationsb40 μ-moll were associated with highest indexes of inflammation whichis consistent with the hypothesis that optimal levels of vitamin Cmay influence immuno-inflammatory activity of alveolar macro-phages and neutrophils Other few studies have examined the effectof supplements containing vitamin C on CF inflammation and oxida-tive stress since the levels of this vitamin do not significantly improvewith supplementation (reviewed in [213]) This highlights the com-mon fate that this hydrosoluble vitamin shares with several fat-soluble counterparts in the ldquomicronutrient paradoxrdquo of CF patients inwhich the need for a correction of their status along the progressionof the disease is frustrated by the poor efficacy of oral supplementa-tion protocols Formulations and appropriate supplementation proto-cols that may produce a better correction of vitamin C status of CFpatients are awaited for further clinical evaluation
362 Selenium and selenium-dependent peroxidasesSelenium is a trace element with marked electrophilicity [214]
that once converted to the organic form of Se-Cys can be introducedin protein structures to play its important role in H2O2 metabolismand signaling [215] As catalytic center of the enzyme GSH-peroxidase (SeGSH-Px) Se plays a crucial role to protect polyunsatu-rated lipids of plasma membrane and circulating lipoproteins formperoxidative insults With other Se-proteins such as the high molecu-lar weight thioredoxin reductases this oligoelement participates tothe control of protein thiol-disulfide oxidoreduction and glutathiony-lation which regulate signaling pathways of crucial importance in theregulation of immunity and inflammation [16] but also the function-ing of other redox-sensitive proteins such as the same CFTR [124]
The activity of SeGSH-Px in blood is considered a functional as-sessment of selenium status even if this assumption has some limita-tions related with the saturation profile that the Se stores show atincreasing doses of Se administration Investigations of the seleniumstatus in CF patients have produced conflicting findings which maydepend on differences in dietary intake ethnicity and environmentalfactors in the diverse patient populations (reviewed in [216217]) CFchildren have been reported to have lowered blood selenium and RBCSeGSH-Px activity [218219] normal plasma selenium and loweredRBC SeGSH-Px [220] and even normal levels of both these two param-eters [221] The supplementation with selenium in combination withother antioxidants was observed to increase the concentrations ofblood selenium that likewise β-carotene and fatty acid were posi-tively correlated with improved lung function [6]
Foucaud et al [218] observed that a defective selenium statuswas associated with lowered levels of other antioxidants that contrib-ute to the anti-peroxidative activity of this microelement such asvitamin E (reviewed in [222]) and the severity of this deficiencywas lower in children with pancreatic enzyme replacement and vita-min E supplementation
Treatments to substitute for exocrine pancreatic insufficiency bypancreatic enzymes from animal sources such as porcine pancreashave been confirmed to be a source of Se [220] These affects RBCSeGSH-Px activity and plasma selenium concentrations which hasto be taken into account when selenium supplements are given toCF patients
Selenium has been used to develop a series of organoseleniumcompounds that may open the way to new therapeutic opportunitiesin CF (see Section 392) These include GPX mimetic drugs and phaseII enzyme inducers which may provide higher antioxidant activity ofASL and cellular protection effects in the airways
363 Zinc and copperZinc and copper (Zn and Cu respectively) are present in many
proteins so that a deficiency of these trace metals could have pleiotro-pic effects in humans As regards antioxidant systems these two oli-goelements contribute an important role being cofactors of two
703F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
isoforms of the superoxide dismutase enzymes eg the extracellularform eg the EC-SOD or Sod 3 and the CundashZn-SOD or Sod 1 that isfound in several tissues and cells [223] The EC-SOD exerts its antiox-idant role also in the lining fluids of the airways [224]
The notion that CF patients have defective concentrations of bloodZn and Cu is controversial As far as Cu status is concerned few datahave been produced and are available in the literature suggestingthe notion that CF patients develop a moderate copper deficiency[225226] That was essentially demonstrated on the bases of a defec-tive activity of Cu-related proteins such as plasma ceruloplasmindiamine oxidase and RBC SOD This defect seems to be refractory toCu and Zn supplementation (see below)
More advanced studies have been carried out in the case of Zn sta-tus in CF Low plasma zinc concentrations were reported in approxi-mately 30 of young infants with CF identified by newbornscreening [227] and an impaired zinc homeostasis in CF patientswas described by Easley et al [228] This is characterized by poor con-servation of the endogenous pool with fecal loss and impaired frac-tional absorption of zinc which are the consequences of pancreaticinsufficiency and persisting steatorrhea These studies suggestedthat in the clinical management of CF patients these defects can beat least in part corrected by exocrine pancreatic enzyme replacement
A series of studies by Van Biervliet et al [229230] demonstratedin a Dutch population of CF infants and children that serum Zn variesin an age-dependent manner but remained unchanged with respectto healthy control levels In CF patients no difference in serum Zn con-centration between pancreatic-sufficient or pancreatic-insufficientpatients was observed and no correlation was found with the nutri-tional status or height z-score Importantly in these studies a signifi-cant correlation of serum Zn was observed with the fat solublevitamins A and E thus confirming the relationship between the ab-normalities of lipid and Zn metabolism in CF This suggests that co-supplementation of Zn and fat-soluble vitamins should be advisedin the presence of pancreatic insufficiency and persisting steatorrhea
Neve et al [219] in a study aimed to assess plasma and erythrocytezinc copper and selenium in CF children showed that mean plasmazinc and copper levels were not different from those in age-matched controls which confirms the observations by Van Biervlietet al described above However plasma zinc concentrations de-creased in patients with moderate-to-severe growth retardation andwith severe pulmonary disease but very low zinc levels occur sporad-ically Erythrocyte zinc and copper levels were significantly higherthan normal while RBC selenium was lower than in age-matchedcontrols These trace element concentrations in erythrocytes werediscussed in relation to the activities of the CuZn-SOD and the Se-enzyme GPx This observation suggests a compensatory upregulationof the erythrocyte CuZn-SOD by the exposure of erythroid precursorsto ROS andor other CF-related stressors
Best et al [225] also studied RBC SOD activity using this as a bio-logical sensor of Cu status in CF patients A lowered activity of thisenzyme was reported in CF together with that of the other Cu-dependent enzyme plasma diamine oxidase while plasma ceruplas-min showed normal activity Degradation rates of copper proteinsare known to be accelerated in conditions of copper deficiencywhich could explain the finding at least in part Anyway when Cuand Zn were supplemented to CF patients either separate or incombination (6 weeks of 3 mg copperd as copper-glycinate and30 mg zincd as zinc-glycinate) any of the copper enzyme activitieswas affected Therefore the moderate copper deficiency of CF patientsappears to be refractory to the intervention by increased copper andor zinc intake
Erythrocyte CuZn-SOD and the plasma levels of Cu and Zn werealso measured in the study of Wood et al [6] in which Australian CFpatients (agegt5 years) were treated with a high-dose antioxidantmultivitamin formulation containing 200 mg vitamin E (as RRR-α-tocopherol) 300 mg vitamin C (as sodium ascorbate) 25 mg β-
carotene (all-trans isomer) 90 μg Se (as selenomethionine) and500 μg vitamin A (as retinyl palmitate) in oil Plasma oligoelementsand particularly Zn were in the normal range at baseline (as com-pared with the data reported in [229230]) and were not affected bythis multivitamin supplement The same was found for the activityof RBC SOD and for plasma 8-iso-PGF2α as surrogate biomarker oflipid peroxidation
In a recent non-randomized small population (n=21) casendashcon-trol study in CF children Zn supplementation was proven to producepositive clinical effects in Zn-deficient patients [196] The supplemen-tation with 5 mgkg Zn sulfateday (maximum 150 mg) significantlydecreased the number of infections and increased the forced expira-tory volume in 1 s energy intake and growth parameters also im-proved These parameters were unaffected in untreated patientsexcept that in the case of the pulmonary function that decreased sig-nificantly These clinical observations on Zn supplementation need tobe confirmed in prospective double-blind randomized control trial
37 Appropriateness and targeting of antioxidant therapies in CF
The choice of the appropriate antioxidant and dose to correct a cer-tain biomarker and its associated biochemical lesion is another impor-tant point that appears to have disregarded in many clinical studiesFor instance unlike vitamin E vitamin C supplementation does notalter F2-IsoPs levels in humans (reviewed in [74]) This appears tobe true also in the antioxidant therapy of CF in which vitamin C(300 mgday) was administered together with other antioxidantsthat included a dose of vitamin E of 200 mgday without any signifi-cant effect on the surrogate biomarker of lipid peroxidation F2-IsoPs[6] When carotenoids are used as supplements to prevent the damag-ing action of ROS in the CF airways it is noteworthy that these are notparticularly good quenchers of peroxyl radicals relative to phenolicsand other antioxidants but are exceptional in quenching singlet oxy-gen at which most other phenolics and antioxidants are relativelyineffective Singlet oxygen is not a radical and does not react via radi-cal mechanisms but reacts mostly by the addition to double bondsforming endoperoxides that can be reduced to alkoxyl radicals that ini-tiate radical chain reactions typical of the peroxidative damage of PUFA[38] In this case the analysis of F2-IsoPs lipid peroxide formation andtransition metal-induced oxidizability of lipoproteins [162180] are allappropriate to evaluate the effect of carotenoids in preventing lipidperoxidation
As far as the dose is concerned clinical pharmacology of vitamin Eas an antioxidant was recently investigated by means of the effect onF2-IsoPs production and doses of α-tocopherol of 1600 IUday orgreater were found to be required to statistically affect plasma F2-IsoPs levels in hypercholeterolemic subjects [176] Several vitamin Esupplementation studies in CF patients have been performed withdoses of lower than 300 IUday regardless of the lowered absorptionby pancreatic and liver defects and the regular supplementationwith these doses does not appear to correct lipid oxidation markersin CF [7]
In the clinical practice and planning trials it has to be taken intoconsideration that in spite of substantial evidence supporting ahigher antioxidant demand in CF interventions with several antioxi-dant formulations produce poor responsiveness particularly in thecase of fat-soluble antioxidants which are poorly absorbed [6162]
Since many oxidants and antioxidants are present in tissuesand biological fluids and these have different chemical and physicalcharacteristics the possibility to produce a successful therapy witha single antioxidant molecule is too far to be realistic Moreover an-tioxidants act by multiple mechanisms in a single system or by adifferent single mechanism depending on the reaction systemresponding in a different manner to different radical or oxidantsources Because multiple reaction characteristics and mechanismsas well as different phase localizations are usually involved no single
704 F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
therapeutic approach will effectively prevent damage by multipleROS sources The defect of physiological antioxidants may also interferewith antioxidant therapies that are based on one or few exogenousantioxidants
Moreover several antioxidant vitamins such as vitamin E and ca-rotenoids have multiple natural forms with different bioavailabilitymetabolism and bioactivity [157167231] As far as the case of vita-min E supplementation concerns α-tocopherol was used as uniquevitamer in the large majority of supplementation trials so far per-formed and is the form used in the nutritional management of CFpatients Moreover several supplements contain the synthetic (or ra-cemic) form of this vitamin that has lower bioavailability than thenatural form Other forms present in nature and abundantly con-tained in vegetables such as tocotrienols and the less methylatedforms of tocopherol are not represented in many of the supplementformulations so far available in clinical centers and the supplementa-tion with α-tocopherol also limits their bioavailability These formsshow markedly higher susceptibility to hepatic metabolism and bili-ary excretion with respect to α-tocopherol eg the most representedform in blood and solid tissues and if co-supplemented these areeasily displaced during liver uptake and excreted with bile bymeans of competition with the same α-tocopherol Notwithstandingthese minor forms have been proposed to play important physiolog-ical roles showing molecular characteristics transcriptional effectsand antioxidant activities that clearly differentiate them in subfam-ilies with distinct biological functions Some of these such as α-tocopherol eg the second vitamin E form as relative abundance inblood and its carboxyethyl-hydroxychroman metabolite [189] ap-pear to have health-related anti-inflammatory effects which are par-ticularly relevant in lung protection [232233] This has suggestedthat such a group of ldquonon-α-tocopherolrdquo forms may represent anoth-er family of vitamins within the family of vitamin E with an impor-tant but often missed contribution to the proposed health effects ofthis vitamin [163]
These aspects may thus limit the possibility to provide CF patientsof optimal levels of this vitamin in all its components even if they areregularly treated with a vitamin E supplement eg withα-tocopherol
Targeted antioxidant therapy with formulations with higher bio-availability and bioactivity has been anticipated in CF New antioxi-dant formulations have been proposed to overcome main limits ofantioxidant therapies so far proposed for these patients Water-miscible α-tocopheryl acetate containing polysorbate propylene gly-col or polyethylene glycol as emulsifiers form micellar structureswere suggested to providing greater bioavailability than the fat-soluble counterparts These were commercialized with the brandnames of E-viminreg Cremophorreg EL and Aquasolreg E but despitethe original positive expectation [234235] some studies failed to ob-serve a higher response in vitamin E levels when these were com-pared with fat-soluble formulations [236237]
In a pilot study by Papas et al [183] a micellar formulation of fat-soluble nutrients and antioxidants was found to improve plasmalevels of β-carotene γ-tocopherol and CoQ(10) reducing at thesame time some inflammatory markers in induced sputum eg mye-loperoxidase and to a lower extent PMN elastase and total cell countswhile lung function and sputum bacterial counts were unaffectedThe same group recently confirmed the possibility to increase the ab-sorption of fat-soluble micronutrients using formulations with higherbioavailability specifically designed for malabsorbing patients such asCF patients that include also vitamin K and commercialized with thebrand name of AquADEKsreg [162] Despite improved vitamin and mi-cronutrient levels in this non-randomized open-label study AquA-DEKsreg produced only modest improvements in weight percentileand pulmonary function Another recent pilot observation [182] hassuggested the beneficial effect of this formulation on antioxidant andoxidative stress parameters of this oral supplement that surely deservesmore clinical investigation by larger randomized controlled trials
Recent multivitaminic formulations have been designed to containalso the minor forms of vitamin E and specifically γ-tocopherol [238]the expected superiority of which with respect to formulations con-taining only α-tocopherol needs to be verified As discussed abovein the section dedicated to vitamin E further advancements in thetherapy of CF inflammation and oxidative stress could be based onsynthetic forms and natural metabolites of this vitamin that havebeen recently identified to possess higher antioxidant and also anti-inflammatory activity than α-tocopherol (reviewed in [163168])
Pre-clinical investigation of these and other fat-soluble agents iscurrently addressed to develop formulations and administration pro-tocols that may increase the therapeutic efficacy in the airways In theantioxidant therapy of lung dysfunction in CF local administrationprotocols may overcome the limits of oral and systemic administra-tion protocols increasing bioavailability and providing targetedapproach to inflammation and oxidative stress Aerosolization of vita-min E and other fat-soluble micronutrients is possible and may allowdirect administration in the airways to prevent toxicity of smokewhich is closely associated with inflammation and oxidative stress[164165] To our knowledge this as well as other strategies of localadministration such as instillation of solutions such as surfactant-like solutions enriched of vitamin E have not been previously inves-tigated in CF patients and other CF model systems
On the contrary inhalation is an administration route widelyadopted in the case of GSH and NAC therapy described above Inthis context Cys formulations alternative to NAC have been proposedfor use as antioxidant and anti-inflammatory agent for inhalationNacystelyn is a lysine adduct of NAC that thanks to a higher proton-ation equilibrium shows increased water solubility and thus betterbioavailability Nacystelyn has been described to influence IL-8 gener-ation and the inflammatory signaling of bronchial epithelial cells[239] and preliminary clinical evaluation has demonstrated the safetyof this drug [240] Further clinical trials aimed to assess the effect onlung symptomatology of CF patients are needed Direct administra-tion in the airways could also be adopted for micronutrient vitaminswith poor absorption and bioavailability due to GI defects
38 Clinical impact of antioxidant therapy in CF
Huge in vitro and pre-clinical evidence has provided the rationaleto support clinical investigation of antioxidant strategies in CF Theseshould aim to restore the oxidantndashantioxidant balance of CF airwaychallenged by chronic infection and inflammatory cell activation
Some observational trials have confirmed that antioxidants usedas either supplements to the diet or drugs for lung administrationby aerosolized formulations may help in relieving progressive lungdamage and other adverse clinical events of CF such as poor growthSo far few studies have examined with sufficient methodologicalrigor the clinical efficacy of antioxidant therapy in CF This was alsoconcluded in a previous review of the literature by Cantin et al [12]that was published in the beginning of 2006 and is confirmed alsoin a recent analysis of clinical trials on antioxidant therapy in CF pa-tients [213] that examined the literature until September 2010using as sources the databases of the Cochrane CF and Genetic Disor-ders Group CF Trials Register PubMed CINAHL and AMED Useful in-formation was retrieved from just four randomized controlled trialsand one quasi-randomized controlled trial on vitamin C vitamin Eβ-carotene and selenium used as supplements administered aloneor in combination Post-hoc data analysis that was possible only inthree studies on a total of 87 CF patients showed the absence ofany significant improvement in lung function that was selected as pri-mary outcome together with quality of life that improved in one trialSecondary outcomes concerning laboratory indices of oxidative stressand antioxidant status showed several improvements These includedan increase of RBC SeGPx by selenium supplementation done as
705F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
individual or combined supplementation and increased levels of allplasma antioxidants except vitamin C that were observed in all thetrials
The message from these studies to pediatricians and nutritionistswithin the clinical staff of CF centers is that in the absence of solid ev-idence regarding the clinical effectiveness of oral formulations of an-tioxidant supplements in CF (including PUFA) their use as a routineclinical practice should be considered with caution keeping clear inmind that this should represent just a complement of one of themost critical interventions in the life-long clinical management pro-gram of CF patients eg providing an adequate nutriture [140] Inthis context compensating energy and protein malnutrition has toremain the first goal of nutritional management programs Providinghigher intakes of antioxidant micronutrients with food naturally-enriched (or functionalized) of micronutrient antioxidants shouldbe preferred in order to have the higher combination of positive nu-tritional factors that are lost during refinement procedures and over-all industrial processing of dietary supplements
Measures of good practice in clinical management of micro-malnutrition in CF patients would include the support of specializedpersonnel and laboratories The centers should have the possibilityto ascertain with appropriate nutritional and laboratory tests whatthe level of deficiency is for the different micronutrients that each pa-tient may suffer from during a dietary program Monitoring dietaryintakes and blood levels of micronutrients is not sufficient to set apersonalized nutritional intervention with supplements or functionalfoods Sub-optimal intakes and the compliance to nutritional inter-ventions should be verified by means of selected biochemical andclinical criteria Unluckily the latter are still not well established forsome micronutrients such as the fat-soluble vitamins E (reviewed in[163173241]) and K [242243] and also for trace elements such asSe [244] For many of the antioxidants used as supplements inhumans we still do not know exactly several of the biological effectsthat these may provide when introduced in a healthy body and weknow less what these can do in disease These aspects hardly impacton the concept of optimal levels of intake that should be identified foreach micronutrient on an individual basis According with the aspectsdiscussed in the previous sections optimal levels of intake for antiox-idant micronutrients are different in CF patients and healthy subjectsand vary with age and several individual factors
Lung administration of antioxidants by means of aerosolized for-mulations so far used for GSH therapy (see above) is a promisingfield of clinical investigation in CF Toxicity issues are currently themain concern and the subject of clinical evaluation by several groups(described above)
Information on future directions of antioxidant therapy in CF canbe inferred by the analysis of pending or recently completed clinicaltrials that have been searched (December 2011) at ClinicalTrialsgovdatabase matching the terms ldquoantioxidant therapyrdquo or ldquoglutathionerdquowith ldquocystic fibrosisrdquo Fifteen trials were retrieved and those directlyrelated to antioxidant therapy (n=12) are presented in Table 1 andinclude efficacy and safety studies of inhaled drugs as GSH sodiumpyruvate NAC and NO and the dietary supplements AquADEKsregan antioxidant-rich multivitamin supplement epigallocatechin gal-late (EGCG)tocotrienol curcuminoids the amino acid glutaminesulforaphane in broccoli sprouts One trial is investigating the flavo-noid quercetin as CFTR modulator
39 Emerging antioxidant and anti-inflammatory approaches in CF
Mediterranean foods such as olive oil and red wine or severalplant extracts such as herbal tea or grape seed extracts contain aseries of natural compounds with important antioxidant and NOscavenging activity that have been widely investigated for the pre-vention of oxidative stress-related diseases [38245] These havebeen long investigated as template molecules to develop antioxidant
and anti-inflammatory drugs Between the multitudes of natural sub-stances most investigated ones include for instance tyrosol hydroxy-tyrosol gallic and caffeic acids belonging to the family of phenolswhile resveratrol of the stilbenes family epicatechin kaempferoland cianidin are examples of flavonoids examples of fat-soluble phe-nolics are those of the family of tocols (vitamin E) and carotenoids Allthese compounds show different metabolisms and signaling effects[246] Antioxidant and cell protection mechanisms are associatedwith different and sometimes concurrent processes as H-atom trans-fer and electron donation radical trapping and chelation of transitionmetals that can be easily investigated at the chemical level [247] Be-sides these direct antioxidant effects metabolic responses and signal-ing effects of natural compounds are also important to producesecond-generation responses that modify the level of antioxidantprotection and the potential for ROS detoxification in cells and bodyfluids These derive from the transcriptional regulation of antioxidantand pro-oxidant genes that coexist with the modulation of cytokinesecretion and inflammatory enzyme activities
Some of these natural plant-derived antioxidants may provide fur-ther pharmacological activities of possible relevance in CF This is thecase for instance of the plant flavonoids genistein apigenin kaemp-ferol quercetin and hesperidin [248ndash251] that fall in the pharmaco-logical category of ldquopotentiatorsrdquo [252] in that these activate at leastto a certain extent CTFR-mediated Cl currents in normal and CF airwayepithelium investigated either in vitro or in vivo in humans and ani-mal models Actually as prototypal flavonoid-derived potentiatorthe tyrosine kinase inhibitor genistein potentiates the gating of wild-type as well as ΔF508 CFTR and G551D CFTR [253] but at higherdoses it inhibits CFTR gating which make this an unlikely clinical can-didate Similar potentiation effects have been reported for the antiox-idant curcumin [250] that shows an additive effect with respect togenistein-induced potentiation Besides CFTR potentiation whichdoes not appear to have a direct influence on GSH and nutrient trans-port in the lung tissue all these natural substances have been usedalone or in combination with other agents as in vivo enhancers oflung antioxidant protection [246254255] In the case of quercetinthiol-reactive phenolic [256] bronchodilation and anti-inflammatoryeffects by a restoration of the Th1Th2 balance have been reportedin inflammatory syndromes of the lung [255257ndash259] but theseeffects have not been explored in CF Pyocyanin toxicity (see abovein the Section 2) could represent an issue for the use of quercetinand other catechols in infectious diseases of the lung [260]
Other natural antioxidants of potential interest in CF therapy in-clude terpenoids [261] such as terpinen-4-ol a major constituentof tea tree oil that is being investigated in the therapy of anti-biotic resistant organisms specifically against methicillin-resistantStaphylococcus aureus (MRSA) [262] a problem in CF [263] Otherthan being lipophilic antioxidants terpenes can prevent oxidativestress of the CF lung secondarily to the antibiotic effect thereby pro-moting a better control of immuno-inflammatory pathways and lungantioxidants
391 Targeting NF-κB with natural compounds resveratrol and plantextracts
Natural compounds were long known to be useful in designinganti-inflammatory drugs and some of these could find an applicationin the control of the transcription factor kappa-B (NF-κB) that maylead to develop advanced pharmacological tools to control inflamma-tion and to produce higher antioxidant protection to CF airwaysInhibitors targeting NF-κB including transcription factors decoymolecules (TFD) are potent down-regulators of gene expressionand release of IL-8 in CF cells infected with P aeruginosa [264265]
Resveratrol (354prime-trihydroxystilbene ldquoErdquo form) is one of the mostinvestigated natural antioxidant with proposed activity as NF-κBinhibitor This is a phytoalexin present in large quantity in red winepreferentially in the skin of grapes being its concentration
706 F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
50ndash100 μgmg of fresh skin and 13ndash3 mgl of red wine [266]Furthermore resveratrol is a constituent of lsquoDarakchasavarsquo (13ndash6 mgl) an ayurvedic medicine from India [267] The antioxidant activity ofresveratrol has been reported in several papers and occurs also in lungtissues suggesting that resveratrol has potential as a therapeuticagent in respiratory disease [268ndash270] Resveratrol can be consideredone of the most interesting molecules from the natural worldexhibiting strong antioxidant activity that at the same time is able toexert anti inflammatory activity through alteration of NF-κB functionsand efficient inhibition of pro-inflammatory genes [271272] As far asthe effects on CF model systems are concerned Cabrini et al [26]reported the effects of resveratrol on P aeruginosa infected CF IB3-1cells The results obtained demonstrate that resveratrol exhibits minoreffects of IB3-1 cell growth and important inhibitory effects on accumu-lation of IL-8 and GRO-α mRNA while minor effects on IL-6 gene ex-pression were observed These data support recently publishedobservations suggesting inhibitory effects of resveratrol in infection-mediated inflammatory processes [273] Interestingly resveratrol hasbeen reported as a potent inhibitor of NF-κB activity and a promisinganti-inflammatory agent [272274] also in combinationwith othermol-ecules [274275] However in vivo translation of this pre-clinical on res-veratrol is hard to be foreseen This natural compound displays poorbioavailability [276] and further characterization of resveratrol pharma-cokinetics is troublesome since it is hardly measurable in vivo [277]Furthermore the regulation of inflammatory responses by resveratrolhas been suggested to be far more complex than simple direct suppres-sion of NF-κB activity Actually some aspects of the immune responsecould be enhanced by this natural substance which may lead tohypothesize broad negative feedback events on immuno-inflammatorypathways [278] In any case and with these cautions in mind the pub-lished observations on cellular model systems support the concept thatresveratrol and resveratrol-containing formulations deserve further con-sideration to determine their possible therapeutic values in CF
Other inhibitors can be identified from systematic studies of naturalproducts and their ability to interfere with NF-κB activity [279ndash281]Recent studies have demonstrated that the whole extract of Aeglemarmelos (Rutaceae) has strong inhibitory effect on the P aeruginosa-dependent IL-8 induction in human CF-derived bronchial IB3-1 cellswithout affecting cell proliferation [280] Molecular analysis of compo-nents contained in A marmelos extracts revealed that three major com-pounds namely 56-dimethoxy-1-indanone 2-hydroxy-cinnamic acidand 5-methoxy psoralen (5-MOP) reproduce the inhibitory effect ob-servedwith thewhole extract [280] A further example has been recent-ly published using extracts from bergamot (Citrus bergamia Risso) Inthis study the extracts were characterized and the main detected con-stituents were assayed for their biological activity [281] The resultsobtained demonstrated that the extracts from bergamot epicarps con-tain components displaying an inhibitory activity on IL-8 Particularlythe most active molecules were bergapten and citropten These effectshave been confirmed by analyzing mRNA levels and protein release inthe CF cellularmodels IB3-1 and CuFi-1 inducedwith TNF-α or exposedto P aeruginosa
A parallel strategy linking NF-κB inhibition and down-regulationof NF-κB-dependent functions is described in recently publishedstudies based on a structured-based virtual screening (VS) of differ-ently substituted furocoumarins and analogues against NF-κB withthe objective of selecting molecules able to inhibit the binding ofthis transcription factor to DNA [282283] Novel compounds wereidentified with this strategy as potent inhibitors of NF-κB dependentbiological functions to be proposed for the control lung inflammationoccurring in patients affected by CF [282ndash284]
392 Scavengers and regulators of H2O2 and NO
3921 Lactoferrin and OSCNmacr The impaired DUOXLPO system of CFpatients could be the target of therapeutic strategies that may
produce concomitant antimicrobial and antioxidant effects This sys-tem described above in Section 22 represents an important compo-nent of innate immunity with a role in bactericidal defense andregulation of H2O2 metabolism of airways [32] CF patients have alsoreported to show lowered LF levels in the ASL [37] that togetherwith a CFTR-dependent defective efflux of SCNmacr and LPO [36] may cre-ate the environment for a sustained flux of H2O2 and for the genera-tion of highly reactive Fenton species [1138] An ideal therapeuticintervention should restore the LPO-dependent generation of bacteri-cidal OSCNmacr from DUOX-derived H2O2 and SCNmacr in the ASL to controlat the same time the microbial biofilm and the flux of H2O2 into theASL An approach close to this therapeutic mechanism was recentlyproposed for the drug Meveolreg This is a complex of LF and OSCNmacrwith proposed in vivo antimicrobial activity [285] to be evaluatedin clinical trials for the aerosol treatment of lung infections in CFpatients The role for this drug in the control of H2O2 levels of ASLremains to be investigated
3922 Organoselenium compounds Organoselenium compoundshave been proposed as therapeutic agents useful in the antioxidanttherapy of inflammatory conditions These include GPX mimetic mol-ecules such as Ebselenreg (2-phenyl-12-benzisoselenazol-3(2H)-one)or other and more recently developed molecules that are still inpre-clinical steps of evaluation [286] Selectively and specificity of ac-tion are main issues in the therapeutic mechanism of this candidateantioxidant drug that thanks to the electrophilic properties of Se[214] reacts with thiols to reduce H2O2 and other species MoreoverEbselenreg has been described to act as potent non-competitive inhib-itor of extracellular nucleoside diphosphokinase (NDPK) having neg-ligible effect on ecto-ATPase and adenyl kinase activities which areother players of the metabolism of extracellular nucleotides [287]This enzyme together with other nucleoside di- and triphosphatescontributes to regulate several components of the mucociliary clear-ance process (MCC) that protects the lung against infections via acti-vation of epithelial purinergic receptors The inhibition of NDPK bythis GPX-mimetic drug may also impact on the energy status of endo-thelial cells [287] This aspect could be further investigated as a cellu-lar protection mechanism in the pulmonary epithelium of CF patientsbeing the control of cell energy of fundamental importance to preventthe activation of death pathways [288]
Further therapeutic mechanisms for these Se-derived drugs mayderive from the marked activity as inducers of phase II enzymessuch as quinone reductase (QR) and glutathione-S-transferase (GST)[289] This induction response also observed with other electrophilsand redox-active molecules such as natural phenolic antioxidantscould produce higher cellular protection by the acquisition of anincreased capability to detoxify endobiotics generated during oxida-tive stress and inflammation [246]
3923 Melatonin and GSNO as NOx regulators Increased markers ofNO-derived biological damage are present in the CF lung suggestingthe abnormal reactivity of NOx in the inflamed lung of CF patients[52] However an impaired metabolism and biological function ofNO in CF airways (see Section 23) suggests a cautious approach tothe use of agents that may influence the levels and chemical behaviorof NO-derived species (NOx) with possible impact on the physiologi-cal roles of NO in vasodilatation innate immunity and H2O2 metabo-lism of the respiratory tract [290291] NO donors also appear toinfluence CFTR function of alveolar epithelium and gland serouscells [292293]
Main physiological role of the pineal gland hormone melatonin isthe synchronization of circadian rhythms including the sleepndashwakecycle but several other functions dealing with immunomodulatoryantioxidant and cellular protection effects have been identified[294] Melatonin receptor stimulation may also influence cyclic AMPsignaling and the regulation of CFTR ion channel [295296]
707F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
A recent randomized double-blind placebo-controlled study hasexamined the effects of short term melatonin administration (3 mgfor 3 weeks) on sleep and oxidative stress markers in CF [297]According with the expected pharmacological effect of this hormonalsubstance the treatment was successful in improving sleep indicesAt the same time nitrite levels determined in exhaled breath conden-sate (EBC) were reduced to suggest a better control of NOmetabolismof CF airways (discussed above in Section 23) but these effects how-ever were not associated with a significant correction of isoprostaneas lipid peroxidation marker measured in EBC Increasing dosages ofmelatonin could be investigated for the pharmacological treatmentof oxidative stress and immune dysfunction of CF patients due tothe absence of adverse effects of this hormonal substance in humans
The S-nitrosation reaction of thiols is another interesting aspect ofNO pharmacology [53] that may find an application in the therapy oflung complications of CF This has been the case for instance of theS-nitrosothiol GSNO that has been used safely in human trials[298299] This endogenous nitrosothiol with proposed regulatory ef-fect on the CFTR of lung epithelia [292293] is well tolerated in pa-tients with CF when administered by aerosolization and mayproduce better oxygenation [299] thereby suggesting that therapyaimed at restoring endogenous GSNO levels in the CF airway maymerit further clinical evaluation Since the administered GSNO de-composes as shown by the increased levels of expired NO in CF pa-tients under treatment with this nitrosothiol [299] furtherinvestigation should be addressed to ascertain whether GSNO thera-py may merely correspond to a GSH therapy
NO dependent effects on CFTR function should be considered toevaluate mechanism of action and specificity of antioxidant therapiesthat target NO metabolism and function in the CF airways
4 Conclusions and future perspectives
The presence of clinical and biochemical symptoms of inflammationand oxidative stress implies that CF patients have a higher demand ofantioxidant protection The combination of the dysfunctional CFTRwith a lowered intake and absorption of dietary antioxidants producesub-optimal levels of protection from both enzymatic and non-enzymatic defense systems The former could be associated with a de-fective glutathionemetabolism and lowered intake of sulfur-containingamino acids and oligoelements such as zinc and possibly seleniumwhile fat-soluble antioxidant vitamins such as vitamin E and caroten-oids and the water-soluble vitamin C are lowered than in healthy sub-jects due to malabsorption and possibly higher consumption
The increased antioxidant demand in CF patients should be evenhigher in the presence of complications of the lung pancreas andliver Lung comorbidity is particularly important in this contextbeing associated with recurrent infections which results in the alter-nation of inflammatory exacerbates and chronic inflammation Thesesustain the flux of ROS in the airways and promote the formation ofsecond-generation byproducts by the damage of biomolecules suchas PUFA and proteins which may diffuse also at the systemic level tofurther promote adverse biological responses and toxic reactions Pan-creatic insufficiency causes malnutrition and may lead to develop en-docrine and metabolic defects associated with diabetes of CF Theseevents can be further aggravated by the concomitance of liver dys-function and a poor nutritional status Malnutrition is strongly associ-ated with poor prognosis as assessed by pulmonary function andsurvival data [138ndash140] The more aggressive nutritional interven-tions seem to produce better clinical outcomes in these patients andthe possibility of achieving higher antioxidant protection in well-nourished patients by dietary factors could be a key aspect to explainsuch a clinical advantage The assumption that food-derived compo-nentsmay help to prevent the damaging effects of oxidative stress im-proving the antioxidant defenses deserves further investigation at theclinical level This together with the investigation of appropriate
laboratory biomarkers could provide critical information to establishintervention criteria for an early nutritional management of newly di-agnosed patients [5] It is expected that a timely secondary preventionstrategy could influence the progression of CF symptoms thusaffecting with a self-feeding mechanism the same extent of malnutri-tion and oxidative stress along the life of CF patients Since severalfactors contribute to impair the nutritional status of CF patients(such as pancreatic insufficiency chronic malabsorption recurrentsinopulmonary infections and progressive lung disease chronic in-flammation increased energy expenditure suboptimal intake multi-therapy) careful monitoring of the antioxidant status should berecommended According with international guidelines fat-solublevitamin supplementation is of utmost importance in daily practice to-gether with energy intake requirements and pancreatic enzyme-replacement therapy Among these vitamin E β-carotene and ω-3FA have observed to alleviate selected biochemical signs of oxidativestress as measured for instance with well established laboratory indi-ces of lipid peroxidation and in some studies these effects werepreliminarily associated with positive clinical outcomes Notwith-standing randomizedndashcontrolled clinical trials on antioxidant supple-ments (including ω-3 FA) so far carried out in CF have failed toconclusively demonstrate significant beneficial effects on respiratorysymptoms and on the consequent impact that these have on the qual-ity of life of these patients (reviewed in [202213]) whichmay provideno support for the use of these supplements in CF An absence of effi-cacy in prevention studies on antioxidant supplements has also beenobserved in other and possibly less severe oxidative stress-relatedconditions particularly in the secondary prevention of cardiovasculardisease and some forms of cancer by vitamin E and other antioxidantssuch as vitamin C selenium and β-carotene (reviewed in [163]) Dif-ferent biases however have been identified in randomize large clini-cal trials that may account for these disappointing findings Theseinclude patient selection criteria (early interventions and primaryprevention could have more chances of success than secondaryprevention) duration and doses of the treatment use of wrong anti-oxidant formulations and administration protocols absence of verifi-cations of the biological compliance to the treatment etc The samebiases apply for the few trials carried out in CF patients Thus the ap-propriateness and efficacy of nutritional interventions with naturalfood-derived or synthetic antioxidants should be verifiedwith respectto the biological pathways of oxidative stress and clinical variablesthat are identified as end-points Profiles of blood and tissue antioxi-dants as well as of reliable surrogate markers of oxidative stresshave to be selected and determined in highly specialized laboratorieswith a well-established experience on these analyses
Well-timed (early) interventions with appropriate antioxidantformulationsprotocols need to be proposed for the next generationof trials and the development of novel CF-tailored antioxidant andanti-inflammatory agents should be promoted
As a consequence of these considerations more clinical investiga-tion is awaited to identify future successful approaches to the antiox-idant therapy as a measure to further enhance quality of life and theoverall clinical outcome of CF patients
Acknowledgments
We are indebted with the Italian Cystic Fibrosis Research Founda-tion for the support that it provided with its grant program to the re-search activity of the authors of this paper This is a scientific initiativeof the ldquoWorking Group on Inflammation in Cystic Fibrosisrdquo (BragonziA Bravo E Cabrini G Conese M Cuzzocrea S Dechecchi MC De Ales-sandri A Evangelista V Galli F Gambari R Lambiase A Lucidi VManca A Melotti P Minicucci L Motta A Pietraforte D Pompella AQuattrucci S Rizzo R Romano M Sorio C Tesse R) of the Italian Soci-ety for Cystic Fibrosis A particular thank goes to the Prof GianniMastella for the critical revision of the manuscript and for the
708 F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
stimulating research environment that he has contributed to createwithin the Italian Cystic Fibrosis Research Foundation
References
[1] BP OSullivan SD Freedman Cystic fibrosis Lancet 373 (2009) 1891ndash1904[2] P Linsdell JW Hanrahan Glutathione permeability of CFTR Am J Physiol 275
(1998) C323ndashC326[3] L Gao KJ Kim JR Yankaskas HJ Forman Abnormal glutathione transport in
cystic fibrosis airway epithelia Am J Physiol 277 (1999) L113ndashL118[4] RK Rowntree A Harris The phenotypic consequences of CFTR mutations Ann
Hum Genet 67 (2003) 471ndash485[5] EI Back C Frindt D Nohr J Frank R Ziebach M Stern M Ranke HK Biesalski
Antioxidant deficiency in cystic fibrosis when is the right time to take actionAm J Clin Nutr 80 (2004) 374ndash384
[6] LG Wood DA Fitzgerald AK Lee ML Garg Improved antioxidant and fattyacid status of patients with cystic fibrosis after antioxidant supplementation islinked to improved lung function Am J Clin Nutr 77 (2003) 150ndash159
[7] L Iuliano R Monticolo G Straface S Zullo F Galli M Boaz S Quattrucci Asso-ciation of cholesterol oxidation and abnormalities in fatty acid metabolism incystic fibrosis Am J Clin Nutr 90 (2009) 477ndash484
[8] C Libetta V Sepe P Esposito F Galli A Dal Canton Oxidative stress and inflam-mation implications in uremia and hemodialysis Clin Biochem 44 (2011)1189ndash1198
[9] G Bartosz Reactive oxygen species destroyers or messengers Biochem Phar-macol 77 (2009) 1303ndash1315
[10] T Ntimbane B Comte G Mailhot Y Berthiaume V Poitout M Prentki RRabasa-Lhoret E Levy Cystic fibrosis-related diabetes from CFTR dysfunctionto oxidative stress Clin Biochem 30 (2009) 153ndash177
[11] A van der Vliet JP Eiserich GP Marelich B Halliwell CE Cross Oxidativestress in cystic fibrosis does it occur and does it matter Adv Pharmacol 38(1997) 491ndash513
[12] AM Cantin TB White CE Cross HJ Forman RJ Sokol D Borowitz Antioxi-dants in cystic fibrosis Conclusions from the CF antioxidant workshop Bethes-da Maryland Free Radic Biol Med 42 (2007) 15ndash31
[13] LT McGrath P Mallon L Dowey B Silke E McClean M McDonnell A DevineS Copeland S Elborn Oxidative stress during acute respiratory exacerbations incystic fibrosis Thorax 54 (1999) 518ndash523
[14] E Thomson S Brennan R Senthilmohan CL Gangell AL Chapman PD SlyAJ Kettle E Balding LJ Berry JB Carlin R Carzino N de Klerk T Douglas CFoo LW Garratt GL Hall J Harrison A Kicic IA Laing KM Logie J MassieLS Mott C Murray F Parsons N Pillarisetti SR Poreddy SC RanganathanCF Robertson R Robins-Browne PJ Robinson B Skoric SM Stick ENSutanto E Williamson Identifying peroxidases and their oxidants in the earlypathology of cystic fibrosis Free Radic Biol Med 49 (2010) 1354ndash1360
[15] SP Range C Dunster AJ Knox FJ Kelly Treatment of pulmonary exacerba-tions of cystic fibrosis leads to improved antioxidant status Eur Respir J 13(1999) 560ndash564
[16] L Coppo P Ghezzi Thiol regulation of pro-inflammatory cytokines and innateimmunity protein S-thiolation as a novel molecular mechanism Biochem SocTrans 39 (2011) 1268ndash1272
[17] C Verhaeghe C Remouchamps B Hennuy A Vanderplasschen A Chariot SPTabruyn C Oury V Bours Role of IKK and ERK pathways in intrinsic inflamma-tion of cystic fibrosis airways Biochem Pharmacol 73 (2007) 1982ndash1994
[18] TL Bonfield JR Panuska MW Konstan KA Hilliard JB Hilliard H Ghnaim MBerger Inflammatory cytokines in cystic fibrosis lungs Am J Respir Crit CareMed 152 (1995) 2111ndash2118
[19] TL Noah HR Black PW Cheng RE Wood MW Leigh Nasal and bronchoal-veolar lavage fluid cytokines in early cystic fibrosis J Infect Dis 175 (1997)638ndash647
[20] MJ Welsh BW Ramsey FJ Accurso GR Cutting Cystic Fibrosis McGraw-HillNew York 2001
[21] TZ Khan JS Wagener T Bost J Martinez FJ Accurso DW Riches Early pul-monary inflammation in infants with cystic fibrosis Am J Respir Crit CareMed 151 (1995) 1075ndash1082
[22] FA Ratjen Cystic fibrosis pathogenesis and future treatment strategies RespirCare 54 (2009) 595ndash605
[23] J Jacquot O Tabary P Le Rouzic A Clement Airway epithelial cell inflamma-tory signalling in cystic fibrosis Int J Biochem Cell Biol 40 (2008)1703ndash1715
[24] CM Greene P Branagan NG McElvaney Toll-like receptors as therapeutic tar-gets in cystic fibrosis Expert Opin Ther Targets 12 (2008) 1481ndash1495
[25] M Rottner JM Freyssinet MC Martinez Mechanisms of the noxious inflam-matory cycle in cystic fibrosis Respir Res 10 (2009) 23
[26] G Cabrini V Bezzerri I Mancini E Nicolis MC Dechecchi A Tamanini ILampronti L Piccagli N Bianchi M Borgatti R Gambari Targeting transcrip-tion factor activity as a strategy to inhibit pro-inflammatory genes involved incystic fibrosis decoy oligonucleotides and low-molecular weight compoundsCurr Med Chem 17 (2010) 4392ndash4404
[27] CM Greene NG McElvaney Proteases and antiproteases in chronic neutrophiliclungdiseasemdash relevance to drug discovery Br J Pharmacol 158 (2009) 1048ndash1058
[28] AM Cantin Potential for antioxidant therapy of cystic fibrosis Curr Opin PulmMed 10 (2004) 531ndash536
[29] JF Chmiel MW Konstan Inflammation and anti-inflammatory therapies forcystic fibrosis Clin Chest Med 28 (2007) 331ndash346
[30] DP Nichols MW Konstan JF Chmiel Anti-inflammatory therapies for cys-tic fibrosis-related lung disease Clin Rev Allergy Immunol 35 (2008)135ndash153
[31] AJ Kettle T Chan I Osberg R Senthilmohan AL Chapman TJ Mocatta JSWagener Myeloperoxidase and protein oxidation in the airways of youngchildren with cystic fibrosis Am J Respir Crit Care Med 170 (2004)1317ndash1323
[32] H Fischer Mechanisms and function of DUOX in epithelia of the lung AntioxidRedox Signal 11 (2009) 2453ndash2465
[33] B Rada TL Leto Oxidative innate immune defenses by NoxDuox familyNADPH oxidases Contrib Microbiol 15 (2008) 164ndash187
[34] P Moskwa D Lorentzen KJ Excoffon J Zabner PB McCray Jr WM NauseefC Dupuy B Banfi A novel host defense system of airways is defective in cysticfibrosis Am J Respir Crit Care Med 175 (2007) 174ndash183
[35] D Lorentzen L Durairaj AA Pezzulo Y Nakano J Launspach DA Stoltz GZamba PB McCray Jr J Zabner MJ Welsh WM Nauseef B Banfi Concentra-tion of the antibacterial precursor thiocyanate in cystic fibrosis airway secre-tions Free Radic Biol Med 50 (2011) 1144ndash1150
[36] Y Xu S Szep Z Lu The antioxidant role of thiocyanate in the pathogenesis ofcystic fibrosis and other inflammation-related diseases Proc Natl Acad Sci US A 106 (2009) 20515ndash20519
[37] MP Rogan CC Taggart CM Greene PG Murphy SJ ONeill NG McElvaneyLoss of microbicidal activity and increased formation of biofilm due to decreasedlactoferrin activity in patients with cystic fibrosis J Infect Dis 190 (2004)1245ndash1253
[38] B Halliwell JM Guttridge Free Radicals in Biology and Medicine Fourth editionOxford University Press New York 2007
[39] B Rada K Lekstrom S Damian C Dupuy TL Leto The Pseudomonastoxin pyocyanin inhibits the dual oxidase-based antimicrobial system as itimposes oxidative stress on airway epithelial cells J Immunol 181 (2008)4883ndash4893
[40] C Schwarzer B Illek JH Suh SJ Remington H Fischer TE Machen Organelleredox of CF and CFTR-corrected airway epithelia Free Radic Biol Med 43(2007) 300ndash316
[41] JH Roum R Buhl NG McElvaney Z Borok RG Crystal Systemic deficiency ofglutathione in cystic fibrosis J Appl Physiol 75 (1993) 2419ndash2424
[42] VM Hudson Rethinking cystic fibrosis pathology the critical role of abnormalreduced glutathione (GSH) transport caused by CFTR mutation Free RadicBiol Med 30 (2001) 1440ndash1461
[43] PJ Barnes RA Dweik AF Gelb PG Gibson SC George H Grasemann IDPavord F Ratjen PE Silkoff DR Taylor N Zamel Exhaled nitric oxide in pul-monary diseases a comprehensive review Chest 138 (2010) 682ndash692
[44] H Grasemann E Michler M Wallot F Ratjen Decreased concentration of ex-haled nitric oxide (NO) in patients with cystic fibrosis Pediatr Pulmonol 24(1997) 173ndash177
[45] H Grasemann F Ratjen Cystic fibrosis lung disease the role of nitric oxidePediatr Pulmonol 28 (1999) 442ndash448
[46] B Gaston F Ratjen JW Vaughan NR Malhotra RG Canady AH Snyder JFHunt S Gaertig JB Goldberg Nitrogen redox balance in the cystic fibrosis air-way effects of antipseudomonal therapy Am J Respir Crit Care Med 165(2002) 387ndash390
[47] H Grasemann I Ioannidis RP Tomkiewicz H de Groot BK Rubin F RatjenNitric oxide metabolites in cystic fibrosis lung disease Arch Dis Child 78(1998) 49ndash53
[48] H Grasemann R Schwiertz S Matthiesen K Racke F Ratjen Increased argi-nase activity in cystic fibrosis airways Am J Respir Crit Care Med 172(2005) 1523ndash1528
[49] H Grasemann S Al-Saleh JA Scott D Shehnaz A Mehl R Amin M Rafii PPencharz J Belik F Ratjen Asymmetric dimethylarginine contributes to airwaynitric oxide deficiency in patients with cystic fibrosis Am J Respir Crit CareMed 183 (2011) 1363ndash1368
[50] H Grasemann F Kurtz F Ratjen Inhaled L-arginine improves exhaled nitricoxide and pulmonary function in patients with cystic fibrosis Am J RespirCrit Care Med 174 (2006) 208ndash212
[51] H Grasemann F Ratjen Emerging therapies for cystic fibrosis lung disease Ex-pert Opin Emerg Drugs 15 (2010) 653ndash659
[52] BM Morrissey K Schilling JV Weil PE Silkoff DM Rodman Nitric oxide andprotein nitration in the cystic fibrosis airway Arch Biochem Biophys 406(2002) 33ndash39
[53] R Radi Nitric oxide oxidants and protein tyrosine nitration Proc Natl AcadSci U S A 101 (2004) 4003ndash4008
[54] J Chen M Kinter S Shank C Cotton TJ Kelley AG Ziady Dysfunction of Nrf-2in CF epithelia leads to excess intracellular H2O2 and inflammatory cytokineproduction PLoS One 3 (2008) e3367
[55] F Galli M Piroddi C Annetti C Aisa E Floridi A Floridi Oxidative stress andreactive oxygen species Contrib Nephrol 149 (2005) 240ndash260
[56] DT Wright LA Cohn H Li B Fischer CM Li KB Adler Interactions of oxygenradicals with airway epithelium Environ Health Perspect 102 (Suppl 10)(1994) 85ndash90
[57] I Rahman SR Yang SK Biswas Current concepts of redox signaling in thelungs Antioxid Redox Signal 8 (2006) 681ndash689
[58] Q Li JF Engelhardt Interleukin-1beta induction of NFκB is partially regulatedby H2O2-mediated activation of NFκB-inducing kinase J Biol Chem 281(2006) 1495ndash1505
709F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
[59] E Boncoeur VS Criq E Bonvin T Roque A Henrion-Caude DC Gruenert AClement J Jacquot O Tabary Oxidative stress induces extracellular signal-regulated kinase 12 mitogen-activated protein kinase in cystic fibrosis lung ep-ithelial cells potential mechanism for excessive IL-8 expression Int J BiochemCell Biol 40 (2008) 432ndash446
[60] B Fischer J Voynow Neutrophil elastase induces MUC5AC messenger RNA ex-pression by an oxidant-dependent mechanism Chest 117 (2000) 317Sndash320S
[61] B Rada P Gardina TG Myers TL Leto Reactive oxygen species mediate in-flammatory cytokine release and EGFR-dependent mucin secretion in airwayepithelial cells exposed to Pseudomonas pyocyanin Mucosal Immunol 4(2011) 158ndash171
[62] C Schwarzer H Fischer EJ Kim KJ Barber AD Mills MJ Kurth DC GruenertJH Suh TE Machen B Illek Oxidative stress caused by pyocyanin impairs CFTRClminus transport in human bronchial epithelial cells Free Radic Biol Med 45(2008) 1653ndash1662
[63] J Hull M South P Phelan K Grimwood Surfactant composition in infants andyoung children with cystic fibrosis Am J Respir Crit Care Med 156 (1997)161ndash165
[64] KC Meyer A Sharma R Brown M Weatherly FR Moya J Lewandoski JJZimmerman Function and composition of pulmonary surfactant andsurfactant-derived fatty acid profiles are altered in young adults with cystic fi-brosis Chest 118 (2000) 164ndash174
[65] MK Pulfer RC Murphy Formation of biologically active oxysterols during ozo-nolysis of cholesterol present in lung surfactant J Biol Chem 279 (2004)26331ndash26338
[66] V Starosta E Rietschel K Paul U Baumann M Griese Oxidative changes ofbronchoalveolar proteins in cystic fibrosis Chest 129 (2006) 431ndash437
[67] V Starosta M Griese Oxidative damage to surfactant protein D in pulmonarydiseases Free Radic Res 40 (2006) 419ndash425
[68] M Griese R Essl R Schmidt E Rietschel F Ratjen M Ballmann K Paul Pulmo-nary surfactant lung function and endobronchial inflammation in cystic fibro-sis Am J Respir Crit Care Med 170 (2004) 1000ndash1005
[69] M Griese R Essl R Schmidt M Ballmann K Paul E Rietschel F Ratjen Se-quential analysis of surfactant lung function and inflammation in cystic fibrosispatients Respir Res 6 (2005) 133
[70] LG Wood DA Fitzgerald PG Gibson DM Cooper ML Garg Increased plasmafatty acid concentrations after respiratory exacerbations are associated with el-evated oxidative stress in cystic fibrosis patients Am J Clin Nutr 75 (2002)668ndash675
[71] P Montuschi SA Kharitonov G Ciabattoni M Corradi L van Rensen DM Ged-des ME Hodson PJ Barnes Exhaled 8-isoprostane as a new non-invasive bio-marker of oxidative stress in cystic fibrosis Thorax 55 (2000) 205ndash209
[72] CE Collins P Quaggiotto L Wood EV OLoughlin RL Henry ML Garg Elevat-ed plasma levels of F2 alpha isoprostane in cystic fibrosis Lipids 34 (1999)551ndash556
[73] D Hartl V Starosta K Maier I Beck-Speier C Rebhan BF Becker P Latzin RFischer F Ratjen RM Huber E Rietschel S Krauss-Etschmann M Griese In-haled glutathione decreases PGE2 and increases lymphocytes in cystic fibrosislungs Free Radic Biol Med 39 (2005) 463ndash472
[74] GL Milne H Yin JD Morrow Human biochemistry of the isoprostane pathwayJ Biol Chem 283 (2008) 15533ndash15537
[75] G Ciabattoni G Davi M Collura L Iapichino F Pardo A Ganci R Romagnoli JMaclouf C Patrono In vivo lipid peroxidation and platelet activation in cystic fi-brosis Am J Respir Crit Care Med 162 (2000) 1195ndash1201
[76] C Garenc P Julien E Levy Oxysterols in biological systems the gastrointestinaltract liver vascular wall and central nervous system Free Radic Res 44 (2011)47ndash73
[77] AM Cantin SL North RC Hubbard RG Crystal Normal alveolar epithelial lin-ing fluid contains high levels of glutathione J Appl Physiol 63 (1987) 152ndash157
[78] R Tirouvanziam CK Conrad T Bottiglieri LA Herzenberg RB Moss High-dose oral N-acetylcysteine a glutathione prodrug modulates inflammation incystic fibrosis Proc Natl Acad Sci U S A 103 (2006) 4628ndash4633
[79] LW Velsor C Kariya R Kachadourian BJ Day Mitochondrial oxidative stressin the lungs of cystic fibrosis transmembrane conductance regulator proteinmutant mice Am J Respir Cell Mol Biol 35 (2006) 579ndash586
[80] M Kelly-Aubert S Trudel J Fritsch T Nguyen-Khoa M Baudouin-Legros SMoriceau L Jeanson F Djouadi C Matar M Conti M Ollero F Brouillard AEdelman GSH monoethyl ester rescues mitochondrial defects in cystic fibrosismodels Hum Mol Genet 20 (2011) 2745ndash2759
[81] P Ghezzi Role of glutathione in immunity and inflammation in the lung Int JGen Med 4 (2011) 105ndash113
[82] N Dauletbaev K Viel R Buhl TO Wagner J Bargon Glutathione and glutathi-one peroxidase in sputum samples of adult patients with cystic fibrosis J CystFibros 3 (2004) 119ndash124
[83] CE Cross A van der Vliet CA ONeill S Louie B Halliwell Oxidants antioxi-dants and respiratory tract lining fluids Environ Health Perspect 102 (Suppl10) (1994) 185ndash191
[84] K Takeyama K Dabbagh J Jeong Shim T Dao-Pick IF Ueki JA Nadel Oxida-tive stress causes mucin synthesis via transactivation of epidermal growth factorreceptor role of neutrophils J Immunol 164 (2000) 1546ndash1552
[85] N Ballatori SM Krance S Notenboom S Shi K Tieu CL Hammond Glutathi-one dysregulation and the etiology and progression of human diseases BiolChem 390 (2009) 191ndash214
[86] SR Soltaninassab KR Sekhar MJ Meredith ML Freeman Multi-faceted regu-lation of gamma-glutamylcysteine synthetase J Cell Physiol 182 (2000)163ndash170
[87] HR Lopez-Mirabal JR Winther Redox characteristics of the eukaryotic cytosolBiochim Biophys Acta 1783 (2008) 629ndash640
[88] C Hwang AJ Sinskey HF Lodish Oxidized redox state of glutathione in the en-doplasmic reticulum Science 257 (1992) 1496ndash1502
[89] M Murphy Mitochondrial thiols in antioxidant protection and redox signallingdistinct roles for glutathionylation and other thiol modifications AntioxidRedox Signal (2011) ahead of print doi101089ars20114289
[90] BJ Day AM van Heeckeren E Min LW Velsor Role for cystic fibrosis trans-membrane conductance regulator protein in a glutathione response to bronch-opulmonary Pseudomonas infection Infect Immun 72 (2004) 2045ndash2051
[91] Y Zhang K Duan Glutathione exhibits antibacterial activity and increases tetra-cycline efficacy against Pseudomonas aeruginosa Sci China C Life Sci 52 (2009)501ndash505
[92] VM Hudson New insights into the pathogenesis of cystic fibrosis pivotal roleof glutathione system dysfunction and implications for therapy Treat RespirMed 3 (2004) 353ndash363
[93] LW Velsor A van Heeckeren BJ Day Antioxidant imbalance in the lungs ofcystic fibrosis transmembrane conductance regulator protein mutant miceAm J Physiol Lung Cell Mol Physiol 281 (2001) L31ndashL38
[94] I Kogan M Ramjeesingh C Li JF Kidd Y Wang EM Leslie SP Cole CE BearCFTR directly mediates nucleotide-regulated glutathione flux EMBO J 22(2003) 1981ndash1989
[95] NS Gould S Gauthier CT Kariya E Min J Huang DJ Brian Hypertonic salineincreases lung epithelial lining fluid glutathione and thiocyanate two protectiveCFTR-dependent thiols against oxidative injury Respir Res 11 (2010) 119
[96] VT Vasu SJ de Cruz JS Houghton KA Hayakawa BM Morrissey CE CrossJP Eiserich Evaluation of thiol-based antioxidant therapeutics in cystic fibrosissputum focus on myeloperoxidase Free Radic Res 45 (2011) 165ndash176
[97] L Roussel G Martel J Berube S Rousseau P aeruginosa drives CXCL8 synthesisvia redundant toll-like receptors and NADPH oxidase in CFTRF508 airway epi-thelial cells J Cyst Fibros 10 (2011) 107ndash113
[98] GW Lau DJ Hassett H Ran F Kong The role of pyocyanin in Pseudomonas aer-uginosa infection Trends Mol Med 10 (2004) 599ndash606
[99] R Wilson DA Sykes D Watson A Rutman GW Taylor PJ Cole Measurementof Pseudomonas aeruginosa phenazine pigments in sputum and assessment oftheir contribution to sputum sol toxicity for respiratory epithelium InfectImmun 56 (1988) 2515ndash2517
[100] M Muller Pyocyanin induces oxidative stress in human endothelial cells andmodulates the glutathione redox cycle Free Radic Biol Med 33 (2002)1527ndash1533
[101] YQ OMalley KJ Reszka BE Britigan Direct oxidation of 2prime7prime-dichlorodihy-drofluorescein by pyocyanin and other redox-active compounds independentof reactive oxygen species production Free Radic Biol Med 36 (2004)90ndash100
[102] CC Caldwell Y Chen HS Goetzmann Y Hao MT Borchers DJ Hassett LRYoung D Mavrodi L Thomashow GW Lau Pseudomonas aeruginosa exotoxinpyocyanin causes cystic fibrosis airway pathogenesis Am J Pathol 175 (2009)2473ndash2488
[103] YQ OMalley KJ Reszka DR Spitz GM Denning BE Britigan Pseudomonasaeruginosa pyocyanin directly oxidizes glutathione and decreases its levels inairway epithelial cells Am J Physiol Lung Cell Mol Physiol 287 (2004)L94ndashL103
[104] M Muller Glutathione modulates the toxicity of but is not a biologically rele-vant reductant for the Pseudomonas aeruginosa redox toxin pyocyanin FreeRadic Biol Med 50 (2011) 971ndash977
[105] R Cheluvappa R Shimmon M Dawson SN Hilmer DG Le Couteur Reactionsof Pseudomonas aeruginosa pyocyanin with reduced glutathione Acta BiochimPol 55 (2008) 571ndash580
[106] JH Widdicombe Transgenic animals may help resolve a sticky situation in cys-tic fibrosis J Clin Invest 120 (2010) 3093ndash3096
[107] X Sun H Sui JT Fisher Z Yan X Liu HJ Cho NS Joo Y Zhang W Zhou Y YiJM Kinyon DC Lei-Butters MA Griffin P Naumann M Luo J Ascher KWang T Frana JJ Wine DK Meyerholz JF Engelhardt Disease phenotype ofa ferret CFTR-knockout model of cystic fibrosis J Clin Invest 120 (2010)3149ndash3160
[108] NS Joo HJ Cho M Khansaheb JJ Wine Hyposecretion of fluid from trachealsubmucosal glands of CFTR-deficient pigs J Clin Invest 120 (2010) 3161ndash3166
[109] A Bragonzi Murine models of acute and chronic lung infection with cystic fibro-sis pathogens IJMM 300 (2010) 584ndash593
[110] AM van Heeckeren MD Schluchter Murine models of chronic Pseudomonasaeruginosa lung infection Lab Anim 36 (2002) 291ndash312
[111] A Bragonzi D Worlitzsch GB Pier P Timpert M Ulrich M Hentzer JB Ander-sen M Givskov M Conese G Doring Nonmucoid Pseudomonas aeruginosa ex-presses alginate in the lungs of patients with cystic fibrosis and in a mousemodel J Infect Dis 192 (2005) 410ndash419
[112] GS CW Bedrossian DB Singer JJ Hansen HS Rosenberg The lung in cysticfibrosis A quantitative study including prevalence of pathologic findingsamong different age groups Hum Pathol 7 (1976) 195ndash204
[113] WD HA Cash B McCullough WG Johanson Jr JA Bass A rat model of chron-ic respiratory infection with Pseudomonas aeruginosa Am Rev Respir Dis 119(1979) 453ndash459
[114] EM JR Starke C Langston CJ Baker A mouse model of chronic pulmonary in-fection with Pseudomonas aeruginosa and Pseudomonas cepacia Pediatr Res 22(1987) 698ndash702
[115] TJ AM van Heeckeren RW Walenga MW Konstan PB Davis B ErokwuMA Haxhiu TW Ferkol Effect of Pseudomonas infection on weight loss lung
710 F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
mechanics and cytokines in mice Am J Respir Crit Care Med 161 (2000)271ndash279
[116] T Aw G Wierzbicka DP Jones Oral glutathione increases tissue glutathione invivo Chem Biol Interact 80 (1991) 89ndash97
[117] F Favilli P Marraccini T Iantomasi MT Vincenzini Effect of orally adminis-tered glutathione on glutathione levels in some organs of rats role of specifictransporters Br J Nutr 78 (1997) 293ndash300
[118] C Kariya H Leitner E Min C van Heeckeren A van Heeckeren BJ Day A rolefor CFTR in the elevation of glutathione levels in the lung by oral glutathione ad-ministration Am J Physiol Lung Cell Mol Physiol 292 (2007) L1590ndashL1597
[119] K Atkuri JJ Mantovani LA Herzenberg LA Herzenberg N-Acetylcysteinemdashasafe antidote for cysteineglutathione deficiency Curr Opin Pharmacol 7(2007) 355ndash359
[120] R De Lisle E Roach K Jansson Effects of laxative and N-acetylcysteine onmucus accumulation bacterial load transit and inflammation in the cystic fi-brosis mouse small intestine Am J Physiol Gastrointest Liver Physiol 293(2007) G577ndashG584
[121] A Luciani VR Villella S Esposito N Brunetti-Pierri D Medina C Settembre MGavina L Pulze I Giardino M Pettoello-Mantovani M DApolito S Guido EMasliah B Spencer S Quaratino V Raia A Ballabio L Maiuri Defective CFTRinduces aggresome formation and lung inflammation in cystic fibrosis throughROS-mediated autophagy inhibition Nat Cell Biol 12 863ndash875
[122] M Griese J Ramakers A Krasselt V Starosta S Van Koningsbruggen R FischerF Ratjen B Mullinger RM Huber K Maier E Rietschel G Scheuch Improve-ment of alveolar glutathione and lung function but not oxidative state in cysticfibrosis Am J Respir Crit Care Med 169 (2004) 822ndash828
[123] C Bishop VM Hudson SC Hilton C Wilde A pilot study of the effect of inhaledbuffered reduced glutathione on the clinical status of patients with cystic fibro-sis Chest 127 (2005) 308ndash317
[124] WWang C Oliva G Li A Holmgren CH Lillig KL Kirk Reversible silencing of CFTRchloride channels by glutathionylation J Gen Physiol 125 (2005) 127ndash141
[125] N Dauletbaev P Fischer B Aulbach J Gross W Kusche U Thyroff-FriesingerTO Wagner J Bargon A phase II study on safety and efficacy of high-dose N-acetylcysteine in patients with cystic fibrosis Eur J Med Res 14 (2009)352ndash358
[126] R Tirouvanziam Y Gernez CK Conrad RB Moss I Schrijver CE Dunn ZADavies LA Herzenberg Profound functional and signaling changes in viable in-flammatory neutrophils homing to cystic fibrosis airways Proc Natl Acad SciU S A 105 (2008) 4335ndash4339
[127] JH Roum Z Borok NG McElvaney GJ Grimes AD Bokser R Buhl RG Crys-tal Glutathione aerosol suppresses lung epithelial surface inflammatory cell-derived oxidants in cystic fibrosis J Appl Physiol 87 (1999) 438ndash443
[128] A Visca CT Bishop SC Hilton VM Hudson Improvement in clinical markersin CF patients using a reduced glutathione regimen an uncontrolled observa-tional study J Cyst Fibros 7 (2008) 433ndash436
[129] EF Nash A Stephenson F Ratjen E Tullis Nebulized and oral thiol derivativesfor pulmonary disease in cystic fibrosis Cochrane Database Syst Rev (2009)CD007168
[130] AC foundation Drug Development Pipeline 2011[131] S Hoshida T Kuzuya N Yamashita M Nishida S Kitahara M Hori T
Kamada M Tada Gamma-glutamylcysteine ethyl ester for myocardial protec-tion in dogs during ischemia and reperfusion J Am Coll Cardiol 24 (1994)1391ndash1397
[132] J Lok W Leung S Zhao S Pallast K van Leyen S Guo X Wang A Yalcin EHLo Gamma-glutamylcysteine ethyl ester protects cerebral endothelial cells dur-ing injury and decreases bloodndashbrain barrier permeability after experimentalbrain trauma J Neurochem 118 (2011) 248ndash255
[133] Z Borok R Buhl GJ Grimes AD Bokser RC Hubbard KJ Holroyd JH RoumDB Czerski AM Cantin RG Crystal Effect of glutathione aerosol on oxidantndashantioxidant imbalance in idiopathic pulmonary fibrosis Lancet 338 (1991)215ndash216
[134] KJ Holroyd R Buhl Z Borok JH Roum AD Bokser GJ Grimes D Czerski AMCantin RG Crystal Correction of glutathione deficiency in the lower respiratorytract of HIV seropositive individuals by glutathione aerosol treatment Thorax 48(1993) 985ndash989
[135] J Hull P Vervaart K Grimwood P Phelan Pulmonary oxidative stress responsein young children with cystic fibrosis Thorax 52 (1997) 557ndash560
[136] A Corti A Paolicchi M Franzini S Dominici AF Casini A Pompella The S-thiolating activity of membrane gamma-glutamyltransferase formation ofcysteinyl-glycine mixed disulfides with cellular proteins and in the cell microen-vironment Antioxid Redox Signal 7 (2005) 911ndash918
[137] A Corti M Franzini AF Casini A Paolicchi A Pompella Vitamin C supply tobronchial epithelial cells linked to glutathione availability in elfmdasha role for se-creted gamma-glutamyltransferase J Cyst Fibros 7 (2008) 174ndash178
[138] A Munck Nutritional considerations in patients with cystic fibrosis Expert RevRespir Med 4 (2010) 47ndash56
[139] JL Matel CE Milla Nutrition in cystic fibrosis Semin Respir Crit Care Med 30(2009) 579ndash586
[140] D Salvatore R Buzzetti E Baldo MP Forneris V Lucidi D Manunza IMarinelli B Messore AS Neri V Raia ML Furnari G Mastella An overviewof international literature from cystic fibrosis registries 2 Neonatal screeningand nutritiongrowth J Cyst Fibros 9 (2010) 75ndash83
[141] KF Joosten JM Hulst Malnutrition in pediatric hospital patients current is-sues Nutrition 27 (2011) 133ndash137
[142] S Fustik T Jacovska L Spirevska S Koceva Protein-energy malnutrition as thefirst manifestation of cystic fibrosis in infancy Pediatr Int 51 (2009) 678ndash683
[143] J Himmelfarb E McMonagle Albumin is the major plasma protein target of ox-idant stress in uremia Kidney Int 60 (2001) 358ndash363
[144] P Stenvinkel JJ Carrero J Axelsson B Lindholm O Heimburger Z MassyEmerging biomarkers for evaluating cardiovascular risk in the chronic kidneydisease patient how do new pieces fit into the uremic puzzle Clin J Am SocNephrol 3 (2008) 505ndash521
[145] M Roche P Rondeau NR Singh E Tarnus E Bourdon The antioxidant proper-ties of serum albumin FEBS Lett 582 (2008) 1783ndash1787
[146] D Giustarini A Milzani I Dalle-Donne R Rossi Red blood cells as a physiolog-ical source of glutathione for extracellular fluids Blood Cells Mol Dis 40 (2008)174ndash179
[147] A Meister ME Anderson Glutathione Annu Rev Biochem 52 (1983) 711ndash760[148] B Alvarez S Carballal L Turell R Radi Formation and reactions of sulfenic acid
in human serum albumin Methods Enzymol 473 (2010) 117ndash136[149] S Carballal B Alvarez L Turell H Botti BA Freeman R Radi Sulfenic acid in
human serum albumin Amino Acids 32 (2007) 543ndash551[150] LR Barclay AM Bailey D Kong The antioxidant activity of alpha-tocopherol-
bovine serum albumin complex in micellar and liposome autoxidations J BiolChem 260 (1985) 15809ndash15814
[151] T Ishii T Ichikawa K Minoda K Kusaka S Ito Y Suzuki M Akagawa K Mochi-zuki T Goda T Nakayama Human serum albumin as an antioxidant in the ox-idation of (minus)-epigallocatechin gallate participation of reversible covalentbinding for interaction and stabilization Biosci Biotechnol Biochem 75(2011) 100ndash106
[152] F Galli S Rovidati S Benedetti U Buoncristiani C Covarelli A Floridi F Canes-trari Overexpression of erythrocyte glutathione S-transferase in uremia and di-alysis Clin Chem 45 (1999) 1781ndash1788
[153] D Borowitz RD Baker V Stallings Consensus report on nutrition for pediat-ric patients with cystic fibrosis J Pediatr Gastroenterol Nutr 35 (2002)246ndash259
[154] LJ Filer Jr SW Wright MP Manning KE Mason Absorption of alpha-tocopherol and tocopherylesters by premature and full term infants and chil-dren in health and disease Pediatrics 8 (1951) 328ndash339
[155] L Lancellotti C DOrazio G Mastella G Mazzi U Lippi Deficiency of vitamins Eand A in cystic fibrosis is independent of pancreatic function and current en-zyme and vitamin supplementation Eur J Pediatr 155 (1996) 281ndash285
[156] MN Sathe AS Patel Update in pediatrics focus on fat-soluble vitamins NutrClin Pract 25 (2010) 340ndash346
[157] MG Traber The ABCs of vitamin E and beta-carotene absorption Am J ClinNutr 80 (2004) 3ndash4
[158] TF Dolan Jr Hemolytic anemia and edema as the initial signs in infants withcystic fibrosis Consider this diagnosis even in absence of pulmonary symptomsClin Pediatr 15 (1976) 597ndash600
[159] DR James M Alfaham MC Goodchild Increased susceptibility to peroxide-induced haemolysis with normal vitamin E concentrations in cystic fibrosisClin Chim Acta 204 (1991) 279ndash290
[160] SA Peters FJ Kelly Vitamin E supplementation in cystic fibrosis J Pediatr Gas-troenterol Nutr 22 (1996) 341ndash345
[161] A Maqbool VA Stallings Update on fat-soluble vitamins in cystic fibrosis CurrOpin Pulm Med 14 (2008) 574ndash581
[162] SD Sagel MK Sontag MM Anthony P Emmett KA Papas Effect of anantioxidant-rich multivitamin supplement in cystic fibrosis J Cyst Fibros 10(2011) 31ndash36
[163] F Galli A Azzi Present trends in vitamin E research Biofactors 36 (2010)33ndash42
[164] A Hamahata P Enkhbaatar ER Kraft M Lange SW Leonard MG Traber RACox FC Schmalstieg HK Hawkins EB Whorton EM Horvath C Szabo LDTraber DN Herndon DL Traber Gamma-tocopherol nebulization by a lipidaerosolization device improves pulmonary function in sheep with burn andsmoke inhalation injury Free Radic Biol Med 45 (2008) 425ndash433
[165] JP Anais N Razzouq M Carvalho C Fernandez A Astier M Paul A AstierH Fessi AM Lorino Development of alpha-tocopherol acetate nanoparti-cles influence of preparative processes Drug Dev Ind Pharm 35 (2009)216ndash223
[166] JM Zingg Molecular and cellular activities of vitamin E analogues Mini RevMed Chem 7 (2007) 543ndash558
[167] V Viola F Pilolli M Piroddi E Pierpaoli F Orlando M Provinciali M Betti FMazzini F Galli Why tocotrienols work better insights into the in vitro anti-cancer mechanism of vitamin E Genes Nutr 7 (2011) 29ndash41
[168] F Galli F Mazzini L Bamonti L Gille S Bohmdorfer M Piroddi T Netscher FJKelly T Rosenau Tocotrienamines and tocopheramines reactions with radicalsand metal ions Bioorg Med Chem 19 (2011) 6483ndash6491
[169] A Kuhad K Chopra Attenuation of diabetic nephropathy by tocotrienol in-volvement of NFκB signaling pathway Life Sci 84 (2009) 296ndash301
[170] Q Jiang X Yin MA Lill ML Danielson H Freiser J Huang Long-chain carbox-ychromanols metabolites of vitamin E are potent inhibitors of cyclooxygenasesProc Natl Acad Sci U S A 105 (2008) 20464ndash20469
[171] ER Miller III R Pastor-Barriuso D Dalal RA Riemersma LJ Appel E GuallarMeta-analysis high-dosage vitamin E supplementation may increase all-causemortality Ann Intern Med 142 (2005) 37ndash46
[172] JN Hathcock A Azzi J Blumberg T Bray A Dickinson B Frei I Jialal CSJohnston FJ Kelly K Kraemer L Packer S Parthasarathy H Sies MG TraberVitamins E and C are safe across a broad range of intakes Am J Clin Nutr 81(2005) 736ndash745
[173] R Brigelius-Flohe F Galli Vitamin E a vitamin still awaiting the detection of itsbiological function Mol Nutr Food Res 54 (2010) 583ndash587
711F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
[174] MG Traber B Frei JS Beckman Vitamin E revisited do new data validate ben-efits for chronic disease prevention Curr Opin Lipidol 19 (2008) 30ndash38
[175] F Galli Meeting report Vitamin E Satellite Symposium (VESS) associated to theAnnual Meeting of the SFRR-Europe Rome 26 August 2009 Free Radic Res 43(2009) 1256ndash1257
[176] LJ Roberts II JA Oates MF Linton S Fazio BP Meador MD Gross Y Shyr JDMorrow The relationship between dose of vitamin E and suppression of oxida-tive stress in humans Free Radic Biol Med 43 (2007) 1388ndash1393
[177] EFSA- EFSA Scientific Opinion of the Panel on Food Additives FlavouringsProcessing Aids and Materials in Contact with Food on a request from the Com-mission on mixed tocopherols tocotrienol tocopherol and tocotrienols assources for vitamin E in EFSA- EFSA (Ed) vol 640 The EFSA Journal2008 pp 1ndash34
[178] P Rust I Eichler S Renner I Elmadfa Long-term oral beta-carotene supple-mentation in patients with cystic fibrosis mdash effects on antioxidative status andpulmonary function Ann Nutr Metab 44 (2000) 30ndash37
[179] G Lepage J Champagne N Ronco A Lamarre I Osberg RJ Sokol CC Roy Sup-plementation with carotenoids corrects increased lipid peroxidation in childrenwith cystic fibrosis Am J Clin Nutr 64 (1996) 87ndash93
[180] BM Winklhofer-Roob H Puhl G Khoschsorur MA vant Hof H EsterbauerDH Shmerling Enhanced resistance to oxidation of low density lipoproteinsand decreased lipid peroxide formation during beta-carotene supplementationin cystic fibrosis Free Radic Biol Med 18 (1995) 849ndash859
[181] RC Graham-Maar JI Schall N Stettler BS Zemel VA Stallings Elevated vita-min A intake and serum retinol in preadolescent children with cystic fibrosisAm J Clin Nutr 84 (2006) 174ndash182
[182] I Sadowska-Woda M Rachel J Pazdan E Bieszczad-Bedrejczuk K PawliszakNutritional supplement attenuates selected oxidative stress markers in pediatricpatients with cystic fibrosis Nutr Res (New York NY) 31 (2011) 509ndash518
[183] KA Papas MK Sontag C Pardee RJ Sokol SD Sagel FJ Accurso JS WagenerA pilot study on the safety and efficacy of a novel antioxidant rich formulation inpatients with cystic fibrosis J Cyst Fibros 7 (2008) 60ndash67
[184] Y Saito A Fukuhara K Nishio M Hayakawa Y Ogawa H Sakamoto K Fujii YYoshida E Niki Characterization of cellular uptake and distribution of coen-zyme Q10 and vitamin E in PC12 cells J Nutr Biochem 20 (2009) 350ndash357
[185] AA Franke CM Morrison JL Bakke LJ Custer X Li RV Cooney CoenzymeQ10 in human blood native levels and determinants of oxidation during proces-sing and storage Free Radic Biol Med 48 (2010) 1610ndash1617
[186] HN Bhagavan RK Chopra Plasma coenzyme Q10 response to oral ingestion ofcoenzyme Q10 formulations Mitochondrion 7 (2007) S78ndashS88 (Suppl)
[187] HN Bhagavan RK Chopra Coenzyme Q10 absorption tissue uptake metabo-lism and pharmacokinetics Free Radic Res 40 (2006) 445ndash453
[188] F Galli R Lee C Dunster FJ Kelly Gas chromatography mass spectrometryanalysis of carboxyethyl-hydroxychroman metabolites of alpha- and gamma-tocopherol in human plasma Free Radic Biol Med 32 (2002) 333ndash340
[189] F Galli R Lee J Atkinson A Floridi FJ Kelly Gamma-tocopherol biokineticsand transformation in humans Free Radic Res 37 (2003) 1225ndash1233
[190] TA Laguna MK Sontag I Osberg JS Wagener FJ Accurso RJ Sokol De-creased total serum coenzyme-Q10 concentrations a longitudinal study in chil-dren with cystic fibrosis J Pediatr 153 (2008) 402ndash407
[191] T Frischer JK Myung G Maurer I Eichler Z Szepfalusi G Lubec Possible dys-regulation of chaperon and metabolic proteins in cystic fibrosis bronchial tissueProteomics 6 (2006) 3381ndash3388
[192] C Andersson MM Zaman AB Jones SD Freedman Alterations in immune re-sponse and PPARLXR regulation in cystic fibrosis macrophages J Cyst Fibros 7(2008) 68ndash78
[193] SD Freedman PG Blanco MM Zaman JC Shea M Ollero IK Hopper DAWeed A Gelrud MM Regan M Laposata JG Alvarez BP OSullivan Associa-tion of cystic fibrosis with abnormalities in fatty acid metabolism N Engl JMed 350 (2004) 560ndash569
[194] S Van Biervliet G Vanbillemont JP Van Biervliet D Declercq E Robberecht AChristophe Relation between fatty acid composition and clinical status or geno-type in cystic fibrosis patients Ann Nutr Metab 51 (2007) 541ndash549
[195] SD Freedman MH Katz EM Parker M Laposata MY Urman JG AlvarezA membrane lipid imbalance plays a role in the phenotypic expression ofcystic fibrosis in cftr(minusminus) mice Proc Natl Acad Sci U S A 96 (1999)13995ndash14000
[196] S Van Biervliet S Vande Velde JP Van Biervliet E Robberecht The effect ofzinc supplements in cystic fibrosis patients Ann Nutr Metab 52 (2008)152ndash156
[197] WR Henderson Jr SJ Astley MM McCready P Kushmerick S Casey JWBecker BW Ramsey Oral absorption of omega-3 fatty acids in patients withcystic fibrosis who have pancreatic insufficiency and in healthy control subjectsJ Pediatr 124 (1994) 400ndash408
[198] I Durieu E Vericel D Guichardant H Roth JP Steghens J Drai RN JosserandE Fontaine M Lagarde G Bellon Fatty acids platelets and oxidative markersfollowing intravenous n-3 fatty acids administration in cystic fibrosis an openpilot observational study J Cyst Fibros 6 (2007) 320ndash326
[199] LG Wood DA Fitzgerald ML Garg Hypothesis vitamin E complements poly-unsaturated fatty acids in essential fatty acid deficiency in cystic fibrosis J AmColl Nutr 22 (2003) 253ndash257
[200] JD Lloyd-Still SB Johnson RT Holman Essential fatty acid status in cystic fi-brosis and the effects of safflower oil supplementation Am J Clin Nutr 34(1981) 1ndash7
[201] A Maqbool JI Schall JF Garcia-Espana BS Zemel B Strandvik VAStallings Serum linoleic acid status as a clinical indicator of essential fatty
acid status in children with cystic fibrosis J Pediatr Gastroenterol Nutr 47(2008) 635ndash644
[202] C Oliver N Jahnke Omega-3 fatty acids for cystic fibrosis Cochrane DatabaseSyst Rev (2011) CD002201
[203] B Strandvik E Gronowitz F Enlund T Martinsson J Wahlstrom Essential fattyacid deficiency in relation to genotype in patients with cystic fibrosis J Pediatr139 (2001) 650ndash655
[204] P Rise S Volpi C Colombo RF Padoan C DOrazio S Ghezzi PMelotti V BennatoC Agostoni BM Assael C Galli Whole blood fatty acid analysis with micromethodin cystic fibrosis and pulmonary disease J Cyst Fibros 9 (2010) 228ndash233
[205] H Cao K Gerhold JR Mayers MM Wiest SM Watkins GS Hotamisligil Iden-tification of a lipokine a lipid hormone linking adipose tissue to systemic me-tabolism Cell 134 (2008) 933ndash944
[206] RR Malapaka SK Khoo J Zhang JH Choi XE Zhou Y Xu Y Gong J Li ELYong MJ Chalmers L Chang JH Resau PR Griffin YE Chen HE Xu Iden-tification and mechanism of a ten carbon fatty acid as a modulating ligand ofperoxisome proliferator activated receptors J Biol Chem 287 (2012)183ndash195
[207] T Hara A Hirasawa A Ichimura I Kimura G Tsujimoto Free fatty acid recep-tors FFAR1 and GPR120 as novel therapeutic targets for metabolic disorders JPharm Sci 100 (2011) 3594ndash3601
[208] R Gupta P Rathi S Bradoo Lipase mediated upgradation of dietary fats andoils Crit Rev Food Sci Nutr 43 (2003) 635ndash644
[209] BH Jennings CC Akoh Lipase-catalyzed modification of rice bran oil to incor-porate capric acid J Agric Food Chem 48 (2000) 4439ndash4443
[210] J Hoeks M Mensink MK Hesselink K Ekroos P Schrauwen Long- andMedium-Chain Fatty Acids Induce Insulin Resistance to a Similar Extent inHumans Despite Marked Differences in Muscle Fat Accumulation J Clin Endo-crinol Metab 97 (2012) 208ndash216
[211] PJ Congden G Bruce MM Rothburn PC Clarke JM Littlewood J KelleherMS Losowsky Vitamin status in treated patients with cystic fibrosis ArchDis Child 56 (1981) 708ndash714
[212] BM Winklhofer-Roob H Ellemunter M Fruhwirth SE Schlegel-Haueter GKhoschsorur MA vant Hof DH Shmerling Plasma vitamin C concentrationsin patients with cystic fibrosis evidence of associations with lung inflammationAm J Clin Nutr 65 (1997) 1858ndash1866
[213] L Shamseer D Adams N Brown JA Johnson S Vohra Antioxidant micronutri-ents for lung disease in cystic fibrosis Cochrane Database Syst Rev (2010)CD007020
[214] C Santi S Santoro Electrophilic Selenium First edition Wiley-VCH VerlagGmbH amp Co KGaA 2012
[215] L Flohe S Toppo G Cozza F Ursini A comparison of thiol peroxidase mecha-nisms Antioxid Redox Signal 15 (2010) 763ndash780
[216] L Flohe JR Andreesen R Brigelius-Flohe M Maiorino F Ursini Selenium theelement of the moon in life on earth IUBMB Life 49 (2000) 411ndash420
[217] V Valdiglesias E Pasaro J Mendez B Laffon In vitro evaluation of seleniumgenotoxic cytotoxic and protective effects a review Arch Toxicol 84(2010) 337ndash351
[218] P Foucaud P Therond M Marchand F Brion JF Demelier J Navarro Seleniumand vitamin E in mucoviscidosis Arch Fr Pediatr 45 (1988) 383ndash386
[219] J Neve R Van Geffel M Hanocq L Molle Plasma and erythrocyte zinc copperand selenium in cystic fibrosis Acta Paediatr Scand 72 (1983) 437ndash440
[220] BM Winklhofer-Roob B Tiran PE Tuchschmid MA vant Hof DH ShmerlingEffects of pancreatic enzyme preparations on erythrocyte glutathione peroxi-dase activities and plasma selenium concentrations in cystic fibrosis FreeRadic Biol Med 25 (1998) 242ndash249
[221] JD Lloyd-Still HE Ganther Selenium and glutathione peroxidase levels in cys-tic fibrosis Pediatrics 65 (1980) 1010ndash1012
[222] D Tsavachidou TJ McDonnell S Wen X Wang F Vakar-Lopez LL Pisters CAPettaway CG Wood KA Do PF Thall C Stephens E Efstathiou R Taylor DGMenter P Troncoso SM Lippman CJ Logothetis J Kim Selenium and vitaminE cell type- and intervention-specific tissue effects in prostate cancer J NatlCancer Inst 101 (2009) 306ndash320
[223] IN Zelko TJ Mariani RJ Folz Superoxide dismutase multigene family acomparison of the CuZn-SOD (SOD1) Mn-SOD (SOD2) and EC-SOD (SOD3)gene structures evolution and expression Free Radic Biol Med 33 (2002)337ndash349
[224] RP Bowler JD Crapo Oxidative stress in airways is there a role for extracellu-lar superoxide dismutase Am J Respir Crit Care Med 166 (2002) S38ndashS43
[225] K Best K McCoy S Gemma RA Disilvestro Copper enzyme activities in cysticfibrosis before and after copper supplementation plus or minus zinc Metabo-lism 53 (2004) 37ndash41
[226] SS Percival GP Kauwell E Bowser M Wagner Altered copper status in adultmen with cystic fibrosis J Am Coll Nutr 18 (1999) 614ndash619
[227] NF Krebs JE Westcott TD Arnold BM Kluger FJ Accurso LV Miller KMHambidge Abnormalities in zinc homeostasis in young infants with cystic fibro-sis Pediatr Res 48 (2000) 256ndash261
[228] D Easley N Krebs M Jefferson L Miller J Erskine F Accurso KM HambidgeEffect of pancreatic enzymes on zinc absorption in cystic fibrosis J Pediatr Gas-troenterol Nutr 26 (1998) 136ndash139
[229] S Van Biervliet JP Van Biervliet E Robberecht Serum zinc in patients with cys-tic fibrosis at diagnosis and after one year of therapy Biol Trace Elem Res 112(2006) 205ndash211
[230] S Van Biervliet JP Van Biervliet S Vande Velde E Robberecht Serum zinc con-centrations in cystic fibrosis patients aged above 4 years a cross-sectional eval-uation Biol Trace Elem Res 119 (2007) 19ndash26
712 F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
[231] F Galli M Cristina Polidori W Stahl P Mecocci FJ Kelly Vitamin E biotransfor-mation in humans Vitam Horm 76 (2007) 263ndash280
[232] J Wiser NE Alexis Q Jiang W Wu C Robinette R Roubey DB Peden In vivogamma-tocopherol supplementation decreases systemic oxidative stress andcytokine responses of human monocytes in normal and asthmatic subjectsFree Radic Biol Med 45 (2008) 40ndash49
[233] JG Wagner Q Jiang JR Harkema B Illek DD Patel BN Ames DB PedenOzone enhancement of lower airway allergic inflammation is prevented bygamma-tocopherol Free Radic Biol Med 43 (2007) 1176ndash1188
[234] JT Harries DP Muller Absorption of different doses of fat soluble and watermiscible preparations of vitamin E in children with cystic fibrosis Arch DisChild 46 (1971) 341ndash344
[235] EI Back C Frindt E Ocenaskova D Nohr M Stern HK Biesalski Can changesin hydrophobicity increase the bioavailability of alpha-tocopherol Eur J Nutr45 (2006) 1ndash6
[236] SZ Nasr MH OLeary C Hillermeier Correction of vitamin E deficiency withfat-soluble versus water-miscible preparations of vitamin E in patients with cys-tic fibrosis J Pediatr 122 (1993) 810ndash812
[237] S Soltani-Frisk E Gronowitz H Andersson B Strandvik Water-miscibletocopherol is not superior to fat-soluble preparation for vitamin E absorptionin cystic fibrosis Acta Paediatr 90 (2001) 1112ndash1115
[238] K Papas J Kalbfleisch R Mohon Bioavailability of a novel water-soluble vi-tamin E formulation in malabsorbing patients Dig Dis Sci 52 (2007)347ndash352
[239] F Antonicelli M Parmentier EM Drost N Hirani I Rahman K Donaldson WMacNee Nacystelyn inhibits oxidant-mediated interleukin-8 expression andNF-kappaB nuclear binding in alveolar epithelial cells Free Radic Biol Med 32(2002) 492ndash502
[240] EM App D Baran I Dab A Malfroot M Coffiner F Vanderbist M King Dose-finding and 24-h monitoring for efficacy and safety of aerosolized Nacystelyn incystic fibrosis Eur Respir J 19 (2002) 294ndash302
[241] MG Traber How much vitamin E hellip Just enough Am J Clin Nutr 84 (2006)959ndash960
[242] JC McCann BN Ames Vitamin K an example of triage theory is micronu-trient inadequacy linked to diseases of aging Am J Clin Nutr 90 (2009)889ndash907
[243] M Fusaro G Crepaldi S Maggi F Galli A DAngelo L Calo S Giannini DMiozzo M Gallieni Vitamin K bone fractures and vascular calcifications inchronic kidney disease an important but poorly studied relationship J Endocri-nol Invest 34 (2010) 317ndash323
[244] JC McCann BN Ames Adaptive dysfunction of selenoproteins from the per-spective of the triage theory why modest selenium deficiency may increaserisk of diseases of aging FASEB J 25 (2011) 1793ndash1814
[245] R Apak K Guclu M Ozyurek B Bektas Oglu M Bener Cupric ion reducing an-tioxidant capacity assay for food antioxidants vitamins polyphenolics and fla-vonoids in food extracts Methods Mol Biol 477 (2008) 163ndash193
[246] F Galli Interactions of polyphenolic compounds with drug disposition and me-tabolism Curr Drug Metab 8 (2007) 830ndash838
[247] RL Prior X Wu K Schaich Standardized methods for the determination of an-tioxidant capacity and phenolics in foods and dietary supplements J Agric FoodChem 53 (2005) 4290ndash4302
[248] C Azbell S Zhang D Skinner J Fortenberry EJ Sorscher BA WoodworthHesperidin stimulates cystic fibrosis transmembrane conductance regulator-mediated chloride secretion and ciliary beat frequency in sinonasal epitheliumOtolaryngol Head Neck Surg 143 (2010) 397ndash404
[249] G Wegrzyn J Jakobkiewicz-Banecka M Gabig-Ciminska E Piotrowska M Nar-ajczyk A Kloska M Malinowska D Dziedzic I Golebiewska M Moskot AWegrzyn Genistein a natural isoflavone with a potential for treatment of ge-netic diseases Biochem Soc Trans 38 (2010) 695ndash701
[250] YC Yu H Miki Y Nakamura A Hanyuda Y Matsuzaki Y Abe M Yasui K Ta-naka TC Hwang SG Bompadre Y Sohma Curcumin and genistein additivelypotentiate G551D-CFTR J Cyst Fibros 10 (2011) 243ndash252
[251] B Illek H Fischer Flavonoids stimulate Cl conductance of human airway epithe-lium in vitro and in vivo Am J Physiol 275 (1998) L902ndashL910
[252] JL Kreindler Cystic fibrosis exploiting its genetic basis in the hunt for newtherapies Pharmacol Ther 125 (2010) 219ndash229
[253] B Illek L Zhang NC Lewis RB Moss JY Dong H Fischer Defective function ofthe cystic fibrosis-causing missense mutation G551D is recovered by genisteinAm J Physiol 277 (1999) C833ndashC839
[254] P Anandakumar S Kamaraj S Jagan G Ramakrishnan R Vinodhkumar TDevaki Capsaicin modulates pulmonary antioxidant defense system during ben-zo(a)pyrene-induced lung cancer in Swiss albinomice Phytother Res 22 (2008)529ndash533
[255] I Rahman Antioxidant therapeutic advances in COPD Ther Adv Respir Dis 2(2008) 351ndash374
[256] AW Boots H Li RP Schins R Duffin JW Heemskerk A Bast GR Haenen Thequercetin paradox Toxicol Appl Pharmacol 222 (2007) 89ndash96
[257] M Joskova S Franova V Sadlonova Acute bronchodilator effect of quercetin inexperimental allergic asthma Bratisl Lek Listy 112 (2011) 9ndash12
[258] HJ Park CM Lee ID Jung JS Lee YI Jeong JH Chang SH Chun MJ Kim IWChoi SC Ahn YK Shin SR Yeom YM Park Quercetin regulates Th1Th2 balancein a murine model of asthma Int Immunopharmacol 9 (2009) 261ndash267
[259] AP Rogerio A Kanashiro C Fontanari EV da Silva YM Lucisano-ValimEG Soares LH Faccioli Anti-inflammatory activity of quercetin and iso-quercitrin in experimental murine allergic asthma Inflamm Res 56 (2007)402ndash408
[260] M Muller Polyphenol cytotoxicity induced by the bacterial toxin pyocyaninrole of NQO1 Free Radic Biol Med 47 (2009) 84ndash91
[261] J Grassmann Terpenoids as plant antioxidants Vitam Horm 72 (2005)505ndash535
[262] P Allen Tea tree oil the science behind the antimicrobial hype Lancet 358(2001) 1245
[263] EC Dasenbrook W Checkley CA Merlo MW Konstan N Lechtzin MP BoyleAssociation between respiratory tract methicillin-resistant Staphylococcus aure-us and survival in cystic fibrosis JAMA 303 (2010) 2386ndash2392
[264] V Bezzerri M Borgatti E Nicolis I Lampronti MC Dechecchi I Mancini PRizzotti R Gambari G Cabrini Transcription factor oligodeoxynucleotides toNF-kappaB inhibit transcription of IL-8 in bronchial cells Am J Respir CellMol Biol 39 (2008) 86ndash96
[265] R Gambari M Borgatti V Bezzerri E Nicolis I Lampronti MC Dechecchi IMancini A Tamanini G Cabrini Decoy oligodeoxyribonucleotides and peptidenucleic acids-DNA chimeras targeting nuclear factor kappa-B inhibition of IL-8 gene expression in cystic fibrosis cells infected with Pseudomonas aeruginosaBiochem Pharmacol 80 (2010) 1887ndash1894
[266] M Adrian P Jeandet AC Douillet-Breuil L Tesson R Bessis Stilbene content ofmature Vitis vinifera berries in response to UV-C elicitation J Agric Food Chem48 (2000) 6103ndash6105
[267] B Paul I Masih J Deopujari C Charpentier Occurrence of resveratrol and pter-ostilbene in age-old darakchasava an ayurvedic medicine from India J Ethno-pharmacol 68 (1999) 71ndash76
[268] I Rahman Antioxidant therapies in COPD Int J Chron Obstruct Pulmon Dis 1(2006) 15ndash29
[269] M Lee S Kim OK Kwon SR Oh HK Lee K Ahn Anti-inflammatory and anti-asthmatic effects of resveratrol a polyphenolic stilbene in a mouse model ofallergic asthma Int Immunopharmacol 9 (2009) 418ndash424
[270] LG Wood PA Wark ML Garg Antioxidant and anti-inflammatory effectsof resveratrol in airway disease Antioxid Redox Signal 13 (2010)1535ndash1548
[271] KV Kiselev Perspectives for production and application of resveratrol ApplMicrobiol Biotechnol 90 (2011) 417ndash425
[272] M Shakibaei C Buhrmann A Mobasheri Resveratrol-mediated SIRT-1 interac-tions with p300 modulate receptor activator of NF-kappaB ligand (RANKL) acti-vation of NF-kappaB signaling and inhibit osteoclastogenesis in bone-derivedcells J Biol Chem 286 (2011) 11492ndash11505
[273] SF Zaidi K Ahmed T Yamamoto T Kondo K Usmanghani M Kadowaki TSugiyama Effect of resveratrol on Helicobacter pylori-induced interleukin-8 secre-tion reactive oxygen species generation and morphological changes in human gas-tric epithelial cells Biol Pharm Bull 32 (2009) 1931ndash1935
[274] JK Kundu YK Shin YJ Surh Resveratrol modulates phorbol ester-inducedpro-inflammatory signal transduction pathways in mouse skin in vivo NF-kappaB and AP-1 as prime targets Biochem Pharmacol 72 (2006)1506ndash1515
[275] NH Nam Naturally occurring NF-kappaB inhibitors Mini Rev Med Chem 6(2006) 945ndash951
[276] JM Smoliga JA Baur HA Hausenblas Resveratrol and healthmdasha comprehen-sive review of human clinical trials Mol Nutr Food Res 55 (2011) 1129ndash1141
[277] ME Juan M Maijo JM Planas Quantification of trans-resveratrol and itsmetabolites in rat plasma and tissues by HPLC J Pharm Biomed Anal 51(2010) 391ndash398
[278] JA Baur DA Sinclair Therapeutic potential of resveratrol the in vivo evidenceNat Rev 5 (2006) 493ndash506
[279] E Nicolis I Lampronti MC Dechecchi M Borgatti A Tamanini N Bianchi VBezzerri I Mancini MG Giri P Rizzotti R Gambari G Cabrini Pyrogallol anactive compound from the medicinal plant Emblica officinalis regulates expres-sion of pro-inflammatory genes in bronchial epithelial cells Int Immunophar-macol 8 (2008) 1672ndash1680
[280] E Nicolis I Lampronti MC Dechecchi M Borgatti A Tamanini V Bezzerri NBianchi M Mazzon I Mancini MG Giri P Rizzotti R Gambari G CabriniModulation of expression of IL-8 gene in bronchial epithelial cells by 5-methoxypsoralen Int Immunopharmacol 9 (2009) 1411ndash1422
[281] M Borgatti I Mancini N Bianchi A Guerrini I Lampronti D Rossi G SacchettiR Gambari Bergamot (Citrus bergamia Risso) fruit extracts and identified com-ponents alter expression of interleukin 8 gene in cystic fibrosis bronchial epithe-lial cell lines BMC Biochem 12 (2011) 15
[282] L Piccagli E Fabbri M Borgatti N Bianchi V Bezzerri I Mancini E Nicolis CMDechecchi I Lampronti G Cabrini R Gambari Virtual screening against p50NF-kappaB transcription factor for the identification of inhibitors of the NF-kappaB-DNA interaction and expression of NF-kappaB upregulated genesChemMedChem 4 (2009) 2024ndash2033
[283] L Piccagli M Borgatti E Nicolis N Bianchi I Mancini I Lampronti D VevaldiF DallAcqua G Cabrini R Gambari Virtual screening against nuclear factorkappaB (NF-kappaB) of a focus library identification of bioactive furocoumarinderivatives inhibiting NF-kappaB dependent biological functions involved incystic fibrosis Bioorg Med Chem 18 (2010) 8341ndash8349
[284] M Borgatti A Chilin L Piccagli I Lampronti N Bianchi I Mancini G Mar-zaro Da Francesco A Guiotto R Gambari Development of a novel furocou-marin derivative inhibiting NF-kappaB dependent biological functionsdesign synthesis and biological effects Eur J Med Chem 46 (2011)4870ndash4877
[285] E Georgy S Le Guellec L Vecellio E Fichant P Stordeur P Bordeau JP PerraudinFeasibility study of OSCN- and lactoferrin (Meveol) nebulization for cysticfibrosis JCyst Fibros 10 (2011) S18
713F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
[286] C Tidei M Piroddi F Galli C Santi Oxidation of thiols promoted by PhSeZnClTetrahedron Lett 53 (2012) 232ndash234
[287] L Semianrio-Vidal C van Hesuden G Mugesh ER Lazarowski Ebselen is a po-tent non-competitive inhibitor of extracellular nucleoside diphosphokinasePurinergic Signal 6 (2010) 383ndash391
[288] C ColussiMC Albertini S Coppola S Rovidati F Galli L Ghibelli H2O2-inducedblockof glycolysis as an active ADP-ribosylation reaction protecting cells from apoptosisFASEB J 14 (2000) 2266ndash2276
[289] H Xiao KL Parkin Induction of phase II enzyme activity by various seleniumcompounds Nutr Cancer 55 (2006) 210ndash223
[290] G Peluffo R Radi Biochemistry of protein tyrosine nitration in cardiovascularpathology Cardiovasc Res 75 (2007) 291ndash302
[291] B Alvarez R Radi Peroxynitrite reactivity with amino acids and proteinsAmino Acids 25 (2003) 295ndash311
[292] B Kamosinska MW Radomski M Duszyk A Radomski SF Man Nitric oxideactivates chloride currents in human lung epithelial cells Am J Physiol 272(1997) L1098ndashL1104
[293] L Chen RP Patel X Teng CA Bosworth JR Lancaster Jr S Matalon Mecha-nisms of cystic fibrosis transmembrane conductance regulator activation by S-nitrosoglutathione J Biol Chem 281 (2006) 9190ndash9199
[294] F Luchetti B CanonicoM BettiM Arcangeletti F PilolliM Piroddi L Canesi S PapaF Galli Melatonin signaling and cell protection function FASEB J 24 (2010)3603ndash3624
[295] MW Bengtsson G Jedstedt G Flemstrom Duodenal bicarbonate secretion inrats stimulation by intra-arterial and luminal guanylin and uroguanylin ActaPhysiol (Oxf) 191 (2007) 309ndash317
[296] CS Nelson JL Marino CN Allen Melatonin receptor potentiation of cyclic AMP andthe cystic fibrosis transmembrane conductance regulator ion channel J Pineal Res 26(1999) 113ndash121
[297] C de Castro-Silva VM de Bruin GM Cunha DM Nunes CAMedeiros PF de BruinMelatonin improves sleep and reduces nitrite in the exhaled breath condensate incystic fibrosismdasha randomized double-blind placebo-controlled study J Pineal Res48 (2010) 65ndash71
[298] I Hornyak E Pankotai L Kiss Z Lacza Current developments in the the-rapeutic potential of S-nitrosoglutathione an endogenous NO-donor mole-cule Curr Pharm Biotechnol (2011) Jan 11 [Epub ahead of print] - PMID21235457
[299] AH Snyder ME McPherson JF Hunt M Johnson JS Stamler B Gaston Acuteeffects of aerosolized S-nitrosoglutathione in cystic fibrosis Am J Respir CritCare Med 165 (2002) 922ndash926

693F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
correction of the defective NO concentration and improvement oflung function in CF patients [49ndash51]
Although exhaled NO is decreased in CF increased immunohisto-chemical staining for nitrotyrosine was demonstrated in lung tissuesfrom CF patients [52] Therefore a decreased production or accelerat-ed metabolism of NO could be present in association with an abnor-mal reactivity of this radical and its derived species (NOx) towardbiomolecular components of the CF airways Peroxynitrite is one ofthe most relevant mediators of the biological activity of NO withtoxic properties and damaging activity on several biomolecules [53]
A third emerging issue takes into consideration the expressionof different enzymatic systems affecting the redox balance in CF bron-chial epithelial cells For instance intracellular concentration of H2O2
has been found abnormally elevated in both immortalized bronchialand primary nasal epithelial cells derived from CF patients bothin the presence and the absence of proinflammatory cytokines [54]This has been accompanied by a marked decrease of expressionof proteins regulating H2O2 levels such as thioredoxin 1 (TRX-1)glutathione-S-transferase pi (GST-pi) peroxyredoxin (PRDX) 6TRX-dependent peroxide reductase (PRDX-1) catalase and con-versely a significant increase of Mn superoxide dismutase (SOD2)[54] Interestingly to link these modifications with CF specific charac-teristics dysfunctional CFTR channel was found associated withreduced activity of the transcription factor Nrf-2 (nuclear factor-erythroid 2 p45 subunit-related factor 2) which could at least inpart explain the differential expression of the enzymatic systemsresulting in the elevated intracellular steady-state concentration ofH2O2 found in CF nasal and bronchial epithelial cells [54] In synthesisthe ASL of CF patients during advanced stages of the lung disease con-tains elevated concentrations of ROS mainly derived from neutro-phils migrated into the airway lumen and a reduced concentrationof NO which can strongly contribute to respiratory tissue injurytogether with the proteases released by the activated neutrophilsThe homeostatic role of the GSH-related defenses appears constitu-tively impaired by the dysfunctional CFTR thus increasing suscepti-bility to develop oxidative stress and lung tissue degeneration(Fig 1) as described in detail in the sections below
24 Conductive airway epithelium as target of ROS
Oxidants can target different biomolecules to damage epithelialcells and extracellular fluids of the airways Lipid peroxidationand post-translational modifications of proteins on both cell mem-branes and extracellular targets are common biomarkers of thisdamage which can occur by the direct reaction between ROS and bio-molecules or through the formation of second-generation reactivebyproducts [955] All levels of this interaction between ROS and bio-logical components can produce toxic and bioactive intermediatesOxidants are known to activate secondmessengers through phospho-lipases A2 C and D and to induce the production of cytokines andmucins a series of molecular events that contribute to progressiveobstructive disease and reduction of lung function [56] Besides thedirect oxidative damage to cellular structures of the bronchial epithe-lial cells the excessive concentration of oxidants in CF both in the ASLlining the apical membranes and inside the bronchial cells has beenstudied in respect to the regulation of the inflammatory response
ROS are often considered a sort of secondmessengers in activatingthe Nuclear Factor (NF)-κB which is in turn involved in the activationof transcription of several proinflammatory cytokines and chemo-kines [57] For instance it has been shown that H2O2 partly controlsNF-κB activation by IL-1beta by facilitating the activation of NIKand subsequent phosphorylation of IKKβ [58] In this respect a directlink has been proposed between the excessive production of intracel-lular H2O2 and the elevated expression of IL-6 and IL-8 the mostabundant pro-inflammatory cytokine and neutrophilic chemokinefound in CF airways [54] which has been further confirmed [59]
Moreover oxidants could be synergic in the induction of mucins aspromoted by neutrophil elastase which further impairs ASL fluidityin CF [60] Finally bacterial infection with P aeruginosa strains releas-ing the toxin pyocyanin (PCN) has been shown to reduce ion trans-port through the CFTR channel thus potentially counteracting thetherapeutic effects of correctors and potentiators of mutated CFTRprotein [6162] In summary excessive oxidants in CF conductive air-ways have different negative effects in the amplification of the al-ready excessive lung inflammation and secretion of mucin togetherwith a direct deleterious effect on CFTR channel function
25 Oxidative stress and surfactant
Oxidative stress and inflammation in cystic fibrosis can affect sur-factant biophysical activity thus leading to early alterations of lungfunction in patients with CF [63] Altered phospholipid-to-protein ra-tios and phospholipid subclasses a modified fatty acid profiles anddecreased association of proteins such as SP-A with lipid componentsof isolated surfactant indicate that components of this fluid are con-siderably altered and dysfunctional in lower respiratory tract secre-tions of CF patients [64]
Oxidative damage of surfactant may involve both lipid and proteincomponents Alteration of lipid components can in turn generatetoxic lipid species with cytotoxic activity towards nearby epithelialcells [65] Altered protein components have been shown in cysticfibrosis [66] Notably surfactant protein D which is an important in-nate host defense molecule becomes unable to agglutinate bacteriawhen it is modified by oxidation which facilitates pathogen coloniza-tion in the lung [67] In a cross-sectional analysis of CF patients withmild lung disease reduced surfactant activity was correlated to in-creased neutrophilic airway inflammation but not to lung function[68] So far longitudinal measurements of surfactant function in CFpatients are lacking and it remains unclear how these alterationsrelate to progression of airway inflammation as well as to the rateof decline of pulmonary function [69]
26 Laboratory indices of oxidative stress in CF
Appropriate biochemical and clinical tools are of importance forthe monitoring of antioxidant therapies in CF and a crucial aspect isthe selection of proper biomarkers and protocols to assess biologicalpathways of oxidation
Pancreatic insufficiency and a diminished bile acid pool cause mal-absorption of important essential nutrients and other dietary compo-nents in CF Of particular significance is the malabsorption of fat-soluble antioxidants such as carotenoids tocopherols and coenzymeQ-10 (CoQ-10) which act as chain breakers in the peroxidation reac-tions of polyunsaturated lipids Accordingly lipid peroxidation is oneof the main signs encountered in the CF plasma buccal mucosal cellsbreath condensate and BALF as measured by the non-enzymaticoxidation product of arachidonic acid 8-iso prostaglandin F2α[570ndash73] Elevations of this and other eicosanoids in human bodyfluids and tissues have been found in a diverse array of human disor-ders including atherosclerosis diabetes obesity cigarette smokingneurodegenerative diseases and many others [74] Further treat-ments for some of these conditions including antioxidant supple-mentation have been shown to decrease the levels of this class ofbiomarkers In CF patients respiratory exacerbations increase plasmalevels of 8-iso-F2α [70] the levels of which in the breath condensatenegatively correlate with respiratory function data [71] At the sametime successful in vivo antioxidant therapy by GSH inhalation hasbeen shown to decreased PGE levels in BALF in association withchanges in the number and activity of leukocyte subpopulations re-sponsible for lung inflammation [73]
Oxysterols a biomarker of cholesterol oxidation were found toincrease in CF plasma as a further proof of the abnormal lipid
694 F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
metabolism and increased susceptibility to oxidation of lipoproteinlipids in CF patients [7] Importantly an increased oxidative burdenof lung and blood lipids may produce bioactive lipid products thatfurther sustain CF symptoms Besides to 8-iso-F2α and other ana-logues with some bioactivity [74] arachidonic acid oxidation maycontribute to persistent platelet activation and pulmonary dysfunc-tion in CF via generation of bioactive isoeicosanoids [75] which pro-vides sufficient rationale for a prevention therapy with fat solubleantioxidants such as vitamin E Evidence has recently accumulatedon the systemic effects of oxysterols on various tissues and organs[76] The role of this lipid oxidation product alone or in combinationwith other factors could be further investigated in the context ofmechanisms and clinical progression of multi-organ failure of CFpatients
The impaired pancreatic and liver functions of CF patients repre-sent the underlying factor for a defective lipoprotein metabolismand hypocholesterolemia which exponentially increase the burdenof damage by cholesterol and other lipids due to reduced blood trans-port of fat-soluble antioxidants with nascent VLDL particles Besidesoxysterol accumulation plasma fatty acid composition is also affected[7] and an increased ratio between unsaturated and saturated fattyacid species may contribute to lower cellular antioxidant defenses
Altogether these findings suggest that lipid oxidation biomarkerscan provide a reliable measure of systemic and lung-specific oxidativestress in CF
Markers of protein damage are also detectable in the airways ofchildren with CF and their levels are observed to parallel the extentof neutrophilic markers and lung dysfunction [143166] Bronchoal-veolar lavage proteins undergo halogenation of Tyr residues aradical-mediated process presumably depending on MPO enzyme ac-tivity and assessed through the analysis of 3-chlorotyrosine and 3-bromotyrosine Thiocyanate and protein carbonyls are also useful bio-markers to assess the inflammation-related injury of BALF proteins inCF [1431]
3 Antioxidants in CF
31 Glutathione and its related defense system
311 Defects in GSH homeostasisOther studies have pointed to alterations in the levels of extracel-
lular antioxidants in respiratory tract lining fluids [3] In particularthe analyses of broncheoalveolar lavages (BAL) have revealed thepresence of decreased levels of GSH in the alveolar epithelial liningfluid of CF patients The normal level of extracellular GSH in thelung is 140 times that present in blood plasma and the lung is a netimporter of circulating GSH [77] As a result GSH concentration inELF is close to 400 μM whereas significantly reduced GSH levels arepresent in adult CF patients [41] Low levels of GSH have been ob-served in plasma and blood neutrophils [4178] suggesting systemicGSH dyshomeostasis in CF Moreover some studies have shown thatat the cellular level the CFTR mutation causes mitochondrial deple-tion of GSH [7980] The consequences of this defect are still difficultto be understood due to our poor knowledge about the exact func-tions of GSH in the lung but there are reasons to believe that thedecrease of GSH in the ASL contributes to lung infection and inflam-mation [4281] At the same time it must be underlined that a recentstudy has shown that the GSH content in sputum samples is higher inCF patients than in healthy people indicating that GSH deficiency inCF is restricted to the lower respiratory tract [82] Several hypotheseshave been proposed to explain such a local increase in GSH includingthe possibility that it may derive from apoptotic neutrophils The re-lease of high levels of GSH may be part of a compensatory mechanismaimed at controlling disulfide bonds-mediated aggregation of mucinsSecretions of the upper respiratory tract contain abundant levels ofthese glycosylated and cysteine-rich proteins likely playing a role in
the airway antioxidant defense Indeed these proteins are potent invitro ROS scavenges [83] and their synthesis is upregulated upon ox-idative stress via epidermal growth factor receptor (EGFR) transacti-vation [84]
GSH a major component of cellular antioxidant defenses exerts im-portant functions related to its electron-donating capacity includingprotection from the damaging effects of ROS and regulation of a pletho-ra of cellular events such as gene expression proliferation and differen-tiation apoptosis and immune response [85] GSH is synthesized by twosequential ATP-dependent reactions catalyzed by γ-glutamylcysteinesynthetase (recently renamed glutamate-cysteine ligase) andGSH syn-thetase The reaction catalyzed by γ-glutamylcysteine synthetase iethe formation of γ-glutamylcysteine from glutamate and cysteine isthe rate-limiting step in GSH synthesis and is feedback regulated byGSH itself In fact this enzyme represents an interesting case of redox-regulation of catalytic activity that is mediated by the reversible forma-tion of disulfide bonds [86] Oxidizing conditions causing GSH depletionpromote the formation of a disulfide bondbetween the catalytic and theregulatory subunits of the enzyme leading to a conformational changewhich favors the binding of glutamate In contrast physiological levelsof GSH reduce this disulfide bond thus explaining GSH feedbackinhibition
Either in intracellular or extracellular compartments GSH is pre-dominantly found in the reduced form although small amounts ofthe oxidized disulfide forms (GSSG or GSSR where a GSH moleculeis linked to a free or a protein thiol) can always be detected GSSG isproduced by the catalysis of glutathione peroxidase during thedetoxification from hydrogen peroxide and other peroxides or bythe direct reactions of GSH with electrophilic compounds such asradical species Despite the bulk of GSH synthesis occurring in thecytoplasm GSH is distributed in intracellular organelles includingthe endoplasmic reticulum mitochondria and nucleus Under physio-logical conditions the GSH to GSSG ratio in these compartments ishigh frequently gt1001 but this may change under conditions of ox-idative stress [87] A major exception is represented by the endoplas-mic reticulum where GSSG is present at much higher levels to favordisulfide bond formation [88] Interestingly the compartmentaliza-tion of GSH in separate pools within organelles allows localized alter-ations in the balance between GSH and GSSG that may haveconsiderable functional and pathological significance [89] Thiscould be particularly important in CF in view of the above mentionedstudies showing that cultured CF cells have an apparent normal GSHGSSG content but are characterized by a marked decrease in mito-chondrial GSH in association to elevated mitochondrial ROS [7980]
Different roles of high levels of GSH in the ELF may be hypothe-sized including a) preventing inflammation and tissue damage byscavenging the ROS spontaneously generated in this highly oxidizingenvironment actively produced by neutrophils during inflammationor originating from lipid peroxidation b) regulating the redox statusof membrane proteins involved in the transduction of signals leadingto changes in the expression of genes involved in the immune re-sponse c) controlling mucus viscosity by breaking disulphide bondsd) modulating the response to bacterial infections This last possibili-ty is suggested by the observation that GSH significantly increasesin the ASL of wild type mice following P aeruginosa infection where-as this response is not observed in CFTR mutant mice [90] Interest-ingly some authors have suggested the ability of GSH to control Paeruginosa growth and resistance to antibiotics although these stud-ies should be considered with some cautions due to the likely use ofunbuffered GSH [91]
Although the decreased levels of GSH in ELF could be due to in-creased consumption during inflammation-related oxidative stress[4192] GSH deficiency in CF ELF likely derives from CFTR channeldysfunction In fact comparable alterations in GSH extracellular con-tent characterize the lung of CFTR knockout mice [93] indicating thatthis defect is correlated to mutations in CFTR
695F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
In particular ELF and lung tissue from CFTR knockout (Cftr KOB6129P2-Cftrtm1Unc) and wild-type mice were compared for GSHcontent and the activities of glutathione-related enzymes [93] Inthe ELF the concentration of GSH was significantly decreased in theCftr KO mice compared to WT whereas tissue concentrations ofGSH were similar [92] In the Cftr KO lung the activities of glutathionereductase and glutathione peroxidase were increased whereas theactivity of γ-glutamyltransferase was unchanged Two indicators ofoxidative stress thiobarbituric acid reactive substances (TBARS) and8-hydroxy-2-deoxyguanosine (8-OHdG) were also increased in theCftr KO lung tissue [90] These data support the hypothesis that a mu-tation in the CFTR gene can affect the antioxidant defenses in the lungand may contribute to the exaggerated inflammatory response ob-served in CF Thereby CFTR could be considered as an importantactor of ELF antioxidant homeostasis and thus an intrinsic cause ofoxidative imbalance in CF airways of human patients as well as CftrKO mice
Moreover CFTR belongs to the MRPABC family of proteins whichincludes several GSH transporters and some in vitro studies have in-dicated that CFTR may mediate GSH export across membranes[2394] Despite these evidences there is still debate about the phys-iological implication of CFTR in GSH transport outside the cells asother studies have raised the possibility that CFTR may not actuallyconduct GSH but regulate its transport indirectly through chloridetransport [85]
312 In vitro studies suggesting a protective role of GSH in CF modelsystems
Possible protective roles of extracellular GSH in the CF lung havebeen long proposed and recent in vitro studies have provided furtherand more robust support to this clue For example it has been sug-gested that GSH may control the levels of chlorinated compoundsformed by the activity of myeloperoxidase a neutrophil-releasedprotein abundantly present in CF patients secretions [9596] and pre-vent NK-κB activation [96] Other studies have suggested that CFTRmutant cells produce higher levels of proinflammatory cytokines inresponse to P aeruginosa diffusible material with respect to wildtype cells through a mechanism involving the activation of NADPHoxidase This effect may be significantly reversed by the addition ofextracellular GSH [97]
GSH could also play an important role in protecting the lung epi-thelia from the toxic effects of pyocyanin (PCN) a redox-active exo-toxin released by P aeruginosa which is supposed to cause a varietyof deleterious effects on the airway physiology [98] PCN levels ashigh as 130 μM have been measured in pulmonary secretions of pa-tients with CF and individuals with chronic bronchiectasis [99] Atconcentrations within the range measured in the sputum from CF pa-tients PCN induces a drastic reduction of intracellular GSH [100101]promotes death of cultured cells [100] and causes pathophysiologicalalterations in the lung of wild type mice that are consistent with thechanges observed in CF patients [102] PCN toxicity likely derivesfrom its ability to accept electrons from cellular reductants and thenreact with oxygen to generate superoxide and other ROS [103] There-fore GSH deficiency is explained either by the reaction of GSH withsuch oxidants or through the direct reaction of PCN with GSH thatleads to the formation of a PCN radical [103] However the electrontransfer from GSH to PCN does not occur at neutral pH and recent ob-servations suggest that extracellular GSH provides significant protec-tion against the toxic effects of PCN [104] Moreover GSH can reactwith PCN to form a stable adduct which is likely redox inactive[105] Although the relationships between extracellular GSH andPCN are still contradictory it is worth mentioning that extracellularGSH increases to millimolar levels in the ELF of wild type miceinfected with P aeruginosa indicating that GSH may be useful to re-sist to bacterial colonization [90] Interestingly in vitro studies have
revealed that extracellular GSH inhibits the ability of Burkholderiacenocepacia to enter epithelial respiratory cells and reduces bacterialinduced expression of proinflammatory cytokines (DOrazio Pacelloand Battistoni 2011 unpublished results)
32 GSH-based antioxidant therapies
321 Preclinical studies in animal models of CFMice genetically modified for the Cftr gene along with acute and
chronic infection induced by CF-related pathogens are a key asset inCF research Although much has been learned through these CFmousemodels limitations in the ability of this species to recapitulatespontaneous lung disease and several other organ abnormalitiesseen in CF humans including few airway mucous glands have creat-ed a need for additional species on which to study CF [106] To thisend pig and ferret CF models have been generated and are currentlybeing characterized [107108] These new larger animal models havephenotypes that appear to closely resemble human CF disease seenin newborns and efforts to characterize their adult phenotypes areongoing However mice have been the dominant species by whichto study CF disease processes in vivo and develop therapies for thepast two decades including GSH-based antioxidant treatment
Despite limitations and significant species differences betweenmice and humans these models proved to be useful tools to mimicthe initial and progressive bronchopulmonary infection typical of CFpatients [109] In particular the model of chronic infection whichchallenge bacterial cells with agar as an immobilizing agent hasbeen extensively characterized and induce the long-term persistenceof the bacterial infection and lung pathology including airway inflam-mation [110111] Lung pathology associatedwith chronic experimen-tal infection resembled some aspects of the advanced chronicpulmonary disease at autopsy in CF patients [112ndash114] Both naturallyoccurring and experimental infections frequently manifest broncho-pneumonia bronchiectasis mucus plugging epithelial metaplasiafibrosis and alveolar exudates with inflammatory cells Lymphoidhyperplasia which was prominent in the infected animals was alsoa common finding in the lungs of CF patients In addition significantdifferences with regard to weight loss BAL neutrophil counts andcytokine concentrations have been detected Infected mice had arapid though transient rise in absolute neutrophil counts TNF-α IL-1β IL-6 MIP-2 and KC in bronchoalveolar lavage (BAL) [110115] Inaddition the generation of CF mice has allowed the possibility of invivo testing of novel therapies before entering in clinical trial Theseinclude the pre-clinical evaluation of antibiotics and biotechnologicaldrugs as well as of natural and synthetic anti-inflammatory agentsthat reduce the excessive recruitment of neutrophils and the progres-sive damage of the respiratory tissue by the unbalanced production ofoxidants
Regarding antioxidants GSH and its pro-drug N-acetylcysteine(NAC) remain the so far most investigated antioxidant agents in CFand several strategies have been proposed to improve systemic andlung GSH status of CF patients based on pre-clinical studies includingthe administration of nebulized GSH by inhalation or the oral supple-mentation of GSH or NAC Oral GSH administration can raise serumand lung tissue GSH levels in rodents [116117] In these studiesGSH was administered to animals dissolved in saline or PBS Thepharmacokinetic profile of an oral bolus dose of GSH (300 mgkg)was determined in mice in other studies [118] Plasma ELF BALcells and lung tissue were analyzed for GSH content There was arapid elevation in the GSH levels that peaked at 30 min in the plasmaand 60 min in the lung ELF and BAL cells after oral GSH dosing OralGSH treatment produced a selective increase in the reduced and ac-tive form of GSH in all lung compartments examined Oral GSSG treat-ment (300 mgkg) resulted in a smaller increase of GSH levels Toevaluate the role of CFTR in this process Cftr KO mice and gut-
Table 1Intervention trials on antioxidant therapy in CF patients found at ClinicalTrialsgov databasea
Rank Title PI Location Recruitment Interventions Age groups Phasesnumberenrolled
Study designsb Outcome measures Start andcompletion date
NCT ID
1 Efficacy and safety studyof inhaled GSH in CFpatients
GrieseM
Germany Completed Drugbull reduced GSH sodium salt
C|A|S II138
1 R|E2 Safetyeff3 PA4 DB (Sub Inv)5 Treatment
bull Differences between inhaled GSHand inhaled normal saline withrespect to the area under the curveof FEV1 predicted within the periodfrom baseline to week 24
bull Treatment changes with respect tothe variablesspirometry peak flowquality-of-life weightheightpercentage of neutrophilsothercell types (induced sputum) inducedsputum levels of GSHinflammatorymediators pulmonary exacerbation
Jul-07May-10
00506688
bull 09 saline (control)
2 A phase I study of inhaledsodium pyruvate for thetreatment of CF
BillingsMCE
United States Terminated Drugbull Inhaled sodium pyruvate
A|S I70
1 R|E2 Safetyeff3 PA4 DB5 Treatment
bull Assessment of safety of inhaled sodiumpyruvate in Subs with CF Subs will beevaluated for the presence of symptomsand safety laboratory measurements
bull Determination of improvement inlungs of CF Subs as determined bymeasurement of FEV1 and measurementof inflammatory markers ininduced sputum
Feb-06na
00332215
3 Inhaled GSH versusplacebo in CF
MarsicoS
Italy Recruiting Drugbull Inhaled reduced GSHbull Physiological solution
C|A III150
1 R|E2 Eff3 PA4 SB (Sub)5 Treatment
bull FEV1bull Small airway function exercise capacityBMI dyspnoea cough quality of lifepulmonary exacerbations markers ofoxidative stress (H2O2)in serum and inEBC epithelial inflammatory markerson BNEC
Jun-10Dec-12
01450267
4 Safety and efficacy ofan antioxidant-richmultivitaminsupplement in CF
SagelSD
United States Completed Dietary supplementbull AquADEKs
C|A IIndashII17
1 NR|E2 Safetyeff3 SGA4 OL5 Treatment
bull Plasma levels of β-carotenebull Plasma levels of coenzyme Q-10retinol (Vitamin A) 25-hydroxy vitaminD α- and γ-tocopherols (Vitamin E)PIVKA-II
Aug-07Nov-09
01018303
5 Efficacy and safety ofepigallocatechin gallate(EGCG)tocotrienol in18 patients with splicing-mutation-mediated CF
KeremE
Israel Not yetrecruiting
Dietary supplementbull EGCGbull Tocotrienolbull EGCG+tocotrienol
A|S na18
2 Safetyeff3 CA4 OL5 Treatment
bull Changes in nasal chloride secretion asassessed by TEPD with assessment ofmean changes in TEPD by drug comparedto baseline and the proportion of patientswith a chloride secretion response bydrug compared to baseline
bull Pulmonary function testing FEV1FVC MEF25-75
Sep-09Jun-11
00889434
6 The effect of inhaledNAC compared tonormal saline onsputum rheology andlung function
VanDaele S
Belgium Terminated Drugbull Acetyl-Cysbull Normal saline
C|A IV19
1 NR|E2 Eff3 CA4 OL5 Treatment
bull Changes in visco-elasticity andlung function
Jan-10Dec-10
00996424
696FG
allietal
Biochimica
etBiophysica
Acta
1822(2012)
690ndash713
7 Safety of orallyadministeredcurcuminoids in adultsubjects with CF
Goss C United States Completed Drugbull Standardized turmericroot extract
A I11
1 NR|E2 Safetyeff3 SGA4 OL5 Treatment
bull Safety and tolerability of 14 days oftreatment with orally administeredcurcuminoids as assessed by adverseevents laboratory parameters andspirometry
bull Pharmacokinetics of repeated dosesof orally administered curcuminoidschange in NPD measurementschange in sweat chloride measurements
Apr-05Jan-06
00219882
8 Nasal potential studiesutilizing CF transmembraneregulator (CFTR) modulators
Rowe S United States Recruiting Other quercetin C|A II46
2 Eff3 SGA4 OL5 BS
bull NPD(NPD) Biomarkerbull Residual CFTR activity
Mar-10Nov-11
01348204
9 Safety and tolerability ofinhaled nitric oxide inpatients with CF
Sagel S United States Completed Drugbull Nitric oxide for inhalationbull Nitrogen
C|A|S IIndashII18
1 R|E2 Saf3 PA4 DB (Sub Care Inv OA)5 Treatment
bull Safety and tolerability of drugassessed by change in methemoglobinlevels oxygensaturation FEV1
bull Assess the difference in sputumbacterial density before and afterNO inhalation and the differencein lower airway inflammatorymeasures before and after NO inhalation
Jul-04Dec-08
00570349
10 NAC Phase IIB a multi-center phase IIBrandomized placebo-controlled DB study ofthe effects of NAC onredox changes and lunginflammation in CF patients
ConradC
United States Completed Drugbull NAC
C|A|S II80
1 R|E2 Eff3 SGA4 DB (Sub Care Inv OA)5 Treatment
bull Change in the logarithm of the levelof human neutrophil elastase(HNE) activity measured in sputum
bull Change in concentration of IL-8measured in sputum and plasmaconcentration of GSH measured inwhole blood the neutrophil countmeasured in sputum
Nov-08Feb-11
00809094
11 Glutamine supplementationin CF
na United States Not yetrecruiting
Dietary supplementbull Glutaminebull L-alanine
A|S II40
1 R3 PA4 DB (Sub Care Inv OA)5 Prev
bull Percent increase in plasma glutamineand GSH redox levels measured atweeks 0 4 8 and 12
Feb-10Feb-11
01051999
12 Effect of sulforaphane inbroccoli sprouts onNrf2 activation
ChmielJF
United States Active notrecruiting
Dietary supplementbull Broccoli sprouts
A na15
3 SGA4 OL5 BS
bull Nrf2 activation in NECbull Measures of lipid peroxidation in NECGSH from blood lymphocytesoxidative stress in urineneutrophil migration into thegingival crevices
Apr-11Sep-11
01315665
AbbreviationsA=adult BC=breath condensate BNEC=brushed nasal epithelial cells BS=basic science C=child CA=crossover assignment Care=caregiver CF=cystic fibrosis DB=double blind EBC=exhaled breath condensate Eff=efficacystudy FEV1=forced expiratory volume in 1 s FVC=forced vital capacity GSH=glutathione Inv=investigator MEF25ndash75=maximal expiratory flow 25ndash75 na=not available NAC=N-acetylcysteine NEC=nasal epithelial cellsNLF=nasal lavage fluid NPD=nasal potential difference NR|E=non-randomized|endpoint OA=outcomes assessor OL=open label PA=parallel assignment PI=principal investigator Prev=prevention R|E=randomized|endpoint S=senior Saf=safety study SB=single blind SGA=single group assignment Sub=subject
a Search was done matching the terms ldquoantioxidant therapyrdquo or ldquoGlutathionerdquo with ldquoCystic Fibrosisrdquob 1 Allocation 2 Classification 3 Intervention model 4 Masking 5 Primary purpose
697FG
allietal
Biochimica
etBiophysica
Acta
1822(2012)
690ndash713
698 F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
corrected Cftr KO-transgenic mice were given an oral bolus dose ofGSH (300 mgkg) and compared with WT mice for changes in GSHlevels in plasma lung ELF and BAL cells There was a twofold in-crease in plasma a twofold increase in lung a fivefold increase inELF and a threefold increase in BAL cell GSH levels at 60 min in WTmice however GSH levels only increased by 40 in the plasma 60in the lung 50 in the ELF and twofold in the BAL cells within thegut-corrected Cftr KO-Tg mice No change in GSH levels was observedin the uncorrected Cftr KO mice These studies suggest that oral GSHadministration can increase plasma and lung compartment GSHlevels in WT mice and to a lesser extent in gut-corrected Cftr KO-Tganimals It also suggests that oral GSH treatment can boost BAL cellGSH levels However since this study failed to show significant in-creases in serum and lung compartment GSH levels in uncorrectedCftr KO mice it is questionable whether oral GSH administration toCF patients with intestinal malabsorption would benefit from thistherapy It was also shown that GSH is rapidly distributed to theserum and lung compartments Kariya et al [118] speculate thatother transporter(s) besides CFTR are responsible of the transport ofGSH and probably of other dietary molecules to the lung whichmay be responsible for dietary deficiencies observed in various lungdiseases
Another strategy is represented by the oral supplementation ofhigh doses of NAC a well known cysteine donor for the synthesis ofglutathione NAC is considered a safe molecule which has beenused successfully to treat GSH deficiency in a wide range of diseases[119] As CF mice display defects in GSH export in the ELF comparableto those of patients they could provide a useful tool to assess the ef-fects of NAC administration on the GSH status However only limitedstudies exploring the effects of NAC on CF animal models have beenso far carried out The effects of NAC have been tested on mucus accu-mulation bacterial load transit and inflammation in the CF mousesmall intestine showing that NAC may reduce intestinal mucus accu-mulation bacterial overgrowth in the gut [120]
Moreover NAC has been reported to restore the accumulationof unwantedmisfolded proteins in aggregates that are associated withthe CF airway phenotype as a cause of lung inflammation [121] Themechanism of this NAC-derived effect seems to involve the restorationof beclin 1 expression and activity in the autophagy pathway of theendoplasmic reticulum that was investigated in vivo using Scnn1b-transgenic and Cftr(F508del) homozygous mice The restoration ofthis pathway also produced a rescued trafficking of CFTR (F508del) tothe cell surface of CF cells obtained from human CF nasal biopsies
Given the defective GSH metabolism of CF reviewed in the previ-ous sections and in [122] and the reduced response to GSH therapyin CF mice [93] some Authors have investigated the influence of bac-terial infections on lung oxidative stress The effects of P aeruginosainfection on ELF and lung tissue antioxidants and the oxidation ofDNA and lipids were investigated in mice challenged with bacterialcells [90] CFTR-KO (B6129P2-Cftrtm1Unc) and WT mice were chal-lenged intratracheally with a clinical isolate of mucoid P aeruginosaembedded in agar beads and on the third day of infection BALF andlung tissue were obtained and analyzed for cytokines antioxidantsand enzyme activities [90] P aeruginosa lung infection increasedlevels of inflammatory cytokines and neutrophils in the ELF This cor-responded with a marked increase in GSH and in urate levels in theELF of P aeruginosa-infected WT mice A twofold increase in uratelevels was also observed among lung tissue antioxidants of Paeruginosa-infected WT mice There were no changes in markers oflung oxidative stress associated with the P aeruginosa lung infectionIn contrast to WT mice the CFTR-KO mice lacked a significant in-crease in ELF GSH when challenged with P aeruginosa and this corre-lated with a decrease in the ratio of reduced to oxidized GSH in theELF a marker of oxidative stress These data would suggest that thelung adapts to infectious agents with elevated ELF GSH and urateTherefore individuals with lung diseases associated with altered
antioxidant transport such as CF might lack the ability to adapt tothe infection which may lead to a more severe inflammatoryresponse
322 Clinical trials on GSHThe discovery of the defect in GSH export has suggested that ther-
apies able to restore or increase GSH levels in the ASL could counteractthe inflammation and oxidative stress conditions typical of CF pa-tients In an attempt to strengthen extracellular defenses againstROS some pilot studies have analyzed the effect of GSH inhalation orthat of oral GSH prodrug N-acetylcysteine (NAC) All these treatmentswere well tolerated by the CF patients and most authors were able tomeasure increased ELF concentrations of GSH in association withsome positive clinical outcomes [4041737896122ndash128] Althoughpotentially promising these findings need stronger clinical evidencein that the majority of these were obtained on very limited numberof patients investigated in non-randomized controlled trials This ishighlighted in a recently published meta-analysis [129] that providesalso a thoroughly analysis of the literature on this aspect of the antiox-idant and anti-inflammatory therapy of CF Among the American CFfoundation sponsored trials two phase II trials on inhaled GSH andoral NAC are in progress in US and Germany (ClinicalTrialsgov Iden-tifier NCT00506688 and NCT00809094 respectively Table 1) andsafety and tolerability of aerosolized glutathione is also matter ofinvestigation by another (not registered) US trial (more informationon this can be found in [130]) Nevertheless the diffusion among CFpatients of NAC preparations for inhalation (Mucomystreg) has in-creased in recent years
γ-Glutamylcysteine ethyl ester (GCEE) is another potentially inter-esting GSH pro-drug which has proved some efficacy in the ameliora-tion of oxidative stress eg in experimental myocardial infarction[131] and central nervous system conditions (see eg [132]) HoweverGCEE has not been investigated in CF yet
33 Limits and potential problems associated to thiol-based therapies
Although the above cited clinical trials may be considered promis-ing attempts to improve the antioxidant levels in the ELF the actualcapacity of these treatments to produce positive clinical effects mustbe considered with caution For example indices of oxidative damagewere found to be unaffected by aerosolized GSH treatment [122]Some in vitro studies have suggested that the reaction of GSH withPCN could produce hydrogen peroxide with potential exacerbationof oxidative damage [101] The exact mechanisms of PCN toxicityand the reaction of this toxin with GSH must be better understoodin order to evaluate the safety of GSH administration to patients col-onized by P aeruginosa
Inhalation of GSH ensures its direct delivery in the airways butsince GSH can rapidly convert to its oxidized form GSSG frequentGSH inhalations are required to maintain a high GSHGSSG As a con-sequence of this limit four separate inhalations have been used inthe study carried out by Bishop et al [123] Unless justified by clearclinical improvements these repeated treatments may represent aburden for patients already undergoing complex therapies Moreoverrepeated inhalations of GSH increase the levels of GSSG in ELF[133134] In the absence of effective homeostatic mechanisms ensur-ing the fast recycling of GSSG to GSH this might produce unwantedeffects and even the exacerbation of CF symptoms being GSSG re-sponsible of the S-glutathiolation and functional inhibition of CFTR[124]
In principle the oral administration of GSH could be considered asafe strategy to prevent GSSG accumulation but this strategy is likelynot feasible due to the substantial inability of this water-soluble mol-ecule to cross biological membranes Moreover a study carried out inmice has established that GSH absorption in the gastrointestinal tractif any is mediated by CFTR itself thus excluding the possibility to
699F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
improve circulating levels of GSH in CF patients through the dietarysupplementation of the antioxidant [127] The limited absorption ofGSH could be overcome by GSH-esters as in vitro studies haveshown that this form of GSH may be specifically useful to rescue mi-tochondrial defects in cystic fibrosis models [80] Safety of these GSHderivatives in humans has been poorly investigated
Two independent studies have shown that the treatment of CF pa-tients with high doses of NAC increases extracellular GSH in sputum[78125] but contrasting results have been reported concerning theeffects of NAC on the concentrations of blood GSH and on the levelsof IL-8 and other markers of inflammation NAC treatments may beuseful to modulate the GSH content in cells but it should be remindedthat an enhanced cysteine supply cannot lead to an increase of GSHabove physiological levels due to the feedback inhibition mechanismof γ-glutamylcysteine synthetase described in the Section 311
331 Gamma-glutamyltransferase and GSH therapySo far none of the studies mentioned above has taken into account
the fact that GSH is degraded by GGT enzyme activity GGT concentra-tions are known to increase several fold in ELF of CF patients even ifthe mechanisms for this effect were not determined [135] and thisphenomenon parallels the above described decrease of GSH levels inELF Preliminary data suggest that a major source of increased ELFGGT is represented by activated neutrophils accumulating in diseasedairways (Corti and Pompella 2011 unpublished observation) Re-gardless of its origin it is likely that increased GGT in ELF would de-grade locally administered GSH to variable extents which couldcontribute to the so far inconclusive results of therapies based onaerosolized GSH Besides its role in GSH catabolism GGT has beenshown to mediate protein S-thiolation [136] suggesting that GSH ad-ministration in the presence of active GGT enzyme might alter CFTRglutathiolation status and function in a potentially unfavorable wayOn the other hand a potential role of GGT in favoring bronchial up-take of antioxidant vitamin C has also been suggested [137]
These controversial findings may add further issues to the ques-tion of whether the therapy of lung oxidative stress by aerosolizedGSH could be safe in all the CF patients regardless of specific strate-gies that would ascertain the extent of lung inflammation Thesestrategies should include the assay of GGT levels in ELF In principleonce an adverse role of ELF GGT in GSH therapies will be confirmedthe association of GGT inhibitors in the GSH formulations for inhala-tion could represent a promising pharmacological strategy
34 Malnutrition as a possible cause of defective thiol-dependentantioxidant protection
Successful nutritional interventions strongly impact on the clinicaloutcome of CF patients [138ndash140] Malnutrition by pancreatic insuffi-ciency and other CF-related factors influence the susceptibility to de-velop recurrent infections and severe inflammatory lesions of thelung tissue If the onset of a defective (sub-optimal) antioxidant sta-tus may represent an underlying component in the clinical effects ofmalnutrition remains a matter of investigation Clinicians have topay particular care to avoid these disturbances and successful proto-cols of nutritional intervention in CF have been developed whichare essentially aimed to avoid the onset of protein-energy malnutri-tion (PEM) [141] Despite this the risk of developing such an unto-ward complication in CF infants and children remains high assuggested by the prevalence data registered in some areas Actuallya prevalence of PEM between 5 and 14 in Moldavian infants was re-cently reported [142] and PEM is associated with poor outcome andparticularly with the risk of developing edema and anemia
Besides lowered intake and absorption of micronutrient antioxi-dants discussed in the other sections malabsorption of dietary proteinand excess fecal amino acid losses result in hypoproteinemiahypoalbu-minemia as key biochemical signs of PEM Hypoalbuminemia is
considered to be linked with a causendasheffect relationship with oxidativestress and is proposed to influence morbidity and mortality in condi-tions associated with chronic inflammation and severe oxidative stress[143144] The human serum albumin (HAS) molecule contains only areactive thiol group eg the Cys 34 the importance of which as an anti-oxidant defense system in blood and for the entire organism is welldocumented [145] This is the second main thiol (and the main proteinthiol) in the circulation (approx 2 mmol in the adult organism assum-ing 5 l of total blood volume anHt of 40 and [HAS] of 45 gl of plasma)being the RBCGSH thefirst thiol in blood (near to 5 mmol assuming thesame parameters of above and an average concentration of GSH inpacked RBC of 25 mM) [146147] The antioxidant role of HSA is notonly a consequence of the relative abundance of its Cys thiol A specificcapability of acting as a sacrificial target for a series of electrophils andmost biologically relevant ROS ie hydrogen peroxide and peroxyni-trite has been demonstrated in a series of studies [145148149] Li-gand binding activity can contribute to promote antioxidant effectsby the HSA molecule [145] Transitions metals particularly copperand also iron in the case of iron-overload diseases bind to HSA Inthis way these are less available to promote the Fenton chemistryand hydroxyl radicals eventually released from this oxidative reactionare mostly directed to the HAS protein sparing more important tar-gets A free radical-trapping activity of HSA has been also demonstratedand this was proposed to be directed toward both hydrophilic and fat-soluble species This activity may result from the interaction withother antioxidants such as α-tocopherol [150] and may influence theantioxidant activity of food-derived phenolic antioxidants [151]
However Cys 34 is considered the main contributor to the antiox-idant function of HAS which plays its role in the antioxidant homeo-stasis of blood thanks to a complex series of interactions with themetabolism and antioxidant function of the pool of free thiols in plas-ma and in the circulating RBC with the latter playing a significantcontribution to the extracellular pool of GSH [146] and to the dynam-ics of inter-organ GSHmetabolism in cooperation with liver and othertissues [147] Immuno-inflammatory cells and the lung tissue areamong the main terminals of this metabolism The RBC contain theentire machinery to synthesize GSH to restore its redox (by enzymat-ic reduction of the oxidized form) and to use this as cofactor of Se-GPx and GSH-S-transferase enzymatic activities that are responsibleof the detoxification of hydroperoxides and alkylating agents thatmay form in or enter the RBC cytosol [147] In this sense the RBC rep-resents a circulating reservoir of GSH that in addition to maintainingthe redox and respiratory function of Hb participates to systemic pro-tection of xenobiotics of endogenous and exogenous origin In consid-eration of these aspects the combination of hypoalbuminemia andanemia may exponentially increase the risk of developing oxidativestress in CF patients as it is supposed to occur in other oxidative stressconditions such as chronic kidney disease [55143152] Additionalclinical investigation should verify the hypothesis that hypoalbumi-nemia together with a defective uptake and metabolism of sulfur-containing amino acids and CF-specific defects of the GSH metabo-lism may represent a causal risk factor for an impaired antioxidantdefense and systemic oxidative stress in CF patients
35 Fat-soluble antioxidants
Pancreatic insufficiency and a diminished bile acid pool cause mal-absorption of important essential nutrients and other dietary compo-nents in CF Of particular significance is the malabsorption of fat-soluble antioxidants such as tocopherols carotenoids and coenzymeQ-10 (Co-Q10) and that of essential fatty acids (EFA)
351 Vitamin EVitamin E therapy in CF has been proposed in several decades of
research as a useful approach to overcome both the lower absorptionof this fat-soluble micronutrient and the increased antioxidant
700 F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
demand by the abnormal generation of ROS in CF tissues (see for in-stance the recommendations by the Cystic Fibrosis Foundation Con-sensus Conference on nutrition [153])
The first report of a vitamin E deficiency in CF appeared in literaturein 1951 by Filer et al [154] In this study the absorption of the mainform of this vitamin eg α-tocopherol and its ester derivatives was in-vestigated in several subsets of infants and children Thanks to a simplebioavailability (or tolerance) test these authors observed that ldquoin-fantshellip diagnosed as fibrocystic disease of the pancreas diarrhea andcirrhosis were characterized by a poor response to the test ie the tol-erance curve was lowrdquo However abnormalities were also observed inother subgroups of infants with a variety of disorders not associatedwith fat or fat-soluble vitamin intolerance such as sprue celiac syn-drome and lupus erythematosus which suggests the general observa-tion that malnutrition and inflammatory and degenerative diseases ofthe GI tract may lead to absorb tocopherols poorly At the same timethese authors reported that ldquoMetabolic disorders with associated hy-percholesterolemia were observed to give abnormally high values forthe area under the curverdquo and that patients responding poorly to to-copherol absorption test did also in vitamin A absorption tests
The finding of lowered (lipid uncorrected) levels of vitamin E wasconfirmed in other studies in which this relative deficiency was foundto occur irrespective of pancreatic comorbidity and in associationwith lowered levels of other liposoluble vitamins such as vitamin Aand D [155] regardless of their different liver metabolism and tissuedelivery mechanisms [156157]
Plasma buccal mucosal cells (BMCs) and breath condensate α-tocopherol decreased significantly with age in association with a de-creased respiratory function [5] This was accompanied by loweredlevels of other antioxidants such as vitamin C and increased oxidativestress markers of different origin such as protein carbonyls thiobarbi-turic acid-reactive substances and F2-IsoPs
Clinical symptoms of vitamin E deficiency in CF have not beenconclusively investigated Dolan et al [158] described that anemiaof CF patients is related to vitamin E deficiency and increasedperoxide-induced hemolysis of RBC Other authors however ob-served an increased susceptibility to peroxide-induced hemolysisalso in the presence of normal levels of vitamin E [159] Peters andKelly [160] observed that RBC vitamin E concentrations were belowthe normal range in almost all unsupplemented patients and roseinto the normal range with a 1-year supplement of 100 mg per daybut not 15 mg per day Since RBC vitamin E concentration has beenshown to correlate well with tissue concentrations of the vitamin inanimals tissue levels of vitamin E are expected to be lower than nor-mal in CF patients
Bioavailability of fat-soluble vitamin is limited in CF Vitamin Edeficiency of CF is also associated with hypocholesterolemia [7] Asa consequence the relative deficiency of this vitamin is compensatedwhen the absolute levels are normalized for cholesterol levels andthis suggests a poor transferring of this vitamin in the circulation bya defective lipid and lipoprotein metabolism Pancreatic insufficiencyand the consequent lipid malnutrition cannot completely explain thisdefect and other possibly CF-specific dysfunctions could play a roleLiver metabolism and specific plasma transport systems of this vita-min need further elucidation in CF
As a consequence of these aspects it is not presently clear whichform and level of supplementation of this vitamin is most appropriateto treat these patients Usingα-tocopherol as a vitamin E supplementPeters et al [160] reported that 100 mg per day are required to nor-malize RBC concentrations Other authors described unsuccessfulsupplementation protocols with higher doses and this has led to de-velop formulations with higher bioavailability in order to achieve bet-ter compliance to oral supplementation (see below and the literaturereviewed in [161ndash163])
Besides absorption and tissue delivery issues specificity of actionis another critical item of antioxidant therapy with fat-soluble agents
in CF As further addressed below this aspect could be themain limit toa successful use of natural forms of vitamin E in the clinical manage-ment of CF inflammation even if a local lung-targeted therapy wouldbe developed according with so far proposed pre-clinical models ofaerosolized vitamin E [164165]
Current pharmacological research is aimed to develop synthetic formsof this and other fat-soluble antioxidants with better radical scavengingproperties at the lipidndashwater interface Type of ROS target and the sitesof action greatly influence the chances of a fat-soluble antioxidant of alle-viating oxidative stress in the airways as well as in other organs such asliver and pancreas These aspects dealing with specificity of action[163166167] have stimulated the search of novel vitamin E-derived an-tioxidants that may help to scavenge radicals at the lipidndashwater interfaceof the epithelial cell membrane and surfactant Amine derivativesof tocopherols and tocotrienols have been recently demonstrated toshow higher antioxidant and free radical scavenging activity than α-tocopherol [168] Further in vitro pharmacological analysis has includedtoxicity evaluations and the detailed investigation of scavenging of azo-and phenolic radicals with different degrees of hydrophobicity and theinhibitory activity on IL-8 gene expression and phospholipase activityin CF cells Comparative evaluation with other synthetic derivativessuch asα-tocopheryl succinate and natural forms of vitamin E suggestedthat these amine derivatives are promising antioxidant and anti-inflammatory agents [Galli F and Pilolli F unpublished observation]deserving further pre-clinical investigation in CF model systems
Anti-inflammatory effects of natural and synthetic analogues of vi-tamin E are also an intriguing pharmacological opportunity currentlyunder investigation by several laboratories [169170]
Recently vitamin E supplementation has been at the center of adispute regarding its safety when used at high dosages in certainpopulations of patients An extensive and speculative debate originat-ed on this subject after a meta-analysis study byMiller et al [171] thatexamined the largest secondary prevention trials on vitamin E trials incardiovascular patients finding a significantly increased mortality riskfor all the causes (about 4 1ndash8 in the 95 interval of confidence)when the patients were treated with doses gt400 IUdie (that areequivalent to 400 mgdie of the synthetic form allrac-α-tocopheroland to 185 mgdie of the natural form RRR-α-tocopherol) This debateresulted in a careful examination of this meta-analysis study by severalother authors and in further revisions of the literature on vitamin E tox-icity in humans [see the literature recently reviewed in [163172ndash174]]that clearly demonstrated the poor consistency of the conclusionsraisedwithMillersmeta-analysis study and the paucity of the concernsthat derived from that These conclusions have been verified in the re-cent international symposium on vitamin E of the Society for Free Rad-ical Research Europe branch of Rome 2009 [173175] Vitamin E used assupplement for humans in all its forms (eg α-tocopherol and othertocopherols and tocotrienols) is safe in abroad range of intakes[172176] The tolerable upper intake level (UL) and the AcceptableDaily Intake (ADI) established by the Joint FAOWHOExpert Committeeon Food Additives for the natural form of vitamin E as α-tocopherolequivalents are of 300 mgdie and 015ndash20 mgkg body weightdierespectively [172177]
352 CarotenoidsLevels of plasma carotenoids such as β-carotene β-cryptoxanthin
and total lycopene are significantly lowered in CF patients and thiswas associated with higher susceptibility to lipid peroxidation[5178ndash180] Rust et al [178] demonstrated that the long-term oralsupplementation with 50 mg β-caroteneday (ie 1 mg β-carotenekg BWday) restored the levels of this carotenoid while sub-optimalsupplementation was observed at doses of 10 mg β-caroteneday orlower thus confirming the need of high doses of this fat-soluble factorto overcome the limited absorption and thus to achieve plasma con-centrations of healthy control subjects Successful high-dose treat-ments appear to lower oxidative stress markers such as TBA-MDA
701F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
complexes and to correct total antioxidant capacity of plasma Inanother study β-carotene supplementation was observed to de-creased lipid peroxide formation as quantitated by malondialdehydeconcentrations in plasma (TBAHPLC method) and to enhance the re-sistance to copper(II) ion-induced oxidation of low density lipopro-teins [180]
At the same time toxicity issues have been raised for human sup-plementation with carotenoid formulations and particularly of water-miscible formulations of preformed vitamin A that is regularly sup-plemented to CF patients which may increase serum retinol andpossible risk of CF-associated liver and bone complications (reviewedin [161181]) However β-carotene supplementation seems to be safesince this does not affect plasma concentrations of other carotenoidsand retinol as well as of other fat-soluble vitamins as α- and γ-tocopherol [178] Recent studies designed to test the clinical efficacyof a CF tailored multivitamin formulation (commercial name AquA-DEKsreg) also tested the safety of this type of formulation and demon-strated that this does not increase vitamin A above the normal levelsobserved in healthy controls [162182183] The normalization of β-carotene levels obtained in these studies was associated only withminor improvements on respiratory and growth parameters whilethe levels of urinary F2-IsoPs used as index of lipid peroxidationwere not affected [162] The surrogate marker of lipid peroxidationMDA was affected together with some selected antioxidant parame-ters (RBC thiols and superoxide dismutase) in another study inwhich this multivitamin formulation was preliminarily evaluated incomparison with standard formulations of vitamin E and A [182]
353 Coenzyme Q-10Coenzyme Q-10 (Q10) is a well-known electron transporter in the
mitochondrial respiratory chain with fundamental role in cellularbioenergetics and scavenging of radical species [184] This lipophilicsubstance is present in the circulation at low levels (serum concentra-tionsle2 μM) mainly as ubiquinol-10 eg the reduced form with anapproximate ratio of 955 with the oxidized form ubiquinone-10[185186] A mechanism for a preferential distribution and accumula-tion in mitochondria has been suggested for both the reduced and ox-idized forms of CoQ10 that are taken up by the cells in a time- andconcentration-dependent Subcellular localization and trafficking ofexogenous Q10 are similar to those of the endogenous form butwere different from that of α-tocopherol that is related with lipidcomposition particularly in the mitochondrial and microsomal frac-tions [184] Ubiquinol-10 readily oxidizes ex vivo by the reactionwith other lipophilic antioxidants such as α-tocopherol and butylatedhydroxytoluene [185] Therefore a higher reduction potential thanother physiological fat-soluble antioxidants such as vitamin E and aselective metabolism and cellular trafficking show peculiar role forthe cell CoQ which may also represent an important lipophilic antiox-idant in cells and body fluids
Human cells synthesize this coenzyme through the cholesterol bio-synthesis pathway so thatmore than two thirds of the tissue levels ap-pear to have an endogenous origin dietary sources provide acontribution to Co-Q10 levels of blood and all solid tissues that variesdepending on the dose applied and type of dietary source [187] How-ever in the case of oral supplements it has to be considered that hy-drophobicity and large molecular weight of this coenzyme influenceits absorption that ultimately is slow and limited [186187] Likewiseto vitamin E pharmacokinetics [188189] Co-Q10 showed T(max) ofaround 6 h that coincides with that of dietary lipids Elimination isclose to that of the more retained form of vitamin E in human bodyeg α-tocopherol with a half-life of about 33 h which suggests poorhepatic metabolism However commercially available formulationsare reported to be safe even at high doses and solubilized formulationsshow enhanced bioavailability In healthy subjects plasma Q10 re-sponse to oral ingestion show saturation profiles with a plateau at a
dose of 2400 mg and the higher plasma concentrations were foundto facilitate uptake by peripheral tissues and also the brain [186187]
Laguna et al [190] recently investigated total serum levels ofcoenzyme Q-10 in a wide population of CF children (n=381) and esti-mated their association with clinical outcome Near to 50 of these CFpatients were deficient of Co-Q10 and this defect was significantlymore prevalent in patients with pancreatic insufficiency and signifi-cantly associated with P aeruginosa colonization in infants (under24 months of age) Importantly low Co-Q10 levels correlated to otherlipid markers of a poor nutritional status such as total lipids and alsothe other fat-soluble antioxidants β-carotene and α-tocopherolwhich confirms the presence of a common defect in the absorptionand metabolic pathways of this coenzyme with dietary lipids
The deficit of Co-Q10 may contribute to the impaired energy func-tion of mitochondria of CF tissues and this may exacerbate CF-linkedinflammation infection and cellular stress response of the lung A sys-tematic analysis of molecular lesions in CF bronchial tissue has beenrecently carried out by proteomic approach [191] Comparative eval-uation of protein expressional pattern in CF and healthy controltissues has revealed aberrant levels of some mitochondrial andenergy-related proteins in CF specimens that included the ubiqui-nolndashcytochrome c reductase complex core protein I and one form ofnidogen a pseudogene of aconitase 2 These changes in CF may reflectmolecular changes which could be associated with an altered mito-chondrial homeostasis and Co-Q10 redox
Multivitamin supplements with high bioavailability containingCo-Q10 have demonstrated to correct the deficit of this antioxidantand were preliminarily observed to improve airway inflammationmarkers in CF patients [183] However further clinical investigationfailed to demonstrate that such an improved biochemical profile isassociated with significant improvements in weight percentile andpulmonary function [162]
354 Fatty acidsA key pathophysiological role in sustaining inflammation in CF has
been attributed to the abnormal polyunsaturated fatty acid (FA) pat-tern Abnormalities in FA profiling are potentially linked to CFTRmutation-driven alterations in the absorption andor metabolism ofdietary lipids [192193] and to the consumption of high oxidizableFA involved in the free radical-mediated lipid peroxidation [7]Among those alterations dysregulation of the docosahexaenoic acidand arachidonic acid balance has been extensively studied with re-portedly significant reduction of DHA in CF and a parallel increasein the levels of AA and inflammatory indices [193ndash195] Actually AAis the progenitor of both enzymatic- and free radical-derived inflam-matory mediators including leukotrienes prostaglandins and iso-prostanes On the other hand n-3 PUFA (eicosapentaenoic acid anddocosahexaenoic acid) are involved in the generation of potent medi-ators namely resolvins and protectins which are able to resolveexudates and to act as organ protective and antifibrotic Secondarilyto their anti-inflammatory action n-3 FA may also produce anantioxidant-like response (eg a reduced demand of antioxidants toachieve an optimal control of oxidative pathways) As a consequencen-3 PUFA have been suggested and widely used as supplements in CFpatients usually under the form of fish oil [196ndash198] It is worth ofnote however that defective levels of DHA in CF patients was notconfirmed in recent studies [7] It was also shown that patients onDHA supplements did not have increased plasma n-3 FA concentra-tions but showed more severe oxidative stress compared to theunsupplemented patients [7] This observation of an increased riskof oxidative stress in CF subjects receiving n-3 fatty acids supple-ments has also been described by other authors [199]
Studies reporting increased AA levels in CF patients have beencontradicted by others [7200201] thus contributing to weakeningthe pathophysiological role of the altered DHAndashAA balance as turnpoint of an upregulated inflammatory status in CF In this context a
702 F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
recent Cochrane meta-analysis on n-3 supplementation in CF patients[202] highlighted the lack of evidence for a significant correction ofthe assessed clinical end points (mainly respiratory symptoms)even when inflammatory indices and other laboratory end pointswere met Taken together these data suggest that there is insufficientevidence to draw firm conclusions or recommend routine use of n-3supplements in CF Notwithstanding it is common belief that n-3supplements provide some benefits for people with CF with relativelyfew adverse effects and thus their use is not discouraged
Further alterations in fatty acid metabolism have been highlight-ed including the consistent findings of an increase in circulatinglevels of saturated and monounsaturated fatty acids [7203204]Decreased levels of essential FA (EFA) ie the FA that have to be in-troduced with the diet correlates with the severity of respiratoryinsufficiency and the same clinical correlation was observed with al-tered proportions of FA species converted by the activity of desatur-ase enzymes (reviewed in [204]) The close relationship betweencertain fatty acids and oxidative stress including the negative correla-tion of C240 and linoleic acid with oxysterol levels point to the needof intensive investigation in CF patients of previously neglected lipidspecies that are emerging candidates in the control of metabolismQuantitative lipidomic analyses have lead to identify C161n7 palmi-toleate as a ldquoprotectiverdquo adipose-derived lipid hormone that stronglystimulates insulin activity in muscle and liver also suppressing in-flammatory cytokine output from mice fat cells [205] Specific meta-bolic activities have been also demonstrated by medium chainsaturated fatty acids caprylic acid (C80) capric acid (C100) and lau-ric acid (C120) Capric acid acts as a direct ligand of PPARγ using abinding pocket different from the binding pocket of thiazolidinedioneor long chain fatty acids [206] Additional activities of medium chainfatty acids which are ligands of free fatty acids receptors detectedin the immune cells the gastrointestinal tract and adipocytes maycontribute to metabolic homeostasis and inflammatory responses[207] These data underscore the importance of a lipid-mediated ldquoen-docrine networkrdquo demonstrating how specific alteration of one orfew serum lipids would be per se sufficient to influence metabolic ho-meostasis Given the relevance of this emerging information and thealteration of lipid metabolism and inflammatory status in CF fattyacid lipidomics need to be deeply investigated in CF
Again these studies have obvious nutritional implications Satu-rated fatty acids with chain lengths higher than C18 are poorlyabsorbed partly because they form insoluble calcium salts [208]Medium chain saturated fatty acids are well known for being highlyabsorbed through the intestine providing rapid delivery of energyvia oxidation of the more hydrophilic short chains and have beensuggested to provide proper nourishment in patients with CF [209]Recent studies have shown that consumption of a high-fat diet richin medium chain fatty acids as opposed to long chain fatty acidsdoes not lead to ectopic fat accumulation in skeletal muscle andliver of both rats and mice [210] In light of the close association be-tween nutritional status inflammation and life expectancy in CF pa-tients the manipulation of dietary lipids in these patients must befurther explored as a possible strategy to provide adequate nutritionand better management of oxidative stress
36 Hydrosoluble antioxidants oligoelements and enzymatic antioxidants
361 Vitamin CVitamin C status in CF patients has been poorly investigated Early
studies suggested a defective vitamin C status that was refractory tooral supplementation [211] Other and more recent studies showednormal or slightly decreased levels of vitamin C in CF patients as com-pared to healthy controls but age- and disease-related decline of thiswater-soluble antioxidant was reported in these patients [5212]In the study of Winklhofer-Roob et al [212] on mid-European CFpatients vitamin C concentrations decreased with age with an
estimated rate of 5 μmollyr and vitamin C concentrationsb40 μ-moll were associated with highest indexes of inflammation whichis consistent with the hypothesis that optimal levels of vitamin Cmay influence immuno-inflammatory activity of alveolar macro-phages and neutrophils Other few studies have examined the effectof supplements containing vitamin C on CF inflammation and oxida-tive stress since the levels of this vitamin do not significantly improvewith supplementation (reviewed in [213]) This highlights the com-mon fate that this hydrosoluble vitamin shares with several fat-soluble counterparts in the ldquomicronutrient paradoxrdquo of CF patients inwhich the need for a correction of their status along the progressionof the disease is frustrated by the poor efficacy of oral supplementa-tion protocols Formulations and appropriate supplementation proto-cols that may produce a better correction of vitamin C status of CFpatients are awaited for further clinical evaluation
362 Selenium and selenium-dependent peroxidasesSelenium is a trace element with marked electrophilicity [214]
that once converted to the organic form of Se-Cys can be introducedin protein structures to play its important role in H2O2 metabolismand signaling [215] As catalytic center of the enzyme GSH-peroxidase (SeGSH-Px) Se plays a crucial role to protect polyunsatu-rated lipids of plasma membrane and circulating lipoproteins formperoxidative insults With other Se-proteins such as the high molecu-lar weight thioredoxin reductases this oligoelement participates tothe control of protein thiol-disulfide oxidoreduction and glutathiony-lation which regulate signaling pathways of crucial importance in theregulation of immunity and inflammation [16] but also the function-ing of other redox-sensitive proteins such as the same CFTR [124]
The activity of SeGSH-Px in blood is considered a functional as-sessment of selenium status even if this assumption has some limita-tions related with the saturation profile that the Se stores show atincreasing doses of Se administration Investigations of the seleniumstatus in CF patients have produced conflicting findings which maydepend on differences in dietary intake ethnicity and environmentalfactors in the diverse patient populations (reviewed in [216217]) CFchildren have been reported to have lowered blood selenium and RBCSeGSH-Px activity [218219] normal plasma selenium and loweredRBC SeGSH-Px [220] and even normal levels of both these two param-eters [221] The supplementation with selenium in combination withother antioxidants was observed to increase the concentrations ofblood selenium that likewise β-carotene and fatty acid were posi-tively correlated with improved lung function [6]
Foucaud et al [218] observed that a defective selenium statuswas associated with lowered levels of other antioxidants that contrib-ute to the anti-peroxidative activity of this microelement such asvitamin E (reviewed in [222]) and the severity of this deficiencywas lower in children with pancreatic enzyme replacement and vita-min E supplementation
Treatments to substitute for exocrine pancreatic insufficiency bypancreatic enzymes from animal sources such as porcine pancreashave been confirmed to be a source of Se [220] These affects RBCSeGSH-Px activity and plasma selenium concentrations which hasto be taken into account when selenium supplements are given toCF patients
Selenium has been used to develop a series of organoseleniumcompounds that may open the way to new therapeutic opportunitiesin CF (see Section 392) These include GPX mimetic drugs and phaseII enzyme inducers which may provide higher antioxidant activity ofASL and cellular protection effects in the airways
363 Zinc and copperZinc and copper (Zn and Cu respectively) are present in many
proteins so that a deficiency of these trace metals could have pleiotro-pic effects in humans As regards antioxidant systems these two oli-goelements contribute an important role being cofactors of two
703F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
isoforms of the superoxide dismutase enzymes eg the extracellularform eg the EC-SOD or Sod 3 and the CundashZn-SOD or Sod 1 that isfound in several tissues and cells [223] The EC-SOD exerts its antiox-idant role also in the lining fluids of the airways [224]
The notion that CF patients have defective concentrations of bloodZn and Cu is controversial As far as Cu status is concerned few datahave been produced and are available in the literature suggestingthe notion that CF patients develop a moderate copper deficiency[225226] That was essentially demonstrated on the bases of a defec-tive activity of Cu-related proteins such as plasma ceruloplasmindiamine oxidase and RBC SOD This defect seems to be refractory toCu and Zn supplementation (see below)
More advanced studies have been carried out in the case of Zn sta-tus in CF Low plasma zinc concentrations were reported in approxi-mately 30 of young infants with CF identified by newbornscreening [227] and an impaired zinc homeostasis in CF patientswas described by Easley et al [228] This is characterized by poor con-servation of the endogenous pool with fecal loss and impaired frac-tional absorption of zinc which are the consequences of pancreaticinsufficiency and persisting steatorrhea These studies suggestedthat in the clinical management of CF patients these defects can beat least in part corrected by exocrine pancreatic enzyme replacement
A series of studies by Van Biervliet et al [229230] demonstratedin a Dutch population of CF infants and children that serum Zn variesin an age-dependent manner but remained unchanged with respectto healthy control levels In CF patients no difference in serum Zn con-centration between pancreatic-sufficient or pancreatic-insufficientpatients was observed and no correlation was found with the nutri-tional status or height z-score Importantly in these studies a signifi-cant correlation of serum Zn was observed with the fat solublevitamins A and E thus confirming the relationship between the ab-normalities of lipid and Zn metabolism in CF This suggests that co-supplementation of Zn and fat-soluble vitamins should be advisedin the presence of pancreatic insufficiency and persisting steatorrhea
Neve et al [219] in a study aimed to assess plasma and erythrocytezinc copper and selenium in CF children showed that mean plasmazinc and copper levels were not different from those in age-matched controls which confirms the observations by Van Biervlietet al described above However plasma zinc concentrations de-creased in patients with moderate-to-severe growth retardation andwith severe pulmonary disease but very low zinc levels occur sporad-ically Erythrocyte zinc and copper levels were significantly higherthan normal while RBC selenium was lower than in age-matchedcontrols These trace element concentrations in erythrocytes werediscussed in relation to the activities of the CuZn-SOD and the Se-enzyme GPx This observation suggests a compensatory upregulationof the erythrocyte CuZn-SOD by the exposure of erythroid precursorsto ROS andor other CF-related stressors
Best et al [225] also studied RBC SOD activity using this as a bio-logical sensor of Cu status in CF patients A lowered activity of thisenzyme was reported in CF together with that of the other Cu-dependent enzyme plasma diamine oxidase while plasma ceruplas-min showed normal activity Degradation rates of copper proteinsare known to be accelerated in conditions of copper deficiencywhich could explain the finding at least in part Anyway when Cuand Zn were supplemented to CF patients either separate or incombination (6 weeks of 3 mg copperd as copper-glycinate and30 mg zincd as zinc-glycinate) any of the copper enzyme activitieswas affected Therefore the moderate copper deficiency of CF patientsappears to be refractory to the intervention by increased copper andor zinc intake
Erythrocyte CuZn-SOD and the plasma levels of Cu and Zn werealso measured in the study of Wood et al [6] in which Australian CFpatients (agegt5 years) were treated with a high-dose antioxidantmultivitamin formulation containing 200 mg vitamin E (as RRR-α-tocopherol) 300 mg vitamin C (as sodium ascorbate) 25 mg β-
carotene (all-trans isomer) 90 μg Se (as selenomethionine) and500 μg vitamin A (as retinyl palmitate) in oil Plasma oligoelementsand particularly Zn were in the normal range at baseline (as com-pared with the data reported in [229230]) and were not affected bythis multivitamin supplement The same was found for the activityof RBC SOD and for plasma 8-iso-PGF2α as surrogate biomarker oflipid peroxidation
In a recent non-randomized small population (n=21) casendashcon-trol study in CF children Zn supplementation was proven to producepositive clinical effects in Zn-deficient patients [196] The supplemen-tation with 5 mgkg Zn sulfateday (maximum 150 mg) significantlydecreased the number of infections and increased the forced expira-tory volume in 1 s energy intake and growth parameters also im-proved These parameters were unaffected in untreated patientsexcept that in the case of the pulmonary function that decreased sig-nificantly These clinical observations on Zn supplementation need tobe confirmed in prospective double-blind randomized control trial
37 Appropriateness and targeting of antioxidant therapies in CF
The choice of the appropriate antioxidant and dose to correct a cer-tain biomarker and its associated biochemical lesion is another impor-tant point that appears to have disregarded in many clinical studiesFor instance unlike vitamin E vitamin C supplementation does notalter F2-IsoPs levels in humans (reviewed in [74]) This appears tobe true also in the antioxidant therapy of CF in which vitamin C(300 mgday) was administered together with other antioxidantsthat included a dose of vitamin E of 200 mgday without any signifi-cant effect on the surrogate biomarker of lipid peroxidation F2-IsoPs[6] When carotenoids are used as supplements to prevent the damag-ing action of ROS in the CF airways it is noteworthy that these are notparticularly good quenchers of peroxyl radicals relative to phenolicsand other antioxidants but are exceptional in quenching singlet oxy-gen at which most other phenolics and antioxidants are relativelyineffective Singlet oxygen is not a radical and does not react via radi-cal mechanisms but reacts mostly by the addition to double bondsforming endoperoxides that can be reduced to alkoxyl radicals that ini-tiate radical chain reactions typical of the peroxidative damage of PUFA[38] In this case the analysis of F2-IsoPs lipid peroxide formation andtransition metal-induced oxidizability of lipoproteins [162180] are allappropriate to evaluate the effect of carotenoids in preventing lipidperoxidation
As far as the dose is concerned clinical pharmacology of vitamin Eas an antioxidant was recently investigated by means of the effect onF2-IsoPs production and doses of α-tocopherol of 1600 IUday orgreater were found to be required to statistically affect plasma F2-IsoPs levels in hypercholeterolemic subjects [176] Several vitamin Esupplementation studies in CF patients have been performed withdoses of lower than 300 IUday regardless of the lowered absorptionby pancreatic and liver defects and the regular supplementationwith these doses does not appear to correct lipid oxidation markersin CF [7]
In the clinical practice and planning trials it has to be taken intoconsideration that in spite of substantial evidence supporting ahigher antioxidant demand in CF interventions with several antioxi-dant formulations produce poor responsiveness particularly in thecase of fat-soluble antioxidants which are poorly absorbed [6162]
Since many oxidants and antioxidants are present in tissuesand biological fluids and these have different chemical and physicalcharacteristics the possibility to produce a successful therapy witha single antioxidant molecule is too far to be realistic Moreover an-tioxidants act by multiple mechanisms in a single system or by adifferent single mechanism depending on the reaction systemresponding in a different manner to different radical or oxidantsources Because multiple reaction characteristics and mechanismsas well as different phase localizations are usually involved no single
704 F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
therapeutic approach will effectively prevent damage by multipleROS sources The defect of physiological antioxidants may also interferewith antioxidant therapies that are based on one or few exogenousantioxidants
Moreover several antioxidant vitamins such as vitamin E and ca-rotenoids have multiple natural forms with different bioavailabilitymetabolism and bioactivity [157167231] As far as the case of vita-min E supplementation concerns α-tocopherol was used as uniquevitamer in the large majority of supplementation trials so far per-formed and is the form used in the nutritional management of CFpatients Moreover several supplements contain the synthetic (or ra-cemic) form of this vitamin that has lower bioavailability than thenatural form Other forms present in nature and abundantly con-tained in vegetables such as tocotrienols and the less methylatedforms of tocopherol are not represented in many of the supplementformulations so far available in clinical centers and the supplementa-tion with α-tocopherol also limits their bioavailability These formsshow markedly higher susceptibility to hepatic metabolism and bili-ary excretion with respect to α-tocopherol eg the most representedform in blood and solid tissues and if co-supplemented these areeasily displaced during liver uptake and excreted with bile bymeans of competition with the same α-tocopherol Notwithstandingthese minor forms have been proposed to play important physiolog-ical roles showing molecular characteristics transcriptional effectsand antioxidant activities that clearly differentiate them in subfam-ilies with distinct biological functions Some of these such as α-tocopherol eg the second vitamin E form as relative abundance inblood and its carboxyethyl-hydroxychroman metabolite [189] ap-pear to have health-related anti-inflammatory effects which are par-ticularly relevant in lung protection [232233] This has suggestedthat such a group of ldquonon-α-tocopherolrdquo forms may represent anoth-er family of vitamins within the family of vitamin E with an impor-tant but often missed contribution to the proposed health effects ofthis vitamin [163]
These aspects may thus limit the possibility to provide CF patientsof optimal levels of this vitamin in all its components even if they areregularly treated with a vitamin E supplement eg withα-tocopherol
Targeted antioxidant therapy with formulations with higher bio-availability and bioactivity has been anticipated in CF New antioxi-dant formulations have been proposed to overcome main limits ofantioxidant therapies so far proposed for these patients Water-miscible α-tocopheryl acetate containing polysorbate propylene gly-col or polyethylene glycol as emulsifiers form micellar structureswere suggested to providing greater bioavailability than the fat-soluble counterparts These were commercialized with the brandnames of E-viminreg Cremophorreg EL and Aquasolreg E but despitethe original positive expectation [234235] some studies failed to ob-serve a higher response in vitamin E levels when these were com-pared with fat-soluble formulations [236237]
In a pilot study by Papas et al [183] a micellar formulation of fat-soluble nutrients and antioxidants was found to improve plasmalevels of β-carotene γ-tocopherol and CoQ(10) reducing at thesame time some inflammatory markers in induced sputum eg mye-loperoxidase and to a lower extent PMN elastase and total cell countswhile lung function and sputum bacterial counts were unaffectedThe same group recently confirmed the possibility to increase the ab-sorption of fat-soluble micronutrients using formulations with higherbioavailability specifically designed for malabsorbing patients such asCF patients that include also vitamin K and commercialized with thebrand name of AquADEKsreg [162] Despite improved vitamin and mi-cronutrient levels in this non-randomized open-label study AquA-DEKsreg produced only modest improvements in weight percentileand pulmonary function Another recent pilot observation [182] hassuggested the beneficial effect of this formulation on antioxidant andoxidative stress parameters of this oral supplement that surely deservesmore clinical investigation by larger randomized controlled trials
Recent multivitaminic formulations have been designed to containalso the minor forms of vitamin E and specifically γ-tocopherol [238]the expected superiority of which with respect to formulations con-taining only α-tocopherol needs to be verified As discussed abovein the section dedicated to vitamin E further advancements in thetherapy of CF inflammation and oxidative stress could be based onsynthetic forms and natural metabolites of this vitamin that havebeen recently identified to possess higher antioxidant and also anti-inflammatory activity than α-tocopherol (reviewed in [163168])
Pre-clinical investigation of these and other fat-soluble agents iscurrently addressed to develop formulations and administration pro-tocols that may increase the therapeutic efficacy in the airways In theantioxidant therapy of lung dysfunction in CF local administrationprotocols may overcome the limits of oral and systemic administra-tion protocols increasing bioavailability and providing targetedapproach to inflammation and oxidative stress Aerosolization of vita-min E and other fat-soluble micronutrients is possible and may allowdirect administration in the airways to prevent toxicity of smokewhich is closely associated with inflammation and oxidative stress[164165] To our knowledge this as well as other strategies of localadministration such as instillation of solutions such as surfactant-like solutions enriched of vitamin E have not been previously inves-tigated in CF patients and other CF model systems
On the contrary inhalation is an administration route widelyadopted in the case of GSH and NAC therapy described above Inthis context Cys formulations alternative to NAC have been proposedfor use as antioxidant and anti-inflammatory agent for inhalationNacystelyn is a lysine adduct of NAC that thanks to a higher proton-ation equilibrium shows increased water solubility and thus betterbioavailability Nacystelyn has been described to influence IL-8 gener-ation and the inflammatory signaling of bronchial epithelial cells[239] and preliminary clinical evaluation has demonstrated the safetyof this drug [240] Further clinical trials aimed to assess the effect onlung symptomatology of CF patients are needed Direct administra-tion in the airways could also be adopted for micronutrient vitaminswith poor absorption and bioavailability due to GI defects
38 Clinical impact of antioxidant therapy in CF
Huge in vitro and pre-clinical evidence has provided the rationaleto support clinical investigation of antioxidant strategies in CF Theseshould aim to restore the oxidantndashantioxidant balance of CF airwaychallenged by chronic infection and inflammatory cell activation
Some observational trials have confirmed that antioxidants usedas either supplements to the diet or drugs for lung administrationby aerosolized formulations may help in relieving progressive lungdamage and other adverse clinical events of CF such as poor growthSo far few studies have examined with sufficient methodologicalrigor the clinical efficacy of antioxidant therapy in CF This was alsoconcluded in a previous review of the literature by Cantin et al [12]that was published in the beginning of 2006 and is confirmed alsoin a recent analysis of clinical trials on antioxidant therapy in CF pa-tients [213] that examined the literature until September 2010using as sources the databases of the Cochrane CF and Genetic Disor-ders Group CF Trials Register PubMed CINAHL and AMED Useful in-formation was retrieved from just four randomized controlled trialsand one quasi-randomized controlled trial on vitamin C vitamin Eβ-carotene and selenium used as supplements administered aloneor in combination Post-hoc data analysis that was possible only inthree studies on a total of 87 CF patients showed the absence ofany significant improvement in lung function that was selected as pri-mary outcome together with quality of life that improved in one trialSecondary outcomes concerning laboratory indices of oxidative stressand antioxidant status showed several improvements These includedan increase of RBC SeGPx by selenium supplementation done as
705F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
individual or combined supplementation and increased levels of allplasma antioxidants except vitamin C that were observed in all thetrials
The message from these studies to pediatricians and nutritionistswithin the clinical staff of CF centers is that in the absence of solid ev-idence regarding the clinical effectiveness of oral formulations of an-tioxidant supplements in CF (including PUFA) their use as a routineclinical practice should be considered with caution keeping clear inmind that this should represent just a complement of one of themost critical interventions in the life-long clinical management pro-gram of CF patients eg providing an adequate nutriture [140] Inthis context compensating energy and protein malnutrition has toremain the first goal of nutritional management programs Providinghigher intakes of antioxidant micronutrients with food naturally-enriched (or functionalized) of micronutrient antioxidants shouldbe preferred in order to have the higher combination of positive nu-tritional factors that are lost during refinement procedures and over-all industrial processing of dietary supplements
Measures of good practice in clinical management of micro-malnutrition in CF patients would include the support of specializedpersonnel and laboratories The centers should have the possibilityto ascertain with appropriate nutritional and laboratory tests whatthe level of deficiency is for the different micronutrients that each pa-tient may suffer from during a dietary program Monitoring dietaryintakes and blood levels of micronutrients is not sufficient to set apersonalized nutritional intervention with supplements or functionalfoods Sub-optimal intakes and the compliance to nutritional inter-ventions should be verified by means of selected biochemical andclinical criteria Unluckily the latter are still not well established forsome micronutrients such as the fat-soluble vitamins E (reviewed in[163173241]) and K [242243] and also for trace elements such asSe [244] For many of the antioxidants used as supplements inhumans we still do not know exactly several of the biological effectsthat these may provide when introduced in a healthy body and weknow less what these can do in disease These aspects hardly impacton the concept of optimal levels of intake that should be identified foreach micronutrient on an individual basis According with the aspectsdiscussed in the previous sections optimal levels of intake for antiox-idant micronutrients are different in CF patients and healthy subjectsand vary with age and several individual factors
Lung administration of antioxidants by means of aerosolized for-mulations so far used for GSH therapy (see above) is a promisingfield of clinical investigation in CF Toxicity issues are currently themain concern and the subject of clinical evaluation by several groups(described above)
Information on future directions of antioxidant therapy in CF canbe inferred by the analysis of pending or recently completed clinicaltrials that have been searched (December 2011) at ClinicalTrialsgovdatabase matching the terms ldquoantioxidant therapyrdquo or ldquoglutathionerdquowith ldquocystic fibrosisrdquo Fifteen trials were retrieved and those directlyrelated to antioxidant therapy (n=12) are presented in Table 1 andinclude efficacy and safety studies of inhaled drugs as GSH sodiumpyruvate NAC and NO and the dietary supplements AquADEKsregan antioxidant-rich multivitamin supplement epigallocatechin gal-late (EGCG)tocotrienol curcuminoids the amino acid glutaminesulforaphane in broccoli sprouts One trial is investigating the flavo-noid quercetin as CFTR modulator
39 Emerging antioxidant and anti-inflammatory approaches in CF
Mediterranean foods such as olive oil and red wine or severalplant extracts such as herbal tea or grape seed extracts contain aseries of natural compounds with important antioxidant and NOscavenging activity that have been widely investigated for the pre-vention of oxidative stress-related diseases [38245] These havebeen long investigated as template molecules to develop antioxidant
and anti-inflammatory drugs Between the multitudes of natural sub-stances most investigated ones include for instance tyrosol hydroxy-tyrosol gallic and caffeic acids belonging to the family of phenolswhile resveratrol of the stilbenes family epicatechin kaempferoland cianidin are examples of flavonoids examples of fat-soluble phe-nolics are those of the family of tocols (vitamin E) and carotenoids Allthese compounds show different metabolisms and signaling effects[246] Antioxidant and cell protection mechanisms are associatedwith different and sometimes concurrent processes as H-atom trans-fer and electron donation radical trapping and chelation of transitionmetals that can be easily investigated at the chemical level [247] Be-sides these direct antioxidant effects metabolic responses and signal-ing effects of natural compounds are also important to producesecond-generation responses that modify the level of antioxidantprotection and the potential for ROS detoxification in cells and bodyfluids These derive from the transcriptional regulation of antioxidantand pro-oxidant genes that coexist with the modulation of cytokinesecretion and inflammatory enzyme activities
Some of these natural plant-derived antioxidants may provide fur-ther pharmacological activities of possible relevance in CF This is thecase for instance of the plant flavonoids genistein apigenin kaemp-ferol quercetin and hesperidin [248ndash251] that fall in the pharmaco-logical category of ldquopotentiatorsrdquo [252] in that these activate at leastto a certain extent CTFR-mediated Cl currents in normal and CF airwayepithelium investigated either in vitro or in vivo in humans and ani-mal models Actually as prototypal flavonoid-derived potentiatorthe tyrosine kinase inhibitor genistein potentiates the gating of wild-type as well as ΔF508 CFTR and G551D CFTR [253] but at higherdoses it inhibits CFTR gating which make this an unlikely clinical can-didate Similar potentiation effects have been reported for the antiox-idant curcumin [250] that shows an additive effect with respect togenistein-induced potentiation Besides CFTR potentiation whichdoes not appear to have a direct influence on GSH and nutrient trans-port in the lung tissue all these natural substances have been usedalone or in combination with other agents as in vivo enhancers oflung antioxidant protection [246254255] In the case of quercetinthiol-reactive phenolic [256] bronchodilation and anti-inflammatoryeffects by a restoration of the Th1Th2 balance have been reportedin inflammatory syndromes of the lung [255257ndash259] but theseeffects have not been explored in CF Pyocyanin toxicity (see abovein the Section 2) could represent an issue for the use of quercetinand other catechols in infectious diseases of the lung [260]
Other natural antioxidants of potential interest in CF therapy in-clude terpenoids [261] such as terpinen-4-ol a major constituentof tea tree oil that is being investigated in the therapy of anti-biotic resistant organisms specifically against methicillin-resistantStaphylococcus aureus (MRSA) [262] a problem in CF [263] Otherthan being lipophilic antioxidants terpenes can prevent oxidativestress of the CF lung secondarily to the antibiotic effect thereby pro-moting a better control of immuno-inflammatory pathways and lungantioxidants
391 Targeting NF-κB with natural compounds resveratrol and plantextracts
Natural compounds were long known to be useful in designinganti-inflammatory drugs and some of these could find an applicationin the control of the transcription factor kappa-B (NF-κB) that maylead to develop advanced pharmacological tools to control inflamma-tion and to produce higher antioxidant protection to CF airwaysInhibitors targeting NF-κB including transcription factors decoymolecules (TFD) are potent down-regulators of gene expressionand release of IL-8 in CF cells infected with P aeruginosa [264265]
Resveratrol (354prime-trihydroxystilbene ldquoErdquo form) is one of the mostinvestigated natural antioxidant with proposed activity as NF-κBinhibitor This is a phytoalexin present in large quantity in red winepreferentially in the skin of grapes being its concentration
706 F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
50ndash100 μgmg of fresh skin and 13ndash3 mgl of red wine [266]Furthermore resveratrol is a constituent of lsquoDarakchasavarsquo (13ndash6 mgl) an ayurvedic medicine from India [267] The antioxidant activity ofresveratrol has been reported in several papers and occurs also in lungtissues suggesting that resveratrol has potential as a therapeuticagent in respiratory disease [268ndash270] Resveratrol can be consideredone of the most interesting molecules from the natural worldexhibiting strong antioxidant activity that at the same time is able toexert anti inflammatory activity through alteration of NF-κB functionsand efficient inhibition of pro-inflammatory genes [271272] As far asthe effects on CF model systems are concerned Cabrini et al [26]reported the effects of resveratrol on P aeruginosa infected CF IB3-1cells The results obtained demonstrate that resveratrol exhibits minoreffects of IB3-1 cell growth and important inhibitory effects on accumu-lation of IL-8 and GRO-α mRNA while minor effects on IL-6 gene ex-pression were observed These data support recently publishedobservations suggesting inhibitory effects of resveratrol in infection-mediated inflammatory processes [273] Interestingly resveratrol hasbeen reported as a potent inhibitor of NF-κB activity and a promisinganti-inflammatory agent [272274] also in combinationwith othermol-ecules [274275] However in vivo translation of this pre-clinical on res-veratrol is hard to be foreseen This natural compound displays poorbioavailability [276] and further characterization of resveratrol pharma-cokinetics is troublesome since it is hardly measurable in vivo [277]Furthermore the regulation of inflammatory responses by resveratrolhas been suggested to be far more complex than simple direct suppres-sion of NF-κB activity Actually some aspects of the immune responsecould be enhanced by this natural substance which may lead tohypothesize broad negative feedback events on immuno-inflammatorypathways [278] In any case and with these cautions in mind the pub-lished observations on cellular model systems support the concept thatresveratrol and resveratrol-containing formulations deserve further con-sideration to determine their possible therapeutic values in CF
Other inhibitors can be identified from systematic studies of naturalproducts and their ability to interfere with NF-κB activity [279ndash281]Recent studies have demonstrated that the whole extract of Aeglemarmelos (Rutaceae) has strong inhibitory effect on the P aeruginosa-dependent IL-8 induction in human CF-derived bronchial IB3-1 cellswithout affecting cell proliferation [280] Molecular analysis of compo-nents contained in A marmelos extracts revealed that three major com-pounds namely 56-dimethoxy-1-indanone 2-hydroxy-cinnamic acidand 5-methoxy psoralen (5-MOP) reproduce the inhibitory effect ob-servedwith thewhole extract [280] A further example has been recent-ly published using extracts from bergamot (Citrus bergamia Risso) Inthis study the extracts were characterized and the main detected con-stituents were assayed for their biological activity [281] The resultsobtained demonstrated that the extracts from bergamot epicarps con-tain components displaying an inhibitory activity on IL-8 Particularlythe most active molecules were bergapten and citropten These effectshave been confirmed by analyzing mRNA levels and protein release inthe CF cellularmodels IB3-1 and CuFi-1 inducedwith TNF-α or exposedto P aeruginosa
A parallel strategy linking NF-κB inhibition and down-regulationof NF-κB-dependent functions is described in recently publishedstudies based on a structured-based virtual screening (VS) of differ-ently substituted furocoumarins and analogues against NF-κB withthe objective of selecting molecules able to inhibit the binding ofthis transcription factor to DNA [282283] Novel compounds wereidentified with this strategy as potent inhibitors of NF-κB dependentbiological functions to be proposed for the control lung inflammationoccurring in patients affected by CF [282ndash284]
392 Scavengers and regulators of H2O2 and NO
3921 Lactoferrin and OSCNmacr The impaired DUOXLPO system of CFpatients could be the target of therapeutic strategies that may
produce concomitant antimicrobial and antioxidant effects This sys-tem described above in Section 22 represents an important compo-nent of innate immunity with a role in bactericidal defense andregulation of H2O2 metabolism of airways [32] CF patients have alsoreported to show lowered LF levels in the ASL [37] that togetherwith a CFTR-dependent defective efflux of SCNmacr and LPO [36] may cre-ate the environment for a sustained flux of H2O2 and for the genera-tion of highly reactive Fenton species [1138] An ideal therapeuticintervention should restore the LPO-dependent generation of bacteri-cidal OSCNmacr from DUOX-derived H2O2 and SCNmacr in the ASL to controlat the same time the microbial biofilm and the flux of H2O2 into theASL An approach close to this therapeutic mechanism was recentlyproposed for the drug Meveolreg This is a complex of LF and OSCNmacrwith proposed in vivo antimicrobial activity [285] to be evaluatedin clinical trials for the aerosol treatment of lung infections in CFpatients The role for this drug in the control of H2O2 levels of ASLremains to be investigated
3922 Organoselenium compounds Organoselenium compoundshave been proposed as therapeutic agents useful in the antioxidanttherapy of inflammatory conditions These include GPX mimetic mol-ecules such as Ebselenreg (2-phenyl-12-benzisoselenazol-3(2H)-one)or other and more recently developed molecules that are still inpre-clinical steps of evaluation [286] Selectively and specificity of ac-tion are main issues in the therapeutic mechanism of this candidateantioxidant drug that thanks to the electrophilic properties of Se[214] reacts with thiols to reduce H2O2 and other species MoreoverEbselenreg has been described to act as potent non-competitive inhib-itor of extracellular nucleoside diphosphokinase (NDPK) having neg-ligible effect on ecto-ATPase and adenyl kinase activities which areother players of the metabolism of extracellular nucleotides [287]This enzyme together with other nucleoside di- and triphosphatescontributes to regulate several components of the mucociliary clear-ance process (MCC) that protects the lung against infections via acti-vation of epithelial purinergic receptors The inhibition of NDPK bythis GPX-mimetic drug may also impact on the energy status of endo-thelial cells [287] This aspect could be further investigated as a cellu-lar protection mechanism in the pulmonary epithelium of CF patientsbeing the control of cell energy of fundamental importance to preventthe activation of death pathways [288]
Further therapeutic mechanisms for these Se-derived drugs mayderive from the marked activity as inducers of phase II enzymessuch as quinone reductase (QR) and glutathione-S-transferase (GST)[289] This induction response also observed with other electrophilsand redox-active molecules such as natural phenolic antioxidantscould produce higher cellular protection by the acquisition of anincreased capability to detoxify endobiotics generated during oxida-tive stress and inflammation [246]
3923 Melatonin and GSNO as NOx regulators Increased markers ofNO-derived biological damage are present in the CF lung suggestingthe abnormal reactivity of NOx in the inflamed lung of CF patients[52] However an impaired metabolism and biological function ofNO in CF airways (see Section 23) suggests a cautious approach tothe use of agents that may influence the levels and chemical behaviorof NO-derived species (NOx) with possible impact on the physiologi-cal roles of NO in vasodilatation innate immunity and H2O2 metabo-lism of the respiratory tract [290291] NO donors also appear toinfluence CFTR function of alveolar epithelium and gland serouscells [292293]
Main physiological role of the pineal gland hormone melatonin isthe synchronization of circadian rhythms including the sleepndashwakecycle but several other functions dealing with immunomodulatoryantioxidant and cellular protection effects have been identified[294] Melatonin receptor stimulation may also influence cyclic AMPsignaling and the regulation of CFTR ion channel [295296]
707F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
A recent randomized double-blind placebo-controlled study hasexamined the effects of short term melatonin administration (3 mgfor 3 weeks) on sleep and oxidative stress markers in CF [297]According with the expected pharmacological effect of this hormonalsubstance the treatment was successful in improving sleep indicesAt the same time nitrite levels determined in exhaled breath conden-sate (EBC) were reduced to suggest a better control of NOmetabolismof CF airways (discussed above in Section 23) but these effects how-ever were not associated with a significant correction of isoprostaneas lipid peroxidation marker measured in EBC Increasing dosages ofmelatonin could be investigated for the pharmacological treatmentof oxidative stress and immune dysfunction of CF patients due tothe absence of adverse effects of this hormonal substance in humans
The S-nitrosation reaction of thiols is another interesting aspect ofNO pharmacology [53] that may find an application in the therapy oflung complications of CF This has been the case for instance of theS-nitrosothiol GSNO that has been used safely in human trials[298299] This endogenous nitrosothiol with proposed regulatory ef-fect on the CFTR of lung epithelia [292293] is well tolerated in pa-tients with CF when administered by aerosolization and mayproduce better oxygenation [299] thereby suggesting that therapyaimed at restoring endogenous GSNO levels in the CF airway maymerit further clinical evaluation Since the administered GSNO de-composes as shown by the increased levels of expired NO in CF pa-tients under treatment with this nitrosothiol [299] furtherinvestigation should be addressed to ascertain whether GSNO thera-py may merely correspond to a GSH therapy
NO dependent effects on CFTR function should be considered toevaluate mechanism of action and specificity of antioxidant therapiesthat target NO metabolism and function in the CF airways
4 Conclusions and future perspectives
The presence of clinical and biochemical symptoms of inflammationand oxidative stress implies that CF patients have a higher demand ofantioxidant protection The combination of the dysfunctional CFTRwith a lowered intake and absorption of dietary antioxidants producesub-optimal levels of protection from both enzymatic and non-enzymatic defense systems The former could be associated with a de-fective glutathionemetabolism and lowered intake of sulfur-containingamino acids and oligoelements such as zinc and possibly seleniumwhile fat-soluble antioxidant vitamins such as vitamin E and caroten-oids and the water-soluble vitamin C are lowered than in healthy sub-jects due to malabsorption and possibly higher consumption
The increased antioxidant demand in CF patients should be evenhigher in the presence of complications of the lung pancreas andliver Lung comorbidity is particularly important in this contextbeing associated with recurrent infections which results in the alter-nation of inflammatory exacerbates and chronic inflammation Thesesustain the flux of ROS in the airways and promote the formation ofsecond-generation byproducts by the damage of biomolecules suchas PUFA and proteins which may diffuse also at the systemic level tofurther promote adverse biological responses and toxic reactions Pan-creatic insufficiency causes malnutrition and may lead to develop en-docrine and metabolic defects associated with diabetes of CF Theseevents can be further aggravated by the concomitance of liver dys-function and a poor nutritional status Malnutrition is strongly associ-ated with poor prognosis as assessed by pulmonary function andsurvival data [138ndash140] The more aggressive nutritional interven-tions seem to produce better clinical outcomes in these patients andthe possibility of achieving higher antioxidant protection in well-nourished patients by dietary factors could be a key aspect to explainsuch a clinical advantage The assumption that food-derived compo-nentsmay help to prevent the damaging effects of oxidative stress im-proving the antioxidant defenses deserves further investigation at theclinical level This together with the investigation of appropriate
laboratory biomarkers could provide critical information to establishintervention criteria for an early nutritional management of newly di-agnosed patients [5] It is expected that a timely secondary preventionstrategy could influence the progression of CF symptoms thusaffecting with a self-feeding mechanism the same extent of malnutri-tion and oxidative stress along the life of CF patients Since severalfactors contribute to impair the nutritional status of CF patients(such as pancreatic insufficiency chronic malabsorption recurrentsinopulmonary infections and progressive lung disease chronic in-flammation increased energy expenditure suboptimal intake multi-therapy) careful monitoring of the antioxidant status should berecommended According with international guidelines fat-solublevitamin supplementation is of utmost importance in daily practice to-gether with energy intake requirements and pancreatic enzyme-replacement therapy Among these vitamin E β-carotene and ω-3FA have observed to alleviate selected biochemical signs of oxidativestress as measured for instance with well established laboratory indi-ces of lipid peroxidation and in some studies these effects werepreliminarily associated with positive clinical outcomes Notwith-standing randomizedndashcontrolled clinical trials on antioxidant supple-ments (including ω-3 FA) so far carried out in CF have failed toconclusively demonstrate significant beneficial effects on respiratorysymptoms and on the consequent impact that these have on the qual-ity of life of these patients (reviewed in [202213]) whichmay provideno support for the use of these supplements in CF An absence of effi-cacy in prevention studies on antioxidant supplements has also beenobserved in other and possibly less severe oxidative stress-relatedconditions particularly in the secondary prevention of cardiovasculardisease and some forms of cancer by vitamin E and other antioxidantssuch as vitamin C selenium and β-carotene (reviewed in [163]) Dif-ferent biases however have been identified in randomize large clini-cal trials that may account for these disappointing findings Theseinclude patient selection criteria (early interventions and primaryprevention could have more chances of success than secondaryprevention) duration and doses of the treatment use of wrong anti-oxidant formulations and administration protocols absence of verifi-cations of the biological compliance to the treatment etc The samebiases apply for the few trials carried out in CF patients Thus the ap-propriateness and efficacy of nutritional interventions with naturalfood-derived or synthetic antioxidants should be verifiedwith respectto the biological pathways of oxidative stress and clinical variablesthat are identified as end-points Profiles of blood and tissue antioxi-dants as well as of reliable surrogate markers of oxidative stresshave to be selected and determined in highly specialized laboratorieswith a well-established experience on these analyses
Well-timed (early) interventions with appropriate antioxidantformulationsprotocols need to be proposed for the next generationof trials and the development of novel CF-tailored antioxidant andanti-inflammatory agents should be promoted
As a consequence of these considerations more clinical investiga-tion is awaited to identify future successful approaches to the antiox-idant therapy as a measure to further enhance quality of life and theoverall clinical outcome of CF patients
Acknowledgments
We are indebted with the Italian Cystic Fibrosis Research Founda-tion for the support that it provided with its grant program to the re-search activity of the authors of this paper This is a scientific initiativeof the ldquoWorking Group on Inflammation in Cystic Fibrosisrdquo (BragonziA Bravo E Cabrini G Conese M Cuzzocrea S Dechecchi MC De Ales-sandri A Evangelista V Galli F Gambari R Lambiase A Lucidi VManca A Melotti P Minicucci L Motta A Pietraforte D Pompella AQuattrucci S Rizzo R Romano M Sorio C Tesse R) of the Italian Soci-ety for Cystic Fibrosis A particular thank goes to the Prof GianniMastella for the critical revision of the manuscript and for the
708 F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
stimulating research environment that he has contributed to createwithin the Italian Cystic Fibrosis Research Foundation
References
[1] BP OSullivan SD Freedman Cystic fibrosis Lancet 373 (2009) 1891ndash1904[2] P Linsdell JW Hanrahan Glutathione permeability of CFTR Am J Physiol 275
(1998) C323ndashC326[3] L Gao KJ Kim JR Yankaskas HJ Forman Abnormal glutathione transport in
cystic fibrosis airway epithelia Am J Physiol 277 (1999) L113ndashL118[4] RK Rowntree A Harris The phenotypic consequences of CFTR mutations Ann
Hum Genet 67 (2003) 471ndash485[5] EI Back C Frindt D Nohr J Frank R Ziebach M Stern M Ranke HK Biesalski
Antioxidant deficiency in cystic fibrosis when is the right time to take actionAm J Clin Nutr 80 (2004) 374ndash384
[6] LG Wood DA Fitzgerald AK Lee ML Garg Improved antioxidant and fattyacid status of patients with cystic fibrosis after antioxidant supplementation islinked to improved lung function Am J Clin Nutr 77 (2003) 150ndash159
[7] L Iuliano R Monticolo G Straface S Zullo F Galli M Boaz S Quattrucci Asso-ciation of cholesterol oxidation and abnormalities in fatty acid metabolism incystic fibrosis Am J Clin Nutr 90 (2009) 477ndash484
[8] C Libetta V Sepe P Esposito F Galli A Dal Canton Oxidative stress and inflam-mation implications in uremia and hemodialysis Clin Biochem 44 (2011)1189ndash1198
[9] G Bartosz Reactive oxygen species destroyers or messengers Biochem Phar-macol 77 (2009) 1303ndash1315
[10] T Ntimbane B Comte G Mailhot Y Berthiaume V Poitout M Prentki RRabasa-Lhoret E Levy Cystic fibrosis-related diabetes from CFTR dysfunctionto oxidative stress Clin Biochem 30 (2009) 153ndash177
[11] A van der Vliet JP Eiserich GP Marelich B Halliwell CE Cross Oxidativestress in cystic fibrosis does it occur and does it matter Adv Pharmacol 38(1997) 491ndash513
[12] AM Cantin TB White CE Cross HJ Forman RJ Sokol D Borowitz Antioxi-dants in cystic fibrosis Conclusions from the CF antioxidant workshop Bethes-da Maryland Free Radic Biol Med 42 (2007) 15ndash31
[13] LT McGrath P Mallon L Dowey B Silke E McClean M McDonnell A DevineS Copeland S Elborn Oxidative stress during acute respiratory exacerbations incystic fibrosis Thorax 54 (1999) 518ndash523
[14] E Thomson S Brennan R Senthilmohan CL Gangell AL Chapman PD SlyAJ Kettle E Balding LJ Berry JB Carlin R Carzino N de Klerk T Douglas CFoo LW Garratt GL Hall J Harrison A Kicic IA Laing KM Logie J MassieLS Mott C Murray F Parsons N Pillarisetti SR Poreddy SC RanganathanCF Robertson R Robins-Browne PJ Robinson B Skoric SM Stick ENSutanto E Williamson Identifying peroxidases and their oxidants in the earlypathology of cystic fibrosis Free Radic Biol Med 49 (2010) 1354ndash1360
[15] SP Range C Dunster AJ Knox FJ Kelly Treatment of pulmonary exacerba-tions of cystic fibrosis leads to improved antioxidant status Eur Respir J 13(1999) 560ndash564
[16] L Coppo P Ghezzi Thiol regulation of pro-inflammatory cytokines and innateimmunity protein S-thiolation as a novel molecular mechanism Biochem SocTrans 39 (2011) 1268ndash1272
[17] C Verhaeghe C Remouchamps B Hennuy A Vanderplasschen A Chariot SPTabruyn C Oury V Bours Role of IKK and ERK pathways in intrinsic inflamma-tion of cystic fibrosis airways Biochem Pharmacol 73 (2007) 1982ndash1994
[18] TL Bonfield JR Panuska MW Konstan KA Hilliard JB Hilliard H Ghnaim MBerger Inflammatory cytokines in cystic fibrosis lungs Am J Respir Crit CareMed 152 (1995) 2111ndash2118
[19] TL Noah HR Black PW Cheng RE Wood MW Leigh Nasal and bronchoal-veolar lavage fluid cytokines in early cystic fibrosis J Infect Dis 175 (1997)638ndash647
[20] MJ Welsh BW Ramsey FJ Accurso GR Cutting Cystic Fibrosis McGraw-HillNew York 2001
[21] TZ Khan JS Wagener T Bost J Martinez FJ Accurso DW Riches Early pul-monary inflammation in infants with cystic fibrosis Am J Respir Crit CareMed 151 (1995) 1075ndash1082
[22] FA Ratjen Cystic fibrosis pathogenesis and future treatment strategies RespirCare 54 (2009) 595ndash605
[23] J Jacquot O Tabary P Le Rouzic A Clement Airway epithelial cell inflamma-tory signalling in cystic fibrosis Int J Biochem Cell Biol 40 (2008)1703ndash1715
[24] CM Greene P Branagan NG McElvaney Toll-like receptors as therapeutic tar-gets in cystic fibrosis Expert Opin Ther Targets 12 (2008) 1481ndash1495
[25] M Rottner JM Freyssinet MC Martinez Mechanisms of the noxious inflam-matory cycle in cystic fibrosis Respir Res 10 (2009) 23
[26] G Cabrini V Bezzerri I Mancini E Nicolis MC Dechecchi A Tamanini ILampronti L Piccagli N Bianchi M Borgatti R Gambari Targeting transcrip-tion factor activity as a strategy to inhibit pro-inflammatory genes involved incystic fibrosis decoy oligonucleotides and low-molecular weight compoundsCurr Med Chem 17 (2010) 4392ndash4404
[27] CM Greene NG McElvaney Proteases and antiproteases in chronic neutrophiliclungdiseasemdash relevance to drug discovery Br J Pharmacol 158 (2009) 1048ndash1058
[28] AM Cantin Potential for antioxidant therapy of cystic fibrosis Curr Opin PulmMed 10 (2004) 531ndash536
[29] JF Chmiel MW Konstan Inflammation and anti-inflammatory therapies forcystic fibrosis Clin Chest Med 28 (2007) 331ndash346
[30] DP Nichols MW Konstan JF Chmiel Anti-inflammatory therapies for cys-tic fibrosis-related lung disease Clin Rev Allergy Immunol 35 (2008)135ndash153
[31] AJ Kettle T Chan I Osberg R Senthilmohan AL Chapman TJ Mocatta JSWagener Myeloperoxidase and protein oxidation in the airways of youngchildren with cystic fibrosis Am J Respir Crit Care Med 170 (2004)1317ndash1323
[32] H Fischer Mechanisms and function of DUOX in epithelia of the lung AntioxidRedox Signal 11 (2009) 2453ndash2465
[33] B Rada TL Leto Oxidative innate immune defenses by NoxDuox familyNADPH oxidases Contrib Microbiol 15 (2008) 164ndash187
[34] P Moskwa D Lorentzen KJ Excoffon J Zabner PB McCray Jr WM NauseefC Dupuy B Banfi A novel host defense system of airways is defective in cysticfibrosis Am J Respir Crit Care Med 175 (2007) 174ndash183
[35] D Lorentzen L Durairaj AA Pezzulo Y Nakano J Launspach DA Stoltz GZamba PB McCray Jr J Zabner MJ Welsh WM Nauseef B Banfi Concentra-tion of the antibacterial precursor thiocyanate in cystic fibrosis airway secre-tions Free Radic Biol Med 50 (2011) 1144ndash1150
[36] Y Xu S Szep Z Lu The antioxidant role of thiocyanate in the pathogenesis ofcystic fibrosis and other inflammation-related diseases Proc Natl Acad Sci US A 106 (2009) 20515ndash20519
[37] MP Rogan CC Taggart CM Greene PG Murphy SJ ONeill NG McElvaneyLoss of microbicidal activity and increased formation of biofilm due to decreasedlactoferrin activity in patients with cystic fibrosis J Infect Dis 190 (2004)1245ndash1253
[38] B Halliwell JM Guttridge Free Radicals in Biology and Medicine Fourth editionOxford University Press New York 2007
[39] B Rada K Lekstrom S Damian C Dupuy TL Leto The Pseudomonastoxin pyocyanin inhibits the dual oxidase-based antimicrobial system as itimposes oxidative stress on airway epithelial cells J Immunol 181 (2008)4883ndash4893
[40] C Schwarzer B Illek JH Suh SJ Remington H Fischer TE Machen Organelleredox of CF and CFTR-corrected airway epithelia Free Radic Biol Med 43(2007) 300ndash316
[41] JH Roum R Buhl NG McElvaney Z Borok RG Crystal Systemic deficiency ofglutathione in cystic fibrosis J Appl Physiol 75 (1993) 2419ndash2424
[42] VM Hudson Rethinking cystic fibrosis pathology the critical role of abnormalreduced glutathione (GSH) transport caused by CFTR mutation Free RadicBiol Med 30 (2001) 1440ndash1461
[43] PJ Barnes RA Dweik AF Gelb PG Gibson SC George H Grasemann IDPavord F Ratjen PE Silkoff DR Taylor N Zamel Exhaled nitric oxide in pul-monary diseases a comprehensive review Chest 138 (2010) 682ndash692
[44] H Grasemann E Michler M Wallot F Ratjen Decreased concentration of ex-haled nitric oxide (NO) in patients with cystic fibrosis Pediatr Pulmonol 24(1997) 173ndash177
[45] H Grasemann F Ratjen Cystic fibrosis lung disease the role of nitric oxidePediatr Pulmonol 28 (1999) 442ndash448
[46] B Gaston F Ratjen JW Vaughan NR Malhotra RG Canady AH Snyder JFHunt S Gaertig JB Goldberg Nitrogen redox balance in the cystic fibrosis air-way effects of antipseudomonal therapy Am J Respir Crit Care Med 165(2002) 387ndash390
[47] H Grasemann I Ioannidis RP Tomkiewicz H de Groot BK Rubin F RatjenNitric oxide metabolites in cystic fibrosis lung disease Arch Dis Child 78(1998) 49ndash53
[48] H Grasemann R Schwiertz S Matthiesen K Racke F Ratjen Increased argi-nase activity in cystic fibrosis airways Am J Respir Crit Care Med 172(2005) 1523ndash1528
[49] H Grasemann S Al-Saleh JA Scott D Shehnaz A Mehl R Amin M Rafii PPencharz J Belik F Ratjen Asymmetric dimethylarginine contributes to airwaynitric oxide deficiency in patients with cystic fibrosis Am J Respir Crit CareMed 183 (2011) 1363ndash1368
[50] H Grasemann F Kurtz F Ratjen Inhaled L-arginine improves exhaled nitricoxide and pulmonary function in patients with cystic fibrosis Am J RespirCrit Care Med 174 (2006) 208ndash212
[51] H Grasemann F Ratjen Emerging therapies for cystic fibrosis lung disease Ex-pert Opin Emerg Drugs 15 (2010) 653ndash659
[52] BM Morrissey K Schilling JV Weil PE Silkoff DM Rodman Nitric oxide andprotein nitration in the cystic fibrosis airway Arch Biochem Biophys 406(2002) 33ndash39
[53] R Radi Nitric oxide oxidants and protein tyrosine nitration Proc Natl AcadSci U S A 101 (2004) 4003ndash4008
[54] J Chen M Kinter S Shank C Cotton TJ Kelley AG Ziady Dysfunction of Nrf-2in CF epithelia leads to excess intracellular H2O2 and inflammatory cytokineproduction PLoS One 3 (2008) e3367
[55] F Galli M Piroddi C Annetti C Aisa E Floridi A Floridi Oxidative stress andreactive oxygen species Contrib Nephrol 149 (2005) 240ndash260
[56] DT Wright LA Cohn H Li B Fischer CM Li KB Adler Interactions of oxygenradicals with airway epithelium Environ Health Perspect 102 (Suppl 10)(1994) 85ndash90
[57] I Rahman SR Yang SK Biswas Current concepts of redox signaling in thelungs Antioxid Redox Signal 8 (2006) 681ndash689
[58] Q Li JF Engelhardt Interleukin-1beta induction of NFκB is partially regulatedby H2O2-mediated activation of NFκB-inducing kinase J Biol Chem 281(2006) 1495ndash1505
709F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
[59] E Boncoeur VS Criq E Bonvin T Roque A Henrion-Caude DC Gruenert AClement J Jacquot O Tabary Oxidative stress induces extracellular signal-regulated kinase 12 mitogen-activated protein kinase in cystic fibrosis lung ep-ithelial cells potential mechanism for excessive IL-8 expression Int J BiochemCell Biol 40 (2008) 432ndash446
[60] B Fischer J Voynow Neutrophil elastase induces MUC5AC messenger RNA ex-pression by an oxidant-dependent mechanism Chest 117 (2000) 317Sndash320S
[61] B Rada P Gardina TG Myers TL Leto Reactive oxygen species mediate in-flammatory cytokine release and EGFR-dependent mucin secretion in airwayepithelial cells exposed to Pseudomonas pyocyanin Mucosal Immunol 4(2011) 158ndash171
[62] C Schwarzer H Fischer EJ Kim KJ Barber AD Mills MJ Kurth DC GruenertJH Suh TE Machen B Illek Oxidative stress caused by pyocyanin impairs CFTRClminus transport in human bronchial epithelial cells Free Radic Biol Med 45(2008) 1653ndash1662
[63] J Hull M South P Phelan K Grimwood Surfactant composition in infants andyoung children with cystic fibrosis Am J Respir Crit Care Med 156 (1997)161ndash165
[64] KC Meyer A Sharma R Brown M Weatherly FR Moya J Lewandoski JJZimmerman Function and composition of pulmonary surfactant andsurfactant-derived fatty acid profiles are altered in young adults with cystic fi-brosis Chest 118 (2000) 164ndash174
[65] MK Pulfer RC Murphy Formation of biologically active oxysterols during ozo-nolysis of cholesterol present in lung surfactant J Biol Chem 279 (2004)26331ndash26338
[66] V Starosta E Rietschel K Paul U Baumann M Griese Oxidative changes ofbronchoalveolar proteins in cystic fibrosis Chest 129 (2006) 431ndash437
[67] V Starosta M Griese Oxidative damage to surfactant protein D in pulmonarydiseases Free Radic Res 40 (2006) 419ndash425
[68] M Griese R Essl R Schmidt E Rietschel F Ratjen M Ballmann K Paul Pulmo-nary surfactant lung function and endobronchial inflammation in cystic fibro-sis Am J Respir Crit Care Med 170 (2004) 1000ndash1005
[69] M Griese R Essl R Schmidt M Ballmann K Paul E Rietschel F Ratjen Se-quential analysis of surfactant lung function and inflammation in cystic fibrosispatients Respir Res 6 (2005) 133
[70] LG Wood DA Fitzgerald PG Gibson DM Cooper ML Garg Increased plasmafatty acid concentrations after respiratory exacerbations are associated with el-evated oxidative stress in cystic fibrosis patients Am J Clin Nutr 75 (2002)668ndash675
[71] P Montuschi SA Kharitonov G Ciabattoni M Corradi L van Rensen DM Ged-des ME Hodson PJ Barnes Exhaled 8-isoprostane as a new non-invasive bio-marker of oxidative stress in cystic fibrosis Thorax 55 (2000) 205ndash209
[72] CE Collins P Quaggiotto L Wood EV OLoughlin RL Henry ML Garg Elevat-ed plasma levels of F2 alpha isoprostane in cystic fibrosis Lipids 34 (1999)551ndash556
[73] D Hartl V Starosta K Maier I Beck-Speier C Rebhan BF Becker P Latzin RFischer F Ratjen RM Huber E Rietschel S Krauss-Etschmann M Griese In-haled glutathione decreases PGE2 and increases lymphocytes in cystic fibrosislungs Free Radic Biol Med 39 (2005) 463ndash472
[74] GL Milne H Yin JD Morrow Human biochemistry of the isoprostane pathwayJ Biol Chem 283 (2008) 15533ndash15537
[75] G Ciabattoni G Davi M Collura L Iapichino F Pardo A Ganci R Romagnoli JMaclouf C Patrono In vivo lipid peroxidation and platelet activation in cystic fi-brosis Am J Respir Crit Care Med 162 (2000) 1195ndash1201
[76] C Garenc P Julien E Levy Oxysterols in biological systems the gastrointestinaltract liver vascular wall and central nervous system Free Radic Res 44 (2011)47ndash73
[77] AM Cantin SL North RC Hubbard RG Crystal Normal alveolar epithelial lin-ing fluid contains high levels of glutathione J Appl Physiol 63 (1987) 152ndash157
[78] R Tirouvanziam CK Conrad T Bottiglieri LA Herzenberg RB Moss High-dose oral N-acetylcysteine a glutathione prodrug modulates inflammation incystic fibrosis Proc Natl Acad Sci U S A 103 (2006) 4628ndash4633
[79] LW Velsor C Kariya R Kachadourian BJ Day Mitochondrial oxidative stressin the lungs of cystic fibrosis transmembrane conductance regulator proteinmutant mice Am J Respir Cell Mol Biol 35 (2006) 579ndash586
[80] M Kelly-Aubert S Trudel J Fritsch T Nguyen-Khoa M Baudouin-Legros SMoriceau L Jeanson F Djouadi C Matar M Conti M Ollero F Brouillard AEdelman GSH monoethyl ester rescues mitochondrial defects in cystic fibrosismodels Hum Mol Genet 20 (2011) 2745ndash2759
[81] P Ghezzi Role of glutathione in immunity and inflammation in the lung Int JGen Med 4 (2011) 105ndash113
[82] N Dauletbaev K Viel R Buhl TO Wagner J Bargon Glutathione and glutathi-one peroxidase in sputum samples of adult patients with cystic fibrosis J CystFibros 3 (2004) 119ndash124
[83] CE Cross A van der Vliet CA ONeill S Louie B Halliwell Oxidants antioxi-dants and respiratory tract lining fluids Environ Health Perspect 102 (Suppl10) (1994) 185ndash191
[84] K Takeyama K Dabbagh J Jeong Shim T Dao-Pick IF Ueki JA Nadel Oxida-tive stress causes mucin synthesis via transactivation of epidermal growth factorreceptor role of neutrophils J Immunol 164 (2000) 1546ndash1552
[85] N Ballatori SM Krance S Notenboom S Shi K Tieu CL Hammond Glutathi-one dysregulation and the etiology and progression of human diseases BiolChem 390 (2009) 191ndash214
[86] SR Soltaninassab KR Sekhar MJ Meredith ML Freeman Multi-faceted regu-lation of gamma-glutamylcysteine synthetase J Cell Physiol 182 (2000)163ndash170
[87] HR Lopez-Mirabal JR Winther Redox characteristics of the eukaryotic cytosolBiochim Biophys Acta 1783 (2008) 629ndash640
[88] C Hwang AJ Sinskey HF Lodish Oxidized redox state of glutathione in the en-doplasmic reticulum Science 257 (1992) 1496ndash1502
[89] M Murphy Mitochondrial thiols in antioxidant protection and redox signallingdistinct roles for glutathionylation and other thiol modifications AntioxidRedox Signal (2011) ahead of print doi101089ars20114289
[90] BJ Day AM van Heeckeren E Min LW Velsor Role for cystic fibrosis trans-membrane conductance regulator protein in a glutathione response to bronch-opulmonary Pseudomonas infection Infect Immun 72 (2004) 2045ndash2051
[91] Y Zhang K Duan Glutathione exhibits antibacterial activity and increases tetra-cycline efficacy against Pseudomonas aeruginosa Sci China C Life Sci 52 (2009)501ndash505
[92] VM Hudson New insights into the pathogenesis of cystic fibrosis pivotal roleof glutathione system dysfunction and implications for therapy Treat RespirMed 3 (2004) 353ndash363
[93] LW Velsor A van Heeckeren BJ Day Antioxidant imbalance in the lungs ofcystic fibrosis transmembrane conductance regulator protein mutant miceAm J Physiol Lung Cell Mol Physiol 281 (2001) L31ndashL38
[94] I Kogan M Ramjeesingh C Li JF Kidd Y Wang EM Leslie SP Cole CE BearCFTR directly mediates nucleotide-regulated glutathione flux EMBO J 22(2003) 1981ndash1989
[95] NS Gould S Gauthier CT Kariya E Min J Huang DJ Brian Hypertonic salineincreases lung epithelial lining fluid glutathione and thiocyanate two protectiveCFTR-dependent thiols against oxidative injury Respir Res 11 (2010) 119
[96] VT Vasu SJ de Cruz JS Houghton KA Hayakawa BM Morrissey CE CrossJP Eiserich Evaluation of thiol-based antioxidant therapeutics in cystic fibrosissputum focus on myeloperoxidase Free Radic Res 45 (2011) 165ndash176
[97] L Roussel G Martel J Berube S Rousseau P aeruginosa drives CXCL8 synthesisvia redundant toll-like receptors and NADPH oxidase in CFTRF508 airway epi-thelial cells J Cyst Fibros 10 (2011) 107ndash113
[98] GW Lau DJ Hassett H Ran F Kong The role of pyocyanin in Pseudomonas aer-uginosa infection Trends Mol Med 10 (2004) 599ndash606
[99] R Wilson DA Sykes D Watson A Rutman GW Taylor PJ Cole Measurementof Pseudomonas aeruginosa phenazine pigments in sputum and assessment oftheir contribution to sputum sol toxicity for respiratory epithelium InfectImmun 56 (1988) 2515ndash2517
[100] M Muller Pyocyanin induces oxidative stress in human endothelial cells andmodulates the glutathione redox cycle Free Radic Biol Med 33 (2002)1527ndash1533
[101] YQ OMalley KJ Reszka BE Britigan Direct oxidation of 2prime7prime-dichlorodihy-drofluorescein by pyocyanin and other redox-active compounds independentof reactive oxygen species production Free Radic Biol Med 36 (2004)90ndash100
[102] CC Caldwell Y Chen HS Goetzmann Y Hao MT Borchers DJ Hassett LRYoung D Mavrodi L Thomashow GW Lau Pseudomonas aeruginosa exotoxinpyocyanin causes cystic fibrosis airway pathogenesis Am J Pathol 175 (2009)2473ndash2488
[103] YQ OMalley KJ Reszka DR Spitz GM Denning BE Britigan Pseudomonasaeruginosa pyocyanin directly oxidizes glutathione and decreases its levels inairway epithelial cells Am J Physiol Lung Cell Mol Physiol 287 (2004)L94ndashL103
[104] M Muller Glutathione modulates the toxicity of but is not a biologically rele-vant reductant for the Pseudomonas aeruginosa redox toxin pyocyanin FreeRadic Biol Med 50 (2011) 971ndash977
[105] R Cheluvappa R Shimmon M Dawson SN Hilmer DG Le Couteur Reactionsof Pseudomonas aeruginosa pyocyanin with reduced glutathione Acta BiochimPol 55 (2008) 571ndash580
[106] JH Widdicombe Transgenic animals may help resolve a sticky situation in cys-tic fibrosis J Clin Invest 120 (2010) 3093ndash3096
[107] X Sun H Sui JT Fisher Z Yan X Liu HJ Cho NS Joo Y Zhang W Zhou Y YiJM Kinyon DC Lei-Butters MA Griffin P Naumann M Luo J Ascher KWang T Frana JJ Wine DK Meyerholz JF Engelhardt Disease phenotype ofa ferret CFTR-knockout model of cystic fibrosis J Clin Invest 120 (2010)3149ndash3160
[108] NS Joo HJ Cho M Khansaheb JJ Wine Hyposecretion of fluid from trachealsubmucosal glands of CFTR-deficient pigs J Clin Invest 120 (2010) 3161ndash3166
[109] A Bragonzi Murine models of acute and chronic lung infection with cystic fibro-sis pathogens IJMM 300 (2010) 584ndash593
[110] AM van Heeckeren MD Schluchter Murine models of chronic Pseudomonasaeruginosa lung infection Lab Anim 36 (2002) 291ndash312
[111] A Bragonzi D Worlitzsch GB Pier P Timpert M Ulrich M Hentzer JB Ander-sen M Givskov M Conese G Doring Nonmucoid Pseudomonas aeruginosa ex-presses alginate in the lungs of patients with cystic fibrosis and in a mousemodel J Infect Dis 192 (2005) 410ndash419
[112] GS CW Bedrossian DB Singer JJ Hansen HS Rosenberg The lung in cysticfibrosis A quantitative study including prevalence of pathologic findingsamong different age groups Hum Pathol 7 (1976) 195ndash204
[113] WD HA Cash B McCullough WG Johanson Jr JA Bass A rat model of chron-ic respiratory infection with Pseudomonas aeruginosa Am Rev Respir Dis 119(1979) 453ndash459
[114] EM JR Starke C Langston CJ Baker A mouse model of chronic pulmonary in-fection with Pseudomonas aeruginosa and Pseudomonas cepacia Pediatr Res 22(1987) 698ndash702
[115] TJ AM van Heeckeren RW Walenga MW Konstan PB Davis B ErokwuMA Haxhiu TW Ferkol Effect of Pseudomonas infection on weight loss lung
710 F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
mechanics and cytokines in mice Am J Respir Crit Care Med 161 (2000)271ndash279
[116] T Aw G Wierzbicka DP Jones Oral glutathione increases tissue glutathione invivo Chem Biol Interact 80 (1991) 89ndash97
[117] F Favilli P Marraccini T Iantomasi MT Vincenzini Effect of orally adminis-tered glutathione on glutathione levels in some organs of rats role of specifictransporters Br J Nutr 78 (1997) 293ndash300
[118] C Kariya H Leitner E Min C van Heeckeren A van Heeckeren BJ Day A rolefor CFTR in the elevation of glutathione levels in the lung by oral glutathione ad-ministration Am J Physiol Lung Cell Mol Physiol 292 (2007) L1590ndashL1597
[119] K Atkuri JJ Mantovani LA Herzenberg LA Herzenberg N-Acetylcysteinemdashasafe antidote for cysteineglutathione deficiency Curr Opin Pharmacol 7(2007) 355ndash359
[120] R De Lisle E Roach K Jansson Effects of laxative and N-acetylcysteine onmucus accumulation bacterial load transit and inflammation in the cystic fi-brosis mouse small intestine Am J Physiol Gastrointest Liver Physiol 293(2007) G577ndashG584
[121] A Luciani VR Villella S Esposito N Brunetti-Pierri D Medina C Settembre MGavina L Pulze I Giardino M Pettoello-Mantovani M DApolito S Guido EMasliah B Spencer S Quaratino V Raia A Ballabio L Maiuri Defective CFTRinduces aggresome formation and lung inflammation in cystic fibrosis throughROS-mediated autophagy inhibition Nat Cell Biol 12 863ndash875
[122] M Griese J Ramakers A Krasselt V Starosta S Van Koningsbruggen R FischerF Ratjen B Mullinger RM Huber K Maier E Rietschel G Scheuch Improve-ment of alveolar glutathione and lung function but not oxidative state in cysticfibrosis Am J Respir Crit Care Med 169 (2004) 822ndash828
[123] C Bishop VM Hudson SC Hilton C Wilde A pilot study of the effect of inhaledbuffered reduced glutathione on the clinical status of patients with cystic fibro-sis Chest 127 (2005) 308ndash317
[124] WWang C Oliva G Li A Holmgren CH Lillig KL Kirk Reversible silencing of CFTRchloride channels by glutathionylation J Gen Physiol 125 (2005) 127ndash141
[125] N Dauletbaev P Fischer B Aulbach J Gross W Kusche U Thyroff-FriesingerTO Wagner J Bargon A phase II study on safety and efficacy of high-dose N-acetylcysteine in patients with cystic fibrosis Eur J Med Res 14 (2009)352ndash358
[126] R Tirouvanziam Y Gernez CK Conrad RB Moss I Schrijver CE Dunn ZADavies LA Herzenberg Profound functional and signaling changes in viable in-flammatory neutrophils homing to cystic fibrosis airways Proc Natl Acad SciU S A 105 (2008) 4335ndash4339
[127] JH Roum Z Borok NG McElvaney GJ Grimes AD Bokser R Buhl RG Crys-tal Glutathione aerosol suppresses lung epithelial surface inflammatory cell-derived oxidants in cystic fibrosis J Appl Physiol 87 (1999) 438ndash443
[128] A Visca CT Bishop SC Hilton VM Hudson Improvement in clinical markersin CF patients using a reduced glutathione regimen an uncontrolled observa-tional study J Cyst Fibros 7 (2008) 433ndash436
[129] EF Nash A Stephenson F Ratjen E Tullis Nebulized and oral thiol derivativesfor pulmonary disease in cystic fibrosis Cochrane Database Syst Rev (2009)CD007168
[130] AC foundation Drug Development Pipeline 2011[131] S Hoshida T Kuzuya N Yamashita M Nishida S Kitahara M Hori T
Kamada M Tada Gamma-glutamylcysteine ethyl ester for myocardial protec-tion in dogs during ischemia and reperfusion J Am Coll Cardiol 24 (1994)1391ndash1397
[132] J Lok W Leung S Zhao S Pallast K van Leyen S Guo X Wang A Yalcin EHLo Gamma-glutamylcysteine ethyl ester protects cerebral endothelial cells dur-ing injury and decreases bloodndashbrain barrier permeability after experimentalbrain trauma J Neurochem 118 (2011) 248ndash255
[133] Z Borok R Buhl GJ Grimes AD Bokser RC Hubbard KJ Holroyd JH RoumDB Czerski AM Cantin RG Crystal Effect of glutathione aerosol on oxidantndashantioxidant imbalance in idiopathic pulmonary fibrosis Lancet 338 (1991)215ndash216
[134] KJ Holroyd R Buhl Z Borok JH Roum AD Bokser GJ Grimes D Czerski AMCantin RG Crystal Correction of glutathione deficiency in the lower respiratorytract of HIV seropositive individuals by glutathione aerosol treatment Thorax 48(1993) 985ndash989
[135] J Hull P Vervaart K Grimwood P Phelan Pulmonary oxidative stress responsein young children with cystic fibrosis Thorax 52 (1997) 557ndash560
[136] A Corti A Paolicchi M Franzini S Dominici AF Casini A Pompella The S-thiolating activity of membrane gamma-glutamyltransferase formation ofcysteinyl-glycine mixed disulfides with cellular proteins and in the cell microen-vironment Antioxid Redox Signal 7 (2005) 911ndash918
[137] A Corti M Franzini AF Casini A Paolicchi A Pompella Vitamin C supply tobronchial epithelial cells linked to glutathione availability in elfmdasha role for se-creted gamma-glutamyltransferase J Cyst Fibros 7 (2008) 174ndash178
[138] A Munck Nutritional considerations in patients with cystic fibrosis Expert RevRespir Med 4 (2010) 47ndash56
[139] JL Matel CE Milla Nutrition in cystic fibrosis Semin Respir Crit Care Med 30(2009) 579ndash586
[140] D Salvatore R Buzzetti E Baldo MP Forneris V Lucidi D Manunza IMarinelli B Messore AS Neri V Raia ML Furnari G Mastella An overviewof international literature from cystic fibrosis registries 2 Neonatal screeningand nutritiongrowth J Cyst Fibros 9 (2010) 75ndash83
[141] KF Joosten JM Hulst Malnutrition in pediatric hospital patients current is-sues Nutrition 27 (2011) 133ndash137
[142] S Fustik T Jacovska L Spirevska S Koceva Protein-energy malnutrition as thefirst manifestation of cystic fibrosis in infancy Pediatr Int 51 (2009) 678ndash683
[143] J Himmelfarb E McMonagle Albumin is the major plasma protein target of ox-idant stress in uremia Kidney Int 60 (2001) 358ndash363
[144] P Stenvinkel JJ Carrero J Axelsson B Lindholm O Heimburger Z MassyEmerging biomarkers for evaluating cardiovascular risk in the chronic kidneydisease patient how do new pieces fit into the uremic puzzle Clin J Am SocNephrol 3 (2008) 505ndash521
[145] M Roche P Rondeau NR Singh E Tarnus E Bourdon The antioxidant proper-ties of serum albumin FEBS Lett 582 (2008) 1783ndash1787
[146] D Giustarini A Milzani I Dalle-Donne R Rossi Red blood cells as a physiolog-ical source of glutathione for extracellular fluids Blood Cells Mol Dis 40 (2008)174ndash179
[147] A Meister ME Anderson Glutathione Annu Rev Biochem 52 (1983) 711ndash760[148] B Alvarez S Carballal L Turell R Radi Formation and reactions of sulfenic acid
in human serum albumin Methods Enzymol 473 (2010) 117ndash136[149] S Carballal B Alvarez L Turell H Botti BA Freeman R Radi Sulfenic acid in
human serum albumin Amino Acids 32 (2007) 543ndash551[150] LR Barclay AM Bailey D Kong The antioxidant activity of alpha-tocopherol-
bovine serum albumin complex in micellar and liposome autoxidations J BiolChem 260 (1985) 15809ndash15814
[151] T Ishii T Ichikawa K Minoda K Kusaka S Ito Y Suzuki M Akagawa K Mochi-zuki T Goda T Nakayama Human serum albumin as an antioxidant in the ox-idation of (minus)-epigallocatechin gallate participation of reversible covalentbinding for interaction and stabilization Biosci Biotechnol Biochem 75(2011) 100ndash106
[152] F Galli S Rovidati S Benedetti U Buoncristiani C Covarelli A Floridi F Canes-trari Overexpression of erythrocyte glutathione S-transferase in uremia and di-alysis Clin Chem 45 (1999) 1781ndash1788
[153] D Borowitz RD Baker V Stallings Consensus report on nutrition for pediat-ric patients with cystic fibrosis J Pediatr Gastroenterol Nutr 35 (2002)246ndash259
[154] LJ Filer Jr SW Wright MP Manning KE Mason Absorption of alpha-tocopherol and tocopherylesters by premature and full term infants and chil-dren in health and disease Pediatrics 8 (1951) 328ndash339
[155] L Lancellotti C DOrazio G Mastella G Mazzi U Lippi Deficiency of vitamins Eand A in cystic fibrosis is independent of pancreatic function and current en-zyme and vitamin supplementation Eur J Pediatr 155 (1996) 281ndash285
[156] MN Sathe AS Patel Update in pediatrics focus on fat-soluble vitamins NutrClin Pract 25 (2010) 340ndash346
[157] MG Traber The ABCs of vitamin E and beta-carotene absorption Am J ClinNutr 80 (2004) 3ndash4
[158] TF Dolan Jr Hemolytic anemia and edema as the initial signs in infants withcystic fibrosis Consider this diagnosis even in absence of pulmonary symptomsClin Pediatr 15 (1976) 597ndash600
[159] DR James M Alfaham MC Goodchild Increased susceptibility to peroxide-induced haemolysis with normal vitamin E concentrations in cystic fibrosisClin Chim Acta 204 (1991) 279ndash290
[160] SA Peters FJ Kelly Vitamin E supplementation in cystic fibrosis J Pediatr Gas-troenterol Nutr 22 (1996) 341ndash345
[161] A Maqbool VA Stallings Update on fat-soluble vitamins in cystic fibrosis CurrOpin Pulm Med 14 (2008) 574ndash581
[162] SD Sagel MK Sontag MM Anthony P Emmett KA Papas Effect of anantioxidant-rich multivitamin supplement in cystic fibrosis J Cyst Fibros 10(2011) 31ndash36
[163] F Galli A Azzi Present trends in vitamin E research Biofactors 36 (2010)33ndash42
[164] A Hamahata P Enkhbaatar ER Kraft M Lange SW Leonard MG Traber RACox FC Schmalstieg HK Hawkins EB Whorton EM Horvath C Szabo LDTraber DN Herndon DL Traber Gamma-tocopherol nebulization by a lipidaerosolization device improves pulmonary function in sheep with burn andsmoke inhalation injury Free Radic Biol Med 45 (2008) 425ndash433
[165] JP Anais N Razzouq M Carvalho C Fernandez A Astier M Paul A AstierH Fessi AM Lorino Development of alpha-tocopherol acetate nanoparti-cles influence of preparative processes Drug Dev Ind Pharm 35 (2009)216ndash223
[166] JM Zingg Molecular and cellular activities of vitamin E analogues Mini RevMed Chem 7 (2007) 543ndash558
[167] V Viola F Pilolli M Piroddi E Pierpaoli F Orlando M Provinciali M Betti FMazzini F Galli Why tocotrienols work better insights into the in vitro anti-cancer mechanism of vitamin E Genes Nutr 7 (2011) 29ndash41
[168] F Galli F Mazzini L Bamonti L Gille S Bohmdorfer M Piroddi T Netscher FJKelly T Rosenau Tocotrienamines and tocopheramines reactions with radicalsand metal ions Bioorg Med Chem 19 (2011) 6483ndash6491
[169] A Kuhad K Chopra Attenuation of diabetic nephropathy by tocotrienol in-volvement of NFκB signaling pathway Life Sci 84 (2009) 296ndash301
[170] Q Jiang X Yin MA Lill ML Danielson H Freiser J Huang Long-chain carbox-ychromanols metabolites of vitamin E are potent inhibitors of cyclooxygenasesProc Natl Acad Sci U S A 105 (2008) 20464ndash20469
[171] ER Miller III R Pastor-Barriuso D Dalal RA Riemersma LJ Appel E GuallarMeta-analysis high-dosage vitamin E supplementation may increase all-causemortality Ann Intern Med 142 (2005) 37ndash46
[172] JN Hathcock A Azzi J Blumberg T Bray A Dickinson B Frei I Jialal CSJohnston FJ Kelly K Kraemer L Packer S Parthasarathy H Sies MG TraberVitamins E and C are safe across a broad range of intakes Am J Clin Nutr 81(2005) 736ndash745
[173] R Brigelius-Flohe F Galli Vitamin E a vitamin still awaiting the detection of itsbiological function Mol Nutr Food Res 54 (2010) 583ndash587
711F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
[174] MG Traber B Frei JS Beckman Vitamin E revisited do new data validate ben-efits for chronic disease prevention Curr Opin Lipidol 19 (2008) 30ndash38
[175] F Galli Meeting report Vitamin E Satellite Symposium (VESS) associated to theAnnual Meeting of the SFRR-Europe Rome 26 August 2009 Free Radic Res 43(2009) 1256ndash1257
[176] LJ Roberts II JA Oates MF Linton S Fazio BP Meador MD Gross Y Shyr JDMorrow The relationship between dose of vitamin E and suppression of oxida-tive stress in humans Free Radic Biol Med 43 (2007) 1388ndash1393
[177] EFSA- EFSA Scientific Opinion of the Panel on Food Additives FlavouringsProcessing Aids and Materials in Contact with Food on a request from the Com-mission on mixed tocopherols tocotrienol tocopherol and tocotrienols assources for vitamin E in EFSA- EFSA (Ed) vol 640 The EFSA Journal2008 pp 1ndash34
[178] P Rust I Eichler S Renner I Elmadfa Long-term oral beta-carotene supple-mentation in patients with cystic fibrosis mdash effects on antioxidative status andpulmonary function Ann Nutr Metab 44 (2000) 30ndash37
[179] G Lepage J Champagne N Ronco A Lamarre I Osberg RJ Sokol CC Roy Sup-plementation with carotenoids corrects increased lipid peroxidation in childrenwith cystic fibrosis Am J Clin Nutr 64 (1996) 87ndash93
[180] BM Winklhofer-Roob H Puhl G Khoschsorur MA vant Hof H EsterbauerDH Shmerling Enhanced resistance to oxidation of low density lipoproteinsand decreased lipid peroxide formation during beta-carotene supplementationin cystic fibrosis Free Radic Biol Med 18 (1995) 849ndash859
[181] RC Graham-Maar JI Schall N Stettler BS Zemel VA Stallings Elevated vita-min A intake and serum retinol in preadolescent children with cystic fibrosisAm J Clin Nutr 84 (2006) 174ndash182
[182] I Sadowska-Woda M Rachel J Pazdan E Bieszczad-Bedrejczuk K PawliszakNutritional supplement attenuates selected oxidative stress markers in pediatricpatients with cystic fibrosis Nutr Res (New York NY) 31 (2011) 509ndash518
[183] KA Papas MK Sontag C Pardee RJ Sokol SD Sagel FJ Accurso JS WagenerA pilot study on the safety and efficacy of a novel antioxidant rich formulation inpatients with cystic fibrosis J Cyst Fibros 7 (2008) 60ndash67
[184] Y Saito A Fukuhara K Nishio M Hayakawa Y Ogawa H Sakamoto K Fujii YYoshida E Niki Characterization of cellular uptake and distribution of coen-zyme Q10 and vitamin E in PC12 cells J Nutr Biochem 20 (2009) 350ndash357
[185] AA Franke CM Morrison JL Bakke LJ Custer X Li RV Cooney CoenzymeQ10 in human blood native levels and determinants of oxidation during proces-sing and storage Free Radic Biol Med 48 (2010) 1610ndash1617
[186] HN Bhagavan RK Chopra Plasma coenzyme Q10 response to oral ingestion ofcoenzyme Q10 formulations Mitochondrion 7 (2007) S78ndashS88 (Suppl)
[187] HN Bhagavan RK Chopra Coenzyme Q10 absorption tissue uptake metabo-lism and pharmacokinetics Free Radic Res 40 (2006) 445ndash453
[188] F Galli R Lee C Dunster FJ Kelly Gas chromatography mass spectrometryanalysis of carboxyethyl-hydroxychroman metabolites of alpha- and gamma-tocopherol in human plasma Free Radic Biol Med 32 (2002) 333ndash340
[189] F Galli R Lee J Atkinson A Floridi FJ Kelly Gamma-tocopherol biokineticsand transformation in humans Free Radic Res 37 (2003) 1225ndash1233
[190] TA Laguna MK Sontag I Osberg JS Wagener FJ Accurso RJ Sokol De-creased total serum coenzyme-Q10 concentrations a longitudinal study in chil-dren with cystic fibrosis J Pediatr 153 (2008) 402ndash407
[191] T Frischer JK Myung G Maurer I Eichler Z Szepfalusi G Lubec Possible dys-regulation of chaperon and metabolic proteins in cystic fibrosis bronchial tissueProteomics 6 (2006) 3381ndash3388
[192] C Andersson MM Zaman AB Jones SD Freedman Alterations in immune re-sponse and PPARLXR regulation in cystic fibrosis macrophages J Cyst Fibros 7(2008) 68ndash78
[193] SD Freedman PG Blanco MM Zaman JC Shea M Ollero IK Hopper DAWeed A Gelrud MM Regan M Laposata JG Alvarez BP OSullivan Associa-tion of cystic fibrosis with abnormalities in fatty acid metabolism N Engl JMed 350 (2004) 560ndash569
[194] S Van Biervliet G Vanbillemont JP Van Biervliet D Declercq E Robberecht AChristophe Relation between fatty acid composition and clinical status or geno-type in cystic fibrosis patients Ann Nutr Metab 51 (2007) 541ndash549
[195] SD Freedman MH Katz EM Parker M Laposata MY Urman JG AlvarezA membrane lipid imbalance plays a role in the phenotypic expression ofcystic fibrosis in cftr(minusminus) mice Proc Natl Acad Sci U S A 96 (1999)13995ndash14000
[196] S Van Biervliet S Vande Velde JP Van Biervliet E Robberecht The effect ofzinc supplements in cystic fibrosis patients Ann Nutr Metab 52 (2008)152ndash156
[197] WR Henderson Jr SJ Astley MM McCready P Kushmerick S Casey JWBecker BW Ramsey Oral absorption of omega-3 fatty acids in patients withcystic fibrosis who have pancreatic insufficiency and in healthy control subjectsJ Pediatr 124 (1994) 400ndash408
[198] I Durieu E Vericel D Guichardant H Roth JP Steghens J Drai RN JosserandE Fontaine M Lagarde G Bellon Fatty acids platelets and oxidative markersfollowing intravenous n-3 fatty acids administration in cystic fibrosis an openpilot observational study J Cyst Fibros 6 (2007) 320ndash326
[199] LG Wood DA Fitzgerald ML Garg Hypothesis vitamin E complements poly-unsaturated fatty acids in essential fatty acid deficiency in cystic fibrosis J AmColl Nutr 22 (2003) 253ndash257
[200] JD Lloyd-Still SB Johnson RT Holman Essential fatty acid status in cystic fi-brosis and the effects of safflower oil supplementation Am J Clin Nutr 34(1981) 1ndash7
[201] A Maqbool JI Schall JF Garcia-Espana BS Zemel B Strandvik VAStallings Serum linoleic acid status as a clinical indicator of essential fatty
acid status in children with cystic fibrosis J Pediatr Gastroenterol Nutr 47(2008) 635ndash644
[202] C Oliver N Jahnke Omega-3 fatty acids for cystic fibrosis Cochrane DatabaseSyst Rev (2011) CD002201
[203] B Strandvik E Gronowitz F Enlund T Martinsson J Wahlstrom Essential fattyacid deficiency in relation to genotype in patients with cystic fibrosis J Pediatr139 (2001) 650ndash655
[204] P Rise S Volpi C Colombo RF Padoan C DOrazio S Ghezzi PMelotti V BennatoC Agostoni BM Assael C Galli Whole blood fatty acid analysis with micromethodin cystic fibrosis and pulmonary disease J Cyst Fibros 9 (2010) 228ndash233
[205] H Cao K Gerhold JR Mayers MM Wiest SM Watkins GS Hotamisligil Iden-tification of a lipokine a lipid hormone linking adipose tissue to systemic me-tabolism Cell 134 (2008) 933ndash944
[206] RR Malapaka SK Khoo J Zhang JH Choi XE Zhou Y Xu Y Gong J Li ELYong MJ Chalmers L Chang JH Resau PR Griffin YE Chen HE Xu Iden-tification and mechanism of a ten carbon fatty acid as a modulating ligand ofperoxisome proliferator activated receptors J Biol Chem 287 (2012)183ndash195
[207] T Hara A Hirasawa A Ichimura I Kimura G Tsujimoto Free fatty acid recep-tors FFAR1 and GPR120 as novel therapeutic targets for metabolic disorders JPharm Sci 100 (2011) 3594ndash3601
[208] R Gupta P Rathi S Bradoo Lipase mediated upgradation of dietary fats andoils Crit Rev Food Sci Nutr 43 (2003) 635ndash644
[209] BH Jennings CC Akoh Lipase-catalyzed modification of rice bran oil to incor-porate capric acid J Agric Food Chem 48 (2000) 4439ndash4443
[210] J Hoeks M Mensink MK Hesselink K Ekroos P Schrauwen Long- andMedium-Chain Fatty Acids Induce Insulin Resistance to a Similar Extent inHumans Despite Marked Differences in Muscle Fat Accumulation J Clin Endo-crinol Metab 97 (2012) 208ndash216
[211] PJ Congden G Bruce MM Rothburn PC Clarke JM Littlewood J KelleherMS Losowsky Vitamin status in treated patients with cystic fibrosis ArchDis Child 56 (1981) 708ndash714
[212] BM Winklhofer-Roob H Ellemunter M Fruhwirth SE Schlegel-Haueter GKhoschsorur MA vant Hof DH Shmerling Plasma vitamin C concentrationsin patients with cystic fibrosis evidence of associations with lung inflammationAm J Clin Nutr 65 (1997) 1858ndash1866
[213] L Shamseer D Adams N Brown JA Johnson S Vohra Antioxidant micronutri-ents for lung disease in cystic fibrosis Cochrane Database Syst Rev (2010)CD007020
[214] C Santi S Santoro Electrophilic Selenium First edition Wiley-VCH VerlagGmbH amp Co KGaA 2012
[215] L Flohe S Toppo G Cozza F Ursini A comparison of thiol peroxidase mecha-nisms Antioxid Redox Signal 15 (2010) 763ndash780
[216] L Flohe JR Andreesen R Brigelius-Flohe M Maiorino F Ursini Selenium theelement of the moon in life on earth IUBMB Life 49 (2000) 411ndash420
[217] V Valdiglesias E Pasaro J Mendez B Laffon In vitro evaluation of seleniumgenotoxic cytotoxic and protective effects a review Arch Toxicol 84(2010) 337ndash351
[218] P Foucaud P Therond M Marchand F Brion JF Demelier J Navarro Seleniumand vitamin E in mucoviscidosis Arch Fr Pediatr 45 (1988) 383ndash386
[219] J Neve R Van Geffel M Hanocq L Molle Plasma and erythrocyte zinc copperand selenium in cystic fibrosis Acta Paediatr Scand 72 (1983) 437ndash440
[220] BM Winklhofer-Roob B Tiran PE Tuchschmid MA vant Hof DH ShmerlingEffects of pancreatic enzyme preparations on erythrocyte glutathione peroxi-dase activities and plasma selenium concentrations in cystic fibrosis FreeRadic Biol Med 25 (1998) 242ndash249
[221] JD Lloyd-Still HE Ganther Selenium and glutathione peroxidase levels in cys-tic fibrosis Pediatrics 65 (1980) 1010ndash1012
[222] D Tsavachidou TJ McDonnell S Wen X Wang F Vakar-Lopez LL Pisters CAPettaway CG Wood KA Do PF Thall C Stephens E Efstathiou R Taylor DGMenter P Troncoso SM Lippman CJ Logothetis J Kim Selenium and vitaminE cell type- and intervention-specific tissue effects in prostate cancer J NatlCancer Inst 101 (2009) 306ndash320
[223] IN Zelko TJ Mariani RJ Folz Superoxide dismutase multigene family acomparison of the CuZn-SOD (SOD1) Mn-SOD (SOD2) and EC-SOD (SOD3)gene structures evolution and expression Free Radic Biol Med 33 (2002)337ndash349
[224] RP Bowler JD Crapo Oxidative stress in airways is there a role for extracellu-lar superoxide dismutase Am J Respir Crit Care Med 166 (2002) S38ndashS43
[225] K Best K McCoy S Gemma RA Disilvestro Copper enzyme activities in cysticfibrosis before and after copper supplementation plus or minus zinc Metabo-lism 53 (2004) 37ndash41
[226] SS Percival GP Kauwell E Bowser M Wagner Altered copper status in adultmen with cystic fibrosis J Am Coll Nutr 18 (1999) 614ndash619
[227] NF Krebs JE Westcott TD Arnold BM Kluger FJ Accurso LV Miller KMHambidge Abnormalities in zinc homeostasis in young infants with cystic fibro-sis Pediatr Res 48 (2000) 256ndash261
[228] D Easley N Krebs M Jefferson L Miller J Erskine F Accurso KM HambidgeEffect of pancreatic enzymes on zinc absorption in cystic fibrosis J Pediatr Gas-troenterol Nutr 26 (1998) 136ndash139
[229] S Van Biervliet JP Van Biervliet E Robberecht Serum zinc in patients with cys-tic fibrosis at diagnosis and after one year of therapy Biol Trace Elem Res 112(2006) 205ndash211
[230] S Van Biervliet JP Van Biervliet S Vande Velde E Robberecht Serum zinc con-centrations in cystic fibrosis patients aged above 4 years a cross-sectional eval-uation Biol Trace Elem Res 119 (2007) 19ndash26
712 F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
[231] F Galli M Cristina Polidori W Stahl P Mecocci FJ Kelly Vitamin E biotransfor-mation in humans Vitam Horm 76 (2007) 263ndash280
[232] J Wiser NE Alexis Q Jiang W Wu C Robinette R Roubey DB Peden In vivogamma-tocopherol supplementation decreases systemic oxidative stress andcytokine responses of human monocytes in normal and asthmatic subjectsFree Radic Biol Med 45 (2008) 40ndash49
[233] JG Wagner Q Jiang JR Harkema B Illek DD Patel BN Ames DB PedenOzone enhancement of lower airway allergic inflammation is prevented bygamma-tocopherol Free Radic Biol Med 43 (2007) 1176ndash1188
[234] JT Harries DP Muller Absorption of different doses of fat soluble and watermiscible preparations of vitamin E in children with cystic fibrosis Arch DisChild 46 (1971) 341ndash344
[235] EI Back C Frindt E Ocenaskova D Nohr M Stern HK Biesalski Can changesin hydrophobicity increase the bioavailability of alpha-tocopherol Eur J Nutr45 (2006) 1ndash6
[236] SZ Nasr MH OLeary C Hillermeier Correction of vitamin E deficiency withfat-soluble versus water-miscible preparations of vitamin E in patients with cys-tic fibrosis J Pediatr 122 (1993) 810ndash812
[237] S Soltani-Frisk E Gronowitz H Andersson B Strandvik Water-miscibletocopherol is not superior to fat-soluble preparation for vitamin E absorptionin cystic fibrosis Acta Paediatr 90 (2001) 1112ndash1115
[238] K Papas J Kalbfleisch R Mohon Bioavailability of a novel water-soluble vi-tamin E formulation in malabsorbing patients Dig Dis Sci 52 (2007)347ndash352
[239] F Antonicelli M Parmentier EM Drost N Hirani I Rahman K Donaldson WMacNee Nacystelyn inhibits oxidant-mediated interleukin-8 expression andNF-kappaB nuclear binding in alveolar epithelial cells Free Radic Biol Med 32(2002) 492ndash502
[240] EM App D Baran I Dab A Malfroot M Coffiner F Vanderbist M King Dose-finding and 24-h monitoring for efficacy and safety of aerosolized Nacystelyn incystic fibrosis Eur Respir J 19 (2002) 294ndash302
[241] MG Traber How much vitamin E hellip Just enough Am J Clin Nutr 84 (2006)959ndash960
[242] JC McCann BN Ames Vitamin K an example of triage theory is micronu-trient inadequacy linked to diseases of aging Am J Clin Nutr 90 (2009)889ndash907
[243] M Fusaro G Crepaldi S Maggi F Galli A DAngelo L Calo S Giannini DMiozzo M Gallieni Vitamin K bone fractures and vascular calcifications inchronic kidney disease an important but poorly studied relationship J Endocri-nol Invest 34 (2010) 317ndash323
[244] JC McCann BN Ames Adaptive dysfunction of selenoproteins from the per-spective of the triage theory why modest selenium deficiency may increaserisk of diseases of aging FASEB J 25 (2011) 1793ndash1814
[245] R Apak K Guclu M Ozyurek B Bektas Oglu M Bener Cupric ion reducing an-tioxidant capacity assay for food antioxidants vitamins polyphenolics and fla-vonoids in food extracts Methods Mol Biol 477 (2008) 163ndash193
[246] F Galli Interactions of polyphenolic compounds with drug disposition and me-tabolism Curr Drug Metab 8 (2007) 830ndash838
[247] RL Prior X Wu K Schaich Standardized methods for the determination of an-tioxidant capacity and phenolics in foods and dietary supplements J Agric FoodChem 53 (2005) 4290ndash4302
[248] C Azbell S Zhang D Skinner J Fortenberry EJ Sorscher BA WoodworthHesperidin stimulates cystic fibrosis transmembrane conductance regulator-mediated chloride secretion and ciliary beat frequency in sinonasal epitheliumOtolaryngol Head Neck Surg 143 (2010) 397ndash404
[249] G Wegrzyn J Jakobkiewicz-Banecka M Gabig-Ciminska E Piotrowska M Nar-ajczyk A Kloska M Malinowska D Dziedzic I Golebiewska M Moskot AWegrzyn Genistein a natural isoflavone with a potential for treatment of ge-netic diseases Biochem Soc Trans 38 (2010) 695ndash701
[250] YC Yu H Miki Y Nakamura A Hanyuda Y Matsuzaki Y Abe M Yasui K Ta-naka TC Hwang SG Bompadre Y Sohma Curcumin and genistein additivelypotentiate G551D-CFTR J Cyst Fibros 10 (2011) 243ndash252
[251] B Illek H Fischer Flavonoids stimulate Cl conductance of human airway epithe-lium in vitro and in vivo Am J Physiol 275 (1998) L902ndashL910
[252] JL Kreindler Cystic fibrosis exploiting its genetic basis in the hunt for newtherapies Pharmacol Ther 125 (2010) 219ndash229
[253] B Illek L Zhang NC Lewis RB Moss JY Dong H Fischer Defective function ofthe cystic fibrosis-causing missense mutation G551D is recovered by genisteinAm J Physiol 277 (1999) C833ndashC839
[254] P Anandakumar S Kamaraj S Jagan G Ramakrishnan R Vinodhkumar TDevaki Capsaicin modulates pulmonary antioxidant defense system during ben-zo(a)pyrene-induced lung cancer in Swiss albinomice Phytother Res 22 (2008)529ndash533
[255] I Rahman Antioxidant therapeutic advances in COPD Ther Adv Respir Dis 2(2008) 351ndash374
[256] AW Boots H Li RP Schins R Duffin JW Heemskerk A Bast GR Haenen Thequercetin paradox Toxicol Appl Pharmacol 222 (2007) 89ndash96
[257] M Joskova S Franova V Sadlonova Acute bronchodilator effect of quercetin inexperimental allergic asthma Bratisl Lek Listy 112 (2011) 9ndash12
[258] HJ Park CM Lee ID Jung JS Lee YI Jeong JH Chang SH Chun MJ Kim IWChoi SC Ahn YK Shin SR Yeom YM Park Quercetin regulates Th1Th2 balancein a murine model of asthma Int Immunopharmacol 9 (2009) 261ndash267
[259] AP Rogerio A Kanashiro C Fontanari EV da Silva YM Lucisano-ValimEG Soares LH Faccioli Anti-inflammatory activity of quercetin and iso-quercitrin in experimental murine allergic asthma Inflamm Res 56 (2007)402ndash408
[260] M Muller Polyphenol cytotoxicity induced by the bacterial toxin pyocyaninrole of NQO1 Free Radic Biol Med 47 (2009) 84ndash91
[261] J Grassmann Terpenoids as plant antioxidants Vitam Horm 72 (2005)505ndash535
[262] P Allen Tea tree oil the science behind the antimicrobial hype Lancet 358(2001) 1245
[263] EC Dasenbrook W Checkley CA Merlo MW Konstan N Lechtzin MP BoyleAssociation between respiratory tract methicillin-resistant Staphylococcus aure-us and survival in cystic fibrosis JAMA 303 (2010) 2386ndash2392
[264] V Bezzerri M Borgatti E Nicolis I Lampronti MC Dechecchi I Mancini PRizzotti R Gambari G Cabrini Transcription factor oligodeoxynucleotides toNF-kappaB inhibit transcription of IL-8 in bronchial cells Am J Respir CellMol Biol 39 (2008) 86ndash96
[265] R Gambari M Borgatti V Bezzerri E Nicolis I Lampronti MC Dechecchi IMancini A Tamanini G Cabrini Decoy oligodeoxyribonucleotides and peptidenucleic acids-DNA chimeras targeting nuclear factor kappa-B inhibition of IL-8 gene expression in cystic fibrosis cells infected with Pseudomonas aeruginosaBiochem Pharmacol 80 (2010) 1887ndash1894
[266] M Adrian P Jeandet AC Douillet-Breuil L Tesson R Bessis Stilbene content ofmature Vitis vinifera berries in response to UV-C elicitation J Agric Food Chem48 (2000) 6103ndash6105
[267] B Paul I Masih J Deopujari C Charpentier Occurrence of resveratrol and pter-ostilbene in age-old darakchasava an ayurvedic medicine from India J Ethno-pharmacol 68 (1999) 71ndash76
[268] I Rahman Antioxidant therapies in COPD Int J Chron Obstruct Pulmon Dis 1(2006) 15ndash29
[269] M Lee S Kim OK Kwon SR Oh HK Lee K Ahn Anti-inflammatory and anti-asthmatic effects of resveratrol a polyphenolic stilbene in a mouse model ofallergic asthma Int Immunopharmacol 9 (2009) 418ndash424
[270] LG Wood PA Wark ML Garg Antioxidant and anti-inflammatory effectsof resveratrol in airway disease Antioxid Redox Signal 13 (2010)1535ndash1548
[271] KV Kiselev Perspectives for production and application of resveratrol ApplMicrobiol Biotechnol 90 (2011) 417ndash425
[272] M Shakibaei C Buhrmann A Mobasheri Resveratrol-mediated SIRT-1 interac-tions with p300 modulate receptor activator of NF-kappaB ligand (RANKL) acti-vation of NF-kappaB signaling and inhibit osteoclastogenesis in bone-derivedcells J Biol Chem 286 (2011) 11492ndash11505
[273] SF Zaidi K Ahmed T Yamamoto T Kondo K Usmanghani M Kadowaki TSugiyama Effect of resveratrol on Helicobacter pylori-induced interleukin-8 secre-tion reactive oxygen species generation and morphological changes in human gas-tric epithelial cells Biol Pharm Bull 32 (2009) 1931ndash1935
[274] JK Kundu YK Shin YJ Surh Resveratrol modulates phorbol ester-inducedpro-inflammatory signal transduction pathways in mouse skin in vivo NF-kappaB and AP-1 as prime targets Biochem Pharmacol 72 (2006)1506ndash1515
[275] NH Nam Naturally occurring NF-kappaB inhibitors Mini Rev Med Chem 6(2006) 945ndash951
[276] JM Smoliga JA Baur HA Hausenblas Resveratrol and healthmdasha comprehen-sive review of human clinical trials Mol Nutr Food Res 55 (2011) 1129ndash1141
[277] ME Juan M Maijo JM Planas Quantification of trans-resveratrol and itsmetabolites in rat plasma and tissues by HPLC J Pharm Biomed Anal 51(2010) 391ndash398
[278] JA Baur DA Sinclair Therapeutic potential of resveratrol the in vivo evidenceNat Rev 5 (2006) 493ndash506
[279] E Nicolis I Lampronti MC Dechecchi M Borgatti A Tamanini N Bianchi VBezzerri I Mancini MG Giri P Rizzotti R Gambari G Cabrini Pyrogallol anactive compound from the medicinal plant Emblica officinalis regulates expres-sion of pro-inflammatory genes in bronchial epithelial cells Int Immunophar-macol 8 (2008) 1672ndash1680
[280] E Nicolis I Lampronti MC Dechecchi M Borgatti A Tamanini V Bezzerri NBianchi M Mazzon I Mancini MG Giri P Rizzotti R Gambari G CabriniModulation of expression of IL-8 gene in bronchial epithelial cells by 5-methoxypsoralen Int Immunopharmacol 9 (2009) 1411ndash1422
[281] M Borgatti I Mancini N Bianchi A Guerrini I Lampronti D Rossi G SacchettiR Gambari Bergamot (Citrus bergamia Risso) fruit extracts and identified com-ponents alter expression of interleukin 8 gene in cystic fibrosis bronchial epithe-lial cell lines BMC Biochem 12 (2011) 15
[282] L Piccagli E Fabbri M Borgatti N Bianchi V Bezzerri I Mancini E Nicolis CMDechecchi I Lampronti G Cabrini R Gambari Virtual screening against p50NF-kappaB transcription factor for the identification of inhibitors of the NF-kappaB-DNA interaction and expression of NF-kappaB upregulated genesChemMedChem 4 (2009) 2024ndash2033
[283] L Piccagli M Borgatti E Nicolis N Bianchi I Mancini I Lampronti D VevaldiF DallAcqua G Cabrini R Gambari Virtual screening against nuclear factorkappaB (NF-kappaB) of a focus library identification of bioactive furocoumarinderivatives inhibiting NF-kappaB dependent biological functions involved incystic fibrosis Bioorg Med Chem 18 (2010) 8341ndash8349
[284] M Borgatti A Chilin L Piccagli I Lampronti N Bianchi I Mancini G Mar-zaro Da Francesco A Guiotto R Gambari Development of a novel furocou-marin derivative inhibiting NF-kappaB dependent biological functionsdesign synthesis and biological effects Eur J Med Chem 46 (2011)4870ndash4877
[285] E Georgy S Le Guellec L Vecellio E Fichant P Stordeur P Bordeau JP PerraudinFeasibility study of OSCN- and lactoferrin (Meveol) nebulization for cysticfibrosis JCyst Fibros 10 (2011) S18
713F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
[286] C Tidei M Piroddi F Galli C Santi Oxidation of thiols promoted by PhSeZnClTetrahedron Lett 53 (2012) 232ndash234
[287] L Semianrio-Vidal C van Hesuden G Mugesh ER Lazarowski Ebselen is a po-tent non-competitive inhibitor of extracellular nucleoside diphosphokinasePurinergic Signal 6 (2010) 383ndash391
[288] C ColussiMC Albertini S Coppola S Rovidati F Galli L Ghibelli H2O2-inducedblockof glycolysis as an active ADP-ribosylation reaction protecting cells from apoptosisFASEB J 14 (2000) 2266ndash2276
[289] H Xiao KL Parkin Induction of phase II enzyme activity by various seleniumcompounds Nutr Cancer 55 (2006) 210ndash223
[290] G Peluffo R Radi Biochemistry of protein tyrosine nitration in cardiovascularpathology Cardiovasc Res 75 (2007) 291ndash302
[291] B Alvarez R Radi Peroxynitrite reactivity with amino acids and proteinsAmino Acids 25 (2003) 295ndash311
[292] B Kamosinska MW Radomski M Duszyk A Radomski SF Man Nitric oxideactivates chloride currents in human lung epithelial cells Am J Physiol 272(1997) L1098ndashL1104
[293] L Chen RP Patel X Teng CA Bosworth JR Lancaster Jr S Matalon Mecha-nisms of cystic fibrosis transmembrane conductance regulator activation by S-nitrosoglutathione J Biol Chem 281 (2006) 9190ndash9199
[294] F Luchetti B CanonicoM BettiM Arcangeletti F PilolliM Piroddi L Canesi S PapaF Galli Melatonin signaling and cell protection function FASEB J 24 (2010)3603ndash3624
[295] MW Bengtsson G Jedstedt G Flemstrom Duodenal bicarbonate secretion inrats stimulation by intra-arterial and luminal guanylin and uroguanylin ActaPhysiol (Oxf) 191 (2007) 309ndash317
[296] CS Nelson JL Marino CN Allen Melatonin receptor potentiation of cyclic AMP andthe cystic fibrosis transmembrane conductance regulator ion channel J Pineal Res 26(1999) 113ndash121
[297] C de Castro-Silva VM de Bruin GM Cunha DM Nunes CAMedeiros PF de BruinMelatonin improves sleep and reduces nitrite in the exhaled breath condensate incystic fibrosismdasha randomized double-blind placebo-controlled study J Pineal Res48 (2010) 65ndash71
[298] I Hornyak E Pankotai L Kiss Z Lacza Current developments in the the-rapeutic potential of S-nitrosoglutathione an endogenous NO-donor mole-cule Curr Pharm Biotechnol (2011) Jan 11 [Epub ahead of print] - PMID21235457
[299] AH Snyder ME McPherson JF Hunt M Johnson JS Stamler B Gaston Acuteeffects of aerosolized S-nitrosoglutathione in cystic fibrosis Am J Respir CritCare Med 165 (2002) 922ndash926

694 F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
metabolism and increased susceptibility to oxidation of lipoproteinlipids in CF patients [7] Importantly an increased oxidative burdenof lung and blood lipids may produce bioactive lipid products thatfurther sustain CF symptoms Besides to 8-iso-F2α and other ana-logues with some bioactivity [74] arachidonic acid oxidation maycontribute to persistent platelet activation and pulmonary dysfunc-tion in CF via generation of bioactive isoeicosanoids [75] which pro-vides sufficient rationale for a prevention therapy with fat solubleantioxidants such as vitamin E Evidence has recently accumulatedon the systemic effects of oxysterols on various tissues and organs[76] The role of this lipid oxidation product alone or in combinationwith other factors could be further investigated in the context ofmechanisms and clinical progression of multi-organ failure of CFpatients
The impaired pancreatic and liver functions of CF patients repre-sent the underlying factor for a defective lipoprotein metabolismand hypocholesterolemia which exponentially increase the burdenof damage by cholesterol and other lipids due to reduced blood trans-port of fat-soluble antioxidants with nascent VLDL particles Besidesoxysterol accumulation plasma fatty acid composition is also affected[7] and an increased ratio between unsaturated and saturated fattyacid species may contribute to lower cellular antioxidant defenses
Altogether these findings suggest that lipid oxidation biomarkerscan provide a reliable measure of systemic and lung-specific oxidativestress in CF
Markers of protein damage are also detectable in the airways ofchildren with CF and their levels are observed to parallel the extentof neutrophilic markers and lung dysfunction [143166] Bronchoal-veolar lavage proteins undergo halogenation of Tyr residues aradical-mediated process presumably depending on MPO enzyme ac-tivity and assessed through the analysis of 3-chlorotyrosine and 3-bromotyrosine Thiocyanate and protein carbonyls are also useful bio-markers to assess the inflammation-related injury of BALF proteins inCF [1431]
3 Antioxidants in CF
31 Glutathione and its related defense system
311 Defects in GSH homeostasisOther studies have pointed to alterations in the levels of extracel-
lular antioxidants in respiratory tract lining fluids [3] In particularthe analyses of broncheoalveolar lavages (BAL) have revealed thepresence of decreased levels of GSH in the alveolar epithelial liningfluid of CF patients The normal level of extracellular GSH in thelung is 140 times that present in blood plasma and the lung is a netimporter of circulating GSH [77] As a result GSH concentration inELF is close to 400 μM whereas significantly reduced GSH levels arepresent in adult CF patients [41] Low levels of GSH have been ob-served in plasma and blood neutrophils [4178] suggesting systemicGSH dyshomeostasis in CF Moreover some studies have shown thatat the cellular level the CFTR mutation causes mitochondrial deple-tion of GSH [7980] The consequences of this defect are still difficultto be understood due to our poor knowledge about the exact func-tions of GSH in the lung but there are reasons to believe that thedecrease of GSH in the ASL contributes to lung infection and inflam-mation [4281] At the same time it must be underlined that a recentstudy has shown that the GSH content in sputum samples is higher inCF patients than in healthy people indicating that GSH deficiency inCF is restricted to the lower respiratory tract [82] Several hypotheseshave been proposed to explain such a local increase in GSH includingthe possibility that it may derive from apoptotic neutrophils The re-lease of high levels of GSH may be part of a compensatory mechanismaimed at controlling disulfide bonds-mediated aggregation of mucinsSecretions of the upper respiratory tract contain abundant levels ofthese glycosylated and cysteine-rich proteins likely playing a role in
the airway antioxidant defense Indeed these proteins are potent invitro ROS scavenges [83] and their synthesis is upregulated upon ox-idative stress via epidermal growth factor receptor (EGFR) transacti-vation [84]
GSH a major component of cellular antioxidant defenses exerts im-portant functions related to its electron-donating capacity includingprotection from the damaging effects of ROS and regulation of a pletho-ra of cellular events such as gene expression proliferation and differen-tiation apoptosis and immune response [85] GSH is synthesized by twosequential ATP-dependent reactions catalyzed by γ-glutamylcysteinesynthetase (recently renamed glutamate-cysteine ligase) andGSH syn-thetase The reaction catalyzed by γ-glutamylcysteine synthetase iethe formation of γ-glutamylcysteine from glutamate and cysteine isthe rate-limiting step in GSH synthesis and is feedback regulated byGSH itself In fact this enzyme represents an interesting case of redox-regulation of catalytic activity that is mediated by the reversible forma-tion of disulfide bonds [86] Oxidizing conditions causing GSH depletionpromote the formation of a disulfide bondbetween the catalytic and theregulatory subunits of the enzyme leading to a conformational changewhich favors the binding of glutamate In contrast physiological levelsof GSH reduce this disulfide bond thus explaining GSH feedbackinhibition
Either in intracellular or extracellular compartments GSH is pre-dominantly found in the reduced form although small amounts ofthe oxidized disulfide forms (GSSG or GSSR where a GSH moleculeis linked to a free or a protein thiol) can always be detected GSSG isproduced by the catalysis of glutathione peroxidase during thedetoxification from hydrogen peroxide and other peroxides or bythe direct reactions of GSH with electrophilic compounds such asradical species Despite the bulk of GSH synthesis occurring in thecytoplasm GSH is distributed in intracellular organelles includingthe endoplasmic reticulum mitochondria and nucleus Under physio-logical conditions the GSH to GSSG ratio in these compartments ishigh frequently gt1001 but this may change under conditions of ox-idative stress [87] A major exception is represented by the endoplas-mic reticulum where GSSG is present at much higher levels to favordisulfide bond formation [88] Interestingly the compartmentaliza-tion of GSH in separate pools within organelles allows localized alter-ations in the balance between GSH and GSSG that may haveconsiderable functional and pathological significance [89] Thiscould be particularly important in CF in view of the above mentionedstudies showing that cultured CF cells have an apparent normal GSHGSSG content but are characterized by a marked decrease in mito-chondrial GSH in association to elevated mitochondrial ROS [7980]
Different roles of high levels of GSH in the ELF may be hypothe-sized including a) preventing inflammation and tissue damage byscavenging the ROS spontaneously generated in this highly oxidizingenvironment actively produced by neutrophils during inflammationor originating from lipid peroxidation b) regulating the redox statusof membrane proteins involved in the transduction of signals leadingto changes in the expression of genes involved in the immune re-sponse c) controlling mucus viscosity by breaking disulphide bondsd) modulating the response to bacterial infections This last possibili-ty is suggested by the observation that GSH significantly increasesin the ASL of wild type mice following P aeruginosa infection where-as this response is not observed in CFTR mutant mice [90] Interest-ingly some authors have suggested the ability of GSH to control Paeruginosa growth and resistance to antibiotics although these stud-ies should be considered with some cautions due to the likely use ofunbuffered GSH [91]
Although the decreased levels of GSH in ELF could be due to in-creased consumption during inflammation-related oxidative stress[4192] GSH deficiency in CF ELF likely derives from CFTR channeldysfunction In fact comparable alterations in GSH extracellular con-tent characterize the lung of CFTR knockout mice [93] indicating thatthis defect is correlated to mutations in CFTR
695F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
In particular ELF and lung tissue from CFTR knockout (Cftr KOB6129P2-Cftrtm1Unc) and wild-type mice were compared for GSHcontent and the activities of glutathione-related enzymes [93] Inthe ELF the concentration of GSH was significantly decreased in theCftr KO mice compared to WT whereas tissue concentrations ofGSH were similar [92] In the Cftr KO lung the activities of glutathionereductase and glutathione peroxidase were increased whereas theactivity of γ-glutamyltransferase was unchanged Two indicators ofoxidative stress thiobarbituric acid reactive substances (TBARS) and8-hydroxy-2-deoxyguanosine (8-OHdG) were also increased in theCftr KO lung tissue [90] These data support the hypothesis that a mu-tation in the CFTR gene can affect the antioxidant defenses in the lungand may contribute to the exaggerated inflammatory response ob-served in CF Thereby CFTR could be considered as an importantactor of ELF antioxidant homeostasis and thus an intrinsic cause ofoxidative imbalance in CF airways of human patients as well as CftrKO mice
Moreover CFTR belongs to the MRPABC family of proteins whichincludes several GSH transporters and some in vitro studies have in-dicated that CFTR may mediate GSH export across membranes[2394] Despite these evidences there is still debate about the phys-iological implication of CFTR in GSH transport outside the cells asother studies have raised the possibility that CFTR may not actuallyconduct GSH but regulate its transport indirectly through chloridetransport [85]
312 In vitro studies suggesting a protective role of GSH in CF modelsystems
Possible protective roles of extracellular GSH in the CF lung havebeen long proposed and recent in vitro studies have provided furtherand more robust support to this clue For example it has been sug-gested that GSH may control the levels of chlorinated compoundsformed by the activity of myeloperoxidase a neutrophil-releasedprotein abundantly present in CF patients secretions [9596] and pre-vent NK-κB activation [96] Other studies have suggested that CFTRmutant cells produce higher levels of proinflammatory cytokines inresponse to P aeruginosa diffusible material with respect to wildtype cells through a mechanism involving the activation of NADPHoxidase This effect may be significantly reversed by the addition ofextracellular GSH [97]
GSH could also play an important role in protecting the lung epi-thelia from the toxic effects of pyocyanin (PCN) a redox-active exo-toxin released by P aeruginosa which is supposed to cause a varietyof deleterious effects on the airway physiology [98] PCN levels ashigh as 130 μM have been measured in pulmonary secretions of pa-tients with CF and individuals with chronic bronchiectasis [99] Atconcentrations within the range measured in the sputum from CF pa-tients PCN induces a drastic reduction of intracellular GSH [100101]promotes death of cultured cells [100] and causes pathophysiologicalalterations in the lung of wild type mice that are consistent with thechanges observed in CF patients [102] PCN toxicity likely derivesfrom its ability to accept electrons from cellular reductants and thenreact with oxygen to generate superoxide and other ROS [103] There-fore GSH deficiency is explained either by the reaction of GSH withsuch oxidants or through the direct reaction of PCN with GSH thatleads to the formation of a PCN radical [103] However the electrontransfer from GSH to PCN does not occur at neutral pH and recent ob-servations suggest that extracellular GSH provides significant protec-tion against the toxic effects of PCN [104] Moreover GSH can reactwith PCN to form a stable adduct which is likely redox inactive[105] Although the relationships between extracellular GSH andPCN are still contradictory it is worth mentioning that extracellularGSH increases to millimolar levels in the ELF of wild type miceinfected with P aeruginosa indicating that GSH may be useful to re-sist to bacterial colonization [90] Interestingly in vitro studies have
revealed that extracellular GSH inhibits the ability of Burkholderiacenocepacia to enter epithelial respiratory cells and reduces bacterialinduced expression of proinflammatory cytokines (DOrazio Pacelloand Battistoni 2011 unpublished results)
32 GSH-based antioxidant therapies
321 Preclinical studies in animal models of CFMice genetically modified for the Cftr gene along with acute and
chronic infection induced by CF-related pathogens are a key asset inCF research Although much has been learned through these CFmousemodels limitations in the ability of this species to recapitulatespontaneous lung disease and several other organ abnormalitiesseen in CF humans including few airway mucous glands have creat-ed a need for additional species on which to study CF [106] To thisend pig and ferret CF models have been generated and are currentlybeing characterized [107108] These new larger animal models havephenotypes that appear to closely resemble human CF disease seenin newborns and efforts to characterize their adult phenotypes areongoing However mice have been the dominant species by whichto study CF disease processes in vivo and develop therapies for thepast two decades including GSH-based antioxidant treatment
Despite limitations and significant species differences betweenmice and humans these models proved to be useful tools to mimicthe initial and progressive bronchopulmonary infection typical of CFpatients [109] In particular the model of chronic infection whichchallenge bacterial cells with agar as an immobilizing agent hasbeen extensively characterized and induce the long-term persistenceof the bacterial infection and lung pathology including airway inflam-mation [110111] Lung pathology associatedwith chronic experimen-tal infection resembled some aspects of the advanced chronicpulmonary disease at autopsy in CF patients [112ndash114] Both naturallyoccurring and experimental infections frequently manifest broncho-pneumonia bronchiectasis mucus plugging epithelial metaplasiafibrosis and alveolar exudates with inflammatory cells Lymphoidhyperplasia which was prominent in the infected animals was alsoa common finding in the lungs of CF patients In addition significantdifferences with regard to weight loss BAL neutrophil counts andcytokine concentrations have been detected Infected mice had arapid though transient rise in absolute neutrophil counts TNF-α IL-1β IL-6 MIP-2 and KC in bronchoalveolar lavage (BAL) [110115] Inaddition the generation of CF mice has allowed the possibility of invivo testing of novel therapies before entering in clinical trial Theseinclude the pre-clinical evaluation of antibiotics and biotechnologicaldrugs as well as of natural and synthetic anti-inflammatory agentsthat reduce the excessive recruitment of neutrophils and the progres-sive damage of the respiratory tissue by the unbalanced production ofoxidants
Regarding antioxidants GSH and its pro-drug N-acetylcysteine(NAC) remain the so far most investigated antioxidant agents in CFand several strategies have been proposed to improve systemic andlung GSH status of CF patients based on pre-clinical studies includingthe administration of nebulized GSH by inhalation or the oral supple-mentation of GSH or NAC Oral GSH administration can raise serumand lung tissue GSH levels in rodents [116117] In these studiesGSH was administered to animals dissolved in saline or PBS Thepharmacokinetic profile of an oral bolus dose of GSH (300 mgkg)was determined in mice in other studies [118] Plasma ELF BALcells and lung tissue were analyzed for GSH content There was arapid elevation in the GSH levels that peaked at 30 min in the plasmaand 60 min in the lung ELF and BAL cells after oral GSH dosing OralGSH treatment produced a selective increase in the reduced and ac-tive form of GSH in all lung compartments examined Oral GSSG treat-ment (300 mgkg) resulted in a smaller increase of GSH levels Toevaluate the role of CFTR in this process Cftr KO mice and gut-
Table 1Intervention trials on antioxidant therapy in CF patients found at ClinicalTrialsgov databasea
Rank Title PI Location Recruitment Interventions Age groups Phasesnumberenrolled
Study designsb Outcome measures Start andcompletion date
NCT ID
1 Efficacy and safety studyof inhaled GSH in CFpatients
GrieseM
Germany Completed Drugbull reduced GSH sodium salt
C|A|S II138
1 R|E2 Safetyeff3 PA4 DB (Sub Inv)5 Treatment
bull Differences between inhaled GSHand inhaled normal saline withrespect to the area under the curveof FEV1 predicted within the periodfrom baseline to week 24
bull Treatment changes with respect tothe variablesspirometry peak flowquality-of-life weightheightpercentage of neutrophilsothercell types (induced sputum) inducedsputum levels of GSHinflammatorymediators pulmonary exacerbation
Jul-07May-10
00506688
bull 09 saline (control)
2 A phase I study of inhaledsodium pyruvate for thetreatment of CF
BillingsMCE
United States Terminated Drugbull Inhaled sodium pyruvate
A|S I70
1 R|E2 Safetyeff3 PA4 DB5 Treatment
bull Assessment of safety of inhaled sodiumpyruvate in Subs with CF Subs will beevaluated for the presence of symptomsand safety laboratory measurements
bull Determination of improvement inlungs of CF Subs as determined bymeasurement of FEV1 and measurementof inflammatory markers ininduced sputum
Feb-06na
00332215
3 Inhaled GSH versusplacebo in CF
MarsicoS
Italy Recruiting Drugbull Inhaled reduced GSHbull Physiological solution
C|A III150
1 R|E2 Eff3 PA4 SB (Sub)5 Treatment
bull FEV1bull Small airway function exercise capacityBMI dyspnoea cough quality of lifepulmonary exacerbations markers ofoxidative stress (H2O2)in serum and inEBC epithelial inflammatory markerson BNEC
Jun-10Dec-12
01450267
4 Safety and efficacy ofan antioxidant-richmultivitaminsupplement in CF
SagelSD
United States Completed Dietary supplementbull AquADEKs
C|A IIndashII17
1 NR|E2 Safetyeff3 SGA4 OL5 Treatment
bull Plasma levels of β-carotenebull Plasma levels of coenzyme Q-10retinol (Vitamin A) 25-hydroxy vitaminD α- and γ-tocopherols (Vitamin E)PIVKA-II
Aug-07Nov-09
01018303
5 Efficacy and safety ofepigallocatechin gallate(EGCG)tocotrienol in18 patients with splicing-mutation-mediated CF
KeremE
Israel Not yetrecruiting
Dietary supplementbull EGCGbull Tocotrienolbull EGCG+tocotrienol
A|S na18
2 Safetyeff3 CA4 OL5 Treatment
bull Changes in nasal chloride secretion asassessed by TEPD with assessment ofmean changes in TEPD by drug comparedto baseline and the proportion of patientswith a chloride secretion response bydrug compared to baseline
bull Pulmonary function testing FEV1FVC MEF25-75
Sep-09Jun-11
00889434
6 The effect of inhaledNAC compared tonormal saline onsputum rheology andlung function
VanDaele S
Belgium Terminated Drugbull Acetyl-Cysbull Normal saline
C|A IV19
1 NR|E2 Eff3 CA4 OL5 Treatment
bull Changes in visco-elasticity andlung function
Jan-10Dec-10
00996424
696FG
allietal
Biochimica
etBiophysica
Acta
1822(2012)
690ndash713
7 Safety of orallyadministeredcurcuminoids in adultsubjects with CF
Goss C United States Completed Drugbull Standardized turmericroot extract
A I11
1 NR|E2 Safetyeff3 SGA4 OL5 Treatment
bull Safety and tolerability of 14 days oftreatment with orally administeredcurcuminoids as assessed by adverseevents laboratory parameters andspirometry
bull Pharmacokinetics of repeated dosesof orally administered curcuminoidschange in NPD measurementschange in sweat chloride measurements
Apr-05Jan-06
00219882
8 Nasal potential studiesutilizing CF transmembraneregulator (CFTR) modulators
Rowe S United States Recruiting Other quercetin C|A II46
2 Eff3 SGA4 OL5 BS
bull NPD(NPD) Biomarkerbull Residual CFTR activity
Mar-10Nov-11
01348204
9 Safety and tolerability ofinhaled nitric oxide inpatients with CF
Sagel S United States Completed Drugbull Nitric oxide for inhalationbull Nitrogen
C|A|S IIndashII18
1 R|E2 Saf3 PA4 DB (Sub Care Inv OA)5 Treatment
bull Safety and tolerability of drugassessed by change in methemoglobinlevels oxygensaturation FEV1
bull Assess the difference in sputumbacterial density before and afterNO inhalation and the differencein lower airway inflammatorymeasures before and after NO inhalation
Jul-04Dec-08
00570349
10 NAC Phase IIB a multi-center phase IIBrandomized placebo-controlled DB study ofthe effects of NAC onredox changes and lunginflammation in CF patients
ConradC
United States Completed Drugbull NAC
C|A|S II80
1 R|E2 Eff3 SGA4 DB (Sub Care Inv OA)5 Treatment
bull Change in the logarithm of the levelof human neutrophil elastase(HNE) activity measured in sputum
bull Change in concentration of IL-8measured in sputum and plasmaconcentration of GSH measured inwhole blood the neutrophil countmeasured in sputum
Nov-08Feb-11
00809094
11 Glutamine supplementationin CF
na United States Not yetrecruiting
Dietary supplementbull Glutaminebull L-alanine
A|S II40
1 R3 PA4 DB (Sub Care Inv OA)5 Prev
bull Percent increase in plasma glutamineand GSH redox levels measured atweeks 0 4 8 and 12
Feb-10Feb-11
01051999
12 Effect of sulforaphane inbroccoli sprouts onNrf2 activation
ChmielJF
United States Active notrecruiting
Dietary supplementbull Broccoli sprouts
A na15
3 SGA4 OL5 BS
bull Nrf2 activation in NECbull Measures of lipid peroxidation in NECGSH from blood lymphocytesoxidative stress in urineneutrophil migration into thegingival crevices
Apr-11Sep-11
01315665
AbbreviationsA=adult BC=breath condensate BNEC=brushed nasal epithelial cells BS=basic science C=child CA=crossover assignment Care=caregiver CF=cystic fibrosis DB=double blind EBC=exhaled breath condensate Eff=efficacystudy FEV1=forced expiratory volume in 1 s FVC=forced vital capacity GSH=glutathione Inv=investigator MEF25ndash75=maximal expiratory flow 25ndash75 na=not available NAC=N-acetylcysteine NEC=nasal epithelial cellsNLF=nasal lavage fluid NPD=nasal potential difference NR|E=non-randomized|endpoint OA=outcomes assessor OL=open label PA=parallel assignment PI=principal investigator Prev=prevention R|E=randomized|endpoint S=senior Saf=safety study SB=single blind SGA=single group assignment Sub=subject
a Search was done matching the terms ldquoantioxidant therapyrdquo or ldquoGlutathionerdquo with ldquoCystic Fibrosisrdquob 1 Allocation 2 Classification 3 Intervention model 4 Masking 5 Primary purpose
697FG
allietal
Biochimica
etBiophysica
Acta
1822(2012)
690ndash713
698 F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
corrected Cftr KO-transgenic mice were given an oral bolus dose ofGSH (300 mgkg) and compared with WT mice for changes in GSHlevels in plasma lung ELF and BAL cells There was a twofold in-crease in plasma a twofold increase in lung a fivefold increase inELF and a threefold increase in BAL cell GSH levels at 60 min in WTmice however GSH levels only increased by 40 in the plasma 60in the lung 50 in the ELF and twofold in the BAL cells within thegut-corrected Cftr KO-Tg mice No change in GSH levels was observedin the uncorrected Cftr KO mice These studies suggest that oral GSHadministration can increase plasma and lung compartment GSHlevels in WT mice and to a lesser extent in gut-corrected Cftr KO-Tganimals It also suggests that oral GSH treatment can boost BAL cellGSH levels However since this study failed to show significant in-creases in serum and lung compartment GSH levels in uncorrectedCftr KO mice it is questionable whether oral GSH administration toCF patients with intestinal malabsorption would benefit from thistherapy It was also shown that GSH is rapidly distributed to theserum and lung compartments Kariya et al [118] speculate thatother transporter(s) besides CFTR are responsible of the transport ofGSH and probably of other dietary molecules to the lung whichmay be responsible for dietary deficiencies observed in various lungdiseases
Another strategy is represented by the oral supplementation ofhigh doses of NAC a well known cysteine donor for the synthesis ofglutathione NAC is considered a safe molecule which has beenused successfully to treat GSH deficiency in a wide range of diseases[119] As CF mice display defects in GSH export in the ELF comparableto those of patients they could provide a useful tool to assess the ef-fects of NAC administration on the GSH status However only limitedstudies exploring the effects of NAC on CF animal models have beenso far carried out The effects of NAC have been tested on mucus accu-mulation bacterial load transit and inflammation in the CF mousesmall intestine showing that NAC may reduce intestinal mucus accu-mulation bacterial overgrowth in the gut [120]
Moreover NAC has been reported to restore the accumulationof unwantedmisfolded proteins in aggregates that are associated withthe CF airway phenotype as a cause of lung inflammation [121] Themechanism of this NAC-derived effect seems to involve the restorationof beclin 1 expression and activity in the autophagy pathway of theendoplasmic reticulum that was investigated in vivo using Scnn1b-transgenic and Cftr(F508del) homozygous mice The restoration ofthis pathway also produced a rescued trafficking of CFTR (F508del) tothe cell surface of CF cells obtained from human CF nasal biopsies
Given the defective GSH metabolism of CF reviewed in the previ-ous sections and in [122] and the reduced response to GSH therapyin CF mice [93] some Authors have investigated the influence of bac-terial infections on lung oxidative stress The effects of P aeruginosainfection on ELF and lung tissue antioxidants and the oxidation ofDNA and lipids were investigated in mice challenged with bacterialcells [90] CFTR-KO (B6129P2-Cftrtm1Unc) and WT mice were chal-lenged intratracheally with a clinical isolate of mucoid P aeruginosaembedded in agar beads and on the third day of infection BALF andlung tissue were obtained and analyzed for cytokines antioxidantsand enzyme activities [90] P aeruginosa lung infection increasedlevels of inflammatory cytokines and neutrophils in the ELF This cor-responded with a marked increase in GSH and in urate levels in theELF of P aeruginosa-infected WT mice A twofold increase in uratelevels was also observed among lung tissue antioxidants of Paeruginosa-infected WT mice There were no changes in markers oflung oxidative stress associated with the P aeruginosa lung infectionIn contrast to WT mice the CFTR-KO mice lacked a significant in-crease in ELF GSH when challenged with P aeruginosa and this corre-lated with a decrease in the ratio of reduced to oxidized GSH in theELF a marker of oxidative stress These data would suggest that thelung adapts to infectious agents with elevated ELF GSH and urateTherefore individuals with lung diseases associated with altered
antioxidant transport such as CF might lack the ability to adapt tothe infection which may lead to a more severe inflammatoryresponse
322 Clinical trials on GSHThe discovery of the defect in GSH export has suggested that ther-
apies able to restore or increase GSH levels in the ASL could counteractthe inflammation and oxidative stress conditions typical of CF pa-tients In an attempt to strengthen extracellular defenses againstROS some pilot studies have analyzed the effect of GSH inhalation orthat of oral GSH prodrug N-acetylcysteine (NAC) All these treatmentswere well tolerated by the CF patients and most authors were able tomeasure increased ELF concentrations of GSH in association withsome positive clinical outcomes [4041737896122ndash128] Althoughpotentially promising these findings need stronger clinical evidencein that the majority of these were obtained on very limited numberof patients investigated in non-randomized controlled trials This ishighlighted in a recently published meta-analysis [129] that providesalso a thoroughly analysis of the literature on this aspect of the antiox-idant and anti-inflammatory therapy of CF Among the American CFfoundation sponsored trials two phase II trials on inhaled GSH andoral NAC are in progress in US and Germany (ClinicalTrialsgov Iden-tifier NCT00506688 and NCT00809094 respectively Table 1) andsafety and tolerability of aerosolized glutathione is also matter ofinvestigation by another (not registered) US trial (more informationon this can be found in [130]) Nevertheless the diffusion among CFpatients of NAC preparations for inhalation (Mucomystreg) has in-creased in recent years
γ-Glutamylcysteine ethyl ester (GCEE) is another potentially inter-esting GSH pro-drug which has proved some efficacy in the ameliora-tion of oxidative stress eg in experimental myocardial infarction[131] and central nervous system conditions (see eg [132]) HoweverGCEE has not been investigated in CF yet
33 Limits and potential problems associated to thiol-based therapies
Although the above cited clinical trials may be considered promis-ing attempts to improve the antioxidant levels in the ELF the actualcapacity of these treatments to produce positive clinical effects mustbe considered with caution For example indices of oxidative damagewere found to be unaffected by aerosolized GSH treatment [122]Some in vitro studies have suggested that the reaction of GSH withPCN could produce hydrogen peroxide with potential exacerbationof oxidative damage [101] The exact mechanisms of PCN toxicityand the reaction of this toxin with GSH must be better understoodin order to evaluate the safety of GSH administration to patients col-onized by P aeruginosa
Inhalation of GSH ensures its direct delivery in the airways butsince GSH can rapidly convert to its oxidized form GSSG frequentGSH inhalations are required to maintain a high GSHGSSG As a con-sequence of this limit four separate inhalations have been used inthe study carried out by Bishop et al [123] Unless justified by clearclinical improvements these repeated treatments may represent aburden for patients already undergoing complex therapies Moreoverrepeated inhalations of GSH increase the levels of GSSG in ELF[133134] In the absence of effective homeostatic mechanisms ensur-ing the fast recycling of GSSG to GSH this might produce unwantedeffects and even the exacerbation of CF symptoms being GSSG re-sponsible of the S-glutathiolation and functional inhibition of CFTR[124]
In principle the oral administration of GSH could be considered asafe strategy to prevent GSSG accumulation but this strategy is likelynot feasible due to the substantial inability of this water-soluble mol-ecule to cross biological membranes Moreover a study carried out inmice has established that GSH absorption in the gastrointestinal tractif any is mediated by CFTR itself thus excluding the possibility to
699F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
improve circulating levels of GSH in CF patients through the dietarysupplementation of the antioxidant [127] The limited absorption ofGSH could be overcome by GSH-esters as in vitro studies haveshown that this form of GSH may be specifically useful to rescue mi-tochondrial defects in cystic fibrosis models [80] Safety of these GSHderivatives in humans has been poorly investigated
Two independent studies have shown that the treatment of CF pa-tients with high doses of NAC increases extracellular GSH in sputum[78125] but contrasting results have been reported concerning theeffects of NAC on the concentrations of blood GSH and on the levelsof IL-8 and other markers of inflammation NAC treatments may beuseful to modulate the GSH content in cells but it should be remindedthat an enhanced cysteine supply cannot lead to an increase of GSHabove physiological levels due to the feedback inhibition mechanismof γ-glutamylcysteine synthetase described in the Section 311
331 Gamma-glutamyltransferase and GSH therapySo far none of the studies mentioned above has taken into account
the fact that GSH is degraded by GGT enzyme activity GGT concentra-tions are known to increase several fold in ELF of CF patients even ifthe mechanisms for this effect were not determined [135] and thisphenomenon parallels the above described decrease of GSH levels inELF Preliminary data suggest that a major source of increased ELFGGT is represented by activated neutrophils accumulating in diseasedairways (Corti and Pompella 2011 unpublished observation) Re-gardless of its origin it is likely that increased GGT in ELF would de-grade locally administered GSH to variable extents which couldcontribute to the so far inconclusive results of therapies based onaerosolized GSH Besides its role in GSH catabolism GGT has beenshown to mediate protein S-thiolation [136] suggesting that GSH ad-ministration in the presence of active GGT enzyme might alter CFTRglutathiolation status and function in a potentially unfavorable wayOn the other hand a potential role of GGT in favoring bronchial up-take of antioxidant vitamin C has also been suggested [137]
These controversial findings may add further issues to the ques-tion of whether the therapy of lung oxidative stress by aerosolizedGSH could be safe in all the CF patients regardless of specific strate-gies that would ascertain the extent of lung inflammation Thesestrategies should include the assay of GGT levels in ELF In principleonce an adverse role of ELF GGT in GSH therapies will be confirmedthe association of GGT inhibitors in the GSH formulations for inhala-tion could represent a promising pharmacological strategy
34 Malnutrition as a possible cause of defective thiol-dependentantioxidant protection
Successful nutritional interventions strongly impact on the clinicaloutcome of CF patients [138ndash140] Malnutrition by pancreatic insuffi-ciency and other CF-related factors influence the susceptibility to de-velop recurrent infections and severe inflammatory lesions of thelung tissue If the onset of a defective (sub-optimal) antioxidant sta-tus may represent an underlying component in the clinical effects ofmalnutrition remains a matter of investigation Clinicians have topay particular care to avoid these disturbances and successful proto-cols of nutritional intervention in CF have been developed whichare essentially aimed to avoid the onset of protein-energy malnutri-tion (PEM) [141] Despite this the risk of developing such an unto-ward complication in CF infants and children remains high assuggested by the prevalence data registered in some areas Actuallya prevalence of PEM between 5 and 14 in Moldavian infants was re-cently reported [142] and PEM is associated with poor outcome andparticularly with the risk of developing edema and anemia
Besides lowered intake and absorption of micronutrient antioxi-dants discussed in the other sections malabsorption of dietary proteinand excess fecal amino acid losses result in hypoproteinemiahypoalbu-minemia as key biochemical signs of PEM Hypoalbuminemia is
considered to be linked with a causendasheffect relationship with oxidativestress and is proposed to influence morbidity and mortality in condi-tions associated with chronic inflammation and severe oxidative stress[143144] The human serum albumin (HAS) molecule contains only areactive thiol group eg the Cys 34 the importance of which as an anti-oxidant defense system in blood and for the entire organism is welldocumented [145] This is the second main thiol (and the main proteinthiol) in the circulation (approx 2 mmol in the adult organism assum-ing 5 l of total blood volume anHt of 40 and [HAS] of 45 gl of plasma)being the RBCGSH thefirst thiol in blood (near to 5 mmol assuming thesame parameters of above and an average concentration of GSH inpacked RBC of 25 mM) [146147] The antioxidant role of HSA is notonly a consequence of the relative abundance of its Cys thiol A specificcapability of acting as a sacrificial target for a series of electrophils andmost biologically relevant ROS ie hydrogen peroxide and peroxyni-trite has been demonstrated in a series of studies [145148149] Li-gand binding activity can contribute to promote antioxidant effectsby the HSA molecule [145] Transitions metals particularly copperand also iron in the case of iron-overload diseases bind to HSA Inthis way these are less available to promote the Fenton chemistryand hydroxyl radicals eventually released from this oxidative reactionare mostly directed to the HAS protein sparing more important tar-gets A free radical-trapping activity of HSA has been also demonstratedand this was proposed to be directed toward both hydrophilic and fat-soluble species This activity may result from the interaction withother antioxidants such as α-tocopherol [150] and may influence theantioxidant activity of food-derived phenolic antioxidants [151]
However Cys 34 is considered the main contributor to the antiox-idant function of HAS which plays its role in the antioxidant homeo-stasis of blood thanks to a complex series of interactions with themetabolism and antioxidant function of the pool of free thiols in plas-ma and in the circulating RBC with the latter playing a significantcontribution to the extracellular pool of GSH [146] and to the dynam-ics of inter-organ GSHmetabolism in cooperation with liver and othertissues [147] Immuno-inflammatory cells and the lung tissue areamong the main terminals of this metabolism The RBC contain theentire machinery to synthesize GSH to restore its redox (by enzymat-ic reduction of the oxidized form) and to use this as cofactor of Se-GPx and GSH-S-transferase enzymatic activities that are responsibleof the detoxification of hydroperoxides and alkylating agents thatmay form in or enter the RBC cytosol [147] In this sense the RBC rep-resents a circulating reservoir of GSH that in addition to maintainingthe redox and respiratory function of Hb participates to systemic pro-tection of xenobiotics of endogenous and exogenous origin In consid-eration of these aspects the combination of hypoalbuminemia andanemia may exponentially increase the risk of developing oxidativestress in CF patients as it is supposed to occur in other oxidative stressconditions such as chronic kidney disease [55143152] Additionalclinical investigation should verify the hypothesis that hypoalbumi-nemia together with a defective uptake and metabolism of sulfur-containing amino acids and CF-specific defects of the GSH metabo-lism may represent a causal risk factor for an impaired antioxidantdefense and systemic oxidative stress in CF patients
35 Fat-soluble antioxidants
Pancreatic insufficiency and a diminished bile acid pool cause mal-absorption of important essential nutrients and other dietary compo-nents in CF Of particular significance is the malabsorption of fat-soluble antioxidants such as tocopherols carotenoids and coenzymeQ-10 (Co-Q10) and that of essential fatty acids (EFA)
351 Vitamin EVitamin E therapy in CF has been proposed in several decades of
research as a useful approach to overcome both the lower absorptionof this fat-soluble micronutrient and the increased antioxidant
700 F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
demand by the abnormal generation of ROS in CF tissues (see for in-stance the recommendations by the Cystic Fibrosis Foundation Con-sensus Conference on nutrition [153])
The first report of a vitamin E deficiency in CF appeared in literaturein 1951 by Filer et al [154] In this study the absorption of the mainform of this vitamin eg α-tocopherol and its ester derivatives was in-vestigated in several subsets of infants and children Thanks to a simplebioavailability (or tolerance) test these authors observed that ldquoin-fantshellip diagnosed as fibrocystic disease of the pancreas diarrhea andcirrhosis were characterized by a poor response to the test ie the tol-erance curve was lowrdquo However abnormalities were also observed inother subgroups of infants with a variety of disorders not associatedwith fat or fat-soluble vitamin intolerance such as sprue celiac syn-drome and lupus erythematosus which suggests the general observa-tion that malnutrition and inflammatory and degenerative diseases ofthe GI tract may lead to absorb tocopherols poorly At the same timethese authors reported that ldquoMetabolic disorders with associated hy-percholesterolemia were observed to give abnormally high values forthe area under the curverdquo and that patients responding poorly to to-copherol absorption test did also in vitamin A absorption tests
The finding of lowered (lipid uncorrected) levels of vitamin E wasconfirmed in other studies in which this relative deficiency was foundto occur irrespective of pancreatic comorbidity and in associationwith lowered levels of other liposoluble vitamins such as vitamin Aand D [155] regardless of their different liver metabolism and tissuedelivery mechanisms [156157]
Plasma buccal mucosal cells (BMCs) and breath condensate α-tocopherol decreased significantly with age in association with a de-creased respiratory function [5] This was accompanied by loweredlevels of other antioxidants such as vitamin C and increased oxidativestress markers of different origin such as protein carbonyls thiobarbi-turic acid-reactive substances and F2-IsoPs
Clinical symptoms of vitamin E deficiency in CF have not beenconclusively investigated Dolan et al [158] described that anemiaof CF patients is related to vitamin E deficiency and increasedperoxide-induced hemolysis of RBC Other authors however ob-served an increased susceptibility to peroxide-induced hemolysisalso in the presence of normal levels of vitamin E [159] Peters andKelly [160] observed that RBC vitamin E concentrations were belowthe normal range in almost all unsupplemented patients and roseinto the normal range with a 1-year supplement of 100 mg per daybut not 15 mg per day Since RBC vitamin E concentration has beenshown to correlate well with tissue concentrations of the vitamin inanimals tissue levels of vitamin E are expected to be lower than nor-mal in CF patients
Bioavailability of fat-soluble vitamin is limited in CF Vitamin Edeficiency of CF is also associated with hypocholesterolemia [7] Asa consequence the relative deficiency of this vitamin is compensatedwhen the absolute levels are normalized for cholesterol levels andthis suggests a poor transferring of this vitamin in the circulation bya defective lipid and lipoprotein metabolism Pancreatic insufficiencyand the consequent lipid malnutrition cannot completely explain thisdefect and other possibly CF-specific dysfunctions could play a roleLiver metabolism and specific plasma transport systems of this vita-min need further elucidation in CF
As a consequence of these aspects it is not presently clear whichform and level of supplementation of this vitamin is most appropriateto treat these patients Usingα-tocopherol as a vitamin E supplementPeters et al [160] reported that 100 mg per day are required to nor-malize RBC concentrations Other authors described unsuccessfulsupplementation protocols with higher doses and this has led to de-velop formulations with higher bioavailability in order to achieve bet-ter compliance to oral supplementation (see below and the literaturereviewed in [161ndash163])
Besides absorption and tissue delivery issues specificity of actionis another critical item of antioxidant therapy with fat-soluble agents
in CF As further addressed below this aspect could be themain limit toa successful use of natural forms of vitamin E in the clinical manage-ment of CF inflammation even if a local lung-targeted therapy wouldbe developed according with so far proposed pre-clinical models ofaerosolized vitamin E [164165]
Current pharmacological research is aimed to develop synthetic formsof this and other fat-soluble antioxidants with better radical scavengingproperties at the lipidndashwater interface Type of ROS target and the sitesof action greatly influence the chances of a fat-soluble antioxidant of alle-viating oxidative stress in the airways as well as in other organs such asliver and pancreas These aspects dealing with specificity of action[163166167] have stimulated the search of novel vitamin E-derived an-tioxidants that may help to scavenge radicals at the lipidndashwater interfaceof the epithelial cell membrane and surfactant Amine derivativesof tocopherols and tocotrienols have been recently demonstrated toshow higher antioxidant and free radical scavenging activity than α-tocopherol [168] Further in vitro pharmacological analysis has includedtoxicity evaluations and the detailed investigation of scavenging of azo-and phenolic radicals with different degrees of hydrophobicity and theinhibitory activity on IL-8 gene expression and phospholipase activityin CF cells Comparative evaluation with other synthetic derivativessuch asα-tocopheryl succinate and natural forms of vitamin E suggestedthat these amine derivatives are promising antioxidant and anti-inflammatory agents [Galli F and Pilolli F unpublished observation]deserving further pre-clinical investigation in CF model systems
Anti-inflammatory effects of natural and synthetic analogues of vi-tamin E are also an intriguing pharmacological opportunity currentlyunder investigation by several laboratories [169170]
Recently vitamin E supplementation has been at the center of adispute regarding its safety when used at high dosages in certainpopulations of patients An extensive and speculative debate originat-ed on this subject after a meta-analysis study byMiller et al [171] thatexamined the largest secondary prevention trials on vitamin E trials incardiovascular patients finding a significantly increased mortality riskfor all the causes (about 4 1ndash8 in the 95 interval of confidence)when the patients were treated with doses gt400 IUdie (that areequivalent to 400 mgdie of the synthetic form allrac-α-tocopheroland to 185 mgdie of the natural form RRR-α-tocopherol) This debateresulted in a careful examination of this meta-analysis study by severalother authors and in further revisions of the literature on vitamin E tox-icity in humans [see the literature recently reviewed in [163172ndash174]]that clearly demonstrated the poor consistency of the conclusionsraisedwithMillersmeta-analysis study and the paucity of the concernsthat derived from that These conclusions have been verified in the re-cent international symposium on vitamin E of the Society for Free Rad-ical Research Europe branch of Rome 2009 [173175] Vitamin E used assupplement for humans in all its forms (eg α-tocopherol and othertocopherols and tocotrienols) is safe in abroad range of intakes[172176] The tolerable upper intake level (UL) and the AcceptableDaily Intake (ADI) established by the Joint FAOWHOExpert Committeeon Food Additives for the natural form of vitamin E as α-tocopherolequivalents are of 300 mgdie and 015ndash20 mgkg body weightdierespectively [172177]
352 CarotenoidsLevels of plasma carotenoids such as β-carotene β-cryptoxanthin
and total lycopene are significantly lowered in CF patients and thiswas associated with higher susceptibility to lipid peroxidation[5178ndash180] Rust et al [178] demonstrated that the long-term oralsupplementation with 50 mg β-caroteneday (ie 1 mg β-carotenekg BWday) restored the levels of this carotenoid while sub-optimalsupplementation was observed at doses of 10 mg β-caroteneday orlower thus confirming the need of high doses of this fat-soluble factorto overcome the limited absorption and thus to achieve plasma con-centrations of healthy control subjects Successful high-dose treat-ments appear to lower oxidative stress markers such as TBA-MDA
701F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
complexes and to correct total antioxidant capacity of plasma Inanother study β-carotene supplementation was observed to de-creased lipid peroxide formation as quantitated by malondialdehydeconcentrations in plasma (TBAHPLC method) and to enhance the re-sistance to copper(II) ion-induced oxidation of low density lipopro-teins [180]
At the same time toxicity issues have been raised for human sup-plementation with carotenoid formulations and particularly of water-miscible formulations of preformed vitamin A that is regularly sup-plemented to CF patients which may increase serum retinol andpossible risk of CF-associated liver and bone complications (reviewedin [161181]) However β-carotene supplementation seems to be safesince this does not affect plasma concentrations of other carotenoidsand retinol as well as of other fat-soluble vitamins as α- and γ-tocopherol [178] Recent studies designed to test the clinical efficacyof a CF tailored multivitamin formulation (commercial name AquA-DEKsreg) also tested the safety of this type of formulation and demon-strated that this does not increase vitamin A above the normal levelsobserved in healthy controls [162182183] The normalization of β-carotene levels obtained in these studies was associated only withminor improvements on respiratory and growth parameters whilethe levels of urinary F2-IsoPs used as index of lipid peroxidationwere not affected [162] The surrogate marker of lipid peroxidationMDA was affected together with some selected antioxidant parame-ters (RBC thiols and superoxide dismutase) in another study inwhich this multivitamin formulation was preliminarily evaluated incomparison with standard formulations of vitamin E and A [182]
353 Coenzyme Q-10Coenzyme Q-10 (Q10) is a well-known electron transporter in the
mitochondrial respiratory chain with fundamental role in cellularbioenergetics and scavenging of radical species [184] This lipophilicsubstance is present in the circulation at low levels (serum concentra-tionsle2 μM) mainly as ubiquinol-10 eg the reduced form with anapproximate ratio of 955 with the oxidized form ubiquinone-10[185186] A mechanism for a preferential distribution and accumula-tion in mitochondria has been suggested for both the reduced and ox-idized forms of CoQ10 that are taken up by the cells in a time- andconcentration-dependent Subcellular localization and trafficking ofexogenous Q10 are similar to those of the endogenous form butwere different from that of α-tocopherol that is related with lipidcomposition particularly in the mitochondrial and microsomal frac-tions [184] Ubiquinol-10 readily oxidizes ex vivo by the reactionwith other lipophilic antioxidants such as α-tocopherol and butylatedhydroxytoluene [185] Therefore a higher reduction potential thanother physiological fat-soluble antioxidants such as vitamin E and aselective metabolism and cellular trafficking show peculiar role forthe cell CoQ which may also represent an important lipophilic antiox-idant in cells and body fluids
Human cells synthesize this coenzyme through the cholesterol bio-synthesis pathway so thatmore than two thirds of the tissue levels ap-pear to have an endogenous origin dietary sources provide acontribution to Co-Q10 levels of blood and all solid tissues that variesdepending on the dose applied and type of dietary source [187] How-ever in the case of oral supplements it has to be considered that hy-drophobicity and large molecular weight of this coenzyme influenceits absorption that ultimately is slow and limited [186187] Likewiseto vitamin E pharmacokinetics [188189] Co-Q10 showed T(max) ofaround 6 h that coincides with that of dietary lipids Elimination isclose to that of the more retained form of vitamin E in human bodyeg α-tocopherol with a half-life of about 33 h which suggests poorhepatic metabolism However commercially available formulationsare reported to be safe even at high doses and solubilized formulationsshow enhanced bioavailability In healthy subjects plasma Q10 re-sponse to oral ingestion show saturation profiles with a plateau at a
dose of 2400 mg and the higher plasma concentrations were foundto facilitate uptake by peripheral tissues and also the brain [186187]
Laguna et al [190] recently investigated total serum levels ofcoenzyme Q-10 in a wide population of CF children (n=381) and esti-mated their association with clinical outcome Near to 50 of these CFpatients were deficient of Co-Q10 and this defect was significantlymore prevalent in patients with pancreatic insufficiency and signifi-cantly associated with P aeruginosa colonization in infants (under24 months of age) Importantly low Co-Q10 levels correlated to otherlipid markers of a poor nutritional status such as total lipids and alsothe other fat-soluble antioxidants β-carotene and α-tocopherolwhich confirms the presence of a common defect in the absorptionand metabolic pathways of this coenzyme with dietary lipids
The deficit of Co-Q10 may contribute to the impaired energy func-tion of mitochondria of CF tissues and this may exacerbate CF-linkedinflammation infection and cellular stress response of the lung A sys-tematic analysis of molecular lesions in CF bronchial tissue has beenrecently carried out by proteomic approach [191] Comparative eval-uation of protein expressional pattern in CF and healthy controltissues has revealed aberrant levels of some mitochondrial andenergy-related proteins in CF specimens that included the ubiqui-nolndashcytochrome c reductase complex core protein I and one form ofnidogen a pseudogene of aconitase 2 These changes in CF may reflectmolecular changes which could be associated with an altered mito-chondrial homeostasis and Co-Q10 redox
Multivitamin supplements with high bioavailability containingCo-Q10 have demonstrated to correct the deficit of this antioxidantand were preliminarily observed to improve airway inflammationmarkers in CF patients [183] However further clinical investigationfailed to demonstrate that such an improved biochemical profile isassociated with significant improvements in weight percentile andpulmonary function [162]
354 Fatty acidsA key pathophysiological role in sustaining inflammation in CF has
been attributed to the abnormal polyunsaturated fatty acid (FA) pat-tern Abnormalities in FA profiling are potentially linked to CFTRmutation-driven alterations in the absorption andor metabolism ofdietary lipids [192193] and to the consumption of high oxidizableFA involved in the free radical-mediated lipid peroxidation [7]Among those alterations dysregulation of the docosahexaenoic acidand arachidonic acid balance has been extensively studied with re-portedly significant reduction of DHA in CF and a parallel increasein the levels of AA and inflammatory indices [193ndash195] Actually AAis the progenitor of both enzymatic- and free radical-derived inflam-matory mediators including leukotrienes prostaglandins and iso-prostanes On the other hand n-3 PUFA (eicosapentaenoic acid anddocosahexaenoic acid) are involved in the generation of potent medi-ators namely resolvins and protectins which are able to resolveexudates and to act as organ protective and antifibrotic Secondarilyto their anti-inflammatory action n-3 FA may also produce anantioxidant-like response (eg a reduced demand of antioxidants toachieve an optimal control of oxidative pathways) As a consequencen-3 PUFA have been suggested and widely used as supplements in CFpatients usually under the form of fish oil [196ndash198] It is worth ofnote however that defective levels of DHA in CF patients was notconfirmed in recent studies [7] It was also shown that patients onDHA supplements did not have increased plasma n-3 FA concentra-tions but showed more severe oxidative stress compared to theunsupplemented patients [7] This observation of an increased riskof oxidative stress in CF subjects receiving n-3 fatty acids supple-ments has also been described by other authors [199]
Studies reporting increased AA levels in CF patients have beencontradicted by others [7200201] thus contributing to weakeningthe pathophysiological role of the altered DHAndashAA balance as turnpoint of an upregulated inflammatory status in CF In this context a
702 F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
recent Cochrane meta-analysis on n-3 supplementation in CF patients[202] highlighted the lack of evidence for a significant correction ofthe assessed clinical end points (mainly respiratory symptoms)even when inflammatory indices and other laboratory end pointswere met Taken together these data suggest that there is insufficientevidence to draw firm conclusions or recommend routine use of n-3supplements in CF Notwithstanding it is common belief that n-3supplements provide some benefits for people with CF with relativelyfew adverse effects and thus their use is not discouraged
Further alterations in fatty acid metabolism have been highlight-ed including the consistent findings of an increase in circulatinglevels of saturated and monounsaturated fatty acids [7203204]Decreased levels of essential FA (EFA) ie the FA that have to be in-troduced with the diet correlates with the severity of respiratoryinsufficiency and the same clinical correlation was observed with al-tered proportions of FA species converted by the activity of desatur-ase enzymes (reviewed in [204]) The close relationship betweencertain fatty acids and oxidative stress including the negative correla-tion of C240 and linoleic acid with oxysterol levels point to the needof intensive investigation in CF patients of previously neglected lipidspecies that are emerging candidates in the control of metabolismQuantitative lipidomic analyses have lead to identify C161n7 palmi-toleate as a ldquoprotectiverdquo adipose-derived lipid hormone that stronglystimulates insulin activity in muscle and liver also suppressing in-flammatory cytokine output from mice fat cells [205] Specific meta-bolic activities have been also demonstrated by medium chainsaturated fatty acids caprylic acid (C80) capric acid (C100) and lau-ric acid (C120) Capric acid acts as a direct ligand of PPARγ using abinding pocket different from the binding pocket of thiazolidinedioneor long chain fatty acids [206] Additional activities of medium chainfatty acids which are ligands of free fatty acids receptors detectedin the immune cells the gastrointestinal tract and adipocytes maycontribute to metabolic homeostasis and inflammatory responses[207] These data underscore the importance of a lipid-mediated ldquoen-docrine networkrdquo demonstrating how specific alteration of one orfew serum lipids would be per se sufficient to influence metabolic ho-meostasis Given the relevance of this emerging information and thealteration of lipid metabolism and inflammatory status in CF fattyacid lipidomics need to be deeply investigated in CF
Again these studies have obvious nutritional implications Satu-rated fatty acids with chain lengths higher than C18 are poorlyabsorbed partly because they form insoluble calcium salts [208]Medium chain saturated fatty acids are well known for being highlyabsorbed through the intestine providing rapid delivery of energyvia oxidation of the more hydrophilic short chains and have beensuggested to provide proper nourishment in patients with CF [209]Recent studies have shown that consumption of a high-fat diet richin medium chain fatty acids as opposed to long chain fatty acidsdoes not lead to ectopic fat accumulation in skeletal muscle andliver of both rats and mice [210] In light of the close association be-tween nutritional status inflammation and life expectancy in CF pa-tients the manipulation of dietary lipids in these patients must befurther explored as a possible strategy to provide adequate nutritionand better management of oxidative stress
36 Hydrosoluble antioxidants oligoelements and enzymatic antioxidants
361 Vitamin CVitamin C status in CF patients has been poorly investigated Early
studies suggested a defective vitamin C status that was refractory tooral supplementation [211] Other and more recent studies showednormal or slightly decreased levels of vitamin C in CF patients as com-pared to healthy controls but age- and disease-related decline of thiswater-soluble antioxidant was reported in these patients [5212]In the study of Winklhofer-Roob et al [212] on mid-European CFpatients vitamin C concentrations decreased with age with an
estimated rate of 5 μmollyr and vitamin C concentrationsb40 μ-moll were associated with highest indexes of inflammation whichis consistent with the hypothesis that optimal levels of vitamin Cmay influence immuno-inflammatory activity of alveolar macro-phages and neutrophils Other few studies have examined the effectof supplements containing vitamin C on CF inflammation and oxida-tive stress since the levels of this vitamin do not significantly improvewith supplementation (reviewed in [213]) This highlights the com-mon fate that this hydrosoluble vitamin shares with several fat-soluble counterparts in the ldquomicronutrient paradoxrdquo of CF patients inwhich the need for a correction of their status along the progressionof the disease is frustrated by the poor efficacy of oral supplementa-tion protocols Formulations and appropriate supplementation proto-cols that may produce a better correction of vitamin C status of CFpatients are awaited for further clinical evaluation
362 Selenium and selenium-dependent peroxidasesSelenium is a trace element with marked electrophilicity [214]
that once converted to the organic form of Se-Cys can be introducedin protein structures to play its important role in H2O2 metabolismand signaling [215] As catalytic center of the enzyme GSH-peroxidase (SeGSH-Px) Se plays a crucial role to protect polyunsatu-rated lipids of plasma membrane and circulating lipoproteins formperoxidative insults With other Se-proteins such as the high molecu-lar weight thioredoxin reductases this oligoelement participates tothe control of protein thiol-disulfide oxidoreduction and glutathiony-lation which regulate signaling pathways of crucial importance in theregulation of immunity and inflammation [16] but also the function-ing of other redox-sensitive proteins such as the same CFTR [124]
The activity of SeGSH-Px in blood is considered a functional as-sessment of selenium status even if this assumption has some limita-tions related with the saturation profile that the Se stores show atincreasing doses of Se administration Investigations of the seleniumstatus in CF patients have produced conflicting findings which maydepend on differences in dietary intake ethnicity and environmentalfactors in the diverse patient populations (reviewed in [216217]) CFchildren have been reported to have lowered blood selenium and RBCSeGSH-Px activity [218219] normal plasma selenium and loweredRBC SeGSH-Px [220] and even normal levels of both these two param-eters [221] The supplementation with selenium in combination withother antioxidants was observed to increase the concentrations ofblood selenium that likewise β-carotene and fatty acid were posi-tively correlated with improved lung function [6]
Foucaud et al [218] observed that a defective selenium statuswas associated with lowered levels of other antioxidants that contrib-ute to the anti-peroxidative activity of this microelement such asvitamin E (reviewed in [222]) and the severity of this deficiencywas lower in children with pancreatic enzyme replacement and vita-min E supplementation
Treatments to substitute for exocrine pancreatic insufficiency bypancreatic enzymes from animal sources such as porcine pancreashave been confirmed to be a source of Se [220] These affects RBCSeGSH-Px activity and plasma selenium concentrations which hasto be taken into account when selenium supplements are given toCF patients
Selenium has been used to develop a series of organoseleniumcompounds that may open the way to new therapeutic opportunitiesin CF (see Section 392) These include GPX mimetic drugs and phaseII enzyme inducers which may provide higher antioxidant activity ofASL and cellular protection effects in the airways
363 Zinc and copperZinc and copper (Zn and Cu respectively) are present in many
proteins so that a deficiency of these trace metals could have pleiotro-pic effects in humans As regards antioxidant systems these two oli-goelements contribute an important role being cofactors of two
703F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
isoforms of the superoxide dismutase enzymes eg the extracellularform eg the EC-SOD or Sod 3 and the CundashZn-SOD or Sod 1 that isfound in several tissues and cells [223] The EC-SOD exerts its antiox-idant role also in the lining fluids of the airways [224]
The notion that CF patients have defective concentrations of bloodZn and Cu is controversial As far as Cu status is concerned few datahave been produced and are available in the literature suggestingthe notion that CF patients develop a moderate copper deficiency[225226] That was essentially demonstrated on the bases of a defec-tive activity of Cu-related proteins such as plasma ceruloplasmindiamine oxidase and RBC SOD This defect seems to be refractory toCu and Zn supplementation (see below)
More advanced studies have been carried out in the case of Zn sta-tus in CF Low plasma zinc concentrations were reported in approxi-mately 30 of young infants with CF identified by newbornscreening [227] and an impaired zinc homeostasis in CF patientswas described by Easley et al [228] This is characterized by poor con-servation of the endogenous pool with fecal loss and impaired frac-tional absorption of zinc which are the consequences of pancreaticinsufficiency and persisting steatorrhea These studies suggestedthat in the clinical management of CF patients these defects can beat least in part corrected by exocrine pancreatic enzyme replacement
A series of studies by Van Biervliet et al [229230] demonstratedin a Dutch population of CF infants and children that serum Zn variesin an age-dependent manner but remained unchanged with respectto healthy control levels In CF patients no difference in serum Zn con-centration between pancreatic-sufficient or pancreatic-insufficientpatients was observed and no correlation was found with the nutri-tional status or height z-score Importantly in these studies a signifi-cant correlation of serum Zn was observed with the fat solublevitamins A and E thus confirming the relationship between the ab-normalities of lipid and Zn metabolism in CF This suggests that co-supplementation of Zn and fat-soluble vitamins should be advisedin the presence of pancreatic insufficiency and persisting steatorrhea
Neve et al [219] in a study aimed to assess plasma and erythrocytezinc copper and selenium in CF children showed that mean plasmazinc and copper levels were not different from those in age-matched controls which confirms the observations by Van Biervlietet al described above However plasma zinc concentrations de-creased in patients with moderate-to-severe growth retardation andwith severe pulmonary disease but very low zinc levels occur sporad-ically Erythrocyte zinc and copper levels were significantly higherthan normal while RBC selenium was lower than in age-matchedcontrols These trace element concentrations in erythrocytes werediscussed in relation to the activities of the CuZn-SOD and the Se-enzyme GPx This observation suggests a compensatory upregulationof the erythrocyte CuZn-SOD by the exposure of erythroid precursorsto ROS andor other CF-related stressors
Best et al [225] also studied RBC SOD activity using this as a bio-logical sensor of Cu status in CF patients A lowered activity of thisenzyme was reported in CF together with that of the other Cu-dependent enzyme plasma diamine oxidase while plasma ceruplas-min showed normal activity Degradation rates of copper proteinsare known to be accelerated in conditions of copper deficiencywhich could explain the finding at least in part Anyway when Cuand Zn were supplemented to CF patients either separate or incombination (6 weeks of 3 mg copperd as copper-glycinate and30 mg zincd as zinc-glycinate) any of the copper enzyme activitieswas affected Therefore the moderate copper deficiency of CF patientsappears to be refractory to the intervention by increased copper andor zinc intake
Erythrocyte CuZn-SOD and the plasma levels of Cu and Zn werealso measured in the study of Wood et al [6] in which Australian CFpatients (agegt5 years) were treated with a high-dose antioxidantmultivitamin formulation containing 200 mg vitamin E (as RRR-α-tocopherol) 300 mg vitamin C (as sodium ascorbate) 25 mg β-
carotene (all-trans isomer) 90 μg Se (as selenomethionine) and500 μg vitamin A (as retinyl palmitate) in oil Plasma oligoelementsand particularly Zn were in the normal range at baseline (as com-pared with the data reported in [229230]) and were not affected bythis multivitamin supplement The same was found for the activityof RBC SOD and for plasma 8-iso-PGF2α as surrogate biomarker oflipid peroxidation
In a recent non-randomized small population (n=21) casendashcon-trol study in CF children Zn supplementation was proven to producepositive clinical effects in Zn-deficient patients [196] The supplemen-tation with 5 mgkg Zn sulfateday (maximum 150 mg) significantlydecreased the number of infections and increased the forced expira-tory volume in 1 s energy intake and growth parameters also im-proved These parameters were unaffected in untreated patientsexcept that in the case of the pulmonary function that decreased sig-nificantly These clinical observations on Zn supplementation need tobe confirmed in prospective double-blind randomized control trial
37 Appropriateness and targeting of antioxidant therapies in CF
The choice of the appropriate antioxidant and dose to correct a cer-tain biomarker and its associated biochemical lesion is another impor-tant point that appears to have disregarded in many clinical studiesFor instance unlike vitamin E vitamin C supplementation does notalter F2-IsoPs levels in humans (reviewed in [74]) This appears tobe true also in the antioxidant therapy of CF in which vitamin C(300 mgday) was administered together with other antioxidantsthat included a dose of vitamin E of 200 mgday without any signifi-cant effect on the surrogate biomarker of lipid peroxidation F2-IsoPs[6] When carotenoids are used as supplements to prevent the damag-ing action of ROS in the CF airways it is noteworthy that these are notparticularly good quenchers of peroxyl radicals relative to phenolicsand other antioxidants but are exceptional in quenching singlet oxy-gen at which most other phenolics and antioxidants are relativelyineffective Singlet oxygen is not a radical and does not react via radi-cal mechanisms but reacts mostly by the addition to double bondsforming endoperoxides that can be reduced to alkoxyl radicals that ini-tiate radical chain reactions typical of the peroxidative damage of PUFA[38] In this case the analysis of F2-IsoPs lipid peroxide formation andtransition metal-induced oxidizability of lipoproteins [162180] are allappropriate to evaluate the effect of carotenoids in preventing lipidperoxidation
As far as the dose is concerned clinical pharmacology of vitamin Eas an antioxidant was recently investigated by means of the effect onF2-IsoPs production and doses of α-tocopherol of 1600 IUday orgreater were found to be required to statistically affect plasma F2-IsoPs levels in hypercholeterolemic subjects [176] Several vitamin Esupplementation studies in CF patients have been performed withdoses of lower than 300 IUday regardless of the lowered absorptionby pancreatic and liver defects and the regular supplementationwith these doses does not appear to correct lipid oxidation markersin CF [7]
In the clinical practice and planning trials it has to be taken intoconsideration that in spite of substantial evidence supporting ahigher antioxidant demand in CF interventions with several antioxi-dant formulations produce poor responsiveness particularly in thecase of fat-soluble antioxidants which are poorly absorbed [6162]
Since many oxidants and antioxidants are present in tissuesand biological fluids and these have different chemical and physicalcharacteristics the possibility to produce a successful therapy witha single antioxidant molecule is too far to be realistic Moreover an-tioxidants act by multiple mechanisms in a single system or by adifferent single mechanism depending on the reaction systemresponding in a different manner to different radical or oxidantsources Because multiple reaction characteristics and mechanismsas well as different phase localizations are usually involved no single
704 F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
therapeutic approach will effectively prevent damage by multipleROS sources The defect of physiological antioxidants may also interferewith antioxidant therapies that are based on one or few exogenousantioxidants
Moreover several antioxidant vitamins such as vitamin E and ca-rotenoids have multiple natural forms with different bioavailabilitymetabolism and bioactivity [157167231] As far as the case of vita-min E supplementation concerns α-tocopherol was used as uniquevitamer in the large majority of supplementation trials so far per-formed and is the form used in the nutritional management of CFpatients Moreover several supplements contain the synthetic (or ra-cemic) form of this vitamin that has lower bioavailability than thenatural form Other forms present in nature and abundantly con-tained in vegetables such as tocotrienols and the less methylatedforms of tocopherol are not represented in many of the supplementformulations so far available in clinical centers and the supplementa-tion with α-tocopherol also limits their bioavailability These formsshow markedly higher susceptibility to hepatic metabolism and bili-ary excretion with respect to α-tocopherol eg the most representedform in blood and solid tissues and if co-supplemented these areeasily displaced during liver uptake and excreted with bile bymeans of competition with the same α-tocopherol Notwithstandingthese minor forms have been proposed to play important physiolog-ical roles showing molecular characteristics transcriptional effectsand antioxidant activities that clearly differentiate them in subfam-ilies with distinct biological functions Some of these such as α-tocopherol eg the second vitamin E form as relative abundance inblood and its carboxyethyl-hydroxychroman metabolite [189] ap-pear to have health-related anti-inflammatory effects which are par-ticularly relevant in lung protection [232233] This has suggestedthat such a group of ldquonon-α-tocopherolrdquo forms may represent anoth-er family of vitamins within the family of vitamin E with an impor-tant but often missed contribution to the proposed health effects ofthis vitamin [163]
These aspects may thus limit the possibility to provide CF patientsof optimal levels of this vitamin in all its components even if they areregularly treated with a vitamin E supplement eg withα-tocopherol
Targeted antioxidant therapy with formulations with higher bio-availability and bioactivity has been anticipated in CF New antioxi-dant formulations have been proposed to overcome main limits ofantioxidant therapies so far proposed for these patients Water-miscible α-tocopheryl acetate containing polysorbate propylene gly-col or polyethylene glycol as emulsifiers form micellar structureswere suggested to providing greater bioavailability than the fat-soluble counterparts These were commercialized with the brandnames of E-viminreg Cremophorreg EL and Aquasolreg E but despitethe original positive expectation [234235] some studies failed to ob-serve a higher response in vitamin E levels when these were com-pared with fat-soluble formulations [236237]
In a pilot study by Papas et al [183] a micellar formulation of fat-soluble nutrients and antioxidants was found to improve plasmalevels of β-carotene γ-tocopherol and CoQ(10) reducing at thesame time some inflammatory markers in induced sputum eg mye-loperoxidase and to a lower extent PMN elastase and total cell countswhile lung function and sputum bacterial counts were unaffectedThe same group recently confirmed the possibility to increase the ab-sorption of fat-soluble micronutrients using formulations with higherbioavailability specifically designed for malabsorbing patients such asCF patients that include also vitamin K and commercialized with thebrand name of AquADEKsreg [162] Despite improved vitamin and mi-cronutrient levels in this non-randomized open-label study AquA-DEKsreg produced only modest improvements in weight percentileand pulmonary function Another recent pilot observation [182] hassuggested the beneficial effect of this formulation on antioxidant andoxidative stress parameters of this oral supplement that surely deservesmore clinical investigation by larger randomized controlled trials
Recent multivitaminic formulations have been designed to containalso the minor forms of vitamin E and specifically γ-tocopherol [238]the expected superiority of which with respect to formulations con-taining only α-tocopherol needs to be verified As discussed abovein the section dedicated to vitamin E further advancements in thetherapy of CF inflammation and oxidative stress could be based onsynthetic forms and natural metabolites of this vitamin that havebeen recently identified to possess higher antioxidant and also anti-inflammatory activity than α-tocopherol (reviewed in [163168])
Pre-clinical investigation of these and other fat-soluble agents iscurrently addressed to develop formulations and administration pro-tocols that may increase the therapeutic efficacy in the airways In theantioxidant therapy of lung dysfunction in CF local administrationprotocols may overcome the limits of oral and systemic administra-tion protocols increasing bioavailability and providing targetedapproach to inflammation and oxidative stress Aerosolization of vita-min E and other fat-soluble micronutrients is possible and may allowdirect administration in the airways to prevent toxicity of smokewhich is closely associated with inflammation and oxidative stress[164165] To our knowledge this as well as other strategies of localadministration such as instillation of solutions such as surfactant-like solutions enriched of vitamin E have not been previously inves-tigated in CF patients and other CF model systems
On the contrary inhalation is an administration route widelyadopted in the case of GSH and NAC therapy described above Inthis context Cys formulations alternative to NAC have been proposedfor use as antioxidant and anti-inflammatory agent for inhalationNacystelyn is a lysine adduct of NAC that thanks to a higher proton-ation equilibrium shows increased water solubility and thus betterbioavailability Nacystelyn has been described to influence IL-8 gener-ation and the inflammatory signaling of bronchial epithelial cells[239] and preliminary clinical evaluation has demonstrated the safetyof this drug [240] Further clinical trials aimed to assess the effect onlung symptomatology of CF patients are needed Direct administra-tion in the airways could also be adopted for micronutrient vitaminswith poor absorption and bioavailability due to GI defects
38 Clinical impact of antioxidant therapy in CF
Huge in vitro and pre-clinical evidence has provided the rationaleto support clinical investigation of antioxidant strategies in CF Theseshould aim to restore the oxidantndashantioxidant balance of CF airwaychallenged by chronic infection and inflammatory cell activation
Some observational trials have confirmed that antioxidants usedas either supplements to the diet or drugs for lung administrationby aerosolized formulations may help in relieving progressive lungdamage and other adverse clinical events of CF such as poor growthSo far few studies have examined with sufficient methodologicalrigor the clinical efficacy of antioxidant therapy in CF This was alsoconcluded in a previous review of the literature by Cantin et al [12]that was published in the beginning of 2006 and is confirmed alsoin a recent analysis of clinical trials on antioxidant therapy in CF pa-tients [213] that examined the literature until September 2010using as sources the databases of the Cochrane CF and Genetic Disor-ders Group CF Trials Register PubMed CINAHL and AMED Useful in-formation was retrieved from just four randomized controlled trialsand one quasi-randomized controlled trial on vitamin C vitamin Eβ-carotene and selenium used as supplements administered aloneor in combination Post-hoc data analysis that was possible only inthree studies on a total of 87 CF patients showed the absence ofany significant improvement in lung function that was selected as pri-mary outcome together with quality of life that improved in one trialSecondary outcomes concerning laboratory indices of oxidative stressand antioxidant status showed several improvements These includedan increase of RBC SeGPx by selenium supplementation done as
705F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
individual or combined supplementation and increased levels of allplasma antioxidants except vitamin C that were observed in all thetrials
The message from these studies to pediatricians and nutritionistswithin the clinical staff of CF centers is that in the absence of solid ev-idence regarding the clinical effectiveness of oral formulations of an-tioxidant supplements in CF (including PUFA) their use as a routineclinical practice should be considered with caution keeping clear inmind that this should represent just a complement of one of themost critical interventions in the life-long clinical management pro-gram of CF patients eg providing an adequate nutriture [140] Inthis context compensating energy and protein malnutrition has toremain the first goal of nutritional management programs Providinghigher intakes of antioxidant micronutrients with food naturally-enriched (or functionalized) of micronutrient antioxidants shouldbe preferred in order to have the higher combination of positive nu-tritional factors that are lost during refinement procedures and over-all industrial processing of dietary supplements
Measures of good practice in clinical management of micro-malnutrition in CF patients would include the support of specializedpersonnel and laboratories The centers should have the possibilityto ascertain with appropriate nutritional and laboratory tests whatthe level of deficiency is for the different micronutrients that each pa-tient may suffer from during a dietary program Monitoring dietaryintakes and blood levels of micronutrients is not sufficient to set apersonalized nutritional intervention with supplements or functionalfoods Sub-optimal intakes and the compliance to nutritional inter-ventions should be verified by means of selected biochemical andclinical criteria Unluckily the latter are still not well established forsome micronutrients such as the fat-soluble vitamins E (reviewed in[163173241]) and K [242243] and also for trace elements such asSe [244] For many of the antioxidants used as supplements inhumans we still do not know exactly several of the biological effectsthat these may provide when introduced in a healthy body and weknow less what these can do in disease These aspects hardly impacton the concept of optimal levels of intake that should be identified foreach micronutrient on an individual basis According with the aspectsdiscussed in the previous sections optimal levels of intake for antiox-idant micronutrients are different in CF patients and healthy subjectsand vary with age and several individual factors
Lung administration of antioxidants by means of aerosolized for-mulations so far used for GSH therapy (see above) is a promisingfield of clinical investigation in CF Toxicity issues are currently themain concern and the subject of clinical evaluation by several groups(described above)
Information on future directions of antioxidant therapy in CF canbe inferred by the analysis of pending or recently completed clinicaltrials that have been searched (December 2011) at ClinicalTrialsgovdatabase matching the terms ldquoantioxidant therapyrdquo or ldquoglutathionerdquowith ldquocystic fibrosisrdquo Fifteen trials were retrieved and those directlyrelated to antioxidant therapy (n=12) are presented in Table 1 andinclude efficacy and safety studies of inhaled drugs as GSH sodiumpyruvate NAC and NO and the dietary supplements AquADEKsregan antioxidant-rich multivitamin supplement epigallocatechin gal-late (EGCG)tocotrienol curcuminoids the amino acid glutaminesulforaphane in broccoli sprouts One trial is investigating the flavo-noid quercetin as CFTR modulator
39 Emerging antioxidant and anti-inflammatory approaches in CF
Mediterranean foods such as olive oil and red wine or severalplant extracts such as herbal tea or grape seed extracts contain aseries of natural compounds with important antioxidant and NOscavenging activity that have been widely investigated for the pre-vention of oxidative stress-related diseases [38245] These havebeen long investigated as template molecules to develop antioxidant
and anti-inflammatory drugs Between the multitudes of natural sub-stances most investigated ones include for instance tyrosol hydroxy-tyrosol gallic and caffeic acids belonging to the family of phenolswhile resveratrol of the stilbenes family epicatechin kaempferoland cianidin are examples of flavonoids examples of fat-soluble phe-nolics are those of the family of tocols (vitamin E) and carotenoids Allthese compounds show different metabolisms and signaling effects[246] Antioxidant and cell protection mechanisms are associatedwith different and sometimes concurrent processes as H-atom trans-fer and electron donation radical trapping and chelation of transitionmetals that can be easily investigated at the chemical level [247] Be-sides these direct antioxidant effects metabolic responses and signal-ing effects of natural compounds are also important to producesecond-generation responses that modify the level of antioxidantprotection and the potential for ROS detoxification in cells and bodyfluids These derive from the transcriptional regulation of antioxidantand pro-oxidant genes that coexist with the modulation of cytokinesecretion and inflammatory enzyme activities
Some of these natural plant-derived antioxidants may provide fur-ther pharmacological activities of possible relevance in CF This is thecase for instance of the plant flavonoids genistein apigenin kaemp-ferol quercetin and hesperidin [248ndash251] that fall in the pharmaco-logical category of ldquopotentiatorsrdquo [252] in that these activate at leastto a certain extent CTFR-mediated Cl currents in normal and CF airwayepithelium investigated either in vitro or in vivo in humans and ani-mal models Actually as prototypal flavonoid-derived potentiatorthe tyrosine kinase inhibitor genistein potentiates the gating of wild-type as well as ΔF508 CFTR and G551D CFTR [253] but at higherdoses it inhibits CFTR gating which make this an unlikely clinical can-didate Similar potentiation effects have been reported for the antiox-idant curcumin [250] that shows an additive effect with respect togenistein-induced potentiation Besides CFTR potentiation whichdoes not appear to have a direct influence on GSH and nutrient trans-port in the lung tissue all these natural substances have been usedalone or in combination with other agents as in vivo enhancers oflung antioxidant protection [246254255] In the case of quercetinthiol-reactive phenolic [256] bronchodilation and anti-inflammatoryeffects by a restoration of the Th1Th2 balance have been reportedin inflammatory syndromes of the lung [255257ndash259] but theseeffects have not been explored in CF Pyocyanin toxicity (see abovein the Section 2) could represent an issue for the use of quercetinand other catechols in infectious diseases of the lung [260]
Other natural antioxidants of potential interest in CF therapy in-clude terpenoids [261] such as terpinen-4-ol a major constituentof tea tree oil that is being investigated in the therapy of anti-biotic resistant organisms specifically against methicillin-resistantStaphylococcus aureus (MRSA) [262] a problem in CF [263] Otherthan being lipophilic antioxidants terpenes can prevent oxidativestress of the CF lung secondarily to the antibiotic effect thereby pro-moting a better control of immuno-inflammatory pathways and lungantioxidants
391 Targeting NF-κB with natural compounds resveratrol and plantextracts
Natural compounds were long known to be useful in designinganti-inflammatory drugs and some of these could find an applicationin the control of the transcription factor kappa-B (NF-κB) that maylead to develop advanced pharmacological tools to control inflamma-tion and to produce higher antioxidant protection to CF airwaysInhibitors targeting NF-κB including transcription factors decoymolecules (TFD) are potent down-regulators of gene expressionand release of IL-8 in CF cells infected with P aeruginosa [264265]
Resveratrol (354prime-trihydroxystilbene ldquoErdquo form) is one of the mostinvestigated natural antioxidant with proposed activity as NF-κBinhibitor This is a phytoalexin present in large quantity in red winepreferentially in the skin of grapes being its concentration
706 F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
50ndash100 μgmg of fresh skin and 13ndash3 mgl of red wine [266]Furthermore resveratrol is a constituent of lsquoDarakchasavarsquo (13ndash6 mgl) an ayurvedic medicine from India [267] The antioxidant activity ofresveratrol has been reported in several papers and occurs also in lungtissues suggesting that resveratrol has potential as a therapeuticagent in respiratory disease [268ndash270] Resveratrol can be consideredone of the most interesting molecules from the natural worldexhibiting strong antioxidant activity that at the same time is able toexert anti inflammatory activity through alteration of NF-κB functionsand efficient inhibition of pro-inflammatory genes [271272] As far asthe effects on CF model systems are concerned Cabrini et al [26]reported the effects of resveratrol on P aeruginosa infected CF IB3-1cells The results obtained demonstrate that resveratrol exhibits minoreffects of IB3-1 cell growth and important inhibitory effects on accumu-lation of IL-8 and GRO-α mRNA while minor effects on IL-6 gene ex-pression were observed These data support recently publishedobservations suggesting inhibitory effects of resveratrol in infection-mediated inflammatory processes [273] Interestingly resveratrol hasbeen reported as a potent inhibitor of NF-κB activity and a promisinganti-inflammatory agent [272274] also in combinationwith othermol-ecules [274275] However in vivo translation of this pre-clinical on res-veratrol is hard to be foreseen This natural compound displays poorbioavailability [276] and further characterization of resveratrol pharma-cokinetics is troublesome since it is hardly measurable in vivo [277]Furthermore the regulation of inflammatory responses by resveratrolhas been suggested to be far more complex than simple direct suppres-sion of NF-κB activity Actually some aspects of the immune responsecould be enhanced by this natural substance which may lead tohypothesize broad negative feedback events on immuno-inflammatorypathways [278] In any case and with these cautions in mind the pub-lished observations on cellular model systems support the concept thatresveratrol and resveratrol-containing formulations deserve further con-sideration to determine their possible therapeutic values in CF
Other inhibitors can be identified from systematic studies of naturalproducts and their ability to interfere with NF-κB activity [279ndash281]Recent studies have demonstrated that the whole extract of Aeglemarmelos (Rutaceae) has strong inhibitory effect on the P aeruginosa-dependent IL-8 induction in human CF-derived bronchial IB3-1 cellswithout affecting cell proliferation [280] Molecular analysis of compo-nents contained in A marmelos extracts revealed that three major com-pounds namely 56-dimethoxy-1-indanone 2-hydroxy-cinnamic acidand 5-methoxy psoralen (5-MOP) reproduce the inhibitory effect ob-servedwith thewhole extract [280] A further example has been recent-ly published using extracts from bergamot (Citrus bergamia Risso) Inthis study the extracts were characterized and the main detected con-stituents were assayed for their biological activity [281] The resultsobtained demonstrated that the extracts from bergamot epicarps con-tain components displaying an inhibitory activity on IL-8 Particularlythe most active molecules were bergapten and citropten These effectshave been confirmed by analyzing mRNA levels and protein release inthe CF cellularmodels IB3-1 and CuFi-1 inducedwith TNF-α or exposedto P aeruginosa
A parallel strategy linking NF-κB inhibition and down-regulationof NF-κB-dependent functions is described in recently publishedstudies based on a structured-based virtual screening (VS) of differ-ently substituted furocoumarins and analogues against NF-κB withthe objective of selecting molecules able to inhibit the binding ofthis transcription factor to DNA [282283] Novel compounds wereidentified with this strategy as potent inhibitors of NF-κB dependentbiological functions to be proposed for the control lung inflammationoccurring in patients affected by CF [282ndash284]
392 Scavengers and regulators of H2O2 and NO
3921 Lactoferrin and OSCNmacr The impaired DUOXLPO system of CFpatients could be the target of therapeutic strategies that may
produce concomitant antimicrobial and antioxidant effects This sys-tem described above in Section 22 represents an important compo-nent of innate immunity with a role in bactericidal defense andregulation of H2O2 metabolism of airways [32] CF patients have alsoreported to show lowered LF levels in the ASL [37] that togetherwith a CFTR-dependent defective efflux of SCNmacr and LPO [36] may cre-ate the environment for a sustained flux of H2O2 and for the genera-tion of highly reactive Fenton species [1138] An ideal therapeuticintervention should restore the LPO-dependent generation of bacteri-cidal OSCNmacr from DUOX-derived H2O2 and SCNmacr in the ASL to controlat the same time the microbial biofilm and the flux of H2O2 into theASL An approach close to this therapeutic mechanism was recentlyproposed for the drug Meveolreg This is a complex of LF and OSCNmacrwith proposed in vivo antimicrobial activity [285] to be evaluatedin clinical trials for the aerosol treatment of lung infections in CFpatients The role for this drug in the control of H2O2 levels of ASLremains to be investigated
3922 Organoselenium compounds Organoselenium compoundshave been proposed as therapeutic agents useful in the antioxidanttherapy of inflammatory conditions These include GPX mimetic mol-ecules such as Ebselenreg (2-phenyl-12-benzisoselenazol-3(2H)-one)or other and more recently developed molecules that are still inpre-clinical steps of evaluation [286] Selectively and specificity of ac-tion are main issues in the therapeutic mechanism of this candidateantioxidant drug that thanks to the electrophilic properties of Se[214] reacts with thiols to reduce H2O2 and other species MoreoverEbselenreg has been described to act as potent non-competitive inhib-itor of extracellular nucleoside diphosphokinase (NDPK) having neg-ligible effect on ecto-ATPase and adenyl kinase activities which areother players of the metabolism of extracellular nucleotides [287]This enzyme together with other nucleoside di- and triphosphatescontributes to regulate several components of the mucociliary clear-ance process (MCC) that protects the lung against infections via acti-vation of epithelial purinergic receptors The inhibition of NDPK bythis GPX-mimetic drug may also impact on the energy status of endo-thelial cells [287] This aspect could be further investigated as a cellu-lar protection mechanism in the pulmonary epithelium of CF patientsbeing the control of cell energy of fundamental importance to preventthe activation of death pathways [288]
Further therapeutic mechanisms for these Se-derived drugs mayderive from the marked activity as inducers of phase II enzymessuch as quinone reductase (QR) and glutathione-S-transferase (GST)[289] This induction response also observed with other electrophilsand redox-active molecules such as natural phenolic antioxidantscould produce higher cellular protection by the acquisition of anincreased capability to detoxify endobiotics generated during oxida-tive stress and inflammation [246]
3923 Melatonin and GSNO as NOx regulators Increased markers ofNO-derived biological damage are present in the CF lung suggestingthe abnormal reactivity of NOx in the inflamed lung of CF patients[52] However an impaired metabolism and biological function ofNO in CF airways (see Section 23) suggests a cautious approach tothe use of agents that may influence the levels and chemical behaviorof NO-derived species (NOx) with possible impact on the physiologi-cal roles of NO in vasodilatation innate immunity and H2O2 metabo-lism of the respiratory tract [290291] NO donors also appear toinfluence CFTR function of alveolar epithelium and gland serouscells [292293]
Main physiological role of the pineal gland hormone melatonin isthe synchronization of circadian rhythms including the sleepndashwakecycle but several other functions dealing with immunomodulatoryantioxidant and cellular protection effects have been identified[294] Melatonin receptor stimulation may also influence cyclic AMPsignaling and the regulation of CFTR ion channel [295296]
707F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
A recent randomized double-blind placebo-controlled study hasexamined the effects of short term melatonin administration (3 mgfor 3 weeks) on sleep and oxidative stress markers in CF [297]According with the expected pharmacological effect of this hormonalsubstance the treatment was successful in improving sleep indicesAt the same time nitrite levels determined in exhaled breath conden-sate (EBC) were reduced to suggest a better control of NOmetabolismof CF airways (discussed above in Section 23) but these effects how-ever were not associated with a significant correction of isoprostaneas lipid peroxidation marker measured in EBC Increasing dosages ofmelatonin could be investigated for the pharmacological treatmentof oxidative stress and immune dysfunction of CF patients due tothe absence of adverse effects of this hormonal substance in humans
The S-nitrosation reaction of thiols is another interesting aspect ofNO pharmacology [53] that may find an application in the therapy oflung complications of CF This has been the case for instance of theS-nitrosothiol GSNO that has been used safely in human trials[298299] This endogenous nitrosothiol with proposed regulatory ef-fect on the CFTR of lung epithelia [292293] is well tolerated in pa-tients with CF when administered by aerosolization and mayproduce better oxygenation [299] thereby suggesting that therapyaimed at restoring endogenous GSNO levels in the CF airway maymerit further clinical evaluation Since the administered GSNO de-composes as shown by the increased levels of expired NO in CF pa-tients under treatment with this nitrosothiol [299] furtherinvestigation should be addressed to ascertain whether GSNO thera-py may merely correspond to a GSH therapy
NO dependent effects on CFTR function should be considered toevaluate mechanism of action and specificity of antioxidant therapiesthat target NO metabolism and function in the CF airways
4 Conclusions and future perspectives
The presence of clinical and biochemical symptoms of inflammationand oxidative stress implies that CF patients have a higher demand ofantioxidant protection The combination of the dysfunctional CFTRwith a lowered intake and absorption of dietary antioxidants producesub-optimal levels of protection from both enzymatic and non-enzymatic defense systems The former could be associated with a de-fective glutathionemetabolism and lowered intake of sulfur-containingamino acids and oligoelements such as zinc and possibly seleniumwhile fat-soluble antioxidant vitamins such as vitamin E and caroten-oids and the water-soluble vitamin C are lowered than in healthy sub-jects due to malabsorption and possibly higher consumption
The increased antioxidant demand in CF patients should be evenhigher in the presence of complications of the lung pancreas andliver Lung comorbidity is particularly important in this contextbeing associated with recurrent infections which results in the alter-nation of inflammatory exacerbates and chronic inflammation Thesesustain the flux of ROS in the airways and promote the formation ofsecond-generation byproducts by the damage of biomolecules suchas PUFA and proteins which may diffuse also at the systemic level tofurther promote adverse biological responses and toxic reactions Pan-creatic insufficiency causes malnutrition and may lead to develop en-docrine and metabolic defects associated with diabetes of CF Theseevents can be further aggravated by the concomitance of liver dys-function and a poor nutritional status Malnutrition is strongly associ-ated with poor prognosis as assessed by pulmonary function andsurvival data [138ndash140] The more aggressive nutritional interven-tions seem to produce better clinical outcomes in these patients andthe possibility of achieving higher antioxidant protection in well-nourished patients by dietary factors could be a key aspect to explainsuch a clinical advantage The assumption that food-derived compo-nentsmay help to prevent the damaging effects of oxidative stress im-proving the antioxidant defenses deserves further investigation at theclinical level This together with the investigation of appropriate
laboratory biomarkers could provide critical information to establishintervention criteria for an early nutritional management of newly di-agnosed patients [5] It is expected that a timely secondary preventionstrategy could influence the progression of CF symptoms thusaffecting with a self-feeding mechanism the same extent of malnutri-tion and oxidative stress along the life of CF patients Since severalfactors contribute to impair the nutritional status of CF patients(such as pancreatic insufficiency chronic malabsorption recurrentsinopulmonary infections and progressive lung disease chronic in-flammation increased energy expenditure suboptimal intake multi-therapy) careful monitoring of the antioxidant status should berecommended According with international guidelines fat-solublevitamin supplementation is of utmost importance in daily practice to-gether with energy intake requirements and pancreatic enzyme-replacement therapy Among these vitamin E β-carotene and ω-3FA have observed to alleviate selected biochemical signs of oxidativestress as measured for instance with well established laboratory indi-ces of lipid peroxidation and in some studies these effects werepreliminarily associated with positive clinical outcomes Notwith-standing randomizedndashcontrolled clinical trials on antioxidant supple-ments (including ω-3 FA) so far carried out in CF have failed toconclusively demonstrate significant beneficial effects on respiratorysymptoms and on the consequent impact that these have on the qual-ity of life of these patients (reviewed in [202213]) whichmay provideno support for the use of these supplements in CF An absence of effi-cacy in prevention studies on antioxidant supplements has also beenobserved in other and possibly less severe oxidative stress-relatedconditions particularly in the secondary prevention of cardiovasculardisease and some forms of cancer by vitamin E and other antioxidantssuch as vitamin C selenium and β-carotene (reviewed in [163]) Dif-ferent biases however have been identified in randomize large clini-cal trials that may account for these disappointing findings Theseinclude patient selection criteria (early interventions and primaryprevention could have more chances of success than secondaryprevention) duration and doses of the treatment use of wrong anti-oxidant formulations and administration protocols absence of verifi-cations of the biological compliance to the treatment etc The samebiases apply for the few trials carried out in CF patients Thus the ap-propriateness and efficacy of nutritional interventions with naturalfood-derived or synthetic antioxidants should be verifiedwith respectto the biological pathways of oxidative stress and clinical variablesthat are identified as end-points Profiles of blood and tissue antioxi-dants as well as of reliable surrogate markers of oxidative stresshave to be selected and determined in highly specialized laboratorieswith a well-established experience on these analyses
Well-timed (early) interventions with appropriate antioxidantformulationsprotocols need to be proposed for the next generationof trials and the development of novel CF-tailored antioxidant andanti-inflammatory agents should be promoted
As a consequence of these considerations more clinical investiga-tion is awaited to identify future successful approaches to the antiox-idant therapy as a measure to further enhance quality of life and theoverall clinical outcome of CF patients
Acknowledgments
We are indebted with the Italian Cystic Fibrosis Research Founda-tion for the support that it provided with its grant program to the re-search activity of the authors of this paper This is a scientific initiativeof the ldquoWorking Group on Inflammation in Cystic Fibrosisrdquo (BragonziA Bravo E Cabrini G Conese M Cuzzocrea S Dechecchi MC De Ales-sandri A Evangelista V Galli F Gambari R Lambiase A Lucidi VManca A Melotti P Minicucci L Motta A Pietraforte D Pompella AQuattrucci S Rizzo R Romano M Sorio C Tesse R) of the Italian Soci-ety for Cystic Fibrosis A particular thank goes to the Prof GianniMastella for the critical revision of the manuscript and for the
708 F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
stimulating research environment that he has contributed to createwithin the Italian Cystic Fibrosis Research Foundation
References
[1] BP OSullivan SD Freedman Cystic fibrosis Lancet 373 (2009) 1891ndash1904[2] P Linsdell JW Hanrahan Glutathione permeability of CFTR Am J Physiol 275
(1998) C323ndashC326[3] L Gao KJ Kim JR Yankaskas HJ Forman Abnormal glutathione transport in
cystic fibrosis airway epithelia Am J Physiol 277 (1999) L113ndashL118[4] RK Rowntree A Harris The phenotypic consequences of CFTR mutations Ann
Hum Genet 67 (2003) 471ndash485[5] EI Back C Frindt D Nohr J Frank R Ziebach M Stern M Ranke HK Biesalski
Antioxidant deficiency in cystic fibrosis when is the right time to take actionAm J Clin Nutr 80 (2004) 374ndash384
[6] LG Wood DA Fitzgerald AK Lee ML Garg Improved antioxidant and fattyacid status of patients with cystic fibrosis after antioxidant supplementation islinked to improved lung function Am J Clin Nutr 77 (2003) 150ndash159
[7] L Iuliano R Monticolo G Straface S Zullo F Galli M Boaz S Quattrucci Asso-ciation of cholesterol oxidation and abnormalities in fatty acid metabolism incystic fibrosis Am J Clin Nutr 90 (2009) 477ndash484
[8] C Libetta V Sepe P Esposito F Galli A Dal Canton Oxidative stress and inflam-mation implications in uremia and hemodialysis Clin Biochem 44 (2011)1189ndash1198
[9] G Bartosz Reactive oxygen species destroyers or messengers Biochem Phar-macol 77 (2009) 1303ndash1315
[10] T Ntimbane B Comte G Mailhot Y Berthiaume V Poitout M Prentki RRabasa-Lhoret E Levy Cystic fibrosis-related diabetes from CFTR dysfunctionto oxidative stress Clin Biochem 30 (2009) 153ndash177
[11] A van der Vliet JP Eiserich GP Marelich B Halliwell CE Cross Oxidativestress in cystic fibrosis does it occur and does it matter Adv Pharmacol 38(1997) 491ndash513
[12] AM Cantin TB White CE Cross HJ Forman RJ Sokol D Borowitz Antioxi-dants in cystic fibrosis Conclusions from the CF antioxidant workshop Bethes-da Maryland Free Radic Biol Med 42 (2007) 15ndash31
[13] LT McGrath P Mallon L Dowey B Silke E McClean M McDonnell A DevineS Copeland S Elborn Oxidative stress during acute respiratory exacerbations incystic fibrosis Thorax 54 (1999) 518ndash523
[14] E Thomson S Brennan R Senthilmohan CL Gangell AL Chapman PD SlyAJ Kettle E Balding LJ Berry JB Carlin R Carzino N de Klerk T Douglas CFoo LW Garratt GL Hall J Harrison A Kicic IA Laing KM Logie J MassieLS Mott C Murray F Parsons N Pillarisetti SR Poreddy SC RanganathanCF Robertson R Robins-Browne PJ Robinson B Skoric SM Stick ENSutanto E Williamson Identifying peroxidases and their oxidants in the earlypathology of cystic fibrosis Free Radic Biol Med 49 (2010) 1354ndash1360
[15] SP Range C Dunster AJ Knox FJ Kelly Treatment of pulmonary exacerba-tions of cystic fibrosis leads to improved antioxidant status Eur Respir J 13(1999) 560ndash564
[16] L Coppo P Ghezzi Thiol regulation of pro-inflammatory cytokines and innateimmunity protein S-thiolation as a novel molecular mechanism Biochem SocTrans 39 (2011) 1268ndash1272
[17] C Verhaeghe C Remouchamps B Hennuy A Vanderplasschen A Chariot SPTabruyn C Oury V Bours Role of IKK and ERK pathways in intrinsic inflamma-tion of cystic fibrosis airways Biochem Pharmacol 73 (2007) 1982ndash1994
[18] TL Bonfield JR Panuska MW Konstan KA Hilliard JB Hilliard H Ghnaim MBerger Inflammatory cytokines in cystic fibrosis lungs Am J Respir Crit CareMed 152 (1995) 2111ndash2118
[19] TL Noah HR Black PW Cheng RE Wood MW Leigh Nasal and bronchoal-veolar lavage fluid cytokines in early cystic fibrosis J Infect Dis 175 (1997)638ndash647
[20] MJ Welsh BW Ramsey FJ Accurso GR Cutting Cystic Fibrosis McGraw-HillNew York 2001
[21] TZ Khan JS Wagener T Bost J Martinez FJ Accurso DW Riches Early pul-monary inflammation in infants with cystic fibrosis Am J Respir Crit CareMed 151 (1995) 1075ndash1082
[22] FA Ratjen Cystic fibrosis pathogenesis and future treatment strategies RespirCare 54 (2009) 595ndash605
[23] J Jacquot O Tabary P Le Rouzic A Clement Airway epithelial cell inflamma-tory signalling in cystic fibrosis Int J Biochem Cell Biol 40 (2008)1703ndash1715
[24] CM Greene P Branagan NG McElvaney Toll-like receptors as therapeutic tar-gets in cystic fibrosis Expert Opin Ther Targets 12 (2008) 1481ndash1495
[25] M Rottner JM Freyssinet MC Martinez Mechanisms of the noxious inflam-matory cycle in cystic fibrosis Respir Res 10 (2009) 23
[26] G Cabrini V Bezzerri I Mancini E Nicolis MC Dechecchi A Tamanini ILampronti L Piccagli N Bianchi M Borgatti R Gambari Targeting transcrip-tion factor activity as a strategy to inhibit pro-inflammatory genes involved incystic fibrosis decoy oligonucleotides and low-molecular weight compoundsCurr Med Chem 17 (2010) 4392ndash4404
[27] CM Greene NG McElvaney Proteases and antiproteases in chronic neutrophiliclungdiseasemdash relevance to drug discovery Br J Pharmacol 158 (2009) 1048ndash1058
[28] AM Cantin Potential for antioxidant therapy of cystic fibrosis Curr Opin PulmMed 10 (2004) 531ndash536
[29] JF Chmiel MW Konstan Inflammation and anti-inflammatory therapies forcystic fibrosis Clin Chest Med 28 (2007) 331ndash346
[30] DP Nichols MW Konstan JF Chmiel Anti-inflammatory therapies for cys-tic fibrosis-related lung disease Clin Rev Allergy Immunol 35 (2008)135ndash153
[31] AJ Kettle T Chan I Osberg R Senthilmohan AL Chapman TJ Mocatta JSWagener Myeloperoxidase and protein oxidation in the airways of youngchildren with cystic fibrosis Am J Respir Crit Care Med 170 (2004)1317ndash1323
[32] H Fischer Mechanisms and function of DUOX in epithelia of the lung AntioxidRedox Signal 11 (2009) 2453ndash2465
[33] B Rada TL Leto Oxidative innate immune defenses by NoxDuox familyNADPH oxidases Contrib Microbiol 15 (2008) 164ndash187
[34] P Moskwa D Lorentzen KJ Excoffon J Zabner PB McCray Jr WM NauseefC Dupuy B Banfi A novel host defense system of airways is defective in cysticfibrosis Am J Respir Crit Care Med 175 (2007) 174ndash183
[35] D Lorentzen L Durairaj AA Pezzulo Y Nakano J Launspach DA Stoltz GZamba PB McCray Jr J Zabner MJ Welsh WM Nauseef B Banfi Concentra-tion of the antibacterial precursor thiocyanate in cystic fibrosis airway secre-tions Free Radic Biol Med 50 (2011) 1144ndash1150
[36] Y Xu S Szep Z Lu The antioxidant role of thiocyanate in the pathogenesis ofcystic fibrosis and other inflammation-related diseases Proc Natl Acad Sci US A 106 (2009) 20515ndash20519
[37] MP Rogan CC Taggart CM Greene PG Murphy SJ ONeill NG McElvaneyLoss of microbicidal activity and increased formation of biofilm due to decreasedlactoferrin activity in patients with cystic fibrosis J Infect Dis 190 (2004)1245ndash1253
[38] B Halliwell JM Guttridge Free Radicals in Biology and Medicine Fourth editionOxford University Press New York 2007
[39] B Rada K Lekstrom S Damian C Dupuy TL Leto The Pseudomonastoxin pyocyanin inhibits the dual oxidase-based antimicrobial system as itimposes oxidative stress on airway epithelial cells J Immunol 181 (2008)4883ndash4893
[40] C Schwarzer B Illek JH Suh SJ Remington H Fischer TE Machen Organelleredox of CF and CFTR-corrected airway epithelia Free Radic Biol Med 43(2007) 300ndash316
[41] JH Roum R Buhl NG McElvaney Z Borok RG Crystal Systemic deficiency ofglutathione in cystic fibrosis J Appl Physiol 75 (1993) 2419ndash2424
[42] VM Hudson Rethinking cystic fibrosis pathology the critical role of abnormalreduced glutathione (GSH) transport caused by CFTR mutation Free RadicBiol Med 30 (2001) 1440ndash1461
[43] PJ Barnes RA Dweik AF Gelb PG Gibson SC George H Grasemann IDPavord F Ratjen PE Silkoff DR Taylor N Zamel Exhaled nitric oxide in pul-monary diseases a comprehensive review Chest 138 (2010) 682ndash692
[44] H Grasemann E Michler M Wallot F Ratjen Decreased concentration of ex-haled nitric oxide (NO) in patients with cystic fibrosis Pediatr Pulmonol 24(1997) 173ndash177
[45] H Grasemann F Ratjen Cystic fibrosis lung disease the role of nitric oxidePediatr Pulmonol 28 (1999) 442ndash448
[46] B Gaston F Ratjen JW Vaughan NR Malhotra RG Canady AH Snyder JFHunt S Gaertig JB Goldberg Nitrogen redox balance in the cystic fibrosis air-way effects of antipseudomonal therapy Am J Respir Crit Care Med 165(2002) 387ndash390
[47] H Grasemann I Ioannidis RP Tomkiewicz H de Groot BK Rubin F RatjenNitric oxide metabolites in cystic fibrosis lung disease Arch Dis Child 78(1998) 49ndash53
[48] H Grasemann R Schwiertz S Matthiesen K Racke F Ratjen Increased argi-nase activity in cystic fibrosis airways Am J Respir Crit Care Med 172(2005) 1523ndash1528
[49] H Grasemann S Al-Saleh JA Scott D Shehnaz A Mehl R Amin M Rafii PPencharz J Belik F Ratjen Asymmetric dimethylarginine contributes to airwaynitric oxide deficiency in patients with cystic fibrosis Am J Respir Crit CareMed 183 (2011) 1363ndash1368
[50] H Grasemann F Kurtz F Ratjen Inhaled L-arginine improves exhaled nitricoxide and pulmonary function in patients with cystic fibrosis Am J RespirCrit Care Med 174 (2006) 208ndash212
[51] H Grasemann F Ratjen Emerging therapies for cystic fibrosis lung disease Ex-pert Opin Emerg Drugs 15 (2010) 653ndash659
[52] BM Morrissey K Schilling JV Weil PE Silkoff DM Rodman Nitric oxide andprotein nitration in the cystic fibrosis airway Arch Biochem Biophys 406(2002) 33ndash39
[53] R Radi Nitric oxide oxidants and protein tyrosine nitration Proc Natl AcadSci U S A 101 (2004) 4003ndash4008
[54] J Chen M Kinter S Shank C Cotton TJ Kelley AG Ziady Dysfunction of Nrf-2in CF epithelia leads to excess intracellular H2O2 and inflammatory cytokineproduction PLoS One 3 (2008) e3367
[55] F Galli M Piroddi C Annetti C Aisa E Floridi A Floridi Oxidative stress andreactive oxygen species Contrib Nephrol 149 (2005) 240ndash260
[56] DT Wright LA Cohn H Li B Fischer CM Li KB Adler Interactions of oxygenradicals with airway epithelium Environ Health Perspect 102 (Suppl 10)(1994) 85ndash90
[57] I Rahman SR Yang SK Biswas Current concepts of redox signaling in thelungs Antioxid Redox Signal 8 (2006) 681ndash689
[58] Q Li JF Engelhardt Interleukin-1beta induction of NFκB is partially regulatedby H2O2-mediated activation of NFκB-inducing kinase J Biol Chem 281(2006) 1495ndash1505
709F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
[59] E Boncoeur VS Criq E Bonvin T Roque A Henrion-Caude DC Gruenert AClement J Jacquot O Tabary Oxidative stress induces extracellular signal-regulated kinase 12 mitogen-activated protein kinase in cystic fibrosis lung ep-ithelial cells potential mechanism for excessive IL-8 expression Int J BiochemCell Biol 40 (2008) 432ndash446
[60] B Fischer J Voynow Neutrophil elastase induces MUC5AC messenger RNA ex-pression by an oxidant-dependent mechanism Chest 117 (2000) 317Sndash320S
[61] B Rada P Gardina TG Myers TL Leto Reactive oxygen species mediate in-flammatory cytokine release and EGFR-dependent mucin secretion in airwayepithelial cells exposed to Pseudomonas pyocyanin Mucosal Immunol 4(2011) 158ndash171
[62] C Schwarzer H Fischer EJ Kim KJ Barber AD Mills MJ Kurth DC GruenertJH Suh TE Machen B Illek Oxidative stress caused by pyocyanin impairs CFTRClminus transport in human bronchial epithelial cells Free Radic Biol Med 45(2008) 1653ndash1662
[63] J Hull M South P Phelan K Grimwood Surfactant composition in infants andyoung children with cystic fibrosis Am J Respir Crit Care Med 156 (1997)161ndash165
[64] KC Meyer A Sharma R Brown M Weatherly FR Moya J Lewandoski JJZimmerman Function and composition of pulmonary surfactant andsurfactant-derived fatty acid profiles are altered in young adults with cystic fi-brosis Chest 118 (2000) 164ndash174
[65] MK Pulfer RC Murphy Formation of biologically active oxysterols during ozo-nolysis of cholesterol present in lung surfactant J Biol Chem 279 (2004)26331ndash26338
[66] V Starosta E Rietschel K Paul U Baumann M Griese Oxidative changes ofbronchoalveolar proteins in cystic fibrosis Chest 129 (2006) 431ndash437
[67] V Starosta M Griese Oxidative damage to surfactant protein D in pulmonarydiseases Free Radic Res 40 (2006) 419ndash425
[68] M Griese R Essl R Schmidt E Rietschel F Ratjen M Ballmann K Paul Pulmo-nary surfactant lung function and endobronchial inflammation in cystic fibro-sis Am J Respir Crit Care Med 170 (2004) 1000ndash1005
[69] M Griese R Essl R Schmidt M Ballmann K Paul E Rietschel F Ratjen Se-quential analysis of surfactant lung function and inflammation in cystic fibrosispatients Respir Res 6 (2005) 133
[70] LG Wood DA Fitzgerald PG Gibson DM Cooper ML Garg Increased plasmafatty acid concentrations after respiratory exacerbations are associated with el-evated oxidative stress in cystic fibrosis patients Am J Clin Nutr 75 (2002)668ndash675
[71] P Montuschi SA Kharitonov G Ciabattoni M Corradi L van Rensen DM Ged-des ME Hodson PJ Barnes Exhaled 8-isoprostane as a new non-invasive bio-marker of oxidative stress in cystic fibrosis Thorax 55 (2000) 205ndash209
[72] CE Collins P Quaggiotto L Wood EV OLoughlin RL Henry ML Garg Elevat-ed plasma levels of F2 alpha isoprostane in cystic fibrosis Lipids 34 (1999)551ndash556
[73] D Hartl V Starosta K Maier I Beck-Speier C Rebhan BF Becker P Latzin RFischer F Ratjen RM Huber E Rietschel S Krauss-Etschmann M Griese In-haled glutathione decreases PGE2 and increases lymphocytes in cystic fibrosislungs Free Radic Biol Med 39 (2005) 463ndash472
[74] GL Milne H Yin JD Morrow Human biochemistry of the isoprostane pathwayJ Biol Chem 283 (2008) 15533ndash15537
[75] G Ciabattoni G Davi M Collura L Iapichino F Pardo A Ganci R Romagnoli JMaclouf C Patrono In vivo lipid peroxidation and platelet activation in cystic fi-brosis Am J Respir Crit Care Med 162 (2000) 1195ndash1201
[76] C Garenc P Julien E Levy Oxysterols in biological systems the gastrointestinaltract liver vascular wall and central nervous system Free Radic Res 44 (2011)47ndash73
[77] AM Cantin SL North RC Hubbard RG Crystal Normal alveolar epithelial lin-ing fluid contains high levels of glutathione J Appl Physiol 63 (1987) 152ndash157
[78] R Tirouvanziam CK Conrad T Bottiglieri LA Herzenberg RB Moss High-dose oral N-acetylcysteine a glutathione prodrug modulates inflammation incystic fibrosis Proc Natl Acad Sci U S A 103 (2006) 4628ndash4633
[79] LW Velsor C Kariya R Kachadourian BJ Day Mitochondrial oxidative stressin the lungs of cystic fibrosis transmembrane conductance regulator proteinmutant mice Am J Respir Cell Mol Biol 35 (2006) 579ndash586
[80] M Kelly-Aubert S Trudel J Fritsch T Nguyen-Khoa M Baudouin-Legros SMoriceau L Jeanson F Djouadi C Matar M Conti M Ollero F Brouillard AEdelman GSH monoethyl ester rescues mitochondrial defects in cystic fibrosismodels Hum Mol Genet 20 (2011) 2745ndash2759
[81] P Ghezzi Role of glutathione in immunity and inflammation in the lung Int JGen Med 4 (2011) 105ndash113
[82] N Dauletbaev K Viel R Buhl TO Wagner J Bargon Glutathione and glutathi-one peroxidase in sputum samples of adult patients with cystic fibrosis J CystFibros 3 (2004) 119ndash124
[83] CE Cross A van der Vliet CA ONeill S Louie B Halliwell Oxidants antioxi-dants and respiratory tract lining fluids Environ Health Perspect 102 (Suppl10) (1994) 185ndash191
[84] K Takeyama K Dabbagh J Jeong Shim T Dao-Pick IF Ueki JA Nadel Oxida-tive stress causes mucin synthesis via transactivation of epidermal growth factorreceptor role of neutrophils J Immunol 164 (2000) 1546ndash1552
[85] N Ballatori SM Krance S Notenboom S Shi K Tieu CL Hammond Glutathi-one dysregulation and the etiology and progression of human diseases BiolChem 390 (2009) 191ndash214
[86] SR Soltaninassab KR Sekhar MJ Meredith ML Freeman Multi-faceted regu-lation of gamma-glutamylcysteine synthetase J Cell Physiol 182 (2000)163ndash170
[87] HR Lopez-Mirabal JR Winther Redox characteristics of the eukaryotic cytosolBiochim Biophys Acta 1783 (2008) 629ndash640
[88] C Hwang AJ Sinskey HF Lodish Oxidized redox state of glutathione in the en-doplasmic reticulum Science 257 (1992) 1496ndash1502
[89] M Murphy Mitochondrial thiols in antioxidant protection and redox signallingdistinct roles for glutathionylation and other thiol modifications AntioxidRedox Signal (2011) ahead of print doi101089ars20114289
[90] BJ Day AM van Heeckeren E Min LW Velsor Role for cystic fibrosis trans-membrane conductance regulator protein in a glutathione response to bronch-opulmonary Pseudomonas infection Infect Immun 72 (2004) 2045ndash2051
[91] Y Zhang K Duan Glutathione exhibits antibacterial activity and increases tetra-cycline efficacy against Pseudomonas aeruginosa Sci China C Life Sci 52 (2009)501ndash505
[92] VM Hudson New insights into the pathogenesis of cystic fibrosis pivotal roleof glutathione system dysfunction and implications for therapy Treat RespirMed 3 (2004) 353ndash363
[93] LW Velsor A van Heeckeren BJ Day Antioxidant imbalance in the lungs ofcystic fibrosis transmembrane conductance regulator protein mutant miceAm J Physiol Lung Cell Mol Physiol 281 (2001) L31ndashL38
[94] I Kogan M Ramjeesingh C Li JF Kidd Y Wang EM Leslie SP Cole CE BearCFTR directly mediates nucleotide-regulated glutathione flux EMBO J 22(2003) 1981ndash1989
[95] NS Gould S Gauthier CT Kariya E Min J Huang DJ Brian Hypertonic salineincreases lung epithelial lining fluid glutathione and thiocyanate two protectiveCFTR-dependent thiols against oxidative injury Respir Res 11 (2010) 119
[96] VT Vasu SJ de Cruz JS Houghton KA Hayakawa BM Morrissey CE CrossJP Eiserich Evaluation of thiol-based antioxidant therapeutics in cystic fibrosissputum focus on myeloperoxidase Free Radic Res 45 (2011) 165ndash176
[97] L Roussel G Martel J Berube S Rousseau P aeruginosa drives CXCL8 synthesisvia redundant toll-like receptors and NADPH oxidase in CFTRF508 airway epi-thelial cells J Cyst Fibros 10 (2011) 107ndash113
[98] GW Lau DJ Hassett H Ran F Kong The role of pyocyanin in Pseudomonas aer-uginosa infection Trends Mol Med 10 (2004) 599ndash606
[99] R Wilson DA Sykes D Watson A Rutman GW Taylor PJ Cole Measurementof Pseudomonas aeruginosa phenazine pigments in sputum and assessment oftheir contribution to sputum sol toxicity for respiratory epithelium InfectImmun 56 (1988) 2515ndash2517
[100] M Muller Pyocyanin induces oxidative stress in human endothelial cells andmodulates the glutathione redox cycle Free Radic Biol Med 33 (2002)1527ndash1533
[101] YQ OMalley KJ Reszka BE Britigan Direct oxidation of 2prime7prime-dichlorodihy-drofluorescein by pyocyanin and other redox-active compounds independentof reactive oxygen species production Free Radic Biol Med 36 (2004)90ndash100
[102] CC Caldwell Y Chen HS Goetzmann Y Hao MT Borchers DJ Hassett LRYoung D Mavrodi L Thomashow GW Lau Pseudomonas aeruginosa exotoxinpyocyanin causes cystic fibrosis airway pathogenesis Am J Pathol 175 (2009)2473ndash2488
[103] YQ OMalley KJ Reszka DR Spitz GM Denning BE Britigan Pseudomonasaeruginosa pyocyanin directly oxidizes glutathione and decreases its levels inairway epithelial cells Am J Physiol Lung Cell Mol Physiol 287 (2004)L94ndashL103
[104] M Muller Glutathione modulates the toxicity of but is not a biologically rele-vant reductant for the Pseudomonas aeruginosa redox toxin pyocyanin FreeRadic Biol Med 50 (2011) 971ndash977
[105] R Cheluvappa R Shimmon M Dawson SN Hilmer DG Le Couteur Reactionsof Pseudomonas aeruginosa pyocyanin with reduced glutathione Acta BiochimPol 55 (2008) 571ndash580
[106] JH Widdicombe Transgenic animals may help resolve a sticky situation in cys-tic fibrosis J Clin Invest 120 (2010) 3093ndash3096
[107] X Sun H Sui JT Fisher Z Yan X Liu HJ Cho NS Joo Y Zhang W Zhou Y YiJM Kinyon DC Lei-Butters MA Griffin P Naumann M Luo J Ascher KWang T Frana JJ Wine DK Meyerholz JF Engelhardt Disease phenotype ofa ferret CFTR-knockout model of cystic fibrosis J Clin Invest 120 (2010)3149ndash3160
[108] NS Joo HJ Cho M Khansaheb JJ Wine Hyposecretion of fluid from trachealsubmucosal glands of CFTR-deficient pigs J Clin Invest 120 (2010) 3161ndash3166
[109] A Bragonzi Murine models of acute and chronic lung infection with cystic fibro-sis pathogens IJMM 300 (2010) 584ndash593
[110] AM van Heeckeren MD Schluchter Murine models of chronic Pseudomonasaeruginosa lung infection Lab Anim 36 (2002) 291ndash312
[111] A Bragonzi D Worlitzsch GB Pier P Timpert M Ulrich M Hentzer JB Ander-sen M Givskov M Conese G Doring Nonmucoid Pseudomonas aeruginosa ex-presses alginate in the lungs of patients with cystic fibrosis and in a mousemodel J Infect Dis 192 (2005) 410ndash419
[112] GS CW Bedrossian DB Singer JJ Hansen HS Rosenberg The lung in cysticfibrosis A quantitative study including prevalence of pathologic findingsamong different age groups Hum Pathol 7 (1976) 195ndash204
[113] WD HA Cash B McCullough WG Johanson Jr JA Bass A rat model of chron-ic respiratory infection with Pseudomonas aeruginosa Am Rev Respir Dis 119(1979) 453ndash459
[114] EM JR Starke C Langston CJ Baker A mouse model of chronic pulmonary in-fection with Pseudomonas aeruginosa and Pseudomonas cepacia Pediatr Res 22(1987) 698ndash702
[115] TJ AM van Heeckeren RW Walenga MW Konstan PB Davis B ErokwuMA Haxhiu TW Ferkol Effect of Pseudomonas infection on weight loss lung
710 F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
mechanics and cytokines in mice Am J Respir Crit Care Med 161 (2000)271ndash279
[116] T Aw G Wierzbicka DP Jones Oral glutathione increases tissue glutathione invivo Chem Biol Interact 80 (1991) 89ndash97
[117] F Favilli P Marraccini T Iantomasi MT Vincenzini Effect of orally adminis-tered glutathione on glutathione levels in some organs of rats role of specifictransporters Br J Nutr 78 (1997) 293ndash300
[118] C Kariya H Leitner E Min C van Heeckeren A van Heeckeren BJ Day A rolefor CFTR in the elevation of glutathione levels in the lung by oral glutathione ad-ministration Am J Physiol Lung Cell Mol Physiol 292 (2007) L1590ndashL1597
[119] K Atkuri JJ Mantovani LA Herzenberg LA Herzenberg N-Acetylcysteinemdashasafe antidote for cysteineglutathione deficiency Curr Opin Pharmacol 7(2007) 355ndash359
[120] R De Lisle E Roach K Jansson Effects of laxative and N-acetylcysteine onmucus accumulation bacterial load transit and inflammation in the cystic fi-brosis mouse small intestine Am J Physiol Gastrointest Liver Physiol 293(2007) G577ndashG584
[121] A Luciani VR Villella S Esposito N Brunetti-Pierri D Medina C Settembre MGavina L Pulze I Giardino M Pettoello-Mantovani M DApolito S Guido EMasliah B Spencer S Quaratino V Raia A Ballabio L Maiuri Defective CFTRinduces aggresome formation and lung inflammation in cystic fibrosis throughROS-mediated autophagy inhibition Nat Cell Biol 12 863ndash875
[122] M Griese J Ramakers A Krasselt V Starosta S Van Koningsbruggen R FischerF Ratjen B Mullinger RM Huber K Maier E Rietschel G Scheuch Improve-ment of alveolar glutathione and lung function but not oxidative state in cysticfibrosis Am J Respir Crit Care Med 169 (2004) 822ndash828
[123] C Bishop VM Hudson SC Hilton C Wilde A pilot study of the effect of inhaledbuffered reduced glutathione on the clinical status of patients with cystic fibro-sis Chest 127 (2005) 308ndash317
[124] WWang C Oliva G Li A Holmgren CH Lillig KL Kirk Reversible silencing of CFTRchloride channels by glutathionylation J Gen Physiol 125 (2005) 127ndash141
[125] N Dauletbaev P Fischer B Aulbach J Gross W Kusche U Thyroff-FriesingerTO Wagner J Bargon A phase II study on safety and efficacy of high-dose N-acetylcysteine in patients with cystic fibrosis Eur J Med Res 14 (2009)352ndash358
[126] R Tirouvanziam Y Gernez CK Conrad RB Moss I Schrijver CE Dunn ZADavies LA Herzenberg Profound functional and signaling changes in viable in-flammatory neutrophils homing to cystic fibrosis airways Proc Natl Acad SciU S A 105 (2008) 4335ndash4339
[127] JH Roum Z Borok NG McElvaney GJ Grimes AD Bokser R Buhl RG Crys-tal Glutathione aerosol suppresses lung epithelial surface inflammatory cell-derived oxidants in cystic fibrosis J Appl Physiol 87 (1999) 438ndash443
[128] A Visca CT Bishop SC Hilton VM Hudson Improvement in clinical markersin CF patients using a reduced glutathione regimen an uncontrolled observa-tional study J Cyst Fibros 7 (2008) 433ndash436
[129] EF Nash A Stephenson F Ratjen E Tullis Nebulized and oral thiol derivativesfor pulmonary disease in cystic fibrosis Cochrane Database Syst Rev (2009)CD007168
[130] AC foundation Drug Development Pipeline 2011[131] S Hoshida T Kuzuya N Yamashita M Nishida S Kitahara M Hori T
Kamada M Tada Gamma-glutamylcysteine ethyl ester for myocardial protec-tion in dogs during ischemia and reperfusion J Am Coll Cardiol 24 (1994)1391ndash1397
[132] J Lok W Leung S Zhao S Pallast K van Leyen S Guo X Wang A Yalcin EHLo Gamma-glutamylcysteine ethyl ester protects cerebral endothelial cells dur-ing injury and decreases bloodndashbrain barrier permeability after experimentalbrain trauma J Neurochem 118 (2011) 248ndash255
[133] Z Borok R Buhl GJ Grimes AD Bokser RC Hubbard KJ Holroyd JH RoumDB Czerski AM Cantin RG Crystal Effect of glutathione aerosol on oxidantndashantioxidant imbalance in idiopathic pulmonary fibrosis Lancet 338 (1991)215ndash216
[134] KJ Holroyd R Buhl Z Borok JH Roum AD Bokser GJ Grimes D Czerski AMCantin RG Crystal Correction of glutathione deficiency in the lower respiratorytract of HIV seropositive individuals by glutathione aerosol treatment Thorax 48(1993) 985ndash989
[135] J Hull P Vervaart K Grimwood P Phelan Pulmonary oxidative stress responsein young children with cystic fibrosis Thorax 52 (1997) 557ndash560
[136] A Corti A Paolicchi M Franzini S Dominici AF Casini A Pompella The S-thiolating activity of membrane gamma-glutamyltransferase formation ofcysteinyl-glycine mixed disulfides with cellular proteins and in the cell microen-vironment Antioxid Redox Signal 7 (2005) 911ndash918
[137] A Corti M Franzini AF Casini A Paolicchi A Pompella Vitamin C supply tobronchial epithelial cells linked to glutathione availability in elfmdasha role for se-creted gamma-glutamyltransferase J Cyst Fibros 7 (2008) 174ndash178
[138] A Munck Nutritional considerations in patients with cystic fibrosis Expert RevRespir Med 4 (2010) 47ndash56
[139] JL Matel CE Milla Nutrition in cystic fibrosis Semin Respir Crit Care Med 30(2009) 579ndash586
[140] D Salvatore R Buzzetti E Baldo MP Forneris V Lucidi D Manunza IMarinelli B Messore AS Neri V Raia ML Furnari G Mastella An overviewof international literature from cystic fibrosis registries 2 Neonatal screeningand nutritiongrowth J Cyst Fibros 9 (2010) 75ndash83
[141] KF Joosten JM Hulst Malnutrition in pediatric hospital patients current is-sues Nutrition 27 (2011) 133ndash137
[142] S Fustik T Jacovska L Spirevska S Koceva Protein-energy malnutrition as thefirst manifestation of cystic fibrosis in infancy Pediatr Int 51 (2009) 678ndash683
[143] J Himmelfarb E McMonagle Albumin is the major plasma protein target of ox-idant stress in uremia Kidney Int 60 (2001) 358ndash363
[144] P Stenvinkel JJ Carrero J Axelsson B Lindholm O Heimburger Z MassyEmerging biomarkers for evaluating cardiovascular risk in the chronic kidneydisease patient how do new pieces fit into the uremic puzzle Clin J Am SocNephrol 3 (2008) 505ndash521
[145] M Roche P Rondeau NR Singh E Tarnus E Bourdon The antioxidant proper-ties of serum albumin FEBS Lett 582 (2008) 1783ndash1787
[146] D Giustarini A Milzani I Dalle-Donne R Rossi Red blood cells as a physiolog-ical source of glutathione for extracellular fluids Blood Cells Mol Dis 40 (2008)174ndash179
[147] A Meister ME Anderson Glutathione Annu Rev Biochem 52 (1983) 711ndash760[148] B Alvarez S Carballal L Turell R Radi Formation and reactions of sulfenic acid
in human serum albumin Methods Enzymol 473 (2010) 117ndash136[149] S Carballal B Alvarez L Turell H Botti BA Freeman R Radi Sulfenic acid in
human serum albumin Amino Acids 32 (2007) 543ndash551[150] LR Barclay AM Bailey D Kong The antioxidant activity of alpha-tocopherol-
bovine serum albumin complex in micellar and liposome autoxidations J BiolChem 260 (1985) 15809ndash15814
[151] T Ishii T Ichikawa K Minoda K Kusaka S Ito Y Suzuki M Akagawa K Mochi-zuki T Goda T Nakayama Human serum albumin as an antioxidant in the ox-idation of (minus)-epigallocatechin gallate participation of reversible covalentbinding for interaction and stabilization Biosci Biotechnol Biochem 75(2011) 100ndash106
[152] F Galli S Rovidati S Benedetti U Buoncristiani C Covarelli A Floridi F Canes-trari Overexpression of erythrocyte glutathione S-transferase in uremia and di-alysis Clin Chem 45 (1999) 1781ndash1788
[153] D Borowitz RD Baker V Stallings Consensus report on nutrition for pediat-ric patients with cystic fibrosis J Pediatr Gastroenterol Nutr 35 (2002)246ndash259
[154] LJ Filer Jr SW Wright MP Manning KE Mason Absorption of alpha-tocopherol and tocopherylesters by premature and full term infants and chil-dren in health and disease Pediatrics 8 (1951) 328ndash339
[155] L Lancellotti C DOrazio G Mastella G Mazzi U Lippi Deficiency of vitamins Eand A in cystic fibrosis is independent of pancreatic function and current en-zyme and vitamin supplementation Eur J Pediatr 155 (1996) 281ndash285
[156] MN Sathe AS Patel Update in pediatrics focus on fat-soluble vitamins NutrClin Pract 25 (2010) 340ndash346
[157] MG Traber The ABCs of vitamin E and beta-carotene absorption Am J ClinNutr 80 (2004) 3ndash4
[158] TF Dolan Jr Hemolytic anemia and edema as the initial signs in infants withcystic fibrosis Consider this diagnosis even in absence of pulmonary symptomsClin Pediatr 15 (1976) 597ndash600
[159] DR James M Alfaham MC Goodchild Increased susceptibility to peroxide-induced haemolysis with normal vitamin E concentrations in cystic fibrosisClin Chim Acta 204 (1991) 279ndash290
[160] SA Peters FJ Kelly Vitamin E supplementation in cystic fibrosis J Pediatr Gas-troenterol Nutr 22 (1996) 341ndash345
[161] A Maqbool VA Stallings Update on fat-soluble vitamins in cystic fibrosis CurrOpin Pulm Med 14 (2008) 574ndash581
[162] SD Sagel MK Sontag MM Anthony P Emmett KA Papas Effect of anantioxidant-rich multivitamin supplement in cystic fibrosis J Cyst Fibros 10(2011) 31ndash36
[163] F Galli A Azzi Present trends in vitamin E research Biofactors 36 (2010)33ndash42
[164] A Hamahata P Enkhbaatar ER Kraft M Lange SW Leonard MG Traber RACox FC Schmalstieg HK Hawkins EB Whorton EM Horvath C Szabo LDTraber DN Herndon DL Traber Gamma-tocopherol nebulization by a lipidaerosolization device improves pulmonary function in sheep with burn andsmoke inhalation injury Free Radic Biol Med 45 (2008) 425ndash433
[165] JP Anais N Razzouq M Carvalho C Fernandez A Astier M Paul A AstierH Fessi AM Lorino Development of alpha-tocopherol acetate nanoparti-cles influence of preparative processes Drug Dev Ind Pharm 35 (2009)216ndash223
[166] JM Zingg Molecular and cellular activities of vitamin E analogues Mini RevMed Chem 7 (2007) 543ndash558
[167] V Viola F Pilolli M Piroddi E Pierpaoli F Orlando M Provinciali M Betti FMazzini F Galli Why tocotrienols work better insights into the in vitro anti-cancer mechanism of vitamin E Genes Nutr 7 (2011) 29ndash41
[168] F Galli F Mazzini L Bamonti L Gille S Bohmdorfer M Piroddi T Netscher FJKelly T Rosenau Tocotrienamines and tocopheramines reactions with radicalsand metal ions Bioorg Med Chem 19 (2011) 6483ndash6491
[169] A Kuhad K Chopra Attenuation of diabetic nephropathy by tocotrienol in-volvement of NFκB signaling pathway Life Sci 84 (2009) 296ndash301
[170] Q Jiang X Yin MA Lill ML Danielson H Freiser J Huang Long-chain carbox-ychromanols metabolites of vitamin E are potent inhibitors of cyclooxygenasesProc Natl Acad Sci U S A 105 (2008) 20464ndash20469
[171] ER Miller III R Pastor-Barriuso D Dalal RA Riemersma LJ Appel E GuallarMeta-analysis high-dosage vitamin E supplementation may increase all-causemortality Ann Intern Med 142 (2005) 37ndash46
[172] JN Hathcock A Azzi J Blumberg T Bray A Dickinson B Frei I Jialal CSJohnston FJ Kelly K Kraemer L Packer S Parthasarathy H Sies MG TraberVitamins E and C are safe across a broad range of intakes Am J Clin Nutr 81(2005) 736ndash745
[173] R Brigelius-Flohe F Galli Vitamin E a vitamin still awaiting the detection of itsbiological function Mol Nutr Food Res 54 (2010) 583ndash587
711F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
[174] MG Traber B Frei JS Beckman Vitamin E revisited do new data validate ben-efits for chronic disease prevention Curr Opin Lipidol 19 (2008) 30ndash38
[175] F Galli Meeting report Vitamin E Satellite Symposium (VESS) associated to theAnnual Meeting of the SFRR-Europe Rome 26 August 2009 Free Radic Res 43(2009) 1256ndash1257
[176] LJ Roberts II JA Oates MF Linton S Fazio BP Meador MD Gross Y Shyr JDMorrow The relationship between dose of vitamin E and suppression of oxida-tive stress in humans Free Radic Biol Med 43 (2007) 1388ndash1393
[177] EFSA- EFSA Scientific Opinion of the Panel on Food Additives FlavouringsProcessing Aids and Materials in Contact with Food on a request from the Com-mission on mixed tocopherols tocotrienol tocopherol and tocotrienols assources for vitamin E in EFSA- EFSA (Ed) vol 640 The EFSA Journal2008 pp 1ndash34
[178] P Rust I Eichler S Renner I Elmadfa Long-term oral beta-carotene supple-mentation in patients with cystic fibrosis mdash effects on antioxidative status andpulmonary function Ann Nutr Metab 44 (2000) 30ndash37
[179] G Lepage J Champagne N Ronco A Lamarre I Osberg RJ Sokol CC Roy Sup-plementation with carotenoids corrects increased lipid peroxidation in childrenwith cystic fibrosis Am J Clin Nutr 64 (1996) 87ndash93
[180] BM Winklhofer-Roob H Puhl G Khoschsorur MA vant Hof H EsterbauerDH Shmerling Enhanced resistance to oxidation of low density lipoproteinsand decreased lipid peroxide formation during beta-carotene supplementationin cystic fibrosis Free Radic Biol Med 18 (1995) 849ndash859
[181] RC Graham-Maar JI Schall N Stettler BS Zemel VA Stallings Elevated vita-min A intake and serum retinol in preadolescent children with cystic fibrosisAm J Clin Nutr 84 (2006) 174ndash182
[182] I Sadowska-Woda M Rachel J Pazdan E Bieszczad-Bedrejczuk K PawliszakNutritional supplement attenuates selected oxidative stress markers in pediatricpatients with cystic fibrosis Nutr Res (New York NY) 31 (2011) 509ndash518
[183] KA Papas MK Sontag C Pardee RJ Sokol SD Sagel FJ Accurso JS WagenerA pilot study on the safety and efficacy of a novel antioxidant rich formulation inpatients with cystic fibrosis J Cyst Fibros 7 (2008) 60ndash67
[184] Y Saito A Fukuhara K Nishio M Hayakawa Y Ogawa H Sakamoto K Fujii YYoshida E Niki Characterization of cellular uptake and distribution of coen-zyme Q10 and vitamin E in PC12 cells J Nutr Biochem 20 (2009) 350ndash357
[185] AA Franke CM Morrison JL Bakke LJ Custer X Li RV Cooney CoenzymeQ10 in human blood native levels and determinants of oxidation during proces-sing and storage Free Radic Biol Med 48 (2010) 1610ndash1617
[186] HN Bhagavan RK Chopra Plasma coenzyme Q10 response to oral ingestion ofcoenzyme Q10 formulations Mitochondrion 7 (2007) S78ndashS88 (Suppl)
[187] HN Bhagavan RK Chopra Coenzyme Q10 absorption tissue uptake metabo-lism and pharmacokinetics Free Radic Res 40 (2006) 445ndash453
[188] F Galli R Lee C Dunster FJ Kelly Gas chromatography mass spectrometryanalysis of carboxyethyl-hydroxychroman metabolites of alpha- and gamma-tocopherol in human plasma Free Radic Biol Med 32 (2002) 333ndash340
[189] F Galli R Lee J Atkinson A Floridi FJ Kelly Gamma-tocopherol biokineticsand transformation in humans Free Radic Res 37 (2003) 1225ndash1233
[190] TA Laguna MK Sontag I Osberg JS Wagener FJ Accurso RJ Sokol De-creased total serum coenzyme-Q10 concentrations a longitudinal study in chil-dren with cystic fibrosis J Pediatr 153 (2008) 402ndash407
[191] T Frischer JK Myung G Maurer I Eichler Z Szepfalusi G Lubec Possible dys-regulation of chaperon and metabolic proteins in cystic fibrosis bronchial tissueProteomics 6 (2006) 3381ndash3388
[192] C Andersson MM Zaman AB Jones SD Freedman Alterations in immune re-sponse and PPARLXR regulation in cystic fibrosis macrophages J Cyst Fibros 7(2008) 68ndash78
[193] SD Freedman PG Blanco MM Zaman JC Shea M Ollero IK Hopper DAWeed A Gelrud MM Regan M Laposata JG Alvarez BP OSullivan Associa-tion of cystic fibrosis with abnormalities in fatty acid metabolism N Engl JMed 350 (2004) 560ndash569
[194] S Van Biervliet G Vanbillemont JP Van Biervliet D Declercq E Robberecht AChristophe Relation between fatty acid composition and clinical status or geno-type in cystic fibrosis patients Ann Nutr Metab 51 (2007) 541ndash549
[195] SD Freedman MH Katz EM Parker M Laposata MY Urman JG AlvarezA membrane lipid imbalance plays a role in the phenotypic expression ofcystic fibrosis in cftr(minusminus) mice Proc Natl Acad Sci U S A 96 (1999)13995ndash14000
[196] S Van Biervliet S Vande Velde JP Van Biervliet E Robberecht The effect ofzinc supplements in cystic fibrosis patients Ann Nutr Metab 52 (2008)152ndash156
[197] WR Henderson Jr SJ Astley MM McCready P Kushmerick S Casey JWBecker BW Ramsey Oral absorption of omega-3 fatty acids in patients withcystic fibrosis who have pancreatic insufficiency and in healthy control subjectsJ Pediatr 124 (1994) 400ndash408
[198] I Durieu E Vericel D Guichardant H Roth JP Steghens J Drai RN JosserandE Fontaine M Lagarde G Bellon Fatty acids platelets and oxidative markersfollowing intravenous n-3 fatty acids administration in cystic fibrosis an openpilot observational study J Cyst Fibros 6 (2007) 320ndash326
[199] LG Wood DA Fitzgerald ML Garg Hypothesis vitamin E complements poly-unsaturated fatty acids in essential fatty acid deficiency in cystic fibrosis J AmColl Nutr 22 (2003) 253ndash257
[200] JD Lloyd-Still SB Johnson RT Holman Essential fatty acid status in cystic fi-brosis and the effects of safflower oil supplementation Am J Clin Nutr 34(1981) 1ndash7
[201] A Maqbool JI Schall JF Garcia-Espana BS Zemel B Strandvik VAStallings Serum linoleic acid status as a clinical indicator of essential fatty
acid status in children with cystic fibrosis J Pediatr Gastroenterol Nutr 47(2008) 635ndash644
[202] C Oliver N Jahnke Omega-3 fatty acids for cystic fibrosis Cochrane DatabaseSyst Rev (2011) CD002201
[203] B Strandvik E Gronowitz F Enlund T Martinsson J Wahlstrom Essential fattyacid deficiency in relation to genotype in patients with cystic fibrosis J Pediatr139 (2001) 650ndash655
[204] P Rise S Volpi C Colombo RF Padoan C DOrazio S Ghezzi PMelotti V BennatoC Agostoni BM Assael C Galli Whole blood fatty acid analysis with micromethodin cystic fibrosis and pulmonary disease J Cyst Fibros 9 (2010) 228ndash233
[205] H Cao K Gerhold JR Mayers MM Wiest SM Watkins GS Hotamisligil Iden-tification of a lipokine a lipid hormone linking adipose tissue to systemic me-tabolism Cell 134 (2008) 933ndash944
[206] RR Malapaka SK Khoo J Zhang JH Choi XE Zhou Y Xu Y Gong J Li ELYong MJ Chalmers L Chang JH Resau PR Griffin YE Chen HE Xu Iden-tification and mechanism of a ten carbon fatty acid as a modulating ligand ofperoxisome proliferator activated receptors J Biol Chem 287 (2012)183ndash195
[207] T Hara A Hirasawa A Ichimura I Kimura G Tsujimoto Free fatty acid recep-tors FFAR1 and GPR120 as novel therapeutic targets for metabolic disorders JPharm Sci 100 (2011) 3594ndash3601
[208] R Gupta P Rathi S Bradoo Lipase mediated upgradation of dietary fats andoils Crit Rev Food Sci Nutr 43 (2003) 635ndash644
[209] BH Jennings CC Akoh Lipase-catalyzed modification of rice bran oil to incor-porate capric acid J Agric Food Chem 48 (2000) 4439ndash4443
[210] J Hoeks M Mensink MK Hesselink K Ekroos P Schrauwen Long- andMedium-Chain Fatty Acids Induce Insulin Resistance to a Similar Extent inHumans Despite Marked Differences in Muscle Fat Accumulation J Clin Endo-crinol Metab 97 (2012) 208ndash216
[211] PJ Congden G Bruce MM Rothburn PC Clarke JM Littlewood J KelleherMS Losowsky Vitamin status in treated patients with cystic fibrosis ArchDis Child 56 (1981) 708ndash714
[212] BM Winklhofer-Roob H Ellemunter M Fruhwirth SE Schlegel-Haueter GKhoschsorur MA vant Hof DH Shmerling Plasma vitamin C concentrationsin patients with cystic fibrosis evidence of associations with lung inflammationAm J Clin Nutr 65 (1997) 1858ndash1866
[213] L Shamseer D Adams N Brown JA Johnson S Vohra Antioxidant micronutri-ents for lung disease in cystic fibrosis Cochrane Database Syst Rev (2010)CD007020
[214] C Santi S Santoro Electrophilic Selenium First edition Wiley-VCH VerlagGmbH amp Co KGaA 2012
[215] L Flohe S Toppo G Cozza F Ursini A comparison of thiol peroxidase mecha-nisms Antioxid Redox Signal 15 (2010) 763ndash780
[216] L Flohe JR Andreesen R Brigelius-Flohe M Maiorino F Ursini Selenium theelement of the moon in life on earth IUBMB Life 49 (2000) 411ndash420
[217] V Valdiglesias E Pasaro J Mendez B Laffon In vitro evaluation of seleniumgenotoxic cytotoxic and protective effects a review Arch Toxicol 84(2010) 337ndash351
[218] P Foucaud P Therond M Marchand F Brion JF Demelier J Navarro Seleniumand vitamin E in mucoviscidosis Arch Fr Pediatr 45 (1988) 383ndash386
[219] J Neve R Van Geffel M Hanocq L Molle Plasma and erythrocyte zinc copperand selenium in cystic fibrosis Acta Paediatr Scand 72 (1983) 437ndash440
[220] BM Winklhofer-Roob B Tiran PE Tuchschmid MA vant Hof DH ShmerlingEffects of pancreatic enzyme preparations on erythrocyte glutathione peroxi-dase activities and plasma selenium concentrations in cystic fibrosis FreeRadic Biol Med 25 (1998) 242ndash249
[221] JD Lloyd-Still HE Ganther Selenium and glutathione peroxidase levels in cys-tic fibrosis Pediatrics 65 (1980) 1010ndash1012
[222] D Tsavachidou TJ McDonnell S Wen X Wang F Vakar-Lopez LL Pisters CAPettaway CG Wood KA Do PF Thall C Stephens E Efstathiou R Taylor DGMenter P Troncoso SM Lippman CJ Logothetis J Kim Selenium and vitaminE cell type- and intervention-specific tissue effects in prostate cancer J NatlCancer Inst 101 (2009) 306ndash320
[223] IN Zelko TJ Mariani RJ Folz Superoxide dismutase multigene family acomparison of the CuZn-SOD (SOD1) Mn-SOD (SOD2) and EC-SOD (SOD3)gene structures evolution and expression Free Radic Biol Med 33 (2002)337ndash349
[224] RP Bowler JD Crapo Oxidative stress in airways is there a role for extracellu-lar superoxide dismutase Am J Respir Crit Care Med 166 (2002) S38ndashS43
[225] K Best K McCoy S Gemma RA Disilvestro Copper enzyme activities in cysticfibrosis before and after copper supplementation plus or minus zinc Metabo-lism 53 (2004) 37ndash41
[226] SS Percival GP Kauwell E Bowser M Wagner Altered copper status in adultmen with cystic fibrosis J Am Coll Nutr 18 (1999) 614ndash619
[227] NF Krebs JE Westcott TD Arnold BM Kluger FJ Accurso LV Miller KMHambidge Abnormalities in zinc homeostasis in young infants with cystic fibro-sis Pediatr Res 48 (2000) 256ndash261
[228] D Easley N Krebs M Jefferson L Miller J Erskine F Accurso KM HambidgeEffect of pancreatic enzymes on zinc absorption in cystic fibrosis J Pediatr Gas-troenterol Nutr 26 (1998) 136ndash139
[229] S Van Biervliet JP Van Biervliet E Robberecht Serum zinc in patients with cys-tic fibrosis at diagnosis and after one year of therapy Biol Trace Elem Res 112(2006) 205ndash211
[230] S Van Biervliet JP Van Biervliet S Vande Velde E Robberecht Serum zinc con-centrations in cystic fibrosis patients aged above 4 years a cross-sectional eval-uation Biol Trace Elem Res 119 (2007) 19ndash26
712 F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
[231] F Galli M Cristina Polidori W Stahl P Mecocci FJ Kelly Vitamin E biotransfor-mation in humans Vitam Horm 76 (2007) 263ndash280
[232] J Wiser NE Alexis Q Jiang W Wu C Robinette R Roubey DB Peden In vivogamma-tocopherol supplementation decreases systemic oxidative stress andcytokine responses of human monocytes in normal and asthmatic subjectsFree Radic Biol Med 45 (2008) 40ndash49
[233] JG Wagner Q Jiang JR Harkema B Illek DD Patel BN Ames DB PedenOzone enhancement of lower airway allergic inflammation is prevented bygamma-tocopherol Free Radic Biol Med 43 (2007) 1176ndash1188
[234] JT Harries DP Muller Absorption of different doses of fat soluble and watermiscible preparations of vitamin E in children with cystic fibrosis Arch DisChild 46 (1971) 341ndash344
[235] EI Back C Frindt E Ocenaskova D Nohr M Stern HK Biesalski Can changesin hydrophobicity increase the bioavailability of alpha-tocopherol Eur J Nutr45 (2006) 1ndash6
[236] SZ Nasr MH OLeary C Hillermeier Correction of vitamin E deficiency withfat-soluble versus water-miscible preparations of vitamin E in patients with cys-tic fibrosis J Pediatr 122 (1993) 810ndash812
[237] S Soltani-Frisk E Gronowitz H Andersson B Strandvik Water-miscibletocopherol is not superior to fat-soluble preparation for vitamin E absorptionin cystic fibrosis Acta Paediatr 90 (2001) 1112ndash1115
[238] K Papas J Kalbfleisch R Mohon Bioavailability of a novel water-soluble vi-tamin E formulation in malabsorbing patients Dig Dis Sci 52 (2007)347ndash352
[239] F Antonicelli M Parmentier EM Drost N Hirani I Rahman K Donaldson WMacNee Nacystelyn inhibits oxidant-mediated interleukin-8 expression andNF-kappaB nuclear binding in alveolar epithelial cells Free Radic Biol Med 32(2002) 492ndash502
[240] EM App D Baran I Dab A Malfroot M Coffiner F Vanderbist M King Dose-finding and 24-h monitoring for efficacy and safety of aerosolized Nacystelyn incystic fibrosis Eur Respir J 19 (2002) 294ndash302
[241] MG Traber How much vitamin E hellip Just enough Am J Clin Nutr 84 (2006)959ndash960
[242] JC McCann BN Ames Vitamin K an example of triage theory is micronu-trient inadequacy linked to diseases of aging Am J Clin Nutr 90 (2009)889ndash907
[243] M Fusaro G Crepaldi S Maggi F Galli A DAngelo L Calo S Giannini DMiozzo M Gallieni Vitamin K bone fractures and vascular calcifications inchronic kidney disease an important but poorly studied relationship J Endocri-nol Invest 34 (2010) 317ndash323
[244] JC McCann BN Ames Adaptive dysfunction of selenoproteins from the per-spective of the triage theory why modest selenium deficiency may increaserisk of diseases of aging FASEB J 25 (2011) 1793ndash1814
[245] R Apak K Guclu M Ozyurek B Bektas Oglu M Bener Cupric ion reducing an-tioxidant capacity assay for food antioxidants vitamins polyphenolics and fla-vonoids in food extracts Methods Mol Biol 477 (2008) 163ndash193
[246] F Galli Interactions of polyphenolic compounds with drug disposition and me-tabolism Curr Drug Metab 8 (2007) 830ndash838
[247] RL Prior X Wu K Schaich Standardized methods for the determination of an-tioxidant capacity and phenolics in foods and dietary supplements J Agric FoodChem 53 (2005) 4290ndash4302
[248] C Azbell S Zhang D Skinner J Fortenberry EJ Sorscher BA WoodworthHesperidin stimulates cystic fibrosis transmembrane conductance regulator-mediated chloride secretion and ciliary beat frequency in sinonasal epitheliumOtolaryngol Head Neck Surg 143 (2010) 397ndash404
[249] G Wegrzyn J Jakobkiewicz-Banecka M Gabig-Ciminska E Piotrowska M Nar-ajczyk A Kloska M Malinowska D Dziedzic I Golebiewska M Moskot AWegrzyn Genistein a natural isoflavone with a potential for treatment of ge-netic diseases Biochem Soc Trans 38 (2010) 695ndash701
[250] YC Yu H Miki Y Nakamura A Hanyuda Y Matsuzaki Y Abe M Yasui K Ta-naka TC Hwang SG Bompadre Y Sohma Curcumin and genistein additivelypotentiate G551D-CFTR J Cyst Fibros 10 (2011) 243ndash252
[251] B Illek H Fischer Flavonoids stimulate Cl conductance of human airway epithe-lium in vitro and in vivo Am J Physiol 275 (1998) L902ndashL910
[252] JL Kreindler Cystic fibrosis exploiting its genetic basis in the hunt for newtherapies Pharmacol Ther 125 (2010) 219ndash229
[253] B Illek L Zhang NC Lewis RB Moss JY Dong H Fischer Defective function ofthe cystic fibrosis-causing missense mutation G551D is recovered by genisteinAm J Physiol 277 (1999) C833ndashC839
[254] P Anandakumar S Kamaraj S Jagan G Ramakrishnan R Vinodhkumar TDevaki Capsaicin modulates pulmonary antioxidant defense system during ben-zo(a)pyrene-induced lung cancer in Swiss albinomice Phytother Res 22 (2008)529ndash533
[255] I Rahman Antioxidant therapeutic advances in COPD Ther Adv Respir Dis 2(2008) 351ndash374
[256] AW Boots H Li RP Schins R Duffin JW Heemskerk A Bast GR Haenen Thequercetin paradox Toxicol Appl Pharmacol 222 (2007) 89ndash96
[257] M Joskova S Franova V Sadlonova Acute bronchodilator effect of quercetin inexperimental allergic asthma Bratisl Lek Listy 112 (2011) 9ndash12
[258] HJ Park CM Lee ID Jung JS Lee YI Jeong JH Chang SH Chun MJ Kim IWChoi SC Ahn YK Shin SR Yeom YM Park Quercetin regulates Th1Th2 balancein a murine model of asthma Int Immunopharmacol 9 (2009) 261ndash267
[259] AP Rogerio A Kanashiro C Fontanari EV da Silva YM Lucisano-ValimEG Soares LH Faccioli Anti-inflammatory activity of quercetin and iso-quercitrin in experimental murine allergic asthma Inflamm Res 56 (2007)402ndash408
[260] M Muller Polyphenol cytotoxicity induced by the bacterial toxin pyocyaninrole of NQO1 Free Radic Biol Med 47 (2009) 84ndash91
[261] J Grassmann Terpenoids as plant antioxidants Vitam Horm 72 (2005)505ndash535
[262] P Allen Tea tree oil the science behind the antimicrobial hype Lancet 358(2001) 1245
[263] EC Dasenbrook W Checkley CA Merlo MW Konstan N Lechtzin MP BoyleAssociation between respiratory tract methicillin-resistant Staphylococcus aure-us and survival in cystic fibrosis JAMA 303 (2010) 2386ndash2392
[264] V Bezzerri M Borgatti E Nicolis I Lampronti MC Dechecchi I Mancini PRizzotti R Gambari G Cabrini Transcription factor oligodeoxynucleotides toNF-kappaB inhibit transcription of IL-8 in bronchial cells Am J Respir CellMol Biol 39 (2008) 86ndash96
[265] R Gambari M Borgatti V Bezzerri E Nicolis I Lampronti MC Dechecchi IMancini A Tamanini G Cabrini Decoy oligodeoxyribonucleotides and peptidenucleic acids-DNA chimeras targeting nuclear factor kappa-B inhibition of IL-8 gene expression in cystic fibrosis cells infected with Pseudomonas aeruginosaBiochem Pharmacol 80 (2010) 1887ndash1894
[266] M Adrian P Jeandet AC Douillet-Breuil L Tesson R Bessis Stilbene content ofmature Vitis vinifera berries in response to UV-C elicitation J Agric Food Chem48 (2000) 6103ndash6105
[267] B Paul I Masih J Deopujari C Charpentier Occurrence of resveratrol and pter-ostilbene in age-old darakchasava an ayurvedic medicine from India J Ethno-pharmacol 68 (1999) 71ndash76
[268] I Rahman Antioxidant therapies in COPD Int J Chron Obstruct Pulmon Dis 1(2006) 15ndash29
[269] M Lee S Kim OK Kwon SR Oh HK Lee K Ahn Anti-inflammatory and anti-asthmatic effects of resveratrol a polyphenolic stilbene in a mouse model ofallergic asthma Int Immunopharmacol 9 (2009) 418ndash424
[270] LG Wood PA Wark ML Garg Antioxidant and anti-inflammatory effectsof resveratrol in airway disease Antioxid Redox Signal 13 (2010)1535ndash1548
[271] KV Kiselev Perspectives for production and application of resveratrol ApplMicrobiol Biotechnol 90 (2011) 417ndash425
[272] M Shakibaei C Buhrmann A Mobasheri Resveratrol-mediated SIRT-1 interac-tions with p300 modulate receptor activator of NF-kappaB ligand (RANKL) acti-vation of NF-kappaB signaling and inhibit osteoclastogenesis in bone-derivedcells J Biol Chem 286 (2011) 11492ndash11505
[273] SF Zaidi K Ahmed T Yamamoto T Kondo K Usmanghani M Kadowaki TSugiyama Effect of resveratrol on Helicobacter pylori-induced interleukin-8 secre-tion reactive oxygen species generation and morphological changes in human gas-tric epithelial cells Biol Pharm Bull 32 (2009) 1931ndash1935
[274] JK Kundu YK Shin YJ Surh Resveratrol modulates phorbol ester-inducedpro-inflammatory signal transduction pathways in mouse skin in vivo NF-kappaB and AP-1 as prime targets Biochem Pharmacol 72 (2006)1506ndash1515
[275] NH Nam Naturally occurring NF-kappaB inhibitors Mini Rev Med Chem 6(2006) 945ndash951
[276] JM Smoliga JA Baur HA Hausenblas Resveratrol and healthmdasha comprehen-sive review of human clinical trials Mol Nutr Food Res 55 (2011) 1129ndash1141
[277] ME Juan M Maijo JM Planas Quantification of trans-resveratrol and itsmetabolites in rat plasma and tissues by HPLC J Pharm Biomed Anal 51(2010) 391ndash398
[278] JA Baur DA Sinclair Therapeutic potential of resveratrol the in vivo evidenceNat Rev 5 (2006) 493ndash506
[279] E Nicolis I Lampronti MC Dechecchi M Borgatti A Tamanini N Bianchi VBezzerri I Mancini MG Giri P Rizzotti R Gambari G Cabrini Pyrogallol anactive compound from the medicinal plant Emblica officinalis regulates expres-sion of pro-inflammatory genes in bronchial epithelial cells Int Immunophar-macol 8 (2008) 1672ndash1680
[280] E Nicolis I Lampronti MC Dechecchi M Borgatti A Tamanini V Bezzerri NBianchi M Mazzon I Mancini MG Giri P Rizzotti R Gambari G CabriniModulation of expression of IL-8 gene in bronchial epithelial cells by 5-methoxypsoralen Int Immunopharmacol 9 (2009) 1411ndash1422
[281] M Borgatti I Mancini N Bianchi A Guerrini I Lampronti D Rossi G SacchettiR Gambari Bergamot (Citrus bergamia Risso) fruit extracts and identified com-ponents alter expression of interleukin 8 gene in cystic fibrosis bronchial epithe-lial cell lines BMC Biochem 12 (2011) 15
[282] L Piccagli E Fabbri M Borgatti N Bianchi V Bezzerri I Mancini E Nicolis CMDechecchi I Lampronti G Cabrini R Gambari Virtual screening against p50NF-kappaB transcription factor for the identification of inhibitors of the NF-kappaB-DNA interaction and expression of NF-kappaB upregulated genesChemMedChem 4 (2009) 2024ndash2033
[283] L Piccagli M Borgatti E Nicolis N Bianchi I Mancini I Lampronti D VevaldiF DallAcqua G Cabrini R Gambari Virtual screening against nuclear factorkappaB (NF-kappaB) of a focus library identification of bioactive furocoumarinderivatives inhibiting NF-kappaB dependent biological functions involved incystic fibrosis Bioorg Med Chem 18 (2010) 8341ndash8349
[284] M Borgatti A Chilin L Piccagli I Lampronti N Bianchi I Mancini G Mar-zaro Da Francesco A Guiotto R Gambari Development of a novel furocou-marin derivative inhibiting NF-kappaB dependent biological functionsdesign synthesis and biological effects Eur J Med Chem 46 (2011)4870ndash4877
[285] E Georgy S Le Guellec L Vecellio E Fichant P Stordeur P Bordeau JP PerraudinFeasibility study of OSCN- and lactoferrin (Meveol) nebulization for cysticfibrosis JCyst Fibros 10 (2011) S18
713F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
[286] C Tidei M Piroddi F Galli C Santi Oxidation of thiols promoted by PhSeZnClTetrahedron Lett 53 (2012) 232ndash234
[287] L Semianrio-Vidal C van Hesuden G Mugesh ER Lazarowski Ebselen is a po-tent non-competitive inhibitor of extracellular nucleoside diphosphokinasePurinergic Signal 6 (2010) 383ndash391
[288] C ColussiMC Albertini S Coppola S Rovidati F Galli L Ghibelli H2O2-inducedblockof glycolysis as an active ADP-ribosylation reaction protecting cells from apoptosisFASEB J 14 (2000) 2266ndash2276
[289] H Xiao KL Parkin Induction of phase II enzyme activity by various seleniumcompounds Nutr Cancer 55 (2006) 210ndash223
[290] G Peluffo R Radi Biochemistry of protein tyrosine nitration in cardiovascularpathology Cardiovasc Res 75 (2007) 291ndash302
[291] B Alvarez R Radi Peroxynitrite reactivity with amino acids and proteinsAmino Acids 25 (2003) 295ndash311
[292] B Kamosinska MW Radomski M Duszyk A Radomski SF Man Nitric oxideactivates chloride currents in human lung epithelial cells Am J Physiol 272(1997) L1098ndashL1104
[293] L Chen RP Patel X Teng CA Bosworth JR Lancaster Jr S Matalon Mecha-nisms of cystic fibrosis transmembrane conductance regulator activation by S-nitrosoglutathione J Biol Chem 281 (2006) 9190ndash9199
[294] F Luchetti B CanonicoM BettiM Arcangeletti F PilolliM Piroddi L Canesi S PapaF Galli Melatonin signaling and cell protection function FASEB J 24 (2010)3603ndash3624
[295] MW Bengtsson G Jedstedt G Flemstrom Duodenal bicarbonate secretion inrats stimulation by intra-arterial and luminal guanylin and uroguanylin ActaPhysiol (Oxf) 191 (2007) 309ndash317
[296] CS Nelson JL Marino CN Allen Melatonin receptor potentiation of cyclic AMP andthe cystic fibrosis transmembrane conductance regulator ion channel J Pineal Res 26(1999) 113ndash121
[297] C de Castro-Silva VM de Bruin GM Cunha DM Nunes CAMedeiros PF de BruinMelatonin improves sleep and reduces nitrite in the exhaled breath condensate incystic fibrosismdasha randomized double-blind placebo-controlled study J Pineal Res48 (2010) 65ndash71
[298] I Hornyak E Pankotai L Kiss Z Lacza Current developments in the the-rapeutic potential of S-nitrosoglutathione an endogenous NO-donor mole-cule Curr Pharm Biotechnol (2011) Jan 11 [Epub ahead of print] - PMID21235457
[299] AH Snyder ME McPherson JF Hunt M Johnson JS Stamler B Gaston Acuteeffects of aerosolized S-nitrosoglutathione in cystic fibrosis Am J Respir CritCare Med 165 (2002) 922ndash926
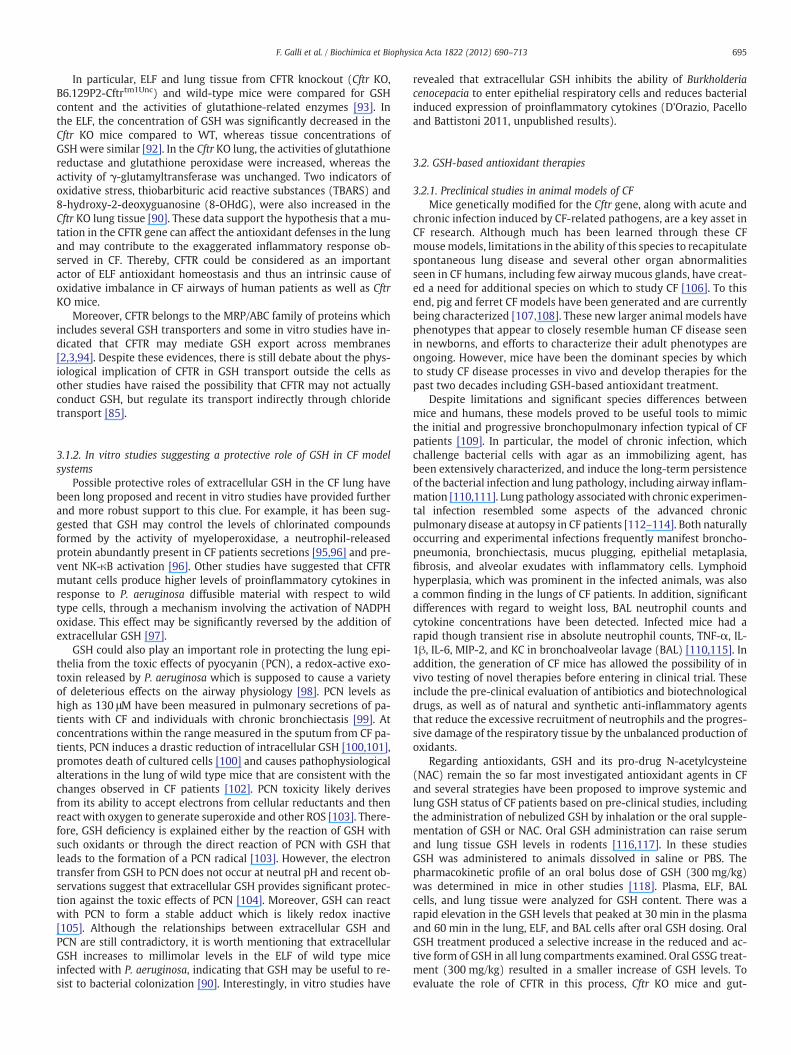
695F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
In particular ELF and lung tissue from CFTR knockout (Cftr KOB6129P2-Cftrtm1Unc) and wild-type mice were compared for GSHcontent and the activities of glutathione-related enzymes [93] Inthe ELF the concentration of GSH was significantly decreased in theCftr KO mice compared to WT whereas tissue concentrations ofGSH were similar [92] In the Cftr KO lung the activities of glutathionereductase and glutathione peroxidase were increased whereas theactivity of γ-glutamyltransferase was unchanged Two indicators ofoxidative stress thiobarbituric acid reactive substances (TBARS) and8-hydroxy-2-deoxyguanosine (8-OHdG) were also increased in theCftr KO lung tissue [90] These data support the hypothesis that a mu-tation in the CFTR gene can affect the antioxidant defenses in the lungand may contribute to the exaggerated inflammatory response ob-served in CF Thereby CFTR could be considered as an importantactor of ELF antioxidant homeostasis and thus an intrinsic cause ofoxidative imbalance in CF airways of human patients as well as CftrKO mice
Moreover CFTR belongs to the MRPABC family of proteins whichincludes several GSH transporters and some in vitro studies have in-dicated that CFTR may mediate GSH export across membranes[2394] Despite these evidences there is still debate about the phys-iological implication of CFTR in GSH transport outside the cells asother studies have raised the possibility that CFTR may not actuallyconduct GSH but regulate its transport indirectly through chloridetransport [85]
312 In vitro studies suggesting a protective role of GSH in CF modelsystems
Possible protective roles of extracellular GSH in the CF lung havebeen long proposed and recent in vitro studies have provided furtherand more robust support to this clue For example it has been sug-gested that GSH may control the levels of chlorinated compoundsformed by the activity of myeloperoxidase a neutrophil-releasedprotein abundantly present in CF patients secretions [9596] and pre-vent NK-κB activation [96] Other studies have suggested that CFTRmutant cells produce higher levels of proinflammatory cytokines inresponse to P aeruginosa diffusible material with respect to wildtype cells through a mechanism involving the activation of NADPHoxidase This effect may be significantly reversed by the addition ofextracellular GSH [97]
GSH could also play an important role in protecting the lung epi-thelia from the toxic effects of pyocyanin (PCN) a redox-active exo-toxin released by P aeruginosa which is supposed to cause a varietyof deleterious effects on the airway physiology [98] PCN levels ashigh as 130 μM have been measured in pulmonary secretions of pa-tients with CF and individuals with chronic bronchiectasis [99] Atconcentrations within the range measured in the sputum from CF pa-tients PCN induces a drastic reduction of intracellular GSH [100101]promotes death of cultured cells [100] and causes pathophysiologicalalterations in the lung of wild type mice that are consistent with thechanges observed in CF patients [102] PCN toxicity likely derivesfrom its ability to accept electrons from cellular reductants and thenreact with oxygen to generate superoxide and other ROS [103] There-fore GSH deficiency is explained either by the reaction of GSH withsuch oxidants or through the direct reaction of PCN with GSH thatleads to the formation of a PCN radical [103] However the electrontransfer from GSH to PCN does not occur at neutral pH and recent ob-servations suggest that extracellular GSH provides significant protec-tion against the toxic effects of PCN [104] Moreover GSH can reactwith PCN to form a stable adduct which is likely redox inactive[105] Although the relationships between extracellular GSH andPCN are still contradictory it is worth mentioning that extracellularGSH increases to millimolar levels in the ELF of wild type miceinfected with P aeruginosa indicating that GSH may be useful to re-sist to bacterial colonization [90] Interestingly in vitro studies have
revealed that extracellular GSH inhibits the ability of Burkholderiacenocepacia to enter epithelial respiratory cells and reduces bacterialinduced expression of proinflammatory cytokines (DOrazio Pacelloand Battistoni 2011 unpublished results)
32 GSH-based antioxidant therapies
321 Preclinical studies in animal models of CFMice genetically modified for the Cftr gene along with acute and
chronic infection induced by CF-related pathogens are a key asset inCF research Although much has been learned through these CFmousemodels limitations in the ability of this species to recapitulatespontaneous lung disease and several other organ abnormalitiesseen in CF humans including few airway mucous glands have creat-ed a need for additional species on which to study CF [106] To thisend pig and ferret CF models have been generated and are currentlybeing characterized [107108] These new larger animal models havephenotypes that appear to closely resemble human CF disease seenin newborns and efforts to characterize their adult phenotypes areongoing However mice have been the dominant species by whichto study CF disease processes in vivo and develop therapies for thepast two decades including GSH-based antioxidant treatment
Despite limitations and significant species differences betweenmice and humans these models proved to be useful tools to mimicthe initial and progressive bronchopulmonary infection typical of CFpatients [109] In particular the model of chronic infection whichchallenge bacterial cells with agar as an immobilizing agent hasbeen extensively characterized and induce the long-term persistenceof the bacterial infection and lung pathology including airway inflam-mation [110111] Lung pathology associatedwith chronic experimen-tal infection resembled some aspects of the advanced chronicpulmonary disease at autopsy in CF patients [112ndash114] Both naturallyoccurring and experimental infections frequently manifest broncho-pneumonia bronchiectasis mucus plugging epithelial metaplasiafibrosis and alveolar exudates with inflammatory cells Lymphoidhyperplasia which was prominent in the infected animals was alsoa common finding in the lungs of CF patients In addition significantdifferences with regard to weight loss BAL neutrophil counts andcytokine concentrations have been detected Infected mice had arapid though transient rise in absolute neutrophil counts TNF-α IL-1β IL-6 MIP-2 and KC in bronchoalveolar lavage (BAL) [110115] Inaddition the generation of CF mice has allowed the possibility of invivo testing of novel therapies before entering in clinical trial Theseinclude the pre-clinical evaluation of antibiotics and biotechnologicaldrugs as well as of natural and synthetic anti-inflammatory agentsthat reduce the excessive recruitment of neutrophils and the progres-sive damage of the respiratory tissue by the unbalanced production ofoxidants
Regarding antioxidants GSH and its pro-drug N-acetylcysteine(NAC) remain the so far most investigated antioxidant agents in CFand several strategies have been proposed to improve systemic andlung GSH status of CF patients based on pre-clinical studies includingthe administration of nebulized GSH by inhalation or the oral supple-mentation of GSH or NAC Oral GSH administration can raise serumand lung tissue GSH levels in rodents [116117] In these studiesGSH was administered to animals dissolved in saline or PBS Thepharmacokinetic profile of an oral bolus dose of GSH (300 mgkg)was determined in mice in other studies [118] Plasma ELF BALcells and lung tissue were analyzed for GSH content There was arapid elevation in the GSH levels that peaked at 30 min in the plasmaand 60 min in the lung ELF and BAL cells after oral GSH dosing OralGSH treatment produced a selective increase in the reduced and ac-tive form of GSH in all lung compartments examined Oral GSSG treat-ment (300 mgkg) resulted in a smaller increase of GSH levels Toevaluate the role of CFTR in this process Cftr KO mice and gut-
Table 1Intervention trials on antioxidant therapy in CF patients found at ClinicalTrialsgov databasea
Rank Title PI Location Recruitment Interventions Age groups Phasesnumberenrolled
Study designsb Outcome measures Start andcompletion date
NCT ID
1 Efficacy and safety studyof inhaled GSH in CFpatients
GrieseM
Germany Completed Drugbull reduced GSH sodium salt
C|A|S II138
1 R|E2 Safetyeff3 PA4 DB (Sub Inv)5 Treatment
bull Differences between inhaled GSHand inhaled normal saline withrespect to the area under the curveof FEV1 predicted within the periodfrom baseline to week 24
bull Treatment changes with respect tothe variablesspirometry peak flowquality-of-life weightheightpercentage of neutrophilsothercell types (induced sputum) inducedsputum levels of GSHinflammatorymediators pulmonary exacerbation
Jul-07May-10
00506688
bull 09 saline (control)
2 A phase I study of inhaledsodium pyruvate for thetreatment of CF
BillingsMCE
United States Terminated Drugbull Inhaled sodium pyruvate
A|S I70
1 R|E2 Safetyeff3 PA4 DB5 Treatment
bull Assessment of safety of inhaled sodiumpyruvate in Subs with CF Subs will beevaluated for the presence of symptomsand safety laboratory measurements
bull Determination of improvement inlungs of CF Subs as determined bymeasurement of FEV1 and measurementof inflammatory markers ininduced sputum
Feb-06na
00332215
3 Inhaled GSH versusplacebo in CF
MarsicoS
Italy Recruiting Drugbull Inhaled reduced GSHbull Physiological solution
C|A III150
1 R|E2 Eff3 PA4 SB (Sub)5 Treatment
bull FEV1bull Small airway function exercise capacityBMI dyspnoea cough quality of lifepulmonary exacerbations markers ofoxidative stress (H2O2)in serum and inEBC epithelial inflammatory markerson BNEC
Jun-10Dec-12
01450267
4 Safety and efficacy ofan antioxidant-richmultivitaminsupplement in CF
SagelSD
United States Completed Dietary supplementbull AquADEKs
C|A IIndashII17
1 NR|E2 Safetyeff3 SGA4 OL5 Treatment
bull Plasma levels of β-carotenebull Plasma levels of coenzyme Q-10retinol (Vitamin A) 25-hydroxy vitaminD α- and γ-tocopherols (Vitamin E)PIVKA-II
Aug-07Nov-09
01018303
5 Efficacy and safety ofepigallocatechin gallate(EGCG)tocotrienol in18 patients with splicing-mutation-mediated CF
KeremE
Israel Not yetrecruiting
Dietary supplementbull EGCGbull Tocotrienolbull EGCG+tocotrienol
A|S na18
2 Safetyeff3 CA4 OL5 Treatment
bull Changes in nasal chloride secretion asassessed by TEPD with assessment ofmean changes in TEPD by drug comparedto baseline and the proportion of patientswith a chloride secretion response bydrug compared to baseline
bull Pulmonary function testing FEV1FVC MEF25-75
Sep-09Jun-11
00889434
6 The effect of inhaledNAC compared tonormal saline onsputum rheology andlung function
VanDaele S
Belgium Terminated Drugbull Acetyl-Cysbull Normal saline
C|A IV19
1 NR|E2 Eff3 CA4 OL5 Treatment
bull Changes in visco-elasticity andlung function
Jan-10Dec-10
00996424
696FG
allietal
Biochimica
etBiophysica
Acta
1822(2012)
690ndash713
7 Safety of orallyadministeredcurcuminoids in adultsubjects with CF
Goss C United States Completed Drugbull Standardized turmericroot extract
A I11
1 NR|E2 Safetyeff3 SGA4 OL5 Treatment
bull Safety and tolerability of 14 days oftreatment with orally administeredcurcuminoids as assessed by adverseevents laboratory parameters andspirometry
bull Pharmacokinetics of repeated dosesof orally administered curcuminoidschange in NPD measurementschange in sweat chloride measurements
Apr-05Jan-06
00219882
8 Nasal potential studiesutilizing CF transmembraneregulator (CFTR) modulators
Rowe S United States Recruiting Other quercetin C|A II46
2 Eff3 SGA4 OL5 BS
bull NPD(NPD) Biomarkerbull Residual CFTR activity
Mar-10Nov-11
01348204
9 Safety and tolerability ofinhaled nitric oxide inpatients with CF
Sagel S United States Completed Drugbull Nitric oxide for inhalationbull Nitrogen
C|A|S IIndashII18
1 R|E2 Saf3 PA4 DB (Sub Care Inv OA)5 Treatment
bull Safety and tolerability of drugassessed by change in methemoglobinlevels oxygensaturation FEV1
bull Assess the difference in sputumbacterial density before and afterNO inhalation and the differencein lower airway inflammatorymeasures before and after NO inhalation
Jul-04Dec-08
00570349
10 NAC Phase IIB a multi-center phase IIBrandomized placebo-controlled DB study ofthe effects of NAC onredox changes and lunginflammation in CF patients
ConradC
United States Completed Drugbull NAC
C|A|S II80
1 R|E2 Eff3 SGA4 DB (Sub Care Inv OA)5 Treatment
bull Change in the logarithm of the levelof human neutrophil elastase(HNE) activity measured in sputum
bull Change in concentration of IL-8measured in sputum and plasmaconcentration of GSH measured inwhole blood the neutrophil countmeasured in sputum
Nov-08Feb-11
00809094
11 Glutamine supplementationin CF
na United States Not yetrecruiting
Dietary supplementbull Glutaminebull L-alanine
A|S II40
1 R3 PA4 DB (Sub Care Inv OA)5 Prev
bull Percent increase in plasma glutamineand GSH redox levels measured atweeks 0 4 8 and 12
Feb-10Feb-11
01051999
12 Effect of sulforaphane inbroccoli sprouts onNrf2 activation
ChmielJF
United States Active notrecruiting
Dietary supplementbull Broccoli sprouts
A na15
3 SGA4 OL5 BS
bull Nrf2 activation in NECbull Measures of lipid peroxidation in NECGSH from blood lymphocytesoxidative stress in urineneutrophil migration into thegingival crevices
Apr-11Sep-11
01315665
AbbreviationsA=adult BC=breath condensate BNEC=brushed nasal epithelial cells BS=basic science C=child CA=crossover assignment Care=caregiver CF=cystic fibrosis DB=double blind EBC=exhaled breath condensate Eff=efficacystudy FEV1=forced expiratory volume in 1 s FVC=forced vital capacity GSH=glutathione Inv=investigator MEF25ndash75=maximal expiratory flow 25ndash75 na=not available NAC=N-acetylcysteine NEC=nasal epithelial cellsNLF=nasal lavage fluid NPD=nasal potential difference NR|E=non-randomized|endpoint OA=outcomes assessor OL=open label PA=parallel assignment PI=principal investigator Prev=prevention R|E=randomized|endpoint S=senior Saf=safety study SB=single blind SGA=single group assignment Sub=subject
a Search was done matching the terms ldquoantioxidant therapyrdquo or ldquoGlutathionerdquo with ldquoCystic Fibrosisrdquob 1 Allocation 2 Classification 3 Intervention model 4 Masking 5 Primary purpose
697FG
allietal
Biochimica
etBiophysica
Acta
1822(2012)
690ndash713
698 F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
corrected Cftr KO-transgenic mice were given an oral bolus dose ofGSH (300 mgkg) and compared with WT mice for changes in GSHlevels in plasma lung ELF and BAL cells There was a twofold in-crease in plasma a twofold increase in lung a fivefold increase inELF and a threefold increase in BAL cell GSH levels at 60 min in WTmice however GSH levels only increased by 40 in the plasma 60in the lung 50 in the ELF and twofold in the BAL cells within thegut-corrected Cftr KO-Tg mice No change in GSH levels was observedin the uncorrected Cftr KO mice These studies suggest that oral GSHadministration can increase plasma and lung compartment GSHlevels in WT mice and to a lesser extent in gut-corrected Cftr KO-Tganimals It also suggests that oral GSH treatment can boost BAL cellGSH levels However since this study failed to show significant in-creases in serum and lung compartment GSH levels in uncorrectedCftr KO mice it is questionable whether oral GSH administration toCF patients with intestinal malabsorption would benefit from thistherapy It was also shown that GSH is rapidly distributed to theserum and lung compartments Kariya et al [118] speculate thatother transporter(s) besides CFTR are responsible of the transport ofGSH and probably of other dietary molecules to the lung whichmay be responsible for dietary deficiencies observed in various lungdiseases
Another strategy is represented by the oral supplementation ofhigh doses of NAC a well known cysteine donor for the synthesis ofglutathione NAC is considered a safe molecule which has beenused successfully to treat GSH deficiency in a wide range of diseases[119] As CF mice display defects in GSH export in the ELF comparableto those of patients they could provide a useful tool to assess the ef-fects of NAC administration on the GSH status However only limitedstudies exploring the effects of NAC on CF animal models have beenso far carried out The effects of NAC have been tested on mucus accu-mulation bacterial load transit and inflammation in the CF mousesmall intestine showing that NAC may reduce intestinal mucus accu-mulation bacterial overgrowth in the gut [120]
Moreover NAC has been reported to restore the accumulationof unwantedmisfolded proteins in aggregates that are associated withthe CF airway phenotype as a cause of lung inflammation [121] Themechanism of this NAC-derived effect seems to involve the restorationof beclin 1 expression and activity in the autophagy pathway of theendoplasmic reticulum that was investigated in vivo using Scnn1b-transgenic and Cftr(F508del) homozygous mice The restoration ofthis pathway also produced a rescued trafficking of CFTR (F508del) tothe cell surface of CF cells obtained from human CF nasal biopsies
Given the defective GSH metabolism of CF reviewed in the previ-ous sections and in [122] and the reduced response to GSH therapyin CF mice [93] some Authors have investigated the influence of bac-terial infections on lung oxidative stress The effects of P aeruginosainfection on ELF and lung tissue antioxidants and the oxidation ofDNA and lipids were investigated in mice challenged with bacterialcells [90] CFTR-KO (B6129P2-Cftrtm1Unc) and WT mice were chal-lenged intratracheally with a clinical isolate of mucoid P aeruginosaembedded in agar beads and on the third day of infection BALF andlung tissue were obtained and analyzed for cytokines antioxidantsand enzyme activities [90] P aeruginosa lung infection increasedlevels of inflammatory cytokines and neutrophils in the ELF This cor-responded with a marked increase in GSH and in urate levels in theELF of P aeruginosa-infected WT mice A twofold increase in uratelevels was also observed among lung tissue antioxidants of Paeruginosa-infected WT mice There were no changes in markers oflung oxidative stress associated with the P aeruginosa lung infectionIn contrast to WT mice the CFTR-KO mice lacked a significant in-crease in ELF GSH when challenged with P aeruginosa and this corre-lated with a decrease in the ratio of reduced to oxidized GSH in theELF a marker of oxidative stress These data would suggest that thelung adapts to infectious agents with elevated ELF GSH and urateTherefore individuals with lung diseases associated with altered
antioxidant transport such as CF might lack the ability to adapt tothe infection which may lead to a more severe inflammatoryresponse
322 Clinical trials on GSHThe discovery of the defect in GSH export has suggested that ther-
apies able to restore or increase GSH levels in the ASL could counteractthe inflammation and oxidative stress conditions typical of CF pa-tients In an attempt to strengthen extracellular defenses againstROS some pilot studies have analyzed the effect of GSH inhalation orthat of oral GSH prodrug N-acetylcysteine (NAC) All these treatmentswere well tolerated by the CF patients and most authors were able tomeasure increased ELF concentrations of GSH in association withsome positive clinical outcomes [4041737896122ndash128] Althoughpotentially promising these findings need stronger clinical evidencein that the majority of these were obtained on very limited numberof patients investigated in non-randomized controlled trials This ishighlighted in a recently published meta-analysis [129] that providesalso a thoroughly analysis of the literature on this aspect of the antiox-idant and anti-inflammatory therapy of CF Among the American CFfoundation sponsored trials two phase II trials on inhaled GSH andoral NAC are in progress in US and Germany (ClinicalTrialsgov Iden-tifier NCT00506688 and NCT00809094 respectively Table 1) andsafety and tolerability of aerosolized glutathione is also matter ofinvestigation by another (not registered) US trial (more informationon this can be found in [130]) Nevertheless the diffusion among CFpatients of NAC preparations for inhalation (Mucomystreg) has in-creased in recent years
γ-Glutamylcysteine ethyl ester (GCEE) is another potentially inter-esting GSH pro-drug which has proved some efficacy in the ameliora-tion of oxidative stress eg in experimental myocardial infarction[131] and central nervous system conditions (see eg [132]) HoweverGCEE has not been investigated in CF yet
33 Limits and potential problems associated to thiol-based therapies
Although the above cited clinical trials may be considered promis-ing attempts to improve the antioxidant levels in the ELF the actualcapacity of these treatments to produce positive clinical effects mustbe considered with caution For example indices of oxidative damagewere found to be unaffected by aerosolized GSH treatment [122]Some in vitro studies have suggested that the reaction of GSH withPCN could produce hydrogen peroxide with potential exacerbationof oxidative damage [101] The exact mechanisms of PCN toxicityand the reaction of this toxin with GSH must be better understoodin order to evaluate the safety of GSH administration to patients col-onized by P aeruginosa
Inhalation of GSH ensures its direct delivery in the airways butsince GSH can rapidly convert to its oxidized form GSSG frequentGSH inhalations are required to maintain a high GSHGSSG As a con-sequence of this limit four separate inhalations have been used inthe study carried out by Bishop et al [123] Unless justified by clearclinical improvements these repeated treatments may represent aburden for patients already undergoing complex therapies Moreoverrepeated inhalations of GSH increase the levels of GSSG in ELF[133134] In the absence of effective homeostatic mechanisms ensur-ing the fast recycling of GSSG to GSH this might produce unwantedeffects and even the exacerbation of CF symptoms being GSSG re-sponsible of the S-glutathiolation and functional inhibition of CFTR[124]
In principle the oral administration of GSH could be considered asafe strategy to prevent GSSG accumulation but this strategy is likelynot feasible due to the substantial inability of this water-soluble mol-ecule to cross biological membranes Moreover a study carried out inmice has established that GSH absorption in the gastrointestinal tractif any is mediated by CFTR itself thus excluding the possibility to
699F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
improve circulating levels of GSH in CF patients through the dietarysupplementation of the antioxidant [127] The limited absorption ofGSH could be overcome by GSH-esters as in vitro studies haveshown that this form of GSH may be specifically useful to rescue mi-tochondrial defects in cystic fibrosis models [80] Safety of these GSHderivatives in humans has been poorly investigated
Two independent studies have shown that the treatment of CF pa-tients with high doses of NAC increases extracellular GSH in sputum[78125] but contrasting results have been reported concerning theeffects of NAC on the concentrations of blood GSH and on the levelsof IL-8 and other markers of inflammation NAC treatments may beuseful to modulate the GSH content in cells but it should be remindedthat an enhanced cysteine supply cannot lead to an increase of GSHabove physiological levels due to the feedback inhibition mechanismof γ-glutamylcysteine synthetase described in the Section 311
331 Gamma-glutamyltransferase and GSH therapySo far none of the studies mentioned above has taken into account
the fact that GSH is degraded by GGT enzyme activity GGT concentra-tions are known to increase several fold in ELF of CF patients even ifthe mechanisms for this effect were not determined [135] and thisphenomenon parallels the above described decrease of GSH levels inELF Preliminary data suggest that a major source of increased ELFGGT is represented by activated neutrophils accumulating in diseasedairways (Corti and Pompella 2011 unpublished observation) Re-gardless of its origin it is likely that increased GGT in ELF would de-grade locally administered GSH to variable extents which couldcontribute to the so far inconclusive results of therapies based onaerosolized GSH Besides its role in GSH catabolism GGT has beenshown to mediate protein S-thiolation [136] suggesting that GSH ad-ministration in the presence of active GGT enzyme might alter CFTRglutathiolation status and function in a potentially unfavorable wayOn the other hand a potential role of GGT in favoring bronchial up-take of antioxidant vitamin C has also been suggested [137]
These controversial findings may add further issues to the ques-tion of whether the therapy of lung oxidative stress by aerosolizedGSH could be safe in all the CF patients regardless of specific strate-gies that would ascertain the extent of lung inflammation Thesestrategies should include the assay of GGT levels in ELF In principleonce an adverse role of ELF GGT in GSH therapies will be confirmedthe association of GGT inhibitors in the GSH formulations for inhala-tion could represent a promising pharmacological strategy
34 Malnutrition as a possible cause of defective thiol-dependentantioxidant protection
Successful nutritional interventions strongly impact on the clinicaloutcome of CF patients [138ndash140] Malnutrition by pancreatic insuffi-ciency and other CF-related factors influence the susceptibility to de-velop recurrent infections and severe inflammatory lesions of thelung tissue If the onset of a defective (sub-optimal) antioxidant sta-tus may represent an underlying component in the clinical effects ofmalnutrition remains a matter of investigation Clinicians have topay particular care to avoid these disturbances and successful proto-cols of nutritional intervention in CF have been developed whichare essentially aimed to avoid the onset of protein-energy malnutri-tion (PEM) [141] Despite this the risk of developing such an unto-ward complication in CF infants and children remains high assuggested by the prevalence data registered in some areas Actuallya prevalence of PEM between 5 and 14 in Moldavian infants was re-cently reported [142] and PEM is associated with poor outcome andparticularly with the risk of developing edema and anemia
Besides lowered intake and absorption of micronutrient antioxi-dants discussed in the other sections malabsorption of dietary proteinand excess fecal amino acid losses result in hypoproteinemiahypoalbu-minemia as key biochemical signs of PEM Hypoalbuminemia is
considered to be linked with a causendasheffect relationship with oxidativestress and is proposed to influence morbidity and mortality in condi-tions associated with chronic inflammation and severe oxidative stress[143144] The human serum albumin (HAS) molecule contains only areactive thiol group eg the Cys 34 the importance of which as an anti-oxidant defense system in blood and for the entire organism is welldocumented [145] This is the second main thiol (and the main proteinthiol) in the circulation (approx 2 mmol in the adult organism assum-ing 5 l of total blood volume anHt of 40 and [HAS] of 45 gl of plasma)being the RBCGSH thefirst thiol in blood (near to 5 mmol assuming thesame parameters of above and an average concentration of GSH inpacked RBC of 25 mM) [146147] The antioxidant role of HSA is notonly a consequence of the relative abundance of its Cys thiol A specificcapability of acting as a sacrificial target for a series of electrophils andmost biologically relevant ROS ie hydrogen peroxide and peroxyni-trite has been demonstrated in a series of studies [145148149] Li-gand binding activity can contribute to promote antioxidant effectsby the HSA molecule [145] Transitions metals particularly copperand also iron in the case of iron-overload diseases bind to HSA Inthis way these are less available to promote the Fenton chemistryand hydroxyl radicals eventually released from this oxidative reactionare mostly directed to the HAS protein sparing more important tar-gets A free radical-trapping activity of HSA has been also demonstratedand this was proposed to be directed toward both hydrophilic and fat-soluble species This activity may result from the interaction withother antioxidants such as α-tocopherol [150] and may influence theantioxidant activity of food-derived phenolic antioxidants [151]
However Cys 34 is considered the main contributor to the antiox-idant function of HAS which plays its role in the antioxidant homeo-stasis of blood thanks to a complex series of interactions with themetabolism and antioxidant function of the pool of free thiols in plas-ma and in the circulating RBC with the latter playing a significantcontribution to the extracellular pool of GSH [146] and to the dynam-ics of inter-organ GSHmetabolism in cooperation with liver and othertissues [147] Immuno-inflammatory cells and the lung tissue areamong the main terminals of this metabolism The RBC contain theentire machinery to synthesize GSH to restore its redox (by enzymat-ic reduction of the oxidized form) and to use this as cofactor of Se-GPx and GSH-S-transferase enzymatic activities that are responsibleof the detoxification of hydroperoxides and alkylating agents thatmay form in or enter the RBC cytosol [147] In this sense the RBC rep-resents a circulating reservoir of GSH that in addition to maintainingthe redox and respiratory function of Hb participates to systemic pro-tection of xenobiotics of endogenous and exogenous origin In consid-eration of these aspects the combination of hypoalbuminemia andanemia may exponentially increase the risk of developing oxidativestress in CF patients as it is supposed to occur in other oxidative stressconditions such as chronic kidney disease [55143152] Additionalclinical investigation should verify the hypothesis that hypoalbumi-nemia together with a defective uptake and metabolism of sulfur-containing amino acids and CF-specific defects of the GSH metabo-lism may represent a causal risk factor for an impaired antioxidantdefense and systemic oxidative stress in CF patients
35 Fat-soluble antioxidants
Pancreatic insufficiency and a diminished bile acid pool cause mal-absorption of important essential nutrients and other dietary compo-nents in CF Of particular significance is the malabsorption of fat-soluble antioxidants such as tocopherols carotenoids and coenzymeQ-10 (Co-Q10) and that of essential fatty acids (EFA)
351 Vitamin EVitamin E therapy in CF has been proposed in several decades of
research as a useful approach to overcome both the lower absorptionof this fat-soluble micronutrient and the increased antioxidant
700 F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
demand by the abnormal generation of ROS in CF tissues (see for in-stance the recommendations by the Cystic Fibrosis Foundation Con-sensus Conference on nutrition [153])
The first report of a vitamin E deficiency in CF appeared in literaturein 1951 by Filer et al [154] In this study the absorption of the mainform of this vitamin eg α-tocopherol and its ester derivatives was in-vestigated in several subsets of infants and children Thanks to a simplebioavailability (or tolerance) test these authors observed that ldquoin-fantshellip diagnosed as fibrocystic disease of the pancreas diarrhea andcirrhosis were characterized by a poor response to the test ie the tol-erance curve was lowrdquo However abnormalities were also observed inother subgroups of infants with a variety of disorders not associatedwith fat or fat-soluble vitamin intolerance such as sprue celiac syn-drome and lupus erythematosus which suggests the general observa-tion that malnutrition and inflammatory and degenerative diseases ofthe GI tract may lead to absorb tocopherols poorly At the same timethese authors reported that ldquoMetabolic disorders with associated hy-percholesterolemia were observed to give abnormally high values forthe area under the curverdquo and that patients responding poorly to to-copherol absorption test did also in vitamin A absorption tests
The finding of lowered (lipid uncorrected) levels of vitamin E wasconfirmed in other studies in which this relative deficiency was foundto occur irrespective of pancreatic comorbidity and in associationwith lowered levels of other liposoluble vitamins such as vitamin Aand D [155] regardless of their different liver metabolism and tissuedelivery mechanisms [156157]
Plasma buccal mucosal cells (BMCs) and breath condensate α-tocopherol decreased significantly with age in association with a de-creased respiratory function [5] This was accompanied by loweredlevels of other antioxidants such as vitamin C and increased oxidativestress markers of different origin such as protein carbonyls thiobarbi-turic acid-reactive substances and F2-IsoPs
Clinical symptoms of vitamin E deficiency in CF have not beenconclusively investigated Dolan et al [158] described that anemiaof CF patients is related to vitamin E deficiency and increasedperoxide-induced hemolysis of RBC Other authors however ob-served an increased susceptibility to peroxide-induced hemolysisalso in the presence of normal levels of vitamin E [159] Peters andKelly [160] observed that RBC vitamin E concentrations were belowthe normal range in almost all unsupplemented patients and roseinto the normal range with a 1-year supplement of 100 mg per daybut not 15 mg per day Since RBC vitamin E concentration has beenshown to correlate well with tissue concentrations of the vitamin inanimals tissue levels of vitamin E are expected to be lower than nor-mal in CF patients
Bioavailability of fat-soluble vitamin is limited in CF Vitamin Edeficiency of CF is also associated with hypocholesterolemia [7] Asa consequence the relative deficiency of this vitamin is compensatedwhen the absolute levels are normalized for cholesterol levels andthis suggests a poor transferring of this vitamin in the circulation bya defective lipid and lipoprotein metabolism Pancreatic insufficiencyand the consequent lipid malnutrition cannot completely explain thisdefect and other possibly CF-specific dysfunctions could play a roleLiver metabolism and specific plasma transport systems of this vita-min need further elucidation in CF
As a consequence of these aspects it is not presently clear whichform and level of supplementation of this vitamin is most appropriateto treat these patients Usingα-tocopherol as a vitamin E supplementPeters et al [160] reported that 100 mg per day are required to nor-malize RBC concentrations Other authors described unsuccessfulsupplementation protocols with higher doses and this has led to de-velop formulations with higher bioavailability in order to achieve bet-ter compliance to oral supplementation (see below and the literaturereviewed in [161ndash163])
Besides absorption and tissue delivery issues specificity of actionis another critical item of antioxidant therapy with fat-soluble agents
in CF As further addressed below this aspect could be themain limit toa successful use of natural forms of vitamin E in the clinical manage-ment of CF inflammation even if a local lung-targeted therapy wouldbe developed according with so far proposed pre-clinical models ofaerosolized vitamin E [164165]
Current pharmacological research is aimed to develop synthetic formsof this and other fat-soluble antioxidants with better radical scavengingproperties at the lipidndashwater interface Type of ROS target and the sitesof action greatly influence the chances of a fat-soluble antioxidant of alle-viating oxidative stress in the airways as well as in other organs such asliver and pancreas These aspects dealing with specificity of action[163166167] have stimulated the search of novel vitamin E-derived an-tioxidants that may help to scavenge radicals at the lipidndashwater interfaceof the epithelial cell membrane and surfactant Amine derivativesof tocopherols and tocotrienols have been recently demonstrated toshow higher antioxidant and free radical scavenging activity than α-tocopherol [168] Further in vitro pharmacological analysis has includedtoxicity evaluations and the detailed investigation of scavenging of azo-and phenolic radicals with different degrees of hydrophobicity and theinhibitory activity on IL-8 gene expression and phospholipase activityin CF cells Comparative evaluation with other synthetic derivativessuch asα-tocopheryl succinate and natural forms of vitamin E suggestedthat these amine derivatives are promising antioxidant and anti-inflammatory agents [Galli F and Pilolli F unpublished observation]deserving further pre-clinical investigation in CF model systems
Anti-inflammatory effects of natural and synthetic analogues of vi-tamin E are also an intriguing pharmacological opportunity currentlyunder investigation by several laboratories [169170]
Recently vitamin E supplementation has been at the center of adispute regarding its safety when used at high dosages in certainpopulations of patients An extensive and speculative debate originat-ed on this subject after a meta-analysis study byMiller et al [171] thatexamined the largest secondary prevention trials on vitamin E trials incardiovascular patients finding a significantly increased mortality riskfor all the causes (about 4 1ndash8 in the 95 interval of confidence)when the patients were treated with doses gt400 IUdie (that areequivalent to 400 mgdie of the synthetic form allrac-α-tocopheroland to 185 mgdie of the natural form RRR-α-tocopherol) This debateresulted in a careful examination of this meta-analysis study by severalother authors and in further revisions of the literature on vitamin E tox-icity in humans [see the literature recently reviewed in [163172ndash174]]that clearly demonstrated the poor consistency of the conclusionsraisedwithMillersmeta-analysis study and the paucity of the concernsthat derived from that These conclusions have been verified in the re-cent international symposium on vitamin E of the Society for Free Rad-ical Research Europe branch of Rome 2009 [173175] Vitamin E used assupplement for humans in all its forms (eg α-tocopherol and othertocopherols and tocotrienols) is safe in abroad range of intakes[172176] The tolerable upper intake level (UL) and the AcceptableDaily Intake (ADI) established by the Joint FAOWHOExpert Committeeon Food Additives for the natural form of vitamin E as α-tocopherolequivalents are of 300 mgdie and 015ndash20 mgkg body weightdierespectively [172177]
352 CarotenoidsLevels of plasma carotenoids such as β-carotene β-cryptoxanthin
and total lycopene are significantly lowered in CF patients and thiswas associated with higher susceptibility to lipid peroxidation[5178ndash180] Rust et al [178] demonstrated that the long-term oralsupplementation with 50 mg β-caroteneday (ie 1 mg β-carotenekg BWday) restored the levels of this carotenoid while sub-optimalsupplementation was observed at doses of 10 mg β-caroteneday orlower thus confirming the need of high doses of this fat-soluble factorto overcome the limited absorption and thus to achieve plasma con-centrations of healthy control subjects Successful high-dose treat-ments appear to lower oxidative stress markers such as TBA-MDA
701F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
complexes and to correct total antioxidant capacity of plasma Inanother study β-carotene supplementation was observed to de-creased lipid peroxide formation as quantitated by malondialdehydeconcentrations in plasma (TBAHPLC method) and to enhance the re-sistance to copper(II) ion-induced oxidation of low density lipopro-teins [180]
At the same time toxicity issues have been raised for human sup-plementation with carotenoid formulations and particularly of water-miscible formulations of preformed vitamin A that is regularly sup-plemented to CF patients which may increase serum retinol andpossible risk of CF-associated liver and bone complications (reviewedin [161181]) However β-carotene supplementation seems to be safesince this does not affect plasma concentrations of other carotenoidsand retinol as well as of other fat-soluble vitamins as α- and γ-tocopherol [178] Recent studies designed to test the clinical efficacyof a CF tailored multivitamin formulation (commercial name AquA-DEKsreg) also tested the safety of this type of formulation and demon-strated that this does not increase vitamin A above the normal levelsobserved in healthy controls [162182183] The normalization of β-carotene levels obtained in these studies was associated only withminor improvements on respiratory and growth parameters whilethe levels of urinary F2-IsoPs used as index of lipid peroxidationwere not affected [162] The surrogate marker of lipid peroxidationMDA was affected together with some selected antioxidant parame-ters (RBC thiols and superoxide dismutase) in another study inwhich this multivitamin formulation was preliminarily evaluated incomparison with standard formulations of vitamin E and A [182]
353 Coenzyme Q-10Coenzyme Q-10 (Q10) is a well-known electron transporter in the
mitochondrial respiratory chain with fundamental role in cellularbioenergetics and scavenging of radical species [184] This lipophilicsubstance is present in the circulation at low levels (serum concentra-tionsle2 μM) mainly as ubiquinol-10 eg the reduced form with anapproximate ratio of 955 with the oxidized form ubiquinone-10[185186] A mechanism for a preferential distribution and accumula-tion in mitochondria has been suggested for both the reduced and ox-idized forms of CoQ10 that are taken up by the cells in a time- andconcentration-dependent Subcellular localization and trafficking ofexogenous Q10 are similar to those of the endogenous form butwere different from that of α-tocopherol that is related with lipidcomposition particularly in the mitochondrial and microsomal frac-tions [184] Ubiquinol-10 readily oxidizes ex vivo by the reactionwith other lipophilic antioxidants such as α-tocopherol and butylatedhydroxytoluene [185] Therefore a higher reduction potential thanother physiological fat-soluble antioxidants such as vitamin E and aselective metabolism and cellular trafficking show peculiar role forthe cell CoQ which may also represent an important lipophilic antiox-idant in cells and body fluids
Human cells synthesize this coenzyme through the cholesterol bio-synthesis pathway so thatmore than two thirds of the tissue levels ap-pear to have an endogenous origin dietary sources provide acontribution to Co-Q10 levels of blood and all solid tissues that variesdepending on the dose applied and type of dietary source [187] How-ever in the case of oral supplements it has to be considered that hy-drophobicity and large molecular weight of this coenzyme influenceits absorption that ultimately is slow and limited [186187] Likewiseto vitamin E pharmacokinetics [188189] Co-Q10 showed T(max) ofaround 6 h that coincides with that of dietary lipids Elimination isclose to that of the more retained form of vitamin E in human bodyeg α-tocopherol with a half-life of about 33 h which suggests poorhepatic metabolism However commercially available formulationsare reported to be safe even at high doses and solubilized formulationsshow enhanced bioavailability In healthy subjects plasma Q10 re-sponse to oral ingestion show saturation profiles with a plateau at a
dose of 2400 mg and the higher plasma concentrations were foundto facilitate uptake by peripheral tissues and also the brain [186187]
Laguna et al [190] recently investigated total serum levels ofcoenzyme Q-10 in a wide population of CF children (n=381) and esti-mated their association with clinical outcome Near to 50 of these CFpatients were deficient of Co-Q10 and this defect was significantlymore prevalent in patients with pancreatic insufficiency and signifi-cantly associated with P aeruginosa colonization in infants (under24 months of age) Importantly low Co-Q10 levels correlated to otherlipid markers of a poor nutritional status such as total lipids and alsothe other fat-soluble antioxidants β-carotene and α-tocopherolwhich confirms the presence of a common defect in the absorptionand metabolic pathways of this coenzyme with dietary lipids
The deficit of Co-Q10 may contribute to the impaired energy func-tion of mitochondria of CF tissues and this may exacerbate CF-linkedinflammation infection and cellular stress response of the lung A sys-tematic analysis of molecular lesions in CF bronchial tissue has beenrecently carried out by proteomic approach [191] Comparative eval-uation of protein expressional pattern in CF and healthy controltissues has revealed aberrant levels of some mitochondrial andenergy-related proteins in CF specimens that included the ubiqui-nolndashcytochrome c reductase complex core protein I and one form ofnidogen a pseudogene of aconitase 2 These changes in CF may reflectmolecular changes which could be associated with an altered mito-chondrial homeostasis and Co-Q10 redox
Multivitamin supplements with high bioavailability containingCo-Q10 have demonstrated to correct the deficit of this antioxidantand were preliminarily observed to improve airway inflammationmarkers in CF patients [183] However further clinical investigationfailed to demonstrate that such an improved biochemical profile isassociated with significant improvements in weight percentile andpulmonary function [162]
354 Fatty acidsA key pathophysiological role in sustaining inflammation in CF has
been attributed to the abnormal polyunsaturated fatty acid (FA) pat-tern Abnormalities in FA profiling are potentially linked to CFTRmutation-driven alterations in the absorption andor metabolism ofdietary lipids [192193] and to the consumption of high oxidizableFA involved in the free radical-mediated lipid peroxidation [7]Among those alterations dysregulation of the docosahexaenoic acidand arachidonic acid balance has been extensively studied with re-portedly significant reduction of DHA in CF and a parallel increasein the levels of AA and inflammatory indices [193ndash195] Actually AAis the progenitor of both enzymatic- and free radical-derived inflam-matory mediators including leukotrienes prostaglandins and iso-prostanes On the other hand n-3 PUFA (eicosapentaenoic acid anddocosahexaenoic acid) are involved in the generation of potent medi-ators namely resolvins and protectins which are able to resolveexudates and to act as organ protective and antifibrotic Secondarilyto their anti-inflammatory action n-3 FA may also produce anantioxidant-like response (eg a reduced demand of antioxidants toachieve an optimal control of oxidative pathways) As a consequencen-3 PUFA have been suggested and widely used as supplements in CFpatients usually under the form of fish oil [196ndash198] It is worth ofnote however that defective levels of DHA in CF patients was notconfirmed in recent studies [7] It was also shown that patients onDHA supplements did not have increased plasma n-3 FA concentra-tions but showed more severe oxidative stress compared to theunsupplemented patients [7] This observation of an increased riskof oxidative stress in CF subjects receiving n-3 fatty acids supple-ments has also been described by other authors [199]
Studies reporting increased AA levels in CF patients have beencontradicted by others [7200201] thus contributing to weakeningthe pathophysiological role of the altered DHAndashAA balance as turnpoint of an upregulated inflammatory status in CF In this context a
702 F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
recent Cochrane meta-analysis on n-3 supplementation in CF patients[202] highlighted the lack of evidence for a significant correction ofthe assessed clinical end points (mainly respiratory symptoms)even when inflammatory indices and other laboratory end pointswere met Taken together these data suggest that there is insufficientevidence to draw firm conclusions or recommend routine use of n-3supplements in CF Notwithstanding it is common belief that n-3supplements provide some benefits for people with CF with relativelyfew adverse effects and thus their use is not discouraged
Further alterations in fatty acid metabolism have been highlight-ed including the consistent findings of an increase in circulatinglevels of saturated and monounsaturated fatty acids [7203204]Decreased levels of essential FA (EFA) ie the FA that have to be in-troduced with the diet correlates with the severity of respiratoryinsufficiency and the same clinical correlation was observed with al-tered proportions of FA species converted by the activity of desatur-ase enzymes (reviewed in [204]) The close relationship betweencertain fatty acids and oxidative stress including the negative correla-tion of C240 and linoleic acid with oxysterol levels point to the needof intensive investigation in CF patients of previously neglected lipidspecies that are emerging candidates in the control of metabolismQuantitative lipidomic analyses have lead to identify C161n7 palmi-toleate as a ldquoprotectiverdquo adipose-derived lipid hormone that stronglystimulates insulin activity in muscle and liver also suppressing in-flammatory cytokine output from mice fat cells [205] Specific meta-bolic activities have been also demonstrated by medium chainsaturated fatty acids caprylic acid (C80) capric acid (C100) and lau-ric acid (C120) Capric acid acts as a direct ligand of PPARγ using abinding pocket different from the binding pocket of thiazolidinedioneor long chain fatty acids [206] Additional activities of medium chainfatty acids which are ligands of free fatty acids receptors detectedin the immune cells the gastrointestinal tract and adipocytes maycontribute to metabolic homeostasis and inflammatory responses[207] These data underscore the importance of a lipid-mediated ldquoen-docrine networkrdquo demonstrating how specific alteration of one orfew serum lipids would be per se sufficient to influence metabolic ho-meostasis Given the relevance of this emerging information and thealteration of lipid metabolism and inflammatory status in CF fattyacid lipidomics need to be deeply investigated in CF
Again these studies have obvious nutritional implications Satu-rated fatty acids with chain lengths higher than C18 are poorlyabsorbed partly because they form insoluble calcium salts [208]Medium chain saturated fatty acids are well known for being highlyabsorbed through the intestine providing rapid delivery of energyvia oxidation of the more hydrophilic short chains and have beensuggested to provide proper nourishment in patients with CF [209]Recent studies have shown that consumption of a high-fat diet richin medium chain fatty acids as opposed to long chain fatty acidsdoes not lead to ectopic fat accumulation in skeletal muscle andliver of both rats and mice [210] In light of the close association be-tween nutritional status inflammation and life expectancy in CF pa-tients the manipulation of dietary lipids in these patients must befurther explored as a possible strategy to provide adequate nutritionand better management of oxidative stress
36 Hydrosoluble antioxidants oligoelements and enzymatic antioxidants
361 Vitamin CVitamin C status in CF patients has been poorly investigated Early
studies suggested a defective vitamin C status that was refractory tooral supplementation [211] Other and more recent studies showednormal or slightly decreased levels of vitamin C in CF patients as com-pared to healthy controls but age- and disease-related decline of thiswater-soluble antioxidant was reported in these patients [5212]In the study of Winklhofer-Roob et al [212] on mid-European CFpatients vitamin C concentrations decreased with age with an
estimated rate of 5 μmollyr and vitamin C concentrationsb40 μ-moll were associated with highest indexes of inflammation whichis consistent with the hypothesis that optimal levels of vitamin Cmay influence immuno-inflammatory activity of alveolar macro-phages and neutrophils Other few studies have examined the effectof supplements containing vitamin C on CF inflammation and oxida-tive stress since the levels of this vitamin do not significantly improvewith supplementation (reviewed in [213]) This highlights the com-mon fate that this hydrosoluble vitamin shares with several fat-soluble counterparts in the ldquomicronutrient paradoxrdquo of CF patients inwhich the need for a correction of their status along the progressionof the disease is frustrated by the poor efficacy of oral supplementa-tion protocols Formulations and appropriate supplementation proto-cols that may produce a better correction of vitamin C status of CFpatients are awaited for further clinical evaluation
362 Selenium and selenium-dependent peroxidasesSelenium is a trace element with marked electrophilicity [214]
that once converted to the organic form of Se-Cys can be introducedin protein structures to play its important role in H2O2 metabolismand signaling [215] As catalytic center of the enzyme GSH-peroxidase (SeGSH-Px) Se plays a crucial role to protect polyunsatu-rated lipids of plasma membrane and circulating lipoproteins formperoxidative insults With other Se-proteins such as the high molecu-lar weight thioredoxin reductases this oligoelement participates tothe control of protein thiol-disulfide oxidoreduction and glutathiony-lation which regulate signaling pathways of crucial importance in theregulation of immunity and inflammation [16] but also the function-ing of other redox-sensitive proteins such as the same CFTR [124]
The activity of SeGSH-Px in blood is considered a functional as-sessment of selenium status even if this assumption has some limita-tions related with the saturation profile that the Se stores show atincreasing doses of Se administration Investigations of the seleniumstatus in CF patients have produced conflicting findings which maydepend on differences in dietary intake ethnicity and environmentalfactors in the diverse patient populations (reviewed in [216217]) CFchildren have been reported to have lowered blood selenium and RBCSeGSH-Px activity [218219] normal plasma selenium and loweredRBC SeGSH-Px [220] and even normal levels of both these two param-eters [221] The supplementation with selenium in combination withother antioxidants was observed to increase the concentrations ofblood selenium that likewise β-carotene and fatty acid were posi-tively correlated with improved lung function [6]
Foucaud et al [218] observed that a defective selenium statuswas associated with lowered levels of other antioxidants that contrib-ute to the anti-peroxidative activity of this microelement such asvitamin E (reviewed in [222]) and the severity of this deficiencywas lower in children with pancreatic enzyme replacement and vita-min E supplementation
Treatments to substitute for exocrine pancreatic insufficiency bypancreatic enzymes from animal sources such as porcine pancreashave been confirmed to be a source of Se [220] These affects RBCSeGSH-Px activity and plasma selenium concentrations which hasto be taken into account when selenium supplements are given toCF patients
Selenium has been used to develop a series of organoseleniumcompounds that may open the way to new therapeutic opportunitiesin CF (see Section 392) These include GPX mimetic drugs and phaseII enzyme inducers which may provide higher antioxidant activity ofASL and cellular protection effects in the airways
363 Zinc and copperZinc and copper (Zn and Cu respectively) are present in many
proteins so that a deficiency of these trace metals could have pleiotro-pic effects in humans As regards antioxidant systems these two oli-goelements contribute an important role being cofactors of two
703F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
isoforms of the superoxide dismutase enzymes eg the extracellularform eg the EC-SOD or Sod 3 and the CundashZn-SOD or Sod 1 that isfound in several tissues and cells [223] The EC-SOD exerts its antiox-idant role also in the lining fluids of the airways [224]
The notion that CF patients have defective concentrations of bloodZn and Cu is controversial As far as Cu status is concerned few datahave been produced and are available in the literature suggestingthe notion that CF patients develop a moderate copper deficiency[225226] That was essentially demonstrated on the bases of a defec-tive activity of Cu-related proteins such as plasma ceruloplasmindiamine oxidase and RBC SOD This defect seems to be refractory toCu and Zn supplementation (see below)
More advanced studies have been carried out in the case of Zn sta-tus in CF Low plasma zinc concentrations were reported in approxi-mately 30 of young infants with CF identified by newbornscreening [227] and an impaired zinc homeostasis in CF patientswas described by Easley et al [228] This is characterized by poor con-servation of the endogenous pool with fecal loss and impaired frac-tional absorption of zinc which are the consequences of pancreaticinsufficiency and persisting steatorrhea These studies suggestedthat in the clinical management of CF patients these defects can beat least in part corrected by exocrine pancreatic enzyme replacement
A series of studies by Van Biervliet et al [229230] demonstratedin a Dutch population of CF infants and children that serum Zn variesin an age-dependent manner but remained unchanged with respectto healthy control levels In CF patients no difference in serum Zn con-centration between pancreatic-sufficient or pancreatic-insufficientpatients was observed and no correlation was found with the nutri-tional status or height z-score Importantly in these studies a signifi-cant correlation of serum Zn was observed with the fat solublevitamins A and E thus confirming the relationship between the ab-normalities of lipid and Zn metabolism in CF This suggests that co-supplementation of Zn and fat-soluble vitamins should be advisedin the presence of pancreatic insufficiency and persisting steatorrhea
Neve et al [219] in a study aimed to assess plasma and erythrocytezinc copper and selenium in CF children showed that mean plasmazinc and copper levels were not different from those in age-matched controls which confirms the observations by Van Biervlietet al described above However plasma zinc concentrations de-creased in patients with moderate-to-severe growth retardation andwith severe pulmonary disease but very low zinc levels occur sporad-ically Erythrocyte zinc and copper levels were significantly higherthan normal while RBC selenium was lower than in age-matchedcontrols These trace element concentrations in erythrocytes werediscussed in relation to the activities of the CuZn-SOD and the Se-enzyme GPx This observation suggests a compensatory upregulationof the erythrocyte CuZn-SOD by the exposure of erythroid precursorsto ROS andor other CF-related stressors
Best et al [225] also studied RBC SOD activity using this as a bio-logical sensor of Cu status in CF patients A lowered activity of thisenzyme was reported in CF together with that of the other Cu-dependent enzyme plasma diamine oxidase while plasma ceruplas-min showed normal activity Degradation rates of copper proteinsare known to be accelerated in conditions of copper deficiencywhich could explain the finding at least in part Anyway when Cuand Zn were supplemented to CF patients either separate or incombination (6 weeks of 3 mg copperd as copper-glycinate and30 mg zincd as zinc-glycinate) any of the copper enzyme activitieswas affected Therefore the moderate copper deficiency of CF patientsappears to be refractory to the intervention by increased copper andor zinc intake
Erythrocyte CuZn-SOD and the plasma levels of Cu and Zn werealso measured in the study of Wood et al [6] in which Australian CFpatients (agegt5 years) were treated with a high-dose antioxidantmultivitamin formulation containing 200 mg vitamin E (as RRR-α-tocopherol) 300 mg vitamin C (as sodium ascorbate) 25 mg β-
carotene (all-trans isomer) 90 μg Se (as selenomethionine) and500 μg vitamin A (as retinyl palmitate) in oil Plasma oligoelementsand particularly Zn were in the normal range at baseline (as com-pared with the data reported in [229230]) and were not affected bythis multivitamin supplement The same was found for the activityof RBC SOD and for plasma 8-iso-PGF2α as surrogate biomarker oflipid peroxidation
In a recent non-randomized small population (n=21) casendashcon-trol study in CF children Zn supplementation was proven to producepositive clinical effects in Zn-deficient patients [196] The supplemen-tation with 5 mgkg Zn sulfateday (maximum 150 mg) significantlydecreased the number of infections and increased the forced expira-tory volume in 1 s energy intake and growth parameters also im-proved These parameters were unaffected in untreated patientsexcept that in the case of the pulmonary function that decreased sig-nificantly These clinical observations on Zn supplementation need tobe confirmed in prospective double-blind randomized control trial
37 Appropriateness and targeting of antioxidant therapies in CF
The choice of the appropriate antioxidant and dose to correct a cer-tain biomarker and its associated biochemical lesion is another impor-tant point that appears to have disregarded in many clinical studiesFor instance unlike vitamin E vitamin C supplementation does notalter F2-IsoPs levels in humans (reviewed in [74]) This appears tobe true also in the antioxidant therapy of CF in which vitamin C(300 mgday) was administered together with other antioxidantsthat included a dose of vitamin E of 200 mgday without any signifi-cant effect on the surrogate biomarker of lipid peroxidation F2-IsoPs[6] When carotenoids are used as supplements to prevent the damag-ing action of ROS in the CF airways it is noteworthy that these are notparticularly good quenchers of peroxyl radicals relative to phenolicsand other antioxidants but are exceptional in quenching singlet oxy-gen at which most other phenolics and antioxidants are relativelyineffective Singlet oxygen is not a radical and does not react via radi-cal mechanisms but reacts mostly by the addition to double bondsforming endoperoxides that can be reduced to alkoxyl radicals that ini-tiate radical chain reactions typical of the peroxidative damage of PUFA[38] In this case the analysis of F2-IsoPs lipid peroxide formation andtransition metal-induced oxidizability of lipoproteins [162180] are allappropriate to evaluate the effect of carotenoids in preventing lipidperoxidation
As far as the dose is concerned clinical pharmacology of vitamin Eas an antioxidant was recently investigated by means of the effect onF2-IsoPs production and doses of α-tocopherol of 1600 IUday orgreater were found to be required to statistically affect plasma F2-IsoPs levels in hypercholeterolemic subjects [176] Several vitamin Esupplementation studies in CF patients have been performed withdoses of lower than 300 IUday regardless of the lowered absorptionby pancreatic and liver defects and the regular supplementationwith these doses does not appear to correct lipid oxidation markersin CF [7]
In the clinical practice and planning trials it has to be taken intoconsideration that in spite of substantial evidence supporting ahigher antioxidant demand in CF interventions with several antioxi-dant formulations produce poor responsiveness particularly in thecase of fat-soluble antioxidants which are poorly absorbed [6162]
Since many oxidants and antioxidants are present in tissuesand biological fluids and these have different chemical and physicalcharacteristics the possibility to produce a successful therapy witha single antioxidant molecule is too far to be realistic Moreover an-tioxidants act by multiple mechanisms in a single system or by adifferent single mechanism depending on the reaction systemresponding in a different manner to different radical or oxidantsources Because multiple reaction characteristics and mechanismsas well as different phase localizations are usually involved no single
704 F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
therapeutic approach will effectively prevent damage by multipleROS sources The defect of physiological antioxidants may also interferewith antioxidant therapies that are based on one or few exogenousantioxidants
Moreover several antioxidant vitamins such as vitamin E and ca-rotenoids have multiple natural forms with different bioavailabilitymetabolism and bioactivity [157167231] As far as the case of vita-min E supplementation concerns α-tocopherol was used as uniquevitamer in the large majority of supplementation trials so far per-formed and is the form used in the nutritional management of CFpatients Moreover several supplements contain the synthetic (or ra-cemic) form of this vitamin that has lower bioavailability than thenatural form Other forms present in nature and abundantly con-tained in vegetables such as tocotrienols and the less methylatedforms of tocopherol are not represented in many of the supplementformulations so far available in clinical centers and the supplementa-tion with α-tocopherol also limits their bioavailability These formsshow markedly higher susceptibility to hepatic metabolism and bili-ary excretion with respect to α-tocopherol eg the most representedform in blood and solid tissues and if co-supplemented these areeasily displaced during liver uptake and excreted with bile bymeans of competition with the same α-tocopherol Notwithstandingthese minor forms have been proposed to play important physiolog-ical roles showing molecular characteristics transcriptional effectsand antioxidant activities that clearly differentiate them in subfam-ilies with distinct biological functions Some of these such as α-tocopherol eg the second vitamin E form as relative abundance inblood and its carboxyethyl-hydroxychroman metabolite [189] ap-pear to have health-related anti-inflammatory effects which are par-ticularly relevant in lung protection [232233] This has suggestedthat such a group of ldquonon-α-tocopherolrdquo forms may represent anoth-er family of vitamins within the family of vitamin E with an impor-tant but often missed contribution to the proposed health effects ofthis vitamin [163]
These aspects may thus limit the possibility to provide CF patientsof optimal levels of this vitamin in all its components even if they areregularly treated with a vitamin E supplement eg withα-tocopherol
Targeted antioxidant therapy with formulations with higher bio-availability and bioactivity has been anticipated in CF New antioxi-dant formulations have been proposed to overcome main limits ofantioxidant therapies so far proposed for these patients Water-miscible α-tocopheryl acetate containing polysorbate propylene gly-col or polyethylene glycol as emulsifiers form micellar structureswere suggested to providing greater bioavailability than the fat-soluble counterparts These were commercialized with the brandnames of E-viminreg Cremophorreg EL and Aquasolreg E but despitethe original positive expectation [234235] some studies failed to ob-serve a higher response in vitamin E levels when these were com-pared with fat-soluble formulations [236237]
In a pilot study by Papas et al [183] a micellar formulation of fat-soluble nutrients and antioxidants was found to improve plasmalevels of β-carotene γ-tocopherol and CoQ(10) reducing at thesame time some inflammatory markers in induced sputum eg mye-loperoxidase and to a lower extent PMN elastase and total cell countswhile lung function and sputum bacterial counts were unaffectedThe same group recently confirmed the possibility to increase the ab-sorption of fat-soluble micronutrients using formulations with higherbioavailability specifically designed for malabsorbing patients such asCF patients that include also vitamin K and commercialized with thebrand name of AquADEKsreg [162] Despite improved vitamin and mi-cronutrient levels in this non-randomized open-label study AquA-DEKsreg produced only modest improvements in weight percentileand pulmonary function Another recent pilot observation [182] hassuggested the beneficial effect of this formulation on antioxidant andoxidative stress parameters of this oral supplement that surely deservesmore clinical investigation by larger randomized controlled trials
Recent multivitaminic formulations have been designed to containalso the minor forms of vitamin E and specifically γ-tocopherol [238]the expected superiority of which with respect to formulations con-taining only α-tocopherol needs to be verified As discussed abovein the section dedicated to vitamin E further advancements in thetherapy of CF inflammation and oxidative stress could be based onsynthetic forms and natural metabolites of this vitamin that havebeen recently identified to possess higher antioxidant and also anti-inflammatory activity than α-tocopherol (reviewed in [163168])
Pre-clinical investigation of these and other fat-soluble agents iscurrently addressed to develop formulations and administration pro-tocols that may increase the therapeutic efficacy in the airways In theantioxidant therapy of lung dysfunction in CF local administrationprotocols may overcome the limits of oral and systemic administra-tion protocols increasing bioavailability and providing targetedapproach to inflammation and oxidative stress Aerosolization of vita-min E and other fat-soluble micronutrients is possible and may allowdirect administration in the airways to prevent toxicity of smokewhich is closely associated with inflammation and oxidative stress[164165] To our knowledge this as well as other strategies of localadministration such as instillation of solutions such as surfactant-like solutions enriched of vitamin E have not been previously inves-tigated in CF patients and other CF model systems
On the contrary inhalation is an administration route widelyadopted in the case of GSH and NAC therapy described above Inthis context Cys formulations alternative to NAC have been proposedfor use as antioxidant and anti-inflammatory agent for inhalationNacystelyn is a lysine adduct of NAC that thanks to a higher proton-ation equilibrium shows increased water solubility and thus betterbioavailability Nacystelyn has been described to influence IL-8 gener-ation and the inflammatory signaling of bronchial epithelial cells[239] and preliminary clinical evaluation has demonstrated the safetyof this drug [240] Further clinical trials aimed to assess the effect onlung symptomatology of CF patients are needed Direct administra-tion in the airways could also be adopted for micronutrient vitaminswith poor absorption and bioavailability due to GI defects
38 Clinical impact of antioxidant therapy in CF
Huge in vitro and pre-clinical evidence has provided the rationaleto support clinical investigation of antioxidant strategies in CF Theseshould aim to restore the oxidantndashantioxidant balance of CF airwaychallenged by chronic infection and inflammatory cell activation
Some observational trials have confirmed that antioxidants usedas either supplements to the diet or drugs for lung administrationby aerosolized formulations may help in relieving progressive lungdamage and other adverse clinical events of CF such as poor growthSo far few studies have examined with sufficient methodologicalrigor the clinical efficacy of antioxidant therapy in CF This was alsoconcluded in a previous review of the literature by Cantin et al [12]that was published in the beginning of 2006 and is confirmed alsoin a recent analysis of clinical trials on antioxidant therapy in CF pa-tients [213] that examined the literature until September 2010using as sources the databases of the Cochrane CF and Genetic Disor-ders Group CF Trials Register PubMed CINAHL and AMED Useful in-formation was retrieved from just four randomized controlled trialsand one quasi-randomized controlled trial on vitamin C vitamin Eβ-carotene and selenium used as supplements administered aloneor in combination Post-hoc data analysis that was possible only inthree studies on a total of 87 CF patients showed the absence ofany significant improvement in lung function that was selected as pri-mary outcome together with quality of life that improved in one trialSecondary outcomes concerning laboratory indices of oxidative stressand antioxidant status showed several improvements These includedan increase of RBC SeGPx by selenium supplementation done as
705F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
individual or combined supplementation and increased levels of allplasma antioxidants except vitamin C that were observed in all thetrials
The message from these studies to pediatricians and nutritionistswithin the clinical staff of CF centers is that in the absence of solid ev-idence regarding the clinical effectiveness of oral formulations of an-tioxidant supplements in CF (including PUFA) their use as a routineclinical practice should be considered with caution keeping clear inmind that this should represent just a complement of one of themost critical interventions in the life-long clinical management pro-gram of CF patients eg providing an adequate nutriture [140] Inthis context compensating energy and protein malnutrition has toremain the first goal of nutritional management programs Providinghigher intakes of antioxidant micronutrients with food naturally-enriched (or functionalized) of micronutrient antioxidants shouldbe preferred in order to have the higher combination of positive nu-tritional factors that are lost during refinement procedures and over-all industrial processing of dietary supplements
Measures of good practice in clinical management of micro-malnutrition in CF patients would include the support of specializedpersonnel and laboratories The centers should have the possibilityto ascertain with appropriate nutritional and laboratory tests whatthe level of deficiency is for the different micronutrients that each pa-tient may suffer from during a dietary program Monitoring dietaryintakes and blood levels of micronutrients is not sufficient to set apersonalized nutritional intervention with supplements or functionalfoods Sub-optimal intakes and the compliance to nutritional inter-ventions should be verified by means of selected biochemical andclinical criteria Unluckily the latter are still not well established forsome micronutrients such as the fat-soluble vitamins E (reviewed in[163173241]) and K [242243] and also for trace elements such asSe [244] For many of the antioxidants used as supplements inhumans we still do not know exactly several of the biological effectsthat these may provide when introduced in a healthy body and weknow less what these can do in disease These aspects hardly impacton the concept of optimal levels of intake that should be identified foreach micronutrient on an individual basis According with the aspectsdiscussed in the previous sections optimal levels of intake for antiox-idant micronutrients are different in CF patients and healthy subjectsand vary with age and several individual factors
Lung administration of antioxidants by means of aerosolized for-mulations so far used for GSH therapy (see above) is a promisingfield of clinical investigation in CF Toxicity issues are currently themain concern and the subject of clinical evaluation by several groups(described above)
Information on future directions of antioxidant therapy in CF canbe inferred by the analysis of pending or recently completed clinicaltrials that have been searched (December 2011) at ClinicalTrialsgovdatabase matching the terms ldquoantioxidant therapyrdquo or ldquoglutathionerdquowith ldquocystic fibrosisrdquo Fifteen trials were retrieved and those directlyrelated to antioxidant therapy (n=12) are presented in Table 1 andinclude efficacy and safety studies of inhaled drugs as GSH sodiumpyruvate NAC and NO and the dietary supplements AquADEKsregan antioxidant-rich multivitamin supplement epigallocatechin gal-late (EGCG)tocotrienol curcuminoids the amino acid glutaminesulforaphane in broccoli sprouts One trial is investigating the flavo-noid quercetin as CFTR modulator
39 Emerging antioxidant and anti-inflammatory approaches in CF
Mediterranean foods such as olive oil and red wine or severalplant extracts such as herbal tea or grape seed extracts contain aseries of natural compounds with important antioxidant and NOscavenging activity that have been widely investigated for the pre-vention of oxidative stress-related diseases [38245] These havebeen long investigated as template molecules to develop antioxidant
and anti-inflammatory drugs Between the multitudes of natural sub-stances most investigated ones include for instance tyrosol hydroxy-tyrosol gallic and caffeic acids belonging to the family of phenolswhile resveratrol of the stilbenes family epicatechin kaempferoland cianidin are examples of flavonoids examples of fat-soluble phe-nolics are those of the family of tocols (vitamin E) and carotenoids Allthese compounds show different metabolisms and signaling effects[246] Antioxidant and cell protection mechanisms are associatedwith different and sometimes concurrent processes as H-atom trans-fer and electron donation radical trapping and chelation of transitionmetals that can be easily investigated at the chemical level [247] Be-sides these direct antioxidant effects metabolic responses and signal-ing effects of natural compounds are also important to producesecond-generation responses that modify the level of antioxidantprotection and the potential for ROS detoxification in cells and bodyfluids These derive from the transcriptional regulation of antioxidantand pro-oxidant genes that coexist with the modulation of cytokinesecretion and inflammatory enzyme activities
Some of these natural plant-derived antioxidants may provide fur-ther pharmacological activities of possible relevance in CF This is thecase for instance of the plant flavonoids genistein apigenin kaemp-ferol quercetin and hesperidin [248ndash251] that fall in the pharmaco-logical category of ldquopotentiatorsrdquo [252] in that these activate at leastto a certain extent CTFR-mediated Cl currents in normal and CF airwayepithelium investigated either in vitro or in vivo in humans and ani-mal models Actually as prototypal flavonoid-derived potentiatorthe tyrosine kinase inhibitor genistein potentiates the gating of wild-type as well as ΔF508 CFTR and G551D CFTR [253] but at higherdoses it inhibits CFTR gating which make this an unlikely clinical can-didate Similar potentiation effects have been reported for the antiox-idant curcumin [250] that shows an additive effect with respect togenistein-induced potentiation Besides CFTR potentiation whichdoes not appear to have a direct influence on GSH and nutrient trans-port in the lung tissue all these natural substances have been usedalone or in combination with other agents as in vivo enhancers oflung antioxidant protection [246254255] In the case of quercetinthiol-reactive phenolic [256] bronchodilation and anti-inflammatoryeffects by a restoration of the Th1Th2 balance have been reportedin inflammatory syndromes of the lung [255257ndash259] but theseeffects have not been explored in CF Pyocyanin toxicity (see abovein the Section 2) could represent an issue for the use of quercetinand other catechols in infectious diseases of the lung [260]
Other natural antioxidants of potential interest in CF therapy in-clude terpenoids [261] such as terpinen-4-ol a major constituentof tea tree oil that is being investigated in the therapy of anti-biotic resistant organisms specifically against methicillin-resistantStaphylococcus aureus (MRSA) [262] a problem in CF [263] Otherthan being lipophilic antioxidants terpenes can prevent oxidativestress of the CF lung secondarily to the antibiotic effect thereby pro-moting a better control of immuno-inflammatory pathways and lungantioxidants
391 Targeting NF-κB with natural compounds resveratrol and plantextracts
Natural compounds were long known to be useful in designinganti-inflammatory drugs and some of these could find an applicationin the control of the transcription factor kappa-B (NF-κB) that maylead to develop advanced pharmacological tools to control inflamma-tion and to produce higher antioxidant protection to CF airwaysInhibitors targeting NF-κB including transcription factors decoymolecules (TFD) are potent down-regulators of gene expressionand release of IL-8 in CF cells infected with P aeruginosa [264265]
Resveratrol (354prime-trihydroxystilbene ldquoErdquo form) is one of the mostinvestigated natural antioxidant with proposed activity as NF-κBinhibitor This is a phytoalexin present in large quantity in red winepreferentially in the skin of grapes being its concentration
706 F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
50ndash100 μgmg of fresh skin and 13ndash3 mgl of red wine [266]Furthermore resveratrol is a constituent of lsquoDarakchasavarsquo (13ndash6 mgl) an ayurvedic medicine from India [267] The antioxidant activity ofresveratrol has been reported in several papers and occurs also in lungtissues suggesting that resveratrol has potential as a therapeuticagent in respiratory disease [268ndash270] Resveratrol can be consideredone of the most interesting molecules from the natural worldexhibiting strong antioxidant activity that at the same time is able toexert anti inflammatory activity through alteration of NF-κB functionsand efficient inhibition of pro-inflammatory genes [271272] As far asthe effects on CF model systems are concerned Cabrini et al [26]reported the effects of resveratrol on P aeruginosa infected CF IB3-1cells The results obtained demonstrate that resveratrol exhibits minoreffects of IB3-1 cell growth and important inhibitory effects on accumu-lation of IL-8 and GRO-α mRNA while minor effects on IL-6 gene ex-pression were observed These data support recently publishedobservations suggesting inhibitory effects of resveratrol in infection-mediated inflammatory processes [273] Interestingly resveratrol hasbeen reported as a potent inhibitor of NF-κB activity and a promisinganti-inflammatory agent [272274] also in combinationwith othermol-ecules [274275] However in vivo translation of this pre-clinical on res-veratrol is hard to be foreseen This natural compound displays poorbioavailability [276] and further characterization of resveratrol pharma-cokinetics is troublesome since it is hardly measurable in vivo [277]Furthermore the regulation of inflammatory responses by resveratrolhas been suggested to be far more complex than simple direct suppres-sion of NF-κB activity Actually some aspects of the immune responsecould be enhanced by this natural substance which may lead tohypothesize broad negative feedback events on immuno-inflammatorypathways [278] In any case and with these cautions in mind the pub-lished observations on cellular model systems support the concept thatresveratrol and resveratrol-containing formulations deserve further con-sideration to determine their possible therapeutic values in CF
Other inhibitors can be identified from systematic studies of naturalproducts and their ability to interfere with NF-κB activity [279ndash281]Recent studies have demonstrated that the whole extract of Aeglemarmelos (Rutaceae) has strong inhibitory effect on the P aeruginosa-dependent IL-8 induction in human CF-derived bronchial IB3-1 cellswithout affecting cell proliferation [280] Molecular analysis of compo-nents contained in A marmelos extracts revealed that three major com-pounds namely 56-dimethoxy-1-indanone 2-hydroxy-cinnamic acidand 5-methoxy psoralen (5-MOP) reproduce the inhibitory effect ob-servedwith thewhole extract [280] A further example has been recent-ly published using extracts from bergamot (Citrus bergamia Risso) Inthis study the extracts were characterized and the main detected con-stituents were assayed for their biological activity [281] The resultsobtained demonstrated that the extracts from bergamot epicarps con-tain components displaying an inhibitory activity on IL-8 Particularlythe most active molecules were bergapten and citropten These effectshave been confirmed by analyzing mRNA levels and protein release inthe CF cellularmodels IB3-1 and CuFi-1 inducedwith TNF-α or exposedto P aeruginosa
A parallel strategy linking NF-κB inhibition and down-regulationof NF-κB-dependent functions is described in recently publishedstudies based on a structured-based virtual screening (VS) of differ-ently substituted furocoumarins and analogues against NF-κB withthe objective of selecting molecules able to inhibit the binding ofthis transcription factor to DNA [282283] Novel compounds wereidentified with this strategy as potent inhibitors of NF-κB dependentbiological functions to be proposed for the control lung inflammationoccurring in patients affected by CF [282ndash284]
392 Scavengers and regulators of H2O2 and NO
3921 Lactoferrin and OSCNmacr The impaired DUOXLPO system of CFpatients could be the target of therapeutic strategies that may
produce concomitant antimicrobial and antioxidant effects This sys-tem described above in Section 22 represents an important compo-nent of innate immunity with a role in bactericidal defense andregulation of H2O2 metabolism of airways [32] CF patients have alsoreported to show lowered LF levels in the ASL [37] that togetherwith a CFTR-dependent defective efflux of SCNmacr and LPO [36] may cre-ate the environment for a sustained flux of H2O2 and for the genera-tion of highly reactive Fenton species [1138] An ideal therapeuticintervention should restore the LPO-dependent generation of bacteri-cidal OSCNmacr from DUOX-derived H2O2 and SCNmacr in the ASL to controlat the same time the microbial biofilm and the flux of H2O2 into theASL An approach close to this therapeutic mechanism was recentlyproposed for the drug Meveolreg This is a complex of LF and OSCNmacrwith proposed in vivo antimicrobial activity [285] to be evaluatedin clinical trials for the aerosol treatment of lung infections in CFpatients The role for this drug in the control of H2O2 levels of ASLremains to be investigated
3922 Organoselenium compounds Organoselenium compoundshave been proposed as therapeutic agents useful in the antioxidanttherapy of inflammatory conditions These include GPX mimetic mol-ecules such as Ebselenreg (2-phenyl-12-benzisoselenazol-3(2H)-one)or other and more recently developed molecules that are still inpre-clinical steps of evaluation [286] Selectively and specificity of ac-tion are main issues in the therapeutic mechanism of this candidateantioxidant drug that thanks to the electrophilic properties of Se[214] reacts with thiols to reduce H2O2 and other species MoreoverEbselenreg has been described to act as potent non-competitive inhib-itor of extracellular nucleoside diphosphokinase (NDPK) having neg-ligible effect on ecto-ATPase and adenyl kinase activities which areother players of the metabolism of extracellular nucleotides [287]This enzyme together with other nucleoside di- and triphosphatescontributes to regulate several components of the mucociliary clear-ance process (MCC) that protects the lung against infections via acti-vation of epithelial purinergic receptors The inhibition of NDPK bythis GPX-mimetic drug may also impact on the energy status of endo-thelial cells [287] This aspect could be further investigated as a cellu-lar protection mechanism in the pulmonary epithelium of CF patientsbeing the control of cell energy of fundamental importance to preventthe activation of death pathways [288]
Further therapeutic mechanisms for these Se-derived drugs mayderive from the marked activity as inducers of phase II enzymessuch as quinone reductase (QR) and glutathione-S-transferase (GST)[289] This induction response also observed with other electrophilsand redox-active molecules such as natural phenolic antioxidantscould produce higher cellular protection by the acquisition of anincreased capability to detoxify endobiotics generated during oxida-tive stress and inflammation [246]
3923 Melatonin and GSNO as NOx regulators Increased markers ofNO-derived biological damage are present in the CF lung suggestingthe abnormal reactivity of NOx in the inflamed lung of CF patients[52] However an impaired metabolism and biological function ofNO in CF airways (see Section 23) suggests a cautious approach tothe use of agents that may influence the levels and chemical behaviorof NO-derived species (NOx) with possible impact on the physiologi-cal roles of NO in vasodilatation innate immunity and H2O2 metabo-lism of the respiratory tract [290291] NO donors also appear toinfluence CFTR function of alveolar epithelium and gland serouscells [292293]
Main physiological role of the pineal gland hormone melatonin isthe synchronization of circadian rhythms including the sleepndashwakecycle but several other functions dealing with immunomodulatoryantioxidant and cellular protection effects have been identified[294] Melatonin receptor stimulation may also influence cyclic AMPsignaling and the regulation of CFTR ion channel [295296]
707F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
A recent randomized double-blind placebo-controlled study hasexamined the effects of short term melatonin administration (3 mgfor 3 weeks) on sleep and oxidative stress markers in CF [297]According with the expected pharmacological effect of this hormonalsubstance the treatment was successful in improving sleep indicesAt the same time nitrite levels determined in exhaled breath conden-sate (EBC) were reduced to suggest a better control of NOmetabolismof CF airways (discussed above in Section 23) but these effects how-ever were not associated with a significant correction of isoprostaneas lipid peroxidation marker measured in EBC Increasing dosages ofmelatonin could be investigated for the pharmacological treatmentof oxidative stress and immune dysfunction of CF patients due tothe absence of adverse effects of this hormonal substance in humans
The S-nitrosation reaction of thiols is another interesting aspect ofNO pharmacology [53] that may find an application in the therapy oflung complications of CF This has been the case for instance of theS-nitrosothiol GSNO that has been used safely in human trials[298299] This endogenous nitrosothiol with proposed regulatory ef-fect on the CFTR of lung epithelia [292293] is well tolerated in pa-tients with CF when administered by aerosolization and mayproduce better oxygenation [299] thereby suggesting that therapyaimed at restoring endogenous GSNO levels in the CF airway maymerit further clinical evaluation Since the administered GSNO de-composes as shown by the increased levels of expired NO in CF pa-tients under treatment with this nitrosothiol [299] furtherinvestigation should be addressed to ascertain whether GSNO thera-py may merely correspond to a GSH therapy
NO dependent effects on CFTR function should be considered toevaluate mechanism of action and specificity of antioxidant therapiesthat target NO metabolism and function in the CF airways
4 Conclusions and future perspectives
The presence of clinical and biochemical symptoms of inflammationand oxidative stress implies that CF patients have a higher demand ofantioxidant protection The combination of the dysfunctional CFTRwith a lowered intake and absorption of dietary antioxidants producesub-optimal levels of protection from both enzymatic and non-enzymatic defense systems The former could be associated with a de-fective glutathionemetabolism and lowered intake of sulfur-containingamino acids and oligoelements such as zinc and possibly seleniumwhile fat-soluble antioxidant vitamins such as vitamin E and caroten-oids and the water-soluble vitamin C are lowered than in healthy sub-jects due to malabsorption and possibly higher consumption
The increased antioxidant demand in CF patients should be evenhigher in the presence of complications of the lung pancreas andliver Lung comorbidity is particularly important in this contextbeing associated with recurrent infections which results in the alter-nation of inflammatory exacerbates and chronic inflammation Thesesustain the flux of ROS in the airways and promote the formation ofsecond-generation byproducts by the damage of biomolecules suchas PUFA and proteins which may diffuse also at the systemic level tofurther promote adverse biological responses and toxic reactions Pan-creatic insufficiency causes malnutrition and may lead to develop en-docrine and metabolic defects associated with diabetes of CF Theseevents can be further aggravated by the concomitance of liver dys-function and a poor nutritional status Malnutrition is strongly associ-ated with poor prognosis as assessed by pulmonary function andsurvival data [138ndash140] The more aggressive nutritional interven-tions seem to produce better clinical outcomes in these patients andthe possibility of achieving higher antioxidant protection in well-nourished patients by dietary factors could be a key aspect to explainsuch a clinical advantage The assumption that food-derived compo-nentsmay help to prevent the damaging effects of oxidative stress im-proving the antioxidant defenses deserves further investigation at theclinical level This together with the investigation of appropriate
laboratory biomarkers could provide critical information to establishintervention criteria for an early nutritional management of newly di-agnosed patients [5] It is expected that a timely secondary preventionstrategy could influence the progression of CF symptoms thusaffecting with a self-feeding mechanism the same extent of malnutri-tion and oxidative stress along the life of CF patients Since severalfactors contribute to impair the nutritional status of CF patients(such as pancreatic insufficiency chronic malabsorption recurrentsinopulmonary infections and progressive lung disease chronic in-flammation increased energy expenditure suboptimal intake multi-therapy) careful monitoring of the antioxidant status should berecommended According with international guidelines fat-solublevitamin supplementation is of utmost importance in daily practice to-gether with energy intake requirements and pancreatic enzyme-replacement therapy Among these vitamin E β-carotene and ω-3FA have observed to alleviate selected biochemical signs of oxidativestress as measured for instance with well established laboratory indi-ces of lipid peroxidation and in some studies these effects werepreliminarily associated with positive clinical outcomes Notwith-standing randomizedndashcontrolled clinical trials on antioxidant supple-ments (including ω-3 FA) so far carried out in CF have failed toconclusively demonstrate significant beneficial effects on respiratorysymptoms and on the consequent impact that these have on the qual-ity of life of these patients (reviewed in [202213]) whichmay provideno support for the use of these supplements in CF An absence of effi-cacy in prevention studies on antioxidant supplements has also beenobserved in other and possibly less severe oxidative stress-relatedconditions particularly in the secondary prevention of cardiovasculardisease and some forms of cancer by vitamin E and other antioxidantssuch as vitamin C selenium and β-carotene (reviewed in [163]) Dif-ferent biases however have been identified in randomize large clini-cal trials that may account for these disappointing findings Theseinclude patient selection criteria (early interventions and primaryprevention could have more chances of success than secondaryprevention) duration and doses of the treatment use of wrong anti-oxidant formulations and administration protocols absence of verifi-cations of the biological compliance to the treatment etc The samebiases apply for the few trials carried out in CF patients Thus the ap-propriateness and efficacy of nutritional interventions with naturalfood-derived or synthetic antioxidants should be verifiedwith respectto the biological pathways of oxidative stress and clinical variablesthat are identified as end-points Profiles of blood and tissue antioxi-dants as well as of reliable surrogate markers of oxidative stresshave to be selected and determined in highly specialized laboratorieswith a well-established experience on these analyses
Well-timed (early) interventions with appropriate antioxidantformulationsprotocols need to be proposed for the next generationof trials and the development of novel CF-tailored antioxidant andanti-inflammatory agents should be promoted
As a consequence of these considerations more clinical investiga-tion is awaited to identify future successful approaches to the antiox-idant therapy as a measure to further enhance quality of life and theoverall clinical outcome of CF patients
Acknowledgments
We are indebted with the Italian Cystic Fibrosis Research Founda-tion for the support that it provided with its grant program to the re-search activity of the authors of this paper This is a scientific initiativeof the ldquoWorking Group on Inflammation in Cystic Fibrosisrdquo (BragonziA Bravo E Cabrini G Conese M Cuzzocrea S Dechecchi MC De Ales-sandri A Evangelista V Galli F Gambari R Lambiase A Lucidi VManca A Melotti P Minicucci L Motta A Pietraforte D Pompella AQuattrucci S Rizzo R Romano M Sorio C Tesse R) of the Italian Soci-ety for Cystic Fibrosis A particular thank goes to the Prof GianniMastella for the critical revision of the manuscript and for the
708 F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
stimulating research environment that he has contributed to createwithin the Italian Cystic Fibrosis Research Foundation
References
[1] BP OSullivan SD Freedman Cystic fibrosis Lancet 373 (2009) 1891ndash1904[2] P Linsdell JW Hanrahan Glutathione permeability of CFTR Am J Physiol 275
(1998) C323ndashC326[3] L Gao KJ Kim JR Yankaskas HJ Forman Abnormal glutathione transport in
cystic fibrosis airway epithelia Am J Physiol 277 (1999) L113ndashL118[4] RK Rowntree A Harris The phenotypic consequences of CFTR mutations Ann
Hum Genet 67 (2003) 471ndash485[5] EI Back C Frindt D Nohr J Frank R Ziebach M Stern M Ranke HK Biesalski
Antioxidant deficiency in cystic fibrosis when is the right time to take actionAm J Clin Nutr 80 (2004) 374ndash384
[6] LG Wood DA Fitzgerald AK Lee ML Garg Improved antioxidant and fattyacid status of patients with cystic fibrosis after antioxidant supplementation islinked to improved lung function Am J Clin Nutr 77 (2003) 150ndash159
[7] L Iuliano R Monticolo G Straface S Zullo F Galli M Boaz S Quattrucci Asso-ciation of cholesterol oxidation and abnormalities in fatty acid metabolism incystic fibrosis Am J Clin Nutr 90 (2009) 477ndash484
[8] C Libetta V Sepe P Esposito F Galli A Dal Canton Oxidative stress and inflam-mation implications in uremia and hemodialysis Clin Biochem 44 (2011)1189ndash1198
[9] G Bartosz Reactive oxygen species destroyers or messengers Biochem Phar-macol 77 (2009) 1303ndash1315
[10] T Ntimbane B Comte G Mailhot Y Berthiaume V Poitout M Prentki RRabasa-Lhoret E Levy Cystic fibrosis-related diabetes from CFTR dysfunctionto oxidative stress Clin Biochem 30 (2009) 153ndash177
[11] A van der Vliet JP Eiserich GP Marelich B Halliwell CE Cross Oxidativestress in cystic fibrosis does it occur and does it matter Adv Pharmacol 38(1997) 491ndash513
[12] AM Cantin TB White CE Cross HJ Forman RJ Sokol D Borowitz Antioxi-dants in cystic fibrosis Conclusions from the CF antioxidant workshop Bethes-da Maryland Free Radic Biol Med 42 (2007) 15ndash31
[13] LT McGrath P Mallon L Dowey B Silke E McClean M McDonnell A DevineS Copeland S Elborn Oxidative stress during acute respiratory exacerbations incystic fibrosis Thorax 54 (1999) 518ndash523
[14] E Thomson S Brennan R Senthilmohan CL Gangell AL Chapman PD SlyAJ Kettle E Balding LJ Berry JB Carlin R Carzino N de Klerk T Douglas CFoo LW Garratt GL Hall J Harrison A Kicic IA Laing KM Logie J MassieLS Mott C Murray F Parsons N Pillarisetti SR Poreddy SC RanganathanCF Robertson R Robins-Browne PJ Robinson B Skoric SM Stick ENSutanto E Williamson Identifying peroxidases and their oxidants in the earlypathology of cystic fibrosis Free Radic Biol Med 49 (2010) 1354ndash1360
[15] SP Range C Dunster AJ Knox FJ Kelly Treatment of pulmonary exacerba-tions of cystic fibrosis leads to improved antioxidant status Eur Respir J 13(1999) 560ndash564
[16] L Coppo P Ghezzi Thiol regulation of pro-inflammatory cytokines and innateimmunity protein S-thiolation as a novel molecular mechanism Biochem SocTrans 39 (2011) 1268ndash1272
[17] C Verhaeghe C Remouchamps B Hennuy A Vanderplasschen A Chariot SPTabruyn C Oury V Bours Role of IKK and ERK pathways in intrinsic inflamma-tion of cystic fibrosis airways Biochem Pharmacol 73 (2007) 1982ndash1994
[18] TL Bonfield JR Panuska MW Konstan KA Hilliard JB Hilliard H Ghnaim MBerger Inflammatory cytokines in cystic fibrosis lungs Am J Respir Crit CareMed 152 (1995) 2111ndash2118
[19] TL Noah HR Black PW Cheng RE Wood MW Leigh Nasal and bronchoal-veolar lavage fluid cytokines in early cystic fibrosis J Infect Dis 175 (1997)638ndash647
[20] MJ Welsh BW Ramsey FJ Accurso GR Cutting Cystic Fibrosis McGraw-HillNew York 2001
[21] TZ Khan JS Wagener T Bost J Martinez FJ Accurso DW Riches Early pul-monary inflammation in infants with cystic fibrosis Am J Respir Crit CareMed 151 (1995) 1075ndash1082
[22] FA Ratjen Cystic fibrosis pathogenesis and future treatment strategies RespirCare 54 (2009) 595ndash605
[23] J Jacquot O Tabary P Le Rouzic A Clement Airway epithelial cell inflamma-tory signalling in cystic fibrosis Int J Biochem Cell Biol 40 (2008)1703ndash1715
[24] CM Greene P Branagan NG McElvaney Toll-like receptors as therapeutic tar-gets in cystic fibrosis Expert Opin Ther Targets 12 (2008) 1481ndash1495
[25] M Rottner JM Freyssinet MC Martinez Mechanisms of the noxious inflam-matory cycle in cystic fibrosis Respir Res 10 (2009) 23
[26] G Cabrini V Bezzerri I Mancini E Nicolis MC Dechecchi A Tamanini ILampronti L Piccagli N Bianchi M Borgatti R Gambari Targeting transcrip-tion factor activity as a strategy to inhibit pro-inflammatory genes involved incystic fibrosis decoy oligonucleotides and low-molecular weight compoundsCurr Med Chem 17 (2010) 4392ndash4404
[27] CM Greene NG McElvaney Proteases and antiproteases in chronic neutrophiliclungdiseasemdash relevance to drug discovery Br J Pharmacol 158 (2009) 1048ndash1058
[28] AM Cantin Potential for antioxidant therapy of cystic fibrosis Curr Opin PulmMed 10 (2004) 531ndash536
[29] JF Chmiel MW Konstan Inflammation and anti-inflammatory therapies forcystic fibrosis Clin Chest Med 28 (2007) 331ndash346
[30] DP Nichols MW Konstan JF Chmiel Anti-inflammatory therapies for cys-tic fibrosis-related lung disease Clin Rev Allergy Immunol 35 (2008)135ndash153
[31] AJ Kettle T Chan I Osberg R Senthilmohan AL Chapman TJ Mocatta JSWagener Myeloperoxidase and protein oxidation in the airways of youngchildren with cystic fibrosis Am J Respir Crit Care Med 170 (2004)1317ndash1323
[32] H Fischer Mechanisms and function of DUOX in epithelia of the lung AntioxidRedox Signal 11 (2009) 2453ndash2465
[33] B Rada TL Leto Oxidative innate immune defenses by NoxDuox familyNADPH oxidases Contrib Microbiol 15 (2008) 164ndash187
[34] P Moskwa D Lorentzen KJ Excoffon J Zabner PB McCray Jr WM NauseefC Dupuy B Banfi A novel host defense system of airways is defective in cysticfibrosis Am J Respir Crit Care Med 175 (2007) 174ndash183
[35] D Lorentzen L Durairaj AA Pezzulo Y Nakano J Launspach DA Stoltz GZamba PB McCray Jr J Zabner MJ Welsh WM Nauseef B Banfi Concentra-tion of the antibacterial precursor thiocyanate in cystic fibrosis airway secre-tions Free Radic Biol Med 50 (2011) 1144ndash1150
[36] Y Xu S Szep Z Lu The antioxidant role of thiocyanate in the pathogenesis ofcystic fibrosis and other inflammation-related diseases Proc Natl Acad Sci US A 106 (2009) 20515ndash20519
[37] MP Rogan CC Taggart CM Greene PG Murphy SJ ONeill NG McElvaneyLoss of microbicidal activity and increased formation of biofilm due to decreasedlactoferrin activity in patients with cystic fibrosis J Infect Dis 190 (2004)1245ndash1253
[38] B Halliwell JM Guttridge Free Radicals in Biology and Medicine Fourth editionOxford University Press New York 2007
[39] B Rada K Lekstrom S Damian C Dupuy TL Leto The Pseudomonastoxin pyocyanin inhibits the dual oxidase-based antimicrobial system as itimposes oxidative stress on airway epithelial cells J Immunol 181 (2008)4883ndash4893
[40] C Schwarzer B Illek JH Suh SJ Remington H Fischer TE Machen Organelleredox of CF and CFTR-corrected airway epithelia Free Radic Biol Med 43(2007) 300ndash316
[41] JH Roum R Buhl NG McElvaney Z Borok RG Crystal Systemic deficiency ofglutathione in cystic fibrosis J Appl Physiol 75 (1993) 2419ndash2424
[42] VM Hudson Rethinking cystic fibrosis pathology the critical role of abnormalreduced glutathione (GSH) transport caused by CFTR mutation Free RadicBiol Med 30 (2001) 1440ndash1461
[43] PJ Barnes RA Dweik AF Gelb PG Gibson SC George H Grasemann IDPavord F Ratjen PE Silkoff DR Taylor N Zamel Exhaled nitric oxide in pul-monary diseases a comprehensive review Chest 138 (2010) 682ndash692
[44] H Grasemann E Michler M Wallot F Ratjen Decreased concentration of ex-haled nitric oxide (NO) in patients with cystic fibrosis Pediatr Pulmonol 24(1997) 173ndash177
[45] H Grasemann F Ratjen Cystic fibrosis lung disease the role of nitric oxidePediatr Pulmonol 28 (1999) 442ndash448
[46] B Gaston F Ratjen JW Vaughan NR Malhotra RG Canady AH Snyder JFHunt S Gaertig JB Goldberg Nitrogen redox balance in the cystic fibrosis air-way effects of antipseudomonal therapy Am J Respir Crit Care Med 165(2002) 387ndash390
[47] H Grasemann I Ioannidis RP Tomkiewicz H de Groot BK Rubin F RatjenNitric oxide metabolites in cystic fibrosis lung disease Arch Dis Child 78(1998) 49ndash53
[48] H Grasemann R Schwiertz S Matthiesen K Racke F Ratjen Increased argi-nase activity in cystic fibrosis airways Am J Respir Crit Care Med 172(2005) 1523ndash1528
[49] H Grasemann S Al-Saleh JA Scott D Shehnaz A Mehl R Amin M Rafii PPencharz J Belik F Ratjen Asymmetric dimethylarginine contributes to airwaynitric oxide deficiency in patients with cystic fibrosis Am J Respir Crit CareMed 183 (2011) 1363ndash1368
[50] H Grasemann F Kurtz F Ratjen Inhaled L-arginine improves exhaled nitricoxide and pulmonary function in patients with cystic fibrosis Am J RespirCrit Care Med 174 (2006) 208ndash212
[51] H Grasemann F Ratjen Emerging therapies for cystic fibrosis lung disease Ex-pert Opin Emerg Drugs 15 (2010) 653ndash659
[52] BM Morrissey K Schilling JV Weil PE Silkoff DM Rodman Nitric oxide andprotein nitration in the cystic fibrosis airway Arch Biochem Biophys 406(2002) 33ndash39
[53] R Radi Nitric oxide oxidants and protein tyrosine nitration Proc Natl AcadSci U S A 101 (2004) 4003ndash4008
[54] J Chen M Kinter S Shank C Cotton TJ Kelley AG Ziady Dysfunction of Nrf-2in CF epithelia leads to excess intracellular H2O2 and inflammatory cytokineproduction PLoS One 3 (2008) e3367
[55] F Galli M Piroddi C Annetti C Aisa E Floridi A Floridi Oxidative stress andreactive oxygen species Contrib Nephrol 149 (2005) 240ndash260
[56] DT Wright LA Cohn H Li B Fischer CM Li KB Adler Interactions of oxygenradicals with airway epithelium Environ Health Perspect 102 (Suppl 10)(1994) 85ndash90
[57] I Rahman SR Yang SK Biswas Current concepts of redox signaling in thelungs Antioxid Redox Signal 8 (2006) 681ndash689
[58] Q Li JF Engelhardt Interleukin-1beta induction of NFκB is partially regulatedby H2O2-mediated activation of NFκB-inducing kinase J Biol Chem 281(2006) 1495ndash1505
709F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
[59] E Boncoeur VS Criq E Bonvin T Roque A Henrion-Caude DC Gruenert AClement J Jacquot O Tabary Oxidative stress induces extracellular signal-regulated kinase 12 mitogen-activated protein kinase in cystic fibrosis lung ep-ithelial cells potential mechanism for excessive IL-8 expression Int J BiochemCell Biol 40 (2008) 432ndash446
[60] B Fischer J Voynow Neutrophil elastase induces MUC5AC messenger RNA ex-pression by an oxidant-dependent mechanism Chest 117 (2000) 317Sndash320S
[61] B Rada P Gardina TG Myers TL Leto Reactive oxygen species mediate in-flammatory cytokine release and EGFR-dependent mucin secretion in airwayepithelial cells exposed to Pseudomonas pyocyanin Mucosal Immunol 4(2011) 158ndash171
[62] C Schwarzer H Fischer EJ Kim KJ Barber AD Mills MJ Kurth DC GruenertJH Suh TE Machen B Illek Oxidative stress caused by pyocyanin impairs CFTRClminus transport in human bronchial epithelial cells Free Radic Biol Med 45(2008) 1653ndash1662
[63] J Hull M South P Phelan K Grimwood Surfactant composition in infants andyoung children with cystic fibrosis Am J Respir Crit Care Med 156 (1997)161ndash165
[64] KC Meyer A Sharma R Brown M Weatherly FR Moya J Lewandoski JJZimmerman Function and composition of pulmonary surfactant andsurfactant-derived fatty acid profiles are altered in young adults with cystic fi-brosis Chest 118 (2000) 164ndash174
[65] MK Pulfer RC Murphy Formation of biologically active oxysterols during ozo-nolysis of cholesterol present in lung surfactant J Biol Chem 279 (2004)26331ndash26338
[66] V Starosta E Rietschel K Paul U Baumann M Griese Oxidative changes ofbronchoalveolar proteins in cystic fibrosis Chest 129 (2006) 431ndash437
[67] V Starosta M Griese Oxidative damage to surfactant protein D in pulmonarydiseases Free Radic Res 40 (2006) 419ndash425
[68] M Griese R Essl R Schmidt E Rietschel F Ratjen M Ballmann K Paul Pulmo-nary surfactant lung function and endobronchial inflammation in cystic fibro-sis Am J Respir Crit Care Med 170 (2004) 1000ndash1005
[69] M Griese R Essl R Schmidt M Ballmann K Paul E Rietschel F Ratjen Se-quential analysis of surfactant lung function and inflammation in cystic fibrosispatients Respir Res 6 (2005) 133
[70] LG Wood DA Fitzgerald PG Gibson DM Cooper ML Garg Increased plasmafatty acid concentrations after respiratory exacerbations are associated with el-evated oxidative stress in cystic fibrosis patients Am J Clin Nutr 75 (2002)668ndash675
[71] P Montuschi SA Kharitonov G Ciabattoni M Corradi L van Rensen DM Ged-des ME Hodson PJ Barnes Exhaled 8-isoprostane as a new non-invasive bio-marker of oxidative stress in cystic fibrosis Thorax 55 (2000) 205ndash209
[72] CE Collins P Quaggiotto L Wood EV OLoughlin RL Henry ML Garg Elevat-ed plasma levels of F2 alpha isoprostane in cystic fibrosis Lipids 34 (1999)551ndash556
[73] D Hartl V Starosta K Maier I Beck-Speier C Rebhan BF Becker P Latzin RFischer F Ratjen RM Huber E Rietschel S Krauss-Etschmann M Griese In-haled glutathione decreases PGE2 and increases lymphocytes in cystic fibrosislungs Free Radic Biol Med 39 (2005) 463ndash472
[74] GL Milne H Yin JD Morrow Human biochemistry of the isoprostane pathwayJ Biol Chem 283 (2008) 15533ndash15537
[75] G Ciabattoni G Davi M Collura L Iapichino F Pardo A Ganci R Romagnoli JMaclouf C Patrono In vivo lipid peroxidation and platelet activation in cystic fi-brosis Am J Respir Crit Care Med 162 (2000) 1195ndash1201
[76] C Garenc P Julien E Levy Oxysterols in biological systems the gastrointestinaltract liver vascular wall and central nervous system Free Radic Res 44 (2011)47ndash73
[77] AM Cantin SL North RC Hubbard RG Crystal Normal alveolar epithelial lin-ing fluid contains high levels of glutathione J Appl Physiol 63 (1987) 152ndash157
[78] R Tirouvanziam CK Conrad T Bottiglieri LA Herzenberg RB Moss High-dose oral N-acetylcysteine a glutathione prodrug modulates inflammation incystic fibrosis Proc Natl Acad Sci U S A 103 (2006) 4628ndash4633
[79] LW Velsor C Kariya R Kachadourian BJ Day Mitochondrial oxidative stressin the lungs of cystic fibrosis transmembrane conductance regulator proteinmutant mice Am J Respir Cell Mol Biol 35 (2006) 579ndash586
[80] M Kelly-Aubert S Trudel J Fritsch T Nguyen-Khoa M Baudouin-Legros SMoriceau L Jeanson F Djouadi C Matar M Conti M Ollero F Brouillard AEdelman GSH monoethyl ester rescues mitochondrial defects in cystic fibrosismodels Hum Mol Genet 20 (2011) 2745ndash2759
[81] P Ghezzi Role of glutathione in immunity and inflammation in the lung Int JGen Med 4 (2011) 105ndash113
[82] N Dauletbaev K Viel R Buhl TO Wagner J Bargon Glutathione and glutathi-one peroxidase in sputum samples of adult patients with cystic fibrosis J CystFibros 3 (2004) 119ndash124
[83] CE Cross A van der Vliet CA ONeill S Louie B Halliwell Oxidants antioxi-dants and respiratory tract lining fluids Environ Health Perspect 102 (Suppl10) (1994) 185ndash191
[84] K Takeyama K Dabbagh J Jeong Shim T Dao-Pick IF Ueki JA Nadel Oxida-tive stress causes mucin synthesis via transactivation of epidermal growth factorreceptor role of neutrophils J Immunol 164 (2000) 1546ndash1552
[85] N Ballatori SM Krance S Notenboom S Shi K Tieu CL Hammond Glutathi-one dysregulation and the etiology and progression of human diseases BiolChem 390 (2009) 191ndash214
[86] SR Soltaninassab KR Sekhar MJ Meredith ML Freeman Multi-faceted regu-lation of gamma-glutamylcysteine synthetase J Cell Physiol 182 (2000)163ndash170
[87] HR Lopez-Mirabal JR Winther Redox characteristics of the eukaryotic cytosolBiochim Biophys Acta 1783 (2008) 629ndash640
[88] C Hwang AJ Sinskey HF Lodish Oxidized redox state of glutathione in the en-doplasmic reticulum Science 257 (1992) 1496ndash1502
[89] M Murphy Mitochondrial thiols in antioxidant protection and redox signallingdistinct roles for glutathionylation and other thiol modifications AntioxidRedox Signal (2011) ahead of print doi101089ars20114289
[90] BJ Day AM van Heeckeren E Min LW Velsor Role for cystic fibrosis trans-membrane conductance regulator protein in a glutathione response to bronch-opulmonary Pseudomonas infection Infect Immun 72 (2004) 2045ndash2051
[91] Y Zhang K Duan Glutathione exhibits antibacterial activity and increases tetra-cycline efficacy against Pseudomonas aeruginosa Sci China C Life Sci 52 (2009)501ndash505
[92] VM Hudson New insights into the pathogenesis of cystic fibrosis pivotal roleof glutathione system dysfunction and implications for therapy Treat RespirMed 3 (2004) 353ndash363
[93] LW Velsor A van Heeckeren BJ Day Antioxidant imbalance in the lungs ofcystic fibrosis transmembrane conductance regulator protein mutant miceAm J Physiol Lung Cell Mol Physiol 281 (2001) L31ndashL38
[94] I Kogan M Ramjeesingh C Li JF Kidd Y Wang EM Leslie SP Cole CE BearCFTR directly mediates nucleotide-regulated glutathione flux EMBO J 22(2003) 1981ndash1989
[95] NS Gould S Gauthier CT Kariya E Min J Huang DJ Brian Hypertonic salineincreases lung epithelial lining fluid glutathione and thiocyanate two protectiveCFTR-dependent thiols against oxidative injury Respir Res 11 (2010) 119
[96] VT Vasu SJ de Cruz JS Houghton KA Hayakawa BM Morrissey CE CrossJP Eiserich Evaluation of thiol-based antioxidant therapeutics in cystic fibrosissputum focus on myeloperoxidase Free Radic Res 45 (2011) 165ndash176
[97] L Roussel G Martel J Berube S Rousseau P aeruginosa drives CXCL8 synthesisvia redundant toll-like receptors and NADPH oxidase in CFTRF508 airway epi-thelial cells J Cyst Fibros 10 (2011) 107ndash113
[98] GW Lau DJ Hassett H Ran F Kong The role of pyocyanin in Pseudomonas aer-uginosa infection Trends Mol Med 10 (2004) 599ndash606
[99] R Wilson DA Sykes D Watson A Rutman GW Taylor PJ Cole Measurementof Pseudomonas aeruginosa phenazine pigments in sputum and assessment oftheir contribution to sputum sol toxicity for respiratory epithelium InfectImmun 56 (1988) 2515ndash2517
[100] M Muller Pyocyanin induces oxidative stress in human endothelial cells andmodulates the glutathione redox cycle Free Radic Biol Med 33 (2002)1527ndash1533
[101] YQ OMalley KJ Reszka BE Britigan Direct oxidation of 2prime7prime-dichlorodihy-drofluorescein by pyocyanin and other redox-active compounds independentof reactive oxygen species production Free Radic Biol Med 36 (2004)90ndash100
[102] CC Caldwell Y Chen HS Goetzmann Y Hao MT Borchers DJ Hassett LRYoung D Mavrodi L Thomashow GW Lau Pseudomonas aeruginosa exotoxinpyocyanin causes cystic fibrosis airway pathogenesis Am J Pathol 175 (2009)2473ndash2488
[103] YQ OMalley KJ Reszka DR Spitz GM Denning BE Britigan Pseudomonasaeruginosa pyocyanin directly oxidizes glutathione and decreases its levels inairway epithelial cells Am J Physiol Lung Cell Mol Physiol 287 (2004)L94ndashL103
[104] M Muller Glutathione modulates the toxicity of but is not a biologically rele-vant reductant for the Pseudomonas aeruginosa redox toxin pyocyanin FreeRadic Biol Med 50 (2011) 971ndash977
[105] R Cheluvappa R Shimmon M Dawson SN Hilmer DG Le Couteur Reactionsof Pseudomonas aeruginosa pyocyanin with reduced glutathione Acta BiochimPol 55 (2008) 571ndash580
[106] JH Widdicombe Transgenic animals may help resolve a sticky situation in cys-tic fibrosis J Clin Invest 120 (2010) 3093ndash3096
[107] X Sun H Sui JT Fisher Z Yan X Liu HJ Cho NS Joo Y Zhang W Zhou Y YiJM Kinyon DC Lei-Butters MA Griffin P Naumann M Luo J Ascher KWang T Frana JJ Wine DK Meyerholz JF Engelhardt Disease phenotype ofa ferret CFTR-knockout model of cystic fibrosis J Clin Invest 120 (2010)3149ndash3160
[108] NS Joo HJ Cho M Khansaheb JJ Wine Hyposecretion of fluid from trachealsubmucosal glands of CFTR-deficient pigs J Clin Invest 120 (2010) 3161ndash3166
[109] A Bragonzi Murine models of acute and chronic lung infection with cystic fibro-sis pathogens IJMM 300 (2010) 584ndash593
[110] AM van Heeckeren MD Schluchter Murine models of chronic Pseudomonasaeruginosa lung infection Lab Anim 36 (2002) 291ndash312
[111] A Bragonzi D Worlitzsch GB Pier P Timpert M Ulrich M Hentzer JB Ander-sen M Givskov M Conese G Doring Nonmucoid Pseudomonas aeruginosa ex-presses alginate in the lungs of patients with cystic fibrosis and in a mousemodel J Infect Dis 192 (2005) 410ndash419
[112] GS CW Bedrossian DB Singer JJ Hansen HS Rosenberg The lung in cysticfibrosis A quantitative study including prevalence of pathologic findingsamong different age groups Hum Pathol 7 (1976) 195ndash204
[113] WD HA Cash B McCullough WG Johanson Jr JA Bass A rat model of chron-ic respiratory infection with Pseudomonas aeruginosa Am Rev Respir Dis 119(1979) 453ndash459
[114] EM JR Starke C Langston CJ Baker A mouse model of chronic pulmonary in-fection with Pseudomonas aeruginosa and Pseudomonas cepacia Pediatr Res 22(1987) 698ndash702
[115] TJ AM van Heeckeren RW Walenga MW Konstan PB Davis B ErokwuMA Haxhiu TW Ferkol Effect of Pseudomonas infection on weight loss lung
710 F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
mechanics and cytokines in mice Am J Respir Crit Care Med 161 (2000)271ndash279
[116] T Aw G Wierzbicka DP Jones Oral glutathione increases tissue glutathione invivo Chem Biol Interact 80 (1991) 89ndash97
[117] F Favilli P Marraccini T Iantomasi MT Vincenzini Effect of orally adminis-tered glutathione on glutathione levels in some organs of rats role of specifictransporters Br J Nutr 78 (1997) 293ndash300
[118] C Kariya H Leitner E Min C van Heeckeren A van Heeckeren BJ Day A rolefor CFTR in the elevation of glutathione levels in the lung by oral glutathione ad-ministration Am J Physiol Lung Cell Mol Physiol 292 (2007) L1590ndashL1597
[119] K Atkuri JJ Mantovani LA Herzenberg LA Herzenberg N-Acetylcysteinemdashasafe antidote for cysteineglutathione deficiency Curr Opin Pharmacol 7(2007) 355ndash359
[120] R De Lisle E Roach K Jansson Effects of laxative and N-acetylcysteine onmucus accumulation bacterial load transit and inflammation in the cystic fi-brosis mouse small intestine Am J Physiol Gastrointest Liver Physiol 293(2007) G577ndashG584
[121] A Luciani VR Villella S Esposito N Brunetti-Pierri D Medina C Settembre MGavina L Pulze I Giardino M Pettoello-Mantovani M DApolito S Guido EMasliah B Spencer S Quaratino V Raia A Ballabio L Maiuri Defective CFTRinduces aggresome formation and lung inflammation in cystic fibrosis throughROS-mediated autophagy inhibition Nat Cell Biol 12 863ndash875
[122] M Griese J Ramakers A Krasselt V Starosta S Van Koningsbruggen R FischerF Ratjen B Mullinger RM Huber K Maier E Rietschel G Scheuch Improve-ment of alveolar glutathione and lung function but not oxidative state in cysticfibrosis Am J Respir Crit Care Med 169 (2004) 822ndash828
[123] C Bishop VM Hudson SC Hilton C Wilde A pilot study of the effect of inhaledbuffered reduced glutathione on the clinical status of patients with cystic fibro-sis Chest 127 (2005) 308ndash317
[124] WWang C Oliva G Li A Holmgren CH Lillig KL Kirk Reversible silencing of CFTRchloride channels by glutathionylation J Gen Physiol 125 (2005) 127ndash141
[125] N Dauletbaev P Fischer B Aulbach J Gross W Kusche U Thyroff-FriesingerTO Wagner J Bargon A phase II study on safety and efficacy of high-dose N-acetylcysteine in patients with cystic fibrosis Eur J Med Res 14 (2009)352ndash358
[126] R Tirouvanziam Y Gernez CK Conrad RB Moss I Schrijver CE Dunn ZADavies LA Herzenberg Profound functional and signaling changes in viable in-flammatory neutrophils homing to cystic fibrosis airways Proc Natl Acad SciU S A 105 (2008) 4335ndash4339
[127] JH Roum Z Borok NG McElvaney GJ Grimes AD Bokser R Buhl RG Crys-tal Glutathione aerosol suppresses lung epithelial surface inflammatory cell-derived oxidants in cystic fibrosis J Appl Physiol 87 (1999) 438ndash443
[128] A Visca CT Bishop SC Hilton VM Hudson Improvement in clinical markersin CF patients using a reduced glutathione regimen an uncontrolled observa-tional study J Cyst Fibros 7 (2008) 433ndash436
[129] EF Nash A Stephenson F Ratjen E Tullis Nebulized and oral thiol derivativesfor pulmonary disease in cystic fibrosis Cochrane Database Syst Rev (2009)CD007168
[130] AC foundation Drug Development Pipeline 2011[131] S Hoshida T Kuzuya N Yamashita M Nishida S Kitahara M Hori T
Kamada M Tada Gamma-glutamylcysteine ethyl ester for myocardial protec-tion in dogs during ischemia and reperfusion J Am Coll Cardiol 24 (1994)1391ndash1397
[132] J Lok W Leung S Zhao S Pallast K van Leyen S Guo X Wang A Yalcin EHLo Gamma-glutamylcysteine ethyl ester protects cerebral endothelial cells dur-ing injury and decreases bloodndashbrain barrier permeability after experimentalbrain trauma J Neurochem 118 (2011) 248ndash255
[133] Z Borok R Buhl GJ Grimes AD Bokser RC Hubbard KJ Holroyd JH RoumDB Czerski AM Cantin RG Crystal Effect of glutathione aerosol on oxidantndashantioxidant imbalance in idiopathic pulmonary fibrosis Lancet 338 (1991)215ndash216
[134] KJ Holroyd R Buhl Z Borok JH Roum AD Bokser GJ Grimes D Czerski AMCantin RG Crystal Correction of glutathione deficiency in the lower respiratorytract of HIV seropositive individuals by glutathione aerosol treatment Thorax 48(1993) 985ndash989
[135] J Hull P Vervaart K Grimwood P Phelan Pulmonary oxidative stress responsein young children with cystic fibrosis Thorax 52 (1997) 557ndash560
[136] A Corti A Paolicchi M Franzini S Dominici AF Casini A Pompella The S-thiolating activity of membrane gamma-glutamyltransferase formation ofcysteinyl-glycine mixed disulfides with cellular proteins and in the cell microen-vironment Antioxid Redox Signal 7 (2005) 911ndash918
[137] A Corti M Franzini AF Casini A Paolicchi A Pompella Vitamin C supply tobronchial epithelial cells linked to glutathione availability in elfmdasha role for se-creted gamma-glutamyltransferase J Cyst Fibros 7 (2008) 174ndash178
[138] A Munck Nutritional considerations in patients with cystic fibrosis Expert RevRespir Med 4 (2010) 47ndash56
[139] JL Matel CE Milla Nutrition in cystic fibrosis Semin Respir Crit Care Med 30(2009) 579ndash586
[140] D Salvatore R Buzzetti E Baldo MP Forneris V Lucidi D Manunza IMarinelli B Messore AS Neri V Raia ML Furnari G Mastella An overviewof international literature from cystic fibrosis registries 2 Neonatal screeningand nutritiongrowth J Cyst Fibros 9 (2010) 75ndash83
[141] KF Joosten JM Hulst Malnutrition in pediatric hospital patients current is-sues Nutrition 27 (2011) 133ndash137
[142] S Fustik T Jacovska L Spirevska S Koceva Protein-energy malnutrition as thefirst manifestation of cystic fibrosis in infancy Pediatr Int 51 (2009) 678ndash683
[143] J Himmelfarb E McMonagle Albumin is the major plasma protein target of ox-idant stress in uremia Kidney Int 60 (2001) 358ndash363
[144] P Stenvinkel JJ Carrero J Axelsson B Lindholm O Heimburger Z MassyEmerging biomarkers for evaluating cardiovascular risk in the chronic kidneydisease patient how do new pieces fit into the uremic puzzle Clin J Am SocNephrol 3 (2008) 505ndash521
[145] M Roche P Rondeau NR Singh E Tarnus E Bourdon The antioxidant proper-ties of serum albumin FEBS Lett 582 (2008) 1783ndash1787
[146] D Giustarini A Milzani I Dalle-Donne R Rossi Red blood cells as a physiolog-ical source of glutathione for extracellular fluids Blood Cells Mol Dis 40 (2008)174ndash179
[147] A Meister ME Anderson Glutathione Annu Rev Biochem 52 (1983) 711ndash760[148] B Alvarez S Carballal L Turell R Radi Formation and reactions of sulfenic acid
in human serum albumin Methods Enzymol 473 (2010) 117ndash136[149] S Carballal B Alvarez L Turell H Botti BA Freeman R Radi Sulfenic acid in
human serum albumin Amino Acids 32 (2007) 543ndash551[150] LR Barclay AM Bailey D Kong The antioxidant activity of alpha-tocopherol-
bovine serum albumin complex in micellar and liposome autoxidations J BiolChem 260 (1985) 15809ndash15814
[151] T Ishii T Ichikawa K Minoda K Kusaka S Ito Y Suzuki M Akagawa K Mochi-zuki T Goda T Nakayama Human serum albumin as an antioxidant in the ox-idation of (minus)-epigallocatechin gallate participation of reversible covalentbinding for interaction and stabilization Biosci Biotechnol Biochem 75(2011) 100ndash106
[152] F Galli S Rovidati S Benedetti U Buoncristiani C Covarelli A Floridi F Canes-trari Overexpression of erythrocyte glutathione S-transferase in uremia and di-alysis Clin Chem 45 (1999) 1781ndash1788
[153] D Borowitz RD Baker V Stallings Consensus report on nutrition for pediat-ric patients with cystic fibrosis J Pediatr Gastroenterol Nutr 35 (2002)246ndash259
[154] LJ Filer Jr SW Wright MP Manning KE Mason Absorption of alpha-tocopherol and tocopherylesters by premature and full term infants and chil-dren in health and disease Pediatrics 8 (1951) 328ndash339
[155] L Lancellotti C DOrazio G Mastella G Mazzi U Lippi Deficiency of vitamins Eand A in cystic fibrosis is independent of pancreatic function and current en-zyme and vitamin supplementation Eur J Pediatr 155 (1996) 281ndash285
[156] MN Sathe AS Patel Update in pediatrics focus on fat-soluble vitamins NutrClin Pract 25 (2010) 340ndash346
[157] MG Traber The ABCs of vitamin E and beta-carotene absorption Am J ClinNutr 80 (2004) 3ndash4
[158] TF Dolan Jr Hemolytic anemia and edema as the initial signs in infants withcystic fibrosis Consider this diagnosis even in absence of pulmonary symptomsClin Pediatr 15 (1976) 597ndash600
[159] DR James M Alfaham MC Goodchild Increased susceptibility to peroxide-induced haemolysis with normal vitamin E concentrations in cystic fibrosisClin Chim Acta 204 (1991) 279ndash290
[160] SA Peters FJ Kelly Vitamin E supplementation in cystic fibrosis J Pediatr Gas-troenterol Nutr 22 (1996) 341ndash345
[161] A Maqbool VA Stallings Update on fat-soluble vitamins in cystic fibrosis CurrOpin Pulm Med 14 (2008) 574ndash581
[162] SD Sagel MK Sontag MM Anthony P Emmett KA Papas Effect of anantioxidant-rich multivitamin supplement in cystic fibrosis J Cyst Fibros 10(2011) 31ndash36
[163] F Galli A Azzi Present trends in vitamin E research Biofactors 36 (2010)33ndash42
[164] A Hamahata P Enkhbaatar ER Kraft M Lange SW Leonard MG Traber RACox FC Schmalstieg HK Hawkins EB Whorton EM Horvath C Szabo LDTraber DN Herndon DL Traber Gamma-tocopherol nebulization by a lipidaerosolization device improves pulmonary function in sheep with burn andsmoke inhalation injury Free Radic Biol Med 45 (2008) 425ndash433
[165] JP Anais N Razzouq M Carvalho C Fernandez A Astier M Paul A AstierH Fessi AM Lorino Development of alpha-tocopherol acetate nanoparti-cles influence of preparative processes Drug Dev Ind Pharm 35 (2009)216ndash223
[166] JM Zingg Molecular and cellular activities of vitamin E analogues Mini RevMed Chem 7 (2007) 543ndash558
[167] V Viola F Pilolli M Piroddi E Pierpaoli F Orlando M Provinciali M Betti FMazzini F Galli Why tocotrienols work better insights into the in vitro anti-cancer mechanism of vitamin E Genes Nutr 7 (2011) 29ndash41
[168] F Galli F Mazzini L Bamonti L Gille S Bohmdorfer M Piroddi T Netscher FJKelly T Rosenau Tocotrienamines and tocopheramines reactions with radicalsand metal ions Bioorg Med Chem 19 (2011) 6483ndash6491
[169] A Kuhad K Chopra Attenuation of diabetic nephropathy by tocotrienol in-volvement of NFκB signaling pathway Life Sci 84 (2009) 296ndash301
[170] Q Jiang X Yin MA Lill ML Danielson H Freiser J Huang Long-chain carbox-ychromanols metabolites of vitamin E are potent inhibitors of cyclooxygenasesProc Natl Acad Sci U S A 105 (2008) 20464ndash20469
[171] ER Miller III R Pastor-Barriuso D Dalal RA Riemersma LJ Appel E GuallarMeta-analysis high-dosage vitamin E supplementation may increase all-causemortality Ann Intern Med 142 (2005) 37ndash46
[172] JN Hathcock A Azzi J Blumberg T Bray A Dickinson B Frei I Jialal CSJohnston FJ Kelly K Kraemer L Packer S Parthasarathy H Sies MG TraberVitamins E and C are safe across a broad range of intakes Am J Clin Nutr 81(2005) 736ndash745
[173] R Brigelius-Flohe F Galli Vitamin E a vitamin still awaiting the detection of itsbiological function Mol Nutr Food Res 54 (2010) 583ndash587
711F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
[174] MG Traber B Frei JS Beckman Vitamin E revisited do new data validate ben-efits for chronic disease prevention Curr Opin Lipidol 19 (2008) 30ndash38
[175] F Galli Meeting report Vitamin E Satellite Symposium (VESS) associated to theAnnual Meeting of the SFRR-Europe Rome 26 August 2009 Free Radic Res 43(2009) 1256ndash1257
[176] LJ Roberts II JA Oates MF Linton S Fazio BP Meador MD Gross Y Shyr JDMorrow The relationship between dose of vitamin E and suppression of oxida-tive stress in humans Free Radic Biol Med 43 (2007) 1388ndash1393
[177] EFSA- EFSA Scientific Opinion of the Panel on Food Additives FlavouringsProcessing Aids and Materials in Contact with Food on a request from the Com-mission on mixed tocopherols tocotrienol tocopherol and tocotrienols assources for vitamin E in EFSA- EFSA (Ed) vol 640 The EFSA Journal2008 pp 1ndash34
[178] P Rust I Eichler S Renner I Elmadfa Long-term oral beta-carotene supple-mentation in patients with cystic fibrosis mdash effects on antioxidative status andpulmonary function Ann Nutr Metab 44 (2000) 30ndash37
[179] G Lepage J Champagne N Ronco A Lamarre I Osberg RJ Sokol CC Roy Sup-plementation with carotenoids corrects increased lipid peroxidation in childrenwith cystic fibrosis Am J Clin Nutr 64 (1996) 87ndash93
[180] BM Winklhofer-Roob H Puhl G Khoschsorur MA vant Hof H EsterbauerDH Shmerling Enhanced resistance to oxidation of low density lipoproteinsand decreased lipid peroxide formation during beta-carotene supplementationin cystic fibrosis Free Radic Biol Med 18 (1995) 849ndash859
[181] RC Graham-Maar JI Schall N Stettler BS Zemel VA Stallings Elevated vita-min A intake and serum retinol in preadolescent children with cystic fibrosisAm J Clin Nutr 84 (2006) 174ndash182
[182] I Sadowska-Woda M Rachel J Pazdan E Bieszczad-Bedrejczuk K PawliszakNutritional supplement attenuates selected oxidative stress markers in pediatricpatients with cystic fibrosis Nutr Res (New York NY) 31 (2011) 509ndash518
[183] KA Papas MK Sontag C Pardee RJ Sokol SD Sagel FJ Accurso JS WagenerA pilot study on the safety and efficacy of a novel antioxidant rich formulation inpatients with cystic fibrosis J Cyst Fibros 7 (2008) 60ndash67
[184] Y Saito A Fukuhara K Nishio M Hayakawa Y Ogawa H Sakamoto K Fujii YYoshida E Niki Characterization of cellular uptake and distribution of coen-zyme Q10 and vitamin E in PC12 cells J Nutr Biochem 20 (2009) 350ndash357
[185] AA Franke CM Morrison JL Bakke LJ Custer X Li RV Cooney CoenzymeQ10 in human blood native levels and determinants of oxidation during proces-sing and storage Free Radic Biol Med 48 (2010) 1610ndash1617
[186] HN Bhagavan RK Chopra Plasma coenzyme Q10 response to oral ingestion ofcoenzyme Q10 formulations Mitochondrion 7 (2007) S78ndashS88 (Suppl)
[187] HN Bhagavan RK Chopra Coenzyme Q10 absorption tissue uptake metabo-lism and pharmacokinetics Free Radic Res 40 (2006) 445ndash453
[188] F Galli R Lee C Dunster FJ Kelly Gas chromatography mass spectrometryanalysis of carboxyethyl-hydroxychroman metabolites of alpha- and gamma-tocopherol in human plasma Free Radic Biol Med 32 (2002) 333ndash340
[189] F Galli R Lee J Atkinson A Floridi FJ Kelly Gamma-tocopherol biokineticsand transformation in humans Free Radic Res 37 (2003) 1225ndash1233
[190] TA Laguna MK Sontag I Osberg JS Wagener FJ Accurso RJ Sokol De-creased total serum coenzyme-Q10 concentrations a longitudinal study in chil-dren with cystic fibrosis J Pediatr 153 (2008) 402ndash407
[191] T Frischer JK Myung G Maurer I Eichler Z Szepfalusi G Lubec Possible dys-regulation of chaperon and metabolic proteins in cystic fibrosis bronchial tissueProteomics 6 (2006) 3381ndash3388
[192] C Andersson MM Zaman AB Jones SD Freedman Alterations in immune re-sponse and PPARLXR regulation in cystic fibrosis macrophages J Cyst Fibros 7(2008) 68ndash78
[193] SD Freedman PG Blanco MM Zaman JC Shea M Ollero IK Hopper DAWeed A Gelrud MM Regan M Laposata JG Alvarez BP OSullivan Associa-tion of cystic fibrosis with abnormalities in fatty acid metabolism N Engl JMed 350 (2004) 560ndash569
[194] S Van Biervliet G Vanbillemont JP Van Biervliet D Declercq E Robberecht AChristophe Relation between fatty acid composition and clinical status or geno-type in cystic fibrosis patients Ann Nutr Metab 51 (2007) 541ndash549
[195] SD Freedman MH Katz EM Parker M Laposata MY Urman JG AlvarezA membrane lipid imbalance plays a role in the phenotypic expression ofcystic fibrosis in cftr(minusminus) mice Proc Natl Acad Sci U S A 96 (1999)13995ndash14000
[196] S Van Biervliet S Vande Velde JP Van Biervliet E Robberecht The effect ofzinc supplements in cystic fibrosis patients Ann Nutr Metab 52 (2008)152ndash156
[197] WR Henderson Jr SJ Astley MM McCready P Kushmerick S Casey JWBecker BW Ramsey Oral absorption of omega-3 fatty acids in patients withcystic fibrosis who have pancreatic insufficiency and in healthy control subjectsJ Pediatr 124 (1994) 400ndash408
[198] I Durieu E Vericel D Guichardant H Roth JP Steghens J Drai RN JosserandE Fontaine M Lagarde G Bellon Fatty acids platelets and oxidative markersfollowing intravenous n-3 fatty acids administration in cystic fibrosis an openpilot observational study J Cyst Fibros 6 (2007) 320ndash326
[199] LG Wood DA Fitzgerald ML Garg Hypothesis vitamin E complements poly-unsaturated fatty acids in essential fatty acid deficiency in cystic fibrosis J AmColl Nutr 22 (2003) 253ndash257
[200] JD Lloyd-Still SB Johnson RT Holman Essential fatty acid status in cystic fi-brosis and the effects of safflower oil supplementation Am J Clin Nutr 34(1981) 1ndash7
[201] A Maqbool JI Schall JF Garcia-Espana BS Zemel B Strandvik VAStallings Serum linoleic acid status as a clinical indicator of essential fatty
acid status in children with cystic fibrosis J Pediatr Gastroenterol Nutr 47(2008) 635ndash644
[202] C Oliver N Jahnke Omega-3 fatty acids for cystic fibrosis Cochrane DatabaseSyst Rev (2011) CD002201
[203] B Strandvik E Gronowitz F Enlund T Martinsson J Wahlstrom Essential fattyacid deficiency in relation to genotype in patients with cystic fibrosis J Pediatr139 (2001) 650ndash655
[204] P Rise S Volpi C Colombo RF Padoan C DOrazio S Ghezzi PMelotti V BennatoC Agostoni BM Assael C Galli Whole blood fatty acid analysis with micromethodin cystic fibrosis and pulmonary disease J Cyst Fibros 9 (2010) 228ndash233
[205] H Cao K Gerhold JR Mayers MM Wiest SM Watkins GS Hotamisligil Iden-tification of a lipokine a lipid hormone linking adipose tissue to systemic me-tabolism Cell 134 (2008) 933ndash944
[206] RR Malapaka SK Khoo J Zhang JH Choi XE Zhou Y Xu Y Gong J Li ELYong MJ Chalmers L Chang JH Resau PR Griffin YE Chen HE Xu Iden-tification and mechanism of a ten carbon fatty acid as a modulating ligand ofperoxisome proliferator activated receptors J Biol Chem 287 (2012)183ndash195
[207] T Hara A Hirasawa A Ichimura I Kimura G Tsujimoto Free fatty acid recep-tors FFAR1 and GPR120 as novel therapeutic targets for metabolic disorders JPharm Sci 100 (2011) 3594ndash3601
[208] R Gupta P Rathi S Bradoo Lipase mediated upgradation of dietary fats andoils Crit Rev Food Sci Nutr 43 (2003) 635ndash644
[209] BH Jennings CC Akoh Lipase-catalyzed modification of rice bran oil to incor-porate capric acid J Agric Food Chem 48 (2000) 4439ndash4443
[210] J Hoeks M Mensink MK Hesselink K Ekroos P Schrauwen Long- andMedium-Chain Fatty Acids Induce Insulin Resistance to a Similar Extent inHumans Despite Marked Differences in Muscle Fat Accumulation J Clin Endo-crinol Metab 97 (2012) 208ndash216
[211] PJ Congden G Bruce MM Rothburn PC Clarke JM Littlewood J KelleherMS Losowsky Vitamin status in treated patients with cystic fibrosis ArchDis Child 56 (1981) 708ndash714
[212] BM Winklhofer-Roob H Ellemunter M Fruhwirth SE Schlegel-Haueter GKhoschsorur MA vant Hof DH Shmerling Plasma vitamin C concentrationsin patients with cystic fibrosis evidence of associations with lung inflammationAm J Clin Nutr 65 (1997) 1858ndash1866
[213] L Shamseer D Adams N Brown JA Johnson S Vohra Antioxidant micronutri-ents for lung disease in cystic fibrosis Cochrane Database Syst Rev (2010)CD007020
[214] C Santi S Santoro Electrophilic Selenium First edition Wiley-VCH VerlagGmbH amp Co KGaA 2012
[215] L Flohe S Toppo G Cozza F Ursini A comparison of thiol peroxidase mecha-nisms Antioxid Redox Signal 15 (2010) 763ndash780
[216] L Flohe JR Andreesen R Brigelius-Flohe M Maiorino F Ursini Selenium theelement of the moon in life on earth IUBMB Life 49 (2000) 411ndash420
[217] V Valdiglesias E Pasaro J Mendez B Laffon In vitro evaluation of seleniumgenotoxic cytotoxic and protective effects a review Arch Toxicol 84(2010) 337ndash351
[218] P Foucaud P Therond M Marchand F Brion JF Demelier J Navarro Seleniumand vitamin E in mucoviscidosis Arch Fr Pediatr 45 (1988) 383ndash386
[219] J Neve R Van Geffel M Hanocq L Molle Plasma and erythrocyte zinc copperand selenium in cystic fibrosis Acta Paediatr Scand 72 (1983) 437ndash440
[220] BM Winklhofer-Roob B Tiran PE Tuchschmid MA vant Hof DH ShmerlingEffects of pancreatic enzyme preparations on erythrocyte glutathione peroxi-dase activities and plasma selenium concentrations in cystic fibrosis FreeRadic Biol Med 25 (1998) 242ndash249
[221] JD Lloyd-Still HE Ganther Selenium and glutathione peroxidase levels in cys-tic fibrosis Pediatrics 65 (1980) 1010ndash1012
[222] D Tsavachidou TJ McDonnell S Wen X Wang F Vakar-Lopez LL Pisters CAPettaway CG Wood KA Do PF Thall C Stephens E Efstathiou R Taylor DGMenter P Troncoso SM Lippman CJ Logothetis J Kim Selenium and vitaminE cell type- and intervention-specific tissue effects in prostate cancer J NatlCancer Inst 101 (2009) 306ndash320
[223] IN Zelko TJ Mariani RJ Folz Superoxide dismutase multigene family acomparison of the CuZn-SOD (SOD1) Mn-SOD (SOD2) and EC-SOD (SOD3)gene structures evolution and expression Free Radic Biol Med 33 (2002)337ndash349
[224] RP Bowler JD Crapo Oxidative stress in airways is there a role for extracellu-lar superoxide dismutase Am J Respir Crit Care Med 166 (2002) S38ndashS43
[225] K Best K McCoy S Gemma RA Disilvestro Copper enzyme activities in cysticfibrosis before and after copper supplementation plus or minus zinc Metabo-lism 53 (2004) 37ndash41
[226] SS Percival GP Kauwell E Bowser M Wagner Altered copper status in adultmen with cystic fibrosis J Am Coll Nutr 18 (1999) 614ndash619
[227] NF Krebs JE Westcott TD Arnold BM Kluger FJ Accurso LV Miller KMHambidge Abnormalities in zinc homeostasis in young infants with cystic fibro-sis Pediatr Res 48 (2000) 256ndash261
[228] D Easley N Krebs M Jefferson L Miller J Erskine F Accurso KM HambidgeEffect of pancreatic enzymes on zinc absorption in cystic fibrosis J Pediatr Gas-troenterol Nutr 26 (1998) 136ndash139
[229] S Van Biervliet JP Van Biervliet E Robberecht Serum zinc in patients with cys-tic fibrosis at diagnosis and after one year of therapy Biol Trace Elem Res 112(2006) 205ndash211
[230] S Van Biervliet JP Van Biervliet S Vande Velde E Robberecht Serum zinc con-centrations in cystic fibrosis patients aged above 4 years a cross-sectional eval-uation Biol Trace Elem Res 119 (2007) 19ndash26
712 F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
[231] F Galli M Cristina Polidori W Stahl P Mecocci FJ Kelly Vitamin E biotransfor-mation in humans Vitam Horm 76 (2007) 263ndash280
[232] J Wiser NE Alexis Q Jiang W Wu C Robinette R Roubey DB Peden In vivogamma-tocopherol supplementation decreases systemic oxidative stress andcytokine responses of human monocytes in normal and asthmatic subjectsFree Radic Biol Med 45 (2008) 40ndash49
[233] JG Wagner Q Jiang JR Harkema B Illek DD Patel BN Ames DB PedenOzone enhancement of lower airway allergic inflammation is prevented bygamma-tocopherol Free Radic Biol Med 43 (2007) 1176ndash1188
[234] JT Harries DP Muller Absorption of different doses of fat soluble and watermiscible preparations of vitamin E in children with cystic fibrosis Arch DisChild 46 (1971) 341ndash344
[235] EI Back C Frindt E Ocenaskova D Nohr M Stern HK Biesalski Can changesin hydrophobicity increase the bioavailability of alpha-tocopherol Eur J Nutr45 (2006) 1ndash6
[236] SZ Nasr MH OLeary C Hillermeier Correction of vitamin E deficiency withfat-soluble versus water-miscible preparations of vitamin E in patients with cys-tic fibrosis J Pediatr 122 (1993) 810ndash812
[237] S Soltani-Frisk E Gronowitz H Andersson B Strandvik Water-miscibletocopherol is not superior to fat-soluble preparation for vitamin E absorptionin cystic fibrosis Acta Paediatr 90 (2001) 1112ndash1115
[238] K Papas J Kalbfleisch R Mohon Bioavailability of a novel water-soluble vi-tamin E formulation in malabsorbing patients Dig Dis Sci 52 (2007)347ndash352
[239] F Antonicelli M Parmentier EM Drost N Hirani I Rahman K Donaldson WMacNee Nacystelyn inhibits oxidant-mediated interleukin-8 expression andNF-kappaB nuclear binding in alveolar epithelial cells Free Radic Biol Med 32(2002) 492ndash502
[240] EM App D Baran I Dab A Malfroot M Coffiner F Vanderbist M King Dose-finding and 24-h monitoring for efficacy and safety of aerosolized Nacystelyn incystic fibrosis Eur Respir J 19 (2002) 294ndash302
[241] MG Traber How much vitamin E hellip Just enough Am J Clin Nutr 84 (2006)959ndash960
[242] JC McCann BN Ames Vitamin K an example of triage theory is micronu-trient inadequacy linked to diseases of aging Am J Clin Nutr 90 (2009)889ndash907
[243] M Fusaro G Crepaldi S Maggi F Galli A DAngelo L Calo S Giannini DMiozzo M Gallieni Vitamin K bone fractures and vascular calcifications inchronic kidney disease an important but poorly studied relationship J Endocri-nol Invest 34 (2010) 317ndash323
[244] JC McCann BN Ames Adaptive dysfunction of selenoproteins from the per-spective of the triage theory why modest selenium deficiency may increaserisk of diseases of aging FASEB J 25 (2011) 1793ndash1814
[245] R Apak K Guclu M Ozyurek B Bektas Oglu M Bener Cupric ion reducing an-tioxidant capacity assay for food antioxidants vitamins polyphenolics and fla-vonoids in food extracts Methods Mol Biol 477 (2008) 163ndash193
[246] F Galli Interactions of polyphenolic compounds with drug disposition and me-tabolism Curr Drug Metab 8 (2007) 830ndash838
[247] RL Prior X Wu K Schaich Standardized methods for the determination of an-tioxidant capacity and phenolics in foods and dietary supplements J Agric FoodChem 53 (2005) 4290ndash4302
[248] C Azbell S Zhang D Skinner J Fortenberry EJ Sorscher BA WoodworthHesperidin stimulates cystic fibrosis transmembrane conductance regulator-mediated chloride secretion and ciliary beat frequency in sinonasal epitheliumOtolaryngol Head Neck Surg 143 (2010) 397ndash404
[249] G Wegrzyn J Jakobkiewicz-Banecka M Gabig-Ciminska E Piotrowska M Nar-ajczyk A Kloska M Malinowska D Dziedzic I Golebiewska M Moskot AWegrzyn Genistein a natural isoflavone with a potential for treatment of ge-netic diseases Biochem Soc Trans 38 (2010) 695ndash701
[250] YC Yu H Miki Y Nakamura A Hanyuda Y Matsuzaki Y Abe M Yasui K Ta-naka TC Hwang SG Bompadre Y Sohma Curcumin and genistein additivelypotentiate G551D-CFTR J Cyst Fibros 10 (2011) 243ndash252
[251] B Illek H Fischer Flavonoids stimulate Cl conductance of human airway epithe-lium in vitro and in vivo Am J Physiol 275 (1998) L902ndashL910
[252] JL Kreindler Cystic fibrosis exploiting its genetic basis in the hunt for newtherapies Pharmacol Ther 125 (2010) 219ndash229
[253] B Illek L Zhang NC Lewis RB Moss JY Dong H Fischer Defective function ofthe cystic fibrosis-causing missense mutation G551D is recovered by genisteinAm J Physiol 277 (1999) C833ndashC839
[254] P Anandakumar S Kamaraj S Jagan G Ramakrishnan R Vinodhkumar TDevaki Capsaicin modulates pulmonary antioxidant defense system during ben-zo(a)pyrene-induced lung cancer in Swiss albinomice Phytother Res 22 (2008)529ndash533
[255] I Rahman Antioxidant therapeutic advances in COPD Ther Adv Respir Dis 2(2008) 351ndash374
[256] AW Boots H Li RP Schins R Duffin JW Heemskerk A Bast GR Haenen Thequercetin paradox Toxicol Appl Pharmacol 222 (2007) 89ndash96
[257] M Joskova S Franova V Sadlonova Acute bronchodilator effect of quercetin inexperimental allergic asthma Bratisl Lek Listy 112 (2011) 9ndash12
[258] HJ Park CM Lee ID Jung JS Lee YI Jeong JH Chang SH Chun MJ Kim IWChoi SC Ahn YK Shin SR Yeom YM Park Quercetin regulates Th1Th2 balancein a murine model of asthma Int Immunopharmacol 9 (2009) 261ndash267
[259] AP Rogerio A Kanashiro C Fontanari EV da Silva YM Lucisano-ValimEG Soares LH Faccioli Anti-inflammatory activity of quercetin and iso-quercitrin in experimental murine allergic asthma Inflamm Res 56 (2007)402ndash408
[260] M Muller Polyphenol cytotoxicity induced by the bacterial toxin pyocyaninrole of NQO1 Free Radic Biol Med 47 (2009) 84ndash91
[261] J Grassmann Terpenoids as plant antioxidants Vitam Horm 72 (2005)505ndash535
[262] P Allen Tea tree oil the science behind the antimicrobial hype Lancet 358(2001) 1245
[263] EC Dasenbrook W Checkley CA Merlo MW Konstan N Lechtzin MP BoyleAssociation between respiratory tract methicillin-resistant Staphylococcus aure-us and survival in cystic fibrosis JAMA 303 (2010) 2386ndash2392
[264] V Bezzerri M Borgatti E Nicolis I Lampronti MC Dechecchi I Mancini PRizzotti R Gambari G Cabrini Transcription factor oligodeoxynucleotides toNF-kappaB inhibit transcription of IL-8 in bronchial cells Am J Respir CellMol Biol 39 (2008) 86ndash96
[265] R Gambari M Borgatti V Bezzerri E Nicolis I Lampronti MC Dechecchi IMancini A Tamanini G Cabrini Decoy oligodeoxyribonucleotides and peptidenucleic acids-DNA chimeras targeting nuclear factor kappa-B inhibition of IL-8 gene expression in cystic fibrosis cells infected with Pseudomonas aeruginosaBiochem Pharmacol 80 (2010) 1887ndash1894
[266] M Adrian P Jeandet AC Douillet-Breuil L Tesson R Bessis Stilbene content ofmature Vitis vinifera berries in response to UV-C elicitation J Agric Food Chem48 (2000) 6103ndash6105
[267] B Paul I Masih J Deopujari C Charpentier Occurrence of resveratrol and pter-ostilbene in age-old darakchasava an ayurvedic medicine from India J Ethno-pharmacol 68 (1999) 71ndash76
[268] I Rahman Antioxidant therapies in COPD Int J Chron Obstruct Pulmon Dis 1(2006) 15ndash29
[269] M Lee S Kim OK Kwon SR Oh HK Lee K Ahn Anti-inflammatory and anti-asthmatic effects of resveratrol a polyphenolic stilbene in a mouse model ofallergic asthma Int Immunopharmacol 9 (2009) 418ndash424
[270] LG Wood PA Wark ML Garg Antioxidant and anti-inflammatory effectsof resveratrol in airway disease Antioxid Redox Signal 13 (2010)1535ndash1548
[271] KV Kiselev Perspectives for production and application of resveratrol ApplMicrobiol Biotechnol 90 (2011) 417ndash425
[272] M Shakibaei C Buhrmann A Mobasheri Resveratrol-mediated SIRT-1 interac-tions with p300 modulate receptor activator of NF-kappaB ligand (RANKL) acti-vation of NF-kappaB signaling and inhibit osteoclastogenesis in bone-derivedcells J Biol Chem 286 (2011) 11492ndash11505
[273] SF Zaidi K Ahmed T Yamamoto T Kondo K Usmanghani M Kadowaki TSugiyama Effect of resveratrol on Helicobacter pylori-induced interleukin-8 secre-tion reactive oxygen species generation and morphological changes in human gas-tric epithelial cells Biol Pharm Bull 32 (2009) 1931ndash1935
[274] JK Kundu YK Shin YJ Surh Resveratrol modulates phorbol ester-inducedpro-inflammatory signal transduction pathways in mouse skin in vivo NF-kappaB and AP-1 as prime targets Biochem Pharmacol 72 (2006)1506ndash1515
[275] NH Nam Naturally occurring NF-kappaB inhibitors Mini Rev Med Chem 6(2006) 945ndash951
[276] JM Smoliga JA Baur HA Hausenblas Resveratrol and healthmdasha comprehen-sive review of human clinical trials Mol Nutr Food Res 55 (2011) 1129ndash1141
[277] ME Juan M Maijo JM Planas Quantification of trans-resveratrol and itsmetabolites in rat plasma and tissues by HPLC J Pharm Biomed Anal 51(2010) 391ndash398
[278] JA Baur DA Sinclair Therapeutic potential of resveratrol the in vivo evidenceNat Rev 5 (2006) 493ndash506
[279] E Nicolis I Lampronti MC Dechecchi M Borgatti A Tamanini N Bianchi VBezzerri I Mancini MG Giri P Rizzotti R Gambari G Cabrini Pyrogallol anactive compound from the medicinal plant Emblica officinalis regulates expres-sion of pro-inflammatory genes in bronchial epithelial cells Int Immunophar-macol 8 (2008) 1672ndash1680
[280] E Nicolis I Lampronti MC Dechecchi M Borgatti A Tamanini V Bezzerri NBianchi M Mazzon I Mancini MG Giri P Rizzotti R Gambari G CabriniModulation of expression of IL-8 gene in bronchial epithelial cells by 5-methoxypsoralen Int Immunopharmacol 9 (2009) 1411ndash1422
[281] M Borgatti I Mancini N Bianchi A Guerrini I Lampronti D Rossi G SacchettiR Gambari Bergamot (Citrus bergamia Risso) fruit extracts and identified com-ponents alter expression of interleukin 8 gene in cystic fibrosis bronchial epithe-lial cell lines BMC Biochem 12 (2011) 15
[282] L Piccagli E Fabbri M Borgatti N Bianchi V Bezzerri I Mancini E Nicolis CMDechecchi I Lampronti G Cabrini R Gambari Virtual screening against p50NF-kappaB transcription factor for the identification of inhibitors of the NF-kappaB-DNA interaction and expression of NF-kappaB upregulated genesChemMedChem 4 (2009) 2024ndash2033
[283] L Piccagli M Borgatti E Nicolis N Bianchi I Mancini I Lampronti D VevaldiF DallAcqua G Cabrini R Gambari Virtual screening against nuclear factorkappaB (NF-kappaB) of a focus library identification of bioactive furocoumarinderivatives inhibiting NF-kappaB dependent biological functions involved incystic fibrosis Bioorg Med Chem 18 (2010) 8341ndash8349
[284] M Borgatti A Chilin L Piccagli I Lampronti N Bianchi I Mancini G Mar-zaro Da Francesco A Guiotto R Gambari Development of a novel furocou-marin derivative inhibiting NF-kappaB dependent biological functionsdesign synthesis and biological effects Eur J Med Chem 46 (2011)4870ndash4877
[285] E Georgy S Le Guellec L Vecellio E Fichant P Stordeur P Bordeau JP PerraudinFeasibility study of OSCN- and lactoferrin (Meveol) nebulization for cysticfibrosis JCyst Fibros 10 (2011) S18
713F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
[286] C Tidei M Piroddi F Galli C Santi Oxidation of thiols promoted by PhSeZnClTetrahedron Lett 53 (2012) 232ndash234
[287] L Semianrio-Vidal C van Hesuden G Mugesh ER Lazarowski Ebselen is a po-tent non-competitive inhibitor of extracellular nucleoside diphosphokinasePurinergic Signal 6 (2010) 383ndash391
[288] C ColussiMC Albertini S Coppola S Rovidati F Galli L Ghibelli H2O2-inducedblockof glycolysis as an active ADP-ribosylation reaction protecting cells from apoptosisFASEB J 14 (2000) 2266ndash2276
[289] H Xiao KL Parkin Induction of phase II enzyme activity by various seleniumcompounds Nutr Cancer 55 (2006) 210ndash223
[290] G Peluffo R Radi Biochemistry of protein tyrosine nitration in cardiovascularpathology Cardiovasc Res 75 (2007) 291ndash302
[291] B Alvarez R Radi Peroxynitrite reactivity with amino acids and proteinsAmino Acids 25 (2003) 295ndash311
[292] B Kamosinska MW Radomski M Duszyk A Radomski SF Man Nitric oxideactivates chloride currents in human lung epithelial cells Am J Physiol 272(1997) L1098ndashL1104
[293] L Chen RP Patel X Teng CA Bosworth JR Lancaster Jr S Matalon Mecha-nisms of cystic fibrosis transmembrane conductance regulator activation by S-nitrosoglutathione J Biol Chem 281 (2006) 9190ndash9199
[294] F Luchetti B CanonicoM BettiM Arcangeletti F PilolliM Piroddi L Canesi S PapaF Galli Melatonin signaling and cell protection function FASEB J 24 (2010)3603ndash3624
[295] MW Bengtsson G Jedstedt G Flemstrom Duodenal bicarbonate secretion inrats stimulation by intra-arterial and luminal guanylin and uroguanylin ActaPhysiol (Oxf) 191 (2007) 309ndash317
[296] CS Nelson JL Marino CN Allen Melatonin receptor potentiation of cyclic AMP andthe cystic fibrosis transmembrane conductance regulator ion channel J Pineal Res 26(1999) 113ndash121
[297] C de Castro-Silva VM de Bruin GM Cunha DM Nunes CAMedeiros PF de BruinMelatonin improves sleep and reduces nitrite in the exhaled breath condensate incystic fibrosismdasha randomized double-blind placebo-controlled study J Pineal Res48 (2010) 65ndash71
[298] I Hornyak E Pankotai L Kiss Z Lacza Current developments in the the-rapeutic potential of S-nitrosoglutathione an endogenous NO-donor mole-cule Curr Pharm Biotechnol (2011) Jan 11 [Epub ahead of print] - PMID21235457
[299] AH Snyder ME McPherson JF Hunt M Johnson JS Stamler B Gaston Acuteeffects of aerosolized S-nitrosoglutathione in cystic fibrosis Am J Respir CritCare Med 165 (2002) 922ndash926
Table 1Intervention trials on antioxidant therapy in CF patients found at ClinicalTrialsgov databasea
Rank Title PI Location Recruitment Interventions Age groups Phasesnumberenrolled
Study designsb Outcome measures Start andcompletion date
NCT ID
1 Efficacy and safety studyof inhaled GSH in CFpatients
GrieseM
Germany Completed Drugbull reduced GSH sodium salt
C|A|S II138
1 R|E2 Safetyeff3 PA4 DB (Sub Inv)5 Treatment
bull Differences between inhaled GSHand inhaled normal saline withrespect to the area under the curveof FEV1 predicted within the periodfrom baseline to week 24
bull Treatment changes with respect tothe variablesspirometry peak flowquality-of-life weightheightpercentage of neutrophilsothercell types (induced sputum) inducedsputum levels of GSHinflammatorymediators pulmonary exacerbation
Jul-07May-10
00506688
bull 09 saline (control)
2 A phase I study of inhaledsodium pyruvate for thetreatment of CF
BillingsMCE
United States Terminated Drugbull Inhaled sodium pyruvate
A|S I70
1 R|E2 Safetyeff3 PA4 DB5 Treatment
bull Assessment of safety of inhaled sodiumpyruvate in Subs with CF Subs will beevaluated for the presence of symptomsand safety laboratory measurements
bull Determination of improvement inlungs of CF Subs as determined bymeasurement of FEV1 and measurementof inflammatory markers ininduced sputum
Feb-06na
00332215
3 Inhaled GSH versusplacebo in CF
MarsicoS
Italy Recruiting Drugbull Inhaled reduced GSHbull Physiological solution
C|A III150
1 R|E2 Eff3 PA4 SB (Sub)5 Treatment
bull FEV1bull Small airway function exercise capacityBMI dyspnoea cough quality of lifepulmonary exacerbations markers ofoxidative stress (H2O2)in serum and inEBC epithelial inflammatory markerson BNEC
Jun-10Dec-12
01450267
4 Safety and efficacy ofan antioxidant-richmultivitaminsupplement in CF
SagelSD
United States Completed Dietary supplementbull AquADEKs
C|A IIndashII17
1 NR|E2 Safetyeff3 SGA4 OL5 Treatment
bull Plasma levels of β-carotenebull Plasma levels of coenzyme Q-10retinol (Vitamin A) 25-hydroxy vitaminD α- and γ-tocopherols (Vitamin E)PIVKA-II
Aug-07Nov-09
01018303
5 Efficacy and safety ofepigallocatechin gallate(EGCG)tocotrienol in18 patients with splicing-mutation-mediated CF
KeremE
Israel Not yetrecruiting
Dietary supplementbull EGCGbull Tocotrienolbull EGCG+tocotrienol
A|S na18
2 Safetyeff3 CA4 OL5 Treatment
bull Changes in nasal chloride secretion asassessed by TEPD with assessment ofmean changes in TEPD by drug comparedto baseline and the proportion of patientswith a chloride secretion response bydrug compared to baseline
bull Pulmonary function testing FEV1FVC MEF25-75
Sep-09Jun-11
00889434
6 The effect of inhaledNAC compared tonormal saline onsputum rheology andlung function
VanDaele S
Belgium Terminated Drugbull Acetyl-Cysbull Normal saline
C|A IV19
1 NR|E2 Eff3 CA4 OL5 Treatment
bull Changes in visco-elasticity andlung function
Jan-10Dec-10
00996424
696FG
allietal
Biochimica
etBiophysica
Acta
1822(2012)
690ndash713
7 Safety of orallyadministeredcurcuminoids in adultsubjects with CF
Goss C United States Completed Drugbull Standardized turmericroot extract
A I11
1 NR|E2 Safetyeff3 SGA4 OL5 Treatment
bull Safety and tolerability of 14 days oftreatment with orally administeredcurcuminoids as assessed by adverseevents laboratory parameters andspirometry
bull Pharmacokinetics of repeated dosesof orally administered curcuminoidschange in NPD measurementschange in sweat chloride measurements
Apr-05Jan-06
00219882
8 Nasal potential studiesutilizing CF transmembraneregulator (CFTR) modulators
Rowe S United States Recruiting Other quercetin C|A II46
2 Eff3 SGA4 OL5 BS
bull NPD(NPD) Biomarkerbull Residual CFTR activity
Mar-10Nov-11
01348204
9 Safety and tolerability ofinhaled nitric oxide inpatients with CF
Sagel S United States Completed Drugbull Nitric oxide for inhalationbull Nitrogen
C|A|S IIndashII18
1 R|E2 Saf3 PA4 DB (Sub Care Inv OA)5 Treatment
bull Safety and tolerability of drugassessed by change in methemoglobinlevels oxygensaturation FEV1
bull Assess the difference in sputumbacterial density before and afterNO inhalation and the differencein lower airway inflammatorymeasures before and after NO inhalation
Jul-04Dec-08
00570349
10 NAC Phase IIB a multi-center phase IIBrandomized placebo-controlled DB study ofthe effects of NAC onredox changes and lunginflammation in CF patients
ConradC
United States Completed Drugbull NAC
C|A|S II80
1 R|E2 Eff3 SGA4 DB (Sub Care Inv OA)5 Treatment
bull Change in the logarithm of the levelof human neutrophil elastase(HNE) activity measured in sputum
bull Change in concentration of IL-8measured in sputum and plasmaconcentration of GSH measured inwhole blood the neutrophil countmeasured in sputum
Nov-08Feb-11
00809094
11 Glutamine supplementationin CF
na United States Not yetrecruiting
Dietary supplementbull Glutaminebull L-alanine
A|S II40
1 R3 PA4 DB (Sub Care Inv OA)5 Prev
bull Percent increase in plasma glutamineand GSH redox levels measured atweeks 0 4 8 and 12
Feb-10Feb-11
01051999
12 Effect of sulforaphane inbroccoli sprouts onNrf2 activation
ChmielJF
United States Active notrecruiting
Dietary supplementbull Broccoli sprouts
A na15
3 SGA4 OL5 BS
bull Nrf2 activation in NECbull Measures of lipid peroxidation in NECGSH from blood lymphocytesoxidative stress in urineneutrophil migration into thegingival crevices
Apr-11Sep-11
01315665
AbbreviationsA=adult BC=breath condensate BNEC=brushed nasal epithelial cells BS=basic science C=child CA=crossover assignment Care=caregiver CF=cystic fibrosis DB=double blind EBC=exhaled breath condensate Eff=efficacystudy FEV1=forced expiratory volume in 1 s FVC=forced vital capacity GSH=glutathione Inv=investigator MEF25ndash75=maximal expiratory flow 25ndash75 na=not available NAC=N-acetylcysteine NEC=nasal epithelial cellsNLF=nasal lavage fluid NPD=nasal potential difference NR|E=non-randomized|endpoint OA=outcomes assessor OL=open label PA=parallel assignment PI=principal investigator Prev=prevention R|E=randomized|endpoint S=senior Saf=safety study SB=single blind SGA=single group assignment Sub=subject
a Search was done matching the terms ldquoantioxidant therapyrdquo or ldquoGlutathionerdquo with ldquoCystic Fibrosisrdquob 1 Allocation 2 Classification 3 Intervention model 4 Masking 5 Primary purpose
697FG
allietal
Biochimica
etBiophysica
Acta
1822(2012)
690ndash713
698 F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
corrected Cftr KO-transgenic mice were given an oral bolus dose ofGSH (300 mgkg) and compared with WT mice for changes in GSHlevels in plasma lung ELF and BAL cells There was a twofold in-crease in plasma a twofold increase in lung a fivefold increase inELF and a threefold increase in BAL cell GSH levels at 60 min in WTmice however GSH levels only increased by 40 in the plasma 60in the lung 50 in the ELF and twofold in the BAL cells within thegut-corrected Cftr KO-Tg mice No change in GSH levels was observedin the uncorrected Cftr KO mice These studies suggest that oral GSHadministration can increase plasma and lung compartment GSHlevels in WT mice and to a lesser extent in gut-corrected Cftr KO-Tganimals It also suggests that oral GSH treatment can boost BAL cellGSH levels However since this study failed to show significant in-creases in serum and lung compartment GSH levels in uncorrectedCftr KO mice it is questionable whether oral GSH administration toCF patients with intestinal malabsorption would benefit from thistherapy It was also shown that GSH is rapidly distributed to theserum and lung compartments Kariya et al [118] speculate thatother transporter(s) besides CFTR are responsible of the transport ofGSH and probably of other dietary molecules to the lung whichmay be responsible for dietary deficiencies observed in various lungdiseases
Another strategy is represented by the oral supplementation ofhigh doses of NAC a well known cysteine donor for the synthesis ofglutathione NAC is considered a safe molecule which has beenused successfully to treat GSH deficiency in a wide range of diseases[119] As CF mice display defects in GSH export in the ELF comparableto those of patients they could provide a useful tool to assess the ef-fects of NAC administration on the GSH status However only limitedstudies exploring the effects of NAC on CF animal models have beenso far carried out The effects of NAC have been tested on mucus accu-mulation bacterial load transit and inflammation in the CF mousesmall intestine showing that NAC may reduce intestinal mucus accu-mulation bacterial overgrowth in the gut [120]
Moreover NAC has been reported to restore the accumulationof unwantedmisfolded proteins in aggregates that are associated withthe CF airway phenotype as a cause of lung inflammation [121] Themechanism of this NAC-derived effect seems to involve the restorationof beclin 1 expression and activity in the autophagy pathway of theendoplasmic reticulum that was investigated in vivo using Scnn1b-transgenic and Cftr(F508del) homozygous mice The restoration ofthis pathway also produced a rescued trafficking of CFTR (F508del) tothe cell surface of CF cells obtained from human CF nasal biopsies
Given the defective GSH metabolism of CF reviewed in the previ-ous sections and in [122] and the reduced response to GSH therapyin CF mice [93] some Authors have investigated the influence of bac-terial infections on lung oxidative stress The effects of P aeruginosainfection on ELF and lung tissue antioxidants and the oxidation ofDNA and lipids were investigated in mice challenged with bacterialcells [90] CFTR-KO (B6129P2-Cftrtm1Unc) and WT mice were chal-lenged intratracheally with a clinical isolate of mucoid P aeruginosaembedded in agar beads and on the third day of infection BALF andlung tissue were obtained and analyzed for cytokines antioxidantsand enzyme activities [90] P aeruginosa lung infection increasedlevels of inflammatory cytokines and neutrophils in the ELF This cor-responded with a marked increase in GSH and in urate levels in theELF of P aeruginosa-infected WT mice A twofold increase in uratelevels was also observed among lung tissue antioxidants of Paeruginosa-infected WT mice There were no changes in markers oflung oxidative stress associated with the P aeruginosa lung infectionIn contrast to WT mice the CFTR-KO mice lacked a significant in-crease in ELF GSH when challenged with P aeruginosa and this corre-lated with a decrease in the ratio of reduced to oxidized GSH in theELF a marker of oxidative stress These data would suggest that thelung adapts to infectious agents with elevated ELF GSH and urateTherefore individuals with lung diseases associated with altered
antioxidant transport such as CF might lack the ability to adapt tothe infection which may lead to a more severe inflammatoryresponse
322 Clinical trials on GSHThe discovery of the defect in GSH export has suggested that ther-
apies able to restore or increase GSH levels in the ASL could counteractthe inflammation and oxidative stress conditions typical of CF pa-tients In an attempt to strengthen extracellular defenses againstROS some pilot studies have analyzed the effect of GSH inhalation orthat of oral GSH prodrug N-acetylcysteine (NAC) All these treatmentswere well tolerated by the CF patients and most authors were able tomeasure increased ELF concentrations of GSH in association withsome positive clinical outcomes [4041737896122ndash128] Althoughpotentially promising these findings need stronger clinical evidencein that the majority of these were obtained on very limited numberof patients investigated in non-randomized controlled trials This ishighlighted in a recently published meta-analysis [129] that providesalso a thoroughly analysis of the literature on this aspect of the antiox-idant and anti-inflammatory therapy of CF Among the American CFfoundation sponsored trials two phase II trials on inhaled GSH andoral NAC are in progress in US and Germany (ClinicalTrialsgov Iden-tifier NCT00506688 and NCT00809094 respectively Table 1) andsafety and tolerability of aerosolized glutathione is also matter ofinvestigation by another (not registered) US trial (more informationon this can be found in [130]) Nevertheless the diffusion among CFpatients of NAC preparations for inhalation (Mucomystreg) has in-creased in recent years
γ-Glutamylcysteine ethyl ester (GCEE) is another potentially inter-esting GSH pro-drug which has proved some efficacy in the ameliora-tion of oxidative stress eg in experimental myocardial infarction[131] and central nervous system conditions (see eg [132]) HoweverGCEE has not been investigated in CF yet
33 Limits and potential problems associated to thiol-based therapies
Although the above cited clinical trials may be considered promis-ing attempts to improve the antioxidant levels in the ELF the actualcapacity of these treatments to produce positive clinical effects mustbe considered with caution For example indices of oxidative damagewere found to be unaffected by aerosolized GSH treatment [122]Some in vitro studies have suggested that the reaction of GSH withPCN could produce hydrogen peroxide with potential exacerbationof oxidative damage [101] The exact mechanisms of PCN toxicityand the reaction of this toxin with GSH must be better understoodin order to evaluate the safety of GSH administration to patients col-onized by P aeruginosa
Inhalation of GSH ensures its direct delivery in the airways butsince GSH can rapidly convert to its oxidized form GSSG frequentGSH inhalations are required to maintain a high GSHGSSG As a con-sequence of this limit four separate inhalations have been used inthe study carried out by Bishop et al [123] Unless justified by clearclinical improvements these repeated treatments may represent aburden for patients already undergoing complex therapies Moreoverrepeated inhalations of GSH increase the levels of GSSG in ELF[133134] In the absence of effective homeostatic mechanisms ensur-ing the fast recycling of GSSG to GSH this might produce unwantedeffects and even the exacerbation of CF symptoms being GSSG re-sponsible of the S-glutathiolation and functional inhibition of CFTR[124]
In principle the oral administration of GSH could be considered asafe strategy to prevent GSSG accumulation but this strategy is likelynot feasible due to the substantial inability of this water-soluble mol-ecule to cross biological membranes Moreover a study carried out inmice has established that GSH absorption in the gastrointestinal tractif any is mediated by CFTR itself thus excluding the possibility to
699F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
improve circulating levels of GSH in CF patients through the dietarysupplementation of the antioxidant [127] The limited absorption ofGSH could be overcome by GSH-esters as in vitro studies haveshown that this form of GSH may be specifically useful to rescue mi-tochondrial defects in cystic fibrosis models [80] Safety of these GSHderivatives in humans has been poorly investigated
Two independent studies have shown that the treatment of CF pa-tients with high doses of NAC increases extracellular GSH in sputum[78125] but contrasting results have been reported concerning theeffects of NAC on the concentrations of blood GSH and on the levelsof IL-8 and other markers of inflammation NAC treatments may beuseful to modulate the GSH content in cells but it should be remindedthat an enhanced cysteine supply cannot lead to an increase of GSHabove physiological levels due to the feedback inhibition mechanismof γ-glutamylcysteine synthetase described in the Section 311
331 Gamma-glutamyltransferase and GSH therapySo far none of the studies mentioned above has taken into account
the fact that GSH is degraded by GGT enzyme activity GGT concentra-tions are known to increase several fold in ELF of CF patients even ifthe mechanisms for this effect were not determined [135] and thisphenomenon parallels the above described decrease of GSH levels inELF Preliminary data suggest that a major source of increased ELFGGT is represented by activated neutrophils accumulating in diseasedairways (Corti and Pompella 2011 unpublished observation) Re-gardless of its origin it is likely that increased GGT in ELF would de-grade locally administered GSH to variable extents which couldcontribute to the so far inconclusive results of therapies based onaerosolized GSH Besides its role in GSH catabolism GGT has beenshown to mediate protein S-thiolation [136] suggesting that GSH ad-ministration in the presence of active GGT enzyme might alter CFTRglutathiolation status and function in a potentially unfavorable wayOn the other hand a potential role of GGT in favoring bronchial up-take of antioxidant vitamin C has also been suggested [137]
These controversial findings may add further issues to the ques-tion of whether the therapy of lung oxidative stress by aerosolizedGSH could be safe in all the CF patients regardless of specific strate-gies that would ascertain the extent of lung inflammation Thesestrategies should include the assay of GGT levels in ELF In principleonce an adverse role of ELF GGT in GSH therapies will be confirmedthe association of GGT inhibitors in the GSH formulations for inhala-tion could represent a promising pharmacological strategy
34 Malnutrition as a possible cause of defective thiol-dependentantioxidant protection
Successful nutritional interventions strongly impact on the clinicaloutcome of CF patients [138ndash140] Malnutrition by pancreatic insuffi-ciency and other CF-related factors influence the susceptibility to de-velop recurrent infections and severe inflammatory lesions of thelung tissue If the onset of a defective (sub-optimal) antioxidant sta-tus may represent an underlying component in the clinical effects ofmalnutrition remains a matter of investigation Clinicians have topay particular care to avoid these disturbances and successful proto-cols of nutritional intervention in CF have been developed whichare essentially aimed to avoid the onset of protein-energy malnutri-tion (PEM) [141] Despite this the risk of developing such an unto-ward complication in CF infants and children remains high assuggested by the prevalence data registered in some areas Actuallya prevalence of PEM between 5 and 14 in Moldavian infants was re-cently reported [142] and PEM is associated with poor outcome andparticularly with the risk of developing edema and anemia
Besides lowered intake and absorption of micronutrient antioxi-dants discussed in the other sections malabsorption of dietary proteinand excess fecal amino acid losses result in hypoproteinemiahypoalbu-minemia as key biochemical signs of PEM Hypoalbuminemia is
considered to be linked with a causendasheffect relationship with oxidativestress and is proposed to influence morbidity and mortality in condi-tions associated with chronic inflammation and severe oxidative stress[143144] The human serum albumin (HAS) molecule contains only areactive thiol group eg the Cys 34 the importance of which as an anti-oxidant defense system in blood and for the entire organism is welldocumented [145] This is the second main thiol (and the main proteinthiol) in the circulation (approx 2 mmol in the adult organism assum-ing 5 l of total blood volume anHt of 40 and [HAS] of 45 gl of plasma)being the RBCGSH thefirst thiol in blood (near to 5 mmol assuming thesame parameters of above and an average concentration of GSH inpacked RBC of 25 mM) [146147] The antioxidant role of HSA is notonly a consequence of the relative abundance of its Cys thiol A specificcapability of acting as a sacrificial target for a series of electrophils andmost biologically relevant ROS ie hydrogen peroxide and peroxyni-trite has been demonstrated in a series of studies [145148149] Li-gand binding activity can contribute to promote antioxidant effectsby the HSA molecule [145] Transitions metals particularly copperand also iron in the case of iron-overload diseases bind to HSA Inthis way these are less available to promote the Fenton chemistryand hydroxyl radicals eventually released from this oxidative reactionare mostly directed to the HAS protein sparing more important tar-gets A free radical-trapping activity of HSA has been also demonstratedand this was proposed to be directed toward both hydrophilic and fat-soluble species This activity may result from the interaction withother antioxidants such as α-tocopherol [150] and may influence theantioxidant activity of food-derived phenolic antioxidants [151]
However Cys 34 is considered the main contributor to the antiox-idant function of HAS which plays its role in the antioxidant homeo-stasis of blood thanks to a complex series of interactions with themetabolism and antioxidant function of the pool of free thiols in plas-ma and in the circulating RBC with the latter playing a significantcontribution to the extracellular pool of GSH [146] and to the dynam-ics of inter-organ GSHmetabolism in cooperation with liver and othertissues [147] Immuno-inflammatory cells and the lung tissue areamong the main terminals of this metabolism The RBC contain theentire machinery to synthesize GSH to restore its redox (by enzymat-ic reduction of the oxidized form) and to use this as cofactor of Se-GPx and GSH-S-transferase enzymatic activities that are responsibleof the detoxification of hydroperoxides and alkylating agents thatmay form in or enter the RBC cytosol [147] In this sense the RBC rep-resents a circulating reservoir of GSH that in addition to maintainingthe redox and respiratory function of Hb participates to systemic pro-tection of xenobiotics of endogenous and exogenous origin In consid-eration of these aspects the combination of hypoalbuminemia andanemia may exponentially increase the risk of developing oxidativestress in CF patients as it is supposed to occur in other oxidative stressconditions such as chronic kidney disease [55143152] Additionalclinical investigation should verify the hypothesis that hypoalbumi-nemia together with a defective uptake and metabolism of sulfur-containing amino acids and CF-specific defects of the GSH metabo-lism may represent a causal risk factor for an impaired antioxidantdefense and systemic oxidative stress in CF patients
35 Fat-soluble antioxidants
Pancreatic insufficiency and a diminished bile acid pool cause mal-absorption of important essential nutrients and other dietary compo-nents in CF Of particular significance is the malabsorption of fat-soluble antioxidants such as tocopherols carotenoids and coenzymeQ-10 (Co-Q10) and that of essential fatty acids (EFA)
351 Vitamin EVitamin E therapy in CF has been proposed in several decades of
research as a useful approach to overcome both the lower absorptionof this fat-soluble micronutrient and the increased antioxidant
700 F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
demand by the abnormal generation of ROS in CF tissues (see for in-stance the recommendations by the Cystic Fibrosis Foundation Con-sensus Conference on nutrition [153])
The first report of a vitamin E deficiency in CF appeared in literaturein 1951 by Filer et al [154] In this study the absorption of the mainform of this vitamin eg α-tocopherol and its ester derivatives was in-vestigated in several subsets of infants and children Thanks to a simplebioavailability (or tolerance) test these authors observed that ldquoin-fantshellip diagnosed as fibrocystic disease of the pancreas diarrhea andcirrhosis were characterized by a poor response to the test ie the tol-erance curve was lowrdquo However abnormalities were also observed inother subgroups of infants with a variety of disorders not associatedwith fat or fat-soluble vitamin intolerance such as sprue celiac syn-drome and lupus erythematosus which suggests the general observa-tion that malnutrition and inflammatory and degenerative diseases ofthe GI tract may lead to absorb tocopherols poorly At the same timethese authors reported that ldquoMetabolic disorders with associated hy-percholesterolemia were observed to give abnormally high values forthe area under the curverdquo and that patients responding poorly to to-copherol absorption test did also in vitamin A absorption tests
The finding of lowered (lipid uncorrected) levels of vitamin E wasconfirmed in other studies in which this relative deficiency was foundto occur irrespective of pancreatic comorbidity and in associationwith lowered levels of other liposoluble vitamins such as vitamin Aand D [155] regardless of their different liver metabolism and tissuedelivery mechanisms [156157]
Plasma buccal mucosal cells (BMCs) and breath condensate α-tocopherol decreased significantly with age in association with a de-creased respiratory function [5] This was accompanied by loweredlevels of other antioxidants such as vitamin C and increased oxidativestress markers of different origin such as protein carbonyls thiobarbi-turic acid-reactive substances and F2-IsoPs
Clinical symptoms of vitamin E deficiency in CF have not beenconclusively investigated Dolan et al [158] described that anemiaof CF patients is related to vitamin E deficiency and increasedperoxide-induced hemolysis of RBC Other authors however ob-served an increased susceptibility to peroxide-induced hemolysisalso in the presence of normal levels of vitamin E [159] Peters andKelly [160] observed that RBC vitamin E concentrations were belowthe normal range in almost all unsupplemented patients and roseinto the normal range with a 1-year supplement of 100 mg per daybut not 15 mg per day Since RBC vitamin E concentration has beenshown to correlate well with tissue concentrations of the vitamin inanimals tissue levels of vitamin E are expected to be lower than nor-mal in CF patients
Bioavailability of fat-soluble vitamin is limited in CF Vitamin Edeficiency of CF is also associated with hypocholesterolemia [7] Asa consequence the relative deficiency of this vitamin is compensatedwhen the absolute levels are normalized for cholesterol levels andthis suggests a poor transferring of this vitamin in the circulation bya defective lipid and lipoprotein metabolism Pancreatic insufficiencyand the consequent lipid malnutrition cannot completely explain thisdefect and other possibly CF-specific dysfunctions could play a roleLiver metabolism and specific plasma transport systems of this vita-min need further elucidation in CF
As a consequence of these aspects it is not presently clear whichform and level of supplementation of this vitamin is most appropriateto treat these patients Usingα-tocopherol as a vitamin E supplementPeters et al [160] reported that 100 mg per day are required to nor-malize RBC concentrations Other authors described unsuccessfulsupplementation protocols with higher doses and this has led to de-velop formulations with higher bioavailability in order to achieve bet-ter compliance to oral supplementation (see below and the literaturereviewed in [161ndash163])
Besides absorption and tissue delivery issues specificity of actionis another critical item of antioxidant therapy with fat-soluble agents
in CF As further addressed below this aspect could be themain limit toa successful use of natural forms of vitamin E in the clinical manage-ment of CF inflammation even if a local lung-targeted therapy wouldbe developed according with so far proposed pre-clinical models ofaerosolized vitamin E [164165]
Current pharmacological research is aimed to develop synthetic formsof this and other fat-soluble antioxidants with better radical scavengingproperties at the lipidndashwater interface Type of ROS target and the sitesof action greatly influence the chances of a fat-soluble antioxidant of alle-viating oxidative stress in the airways as well as in other organs such asliver and pancreas These aspects dealing with specificity of action[163166167] have stimulated the search of novel vitamin E-derived an-tioxidants that may help to scavenge radicals at the lipidndashwater interfaceof the epithelial cell membrane and surfactant Amine derivativesof tocopherols and tocotrienols have been recently demonstrated toshow higher antioxidant and free radical scavenging activity than α-tocopherol [168] Further in vitro pharmacological analysis has includedtoxicity evaluations and the detailed investigation of scavenging of azo-and phenolic radicals with different degrees of hydrophobicity and theinhibitory activity on IL-8 gene expression and phospholipase activityin CF cells Comparative evaluation with other synthetic derivativessuch asα-tocopheryl succinate and natural forms of vitamin E suggestedthat these amine derivatives are promising antioxidant and anti-inflammatory agents [Galli F and Pilolli F unpublished observation]deserving further pre-clinical investigation in CF model systems
Anti-inflammatory effects of natural and synthetic analogues of vi-tamin E are also an intriguing pharmacological opportunity currentlyunder investigation by several laboratories [169170]
Recently vitamin E supplementation has been at the center of adispute regarding its safety when used at high dosages in certainpopulations of patients An extensive and speculative debate originat-ed on this subject after a meta-analysis study byMiller et al [171] thatexamined the largest secondary prevention trials on vitamin E trials incardiovascular patients finding a significantly increased mortality riskfor all the causes (about 4 1ndash8 in the 95 interval of confidence)when the patients were treated with doses gt400 IUdie (that areequivalent to 400 mgdie of the synthetic form allrac-α-tocopheroland to 185 mgdie of the natural form RRR-α-tocopherol) This debateresulted in a careful examination of this meta-analysis study by severalother authors and in further revisions of the literature on vitamin E tox-icity in humans [see the literature recently reviewed in [163172ndash174]]that clearly demonstrated the poor consistency of the conclusionsraisedwithMillersmeta-analysis study and the paucity of the concernsthat derived from that These conclusions have been verified in the re-cent international symposium on vitamin E of the Society for Free Rad-ical Research Europe branch of Rome 2009 [173175] Vitamin E used assupplement for humans in all its forms (eg α-tocopherol and othertocopherols and tocotrienols) is safe in abroad range of intakes[172176] The tolerable upper intake level (UL) and the AcceptableDaily Intake (ADI) established by the Joint FAOWHOExpert Committeeon Food Additives for the natural form of vitamin E as α-tocopherolequivalents are of 300 mgdie and 015ndash20 mgkg body weightdierespectively [172177]
352 CarotenoidsLevels of plasma carotenoids such as β-carotene β-cryptoxanthin
and total lycopene are significantly lowered in CF patients and thiswas associated with higher susceptibility to lipid peroxidation[5178ndash180] Rust et al [178] demonstrated that the long-term oralsupplementation with 50 mg β-caroteneday (ie 1 mg β-carotenekg BWday) restored the levels of this carotenoid while sub-optimalsupplementation was observed at doses of 10 mg β-caroteneday orlower thus confirming the need of high doses of this fat-soluble factorto overcome the limited absorption and thus to achieve plasma con-centrations of healthy control subjects Successful high-dose treat-ments appear to lower oxidative stress markers such as TBA-MDA
701F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
complexes and to correct total antioxidant capacity of plasma Inanother study β-carotene supplementation was observed to de-creased lipid peroxide formation as quantitated by malondialdehydeconcentrations in plasma (TBAHPLC method) and to enhance the re-sistance to copper(II) ion-induced oxidation of low density lipopro-teins [180]
At the same time toxicity issues have been raised for human sup-plementation with carotenoid formulations and particularly of water-miscible formulations of preformed vitamin A that is regularly sup-plemented to CF patients which may increase serum retinol andpossible risk of CF-associated liver and bone complications (reviewedin [161181]) However β-carotene supplementation seems to be safesince this does not affect plasma concentrations of other carotenoidsand retinol as well as of other fat-soluble vitamins as α- and γ-tocopherol [178] Recent studies designed to test the clinical efficacyof a CF tailored multivitamin formulation (commercial name AquA-DEKsreg) also tested the safety of this type of formulation and demon-strated that this does not increase vitamin A above the normal levelsobserved in healthy controls [162182183] The normalization of β-carotene levels obtained in these studies was associated only withminor improvements on respiratory and growth parameters whilethe levels of urinary F2-IsoPs used as index of lipid peroxidationwere not affected [162] The surrogate marker of lipid peroxidationMDA was affected together with some selected antioxidant parame-ters (RBC thiols and superoxide dismutase) in another study inwhich this multivitamin formulation was preliminarily evaluated incomparison with standard formulations of vitamin E and A [182]
353 Coenzyme Q-10Coenzyme Q-10 (Q10) is a well-known electron transporter in the
mitochondrial respiratory chain with fundamental role in cellularbioenergetics and scavenging of radical species [184] This lipophilicsubstance is present in the circulation at low levels (serum concentra-tionsle2 μM) mainly as ubiquinol-10 eg the reduced form with anapproximate ratio of 955 with the oxidized form ubiquinone-10[185186] A mechanism for a preferential distribution and accumula-tion in mitochondria has been suggested for both the reduced and ox-idized forms of CoQ10 that are taken up by the cells in a time- andconcentration-dependent Subcellular localization and trafficking ofexogenous Q10 are similar to those of the endogenous form butwere different from that of α-tocopherol that is related with lipidcomposition particularly in the mitochondrial and microsomal frac-tions [184] Ubiquinol-10 readily oxidizes ex vivo by the reactionwith other lipophilic antioxidants such as α-tocopherol and butylatedhydroxytoluene [185] Therefore a higher reduction potential thanother physiological fat-soluble antioxidants such as vitamin E and aselective metabolism and cellular trafficking show peculiar role forthe cell CoQ which may also represent an important lipophilic antiox-idant in cells and body fluids
Human cells synthesize this coenzyme through the cholesterol bio-synthesis pathway so thatmore than two thirds of the tissue levels ap-pear to have an endogenous origin dietary sources provide acontribution to Co-Q10 levels of blood and all solid tissues that variesdepending on the dose applied and type of dietary source [187] How-ever in the case of oral supplements it has to be considered that hy-drophobicity and large molecular weight of this coenzyme influenceits absorption that ultimately is slow and limited [186187] Likewiseto vitamin E pharmacokinetics [188189] Co-Q10 showed T(max) ofaround 6 h that coincides with that of dietary lipids Elimination isclose to that of the more retained form of vitamin E in human bodyeg α-tocopherol with a half-life of about 33 h which suggests poorhepatic metabolism However commercially available formulationsare reported to be safe even at high doses and solubilized formulationsshow enhanced bioavailability In healthy subjects plasma Q10 re-sponse to oral ingestion show saturation profiles with a plateau at a
dose of 2400 mg and the higher plasma concentrations were foundto facilitate uptake by peripheral tissues and also the brain [186187]
Laguna et al [190] recently investigated total serum levels ofcoenzyme Q-10 in a wide population of CF children (n=381) and esti-mated their association with clinical outcome Near to 50 of these CFpatients were deficient of Co-Q10 and this defect was significantlymore prevalent in patients with pancreatic insufficiency and signifi-cantly associated with P aeruginosa colonization in infants (under24 months of age) Importantly low Co-Q10 levels correlated to otherlipid markers of a poor nutritional status such as total lipids and alsothe other fat-soluble antioxidants β-carotene and α-tocopherolwhich confirms the presence of a common defect in the absorptionand metabolic pathways of this coenzyme with dietary lipids
The deficit of Co-Q10 may contribute to the impaired energy func-tion of mitochondria of CF tissues and this may exacerbate CF-linkedinflammation infection and cellular stress response of the lung A sys-tematic analysis of molecular lesions in CF bronchial tissue has beenrecently carried out by proteomic approach [191] Comparative eval-uation of protein expressional pattern in CF and healthy controltissues has revealed aberrant levels of some mitochondrial andenergy-related proteins in CF specimens that included the ubiqui-nolndashcytochrome c reductase complex core protein I and one form ofnidogen a pseudogene of aconitase 2 These changes in CF may reflectmolecular changes which could be associated with an altered mito-chondrial homeostasis and Co-Q10 redox
Multivitamin supplements with high bioavailability containingCo-Q10 have demonstrated to correct the deficit of this antioxidantand were preliminarily observed to improve airway inflammationmarkers in CF patients [183] However further clinical investigationfailed to demonstrate that such an improved biochemical profile isassociated with significant improvements in weight percentile andpulmonary function [162]
354 Fatty acidsA key pathophysiological role in sustaining inflammation in CF has
been attributed to the abnormal polyunsaturated fatty acid (FA) pat-tern Abnormalities in FA profiling are potentially linked to CFTRmutation-driven alterations in the absorption andor metabolism ofdietary lipids [192193] and to the consumption of high oxidizableFA involved in the free radical-mediated lipid peroxidation [7]Among those alterations dysregulation of the docosahexaenoic acidand arachidonic acid balance has been extensively studied with re-portedly significant reduction of DHA in CF and a parallel increasein the levels of AA and inflammatory indices [193ndash195] Actually AAis the progenitor of both enzymatic- and free radical-derived inflam-matory mediators including leukotrienes prostaglandins and iso-prostanes On the other hand n-3 PUFA (eicosapentaenoic acid anddocosahexaenoic acid) are involved in the generation of potent medi-ators namely resolvins and protectins which are able to resolveexudates and to act as organ protective and antifibrotic Secondarilyto their anti-inflammatory action n-3 FA may also produce anantioxidant-like response (eg a reduced demand of antioxidants toachieve an optimal control of oxidative pathways) As a consequencen-3 PUFA have been suggested and widely used as supplements in CFpatients usually under the form of fish oil [196ndash198] It is worth ofnote however that defective levels of DHA in CF patients was notconfirmed in recent studies [7] It was also shown that patients onDHA supplements did not have increased plasma n-3 FA concentra-tions but showed more severe oxidative stress compared to theunsupplemented patients [7] This observation of an increased riskof oxidative stress in CF subjects receiving n-3 fatty acids supple-ments has also been described by other authors [199]
Studies reporting increased AA levels in CF patients have beencontradicted by others [7200201] thus contributing to weakeningthe pathophysiological role of the altered DHAndashAA balance as turnpoint of an upregulated inflammatory status in CF In this context a
702 F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
recent Cochrane meta-analysis on n-3 supplementation in CF patients[202] highlighted the lack of evidence for a significant correction ofthe assessed clinical end points (mainly respiratory symptoms)even when inflammatory indices and other laboratory end pointswere met Taken together these data suggest that there is insufficientevidence to draw firm conclusions or recommend routine use of n-3supplements in CF Notwithstanding it is common belief that n-3supplements provide some benefits for people with CF with relativelyfew adverse effects and thus their use is not discouraged
Further alterations in fatty acid metabolism have been highlight-ed including the consistent findings of an increase in circulatinglevels of saturated and monounsaturated fatty acids [7203204]Decreased levels of essential FA (EFA) ie the FA that have to be in-troduced with the diet correlates with the severity of respiratoryinsufficiency and the same clinical correlation was observed with al-tered proportions of FA species converted by the activity of desatur-ase enzymes (reviewed in [204]) The close relationship betweencertain fatty acids and oxidative stress including the negative correla-tion of C240 and linoleic acid with oxysterol levels point to the needof intensive investigation in CF patients of previously neglected lipidspecies that are emerging candidates in the control of metabolismQuantitative lipidomic analyses have lead to identify C161n7 palmi-toleate as a ldquoprotectiverdquo adipose-derived lipid hormone that stronglystimulates insulin activity in muscle and liver also suppressing in-flammatory cytokine output from mice fat cells [205] Specific meta-bolic activities have been also demonstrated by medium chainsaturated fatty acids caprylic acid (C80) capric acid (C100) and lau-ric acid (C120) Capric acid acts as a direct ligand of PPARγ using abinding pocket different from the binding pocket of thiazolidinedioneor long chain fatty acids [206] Additional activities of medium chainfatty acids which are ligands of free fatty acids receptors detectedin the immune cells the gastrointestinal tract and adipocytes maycontribute to metabolic homeostasis and inflammatory responses[207] These data underscore the importance of a lipid-mediated ldquoen-docrine networkrdquo demonstrating how specific alteration of one orfew serum lipids would be per se sufficient to influence metabolic ho-meostasis Given the relevance of this emerging information and thealteration of lipid metabolism and inflammatory status in CF fattyacid lipidomics need to be deeply investigated in CF
Again these studies have obvious nutritional implications Satu-rated fatty acids with chain lengths higher than C18 are poorlyabsorbed partly because they form insoluble calcium salts [208]Medium chain saturated fatty acids are well known for being highlyabsorbed through the intestine providing rapid delivery of energyvia oxidation of the more hydrophilic short chains and have beensuggested to provide proper nourishment in patients with CF [209]Recent studies have shown that consumption of a high-fat diet richin medium chain fatty acids as opposed to long chain fatty acidsdoes not lead to ectopic fat accumulation in skeletal muscle andliver of both rats and mice [210] In light of the close association be-tween nutritional status inflammation and life expectancy in CF pa-tients the manipulation of dietary lipids in these patients must befurther explored as a possible strategy to provide adequate nutritionand better management of oxidative stress
36 Hydrosoluble antioxidants oligoelements and enzymatic antioxidants
361 Vitamin CVitamin C status in CF patients has been poorly investigated Early
studies suggested a defective vitamin C status that was refractory tooral supplementation [211] Other and more recent studies showednormal or slightly decreased levels of vitamin C in CF patients as com-pared to healthy controls but age- and disease-related decline of thiswater-soluble antioxidant was reported in these patients [5212]In the study of Winklhofer-Roob et al [212] on mid-European CFpatients vitamin C concentrations decreased with age with an
estimated rate of 5 μmollyr and vitamin C concentrationsb40 μ-moll were associated with highest indexes of inflammation whichis consistent with the hypothesis that optimal levels of vitamin Cmay influence immuno-inflammatory activity of alveolar macro-phages and neutrophils Other few studies have examined the effectof supplements containing vitamin C on CF inflammation and oxida-tive stress since the levels of this vitamin do not significantly improvewith supplementation (reviewed in [213]) This highlights the com-mon fate that this hydrosoluble vitamin shares with several fat-soluble counterparts in the ldquomicronutrient paradoxrdquo of CF patients inwhich the need for a correction of their status along the progressionof the disease is frustrated by the poor efficacy of oral supplementa-tion protocols Formulations and appropriate supplementation proto-cols that may produce a better correction of vitamin C status of CFpatients are awaited for further clinical evaluation
362 Selenium and selenium-dependent peroxidasesSelenium is a trace element with marked electrophilicity [214]
that once converted to the organic form of Se-Cys can be introducedin protein structures to play its important role in H2O2 metabolismand signaling [215] As catalytic center of the enzyme GSH-peroxidase (SeGSH-Px) Se plays a crucial role to protect polyunsatu-rated lipids of plasma membrane and circulating lipoproteins formperoxidative insults With other Se-proteins such as the high molecu-lar weight thioredoxin reductases this oligoelement participates tothe control of protein thiol-disulfide oxidoreduction and glutathiony-lation which regulate signaling pathways of crucial importance in theregulation of immunity and inflammation [16] but also the function-ing of other redox-sensitive proteins such as the same CFTR [124]
The activity of SeGSH-Px in blood is considered a functional as-sessment of selenium status even if this assumption has some limita-tions related with the saturation profile that the Se stores show atincreasing doses of Se administration Investigations of the seleniumstatus in CF patients have produced conflicting findings which maydepend on differences in dietary intake ethnicity and environmentalfactors in the diverse patient populations (reviewed in [216217]) CFchildren have been reported to have lowered blood selenium and RBCSeGSH-Px activity [218219] normal plasma selenium and loweredRBC SeGSH-Px [220] and even normal levels of both these two param-eters [221] The supplementation with selenium in combination withother antioxidants was observed to increase the concentrations ofblood selenium that likewise β-carotene and fatty acid were posi-tively correlated with improved lung function [6]
Foucaud et al [218] observed that a defective selenium statuswas associated with lowered levels of other antioxidants that contrib-ute to the anti-peroxidative activity of this microelement such asvitamin E (reviewed in [222]) and the severity of this deficiencywas lower in children with pancreatic enzyme replacement and vita-min E supplementation
Treatments to substitute for exocrine pancreatic insufficiency bypancreatic enzymes from animal sources such as porcine pancreashave been confirmed to be a source of Se [220] These affects RBCSeGSH-Px activity and plasma selenium concentrations which hasto be taken into account when selenium supplements are given toCF patients
Selenium has been used to develop a series of organoseleniumcompounds that may open the way to new therapeutic opportunitiesin CF (see Section 392) These include GPX mimetic drugs and phaseII enzyme inducers which may provide higher antioxidant activity ofASL and cellular protection effects in the airways
363 Zinc and copperZinc and copper (Zn and Cu respectively) are present in many
proteins so that a deficiency of these trace metals could have pleiotro-pic effects in humans As regards antioxidant systems these two oli-goelements contribute an important role being cofactors of two
703F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
isoforms of the superoxide dismutase enzymes eg the extracellularform eg the EC-SOD or Sod 3 and the CundashZn-SOD or Sod 1 that isfound in several tissues and cells [223] The EC-SOD exerts its antiox-idant role also in the lining fluids of the airways [224]
The notion that CF patients have defective concentrations of bloodZn and Cu is controversial As far as Cu status is concerned few datahave been produced and are available in the literature suggestingthe notion that CF patients develop a moderate copper deficiency[225226] That was essentially demonstrated on the bases of a defec-tive activity of Cu-related proteins such as plasma ceruloplasmindiamine oxidase and RBC SOD This defect seems to be refractory toCu and Zn supplementation (see below)
More advanced studies have been carried out in the case of Zn sta-tus in CF Low plasma zinc concentrations were reported in approxi-mately 30 of young infants with CF identified by newbornscreening [227] and an impaired zinc homeostasis in CF patientswas described by Easley et al [228] This is characterized by poor con-servation of the endogenous pool with fecal loss and impaired frac-tional absorption of zinc which are the consequences of pancreaticinsufficiency and persisting steatorrhea These studies suggestedthat in the clinical management of CF patients these defects can beat least in part corrected by exocrine pancreatic enzyme replacement
A series of studies by Van Biervliet et al [229230] demonstratedin a Dutch population of CF infants and children that serum Zn variesin an age-dependent manner but remained unchanged with respectto healthy control levels In CF patients no difference in serum Zn con-centration between pancreatic-sufficient or pancreatic-insufficientpatients was observed and no correlation was found with the nutri-tional status or height z-score Importantly in these studies a signifi-cant correlation of serum Zn was observed with the fat solublevitamins A and E thus confirming the relationship between the ab-normalities of lipid and Zn metabolism in CF This suggests that co-supplementation of Zn and fat-soluble vitamins should be advisedin the presence of pancreatic insufficiency and persisting steatorrhea
Neve et al [219] in a study aimed to assess plasma and erythrocytezinc copper and selenium in CF children showed that mean plasmazinc and copper levels were not different from those in age-matched controls which confirms the observations by Van Biervlietet al described above However plasma zinc concentrations de-creased in patients with moderate-to-severe growth retardation andwith severe pulmonary disease but very low zinc levels occur sporad-ically Erythrocyte zinc and copper levels were significantly higherthan normal while RBC selenium was lower than in age-matchedcontrols These trace element concentrations in erythrocytes werediscussed in relation to the activities of the CuZn-SOD and the Se-enzyme GPx This observation suggests a compensatory upregulationof the erythrocyte CuZn-SOD by the exposure of erythroid precursorsto ROS andor other CF-related stressors
Best et al [225] also studied RBC SOD activity using this as a bio-logical sensor of Cu status in CF patients A lowered activity of thisenzyme was reported in CF together with that of the other Cu-dependent enzyme plasma diamine oxidase while plasma ceruplas-min showed normal activity Degradation rates of copper proteinsare known to be accelerated in conditions of copper deficiencywhich could explain the finding at least in part Anyway when Cuand Zn were supplemented to CF patients either separate or incombination (6 weeks of 3 mg copperd as copper-glycinate and30 mg zincd as zinc-glycinate) any of the copper enzyme activitieswas affected Therefore the moderate copper deficiency of CF patientsappears to be refractory to the intervention by increased copper andor zinc intake
Erythrocyte CuZn-SOD and the plasma levels of Cu and Zn werealso measured in the study of Wood et al [6] in which Australian CFpatients (agegt5 years) were treated with a high-dose antioxidantmultivitamin formulation containing 200 mg vitamin E (as RRR-α-tocopherol) 300 mg vitamin C (as sodium ascorbate) 25 mg β-
carotene (all-trans isomer) 90 μg Se (as selenomethionine) and500 μg vitamin A (as retinyl palmitate) in oil Plasma oligoelementsand particularly Zn were in the normal range at baseline (as com-pared with the data reported in [229230]) and were not affected bythis multivitamin supplement The same was found for the activityof RBC SOD and for plasma 8-iso-PGF2α as surrogate biomarker oflipid peroxidation
In a recent non-randomized small population (n=21) casendashcon-trol study in CF children Zn supplementation was proven to producepositive clinical effects in Zn-deficient patients [196] The supplemen-tation with 5 mgkg Zn sulfateday (maximum 150 mg) significantlydecreased the number of infections and increased the forced expira-tory volume in 1 s energy intake and growth parameters also im-proved These parameters were unaffected in untreated patientsexcept that in the case of the pulmonary function that decreased sig-nificantly These clinical observations on Zn supplementation need tobe confirmed in prospective double-blind randomized control trial
37 Appropriateness and targeting of antioxidant therapies in CF
The choice of the appropriate antioxidant and dose to correct a cer-tain biomarker and its associated biochemical lesion is another impor-tant point that appears to have disregarded in many clinical studiesFor instance unlike vitamin E vitamin C supplementation does notalter F2-IsoPs levels in humans (reviewed in [74]) This appears tobe true also in the antioxidant therapy of CF in which vitamin C(300 mgday) was administered together with other antioxidantsthat included a dose of vitamin E of 200 mgday without any signifi-cant effect on the surrogate biomarker of lipid peroxidation F2-IsoPs[6] When carotenoids are used as supplements to prevent the damag-ing action of ROS in the CF airways it is noteworthy that these are notparticularly good quenchers of peroxyl radicals relative to phenolicsand other antioxidants but are exceptional in quenching singlet oxy-gen at which most other phenolics and antioxidants are relativelyineffective Singlet oxygen is not a radical and does not react via radi-cal mechanisms but reacts mostly by the addition to double bondsforming endoperoxides that can be reduced to alkoxyl radicals that ini-tiate radical chain reactions typical of the peroxidative damage of PUFA[38] In this case the analysis of F2-IsoPs lipid peroxide formation andtransition metal-induced oxidizability of lipoproteins [162180] are allappropriate to evaluate the effect of carotenoids in preventing lipidperoxidation
As far as the dose is concerned clinical pharmacology of vitamin Eas an antioxidant was recently investigated by means of the effect onF2-IsoPs production and doses of α-tocopherol of 1600 IUday orgreater were found to be required to statistically affect plasma F2-IsoPs levels in hypercholeterolemic subjects [176] Several vitamin Esupplementation studies in CF patients have been performed withdoses of lower than 300 IUday regardless of the lowered absorptionby pancreatic and liver defects and the regular supplementationwith these doses does not appear to correct lipid oxidation markersin CF [7]
In the clinical practice and planning trials it has to be taken intoconsideration that in spite of substantial evidence supporting ahigher antioxidant demand in CF interventions with several antioxi-dant formulations produce poor responsiveness particularly in thecase of fat-soluble antioxidants which are poorly absorbed [6162]
Since many oxidants and antioxidants are present in tissuesand biological fluids and these have different chemical and physicalcharacteristics the possibility to produce a successful therapy witha single antioxidant molecule is too far to be realistic Moreover an-tioxidants act by multiple mechanisms in a single system or by adifferent single mechanism depending on the reaction systemresponding in a different manner to different radical or oxidantsources Because multiple reaction characteristics and mechanismsas well as different phase localizations are usually involved no single
704 F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
therapeutic approach will effectively prevent damage by multipleROS sources The defect of physiological antioxidants may also interferewith antioxidant therapies that are based on one or few exogenousantioxidants
Moreover several antioxidant vitamins such as vitamin E and ca-rotenoids have multiple natural forms with different bioavailabilitymetabolism and bioactivity [157167231] As far as the case of vita-min E supplementation concerns α-tocopherol was used as uniquevitamer in the large majority of supplementation trials so far per-formed and is the form used in the nutritional management of CFpatients Moreover several supplements contain the synthetic (or ra-cemic) form of this vitamin that has lower bioavailability than thenatural form Other forms present in nature and abundantly con-tained in vegetables such as tocotrienols and the less methylatedforms of tocopherol are not represented in many of the supplementformulations so far available in clinical centers and the supplementa-tion with α-tocopherol also limits their bioavailability These formsshow markedly higher susceptibility to hepatic metabolism and bili-ary excretion with respect to α-tocopherol eg the most representedform in blood and solid tissues and if co-supplemented these areeasily displaced during liver uptake and excreted with bile bymeans of competition with the same α-tocopherol Notwithstandingthese minor forms have been proposed to play important physiolog-ical roles showing molecular characteristics transcriptional effectsand antioxidant activities that clearly differentiate them in subfam-ilies with distinct biological functions Some of these such as α-tocopherol eg the second vitamin E form as relative abundance inblood and its carboxyethyl-hydroxychroman metabolite [189] ap-pear to have health-related anti-inflammatory effects which are par-ticularly relevant in lung protection [232233] This has suggestedthat such a group of ldquonon-α-tocopherolrdquo forms may represent anoth-er family of vitamins within the family of vitamin E with an impor-tant but often missed contribution to the proposed health effects ofthis vitamin [163]
These aspects may thus limit the possibility to provide CF patientsof optimal levels of this vitamin in all its components even if they areregularly treated with a vitamin E supplement eg withα-tocopherol
Targeted antioxidant therapy with formulations with higher bio-availability and bioactivity has been anticipated in CF New antioxi-dant formulations have been proposed to overcome main limits ofantioxidant therapies so far proposed for these patients Water-miscible α-tocopheryl acetate containing polysorbate propylene gly-col or polyethylene glycol as emulsifiers form micellar structureswere suggested to providing greater bioavailability than the fat-soluble counterparts These were commercialized with the brandnames of E-viminreg Cremophorreg EL and Aquasolreg E but despitethe original positive expectation [234235] some studies failed to ob-serve a higher response in vitamin E levels when these were com-pared with fat-soluble formulations [236237]
In a pilot study by Papas et al [183] a micellar formulation of fat-soluble nutrients and antioxidants was found to improve plasmalevels of β-carotene γ-tocopherol and CoQ(10) reducing at thesame time some inflammatory markers in induced sputum eg mye-loperoxidase and to a lower extent PMN elastase and total cell countswhile lung function and sputum bacterial counts were unaffectedThe same group recently confirmed the possibility to increase the ab-sorption of fat-soluble micronutrients using formulations with higherbioavailability specifically designed for malabsorbing patients such asCF patients that include also vitamin K and commercialized with thebrand name of AquADEKsreg [162] Despite improved vitamin and mi-cronutrient levels in this non-randomized open-label study AquA-DEKsreg produced only modest improvements in weight percentileand pulmonary function Another recent pilot observation [182] hassuggested the beneficial effect of this formulation on antioxidant andoxidative stress parameters of this oral supplement that surely deservesmore clinical investigation by larger randomized controlled trials
Recent multivitaminic formulations have been designed to containalso the minor forms of vitamin E and specifically γ-tocopherol [238]the expected superiority of which with respect to formulations con-taining only α-tocopherol needs to be verified As discussed abovein the section dedicated to vitamin E further advancements in thetherapy of CF inflammation and oxidative stress could be based onsynthetic forms and natural metabolites of this vitamin that havebeen recently identified to possess higher antioxidant and also anti-inflammatory activity than α-tocopherol (reviewed in [163168])
Pre-clinical investigation of these and other fat-soluble agents iscurrently addressed to develop formulations and administration pro-tocols that may increase the therapeutic efficacy in the airways In theantioxidant therapy of lung dysfunction in CF local administrationprotocols may overcome the limits of oral and systemic administra-tion protocols increasing bioavailability and providing targetedapproach to inflammation and oxidative stress Aerosolization of vita-min E and other fat-soluble micronutrients is possible and may allowdirect administration in the airways to prevent toxicity of smokewhich is closely associated with inflammation and oxidative stress[164165] To our knowledge this as well as other strategies of localadministration such as instillation of solutions such as surfactant-like solutions enriched of vitamin E have not been previously inves-tigated in CF patients and other CF model systems
On the contrary inhalation is an administration route widelyadopted in the case of GSH and NAC therapy described above Inthis context Cys formulations alternative to NAC have been proposedfor use as antioxidant and anti-inflammatory agent for inhalationNacystelyn is a lysine adduct of NAC that thanks to a higher proton-ation equilibrium shows increased water solubility and thus betterbioavailability Nacystelyn has been described to influence IL-8 gener-ation and the inflammatory signaling of bronchial epithelial cells[239] and preliminary clinical evaluation has demonstrated the safetyof this drug [240] Further clinical trials aimed to assess the effect onlung symptomatology of CF patients are needed Direct administra-tion in the airways could also be adopted for micronutrient vitaminswith poor absorption and bioavailability due to GI defects
38 Clinical impact of antioxidant therapy in CF
Huge in vitro and pre-clinical evidence has provided the rationaleto support clinical investigation of antioxidant strategies in CF Theseshould aim to restore the oxidantndashantioxidant balance of CF airwaychallenged by chronic infection and inflammatory cell activation
Some observational trials have confirmed that antioxidants usedas either supplements to the diet or drugs for lung administrationby aerosolized formulations may help in relieving progressive lungdamage and other adverse clinical events of CF such as poor growthSo far few studies have examined with sufficient methodologicalrigor the clinical efficacy of antioxidant therapy in CF This was alsoconcluded in a previous review of the literature by Cantin et al [12]that was published in the beginning of 2006 and is confirmed alsoin a recent analysis of clinical trials on antioxidant therapy in CF pa-tients [213] that examined the literature until September 2010using as sources the databases of the Cochrane CF and Genetic Disor-ders Group CF Trials Register PubMed CINAHL and AMED Useful in-formation was retrieved from just four randomized controlled trialsand one quasi-randomized controlled trial on vitamin C vitamin Eβ-carotene and selenium used as supplements administered aloneor in combination Post-hoc data analysis that was possible only inthree studies on a total of 87 CF patients showed the absence ofany significant improvement in lung function that was selected as pri-mary outcome together with quality of life that improved in one trialSecondary outcomes concerning laboratory indices of oxidative stressand antioxidant status showed several improvements These includedan increase of RBC SeGPx by selenium supplementation done as
705F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
individual or combined supplementation and increased levels of allplasma antioxidants except vitamin C that were observed in all thetrials
The message from these studies to pediatricians and nutritionistswithin the clinical staff of CF centers is that in the absence of solid ev-idence regarding the clinical effectiveness of oral formulations of an-tioxidant supplements in CF (including PUFA) their use as a routineclinical practice should be considered with caution keeping clear inmind that this should represent just a complement of one of themost critical interventions in the life-long clinical management pro-gram of CF patients eg providing an adequate nutriture [140] Inthis context compensating energy and protein malnutrition has toremain the first goal of nutritional management programs Providinghigher intakes of antioxidant micronutrients with food naturally-enriched (or functionalized) of micronutrient antioxidants shouldbe preferred in order to have the higher combination of positive nu-tritional factors that are lost during refinement procedures and over-all industrial processing of dietary supplements
Measures of good practice in clinical management of micro-malnutrition in CF patients would include the support of specializedpersonnel and laboratories The centers should have the possibilityto ascertain with appropriate nutritional and laboratory tests whatthe level of deficiency is for the different micronutrients that each pa-tient may suffer from during a dietary program Monitoring dietaryintakes and blood levels of micronutrients is not sufficient to set apersonalized nutritional intervention with supplements or functionalfoods Sub-optimal intakes and the compliance to nutritional inter-ventions should be verified by means of selected biochemical andclinical criteria Unluckily the latter are still not well established forsome micronutrients such as the fat-soluble vitamins E (reviewed in[163173241]) and K [242243] and also for trace elements such asSe [244] For many of the antioxidants used as supplements inhumans we still do not know exactly several of the biological effectsthat these may provide when introduced in a healthy body and weknow less what these can do in disease These aspects hardly impacton the concept of optimal levels of intake that should be identified foreach micronutrient on an individual basis According with the aspectsdiscussed in the previous sections optimal levels of intake for antiox-idant micronutrients are different in CF patients and healthy subjectsand vary with age and several individual factors
Lung administration of antioxidants by means of aerosolized for-mulations so far used for GSH therapy (see above) is a promisingfield of clinical investigation in CF Toxicity issues are currently themain concern and the subject of clinical evaluation by several groups(described above)
Information on future directions of antioxidant therapy in CF canbe inferred by the analysis of pending or recently completed clinicaltrials that have been searched (December 2011) at ClinicalTrialsgovdatabase matching the terms ldquoantioxidant therapyrdquo or ldquoglutathionerdquowith ldquocystic fibrosisrdquo Fifteen trials were retrieved and those directlyrelated to antioxidant therapy (n=12) are presented in Table 1 andinclude efficacy and safety studies of inhaled drugs as GSH sodiumpyruvate NAC and NO and the dietary supplements AquADEKsregan antioxidant-rich multivitamin supplement epigallocatechin gal-late (EGCG)tocotrienol curcuminoids the amino acid glutaminesulforaphane in broccoli sprouts One trial is investigating the flavo-noid quercetin as CFTR modulator
39 Emerging antioxidant and anti-inflammatory approaches in CF
Mediterranean foods such as olive oil and red wine or severalplant extracts such as herbal tea or grape seed extracts contain aseries of natural compounds with important antioxidant and NOscavenging activity that have been widely investigated for the pre-vention of oxidative stress-related diseases [38245] These havebeen long investigated as template molecules to develop antioxidant
and anti-inflammatory drugs Between the multitudes of natural sub-stances most investigated ones include for instance tyrosol hydroxy-tyrosol gallic and caffeic acids belonging to the family of phenolswhile resveratrol of the stilbenes family epicatechin kaempferoland cianidin are examples of flavonoids examples of fat-soluble phe-nolics are those of the family of tocols (vitamin E) and carotenoids Allthese compounds show different metabolisms and signaling effects[246] Antioxidant and cell protection mechanisms are associatedwith different and sometimes concurrent processes as H-atom trans-fer and electron donation radical trapping and chelation of transitionmetals that can be easily investigated at the chemical level [247] Be-sides these direct antioxidant effects metabolic responses and signal-ing effects of natural compounds are also important to producesecond-generation responses that modify the level of antioxidantprotection and the potential for ROS detoxification in cells and bodyfluids These derive from the transcriptional regulation of antioxidantand pro-oxidant genes that coexist with the modulation of cytokinesecretion and inflammatory enzyme activities
Some of these natural plant-derived antioxidants may provide fur-ther pharmacological activities of possible relevance in CF This is thecase for instance of the plant flavonoids genistein apigenin kaemp-ferol quercetin and hesperidin [248ndash251] that fall in the pharmaco-logical category of ldquopotentiatorsrdquo [252] in that these activate at leastto a certain extent CTFR-mediated Cl currents in normal and CF airwayepithelium investigated either in vitro or in vivo in humans and ani-mal models Actually as prototypal flavonoid-derived potentiatorthe tyrosine kinase inhibitor genistein potentiates the gating of wild-type as well as ΔF508 CFTR and G551D CFTR [253] but at higherdoses it inhibits CFTR gating which make this an unlikely clinical can-didate Similar potentiation effects have been reported for the antiox-idant curcumin [250] that shows an additive effect with respect togenistein-induced potentiation Besides CFTR potentiation whichdoes not appear to have a direct influence on GSH and nutrient trans-port in the lung tissue all these natural substances have been usedalone or in combination with other agents as in vivo enhancers oflung antioxidant protection [246254255] In the case of quercetinthiol-reactive phenolic [256] bronchodilation and anti-inflammatoryeffects by a restoration of the Th1Th2 balance have been reportedin inflammatory syndromes of the lung [255257ndash259] but theseeffects have not been explored in CF Pyocyanin toxicity (see abovein the Section 2) could represent an issue for the use of quercetinand other catechols in infectious diseases of the lung [260]
Other natural antioxidants of potential interest in CF therapy in-clude terpenoids [261] such as terpinen-4-ol a major constituentof tea tree oil that is being investigated in the therapy of anti-biotic resistant organisms specifically against methicillin-resistantStaphylococcus aureus (MRSA) [262] a problem in CF [263] Otherthan being lipophilic antioxidants terpenes can prevent oxidativestress of the CF lung secondarily to the antibiotic effect thereby pro-moting a better control of immuno-inflammatory pathways and lungantioxidants
391 Targeting NF-κB with natural compounds resveratrol and plantextracts
Natural compounds were long known to be useful in designinganti-inflammatory drugs and some of these could find an applicationin the control of the transcription factor kappa-B (NF-κB) that maylead to develop advanced pharmacological tools to control inflamma-tion and to produce higher antioxidant protection to CF airwaysInhibitors targeting NF-κB including transcription factors decoymolecules (TFD) are potent down-regulators of gene expressionand release of IL-8 in CF cells infected with P aeruginosa [264265]
Resveratrol (354prime-trihydroxystilbene ldquoErdquo form) is one of the mostinvestigated natural antioxidant with proposed activity as NF-κBinhibitor This is a phytoalexin present in large quantity in red winepreferentially in the skin of grapes being its concentration
706 F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
50ndash100 μgmg of fresh skin and 13ndash3 mgl of red wine [266]Furthermore resveratrol is a constituent of lsquoDarakchasavarsquo (13ndash6 mgl) an ayurvedic medicine from India [267] The antioxidant activity ofresveratrol has been reported in several papers and occurs also in lungtissues suggesting that resveratrol has potential as a therapeuticagent in respiratory disease [268ndash270] Resveratrol can be consideredone of the most interesting molecules from the natural worldexhibiting strong antioxidant activity that at the same time is able toexert anti inflammatory activity through alteration of NF-κB functionsand efficient inhibition of pro-inflammatory genes [271272] As far asthe effects on CF model systems are concerned Cabrini et al [26]reported the effects of resveratrol on P aeruginosa infected CF IB3-1cells The results obtained demonstrate that resveratrol exhibits minoreffects of IB3-1 cell growth and important inhibitory effects on accumu-lation of IL-8 and GRO-α mRNA while minor effects on IL-6 gene ex-pression were observed These data support recently publishedobservations suggesting inhibitory effects of resveratrol in infection-mediated inflammatory processes [273] Interestingly resveratrol hasbeen reported as a potent inhibitor of NF-κB activity and a promisinganti-inflammatory agent [272274] also in combinationwith othermol-ecules [274275] However in vivo translation of this pre-clinical on res-veratrol is hard to be foreseen This natural compound displays poorbioavailability [276] and further characterization of resveratrol pharma-cokinetics is troublesome since it is hardly measurable in vivo [277]Furthermore the regulation of inflammatory responses by resveratrolhas been suggested to be far more complex than simple direct suppres-sion of NF-κB activity Actually some aspects of the immune responsecould be enhanced by this natural substance which may lead tohypothesize broad negative feedback events on immuno-inflammatorypathways [278] In any case and with these cautions in mind the pub-lished observations on cellular model systems support the concept thatresveratrol and resveratrol-containing formulations deserve further con-sideration to determine their possible therapeutic values in CF
Other inhibitors can be identified from systematic studies of naturalproducts and their ability to interfere with NF-κB activity [279ndash281]Recent studies have demonstrated that the whole extract of Aeglemarmelos (Rutaceae) has strong inhibitory effect on the P aeruginosa-dependent IL-8 induction in human CF-derived bronchial IB3-1 cellswithout affecting cell proliferation [280] Molecular analysis of compo-nents contained in A marmelos extracts revealed that three major com-pounds namely 56-dimethoxy-1-indanone 2-hydroxy-cinnamic acidand 5-methoxy psoralen (5-MOP) reproduce the inhibitory effect ob-servedwith thewhole extract [280] A further example has been recent-ly published using extracts from bergamot (Citrus bergamia Risso) Inthis study the extracts were characterized and the main detected con-stituents were assayed for their biological activity [281] The resultsobtained demonstrated that the extracts from bergamot epicarps con-tain components displaying an inhibitory activity on IL-8 Particularlythe most active molecules were bergapten and citropten These effectshave been confirmed by analyzing mRNA levels and protein release inthe CF cellularmodels IB3-1 and CuFi-1 inducedwith TNF-α or exposedto P aeruginosa
A parallel strategy linking NF-κB inhibition and down-regulationof NF-κB-dependent functions is described in recently publishedstudies based on a structured-based virtual screening (VS) of differ-ently substituted furocoumarins and analogues against NF-κB withthe objective of selecting molecules able to inhibit the binding ofthis transcription factor to DNA [282283] Novel compounds wereidentified with this strategy as potent inhibitors of NF-κB dependentbiological functions to be proposed for the control lung inflammationoccurring in patients affected by CF [282ndash284]
392 Scavengers and regulators of H2O2 and NO
3921 Lactoferrin and OSCNmacr The impaired DUOXLPO system of CFpatients could be the target of therapeutic strategies that may
produce concomitant antimicrobial and antioxidant effects This sys-tem described above in Section 22 represents an important compo-nent of innate immunity with a role in bactericidal defense andregulation of H2O2 metabolism of airways [32] CF patients have alsoreported to show lowered LF levels in the ASL [37] that togetherwith a CFTR-dependent defective efflux of SCNmacr and LPO [36] may cre-ate the environment for a sustained flux of H2O2 and for the genera-tion of highly reactive Fenton species [1138] An ideal therapeuticintervention should restore the LPO-dependent generation of bacteri-cidal OSCNmacr from DUOX-derived H2O2 and SCNmacr in the ASL to controlat the same time the microbial biofilm and the flux of H2O2 into theASL An approach close to this therapeutic mechanism was recentlyproposed for the drug Meveolreg This is a complex of LF and OSCNmacrwith proposed in vivo antimicrobial activity [285] to be evaluatedin clinical trials for the aerosol treatment of lung infections in CFpatients The role for this drug in the control of H2O2 levels of ASLremains to be investigated
3922 Organoselenium compounds Organoselenium compoundshave been proposed as therapeutic agents useful in the antioxidanttherapy of inflammatory conditions These include GPX mimetic mol-ecules such as Ebselenreg (2-phenyl-12-benzisoselenazol-3(2H)-one)or other and more recently developed molecules that are still inpre-clinical steps of evaluation [286] Selectively and specificity of ac-tion are main issues in the therapeutic mechanism of this candidateantioxidant drug that thanks to the electrophilic properties of Se[214] reacts with thiols to reduce H2O2 and other species MoreoverEbselenreg has been described to act as potent non-competitive inhib-itor of extracellular nucleoside diphosphokinase (NDPK) having neg-ligible effect on ecto-ATPase and adenyl kinase activities which areother players of the metabolism of extracellular nucleotides [287]This enzyme together with other nucleoside di- and triphosphatescontributes to regulate several components of the mucociliary clear-ance process (MCC) that protects the lung against infections via acti-vation of epithelial purinergic receptors The inhibition of NDPK bythis GPX-mimetic drug may also impact on the energy status of endo-thelial cells [287] This aspect could be further investigated as a cellu-lar protection mechanism in the pulmonary epithelium of CF patientsbeing the control of cell energy of fundamental importance to preventthe activation of death pathways [288]
Further therapeutic mechanisms for these Se-derived drugs mayderive from the marked activity as inducers of phase II enzymessuch as quinone reductase (QR) and glutathione-S-transferase (GST)[289] This induction response also observed with other electrophilsand redox-active molecules such as natural phenolic antioxidantscould produce higher cellular protection by the acquisition of anincreased capability to detoxify endobiotics generated during oxida-tive stress and inflammation [246]
3923 Melatonin and GSNO as NOx regulators Increased markers ofNO-derived biological damage are present in the CF lung suggestingthe abnormal reactivity of NOx in the inflamed lung of CF patients[52] However an impaired metabolism and biological function ofNO in CF airways (see Section 23) suggests a cautious approach tothe use of agents that may influence the levels and chemical behaviorof NO-derived species (NOx) with possible impact on the physiologi-cal roles of NO in vasodilatation innate immunity and H2O2 metabo-lism of the respiratory tract [290291] NO donors also appear toinfluence CFTR function of alveolar epithelium and gland serouscells [292293]
Main physiological role of the pineal gland hormone melatonin isthe synchronization of circadian rhythms including the sleepndashwakecycle but several other functions dealing with immunomodulatoryantioxidant and cellular protection effects have been identified[294] Melatonin receptor stimulation may also influence cyclic AMPsignaling and the regulation of CFTR ion channel [295296]
707F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
A recent randomized double-blind placebo-controlled study hasexamined the effects of short term melatonin administration (3 mgfor 3 weeks) on sleep and oxidative stress markers in CF [297]According with the expected pharmacological effect of this hormonalsubstance the treatment was successful in improving sleep indicesAt the same time nitrite levels determined in exhaled breath conden-sate (EBC) were reduced to suggest a better control of NOmetabolismof CF airways (discussed above in Section 23) but these effects how-ever were not associated with a significant correction of isoprostaneas lipid peroxidation marker measured in EBC Increasing dosages ofmelatonin could be investigated for the pharmacological treatmentof oxidative stress and immune dysfunction of CF patients due tothe absence of adverse effects of this hormonal substance in humans
The S-nitrosation reaction of thiols is another interesting aspect ofNO pharmacology [53] that may find an application in the therapy oflung complications of CF This has been the case for instance of theS-nitrosothiol GSNO that has been used safely in human trials[298299] This endogenous nitrosothiol with proposed regulatory ef-fect on the CFTR of lung epithelia [292293] is well tolerated in pa-tients with CF when administered by aerosolization and mayproduce better oxygenation [299] thereby suggesting that therapyaimed at restoring endogenous GSNO levels in the CF airway maymerit further clinical evaluation Since the administered GSNO de-composes as shown by the increased levels of expired NO in CF pa-tients under treatment with this nitrosothiol [299] furtherinvestigation should be addressed to ascertain whether GSNO thera-py may merely correspond to a GSH therapy
NO dependent effects on CFTR function should be considered toevaluate mechanism of action and specificity of antioxidant therapiesthat target NO metabolism and function in the CF airways
4 Conclusions and future perspectives
The presence of clinical and biochemical symptoms of inflammationand oxidative stress implies that CF patients have a higher demand ofantioxidant protection The combination of the dysfunctional CFTRwith a lowered intake and absorption of dietary antioxidants producesub-optimal levels of protection from both enzymatic and non-enzymatic defense systems The former could be associated with a de-fective glutathionemetabolism and lowered intake of sulfur-containingamino acids and oligoelements such as zinc and possibly seleniumwhile fat-soluble antioxidant vitamins such as vitamin E and caroten-oids and the water-soluble vitamin C are lowered than in healthy sub-jects due to malabsorption and possibly higher consumption
The increased antioxidant demand in CF patients should be evenhigher in the presence of complications of the lung pancreas andliver Lung comorbidity is particularly important in this contextbeing associated with recurrent infections which results in the alter-nation of inflammatory exacerbates and chronic inflammation Thesesustain the flux of ROS in the airways and promote the formation ofsecond-generation byproducts by the damage of biomolecules suchas PUFA and proteins which may diffuse also at the systemic level tofurther promote adverse biological responses and toxic reactions Pan-creatic insufficiency causes malnutrition and may lead to develop en-docrine and metabolic defects associated with diabetes of CF Theseevents can be further aggravated by the concomitance of liver dys-function and a poor nutritional status Malnutrition is strongly associ-ated with poor prognosis as assessed by pulmonary function andsurvival data [138ndash140] The more aggressive nutritional interven-tions seem to produce better clinical outcomes in these patients andthe possibility of achieving higher antioxidant protection in well-nourished patients by dietary factors could be a key aspect to explainsuch a clinical advantage The assumption that food-derived compo-nentsmay help to prevent the damaging effects of oxidative stress im-proving the antioxidant defenses deserves further investigation at theclinical level This together with the investigation of appropriate
laboratory biomarkers could provide critical information to establishintervention criteria for an early nutritional management of newly di-agnosed patients [5] It is expected that a timely secondary preventionstrategy could influence the progression of CF symptoms thusaffecting with a self-feeding mechanism the same extent of malnutri-tion and oxidative stress along the life of CF patients Since severalfactors contribute to impair the nutritional status of CF patients(such as pancreatic insufficiency chronic malabsorption recurrentsinopulmonary infections and progressive lung disease chronic in-flammation increased energy expenditure suboptimal intake multi-therapy) careful monitoring of the antioxidant status should berecommended According with international guidelines fat-solublevitamin supplementation is of utmost importance in daily practice to-gether with energy intake requirements and pancreatic enzyme-replacement therapy Among these vitamin E β-carotene and ω-3FA have observed to alleviate selected biochemical signs of oxidativestress as measured for instance with well established laboratory indi-ces of lipid peroxidation and in some studies these effects werepreliminarily associated with positive clinical outcomes Notwith-standing randomizedndashcontrolled clinical trials on antioxidant supple-ments (including ω-3 FA) so far carried out in CF have failed toconclusively demonstrate significant beneficial effects on respiratorysymptoms and on the consequent impact that these have on the qual-ity of life of these patients (reviewed in [202213]) whichmay provideno support for the use of these supplements in CF An absence of effi-cacy in prevention studies on antioxidant supplements has also beenobserved in other and possibly less severe oxidative stress-relatedconditions particularly in the secondary prevention of cardiovasculardisease and some forms of cancer by vitamin E and other antioxidantssuch as vitamin C selenium and β-carotene (reviewed in [163]) Dif-ferent biases however have been identified in randomize large clini-cal trials that may account for these disappointing findings Theseinclude patient selection criteria (early interventions and primaryprevention could have more chances of success than secondaryprevention) duration and doses of the treatment use of wrong anti-oxidant formulations and administration protocols absence of verifi-cations of the biological compliance to the treatment etc The samebiases apply for the few trials carried out in CF patients Thus the ap-propriateness and efficacy of nutritional interventions with naturalfood-derived or synthetic antioxidants should be verifiedwith respectto the biological pathways of oxidative stress and clinical variablesthat are identified as end-points Profiles of blood and tissue antioxi-dants as well as of reliable surrogate markers of oxidative stresshave to be selected and determined in highly specialized laboratorieswith a well-established experience on these analyses
Well-timed (early) interventions with appropriate antioxidantformulationsprotocols need to be proposed for the next generationof trials and the development of novel CF-tailored antioxidant andanti-inflammatory agents should be promoted
As a consequence of these considerations more clinical investiga-tion is awaited to identify future successful approaches to the antiox-idant therapy as a measure to further enhance quality of life and theoverall clinical outcome of CF patients
Acknowledgments
We are indebted with the Italian Cystic Fibrosis Research Founda-tion for the support that it provided with its grant program to the re-search activity of the authors of this paper This is a scientific initiativeof the ldquoWorking Group on Inflammation in Cystic Fibrosisrdquo (BragonziA Bravo E Cabrini G Conese M Cuzzocrea S Dechecchi MC De Ales-sandri A Evangelista V Galli F Gambari R Lambiase A Lucidi VManca A Melotti P Minicucci L Motta A Pietraforte D Pompella AQuattrucci S Rizzo R Romano M Sorio C Tesse R) of the Italian Soci-ety for Cystic Fibrosis A particular thank goes to the Prof GianniMastella for the critical revision of the manuscript and for the
708 F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
stimulating research environment that he has contributed to createwithin the Italian Cystic Fibrosis Research Foundation
References
[1] BP OSullivan SD Freedman Cystic fibrosis Lancet 373 (2009) 1891ndash1904[2] P Linsdell JW Hanrahan Glutathione permeability of CFTR Am J Physiol 275
(1998) C323ndashC326[3] L Gao KJ Kim JR Yankaskas HJ Forman Abnormal glutathione transport in
cystic fibrosis airway epithelia Am J Physiol 277 (1999) L113ndashL118[4] RK Rowntree A Harris The phenotypic consequences of CFTR mutations Ann
Hum Genet 67 (2003) 471ndash485[5] EI Back C Frindt D Nohr J Frank R Ziebach M Stern M Ranke HK Biesalski
Antioxidant deficiency in cystic fibrosis when is the right time to take actionAm J Clin Nutr 80 (2004) 374ndash384
[6] LG Wood DA Fitzgerald AK Lee ML Garg Improved antioxidant and fattyacid status of patients with cystic fibrosis after antioxidant supplementation islinked to improved lung function Am J Clin Nutr 77 (2003) 150ndash159
[7] L Iuliano R Monticolo G Straface S Zullo F Galli M Boaz S Quattrucci Asso-ciation of cholesterol oxidation and abnormalities in fatty acid metabolism incystic fibrosis Am J Clin Nutr 90 (2009) 477ndash484
[8] C Libetta V Sepe P Esposito F Galli A Dal Canton Oxidative stress and inflam-mation implications in uremia and hemodialysis Clin Biochem 44 (2011)1189ndash1198
[9] G Bartosz Reactive oxygen species destroyers or messengers Biochem Phar-macol 77 (2009) 1303ndash1315
[10] T Ntimbane B Comte G Mailhot Y Berthiaume V Poitout M Prentki RRabasa-Lhoret E Levy Cystic fibrosis-related diabetes from CFTR dysfunctionto oxidative stress Clin Biochem 30 (2009) 153ndash177
[11] A van der Vliet JP Eiserich GP Marelich B Halliwell CE Cross Oxidativestress in cystic fibrosis does it occur and does it matter Adv Pharmacol 38(1997) 491ndash513
[12] AM Cantin TB White CE Cross HJ Forman RJ Sokol D Borowitz Antioxi-dants in cystic fibrosis Conclusions from the CF antioxidant workshop Bethes-da Maryland Free Radic Biol Med 42 (2007) 15ndash31
[13] LT McGrath P Mallon L Dowey B Silke E McClean M McDonnell A DevineS Copeland S Elborn Oxidative stress during acute respiratory exacerbations incystic fibrosis Thorax 54 (1999) 518ndash523
[14] E Thomson S Brennan R Senthilmohan CL Gangell AL Chapman PD SlyAJ Kettle E Balding LJ Berry JB Carlin R Carzino N de Klerk T Douglas CFoo LW Garratt GL Hall J Harrison A Kicic IA Laing KM Logie J MassieLS Mott C Murray F Parsons N Pillarisetti SR Poreddy SC RanganathanCF Robertson R Robins-Browne PJ Robinson B Skoric SM Stick ENSutanto E Williamson Identifying peroxidases and their oxidants in the earlypathology of cystic fibrosis Free Radic Biol Med 49 (2010) 1354ndash1360
[15] SP Range C Dunster AJ Knox FJ Kelly Treatment of pulmonary exacerba-tions of cystic fibrosis leads to improved antioxidant status Eur Respir J 13(1999) 560ndash564
[16] L Coppo P Ghezzi Thiol regulation of pro-inflammatory cytokines and innateimmunity protein S-thiolation as a novel molecular mechanism Biochem SocTrans 39 (2011) 1268ndash1272
[17] C Verhaeghe C Remouchamps B Hennuy A Vanderplasschen A Chariot SPTabruyn C Oury V Bours Role of IKK and ERK pathways in intrinsic inflamma-tion of cystic fibrosis airways Biochem Pharmacol 73 (2007) 1982ndash1994
[18] TL Bonfield JR Panuska MW Konstan KA Hilliard JB Hilliard H Ghnaim MBerger Inflammatory cytokines in cystic fibrosis lungs Am J Respir Crit CareMed 152 (1995) 2111ndash2118
[19] TL Noah HR Black PW Cheng RE Wood MW Leigh Nasal and bronchoal-veolar lavage fluid cytokines in early cystic fibrosis J Infect Dis 175 (1997)638ndash647
[20] MJ Welsh BW Ramsey FJ Accurso GR Cutting Cystic Fibrosis McGraw-HillNew York 2001
[21] TZ Khan JS Wagener T Bost J Martinez FJ Accurso DW Riches Early pul-monary inflammation in infants with cystic fibrosis Am J Respir Crit CareMed 151 (1995) 1075ndash1082
[22] FA Ratjen Cystic fibrosis pathogenesis and future treatment strategies RespirCare 54 (2009) 595ndash605
[23] J Jacquot O Tabary P Le Rouzic A Clement Airway epithelial cell inflamma-tory signalling in cystic fibrosis Int J Biochem Cell Biol 40 (2008)1703ndash1715
[24] CM Greene P Branagan NG McElvaney Toll-like receptors as therapeutic tar-gets in cystic fibrosis Expert Opin Ther Targets 12 (2008) 1481ndash1495
[25] M Rottner JM Freyssinet MC Martinez Mechanisms of the noxious inflam-matory cycle in cystic fibrosis Respir Res 10 (2009) 23
[26] G Cabrini V Bezzerri I Mancini E Nicolis MC Dechecchi A Tamanini ILampronti L Piccagli N Bianchi M Borgatti R Gambari Targeting transcrip-tion factor activity as a strategy to inhibit pro-inflammatory genes involved incystic fibrosis decoy oligonucleotides and low-molecular weight compoundsCurr Med Chem 17 (2010) 4392ndash4404
[27] CM Greene NG McElvaney Proteases and antiproteases in chronic neutrophiliclungdiseasemdash relevance to drug discovery Br J Pharmacol 158 (2009) 1048ndash1058
[28] AM Cantin Potential for antioxidant therapy of cystic fibrosis Curr Opin PulmMed 10 (2004) 531ndash536
[29] JF Chmiel MW Konstan Inflammation and anti-inflammatory therapies forcystic fibrosis Clin Chest Med 28 (2007) 331ndash346
[30] DP Nichols MW Konstan JF Chmiel Anti-inflammatory therapies for cys-tic fibrosis-related lung disease Clin Rev Allergy Immunol 35 (2008)135ndash153
[31] AJ Kettle T Chan I Osberg R Senthilmohan AL Chapman TJ Mocatta JSWagener Myeloperoxidase and protein oxidation in the airways of youngchildren with cystic fibrosis Am J Respir Crit Care Med 170 (2004)1317ndash1323
[32] H Fischer Mechanisms and function of DUOX in epithelia of the lung AntioxidRedox Signal 11 (2009) 2453ndash2465
[33] B Rada TL Leto Oxidative innate immune defenses by NoxDuox familyNADPH oxidases Contrib Microbiol 15 (2008) 164ndash187
[34] P Moskwa D Lorentzen KJ Excoffon J Zabner PB McCray Jr WM NauseefC Dupuy B Banfi A novel host defense system of airways is defective in cysticfibrosis Am J Respir Crit Care Med 175 (2007) 174ndash183
[35] D Lorentzen L Durairaj AA Pezzulo Y Nakano J Launspach DA Stoltz GZamba PB McCray Jr J Zabner MJ Welsh WM Nauseef B Banfi Concentra-tion of the antibacterial precursor thiocyanate in cystic fibrosis airway secre-tions Free Radic Biol Med 50 (2011) 1144ndash1150
[36] Y Xu S Szep Z Lu The antioxidant role of thiocyanate in the pathogenesis ofcystic fibrosis and other inflammation-related diseases Proc Natl Acad Sci US A 106 (2009) 20515ndash20519
[37] MP Rogan CC Taggart CM Greene PG Murphy SJ ONeill NG McElvaneyLoss of microbicidal activity and increased formation of biofilm due to decreasedlactoferrin activity in patients with cystic fibrosis J Infect Dis 190 (2004)1245ndash1253
[38] B Halliwell JM Guttridge Free Radicals in Biology and Medicine Fourth editionOxford University Press New York 2007
[39] B Rada K Lekstrom S Damian C Dupuy TL Leto The Pseudomonastoxin pyocyanin inhibits the dual oxidase-based antimicrobial system as itimposes oxidative stress on airway epithelial cells J Immunol 181 (2008)4883ndash4893
[40] C Schwarzer B Illek JH Suh SJ Remington H Fischer TE Machen Organelleredox of CF and CFTR-corrected airway epithelia Free Radic Biol Med 43(2007) 300ndash316
[41] JH Roum R Buhl NG McElvaney Z Borok RG Crystal Systemic deficiency ofglutathione in cystic fibrosis J Appl Physiol 75 (1993) 2419ndash2424
[42] VM Hudson Rethinking cystic fibrosis pathology the critical role of abnormalreduced glutathione (GSH) transport caused by CFTR mutation Free RadicBiol Med 30 (2001) 1440ndash1461
[43] PJ Barnes RA Dweik AF Gelb PG Gibson SC George H Grasemann IDPavord F Ratjen PE Silkoff DR Taylor N Zamel Exhaled nitric oxide in pul-monary diseases a comprehensive review Chest 138 (2010) 682ndash692
[44] H Grasemann E Michler M Wallot F Ratjen Decreased concentration of ex-haled nitric oxide (NO) in patients with cystic fibrosis Pediatr Pulmonol 24(1997) 173ndash177
[45] H Grasemann F Ratjen Cystic fibrosis lung disease the role of nitric oxidePediatr Pulmonol 28 (1999) 442ndash448
[46] B Gaston F Ratjen JW Vaughan NR Malhotra RG Canady AH Snyder JFHunt S Gaertig JB Goldberg Nitrogen redox balance in the cystic fibrosis air-way effects of antipseudomonal therapy Am J Respir Crit Care Med 165(2002) 387ndash390
[47] H Grasemann I Ioannidis RP Tomkiewicz H de Groot BK Rubin F RatjenNitric oxide metabolites in cystic fibrosis lung disease Arch Dis Child 78(1998) 49ndash53
[48] H Grasemann R Schwiertz S Matthiesen K Racke F Ratjen Increased argi-nase activity in cystic fibrosis airways Am J Respir Crit Care Med 172(2005) 1523ndash1528
[49] H Grasemann S Al-Saleh JA Scott D Shehnaz A Mehl R Amin M Rafii PPencharz J Belik F Ratjen Asymmetric dimethylarginine contributes to airwaynitric oxide deficiency in patients with cystic fibrosis Am J Respir Crit CareMed 183 (2011) 1363ndash1368
[50] H Grasemann F Kurtz F Ratjen Inhaled L-arginine improves exhaled nitricoxide and pulmonary function in patients with cystic fibrosis Am J RespirCrit Care Med 174 (2006) 208ndash212
[51] H Grasemann F Ratjen Emerging therapies for cystic fibrosis lung disease Ex-pert Opin Emerg Drugs 15 (2010) 653ndash659
[52] BM Morrissey K Schilling JV Weil PE Silkoff DM Rodman Nitric oxide andprotein nitration in the cystic fibrosis airway Arch Biochem Biophys 406(2002) 33ndash39
[53] R Radi Nitric oxide oxidants and protein tyrosine nitration Proc Natl AcadSci U S A 101 (2004) 4003ndash4008
[54] J Chen M Kinter S Shank C Cotton TJ Kelley AG Ziady Dysfunction of Nrf-2in CF epithelia leads to excess intracellular H2O2 and inflammatory cytokineproduction PLoS One 3 (2008) e3367
[55] F Galli M Piroddi C Annetti C Aisa E Floridi A Floridi Oxidative stress andreactive oxygen species Contrib Nephrol 149 (2005) 240ndash260
[56] DT Wright LA Cohn H Li B Fischer CM Li KB Adler Interactions of oxygenradicals with airway epithelium Environ Health Perspect 102 (Suppl 10)(1994) 85ndash90
[57] I Rahman SR Yang SK Biswas Current concepts of redox signaling in thelungs Antioxid Redox Signal 8 (2006) 681ndash689
[58] Q Li JF Engelhardt Interleukin-1beta induction of NFκB is partially regulatedby H2O2-mediated activation of NFκB-inducing kinase J Biol Chem 281(2006) 1495ndash1505
709F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
[59] E Boncoeur VS Criq E Bonvin T Roque A Henrion-Caude DC Gruenert AClement J Jacquot O Tabary Oxidative stress induces extracellular signal-regulated kinase 12 mitogen-activated protein kinase in cystic fibrosis lung ep-ithelial cells potential mechanism for excessive IL-8 expression Int J BiochemCell Biol 40 (2008) 432ndash446
[60] B Fischer J Voynow Neutrophil elastase induces MUC5AC messenger RNA ex-pression by an oxidant-dependent mechanism Chest 117 (2000) 317Sndash320S
[61] B Rada P Gardina TG Myers TL Leto Reactive oxygen species mediate in-flammatory cytokine release and EGFR-dependent mucin secretion in airwayepithelial cells exposed to Pseudomonas pyocyanin Mucosal Immunol 4(2011) 158ndash171
[62] C Schwarzer H Fischer EJ Kim KJ Barber AD Mills MJ Kurth DC GruenertJH Suh TE Machen B Illek Oxidative stress caused by pyocyanin impairs CFTRClminus transport in human bronchial epithelial cells Free Radic Biol Med 45(2008) 1653ndash1662
[63] J Hull M South P Phelan K Grimwood Surfactant composition in infants andyoung children with cystic fibrosis Am J Respir Crit Care Med 156 (1997)161ndash165
[64] KC Meyer A Sharma R Brown M Weatherly FR Moya J Lewandoski JJZimmerman Function and composition of pulmonary surfactant andsurfactant-derived fatty acid profiles are altered in young adults with cystic fi-brosis Chest 118 (2000) 164ndash174
[65] MK Pulfer RC Murphy Formation of biologically active oxysterols during ozo-nolysis of cholesterol present in lung surfactant J Biol Chem 279 (2004)26331ndash26338
[66] V Starosta E Rietschel K Paul U Baumann M Griese Oxidative changes ofbronchoalveolar proteins in cystic fibrosis Chest 129 (2006) 431ndash437
[67] V Starosta M Griese Oxidative damage to surfactant protein D in pulmonarydiseases Free Radic Res 40 (2006) 419ndash425
[68] M Griese R Essl R Schmidt E Rietschel F Ratjen M Ballmann K Paul Pulmo-nary surfactant lung function and endobronchial inflammation in cystic fibro-sis Am J Respir Crit Care Med 170 (2004) 1000ndash1005
[69] M Griese R Essl R Schmidt M Ballmann K Paul E Rietschel F Ratjen Se-quential analysis of surfactant lung function and inflammation in cystic fibrosispatients Respir Res 6 (2005) 133
[70] LG Wood DA Fitzgerald PG Gibson DM Cooper ML Garg Increased plasmafatty acid concentrations after respiratory exacerbations are associated with el-evated oxidative stress in cystic fibrosis patients Am J Clin Nutr 75 (2002)668ndash675
[71] P Montuschi SA Kharitonov G Ciabattoni M Corradi L van Rensen DM Ged-des ME Hodson PJ Barnes Exhaled 8-isoprostane as a new non-invasive bio-marker of oxidative stress in cystic fibrosis Thorax 55 (2000) 205ndash209
[72] CE Collins P Quaggiotto L Wood EV OLoughlin RL Henry ML Garg Elevat-ed plasma levels of F2 alpha isoprostane in cystic fibrosis Lipids 34 (1999)551ndash556
[73] D Hartl V Starosta K Maier I Beck-Speier C Rebhan BF Becker P Latzin RFischer F Ratjen RM Huber E Rietschel S Krauss-Etschmann M Griese In-haled glutathione decreases PGE2 and increases lymphocytes in cystic fibrosislungs Free Radic Biol Med 39 (2005) 463ndash472
[74] GL Milne H Yin JD Morrow Human biochemistry of the isoprostane pathwayJ Biol Chem 283 (2008) 15533ndash15537
[75] G Ciabattoni G Davi M Collura L Iapichino F Pardo A Ganci R Romagnoli JMaclouf C Patrono In vivo lipid peroxidation and platelet activation in cystic fi-brosis Am J Respir Crit Care Med 162 (2000) 1195ndash1201
[76] C Garenc P Julien E Levy Oxysterols in biological systems the gastrointestinaltract liver vascular wall and central nervous system Free Radic Res 44 (2011)47ndash73
[77] AM Cantin SL North RC Hubbard RG Crystal Normal alveolar epithelial lin-ing fluid contains high levels of glutathione J Appl Physiol 63 (1987) 152ndash157
[78] R Tirouvanziam CK Conrad T Bottiglieri LA Herzenberg RB Moss High-dose oral N-acetylcysteine a glutathione prodrug modulates inflammation incystic fibrosis Proc Natl Acad Sci U S A 103 (2006) 4628ndash4633
[79] LW Velsor C Kariya R Kachadourian BJ Day Mitochondrial oxidative stressin the lungs of cystic fibrosis transmembrane conductance regulator proteinmutant mice Am J Respir Cell Mol Biol 35 (2006) 579ndash586
[80] M Kelly-Aubert S Trudel J Fritsch T Nguyen-Khoa M Baudouin-Legros SMoriceau L Jeanson F Djouadi C Matar M Conti M Ollero F Brouillard AEdelman GSH monoethyl ester rescues mitochondrial defects in cystic fibrosismodels Hum Mol Genet 20 (2011) 2745ndash2759
[81] P Ghezzi Role of glutathione in immunity and inflammation in the lung Int JGen Med 4 (2011) 105ndash113
[82] N Dauletbaev K Viel R Buhl TO Wagner J Bargon Glutathione and glutathi-one peroxidase in sputum samples of adult patients with cystic fibrosis J CystFibros 3 (2004) 119ndash124
[83] CE Cross A van der Vliet CA ONeill S Louie B Halliwell Oxidants antioxi-dants and respiratory tract lining fluids Environ Health Perspect 102 (Suppl10) (1994) 185ndash191
[84] K Takeyama K Dabbagh J Jeong Shim T Dao-Pick IF Ueki JA Nadel Oxida-tive stress causes mucin synthesis via transactivation of epidermal growth factorreceptor role of neutrophils J Immunol 164 (2000) 1546ndash1552
[85] N Ballatori SM Krance S Notenboom S Shi K Tieu CL Hammond Glutathi-one dysregulation and the etiology and progression of human diseases BiolChem 390 (2009) 191ndash214
[86] SR Soltaninassab KR Sekhar MJ Meredith ML Freeman Multi-faceted regu-lation of gamma-glutamylcysteine synthetase J Cell Physiol 182 (2000)163ndash170
[87] HR Lopez-Mirabal JR Winther Redox characteristics of the eukaryotic cytosolBiochim Biophys Acta 1783 (2008) 629ndash640
[88] C Hwang AJ Sinskey HF Lodish Oxidized redox state of glutathione in the en-doplasmic reticulum Science 257 (1992) 1496ndash1502
[89] M Murphy Mitochondrial thiols in antioxidant protection and redox signallingdistinct roles for glutathionylation and other thiol modifications AntioxidRedox Signal (2011) ahead of print doi101089ars20114289
[90] BJ Day AM van Heeckeren E Min LW Velsor Role for cystic fibrosis trans-membrane conductance regulator protein in a glutathione response to bronch-opulmonary Pseudomonas infection Infect Immun 72 (2004) 2045ndash2051
[91] Y Zhang K Duan Glutathione exhibits antibacterial activity and increases tetra-cycline efficacy against Pseudomonas aeruginosa Sci China C Life Sci 52 (2009)501ndash505
[92] VM Hudson New insights into the pathogenesis of cystic fibrosis pivotal roleof glutathione system dysfunction and implications for therapy Treat RespirMed 3 (2004) 353ndash363
[93] LW Velsor A van Heeckeren BJ Day Antioxidant imbalance in the lungs ofcystic fibrosis transmembrane conductance regulator protein mutant miceAm J Physiol Lung Cell Mol Physiol 281 (2001) L31ndashL38
[94] I Kogan M Ramjeesingh C Li JF Kidd Y Wang EM Leslie SP Cole CE BearCFTR directly mediates nucleotide-regulated glutathione flux EMBO J 22(2003) 1981ndash1989
[95] NS Gould S Gauthier CT Kariya E Min J Huang DJ Brian Hypertonic salineincreases lung epithelial lining fluid glutathione and thiocyanate two protectiveCFTR-dependent thiols against oxidative injury Respir Res 11 (2010) 119
[96] VT Vasu SJ de Cruz JS Houghton KA Hayakawa BM Morrissey CE CrossJP Eiserich Evaluation of thiol-based antioxidant therapeutics in cystic fibrosissputum focus on myeloperoxidase Free Radic Res 45 (2011) 165ndash176
[97] L Roussel G Martel J Berube S Rousseau P aeruginosa drives CXCL8 synthesisvia redundant toll-like receptors and NADPH oxidase in CFTRF508 airway epi-thelial cells J Cyst Fibros 10 (2011) 107ndash113
[98] GW Lau DJ Hassett H Ran F Kong The role of pyocyanin in Pseudomonas aer-uginosa infection Trends Mol Med 10 (2004) 599ndash606
[99] R Wilson DA Sykes D Watson A Rutman GW Taylor PJ Cole Measurementof Pseudomonas aeruginosa phenazine pigments in sputum and assessment oftheir contribution to sputum sol toxicity for respiratory epithelium InfectImmun 56 (1988) 2515ndash2517
[100] M Muller Pyocyanin induces oxidative stress in human endothelial cells andmodulates the glutathione redox cycle Free Radic Biol Med 33 (2002)1527ndash1533
[101] YQ OMalley KJ Reszka BE Britigan Direct oxidation of 2prime7prime-dichlorodihy-drofluorescein by pyocyanin and other redox-active compounds independentof reactive oxygen species production Free Radic Biol Med 36 (2004)90ndash100
[102] CC Caldwell Y Chen HS Goetzmann Y Hao MT Borchers DJ Hassett LRYoung D Mavrodi L Thomashow GW Lau Pseudomonas aeruginosa exotoxinpyocyanin causes cystic fibrosis airway pathogenesis Am J Pathol 175 (2009)2473ndash2488
[103] YQ OMalley KJ Reszka DR Spitz GM Denning BE Britigan Pseudomonasaeruginosa pyocyanin directly oxidizes glutathione and decreases its levels inairway epithelial cells Am J Physiol Lung Cell Mol Physiol 287 (2004)L94ndashL103
[104] M Muller Glutathione modulates the toxicity of but is not a biologically rele-vant reductant for the Pseudomonas aeruginosa redox toxin pyocyanin FreeRadic Biol Med 50 (2011) 971ndash977
[105] R Cheluvappa R Shimmon M Dawson SN Hilmer DG Le Couteur Reactionsof Pseudomonas aeruginosa pyocyanin with reduced glutathione Acta BiochimPol 55 (2008) 571ndash580
[106] JH Widdicombe Transgenic animals may help resolve a sticky situation in cys-tic fibrosis J Clin Invest 120 (2010) 3093ndash3096
[107] X Sun H Sui JT Fisher Z Yan X Liu HJ Cho NS Joo Y Zhang W Zhou Y YiJM Kinyon DC Lei-Butters MA Griffin P Naumann M Luo J Ascher KWang T Frana JJ Wine DK Meyerholz JF Engelhardt Disease phenotype ofa ferret CFTR-knockout model of cystic fibrosis J Clin Invest 120 (2010)3149ndash3160
[108] NS Joo HJ Cho M Khansaheb JJ Wine Hyposecretion of fluid from trachealsubmucosal glands of CFTR-deficient pigs J Clin Invest 120 (2010) 3161ndash3166
[109] A Bragonzi Murine models of acute and chronic lung infection with cystic fibro-sis pathogens IJMM 300 (2010) 584ndash593
[110] AM van Heeckeren MD Schluchter Murine models of chronic Pseudomonasaeruginosa lung infection Lab Anim 36 (2002) 291ndash312
[111] A Bragonzi D Worlitzsch GB Pier P Timpert M Ulrich M Hentzer JB Ander-sen M Givskov M Conese G Doring Nonmucoid Pseudomonas aeruginosa ex-presses alginate in the lungs of patients with cystic fibrosis and in a mousemodel J Infect Dis 192 (2005) 410ndash419
[112] GS CW Bedrossian DB Singer JJ Hansen HS Rosenberg The lung in cysticfibrosis A quantitative study including prevalence of pathologic findingsamong different age groups Hum Pathol 7 (1976) 195ndash204
[113] WD HA Cash B McCullough WG Johanson Jr JA Bass A rat model of chron-ic respiratory infection with Pseudomonas aeruginosa Am Rev Respir Dis 119(1979) 453ndash459
[114] EM JR Starke C Langston CJ Baker A mouse model of chronic pulmonary in-fection with Pseudomonas aeruginosa and Pseudomonas cepacia Pediatr Res 22(1987) 698ndash702
[115] TJ AM van Heeckeren RW Walenga MW Konstan PB Davis B ErokwuMA Haxhiu TW Ferkol Effect of Pseudomonas infection on weight loss lung
710 F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
mechanics and cytokines in mice Am J Respir Crit Care Med 161 (2000)271ndash279
[116] T Aw G Wierzbicka DP Jones Oral glutathione increases tissue glutathione invivo Chem Biol Interact 80 (1991) 89ndash97
[117] F Favilli P Marraccini T Iantomasi MT Vincenzini Effect of orally adminis-tered glutathione on glutathione levels in some organs of rats role of specifictransporters Br J Nutr 78 (1997) 293ndash300
[118] C Kariya H Leitner E Min C van Heeckeren A van Heeckeren BJ Day A rolefor CFTR in the elevation of glutathione levels in the lung by oral glutathione ad-ministration Am J Physiol Lung Cell Mol Physiol 292 (2007) L1590ndashL1597
[119] K Atkuri JJ Mantovani LA Herzenberg LA Herzenberg N-Acetylcysteinemdashasafe antidote for cysteineglutathione deficiency Curr Opin Pharmacol 7(2007) 355ndash359
[120] R De Lisle E Roach K Jansson Effects of laxative and N-acetylcysteine onmucus accumulation bacterial load transit and inflammation in the cystic fi-brosis mouse small intestine Am J Physiol Gastrointest Liver Physiol 293(2007) G577ndashG584
[121] A Luciani VR Villella S Esposito N Brunetti-Pierri D Medina C Settembre MGavina L Pulze I Giardino M Pettoello-Mantovani M DApolito S Guido EMasliah B Spencer S Quaratino V Raia A Ballabio L Maiuri Defective CFTRinduces aggresome formation and lung inflammation in cystic fibrosis throughROS-mediated autophagy inhibition Nat Cell Biol 12 863ndash875
[122] M Griese J Ramakers A Krasselt V Starosta S Van Koningsbruggen R FischerF Ratjen B Mullinger RM Huber K Maier E Rietschel G Scheuch Improve-ment of alveolar glutathione and lung function but not oxidative state in cysticfibrosis Am J Respir Crit Care Med 169 (2004) 822ndash828
[123] C Bishop VM Hudson SC Hilton C Wilde A pilot study of the effect of inhaledbuffered reduced glutathione on the clinical status of patients with cystic fibro-sis Chest 127 (2005) 308ndash317
[124] WWang C Oliva G Li A Holmgren CH Lillig KL Kirk Reversible silencing of CFTRchloride channels by glutathionylation J Gen Physiol 125 (2005) 127ndash141
[125] N Dauletbaev P Fischer B Aulbach J Gross W Kusche U Thyroff-FriesingerTO Wagner J Bargon A phase II study on safety and efficacy of high-dose N-acetylcysteine in patients with cystic fibrosis Eur J Med Res 14 (2009)352ndash358
[126] R Tirouvanziam Y Gernez CK Conrad RB Moss I Schrijver CE Dunn ZADavies LA Herzenberg Profound functional and signaling changes in viable in-flammatory neutrophils homing to cystic fibrosis airways Proc Natl Acad SciU S A 105 (2008) 4335ndash4339
[127] JH Roum Z Borok NG McElvaney GJ Grimes AD Bokser R Buhl RG Crys-tal Glutathione aerosol suppresses lung epithelial surface inflammatory cell-derived oxidants in cystic fibrosis J Appl Physiol 87 (1999) 438ndash443
[128] A Visca CT Bishop SC Hilton VM Hudson Improvement in clinical markersin CF patients using a reduced glutathione regimen an uncontrolled observa-tional study J Cyst Fibros 7 (2008) 433ndash436
[129] EF Nash A Stephenson F Ratjen E Tullis Nebulized and oral thiol derivativesfor pulmonary disease in cystic fibrosis Cochrane Database Syst Rev (2009)CD007168
[130] AC foundation Drug Development Pipeline 2011[131] S Hoshida T Kuzuya N Yamashita M Nishida S Kitahara M Hori T
Kamada M Tada Gamma-glutamylcysteine ethyl ester for myocardial protec-tion in dogs during ischemia and reperfusion J Am Coll Cardiol 24 (1994)1391ndash1397
[132] J Lok W Leung S Zhao S Pallast K van Leyen S Guo X Wang A Yalcin EHLo Gamma-glutamylcysteine ethyl ester protects cerebral endothelial cells dur-ing injury and decreases bloodndashbrain barrier permeability after experimentalbrain trauma J Neurochem 118 (2011) 248ndash255
[133] Z Borok R Buhl GJ Grimes AD Bokser RC Hubbard KJ Holroyd JH RoumDB Czerski AM Cantin RG Crystal Effect of glutathione aerosol on oxidantndashantioxidant imbalance in idiopathic pulmonary fibrosis Lancet 338 (1991)215ndash216
[134] KJ Holroyd R Buhl Z Borok JH Roum AD Bokser GJ Grimes D Czerski AMCantin RG Crystal Correction of glutathione deficiency in the lower respiratorytract of HIV seropositive individuals by glutathione aerosol treatment Thorax 48(1993) 985ndash989
[135] J Hull P Vervaart K Grimwood P Phelan Pulmonary oxidative stress responsein young children with cystic fibrosis Thorax 52 (1997) 557ndash560
[136] A Corti A Paolicchi M Franzini S Dominici AF Casini A Pompella The S-thiolating activity of membrane gamma-glutamyltransferase formation ofcysteinyl-glycine mixed disulfides with cellular proteins and in the cell microen-vironment Antioxid Redox Signal 7 (2005) 911ndash918
[137] A Corti M Franzini AF Casini A Paolicchi A Pompella Vitamin C supply tobronchial epithelial cells linked to glutathione availability in elfmdasha role for se-creted gamma-glutamyltransferase J Cyst Fibros 7 (2008) 174ndash178
[138] A Munck Nutritional considerations in patients with cystic fibrosis Expert RevRespir Med 4 (2010) 47ndash56
[139] JL Matel CE Milla Nutrition in cystic fibrosis Semin Respir Crit Care Med 30(2009) 579ndash586
[140] D Salvatore R Buzzetti E Baldo MP Forneris V Lucidi D Manunza IMarinelli B Messore AS Neri V Raia ML Furnari G Mastella An overviewof international literature from cystic fibrosis registries 2 Neonatal screeningand nutritiongrowth J Cyst Fibros 9 (2010) 75ndash83
[141] KF Joosten JM Hulst Malnutrition in pediatric hospital patients current is-sues Nutrition 27 (2011) 133ndash137
[142] S Fustik T Jacovska L Spirevska S Koceva Protein-energy malnutrition as thefirst manifestation of cystic fibrosis in infancy Pediatr Int 51 (2009) 678ndash683
[143] J Himmelfarb E McMonagle Albumin is the major plasma protein target of ox-idant stress in uremia Kidney Int 60 (2001) 358ndash363
[144] P Stenvinkel JJ Carrero J Axelsson B Lindholm O Heimburger Z MassyEmerging biomarkers for evaluating cardiovascular risk in the chronic kidneydisease patient how do new pieces fit into the uremic puzzle Clin J Am SocNephrol 3 (2008) 505ndash521
[145] M Roche P Rondeau NR Singh E Tarnus E Bourdon The antioxidant proper-ties of serum albumin FEBS Lett 582 (2008) 1783ndash1787
[146] D Giustarini A Milzani I Dalle-Donne R Rossi Red blood cells as a physiolog-ical source of glutathione for extracellular fluids Blood Cells Mol Dis 40 (2008)174ndash179
[147] A Meister ME Anderson Glutathione Annu Rev Biochem 52 (1983) 711ndash760[148] B Alvarez S Carballal L Turell R Radi Formation and reactions of sulfenic acid
in human serum albumin Methods Enzymol 473 (2010) 117ndash136[149] S Carballal B Alvarez L Turell H Botti BA Freeman R Radi Sulfenic acid in
human serum albumin Amino Acids 32 (2007) 543ndash551[150] LR Barclay AM Bailey D Kong The antioxidant activity of alpha-tocopherol-
bovine serum albumin complex in micellar and liposome autoxidations J BiolChem 260 (1985) 15809ndash15814
[151] T Ishii T Ichikawa K Minoda K Kusaka S Ito Y Suzuki M Akagawa K Mochi-zuki T Goda T Nakayama Human serum albumin as an antioxidant in the ox-idation of (minus)-epigallocatechin gallate participation of reversible covalentbinding for interaction and stabilization Biosci Biotechnol Biochem 75(2011) 100ndash106
[152] F Galli S Rovidati S Benedetti U Buoncristiani C Covarelli A Floridi F Canes-trari Overexpression of erythrocyte glutathione S-transferase in uremia and di-alysis Clin Chem 45 (1999) 1781ndash1788
[153] D Borowitz RD Baker V Stallings Consensus report on nutrition for pediat-ric patients with cystic fibrosis J Pediatr Gastroenterol Nutr 35 (2002)246ndash259
[154] LJ Filer Jr SW Wright MP Manning KE Mason Absorption of alpha-tocopherol and tocopherylesters by premature and full term infants and chil-dren in health and disease Pediatrics 8 (1951) 328ndash339
[155] L Lancellotti C DOrazio G Mastella G Mazzi U Lippi Deficiency of vitamins Eand A in cystic fibrosis is independent of pancreatic function and current en-zyme and vitamin supplementation Eur J Pediatr 155 (1996) 281ndash285
[156] MN Sathe AS Patel Update in pediatrics focus on fat-soluble vitamins NutrClin Pract 25 (2010) 340ndash346
[157] MG Traber The ABCs of vitamin E and beta-carotene absorption Am J ClinNutr 80 (2004) 3ndash4
[158] TF Dolan Jr Hemolytic anemia and edema as the initial signs in infants withcystic fibrosis Consider this diagnosis even in absence of pulmonary symptomsClin Pediatr 15 (1976) 597ndash600
[159] DR James M Alfaham MC Goodchild Increased susceptibility to peroxide-induced haemolysis with normal vitamin E concentrations in cystic fibrosisClin Chim Acta 204 (1991) 279ndash290
[160] SA Peters FJ Kelly Vitamin E supplementation in cystic fibrosis J Pediatr Gas-troenterol Nutr 22 (1996) 341ndash345
[161] A Maqbool VA Stallings Update on fat-soluble vitamins in cystic fibrosis CurrOpin Pulm Med 14 (2008) 574ndash581
[162] SD Sagel MK Sontag MM Anthony P Emmett KA Papas Effect of anantioxidant-rich multivitamin supplement in cystic fibrosis J Cyst Fibros 10(2011) 31ndash36
[163] F Galli A Azzi Present trends in vitamin E research Biofactors 36 (2010)33ndash42
[164] A Hamahata P Enkhbaatar ER Kraft M Lange SW Leonard MG Traber RACox FC Schmalstieg HK Hawkins EB Whorton EM Horvath C Szabo LDTraber DN Herndon DL Traber Gamma-tocopherol nebulization by a lipidaerosolization device improves pulmonary function in sheep with burn andsmoke inhalation injury Free Radic Biol Med 45 (2008) 425ndash433
[165] JP Anais N Razzouq M Carvalho C Fernandez A Astier M Paul A AstierH Fessi AM Lorino Development of alpha-tocopherol acetate nanoparti-cles influence of preparative processes Drug Dev Ind Pharm 35 (2009)216ndash223
[166] JM Zingg Molecular and cellular activities of vitamin E analogues Mini RevMed Chem 7 (2007) 543ndash558
[167] V Viola F Pilolli M Piroddi E Pierpaoli F Orlando M Provinciali M Betti FMazzini F Galli Why tocotrienols work better insights into the in vitro anti-cancer mechanism of vitamin E Genes Nutr 7 (2011) 29ndash41
[168] F Galli F Mazzini L Bamonti L Gille S Bohmdorfer M Piroddi T Netscher FJKelly T Rosenau Tocotrienamines and tocopheramines reactions with radicalsand metal ions Bioorg Med Chem 19 (2011) 6483ndash6491
[169] A Kuhad K Chopra Attenuation of diabetic nephropathy by tocotrienol in-volvement of NFκB signaling pathway Life Sci 84 (2009) 296ndash301
[170] Q Jiang X Yin MA Lill ML Danielson H Freiser J Huang Long-chain carbox-ychromanols metabolites of vitamin E are potent inhibitors of cyclooxygenasesProc Natl Acad Sci U S A 105 (2008) 20464ndash20469
[171] ER Miller III R Pastor-Barriuso D Dalal RA Riemersma LJ Appel E GuallarMeta-analysis high-dosage vitamin E supplementation may increase all-causemortality Ann Intern Med 142 (2005) 37ndash46
[172] JN Hathcock A Azzi J Blumberg T Bray A Dickinson B Frei I Jialal CSJohnston FJ Kelly K Kraemer L Packer S Parthasarathy H Sies MG TraberVitamins E and C are safe across a broad range of intakes Am J Clin Nutr 81(2005) 736ndash745
[173] R Brigelius-Flohe F Galli Vitamin E a vitamin still awaiting the detection of itsbiological function Mol Nutr Food Res 54 (2010) 583ndash587
711F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
[174] MG Traber B Frei JS Beckman Vitamin E revisited do new data validate ben-efits for chronic disease prevention Curr Opin Lipidol 19 (2008) 30ndash38
[175] F Galli Meeting report Vitamin E Satellite Symposium (VESS) associated to theAnnual Meeting of the SFRR-Europe Rome 26 August 2009 Free Radic Res 43(2009) 1256ndash1257
[176] LJ Roberts II JA Oates MF Linton S Fazio BP Meador MD Gross Y Shyr JDMorrow The relationship between dose of vitamin E and suppression of oxida-tive stress in humans Free Radic Biol Med 43 (2007) 1388ndash1393
[177] EFSA- EFSA Scientific Opinion of the Panel on Food Additives FlavouringsProcessing Aids and Materials in Contact with Food on a request from the Com-mission on mixed tocopherols tocotrienol tocopherol and tocotrienols assources for vitamin E in EFSA- EFSA (Ed) vol 640 The EFSA Journal2008 pp 1ndash34
[178] P Rust I Eichler S Renner I Elmadfa Long-term oral beta-carotene supple-mentation in patients with cystic fibrosis mdash effects on antioxidative status andpulmonary function Ann Nutr Metab 44 (2000) 30ndash37
[179] G Lepage J Champagne N Ronco A Lamarre I Osberg RJ Sokol CC Roy Sup-plementation with carotenoids corrects increased lipid peroxidation in childrenwith cystic fibrosis Am J Clin Nutr 64 (1996) 87ndash93
[180] BM Winklhofer-Roob H Puhl G Khoschsorur MA vant Hof H EsterbauerDH Shmerling Enhanced resistance to oxidation of low density lipoproteinsand decreased lipid peroxide formation during beta-carotene supplementationin cystic fibrosis Free Radic Biol Med 18 (1995) 849ndash859
[181] RC Graham-Maar JI Schall N Stettler BS Zemel VA Stallings Elevated vita-min A intake and serum retinol in preadolescent children with cystic fibrosisAm J Clin Nutr 84 (2006) 174ndash182
[182] I Sadowska-Woda M Rachel J Pazdan E Bieszczad-Bedrejczuk K PawliszakNutritional supplement attenuates selected oxidative stress markers in pediatricpatients with cystic fibrosis Nutr Res (New York NY) 31 (2011) 509ndash518
[183] KA Papas MK Sontag C Pardee RJ Sokol SD Sagel FJ Accurso JS WagenerA pilot study on the safety and efficacy of a novel antioxidant rich formulation inpatients with cystic fibrosis J Cyst Fibros 7 (2008) 60ndash67
[184] Y Saito A Fukuhara K Nishio M Hayakawa Y Ogawa H Sakamoto K Fujii YYoshida E Niki Characterization of cellular uptake and distribution of coen-zyme Q10 and vitamin E in PC12 cells J Nutr Biochem 20 (2009) 350ndash357
[185] AA Franke CM Morrison JL Bakke LJ Custer X Li RV Cooney CoenzymeQ10 in human blood native levels and determinants of oxidation during proces-sing and storage Free Radic Biol Med 48 (2010) 1610ndash1617
[186] HN Bhagavan RK Chopra Plasma coenzyme Q10 response to oral ingestion ofcoenzyme Q10 formulations Mitochondrion 7 (2007) S78ndashS88 (Suppl)
[187] HN Bhagavan RK Chopra Coenzyme Q10 absorption tissue uptake metabo-lism and pharmacokinetics Free Radic Res 40 (2006) 445ndash453
[188] F Galli R Lee C Dunster FJ Kelly Gas chromatography mass spectrometryanalysis of carboxyethyl-hydroxychroman metabolites of alpha- and gamma-tocopherol in human plasma Free Radic Biol Med 32 (2002) 333ndash340
[189] F Galli R Lee J Atkinson A Floridi FJ Kelly Gamma-tocopherol biokineticsand transformation in humans Free Radic Res 37 (2003) 1225ndash1233
[190] TA Laguna MK Sontag I Osberg JS Wagener FJ Accurso RJ Sokol De-creased total serum coenzyme-Q10 concentrations a longitudinal study in chil-dren with cystic fibrosis J Pediatr 153 (2008) 402ndash407
[191] T Frischer JK Myung G Maurer I Eichler Z Szepfalusi G Lubec Possible dys-regulation of chaperon and metabolic proteins in cystic fibrosis bronchial tissueProteomics 6 (2006) 3381ndash3388
[192] C Andersson MM Zaman AB Jones SD Freedman Alterations in immune re-sponse and PPARLXR regulation in cystic fibrosis macrophages J Cyst Fibros 7(2008) 68ndash78
[193] SD Freedman PG Blanco MM Zaman JC Shea M Ollero IK Hopper DAWeed A Gelrud MM Regan M Laposata JG Alvarez BP OSullivan Associa-tion of cystic fibrosis with abnormalities in fatty acid metabolism N Engl JMed 350 (2004) 560ndash569
[194] S Van Biervliet G Vanbillemont JP Van Biervliet D Declercq E Robberecht AChristophe Relation between fatty acid composition and clinical status or geno-type in cystic fibrosis patients Ann Nutr Metab 51 (2007) 541ndash549
[195] SD Freedman MH Katz EM Parker M Laposata MY Urman JG AlvarezA membrane lipid imbalance plays a role in the phenotypic expression ofcystic fibrosis in cftr(minusminus) mice Proc Natl Acad Sci U S A 96 (1999)13995ndash14000
[196] S Van Biervliet S Vande Velde JP Van Biervliet E Robberecht The effect ofzinc supplements in cystic fibrosis patients Ann Nutr Metab 52 (2008)152ndash156
[197] WR Henderson Jr SJ Astley MM McCready P Kushmerick S Casey JWBecker BW Ramsey Oral absorption of omega-3 fatty acids in patients withcystic fibrosis who have pancreatic insufficiency and in healthy control subjectsJ Pediatr 124 (1994) 400ndash408
[198] I Durieu E Vericel D Guichardant H Roth JP Steghens J Drai RN JosserandE Fontaine M Lagarde G Bellon Fatty acids platelets and oxidative markersfollowing intravenous n-3 fatty acids administration in cystic fibrosis an openpilot observational study J Cyst Fibros 6 (2007) 320ndash326
[199] LG Wood DA Fitzgerald ML Garg Hypothesis vitamin E complements poly-unsaturated fatty acids in essential fatty acid deficiency in cystic fibrosis J AmColl Nutr 22 (2003) 253ndash257
[200] JD Lloyd-Still SB Johnson RT Holman Essential fatty acid status in cystic fi-brosis and the effects of safflower oil supplementation Am J Clin Nutr 34(1981) 1ndash7
[201] A Maqbool JI Schall JF Garcia-Espana BS Zemel B Strandvik VAStallings Serum linoleic acid status as a clinical indicator of essential fatty
acid status in children with cystic fibrosis J Pediatr Gastroenterol Nutr 47(2008) 635ndash644
[202] C Oliver N Jahnke Omega-3 fatty acids for cystic fibrosis Cochrane DatabaseSyst Rev (2011) CD002201
[203] B Strandvik E Gronowitz F Enlund T Martinsson J Wahlstrom Essential fattyacid deficiency in relation to genotype in patients with cystic fibrosis J Pediatr139 (2001) 650ndash655
[204] P Rise S Volpi C Colombo RF Padoan C DOrazio S Ghezzi PMelotti V BennatoC Agostoni BM Assael C Galli Whole blood fatty acid analysis with micromethodin cystic fibrosis and pulmonary disease J Cyst Fibros 9 (2010) 228ndash233
[205] H Cao K Gerhold JR Mayers MM Wiest SM Watkins GS Hotamisligil Iden-tification of a lipokine a lipid hormone linking adipose tissue to systemic me-tabolism Cell 134 (2008) 933ndash944
[206] RR Malapaka SK Khoo J Zhang JH Choi XE Zhou Y Xu Y Gong J Li ELYong MJ Chalmers L Chang JH Resau PR Griffin YE Chen HE Xu Iden-tification and mechanism of a ten carbon fatty acid as a modulating ligand ofperoxisome proliferator activated receptors J Biol Chem 287 (2012)183ndash195
[207] T Hara A Hirasawa A Ichimura I Kimura G Tsujimoto Free fatty acid recep-tors FFAR1 and GPR120 as novel therapeutic targets for metabolic disorders JPharm Sci 100 (2011) 3594ndash3601
[208] R Gupta P Rathi S Bradoo Lipase mediated upgradation of dietary fats andoils Crit Rev Food Sci Nutr 43 (2003) 635ndash644
[209] BH Jennings CC Akoh Lipase-catalyzed modification of rice bran oil to incor-porate capric acid J Agric Food Chem 48 (2000) 4439ndash4443
[210] J Hoeks M Mensink MK Hesselink K Ekroos P Schrauwen Long- andMedium-Chain Fatty Acids Induce Insulin Resistance to a Similar Extent inHumans Despite Marked Differences in Muscle Fat Accumulation J Clin Endo-crinol Metab 97 (2012) 208ndash216
[211] PJ Congden G Bruce MM Rothburn PC Clarke JM Littlewood J KelleherMS Losowsky Vitamin status in treated patients with cystic fibrosis ArchDis Child 56 (1981) 708ndash714
[212] BM Winklhofer-Roob H Ellemunter M Fruhwirth SE Schlegel-Haueter GKhoschsorur MA vant Hof DH Shmerling Plasma vitamin C concentrationsin patients with cystic fibrosis evidence of associations with lung inflammationAm J Clin Nutr 65 (1997) 1858ndash1866
[213] L Shamseer D Adams N Brown JA Johnson S Vohra Antioxidant micronutri-ents for lung disease in cystic fibrosis Cochrane Database Syst Rev (2010)CD007020
[214] C Santi S Santoro Electrophilic Selenium First edition Wiley-VCH VerlagGmbH amp Co KGaA 2012
[215] L Flohe S Toppo G Cozza F Ursini A comparison of thiol peroxidase mecha-nisms Antioxid Redox Signal 15 (2010) 763ndash780
[216] L Flohe JR Andreesen R Brigelius-Flohe M Maiorino F Ursini Selenium theelement of the moon in life on earth IUBMB Life 49 (2000) 411ndash420
[217] V Valdiglesias E Pasaro J Mendez B Laffon In vitro evaluation of seleniumgenotoxic cytotoxic and protective effects a review Arch Toxicol 84(2010) 337ndash351
[218] P Foucaud P Therond M Marchand F Brion JF Demelier J Navarro Seleniumand vitamin E in mucoviscidosis Arch Fr Pediatr 45 (1988) 383ndash386
[219] J Neve R Van Geffel M Hanocq L Molle Plasma and erythrocyte zinc copperand selenium in cystic fibrosis Acta Paediatr Scand 72 (1983) 437ndash440
[220] BM Winklhofer-Roob B Tiran PE Tuchschmid MA vant Hof DH ShmerlingEffects of pancreatic enzyme preparations on erythrocyte glutathione peroxi-dase activities and plasma selenium concentrations in cystic fibrosis FreeRadic Biol Med 25 (1998) 242ndash249
[221] JD Lloyd-Still HE Ganther Selenium and glutathione peroxidase levels in cys-tic fibrosis Pediatrics 65 (1980) 1010ndash1012
[222] D Tsavachidou TJ McDonnell S Wen X Wang F Vakar-Lopez LL Pisters CAPettaway CG Wood KA Do PF Thall C Stephens E Efstathiou R Taylor DGMenter P Troncoso SM Lippman CJ Logothetis J Kim Selenium and vitaminE cell type- and intervention-specific tissue effects in prostate cancer J NatlCancer Inst 101 (2009) 306ndash320
[223] IN Zelko TJ Mariani RJ Folz Superoxide dismutase multigene family acomparison of the CuZn-SOD (SOD1) Mn-SOD (SOD2) and EC-SOD (SOD3)gene structures evolution and expression Free Radic Biol Med 33 (2002)337ndash349
[224] RP Bowler JD Crapo Oxidative stress in airways is there a role for extracellu-lar superoxide dismutase Am J Respir Crit Care Med 166 (2002) S38ndashS43
[225] K Best K McCoy S Gemma RA Disilvestro Copper enzyme activities in cysticfibrosis before and after copper supplementation plus or minus zinc Metabo-lism 53 (2004) 37ndash41
[226] SS Percival GP Kauwell E Bowser M Wagner Altered copper status in adultmen with cystic fibrosis J Am Coll Nutr 18 (1999) 614ndash619
[227] NF Krebs JE Westcott TD Arnold BM Kluger FJ Accurso LV Miller KMHambidge Abnormalities in zinc homeostasis in young infants with cystic fibro-sis Pediatr Res 48 (2000) 256ndash261
[228] D Easley N Krebs M Jefferson L Miller J Erskine F Accurso KM HambidgeEffect of pancreatic enzymes on zinc absorption in cystic fibrosis J Pediatr Gas-troenterol Nutr 26 (1998) 136ndash139
[229] S Van Biervliet JP Van Biervliet E Robberecht Serum zinc in patients with cys-tic fibrosis at diagnosis and after one year of therapy Biol Trace Elem Res 112(2006) 205ndash211
[230] S Van Biervliet JP Van Biervliet S Vande Velde E Robberecht Serum zinc con-centrations in cystic fibrosis patients aged above 4 years a cross-sectional eval-uation Biol Trace Elem Res 119 (2007) 19ndash26
712 F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
[231] F Galli M Cristina Polidori W Stahl P Mecocci FJ Kelly Vitamin E biotransfor-mation in humans Vitam Horm 76 (2007) 263ndash280
[232] J Wiser NE Alexis Q Jiang W Wu C Robinette R Roubey DB Peden In vivogamma-tocopherol supplementation decreases systemic oxidative stress andcytokine responses of human monocytes in normal and asthmatic subjectsFree Radic Biol Med 45 (2008) 40ndash49
[233] JG Wagner Q Jiang JR Harkema B Illek DD Patel BN Ames DB PedenOzone enhancement of lower airway allergic inflammation is prevented bygamma-tocopherol Free Radic Biol Med 43 (2007) 1176ndash1188
[234] JT Harries DP Muller Absorption of different doses of fat soluble and watermiscible preparations of vitamin E in children with cystic fibrosis Arch DisChild 46 (1971) 341ndash344
[235] EI Back C Frindt E Ocenaskova D Nohr M Stern HK Biesalski Can changesin hydrophobicity increase the bioavailability of alpha-tocopherol Eur J Nutr45 (2006) 1ndash6
[236] SZ Nasr MH OLeary C Hillermeier Correction of vitamin E deficiency withfat-soluble versus water-miscible preparations of vitamin E in patients with cys-tic fibrosis J Pediatr 122 (1993) 810ndash812
[237] S Soltani-Frisk E Gronowitz H Andersson B Strandvik Water-miscibletocopherol is not superior to fat-soluble preparation for vitamin E absorptionin cystic fibrosis Acta Paediatr 90 (2001) 1112ndash1115
[238] K Papas J Kalbfleisch R Mohon Bioavailability of a novel water-soluble vi-tamin E formulation in malabsorbing patients Dig Dis Sci 52 (2007)347ndash352
[239] F Antonicelli M Parmentier EM Drost N Hirani I Rahman K Donaldson WMacNee Nacystelyn inhibits oxidant-mediated interleukin-8 expression andNF-kappaB nuclear binding in alveolar epithelial cells Free Radic Biol Med 32(2002) 492ndash502
[240] EM App D Baran I Dab A Malfroot M Coffiner F Vanderbist M King Dose-finding and 24-h monitoring for efficacy and safety of aerosolized Nacystelyn incystic fibrosis Eur Respir J 19 (2002) 294ndash302
[241] MG Traber How much vitamin E hellip Just enough Am J Clin Nutr 84 (2006)959ndash960
[242] JC McCann BN Ames Vitamin K an example of triage theory is micronu-trient inadequacy linked to diseases of aging Am J Clin Nutr 90 (2009)889ndash907
[243] M Fusaro G Crepaldi S Maggi F Galli A DAngelo L Calo S Giannini DMiozzo M Gallieni Vitamin K bone fractures and vascular calcifications inchronic kidney disease an important but poorly studied relationship J Endocri-nol Invest 34 (2010) 317ndash323
[244] JC McCann BN Ames Adaptive dysfunction of selenoproteins from the per-spective of the triage theory why modest selenium deficiency may increaserisk of diseases of aging FASEB J 25 (2011) 1793ndash1814
[245] R Apak K Guclu M Ozyurek B Bektas Oglu M Bener Cupric ion reducing an-tioxidant capacity assay for food antioxidants vitamins polyphenolics and fla-vonoids in food extracts Methods Mol Biol 477 (2008) 163ndash193
[246] F Galli Interactions of polyphenolic compounds with drug disposition and me-tabolism Curr Drug Metab 8 (2007) 830ndash838
[247] RL Prior X Wu K Schaich Standardized methods for the determination of an-tioxidant capacity and phenolics in foods and dietary supplements J Agric FoodChem 53 (2005) 4290ndash4302
[248] C Azbell S Zhang D Skinner J Fortenberry EJ Sorscher BA WoodworthHesperidin stimulates cystic fibrosis transmembrane conductance regulator-mediated chloride secretion and ciliary beat frequency in sinonasal epitheliumOtolaryngol Head Neck Surg 143 (2010) 397ndash404
[249] G Wegrzyn J Jakobkiewicz-Banecka M Gabig-Ciminska E Piotrowska M Nar-ajczyk A Kloska M Malinowska D Dziedzic I Golebiewska M Moskot AWegrzyn Genistein a natural isoflavone with a potential for treatment of ge-netic diseases Biochem Soc Trans 38 (2010) 695ndash701
[250] YC Yu H Miki Y Nakamura A Hanyuda Y Matsuzaki Y Abe M Yasui K Ta-naka TC Hwang SG Bompadre Y Sohma Curcumin and genistein additivelypotentiate G551D-CFTR J Cyst Fibros 10 (2011) 243ndash252
[251] B Illek H Fischer Flavonoids stimulate Cl conductance of human airway epithe-lium in vitro and in vivo Am J Physiol 275 (1998) L902ndashL910
[252] JL Kreindler Cystic fibrosis exploiting its genetic basis in the hunt for newtherapies Pharmacol Ther 125 (2010) 219ndash229
[253] B Illek L Zhang NC Lewis RB Moss JY Dong H Fischer Defective function ofthe cystic fibrosis-causing missense mutation G551D is recovered by genisteinAm J Physiol 277 (1999) C833ndashC839
[254] P Anandakumar S Kamaraj S Jagan G Ramakrishnan R Vinodhkumar TDevaki Capsaicin modulates pulmonary antioxidant defense system during ben-zo(a)pyrene-induced lung cancer in Swiss albinomice Phytother Res 22 (2008)529ndash533
[255] I Rahman Antioxidant therapeutic advances in COPD Ther Adv Respir Dis 2(2008) 351ndash374
[256] AW Boots H Li RP Schins R Duffin JW Heemskerk A Bast GR Haenen Thequercetin paradox Toxicol Appl Pharmacol 222 (2007) 89ndash96
[257] M Joskova S Franova V Sadlonova Acute bronchodilator effect of quercetin inexperimental allergic asthma Bratisl Lek Listy 112 (2011) 9ndash12
[258] HJ Park CM Lee ID Jung JS Lee YI Jeong JH Chang SH Chun MJ Kim IWChoi SC Ahn YK Shin SR Yeom YM Park Quercetin regulates Th1Th2 balancein a murine model of asthma Int Immunopharmacol 9 (2009) 261ndash267
[259] AP Rogerio A Kanashiro C Fontanari EV da Silva YM Lucisano-ValimEG Soares LH Faccioli Anti-inflammatory activity of quercetin and iso-quercitrin in experimental murine allergic asthma Inflamm Res 56 (2007)402ndash408
[260] M Muller Polyphenol cytotoxicity induced by the bacterial toxin pyocyaninrole of NQO1 Free Radic Biol Med 47 (2009) 84ndash91
[261] J Grassmann Terpenoids as plant antioxidants Vitam Horm 72 (2005)505ndash535
[262] P Allen Tea tree oil the science behind the antimicrobial hype Lancet 358(2001) 1245
[263] EC Dasenbrook W Checkley CA Merlo MW Konstan N Lechtzin MP BoyleAssociation between respiratory tract methicillin-resistant Staphylococcus aure-us and survival in cystic fibrosis JAMA 303 (2010) 2386ndash2392
[264] V Bezzerri M Borgatti E Nicolis I Lampronti MC Dechecchi I Mancini PRizzotti R Gambari G Cabrini Transcription factor oligodeoxynucleotides toNF-kappaB inhibit transcription of IL-8 in bronchial cells Am J Respir CellMol Biol 39 (2008) 86ndash96
[265] R Gambari M Borgatti V Bezzerri E Nicolis I Lampronti MC Dechecchi IMancini A Tamanini G Cabrini Decoy oligodeoxyribonucleotides and peptidenucleic acids-DNA chimeras targeting nuclear factor kappa-B inhibition of IL-8 gene expression in cystic fibrosis cells infected with Pseudomonas aeruginosaBiochem Pharmacol 80 (2010) 1887ndash1894
[266] M Adrian P Jeandet AC Douillet-Breuil L Tesson R Bessis Stilbene content ofmature Vitis vinifera berries in response to UV-C elicitation J Agric Food Chem48 (2000) 6103ndash6105
[267] B Paul I Masih J Deopujari C Charpentier Occurrence of resveratrol and pter-ostilbene in age-old darakchasava an ayurvedic medicine from India J Ethno-pharmacol 68 (1999) 71ndash76
[268] I Rahman Antioxidant therapies in COPD Int J Chron Obstruct Pulmon Dis 1(2006) 15ndash29
[269] M Lee S Kim OK Kwon SR Oh HK Lee K Ahn Anti-inflammatory and anti-asthmatic effects of resveratrol a polyphenolic stilbene in a mouse model ofallergic asthma Int Immunopharmacol 9 (2009) 418ndash424
[270] LG Wood PA Wark ML Garg Antioxidant and anti-inflammatory effectsof resveratrol in airway disease Antioxid Redox Signal 13 (2010)1535ndash1548
[271] KV Kiselev Perspectives for production and application of resveratrol ApplMicrobiol Biotechnol 90 (2011) 417ndash425
[272] M Shakibaei C Buhrmann A Mobasheri Resveratrol-mediated SIRT-1 interac-tions with p300 modulate receptor activator of NF-kappaB ligand (RANKL) acti-vation of NF-kappaB signaling and inhibit osteoclastogenesis in bone-derivedcells J Biol Chem 286 (2011) 11492ndash11505
[273] SF Zaidi K Ahmed T Yamamoto T Kondo K Usmanghani M Kadowaki TSugiyama Effect of resveratrol on Helicobacter pylori-induced interleukin-8 secre-tion reactive oxygen species generation and morphological changes in human gas-tric epithelial cells Biol Pharm Bull 32 (2009) 1931ndash1935
[274] JK Kundu YK Shin YJ Surh Resveratrol modulates phorbol ester-inducedpro-inflammatory signal transduction pathways in mouse skin in vivo NF-kappaB and AP-1 as prime targets Biochem Pharmacol 72 (2006)1506ndash1515
[275] NH Nam Naturally occurring NF-kappaB inhibitors Mini Rev Med Chem 6(2006) 945ndash951
[276] JM Smoliga JA Baur HA Hausenblas Resveratrol and healthmdasha comprehen-sive review of human clinical trials Mol Nutr Food Res 55 (2011) 1129ndash1141
[277] ME Juan M Maijo JM Planas Quantification of trans-resveratrol and itsmetabolites in rat plasma and tissues by HPLC J Pharm Biomed Anal 51(2010) 391ndash398
[278] JA Baur DA Sinclair Therapeutic potential of resveratrol the in vivo evidenceNat Rev 5 (2006) 493ndash506
[279] E Nicolis I Lampronti MC Dechecchi M Borgatti A Tamanini N Bianchi VBezzerri I Mancini MG Giri P Rizzotti R Gambari G Cabrini Pyrogallol anactive compound from the medicinal plant Emblica officinalis regulates expres-sion of pro-inflammatory genes in bronchial epithelial cells Int Immunophar-macol 8 (2008) 1672ndash1680
[280] E Nicolis I Lampronti MC Dechecchi M Borgatti A Tamanini V Bezzerri NBianchi M Mazzon I Mancini MG Giri P Rizzotti R Gambari G CabriniModulation of expression of IL-8 gene in bronchial epithelial cells by 5-methoxypsoralen Int Immunopharmacol 9 (2009) 1411ndash1422
[281] M Borgatti I Mancini N Bianchi A Guerrini I Lampronti D Rossi G SacchettiR Gambari Bergamot (Citrus bergamia Risso) fruit extracts and identified com-ponents alter expression of interleukin 8 gene in cystic fibrosis bronchial epithe-lial cell lines BMC Biochem 12 (2011) 15
[282] L Piccagli E Fabbri M Borgatti N Bianchi V Bezzerri I Mancini E Nicolis CMDechecchi I Lampronti G Cabrini R Gambari Virtual screening against p50NF-kappaB transcription factor for the identification of inhibitors of the NF-kappaB-DNA interaction and expression of NF-kappaB upregulated genesChemMedChem 4 (2009) 2024ndash2033
[283] L Piccagli M Borgatti E Nicolis N Bianchi I Mancini I Lampronti D VevaldiF DallAcqua G Cabrini R Gambari Virtual screening against nuclear factorkappaB (NF-kappaB) of a focus library identification of bioactive furocoumarinderivatives inhibiting NF-kappaB dependent biological functions involved incystic fibrosis Bioorg Med Chem 18 (2010) 8341ndash8349
[284] M Borgatti A Chilin L Piccagli I Lampronti N Bianchi I Mancini G Mar-zaro Da Francesco A Guiotto R Gambari Development of a novel furocou-marin derivative inhibiting NF-kappaB dependent biological functionsdesign synthesis and biological effects Eur J Med Chem 46 (2011)4870ndash4877
[285] E Georgy S Le Guellec L Vecellio E Fichant P Stordeur P Bordeau JP PerraudinFeasibility study of OSCN- and lactoferrin (Meveol) nebulization for cysticfibrosis JCyst Fibros 10 (2011) S18
713F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
[286] C Tidei M Piroddi F Galli C Santi Oxidation of thiols promoted by PhSeZnClTetrahedron Lett 53 (2012) 232ndash234
[287] L Semianrio-Vidal C van Hesuden G Mugesh ER Lazarowski Ebselen is a po-tent non-competitive inhibitor of extracellular nucleoside diphosphokinasePurinergic Signal 6 (2010) 383ndash391
[288] C ColussiMC Albertini S Coppola S Rovidati F Galli L Ghibelli H2O2-inducedblockof glycolysis as an active ADP-ribosylation reaction protecting cells from apoptosisFASEB J 14 (2000) 2266ndash2276
[289] H Xiao KL Parkin Induction of phase II enzyme activity by various seleniumcompounds Nutr Cancer 55 (2006) 210ndash223
[290] G Peluffo R Radi Biochemistry of protein tyrosine nitration in cardiovascularpathology Cardiovasc Res 75 (2007) 291ndash302
[291] B Alvarez R Radi Peroxynitrite reactivity with amino acids and proteinsAmino Acids 25 (2003) 295ndash311
[292] B Kamosinska MW Radomski M Duszyk A Radomski SF Man Nitric oxideactivates chloride currents in human lung epithelial cells Am J Physiol 272(1997) L1098ndashL1104
[293] L Chen RP Patel X Teng CA Bosworth JR Lancaster Jr S Matalon Mecha-nisms of cystic fibrosis transmembrane conductance regulator activation by S-nitrosoglutathione J Biol Chem 281 (2006) 9190ndash9199
[294] F Luchetti B CanonicoM BettiM Arcangeletti F PilolliM Piroddi L Canesi S PapaF Galli Melatonin signaling and cell protection function FASEB J 24 (2010)3603ndash3624
[295] MW Bengtsson G Jedstedt G Flemstrom Duodenal bicarbonate secretion inrats stimulation by intra-arterial and luminal guanylin and uroguanylin ActaPhysiol (Oxf) 191 (2007) 309ndash317
[296] CS Nelson JL Marino CN Allen Melatonin receptor potentiation of cyclic AMP andthe cystic fibrosis transmembrane conductance regulator ion channel J Pineal Res 26(1999) 113ndash121
[297] C de Castro-Silva VM de Bruin GM Cunha DM Nunes CAMedeiros PF de BruinMelatonin improves sleep and reduces nitrite in the exhaled breath condensate incystic fibrosismdasha randomized double-blind placebo-controlled study J Pineal Res48 (2010) 65ndash71
[298] I Hornyak E Pankotai L Kiss Z Lacza Current developments in the the-rapeutic potential of S-nitrosoglutathione an endogenous NO-donor mole-cule Curr Pharm Biotechnol (2011) Jan 11 [Epub ahead of print] - PMID21235457
[299] AH Snyder ME McPherson JF Hunt M Johnson JS Stamler B Gaston Acuteeffects of aerosolized S-nitrosoglutathione in cystic fibrosis Am J Respir CritCare Med 165 (2002) 922ndash926
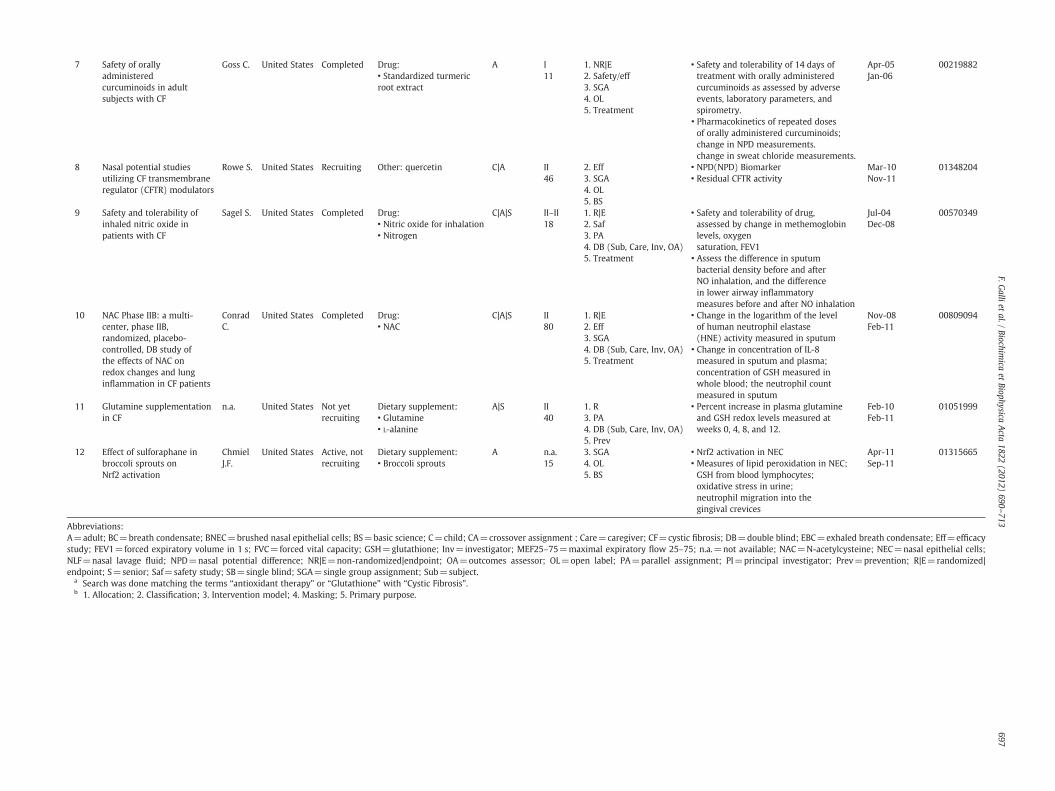
7 Safety of orallyadministeredcurcuminoids in adultsubjects with CF
Goss C United States Completed Drugbull Standardized turmericroot extract
A I11
1 NR|E2 Safetyeff3 SGA4 OL5 Treatment
bull Safety and tolerability of 14 days oftreatment with orally administeredcurcuminoids as assessed by adverseevents laboratory parameters andspirometry
bull Pharmacokinetics of repeated dosesof orally administered curcuminoidschange in NPD measurementschange in sweat chloride measurements
Apr-05Jan-06
00219882
8 Nasal potential studiesutilizing CF transmembraneregulator (CFTR) modulators
Rowe S United States Recruiting Other quercetin C|A II46
2 Eff3 SGA4 OL5 BS
bull NPD(NPD) Biomarkerbull Residual CFTR activity
Mar-10Nov-11
01348204
9 Safety and tolerability ofinhaled nitric oxide inpatients with CF
Sagel S United States Completed Drugbull Nitric oxide for inhalationbull Nitrogen
C|A|S IIndashII18
1 R|E2 Saf3 PA4 DB (Sub Care Inv OA)5 Treatment
bull Safety and tolerability of drugassessed by change in methemoglobinlevels oxygensaturation FEV1
bull Assess the difference in sputumbacterial density before and afterNO inhalation and the differencein lower airway inflammatorymeasures before and after NO inhalation
Jul-04Dec-08
00570349
10 NAC Phase IIB a multi-center phase IIBrandomized placebo-controlled DB study ofthe effects of NAC onredox changes and lunginflammation in CF patients
ConradC
United States Completed Drugbull NAC
C|A|S II80
1 R|E2 Eff3 SGA4 DB (Sub Care Inv OA)5 Treatment
bull Change in the logarithm of the levelof human neutrophil elastase(HNE) activity measured in sputum
bull Change in concentration of IL-8measured in sputum and plasmaconcentration of GSH measured inwhole blood the neutrophil countmeasured in sputum
Nov-08Feb-11
00809094
11 Glutamine supplementationin CF
na United States Not yetrecruiting
Dietary supplementbull Glutaminebull L-alanine
A|S II40
1 R3 PA4 DB (Sub Care Inv OA)5 Prev
bull Percent increase in plasma glutamineand GSH redox levels measured atweeks 0 4 8 and 12
Feb-10Feb-11
01051999
12 Effect of sulforaphane inbroccoli sprouts onNrf2 activation
ChmielJF
United States Active notrecruiting
Dietary supplementbull Broccoli sprouts
A na15
3 SGA4 OL5 BS
bull Nrf2 activation in NECbull Measures of lipid peroxidation in NECGSH from blood lymphocytesoxidative stress in urineneutrophil migration into thegingival crevices
Apr-11Sep-11
01315665
AbbreviationsA=adult BC=breath condensate BNEC=brushed nasal epithelial cells BS=basic science C=child CA=crossover assignment Care=caregiver CF=cystic fibrosis DB=double blind EBC=exhaled breath condensate Eff=efficacystudy FEV1=forced expiratory volume in 1 s FVC=forced vital capacity GSH=glutathione Inv=investigator MEF25ndash75=maximal expiratory flow 25ndash75 na=not available NAC=N-acetylcysteine NEC=nasal epithelial cellsNLF=nasal lavage fluid NPD=nasal potential difference NR|E=non-randomized|endpoint OA=outcomes assessor OL=open label PA=parallel assignment PI=principal investigator Prev=prevention R|E=randomized|endpoint S=senior Saf=safety study SB=single blind SGA=single group assignment Sub=subject
a Search was done matching the terms ldquoantioxidant therapyrdquo or ldquoGlutathionerdquo with ldquoCystic Fibrosisrdquob 1 Allocation 2 Classification 3 Intervention model 4 Masking 5 Primary purpose
697FG
allietal
Biochimica
etBiophysica
Acta
1822(2012)
690ndash713
698 F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
corrected Cftr KO-transgenic mice were given an oral bolus dose ofGSH (300 mgkg) and compared with WT mice for changes in GSHlevels in plasma lung ELF and BAL cells There was a twofold in-crease in plasma a twofold increase in lung a fivefold increase inELF and a threefold increase in BAL cell GSH levels at 60 min in WTmice however GSH levels only increased by 40 in the plasma 60in the lung 50 in the ELF and twofold in the BAL cells within thegut-corrected Cftr KO-Tg mice No change in GSH levels was observedin the uncorrected Cftr KO mice These studies suggest that oral GSHadministration can increase plasma and lung compartment GSHlevels in WT mice and to a lesser extent in gut-corrected Cftr KO-Tganimals It also suggests that oral GSH treatment can boost BAL cellGSH levels However since this study failed to show significant in-creases in serum and lung compartment GSH levels in uncorrectedCftr KO mice it is questionable whether oral GSH administration toCF patients with intestinal malabsorption would benefit from thistherapy It was also shown that GSH is rapidly distributed to theserum and lung compartments Kariya et al [118] speculate thatother transporter(s) besides CFTR are responsible of the transport ofGSH and probably of other dietary molecules to the lung whichmay be responsible for dietary deficiencies observed in various lungdiseases
Another strategy is represented by the oral supplementation ofhigh doses of NAC a well known cysteine donor for the synthesis ofglutathione NAC is considered a safe molecule which has beenused successfully to treat GSH deficiency in a wide range of diseases[119] As CF mice display defects in GSH export in the ELF comparableto those of patients they could provide a useful tool to assess the ef-fects of NAC administration on the GSH status However only limitedstudies exploring the effects of NAC on CF animal models have beenso far carried out The effects of NAC have been tested on mucus accu-mulation bacterial load transit and inflammation in the CF mousesmall intestine showing that NAC may reduce intestinal mucus accu-mulation bacterial overgrowth in the gut [120]
Moreover NAC has been reported to restore the accumulationof unwantedmisfolded proteins in aggregates that are associated withthe CF airway phenotype as a cause of lung inflammation [121] Themechanism of this NAC-derived effect seems to involve the restorationof beclin 1 expression and activity in the autophagy pathway of theendoplasmic reticulum that was investigated in vivo using Scnn1b-transgenic and Cftr(F508del) homozygous mice The restoration ofthis pathway also produced a rescued trafficking of CFTR (F508del) tothe cell surface of CF cells obtained from human CF nasal biopsies
Given the defective GSH metabolism of CF reviewed in the previ-ous sections and in [122] and the reduced response to GSH therapyin CF mice [93] some Authors have investigated the influence of bac-terial infections on lung oxidative stress The effects of P aeruginosainfection on ELF and lung tissue antioxidants and the oxidation ofDNA and lipids were investigated in mice challenged with bacterialcells [90] CFTR-KO (B6129P2-Cftrtm1Unc) and WT mice were chal-lenged intratracheally with a clinical isolate of mucoid P aeruginosaembedded in agar beads and on the third day of infection BALF andlung tissue were obtained and analyzed for cytokines antioxidantsand enzyme activities [90] P aeruginosa lung infection increasedlevels of inflammatory cytokines and neutrophils in the ELF This cor-responded with a marked increase in GSH and in urate levels in theELF of P aeruginosa-infected WT mice A twofold increase in uratelevels was also observed among lung tissue antioxidants of Paeruginosa-infected WT mice There were no changes in markers oflung oxidative stress associated with the P aeruginosa lung infectionIn contrast to WT mice the CFTR-KO mice lacked a significant in-crease in ELF GSH when challenged with P aeruginosa and this corre-lated with a decrease in the ratio of reduced to oxidized GSH in theELF a marker of oxidative stress These data would suggest that thelung adapts to infectious agents with elevated ELF GSH and urateTherefore individuals with lung diseases associated with altered
antioxidant transport such as CF might lack the ability to adapt tothe infection which may lead to a more severe inflammatoryresponse
322 Clinical trials on GSHThe discovery of the defect in GSH export has suggested that ther-
apies able to restore or increase GSH levels in the ASL could counteractthe inflammation and oxidative stress conditions typical of CF pa-tients In an attempt to strengthen extracellular defenses againstROS some pilot studies have analyzed the effect of GSH inhalation orthat of oral GSH prodrug N-acetylcysteine (NAC) All these treatmentswere well tolerated by the CF patients and most authors were able tomeasure increased ELF concentrations of GSH in association withsome positive clinical outcomes [4041737896122ndash128] Althoughpotentially promising these findings need stronger clinical evidencein that the majority of these were obtained on very limited numberof patients investigated in non-randomized controlled trials This ishighlighted in a recently published meta-analysis [129] that providesalso a thoroughly analysis of the literature on this aspect of the antiox-idant and anti-inflammatory therapy of CF Among the American CFfoundation sponsored trials two phase II trials on inhaled GSH andoral NAC are in progress in US and Germany (ClinicalTrialsgov Iden-tifier NCT00506688 and NCT00809094 respectively Table 1) andsafety and tolerability of aerosolized glutathione is also matter ofinvestigation by another (not registered) US trial (more informationon this can be found in [130]) Nevertheless the diffusion among CFpatients of NAC preparations for inhalation (Mucomystreg) has in-creased in recent years
γ-Glutamylcysteine ethyl ester (GCEE) is another potentially inter-esting GSH pro-drug which has proved some efficacy in the ameliora-tion of oxidative stress eg in experimental myocardial infarction[131] and central nervous system conditions (see eg [132]) HoweverGCEE has not been investigated in CF yet
33 Limits and potential problems associated to thiol-based therapies
Although the above cited clinical trials may be considered promis-ing attempts to improve the antioxidant levels in the ELF the actualcapacity of these treatments to produce positive clinical effects mustbe considered with caution For example indices of oxidative damagewere found to be unaffected by aerosolized GSH treatment [122]Some in vitro studies have suggested that the reaction of GSH withPCN could produce hydrogen peroxide with potential exacerbationof oxidative damage [101] The exact mechanisms of PCN toxicityand the reaction of this toxin with GSH must be better understoodin order to evaluate the safety of GSH administration to patients col-onized by P aeruginosa
Inhalation of GSH ensures its direct delivery in the airways butsince GSH can rapidly convert to its oxidized form GSSG frequentGSH inhalations are required to maintain a high GSHGSSG As a con-sequence of this limit four separate inhalations have been used inthe study carried out by Bishop et al [123] Unless justified by clearclinical improvements these repeated treatments may represent aburden for patients already undergoing complex therapies Moreoverrepeated inhalations of GSH increase the levels of GSSG in ELF[133134] In the absence of effective homeostatic mechanisms ensur-ing the fast recycling of GSSG to GSH this might produce unwantedeffects and even the exacerbation of CF symptoms being GSSG re-sponsible of the S-glutathiolation and functional inhibition of CFTR[124]
In principle the oral administration of GSH could be considered asafe strategy to prevent GSSG accumulation but this strategy is likelynot feasible due to the substantial inability of this water-soluble mol-ecule to cross biological membranes Moreover a study carried out inmice has established that GSH absorption in the gastrointestinal tractif any is mediated by CFTR itself thus excluding the possibility to
699F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
improve circulating levels of GSH in CF patients through the dietarysupplementation of the antioxidant [127] The limited absorption ofGSH could be overcome by GSH-esters as in vitro studies haveshown that this form of GSH may be specifically useful to rescue mi-tochondrial defects in cystic fibrosis models [80] Safety of these GSHderivatives in humans has been poorly investigated
Two independent studies have shown that the treatment of CF pa-tients with high doses of NAC increases extracellular GSH in sputum[78125] but contrasting results have been reported concerning theeffects of NAC on the concentrations of blood GSH and on the levelsof IL-8 and other markers of inflammation NAC treatments may beuseful to modulate the GSH content in cells but it should be remindedthat an enhanced cysteine supply cannot lead to an increase of GSHabove physiological levels due to the feedback inhibition mechanismof γ-glutamylcysteine synthetase described in the Section 311
331 Gamma-glutamyltransferase and GSH therapySo far none of the studies mentioned above has taken into account
the fact that GSH is degraded by GGT enzyme activity GGT concentra-tions are known to increase several fold in ELF of CF patients even ifthe mechanisms for this effect were not determined [135] and thisphenomenon parallels the above described decrease of GSH levels inELF Preliminary data suggest that a major source of increased ELFGGT is represented by activated neutrophils accumulating in diseasedairways (Corti and Pompella 2011 unpublished observation) Re-gardless of its origin it is likely that increased GGT in ELF would de-grade locally administered GSH to variable extents which couldcontribute to the so far inconclusive results of therapies based onaerosolized GSH Besides its role in GSH catabolism GGT has beenshown to mediate protein S-thiolation [136] suggesting that GSH ad-ministration in the presence of active GGT enzyme might alter CFTRglutathiolation status and function in a potentially unfavorable wayOn the other hand a potential role of GGT in favoring bronchial up-take of antioxidant vitamin C has also been suggested [137]
These controversial findings may add further issues to the ques-tion of whether the therapy of lung oxidative stress by aerosolizedGSH could be safe in all the CF patients regardless of specific strate-gies that would ascertain the extent of lung inflammation Thesestrategies should include the assay of GGT levels in ELF In principleonce an adverse role of ELF GGT in GSH therapies will be confirmedthe association of GGT inhibitors in the GSH formulations for inhala-tion could represent a promising pharmacological strategy
34 Malnutrition as a possible cause of defective thiol-dependentantioxidant protection
Successful nutritional interventions strongly impact on the clinicaloutcome of CF patients [138ndash140] Malnutrition by pancreatic insuffi-ciency and other CF-related factors influence the susceptibility to de-velop recurrent infections and severe inflammatory lesions of thelung tissue If the onset of a defective (sub-optimal) antioxidant sta-tus may represent an underlying component in the clinical effects ofmalnutrition remains a matter of investigation Clinicians have topay particular care to avoid these disturbances and successful proto-cols of nutritional intervention in CF have been developed whichare essentially aimed to avoid the onset of protein-energy malnutri-tion (PEM) [141] Despite this the risk of developing such an unto-ward complication in CF infants and children remains high assuggested by the prevalence data registered in some areas Actuallya prevalence of PEM between 5 and 14 in Moldavian infants was re-cently reported [142] and PEM is associated with poor outcome andparticularly with the risk of developing edema and anemia
Besides lowered intake and absorption of micronutrient antioxi-dants discussed in the other sections malabsorption of dietary proteinand excess fecal amino acid losses result in hypoproteinemiahypoalbu-minemia as key biochemical signs of PEM Hypoalbuminemia is
considered to be linked with a causendasheffect relationship with oxidativestress and is proposed to influence morbidity and mortality in condi-tions associated with chronic inflammation and severe oxidative stress[143144] The human serum albumin (HAS) molecule contains only areactive thiol group eg the Cys 34 the importance of which as an anti-oxidant defense system in blood and for the entire organism is welldocumented [145] This is the second main thiol (and the main proteinthiol) in the circulation (approx 2 mmol in the adult organism assum-ing 5 l of total blood volume anHt of 40 and [HAS] of 45 gl of plasma)being the RBCGSH thefirst thiol in blood (near to 5 mmol assuming thesame parameters of above and an average concentration of GSH inpacked RBC of 25 mM) [146147] The antioxidant role of HSA is notonly a consequence of the relative abundance of its Cys thiol A specificcapability of acting as a sacrificial target for a series of electrophils andmost biologically relevant ROS ie hydrogen peroxide and peroxyni-trite has been demonstrated in a series of studies [145148149] Li-gand binding activity can contribute to promote antioxidant effectsby the HSA molecule [145] Transitions metals particularly copperand also iron in the case of iron-overload diseases bind to HSA Inthis way these are less available to promote the Fenton chemistryand hydroxyl radicals eventually released from this oxidative reactionare mostly directed to the HAS protein sparing more important tar-gets A free radical-trapping activity of HSA has been also demonstratedand this was proposed to be directed toward both hydrophilic and fat-soluble species This activity may result from the interaction withother antioxidants such as α-tocopherol [150] and may influence theantioxidant activity of food-derived phenolic antioxidants [151]
However Cys 34 is considered the main contributor to the antiox-idant function of HAS which plays its role in the antioxidant homeo-stasis of blood thanks to a complex series of interactions with themetabolism and antioxidant function of the pool of free thiols in plas-ma and in the circulating RBC with the latter playing a significantcontribution to the extracellular pool of GSH [146] and to the dynam-ics of inter-organ GSHmetabolism in cooperation with liver and othertissues [147] Immuno-inflammatory cells and the lung tissue areamong the main terminals of this metabolism The RBC contain theentire machinery to synthesize GSH to restore its redox (by enzymat-ic reduction of the oxidized form) and to use this as cofactor of Se-GPx and GSH-S-transferase enzymatic activities that are responsibleof the detoxification of hydroperoxides and alkylating agents thatmay form in or enter the RBC cytosol [147] In this sense the RBC rep-resents a circulating reservoir of GSH that in addition to maintainingthe redox and respiratory function of Hb participates to systemic pro-tection of xenobiotics of endogenous and exogenous origin In consid-eration of these aspects the combination of hypoalbuminemia andanemia may exponentially increase the risk of developing oxidativestress in CF patients as it is supposed to occur in other oxidative stressconditions such as chronic kidney disease [55143152] Additionalclinical investigation should verify the hypothesis that hypoalbumi-nemia together with a defective uptake and metabolism of sulfur-containing amino acids and CF-specific defects of the GSH metabo-lism may represent a causal risk factor for an impaired antioxidantdefense and systemic oxidative stress in CF patients
35 Fat-soluble antioxidants
Pancreatic insufficiency and a diminished bile acid pool cause mal-absorption of important essential nutrients and other dietary compo-nents in CF Of particular significance is the malabsorption of fat-soluble antioxidants such as tocopherols carotenoids and coenzymeQ-10 (Co-Q10) and that of essential fatty acids (EFA)
351 Vitamin EVitamin E therapy in CF has been proposed in several decades of
research as a useful approach to overcome both the lower absorptionof this fat-soluble micronutrient and the increased antioxidant
700 F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
demand by the abnormal generation of ROS in CF tissues (see for in-stance the recommendations by the Cystic Fibrosis Foundation Con-sensus Conference on nutrition [153])
The first report of a vitamin E deficiency in CF appeared in literaturein 1951 by Filer et al [154] In this study the absorption of the mainform of this vitamin eg α-tocopherol and its ester derivatives was in-vestigated in several subsets of infants and children Thanks to a simplebioavailability (or tolerance) test these authors observed that ldquoin-fantshellip diagnosed as fibrocystic disease of the pancreas diarrhea andcirrhosis were characterized by a poor response to the test ie the tol-erance curve was lowrdquo However abnormalities were also observed inother subgroups of infants with a variety of disorders not associatedwith fat or fat-soluble vitamin intolerance such as sprue celiac syn-drome and lupus erythematosus which suggests the general observa-tion that malnutrition and inflammatory and degenerative diseases ofthe GI tract may lead to absorb tocopherols poorly At the same timethese authors reported that ldquoMetabolic disorders with associated hy-percholesterolemia were observed to give abnormally high values forthe area under the curverdquo and that patients responding poorly to to-copherol absorption test did also in vitamin A absorption tests
The finding of lowered (lipid uncorrected) levels of vitamin E wasconfirmed in other studies in which this relative deficiency was foundto occur irrespective of pancreatic comorbidity and in associationwith lowered levels of other liposoluble vitamins such as vitamin Aand D [155] regardless of their different liver metabolism and tissuedelivery mechanisms [156157]
Plasma buccal mucosal cells (BMCs) and breath condensate α-tocopherol decreased significantly with age in association with a de-creased respiratory function [5] This was accompanied by loweredlevels of other antioxidants such as vitamin C and increased oxidativestress markers of different origin such as protein carbonyls thiobarbi-turic acid-reactive substances and F2-IsoPs
Clinical symptoms of vitamin E deficiency in CF have not beenconclusively investigated Dolan et al [158] described that anemiaof CF patients is related to vitamin E deficiency and increasedperoxide-induced hemolysis of RBC Other authors however ob-served an increased susceptibility to peroxide-induced hemolysisalso in the presence of normal levels of vitamin E [159] Peters andKelly [160] observed that RBC vitamin E concentrations were belowthe normal range in almost all unsupplemented patients and roseinto the normal range with a 1-year supplement of 100 mg per daybut not 15 mg per day Since RBC vitamin E concentration has beenshown to correlate well with tissue concentrations of the vitamin inanimals tissue levels of vitamin E are expected to be lower than nor-mal in CF patients
Bioavailability of fat-soluble vitamin is limited in CF Vitamin Edeficiency of CF is also associated with hypocholesterolemia [7] Asa consequence the relative deficiency of this vitamin is compensatedwhen the absolute levels are normalized for cholesterol levels andthis suggests a poor transferring of this vitamin in the circulation bya defective lipid and lipoprotein metabolism Pancreatic insufficiencyand the consequent lipid malnutrition cannot completely explain thisdefect and other possibly CF-specific dysfunctions could play a roleLiver metabolism and specific plasma transport systems of this vita-min need further elucidation in CF
As a consequence of these aspects it is not presently clear whichform and level of supplementation of this vitamin is most appropriateto treat these patients Usingα-tocopherol as a vitamin E supplementPeters et al [160] reported that 100 mg per day are required to nor-malize RBC concentrations Other authors described unsuccessfulsupplementation protocols with higher doses and this has led to de-velop formulations with higher bioavailability in order to achieve bet-ter compliance to oral supplementation (see below and the literaturereviewed in [161ndash163])
Besides absorption and tissue delivery issues specificity of actionis another critical item of antioxidant therapy with fat-soluble agents
in CF As further addressed below this aspect could be themain limit toa successful use of natural forms of vitamin E in the clinical manage-ment of CF inflammation even if a local lung-targeted therapy wouldbe developed according with so far proposed pre-clinical models ofaerosolized vitamin E [164165]
Current pharmacological research is aimed to develop synthetic formsof this and other fat-soluble antioxidants with better radical scavengingproperties at the lipidndashwater interface Type of ROS target and the sitesof action greatly influence the chances of a fat-soluble antioxidant of alle-viating oxidative stress in the airways as well as in other organs such asliver and pancreas These aspects dealing with specificity of action[163166167] have stimulated the search of novel vitamin E-derived an-tioxidants that may help to scavenge radicals at the lipidndashwater interfaceof the epithelial cell membrane and surfactant Amine derivativesof tocopherols and tocotrienols have been recently demonstrated toshow higher antioxidant and free radical scavenging activity than α-tocopherol [168] Further in vitro pharmacological analysis has includedtoxicity evaluations and the detailed investigation of scavenging of azo-and phenolic radicals with different degrees of hydrophobicity and theinhibitory activity on IL-8 gene expression and phospholipase activityin CF cells Comparative evaluation with other synthetic derivativessuch asα-tocopheryl succinate and natural forms of vitamin E suggestedthat these amine derivatives are promising antioxidant and anti-inflammatory agents [Galli F and Pilolli F unpublished observation]deserving further pre-clinical investigation in CF model systems
Anti-inflammatory effects of natural and synthetic analogues of vi-tamin E are also an intriguing pharmacological opportunity currentlyunder investigation by several laboratories [169170]
Recently vitamin E supplementation has been at the center of adispute regarding its safety when used at high dosages in certainpopulations of patients An extensive and speculative debate originat-ed on this subject after a meta-analysis study byMiller et al [171] thatexamined the largest secondary prevention trials on vitamin E trials incardiovascular patients finding a significantly increased mortality riskfor all the causes (about 4 1ndash8 in the 95 interval of confidence)when the patients were treated with doses gt400 IUdie (that areequivalent to 400 mgdie of the synthetic form allrac-α-tocopheroland to 185 mgdie of the natural form RRR-α-tocopherol) This debateresulted in a careful examination of this meta-analysis study by severalother authors and in further revisions of the literature on vitamin E tox-icity in humans [see the literature recently reviewed in [163172ndash174]]that clearly demonstrated the poor consistency of the conclusionsraisedwithMillersmeta-analysis study and the paucity of the concernsthat derived from that These conclusions have been verified in the re-cent international symposium on vitamin E of the Society for Free Rad-ical Research Europe branch of Rome 2009 [173175] Vitamin E used assupplement for humans in all its forms (eg α-tocopherol and othertocopherols and tocotrienols) is safe in abroad range of intakes[172176] The tolerable upper intake level (UL) and the AcceptableDaily Intake (ADI) established by the Joint FAOWHOExpert Committeeon Food Additives for the natural form of vitamin E as α-tocopherolequivalents are of 300 mgdie and 015ndash20 mgkg body weightdierespectively [172177]
352 CarotenoidsLevels of plasma carotenoids such as β-carotene β-cryptoxanthin
and total lycopene are significantly lowered in CF patients and thiswas associated with higher susceptibility to lipid peroxidation[5178ndash180] Rust et al [178] demonstrated that the long-term oralsupplementation with 50 mg β-caroteneday (ie 1 mg β-carotenekg BWday) restored the levels of this carotenoid while sub-optimalsupplementation was observed at doses of 10 mg β-caroteneday orlower thus confirming the need of high doses of this fat-soluble factorto overcome the limited absorption and thus to achieve plasma con-centrations of healthy control subjects Successful high-dose treat-ments appear to lower oxidative stress markers such as TBA-MDA
701F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
complexes and to correct total antioxidant capacity of plasma Inanother study β-carotene supplementation was observed to de-creased lipid peroxide formation as quantitated by malondialdehydeconcentrations in plasma (TBAHPLC method) and to enhance the re-sistance to copper(II) ion-induced oxidation of low density lipopro-teins [180]
At the same time toxicity issues have been raised for human sup-plementation with carotenoid formulations and particularly of water-miscible formulations of preformed vitamin A that is regularly sup-plemented to CF patients which may increase serum retinol andpossible risk of CF-associated liver and bone complications (reviewedin [161181]) However β-carotene supplementation seems to be safesince this does not affect plasma concentrations of other carotenoidsand retinol as well as of other fat-soluble vitamins as α- and γ-tocopherol [178] Recent studies designed to test the clinical efficacyof a CF tailored multivitamin formulation (commercial name AquA-DEKsreg) also tested the safety of this type of formulation and demon-strated that this does not increase vitamin A above the normal levelsobserved in healthy controls [162182183] The normalization of β-carotene levels obtained in these studies was associated only withminor improvements on respiratory and growth parameters whilethe levels of urinary F2-IsoPs used as index of lipid peroxidationwere not affected [162] The surrogate marker of lipid peroxidationMDA was affected together with some selected antioxidant parame-ters (RBC thiols and superoxide dismutase) in another study inwhich this multivitamin formulation was preliminarily evaluated incomparison with standard formulations of vitamin E and A [182]
353 Coenzyme Q-10Coenzyme Q-10 (Q10) is a well-known electron transporter in the
mitochondrial respiratory chain with fundamental role in cellularbioenergetics and scavenging of radical species [184] This lipophilicsubstance is present in the circulation at low levels (serum concentra-tionsle2 μM) mainly as ubiquinol-10 eg the reduced form with anapproximate ratio of 955 with the oxidized form ubiquinone-10[185186] A mechanism for a preferential distribution and accumula-tion in mitochondria has been suggested for both the reduced and ox-idized forms of CoQ10 that are taken up by the cells in a time- andconcentration-dependent Subcellular localization and trafficking ofexogenous Q10 are similar to those of the endogenous form butwere different from that of α-tocopherol that is related with lipidcomposition particularly in the mitochondrial and microsomal frac-tions [184] Ubiquinol-10 readily oxidizes ex vivo by the reactionwith other lipophilic antioxidants such as α-tocopherol and butylatedhydroxytoluene [185] Therefore a higher reduction potential thanother physiological fat-soluble antioxidants such as vitamin E and aselective metabolism and cellular trafficking show peculiar role forthe cell CoQ which may also represent an important lipophilic antiox-idant in cells and body fluids
Human cells synthesize this coenzyme through the cholesterol bio-synthesis pathway so thatmore than two thirds of the tissue levels ap-pear to have an endogenous origin dietary sources provide acontribution to Co-Q10 levels of blood and all solid tissues that variesdepending on the dose applied and type of dietary source [187] How-ever in the case of oral supplements it has to be considered that hy-drophobicity and large molecular weight of this coenzyme influenceits absorption that ultimately is slow and limited [186187] Likewiseto vitamin E pharmacokinetics [188189] Co-Q10 showed T(max) ofaround 6 h that coincides with that of dietary lipids Elimination isclose to that of the more retained form of vitamin E in human bodyeg α-tocopherol with a half-life of about 33 h which suggests poorhepatic metabolism However commercially available formulationsare reported to be safe even at high doses and solubilized formulationsshow enhanced bioavailability In healthy subjects plasma Q10 re-sponse to oral ingestion show saturation profiles with a plateau at a
dose of 2400 mg and the higher plasma concentrations were foundto facilitate uptake by peripheral tissues and also the brain [186187]
Laguna et al [190] recently investigated total serum levels ofcoenzyme Q-10 in a wide population of CF children (n=381) and esti-mated their association with clinical outcome Near to 50 of these CFpatients were deficient of Co-Q10 and this defect was significantlymore prevalent in patients with pancreatic insufficiency and signifi-cantly associated with P aeruginosa colonization in infants (under24 months of age) Importantly low Co-Q10 levels correlated to otherlipid markers of a poor nutritional status such as total lipids and alsothe other fat-soluble antioxidants β-carotene and α-tocopherolwhich confirms the presence of a common defect in the absorptionand metabolic pathways of this coenzyme with dietary lipids
The deficit of Co-Q10 may contribute to the impaired energy func-tion of mitochondria of CF tissues and this may exacerbate CF-linkedinflammation infection and cellular stress response of the lung A sys-tematic analysis of molecular lesions in CF bronchial tissue has beenrecently carried out by proteomic approach [191] Comparative eval-uation of protein expressional pattern in CF and healthy controltissues has revealed aberrant levels of some mitochondrial andenergy-related proteins in CF specimens that included the ubiqui-nolndashcytochrome c reductase complex core protein I and one form ofnidogen a pseudogene of aconitase 2 These changes in CF may reflectmolecular changes which could be associated with an altered mito-chondrial homeostasis and Co-Q10 redox
Multivitamin supplements with high bioavailability containingCo-Q10 have demonstrated to correct the deficit of this antioxidantand were preliminarily observed to improve airway inflammationmarkers in CF patients [183] However further clinical investigationfailed to demonstrate that such an improved biochemical profile isassociated with significant improvements in weight percentile andpulmonary function [162]
354 Fatty acidsA key pathophysiological role in sustaining inflammation in CF has
been attributed to the abnormal polyunsaturated fatty acid (FA) pat-tern Abnormalities in FA profiling are potentially linked to CFTRmutation-driven alterations in the absorption andor metabolism ofdietary lipids [192193] and to the consumption of high oxidizableFA involved in the free radical-mediated lipid peroxidation [7]Among those alterations dysregulation of the docosahexaenoic acidand arachidonic acid balance has been extensively studied with re-portedly significant reduction of DHA in CF and a parallel increasein the levels of AA and inflammatory indices [193ndash195] Actually AAis the progenitor of both enzymatic- and free radical-derived inflam-matory mediators including leukotrienes prostaglandins and iso-prostanes On the other hand n-3 PUFA (eicosapentaenoic acid anddocosahexaenoic acid) are involved in the generation of potent medi-ators namely resolvins and protectins which are able to resolveexudates and to act as organ protective and antifibrotic Secondarilyto their anti-inflammatory action n-3 FA may also produce anantioxidant-like response (eg a reduced demand of antioxidants toachieve an optimal control of oxidative pathways) As a consequencen-3 PUFA have been suggested and widely used as supplements in CFpatients usually under the form of fish oil [196ndash198] It is worth ofnote however that defective levels of DHA in CF patients was notconfirmed in recent studies [7] It was also shown that patients onDHA supplements did not have increased plasma n-3 FA concentra-tions but showed more severe oxidative stress compared to theunsupplemented patients [7] This observation of an increased riskof oxidative stress in CF subjects receiving n-3 fatty acids supple-ments has also been described by other authors [199]
Studies reporting increased AA levels in CF patients have beencontradicted by others [7200201] thus contributing to weakeningthe pathophysiological role of the altered DHAndashAA balance as turnpoint of an upregulated inflammatory status in CF In this context a
702 F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
recent Cochrane meta-analysis on n-3 supplementation in CF patients[202] highlighted the lack of evidence for a significant correction ofthe assessed clinical end points (mainly respiratory symptoms)even when inflammatory indices and other laboratory end pointswere met Taken together these data suggest that there is insufficientevidence to draw firm conclusions or recommend routine use of n-3supplements in CF Notwithstanding it is common belief that n-3supplements provide some benefits for people with CF with relativelyfew adverse effects and thus their use is not discouraged
Further alterations in fatty acid metabolism have been highlight-ed including the consistent findings of an increase in circulatinglevels of saturated and monounsaturated fatty acids [7203204]Decreased levels of essential FA (EFA) ie the FA that have to be in-troduced with the diet correlates with the severity of respiratoryinsufficiency and the same clinical correlation was observed with al-tered proportions of FA species converted by the activity of desatur-ase enzymes (reviewed in [204]) The close relationship betweencertain fatty acids and oxidative stress including the negative correla-tion of C240 and linoleic acid with oxysterol levels point to the needof intensive investigation in CF patients of previously neglected lipidspecies that are emerging candidates in the control of metabolismQuantitative lipidomic analyses have lead to identify C161n7 palmi-toleate as a ldquoprotectiverdquo adipose-derived lipid hormone that stronglystimulates insulin activity in muscle and liver also suppressing in-flammatory cytokine output from mice fat cells [205] Specific meta-bolic activities have been also demonstrated by medium chainsaturated fatty acids caprylic acid (C80) capric acid (C100) and lau-ric acid (C120) Capric acid acts as a direct ligand of PPARγ using abinding pocket different from the binding pocket of thiazolidinedioneor long chain fatty acids [206] Additional activities of medium chainfatty acids which are ligands of free fatty acids receptors detectedin the immune cells the gastrointestinal tract and adipocytes maycontribute to metabolic homeostasis and inflammatory responses[207] These data underscore the importance of a lipid-mediated ldquoen-docrine networkrdquo demonstrating how specific alteration of one orfew serum lipids would be per se sufficient to influence metabolic ho-meostasis Given the relevance of this emerging information and thealteration of lipid metabolism and inflammatory status in CF fattyacid lipidomics need to be deeply investigated in CF
Again these studies have obvious nutritional implications Satu-rated fatty acids with chain lengths higher than C18 are poorlyabsorbed partly because they form insoluble calcium salts [208]Medium chain saturated fatty acids are well known for being highlyabsorbed through the intestine providing rapid delivery of energyvia oxidation of the more hydrophilic short chains and have beensuggested to provide proper nourishment in patients with CF [209]Recent studies have shown that consumption of a high-fat diet richin medium chain fatty acids as opposed to long chain fatty acidsdoes not lead to ectopic fat accumulation in skeletal muscle andliver of both rats and mice [210] In light of the close association be-tween nutritional status inflammation and life expectancy in CF pa-tients the manipulation of dietary lipids in these patients must befurther explored as a possible strategy to provide adequate nutritionand better management of oxidative stress
36 Hydrosoluble antioxidants oligoelements and enzymatic antioxidants
361 Vitamin CVitamin C status in CF patients has been poorly investigated Early
studies suggested a defective vitamin C status that was refractory tooral supplementation [211] Other and more recent studies showednormal or slightly decreased levels of vitamin C in CF patients as com-pared to healthy controls but age- and disease-related decline of thiswater-soluble antioxidant was reported in these patients [5212]In the study of Winklhofer-Roob et al [212] on mid-European CFpatients vitamin C concentrations decreased with age with an
estimated rate of 5 μmollyr and vitamin C concentrationsb40 μ-moll were associated with highest indexes of inflammation whichis consistent with the hypothesis that optimal levels of vitamin Cmay influence immuno-inflammatory activity of alveolar macro-phages and neutrophils Other few studies have examined the effectof supplements containing vitamin C on CF inflammation and oxida-tive stress since the levels of this vitamin do not significantly improvewith supplementation (reviewed in [213]) This highlights the com-mon fate that this hydrosoluble vitamin shares with several fat-soluble counterparts in the ldquomicronutrient paradoxrdquo of CF patients inwhich the need for a correction of their status along the progressionof the disease is frustrated by the poor efficacy of oral supplementa-tion protocols Formulations and appropriate supplementation proto-cols that may produce a better correction of vitamin C status of CFpatients are awaited for further clinical evaluation
362 Selenium and selenium-dependent peroxidasesSelenium is a trace element with marked electrophilicity [214]
that once converted to the organic form of Se-Cys can be introducedin protein structures to play its important role in H2O2 metabolismand signaling [215] As catalytic center of the enzyme GSH-peroxidase (SeGSH-Px) Se plays a crucial role to protect polyunsatu-rated lipids of plasma membrane and circulating lipoproteins formperoxidative insults With other Se-proteins such as the high molecu-lar weight thioredoxin reductases this oligoelement participates tothe control of protein thiol-disulfide oxidoreduction and glutathiony-lation which regulate signaling pathways of crucial importance in theregulation of immunity and inflammation [16] but also the function-ing of other redox-sensitive proteins such as the same CFTR [124]
The activity of SeGSH-Px in blood is considered a functional as-sessment of selenium status even if this assumption has some limita-tions related with the saturation profile that the Se stores show atincreasing doses of Se administration Investigations of the seleniumstatus in CF patients have produced conflicting findings which maydepend on differences in dietary intake ethnicity and environmentalfactors in the diverse patient populations (reviewed in [216217]) CFchildren have been reported to have lowered blood selenium and RBCSeGSH-Px activity [218219] normal plasma selenium and loweredRBC SeGSH-Px [220] and even normal levels of both these two param-eters [221] The supplementation with selenium in combination withother antioxidants was observed to increase the concentrations ofblood selenium that likewise β-carotene and fatty acid were posi-tively correlated with improved lung function [6]
Foucaud et al [218] observed that a defective selenium statuswas associated with lowered levels of other antioxidants that contrib-ute to the anti-peroxidative activity of this microelement such asvitamin E (reviewed in [222]) and the severity of this deficiencywas lower in children with pancreatic enzyme replacement and vita-min E supplementation
Treatments to substitute for exocrine pancreatic insufficiency bypancreatic enzymes from animal sources such as porcine pancreashave been confirmed to be a source of Se [220] These affects RBCSeGSH-Px activity and plasma selenium concentrations which hasto be taken into account when selenium supplements are given toCF patients
Selenium has been used to develop a series of organoseleniumcompounds that may open the way to new therapeutic opportunitiesin CF (see Section 392) These include GPX mimetic drugs and phaseII enzyme inducers which may provide higher antioxidant activity ofASL and cellular protection effects in the airways
363 Zinc and copperZinc and copper (Zn and Cu respectively) are present in many
proteins so that a deficiency of these trace metals could have pleiotro-pic effects in humans As regards antioxidant systems these two oli-goelements contribute an important role being cofactors of two
703F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
isoforms of the superoxide dismutase enzymes eg the extracellularform eg the EC-SOD or Sod 3 and the CundashZn-SOD or Sod 1 that isfound in several tissues and cells [223] The EC-SOD exerts its antiox-idant role also in the lining fluids of the airways [224]
The notion that CF patients have defective concentrations of bloodZn and Cu is controversial As far as Cu status is concerned few datahave been produced and are available in the literature suggestingthe notion that CF patients develop a moderate copper deficiency[225226] That was essentially demonstrated on the bases of a defec-tive activity of Cu-related proteins such as plasma ceruloplasmindiamine oxidase and RBC SOD This defect seems to be refractory toCu and Zn supplementation (see below)
More advanced studies have been carried out in the case of Zn sta-tus in CF Low plasma zinc concentrations were reported in approxi-mately 30 of young infants with CF identified by newbornscreening [227] and an impaired zinc homeostasis in CF patientswas described by Easley et al [228] This is characterized by poor con-servation of the endogenous pool with fecal loss and impaired frac-tional absorption of zinc which are the consequences of pancreaticinsufficiency and persisting steatorrhea These studies suggestedthat in the clinical management of CF patients these defects can beat least in part corrected by exocrine pancreatic enzyme replacement
A series of studies by Van Biervliet et al [229230] demonstratedin a Dutch population of CF infants and children that serum Zn variesin an age-dependent manner but remained unchanged with respectto healthy control levels In CF patients no difference in serum Zn con-centration between pancreatic-sufficient or pancreatic-insufficientpatients was observed and no correlation was found with the nutri-tional status or height z-score Importantly in these studies a signifi-cant correlation of serum Zn was observed with the fat solublevitamins A and E thus confirming the relationship between the ab-normalities of lipid and Zn metabolism in CF This suggests that co-supplementation of Zn and fat-soluble vitamins should be advisedin the presence of pancreatic insufficiency and persisting steatorrhea
Neve et al [219] in a study aimed to assess plasma and erythrocytezinc copper and selenium in CF children showed that mean plasmazinc and copper levels were not different from those in age-matched controls which confirms the observations by Van Biervlietet al described above However plasma zinc concentrations de-creased in patients with moderate-to-severe growth retardation andwith severe pulmonary disease but very low zinc levels occur sporad-ically Erythrocyte zinc and copper levels were significantly higherthan normal while RBC selenium was lower than in age-matchedcontrols These trace element concentrations in erythrocytes werediscussed in relation to the activities of the CuZn-SOD and the Se-enzyme GPx This observation suggests a compensatory upregulationof the erythrocyte CuZn-SOD by the exposure of erythroid precursorsto ROS andor other CF-related stressors
Best et al [225] also studied RBC SOD activity using this as a bio-logical sensor of Cu status in CF patients A lowered activity of thisenzyme was reported in CF together with that of the other Cu-dependent enzyme plasma diamine oxidase while plasma ceruplas-min showed normal activity Degradation rates of copper proteinsare known to be accelerated in conditions of copper deficiencywhich could explain the finding at least in part Anyway when Cuand Zn were supplemented to CF patients either separate or incombination (6 weeks of 3 mg copperd as copper-glycinate and30 mg zincd as zinc-glycinate) any of the copper enzyme activitieswas affected Therefore the moderate copper deficiency of CF patientsappears to be refractory to the intervention by increased copper andor zinc intake
Erythrocyte CuZn-SOD and the plasma levels of Cu and Zn werealso measured in the study of Wood et al [6] in which Australian CFpatients (agegt5 years) were treated with a high-dose antioxidantmultivitamin formulation containing 200 mg vitamin E (as RRR-α-tocopherol) 300 mg vitamin C (as sodium ascorbate) 25 mg β-
carotene (all-trans isomer) 90 μg Se (as selenomethionine) and500 μg vitamin A (as retinyl palmitate) in oil Plasma oligoelementsand particularly Zn were in the normal range at baseline (as com-pared with the data reported in [229230]) and were not affected bythis multivitamin supplement The same was found for the activityof RBC SOD and for plasma 8-iso-PGF2α as surrogate biomarker oflipid peroxidation
In a recent non-randomized small population (n=21) casendashcon-trol study in CF children Zn supplementation was proven to producepositive clinical effects in Zn-deficient patients [196] The supplemen-tation with 5 mgkg Zn sulfateday (maximum 150 mg) significantlydecreased the number of infections and increased the forced expira-tory volume in 1 s energy intake and growth parameters also im-proved These parameters were unaffected in untreated patientsexcept that in the case of the pulmonary function that decreased sig-nificantly These clinical observations on Zn supplementation need tobe confirmed in prospective double-blind randomized control trial
37 Appropriateness and targeting of antioxidant therapies in CF
The choice of the appropriate antioxidant and dose to correct a cer-tain biomarker and its associated biochemical lesion is another impor-tant point that appears to have disregarded in many clinical studiesFor instance unlike vitamin E vitamin C supplementation does notalter F2-IsoPs levels in humans (reviewed in [74]) This appears tobe true also in the antioxidant therapy of CF in which vitamin C(300 mgday) was administered together with other antioxidantsthat included a dose of vitamin E of 200 mgday without any signifi-cant effect on the surrogate biomarker of lipid peroxidation F2-IsoPs[6] When carotenoids are used as supplements to prevent the damag-ing action of ROS in the CF airways it is noteworthy that these are notparticularly good quenchers of peroxyl radicals relative to phenolicsand other antioxidants but are exceptional in quenching singlet oxy-gen at which most other phenolics and antioxidants are relativelyineffective Singlet oxygen is not a radical and does not react via radi-cal mechanisms but reacts mostly by the addition to double bondsforming endoperoxides that can be reduced to alkoxyl radicals that ini-tiate radical chain reactions typical of the peroxidative damage of PUFA[38] In this case the analysis of F2-IsoPs lipid peroxide formation andtransition metal-induced oxidizability of lipoproteins [162180] are allappropriate to evaluate the effect of carotenoids in preventing lipidperoxidation
As far as the dose is concerned clinical pharmacology of vitamin Eas an antioxidant was recently investigated by means of the effect onF2-IsoPs production and doses of α-tocopherol of 1600 IUday orgreater were found to be required to statistically affect plasma F2-IsoPs levels in hypercholeterolemic subjects [176] Several vitamin Esupplementation studies in CF patients have been performed withdoses of lower than 300 IUday regardless of the lowered absorptionby pancreatic and liver defects and the regular supplementationwith these doses does not appear to correct lipid oxidation markersin CF [7]
In the clinical practice and planning trials it has to be taken intoconsideration that in spite of substantial evidence supporting ahigher antioxidant demand in CF interventions with several antioxi-dant formulations produce poor responsiveness particularly in thecase of fat-soluble antioxidants which are poorly absorbed [6162]
Since many oxidants and antioxidants are present in tissuesand biological fluids and these have different chemical and physicalcharacteristics the possibility to produce a successful therapy witha single antioxidant molecule is too far to be realistic Moreover an-tioxidants act by multiple mechanisms in a single system or by adifferent single mechanism depending on the reaction systemresponding in a different manner to different radical or oxidantsources Because multiple reaction characteristics and mechanismsas well as different phase localizations are usually involved no single
704 F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
therapeutic approach will effectively prevent damage by multipleROS sources The defect of physiological antioxidants may also interferewith antioxidant therapies that are based on one or few exogenousantioxidants
Moreover several antioxidant vitamins such as vitamin E and ca-rotenoids have multiple natural forms with different bioavailabilitymetabolism and bioactivity [157167231] As far as the case of vita-min E supplementation concerns α-tocopherol was used as uniquevitamer in the large majority of supplementation trials so far per-formed and is the form used in the nutritional management of CFpatients Moreover several supplements contain the synthetic (or ra-cemic) form of this vitamin that has lower bioavailability than thenatural form Other forms present in nature and abundantly con-tained in vegetables such as tocotrienols and the less methylatedforms of tocopherol are not represented in many of the supplementformulations so far available in clinical centers and the supplementa-tion with α-tocopherol also limits their bioavailability These formsshow markedly higher susceptibility to hepatic metabolism and bili-ary excretion with respect to α-tocopherol eg the most representedform in blood and solid tissues and if co-supplemented these areeasily displaced during liver uptake and excreted with bile bymeans of competition with the same α-tocopherol Notwithstandingthese minor forms have been proposed to play important physiolog-ical roles showing molecular characteristics transcriptional effectsand antioxidant activities that clearly differentiate them in subfam-ilies with distinct biological functions Some of these such as α-tocopherol eg the second vitamin E form as relative abundance inblood and its carboxyethyl-hydroxychroman metabolite [189] ap-pear to have health-related anti-inflammatory effects which are par-ticularly relevant in lung protection [232233] This has suggestedthat such a group of ldquonon-α-tocopherolrdquo forms may represent anoth-er family of vitamins within the family of vitamin E with an impor-tant but often missed contribution to the proposed health effects ofthis vitamin [163]
These aspects may thus limit the possibility to provide CF patientsof optimal levels of this vitamin in all its components even if they areregularly treated with a vitamin E supplement eg withα-tocopherol
Targeted antioxidant therapy with formulations with higher bio-availability and bioactivity has been anticipated in CF New antioxi-dant formulations have been proposed to overcome main limits ofantioxidant therapies so far proposed for these patients Water-miscible α-tocopheryl acetate containing polysorbate propylene gly-col or polyethylene glycol as emulsifiers form micellar structureswere suggested to providing greater bioavailability than the fat-soluble counterparts These were commercialized with the brandnames of E-viminreg Cremophorreg EL and Aquasolreg E but despitethe original positive expectation [234235] some studies failed to ob-serve a higher response in vitamin E levels when these were com-pared with fat-soluble formulations [236237]
In a pilot study by Papas et al [183] a micellar formulation of fat-soluble nutrients and antioxidants was found to improve plasmalevels of β-carotene γ-tocopherol and CoQ(10) reducing at thesame time some inflammatory markers in induced sputum eg mye-loperoxidase and to a lower extent PMN elastase and total cell countswhile lung function and sputum bacterial counts were unaffectedThe same group recently confirmed the possibility to increase the ab-sorption of fat-soluble micronutrients using formulations with higherbioavailability specifically designed for malabsorbing patients such asCF patients that include also vitamin K and commercialized with thebrand name of AquADEKsreg [162] Despite improved vitamin and mi-cronutrient levels in this non-randomized open-label study AquA-DEKsreg produced only modest improvements in weight percentileand pulmonary function Another recent pilot observation [182] hassuggested the beneficial effect of this formulation on antioxidant andoxidative stress parameters of this oral supplement that surely deservesmore clinical investigation by larger randomized controlled trials
Recent multivitaminic formulations have been designed to containalso the minor forms of vitamin E and specifically γ-tocopherol [238]the expected superiority of which with respect to formulations con-taining only α-tocopherol needs to be verified As discussed abovein the section dedicated to vitamin E further advancements in thetherapy of CF inflammation and oxidative stress could be based onsynthetic forms and natural metabolites of this vitamin that havebeen recently identified to possess higher antioxidant and also anti-inflammatory activity than α-tocopherol (reviewed in [163168])
Pre-clinical investigation of these and other fat-soluble agents iscurrently addressed to develop formulations and administration pro-tocols that may increase the therapeutic efficacy in the airways In theantioxidant therapy of lung dysfunction in CF local administrationprotocols may overcome the limits of oral and systemic administra-tion protocols increasing bioavailability and providing targetedapproach to inflammation and oxidative stress Aerosolization of vita-min E and other fat-soluble micronutrients is possible and may allowdirect administration in the airways to prevent toxicity of smokewhich is closely associated with inflammation and oxidative stress[164165] To our knowledge this as well as other strategies of localadministration such as instillation of solutions such as surfactant-like solutions enriched of vitamin E have not been previously inves-tigated in CF patients and other CF model systems
On the contrary inhalation is an administration route widelyadopted in the case of GSH and NAC therapy described above Inthis context Cys formulations alternative to NAC have been proposedfor use as antioxidant and anti-inflammatory agent for inhalationNacystelyn is a lysine adduct of NAC that thanks to a higher proton-ation equilibrium shows increased water solubility and thus betterbioavailability Nacystelyn has been described to influence IL-8 gener-ation and the inflammatory signaling of bronchial epithelial cells[239] and preliminary clinical evaluation has demonstrated the safetyof this drug [240] Further clinical trials aimed to assess the effect onlung symptomatology of CF patients are needed Direct administra-tion in the airways could also be adopted for micronutrient vitaminswith poor absorption and bioavailability due to GI defects
38 Clinical impact of antioxidant therapy in CF
Huge in vitro and pre-clinical evidence has provided the rationaleto support clinical investigation of antioxidant strategies in CF Theseshould aim to restore the oxidantndashantioxidant balance of CF airwaychallenged by chronic infection and inflammatory cell activation
Some observational trials have confirmed that antioxidants usedas either supplements to the diet or drugs for lung administrationby aerosolized formulations may help in relieving progressive lungdamage and other adverse clinical events of CF such as poor growthSo far few studies have examined with sufficient methodologicalrigor the clinical efficacy of antioxidant therapy in CF This was alsoconcluded in a previous review of the literature by Cantin et al [12]that was published in the beginning of 2006 and is confirmed alsoin a recent analysis of clinical trials on antioxidant therapy in CF pa-tients [213] that examined the literature until September 2010using as sources the databases of the Cochrane CF and Genetic Disor-ders Group CF Trials Register PubMed CINAHL and AMED Useful in-formation was retrieved from just four randomized controlled trialsand one quasi-randomized controlled trial on vitamin C vitamin Eβ-carotene and selenium used as supplements administered aloneor in combination Post-hoc data analysis that was possible only inthree studies on a total of 87 CF patients showed the absence ofany significant improvement in lung function that was selected as pri-mary outcome together with quality of life that improved in one trialSecondary outcomes concerning laboratory indices of oxidative stressand antioxidant status showed several improvements These includedan increase of RBC SeGPx by selenium supplementation done as
705F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
individual or combined supplementation and increased levels of allplasma antioxidants except vitamin C that were observed in all thetrials
The message from these studies to pediatricians and nutritionistswithin the clinical staff of CF centers is that in the absence of solid ev-idence regarding the clinical effectiveness of oral formulations of an-tioxidant supplements in CF (including PUFA) their use as a routineclinical practice should be considered with caution keeping clear inmind that this should represent just a complement of one of themost critical interventions in the life-long clinical management pro-gram of CF patients eg providing an adequate nutriture [140] Inthis context compensating energy and protein malnutrition has toremain the first goal of nutritional management programs Providinghigher intakes of antioxidant micronutrients with food naturally-enriched (or functionalized) of micronutrient antioxidants shouldbe preferred in order to have the higher combination of positive nu-tritional factors that are lost during refinement procedures and over-all industrial processing of dietary supplements
Measures of good practice in clinical management of micro-malnutrition in CF patients would include the support of specializedpersonnel and laboratories The centers should have the possibilityto ascertain with appropriate nutritional and laboratory tests whatthe level of deficiency is for the different micronutrients that each pa-tient may suffer from during a dietary program Monitoring dietaryintakes and blood levels of micronutrients is not sufficient to set apersonalized nutritional intervention with supplements or functionalfoods Sub-optimal intakes and the compliance to nutritional inter-ventions should be verified by means of selected biochemical andclinical criteria Unluckily the latter are still not well established forsome micronutrients such as the fat-soluble vitamins E (reviewed in[163173241]) and K [242243] and also for trace elements such asSe [244] For many of the antioxidants used as supplements inhumans we still do not know exactly several of the biological effectsthat these may provide when introduced in a healthy body and weknow less what these can do in disease These aspects hardly impacton the concept of optimal levels of intake that should be identified foreach micronutrient on an individual basis According with the aspectsdiscussed in the previous sections optimal levels of intake for antiox-idant micronutrients are different in CF patients and healthy subjectsand vary with age and several individual factors
Lung administration of antioxidants by means of aerosolized for-mulations so far used for GSH therapy (see above) is a promisingfield of clinical investigation in CF Toxicity issues are currently themain concern and the subject of clinical evaluation by several groups(described above)
Information on future directions of antioxidant therapy in CF canbe inferred by the analysis of pending or recently completed clinicaltrials that have been searched (December 2011) at ClinicalTrialsgovdatabase matching the terms ldquoantioxidant therapyrdquo or ldquoglutathionerdquowith ldquocystic fibrosisrdquo Fifteen trials were retrieved and those directlyrelated to antioxidant therapy (n=12) are presented in Table 1 andinclude efficacy and safety studies of inhaled drugs as GSH sodiumpyruvate NAC and NO and the dietary supplements AquADEKsregan antioxidant-rich multivitamin supplement epigallocatechin gal-late (EGCG)tocotrienol curcuminoids the amino acid glutaminesulforaphane in broccoli sprouts One trial is investigating the flavo-noid quercetin as CFTR modulator
39 Emerging antioxidant and anti-inflammatory approaches in CF
Mediterranean foods such as olive oil and red wine or severalplant extracts such as herbal tea or grape seed extracts contain aseries of natural compounds with important antioxidant and NOscavenging activity that have been widely investigated for the pre-vention of oxidative stress-related diseases [38245] These havebeen long investigated as template molecules to develop antioxidant
and anti-inflammatory drugs Between the multitudes of natural sub-stances most investigated ones include for instance tyrosol hydroxy-tyrosol gallic and caffeic acids belonging to the family of phenolswhile resveratrol of the stilbenes family epicatechin kaempferoland cianidin are examples of flavonoids examples of fat-soluble phe-nolics are those of the family of tocols (vitamin E) and carotenoids Allthese compounds show different metabolisms and signaling effects[246] Antioxidant and cell protection mechanisms are associatedwith different and sometimes concurrent processes as H-atom trans-fer and electron donation radical trapping and chelation of transitionmetals that can be easily investigated at the chemical level [247] Be-sides these direct antioxidant effects metabolic responses and signal-ing effects of natural compounds are also important to producesecond-generation responses that modify the level of antioxidantprotection and the potential for ROS detoxification in cells and bodyfluids These derive from the transcriptional regulation of antioxidantand pro-oxidant genes that coexist with the modulation of cytokinesecretion and inflammatory enzyme activities
Some of these natural plant-derived antioxidants may provide fur-ther pharmacological activities of possible relevance in CF This is thecase for instance of the plant flavonoids genistein apigenin kaemp-ferol quercetin and hesperidin [248ndash251] that fall in the pharmaco-logical category of ldquopotentiatorsrdquo [252] in that these activate at leastto a certain extent CTFR-mediated Cl currents in normal and CF airwayepithelium investigated either in vitro or in vivo in humans and ani-mal models Actually as prototypal flavonoid-derived potentiatorthe tyrosine kinase inhibitor genistein potentiates the gating of wild-type as well as ΔF508 CFTR and G551D CFTR [253] but at higherdoses it inhibits CFTR gating which make this an unlikely clinical can-didate Similar potentiation effects have been reported for the antiox-idant curcumin [250] that shows an additive effect with respect togenistein-induced potentiation Besides CFTR potentiation whichdoes not appear to have a direct influence on GSH and nutrient trans-port in the lung tissue all these natural substances have been usedalone or in combination with other agents as in vivo enhancers oflung antioxidant protection [246254255] In the case of quercetinthiol-reactive phenolic [256] bronchodilation and anti-inflammatoryeffects by a restoration of the Th1Th2 balance have been reportedin inflammatory syndromes of the lung [255257ndash259] but theseeffects have not been explored in CF Pyocyanin toxicity (see abovein the Section 2) could represent an issue for the use of quercetinand other catechols in infectious diseases of the lung [260]
Other natural antioxidants of potential interest in CF therapy in-clude terpenoids [261] such as terpinen-4-ol a major constituentof tea tree oil that is being investigated in the therapy of anti-biotic resistant organisms specifically against methicillin-resistantStaphylococcus aureus (MRSA) [262] a problem in CF [263] Otherthan being lipophilic antioxidants terpenes can prevent oxidativestress of the CF lung secondarily to the antibiotic effect thereby pro-moting a better control of immuno-inflammatory pathways and lungantioxidants
391 Targeting NF-κB with natural compounds resveratrol and plantextracts
Natural compounds were long known to be useful in designinganti-inflammatory drugs and some of these could find an applicationin the control of the transcription factor kappa-B (NF-κB) that maylead to develop advanced pharmacological tools to control inflamma-tion and to produce higher antioxidant protection to CF airwaysInhibitors targeting NF-κB including transcription factors decoymolecules (TFD) are potent down-regulators of gene expressionand release of IL-8 in CF cells infected with P aeruginosa [264265]
Resveratrol (354prime-trihydroxystilbene ldquoErdquo form) is one of the mostinvestigated natural antioxidant with proposed activity as NF-κBinhibitor This is a phytoalexin present in large quantity in red winepreferentially in the skin of grapes being its concentration
706 F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
50ndash100 μgmg of fresh skin and 13ndash3 mgl of red wine [266]Furthermore resveratrol is a constituent of lsquoDarakchasavarsquo (13ndash6 mgl) an ayurvedic medicine from India [267] The antioxidant activity ofresveratrol has been reported in several papers and occurs also in lungtissues suggesting that resveratrol has potential as a therapeuticagent in respiratory disease [268ndash270] Resveratrol can be consideredone of the most interesting molecules from the natural worldexhibiting strong antioxidant activity that at the same time is able toexert anti inflammatory activity through alteration of NF-κB functionsand efficient inhibition of pro-inflammatory genes [271272] As far asthe effects on CF model systems are concerned Cabrini et al [26]reported the effects of resveratrol on P aeruginosa infected CF IB3-1cells The results obtained demonstrate that resveratrol exhibits minoreffects of IB3-1 cell growth and important inhibitory effects on accumu-lation of IL-8 and GRO-α mRNA while minor effects on IL-6 gene ex-pression were observed These data support recently publishedobservations suggesting inhibitory effects of resveratrol in infection-mediated inflammatory processes [273] Interestingly resveratrol hasbeen reported as a potent inhibitor of NF-κB activity and a promisinganti-inflammatory agent [272274] also in combinationwith othermol-ecules [274275] However in vivo translation of this pre-clinical on res-veratrol is hard to be foreseen This natural compound displays poorbioavailability [276] and further characterization of resveratrol pharma-cokinetics is troublesome since it is hardly measurable in vivo [277]Furthermore the regulation of inflammatory responses by resveratrolhas been suggested to be far more complex than simple direct suppres-sion of NF-κB activity Actually some aspects of the immune responsecould be enhanced by this natural substance which may lead tohypothesize broad negative feedback events on immuno-inflammatorypathways [278] In any case and with these cautions in mind the pub-lished observations on cellular model systems support the concept thatresveratrol and resveratrol-containing formulations deserve further con-sideration to determine their possible therapeutic values in CF
Other inhibitors can be identified from systematic studies of naturalproducts and their ability to interfere with NF-κB activity [279ndash281]Recent studies have demonstrated that the whole extract of Aeglemarmelos (Rutaceae) has strong inhibitory effect on the P aeruginosa-dependent IL-8 induction in human CF-derived bronchial IB3-1 cellswithout affecting cell proliferation [280] Molecular analysis of compo-nents contained in A marmelos extracts revealed that three major com-pounds namely 56-dimethoxy-1-indanone 2-hydroxy-cinnamic acidand 5-methoxy psoralen (5-MOP) reproduce the inhibitory effect ob-servedwith thewhole extract [280] A further example has been recent-ly published using extracts from bergamot (Citrus bergamia Risso) Inthis study the extracts were characterized and the main detected con-stituents were assayed for their biological activity [281] The resultsobtained demonstrated that the extracts from bergamot epicarps con-tain components displaying an inhibitory activity on IL-8 Particularlythe most active molecules were bergapten and citropten These effectshave been confirmed by analyzing mRNA levels and protein release inthe CF cellularmodels IB3-1 and CuFi-1 inducedwith TNF-α or exposedto P aeruginosa
A parallel strategy linking NF-κB inhibition and down-regulationof NF-κB-dependent functions is described in recently publishedstudies based on a structured-based virtual screening (VS) of differ-ently substituted furocoumarins and analogues against NF-κB withthe objective of selecting molecules able to inhibit the binding ofthis transcription factor to DNA [282283] Novel compounds wereidentified with this strategy as potent inhibitors of NF-κB dependentbiological functions to be proposed for the control lung inflammationoccurring in patients affected by CF [282ndash284]
392 Scavengers and regulators of H2O2 and NO
3921 Lactoferrin and OSCNmacr The impaired DUOXLPO system of CFpatients could be the target of therapeutic strategies that may
produce concomitant antimicrobial and antioxidant effects This sys-tem described above in Section 22 represents an important compo-nent of innate immunity with a role in bactericidal defense andregulation of H2O2 metabolism of airways [32] CF patients have alsoreported to show lowered LF levels in the ASL [37] that togetherwith a CFTR-dependent defective efflux of SCNmacr and LPO [36] may cre-ate the environment for a sustained flux of H2O2 and for the genera-tion of highly reactive Fenton species [1138] An ideal therapeuticintervention should restore the LPO-dependent generation of bacteri-cidal OSCNmacr from DUOX-derived H2O2 and SCNmacr in the ASL to controlat the same time the microbial biofilm and the flux of H2O2 into theASL An approach close to this therapeutic mechanism was recentlyproposed for the drug Meveolreg This is a complex of LF and OSCNmacrwith proposed in vivo antimicrobial activity [285] to be evaluatedin clinical trials for the aerosol treatment of lung infections in CFpatients The role for this drug in the control of H2O2 levels of ASLremains to be investigated
3922 Organoselenium compounds Organoselenium compoundshave been proposed as therapeutic agents useful in the antioxidanttherapy of inflammatory conditions These include GPX mimetic mol-ecules such as Ebselenreg (2-phenyl-12-benzisoselenazol-3(2H)-one)or other and more recently developed molecules that are still inpre-clinical steps of evaluation [286] Selectively and specificity of ac-tion are main issues in the therapeutic mechanism of this candidateantioxidant drug that thanks to the electrophilic properties of Se[214] reacts with thiols to reduce H2O2 and other species MoreoverEbselenreg has been described to act as potent non-competitive inhib-itor of extracellular nucleoside diphosphokinase (NDPK) having neg-ligible effect on ecto-ATPase and adenyl kinase activities which areother players of the metabolism of extracellular nucleotides [287]This enzyme together with other nucleoside di- and triphosphatescontributes to regulate several components of the mucociliary clear-ance process (MCC) that protects the lung against infections via acti-vation of epithelial purinergic receptors The inhibition of NDPK bythis GPX-mimetic drug may also impact on the energy status of endo-thelial cells [287] This aspect could be further investigated as a cellu-lar protection mechanism in the pulmonary epithelium of CF patientsbeing the control of cell energy of fundamental importance to preventthe activation of death pathways [288]
Further therapeutic mechanisms for these Se-derived drugs mayderive from the marked activity as inducers of phase II enzymessuch as quinone reductase (QR) and glutathione-S-transferase (GST)[289] This induction response also observed with other electrophilsand redox-active molecules such as natural phenolic antioxidantscould produce higher cellular protection by the acquisition of anincreased capability to detoxify endobiotics generated during oxida-tive stress and inflammation [246]
3923 Melatonin and GSNO as NOx regulators Increased markers ofNO-derived biological damage are present in the CF lung suggestingthe abnormal reactivity of NOx in the inflamed lung of CF patients[52] However an impaired metabolism and biological function ofNO in CF airways (see Section 23) suggests a cautious approach tothe use of agents that may influence the levels and chemical behaviorof NO-derived species (NOx) with possible impact on the physiologi-cal roles of NO in vasodilatation innate immunity and H2O2 metabo-lism of the respiratory tract [290291] NO donors also appear toinfluence CFTR function of alveolar epithelium and gland serouscells [292293]
Main physiological role of the pineal gland hormone melatonin isthe synchronization of circadian rhythms including the sleepndashwakecycle but several other functions dealing with immunomodulatoryantioxidant and cellular protection effects have been identified[294] Melatonin receptor stimulation may also influence cyclic AMPsignaling and the regulation of CFTR ion channel [295296]
707F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
A recent randomized double-blind placebo-controlled study hasexamined the effects of short term melatonin administration (3 mgfor 3 weeks) on sleep and oxidative stress markers in CF [297]According with the expected pharmacological effect of this hormonalsubstance the treatment was successful in improving sleep indicesAt the same time nitrite levels determined in exhaled breath conden-sate (EBC) were reduced to suggest a better control of NOmetabolismof CF airways (discussed above in Section 23) but these effects how-ever were not associated with a significant correction of isoprostaneas lipid peroxidation marker measured in EBC Increasing dosages ofmelatonin could be investigated for the pharmacological treatmentof oxidative stress and immune dysfunction of CF patients due tothe absence of adverse effects of this hormonal substance in humans
The S-nitrosation reaction of thiols is another interesting aspect ofNO pharmacology [53] that may find an application in the therapy oflung complications of CF This has been the case for instance of theS-nitrosothiol GSNO that has been used safely in human trials[298299] This endogenous nitrosothiol with proposed regulatory ef-fect on the CFTR of lung epithelia [292293] is well tolerated in pa-tients with CF when administered by aerosolization and mayproduce better oxygenation [299] thereby suggesting that therapyaimed at restoring endogenous GSNO levels in the CF airway maymerit further clinical evaluation Since the administered GSNO de-composes as shown by the increased levels of expired NO in CF pa-tients under treatment with this nitrosothiol [299] furtherinvestigation should be addressed to ascertain whether GSNO thera-py may merely correspond to a GSH therapy
NO dependent effects on CFTR function should be considered toevaluate mechanism of action and specificity of antioxidant therapiesthat target NO metabolism and function in the CF airways
4 Conclusions and future perspectives
The presence of clinical and biochemical symptoms of inflammationand oxidative stress implies that CF patients have a higher demand ofantioxidant protection The combination of the dysfunctional CFTRwith a lowered intake and absorption of dietary antioxidants producesub-optimal levels of protection from both enzymatic and non-enzymatic defense systems The former could be associated with a de-fective glutathionemetabolism and lowered intake of sulfur-containingamino acids and oligoelements such as zinc and possibly seleniumwhile fat-soluble antioxidant vitamins such as vitamin E and caroten-oids and the water-soluble vitamin C are lowered than in healthy sub-jects due to malabsorption and possibly higher consumption
The increased antioxidant demand in CF patients should be evenhigher in the presence of complications of the lung pancreas andliver Lung comorbidity is particularly important in this contextbeing associated with recurrent infections which results in the alter-nation of inflammatory exacerbates and chronic inflammation Thesesustain the flux of ROS in the airways and promote the formation ofsecond-generation byproducts by the damage of biomolecules suchas PUFA and proteins which may diffuse also at the systemic level tofurther promote adverse biological responses and toxic reactions Pan-creatic insufficiency causes malnutrition and may lead to develop en-docrine and metabolic defects associated with diabetes of CF Theseevents can be further aggravated by the concomitance of liver dys-function and a poor nutritional status Malnutrition is strongly associ-ated with poor prognosis as assessed by pulmonary function andsurvival data [138ndash140] The more aggressive nutritional interven-tions seem to produce better clinical outcomes in these patients andthe possibility of achieving higher antioxidant protection in well-nourished patients by dietary factors could be a key aspect to explainsuch a clinical advantage The assumption that food-derived compo-nentsmay help to prevent the damaging effects of oxidative stress im-proving the antioxidant defenses deserves further investigation at theclinical level This together with the investigation of appropriate
laboratory biomarkers could provide critical information to establishintervention criteria for an early nutritional management of newly di-agnosed patients [5] It is expected that a timely secondary preventionstrategy could influence the progression of CF symptoms thusaffecting with a self-feeding mechanism the same extent of malnutri-tion and oxidative stress along the life of CF patients Since severalfactors contribute to impair the nutritional status of CF patients(such as pancreatic insufficiency chronic malabsorption recurrentsinopulmonary infections and progressive lung disease chronic in-flammation increased energy expenditure suboptimal intake multi-therapy) careful monitoring of the antioxidant status should berecommended According with international guidelines fat-solublevitamin supplementation is of utmost importance in daily practice to-gether with energy intake requirements and pancreatic enzyme-replacement therapy Among these vitamin E β-carotene and ω-3FA have observed to alleviate selected biochemical signs of oxidativestress as measured for instance with well established laboratory indi-ces of lipid peroxidation and in some studies these effects werepreliminarily associated with positive clinical outcomes Notwith-standing randomizedndashcontrolled clinical trials on antioxidant supple-ments (including ω-3 FA) so far carried out in CF have failed toconclusively demonstrate significant beneficial effects on respiratorysymptoms and on the consequent impact that these have on the qual-ity of life of these patients (reviewed in [202213]) whichmay provideno support for the use of these supplements in CF An absence of effi-cacy in prevention studies on antioxidant supplements has also beenobserved in other and possibly less severe oxidative stress-relatedconditions particularly in the secondary prevention of cardiovasculardisease and some forms of cancer by vitamin E and other antioxidantssuch as vitamin C selenium and β-carotene (reviewed in [163]) Dif-ferent biases however have been identified in randomize large clini-cal trials that may account for these disappointing findings Theseinclude patient selection criteria (early interventions and primaryprevention could have more chances of success than secondaryprevention) duration and doses of the treatment use of wrong anti-oxidant formulations and administration protocols absence of verifi-cations of the biological compliance to the treatment etc The samebiases apply for the few trials carried out in CF patients Thus the ap-propriateness and efficacy of nutritional interventions with naturalfood-derived or synthetic antioxidants should be verifiedwith respectto the biological pathways of oxidative stress and clinical variablesthat are identified as end-points Profiles of blood and tissue antioxi-dants as well as of reliable surrogate markers of oxidative stresshave to be selected and determined in highly specialized laboratorieswith a well-established experience on these analyses
Well-timed (early) interventions with appropriate antioxidantformulationsprotocols need to be proposed for the next generationof trials and the development of novel CF-tailored antioxidant andanti-inflammatory agents should be promoted
As a consequence of these considerations more clinical investiga-tion is awaited to identify future successful approaches to the antiox-idant therapy as a measure to further enhance quality of life and theoverall clinical outcome of CF patients
Acknowledgments
We are indebted with the Italian Cystic Fibrosis Research Founda-tion for the support that it provided with its grant program to the re-search activity of the authors of this paper This is a scientific initiativeof the ldquoWorking Group on Inflammation in Cystic Fibrosisrdquo (BragonziA Bravo E Cabrini G Conese M Cuzzocrea S Dechecchi MC De Ales-sandri A Evangelista V Galli F Gambari R Lambiase A Lucidi VManca A Melotti P Minicucci L Motta A Pietraforte D Pompella AQuattrucci S Rizzo R Romano M Sorio C Tesse R) of the Italian Soci-ety for Cystic Fibrosis A particular thank goes to the Prof GianniMastella for the critical revision of the manuscript and for the
708 F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
stimulating research environment that he has contributed to createwithin the Italian Cystic Fibrosis Research Foundation
References
[1] BP OSullivan SD Freedman Cystic fibrosis Lancet 373 (2009) 1891ndash1904[2] P Linsdell JW Hanrahan Glutathione permeability of CFTR Am J Physiol 275
(1998) C323ndashC326[3] L Gao KJ Kim JR Yankaskas HJ Forman Abnormal glutathione transport in
cystic fibrosis airway epithelia Am J Physiol 277 (1999) L113ndashL118[4] RK Rowntree A Harris The phenotypic consequences of CFTR mutations Ann
Hum Genet 67 (2003) 471ndash485[5] EI Back C Frindt D Nohr J Frank R Ziebach M Stern M Ranke HK Biesalski
Antioxidant deficiency in cystic fibrosis when is the right time to take actionAm J Clin Nutr 80 (2004) 374ndash384
[6] LG Wood DA Fitzgerald AK Lee ML Garg Improved antioxidant and fattyacid status of patients with cystic fibrosis after antioxidant supplementation islinked to improved lung function Am J Clin Nutr 77 (2003) 150ndash159
[7] L Iuliano R Monticolo G Straface S Zullo F Galli M Boaz S Quattrucci Asso-ciation of cholesterol oxidation and abnormalities in fatty acid metabolism incystic fibrosis Am J Clin Nutr 90 (2009) 477ndash484
[8] C Libetta V Sepe P Esposito F Galli A Dal Canton Oxidative stress and inflam-mation implications in uremia and hemodialysis Clin Biochem 44 (2011)1189ndash1198
[9] G Bartosz Reactive oxygen species destroyers or messengers Biochem Phar-macol 77 (2009) 1303ndash1315
[10] T Ntimbane B Comte G Mailhot Y Berthiaume V Poitout M Prentki RRabasa-Lhoret E Levy Cystic fibrosis-related diabetes from CFTR dysfunctionto oxidative stress Clin Biochem 30 (2009) 153ndash177
[11] A van der Vliet JP Eiserich GP Marelich B Halliwell CE Cross Oxidativestress in cystic fibrosis does it occur and does it matter Adv Pharmacol 38(1997) 491ndash513
[12] AM Cantin TB White CE Cross HJ Forman RJ Sokol D Borowitz Antioxi-dants in cystic fibrosis Conclusions from the CF antioxidant workshop Bethes-da Maryland Free Radic Biol Med 42 (2007) 15ndash31
[13] LT McGrath P Mallon L Dowey B Silke E McClean M McDonnell A DevineS Copeland S Elborn Oxidative stress during acute respiratory exacerbations incystic fibrosis Thorax 54 (1999) 518ndash523
[14] E Thomson S Brennan R Senthilmohan CL Gangell AL Chapman PD SlyAJ Kettle E Balding LJ Berry JB Carlin R Carzino N de Klerk T Douglas CFoo LW Garratt GL Hall J Harrison A Kicic IA Laing KM Logie J MassieLS Mott C Murray F Parsons N Pillarisetti SR Poreddy SC RanganathanCF Robertson R Robins-Browne PJ Robinson B Skoric SM Stick ENSutanto E Williamson Identifying peroxidases and their oxidants in the earlypathology of cystic fibrosis Free Radic Biol Med 49 (2010) 1354ndash1360
[15] SP Range C Dunster AJ Knox FJ Kelly Treatment of pulmonary exacerba-tions of cystic fibrosis leads to improved antioxidant status Eur Respir J 13(1999) 560ndash564
[16] L Coppo P Ghezzi Thiol regulation of pro-inflammatory cytokines and innateimmunity protein S-thiolation as a novel molecular mechanism Biochem SocTrans 39 (2011) 1268ndash1272
[17] C Verhaeghe C Remouchamps B Hennuy A Vanderplasschen A Chariot SPTabruyn C Oury V Bours Role of IKK and ERK pathways in intrinsic inflamma-tion of cystic fibrosis airways Biochem Pharmacol 73 (2007) 1982ndash1994
[18] TL Bonfield JR Panuska MW Konstan KA Hilliard JB Hilliard H Ghnaim MBerger Inflammatory cytokines in cystic fibrosis lungs Am J Respir Crit CareMed 152 (1995) 2111ndash2118
[19] TL Noah HR Black PW Cheng RE Wood MW Leigh Nasal and bronchoal-veolar lavage fluid cytokines in early cystic fibrosis J Infect Dis 175 (1997)638ndash647
[20] MJ Welsh BW Ramsey FJ Accurso GR Cutting Cystic Fibrosis McGraw-HillNew York 2001
[21] TZ Khan JS Wagener T Bost J Martinez FJ Accurso DW Riches Early pul-monary inflammation in infants with cystic fibrosis Am J Respir Crit CareMed 151 (1995) 1075ndash1082
[22] FA Ratjen Cystic fibrosis pathogenesis and future treatment strategies RespirCare 54 (2009) 595ndash605
[23] J Jacquot O Tabary P Le Rouzic A Clement Airway epithelial cell inflamma-tory signalling in cystic fibrosis Int J Biochem Cell Biol 40 (2008)1703ndash1715
[24] CM Greene P Branagan NG McElvaney Toll-like receptors as therapeutic tar-gets in cystic fibrosis Expert Opin Ther Targets 12 (2008) 1481ndash1495
[25] M Rottner JM Freyssinet MC Martinez Mechanisms of the noxious inflam-matory cycle in cystic fibrosis Respir Res 10 (2009) 23
[26] G Cabrini V Bezzerri I Mancini E Nicolis MC Dechecchi A Tamanini ILampronti L Piccagli N Bianchi M Borgatti R Gambari Targeting transcrip-tion factor activity as a strategy to inhibit pro-inflammatory genes involved incystic fibrosis decoy oligonucleotides and low-molecular weight compoundsCurr Med Chem 17 (2010) 4392ndash4404
[27] CM Greene NG McElvaney Proteases and antiproteases in chronic neutrophiliclungdiseasemdash relevance to drug discovery Br J Pharmacol 158 (2009) 1048ndash1058
[28] AM Cantin Potential for antioxidant therapy of cystic fibrosis Curr Opin PulmMed 10 (2004) 531ndash536
[29] JF Chmiel MW Konstan Inflammation and anti-inflammatory therapies forcystic fibrosis Clin Chest Med 28 (2007) 331ndash346
[30] DP Nichols MW Konstan JF Chmiel Anti-inflammatory therapies for cys-tic fibrosis-related lung disease Clin Rev Allergy Immunol 35 (2008)135ndash153
[31] AJ Kettle T Chan I Osberg R Senthilmohan AL Chapman TJ Mocatta JSWagener Myeloperoxidase and protein oxidation in the airways of youngchildren with cystic fibrosis Am J Respir Crit Care Med 170 (2004)1317ndash1323
[32] H Fischer Mechanisms and function of DUOX in epithelia of the lung AntioxidRedox Signal 11 (2009) 2453ndash2465
[33] B Rada TL Leto Oxidative innate immune defenses by NoxDuox familyNADPH oxidases Contrib Microbiol 15 (2008) 164ndash187
[34] P Moskwa D Lorentzen KJ Excoffon J Zabner PB McCray Jr WM NauseefC Dupuy B Banfi A novel host defense system of airways is defective in cysticfibrosis Am J Respir Crit Care Med 175 (2007) 174ndash183
[35] D Lorentzen L Durairaj AA Pezzulo Y Nakano J Launspach DA Stoltz GZamba PB McCray Jr J Zabner MJ Welsh WM Nauseef B Banfi Concentra-tion of the antibacterial precursor thiocyanate in cystic fibrosis airway secre-tions Free Radic Biol Med 50 (2011) 1144ndash1150
[36] Y Xu S Szep Z Lu The antioxidant role of thiocyanate in the pathogenesis ofcystic fibrosis and other inflammation-related diseases Proc Natl Acad Sci US A 106 (2009) 20515ndash20519
[37] MP Rogan CC Taggart CM Greene PG Murphy SJ ONeill NG McElvaneyLoss of microbicidal activity and increased formation of biofilm due to decreasedlactoferrin activity in patients with cystic fibrosis J Infect Dis 190 (2004)1245ndash1253
[38] B Halliwell JM Guttridge Free Radicals in Biology and Medicine Fourth editionOxford University Press New York 2007
[39] B Rada K Lekstrom S Damian C Dupuy TL Leto The Pseudomonastoxin pyocyanin inhibits the dual oxidase-based antimicrobial system as itimposes oxidative stress on airway epithelial cells J Immunol 181 (2008)4883ndash4893
[40] C Schwarzer B Illek JH Suh SJ Remington H Fischer TE Machen Organelleredox of CF and CFTR-corrected airway epithelia Free Radic Biol Med 43(2007) 300ndash316
[41] JH Roum R Buhl NG McElvaney Z Borok RG Crystal Systemic deficiency ofglutathione in cystic fibrosis J Appl Physiol 75 (1993) 2419ndash2424
[42] VM Hudson Rethinking cystic fibrosis pathology the critical role of abnormalreduced glutathione (GSH) transport caused by CFTR mutation Free RadicBiol Med 30 (2001) 1440ndash1461
[43] PJ Barnes RA Dweik AF Gelb PG Gibson SC George H Grasemann IDPavord F Ratjen PE Silkoff DR Taylor N Zamel Exhaled nitric oxide in pul-monary diseases a comprehensive review Chest 138 (2010) 682ndash692
[44] H Grasemann E Michler M Wallot F Ratjen Decreased concentration of ex-haled nitric oxide (NO) in patients with cystic fibrosis Pediatr Pulmonol 24(1997) 173ndash177
[45] H Grasemann F Ratjen Cystic fibrosis lung disease the role of nitric oxidePediatr Pulmonol 28 (1999) 442ndash448
[46] B Gaston F Ratjen JW Vaughan NR Malhotra RG Canady AH Snyder JFHunt S Gaertig JB Goldberg Nitrogen redox balance in the cystic fibrosis air-way effects of antipseudomonal therapy Am J Respir Crit Care Med 165(2002) 387ndash390
[47] H Grasemann I Ioannidis RP Tomkiewicz H de Groot BK Rubin F RatjenNitric oxide metabolites in cystic fibrosis lung disease Arch Dis Child 78(1998) 49ndash53
[48] H Grasemann R Schwiertz S Matthiesen K Racke F Ratjen Increased argi-nase activity in cystic fibrosis airways Am J Respir Crit Care Med 172(2005) 1523ndash1528
[49] H Grasemann S Al-Saleh JA Scott D Shehnaz A Mehl R Amin M Rafii PPencharz J Belik F Ratjen Asymmetric dimethylarginine contributes to airwaynitric oxide deficiency in patients with cystic fibrosis Am J Respir Crit CareMed 183 (2011) 1363ndash1368
[50] H Grasemann F Kurtz F Ratjen Inhaled L-arginine improves exhaled nitricoxide and pulmonary function in patients with cystic fibrosis Am J RespirCrit Care Med 174 (2006) 208ndash212
[51] H Grasemann F Ratjen Emerging therapies for cystic fibrosis lung disease Ex-pert Opin Emerg Drugs 15 (2010) 653ndash659
[52] BM Morrissey K Schilling JV Weil PE Silkoff DM Rodman Nitric oxide andprotein nitration in the cystic fibrosis airway Arch Biochem Biophys 406(2002) 33ndash39
[53] R Radi Nitric oxide oxidants and protein tyrosine nitration Proc Natl AcadSci U S A 101 (2004) 4003ndash4008
[54] J Chen M Kinter S Shank C Cotton TJ Kelley AG Ziady Dysfunction of Nrf-2in CF epithelia leads to excess intracellular H2O2 and inflammatory cytokineproduction PLoS One 3 (2008) e3367
[55] F Galli M Piroddi C Annetti C Aisa E Floridi A Floridi Oxidative stress andreactive oxygen species Contrib Nephrol 149 (2005) 240ndash260
[56] DT Wright LA Cohn H Li B Fischer CM Li KB Adler Interactions of oxygenradicals with airway epithelium Environ Health Perspect 102 (Suppl 10)(1994) 85ndash90
[57] I Rahman SR Yang SK Biswas Current concepts of redox signaling in thelungs Antioxid Redox Signal 8 (2006) 681ndash689
[58] Q Li JF Engelhardt Interleukin-1beta induction of NFκB is partially regulatedby H2O2-mediated activation of NFκB-inducing kinase J Biol Chem 281(2006) 1495ndash1505
709F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
[59] E Boncoeur VS Criq E Bonvin T Roque A Henrion-Caude DC Gruenert AClement J Jacquot O Tabary Oxidative stress induces extracellular signal-regulated kinase 12 mitogen-activated protein kinase in cystic fibrosis lung ep-ithelial cells potential mechanism for excessive IL-8 expression Int J BiochemCell Biol 40 (2008) 432ndash446
[60] B Fischer J Voynow Neutrophil elastase induces MUC5AC messenger RNA ex-pression by an oxidant-dependent mechanism Chest 117 (2000) 317Sndash320S
[61] B Rada P Gardina TG Myers TL Leto Reactive oxygen species mediate in-flammatory cytokine release and EGFR-dependent mucin secretion in airwayepithelial cells exposed to Pseudomonas pyocyanin Mucosal Immunol 4(2011) 158ndash171
[62] C Schwarzer H Fischer EJ Kim KJ Barber AD Mills MJ Kurth DC GruenertJH Suh TE Machen B Illek Oxidative stress caused by pyocyanin impairs CFTRClminus transport in human bronchial epithelial cells Free Radic Biol Med 45(2008) 1653ndash1662
[63] J Hull M South P Phelan K Grimwood Surfactant composition in infants andyoung children with cystic fibrosis Am J Respir Crit Care Med 156 (1997)161ndash165
[64] KC Meyer A Sharma R Brown M Weatherly FR Moya J Lewandoski JJZimmerman Function and composition of pulmonary surfactant andsurfactant-derived fatty acid profiles are altered in young adults with cystic fi-brosis Chest 118 (2000) 164ndash174
[65] MK Pulfer RC Murphy Formation of biologically active oxysterols during ozo-nolysis of cholesterol present in lung surfactant J Biol Chem 279 (2004)26331ndash26338
[66] V Starosta E Rietschel K Paul U Baumann M Griese Oxidative changes ofbronchoalveolar proteins in cystic fibrosis Chest 129 (2006) 431ndash437
[67] V Starosta M Griese Oxidative damage to surfactant protein D in pulmonarydiseases Free Radic Res 40 (2006) 419ndash425
[68] M Griese R Essl R Schmidt E Rietschel F Ratjen M Ballmann K Paul Pulmo-nary surfactant lung function and endobronchial inflammation in cystic fibro-sis Am J Respir Crit Care Med 170 (2004) 1000ndash1005
[69] M Griese R Essl R Schmidt M Ballmann K Paul E Rietschel F Ratjen Se-quential analysis of surfactant lung function and inflammation in cystic fibrosispatients Respir Res 6 (2005) 133
[70] LG Wood DA Fitzgerald PG Gibson DM Cooper ML Garg Increased plasmafatty acid concentrations after respiratory exacerbations are associated with el-evated oxidative stress in cystic fibrosis patients Am J Clin Nutr 75 (2002)668ndash675
[71] P Montuschi SA Kharitonov G Ciabattoni M Corradi L van Rensen DM Ged-des ME Hodson PJ Barnes Exhaled 8-isoprostane as a new non-invasive bio-marker of oxidative stress in cystic fibrosis Thorax 55 (2000) 205ndash209
[72] CE Collins P Quaggiotto L Wood EV OLoughlin RL Henry ML Garg Elevat-ed plasma levels of F2 alpha isoprostane in cystic fibrosis Lipids 34 (1999)551ndash556
[73] D Hartl V Starosta K Maier I Beck-Speier C Rebhan BF Becker P Latzin RFischer F Ratjen RM Huber E Rietschel S Krauss-Etschmann M Griese In-haled glutathione decreases PGE2 and increases lymphocytes in cystic fibrosislungs Free Radic Biol Med 39 (2005) 463ndash472
[74] GL Milne H Yin JD Morrow Human biochemistry of the isoprostane pathwayJ Biol Chem 283 (2008) 15533ndash15537
[75] G Ciabattoni G Davi M Collura L Iapichino F Pardo A Ganci R Romagnoli JMaclouf C Patrono In vivo lipid peroxidation and platelet activation in cystic fi-brosis Am J Respir Crit Care Med 162 (2000) 1195ndash1201
[76] C Garenc P Julien E Levy Oxysterols in biological systems the gastrointestinaltract liver vascular wall and central nervous system Free Radic Res 44 (2011)47ndash73
[77] AM Cantin SL North RC Hubbard RG Crystal Normal alveolar epithelial lin-ing fluid contains high levels of glutathione J Appl Physiol 63 (1987) 152ndash157
[78] R Tirouvanziam CK Conrad T Bottiglieri LA Herzenberg RB Moss High-dose oral N-acetylcysteine a glutathione prodrug modulates inflammation incystic fibrosis Proc Natl Acad Sci U S A 103 (2006) 4628ndash4633
[79] LW Velsor C Kariya R Kachadourian BJ Day Mitochondrial oxidative stressin the lungs of cystic fibrosis transmembrane conductance regulator proteinmutant mice Am J Respir Cell Mol Biol 35 (2006) 579ndash586
[80] M Kelly-Aubert S Trudel J Fritsch T Nguyen-Khoa M Baudouin-Legros SMoriceau L Jeanson F Djouadi C Matar M Conti M Ollero F Brouillard AEdelman GSH monoethyl ester rescues mitochondrial defects in cystic fibrosismodels Hum Mol Genet 20 (2011) 2745ndash2759
[81] P Ghezzi Role of glutathione in immunity and inflammation in the lung Int JGen Med 4 (2011) 105ndash113
[82] N Dauletbaev K Viel R Buhl TO Wagner J Bargon Glutathione and glutathi-one peroxidase in sputum samples of adult patients with cystic fibrosis J CystFibros 3 (2004) 119ndash124
[83] CE Cross A van der Vliet CA ONeill S Louie B Halliwell Oxidants antioxi-dants and respiratory tract lining fluids Environ Health Perspect 102 (Suppl10) (1994) 185ndash191
[84] K Takeyama K Dabbagh J Jeong Shim T Dao-Pick IF Ueki JA Nadel Oxida-tive stress causes mucin synthesis via transactivation of epidermal growth factorreceptor role of neutrophils J Immunol 164 (2000) 1546ndash1552
[85] N Ballatori SM Krance S Notenboom S Shi K Tieu CL Hammond Glutathi-one dysregulation and the etiology and progression of human diseases BiolChem 390 (2009) 191ndash214
[86] SR Soltaninassab KR Sekhar MJ Meredith ML Freeman Multi-faceted regu-lation of gamma-glutamylcysteine synthetase J Cell Physiol 182 (2000)163ndash170
[87] HR Lopez-Mirabal JR Winther Redox characteristics of the eukaryotic cytosolBiochim Biophys Acta 1783 (2008) 629ndash640
[88] C Hwang AJ Sinskey HF Lodish Oxidized redox state of glutathione in the en-doplasmic reticulum Science 257 (1992) 1496ndash1502
[89] M Murphy Mitochondrial thiols in antioxidant protection and redox signallingdistinct roles for glutathionylation and other thiol modifications AntioxidRedox Signal (2011) ahead of print doi101089ars20114289
[90] BJ Day AM van Heeckeren E Min LW Velsor Role for cystic fibrosis trans-membrane conductance regulator protein in a glutathione response to bronch-opulmonary Pseudomonas infection Infect Immun 72 (2004) 2045ndash2051
[91] Y Zhang K Duan Glutathione exhibits antibacterial activity and increases tetra-cycline efficacy against Pseudomonas aeruginosa Sci China C Life Sci 52 (2009)501ndash505
[92] VM Hudson New insights into the pathogenesis of cystic fibrosis pivotal roleof glutathione system dysfunction and implications for therapy Treat RespirMed 3 (2004) 353ndash363
[93] LW Velsor A van Heeckeren BJ Day Antioxidant imbalance in the lungs ofcystic fibrosis transmembrane conductance regulator protein mutant miceAm J Physiol Lung Cell Mol Physiol 281 (2001) L31ndashL38
[94] I Kogan M Ramjeesingh C Li JF Kidd Y Wang EM Leslie SP Cole CE BearCFTR directly mediates nucleotide-regulated glutathione flux EMBO J 22(2003) 1981ndash1989
[95] NS Gould S Gauthier CT Kariya E Min J Huang DJ Brian Hypertonic salineincreases lung epithelial lining fluid glutathione and thiocyanate two protectiveCFTR-dependent thiols against oxidative injury Respir Res 11 (2010) 119
[96] VT Vasu SJ de Cruz JS Houghton KA Hayakawa BM Morrissey CE CrossJP Eiserich Evaluation of thiol-based antioxidant therapeutics in cystic fibrosissputum focus on myeloperoxidase Free Radic Res 45 (2011) 165ndash176
[97] L Roussel G Martel J Berube S Rousseau P aeruginosa drives CXCL8 synthesisvia redundant toll-like receptors and NADPH oxidase in CFTRF508 airway epi-thelial cells J Cyst Fibros 10 (2011) 107ndash113
[98] GW Lau DJ Hassett H Ran F Kong The role of pyocyanin in Pseudomonas aer-uginosa infection Trends Mol Med 10 (2004) 599ndash606
[99] R Wilson DA Sykes D Watson A Rutman GW Taylor PJ Cole Measurementof Pseudomonas aeruginosa phenazine pigments in sputum and assessment oftheir contribution to sputum sol toxicity for respiratory epithelium InfectImmun 56 (1988) 2515ndash2517
[100] M Muller Pyocyanin induces oxidative stress in human endothelial cells andmodulates the glutathione redox cycle Free Radic Biol Med 33 (2002)1527ndash1533
[101] YQ OMalley KJ Reszka BE Britigan Direct oxidation of 2prime7prime-dichlorodihy-drofluorescein by pyocyanin and other redox-active compounds independentof reactive oxygen species production Free Radic Biol Med 36 (2004)90ndash100
[102] CC Caldwell Y Chen HS Goetzmann Y Hao MT Borchers DJ Hassett LRYoung D Mavrodi L Thomashow GW Lau Pseudomonas aeruginosa exotoxinpyocyanin causes cystic fibrosis airway pathogenesis Am J Pathol 175 (2009)2473ndash2488
[103] YQ OMalley KJ Reszka DR Spitz GM Denning BE Britigan Pseudomonasaeruginosa pyocyanin directly oxidizes glutathione and decreases its levels inairway epithelial cells Am J Physiol Lung Cell Mol Physiol 287 (2004)L94ndashL103
[104] M Muller Glutathione modulates the toxicity of but is not a biologically rele-vant reductant for the Pseudomonas aeruginosa redox toxin pyocyanin FreeRadic Biol Med 50 (2011) 971ndash977
[105] R Cheluvappa R Shimmon M Dawson SN Hilmer DG Le Couteur Reactionsof Pseudomonas aeruginosa pyocyanin with reduced glutathione Acta BiochimPol 55 (2008) 571ndash580
[106] JH Widdicombe Transgenic animals may help resolve a sticky situation in cys-tic fibrosis J Clin Invest 120 (2010) 3093ndash3096
[107] X Sun H Sui JT Fisher Z Yan X Liu HJ Cho NS Joo Y Zhang W Zhou Y YiJM Kinyon DC Lei-Butters MA Griffin P Naumann M Luo J Ascher KWang T Frana JJ Wine DK Meyerholz JF Engelhardt Disease phenotype ofa ferret CFTR-knockout model of cystic fibrosis J Clin Invest 120 (2010)3149ndash3160
[108] NS Joo HJ Cho M Khansaheb JJ Wine Hyposecretion of fluid from trachealsubmucosal glands of CFTR-deficient pigs J Clin Invest 120 (2010) 3161ndash3166
[109] A Bragonzi Murine models of acute and chronic lung infection with cystic fibro-sis pathogens IJMM 300 (2010) 584ndash593
[110] AM van Heeckeren MD Schluchter Murine models of chronic Pseudomonasaeruginosa lung infection Lab Anim 36 (2002) 291ndash312
[111] A Bragonzi D Worlitzsch GB Pier P Timpert M Ulrich M Hentzer JB Ander-sen M Givskov M Conese G Doring Nonmucoid Pseudomonas aeruginosa ex-presses alginate in the lungs of patients with cystic fibrosis and in a mousemodel J Infect Dis 192 (2005) 410ndash419
[112] GS CW Bedrossian DB Singer JJ Hansen HS Rosenberg The lung in cysticfibrosis A quantitative study including prevalence of pathologic findingsamong different age groups Hum Pathol 7 (1976) 195ndash204
[113] WD HA Cash B McCullough WG Johanson Jr JA Bass A rat model of chron-ic respiratory infection with Pseudomonas aeruginosa Am Rev Respir Dis 119(1979) 453ndash459
[114] EM JR Starke C Langston CJ Baker A mouse model of chronic pulmonary in-fection with Pseudomonas aeruginosa and Pseudomonas cepacia Pediatr Res 22(1987) 698ndash702
[115] TJ AM van Heeckeren RW Walenga MW Konstan PB Davis B ErokwuMA Haxhiu TW Ferkol Effect of Pseudomonas infection on weight loss lung
710 F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
mechanics and cytokines in mice Am J Respir Crit Care Med 161 (2000)271ndash279
[116] T Aw G Wierzbicka DP Jones Oral glutathione increases tissue glutathione invivo Chem Biol Interact 80 (1991) 89ndash97
[117] F Favilli P Marraccini T Iantomasi MT Vincenzini Effect of orally adminis-tered glutathione on glutathione levels in some organs of rats role of specifictransporters Br J Nutr 78 (1997) 293ndash300
[118] C Kariya H Leitner E Min C van Heeckeren A van Heeckeren BJ Day A rolefor CFTR in the elevation of glutathione levels in the lung by oral glutathione ad-ministration Am J Physiol Lung Cell Mol Physiol 292 (2007) L1590ndashL1597
[119] K Atkuri JJ Mantovani LA Herzenberg LA Herzenberg N-Acetylcysteinemdashasafe antidote for cysteineglutathione deficiency Curr Opin Pharmacol 7(2007) 355ndash359
[120] R De Lisle E Roach K Jansson Effects of laxative and N-acetylcysteine onmucus accumulation bacterial load transit and inflammation in the cystic fi-brosis mouse small intestine Am J Physiol Gastrointest Liver Physiol 293(2007) G577ndashG584
[121] A Luciani VR Villella S Esposito N Brunetti-Pierri D Medina C Settembre MGavina L Pulze I Giardino M Pettoello-Mantovani M DApolito S Guido EMasliah B Spencer S Quaratino V Raia A Ballabio L Maiuri Defective CFTRinduces aggresome formation and lung inflammation in cystic fibrosis throughROS-mediated autophagy inhibition Nat Cell Biol 12 863ndash875
[122] M Griese J Ramakers A Krasselt V Starosta S Van Koningsbruggen R FischerF Ratjen B Mullinger RM Huber K Maier E Rietschel G Scheuch Improve-ment of alveolar glutathione and lung function but not oxidative state in cysticfibrosis Am J Respir Crit Care Med 169 (2004) 822ndash828
[123] C Bishop VM Hudson SC Hilton C Wilde A pilot study of the effect of inhaledbuffered reduced glutathione on the clinical status of patients with cystic fibro-sis Chest 127 (2005) 308ndash317
[124] WWang C Oliva G Li A Holmgren CH Lillig KL Kirk Reversible silencing of CFTRchloride channels by glutathionylation J Gen Physiol 125 (2005) 127ndash141
[125] N Dauletbaev P Fischer B Aulbach J Gross W Kusche U Thyroff-FriesingerTO Wagner J Bargon A phase II study on safety and efficacy of high-dose N-acetylcysteine in patients with cystic fibrosis Eur J Med Res 14 (2009)352ndash358
[126] R Tirouvanziam Y Gernez CK Conrad RB Moss I Schrijver CE Dunn ZADavies LA Herzenberg Profound functional and signaling changes in viable in-flammatory neutrophils homing to cystic fibrosis airways Proc Natl Acad SciU S A 105 (2008) 4335ndash4339
[127] JH Roum Z Borok NG McElvaney GJ Grimes AD Bokser R Buhl RG Crys-tal Glutathione aerosol suppresses lung epithelial surface inflammatory cell-derived oxidants in cystic fibrosis J Appl Physiol 87 (1999) 438ndash443
[128] A Visca CT Bishop SC Hilton VM Hudson Improvement in clinical markersin CF patients using a reduced glutathione regimen an uncontrolled observa-tional study J Cyst Fibros 7 (2008) 433ndash436
[129] EF Nash A Stephenson F Ratjen E Tullis Nebulized and oral thiol derivativesfor pulmonary disease in cystic fibrosis Cochrane Database Syst Rev (2009)CD007168
[130] AC foundation Drug Development Pipeline 2011[131] S Hoshida T Kuzuya N Yamashita M Nishida S Kitahara M Hori T
Kamada M Tada Gamma-glutamylcysteine ethyl ester for myocardial protec-tion in dogs during ischemia and reperfusion J Am Coll Cardiol 24 (1994)1391ndash1397
[132] J Lok W Leung S Zhao S Pallast K van Leyen S Guo X Wang A Yalcin EHLo Gamma-glutamylcysteine ethyl ester protects cerebral endothelial cells dur-ing injury and decreases bloodndashbrain barrier permeability after experimentalbrain trauma J Neurochem 118 (2011) 248ndash255
[133] Z Borok R Buhl GJ Grimes AD Bokser RC Hubbard KJ Holroyd JH RoumDB Czerski AM Cantin RG Crystal Effect of glutathione aerosol on oxidantndashantioxidant imbalance in idiopathic pulmonary fibrosis Lancet 338 (1991)215ndash216
[134] KJ Holroyd R Buhl Z Borok JH Roum AD Bokser GJ Grimes D Czerski AMCantin RG Crystal Correction of glutathione deficiency in the lower respiratorytract of HIV seropositive individuals by glutathione aerosol treatment Thorax 48(1993) 985ndash989
[135] J Hull P Vervaart K Grimwood P Phelan Pulmonary oxidative stress responsein young children with cystic fibrosis Thorax 52 (1997) 557ndash560
[136] A Corti A Paolicchi M Franzini S Dominici AF Casini A Pompella The S-thiolating activity of membrane gamma-glutamyltransferase formation ofcysteinyl-glycine mixed disulfides with cellular proteins and in the cell microen-vironment Antioxid Redox Signal 7 (2005) 911ndash918
[137] A Corti M Franzini AF Casini A Paolicchi A Pompella Vitamin C supply tobronchial epithelial cells linked to glutathione availability in elfmdasha role for se-creted gamma-glutamyltransferase J Cyst Fibros 7 (2008) 174ndash178
[138] A Munck Nutritional considerations in patients with cystic fibrosis Expert RevRespir Med 4 (2010) 47ndash56
[139] JL Matel CE Milla Nutrition in cystic fibrosis Semin Respir Crit Care Med 30(2009) 579ndash586
[140] D Salvatore R Buzzetti E Baldo MP Forneris V Lucidi D Manunza IMarinelli B Messore AS Neri V Raia ML Furnari G Mastella An overviewof international literature from cystic fibrosis registries 2 Neonatal screeningand nutritiongrowth J Cyst Fibros 9 (2010) 75ndash83
[141] KF Joosten JM Hulst Malnutrition in pediatric hospital patients current is-sues Nutrition 27 (2011) 133ndash137
[142] S Fustik T Jacovska L Spirevska S Koceva Protein-energy malnutrition as thefirst manifestation of cystic fibrosis in infancy Pediatr Int 51 (2009) 678ndash683
[143] J Himmelfarb E McMonagle Albumin is the major plasma protein target of ox-idant stress in uremia Kidney Int 60 (2001) 358ndash363
[144] P Stenvinkel JJ Carrero J Axelsson B Lindholm O Heimburger Z MassyEmerging biomarkers for evaluating cardiovascular risk in the chronic kidneydisease patient how do new pieces fit into the uremic puzzle Clin J Am SocNephrol 3 (2008) 505ndash521
[145] M Roche P Rondeau NR Singh E Tarnus E Bourdon The antioxidant proper-ties of serum albumin FEBS Lett 582 (2008) 1783ndash1787
[146] D Giustarini A Milzani I Dalle-Donne R Rossi Red blood cells as a physiolog-ical source of glutathione for extracellular fluids Blood Cells Mol Dis 40 (2008)174ndash179
[147] A Meister ME Anderson Glutathione Annu Rev Biochem 52 (1983) 711ndash760[148] B Alvarez S Carballal L Turell R Radi Formation and reactions of sulfenic acid
in human serum albumin Methods Enzymol 473 (2010) 117ndash136[149] S Carballal B Alvarez L Turell H Botti BA Freeman R Radi Sulfenic acid in
human serum albumin Amino Acids 32 (2007) 543ndash551[150] LR Barclay AM Bailey D Kong The antioxidant activity of alpha-tocopherol-
bovine serum albumin complex in micellar and liposome autoxidations J BiolChem 260 (1985) 15809ndash15814
[151] T Ishii T Ichikawa K Minoda K Kusaka S Ito Y Suzuki M Akagawa K Mochi-zuki T Goda T Nakayama Human serum albumin as an antioxidant in the ox-idation of (minus)-epigallocatechin gallate participation of reversible covalentbinding for interaction and stabilization Biosci Biotechnol Biochem 75(2011) 100ndash106
[152] F Galli S Rovidati S Benedetti U Buoncristiani C Covarelli A Floridi F Canes-trari Overexpression of erythrocyte glutathione S-transferase in uremia and di-alysis Clin Chem 45 (1999) 1781ndash1788
[153] D Borowitz RD Baker V Stallings Consensus report on nutrition for pediat-ric patients with cystic fibrosis J Pediatr Gastroenterol Nutr 35 (2002)246ndash259
[154] LJ Filer Jr SW Wright MP Manning KE Mason Absorption of alpha-tocopherol and tocopherylesters by premature and full term infants and chil-dren in health and disease Pediatrics 8 (1951) 328ndash339
[155] L Lancellotti C DOrazio G Mastella G Mazzi U Lippi Deficiency of vitamins Eand A in cystic fibrosis is independent of pancreatic function and current en-zyme and vitamin supplementation Eur J Pediatr 155 (1996) 281ndash285
[156] MN Sathe AS Patel Update in pediatrics focus on fat-soluble vitamins NutrClin Pract 25 (2010) 340ndash346
[157] MG Traber The ABCs of vitamin E and beta-carotene absorption Am J ClinNutr 80 (2004) 3ndash4
[158] TF Dolan Jr Hemolytic anemia and edema as the initial signs in infants withcystic fibrosis Consider this diagnosis even in absence of pulmonary symptomsClin Pediatr 15 (1976) 597ndash600
[159] DR James M Alfaham MC Goodchild Increased susceptibility to peroxide-induced haemolysis with normal vitamin E concentrations in cystic fibrosisClin Chim Acta 204 (1991) 279ndash290
[160] SA Peters FJ Kelly Vitamin E supplementation in cystic fibrosis J Pediatr Gas-troenterol Nutr 22 (1996) 341ndash345
[161] A Maqbool VA Stallings Update on fat-soluble vitamins in cystic fibrosis CurrOpin Pulm Med 14 (2008) 574ndash581
[162] SD Sagel MK Sontag MM Anthony P Emmett KA Papas Effect of anantioxidant-rich multivitamin supplement in cystic fibrosis J Cyst Fibros 10(2011) 31ndash36
[163] F Galli A Azzi Present trends in vitamin E research Biofactors 36 (2010)33ndash42
[164] A Hamahata P Enkhbaatar ER Kraft M Lange SW Leonard MG Traber RACox FC Schmalstieg HK Hawkins EB Whorton EM Horvath C Szabo LDTraber DN Herndon DL Traber Gamma-tocopherol nebulization by a lipidaerosolization device improves pulmonary function in sheep with burn andsmoke inhalation injury Free Radic Biol Med 45 (2008) 425ndash433
[165] JP Anais N Razzouq M Carvalho C Fernandez A Astier M Paul A AstierH Fessi AM Lorino Development of alpha-tocopherol acetate nanoparti-cles influence of preparative processes Drug Dev Ind Pharm 35 (2009)216ndash223
[166] JM Zingg Molecular and cellular activities of vitamin E analogues Mini RevMed Chem 7 (2007) 543ndash558
[167] V Viola F Pilolli M Piroddi E Pierpaoli F Orlando M Provinciali M Betti FMazzini F Galli Why tocotrienols work better insights into the in vitro anti-cancer mechanism of vitamin E Genes Nutr 7 (2011) 29ndash41
[168] F Galli F Mazzini L Bamonti L Gille S Bohmdorfer M Piroddi T Netscher FJKelly T Rosenau Tocotrienamines and tocopheramines reactions with radicalsand metal ions Bioorg Med Chem 19 (2011) 6483ndash6491
[169] A Kuhad K Chopra Attenuation of diabetic nephropathy by tocotrienol in-volvement of NFκB signaling pathway Life Sci 84 (2009) 296ndash301
[170] Q Jiang X Yin MA Lill ML Danielson H Freiser J Huang Long-chain carbox-ychromanols metabolites of vitamin E are potent inhibitors of cyclooxygenasesProc Natl Acad Sci U S A 105 (2008) 20464ndash20469
[171] ER Miller III R Pastor-Barriuso D Dalal RA Riemersma LJ Appel E GuallarMeta-analysis high-dosage vitamin E supplementation may increase all-causemortality Ann Intern Med 142 (2005) 37ndash46
[172] JN Hathcock A Azzi J Blumberg T Bray A Dickinson B Frei I Jialal CSJohnston FJ Kelly K Kraemer L Packer S Parthasarathy H Sies MG TraberVitamins E and C are safe across a broad range of intakes Am J Clin Nutr 81(2005) 736ndash745
[173] R Brigelius-Flohe F Galli Vitamin E a vitamin still awaiting the detection of itsbiological function Mol Nutr Food Res 54 (2010) 583ndash587
711F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
[174] MG Traber B Frei JS Beckman Vitamin E revisited do new data validate ben-efits for chronic disease prevention Curr Opin Lipidol 19 (2008) 30ndash38
[175] F Galli Meeting report Vitamin E Satellite Symposium (VESS) associated to theAnnual Meeting of the SFRR-Europe Rome 26 August 2009 Free Radic Res 43(2009) 1256ndash1257
[176] LJ Roberts II JA Oates MF Linton S Fazio BP Meador MD Gross Y Shyr JDMorrow The relationship between dose of vitamin E and suppression of oxida-tive stress in humans Free Radic Biol Med 43 (2007) 1388ndash1393
[177] EFSA- EFSA Scientific Opinion of the Panel on Food Additives FlavouringsProcessing Aids and Materials in Contact with Food on a request from the Com-mission on mixed tocopherols tocotrienol tocopherol and tocotrienols assources for vitamin E in EFSA- EFSA (Ed) vol 640 The EFSA Journal2008 pp 1ndash34
[178] P Rust I Eichler S Renner I Elmadfa Long-term oral beta-carotene supple-mentation in patients with cystic fibrosis mdash effects on antioxidative status andpulmonary function Ann Nutr Metab 44 (2000) 30ndash37
[179] G Lepage J Champagne N Ronco A Lamarre I Osberg RJ Sokol CC Roy Sup-plementation with carotenoids corrects increased lipid peroxidation in childrenwith cystic fibrosis Am J Clin Nutr 64 (1996) 87ndash93
[180] BM Winklhofer-Roob H Puhl G Khoschsorur MA vant Hof H EsterbauerDH Shmerling Enhanced resistance to oxidation of low density lipoproteinsand decreased lipid peroxide formation during beta-carotene supplementationin cystic fibrosis Free Radic Biol Med 18 (1995) 849ndash859
[181] RC Graham-Maar JI Schall N Stettler BS Zemel VA Stallings Elevated vita-min A intake and serum retinol in preadolescent children with cystic fibrosisAm J Clin Nutr 84 (2006) 174ndash182
[182] I Sadowska-Woda M Rachel J Pazdan E Bieszczad-Bedrejczuk K PawliszakNutritional supplement attenuates selected oxidative stress markers in pediatricpatients with cystic fibrosis Nutr Res (New York NY) 31 (2011) 509ndash518
[183] KA Papas MK Sontag C Pardee RJ Sokol SD Sagel FJ Accurso JS WagenerA pilot study on the safety and efficacy of a novel antioxidant rich formulation inpatients with cystic fibrosis J Cyst Fibros 7 (2008) 60ndash67
[184] Y Saito A Fukuhara K Nishio M Hayakawa Y Ogawa H Sakamoto K Fujii YYoshida E Niki Characterization of cellular uptake and distribution of coen-zyme Q10 and vitamin E in PC12 cells J Nutr Biochem 20 (2009) 350ndash357
[185] AA Franke CM Morrison JL Bakke LJ Custer X Li RV Cooney CoenzymeQ10 in human blood native levels and determinants of oxidation during proces-sing and storage Free Radic Biol Med 48 (2010) 1610ndash1617
[186] HN Bhagavan RK Chopra Plasma coenzyme Q10 response to oral ingestion ofcoenzyme Q10 formulations Mitochondrion 7 (2007) S78ndashS88 (Suppl)
[187] HN Bhagavan RK Chopra Coenzyme Q10 absorption tissue uptake metabo-lism and pharmacokinetics Free Radic Res 40 (2006) 445ndash453
[188] F Galli R Lee C Dunster FJ Kelly Gas chromatography mass spectrometryanalysis of carboxyethyl-hydroxychroman metabolites of alpha- and gamma-tocopherol in human plasma Free Radic Biol Med 32 (2002) 333ndash340
[189] F Galli R Lee J Atkinson A Floridi FJ Kelly Gamma-tocopherol biokineticsand transformation in humans Free Radic Res 37 (2003) 1225ndash1233
[190] TA Laguna MK Sontag I Osberg JS Wagener FJ Accurso RJ Sokol De-creased total serum coenzyme-Q10 concentrations a longitudinal study in chil-dren with cystic fibrosis J Pediatr 153 (2008) 402ndash407
[191] T Frischer JK Myung G Maurer I Eichler Z Szepfalusi G Lubec Possible dys-regulation of chaperon and metabolic proteins in cystic fibrosis bronchial tissueProteomics 6 (2006) 3381ndash3388
[192] C Andersson MM Zaman AB Jones SD Freedman Alterations in immune re-sponse and PPARLXR regulation in cystic fibrosis macrophages J Cyst Fibros 7(2008) 68ndash78
[193] SD Freedman PG Blanco MM Zaman JC Shea M Ollero IK Hopper DAWeed A Gelrud MM Regan M Laposata JG Alvarez BP OSullivan Associa-tion of cystic fibrosis with abnormalities in fatty acid metabolism N Engl JMed 350 (2004) 560ndash569
[194] S Van Biervliet G Vanbillemont JP Van Biervliet D Declercq E Robberecht AChristophe Relation between fatty acid composition and clinical status or geno-type in cystic fibrosis patients Ann Nutr Metab 51 (2007) 541ndash549
[195] SD Freedman MH Katz EM Parker M Laposata MY Urman JG AlvarezA membrane lipid imbalance plays a role in the phenotypic expression ofcystic fibrosis in cftr(minusminus) mice Proc Natl Acad Sci U S A 96 (1999)13995ndash14000
[196] S Van Biervliet S Vande Velde JP Van Biervliet E Robberecht The effect ofzinc supplements in cystic fibrosis patients Ann Nutr Metab 52 (2008)152ndash156
[197] WR Henderson Jr SJ Astley MM McCready P Kushmerick S Casey JWBecker BW Ramsey Oral absorption of omega-3 fatty acids in patients withcystic fibrosis who have pancreatic insufficiency and in healthy control subjectsJ Pediatr 124 (1994) 400ndash408
[198] I Durieu E Vericel D Guichardant H Roth JP Steghens J Drai RN JosserandE Fontaine M Lagarde G Bellon Fatty acids platelets and oxidative markersfollowing intravenous n-3 fatty acids administration in cystic fibrosis an openpilot observational study J Cyst Fibros 6 (2007) 320ndash326
[199] LG Wood DA Fitzgerald ML Garg Hypothesis vitamin E complements poly-unsaturated fatty acids in essential fatty acid deficiency in cystic fibrosis J AmColl Nutr 22 (2003) 253ndash257
[200] JD Lloyd-Still SB Johnson RT Holman Essential fatty acid status in cystic fi-brosis and the effects of safflower oil supplementation Am J Clin Nutr 34(1981) 1ndash7
[201] A Maqbool JI Schall JF Garcia-Espana BS Zemel B Strandvik VAStallings Serum linoleic acid status as a clinical indicator of essential fatty
acid status in children with cystic fibrosis J Pediatr Gastroenterol Nutr 47(2008) 635ndash644
[202] C Oliver N Jahnke Omega-3 fatty acids for cystic fibrosis Cochrane DatabaseSyst Rev (2011) CD002201
[203] B Strandvik E Gronowitz F Enlund T Martinsson J Wahlstrom Essential fattyacid deficiency in relation to genotype in patients with cystic fibrosis J Pediatr139 (2001) 650ndash655
[204] P Rise S Volpi C Colombo RF Padoan C DOrazio S Ghezzi PMelotti V BennatoC Agostoni BM Assael C Galli Whole blood fatty acid analysis with micromethodin cystic fibrosis and pulmonary disease J Cyst Fibros 9 (2010) 228ndash233
[205] H Cao K Gerhold JR Mayers MM Wiest SM Watkins GS Hotamisligil Iden-tification of a lipokine a lipid hormone linking adipose tissue to systemic me-tabolism Cell 134 (2008) 933ndash944
[206] RR Malapaka SK Khoo J Zhang JH Choi XE Zhou Y Xu Y Gong J Li ELYong MJ Chalmers L Chang JH Resau PR Griffin YE Chen HE Xu Iden-tification and mechanism of a ten carbon fatty acid as a modulating ligand ofperoxisome proliferator activated receptors J Biol Chem 287 (2012)183ndash195
[207] T Hara A Hirasawa A Ichimura I Kimura G Tsujimoto Free fatty acid recep-tors FFAR1 and GPR120 as novel therapeutic targets for metabolic disorders JPharm Sci 100 (2011) 3594ndash3601
[208] R Gupta P Rathi S Bradoo Lipase mediated upgradation of dietary fats andoils Crit Rev Food Sci Nutr 43 (2003) 635ndash644
[209] BH Jennings CC Akoh Lipase-catalyzed modification of rice bran oil to incor-porate capric acid J Agric Food Chem 48 (2000) 4439ndash4443
[210] J Hoeks M Mensink MK Hesselink K Ekroos P Schrauwen Long- andMedium-Chain Fatty Acids Induce Insulin Resistance to a Similar Extent inHumans Despite Marked Differences in Muscle Fat Accumulation J Clin Endo-crinol Metab 97 (2012) 208ndash216
[211] PJ Congden G Bruce MM Rothburn PC Clarke JM Littlewood J KelleherMS Losowsky Vitamin status in treated patients with cystic fibrosis ArchDis Child 56 (1981) 708ndash714
[212] BM Winklhofer-Roob H Ellemunter M Fruhwirth SE Schlegel-Haueter GKhoschsorur MA vant Hof DH Shmerling Plasma vitamin C concentrationsin patients with cystic fibrosis evidence of associations with lung inflammationAm J Clin Nutr 65 (1997) 1858ndash1866
[213] L Shamseer D Adams N Brown JA Johnson S Vohra Antioxidant micronutri-ents for lung disease in cystic fibrosis Cochrane Database Syst Rev (2010)CD007020
[214] C Santi S Santoro Electrophilic Selenium First edition Wiley-VCH VerlagGmbH amp Co KGaA 2012
[215] L Flohe S Toppo G Cozza F Ursini A comparison of thiol peroxidase mecha-nisms Antioxid Redox Signal 15 (2010) 763ndash780
[216] L Flohe JR Andreesen R Brigelius-Flohe M Maiorino F Ursini Selenium theelement of the moon in life on earth IUBMB Life 49 (2000) 411ndash420
[217] V Valdiglesias E Pasaro J Mendez B Laffon In vitro evaluation of seleniumgenotoxic cytotoxic and protective effects a review Arch Toxicol 84(2010) 337ndash351
[218] P Foucaud P Therond M Marchand F Brion JF Demelier J Navarro Seleniumand vitamin E in mucoviscidosis Arch Fr Pediatr 45 (1988) 383ndash386
[219] J Neve R Van Geffel M Hanocq L Molle Plasma and erythrocyte zinc copperand selenium in cystic fibrosis Acta Paediatr Scand 72 (1983) 437ndash440
[220] BM Winklhofer-Roob B Tiran PE Tuchschmid MA vant Hof DH ShmerlingEffects of pancreatic enzyme preparations on erythrocyte glutathione peroxi-dase activities and plasma selenium concentrations in cystic fibrosis FreeRadic Biol Med 25 (1998) 242ndash249
[221] JD Lloyd-Still HE Ganther Selenium and glutathione peroxidase levels in cys-tic fibrosis Pediatrics 65 (1980) 1010ndash1012
[222] D Tsavachidou TJ McDonnell S Wen X Wang F Vakar-Lopez LL Pisters CAPettaway CG Wood KA Do PF Thall C Stephens E Efstathiou R Taylor DGMenter P Troncoso SM Lippman CJ Logothetis J Kim Selenium and vitaminE cell type- and intervention-specific tissue effects in prostate cancer J NatlCancer Inst 101 (2009) 306ndash320
[223] IN Zelko TJ Mariani RJ Folz Superoxide dismutase multigene family acomparison of the CuZn-SOD (SOD1) Mn-SOD (SOD2) and EC-SOD (SOD3)gene structures evolution and expression Free Radic Biol Med 33 (2002)337ndash349
[224] RP Bowler JD Crapo Oxidative stress in airways is there a role for extracellu-lar superoxide dismutase Am J Respir Crit Care Med 166 (2002) S38ndashS43
[225] K Best K McCoy S Gemma RA Disilvestro Copper enzyme activities in cysticfibrosis before and after copper supplementation plus or minus zinc Metabo-lism 53 (2004) 37ndash41
[226] SS Percival GP Kauwell E Bowser M Wagner Altered copper status in adultmen with cystic fibrosis J Am Coll Nutr 18 (1999) 614ndash619
[227] NF Krebs JE Westcott TD Arnold BM Kluger FJ Accurso LV Miller KMHambidge Abnormalities in zinc homeostasis in young infants with cystic fibro-sis Pediatr Res 48 (2000) 256ndash261
[228] D Easley N Krebs M Jefferson L Miller J Erskine F Accurso KM HambidgeEffect of pancreatic enzymes on zinc absorption in cystic fibrosis J Pediatr Gas-troenterol Nutr 26 (1998) 136ndash139
[229] S Van Biervliet JP Van Biervliet E Robberecht Serum zinc in patients with cys-tic fibrosis at diagnosis and after one year of therapy Biol Trace Elem Res 112(2006) 205ndash211
[230] S Van Biervliet JP Van Biervliet S Vande Velde E Robberecht Serum zinc con-centrations in cystic fibrosis patients aged above 4 years a cross-sectional eval-uation Biol Trace Elem Res 119 (2007) 19ndash26
712 F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
[231] F Galli M Cristina Polidori W Stahl P Mecocci FJ Kelly Vitamin E biotransfor-mation in humans Vitam Horm 76 (2007) 263ndash280
[232] J Wiser NE Alexis Q Jiang W Wu C Robinette R Roubey DB Peden In vivogamma-tocopherol supplementation decreases systemic oxidative stress andcytokine responses of human monocytes in normal and asthmatic subjectsFree Radic Biol Med 45 (2008) 40ndash49
[233] JG Wagner Q Jiang JR Harkema B Illek DD Patel BN Ames DB PedenOzone enhancement of lower airway allergic inflammation is prevented bygamma-tocopherol Free Radic Biol Med 43 (2007) 1176ndash1188
[234] JT Harries DP Muller Absorption of different doses of fat soluble and watermiscible preparations of vitamin E in children with cystic fibrosis Arch DisChild 46 (1971) 341ndash344
[235] EI Back C Frindt E Ocenaskova D Nohr M Stern HK Biesalski Can changesin hydrophobicity increase the bioavailability of alpha-tocopherol Eur J Nutr45 (2006) 1ndash6
[236] SZ Nasr MH OLeary C Hillermeier Correction of vitamin E deficiency withfat-soluble versus water-miscible preparations of vitamin E in patients with cys-tic fibrosis J Pediatr 122 (1993) 810ndash812
[237] S Soltani-Frisk E Gronowitz H Andersson B Strandvik Water-miscibletocopherol is not superior to fat-soluble preparation for vitamin E absorptionin cystic fibrosis Acta Paediatr 90 (2001) 1112ndash1115
[238] K Papas J Kalbfleisch R Mohon Bioavailability of a novel water-soluble vi-tamin E formulation in malabsorbing patients Dig Dis Sci 52 (2007)347ndash352
[239] F Antonicelli M Parmentier EM Drost N Hirani I Rahman K Donaldson WMacNee Nacystelyn inhibits oxidant-mediated interleukin-8 expression andNF-kappaB nuclear binding in alveolar epithelial cells Free Radic Biol Med 32(2002) 492ndash502
[240] EM App D Baran I Dab A Malfroot M Coffiner F Vanderbist M King Dose-finding and 24-h monitoring for efficacy and safety of aerosolized Nacystelyn incystic fibrosis Eur Respir J 19 (2002) 294ndash302
[241] MG Traber How much vitamin E hellip Just enough Am J Clin Nutr 84 (2006)959ndash960
[242] JC McCann BN Ames Vitamin K an example of triage theory is micronu-trient inadequacy linked to diseases of aging Am J Clin Nutr 90 (2009)889ndash907
[243] M Fusaro G Crepaldi S Maggi F Galli A DAngelo L Calo S Giannini DMiozzo M Gallieni Vitamin K bone fractures and vascular calcifications inchronic kidney disease an important but poorly studied relationship J Endocri-nol Invest 34 (2010) 317ndash323
[244] JC McCann BN Ames Adaptive dysfunction of selenoproteins from the per-spective of the triage theory why modest selenium deficiency may increaserisk of diseases of aging FASEB J 25 (2011) 1793ndash1814
[245] R Apak K Guclu M Ozyurek B Bektas Oglu M Bener Cupric ion reducing an-tioxidant capacity assay for food antioxidants vitamins polyphenolics and fla-vonoids in food extracts Methods Mol Biol 477 (2008) 163ndash193
[246] F Galli Interactions of polyphenolic compounds with drug disposition and me-tabolism Curr Drug Metab 8 (2007) 830ndash838
[247] RL Prior X Wu K Schaich Standardized methods for the determination of an-tioxidant capacity and phenolics in foods and dietary supplements J Agric FoodChem 53 (2005) 4290ndash4302
[248] C Azbell S Zhang D Skinner J Fortenberry EJ Sorscher BA WoodworthHesperidin stimulates cystic fibrosis transmembrane conductance regulator-mediated chloride secretion and ciliary beat frequency in sinonasal epitheliumOtolaryngol Head Neck Surg 143 (2010) 397ndash404
[249] G Wegrzyn J Jakobkiewicz-Banecka M Gabig-Ciminska E Piotrowska M Nar-ajczyk A Kloska M Malinowska D Dziedzic I Golebiewska M Moskot AWegrzyn Genistein a natural isoflavone with a potential for treatment of ge-netic diseases Biochem Soc Trans 38 (2010) 695ndash701
[250] YC Yu H Miki Y Nakamura A Hanyuda Y Matsuzaki Y Abe M Yasui K Ta-naka TC Hwang SG Bompadre Y Sohma Curcumin and genistein additivelypotentiate G551D-CFTR J Cyst Fibros 10 (2011) 243ndash252
[251] B Illek H Fischer Flavonoids stimulate Cl conductance of human airway epithe-lium in vitro and in vivo Am J Physiol 275 (1998) L902ndashL910
[252] JL Kreindler Cystic fibrosis exploiting its genetic basis in the hunt for newtherapies Pharmacol Ther 125 (2010) 219ndash229
[253] B Illek L Zhang NC Lewis RB Moss JY Dong H Fischer Defective function ofthe cystic fibrosis-causing missense mutation G551D is recovered by genisteinAm J Physiol 277 (1999) C833ndashC839
[254] P Anandakumar S Kamaraj S Jagan G Ramakrishnan R Vinodhkumar TDevaki Capsaicin modulates pulmonary antioxidant defense system during ben-zo(a)pyrene-induced lung cancer in Swiss albinomice Phytother Res 22 (2008)529ndash533
[255] I Rahman Antioxidant therapeutic advances in COPD Ther Adv Respir Dis 2(2008) 351ndash374
[256] AW Boots H Li RP Schins R Duffin JW Heemskerk A Bast GR Haenen Thequercetin paradox Toxicol Appl Pharmacol 222 (2007) 89ndash96
[257] M Joskova S Franova V Sadlonova Acute bronchodilator effect of quercetin inexperimental allergic asthma Bratisl Lek Listy 112 (2011) 9ndash12
[258] HJ Park CM Lee ID Jung JS Lee YI Jeong JH Chang SH Chun MJ Kim IWChoi SC Ahn YK Shin SR Yeom YM Park Quercetin regulates Th1Th2 balancein a murine model of asthma Int Immunopharmacol 9 (2009) 261ndash267
[259] AP Rogerio A Kanashiro C Fontanari EV da Silva YM Lucisano-ValimEG Soares LH Faccioli Anti-inflammatory activity of quercetin and iso-quercitrin in experimental murine allergic asthma Inflamm Res 56 (2007)402ndash408
[260] M Muller Polyphenol cytotoxicity induced by the bacterial toxin pyocyaninrole of NQO1 Free Radic Biol Med 47 (2009) 84ndash91
[261] J Grassmann Terpenoids as plant antioxidants Vitam Horm 72 (2005)505ndash535
[262] P Allen Tea tree oil the science behind the antimicrobial hype Lancet 358(2001) 1245
[263] EC Dasenbrook W Checkley CA Merlo MW Konstan N Lechtzin MP BoyleAssociation between respiratory tract methicillin-resistant Staphylococcus aure-us and survival in cystic fibrosis JAMA 303 (2010) 2386ndash2392
[264] V Bezzerri M Borgatti E Nicolis I Lampronti MC Dechecchi I Mancini PRizzotti R Gambari G Cabrini Transcription factor oligodeoxynucleotides toNF-kappaB inhibit transcription of IL-8 in bronchial cells Am J Respir CellMol Biol 39 (2008) 86ndash96
[265] R Gambari M Borgatti V Bezzerri E Nicolis I Lampronti MC Dechecchi IMancini A Tamanini G Cabrini Decoy oligodeoxyribonucleotides and peptidenucleic acids-DNA chimeras targeting nuclear factor kappa-B inhibition of IL-8 gene expression in cystic fibrosis cells infected with Pseudomonas aeruginosaBiochem Pharmacol 80 (2010) 1887ndash1894
[266] M Adrian P Jeandet AC Douillet-Breuil L Tesson R Bessis Stilbene content ofmature Vitis vinifera berries in response to UV-C elicitation J Agric Food Chem48 (2000) 6103ndash6105
[267] B Paul I Masih J Deopujari C Charpentier Occurrence of resveratrol and pter-ostilbene in age-old darakchasava an ayurvedic medicine from India J Ethno-pharmacol 68 (1999) 71ndash76
[268] I Rahman Antioxidant therapies in COPD Int J Chron Obstruct Pulmon Dis 1(2006) 15ndash29
[269] M Lee S Kim OK Kwon SR Oh HK Lee K Ahn Anti-inflammatory and anti-asthmatic effects of resveratrol a polyphenolic stilbene in a mouse model ofallergic asthma Int Immunopharmacol 9 (2009) 418ndash424
[270] LG Wood PA Wark ML Garg Antioxidant and anti-inflammatory effectsof resveratrol in airway disease Antioxid Redox Signal 13 (2010)1535ndash1548
[271] KV Kiselev Perspectives for production and application of resveratrol ApplMicrobiol Biotechnol 90 (2011) 417ndash425
[272] M Shakibaei C Buhrmann A Mobasheri Resveratrol-mediated SIRT-1 interac-tions with p300 modulate receptor activator of NF-kappaB ligand (RANKL) acti-vation of NF-kappaB signaling and inhibit osteoclastogenesis in bone-derivedcells J Biol Chem 286 (2011) 11492ndash11505
[273] SF Zaidi K Ahmed T Yamamoto T Kondo K Usmanghani M Kadowaki TSugiyama Effect of resveratrol on Helicobacter pylori-induced interleukin-8 secre-tion reactive oxygen species generation and morphological changes in human gas-tric epithelial cells Biol Pharm Bull 32 (2009) 1931ndash1935
[274] JK Kundu YK Shin YJ Surh Resveratrol modulates phorbol ester-inducedpro-inflammatory signal transduction pathways in mouse skin in vivo NF-kappaB and AP-1 as prime targets Biochem Pharmacol 72 (2006)1506ndash1515
[275] NH Nam Naturally occurring NF-kappaB inhibitors Mini Rev Med Chem 6(2006) 945ndash951
[276] JM Smoliga JA Baur HA Hausenblas Resveratrol and healthmdasha comprehen-sive review of human clinical trials Mol Nutr Food Res 55 (2011) 1129ndash1141
[277] ME Juan M Maijo JM Planas Quantification of trans-resveratrol and itsmetabolites in rat plasma and tissues by HPLC J Pharm Biomed Anal 51(2010) 391ndash398
[278] JA Baur DA Sinclair Therapeutic potential of resveratrol the in vivo evidenceNat Rev 5 (2006) 493ndash506
[279] E Nicolis I Lampronti MC Dechecchi M Borgatti A Tamanini N Bianchi VBezzerri I Mancini MG Giri P Rizzotti R Gambari G Cabrini Pyrogallol anactive compound from the medicinal plant Emblica officinalis regulates expres-sion of pro-inflammatory genes in bronchial epithelial cells Int Immunophar-macol 8 (2008) 1672ndash1680
[280] E Nicolis I Lampronti MC Dechecchi M Borgatti A Tamanini V Bezzerri NBianchi M Mazzon I Mancini MG Giri P Rizzotti R Gambari G CabriniModulation of expression of IL-8 gene in bronchial epithelial cells by 5-methoxypsoralen Int Immunopharmacol 9 (2009) 1411ndash1422
[281] M Borgatti I Mancini N Bianchi A Guerrini I Lampronti D Rossi G SacchettiR Gambari Bergamot (Citrus bergamia Risso) fruit extracts and identified com-ponents alter expression of interleukin 8 gene in cystic fibrosis bronchial epithe-lial cell lines BMC Biochem 12 (2011) 15
[282] L Piccagli E Fabbri M Borgatti N Bianchi V Bezzerri I Mancini E Nicolis CMDechecchi I Lampronti G Cabrini R Gambari Virtual screening against p50NF-kappaB transcription factor for the identification of inhibitors of the NF-kappaB-DNA interaction and expression of NF-kappaB upregulated genesChemMedChem 4 (2009) 2024ndash2033
[283] L Piccagli M Borgatti E Nicolis N Bianchi I Mancini I Lampronti D VevaldiF DallAcqua G Cabrini R Gambari Virtual screening against nuclear factorkappaB (NF-kappaB) of a focus library identification of bioactive furocoumarinderivatives inhibiting NF-kappaB dependent biological functions involved incystic fibrosis Bioorg Med Chem 18 (2010) 8341ndash8349
[284] M Borgatti A Chilin L Piccagli I Lampronti N Bianchi I Mancini G Mar-zaro Da Francesco A Guiotto R Gambari Development of a novel furocou-marin derivative inhibiting NF-kappaB dependent biological functionsdesign synthesis and biological effects Eur J Med Chem 46 (2011)4870ndash4877
[285] E Georgy S Le Guellec L Vecellio E Fichant P Stordeur P Bordeau JP PerraudinFeasibility study of OSCN- and lactoferrin (Meveol) nebulization for cysticfibrosis JCyst Fibros 10 (2011) S18
713F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
[286] C Tidei M Piroddi F Galli C Santi Oxidation of thiols promoted by PhSeZnClTetrahedron Lett 53 (2012) 232ndash234
[287] L Semianrio-Vidal C van Hesuden G Mugesh ER Lazarowski Ebselen is a po-tent non-competitive inhibitor of extracellular nucleoside diphosphokinasePurinergic Signal 6 (2010) 383ndash391
[288] C ColussiMC Albertini S Coppola S Rovidati F Galli L Ghibelli H2O2-inducedblockof glycolysis as an active ADP-ribosylation reaction protecting cells from apoptosisFASEB J 14 (2000) 2266ndash2276
[289] H Xiao KL Parkin Induction of phase II enzyme activity by various seleniumcompounds Nutr Cancer 55 (2006) 210ndash223
[290] G Peluffo R Radi Biochemistry of protein tyrosine nitration in cardiovascularpathology Cardiovasc Res 75 (2007) 291ndash302
[291] B Alvarez R Radi Peroxynitrite reactivity with amino acids and proteinsAmino Acids 25 (2003) 295ndash311
[292] B Kamosinska MW Radomski M Duszyk A Radomski SF Man Nitric oxideactivates chloride currents in human lung epithelial cells Am J Physiol 272(1997) L1098ndashL1104
[293] L Chen RP Patel X Teng CA Bosworth JR Lancaster Jr S Matalon Mecha-nisms of cystic fibrosis transmembrane conductance regulator activation by S-nitrosoglutathione J Biol Chem 281 (2006) 9190ndash9199
[294] F Luchetti B CanonicoM BettiM Arcangeletti F PilolliM Piroddi L Canesi S PapaF Galli Melatonin signaling and cell protection function FASEB J 24 (2010)3603ndash3624
[295] MW Bengtsson G Jedstedt G Flemstrom Duodenal bicarbonate secretion inrats stimulation by intra-arterial and luminal guanylin and uroguanylin ActaPhysiol (Oxf) 191 (2007) 309ndash317
[296] CS Nelson JL Marino CN Allen Melatonin receptor potentiation of cyclic AMP andthe cystic fibrosis transmembrane conductance regulator ion channel J Pineal Res 26(1999) 113ndash121
[297] C de Castro-Silva VM de Bruin GM Cunha DM Nunes CAMedeiros PF de BruinMelatonin improves sleep and reduces nitrite in the exhaled breath condensate incystic fibrosismdasha randomized double-blind placebo-controlled study J Pineal Res48 (2010) 65ndash71
[298] I Hornyak E Pankotai L Kiss Z Lacza Current developments in the the-rapeutic potential of S-nitrosoglutathione an endogenous NO-donor mole-cule Curr Pharm Biotechnol (2011) Jan 11 [Epub ahead of print] - PMID21235457
[299] AH Snyder ME McPherson JF Hunt M Johnson JS Stamler B Gaston Acuteeffects of aerosolized S-nitrosoglutathione in cystic fibrosis Am J Respir CritCare Med 165 (2002) 922ndash926

698 F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
corrected Cftr KO-transgenic mice were given an oral bolus dose ofGSH (300 mgkg) and compared with WT mice for changes in GSHlevels in plasma lung ELF and BAL cells There was a twofold in-crease in plasma a twofold increase in lung a fivefold increase inELF and a threefold increase in BAL cell GSH levels at 60 min in WTmice however GSH levels only increased by 40 in the plasma 60in the lung 50 in the ELF and twofold in the BAL cells within thegut-corrected Cftr KO-Tg mice No change in GSH levels was observedin the uncorrected Cftr KO mice These studies suggest that oral GSHadministration can increase plasma and lung compartment GSHlevels in WT mice and to a lesser extent in gut-corrected Cftr KO-Tganimals It also suggests that oral GSH treatment can boost BAL cellGSH levels However since this study failed to show significant in-creases in serum and lung compartment GSH levels in uncorrectedCftr KO mice it is questionable whether oral GSH administration toCF patients with intestinal malabsorption would benefit from thistherapy It was also shown that GSH is rapidly distributed to theserum and lung compartments Kariya et al [118] speculate thatother transporter(s) besides CFTR are responsible of the transport ofGSH and probably of other dietary molecules to the lung whichmay be responsible for dietary deficiencies observed in various lungdiseases
Another strategy is represented by the oral supplementation ofhigh doses of NAC a well known cysteine donor for the synthesis ofglutathione NAC is considered a safe molecule which has beenused successfully to treat GSH deficiency in a wide range of diseases[119] As CF mice display defects in GSH export in the ELF comparableto those of patients they could provide a useful tool to assess the ef-fects of NAC administration on the GSH status However only limitedstudies exploring the effects of NAC on CF animal models have beenso far carried out The effects of NAC have been tested on mucus accu-mulation bacterial load transit and inflammation in the CF mousesmall intestine showing that NAC may reduce intestinal mucus accu-mulation bacterial overgrowth in the gut [120]
Moreover NAC has been reported to restore the accumulationof unwantedmisfolded proteins in aggregates that are associated withthe CF airway phenotype as a cause of lung inflammation [121] Themechanism of this NAC-derived effect seems to involve the restorationof beclin 1 expression and activity in the autophagy pathway of theendoplasmic reticulum that was investigated in vivo using Scnn1b-transgenic and Cftr(F508del) homozygous mice The restoration ofthis pathway also produced a rescued trafficking of CFTR (F508del) tothe cell surface of CF cells obtained from human CF nasal biopsies
Given the defective GSH metabolism of CF reviewed in the previ-ous sections and in [122] and the reduced response to GSH therapyin CF mice [93] some Authors have investigated the influence of bac-terial infections on lung oxidative stress The effects of P aeruginosainfection on ELF and lung tissue antioxidants and the oxidation ofDNA and lipids were investigated in mice challenged with bacterialcells [90] CFTR-KO (B6129P2-Cftrtm1Unc) and WT mice were chal-lenged intratracheally with a clinical isolate of mucoid P aeruginosaembedded in agar beads and on the third day of infection BALF andlung tissue were obtained and analyzed for cytokines antioxidantsand enzyme activities [90] P aeruginosa lung infection increasedlevels of inflammatory cytokines and neutrophils in the ELF This cor-responded with a marked increase in GSH and in urate levels in theELF of P aeruginosa-infected WT mice A twofold increase in uratelevels was also observed among lung tissue antioxidants of Paeruginosa-infected WT mice There were no changes in markers oflung oxidative stress associated with the P aeruginosa lung infectionIn contrast to WT mice the CFTR-KO mice lacked a significant in-crease in ELF GSH when challenged with P aeruginosa and this corre-lated with a decrease in the ratio of reduced to oxidized GSH in theELF a marker of oxidative stress These data would suggest that thelung adapts to infectious agents with elevated ELF GSH and urateTherefore individuals with lung diseases associated with altered
antioxidant transport such as CF might lack the ability to adapt tothe infection which may lead to a more severe inflammatoryresponse
322 Clinical trials on GSHThe discovery of the defect in GSH export has suggested that ther-
apies able to restore or increase GSH levels in the ASL could counteractthe inflammation and oxidative stress conditions typical of CF pa-tients In an attempt to strengthen extracellular defenses againstROS some pilot studies have analyzed the effect of GSH inhalation orthat of oral GSH prodrug N-acetylcysteine (NAC) All these treatmentswere well tolerated by the CF patients and most authors were able tomeasure increased ELF concentrations of GSH in association withsome positive clinical outcomes [4041737896122ndash128] Althoughpotentially promising these findings need stronger clinical evidencein that the majority of these were obtained on very limited numberof patients investigated in non-randomized controlled trials This ishighlighted in a recently published meta-analysis [129] that providesalso a thoroughly analysis of the literature on this aspect of the antiox-idant and anti-inflammatory therapy of CF Among the American CFfoundation sponsored trials two phase II trials on inhaled GSH andoral NAC are in progress in US and Germany (ClinicalTrialsgov Iden-tifier NCT00506688 and NCT00809094 respectively Table 1) andsafety and tolerability of aerosolized glutathione is also matter ofinvestigation by another (not registered) US trial (more informationon this can be found in [130]) Nevertheless the diffusion among CFpatients of NAC preparations for inhalation (Mucomystreg) has in-creased in recent years
γ-Glutamylcysteine ethyl ester (GCEE) is another potentially inter-esting GSH pro-drug which has proved some efficacy in the ameliora-tion of oxidative stress eg in experimental myocardial infarction[131] and central nervous system conditions (see eg [132]) HoweverGCEE has not been investigated in CF yet
33 Limits and potential problems associated to thiol-based therapies
Although the above cited clinical trials may be considered promis-ing attempts to improve the antioxidant levels in the ELF the actualcapacity of these treatments to produce positive clinical effects mustbe considered with caution For example indices of oxidative damagewere found to be unaffected by aerosolized GSH treatment [122]Some in vitro studies have suggested that the reaction of GSH withPCN could produce hydrogen peroxide with potential exacerbationof oxidative damage [101] The exact mechanisms of PCN toxicityand the reaction of this toxin with GSH must be better understoodin order to evaluate the safety of GSH administration to patients col-onized by P aeruginosa
Inhalation of GSH ensures its direct delivery in the airways butsince GSH can rapidly convert to its oxidized form GSSG frequentGSH inhalations are required to maintain a high GSHGSSG As a con-sequence of this limit four separate inhalations have been used inthe study carried out by Bishop et al [123] Unless justified by clearclinical improvements these repeated treatments may represent aburden for patients already undergoing complex therapies Moreoverrepeated inhalations of GSH increase the levels of GSSG in ELF[133134] In the absence of effective homeostatic mechanisms ensur-ing the fast recycling of GSSG to GSH this might produce unwantedeffects and even the exacerbation of CF symptoms being GSSG re-sponsible of the S-glutathiolation and functional inhibition of CFTR[124]
In principle the oral administration of GSH could be considered asafe strategy to prevent GSSG accumulation but this strategy is likelynot feasible due to the substantial inability of this water-soluble mol-ecule to cross biological membranes Moreover a study carried out inmice has established that GSH absorption in the gastrointestinal tractif any is mediated by CFTR itself thus excluding the possibility to
699F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
improve circulating levels of GSH in CF patients through the dietarysupplementation of the antioxidant [127] The limited absorption ofGSH could be overcome by GSH-esters as in vitro studies haveshown that this form of GSH may be specifically useful to rescue mi-tochondrial defects in cystic fibrosis models [80] Safety of these GSHderivatives in humans has been poorly investigated
Two independent studies have shown that the treatment of CF pa-tients with high doses of NAC increases extracellular GSH in sputum[78125] but contrasting results have been reported concerning theeffects of NAC on the concentrations of blood GSH and on the levelsof IL-8 and other markers of inflammation NAC treatments may beuseful to modulate the GSH content in cells but it should be remindedthat an enhanced cysteine supply cannot lead to an increase of GSHabove physiological levels due to the feedback inhibition mechanismof γ-glutamylcysteine synthetase described in the Section 311
331 Gamma-glutamyltransferase and GSH therapySo far none of the studies mentioned above has taken into account
the fact that GSH is degraded by GGT enzyme activity GGT concentra-tions are known to increase several fold in ELF of CF patients even ifthe mechanisms for this effect were not determined [135] and thisphenomenon parallels the above described decrease of GSH levels inELF Preliminary data suggest that a major source of increased ELFGGT is represented by activated neutrophils accumulating in diseasedairways (Corti and Pompella 2011 unpublished observation) Re-gardless of its origin it is likely that increased GGT in ELF would de-grade locally administered GSH to variable extents which couldcontribute to the so far inconclusive results of therapies based onaerosolized GSH Besides its role in GSH catabolism GGT has beenshown to mediate protein S-thiolation [136] suggesting that GSH ad-ministration in the presence of active GGT enzyme might alter CFTRglutathiolation status and function in a potentially unfavorable wayOn the other hand a potential role of GGT in favoring bronchial up-take of antioxidant vitamin C has also been suggested [137]
These controversial findings may add further issues to the ques-tion of whether the therapy of lung oxidative stress by aerosolizedGSH could be safe in all the CF patients regardless of specific strate-gies that would ascertain the extent of lung inflammation Thesestrategies should include the assay of GGT levels in ELF In principleonce an adverse role of ELF GGT in GSH therapies will be confirmedthe association of GGT inhibitors in the GSH formulations for inhala-tion could represent a promising pharmacological strategy
34 Malnutrition as a possible cause of defective thiol-dependentantioxidant protection
Successful nutritional interventions strongly impact on the clinicaloutcome of CF patients [138ndash140] Malnutrition by pancreatic insuffi-ciency and other CF-related factors influence the susceptibility to de-velop recurrent infections and severe inflammatory lesions of thelung tissue If the onset of a defective (sub-optimal) antioxidant sta-tus may represent an underlying component in the clinical effects ofmalnutrition remains a matter of investigation Clinicians have topay particular care to avoid these disturbances and successful proto-cols of nutritional intervention in CF have been developed whichare essentially aimed to avoid the onset of protein-energy malnutri-tion (PEM) [141] Despite this the risk of developing such an unto-ward complication in CF infants and children remains high assuggested by the prevalence data registered in some areas Actuallya prevalence of PEM between 5 and 14 in Moldavian infants was re-cently reported [142] and PEM is associated with poor outcome andparticularly with the risk of developing edema and anemia
Besides lowered intake and absorption of micronutrient antioxi-dants discussed in the other sections malabsorption of dietary proteinand excess fecal amino acid losses result in hypoproteinemiahypoalbu-minemia as key biochemical signs of PEM Hypoalbuminemia is
considered to be linked with a causendasheffect relationship with oxidativestress and is proposed to influence morbidity and mortality in condi-tions associated with chronic inflammation and severe oxidative stress[143144] The human serum albumin (HAS) molecule contains only areactive thiol group eg the Cys 34 the importance of which as an anti-oxidant defense system in blood and for the entire organism is welldocumented [145] This is the second main thiol (and the main proteinthiol) in the circulation (approx 2 mmol in the adult organism assum-ing 5 l of total blood volume anHt of 40 and [HAS] of 45 gl of plasma)being the RBCGSH thefirst thiol in blood (near to 5 mmol assuming thesame parameters of above and an average concentration of GSH inpacked RBC of 25 mM) [146147] The antioxidant role of HSA is notonly a consequence of the relative abundance of its Cys thiol A specificcapability of acting as a sacrificial target for a series of electrophils andmost biologically relevant ROS ie hydrogen peroxide and peroxyni-trite has been demonstrated in a series of studies [145148149] Li-gand binding activity can contribute to promote antioxidant effectsby the HSA molecule [145] Transitions metals particularly copperand also iron in the case of iron-overload diseases bind to HSA Inthis way these are less available to promote the Fenton chemistryand hydroxyl radicals eventually released from this oxidative reactionare mostly directed to the HAS protein sparing more important tar-gets A free radical-trapping activity of HSA has been also demonstratedand this was proposed to be directed toward both hydrophilic and fat-soluble species This activity may result from the interaction withother antioxidants such as α-tocopherol [150] and may influence theantioxidant activity of food-derived phenolic antioxidants [151]
However Cys 34 is considered the main contributor to the antiox-idant function of HAS which plays its role in the antioxidant homeo-stasis of blood thanks to a complex series of interactions with themetabolism and antioxidant function of the pool of free thiols in plas-ma and in the circulating RBC with the latter playing a significantcontribution to the extracellular pool of GSH [146] and to the dynam-ics of inter-organ GSHmetabolism in cooperation with liver and othertissues [147] Immuno-inflammatory cells and the lung tissue areamong the main terminals of this metabolism The RBC contain theentire machinery to synthesize GSH to restore its redox (by enzymat-ic reduction of the oxidized form) and to use this as cofactor of Se-GPx and GSH-S-transferase enzymatic activities that are responsibleof the detoxification of hydroperoxides and alkylating agents thatmay form in or enter the RBC cytosol [147] In this sense the RBC rep-resents a circulating reservoir of GSH that in addition to maintainingthe redox and respiratory function of Hb participates to systemic pro-tection of xenobiotics of endogenous and exogenous origin In consid-eration of these aspects the combination of hypoalbuminemia andanemia may exponentially increase the risk of developing oxidativestress in CF patients as it is supposed to occur in other oxidative stressconditions such as chronic kidney disease [55143152] Additionalclinical investigation should verify the hypothesis that hypoalbumi-nemia together with a defective uptake and metabolism of sulfur-containing amino acids and CF-specific defects of the GSH metabo-lism may represent a causal risk factor for an impaired antioxidantdefense and systemic oxidative stress in CF patients
35 Fat-soluble antioxidants
Pancreatic insufficiency and a diminished bile acid pool cause mal-absorption of important essential nutrients and other dietary compo-nents in CF Of particular significance is the malabsorption of fat-soluble antioxidants such as tocopherols carotenoids and coenzymeQ-10 (Co-Q10) and that of essential fatty acids (EFA)
351 Vitamin EVitamin E therapy in CF has been proposed in several decades of
research as a useful approach to overcome both the lower absorptionof this fat-soluble micronutrient and the increased antioxidant
700 F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
demand by the abnormal generation of ROS in CF tissues (see for in-stance the recommendations by the Cystic Fibrosis Foundation Con-sensus Conference on nutrition [153])
The first report of a vitamin E deficiency in CF appeared in literaturein 1951 by Filer et al [154] In this study the absorption of the mainform of this vitamin eg α-tocopherol and its ester derivatives was in-vestigated in several subsets of infants and children Thanks to a simplebioavailability (or tolerance) test these authors observed that ldquoin-fantshellip diagnosed as fibrocystic disease of the pancreas diarrhea andcirrhosis were characterized by a poor response to the test ie the tol-erance curve was lowrdquo However abnormalities were also observed inother subgroups of infants with a variety of disorders not associatedwith fat or fat-soluble vitamin intolerance such as sprue celiac syn-drome and lupus erythematosus which suggests the general observa-tion that malnutrition and inflammatory and degenerative diseases ofthe GI tract may lead to absorb tocopherols poorly At the same timethese authors reported that ldquoMetabolic disorders with associated hy-percholesterolemia were observed to give abnormally high values forthe area under the curverdquo and that patients responding poorly to to-copherol absorption test did also in vitamin A absorption tests
The finding of lowered (lipid uncorrected) levels of vitamin E wasconfirmed in other studies in which this relative deficiency was foundto occur irrespective of pancreatic comorbidity and in associationwith lowered levels of other liposoluble vitamins such as vitamin Aand D [155] regardless of their different liver metabolism and tissuedelivery mechanisms [156157]
Plasma buccal mucosal cells (BMCs) and breath condensate α-tocopherol decreased significantly with age in association with a de-creased respiratory function [5] This was accompanied by loweredlevels of other antioxidants such as vitamin C and increased oxidativestress markers of different origin such as protein carbonyls thiobarbi-turic acid-reactive substances and F2-IsoPs
Clinical symptoms of vitamin E deficiency in CF have not beenconclusively investigated Dolan et al [158] described that anemiaof CF patients is related to vitamin E deficiency and increasedperoxide-induced hemolysis of RBC Other authors however ob-served an increased susceptibility to peroxide-induced hemolysisalso in the presence of normal levels of vitamin E [159] Peters andKelly [160] observed that RBC vitamin E concentrations were belowthe normal range in almost all unsupplemented patients and roseinto the normal range with a 1-year supplement of 100 mg per daybut not 15 mg per day Since RBC vitamin E concentration has beenshown to correlate well with tissue concentrations of the vitamin inanimals tissue levels of vitamin E are expected to be lower than nor-mal in CF patients
Bioavailability of fat-soluble vitamin is limited in CF Vitamin Edeficiency of CF is also associated with hypocholesterolemia [7] Asa consequence the relative deficiency of this vitamin is compensatedwhen the absolute levels are normalized for cholesterol levels andthis suggests a poor transferring of this vitamin in the circulation bya defective lipid and lipoprotein metabolism Pancreatic insufficiencyand the consequent lipid malnutrition cannot completely explain thisdefect and other possibly CF-specific dysfunctions could play a roleLiver metabolism and specific plasma transport systems of this vita-min need further elucidation in CF
As a consequence of these aspects it is not presently clear whichform and level of supplementation of this vitamin is most appropriateto treat these patients Usingα-tocopherol as a vitamin E supplementPeters et al [160] reported that 100 mg per day are required to nor-malize RBC concentrations Other authors described unsuccessfulsupplementation protocols with higher doses and this has led to de-velop formulations with higher bioavailability in order to achieve bet-ter compliance to oral supplementation (see below and the literaturereviewed in [161ndash163])
Besides absorption and tissue delivery issues specificity of actionis another critical item of antioxidant therapy with fat-soluble agents
in CF As further addressed below this aspect could be themain limit toa successful use of natural forms of vitamin E in the clinical manage-ment of CF inflammation even if a local lung-targeted therapy wouldbe developed according with so far proposed pre-clinical models ofaerosolized vitamin E [164165]
Current pharmacological research is aimed to develop synthetic formsof this and other fat-soluble antioxidants with better radical scavengingproperties at the lipidndashwater interface Type of ROS target and the sitesof action greatly influence the chances of a fat-soluble antioxidant of alle-viating oxidative stress in the airways as well as in other organs such asliver and pancreas These aspects dealing with specificity of action[163166167] have stimulated the search of novel vitamin E-derived an-tioxidants that may help to scavenge radicals at the lipidndashwater interfaceof the epithelial cell membrane and surfactant Amine derivativesof tocopherols and tocotrienols have been recently demonstrated toshow higher antioxidant and free radical scavenging activity than α-tocopherol [168] Further in vitro pharmacological analysis has includedtoxicity evaluations and the detailed investigation of scavenging of azo-and phenolic radicals with different degrees of hydrophobicity and theinhibitory activity on IL-8 gene expression and phospholipase activityin CF cells Comparative evaluation with other synthetic derivativessuch asα-tocopheryl succinate and natural forms of vitamin E suggestedthat these amine derivatives are promising antioxidant and anti-inflammatory agents [Galli F and Pilolli F unpublished observation]deserving further pre-clinical investigation in CF model systems
Anti-inflammatory effects of natural and synthetic analogues of vi-tamin E are also an intriguing pharmacological opportunity currentlyunder investigation by several laboratories [169170]
Recently vitamin E supplementation has been at the center of adispute regarding its safety when used at high dosages in certainpopulations of patients An extensive and speculative debate originat-ed on this subject after a meta-analysis study byMiller et al [171] thatexamined the largest secondary prevention trials on vitamin E trials incardiovascular patients finding a significantly increased mortality riskfor all the causes (about 4 1ndash8 in the 95 interval of confidence)when the patients were treated with doses gt400 IUdie (that areequivalent to 400 mgdie of the synthetic form allrac-α-tocopheroland to 185 mgdie of the natural form RRR-α-tocopherol) This debateresulted in a careful examination of this meta-analysis study by severalother authors and in further revisions of the literature on vitamin E tox-icity in humans [see the literature recently reviewed in [163172ndash174]]that clearly demonstrated the poor consistency of the conclusionsraisedwithMillersmeta-analysis study and the paucity of the concernsthat derived from that These conclusions have been verified in the re-cent international symposium on vitamin E of the Society for Free Rad-ical Research Europe branch of Rome 2009 [173175] Vitamin E used assupplement for humans in all its forms (eg α-tocopherol and othertocopherols and tocotrienols) is safe in abroad range of intakes[172176] The tolerable upper intake level (UL) and the AcceptableDaily Intake (ADI) established by the Joint FAOWHOExpert Committeeon Food Additives for the natural form of vitamin E as α-tocopherolequivalents are of 300 mgdie and 015ndash20 mgkg body weightdierespectively [172177]
352 CarotenoidsLevels of plasma carotenoids such as β-carotene β-cryptoxanthin
and total lycopene are significantly lowered in CF patients and thiswas associated with higher susceptibility to lipid peroxidation[5178ndash180] Rust et al [178] demonstrated that the long-term oralsupplementation with 50 mg β-caroteneday (ie 1 mg β-carotenekg BWday) restored the levels of this carotenoid while sub-optimalsupplementation was observed at doses of 10 mg β-caroteneday orlower thus confirming the need of high doses of this fat-soluble factorto overcome the limited absorption and thus to achieve plasma con-centrations of healthy control subjects Successful high-dose treat-ments appear to lower oxidative stress markers such as TBA-MDA
701F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
complexes and to correct total antioxidant capacity of plasma Inanother study β-carotene supplementation was observed to de-creased lipid peroxide formation as quantitated by malondialdehydeconcentrations in plasma (TBAHPLC method) and to enhance the re-sistance to copper(II) ion-induced oxidation of low density lipopro-teins [180]
At the same time toxicity issues have been raised for human sup-plementation with carotenoid formulations and particularly of water-miscible formulations of preformed vitamin A that is regularly sup-plemented to CF patients which may increase serum retinol andpossible risk of CF-associated liver and bone complications (reviewedin [161181]) However β-carotene supplementation seems to be safesince this does not affect plasma concentrations of other carotenoidsand retinol as well as of other fat-soluble vitamins as α- and γ-tocopherol [178] Recent studies designed to test the clinical efficacyof a CF tailored multivitamin formulation (commercial name AquA-DEKsreg) also tested the safety of this type of formulation and demon-strated that this does not increase vitamin A above the normal levelsobserved in healthy controls [162182183] The normalization of β-carotene levels obtained in these studies was associated only withminor improvements on respiratory and growth parameters whilethe levels of urinary F2-IsoPs used as index of lipid peroxidationwere not affected [162] The surrogate marker of lipid peroxidationMDA was affected together with some selected antioxidant parame-ters (RBC thiols and superoxide dismutase) in another study inwhich this multivitamin formulation was preliminarily evaluated incomparison with standard formulations of vitamin E and A [182]
353 Coenzyme Q-10Coenzyme Q-10 (Q10) is a well-known electron transporter in the
mitochondrial respiratory chain with fundamental role in cellularbioenergetics and scavenging of radical species [184] This lipophilicsubstance is present in the circulation at low levels (serum concentra-tionsle2 μM) mainly as ubiquinol-10 eg the reduced form with anapproximate ratio of 955 with the oxidized form ubiquinone-10[185186] A mechanism for a preferential distribution and accumula-tion in mitochondria has been suggested for both the reduced and ox-idized forms of CoQ10 that are taken up by the cells in a time- andconcentration-dependent Subcellular localization and trafficking ofexogenous Q10 are similar to those of the endogenous form butwere different from that of α-tocopherol that is related with lipidcomposition particularly in the mitochondrial and microsomal frac-tions [184] Ubiquinol-10 readily oxidizes ex vivo by the reactionwith other lipophilic antioxidants such as α-tocopherol and butylatedhydroxytoluene [185] Therefore a higher reduction potential thanother physiological fat-soluble antioxidants such as vitamin E and aselective metabolism and cellular trafficking show peculiar role forthe cell CoQ which may also represent an important lipophilic antiox-idant in cells and body fluids
Human cells synthesize this coenzyme through the cholesterol bio-synthesis pathway so thatmore than two thirds of the tissue levels ap-pear to have an endogenous origin dietary sources provide acontribution to Co-Q10 levels of blood and all solid tissues that variesdepending on the dose applied and type of dietary source [187] How-ever in the case of oral supplements it has to be considered that hy-drophobicity and large molecular weight of this coenzyme influenceits absorption that ultimately is slow and limited [186187] Likewiseto vitamin E pharmacokinetics [188189] Co-Q10 showed T(max) ofaround 6 h that coincides with that of dietary lipids Elimination isclose to that of the more retained form of vitamin E in human bodyeg α-tocopherol with a half-life of about 33 h which suggests poorhepatic metabolism However commercially available formulationsare reported to be safe even at high doses and solubilized formulationsshow enhanced bioavailability In healthy subjects plasma Q10 re-sponse to oral ingestion show saturation profiles with a plateau at a
dose of 2400 mg and the higher plasma concentrations were foundto facilitate uptake by peripheral tissues and also the brain [186187]
Laguna et al [190] recently investigated total serum levels ofcoenzyme Q-10 in a wide population of CF children (n=381) and esti-mated their association with clinical outcome Near to 50 of these CFpatients were deficient of Co-Q10 and this defect was significantlymore prevalent in patients with pancreatic insufficiency and signifi-cantly associated with P aeruginosa colonization in infants (under24 months of age) Importantly low Co-Q10 levels correlated to otherlipid markers of a poor nutritional status such as total lipids and alsothe other fat-soluble antioxidants β-carotene and α-tocopherolwhich confirms the presence of a common defect in the absorptionand metabolic pathways of this coenzyme with dietary lipids
The deficit of Co-Q10 may contribute to the impaired energy func-tion of mitochondria of CF tissues and this may exacerbate CF-linkedinflammation infection and cellular stress response of the lung A sys-tematic analysis of molecular lesions in CF bronchial tissue has beenrecently carried out by proteomic approach [191] Comparative eval-uation of protein expressional pattern in CF and healthy controltissues has revealed aberrant levels of some mitochondrial andenergy-related proteins in CF specimens that included the ubiqui-nolndashcytochrome c reductase complex core protein I and one form ofnidogen a pseudogene of aconitase 2 These changes in CF may reflectmolecular changes which could be associated with an altered mito-chondrial homeostasis and Co-Q10 redox
Multivitamin supplements with high bioavailability containingCo-Q10 have demonstrated to correct the deficit of this antioxidantand were preliminarily observed to improve airway inflammationmarkers in CF patients [183] However further clinical investigationfailed to demonstrate that such an improved biochemical profile isassociated with significant improvements in weight percentile andpulmonary function [162]
354 Fatty acidsA key pathophysiological role in sustaining inflammation in CF has
been attributed to the abnormal polyunsaturated fatty acid (FA) pat-tern Abnormalities in FA profiling are potentially linked to CFTRmutation-driven alterations in the absorption andor metabolism ofdietary lipids [192193] and to the consumption of high oxidizableFA involved in the free radical-mediated lipid peroxidation [7]Among those alterations dysregulation of the docosahexaenoic acidand arachidonic acid balance has been extensively studied with re-portedly significant reduction of DHA in CF and a parallel increasein the levels of AA and inflammatory indices [193ndash195] Actually AAis the progenitor of both enzymatic- and free radical-derived inflam-matory mediators including leukotrienes prostaglandins and iso-prostanes On the other hand n-3 PUFA (eicosapentaenoic acid anddocosahexaenoic acid) are involved in the generation of potent medi-ators namely resolvins and protectins which are able to resolveexudates and to act as organ protective and antifibrotic Secondarilyto their anti-inflammatory action n-3 FA may also produce anantioxidant-like response (eg a reduced demand of antioxidants toachieve an optimal control of oxidative pathways) As a consequencen-3 PUFA have been suggested and widely used as supplements in CFpatients usually under the form of fish oil [196ndash198] It is worth ofnote however that defective levels of DHA in CF patients was notconfirmed in recent studies [7] It was also shown that patients onDHA supplements did not have increased plasma n-3 FA concentra-tions but showed more severe oxidative stress compared to theunsupplemented patients [7] This observation of an increased riskof oxidative stress in CF subjects receiving n-3 fatty acids supple-ments has also been described by other authors [199]
Studies reporting increased AA levels in CF patients have beencontradicted by others [7200201] thus contributing to weakeningthe pathophysiological role of the altered DHAndashAA balance as turnpoint of an upregulated inflammatory status in CF In this context a
702 F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
recent Cochrane meta-analysis on n-3 supplementation in CF patients[202] highlighted the lack of evidence for a significant correction ofthe assessed clinical end points (mainly respiratory symptoms)even when inflammatory indices and other laboratory end pointswere met Taken together these data suggest that there is insufficientevidence to draw firm conclusions or recommend routine use of n-3supplements in CF Notwithstanding it is common belief that n-3supplements provide some benefits for people with CF with relativelyfew adverse effects and thus their use is not discouraged
Further alterations in fatty acid metabolism have been highlight-ed including the consistent findings of an increase in circulatinglevels of saturated and monounsaturated fatty acids [7203204]Decreased levels of essential FA (EFA) ie the FA that have to be in-troduced with the diet correlates with the severity of respiratoryinsufficiency and the same clinical correlation was observed with al-tered proportions of FA species converted by the activity of desatur-ase enzymes (reviewed in [204]) The close relationship betweencertain fatty acids and oxidative stress including the negative correla-tion of C240 and linoleic acid with oxysterol levels point to the needof intensive investigation in CF patients of previously neglected lipidspecies that are emerging candidates in the control of metabolismQuantitative lipidomic analyses have lead to identify C161n7 palmi-toleate as a ldquoprotectiverdquo adipose-derived lipid hormone that stronglystimulates insulin activity in muscle and liver also suppressing in-flammatory cytokine output from mice fat cells [205] Specific meta-bolic activities have been also demonstrated by medium chainsaturated fatty acids caprylic acid (C80) capric acid (C100) and lau-ric acid (C120) Capric acid acts as a direct ligand of PPARγ using abinding pocket different from the binding pocket of thiazolidinedioneor long chain fatty acids [206] Additional activities of medium chainfatty acids which are ligands of free fatty acids receptors detectedin the immune cells the gastrointestinal tract and adipocytes maycontribute to metabolic homeostasis and inflammatory responses[207] These data underscore the importance of a lipid-mediated ldquoen-docrine networkrdquo demonstrating how specific alteration of one orfew serum lipids would be per se sufficient to influence metabolic ho-meostasis Given the relevance of this emerging information and thealteration of lipid metabolism and inflammatory status in CF fattyacid lipidomics need to be deeply investigated in CF
Again these studies have obvious nutritional implications Satu-rated fatty acids with chain lengths higher than C18 are poorlyabsorbed partly because they form insoluble calcium salts [208]Medium chain saturated fatty acids are well known for being highlyabsorbed through the intestine providing rapid delivery of energyvia oxidation of the more hydrophilic short chains and have beensuggested to provide proper nourishment in patients with CF [209]Recent studies have shown that consumption of a high-fat diet richin medium chain fatty acids as opposed to long chain fatty acidsdoes not lead to ectopic fat accumulation in skeletal muscle andliver of both rats and mice [210] In light of the close association be-tween nutritional status inflammation and life expectancy in CF pa-tients the manipulation of dietary lipids in these patients must befurther explored as a possible strategy to provide adequate nutritionand better management of oxidative stress
36 Hydrosoluble antioxidants oligoelements and enzymatic antioxidants
361 Vitamin CVitamin C status in CF patients has been poorly investigated Early
studies suggested a defective vitamin C status that was refractory tooral supplementation [211] Other and more recent studies showednormal or slightly decreased levels of vitamin C in CF patients as com-pared to healthy controls but age- and disease-related decline of thiswater-soluble antioxidant was reported in these patients [5212]In the study of Winklhofer-Roob et al [212] on mid-European CFpatients vitamin C concentrations decreased with age with an
estimated rate of 5 μmollyr and vitamin C concentrationsb40 μ-moll were associated with highest indexes of inflammation whichis consistent with the hypothesis that optimal levels of vitamin Cmay influence immuno-inflammatory activity of alveolar macro-phages and neutrophils Other few studies have examined the effectof supplements containing vitamin C on CF inflammation and oxida-tive stress since the levels of this vitamin do not significantly improvewith supplementation (reviewed in [213]) This highlights the com-mon fate that this hydrosoluble vitamin shares with several fat-soluble counterparts in the ldquomicronutrient paradoxrdquo of CF patients inwhich the need for a correction of their status along the progressionof the disease is frustrated by the poor efficacy of oral supplementa-tion protocols Formulations and appropriate supplementation proto-cols that may produce a better correction of vitamin C status of CFpatients are awaited for further clinical evaluation
362 Selenium and selenium-dependent peroxidasesSelenium is a trace element with marked electrophilicity [214]
that once converted to the organic form of Se-Cys can be introducedin protein structures to play its important role in H2O2 metabolismand signaling [215] As catalytic center of the enzyme GSH-peroxidase (SeGSH-Px) Se plays a crucial role to protect polyunsatu-rated lipids of plasma membrane and circulating lipoproteins formperoxidative insults With other Se-proteins such as the high molecu-lar weight thioredoxin reductases this oligoelement participates tothe control of protein thiol-disulfide oxidoreduction and glutathiony-lation which regulate signaling pathways of crucial importance in theregulation of immunity and inflammation [16] but also the function-ing of other redox-sensitive proteins such as the same CFTR [124]
The activity of SeGSH-Px in blood is considered a functional as-sessment of selenium status even if this assumption has some limita-tions related with the saturation profile that the Se stores show atincreasing doses of Se administration Investigations of the seleniumstatus in CF patients have produced conflicting findings which maydepend on differences in dietary intake ethnicity and environmentalfactors in the diverse patient populations (reviewed in [216217]) CFchildren have been reported to have lowered blood selenium and RBCSeGSH-Px activity [218219] normal plasma selenium and loweredRBC SeGSH-Px [220] and even normal levels of both these two param-eters [221] The supplementation with selenium in combination withother antioxidants was observed to increase the concentrations ofblood selenium that likewise β-carotene and fatty acid were posi-tively correlated with improved lung function [6]
Foucaud et al [218] observed that a defective selenium statuswas associated with lowered levels of other antioxidants that contrib-ute to the anti-peroxidative activity of this microelement such asvitamin E (reviewed in [222]) and the severity of this deficiencywas lower in children with pancreatic enzyme replacement and vita-min E supplementation
Treatments to substitute for exocrine pancreatic insufficiency bypancreatic enzymes from animal sources such as porcine pancreashave been confirmed to be a source of Se [220] These affects RBCSeGSH-Px activity and plasma selenium concentrations which hasto be taken into account when selenium supplements are given toCF patients
Selenium has been used to develop a series of organoseleniumcompounds that may open the way to new therapeutic opportunitiesin CF (see Section 392) These include GPX mimetic drugs and phaseII enzyme inducers which may provide higher antioxidant activity ofASL and cellular protection effects in the airways
363 Zinc and copperZinc and copper (Zn and Cu respectively) are present in many
proteins so that a deficiency of these trace metals could have pleiotro-pic effects in humans As regards antioxidant systems these two oli-goelements contribute an important role being cofactors of two
703F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
isoforms of the superoxide dismutase enzymes eg the extracellularform eg the EC-SOD or Sod 3 and the CundashZn-SOD or Sod 1 that isfound in several tissues and cells [223] The EC-SOD exerts its antiox-idant role also in the lining fluids of the airways [224]
The notion that CF patients have defective concentrations of bloodZn and Cu is controversial As far as Cu status is concerned few datahave been produced and are available in the literature suggestingthe notion that CF patients develop a moderate copper deficiency[225226] That was essentially demonstrated on the bases of a defec-tive activity of Cu-related proteins such as plasma ceruloplasmindiamine oxidase and RBC SOD This defect seems to be refractory toCu and Zn supplementation (see below)
More advanced studies have been carried out in the case of Zn sta-tus in CF Low plasma zinc concentrations were reported in approxi-mately 30 of young infants with CF identified by newbornscreening [227] and an impaired zinc homeostasis in CF patientswas described by Easley et al [228] This is characterized by poor con-servation of the endogenous pool with fecal loss and impaired frac-tional absorption of zinc which are the consequences of pancreaticinsufficiency and persisting steatorrhea These studies suggestedthat in the clinical management of CF patients these defects can beat least in part corrected by exocrine pancreatic enzyme replacement
A series of studies by Van Biervliet et al [229230] demonstratedin a Dutch population of CF infants and children that serum Zn variesin an age-dependent manner but remained unchanged with respectto healthy control levels In CF patients no difference in serum Zn con-centration between pancreatic-sufficient or pancreatic-insufficientpatients was observed and no correlation was found with the nutri-tional status or height z-score Importantly in these studies a signifi-cant correlation of serum Zn was observed with the fat solublevitamins A and E thus confirming the relationship between the ab-normalities of lipid and Zn metabolism in CF This suggests that co-supplementation of Zn and fat-soluble vitamins should be advisedin the presence of pancreatic insufficiency and persisting steatorrhea
Neve et al [219] in a study aimed to assess plasma and erythrocytezinc copper and selenium in CF children showed that mean plasmazinc and copper levels were not different from those in age-matched controls which confirms the observations by Van Biervlietet al described above However plasma zinc concentrations de-creased in patients with moderate-to-severe growth retardation andwith severe pulmonary disease but very low zinc levels occur sporad-ically Erythrocyte zinc and copper levels were significantly higherthan normal while RBC selenium was lower than in age-matchedcontrols These trace element concentrations in erythrocytes werediscussed in relation to the activities of the CuZn-SOD and the Se-enzyme GPx This observation suggests a compensatory upregulationof the erythrocyte CuZn-SOD by the exposure of erythroid precursorsto ROS andor other CF-related stressors
Best et al [225] also studied RBC SOD activity using this as a bio-logical sensor of Cu status in CF patients A lowered activity of thisenzyme was reported in CF together with that of the other Cu-dependent enzyme plasma diamine oxidase while plasma ceruplas-min showed normal activity Degradation rates of copper proteinsare known to be accelerated in conditions of copper deficiencywhich could explain the finding at least in part Anyway when Cuand Zn were supplemented to CF patients either separate or incombination (6 weeks of 3 mg copperd as copper-glycinate and30 mg zincd as zinc-glycinate) any of the copper enzyme activitieswas affected Therefore the moderate copper deficiency of CF patientsappears to be refractory to the intervention by increased copper andor zinc intake
Erythrocyte CuZn-SOD and the plasma levels of Cu and Zn werealso measured in the study of Wood et al [6] in which Australian CFpatients (agegt5 years) were treated with a high-dose antioxidantmultivitamin formulation containing 200 mg vitamin E (as RRR-α-tocopherol) 300 mg vitamin C (as sodium ascorbate) 25 mg β-
carotene (all-trans isomer) 90 μg Se (as selenomethionine) and500 μg vitamin A (as retinyl palmitate) in oil Plasma oligoelementsand particularly Zn were in the normal range at baseline (as com-pared with the data reported in [229230]) and were not affected bythis multivitamin supplement The same was found for the activityof RBC SOD and for plasma 8-iso-PGF2α as surrogate biomarker oflipid peroxidation
In a recent non-randomized small population (n=21) casendashcon-trol study in CF children Zn supplementation was proven to producepositive clinical effects in Zn-deficient patients [196] The supplemen-tation with 5 mgkg Zn sulfateday (maximum 150 mg) significantlydecreased the number of infections and increased the forced expira-tory volume in 1 s energy intake and growth parameters also im-proved These parameters were unaffected in untreated patientsexcept that in the case of the pulmonary function that decreased sig-nificantly These clinical observations on Zn supplementation need tobe confirmed in prospective double-blind randomized control trial
37 Appropriateness and targeting of antioxidant therapies in CF
The choice of the appropriate antioxidant and dose to correct a cer-tain biomarker and its associated biochemical lesion is another impor-tant point that appears to have disregarded in many clinical studiesFor instance unlike vitamin E vitamin C supplementation does notalter F2-IsoPs levels in humans (reviewed in [74]) This appears tobe true also in the antioxidant therapy of CF in which vitamin C(300 mgday) was administered together with other antioxidantsthat included a dose of vitamin E of 200 mgday without any signifi-cant effect on the surrogate biomarker of lipid peroxidation F2-IsoPs[6] When carotenoids are used as supplements to prevent the damag-ing action of ROS in the CF airways it is noteworthy that these are notparticularly good quenchers of peroxyl radicals relative to phenolicsand other antioxidants but are exceptional in quenching singlet oxy-gen at which most other phenolics and antioxidants are relativelyineffective Singlet oxygen is not a radical and does not react via radi-cal mechanisms but reacts mostly by the addition to double bondsforming endoperoxides that can be reduced to alkoxyl radicals that ini-tiate radical chain reactions typical of the peroxidative damage of PUFA[38] In this case the analysis of F2-IsoPs lipid peroxide formation andtransition metal-induced oxidizability of lipoproteins [162180] are allappropriate to evaluate the effect of carotenoids in preventing lipidperoxidation
As far as the dose is concerned clinical pharmacology of vitamin Eas an antioxidant was recently investigated by means of the effect onF2-IsoPs production and doses of α-tocopherol of 1600 IUday orgreater were found to be required to statistically affect plasma F2-IsoPs levels in hypercholeterolemic subjects [176] Several vitamin Esupplementation studies in CF patients have been performed withdoses of lower than 300 IUday regardless of the lowered absorptionby pancreatic and liver defects and the regular supplementationwith these doses does not appear to correct lipid oxidation markersin CF [7]
In the clinical practice and planning trials it has to be taken intoconsideration that in spite of substantial evidence supporting ahigher antioxidant demand in CF interventions with several antioxi-dant formulations produce poor responsiveness particularly in thecase of fat-soluble antioxidants which are poorly absorbed [6162]
Since many oxidants and antioxidants are present in tissuesand biological fluids and these have different chemical and physicalcharacteristics the possibility to produce a successful therapy witha single antioxidant molecule is too far to be realistic Moreover an-tioxidants act by multiple mechanisms in a single system or by adifferent single mechanism depending on the reaction systemresponding in a different manner to different radical or oxidantsources Because multiple reaction characteristics and mechanismsas well as different phase localizations are usually involved no single
704 F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
therapeutic approach will effectively prevent damage by multipleROS sources The defect of physiological antioxidants may also interferewith antioxidant therapies that are based on one or few exogenousantioxidants
Moreover several antioxidant vitamins such as vitamin E and ca-rotenoids have multiple natural forms with different bioavailabilitymetabolism and bioactivity [157167231] As far as the case of vita-min E supplementation concerns α-tocopherol was used as uniquevitamer in the large majority of supplementation trials so far per-formed and is the form used in the nutritional management of CFpatients Moreover several supplements contain the synthetic (or ra-cemic) form of this vitamin that has lower bioavailability than thenatural form Other forms present in nature and abundantly con-tained in vegetables such as tocotrienols and the less methylatedforms of tocopherol are not represented in many of the supplementformulations so far available in clinical centers and the supplementa-tion with α-tocopherol also limits their bioavailability These formsshow markedly higher susceptibility to hepatic metabolism and bili-ary excretion with respect to α-tocopherol eg the most representedform in blood and solid tissues and if co-supplemented these areeasily displaced during liver uptake and excreted with bile bymeans of competition with the same α-tocopherol Notwithstandingthese minor forms have been proposed to play important physiolog-ical roles showing molecular characteristics transcriptional effectsand antioxidant activities that clearly differentiate them in subfam-ilies with distinct biological functions Some of these such as α-tocopherol eg the second vitamin E form as relative abundance inblood and its carboxyethyl-hydroxychroman metabolite [189] ap-pear to have health-related anti-inflammatory effects which are par-ticularly relevant in lung protection [232233] This has suggestedthat such a group of ldquonon-α-tocopherolrdquo forms may represent anoth-er family of vitamins within the family of vitamin E with an impor-tant but often missed contribution to the proposed health effects ofthis vitamin [163]
These aspects may thus limit the possibility to provide CF patientsof optimal levels of this vitamin in all its components even if they areregularly treated with a vitamin E supplement eg withα-tocopherol
Targeted antioxidant therapy with formulations with higher bio-availability and bioactivity has been anticipated in CF New antioxi-dant formulations have been proposed to overcome main limits ofantioxidant therapies so far proposed for these patients Water-miscible α-tocopheryl acetate containing polysorbate propylene gly-col or polyethylene glycol as emulsifiers form micellar structureswere suggested to providing greater bioavailability than the fat-soluble counterparts These were commercialized with the brandnames of E-viminreg Cremophorreg EL and Aquasolreg E but despitethe original positive expectation [234235] some studies failed to ob-serve a higher response in vitamin E levels when these were com-pared with fat-soluble formulations [236237]
In a pilot study by Papas et al [183] a micellar formulation of fat-soluble nutrients and antioxidants was found to improve plasmalevels of β-carotene γ-tocopherol and CoQ(10) reducing at thesame time some inflammatory markers in induced sputum eg mye-loperoxidase and to a lower extent PMN elastase and total cell countswhile lung function and sputum bacterial counts were unaffectedThe same group recently confirmed the possibility to increase the ab-sorption of fat-soluble micronutrients using formulations with higherbioavailability specifically designed for malabsorbing patients such asCF patients that include also vitamin K and commercialized with thebrand name of AquADEKsreg [162] Despite improved vitamin and mi-cronutrient levels in this non-randomized open-label study AquA-DEKsreg produced only modest improvements in weight percentileand pulmonary function Another recent pilot observation [182] hassuggested the beneficial effect of this formulation on antioxidant andoxidative stress parameters of this oral supplement that surely deservesmore clinical investigation by larger randomized controlled trials
Recent multivitaminic formulations have been designed to containalso the minor forms of vitamin E and specifically γ-tocopherol [238]the expected superiority of which with respect to formulations con-taining only α-tocopherol needs to be verified As discussed abovein the section dedicated to vitamin E further advancements in thetherapy of CF inflammation and oxidative stress could be based onsynthetic forms and natural metabolites of this vitamin that havebeen recently identified to possess higher antioxidant and also anti-inflammatory activity than α-tocopherol (reviewed in [163168])
Pre-clinical investigation of these and other fat-soluble agents iscurrently addressed to develop formulations and administration pro-tocols that may increase the therapeutic efficacy in the airways In theantioxidant therapy of lung dysfunction in CF local administrationprotocols may overcome the limits of oral and systemic administra-tion protocols increasing bioavailability and providing targetedapproach to inflammation and oxidative stress Aerosolization of vita-min E and other fat-soluble micronutrients is possible and may allowdirect administration in the airways to prevent toxicity of smokewhich is closely associated with inflammation and oxidative stress[164165] To our knowledge this as well as other strategies of localadministration such as instillation of solutions such as surfactant-like solutions enriched of vitamin E have not been previously inves-tigated in CF patients and other CF model systems
On the contrary inhalation is an administration route widelyadopted in the case of GSH and NAC therapy described above Inthis context Cys formulations alternative to NAC have been proposedfor use as antioxidant and anti-inflammatory agent for inhalationNacystelyn is a lysine adduct of NAC that thanks to a higher proton-ation equilibrium shows increased water solubility and thus betterbioavailability Nacystelyn has been described to influence IL-8 gener-ation and the inflammatory signaling of bronchial epithelial cells[239] and preliminary clinical evaluation has demonstrated the safetyof this drug [240] Further clinical trials aimed to assess the effect onlung symptomatology of CF patients are needed Direct administra-tion in the airways could also be adopted for micronutrient vitaminswith poor absorption and bioavailability due to GI defects
38 Clinical impact of antioxidant therapy in CF
Huge in vitro and pre-clinical evidence has provided the rationaleto support clinical investigation of antioxidant strategies in CF Theseshould aim to restore the oxidantndashantioxidant balance of CF airwaychallenged by chronic infection and inflammatory cell activation
Some observational trials have confirmed that antioxidants usedas either supplements to the diet or drugs for lung administrationby aerosolized formulations may help in relieving progressive lungdamage and other adverse clinical events of CF such as poor growthSo far few studies have examined with sufficient methodologicalrigor the clinical efficacy of antioxidant therapy in CF This was alsoconcluded in a previous review of the literature by Cantin et al [12]that was published in the beginning of 2006 and is confirmed alsoin a recent analysis of clinical trials on antioxidant therapy in CF pa-tients [213] that examined the literature until September 2010using as sources the databases of the Cochrane CF and Genetic Disor-ders Group CF Trials Register PubMed CINAHL and AMED Useful in-formation was retrieved from just four randomized controlled trialsand one quasi-randomized controlled trial on vitamin C vitamin Eβ-carotene and selenium used as supplements administered aloneor in combination Post-hoc data analysis that was possible only inthree studies on a total of 87 CF patients showed the absence ofany significant improvement in lung function that was selected as pri-mary outcome together with quality of life that improved in one trialSecondary outcomes concerning laboratory indices of oxidative stressand antioxidant status showed several improvements These includedan increase of RBC SeGPx by selenium supplementation done as
705F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
individual or combined supplementation and increased levels of allplasma antioxidants except vitamin C that were observed in all thetrials
The message from these studies to pediatricians and nutritionistswithin the clinical staff of CF centers is that in the absence of solid ev-idence regarding the clinical effectiveness of oral formulations of an-tioxidant supplements in CF (including PUFA) their use as a routineclinical practice should be considered with caution keeping clear inmind that this should represent just a complement of one of themost critical interventions in the life-long clinical management pro-gram of CF patients eg providing an adequate nutriture [140] Inthis context compensating energy and protein malnutrition has toremain the first goal of nutritional management programs Providinghigher intakes of antioxidant micronutrients with food naturally-enriched (or functionalized) of micronutrient antioxidants shouldbe preferred in order to have the higher combination of positive nu-tritional factors that are lost during refinement procedures and over-all industrial processing of dietary supplements
Measures of good practice in clinical management of micro-malnutrition in CF patients would include the support of specializedpersonnel and laboratories The centers should have the possibilityto ascertain with appropriate nutritional and laboratory tests whatthe level of deficiency is for the different micronutrients that each pa-tient may suffer from during a dietary program Monitoring dietaryintakes and blood levels of micronutrients is not sufficient to set apersonalized nutritional intervention with supplements or functionalfoods Sub-optimal intakes and the compliance to nutritional inter-ventions should be verified by means of selected biochemical andclinical criteria Unluckily the latter are still not well established forsome micronutrients such as the fat-soluble vitamins E (reviewed in[163173241]) and K [242243] and also for trace elements such asSe [244] For many of the antioxidants used as supplements inhumans we still do not know exactly several of the biological effectsthat these may provide when introduced in a healthy body and weknow less what these can do in disease These aspects hardly impacton the concept of optimal levels of intake that should be identified foreach micronutrient on an individual basis According with the aspectsdiscussed in the previous sections optimal levels of intake for antiox-idant micronutrients are different in CF patients and healthy subjectsand vary with age and several individual factors
Lung administration of antioxidants by means of aerosolized for-mulations so far used for GSH therapy (see above) is a promisingfield of clinical investigation in CF Toxicity issues are currently themain concern and the subject of clinical evaluation by several groups(described above)
Information on future directions of antioxidant therapy in CF canbe inferred by the analysis of pending or recently completed clinicaltrials that have been searched (December 2011) at ClinicalTrialsgovdatabase matching the terms ldquoantioxidant therapyrdquo or ldquoglutathionerdquowith ldquocystic fibrosisrdquo Fifteen trials were retrieved and those directlyrelated to antioxidant therapy (n=12) are presented in Table 1 andinclude efficacy and safety studies of inhaled drugs as GSH sodiumpyruvate NAC and NO and the dietary supplements AquADEKsregan antioxidant-rich multivitamin supplement epigallocatechin gal-late (EGCG)tocotrienol curcuminoids the amino acid glutaminesulforaphane in broccoli sprouts One trial is investigating the flavo-noid quercetin as CFTR modulator
39 Emerging antioxidant and anti-inflammatory approaches in CF
Mediterranean foods such as olive oil and red wine or severalplant extracts such as herbal tea or grape seed extracts contain aseries of natural compounds with important antioxidant and NOscavenging activity that have been widely investigated for the pre-vention of oxidative stress-related diseases [38245] These havebeen long investigated as template molecules to develop antioxidant
and anti-inflammatory drugs Between the multitudes of natural sub-stances most investigated ones include for instance tyrosol hydroxy-tyrosol gallic and caffeic acids belonging to the family of phenolswhile resveratrol of the stilbenes family epicatechin kaempferoland cianidin are examples of flavonoids examples of fat-soluble phe-nolics are those of the family of tocols (vitamin E) and carotenoids Allthese compounds show different metabolisms and signaling effects[246] Antioxidant and cell protection mechanisms are associatedwith different and sometimes concurrent processes as H-atom trans-fer and electron donation radical trapping and chelation of transitionmetals that can be easily investigated at the chemical level [247] Be-sides these direct antioxidant effects metabolic responses and signal-ing effects of natural compounds are also important to producesecond-generation responses that modify the level of antioxidantprotection and the potential for ROS detoxification in cells and bodyfluids These derive from the transcriptional regulation of antioxidantand pro-oxidant genes that coexist with the modulation of cytokinesecretion and inflammatory enzyme activities
Some of these natural plant-derived antioxidants may provide fur-ther pharmacological activities of possible relevance in CF This is thecase for instance of the plant flavonoids genistein apigenin kaemp-ferol quercetin and hesperidin [248ndash251] that fall in the pharmaco-logical category of ldquopotentiatorsrdquo [252] in that these activate at leastto a certain extent CTFR-mediated Cl currents in normal and CF airwayepithelium investigated either in vitro or in vivo in humans and ani-mal models Actually as prototypal flavonoid-derived potentiatorthe tyrosine kinase inhibitor genistein potentiates the gating of wild-type as well as ΔF508 CFTR and G551D CFTR [253] but at higherdoses it inhibits CFTR gating which make this an unlikely clinical can-didate Similar potentiation effects have been reported for the antiox-idant curcumin [250] that shows an additive effect with respect togenistein-induced potentiation Besides CFTR potentiation whichdoes not appear to have a direct influence on GSH and nutrient trans-port in the lung tissue all these natural substances have been usedalone or in combination with other agents as in vivo enhancers oflung antioxidant protection [246254255] In the case of quercetinthiol-reactive phenolic [256] bronchodilation and anti-inflammatoryeffects by a restoration of the Th1Th2 balance have been reportedin inflammatory syndromes of the lung [255257ndash259] but theseeffects have not been explored in CF Pyocyanin toxicity (see abovein the Section 2) could represent an issue for the use of quercetinand other catechols in infectious diseases of the lung [260]
Other natural antioxidants of potential interest in CF therapy in-clude terpenoids [261] such as terpinen-4-ol a major constituentof tea tree oil that is being investigated in the therapy of anti-biotic resistant organisms specifically against methicillin-resistantStaphylococcus aureus (MRSA) [262] a problem in CF [263] Otherthan being lipophilic antioxidants terpenes can prevent oxidativestress of the CF lung secondarily to the antibiotic effect thereby pro-moting a better control of immuno-inflammatory pathways and lungantioxidants
391 Targeting NF-κB with natural compounds resveratrol and plantextracts
Natural compounds were long known to be useful in designinganti-inflammatory drugs and some of these could find an applicationin the control of the transcription factor kappa-B (NF-κB) that maylead to develop advanced pharmacological tools to control inflamma-tion and to produce higher antioxidant protection to CF airwaysInhibitors targeting NF-κB including transcription factors decoymolecules (TFD) are potent down-regulators of gene expressionand release of IL-8 in CF cells infected with P aeruginosa [264265]
Resveratrol (354prime-trihydroxystilbene ldquoErdquo form) is one of the mostinvestigated natural antioxidant with proposed activity as NF-κBinhibitor This is a phytoalexin present in large quantity in red winepreferentially in the skin of grapes being its concentration
706 F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
50ndash100 μgmg of fresh skin and 13ndash3 mgl of red wine [266]Furthermore resveratrol is a constituent of lsquoDarakchasavarsquo (13ndash6 mgl) an ayurvedic medicine from India [267] The antioxidant activity ofresveratrol has been reported in several papers and occurs also in lungtissues suggesting that resveratrol has potential as a therapeuticagent in respiratory disease [268ndash270] Resveratrol can be consideredone of the most interesting molecules from the natural worldexhibiting strong antioxidant activity that at the same time is able toexert anti inflammatory activity through alteration of NF-κB functionsand efficient inhibition of pro-inflammatory genes [271272] As far asthe effects on CF model systems are concerned Cabrini et al [26]reported the effects of resveratrol on P aeruginosa infected CF IB3-1cells The results obtained demonstrate that resveratrol exhibits minoreffects of IB3-1 cell growth and important inhibitory effects on accumu-lation of IL-8 and GRO-α mRNA while minor effects on IL-6 gene ex-pression were observed These data support recently publishedobservations suggesting inhibitory effects of resveratrol in infection-mediated inflammatory processes [273] Interestingly resveratrol hasbeen reported as a potent inhibitor of NF-κB activity and a promisinganti-inflammatory agent [272274] also in combinationwith othermol-ecules [274275] However in vivo translation of this pre-clinical on res-veratrol is hard to be foreseen This natural compound displays poorbioavailability [276] and further characterization of resveratrol pharma-cokinetics is troublesome since it is hardly measurable in vivo [277]Furthermore the regulation of inflammatory responses by resveratrolhas been suggested to be far more complex than simple direct suppres-sion of NF-κB activity Actually some aspects of the immune responsecould be enhanced by this natural substance which may lead tohypothesize broad negative feedback events on immuno-inflammatorypathways [278] In any case and with these cautions in mind the pub-lished observations on cellular model systems support the concept thatresveratrol and resveratrol-containing formulations deserve further con-sideration to determine their possible therapeutic values in CF
Other inhibitors can be identified from systematic studies of naturalproducts and their ability to interfere with NF-κB activity [279ndash281]Recent studies have demonstrated that the whole extract of Aeglemarmelos (Rutaceae) has strong inhibitory effect on the P aeruginosa-dependent IL-8 induction in human CF-derived bronchial IB3-1 cellswithout affecting cell proliferation [280] Molecular analysis of compo-nents contained in A marmelos extracts revealed that three major com-pounds namely 56-dimethoxy-1-indanone 2-hydroxy-cinnamic acidand 5-methoxy psoralen (5-MOP) reproduce the inhibitory effect ob-servedwith thewhole extract [280] A further example has been recent-ly published using extracts from bergamot (Citrus bergamia Risso) Inthis study the extracts were characterized and the main detected con-stituents were assayed for their biological activity [281] The resultsobtained demonstrated that the extracts from bergamot epicarps con-tain components displaying an inhibitory activity on IL-8 Particularlythe most active molecules were bergapten and citropten These effectshave been confirmed by analyzing mRNA levels and protein release inthe CF cellularmodels IB3-1 and CuFi-1 inducedwith TNF-α or exposedto P aeruginosa
A parallel strategy linking NF-κB inhibition and down-regulationof NF-κB-dependent functions is described in recently publishedstudies based on a structured-based virtual screening (VS) of differ-ently substituted furocoumarins and analogues against NF-κB withthe objective of selecting molecules able to inhibit the binding ofthis transcription factor to DNA [282283] Novel compounds wereidentified with this strategy as potent inhibitors of NF-κB dependentbiological functions to be proposed for the control lung inflammationoccurring in patients affected by CF [282ndash284]
392 Scavengers and regulators of H2O2 and NO
3921 Lactoferrin and OSCNmacr The impaired DUOXLPO system of CFpatients could be the target of therapeutic strategies that may
produce concomitant antimicrobial and antioxidant effects This sys-tem described above in Section 22 represents an important compo-nent of innate immunity with a role in bactericidal defense andregulation of H2O2 metabolism of airways [32] CF patients have alsoreported to show lowered LF levels in the ASL [37] that togetherwith a CFTR-dependent defective efflux of SCNmacr and LPO [36] may cre-ate the environment for a sustained flux of H2O2 and for the genera-tion of highly reactive Fenton species [1138] An ideal therapeuticintervention should restore the LPO-dependent generation of bacteri-cidal OSCNmacr from DUOX-derived H2O2 and SCNmacr in the ASL to controlat the same time the microbial biofilm and the flux of H2O2 into theASL An approach close to this therapeutic mechanism was recentlyproposed for the drug Meveolreg This is a complex of LF and OSCNmacrwith proposed in vivo antimicrobial activity [285] to be evaluatedin clinical trials for the aerosol treatment of lung infections in CFpatients The role for this drug in the control of H2O2 levels of ASLremains to be investigated
3922 Organoselenium compounds Organoselenium compoundshave been proposed as therapeutic agents useful in the antioxidanttherapy of inflammatory conditions These include GPX mimetic mol-ecules such as Ebselenreg (2-phenyl-12-benzisoselenazol-3(2H)-one)or other and more recently developed molecules that are still inpre-clinical steps of evaluation [286] Selectively and specificity of ac-tion are main issues in the therapeutic mechanism of this candidateantioxidant drug that thanks to the electrophilic properties of Se[214] reacts with thiols to reduce H2O2 and other species MoreoverEbselenreg has been described to act as potent non-competitive inhib-itor of extracellular nucleoside diphosphokinase (NDPK) having neg-ligible effect on ecto-ATPase and adenyl kinase activities which areother players of the metabolism of extracellular nucleotides [287]This enzyme together with other nucleoside di- and triphosphatescontributes to regulate several components of the mucociliary clear-ance process (MCC) that protects the lung against infections via acti-vation of epithelial purinergic receptors The inhibition of NDPK bythis GPX-mimetic drug may also impact on the energy status of endo-thelial cells [287] This aspect could be further investigated as a cellu-lar protection mechanism in the pulmonary epithelium of CF patientsbeing the control of cell energy of fundamental importance to preventthe activation of death pathways [288]
Further therapeutic mechanisms for these Se-derived drugs mayderive from the marked activity as inducers of phase II enzymessuch as quinone reductase (QR) and glutathione-S-transferase (GST)[289] This induction response also observed with other electrophilsand redox-active molecules such as natural phenolic antioxidantscould produce higher cellular protection by the acquisition of anincreased capability to detoxify endobiotics generated during oxida-tive stress and inflammation [246]
3923 Melatonin and GSNO as NOx regulators Increased markers ofNO-derived biological damage are present in the CF lung suggestingthe abnormal reactivity of NOx in the inflamed lung of CF patients[52] However an impaired metabolism and biological function ofNO in CF airways (see Section 23) suggests a cautious approach tothe use of agents that may influence the levels and chemical behaviorof NO-derived species (NOx) with possible impact on the physiologi-cal roles of NO in vasodilatation innate immunity and H2O2 metabo-lism of the respiratory tract [290291] NO donors also appear toinfluence CFTR function of alveolar epithelium and gland serouscells [292293]
Main physiological role of the pineal gland hormone melatonin isthe synchronization of circadian rhythms including the sleepndashwakecycle but several other functions dealing with immunomodulatoryantioxidant and cellular protection effects have been identified[294] Melatonin receptor stimulation may also influence cyclic AMPsignaling and the regulation of CFTR ion channel [295296]
707F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
A recent randomized double-blind placebo-controlled study hasexamined the effects of short term melatonin administration (3 mgfor 3 weeks) on sleep and oxidative stress markers in CF [297]According with the expected pharmacological effect of this hormonalsubstance the treatment was successful in improving sleep indicesAt the same time nitrite levels determined in exhaled breath conden-sate (EBC) were reduced to suggest a better control of NOmetabolismof CF airways (discussed above in Section 23) but these effects how-ever were not associated with a significant correction of isoprostaneas lipid peroxidation marker measured in EBC Increasing dosages ofmelatonin could be investigated for the pharmacological treatmentof oxidative stress and immune dysfunction of CF patients due tothe absence of adverse effects of this hormonal substance in humans
The S-nitrosation reaction of thiols is another interesting aspect ofNO pharmacology [53] that may find an application in the therapy oflung complications of CF This has been the case for instance of theS-nitrosothiol GSNO that has been used safely in human trials[298299] This endogenous nitrosothiol with proposed regulatory ef-fect on the CFTR of lung epithelia [292293] is well tolerated in pa-tients with CF when administered by aerosolization and mayproduce better oxygenation [299] thereby suggesting that therapyaimed at restoring endogenous GSNO levels in the CF airway maymerit further clinical evaluation Since the administered GSNO de-composes as shown by the increased levels of expired NO in CF pa-tients under treatment with this nitrosothiol [299] furtherinvestigation should be addressed to ascertain whether GSNO thera-py may merely correspond to a GSH therapy
NO dependent effects on CFTR function should be considered toevaluate mechanism of action and specificity of antioxidant therapiesthat target NO metabolism and function in the CF airways
4 Conclusions and future perspectives
The presence of clinical and biochemical symptoms of inflammationand oxidative stress implies that CF patients have a higher demand ofantioxidant protection The combination of the dysfunctional CFTRwith a lowered intake and absorption of dietary antioxidants producesub-optimal levels of protection from both enzymatic and non-enzymatic defense systems The former could be associated with a de-fective glutathionemetabolism and lowered intake of sulfur-containingamino acids and oligoelements such as zinc and possibly seleniumwhile fat-soluble antioxidant vitamins such as vitamin E and caroten-oids and the water-soluble vitamin C are lowered than in healthy sub-jects due to malabsorption and possibly higher consumption
The increased antioxidant demand in CF patients should be evenhigher in the presence of complications of the lung pancreas andliver Lung comorbidity is particularly important in this contextbeing associated with recurrent infections which results in the alter-nation of inflammatory exacerbates and chronic inflammation Thesesustain the flux of ROS in the airways and promote the formation ofsecond-generation byproducts by the damage of biomolecules suchas PUFA and proteins which may diffuse also at the systemic level tofurther promote adverse biological responses and toxic reactions Pan-creatic insufficiency causes malnutrition and may lead to develop en-docrine and metabolic defects associated with diabetes of CF Theseevents can be further aggravated by the concomitance of liver dys-function and a poor nutritional status Malnutrition is strongly associ-ated with poor prognosis as assessed by pulmonary function andsurvival data [138ndash140] The more aggressive nutritional interven-tions seem to produce better clinical outcomes in these patients andthe possibility of achieving higher antioxidant protection in well-nourished patients by dietary factors could be a key aspect to explainsuch a clinical advantage The assumption that food-derived compo-nentsmay help to prevent the damaging effects of oxidative stress im-proving the antioxidant defenses deserves further investigation at theclinical level This together with the investigation of appropriate
laboratory biomarkers could provide critical information to establishintervention criteria for an early nutritional management of newly di-agnosed patients [5] It is expected that a timely secondary preventionstrategy could influence the progression of CF symptoms thusaffecting with a self-feeding mechanism the same extent of malnutri-tion and oxidative stress along the life of CF patients Since severalfactors contribute to impair the nutritional status of CF patients(such as pancreatic insufficiency chronic malabsorption recurrentsinopulmonary infections and progressive lung disease chronic in-flammation increased energy expenditure suboptimal intake multi-therapy) careful monitoring of the antioxidant status should berecommended According with international guidelines fat-solublevitamin supplementation is of utmost importance in daily practice to-gether with energy intake requirements and pancreatic enzyme-replacement therapy Among these vitamin E β-carotene and ω-3FA have observed to alleviate selected biochemical signs of oxidativestress as measured for instance with well established laboratory indi-ces of lipid peroxidation and in some studies these effects werepreliminarily associated with positive clinical outcomes Notwith-standing randomizedndashcontrolled clinical trials on antioxidant supple-ments (including ω-3 FA) so far carried out in CF have failed toconclusively demonstrate significant beneficial effects on respiratorysymptoms and on the consequent impact that these have on the qual-ity of life of these patients (reviewed in [202213]) whichmay provideno support for the use of these supplements in CF An absence of effi-cacy in prevention studies on antioxidant supplements has also beenobserved in other and possibly less severe oxidative stress-relatedconditions particularly in the secondary prevention of cardiovasculardisease and some forms of cancer by vitamin E and other antioxidantssuch as vitamin C selenium and β-carotene (reviewed in [163]) Dif-ferent biases however have been identified in randomize large clini-cal trials that may account for these disappointing findings Theseinclude patient selection criteria (early interventions and primaryprevention could have more chances of success than secondaryprevention) duration and doses of the treatment use of wrong anti-oxidant formulations and administration protocols absence of verifi-cations of the biological compliance to the treatment etc The samebiases apply for the few trials carried out in CF patients Thus the ap-propriateness and efficacy of nutritional interventions with naturalfood-derived or synthetic antioxidants should be verifiedwith respectto the biological pathways of oxidative stress and clinical variablesthat are identified as end-points Profiles of blood and tissue antioxi-dants as well as of reliable surrogate markers of oxidative stresshave to be selected and determined in highly specialized laboratorieswith a well-established experience on these analyses
Well-timed (early) interventions with appropriate antioxidantformulationsprotocols need to be proposed for the next generationof trials and the development of novel CF-tailored antioxidant andanti-inflammatory agents should be promoted
As a consequence of these considerations more clinical investiga-tion is awaited to identify future successful approaches to the antiox-idant therapy as a measure to further enhance quality of life and theoverall clinical outcome of CF patients
Acknowledgments
We are indebted with the Italian Cystic Fibrosis Research Founda-tion for the support that it provided with its grant program to the re-search activity of the authors of this paper This is a scientific initiativeof the ldquoWorking Group on Inflammation in Cystic Fibrosisrdquo (BragonziA Bravo E Cabrini G Conese M Cuzzocrea S Dechecchi MC De Ales-sandri A Evangelista V Galli F Gambari R Lambiase A Lucidi VManca A Melotti P Minicucci L Motta A Pietraforte D Pompella AQuattrucci S Rizzo R Romano M Sorio C Tesse R) of the Italian Soci-ety for Cystic Fibrosis A particular thank goes to the Prof GianniMastella for the critical revision of the manuscript and for the
708 F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
stimulating research environment that he has contributed to createwithin the Italian Cystic Fibrosis Research Foundation
References
[1] BP OSullivan SD Freedman Cystic fibrosis Lancet 373 (2009) 1891ndash1904[2] P Linsdell JW Hanrahan Glutathione permeability of CFTR Am J Physiol 275
(1998) C323ndashC326[3] L Gao KJ Kim JR Yankaskas HJ Forman Abnormal glutathione transport in
cystic fibrosis airway epithelia Am J Physiol 277 (1999) L113ndashL118[4] RK Rowntree A Harris The phenotypic consequences of CFTR mutations Ann
Hum Genet 67 (2003) 471ndash485[5] EI Back C Frindt D Nohr J Frank R Ziebach M Stern M Ranke HK Biesalski
Antioxidant deficiency in cystic fibrosis when is the right time to take actionAm J Clin Nutr 80 (2004) 374ndash384
[6] LG Wood DA Fitzgerald AK Lee ML Garg Improved antioxidant and fattyacid status of patients with cystic fibrosis after antioxidant supplementation islinked to improved lung function Am J Clin Nutr 77 (2003) 150ndash159
[7] L Iuliano R Monticolo G Straface S Zullo F Galli M Boaz S Quattrucci Asso-ciation of cholesterol oxidation and abnormalities in fatty acid metabolism incystic fibrosis Am J Clin Nutr 90 (2009) 477ndash484
[8] C Libetta V Sepe P Esposito F Galli A Dal Canton Oxidative stress and inflam-mation implications in uremia and hemodialysis Clin Biochem 44 (2011)1189ndash1198
[9] G Bartosz Reactive oxygen species destroyers or messengers Biochem Phar-macol 77 (2009) 1303ndash1315
[10] T Ntimbane B Comte G Mailhot Y Berthiaume V Poitout M Prentki RRabasa-Lhoret E Levy Cystic fibrosis-related diabetes from CFTR dysfunctionto oxidative stress Clin Biochem 30 (2009) 153ndash177
[11] A van der Vliet JP Eiserich GP Marelich B Halliwell CE Cross Oxidativestress in cystic fibrosis does it occur and does it matter Adv Pharmacol 38(1997) 491ndash513
[12] AM Cantin TB White CE Cross HJ Forman RJ Sokol D Borowitz Antioxi-dants in cystic fibrosis Conclusions from the CF antioxidant workshop Bethes-da Maryland Free Radic Biol Med 42 (2007) 15ndash31
[13] LT McGrath P Mallon L Dowey B Silke E McClean M McDonnell A DevineS Copeland S Elborn Oxidative stress during acute respiratory exacerbations incystic fibrosis Thorax 54 (1999) 518ndash523
[14] E Thomson S Brennan R Senthilmohan CL Gangell AL Chapman PD SlyAJ Kettle E Balding LJ Berry JB Carlin R Carzino N de Klerk T Douglas CFoo LW Garratt GL Hall J Harrison A Kicic IA Laing KM Logie J MassieLS Mott C Murray F Parsons N Pillarisetti SR Poreddy SC RanganathanCF Robertson R Robins-Browne PJ Robinson B Skoric SM Stick ENSutanto E Williamson Identifying peroxidases and their oxidants in the earlypathology of cystic fibrosis Free Radic Biol Med 49 (2010) 1354ndash1360
[15] SP Range C Dunster AJ Knox FJ Kelly Treatment of pulmonary exacerba-tions of cystic fibrosis leads to improved antioxidant status Eur Respir J 13(1999) 560ndash564
[16] L Coppo P Ghezzi Thiol regulation of pro-inflammatory cytokines and innateimmunity protein S-thiolation as a novel molecular mechanism Biochem SocTrans 39 (2011) 1268ndash1272
[17] C Verhaeghe C Remouchamps B Hennuy A Vanderplasschen A Chariot SPTabruyn C Oury V Bours Role of IKK and ERK pathways in intrinsic inflamma-tion of cystic fibrosis airways Biochem Pharmacol 73 (2007) 1982ndash1994
[18] TL Bonfield JR Panuska MW Konstan KA Hilliard JB Hilliard H Ghnaim MBerger Inflammatory cytokines in cystic fibrosis lungs Am J Respir Crit CareMed 152 (1995) 2111ndash2118
[19] TL Noah HR Black PW Cheng RE Wood MW Leigh Nasal and bronchoal-veolar lavage fluid cytokines in early cystic fibrosis J Infect Dis 175 (1997)638ndash647
[20] MJ Welsh BW Ramsey FJ Accurso GR Cutting Cystic Fibrosis McGraw-HillNew York 2001
[21] TZ Khan JS Wagener T Bost J Martinez FJ Accurso DW Riches Early pul-monary inflammation in infants with cystic fibrosis Am J Respir Crit CareMed 151 (1995) 1075ndash1082
[22] FA Ratjen Cystic fibrosis pathogenesis and future treatment strategies RespirCare 54 (2009) 595ndash605
[23] J Jacquot O Tabary P Le Rouzic A Clement Airway epithelial cell inflamma-tory signalling in cystic fibrosis Int J Biochem Cell Biol 40 (2008)1703ndash1715
[24] CM Greene P Branagan NG McElvaney Toll-like receptors as therapeutic tar-gets in cystic fibrosis Expert Opin Ther Targets 12 (2008) 1481ndash1495
[25] M Rottner JM Freyssinet MC Martinez Mechanisms of the noxious inflam-matory cycle in cystic fibrosis Respir Res 10 (2009) 23
[26] G Cabrini V Bezzerri I Mancini E Nicolis MC Dechecchi A Tamanini ILampronti L Piccagli N Bianchi M Borgatti R Gambari Targeting transcrip-tion factor activity as a strategy to inhibit pro-inflammatory genes involved incystic fibrosis decoy oligonucleotides and low-molecular weight compoundsCurr Med Chem 17 (2010) 4392ndash4404
[27] CM Greene NG McElvaney Proteases and antiproteases in chronic neutrophiliclungdiseasemdash relevance to drug discovery Br J Pharmacol 158 (2009) 1048ndash1058
[28] AM Cantin Potential for antioxidant therapy of cystic fibrosis Curr Opin PulmMed 10 (2004) 531ndash536
[29] JF Chmiel MW Konstan Inflammation and anti-inflammatory therapies forcystic fibrosis Clin Chest Med 28 (2007) 331ndash346
[30] DP Nichols MW Konstan JF Chmiel Anti-inflammatory therapies for cys-tic fibrosis-related lung disease Clin Rev Allergy Immunol 35 (2008)135ndash153
[31] AJ Kettle T Chan I Osberg R Senthilmohan AL Chapman TJ Mocatta JSWagener Myeloperoxidase and protein oxidation in the airways of youngchildren with cystic fibrosis Am J Respir Crit Care Med 170 (2004)1317ndash1323
[32] H Fischer Mechanisms and function of DUOX in epithelia of the lung AntioxidRedox Signal 11 (2009) 2453ndash2465
[33] B Rada TL Leto Oxidative innate immune defenses by NoxDuox familyNADPH oxidases Contrib Microbiol 15 (2008) 164ndash187
[34] P Moskwa D Lorentzen KJ Excoffon J Zabner PB McCray Jr WM NauseefC Dupuy B Banfi A novel host defense system of airways is defective in cysticfibrosis Am J Respir Crit Care Med 175 (2007) 174ndash183
[35] D Lorentzen L Durairaj AA Pezzulo Y Nakano J Launspach DA Stoltz GZamba PB McCray Jr J Zabner MJ Welsh WM Nauseef B Banfi Concentra-tion of the antibacterial precursor thiocyanate in cystic fibrosis airway secre-tions Free Radic Biol Med 50 (2011) 1144ndash1150
[36] Y Xu S Szep Z Lu The antioxidant role of thiocyanate in the pathogenesis ofcystic fibrosis and other inflammation-related diseases Proc Natl Acad Sci US A 106 (2009) 20515ndash20519
[37] MP Rogan CC Taggart CM Greene PG Murphy SJ ONeill NG McElvaneyLoss of microbicidal activity and increased formation of biofilm due to decreasedlactoferrin activity in patients with cystic fibrosis J Infect Dis 190 (2004)1245ndash1253
[38] B Halliwell JM Guttridge Free Radicals in Biology and Medicine Fourth editionOxford University Press New York 2007
[39] B Rada K Lekstrom S Damian C Dupuy TL Leto The Pseudomonastoxin pyocyanin inhibits the dual oxidase-based antimicrobial system as itimposes oxidative stress on airway epithelial cells J Immunol 181 (2008)4883ndash4893
[40] C Schwarzer B Illek JH Suh SJ Remington H Fischer TE Machen Organelleredox of CF and CFTR-corrected airway epithelia Free Radic Biol Med 43(2007) 300ndash316
[41] JH Roum R Buhl NG McElvaney Z Borok RG Crystal Systemic deficiency ofglutathione in cystic fibrosis J Appl Physiol 75 (1993) 2419ndash2424
[42] VM Hudson Rethinking cystic fibrosis pathology the critical role of abnormalreduced glutathione (GSH) transport caused by CFTR mutation Free RadicBiol Med 30 (2001) 1440ndash1461
[43] PJ Barnes RA Dweik AF Gelb PG Gibson SC George H Grasemann IDPavord F Ratjen PE Silkoff DR Taylor N Zamel Exhaled nitric oxide in pul-monary diseases a comprehensive review Chest 138 (2010) 682ndash692
[44] H Grasemann E Michler M Wallot F Ratjen Decreased concentration of ex-haled nitric oxide (NO) in patients with cystic fibrosis Pediatr Pulmonol 24(1997) 173ndash177
[45] H Grasemann F Ratjen Cystic fibrosis lung disease the role of nitric oxidePediatr Pulmonol 28 (1999) 442ndash448
[46] B Gaston F Ratjen JW Vaughan NR Malhotra RG Canady AH Snyder JFHunt S Gaertig JB Goldberg Nitrogen redox balance in the cystic fibrosis air-way effects of antipseudomonal therapy Am J Respir Crit Care Med 165(2002) 387ndash390
[47] H Grasemann I Ioannidis RP Tomkiewicz H de Groot BK Rubin F RatjenNitric oxide metabolites in cystic fibrosis lung disease Arch Dis Child 78(1998) 49ndash53
[48] H Grasemann R Schwiertz S Matthiesen K Racke F Ratjen Increased argi-nase activity in cystic fibrosis airways Am J Respir Crit Care Med 172(2005) 1523ndash1528
[49] H Grasemann S Al-Saleh JA Scott D Shehnaz A Mehl R Amin M Rafii PPencharz J Belik F Ratjen Asymmetric dimethylarginine contributes to airwaynitric oxide deficiency in patients with cystic fibrosis Am J Respir Crit CareMed 183 (2011) 1363ndash1368
[50] H Grasemann F Kurtz F Ratjen Inhaled L-arginine improves exhaled nitricoxide and pulmonary function in patients with cystic fibrosis Am J RespirCrit Care Med 174 (2006) 208ndash212
[51] H Grasemann F Ratjen Emerging therapies for cystic fibrosis lung disease Ex-pert Opin Emerg Drugs 15 (2010) 653ndash659
[52] BM Morrissey K Schilling JV Weil PE Silkoff DM Rodman Nitric oxide andprotein nitration in the cystic fibrosis airway Arch Biochem Biophys 406(2002) 33ndash39
[53] R Radi Nitric oxide oxidants and protein tyrosine nitration Proc Natl AcadSci U S A 101 (2004) 4003ndash4008
[54] J Chen M Kinter S Shank C Cotton TJ Kelley AG Ziady Dysfunction of Nrf-2in CF epithelia leads to excess intracellular H2O2 and inflammatory cytokineproduction PLoS One 3 (2008) e3367
[55] F Galli M Piroddi C Annetti C Aisa E Floridi A Floridi Oxidative stress andreactive oxygen species Contrib Nephrol 149 (2005) 240ndash260
[56] DT Wright LA Cohn H Li B Fischer CM Li KB Adler Interactions of oxygenradicals with airway epithelium Environ Health Perspect 102 (Suppl 10)(1994) 85ndash90
[57] I Rahman SR Yang SK Biswas Current concepts of redox signaling in thelungs Antioxid Redox Signal 8 (2006) 681ndash689
[58] Q Li JF Engelhardt Interleukin-1beta induction of NFκB is partially regulatedby H2O2-mediated activation of NFκB-inducing kinase J Biol Chem 281(2006) 1495ndash1505
709F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
[59] E Boncoeur VS Criq E Bonvin T Roque A Henrion-Caude DC Gruenert AClement J Jacquot O Tabary Oxidative stress induces extracellular signal-regulated kinase 12 mitogen-activated protein kinase in cystic fibrosis lung ep-ithelial cells potential mechanism for excessive IL-8 expression Int J BiochemCell Biol 40 (2008) 432ndash446
[60] B Fischer J Voynow Neutrophil elastase induces MUC5AC messenger RNA ex-pression by an oxidant-dependent mechanism Chest 117 (2000) 317Sndash320S
[61] B Rada P Gardina TG Myers TL Leto Reactive oxygen species mediate in-flammatory cytokine release and EGFR-dependent mucin secretion in airwayepithelial cells exposed to Pseudomonas pyocyanin Mucosal Immunol 4(2011) 158ndash171
[62] C Schwarzer H Fischer EJ Kim KJ Barber AD Mills MJ Kurth DC GruenertJH Suh TE Machen B Illek Oxidative stress caused by pyocyanin impairs CFTRClminus transport in human bronchial epithelial cells Free Radic Biol Med 45(2008) 1653ndash1662
[63] J Hull M South P Phelan K Grimwood Surfactant composition in infants andyoung children with cystic fibrosis Am J Respir Crit Care Med 156 (1997)161ndash165
[64] KC Meyer A Sharma R Brown M Weatherly FR Moya J Lewandoski JJZimmerman Function and composition of pulmonary surfactant andsurfactant-derived fatty acid profiles are altered in young adults with cystic fi-brosis Chest 118 (2000) 164ndash174
[65] MK Pulfer RC Murphy Formation of biologically active oxysterols during ozo-nolysis of cholesterol present in lung surfactant J Biol Chem 279 (2004)26331ndash26338
[66] V Starosta E Rietschel K Paul U Baumann M Griese Oxidative changes ofbronchoalveolar proteins in cystic fibrosis Chest 129 (2006) 431ndash437
[67] V Starosta M Griese Oxidative damage to surfactant protein D in pulmonarydiseases Free Radic Res 40 (2006) 419ndash425
[68] M Griese R Essl R Schmidt E Rietschel F Ratjen M Ballmann K Paul Pulmo-nary surfactant lung function and endobronchial inflammation in cystic fibro-sis Am J Respir Crit Care Med 170 (2004) 1000ndash1005
[69] M Griese R Essl R Schmidt M Ballmann K Paul E Rietschel F Ratjen Se-quential analysis of surfactant lung function and inflammation in cystic fibrosispatients Respir Res 6 (2005) 133
[70] LG Wood DA Fitzgerald PG Gibson DM Cooper ML Garg Increased plasmafatty acid concentrations after respiratory exacerbations are associated with el-evated oxidative stress in cystic fibrosis patients Am J Clin Nutr 75 (2002)668ndash675
[71] P Montuschi SA Kharitonov G Ciabattoni M Corradi L van Rensen DM Ged-des ME Hodson PJ Barnes Exhaled 8-isoprostane as a new non-invasive bio-marker of oxidative stress in cystic fibrosis Thorax 55 (2000) 205ndash209
[72] CE Collins P Quaggiotto L Wood EV OLoughlin RL Henry ML Garg Elevat-ed plasma levels of F2 alpha isoprostane in cystic fibrosis Lipids 34 (1999)551ndash556
[73] D Hartl V Starosta K Maier I Beck-Speier C Rebhan BF Becker P Latzin RFischer F Ratjen RM Huber E Rietschel S Krauss-Etschmann M Griese In-haled glutathione decreases PGE2 and increases lymphocytes in cystic fibrosislungs Free Radic Biol Med 39 (2005) 463ndash472
[74] GL Milne H Yin JD Morrow Human biochemistry of the isoprostane pathwayJ Biol Chem 283 (2008) 15533ndash15537
[75] G Ciabattoni G Davi M Collura L Iapichino F Pardo A Ganci R Romagnoli JMaclouf C Patrono In vivo lipid peroxidation and platelet activation in cystic fi-brosis Am J Respir Crit Care Med 162 (2000) 1195ndash1201
[76] C Garenc P Julien E Levy Oxysterols in biological systems the gastrointestinaltract liver vascular wall and central nervous system Free Radic Res 44 (2011)47ndash73
[77] AM Cantin SL North RC Hubbard RG Crystal Normal alveolar epithelial lin-ing fluid contains high levels of glutathione J Appl Physiol 63 (1987) 152ndash157
[78] R Tirouvanziam CK Conrad T Bottiglieri LA Herzenberg RB Moss High-dose oral N-acetylcysteine a glutathione prodrug modulates inflammation incystic fibrosis Proc Natl Acad Sci U S A 103 (2006) 4628ndash4633
[79] LW Velsor C Kariya R Kachadourian BJ Day Mitochondrial oxidative stressin the lungs of cystic fibrosis transmembrane conductance regulator proteinmutant mice Am J Respir Cell Mol Biol 35 (2006) 579ndash586
[80] M Kelly-Aubert S Trudel J Fritsch T Nguyen-Khoa M Baudouin-Legros SMoriceau L Jeanson F Djouadi C Matar M Conti M Ollero F Brouillard AEdelman GSH monoethyl ester rescues mitochondrial defects in cystic fibrosismodels Hum Mol Genet 20 (2011) 2745ndash2759
[81] P Ghezzi Role of glutathione in immunity and inflammation in the lung Int JGen Med 4 (2011) 105ndash113
[82] N Dauletbaev K Viel R Buhl TO Wagner J Bargon Glutathione and glutathi-one peroxidase in sputum samples of adult patients with cystic fibrosis J CystFibros 3 (2004) 119ndash124
[83] CE Cross A van der Vliet CA ONeill S Louie B Halliwell Oxidants antioxi-dants and respiratory tract lining fluids Environ Health Perspect 102 (Suppl10) (1994) 185ndash191
[84] K Takeyama K Dabbagh J Jeong Shim T Dao-Pick IF Ueki JA Nadel Oxida-tive stress causes mucin synthesis via transactivation of epidermal growth factorreceptor role of neutrophils J Immunol 164 (2000) 1546ndash1552
[85] N Ballatori SM Krance S Notenboom S Shi K Tieu CL Hammond Glutathi-one dysregulation and the etiology and progression of human diseases BiolChem 390 (2009) 191ndash214
[86] SR Soltaninassab KR Sekhar MJ Meredith ML Freeman Multi-faceted regu-lation of gamma-glutamylcysteine synthetase J Cell Physiol 182 (2000)163ndash170
[87] HR Lopez-Mirabal JR Winther Redox characteristics of the eukaryotic cytosolBiochim Biophys Acta 1783 (2008) 629ndash640
[88] C Hwang AJ Sinskey HF Lodish Oxidized redox state of glutathione in the en-doplasmic reticulum Science 257 (1992) 1496ndash1502
[89] M Murphy Mitochondrial thiols in antioxidant protection and redox signallingdistinct roles for glutathionylation and other thiol modifications AntioxidRedox Signal (2011) ahead of print doi101089ars20114289
[90] BJ Day AM van Heeckeren E Min LW Velsor Role for cystic fibrosis trans-membrane conductance regulator protein in a glutathione response to bronch-opulmonary Pseudomonas infection Infect Immun 72 (2004) 2045ndash2051
[91] Y Zhang K Duan Glutathione exhibits antibacterial activity and increases tetra-cycline efficacy against Pseudomonas aeruginosa Sci China C Life Sci 52 (2009)501ndash505
[92] VM Hudson New insights into the pathogenesis of cystic fibrosis pivotal roleof glutathione system dysfunction and implications for therapy Treat RespirMed 3 (2004) 353ndash363
[93] LW Velsor A van Heeckeren BJ Day Antioxidant imbalance in the lungs ofcystic fibrosis transmembrane conductance regulator protein mutant miceAm J Physiol Lung Cell Mol Physiol 281 (2001) L31ndashL38
[94] I Kogan M Ramjeesingh C Li JF Kidd Y Wang EM Leslie SP Cole CE BearCFTR directly mediates nucleotide-regulated glutathione flux EMBO J 22(2003) 1981ndash1989
[95] NS Gould S Gauthier CT Kariya E Min J Huang DJ Brian Hypertonic salineincreases lung epithelial lining fluid glutathione and thiocyanate two protectiveCFTR-dependent thiols against oxidative injury Respir Res 11 (2010) 119
[96] VT Vasu SJ de Cruz JS Houghton KA Hayakawa BM Morrissey CE CrossJP Eiserich Evaluation of thiol-based antioxidant therapeutics in cystic fibrosissputum focus on myeloperoxidase Free Radic Res 45 (2011) 165ndash176
[97] L Roussel G Martel J Berube S Rousseau P aeruginosa drives CXCL8 synthesisvia redundant toll-like receptors and NADPH oxidase in CFTRF508 airway epi-thelial cells J Cyst Fibros 10 (2011) 107ndash113
[98] GW Lau DJ Hassett H Ran F Kong The role of pyocyanin in Pseudomonas aer-uginosa infection Trends Mol Med 10 (2004) 599ndash606
[99] R Wilson DA Sykes D Watson A Rutman GW Taylor PJ Cole Measurementof Pseudomonas aeruginosa phenazine pigments in sputum and assessment oftheir contribution to sputum sol toxicity for respiratory epithelium InfectImmun 56 (1988) 2515ndash2517
[100] M Muller Pyocyanin induces oxidative stress in human endothelial cells andmodulates the glutathione redox cycle Free Radic Biol Med 33 (2002)1527ndash1533
[101] YQ OMalley KJ Reszka BE Britigan Direct oxidation of 2prime7prime-dichlorodihy-drofluorescein by pyocyanin and other redox-active compounds independentof reactive oxygen species production Free Radic Biol Med 36 (2004)90ndash100
[102] CC Caldwell Y Chen HS Goetzmann Y Hao MT Borchers DJ Hassett LRYoung D Mavrodi L Thomashow GW Lau Pseudomonas aeruginosa exotoxinpyocyanin causes cystic fibrosis airway pathogenesis Am J Pathol 175 (2009)2473ndash2488
[103] YQ OMalley KJ Reszka DR Spitz GM Denning BE Britigan Pseudomonasaeruginosa pyocyanin directly oxidizes glutathione and decreases its levels inairway epithelial cells Am J Physiol Lung Cell Mol Physiol 287 (2004)L94ndashL103
[104] M Muller Glutathione modulates the toxicity of but is not a biologically rele-vant reductant for the Pseudomonas aeruginosa redox toxin pyocyanin FreeRadic Biol Med 50 (2011) 971ndash977
[105] R Cheluvappa R Shimmon M Dawson SN Hilmer DG Le Couteur Reactionsof Pseudomonas aeruginosa pyocyanin with reduced glutathione Acta BiochimPol 55 (2008) 571ndash580
[106] JH Widdicombe Transgenic animals may help resolve a sticky situation in cys-tic fibrosis J Clin Invest 120 (2010) 3093ndash3096
[107] X Sun H Sui JT Fisher Z Yan X Liu HJ Cho NS Joo Y Zhang W Zhou Y YiJM Kinyon DC Lei-Butters MA Griffin P Naumann M Luo J Ascher KWang T Frana JJ Wine DK Meyerholz JF Engelhardt Disease phenotype ofa ferret CFTR-knockout model of cystic fibrosis J Clin Invest 120 (2010)3149ndash3160
[108] NS Joo HJ Cho M Khansaheb JJ Wine Hyposecretion of fluid from trachealsubmucosal glands of CFTR-deficient pigs J Clin Invest 120 (2010) 3161ndash3166
[109] A Bragonzi Murine models of acute and chronic lung infection with cystic fibro-sis pathogens IJMM 300 (2010) 584ndash593
[110] AM van Heeckeren MD Schluchter Murine models of chronic Pseudomonasaeruginosa lung infection Lab Anim 36 (2002) 291ndash312
[111] A Bragonzi D Worlitzsch GB Pier P Timpert M Ulrich M Hentzer JB Ander-sen M Givskov M Conese G Doring Nonmucoid Pseudomonas aeruginosa ex-presses alginate in the lungs of patients with cystic fibrosis and in a mousemodel J Infect Dis 192 (2005) 410ndash419
[112] GS CW Bedrossian DB Singer JJ Hansen HS Rosenberg The lung in cysticfibrosis A quantitative study including prevalence of pathologic findingsamong different age groups Hum Pathol 7 (1976) 195ndash204
[113] WD HA Cash B McCullough WG Johanson Jr JA Bass A rat model of chron-ic respiratory infection with Pseudomonas aeruginosa Am Rev Respir Dis 119(1979) 453ndash459
[114] EM JR Starke C Langston CJ Baker A mouse model of chronic pulmonary in-fection with Pseudomonas aeruginosa and Pseudomonas cepacia Pediatr Res 22(1987) 698ndash702
[115] TJ AM van Heeckeren RW Walenga MW Konstan PB Davis B ErokwuMA Haxhiu TW Ferkol Effect of Pseudomonas infection on weight loss lung
710 F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
mechanics and cytokines in mice Am J Respir Crit Care Med 161 (2000)271ndash279
[116] T Aw G Wierzbicka DP Jones Oral glutathione increases tissue glutathione invivo Chem Biol Interact 80 (1991) 89ndash97
[117] F Favilli P Marraccini T Iantomasi MT Vincenzini Effect of orally adminis-tered glutathione on glutathione levels in some organs of rats role of specifictransporters Br J Nutr 78 (1997) 293ndash300
[118] C Kariya H Leitner E Min C van Heeckeren A van Heeckeren BJ Day A rolefor CFTR in the elevation of glutathione levels in the lung by oral glutathione ad-ministration Am J Physiol Lung Cell Mol Physiol 292 (2007) L1590ndashL1597
[119] K Atkuri JJ Mantovani LA Herzenberg LA Herzenberg N-Acetylcysteinemdashasafe antidote for cysteineglutathione deficiency Curr Opin Pharmacol 7(2007) 355ndash359
[120] R De Lisle E Roach K Jansson Effects of laxative and N-acetylcysteine onmucus accumulation bacterial load transit and inflammation in the cystic fi-brosis mouse small intestine Am J Physiol Gastrointest Liver Physiol 293(2007) G577ndashG584
[121] A Luciani VR Villella S Esposito N Brunetti-Pierri D Medina C Settembre MGavina L Pulze I Giardino M Pettoello-Mantovani M DApolito S Guido EMasliah B Spencer S Quaratino V Raia A Ballabio L Maiuri Defective CFTRinduces aggresome formation and lung inflammation in cystic fibrosis throughROS-mediated autophagy inhibition Nat Cell Biol 12 863ndash875
[122] M Griese J Ramakers A Krasselt V Starosta S Van Koningsbruggen R FischerF Ratjen B Mullinger RM Huber K Maier E Rietschel G Scheuch Improve-ment of alveolar glutathione and lung function but not oxidative state in cysticfibrosis Am J Respir Crit Care Med 169 (2004) 822ndash828
[123] C Bishop VM Hudson SC Hilton C Wilde A pilot study of the effect of inhaledbuffered reduced glutathione on the clinical status of patients with cystic fibro-sis Chest 127 (2005) 308ndash317
[124] WWang C Oliva G Li A Holmgren CH Lillig KL Kirk Reversible silencing of CFTRchloride channels by glutathionylation J Gen Physiol 125 (2005) 127ndash141
[125] N Dauletbaev P Fischer B Aulbach J Gross W Kusche U Thyroff-FriesingerTO Wagner J Bargon A phase II study on safety and efficacy of high-dose N-acetylcysteine in patients with cystic fibrosis Eur J Med Res 14 (2009)352ndash358
[126] R Tirouvanziam Y Gernez CK Conrad RB Moss I Schrijver CE Dunn ZADavies LA Herzenberg Profound functional and signaling changes in viable in-flammatory neutrophils homing to cystic fibrosis airways Proc Natl Acad SciU S A 105 (2008) 4335ndash4339
[127] JH Roum Z Borok NG McElvaney GJ Grimes AD Bokser R Buhl RG Crys-tal Glutathione aerosol suppresses lung epithelial surface inflammatory cell-derived oxidants in cystic fibrosis J Appl Physiol 87 (1999) 438ndash443
[128] A Visca CT Bishop SC Hilton VM Hudson Improvement in clinical markersin CF patients using a reduced glutathione regimen an uncontrolled observa-tional study J Cyst Fibros 7 (2008) 433ndash436
[129] EF Nash A Stephenson F Ratjen E Tullis Nebulized and oral thiol derivativesfor pulmonary disease in cystic fibrosis Cochrane Database Syst Rev (2009)CD007168
[130] AC foundation Drug Development Pipeline 2011[131] S Hoshida T Kuzuya N Yamashita M Nishida S Kitahara M Hori T
Kamada M Tada Gamma-glutamylcysteine ethyl ester for myocardial protec-tion in dogs during ischemia and reperfusion J Am Coll Cardiol 24 (1994)1391ndash1397
[132] J Lok W Leung S Zhao S Pallast K van Leyen S Guo X Wang A Yalcin EHLo Gamma-glutamylcysteine ethyl ester protects cerebral endothelial cells dur-ing injury and decreases bloodndashbrain barrier permeability after experimentalbrain trauma J Neurochem 118 (2011) 248ndash255
[133] Z Borok R Buhl GJ Grimes AD Bokser RC Hubbard KJ Holroyd JH RoumDB Czerski AM Cantin RG Crystal Effect of glutathione aerosol on oxidantndashantioxidant imbalance in idiopathic pulmonary fibrosis Lancet 338 (1991)215ndash216
[134] KJ Holroyd R Buhl Z Borok JH Roum AD Bokser GJ Grimes D Czerski AMCantin RG Crystal Correction of glutathione deficiency in the lower respiratorytract of HIV seropositive individuals by glutathione aerosol treatment Thorax 48(1993) 985ndash989
[135] J Hull P Vervaart K Grimwood P Phelan Pulmonary oxidative stress responsein young children with cystic fibrosis Thorax 52 (1997) 557ndash560
[136] A Corti A Paolicchi M Franzini S Dominici AF Casini A Pompella The S-thiolating activity of membrane gamma-glutamyltransferase formation ofcysteinyl-glycine mixed disulfides with cellular proteins and in the cell microen-vironment Antioxid Redox Signal 7 (2005) 911ndash918
[137] A Corti M Franzini AF Casini A Paolicchi A Pompella Vitamin C supply tobronchial epithelial cells linked to glutathione availability in elfmdasha role for se-creted gamma-glutamyltransferase J Cyst Fibros 7 (2008) 174ndash178
[138] A Munck Nutritional considerations in patients with cystic fibrosis Expert RevRespir Med 4 (2010) 47ndash56
[139] JL Matel CE Milla Nutrition in cystic fibrosis Semin Respir Crit Care Med 30(2009) 579ndash586
[140] D Salvatore R Buzzetti E Baldo MP Forneris V Lucidi D Manunza IMarinelli B Messore AS Neri V Raia ML Furnari G Mastella An overviewof international literature from cystic fibrosis registries 2 Neonatal screeningand nutritiongrowth J Cyst Fibros 9 (2010) 75ndash83
[141] KF Joosten JM Hulst Malnutrition in pediatric hospital patients current is-sues Nutrition 27 (2011) 133ndash137
[142] S Fustik T Jacovska L Spirevska S Koceva Protein-energy malnutrition as thefirst manifestation of cystic fibrosis in infancy Pediatr Int 51 (2009) 678ndash683
[143] J Himmelfarb E McMonagle Albumin is the major plasma protein target of ox-idant stress in uremia Kidney Int 60 (2001) 358ndash363
[144] P Stenvinkel JJ Carrero J Axelsson B Lindholm O Heimburger Z MassyEmerging biomarkers for evaluating cardiovascular risk in the chronic kidneydisease patient how do new pieces fit into the uremic puzzle Clin J Am SocNephrol 3 (2008) 505ndash521
[145] M Roche P Rondeau NR Singh E Tarnus E Bourdon The antioxidant proper-ties of serum albumin FEBS Lett 582 (2008) 1783ndash1787
[146] D Giustarini A Milzani I Dalle-Donne R Rossi Red blood cells as a physiolog-ical source of glutathione for extracellular fluids Blood Cells Mol Dis 40 (2008)174ndash179
[147] A Meister ME Anderson Glutathione Annu Rev Biochem 52 (1983) 711ndash760[148] B Alvarez S Carballal L Turell R Radi Formation and reactions of sulfenic acid
in human serum albumin Methods Enzymol 473 (2010) 117ndash136[149] S Carballal B Alvarez L Turell H Botti BA Freeman R Radi Sulfenic acid in
human serum albumin Amino Acids 32 (2007) 543ndash551[150] LR Barclay AM Bailey D Kong The antioxidant activity of alpha-tocopherol-
bovine serum albumin complex in micellar and liposome autoxidations J BiolChem 260 (1985) 15809ndash15814
[151] T Ishii T Ichikawa K Minoda K Kusaka S Ito Y Suzuki M Akagawa K Mochi-zuki T Goda T Nakayama Human serum albumin as an antioxidant in the ox-idation of (minus)-epigallocatechin gallate participation of reversible covalentbinding for interaction and stabilization Biosci Biotechnol Biochem 75(2011) 100ndash106
[152] F Galli S Rovidati S Benedetti U Buoncristiani C Covarelli A Floridi F Canes-trari Overexpression of erythrocyte glutathione S-transferase in uremia and di-alysis Clin Chem 45 (1999) 1781ndash1788
[153] D Borowitz RD Baker V Stallings Consensus report on nutrition for pediat-ric patients with cystic fibrosis J Pediatr Gastroenterol Nutr 35 (2002)246ndash259
[154] LJ Filer Jr SW Wright MP Manning KE Mason Absorption of alpha-tocopherol and tocopherylesters by premature and full term infants and chil-dren in health and disease Pediatrics 8 (1951) 328ndash339
[155] L Lancellotti C DOrazio G Mastella G Mazzi U Lippi Deficiency of vitamins Eand A in cystic fibrosis is independent of pancreatic function and current en-zyme and vitamin supplementation Eur J Pediatr 155 (1996) 281ndash285
[156] MN Sathe AS Patel Update in pediatrics focus on fat-soluble vitamins NutrClin Pract 25 (2010) 340ndash346
[157] MG Traber The ABCs of vitamin E and beta-carotene absorption Am J ClinNutr 80 (2004) 3ndash4
[158] TF Dolan Jr Hemolytic anemia and edema as the initial signs in infants withcystic fibrosis Consider this diagnosis even in absence of pulmonary symptomsClin Pediatr 15 (1976) 597ndash600
[159] DR James M Alfaham MC Goodchild Increased susceptibility to peroxide-induced haemolysis with normal vitamin E concentrations in cystic fibrosisClin Chim Acta 204 (1991) 279ndash290
[160] SA Peters FJ Kelly Vitamin E supplementation in cystic fibrosis J Pediatr Gas-troenterol Nutr 22 (1996) 341ndash345
[161] A Maqbool VA Stallings Update on fat-soluble vitamins in cystic fibrosis CurrOpin Pulm Med 14 (2008) 574ndash581
[162] SD Sagel MK Sontag MM Anthony P Emmett KA Papas Effect of anantioxidant-rich multivitamin supplement in cystic fibrosis J Cyst Fibros 10(2011) 31ndash36
[163] F Galli A Azzi Present trends in vitamin E research Biofactors 36 (2010)33ndash42
[164] A Hamahata P Enkhbaatar ER Kraft M Lange SW Leonard MG Traber RACox FC Schmalstieg HK Hawkins EB Whorton EM Horvath C Szabo LDTraber DN Herndon DL Traber Gamma-tocopherol nebulization by a lipidaerosolization device improves pulmonary function in sheep with burn andsmoke inhalation injury Free Radic Biol Med 45 (2008) 425ndash433
[165] JP Anais N Razzouq M Carvalho C Fernandez A Astier M Paul A AstierH Fessi AM Lorino Development of alpha-tocopherol acetate nanoparti-cles influence of preparative processes Drug Dev Ind Pharm 35 (2009)216ndash223
[166] JM Zingg Molecular and cellular activities of vitamin E analogues Mini RevMed Chem 7 (2007) 543ndash558
[167] V Viola F Pilolli M Piroddi E Pierpaoli F Orlando M Provinciali M Betti FMazzini F Galli Why tocotrienols work better insights into the in vitro anti-cancer mechanism of vitamin E Genes Nutr 7 (2011) 29ndash41
[168] F Galli F Mazzini L Bamonti L Gille S Bohmdorfer M Piroddi T Netscher FJKelly T Rosenau Tocotrienamines and tocopheramines reactions with radicalsand metal ions Bioorg Med Chem 19 (2011) 6483ndash6491
[169] A Kuhad K Chopra Attenuation of diabetic nephropathy by tocotrienol in-volvement of NFκB signaling pathway Life Sci 84 (2009) 296ndash301
[170] Q Jiang X Yin MA Lill ML Danielson H Freiser J Huang Long-chain carbox-ychromanols metabolites of vitamin E are potent inhibitors of cyclooxygenasesProc Natl Acad Sci U S A 105 (2008) 20464ndash20469
[171] ER Miller III R Pastor-Barriuso D Dalal RA Riemersma LJ Appel E GuallarMeta-analysis high-dosage vitamin E supplementation may increase all-causemortality Ann Intern Med 142 (2005) 37ndash46
[172] JN Hathcock A Azzi J Blumberg T Bray A Dickinson B Frei I Jialal CSJohnston FJ Kelly K Kraemer L Packer S Parthasarathy H Sies MG TraberVitamins E and C are safe across a broad range of intakes Am J Clin Nutr 81(2005) 736ndash745
[173] R Brigelius-Flohe F Galli Vitamin E a vitamin still awaiting the detection of itsbiological function Mol Nutr Food Res 54 (2010) 583ndash587
711F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
[174] MG Traber B Frei JS Beckman Vitamin E revisited do new data validate ben-efits for chronic disease prevention Curr Opin Lipidol 19 (2008) 30ndash38
[175] F Galli Meeting report Vitamin E Satellite Symposium (VESS) associated to theAnnual Meeting of the SFRR-Europe Rome 26 August 2009 Free Radic Res 43(2009) 1256ndash1257
[176] LJ Roberts II JA Oates MF Linton S Fazio BP Meador MD Gross Y Shyr JDMorrow The relationship between dose of vitamin E and suppression of oxida-tive stress in humans Free Radic Biol Med 43 (2007) 1388ndash1393
[177] EFSA- EFSA Scientific Opinion of the Panel on Food Additives FlavouringsProcessing Aids and Materials in Contact with Food on a request from the Com-mission on mixed tocopherols tocotrienol tocopherol and tocotrienols assources for vitamin E in EFSA- EFSA (Ed) vol 640 The EFSA Journal2008 pp 1ndash34
[178] P Rust I Eichler S Renner I Elmadfa Long-term oral beta-carotene supple-mentation in patients with cystic fibrosis mdash effects on antioxidative status andpulmonary function Ann Nutr Metab 44 (2000) 30ndash37
[179] G Lepage J Champagne N Ronco A Lamarre I Osberg RJ Sokol CC Roy Sup-plementation with carotenoids corrects increased lipid peroxidation in childrenwith cystic fibrosis Am J Clin Nutr 64 (1996) 87ndash93
[180] BM Winklhofer-Roob H Puhl G Khoschsorur MA vant Hof H EsterbauerDH Shmerling Enhanced resistance to oxidation of low density lipoproteinsand decreased lipid peroxide formation during beta-carotene supplementationin cystic fibrosis Free Radic Biol Med 18 (1995) 849ndash859
[181] RC Graham-Maar JI Schall N Stettler BS Zemel VA Stallings Elevated vita-min A intake and serum retinol in preadolescent children with cystic fibrosisAm J Clin Nutr 84 (2006) 174ndash182
[182] I Sadowska-Woda M Rachel J Pazdan E Bieszczad-Bedrejczuk K PawliszakNutritional supplement attenuates selected oxidative stress markers in pediatricpatients with cystic fibrosis Nutr Res (New York NY) 31 (2011) 509ndash518
[183] KA Papas MK Sontag C Pardee RJ Sokol SD Sagel FJ Accurso JS WagenerA pilot study on the safety and efficacy of a novel antioxidant rich formulation inpatients with cystic fibrosis J Cyst Fibros 7 (2008) 60ndash67
[184] Y Saito A Fukuhara K Nishio M Hayakawa Y Ogawa H Sakamoto K Fujii YYoshida E Niki Characterization of cellular uptake and distribution of coen-zyme Q10 and vitamin E in PC12 cells J Nutr Biochem 20 (2009) 350ndash357
[185] AA Franke CM Morrison JL Bakke LJ Custer X Li RV Cooney CoenzymeQ10 in human blood native levels and determinants of oxidation during proces-sing and storage Free Radic Biol Med 48 (2010) 1610ndash1617
[186] HN Bhagavan RK Chopra Plasma coenzyme Q10 response to oral ingestion ofcoenzyme Q10 formulations Mitochondrion 7 (2007) S78ndashS88 (Suppl)
[187] HN Bhagavan RK Chopra Coenzyme Q10 absorption tissue uptake metabo-lism and pharmacokinetics Free Radic Res 40 (2006) 445ndash453
[188] F Galli R Lee C Dunster FJ Kelly Gas chromatography mass spectrometryanalysis of carboxyethyl-hydroxychroman metabolites of alpha- and gamma-tocopherol in human plasma Free Radic Biol Med 32 (2002) 333ndash340
[189] F Galli R Lee J Atkinson A Floridi FJ Kelly Gamma-tocopherol biokineticsand transformation in humans Free Radic Res 37 (2003) 1225ndash1233
[190] TA Laguna MK Sontag I Osberg JS Wagener FJ Accurso RJ Sokol De-creased total serum coenzyme-Q10 concentrations a longitudinal study in chil-dren with cystic fibrosis J Pediatr 153 (2008) 402ndash407
[191] T Frischer JK Myung G Maurer I Eichler Z Szepfalusi G Lubec Possible dys-regulation of chaperon and metabolic proteins in cystic fibrosis bronchial tissueProteomics 6 (2006) 3381ndash3388
[192] C Andersson MM Zaman AB Jones SD Freedman Alterations in immune re-sponse and PPARLXR regulation in cystic fibrosis macrophages J Cyst Fibros 7(2008) 68ndash78
[193] SD Freedman PG Blanco MM Zaman JC Shea M Ollero IK Hopper DAWeed A Gelrud MM Regan M Laposata JG Alvarez BP OSullivan Associa-tion of cystic fibrosis with abnormalities in fatty acid metabolism N Engl JMed 350 (2004) 560ndash569
[194] S Van Biervliet G Vanbillemont JP Van Biervliet D Declercq E Robberecht AChristophe Relation between fatty acid composition and clinical status or geno-type in cystic fibrosis patients Ann Nutr Metab 51 (2007) 541ndash549
[195] SD Freedman MH Katz EM Parker M Laposata MY Urman JG AlvarezA membrane lipid imbalance plays a role in the phenotypic expression ofcystic fibrosis in cftr(minusminus) mice Proc Natl Acad Sci U S A 96 (1999)13995ndash14000
[196] S Van Biervliet S Vande Velde JP Van Biervliet E Robberecht The effect ofzinc supplements in cystic fibrosis patients Ann Nutr Metab 52 (2008)152ndash156
[197] WR Henderson Jr SJ Astley MM McCready P Kushmerick S Casey JWBecker BW Ramsey Oral absorption of omega-3 fatty acids in patients withcystic fibrosis who have pancreatic insufficiency and in healthy control subjectsJ Pediatr 124 (1994) 400ndash408
[198] I Durieu E Vericel D Guichardant H Roth JP Steghens J Drai RN JosserandE Fontaine M Lagarde G Bellon Fatty acids platelets and oxidative markersfollowing intravenous n-3 fatty acids administration in cystic fibrosis an openpilot observational study J Cyst Fibros 6 (2007) 320ndash326
[199] LG Wood DA Fitzgerald ML Garg Hypothesis vitamin E complements poly-unsaturated fatty acids in essential fatty acid deficiency in cystic fibrosis J AmColl Nutr 22 (2003) 253ndash257
[200] JD Lloyd-Still SB Johnson RT Holman Essential fatty acid status in cystic fi-brosis and the effects of safflower oil supplementation Am J Clin Nutr 34(1981) 1ndash7
[201] A Maqbool JI Schall JF Garcia-Espana BS Zemel B Strandvik VAStallings Serum linoleic acid status as a clinical indicator of essential fatty
acid status in children with cystic fibrosis J Pediatr Gastroenterol Nutr 47(2008) 635ndash644
[202] C Oliver N Jahnke Omega-3 fatty acids for cystic fibrosis Cochrane DatabaseSyst Rev (2011) CD002201
[203] B Strandvik E Gronowitz F Enlund T Martinsson J Wahlstrom Essential fattyacid deficiency in relation to genotype in patients with cystic fibrosis J Pediatr139 (2001) 650ndash655
[204] P Rise S Volpi C Colombo RF Padoan C DOrazio S Ghezzi PMelotti V BennatoC Agostoni BM Assael C Galli Whole blood fatty acid analysis with micromethodin cystic fibrosis and pulmonary disease J Cyst Fibros 9 (2010) 228ndash233
[205] H Cao K Gerhold JR Mayers MM Wiest SM Watkins GS Hotamisligil Iden-tification of a lipokine a lipid hormone linking adipose tissue to systemic me-tabolism Cell 134 (2008) 933ndash944
[206] RR Malapaka SK Khoo J Zhang JH Choi XE Zhou Y Xu Y Gong J Li ELYong MJ Chalmers L Chang JH Resau PR Griffin YE Chen HE Xu Iden-tification and mechanism of a ten carbon fatty acid as a modulating ligand ofperoxisome proliferator activated receptors J Biol Chem 287 (2012)183ndash195
[207] T Hara A Hirasawa A Ichimura I Kimura G Tsujimoto Free fatty acid recep-tors FFAR1 and GPR120 as novel therapeutic targets for metabolic disorders JPharm Sci 100 (2011) 3594ndash3601
[208] R Gupta P Rathi S Bradoo Lipase mediated upgradation of dietary fats andoils Crit Rev Food Sci Nutr 43 (2003) 635ndash644
[209] BH Jennings CC Akoh Lipase-catalyzed modification of rice bran oil to incor-porate capric acid J Agric Food Chem 48 (2000) 4439ndash4443
[210] J Hoeks M Mensink MK Hesselink K Ekroos P Schrauwen Long- andMedium-Chain Fatty Acids Induce Insulin Resistance to a Similar Extent inHumans Despite Marked Differences in Muscle Fat Accumulation J Clin Endo-crinol Metab 97 (2012) 208ndash216
[211] PJ Congden G Bruce MM Rothburn PC Clarke JM Littlewood J KelleherMS Losowsky Vitamin status in treated patients with cystic fibrosis ArchDis Child 56 (1981) 708ndash714
[212] BM Winklhofer-Roob H Ellemunter M Fruhwirth SE Schlegel-Haueter GKhoschsorur MA vant Hof DH Shmerling Plasma vitamin C concentrationsin patients with cystic fibrosis evidence of associations with lung inflammationAm J Clin Nutr 65 (1997) 1858ndash1866
[213] L Shamseer D Adams N Brown JA Johnson S Vohra Antioxidant micronutri-ents for lung disease in cystic fibrosis Cochrane Database Syst Rev (2010)CD007020
[214] C Santi S Santoro Electrophilic Selenium First edition Wiley-VCH VerlagGmbH amp Co KGaA 2012
[215] L Flohe S Toppo G Cozza F Ursini A comparison of thiol peroxidase mecha-nisms Antioxid Redox Signal 15 (2010) 763ndash780
[216] L Flohe JR Andreesen R Brigelius-Flohe M Maiorino F Ursini Selenium theelement of the moon in life on earth IUBMB Life 49 (2000) 411ndash420
[217] V Valdiglesias E Pasaro J Mendez B Laffon In vitro evaluation of seleniumgenotoxic cytotoxic and protective effects a review Arch Toxicol 84(2010) 337ndash351
[218] P Foucaud P Therond M Marchand F Brion JF Demelier J Navarro Seleniumand vitamin E in mucoviscidosis Arch Fr Pediatr 45 (1988) 383ndash386
[219] J Neve R Van Geffel M Hanocq L Molle Plasma and erythrocyte zinc copperand selenium in cystic fibrosis Acta Paediatr Scand 72 (1983) 437ndash440
[220] BM Winklhofer-Roob B Tiran PE Tuchschmid MA vant Hof DH ShmerlingEffects of pancreatic enzyme preparations on erythrocyte glutathione peroxi-dase activities and plasma selenium concentrations in cystic fibrosis FreeRadic Biol Med 25 (1998) 242ndash249
[221] JD Lloyd-Still HE Ganther Selenium and glutathione peroxidase levels in cys-tic fibrosis Pediatrics 65 (1980) 1010ndash1012
[222] D Tsavachidou TJ McDonnell S Wen X Wang F Vakar-Lopez LL Pisters CAPettaway CG Wood KA Do PF Thall C Stephens E Efstathiou R Taylor DGMenter P Troncoso SM Lippman CJ Logothetis J Kim Selenium and vitaminE cell type- and intervention-specific tissue effects in prostate cancer J NatlCancer Inst 101 (2009) 306ndash320
[223] IN Zelko TJ Mariani RJ Folz Superoxide dismutase multigene family acomparison of the CuZn-SOD (SOD1) Mn-SOD (SOD2) and EC-SOD (SOD3)gene structures evolution and expression Free Radic Biol Med 33 (2002)337ndash349
[224] RP Bowler JD Crapo Oxidative stress in airways is there a role for extracellu-lar superoxide dismutase Am J Respir Crit Care Med 166 (2002) S38ndashS43
[225] K Best K McCoy S Gemma RA Disilvestro Copper enzyme activities in cysticfibrosis before and after copper supplementation plus or minus zinc Metabo-lism 53 (2004) 37ndash41
[226] SS Percival GP Kauwell E Bowser M Wagner Altered copper status in adultmen with cystic fibrosis J Am Coll Nutr 18 (1999) 614ndash619
[227] NF Krebs JE Westcott TD Arnold BM Kluger FJ Accurso LV Miller KMHambidge Abnormalities in zinc homeostasis in young infants with cystic fibro-sis Pediatr Res 48 (2000) 256ndash261
[228] D Easley N Krebs M Jefferson L Miller J Erskine F Accurso KM HambidgeEffect of pancreatic enzymes on zinc absorption in cystic fibrosis J Pediatr Gas-troenterol Nutr 26 (1998) 136ndash139
[229] S Van Biervliet JP Van Biervliet E Robberecht Serum zinc in patients with cys-tic fibrosis at diagnosis and after one year of therapy Biol Trace Elem Res 112(2006) 205ndash211
[230] S Van Biervliet JP Van Biervliet S Vande Velde E Robberecht Serum zinc con-centrations in cystic fibrosis patients aged above 4 years a cross-sectional eval-uation Biol Trace Elem Res 119 (2007) 19ndash26
712 F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
[231] F Galli M Cristina Polidori W Stahl P Mecocci FJ Kelly Vitamin E biotransfor-mation in humans Vitam Horm 76 (2007) 263ndash280
[232] J Wiser NE Alexis Q Jiang W Wu C Robinette R Roubey DB Peden In vivogamma-tocopherol supplementation decreases systemic oxidative stress andcytokine responses of human monocytes in normal and asthmatic subjectsFree Radic Biol Med 45 (2008) 40ndash49
[233] JG Wagner Q Jiang JR Harkema B Illek DD Patel BN Ames DB PedenOzone enhancement of lower airway allergic inflammation is prevented bygamma-tocopherol Free Radic Biol Med 43 (2007) 1176ndash1188
[234] JT Harries DP Muller Absorption of different doses of fat soluble and watermiscible preparations of vitamin E in children with cystic fibrosis Arch DisChild 46 (1971) 341ndash344
[235] EI Back C Frindt E Ocenaskova D Nohr M Stern HK Biesalski Can changesin hydrophobicity increase the bioavailability of alpha-tocopherol Eur J Nutr45 (2006) 1ndash6
[236] SZ Nasr MH OLeary C Hillermeier Correction of vitamin E deficiency withfat-soluble versus water-miscible preparations of vitamin E in patients with cys-tic fibrosis J Pediatr 122 (1993) 810ndash812
[237] S Soltani-Frisk E Gronowitz H Andersson B Strandvik Water-miscibletocopherol is not superior to fat-soluble preparation for vitamin E absorptionin cystic fibrosis Acta Paediatr 90 (2001) 1112ndash1115
[238] K Papas J Kalbfleisch R Mohon Bioavailability of a novel water-soluble vi-tamin E formulation in malabsorbing patients Dig Dis Sci 52 (2007)347ndash352
[239] F Antonicelli M Parmentier EM Drost N Hirani I Rahman K Donaldson WMacNee Nacystelyn inhibits oxidant-mediated interleukin-8 expression andNF-kappaB nuclear binding in alveolar epithelial cells Free Radic Biol Med 32(2002) 492ndash502
[240] EM App D Baran I Dab A Malfroot M Coffiner F Vanderbist M King Dose-finding and 24-h monitoring for efficacy and safety of aerosolized Nacystelyn incystic fibrosis Eur Respir J 19 (2002) 294ndash302
[241] MG Traber How much vitamin E hellip Just enough Am J Clin Nutr 84 (2006)959ndash960
[242] JC McCann BN Ames Vitamin K an example of triage theory is micronu-trient inadequacy linked to diseases of aging Am J Clin Nutr 90 (2009)889ndash907
[243] M Fusaro G Crepaldi S Maggi F Galli A DAngelo L Calo S Giannini DMiozzo M Gallieni Vitamin K bone fractures and vascular calcifications inchronic kidney disease an important but poorly studied relationship J Endocri-nol Invest 34 (2010) 317ndash323
[244] JC McCann BN Ames Adaptive dysfunction of selenoproteins from the per-spective of the triage theory why modest selenium deficiency may increaserisk of diseases of aging FASEB J 25 (2011) 1793ndash1814
[245] R Apak K Guclu M Ozyurek B Bektas Oglu M Bener Cupric ion reducing an-tioxidant capacity assay for food antioxidants vitamins polyphenolics and fla-vonoids in food extracts Methods Mol Biol 477 (2008) 163ndash193
[246] F Galli Interactions of polyphenolic compounds with drug disposition and me-tabolism Curr Drug Metab 8 (2007) 830ndash838
[247] RL Prior X Wu K Schaich Standardized methods for the determination of an-tioxidant capacity and phenolics in foods and dietary supplements J Agric FoodChem 53 (2005) 4290ndash4302
[248] C Azbell S Zhang D Skinner J Fortenberry EJ Sorscher BA WoodworthHesperidin stimulates cystic fibrosis transmembrane conductance regulator-mediated chloride secretion and ciliary beat frequency in sinonasal epitheliumOtolaryngol Head Neck Surg 143 (2010) 397ndash404
[249] G Wegrzyn J Jakobkiewicz-Banecka M Gabig-Ciminska E Piotrowska M Nar-ajczyk A Kloska M Malinowska D Dziedzic I Golebiewska M Moskot AWegrzyn Genistein a natural isoflavone with a potential for treatment of ge-netic diseases Biochem Soc Trans 38 (2010) 695ndash701
[250] YC Yu H Miki Y Nakamura A Hanyuda Y Matsuzaki Y Abe M Yasui K Ta-naka TC Hwang SG Bompadre Y Sohma Curcumin and genistein additivelypotentiate G551D-CFTR J Cyst Fibros 10 (2011) 243ndash252
[251] B Illek H Fischer Flavonoids stimulate Cl conductance of human airway epithe-lium in vitro and in vivo Am J Physiol 275 (1998) L902ndashL910
[252] JL Kreindler Cystic fibrosis exploiting its genetic basis in the hunt for newtherapies Pharmacol Ther 125 (2010) 219ndash229
[253] B Illek L Zhang NC Lewis RB Moss JY Dong H Fischer Defective function ofthe cystic fibrosis-causing missense mutation G551D is recovered by genisteinAm J Physiol 277 (1999) C833ndashC839
[254] P Anandakumar S Kamaraj S Jagan G Ramakrishnan R Vinodhkumar TDevaki Capsaicin modulates pulmonary antioxidant defense system during ben-zo(a)pyrene-induced lung cancer in Swiss albinomice Phytother Res 22 (2008)529ndash533
[255] I Rahman Antioxidant therapeutic advances in COPD Ther Adv Respir Dis 2(2008) 351ndash374
[256] AW Boots H Li RP Schins R Duffin JW Heemskerk A Bast GR Haenen Thequercetin paradox Toxicol Appl Pharmacol 222 (2007) 89ndash96
[257] M Joskova S Franova V Sadlonova Acute bronchodilator effect of quercetin inexperimental allergic asthma Bratisl Lek Listy 112 (2011) 9ndash12
[258] HJ Park CM Lee ID Jung JS Lee YI Jeong JH Chang SH Chun MJ Kim IWChoi SC Ahn YK Shin SR Yeom YM Park Quercetin regulates Th1Th2 balancein a murine model of asthma Int Immunopharmacol 9 (2009) 261ndash267
[259] AP Rogerio A Kanashiro C Fontanari EV da Silva YM Lucisano-ValimEG Soares LH Faccioli Anti-inflammatory activity of quercetin and iso-quercitrin in experimental murine allergic asthma Inflamm Res 56 (2007)402ndash408
[260] M Muller Polyphenol cytotoxicity induced by the bacterial toxin pyocyaninrole of NQO1 Free Radic Biol Med 47 (2009) 84ndash91
[261] J Grassmann Terpenoids as plant antioxidants Vitam Horm 72 (2005)505ndash535
[262] P Allen Tea tree oil the science behind the antimicrobial hype Lancet 358(2001) 1245
[263] EC Dasenbrook W Checkley CA Merlo MW Konstan N Lechtzin MP BoyleAssociation between respiratory tract methicillin-resistant Staphylococcus aure-us and survival in cystic fibrosis JAMA 303 (2010) 2386ndash2392
[264] V Bezzerri M Borgatti E Nicolis I Lampronti MC Dechecchi I Mancini PRizzotti R Gambari G Cabrini Transcription factor oligodeoxynucleotides toNF-kappaB inhibit transcription of IL-8 in bronchial cells Am J Respir CellMol Biol 39 (2008) 86ndash96
[265] R Gambari M Borgatti V Bezzerri E Nicolis I Lampronti MC Dechecchi IMancini A Tamanini G Cabrini Decoy oligodeoxyribonucleotides and peptidenucleic acids-DNA chimeras targeting nuclear factor kappa-B inhibition of IL-8 gene expression in cystic fibrosis cells infected with Pseudomonas aeruginosaBiochem Pharmacol 80 (2010) 1887ndash1894
[266] M Adrian P Jeandet AC Douillet-Breuil L Tesson R Bessis Stilbene content ofmature Vitis vinifera berries in response to UV-C elicitation J Agric Food Chem48 (2000) 6103ndash6105
[267] B Paul I Masih J Deopujari C Charpentier Occurrence of resveratrol and pter-ostilbene in age-old darakchasava an ayurvedic medicine from India J Ethno-pharmacol 68 (1999) 71ndash76
[268] I Rahman Antioxidant therapies in COPD Int J Chron Obstruct Pulmon Dis 1(2006) 15ndash29
[269] M Lee S Kim OK Kwon SR Oh HK Lee K Ahn Anti-inflammatory and anti-asthmatic effects of resveratrol a polyphenolic stilbene in a mouse model ofallergic asthma Int Immunopharmacol 9 (2009) 418ndash424
[270] LG Wood PA Wark ML Garg Antioxidant and anti-inflammatory effectsof resveratrol in airway disease Antioxid Redox Signal 13 (2010)1535ndash1548
[271] KV Kiselev Perspectives for production and application of resveratrol ApplMicrobiol Biotechnol 90 (2011) 417ndash425
[272] M Shakibaei C Buhrmann A Mobasheri Resveratrol-mediated SIRT-1 interac-tions with p300 modulate receptor activator of NF-kappaB ligand (RANKL) acti-vation of NF-kappaB signaling and inhibit osteoclastogenesis in bone-derivedcells J Biol Chem 286 (2011) 11492ndash11505
[273] SF Zaidi K Ahmed T Yamamoto T Kondo K Usmanghani M Kadowaki TSugiyama Effect of resveratrol on Helicobacter pylori-induced interleukin-8 secre-tion reactive oxygen species generation and morphological changes in human gas-tric epithelial cells Biol Pharm Bull 32 (2009) 1931ndash1935
[274] JK Kundu YK Shin YJ Surh Resveratrol modulates phorbol ester-inducedpro-inflammatory signal transduction pathways in mouse skin in vivo NF-kappaB and AP-1 as prime targets Biochem Pharmacol 72 (2006)1506ndash1515
[275] NH Nam Naturally occurring NF-kappaB inhibitors Mini Rev Med Chem 6(2006) 945ndash951
[276] JM Smoliga JA Baur HA Hausenblas Resveratrol and healthmdasha comprehen-sive review of human clinical trials Mol Nutr Food Res 55 (2011) 1129ndash1141
[277] ME Juan M Maijo JM Planas Quantification of trans-resveratrol and itsmetabolites in rat plasma and tissues by HPLC J Pharm Biomed Anal 51(2010) 391ndash398
[278] JA Baur DA Sinclair Therapeutic potential of resveratrol the in vivo evidenceNat Rev 5 (2006) 493ndash506
[279] E Nicolis I Lampronti MC Dechecchi M Borgatti A Tamanini N Bianchi VBezzerri I Mancini MG Giri P Rizzotti R Gambari G Cabrini Pyrogallol anactive compound from the medicinal plant Emblica officinalis regulates expres-sion of pro-inflammatory genes in bronchial epithelial cells Int Immunophar-macol 8 (2008) 1672ndash1680
[280] E Nicolis I Lampronti MC Dechecchi M Borgatti A Tamanini V Bezzerri NBianchi M Mazzon I Mancini MG Giri P Rizzotti R Gambari G CabriniModulation of expression of IL-8 gene in bronchial epithelial cells by 5-methoxypsoralen Int Immunopharmacol 9 (2009) 1411ndash1422
[281] M Borgatti I Mancini N Bianchi A Guerrini I Lampronti D Rossi G SacchettiR Gambari Bergamot (Citrus bergamia Risso) fruit extracts and identified com-ponents alter expression of interleukin 8 gene in cystic fibrosis bronchial epithe-lial cell lines BMC Biochem 12 (2011) 15
[282] L Piccagli E Fabbri M Borgatti N Bianchi V Bezzerri I Mancini E Nicolis CMDechecchi I Lampronti G Cabrini R Gambari Virtual screening against p50NF-kappaB transcription factor for the identification of inhibitors of the NF-kappaB-DNA interaction and expression of NF-kappaB upregulated genesChemMedChem 4 (2009) 2024ndash2033
[283] L Piccagli M Borgatti E Nicolis N Bianchi I Mancini I Lampronti D VevaldiF DallAcqua G Cabrini R Gambari Virtual screening against nuclear factorkappaB (NF-kappaB) of a focus library identification of bioactive furocoumarinderivatives inhibiting NF-kappaB dependent biological functions involved incystic fibrosis Bioorg Med Chem 18 (2010) 8341ndash8349
[284] M Borgatti A Chilin L Piccagli I Lampronti N Bianchi I Mancini G Mar-zaro Da Francesco A Guiotto R Gambari Development of a novel furocou-marin derivative inhibiting NF-kappaB dependent biological functionsdesign synthesis and biological effects Eur J Med Chem 46 (2011)4870ndash4877
[285] E Georgy S Le Guellec L Vecellio E Fichant P Stordeur P Bordeau JP PerraudinFeasibility study of OSCN- and lactoferrin (Meveol) nebulization for cysticfibrosis JCyst Fibros 10 (2011) S18
713F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
[286] C Tidei M Piroddi F Galli C Santi Oxidation of thiols promoted by PhSeZnClTetrahedron Lett 53 (2012) 232ndash234
[287] L Semianrio-Vidal C van Hesuden G Mugesh ER Lazarowski Ebselen is a po-tent non-competitive inhibitor of extracellular nucleoside diphosphokinasePurinergic Signal 6 (2010) 383ndash391
[288] C ColussiMC Albertini S Coppola S Rovidati F Galli L Ghibelli H2O2-inducedblockof glycolysis as an active ADP-ribosylation reaction protecting cells from apoptosisFASEB J 14 (2000) 2266ndash2276
[289] H Xiao KL Parkin Induction of phase II enzyme activity by various seleniumcompounds Nutr Cancer 55 (2006) 210ndash223
[290] G Peluffo R Radi Biochemistry of protein tyrosine nitration in cardiovascularpathology Cardiovasc Res 75 (2007) 291ndash302
[291] B Alvarez R Radi Peroxynitrite reactivity with amino acids and proteinsAmino Acids 25 (2003) 295ndash311
[292] B Kamosinska MW Radomski M Duszyk A Radomski SF Man Nitric oxideactivates chloride currents in human lung epithelial cells Am J Physiol 272(1997) L1098ndashL1104
[293] L Chen RP Patel X Teng CA Bosworth JR Lancaster Jr S Matalon Mecha-nisms of cystic fibrosis transmembrane conductance regulator activation by S-nitrosoglutathione J Biol Chem 281 (2006) 9190ndash9199
[294] F Luchetti B CanonicoM BettiM Arcangeletti F PilolliM Piroddi L Canesi S PapaF Galli Melatonin signaling and cell protection function FASEB J 24 (2010)3603ndash3624
[295] MW Bengtsson G Jedstedt G Flemstrom Duodenal bicarbonate secretion inrats stimulation by intra-arterial and luminal guanylin and uroguanylin ActaPhysiol (Oxf) 191 (2007) 309ndash317
[296] CS Nelson JL Marino CN Allen Melatonin receptor potentiation of cyclic AMP andthe cystic fibrosis transmembrane conductance regulator ion channel J Pineal Res 26(1999) 113ndash121
[297] C de Castro-Silva VM de Bruin GM Cunha DM Nunes CAMedeiros PF de BruinMelatonin improves sleep and reduces nitrite in the exhaled breath condensate incystic fibrosismdasha randomized double-blind placebo-controlled study J Pineal Res48 (2010) 65ndash71
[298] I Hornyak E Pankotai L Kiss Z Lacza Current developments in the the-rapeutic potential of S-nitrosoglutathione an endogenous NO-donor mole-cule Curr Pharm Biotechnol (2011) Jan 11 [Epub ahead of print] - PMID21235457
[299] AH Snyder ME McPherson JF Hunt M Johnson JS Stamler B Gaston Acuteeffects of aerosolized S-nitrosoglutathione in cystic fibrosis Am J Respir CritCare Med 165 (2002) 922ndash926

699F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
improve circulating levels of GSH in CF patients through the dietarysupplementation of the antioxidant [127] The limited absorption ofGSH could be overcome by GSH-esters as in vitro studies haveshown that this form of GSH may be specifically useful to rescue mi-tochondrial defects in cystic fibrosis models [80] Safety of these GSHderivatives in humans has been poorly investigated
Two independent studies have shown that the treatment of CF pa-tients with high doses of NAC increases extracellular GSH in sputum[78125] but contrasting results have been reported concerning theeffects of NAC on the concentrations of blood GSH and on the levelsof IL-8 and other markers of inflammation NAC treatments may beuseful to modulate the GSH content in cells but it should be remindedthat an enhanced cysteine supply cannot lead to an increase of GSHabove physiological levels due to the feedback inhibition mechanismof γ-glutamylcysteine synthetase described in the Section 311
331 Gamma-glutamyltransferase and GSH therapySo far none of the studies mentioned above has taken into account
the fact that GSH is degraded by GGT enzyme activity GGT concentra-tions are known to increase several fold in ELF of CF patients even ifthe mechanisms for this effect were not determined [135] and thisphenomenon parallels the above described decrease of GSH levels inELF Preliminary data suggest that a major source of increased ELFGGT is represented by activated neutrophils accumulating in diseasedairways (Corti and Pompella 2011 unpublished observation) Re-gardless of its origin it is likely that increased GGT in ELF would de-grade locally administered GSH to variable extents which couldcontribute to the so far inconclusive results of therapies based onaerosolized GSH Besides its role in GSH catabolism GGT has beenshown to mediate protein S-thiolation [136] suggesting that GSH ad-ministration in the presence of active GGT enzyme might alter CFTRglutathiolation status and function in a potentially unfavorable wayOn the other hand a potential role of GGT in favoring bronchial up-take of antioxidant vitamin C has also been suggested [137]
These controversial findings may add further issues to the ques-tion of whether the therapy of lung oxidative stress by aerosolizedGSH could be safe in all the CF patients regardless of specific strate-gies that would ascertain the extent of lung inflammation Thesestrategies should include the assay of GGT levels in ELF In principleonce an adverse role of ELF GGT in GSH therapies will be confirmedthe association of GGT inhibitors in the GSH formulations for inhala-tion could represent a promising pharmacological strategy
34 Malnutrition as a possible cause of defective thiol-dependentantioxidant protection
Successful nutritional interventions strongly impact on the clinicaloutcome of CF patients [138ndash140] Malnutrition by pancreatic insuffi-ciency and other CF-related factors influence the susceptibility to de-velop recurrent infections and severe inflammatory lesions of thelung tissue If the onset of a defective (sub-optimal) antioxidant sta-tus may represent an underlying component in the clinical effects ofmalnutrition remains a matter of investigation Clinicians have topay particular care to avoid these disturbances and successful proto-cols of nutritional intervention in CF have been developed whichare essentially aimed to avoid the onset of protein-energy malnutri-tion (PEM) [141] Despite this the risk of developing such an unto-ward complication in CF infants and children remains high assuggested by the prevalence data registered in some areas Actuallya prevalence of PEM between 5 and 14 in Moldavian infants was re-cently reported [142] and PEM is associated with poor outcome andparticularly with the risk of developing edema and anemia
Besides lowered intake and absorption of micronutrient antioxi-dants discussed in the other sections malabsorption of dietary proteinand excess fecal amino acid losses result in hypoproteinemiahypoalbu-minemia as key biochemical signs of PEM Hypoalbuminemia is
considered to be linked with a causendasheffect relationship with oxidativestress and is proposed to influence morbidity and mortality in condi-tions associated with chronic inflammation and severe oxidative stress[143144] The human serum albumin (HAS) molecule contains only areactive thiol group eg the Cys 34 the importance of which as an anti-oxidant defense system in blood and for the entire organism is welldocumented [145] This is the second main thiol (and the main proteinthiol) in the circulation (approx 2 mmol in the adult organism assum-ing 5 l of total blood volume anHt of 40 and [HAS] of 45 gl of plasma)being the RBCGSH thefirst thiol in blood (near to 5 mmol assuming thesame parameters of above and an average concentration of GSH inpacked RBC of 25 mM) [146147] The antioxidant role of HSA is notonly a consequence of the relative abundance of its Cys thiol A specificcapability of acting as a sacrificial target for a series of electrophils andmost biologically relevant ROS ie hydrogen peroxide and peroxyni-trite has been demonstrated in a series of studies [145148149] Li-gand binding activity can contribute to promote antioxidant effectsby the HSA molecule [145] Transitions metals particularly copperand also iron in the case of iron-overload diseases bind to HSA Inthis way these are less available to promote the Fenton chemistryand hydroxyl radicals eventually released from this oxidative reactionare mostly directed to the HAS protein sparing more important tar-gets A free radical-trapping activity of HSA has been also demonstratedand this was proposed to be directed toward both hydrophilic and fat-soluble species This activity may result from the interaction withother antioxidants such as α-tocopherol [150] and may influence theantioxidant activity of food-derived phenolic antioxidants [151]
However Cys 34 is considered the main contributor to the antiox-idant function of HAS which plays its role in the antioxidant homeo-stasis of blood thanks to a complex series of interactions with themetabolism and antioxidant function of the pool of free thiols in plas-ma and in the circulating RBC with the latter playing a significantcontribution to the extracellular pool of GSH [146] and to the dynam-ics of inter-organ GSHmetabolism in cooperation with liver and othertissues [147] Immuno-inflammatory cells and the lung tissue areamong the main terminals of this metabolism The RBC contain theentire machinery to synthesize GSH to restore its redox (by enzymat-ic reduction of the oxidized form) and to use this as cofactor of Se-GPx and GSH-S-transferase enzymatic activities that are responsibleof the detoxification of hydroperoxides and alkylating agents thatmay form in or enter the RBC cytosol [147] In this sense the RBC rep-resents a circulating reservoir of GSH that in addition to maintainingthe redox and respiratory function of Hb participates to systemic pro-tection of xenobiotics of endogenous and exogenous origin In consid-eration of these aspects the combination of hypoalbuminemia andanemia may exponentially increase the risk of developing oxidativestress in CF patients as it is supposed to occur in other oxidative stressconditions such as chronic kidney disease [55143152] Additionalclinical investigation should verify the hypothesis that hypoalbumi-nemia together with a defective uptake and metabolism of sulfur-containing amino acids and CF-specific defects of the GSH metabo-lism may represent a causal risk factor for an impaired antioxidantdefense and systemic oxidative stress in CF patients
35 Fat-soluble antioxidants
Pancreatic insufficiency and a diminished bile acid pool cause mal-absorption of important essential nutrients and other dietary compo-nents in CF Of particular significance is the malabsorption of fat-soluble antioxidants such as tocopherols carotenoids and coenzymeQ-10 (Co-Q10) and that of essential fatty acids (EFA)
351 Vitamin EVitamin E therapy in CF has been proposed in several decades of
research as a useful approach to overcome both the lower absorptionof this fat-soluble micronutrient and the increased antioxidant
700 F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
demand by the abnormal generation of ROS in CF tissues (see for in-stance the recommendations by the Cystic Fibrosis Foundation Con-sensus Conference on nutrition [153])
The first report of a vitamin E deficiency in CF appeared in literaturein 1951 by Filer et al [154] In this study the absorption of the mainform of this vitamin eg α-tocopherol and its ester derivatives was in-vestigated in several subsets of infants and children Thanks to a simplebioavailability (or tolerance) test these authors observed that ldquoin-fantshellip diagnosed as fibrocystic disease of the pancreas diarrhea andcirrhosis were characterized by a poor response to the test ie the tol-erance curve was lowrdquo However abnormalities were also observed inother subgroups of infants with a variety of disorders not associatedwith fat or fat-soluble vitamin intolerance such as sprue celiac syn-drome and lupus erythematosus which suggests the general observa-tion that malnutrition and inflammatory and degenerative diseases ofthe GI tract may lead to absorb tocopherols poorly At the same timethese authors reported that ldquoMetabolic disorders with associated hy-percholesterolemia were observed to give abnormally high values forthe area under the curverdquo and that patients responding poorly to to-copherol absorption test did also in vitamin A absorption tests
The finding of lowered (lipid uncorrected) levels of vitamin E wasconfirmed in other studies in which this relative deficiency was foundto occur irrespective of pancreatic comorbidity and in associationwith lowered levels of other liposoluble vitamins such as vitamin Aand D [155] regardless of their different liver metabolism and tissuedelivery mechanisms [156157]
Plasma buccal mucosal cells (BMCs) and breath condensate α-tocopherol decreased significantly with age in association with a de-creased respiratory function [5] This was accompanied by loweredlevels of other antioxidants such as vitamin C and increased oxidativestress markers of different origin such as protein carbonyls thiobarbi-turic acid-reactive substances and F2-IsoPs
Clinical symptoms of vitamin E deficiency in CF have not beenconclusively investigated Dolan et al [158] described that anemiaof CF patients is related to vitamin E deficiency and increasedperoxide-induced hemolysis of RBC Other authors however ob-served an increased susceptibility to peroxide-induced hemolysisalso in the presence of normal levels of vitamin E [159] Peters andKelly [160] observed that RBC vitamin E concentrations were belowthe normal range in almost all unsupplemented patients and roseinto the normal range with a 1-year supplement of 100 mg per daybut not 15 mg per day Since RBC vitamin E concentration has beenshown to correlate well with tissue concentrations of the vitamin inanimals tissue levels of vitamin E are expected to be lower than nor-mal in CF patients
Bioavailability of fat-soluble vitamin is limited in CF Vitamin Edeficiency of CF is also associated with hypocholesterolemia [7] Asa consequence the relative deficiency of this vitamin is compensatedwhen the absolute levels are normalized for cholesterol levels andthis suggests a poor transferring of this vitamin in the circulation bya defective lipid and lipoprotein metabolism Pancreatic insufficiencyand the consequent lipid malnutrition cannot completely explain thisdefect and other possibly CF-specific dysfunctions could play a roleLiver metabolism and specific plasma transport systems of this vita-min need further elucidation in CF
As a consequence of these aspects it is not presently clear whichform and level of supplementation of this vitamin is most appropriateto treat these patients Usingα-tocopherol as a vitamin E supplementPeters et al [160] reported that 100 mg per day are required to nor-malize RBC concentrations Other authors described unsuccessfulsupplementation protocols with higher doses and this has led to de-velop formulations with higher bioavailability in order to achieve bet-ter compliance to oral supplementation (see below and the literaturereviewed in [161ndash163])
Besides absorption and tissue delivery issues specificity of actionis another critical item of antioxidant therapy with fat-soluble agents
in CF As further addressed below this aspect could be themain limit toa successful use of natural forms of vitamin E in the clinical manage-ment of CF inflammation even if a local lung-targeted therapy wouldbe developed according with so far proposed pre-clinical models ofaerosolized vitamin E [164165]
Current pharmacological research is aimed to develop synthetic formsof this and other fat-soluble antioxidants with better radical scavengingproperties at the lipidndashwater interface Type of ROS target and the sitesof action greatly influence the chances of a fat-soluble antioxidant of alle-viating oxidative stress in the airways as well as in other organs such asliver and pancreas These aspects dealing with specificity of action[163166167] have stimulated the search of novel vitamin E-derived an-tioxidants that may help to scavenge radicals at the lipidndashwater interfaceof the epithelial cell membrane and surfactant Amine derivativesof tocopherols and tocotrienols have been recently demonstrated toshow higher antioxidant and free radical scavenging activity than α-tocopherol [168] Further in vitro pharmacological analysis has includedtoxicity evaluations and the detailed investigation of scavenging of azo-and phenolic radicals with different degrees of hydrophobicity and theinhibitory activity on IL-8 gene expression and phospholipase activityin CF cells Comparative evaluation with other synthetic derivativessuch asα-tocopheryl succinate and natural forms of vitamin E suggestedthat these amine derivatives are promising antioxidant and anti-inflammatory agents [Galli F and Pilolli F unpublished observation]deserving further pre-clinical investigation in CF model systems
Anti-inflammatory effects of natural and synthetic analogues of vi-tamin E are also an intriguing pharmacological opportunity currentlyunder investigation by several laboratories [169170]
Recently vitamin E supplementation has been at the center of adispute regarding its safety when used at high dosages in certainpopulations of patients An extensive and speculative debate originat-ed on this subject after a meta-analysis study byMiller et al [171] thatexamined the largest secondary prevention trials on vitamin E trials incardiovascular patients finding a significantly increased mortality riskfor all the causes (about 4 1ndash8 in the 95 interval of confidence)when the patients were treated with doses gt400 IUdie (that areequivalent to 400 mgdie of the synthetic form allrac-α-tocopheroland to 185 mgdie of the natural form RRR-α-tocopherol) This debateresulted in a careful examination of this meta-analysis study by severalother authors and in further revisions of the literature on vitamin E tox-icity in humans [see the literature recently reviewed in [163172ndash174]]that clearly demonstrated the poor consistency of the conclusionsraisedwithMillersmeta-analysis study and the paucity of the concernsthat derived from that These conclusions have been verified in the re-cent international symposium on vitamin E of the Society for Free Rad-ical Research Europe branch of Rome 2009 [173175] Vitamin E used assupplement for humans in all its forms (eg α-tocopherol and othertocopherols and tocotrienols) is safe in abroad range of intakes[172176] The tolerable upper intake level (UL) and the AcceptableDaily Intake (ADI) established by the Joint FAOWHOExpert Committeeon Food Additives for the natural form of vitamin E as α-tocopherolequivalents are of 300 mgdie and 015ndash20 mgkg body weightdierespectively [172177]
352 CarotenoidsLevels of plasma carotenoids such as β-carotene β-cryptoxanthin
and total lycopene are significantly lowered in CF patients and thiswas associated with higher susceptibility to lipid peroxidation[5178ndash180] Rust et al [178] demonstrated that the long-term oralsupplementation with 50 mg β-caroteneday (ie 1 mg β-carotenekg BWday) restored the levels of this carotenoid while sub-optimalsupplementation was observed at doses of 10 mg β-caroteneday orlower thus confirming the need of high doses of this fat-soluble factorto overcome the limited absorption and thus to achieve plasma con-centrations of healthy control subjects Successful high-dose treat-ments appear to lower oxidative stress markers such as TBA-MDA
701F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
complexes and to correct total antioxidant capacity of plasma Inanother study β-carotene supplementation was observed to de-creased lipid peroxide formation as quantitated by malondialdehydeconcentrations in plasma (TBAHPLC method) and to enhance the re-sistance to copper(II) ion-induced oxidation of low density lipopro-teins [180]
At the same time toxicity issues have been raised for human sup-plementation with carotenoid formulations and particularly of water-miscible formulations of preformed vitamin A that is regularly sup-plemented to CF patients which may increase serum retinol andpossible risk of CF-associated liver and bone complications (reviewedin [161181]) However β-carotene supplementation seems to be safesince this does not affect plasma concentrations of other carotenoidsand retinol as well as of other fat-soluble vitamins as α- and γ-tocopherol [178] Recent studies designed to test the clinical efficacyof a CF tailored multivitamin formulation (commercial name AquA-DEKsreg) also tested the safety of this type of formulation and demon-strated that this does not increase vitamin A above the normal levelsobserved in healthy controls [162182183] The normalization of β-carotene levels obtained in these studies was associated only withminor improvements on respiratory and growth parameters whilethe levels of urinary F2-IsoPs used as index of lipid peroxidationwere not affected [162] The surrogate marker of lipid peroxidationMDA was affected together with some selected antioxidant parame-ters (RBC thiols and superoxide dismutase) in another study inwhich this multivitamin formulation was preliminarily evaluated incomparison with standard formulations of vitamin E and A [182]
353 Coenzyme Q-10Coenzyme Q-10 (Q10) is a well-known electron transporter in the
mitochondrial respiratory chain with fundamental role in cellularbioenergetics and scavenging of radical species [184] This lipophilicsubstance is present in the circulation at low levels (serum concentra-tionsle2 μM) mainly as ubiquinol-10 eg the reduced form with anapproximate ratio of 955 with the oxidized form ubiquinone-10[185186] A mechanism for a preferential distribution and accumula-tion in mitochondria has been suggested for both the reduced and ox-idized forms of CoQ10 that are taken up by the cells in a time- andconcentration-dependent Subcellular localization and trafficking ofexogenous Q10 are similar to those of the endogenous form butwere different from that of α-tocopherol that is related with lipidcomposition particularly in the mitochondrial and microsomal frac-tions [184] Ubiquinol-10 readily oxidizes ex vivo by the reactionwith other lipophilic antioxidants such as α-tocopherol and butylatedhydroxytoluene [185] Therefore a higher reduction potential thanother physiological fat-soluble antioxidants such as vitamin E and aselective metabolism and cellular trafficking show peculiar role forthe cell CoQ which may also represent an important lipophilic antiox-idant in cells and body fluids
Human cells synthesize this coenzyme through the cholesterol bio-synthesis pathway so thatmore than two thirds of the tissue levels ap-pear to have an endogenous origin dietary sources provide acontribution to Co-Q10 levels of blood and all solid tissues that variesdepending on the dose applied and type of dietary source [187] How-ever in the case of oral supplements it has to be considered that hy-drophobicity and large molecular weight of this coenzyme influenceits absorption that ultimately is slow and limited [186187] Likewiseto vitamin E pharmacokinetics [188189] Co-Q10 showed T(max) ofaround 6 h that coincides with that of dietary lipids Elimination isclose to that of the more retained form of vitamin E in human bodyeg α-tocopherol with a half-life of about 33 h which suggests poorhepatic metabolism However commercially available formulationsare reported to be safe even at high doses and solubilized formulationsshow enhanced bioavailability In healthy subjects plasma Q10 re-sponse to oral ingestion show saturation profiles with a plateau at a
dose of 2400 mg and the higher plasma concentrations were foundto facilitate uptake by peripheral tissues and also the brain [186187]
Laguna et al [190] recently investigated total serum levels ofcoenzyme Q-10 in a wide population of CF children (n=381) and esti-mated their association with clinical outcome Near to 50 of these CFpatients were deficient of Co-Q10 and this defect was significantlymore prevalent in patients with pancreatic insufficiency and signifi-cantly associated with P aeruginosa colonization in infants (under24 months of age) Importantly low Co-Q10 levels correlated to otherlipid markers of a poor nutritional status such as total lipids and alsothe other fat-soluble antioxidants β-carotene and α-tocopherolwhich confirms the presence of a common defect in the absorptionand metabolic pathways of this coenzyme with dietary lipids
The deficit of Co-Q10 may contribute to the impaired energy func-tion of mitochondria of CF tissues and this may exacerbate CF-linkedinflammation infection and cellular stress response of the lung A sys-tematic analysis of molecular lesions in CF bronchial tissue has beenrecently carried out by proteomic approach [191] Comparative eval-uation of protein expressional pattern in CF and healthy controltissues has revealed aberrant levels of some mitochondrial andenergy-related proteins in CF specimens that included the ubiqui-nolndashcytochrome c reductase complex core protein I and one form ofnidogen a pseudogene of aconitase 2 These changes in CF may reflectmolecular changes which could be associated with an altered mito-chondrial homeostasis and Co-Q10 redox
Multivitamin supplements with high bioavailability containingCo-Q10 have demonstrated to correct the deficit of this antioxidantand were preliminarily observed to improve airway inflammationmarkers in CF patients [183] However further clinical investigationfailed to demonstrate that such an improved biochemical profile isassociated with significant improvements in weight percentile andpulmonary function [162]
354 Fatty acidsA key pathophysiological role in sustaining inflammation in CF has
been attributed to the abnormal polyunsaturated fatty acid (FA) pat-tern Abnormalities in FA profiling are potentially linked to CFTRmutation-driven alterations in the absorption andor metabolism ofdietary lipids [192193] and to the consumption of high oxidizableFA involved in the free radical-mediated lipid peroxidation [7]Among those alterations dysregulation of the docosahexaenoic acidand arachidonic acid balance has been extensively studied with re-portedly significant reduction of DHA in CF and a parallel increasein the levels of AA and inflammatory indices [193ndash195] Actually AAis the progenitor of both enzymatic- and free radical-derived inflam-matory mediators including leukotrienes prostaglandins and iso-prostanes On the other hand n-3 PUFA (eicosapentaenoic acid anddocosahexaenoic acid) are involved in the generation of potent medi-ators namely resolvins and protectins which are able to resolveexudates and to act as organ protective and antifibrotic Secondarilyto their anti-inflammatory action n-3 FA may also produce anantioxidant-like response (eg a reduced demand of antioxidants toachieve an optimal control of oxidative pathways) As a consequencen-3 PUFA have been suggested and widely used as supplements in CFpatients usually under the form of fish oil [196ndash198] It is worth ofnote however that defective levels of DHA in CF patients was notconfirmed in recent studies [7] It was also shown that patients onDHA supplements did not have increased plasma n-3 FA concentra-tions but showed more severe oxidative stress compared to theunsupplemented patients [7] This observation of an increased riskof oxidative stress in CF subjects receiving n-3 fatty acids supple-ments has also been described by other authors [199]
Studies reporting increased AA levels in CF patients have beencontradicted by others [7200201] thus contributing to weakeningthe pathophysiological role of the altered DHAndashAA balance as turnpoint of an upregulated inflammatory status in CF In this context a
702 F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
recent Cochrane meta-analysis on n-3 supplementation in CF patients[202] highlighted the lack of evidence for a significant correction ofthe assessed clinical end points (mainly respiratory symptoms)even when inflammatory indices and other laboratory end pointswere met Taken together these data suggest that there is insufficientevidence to draw firm conclusions or recommend routine use of n-3supplements in CF Notwithstanding it is common belief that n-3supplements provide some benefits for people with CF with relativelyfew adverse effects and thus their use is not discouraged
Further alterations in fatty acid metabolism have been highlight-ed including the consistent findings of an increase in circulatinglevels of saturated and monounsaturated fatty acids [7203204]Decreased levels of essential FA (EFA) ie the FA that have to be in-troduced with the diet correlates with the severity of respiratoryinsufficiency and the same clinical correlation was observed with al-tered proportions of FA species converted by the activity of desatur-ase enzymes (reviewed in [204]) The close relationship betweencertain fatty acids and oxidative stress including the negative correla-tion of C240 and linoleic acid with oxysterol levels point to the needof intensive investigation in CF patients of previously neglected lipidspecies that are emerging candidates in the control of metabolismQuantitative lipidomic analyses have lead to identify C161n7 palmi-toleate as a ldquoprotectiverdquo adipose-derived lipid hormone that stronglystimulates insulin activity in muscle and liver also suppressing in-flammatory cytokine output from mice fat cells [205] Specific meta-bolic activities have been also demonstrated by medium chainsaturated fatty acids caprylic acid (C80) capric acid (C100) and lau-ric acid (C120) Capric acid acts as a direct ligand of PPARγ using abinding pocket different from the binding pocket of thiazolidinedioneor long chain fatty acids [206] Additional activities of medium chainfatty acids which are ligands of free fatty acids receptors detectedin the immune cells the gastrointestinal tract and adipocytes maycontribute to metabolic homeostasis and inflammatory responses[207] These data underscore the importance of a lipid-mediated ldquoen-docrine networkrdquo demonstrating how specific alteration of one orfew serum lipids would be per se sufficient to influence metabolic ho-meostasis Given the relevance of this emerging information and thealteration of lipid metabolism and inflammatory status in CF fattyacid lipidomics need to be deeply investigated in CF
Again these studies have obvious nutritional implications Satu-rated fatty acids with chain lengths higher than C18 are poorlyabsorbed partly because they form insoluble calcium salts [208]Medium chain saturated fatty acids are well known for being highlyabsorbed through the intestine providing rapid delivery of energyvia oxidation of the more hydrophilic short chains and have beensuggested to provide proper nourishment in patients with CF [209]Recent studies have shown that consumption of a high-fat diet richin medium chain fatty acids as opposed to long chain fatty acidsdoes not lead to ectopic fat accumulation in skeletal muscle andliver of both rats and mice [210] In light of the close association be-tween nutritional status inflammation and life expectancy in CF pa-tients the manipulation of dietary lipids in these patients must befurther explored as a possible strategy to provide adequate nutritionand better management of oxidative stress
36 Hydrosoluble antioxidants oligoelements and enzymatic antioxidants
361 Vitamin CVitamin C status in CF patients has been poorly investigated Early
studies suggested a defective vitamin C status that was refractory tooral supplementation [211] Other and more recent studies showednormal or slightly decreased levels of vitamin C in CF patients as com-pared to healthy controls but age- and disease-related decline of thiswater-soluble antioxidant was reported in these patients [5212]In the study of Winklhofer-Roob et al [212] on mid-European CFpatients vitamin C concentrations decreased with age with an
estimated rate of 5 μmollyr and vitamin C concentrationsb40 μ-moll were associated with highest indexes of inflammation whichis consistent with the hypothesis that optimal levels of vitamin Cmay influence immuno-inflammatory activity of alveolar macro-phages and neutrophils Other few studies have examined the effectof supplements containing vitamin C on CF inflammation and oxida-tive stress since the levels of this vitamin do not significantly improvewith supplementation (reviewed in [213]) This highlights the com-mon fate that this hydrosoluble vitamin shares with several fat-soluble counterparts in the ldquomicronutrient paradoxrdquo of CF patients inwhich the need for a correction of their status along the progressionof the disease is frustrated by the poor efficacy of oral supplementa-tion protocols Formulations and appropriate supplementation proto-cols that may produce a better correction of vitamin C status of CFpatients are awaited for further clinical evaluation
362 Selenium and selenium-dependent peroxidasesSelenium is a trace element with marked electrophilicity [214]
that once converted to the organic form of Se-Cys can be introducedin protein structures to play its important role in H2O2 metabolismand signaling [215] As catalytic center of the enzyme GSH-peroxidase (SeGSH-Px) Se plays a crucial role to protect polyunsatu-rated lipids of plasma membrane and circulating lipoproteins formperoxidative insults With other Se-proteins such as the high molecu-lar weight thioredoxin reductases this oligoelement participates tothe control of protein thiol-disulfide oxidoreduction and glutathiony-lation which regulate signaling pathways of crucial importance in theregulation of immunity and inflammation [16] but also the function-ing of other redox-sensitive proteins such as the same CFTR [124]
The activity of SeGSH-Px in blood is considered a functional as-sessment of selenium status even if this assumption has some limita-tions related with the saturation profile that the Se stores show atincreasing doses of Se administration Investigations of the seleniumstatus in CF patients have produced conflicting findings which maydepend on differences in dietary intake ethnicity and environmentalfactors in the diverse patient populations (reviewed in [216217]) CFchildren have been reported to have lowered blood selenium and RBCSeGSH-Px activity [218219] normal plasma selenium and loweredRBC SeGSH-Px [220] and even normal levels of both these two param-eters [221] The supplementation with selenium in combination withother antioxidants was observed to increase the concentrations ofblood selenium that likewise β-carotene and fatty acid were posi-tively correlated with improved lung function [6]
Foucaud et al [218] observed that a defective selenium statuswas associated with lowered levels of other antioxidants that contrib-ute to the anti-peroxidative activity of this microelement such asvitamin E (reviewed in [222]) and the severity of this deficiencywas lower in children with pancreatic enzyme replacement and vita-min E supplementation
Treatments to substitute for exocrine pancreatic insufficiency bypancreatic enzymes from animal sources such as porcine pancreashave been confirmed to be a source of Se [220] These affects RBCSeGSH-Px activity and plasma selenium concentrations which hasto be taken into account when selenium supplements are given toCF patients
Selenium has been used to develop a series of organoseleniumcompounds that may open the way to new therapeutic opportunitiesin CF (see Section 392) These include GPX mimetic drugs and phaseII enzyme inducers which may provide higher antioxidant activity ofASL and cellular protection effects in the airways
363 Zinc and copperZinc and copper (Zn and Cu respectively) are present in many
proteins so that a deficiency of these trace metals could have pleiotro-pic effects in humans As regards antioxidant systems these two oli-goelements contribute an important role being cofactors of two
703F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
isoforms of the superoxide dismutase enzymes eg the extracellularform eg the EC-SOD or Sod 3 and the CundashZn-SOD or Sod 1 that isfound in several tissues and cells [223] The EC-SOD exerts its antiox-idant role also in the lining fluids of the airways [224]
The notion that CF patients have defective concentrations of bloodZn and Cu is controversial As far as Cu status is concerned few datahave been produced and are available in the literature suggestingthe notion that CF patients develop a moderate copper deficiency[225226] That was essentially demonstrated on the bases of a defec-tive activity of Cu-related proteins such as plasma ceruloplasmindiamine oxidase and RBC SOD This defect seems to be refractory toCu and Zn supplementation (see below)
More advanced studies have been carried out in the case of Zn sta-tus in CF Low plasma zinc concentrations were reported in approxi-mately 30 of young infants with CF identified by newbornscreening [227] and an impaired zinc homeostasis in CF patientswas described by Easley et al [228] This is characterized by poor con-servation of the endogenous pool with fecal loss and impaired frac-tional absorption of zinc which are the consequences of pancreaticinsufficiency and persisting steatorrhea These studies suggestedthat in the clinical management of CF patients these defects can beat least in part corrected by exocrine pancreatic enzyme replacement
A series of studies by Van Biervliet et al [229230] demonstratedin a Dutch population of CF infants and children that serum Zn variesin an age-dependent manner but remained unchanged with respectto healthy control levels In CF patients no difference in serum Zn con-centration between pancreatic-sufficient or pancreatic-insufficientpatients was observed and no correlation was found with the nutri-tional status or height z-score Importantly in these studies a signifi-cant correlation of serum Zn was observed with the fat solublevitamins A and E thus confirming the relationship between the ab-normalities of lipid and Zn metabolism in CF This suggests that co-supplementation of Zn and fat-soluble vitamins should be advisedin the presence of pancreatic insufficiency and persisting steatorrhea
Neve et al [219] in a study aimed to assess plasma and erythrocytezinc copper and selenium in CF children showed that mean plasmazinc and copper levels were not different from those in age-matched controls which confirms the observations by Van Biervlietet al described above However plasma zinc concentrations de-creased in patients with moderate-to-severe growth retardation andwith severe pulmonary disease but very low zinc levels occur sporad-ically Erythrocyte zinc and copper levels were significantly higherthan normal while RBC selenium was lower than in age-matchedcontrols These trace element concentrations in erythrocytes werediscussed in relation to the activities of the CuZn-SOD and the Se-enzyme GPx This observation suggests a compensatory upregulationof the erythrocyte CuZn-SOD by the exposure of erythroid precursorsto ROS andor other CF-related stressors
Best et al [225] also studied RBC SOD activity using this as a bio-logical sensor of Cu status in CF patients A lowered activity of thisenzyme was reported in CF together with that of the other Cu-dependent enzyme plasma diamine oxidase while plasma ceruplas-min showed normal activity Degradation rates of copper proteinsare known to be accelerated in conditions of copper deficiencywhich could explain the finding at least in part Anyway when Cuand Zn were supplemented to CF patients either separate or incombination (6 weeks of 3 mg copperd as copper-glycinate and30 mg zincd as zinc-glycinate) any of the copper enzyme activitieswas affected Therefore the moderate copper deficiency of CF patientsappears to be refractory to the intervention by increased copper andor zinc intake
Erythrocyte CuZn-SOD and the plasma levels of Cu and Zn werealso measured in the study of Wood et al [6] in which Australian CFpatients (agegt5 years) were treated with a high-dose antioxidantmultivitamin formulation containing 200 mg vitamin E (as RRR-α-tocopherol) 300 mg vitamin C (as sodium ascorbate) 25 mg β-
carotene (all-trans isomer) 90 μg Se (as selenomethionine) and500 μg vitamin A (as retinyl palmitate) in oil Plasma oligoelementsand particularly Zn were in the normal range at baseline (as com-pared with the data reported in [229230]) and were not affected bythis multivitamin supplement The same was found for the activityof RBC SOD and for plasma 8-iso-PGF2α as surrogate biomarker oflipid peroxidation
In a recent non-randomized small population (n=21) casendashcon-trol study in CF children Zn supplementation was proven to producepositive clinical effects in Zn-deficient patients [196] The supplemen-tation with 5 mgkg Zn sulfateday (maximum 150 mg) significantlydecreased the number of infections and increased the forced expira-tory volume in 1 s energy intake and growth parameters also im-proved These parameters were unaffected in untreated patientsexcept that in the case of the pulmonary function that decreased sig-nificantly These clinical observations on Zn supplementation need tobe confirmed in prospective double-blind randomized control trial
37 Appropriateness and targeting of antioxidant therapies in CF
The choice of the appropriate antioxidant and dose to correct a cer-tain biomarker and its associated biochemical lesion is another impor-tant point that appears to have disregarded in many clinical studiesFor instance unlike vitamin E vitamin C supplementation does notalter F2-IsoPs levels in humans (reviewed in [74]) This appears tobe true also in the antioxidant therapy of CF in which vitamin C(300 mgday) was administered together with other antioxidantsthat included a dose of vitamin E of 200 mgday without any signifi-cant effect on the surrogate biomarker of lipid peroxidation F2-IsoPs[6] When carotenoids are used as supplements to prevent the damag-ing action of ROS in the CF airways it is noteworthy that these are notparticularly good quenchers of peroxyl radicals relative to phenolicsand other antioxidants but are exceptional in quenching singlet oxy-gen at which most other phenolics and antioxidants are relativelyineffective Singlet oxygen is not a radical and does not react via radi-cal mechanisms but reacts mostly by the addition to double bondsforming endoperoxides that can be reduced to alkoxyl radicals that ini-tiate radical chain reactions typical of the peroxidative damage of PUFA[38] In this case the analysis of F2-IsoPs lipid peroxide formation andtransition metal-induced oxidizability of lipoproteins [162180] are allappropriate to evaluate the effect of carotenoids in preventing lipidperoxidation
As far as the dose is concerned clinical pharmacology of vitamin Eas an antioxidant was recently investigated by means of the effect onF2-IsoPs production and doses of α-tocopherol of 1600 IUday orgreater were found to be required to statistically affect plasma F2-IsoPs levels in hypercholeterolemic subjects [176] Several vitamin Esupplementation studies in CF patients have been performed withdoses of lower than 300 IUday regardless of the lowered absorptionby pancreatic and liver defects and the regular supplementationwith these doses does not appear to correct lipid oxidation markersin CF [7]
In the clinical practice and planning trials it has to be taken intoconsideration that in spite of substantial evidence supporting ahigher antioxidant demand in CF interventions with several antioxi-dant formulations produce poor responsiveness particularly in thecase of fat-soluble antioxidants which are poorly absorbed [6162]
Since many oxidants and antioxidants are present in tissuesand biological fluids and these have different chemical and physicalcharacteristics the possibility to produce a successful therapy witha single antioxidant molecule is too far to be realistic Moreover an-tioxidants act by multiple mechanisms in a single system or by adifferent single mechanism depending on the reaction systemresponding in a different manner to different radical or oxidantsources Because multiple reaction characteristics and mechanismsas well as different phase localizations are usually involved no single
704 F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
therapeutic approach will effectively prevent damage by multipleROS sources The defect of physiological antioxidants may also interferewith antioxidant therapies that are based on one or few exogenousantioxidants
Moreover several antioxidant vitamins such as vitamin E and ca-rotenoids have multiple natural forms with different bioavailabilitymetabolism and bioactivity [157167231] As far as the case of vita-min E supplementation concerns α-tocopherol was used as uniquevitamer in the large majority of supplementation trials so far per-formed and is the form used in the nutritional management of CFpatients Moreover several supplements contain the synthetic (or ra-cemic) form of this vitamin that has lower bioavailability than thenatural form Other forms present in nature and abundantly con-tained in vegetables such as tocotrienols and the less methylatedforms of tocopherol are not represented in many of the supplementformulations so far available in clinical centers and the supplementa-tion with α-tocopherol also limits their bioavailability These formsshow markedly higher susceptibility to hepatic metabolism and bili-ary excretion with respect to α-tocopherol eg the most representedform in blood and solid tissues and if co-supplemented these areeasily displaced during liver uptake and excreted with bile bymeans of competition with the same α-tocopherol Notwithstandingthese minor forms have been proposed to play important physiolog-ical roles showing molecular characteristics transcriptional effectsand antioxidant activities that clearly differentiate them in subfam-ilies with distinct biological functions Some of these such as α-tocopherol eg the second vitamin E form as relative abundance inblood and its carboxyethyl-hydroxychroman metabolite [189] ap-pear to have health-related anti-inflammatory effects which are par-ticularly relevant in lung protection [232233] This has suggestedthat such a group of ldquonon-α-tocopherolrdquo forms may represent anoth-er family of vitamins within the family of vitamin E with an impor-tant but often missed contribution to the proposed health effects ofthis vitamin [163]
These aspects may thus limit the possibility to provide CF patientsof optimal levels of this vitamin in all its components even if they areregularly treated with a vitamin E supplement eg withα-tocopherol
Targeted antioxidant therapy with formulations with higher bio-availability and bioactivity has been anticipated in CF New antioxi-dant formulations have been proposed to overcome main limits ofantioxidant therapies so far proposed for these patients Water-miscible α-tocopheryl acetate containing polysorbate propylene gly-col or polyethylene glycol as emulsifiers form micellar structureswere suggested to providing greater bioavailability than the fat-soluble counterparts These were commercialized with the brandnames of E-viminreg Cremophorreg EL and Aquasolreg E but despitethe original positive expectation [234235] some studies failed to ob-serve a higher response in vitamin E levels when these were com-pared with fat-soluble formulations [236237]
In a pilot study by Papas et al [183] a micellar formulation of fat-soluble nutrients and antioxidants was found to improve plasmalevels of β-carotene γ-tocopherol and CoQ(10) reducing at thesame time some inflammatory markers in induced sputum eg mye-loperoxidase and to a lower extent PMN elastase and total cell countswhile lung function and sputum bacterial counts were unaffectedThe same group recently confirmed the possibility to increase the ab-sorption of fat-soluble micronutrients using formulations with higherbioavailability specifically designed for malabsorbing patients such asCF patients that include also vitamin K and commercialized with thebrand name of AquADEKsreg [162] Despite improved vitamin and mi-cronutrient levels in this non-randomized open-label study AquA-DEKsreg produced only modest improvements in weight percentileand pulmonary function Another recent pilot observation [182] hassuggested the beneficial effect of this formulation on antioxidant andoxidative stress parameters of this oral supplement that surely deservesmore clinical investigation by larger randomized controlled trials
Recent multivitaminic formulations have been designed to containalso the minor forms of vitamin E and specifically γ-tocopherol [238]the expected superiority of which with respect to formulations con-taining only α-tocopherol needs to be verified As discussed abovein the section dedicated to vitamin E further advancements in thetherapy of CF inflammation and oxidative stress could be based onsynthetic forms and natural metabolites of this vitamin that havebeen recently identified to possess higher antioxidant and also anti-inflammatory activity than α-tocopherol (reviewed in [163168])
Pre-clinical investigation of these and other fat-soluble agents iscurrently addressed to develop formulations and administration pro-tocols that may increase the therapeutic efficacy in the airways In theantioxidant therapy of lung dysfunction in CF local administrationprotocols may overcome the limits of oral and systemic administra-tion protocols increasing bioavailability and providing targetedapproach to inflammation and oxidative stress Aerosolization of vita-min E and other fat-soluble micronutrients is possible and may allowdirect administration in the airways to prevent toxicity of smokewhich is closely associated with inflammation and oxidative stress[164165] To our knowledge this as well as other strategies of localadministration such as instillation of solutions such as surfactant-like solutions enriched of vitamin E have not been previously inves-tigated in CF patients and other CF model systems
On the contrary inhalation is an administration route widelyadopted in the case of GSH and NAC therapy described above Inthis context Cys formulations alternative to NAC have been proposedfor use as antioxidant and anti-inflammatory agent for inhalationNacystelyn is a lysine adduct of NAC that thanks to a higher proton-ation equilibrium shows increased water solubility and thus betterbioavailability Nacystelyn has been described to influence IL-8 gener-ation and the inflammatory signaling of bronchial epithelial cells[239] and preliminary clinical evaluation has demonstrated the safetyof this drug [240] Further clinical trials aimed to assess the effect onlung symptomatology of CF patients are needed Direct administra-tion in the airways could also be adopted for micronutrient vitaminswith poor absorption and bioavailability due to GI defects
38 Clinical impact of antioxidant therapy in CF
Huge in vitro and pre-clinical evidence has provided the rationaleto support clinical investigation of antioxidant strategies in CF Theseshould aim to restore the oxidantndashantioxidant balance of CF airwaychallenged by chronic infection and inflammatory cell activation
Some observational trials have confirmed that antioxidants usedas either supplements to the diet or drugs for lung administrationby aerosolized formulations may help in relieving progressive lungdamage and other adverse clinical events of CF such as poor growthSo far few studies have examined with sufficient methodologicalrigor the clinical efficacy of antioxidant therapy in CF This was alsoconcluded in a previous review of the literature by Cantin et al [12]that was published in the beginning of 2006 and is confirmed alsoin a recent analysis of clinical trials on antioxidant therapy in CF pa-tients [213] that examined the literature until September 2010using as sources the databases of the Cochrane CF and Genetic Disor-ders Group CF Trials Register PubMed CINAHL and AMED Useful in-formation was retrieved from just four randomized controlled trialsand one quasi-randomized controlled trial on vitamin C vitamin Eβ-carotene and selenium used as supplements administered aloneor in combination Post-hoc data analysis that was possible only inthree studies on a total of 87 CF patients showed the absence ofany significant improvement in lung function that was selected as pri-mary outcome together with quality of life that improved in one trialSecondary outcomes concerning laboratory indices of oxidative stressand antioxidant status showed several improvements These includedan increase of RBC SeGPx by selenium supplementation done as
705F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
individual or combined supplementation and increased levels of allplasma antioxidants except vitamin C that were observed in all thetrials
The message from these studies to pediatricians and nutritionistswithin the clinical staff of CF centers is that in the absence of solid ev-idence regarding the clinical effectiveness of oral formulations of an-tioxidant supplements in CF (including PUFA) their use as a routineclinical practice should be considered with caution keeping clear inmind that this should represent just a complement of one of themost critical interventions in the life-long clinical management pro-gram of CF patients eg providing an adequate nutriture [140] Inthis context compensating energy and protein malnutrition has toremain the first goal of nutritional management programs Providinghigher intakes of antioxidant micronutrients with food naturally-enriched (or functionalized) of micronutrient antioxidants shouldbe preferred in order to have the higher combination of positive nu-tritional factors that are lost during refinement procedures and over-all industrial processing of dietary supplements
Measures of good practice in clinical management of micro-malnutrition in CF patients would include the support of specializedpersonnel and laboratories The centers should have the possibilityto ascertain with appropriate nutritional and laboratory tests whatthe level of deficiency is for the different micronutrients that each pa-tient may suffer from during a dietary program Monitoring dietaryintakes and blood levels of micronutrients is not sufficient to set apersonalized nutritional intervention with supplements or functionalfoods Sub-optimal intakes and the compliance to nutritional inter-ventions should be verified by means of selected biochemical andclinical criteria Unluckily the latter are still not well established forsome micronutrients such as the fat-soluble vitamins E (reviewed in[163173241]) and K [242243] and also for trace elements such asSe [244] For many of the antioxidants used as supplements inhumans we still do not know exactly several of the biological effectsthat these may provide when introduced in a healthy body and weknow less what these can do in disease These aspects hardly impacton the concept of optimal levels of intake that should be identified foreach micronutrient on an individual basis According with the aspectsdiscussed in the previous sections optimal levels of intake for antiox-idant micronutrients are different in CF patients and healthy subjectsand vary with age and several individual factors
Lung administration of antioxidants by means of aerosolized for-mulations so far used for GSH therapy (see above) is a promisingfield of clinical investigation in CF Toxicity issues are currently themain concern and the subject of clinical evaluation by several groups(described above)
Information on future directions of antioxidant therapy in CF canbe inferred by the analysis of pending or recently completed clinicaltrials that have been searched (December 2011) at ClinicalTrialsgovdatabase matching the terms ldquoantioxidant therapyrdquo or ldquoglutathionerdquowith ldquocystic fibrosisrdquo Fifteen trials were retrieved and those directlyrelated to antioxidant therapy (n=12) are presented in Table 1 andinclude efficacy and safety studies of inhaled drugs as GSH sodiumpyruvate NAC and NO and the dietary supplements AquADEKsregan antioxidant-rich multivitamin supplement epigallocatechin gal-late (EGCG)tocotrienol curcuminoids the amino acid glutaminesulforaphane in broccoli sprouts One trial is investigating the flavo-noid quercetin as CFTR modulator
39 Emerging antioxidant and anti-inflammatory approaches in CF
Mediterranean foods such as olive oil and red wine or severalplant extracts such as herbal tea or grape seed extracts contain aseries of natural compounds with important antioxidant and NOscavenging activity that have been widely investigated for the pre-vention of oxidative stress-related diseases [38245] These havebeen long investigated as template molecules to develop antioxidant
and anti-inflammatory drugs Between the multitudes of natural sub-stances most investigated ones include for instance tyrosol hydroxy-tyrosol gallic and caffeic acids belonging to the family of phenolswhile resveratrol of the stilbenes family epicatechin kaempferoland cianidin are examples of flavonoids examples of fat-soluble phe-nolics are those of the family of tocols (vitamin E) and carotenoids Allthese compounds show different metabolisms and signaling effects[246] Antioxidant and cell protection mechanisms are associatedwith different and sometimes concurrent processes as H-atom trans-fer and electron donation radical trapping and chelation of transitionmetals that can be easily investigated at the chemical level [247] Be-sides these direct antioxidant effects metabolic responses and signal-ing effects of natural compounds are also important to producesecond-generation responses that modify the level of antioxidantprotection and the potential for ROS detoxification in cells and bodyfluids These derive from the transcriptional regulation of antioxidantand pro-oxidant genes that coexist with the modulation of cytokinesecretion and inflammatory enzyme activities
Some of these natural plant-derived antioxidants may provide fur-ther pharmacological activities of possible relevance in CF This is thecase for instance of the plant flavonoids genistein apigenin kaemp-ferol quercetin and hesperidin [248ndash251] that fall in the pharmaco-logical category of ldquopotentiatorsrdquo [252] in that these activate at leastto a certain extent CTFR-mediated Cl currents in normal and CF airwayepithelium investigated either in vitro or in vivo in humans and ani-mal models Actually as prototypal flavonoid-derived potentiatorthe tyrosine kinase inhibitor genistein potentiates the gating of wild-type as well as ΔF508 CFTR and G551D CFTR [253] but at higherdoses it inhibits CFTR gating which make this an unlikely clinical can-didate Similar potentiation effects have been reported for the antiox-idant curcumin [250] that shows an additive effect with respect togenistein-induced potentiation Besides CFTR potentiation whichdoes not appear to have a direct influence on GSH and nutrient trans-port in the lung tissue all these natural substances have been usedalone or in combination with other agents as in vivo enhancers oflung antioxidant protection [246254255] In the case of quercetinthiol-reactive phenolic [256] bronchodilation and anti-inflammatoryeffects by a restoration of the Th1Th2 balance have been reportedin inflammatory syndromes of the lung [255257ndash259] but theseeffects have not been explored in CF Pyocyanin toxicity (see abovein the Section 2) could represent an issue for the use of quercetinand other catechols in infectious diseases of the lung [260]
Other natural antioxidants of potential interest in CF therapy in-clude terpenoids [261] such as terpinen-4-ol a major constituentof tea tree oil that is being investigated in the therapy of anti-biotic resistant organisms specifically against methicillin-resistantStaphylococcus aureus (MRSA) [262] a problem in CF [263] Otherthan being lipophilic antioxidants terpenes can prevent oxidativestress of the CF lung secondarily to the antibiotic effect thereby pro-moting a better control of immuno-inflammatory pathways and lungantioxidants
391 Targeting NF-κB with natural compounds resveratrol and plantextracts
Natural compounds were long known to be useful in designinganti-inflammatory drugs and some of these could find an applicationin the control of the transcription factor kappa-B (NF-κB) that maylead to develop advanced pharmacological tools to control inflamma-tion and to produce higher antioxidant protection to CF airwaysInhibitors targeting NF-κB including transcription factors decoymolecules (TFD) are potent down-regulators of gene expressionand release of IL-8 in CF cells infected with P aeruginosa [264265]
Resveratrol (354prime-trihydroxystilbene ldquoErdquo form) is one of the mostinvestigated natural antioxidant with proposed activity as NF-κBinhibitor This is a phytoalexin present in large quantity in red winepreferentially in the skin of grapes being its concentration
706 F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
50ndash100 μgmg of fresh skin and 13ndash3 mgl of red wine [266]Furthermore resveratrol is a constituent of lsquoDarakchasavarsquo (13ndash6 mgl) an ayurvedic medicine from India [267] The antioxidant activity ofresveratrol has been reported in several papers and occurs also in lungtissues suggesting that resveratrol has potential as a therapeuticagent in respiratory disease [268ndash270] Resveratrol can be consideredone of the most interesting molecules from the natural worldexhibiting strong antioxidant activity that at the same time is able toexert anti inflammatory activity through alteration of NF-κB functionsand efficient inhibition of pro-inflammatory genes [271272] As far asthe effects on CF model systems are concerned Cabrini et al [26]reported the effects of resveratrol on P aeruginosa infected CF IB3-1cells The results obtained demonstrate that resveratrol exhibits minoreffects of IB3-1 cell growth and important inhibitory effects on accumu-lation of IL-8 and GRO-α mRNA while minor effects on IL-6 gene ex-pression were observed These data support recently publishedobservations suggesting inhibitory effects of resveratrol in infection-mediated inflammatory processes [273] Interestingly resveratrol hasbeen reported as a potent inhibitor of NF-κB activity and a promisinganti-inflammatory agent [272274] also in combinationwith othermol-ecules [274275] However in vivo translation of this pre-clinical on res-veratrol is hard to be foreseen This natural compound displays poorbioavailability [276] and further characterization of resveratrol pharma-cokinetics is troublesome since it is hardly measurable in vivo [277]Furthermore the regulation of inflammatory responses by resveratrolhas been suggested to be far more complex than simple direct suppres-sion of NF-κB activity Actually some aspects of the immune responsecould be enhanced by this natural substance which may lead tohypothesize broad negative feedback events on immuno-inflammatorypathways [278] In any case and with these cautions in mind the pub-lished observations on cellular model systems support the concept thatresveratrol and resveratrol-containing formulations deserve further con-sideration to determine their possible therapeutic values in CF
Other inhibitors can be identified from systematic studies of naturalproducts and their ability to interfere with NF-κB activity [279ndash281]Recent studies have demonstrated that the whole extract of Aeglemarmelos (Rutaceae) has strong inhibitory effect on the P aeruginosa-dependent IL-8 induction in human CF-derived bronchial IB3-1 cellswithout affecting cell proliferation [280] Molecular analysis of compo-nents contained in A marmelos extracts revealed that three major com-pounds namely 56-dimethoxy-1-indanone 2-hydroxy-cinnamic acidand 5-methoxy psoralen (5-MOP) reproduce the inhibitory effect ob-servedwith thewhole extract [280] A further example has been recent-ly published using extracts from bergamot (Citrus bergamia Risso) Inthis study the extracts were characterized and the main detected con-stituents were assayed for their biological activity [281] The resultsobtained demonstrated that the extracts from bergamot epicarps con-tain components displaying an inhibitory activity on IL-8 Particularlythe most active molecules were bergapten and citropten These effectshave been confirmed by analyzing mRNA levels and protein release inthe CF cellularmodels IB3-1 and CuFi-1 inducedwith TNF-α or exposedto P aeruginosa
A parallel strategy linking NF-κB inhibition and down-regulationof NF-κB-dependent functions is described in recently publishedstudies based on a structured-based virtual screening (VS) of differ-ently substituted furocoumarins and analogues against NF-κB withthe objective of selecting molecules able to inhibit the binding ofthis transcription factor to DNA [282283] Novel compounds wereidentified with this strategy as potent inhibitors of NF-κB dependentbiological functions to be proposed for the control lung inflammationoccurring in patients affected by CF [282ndash284]
392 Scavengers and regulators of H2O2 and NO
3921 Lactoferrin and OSCNmacr The impaired DUOXLPO system of CFpatients could be the target of therapeutic strategies that may
produce concomitant antimicrobial and antioxidant effects This sys-tem described above in Section 22 represents an important compo-nent of innate immunity with a role in bactericidal defense andregulation of H2O2 metabolism of airways [32] CF patients have alsoreported to show lowered LF levels in the ASL [37] that togetherwith a CFTR-dependent defective efflux of SCNmacr and LPO [36] may cre-ate the environment for a sustained flux of H2O2 and for the genera-tion of highly reactive Fenton species [1138] An ideal therapeuticintervention should restore the LPO-dependent generation of bacteri-cidal OSCNmacr from DUOX-derived H2O2 and SCNmacr in the ASL to controlat the same time the microbial biofilm and the flux of H2O2 into theASL An approach close to this therapeutic mechanism was recentlyproposed for the drug Meveolreg This is a complex of LF and OSCNmacrwith proposed in vivo antimicrobial activity [285] to be evaluatedin clinical trials for the aerosol treatment of lung infections in CFpatients The role for this drug in the control of H2O2 levels of ASLremains to be investigated
3922 Organoselenium compounds Organoselenium compoundshave been proposed as therapeutic agents useful in the antioxidanttherapy of inflammatory conditions These include GPX mimetic mol-ecules such as Ebselenreg (2-phenyl-12-benzisoselenazol-3(2H)-one)or other and more recently developed molecules that are still inpre-clinical steps of evaluation [286] Selectively and specificity of ac-tion are main issues in the therapeutic mechanism of this candidateantioxidant drug that thanks to the electrophilic properties of Se[214] reacts with thiols to reduce H2O2 and other species MoreoverEbselenreg has been described to act as potent non-competitive inhib-itor of extracellular nucleoside diphosphokinase (NDPK) having neg-ligible effect on ecto-ATPase and adenyl kinase activities which areother players of the metabolism of extracellular nucleotides [287]This enzyme together with other nucleoside di- and triphosphatescontributes to regulate several components of the mucociliary clear-ance process (MCC) that protects the lung against infections via acti-vation of epithelial purinergic receptors The inhibition of NDPK bythis GPX-mimetic drug may also impact on the energy status of endo-thelial cells [287] This aspect could be further investigated as a cellu-lar protection mechanism in the pulmonary epithelium of CF patientsbeing the control of cell energy of fundamental importance to preventthe activation of death pathways [288]
Further therapeutic mechanisms for these Se-derived drugs mayderive from the marked activity as inducers of phase II enzymessuch as quinone reductase (QR) and glutathione-S-transferase (GST)[289] This induction response also observed with other electrophilsand redox-active molecules such as natural phenolic antioxidantscould produce higher cellular protection by the acquisition of anincreased capability to detoxify endobiotics generated during oxida-tive stress and inflammation [246]
3923 Melatonin and GSNO as NOx regulators Increased markers ofNO-derived biological damage are present in the CF lung suggestingthe abnormal reactivity of NOx in the inflamed lung of CF patients[52] However an impaired metabolism and biological function ofNO in CF airways (see Section 23) suggests a cautious approach tothe use of agents that may influence the levels and chemical behaviorof NO-derived species (NOx) with possible impact on the physiologi-cal roles of NO in vasodilatation innate immunity and H2O2 metabo-lism of the respiratory tract [290291] NO donors also appear toinfluence CFTR function of alveolar epithelium and gland serouscells [292293]
Main physiological role of the pineal gland hormone melatonin isthe synchronization of circadian rhythms including the sleepndashwakecycle but several other functions dealing with immunomodulatoryantioxidant and cellular protection effects have been identified[294] Melatonin receptor stimulation may also influence cyclic AMPsignaling and the regulation of CFTR ion channel [295296]
707F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
A recent randomized double-blind placebo-controlled study hasexamined the effects of short term melatonin administration (3 mgfor 3 weeks) on sleep and oxidative stress markers in CF [297]According with the expected pharmacological effect of this hormonalsubstance the treatment was successful in improving sleep indicesAt the same time nitrite levels determined in exhaled breath conden-sate (EBC) were reduced to suggest a better control of NOmetabolismof CF airways (discussed above in Section 23) but these effects how-ever were not associated with a significant correction of isoprostaneas lipid peroxidation marker measured in EBC Increasing dosages ofmelatonin could be investigated for the pharmacological treatmentof oxidative stress and immune dysfunction of CF patients due tothe absence of adverse effects of this hormonal substance in humans
The S-nitrosation reaction of thiols is another interesting aspect ofNO pharmacology [53] that may find an application in the therapy oflung complications of CF This has been the case for instance of theS-nitrosothiol GSNO that has been used safely in human trials[298299] This endogenous nitrosothiol with proposed regulatory ef-fect on the CFTR of lung epithelia [292293] is well tolerated in pa-tients with CF when administered by aerosolization and mayproduce better oxygenation [299] thereby suggesting that therapyaimed at restoring endogenous GSNO levels in the CF airway maymerit further clinical evaluation Since the administered GSNO de-composes as shown by the increased levels of expired NO in CF pa-tients under treatment with this nitrosothiol [299] furtherinvestigation should be addressed to ascertain whether GSNO thera-py may merely correspond to a GSH therapy
NO dependent effects on CFTR function should be considered toevaluate mechanism of action and specificity of antioxidant therapiesthat target NO metabolism and function in the CF airways
4 Conclusions and future perspectives
The presence of clinical and biochemical symptoms of inflammationand oxidative stress implies that CF patients have a higher demand ofantioxidant protection The combination of the dysfunctional CFTRwith a lowered intake and absorption of dietary antioxidants producesub-optimal levels of protection from both enzymatic and non-enzymatic defense systems The former could be associated with a de-fective glutathionemetabolism and lowered intake of sulfur-containingamino acids and oligoelements such as zinc and possibly seleniumwhile fat-soluble antioxidant vitamins such as vitamin E and caroten-oids and the water-soluble vitamin C are lowered than in healthy sub-jects due to malabsorption and possibly higher consumption
The increased antioxidant demand in CF patients should be evenhigher in the presence of complications of the lung pancreas andliver Lung comorbidity is particularly important in this contextbeing associated with recurrent infections which results in the alter-nation of inflammatory exacerbates and chronic inflammation Thesesustain the flux of ROS in the airways and promote the formation ofsecond-generation byproducts by the damage of biomolecules suchas PUFA and proteins which may diffuse also at the systemic level tofurther promote adverse biological responses and toxic reactions Pan-creatic insufficiency causes malnutrition and may lead to develop en-docrine and metabolic defects associated with diabetes of CF Theseevents can be further aggravated by the concomitance of liver dys-function and a poor nutritional status Malnutrition is strongly associ-ated with poor prognosis as assessed by pulmonary function andsurvival data [138ndash140] The more aggressive nutritional interven-tions seem to produce better clinical outcomes in these patients andthe possibility of achieving higher antioxidant protection in well-nourished patients by dietary factors could be a key aspect to explainsuch a clinical advantage The assumption that food-derived compo-nentsmay help to prevent the damaging effects of oxidative stress im-proving the antioxidant defenses deserves further investigation at theclinical level This together with the investigation of appropriate
laboratory biomarkers could provide critical information to establishintervention criteria for an early nutritional management of newly di-agnosed patients [5] It is expected that a timely secondary preventionstrategy could influence the progression of CF symptoms thusaffecting with a self-feeding mechanism the same extent of malnutri-tion and oxidative stress along the life of CF patients Since severalfactors contribute to impair the nutritional status of CF patients(such as pancreatic insufficiency chronic malabsorption recurrentsinopulmonary infections and progressive lung disease chronic in-flammation increased energy expenditure suboptimal intake multi-therapy) careful monitoring of the antioxidant status should berecommended According with international guidelines fat-solublevitamin supplementation is of utmost importance in daily practice to-gether with energy intake requirements and pancreatic enzyme-replacement therapy Among these vitamin E β-carotene and ω-3FA have observed to alleviate selected biochemical signs of oxidativestress as measured for instance with well established laboratory indi-ces of lipid peroxidation and in some studies these effects werepreliminarily associated with positive clinical outcomes Notwith-standing randomizedndashcontrolled clinical trials on antioxidant supple-ments (including ω-3 FA) so far carried out in CF have failed toconclusively demonstrate significant beneficial effects on respiratorysymptoms and on the consequent impact that these have on the qual-ity of life of these patients (reviewed in [202213]) whichmay provideno support for the use of these supplements in CF An absence of effi-cacy in prevention studies on antioxidant supplements has also beenobserved in other and possibly less severe oxidative stress-relatedconditions particularly in the secondary prevention of cardiovasculardisease and some forms of cancer by vitamin E and other antioxidantssuch as vitamin C selenium and β-carotene (reviewed in [163]) Dif-ferent biases however have been identified in randomize large clini-cal trials that may account for these disappointing findings Theseinclude patient selection criteria (early interventions and primaryprevention could have more chances of success than secondaryprevention) duration and doses of the treatment use of wrong anti-oxidant formulations and administration protocols absence of verifi-cations of the biological compliance to the treatment etc The samebiases apply for the few trials carried out in CF patients Thus the ap-propriateness and efficacy of nutritional interventions with naturalfood-derived or synthetic antioxidants should be verifiedwith respectto the biological pathways of oxidative stress and clinical variablesthat are identified as end-points Profiles of blood and tissue antioxi-dants as well as of reliable surrogate markers of oxidative stresshave to be selected and determined in highly specialized laboratorieswith a well-established experience on these analyses
Well-timed (early) interventions with appropriate antioxidantformulationsprotocols need to be proposed for the next generationof trials and the development of novel CF-tailored antioxidant andanti-inflammatory agents should be promoted
As a consequence of these considerations more clinical investiga-tion is awaited to identify future successful approaches to the antiox-idant therapy as a measure to further enhance quality of life and theoverall clinical outcome of CF patients
Acknowledgments
We are indebted with the Italian Cystic Fibrosis Research Founda-tion for the support that it provided with its grant program to the re-search activity of the authors of this paper This is a scientific initiativeof the ldquoWorking Group on Inflammation in Cystic Fibrosisrdquo (BragonziA Bravo E Cabrini G Conese M Cuzzocrea S Dechecchi MC De Ales-sandri A Evangelista V Galli F Gambari R Lambiase A Lucidi VManca A Melotti P Minicucci L Motta A Pietraforte D Pompella AQuattrucci S Rizzo R Romano M Sorio C Tesse R) of the Italian Soci-ety for Cystic Fibrosis A particular thank goes to the Prof GianniMastella for the critical revision of the manuscript and for the
708 F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
stimulating research environment that he has contributed to createwithin the Italian Cystic Fibrosis Research Foundation
References
[1] BP OSullivan SD Freedman Cystic fibrosis Lancet 373 (2009) 1891ndash1904[2] P Linsdell JW Hanrahan Glutathione permeability of CFTR Am J Physiol 275
(1998) C323ndashC326[3] L Gao KJ Kim JR Yankaskas HJ Forman Abnormal glutathione transport in
cystic fibrosis airway epithelia Am J Physiol 277 (1999) L113ndashL118[4] RK Rowntree A Harris The phenotypic consequences of CFTR mutations Ann
Hum Genet 67 (2003) 471ndash485[5] EI Back C Frindt D Nohr J Frank R Ziebach M Stern M Ranke HK Biesalski
Antioxidant deficiency in cystic fibrosis when is the right time to take actionAm J Clin Nutr 80 (2004) 374ndash384
[6] LG Wood DA Fitzgerald AK Lee ML Garg Improved antioxidant and fattyacid status of patients with cystic fibrosis after antioxidant supplementation islinked to improved lung function Am J Clin Nutr 77 (2003) 150ndash159
[7] L Iuliano R Monticolo G Straface S Zullo F Galli M Boaz S Quattrucci Asso-ciation of cholesterol oxidation and abnormalities in fatty acid metabolism incystic fibrosis Am J Clin Nutr 90 (2009) 477ndash484
[8] C Libetta V Sepe P Esposito F Galli A Dal Canton Oxidative stress and inflam-mation implications in uremia and hemodialysis Clin Biochem 44 (2011)1189ndash1198
[9] G Bartosz Reactive oxygen species destroyers or messengers Biochem Phar-macol 77 (2009) 1303ndash1315
[10] T Ntimbane B Comte G Mailhot Y Berthiaume V Poitout M Prentki RRabasa-Lhoret E Levy Cystic fibrosis-related diabetes from CFTR dysfunctionto oxidative stress Clin Biochem 30 (2009) 153ndash177
[11] A van der Vliet JP Eiserich GP Marelich B Halliwell CE Cross Oxidativestress in cystic fibrosis does it occur and does it matter Adv Pharmacol 38(1997) 491ndash513
[12] AM Cantin TB White CE Cross HJ Forman RJ Sokol D Borowitz Antioxi-dants in cystic fibrosis Conclusions from the CF antioxidant workshop Bethes-da Maryland Free Radic Biol Med 42 (2007) 15ndash31
[13] LT McGrath P Mallon L Dowey B Silke E McClean M McDonnell A DevineS Copeland S Elborn Oxidative stress during acute respiratory exacerbations incystic fibrosis Thorax 54 (1999) 518ndash523
[14] E Thomson S Brennan R Senthilmohan CL Gangell AL Chapman PD SlyAJ Kettle E Balding LJ Berry JB Carlin R Carzino N de Klerk T Douglas CFoo LW Garratt GL Hall J Harrison A Kicic IA Laing KM Logie J MassieLS Mott C Murray F Parsons N Pillarisetti SR Poreddy SC RanganathanCF Robertson R Robins-Browne PJ Robinson B Skoric SM Stick ENSutanto E Williamson Identifying peroxidases and their oxidants in the earlypathology of cystic fibrosis Free Radic Biol Med 49 (2010) 1354ndash1360
[15] SP Range C Dunster AJ Knox FJ Kelly Treatment of pulmonary exacerba-tions of cystic fibrosis leads to improved antioxidant status Eur Respir J 13(1999) 560ndash564
[16] L Coppo P Ghezzi Thiol regulation of pro-inflammatory cytokines and innateimmunity protein S-thiolation as a novel molecular mechanism Biochem SocTrans 39 (2011) 1268ndash1272
[17] C Verhaeghe C Remouchamps B Hennuy A Vanderplasschen A Chariot SPTabruyn C Oury V Bours Role of IKK and ERK pathways in intrinsic inflamma-tion of cystic fibrosis airways Biochem Pharmacol 73 (2007) 1982ndash1994
[18] TL Bonfield JR Panuska MW Konstan KA Hilliard JB Hilliard H Ghnaim MBerger Inflammatory cytokines in cystic fibrosis lungs Am J Respir Crit CareMed 152 (1995) 2111ndash2118
[19] TL Noah HR Black PW Cheng RE Wood MW Leigh Nasal and bronchoal-veolar lavage fluid cytokines in early cystic fibrosis J Infect Dis 175 (1997)638ndash647
[20] MJ Welsh BW Ramsey FJ Accurso GR Cutting Cystic Fibrosis McGraw-HillNew York 2001
[21] TZ Khan JS Wagener T Bost J Martinez FJ Accurso DW Riches Early pul-monary inflammation in infants with cystic fibrosis Am J Respir Crit CareMed 151 (1995) 1075ndash1082
[22] FA Ratjen Cystic fibrosis pathogenesis and future treatment strategies RespirCare 54 (2009) 595ndash605
[23] J Jacquot O Tabary P Le Rouzic A Clement Airway epithelial cell inflamma-tory signalling in cystic fibrosis Int J Biochem Cell Biol 40 (2008)1703ndash1715
[24] CM Greene P Branagan NG McElvaney Toll-like receptors as therapeutic tar-gets in cystic fibrosis Expert Opin Ther Targets 12 (2008) 1481ndash1495
[25] M Rottner JM Freyssinet MC Martinez Mechanisms of the noxious inflam-matory cycle in cystic fibrosis Respir Res 10 (2009) 23
[26] G Cabrini V Bezzerri I Mancini E Nicolis MC Dechecchi A Tamanini ILampronti L Piccagli N Bianchi M Borgatti R Gambari Targeting transcrip-tion factor activity as a strategy to inhibit pro-inflammatory genes involved incystic fibrosis decoy oligonucleotides and low-molecular weight compoundsCurr Med Chem 17 (2010) 4392ndash4404
[27] CM Greene NG McElvaney Proteases and antiproteases in chronic neutrophiliclungdiseasemdash relevance to drug discovery Br J Pharmacol 158 (2009) 1048ndash1058
[28] AM Cantin Potential for antioxidant therapy of cystic fibrosis Curr Opin PulmMed 10 (2004) 531ndash536
[29] JF Chmiel MW Konstan Inflammation and anti-inflammatory therapies forcystic fibrosis Clin Chest Med 28 (2007) 331ndash346
[30] DP Nichols MW Konstan JF Chmiel Anti-inflammatory therapies for cys-tic fibrosis-related lung disease Clin Rev Allergy Immunol 35 (2008)135ndash153
[31] AJ Kettle T Chan I Osberg R Senthilmohan AL Chapman TJ Mocatta JSWagener Myeloperoxidase and protein oxidation in the airways of youngchildren with cystic fibrosis Am J Respir Crit Care Med 170 (2004)1317ndash1323
[32] H Fischer Mechanisms and function of DUOX in epithelia of the lung AntioxidRedox Signal 11 (2009) 2453ndash2465
[33] B Rada TL Leto Oxidative innate immune defenses by NoxDuox familyNADPH oxidases Contrib Microbiol 15 (2008) 164ndash187
[34] P Moskwa D Lorentzen KJ Excoffon J Zabner PB McCray Jr WM NauseefC Dupuy B Banfi A novel host defense system of airways is defective in cysticfibrosis Am J Respir Crit Care Med 175 (2007) 174ndash183
[35] D Lorentzen L Durairaj AA Pezzulo Y Nakano J Launspach DA Stoltz GZamba PB McCray Jr J Zabner MJ Welsh WM Nauseef B Banfi Concentra-tion of the antibacterial precursor thiocyanate in cystic fibrosis airway secre-tions Free Radic Biol Med 50 (2011) 1144ndash1150
[36] Y Xu S Szep Z Lu The antioxidant role of thiocyanate in the pathogenesis ofcystic fibrosis and other inflammation-related diseases Proc Natl Acad Sci US A 106 (2009) 20515ndash20519
[37] MP Rogan CC Taggart CM Greene PG Murphy SJ ONeill NG McElvaneyLoss of microbicidal activity and increased formation of biofilm due to decreasedlactoferrin activity in patients with cystic fibrosis J Infect Dis 190 (2004)1245ndash1253
[38] B Halliwell JM Guttridge Free Radicals in Biology and Medicine Fourth editionOxford University Press New York 2007
[39] B Rada K Lekstrom S Damian C Dupuy TL Leto The Pseudomonastoxin pyocyanin inhibits the dual oxidase-based antimicrobial system as itimposes oxidative stress on airway epithelial cells J Immunol 181 (2008)4883ndash4893
[40] C Schwarzer B Illek JH Suh SJ Remington H Fischer TE Machen Organelleredox of CF and CFTR-corrected airway epithelia Free Radic Biol Med 43(2007) 300ndash316
[41] JH Roum R Buhl NG McElvaney Z Borok RG Crystal Systemic deficiency ofglutathione in cystic fibrosis J Appl Physiol 75 (1993) 2419ndash2424
[42] VM Hudson Rethinking cystic fibrosis pathology the critical role of abnormalreduced glutathione (GSH) transport caused by CFTR mutation Free RadicBiol Med 30 (2001) 1440ndash1461
[43] PJ Barnes RA Dweik AF Gelb PG Gibson SC George H Grasemann IDPavord F Ratjen PE Silkoff DR Taylor N Zamel Exhaled nitric oxide in pul-monary diseases a comprehensive review Chest 138 (2010) 682ndash692
[44] H Grasemann E Michler M Wallot F Ratjen Decreased concentration of ex-haled nitric oxide (NO) in patients with cystic fibrosis Pediatr Pulmonol 24(1997) 173ndash177
[45] H Grasemann F Ratjen Cystic fibrosis lung disease the role of nitric oxidePediatr Pulmonol 28 (1999) 442ndash448
[46] B Gaston F Ratjen JW Vaughan NR Malhotra RG Canady AH Snyder JFHunt S Gaertig JB Goldberg Nitrogen redox balance in the cystic fibrosis air-way effects of antipseudomonal therapy Am J Respir Crit Care Med 165(2002) 387ndash390
[47] H Grasemann I Ioannidis RP Tomkiewicz H de Groot BK Rubin F RatjenNitric oxide metabolites in cystic fibrosis lung disease Arch Dis Child 78(1998) 49ndash53
[48] H Grasemann R Schwiertz S Matthiesen K Racke F Ratjen Increased argi-nase activity in cystic fibrosis airways Am J Respir Crit Care Med 172(2005) 1523ndash1528
[49] H Grasemann S Al-Saleh JA Scott D Shehnaz A Mehl R Amin M Rafii PPencharz J Belik F Ratjen Asymmetric dimethylarginine contributes to airwaynitric oxide deficiency in patients with cystic fibrosis Am J Respir Crit CareMed 183 (2011) 1363ndash1368
[50] H Grasemann F Kurtz F Ratjen Inhaled L-arginine improves exhaled nitricoxide and pulmonary function in patients with cystic fibrosis Am J RespirCrit Care Med 174 (2006) 208ndash212
[51] H Grasemann F Ratjen Emerging therapies for cystic fibrosis lung disease Ex-pert Opin Emerg Drugs 15 (2010) 653ndash659
[52] BM Morrissey K Schilling JV Weil PE Silkoff DM Rodman Nitric oxide andprotein nitration in the cystic fibrosis airway Arch Biochem Biophys 406(2002) 33ndash39
[53] R Radi Nitric oxide oxidants and protein tyrosine nitration Proc Natl AcadSci U S A 101 (2004) 4003ndash4008
[54] J Chen M Kinter S Shank C Cotton TJ Kelley AG Ziady Dysfunction of Nrf-2in CF epithelia leads to excess intracellular H2O2 and inflammatory cytokineproduction PLoS One 3 (2008) e3367
[55] F Galli M Piroddi C Annetti C Aisa E Floridi A Floridi Oxidative stress andreactive oxygen species Contrib Nephrol 149 (2005) 240ndash260
[56] DT Wright LA Cohn H Li B Fischer CM Li KB Adler Interactions of oxygenradicals with airway epithelium Environ Health Perspect 102 (Suppl 10)(1994) 85ndash90
[57] I Rahman SR Yang SK Biswas Current concepts of redox signaling in thelungs Antioxid Redox Signal 8 (2006) 681ndash689
[58] Q Li JF Engelhardt Interleukin-1beta induction of NFκB is partially regulatedby H2O2-mediated activation of NFκB-inducing kinase J Biol Chem 281(2006) 1495ndash1505
709F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
[59] E Boncoeur VS Criq E Bonvin T Roque A Henrion-Caude DC Gruenert AClement J Jacquot O Tabary Oxidative stress induces extracellular signal-regulated kinase 12 mitogen-activated protein kinase in cystic fibrosis lung ep-ithelial cells potential mechanism for excessive IL-8 expression Int J BiochemCell Biol 40 (2008) 432ndash446
[60] B Fischer J Voynow Neutrophil elastase induces MUC5AC messenger RNA ex-pression by an oxidant-dependent mechanism Chest 117 (2000) 317Sndash320S
[61] B Rada P Gardina TG Myers TL Leto Reactive oxygen species mediate in-flammatory cytokine release and EGFR-dependent mucin secretion in airwayepithelial cells exposed to Pseudomonas pyocyanin Mucosal Immunol 4(2011) 158ndash171
[62] C Schwarzer H Fischer EJ Kim KJ Barber AD Mills MJ Kurth DC GruenertJH Suh TE Machen B Illek Oxidative stress caused by pyocyanin impairs CFTRClminus transport in human bronchial epithelial cells Free Radic Biol Med 45(2008) 1653ndash1662
[63] J Hull M South P Phelan K Grimwood Surfactant composition in infants andyoung children with cystic fibrosis Am J Respir Crit Care Med 156 (1997)161ndash165
[64] KC Meyer A Sharma R Brown M Weatherly FR Moya J Lewandoski JJZimmerman Function and composition of pulmonary surfactant andsurfactant-derived fatty acid profiles are altered in young adults with cystic fi-brosis Chest 118 (2000) 164ndash174
[65] MK Pulfer RC Murphy Formation of biologically active oxysterols during ozo-nolysis of cholesterol present in lung surfactant J Biol Chem 279 (2004)26331ndash26338
[66] V Starosta E Rietschel K Paul U Baumann M Griese Oxidative changes ofbronchoalveolar proteins in cystic fibrosis Chest 129 (2006) 431ndash437
[67] V Starosta M Griese Oxidative damage to surfactant protein D in pulmonarydiseases Free Radic Res 40 (2006) 419ndash425
[68] M Griese R Essl R Schmidt E Rietschel F Ratjen M Ballmann K Paul Pulmo-nary surfactant lung function and endobronchial inflammation in cystic fibro-sis Am J Respir Crit Care Med 170 (2004) 1000ndash1005
[69] M Griese R Essl R Schmidt M Ballmann K Paul E Rietschel F Ratjen Se-quential analysis of surfactant lung function and inflammation in cystic fibrosispatients Respir Res 6 (2005) 133
[70] LG Wood DA Fitzgerald PG Gibson DM Cooper ML Garg Increased plasmafatty acid concentrations after respiratory exacerbations are associated with el-evated oxidative stress in cystic fibrosis patients Am J Clin Nutr 75 (2002)668ndash675
[71] P Montuschi SA Kharitonov G Ciabattoni M Corradi L van Rensen DM Ged-des ME Hodson PJ Barnes Exhaled 8-isoprostane as a new non-invasive bio-marker of oxidative stress in cystic fibrosis Thorax 55 (2000) 205ndash209
[72] CE Collins P Quaggiotto L Wood EV OLoughlin RL Henry ML Garg Elevat-ed plasma levels of F2 alpha isoprostane in cystic fibrosis Lipids 34 (1999)551ndash556
[73] D Hartl V Starosta K Maier I Beck-Speier C Rebhan BF Becker P Latzin RFischer F Ratjen RM Huber E Rietschel S Krauss-Etschmann M Griese In-haled glutathione decreases PGE2 and increases lymphocytes in cystic fibrosislungs Free Radic Biol Med 39 (2005) 463ndash472
[74] GL Milne H Yin JD Morrow Human biochemistry of the isoprostane pathwayJ Biol Chem 283 (2008) 15533ndash15537
[75] G Ciabattoni G Davi M Collura L Iapichino F Pardo A Ganci R Romagnoli JMaclouf C Patrono In vivo lipid peroxidation and platelet activation in cystic fi-brosis Am J Respir Crit Care Med 162 (2000) 1195ndash1201
[76] C Garenc P Julien E Levy Oxysterols in biological systems the gastrointestinaltract liver vascular wall and central nervous system Free Radic Res 44 (2011)47ndash73
[77] AM Cantin SL North RC Hubbard RG Crystal Normal alveolar epithelial lin-ing fluid contains high levels of glutathione J Appl Physiol 63 (1987) 152ndash157
[78] R Tirouvanziam CK Conrad T Bottiglieri LA Herzenberg RB Moss High-dose oral N-acetylcysteine a glutathione prodrug modulates inflammation incystic fibrosis Proc Natl Acad Sci U S A 103 (2006) 4628ndash4633
[79] LW Velsor C Kariya R Kachadourian BJ Day Mitochondrial oxidative stressin the lungs of cystic fibrosis transmembrane conductance regulator proteinmutant mice Am J Respir Cell Mol Biol 35 (2006) 579ndash586
[80] M Kelly-Aubert S Trudel J Fritsch T Nguyen-Khoa M Baudouin-Legros SMoriceau L Jeanson F Djouadi C Matar M Conti M Ollero F Brouillard AEdelman GSH monoethyl ester rescues mitochondrial defects in cystic fibrosismodels Hum Mol Genet 20 (2011) 2745ndash2759
[81] P Ghezzi Role of glutathione in immunity and inflammation in the lung Int JGen Med 4 (2011) 105ndash113
[82] N Dauletbaev K Viel R Buhl TO Wagner J Bargon Glutathione and glutathi-one peroxidase in sputum samples of adult patients with cystic fibrosis J CystFibros 3 (2004) 119ndash124
[83] CE Cross A van der Vliet CA ONeill S Louie B Halliwell Oxidants antioxi-dants and respiratory tract lining fluids Environ Health Perspect 102 (Suppl10) (1994) 185ndash191
[84] K Takeyama K Dabbagh J Jeong Shim T Dao-Pick IF Ueki JA Nadel Oxida-tive stress causes mucin synthesis via transactivation of epidermal growth factorreceptor role of neutrophils J Immunol 164 (2000) 1546ndash1552
[85] N Ballatori SM Krance S Notenboom S Shi K Tieu CL Hammond Glutathi-one dysregulation and the etiology and progression of human diseases BiolChem 390 (2009) 191ndash214
[86] SR Soltaninassab KR Sekhar MJ Meredith ML Freeman Multi-faceted regu-lation of gamma-glutamylcysteine synthetase J Cell Physiol 182 (2000)163ndash170
[87] HR Lopez-Mirabal JR Winther Redox characteristics of the eukaryotic cytosolBiochim Biophys Acta 1783 (2008) 629ndash640
[88] C Hwang AJ Sinskey HF Lodish Oxidized redox state of glutathione in the en-doplasmic reticulum Science 257 (1992) 1496ndash1502
[89] M Murphy Mitochondrial thiols in antioxidant protection and redox signallingdistinct roles for glutathionylation and other thiol modifications AntioxidRedox Signal (2011) ahead of print doi101089ars20114289
[90] BJ Day AM van Heeckeren E Min LW Velsor Role for cystic fibrosis trans-membrane conductance regulator protein in a glutathione response to bronch-opulmonary Pseudomonas infection Infect Immun 72 (2004) 2045ndash2051
[91] Y Zhang K Duan Glutathione exhibits antibacterial activity and increases tetra-cycline efficacy against Pseudomonas aeruginosa Sci China C Life Sci 52 (2009)501ndash505
[92] VM Hudson New insights into the pathogenesis of cystic fibrosis pivotal roleof glutathione system dysfunction and implications for therapy Treat RespirMed 3 (2004) 353ndash363
[93] LW Velsor A van Heeckeren BJ Day Antioxidant imbalance in the lungs ofcystic fibrosis transmembrane conductance regulator protein mutant miceAm J Physiol Lung Cell Mol Physiol 281 (2001) L31ndashL38
[94] I Kogan M Ramjeesingh C Li JF Kidd Y Wang EM Leslie SP Cole CE BearCFTR directly mediates nucleotide-regulated glutathione flux EMBO J 22(2003) 1981ndash1989
[95] NS Gould S Gauthier CT Kariya E Min J Huang DJ Brian Hypertonic salineincreases lung epithelial lining fluid glutathione and thiocyanate two protectiveCFTR-dependent thiols against oxidative injury Respir Res 11 (2010) 119
[96] VT Vasu SJ de Cruz JS Houghton KA Hayakawa BM Morrissey CE CrossJP Eiserich Evaluation of thiol-based antioxidant therapeutics in cystic fibrosissputum focus on myeloperoxidase Free Radic Res 45 (2011) 165ndash176
[97] L Roussel G Martel J Berube S Rousseau P aeruginosa drives CXCL8 synthesisvia redundant toll-like receptors and NADPH oxidase in CFTRF508 airway epi-thelial cells J Cyst Fibros 10 (2011) 107ndash113
[98] GW Lau DJ Hassett H Ran F Kong The role of pyocyanin in Pseudomonas aer-uginosa infection Trends Mol Med 10 (2004) 599ndash606
[99] R Wilson DA Sykes D Watson A Rutman GW Taylor PJ Cole Measurementof Pseudomonas aeruginosa phenazine pigments in sputum and assessment oftheir contribution to sputum sol toxicity for respiratory epithelium InfectImmun 56 (1988) 2515ndash2517
[100] M Muller Pyocyanin induces oxidative stress in human endothelial cells andmodulates the glutathione redox cycle Free Radic Biol Med 33 (2002)1527ndash1533
[101] YQ OMalley KJ Reszka BE Britigan Direct oxidation of 2prime7prime-dichlorodihy-drofluorescein by pyocyanin and other redox-active compounds independentof reactive oxygen species production Free Radic Biol Med 36 (2004)90ndash100
[102] CC Caldwell Y Chen HS Goetzmann Y Hao MT Borchers DJ Hassett LRYoung D Mavrodi L Thomashow GW Lau Pseudomonas aeruginosa exotoxinpyocyanin causes cystic fibrosis airway pathogenesis Am J Pathol 175 (2009)2473ndash2488
[103] YQ OMalley KJ Reszka DR Spitz GM Denning BE Britigan Pseudomonasaeruginosa pyocyanin directly oxidizes glutathione and decreases its levels inairway epithelial cells Am J Physiol Lung Cell Mol Physiol 287 (2004)L94ndashL103
[104] M Muller Glutathione modulates the toxicity of but is not a biologically rele-vant reductant for the Pseudomonas aeruginosa redox toxin pyocyanin FreeRadic Biol Med 50 (2011) 971ndash977
[105] R Cheluvappa R Shimmon M Dawson SN Hilmer DG Le Couteur Reactionsof Pseudomonas aeruginosa pyocyanin with reduced glutathione Acta BiochimPol 55 (2008) 571ndash580
[106] JH Widdicombe Transgenic animals may help resolve a sticky situation in cys-tic fibrosis J Clin Invest 120 (2010) 3093ndash3096
[107] X Sun H Sui JT Fisher Z Yan X Liu HJ Cho NS Joo Y Zhang W Zhou Y YiJM Kinyon DC Lei-Butters MA Griffin P Naumann M Luo J Ascher KWang T Frana JJ Wine DK Meyerholz JF Engelhardt Disease phenotype ofa ferret CFTR-knockout model of cystic fibrosis J Clin Invest 120 (2010)3149ndash3160
[108] NS Joo HJ Cho M Khansaheb JJ Wine Hyposecretion of fluid from trachealsubmucosal glands of CFTR-deficient pigs J Clin Invest 120 (2010) 3161ndash3166
[109] A Bragonzi Murine models of acute and chronic lung infection with cystic fibro-sis pathogens IJMM 300 (2010) 584ndash593
[110] AM van Heeckeren MD Schluchter Murine models of chronic Pseudomonasaeruginosa lung infection Lab Anim 36 (2002) 291ndash312
[111] A Bragonzi D Worlitzsch GB Pier P Timpert M Ulrich M Hentzer JB Ander-sen M Givskov M Conese G Doring Nonmucoid Pseudomonas aeruginosa ex-presses alginate in the lungs of patients with cystic fibrosis and in a mousemodel J Infect Dis 192 (2005) 410ndash419
[112] GS CW Bedrossian DB Singer JJ Hansen HS Rosenberg The lung in cysticfibrosis A quantitative study including prevalence of pathologic findingsamong different age groups Hum Pathol 7 (1976) 195ndash204
[113] WD HA Cash B McCullough WG Johanson Jr JA Bass A rat model of chron-ic respiratory infection with Pseudomonas aeruginosa Am Rev Respir Dis 119(1979) 453ndash459
[114] EM JR Starke C Langston CJ Baker A mouse model of chronic pulmonary in-fection with Pseudomonas aeruginosa and Pseudomonas cepacia Pediatr Res 22(1987) 698ndash702
[115] TJ AM van Heeckeren RW Walenga MW Konstan PB Davis B ErokwuMA Haxhiu TW Ferkol Effect of Pseudomonas infection on weight loss lung
710 F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
mechanics and cytokines in mice Am J Respir Crit Care Med 161 (2000)271ndash279
[116] T Aw G Wierzbicka DP Jones Oral glutathione increases tissue glutathione invivo Chem Biol Interact 80 (1991) 89ndash97
[117] F Favilli P Marraccini T Iantomasi MT Vincenzini Effect of orally adminis-tered glutathione on glutathione levels in some organs of rats role of specifictransporters Br J Nutr 78 (1997) 293ndash300
[118] C Kariya H Leitner E Min C van Heeckeren A van Heeckeren BJ Day A rolefor CFTR in the elevation of glutathione levels in the lung by oral glutathione ad-ministration Am J Physiol Lung Cell Mol Physiol 292 (2007) L1590ndashL1597
[119] K Atkuri JJ Mantovani LA Herzenberg LA Herzenberg N-Acetylcysteinemdashasafe antidote for cysteineglutathione deficiency Curr Opin Pharmacol 7(2007) 355ndash359
[120] R De Lisle E Roach K Jansson Effects of laxative and N-acetylcysteine onmucus accumulation bacterial load transit and inflammation in the cystic fi-brosis mouse small intestine Am J Physiol Gastrointest Liver Physiol 293(2007) G577ndashG584
[121] A Luciani VR Villella S Esposito N Brunetti-Pierri D Medina C Settembre MGavina L Pulze I Giardino M Pettoello-Mantovani M DApolito S Guido EMasliah B Spencer S Quaratino V Raia A Ballabio L Maiuri Defective CFTRinduces aggresome formation and lung inflammation in cystic fibrosis throughROS-mediated autophagy inhibition Nat Cell Biol 12 863ndash875
[122] M Griese J Ramakers A Krasselt V Starosta S Van Koningsbruggen R FischerF Ratjen B Mullinger RM Huber K Maier E Rietschel G Scheuch Improve-ment of alveolar glutathione and lung function but not oxidative state in cysticfibrosis Am J Respir Crit Care Med 169 (2004) 822ndash828
[123] C Bishop VM Hudson SC Hilton C Wilde A pilot study of the effect of inhaledbuffered reduced glutathione on the clinical status of patients with cystic fibro-sis Chest 127 (2005) 308ndash317
[124] WWang C Oliva G Li A Holmgren CH Lillig KL Kirk Reversible silencing of CFTRchloride channels by glutathionylation J Gen Physiol 125 (2005) 127ndash141
[125] N Dauletbaev P Fischer B Aulbach J Gross W Kusche U Thyroff-FriesingerTO Wagner J Bargon A phase II study on safety and efficacy of high-dose N-acetylcysteine in patients with cystic fibrosis Eur J Med Res 14 (2009)352ndash358
[126] R Tirouvanziam Y Gernez CK Conrad RB Moss I Schrijver CE Dunn ZADavies LA Herzenberg Profound functional and signaling changes in viable in-flammatory neutrophils homing to cystic fibrosis airways Proc Natl Acad SciU S A 105 (2008) 4335ndash4339
[127] JH Roum Z Borok NG McElvaney GJ Grimes AD Bokser R Buhl RG Crys-tal Glutathione aerosol suppresses lung epithelial surface inflammatory cell-derived oxidants in cystic fibrosis J Appl Physiol 87 (1999) 438ndash443
[128] A Visca CT Bishop SC Hilton VM Hudson Improvement in clinical markersin CF patients using a reduced glutathione regimen an uncontrolled observa-tional study J Cyst Fibros 7 (2008) 433ndash436
[129] EF Nash A Stephenson F Ratjen E Tullis Nebulized and oral thiol derivativesfor pulmonary disease in cystic fibrosis Cochrane Database Syst Rev (2009)CD007168
[130] AC foundation Drug Development Pipeline 2011[131] S Hoshida T Kuzuya N Yamashita M Nishida S Kitahara M Hori T
Kamada M Tada Gamma-glutamylcysteine ethyl ester for myocardial protec-tion in dogs during ischemia and reperfusion J Am Coll Cardiol 24 (1994)1391ndash1397
[132] J Lok W Leung S Zhao S Pallast K van Leyen S Guo X Wang A Yalcin EHLo Gamma-glutamylcysteine ethyl ester protects cerebral endothelial cells dur-ing injury and decreases bloodndashbrain barrier permeability after experimentalbrain trauma J Neurochem 118 (2011) 248ndash255
[133] Z Borok R Buhl GJ Grimes AD Bokser RC Hubbard KJ Holroyd JH RoumDB Czerski AM Cantin RG Crystal Effect of glutathione aerosol on oxidantndashantioxidant imbalance in idiopathic pulmonary fibrosis Lancet 338 (1991)215ndash216
[134] KJ Holroyd R Buhl Z Borok JH Roum AD Bokser GJ Grimes D Czerski AMCantin RG Crystal Correction of glutathione deficiency in the lower respiratorytract of HIV seropositive individuals by glutathione aerosol treatment Thorax 48(1993) 985ndash989
[135] J Hull P Vervaart K Grimwood P Phelan Pulmonary oxidative stress responsein young children with cystic fibrosis Thorax 52 (1997) 557ndash560
[136] A Corti A Paolicchi M Franzini S Dominici AF Casini A Pompella The S-thiolating activity of membrane gamma-glutamyltransferase formation ofcysteinyl-glycine mixed disulfides with cellular proteins and in the cell microen-vironment Antioxid Redox Signal 7 (2005) 911ndash918
[137] A Corti M Franzini AF Casini A Paolicchi A Pompella Vitamin C supply tobronchial epithelial cells linked to glutathione availability in elfmdasha role for se-creted gamma-glutamyltransferase J Cyst Fibros 7 (2008) 174ndash178
[138] A Munck Nutritional considerations in patients with cystic fibrosis Expert RevRespir Med 4 (2010) 47ndash56
[139] JL Matel CE Milla Nutrition in cystic fibrosis Semin Respir Crit Care Med 30(2009) 579ndash586
[140] D Salvatore R Buzzetti E Baldo MP Forneris V Lucidi D Manunza IMarinelli B Messore AS Neri V Raia ML Furnari G Mastella An overviewof international literature from cystic fibrosis registries 2 Neonatal screeningand nutritiongrowth J Cyst Fibros 9 (2010) 75ndash83
[141] KF Joosten JM Hulst Malnutrition in pediatric hospital patients current is-sues Nutrition 27 (2011) 133ndash137
[142] S Fustik T Jacovska L Spirevska S Koceva Protein-energy malnutrition as thefirst manifestation of cystic fibrosis in infancy Pediatr Int 51 (2009) 678ndash683
[143] J Himmelfarb E McMonagle Albumin is the major plasma protein target of ox-idant stress in uremia Kidney Int 60 (2001) 358ndash363
[144] P Stenvinkel JJ Carrero J Axelsson B Lindholm O Heimburger Z MassyEmerging biomarkers for evaluating cardiovascular risk in the chronic kidneydisease patient how do new pieces fit into the uremic puzzle Clin J Am SocNephrol 3 (2008) 505ndash521
[145] M Roche P Rondeau NR Singh E Tarnus E Bourdon The antioxidant proper-ties of serum albumin FEBS Lett 582 (2008) 1783ndash1787
[146] D Giustarini A Milzani I Dalle-Donne R Rossi Red blood cells as a physiolog-ical source of glutathione for extracellular fluids Blood Cells Mol Dis 40 (2008)174ndash179
[147] A Meister ME Anderson Glutathione Annu Rev Biochem 52 (1983) 711ndash760[148] B Alvarez S Carballal L Turell R Radi Formation and reactions of sulfenic acid
in human serum albumin Methods Enzymol 473 (2010) 117ndash136[149] S Carballal B Alvarez L Turell H Botti BA Freeman R Radi Sulfenic acid in
human serum albumin Amino Acids 32 (2007) 543ndash551[150] LR Barclay AM Bailey D Kong The antioxidant activity of alpha-tocopherol-
bovine serum albumin complex in micellar and liposome autoxidations J BiolChem 260 (1985) 15809ndash15814
[151] T Ishii T Ichikawa K Minoda K Kusaka S Ito Y Suzuki M Akagawa K Mochi-zuki T Goda T Nakayama Human serum albumin as an antioxidant in the ox-idation of (minus)-epigallocatechin gallate participation of reversible covalentbinding for interaction and stabilization Biosci Biotechnol Biochem 75(2011) 100ndash106
[152] F Galli S Rovidati S Benedetti U Buoncristiani C Covarelli A Floridi F Canes-trari Overexpression of erythrocyte glutathione S-transferase in uremia and di-alysis Clin Chem 45 (1999) 1781ndash1788
[153] D Borowitz RD Baker V Stallings Consensus report on nutrition for pediat-ric patients with cystic fibrosis J Pediatr Gastroenterol Nutr 35 (2002)246ndash259
[154] LJ Filer Jr SW Wright MP Manning KE Mason Absorption of alpha-tocopherol and tocopherylesters by premature and full term infants and chil-dren in health and disease Pediatrics 8 (1951) 328ndash339
[155] L Lancellotti C DOrazio G Mastella G Mazzi U Lippi Deficiency of vitamins Eand A in cystic fibrosis is independent of pancreatic function and current en-zyme and vitamin supplementation Eur J Pediatr 155 (1996) 281ndash285
[156] MN Sathe AS Patel Update in pediatrics focus on fat-soluble vitamins NutrClin Pract 25 (2010) 340ndash346
[157] MG Traber The ABCs of vitamin E and beta-carotene absorption Am J ClinNutr 80 (2004) 3ndash4
[158] TF Dolan Jr Hemolytic anemia and edema as the initial signs in infants withcystic fibrosis Consider this diagnosis even in absence of pulmonary symptomsClin Pediatr 15 (1976) 597ndash600
[159] DR James M Alfaham MC Goodchild Increased susceptibility to peroxide-induced haemolysis with normal vitamin E concentrations in cystic fibrosisClin Chim Acta 204 (1991) 279ndash290
[160] SA Peters FJ Kelly Vitamin E supplementation in cystic fibrosis J Pediatr Gas-troenterol Nutr 22 (1996) 341ndash345
[161] A Maqbool VA Stallings Update on fat-soluble vitamins in cystic fibrosis CurrOpin Pulm Med 14 (2008) 574ndash581
[162] SD Sagel MK Sontag MM Anthony P Emmett KA Papas Effect of anantioxidant-rich multivitamin supplement in cystic fibrosis J Cyst Fibros 10(2011) 31ndash36
[163] F Galli A Azzi Present trends in vitamin E research Biofactors 36 (2010)33ndash42
[164] A Hamahata P Enkhbaatar ER Kraft M Lange SW Leonard MG Traber RACox FC Schmalstieg HK Hawkins EB Whorton EM Horvath C Szabo LDTraber DN Herndon DL Traber Gamma-tocopherol nebulization by a lipidaerosolization device improves pulmonary function in sheep with burn andsmoke inhalation injury Free Radic Biol Med 45 (2008) 425ndash433
[165] JP Anais N Razzouq M Carvalho C Fernandez A Astier M Paul A AstierH Fessi AM Lorino Development of alpha-tocopherol acetate nanoparti-cles influence of preparative processes Drug Dev Ind Pharm 35 (2009)216ndash223
[166] JM Zingg Molecular and cellular activities of vitamin E analogues Mini RevMed Chem 7 (2007) 543ndash558
[167] V Viola F Pilolli M Piroddi E Pierpaoli F Orlando M Provinciali M Betti FMazzini F Galli Why tocotrienols work better insights into the in vitro anti-cancer mechanism of vitamin E Genes Nutr 7 (2011) 29ndash41
[168] F Galli F Mazzini L Bamonti L Gille S Bohmdorfer M Piroddi T Netscher FJKelly T Rosenau Tocotrienamines and tocopheramines reactions with radicalsand metal ions Bioorg Med Chem 19 (2011) 6483ndash6491
[169] A Kuhad K Chopra Attenuation of diabetic nephropathy by tocotrienol in-volvement of NFκB signaling pathway Life Sci 84 (2009) 296ndash301
[170] Q Jiang X Yin MA Lill ML Danielson H Freiser J Huang Long-chain carbox-ychromanols metabolites of vitamin E are potent inhibitors of cyclooxygenasesProc Natl Acad Sci U S A 105 (2008) 20464ndash20469
[171] ER Miller III R Pastor-Barriuso D Dalal RA Riemersma LJ Appel E GuallarMeta-analysis high-dosage vitamin E supplementation may increase all-causemortality Ann Intern Med 142 (2005) 37ndash46
[172] JN Hathcock A Azzi J Blumberg T Bray A Dickinson B Frei I Jialal CSJohnston FJ Kelly K Kraemer L Packer S Parthasarathy H Sies MG TraberVitamins E and C are safe across a broad range of intakes Am J Clin Nutr 81(2005) 736ndash745
[173] R Brigelius-Flohe F Galli Vitamin E a vitamin still awaiting the detection of itsbiological function Mol Nutr Food Res 54 (2010) 583ndash587
711F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
[174] MG Traber B Frei JS Beckman Vitamin E revisited do new data validate ben-efits for chronic disease prevention Curr Opin Lipidol 19 (2008) 30ndash38
[175] F Galli Meeting report Vitamin E Satellite Symposium (VESS) associated to theAnnual Meeting of the SFRR-Europe Rome 26 August 2009 Free Radic Res 43(2009) 1256ndash1257
[176] LJ Roberts II JA Oates MF Linton S Fazio BP Meador MD Gross Y Shyr JDMorrow The relationship between dose of vitamin E and suppression of oxida-tive stress in humans Free Radic Biol Med 43 (2007) 1388ndash1393
[177] EFSA- EFSA Scientific Opinion of the Panel on Food Additives FlavouringsProcessing Aids and Materials in Contact with Food on a request from the Com-mission on mixed tocopherols tocotrienol tocopherol and tocotrienols assources for vitamin E in EFSA- EFSA (Ed) vol 640 The EFSA Journal2008 pp 1ndash34
[178] P Rust I Eichler S Renner I Elmadfa Long-term oral beta-carotene supple-mentation in patients with cystic fibrosis mdash effects on antioxidative status andpulmonary function Ann Nutr Metab 44 (2000) 30ndash37
[179] G Lepage J Champagne N Ronco A Lamarre I Osberg RJ Sokol CC Roy Sup-plementation with carotenoids corrects increased lipid peroxidation in childrenwith cystic fibrosis Am J Clin Nutr 64 (1996) 87ndash93
[180] BM Winklhofer-Roob H Puhl G Khoschsorur MA vant Hof H EsterbauerDH Shmerling Enhanced resistance to oxidation of low density lipoproteinsand decreased lipid peroxide formation during beta-carotene supplementationin cystic fibrosis Free Radic Biol Med 18 (1995) 849ndash859
[181] RC Graham-Maar JI Schall N Stettler BS Zemel VA Stallings Elevated vita-min A intake and serum retinol in preadolescent children with cystic fibrosisAm J Clin Nutr 84 (2006) 174ndash182
[182] I Sadowska-Woda M Rachel J Pazdan E Bieszczad-Bedrejczuk K PawliszakNutritional supplement attenuates selected oxidative stress markers in pediatricpatients with cystic fibrosis Nutr Res (New York NY) 31 (2011) 509ndash518
[183] KA Papas MK Sontag C Pardee RJ Sokol SD Sagel FJ Accurso JS WagenerA pilot study on the safety and efficacy of a novel antioxidant rich formulation inpatients with cystic fibrosis J Cyst Fibros 7 (2008) 60ndash67
[184] Y Saito A Fukuhara K Nishio M Hayakawa Y Ogawa H Sakamoto K Fujii YYoshida E Niki Characterization of cellular uptake and distribution of coen-zyme Q10 and vitamin E in PC12 cells J Nutr Biochem 20 (2009) 350ndash357
[185] AA Franke CM Morrison JL Bakke LJ Custer X Li RV Cooney CoenzymeQ10 in human blood native levels and determinants of oxidation during proces-sing and storage Free Radic Biol Med 48 (2010) 1610ndash1617
[186] HN Bhagavan RK Chopra Plasma coenzyme Q10 response to oral ingestion ofcoenzyme Q10 formulations Mitochondrion 7 (2007) S78ndashS88 (Suppl)
[187] HN Bhagavan RK Chopra Coenzyme Q10 absorption tissue uptake metabo-lism and pharmacokinetics Free Radic Res 40 (2006) 445ndash453
[188] F Galli R Lee C Dunster FJ Kelly Gas chromatography mass spectrometryanalysis of carboxyethyl-hydroxychroman metabolites of alpha- and gamma-tocopherol in human plasma Free Radic Biol Med 32 (2002) 333ndash340
[189] F Galli R Lee J Atkinson A Floridi FJ Kelly Gamma-tocopherol biokineticsand transformation in humans Free Radic Res 37 (2003) 1225ndash1233
[190] TA Laguna MK Sontag I Osberg JS Wagener FJ Accurso RJ Sokol De-creased total serum coenzyme-Q10 concentrations a longitudinal study in chil-dren with cystic fibrosis J Pediatr 153 (2008) 402ndash407
[191] T Frischer JK Myung G Maurer I Eichler Z Szepfalusi G Lubec Possible dys-regulation of chaperon and metabolic proteins in cystic fibrosis bronchial tissueProteomics 6 (2006) 3381ndash3388
[192] C Andersson MM Zaman AB Jones SD Freedman Alterations in immune re-sponse and PPARLXR regulation in cystic fibrosis macrophages J Cyst Fibros 7(2008) 68ndash78
[193] SD Freedman PG Blanco MM Zaman JC Shea M Ollero IK Hopper DAWeed A Gelrud MM Regan M Laposata JG Alvarez BP OSullivan Associa-tion of cystic fibrosis with abnormalities in fatty acid metabolism N Engl JMed 350 (2004) 560ndash569
[194] S Van Biervliet G Vanbillemont JP Van Biervliet D Declercq E Robberecht AChristophe Relation between fatty acid composition and clinical status or geno-type in cystic fibrosis patients Ann Nutr Metab 51 (2007) 541ndash549
[195] SD Freedman MH Katz EM Parker M Laposata MY Urman JG AlvarezA membrane lipid imbalance plays a role in the phenotypic expression ofcystic fibrosis in cftr(minusminus) mice Proc Natl Acad Sci U S A 96 (1999)13995ndash14000
[196] S Van Biervliet S Vande Velde JP Van Biervliet E Robberecht The effect ofzinc supplements in cystic fibrosis patients Ann Nutr Metab 52 (2008)152ndash156
[197] WR Henderson Jr SJ Astley MM McCready P Kushmerick S Casey JWBecker BW Ramsey Oral absorption of omega-3 fatty acids in patients withcystic fibrosis who have pancreatic insufficiency and in healthy control subjectsJ Pediatr 124 (1994) 400ndash408
[198] I Durieu E Vericel D Guichardant H Roth JP Steghens J Drai RN JosserandE Fontaine M Lagarde G Bellon Fatty acids platelets and oxidative markersfollowing intravenous n-3 fatty acids administration in cystic fibrosis an openpilot observational study J Cyst Fibros 6 (2007) 320ndash326
[199] LG Wood DA Fitzgerald ML Garg Hypothesis vitamin E complements poly-unsaturated fatty acids in essential fatty acid deficiency in cystic fibrosis J AmColl Nutr 22 (2003) 253ndash257
[200] JD Lloyd-Still SB Johnson RT Holman Essential fatty acid status in cystic fi-brosis and the effects of safflower oil supplementation Am J Clin Nutr 34(1981) 1ndash7
[201] A Maqbool JI Schall JF Garcia-Espana BS Zemel B Strandvik VAStallings Serum linoleic acid status as a clinical indicator of essential fatty
acid status in children with cystic fibrosis J Pediatr Gastroenterol Nutr 47(2008) 635ndash644
[202] C Oliver N Jahnke Omega-3 fatty acids for cystic fibrosis Cochrane DatabaseSyst Rev (2011) CD002201
[203] B Strandvik E Gronowitz F Enlund T Martinsson J Wahlstrom Essential fattyacid deficiency in relation to genotype in patients with cystic fibrosis J Pediatr139 (2001) 650ndash655
[204] P Rise S Volpi C Colombo RF Padoan C DOrazio S Ghezzi PMelotti V BennatoC Agostoni BM Assael C Galli Whole blood fatty acid analysis with micromethodin cystic fibrosis and pulmonary disease J Cyst Fibros 9 (2010) 228ndash233
[205] H Cao K Gerhold JR Mayers MM Wiest SM Watkins GS Hotamisligil Iden-tification of a lipokine a lipid hormone linking adipose tissue to systemic me-tabolism Cell 134 (2008) 933ndash944
[206] RR Malapaka SK Khoo J Zhang JH Choi XE Zhou Y Xu Y Gong J Li ELYong MJ Chalmers L Chang JH Resau PR Griffin YE Chen HE Xu Iden-tification and mechanism of a ten carbon fatty acid as a modulating ligand ofperoxisome proliferator activated receptors J Biol Chem 287 (2012)183ndash195
[207] T Hara A Hirasawa A Ichimura I Kimura G Tsujimoto Free fatty acid recep-tors FFAR1 and GPR120 as novel therapeutic targets for metabolic disorders JPharm Sci 100 (2011) 3594ndash3601
[208] R Gupta P Rathi S Bradoo Lipase mediated upgradation of dietary fats andoils Crit Rev Food Sci Nutr 43 (2003) 635ndash644
[209] BH Jennings CC Akoh Lipase-catalyzed modification of rice bran oil to incor-porate capric acid J Agric Food Chem 48 (2000) 4439ndash4443
[210] J Hoeks M Mensink MK Hesselink K Ekroos P Schrauwen Long- andMedium-Chain Fatty Acids Induce Insulin Resistance to a Similar Extent inHumans Despite Marked Differences in Muscle Fat Accumulation J Clin Endo-crinol Metab 97 (2012) 208ndash216
[211] PJ Congden G Bruce MM Rothburn PC Clarke JM Littlewood J KelleherMS Losowsky Vitamin status in treated patients with cystic fibrosis ArchDis Child 56 (1981) 708ndash714
[212] BM Winklhofer-Roob H Ellemunter M Fruhwirth SE Schlegel-Haueter GKhoschsorur MA vant Hof DH Shmerling Plasma vitamin C concentrationsin patients with cystic fibrosis evidence of associations with lung inflammationAm J Clin Nutr 65 (1997) 1858ndash1866
[213] L Shamseer D Adams N Brown JA Johnson S Vohra Antioxidant micronutri-ents for lung disease in cystic fibrosis Cochrane Database Syst Rev (2010)CD007020
[214] C Santi S Santoro Electrophilic Selenium First edition Wiley-VCH VerlagGmbH amp Co KGaA 2012
[215] L Flohe S Toppo G Cozza F Ursini A comparison of thiol peroxidase mecha-nisms Antioxid Redox Signal 15 (2010) 763ndash780
[216] L Flohe JR Andreesen R Brigelius-Flohe M Maiorino F Ursini Selenium theelement of the moon in life on earth IUBMB Life 49 (2000) 411ndash420
[217] V Valdiglesias E Pasaro J Mendez B Laffon In vitro evaluation of seleniumgenotoxic cytotoxic and protective effects a review Arch Toxicol 84(2010) 337ndash351
[218] P Foucaud P Therond M Marchand F Brion JF Demelier J Navarro Seleniumand vitamin E in mucoviscidosis Arch Fr Pediatr 45 (1988) 383ndash386
[219] J Neve R Van Geffel M Hanocq L Molle Plasma and erythrocyte zinc copperand selenium in cystic fibrosis Acta Paediatr Scand 72 (1983) 437ndash440
[220] BM Winklhofer-Roob B Tiran PE Tuchschmid MA vant Hof DH ShmerlingEffects of pancreatic enzyme preparations on erythrocyte glutathione peroxi-dase activities and plasma selenium concentrations in cystic fibrosis FreeRadic Biol Med 25 (1998) 242ndash249
[221] JD Lloyd-Still HE Ganther Selenium and glutathione peroxidase levels in cys-tic fibrosis Pediatrics 65 (1980) 1010ndash1012
[222] D Tsavachidou TJ McDonnell S Wen X Wang F Vakar-Lopez LL Pisters CAPettaway CG Wood KA Do PF Thall C Stephens E Efstathiou R Taylor DGMenter P Troncoso SM Lippman CJ Logothetis J Kim Selenium and vitaminE cell type- and intervention-specific tissue effects in prostate cancer J NatlCancer Inst 101 (2009) 306ndash320
[223] IN Zelko TJ Mariani RJ Folz Superoxide dismutase multigene family acomparison of the CuZn-SOD (SOD1) Mn-SOD (SOD2) and EC-SOD (SOD3)gene structures evolution and expression Free Radic Biol Med 33 (2002)337ndash349
[224] RP Bowler JD Crapo Oxidative stress in airways is there a role for extracellu-lar superoxide dismutase Am J Respir Crit Care Med 166 (2002) S38ndashS43
[225] K Best K McCoy S Gemma RA Disilvestro Copper enzyme activities in cysticfibrosis before and after copper supplementation plus or minus zinc Metabo-lism 53 (2004) 37ndash41
[226] SS Percival GP Kauwell E Bowser M Wagner Altered copper status in adultmen with cystic fibrosis J Am Coll Nutr 18 (1999) 614ndash619
[227] NF Krebs JE Westcott TD Arnold BM Kluger FJ Accurso LV Miller KMHambidge Abnormalities in zinc homeostasis in young infants with cystic fibro-sis Pediatr Res 48 (2000) 256ndash261
[228] D Easley N Krebs M Jefferson L Miller J Erskine F Accurso KM HambidgeEffect of pancreatic enzymes on zinc absorption in cystic fibrosis J Pediatr Gas-troenterol Nutr 26 (1998) 136ndash139
[229] S Van Biervliet JP Van Biervliet E Robberecht Serum zinc in patients with cys-tic fibrosis at diagnosis and after one year of therapy Biol Trace Elem Res 112(2006) 205ndash211
[230] S Van Biervliet JP Van Biervliet S Vande Velde E Robberecht Serum zinc con-centrations in cystic fibrosis patients aged above 4 years a cross-sectional eval-uation Biol Trace Elem Res 119 (2007) 19ndash26
712 F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
[231] F Galli M Cristina Polidori W Stahl P Mecocci FJ Kelly Vitamin E biotransfor-mation in humans Vitam Horm 76 (2007) 263ndash280
[232] J Wiser NE Alexis Q Jiang W Wu C Robinette R Roubey DB Peden In vivogamma-tocopherol supplementation decreases systemic oxidative stress andcytokine responses of human monocytes in normal and asthmatic subjectsFree Radic Biol Med 45 (2008) 40ndash49
[233] JG Wagner Q Jiang JR Harkema B Illek DD Patel BN Ames DB PedenOzone enhancement of lower airway allergic inflammation is prevented bygamma-tocopherol Free Radic Biol Med 43 (2007) 1176ndash1188
[234] JT Harries DP Muller Absorption of different doses of fat soluble and watermiscible preparations of vitamin E in children with cystic fibrosis Arch DisChild 46 (1971) 341ndash344
[235] EI Back C Frindt E Ocenaskova D Nohr M Stern HK Biesalski Can changesin hydrophobicity increase the bioavailability of alpha-tocopherol Eur J Nutr45 (2006) 1ndash6
[236] SZ Nasr MH OLeary C Hillermeier Correction of vitamin E deficiency withfat-soluble versus water-miscible preparations of vitamin E in patients with cys-tic fibrosis J Pediatr 122 (1993) 810ndash812
[237] S Soltani-Frisk E Gronowitz H Andersson B Strandvik Water-miscibletocopherol is not superior to fat-soluble preparation for vitamin E absorptionin cystic fibrosis Acta Paediatr 90 (2001) 1112ndash1115
[238] K Papas J Kalbfleisch R Mohon Bioavailability of a novel water-soluble vi-tamin E formulation in malabsorbing patients Dig Dis Sci 52 (2007)347ndash352
[239] F Antonicelli M Parmentier EM Drost N Hirani I Rahman K Donaldson WMacNee Nacystelyn inhibits oxidant-mediated interleukin-8 expression andNF-kappaB nuclear binding in alveolar epithelial cells Free Radic Biol Med 32(2002) 492ndash502
[240] EM App D Baran I Dab A Malfroot M Coffiner F Vanderbist M King Dose-finding and 24-h monitoring for efficacy and safety of aerosolized Nacystelyn incystic fibrosis Eur Respir J 19 (2002) 294ndash302
[241] MG Traber How much vitamin E hellip Just enough Am J Clin Nutr 84 (2006)959ndash960
[242] JC McCann BN Ames Vitamin K an example of triage theory is micronu-trient inadequacy linked to diseases of aging Am J Clin Nutr 90 (2009)889ndash907
[243] M Fusaro G Crepaldi S Maggi F Galli A DAngelo L Calo S Giannini DMiozzo M Gallieni Vitamin K bone fractures and vascular calcifications inchronic kidney disease an important but poorly studied relationship J Endocri-nol Invest 34 (2010) 317ndash323
[244] JC McCann BN Ames Adaptive dysfunction of selenoproteins from the per-spective of the triage theory why modest selenium deficiency may increaserisk of diseases of aging FASEB J 25 (2011) 1793ndash1814
[245] R Apak K Guclu M Ozyurek B Bektas Oglu M Bener Cupric ion reducing an-tioxidant capacity assay for food antioxidants vitamins polyphenolics and fla-vonoids in food extracts Methods Mol Biol 477 (2008) 163ndash193
[246] F Galli Interactions of polyphenolic compounds with drug disposition and me-tabolism Curr Drug Metab 8 (2007) 830ndash838
[247] RL Prior X Wu K Schaich Standardized methods for the determination of an-tioxidant capacity and phenolics in foods and dietary supplements J Agric FoodChem 53 (2005) 4290ndash4302
[248] C Azbell S Zhang D Skinner J Fortenberry EJ Sorscher BA WoodworthHesperidin stimulates cystic fibrosis transmembrane conductance regulator-mediated chloride secretion and ciliary beat frequency in sinonasal epitheliumOtolaryngol Head Neck Surg 143 (2010) 397ndash404
[249] G Wegrzyn J Jakobkiewicz-Banecka M Gabig-Ciminska E Piotrowska M Nar-ajczyk A Kloska M Malinowska D Dziedzic I Golebiewska M Moskot AWegrzyn Genistein a natural isoflavone with a potential for treatment of ge-netic diseases Biochem Soc Trans 38 (2010) 695ndash701
[250] YC Yu H Miki Y Nakamura A Hanyuda Y Matsuzaki Y Abe M Yasui K Ta-naka TC Hwang SG Bompadre Y Sohma Curcumin and genistein additivelypotentiate G551D-CFTR J Cyst Fibros 10 (2011) 243ndash252
[251] B Illek H Fischer Flavonoids stimulate Cl conductance of human airway epithe-lium in vitro and in vivo Am J Physiol 275 (1998) L902ndashL910
[252] JL Kreindler Cystic fibrosis exploiting its genetic basis in the hunt for newtherapies Pharmacol Ther 125 (2010) 219ndash229
[253] B Illek L Zhang NC Lewis RB Moss JY Dong H Fischer Defective function ofthe cystic fibrosis-causing missense mutation G551D is recovered by genisteinAm J Physiol 277 (1999) C833ndashC839
[254] P Anandakumar S Kamaraj S Jagan G Ramakrishnan R Vinodhkumar TDevaki Capsaicin modulates pulmonary antioxidant defense system during ben-zo(a)pyrene-induced lung cancer in Swiss albinomice Phytother Res 22 (2008)529ndash533
[255] I Rahman Antioxidant therapeutic advances in COPD Ther Adv Respir Dis 2(2008) 351ndash374
[256] AW Boots H Li RP Schins R Duffin JW Heemskerk A Bast GR Haenen Thequercetin paradox Toxicol Appl Pharmacol 222 (2007) 89ndash96
[257] M Joskova S Franova V Sadlonova Acute bronchodilator effect of quercetin inexperimental allergic asthma Bratisl Lek Listy 112 (2011) 9ndash12
[258] HJ Park CM Lee ID Jung JS Lee YI Jeong JH Chang SH Chun MJ Kim IWChoi SC Ahn YK Shin SR Yeom YM Park Quercetin regulates Th1Th2 balancein a murine model of asthma Int Immunopharmacol 9 (2009) 261ndash267
[259] AP Rogerio A Kanashiro C Fontanari EV da Silva YM Lucisano-ValimEG Soares LH Faccioli Anti-inflammatory activity of quercetin and iso-quercitrin in experimental murine allergic asthma Inflamm Res 56 (2007)402ndash408
[260] M Muller Polyphenol cytotoxicity induced by the bacterial toxin pyocyaninrole of NQO1 Free Radic Biol Med 47 (2009) 84ndash91
[261] J Grassmann Terpenoids as plant antioxidants Vitam Horm 72 (2005)505ndash535
[262] P Allen Tea tree oil the science behind the antimicrobial hype Lancet 358(2001) 1245
[263] EC Dasenbrook W Checkley CA Merlo MW Konstan N Lechtzin MP BoyleAssociation between respiratory tract methicillin-resistant Staphylococcus aure-us and survival in cystic fibrosis JAMA 303 (2010) 2386ndash2392
[264] V Bezzerri M Borgatti E Nicolis I Lampronti MC Dechecchi I Mancini PRizzotti R Gambari G Cabrini Transcription factor oligodeoxynucleotides toNF-kappaB inhibit transcription of IL-8 in bronchial cells Am J Respir CellMol Biol 39 (2008) 86ndash96
[265] R Gambari M Borgatti V Bezzerri E Nicolis I Lampronti MC Dechecchi IMancini A Tamanini G Cabrini Decoy oligodeoxyribonucleotides and peptidenucleic acids-DNA chimeras targeting nuclear factor kappa-B inhibition of IL-8 gene expression in cystic fibrosis cells infected with Pseudomonas aeruginosaBiochem Pharmacol 80 (2010) 1887ndash1894
[266] M Adrian P Jeandet AC Douillet-Breuil L Tesson R Bessis Stilbene content ofmature Vitis vinifera berries in response to UV-C elicitation J Agric Food Chem48 (2000) 6103ndash6105
[267] B Paul I Masih J Deopujari C Charpentier Occurrence of resveratrol and pter-ostilbene in age-old darakchasava an ayurvedic medicine from India J Ethno-pharmacol 68 (1999) 71ndash76
[268] I Rahman Antioxidant therapies in COPD Int J Chron Obstruct Pulmon Dis 1(2006) 15ndash29
[269] M Lee S Kim OK Kwon SR Oh HK Lee K Ahn Anti-inflammatory and anti-asthmatic effects of resveratrol a polyphenolic stilbene in a mouse model ofallergic asthma Int Immunopharmacol 9 (2009) 418ndash424
[270] LG Wood PA Wark ML Garg Antioxidant and anti-inflammatory effectsof resveratrol in airway disease Antioxid Redox Signal 13 (2010)1535ndash1548
[271] KV Kiselev Perspectives for production and application of resveratrol ApplMicrobiol Biotechnol 90 (2011) 417ndash425
[272] M Shakibaei C Buhrmann A Mobasheri Resveratrol-mediated SIRT-1 interac-tions with p300 modulate receptor activator of NF-kappaB ligand (RANKL) acti-vation of NF-kappaB signaling and inhibit osteoclastogenesis in bone-derivedcells J Biol Chem 286 (2011) 11492ndash11505
[273] SF Zaidi K Ahmed T Yamamoto T Kondo K Usmanghani M Kadowaki TSugiyama Effect of resveratrol on Helicobacter pylori-induced interleukin-8 secre-tion reactive oxygen species generation and morphological changes in human gas-tric epithelial cells Biol Pharm Bull 32 (2009) 1931ndash1935
[274] JK Kundu YK Shin YJ Surh Resveratrol modulates phorbol ester-inducedpro-inflammatory signal transduction pathways in mouse skin in vivo NF-kappaB and AP-1 as prime targets Biochem Pharmacol 72 (2006)1506ndash1515
[275] NH Nam Naturally occurring NF-kappaB inhibitors Mini Rev Med Chem 6(2006) 945ndash951
[276] JM Smoliga JA Baur HA Hausenblas Resveratrol and healthmdasha comprehen-sive review of human clinical trials Mol Nutr Food Res 55 (2011) 1129ndash1141
[277] ME Juan M Maijo JM Planas Quantification of trans-resveratrol and itsmetabolites in rat plasma and tissues by HPLC J Pharm Biomed Anal 51(2010) 391ndash398
[278] JA Baur DA Sinclair Therapeutic potential of resveratrol the in vivo evidenceNat Rev 5 (2006) 493ndash506
[279] E Nicolis I Lampronti MC Dechecchi M Borgatti A Tamanini N Bianchi VBezzerri I Mancini MG Giri P Rizzotti R Gambari G Cabrini Pyrogallol anactive compound from the medicinal plant Emblica officinalis regulates expres-sion of pro-inflammatory genes in bronchial epithelial cells Int Immunophar-macol 8 (2008) 1672ndash1680
[280] E Nicolis I Lampronti MC Dechecchi M Borgatti A Tamanini V Bezzerri NBianchi M Mazzon I Mancini MG Giri P Rizzotti R Gambari G CabriniModulation of expression of IL-8 gene in bronchial epithelial cells by 5-methoxypsoralen Int Immunopharmacol 9 (2009) 1411ndash1422
[281] M Borgatti I Mancini N Bianchi A Guerrini I Lampronti D Rossi G SacchettiR Gambari Bergamot (Citrus bergamia Risso) fruit extracts and identified com-ponents alter expression of interleukin 8 gene in cystic fibrosis bronchial epithe-lial cell lines BMC Biochem 12 (2011) 15
[282] L Piccagli E Fabbri M Borgatti N Bianchi V Bezzerri I Mancini E Nicolis CMDechecchi I Lampronti G Cabrini R Gambari Virtual screening against p50NF-kappaB transcription factor for the identification of inhibitors of the NF-kappaB-DNA interaction and expression of NF-kappaB upregulated genesChemMedChem 4 (2009) 2024ndash2033
[283] L Piccagli M Borgatti E Nicolis N Bianchi I Mancini I Lampronti D VevaldiF DallAcqua G Cabrini R Gambari Virtual screening against nuclear factorkappaB (NF-kappaB) of a focus library identification of bioactive furocoumarinderivatives inhibiting NF-kappaB dependent biological functions involved incystic fibrosis Bioorg Med Chem 18 (2010) 8341ndash8349
[284] M Borgatti A Chilin L Piccagli I Lampronti N Bianchi I Mancini G Mar-zaro Da Francesco A Guiotto R Gambari Development of a novel furocou-marin derivative inhibiting NF-kappaB dependent biological functionsdesign synthesis and biological effects Eur J Med Chem 46 (2011)4870ndash4877
[285] E Georgy S Le Guellec L Vecellio E Fichant P Stordeur P Bordeau JP PerraudinFeasibility study of OSCN- and lactoferrin (Meveol) nebulization for cysticfibrosis JCyst Fibros 10 (2011) S18
713F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
[286] C Tidei M Piroddi F Galli C Santi Oxidation of thiols promoted by PhSeZnClTetrahedron Lett 53 (2012) 232ndash234
[287] L Semianrio-Vidal C van Hesuden G Mugesh ER Lazarowski Ebselen is a po-tent non-competitive inhibitor of extracellular nucleoside diphosphokinasePurinergic Signal 6 (2010) 383ndash391
[288] C ColussiMC Albertini S Coppola S Rovidati F Galli L Ghibelli H2O2-inducedblockof glycolysis as an active ADP-ribosylation reaction protecting cells from apoptosisFASEB J 14 (2000) 2266ndash2276
[289] H Xiao KL Parkin Induction of phase II enzyme activity by various seleniumcompounds Nutr Cancer 55 (2006) 210ndash223
[290] G Peluffo R Radi Biochemistry of protein tyrosine nitration in cardiovascularpathology Cardiovasc Res 75 (2007) 291ndash302
[291] B Alvarez R Radi Peroxynitrite reactivity with amino acids and proteinsAmino Acids 25 (2003) 295ndash311
[292] B Kamosinska MW Radomski M Duszyk A Radomski SF Man Nitric oxideactivates chloride currents in human lung epithelial cells Am J Physiol 272(1997) L1098ndashL1104
[293] L Chen RP Patel X Teng CA Bosworth JR Lancaster Jr S Matalon Mecha-nisms of cystic fibrosis transmembrane conductance regulator activation by S-nitrosoglutathione J Biol Chem 281 (2006) 9190ndash9199
[294] F Luchetti B CanonicoM BettiM Arcangeletti F PilolliM Piroddi L Canesi S PapaF Galli Melatonin signaling and cell protection function FASEB J 24 (2010)3603ndash3624
[295] MW Bengtsson G Jedstedt G Flemstrom Duodenal bicarbonate secretion inrats stimulation by intra-arterial and luminal guanylin and uroguanylin ActaPhysiol (Oxf) 191 (2007) 309ndash317
[296] CS Nelson JL Marino CN Allen Melatonin receptor potentiation of cyclic AMP andthe cystic fibrosis transmembrane conductance regulator ion channel J Pineal Res 26(1999) 113ndash121
[297] C de Castro-Silva VM de Bruin GM Cunha DM Nunes CAMedeiros PF de BruinMelatonin improves sleep and reduces nitrite in the exhaled breath condensate incystic fibrosismdasha randomized double-blind placebo-controlled study J Pineal Res48 (2010) 65ndash71
[298] I Hornyak E Pankotai L Kiss Z Lacza Current developments in the the-rapeutic potential of S-nitrosoglutathione an endogenous NO-donor mole-cule Curr Pharm Biotechnol (2011) Jan 11 [Epub ahead of print] - PMID21235457
[299] AH Snyder ME McPherson JF Hunt M Johnson JS Stamler B Gaston Acuteeffects of aerosolized S-nitrosoglutathione in cystic fibrosis Am J Respir CritCare Med 165 (2002) 922ndash926

700 F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
demand by the abnormal generation of ROS in CF tissues (see for in-stance the recommendations by the Cystic Fibrosis Foundation Con-sensus Conference on nutrition [153])
The first report of a vitamin E deficiency in CF appeared in literaturein 1951 by Filer et al [154] In this study the absorption of the mainform of this vitamin eg α-tocopherol and its ester derivatives was in-vestigated in several subsets of infants and children Thanks to a simplebioavailability (or tolerance) test these authors observed that ldquoin-fantshellip diagnosed as fibrocystic disease of the pancreas diarrhea andcirrhosis were characterized by a poor response to the test ie the tol-erance curve was lowrdquo However abnormalities were also observed inother subgroups of infants with a variety of disorders not associatedwith fat or fat-soluble vitamin intolerance such as sprue celiac syn-drome and lupus erythematosus which suggests the general observa-tion that malnutrition and inflammatory and degenerative diseases ofthe GI tract may lead to absorb tocopherols poorly At the same timethese authors reported that ldquoMetabolic disorders with associated hy-percholesterolemia were observed to give abnormally high values forthe area under the curverdquo and that patients responding poorly to to-copherol absorption test did also in vitamin A absorption tests
The finding of lowered (lipid uncorrected) levels of vitamin E wasconfirmed in other studies in which this relative deficiency was foundto occur irrespective of pancreatic comorbidity and in associationwith lowered levels of other liposoluble vitamins such as vitamin Aand D [155] regardless of their different liver metabolism and tissuedelivery mechanisms [156157]
Plasma buccal mucosal cells (BMCs) and breath condensate α-tocopherol decreased significantly with age in association with a de-creased respiratory function [5] This was accompanied by loweredlevels of other antioxidants such as vitamin C and increased oxidativestress markers of different origin such as protein carbonyls thiobarbi-turic acid-reactive substances and F2-IsoPs
Clinical symptoms of vitamin E deficiency in CF have not beenconclusively investigated Dolan et al [158] described that anemiaof CF patients is related to vitamin E deficiency and increasedperoxide-induced hemolysis of RBC Other authors however ob-served an increased susceptibility to peroxide-induced hemolysisalso in the presence of normal levels of vitamin E [159] Peters andKelly [160] observed that RBC vitamin E concentrations were belowthe normal range in almost all unsupplemented patients and roseinto the normal range with a 1-year supplement of 100 mg per daybut not 15 mg per day Since RBC vitamin E concentration has beenshown to correlate well with tissue concentrations of the vitamin inanimals tissue levels of vitamin E are expected to be lower than nor-mal in CF patients
Bioavailability of fat-soluble vitamin is limited in CF Vitamin Edeficiency of CF is also associated with hypocholesterolemia [7] Asa consequence the relative deficiency of this vitamin is compensatedwhen the absolute levels are normalized for cholesterol levels andthis suggests a poor transferring of this vitamin in the circulation bya defective lipid and lipoprotein metabolism Pancreatic insufficiencyand the consequent lipid malnutrition cannot completely explain thisdefect and other possibly CF-specific dysfunctions could play a roleLiver metabolism and specific plasma transport systems of this vita-min need further elucidation in CF
As a consequence of these aspects it is not presently clear whichform and level of supplementation of this vitamin is most appropriateto treat these patients Usingα-tocopherol as a vitamin E supplementPeters et al [160] reported that 100 mg per day are required to nor-malize RBC concentrations Other authors described unsuccessfulsupplementation protocols with higher doses and this has led to de-velop formulations with higher bioavailability in order to achieve bet-ter compliance to oral supplementation (see below and the literaturereviewed in [161ndash163])
Besides absorption and tissue delivery issues specificity of actionis another critical item of antioxidant therapy with fat-soluble agents
in CF As further addressed below this aspect could be themain limit toa successful use of natural forms of vitamin E in the clinical manage-ment of CF inflammation even if a local lung-targeted therapy wouldbe developed according with so far proposed pre-clinical models ofaerosolized vitamin E [164165]
Current pharmacological research is aimed to develop synthetic formsof this and other fat-soluble antioxidants with better radical scavengingproperties at the lipidndashwater interface Type of ROS target and the sitesof action greatly influence the chances of a fat-soluble antioxidant of alle-viating oxidative stress in the airways as well as in other organs such asliver and pancreas These aspects dealing with specificity of action[163166167] have stimulated the search of novel vitamin E-derived an-tioxidants that may help to scavenge radicals at the lipidndashwater interfaceof the epithelial cell membrane and surfactant Amine derivativesof tocopherols and tocotrienols have been recently demonstrated toshow higher antioxidant and free radical scavenging activity than α-tocopherol [168] Further in vitro pharmacological analysis has includedtoxicity evaluations and the detailed investigation of scavenging of azo-and phenolic radicals with different degrees of hydrophobicity and theinhibitory activity on IL-8 gene expression and phospholipase activityin CF cells Comparative evaluation with other synthetic derivativessuch asα-tocopheryl succinate and natural forms of vitamin E suggestedthat these amine derivatives are promising antioxidant and anti-inflammatory agents [Galli F and Pilolli F unpublished observation]deserving further pre-clinical investigation in CF model systems
Anti-inflammatory effects of natural and synthetic analogues of vi-tamin E are also an intriguing pharmacological opportunity currentlyunder investigation by several laboratories [169170]
Recently vitamin E supplementation has been at the center of adispute regarding its safety when used at high dosages in certainpopulations of patients An extensive and speculative debate originat-ed on this subject after a meta-analysis study byMiller et al [171] thatexamined the largest secondary prevention trials on vitamin E trials incardiovascular patients finding a significantly increased mortality riskfor all the causes (about 4 1ndash8 in the 95 interval of confidence)when the patients were treated with doses gt400 IUdie (that areequivalent to 400 mgdie of the synthetic form allrac-α-tocopheroland to 185 mgdie of the natural form RRR-α-tocopherol) This debateresulted in a careful examination of this meta-analysis study by severalother authors and in further revisions of the literature on vitamin E tox-icity in humans [see the literature recently reviewed in [163172ndash174]]that clearly demonstrated the poor consistency of the conclusionsraisedwithMillersmeta-analysis study and the paucity of the concernsthat derived from that These conclusions have been verified in the re-cent international symposium on vitamin E of the Society for Free Rad-ical Research Europe branch of Rome 2009 [173175] Vitamin E used assupplement for humans in all its forms (eg α-tocopherol and othertocopherols and tocotrienols) is safe in abroad range of intakes[172176] The tolerable upper intake level (UL) and the AcceptableDaily Intake (ADI) established by the Joint FAOWHOExpert Committeeon Food Additives for the natural form of vitamin E as α-tocopherolequivalents are of 300 mgdie and 015ndash20 mgkg body weightdierespectively [172177]
352 CarotenoidsLevels of plasma carotenoids such as β-carotene β-cryptoxanthin
and total lycopene are significantly lowered in CF patients and thiswas associated with higher susceptibility to lipid peroxidation[5178ndash180] Rust et al [178] demonstrated that the long-term oralsupplementation with 50 mg β-caroteneday (ie 1 mg β-carotenekg BWday) restored the levels of this carotenoid while sub-optimalsupplementation was observed at doses of 10 mg β-caroteneday orlower thus confirming the need of high doses of this fat-soluble factorto overcome the limited absorption and thus to achieve plasma con-centrations of healthy control subjects Successful high-dose treat-ments appear to lower oxidative stress markers such as TBA-MDA
701F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
complexes and to correct total antioxidant capacity of plasma Inanother study β-carotene supplementation was observed to de-creased lipid peroxide formation as quantitated by malondialdehydeconcentrations in plasma (TBAHPLC method) and to enhance the re-sistance to copper(II) ion-induced oxidation of low density lipopro-teins [180]
At the same time toxicity issues have been raised for human sup-plementation with carotenoid formulations and particularly of water-miscible formulations of preformed vitamin A that is regularly sup-plemented to CF patients which may increase serum retinol andpossible risk of CF-associated liver and bone complications (reviewedin [161181]) However β-carotene supplementation seems to be safesince this does not affect plasma concentrations of other carotenoidsand retinol as well as of other fat-soluble vitamins as α- and γ-tocopherol [178] Recent studies designed to test the clinical efficacyof a CF tailored multivitamin formulation (commercial name AquA-DEKsreg) also tested the safety of this type of formulation and demon-strated that this does not increase vitamin A above the normal levelsobserved in healthy controls [162182183] The normalization of β-carotene levels obtained in these studies was associated only withminor improvements on respiratory and growth parameters whilethe levels of urinary F2-IsoPs used as index of lipid peroxidationwere not affected [162] The surrogate marker of lipid peroxidationMDA was affected together with some selected antioxidant parame-ters (RBC thiols and superoxide dismutase) in another study inwhich this multivitamin formulation was preliminarily evaluated incomparison with standard formulations of vitamin E and A [182]
353 Coenzyme Q-10Coenzyme Q-10 (Q10) is a well-known electron transporter in the
mitochondrial respiratory chain with fundamental role in cellularbioenergetics and scavenging of radical species [184] This lipophilicsubstance is present in the circulation at low levels (serum concentra-tionsle2 μM) mainly as ubiquinol-10 eg the reduced form with anapproximate ratio of 955 with the oxidized form ubiquinone-10[185186] A mechanism for a preferential distribution and accumula-tion in mitochondria has been suggested for both the reduced and ox-idized forms of CoQ10 that are taken up by the cells in a time- andconcentration-dependent Subcellular localization and trafficking ofexogenous Q10 are similar to those of the endogenous form butwere different from that of α-tocopherol that is related with lipidcomposition particularly in the mitochondrial and microsomal frac-tions [184] Ubiquinol-10 readily oxidizes ex vivo by the reactionwith other lipophilic antioxidants such as α-tocopherol and butylatedhydroxytoluene [185] Therefore a higher reduction potential thanother physiological fat-soluble antioxidants such as vitamin E and aselective metabolism and cellular trafficking show peculiar role forthe cell CoQ which may also represent an important lipophilic antiox-idant in cells and body fluids
Human cells synthesize this coenzyme through the cholesterol bio-synthesis pathway so thatmore than two thirds of the tissue levels ap-pear to have an endogenous origin dietary sources provide acontribution to Co-Q10 levels of blood and all solid tissues that variesdepending on the dose applied and type of dietary source [187] How-ever in the case of oral supplements it has to be considered that hy-drophobicity and large molecular weight of this coenzyme influenceits absorption that ultimately is slow and limited [186187] Likewiseto vitamin E pharmacokinetics [188189] Co-Q10 showed T(max) ofaround 6 h that coincides with that of dietary lipids Elimination isclose to that of the more retained form of vitamin E in human bodyeg α-tocopherol with a half-life of about 33 h which suggests poorhepatic metabolism However commercially available formulationsare reported to be safe even at high doses and solubilized formulationsshow enhanced bioavailability In healthy subjects plasma Q10 re-sponse to oral ingestion show saturation profiles with a plateau at a
dose of 2400 mg and the higher plasma concentrations were foundto facilitate uptake by peripheral tissues and also the brain [186187]
Laguna et al [190] recently investigated total serum levels ofcoenzyme Q-10 in a wide population of CF children (n=381) and esti-mated their association with clinical outcome Near to 50 of these CFpatients were deficient of Co-Q10 and this defect was significantlymore prevalent in patients with pancreatic insufficiency and signifi-cantly associated with P aeruginosa colonization in infants (under24 months of age) Importantly low Co-Q10 levels correlated to otherlipid markers of a poor nutritional status such as total lipids and alsothe other fat-soluble antioxidants β-carotene and α-tocopherolwhich confirms the presence of a common defect in the absorptionand metabolic pathways of this coenzyme with dietary lipids
The deficit of Co-Q10 may contribute to the impaired energy func-tion of mitochondria of CF tissues and this may exacerbate CF-linkedinflammation infection and cellular stress response of the lung A sys-tematic analysis of molecular lesions in CF bronchial tissue has beenrecently carried out by proteomic approach [191] Comparative eval-uation of protein expressional pattern in CF and healthy controltissues has revealed aberrant levels of some mitochondrial andenergy-related proteins in CF specimens that included the ubiqui-nolndashcytochrome c reductase complex core protein I and one form ofnidogen a pseudogene of aconitase 2 These changes in CF may reflectmolecular changes which could be associated with an altered mito-chondrial homeostasis and Co-Q10 redox
Multivitamin supplements with high bioavailability containingCo-Q10 have demonstrated to correct the deficit of this antioxidantand were preliminarily observed to improve airway inflammationmarkers in CF patients [183] However further clinical investigationfailed to demonstrate that such an improved biochemical profile isassociated with significant improvements in weight percentile andpulmonary function [162]
354 Fatty acidsA key pathophysiological role in sustaining inflammation in CF has
been attributed to the abnormal polyunsaturated fatty acid (FA) pat-tern Abnormalities in FA profiling are potentially linked to CFTRmutation-driven alterations in the absorption andor metabolism ofdietary lipids [192193] and to the consumption of high oxidizableFA involved in the free radical-mediated lipid peroxidation [7]Among those alterations dysregulation of the docosahexaenoic acidand arachidonic acid balance has been extensively studied with re-portedly significant reduction of DHA in CF and a parallel increasein the levels of AA and inflammatory indices [193ndash195] Actually AAis the progenitor of both enzymatic- and free radical-derived inflam-matory mediators including leukotrienes prostaglandins and iso-prostanes On the other hand n-3 PUFA (eicosapentaenoic acid anddocosahexaenoic acid) are involved in the generation of potent medi-ators namely resolvins and protectins which are able to resolveexudates and to act as organ protective and antifibrotic Secondarilyto their anti-inflammatory action n-3 FA may also produce anantioxidant-like response (eg a reduced demand of antioxidants toachieve an optimal control of oxidative pathways) As a consequencen-3 PUFA have been suggested and widely used as supplements in CFpatients usually under the form of fish oil [196ndash198] It is worth ofnote however that defective levels of DHA in CF patients was notconfirmed in recent studies [7] It was also shown that patients onDHA supplements did not have increased plasma n-3 FA concentra-tions but showed more severe oxidative stress compared to theunsupplemented patients [7] This observation of an increased riskof oxidative stress in CF subjects receiving n-3 fatty acids supple-ments has also been described by other authors [199]
Studies reporting increased AA levels in CF patients have beencontradicted by others [7200201] thus contributing to weakeningthe pathophysiological role of the altered DHAndashAA balance as turnpoint of an upregulated inflammatory status in CF In this context a
702 F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
recent Cochrane meta-analysis on n-3 supplementation in CF patients[202] highlighted the lack of evidence for a significant correction ofthe assessed clinical end points (mainly respiratory symptoms)even when inflammatory indices and other laboratory end pointswere met Taken together these data suggest that there is insufficientevidence to draw firm conclusions or recommend routine use of n-3supplements in CF Notwithstanding it is common belief that n-3supplements provide some benefits for people with CF with relativelyfew adverse effects and thus their use is not discouraged
Further alterations in fatty acid metabolism have been highlight-ed including the consistent findings of an increase in circulatinglevels of saturated and monounsaturated fatty acids [7203204]Decreased levels of essential FA (EFA) ie the FA that have to be in-troduced with the diet correlates with the severity of respiratoryinsufficiency and the same clinical correlation was observed with al-tered proportions of FA species converted by the activity of desatur-ase enzymes (reviewed in [204]) The close relationship betweencertain fatty acids and oxidative stress including the negative correla-tion of C240 and linoleic acid with oxysterol levels point to the needof intensive investigation in CF patients of previously neglected lipidspecies that are emerging candidates in the control of metabolismQuantitative lipidomic analyses have lead to identify C161n7 palmi-toleate as a ldquoprotectiverdquo adipose-derived lipid hormone that stronglystimulates insulin activity in muscle and liver also suppressing in-flammatory cytokine output from mice fat cells [205] Specific meta-bolic activities have been also demonstrated by medium chainsaturated fatty acids caprylic acid (C80) capric acid (C100) and lau-ric acid (C120) Capric acid acts as a direct ligand of PPARγ using abinding pocket different from the binding pocket of thiazolidinedioneor long chain fatty acids [206] Additional activities of medium chainfatty acids which are ligands of free fatty acids receptors detectedin the immune cells the gastrointestinal tract and adipocytes maycontribute to metabolic homeostasis and inflammatory responses[207] These data underscore the importance of a lipid-mediated ldquoen-docrine networkrdquo demonstrating how specific alteration of one orfew serum lipids would be per se sufficient to influence metabolic ho-meostasis Given the relevance of this emerging information and thealteration of lipid metabolism and inflammatory status in CF fattyacid lipidomics need to be deeply investigated in CF
Again these studies have obvious nutritional implications Satu-rated fatty acids with chain lengths higher than C18 are poorlyabsorbed partly because they form insoluble calcium salts [208]Medium chain saturated fatty acids are well known for being highlyabsorbed through the intestine providing rapid delivery of energyvia oxidation of the more hydrophilic short chains and have beensuggested to provide proper nourishment in patients with CF [209]Recent studies have shown that consumption of a high-fat diet richin medium chain fatty acids as opposed to long chain fatty acidsdoes not lead to ectopic fat accumulation in skeletal muscle andliver of both rats and mice [210] In light of the close association be-tween nutritional status inflammation and life expectancy in CF pa-tients the manipulation of dietary lipids in these patients must befurther explored as a possible strategy to provide adequate nutritionand better management of oxidative stress
36 Hydrosoluble antioxidants oligoelements and enzymatic antioxidants
361 Vitamin CVitamin C status in CF patients has been poorly investigated Early
studies suggested a defective vitamin C status that was refractory tooral supplementation [211] Other and more recent studies showednormal or slightly decreased levels of vitamin C in CF patients as com-pared to healthy controls but age- and disease-related decline of thiswater-soluble antioxidant was reported in these patients [5212]In the study of Winklhofer-Roob et al [212] on mid-European CFpatients vitamin C concentrations decreased with age with an
estimated rate of 5 μmollyr and vitamin C concentrationsb40 μ-moll were associated with highest indexes of inflammation whichis consistent with the hypothesis that optimal levels of vitamin Cmay influence immuno-inflammatory activity of alveolar macro-phages and neutrophils Other few studies have examined the effectof supplements containing vitamin C on CF inflammation and oxida-tive stress since the levels of this vitamin do not significantly improvewith supplementation (reviewed in [213]) This highlights the com-mon fate that this hydrosoluble vitamin shares with several fat-soluble counterparts in the ldquomicronutrient paradoxrdquo of CF patients inwhich the need for a correction of their status along the progressionof the disease is frustrated by the poor efficacy of oral supplementa-tion protocols Formulations and appropriate supplementation proto-cols that may produce a better correction of vitamin C status of CFpatients are awaited for further clinical evaluation
362 Selenium and selenium-dependent peroxidasesSelenium is a trace element with marked electrophilicity [214]
that once converted to the organic form of Se-Cys can be introducedin protein structures to play its important role in H2O2 metabolismand signaling [215] As catalytic center of the enzyme GSH-peroxidase (SeGSH-Px) Se plays a crucial role to protect polyunsatu-rated lipids of plasma membrane and circulating lipoproteins formperoxidative insults With other Se-proteins such as the high molecu-lar weight thioredoxin reductases this oligoelement participates tothe control of protein thiol-disulfide oxidoreduction and glutathiony-lation which regulate signaling pathways of crucial importance in theregulation of immunity and inflammation [16] but also the function-ing of other redox-sensitive proteins such as the same CFTR [124]
The activity of SeGSH-Px in blood is considered a functional as-sessment of selenium status even if this assumption has some limita-tions related with the saturation profile that the Se stores show atincreasing doses of Se administration Investigations of the seleniumstatus in CF patients have produced conflicting findings which maydepend on differences in dietary intake ethnicity and environmentalfactors in the diverse patient populations (reviewed in [216217]) CFchildren have been reported to have lowered blood selenium and RBCSeGSH-Px activity [218219] normal plasma selenium and loweredRBC SeGSH-Px [220] and even normal levels of both these two param-eters [221] The supplementation with selenium in combination withother antioxidants was observed to increase the concentrations ofblood selenium that likewise β-carotene and fatty acid were posi-tively correlated with improved lung function [6]
Foucaud et al [218] observed that a defective selenium statuswas associated with lowered levels of other antioxidants that contrib-ute to the anti-peroxidative activity of this microelement such asvitamin E (reviewed in [222]) and the severity of this deficiencywas lower in children with pancreatic enzyme replacement and vita-min E supplementation
Treatments to substitute for exocrine pancreatic insufficiency bypancreatic enzymes from animal sources such as porcine pancreashave been confirmed to be a source of Se [220] These affects RBCSeGSH-Px activity and plasma selenium concentrations which hasto be taken into account when selenium supplements are given toCF patients
Selenium has been used to develop a series of organoseleniumcompounds that may open the way to new therapeutic opportunitiesin CF (see Section 392) These include GPX mimetic drugs and phaseII enzyme inducers which may provide higher antioxidant activity ofASL and cellular protection effects in the airways
363 Zinc and copperZinc and copper (Zn and Cu respectively) are present in many
proteins so that a deficiency of these trace metals could have pleiotro-pic effects in humans As regards antioxidant systems these two oli-goelements contribute an important role being cofactors of two
703F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
isoforms of the superoxide dismutase enzymes eg the extracellularform eg the EC-SOD or Sod 3 and the CundashZn-SOD or Sod 1 that isfound in several tissues and cells [223] The EC-SOD exerts its antiox-idant role also in the lining fluids of the airways [224]
The notion that CF patients have defective concentrations of bloodZn and Cu is controversial As far as Cu status is concerned few datahave been produced and are available in the literature suggestingthe notion that CF patients develop a moderate copper deficiency[225226] That was essentially demonstrated on the bases of a defec-tive activity of Cu-related proteins such as plasma ceruloplasmindiamine oxidase and RBC SOD This defect seems to be refractory toCu and Zn supplementation (see below)
More advanced studies have been carried out in the case of Zn sta-tus in CF Low plasma zinc concentrations were reported in approxi-mately 30 of young infants with CF identified by newbornscreening [227] and an impaired zinc homeostasis in CF patientswas described by Easley et al [228] This is characterized by poor con-servation of the endogenous pool with fecal loss and impaired frac-tional absorption of zinc which are the consequences of pancreaticinsufficiency and persisting steatorrhea These studies suggestedthat in the clinical management of CF patients these defects can beat least in part corrected by exocrine pancreatic enzyme replacement
A series of studies by Van Biervliet et al [229230] demonstratedin a Dutch population of CF infants and children that serum Zn variesin an age-dependent manner but remained unchanged with respectto healthy control levels In CF patients no difference in serum Zn con-centration between pancreatic-sufficient or pancreatic-insufficientpatients was observed and no correlation was found with the nutri-tional status or height z-score Importantly in these studies a signifi-cant correlation of serum Zn was observed with the fat solublevitamins A and E thus confirming the relationship between the ab-normalities of lipid and Zn metabolism in CF This suggests that co-supplementation of Zn and fat-soluble vitamins should be advisedin the presence of pancreatic insufficiency and persisting steatorrhea
Neve et al [219] in a study aimed to assess plasma and erythrocytezinc copper and selenium in CF children showed that mean plasmazinc and copper levels were not different from those in age-matched controls which confirms the observations by Van Biervlietet al described above However plasma zinc concentrations de-creased in patients with moderate-to-severe growth retardation andwith severe pulmonary disease but very low zinc levels occur sporad-ically Erythrocyte zinc and copper levels were significantly higherthan normal while RBC selenium was lower than in age-matchedcontrols These trace element concentrations in erythrocytes werediscussed in relation to the activities of the CuZn-SOD and the Se-enzyme GPx This observation suggests a compensatory upregulationof the erythrocyte CuZn-SOD by the exposure of erythroid precursorsto ROS andor other CF-related stressors
Best et al [225] also studied RBC SOD activity using this as a bio-logical sensor of Cu status in CF patients A lowered activity of thisenzyme was reported in CF together with that of the other Cu-dependent enzyme plasma diamine oxidase while plasma ceruplas-min showed normal activity Degradation rates of copper proteinsare known to be accelerated in conditions of copper deficiencywhich could explain the finding at least in part Anyway when Cuand Zn were supplemented to CF patients either separate or incombination (6 weeks of 3 mg copperd as copper-glycinate and30 mg zincd as zinc-glycinate) any of the copper enzyme activitieswas affected Therefore the moderate copper deficiency of CF patientsappears to be refractory to the intervention by increased copper andor zinc intake
Erythrocyte CuZn-SOD and the plasma levels of Cu and Zn werealso measured in the study of Wood et al [6] in which Australian CFpatients (agegt5 years) were treated with a high-dose antioxidantmultivitamin formulation containing 200 mg vitamin E (as RRR-α-tocopherol) 300 mg vitamin C (as sodium ascorbate) 25 mg β-
carotene (all-trans isomer) 90 μg Se (as selenomethionine) and500 μg vitamin A (as retinyl palmitate) in oil Plasma oligoelementsand particularly Zn were in the normal range at baseline (as com-pared with the data reported in [229230]) and were not affected bythis multivitamin supplement The same was found for the activityof RBC SOD and for plasma 8-iso-PGF2α as surrogate biomarker oflipid peroxidation
In a recent non-randomized small population (n=21) casendashcon-trol study in CF children Zn supplementation was proven to producepositive clinical effects in Zn-deficient patients [196] The supplemen-tation with 5 mgkg Zn sulfateday (maximum 150 mg) significantlydecreased the number of infections and increased the forced expira-tory volume in 1 s energy intake and growth parameters also im-proved These parameters were unaffected in untreated patientsexcept that in the case of the pulmonary function that decreased sig-nificantly These clinical observations on Zn supplementation need tobe confirmed in prospective double-blind randomized control trial
37 Appropriateness and targeting of antioxidant therapies in CF
The choice of the appropriate antioxidant and dose to correct a cer-tain biomarker and its associated biochemical lesion is another impor-tant point that appears to have disregarded in many clinical studiesFor instance unlike vitamin E vitamin C supplementation does notalter F2-IsoPs levels in humans (reviewed in [74]) This appears tobe true also in the antioxidant therapy of CF in which vitamin C(300 mgday) was administered together with other antioxidantsthat included a dose of vitamin E of 200 mgday without any signifi-cant effect on the surrogate biomarker of lipid peroxidation F2-IsoPs[6] When carotenoids are used as supplements to prevent the damag-ing action of ROS in the CF airways it is noteworthy that these are notparticularly good quenchers of peroxyl radicals relative to phenolicsand other antioxidants but are exceptional in quenching singlet oxy-gen at which most other phenolics and antioxidants are relativelyineffective Singlet oxygen is not a radical and does not react via radi-cal mechanisms but reacts mostly by the addition to double bondsforming endoperoxides that can be reduced to alkoxyl radicals that ini-tiate radical chain reactions typical of the peroxidative damage of PUFA[38] In this case the analysis of F2-IsoPs lipid peroxide formation andtransition metal-induced oxidizability of lipoproteins [162180] are allappropriate to evaluate the effect of carotenoids in preventing lipidperoxidation
As far as the dose is concerned clinical pharmacology of vitamin Eas an antioxidant was recently investigated by means of the effect onF2-IsoPs production and doses of α-tocopherol of 1600 IUday orgreater were found to be required to statistically affect plasma F2-IsoPs levels in hypercholeterolemic subjects [176] Several vitamin Esupplementation studies in CF patients have been performed withdoses of lower than 300 IUday regardless of the lowered absorptionby pancreatic and liver defects and the regular supplementationwith these doses does not appear to correct lipid oxidation markersin CF [7]
In the clinical practice and planning trials it has to be taken intoconsideration that in spite of substantial evidence supporting ahigher antioxidant demand in CF interventions with several antioxi-dant formulations produce poor responsiveness particularly in thecase of fat-soluble antioxidants which are poorly absorbed [6162]
Since many oxidants and antioxidants are present in tissuesand biological fluids and these have different chemical and physicalcharacteristics the possibility to produce a successful therapy witha single antioxidant molecule is too far to be realistic Moreover an-tioxidants act by multiple mechanisms in a single system or by adifferent single mechanism depending on the reaction systemresponding in a different manner to different radical or oxidantsources Because multiple reaction characteristics and mechanismsas well as different phase localizations are usually involved no single
704 F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
therapeutic approach will effectively prevent damage by multipleROS sources The defect of physiological antioxidants may also interferewith antioxidant therapies that are based on one or few exogenousantioxidants
Moreover several antioxidant vitamins such as vitamin E and ca-rotenoids have multiple natural forms with different bioavailabilitymetabolism and bioactivity [157167231] As far as the case of vita-min E supplementation concerns α-tocopherol was used as uniquevitamer in the large majority of supplementation trials so far per-formed and is the form used in the nutritional management of CFpatients Moreover several supplements contain the synthetic (or ra-cemic) form of this vitamin that has lower bioavailability than thenatural form Other forms present in nature and abundantly con-tained in vegetables such as tocotrienols and the less methylatedforms of tocopherol are not represented in many of the supplementformulations so far available in clinical centers and the supplementa-tion with α-tocopherol also limits their bioavailability These formsshow markedly higher susceptibility to hepatic metabolism and bili-ary excretion with respect to α-tocopherol eg the most representedform in blood and solid tissues and if co-supplemented these areeasily displaced during liver uptake and excreted with bile bymeans of competition with the same α-tocopherol Notwithstandingthese minor forms have been proposed to play important physiolog-ical roles showing molecular characteristics transcriptional effectsand antioxidant activities that clearly differentiate them in subfam-ilies with distinct biological functions Some of these such as α-tocopherol eg the second vitamin E form as relative abundance inblood and its carboxyethyl-hydroxychroman metabolite [189] ap-pear to have health-related anti-inflammatory effects which are par-ticularly relevant in lung protection [232233] This has suggestedthat such a group of ldquonon-α-tocopherolrdquo forms may represent anoth-er family of vitamins within the family of vitamin E with an impor-tant but often missed contribution to the proposed health effects ofthis vitamin [163]
These aspects may thus limit the possibility to provide CF patientsof optimal levels of this vitamin in all its components even if they areregularly treated with a vitamin E supplement eg withα-tocopherol
Targeted antioxidant therapy with formulations with higher bio-availability and bioactivity has been anticipated in CF New antioxi-dant formulations have been proposed to overcome main limits ofantioxidant therapies so far proposed for these patients Water-miscible α-tocopheryl acetate containing polysorbate propylene gly-col or polyethylene glycol as emulsifiers form micellar structureswere suggested to providing greater bioavailability than the fat-soluble counterparts These were commercialized with the brandnames of E-viminreg Cremophorreg EL and Aquasolreg E but despitethe original positive expectation [234235] some studies failed to ob-serve a higher response in vitamin E levels when these were com-pared with fat-soluble formulations [236237]
In a pilot study by Papas et al [183] a micellar formulation of fat-soluble nutrients and antioxidants was found to improve plasmalevels of β-carotene γ-tocopherol and CoQ(10) reducing at thesame time some inflammatory markers in induced sputum eg mye-loperoxidase and to a lower extent PMN elastase and total cell countswhile lung function and sputum bacterial counts were unaffectedThe same group recently confirmed the possibility to increase the ab-sorption of fat-soluble micronutrients using formulations with higherbioavailability specifically designed for malabsorbing patients such asCF patients that include also vitamin K and commercialized with thebrand name of AquADEKsreg [162] Despite improved vitamin and mi-cronutrient levels in this non-randomized open-label study AquA-DEKsreg produced only modest improvements in weight percentileand pulmonary function Another recent pilot observation [182] hassuggested the beneficial effect of this formulation on antioxidant andoxidative stress parameters of this oral supplement that surely deservesmore clinical investigation by larger randomized controlled trials
Recent multivitaminic formulations have been designed to containalso the minor forms of vitamin E and specifically γ-tocopherol [238]the expected superiority of which with respect to formulations con-taining only α-tocopherol needs to be verified As discussed abovein the section dedicated to vitamin E further advancements in thetherapy of CF inflammation and oxidative stress could be based onsynthetic forms and natural metabolites of this vitamin that havebeen recently identified to possess higher antioxidant and also anti-inflammatory activity than α-tocopherol (reviewed in [163168])
Pre-clinical investigation of these and other fat-soluble agents iscurrently addressed to develop formulations and administration pro-tocols that may increase the therapeutic efficacy in the airways In theantioxidant therapy of lung dysfunction in CF local administrationprotocols may overcome the limits of oral and systemic administra-tion protocols increasing bioavailability and providing targetedapproach to inflammation and oxidative stress Aerosolization of vita-min E and other fat-soluble micronutrients is possible and may allowdirect administration in the airways to prevent toxicity of smokewhich is closely associated with inflammation and oxidative stress[164165] To our knowledge this as well as other strategies of localadministration such as instillation of solutions such as surfactant-like solutions enriched of vitamin E have not been previously inves-tigated in CF patients and other CF model systems
On the contrary inhalation is an administration route widelyadopted in the case of GSH and NAC therapy described above Inthis context Cys formulations alternative to NAC have been proposedfor use as antioxidant and anti-inflammatory agent for inhalationNacystelyn is a lysine adduct of NAC that thanks to a higher proton-ation equilibrium shows increased water solubility and thus betterbioavailability Nacystelyn has been described to influence IL-8 gener-ation and the inflammatory signaling of bronchial epithelial cells[239] and preliminary clinical evaluation has demonstrated the safetyof this drug [240] Further clinical trials aimed to assess the effect onlung symptomatology of CF patients are needed Direct administra-tion in the airways could also be adopted for micronutrient vitaminswith poor absorption and bioavailability due to GI defects
38 Clinical impact of antioxidant therapy in CF
Huge in vitro and pre-clinical evidence has provided the rationaleto support clinical investigation of antioxidant strategies in CF Theseshould aim to restore the oxidantndashantioxidant balance of CF airwaychallenged by chronic infection and inflammatory cell activation
Some observational trials have confirmed that antioxidants usedas either supplements to the diet or drugs for lung administrationby aerosolized formulations may help in relieving progressive lungdamage and other adverse clinical events of CF such as poor growthSo far few studies have examined with sufficient methodologicalrigor the clinical efficacy of antioxidant therapy in CF This was alsoconcluded in a previous review of the literature by Cantin et al [12]that was published in the beginning of 2006 and is confirmed alsoin a recent analysis of clinical trials on antioxidant therapy in CF pa-tients [213] that examined the literature until September 2010using as sources the databases of the Cochrane CF and Genetic Disor-ders Group CF Trials Register PubMed CINAHL and AMED Useful in-formation was retrieved from just four randomized controlled trialsand one quasi-randomized controlled trial on vitamin C vitamin Eβ-carotene and selenium used as supplements administered aloneor in combination Post-hoc data analysis that was possible only inthree studies on a total of 87 CF patients showed the absence ofany significant improvement in lung function that was selected as pri-mary outcome together with quality of life that improved in one trialSecondary outcomes concerning laboratory indices of oxidative stressand antioxidant status showed several improvements These includedan increase of RBC SeGPx by selenium supplementation done as
705F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
individual or combined supplementation and increased levels of allplasma antioxidants except vitamin C that were observed in all thetrials
The message from these studies to pediatricians and nutritionistswithin the clinical staff of CF centers is that in the absence of solid ev-idence regarding the clinical effectiveness of oral formulations of an-tioxidant supplements in CF (including PUFA) their use as a routineclinical practice should be considered with caution keeping clear inmind that this should represent just a complement of one of themost critical interventions in the life-long clinical management pro-gram of CF patients eg providing an adequate nutriture [140] Inthis context compensating energy and protein malnutrition has toremain the first goal of nutritional management programs Providinghigher intakes of antioxidant micronutrients with food naturally-enriched (or functionalized) of micronutrient antioxidants shouldbe preferred in order to have the higher combination of positive nu-tritional factors that are lost during refinement procedures and over-all industrial processing of dietary supplements
Measures of good practice in clinical management of micro-malnutrition in CF patients would include the support of specializedpersonnel and laboratories The centers should have the possibilityto ascertain with appropriate nutritional and laboratory tests whatthe level of deficiency is for the different micronutrients that each pa-tient may suffer from during a dietary program Monitoring dietaryintakes and blood levels of micronutrients is not sufficient to set apersonalized nutritional intervention with supplements or functionalfoods Sub-optimal intakes and the compliance to nutritional inter-ventions should be verified by means of selected biochemical andclinical criteria Unluckily the latter are still not well established forsome micronutrients such as the fat-soluble vitamins E (reviewed in[163173241]) and K [242243] and also for trace elements such asSe [244] For many of the antioxidants used as supplements inhumans we still do not know exactly several of the biological effectsthat these may provide when introduced in a healthy body and weknow less what these can do in disease These aspects hardly impacton the concept of optimal levels of intake that should be identified foreach micronutrient on an individual basis According with the aspectsdiscussed in the previous sections optimal levels of intake for antiox-idant micronutrients are different in CF patients and healthy subjectsand vary with age and several individual factors
Lung administration of antioxidants by means of aerosolized for-mulations so far used for GSH therapy (see above) is a promisingfield of clinical investigation in CF Toxicity issues are currently themain concern and the subject of clinical evaluation by several groups(described above)
Information on future directions of antioxidant therapy in CF canbe inferred by the analysis of pending or recently completed clinicaltrials that have been searched (December 2011) at ClinicalTrialsgovdatabase matching the terms ldquoantioxidant therapyrdquo or ldquoglutathionerdquowith ldquocystic fibrosisrdquo Fifteen trials were retrieved and those directlyrelated to antioxidant therapy (n=12) are presented in Table 1 andinclude efficacy and safety studies of inhaled drugs as GSH sodiumpyruvate NAC and NO and the dietary supplements AquADEKsregan antioxidant-rich multivitamin supplement epigallocatechin gal-late (EGCG)tocotrienol curcuminoids the amino acid glutaminesulforaphane in broccoli sprouts One trial is investigating the flavo-noid quercetin as CFTR modulator
39 Emerging antioxidant and anti-inflammatory approaches in CF
Mediterranean foods such as olive oil and red wine or severalplant extracts such as herbal tea or grape seed extracts contain aseries of natural compounds with important antioxidant and NOscavenging activity that have been widely investigated for the pre-vention of oxidative stress-related diseases [38245] These havebeen long investigated as template molecules to develop antioxidant
and anti-inflammatory drugs Between the multitudes of natural sub-stances most investigated ones include for instance tyrosol hydroxy-tyrosol gallic and caffeic acids belonging to the family of phenolswhile resveratrol of the stilbenes family epicatechin kaempferoland cianidin are examples of flavonoids examples of fat-soluble phe-nolics are those of the family of tocols (vitamin E) and carotenoids Allthese compounds show different metabolisms and signaling effects[246] Antioxidant and cell protection mechanisms are associatedwith different and sometimes concurrent processes as H-atom trans-fer and electron donation radical trapping and chelation of transitionmetals that can be easily investigated at the chemical level [247] Be-sides these direct antioxidant effects metabolic responses and signal-ing effects of natural compounds are also important to producesecond-generation responses that modify the level of antioxidantprotection and the potential for ROS detoxification in cells and bodyfluids These derive from the transcriptional regulation of antioxidantand pro-oxidant genes that coexist with the modulation of cytokinesecretion and inflammatory enzyme activities
Some of these natural plant-derived antioxidants may provide fur-ther pharmacological activities of possible relevance in CF This is thecase for instance of the plant flavonoids genistein apigenin kaemp-ferol quercetin and hesperidin [248ndash251] that fall in the pharmaco-logical category of ldquopotentiatorsrdquo [252] in that these activate at leastto a certain extent CTFR-mediated Cl currents in normal and CF airwayepithelium investigated either in vitro or in vivo in humans and ani-mal models Actually as prototypal flavonoid-derived potentiatorthe tyrosine kinase inhibitor genistein potentiates the gating of wild-type as well as ΔF508 CFTR and G551D CFTR [253] but at higherdoses it inhibits CFTR gating which make this an unlikely clinical can-didate Similar potentiation effects have been reported for the antiox-idant curcumin [250] that shows an additive effect with respect togenistein-induced potentiation Besides CFTR potentiation whichdoes not appear to have a direct influence on GSH and nutrient trans-port in the lung tissue all these natural substances have been usedalone or in combination with other agents as in vivo enhancers oflung antioxidant protection [246254255] In the case of quercetinthiol-reactive phenolic [256] bronchodilation and anti-inflammatoryeffects by a restoration of the Th1Th2 balance have been reportedin inflammatory syndromes of the lung [255257ndash259] but theseeffects have not been explored in CF Pyocyanin toxicity (see abovein the Section 2) could represent an issue for the use of quercetinand other catechols in infectious diseases of the lung [260]
Other natural antioxidants of potential interest in CF therapy in-clude terpenoids [261] such as terpinen-4-ol a major constituentof tea tree oil that is being investigated in the therapy of anti-biotic resistant organisms specifically against methicillin-resistantStaphylococcus aureus (MRSA) [262] a problem in CF [263] Otherthan being lipophilic antioxidants terpenes can prevent oxidativestress of the CF lung secondarily to the antibiotic effect thereby pro-moting a better control of immuno-inflammatory pathways and lungantioxidants
391 Targeting NF-κB with natural compounds resveratrol and plantextracts
Natural compounds were long known to be useful in designinganti-inflammatory drugs and some of these could find an applicationin the control of the transcription factor kappa-B (NF-κB) that maylead to develop advanced pharmacological tools to control inflamma-tion and to produce higher antioxidant protection to CF airwaysInhibitors targeting NF-κB including transcription factors decoymolecules (TFD) are potent down-regulators of gene expressionand release of IL-8 in CF cells infected with P aeruginosa [264265]
Resveratrol (354prime-trihydroxystilbene ldquoErdquo form) is one of the mostinvestigated natural antioxidant with proposed activity as NF-κBinhibitor This is a phytoalexin present in large quantity in red winepreferentially in the skin of grapes being its concentration
706 F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
50ndash100 μgmg of fresh skin and 13ndash3 mgl of red wine [266]Furthermore resveratrol is a constituent of lsquoDarakchasavarsquo (13ndash6 mgl) an ayurvedic medicine from India [267] The antioxidant activity ofresveratrol has been reported in several papers and occurs also in lungtissues suggesting that resveratrol has potential as a therapeuticagent in respiratory disease [268ndash270] Resveratrol can be consideredone of the most interesting molecules from the natural worldexhibiting strong antioxidant activity that at the same time is able toexert anti inflammatory activity through alteration of NF-κB functionsand efficient inhibition of pro-inflammatory genes [271272] As far asthe effects on CF model systems are concerned Cabrini et al [26]reported the effects of resveratrol on P aeruginosa infected CF IB3-1cells The results obtained demonstrate that resveratrol exhibits minoreffects of IB3-1 cell growth and important inhibitory effects on accumu-lation of IL-8 and GRO-α mRNA while minor effects on IL-6 gene ex-pression were observed These data support recently publishedobservations suggesting inhibitory effects of resveratrol in infection-mediated inflammatory processes [273] Interestingly resveratrol hasbeen reported as a potent inhibitor of NF-κB activity and a promisinganti-inflammatory agent [272274] also in combinationwith othermol-ecules [274275] However in vivo translation of this pre-clinical on res-veratrol is hard to be foreseen This natural compound displays poorbioavailability [276] and further characterization of resveratrol pharma-cokinetics is troublesome since it is hardly measurable in vivo [277]Furthermore the regulation of inflammatory responses by resveratrolhas been suggested to be far more complex than simple direct suppres-sion of NF-κB activity Actually some aspects of the immune responsecould be enhanced by this natural substance which may lead tohypothesize broad negative feedback events on immuno-inflammatorypathways [278] In any case and with these cautions in mind the pub-lished observations on cellular model systems support the concept thatresveratrol and resveratrol-containing formulations deserve further con-sideration to determine their possible therapeutic values in CF
Other inhibitors can be identified from systematic studies of naturalproducts and their ability to interfere with NF-κB activity [279ndash281]Recent studies have demonstrated that the whole extract of Aeglemarmelos (Rutaceae) has strong inhibitory effect on the P aeruginosa-dependent IL-8 induction in human CF-derived bronchial IB3-1 cellswithout affecting cell proliferation [280] Molecular analysis of compo-nents contained in A marmelos extracts revealed that three major com-pounds namely 56-dimethoxy-1-indanone 2-hydroxy-cinnamic acidand 5-methoxy psoralen (5-MOP) reproduce the inhibitory effect ob-servedwith thewhole extract [280] A further example has been recent-ly published using extracts from bergamot (Citrus bergamia Risso) Inthis study the extracts were characterized and the main detected con-stituents were assayed for their biological activity [281] The resultsobtained demonstrated that the extracts from bergamot epicarps con-tain components displaying an inhibitory activity on IL-8 Particularlythe most active molecules were bergapten and citropten These effectshave been confirmed by analyzing mRNA levels and protein release inthe CF cellularmodels IB3-1 and CuFi-1 inducedwith TNF-α or exposedto P aeruginosa
A parallel strategy linking NF-κB inhibition and down-regulationof NF-κB-dependent functions is described in recently publishedstudies based on a structured-based virtual screening (VS) of differ-ently substituted furocoumarins and analogues against NF-κB withthe objective of selecting molecules able to inhibit the binding ofthis transcription factor to DNA [282283] Novel compounds wereidentified with this strategy as potent inhibitors of NF-κB dependentbiological functions to be proposed for the control lung inflammationoccurring in patients affected by CF [282ndash284]
392 Scavengers and regulators of H2O2 and NO
3921 Lactoferrin and OSCNmacr The impaired DUOXLPO system of CFpatients could be the target of therapeutic strategies that may
produce concomitant antimicrobial and antioxidant effects This sys-tem described above in Section 22 represents an important compo-nent of innate immunity with a role in bactericidal defense andregulation of H2O2 metabolism of airways [32] CF patients have alsoreported to show lowered LF levels in the ASL [37] that togetherwith a CFTR-dependent defective efflux of SCNmacr and LPO [36] may cre-ate the environment for a sustained flux of H2O2 and for the genera-tion of highly reactive Fenton species [1138] An ideal therapeuticintervention should restore the LPO-dependent generation of bacteri-cidal OSCNmacr from DUOX-derived H2O2 and SCNmacr in the ASL to controlat the same time the microbial biofilm and the flux of H2O2 into theASL An approach close to this therapeutic mechanism was recentlyproposed for the drug Meveolreg This is a complex of LF and OSCNmacrwith proposed in vivo antimicrobial activity [285] to be evaluatedin clinical trials for the aerosol treatment of lung infections in CFpatients The role for this drug in the control of H2O2 levels of ASLremains to be investigated
3922 Organoselenium compounds Organoselenium compoundshave been proposed as therapeutic agents useful in the antioxidanttherapy of inflammatory conditions These include GPX mimetic mol-ecules such as Ebselenreg (2-phenyl-12-benzisoselenazol-3(2H)-one)or other and more recently developed molecules that are still inpre-clinical steps of evaluation [286] Selectively and specificity of ac-tion are main issues in the therapeutic mechanism of this candidateantioxidant drug that thanks to the electrophilic properties of Se[214] reacts with thiols to reduce H2O2 and other species MoreoverEbselenreg has been described to act as potent non-competitive inhib-itor of extracellular nucleoside diphosphokinase (NDPK) having neg-ligible effect on ecto-ATPase and adenyl kinase activities which areother players of the metabolism of extracellular nucleotides [287]This enzyme together with other nucleoside di- and triphosphatescontributes to regulate several components of the mucociliary clear-ance process (MCC) that protects the lung against infections via acti-vation of epithelial purinergic receptors The inhibition of NDPK bythis GPX-mimetic drug may also impact on the energy status of endo-thelial cells [287] This aspect could be further investigated as a cellu-lar protection mechanism in the pulmonary epithelium of CF patientsbeing the control of cell energy of fundamental importance to preventthe activation of death pathways [288]
Further therapeutic mechanisms for these Se-derived drugs mayderive from the marked activity as inducers of phase II enzymessuch as quinone reductase (QR) and glutathione-S-transferase (GST)[289] This induction response also observed with other electrophilsand redox-active molecules such as natural phenolic antioxidantscould produce higher cellular protection by the acquisition of anincreased capability to detoxify endobiotics generated during oxida-tive stress and inflammation [246]
3923 Melatonin and GSNO as NOx regulators Increased markers ofNO-derived biological damage are present in the CF lung suggestingthe abnormal reactivity of NOx in the inflamed lung of CF patients[52] However an impaired metabolism and biological function ofNO in CF airways (see Section 23) suggests a cautious approach tothe use of agents that may influence the levels and chemical behaviorof NO-derived species (NOx) with possible impact on the physiologi-cal roles of NO in vasodilatation innate immunity and H2O2 metabo-lism of the respiratory tract [290291] NO donors also appear toinfluence CFTR function of alveolar epithelium and gland serouscells [292293]
Main physiological role of the pineal gland hormone melatonin isthe synchronization of circadian rhythms including the sleepndashwakecycle but several other functions dealing with immunomodulatoryantioxidant and cellular protection effects have been identified[294] Melatonin receptor stimulation may also influence cyclic AMPsignaling and the regulation of CFTR ion channel [295296]
707F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
A recent randomized double-blind placebo-controlled study hasexamined the effects of short term melatonin administration (3 mgfor 3 weeks) on sleep and oxidative stress markers in CF [297]According with the expected pharmacological effect of this hormonalsubstance the treatment was successful in improving sleep indicesAt the same time nitrite levels determined in exhaled breath conden-sate (EBC) were reduced to suggest a better control of NOmetabolismof CF airways (discussed above in Section 23) but these effects how-ever were not associated with a significant correction of isoprostaneas lipid peroxidation marker measured in EBC Increasing dosages ofmelatonin could be investigated for the pharmacological treatmentof oxidative stress and immune dysfunction of CF patients due tothe absence of adverse effects of this hormonal substance in humans
The S-nitrosation reaction of thiols is another interesting aspect ofNO pharmacology [53] that may find an application in the therapy oflung complications of CF This has been the case for instance of theS-nitrosothiol GSNO that has been used safely in human trials[298299] This endogenous nitrosothiol with proposed regulatory ef-fect on the CFTR of lung epithelia [292293] is well tolerated in pa-tients with CF when administered by aerosolization and mayproduce better oxygenation [299] thereby suggesting that therapyaimed at restoring endogenous GSNO levels in the CF airway maymerit further clinical evaluation Since the administered GSNO de-composes as shown by the increased levels of expired NO in CF pa-tients under treatment with this nitrosothiol [299] furtherinvestigation should be addressed to ascertain whether GSNO thera-py may merely correspond to a GSH therapy
NO dependent effects on CFTR function should be considered toevaluate mechanism of action and specificity of antioxidant therapiesthat target NO metabolism and function in the CF airways
4 Conclusions and future perspectives
The presence of clinical and biochemical symptoms of inflammationand oxidative stress implies that CF patients have a higher demand ofantioxidant protection The combination of the dysfunctional CFTRwith a lowered intake and absorption of dietary antioxidants producesub-optimal levels of protection from both enzymatic and non-enzymatic defense systems The former could be associated with a de-fective glutathionemetabolism and lowered intake of sulfur-containingamino acids and oligoelements such as zinc and possibly seleniumwhile fat-soluble antioxidant vitamins such as vitamin E and caroten-oids and the water-soluble vitamin C are lowered than in healthy sub-jects due to malabsorption and possibly higher consumption
The increased antioxidant demand in CF patients should be evenhigher in the presence of complications of the lung pancreas andliver Lung comorbidity is particularly important in this contextbeing associated with recurrent infections which results in the alter-nation of inflammatory exacerbates and chronic inflammation Thesesustain the flux of ROS in the airways and promote the formation ofsecond-generation byproducts by the damage of biomolecules suchas PUFA and proteins which may diffuse also at the systemic level tofurther promote adverse biological responses and toxic reactions Pan-creatic insufficiency causes malnutrition and may lead to develop en-docrine and metabolic defects associated with diabetes of CF Theseevents can be further aggravated by the concomitance of liver dys-function and a poor nutritional status Malnutrition is strongly associ-ated with poor prognosis as assessed by pulmonary function andsurvival data [138ndash140] The more aggressive nutritional interven-tions seem to produce better clinical outcomes in these patients andthe possibility of achieving higher antioxidant protection in well-nourished patients by dietary factors could be a key aspect to explainsuch a clinical advantage The assumption that food-derived compo-nentsmay help to prevent the damaging effects of oxidative stress im-proving the antioxidant defenses deserves further investigation at theclinical level This together with the investigation of appropriate
laboratory biomarkers could provide critical information to establishintervention criteria for an early nutritional management of newly di-agnosed patients [5] It is expected that a timely secondary preventionstrategy could influence the progression of CF symptoms thusaffecting with a self-feeding mechanism the same extent of malnutri-tion and oxidative stress along the life of CF patients Since severalfactors contribute to impair the nutritional status of CF patients(such as pancreatic insufficiency chronic malabsorption recurrentsinopulmonary infections and progressive lung disease chronic in-flammation increased energy expenditure suboptimal intake multi-therapy) careful monitoring of the antioxidant status should berecommended According with international guidelines fat-solublevitamin supplementation is of utmost importance in daily practice to-gether with energy intake requirements and pancreatic enzyme-replacement therapy Among these vitamin E β-carotene and ω-3FA have observed to alleviate selected biochemical signs of oxidativestress as measured for instance with well established laboratory indi-ces of lipid peroxidation and in some studies these effects werepreliminarily associated with positive clinical outcomes Notwith-standing randomizedndashcontrolled clinical trials on antioxidant supple-ments (including ω-3 FA) so far carried out in CF have failed toconclusively demonstrate significant beneficial effects on respiratorysymptoms and on the consequent impact that these have on the qual-ity of life of these patients (reviewed in [202213]) whichmay provideno support for the use of these supplements in CF An absence of effi-cacy in prevention studies on antioxidant supplements has also beenobserved in other and possibly less severe oxidative stress-relatedconditions particularly in the secondary prevention of cardiovasculardisease and some forms of cancer by vitamin E and other antioxidantssuch as vitamin C selenium and β-carotene (reviewed in [163]) Dif-ferent biases however have been identified in randomize large clini-cal trials that may account for these disappointing findings Theseinclude patient selection criteria (early interventions and primaryprevention could have more chances of success than secondaryprevention) duration and doses of the treatment use of wrong anti-oxidant formulations and administration protocols absence of verifi-cations of the biological compliance to the treatment etc The samebiases apply for the few trials carried out in CF patients Thus the ap-propriateness and efficacy of nutritional interventions with naturalfood-derived or synthetic antioxidants should be verifiedwith respectto the biological pathways of oxidative stress and clinical variablesthat are identified as end-points Profiles of blood and tissue antioxi-dants as well as of reliable surrogate markers of oxidative stresshave to be selected and determined in highly specialized laboratorieswith a well-established experience on these analyses
Well-timed (early) interventions with appropriate antioxidantformulationsprotocols need to be proposed for the next generationof trials and the development of novel CF-tailored antioxidant andanti-inflammatory agents should be promoted
As a consequence of these considerations more clinical investiga-tion is awaited to identify future successful approaches to the antiox-idant therapy as a measure to further enhance quality of life and theoverall clinical outcome of CF patients
Acknowledgments
We are indebted with the Italian Cystic Fibrosis Research Founda-tion for the support that it provided with its grant program to the re-search activity of the authors of this paper This is a scientific initiativeof the ldquoWorking Group on Inflammation in Cystic Fibrosisrdquo (BragonziA Bravo E Cabrini G Conese M Cuzzocrea S Dechecchi MC De Ales-sandri A Evangelista V Galli F Gambari R Lambiase A Lucidi VManca A Melotti P Minicucci L Motta A Pietraforte D Pompella AQuattrucci S Rizzo R Romano M Sorio C Tesse R) of the Italian Soci-ety for Cystic Fibrosis A particular thank goes to the Prof GianniMastella for the critical revision of the manuscript and for the
708 F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
stimulating research environment that he has contributed to createwithin the Italian Cystic Fibrosis Research Foundation
References
[1] BP OSullivan SD Freedman Cystic fibrosis Lancet 373 (2009) 1891ndash1904[2] P Linsdell JW Hanrahan Glutathione permeability of CFTR Am J Physiol 275
(1998) C323ndashC326[3] L Gao KJ Kim JR Yankaskas HJ Forman Abnormal glutathione transport in
cystic fibrosis airway epithelia Am J Physiol 277 (1999) L113ndashL118[4] RK Rowntree A Harris The phenotypic consequences of CFTR mutations Ann
Hum Genet 67 (2003) 471ndash485[5] EI Back C Frindt D Nohr J Frank R Ziebach M Stern M Ranke HK Biesalski
Antioxidant deficiency in cystic fibrosis when is the right time to take actionAm J Clin Nutr 80 (2004) 374ndash384
[6] LG Wood DA Fitzgerald AK Lee ML Garg Improved antioxidant and fattyacid status of patients with cystic fibrosis after antioxidant supplementation islinked to improved lung function Am J Clin Nutr 77 (2003) 150ndash159
[7] L Iuliano R Monticolo G Straface S Zullo F Galli M Boaz S Quattrucci Asso-ciation of cholesterol oxidation and abnormalities in fatty acid metabolism incystic fibrosis Am J Clin Nutr 90 (2009) 477ndash484
[8] C Libetta V Sepe P Esposito F Galli A Dal Canton Oxidative stress and inflam-mation implications in uremia and hemodialysis Clin Biochem 44 (2011)1189ndash1198
[9] G Bartosz Reactive oxygen species destroyers or messengers Biochem Phar-macol 77 (2009) 1303ndash1315
[10] T Ntimbane B Comte G Mailhot Y Berthiaume V Poitout M Prentki RRabasa-Lhoret E Levy Cystic fibrosis-related diabetes from CFTR dysfunctionto oxidative stress Clin Biochem 30 (2009) 153ndash177
[11] A van der Vliet JP Eiserich GP Marelich B Halliwell CE Cross Oxidativestress in cystic fibrosis does it occur and does it matter Adv Pharmacol 38(1997) 491ndash513
[12] AM Cantin TB White CE Cross HJ Forman RJ Sokol D Borowitz Antioxi-dants in cystic fibrosis Conclusions from the CF antioxidant workshop Bethes-da Maryland Free Radic Biol Med 42 (2007) 15ndash31
[13] LT McGrath P Mallon L Dowey B Silke E McClean M McDonnell A DevineS Copeland S Elborn Oxidative stress during acute respiratory exacerbations incystic fibrosis Thorax 54 (1999) 518ndash523
[14] E Thomson S Brennan R Senthilmohan CL Gangell AL Chapman PD SlyAJ Kettle E Balding LJ Berry JB Carlin R Carzino N de Klerk T Douglas CFoo LW Garratt GL Hall J Harrison A Kicic IA Laing KM Logie J MassieLS Mott C Murray F Parsons N Pillarisetti SR Poreddy SC RanganathanCF Robertson R Robins-Browne PJ Robinson B Skoric SM Stick ENSutanto E Williamson Identifying peroxidases and their oxidants in the earlypathology of cystic fibrosis Free Radic Biol Med 49 (2010) 1354ndash1360
[15] SP Range C Dunster AJ Knox FJ Kelly Treatment of pulmonary exacerba-tions of cystic fibrosis leads to improved antioxidant status Eur Respir J 13(1999) 560ndash564
[16] L Coppo P Ghezzi Thiol regulation of pro-inflammatory cytokines and innateimmunity protein S-thiolation as a novel molecular mechanism Biochem SocTrans 39 (2011) 1268ndash1272
[17] C Verhaeghe C Remouchamps B Hennuy A Vanderplasschen A Chariot SPTabruyn C Oury V Bours Role of IKK and ERK pathways in intrinsic inflamma-tion of cystic fibrosis airways Biochem Pharmacol 73 (2007) 1982ndash1994
[18] TL Bonfield JR Panuska MW Konstan KA Hilliard JB Hilliard H Ghnaim MBerger Inflammatory cytokines in cystic fibrosis lungs Am J Respir Crit CareMed 152 (1995) 2111ndash2118
[19] TL Noah HR Black PW Cheng RE Wood MW Leigh Nasal and bronchoal-veolar lavage fluid cytokines in early cystic fibrosis J Infect Dis 175 (1997)638ndash647
[20] MJ Welsh BW Ramsey FJ Accurso GR Cutting Cystic Fibrosis McGraw-HillNew York 2001
[21] TZ Khan JS Wagener T Bost J Martinez FJ Accurso DW Riches Early pul-monary inflammation in infants with cystic fibrosis Am J Respir Crit CareMed 151 (1995) 1075ndash1082
[22] FA Ratjen Cystic fibrosis pathogenesis and future treatment strategies RespirCare 54 (2009) 595ndash605
[23] J Jacquot O Tabary P Le Rouzic A Clement Airway epithelial cell inflamma-tory signalling in cystic fibrosis Int J Biochem Cell Biol 40 (2008)1703ndash1715
[24] CM Greene P Branagan NG McElvaney Toll-like receptors as therapeutic tar-gets in cystic fibrosis Expert Opin Ther Targets 12 (2008) 1481ndash1495
[25] M Rottner JM Freyssinet MC Martinez Mechanisms of the noxious inflam-matory cycle in cystic fibrosis Respir Res 10 (2009) 23
[26] G Cabrini V Bezzerri I Mancini E Nicolis MC Dechecchi A Tamanini ILampronti L Piccagli N Bianchi M Borgatti R Gambari Targeting transcrip-tion factor activity as a strategy to inhibit pro-inflammatory genes involved incystic fibrosis decoy oligonucleotides and low-molecular weight compoundsCurr Med Chem 17 (2010) 4392ndash4404
[27] CM Greene NG McElvaney Proteases and antiproteases in chronic neutrophiliclungdiseasemdash relevance to drug discovery Br J Pharmacol 158 (2009) 1048ndash1058
[28] AM Cantin Potential for antioxidant therapy of cystic fibrosis Curr Opin PulmMed 10 (2004) 531ndash536
[29] JF Chmiel MW Konstan Inflammation and anti-inflammatory therapies forcystic fibrosis Clin Chest Med 28 (2007) 331ndash346
[30] DP Nichols MW Konstan JF Chmiel Anti-inflammatory therapies for cys-tic fibrosis-related lung disease Clin Rev Allergy Immunol 35 (2008)135ndash153
[31] AJ Kettle T Chan I Osberg R Senthilmohan AL Chapman TJ Mocatta JSWagener Myeloperoxidase and protein oxidation in the airways of youngchildren with cystic fibrosis Am J Respir Crit Care Med 170 (2004)1317ndash1323
[32] H Fischer Mechanisms and function of DUOX in epithelia of the lung AntioxidRedox Signal 11 (2009) 2453ndash2465
[33] B Rada TL Leto Oxidative innate immune defenses by NoxDuox familyNADPH oxidases Contrib Microbiol 15 (2008) 164ndash187
[34] P Moskwa D Lorentzen KJ Excoffon J Zabner PB McCray Jr WM NauseefC Dupuy B Banfi A novel host defense system of airways is defective in cysticfibrosis Am J Respir Crit Care Med 175 (2007) 174ndash183
[35] D Lorentzen L Durairaj AA Pezzulo Y Nakano J Launspach DA Stoltz GZamba PB McCray Jr J Zabner MJ Welsh WM Nauseef B Banfi Concentra-tion of the antibacterial precursor thiocyanate in cystic fibrosis airway secre-tions Free Radic Biol Med 50 (2011) 1144ndash1150
[36] Y Xu S Szep Z Lu The antioxidant role of thiocyanate in the pathogenesis ofcystic fibrosis and other inflammation-related diseases Proc Natl Acad Sci US A 106 (2009) 20515ndash20519
[37] MP Rogan CC Taggart CM Greene PG Murphy SJ ONeill NG McElvaneyLoss of microbicidal activity and increased formation of biofilm due to decreasedlactoferrin activity in patients with cystic fibrosis J Infect Dis 190 (2004)1245ndash1253
[38] B Halliwell JM Guttridge Free Radicals in Biology and Medicine Fourth editionOxford University Press New York 2007
[39] B Rada K Lekstrom S Damian C Dupuy TL Leto The Pseudomonastoxin pyocyanin inhibits the dual oxidase-based antimicrobial system as itimposes oxidative stress on airway epithelial cells J Immunol 181 (2008)4883ndash4893
[40] C Schwarzer B Illek JH Suh SJ Remington H Fischer TE Machen Organelleredox of CF and CFTR-corrected airway epithelia Free Radic Biol Med 43(2007) 300ndash316
[41] JH Roum R Buhl NG McElvaney Z Borok RG Crystal Systemic deficiency ofglutathione in cystic fibrosis J Appl Physiol 75 (1993) 2419ndash2424
[42] VM Hudson Rethinking cystic fibrosis pathology the critical role of abnormalreduced glutathione (GSH) transport caused by CFTR mutation Free RadicBiol Med 30 (2001) 1440ndash1461
[43] PJ Barnes RA Dweik AF Gelb PG Gibson SC George H Grasemann IDPavord F Ratjen PE Silkoff DR Taylor N Zamel Exhaled nitric oxide in pul-monary diseases a comprehensive review Chest 138 (2010) 682ndash692
[44] H Grasemann E Michler M Wallot F Ratjen Decreased concentration of ex-haled nitric oxide (NO) in patients with cystic fibrosis Pediatr Pulmonol 24(1997) 173ndash177
[45] H Grasemann F Ratjen Cystic fibrosis lung disease the role of nitric oxidePediatr Pulmonol 28 (1999) 442ndash448
[46] B Gaston F Ratjen JW Vaughan NR Malhotra RG Canady AH Snyder JFHunt S Gaertig JB Goldberg Nitrogen redox balance in the cystic fibrosis air-way effects of antipseudomonal therapy Am J Respir Crit Care Med 165(2002) 387ndash390
[47] H Grasemann I Ioannidis RP Tomkiewicz H de Groot BK Rubin F RatjenNitric oxide metabolites in cystic fibrosis lung disease Arch Dis Child 78(1998) 49ndash53
[48] H Grasemann R Schwiertz S Matthiesen K Racke F Ratjen Increased argi-nase activity in cystic fibrosis airways Am J Respir Crit Care Med 172(2005) 1523ndash1528
[49] H Grasemann S Al-Saleh JA Scott D Shehnaz A Mehl R Amin M Rafii PPencharz J Belik F Ratjen Asymmetric dimethylarginine contributes to airwaynitric oxide deficiency in patients with cystic fibrosis Am J Respir Crit CareMed 183 (2011) 1363ndash1368
[50] H Grasemann F Kurtz F Ratjen Inhaled L-arginine improves exhaled nitricoxide and pulmonary function in patients with cystic fibrosis Am J RespirCrit Care Med 174 (2006) 208ndash212
[51] H Grasemann F Ratjen Emerging therapies for cystic fibrosis lung disease Ex-pert Opin Emerg Drugs 15 (2010) 653ndash659
[52] BM Morrissey K Schilling JV Weil PE Silkoff DM Rodman Nitric oxide andprotein nitration in the cystic fibrosis airway Arch Biochem Biophys 406(2002) 33ndash39
[53] R Radi Nitric oxide oxidants and protein tyrosine nitration Proc Natl AcadSci U S A 101 (2004) 4003ndash4008
[54] J Chen M Kinter S Shank C Cotton TJ Kelley AG Ziady Dysfunction of Nrf-2in CF epithelia leads to excess intracellular H2O2 and inflammatory cytokineproduction PLoS One 3 (2008) e3367
[55] F Galli M Piroddi C Annetti C Aisa E Floridi A Floridi Oxidative stress andreactive oxygen species Contrib Nephrol 149 (2005) 240ndash260
[56] DT Wright LA Cohn H Li B Fischer CM Li KB Adler Interactions of oxygenradicals with airway epithelium Environ Health Perspect 102 (Suppl 10)(1994) 85ndash90
[57] I Rahman SR Yang SK Biswas Current concepts of redox signaling in thelungs Antioxid Redox Signal 8 (2006) 681ndash689
[58] Q Li JF Engelhardt Interleukin-1beta induction of NFκB is partially regulatedby H2O2-mediated activation of NFκB-inducing kinase J Biol Chem 281(2006) 1495ndash1505
709F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
[59] E Boncoeur VS Criq E Bonvin T Roque A Henrion-Caude DC Gruenert AClement J Jacquot O Tabary Oxidative stress induces extracellular signal-regulated kinase 12 mitogen-activated protein kinase in cystic fibrosis lung ep-ithelial cells potential mechanism for excessive IL-8 expression Int J BiochemCell Biol 40 (2008) 432ndash446
[60] B Fischer J Voynow Neutrophil elastase induces MUC5AC messenger RNA ex-pression by an oxidant-dependent mechanism Chest 117 (2000) 317Sndash320S
[61] B Rada P Gardina TG Myers TL Leto Reactive oxygen species mediate in-flammatory cytokine release and EGFR-dependent mucin secretion in airwayepithelial cells exposed to Pseudomonas pyocyanin Mucosal Immunol 4(2011) 158ndash171
[62] C Schwarzer H Fischer EJ Kim KJ Barber AD Mills MJ Kurth DC GruenertJH Suh TE Machen B Illek Oxidative stress caused by pyocyanin impairs CFTRClminus transport in human bronchial epithelial cells Free Radic Biol Med 45(2008) 1653ndash1662
[63] J Hull M South P Phelan K Grimwood Surfactant composition in infants andyoung children with cystic fibrosis Am J Respir Crit Care Med 156 (1997)161ndash165
[64] KC Meyer A Sharma R Brown M Weatherly FR Moya J Lewandoski JJZimmerman Function and composition of pulmonary surfactant andsurfactant-derived fatty acid profiles are altered in young adults with cystic fi-brosis Chest 118 (2000) 164ndash174
[65] MK Pulfer RC Murphy Formation of biologically active oxysterols during ozo-nolysis of cholesterol present in lung surfactant J Biol Chem 279 (2004)26331ndash26338
[66] V Starosta E Rietschel K Paul U Baumann M Griese Oxidative changes ofbronchoalveolar proteins in cystic fibrosis Chest 129 (2006) 431ndash437
[67] V Starosta M Griese Oxidative damage to surfactant protein D in pulmonarydiseases Free Radic Res 40 (2006) 419ndash425
[68] M Griese R Essl R Schmidt E Rietschel F Ratjen M Ballmann K Paul Pulmo-nary surfactant lung function and endobronchial inflammation in cystic fibro-sis Am J Respir Crit Care Med 170 (2004) 1000ndash1005
[69] M Griese R Essl R Schmidt M Ballmann K Paul E Rietschel F Ratjen Se-quential analysis of surfactant lung function and inflammation in cystic fibrosispatients Respir Res 6 (2005) 133
[70] LG Wood DA Fitzgerald PG Gibson DM Cooper ML Garg Increased plasmafatty acid concentrations after respiratory exacerbations are associated with el-evated oxidative stress in cystic fibrosis patients Am J Clin Nutr 75 (2002)668ndash675
[71] P Montuschi SA Kharitonov G Ciabattoni M Corradi L van Rensen DM Ged-des ME Hodson PJ Barnes Exhaled 8-isoprostane as a new non-invasive bio-marker of oxidative stress in cystic fibrosis Thorax 55 (2000) 205ndash209
[72] CE Collins P Quaggiotto L Wood EV OLoughlin RL Henry ML Garg Elevat-ed plasma levels of F2 alpha isoprostane in cystic fibrosis Lipids 34 (1999)551ndash556
[73] D Hartl V Starosta K Maier I Beck-Speier C Rebhan BF Becker P Latzin RFischer F Ratjen RM Huber E Rietschel S Krauss-Etschmann M Griese In-haled glutathione decreases PGE2 and increases lymphocytes in cystic fibrosislungs Free Radic Biol Med 39 (2005) 463ndash472
[74] GL Milne H Yin JD Morrow Human biochemistry of the isoprostane pathwayJ Biol Chem 283 (2008) 15533ndash15537
[75] G Ciabattoni G Davi M Collura L Iapichino F Pardo A Ganci R Romagnoli JMaclouf C Patrono In vivo lipid peroxidation and platelet activation in cystic fi-brosis Am J Respir Crit Care Med 162 (2000) 1195ndash1201
[76] C Garenc P Julien E Levy Oxysterols in biological systems the gastrointestinaltract liver vascular wall and central nervous system Free Radic Res 44 (2011)47ndash73
[77] AM Cantin SL North RC Hubbard RG Crystal Normal alveolar epithelial lin-ing fluid contains high levels of glutathione J Appl Physiol 63 (1987) 152ndash157
[78] R Tirouvanziam CK Conrad T Bottiglieri LA Herzenberg RB Moss High-dose oral N-acetylcysteine a glutathione prodrug modulates inflammation incystic fibrosis Proc Natl Acad Sci U S A 103 (2006) 4628ndash4633
[79] LW Velsor C Kariya R Kachadourian BJ Day Mitochondrial oxidative stressin the lungs of cystic fibrosis transmembrane conductance regulator proteinmutant mice Am J Respir Cell Mol Biol 35 (2006) 579ndash586
[80] M Kelly-Aubert S Trudel J Fritsch T Nguyen-Khoa M Baudouin-Legros SMoriceau L Jeanson F Djouadi C Matar M Conti M Ollero F Brouillard AEdelman GSH monoethyl ester rescues mitochondrial defects in cystic fibrosismodels Hum Mol Genet 20 (2011) 2745ndash2759
[81] P Ghezzi Role of glutathione in immunity and inflammation in the lung Int JGen Med 4 (2011) 105ndash113
[82] N Dauletbaev K Viel R Buhl TO Wagner J Bargon Glutathione and glutathi-one peroxidase in sputum samples of adult patients with cystic fibrosis J CystFibros 3 (2004) 119ndash124
[83] CE Cross A van der Vliet CA ONeill S Louie B Halliwell Oxidants antioxi-dants and respiratory tract lining fluids Environ Health Perspect 102 (Suppl10) (1994) 185ndash191
[84] K Takeyama K Dabbagh J Jeong Shim T Dao-Pick IF Ueki JA Nadel Oxida-tive stress causes mucin synthesis via transactivation of epidermal growth factorreceptor role of neutrophils J Immunol 164 (2000) 1546ndash1552
[85] N Ballatori SM Krance S Notenboom S Shi K Tieu CL Hammond Glutathi-one dysregulation and the etiology and progression of human diseases BiolChem 390 (2009) 191ndash214
[86] SR Soltaninassab KR Sekhar MJ Meredith ML Freeman Multi-faceted regu-lation of gamma-glutamylcysteine synthetase J Cell Physiol 182 (2000)163ndash170
[87] HR Lopez-Mirabal JR Winther Redox characteristics of the eukaryotic cytosolBiochim Biophys Acta 1783 (2008) 629ndash640
[88] C Hwang AJ Sinskey HF Lodish Oxidized redox state of glutathione in the en-doplasmic reticulum Science 257 (1992) 1496ndash1502
[89] M Murphy Mitochondrial thiols in antioxidant protection and redox signallingdistinct roles for glutathionylation and other thiol modifications AntioxidRedox Signal (2011) ahead of print doi101089ars20114289
[90] BJ Day AM van Heeckeren E Min LW Velsor Role for cystic fibrosis trans-membrane conductance regulator protein in a glutathione response to bronch-opulmonary Pseudomonas infection Infect Immun 72 (2004) 2045ndash2051
[91] Y Zhang K Duan Glutathione exhibits antibacterial activity and increases tetra-cycline efficacy against Pseudomonas aeruginosa Sci China C Life Sci 52 (2009)501ndash505
[92] VM Hudson New insights into the pathogenesis of cystic fibrosis pivotal roleof glutathione system dysfunction and implications for therapy Treat RespirMed 3 (2004) 353ndash363
[93] LW Velsor A van Heeckeren BJ Day Antioxidant imbalance in the lungs ofcystic fibrosis transmembrane conductance regulator protein mutant miceAm J Physiol Lung Cell Mol Physiol 281 (2001) L31ndashL38
[94] I Kogan M Ramjeesingh C Li JF Kidd Y Wang EM Leslie SP Cole CE BearCFTR directly mediates nucleotide-regulated glutathione flux EMBO J 22(2003) 1981ndash1989
[95] NS Gould S Gauthier CT Kariya E Min J Huang DJ Brian Hypertonic salineincreases lung epithelial lining fluid glutathione and thiocyanate two protectiveCFTR-dependent thiols against oxidative injury Respir Res 11 (2010) 119
[96] VT Vasu SJ de Cruz JS Houghton KA Hayakawa BM Morrissey CE CrossJP Eiserich Evaluation of thiol-based antioxidant therapeutics in cystic fibrosissputum focus on myeloperoxidase Free Radic Res 45 (2011) 165ndash176
[97] L Roussel G Martel J Berube S Rousseau P aeruginosa drives CXCL8 synthesisvia redundant toll-like receptors and NADPH oxidase in CFTRF508 airway epi-thelial cells J Cyst Fibros 10 (2011) 107ndash113
[98] GW Lau DJ Hassett H Ran F Kong The role of pyocyanin in Pseudomonas aer-uginosa infection Trends Mol Med 10 (2004) 599ndash606
[99] R Wilson DA Sykes D Watson A Rutman GW Taylor PJ Cole Measurementof Pseudomonas aeruginosa phenazine pigments in sputum and assessment oftheir contribution to sputum sol toxicity for respiratory epithelium InfectImmun 56 (1988) 2515ndash2517
[100] M Muller Pyocyanin induces oxidative stress in human endothelial cells andmodulates the glutathione redox cycle Free Radic Biol Med 33 (2002)1527ndash1533
[101] YQ OMalley KJ Reszka BE Britigan Direct oxidation of 2prime7prime-dichlorodihy-drofluorescein by pyocyanin and other redox-active compounds independentof reactive oxygen species production Free Radic Biol Med 36 (2004)90ndash100
[102] CC Caldwell Y Chen HS Goetzmann Y Hao MT Borchers DJ Hassett LRYoung D Mavrodi L Thomashow GW Lau Pseudomonas aeruginosa exotoxinpyocyanin causes cystic fibrosis airway pathogenesis Am J Pathol 175 (2009)2473ndash2488
[103] YQ OMalley KJ Reszka DR Spitz GM Denning BE Britigan Pseudomonasaeruginosa pyocyanin directly oxidizes glutathione and decreases its levels inairway epithelial cells Am J Physiol Lung Cell Mol Physiol 287 (2004)L94ndashL103
[104] M Muller Glutathione modulates the toxicity of but is not a biologically rele-vant reductant for the Pseudomonas aeruginosa redox toxin pyocyanin FreeRadic Biol Med 50 (2011) 971ndash977
[105] R Cheluvappa R Shimmon M Dawson SN Hilmer DG Le Couteur Reactionsof Pseudomonas aeruginosa pyocyanin with reduced glutathione Acta BiochimPol 55 (2008) 571ndash580
[106] JH Widdicombe Transgenic animals may help resolve a sticky situation in cys-tic fibrosis J Clin Invest 120 (2010) 3093ndash3096
[107] X Sun H Sui JT Fisher Z Yan X Liu HJ Cho NS Joo Y Zhang W Zhou Y YiJM Kinyon DC Lei-Butters MA Griffin P Naumann M Luo J Ascher KWang T Frana JJ Wine DK Meyerholz JF Engelhardt Disease phenotype ofa ferret CFTR-knockout model of cystic fibrosis J Clin Invest 120 (2010)3149ndash3160
[108] NS Joo HJ Cho M Khansaheb JJ Wine Hyposecretion of fluid from trachealsubmucosal glands of CFTR-deficient pigs J Clin Invest 120 (2010) 3161ndash3166
[109] A Bragonzi Murine models of acute and chronic lung infection with cystic fibro-sis pathogens IJMM 300 (2010) 584ndash593
[110] AM van Heeckeren MD Schluchter Murine models of chronic Pseudomonasaeruginosa lung infection Lab Anim 36 (2002) 291ndash312
[111] A Bragonzi D Worlitzsch GB Pier P Timpert M Ulrich M Hentzer JB Ander-sen M Givskov M Conese G Doring Nonmucoid Pseudomonas aeruginosa ex-presses alginate in the lungs of patients with cystic fibrosis and in a mousemodel J Infect Dis 192 (2005) 410ndash419
[112] GS CW Bedrossian DB Singer JJ Hansen HS Rosenberg The lung in cysticfibrosis A quantitative study including prevalence of pathologic findingsamong different age groups Hum Pathol 7 (1976) 195ndash204
[113] WD HA Cash B McCullough WG Johanson Jr JA Bass A rat model of chron-ic respiratory infection with Pseudomonas aeruginosa Am Rev Respir Dis 119(1979) 453ndash459
[114] EM JR Starke C Langston CJ Baker A mouse model of chronic pulmonary in-fection with Pseudomonas aeruginosa and Pseudomonas cepacia Pediatr Res 22(1987) 698ndash702
[115] TJ AM van Heeckeren RW Walenga MW Konstan PB Davis B ErokwuMA Haxhiu TW Ferkol Effect of Pseudomonas infection on weight loss lung
710 F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
mechanics and cytokines in mice Am J Respir Crit Care Med 161 (2000)271ndash279
[116] T Aw G Wierzbicka DP Jones Oral glutathione increases tissue glutathione invivo Chem Biol Interact 80 (1991) 89ndash97
[117] F Favilli P Marraccini T Iantomasi MT Vincenzini Effect of orally adminis-tered glutathione on glutathione levels in some organs of rats role of specifictransporters Br J Nutr 78 (1997) 293ndash300
[118] C Kariya H Leitner E Min C van Heeckeren A van Heeckeren BJ Day A rolefor CFTR in the elevation of glutathione levels in the lung by oral glutathione ad-ministration Am J Physiol Lung Cell Mol Physiol 292 (2007) L1590ndashL1597
[119] K Atkuri JJ Mantovani LA Herzenberg LA Herzenberg N-Acetylcysteinemdashasafe antidote for cysteineglutathione deficiency Curr Opin Pharmacol 7(2007) 355ndash359
[120] R De Lisle E Roach K Jansson Effects of laxative and N-acetylcysteine onmucus accumulation bacterial load transit and inflammation in the cystic fi-brosis mouse small intestine Am J Physiol Gastrointest Liver Physiol 293(2007) G577ndashG584
[121] A Luciani VR Villella S Esposito N Brunetti-Pierri D Medina C Settembre MGavina L Pulze I Giardino M Pettoello-Mantovani M DApolito S Guido EMasliah B Spencer S Quaratino V Raia A Ballabio L Maiuri Defective CFTRinduces aggresome formation and lung inflammation in cystic fibrosis throughROS-mediated autophagy inhibition Nat Cell Biol 12 863ndash875
[122] M Griese J Ramakers A Krasselt V Starosta S Van Koningsbruggen R FischerF Ratjen B Mullinger RM Huber K Maier E Rietschel G Scheuch Improve-ment of alveolar glutathione and lung function but not oxidative state in cysticfibrosis Am J Respir Crit Care Med 169 (2004) 822ndash828
[123] C Bishop VM Hudson SC Hilton C Wilde A pilot study of the effect of inhaledbuffered reduced glutathione on the clinical status of patients with cystic fibro-sis Chest 127 (2005) 308ndash317
[124] WWang C Oliva G Li A Holmgren CH Lillig KL Kirk Reversible silencing of CFTRchloride channels by glutathionylation J Gen Physiol 125 (2005) 127ndash141
[125] N Dauletbaev P Fischer B Aulbach J Gross W Kusche U Thyroff-FriesingerTO Wagner J Bargon A phase II study on safety and efficacy of high-dose N-acetylcysteine in patients with cystic fibrosis Eur J Med Res 14 (2009)352ndash358
[126] R Tirouvanziam Y Gernez CK Conrad RB Moss I Schrijver CE Dunn ZADavies LA Herzenberg Profound functional and signaling changes in viable in-flammatory neutrophils homing to cystic fibrosis airways Proc Natl Acad SciU S A 105 (2008) 4335ndash4339
[127] JH Roum Z Borok NG McElvaney GJ Grimes AD Bokser R Buhl RG Crys-tal Glutathione aerosol suppresses lung epithelial surface inflammatory cell-derived oxidants in cystic fibrosis J Appl Physiol 87 (1999) 438ndash443
[128] A Visca CT Bishop SC Hilton VM Hudson Improvement in clinical markersin CF patients using a reduced glutathione regimen an uncontrolled observa-tional study J Cyst Fibros 7 (2008) 433ndash436
[129] EF Nash A Stephenson F Ratjen E Tullis Nebulized and oral thiol derivativesfor pulmonary disease in cystic fibrosis Cochrane Database Syst Rev (2009)CD007168
[130] AC foundation Drug Development Pipeline 2011[131] S Hoshida T Kuzuya N Yamashita M Nishida S Kitahara M Hori T
Kamada M Tada Gamma-glutamylcysteine ethyl ester for myocardial protec-tion in dogs during ischemia and reperfusion J Am Coll Cardiol 24 (1994)1391ndash1397
[132] J Lok W Leung S Zhao S Pallast K van Leyen S Guo X Wang A Yalcin EHLo Gamma-glutamylcysteine ethyl ester protects cerebral endothelial cells dur-ing injury and decreases bloodndashbrain barrier permeability after experimentalbrain trauma J Neurochem 118 (2011) 248ndash255
[133] Z Borok R Buhl GJ Grimes AD Bokser RC Hubbard KJ Holroyd JH RoumDB Czerski AM Cantin RG Crystal Effect of glutathione aerosol on oxidantndashantioxidant imbalance in idiopathic pulmonary fibrosis Lancet 338 (1991)215ndash216
[134] KJ Holroyd R Buhl Z Borok JH Roum AD Bokser GJ Grimes D Czerski AMCantin RG Crystal Correction of glutathione deficiency in the lower respiratorytract of HIV seropositive individuals by glutathione aerosol treatment Thorax 48(1993) 985ndash989
[135] J Hull P Vervaart K Grimwood P Phelan Pulmonary oxidative stress responsein young children with cystic fibrosis Thorax 52 (1997) 557ndash560
[136] A Corti A Paolicchi M Franzini S Dominici AF Casini A Pompella The S-thiolating activity of membrane gamma-glutamyltransferase formation ofcysteinyl-glycine mixed disulfides with cellular proteins and in the cell microen-vironment Antioxid Redox Signal 7 (2005) 911ndash918
[137] A Corti M Franzini AF Casini A Paolicchi A Pompella Vitamin C supply tobronchial epithelial cells linked to glutathione availability in elfmdasha role for se-creted gamma-glutamyltransferase J Cyst Fibros 7 (2008) 174ndash178
[138] A Munck Nutritional considerations in patients with cystic fibrosis Expert RevRespir Med 4 (2010) 47ndash56
[139] JL Matel CE Milla Nutrition in cystic fibrosis Semin Respir Crit Care Med 30(2009) 579ndash586
[140] D Salvatore R Buzzetti E Baldo MP Forneris V Lucidi D Manunza IMarinelli B Messore AS Neri V Raia ML Furnari G Mastella An overviewof international literature from cystic fibrosis registries 2 Neonatal screeningand nutritiongrowth J Cyst Fibros 9 (2010) 75ndash83
[141] KF Joosten JM Hulst Malnutrition in pediatric hospital patients current is-sues Nutrition 27 (2011) 133ndash137
[142] S Fustik T Jacovska L Spirevska S Koceva Protein-energy malnutrition as thefirst manifestation of cystic fibrosis in infancy Pediatr Int 51 (2009) 678ndash683
[143] J Himmelfarb E McMonagle Albumin is the major plasma protein target of ox-idant stress in uremia Kidney Int 60 (2001) 358ndash363
[144] P Stenvinkel JJ Carrero J Axelsson B Lindholm O Heimburger Z MassyEmerging biomarkers for evaluating cardiovascular risk in the chronic kidneydisease patient how do new pieces fit into the uremic puzzle Clin J Am SocNephrol 3 (2008) 505ndash521
[145] M Roche P Rondeau NR Singh E Tarnus E Bourdon The antioxidant proper-ties of serum albumin FEBS Lett 582 (2008) 1783ndash1787
[146] D Giustarini A Milzani I Dalle-Donne R Rossi Red blood cells as a physiolog-ical source of glutathione for extracellular fluids Blood Cells Mol Dis 40 (2008)174ndash179
[147] A Meister ME Anderson Glutathione Annu Rev Biochem 52 (1983) 711ndash760[148] B Alvarez S Carballal L Turell R Radi Formation and reactions of sulfenic acid
in human serum albumin Methods Enzymol 473 (2010) 117ndash136[149] S Carballal B Alvarez L Turell H Botti BA Freeman R Radi Sulfenic acid in
human serum albumin Amino Acids 32 (2007) 543ndash551[150] LR Barclay AM Bailey D Kong The antioxidant activity of alpha-tocopherol-
bovine serum albumin complex in micellar and liposome autoxidations J BiolChem 260 (1985) 15809ndash15814
[151] T Ishii T Ichikawa K Minoda K Kusaka S Ito Y Suzuki M Akagawa K Mochi-zuki T Goda T Nakayama Human serum albumin as an antioxidant in the ox-idation of (minus)-epigallocatechin gallate participation of reversible covalentbinding for interaction and stabilization Biosci Biotechnol Biochem 75(2011) 100ndash106
[152] F Galli S Rovidati S Benedetti U Buoncristiani C Covarelli A Floridi F Canes-trari Overexpression of erythrocyte glutathione S-transferase in uremia and di-alysis Clin Chem 45 (1999) 1781ndash1788
[153] D Borowitz RD Baker V Stallings Consensus report on nutrition for pediat-ric patients with cystic fibrosis J Pediatr Gastroenterol Nutr 35 (2002)246ndash259
[154] LJ Filer Jr SW Wright MP Manning KE Mason Absorption of alpha-tocopherol and tocopherylesters by premature and full term infants and chil-dren in health and disease Pediatrics 8 (1951) 328ndash339
[155] L Lancellotti C DOrazio G Mastella G Mazzi U Lippi Deficiency of vitamins Eand A in cystic fibrosis is independent of pancreatic function and current en-zyme and vitamin supplementation Eur J Pediatr 155 (1996) 281ndash285
[156] MN Sathe AS Patel Update in pediatrics focus on fat-soluble vitamins NutrClin Pract 25 (2010) 340ndash346
[157] MG Traber The ABCs of vitamin E and beta-carotene absorption Am J ClinNutr 80 (2004) 3ndash4
[158] TF Dolan Jr Hemolytic anemia and edema as the initial signs in infants withcystic fibrosis Consider this diagnosis even in absence of pulmonary symptomsClin Pediatr 15 (1976) 597ndash600
[159] DR James M Alfaham MC Goodchild Increased susceptibility to peroxide-induced haemolysis with normal vitamin E concentrations in cystic fibrosisClin Chim Acta 204 (1991) 279ndash290
[160] SA Peters FJ Kelly Vitamin E supplementation in cystic fibrosis J Pediatr Gas-troenterol Nutr 22 (1996) 341ndash345
[161] A Maqbool VA Stallings Update on fat-soluble vitamins in cystic fibrosis CurrOpin Pulm Med 14 (2008) 574ndash581
[162] SD Sagel MK Sontag MM Anthony P Emmett KA Papas Effect of anantioxidant-rich multivitamin supplement in cystic fibrosis J Cyst Fibros 10(2011) 31ndash36
[163] F Galli A Azzi Present trends in vitamin E research Biofactors 36 (2010)33ndash42
[164] A Hamahata P Enkhbaatar ER Kraft M Lange SW Leonard MG Traber RACox FC Schmalstieg HK Hawkins EB Whorton EM Horvath C Szabo LDTraber DN Herndon DL Traber Gamma-tocopherol nebulization by a lipidaerosolization device improves pulmonary function in sheep with burn andsmoke inhalation injury Free Radic Biol Med 45 (2008) 425ndash433
[165] JP Anais N Razzouq M Carvalho C Fernandez A Astier M Paul A AstierH Fessi AM Lorino Development of alpha-tocopherol acetate nanoparti-cles influence of preparative processes Drug Dev Ind Pharm 35 (2009)216ndash223
[166] JM Zingg Molecular and cellular activities of vitamin E analogues Mini RevMed Chem 7 (2007) 543ndash558
[167] V Viola F Pilolli M Piroddi E Pierpaoli F Orlando M Provinciali M Betti FMazzini F Galli Why tocotrienols work better insights into the in vitro anti-cancer mechanism of vitamin E Genes Nutr 7 (2011) 29ndash41
[168] F Galli F Mazzini L Bamonti L Gille S Bohmdorfer M Piroddi T Netscher FJKelly T Rosenau Tocotrienamines and tocopheramines reactions with radicalsand metal ions Bioorg Med Chem 19 (2011) 6483ndash6491
[169] A Kuhad K Chopra Attenuation of diabetic nephropathy by tocotrienol in-volvement of NFκB signaling pathway Life Sci 84 (2009) 296ndash301
[170] Q Jiang X Yin MA Lill ML Danielson H Freiser J Huang Long-chain carbox-ychromanols metabolites of vitamin E are potent inhibitors of cyclooxygenasesProc Natl Acad Sci U S A 105 (2008) 20464ndash20469
[171] ER Miller III R Pastor-Barriuso D Dalal RA Riemersma LJ Appel E GuallarMeta-analysis high-dosage vitamin E supplementation may increase all-causemortality Ann Intern Med 142 (2005) 37ndash46
[172] JN Hathcock A Azzi J Blumberg T Bray A Dickinson B Frei I Jialal CSJohnston FJ Kelly K Kraemer L Packer S Parthasarathy H Sies MG TraberVitamins E and C are safe across a broad range of intakes Am J Clin Nutr 81(2005) 736ndash745
[173] R Brigelius-Flohe F Galli Vitamin E a vitamin still awaiting the detection of itsbiological function Mol Nutr Food Res 54 (2010) 583ndash587
711F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
[174] MG Traber B Frei JS Beckman Vitamin E revisited do new data validate ben-efits for chronic disease prevention Curr Opin Lipidol 19 (2008) 30ndash38
[175] F Galli Meeting report Vitamin E Satellite Symposium (VESS) associated to theAnnual Meeting of the SFRR-Europe Rome 26 August 2009 Free Radic Res 43(2009) 1256ndash1257
[176] LJ Roberts II JA Oates MF Linton S Fazio BP Meador MD Gross Y Shyr JDMorrow The relationship between dose of vitamin E and suppression of oxida-tive stress in humans Free Radic Biol Med 43 (2007) 1388ndash1393
[177] EFSA- EFSA Scientific Opinion of the Panel on Food Additives FlavouringsProcessing Aids and Materials in Contact with Food on a request from the Com-mission on mixed tocopherols tocotrienol tocopherol and tocotrienols assources for vitamin E in EFSA- EFSA (Ed) vol 640 The EFSA Journal2008 pp 1ndash34
[178] P Rust I Eichler S Renner I Elmadfa Long-term oral beta-carotene supple-mentation in patients with cystic fibrosis mdash effects on antioxidative status andpulmonary function Ann Nutr Metab 44 (2000) 30ndash37
[179] G Lepage J Champagne N Ronco A Lamarre I Osberg RJ Sokol CC Roy Sup-plementation with carotenoids corrects increased lipid peroxidation in childrenwith cystic fibrosis Am J Clin Nutr 64 (1996) 87ndash93
[180] BM Winklhofer-Roob H Puhl G Khoschsorur MA vant Hof H EsterbauerDH Shmerling Enhanced resistance to oxidation of low density lipoproteinsand decreased lipid peroxide formation during beta-carotene supplementationin cystic fibrosis Free Radic Biol Med 18 (1995) 849ndash859
[181] RC Graham-Maar JI Schall N Stettler BS Zemel VA Stallings Elevated vita-min A intake and serum retinol in preadolescent children with cystic fibrosisAm J Clin Nutr 84 (2006) 174ndash182
[182] I Sadowska-Woda M Rachel J Pazdan E Bieszczad-Bedrejczuk K PawliszakNutritional supplement attenuates selected oxidative stress markers in pediatricpatients with cystic fibrosis Nutr Res (New York NY) 31 (2011) 509ndash518
[183] KA Papas MK Sontag C Pardee RJ Sokol SD Sagel FJ Accurso JS WagenerA pilot study on the safety and efficacy of a novel antioxidant rich formulation inpatients with cystic fibrosis J Cyst Fibros 7 (2008) 60ndash67
[184] Y Saito A Fukuhara K Nishio M Hayakawa Y Ogawa H Sakamoto K Fujii YYoshida E Niki Characterization of cellular uptake and distribution of coen-zyme Q10 and vitamin E in PC12 cells J Nutr Biochem 20 (2009) 350ndash357
[185] AA Franke CM Morrison JL Bakke LJ Custer X Li RV Cooney CoenzymeQ10 in human blood native levels and determinants of oxidation during proces-sing and storage Free Radic Biol Med 48 (2010) 1610ndash1617
[186] HN Bhagavan RK Chopra Plasma coenzyme Q10 response to oral ingestion ofcoenzyme Q10 formulations Mitochondrion 7 (2007) S78ndashS88 (Suppl)
[187] HN Bhagavan RK Chopra Coenzyme Q10 absorption tissue uptake metabo-lism and pharmacokinetics Free Radic Res 40 (2006) 445ndash453
[188] F Galli R Lee C Dunster FJ Kelly Gas chromatography mass spectrometryanalysis of carboxyethyl-hydroxychroman metabolites of alpha- and gamma-tocopherol in human plasma Free Radic Biol Med 32 (2002) 333ndash340
[189] F Galli R Lee J Atkinson A Floridi FJ Kelly Gamma-tocopherol biokineticsand transformation in humans Free Radic Res 37 (2003) 1225ndash1233
[190] TA Laguna MK Sontag I Osberg JS Wagener FJ Accurso RJ Sokol De-creased total serum coenzyme-Q10 concentrations a longitudinal study in chil-dren with cystic fibrosis J Pediatr 153 (2008) 402ndash407
[191] T Frischer JK Myung G Maurer I Eichler Z Szepfalusi G Lubec Possible dys-regulation of chaperon and metabolic proteins in cystic fibrosis bronchial tissueProteomics 6 (2006) 3381ndash3388
[192] C Andersson MM Zaman AB Jones SD Freedman Alterations in immune re-sponse and PPARLXR regulation in cystic fibrosis macrophages J Cyst Fibros 7(2008) 68ndash78
[193] SD Freedman PG Blanco MM Zaman JC Shea M Ollero IK Hopper DAWeed A Gelrud MM Regan M Laposata JG Alvarez BP OSullivan Associa-tion of cystic fibrosis with abnormalities in fatty acid metabolism N Engl JMed 350 (2004) 560ndash569
[194] S Van Biervliet G Vanbillemont JP Van Biervliet D Declercq E Robberecht AChristophe Relation between fatty acid composition and clinical status or geno-type in cystic fibrosis patients Ann Nutr Metab 51 (2007) 541ndash549
[195] SD Freedman MH Katz EM Parker M Laposata MY Urman JG AlvarezA membrane lipid imbalance plays a role in the phenotypic expression ofcystic fibrosis in cftr(minusminus) mice Proc Natl Acad Sci U S A 96 (1999)13995ndash14000
[196] S Van Biervliet S Vande Velde JP Van Biervliet E Robberecht The effect ofzinc supplements in cystic fibrosis patients Ann Nutr Metab 52 (2008)152ndash156
[197] WR Henderson Jr SJ Astley MM McCready P Kushmerick S Casey JWBecker BW Ramsey Oral absorption of omega-3 fatty acids in patients withcystic fibrosis who have pancreatic insufficiency and in healthy control subjectsJ Pediatr 124 (1994) 400ndash408
[198] I Durieu E Vericel D Guichardant H Roth JP Steghens J Drai RN JosserandE Fontaine M Lagarde G Bellon Fatty acids platelets and oxidative markersfollowing intravenous n-3 fatty acids administration in cystic fibrosis an openpilot observational study J Cyst Fibros 6 (2007) 320ndash326
[199] LG Wood DA Fitzgerald ML Garg Hypothesis vitamin E complements poly-unsaturated fatty acids in essential fatty acid deficiency in cystic fibrosis J AmColl Nutr 22 (2003) 253ndash257
[200] JD Lloyd-Still SB Johnson RT Holman Essential fatty acid status in cystic fi-brosis and the effects of safflower oil supplementation Am J Clin Nutr 34(1981) 1ndash7
[201] A Maqbool JI Schall JF Garcia-Espana BS Zemel B Strandvik VAStallings Serum linoleic acid status as a clinical indicator of essential fatty
acid status in children with cystic fibrosis J Pediatr Gastroenterol Nutr 47(2008) 635ndash644
[202] C Oliver N Jahnke Omega-3 fatty acids for cystic fibrosis Cochrane DatabaseSyst Rev (2011) CD002201
[203] B Strandvik E Gronowitz F Enlund T Martinsson J Wahlstrom Essential fattyacid deficiency in relation to genotype in patients with cystic fibrosis J Pediatr139 (2001) 650ndash655
[204] P Rise S Volpi C Colombo RF Padoan C DOrazio S Ghezzi PMelotti V BennatoC Agostoni BM Assael C Galli Whole blood fatty acid analysis with micromethodin cystic fibrosis and pulmonary disease J Cyst Fibros 9 (2010) 228ndash233
[205] H Cao K Gerhold JR Mayers MM Wiest SM Watkins GS Hotamisligil Iden-tification of a lipokine a lipid hormone linking adipose tissue to systemic me-tabolism Cell 134 (2008) 933ndash944
[206] RR Malapaka SK Khoo J Zhang JH Choi XE Zhou Y Xu Y Gong J Li ELYong MJ Chalmers L Chang JH Resau PR Griffin YE Chen HE Xu Iden-tification and mechanism of a ten carbon fatty acid as a modulating ligand ofperoxisome proliferator activated receptors J Biol Chem 287 (2012)183ndash195
[207] T Hara A Hirasawa A Ichimura I Kimura G Tsujimoto Free fatty acid recep-tors FFAR1 and GPR120 as novel therapeutic targets for metabolic disorders JPharm Sci 100 (2011) 3594ndash3601
[208] R Gupta P Rathi S Bradoo Lipase mediated upgradation of dietary fats andoils Crit Rev Food Sci Nutr 43 (2003) 635ndash644
[209] BH Jennings CC Akoh Lipase-catalyzed modification of rice bran oil to incor-porate capric acid J Agric Food Chem 48 (2000) 4439ndash4443
[210] J Hoeks M Mensink MK Hesselink K Ekroos P Schrauwen Long- andMedium-Chain Fatty Acids Induce Insulin Resistance to a Similar Extent inHumans Despite Marked Differences in Muscle Fat Accumulation J Clin Endo-crinol Metab 97 (2012) 208ndash216
[211] PJ Congden G Bruce MM Rothburn PC Clarke JM Littlewood J KelleherMS Losowsky Vitamin status in treated patients with cystic fibrosis ArchDis Child 56 (1981) 708ndash714
[212] BM Winklhofer-Roob H Ellemunter M Fruhwirth SE Schlegel-Haueter GKhoschsorur MA vant Hof DH Shmerling Plasma vitamin C concentrationsin patients with cystic fibrosis evidence of associations with lung inflammationAm J Clin Nutr 65 (1997) 1858ndash1866
[213] L Shamseer D Adams N Brown JA Johnson S Vohra Antioxidant micronutri-ents for lung disease in cystic fibrosis Cochrane Database Syst Rev (2010)CD007020
[214] C Santi S Santoro Electrophilic Selenium First edition Wiley-VCH VerlagGmbH amp Co KGaA 2012
[215] L Flohe S Toppo G Cozza F Ursini A comparison of thiol peroxidase mecha-nisms Antioxid Redox Signal 15 (2010) 763ndash780
[216] L Flohe JR Andreesen R Brigelius-Flohe M Maiorino F Ursini Selenium theelement of the moon in life on earth IUBMB Life 49 (2000) 411ndash420
[217] V Valdiglesias E Pasaro J Mendez B Laffon In vitro evaluation of seleniumgenotoxic cytotoxic and protective effects a review Arch Toxicol 84(2010) 337ndash351
[218] P Foucaud P Therond M Marchand F Brion JF Demelier J Navarro Seleniumand vitamin E in mucoviscidosis Arch Fr Pediatr 45 (1988) 383ndash386
[219] J Neve R Van Geffel M Hanocq L Molle Plasma and erythrocyte zinc copperand selenium in cystic fibrosis Acta Paediatr Scand 72 (1983) 437ndash440
[220] BM Winklhofer-Roob B Tiran PE Tuchschmid MA vant Hof DH ShmerlingEffects of pancreatic enzyme preparations on erythrocyte glutathione peroxi-dase activities and plasma selenium concentrations in cystic fibrosis FreeRadic Biol Med 25 (1998) 242ndash249
[221] JD Lloyd-Still HE Ganther Selenium and glutathione peroxidase levels in cys-tic fibrosis Pediatrics 65 (1980) 1010ndash1012
[222] D Tsavachidou TJ McDonnell S Wen X Wang F Vakar-Lopez LL Pisters CAPettaway CG Wood KA Do PF Thall C Stephens E Efstathiou R Taylor DGMenter P Troncoso SM Lippman CJ Logothetis J Kim Selenium and vitaminE cell type- and intervention-specific tissue effects in prostate cancer J NatlCancer Inst 101 (2009) 306ndash320
[223] IN Zelko TJ Mariani RJ Folz Superoxide dismutase multigene family acomparison of the CuZn-SOD (SOD1) Mn-SOD (SOD2) and EC-SOD (SOD3)gene structures evolution and expression Free Radic Biol Med 33 (2002)337ndash349
[224] RP Bowler JD Crapo Oxidative stress in airways is there a role for extracellu-lar superoxide dismutase Am J Respir Crit Care Med 166 (2002) S38ndashS43
[225] K Best K McCoy S Gemma RA Disilvestro Copper enzyme activities in cysticfibrosis before and after copper supplementation plus or minus zinc Metabo-lism 53 (2004) 37ndash41
[226] SS Percival GP Kauwell E Bowser M Wagner Altered copper status in adultmen with cystic fibrosis J Am Coll Nutr 18 (1999) 614ndash619
[227] NF Krebs JE Westcott TD Arnold BM Kluger FJ Accurso LV Miller KMHambidge Abnormalities in zinc homeostasis in young infants with cystic fibro-sis Pediatr Res 48 (2000) 256ndash261
[228] D Easley N Krebs M Jefferson L Miller J Erskine F Accurso KM HambidgeEffect of pancreatic enzymes on zinc absorption in cystic fibrosis J Pediatr Gas-troenterol Nutr 26 (1998) 136ndash139
[229] S Van Biervliet JP Van Biervliet E Robberecht Serum zinc in patients with cys-tic fibrosis at diagnosis and after one year of therapy Biol Trace Elem Res 112(2006) 205ndash211
[230] S Van Biervliet JP Van Biervliet S Vande Velde E Robberecht Serum zinc con-centrations in cystic fibrosis patients aged above 4 years a cross-sectional eval-uation Biol Trace Elem Res 119 (2007) 19ndash26
712 F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
[231] F Galli M Cristina Polidori W Stahl P Mecocci FJ Kelly Vitamin E biotransfor-mation in humans Vitam Horm 76 (2007) 263ndash280
[232] J Wiser NE Alexis Q Jiang W Wu C Robinette R Roubey DB Peden In vivogamma-tocopherol supplementation decreases systemic oxidative stress andcytokine responses of human monocytes in normal and asthmatic subjectsFree Radic Biol Med 45 (2008) 40ndash49
[233] JG Wagner Q Jiang JR Harkema B Illek DD Patel BN Ames DB PedenOzone enhancement of lower airway allergic inflammation is prevented bygamma-tocopherol Free Radic Biol Med 43 (2007) 1176ndash1188
[234] JT Harries DP Muller Absorption of different doses of fat soluble and watermiscible preparations of vitamin E in children with cystic fibrosis Arch DisChild 46 (1971) 341ndash344
[235] EI Back C Frindt E Ocenaskova D Nohr M Stern HK Biesalski Can changesin hydrophobicity increase the bioavailability of alpha-tocopherol Eur J Nutr45 (2006) 1ndash6
[236] SZ Nasr MH OLeary C Hillermeier Correction of vitamin E deficiency withfat-soluble versus water-miscible preparations of vitamin E in patients with cys-tic fibrosis J Pediatr 122 (1993) 810ndash812
[237] S Soltani-Frisk E Gronowitz H Andersson B Strandvik Water-miscibletocopherol is not superior to fat-soluble preparation for vitamin E absorptionin cystic fibrosis Acta Paediatr 90 (2001) 1112ndash1115
[238] K Papas J Kalbfleisch R Mohon Bioavailability of a novel water-soluble vi-tamin E formulation in malabsorbing patients Dig Dis Sci 52 (2007)347ndash352
[239] F Antonicelli M Parmentier EM Drost N Hirani I Rahman K Donaldson WMacNee Nacystelyn inhibits oxidant-mediated interleukin-8 expression andNF-kappaB nuclear binding in alveolar epithelial cells Free Radic Biol Med 32(2002) 492ndash502
[240] EM App D Baran I Dab A Malfroot M Coffiner F Vanderbist M King Dose-finding and 24-h monitoring for efficacy and safety of aerosolized Nacystelyn incystic fibrosis Eur Respir J 19 (2002) 294ndash302
[241] MG Traber How much vitamin E hellip Just enough Am J Clin Nutr 84 (2006)959ndash960
[242] JC McCann BN Ames Vitamin K an example of triage theory is micronu-trient inadequacy linked to diseases of aging Am J Clin Nutr 90 (2009)889ndash907
[243] M Fusaro G Crepaldi S Maggi F Galli A DAngelo L Calo S Giannini DMiozzo M Gallieni Vitamin K bone fractures and vascular calcifications inchronic kidney disease an important but poorly studied relationship J Endocri-nol Invest 34 (2010) 317ndash323
[244] JC McCann BN Ames Adaptive dysfunction of selenoproteins from the per-spective of the triage theory why modest selenium deficiency may increaserisk of diseases of aging FASEB J 25 (2011) 1793ndash1814
[245] R Apak K Guclu M Ozyurek B Bektas Oglu M Bener Cupric ion reducing an-tioxidant capacity assay for food antioxidants vitamins polyphenolics and fla-vonoids in food extracts Methods Mol Biol 477 (2008) 163ndash193
[246] F Galli Interactions of polyphenolic compounds with drug disposition and me-tabolism Curr Drug Metab 8 (2007) 830ndash838
[247] RL Prior X Wu K Schaich Standardized methods for the determination of an-tioxidant capacity and phenolics in foods and dietary supplements J Agric FoodChem 53 (2005) 4290ndash4302
[248] C Azbell S Zhang D Skinner J Fortenberry EJ Sorscher BA WoodworthHesperidin stimulates cystic fibrosis transmembrane conductance regulator-mediated chloride secretion and ciliary beat frequency in sinonasal epitheliumOtolaryngol Head Neck Surg 143 (2010) 397ndash404
[249] G Wegrzyn J Jakobkiewicz-Banecka M Gabig-Ciminska E Piotrowska M Nar-ajczyk A Kloska M Malinowska D Dziedzic I Golebiewska M Moskot AWegrzyn Genistein a natural isoflavone with a potential for treatment of ge-netic diseases Biochem Soc Trans 38 (2010) 695ndash701
[250] YC Yu H Miki Y Nakamura A Hanyuda Y Matsuzaki Y Abe M Yasui K Ta-naka TC Hwang SG Bompadre Y Sohma Curcumin and genistein additivelypotentiate G551D-CFTR J Cyst Fibros 10 (2011) 243ndash252
[251] B Illek H Fischer Flavonoids stimulate Cl conductance of human airway epithe-lium in vitro and in vivo Am J Physiol 275 (1998) L902ndashL910
[252] JL Kreindler Cystic fibrosis exploiting its genetic basis in the hunt for newtherapies Pharmacol Ther 125 (2010) 219ndash229
[253] B Illek L Zhang NC Lewis RB Moss JY Dong H Fischer Defective function ofthe cystic fibrosis-causing missense mutation G551D is recovered by genisteinAm J Physiol 277 (1999) C833ndashC839
[254] P Anandakumar S Kamaraj S Jagan G Ramakrishnan R Vinodhkumar TDevaki Capsaicin modulates pulmonary antioxidant defense system during ben-zo(a)pyrene-induced lung cancer in Swiss albinomice Phytother Res 22 (2008)529ndash533
[255] I Rahman Antioxidant therapeutic advances in COPD Ther Adv Respir Dis 2(2008) 351ndash374
[256] AW Boots H Li RP Schins R Duffin JW Heemskerk A Bast GR Haenen Thequercetin paradox Toxicol Appl Pharmacol 222 (2007) 89ndash96
[257] M Joskova S Franova V Sadlonova Acute bronchodilator effect of quercetin inexperimental allergic asthma Bratisl Lek Listy 112 (2011) 9ndash12
[258] HJ Park CM Lee ID Jung JS Lee YI Jeong JH Chang SH Chun MJ Kim IWChoi SC Ahn YK Shin SR Yeom YM Park Quercetin regulates Th1Th2 balancein a murine model of asthma Int Immunopharmacol 9 (2009) 261ndash267
[259] AP Rogerio A Kanashiro C Fontanari EV da Silva YM Lucisano-ValimEG Soares LH Faccioli Anti-inflammatory activity of quercetin and iso-quercitrin in experimental murine allergic asthma Inflamm Res 56 (2007)402ndash408
[260] M Muller Polyphenol cytotoxicity induced by the bacterial toxin pyocyaninrole of NQO1 Free Radic Biol Med 47 (2009) 84ndash91
[261] J Grassmann Terpenoids as plant antioxidants Vitam Horm 72 (2005)505ndash535
[262] P Allen Tea tree oil the science behind the antimicrobial hype Lancet 358(2001) 1245
[263] EC Dasenbrook W Checkley CA Merlo MW Konstan N Lechtzin MP BoyleAssociation between respiratory tract methicillin-resistant Staphylococcus aure-us and survival in cystic fibrosis JAMA 303 (2010) 2386ndash2392
[264] V Bezzerri M Borgatti E Nicolis I Lampronti MC Dechecchi I Mancini PRizzotti R Gambari G Cabrini Transcription factor oligodeoxynucleotides toNF-kappaB inhibit transcription of IL-8 in bronchial cells Am J Respir CellMol Biol 39 (2008) 86ndash96
[265] R Gambari M Borgatti V Bezzerri E Nicolis I Lampronti MC Dechecchi IMancini A Tamanini G Cabrini Decoy oligodeoxyribonucleotides and peptidenucleic acids-DNA chimeras targeting nuclear factor kappa-B inhibition of IL-8 gene expression in cystic fibrosis cells infected with Pseudomonas aeruginosaBiochem Pharmacol 80 (2010) 1887ndash1894
[266] M Adrian P Jeandet AC Douillet-Breuil L Tesson R Bessis Stilbene content ofmature Vitis vinifera berries in response to UV-C elicitation J Agric Food Chem48 (2000) 6103ndash6105
[267] B Paul I Masih J Deopujari C Charpentier Occurrence of resveratrol and pter-ostilbene in age-old darakchasava an ayurvedic medicine from India J Ethno-pharmacol 68 (1999) 71ndash76
[268] I Rahman Antioxidant therapies in COPD Int J Chron Obstruct Pulmon Dis 1(2006) 15ndash29
[269] M Lee S Kim OK Kwon SR Oh HK Lee K Ahn Anti-inflammatory and anti-asthmatic effects of resveratrol a polyphenolic stilbene in a mouse model ofallergic asthma Int Immunopharmacol 9 (2009) 418ndash424
[270] LG Wood PA Wark ML Garg Antioxidant and anti-inflammatory effectsof resveratrol in airway disease Antioxid Redox Signal 13 (2010)1535ndash1548
[271] KV Kiselev Perspectives for production and application of resveratrol ApplMicrobiol Biotechnol 90 (2011) 417ndash425
[272] M Shakibaei C Buhrmann A Mobasheri Resveratrol-mediated SIRT-1 interac-tions with p300 modulate receptor activator of NF-kappaB ligand (RANKL) acti-vation of NF-kappaB signaling and inhibit osteoclastogenesis in bone-derivedcells J Biol Chem 286 (2011) 11492ndash11505
[273] SF Zaidi K Ahmed T Yamamoto T Kondo K Usmanghani M Kadowaki TSugiyama Effect of resveratrol on Helicobacter pylori-induced interleukin-8 secre-tion reactive oxygen species generation and morphological changes in human gas-tric epithelial cells Biol Pharm Bull 32 (2009) 1931ndash1935
[274] JK Kundu YK Shin YJ Surh Resveratrol modulates phorbol ester-inducedpro-inflammatory signal transduction pathways in mouse skin in vivo NF-kappaB and AP-1 as prime targets Biochem Pharmacol 72 (2006)1506ndash1515
[275] NH Nam Naturally occurring NF-kappaB inhibitors Mini Rev Med Chem 6(2006) 945ndash951
[276] JM Smoliga JA Baur HA Hausenblas Resveratrol and healthmdasha comprehen-sive review of human clinical trials Mol Nutr Food Res 55 (2011) 1129ndash1141
[277] ME Juan M Maijo JM Planas Quantification of trans-resveratrol and itsmetabolites in rat plasma and tissues by HPLC J Pharm Biomed Anal 51(2010) 391ndash398
[278] JA Baur DA Sinclair Therapeutic potential of resveratrol the in vivo evidenceNat Rev 5 (2006) 493ndash506
[279] E Nicolis I Lampronti MC Dechecchi M Borgatti A Tamanini N Bianchi VBezzerri I Mancini MG Giri P Rizzotti R Gambari G Cabrini Pyrogallol anactive compound from the medicinal plant Emblica officinalis regulates expres-sion of pro-inflammatory genes in bronchial epithelial cells Int Immunophar-macol 8 (2008) 1672ndash1680
[280] E Nicolis I Lampronti MC Dechecchi M Borgatti A Tamanini V Bezzerri NBianchi M Mazzon I Mancini MG Giri P Rizzotti R Gambari G CabriniModulation of expression of IL-8 gene in bronchial epithelial cells by 5-methoxypsoralen Int Immunopharmacol 9 (2009) 1411ndash1422
[281] M Borgatti I Mancini N Bianchi A Guerrini I Lampronti D Rossi G SacchettiR Gambari Bergamot (Citrus bergamia Risso) fruit extracts and identified com-ponents alter expression of interleukin 8 gene in cystic fibrosis bronchial epithe-lial cell lines BMC Biochem 12 (2011) 15
[282] L Piccagli E Fabbri M Borgatti N Bianchi V Bezzerri I Mancini E Nicolis CMDechecchi I Lampronti G Cabrini R Gambari Virtual screening against p50NF-kappaB transcription factor for the identification of inhibitors of the NF-kappaB-DNA interaction and expression of NF-kappaB upregulated genesChemMedChem 4 (2009) 2024ndash2033
[283] L Piccagli M Borgatti E Nicolis N Bianchi I Mancini I Lampronti D VevaldiF DallAcqua G Cabrini R Gambari Virtual screening against nuclear factorkappaB (NF-kappaB) of a focus library identification of bioactive furocoumarinderivatives inhibiting NF-kappaB dependent biological functions involved incystic fibrosis Bioorg Med Chem 18 (2010) 8341ndash8349
[284] M Borgatti A Chilin L Piccagli I Lampronti N Bianchi I Mancini G Mar-zaro Da Francesco A Guiotto R Gambari Development of a novel furocou-marin derivative inhibiting NF-kappaB dependent biological functionsdesign synthesis and biological effects Eur J Med Chem 46 (2011)4870ndash4877
[285] E Georgy S Le Guellec L Vecellio E Fichant P Stordeur P Bordeau JP PerraudinFeasibility study of OSCN- and lactoferrin (Meveol) nebulization for cysticfibrosis JCyst Fibros 10 (2011) S18
713F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
[286] C Tidei M Piroddi F Galli C Santi Oxidation of thiols promoted by PhSeZnClTetrahedron Lett 53 (2012) 232ndash234
[287] L Semianrio-Vidal C van Hesuden G Mugesh ER Lazarowski Ebselen is a po-tent non-competitive inhibitor of extracellular nucleoside diphosphokinasePurinergic Signal 6 (2010) 383ndash391
[288] C ColussiMC Albertini S Coppola S Rovidati F Galli L Ghibelli H2O2-inducedblockof glycolysis as an active ADP-ribosylation reaction protecting cells from apoptosisFASEB J 14 (2000) 2266ndash2276
[289] H Xiao KL Parkin Induction of phase II enzyme activity by various seleniumcompounds Nutr Cancer 55 (2006) 210ndash223
[290] G Peluffo R Radi Biochemistry of protein tyrosine nitration in cardiovascularpathology Cardiovasc Res 75 (2007) 291ndash302
[291] B Alvarez R Radi Peroxynitrite reactivity with amino acids and proteinsAmino Acids 25 (2003) 295ndash311
[292] B Kamosinska MW Radomski M Duszyk A Radomski SF Man Nitric oxideactivates chloride currents in human lung epithelial cells Am J Physiol 272(1997) L1098ndashL1104
[293] L Chen RP Patel X Teng CA Bosworth JR Lancaster Jr S Matalon Mecha-nisms of cystic fibrosis transmembrane conductance regulator activation by S-nitrosoglutathione J Biol Chem 281 (2006) 9190ndash9199
[294] F Luchetti B CanonicoM BettiM Arcangeletti F PilolliM Piroddi L Canesi S PapaF Galli Melatonin signaling and cell protection function FASEB J 24 (2010)3603ndash3624
[295] MW Bengtsson G Jedstedt G Flemstrom Duodenal bicarbonate secretion inrats stimulation by intra-arterial and luminal guanylin and uroguanylin ActaPhysiol (Oxf) 191 (2007) 309ndash317
[296] CS Nelson JL Marino CN Allen Melatonin receptor potentiation of cyclic AMP andthe cystic fibrosis transmembrane conductance regulator ion channel J Pineal Res 26(1999) 113ndash121
[297] C de Castro-Silva VM de Bruin GM Cunha DM Nunes CAMedeiros PF de BruinMelatonin improves sleep and reduces nitrite in the exhaled breath condensate incystic fibrosismdasha randomized double-blind placebo-controlled study J Pineal Res48 (2010) 65ndash71
[298] I Hornyak E Pankotai L Kiss Z Lacza Current developments in the the-rapeutic potential of S-nitrosoglutathione an endogenous NO-donor mole-cule Curr Pharm Biotechnol (2011) Jan 11 [Epub ahead of print] - PMID21235457
[299] AH Snyder ME McPherson JF Hunt M Johnson JS Stamler B Gaston Acuteeffects of aerosolized S-nitrosoglutathione in cystic fibrosis Am J Respir CritCare Med 165 (2002) 922ndash926

701F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
complexes and to correct total antioxidant capacity of plasma Inanother study β-carotene supplementation was observed to de-creased lipid peroxide formation as quantitated by malondialdehydeconcentrations in plasma (TBAHPLC method) and to enhance the re-sistance to copper(II) ion-induced oxidation of low density lipopro-teins [180]
At the same time toxicity issues have been raised for human sup-plementation with carotenoid formulations and particularly of water-miscible formulations of preformed vitamin A that is regularly sup-plemented to CF patients which may increase serum retinol andpossible risk of CF-associated liver and bone complications (reviewedin [161181]) However β-carotene supplementation seems to be safesince this does not affect plasma concentrations of other carotenoidsand retinol as well as of other fat-soluble vitamins as α- and γ-tocopherol [178] Recent studies designed to test the clinical efficacyof a CF tailored multivitamin formulation (commercial name AquA-DEKsreg) also tested the safety of this type of formulation and demon-strated that this does not increase vitamin A above the normal levelsobserved in healthy controls [162182183] The normalization of β-carotene levels obtained in these studies was associated only withminor improvements on respiratory and growth parameters whilethe levels of urinary F2-IsoPs used as index of lipid peroxidationwere not affected [162] The surrogate marker of lipid peroxidationMDA was affected together with some selected antioxidant parame-ters (RBC thiols and superoxide dismutase) in another study inwhich this multivitamin formulation was preliminarily evaluated incomparison with standard formulations of vitamin E and A [182]
353 Coenzyme Q-10Coenzyme Q-10 (Q10) is a well-known electron transporter in the
mitochondrial respiratory chain with fundamental role in cellularbioenergetics and scavenging of radical species [184] This lipophilicsubstance is present in the circulation at low levels (serum concentra-tionsle2 μM) mainly as ubiquinol-10 eg the reduced form with anapproximate ratio of 955 with the oxidized form ubiquinone-10[185186] A mechanism for a preferential distribution and accumula-tion in mitochondria has been suggested for both the reduced and ox-idized forms of CoQ10 that are taken up by the cells in a time- andconcentration-dependent Subcellular localization and trafficking ofexogenous Q10 are similar to those of the endogenous form butwere different from that of α-tocopherol that is related with lipidcomposition particularly in the mitochondrial and microsomal frac-tions [184] Ubiquinol-10 readily oxidizes ex vivo by the reactionwith other lipophilic antioxidants such as α-tocopherol and butylatedhydroxytoluene [185] Therefore a higher reduction potential thanother physiological fat-soluble antioxidants such as vitamin E and aselective metabolism and cellular trafficking show peculiar role forthe cell CoQ which may also represent an important lipophilic antiox-idant in cells and body fluids
Human cells synthesize this coenzyme through the cholesterol bio-synthesis pathway so thatmore than two thirds of the tissue levels ap-pear to have an endogenous origin dietary sources provide acontribution to Co-Q10 levels of blood and all solid tissues that variesdepending on the dose applied and type of dietary source [187] How-ever in the case of oral supplements it has to be considered that hy-drophobicity and large molecular weight of this coenzyme influenceits absorption that ultimately is slow and limited [186187] Likewiseto vitamin E pharmacokinetics [188189] Co-Q10 showed T(max) ofaround 6 h that coincides with that of dietary lipids Elimination isclose to that of the more retained form of vitamin E in human bodyeg α-tocopherol with a half-life of about 33 h which suggests poorhepatic metabolism However commercially available formulationsare reported to be safe even at high doses and solubilized formulationsshow enhanced bioavailability In healthy subjects plasma Q10 re-sponse to oral ingestion show saturation profiles with a plateau at a
dose of 2400 mg and the higher plasma concentrations were foundto facilitate uptake by peripheral tissues and also the brain [186187]
Laguna et al [190] recently investigated total serum levels ofcoenzyme Q-10 in a wide population of CF children (n=381) and esti-mated their association with clinical outcome Near to 50 of these CFpatients were deficient of Co-Q10 and this defect was significantlymore prevalent in patients with pancreatic insufficiency and signifi-cantly associated with P aeruginosa colonization in infants (under24 months of age) Importantly low Co-Q10 levels correlated to otherlipid markers of a poor nutritional status such as total lipids and alsothe other fat-soluble antioxidants β-carotene and α-tocopherolwhich confirms the presence of a common defect in the absorptionand metabolic pathways of this coenzyme with dietary lipids
The deficit of Co-Q10 may contribute to the impaired energy func-tion of mitochondria of CF tissues and this may exacerbate CF-linkedinflammation infection and cellular stress response of the lung A sys-tematic analysis of molecular lesions in CF bronchial tissue has beenrecently carried out by proteomic approach [191] Comparative eval-uation of protein expressional pattern in CF and healthy controltissues has revealed aberrant levels of some mitochondrial andenergy-related proteins in CF specimens that included the ubiqui-nolndashcytochrome c reductase complex core protein I and one form ofnidogen a pseudogene of aconitase 2 These changes in CF may reflectmolecular changes which could be associated with an altered mito-chondrial homeostasis and Co-Q10 redox
Multivitamin supplements with high bioavailability containingCo-Q10 have demonstrated to correct the deficit of this antioxidantand were preliminarily observed to improve airway inflammationmarkers in CF patients [183] However further clinical investigationfailed to demonstrate that such an improved biochemical profile isassociated with significant improvements in weight percentile andpulmonary function [162]
354 Fatty acidsA key pathophysiological role in sustaining inflammation in CF has
been attributed to the abnormal polyunsaturated fatty acid (FA) pat-tern Abnormalities in FA profiling are potentially linked to CFTRmutation-driven alterations in the absorption andor metabolism ofdietary lipids [192193] and to the consumption of high oxidizableFA involved in the free radical-mediated lipid peroxidation [7]Among those alterations dysregulation of the docosahexaenoic acidand arachidonic acid balance has been extensively studied with re-portedly significant reduction of DHA in CF and a parallel increasein the levels of AA and inflammatory indices [193ndash195] Actually AAis the progenitor of both enzymatic- and free radical-derived inflam-matory mediators including leukotrienes prostaglandins and iso-prostanes On the other hand n-3 PUFA (eicosapentaenoic acid anddocosahexaenoic acid) are involved in the generation of potent medi-ators namely resolvins and protectins which are able to resolveexudates and to act as organ protective and antifibrotic Secondarilyto their anti-inflammatory action n-3 FA may also produce anantioxidant-like response (eg a reduced demand of antioxidants toachieve an optimal control of oxidative pathways) As a consequencen-3 PUFA have been suggested and widely used as supplements in CFpatients usually under the form of fish oil [196ndash198] It is worth ofnote however that defective levels of DHA in CF patients was notconfirmed in recent studies [7] It was also shown that patients onDHA supplements did not have increased plasma n-3 FA concentra-tions but showed more severe oxidative stress compared to theunsupplemented patients [7] This observation of an increased riskof oxidative stress in CF subjects receiving n-3 fatty acids supple-ments has also been described by other authors [199]
Studies reporting increased AA levels in CF patients have beencontradicted by others [7200201] thus contributing to weakeningthe pathophysiological role of the altered DHAndashAA balance as turnpoint of an upregulated inflammatory status in CF In this context a
702 F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
recent Cochrane meta-analysis on n-3 supplementation in CF patients[202] highlighted the lack of evidence for a significant correction ofthe assessed clinical end points (mainly respiratory symptoms)even when inflammatory indices and other laboratory end pointswere met Taken together these data suggest that there is insufficientevidence to draw firm conclusions or recommend routine use of n-3supplements in CF Notwithstanding it is common belief that n-3supplements provide some benefits for people with CF with relativelyfew adverse effects and thus their use is not discouraged
Further alterations in fatty acid metabolism have been highlight-ed including the consistent findings of an increase in circulatinglevels of saturated and monounsaturated fatty acids [7203204]Decreased levels of essential FA (EFA) ie the FA that have to be in-troduced with the diet correlates with the severity of respiratoryinsufficiency and the same clinical correlation was observed with al-tered proportions of FA species converted by the activity of desatur-ase enzymes (reviewed in [204]) The close relationship betweencertain fatty acids and oxidative stress including the negative correla-tion of C240 and linoleic acid with oxysterol levels point to the needof intensive investigation in CF patients of previously neglected lipidspecies that are emerging candidates in the control of metabolismQuantitative lipidomic analyses have lead to identify C161n7 palmi-toleate as a ldquoprotectiverdquo adipose-derived lipid hormone that stronglystimulates insulin activity in muscle and liver also suppressing in-flammatory cytokine output from mice fat cells [205] Specific meta-bolic activities have been also demonstrated by medium chainsaturated fatty acids caprylic acid (C80) capric acid (C100) and lau-ric acid (C120) Capric acid acts as a direct ligand of PPARγ using abinding pocket different from the binding pocket of thiazolidinedioneor long chain fatty acids [206] Additional activities of medium chainfatty acids which are ligands of free fatty acids receptors detectedin the immune cells the gastrointestinal tract and adipocytes maycontribute to metabolic homeostasis and inflammatory responses[207] These data underscore the importance of a lipid-mediated ldquoen-docrine networkrdquo demonstrating how specific alteration of one orfew serum lipids would be per se sufficient to influence metabolic ho-meostasis Given the relevance of this emerging information and thealteration of lipid metabolism and inflammatory status in CF fattyacid lipidomics need to be deeply investigated in CF
Again these studies have obvious nutritional implications Satu-rated fatty acids with chain lengths higher than C18 are poorlyabsorbed partly because they form insoluble calcium salts [208]Medium chain saturated fatty acids are well known for being highlyabsorbed through the intestine providing rapid delivery of energyvia oxidation of the more hydrophilic short chains and have beensuggested to provide proper nourishment in patients with CF [209]Recent studies have shown that consumption of a high-fat diet richin medium chain fatty acids as opposed to long chain fatty acidsdoes not lead to ectopic fat accumulation in skeletal muscle andliver of both rats and mice [210] In light of the close association be-tween nutritional status inflammation and life expectancy in CF pa-tients the manipulation of dietary lipids in these patients must befurther explored as a possible strategy to provide adequate nutritionand better management of oxidative stress
36 Hydrosoluble antioxidants oligoelements and enzymatic antioxidants
361 Vitamin CVitamin C status in CF patients has been poorly investigated Early
studies suggested a defective vitamin C status that was refractory tooral supplementation [211] Other and more recent studies showednormal or slightly decreased levels of vitamin C in CF patients as com-pared to healthy controls but age- and disease-related decline of thiswater-soluble antioxidant was reported in these patients [5212]In the study of Winklhofer-Roob et al [212] on mid-European CFpatients vitamin C concentrations decreased with age with an
estimated rate of 5 μmollyr and vitamin C concentrationsb40 μ-moll were associated with highest indexes of inflammation whichis consistent with the hypothesis that optimal levels of vitamin Cmay influence immuno-inflammatory activity of alveolar macro-phages and neutrophils Other few studies have examined the effectof supplements containing vitamin C on CF inflammation and oxida-tive stress since the levels of this vitamin do not significantly improvewith supplementation (reviewed in [213]) This highlights the com-mon fate that this hydrosoluble vitamin shares with several fat-soluble counterparts in the ldquomicronutrient paradoxrdquo of CF patients inwhich the need for a correction of their status along the progressionof the disease is frustrated by the poor efficacy of oral supplementa-tion protocols Formulations and appropriate supplementation proto-cols that may produce a better correction of vitamin C status of CFpatients are awaited for further clinical evaluation
362 Selenium and selenium-dependent peroxidasesSelenium is a trace element with marked electrophilicity [214]
that once converted to the organic form of Se-Cys can be introducedin protein structures to play its important role in H2O2 metabolismand signaling [215] As catalytic center of the enzyme GSH-peroxidase (SeGSH-Px) Se plays a crucial role to protect polyunsatu-rated lipids of plasma membrane and circulating lipoproteins formperoxidative insults With other Se-proteins such as the high molecu-lar weight thioredoxin reductases this oligoelement participates tothe control of protein thiol-disulfide oxidoreduction and glutathiony-lation which regulate signaling pathways of crucial importance in theregulation of immunity and inflammation [16] but also the function-ing of other redox-sensitive proteins such as the same CFTR [124]
The activity of SeGSH-Px in blood is considered a functional as-sessment of selenium status even if this assumption has some limita-tions related with the saturation profile that the Se stores show atincreasing doses of Se administration Investigations of the seleniumstatus in CF patients have produced conflicting findings which maydepend on differences in dietary intake ethnicity and environmentalfactors in the diverse patient populations (reviewed in [216217]) CFchildren have been reported to have lowered blood selenium and RBCSeGSH-Px activity [218219] normal plasma selenium and loweredRBC SeGSH-Px [220] and even normal levels of both these two param-eters [221] The supplementation with selenium in combination withother antioxidants was observed to increase the concentrations ofblood selenium that likewise β-carotene and fatty acid were posi-tively correlated with improved lung function [6]
Foucaud et al [218] observed that a defective selenium statuswas associated with lowered levels of other antioxidants that contrib-ute to the anti-peroxidative activity of this microelement such asvitamin E (reviewed in [222]) and the severity of this deficiencywas lower in children with pancreatic enzyme replacement and vita-min E supplementation
Treatments to substitute for exocrine pancreatic insufficiency bypancreatic enzymes from animal sources such as porcine pancreashave been confirmed to be a source of Se [220] These affects RBCSeGSH-Px activity and plasma selenium concentrations which hasto be taken into account when selenium supplements are given toCF patients
Selenium has been used to develop a series of organoseleniumcompounds that may open the way to new therapeutic opportunitiesin CF (see Section 392) These include GPX mimetic drugs and phaseII enzyme inducers which may provide higher antioxidant activity ofASL and cellular protection effects in the airways
363 Zinc and copperZinc and copper (Zn and Cu respectively) are present in many
proteins so that a deficiency of these trace metals could have pleiotro-pic effects in humans As regards antioxidant systems these two oli-goelements contribute an important role being cofactors of two
703F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
isoforms of the superoxide dismutase enzymes eg the extracellularform eg the EC-SOD or Sod 3 and the CundashZn-SOD or Sod 1 that isfound in several tissues and cells [223] The EC-SOD exerts its antiox-idant role also in the lining fluids of the airways [224]
The notion that CF patients have defective concentrations of bloodZn and Cu is controversial As far as Cu status is concerned few datahave been produced and are available in the literature suggestingthe notion that CF patients develop a moderate copper deficiency[225226] That was essentially demonstrated on the bases of a defec-tive activity of Cu-related proteins such as plasma ceruloplasmindiamine oxidase and RBC SOD This defect seems to be refractory toCu and Zn supplementation (see below)
More advanced studies have been carried out in the case of Zn sta-tus in CF Low plasma zinc concentrations were reported in approxi-mately 30 of young infants with CF identified by newbornscreening [227] and an impaired zinc homeostasis in CF patientswas described by Easley et al [228] This is characterized by poor con-servation of the endogenous pool with fecal loss and impaired frac-tional absorption of zinc which are the consequences of pancreaticinsufficiency and persisting steatorrhea These studies suggestedthat in the clinical management of CF patients these defects can beat least in part corrected by exocrine pancreatic enzyme replacement
A series of studies by Van Biervliet et al [229230] demonstratedin a Dutch population of CF infants and children that serum Zn variesin an age-dependent manner but remained unchanged with respectto healthy control levels In CF patients no difference in serum Zn con-centration between pancreatic-sufficient or pancreatic-insufficientpatients was observed and no correlation was found with the nutri-tional status or height z-score Importantly in these studies a signifi-cant correlation of serum Zn was observed with the fat solublevitamins A and E thus confirming the relationship between the ab-normalities of lipid and Zn metabolism in CF This suggests that co-supplementation of Zn and fat-soluble vitamins should be advisedin the presence of pancreatic insufficiency and persisting steatorrhea
Neve et al [219] in a study aimed to assess plasma and erythrocytezinc copper and selenium in CF children showed that mean plasmazinc and copper levels were not different from those in age-matched controls which confirms the observations by Van Biervlietet al described above However plasma zinc concentrations de-creased in patients with moderate-to-severe growth retardation andwith severe pulmonary disease but very low zinc levels occur sporad-ically Erythrocyte zinc and copper levels were significantly higherthan normal while RBC selenium was lower than in age-matchedcontrols These trace element concentrations in erythrocytes werediscussed in relation to the activities of the CuZn-SOD and the Se-enzyme GPx This observation suggests a compensatory upregulationof the erythrocyte CuZn-SOD by the exposure of erythroid precursorsto ROS andor other CF-related stressors
Best et al [225] also studied RBC SOD activity using this as a bio-logical sensor of Cu status in CF patients A lowered activity of thisenzyme was reported in CF together with that of the other Cu-dependent enzyme plasma diamine oxidase while plasma ceruplas-min showed normal activity Degradation rates of copper proteinsare known to be accelerated in conditions of copper deficiencywhich could explain the finding at least in part Anyway when Cuand Zn were supplemented to CF patients either separate or incombination (6 weeks of 3 mg copperd as copper-glycinate and30 mg zincd as zinc-glycinate) any of the copper enzyme activitieswas affected Therefore the moderate copper deficiency of CF patientsappears to be refractory to the intervention by increased copper andor zinc intake
Erythrocyte CuZn-SOD and the plasma levels of Cu and Zn werealso measured in the study of Wood et al [6] in which Australian CFpatients (agegt5 years) were treated with a high-dose antioxidantmultivitamin formulation containing 200 mg vitamin E (as RRR-α-tocopherol) 300 mg vitamin C (as sodium ascorbate) 25 mg β-
carotene (all-trans isomer) 90 μg Se (as selenomethionine) and500 μg vitamin A (as retinyl palmitate) in oil Plasma oligoelementsand particularly Zn were in the normal range at baseline (as com-pared with the data reported in [229230]) and were not affected bythis multivitamin supplement The same was found for the activityof RBC SOD and for plasma 8-iso-PGF2α as surrogate biomarker oflipid peroxidation
In a recent non-randomized small population (n=21) casendashcon-trol study in CF children Zn supplementation was proven to producepositive clinical effects in Zn-deficient patients [196] The supplemen-tation with 5 mgkg Zn sulfateday (maximum 150 mg) significantlydecreased the number of infections and increased the forced expira-tory volume in 1 s energy intake and growth parameters also im-proved These parameters were unaffected in untreated patientsexcept that in the case of the pulmonary function that decreased sig-nificantly These clinical observations on Zn supplementation need tobe confirmed in prospective double-blind randomized control trial
37 Appropriateness and targeting of antioxidant therapies in CF
The choice of the appropriate antioxidant and dose to correct a cer-tain biomarker and its associated biochemical lesion is another impor-tant point that appears to have disregarded in many clinical studiesFor instance unlike vitamin E vitamin C supplementation does notalter F2-IsoPs levels in humans (reviewed in [74]) This appears tobe true also in the antioxidant therapy of CF in which vitamin C(300 mgday) was administered together with other antioxidantsthat included a dose of vitamin E of 200 mgday without any signifi-cant effect on the surrogate biomarker of lipid peroxidation F2-IsoPs[6] When carotenoids are used as supplements to prevent the damag-ing action of ROS in the CF airways it is noteworthy that these are notparticularly good quenchers of peroxyl radicals relative to phenolicsand other antioxidants but are exceptional in quenching singlet oxy-gen at which most other phenolics and antioxidants are relativelyineffective Singlet oxygen is not a radical and does not react via radi-cal mechanisms but reacts mostly by the addition to double bondsforming endoperoxides that can be reduced to alkoxyl radicals that ini-tiate radical chain reactions typical of the peroxidative damage of PUFA[38] In this case the analysis of F2-IsoPs lipid peroxide formation andtransition metal-induced oxidizability of lipoproteins [162180] are allappropriate to evaluate the effect of carotenoids in preventing lipidperoxidation
As far as the dose is concerned clinical pharmacology of vitamin Eas an antioxidant was recently investigated by means of the effect onF2-IsoPs production and doses of α-tocopherol of 1600 IUday orgreater were found to be required to statistically affect plasma F2-IsoPs levels in hypercholeterolemic subjects [176] Several vitamin Esupplementation studies in CF patients have been performed withdoses of lower than 300 IUday regardless of the lowered absorptionby pancreatic and liver defects and the regular supplementationwith these doses does not appear to correct lipid oxidation markersin CF [7]
In the clinical practice and planning trials it has to be taken intoconsideration that in spite of substantial evidence supporting ahigher antioxidant demand in CF interventions with several antioxi-dant formulations produce poor responsiveness particularly in thecase of fat-soluble antioxidants which are poorly absorbed [6162]
Since many oxidants and antioxidants are present in tissuesand biological fluids and these have different chemical and physicalcharacteristics the possibility to produce a successful therapy witha single antioxidant molecule is too far to be realistic Moreover an-tioxidants act by multiple mechanisms in a single system or by adifferent single mechanism depending on the reaction systemresponding in a different manner to different radical or oxidantsources Because multiple reaction characteristics and mechanismsas well as different phase localizations are usually involved no single
704 F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
therapeutic approach will effectively prevent damage by multipleROS sources The defect of physiological antioxidants may also interferewith antioxidant therapies that are based on one or few exogenousantioxidants
Moreover several antioxidant vitamins such as vitamin E and ca-rotenoids have multiple natural forms with different bioavailabilitymetabolism and bioactivity [157167231] As far as the case of vita-min E supplementation concerns α-tocopherol was used as uniquevitamer in the large majority of supplementation trials so far per-formed and is the form used in the nutritional management of CFpatients Moreover several supplements contain the synthetic (or ra-cemic) form of this vitamin that has lower bioavailability than thenatural form Other forms present in nature and abundantly con-tained in vegetables such as tocotrienols and the less methylatedforms of tocopherol are not represented in many of the supplementformulations so far available in clinical centers and the supplementa-tion with α-tocopherol also limits their bioavailability These formsshow markedly higher susceptibility to hepatic metabolism and bili-ary excretion with respect to α-tocopherol eg the most representedform in blood and solid tissues and if co-supplemented these areeasily displaced during liver uptake and excreted with bile bymeans of competition with the same α-tocopherol Notwithstandingthese minor forms have been proposed to play important physiolog-ical roles showing molecular characteristics transcriptional effectsand antioxidant activities that clearly differentiate them in subfam-ilies with distinct biological functions Some of these such as α-tocopherol eg the second vitamin E form as relative abundance inblood and its carboxyethyl-hydroxychroman metabolite [189] ap-pear to have health-related anti-inflammatory effects which are par-ticularly relevant in lung protection [232233] This has suggestedthat such a group of ldquonon-α-tocopherolrdquo forms may represent anoth-er family of vitamins within the family of vitamin E with an impor-tant but often missed contribution to the proposed health effects ofthis vitamin [163]
These aspects may thus limit the possibility to provide CF patientsof optimal levels of this vitamin in all its components even if they areregularly treated with a vitamin E supplement eg withα-tocopherol
Targeted antioxidant therapy with formulations with higher bio-availability and bioactivity has been anticipated in CF New antioxi-dant formulations have been proposed to overcome main limits ofantioxidant therapies so far proposed for these patients Water-miscible α-tocopheryl acetate containing polysorbate propylene gly-col or polyethylene glycol as emulsifiers form micellar structureswere suggested to providing greater bioavailability than the fat-soluble counterparts These were commercialized with the brandnames of E-viminreg Cremophorreg EL and Aquasolreg E but despitethe original positive expectation [234235] some studies failed to ob-serve a higher response in vitamin E levels when these were com-pared with fat-soluble formulations [236237]
In a pilot study by Papas et al [183] a micellar formulation of fat-soluble nutrients and antioxidants was found to improve plasmalevels of β-carotene γ-tocopherol and CoQ(10) reducing at thesame time some inflammatory markers in induced sputum eg mye-loperoxidase and to a lower extent PMN elastase and total cell countswhile lung function and sputum bacterial counts were unaffectedThe same group recently confirmed the possibility to increase the ab-sorption of fat-soluble micronutrients using formulations with higherbioavailability specifically designed for malabsorbing patients such asCF patients that include also vitamin K and commercialized with thebrand name of AquADEKsreg [162] Despite improved vitamin and mi-cronutrient levels in this non-randomized open-label study AquA-DEKsreg produced only modest improvements in weight percentileand pulmonary function Another recent pilot observation [182] hassuggested the beneficial effect of this formulation on antioxidant andoxidative stress parameters of this oral supplement that surely deservesmore clinical investigation by larger randomized controlled trials
Recent multivitaminic formulations have been designed to containalso the minor forms of vitamin E and specifically γ-tocopherol [238]the expected superiority of which with respect to formulations con-taining only α-tocopherol needs to be verified As discussed abovein the section dedicated to vitamin E further advancements in thetherapy of CF inflammation and oxidative stress could be based onsynthetic forms and natural metabolites of this vitamin that havebeen recently identified to possess higher antioxidant and also anti-inflammatory activity than α-tocopherol (reviewed in [163168])
Pre-clinical investigation of these and other fat-soluble agents iscurrently addressed to develop formulations and administration pro-tocols that may increase the therapeutic efficacy in the airways In theantioxidant therapy of lung dysfunction in CF local administrationprotocols may overcome the limits of oral and systemic administra-tion protocols increasing bioavailability and providing targetedapproach to inflammation and oxidative stress Aerosolization of vita-min E and other fat-soluble micronutrients is possible and may allowdirect administration in the airways to prevent toxicity of smokewhich is closely associated with inflammation and oxidative stress[164165] To our knowledge this as well as other strategies of localadministration such as instillation of solutions such as surfactant-like solutions enriched of vitamin E have not been previously inves-tigated in CF patients and other CF model systems
On the contrary inhalation is an administration route widelyadopted in the case of GSH and NAC therapy described above Inthis context Cys formulations alternative to NAC have been proposedfor use as antioxidant and anti-inflammatory agent for inhalationNacystelyn is a lysine adduct of NAC that thanks to a higher proton-ation equilibrium shows increased water solubility and thus betterbioavailability Nacystelyn has been described to influence IL-8 gener-ation and the inflammatory signaling of bronchial epithelial cells[239] and preliminary clinical evaluation has demonstrated the safetyof this drug [240] Further clinical trials aimed to assess the effect onlung symptomatology of CF patients are needed Direct administra-tion in the airways could also be adopted for micronutrient vitaminswith poor absorption and bioavailability due to GI defects
38 Clinical impact of antioxidant therapy in CF
Huge in vitro and pre-clinical evidence has provided the rationaleto support clinical investigation of antioxidant strategies in CF Theseshould aim to restore the oxidantndashantioxidant balance of CF airwaychallenged by chronic infection and inflammatory cell activation
Some observational trials have confirmed that antioxidants usedas either supplements to the diet or drugs for lung administrationby aerosolized formulations may help in relieving progressive lungdamage and other adverse clinical events of CF such as poor growthSo far few studies have examined with sufficient methodologicalrigor the clinical efficacy of antioxidant therapy in CF This was alsoconcluded in a previous review of the literature by Cantin et al [12]that was published in the beginning of 2006 and is confirmed alsoin a recent analysis of clinical trials on antioxidant therapy in CF pa-tients [213] that examined the literature until September 2010using as sources the databases of the Cochrane CF and Genetic Disor-ders Group CF Trials Register PubMed CINAHL and AMED Useful in-formation was retrieved from just four randomized controlled trialsand one quasi-randomized controlled trial on vitamin C vitamin Eβ-carotene and selenium used as supplements administered aloneor in combination Post-hoc data analysis that was possible only inthree studies on a total of 87 CF patients showed the absence ofany significant improvement in lung function that was selected as pri-mary outcome together with quality of life that improved in one trialSecondary outcomes concerning laboratory indices of oxidative stressand antioxidant status showed several improvements These includedan increase of RBC SeGPx by selenium supplementation done as
705F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
individual or combined supplementation and increased levels of allplasma antioxidants except vitamin C that were observed in all thetrials
The message from these studies to pediatricians and nutritionistswithin the clinical staff of CF centers is that in the absence of solid ev-idence regarding the clinical effectiveness of oral formulations of an-tioxidant supplements in CF (including PUFA) their use as a routineclinical practice should be considered with caution keeping clear inmind that this should represent just a complement of one of themost critical interventions in the life-long clinical management pro-gram of CF patients eg providing an adequate nutriture [140] Inthis context compensating energy and protein malnutrition has toremain the first goal of nutritional management programs Providinghigher intakes of antioxidant micronutrients with food naturally-enriched (or functionalized) of micronutrient antioxidants shouldbe preferred in order to have the higher combination of positive nu-tritional factors that are lost during refinement procedures and over-all industrial processing of dietary supplements
Measures of good practice in clinical management of micro-malnutrition in CF patients would include the support of specializedpersonnel and laboratories The centers should have the possibilityto ascertain with appropriate nutritional and laboratory tests whatthe level of deficiency is for the different micronutrients that each pa-tient may suffer from during a dietary program Monitoring dietaryintakes and blood levels of micronutrients is not sufficient to set apersonalized nutritional intervention with supplements or functionalfoods Sub-optimal intakes and the compliance to nutritional inter-ventions should be verified by means of selected biochemical andclinical criteria Unluckily the latter are still not well established forsome micronutrients such as the fat-soluble vitamins E (reviewed in[163173241]) and K [242243] and also for trace elements such asSe [244] For many of the antioxidants used as supplements inhumans we still do not know exactly several of the biological effectsthat these may provide when introduced in a healthy body and weknow less what these can do in disease These aspects hardly impacton the concept of optimal levels of intake that should be identified foreach micronutrient on an individual basis According with the aspectsdiscussed in the previous sections optimal levels of intake for antiox-idant micronutrients are different in CF patients and healthy subjectsand vary with age and several individual factors
Lung administration of antioxidants by means of aerosolized for-mulations so far used for GSH therapy (see above) is a promisingfield of clinical investigation in CF Toxicity issues are currently themain concern and the subject of clinical evaluation by several groups(described above)
Information on future directions of antioxidant therapy in CF canbe inferred by the analysis of pending or recently completed clinicaltrials that have been searched (December 2011) at ClinicalTrialsgovdatabase matching the terms ldquoantioxidant therapyrdquo or ldquoglutathionerdquowith ldquocystic fibrosisrdquo Fifteen trials were retrieved and those directlyrelated to antioxidant therapy (n=12) are presented in Table 1 andinclude efficacy and safety studies of inhaled drugs as GSH sodiumpyruvate NAC and NO and the dietary supplements AquADEKsregan antioxidant-rich multivitamin supplement epigallocatechin gal-late (EGCG)tocotrienol curcuminoids the amino acid glutaminesulforaphane in broccoli sprouts One trial is investigating the flavo-noid quercetin as CFTR modulator
39 Emerging antioxidant and anti-inflammatory approaches in CF
Mediterranean foods such as olive oil and red wine or severalplant extracts such as herbal tea or grape seed extracts contain aseries of natural compounds with important antioxidant and NOscavenging activity that have been widely investigated for the pre-vention of oxidative stress-related diseases [38245] These havebeen long investigated as template molecules to develop antioxidant
and anti-inflammatory drugs Between the multitudes of natural sub-stances most investigated ones include for instance tyrosol hydroxy-tyrosol gallic and caffeic acids belonging to the family of phenolswhile resveratrol of the stilbenes family epicatechin kaempferoland cianidin are examples of flavonoids examples of fat-soluble phe-nolics are those of the family of tocols (vitamin E) and carotenoids Allthese compounds show different metabolisms and signaling effects[246] Antioxidant and cell protection mechanisms are associatedwith different and sometimes concurrent processes as H-atom trans-fer and electron donation radical trapping and chelation of transitionmetals that can be easily investigated at the chemical level [247] Be-sides these direct antioxidant effects metabolic responses and signal-ing effects of natural compounds are also important to producesecond-generation responses that modify the level of antioxidantprotection and the potential for ROS detoxification in cells and bodyfluids These derive from the transcriptional regulation of antioxidantand pro-oxidant genes that coexist with the modulation of cytokinesecretion and inflammatory enzyme activities
Some of these natural plant-derived antioxidants may provide fur-ther pharmacological activities of possible relevance in CF This is thecase for instance of the plant flavonoids genistein apigenin kaemp-ferol quercetin and hesperidin [248ndash251] that fall in the pharmaco-logical category of ldquopotentiatorsrdquo [252] in that these activate at leastto a certain extent CTFR-mediated Cl currents in normal and CF airwayepithelium investigated either in vitro or in vivo in humans and ani-mal models Actually as prototypal flavonoid-derived potentiatorthe tyrosine kinase inhibitor genistein potentiates the gating of wild-type as well as ΔF508 CFTR and G551D CFTR [253] but at higherdoses it inhibits CFTR gating which make this an unlikely clinical can-didate Similar potentiation effects have been reported for the antiox-idant curcumin [250] that shows an additive effect with respect togenistein-induced potentiation Besides CFTR potentiation whichdoes not appear to have a direct influence on GSH and nutrient trans-port in the lung tissue all these natural substances have been usedalone or in combination with other agents as in vivo enhancers oflung antioxidant protection [246254255] In the case of quercetinthiol-reactive phenolic [256] bronchodilation and anti-inflammatoryeffects by a restoration of the Th1Th2 balance have been reportedin inflammatory syndromes of the lung [255257ndash259] but theseeffects have not been explored in CF Pyocyanin toxicity (see abovein the Section 2) could represent an issue for the use of quercetinand other catechols in infectious diseases of the lung [260]
Other natural antioxidants of potential interest in CF therapy in-clude terpenoids [261] such as terpinen-4-ol a major constituentof tea tree oil that is being investigated in the therapy of anti-biotic resistant organisms specifically against methicillin-resistantStaphylococcus aureus (MRSA) [262] a problem in CF [263] Otherthan being lipophilic antioxidants terpenes can prevent oxidativestress of the CF lung secondarily to the antibiotic effect thereby pro-moting a better control of immuno-inflammatory pathways and lungantioxidants
391 Targeting NF-κB with natural compounds resveratrol and plantextracts
Natural compounds were long known to be useful in designinganti-inflammatory drugs and some of these could find an applicationin the control of the transcription factor kappa-B (NF-κB) that maylead to develop advanced pharmacological tools to control inflamma-tion and to produce higher antioxidant protection to CF airwaysInhibitors targeting NF-κB including transcription factors decoymolecules (TFD) are potent down-regulators of gene expressionand release of IL-8 in CF cells infected with P aeruginosa [264265]
Resveratrol (354prime-trihydroxystilbene ldquoErdquo form) is one of the mostinvestigated natural antioxidant with proposed activity as NF-κBinhibitor This is a phytoalexin present in large quantity in red winepreferentially in the skin of grapes being its concentration
706 F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
50ndash100 μgmg of fresh skin and 13ndash3 mgl of red wine [266]Furthermore resveratrol is a constituent of lsquoDarakchasavarsquo (13ndash6 mgl) an ayurvedic medicine from India [267] The antioxidant activity ofresveratrol has been reported in several papers and occurs also in lungtissues suggesting that resveratrol has potential as a therapeuticagent in respiratory disease [268ndash270] Resveratrol can be consideredone of the most interesting molecules from the natural worldexhibiting strong antioxidant activity that at the same time is able toexert anti inflammatory activity through alteration of NF-κB functionsand efficient inhibition of pro-inflammatory genes [271272] As far asthe effects on CF model systems are concerned Cabrini et al [26]reported the effects of resveratrol on P aeruginosa infected CF IB3-1cells The results obtained demonstrate that resveratrol exhibits minoreffects of IB3-1 cell growth and important inhibitory effects on accumu-lation of IL-8 and GRO-α mRNA while minor effects on IL-6 gene ex-pression were observed These data support recently publishedobservations suggesting inhibitory effects of resveratrol in infection-mediated inflammatory processes [273] Interestingly resveratrol hasbeen reported as a potent inhibitor of NF-κB activity and a promisinganti-inflammatory agent [272274] also in combinationwith othermol-ecules [274275] However in vivo translation of this pre-clinical on res-veratrol is hard to be foreseen This natural compound displays poorbioavailability [276] and further characterization of resveratrol pharma-cokinetics is troublesome since it is hardly measurable in vivo [277]Furthermore the regulation of inflammatory responses by resveratrolhas been suggested to be far more complex than simple direct suppres-sion of NF-κB activity Actually some aspects of the immune responsecould be enhanced by this natural substance which may lead tohypothesize broad negative feedback events on immuno-inflammatorypathways [278] In any case and with these cautions in mind the pub-lished observations on cellular model systems support the concept thatresveratrol and resveratrol-containing formulations deserve further con-sideration to determine their possible therapeutic values in CF
Other inhibitors can be identified from systematic studies of naturalproducts and their ability to interfere with NF-κB activity [279ndash281]Recent studies have demonstrated that the whole extract of Aeglemarmelos (Rutaceae) has strong inhibitory effect on the P aeruginosa-dependent IL-8 induction in human CF-derived bronchial IB3-1 cellswithout affecting cell proliferation [280] Molecular analysis of compo-nents contained in A marmelos extracts revealed that three major com-pounds namely 56-dimethoxy-1-indanone 2-hydroxy-cinnamic acidand 5-methoxy psoralen (5-MOP) reproduce the inhibitory effect ob-servedwith thewhole extract [280] A further example has been recent-ly published using extracts from bergamot (Citrus bergamia Risso) Inthis study the extracts were characterized and the main detected con-stituents were assayed for their biological activity [281] The resultsobtained demonstrated that the extracts from bergamot epicarps con-tain components displaying an inhibitory activity on IL-8 Particularlythe most active molecules were bergapten and citropten These effectshave been confirmed by analyzing mRNA levels and protein release inthe CF cellularmodels IB3-1 and CuFi-1 inducedwith TNF-α or exposedto P aeruginosa
A parallel strategy linking NF-κB inhibition and down-regulationof NF-κB-dependent functions is described in recently publishedstudies based on a structured-based virtual screening (VS) of differ-ently substituted furocoumarins and analogues against NF-κB withthe objective of selecting molecules able to inhibit the binding ofthis transcription factor to DNA [282283] Novel compounds wereidentified with this strategy as potent inhibitors of NF-κB dependentbiological functions to be proposed for the control lung inflammationoccurring in patients affected by CF [282ndash284]
392 Scavengers and regulators of H2O2 and NO
3921 Lactoferrin and OSCNmacr The impaired DUOXLPO system of CFpatients could be the target of therapeutic strategies that may
produce concomitant antimicrobial and antioxidant effects This sys-tem described above in Section 22 represents an important compo-nent of innate immunity with a role in bactericidal defense andregulation of H2O2 metabolism of airways [32] CF patients have alsoreported to show lowered LF levels in the ASL [37] that togetherwith a CFTR-dependent defective efflux of SCNmacr and LPO [36] may cre-ate the environment for a sustained flux of H2O2 and for the genera-tion of highly reactive Fenton species [1138] An ideal therapeuticintervention should restore the LPO-dependent generation of bacteri-cidal OSCNmacr from DUOX-derived H2O2 and SCNmacr in the ASL to controlat the same time the microbial biofilm and the flux of H2O2 into theASL An approach close to this therapeutic mechanism was recentlyproposed for the drug Meveolreg This is a complex of LF and OSCNmacrwith proposed in vivo antimicrobial activity [285] to be evaluatedin clinical trials for the aerosol treatment of lung infections in CFpatients The role for this drug in the control of H2O2 levels of ASLremains to be investigated
3922 Organoselenium compounds Organoselenium compoundshave been proposed as therapeutic agents useful in the antioxidanttherapy of inflammatory conditions These include GPX mimetic mol-ecules such as Ebselenreg (2-phenyl-12-benzisoselenazol-3(2H)-one)or other and more recently developed molecules that are still inpre-clinical steps of evaluation [286] Selectively and specificity of ac-tion are main issues in the therapeutic mechanism of this candidateantioxidant drug that thanks to the electrophilic properties of Se[214] reacts with thiols to reduce H2O2 and other species MoreoverEbselenreg has been described to act as potent non-competitive inhib-itor of extracellular nucleoside diphosphokinase (NDPK) having neg-ligible effect on ecto-ATPase and adenyl kinase activities which areother players of the metabolism of extracellular nucleotides [287]This enzyme together with other nucleoside di- and triphosphatescontributes to regulate several components of the mucociliary clear-ance process (MCC) that protects the lung against infections via acti-vation of epithelial purinergic receptors The inhibition of NDPK bythis GPX-mimetic drug may also impact on the energy status of endo-thelial cells [287] This aspect could be further investigated as a cellu-lar protection mechanism in the pulmonary epithelium of CF patientsbeing the control of cell energy of fundamental importance to preventthe activation of death pathways [288]
Further therapeutic mechanisms for these Se-derived drugs mayderive from the marked activity as inducers of phase II enzymessuch as quinone reductase (QR) and glutathione-S-transferase (GST)[289] This induction response also observed with other electrophilsand redox-active molecules such as natural phenolic antioxidantscould produce higher cellular protection by the acquisition of anincreased capability to detoxify endobiotics generated during oxida-tive stress and inflammation [246]
3923 Melatonin and GSNO as NOx regulators Increased markers ofNO-derived biological damage are present in the CF lung suggestingthe abnormal reactivity of NOx in the inflamed lung of CF patients[52] However an impaired metabolism and biological function ofNO in CF airways (see Section 23) suggests a cautious approach tothe use of agents that may influence the levels and chemical behaviorof NO-derived species (NOx) with possible impact on the physiologi-cal roles of NO in vasodilatation innate immunity and H2O2 metabo-lism of the respiratory tract [290291] NO donors also appear toinfluence CFTR function of alveolar epithelium and gland serouscells [292293]
Main physiological role of the pineal gland hormone melatonin isthe synchronization of circadian rhythms including the sleepndashwakecycle but several other functions dealing with immunomodulatoryantioxidant and cellular protection effects have been identified[294] Melatonin receptor stimulation may also influence cyclic AMPsignaling and the regulation of CFTR ion channel [295296]
707F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
A recent randomized double-blind placebo-controlled study hasexamined the effects of short term melatonin administration (3 mgfor 3 weeks) on sleep and oxidative stress markers in CF [297]According with the expected pharmacological effect of this hormonalsubstance the treatment was successful in improving sleep indicesAt the same time nitrite levels determined in exhaled breath conden-sate (EBC) were reduced to suggest a better control of NOmetabolismof CF airways (discussed above in Section 23) but these effects how-ever were not associated with a significant correction of isoprostaneas lipid peroxidation marker measured in EBC Increasing dosages ofmelatonin could be investigated for the pharmacological treatmentof oxidative stress and immune dysfunction of CF patients due tothe absence of adverse effects of this hormonal substance in humans
The S-nitrosation reaction of thiols is another interesting aspect ofNO pharmacology [53] that may find an application in the therapy oflung complications of CF This has been the case for instance of theS-nitrosothiol GSNO that has been used safely in human trials[298299] This endogenous nitrosothiol with proposed regulatory ef-fect on the CFTR of lung epithelia [292293] is well tolerated in pa-tients with CF when administered by aerosolization and mayproduce better oxygenation [299] thereby suggesting that therapyaimed at restoring endogenous GSNO levels in the CF airway maymerit further clinical evaluation Since the administered GSNO de-composes as shown by the increased levels of expired NO in CF pa-tients under treatment with this nitrosothiol [299] furtherinvestigation should be addressed to ascertain whether GSNO thera-py may merely correspond to a GSH therapy
NO dependent effects on CFTR function should be considered toevaluate mechanism of action and specificity of antioxidant therapiesthat target NO metabolism and function in the CF airways
4 Conclusions and future perspectives
The presence of clinical and biochemical symptoms of inflammationand oxidative stress implies that CF patients have a higher demand ofantioxidant protection The combination of the dysfunctional CFTRwith a lowered intake and absorption of dietary antioxidants producesub-optimal levels of protection from both enzymatic and non-enzymatic defense systems The former could be associated with a de-fective glutathionemetabolism and lowered intake of sulfur-containingamino acids and oligoelements such as zinc and possibly seleniumwhile fat-soluble antioxidant vitamins such as vitamin E and caroten-oids and the water-soluble vitamin C are lowered than in healthy sub-jects due to malabsorption and possibly higher consumption
The increased antioxidant demand in CF patients should be evenhigher in the presence of complications of the lung pancreas andliver Lung comorbidity is particularly important in this contextbeing associated with recurrent infections which results in the alter-nation of inflammatory exacerbates and chronic inflammation Thesesustain the flux of ROS in the airways and promote the formation ofsecond-generation byproducts by the damage of biomolecules suchas PUFA and proteins which may diffuse also at the systemic level tofurther promote adverse biological responses and toxic reactions Pan-creatic insufficiency causes malnutrition and may lead to develop en-docrine and metabolic defects associated with diabetes of CF Theseevents can be further aggravated by the concomitance of liver dys-function and a poor nutritional status Malnutrition is strongly associ-ated with poor prognosis as assessed by pulmonary function andsurvival data [138ndash140] The more aggressive nutritional interven-tions seem to produce better clinical outcomes in these patients andthe possibility of achieving higher antioxidant protection in well-nourished patients by dietary factors could be a key aspect to explainsuch a clinical advantage The assumption that food-derived compo-nentsmay help to prevent the damaging effects of oxidative stress im-proving the antioxidant defenses deserves further investigation at theclinical level This together with the investigation of appropriate
laboratory biomarkers could provide critical information to establishintervention criteria for an early nutritional management of newly di-agnosed patients [5] It is expected that a timely secondary preventionstrategy could influence the progression of CF symptoms thusaffecting with a self-feeding mechanism the same extent of malnutri-tion and oxidative stress along the life of CF patients Since severalfactors contribute to impair the nutritional status of CF patients(such as pancreatic insufficiency chronic malabsorption recurrentsinopulmonary infections and progressive lung disease chronic in-flammation increased energy expenditure suboptimal intake multi-therapy) careful monitoring of the antioxidant status should berecommended According with international guidelines fat-solublevitamin supplementation is of utmost importance in daily practice to-gether with energy intake requirements and pancreatic enzyme-replacement therapy Among these vitamin E β-carotene and ω-3FA have observed to alleviate selected biochemical signs of oxidativestress as measured for instance with well established laboratory indi-ces of lipid peroxidation and in some studies these effects werepreliminarily associated with positive clinical outcomes Notwith-standing randomizedndashcontrolled clinical trials on antioxidant supple-ments (including ω-3 FA) so far carried out in CF have failed toconclusively demonstrate significant beneficial effects on respiratorysymptoms and on the consequent impact that these have on the qual-ity of life of these patients (reviewed in [202213]) whichmay provideno support for the use of these supplements in CF An absence of effi-cacy in prevention studies on antioxidant supplements has also beenobserved in other and possibly less severe oxidative stress-relatedconditions particularly in the secondary prevention of cardiovasculardisease and some forms of cancer by vitamin E and other antioxidantssuch as vitamin C selenium and β-carotene (reviewed in [163]) Dif-ferent biases however have been identified in randomize large clini-cal trials that may account for these disappointing findings Theseinclude patient selection criteria (early interventions and primaryprevention could have more chances of success than secondaryprevention) duration and doses of the treatment use of wrong anti-oxidant formulations and administration protocols absence of verifi-cations of the biological compliance to the treatment etc The samebiases apply for the few trials carried out in CF patients Thus the ap-propriateness and efficacy of nutritional interventions with naturalfood-derived or synthetic antioxidants should be verifiedwith respectto the biological pathways of oxidative stress and clinical variablesthat are identified as end-points Profiles of blood and tissue antioxi-dants as well as of reliable surrogate markers of oxidative stresshave to be selected and determined in highly specialized laboratorieswith a well-established experience on these analyses
Well-timed (early) interventions with appropriate antioxidantformulationsprotocols need to be proposed for the next generationof trials and the development of novel CF-tailored antioxidant andanti-inflammatory agents should be promoted
As a consequence of these considerations more clinical investiga-tion is awaited to identify future successful approaches to the antiox-idant therapy as a measure to further enhance quality of life and theoverall clinical outcome of CF patients
Acknowledgments
We are indebted with the Italian Cystic Fibrosis Research Founda-tion for the support that it provided with its grant program to the re-search activity of the authors of this paper This is a scientific initiativeof the ldquoWorking Group on Inflammation in Cystic Fibrosisrdquo (BragonziA Bravo E Cabrini G Conese M Cuzzocrea S Dechecchi MC De Ales-sandri A Evangelista V Galli F Gambari R Lambiase A Lucidi VManca A Melotti P Minicucci L Motta A Pietraforte D Pompella AQuattrucci S Rizzo R Romano M Sorio C Tesse R) of the Italian Soci-ety for Cystic Fibrosis A particular thank goes to the Prof GianniMastella for the critical revision of the manuscript and for the
708 F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
stimulating research environment that he has contributed to createwithin the Italian Cystic Fibrosis Research Foundation
References
[1] BP OSullivan SD Freedman Cystic fibrosis Lancet 373 (2009) 1891ndash1904[2] P Linsdell JW Hanrahan Glutathione permeability of CFTR Am J Physiol 275
(1998) C323ndashC326[3] L Gao KJ Kim JR Yankaskas HJ Forman Abnormal glutathione transport in
cystic fibrosis airway epithelia Am J Physiol 277 (1999) L113ndashL118[4] RK Rowntree A Harris The phenotypic consequences of CFTR mutations Ann
Hum Genet 67 (2003) 471ndash485[5] EI Back C Frindt D Nohr J Frank R Ziebach M Stern M Ranke HK Biesalski
Antioxidant deficiency in cystic fibrosis when is the right time to take actionAm J Clin Nutr 80 (2004) 374ndash384
[6] LG Wood DA Fitzgerald AK Lee ML Garg Improved antioxidant and fattyacid status of patients with cystic fibrosis after antioxidant supplementation islinked to improved lung function Am J Clin Nutr 77 (2003) 150ndash159
[7] L Iuliano R Monticolo G Straface S Zullo F Galli M Boaz S Quattrucci Asso-ciation of cholesterol oxidation and abnormalities in fatty acid metabolism incystic fibrosis Am J Clin Nutr 90 (2009) 477ndash484
[8] C Libetta V Sepe P Esposito F Galli A Dal Canton Oxidative stress and inflam-mation implications in uremia and hemodialysis Clin Biochem 44 (2011)1189ndash1198
[9] G Bartosz Reactive oxygen species destroyers or messengers Biochem Phar-macol 77 (2009) 1303ndash1315
[10] T Ntimbane B Comte G Mailhot Y Berthiaume V Poitout M Prentki RRabasa-Lhoret E Levy Cystic fibrosis-related diabetes from CFTR dysfunctionto oxidative stress Clin Biochem 30 (2009) 153ndash177
[11] A van der Vliet JP Eiserich GP Marelich B Halliwell CE Cross Oxidativestress in cystic fibrosis does it occur and does it matter Adv Pharmacol 38(1997) 491ndash513
[12] AM Cantin TB White CE Cross HJ Forman RJ Sokol D Borowitz Antioxi-dants in cystic fibrosis Conclusions from the CF antioxidant workshop Bethes-da Maryland Free Radic Biol Med 42 (2007) 15ndash31
[13] LT McGrath P Mallon L Dowey B Silke E McClean M McDonnell A DevineS Copeland S Elborn Oxidative stress during acute respiratory exacerbations incystic fibrosis Thorax 54 (1999) 518ndash523
[14] E Thomson S Brennan R Senthilmohan CL Gangell AL Chapman PD SlyAJ Kettle E Balding LJ Berry JB Carlin R Carzino N de Klerk T Douglas CFoo LW Garratt GL Hall J Harrison A Kicic IA Laing KM Logie J MassieLS Mott C Murray F Parsons N Pillarisetti SR Poreddy SC RanganathanCF Robertson R Robins-Browne PJ Robinson B Skoric SM Stick ENSutanto E Williamson Identifying peroxidases and their oxidants in the earlypathology of cystic fibrosis Free Radic Biol Med 49 (2010) 1354ndash1360
[15] SP Range C Dunster AJ Knox FJ Kelly Treatment of pulmonary exacerba-tions of cystic fibrosis leads to improved antioxidant status Eur Respir J 13(1999) 560ndash564
[16] L Coppo P Ghezzi Thiol regulation of pro-inflammatory cytokines and innateimmunity protein S-thiolation as a novel molecular mechanism Biochem SocTrans 39 (2011) 1268ndash1272
[17] C Verhaeghe C Remouchamps B Hennuy A Vanderplasschen A Chariot SPTabruyn C Oury V Bours Role of IKK and ERK pathways in intrinsic inflamma-tion of cystic fibrosis airways Biochem Pharmacol 73 (2007) 1982ndash1994
[18] TL Bonfield JR Panuska MW Konstan KA Hilliard JB Hilliard H Ghnaim MBerger Inflammatory cytokines in cystic fibrosis lungs Am J Respir Crit CareMed 152 (1995) 2111ndash2118
[19] TL Noah HR Black PW Cheng RE Wood MW Leigh Nasal and bronchoal-veolar lavage fluid cytokines in early cystic fibrosis J Infect Dis 175 (1997)638ndash647
[20] MJ Welsh BW Ramsey FJ Accurso GR Cutting Cystic Fibrosis McGraw-HillNew York 2001
[21] TZ Khan JS Wagener T Bost J Martinez FJ Accurso DW Riches Early pul-monary inflammation in infants with cystic fibrosis Am J Respir Crit CareMed 151 (1995) 1075ndash1082
[22] FA Ratjen Cystic fibrosis pathogenesis and future treatment strategies RespirCare 54 (2009) 595ndash605
[23] J Jacquot O Tabary P Le Rouzic A Clement Airway epithelial cell inflamma-tory signalling in cystic fibrosis Int J Biochem Cell Biol 40 (2008)1703ndash1715
[24] CM Greene P Branagan NG McElvaney Toll-like receptors as therapeutic tar-gets in cystic fibrosis Expert Opin Ther Targets 12 (2008) 1481ndash1495
[25] M Rottner JM Freyssinet MC Martinez Mechanisms of the noxious inflam-matory cycle in cystic fibrosis Respir Res 10 (2009) 23
[26] G Cabrini V Bezzerri I Mancini E Nicolis MC Dechecchi A Tamanini ILampronti L Piccagli N Bianchi M Borgatti R Gambari Targeting transcrip-tion factor activity as a strategy to inhibit pro-inflammatory genes involved incystic fibrosis decoy oligonucleotides and low-molecular weight compoundsCurr Med Chem 17 (2010) 4392ndash4404
[27] CM Greene NG McElvaney Proteases and antiproteases in chronic neutrophiliclungdiseasemdash relevance to drug discovery Br J Pharmacol 158 (2009) 1048ndash1058
[28] AM Cantin Potential for antioxidant therapy of cystic fibrosis Curr Opin PulmMed 10 (2004) 531ndash536
[29] JF Chmiel MW Konstan Inflammation and anti-inflammatory therapies forcystic fibrosis Clin Chest Med 28 (2007) 331ndash346
[30] DP Nichols MW Konstan JF Chmiel Anti-inflammatory therapies for cys-tic fibrosis-related lung disease Clin Rev Allergy Immunol 35 (2008)135ndash153
[31] AJ Kettle T Chan I Osberg R Senthilmohan AL Chapman TJ Mocatta JSWagener Myeloperoxidase and protein oxidation in the airways of youngchildren with cystic fibrosis Am J Respir Crit Care Med 170 (2004)1317ndash1323
[32] H Fischer Mechanisms and function of DUOX in epithelia of the lung AntioxidRedox Signal 11 (2009) 2453ndash2465
[33] B Rada TL Leto Oxidative innate immune defenses by NoxDuox familyNADPH oxidases Contrib Microbiol 15 (2008) 164ndash187
[34] P Moskwa D Lorentzen KJ Excoffon J Zabner PB McCray Jr WM NauseefC Dupuy B Banfi A novel host defense system of airways is defective in cysticfibrosis Am J Respir Crit Care Med 175 (2007) 174ndash183
[35] D Lorentzen L Durairaj AA Pezzulo Y Nakano J Launspach DA Stoltz GZamba PB McCray Jr J Zabner MJ Welsh WM Nauseef B Banfi Concentra-tion of the antibacterial precursor thiocyanate in cystic fibrosis airway secre-tions Free Radic Biol Med 50 (2011) 1144ndash1150
[36] Y Xu S Szep Z Lu The antioxidant role of thiocyanate in the pathogenesis ofcystic fibrosis and other inflammation-related diseases Proc Natl Acad Sci US A 106 (2009) 20515ndash20519
[37] MP Rogan CC Taggart CM Greene PG Murphy SJ ONeill NG McElvaneyLoss of microbicidal activity and increased formation of biofilm due to decreasedlactoferrin activity in patients with cystic fibrosis J Infect Dis 190 (2004)1245ndash1253
[38] B Halliwell JM Guttridge Free Radicals in Biology and Medicine Fourth editionOxford University Press New York 2007
[39] B Rada K Lekstrom S Damian C Dupuy TL Leto The Pseudomonastoxin pyocyanin inhibits the dual oxidase-based antimicrobial system as itimposes oxidative stress on airway epithelial cells J Immunol 181 (2008)4883ndash4893
[40] C Schwarzer B Illek JH Suh SJ Remington H Fischer TE Machen Organelleredox of CF and CFTR-corrected airway epithelia Free Radic Biol Med 43(2007) 300ndash316
[41] JH Roum R Buhl NG McElvaney Z Borok RG Crystal Systemic deficiency ofglutathione in cystic fibrosis J Appl Physiol 75 (1993) 2419ndash2424
[42] VM Hudson Rethinking cystic fibrosis pathology the critical role of abnormalreduced glutathione (GSH) transport caused by CFTR mutation Free RadicBiol Med 30 (2001) 1440ndash1461
[43] PJ Barnes RA Dweik AF Gelb PG Gibson SC George H Grasemann IDPavord F Ratjen PE Silkoff DR Taylor N Zamel Exhaled nitric oxide in pul-monary diseases a comprehensive review Chest 138 (2010) 682ndash692
[44] H Grasemann E Michler M Wallot F Ratjen Decreased concentration of ex-haled nitric oxide (NO) in patients with cystic fibrosis Pediatr Pulmonol 24(1997) 173ndash177
[45] H Grasemann F Ratjen Cystic fibrosis lung disease the role of nitric oxidePediatr Pulmonol 28 (1999) 442ndash448
[46] B Gaston F Ratjen JW Vaughan NR Malhotra RG Canady AH Snyder JFHunt S Gaertig JB Goldberg Nitrogen redox balance in the cystic fibrosis air-way effects of antipseudomonal therapy Am J Respir Crit Care Med 165(2002) 387ndash390
[47] H Grasemann I Ioannidis RP Tomkiewicz H de Groot BK Rubin F RatjenNitric oxide metabolites in cystic fibrosis lung disease Arch Dis Child 78(1998) 49ndash53
[48] H Grasemann R Schwiertz S Matthiesen K Racke F Ratjen Increased argi-nase activity in cystic fibrosis airways Am J Respir Crit Care Med 172(2005) 1523ndash1528
[49] H Grasemann S Al-Saleh JA Scott D Shehnaz A Mehl R Amin M Rafii PPencharz J Belik F Ratjen Asymmetric dimethylarginine contributes to airwaynitric oxide deficiency in patients with cystic fibrosis Am J Respir Crit CareMed 183 (2011) 1363ndash1368
[50] H Grasemann F Kurtz F Ratjen Inhaled L-arginine improves exhaled nitricoxide and pulmonary function in patients with cystic fibrosis Am J RespirCrit Care Med 174 (2006) 208ndash212
[51] H Grasemann F Ratjen Emerging therapies for cystic fibrosis lung disease Ex-pert Opin Emerg Drugs 15 (2010) 653ndash659
[52] BM Morrissey K Schilling JV Weil PE Silkoff DM Rodman Nitric oxide andprotein nitration in the cystic fibrosis airway Arch Biochem Biophys 406(2002) 33ndash39
[53] R Radi Nitric oxide oxidants and protein tyrosine nitration Proc Natl AcadSci U S A 101 (2004) 4003ndash4008
[54] J Chen M Kinter S Shank C Cotton TJ Kelley AG Ziady Dysfunction of Nrf-2in CF epithelia leads to excess intracellular H2O2 and inflammatory cytokineproduction PLoS One 3 (2008) e3367
[55] F Galli M Piroddi C Annetti C Aisa E Floridi A Floridi Oxidative stress andreactive oxygen species Contrib Nephrol 149 (2005) 240ndash260
[56] DT Wright LA Cohn H Li B Fischer CM Li KB Adler Interactions of oxygenradicals with airway epithelium Environ Health Perspect 102 (Suppl 10)(1994) 85ndash90
[57] I Rahman SR Yang SK Biswas Current concepts of redox signaling in thelungs Antioxid Redox Signal 8 (2006) 681ndash689
[58] Q Li JF Engelhardt Interleukin-1beta induction of NFκB is partially regulatedby H2O2-mediated activation of NFκB-inducing kinase J Biol Chem 281(2006) 1495ndash1505
709F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
[59] E Boncoeur VS Criq E Bonvin T Roque A Henrion-Caude DC Gruenert AClement J Jacquot O Tabary Oxidative stress induces extracellular signal-regulated kinase 12 mitogen-activated protein kinase in cystic fibrosis lung ep-ithelial cells potential mechanism for excessive IL-8 expression Int J BiochemCell Biol 40 (2008) 432ndash446
[60] B Fischer J Voynow Neutrophil elastase induces MUC5AC messenger RNA ex-pression by an oxidant-dependent mechanism Chest 117 (2000) 317Sndash320S
[61] B Rada P Gardina TG Myers TL Leto Reactive oxygen species mediate in-flammatory cytokine release and EGFR-dependent mucin secretion in airwayepithelial cells exposed to Pseudomonas pyocyanin Mucosal Immunol 4(2011) 158ndash171
[62] C Schwarzer H Fischer EJ Kim KJ Barber AD Mills MJ Kurth DC GruenertJH Suh TE Machen B Illek Oxidative stress caused by pyocyanin impairs CFTRClminus transport in human bronchial epithelial cells Free Radic Biol Med 45(2008) 1653ndash1662
[63] J Hull M South P Phelan K Grimwood Surfactant composition in infants andyoung children with cystic fibrosis Am J Respir Crit Care Med 156 (1997)161ndash165
[64] KC Meyer A Sharma R Brown M Weatherly FR Moya J Lewandoski JJZimmerman Function and composition of pulmonary surfactant andsurfactant-derived fatty acid profiles are altered in young adults with cystic fi-brosis Chest 118 (2000) 164ndash174
[65] MK Pulfer RC Murphy Formation of biologically active oxysterols during ozo-nolysis of cholesterol present in lung surfactant J Biol Chem 279 (2004)26331ndash26338
[66] V Starosta E Rietschel K Paul U Baumann M Griese Oxidative changes ofbronchoalveolar proteins in cystic fibrosis Chest 129 (2006) 431ndash437
[67] V Starosta M Griese Oxidative damage to surfactant protein D in pulmonarydiseases Free Radic Res 40 (2006) 419ndash425
[68] M Griese R Essl R Schmidt E Rietschel F Ratjen M Ballmann K Paul Pulmo-nary surfactant lung function and endobronchial inflammation in cystic fibro-sis Am J Respir Crit Care Med 170 (2004) 1000ndash1005
[69] M Griese R Essl R Schmidt M Ballmann K Paul E Rietschel F Ratjen Se-quential analysis of surfactant lung function and inflammation in cystic fibrosispatients Respir Res 6 (2005) 133
[70] LG Wood DA Fitzgerald PG Gibson DM Cooper ML Garg Increased plasmafatty acid concentrations after respiratory exacerbations are associated with el-evated oxidative stress in cystic fibrosis patients Am J Clin Nutr 75 (2002)668ndash675
[71] P Montuschi SA Kharitonov G Ciabattoni M Corradi L van Rensen DM Ged-des ME Hodson PJ Barnes Exhaled 8-isoprostane as a new non-invasive bio-marker of oxidative stress in cystic fibrosis Thorax 55 (2000) 205ndash209
[72] CE Collins P Quaggiotto L Wood EV OLoughlin RL Henry ML Garg Elevat-ed plasma levels of F2 alpha isoprostane in cystic fibrosis Lipids 34 (1999)551ndash556
[73] D Hartl V Starosta K Maier I Beck-Speier C Rebhan BF Becker P Latzin RFischer F Ratjen RM Huber E Rietschel S Krauss-Etschmann M Griese In-haled glutathione decreases PGE2 and increases lymphocytes in cystic fibrosislungs Free Radic Biol Med 39 (2005) 463ndash472
[74] GL Milne H Yin JD Morrow Human biochemistry of the isoprostane pathwayJ Biol Chem 283 (2008) 15533ndash15537
[75] G Ciabattoni G Davi M Collura L Iapichino F Pardo A Ganci R Romagnoli JMaclouf C Patrono In vivo lipid peroxidation and platelet activation in cystic fi-brosis Am J Respir Crit Care Med 162 (2000) 1195ndash1201
[76] C Garenc P Julien E Levy Oxysterols in biological systems the gastrointestinaltract liver vascular wall and central nervous system Free Radic Res 44 (2011)47ndash73
[77] AM Cantin SL North RC Hubbard RG Crystal Normal alveolar epithelial lin-ing fluid contains high levels of glutathione J Appl Physiol 63 (1987) 152ndash157
[78] R Tirouvanziam CK Conrad T Bottiglieri LA Herzenberg RB Moss High-dose oral N-acetylcysteine a glutathione prodrug modulates inflammation incystic fibrosis Proc Natl Acad Sci U S A 103 (2006) 4628ndash4633
[79] LW Velsor C Kariya R Kachadourian BJ Day Mitochondrial oxidative stressin the lungs of cystic fibrosis transmembrane conductance regulator proteinmutant mice Am J Respir Cell Mol Biol 35 (2006) 579ndash586
[80] M Kelly-Aubert S Trudel J Fritsch T Nguyen-Khoa M Baudouin-Legros SMoriceau L Jeanson F Djouadi C Matar M Conti M Ollero F Brouillard AEdelman GSH monoethyl ester rescues mitochondrial defects in cystic fibrosismodels Hum Mol Genet 20 (2011) 2745ndash2759
[81] P Ghezzi Role of glutathione in immunity and inflammation in the lung Int JGen Med 4 (2011) 105ndash113
[82] N Dauletbaev K Viel R Buhl TO Wagner J Bargon Glutathione and glutathi-one peroxidase in sputum samples of adult patients with cystic fibrosis J CystFibros 3 (2004) 119ndash124
[83] CE Cross A van der Vliet CA ONeill S Louie B Halliwell Oxidants antioxi-dants and respiratory tract lining fluids Environ Health Perspect 102 (Suppl10) (1994) 185ndash191
[84] K Takeyama K Dabbagh J Jeong Shim T Dao-Pick IF Ueki JA Nadel Oxida-tive stress causes mucin synthesis via transactivation of epidermal growth factorreceptor role of neutrophils J Immunol 164 (2000) 1546ndash1552
[85] N Ballatori SM Krance S Notenboom S Shi K Tieu CL Hammond Glutathi-one dysregulation and the etiology and progression of human diseases BiolChem 390 (2009) 191ndash214
[86] SR Soltaninassab KR Sekhar MJ Meredith ML Freeman Multi-faceted regu-lation of gamma-glutamylcysteine synthetase J Cell Physiol 182 (2000)163ndash170
[87] HR Lopez-Mirabal JR Winther Redox characteristics of the eukaryotic cytosolBiochim Biophys Acta 1783 (2008) 629ndash640
[88] C Hwang AJ Sinskey HF Lodish Oxidized redox state of glutathione in the en-doplasmic reticulum Science 257 (1992) 1496ndash1502
[89] M Murphy Mitochondrial thiols in antioxidant protection and redox signallingdistinct roles for glutathionylation and other thiol modifications AntioxidRedox Signal (2011) ahead of print doi101089ars20114289
[90] BJ Day AM van Heeckeren E Min LW Velsor Role for cystic fibrosis trans-membrane conductance regulator protein in a glutathione response to bronch-opulmonary Pseudomonas infection Infect Immun 72 (2004) 2045ndash2051
[91] Y Zhang K Duan Glutathione exhibits antibacterial activity and increases tetra-cycline efficacy against Pseudomonas aeruginosa Sci China C Life Sci 52 (2009)501ndash505
[92] VM Hudson New insights into the pathogenesis of cystic fibrosis pivotal roleof glutathione system dysfunction and implications for therapy Treat RespirMed 3 (2004) 353ndash363
[93] LW Velsor A van Heeckeren BJ Day Antioxidant imbalance in the lungs ofcystic fibrosis transmembrane conductance regulator protein mutant miceAm J Physiol Lung Cell Mol Physiol 281 (2001) L31ndashL38
[94] I Kogan M Ramjeesingh C Li JF Kidd Y Wang EM Leslie SP Cole CE BearCFTR directly mediates nucleotide-regulated glutathione flux EMBO J 22(2003) 1981ndash1989
[95] NS Gould S Gauthier CT Kariya E Min J Huang DJ Brian Hypertonic salineincreases lung epithelial lining fluid glutathione and thiocyanate two protectiveCFTR-dependent thiols against oxidative injury Respir Res 11 (2010) 119
[96] VT Vasu SJ de Cruz JS Houghton KA Hayakawa BM Morrissey CE CrossJP Eiserich Evaluation of thiol-based antioxidant therapeutics in cystic fibrosissputum focus on myeloperoxidase Free Radic Res 45 (2011) 165ndash176
[97] L Roussel G Martel J Berube S Rousseau P aeruginosa drives CXCL8 synthesisvia redundant toll-like receptors and NADPH oxidase in CFTRF508 airway epi-thelial cells J Cyst Fibros 10 (2011) 107ndash113
[98] GW Lau DJ Hassett H Ran F Kong The role of pyocyanin in Pseudomonas aer-uginosa infection Trends Mol Med 10 (2004) 599ndash606
[99] R Wilson DA Sykes D Watson A Rutman GW Taylor PJ Cole Measurementof Pseudomonas aeruginosa phenazine pigments in sputum and assessment oftheir contribution to sputum sol toxicity for respiratory epithelium InfectImmun 56 (1988) 2515ndash2517
[100] M Muller Pyocyanin induces oxidative stress in human endothelial cells andmodulates the glutathione redox cycle Free Radic Biol Med 33 (2002)1527ndash1533
[101] YQ OMalley KJ Reszka BE Britigan Direct oxidation of 2prime7prime-dichlorodihy-drofluorescein by pyocyanin and other redox-active compounds independentof reactive oxygen species production Free Radic Biol Med 36 (2004)90ndash100
[102] CC Caldwell Y Chen HS Goetzmann Y Hao MT Borchers DJ Hassett LRYoung D Mavrodi L Thomashow GW Lau Pseudomonas aeruginosa exotoxinpyocyanin causes cystic fibrosis airway pathogenesis Am J Pathol 175 (2009)2473ndash2488
[103] YQ OMalley KJ Reszka DR Spitz GM Denning BE Britigan Pseudomonasaeruginosa pyocyanin directly oxidizes glutathione and decreases its levels inairway epithelial cells Am J Physiol Lung Cell Mol Physiol 287 (2004)L94ndashL103
[104] M Muller Glutathione modulates the toxicity of but is not a biologically rele-vant reductant for the Pseudomonas aeruginosa redox toxin pyocyanin FreeRadic Biol Med 50 (2011) 971ndash977
[105] R Cheluvappa R Shimmon M Dawson SN Hilmer DG Le Couteur Reactionsof Pseudomonas aeruginosa pyocyanin with reduced glutathione Acta BiochimPol 55 (2008) 571ndash580
[106] JH Widdicombe Transgenic animals may help resolve a sticky situation in cys-tic fibrosis J Clin Invest 120 (2010) 3093ndash3096
[107] X Sun H Sui JT Fisher Z Yan X Liu HJ Cho NS Joo Y Zhang W Zhou Y YiJM Kinyon DC Lei-Butters MA Griffin P Naumann M Luo J Ascher KWang T Frana JJ Wine DK Meyerholz JF Engelhardt Disease phenotype ofa ferret CFTR-knockout model of cystic fibrosis J Clin Invest 120 (2010)3149ndash3160
[108] NS Joo HJ Cho M Khansaheb JJ Wine Hyposecretion of fluid from trachealsubmucosal glands of CFTR-deficient pigs J Clin Invest 120 (2010) 3161ndash3166
[109] A Bragonzi Murine models of acute and chronic lung infection with cystic fibro-sis pathogens IJMM 300 (2010) 584ndash593
[110] AM van Heeckeren MD Schluchter Murine models of chronic Pseudomonasaeruginosa lung infection Lab Anim 36 (2002) 291ndash312
[111] A Bragonzi D Worlitzsch GB Pier P Timpert M Ulrich M Hentzer JB Ander-sen M Givskov M Conese G Doring Nonmucoid Pseudomonas aeruginosa ex-presses alginate in the lungs of patients with cystic fibrosis and in a mousemodel J Infect Dis 192 (2005) 410ndash419
[112] GS CW Bedrossian DB Singer JJ Hansen HS Rosenberg The lung in cysticfibrosis A quantitative study including prevalence of pathologic findingsamong different age groups Hum Pathol 7 (1976) 195ndash204
[113] WD HA Cash B McCullough WG Johanson Jr JA Bass A rat model of chron-ic respiratory infection with Pseudomonas aeruginosa Am Rev Respir Dis 119(1979) 453ndash459
[114] EM JR Starke C Langston CJ Baker A mouse model of chronic pulmonary in-fection with Pseudomonas aeruginosa and Pseudomonas cepacia Pediatr Res 22(1987) 698ndash702
[115] TJ AM van Heeckeren RW Walenga MW Konstan PB Davis B ErokwuMA Haxhiu TW Ferkol Effect of Pseudomonas infection on weight loss lung
710 F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
mechanics and cytokines in mice Am J Respir Crit Care Med 161 (2000)271ndash279
[116] T Aw G Wierzbicka DP Jones Oral glutathione increases tissue glutathione invivo Chem Biol Interact 80 (1991) 89ndash97
[117] F Favilli P Marraccini T Iantomasi MT Vincenzini Effect of orally adminis-tered glutathione on glutathione levels in some organs of rats role of specifictransporters Br J Nutr 78 (1997) 293ndash300
[118] C Kariya H Leitner E Min C van Heeckeren A van Heeckeren BJ Day A rolefor CFTR in the elevation of glutathione levels in the lung by oral glutathione ad-ministration Am J Physiol Lung Cell Mol Physiol 292 (2007) L1590ndashL1597
[119] K Atkuri JJ Mantovani LA Herzenberg LA Herzenberg N-Acetylcysteinemdashasafe antidote for cysteineglutathione deficiency Curr Opin Pharmacol 7(2007) 355ndash359
[120] R De Lisle E Roach K Jansson Effects of laxative and N-acetylcysteine onmucus accumulation bacterial load transit and inflammation in the cystic fi-brosis mouse small intestine Am J Physiol Gastrointest Liver Physiol 293(2007) G577ndashG584
[121] A Luciani VR Villella S Esposito N Brunetti-Pierri D Medina C Settembre MGavina L Pulze I Giardino M Pettoello-Mantovani M DApolito S Guido EMasliah B Spencer S Quaratino V Raia A Ballabio L Maiuri Defective CFTRinduces aggresome formation and lung inflammation in cystic fibrosis throughROS-mediated autophagy inhibition Nat Cell Biol 12 863ndash875
[122] M Griese J Ramakers A Krasselt V Starosta S Van Koningsbruggen R FischerF Ratjen B Mullinger RM Huber K Maier E Rietschel G Scheuch Improve-ment of alveolar glutathione and lung function but not oxidative state in cysticfibrosis Am J Respir Crit Care Med 169 (2004) 822ndash828
[123] C Bishop VM Hudson SC Hilton C Wilde A pilot study of the effect of inhaledbuffered reduced glutathione on the clinical status of patients with cystic fibro-sis Chest 127 (2005) 308ndash317
[124] WWang C Oliva G Li A Holmgren CH Lillig KL Kirk Reversible silencing of CFTRchloride channels by glutathionylation J Gen Physiol 125 (2005) 127ndash141
[125] N Dauletbaev P Fischer B Aulbach J Gross W Kusche U Thyroff-FriesingerTO Wagner J Bargon A phase II study on safety and efficacy of high-dose N-acetylcysteine in patients with cystic fibrosis Eur J Med Res 14 (2009)352ndash358
[126] R Tirouvanziam Y Gernez CK Conrad RB Moss I Schrijver CE Dunn ZADavies LA Herzenberg Profound functional and signaling changes in viable in-flammatory neutrophils homing to cystic fibrosis airways Proc Natl Acad SciU S A 105 (2008) 4335ndash4339
[127] JH Roum Z Borok NG McElvaney GJ Grimes AD Bokser R Buhl RG Crys-tal Glutathione aerosol suppresses lung epithelial surface inflammatory cell-derived oxidants in cystic fibrosis J Appl Physiol 87 (1999) 438ndash443
[128] A Visca CT Bishop SC Hilton VM Hudson Improvement in clinical markersin CF patients using a reduced glutathione regimen an uncontrolled observa-tional study J Cyst Fibros 7 (2008) 433ndash436
[129] EF Nash A Stephenson F Ratjen E Tullis Nebulized and oral thiol derivativesfor pulmonary disease in cystic fibrosis Cochrane Database Syst Rev (2009)CD007168
[130] AC foundation Drug Development Pipeline 2011[131] S Hoshida T Kuzuya N Yamashita M Nishida S Kitahara M Hori T
Kamada M Tada Gamma-glutamylcysteine ethyl ester for myocardial protec-tion in dogs during ischemia and reperfusion J Am Coll Cardiol 24 (1994)1391ndash1397
[132] J Lok W Leung S Zhao S Pallast K van Leyen S Guo X Wang A Yalcin EHLo Gamma-glutamylcysteine ethyl ester protects cerebral endothelial cells dur-ing injury and decreases bloodndashbrain barrier permeability after experimentalbrain trauma J Neurochem 118 (2011) 248ndash255
[133] Z Borok R Buhl GJ Grimes AD Bokser RC Hubbard KJ Holroyd JH RoumDB Czerski AM Cantin RG Crystal Effect of glutathione aerosol on oxidantndashantioxidant imbalance in idiopathic pulmonary fibrosis Lancet 338 (1991)215ndash216
[134] KJ Holroyd R Buhl Z Borok JH Roum AD Bokser GJ Grimes D Czerski AMCantin RG Crystal Correction of glutathione deficiency in the lower respiratorytract of HIV seropositive individuals by glutathione aerosol treatment Thorax 48(1993) 985ndash989
[135] J Hull P Vervaart K Grimwood P Phelan Pulmonary oxidative stress responsein young children with cystic fibrosis Thorax 52 (1997) 557ndash560
[136] A Corti A Paolicchi M Franzini S Dominici AF Casini A Pompella The S-thiolating activity of membrane gamma-glutamyltransferase formation ofcysteinyl-glycine mixed disulfides with cellular proteins and in the cell microen-vironment Antioxid Redox Signal 7 (2005) 911ndash918
[137] A Corti M Franzini AF Casini A Paolicchi A Pompella Vitamin C supply tobronchial epithelial cells linked to glutathione availability in elfmdasha role for se-creted gamma-glutamyltransferase J Cyst Fibros 7 (2008) 174ndash178
[138] A Munck Nutritional considerations in patients with cystic fibrosis Expert RevRespir Med 4 (2010) 47ndash56
[139] JL Matel CE Milla Nutrition in cystic fibrosis Semin Respir Crit Care Med 30(2009) 579ndash586
[140] D Salvatore R Buzzetti E Baldo MP Forneris V Lucidi D Manunza IMarinelli B Messore AS Neri V Raia ML Furnari G Mastella An overviewof international literature from cystic fibrosis registries 2 Neonatal screeningand nutritiongrowth J Cyst Fibros 9 (2010) 75ndash83
[141] KF Joosten JM Hulst Malnutrition in pediatric hospital patients current is-sues Nutrition 27 (2011) 133ndash137
[142] S Fustik T Jacovska L Spirevska S Koceva Protein-energy malnutrition as thefirst manifestation of cystic fibrosis in infancy Pediatr Int 51 (2009) 678ndash683
[143] J Himmelfarb E McMonagle Albumin is the major plasma protein target of ox-idant stress in uremia Kidney Int 60 (2001) 358ndash363
[144] P Stenvinkel JJ Carrero J Axelsson B Lindholm O Heimburger Z MassyEmerging biomarkers for evaluating cardiovascular risk in the chronic kidneydisease patient how do new pieces fit into the uremic puzzle Clin J Am SocNephrol 3 (2008) 505ndash521
[145] M Roche P Rondeau NR Singh E Tarnus E Bourdon The antioxidant proper-ties of serum albumin FEBS Lett 582 (2008) 1783ndash1787
[146] D Giustarini A Milzani I Dalle-Donne R Rossi Red blood cells as a physiolog-ical source of glutathione for extracellular fluids Blood Cells Mol Dis 40 (2008)174ndash179
[147] A Meister ME Anderson Glutathione Annu Rev Biochem 52 (1983) 711ndash760[148] B Alvarez S Carballal L Turell R Radi Formation and reactions of sulfenic acid
in human serum albumin Methods Enzymol 473 (2010) 117ndash136[149] S Carballal B Alvarez L Turell H Botti BA Freeman R Radi Sulfenic acid in
human serum albumin Amino Acids 32 (2007) 543ndash551[150] LR Barclay AM Bailey D Kong The antioxidant activity of alpha-tocopherol-
bovine serum albumin complex in micellar and liposome autoxidations J BiolChem 260 (1985) 15809ndash15814
[151] T Ishii T Ichikawa K Minoda K Kusaka S Ito Y Suzuki M Akagawa K Mochi-zuki T Goda T Nakayama Human serum albumin as an antioxidant in the ox-idation of (minus)-epigallocatechin gallate participation of reversible covalentbinding for interaction and stabilization Biosci Biotechnol Biochem 75(2011) 100ndash106
[152] F Galli S Rovidati S Benedetti U Buoncristiani C Covarelli A Floridi F Canes-trari Overexpression of erythrocyte glutathione S-transferase in uremia and di-alysis Clin Chem 45 (1999) 1781ndash1788
[153] D Borowitz RD Baker V Stallings Consensus report on nutrition for pediat-ric patients with cystic fibrosis J Pediatr Gastroenterol Nutr 35 (2002)246ndash259
[154] LJ Filer Jr SW Wright MP Manning KE Mason Absorption of alpha-tocopherol and tocopherylesters by premature and full term infants and chil-dren in health and disease Pediatrics 8 (1951) 328ndash339
[155] L Lancellotti C DOrazio G Mastella G Mazzi U Lippi Deficiency of vitamins Eand A in cystic fibrosis is independent of pancreatic function and current en-zyme and vitamin supplementation Eur J Pediatr 155 (1996) 281ndash285
[156] MN Sathe AS Patel Update in pediatrics focus on fat-soluble vitamins NutrClin Pract 25 (2010) 340ndash346
[157] MG Traber The ABCs of vitamin E and beta-carotene absorption Am J ClinNutr 80 (2004) 3ndash4
[158] TF Dolan Jr Hemolytic anemia and edema as the initial signs in infants withcystic fibrosis Consider this diagnosis even in absence of pulmonary symptomsClin Pediatr 15 (1976) 597ndash600
[159] DR James M Alfaham MC Goodchild Increased susceptibility to peroxide-induced haemolysis with normal vitamin E concentrations in cystic fibrosisClin Chim Acta 204 (1991) 279ndash290
[160] SA Peters FJ Kelly Vitamin E supplementation in cystic fibrosis J Pediatr Gas-troenterol Nutr 22 (1996) 341ndash345
[161] A Maqbool VA Stallings Update on fat-soluble vitamins in cystic fibrosis CurrOpin Pulm Med 14 (2008) 574ndash581
[162] SD Sagel MK Sontag MM Anthony P Emmett KA Papas Effect of anantioxidant-rich multivitamin supplement in cystic fibrosis J Cyst Fibros 10(2011) 31ndash36
[163] F Galli A Azzi Present trends in vitamin E research Biofactors 36 (2010)33ndash42
[164] A Hamahata P Enkhbaatar ER Kraft M Lange SW Leonard MG Traber RACox FC Schmalstieg HK Hawkins EB Whorton EM Horvath C Szabo LDTraber DN Herndon DL Traber Gamma-tocopherol nebulization by a lipidaerosolization device improves pulmonary function in sheep with burn andsmoke inhalation injury Free Radic Biol Med 45 (2008) 425ndash433
[165] JP Anais N Razzouq M Carvalho C Fernandez A Astier M Paul A AstierH Fessi AM Lorino Development of alpha-tocopherol acetate nanoparti-cles influence of preparative processes Drug Dev Ind Pharm 35 (2009)216ndash223
[166] JM Zingg Molecular and cellular activities of vitamin E analogues Mini RevMed Chem 7 (2007) 543ndash558
[167] V Viola F Pilolli M Piroddi E Pierpaoli F Orlando M Provinciali M Betti FMazzini F Galli Why tocotrienols work better insights into the in vitro anti-cancer mechanism of vitamin E Genes Nutr 7 (2011) 29ndash41
[168] F Galli F Mazzini L Bamonti L Gille S Bohmdorfer M Piroddi T Netscher FJKelly T Rosenau Tocotrienamines and tocopheramines reactions with radicalsand metal ions Bioorg Med Chem 19 (2011) 6483ndash6491
[169] A Kuhad K Chopra Attenuation of diabetic nephropathy by tocotrienol in-volvement of NFκB signaling pathway Life Sci 84 (2009) 296ndash301
[170] Q Jiang X Yin MA Lill ML Danielson H Freiser J Huang Long-chain carbox-ychromanols metabolites of vitamin E are potent inhibitors of cyclooxygenasesProc Natl Acad Sci U S A 105 (2008) 20464ndash20469
[171] ER Miller III R Pastor-Barriuso D Dalal RA Riemersma LJ Appel E GuallarMeta-analysis high-dosage vitamin E supplementation may increase all-causemortality Ann Intern Med 142 (2005) 37ndash46
[172] JN Hathcock A Azzi J Blumberg T Bray A Dickinson B Frei I Jialal CSJohnston FJ Kelly K Kraemer L Packer S Parthasarathy H Sies MG TraberVitamins E and C are safe across a broad range of intakes Am J Clin Nutr 81(2005) 736ndash745
[173] R Brigelius-Flohe F Galli Vitamin E a vitamin still awaiting the detection of itsbiological function Mol Nutr Food Res 54 (2010) 583ndash587
711F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
[174] MG Traber B Frei JS Beckman Vitamin E revisited do new data validate ben-efits for chronic disease prevention Curr Opin Lipidol 19 (2008) 30ndash38
[175] F Galli Meeting report Vitamin E Satellite Symposium (VESS) associated to theAnnual Meeting of the SFRR-Europe Rome 26 August 2009 Free Radic Res 43(2009) 1256ndash1257
[176] LJ Roberts II JA Oates MF Linton S Fazio BP Meador MD Gross Y Shyr JDMorrow The relationship between dose of vitamin E and suppression of oxida-tive stress in humans Free Radic Biol Med 43 (2007) 1388ndash1393
[177] EFSA- EFSA Scientific Opinion of the Panel on Food Additives FlavouringsProcessing Aids and Materials in Contact with Food on a request from the Com-mission on mixed tocopherols tocotrienol tocopherol and tocotrienols assources for vitamin E in EFSA- EFSA (Ed) vol 640 The EFSA Journal2008 pp 1ndash34
[178] P Rust I Eichler S Renner I Elmadfa Long-term oral beta-carotene supple-mentation in patients with cystic fibrosis mdash effects on antioxidative status andpulmonary function Ann Nutr Metab 44 (2000) 30ndash37
[179] G Lepage J Champagne N Ronco A Lamarre I Osberg RJ Sokol CC Roy Sup-plementation with carotenoids corrects increased lipid peroxidation in childrenwith cystic fibrosis Am J Clin Nutr 64 (1996) 87ndash93
[180] BM Winklhofer-Roob H Puhl G Khoschsorur MA vant Hof H EsterbauerDH Shmerling Enhanced resistance to oxidation of low density lipoproteinsand decreased lipid peroxide formation during beta-carotene supplementationin cystic fibrosis Free Radic Biol Med 18 (1995) 849ndash859
[181] RC Graham-Maar JI Schall N Stettler BS Zemel VA Stallings Elevated vita-min A intake and serum retinol in preadolescent children with cystic fibrosisAm J Clin Nutr 84 (2006) 174ndash182
[182] I Sadowska-Woda M Rachel J Pazdan E Bieszczad-Bedrejczuk K PawliszakNutritional supplement attenuates selected oxidative stress markers in pediatricpatients with cystic fibrosis Nutr Res (New York NY) 31 (2011) 509ndash518
[183] KA Papas MK Sontag C Pardee RJ Sokol SD Sagel FJ Accurso JS WagenerA pilot study on the safety and efficacy of a novel antioxidant rich formulation inpatients with cystic fibrosis J Cyst Fibros 7 (2008) 60ndash67
[184] Y Saito A Fukuhara K Nishio M Hayakawa Y Ogawa H Sakamoto K Fujii YYoshida E Niki Characterization of cellular uptake and distribution of coen-zyme Q10 and vitamin E in PC12 cells J Nutr Biochem 20 (2009) 350ndash357
[185] AA Franke CM Morrison JL Bakke LJ Custer X Li RV Cooney CoenzymeQ10 in human blood native levels and determinants of oxidation during proces-sing and storage Free Radic Biol Med 48 (2010) 1610ndash1617
[186] HN Bhagavan RK Chopra Plasma coenzyme Q10 response to oral ingestion ofcoenzyme Q10 formulations Mitochondrion 7 (2007) S78ndashS88 (Suppl)
[187] HN Bhagavan RK Chopra Coenzyme Q10 absorption tissue uptake metabo-lism and pharmacokinetics Free Radic Res 40 (2006) 445ndash453
[188] F Galli R Lee C Dunster FJ Kelly Gas chromatography mass spectrometryanalysis of carboxyethyl-hydroxychroman metabolites of alpha- and gamma-tocopherol in human plasma Free Radic Biol Med 32 (2002) 333ndash340
[189] F Galli R Lee J Atkinson A Floridi FJ Kelly Gamma-tocopherol biokineticsand transformation in humans Free Radic Res 37 (2003) 1225ndash1233
[190] TA Laguna MK Sontag I Osberg JS Wagener FJ Accurso RJ Sokol De-creased total serum coenzyme-Q10 concentrations a longitudinal study in chil-dren with cystic fibrosis J Pediatr 153 (2008) 402ndash407
[191] T Frischer JK Myung G Maurer I Eichler Z Szepfalusi G Lubec Possible dys-regulation of chaperon and metabolic proteins in cystic fibrosis bronchial tissueProteomics 6 (2006) 3381ndash3388
[192] C Andersson MM Zaman AB Jones SD Freedman Alterations in immune re-sponse and PPARLXR regulation in cystic fibrosis macrophages J Cyst Fibros 7(2008) 68ndash78
[193] SD Freedman PG Blanco MM Zaman JC Shea M Ollero IK Hopper DAWeed A Gelrud MM Regan M Laposata JG Alvarez BP OSullivan Associa-tion of cystic fibrosis with abnormalities in fatty acid metabolism N Engl JMed 350 (2004) 560ndash569
[194] S Van Biervliet G Vanbillemont JP Van Biervliet D Declercq E Robberecht AChristophe Relation between fatty acid composition and clinical status or geno-type in cystic fibrosis patients Ann Nutr Metab 51 (2007) 541ndash549
[195] SD Freedman MH Katz EM Parker M Laposata MY Urman JG AlvarezA membrane lipid imbalance plays a role in the phenotypic expression ofcystic fibrosis in cftr(minusminus) mice Proc Natl Acad Sci U S A 96 (1999)13995ndash14000
[196] S Van Biervliet S Vande Velde JP Van Biervliet E Robberecht The effect ofzinc supplements in cystic fibrosis patients Ann Nutr Metab 52 (2008)152ndash156
[197] WR Henderson Jr SJ Astley MM McCready P Kushmerick S Casey JWBecker BW Ramsey Oral absorption of omega-3 fatty acids in patients withcystic fibrosis who have pancreatic insufficiency and in healthy control subjectsJ Pediatr 124 (1994) 400ndash408
[198] I Durieu E Vericel D Guichardant H Roth JP Steghens J Drai RN JosserandE Fontaine M Lagarde G Bellon Fatty acids platelets and oxidative markersfollowing intravenous n-3 fatty acids administration in cystic fibrosis an openpilot observational study J Cyst Fibros 6 (2007) 320ndash326
[199] LG Wood DA Fitzgerald ML Garg Hypothesis vitamin E complements poly-unsaturated fatty acids in essential fatty acid deficiency in cystic fibrosis J AmColl Nutr 22 (2003) 253ndash257
[200] JD Lloyd-Still SB Johnson RT Holman Essential fatty acid status in cystic fi-brosis and the effects of safflower oil supplementation Am J Clin Nutr 34(1981) 1ndash7
[201] A Maqbool JI Schall JF Garcia-Espana BS Zemel B Strandvik VAStallings Serum linoleic acid status as a clinical indicator of essential fatty
acid status in children with cystic fibrosis J Pediatr Gastroenterol Nutr 47(2008) 635ndash644
[202] C Oliver N Jahnke Omega-3 fatty acids for cystic fibrosis Cochrane DatabaseSyst Rev (2011) CD002201
[203] B Strandvik E Gronowitz F Enlund T Martinsson J Wahlstrom Essential fattyacid deficiency in relation to genotype in patients with cystic fibrosis J Pediatr139 (2001) 650ndash655
[204] P Rise S Volpi C Colombo RF Padoan C DOrazio S Ghezzi PMelotti V BennatoC Agostoni BM Assael C Galli Whole blood fatty acid analysis with micromethodin cystic fibrosis and pulmonary disease J Cyst Fibros 9 (2010) 228ndash233
[205] H Cao K Gerhold JR Mayers MM Wiest SM Watkins GS Hotamisligil Iden-tification of a lipokine a lipid hormone linking adipose tissue to systemic me-tabolism Cell 134 (2008) 933ndash944
[206] RR Malapaka SK Khoo J Zhang JH Choi XE Zhou Y Xu Y Gong J Li ELYong MJ Chalmers L Chang JH Resau PR Griffin YE Chen HE Xu Iden-tification and mechanism of a ten carbon fatty acid as a modulating ligand ofperoxisome proliferator activated receptors J Biol Chem 287 (2012)183ndash195
[207] T Hara A Hirasawa A Ichimura I Kimura G Tsujimoto Free fatty acid recep-tors FFAR1 and GPR120 as novel therapeutic targets for metabolic disorders JPharm Sci 100 (2011) 3594ndash3601
[208] R Gupta P Rathi S Bradoo Lipase mediated upgradation of dietary fats andoils Crit Rev Food Sci Nutr 43 (2003) 635ndash644
[209] BH Jennings CC Akoh Lipase-catalyzed modification of rice bran oil to incor-porate capric acid J Agric Food Chem 48 (2000) 4439ndash4443
[210] J Hoeks M Mensink MK Hesselink K Ekroos P Schrauwen Long- andMedium-Chain Fatty Acids Induce Insulin Resistance to a Similar Extent inHumans Despite Marked Differences in Muscle Fat Accumulation J Clin Endo-crinol Metab 97 (2012) 208ndash216
[211] PJ Congden G Bruce MM Rothburn PC Clarke JM Littlewood J KelleherMS Losowsky Vitamin status in treated patients with cystic fibrosis ArchDis Child 56 (1981) 708ndash714
[212] BM Winklhofer-Roob H Ellemunter M Fruhwirth SE Schlegel-Haueter GKhoschsorur MA vant Hof DH Shmerling Plasma vitamin C concentrationsin patients with cystic fibrosis evidence of associations with lung inflammationAm J Clin Nutr 65 (1997) 1858ndash1866
[213] L Shamseer D Adams N Brown JA Johnson S Vohra Antioxidant micronutri-ents for lung disease in cystic fibrosis Cochrane Database Syst Rev (2010)CD007020
[214] C Santi S Santoro Electrophilic Selenium First edition Wiley-VCH VerlagGmbH amp Co KGaA 2012
[215] L Flohe S Toppo G Cozza F Ursini A comparison of thiol peroxidase mecha-nisms Antioxid Redox Signal 15 (2010) 763ndash780
[216] L Flohe JR Andreesen R Brigelius-Flohe M Maiorino F Ursini Selenium theelement of the moon in life on earth IUBMB Life 49 (2000) 411ndash420
[217] V Valdiglesias E Pasaro J Mendez B Laffon In vitro evaluation of seleniumgenotoxic cytotoxic and protective effects a review Arch Toxicol 84(2010) 337ndash351
[218] P Foucaud P Therond M Marchand F Brion JF Demelier J Navarro Seleniumand vitamin E in mucoviscidosis Arch Fr Pediatr 45 (1988) 383ndash386
[219] J Neve R Van Geffel M Hanocq L Molle Plasma and erythrocyte zinc copperand selenium in cystic fibrosis Acta Paediatr Scand 72 (1983) 437ndash440
[220] BM Winklhofer-Roob B Tiran PE Tuchschmid MA vant Hof DH ShmerlingEffects of pancreatic enzyme preparations on erythrocyte glutathione peroxi-dase activities and plasma selenium concentrations in cystic fibrosis FreeRadic Biol Med 25 (1998) 242ndash249
[221] JD Lloyd-Still HE Ganther Selenium and glutathione peroxidase levels in cys-tic fibrosis Pediatrics 65 (1980) 1010ndash1012
[222] D Tsavachidou TJ McDonnell S Wen X Wang F Vakar-Lopez LL Pisters CAPettaway CG Wood KA Do PF Thall C Stephens E Efstathiou R Taylor DGMenter P Troncoso SM Lippman CJ Logothetis J Kim Selenium and vitaminE cell type- and intervention-specific tissue effects in prostate cancer J NatlCancer Inst 101 (2009) 306ndash320
[223] IN Zelko TJ Mariani RJ Folz Superoxide dismutase multigene family acomparison of the CuZn-SOD (SOD1) Mn-SOD (SOD2) and EC-SOD (SOD3)gene structures evolution and expression Free Radic Biol Med 33 (2002)337ndash349
[224] RP Bowler JD Crapo Oxidative stress in airways is there a role for extracellu-lar superoxide dismutase Am J Respir Crit Care Med 166 (2002) S38ndashS43
[225] K Best K McCoy S Gemma RA Disilvestro Copper enzyme activities in cysticfibrosis before and after copper supplementation plus or minus zinc Metabo-lism 53 (2004) 37ndash41
[226] SS Percival GP Kauwell E Bowser M Wagner Altered copper status in adultmen with cystic fibrosis J Am Coll Nutr 18 (1999) 614ndash619
[227] NF Krebs JE Westcott TD Arnold BM Kluger FJ Accurso LV Miller KMHambidge Abnormalities in zinc homeostasis in young infants with cystic fibro-sis Pediatr Res 48 (2000) 256ndash261
[228] D Easley N Krebs M Jefferson L Miller J Erskine F Accurso KM HambidgeEffect of pancreatic enzymes on zinc absorption in cystic fibrosis J Pediatr Gas-troenterol Nutr 26 (1998) 136ndash139
[229] S Van Biervliet JP Van Biervliet E Robberecht Serum zinc in patients with cys-tic fibrosis at diagnosis and after one year of therapy Biol Trace Elem Res 112(2006) 205ndash211
[230] S Van Biervliet JP Van Biervliet S Vande Velde E Robberecht Serum zinc con-centrations in cystic fibrosis patients aged above 4 years a cross-sectional eval-uation Biol Trace Elem Res 119 (2007) 19ndash26
712 F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
[231] F Galli M Cristina Polidori W Stahl P Mecocci FJ Kelly Vitamin E biotransfor-mation in humans Vitam Horm 76 (2007) 263ndash280
[232] J Wiser NE Alexis Q Jiang W Wu C Robinette R Roubey DB Peden In vivogamma-tocopherol supplementation decreases systemic oxidative stress andcytokine responses of human monocytes in normal and asthmatic subjectsFree Radic Biol Med 45 (2008) 40ndash49
[233] JG Wagner Q Jiang JR Harkema B Illek DD Patel BN Ames DB PedenOzone enhancement of lower airway allergic inflammation is prevented bygamma-tocopherol Free Radic Biol Med 43 (2007) 1176ndash1188
[234] JT Harries DP Muller Absorption of different doses of fat soluble and watermiscible preparations of vitamin E in children with cystic fibrosis Arch DisChild 46 (1971) 341ndash344
[235] EI Back C Frindt E Ocenaskova D Nohr M Stern HK Biesalski Can changesin hydrophobicity increase the bioavailability of alpha-tocopherol Eur J Nutr45 (2006) 1ndash6
[236] SZ Nasr MH OLeary C Hillermeier Correction of vitamin E deficiency withfat-soluble versus water-miscible preparations of vitamin E in patients with cys-tic fibrosis J Pediatr 122 (1993) 810ndash812
[237] S Soltani-Frisk E Gronowitz H Andersson B Strandvik Water-miscibletocopherol is not superior to fat-soluble preparation for vitamin E absorptionin cystic fibrosis Acta Paediatr 90 (2001) 1112ndash1115
[238] K Papas J Kalbfleisch R Mohon Bioavailability of a novel water-soluble vi-tamin E formulation in malabsorbing patients Dig Dis Sci 52 (2007)347ndash352
[239] F Antonicelli M Parmentier EM Drost N Hirani I Rahman K Donaldson WMacNee Nacystelyn inhibits oxidant-mediated interleukin-8 expression andNF-kappaB nuclear binding in alveolar epithelial cells Free Radic Biol Med 32(2002) 492ndash502
[240] EM App D Baran I Dab A Malfroot M Coffiner F Vanderbist M King Dose-finding and 24-h monitoring for efficacy and safety of aerosolized Nacystelyn incystic fibrosis Eur Respir J 19 (2002) 294ndash302
[241] MG Traber How much vitamin E hellip Just enough Am J Clin Nutr 84 (2006)959ndash960
[242] JC McCann BN Ames Vitamin K an example of triage theory is micronu-trient inadequacy linked to diseases of aging Am J Clin Nutr 90 (2009)889ndash907
[243] M Fusaro G Crepaldi S Maggi F Galli A DAngelo L Calo S Giannini DMiozzo M Gallieni Vitamin K bone fractures and vascular calcifications inchronic kidney disease an important but poorly studied relationship J Endocri-nol Invest 34 (2010) 317ndash323
[244] JC McCann BN Ames Adaptive dysfunction of selenoproteins from the per-spective of the triage theory why modest selenium deficiency may increaserisk of diseases of aging FASEB J 25 (2011) 1793ndash1814
[245] R Apak K Guclu M Ozyurek B Bektas Oglu M Bener Cupric ion reducing an-tioxidant capacity assay for food antioxidants vitamins polyphenolics and fla-vonoids in food extracts Methods Mol Biol 477 (2008) 163ndash193
[246] F Galli Interactions of polyphenolic compounds with drug disposition and me-tabolism Curr Drug Metab 8 (2007) 830ndash838
[247] RL Prior X Wu K Schaich Standardized methods for the determination of an-tioxidant capacity and phenolics in foods and dietary supplements J Agric FoodChem 53 (2005) 4290ndash4302
[248] C Azbell S Zhang D Skinner J Fortenberry EJ Sorscher BA WoodworthHesperidin stimulates cystic fibrosis transmembrane conductance regulator-mediated chloride secretion and ciliary beat frequency in sinonasal epitheliumOtolaryngol Head Neck Surg 143 (2010) 397ndash404
[249] G Wegrzyn J Jakobkiewicz-Banecka M Gabig-Ciminska E Piotrowska M Nar-ajczyk A Kloska M Malinowska D Dziedzic I Golebiewska M Moskot AWegrzyn Genistein a natural isoflavone with a potential for treatment of ge-netic diseases Biochem Soc Trans 38 (2010) 695ndash701
[250] YC Yu H Miki Y Nakamura A Hanyuda Y Matsuzaki Y Abe M Yasui K Ta-naka TC Hwang SG Bompadre Y Sohma Curcumin and genistein additivelypotentiate G551D-CFTR J Cyst Fibros 10 (2011) 243ndash252
[251] B Illek H Fischer Flavonoids stimulate Cl conductance of human airway epithe-lium in vitro and in vivo Am J Physiol 275 (1998) L902ndashL910
[252] JL Kreindler Cystic fibrosis exploiting its genetic basis in the hunt for newtherapies Pharmacol Ther 125 (2010) 219ndash229
[253] B Illek L Zhang NC Lewis RB Moss JY Dong H Fischer Defective function ofthe cystic fibrosis-causing missense mutation G551D is recovered by genisteinAm J Physiol 277 (1999) C833ndashC839
[254] P Anandakumar S Kamaraj S Jagan G Ramakrishnan R Vinodhkumar TDevaki Capsaicin modulates pulmonary antioxidant defense system during ben-zo(a)pyrene-induced lung cancer in Swiss albinomice Phytother Res 22 (2008)529ndash533
[255] I Rahman Antioxidant therapeutic advances in COPD Ther Adv Respir Dis 2(2008) 351ndash374
[256] AW Boots H Li RP Schins R Duffin JW Heemskerk A Bast GR Haenen Thequercetin paradox Toxicol Appl Pharmacol 222 (2007) 89ndash96
[257] M Joskova S Franova V Sadlonova Acute bronchodilator effect of quercetin inexperimental allergic asthma Bratisl Lek Listy 112 (2011) 9ndash12
[258] HJ Park CM Lee ID Jung JS Lee YI Jeong JH Chang SH Chun MJ Kim IWChoi SC Ahn YK Shin SR Yeom YM Park Quercetin regulates Th1Th2 balancein a murine model of asthma Int Immunopharmacol 9 (2009) 261ndash267
[259] AP Rogerio A Kanashiro C Fontanari EV da Silva YM Lucisano-ValimEG Soares LH Faccioli Anti-inflammatory activity of quercetin and iso-quercitrin in experimental murine allergic asthma Inflamm Res 56 (2007)402ndash408
[260] M Muller Polyphenol cytotoxicity induced by the bacterial toxin pyocyaninrole of NQO1 Free Radic Biol Med 47 (2009) 84ndash91
[261] J Grassmann Terpenoids as plant antioxidants Vitam Horm 72 (2005)505ndash535
[262] P Allen Tea tree oil the science behind the antimicrobial hype Lancet 358(2001) 1245
[263] EC Dasenbrook W Checkley CA Merlo MW Konstan N Lechtzin MP BoyleAssociation between respiratory tract methicillin-resistant Staphylococcus aure-us and survival in cystic fibrosis JAMA 303 (2010) 2386ndash2392
[264] V Bezzerri M Borgatti E Nicolis I Lampronti MC Dechecchi I Mancini PRizzotti R Gambari G Cabrini Transcription factor oligodeoxynucleotides toNF-kappaB inhibit transcription of IL-8 in bronchial cells Am J Respir CellMol Biol 39 (2008) 86ndash96
[265] R Gambari M Borgatti V Bezzerri E Nicolis I Lampronti MC Dechecchi IMancini A Tamanini G Cabrini Decoy oligodeoxyribonucleotides and peptidenucleic acids-DNA chimeras targeting nuclear factor kappa-B inhibition of IL-8 gene expression in cystic fibrosis cells infected with Pseudomonas aeruginosaBiochem Pharmacol 80 (2010) 1887ndash1894
[266] M Adrian P Jeandet AC Douillet-Breuil L Tesson R Bessis Stilbene content ofmature Vitis vinifera berries in response to UV-C elicitation J Agric Food Chem48 (2000) 6103ndash6105
[267] B Paul I Masih J Deopujari C Charpentier Occurrence of resveratrol and pter-ostilbene in age-old darakchasava an ayurvedic medicine from India J Ethno-pharmacol 68 (1999) 71ndash76
[268] I Rahman Antioxidant therapies in COPD Int J Chron Obstruct Pulmon Dis 1(2006) 15ndash29
[269] M Lee S Kim OK Kwon SR Oh HK Lee K Ahn Anti-inflammatory and anti-asthmatic effects of resveratrol a polyphenolic stilbene in a mouse model ofallergic asthma Int Immunopharmacol 9 (2009) 418ndash424
[270] LG Wood PA Wark ML Garg Antioxidant and anti-inflammatory effectsof resveratrol in airway disease Antioxid Redox Signal 13 (2010)1535ndash1548
[271] KV Kiselev Perspectives for production and application of resveratrol ApplMicrobiol Biotechnol 90 (2011) 417ndash425
[272] M Shakibaei C Buhrmann A Mobasheri Resveratrol-mediated SIRT-1 interac-tions with p300 modulate receptor activator of NF-kappaB ligand (RANKL) acti-vation of NF-kappaB signaling and inhibit osteoclastogenesis in bone-derivedcells J Biol Chem 286 (2011) 11492ndash11505
[273] SF Zaidi K Ahmed T Yamamoto T Kondo K Usmanghani M Kadowaki TSugiyama Effect of resveratrol on Helicobacter pylori-induced interleukin-8 secre-tion reactive oxygen species generation and morphological changes in human gas-tric epithelial cells Biol Pharm Bull 32 (2009) 1931ndash1935
[274] JK Kundu YK Shin YJ Surh Resveratrol modulates phorbol ester-inducedpro-inflammatory signal transduction pathways in mouse skin in vivo NF-kappaB and AP-1 as prime targets Biochem Pharmacol 72 (2006)1506ndash1515
[275] NH Nam Naturally occurring NF-kappaB inhibitors Mini Rev Med Chem 6(2006) 945ndash951
[276] JM Smoliga JA Baur HA Hausenblas Resveratrol and healthmdasha comprehen-sive review of human clinical trials Mol Nutr Food Res 55 (2011) 1129ndash1141
[277] ME Juan M Maijo JM Planas Quantification of trans-resveratrol and itsmetabolites in rat plasma and tissues by HPLC J Pharm Biomed Anal 51(2010) 391ndash398
[278] JA Baur DA Sinclair Therapeutic potential of resveratrol the in vivo evidenceNat Rev 5 (2006) 493ndash506
[279] E Nicolis I Lampronti MC Dechecchi M Borgatti A Tamanini N Bianchi VBezzerri I Mancini MG Giri P Rizzotti R Gambari G Cabrini Pyrogallol anactive compound from the medicinal plant Emblica officinalis regulates expres-sion of pro-inflammatory genes in bronchial epithelial cells Int Immunophar-macol 8 (2008) 1672ndash1680
[280] E Nicolis I Lampronti MC Dechecchi M Borgatti A Tamanini V Bezzerri NBianchi M Mazzon I Mancini MG Giri P Rizzotti R Gambari G CabriniModulation of expression of IL-8 gene in bronchial epithelial cells by 5-methoxypsoralen Int Immunopharmacol 9 (2009) 1411ndash1422
[281] M Borgatti I Mancini N Bianchi A Guerrini I Lampronti D Rossi G SacchettiR Gambari Bergamot (Citrus bergamia Risso) fruit extracts and identified com-ponents alter expression of interleukin 8 gene in cystic fibrosis bronchial epithe-lial cell lines BMC Biochem 12 (2011) 15
[282] L Piccagli E Fabbri M Borgatti N Bianchi V Bezzerri I Mancini E Nicolis CMDechecchi I Lampronti G Cabrini R Gambari Virtual screening against p50NF-kappaB transcription factor for the identification of inhibitors of the NF-kappaB-DNA interaction and expression of NF-kappaB upregulated genesChemMedChem 4 (2009) 2024ndash2033
[283] L Piccagli M Borgatti E Nicolis N Bianchi I Mancini I Lampronti D VevaldiF DallAcqua G Cabrini R Gambari Virtual screening against nuclear factorkappaB (NF-kappaB) of a focus library identification of bioactive furocoumarinderivatives inhibiting NF-kappaB dependent biological functions involved incystic fibrosis Bioorg Med Chem 18 (2010) 8341ndash8349
[284] M Borgatti A Chilin L Piccagli I Lampronti N Bianchi I Mancini G Mar-zaro Da Francesco A Guiotto R Gambari Development of a novel furocou-marin derivative inhibiting NF-kappaB dependent biological functionsdesign synthesis and biological effects Eur J Med Chem 46 (2011)4870ndash4877
[285] E Georgy S Le Guellec L Vecellio E Fichant P Stordeur P Bordeau JP PerraudinFeasibility study of OSCN- and lactoferrin (Meveol) nebulization for cysticfibrosis JCyst Fibros 10 (2011) S18
713F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
[286] C Tidei M Piroddi F Galli C Santi Oxidation of thiols promoted by PhSeZnClTetrahedron Lett 53 (2012) 232ndash234
[287] L Semianrio-Vidal C van Hesuden G Mugesh ER Lazarowski Ebselen is a po-tent non-competitive inhibitor of extracellular nucleoside diphosphokinasePurinergic Signal 6 (2010) 383ndash391
[288] C ColussiMC Albertini S Coppola S Rovidati F Galli L Ghibelli H2O2-inducedblockof glycolysis as an active ADP-ribosylation reaction protecting cells from apoptosisFASEB J 14 (2000) 2266ndash2276
[289] H Xiao KL Parkin Induction of phase II enzyme activity by various seleniumcompounds Nutr Cancer 55 (2006) 210ndash223
[290] G Peluffo R Radi Biochemistry of protein tyrosine nitration in cardiovascularpathology Cardiovasc Res 75 (2007) 291ndash302
[291] B Alvarez R Radi Peroxynitrite reactivity with amino acids and proteinsAmino Acids 25 (2003) 295ndash311
[292] B Kamosinska MW Radomski M Duszyk A Radomski SF Man Nitric oxideactivates chloride currents in human lung epithelial cells Am J Physiol 272(1997) L1098ndashL1104
[293] L Chen RP Patel X Teng CA Bosworth JR Lancaster Jr S Matalon Mecha-nisms of cystic fibrosis transmembrane conductance regulator activation by S-nitrosoglutathione J Biol Chem 281 (2006) 9190ndash9199
[294] F Luchetti B CanonicoM BettiM Arcangeletti F PilolliM Piroddi L Canesi S PapaF Galli Melatonin signaling and cell protection function FASEB J 24 (2010)3603ndash3624
[295] MW Bengtsson G Jedstedt G Flemstrom Duodenal bicarbonate secretion inrats stimulation by intra-arterial and luminal guanylin and uroguanylin ActaPhysiol (Oxf) 191 (2007) 309ndash317
[296] CS Nelson JL Marino CN Allen Melatonin receptor potentiation of cyclic AMP andthe cystic fibrosis transmembrane conductance regulator ion channel J Pineal Res 26(1999) 113ndash121
[297] C de Castro-Silva VM de Bruin GM Cunha DM Nunes CAMedeiros PF de BruinMelatonin improves sleep and reduces nitrite in the exhaled breath condensate incystic fibrosismdasha randomized double-blind placebo-controlled study J Pineal Res48 (2010) 65ndash71
[298] I Hornyak E Pankotai L Kiss Z Lacza Current developments in the the-rapeutic potential of S-nitrosoglutathione an endogenous NO-donor mole-cule Curr Pharm Biotechnol (2011) Jan 11 [Epub ahead of print] - PMID21235457
[299] AH Snyder ME McPherson JF Hunt M Johnson JS Stamler B Gaston Acuteeffects of aerosolized S-nitrosoglutathione in cystic fibrosis Am J Respir CritCare Med 165 (2002) 922ndash926

702 F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
recent Cochrane meta-analysis on n-3 supplementation in CF patients[202] highlighted the lack of evidence for a significant correction ofthe assessed clinical end points (mainly respiratory symptoms)even when inflammatory indices and other laboratory end pointswere met Taken together these data suggest that there is insufficientevidence to draw firm conclusions or recommend routine use of n-3supplements in CF Notwithstanding it is common belief that n-3supplements provide some benefits for people with CF with relativelyfew adverse effects and thus their use is not discouraged
Further alterations in fatty acid metabolism have been highlight-ed including the consistent findings of an increase in circulatinglevels of saturated and monounsaturated fatty acids [7203204]Decreased levels of essential FA (EFA) ie the FA that have to be in-troduced with the diet correlates with the severity of respiratoryinsufficiency and the same clinical correlation was observed with al-tered proportions of FA species converted by the activity of desatur-ase enzymes (reviewed in [204]) The close relationship betweencertain fatty acids and oxidative stress including the negative correla-tion of C240 and linoleic acid with oxysterol levels point to the needof intensive investigation in CF patients of previously neglected lipidspecies that are emerging candidates in the control of metabolismQuantitative lipidomic analyses have lead to identify C161n7 palmi-toleate as a ldquoprotectiverdquo adipose-derived lipid hormone that stronglystimulates insulin activity in muscle and liver also suppressing in-flammatory cytokine output from mice fat cells [205] Specific meta-bolic activities have been also demonstrated by medium chainsaturated fatty acids caprylic acid (C80) capric acid (C100) and lau-ric acid (C120) Capric acid acts as a direct ligand of PPARγ using abinding pocket different from the binding pocket of thiazolidinedioneor long chain fatty acids [206] Additional activities of medium chainfatty acids which are ligands of free fatty acids receptors detectedin the immune cells the gastrointestinal tract and adipocytes maycontribute to metabolic homeostasis and inflammatory responses[207] These data underscore the importance of a lipid-mediated ldquoen-docrine networkrdquo demonstrating how specific alteration of one orfew serum lipids would be per se sufficient to influence metabolic ho-meostasis Given the relevance of this emerging information and thealteration of lipid metabolism and inflammatory status in CF fattyacid lipidomics need to be deeply investigated in CF
Again these studies have obvious nutritional implications Satu-rated fatty acids with chain lengths higher than C18 are poorlyabsorbed partly because they form insoluble calcium salts [208]Medium chain saturated fatty acids are well known for being highlyabsorbed through the intestine providing rapid delivery of energyvia oxidation of the more hydrophilic short chains and have beensuggested to provide proper nourishment in patients with CF [209]Recent studies have shown that consumption of a high-fat diet richin medium chain fatty acids as opposed to long chain fatty acidsdoes not lead to ectopic fat accumulation in skeletal muscle andliver of both rats and mice [210] In light of the close association be-tween nutritional status inflammation and life expectancy in CF pa-tients the manipulation of dietary lipids in these patients must befurther explored as a possible strategy to provide adequate nutritionand better management of oxidative stress
36 Hydrosoluble antioxidants oligoelements and enzymatic antioxidants
361 Vitamin CVitamin C status in CF patients has been poorly investigated Early
studies suggested a defective vitamin C status that was refractory tooral supplementation [211] Other and more recent studies showednormal or slightly decreased levels of vitamin C in CF patients as com-pared to healthy controls but age- and disease-related decline of thiswater-soluble antioxidant was reported in these patients [5212]In the study of Winklhofer-Roob et al [212] on mid-European CFpatients vitamin C concentrations decreased with age with an
estimated rate of 5 μmollyr and vitamin C concentrationsb40 μ-moll were associated with highest indexes of inflammation whichis consistent with the hypothesis that optimal levels of vitamin Cmay influence immuno-inflammatory activity of alveolar macro-phages and neutrophils Other few studies have examined the effectof supplements containing vitamin C on CF inflammation and oxida-tive stress since the levels of this vitamin do not significantly improvewith supplementation (reviewed in [213]) This highlights the com-mon fate that this hydrosoluble vitamin shares with several fat-soluble counterparts in the ldquomicronutrient paradoxrdquo of CF patients inwhich the need for a correction of their status along the progressionof the disease is frustrated by the poor efficacy of oral supplementa-tion protocols Formulations and appropriate supplementation proto-cols that may produce a better correction of vitamin C status of CFpatients are awaited for further clinical evaluation
362 Selenium and selenium-dependent peroxidasesSelenium is a trace element with marked electrophilicity [214]
that once converted to the organic form of Se-Cys can be introducedin protein structures to play its important role in H2O2 metabolismand signaling [215] As catalytic center of the enzyme GSH-peroxidase (SeGSH-Px) Se plays a crucial role to protect polyunsatu-rated lipids of plasma membrane and circulating lipoproteins formperoxidative insults With other Se-proteins such as the high molecu-lar weight thioredoxin reductases this oligoelement participates tothe control of protein thiol-disulfide oxidoreduction and glutathiony-lation which regulate signaling pathways of crucial importance in theregulation of immunity and inflammation [16] but also the function-ing of other redox-sensitive proteins such as the same CFTR [124]
The activity of SeGSH-Px in blood is considered a functional as-sessment of selenium status even if this assumption has some limita-tions related with the saturation profile that the Se stores show atincreasing doses of Se administration Investigations of the seleniumstatus in CF patients have produced conflicting findings which maydepend on differences in dietary intake ethnicity and environmentalfactors in the diverse patient populations (reviewed in [216217]) CFchildren have been reported to have lowered blood selenium and RBCSeGSH-Px activity [218219] normal plasma selenium and loweredRBC SeGSH-Px [220] and even normal levels of both these two param-eters [221] The supplementation with selenium in combination withother antioxidants was observed to increase the concentrations ofblood selenium that likewise β-carotene and fatty acid were posi-tively correlated with improved lung function [6]
Foucaud et al [218] observed that a defective selenium statuswas associated with lowered levels of other antioxidants that contrib-ute to the anti-peroxidative activity of this microelement such asvitamin E (reviewed in [222]) and the severity of this deficiencywas lower in children with pancreatic enzyme replacement and vita-min E supplementation
Treatments to substitute for exocrine pancreatic insufficiency bypancreatic enzymes from animal sources such as porcine pancreashave been confirmed to be a source of Se [220] These affects RBCSeGSH-Px activity and plasma selenium concentrations which hasto be taken into account when selenium supplements are given toCF patients
Selenium has been used to develop a series of organoseleniumcompounds that may open the way to new therapeutic opportunitiesin CF (see Section 392) These include GPX mimetic drugs and phaseII enzyme inducers which may provide higher antioxidant activity ofASL and cellular protection effects in the airways
363 Zinc and copperZinc and copper (Zn and Cu respectively) are present in many
proteins so that a deficiency of these trace metals could have pleiotro-pic effects in humans As regards antioxidant systems these two oli-goelements contribute an important role being cofactors of two
703F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
isoforms of the superoxide dismutase enzymes eg the extracellularform eg the EC-SOD or Sod 3 and the CundashZn-SOD or Sod 1 that isfound in several tissues and cells [223] The EC-SOD exerts its antiox-idant role also in the lining fluids of the airways [224]
The notion that CF patients have defective concentrations of bloodZn and Cu is controversial As far as Cu status is concerned few datahave been produced and are available in the literature suggestingthe notion that CF patients develop a moderate copper deficiency[225226] That was essentially demonstrated on the bases of a defec-tive activity of Cu-related proteins such as plasma ceruloplasmindiamine oxidase and RBC SOD This defect seems to be refractory toCu and Zn supplementation (see below)
More advanced studies have been carried out in the case of Zn sta-tus in CF Low plasma zinc concentrations were reported in approxi-mately 30 of young infants with CF identified by newbornscreening [227] and an impaired zinc homeostasis in CF patientswas described by Easley et al [228] This is characterized by poor con-servation of the endogenous pool with fecal loss and impaired frac-tional absorption of zinc which are the consequences of pancreaticinsufficiency and persisting steatorrhea These studies suggestedthat in the clinical management of CF patients these defects can beat least in part corrected by exocrine pancreatic enzyme replacement
A series of studies by Van Biervliet et al [229230] demonstratedin a Dutch population of CF infants and children that serum Zn variesin an age-dependent manner but remained unchanged with respectto healthy control levels In CF patients no difference in serum Zn con-centration between pancreatic-sufficient or pancreatic-insufficientpatients was observed and no correlation was found with the nutri-tional status or height z-score Importantly in these studies a signifi-cant correlation of serum Zn was observed with the fat solublevitamins A and E thus confirming the relationship between the ab-normalities of lipid and Zn metabolism in CF This suggests that co-supplementation of Zn and fat-soluble vitamins should be advisedin the presence of pancreatic insufficiency and persisting steatorrhea
Neve et al [219] in a study aimed to assess plasma and erythrocytezinc copper and selenium in CF children showed that mean plasmazinc and copper levels were not different from those in age-matched controls which confirms the observations by Van Biervlietet al described above However plasma zinc concentrations de-creased in patients with moderate-to-severe growth retardation andwith severe pulmonary disease but very low zinc levels occur sporad-ically Erythrocyte zinc and copper levels were significantly higherthan normal while RBC selenium was lower than in age-matchedcontrols These trace element concentrations in erythrocytes werediscussed in relation to the activities of the CuZn-SOD and the Se-enzyme GPx This observation suggests a compensatory upregulationof the erythrocyte CuZn-SOD by the exposure of erythroid precursorsto ROS andor other CF-related stressors
Best et al [225] also studied RBC SOD activity using this as a bio-logical sensor of Cu status in CF patients A lowered activity of thisenzyme was reported in CF together with that of the other Cu-dependent enzyme plasma diamine oxidase while plasma ceruplas-min showed normal activity Degradation rates of copper proteinsare known to be accelerated in conditions of copper deficiencywhich could explain the finding at least in part Anyway when Cuand Zn were supplemented to CF patients either separate or incombination (6 weeks of 3 mg copperd as copper-glycinate and30 mg zincd as zinc-glycinate) any of the copper enzyme activitieswas affected Therefore the moderate copper deficiency of CF patientsappears to be refractory to the intervention by increased copper andor zinc intake
Erythrocyte CuZn-SOD and the plasma levels of Cu and Zn werealso measured in the study of Wood et al [6] in which Australian CFpatients (agegt5 years) were treated with a high-dose antioxidantmultivitamin formulation containing 200 mg vitamin E (as RRR-α-tocopherol) 300 mg vitamin C (as sodium ascorbate) 25 mg β-
carotene (all-trans isomer) 90 μg Se (as selenomethionine) and500 μg vitamin A (as retinyl palmitate) in oil Plasma oligoelementsand particularly Zn were in the normal range at baseline (as com-pared with the data reported in [229230]) and were not affected bythis multivitamin supplement The same was found for the activityof RBC SOD and for plasma 8-iso-PGF2α as surrogate biomarker oflipid peroxidation
In a recent non-randomized small population (n=21) casendashcon-trol study in CF children Zn supplementation was proven to producepositive clinical effects in Zn-deficient patients [196] The supplemen-tation with 5 mgkg Zn sulfateday (maximum 150 mg) significantlydecreased the number of infections and increased the forced expira-tory volume in 1 s energy intake and growth parameters also im-proved These parameters were unaffected in untreated patientsexcept that in the case of the pulmonary function that decreased sig-nificantly These clinical observations on Zn supplementation need tobe confirmed in prospective double-blind randomized control trial
37 Appropriateness and targeting of antioxidant therapies in CF
The choice of the appropriate antioxidant and dose to correct a cer-tain biomarker and its associated biochemical lesion is another impor-tant point that appears to have disregarded in many clinical studiesFor instance unlike vitamin E vitamin C supplementation does notalter F2-IsoPs levels in humans (reviewed in [74]) This appears tobe true also in the antioxidant therapy of CF in which vitamin C(300 mgday) was administered together with other antioxidantsthat included a dose of vitamin E of 200 mgday without any signifi-cant effect on the surrogate biomarker of lipid peroxidation F2-IsoPs[6] When carotenoids are used as supplements to prevent the damag-ing action of ROS in the CF airways it is noteworthy that these are notparticularly good quenchers of peroxyl radicals relative to phenolicsand other antioxidants but are exceptional in quenching singlet oxy-gen at which most other phenolics and antioxidants are relativelyineffective Singlet oxygen is not a radical and does not react via radi-cal mechanisms but reacts mostly by the addition to double bondsforming endoperoxides that can be reduced to alkoxyl radicals that ini-tiate radical chain reactions typical of the peroxidative damage of PUFA[38] In this case the analysis of F2-IsoPs lipid peroxide formation andtransition metal-induced oxidizability of lipoproteins [162180] are allappropriate to evaluate the effect of carotenoids in preventing lipidperoxidation
As far as the dose is concerned clinical pharmacology of vitamin Eas an antioxidant was recently investigated by means of the effect onF2-IsoPs production and doses of α-tocopherol of 1600 IUday orgreater were found to be required to statistically affect plasma F2-IsoPs levels in hypercholeterolemic subjects [176] Several vitamin Esupplementation studies in CF patients have been performed withdoses of lower than 300 IUday regardless of the lowered absorptionby pancreatic and liver defects and the regular supplementationwith these doses does not appear to correct lipid oxidation markersin CF [7]
In the clinical practice and planning trials it has to be taken intoconsideration that in spite of substantial evidence supporting ahigher antioxidant demand in CF interventions with several antioxi-dant formulations produce poor responsiveness particularly in thecase of fat-soluble antioxidants which are poorly absorbed [6162]
Since many oxidants and antioxidants are present in tissuesand biological fluids and these have different chemical and physicalcharacteristics the possibility to produce a successful therapy witha single antioxidant molecule is too far to be realistic Moreover an-tioxidants act by multiple mechanisms in a single system or by adifferent single mechanism depending on the reaction systemresponding in a different manner to different radical or oxidantsources Because multiple reaction characteristics and mechanismsas well as different phase localizations are usually involved no single
704 F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
therapeutic approach will effectively prevent damage by multipleROS sources The defect of physiological antioxidants may also interferewith antioxidant therapies that are based on one or few exogenousantioxidants
Moreover several antioxidant vitamins such as vitamin E and ca-rotenoids have multiple natural forms with different bioavailabilitymetabolism and bioactivity [157167231] As far as the case of vita-min E supplementation concerns α-tocopherol was used as uniquevitamer in the large majority of supplementation trials so far per-formed and is the form used in the nutritional management of CFpatients Moreover several supplements contain the synthetic (or ra-cemic) form of this vitamin that has lower bioavailability than thenatural form Other forms present in nature and abundantly con-tained in vegetables such as tocotrienols and the less methylatedforms of tocopherol are not represented in many of the supplementformulations so far available in clinical centers and the supplementa-tion with α-tocopherol also limits their bioavailability These formsshow markedly higher susceptibility to hepatic metabolism and bili-ary excretion with respect to α-tocopherol eg the most representedform in blood and solid tissues and if co-supplemented these areeasily displaced during liver uptake and excreted with bile bymeans of competition with the same α-tocopherol Notwithstandingthese minor forms have been proposed to play important physiolog-ical roles showing molecular characteristics transcriptional effectsand antioxidant activities that clearly differentiate them in subfam-ilies with distinct biological functions Some of these such as α-tocopherol eg the second vitamin E form as relative abundance inblood and its carboxyethyl-hydroxychroman metabolite [189] ap-pear to have health-related anti-inflammatory effects which are par-ticularly relevant in lung protection [232233] This has suggestedthat such a group of ldquonon-α-tocopherolrdquo forms may represent anoth-er family of vitamins within the family of vitamin E with an impor-tant but often missed contribution to the proposed health effects ofthis vitamin [163]
These aspects may thus limit the possibility to provide CF patientsof optimal levels of this vitamin in all its components even if they areregularly treated with a vitamin E supplement eg withα-tocopherol
Targeted antioxidant therapy with formulations with higher bio-availability and bioactivity has been anticipated in CF New antioxi-dant formulations have been proposed to overcome main limits ofantioxidant therapies so far proposed for these patients Water-miscible α-tocopheryl acetate containing polysorbate propylene gly-col or polyethylene glycol as emulsifiers form micellar structureswere suggested to providing greater bioavailability than the fat-soluble counterparts These were commercialized with the brandnames of E-viminreg Cremophorreg EL and Aquasolreg E but despitethe original positive expectation [234235] some studies failed to ob-serve a higher response in vitamin E levels when these were com-pared with fat-soluble formulations [236237]
In a pilot study by Papas et al [183] a micellar formulation of fat-soluble nutrients and antioxidants was found to improve plasmalevels of β-carotene γ-tocopherol and CoQ(10) reducing at thesame time some inflammatory markers in induced sputum eg mye-loperoxidase and to a lower extent PMN elastase and total cell countswhile lung function and sputum bacterial counts were unaffectedThe same group recently confirmed the possibility to increase the ab-sorption of fat-soluble micronutrients using formulations with higherbioavailability specifically designed for malabsorbing patients such asCF patients that include also vitamin K and commercialized with thebrand name of AquADEKsreg [162] Despite improved vitamin and mi-cronutrient levels in this non-randomized open-label study AquA-DEKsreg produced only modest improvements in weight percentileand pulmonary function Another recent pilot observation [182] hassuggested the beneficial effect of this formulation on antioxidant andoxidative stress parameters of this oral supplement that surely deservesmore clinical investigation by larger randomized controlled trials
Recent multivitaminic formulations have been designed to containalso the minor forms of vitamin E and specifically γ-tocopherol [238]the expected superiority of which with respect to formulations con-taining only α-tocopherol needs to be verified As discussed abovein the section dedicated to vitamin E further advancements in thetherapy of CF inflammation and oxidative stress could be based onsynthetic forms and natural metabolites of this vitamin that havebeen recently identified to possess higher antioxidant and also anti-inflammatory activity than α-tocopherol (reviewed in [163168])
Pre-clinical investigation of these and other fat-soluble agents iscurrently addressed to develop formulations and administration pro-tocols that may increase the therapeutic efficacy in the airways In theantioxidant therapy of lung dysfunction in CF local administrationprotocols may overcome the limits of oral and systemic administra-tion protocols increasing bioavailability and providing targetedapproach to inflammation and oxidative stress Aerosolization of vita-min E and other fat-soluble micronutrients is possible and may allowdirect administration in the airways to prevent toxicity of smokewhich is closely associated with inflammation and oxidative stress[164165] To our knowledge this as well as other strategies of localadministration such as instillation of solutions such as surfactant-like solutions enriched of vitamin E have not been previously inves-tigated in CF patients and other CF model systems
On the contrary inhalation is an administration route widelyadopted in the case of GSH and NAC therapy described above Inthis context Cys formulations alternative to NAC have been proposedfor use as antioxidant and anti-inflammatory agent for inhalationNacystelyn is a lysine adduct of NAC that thanks to a higher proton-ation equilibrium shows increased water solubility and thus betterbioavailability Nacystelyn has been described to influence IL-8 gener-ation and the inflammatory signaling of bronchial epithelial cells[239] and preliminary clinical evaluation has demonstrated the safetyof this drug [240] Further clinical trials aimed to assess the effect onlung symptomatology of CF patients are needed Direct administra-tion in the airways could also be adopted for micronutrient vitaminswith poor absorption and bioavailability due to GI defects
38 Clinical impact of antioxidant therapy in CF
Huge in vitro and pre-clinical evidence has provided the rationaleto support clinical investigation of antioxidant strategies in CF Theseshould aim to restore the oxidantndashantioxidant balance of CF airwaychallenged by chronic infection and inflammatory cell activation
Some observational trials have confirmed that antioxidants usedas either supplements to the diet or drugs for lung administrationby aerosolized formulations may help in relieving progressive lungdamage and other adverse clinical events of CF such as poor growthSo far few studies have examined with sufficient methodologicalrigor the clinical efficacy of antioxidant therapy in CF This was alsoconcluded in a previous review of the literature by Cantin et al [12]that was published in the beginning of 2006 and is confirmed alsoin a recent analysis of clinical trials on antioxidant therapy in CF pa-tients [213] that examined the literature until September 2010using as sources the databases of the Cochrane CF and Genetic Disor-ders Group CF Trials Register PubMed CINAHL and AMED Useful in-formation was retrieved from just four randomized controlled trialsand one quasi-randomized controlled trial on vitamin C vitamin Eβ-carotene and selenium used as supplements administered aloneor in combination Post-hoc data analysis that was possible only inthree studies on a total of 87 CF patients showed the absence ofany significant improvement in lung function that was selected as pri-mary outcome together with quality of life that improved in one trialSecondary outcomes concerning laboratory indices of oxidative stressand antioxidant status showed several improvements These includedan increase of RBC SeGPx by selenium supplementation done as
705F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
individual or combined supplementation and increased levels of allplasma antioxidants except vitamin C that were observed in all thetrials
The message from these studies to pediatricians and nutritionistswithin the clinical staff of CF centers is that in the absence of solid ev-idence regarding the clinical effectiveness of oral formulations of an-tioxidant supplements in CF (including PUFA) their use as a routineclinical practice should be considered with caution keeping clear inmind that this should represent just a complement of one of themost critical interventions in the life-long clinical management pro-gram of CF patients eg providing an adequate nutriture [140] Inthis context compensating energy and protein malnutrition has toremain the first goal of nutritional management programs Providinghigher intakes of antioxidant micronutrients with food naturally-enriched (or functionalized) of micronutrient antioxidants shouldbe preferred in order to have the higher combination of positive nu-tritional factors that are lost during refinement procedures and over-all industrial processing of dietary supplements
Measures of good practice in clinical management of micro-malnutrition in CF patients would include the support of specializedpersonnel and laboratories The centers should have the possibilityto ascertain with appropriate nutritional and laboratory tests whatthe level of deficiency is for the different micronutrients that each pa-tient may suffer from during a dietary program Monitoring dietaryintakes and blood levels of micronutrients is not sufficient to set apersonalized nutritional intervention with supplements or functionalfoods Sub-optimal intakes and the compliance to nutritional inter-ventions should be verified by means of selected biochemical andclinical criteria Unluckily the latter are still not well established forsome micronutrients such as the fat-soluble vitamins E (reviewed in[163173241]) and K [242243] and also for trace elements such asSe [244] For many of the antioxidants used as supplements inhumans we still do not know exactly several of the biological effectsthat these may provide when introduced in a healthy body and weknow less what these can do in disease These aspects hardly impacton the concept of optimal levels of intake that should be identified foreach micronutrient on an individual basis According with the aspectsdiscussed in the previous sections optimal levels of intake for antiox-idant micronutrients are different in CF patients and healthy subjectsand vary with age and several individual factors
Lung administration of antioxidants by means of aerosolized for-mulations so far used for GSH therapy (see above) is a promisingfield of clinical investigation in CF Toxicity issues are currently themain concern and the subject of clinical evaluation by several groups(described above)
Information on future directions of antioxidant therapy in CF canbe inferred by the analysis of pending or recently completed clinicaltrials that have been searched (December 2011) at ClinicalTrialsgovdatabase matching the terms ldquoantioxidant therapyrdquo or ldquoglutathionerdquowith ldquocystic fibrosisrdquo Fifteen trials were retrieved and those directlyrelated to antioxidant therapy (n=12) are presented in Table 1 andinclude efficacy and safety studies of inhaled drugs as GSH sodiumpyruvate NAC and NO and the dietary supplements AquADEKsregan antioxidant-rich multivitamin supplement epigallocatechin gal-late (EGCG)tocotrienol curcuminoids the amino acid glutaminesulforaphane in broccoli sprouts One trial is investigating the flavo-noid quercetin as CFTR modulator
39 Emerging antioxidant and anti-inflammatory approaches in CF
Mediterranean foods such as olive oil and red wine or severalplant extracts such as herbal tea or grape seed extracts contain aseries of natural compounds with important antioxidant and NOscavenging activity that have been widely investigated for the pre-vention of oxidative stress-related diseases [38245] These havebeen long investigated as template molecules to develop antioxidant
and anti-inflammatory drugs Between the multitudes of natural sub-stances most investigated ones include for instance tyrosol hydroxy-tyrosol gallic and caffeic acids belonging to the family of phenolswhile resveratrol of the stilbenes family epicatechin kaempferoland cianidin are examples of flavonoids examples of fat-soluble phe-nolics are those of the family of tocols (vitamin E) and carotenoids Allthese compounds show different metabolisms and signaling effects[246] Antioxidant and cell protection mechanisms are associatedwith different and sometimes concurrent processes as H-atom trans-fer and electron donation radical trapping and chelation of transitionmetals that can be easily investigated at the chemical level [247] Be-sides these direct antioxidant effects metabolic responses and signal-ing effects of natural compounds are also important to producesecond-generation responses that modify the level of antioxidantprotection and the potential for ROS detoxification in cells and bodyfluids These derive from the transcriptional regulation of antioxidantand pro-oxidant genes that coexist with the modulation of cytokinesecretion and inflammatory enzyme activities
Some of these natural plant-derived antioxidants may provide fur-ther pharmacological activities of possible relevance in CF This is thecase for instance of the plant flavonoids genistein apigenin kaemp-ferol quercetin and hesperidin [248ndash251] that fall in the pharmaco-logical category of ldquopotentiatorsrdquo [252] in that these activate at leastto a certain extent CTFR-mediated Cl currents in normal and CF airwayepithelium investigated either in vitro or in vivo in humans and ani-mal models Actually as prototypal flavonoid-derived potentiatorthe tyrosine kinase inhibitor genistein potentiates the gating of wild-type as well as ΔF508 CFTR and G551D CFTR [253] but at higherdoses it inhibits CFTR gating which make this an unlikely clinical can-didate Similar potentiation effects have been reported for the antiox-idant curcumin [250] that shows an additive effect with respect togenistein-induced potentiation Besides CFTR potentiation whichdoes not appear to have a direct influence on GSH and nutrient trans-port in the lung tissue all these natural substances have been usedalone or in combination with other agents as in vivo enhancers oflung antioxidant protection [246254255] In the case of quercetinthiol-reactive phenolic [256] bronchodilation and anti-inflammatoryeffects by a restoration of the Th1Th2 balance have been reportedin inflammatory syndromes of the lung [255257ndash259] but theseeffects have not been explored in CF Pyocyanin toxicity (see abovein the Section 2) could represent an issue for the use of quercetinand other catechols in infectious diseases of the lung [260]
Other natural antioxidants of potential interest in CF therapy in-clude terpenoids [261] such as terpinen-4-ol a major constituentof tea tree oil that is being investigated in the therapy of anti-biotic resistant organisms specifically against methicillin-resistantStaphylococcus aureus (MRSA) [262] a problem in CF [263] Otherthan being lipophilic antioxidants terpenes can prevent oxidativestress of the CF lung secondarily to the antibiotic effect thereby pro-moting a better control of immuno-inflammatory pathways and lungantioxidants
391 Targeting NF-κB with natural compounds resveratrol and plantextracts
Natural compounds were long known to be useful in designinganti-inflammatory drugs and some of these could find an applicationin the control of the transcription factor kappa-B (NF-κB) that maylead to develop advanced pharmacological tools to control inflamma-tion and to produce higher antioxidant protection to CF airwaysInhibitors targeting NF-κB including transcription factors decoymolecules (TFD) are potent down-regulators of gene expressionand release of IL-8 in CF cells infected with P aeruginosa [264265]
Resveratrol (354prime-trihydroxystilbene ldquoErdquo form) is one of the mostinvestigated natural antioxidant with proposed activity as NF-κBinhibitor This is a phytoalexin present in large quantity in red winepreferentially in the skin of grapes being its concentration
706 F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
50ndash100 μgmg of fresh skin and 13ndash3 mgl of red wine [266]Furthermore resveratrol is a constituent of lsquoDarakchasavarsquo (13ndash6 mgl) an ayurvedic medicine from India [267] The antioxidant activity ofresveratrol has been reported in several papers and occurs also in lungtissues suggesting that resveratrol has potential as a therapeuticagent in respiratory disease [268ndash270] Resveratrol can be consideredone of the most interesting molecules from the natural worldexhibiting strong antioxidant activity that at the same time is able toexert anti inflammatory activity through alteration of NF-κB functionsand efficient inhibition of pro-inflammatory genes [271272] As far asthe effects on CF model systems are concerned Cabrini et al [26]reported the effects of resveratrol on P aeruginosa infected CF IB3-1cells The results obtained demonstrate that resveratrol exhibits minoreffects of IB3-1 cell growth and important inhibitory effects on accumu-lation of IL-8 and GRO-α mRNA while minor effects on IL-6 gene ex-pression were observed These data support recently publishedobservations suggesting inhibitory effects of resveratrol in infection-mediated inflammatory processes [273] Interestingly resveratrol hasbeen reported as a potent inhibitor of NF-κB activity and a promisinganti-inflammatory agent [272274] also in combinationwith othermol-ecules [274275] However in vivo translation of this pre-clinical on res-veratrol is hard to be foreseen This natural compound displays poorbioavailability [276] and further characterization of resveratrol pharma-cokinetics is troublesome since it is hardly measurable in vivo [277]Furthermore the regulation of inflammatory responses by resveratrolhas been suggested to be far more complex than simple direct suppres-sion of NF-κB activity Actually some aspects of the immune responsecould be enhanced by this natural substance which may lead tohypothesize broad negative feedback events on immuno-inflammatorypathways [278] In any case and with these cautions in mind the pub-lished observations on cellular model systems support the concept thatresveratrol and resveratrol-containing formulations deserve further con-sideration to determine their possible therapeutic values in CF
Other inhibitors can be identified from systematic studies of naturalproducts and their ability to interfere with NF-κB activity [279ndash281]Recent studies have demonstrated that the whole extract of Aeglemarmelos (Rutaceae) has strong inhibitory effect on the P aeruginosa-dependent IL-8 induction in human CF-derived bronchial IB3-1 cellswithout affecting cell proliferation [280] Molecular analysis of compo-nents contained in A marmelos extracts revealed that three major com-pounds namely 56-dimethoxy-1-indanone 2-hydroxy-cinnamic acidand 5-methoxy psoralen (5-MOP) reproduce the inhibitory effect ob-servedwith thewhole extract [280] A further example has been recent-ly published using extracts from bergamot (Citrus bergamia Risso) Inthis study the extracts were characterized and the main detected con-stituents were assayed for their biological activity [281] The resultsobtained demonstrated that the extracts from bergamot epicarps con-tain components displaying an inhibitory activity on IL-8 Particularlythe most active molecules were bergapten and citropten These effectshave been confirmed by analyzing mRNA levels and protein release inthe CF cellularmodels IB3-1 and CuFi-1 inducedwith TNF-α or exposedto P aeruginosa
A parallel strategy linking NF-κB inhibition and down-regulationof NF-κB-dependent functions is described in recently publishedstudies based on a structured-based virtual screening (VS) of differ-ently substituted furocoumarins and analogues against NF-κB withthe objective of selecting molecules able to inhibit the binding ofthis transcription factor to DNA [282283] Novel compounds wereidentified with this strategy as potent inhibitors of NF-κB dependentbiological functions to be proposed for the control lung inflammationoccurring in patients affected by CF [282ndash284]
392 Scavengers and regulators of H2O2 and NO
3921 Lactoferrin and OSCNmacr The impaired DUOXLPO system of CFpatients could be the target of therapeutic strategies that may
produce concomitant antimicrobial and antioxidant effects This sys-tem described above in Section 22 represents an important compo-nent of innate immunity with a role in bactericidal defense andregulation of H2O2 metabolism of airways [32] CF patients have alsoreported to show lowered LF levels in the ASL [37] that togetherwith a CFTR-dependent defective efflux of SCNmacr and LPO [36] may cre-ate the environment for a sustained flux of H2O2 and for the genera-tion of highly reactive Fenton species [1138] An ideal therapeuticintervention should restore the LPO-dependent generation of bacteri-cidal OSCNmacr from DUOX-derived H2O2 and SCNmacr in the ASL to controlat the same time the microbial biofilm and the flux of H2O2 into theASL An approach close to this therapeutic mechanism was recentlyproposed for the drug Meveolreg This is a complex of LF and OSCNmacrwith proposed in vivo antimicrobial activity [285] to be evaluatedin clinical trials for the aerosol treatment of lung infections in CFpatients The role for this drug in the control of H2O2 levels of ASLremains to be investigated
3922 Organoselenium compounds Organoselenium compoundshave been proposed as therapeutic agents useful in the antioxidanttherapy of inflammatory conditions These include GPX mimetic mol-ecules such as Ebselenreg (2-phenyl-12-benzisoselenazol-3(2H)-one)or other and more recently developed molecules that are still inpre-clinical steps of evaluation [286] Selectively and specificity of ac-tion are main issues in the therapeutic mechanism of this candidateantioxidant drug that thanks to the electrophilic properties of Se[214] reacts with thiols to reduce H2O2 and other species MoreoverEbselenreg has been described to act as potent non-competitive inhib-itor of extracellular nucleoside diphosphokinase (NDPK) having neg-ligible effect on ecto-ATPase and adenyl kinase activities which areother players of the metabolism of extracellular nucleotides [287]This enzyme together with other nucleoside di- and triphosphatescontributes to regulate several components of the mucociliary clear-ance process (MCC) that protects the lung against infections via acti-vation of epithelial purinergic receptors The inhibition of NDPK bythis GPX-mimetic drug may also impact on the energy status of endo-thelial cells [287] This aspect could be further investigated as a cellu-lar protection mechanism in the pulmonary epithelium of CF patientsbeing the control of cell energy of fundamental importance to preventthe activation of death pathways [288]
Further therapeutic mechanisms for these Se-derived drugs mayderive from the marked activity as inducers of phase II enzymessuch as quinone reductase (QR) and glutathione-S-transferase (GST)[289] This induction response also observed with other electrophilsand redox-active molecules such as natural phenolic antioxidantscould produce higher cellular protection by the acquisition of anincreased capability to detoxify endobiotics generated during oxida-tive stress and inflammation [246]
3923 Melatonin and GSNO as NOx regulators Increased markers ofNO-derived biological damage are present in the CF lung suggestingthe abnormal reactivity of NOx in the inflamed lung of CF patients[52] However an impaired metabolism and biological function ofNO in CF airways (see Section 23) suggests a cautious approach tothe use of agents that may influence the levels and chemical behaviorof NO-derived species (NOx) with possible impact on the physiologi-cal roles of NO in vasodilatation innate immunity and H2O2 metabo-lism of the respiratory tract [290291] NO donors also appear toinfluence CFTR function of alveolar epithelium and gland serouscells [292293]
Main physiological role of the pineal gland hormone melatonin isthe synchronization of circadian rhythms including the sleepndashwakecycle but several other functions dealing with immunomodulatoryantioxidant and cellular protection effects have been identified[294] Melatonin receptor stimulation may also influence cyclic AMPsignaling and the regulation of CFTR ion channel [295296]
707F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
A recent randomized double-blind placebo-controlled study hasexamined the effects of short term melatonin administration (3 mgfor 3 weeks) on sleep and oxidative stress markers in CF [297]According with the expected pharmacological effect of this hormonalsubstance the treatment was successful in improving sleep indicesAt the same time nitrite levels determined in exhaled breath conden-sate (EBC) were reduced to suggest a better control of NOmetabolismof CF airways (discussed above in Section 23) but these effects how-ever were not associated with a significant correction of isoprostaneas lipid peroxidation marker measured in EBC Increasing dosages ofmelatonin could be investigated for the pharmacological treatmentof oxidative stress and immune dysfunction of CF patients due tothe absence of adverse effects of this hormonal substance in humans
The S-nitrosation reaction of thiols is another interesting aspect ofNO pharmacology [53] that may find an application in the therapy oflung complications of CF This has been the case for instance of theS-nitrosothiol GSNO that has been used safely in human trials[298299] This endogenous nitrosothiol with proposed regulatory ef-fect on the CFTR of lung epithelia [292293] is well tolerated in pa-tients with CF when administered by aerosolization and mayproduce better oxygenation [299] thereby suggesting that therapyaimed at restoring endogenous GSNO levels in the CF airway maymerit further clinical evaluation Since the administered GSNO de-composes as shown by the increased levels of expired NO in CF pa-tients under treatment with this nitrosothiol [299] furtherinvestigation should be addressed to ascertain whether GSNO thera-py may merely correspond to a GSH therapy
NO dependent effects on CFTR function should be considered toevaluate mechanism of action and specificity of antioxidant therapiesthat target NO metabolism and function in the CF airways
4 Conclusions and future perspectives
The presence of clinical and biochemical symptoms of inflammationand oxidative stress implies that CF patients have a higher demand ofantioxidant protection The combination of the dysfunctional CFTRwith a lowered intake and absorption of dietary antioxidants producesub-optimal levels of protection from both enzymatic and non-enzymatic defense systems The former could be associated with a de-fective glutathionemetabolism and lowered intake of sulfur-containingamino acids and oligoelements such as zinc and possibly seleniumwhile fat-soluble antioxidant vitamins such as vitamin E and caroten-oids and the water-soluble vitamin C are lowered than in healthy sub-jects due to malabsorption and possibly higher consumption
The increased antioxidant demand in CF patients should be evenhigher in the presence of complications of the lung pancreas andliver Lung comorbidity is particularly important in this contextbeing associated with recurrent infections which results in the alter-nation of inflammatory exacerbates and chronic inflammation Thesesustain the flux of ROS in the airways and promote the formation ofsecond-generation byproducts by the damage of biomolecules suchas PUFA and proteins which may diffuse also at the systemic level tofurther promote adverse biological responses and toxic reactions Pan-creatic insufficiency causes malnutrition and may lead to develop en-docrine and metabolic defects associated with diabetes of CF Theseevents can be further aggravated by the concomitance of liver dys-function and a poor nutritional status Malnutrition is strongly associ-ated with poor prognosis as assessed by pulmonary function andsurvival data [138ndash140] The more aggressive nutritional interven-tions seem to produce better clinical outcomes in these patients andthe possibility of achieving higher antioxidant protection in well-nourished patients by dietary factors could be a key aspect to explainsuch a clinical advantage The assumption that food-derived compo-nentsmay help to prevent the damaging effects of oxidative stress im-proving the antioxidant defenses deserves further investigation at theclinical level This together with the investigation of appropriate
laboratory biomarkers could provide critical information to establishintervention criteria for an early nutritional management of newly di-agnosed patients [5] It is expected that a timely secondary preventionstrategy could influence the progression of CF symptoms thusaffecting with a self-feeding mechanism the same extent of malnutri-tion and oxidative stress along the life of CF patients Since severalfactors contribute to impair the nutritional status of CF patients(such as pancreatic insufficiency chronic malabsorption recurrentsinopulmonary infections and progressive lung disease chronic in-flammation increased energy expenditure suboptimal intake multi-therapy) careful monitoring of the antioxidant status should berecommended According with international guidelines fat-solublevitamin supplementation is of utmost importance in daily practice to-gether with energy intake requirements and pancreatic enzyme-replacement therapy Among these vitamin E β-carotene and ω-3FA have observed to alleviate selected biochemical signs of oxidativestress as measured for instance with well established laboratory indi-ces of lipid peroxidation and in some studies these effects werepreliminarily associated with positive clinical outcomes Notwith-standing randomizedndashcontrolled clinical trials on antioxidant supple-ments (including ω-3 FA) so far carried out in CF have failed toconclusively demonstrate significant beneficial effects on respiratorysymptoms and on the consequent impact that these have on the qual-ity of life of these patients (reviewed in [202213]) whichmay provideno support for the use of these supplements in CF An absence of effi-cacy in prevention studies on antioxidant supplements has also beenobserved in other and possibly less severe oxidative stress-relatedconditions particularly in the secondary prevention of cardiovasculardisease and some forms of cancer by vitamin E and other antioxidantssuch as vitamin C selenium and β-carotene (reviewed in [163]) Dif-ferent biases however have been identified in randomize large clini-cal trials that may account for these disappointing findings Theseinclude patient selection criteria (early interventions and primaryprevention could have more chances of success than secondaryprevention) duration and doses of the treatment use of wrong anti-oxidant formulations and administration protocols absence of verifi-cations of the biological compliance to the treatment etc The samebiases apply for the few trials carried out in CF patients Thus the ap-propriateness and efficacy of nutritional interventions with naturalfood-derived or synthetic antioxidants should be verifiedwith respectto the biological pathways of oxidative stress and clinical variablesthat are identified as end-points Profiles of blood and tissue antioxi-dants as well as of reliable surrogate markers of oxidative stresshave to be selected and determined in highly specialized laboratorieswith a well-established experience on these analyses
Well-timed (early) interventions with appropriate antioxidantformulationsprotocols need to be proposed for the next generationof trials and the development of novel CF-tailored antioxidant andanti-inflammatory agents should be promoted
As a consequence of these considerations more clinical investiga-tion is awaited to identify future successful approaches to the antiox-idant therapy as a measure to further enhance quality of life and theoverall clinical outcome of CF patients
Acknowledgments
We are indebted with the Italian Cystic Fibrosis Research Founda-tion for the support that it provided with its grant program to the re-search activity of the authors of this paper This is a scientific initiativeof the ldquoWorking Group on Inflammation in Cystic Fibrosisrdquo (BragonziA Bravo E Cabrini G Conese M Cuzzocrea S Dechecchi MC De Ales-sandri A Evangelista V Galli F Gambari R Lambiase A Lucidi VManca A Melotti P Minicucci L Motta A Pietraforte D Pompella AQuattrucci S Rizzo R Romano M Sorio C Tesse R) of the Italian Soci-ety for Cystic Fibrosis A particular thank goes to the Prof GianniMastella for the critical revision of the manuscript and for the
708 F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
stimulating research environment that he has contributed to createwithin the Italian Cystic Fibrosis Research Foundation
References
[1] BP OSullivan SD Freedman Cystic fibrosis Lancet 373 (2009) 1891ndash1904[2] P Linsdell JW Hanrahan Glutathione permeability of CFTR Am J Physiol 275
(1998) C323ndashC326[3] L Gao KJ Kim JR Yankaskas HJ Forman Abnormal glutathione transport in
cystic fibrosis airway epithelia Am J Physiol 277 (1999) L113ndashL118[4] RK Rowntree A Harris The phenotypic consequences of CFTR mutations Ann
Hum Genet 67 (2003) 471ndash485[5] EI Back C Frindt D Nohr J Frank R Ziebach M Stern M Ranke HK Biesalski
Antioxidant deficiency in cystic fibrosis when is the right time to take actionAm J Clin Nutr 80 (2004) 374ndash384
[6] LG Wood DA Fitzgerald AK Lee ML Garg Improved antioxidant and fattyacid status of patients with cystic fibrosis after antioxidant supplementation islinked to improved lung function Am J Clin Nutr 77 (2003) 150ndash159
[7] L Iuliano R Monticolo G Straface S Zullo F Galli M Boaz S Quattrucci Asso-ciation of cholesterol oxidation and abnormalities in fatty acid metabolism incystic fibrosis Am J Clin Nutr 90 (2009) 477ndash484
[8] C Libetta V Sepe P Esposito F Galli A Dal Canton Oxidative stress and inflam-mation implications in uremia and hemodialysis Clin Biochem 44 (2011)1189ndash1198
[9] G Bartosz Reactive oxygen species destroyers or messengers Biochem Phar-macol 77 (2009) 1303ndash1315
[10] T Ntimbane B Comte G Mailhot Y Berthiaume V Poitout M Prentki RRabasa-Lhoret E Levy Cystic fibrosis-related diabetes from CFTR dysfunctionto oxidative stress Clin Biochem 30 (2009) 153ndash177
[11] A van der Vliet JP Eiserich GP Marelich B Halliwell CE Cross Oxidativestress in cystic fibrosis does it occur and does it matter Adv Pharmacol 38(1997) 491ndash513
[12] AM Cantin TB White CE Cross HJ Forman RJ Sokol D Borowitz Antioxi-dants in cystic fibrosis Conclusions from the CF antioxidant workshop Bethes-da Maryland Free Radic Biol Med 42 (2007) 15ndash31
[13] LT McGrath P Mallon L Dowey B Silke E McClean M McDonnell A DevineS Copeland S Elborn Oxidative stress during acute respiratory exacerbations incystic fibrosis Thorax 54 (1999) 518ndash523
[14] E Thomson S Brennan R Senthilmohan CL Gangell AL Chapman PD SlyAJ Kettle E Balding LJ Berry JB Carlin R Carzino N de Klerk T Douglas CFoo LW Garratt GL Hall J Harrison A Kicic IA Laing KM Logie J MassieLS Mott C Murray F Parsons N Pillarisetti SR Poreddy SC RanganathanCF Robertson R Robins-Browne PJ Robinson B Skoric SM Stick ENSutanto E Williamson Identifying peroxidases and their oxidants in the earlypathology of cystic fibrosis Free Radic Biol Med 49 (2010) 1354ndash1360
[15] SP Range C Dunster AJ Knox FJ Kelly Treatment of pulmonary exacerba-tions of cystic fibrosis leads to improved antioxidant status Eur Respir J 13(1999) 560ndash564
[16] L Coppo P Ghezzi Thiol regulation of pro-inflammatory cytokines and innateimmunity protein S-thiolation as a novel molecular mechanism Biochem SocTrans 39 (2011) 1268ndash1272
[17] C Verhaeghe C Remouchamps B Hennuy A Vanderplasschen A Chariot SPTabruyn C Oury V Bours Role of IKK and ERK pathways in intrinsic inflamma-tion of cystic fibrosis airways Biochem Pharmacol 73 (2007) 1982ndash1994
[18] TL Bonfield JR Panuska MW Konstan KA Hilliard JB Hilliard H Ghnaim MBerger Inflammatory cytokines in cystic fibrosis lungs Am J Respir Crit CareMed 152 (1995) 2111ndash2118
[19] TL Noah HR Black PW Cheng RE Wood MW Leigh Nasal and bronchoal-veolar lavage fluid cytokines in early cystic fibrosis J Infect Dis 175 (1997)638ndash647
[20] MJ Welsh BW Ramsey FJ Accurso GR Cutting Cystic Fibrosis McGraw-HillNew York 2001
[21] TZ Khan JS Wagener T Bost J Martinez FJ Accurso DW Riches Early pul-monary inflammation in infants with cystic fibrosis Am J Respir Crit CareMed 151 (1995) 1075ndash1082
[22] FA Ratjen Cystic fibrosis pathogenesis and future treatment strategies RespirCare 54 (2009) 595ndash605
[23] J Jacquot O Tabary P Le Rouzic A Clement Airway epithelial cell inflamma-tory signalling in cystic fibrosis Int J Biochem Cell Biol 40 (2008)1703ndash1715
[24] CM Greene P Branagan NG McElvaney Toll-like receptors as therapeutic tar-gets in cystic fibrosis Expert Opin Ther Targets 12 (2008) 1481ndash1495
[25] M Rottner JM Freyssinet MC Martinez Mechanisms of the noxious inflam-matory cycle in cystic fibrosis Respir Res 10 (2009) 23
[26] G Cabrini V Bezzerri I Mancini E Nicolis MC Dechecchi A Tamanini ILampronti L Piccagli N Bianchi M Borgatti R Gambari Targeting transcrip-tion factor activity as a strategy to inhibit pro-inflammatory genes involved incystic fibrosis decoy oligonucleotides and low-molecular weight compoundsCurr Med Chem 17 (2010) 4392ndash4404
[27] CM Greene NG McElvaney Proteases and antiproteases in chronic neutrophiliclungdiseasemdash relevance to drug discovery Br J Pharmacol 158 (2009) 1048ndash1058
[28] AM Cantin Potential for antioxidant therapy of cystic fibrosis Curr Opin PulmMed 10 (2004) 531ndash536
[29] JF Chmiel MW Konstan Inflammation and anti-inflammatory therapies forcystic fibrosis Clin Chest Med 28 (2007) 331ndash346
[30] DP Nichols MW Konstan JF Chmiel Anti-inflammatory therapies for cys-tic fibrosis-related lung disease Clin Rev Allergy Immunol 35 (2008)135ndash153
[31] AJ Kettle T Chan I Osberg R Senthilmohan AL Chapman TJ Mocatta JSWagener Myeloperoxidase and protein oxidation in the airways of youngchildren with cystic fibrosis Am J Respir Crit Care Med 170 (2004)1317ndash1323
[32] H Fischer Mechanisms and function of DUOX in epithelia of the lung AntioxidRedox Signal 11 (2009) 2453ndash2465
[33] B Rada TL Leto Oxidative innate immune defenses by NoxDuox familyNADPH oxidases Contrib Microbiol 15 (2008) 164ndash187
[34] P Moskwa D Lorentzen KJ Excoffon J Zabner PB McCray Jr WM NauseefC Dupuy B Banfi A novel host defense system of airways is defective in cysticfibrosis Am J Respir Crit Care Med 175 (2007) 174ndash183
[35] D Lorentzen L Durairaj AA Pezzulo Y Nakano J Launspach DA Stoltz GZamba PB McCray Jr J Zabner MJ Welsh WM Nauseef B Banfi Concentra-tion of the antibacterial precursor thiocyanate in cystic fibrosis airway secre-tions Free Radic Biol Med 50 (2011) 1144ndash1150
[36] Y Xu S Szep Z Lu The antioxidant role of thiocyanate in the pathogenesis ofcystic fibrosis and other inflammation-related diseases Proc Natl Acad Sci US A 106 (2009) 20515ndash20519
[37] MP Rogan CC Taggart CM Greene PG Murphy SJ ONeill NG McElvaneyLoss of microbicidal activity and increased formation of biofilm due to decreasedlactoferrin activity in patients with cystic fibrosis J Infect Dis 190 (2004)1245ndash1253
[38] B Halliwell JM Guttridge Free Radicals in Biology and Medicine Fourth editionOxford University Press New York 2007
[39] B Rada K Lekstrom S Damian C Dupuy TL Leto The Pseudomonastoxin pyocyanin inhibits the dual oxidase-based antimicrobial system as itimposes oxidative stress on airway epithelial cells J Immunol 181 (2008)4883ndash4893
[40] C Schwarzer B Illek JH Suh SJ Remington H Fischer TE Machen Organelleredox of CF and CFTR-corrected airway epithelia Free Radic Biol Med 43(2007) 300ndash316
[41] JH Roum R Buhl NG McElvaney Z Borok RG Crystal Systemic deficiency ofglutathione in cystic fibrosis J Appl Physiol 75 (1993) 2419ndash2424
[42] VM Hudson Rethinking cystic fibrosis pathology the critical role of abnormalreduced glutathione (GSH) transport caused by CFTR mutation Free RadicBiol Med 30 (2001) 1440ndash1461
[43] PJ Barnes RA Dweik AF Gelb PG Gibson SC George H Grasemann IDPavord F Ratjen PE Silkoff DR Taylor N Zamel Exhaled nitric oxide in pul-monary diseases a comprehensive review Chest 138 (2010) 682ndash692
[44] H Grasemann E Michler M Wallot F Ratjen Decreased concentration of ex-haled nitric oxide (NO) in patients with cystic fibrosis Pediatr Pulmonol 24(1997) 173ndash177
[45] H Grasemann F Ratjen Cystic fibrosis lung disease the role of nitric oxidePediatr Pulmonol 28 (1999) 442ndash448
[46] B Gaston F Ratjen JW Vaughan NR Malhotra RG Canady AH Snyder JFHunt S Gaertig JB Goldberg Nitrogen redox balance in the cystic fibrosis air-way effects of antipseudomonal therapy Am J Respir Crit Care Med 165(2002) 387ndash390
[47] H Grasemann I Ioannidis RP Tomkiewicz H de Groot BK Rubin F RatjenNitric oxide metabolites in cystic fibrosis lung disease Arch Dis Child 78(1998) 49ndash53
[48] H Grasemann R Schwiertz S Matthiesen K Racke F Ratjen Increased argi-nase activity in cystic fibrosis airways Am J Respir Crit Care Med 172(2005) 1523ndash1528
[49] H Grasemann S Al-Saleh JA Scott D Shehnaz A Mehl R Amin M Rafii PPencharz J Belik F Ratjen Asymmetric dimethylarginine contributes to airwaynitric oxide deficiency in patients with cystic fibrosis Am J Respir Crit CareMed 183 (2011) 1363ndash1368
[50] H Grasemann F Kurtz F Ratjen Inhaled L-arginine improves exhaled nitricoxide and pulmonary function in patients with cystic fibrosis Am J RespirCrit Care Med 174 (2006) 208ndash212
[51] H Grasemann F Ratjen Emerging therapies for cystic fibrosis lung disease Ex-pert Opin Emerg Drugs 15 (2010) 653ndash659
[52] BM Morrissey K Schilling JV Weil PE Silkoff DM Rodman Nitric oxide andprotein nitration in the cystic fibrosis airway Arch Biochem Biophys 406(2002) 33ndash39
[53] R Radi Nitric oxide oxidants and protein tyrosine nitration Proc Natl AcadSci U S A 101 (2004) 4003ndash4008
[54] J Chen M Kinter S Shank C Cotton TJ Kelley AG Ziady Dysfunction of Nrf-2in CF epithelia leads to excess intracellular H2O2 and inflammatory cytokineproduction PLoS One 3 (2008) e3367
[55] F Galli M Piroddi C Annetti C Aisa E Floridi A Floridi Oxidative stress andreactive oxygen species Contrib Nephrol 149 (2005) 240ndash260
[56] DT Wright LA Cohn H Li B Fischer CM Li KB Adler Interactions of oxygenradicals with airway epithelium Environ Health Perspect 102 (Suppl 10)(1994) 85ndash90
[57] I Rahman SR Yang SK Biswas Current concepts of redox signaling in thelungs Antioxid Redox Signal 8 (2006) 681ndash689
[58] Q Li JF Engelhardt Interleukin-1beta induction of NFκB is partially regulatedby H2O2-mediated activation of NFκB-inducing kinase J Biol Chem 281(2006) 1495ndash1505
709F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
[59] E Boncoeur VS Criq E Bonvin T Roque A Henrion-Caude DC Gruenert AClement J Jacquot O Tabary Oxidative stress induces extracellular signal-regulated kinase 12 mitogen-activated protein kinase in cystic fibrosis lung ep-ithelial cells potential mechanism for excessive IL-8 expression Int J BiochemCell Biol 40 (2008) 432ndash446
[60] B Fischer J Voynow Neutrophil elastase induces MUC5AC messenger RNA ex-pression by an oxidant-dependent mechanism Chest 117 (2000) 317Sndash320S
[61] B Rada P Gardina TG Myers TL Leto Reactive oxygen species mediate in-flammatory cytokine release and EGFR-dependent mucin secretion in airwayepithelial cells exposed to Pseudomonas pyocyanin Mucosal Immunol 4(2011) 158ndash171
[62] C Schwarzer H Fischer EJ Kim KJ Barber AD Mills MJ Kurth DC GruenertJH Suh TE Machen B Illek Oxidative stress caused by pyocyanin impairs CFTRClminus transport in human bronchial epithelial cells Free Radic Biol Med 45(2008) 1653ndash1662
[63] J Hull M South P Phelan K Grimwood Surfactant composition in infants andyoung children with cystic fibrosis Am J Respir Crit Care Med 156 (1997)161ndash165
[64] KC Meyer A Sharma R Brown M Weatherly FR Moya J Lewandoski JJZimmerman Function and composition of pulmonary surfactant andsurfactant-derived fatty acid profiles are altered in young adults with cystic fi-brosis Chest 118 (2000) 164ndash174
[65] MK Pulfer RC Murphy Formation of biologically active oxysterols during ozo-nolysis of cholesterol present in lung surfactant J Biol Chem 279 (2004)26331ndash26338
[66] V Starosta E Rietschel K Paul U Baumann M Griese Oxidative changes ofbronchoalveolar proteins in cystic fibrosis Chest 129 (2006) 431ndash437
[67] V Starosta M Griese Oxidative damage to surfactant protein D in pulmonarydiseases Free Radic Res 40 (2006) 419ndash425
[68] M Griese R Essl R Schmidt E Rietschel F Ratjen M Ballmann K Paul Pulmo-nary surfactant lung function and endobronchial inflammation in cystic fibro-sis Am J Respir Crit Care Med 170 (2004) 1000ndash1005
[69] M Griese R Essl R Schmidt M Ballmann K Paul E Rietschel F Ratjen Se-quential analysis of surfactant lung function and inflammation in cystic fibrosispatients Respir Res 6 (2005) 133
[70] LG Wood DA Fitzgerald PG Gibson DM Cooper ML Garg Increased plasmafatty acid concentrations after respiratory exacerbations are associated with el-evated oxidative stress in cystic fibrosis patients Am J Clin Nutr 75 (2002)668ndash675
[71] P Montuschi SA Kharitonov G Ciabattoni M Corradi L van Rensen DM Ged-des ME Hodson PJ Barnes Exhaled 8-isoprostane as a new non-invasive bio-marker of oxidative stress in cystic fibrosis Thorax 55 (2000) 205ndash209
[72] CE Collins P Quaggiotto L Wood EV OLoughlin RL Henry ML Garg Elevat-ed plasma levels of F2 alpha isoprostane in cystic fibrosis Lipids 34 (1999)551ndash556
[73] D Hartl V Starosta K Maier I Beck-Speier C Rebhan BF Becker P Latzin RFischer F Ratjen RM Huber E Rietschel S Krauss-Etschmann M Griese In-haled glutathione decreases PGE2 and increases lymphocytes in cystic fibrosislungs Free Radic Biol Med 39 (2005) 463ndash472
[74] GL Milne H Yin JD Morrow Human biochemistry of the isoprostane pathwayJ Biol Chem 283 (2008) 15533ndash15537
[75] G Ciabattoni G Davi M Collura L Iapichino F Pardo A Ganci R Romagnoli JMaclouf C Patrono In vivo lipid peroxidation and platelet activation in cystic fi-brosis Am J Respir Crit Care Med 162 (2000) 1195ndash1201
[76] C Garenc P Julien E Levy Oxysterols in biological systems the gastrointestinaltract liver vascular wall and central nervous system Free Radic Res 44 (2011)47ndash73
[77] AM Cantin SL North RC Hubbard RG Crystal Normal alveolar epithelial lin-ing fluid contains high levels of glutathione J Appl Physiol 63 (1987) 152ndash157
[78] R Tirouvanziam CK Conrad T Bottiglieri LA Herzenberg RB Moss High-dose oral N-acetylcysteine a glutathione prodrug modulates inflammation incystic fibrosis Proc Natl Acad Sci U S A 103 (2006) 4628ndash4633
[79] LW Velsor C Kariya R Kachadourian BJ Day Mitochondrial oxidative stressin the lungs of cystic fibrosis transmembrane conductance regulator proteinmutant mice Am J Respir Cell Mol Biol 35 (2006) 579ndash586
[80] M Kelly-Aubert S Trudel J Fritsch T Nguyen-Khoa M Baudouin-Legros SMoriceau L Jeanson F Djouadi C Matar M Conti M Ollero F Brouillard AEdelman GSH monoethyl ester rescues mitochondrial defects in cystic fibrosismodels Hum Mol Genet 20 (2011) 2745ndash2759
[81] P Ghezzi Role of glutathione in immunity and inflammation in the lung Int JGen Med 4 (2011) 105ndash113
[82] N Dauletbaev K Viel R Buhl TO Wagner J Bargon Glutathione and glutathi-one peroxidase in sputum samples of adult patients with cystic fibrosis J CystFibros 3 (2004) 119ndash124
[83] CE Cross A van der Vliet CA ONeill S Louie B Halliwell Oxidants antioxi-dants and respiratory tract lining fluids Environ Health Perspect 102 (Suppl10) (1994) 185ndash191
[84] K Takeyama K Dabbagh J Jeong Shim T Dao-Pick IF Ueki JA Nadel Oxida-tive stress causes mucin synthesis via transactivation of epidermal growth factorreceptor role of neutrophils J Immunol 164 (2000) 1546ndash1552
[85] N Ballatori SM Krance S Notenboom S Shi K Tieu CL Hammond Glutathi-one dysregulation and the etiology and progression of human diseases BiolChem 390 (2009) 191ndash214
[86] SR Soltaninassab KR Sekhar MJ Meredith ML Freeman Multi-faceted regu-lation of gamma-glutamylcysteine synthetase J Cell Physiol 182 (2000)163ndash170
[87] HR Lopez-Mirabal JR Winther Redox characteristics of the eukaryotic cytosolBiochim Biophys Acta 1783 (2008) 629ndash640
[88] C Hwang AJ Sinskey HF Lodish Oxidized redox state of glutathione in the en-doplasmic reticulum Science 257 (1992) 1496ndash1502
[89] M Murphy Mitochondrial thiols in antioxidant protection and redox signallingdistinct roles for glutathionylation and other thiol modifications AntioxidRedox Signal (2011) ahead of print doi101089ars20114289
[90] BJ Day AM van Heeckeren E Min LW Velsor Role for cystic fibrosis trans-membrane conductance regulator protein in a glutathione response to bronch-opulmonary Pseudomonas infection Infect Immun 72 (2004) 2045ndash2051
[91] Y Zhang K Duan Glutathione exhibits antibacterial activity and increases tetra-cycline efficacy against Pseudomonas aeruginosa Sci China C Life Sci 52 (2009)501ndash505
[92] VM Hudson New insights into the pathogenesis of cystic fibrosis pivotal roleof glutathione system dysfunction and implications for therapy Treat RespirMed 3 (2004) 353ndash363
[93] LW Velsor A van Heeckeren BJ Day Antioxidant imbalance in the lungs ofcystic fibrosis transmembrane conductance regulator protein mutant miceAm J Physiol Lung Cell Mol Physiol 281 (2001) L31ndashL38
[94] I Kogan M Ramjeesingh C Li JF Kidd Y Wang EM Leslie SP Cole CE BearCFTR directly mediates nucleotide-regulated glutathione flux EMBO J 22(2003) 1981ndash1989
[95] NS Gould S Gauthier CT Kariya E Min J Huang DJ Brian Hypertonic salineincreases lung epithelial lining fluid glutathione and thiocyanate two protectiveCFTR-dependent thiols against oxidative injury Respir Res 11 (2010) 119
[96] VT Vasu SJ de Cruz JS Houghton KA Hayakawa BM Morrissey CE CrossJP Eiserich Evaluation of thiol-based antioxidant therapeutics in cystic fibrosissputum focus on myeloperoxidase Free Radic Res 45 (2011) 165ndash176
[97] L Roussel G Martel J Berube S Rousseau P aeruginosa drives CXCL8 synthesisvia redundant toll-like receptors and NADPH oxidase in CFTRF508 airway epi-thelial cells J Cyst Fibros 10 (2011) 107ndash113
[98] GW Lau DJ Hassett H Ran F Kong The role of pyocyanin in Pseudomonas aer-uginosa infection Trends Mol Med 10 (2004) 599ndash606
[99] R Wilson DA Sykes D Watson A Rutman GW Taylor PJ Cole Measurementof Pseudomonas aeruginosa phenazine pigments in sputum and assessment oftheir contribution to sputum sol toxicity for respiratory epithelium InfectImmun 56 (1988) 2515ndash2517
[100] M Muller Pyocyanin induces oxidative stress in human endothelial cells andmodulates the glutathione redox cycle Free Radic Biol Med 33 (2002)1527ndash1533
[101] YQ OMalley KJ Reszka BE Britigan Direct oxidation of 2prime7prime-dichlorodihy-drofluorescein by pyocyanin and other redox-active compounds independentof reactive oxygen species production Free Radic Biol Med 36 (2004)90ndash100
[102] CC Caldwell Y Chen HS Goetzmann Y Hao MT Borchers DJ Hassett LRYoung D Mavrodi L Thomashow GW Lau Pseudomonas aeruginosa exotoxinpyocyanin causes cystic fibrosis airway pathogenesis Am J Pathol 175 (2009)2473ndash2488
[103] YQ OMalley KJ Reszka DR Spitz GM Denning BE Britigan Pseudomonasaeruginosa pyocyanin directly oxidizes glutathione and decreases its levels inairway epithelial cells Am J Physiol Lung Cell Mol Physiol 287 (2004)L94ndashL103
[104] M Muller Glutathione modulates the toxicity of but is not a biologically rele-vant reductant for the Pseudomonas aeruginosa redox toxin pyocyanin FreeRadic Biol Med 50 (2011) 971ndash977
[105] R Cheluvappa R Shimmon M Dawson SN Hilmer DG Le Couteur Reactionsof Pseudomonas aeruginosa pyocyanin with reduced glutathione Acta BiochimPol 55 (2008) 571ndash580
[106] JH Widdicombe Transgenic animals may help resolve a sticky situation in cys-tic fibrosis J Clin Invest 120 (2010) 3093ndash3096
[107] X Sun H Sui JT Fisher Z Yan X Liu HJ Cho NS Joo Y Zhang W Zhou Y YiJM Kinyon DC Lei-Butters MA Griffin P Naumann M Luo J Ascher KWang T Frana JJ Wine DK Meyerholz JF Engelhardt Disease phenotype ofa ferret CFTR-knockout model of cystic fibrosis J Clin Invest 120 (2010)3149ndash3160
[108] NS Joo HJ Cho M Khansaheb JJ Wine Hyposecretion of fluid from trachealsubmucosal glands of CFTR-deficient pigs J Clin Invest 120 (2010) 3161ndash3166
[109] A Bragonzi Murine models of acute and chronic lung infection with cystic fibro-sis pathogens IJMM 300 (2010) 584ndash593
[110] AM van Heeckeren MD Schluchter Murine models of chronic Pseudomonasaeruginosa lung infection Lab Anim 36 (2002) 291ndash312
[111] A Bragonzi D Worlitzsch GB Pier P Timpert M Ulrich M Hentzer JB Ander-sen M Givskov M Conese G Doring Nonmucoid Pseudomonas aeruginosa ex-presses alginate in the lungs of patients with cystic fibrosis and in a mousemodel J Infect Dis 192 (2005) 410ndash419
[112] GS CW Bedrossian DB Singer JJ Hansen HS Rosenberg The lung in cysticfibrosis A quantitative study including prevalence of pathologic findingsamong different age groups Hum Pathol 7 (1976) 195ndash204
[113] WD HA Cash B McCullough WG Johanson Jr JA Bass A rat model of chron-ic respiratory infection with Pseudomonas aeruginosa Am Rev Respir Dis 119(1979) 453ndash459
[114] EM JR Starke C Langston CJ Baker A mouse model of chronic pulmonary in-fection with Pseudomonas aeruginosa and Pseudomonas cepacia Pediatr Res 22(1987) 698ndash702
[115] TJ AM van Heeckeren RW Walenga MW Konstan PB Davis B ErokwuMA Haxhiu TW Ferkol Effect of Pseudomonas infection on weight loss lung
710 F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
mechanics and cytokines in mice Am J Respir Crit Care Med 161 (2000)271ndash279
[116] T Aw G Wierzbicka DP Jones Oral glutathione increases tissue glutathione invivo Chem Biol Interact 80 (1991) 89ndash97
[117] F Favilli P Marraccini T Iantomasi MT Vincenzini Effect of orally adminis-tered glutathione on glutathione levels in some organs of rats role of specifictransporters Br J Nutr 78 (1997) 293ndash300
[118] C Kariya H Leitner E Min C van Heeckeren A van Heeckeren BJ Day A rolefor CFTR in the elevation of glutathione levels in the lung by oral glutathione ad-ministration Am J Physiol Lung Cell Mol Physiol 292 (2007) L1590ndashL1597
[119] K Atkuri JJ Mantovani LA Herzenberg LA Herzenberg N-Acetylcysteinemdashasafe antidote for cysteineglutathione deficiency Curr Opin Pharmacol 7(2007) 355ndash359
[120] R De Lisle E Roach K Jansson Effects of laxative and N-acetylcysteine onmucus accumulation bacterial load transit and inflammation in the cystic fi-brosis mouse small intestine Am J Physiol Gastrointest Liver Physiol 293(2007) G577ndashG584
[121] A Luciani VR Villella S Esposito N Brunetti-Pierri D Medina C Settembre MGavina L Pulze I Giardino M Pettoello-Mantovani M DApolito S Guido EMasliah B Spencer S Quaratino V Raia A Ballabio L Maiuri Defective CFTRinduces aggresome formation and lung inflammation in cystic fibrosis throughROS-mediated autophagy inhibition Nat Cell Biol 12 863ndash875
[122] M Griese J Ramakers A Krasselt V Starosta S Van Koningsbruggen R FischerF Ratjen B Mullinger RM Huber K Maier E Rietschel G Scheuch Improve-ment of alveolar glutathione and lung function but not oxidative state in cysticfibrosis Am J Respir Crit Care Med 169 (2004) 822ndash828
[123] C Bishop VM Hudson SC Hilton C Wilde A pilot study of the effect of inhaledbuffered reduced glutathione on the clinical status of patients with cystic fibro-sis Chest 127 (2005) 308ndash317
[124] WWang C Oliva G Li A Holmgren CH Lillig KL Kirk Reversible silencing of CFTRchloride channels by glutathionylation J Gen Physiol 125 (2005) 127ndash141
[125] N Dauletbaev P Fischer B Aulbach J Gross W Kusche U Thyroff-FriesingerTO Wagner J Bargon A phase II study on safety and efficacy of high-dose N-acetylcysteine in patients with cystic fibrosis Eur J Med Res 14 (2009)352ndash358
[126] R Tirouvanziam Y Gernez CK Conrad RB Moss I Schrijver CE Dunn ZADavies LA Herzenberg Profound functional and signaling changes in viable in-flammatory neutrophils homing to cystic fibrosis airways Proc Natl Acad SciU S A 105 (2008) 4335ndash4339
[127] JH Roum Z Borok NG McElvaney GJ Grimes AD Bokser R Buhl RG Crys-tal Glutathione aerosol suppresses lung epithelial surface inflammatory cell-derived oxidants in cystic fibrosis J Appl Physiol 87 (1999) 438ndash443
[128] A Visca CT Bishop SC Hilton VM Hudson Improvement in clinical markersin CF patients using a reduced glutathione regimen an uncontrolled observa-tional study J Cyst Fibros 7 (2008) 433ndash436
[129] EF Nash A Stephenson F Ratjen E Tullis Nebulized and oral thiol derivativesfor pulmonary disease in cystic fibrosis Cochrane Database Syst Rev (2009)CD007168
[130] AC foundation Drug Development Pipeline 2011[131] S Hoshida T Kuzuya N Yamashita M Nishida S Kitahara M Hori T
Kamada M Tada Gamma-glutamylcysteine ethyl ester for myocardial protec-tion in dogs during ischemia and reperfusion J Am Coll Cardiol 24 (1994)1391ndash1397
[132] J Lok W Leung S Zhao S Pallast K van Leyen S Guo X Wang A Yalcin EHLo Gamma-glutamylcysteine ethyl ester protects cerebral endothelial cells dur-ing injury and decreases bloodndashbrain barrier permeability after experimentalbrain trauma J Neurochem 118 (2011) 248ndash255
[133] Z Borok R Buhl GJ Grimes AD Bokser RC Hubbard KJ Holroyd JH RoumDB Czerski AM Cantin RG Crystal Effect of glutathione aerosol on oxidantndashantioxidant imbalance in idiopathic pulmonary fibrosis Lancet 338 (1991)215ndash216
[134] KJ Holroyd R Buhl Z Borok JH Roum AD Bokser GJ Grimes D Czerski AMCantin RG Crystal Correction of glutathione deficiency in the lower respiratorytract of HIV seropositive individuals by glutathione aerosol treatment Thorax 48(1993) 985ndash989
[135] J Hull P Vervaart K Grimwood P Phelan Pulmonary oxidative stress responsein young children with cystic fibrosis Thorax 52 (1997) 557ndash560
[136] A Corti A Paolicchi M Franzini S Dominici AF Casini A Pompella The S-thiolating activity of membrane gamma-glutamyltransferase formation ofcysteinyl-glycine mixed disulfides with cellular proteins and in the cell microen-vironment Antioxid Redox Signal 7 (2005) 911ndash918
[137] A Corti M Franzini AF Casini A Paolicchi A Pompella Vitamin C supply tobronchial epithelial cells linked to glutathione availability in elfmdasha role for se-creted gamma-glutamyltransferase J Cyst Fibros 7 (2008) 174ndash178
[138] A Munck Nutritional considerations in patients with cystic fibrosis Expert RevRespir Med 4 (2010) 47ndash56
[139] JL Matel CE Milla Nutrition in cystic fibrosis Semin Respir Crit Care Med 30(2009) 579ndash586
[140] D Salvatore R Buzzetti E Baldo MP Forneris V Lucidi D Manunza IMarinelli B Messore AS Neri V Raia ML Furnari G Mastella An overviewof international literature from cystic fibrosis registries 2 Neonatal screeningand nutritiongrowth J Cyst Fibros 9 (2010) 75ndash83
[141] KF Joosten JM Hulst Malnutrition in pediatric hospital patients current is-sues Nutrition 27 (2011) 133ndash137
[142] S Fustik T Jacovska L Spirevska S Koceva Protein-energy malnutrition as thefirst manifestation of cystic fibrosis in infancy Pediatr Int 51 (2009) 678ndash683
[143] J Himmelfarb E McMonagle Albumin is the major plasma protein target of ox-idant stress in uremia Kidney Int 60 (2001) 358ndash363
[144] P Stenvinkel JJ Carrero J Axelsson B Lindholm O Heimburger Z MassyEmerging biomarkers for evaluating cardiovascular risk in the chronic kidneydisease patient how do new pieces fit into the uremic puzzle Clin J Am SocNephrol 3 (2008) 505ndash521
[145] M Roche P Rondeau NR Singh E Tarnus E Bourdon The antioxidant proper-ties of serum albumin FEBS Lett 582 (2008) 1783ndash1787
[146] D Giustarini A Milzani I Dalle-Donne R Rossi Red blood cells as a physiolog-ical source of glutathione for extracellular fluids Blood Cells Mol Dis 40 (2008)174ndash179
[147] A Meister ME Anderson Glutathione Annu Rev Biochem 52 (1983) 711ndash760[148] B Alvarez S Carballal L Turell R Radi Formation and reactions of sulfenic acid
in human serum albumin Methods Enzymol 473 (2010) 117ndash136[149] S Carballal B Alvarez L Turell H Botti BA Freeman R Radi Sulfenic acid in
human serum albumin Amino Acids 32 (2007) 543ndash551[150] LR Barclay AM Bailey D Kong The antioxidant activity of alpha-tocopherol-
bovine serum albumin complex in micellar and liposome autoxidations J BiolChem 260 (1985) 15809ndash15814
[151] T Ishii T Ichikawa K Minoda K Kusaka S Ito Y Suzuki M Akagawa K Mochi-zuki T Goda T Nakayama Human serum albumin as an antioxidant in the ox-idation of (minus)-epigallocatechin gallate participation of reversible covalentbinding for interaction and stabilization Biosci Biotechnol Biochem 75(2011) 100ndash106
[152] F Galli S Rovidati S Benedetti U Buoncristiani C Covarelli A Floridi F Canes-trari Overexpression of erythrocyte glutathione S-transferase in uremia and di-alysis Clin Chem 45 (1999) 1781ndash1788
[153] D Borowitz RD Baker V Stallings Consensus report on nutrition for pediat-ric patients with cystic fibrosis J Pediatr Gastroenterol Nutr 35 (2002)246ndash259
[154] LJ Filer Jr SW Wright MP Manning KE Mason Absorption of alpha-tocopherol and tocopherylesters by premature and full term infants and chil-dren in health and disease Pediatrics 8 (1951) 328ndash339
[155] L Lancellotti C DOrazio G Mastella G Mazzi U Lippi Deficiency of vitamins Eand A in cystic fibrosis is independent of pancreatic function and current en-zyme and vitamin supplementation Eur J Pediatr 155 (1996) 281ndash285
[156] MN Sathe AS Patel Update in pediatrics focus on fat-soluble vitamins NutrClin Pract 25 (2010) 340ndash346
[157] MG Traber The ABCs of vitamin E and beta-carotene absorption Am J ClinNutr 80 (2004) 3ndash4
[158] TF Dolan Jr Hemolytic anemia and edema as the initial signs in infants withcystic fibrosis Consider this diagnosis even in absence of pulmonary symptomsClin Pediatr 15 (1976) 597ndash600
[159] DR James M Alfaham MC Goodchild Increased susceptibility to peroxide-induced haemolysis with normal vitamin E concentrations in cystic fibrosisClin Chim Acta 204 (1991) 279ndash290
[160] SA Peters FJ Kelly Vitamin E supplementation in cystic fibrosis J Pediatr Gas-troenterol Nutr 22 (1996) 341ndash345
[161] A Maqbool VA Stallings Update on fat-soluble vitamins in cystic fibrosis CurrOpin Pulm Med 14 (2008) 574ndash581
[162] SD Sagel MK Sontag MM Anthony P Emmett KA Papas Effect of anantioxidant-rich multivitamin supplement in cystic fibrosis J Cyst Fibros 10(2011) 31ndash36
[163] F Galli A Azzi Present trends in vitamin E research Biofactors 36 (2010)33ndash42
[164] A Hamahata P Enkhbaatar ER Kraft M Lange SW Leonard MG Traber RACox FC Schmalstieg HK Hawkins EB Whorton EM Horvath C Szabo LDTraber DN Herndon DL Traber Gamma-tocopherol nebulization by a lipidaerosolization device improves pulmonary function in sheep with burn andsmoke inhalation injury Free Radic Biol Med 45 (2008) 425ndash433
[165] JP Anais N Razzouq M Carvalho C Fernandez A Astier M Paul A AstierH Fessi AM Lorino Development of alpha-tocopherol acetate nanoparti-cles influence of preparative processes Drug Dev Ind Pharm 35 (2009)216ndash223
[166] JM Zingg Molecular and cellular activities of vitamin E analogues Mini RevMed Chem 7 (2007) 543ndash558
[167] V Viola F Pilolli M Piroddi E Pierpaoli F Orlando M Provinciali M Betti FMazzini F Galli Why tocotrienols work better insights into the in vitro anti-cancer mechanism of vitamin E Genes Nutr 7 (2011) 29ndash41
[168] F Galli F Mazzini L Bamonti L Gille S Bohmdorfer M Piroddi T Netscher FJKelly T Rosenau Tocotrienamines and tocopheramines reactions with radicalsand metal ions Bioorg Med Chem 19 (2011) 6483ndash6491
[169] A Kuhad K Chopra Attenuation of diabetic nephropathy by tocotrienol in-volvement of NFκB signaling pathway Life Sci 84 (2009) 296ndash301
[170] Q Jiang X Yin MA Lill ML Danielson H Freiser J Huang Long-chain carbox-ychromanols metabolites of vitamin E are potent inhibitors of cyclooxygenasesProc Natl Acad Sci U S A 105 (2008) 20464ndash20469
[171] ER Miller III R Pastor-Barriuso D Dalal RA Riemersma LJ Appel E GuallarMeta-analysis high-dosage vitamin E supplementation may increase all-causemortality Ann Intern Med 142 (2005) 37ndash46
[172] JN Hathcock A Azzi J Blumberg T Bray A Dickinson B Frei I Jialal CSJohnston FJ Kelly K Kraemer L Packer S Parthasarathy H Sies MG TraberVitamins E and C are safe across a broad range of intakes Am J Clin Nutr 81(2005) 736ndash745
[173] R Brigelius-Flohe F Galli Vitamin E a vitamin still awaiting the detection of itsbiological function Mol Nutr Food Res 54 (2010) 583ndash587
711F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
[174] MG Traber B Frei JS Beckman Vitamin E revisited do new data validate ben-efits for chronic disease prevention Curr Opin Lipidol 19 (2008) 30ndash38
[175] F Galli Meeting report Vitamin E Satellite Symposium (VESS) associated to theAnnual Meeting of the SFRR-Europe Rome 26 August 2009 Free Radic Res 43(2009) 1256ndash1257
[176] LJ Roberts II JA Oates MF Linton S Fazio BP Meador MD Gross Y Shyr JDMorrow The relationship between dose of vitamin E and suppression of oxida-tive stress in humans Free Radic Biol Med 43 (2007) 1388ndash1393
[177] EFSA- EFSA Scientific Opinion of the Panel on Food Additives FlavouringsProcessing Aids and Materials in Contact with Food on a request from the Com-mission on mixed tocopherols tocotrienol tocopherol and tocotrienols assources for vitamin E in EFSA- EFSA (Ed) vol 640 The EFSA Journal2008 pp 1ndash34
[178] P Rust I Eichler S Renner I Elmadfa Long-term oral beta-carotene supple-mentation in patients with cystic fibrosis mdash effects on antioxidative status andpulmonary function Ann Nutr Metab 44 (2000) 30ndash37
[179] G Lepage J Champagne N Ronco A Lamarre I Osberg RJ Sokol CC Roy Sup-plementation with carotenoids corrects increased lipid peroxidation in childrenwith cystic fibrosis Am J Clin Nutr 64 (1996) 87ndash93
[180] BM Winklhofer-Roob H Puhl G Khoschsorur MA vant Hof H EsterbauerDH Shmerling Enhanced resistance to oxidation of low density lipoproteinsand decreased lipid peroxide formation during beta-carotene supplementationin cystic fibrosis Free Radic Biol Med 18 (1995) 849ndash859
[181] RC Graham-Maar JI Schall N Stettler BS Zemel VA Stallings Elevated vita-min A intake and serum retinol in preadolescent children with cystic fibrosisAm J Clin Nutr 84 (2006) 174ndash182
[182] I Sadowska-Woda M Rachel J Pazdan E Bieszczad-Bedrejczuk K PawliszakNutritional supplement attenuates selected oxidative stress markers in pediatricpatients with cystic fibrosis Nutr Res (New York NY) 31 (2011) 509ndash518
[183] KA Papas MK Sontag C Pardee RJ Sokol SD Sagel FJ Accurso JS WagenerA pilot study on the safety and efficacy of a novel antioxidant rich formulation inpatients with cystic fibrosis J Cyst Fibros 7 (2008) 60ndash67
[184] Y Saito A Fukuhara K Nishio M Hayakawa Y Ogawa H Sakamoto K Fujii YYoshida E Niki Characterization of cellular uptake and distribution of coen-zyme Q10 and vitamin E in PC12 cells J Nutr Biochem 20 (2009) 350ndash357
[185] AA Franke CM Morrison JL Bakke LJ Custer X Li RV Cooney CoenzymeQ10 in human blood native levels and determinants of oxidation during proces-sing and storage Free Radic Biol Med 48 (2010) 1610ndash1617
[186] HN Bhagavan RK Chopra Plasma coenzyme Q10 response to oral ingestion ofcoenzyme Q10 formulations Mitochondrion 7 (2007) S78ndashS88 (Suppl)
[187] HN Bhagavan RK Chopra Coenzyme Q10 absorption tissue uptake metabo-lism and pharmacokinetics Free Radic Res 40 (2006) 445ndash453
[188] F Galli R Lee C Dunster FJ Kelly Gas chromatography mass spectrometryanalysis of carboxyethyl-hydroxychroman metabolites of alpha- and gamma-tocopherol in human plasma Free Radic Biol Med 32 (2002) 333ndash340
[189] F Galli R Lee J Atkinson A Floridi FJ Kelly Gamma-tocopherol biokineticsand transformation in humans Free Radic Res 37 (2003) 1225ndash1233
[190] TA Laguna MK Sontag I Osberg JS Wagener FJ Accurso RJ Sokol De-creased total serum coenzyme-Q10 concentrations a longitudinal study in chil-dren with cystic fibrosis J Pediatr 153 (2008) 402ndash407
[191] T Frischer JK Myung G Maurer I Eichler Z Szepfalusi G Lubec Possible dys-regulation of chaperon and metabolic proteins in cystic fibrosis bronchial tissueProteomics 6 (2006) 3381ndash3388
[192] C Andersson MM Zaman AB Jones SD Freedman Alterations in immune re-sponse and PPARLXR regulation in cystic fibrosis macrophages J Cyst Fibros 7(2008) 68ndash78
[193] SD Freedman PG Blanco MM Zaman JC Shea M Ollero IK Hopper DAWeed A Gelrud MM Regan M Laposata JG Alvarez BP OSullivan Associa-tion of cystic fibrosis with abnormalities in fatty acid metabolism N Engl JMed 350 (2004) 560ndash569
[194] S Van Biervliet G Vanbillemont JP Van Biervliet D Declercq E Robberecht AChristophe Relation between fatty acid composition and clinical status or geno-type in cystic fibrosis patients Ann Nutr Metab 51 (2007) 541ndash549
[195] SD Freedman MH Katz EM Parker M Laposata MY Urman JG AlvarezA membrane lipid imbalance plays a role in the phenotypic expression ofcystic fibrosis in cftr(minusminus) mice Proc Natl Acad Sci U S A 96 (1999)13995ndash14000
[196] S Van Biervliet S Vande Velde JP Van Biervliet E Robberecht The effect ofzinc supplements in cystic fibrosis patients Ann Nutr Metab 52 (2008)152ndash156
[197] WR Henderson Jr SJ Astley MM McCready P Kushmerick S Casey JWBecker BW Ramsey Oral absorption of omega-3 fatty acids in patients withcystic fibrosis who have pancreatic insufficiency and in healthy control subjectsJ Pediatr 124 (1994) 400ndash408
[198] I Durieu E Vericel D Guichardant H Roth JP Steghens J Drai RN JosserandE Fontaine M Lagarde G Bellon Fatty acids platelets and oxidative markersfollowing intravenous n-3 fatty acids administration in cystic fibrosis an openpilot observational study J Cyst Fibros 6 (2007) 320ndash326
[199] LG Wood DA Fitzgerald ML Garg Hypothesis vitamin E complements poly-unsaturated fatty acids in essential fatty acid deficiency in cystic fibrosis J AmColl Nutr 22 (2003) 253ndash257
[200] JD Lloyd-Still SB Johnson RT Holman Essential fatty acid status in cystic fi-brosis and the effects of safflower oil supplementation Am J Clin Nutr 34(1981) 1ndash7
[201] A Maqbool JI Schall JF Garcia-Espana BS Zemel B Strandvik VAStallings Serum linoleic acid status as a clinical indicator of essential fatty
acid status in children with cystic fibrosis J Pediatr Gastroenterol Nutr 47(2008) 635ndash644
[202] C Oliver N Jahnke Omega-3 fatty acids for cystic fibrosis Cochrane DatabaseSyst Rev (2011) CD002201
[203] B Strandvik E Gronowitz F Enlund T Martinsson J Wahlstrom Essential fattyacid deficiency in relation to genotype in patients with cystic fibrosis J Pediatr139 (2001) 650ndash655
[204] P Rise S Volpi C Colombo RF Padoan C DOrazio S Ghezzi PMelotti V BennatoC Agostoni BM Assael C Galli Whole blood fatty acid analysis with micromethodin cystic fibrosis and pulmonary disease J Cyst Fibros 9 (2010) 228ndash233
[205] H Cao K Gerhold JR Mayers MM Wiest SM Watkins GS Hotamisligil Iden-tification of a lipokine a lipid hormone linking adipose tissue to systemic me-tabolism Cell 134 (2008) 933ndash944
[206] RR Malapaka SK Khoo J Zhang JH Choi XE Zhou Y Xu Y Gong J Li ELYong MJ Chalmers L Chang JH Resau PR Griffin YE Chen HE Xu Iden-tification and mechanism of a ten carbon fatty acid as a modulating ligand ofperoxisome proliferator activated receptors J Biol Chem 287 (2012)183ndash195
[207] T Hara A Hirasawa A Ichimura I Kimura G Tsujimoto Free fatty acid recep-tors FFAR1 and GPR120 as novel therapeutic targets for metabolic disorders JPharm Sci 100 (2011) 3594ndash3601
[208] R Gupta P Rathi S Bradoo Lipase mediated upgradation of dietary fats andoils Crit Rev Food Sci Nutr 43 (2003) 635ndash644
[209] BH Jennings CC Akoh Lipase-catalyzed modification of rice bran oil to incor-porate capric acid J Agric Food Chem 48 (2000) 4439ndash4443
[210] J Hoeks M Mensink MK Hesselink K Ekroos P Schrauwen Long- andMedium-Chain Fatty Acids Induce Insulin Resistance to a Similar Extent inHumans Despite Marked Differences in Muscle Fat Accumulation J Clin Endo-crinol Metab 97 (2012) 208ndash216
[211] PJ Congden G Bruce MM Rothburn PC Clarke JM Littlewood J KelleherMS Losowsky Vitamin status in treated patients with cystic fibrosis ArchDis Child 56 (1981) 708ndash714
[212] BM Winklhofer-Roob H Ellemunter M Fruhwirth SE Schlegel-Haueter GKhoschsorur MA vant Hof DH Shmerling Plasma vitamin C concentrationsin patients with cystic fibrosis evidence of associations with lung inflammationAm J Clin Nutr 65 (1997) 1858ndash1866
[213] L Shamseer D Adams N Brown JA Johnson S Vohra Antioxidant micronutri-ents for lung disease in cystic fibrosis Cochrane Database Syst Rev (2010)CD007020
[214] C Santi S Santoro Electrophilic Selenium First edition Wiley-VCH VerlagGmbH amp Co KGaA 2012
[215] L Flohe S Toppo G Cozza F Ursini A comparison of thiol peroxidase mecha-nisms Antioxid Redox Signal 15 (2010) 763ndash780
[216] L Flohe JR Andreesen R Brigelius-Flohe M Maiorino F Ursini Selenium theelement of the moon in life on earth IUBMB Life 49 (2000) 411ndash420
[217] V Valdiglesias E Pasaro J Mendez B Laffon In vitro evaluation of seleniumgenotoxic cytotoxic and protective effects a review Arch Toxicol 84(2010) 337ndash351
[218] P Foucaud P Therond M Marchand F Brion JF Demelier J Navarro Seleniumand vitamin E in mucoviscidosis Arch Fr Pediatr 45 (1988) 383ndash386
[219] J Neve R Van Geffel M Hanocq L Molle Plasma and erythrocyte zinc copperand selenium in cystic fibrosis Acta Paediatr Scand 72 (1983) 437ndash440
[220] BM Winklhofer-Roob B Tiran PE Tuchschmid MA vant Hof DH ShmerlingEffects of pancreatic enzyme preparations on erythrocyte glutathione peroxi-dase activities and plasma selenium concentrations in cystic fibrosis FreeRadic Biol Med 25 (1998) 242ndash249
[221] JD Lloyd-Still HE Ganther Selenium and glutathione peroxidase levels in cys-tic fibrosis Pediatrics 65 (1980) 1010ndash1012
[222] D Tsavachidou TJ McDonnell S Wen X Wang F Vakar-Lopez LL Pisters CAPettaway CG Wood KA Do PF Thall C Stephens E Efstathiou R Taylor DGMenter P Troncoso SM Lippman CJ Logothetis J Kim Selenium and vitaminE cell type- and intervention-specific tissue effects in prostate cancer J NatlCancer Inst 101 (2009) 306ndash320
[223] IN Zelko TJ Mariani RJ Folz Superoxide dismutase multigene family acomparison of the CuZn-SOD (SOD1) Mn-SOD (SOD2) and EC-SOD (SOD3)gene structures evolution and expression Free Radic Biol Med 33 (2002)337ndash349
[224] RP Bowler JD Crapo Oxidative stress in airways is there a role for extracellu-lar superoxide dismutase Am J Respir Crit Care Med 166 (2002) S38ndashS43
[225] K Best K McCoy S Gemma RA Disilvestro Copper enzyme activities in cysticfibrosis before and after copper supplementation plus or minus zinc Metabo-lism 53 (2004) 37ndash41
[226] SS Percival GP Kauwell E Bowser M Wagner Altered copper status in adultmen with cystic fibrosis J Am Coll Nutr 18 (1999) 614ndash619
[227] NF Krebs JE Westcott TD Arnold BM Kluger FJ Accurso LV Miller KMHambidge Abnormalities in zinc homeostasis in young infants with cystic fibro-sis Pediatr Res 48 (2000) 256ndash261
[228] D Easley N Krebs M Jefferson L Miller J Erskine F Accurso KM HambidgeEffect of pancreatic enzymes on zinc absorption in cystic fibrosis J Pediatr Gas-troenterol Nutr 26 (1998) 136ndash139
[229] S Van Biervliet JP Van Biervliet E Robberecht Serum zinc in patients with cys-tic fibrosis at diagnosis and after one year of therapy Biol Trace Elem Res 112(2006) 205ndash211
[230] S Van Biervliet JP Van Biervliet S Vande Velde E Robberecht Serum zinc con-centrations in cystic fibrosis patients aged above 4 years a cross-sectional eval-uation Biol Trace Elem Res 119 (2007) 19ndash26
712 F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
[231] F Galli M Cristina Polidori W Stahl P Mecocci FJ Kelly Vitamin E biotransfor-mation in humans Vitam Horm 76 (2007) 263ndash280
[232] J Wiser NE Alexis Q Jiang W Wu C Robinette R Roubey DB Peden In vivogamma-tocopherol supplementation decreases systemic oxidative stress andcytokine responses of human monocytes in normal and asthmatic subjectsFree Radic Biol Med 45 (2008) 40ndash49
[233] JG Wagner Q Jiang JR Harkema B Illek DD Patel BN Ames DB PedenOzone enhancement of lower airway allergic inflammation is prevented bygamma-tocopherol Free Radic Biol Med 43 (2007) 1176ndash1188
[234] JT Harries DP Muller Absorption of different doses of fat soluble and watermiscible preparations of vitamin E in children with cystic fibrosis Arch DisChild 46 (1971) 341ndash344
[235] EI Back C Frindt E Ocenaskova D Nohr M Stern HK Biesalski Can changesin hydrophobicity increase the bioavailability of alpha-tocopherol Eur J Nutr45 (2006) 1ndash6
[236] SZ Nasr MH OLeary C Hillermeier Correction of vitamin E deficiency withfat-soluble versus water-miscible preparations of vitamin E in patients with cys-tic fibrosis J Pediatr 122 (1993) 810ndash812
[237] S Soltani-Frisk E Gronowitz H Andersson B Strandvik Water-miscibletocopherol is not superior to fat-soluble preparation for vitamin E absorptionin cystic fibrosis Acta Paediatr 90 (2001) 1112ndash1115
[238] K Papas J Kalbfleisch R Mohon Bioavailability of a novel water-soluble vi-tamin E formulation in malabsorbing patients Dig Dis Sci 52 (2007)347ndash352
[239] F Antonicelli M Parmentier EM Drost N Hirani I Rahman K Donaldson WMacNee Nacystelyn inhibits oxidant-mediated interleukin-8 expression andNF-kappaB nuclear binding in alveolar epithelial cells Free Radic Biol Med 32(2002) 492ndash502
[240] EM App D Baran I Dab A Malfroot M Coffiner F Vanderbist M King Dose-finding and 24-h monitoring for efficacy and safety of aerosolized Nacystelyn incystic fibrosis Eur Respir J 19 (2002) 294ndash302
[241] MG Traber How much vitamin E hellip Just enough Am J Clin Nutr 84 (2006)959ndash960
[242] JC McCann BN Ames Vitamin K an example of triage theory is micronu-trient inadequacy linked to diseases of aging Am J Clin Nutr 90 (2009)889ndash907
[243] M Fusaro G Crepaldi S Maggi F Galli A DAngelo L Calo S Giannini DMiozzo M Gallieni Vitamin K bone fractures and vascular calcifications inchronic kidney disease an important but poorly studied relationship J Endocri-nol Invest 34 (2010) 317ndash323
[244] JC McCann BN Ames Adaptive dysfunction of selenoproteins from the per-spective of the triage theory why modest selenium deficiency may increaserisk of diseases of aging FASEB J 25 (2011) 1793ndash1814
[245] R Apak K Guclu M Ozyurek B Bektas Oglu M Bener Cupric ion reducing an-tioxidant capacity assay for food antioxidants vitamins polyphenolics and fla-vonoids in food extracts Methods Mol Biol 477 (2008) 163ndash193
[246] F Galli Interactions of polyphenolic compounds with drug disposition and me-tabolism Curr Drug Metab 8 (2007) 830ndash838
[247] RL Prior X Wu K Schaich Standardized methods for the determination of an-tioxidant capacity and phenolics in foods and dietary supplements J Agric FoodChem 53 (2005) 4290ndash4302
[248] C Azbell S Zhang D Skinner J Fortenberry EJ Sorscher BA WoodworthHesperidin stimulates cystic fibrosis transmembrane conductance regulator-mediated chloride secretion and ciliary beat frequency in sinonasal epitheliumOtolaryngol Head Neck Surg 143 (2010) 397ndash404
[249] G Wegrzyn J Jakobkiewicz-Banecka M Gabig-Ciminska E Piotrowska M Nar-ajczyk A Kloska M Malinowska D Dziedzic I Golebiewska M Moskot AWegrzyn Genistein a natural isoflavone with a potential for treatment of ge-netic diseases Biochem Soc Trans 38 (2010) 695ndash701
[250] YC Yu H Miki Y Nakamura A Hanyuda Y Matsuzaki Y Abe M Yasui K Ta-naka TC Hwang SG Bompadre Y Sohma Curcumin and genistein additivelypotentiate G551D-CFTR J Cyst Fibros 10 (2011) 243ndash252
[251] B Illek H Fischer Flavonoids stimulate Cl conductance of human airway epithe-lium in vitro and in vivo Am J Physiol 275 (1998) L902ndashL910
[252] JL Kreindler Cystic fibrosis exploiting its genetic basis in the hunt for newtherapies Pharmacol Ther 125 (2010) 219ndash229
[253] B Illek L Zhang NC Lewis RB Moss JY Dong H Fischer Defective function ofthe cystic fibrosis-causing missense mutation G551D is recovered by genisteinAm J Physiol 277 (1999) C833ndashC839
[254] P Anandakumar S Kamaraj S Jagan G Ramakrishnan R Vinodhkumar TDevaki Capsaicin modulates pulmonary antioxidant defense system during ben-zo(a)pyrene-induced lung cancer in Swiss albinomice Phytother Res 22 (2008)529ndash533
[255] I Rahman Antioxidant therapeutic advances in COPD Ther Adv Respir Dis 2(2008) 351ndash374
[256] AW Boots H Li RP Schins R Duffin JW Heemskerk A Bast GR Haenen Thequercetin paradox Toxicol Appl Pharmacol 222 (2007) 89ndash96
[257] M Joskova S Franova V Sadlonova Acute bronchodilator effect of quercetin inexperimental allergic asthma Bratisl Lek Listy 112 (2011) 9ndash12
[258] HJ Park CM Lee ID Jung JS Lee YI Jeong JH Chang SH Chun MJ Kim IWChoi SC Ahn YK Shin SR Yeom YM Park Quercetin regulates Th1Th2 balancein a murine model of asthma Int Immunopharmacol 9 (2009) 261ndash267
[259] AP Rogerio A Kanashiro C Fontanari EV da Silva YM Lucisano-ValimEG Soares LH Faccioli Anti-inflammatory activity of quercetin and iso-quercitrin in experimental murine allergic asthma Inflamm Res 56 (2007)402ndash408
[260] M Muller Polyphenol cytotoxicity induced by the bacterial toxin pyocyaninrole of NQO1 Free Radic Biol Med 47 (2009) 84ndash91
[261] J Grassmann Terpenoids as plant antioxidants Vitam Horm 72 (2005)505ndash535
[262] P Allen Tea tree oil the science behind the antimicrobial hype Lancet 358(2001) 1245
[263] EC Dasenbrook W Checkley CA Merlo MW Konstan N Lechtzin MP BoyleAssociation between respiratory tract methicillin-resistant Staphylococcus aure-us and survival in cystic fibrosis JAMA 303 (2010) 2386ndash2392
[264] V Bezzerri M Borgatti E Nicolis I Lampronti MC Dechecchi I Mancini PRizzotti R Gambari G Cabrini Transcription factor oligodeoxynucleotides toNF-kappaB inhibit transcription of IL-8 in bronchial cells Am J Respir CellMol Biol 39 (2008) 86ndash96
[265] R Gambari M Borgatti V Bezzerri E Nicolis I Lampronti MC Dechecchi IMancini A Tamanini G Cabrini Decoy oligodeoxyribonucleotides and peptidenucleic acids-DNA chimeras targeting nuclear factor kappa-B inhibition of IL-8 gene expression in cystic fibrosis cells infected with Pseudomonas aeruginosaBiochem Pharmacol 80 (2010) 1887ndash1894
[266] M Adrian P Jeandet AC Douillet-Breuil L Tesson R Bessis Stilbene content ofmature Vitis vinifera berries in response to UV-C elicitation J Agric Food Chem48 (2000) 6103ndash6105
[267] B Paul I Masih J Deopujari C Charpentier Occurrence of resveratrol and pter-ostilbene in age-old darakchasava an ayurvedic medicine from India J Ethno-pharmacol 68 (1999) 71ndash76
[268] I Rahman Antioxidant therapies in COPD Int J Chron Obstruct Pulmon Dis 1(2006) 15ndash29
[269] M Lee S Kim OK Kwon SR Oh HK Lee K Ahn Anti-inflammatory and anti-asthmatic effects of resveratrol a polyphenolic stilbene in a mouse model ofallergic asthma Int Immunopharmacol 9 (2009) 418ndash424
[270] LG Wood PA Wark ML Garg Antioxidant and anti-inflammatory effectsof resveratrol in airway disease Antioxid Redox Signal 13 (2010)1535ndash1548
[271] KV Kiselev Perspectives for production and application of resveratrol ApplMicrobiol Biotechnol 90 (2011) 417ndash425
[272] M Shakibaei C Buhrmann A Mobasheri Resveratrol-mediated SIRT-1 interac-tions with p300 modulate receptor activator of NF-kappaB ligand (RANKL) acti-vation of NF-kappaB signaling and inhibit osteoclastogenesis in bone-derivedcells J Biol Chem 286 (2011) 11492ndash11505
[273] SF Zaidi K Ahmed T Yamamoto T Kondo K Usmanghani M Kadowaki TSugiyama Effect of resveratrol on Helicobacter pylori-induced interleukin-8 secre-tion reactive oxygen species generation and morphological changes in human gas-tric epithelial cells Biol Pharm Bull 32 (2009) 1931ndash1935
[274] JK Kundu YK Shin YJ Surh Resveratrol modulates phorbol ester-inducedpro-inflammatory signal transduction pathways in mouse skin in vivo NF-kappaB and AP-1 as prime targets Biochem Pharmacol 72 (2006)1506ndash1515
[275] NH Nam Naturally occurring NF-kappaB inhibitors Mini Rev Med Chem 6(2006) 945ndash951
[276] JM Smoliga JA Baur HA Hausenblas Resveratrol and healthmdasha comprehen-sive review of human clinical trials Mol Nutr Food Res 55 (2011) 1129ndash1141
[277] ME Juan M Maijo JM Planas Quantification of trans-resveratrol and itsmetabolites in rat plasma and tissues by HPLC J Pharm Biomed Anal 51(2010) 391ndash398
[278] JA Baur DA Sinclair Therapeutic potential of resveratrol the in vivo evidenceNat Rev 5 (2006) 493ndash506
[279] E Nicolis I Lampronti MC Dechecchi M Borgatti A Tamanini N Bianchi VBezzerri I Mancini MG Giri P Rizzotti R Gambari G Cabrini Pyrogallol anactive compound from the medicinal plant Emblica officinalis regulates expres-sion of pro-inflammatory genes in bronchial epithelial cells Int Immunophar-macol 8 (2008) 1672ndash1680
[280] E Nicolis I Lampronti MC Dechecchi M Borgatti A Tamanini V Bezzerri NBianchi M Mazzon I Mancini MG Giri P Rizzotti R Gambari G CabriniModulation of expression of IL-8 gene in bronchial epithelial cells by 5-methoxypsoralen Int Immunopharmacol 9 (2009) 1411ndash1422
[281] M Borgatti I Mancini N Bianchi A Guerrini I Lampronti D Rossi G SacchettiR Gambari Bergamot (Citrus bergamia Risso) fruit extracts and identified com-ponents alter expression of interleukin 8 gene in cystic fibrosis bronchial epithe-lial cell lines BMC Biochem 12 (2011) 15
[282] L Piccagli E Fabbri M Borgatti N Bianchi V Bezzerri I Mancini E Nicolis CMDechecchi I Lampronti G Cabrini R Gambari Virtual screening against p50NF-kappaB transcription factor for the identification of inhibitors of the NF-kappaB-DNA interaction and expression of NF-kappaB upregulated genesChemMedChem 4 (2009) 2024ndash2033
[283] L Piccagli M Borgatti E Nicolis N Bianchi I Mancini I Lampronti D VevaldiF DallAcqua G Cabrini R Gambari Virtual screening against nuclear factorkappaB (NF-kappaB) of a focus library identification of bioactive furocoumarinderivatives inhibiting NF-kappaB dependent biological functions involved incystic fibrosis Bioorg Med Chem 18 (2010) 8341ndash8349
[284] M Borgatti A Chilin L Piccagli I Lampronti N Bianchi I Mancini G Mar-zaro Da Francesco A Guiotto R Gambari Development of a novel furocou-marin derivative inhibiting NF-kappaB dependent biological functionsdesign synthesis and biological effects Eur J Med Chem 46 (2011)4870ndash4877
[285] E Georgy S Le Guellec L Vecellio E Fichant P Stordeur P Bordeau JP PerraudinFeasibility study of OSCN- and lactoferrin (Meveol) nebulization for cysticfibrosis JCyst Fibros 10 (2011) S18
713F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
[286] C Tidei M Piroddi F Galli C Santi Oxidation of thiols promoted by PhSeZnClTetrahedron Lett 53 (2012) 232ndash234
[287] L Semianrio-Vidal C van Hesuden G Mugesh ER Lazarowski Ebselen is a po-tent non-competitive inhibitor of extracellular nucleoside diphosphokinasePurinergic Signal 6 (2010) 383ndash391
[288] C ColussiMC Albertini S Coppola S Rovidati F Galli L Ghibelli H2O2-inducedblockof glycolysis as an active ADP-ribosylation reaction protecting cells from apoptosisFASEB J 14 (2000) 2266ndash2276
[289] H Xiao KL Parkin Induction of phase II enzyme activity by various seleniumcompounds Nutr Cancer 55 (2006) 210ndash223
[290] G Peluffo R Radi Biochemistry of protein tyrosine nitration in cardiovascularpathology Cardiovasc Res 75 (2007) 291ndash302
[291] B Alvarez R Radi Peroxynitrite reactivity with amino acids and proteinsAmino Acids 25 (2003) 295ndash311
[292] B Kamosinska MW Radomski M Duszyk A Radomski SF Man Nitric oxideactivates chloride currents in human lung epithelial cells Am J Physiol 272(1997) L1098ndashL1104
[293] L Chen RP Patel X Teng CA Bosworth JR Lancaster Jr S Matalon Mecha-nisms of cystic fibrosis transmembrane conductance regulator activation by S-nitrosoglutathione J Biol Chem 281 (2006) 9190ndash9199
[294] F Luchetti B CanonicoM BettiM Arcangeletti F PilolliM Piroddi L Canesi S PapaF Galli Melatonin signaling and cell protection function FASEB J 24 (2010)3603ndash3624
[295] MW Bengtsson G Jedstedt G Flemstrom Duodenal bicarbonate secretion inrats stimulation by intra-arterial and luminal guanylin and uroguanylin ActaPhysiol (Oxf) 191 (2007) 309ndash317
[296] CS Nelson JL Marino CN Allen Melatonin receptor potentiation of cyclic AMP andthe cystic fibrosis transmembrane conductance regulator ion channel J Pineal Res 26(1999) 113ndash121
[297] C de Castro-Silva VM de Bruin GM Cunha DM Nunes CAMedeiros PF de BruinMelatonin improves sleep and reduces nitrite in the exhaled breath condensate incystic fibrosismdasha randomized double-blind placebo-controlled study J Pineal Res48 (2010) 65ndash71
[298] I Hornyak E Pankotai L Kiss Z Lacza Current developments in the the-rapeutic potential of S-nitrosoglutathione an endogenous NO-donor mole-cule Curr Pharm Biotechnol (2011) Jan 11 [Epub ahead of print] - PMID21235457
[299] AH Snyder ME McPherson JF Hunt M Johnson JS Stamler B Gaston Acuteeffects of aerosolized S-nitrosoglutathione in cystic fibrosis Am J Respir CritCare Med 165 (2002) 922ndash926

703F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
isoforms of the superoxide dismutase enzymes eg the extracellularform eg the EC-SOD or Sod 3 and the CundashZn-SOD or Sod 1 that isfound in several tissues and cells [223] The EC-SOD exerts its antiox-idant role also in the lining fluids of the airways [224]
The notion that CF patients have defective concentrations of bloodZn and Cu is controversial As far as Cu status is concerned few datahave been produced and are available in the literature suggestingthe notion that CF patients develop a moderate copper deficiency[225226] That was essentially demonstrated on the bases of a defec-tive activity of Cu-related proteins such as plasma ceruloplasmindiamine oxidase and RBC SOD This defect seems to be refractory toCu and Zn supplementation (see below)
More advanced studies have been carried out in the case of Zn sta-tus in CF Low plasma zinc concentrations were reported in approxi-mately 30 of young infants with CF identified by newbornscreening [227] and an impaired zinc homeostasis in CF patientswas described by Easley et al [228] This is characterized by poor con-servation of the endogenous pool with fecal loss and impaired frac-tional absorption of zinc which are the consequences of pancreaticinsufficiency and persisting steatorrhea These studies suggestedthat in the clinical management of CF patients these defects can beat least in part corrected by exocrine pancreatic enzyme replacement
A series of studies by Van Biervliet et al [229230] demonstratedin a Dutch population of CF infants and children that serum Zn variesin an age-dependent manner but remained unchanged with respectto healthy control levels In CF patients no difference in serum Zn con-centration between pancreatic-sufficient or pancreatic-insufficientpatients was observed and no correlation was found with the nutri-tional status or height z-score Importantly in these studies a signifi-cant correlation of serum Zn was observed with the fat solublevitamins A and E thus confirming the relationship between the ab-normalities of lipid and Zn metabolism in CF This suggests that co-supplementation of Zn and fat-soluble vitamins should be advisedin the presence of pancreatic insufficiency and persisting steatorrhea
Neve et al [219] in a study aimed to assess plasma and erythrocytezinc copper and selenium in CF children showed that mean plasmazinc and copper levels were not different from those in age-matched controls which confirms the observations by Van Biervlietet al described above However plasma zinc concentrations de-creased in patients with moderate-to-severe growth retardation andwith severe pulmonary disease but very low zinc levels occur sporad-ically Erythrocyte zinc and copper levels were significantly higherthan normal while RBC selenium was lower than in age-matchedcontrols These trace element concentrations in erythrocytes werediscussed in relation to the activities of the CuZn-SOD and the Se-enzyme GPx This observation suggests a compensatory upregulationof the erythrocyte CuZn-SOD by the exposure of erythroid precursorsto ROS andor other CF-related stressors
Best et al [225] also studied RBC SOD activity using this as a bio-logical sensor of Cu status in CF patients A lowered activity of thisenzyme was reported in CF together with that of the other Cu-dependent enzyme plasma diamine oxidase while plasma ceruplas-min showed normal activity Degradation rates of copper proteinsare known to be accelerated in conditions of copper deficiencywhich could explain the finding at least in part Anyway when Cuand Zn were supplemented to CF patients either separate or incombination (6 weeks of 3 mg copperd as copper-glycinate and30 mg zincd as zinc-glycinate) any of the copper enzyme activitieswas affected Therefore the moderate copper deficiency of CF patientsappears to be refractory to the intervention by increased copper andor zinc intake
Erythrocyte CuZn-SOD and the plasma levels of Cu and Zn werealso measured in the study of Wood et al [6] in which Australian CFpatients (agegt5 years) were treated with a high-dose antioxidantmultivitamin formulation containing 200 mg vitamin E (as RRR-α-tocopherol) 300 mg vitamin C (as sodium ascorbate) 25 mg β-
carotene (all-trans isomer) 90 μg Se (as selenomethionine) and500 μg vitamin A (as retinyl palmitate) in oil Plasma oligoelementsand particularly Zn were in the normal range at baseline (as com-pared with the data reported in [229230]) and were not affected bythis multivitamin supplement The same was found for the activityof RBC SOD and for plasma 8-iso-PGF2α as surrogate biomarker oflipid peroxidation
In a recent non-randomized small population (n=21) casendashcon-trol study in CF children Zn supplementation was proven to producepositive clinical effects in Zn-deficient patients [196] The supplemen-tation with 5 mgkg Zn sulfateday (maximum 150 mg) significantlydecreased the number of infections and increased the forced expira-tory volume in 1 s energy intake and growth parameters also im-proved These parameters were unaffected in untreated patientsexcept that in the case of the pulmonary function that decreased sig-nificantly These clinical observations on Zn supplementation need tobe confirmed in prospective double-blind randomized control trial
37 Appropriateness and targeting of antioxidant therapies in CF
The choice of the appropriate antioxidant and dose to correct a cer-tain biomarker and its associated biochemical lesion is another impor-tant point that appears to have disregarded in many clinical studiesFor instance unlike vitamin E vitamin C supplementation does notalter F2-IsoPs levels in humans (reviewed in [74]) This appears tobe true also in the antioxidant therapy of CF in which vitamin C(300 mgday) was administered together with other antioxidantsthat included a dose of vitamin E of 200 mgday without any signifi-cant effect on the surrogate biomarker of lipid peroxidation F2-IsoPs[6] When carotenoids are used as supplements to prevent the damag-ing action of ROS in the CF airways it is noteworthy that these are notparticularly good quenchers of peroxyl radicals relative to phenolicsand other antioxidants but are exceptional in quenching singlet oxy-gen at which most other phenolics and antioxidants are relativelyineffective Singlet oxygen is not a radical and does not react via radi-cal mechanisms but reacts mostly by the addition to double bondsforming endoperoxides that can be reduced to alkoxyl radicals that ini-tiate radical chain reactions typical of the peroxidative damage of PUFA[38] In this case the analysis of F2-IsoPs lipid peroxide formation andtransition metal-induced oxidizability of lipoproteins [162180] are allappropriate to evaluate the effect of carotenoids in preventing lipidperoxidation
As far as the dose is concerned clinical pharmacology of vitamin Eas an antioxidant was recently investigated by means of the effect onF2-IsoPs production and doses of α-tocopherol of 1600 IUday orgreater were found to be required to statistically affect plasma F2-IsoPs levels in hypercholeterolemic subjects [176] Several vitamin Esupplementation studies in CF patients have been performed withdoses of lower than 300 IUday regardless of the lowered absorptionby pancreatic and liver defects and the regular supplementationwith these doses does not appear to correct lipid oxidation markersin CF [7]
In the clinical practice and planning trials it has to be taken intoconsideration that in spite of substantial evidence supporting ahigher antioxidant demand in CF interventions with several antioxi-dant formulations produce poor responsiveness particularly in thecase of fat-soluble antioxidants which are poorly absorbed [6162]
Since many oxidants and antioxidants are present in tissuesand biological fluids and these have different chemical and physicalcharacteristics the possibility to produce a successful therapy witha single antioxidant molecule is too far to be realistic Moreover an-tioxidants act by multiple mechanisms in a single system or by adifferent single mechanism depending on the reaction systemresponding in a different manner to different radical or oxidantsources Because multiple reaction characteristics and mechanismsas well as different phase localizations are usually involved no single
704 F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
therapeutic approach will effectively prevent damage by multipleROS sources The defect of physiological antioxidants may also interferewith antioxidant therapies that are based on one or few exogenousantioxidants
Moreover several antioxidant vitamins such as vitamin E and ca-rotenoids have multiple natural forms with different bioavailabilitymetabolism and bioactivity [157167231] As far as the case of vita-min E supplementation concerns α-tocopherol was used as uniquevitamer in the large majority of supplementation trials so far per-formed and is the form used in the nutritional management of CFpatients Moreover several supplements contain the synthetic (or ra-cemic) form of this vitamin that has lower bioavailability than thenatural form Other forms present in nature and abundantly con-tained in vegetables such as tocotrienols and the less methylatedforms of tocopherol are not represented in many of the supplementformulations so far available in clinical centers and the supplementa-tion with α-tocopherol also limits their bioavailability These formsshow markedly higher susceptibility to hepatic metabolism and bili-ary excretion with respect to α-tocopherol eg the most representedform in blood and solid tissues and if co-supplemented these areeasily displaced during liver uptake and excreted with bile bymeans of competition with the same α-tocopherol Notwithstandingthese minor forms have been proposed to play important physiolog-ical roles showing molecular characteristics transcriptional effectsand antioxidant activities that clearly differentiate them in subfam-ilies with distinct biological functions Some of these such as α-tocopherol eg the second vitamin E form as relative abundance inblood and its carboxyethyl-hydroxychroman metabolite [189] ap-pear to have health-related anti-inflammatory effects which are par-ticularly relevant in lung protection [232233] This has suggestedthat such a group of ldquonon-α-tocopherolrdquo forms may represent anoth-er family of vitamins within the family of vitamin E with an impor-tant but often missed contribution to the proposed health effects ofthis vitamin [163]
These aspects may thus limit the possibility to provide CF patientsof optimal levels of this vitamin in all its components even if they areregularly treated with a vitamin E supplement eg withα-tocopherol
Targeted antioxidant therapy with formulations with higher bio-availability and bioactivity has been anticipated in CF New antioxi-dant formulations have been proposed to overcome main limits ofantioxidant therapies so far proposed for these patients Water-miscible α-tocopheryl acetate containing polysorbate propylene gly-col or polyethylene glycol as emulsifiers form micellar structureswere suggested to providing greater bioavailability than the fat-soluble counterparts These were commercialized with the brandnames of E-viminreg Cremophorreg EL and Aquasolreg E but despitethe original positive expectation [234235] some studies failed to ob-serve a higher response in vitamin E levels when these were com-pared with fat-soluble formulations [236237]
In a pilot study by Papas et al [183] a micellar formulation of fat-soluble nutrients and antioxidants was found to improve plasmalevels of β-carotene γ-tocopherol and CoQ(10) reducing at thesame time some inflammatory markers in induced sputum eg mye-loperoxidase and to a lower extent PMN elastase and total cell countswhile lung function and sputum bacterial counts were unaffectedThe same group recently confirmed the possibility to increase the ab-sorption of fat-soluble micronutrients using formulations with higherbioavailability specifically designed for malabsorbing patients such asCF patients that include also vitamin K and commercialized with thebrand name of AquADEKsreg [162] Despite improved vitamin and mi-cronutrient levels in this non-randomized open-label study AquA-DEKsreg produced only modest improvements in weight percentileand pulmonary function Another recent pilot observation [182] hassuggested the beneficial effect of this formulation on antioxidant andoxidative stress parameters of this oral supplement that surely deservesmore clinical investigation by larger randomized controlled trials
Recent multivitaminic formulations have been designed to containalso the minor forms of vitamin E and specifically γ-tocopherol [238]the expected superiority of which with respect to formulations con-taining only α-tocopherol needs to be verified As discussed abovein the section dedicated to vitamin E further advancements in thetherapy of CF inflammation and oxidative stress could be based onsynthetic forms and natural metabolites of this vitamin that havebeen recently identified to possess higher antioxidant and also anti-inflammatory activity than α-tocopherol (reviewed in [163168])
Pre-clinical investigation of these and other fat-soluble agents iscurrently addressed to develop formulations and administration pro-tocols that may increase the therapeutic efficacy in the airways In theantioxidant therapy of lung dysfunction in CF local administrationprotocols may overcome the limits of oral and systemic administra-tion protocols increasing bioavailability and providing targetedapproach to inflammation and oxidative stress Aerosolization of vita-min E and other fat-soluble micronutrients is possible and may allowdirect administration in the airways to prevent toxicity of smokewhich is closely associated with inflammation and oxidative stress[164165] To our knowledge this as well as other strategies of localadministration such as instillation of solutions such as surfactant-like solutions enriched of vitamin E have not been previously inves-tigated in CF patients and other CF model systems
On the contrary inhalation is an administration route widelyadopted in the case of GSH and NAC therapy described above Inthis context Cys formulations alternative to NAC have been proposedfor use as antioxidant and anti-inflammatory agent for inhalationNacystelyn is a lysine adduct of NAC that thanks to a higher proton-ation equilibrium shows increased water solubility and thus betterbioavailability Nacystelyn has been described to influence IL-8 gener-ation and the inflammatory signaling of bronchial epithelial cells[239] and preliminary clinical evaluation has demonstrated the safetyof this drug [240] Further clinical trials aimed to assess the effect onlung symptomatology of CF patients are needed Direct administra-tion in the airways could also be adopted for micronutrient vitaminswith poor absorption and bioavailability due to GI defects
38 Clinical impact of antioxidant therapy in CF
Huge in vitro and pre-clinical evidence has provided the rationaleto support clinical investigation of antioxidant strategies in CF Theseshould aim to restore the oxidantndashantioxidant balance of CF airwaychallenged by chronic infection and inflammatory cell activation
Some observational trials have confirmed that antioxidants usedas either supplements to the diet or drugs for lung administrationby aerosolized formulations may help in relieving progressive lungdamage and other adverse clinical events of CF such as poor growthSo far few studies have examined with sufficient methodologicalrigor the clinical efficacy of antioxidant therapy in CF This was alsoconcluded in a previous review of the literature by Cantin et al [12]that was published in the beginning of 2006 and is confirmed alsoin a recent analysis of clinical trials on antioxidant therapy in CF pa-tients [213] that examined the literature until September 2010using as sources the databases of the Cochrane CF and Genetic Disor-ders Group CF Trials Register PubMed CINAHL and AMED Useful in-formation was retrieved from just four randomized controlled trialsand one quasi-randomized controlled trial on vitamin C vitamin Eβ-carotene and selenium used as supplements administered aloneor in combination Post-hoc data analysis that was possible only inthree studies on a total of 87 CF patients showed the absence ofany significant improvement in lung function that was selected as pri-mary outcome together with quality of life that improved in one trialSecondary outcomes concerning laboratory indices of oxidative stressand antioxidant status showed several improvements These includedan increase of RBC SeGPx by selenium supplementation done as
705F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
individual or combined supplementation and increased levels of allplasma antioxidants except vitamin C that were observed in all thetrials
The message from these studies to pediatricians and nutritionistswithin the clinical staff of CF centers is that in the absence of solid ev-idence regarding the clinical effectiveness of oral formulations of an-tioxidant supplements in CF (including PUFA) their use as a routineclinical practice should be considered with caution keeping clear inmind that this should represent just a complement of one of themost critical interventions in the life-long clinical management pro-gram of CF patients eg providing an adequate nutriture [140] Inthis context compensating energy and protein malnutrition has toremain the first goal of nutritional management programs Providinghigher intakes of antioxidant micronutrients with food naturally-enriched (or functionalized) of micronutrient antioxidants shouldbe preferred in order to have the higher combination of positive nu-tritional factors that are lost during refinement procedures and over-all industrial processing of dietary supplements
Measures of good practice in clinical management of micro-malnutrition in CF patients would include the support of specializedpersonnel and laboratories The centers should have the possibilityto ascertain with appropriate nutritional and laboratory tests whatthe level of deficiency is for the different micronutrients that each pa-tient may suffer from during a dietary program Monitoring dietaryintakes and blood levels of micronutrients is not sufficient to set apersonalized nutritional intervention with supplements or functionalfoods Sub-optimal intakes and the compliance to nutritional inter-ventions should be verified by means of selected biochemical andclinical criteria Unluckily the latter are still not well established forsome micronutrients such as the fat-soluble vitamins E (reviewed in[163173241]) and K [242243] and also for trace elements such asSe [244] For many of the antioxidants used as supplements inhumans we still do not know exactly several of the biological effectsthat these may provide when introduced in a healthy body and weknow less what these can do in disease These aspects hardly impacton the concept of optimal levels of intake that should be identified foreach micronutrient on an individual basis According with the aspectsdiscussed in the previous sections optimal levels of intake for antiox-idant micronutrients are different in CF patients and healthy subjectsand vary with age and several individual factors
Lung administration of antioxidants by means of aerosolized for-mulations so far used for GSH therapy (see above) is a promisingfield of clinical investigation in CF Toxicity issues are currently themain concern and the subject of clinical evaluation by several groups(described above)
Information on future directions of antioxidant therapy in CF canbe inferred by the analysis of pending or recently completed clinicaltrials that have been searched (December 2011) at ClinicalTrialsgovdatabase matching the terms ldquoantioxidant therapyrdquo or ldquoglutathionerdquowith ldquocystic fibrosisrdquo Fifteen trials were retrieved and those directlyrelated to antioxidant therapy (n=12) are presented in Table 1 andinclude efficacy and safety studies of inhaled drugs as GSH sodiumpyruvate NAC and NO and the dietary supplements AquADEKsregan antioxidant-rich multivitamin supplement epigallocatechin gal-late (EGCG)tocotrienol curcuminoids the amino acid glutaminesulforaphane in broccoli sprouts One trial is investigating the flavo-noid quercetin as CFTR modulator
39 Emerging antioxidant and anti-inflammatory approaches in CF
Mediterranean foods such as olive oil and red wine or severalplant extracts such as herbal tea or grape seed extracts contain aseries of natural compounds with important antioxidant and NOscavenging activity that have been widely investigated for the pre-vention of oxidative stress-related diseases [38245] These havebeen long investigated as template molecules to develop antioxidant
and anti-inflammatory drugs Between the multitudes of natural sub-stances most investigated ones include for instance tyrosol hydroxy-tyrosol gallic and caffeic acids belonging to the family of phenolswhile resveratrol of the stilbenes family epicatechin kaempferoland cianidin are examples of flavonoids examples of fat-soluble phe-nolics are those of the family of tocols (vitamin E) and carotenoids Allthese compounds show different metabolisms and signaling effects[246] Antioxidant and cell protection mechanisms are associatedwith different and sometimes concurrent processes as H-atom trans-fer and electron donation radical trapping and chelation of transitionmetals that can be easily investigated at the chemical level [247] Be-sides these direct antioxidant effects metabolic responses and signal-ing effects of natural compounds are also important to producesecond-generation responses that modify the level of antioxidantprotection and the potential for ROS detoxification in cells and bodyfluids These derive from the transcriptional regulation of antioxidantand pro-oxidant genes that coexist with the modulation of cytokinesecretion and inflammatory enzyme activities
Some of these natural plant-derived antioxidants may provide fur-ther pharmacological activities of possible relevance in CF This is thecase for instance of the plant flavonoids genistein apigenin kaemp-ferol quercetin and hesperidin [248ndash251] that fall in the pharmaco-logical category of ldquopotentiatorsrdquo [252] in that these activate at leastto a certain extent CTFR-mediated Cl currents in normal and CF airwayepithelium investigated either in vitro or in vivo in humans and ani-mal models Actually as prototypal flavonoid-derived potentiatorthe tyrosine kinase inhibitor genistein potentiates the gating of wild-type as well as ΔF508 CFTR and G551D CFTR [253] but at higherdoses it inhibits CFTR gating which make this an unlikely clinical can-didate Similar potentiation effects have been reported for the antiox-idant curcumin [250] that shows an additive effect with respect togenistein-induced potentiation Besides CFTR potentiation whichdoes not appear to have a direct influence on GSH and nutrient trans-port in the lung tissue all these natural substances have been usedalone or in combination with other agents as in vivo enhancers oflung antioxidant protection [246254255] In the case of quercetinthiol-reactive phenolic [256] bronchodilation and anti-inflammatoryeffects by a restoration of the Th1Th2 balance have been reportedin inflammatory syndromes of the lung [255257ndash259] but theseeffects have not been explored in CF Pyocyanin toxicity (see abovein the Section 2) could represent an issue for the use of quercetinand other catechols in infectious diseases of the lung [260]
Other natural antioxidants of potential interest in CF therapy in-clude terpenoids [261] such as terpinen-4-ol a major constituentof tea tree oil that is being investigated in the therapy of anti-biotic resistant organisms specifically against methicillin-resistantStaphylococcus aureus (MRSA) [262] a problem in CF [263] Otherthan being lipophilic antioxidants terpenes can prevent oxidativestress of the CF lung secondarily to the antibiotic effect thereby pro-moting a better control of immuno-inflammatory pathways and lungantioxidants
391 Targeting NF-κB with natural compounds resveratrol and plantextracts
Natural compounds were long known to be useful in designinganti-inflammatory drugs and some of these could find an applicationin the control of the transcription factor kappa-B (NF-κB) that maylead to develop advanced pharmacological tools to control inflamma-tion and to produce higher antioxidant protection to CF airwaysInhibitors targeting NF-κB including transcription factors decoymolecules (TFD) are potent down-regulators of gene expressionand release of IL-8 in CF cells infected with P aeruginosa [264265]
Resveratrol (354prime-trihydroxystilbene ldquoErdquo form) is one of the mostinvestigated natural antioxidant with proposed activity as NF-κBinhibitor This is a phytoalexin present in large quantity in red winepreferentially in the skin of grapes being its concentration
706 F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
50ndash100 μgmg of fresh skin and 13ndash3 mgl of red wine [266]Furthermore resveratrol is a constituent of lsquoDarakchasavarsquo (13ndash6 mgl) an ayurvedic medicine from India [267] The antioxidant activity ofresveratrol has been reported in several papers and occurs also in lungtissues suggesting that resveratrol has potential as a therapeuticagent in respiratory disease [268ndash270] Resveratrol can be consideredone of the most interesting molecules from the natural worldexhibiting strong antioxidant activity that at the same time is able toexert anti inflammatory activity through alteration of NF-κB functionsand efficient inhibition of pro-inflammatory genes [271272] As far asthe effects on CF model systems are concerned Cabrini et al [26]reported the effects of resveratrol on P aeruginosa infected CF IB3-1cells The results obtained demonstrate that resveratrol exhibits minoreffects of IB3-1 cell growth and important inhibitory effects on accumu-lation of IL-8 and GRO-α mRNA while minor effects on IL-6 gene ex-pression were observed These data support recently publishedobservations suggesting inhibitory effects of resveratrol in infection-mediated inflammatory processes [273] Interestingly resveratrol hasbeen reported as a potent inhibitor of NF-κB activity and a promisinganti-inflammatory agent [272274] also in combinationwith othermol-ecules [274275] However in vivo translation of this pre-clinical on res-veratrol is hard to be foreseen This natural compound displays poorbioavailability [276] and further characterization of resveratrol pharma-cokinetics is troublesome since it is hardly measurable in vivo [277]Furthermore the regulation of inflammatory responses by resveratrolhas been suggested to be far more complex than simple direct suppres-sion of NF-κB activity Actually some aspects of the immune responsecould be enhanced by this natural substance which may lead tohypothesize broad negative feedback events on immuno-inflammatorypathways [278] In any case and with these cautions in mind the pub-lished observations on cellular model systems support the concept thatresveratrol and resveratrol-containing formulations deserve further con-sideration to determine their possible therapeutic values in CF
Other inhibitors can be identified from systematic studies of naturalproducts and their ability to interfere with NF-κB activity [279ndash281]Recent studies have demonstrated that the whole extract of Aeglemarmelos (Rutaceae) has strong inhibitory effect on the P aeruginosa-dependent IL-8 induction in human CF-derived bronchial IB3-1 cellswithout affecting cell proliferation [280] Molecular analysis of compo-nents contained in A marmelos extracts revealed that three major com-pounds namely 56-dimethoxy-1-indanone 2-hydroxy-cinnamic acidand 5-methoxy psoralen (5-MOP) reproduce the inhibitory effect ob-servedwith thewhole extract [280] A further example has been recent-ly published using extracts from bergamot (Citrus bergamia Risso) Inthis study the extracts were characterized and the main detected con-stituents were assayed for their biological activity [281] The resultsobtained demonstrated that the extracts from bergamot epicarps con-tain components displaying an inhibitory activity on IL-8 Particularlythe most active molecules were bergapten and citropten These effectshave been confirmed by analyzing mRNA levels and protein release inthe CF cellularmodels IB3-1 and CuFi-1 inducedwith TNF-α or exposedto P aeruginosa
A parallel strategy linking NF-κB inhibition and down-regulationof NF-κB-dependent functions is described in recently publishedstudies based on a structured-based virtual screening (VS) of differ-ently substituted furocoumarins and analogues against NF-κB withthe objective of selecting molecules able to inhibit the binding ofthis transcription factor to DNA [282283] Novel compounds wereidentified with this strategy as potent inhibitors of NF-κB dependentbiological functions to be proposed for the control lung inflammationoccurring in patients affected by CF [282ndash284]
392 Scavengers and regulators of H2O2 and NO
3921 Lactoferrin and OSCNmacr The impaired DUOXLPO system of CFpatients could be the target of therapeutic strategies that may
produce concomitant antimicrobial and antioxidant effects This sys-tem described above in Section 22 represents an important compo-nent of innate immunity with a role in bactericidal defense andregulation of H2O2 metabolism of airways [32] CF patients have alsoreported to show lowered LF levels in the ASL [37] that togetherwith a CFTR-dependent defective efflux of SCNmacr and LPO [36] may cre-ate the environment for a sustained flux of H2O2 and for the genera-tion of highly reactive Fenton species [1138] An ideal therapeuticintervention should restore the LPO-dependent generation of bacteri-cidal OSCNmacr from DUOX-derived H2O2 and SCNmacr in the ASL to controlat the same time the microbial biofilm and the flux of H2O2 into theASL An approach close to this therapeutic mechanism was recentlyproposed for the drug Meveolreg This is a complex of LF and OSCNmacrwith proposed in vivo antimicrobial activity [285] to be evaluatedin clinical trials for the aerosol treatment of lung infections in CFpatients The role for this drug in the control of H2O2 levels of ASLremains to be investigated
3922 Organoselenium compounds Organoselenium compoundshave been proposed as therapeutic agents useful in the antioxidanttherapy of inflammatory conditions These include GPX mimetic mol-ecules such as Ebselenreg (2-phenyl-12-benzisoselenazol-3(2H)-one)or other and more recently developed molecules that are still inpre-clinical steps of evaluation [286] Selectively and specificity of ac-tion are main issues in the therapeutic mechanism of this candidateantioxidant drug that thanks to the electrophilic properties of Se[214] reacts with thiols to reduce H2O2 and other species MoreoverEbselenreg has been described to act as potent non-competitive inhib-itor of extracellular nucleoside diphosphokinase (NDPK) having neg-ligible effect on ecto-ATPase and adenyl kinase activities which areother players of the metabolism of extracellular nucleotides [287]This enzyme together with other nucleoside di- and triphosphatescontributes to regulate several components of the mucociliary clear-ance process (MCC) that protects the lung against infections via acti-vation of epithelial purinergic receptors The inhibition of NDPK bythis GPX-mimetic drug may also impact on the energy status of endo-thelial cells [287] This aspect could be further investigated as a cellu-lar protection mechanism in the pulmonary epithelium of CF patientsbeing the control of cell energy of fundamental importance to preventthe activation of death pathways [288]
Further therapeutic mechanisms for these Se-derived drugs mayderive from the marked activity as inducers of phase II enzymessuch as quinone reductase (QR) and glutathione-S-transferase (GST)[289] This induction response also observed with other electrophilsand redox-active molecules such as natural phenolic antioxidantscould produce higher cellular protection by the acquisition of anincreased capability to detoxify endobiotics generated during oxida-tive stress and inflammation [246]
3923 Melatonin and GSNO as NOx regulators Increased markers ofNO-derived biological damage are present in the CF lung suggestingthe abnormal reactivity of NOx in the inflamed lung of CF patients[52] However an impaired metabolism and biological function ofNO in CF airways (see Section 23) suggests a cautious approach tothe use of agents that may influence the levels and chemical behaviorof NO-derived species (NOx) with possible impact on the physiologi-cal roles of NO in vasodilatation innate immunity and H2O2 metabo-lism of the respiratory tract [290291] NO donors also appear toinfluence CFTR function of alveolar epithelium and gland serouscells [292293]
Main physiological role of the pineal gland hormone melatonin isthe synchronization of circadian rhythms including the sleepndashwakecycle but several other functions dealing with immunomodulatoryantioxidant and cellular protection effects have been identified[294] Melatonin receptor stimulation may also influence cyclic AMPsignaling and the regulation of CFTR ion channel [295296]
707F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
A recent randomized double-blind placebo-controlled study hasexamined the effects of short term melatonin administration (3 mgfor 3 weeks) on sleep and oxidative stress markers in CF [297]According with the expected pharmacological effect of this hormonalsubstance the treatment was successful in improving sleep indicesAt the same time nitrite levels determined in exhaled breath conden-sate (EBC) were reduced to suggest a better control of NOmetabolismof CF airways (discussed above in Section 23) but these effects how-ever were not associated with a significant correction of isoprostaneas lipid peroxidation marker measured in EBC Increasing dosages ofmelatonin could be investigated for the pharmacological treatmentof oxidative stress and immune dysfunction of CF patients due tothe absence of adverse effects of this hormonal substance in humans
The S-nitrosation reaction of thiols is another interesting aspect ofNO pharmacology [53] that may find an application in the therapy oflung complications of CF This has been the case for instance of theS-nitrosothiol GSNO that has been used safely in human trials[298299] This endogenous nitrosothiol with proposed regulatory ef-fect on the CFTR of lung epithelia [292293] is well tolerated in pa-tients with CF when administered by aerosolization and mayproduce better oxygenation [299] thereby suggesting that therapyaimed at restoring endogenous GSNO levels in the CF airway maymerit further clinical evaluation Since the administered GSNO de-composes as shown by the increased levels of expired NO in CF pa-tients under treatment with this nitrosothiol [299] furtherinvestigation should be addressed to ascertain whether GSNO thera-py may merely correspond to a GSH therapy
NO dependent effects on CFTR function should be considered toevaluate mechanism of action and specificity of antioxidant therapiesthat target NO metabolism and function in the CF airways
4 Conclusions and future perspectives
The presence of clinical and biochemical symptoms of inflammationand oxidative stress implies that CF patients have a higher demand ofantioxidant protection The combination of the dysfunctional CFTRwith a lowered intake and absorption of dietary antioxidants producesub-optimal levels of protection from both enzymatic and non-enzymatic defense systems The former could be associated with a de-fective glutathionemetabolism and lowered intake of sulfur-containingamino acids and oligoelements such as zinc and possibly seleniumwhile fat-soluble antioxidant vitamins such as vitamin E and caroten-oids and the water-soluble vitamin C are lowered than in healthy sub-jects due to malabsorption and possibly higher consumption
The increased antioxidant demand in CF patients should be evenhigher in the presence of complications of the lung pancreas andliver Lung comorbidity is particularly important in this contextbeing associated with recurrent infections which results in the alter-nation of inflammatory exacerbates and chronic inflammation Thesesustain the flux of ROS in the airways and promote the formation ofsecond-generation byproducts by the damage of biomolecules suchas PUFA and proteins which may diffuse also at the systemic level tofurther promote adverse biological responses and toxic reactions Pan-creatic insufficiency causes malnutrition and may lead to develop en-docrine and metabolic defects associated with diabetes of CF Theseevents can be further aggravated by the concomitance of liver dys-function and a poor nutritional status Malnutrition is strongly associ-ated with poor prognosis as assessed by pulmonary function andsurvival data [138ndash140] The more aggressive nutritional interven-tions seem to produce better clinical outcomes in these patients andthe possibility of achieving higher antioxidant protection in well-nourished patients by dietary factors could be a key aspect to explainsuch a clinical advantage The assumption that food-derived compo-nentsmay help to prevent the damaging effects of oxidative stress im-proving the antioxidant defenses deserves further investigation at theclinical level This together with the investigation of appropriate
laboratory biomarkers could provide critical information to establishintervention criteria for an early nutritional management of newly di-agnosed patients [5] It is expected that a timely secondary preventionstrategy could influence the progression of CF symptoms thusaffecting with a self-feeding mechanism the same extent of malnutri-tion and oxidative stress along the life of CF patients Since severalfactors contribute to impair the nutritional status of CF patients(such as pancreatic insufficiency chronic malabsorption recurrentsinopulmonary infections and progressive lung disease chronic in-flammation increased energy expenditure suboptimal intake multi-therapy) careful monitoring of the antioxidant status should berecommended According with international guidelines fat-solublevitamin supplementation is of utmost importance in daily practice to-gether with energy intake requirements and pancreatic enzyme-replacement therapy Among these vitamin E β-carotene and ω-3FA have observed to alleviate selected biochemical signs of oxidativestress as measured for instance with well established laboratory indi-ces of lipid peroxidation and in some studies these effects werepreliminarily associated with positive clinical outcomes Notwith-standing randomizedndashcontrolled clinical trials on antioxidant supple-ments (including ω-3 FA) so far carried out in CF have failed toconclusively demonstrate significant beneficial effects on respiratorysymptoms and on the consequent impact that these have on the qual-ity of life of these patients (reviewed in [202213]) whichmay provideno support for the use of these supplements in CF An absence of effi-cacy in prevention studies on antioxidant supplements has also beenobserved in other and possibly less severe oxidative stress-relatedconditions particularly in the secondary prevention of cardiovasculardisease and some forms of cancer by vitamin E and other antioxidantssuch as vitamin C selenium and β-carotene (reviewed in [163]) Dif-ferent biases however have been identified in randomize large clini-cal trials that may account for these disappointing findings Theseinclude patient selection criteria (early interventions and primaryprevention could have more chances of success than secondaryprevention) duration and doses of the treatment use of wrong anti-oxidant formulations and administration protocols absence of verifi-cations of the biological compliance to the treatment etc The samebiases apply for the few trials carried out in CF patients Thus the ap-propriateness and efficacy of nutritional interventions with naturalfood-derived or synthetic antioxidants should be verifiedwith respectto the biological pathways of oxidative stress and clinical variablesthat are identified as end-points Profiles of blood and tissue antioxi-dants as well as of reliable surrogate markers of oxidative stresshave to be selected and determined in highly specialized laboratorieswith a well-established experience on these analyses
Well-timed (early) interventions with appropriate antioxidantformulationsprotocols need to be proposed for the next generationof trials and the development of novel CF-tailored antioxidant andanti-inflammatory agents should be promoted
As a consequence of these considerations more clinical investiga-tion is awaited to identify future successful approaches to the antiox-idant therapy as a measure to further enhance quality of life and theoverall clinical outcome of CF patients
Acknowledgments
We are indebted with the Italian Cystic Fibrosis Research Founda-tion for the support that it provided with its grant program to the re-search activity of the authors of this paper This is a scientific initiativeof the ldquoWorking Group on Inflammation in Cystic Fibrosisrdquo (BragonziA Bravo E Cabrini G Conese M Cuzzocrea S Dechecchi MC De Ales-sandri A Evangelista V Galli F Gambari R Lambiase A Lucidi VManca A Melotti P Minicucci L Motta A Pietraforte D Pompella AQuattrucci S Rizzo R Romano M Sorio C Tesse R) of the Italian Soci-ety for Cystic Fibrosis A particular thank goes to the Prof GianniMastella for the critical revision of the manuscript and for the
708 F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
stimulating research environment that he has contributed to createwithin the Italian Cystic Fibrosis Research Foundation
References
[1] BP OSullivan SD Freedman Cystic fibrosis Lancet 373 (2009) 1891ndash1904[2] P Linsdell JW Hanrahan Glutathione permeability of CFTR Am J Physiol 275
(1998) C323ndashC326[3] L Gao KJ Kim JR Yankaskas HJ Forman Abnormal glutathione transport in
cystic fibrosis airway epithelia Am J Physiol 277 (1999) L113ndashL118[4] RK Rowntree A Harris The phenotypic consequences of CFTR mutations Ann
Hum Genet 67 (2003) 471ndash485[5] EI Back C Frindt D Nohr J Frank R Ziebach M Stern M Ranke HK Biesalski
Antioxidant deficiency in cystic fibrosis when is the right time to take actionAm J Clin Nutr 80 (2004) 374ndash384
[6] LG Wood DA Fitzgerald AK Lee ML Garg Improved antioxidant and fattyacid status of patients with cystic fibrosis after antioxidant supplementation islinked to improved lung function Am J Clin Nutr 77 (2003) 150ndash159
[7] L Iuliano R Monticolo G Straface S Zullo F Galli M Boaz S Quattrucci Asso-ciation of cholesterol oxidation and abnormalities in fatty acid metabolism incystic fibrosis Am J Clin Nutr 90 (2009) 477ndash484
[8] C Libetta V Sepe P Esposito F Galli A Dal Canton Oxidative stress and inflam-mation implications in uremia and hemodialysis Clin Biochem 44 (2011)1189ndash1198
[9] G Bartosz Reactive oxygen species destroyers or messengers Biochem Phar-macol 77 (2009) 1303ndash1315
[10] T Ntimbane B Comte G Mailhot Y Berthiaume V Poitout M Prentki RRabasa-Lhoret E Levy Cystic fibrosis-related diabetes from CFTR dysfunctionto oxidative stress Clin Biochem 30 (2009) 153ndash177
[11] A van der Vliet JP Eiserich GP Marelich B Halliwell CE Cross Oxidativestress in cystic fibrosis does it occur and does it matter Adv Pharmacol 38(1997) 491ndash513
[12] AM Cantin TB White CE Cross HJ Forman RJ Sokol D Borowitz Antioxi-dants in cystic fibrosis Conclusions from the CF antioxidant workshop Bethes-da Maryland Free Radic Biol Med 42 (2007) 15ndash31
[13] LT McGrath P Mallon L Dowey B Silke E McClean M McDonnell A DevineS Copeland S Elborn Oxidative stress during acute respiratory exacerbations incystic fibrosis Thorax 54 (1999) 518ndash523
[14] E Thomson S Brennan R Senthilmohan CL Gangell AL Chapman PD SlyAJ Kettle E Balding LJ Berry JB Carlin R Carzino N de Klerk T Douglas CFoo LW Garratt GL Hall J Harrison A Kicic IA Laing KM Logie J MassieLS Mott C Murray F Parsons N Pillarisetti SR Poreddy SC RanganathanCF Robertson R Robins-Browne PJ Robinson B Skoric SM Stick ENSutanto E Williamson Identifying peroxidases and their oxidants in the earlypathology of cystic fibrosis Free Radic Biol Med 49 (2010) 1354ndash1360
[15] SP Range C Dunster AJ Knox FJ Kelly Treatment of pulmonary exacerba-tions of cystic fibrosis leads to improved antioxidant status Eur Respir J 13(1999) 560ndash564
[16] L Coppo P Ghezzi Thiol regulation of pro-inflammatory cytokines and innateimmunity protein S-thiolation as a novel molecular mechanism Biochem SocTrans 39 (2011) 1268ndash1272
[17] C Verhaeghe C Remouchamps B Hennuy A Vanderplasschen A Chariot SPTabruyn C Oury V Bours Role of IKK and ERK pathways in intrinsic inflamma-tion of cystic fibrosis airways Biochem Pharmacol 73 (2007) 1982ndash1994
[18] TL Bonfield JR Panuska MW Konstan KA Hilliard JB Hilliard H Ghnaim MBerger Inflammatory cytokines in cystic fibrosis lungs Am J Respir Crit CareMed 152 (1995) 2111ndash2118
[19] TL Noah HR Black PW Cheng RE Wood MW Leigh Nasal and bronchoal-veolar lavage fluid cytokines in early cystic fibrosis J Infect Dis 175 (1997)638ndash647
[20] MJ Welsh BW Ramsey FJ Accurso GR Cutting Cystic Fibrosis McGraw-HillNew York 2001
[21] TZ Khan JS Wagener T Bost J Martinez FJ Accurso DW Riches Early pul-monary inflammation in infants with cystic fibrosis Am J Respir Crit CareMed 151 (1995) 1075ndash1082
[22] FA Ratjen Cystic fibrosis pathogenesis and future treatment strategies RespirCare 54 (2009) 595ndash605
[23] J Jacquot O Tabary P Le Rouzic A Clement Airway epithelial cell inflamma-tory signalling in cystic fibrosis Int J Biochem Cell Biol 40 (2008)1703ndash1715
[24] CM Greene P Branagan NG McElvaney Toll-like receptors as therapeutic tar-gets in cystic fibrosis Expert Opin Ther Targets 12 (2008) 1481ndash1495
[25] M Rottner JM Freyssinet MC Martinez Mechanisms of the noxious inflam-matory cycle in cystic fibrosis Respir Res 10 (2009) 23
[26] G Cabrini V Bezzerri I Mancini E Nicolis MC Dechecchi A Tamanini ILampronti L Piccagli N Bianchi M Borgatti R Gambari Targeting transcrip-tion factor activity as a strategy to inhibit pro-inflammatory genes involved incystic fibrosis decoy oligonucleotides and low-molecular weight compoundsCurr Med Chem 17 (2010) 4392ndash4404
[27] CM Greene NG McElvaney Proteases and antiproteases in chronic neutrophiliclungdiseasemdash relevance to drug discovery Br J Pharmacol 158 (2009) 1048ndash1058
[28] AM Cantin Potential for antioxidant therapy of cystic fibrosis Curr Opin PulmMed 10 (2004) 531ndash536
[29] JF Chmiel MW Konstan Inflammation and anti-inflammatory therapies forcystic fibrosis Clin Chest Med 28 (2007) 331ndash346
[30] DP Nichols MW Konstan JF Chmiel Anti-inflammatory therapies for cys-tic fibrosis-related lung disease Clin Rev Allergy Immunol 35 (2008)135ndash153
[31] AJ Kettle T Chan I Osberg R Senthilmohan AL Chapman TJ Mocatta JSWagener Myeloperoxidase and protein oxidation in the airways of youngchildren with cystic fibrosis Am J Respir Crit Care Med 170 (2004)1317ndash1323
[32] H Fischer Mechanisms and function of DUOX in epithelia of the lung AntioxidRedox Signal 11 (2009) 2453ndash2465
[33] B Rada TL Leto Oxidative innate immune defenses by NoxDuox familyNADPH oxidases Contrib Microbiol 15 (2008) 164ndash187
[34] P Moskwa D Lorentzen KJ Excoffon J Zabner PB McCray Jr WM NauseefC Dupuy B Banfi A novel host defense system of airways is defective in cysticfibrosis Am J Respir Crit Care Med 175 (2007) 174ndash183
[35] D Lorentzen L Durairaj AA Pezzulo Y Nakano J Launspach DA Stoltz GZamba PB McCray Jr J Zabner MJ Welsh WM Nauseef B Banfi Concentra-tion of the antibacterial precursor thiocyanate in cystic fibrosis airway secre-tions Free Radic Biol Med 50 (2011) 1144ndash1150
[36] Y Xu S Szep Z Lu The antioxidant role of thiocyanate in the pathogenesis ofcystic fibrosis and other inflammation-related diseases Proc Natl Acad Sci US A 106 (2009) 20515ndash20519
[37] MP Rogan CC Taggart CM Greene PG Murphy SJ ONeill NG McElvaneyLoss of microbicidal activity and increased formation of biofilm due to decreasedlactoferrin activity in patients with cystic fibrosis J Infect Dis 190 (2004)1245ndash1253
[38] B Halliwell JM Guttridge Free Radicals in Biology and Medicine Fourth editionOxford University Press New York 2007
[39] B Rada K Lekstrom S Damian C Dupuy TL Leto The Pseudomonastoxin pyocyanin inhibits the dual oxidase-based antimicrobial system as itimposes oxidative stress on airway epithelial cells J Immunol 181 (2008)4883ndash4893
[40] C Schwarzer B Illek JH Suh SJ Remington H Fischer TE Machen Organelleredox of CF and CFTR-corrected airway epithelia Free Radic Biol Med 43(2007) 300ndash316
[41] JH Roum R Buhl NG McElvaney Z Borok RG Crystal Systemic deficiency ofglutathione in cystic fibrosis J Appl Physiol 75 (1993) 2419ndash2424
[42] VM Hudson Rethinking cystic fibrosis pathology the critical role of abnormalreduced glutathione (GSH) transport caused by CFTR mutation Free RadicBiol Med 30 (2001) 1440ndash1461
[43] PJ Barnes RA Dweik AF Gelb PG Gibson SC George H Grasemann IDPavord F Ratjen PE Silkoff DR Taylor N Zamel Exhaled nitric oxide in pul-monary diseases a comprehensive review Chest 138 (2010) 682ndash692
[44] H Grasemann E Michler M Wallot F Ratjen Decreased concentration of ex-haled nitric oxide (NO) in patients with cystic fibrosis Pediatr Pulmonol 24(1997) 173ndash177
[45] H Grasemann F Ratjen Cystic fibrosis lung disease the role of nitric oxidePediatr Pulmonol 28 (1999) 442ndash448
[46] B Gaston F Ratjen JW Vaughan NR Malhotra RG Canady AH Snyder JFHunt S Gaertig JB Goldberg Nitrogen redox balance in the cystic fibrosis air-way effects of antipseudomonal therapy Am J Respir Crit Care Med 165(2002) 387ndash390
[47] H Grasemann I Ioannidis RP Tomkiewicz H de Groot BK Rubin F RatjenNitric oxide metabolites in cystic fibrosis lung disease Arch Dis Child 78(1998) 49ndash53
[48] H Grasemann R Schwiertz S Matthiesen K Racke F Ratjen Increased argi-nase activity in cystic fibrosis airways Am J Respir Crit Care Med 172(2005) 1523ndash1528
[49] H Grasemann S Al-Saleh JA Scott D Shehnaz A Mehl R Amin M Rafii PPencharz J Belik F Ratjen Asymmetric dimethylarginine contributes to airwaynitric oxide deficiency in patients with cystic fibrosis Am J Respir Crit CareMed 183 (2011) 1363ndash1368
[50] H Grasemann F Kurtz F Ratjen Inhaled L-arginine improves exhaled nitricoxide and pulmonary function in patients with cystic fibrosis Am J RespirCrit Care Med 174 (2006) 208ndash212
[51] H Grasemann F Ratjen Emerging therapies for cystic fibrosis lung disease Ex-pert Opin Emerg Drugs 15 (2010) 653ndash659
[52] BM Morrissey K Schilling JV Weil PE Silkoff DM Rodman Nitric oxide andprotein nitration in the cystic fibrosis airway Arch Biochem Biophys 406(2002) 33ndash39
[53] R Radi Nitric oxide oxidants and protein tyrosine nitration Proc Natl AcadSci U S A 101 (2004) 4003ndash4008
[54] J Chen M Kinter S Shank C Cotton TJ Kelley AG Ziady Dysfunction of Nrf-2in CF epithelia leads to excess intracellular H2O2 and inflammatory cytokineproduction PLoS One 3 (2008) e3367
[55] F Galli M Piroddi C Annetti C Aisa E Floridi A Floridi Oxidative stress andreactive oxygen species Contrib Nephrol 149 (2005) 240ndash260
[56] DT Wright LA Cohn H Li B Fischer CM Li KB Adler Interactions of oxygenradicals with airway epithelium Environ Health Perspect 102 (Suppl 10)(1994) 85ndash90
[57] I Rahman SR Yang SK Biswas Current concepts of redox signaling in thelungs Antioxid Redox Signal 8 (2006) 681ndash689
[58] Q Li JF Engelhardt Interleukin-1beta induction of NFκB is partially regulatedby H2O2-mediated activation of NFκB-inducing kinase J Biol Chem 281(2006) 1495ndash1505
709F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
[59] E Boncoeur VS Criq E Bonvin T Roque A Henrion-Caude DC Gruenert AClement J Jacquot O Tabary Oxidative stress induces extracellular signal-regulated kinase 12 mitogen-activated protein kinase in cystic fibrosis lung ep-ithelial cells potential mechanism for excessive IL-8 expression Int J BiochemCell Biol 40 (2008) 432ndash446
[60] B Fischer J Voynow Neutrophil elastase induces MUC5AC messenger RNA ex-pression by an oxidant-dependent mechanism Chest 117 (2000) 317Sndash320S
[61] B Rada P Gardina TG Myers TL Leto Reactive oxygen species mediate in-flammatory cytokine release and EGFR-dependent mucin secretion in airwayepithelial cells exposed to Pseudomonas pyocyanin Mucosal Immunol 4(2011) 158ndash171
[62] C Schwarzer H Fischer EJ Kim KJ Barber AD Mills MJ Kurth DC GruenertJH Suh TE Machen B Illek Oxidative stress caused by pyocyanin impairs CFTRClminus transport in human bronchial epithelial cells Free Radic Biol Med 45(2008) 1653ndash1662
[63] J Hull M South P Phelan K Grimwood Surfactant composition in infants andyoung children with cystic fibrosis Am J Respir Crit Care Med 156 (1997)161ndash165
[64] KC Meyer A Sharma R Brown M Weatherly FR Moya J Lewandoski JJZimmerman Function and composition of pulmonary surfactant andsurfactant-derived fatty acid profiles are altered in young adults with cystic fi-brosis Chest 118 (2000) 164ndash174
[65] MK Pulfer RC Murphy Formation of biologically active oxysterols during ozo-nolysis of cholesterol present in lung surfactant J Biol Chem 279 (2004)26331ndash26338
[66] V Starosta E Rietschel K Paul U Baumann M Griese Oxidative changes ofbronchoalveolar proteins in cystic fibrosis Chest 129 (2006) 431ndash437
[67] V Starosta M Griese Oxidative damage to surfactant protein D in pulmonarydiseases Free Radic Res 40 (2006) 419ndash425
[68] M Griese R Essl R Schmidt E Rietschel F Ratjen M Ballmann K Paul Pulmo-nary surfactant lung function and endobronchial inflammation in cystic fibro-sis Am J Respir Crit Care Med 170 (2004) 1000ndash1005
[69] M Griese R Essl R Schmidt M Ballmann K Paul E Rietschel F Ratjen Se-quential analysis of surfactant lung function and inflammation in cystic fibrosispatients Respir Res 6 (2005) 133
[70] LG Wood DA Fitzgerald PG Gibson DM Cooper ML Garg Increased plasmafatty acid concentrations after respiratory exacerbations are associated with el-evated oxidative stress in cystic fibrosis patients Am J Clin Nutr 75 (2002)668ndash675
[71] P Montuschi SA Kharitonov G Ciabattoni M Corradi L van Rensen DM Ged-des ME Hodson PJ Barnes Exhaled 8-isoprostane as a new non-invasive bio-marker of oxidative stress in cystic fibrosis Thorax 55 (2000) 205ndash209
[72] CE Collins P Quaggiotto L Wood EV OLoughlin RL Henry ML Garg Elevat-ed plasma levels of F2 alpha isoprostane in cystic fibrosis Lipids 34 (1999)551ndash556
[73] D Hartl V Starosta K Maier I Beck-Speier C Rebhan BF Becker P Latzin RFischer F Ratjen RM Huber E Rietschel S Krauss-Etschmann M Griese In-haled glutathione decreases PGE2 and increases lymphocytes in cystic fibrosislungs Free Radic Biol Med 39 (2005) 463ndash472
[74] GL Milne H Yin JD Morrow Human biochemistry of the isoprostane pathwayJ Biol Chem 283 (2008) 15533ndash15537
[75] G Ciabattoni G Davi M Collura L Iapichino F Pardo A Ganci R Romagnoli JMaclouf C Patrono In vivo lipid peroxidation and platelet activation in cystic fi-brosis Am J Respir Crit Care Med 162 (2000) 1195ndash1201
[76] C Garenc P Julien E Levy Oxysterols in biological systems the gastrointestinaltract liver vascular wall and central nervous system Free Radic Res 44 (2011)47ndash73
[77] AM Cantin SL North RC Hubbard RG Crystal Normal alveolar epithelial lin-ing fluid contains high levels of glutathione J Appl Physiol 63 (1987) 152ndash157
[78] R Tirouvanziam CK Conrad T Bottiglieri LA Herzenberg RB Moss High-dose oral N-acetylcysteine a glutathione prodrug modulates inflammation incystic fibrosis Proc Natl Acad Sci U S A 103 (2006) 4628ndash4633
[79] LW Velsor C Kariya R Kachadourian BJ Day Mitochondrial oxidative stressin the lungs of cystic fibrosis transmembrane conductance regulator proteinmutant mice Am J Respir Cell Mol Biol 35 (2006) 579ndash586
[80] M Kelly-Aubert S Trudel J Fritsch T Nguyen-Khoa M Baudouin-Legros SMoriceau L Jeanson F Djouadi C Matar M Conti M Ollero F Brouillard AEdelman GSH monoethyl ester rescues mitochondrial defects in cystic fibrosismodels Hum Mol Genet 20 (2011) 2745ndash2759
[81] P Ghezzi Role of glutathione in immunity and inflammation in the lung Int JGen Med 4 (2011) 105ndash113
[82] N Dauletbaev K Viel R Buhl TO Wagner J Bargon Glutathione and glutathi-one peroxidase in sputum samples of adult patients with cystic fibrosis J CystFibros 3 (2004) 119ndash124
[83] CE Cross A van der Vliet CA ONeill S Louie B Halliwell Oxidants antioxi-dants and respiratory tract lining fluids Environ Health Perspect 102 (Suppl10) (1994) 185ndash191
[84] K Takeyama K Dabbagh J Jeong Shim T Dao-Pick IF Ueki JA Nadel Oxida-tive stress causes mucin synthesis via transactivation of epidermal growth factorreceptor role of neutrophils J Immunol 164 (2000) 1546ndash1552
[85] N Ballatori SM Krance S Notenboom S Shi K Tieu CL Hammond Glutathi-one dysregulation and the etiology and progression of human diseases BiolChem 390 (2009) 191ndash214
[86] SR Soltaninassab KR Sekhar MJ Meredith ML Freeman Multi-faceted regu-lation of gamma-glutamylcysteine synthetase J Cell Physiol 182 (2000)163ndash170
[87] HR Lopez-Mirabal JR Winther Redox characteristics of the eukaryotic cytosolBiochim Biophys Acta 1783 (2008) 629ndash640
[88] C Hwang AJ Sinskey HF Lodish Oxidized redox state of glutathione in the en-doplasmic reticulum Science 257 (1992) 1496ndash1502
[89] M Murphy Mitochondrial thiols in antioxidant protection and redox signallingdistinct roles for glutathionylation and other thiol modifications AntioxidRedox Signal (2011) ahead of print doi101089ars20114289
[90] BJ Day AM van Heeckeren E Min LW Velsor Role for cystic fibrosis trans-membrane conductance regulator protein in a glutathione response to bronch-opulmonary Pseudomonas infection Infect Immun 72 (2004) 2045ndash2051
[91] Y Zhang K Duan Glutathione exhibits antibacterial activity and increases tetra-cycline efficacy against Pseudomonas aeruginosa Sci China C Life Sci 52 (2009)501ndash505
[92] VM Hudson New insights into the pathogenesis of cystic fibrosis pivotal roleof glutathione system dysfunction and implications for therapy Treat RespirMed 3 (2004) 353ndash363
[93] LW Velsor A van Heeckeren BJ Day Antioxidant imbalance in the lungs ofcystic fibrosis transmembrane conductance regulator protein mutant miceAm J Physiol Lung Cell Mol Physiol 281 (2001) L31ndashL38
[94] I Kogan M Ramjeesingh C Li JF Kidd Y Wang EM Leslie SP Cole CE BearCFTR directly mediates nucleotide-regulated glutathione flux EMBO J 22(2003) 1981ndash1989
[95] NS Gould S Gauthier CT Kariya E Min J Huang DJ Brian Hypertonic salineincreases lung epithelial lining fluid glutathione and thiocyanate two protectiveCFTR-dependent thiols against oxidative injury Respir Res 11 (2010) 119
[96] VT Vasu SJ de Cruz JS Houghton KA Hayakawa BM Morrissey CE CrossJP Eiserich Evaluation of thiol-based antioxidant therapeutics in cystic fibrosissputum focus on myeloperoxidase Free Radic Res 45 (2011) 165ndash176
[97] L Roussel G Martel J Berube S Rousseau P aeruginosa drives CXCL8 synthesisvia redundant toll-like receptors and NADPH oxidase in CFTRF508 airway epi-thelial cells J Cyst Fibros 10 (2011) 107ndash113
[98] GW Lau DJ Hassett H Ran F Kong The role of pyocyanin in Pseudomonas aer-uginosa infection Trends Mol Med 10 (2004) 599ndash606
[99] R Wilson DA Sykes D Watson A Rutman GW Taylor PJ Cole Measurementof Pseudomonas aeruginosa phenazine pigments in sputum and assessment oftheir contribution to sputum sol toxicity for respiratory epithelium InfectImmun 56 (1988) 2515ndash2517
[100] M Muller Pyocyanin induces oxidative stress in human endothelial cells andmodulates the glutathione redox cycle Free Radic Biol Med 33 (2002)1527ndash1533
[101] YQ OMalley KJ Reszka BE Britigan Direct oxidation of 2prime7prime-dichlorodihy-drofluorescein by pyocyanin and other redox-active compounds independentof reactive oxygen species production Free Radic Biol Med 36 (2004)90ndash100
[102] CC Caldwell Y Chen HS Goetzmann Y Hao MT Borchers DJ Hassett LRYoung D Mavrodi L Thomashow GW Lau Pseudomonas aeruginosa exotoxinpyocyanin causes cystic fibrosis airway pathogenesis Am J Pathol 175 (2009)2473ndash2488
[103] YQ OMalley KJ Reszka DR Spitz GM Denning BE Britigan Pseudomonasaeruginosa pyocyanin directly oxidizes glutathione and decreases its levels inairway epithelial cells Am J Physiol Lung Cell Mol Physiol 287 (2004)L94ndashL103
[104] M Muller Glutathione modulates the toxicity of but is not a biologically rele-vant reductant for the Pseudomonas aeruginosa redox toxin pyocyanin FreeRadic Biol Med 50 (2011) 971ndash977
[105] R Cheluvappa R Shimmon M Dawson SN Hilmer DG Le Couteur Reactionsof Pseudomonas aeruginosa pyocyanin with reduced glutathione Acta BiochimPol 55 (2008) 571ndash580
[106] JH Widdicombe Transgenic animals may help resolve a sticky situation in cys-tic fibrosis J Clin Invest 120 (2010) 3093ndash3096
[107] X Sun H Sui JT Fisher Z Yan X Liu HJ Cho NS Joo Y Zhang W Zhou Y YiJM Kinyon DC Lei-Butters MA Griffin P Naumann M Luo J Ascher KWang T Frana JJ Wine DK Meyerholz JF Engelhardt Disease phenotype ofa ferret CFTR-knockout model of cystic fibrosis J Clin Invest 120 (2010)3149ndash3160
[108] NS Joo HJ Cho M Khansaheb JJ Wine Hyposecretion of fluid from trachealsubmucosal glands of CFTR-deficient pigs J Clin Invest 120 (2010) 3161ndash3166
[109] A Bragonzi Murine models of acute and chronic lung infection with cystic fibro-sis pathogens IJMM 300 (2010) 584ndash593
[110] AM van Heeckeren MD Schluchter Murine models of chronic Pseudomonasaeruginosa lung infection Lab Anim 36 (2002) 291ndash312
[111] A Bragonzi D Worlitzsch GB Pier P Timpert M Ulrich M Hentzer JB Ander-sen M Givskov M Conese G Doring Nonmucoid Pseudomonas aeruginosa ex-presses alginate in the lungs of patients with cystic fibrosis and in a mousemodel J Infect Dis 192 (2005) 410ndash419
[112] GS CW Bedrossian DB Singer JJ Hansen HS Rosenberg The lung in cysticfibrosis A quantitative study including prevalence of pathologic findingsamong different age groups Hum Pathol 7 (1976) 195ndash204
[113] WD HA Cash B McCullough WG Johanson Jr JA Bass A rat model of chron-ic respiratory infection with Pseudomonas aeruginosa Am Rev Respir Dis 119(1979) 453ndash459
[114] EM JR Starke C Langston CJ Baker A mouse model of chronic pulmonary in-fection with Pseudomonas aeruginosa and Pseudomonas cepacia Pediatr Res 22(1987) 698ndash702
[115] TJ AM van Heeckeren RW Walenga MW Konstan PB Davis B ErokwuMA Haxhiu TW Ferkol Effect of Pseudomonas infection on weight loss lung
710 F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
mechanics and cytokines in mice Am J Respir Crit Care Med 161 (2000)271ndash279
[116] T Aw G Wierzbicka DP Jones Oral glutathione increases tissue glutathione invivo Chem Biol Interact 80 (1991) 89ndash97
[117] F Favilli P Marraccini T Iantomasi MT Vincenzini Effect of orally adminis-tered glutathione on glutathione levels in some organs of rats role of specifictransporters Br J Nutr 78 (1997) 293ndash300
[118] C Kariya H Leitner E Min C van Heeckeren A van Heeckeren BJ Day A rolefor CFTR in the elevation of glutathione levels in the lung by oral glutathione ad-ministration Am J Physiol Lung Cell Mol Physiol 292 (2007) L1590ndashL1597
[119] K Atkuri JJ Mantovani LA Herzenberg LA Herzenberg N-Acetylcysteinemdashasafe antidote for cysteineglutathione deficiency Curr Opin Pharmacol 7(2007) 355ndash359
[120] R De Lisle E Roach K Jansson Effects of laxative and N-acetylcysteine onmucus accumulation bacterial load transit and inflammation in the cystic fi-brosis mouse small intestine Am J Physiol Gastrointest Liver Physiol 293(2007) G577ndashG584
[121] A Luciani VR Villella S Esposito N Brunetti-Pierri D Medina C Settembre MGavina L Pulze I Giardino M Pettoello-Mantovani M DApolito S Guido EMasliah B Spencer S Quaratino V Raia A Ballabio L Maiuri Defective CFTRinduces aggresome formation and lung inflammation in cystic fibrosis throughROS-mediated autophagy inhibition Nat Cell Biol 12 863ndash875
[122] M Griese J Ramakers A Krasselt V Starosta S Van Koningsbruggen R FischerF Ratjen B Mullinger RM Huber K Maier E Rietschel G Scheuch Improve-ment of alveolar glutathione and lung function but not oxidative state in cysticfibrosis Am J Respir Crit Care Med 169 (2004) 822ndash828
[123] C Bishop VM Hudson SC Hilton C Wilde A pilot study of the effect of inhaledbuffered reduced glutathione on the clinical status of patients with cystic fibro-sis Chest 127 (2005) 308ndash317
[124] WWang C Oliva G Li A Holmgren CH Lillig KL Kirk Reversible silencing of CFTRchloride channels by glutathionylation J Gen Physiol 125 (2005) 127ndash141
[125] N Dauletbaev P Fischer B Aulbach J Gross W Kusche U Thyroff-FriesingerTO Wagner J Bargon A phase II study on safety and efficacy of high-dose N-acetylcysteine in patients with cystic fibrosis Eur J Med Res 14 (2009)352ndash358
[126] R Tirouvanziam Y Gernez CK Conrad RB Moss I Schrijver CE Dunn ZADavies LA Herzenberg Profound functional and signaling changes in viable in-flammatory neutrophils homing to cystic fibrosis airways Proc Natl Acad SciU S A 105 (2008) 4335ndash4339
[127] JH Roum Z Borok NG McElvaney GJ Grimes AD Bokser R Buhl RG Crys-tal Glutathione aerosol suppresses lung epithelial surface inflammatory cell-derived oxidants in cystic fibrosis J Appl Physiol 87 (1999) 438ndash443
[128] A Visca CT Bishop SC Hilton VM Hudson Improvement in clinical markersin CF patients using a reduced glutathione regimen an uncontrolled observa-tional study J Cyst Fibros 7 (2008) 433ndash436
[129] EF Nash A Stephenson F Ratjen E Tullis Nebulized and oral thiol derivativesfor pulmonary disease in cystic fibrosis Cochrane Database Syst Rev (2009)CD007168
[130] AC foundation Drug Development Pipeline 2011[131] S Hoshida T Kuzuya N Yamashita M Nishida S Kitahara M Hori T
Kamada M Tada Gamma-glutamylcysteine ethyl ester for myocardial protec-tion in dogs during ischemia and reperfusion J Am Coll Cardiol 24 (1994)1391ndash1397
[132] J Lok W Leung S Zhao S Pallast K van Leyen S Guo X Wang A Yalcin EHLo Gamma-glutamylcysteine ethyl ester protects cerebral endothelial cells dur-ing injury and decreases bloodndashbrain barrier permeability after experimentalbrain trauma J Neurochem 118 (2011) 248ndash255
[133] Z Borok R Buhl GJ Grimes AD Bokser RC Hubbard KJ Holroyd JH RoumDB Czerski AM Cantin RG Crystal Effect of glutathione aerosol on oxidantndashantioxidant imbalance in idiopathic pulmonary fibrosis Lancet 338 (1991)215ndash216
[134] KJ Holroyd R Buhl Z Borok JH Roum AD Bokser GJ Grimes D Czerski AMCantin RG Crystal Correction of glutathione deficiency in the lower respiratorytract of HIV seropositive individuals by glutathione aerosol treatment Thorax 48(1993) 985ndash989
[135] J Hull P Vervaart K Grimwood P Phelan Pulmonary oxidative stress responsein young children with cystic fibrosis Thorax 52 (1997) 557ndash560
[136] A Corti A Paolicchi M Franzini S Dominici AF Casini A Pompella The S-thiolating activity of membrane gamma-glutamyltransferase formation ofcysteinyl-glycine mixed disulfides with cellular proteins and in the cell microen-vironment Antioxid Redox Signal 7 (2005) 911ndash918
[137] A Corti M Franzini AF Casini A Paolicchi A Pompella Vitamin C supply tobronchial epithelial cells linked to glutathione availability in elfmdasha role for se-creted gamma-glutamyltransferase J Cyst Fibros 7 (2008) 174ndash178
[138] A Munck Nutritional considerations in patients with cystic fibrosis Expert RevRespir Med 4 (2010) 47ndash56
[139] JL Matel CE Milla Nutrition in cystic fibrosis Semin Respir Crit Care Med 30(2009) 579ndash586
[140] D Salvatore R Buzzetti E Baldo MP Forneris V Lucidi D Manunza IMarinelli B Messore AS Neri V Raia ML Furnari G Mastella An overviewof international literature from cystic fibrosis registries 2 Neonatal screeningand nutritiongrowth J Cyst Fibros 9 (2010) 75ndash83
[141] KF Joosten JM Hulst Malnutrition in pediatric hospital patients current is-sues Nutrition 27 (2011) 133ndash137
[142] S Fustik T Jacovska L Spirevska S Koceva Protein-energy malnutrition as thefirst manifestation of cystic fibrosis in infancy Pediatr Int 51 (2009) 678ndash683
[143] J Himmelfarb E McMonagle Albumin is the major plasma protein target of ox-idant stress in uremia Kidney Int 60 (2001) 358ndash363
[144] P Stenvinkel JJ Carrero J Axelsson B Lindholm O Heimburger Z MassyEmerging biomarkers for evaluating cardiovascular risk in the chronic kidneydisease patient how do new pieces fit into the uremic puzzle Clin J Am SocNephrol 3 (2008) 505ndash521
[145] M Roche P Rondeau NR Singh E Tarnus E Bourdon The antioxidant proper-ties of serum albumin FEBS Lett 582 (2008) 1783ndash1787
[146] D Giustarini A Milzani I Dalle-Donne R Rossi Red blood cells as a physiolog-ical source of glutathione for extracellular fluids Blood Cells Mol Dis 40 (2008)174ndash179
[147] A Meister ME Anderson Glutathione Annu Rev Biochem 52 (1983) 711ndash760[148] B Alvarez S Carballal L Turell R Radi Formation and reactions of sulfenic acid
in human serum albumin Methods Enzymol 473 (2010) 117ndash136[149] S Carballal B Alvarez L Turell H Botti BA Freeman R Radi Sulfenic acid in
human serum albumin Amino Acids 32 (2007) 543ndash551[150] LR Barclay AM Bailey D Kong The antioxidant activity of alpha-tocopherol-
bovine serum albumin complex in micellar and liposome autoxidations J BiolChem 260 (1985) 15809ndash15814
[151] T Ishii T Ichikawa K Minoda K Kusaka S Ito Y Suzuki M Akagawa K Mochi-zuki T Goda T Nakayama Human serum albumin as an antioxidant in the ox-idation of (minus)-epigallocatechin gallate participation of reversible covalentbinding for interaction and stabilization Biosci Biotechnol Biochem 75(2011) 100ndash106
[152] F Galli S Rovidati S Benedetti U Buoncristiani C Covarelli A Floridi F Canes-trari Overexpression of erythrocyte glutathione S-transferase in uremia and di-alysis Clin Chem 45 (1999) 1781ndash1788
[153] D Borowitz RD Baker V Stallings Consensus report on nutrition for pediat-ric patients with cystic fibrosis J Pediatr Gastroenterol Nutr 35 (2002)246ndash259
[154] LJ Filer Jr SW Wright MP Manning KE Mason Absorption of alpha-tocopherol and tocopherylesters by premature and full term infants and chil-dren in health and disease Pediatrics 8 (1951) 328ndash339
[155] L Lancellotti C DOrazio G Mastella G Mazzi U Lippi Deficiency of vitamins Eand A in cystic fibrosis is independent of pancreatic function and current en-zyme and vitamin supplementation Eur J Pediatr 155 (1996) 281ndash285
[156] MN Sathe AS Patel Update in pediatrics focus on fat-soluble vitamins NutrClin Pract 25 (2010) 340ndash346
[157] MG Traber The ABCs of vitamin E and beta-carotene absorption Am J ClinNutr 80 (2004) 3ndash4
[158] TF Dolan Jr Hemolytic anemia and edema as the initial signs in infants withcystic fibrosis Consider this diagnosis even in absence of pulmonary symptomsClin Pediatr 15 (1976) 597ndash600
[159] DR James M Alfaham MC Goodchild Increased susceptibility to peroxide-induced haemolysis with normal vitamin E concentrations in cystic fibrosisClin Chim Acta 204 (1991) 279ndash290
[160] SA Peters FJ Kelly Vitamin E supplementation in cystic fibrosis J Pediatr Gas-troenterol Nutr 22 (1996) 341ndash345
[161] A Maqbool VA Stallings Update on fat-soluble vitamins in cystic fibrosis CurrOpin Pulm Med 14 (2008) 574ndash581
[162] SD Sagel MK Sontag MM Anthony P Emmett KA Papas Effect of anantioxidant-rich multivitamin supplement in cystic fibrosis J Cyst Fibros 10(2011) 31ndash36
[163] F Galli A Azzi Present trends in vitamin E research Biofactors 36 (2010)33ndash42
[164] A Hamahata P Enkhbaatar ER Kraft M Lange SW Leonard MG Traber RACox FC Schmalstieg HK Hawkins EB Whorton EM Horvath C Szabo LDTraber DN Herndon DL Traber Gamma-tocopherol nebulization by a lipidaerosolization device improves pulmonary function in sheep with burn andsmoke inhalation injury Free Radic Biol Med 45 (2008) 425ndash433
[165] JP Anais N Razzouq M Carvalho C Fernandez A Astier M Paul A AstierH Fessi AM Lorino Development of alpha-tocopherol acetate nanoparti-cles influence of preparative processes Drug Dev Ind Pharm 35 (2009)216ndash223
[166] JM Zingg Molecular and cellular activities of vitamin E analogues Mini RevMed Chem 7 (2007) 543ndash558
[167] V Viola F Pilolli M Piroddi E Pierpaoli F Orlando M Provinciali M Betti FMazzini F Galli Why tocotrienols work better insights into the in vitro anti-cancer mechanism of vitamin E Genes Nutr 7 (2011) 29ndash41
[168] F Galli F Mazzini L Bamonti L Gille S Bohmdorfer M Piroddi T Netscher FJKelly T Rosenau Tocotrienamines and tocopheramines reactions with radicalsand metal ions Bioorg Med Chem 19 (2011) 6483ndash6491
[169] A Kuhad K Chopra Attenuation of diabetic nephropathy by tocotrienol in-volvement of NFκB signaling pathway Life Sci 84 (2009) 296ndash301
[170] Q Jiang X Yin MA Lill ML Danielson H Freiser J Huang Long-chain carbox-ychromanols metabolites of vitamin E are potent inhibitors of cyclooxygenasesProc Natl Acad Sci U S A 105 (2008) 20464ndash20469
[171] ER Miller III R Pastor-Barriuso D Dalal RA Riemersma LJ Appel E GuallarMeta-analysis high-dosage vitamin E supplementation may increase all-causemortality Ann Intern Med 142 (2005) 37ndash46
[172] JN Hathcock A Azzi J Blumberg T Bray A Dickinson B Frei I Jialal CSJohnston FJ Kelly K Kraemer L Packer S Parthasarathy H Sies MG TraberVitamins E and C are safe across a broad range of intakes Am J Clin Nutr 81(2005) 736ndash745
[173] R Brigelius-Flohe F Galli Vitamin E a vitamin still awaiting the detection of itsbiological function Mol Nutr Food Res 54 (2010) 583ndash587
711F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
[174] MG Traber B Frei JS Beckman Vitamin E revisited do new data validate ben-efits for chronic disease prevention Curr Opin Lipidol 19 (2008) 30ndash38
[175] F Galli Meeting report Vitamin E Satellite Symposium (VESS) associated to theAnnual Meeting of the SFRR-Europe Rome 26 August 2009 Free Radic Res 43(2009) 1256ndash1257
[176] LJ Roberts II JA Oates MF Linton S Fazio BP Meador MD Gross Y Shyr JDMorrow The relationship between dose of vitamin E and suppression of oxida-tive stress in humans Free Radic Biol Med 43 (2007) 1388ndash1393
[177] EFSA- EFSA Scientific Opinion of the Panel on Food Additives FlavouringsProcessing Aids and Materials in Contact with Food on a request from the Com-mission on mixed tocopherols tocotrienol tocopherol and tocotrienols assources for vitamin E in EFSA- EFSA (Ed) vol 640 The EFSA Journal2008 pp 1ndash34
[178] P Rust I Eichler S Renner I Elmadfa Long-term oral beta-carotene supple-mentation in patients with cystic fibrosis mdash effects on antioxidative status andpulmonary function Ann Nutr Metab 44 (2000) 30ndash37
[179] G Lepage J Champagne N Ronco A Lamarre I Osberg RJ Sokol CC Roy Sup-plementation with carotenoids corrects increased lipid peroxidation in childrenwith cystic fibrosis Am J Clin Nutr 64 (1996) 87ndash93
[180] BM Winklhofer-Roob H Puhl G Khoschsorur MA vant Hof H EsterbauerDH Shmerling Enhanced resistance to oxidation of low density lipoproteinsand decreased lipid peroxide formation during beta-carotene supplementationin cystic fibrosis Free Radic Biol Med 18 (1995) 849ndash859
[181] RC Graham-Maar JI Schall N Stettler BS Zemel VA Stallings Elevated vita-min A intake and serum retinol in preadolescent children with cystic fibrosisAm J Clin Nutr 84 (2006) 174ndash182
[182] I Sadowska-Woda M Rachel J Pazdan E Bieszczad-Bedrejczuk K PawliszakNutritional supplement attenuates selected oxidative stress markers in pediatricpatients with cystic fibrosis Nutr Res (New York NY) 31 (2011) 509ndash518
[183] KA Papas MK Sontag C Pardee RJ Sokol SD Sagel FJ Accurso JS WagenerA pilot study on the safety and efficacy of a novel antioxidant rich formulation inpatients with cystic fibrosis J Cyst Fibros 7 (2008) 60ndash67
[184] Y Saito A Fukuhara K Nishio M Hayakawa Y Ogawa H Sakamoto K Fujii YYoshida E Niki Characterization of cellular uptake and distribution of coen-zyme Q10 and vitamin E in PC12 cells J Nutr Biochem 20 (2009) 350ndash357
[185] AA Franke CM Morrison JL Bakke LJ Custer X Li RV Cooney CoenzymeQ10 in human blood native levels and determinants of oxidation during proces-sing and storage Free Radic Biol Med 48 (2010) 1610ndash1617
[186] HN Bhagavan RK Chopra Plasma coenzyme Q10 response to oral ingestion ofcoenzyme Q10 formulations Mitochondrion 7 (2007) S78ndashS88 (Suppl)
[187] HN Bhagavan RK Chopra Coenzyme Q10 absorption tissue uptake metabo-lism and pharmacokinetics Free Radic Res 40 (2006) 445ndash453
[188] F Galli R Lee C Dunster FJ Kelly Gas chromatography mass spectrometryanalysis of carboxyethyl-hydroxychroman metabolites of alpha- and gamma-tocopherol in human plasma Free Radic Biol Med 32 (2002) 333ndash340
[189] F Galli R Lee J Atkinson A Floridi FJ Kelly Gamma-tocopherol biokineticsand transformation in humans Free Radic Res 37 (2003) 1225ndash1233
[190] TA Laguna MK Sontag I Osberg JS Wagener FJ Accurso RJ Sokol De-creased total serum coenzyme-Q10 concentrations a longitudinal study in chil-dren with cystic fibrosis J Pediatr 153 (2008) 402ndash407
[191] T Frischer JK Myung G Maurer I Eichler Z Szepfalusi G Lubec Possible dys-regulation of chaperon and metabolic proteins in cystic fibrosis bronchial tissueProteomics 6 (2006) 3381ndash3388
[192] C Andersson MM Zaman AB Jones SD Freedman Alterations in immune re-sponse and PPARLXR regulation in cystic fibrosis macrophages J Cyst Fibros 7(2008) 68ndash78
[193] SD Freedman PG Blanco MM Zaman JC Shea M Ollero IK Hopper DAWeed A Gelrud MM Regan M Laposata JG Alvarez BP OSullivan Associa-tion of cystic fibrosis with abnormalities in fatty acid metabolism N Engl JMed 350 (2004) 560ndash569
[194] S Van Biervliet G Vanbillemont JP Van Biervliet D Declercq E Robberecht AChristophe Relation between fatty acid composition and clinical status or geno-type in cystic fibrosis patients Ann Nutr Metab 51 (2007) 541ndash549
[195] SD Freedman MH Katz EM Parker M Laposata MY Urman JG AlvarezA membrane lipid imbalance plays a role in the phenotypic expression ofcystic fibrosis in cftr(minusminus) mice Proc Natl Acad Sci U S A 96 (1999)13995ndash14000
[196] S Van Biervliet S Vande Velde JP Van Biervliet E Robberecht The effect ofzinc supplements in cystic fibrosis patients Ann Nutr Metab 52 (2008)152ndash156
[197] WR Henderson Jr SJ Astley MM McCready P Kushmerick S Casey JWBecker BW Ramsey Oral absorption of omega-3 fatty acids in patients withcystic fibrosis who have pancreatic insufficiency and in healthy control subjectsJ Pediatr 124 (1994) 400ndash408
[198] I Durieu E Vericel D Guichardant H Roth JP Steghens J Drai RN JosserandE Fontaine M Lagarde G Bellon Fatty acids platelets and oxidative markersfollowing intravenous n-3 fatty acids administration in cystic fibrosis an openpilot observational study J Cyst Fibros 6 (2007) 320ndash326
[199] LG Wood DA Fitzgerald ML Garg Hypothesis vitamin E complements poly-unsaturated fatty acids in essential fatty acid deficiency in cystic fibrosis J AmColl Nutr 22 (2003) 253ndash257
[200] JD Lloyd-Still SB Johnson RT Holman Essential fatty acid status in cystic fi-brosis and the effects of safflower oil supplementation Am J Clin Nutr 34(1981) 1ndash7
[201] A Maqbool JI Schall JF Garcia-Espana BS Zemel B Strandvik VAStallings Serum linoleic acid status as a clinical indicator of essential fatty
acid status in children with cystic fibrosis J Pediatr Gastroenterol Nutr 47(2008) 635ndash644
[202] C Oliver N Jahnke Omega-3 fatty acids for cystic fibrosis Cochrane DatabaseSyst Rev (2011) CD002201
[203] B Strandvik E Gronowitz F Enlund T Martinsson J Wahlstrom Essential fattyacid deficiency in relation to genotype in patients with cystic fibrosis J Pediatr139 (2001) 650ndash655
[204] P Rise S Volpi C Colombo RF Padoan C DOrazio S Ghezzi PMelotti V BennatoC Agostoni BM Assael C Galli Whole blood fatty acid analysis with micromethodin cystic fibrosis and pulmonary disease J Cyst Fibros 9 (2010) 228ndash233
[205] H Cao K Gerhold JR Mayers MM Wiest SM Watkins GS Hotamisligil Iden-tification of a lipokine a lipid hormone linking adipose tissue to systemic me-tabolism Cell 134 (2008) 933ndash944
[206] RR Malapaka SK Khoo J Zhang JH Choi XE Zhou Y Xu Y Gong J Li ELYong MJ Chalmers L Chang JH Resau PR Griffin YE Chen HE Xu Iden-tification and mechanism of a ten carbon fatty acid as a modulating ligand ofperoxisome proliferator activated receptors J Biol Chem 287 (2012)183ndash195
[207] T Hara A Hirasawa A Ichimura I Kimura G Tsujimoto Free fatty acid recep-tors FFAR1 and GPR120 as novel therapeutic targets for metabolic disorders JPharm Sci 100 (2011) 3594ndash3601
[208] R Gupta P Rathi S Bradoo Lipase mediated upgradation of dietary fats andoils Crit Rev Food Sci Nutr 43 (2003) 635ndash644
[209] BH Jennings CC Akoh Lipase-catalyzed modification of rice bran oil to incor-porate capric acid J Agric Food Chem 48 (2000) 4439ndash4443
[210] J Hoeks M Mensink MK Hesselink K Ekroos P Schrauwen Long- andMedium-Chain Fatty Acids Induce Insulin Resistance to a Similar Extent inHumans Despite Marked Differences in Muscle Fat Accumulation J Clin Endo-crinol Metab 97 (2012) 208ndash216
[211] PJ Congden G Bruce MM Rothburn PC Clarke JM Littlewood J KelleherMS Losowsky Vitamin status in treated patients with cystic fibrosis ArchDis Child 56 (1981) 708ndash714
[212] BM Winklhofer-Roob H Ellemunter M Fruhwirth SE Schlegel-Haueter GKhoschsorur MA vant Hof DH Shmerling Plasma vitamin C concentrationsin patients with cystic fibrosis evidence of associations with lung inflammationAm J Clin Nutr 65 (1997) 1858ndash1866
[213] L Shamseer D Adams N Brown JA Johnson S Vohra Antioxidant micronutri-ents for lung disease in cystic fibrosis Cochrane Database Syst Rev (2010)CD007020
[214] C Santi S Santoro Electrophilic Selenium First edition Wiley-VCH VerlagGmbH amp Co KGaA 2012
[215] L Flohe S Toppo G Cozza F Ursini A comparison of thiol peroxidase mecha-nisms Antioxid Redox Signal 15 (2010) 763ndash780
[216] L Flohe JR Andreesen R Brigelius-Flohe M Maiorino F Ursini Selenium theelement of the moon in life on earth IUBMB Life 49 (2000) 411ndash420
[217] V Valdiglesias E Pasaro J Mendez B Laffon In vitro evaluation of seleniumgenotoxic cytotoxic and protective effects a review Arch Toxicol 84(2010) 337ndash351
[218] P Foucaud P Therond M Marchand F Brion JF Demelier J Navarro Seleniumand vitamin E in mucoviscidosis Arch Fr Pediatr 45 (1988) 383ndash386
[219] J Neve R Van Geffel M Hanocq L Molle Plasma and erythrocyte zinc copperand selenium in cystic fibrosis Acta Paediatr Scand 72 (1983) 437ndash440
[220] BM Winklhofer-Roob B Tiran PE Tuchschmid MA vant Hof DH ShmerlingEffects of pancreatic enzyme preparations on erythrocyte glutathione peroxi-dase activities and plasma selenium concentrations in cystic fibrosis FreeRadic Biol Med 25 (1998) 242ndash249
[221] JD Lloyd-Still HE Ganther Selenium and glutathione peroxidase levels in cys-tic fibrosis Pediatrics 65 (1980) 1010ndash1012
[222] D Tsavachidou TJ McDonnell S Wen X Wang F Vakar-Lopez LL Pisters CAPettaway CG Wood KA Do PF Thall C Stephens E Efstathiou R Taylor DGMenter P Troncoso SM Lippman CJ Logothetis J Kim Selenium and vitaminE cell type- and intervention-specific tissue effects in prostate cancer J NatlCancer Inst 101 (2009) 306ndash320
[223] IN Zelko TJ Mariani RJ Folz Superoxide dismutase multigene family acomparison of the CuZn-SOD (SOD1) Mn-SOD (SOD2) and EC-SOD (SOD3)gene structures evolution and expression Free Radic Biol Med 33 (2002)337ndash349
[224] RP Bowler JD Crapo Oxidative stress in airways is there a role for extracellu-lar superoxide dismutase Am J Respir Crit Care Med 166 (2002) S38ndashS43
[225] K Best K McCoy S Gemma RA Disilvestro Copper enzyme activities in cysticfibrosis before and after copper supplementation plus or minus zinc Metabo-lism 53 (2004) 37ndash41
[226] SS Percival GP Kauwell E Bowser M Wagner Altered copper status in adultmen with cystic fibrosis J Am Coll Nutr 18 (1999) 614ndash619
[227] NF Krebs JE Westcott TD Arnold BM Kluger FJ Accurso LV Miller KMHambidge Abnormalities in zinc homeostasis in young infants with cystic fibro-sis Pediatr Res 48 (2000) 256ndash261
[228] D Easley N Krebs M Jefferson L Miller J Erskine F Accurso KM HambidgeEffect of pancreatic enzymes on zinc absorption in cystic fibrosis J Pediatr Gas-troenterol Nutr 26 (1998) 136ndash139
[229] S Van Biervliet JP Van Biervliet E Robberecht Serum zinc in patients with cys-tic fibrosis at diagnosis and after one year of therapy Biol Trace Elem Res 112(2006) 205ndash211
[230] S Van Biervliet JP Van Biervliet S Vande Velde E Robberecht Serum zinc con-centrations in cystic fibrosis patients aged above 4 years a cross-sectional eval-uation Biol Trace Elem Res 119 (2007) 19ndash26
712 F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
[231] F Galli M Cristina Polidori W Stahl P Mecocci FJ Kelly Vitamin E biotransfor-mation in humans Vitam Horm 76 (2007) 263ndash280
[232] J Wiser NE Alexis Q Jiang W Wu C Robinette R Roubey DB Peden In vivogamma-tocopherol supplementation decreases systemic oxidative stress andcytokine responses of human monocytes in normal and asthmatic subjectsFree Radic Biol Med 45 (2008) 40ndash49
[233] JG Wagner Q Jiang JR Harkema B Illek DD Patel BN Ames DB PedenOzone enhancement of lower airway allergic inflammation is prevented bygamma-tocopherol Free Radic Biol Med 43 (2007) 1176ndash1188
[234] JT Harries DP Muller Absorption of different doses of fat soluble and watermiscible preparations of vitamin E in children with cystic fibrosis Arch DisChild 46 (1971) 341ndash344
[235] EI Back C Frindt E Ocenaskova D Nohr M Stern HK Biesalski Can changesin hydrophobicity increase the bioavailability of alpha-tocopherol Eur J Nutr45 (2006) 1ndash6
[236] SZ Nasr MH OLeary C Hillermeier Correction of vitamin E deficiency withfat-soluble versus water-miscible preparations of vitamin E in patients with cys-tic fibrosis J Pediatr 122 (1993) 810ndash812
[237] S Soltani-Frisk E Gronowitz H Andersson B Strandvik Water-miscibletocopherol is not superior to fat-soluble preparation for vitamin E absorptionin cystic fibrosis Acta Paediatr 90 (2001) 1112ndash1115
[238] K Papas J Kalbfleisch R Mohon Bioavailability of a novel water-soluble vi-tamin E formulation in malabsorbing patients Dig Dis Sci 52 (2007)347ndash352
[239] F Antonicelli M Parmentier EM Drost N Hirani I Rahman K Donaldson WMacNee Nacystelyn inhibits oxidant-mediated interleukin-8 expression andNF-kappaB nuclear binding in alveolar epithelial cells Free Radic Biol Med 32(2002) 492ndash502
[240] EM App D Baran I Dab A Malfroot M Coffiner F Vanderbist M King Dose-finding and 24-h monitoring for efficacy and safety of aerosolized Nacystelyn incystic fibrosis Eur Respir J 19 (2002) 294ndash302
[241] MG Traber How much vitamin E hellip Just enough Am J Clin Nutr 84 (2006)959ndash960
[242] JC McCann BN Ames Vitamin K an example of triage theory is micronu-trient inadequacy linked to diseases of aging Am J Clin Nutr 90 (2009)889ndash907
[243] M Fusaro G Crepaldi S Maggi F Galli A DAngelo L Calo S Giannini DMiozzo M Gallieni Vitamin K bone fractures and vascular calcifications inchronic kidney disease an important but poorly studied relationship J Endocri-nol Invest 34 (2010) 317ndash323
[244] JC McCann BN Ames Adaptive dysfunction of selenoproteins from the per-spective of the triage theory why modest selenium deficiency may increaserisk of diseases of aging FASEB J 25 (2011) 1793ndash1814
[245] R Apak K Guclu M Ozyurek B Bektas Oglu M Bener Cupric ion reducing an-tioxidant capacity assay for food antioxidants vitamins polyphenolics and fla-vonoids in food extracts Methods Mol Biol 477 (2008) 163ndash193
[246] F Galli Interactions of polyphenolic compounds with drug disposition and me-tabolism Curr Drug Metab 8 (2007) 830ndash838
[247] RL Prior X Wu K Schaich Standardized methods for the determination of an-tioxidant capacity and phenolics in foods and dietary supplements J Agric FoodChem 53 (2005) 4290ndash4302
[248] C Azbell S Zhang D Skinner J Fortenberry EJ Sorscher BA WoodworthHesperidin stimulates cystic fibrosis transmembrane conductance regulator-mediated chloride secretion and ciliary beat frequency in sinonasal epitheliumOtolaryngol Head Neck Surg 143 (2010) 397ndash404
[249] G Wegrzyn J Jakobkiewicz-Banecka M Gabig-Ciminska E Piotrowska M Nar-ajczyk A Kloska M Malinowska D Dziedzic I Golebiewska M Moskot AWegrzyn Genistein a natural isoflavone with a potential for treatment of ge-netic diseases Biochem Soc Trans 38 (2010) 695ndash701
[250] YC Yu H Miki Y Nakamura A Hanyuda Y Matsuzaki Y Abe M Yasui K Ta-naka TC Hwang SG Bompadre Y Sohma Curcumin and genistein additivelypotentiate G551D-CFTR J Cyst Fibros 10 (2011) 243ndash252
[251] B Illek H Fischer Flavonoids stimulate Cl conductance of human airway epithe-lium in vitro and in vivo Am J Physiol 275 (1998) L902ndashL910
[252] JL Kreindler Cystic fibrosis exploiting its genetic basis in the hunt for newtherapies Pharmacol Ther 125 (2010) 219ndash229
[253] B Illek L Zhang NC Lewis RB Moss JY Dong H Fischer Defective function ofthe cystic fibrosis-causing missense mutation G551D is recovered by genisteinAm J Physiol 277 (1999) C833ndashC839
[254] P Anandakumar S Kamaraj S Jagan G Ramakrishnan R Vinodhkumar TDevaki Capsaicin modulates pulmonary antioxidant defense system during ben-zo(a)pyrene-induced lung cancer in Swiss albinomice Phytother Res 22 (2008)529ndash533
[255] I Rahman Antioxidant therapeutic advances in COPD Ther Adv Respir Dis 2(2008) 351ndash374
[256] AW Boots H Li RP Schins R Duffin JW Heemskerk A Bast GR Haenen Thequercetin paradox Toxicol Appl Pharmacol 222 (2007) 89ndash96
[257] M Joskova S Franova V Sadlonova Acute bronchodilator effect of quercetin inexperimental allergic asthma Bratisl Lek Listy 112 (2011) 9ndash12
[258] HJ Park CM Lee ID Jung JS Lee YI Jeong JH Chang SH Chun MJ Kim IWChoi SC Ahn YK Shin SR Yeom YM Park Quercetin regulates Th1Th2 balancein a murine model of asthma Int Immunopharmacol 9 (2009) 261ndash267
[259] AP Rogerio A Kanashiro C Fontanari EV da Silva YM Lucisano-ValimEG Soares LH Faccioli Anti-inflammatory activity of quercetin and iso-quercitrin in experimental murine allergic asthma Inflamm Res 56 (2007)402ndash408
[260] M Muller Polyphenol cytotoxicity induced by the bacterial toxin pyocyaninrole of NQO1 Free Radic Biol Med 47 (2009) 84ndash91
[261] J Grassmann Terpenoids as plant antioxidants Vitam Horm 72 (2005)505ndash535
[262] P Allen Tea tree oil the science behind the antimicrobial hype Lancet 358(2001) 1245
[263] EC Dasenbrook W Checkley CA Merlo MW Konstan N Lechtzin MP BoyleAssociation between respiratory tract methicillin-resistant Staphylococcus aure-us and survival in cystic fibrosis JAMA 303 (2010) 2386ndash2392
[264] V Bezzerri M Borgatti E Nicolis I Lampronti MC Dechecchi I Mancini PRizzotti R Gambari G Cabrini Transcription factor oligodeoxynucleotides toNF-kappaB inhibit transcription of IL-8 in bronchial cells Am J Respir CellMol Biol 39 (2008) 86ndash96
[265] R Gambari M Borgatti V Bezzerri E Nicolis I Lampronti MC Dechecchi IMancini A Tamanini G Cabrini Decoy oligodeoxyribonucleotides and peptidenucleic acids-DNA chimeras targeting nuclear factor kappa-B inhibition of IL-8 gene expression in cystic fibrosis cells infected with Pseudomonas aeruginosaBiochem Pharmacol 80 (2010) 1887ndash1894
[266] M Adrian P Jeandet AC Douillet-Breuil L Tesson R Bessis Stilbene content ofmature Vitis vinifera berries in response to UV-C elicitation J Agric Food Chem48 (2000) 6103ndash6105
[267] B Paul I Masih J Deopujari C Charpentier Occurrence of resveratrol and pter-ostilbene in age-old darakchasava an ayurvedic medicine from India J Ethno-pharmacol 68 (1999) 71ndash76
[268] I Rahman Antioxidant therapies in COPD Int J Chron Obstruct Pulmon Dis 1(2006) 15ndash29
[269] M Lee S Kim OK Kwon SR Oh HK Lee K Ahn Anti-inflammatory and anti-asthmatic effects of resveratrol a polyphenolic stilbene in a mouse model ofallergic asthma Int Immunopharmacol 9 (2009) 418ndash424
[270] LG Wood PA Wark ML Garg Antioxidant and anti-inflammatory effectsof resveratrol in airway disease Antioxid Redox Signal 13 (2010)1535ndash1548
[271] KV Kiselev Perspectives for production and application of resveratrol ApplMicrobiol Biotechnol 90 (2011) 417ndash425
[272] M Shakibaei C Buhrmann A Mobasheri Resveratrol-mediated SIRT-1 interac-tions with p300 modulate receptor activator of NF-kappaB ligand (RANKL) acti-vation of NF-kappaB signaling and inhibit osteoclastogenesis in bone-derivedcells J Biol Chem 286 (2011) 11492ndash11505
[273] SF Zaidi K Ahmed T Yamamoto T Kondo K Usmanghani M Kadowaki TSugiyama Effect of resveratrol on Helicobacter pylori-induced interleukin-8 secre-tion reactive oxygen species generation and morphological changes in human gas-tric epithelial cells Biol Pharm Bull 32 (2009) 1931ndash1935
[274] JK Kundu YK Shin YJ Surh Resveratrol modulates phorbol ester-inducedpro-inflammatory signal transduction pathways in mouse skin in vivo NF-kappaB and AP-1 as prime targets Biochem Pharmacol 72 (2006)1506ndash1515
[275] NH Nam Naturally occurring NF-kappaB inhibitors Mini Rev Med Chem 6(2006) 945ndash951
[276] JM Smoliga JA Baur HA Hausenblas Resveratrol and healthmdasha comprehen-sive review of human clinical trials Mol Nutr Food Res 55 (2011) 1129ndash1141
[277] ME Juan M Maijo JM Planas Quantification of trans-resveratrol and itsmetabolites in rat plasma and tissues by HPLC J Pharm Biomed Anal 51(2010) 391ndash398
[278] JA Baur DA Sinclair Therapeutic potential of resveratrol the in vivo evidenceNat Rev 5 (2006) 493ndash506
[279] E Nicolis I Lampronti MC Dechecchi M Borgatti A Tamanini N Bianchi VBezzerri I Mancini MG Giri P Rizzotti R Gambari G Cabrini Pyrogallol anactive compound from the medicinal plant Emblica officinalis regulates expres-sion of pro-inflammatory genes in bronchial epithelial cells Int Immunophar-macol 8 (2008) 1672ndash1680
[280] E Nicolis I Lampronti MC Dechecchi M Borgatti A Tamanini V Bezzerri NBianchi M Mazzon I Mancini MG Giri P Rizzotti R Gambari G CabriniModulation of expression of IL-8 gene in bronchial epithelial cells by 5-methoxypsoralen Int Immunopharmacol 9 (2009) 1411ndash1422
[281] M Borgatti I Mancini N Bianchi A Guerrini I Lampronti D Rossi G SacchettiR Gambari Bergamot (Citrus bergamia Risso) fruit extracts and identified com-ponents alter expression of interleukin 8 gene in cystic fibrosis bronchial epithe-lial cell lines BMC Biochem 12 (2011) 15
[282] L Piccagli E Fabbri M Borgatti N Bianchi V Bezzerri I Mancini E Nicolis CMDechecchi I Lampronti G Cabrini R Gambari Virtual screening against p50NF-kappaB transcription factor for the identification of inhibitors of the NF-kappaB-DNA interaction and expression of NF-kappaB upregulated genesChemMedChem 4 (2009) 2024ndash2033
[283] L Piccagli M Borgatti E Nicolis N Bianchi I Mancini I Lampronti D VevaldiF DallAcqua G Cabrini R Gambari Virtual screening against nuclear factorkappaB (NF-kappaB) of a focus library identification of bioactive furocoumarinderivatives inhibiting NF-kappaB dependent biological functions involved incystic fibrosis Bioorg Med Chem 18 (2010) 8341ndash8349
[284] M Borgatti A Chilin L Piccagli I Lampronti N Bianchi I Mancini G Mar-zaro Da Francesco A Guiotto R Gambari Development of a novel furocou-marin derivative inhibiting NF-kappaB dependent biological functionsdesign synthesis and biological effects Eur J Med Chem 46 (2011)4870ndash4877
[285] E Georgy S Le Guellec L Vecellio E Fichant P Stordeur P Bordeau JP PerraudinFeasibility study of OSCN- and lactoferrin (Meveol) nebulization for cysticfibrosis JCyst Fibros 10 (2011) S18
713F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
[286] C Tidei M Piroddi F Galli C Santi Oxidation of thiols promoted by PhSeZnClTetrahedron Lett 53 (2012) 232ndash234
[287] L Semianrio-Vidal C van Hesuden G Mugesh ER Lazarowski Ebselen is a po-tent non-competitive inhibitor of extracellular nucleoside diphosphokinasePurinergic Signal 6 (2010) 383ndash391
[288] C ColussiMC Albertini S Coppola S Rovidati F Galli L Ghibelli H2O2-inducedblockof glycolysis as an active ADP-ribosylation reaction protecting cells from apoptosisFASEB J 14 (2000) 2266ndash2276
[289] H Xiao KL Parkin Induction of phase II enzyme activity by various seleniumcompounds Nutr Cancer 55 (2006) 210ndash223
[290] G Peluffo R Radi Biochemistry of protein tyrosine nitration in cardiovascularpathology Cardiovasc Res 75 (2007) 291ndash302
[291] B Alvarez R Radi Peroxynitrite reactivity with amino acids and proteinsAmino Acids 25 (2003) 295ndash311
[292] B Kamosinska MW Radomski M Duszyk A Radomski SF Man Nitric oxideactivates chloride currents in human lung epithelial cells Am J Physiol 272(1997) L1098ndashL1104
[293] L Chen RP Patel X Teng CA Bosworth JR Lancaster Jr S Matalon Mecha-nisms of cystic fibrosis transmembrane conductance regulator activation by S-nitrosoglutathione J Biol Chem 281 (2006) 9190ndash9199
[294] F Luchetti B CanonicoM BettiM Arcangeletti F PilolliM Piroddi L Canesi S PapaF Galli Melatonin signaling and cell protection function FASEB J 24 (2010)3603ndash3624
[295] MW Bengtsson G Jedstedt G Flemstrom Duodenal bicarbonate secretion inrats stimulation by intra-arterial and luminal guanylin and uroguanylin ActaPhysiol (Oxf) 191 (2007) 309ndash317
[296] CS Nelson JL Marino CN Allen Melatonin receptor potentiation of cyclic AMP andthe cystic fibrosis transmembrane conductance regulator ion channel J Pineal Res 26(1999) 113ndash121
[297] C de Castro-Silva VM de Bruin GM Cunha DM Nunes CAMedeiros PF de BruinMelatonin improves sleep and reduces nitrite in the exhaled breath condensate incystic fibrosismdasha randomized double-blind placebo-controlled study J Pineal Res48 (2010) 65ndash71
[298] I Hornyak E Pankotai L Kiss Z Lacza Current developments in the the-rapeutic potential of S-nitrosoglutathione an endogenous NO-donor mole-cule Curr Pharm Biotechnol (2011) Jan 11 [Epub ahead of print] - PMID21235457
[299] AH Snyder ME McPherson JF Hunt M Johnson JS Stamler B Gaston Acuteeffects of aerosolized S-nitrosoglutathione in cystic fibrosis Am J Respir CritCare Med 165 (2002) 922ndash926

704 F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
therapeutic approach will effectively prevent damage by multipleROS sources The defect of physiological antioxidants may also interferewith antioxidant therapies that are based on one or few exogenousantioxidants
Moreover several antioxidant vitamins such as vitamin E and ca-rotenoids have multiple natural forms with different bioavailabilitymetabolism and bioactivity [157167231] As far as the case of vita-min E supplementation concerns α-tocopherol was used as uniquevitamer in the large majority of supplementation trials so far per-formed and is the form used in the nutritional management of CFpatients Moreover several supplements contain the synthetic (or ra-cemic) form of this vitamin that has lower bioavailability than thenatural form Other forms present in nature and abundantly con-tained in vegetables such as tocotrienols and the less methylatedforms of tocopherol are not represented in many of the supplementformulations so far available in clinical centers and the supplementa-tion with α-tocopherol also limits their bioavailability These formsshow markedly higher susceptibility to hepatic metabolism and bili-ary excretion with respect to α-tocopherol eg the most representedform in blood and solid tissues and if co-supplemented these areeasily displaced during liver uptake and excreted with bile bymeans of competition with the same α-tocopherol Notwithstandingthese minor forms have been proposed to play important physiolog-ical roles showing molecular characteristics transcriptional effectsand antioxidant activities that clearly differentiate them in subfam-ilies with distinct biological functions Some of these such as α-tocopherol eg the second vitamin E form as relative abundance inblood and its carboxyethyl-hydroxychroman metabolite [189] ap-pear to have health-related anti-inflammatory effects which are par-ticularly relevant in lung protection [232233] This has suggestedthat such a group of ldquonon-α-tocopherolrdquo forms may represent anoth-er family of vitamins within the family of vitamin E with an impor-tant but often missed contribution to the proposed health effects ofthis vitamin [163]
These aspects may thus limit the possibility to provide CF patientsof optimal levels of this vitamin in all its components even if they areregularly treated with a vitamin E supplement eg withα-tocopherol
Targeted antioxidant therapy with formulations with higher bio-availability and bioactivity has been anticipated in CF New antioxi-dant formulations have been proposed to overcome main limits ofantioxidant therapies so far proposed for these patients Water-miscible α-tocopheryl acetate containing polysorbate propylene gly-col or polyethylene glycol as emulsifiers form micellar structureswere suggested to providing greater bioavailability than the fat-soluble counterparts These were commercialized with the brandnames of E-viminreg Cremophorreg EL and Aquasolreg E but despitethe original positive expectation [234235] some studies failed to ob-serve a higher response in vitamin E levels when these were com-pared with fat-soluble formulations [236237]
In a pilot study by Papas et al [183] a micellar formulation of fat-soluble nutrients and antioxidants was found to improve plasmalevels of β-carotene γ-tocopherol and CoQ(10) reducing at thesame time some inflammatory markers in induced sputum eg mye-loperoxidase and to a lower extent PMN elastase and total cell countswhile lung function and sputum bacterial counts were unaffectedThe same group recently confirmed the possibility to increase the ab-sorption of fat-soluble micronutrients using formulations with higherbioavailability specifically designed for malabsorbing patients such asCF patients that include also vitamin K and commercialized with thebrand name of AquADEKsreg [162] Despite improved vitamin and mi-cronutrient levels in this non-randomized open-label study AquA-DEKsreg produced only modest improvements in weight percentileand pulmonary function Another recent pilot observation [182] hassuggested the beneficial effect of this formulation on antioxidant andoxidative stress parameters of this oral supplement that surely deservesmore clinical investigation by larger randomized controlled trials
Recent multivitaminic formulations have been designed to containalso the minor forms of vitamin E and specifically γ-tocopherol [238]the expected superiority of which with respect to formulations con-taining only α-tocopherol needs to be verified As discussed abovein the section dedicated to vitamin E further advancements in thetherapy of CF inflammation and oxidative stress could be based onsynthetic forms and natural metabolites of this vitamin that havebeen recently identified to possess higher antioxidant and also anti-inflammatory activity than α-tocopherol (reviewed in [163168])
Pre-clinical investigation of these and other fat-soluble agents iscurrently addressed to develop formulations and administration pro-tocols that may increase the therapeutic efficacy in the airways In theantioxidant therapy of lung dysfunction in CF local administrationprotocols may overcome the limits of oral and systemic administra-tion protocols increasing bioavailability and providing targetedapproach to inflammation and oxidative stress Aerosolization of vita-min E and other fat-soluble micronutrients is possible and may allowdirect administration in the airways to prevent toxicity of smokewhich is closely associated with inflammation and oxidative stress[164165] To our knowledge this as well as other strategies of localadministration such as instillation of solutions such as surfactant-like solutions enriched of vitamin E have not been previously inves-tigated in CF patients and other CF model systems
On the contrary inhalation is an administration route widelyadopted in the case of GSH and NAC therapy described above Inthis context Cys formulations alternative to NAC have been proposedfor use as antioxidant and anti-inflammatory agent for inhalationNacystelyn is a lysine adduct of NAC that thanks to a higher proton-ation equilibrium shows increased water solubility and thus betterbioavailability Nacystelyn has been described to influence IL-8 gener-ation and the inflammatory signaling of bronchial epithelial cells[239] and preliminary clinical evaluation has demonstrated the safetyof this drug [240] Further clinical trials aimed to assess the effect onlung symptomatology of CF patients are needed Direct administra-tion in the airways could also be adopted for micronutrient vitaminswith poor absorption and bioavailability due to GI defects
38 Clinical impact of antioxidant therapy in CF
Huge in vitro and pre-clinical evidence has provided the rationaleto support clinical investigation of antioxidant strategies in CF Theseshould aim to restore the oxidantndashantioxidant balance of CF airwaychallenged by chronic infection and inflammatory cell activation
Some observational trials have confirmed that antioxidants usedas either supplements to the diet or drugs for lung administrationby aerosolized formulations may help in relieving progressive lungdamage and other adverse clinical events of CF such as poor growthSo far few studies have examined with sufficient methodologicalrigor the clinical efficacy of antioxidant therapy in CF This was alsoconcluded in a previous review of the literature by Cantin et al [12]that was published in the beginning of 2006 and is confirmed alsoin a recent analysis of clinical trials on antioxidant therapy in CF pa-tients [213] that examined the literature until September 2010using as sources the databases of the Cochrane CF and Genetic Disor-ders Group CF Trials Register PubMed CINAHL and AMED Useful in-formation was retrieved from just four randomized controlled trialsand one quasi-randomized controlled trial on vitamin C vitamin Eβ-carotene and selenium used as supplements administered aloneor in combination Post-hoc data analysis that was possible only inthree studies on a total of 87 CF patients showed the absence ofany significant improvement in lung function that was selected as pri-mary outcome together with quality of life that improved in one trialSecondary outcomes concerning laboratory indices of oxidative stressand antioxidant status showed several improvements These includedan increase of RBC SeGPx by selenium supplementation done as
705F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
individual or combined supplementation and increased levels of allplasma antioxidants except vitamin C that were observed in all thetrials
The message from these studies to pediatricians and nutritionistswithin the clinical staff of CF centers is that in the absence of solid ev-idence regarding the clinical effectiveness of oral formulations of an-tioxidant supplements in CF (including PUFA) their use as a routineclinical practice should be considered with caution keeping clear inmind that this should represent just a complement of one of themost critical interventions in the life-long clinical management pro-gram of CF patients eg providing an adequate nutriture [140] Inthis context compensating energy and protein malnutrition has toremain the first goal of nutritional management programs Providinghigher intakes of antioxidant micronutrients with food naturally-enriched (or functionalized) of micronutrient antioxidants shouldbe preferred in order to have the higher combination of positive nu-tritional factors that are lost during refinement procedures and over-all industrial processing of dietary supplements
Measures of good practice in clinical management of micro-malnutrition in CF patients would include the support of specializedpersonnel and laboratories The centers should have the possibilityto ascertain with appropriate nutritional and laboratory tests whatthe level of deficiency is for the different micronutrients that each pa-tient may suffer from during a dietary program Monitoring dietaryintakes and blood levels of micronutrients is not sufficient to set apersonalized nutritional intervention with supplements or functionalfoods Sub-optimal intakes and the compliance to nutritional inter-ventions should be verified by means of selected biochemical andclinical criteria Unluckily the latter are still not well established forsome micronutrients such as the fat-soluble vitamins E (reviewed in[163173241]) and K [242243] and also for trace elements such asSe [244] For many of the antioxidants used as supplements inhumans we still do not know exactly several of the biological effectsthat these may provide when introduced in a healthy body and weknow less what these can do in disease These aspects hardly impacton the concept of optimal levels of intake that should be identified foreach micronutrient on an individual basis According with the aspectsdiscussed in the previous sections optimal levels of intake for antiox-idant micronutrients are different in CF patients and healthy subjectsand vary with age and several individual factors
Lung administration of antioxidants by means of aerosolized for-mulations so far used for GSH therapy (see above) is a promisingfield of clinical investigation in CF Toxicity issues are currently themain concern and the subject of clinical evaluation by several groups(described above)
Information on future directions of antioxidant therapy in CF canbe inferred by the analysis of pending or recently completed clinicaltrials that have been searched (December 2011) at ClinicalTrialsgovdatabase matching the terms ldquoantioxidant therapyrdquo or ldquoglutathionerdquowith ldquocystic fibrosisrdquo Fifteen trials were retrieved and those directlyrelated to antioxidant therapy (n=12) are presented in Table 1 andinclude efficacy and safety studies of inhaled drugs as GSH sodiumpyruvate NAC and NO and the dietary supplements AquADEKsregan antioxidant-rich multivitamin supplement epigallocatechin gal-late (EGCG)tocotrienol curcuminoids the amino acid glutaminesulforaphane in broccoli sprouts One trial is investigating the flavo-noid quercetin as CFTR modulator
39 Emerging antioxidant and anti-inflammatory approaches in CF
Mediterranean foods such as olive oil and red wine or severalplant extracts such as herbal tea or grape seed extracts contain aseries of natural compounds with important antioxidant and NOscavenging activity that have been widely investigated for the pre-vention of oxidative stress-related diseases [38245] These havebeen long investigated as template molecules to develop antioxidant
and anti-inflammatory drugs Between the multitudes of natural sub-stances most investigated ones include for instance tyrosol hydroxy-tyrosol gallic and caffeic acids belonging to the family of phenolswhile resveratrol of the stilbenes family epicatechin kaempferoland cianidin are examples of flavonoids examples of fat-soluble phe-nolics are those of the family of tocols (vitamin E) and carotenoids Allthese compounds show different metabolisms and signaling effects[246] Antioxidant and cell protection mechanisms are associatedwith different and sometimes concurrent processes as H-atom trans-fer and electron donation radical trapping and chelation of transitionmetals that can be easily investigated at the chemical level [247] Be-sides these direct antioxidant effects metabolic responses and signal-ing effects of natural compounds are also important to producesecond-generation responses that modify the level of antioxidantprotection and the potential for ROS detoxification in cells and bodyfluids These derive from the transcriptional regulation of antioxidantand pro-oxidant genes that coexist with the modulation of cytokinesecretion and inflammatory enzyme activities
Some of these natural plant-derived antioxidants may provide fur-ther pharmacological activities of possible relevance in CF This is thecase for instance of the plant flavonoids genistein apigenin kaemp-ferol quercetin and hesperidin [248ndash251] that fall in the pharmaco-logical category of ldquopotentiatorsrdquo [252] in that these activate at leastto a certain extent CTFR-mediated Cl currents in normal and CF airwayepithelium investigated either in vitro or in vivo in humans and ani-mal models Actually as prototypal flavonoid-derived potentiatorthe tyrosine kinase inhibitor genistein potentiates the gating of wild-type as well as ΔF508 CFTR and G551D CFTR [253] but at higherdoses it inhibits CFTR gating which make this an unlikely clinical can-didate Similar potentiation effects have been reported for the antiox-idant curcumin [250] that shows an additive effect with respect togenistein-induced potentiation Besides CFTR potentiation whichdoes not appear to have a direct influence on GSH and nutrient trans-port in the lung tissue all these natural substances have been usedalone or in combination with other agents as in vivo enhancers oflung antioxidant protection [246254255] In the case of quercetinthiol-reactive phenolic [256] bronchodilation and anti-inflammatoryeffects by a restoration of the Th1Th2 balance have been reportedin inflammatory syndromes of the lung [255257ndash259] but theseeffects have not been explored in CF Pyocyanin toxicity (see abovein the Section 2) could represent an issue for the use of quercetinand other catechols in infectious diseases of the lung [260]
Other natural antioxidants of potential interest in CF therapy in-clude terpenoids [261] such as terpinen-4-ol a major constituentof tea tree oil that is being investigated in the therapy of anti-biotic resistant organisms specifically against methicillin-resistantStaphylococcus aureus (MRSA) [262] a problem in CF [263] Otherthan being lipophilic antioxidants terpenes can prevent oxidativestress of the CF lung secondarily to the antibiotic effect thereby pro-moting a better control of immuno-inflammatory pathways and lungantioxidants
391 Targeting NF-κB with natural compounds resveratrol and plantextracts
Natural compounds were long known to be useful in designinganti-inflammatory drugs and some of these could find an applicationin the control of the transcription factor kappa-B (NF-κB) that maylead to develop advanced pharmacological tools to control inflamma-tion and to produce higher antioxidant protection to CF airwaysInhibitors targeting NF-κB including transcription factors decoymolecules (TFD) are potent down-regulators of gene expressionand release of IL-8 in CF cells infected with P aeruginosa [264265]
Resveratrol (354prime-trihydroxystilbene ldquoErdquo form) is one of the mostinvestigated natural antioxidant with proposed activity as NF-κBinhibitor This is a phytoalexin present in large quantity in red winepreferentially in the skin of grapes being its concentration
706 F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
50ndash100 μgmg of fresh skin and 13ndash3 mgl of red wine [266]Furthermore resveratrol is a constituent of lsquoDarakchasavarsquo (13ndash6 mgl) an ayurvedic medicine from India [267] The antioxidant activity ofresveratrol has been reported in several papers and occurs also in lungtissues suggesting that resveratrol has potential as a therapeuticagent in respiratory disease [268ndash270] Resveratrol can be consideredone of the most interesting molecules from the natural worldexhibiting strong antioxidant activity that at the same time is able toexert anti inflammatory activity through alteration of NF-κB functionsand efficient inhibition of pro-inflammatory genes [271272] As far asthe effects on CF model systems are concerned Cabrini et al [26]reported the effects of resveratrol on P aeruginosa infected CF IB3-1cells The results obtained demonstrate that resveratrol exhibits minoreffects of IB3-1 cell growth and important inhibitory effects on accumu-lation of IL-8 and GRO-α mRNA while minor effects on IL-6 gene ex-pression were observed These data support recently publishedobservations suggesting inhibitory effects of resveratrol in infection-mediated inflammatory processes [273] Interestingly resveratrol hasbeen reported as a potent inhibitor of NF-κB activity and a promisinganti-inflammatory agent [272274] also in combinationwith othermol-ecules [274275] However in vivo translation of this pre-clinical on res-veratrol is hard to be foreseen This natural compound displays poorbioavailability [276] and further characterization of resveratrol pharma-cokinetics is troublesome since it is hardly measurable in vivo [277]Furthermore the regulation of inflammatory responses by resveratrolhas been suggested to be far more complex than simple direct suppres-sion of NF-κB activity Actually some aspects of the immune responsecould be enhanced by this natural substance which may lead tohypothesize broad negative feedback events on immuno-inflammatorypathways [278] In any case and with these cautions in mind the pub-lished observations on cellular model systems support the concept thatresveratrol and resveratrol-containing formulations deserve further con-sideration to determine their possible therapeutic values in CF
Other inhibitors can be identified from systematic studies of naturalproducts and their ability to interfere with NF-κB activity [279ndash281]Recent studies have demonstrated that the whole extract of Aeglemarmelos (Rutaceae) has strong inhibitory effect on the P aeruginosa-dependent IL-8 induction in human CF-derived bronchial IB3-1 cellswithout affecting cell proliferation [280] Molecular analysis of compo-nents contained in A marmelos extracts revealed that three major com-pounds namely 56-dimethoxy-1-indanone 2-hydroxy-cinnamic acidand 5-methoxy psoralen (5-MOP) reproduce the inhibitory effect ob-servedwith thewhole extract [280] A further example has been recent-ly published using extracts from bergamot (Citrus bergamia Risso) Inthis study the extracts were characterized and the main detected con-stituents were assayed for their biological activity [281] The resultsobtained demonstrated that the extracts from bergamot epicarps con-tain components displaying an inhibitory activity on IL-8 Particularlythe most active molecules were bergapten and citropten These effectshave been confirmed by analyzing mRNA levels and protein release inthe CF cellularmodels IB3-1 and CuFi-1 inducedwith TNF-α or exposedto P aeruginosa
A parallel strategy linking NF-κB inhibition and down-regulationof NF-κB-dependent functions is described in recently publishedstudies based on a structured-based virtual screening (VS) of differ-ently substituted furocoumarins and analogues against NF-κB withthe objective of selecting molecules able to inhibit the binding ofthis transcription factor to DNA [282283] Novel compounds wereidentified with this strategy as potent inhibitors of NF-κB dependentbiological functions to be proposed for the control lung inflammationoccurring in patients affected by CF [282ndash284]
392 Scavengers and regulators of H2O2 and NO
3921 Lactoferrin and OSCNmacr The impaired DUOXLPO system of CFpatients could be the target of therapeutic strategies that may
produce concomitant antimicrobial and antioxidant effects This sys-tem described above in Section 22 represents an important compo-nent of innate immunity with a role in bactericidal defense andregulation of H2O2 metabolism of airways [32] CF patients have alsoreported to show lowered LF levels in the ASL [37] that togetherwith a CFTR-dependent defective efflux of SCNmacr and LPO [36] may cre-ate the environment for a sustained flux of H2O2 and for the genera-tion of highly reactive Fenton species [1138] An ideal therapeuticintervention should restore the LPO-dependent generation of bacteri-cidal OSCNmacr from DUOX-derived H2O2 and SCNmacr in the ASL to controlat the same time the microbial biofilm and the flux of H2O2 into theASL An approach close to this therapeutic mechanism was recentlyproposed for the drug Meveolreg This is a complex of LF and OSCNmacrwith proposed in vivo antimicrobial activity [285] to be evaluatedin clinical trials for the aerosol treatment of lung infections in CFpatients The role for this drug in the control of H2O2 levels of ASLremains to be investigated
3922 Organoselenium compounds Organoselenium compoundshave been proposed as therapeutic agents useful in the antioxidanttherapy of inflammatory conditions These include GPX mimetic mol-ecules such as Ebselenreg (2-phenyl-12-benzisoselenazol-3(2H)-one)or other and more recently developed molecules that are still inpre-clinical steps of evaluation [286] Selectively and specificity of ac-tion are main issues in the therapeutic mechanism of this candidateantioxidant drug that thanks to the electrophilic properties of Se[214] reacts with thiols to reduce H2O2 and other species MoreoverEbselenreg has been described to act as potent non-competitive inhib-itor of extracellular nucleoside diphosphokinase (NDPK) having neg-ligible effect on ecto-ATPase and adenyl kinase activities which areother players of the metabolism of extracellular nucleotides [287]This enzyme together with other nucleoside di- and triphosphatescontributes to regulate several components of the mucociliary clear-ance process (MCC) that protects the lung against infections via acti-vation of epithelial purinergic receptors The inhibition of NDPK bythis GPX-mimetic drug may also impact on the energy status of endo-thelial cells [287] This aspect could be further investigated as a cellu-lar protection mechanism in the pulmonary epithelium of CF patientsbeing the control of cell energy of fundamental importance to preventthe activation of death pathways [288]
Further therapeutic mechanisms for these Se-derived drugs mayderive from the marked activity as inducers of phase II enzymessuch as quinone reductase (QR) and glutathione-S-transferase (GST)[289] This induction response also observed with other electrophilsand redox-active molecules such as natural phenolic antioxidantscould produce higher cellular protection by the acquisition of anincreased capability to detoxify endobiotics generated during oxida-tive stress and inflammation [246]
3923 Melatonin and GSNO as NOx regulators Increased markers ofNO-derived biological damage are present in the CF lung suggestingthe abnormal reactivity of NOx in the inflamed lung of CF patients[52] However an impaired metabolism and biological function ofNO in CF airways (see Section 23) suggests a cautious approach tothe use of agents that may influence the levels and chemical behaviorof NO-derived species (NOx) with possible impact on the physiologi-cal roles of NO in vasodilatation innate immunity and H2O2 metabo-lism of the respiratory tract [290291] NO donors also appear toinfluence CFTR function of alveolar epithelium and gland serouscells [292293]
Main physiological role of the pineal gland hormone melatonin isthe synchronization of circadian rhythms including the sleepndashwakecycle but several other functions dealing with immunomodulatoryantioxidant and cellular protection effects have been identified[294] Melatonin receptor stimulation may also influence cyclic AMPsignaling and the regulation of CFTR ion channel [295296]
707F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
A recent randomized double-blind placebo-controlled study hasexamined the effects of short term melatonin administration (3 mgfor 3 weeks) on sleep and oxidative stress markers in CF [297]According with the expected pharmacological effect of this hormonalsubstance the treatment was successful in improving sleep indicesAt the same time nitrite levels determined in exhaled breath conden-sate (EBC) were reduced to suggest a better control of NOmetabolismof CF airways (discussed above in Section 23) but these effects how-ever were not associated with a significant correction of isoprostaneas lipid peroxidation marker measured in EBC Increasing dosages ofmelatonin could be investigated for the pharmacological treatmentof oxidative stress and immune dysfunction of CF patients due tothe absence of adverse effects of this hormonal substance in humans
The S-nitrosation reaction of thiols is another interesting aspect ofNO pharmacology [53] that may find an application in the therapy oflung complications of CF This has been the case for instance of theS-nitrosothiol GSNO that has been used safely in human trials[298299] This endogenous nitrosothiol with proposed regulatory ef-fect on the CFTR of lung epithelia [292293] is well tolerated in pa-tients with CF when administered by aerosolization and mayproduce better oxygenation [299] thereby suggesting that therapyaimed at restoring endogenous GSNO levels in the CF airway maymerit further clinical evaluation Since the administered GSNO de-composes as shown by the increased levels of expired NO in CF pa-tients under treatment with this nitrosothiol [299] furtherinvestigation should be addressed to ascertain whether GSNO thera-py may merely correspond to a GSH therapy
NO dependent effects on CFTR function should be considered toevaluate mechanism of action and specificity of antioxidant therapiesthat target NO metabolism and function in the CF airways
4 Conclusions and future perspectives
The presence of clinical and biochemical symptoms of inflammationand oxidative stress implies that CF patients have a higher demand ofantioxidant protection The combination of the dysfunctional CFTRwith a lowered intake and absorption of dietary antioxidants producesub-optimal levels of protection from both enzymatic and non-enzymatic defense systems The former could be associated with a de-fective glutathionemetabolism and lowered intake of sulfur-containingamino acids and oligoelements such as zinc and possibly seleniumwhile fat-soluble antioxidant vitamins such as vitamin E and caroten-oids and the water-soluble vitamin C are lowered than in healthy sub-jects due to malabsorption and possibly higher consumption
The increased antioxidant demand in CF patients should be evenhigher in the presence of complications of the lung pancreas andliver Lung comorbidity is particularly important in this contextbeing associated with recurrent infections which results in the alter-nation of inflammatory exacerbates and chronic inflammation Thesesustain the flux of ROS in the airways and promote the formation ofsecond-generation byproducts by the damage of biomolecules suchas PUFA and proteins which may diffuse also at the systemic level tofurther promote adverse biological responses and toxic reactions Pan-creatic insufficiency causes malnutrition and may lead to develop en-docrine and metabolic defects associated with diabetes of CF Theseevents can be further aggravated by the concomitance of liver dys-function and a poor nutritional status Malnutrition is strongly associ-ated with poor prognosis as assessed by pulmonary function andsurvival data [138ndash140] The more aggressive nutritional interven-tions seem to produce better clinical outcomes in these patients andthe possibility of achieving higher antioxidant protection in well-nourished patients by dietary factors could be a key aspect to explainsuch a clinical advantage The assumption that food-derived compo-nentsmay help to prevent the damaging effects of oxidative stress im-proving the antioxidant defenses deserves further investigation at theclinical level This together with the investigation of appropriate
laboratory biomarkers could provide critical information to establishintervention criteria for an early nutritional management of newly di-agnosed patients [5] It is expected that a timely secondary preventionstrategy could influence the progression of CF symptoms thusaffecting with a self-feeding mechanism the same extent of malnutri-tion and oxidative stress along the life of CF patients Since severalfactors contribute to impair the nutritional status of CF patients(such as pancreatic insufficiency chronic malabsorption recurrentsinopulmonary infections and progressive lung disease chronic in-flammation increased energy expenditure suboptimal intake multi-therapy) careful monitoring of the antioxidant status should berecommended According with international guidelines fat-solublevitamin supplementation is of utmost importance in daily practice to-gether with energy intake requirements and pancreatic enzyme-replacement therapy Among these vitamin E β-carotene and ω-3FA have observed to alleviate selected biochemical signs of oxidativestress as measured for instance with well established laboratory indi-ces of lipid peroxidation and in some studies these effects werepreliminarily associated with positive clinical outcomes Notwith-standing randomizedndashcontrolled clinical trials on antioxidant supple-ments (including ω-3 FA) so far carried out in CF have failed toconclusively demonstrate significant beneficial effects on respiratorysymptoms and on the consequent impact that these have on the qual-ity of life of these patients (reviewed in [202213]) whichmay provideno support for the use of these supplements in CF An absence of effi-cacy in prevention studies on antioxidant supplements has also beenobserved in other and possibly less severe oxidative stress-relatedconditions particularly in the secondary prevention of cardiovasculardisease and some forms of cancer by vitamin E and other antioxidantssuch as vitamin C selenium and β-carotene (reviewed in [163]) Dif-ferent biases however have been identified in randomize large clini-cal trials that may account for these disappointing findings Theseinclude patient selection criteria (early interventions and primaryprevention could have more chances of success than secondaryprevention) duration and doses of the treatment use of wrong anti-oxidant formulations and administration protocols absence of verifi-cations of the biological compliance to the treatment etc The samebiases apply for the few trials carried out in CF patients Thus the ap-propriateness and efficacy of nutritional interventions with naturalfood-derived or synthetic antioxidants should be verifiedwith respectto the biological pathways of oxidative stress and clinical variablesthat are identified as end-points Profiles of blood and tissue antioxi-dants as well as of reliable surrogate markers of oxidative stresshave to be selected and determined in highly specialized laboratorieswith a well-established experience on these analyses
Well-timed (early) interventions with appropriate antioxidantformulationsprotocols need to be proposed for the next generationof trials and the development of novel CF-tailored antioxidant andanti-inflammatory agents should be promoted
As a consequence of these considerations more clinical investiga-tion is awaited to identify future successful approaches to the antiox-idant therapy as a measure to further enhance quality of life and theoverall clinical outcome of CF patients
Acknowledgments
We are indebted with the Italian Cystic Fibrosis Research Founda-tion for the support that it provided with its grant program to the re-search activity of the authors of this paper This is a scientific initiativeof the ldquoWorking Group on Inflammation in Cystic Fibrosisrdquo (BragonziA Bravo E Cabrini G Conese M Cuzzocrea S Dechecchi MC De Ales-sandri A Evangelista V Galli F Gambari R Lambiase A Lucidi VManca A Melotti P Minicucci L Motta A Pietraforte D Pompella AQuattrucci S Rizzo R Romano M Sorio C Tesse R) of the Italian Soci-ety for Cystic Fibrosis A particular thank goes to the Prof GianniMastella for the critical revision of the manuscript and for the
708 F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
stimulating research environment that he has contributed to createwithin the Italian Cystic Fibrosis Research Foundation
References
[1] BP OSullivan SD Freedman Cystic fibrosis Lancet 373 (2009) 1891ndash1904[2] P Linsdell JW Hanrahan Glutathione permeability of CFTR Am J Physiol 275
(1998) C323ndashC326[3] L Gao KJ Kim JR Yankaskas HJ Forman Abnormal glutathione transport in
cystic fibrosis airway epithelia Am J Physiol 277 (1999) L113ndashL118[4] RK Rowntree A Harris The phenotypic consequences of CFTR mutations Ann
Hum Genet 67 (2003) 471ndash485[5] EI Back C Frindt D Nohr J Frank R Ziebach M Stern M Ranke HK Biesalski
Antioxidant deficiency in cystic fibrosis when is the right time to take actionAm J Clin Nutr 80 (2004) 374ndash384
[6] LG Wood DA Fitzgerald AK Lee ML Garg Improved antioxidant and fattyacid status of patients with cystic fibrosis after antioxidant supplementation islinked to improved lung function Am J Clin Nutr 77 (2003) 150ndash159
[7] L Iuliano R Monticolo G Straface S Zullo F Galli M Boaz S Quattrucci Asso-ciation of cholesterol oxidation and abnormalities in fatty acid metabolism incystic fibrosis Am J Clin Nutr 90 (2009) 477ndash484
[8] C Libetta V Sepe P Esposito F Galli A Dal Canton Oxidative stress and inflam-mation implications in uremia and hemodialysis Clin Biochem 44 (2011)1189ndash1198
[9] G Bartosz Reactive oxygen species destroyers or messengers Biochem Phar-macol 77 (2009) 1303ndash1315
[10] T Ntimbane B Comte G Mailhot Y Berthiaume V Poitout M Prentki RRabasa-Lhoret E Levy Cystic fibrosis-related diabetes from CFTR dysfunctionto oxidative stress Clin Biochem 30 (2009) 153ndash177
[11] A van der Vliet JP Eiserich GP Marelich B Halliwell CE Cross Oxidativestress in cystic fibrosis does it occur and does it matter Adv Pharmacol 38(1997) 491ndash513
[12] AM Cantin TB White CE Cross HJ Forman RJ Sokol D Borowitz Antioxi-dants in cystic fibrosis Conclusions from the CF antioxidant workshop Bethes-da Maryland Free Radic Biol Med 42 (2007) 15ndash31
[13] LT McGrath P Mallon L Dowey B Silke E McClean M McDonnell A DevineS Copeland S Elborn Oxidative stress during acute respiratory exacerbations incystic fibrosis Thorax 54 (1999) 518ndash523
[14] E Thomson S Brennan R Senthilmohan CL Gangell AL Chapman PD SlyAJ Kettle E Balding LJ Berry JB Carlin R Carzino N de Klerk T Douglas CFoo LW Garratt GL Hall J Harrison A Kicic IA Laing KM Logie J MassieLS Mott C Murray F Parsons N Pillarisetti SR Poreddy SC RanganathanCF Robertson R Robins-Browne PJ Robinson B Skoric SM Stick ENSutanto E Williamson Identifying peroxidases and their oxidants in the earlypathology of cystic fibrosis Free Radic Biol Med 49 (2010) 1354ndash1360
[15] SP Range C Dunster AJ Knox FJ Kelly Treatment of pulmonary exacerba-tions of cystic fibrosis leads to improved antioxidant status Eur Respir J 13(1999) 560ndash564
[16] L Coppo P Ghezzi Thiol regulation of pro-inflammatory cytokines and innateimmunity protein S-thiolation as a novel molecular mechanism Biochem SocTrans 39 (2011) 1268ndash1272
[17] C Verhaeghe C Remouchamps B Hennuy A Vanderplasschen A Chariot SPTabruyn C Oury V Bours Role of IKK and ERK pathways in intrinsic inflamma-tion of cystic fibrosis airways Biochem Pharmacol 73 (2007) 1982ndash1994
[18] TL Bonfield JR Panuska MW Konstan KA Hilliard JB Hilliard H Ghnaim MBerger Inflammatory cytokines in cystic fibrosis lungs Am J Respir Crit CareMed 152 (1995) 2111ndash2118
[19] TL Noah HR Black PW Cheng RE Wood MW Leigh Nasal and bronchoal-veolar lavage fluid cytokines in early cystic fibrosis J Infect Dis 175 (1997)638ndash647
[20] MJ Welsh BW Ramsey FJ Accurso GR Cutting Cystic Fibrosis McGraw-HillNew York 2001
[21] TZ Khan JS Wagener T Bost J Martinez FJ Accurso DW Riches Early pul-monary inflammation in infants with cystic fibrosis Am J Respir Crit CareMed 151 (1995) 1075ndash1082
[22] FA Ratjen Cystic fibrosis pathogenesis and future treatment strategies RespirCare 54 (2009) 595ndash605
[23] J Jacquot O Tabary P Le Rouzic A Clement Airway epithelial cell inflamma-tory signalling in cystic fibrosis Int J Biochem Cell Biol 40 (2008)1703ndash1715
[24] CM Greene P Branagan NG McElvaney Toll-like receptors as therapeutic tar-gets in cystic fibrosis Expert Opin Ther Targets 12 (2008) 1481ndash1495
[25] M Rottner JM Freyssinet MC Martinez Mechanisms of the noxious inflam-matory cycle in cystic fibrosis Respir Res 10 (2009) 23
[26] G Cabrini V Bezzerri I Mancini E Nicolis MC Dechecchi A Tamanini ILampronti L Piccagli N Bianchi M Borgatti R Gambari Targeting transcrip-tion factor activity as a strategy to inhibit pro-inflammatory genes involved incystic fibrosis decoy oligonucleotides and low-molecular weight compoundsCurr Med Chem 17 (2010) 4392ndash4404
[27] CM Greene NG McElvaney Proteases and antiproteases in chronic neutrophiliclungdiseasemdash relevance to drug discovery Br J Pharmacol 158 (2009) 1048ndash1058
[28] AM Cantin Potential for antioxidant therapy of cystic fibrosis Curr Opin PulmMed 10 (2004) 531ndash536
[29] JF Chmiel MW Konstan Inflammation and anti-inflammatory therapies forcystic fibrosis Clin Chest Med 28 (2007) 331ndash346
[30] DP Nichols MW Konstan JF Chmiel Anti-inflammatory therapies for cys-tic fibrosis-related lung disease Clin Rev Allergy Immunol 35 (2008)135ndash153
[31] AJ Kettle T Chan I Osberg R Senthilmohan AL Chapman TJ Mocatta JSWagener Myeloperoxidase and protein oxidation in the airways of youngchildren with cystic fibrosis Am J Respir Crit Care Med 170 (2004)1317ndash1323
[32] H Fischer Mechanisms and function of DUOX in epithelia of the lung AntioxidRedox Signal 11 (2009) 2453ndash2465
[33] B Rada TL Leto Oxidative innate immune defenses by NoxDuox familyNADPH oxidases Contrib Microbiol 15 (2008) 164ndash187
[34] P Moskwa D Lorentzen KJ Excoffon J Zabner PB McCray Jr WM NauseefC Dupuy B Banfi A novel host defense system of airways is defective in cysticfibrosis Am J Respir Crit Care Med 175 (2007) 174ndash183
[35] D Lorentzen L Durairaj AA Pezzulo Y Nakano J Launspach DA Stoltz GZamba PB McCray Jr J Zabner MJ Welsh WM Nauseef B Banfi Concentra-tion of the antibacterial precursor thiocyanate in cystic fibrosis airway secre-tions Free Radic Biol Med 50 (2011) 1144ndash1150
[36] Y Xu S Szep Z Lu The antioxidant role of thiocyanate in the pathogenesis ofcystic fibrosis and other inflammation-related diseases Proc Natl Acad Sci US A 106 (2009) 20515ndash20519
[37] MP Rogan CC Taggart CM Greene PG Murphy SJ ONeill NG McElvaneyLoss of microbicidal activity and increased formation of biofilm due to decreasedlactoferrin activity in patients with cystic fibrosis J Infect Dis 190 (2004)1245ndash1253
[38] B Halliwell JM Guttridge Free Radicals in Biology and Medicine Fourth editionOxford University Press New York 2007
[39] B Rada K Lekstrom S Damian C Dupuy TL Leto The Pseudomonastoxin pyocyanin inhibits the dual oxidase-based antimicrobial system as itimposes oxidative stress on airway epithelial cells J Immunol 181 (2008)4883ndash4893
[40] C Schwarzer B Illek JH Suh SJ Remington H Fischer TE Machen Organelleredox of CF and CFTR-corrected airway epithelia Free Radic Biol Med 43(2007) 300ndash316
[41] JH Roum R Buhl NG McElvaney Z Borok RG Crystal Systemic deficiency ofglutathione in cystic fibrosis J Appl Physiol 75 (1993) 2419ndash2424
[42] VM Hudson Rethinking cystic fibrosis pathology the critical role of abnormalreduced glutathione (GSH) transport caused by CFTR mutation Free RadicBiol Med 30 (2001) 1440ndash1461
[43] PJ Barnes RA Dweik AF Gelb PG Gibson SC George H Grasemann IDPavord F Ratjen PE Silkoff DR Taylor N Zamel Exhaled nitric oxide in pul-monary diseases a comprehensive review Chest 138 (2010) 682ndash692
[44] H Grasemann E Michler M Wallot F Ratjen Decreased concentration of ex-haled nitric oxide (NO) in patients with cystic fibrosis Pediatr Pulmonol 24(1997) 173ndash177
[45] H Grasemann F Ratjen Cystic fibrosis lung disease the role of nitric oxidePediatr Pulmonol 28 (1999) 442ndash448
[46] B Gaston F Ratjen JW Vaughan NR Malhotra RG Canady AH Snyder JFHunt S Gaertig JB Goldberg Nitrogen redox balance in the cystic fibrosis air-way effects of antipseudomonal therapy Am J Respir Crit Care Med 165(2002) 387ndash390
[47] H Grasemann I Ioannidis RP Tomkiewicz H de Groot BK Rubin F RatjenNitric oxide metabolites in cystic fibrosis lung disease Arch Dis Child 78(1998) 49ndash53
[48] H Grasemann R Schwiertz S Matthiesen K Racke F Ratjen Increased argi-nase activity in cystic fibrosis airways Am J Respir Crit Care Med 172(2005) 1523ndash1528
[49] H Grasemann S Al-Saleh JA Scott D Shehnaz A Mehl R Amin M Rafii PPencharz J Belik F Ratjen Asymmetric dimethylarginine contributes to airwaynitric oxide deficiency in patients with cystic fibrosis Am J Respir Crit CareMed 183 (2011) 1363ndash1368
[50] H Grasemann F Kurtz F Ratjen Inhaled L-arginine improves exhaled nitricoxide and pulmonary function in patients with cystic fibrosis Am J RespirCrit Care Med 174 (2006) 208ndash212
[51] H Grasemann F Ratjen Emerging therapies for cystic fibrosis lung disease Ex-pert Opin Emerg Drugs 15 (2010) 653ndash659
[52] BM Morrissey K Schilling JV Weil PE Silkoff DM Rodman Nitric oxide andprotein nitration in the cystic fibrosis airway Arch Biochem Biophys 406(2002) 33ndash39
[53] R Radi Nitric oxide oxidants and protein tyrosine nitration Proc Natl AcadSci U S A 101 (2004) 4003ndash4008
[54] J Chen M Kinter S Shank C Cotton TJ Kelley AG Ziady Dysfunction of Nrf-2in CF epithelia leads to excess intracellular H2O2 and inflammatory cytokineproduction PLoS One 3 (2008) e3367
[55] F Galli M Piroddi C Annetti C Aisa E Floridi A Floridi Oxidative stress andreactive oxygen species Contrib Nephrol 149 (2005) 240ndash260
[56] DT Wright LA Cohn H Li B Fischer CM Li KB Adler Interactions of oxygenradicals with airway epithelium Environ Health Perspect 102 (Suppl 10)(1994) 85ndash90
[57] I Rahman SR Yang SK Biswas Current concepts of redox signaling in thelungs Antioxid Redox Signal 8 (2006) 681ndash689
[58] Q Li JF Engelhardt Interleukin-1beta induction of NFκB is partially regulatedby H2O2-mediated activation of NFκB-inducing kinase J Biol Chem 281(2006) 1495ndash1505
709F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
[59] E Boncoeur VS Criq E Bonvin T Roque A Henrion-Caude DC Gruenert AClement J Jacquot O Tabary Oxidative stress induces extracellular signal-regulated kinase 12 mitogen-activated protein kinase in cystic fibrosis lung ep-ithelial cells potential mechanism for excessive IL-8 expression Int J BiochemCell Biol 40 (2008) 432ndash446
[60] B Fischer J Voynow Neutrophil elastase induces MUC5AC messenger RNA ex-pression by an oxidant-dependent mechanism Chest 117 (2000) 317Sndash320S
[61] B Rada P Gardina TG Myers TL Leto Reactive oxygen species mediate in-flammatory cytokine release and EGFR-dependent mucin secretion in airwayepithelial cells exposed to Pseudomonas pyocyanin Mucosal Immunol 4(2011) 158ndash171
[62] C Schwarzer H Fischer EJ Kim KJ Barber AD Mills MJ Kurth DC GruenertJH Suh TE Machen B Illek Oxidative stress caused by pyocyanin impairs CFTRClminus transport in human bronchial epithelial cells Free Radic Biol Med 45(2008) 1653ndash1662
[63] J Hull M South P Phelan K Grimwood Surfactant composition in infants andyoung children with cystic fibrosis Am J Respir Crit Care Med 156 (1997)161ndash165
[64] KC Meyer A Sharma R Brown M Weatherly FR Moya J Lewandoski JJZimmerman Function and composition of pulmonary surfactant andsurfactant-derived fatty acid profiles are altered in young adults with cystic fi-brosis Chest 118 (2000) 164ndash174
[65] MK Pulfer RC Murphy Formation of biologically active oxysterols during ozo-nolysis of cholesterol present in lung surfactant J Biol Chem 279 (2004)26331ndash26338
[66] V Starosta E Rietschel K Paul U Baumann M Griese Oxidative changes ofbronchoalveolar proteins in cystic fibrosis Chest 129 (2006) 431ndash437
[67] V Starosta M Griese Oxidative damage to surfactant protein D in pulmonarydiseases Free Radic Res 40 (2006) 419ndash425
[68] M Griese R Essl R Schmidt E Rietschel F Ratjen M Ballmann K Paul Pulmo-nary surfactant lung function and endobronchial inflammation in cystic fibro-sis Am J Respir Crit Care Med 170 (2004) 1000ndash1005
[69] M Griese R Essl R Schmidt M Ballmann K Paul E Rietschel F Ratjen Se-quential analysis of surfactant lung function and inflammation in cystic fibrosispatients Respir Res 6 (2005) 133
[70] LG Wood DA Fitzgerald PG Gibson DM Cooper ML Garg Increased plasmafatty acid concentrations after respiratory exacerbations are associated with el-evated oxidative stress in cystic fibrosis patients Am J Clin Nutr 75 (2002)668ndash675
[71] P Montuschi SA Kharitonov G Ciabattoni M Corradi L van Rensen DM Ged-des ME Hodson PJ Barnes Exhaled 8-isoprostane as a new non-invasive bio-marker of oxidative stress in cystic fibrosis Thorax 55 (2000) 205ndash209
[72] CE Collins P Quaggiotto L Wood EV OLoughlin RL Henry ML Garg Elevat-ed plasma levels of F2 alpha isoprostane in cystic fibrosis Lipids 34 (1999)551ndash556
[73] D Hartl V Starosta K Maier I Beck-Speier C Rebhan BF Becker P Latzin RFischer F Ratjen RM Huber E Rietschel S Krauss-Etschmann M Griese In-haled glutathione decreases PGE2 and increases lymphocytes in cystic fibrosislungs Free Radic Biol Med 39 (2005) 463ndash472
[74] GL Milne H Yin JD Morrow Human biochemistry of the isoprostane pathwayJ Biol Chem 283 (2008) 15533ndash15537
[75] G Ciabattoni G Davi M Collura L Iapichino F Pardo A Ganci R Romagnoli JMaclouf C Patrono In vivo lipid peroxidation and platelet activation in cystic fi-brosis Am J Respir Crit Care Med 162 (2000) 1195ndash1201
[76] C Garenc P Julien E Levy Oxysterols in biological systems the gastrointestinaltract liver vascular wall and central nervous system Free Radic Res 44 (2011)47ndash73
[77] AM Cantin SL North RC Hubbard RG Crystal Normal alveolar epithelial lin-ing fluid contains high levels of glutathione J Appl Physiol 63 (1987) 152ndash157
[78] R Tirouvanziam CK Conrad T Bottiglieri LA Herzenberg RB Moss High-dose oral N-acetylcysteine a glutathione prodrug modulates inflammation incystic fibrosis Proc Natl Acad Sci U S A 103 (2006) 4628ndash4633
[79] LW Velsor C Kariya R Kachadourian BJ Day Mitochondrial oxidative stressin the lungs of cystic fibrosis transmembrane conductance regulator proteinmutant mice Am J Respir Cell Mol Biol 35 (2006) 579ndash586
[80] M Kelly-Aubert S Trudel J Fritsch T Nguyen-Khoa M Baudouin-Legros SMoriceau L Jeanson F Djouadi C Matar M Conti M Ollero F Brouillard AEdelman GSH monoethyl ester rescues mitochondrial defects in cystic fibrosismodels Hum Mol Genet 20 (2011) 2745ndash2759
[81] P Ghezzi Role of glutathione in immunity and inflammation in the lung Int JGen Med 4 (2011) 105ndash113
[82] N Dauletbaev K Viel R Buhl TO Wagner J Bargon Glutathione and glutathi-one peroxidase in sputum samples of adult patients with cystic fibrosis J CystFibros 3 (2004) 119ndash124
[83] CE Cross A van der Vliet CA ONeill S Louie B Halliwell Oxidants antioxi-dants and respiratory tract lining fluids Environ Health Perspect 102 (Suppl10) (1994) 185ndash191
[84] K Takeyama K Dabbagh J Jeong Shim T Dao-Pick IF Ueki JA Nadel Oxida-tive stress causes mucin synthesis via transactivation of epidermal growth factorreceptor role of neutrophils J Immunol 164 (2000) 1546ndash1552
[85] N Ballatori SM Krance S Notenboom S Shi K Tieu CL Hammond Glutathi-one dysregulation and the etiology and progression of human diseases BiolChem 390 (2009) 191ndash214
[86] SR Soltaninassab KR Sekhar MJ Meredith ML Freeman Multi-faceted regu-lation of gamma-glutamylcysteine synthetase J Cell Physiol 182 (2000)163ndash170
[87] HR Lopez-Mirabal JR Winther Redox characteristics of the eukaryotic cytosolBiochim Biophys Acta 1783 (2008) 629ndash640
[88] C Hwang AJ Sinskey HF Lodish Oxidized redox state of glutathione in the en-doplasmic reticulum Science 257 (1992) 1496ndash1502
[89] M Murphy Mitochondrial thiols in antioxidant protection and redox signallingdistinct roles for glutathionylation and other thiol modifications AntioxidRedox Signal (2011) ahead of print doi101089ars20114289
[90] BJ Day AM van Heeckeren E Min LW Velsor Role for cystic fibrosis trans-membrane conductance regulator protein in a glutathione response to bronch-opulmonary Pseudomonas infection Infect Immun 72 (2004) 2045ndash2051
[91] Y Zhang K Duan Glutathione exhibits antibacterial activity and increases tetra-cycline efficacy against Pseudomonas aeruginosa Sci China C Life Sci 52 (2009)501ndash505
[92] VM Hudson New insights into the pathogenesis of cystic fibrosis pivotal roleof glutathione system dysfunction and implications for therapy Treat RespirMed 3 (2004) 353ndash363
[93] LW Velsor A van Heeckeren BJ Day Antioxidant imbalance in the lungs ofcystic fibrosis transmembrane conductance regulator protein mutant miceAm J Physiol Lung Cell Mol Physiol 281 (2001) L31ndashL38
[94] I Kogan M Ramjeesingh C Li JF Kidd Y Wang EM Leslie SP Cole CE BearCFTR directly mediates nucleotide-regulated glutathione flux EMBO J 22(2003) 1981ndash1989
[95] NS Gould S Gauthier CT Kariya E Min J Huang DJ Brian Hypertonic salineincreases lung epithelial lining fluid glutathione and thiocyanate two protectiveCFTR-dependent thiols against oxidative injury Respir Res 11 (2010) 119
[96] VT Vasu SJ de Cruz JS Houghton KA Hayakawa BM Morrissey CE CrossJP Eiserich Evaluation of thiol-based antioxidant therapeutics in cystic fibrosissputum focus on myeloperoxidase Free Radic Res 45 (2011) 165ndash176
[97] L Roussel G Martel J Berube S Rousseau P aeruginosa drives CXCL8 synthesisvia redundant toll-like receptors and NADPH oxidase in CFTRF508 airway epi-thelial cells J Cyst Fibros 10 (2011) 107ndash113
[98] GW Lau DJ Hassett H Ran F Kong The role of pyocyanin in Pseudomonas aer-uginosa infection Trends Mol Med 10 (2004) 599ndash606
[99] R Wilson DA Sykes D Watson A Rutman GW Taylor PJ Cole Measurementof Pseudomonas aeruginosa phenazine pigments in sputum and assessment oftheir contribution to sputum sol toxicity for respiratory epithelium InfectImmun 56 (1988) 2515ndash2517
[100] M Muller Pyocyanin induces oxidative stress in human endothelial cells andmodulates the glutathione redox cycle Free Radic Biol Med 33 (2002)1527ndash1533
[101] YQ OMalley KJ Reszka BE Britigan Direct oxidation of 2prime7prime-dichlorodihy-drofluorescein by pyocyanin and other redox-active compounds independentof reactive oxygen species production Free Radic Biol Med 36 (2004)90ndash100
[102] CC Caldwell Y Chen HS Goetzmann Y Hao MT Borchers DJ Hassett LRYoung D Mavrodi L Thomashow GW Lau Pseudomonas aeruginosa exotoxinpyocyanin causes cystic fibrosis airway pathogenesis Am J Pathol 175 (2009)2473ndash2488
[103] YQ OMalley KJ Reszka DR Spitz GM Denning BE Britigan Pseudomonasaeruginosa pyocyanin directly oxidizes glutathione and decreases its levels inairway epithelial cells Am J Physiol Lung Cell Mol Physiol 287 (2004)L94ndashL103
[104] M Muller Glutathione modulates the toxicity of but is not a biologically rele-vant reductant for the Pseudomonas aeruginosa redox toxin pyocyanin FreeRadic Biol Med 50 (2011) 971ndash977
[105] R Cheluvappa R Shimmon M Dawson SN Hilmer DG Le Couteur Reactionsof Pseudomonas aeruginosa pyocyanin with reduced glutathione Acta BiochimPol 55 (2008) 571ndash580
[106] JH Widdicombe Transgenic animals may help resolve a sticky situation in cys-tic fibrosis J Clin Invest 120 (2010) 3093ndash3096
[107] X Sun H Sui JT Fisher Z Yan X Liu HJ Cho NS Joo Y Zhang W Zhou Y YiJM Kinyon DC Lei-Butters MA Griffin P Naumann M Luo J Ascher KWang T Frana JJ Wine DK Meyerholz JF Engelhardt Disease phenotype ofa ferret CFTR-knockout model of cystic fibrosis J Clin Invest 120 (2010)3149ndash3160
[108] NS Joo HJ Cho M Khansaheb JJ Wine Hyposecretion of fluid from trachealsubmucosal glands of CFTR-deficient pigs J Clin Invest 120 (2010) 3161ndash3166
[109] A Bragonzi Murine models of acute and chronic lung infection with cystic fibro-sis pathogens IJMM 300 (2010) 584ndash593
[110] AM van Heeckeren MD Schluchter Murine models of chronic Pseudomonasaeruginosa lung infection Lab Anim 36 (2002) 291ndash312
[111] A Bragonzi D Worlitzsch GB Pier P Timpert M Ulrich M Hentzer JB Ander-sen M Givskov M Conese G Doring Nonmucoid Pseudomonas aeruginosa ex-presses alginate in the lungs of patients with cystic fibrosis and in a mousemodel J Infect Dis 192 (2005) 410ndash419
[112] GS CW Bedrossian DB Singer JJ Hansen HS Rosenberg The lung in cysticfibrosis A quantitative study including prevalence of pathologic findingsamong different age groups Hum Pathol 7 (1976) 195ndash204
[113] WD HA Cash B McCullough WG Johanson Jr JA Bass A rat model of chron-ic respiratory infection with Pseudomonas aeruginosa Am Rev Respir Dis 119(1979) 453ndash459
[114] EM JR Starke C Langston CJ Baker A mouse model of chronic pulmonary in-fection with Pseudomonas aeruginosa and Pseudomonas cepacia Pediatr Res 22(1987) 698ndash702
[115] TJ AM van Heeckeren RW Walenga MW Konstan PB Davis B ErokwuMA Haxhiu TW Ferkol Effect of Pseudomonas infection on weight loss lung
710 F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
mechanics and cytokines in mice Am J Respir Crit Care Med 161 (2000)271ndash279
[116] T Aw G Wierzbicka DP Jones Oral glutathione increases tissue glutathione invivo Chem Biol Interact 80 (1991) 89ndash97
[117] F Favilli P Marraccini T Iantomasi MT Vincenzini Effect of orally adminis-tered glutathione on glutathione levels in some organs of rats role of specifictransporters Br J Nutr 78 (1997) 293ndash300
[118] C Kariya H Leitner E Min C van Heeckeren A van Heeckeren BJ Day A rolefor CFTR in the elevation of glutathione levels in the lung by oral glutathione ad-ministration Am J Physiol Lung Cell Mol Physiol 292 (2007) L1590ndashL1597
[119] K Atkuri JJ Mantovani LA Herzenberg LA Herzenberg N-Acetylcysteinemdashasafe antidote for cysteineglutathione deficiency Curr Opin Pharmacol 7(2007) 355ndash359
[120] R De Lisle E Roach K Jansson Effects of laxative and N-acetylcysteine onmucus accumulation bacterial load transit and inflammation in the cystic fi-brosis mouse small intestine Am J Physiol Gastrointest Liver Physiol 293(2007) G577ndashG584
[121] A Luciani VR Villella S Esposito N Brunetti-Pierri D Medina C Settembre MGavina L Pulze I Giardino M Pettoello-Mantovani M DApolito S Guido EMasliah B Spencer S Quaratino V Raia A Ballabio L Maiuri Defective CFTRinduces aggresome formation and lung inflammation in cystic fibrosis throughROS-mediated autophagy inhibition Nat Cell Biol 12 863ndash875
[122] M Griese J Ramakers A Krasselt V Starosta S Van Koningsbruggen R FischerF Ratjen B Mullinger RM Huber K Maier E Rietschel G Scheuch Improve-ment of alveolar glutathione and lung function but not oxidative state in cysticfibrosis Am J Respir Crit Care Med 169 (2004) 822ndash828
[123] C Bishop VM Hudson SC Hilton C Wilde A pilot study of the effect of inhaledbuffered reduced glutathione on the clinical status of patients with cystic fibro-sis Chest 127 (2005) 308ndash317
[124] WWang C Oliva G Li A Holmgren CH Lillig KL Kirk Reversible silencing of CFTRchloride channels by glutathionylation J Gen Physiol 125 (2005) 127ndash141
[125] N Dauletbaev P Fischer B Aulbach J Gross W Kusche U Thyroff-FriesingerTO Wagner J Bargon A phase II study on safety and efficacy of high-dose N-acetylcysteine in patients with cystic fibrosis Eur J Med Res 14 (2009)352ndash358
[126] R Tirouvanziam Y Gernez CK Conrad RB Moss I Schrijver CE Dunn ZADavies LA Herzenberg Profound functional and signaling changes in viable in-flammatory neutrophils homing to cystic fibrosis airways Proc Natl Acad SciU S A 105 (2008) 4335ndash4339
[127] JH Roum Z Borok NG McElvaney GJ Grimes AD Bokser R Buhl RG Crys-tal Glutathione aerosol suppresses lung epithelial surface inflammatory cell-derived oxidants in cystic fibrosis J Appl Physiol 87 (1999) 438ndash443
[128] A Visca CT Bishop SC Hilton VM Hudson Improvement in clinical markersin CF patients using a reduced glutathione regimen an uncontrolled observa-tional study J Cyst Fibros 7 (2008) 433ndash436
[129] EF Nash A Stephenson F Ratjen E Tullis Nebulized and oral thiol derivativesfor pulmonary disease in cystic fibrosis Cochrane Database Syst Rev (2009)CD007168
[130] AC foundation Drug Development Pipeline 2011[131] S Hoshida T Kuzuya N Yamashita M Nishida S Kitahara M Hori T
Kamada M Tada Gamma-glutamylcysteine ethyl ester for myocardial protec-tion in dogs during ischemia and reperfusion J Am Coll Cardiol 24 (1994)1391ndash1397
[132] J Lok W Leung S Zhao S Pallast K van Leyen S Guo X Wang A Yalcin EHLo Gamma-glutamylcysteine ethyl ester protects cerebral endothelial cells dur-ing injury and decreases bloodndashbrain barrier permeability after experimentalbrain trauma J Neurochem 118 (2011) 248ndash255
[133] Z Borok R Buhl GJ Grimes AD Bokser RC Hubbard KJ Holroyd JH RoumDB Czerski AM Cantin RG Crystal Effect of glutathione aerosol on oxidantndashantioxidant imbalance in idiopathic pulmonary fibrosis Lancet 338 (1991)215ndash216
[134] KJ Holroyd R Buhl Z Borok JH Roum AD Bokser GJ Grimes D Czerski AMCantin RG Crystal Correction of glutathione deficiency in the lower respiratorytract of HIV seropositive individuals by glutathione aerosol treatment Thorax 48(1993) 985ndash989
[135] J Hull P Vervaart K Grimwood P Phelan Pulmonary oxidative stress responsein young children with cystic fibrosis Thorax 52 (1997) 557ndash560
[136] A Corti A Paolicchi M Franzini S Dominici AF Casini A Pompella The S-thiolating activity of membrane gamma-glutamyltransferase formation ofcysteinyl-glycine mixed disulfides with cellular proteins and in the cell microen-vironment Antioxid Redox Signal 7 (2005) 911ndash918
[137] A Corti M Franzini AF Casini A Paolicchi A Pompella Vitamin C supply tobronchial epithelial cells linked to glutathione availability in elfmdasha role for se-creted gamma-glutamyltransferase J Cyst Fibros 7 (2008) 174ndash178
[138] A Munck Nutritional considerations in patients with cystic fibrosis Expert RevRespir Med 4 (2010) 47ndash56
[139] JL Matel CE Milla Nutrition in cystic fibrosis Semin Respir Crit Care Med 30(2009) 579ndash586
[140] D Salvatore R Buzzetti E Baldo MP Forneris V Lucidi D Manunza IMarinelli B Messore AS Neri V Raia ML Furnari G Mastella An overviewof international literature from cystic fibrosis registries 2 Neonatal screeningand nutritiongrowth J Cyst Fibros 9 (2010) 75ndash83
[141] KF Joosten JM Hulst Malnutrition in pediatric hospital patients current is-sues Nutrition 27 (2011) 133ndash137
[142] S Fustik T Jacovska L Spirevska S Koceva Protein-energy malnutrition as thefirst manifestation of cystic fibrosis in infancy Pediatr Int 51 (2009) 678ndash683
[143] J Himmelfarb E McMonagle Albumin is the major plasma protein target of ox-idant stress in uremia Kidney Int 60 (2001) 358ndash363
[144] P Stenvinkel JJ Carrero J Axelsson B Lindholm O Heimburger Z MassyEmerging biomarkers for evaluating cardiovascular risk in the chronic kidneydisease patient how do new pieces fit into the uremic puzzle Clin J Am SocNephrol 3 (2008) 505ndash521
[145] M Roche P Rondeau NR Singh E Tarnus E Bourdon The antioxidant proper-ties of serum albumin FEBS Lett 582 (2008) 1783ndash1787
[146] D Giustarini A Milzani I Dalle-Donne R Rossi Red blood cells as a physiolog-ical source of glutathione for extracellular fluids Blood Cells Mol Dis 40 (2008)174ndash179
[147] A Meister ME Anderson Glutathione Annu Rev Biochem 52 (1983) 711ndash760[148] B Alvarez S Carballal L Turell R Radi Formation and reactions of sulfenic acid
in human serum albumin Methods Enzymol 473 (2010) 117ndash136[149] S Carballal B Alvarez L Turell H Botti BA Freeman R Radi Sulfenic acid in
human serum albumin Amino Acids 32 (2007) 543ndash551[150] LR Barclay AM Bailey D Kong The antioxidant activity of alpha-tocopherol-
bovine serum albumin complex in micellar and liposome autoxidations J BiolChem 260 (1985) 15809ndash15814
[151] T Ishii T Ichikawa K Minoda K Kusaka S Ito Y Suzuki M Akagawa K Mochi-zuki T Goda T Nakayama Human serum albumin as an antioxidant in the ox-idation of (minus)-epigallocatechin gallate participation of reversible covalentbinding for interaction and stabilization Biosci Biotechnol Biochem 75(2011) 100ndash106
[152] F Galli S Rovidati S Benedetti U Buoncristiani C Covarelli A Floridi F Canes-trari Overexpression of erythrocyte glutathione S-transferase in uremia and di-alysis Clin Chem 45 (1999) 1781ndash1788
[153] D Borowitz RD Baker V Stallings Consensus report on nutrition for pediat-ric patients with cystic fibrosis J Pediatr Gastroenterol Nutr 35 (2002)246ndash259
[154] LJ Filer Jr SW Wright MP Manning KE Mason Absorption of alpha-tocopherol and tocopherylesters by premature and full term infants and chil-dren in health and disease Pediatrics 8 (1951) 328ndash339
[155] L Lancellotti C DOrazio G Mastella G Mazzi U Lippi Deficiency of vitamins Eand A in cystic fibrosis is independent of pancreatic function and current en-zyme and vitamin supplementation Eur J Pediatr 155 (1996) 281ndash285
[156] MN Sathe AS Patel Update in pediatrics focus on fat-soluble vitamins NutrClin Pract 25 (2010) 340ndash346
[157] MG Traber The ABCs of vitamin E and beta-carotene absorption Am J ClinNutr 80 (2004) 3ndash4
[158] TF Dolan Jr Hemolytic anemia and edema as the initial signs in infants withcystic fibrosis Consider this diagnosis even in absence of pulmonary symptomsClin Pediatr 15 (1976) 597ndash600
[159] DR James M Alfaham MC Goodchild Increased susceptibility to peroxide-induced haemolysis with normal vitamin E concentrations in cystic fibrosisClin Chim Acta 204 (1991) 279ndash290
[160] SA Peters FJ Kelly Vitamin E supplementation in cystic fibrosis J Pediatr Gas-troenterol Nutr 22 (1996) 341ndash345
[161] A Maqbool VA Stallings Update on fat-soluble vitamins in cystic fibrosis CurrOpin Pulm Med 14 (2008) 574ndash581
[162] SD Sagel MK Sontag MM Anthony P Emmett KA Papas Effect of anantioxidant-rich multivitamin supplement in cystic fibrosis J Cyst Fibros 10(2011) 31ndash36
[163] F Galli A Azzi Present trends in vitamin E research Biofactors 36 (2010)33ndash42
[164] A Hamahata P Enkhbaatar ER Kraft M Lange SW Leonard MG Traber RACox FC Schmalstieg HK Hawkins EB Whorton EM Horvath C Szabo LDTraber DN Herndon DL Traber Gamma-tocopherol nebulization by a lipidaerosolization device improves pulmonary function in sheep with burn andsmoke inhalation injury Free Radic Biol Med 45 (2008) 425ndash433
[165] JP Anais N Razzouq M Carvalho C Fernandez A Astier M Paul A AstierH Fessi AM Lorino Development of alpha-tocopherol acetate nanoparti-cles influence of preparative processes Drug Dev Ind Pharm 35 (2009)216ndash223
[166] JM Zingg Molecular and cellular activities of vitamin E analogues Mini RevMed Chem 7 (2007) 543ndash558
[167] V Viola F Pilolli M Piroddi E Pierpaoli F Orlando M Provinciali M Betti FMazzini F Galli Why tocotrienols work better insights into the in vitro anti-cancer mechanism of vitamin E Genes Nutr 7 (2011) 29ndash41
[168] F Galli F Mazzini L Bamonti L Gille S Bohmdorfer M Piroddi T Netscher FJKelly T Rosenau Tocotrienamines and tocopheramines reactions with radicalsand metal ions Bioorg Med Chem 19 (2011) 6483ndash6491
[169] A Kuhad K Chopra Attenuation of diabetic nephropathy by tocotrienol in-volvement of NFκB signaling pathway Life Sci 84 (2009) 296ndash301
[170] Q Jiang X Yin MA Lill ML Danielson H Freiser J Huang Long-chain carbox-ychromanols metabolites of vitamin E are potent inhibitors of cyclooxygenasesProc Natl Acad Sci U S A 105 (2008) 20464ndash20469
[171] ER Miller III R Pastor-Barriuso D Dalal RA Riemersma LJ Appel E GuallarMeta-analysis high-dosage vitamin E supplementation may increase all-causemortality Ann Intern Med 142 (2005) 37ndash46
[172] JN Hathcock A Azzi J Blumberg T Bray A Dickinson B Frei I Jialal CSJohnston FJ Kelly K Kraemer L Packer S Parthasarathy H Sies MG TraberVitamins E and C are safe across a broad range of intakes Am J Clin Nutr 81(2005) 736ndash745
[173] R Brigelius-Flohe F Galli Vitamin E a vitamin still awaiting the detection of itsbiological function Mol Nutr Food Res 54 (2010) 583ndash587
711F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
[174] MG Traber B Frei JS Beckman Vitamin E revisited do new data validate ben-efits for chronic disease prevention Curr Opin Lipidol 19 (2008) 30ndash38
[175] F Galli Meeting report Vitamin E Satellite Symposium (VESS) associated to theAnnual Meeting of the SFRR-Europe Rome 26 August 2009 Free Radic Res 43(2009) 1256ndash1257
[176] LJ Roberts II JA Oates MF Linton S Fazio BP Meador MD Gross Y Shyr JDMorrow The relationship between dose of vitamin E and suppression of oxida-tive stress in humans Free Radic Biol Med 43 (2007) 1388ndash1393
[177] EFSA- EFSA Scientific Opinion of the Panel on Food Additives FlavouringsProcessing Aids and Materials in Contact with Food on a request from the Com-mission on mixed tocopherols tocotrienol tocopherol and tocotrienols assources for vitamin E in EFSA- EFSA (Ed) vol 640 The EFSA Journal2008 pp 1ndash34
[178] P Rust I Eichler S Renner I Elmadfa Long-term oral beta-carotene supple-mentation in patients with cystic fibrosis mdash effects on antioxidative status andpulmonary function Ann Nutr Metab 44 (2000) 30ndash37
[179] G Lepage J Champagne N Ronco A Lamarre I Osberg RJ Sokol CC Roy Sup-plementation with carotenoids corrects increased lipid peroxidation in childrenwith cystic fibrosis Am J Clin Nutr 64 (1996) 87ndash93
[180] BM Winklhofer-Roob H Puhl G Khoschsorur MA vant Hof H EsterbauerDH Shmerling Enhanced resistance to oxidation of low density lipoproteinsand decreased lipid peroxide formation during beta-carotene supplementationin cystic fibrosis Free Radic Biol Med 18 (1995) 849ndash859
[181] RC Graham-Maar JI Schall N Stettler BS Zemel VA Stallings Elevated vita-min A intake and serum retinol in preadolescent children with cystic fibrosisAm J Clin Nutr 84 (2006) 174ndash182
[182] I Sadowska-Woda M Rachel J Pazdan E Bieszczad-Bedrejczuk K PawliszakNutritional supplement attenuates selected oxidative stress markers in pediatricpatients with cystic fibrosis Nutr Res (New York NY) 31 (2011) 509ndash518
[183] KA Papas MK Sontag C Pardee RJ Sokol SD Sagel FJ Accurso JS WagenerA pilot study on the safety and efficacy of a novel antioxidant rich formulation inpatients with cystic fibrosis J Cyst Fibros 7 (2008) 60ndash67
[184] Y Saito A Fukuhara K Nishio M Hayakawa Y Ogawa H Sakamoto K Fujii YYoshida E Niki Characterization of cellular uptake and distribution of coen-zyme Q10 and vitamin E in PC12 cells J Nutr Biochem 20 (2009) 350ndash357
[185] AA Franke CM Morrison JL Bakke LJ Custer X Li RV Cooney CoenzymeQ10 in human blood native levels and determinants of oxidation during proces-sing and storage Free Radic Biol Med 48 (2010) 1610ndash1617
[186] HN Bhagavan RK Chopra Plasma coenzyme Q10 response to oral ingestion ofcoenzyme Q10 formulations Mitochondrion 7 (2007) S78ndashS88 (Suppl)
[187] HN Bhagavan RK Chopra Coenzyme Q10 absorption tissue uptake metabo-lism and pharmacokinetics Free Radic Res 40 (2006) 445ndash453
[188] F Galli R Lee C Dunster FJ Kelly Gas chromatography mass spectrometryanalysis of carboxyethyl-hydroxychroman metabolites of alpha- and gamma-tocopherol in human plasma Free Radic Biol Med 32 (2002) 333ndash340
[189] F Galli R Lee J Atkinson A Floridi FJ Kelly Gamma-tocopherol biokineticsand transformation in humans Free Radic Res 37 (2003) 1225ndash1233
[190] TA Laguna MK Sontag I Osberg JS Wagener FJ Accurso RJ Sokol De-creased total serum coenzyme-Q10 concentrations a longitudinal study in chil-dren with cystic fibrosis J Pediatr 153 (2008) 402ndash407
[191] T Frischer JK Myung G Maurer I Eichler Z Szepfalusi G Lubec Possible dys-regulation of chaperon and metabolic proteins in cystic fibrosis bronchial tissueProteomics 6 (2006) 3381ndash3388
[192] C Andersson MM Zaman AB Jones SD Freedman Alterations in immune re-sponse and PPARLXR regulation in cystic fibrosis macrophages J Cyst Fibros 7(2008) 68ndash78
[193] SD Freedman PG Blanco MM Zaman JC Shea M Ollero IK Hopper DAWeed A Gelrud MM Regan M Laposata JG Alvarez BP OSullivan Associa-tion of cystic fibrosis with abnormalities in fatty acid metabolism N Engl JMed 350 (2004) 560ndash569
[194] S Van Biervliet G Vanbillemont JP Van Biervliet D Declercq E Robberecht AChristophe Relation between fatty acid composition and clinical status or geno-type in cystic fibrosis patients Ann Nutr Metab 51 (2007) 541ndash549
[195] SD Freedman MH Katz EM Parker M Laposata MY Urman JG AlvarezA membrane lipid imbalance plays a role in the phenotypic expression ofcystic fibrosis in cftr(minusminus) mice Proc Natl Acad Sci U S A 96 (1999)13995ndash14000
[196] S Van Biervliet S Vande Velde JP Van Biervliet E Robberecht The effect ofzinc supplements in cystic fibrosis patients Ann Nutr Metab 52 (2008)152ndash156
[197] WR Henderson Jr SJ Astley MM McCready P Kushmerick S Casey JWBecker BW Ramsey Oral absorption of omega-3 fatty acids in patients withcystic fibrosis who have pancreatic insufficiency and in healthy control subjectsJ Pediatr 124 (1994) 400ndash408
[198] I Durieu E Vericel D Guichardant H Roth JP Steghens J Drai RN JosserandE Fontaine M Lagarde G Bellon Fatty acids platelets and oxidative markersfollowing intravenous n-3 fatty acids administration in cystic fibrosis an openpilot observational study J Cyst Fibros 6 (2007) 320ndash326
[199] LG Wood DA Fitzgerald ML Garg Hypothesis vitamin E complements poly-unsaturated fatty acids in essential fatty acid deficiency in cystic fibrosis J AmColl Nutr 22 (2003) 253ndash257
[200] JD Lloyd-Still SB Johnson RT Holman Essential fatty acid status in cystic fi-brosis and the effects of safflower oil supplementation Am J Clin Nutr 34(1981) 1ndash7
[201] A Maqbool JI Schall JF Garcia-Espana BS Zemel B Strandvik VAStallings Serum linoleic acid status as a clinical indicator of essential fatty
acid status in children with cystic fibrosis J Pediatr Gastroenterol Nutr 47(2008) 635ndash644
[202] C Oliver N Jahnke Omega-3 fatty acids for cystic fibrosis Cochrane DatabaseSyst Rev (2011) CD002201
[203] B Strandvik E Gronowitz F Enlund T Martinsson J Wahlstrom Essential fattyacid deficiency in relation to genotype in patients with cystic fibrosis J Pediatr139 (2001) 650ndash655
[204] P Rise S Volpi C Colombo RF Padoan C DOrazio S Ghezzi PMelotti V BennatoC Agostoni BM Assael C Galli Whole blood fatty acid analysis with micromethodin cystic fibrosis and pulmonary disease J Cyst Fibros 9 (2010) 228ndash233
[205] H Cao K Gerhold JR Mayers MM Wiest SM Watkins GS Hotamisligil Iden-tification of a lipokine a lipid hormone linking adipose tissue to systemic me-tabolism Cell 134 (2008) 933ndash944
[206] RR Malapaka SK Khoo J Zhang JH Choi XE Zhou Y Xu Y Gong J Li ELYong MJ Chalmers L Chang JH Resau PR Griffin YE Chen HE Xu Iden-tification and mechanism of a ten carbon fatty acid as a modulating ligand ofperoxisome proliferator activated receptors J Biol Chem 287 (2012)183ndash195
[207] T Hara A Hirasawa A Ichimura I Kimura G Tsujimoto Free fatty acid recep-tors FFAR1 and GPR120 as novel therapeutic targets for metabolic disorders JPharm Sci 100 (2011) 3594ndash3601
[208] R Gupta P Rathi S Bradoo Lipase mediated upgradation of dietary fats andoils Crit Rev Food Sci Nutr 43 (2003) 635ndash644
[209] BH Jennings CC Akoh Lipase-catalyzed modification of rice bran oil to incor-porate capric acid J Agric Food Chem 48 (2000) 4439ndash4443
[210] J Hoeks M Mensink MK Hesselink K Ekroos P Schrauwen Long- andMedium-Chain Fatty Acids Induce Insulin Resistance to a Similar Extent inHumans Despite Marked Differences in Muscle Fat Accumulation J Clin Endo-crinol Metab 97 (2012) 208ndash216
[211] PJ Congden G Bruce MM Rothburn PC Clarke JM Littlewood J KelleherMS Losowsky Vitamin status in treated patients with cystic fibrosis ArchDis Child 56 (1981) 708ndash714
[212] BM Winklhofer-Roob H Ellemunter M Fruhwirth SE Schlegel-Haueter GKhoschsorur MA vant Hof DH Shmerling Plasma vitamin C concentrationsin patients with cystic fibrosis evidence of associations with lung inflammationAm J Clin Nutr 65 (1997) 1858ndash1866
[213] L Shamseer D Adams N Brown JA Johnson S Vohra Antioxidant micronutri-ents for lung disease in cystic fibrosis Cochrane Database Syst Rev (2010)CD007020
[214] C Santi S Santoro Electrophilic Selenium First edition Wiley-VCH VerlagGmbH amp Co KGaA 2012
[215] L Flohe S Toppo G Cozza F Ursini A comparison of thiol peroxidase mecha-nisms Antioxid Redox Signal 15 (2010) 763ndash780
[216] L Flohe JR Andreesen R Brigelius-Flohe M Maiorino F Ursini Selenium theelement of the moon in life on earth IUBMB Life 49 (2000) 411ndash420
[217] V Valdiglesias E Pasaro J Mendez B Laffon In vitro evaluation of seleniumgenotoxic cytotoxic and protective effects a review Arch Toxicol 84(2010) 337ndash351
[218] P Foucaud P Therond M Marchand F Brion JF Demelier J Navarro Seleniumand vitamin E in mucoviscidosis Arch Fr Pediatr 45 (1988) 383ndash386
[219] J Neve R Van Geffel M Hanocq L Molle Plasma and erythrocyte zinc copperand selenium in cystic fibrosis Acta Paediatr Scand 72 (1983) 437ndash440
[220] BM Winklhofer-Roob B Tiran PE Tuchschmid MA vant Hof DH ShmerlingEffects of pancreatic enzyme preparations on erythrocyte glutathione peroxi-dase activities and plasma selenium concentrations in cystic fibrosis FreeRadic Biol Med 25 (1998) 242ndash249
[221] JD Lloyd-Still HE Ganther Selenium and glutathione peroxidase levels in cys-tic fibrosis Pediatrics 65 (1980) 1010ndash1012
[222] D Tsavachidou TJ McDonnell S Wen X Wang F Vakar-Lopez LL Pisters CAPettaway CG Wood KA Do PF Thall C Stephens E Efstathiou R Taylor DGMenter P Troncoso SM Lippman CJ Logothetis J Kim Selenium and vitaminE cell type- and intervention-specific tissue effects in prostate cancer J NatlCancer Inst 101 (2009) 306ndash320
[223] IN Zelko TJ Mariani RJ Folz Superoxide dismutase multigene family acomparison of the CuZn-SOD (SOD1) Mn-SOD (SOD2) and EC-SOD (SOD3)gene structures evolution and expression Free Radic Biol Med 33 (2002)337ndash349
[224] RP Bowler JD Crapo Oxidative stress in airways is there a role for extracellu-lar superoxide dismutase Am J Respir Crit Care Med 166 (2002) S38ndashS43
[225] K Best K McCoy S Gemma RA Disilvestro Copper enzyme activities in cysticfibrosis before and after copper supplementation plus or minus zinc Metabo-lism 53 (2004) 37ndash41
[226] SS Percival GP Kauwell E Bowser M Wagner Altered copper status in adultmen with cystic fibrosis J Am Coll Nutr 18 (1999) 614ndash619
[227] NF Krebs JE Westcott TD Arnold BM Kluger FJ Accurso LV Miller KMHambidge Abnormalities in zinc homeostasis in young infants with cystic fibro-sis Pediatr Res 48 (2000) 256ndash261
[228] D Easley N Krebs M Jefferson L Miller J Erskine F Accurso KM HambidgeEffect of pancreatic enzymes on zinc absorption in cystic fibrosis J Pediatr Gas-troenterol Nutr 26 (1998) 136ndash139
[229] S Van Biervliet JP Van Biervliet E Robberecht Serum zinc in patients with cys-tic fibrosis at diagnosis and after one year of therapy Biol Trace Elem Res 112(2006) 205ndash211
[230] S Van Biervliet JP Van Biervliet S Vande Velde E Robberecht Serum zinc con-centrations in cystic fibrosis patients aged above 4 years a cross-sectional eval-uation Biol Trace Elem Res 119 (2007) 19ndash26
712 F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
[231] F Galli M Cristina Polidori W Stahl P Mecocci FJ Kelly Vitamin E biotransfor-mation in humans Vitam Horm 76 (2007) 263ndash280
[232] J Wiser NE Alexis Q Jiang W Wu C Robinette R Roubey DB Peden In vivogamma-tocopherol supplementation decreases systemic oxidative stress andcytokine responses of human monocytes in normal and asthmatic subjectsFree Radic Biol Med 45 (2008) 40ndash49
[233] JG Wagner Q Jiang JR Harkema B Illek DD Patel BN Ames DB PedenOzone enhancement of lower airway allergic inflammation is prevented bygamma-tocopherol Free Radic Biol Med 43 (2007) 1176ndash1188
[234] JT Harries DP Muller Absorption of different doses of fat soluble and watermiscible preparations of vitamin E in children with cystic fibrosis Arch DisChild 46 (1971) 341ndash344
[235] EI Back C Frindt E Ocenaskova D Nohr M Stern HK Biesalski Can changesin hydrophobicity increase the bioavailability of alpha-tocopherol Eur J Nutr45 (2006) 1ndash6
[236] SZ Nasr MH OLeary C Hillermeier Correction of vitamin E deficiency withfat-soluble versus water-miscible preparations of vitamin E in patients with cys-tic fibrosis J Pediatr 122 (1993) 810ndash812
[237] S Soltani-Frisk E Gronowitz H Andersson B Strandvik Water-miscibletocopherol is not superior to fat-soluble preparation for vitamin E absorptionin cystic fibrosis Acta Paediatr 90 (2001) 1112ndash1115
[238] K Papas J Kalbfleisch R Mohon Bioavailability of a novel water-soluble vi-tamin E formulation in malabsorbing patients Dig Dis Sci 52 (2007)347ndash352
[239] F Antonicelli M Parmentier EM Drost N Hirani I Rahman K Donaldson WMacNee Nacystelyn inhibits oxidant-mediated interleukin-8 expression andNF-kappaB nuclear binding in alveolar epithelial cells Free Radic Biol Med 32(2002) 492ndash502
[240] EM App D Baran I Dab A Malfroot M Coffiner F Vanderbist M King Dose-finding and 24-h monitoring for efficacy and safety of aerosolized Nacystelyn incystic fibrosis Eur Respir J 19 (2002) 294ndash302
[241] MG Traber How much vitamin E hellip Just enough Am J Clin Nutr 84 (2006)959ndash960
[242] JC McCann BN Ames Vitamin K an example of triage theory is micronu-trient inadequacy linked to diseases of aging Am J Clin Nutr 90 (2009)889ndash907
[243] M Fusaro G Crepaldi S Maggi F Galli A DAngelo L Calo S Giannini DMiozzo M Gallieni Vitamin K bone fractures and vascular calcifications inchronic kidney disease an important but poorly studied relationship J Endocri-nol Invest 34 (2010) 317ndash323
[244] JC McCann BN Ames Adaptive dysfunction of selenoproteins from the per-spective of the triage theory why modest selenium deficiency may increaserisk of diseases of aging FASEB J 25 (2011) 1793ndash1814
[245] R Apak K Guclu M Ozyurek B Bektas Oglu M Bener Cupric ion reducing an-tioxidant capacity assay for food antioxidants vitamins polyphenolics and fla-vonoids in food extracts Methods Mol Biol 477 (2008) 163ndash193
[246] F Galli Interactions of polyphenolic compounds with drug disposition and me-tabolism Curr Drug Metab 8 (2007) 830ndash838
[247] RL Prior X Wu K Schaich Standardized methods for the determination of an-tioxidant capacity and phenolics in foods and dietary supplements J Agric FoodChem 53 (2005) 4290ndash4302
[248] C Azbell S Zhang D Skinner J Fortenberry EJ Sorscher BA WoodworthHesperidin stimulates cystic fibrosis transmembrane conductance regulator-mediated chloride secretion and ciliary beat frequency in sinonasal epitheliumOtolaryngol Head Neck Surg 143 (2010) 397ndash404
[249] G Wegrzyn J Jakobkiewicz-Banecka M Gabig-Ciminska E Piotrowska M Nar-ajczyk A Kloska M Malinowska D Dziedzic I Golebiewska M Moskot AWegrzyn Genistein a natural isoflavone with a potential for treatment of ge-netic diseases Biochem Soc Trans 38 (2010) 695ndash701
[250] YC Yu H Miki Y Nakamura A Hanyuda Y Matsuzaki Y Abe M Yasui K Ta-naka TC Hwang SG Bompadre Y Sohma Curcumin and genistein additivelypotentiate G551D-CFTR J Cyst Fibros 10 (2011) 243ndash252
[251] B Illek H Fischer Flavonoids stimulate Cl conductance of human airway epithe-lium in vitro and in vivo Am J Physiol 275 (1998) L902ndashL910
[252] JL Kreindler Cystic fibrosis exploiting its genetic basis in the hunt for newtherapies Pharmacol Ther 125 (2010) 219ndash229
[253] B Illek L Zhang NC Lewis RB Moss JY Dong H Fischer Defective function ofthe cystic fibrosis-causing missense mutation G551D is recovered by genisteinAm J Physiol 277 (1999) C833ndashC839
[254] P Anandakumar S Kamaraj S Jagan G Ramakrishnan R Vinodhkumar TDevaki Capsaicin modulates pulmonary antioxidant defense system during ben-zo(a)pyrene-induced lung cancer in Swiss albinomice Phytother Res 22 (2008)529ndash533
[255] I Rahman Antioxidant therapeutic advances in COPD Ther Adv Respir Dis 2(2008) 351ndash374
[256] AW Boots H Li RP Schins R Duffin JW Heemskerk A Bast GR Haenen Thequercetin paradox Toxicol Appl Pharmacol 222 (2007) 89ndash96
[257] M Joskova S Franova V Sadlonova Acute bronchodilator effect of quercetin inexperimental allergic asthma Bratisl Lek Listy 112 (2011) 9ndash12
[258] HJ Park CM Lee ID Jung JS Lee YI Jeong JH Chang SH Chun MJ Kim IWChoi SC Ahn YK Shin SR Yeom YM Park Quercetin regulates Th1Th2 balancein a murine model of asthma Int Immunopharmacol 9 (2009) 261ndash267
[259] AP Rogerio A Kanashiro C Fontanari EV da Silva YM Lucisano-ValimEG Soares LH Faccioli Anti-inflammatory activity of quercetin and iso-quercitrin in experimental murine allergic asthma Inflamm Res 56 (2007)402ndash408
[260] M Muller Polyphenol cytotoxicity induced by the bacterial toxin pyocyaninrole of NQO1 Free Radic Biol Med 47 (2009) 84ndash91
[261] J Grassmann Terpenoids as plant antioxidants Vitam Horm 72 (2005)505ndash535
[262] P Allen Tea tree oil the science behind the antimicrobial hype Lancet 358(2001) 1245
[263] EC Dasenbrook W Checkley CA Merlo MW Konstan N Lechtzin MP BoyleAssociation between respiratory tract methicillin-resistant Staphylococcus aure-us and survival in cystic fibrosis JAMA 303 (2010) 2386ndash2392
[264] V Bezzerri M Borgatti E Nicolis I Lampronti MC Dechecchi I Mancini PRizzotti R Gambari G Cabrini Transcription factor oligodeoxynucleotides toNF-kappaB inhibit transcription of IL-8 in bronchial cells Am J Respir CellMol Biol 39 (2008) 86ndash96
[265] R Gambari M Borgatti V Bezzerri E Nicolis I Lampronti MC Dechecchi IMancini A Tamanini G Cabrini Decoy oligodeoxyribonucleotides and peptidenucleic acids-DNA chimeras targeting nuclear factor kappa-B inhibition of IL-8 gene expression in cystic fibrosis cells infected with Pseudomonas aeruginosaBiochem Pharmacol 80 (2010) 1887ndash1894
[266] M Adrian P Jeandet AC Douillet-Breuil L Tesson R Bessis Stilbene content ofmature Vitis vinifera berries in response to UV-C elicitation J Agric Food Chem48 (2000) 6103ndash6105
[267] B Paul I Masih J Deopujari C Charpentier Occurrence of resveratrol and pter-ostilbene in age-old darakchasava an ayurvedic medicine from India J Ethno-pharmacol 68 (1999) 71ndash76
[268] I Rahman Antioxidant therapies in COPD Int J Chron Obstruct Pulmon Dis 1(2006) 15ndash29
[269] M Lee S Kim OK Kwon SR Oh HK Lee K Ahn Anti-inflammatory and anti-asthmatic effects of resveratrol a polyphenolic stilbene in a mouse model ofallergic asthma Int Immunopharmacol 9 (2009) 418ndash424
[270] LG Wood PA Wark ML Garg Antioxidant and anti-inflammatory effectsof resveratrol in airway disease Antioxid Redox Signal 13 (2010)1535ndash1548
[271] KV Kiselev Perspectives for production and application of resveratrol ApplMicrobiol Biotechnol 90 (2011) 417ndash425
[272] M Shakibaei C Buhrmann A Mobasheri Resveratrol-mediated SIRT-1 interac-tions with p300 modulate receptor activator of NF-kappaB ligand (RANKL) acti-vation of NF-kappaB signaling and inhibit osteoclastogenesis in bone-derivedcells J Biol Chem 286 (2011) 11492ndash11505
[273] SF Zaidi K Ahmed T Yamamoto T Kondo K Usmanghani M Kadowaki TSugiyama Effect of resveratrol on Helicobacter pylori-induced interleukin-8 secre-tion reactive oxygen species generation and morphological changes in human gas-tric epithelial cells Biol Pharm Bull 32 (2009) 1931ndash1935
[274] JK Kundu YK Shin YJ Surh Resveratrol modulates phorbol ester-inducedpro-inflammatory signal transduction pathways in mouse skin in vivo NF-kappaB and AP-1 as prime targets Biochem Pharmacol 72 (2006)1506ndash1515
[275] NH Nam Naturally occurring NF-kappaB inhibitors Mini Rev Med Chem 6(2006) 945ndash951
[276] JM Smoliga JA Baur HA Hausenblas Resveratrol and healthmdasha comprehen-sive review of human clinical trials Mol Nutr Food Res 55 (2011) 1129ndash1141
[277] ME Juan M Maijo JM Planas Quantification of trans-resveratrol and itsmetabolites in rat plasma and tissues by HPLC J Pharm Biomed Anal 51(2010) 391ndash398
[278] JA Baur DA Sinclair Therapeutic potential of resveratrol the in vivo evidenceNat Rev 5 (2006) 493ndash506
[279] E Nicolis I Lampronti MC Dechecchi M Borgatti A Tamanini N Bianchi VBezzerri I Mancini MG Giri P Rizzotti R Gambari G Cabrini Pyrogallol anactive compound from the medicinal plant Emblica officinalis regulates expres-sion of pro-inflammatory genes in bronchial epithelial cells Int Immunophar-macol 8 (2008) 1672ndash1680
[280] E Nicolis I Lampronti MC Dechecchi M Borgatti A Tamanini V Bezzerri NBianchi M Mazzon I Mancini MG Giri P Rizzotti R Gambari G CabriniModulation of expression of IL-8 gene in bronchial epithelial cells by 5-methoxypsoralen Int Immunopharmacol 9 (2009) 1411ndash1422
[281] M Borgatti I Mancini N Bianchi A Guerrini I Lampronti D Rossi G SacchettiR Gambari Bergamot (Citrus bergamia Risso) fruit extracts and identified com-ponents alter expression of interleukin 8 gene in cystic fibrosis bronchial epithe-lial cell lines BMC Biochem 12 (2011) 15
[282] L Piccagli E Fabbri M Borgatti N Bianchi V Bezzerri I Mancini E Nicolis CMDechecchi I Lampronti G Cabrini R Gambari Virtual screening against p50NF-kappaB transcription factor for the identification of inhibitors of the NF-kappaB-DNA interaction and expression of NF-kappaB upregulated genesChemMedChem 4 (2009) 2024ndash2033
[283] L Piccagli M Borgatti E Nicolis N Bianchi I Mancini I Lampronti D VevaldiF DallAcqua G Cabrini R Gambari Virtual screening against nuclear factorkappaB (NF-kappaB) of a focus library identification of bioactive furocoumarinderivatives inhibiting NF-kappaB dependent biological functions involved incystic fibrosis Bioorg Med Chem 18 (2010) 8341ndash8349
[284] M Borgatti A Chilin L Piccagli I Lampronti N Bianchi I Mancini G Mar-zaro Da Francesco A Guiotto R Gambari Development of a novel furocou-marin derivative inhibiting NF-kappaB dependent biological functionsdesign synthesis and biological effects Eur J Med Chem 46 (2011)4870ndash4877
[285] E Georgy S Le Guellec L Vecellio E Fichant P Stordeur P Bordeau JP PerraudinFeasibility study of OSCN- and lactoferrin (Meveol) nebulization for cysticfibrosis JCyst Fibros 10 (2011) S18
713F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
[286] C Tidei M Piroddi F Galli C Santi Oxidation of thiols promoted by PhSeZnClTetrahedron Lett 53 (2012) 232ndash234
[287] L Semianrio-Vidal C van Hesuden G Mugesh ER Lazarowski Ebselen is a po-tent non-competitive inhibitor of extracellular nucleoside diphosphokinasePurinergic Signal 6 (2010) 383ndash391
[288] C ColussiMC Albertini S Coppola S Rovidati F Galli L Ghibelli H2O2-inducedblockof glycolysis as an active ADP-ribosylation reaction protecting cells from apoptosisFASEB J 14 (2000) 2266ndash2276
[289] H Xiao KL Parkin Induction of phase II enzyme activity by various seleniumcompounds Nutr Cancer 55 (2006) 210ndash223
[290] G Peluffo R Radi Biochemistry of protein tyrosine nitration in cardiovascularpathology Cardiovasc Res 75 (2007) 291ndash302
[291] B Alvarez R Radi Peroxynitrite reactivity with amino acids and proteinsAmino Acids 25 (2003) 295ndash311
[292] B Kamosinska MW Radomski M Duszyk A Radomski SF Man Nitric oxideactivates chloride currents in human lung epithelial cells Am J Physiol 272(1997) L1098ndashL1104
[293] L Chen RP Patel X Teng CA Bosworth JR Lancaster Jr S Matalon Mecha-nisms of cystic fibrosis transmembrane conductance regulator activation by S-nitrosoglutathione J Biol Chem 281 (2006) 9190ndash9199
[294] F Luchetti B CanonicoM BettiM Arcangeletti F PilolliM Piroddi L Canesi S PapaF Galli Melatonin signaling and cell protection function FASEB J 24 (2010)3603ndash3624
[295] MW Bengtsson G Jedstedt G Flemstrom Duodenal bicarbonate secretion inrats stimulation by intra-arterial and luminal guanylin and uroguanylin ActaPhysiol (Oxf) 191 (2007) 309ndash317
[296] CS Nelson JL Marino CN Allen Melatonin receptor potentiation of cyclic AMP andthe cystic fibrosis transmembrane conductance regulator ion channel J Pineal Res 26(1999) 113ndash121
[297] C de Castro-Silva VM de Bruin GM Cunha DM Nunes CAMedeiros PF de BruinMelatonin improves sleep and reduces nitrite in the exhaled breath condensate incystic fibrosismdasha randomized double-blind placebo-controlled study J Pineal Res48 (2010) 65ndash71
[298] I Hornyak E Pankotai L Kiss Z Lacza Current developments in the the-rapeutic potential of S-nitrosoglutathione an endogenous NO-donor mole-cule Curr Pharm Biotechnol (2011) Jan 11 [Epub ahead of print] - PMID21235457
[299] AH Snyder ME McPherson JF Hunt M Johnson JS Stamler B Gaston Acuteeffects of aerosolized S-nitrosoglutathione in cystic fibrosis Am J Respir CritCare Med 165 (2002) 922ndash926

705F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
individual or combined supplementation and increased levels of allplasma antioxidants except vitamin C that were observed in all thetrials
The message from these studies to pediatricians and nutritionistswithin the clinical staff of CF centers is that in the absence of solid ev-idence regarding the clinical effectiveness of oral formulations of an-tioxidant supplements in CF (including PUFA) their use as a routineclinical practice should be considered with caution keeping clear inmind that this should represent just a complement of one of themost critical interventions in the life-long clinical management pro-gram of CF patients eg providing an adequate nutriture [140] Inthis context compensating energy and protein malnutrition has toremain the first goal of nutritional management programs Providinghigher intakes of antioxidant micronutrients with food naturally-enriched (or functionalized) of micronutrient antioxidants shouldbe preferred in order to have the higher combination of positive nu-tritional factors that are lost during refinement procedures and over-all industrial processing of dietary supplements
Measures of good practice in clinical management of micro-malnutrition in CF patients would include the support of specializedpersonnel and laboratories The centers should have the possibilityto ascertain with appropriate nutritional and laboratory tests whatthe level of deficiency is for the different micronutrients that each pa-tient may suffer from during a dietary program Monitoring dietaryintakes and blood levels of micronutrients is not sufficient to set apersonalized nutritional intervention with supplements or functionalfoods Sub-optimal intakes and the compliance to nutritional inter-ventions should be verified by means of selected biochemical andclinical criteria Unluckily the latter are still not well established forsome micronutrients such as the fat-soluble vitamins E (reviewed in[163173241]) and K [242243] and also for trace elements such asSe [244] For many of the antioxidants used as supplements inhumans we still do not know exactly several of the biological effectsthat these may provide when introduced in a healthy body and weknow less what these can do in disease These aspects hardly impacton the concept of optimal levels of intake that should be identified foreach micronutrient on an individual basis According with the aspectsdiscussed in the previous sections optimal levels of intake for antiox-idant micronutrients are different in CF patients and healthy subjectsand vary with age and several individual factors
Lung administration of antioxidants by means of aerosolized for-mulations so far used for GSH therapy (see above) is a promisingfield of clinical investigation in CF Toxicity issues are currently themain concern and the subject of clinical evaluation by several groups(described above)
Information on future directions of antioxidant therapy in CF canbe inferred by the analysis of pending or recently completed clinicaltrials that have been searched (December 2011) at ClinicalTrialsgovdatabase matching the terms ldquoantioxidant therapyrdquo or ldquoglutathionerdquowith ldquocystic fibrosisrdquo Fifteen trials were retrieved and those directlyrelated to antioxidant therapy (n=12) are presented in Table 1 andinclude efficacy and safety studies of inhaled drugs as GSH sodiumpyruvate NAC and NO and the dietary supplements AquADEKsregan antioxidant-rich multivitamin supplement epigallocatechin gal-late (EGCG)tocotrienol curcuminoids the amino acid glutaminesulforaphane in broccoli sprouts One trial is investigating the flavo-noid quercetin as CFTR modulator
39 Emerging antioxidant and anti-inflammatory approaches in CF
Mediterranean foods such as olive oil and red wine or severalplant extracts such as herbal tea or grape seed extracts contain aseries of natural compounds with important antioxidant and NOscavenging activity that have been widely investigated for the pre-vention of oxidative stress-related diseases [38245] These havebeen long investigated as template molecules to develop antioxidant
and anti-inflammatory drugs Between the multitudes of natural sub-stances most investigated ones include for instance tyrosol hydroxy-tyrosol gallic and caffeic acids belonging to the family of phenolswhile resveratrol of the stilbenes family epicatechin kaempferoland cianidin are examples of flavonoids examples of fat-soluble phe-nolics are those of the family of tocols (vitamin E) and carotenoids Allthese compounds show different metabolisms and signaling effects[246] Antioxidant and cell protection mechanisms are associatedwith different and sometimes concurrent processes as H-atom trans-fer and electron donation radical trapping and chelation of transitionmetals that can be easily investigated at the chemical level [247] Be-sides these direct antioxidant effects metabolic responses and signal-ing effects of natural compounds are also important to producesecond-generation responses that modify the level of antioxidantprotection and the potential for ROS detoxification in cells and bodyfluids These derive from the transcriptional regulation of antioxidantand pro-oxidant genes that coexist with the modulation of cytokinesecretion and inflammatory enzyme activities
Some of these natural plant-derived antioxidants may provide fur-ther pharmacological activities of possible relevance in CF This is thecase for instance of the plant flavonoids genistein apigenin kaemp-ferol quercetin and hesperidin [248ndash251] that fall in the pharmaco-logical category of ldquopotentiatorsrdquo [252] in that these activate at leastto a certain extent CTFR-mediated Cl currents in normal and CF airwayepithelium investigated either in vitro or in vivo in humans and ani-mal models Actually as prototypal flavonoid-derived potentiatorthe tyrosine kinase inhibitor genistein potentiates the gating of wild-type as well as ΔF508 CFTR and G551D CFTR [253] but at higherdoses it inhibits CFTR gating which make this an unlikely clinical can-didate Similar potentiation effects have been reported for the antiox-idant curcumin [250] that shows an additive effect with respect togenistein-induced potentiation Besides CFTR potentiation whichdoes not appear to have a direct influence on GSH and nutrient trans-port in the lung tissue all these natural substances have been usedalone or in combination with other agents as in vivo enhancers oflung antioxidant protection [246254255] In the case of quercetinthiol-reactive phenolic [256] bronchodilation and anti-inflammatoryeffects by a restoration of the Th1Th2 balance have been reportedin inflammatory syndromes of the lung [255257ndash259] but theseeffects have not been explored in CF Pyocyanin toxicity (see abovein the Section 2) could represent an issue for the use of quercetinand other catechols in infectious diseases of the lung [260]
Other natural antioxidants of potential interest in CF therapy in-clude terpenoids [261] such as terpinen-4-ol a major constituentof tea tree oil that is being investigated in the therapy of anti-biotic resistant organisms specifically against methicillin-resistantStaphylococcus aureus (MRSA) [262] a problem in CF [263] Otherthan being lipophilic antioxidants terpenes can prevent oxidativestress of the CF lung secondarily to the antibiotic effect thereby pro-moting a better control of immuno-inflammatory pathways and lungantioxidants
391 Targeting NF-κB with natural compounds resveratrol and plantextracts
Natural compounds were long known to be useful in designinganti-inflammatory drugs and some of these could find an applicationin the control of the transcription factor kappa-B (NF-κB) that maylead to develop advanced pharmacological tools to control inflamma-tion and to produce higher antioxidant protection to CF airwaysInhibitors targeting NF-κB including transcription factors decoymolecules (TFD) are potent down-regulators of gene expressionand release of IL-8 in CF cells infected with P aeruginosa [264265]
Resveratrol (354prime-trihydroxystilbene ldquoErdquo form) is one of the mostinvestigated natural antioxidant with proposed activity as NF-κBinhibitor This is a phytoalexin present in large quantity in red winepreferentially in the skin of grapes being its concentration
706 F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
50ndash100 μgmg of fresh skin and 13ndash3 mgl of red wine [266]Furthermore resveratrol is a constituent of lsquoDarakchasavarsquo (13ndash6 mgl) an ayurvedic medicine from India [267] The antioxidant activity ofresveratrol has been reported in several papers and occurs also in lungtissues suggesting that resveratrol has potential as a therapeuticagent in respiratory disease [268ndash270] Resveratrol can be consideredone of the most interesting molecules from the natural worldexhibiting strong antioxidant activity that at the same time is able toexert anti inflammatory activity through alteration of NF-κB functionsand efficient inhibition of pro-inflammatory genes [271272] As far asthe effects on CF model systems are concerned Cabrini et al [26]reported the effects of resveratrol on P aeruginosa infected CF IB3-1cells The results obtained demonstrate that resveratrol exhibits minoreffects of IB3-1 cell growth and important inhibitory effects on accumu-lation of IL-8 and GRO-α mRNA while minor effects on IL-6 gene ex-pression were observed These data support recently publishedobservations suggesting inhibitory effects of resveratrol in infection-mediated inflammatory processes [273] Interestingly resveratrol hasbeen reported as a potent inhibitor of NF-κB activity and a promisinganti-inflammatory agent [272274] also in combinationwith othermol-ecules [274275] However in vivo translation of this pre-clinical on res-veratrol is hard to be foreseen This natural compound displays poorbioavailability [276] and further characterization of resveratrol pharma-cokinetics is troublesome since it is hardly measurable in vivo [277]Furthermore the regulation of inflammatory responses by resveratrolhas been suggested to be far more complex than simple direct suppres-sion of NF-κB activity Actually some aspects of the immune responsecould be enhanced by this natural substance which may lead tohypothesize broad negative feedback events on immuno-inflammatorypathways [278] In any case and with these cautions in mind the pub-lished observations on cellular model systems support the concept thatresveratrol and resveratrol-containing formulations deserve further con-sideration to determine their possible therapeutic values in CF
Other inhibitors can be identified from systematic studies of naturalproducts and their ability to interfere with NF-κB activity [279ndash281]Recent studies have demonstrated that the whole extract of Aeglemarmelos (Rutaceae) has strong inhibitory effect on the P aeruginosa-dependent IL-8 induction in human CF-derived bronchial IB3-1 cellswithout affecting cell proliferation [280] Molecular analysis of compo-nents contained in A marmelos extracts revealed that three major com-pounds namely 56-dimethoxy-1-indanone 2-hydroxy-cinnamic acidand 5-methoxy psoralen (5-MOP) reproduce the inhibitory effect ob-servedwith thewhole extract [280] A further example has been recent-ly published using extracts from bergamot (Citrus bergamia Risso) Inthis study the extracts were characterized and the main detected con-stituents were assayed for their biological activity [281] The resultsobtained demonstrated that the extracts from bergamot epicarps con-tain components displaying an inhibitory activity on IL-8 Particularlythe most active molecules were bergapten and citropten These effectshave been confirmed by analyzing mRNA levels and protein release inthe CF cellularmodels IB3-1 and CuFi-1 inducedwith TNF-α or exposedto P aeruginosa
A parallel strategy linking NF-κB inhibition and down-regulationof NF-κB-dependent functions is described in recently publishedstudies based on a structured-based virtual screening (VS) of differ-ently substituted furocoumarins and analogues against NF-κB withthe objective of selecting molecules able to inhibit the binding ofthis transcription factor to DNA [282283] Novel compounds wereidentified with this strategy as potent inhibitors of NF-κB dependentbiological functions to be proposed for the control lung inflammationoccurring in patients affected by CF [282ndash284]
392 Scavengers and regulators of H2O2 and NO
3921 Lactoferrin and OSCNmacr The impaired DUOXLPO system of CFpatients could be the target of therapeutic strategies that may
produce concomitant antimicrobial and antioxidant effects This sys-tem described above in Section 22 represents an important compo-nent of innate immunity with a role in bactericidal defense andregulation of H2O2 metabolism of airways [32] CF patients have alsoreported to show lowered LF levels in the ASL [37] that togetherwith a CFTR-dependent defective efflux of SCNmacr and LPO [36] may cre-ate the environment for a sustained flux of H2O2 and for the genera-tion of highly reactive Fenton species [1138] An ideal therapeuticintervention should restore the LPO-dependent generation of bacteri-cidal OSCNmacr from DUOX-derived H2O2 and SCNmacr in the ASL to controlat the same time the microbial biofilm and the flux of H2O2 into theASL An approach close to this therapeutic mechanism was recentlyproposed for the drug Meveolreg This is a complex of LF and OSCNmacrwith proposed in vivo antimicrobial activity [285] to be evaluatedin clinical trials for the aerosol treatment of lung infections in CFpatients The role for this drug in the control of H2O2 levels of ASLremains to be investigated
3922 Organoselenium compounds Organoselenium compoundshave been proposed as therapeutic agents useful in the antioxidanttherapy of inflammatory conditions These include GPX mimetic mol-ecules such as Ebselenreg (2-phenyl-12-benzisoselenazol-3(2H)-one)or other and more recently developed molecules that are still inpre-clinical steps of evaluation [286] Selectively and specificity of ac-tion are main issues in the therapeutic mechanism of this candidateantioxidant drug that thanks to the electrophilic properties of Se[214] reacts with thiols to reduce H2O2 and other species MoreoverEbselenreg has been described to act as potent non-competitive inhib-itor of extracellular nucleoside diphosphokinase (NDPK) having neg-ligible effect on ecto-ATPase and adenyl kinase activities which areother players of the metabolism of extracellular nucleotides [287]This enzyme together with other nucleoside di- and triphosphatescontributes to regulate several components of the mucociliary clear-ance process (MCC) that protects the lung against infections via acti-vation of epithelial purinergic receptors The inhibition of NDPK bythis GPX-mimetic drug may also impact on the energy status of endo-thelial cells [287] This aspect could be further investigated as a cellu-lar protection mechanism in the pulmonary epithelium of CF patientsbeing the control of cell energy of fundamental importance to preventthe activation of death pathways [288]
Further therapeutic mechanisms for these Se-derived drugs mayderive from the marked activity as inducers of phase II enzymessuch as quinone reductase (QR) and glutathione-S-transferase (GST)[289] This induction response also observed with other electrophilsand redox-active molecules such as natural phenolic antioxidantscould produce higher cellular protection by the acquisition of anincreased capability to detoxify endobiotics generated during oxida-tive stress and inflammation [246]
3923 Melatonin and GSNO as NOx regulators Increased markers ofNO-derived biological damage are present in the CF lung suggestingthe abnormal reactivity of NOx in the inflamed lung of CF patients[52] However an impaired metabolism and biological function ofNO in CF airways (see Section 23) suggests a cautious approach tothe use of agents that may influence the levels and chemical behaviorof NO-derived species (NOx) with possible impact on the physiologi-cal roles of NO in vasodilatation innate immunity and H2O2 metabo-lism of the respiratory tract [290291] NO donors also appear toinfluence CFTR function of alveolar epithelium and gland serouscells [292293]
Main physiological role of the pineal gland hormone melatonin isthe synchronization of circadian rhythms including the sleepndashwakecycle but several other functions dealing with immunomodulatoryantioxidant and cellular protection effects have been identified[294] Melatonin receptor stimulation may also influence cyclic AMPsignaling and the regulation of CFTR ion channel [295296]
707F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
A recent randomized double-blind placebo-controlled study hasexamined the effects of short term melatonin administration (3 mgfor 3 weeks) on sleep and oxidative stress markers in CF [297]According with the expected pharmacological effect of this hormonalsubstance the treatment was successful in improving sleep indicesAt the same time nitrite levels determined in exhaled breath conden-sate (EBC) were reduced to suggest a better control of NOmetabolismof CF airways (discussed above in Section 23) but these effects how-ever were not associated with a significant correction of isoprostaneas lipid peroxidation marker measured in EBC Increasing dosages ofmelatonin could be investigated for the pharmacological treatmentof oxidative stress and immune dysfunction of CF patients due tothe absence of adverse effects of this hormonal substance in humans
The S-nitrosation reaction of thiols is another interesting aspect ofNO pharmacology [53] that may find an application in the therapy oflung complications of CF This has been the case for instance of theS-nitrosothiol GSNO that has been used safely in human trials[298299] This endogenous nitrosothiol with proposed regulatory ef-fect on the CFTR of lung epithelia [292293] is well tolerated in pa-tients with CF when administered by aerosolization and mayproduce better oxygenation [299] thereby suggesting that therapyaimed at restoring endogenous GSNO levels in the CF airway maymerit further clinical evaluation Since the administered GSNO de-composes as shown by the increased levels of expired NO in CF pa-tients under treatment with this nitrosothiol [299] furtherinvestigation should be addressed to ascertain whether GSNO thera-py may merely correspond to a GSH therapy
NO dependent effects on CFTR function should be considered toevaluate mechanism of action and specificity of antioxidant therapiesthat target NO metabolism and function in the CF airways
4 Conclusions and future perspectives
The presence of clinical and biochemical symptoms of inflammationand oxidative stress implies that CF patients have a higher demand ofantioxidant protection The combination of the dysfunctional CFTRwith a lowered intake and absorption of dietary antioxidants producesub-optimal levels of protection from both enzymatic and non-enzymatic defense systems The former could be associated with a de-fective glutathionemetabolism and lowered intake of sulfur-containingamino acids and oligoelements such as zinc and possibly seleniumwhile fat-soluble antioxidant vitamins such as vitamin E and caroten-oids and the water-soluble vitamin C are lowered than in healthy sub-jects due to malabsorption and possibly higher consumption
The increased antioxidant demand in CF patients should be evenhigher in the presence of complications of the lung pancreas andliver Lung comorbidity is particularly important in this contextbeing associated with recurrent infections which results in the alter-nation of inflammatory exacerbates and chronic inflammation Thesesustain the flux of ROS in the airways and promote the formation ofsecond-generation byproducts by the damage of biomolecules suchas PUFA and proteins which may diffuse also at the systemic level tofurther promote adverse biological responses and toxic reactions Pan-creatic insufficiency causes malnutrition and may lead to develop en-docrine and metabolic defects associated with diabetes of CF Theseevents can be further aggravated by the concomitance of liver dys-function and a poor nutritional status Malnutrition is strongly associ-ated with poor prognosis as assessed by pulmonary function andsurvival data [138ndash140] The more aggressive nutritional interven-tions seem to produce better clinical outcomes in these patients andthe possibility of achieving higher antioxidant protection in well-nourished patients by dietary factors could be a key aspect to explainsuch a clinical advantage The assumption that food-derived compo-nentsmay help to prevent the damaging effects of oxidative stress im-proving the antioxidant defenses deserves further investigation at theclinical level This together with the investigation of appropriate
laboratory biomarkers could provide critical information to establishintervention criteria for an early nutritional management of newly di-agnosed patients [5] It is expected that a timely secondary preventionstrategy could influence the progression of CF symptoms thusaffecting with a self-feeding mechanism the same extent of malnutri-tion and oxidative stress along the life of CF patients Since severalfactors contribute to impair the nutritional status of CF patients(such as pancreatic insufficiency chronic malabsorption recurrentsinopulmonary infections and progressive lung disease chronic in-flammation increased energy expenditure suboptimal intake multi-therapy) careful monitoring of the antioxidant status should berecommended According with international guidelines fat-solublevitamin supplementation is of utmost importance in daily practice to-gether with energy intake requirements and pancreatic enzyme-replacement therapy Among these vitamin E β-carotene and ω-3FA have observed to alleviate selected biochemical signs of oxidativestress as measured for instance with well established laboratory indi-ces of lipid peroxidation and in some studies these effects werepreliminarily associated with positive clinical outcomes Notwith-standing randomizedndashcontrolled clinical trials on antioxidant supple-ments (including ω-3 FA) so far carried out in CF have failed toconclusively demonstrate significant beneficial effects on respiratorysymptoms and on the consequent impact that these have on the qual-ity of life of these patients (reviewed in [202213]) whichmay provideno support for the use of these supplements in CF An absence of effi-cacy in prevention studies on antioxidant supplements has also beenobserved in other and possibly less severe oxidative stress-relatedconditions particularly in the secondary prevention of cardiovasculardisease and some forms of cancer by vitamin E and other antioxidantssuch as vitamin C selenium and β-carotene (reviewed in [163]) Dif-ferent biases however have been identified in randomize large clini-cal trials that may account for these disappointing findings Theseinclude patient selection criteria (early interventions and primaryprevention could have more chances of success than secondaryprevention) duration and doses of the treatment use of wrong anti-oxidant formulations and administration protocols absence of verifi-cations of the biological compliance to the treatment etc The samebiases apply for the few trials carried out in CF patients Thus the ap-propriateness and efficacy of nutritional interventions with naturalfood-derived or synthetic antioxidants should be verifiedwith respectto the biological pathways of oxidative stress and clinical variablesthat are identified as end-points Profiles of blood and tissue antioxi-dants as well as of reliable surrogate markers of oxidative stresshave to be selected and determined in highly specialized laboratorieswith a well-established experience on these analyses
Well-timed (early) interventions with appropriate antioxidantformulationsprotocols need to be proposed for the next generationof trials and the development of novel CF-tailored antioxidant andanti-inflammatory agents should be promoted
As a consequence of these considerations more clinical investiga-tion is awaited to identify future successful approaches to the antiox-idant therapy as a measure to further enhance quality of life and theoverall clinical outcome of CF patients
Acknowledgments
We are indebted with the Italian Cystic Fibrosis Research Founda-tion for the support that it provided with its grant program to the re-search activity of the authors of this paper This is a scientific initiativeof the ldquoWorking Group on Inflammation in Cystic Fibrosisrdquo (BragonziA Bravo E Cabrini G Conese M Cuzzocrea S Dechecchi MC De Ales-sandri A Evangelista V Galli F Gambari R Lambiase A Lucidi VManca A Melotti P Minicucci L Motta A Pietraforte D Pompella AQuattrucci S Rizzo R Romano M Sorio C Tesse R) of the Italian Soci-ety for Cystic Fibrosis A particular thank goes to the Prof GianniMastella for the critical revision of the manuscript and for the
708 F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
stimulating research environment that he has contributed to createwithin the Italian Cystic Fibrosis Research Foundation
References
[1] BP OSullivan SD Freedman Cystic fibrosis Lancet 373 (2009) 1891ndash1904[2] P Linsdell JW Hanrahan Glutathione permeability of CFTR Am J Physiol 275
(1998) C323ndashC326[3] L Gao KJ Kim JR Yankaskas HJ Forman Abnormal glutathione transport in
cystic fibrosis airway epithelia Am J Physiol 277 (1999) L113ndashL118[4] RK Rowntree A Harris The phenotypic consequences of CFTR mutations Ann
Hum Genet 67 (2003) 471ndash485[5] EI Back C Frindt D Nohr J Frank R Ziebach M Stern M Ranke HK Biesalski
Antioxidant deficiency in cystic fibrosis when is the right time to take actionAm J Clin Nutr 80 (2004) 374ndash384
[6] LG Wood DA Fitzgerald AK Lee ML Garg Improved antioxidant and fattyacid status of patients with cystic fibrosis after antioxidant supplementation islinked to improved lung function Am J Clin Nutr 77 (2003) 150ndash159
[7] L Iuliano R Monticolo G Straface S Zullo F Galli M Boaz S Quattrucci Asso-ciation of cholesterol oxidation and abnormalities in fatty acid metabolism incystic fibrosis Am J Clin Nutr 90 (2009) 477ndash484
[8] C Libetta V Sepe P Esposito F Galli A Dal Canton Oxidative stress and inflam-mation implications in uremia and hemodialysis Clin Biochem 44 (2011)1189ndash1198
[9] G Bartosz Reactive oxygen species destroyers or messengers Biochem Phar-macol 77 (2009) 1303ndash1315
[10] T Ntimbane B Comte G Mailhot Y Berthiaume V Poitout M Prentki RRabasa-Lhoret E Levy Cystic fibrosis-related diabetes from CFTR dysfunctionto oxidative stress Clin Biochem 30 (2009) 153ndash177
[11] A van der Vliet JP Eiserich GP Marelich B Halliwell CE Cross Oxidativestress in cystic fibrosis does it occur and does it matter Adv Pharmacol 38(1997) 491ndash513
[12] AM Cantin TB White CE Cross HJ Forman RJ Sokol D Borowitz Antioxi-dants in cystic fibrosis Conclusions from the CF antioxidant workshop Bethes-da Maryland Free Radic Biol Med 42 (2007) 15ndash31
[13] LT McGrath P Mallon L Dowey B Silke E McClean M McDonnell A DevineS Copeland S Elborn Oxidative stress during acute respiratory exacerbations incystic fibrosis Thorax 54 (1999) 518ndash523
[14] E Thomson S Brennan R Senthilmohan CL Gangell AL Chapman PD SlyAJ Kettle E Balding LJ Berry JB Carlin R Carzino N de Klerk T Douglas CFoo LW Garratt GL Hall J Harrison A Kicic IA Laing KM Logie J MassieLS Mott C Murray F Parsons N Pillarisetti SR Poreddy SC RanganathanCF Robertson R Robins-Browne PJ Robinson B Skoric SM Stick ENSutanto E Williamson Identifying peroxidases and their oxidants in the earlypathology of cystic fibrosis Free Radic Biol Med 49 (2010) 1354ndash1360
[15] SP Range C Dunster AJ Knox FJ Kelly Treatment of pulmonary exacerba-tions of cystic fibrosis leads to improved antioxidant status Eur Respir J 13(1999) 560ndash564
[16] L Coppo P Ghezzi Thiol regulation of pro-inflammatory cytokines and innateimmunity protein S-thiolation as a novel molecular mechanism Biochem SocTrans 39 (2011) 1268ndash1272
[17] C Verhaeghe C Remouchamps B Hennuy A Vanderplasschen A Chariot SPTabruyn C Oury V Bours Role of IKK and ERK pathways in intrinsic inflamma-tion of cystic fibrosis airways Biochem Pharmacol 73 (2007) 1982ndash1994
[18] TL Bonfield JR Panuska MW Konstan KA Hilliard JB Hilliard H Ghnaim MBerger Inflammatory cytokines in cystic fibrosis lungs Am J Respir Crit CareMed 152 (1995) 2111ndash2118
[19] TL Noah HR Black PW Cheng RE Wood MW Leigh Nasal and bronchoal-veolar lavage fluid cytokines in early cystic fibrosis J Infect Dis 175 (1997)638ndash647
[20] MJ Welsh BW Ramsey FJ Accurso GR Cutting Cystic Fibrosis McGraw-HillNew York 2001
[21] TZ Khan JS Wagener T Bost J Martinez FJ Accurso DW Riches Early pul-monary inflammation in infants with cystic fibrosis Am J Respir Crit CareMed 151 (1995) 1075ndash1082
[22] FA Ratjen Cystic fibrosis pathogenesis and future treatment strategies RespirCare 54 (2009) 595ndash605
[23] J Jacquot O Tabary P Le Rouzic A Clement Airway epithelial cell inflamma-tory signalling in cystic fibrosis Int J Biochem Cell Biol 40 (2008)1703ndash1715
[24] CM Greene P Branagan NG McElvaney Toll-like receptors as therapeutic tar-gets in cystic fibrosis Expert Opin Ther Targets 12 (2008) 1481ndash1495
[25] M Rottner JM Freyssinet MC Martinez Mechanisms of the noxious inflam-matory cycle in cystic fibrosis Respir Res 10 (2009) 23
[26] G Cabrini V Bezzerri I Mancini E Nicolis MC Dechecchi A Tamanini ILampronti L Piccagli N Bianchi M Borgatti R Gambari Targeting transcrip-tion factor activity as a strategy to inhibit pro-inflammatory genes involved incystic fibrosis decoy oligonucleotides and low-molecular weight compoundsCurr Med Chem 17 (2010) 4392ndash4404
[27] CM Greene NG McElvaney Proteases and antiproteases in chronic neutrophiliclungdiseasemdash relevance to drug discovery Br J Pharmacol 158 (2009) 1048ndash1058
[28] AM Cantin Potential for antioxidant therapy of cystic fibrosis Curr Opin PulmMed 10 (2004) 531ndash536
[29] JF Chmiel MW Konstan Inflammation and anti-inflammatory therapies forcystic fibrosis Clin Chest Med 28 (2007) 331ndash346
[30] DP Nichols MW Konstan JF Chmiel Anti-inflammatory therapies for cys-tic fibrosis-related lung disease Clin Rev Allergy Immunol 35 (2008)135ndash153
[31] AJ Kettle T Chan I Osberg R Senthilmohan AL Chapman TJ Mocatta JSWagener Myeloperoxidase and protein oxidation in the airways of youngchildren with cystic fibrosis Am J Respir Crit Care Med 170 (2004)1317ndash1323
[32] H Fischer Mechanisms and function of DUOX in epithelia of the lung AntioxidRedox Signal 11 (2009) 2453ndash2465
[33] B Rada TL Leto Oxidative innate immune defenses by NoxDuox familyNADPH oxidases Contrib Microbiol 15 (2008) 164ndash187
[34] P Moskwa D Lorentzen KJ Excoffon J Zabner PB McCray Jr WM NauseefC Dupuy B Banfi A novel host defense system of airways is defective in cysticfibrosis Am J Respir Crit Care Med 175 (2007) 174ndash183
[35] D Lorentzen L Durairaj AA Pezzulo Y Nakano J Launspach DA Stoltz GZamba PB McCray Jr J Zabner MJ Welsh WM Nauseef B Banfi Concentra-tion of the antibacterial precursor thiocyanate in cystic fibrosis airway secre-tions Free Radic Biol Med 50 (2011) 1144ndash1150
[36] Y Xu S Szep Z Lu The antioxidant role of thiocyanate in the pathogenesis ofcystic fibrosis and other inflammation-related diseases Proc Natl Acad Sci US A 106 (2009) 20515ndash20519
[37] MP Rogan CC Taggart CM Greene PG Murphy SJ ONeill NG McElvaneyLoss of microbicidal activity and increased formation of biofilm due to decreasedlactoferrin activity in patients with cystic fibrosis J Infect Dis 190 (2004)1245ndash1253
[38] B Halliwell JM Guttridge Free Radicals in Biology and Medicine Fourth editionOxford University Press New York 2007
[39] B Rada K Lekstrom S Damian C Dupuy TL Leto The Pseudomonastoxin pyocyanin inhibits the dual oxidase-based antimicrobial system as itimposes oxidative stress on airway epithelial cells J Immunol 181 (2008)4883ndash4893
[40] C Schwarzer B Illek JH Suh SJ Remington H Fischer TE Machen Organelleredox of CF and CFTR-corrected airway epithelia Free Radic Biol Med 43(2007) 300ndash316
[41] JH Roum R Buhl NG McElvaney Z Borok RG Crystal Systemic deficiency ofglutathione in cystic fibrosis J Appl Physiol 75 (1993) 2419ndash2424
[42] VM Hudson Rethinking cystic fibrosis pathology the critical role of abnormalreduced glutathione (GSH) transport caused by CFTR mutation Free RadicBiol Med 30 (2001) 1440ndash1461
[43] PJ Barnes RA Dweik AF Gelb PG Gibson SC George H Grasemann IDPavord F Ratjen PE Silkoff DR Taylor N Zamel Exhaled nitric oxide in pul-monary diseases a comprehensive review Chest 138 (2010) 682ndash692
[44] H Grasemann E Michler M Wallot F Ratjen Decreased concentration of ex-haled nitric oxide (NO) in patients with cystic fibrosis Pediatr Pulmonol 24(1997) 173ndash177
[45] H Grasemann F Ratjen Cystic fibrosis lung disease the role of nitric oxidePediatr Pulmonol 28 (1999) 442ndash448
[46] B Gaston F Ratjen JW Vaughan NR Malhotra RG Canady AH Snyder JFHunt S Gaertig JB Goldberg Nitrogen redox balance in the cystic fibrosis air-way effects of antipseudomonal therapy Am J Respir Crit Care Med 165(2002) 387ndash390
[47] H Grasemann I Ioannidis RP Tomkiewicz H de Groot BK Rubin F RatjenNitric oxide metabolites in cystic fibrosis lung disease Arch Dis Child 78(1998) 49ndash53
[48] H Grasemann R Schwiertz S Matthiesen K Racke F Ratjen Increased argi-nase activity in cystic fibrosis airways Am J Respir Crit Care Med 172(2005) 1523ndash1528
[49] H Grasemann S Al-Saleh JA Scott D Shehnaz A Mehl R Amin M Rafii PPencharz J Belik F Ratjen Asymmetric dimethylarginine contributes to airwaynitric oxide deficiency in patients with cystic fibrosis Am J Respir Crit CareMed 183 (2011) 1363ndash1368
[50] H Grasemann F Kurtz F Ratjen Inhaled L-arginine improves exhaled nitricoxide and pulmonary function in patients with cystic fibrosis Am J RespirCrit Care Med 174 (2006) 208ndash212
[51] H Grasemann F Ratjen Emerging therapies for cystic fibrosis lung disease Ex-pert Opin Emerg Drugs 15 (2010) 653ndash659
[52] BM Morrissey K Schilling JV Weil PE Silkoff DM Rodman Nitric oxide andprotein nitration in the cystic fibrosis airway Arch Biochem Biophys 406(2002) 33ndash39
[53] R Radi Nitric oxide oxidants and protein tyrosine nitration Proc Natl AcadSci U S A 101 (2004) 4003ndash4008
[54] J Chen M Kinter S Shank C Cotton TJ Kelley AG Ziady Dysfunction of Nrf-2in CF epithelia leads to excess intracellular H2O2 and inflammatory cytokineproduction PLoS One 3 (2008) e3367
[55] F Galli M Piroddi C Annetti C Aisa E Floridi A Floridi Oxidative stress andreactive oxygen species Contrib Nephrol 149 (2005) 240ndash260
[56] DT Wright LA Cohn H Li B Fischer CM Li KB Adler Interactions of oxygenradicals with airway epithelium Environ Health Perspect 102 (Suppl 10)(1994) 85ndash90
[57] I Rahman SR Yang SK Biswas Current concepts of redox signaling in thelungs Antioxid Redox Signal 8 (2006) 681ndash689
[58] Q Li JF Engelhardt Interleukin-1beta induction of NFκB is partially regulatedby H2O2-mediated activation of NFκB-inducing kinase J Biol Chem 281(2006) 1495ndash1505
709F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
[59] E Boncoeur VS Criq E Bonvin T Roque A Henrion-Caude DC Gruenert AClement J Jacquot O Tabary Oxidative stress induces extracellular signal-regulated kinase 12 mitogen-activated protein kinase in cystic fibrosis lung ep-ithelial cells potential mechanism for excessive IL-8 expression Int J BiochemCell Biol 40 (2008) 432ndash446
[60] B Fischer J Voynow Neutrophil elastase induces MUC5AC messenger RNA ex-pression by an oxidant-dependent mechanism Chest 117 (2000) 317Sndash320S
[61] B Rada P Gardina TG Myers TL Leto Reactive oxygen species mediate in-flammatory cytokine release and EGFR-dependent mucin secretion in airwayepithelial cells exposed to Pseudomonas pyocyanin Mucosal Immunol 4(2011) 158ndash171
[62] C Schwarzer H Fischer EJ Kim KJ Barber AD Mills MJ Kurth DC GruenertJH Suh TE Machen B Illek Oxidative stress caused by pyocyanin impairs CFTRClminus transport in human bronchial epithelial cells Free Radic Biol Med 45(2008) 1653ndash1662
[63] J Hull M South P Phelan K Grimwood Surfactant composition in infants andyoung children with cystic fibrosis Am J Respir Crit Care Med 156 (1997)161ndash165
[64] KC Meyer A Sharma R Brown M Weatherly FR Moya J Lewandoski JJZimmerman Function and composition of pulmonary surfactant andsurfactant-derived fatty acid profiles are altered in young adults with cystic fi-brosis Chest 118 (2000) 164ndash174
[65] MK Pulfer RC Murphy Formation of biologically active oxysterols during ozo-nolysis of cholesterol present in lung surfactant J Biol Chem 279 (2004)26331ndash26338
[66] V Starosta E Rietschel K Paul U Baumann M Griese Oxidative changes ofbronchoalveolar proteins in cystic fibrosis Chest 129 (2006) 431ndash437
[67] V Starosta M Griese Oxidative damage to surfactant protein D in pulmonarydiseases Free Radic Res 40 (2006) 419ndash425
[68] M Griese R Essl R Schmidt E Rietschel F Ratjen M Ballmann K Paul Pulmo-nary surfactant lung function and endobronchial inflammation in cystic fibro-sis Am J Respir Crit Care Med 170 (2004) 1000ndash1005
[69] M Griese R Essl R Schmidt M Ballmann K Paul E Rietschel F Ratjen Se-quential analysis of surfactant lung function and inflammation in cystic fibrosispatients Respir Res 6 (2005) 133
[70] LG Wood DA Fitzgerald PG Gibson DM Cooper ML Garg Increased plasmafatty acid concentrations after respiratory exacerbations are associated with el-evated oxidative stress in cystic fibrosis patients Am J Clin Nutr 75 (2002)668ndash675
[71] P Montuschi SA Kharitonov G Ciabattoni M Corradi L van Rensen DM Ged-des ME Hodson PJ Barnes Exhaled 8-isoprostane as a new non-invasive bio-marker of oxidative stress in cystic fibrosis Thorax 55 (2000) 205ndash209
[72] CE Collins P Quaggiotto L Wood EV OLoughlin RL Henry ML Garg Elevat-ed plasma levels of F2 alpha isoprostane in cystic fibrosis Lipids 34 (1999)551ndash556
[73] D Hartl V Starosta K Maier I Beck-Speier C Rebhan BF Becker P Latzin RFischer F Ratjen RM Huber E Rietschel S Krauss-Etschmann M Griese In-haled glutathione decreases PGE2 and increases lymphocytes in cystic fibrosislungs Free Radic Biol Med 39 (2005) 463ndash472
[74] GL Milne H Yin JD Morrow Human biochemistry of the isoprostane pathwayJ Biol Chem 283 (2008) 15533ndash15537
[75] G Ciabattoni G Davi M Collura L Iapichino F Pardo A Ganci R Romagnoli JMaclouf C Patrono In vivo lipid peroxidation and platelet activation in cystic fi-brosis Am J Respir Crit Care Med 162 (2000) 1195ndash1201
[76] C Garenc P Julien E Levy Oxysterols in biological systems the gastrointestinaltract liver vascular wall and central nervous system Free Radic Res 44 (2011)47ndash73
[77] AM Cantin SL North RC Hubbard RG Crystal Normal alveolar epithelial lin-ing fluid contains high levels of glutathione J Appl Physiol 63 (1987) 152ndash157
[78] R Tirouvanziam CK Conrad T Bottiglieri LA Herzenberg RB Moss High-dose oral N-acetylcysteine a glutathione prodrug modulates inflammation incystic fibrosis Proc Natl Acad Sci U S A 103 (2006) 4628ndash4633
[79] LW Velsor C Kariya R Kachadourian BJ Day Mitochondrial oxidative stressin the lungs of cystic fibrosis transmembrane conductance regulator proteinmutant mice Am J Respir Cell Mol Biol 35 (2006) 579ndash586
[80] M Kelly-Aubert S Trudel J Fritsch T Nguyen-Khoa M Baudouin-Legros SMoriceau L Jeanson F Djouadi C Matar M Conti M Ollero F Brouillard AEdelman GSH monoethyl ester rescues mitochondrial defects in cystic fibrosismodels Hum Mol Genet 20 (2011) 2745ndash2759
[81] P Ghezzi Role of glutathione in immunity and inflammation in the lung Int JGen Med 4 (2011) 105ndash113
[82] N Dauletbaev K Viel R Buhl TO Wagner J Bargon Glutathione and glutathi-one peroxidase in sputum samples of adult patients with cystic fibrosis J CystFibros 3 (2004) 119ndash124
[83] CE Cross A van der Vliet CA ONeill S Louie B Halliwell Oxidants antioxi-dants and respiratory tract lining fluids Environ Health Perspect 102 (Suppl10) (1994) 185ndash191
[84] K Takeyama K Dabbagh J Jeong Shim T Dao-Pick IF Ueki JA Nadel Oxida-tive stress causes mucin synthesis via transactivation of epidermal growth factorreceptor role of neutrophils J Immunol 164 (2000) 1546ndash1552
[85] N Ballatori SM Krance S Notenboom S Shi K Tieu CL Hammond Glutathi-one dysregulation and the etiology and progression of human diseases BiolChem 390 (2009) 191ndash214
[86] SR Soltaninassab KR Sekhar MJ Meredith ML Freeman Multi-faceted regu-lation of gamma-glutamylcysteine synthetase J Cell Physiol 182 (2000)163ndash170
[87] HR Lopez-Mirabal JR Winther Redox characteristics of the eukaryotic cytosolBiochim Biophys Acta 1783 (2008) 629ndash640
[88] C Hwang AJ Sinskey HF Lodish Oxidized redox state of glutathione in the en-doplasmic reticulum Science 257 (1992) 1496ndash1502
[89] M Murphy Mitochondrial thiols in antioxidant protection and redox signallingdistinct roles for glutathionylation and other thiol modifications AntioxidRedox Signal (2011) ahead of print doi101089ars20114289
[90] BJ Day AM van Heeckeren E Min LW Velsor Role for cystic fibrosis trans-membrane conductance regulator protein in a glutathione response to bronch-opulmonary Pseudomonas infection Infect Immun 72 (2004) 2045ndash2051
[91] Y Zhang K Duan Glutathione exhibits antibacterial activity and increases tetra-cycline efficacy against Pseudomonas aeruginosa Sci China C Life Sci 52 (2009)501ndash505
[92] VM Hudson New insights into the pathogenesis of cystic fibrosis pivotal roleof glutathione system dysfunction and implications for therapy Treat RespirMed 3 (2004) 353ndash363
[93] LW Velsor A van Heeckeren BJ Day Antioxidant imbalance in the lungs ofcystic fibrosis transmembrane conductance regulator protein mutant miceAm J Physiol Lung Cell Mol Physiol 281 (2001) L31ndashL38
[94] I Kogan M Ramjeesingh C Li JF Kidd Y Wang EM Leslie SP Cole CE BearCFTR directly mediates nucleotide-regulated glutathione flux EMBO J 22(2003) 1981ndash1989
[95] NS Gould S Gauthier CT Kariya E Min J Huang DJ Brian Hypertonic salineincreases lung epithelial lining fluid glutathione and thiocyanate two protectiveCFTR-dependent thiols against oxidative injury Respir Res 11 (2010) 119
[96] VT Vasu SJ de Cruz JS Houghton KA Hayakawa BM Morrissey CE CrossJP Eiserich Evaluation of thiol-based antioxidant therapeutics in cystic fibrosissputum focus on myeloperoxidase Free Radic Res 45 (2011) 165ndash176
[97] L Roussel G Martel J Berube S Rousseau P aeruginosa drives CXCL8 synthesisvia redundant toll-like receptors and NADPH oxidase in CFTRF508 airway epi-thelial cells J Cyst Fibros 10 (2011) 107ndash113
[98] GW Lau DJ Hassett H Ran F Kong The role of pyocyanin in Pseudomonas aer-uginosa infection Trends Mol Med 10 (2004) 599ndash606
[99] R Wilson DA Sykes D Watson A Rutman GW Taylor PJ Cole Measurementof Pseudomonas aeruginosa phenazine pigments in sputum and assessment oftheir contribution to sputum sol toxicity for respiratory epithelium InfectImmun 56 (1988) 2515ndash2517
[100] M Muller Pyocyanin induces oxidative stress in human endothelial cells andmodulates the glutathione redox cycle Free Radic Biol Med 33 (2002)1527ndash1533
[101] YQ OMalley KJ Reszka BE Britigan Direct oxidation of 2prime7prime-dichlorodihy-drofluorescein by pyocyanin and other redox-active compounds independentof reactive oxygen species production Free Radic Biol Med 36 (2004)90ndash100
[102] CC Caldwell Y Chen HS Goetzmann Y Hao MT Borchers DJ Hassett LRYoung D Mavrodi L Thomashow GW Lau Pseudomonas aeruginosa exotoxinpyocyanin causes cystic fibrosis airway pathogenesis Am J Pathol 175 (2009)2473ndash2488
[103] YQ OMalley KJ Reszka DR Spitz GM Denning BE Britigan Pseudomonasaeruginosa pyocyanin directly oxidizes glutathione and decreases its levels inairway epithelial cells Am J Physiol Lung Cell Mol Physiol 287 (2004)L94ndashL103
[104] M Muller Glutathione modulates the toxicity of but is not a biologically rele-vant reductant for the Pseudomonas aeruginosa redox toxin pyocyanin FreeRadic Biol Med 50 (2011) 971ndash977
[105] R Cheluvappa R Shimmon M Dawson SN Hilmer DG Le Couteur Reactionsof Pseudomonas aeruginosa pyocyanin with reduced glutathione Acta BiochimPol 55 (2008) 571ndash580
[106] JH Widdicombe Transgenic animals may help resolve a sticky situation in cys-tic fibrosis J Clin Invest 120 (2010) 3093ndash3096
[107] X Sun H Sui JT Fisher Z Yan X Liu HJ Cho NS Joo Y Zhang W Zhou Y YiJM Kinyon DC Lei-Butters MA Griffin P Naumann M Luo J Ascher KWang T Frana JJ Wine DK Meyerholz JF Engelhardt Disease phenotype ofa ferret CFTR-knockout model of cystic fibrosis J Clin Invest 120 (2010)3149ndash3160
[108] NS Joo HJ Cho M Khansaheb JJ Wine Hyposecretion of fluid from trachealsubmucosal glands of CFTR-deficient pigs J Clin Invest 120 (2010) 3161ndash3166
[109] A Bragonzi Murine models of acute and chronic lung infection with cystic fibro-sis pathogens IJMM 300 (2010) 584ndash593
[110] AM van Heeckeren MD Schluchter Murine models of chronic Pseudomonasaeruginosa lung infection Lab Anim 36 (2002) 291ndash312
[111] A Bragonzi D Worlitzsch GB Pier P Timpert M Ulrich M Hentzer JB Ander-sen M Givskov M Conese G Doring Nonmucoid Pseudomonas aeruginosa ex-presses alginate in the lungs of patients with cystic fibrosis and in a mousemodel J Infect Dis 192 (2005) 410ndash419
[112] GS CW Bedrossian DB Singer JJ Hansen HS Rosenberg The lung in cysticfibrosis A quantitative study including prevalence of pathologic findingsamong different age groups Hum Pathol 7 (1976) 195ndash204
[113] WD HA Cash B McCullough WG Johanson Jr JA Bass A rat model of chron-ic respiratory infection with Pseudomonas aeruginosa Am Rev Respir Dis 119(1979) 453ndash459
[114] EM JR Starke C Langston CJ Baker A mouse model of chronic pulmonary in-fection with Pseudomonas aeruginosa and Pseudomonas cepacia Pediatr Res 22(1987) 698ndash702
[115] TJ AM van Heeckeren RW Walenga MW Konstan PB Davis B ErokwuMA Haxhiu TW Ferkol Effect of Pseudomonas infection on weight loss lung
710 F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
mechanics and cytokines in mice Am J Respir Crit Care Med 161 (2000)271ndash279
[116] T Aw G Wierzbicka DP Jones Oral glutathione increases tissue glutathione invivo Chem Biol Interact 80 (1991) 89ndash97
[117] F Favilli P Marraccini T Iantomasi MT Vincenzini Effect of orally adminis-tered glutathione on glutathione levels in some organs of rats role of specifictransporters Br J Nutr 78 (1997) 293ndash300
[118] C Kariya H Leitner E Min C van Heeckeren A van Heeckeren BJ Day A rolefor CFTR in the elevation of glutathione levels in the lung by oral glutathione ad-ministration Am J Physiol Lung Cell Mol Physiol 292 (2007) L1590ndashL1597
[119] K Atkuri JJ Mantovani LA Herzenberg LA Herzenberg N-Acetylcysteinemdashasafe antidote for cysteineglutathione deficiency Curr Opin Pharmacol 7(2007) 355ndash359
[120] R De Lisle E Roach K Jansson Effects of laxative and N-acetylcysteine onmucus accumulation bacterial load transit and inflammation in the cystic fi-brosis mouse small intestine Am J Physiol Gastrointest Liver Physiol 293(2007) G577ndashG584
[121] A Luciani VR Villella S Esposito N Brunetti-Pierri D Medina C Settembre MGavina L Pulze I Giardino M Pettoello-Mantovani M DApolito S Guido EMasliah B Spencer S Quaratino V Raia A Ballabio L Maiuri Defective CFTRinduces aggresome formation and lung inflammation in cystic fibrosis throughROS-mediated autophagy inhibition Nat Cell Biol 12 863ndash875
[122] M Griese J Ramakers A Krasselt V Starosta S Van Koningsbruggen R FischerF Ratjen B Mullinger RM Huber K Maier E Rietschel G Scheuch Improve-ment of alveolar glutathione and lung function but not oxidative state in cysticfibrosis Am J Respir Crit Care Med 169 (2004) 822ndash828
[123] C Bishop VM Hudson SC Hilton C Wilde A pilot study of the effect of inhaledbuffered reduced glutathione on the clinical status of patients with cystic fibro-sis Chest 127 (2005) 308ndash317
[124] WWang C Oliva G Li A Holmgren CH Lillig KL Kirk Reversible silencing of CFTRchloride channels by glutathionylation J Gen Physiol 125 (2005) 127ndash141
[125] N Dauletbaev P Fischer B Aulbach J Gross W Kusche U Thyroff-FriesingerTO Wagner J Bargon A phase II study on safety and efficacy of high-dose N-acetylcysteine in patients with cystic fibrosis Eur J Med Res 14 (2009)352ndash358
[126] R Tirouvanziam Y Gernez CK Conrad RB Moss I Schrijver CE Dunn ZADavies LA Herzenberg Profound functional and signaling changes in viable in-flammatory neutrophils homing to cystic fibrosis airways Proc Natl Acad SciU S A 105 (2008) 4335ndash4339
[127] JH Roum Z Borok NG McElvaney GJ Grimes AD Bokser R Buhl RG Crys-tal Glutathione aerosol suppresses lung epithelial surface inflammatory cell-derived oxidants in cystic fibrosis J Appl Physiol 87 (1999) 438ndash443
[128] A Visca CT Bishop SC Hilton VM Hudson Improvement in clinical markersin CF patients using a reduced glutathione regimen an uncontrolled observa-tional study J Cyst Fibros 7 (2008) 433ndash436
[129] EF Nash A Stephenson F Ratjen E Tullis Nebulized and oral thiol derivativesfor pulmonary disease in cystic fibrosis Cochrane Database Syst Rev (2009)CD007168
[130] AC foundation Drug Development Pipeline 2011[131] S Hoshida T Kuzuya N Yamashita M Nishida S Kitahara M Hori T
Kamada M Tada Gamma-glutamylcysteine ethyl ester for myocardial protec-tion in dogs during ischemia and reperfusion J Am Coll Cardiol 24 (1994)1391ndash1397
[132] J Lok W Leung S Zhao S Pallast K van Leyen S Guo X Wang A Yalcin EHLo Gamma-glutamylcysteine ethyl ester protects cerebral endothelial cells dur-ing injury and decreases bloodndashbrain barrier permeability after experimentalbrain trauma J Neurochem 118 (2011) 248ndash255
[133] Z Borok R Buhl GJ Grimes AD Bokser RC Hubbard KJ Holroyd JH RoumDB Czerski AM Cantin RG Crystal Effect of glutathione aerosol on oxidantndashantioxidant imbalance in idiopathic pulmonary fibrosis Lancet 338 (1991)215ndash216
[134] KJ Holroyd R Buhl Z Borok JH Roum AD Bokser GJ Grimes D Czerski AMCantin RG Crystal Correction of glutathione deficiency in the lower respiratorytract of HIV seropositive individuals by glutathione aerosol treatment Thorax 48(1993) 985ndash989
[135] J Hull P Vervaart K Grimwood P Phelan Pulmonary oxidative stress responsein young children with cystic fibrosis Thorax 52 (1997) 557ndash560
[136] A Corti A Paolicchi M Franzini S Dominici AF Casini A Pompella The S-thiolating activity of membrane gamma-glutamyltransferase formation ofcysteinyl-glycine mixed disulfides with cellular proteins and in the cell microen-vironment Antioxid Redox Signal 7 (2005) 911ndash918
[137] A Corti M Franzini AF Casini A Paolicchi A Pompella Vitamin C supply tobronchial epithelial cells linked to glutathione availability in elfmdasha role for se-creted gamma-glutamyltransferase J Cyst Fibros 7 (2008) 174ndash178
[138] A Munck Nutritional considerations in patients with cystic fibrosis Expert RevRespir Med 4 (2010) 47ndash56
[139] JL Matel CE Milla Nutrition in cystic fibrosis Semin Respir Crit Care Med 30(2009) 579ndash586
[140] D Salvatore R Buzzetti E Baldo MP Forneris V Lucidi D Manunza IMarinelli B Messore AS Neri V Raia ML Furnari G Mastella An overviewof international literature from cystic fibrosis registries 2 Neonatal screeningand nutritiongrowth J Cyst Fibros 9 (2010) 75ndash83
[141] KF Joosten JM Hulst Malnutrition in pediatric hospital patients current is-sues Nutrition 27 (2011) 133ndash137
[142] S Fustik T Jacovska L Spirevska S Koceva Protein-energy malnutrition as thefirst manifestation of cystic fibrosis in infancy Pediatr Int 51 (2009) 678ndash683
[143] J Himmelfarb E McMonagle Albumin is the major plasma protein target of ox-idant stress in uremia Kidney Int 60 (2001) 358ndash363
[144] P Stenvinkel JJ Carrero J Axelsson B Lindholm O Heimburger Z MassyEmerging biomarkers for evaluating cardiovascular risk in the chronic kidneydisease patient how do new pieces fit into the uremic puzzle Clin J Am SocNephrol 3 (2008) 505ndash521
[145] M Roche P Rondeau NR Singh E Tarnus E Bourdon The antioxidant proper-ties of serum albumin FEBS Lett 582 (2008) 1783ndash1787
[146] D Giustarini A Milzani I Dalle-Donne R Rossi Red blood cells as a physiolog-ical source of glutathione for extracellular fluids Blood Cells Mol Dis 40 (2008)174ndash179
[147] A Meister ME Anderson Glutathione Annu Rev Biochem 52 (1983) 711ndash760[148] B Alvarez S Carballal L Turell R Radi Formation and reactions of sulfenic acid
in human serum albumin Methods Enzymol 473 (2010) 117ndash136[149] S Carballal B Alvarez L Turell H Botti BA Freeman R Radi Sulfenic acid in
human serum albumin Amino Acids 32 (2007) 543ndash551[150] LR Barclay AM Bailey D Kong The antioxidant activity of alpha-tocopherol-
bovine serum albumin complex in micellar and liposome autoxidations J BiolChem 260 (1985) 15809ndash15814
[151] T Ishii T Ichikawa K Minoda K Kusaka S Ito Y Suzuki M Akagawa K Mochi-zuki T Goda T Nakayama Human serum albumin as an antioxidant in the ox-idation of (minus)-epigallocatechin gallate participation of reversible covalentbinding for interaction and stabilization Biosci Biotechnol Biochem 75(2011) 100ndash106
[152] F Galli S Rovidati S Benedetti U Buoncristiani C Covarelli A Floridi F Canes-trari Overexpression of erythrocyte glutathione S-transferase in uremia and di-alysis Clin Chem 45 (1999) 1781ndash1788
[153] D Borowitz RD Baker V Stallings Consensus report on nutrition for pediat-ric patients with cystic fibrosis J Pediatr Gastroenterol Nutr 35 (2002)246ndash259
[154] LJ Filer Jr SW Wright MP Manning KE Mason Absorption of alpha-tocopherol and tocopherylesters by premature and full term infants and chil-dren in health and disease Pediatrics 8 (1951) 328ndash339
[155] L Lancellotti C DOrazio G Mastella G Mazzi U Lippi Deficiency of vitamins Eand A in cystic fibrosis is independent of pancreatic function and current en-zyme and vitamin supplementation Eur J Pediatr 155 (1996) 281ndash285
[156] MN Sathe AS Patel Update in pediatrics focus on fat-soluble vitamins NutrClin Pract 25 (2010) 340ndash346
[157] MG Traber The ABCs of vitamin E and beta-carotene absorption Am J ClinNutr 80 (2004) 3ndash4
[158] TF Dolan Jr Hemolytic anemia and edema as the initial signs in infants withcystic fibrosis Consider this diagnosis even in absence of pulmonary symptomsClin Pediatr 15 (1976) 597ndash600
[159] DR James M Alfaham MC Goodchild Increased susceptibility to peroxide-induced haemolysis with normal vitamin E concentrations in cystic fibrosisClin Chim Acta 204 (1991) 279ndash290
[160] SA Peters FJ Kelly Vitamin E supplementation in cystic fibrosis J Pediatr Gas-troenterol Nutr 22 (1996) 341ndash345
[161] A Maqbool VA Stallings Update on fat-soluble vitamins in cystic fibrosis CurrOpin Pulm Med 14 (2008) 574ndash581
[162] SD Sagel MK Sontag MM Anthony P Emmett KA Papas Effect of anantioxidant-rich multivitamin supplement in cystic fibrosis J Cyst Fibros 10(2011) 31ndash36
[163] F Galli A Azzi Present trends in vitamin E research Biofactors 36 (2010)33ndash42
[164] A Hamahata P Enkhbaatar ER Kraft M Lange SW Leonard MG Traber RACox FC Schmalstieg HK Hawkins EB Whorton EM Horvath C Szabo LDTraber DN Herndon DL Traber Gamma-tocopherol nebulization by a lipidaerosolization device improves pulmonary function in sheep with burn andsmoke inhalation injury Free Radic Biol Med 45 (2008) 425ndash433
[165] JP Anais N Razzouq M Carvalho C Fernandez A Astier M Paul A AstierH Fessi AM Lorino Development of alpha-tocopherol acetate nanoparti-cles influence of preparative processes Drug Dev Ind Pharm 35 (2009)216ndash223
[166] JM Zingg Molecular and cellular activities of vitamin E analogues Mini RevMed Chem 7 (2007) 543ndash558
[167] V Viola F Pilolli M Piroddi E Pierpaoli F Orlando M Provinciali M Betti FMazzini F Galli Why tocotrienols work better insights into the in vitro anti-cancer mechanism of vitamin E Genes Nutr 7 (2011) 29ndash41
[168] F Galli F Mazzini L Bamonti L Gille S Bohmdorfer M Piroddi T Netscher FJKelly T Rosenau Tocotrienamines and tocopheramines reactions with radicalsand metal ions Bioorg Med Chem 19 (2011) 6483ndash6491
[169] A Kuhad K Chopra Attenuation of diabetic nephropathy by tocotrienol in-volvement of NFκB signaling pathway Life Sci 84 (2009) 296ndash301
[170] Q Jiang X Yin MA Lill ML Danielson H Freiser J Huang Long-chain carbox-ychromanols metabolites of vitamin E are potent inhibitors of cyclooxygenasesProc Natl Acad Sci U S A 105 (2008) 20464ndash20469
[171] ER Miller III R Pastor-Barriuso D Dalal RA Riemersma LJ Appel E GuallarMeta-analysis high-dosage vitamin E supplementation may increase all-causemortality Ann Intern Med 142 (2005) 37ndash46
[172] JN Hathcock A Azzi J Blumberg T Bray A Dickinson B Frei I Jialal CSJohnston FJ Kelly K Kraemer L Packer S Parthasarathy H Sies MG TraberVitamins E and C are safe across a broad range of intakes Am J Clin Nutr 81(2005) 736ndash745
[173] R Brigelius-Flohe F Galli Vitamin E a vitamin still awaiting the detection of itsbiological function Mol Nutr Food Res 54 (2010) 583ndash587
711F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
[174] MG Traber B Frei JS Beckman Vitamin E revisited do new data validate ben-efits for chronic disease prevention Curr Opin Lipidol 19 (2008) 30ndash38
[175] F Galli Meeting report Vitamin E Satellite Symposium (VESS) associated to theAnnual Meeting of the SFRR-Europe Rome 26 August 2009 Free Radic Res 43(2009) 1256ndash1257
[176] LJ Roberts II JA Oates MF Linton S Fazio BP Meador MD Gross Y Shyr JDMorrow The relationship between dose of vitamin E and suppression of oxida-tive stress in humans Free Radic Biol Med 43 (2007) 1388ndash1393
[177] EFSA- EFSA Scientific Opinion of the Panel on Food Additives FlavouringsProcessing Aids and Materials in Contact with Food on a request from the Com-mission on mixed tocopherols tocotrienol tocopherol and tocotrienols assources for vitamin E in EFSA- EFSA (Ed) vol 640 The EFSA Journal2008 pp 1ndash34
[178] P Rust I Eichler S Renner I Elmadfa Long-term oral beta-carotene supple-mentation in patients with cystic fibrosis mdash effects on antioxidative status andpulmonary function Ann Nutr Metab 44 (2000) 30ndash37
[179] G Lepage J Champagne N Ronco A Lamarre I Osberg RJ Sokol CC Roy Sup-plementation with carotenoids corrects increased lipid peroxidation in childrenwith cystic fibrosis Am J Clin Nutr 64 (1996) 87ndash93
[180] BM Winklhofer-Roob H Puhl G Khoschsorur MA vant Hof H EsterbauerDH Shmerling Enhanced resistance to oxidation of low density lipoproteinsand decreased lipid peroxide formation during beta-carotene supplementationin cystic fibrosis Free Radic Biol Med 18 (1995) 849ndash859
[181] RC Graham-Maar JI Schall N Stettler BS Zemel VA Stallings Elevated vita-min A intake and serum retinol in preadolescent children with cystic fibrosisAm J Clin Nutr 84 (2006) 174ndash182
[182] I Sadowska-Woda M Rachel J Pazdan E Bieszczad-Bedrejczuk K PawliszakNutritional supplement attenuates selected oxidative stress markers in pediatricpatients with cystic fibrosis Nutr Res (New York NY) 31 (2011) 509ndash518
[183] KA Papas MK Sontag C Pardee RJ Sokol SD Sagel FJ Accurso JS WagenerA pilot study on the safety and efficacy of a novel antioxidant rich formulation inpatients with cystic fibrosis J Cyst Fibros 7 (2008) 60ndash67
[184] Y Saito A Fukuhara K Nishio M Hayakawa Y Ogawa H Sakamoto K Fujii YYoshida E Niki Characterization of cellular uptake and distribution of coen-zyme Q10 and vitamin E in PC12 cells J Nutr Biochem 20 (2009) 350ndash357
[185] AA Franke CM Morrison JL Bakke LJ Custer X Li RV Cooney CoenzymeQ10 in human blood native levels and determinants of oxidation during proces-sing and storage Free Radic Biol Med 48 (2010) 1610ndash1617
[186] HN Bhagavan RK Chopra Plasma coenzyme Q10 response to oral ingestion ofcoenzyme Q10 formulations Mitochondrion 7 (2007) S78ndashS88 (Suppl)
[187] HN Bhagavan RK Chopra Coenzyme Q10 absorption tissue uptake metabo-lism and pharmacokinetics Free Radic Res 40 (2006) 445ndash453
[188] F Galli R Lee C Dunster FJ Kelly Gas chromatography mass spectrometryanalysis of carboxyethyl-hydroxychroman metabolites of alpha- and gamma-tocopherol in human plasma Free Radic Biol Med 32 (2002) 333ndash340
[189] F Galli R Lee J Atkinson A Floridi FJ Kelly Gamma-tocopherol biokineticsand transformation in humans Free Radic Res 37 (2003) 1225ndash1233
[190] TA Laguna MK Sontag I Osberg JS Wagener FJ Accurso RJ Sokol De-creased total serum coenzyme-Q10 concentrations a longitudinal study in chil-dren with cystic fibrosis J Pediatr 153 (2008) 402ndash407
[191] T Frischer JK Myung G Maurer I Eichler Z Szepfalusi G Lubec Possible dys-regulation of chaperon and metabolic proteins in cystic fibrosis bronchial tissueProteomics 6 (2006) 3381ndash3388
[192] C Andersson MM Zaman AB Jones SD Freedman Alterations in immune re-sponse and PPARLXR regulation in cystic fibrosis macrophages J Cyst Fibros 7(2008) 68ndash78
[193] SD Freedman PG Blanco MM Zaman JC Shea M Ollero IK Hopper DAWeed A Gelrud MM Regan M Laposata JG Alvarez BP OSullivan Associa-tion of cystic fibrosis with abnormalities in fatty acid metabolism N Engl JMed 350 (2004) 560ndash569
[194] S Van Biervliet G Vanbillemont JP Van Biervliet D Declercq E Robberecht AChristophe Relation between fatty acid composition and clinical status or geno-type in cystic fibrosis patients Ann Nutr Metab 51 (2007) 541ndash549
[195] SD Freedman MH Katz EM Parker M Laposata MY Urman JG AlvarezA membrane lipid imbalance plays a role in the phenotypic expression ofcystic fibrosis in cftr(minusminus) mice Proc Natl Acad Sci U S A 96 (1999)13995ndash14000
[196] S Van Biervliet S Vande Velde JP Van Biervliet E Robberecht The effect ofzinc supplements in cystic fibrosis patients Ann Nutr Metab 52 (2008)152ndash156
[197] WR Henderson Jr SJ Astley MM McCready P Kushmerick S Casey JWBecker BW Ramsey Oral absorption of omega-3 fatty acids in patients withcystic fibrosis who have pancreatic insufficiency and in healthy control subjectsJ Pediatr 124 (1994) 400ndash408
[198] I Durieu E Vericel D Guichardant H Roth JP Steghens J Drai RN JosserandE Fontaine M Lagarde G Bellon Fatty acids platelets and oxidative markersfollowing intravenous n-3 fatty acids administration in cystic fibrosis an openpilot observational study J Cyst Fibros 6 (2007) 320ndash326
[199] LG Wood DA Fitzgerald ML Garg Hypothesis vitamin E complements poly-unsaturated fatty acids in essential fatty acid deficiency in cystic fibrosis J AmColl Nutr 22 (2003) 253ndash257
[200] JD Lloyd-Still SB Johnson RT Holman Essential fatty acid status in cystic fi-brosis and the effects of safflower oil supplementation Am J Clin Nutr 34(1981) 1ndash7
[201] A Maqbool JI Schall JF Garcia-Espana BS Zemel B Strandvik VAStallings Serum linoleic acid status as a clinical indicator of essential fatty
acid status in children with cystic fibrosis J Pediatr Gastroenterol Nutr 47(2008) 635ndash644
[202] C Oliver N Jahnke Omega-3 fatty acids for cystic fibrosis Cochrane DatabaseSyst Rev (2011) CD002201
[203] B Strandvik E Gronowitz F Enlund T Martinsson J Wahlstrom Essential fattyacid deficiency in relation to genotype in patients with cystic fibrosis J Pediatr139 (2001) 650ndash655
[204] P Rise S Volpi C Colombo RF Padoan C DOrazio S Ghezzi PMelotti V BennatoC Agostoni BM Assael C Galli Whole blood fatty acid analysis with micromethodin cystic fibrosis and pulmonary disease J Cyst Fibros 9 (2010) 228ndash233
[205] H Cao K Gerhold JR Mayers MM Wiest SM Watkins GS Hotamisligil Iden-tification of a lipokine a lipid hormone linking adipose tissue to systemic me-tabolism Cell 134 (2008) 933ndash944
[206] RR Malapaka SK Khoo J Zhang JH Choi XE Zhou Y Xu Y Gong J Li ELYong MJ Chalmers L Chang JH Resau PR Griffin YE Chen HE Xu Iden-tification and mechanism of a ten carbon fatty acid as a modulating ligand ofperoxisome proliferator activated receptors J Biol Chem 287 (2012)183ndash195
[207] T Hara A Hirasawa A Ichimura I Kimura G Tsujimoto Free fatty acid recep-tors FFAR1 and GPR120 as novel therapeutic targets for metabolic disorders JPharm Sci 100 (2011) 3594ndash3601
[208] R Gupta P Rathi S Bradoo Lipase mediated upgradation of dietary fats andoils Crit Rev Food Sci Nutr 43 (2003) 635ndash644
[209] BH Jennings CC Akoh Lipase-catalyzed modification of rice bran oil to incor-porate capric acid J Agric Food Chem 48 (2000) 4439ndash4443
[210] J Hoeks M Mensink MK Hesselink K Ekroos P Schrauwen Long- andMedium-Chain Fatty Acids Induce Insulin Resistance to a Similar Extent inHumans Despite Marked Differences in Muscle Fat Accumulation J Clin Endo-crinol Metab 97 (2012) 208ndash216
[211] PJ Congden G Bruce MM Rothburn PC Clarke JM Littlewood J KelleherMS Losowsky Vitamin status in treated patients with cystic fibrosis ArchDis Child 56 (1981) 708ndash714
[212] BM Winklhofer-Roob H Ellemunter M Fruhwirth SE Schlegel-Haueter GKhoschsorur MA vant Hof DH Shmerling Plasma vitamin C concentrationsin patients with cystic fibrosis evidence of associations with lung inflammationAm J Clin Nutr 65 (1997) 1858ndash1866
[213] L Shamseer D Adams N Brown JA Johnson S Vohra Antioxidant micronutri-ents for lung disease in cystic fibrosis Cochrane Database Syst Rev (2010)CD007020
[214] C Santi S Santoro Electrophilic Selenium First edition Wiley-VCH VerlagGmbH amp Co KGaA 2012
[215] L Flohe S Toppo G Cozza F Ursini A comparison of thiol peroxidase mecha-nisms Antioxid Redox Signal 15 (2010) 763ndash780
[216] L Flohe JR Andreesen R Brigelius-Flohe M Maiorino F Ursini Selenium theelement of the moon in life on earth IUBMB Life 49 (2000) 411ndash420
[217] V Valdiglesias E Pasaro J Mendez B Laffon In vitro evaluation of seleniumgenotoxic cytotoxic and protective effects a review Arch Toxicol 84(2010) 337ndash351
[218] P Foucaud P Therond M Marchand F Brion JF Demelier J Navarro Seleniumand vitamin E in mucoviscidosis Arch Fr Pediatr 45 (1988) 383ndash386
[219] J Neve R Van Geffel M Hanocq L Molle Plasma and erythrocyte zinc copperand selenium in cystic fibrosis Acta Paediatr Scand 72 (1983) 437ndash440
[220] BM Winklhofer-Roob B Tiran PE Tuchschmid MA vant Hof DH ShmerlingEffects of pancreatic enzyme preparations on erythrocyte glutathione peroxi-dase activities and plasma selenium concentrations in cystic fibrosis FreeRadic Biol Med 25 (1998) 242ndash249
[221] JD Lloyd-Still HE Ganther Selenium and glutathione peroxidase levels in cys-tic fibrosis Pediatrics 65 (1980) 1010ndash1012
[222] D Tsavachidou TJ McDonnell S Wen X Wang F Vakar-Lopez LL Pisters CAPettaway CG Wood KA Do PF Thall C Stephens E Efstathiou R Taylor DGMenter P Troncoso SM Lippman CJ Logothetis J Kim Selenium and vitaminE cell type- and intervention-specific tissue effects in prostate cancer J NatlCancer Inst 101 (2009) 306ndash320
[223] IN Zelko TJ Mariani RJ Folz Superoxide dismutase multigene family acomparison of the CuZn-SOD (SOD1) Mn-SOD (SOD2) and EC-SOD (SOD3)gene structures evolution and expression Free Radic Biol Med 33 (2002)337ndash349
[224] RP Bowler JD Crapo Oxidative stress in airways is there a role for extracellu-lar superoxide dismutase Am J Respir Crit Care Med 166 (2002) S38ndashS43
[225] K Best K McCoy S Gemma RA Disilvestro Copper enzyme activities in cysticfibrosis before and after copper supplementation plus or minus zinc Metabo-lism 53 (2004) 37ndash41
[226] SS Percival GP Kauwell E Bowser M Wagner Altered copper status in adultmen with cystic fibrosis J Am Coll Nutr 18 (1999) 614ndash619
[227] NF Krebs JE Westcott TD Arnold BM Kluger FJ Accurso LV Miller KMHambidge Abnormalities in zinc homeostasis in young infants with cystic fibro-sis Pediatr Res 48 (2000) 256ndash261
[228] D Easley N Krebs M Jefferson L Miller J Erskine F Accurso KM HambidgeEffect of pancreatic enzymes on zinc absorption in cystic fibrosis J Pediatr Gas-troenterol Nutr 26 (1998) 136ndash139
[229] S Van Biervliet JP Van Biervliet E Robberecht Serum zinc in patients with cys-tic fibrosis at diagnosis and after one year of therapy Biol Trace Elem Res 112(2006) 205ndash211
[230] S Van Biervliet JP Van Biervliet S Vande Velde E Robberecht Serum zinc con-centrations in cystic fibrosis patients aged above 4 years a cross-sectional eval-uation Biol Trace Elem Res 119 (2007) 19ndash26
712 F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
[231] F Galli M Cristina Polidori W Stahl P Mecocci FJ Kelly Vitamin E biotransfor-mation in humans Vitam Horm 76 (2007) 263ndash280
[232] J Wiser NE Alexis Q Jiang W Wu C Robinette R Roubey DB Peden In vivogamma-tocopherol supplementation decreases systemic oxidative stress andcytokine responses of human monocytes in normal and asthmatic subjectsFree Radic Biol Med 45 (2008) 40ndash49
[233] JG Wagner Q Jiang JR Harkema B Illek DD Patel BN Ames DB PedenOzone enhancement of lower airway allergic inflammation is prevented bygamma-tocopherol Free Radic Biol Med 43 (2007) 1176ndash1188
[234] JT Harries DP Muller Absorption of different doses of fat soluble and watermiscible preparations of vitamin E in children with cystic fibrosis Arch DisChild 46 (1971) 341ndash344
[235] EI Back C Frindt E Ocenaskova D Nohr M Stern HK Biesalski Can changesin hydrophobicity increase the bioavailability of alpha-tocopherol Eur J Nutr45 (2006) 1ndash6
[236] SZ Nasr MH OLeary C Hillermeier Correction of vitamin E deficiency withfat-soluble versus water-miscible preparations of vitamin E in patients with cys-tic fibrosis J Pediatr 122 (1993) 810ndash812
[237] S Soltani-Frisk E Gronowitz H Andersson B Strandvik Water-miscibletocopherol is not superior to fat-soluble preparation for vitamin E absorptionin cystic fibrosis Acta Paediatr 90 (2001) 1112ndash1115
[238] K Papas J Kalbfleisch R Mohon Bioavailability of a novel water-soluble vi-tamin E formulation in malabsorbing patients Dig Dis Sci 52 (2007)347ndash352
[239] F Antonicelli M Parmentier EM Drost N Hirani I Rahman K Donaldson WMacNee Nacystelyn inhibits oxidant-mediated interleukin-8 expression andNF-kappaB nuclear binding in alveolar epithelial cells Free Radic Biol Med 32(2002) 492ndash502
[240] EM App D Baran I Dab A Malfroot M Coffiner F Vanderbist M King Dose-finding and 24-h monitoring for efficacy and safety of aerosolized Nacystelyn incystic fibrosis Eur Respir J 19 (2002) 294ndash302
[241] MG Traber How much vitamin E hellip Just enough Am J Clin Nutr 84 (2006)959ndash960
[242] JC McCann BN Ames Vitamin K an example of triage theory is micronu-trient inadequacy linked to diseases of aging Am J Clin Nutr 90 (2009)889ndash907
[243] M Fusaro G Crepaldi S Maggi F Galli A DAngelo L Calo S Giannini DMiozzo M Gallieni Vitamin K bone fractures and vascular calcifications inchronic kidney disease an important but poorly studied relationship J Endocri-nol Invest 34 (2010) 317ndash323
[244] JC McCann BN Ames Adaptive dysfunction of selenoproteins from the per-spective of the triage theory why modest selenium deficiency may increaserisk of diseases of aging FASEB J 25 (2011) 1793ndash1814
[245] R Apak K Guclu M Ozyurek B Bektas Oglu M Bener Cupric ion reducing an-tioxidant capacity assay for food antioxidants vitamins polyphenolics and fla-vonoids in food extracts Methods Mol Biol 477 (2008) 163ndash193
[246] F Galli Interactions of polyphenolic compounds with drug disposition and me-tabolism Curr Drug Metab 8 (2007) 830ndash838
[247] RL Prior X Wu K Schaich Standardized methods for the determination of an-tioxidant capacity and phenolics in foods and dietary supplements J Agric FoodChem 53 (2005) 4290ndash4302
[248] C Azbell S Zhang D Skinner J Fortenberry EJ Sorscher BA WoodworthHesperidin stimulates cystic fibrosis transmembrane conductance regulator-mediated chloride secretion and ciliary beat frequency in sinonasal epitheliumOtolaryngol Head Neck Surg 143 (2010) 397ndash404
[249] G Wegrzyn J Jakobkiewicz-Banecka M Gabig-Ciminska E Piotrowska M Nar-ajczyk A Kloska M Malinowska D Dziedzic I Golebiewska M Moskot AWegrzyn Genistein a natural isoflavone with a potential for treatment of ge-netic diseases Biochem Soc Trans 38 (2010) 695ndash701
[250] YC Yu H Miki Y Nakamura A Hanyuda Y Matsuzaki Y Abe M Yasui K Ta-naka TC Hwang SG Bompadre Y Sohma Curcumin and genistein additivelypotentiate G551D-CFTR J Cyst Fibros 10 (2011) 243ndash252
[251] B Illek H Fischer Flavonoids stimulate Cl conductance of human airway epithe-lium in vitro and in vivo Am J Physiol 275 (1998) L902ndashL910
[252] JL Kreindler Cystic fibrosis exploiting its genetic basis in the hunt for newtherapies Pharmacol Ther 125 (2010) 219ndash229
[253] B Illek L Zhang NC Lewis RB Moss JY Dong H Fischer Defective function ofthe cystic fibrosis-causing missense mutation G551D is recovered by genisteinAm J Physiol 277 (1999) C833ndashC839
[254] P Anandakumar S Kamaraj S Jagan G Ramakrishnan R Vinodhkumar TDevaki Capsaicin modulates pulmonary antioxidant defense system during ben-zo(a)pyrene-induced lung cancer in Swiss albinomice Phytother Res 22 (2008)529ndash533
[255] I Rahman Antioxidant therapeutic advances in COPD Ther Adv Respir Dis 2(2008) 351ndash374
[256] AW Boots H Li RP Schins R Duffin JW Heemskerk A Bast GR Haenen Thequercetin paradox Toxicol Appl Pharmacol 222 (2007) 89ndash96
[257] M Joskova S Franova V Sadlonova Acute bronchodilator effect of quercetin inexperimental allergic asthma Bratisl Lek Listy 112 (2011) 9ndash12
[258] HJ Park CM Lee ID Jung JS Lee YI Jeong JH Chang SH Chun MJ Kim IWChoi SC Ahn YK Shin SR Yeom YM Park Quercetin regulates Th1Th2 balancein a murine model of asthma Int Immunopharmacol 9 (2009) 261ndash267
[259] AP Rogerio A Kanashiro C Fontanari EV da Silva YM Lucisano-ValimEG Soares LH Faccioli Anti-inflammatory activity of quercetin and iso-quercitrin in experimental murine allergic asthma Inflamm Res 56 (2007)402ndash408
[260] M Muller Polyphenol cytotoxicity induced by the bacterial toxin pyocyaninrole of NQO1 Free Radic Biol Med 47 (2009) 84ndash91
[261] J Grassmann Terpenoids as plant antioxidants Vitam Horm 72 (2005)505ndash535
[262] P Allen Tea tree oil the science behind the antimicrobial hype Lancet 358(2001) 1245
[263] EC Dasenbrook W Checkley CA Merlo MW Konstan N Lechtzin MP BoyleAssociation between respiratory tract methicillin-resistant Staphylococcus aure-us and survival in cystic fibrosis JAMA 303 (2010) 2386ndash2392
[264] V Bezzerri M Borgatti E Nicolis I Lampronti MC Dechecchi I Mancini PRizzotti R Gambari G Cabrini Transcription factor oligodeoxynucleotides toNF-kappaB inhibit transcription of IL-8 in bronchial cells Am J Respir CellMol Biol 39 (2008) 86ndash96
[265] R Gambari M Borgatti V Bezzerri E Nicolis I Lampronti MC Dechecchi IMancini A Tamanini G Cabrini Decoy oligodeoxyribonucleotides and peptidenucleic acids-DNA chimeras targeting nuclear factor kappa-B inhibition of IL-8 gene expression in cystic fibrosis cells infected with Pseudomonas aeruginosaBiochem Pharmacol 80 (2010) 1887ndash1894
[266] M Adrian P Jeandet AC Douillet-Breuil L Tesson R Bessis Stilbene content ofmature Vitis vinifera berries in response to UV-C elicitation J Agric Food Chem48 (2000) 6103ndash6105
[267] B Paul I Masih J Deopujari C Charpentier Occurrence of resveratrol and pter-ostilbene in age-old darakchasava an ayurvedic medicine from India J Ethno-pharmacol 68 (1999) 71ndash76
[268] I Rahman Antioxidant therapies in COPD Int J Chron Obstruct Pulmon Dis 1(2006) 15ndash29
[269] M Lee S Kim OK Kwon SR Oh HK Lee K Ahn Anti-inflammatory and anti-asthmatic effects of resveratrol a polyphenolic stilbene in a mouse model ofallergic asthma Int Immunopharmacol 9 (2009) 418ndash424
[270] LG Wood PA Wark ML Garg Antioxidant and anti-inflammatory effectsof resveratrol in airway disease Antioxid Redox Signal 13 (2010)1535ndash1548
[271] KV Kiselev Perspectives for production and application of resveratrol ApplMicrobiol Biotechnol 90 (2011) 417ndash425
[272] M Shakibaei C Buhrmann A Mobasheri Resveratrol-mediated SIRT-1 interac-tions with p300 modulate receptor activator of NF-kappaB ligand (RANKL) acti-vation of NF-kappaB signaling and inhibit osteoclastogenesis in bone-derivedcells J Biol Chem 286 (2011) 11492ndash11505
[273] SF Zaidi K Ahmed T Yamamoto T Kondo K Usmanghani M Kadowaki TSugiyama Effect of resveratrol on Helicobacter pylori-induced interleukin-8 secre-tion reactive oxygen species generation and morphological changes in human gas-tric epithelial cells Biol Pharm Bull 32 (2009) 1931ndash1935
[274] JK Kundu YK Shin YJ Surh Resveratrol modulates phorbol ester-inducedpro-inflammatory signal transduction pathways in mouse skin in vivo NF-kappaB and AP-1 as prime targets Biochem Pharmacol 72 (2006)1506ndash1515
[275] NH Nam Naturally occurring NF-kappaB inhibitors Mini Rev Med Chem 6(2006) 945ndash951
[276] JM Smoliga JA Baur HA Hausenblas Resveratrol and healthmdasha comprehen-sive review of human clinical trials Mol Nutr Food Res 55 (2011) 1129ndash1141
[277] ME Juan M Maijo JM Planas Quantification of trans-resveratrol and itsmetabolites in rat plasma and tissues by HPLC J Pharm Biomed Anal 51(2010) 391ndash398
[278] JA Baur DA Sinclair Therapeutic potential of resveratrol the in vivo evidenceNat Rev 5 (2006) 493ndash506
[279] E Nicolis I Lampronti MC Dechecchi M Borgatti A Tamanini N Bianchi VBezzerri I Mancini MG Giri P Rizzotti R Gambari G Cabrini Pyrogallol anactive compound from the medicinal plant Emblica officinalis regulates expres-sion of pro-inflammatory genes in bronchial epithelial cells Int Immunophar-macol 8 (2008) 1672ndash1680
[280] E Nicolis I Lampronti MC Dechecchi M Borgatti A Tamanini V Bezzerri NBianchi M Mazzon I Mancini MG Giri P Rizzotti R Gambari G CabriniModulation of expression of IL-8 gene in bronchial epithelial cells by 5-methoxypsoralen Int Immunopharmacol 9 (2009) 1411ndash1422
[281] M Borgatti I Mancini N Bianchi A Guerrini I Lampronti D Rossi G SacchettiR Gambari Bergamot (Citrus bergamia Risso) fruit extracts and identified com-ponents alter expression of interleukin 8 gene in cystic fibrosis bronchial epithe-lial cell lines BMC Biochem 12 (2011) 15
[282] L Piccagli E Fabbri M Borgatti N Bianchi V Bezzerri I Mancini E Nicolis CMDechecchi I Lampronti G Cabrini R Gambari Virtual screening against p50NF-kappaB transcription factor for the identification of inhibitors of the NF-kappaB-DNA interaction and expression of NF-kappaB upregulated genesChemMedChem 4 (2009) 2024ndash2033
[283] L Piccagli M Borgatti E Nicolis N Bianchi I Mancini I Lampronti D VevaldiF DallAcqua G Cabrini R Gambari Virtual screening against nuclear factorkappaB (NF-kappaB) of a focus library identification of bioactive furocoumarinderivatives inhibiting NF-kappaB dependent biological functions involved incystic fibrosis Bioorg Med Chem 18 (2010) 8341ndash8349
[284] M Borgatti A Chilin L Piccagli I Lampronti N Bianchi I Mancini G Mar-zaro Da Francesco A Guiotto R Gambari Development of a novel furocou-marin derivative inhibiting NF-kappaB dependent biological functionsdesign synthesis and biological effects Eur J Med Chem 46 (2011)4870ndash4877
[285] E Georgy S Le Guellec L Vecellio E Fichant P Stordeur P Bordeau JP PerraudinFeasibility study of OSCN- and lactoferrin (Meveol) nebulization for cysticfibrosis JCyst Fibros 10 (2011) S18
713F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
[286] C Tidei M Piroddi F Galli C Santi Oxidation of thiols promoted by PhSeZnClTetrahedron Lett 53 (2012) 232ndash234
[287] L Semianrio-Vidal C van Hesuden G Mugesh ER Lazarowski Ebselen is a po-tent non-competitive inhibitor of extracellular nucleoside diphosphokinasePurinergic Signal 6 (2010) 383ndash391
[288] C ColussiMC Albertini S Coppola S Rovidati F Galli L Ghibelli H2O2-inducedblockof glycolysis as an active ADP-ribosylation reaction protecting cells from apoptosisFASEB J 14 (2000) 2266ndash2276
[289] H Xiao KL Parkin Induction of phase II enzyme activity by various seleniumcompounds Nutr Cancer 55 (2006) 210ndash223
[290] G Peluffo R Radi Biochemistry of protein tyrosine nitration in cardiovascularpathology Cardiovasc Res 75 (2007) 291ndash302
[291] B Alvarez R Radi Peroxynitrite reactivity with amino acids and proteinsAmino Acids 25 (2003) 295ndash311
[292] B Kamosinska MW Radomski M Duszyk A Radomski SF Man Nitric oxideactivates chloride currents in human lung epithelial cells Am J Physiol 272(1997) L1098ndashL1104
[293] L Chen RP Patel X Teng CA Bosworth JR Lancaster Jr S Matalon Mecha-nisms of cystic fibrosis transmembrane conductance regulator activation by S-nitrosoglutathione J Biol Chem 281 (2006) 9190ndash9199
[294] F Luchetti B CanonicoM BettiM Arcangeletti F PilolliM Piroddi L Canesi S PapaF Galli Melatonin signaling and cell protection function FASEB J 24 (2010)3603ndash3624
[295] MW Bengtsson G Jedstedt G Flemstrom Duodenal bicarbonate secretion inrats stimulation by intra-arterial and luminal guanylin and uroguanylin ActaPhysiol (Oxf) 191 (2007) 309ndash317
[296] CS Nelson JL Marino CN Allen Melatonin receptor potentiation of cyclic AMP andthe cystic fibrosis transmembrane conductance regulator ion channel J Pineal Res 26(1999) 113ndash121
[297] C de Castro-Silva VM de Bruin GM Cunha DM Nunes CAMedeiros PF de BruinMelatonin improves sleep and reduces nitrite in the exhaled breath condensate incystic fibrosismdasha randomized double-blind placebo-controlled study J Pineal Res48 (2010) 65ndash71
[298] I Hornyak E Pankotai L Kiss Z Lacza Current developments in the the-rapeutic potential of S-nitrosoglutathione an endogenous NO-donor mole-cule Curr Pharm Biotechnol (2011) Jan 11 [Epub ahead of print] - PMID21235457
[299] AH Snyder ME McPherson JF Hunt M Johnson JS Stamler B Gaston Acuteeffects of aerosolized S-nitrosoglutathione in cystic fibrosis Am J Respir CritCare Med 165 (2002) 922ndash926

706 F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
50ndash100 μgmg of fresh skin and 13ndash3 mgl of red wine [266]Furthermore resveratrol is a constituent of lsquoDarakchasavarsquo (13ndash6 mgl) an ayurvedic medicine from India [267] The antioxidant activity ofresveratrol has been reported in several papers and occurs also in lungtissues suggesting that resveratrol has potential as a therapeuticagent in respiratory disease [268ndash270] Resveratrol can be consideredone of the most interesting molecules from the natural worldexhibiting strong antioxidant activity that at the same time is able toexert anti inflammatory activity through alteration of NF-κB functionsand efficient inhibition of pro-inflammatory genes [271272] As far asthe effects on CF model systems are concerned Cabrini et al [26]reported the effects of resveratrol on P aeruginosa infected CF IB3-1cells The results obtained demonstrate that resveratrol exhibits minoreffects of IB3-1 cell growth and important inhibitory effects on accumu-lation of IL-8 and GRO-α mRNA while minor effects on IL-6 gene ex-pression were observed These data support recently publishedobservations suggesting inhibitory effects of resveratrol in infection-mediated inflammatory processes [273] Interestingly resveratrol hasbeen reported as a potent inhibitor of NF-κB activity and a promisinganti-inflammatory agent [272274] also in combinationwith othermol-ecules [274275] However in vivo translation of this pre-clinical on res-veratrol is hard to be foreseen This natural compound displays poorbioavailability [276] and further characterization of resveratrol pharma-cokinetics is troublesome since it is hardly measurable in vivo [277]Furthermore the regulation of inflammatory responses by resveratrolhas been suggested to be far more complex than simple direct suppres-sion of NF-κB activity Actually some aspects of the immune responsecould be enhanced by this natural substance which may lead tohypothesize broad negative feedback events on immuno-inflammatorypathways [278] In any case and with these cautions in mind the pub-lished observations on cellular model systems support the concept thatresveratrol and resveratrol-containing formulations deserve further con-sideration to determine their possible therapeutic values in CF
Other inhibitors can be identified from systematic studies of naturalproducts and their ability to interfere with NF-κB activity [279ndash281]Recent studies have demonstrated that the whole extract of Aeglemarmelos (Rutaceae) has strong inhibitory effect on the P aeruginosa-dependent IL-8 induction in human CF-derived bronchial IB3-1 cellswithout affecting cell proliferation [280] Molecular analysis of compo-nents contained in A marmelos extracts revealed that three major com-pounds namely 56-dimethoxy-1-indanone 2-hydroxy-cinnamic acidand 5-methoxy psoralen (5-MOP) reproduce the inhibitory effect ob-servedwith thewhole extract [280] A further example has been recent-ly published using extracts from bergamot (Citrus bergamia Risso) Inthis study the extracts were characterized and the main detected con-stituents were assayed for their biological activity [281] The resultsobtained demonstrated that the extracts from bergamot epicarps con-tain components displaying an inhibitory activity on IL-8 Particularlythe most active molecules were bergapten and citropten These effectshave been confirmed by analyzing mRNA levels and protein release inthe CF cellularmodels IB3-1 and CuFi-1 inducedwith TNF-α or exposedto P aeruginosa
A parallel strategy linking NF-κB inhibition and down-regulationof NF-κB-dependent functions is described in recently publishedstudies based on a structured-based virtual screening (VS) of differ-ently substituted furocoumarins and analogues against NF-κB withthe objective of selecting molecules able to inhibit the binding ofthis transcription factor to DNA [282283] Novel compounds wereidentified with this strategy as potent inhibitors of NF-κB dependentbiological functions to be proposed for the control lung inflammationoccurring in patients affected by CF [282ndash284]
392 Scavengers and regulators of H2O2 and NO
3921 Lactoferrin and OSCNmacr The impaired DUOXLPO system of CFpatients could be the target of therapeutic strategies that may
produce concomitant antimicrobial and antioxidant effects This sys-tem described above in Section 22 represents an important compo-nent of innate immunity with a role in bactericidal defense andregulation of H2O2 metabolism of airways [32] CF patients have alsoreported to show lowered LF levels in the ASL [37] that togetherwith a CFTR-dependent defective efflux of SCNmacr and LPO [36] may cre-ate the environment for a sustained flux of H2O2 and for the genera-tion of highly reactive Fenton species [1138] An ideal therapeuticintervention should restore the LPO-dependent generation of bacteri-cidal OSCNmacr from DUOX-derived H2O2 and SCNmacr in the ASL to controlat the same time the microbial biofilm and the flux of H2O2 into theASL An approach close to this therapeutic mechanism was recentlyproposed for the drug Meveolreg This is a complex of LF and OSCNmacrwith proposed in vivo antimicrobial activity [285] to be evaluatedin clinical trials for the aerosol treatment of lung infections in CFpatients The role for this drug in the control of H2O2 levels of ASLremains to be investigated
3922 Organoselenium compounds Organoselenium compoundshave been proposed as therapeutic agents useful in the antioxidanttherapy of inflammatory conditions These include GPX mimetic mol-ecules such as Ebselenreg (2-phenyl-12-benzisoselenazol-3(2H)-one)or other and more recently developed molecules that are still inpre-clinical steps of evaluation [286] Selectively and specificity of ac-tion are main issues in the therapeutic mechanism of this candidateantioxidant drug that thanks to the electrophilic properties of Se[214] reacts with thiols to reduce H2O2 and other species MoreoverEbselenreg has been described to act as potent non-competitive inhib-itor of extracellular nucleoside diphosphokinase (NDPK) having neg-ligible effect on ecto-ATPase and adenyl kinase activities which areother players of the metabolism of extracellular nucleotides [287]This enzyme together with other nucleoside di- and triphosphatescontributes to regulate several components of the mucociliary clear-ance process (MCC) that protects the lung against infections via acti-vation of epithelial purinergic receptors The inhibition of NDPK bythis GPX-mimetic drug may also impact on the energy status of endo-thelial cells [287] This aspect could be further investigated as a cellu-lar protection mechanism in the pulmonary epithelium of CF patientsbeing the control of cell energy of fundamental importance to preventthe activation of death pathways [288]
Further therapeutic mechanisms for these Se-derived drugs mayderive from the marked activity as inducers of phase II enzymessuch as quinone reductase (QR) and glutathione-S-transferase (GST)[289] This induction response also observed with other electrophilsand redox-active molecules such as natural phenolic antioxidantscould produce higher cellular protection by the acquisition of anincreased capability to detoxify endobiotics generated during oxida-tive stress and inflammation [246]
3923 Melatonin and GSNO as NOx regulators Increased markers ofNO-derived biological damage are present in the CF lung suggestingthe abnormal reactivity of NOx in the inflamed lung of CF patients[52] However an impaired metabolism and biological function ofNO in CF airways (see Section 23) suggests a cautious approach tothe use of agents that may influence the levels and chemical behaviorof NO-derived species (NOx) with possible impact on the physiologi-cal roles of NO in vasodilatation innate immunity and H2O2 metabo-lism of the respiratory tract [290291] NO donors also appear toinfluence CFTR function of alveolar epithelium and gland serouscells [292293]
Main physiological role of the pineal gland hormone melatonin isthe synchronization of circadian rhythms including the sleepndashwakecycle but several other functions dealing with immunomodulatoryantioxidant and cellular protection effects have been identified[294] Melatonin receptor stimulation may also influence cyclic AMPsignaling and the regulation of CFTR ion channel [295296]
707F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
A recent randomized double-blind placebo-controlled study hasexamined the effects of short term melatonin administration (3 mgfor 3 weeks) on sleep and oxidative stress markers in CF [297]According with the expected pharmacological effect of this hormonalsubstance the treatment was successful in improving sleep indicesAt the same time nitrite levels determined in exhaled breath conden-sate (EBC) were reduced to suggest a better control of NOmetabolismof CF airways (discussed above in Section 23) but these effects how-ever were not associated with a significant correction of isoprostaneas lipid peroxidation marker measured in EBC Increasing dosages ofmelatonin could be investigated for the pharmacological treatmentof oxidative stress and immune dysfunction of CF patients due tothe absence of adverse effects of this hormonal substance in humans
The S-nitrosation reaction of thiols is another interesting aspect ofNO pharmacology [53] that may find an application in the therapy oflung complications of CF This has been the case for instance of theS-nitrosothiol GSNO that has been used safely in human trials[298299] This endogenous nitrosothiol with proposed regulatory ef-fect on the CFTR of lung epithelia [292293] is well tolerated in pa-tients with CF when administered by aerosolization and mayproduce better oxygenation [299] thereby suggesting that therapyaimed at restoring endogenous GSNO levels in the CF airway maymerit further clinical evaluation Since the administered GSNO de-composes as shown by the increased levels of expired NO in CF pa-tients under treatment with this nitrosothiol [299] furtherinvestigation should be addressed to ascertain whether GSNO thera-py may merely correspond to a GSH therapy
NO dependent effects on CFTR function should be considered toevaluate mechanism of action and specificity of antioxidant therapiesthat target NO metabolism and function in the CF airways
4 Conclusions and future perspectives
The presence of clinical and biochemical symptoms of inflammationand oxidative stress implies that CF patients have a higher demand ofantioxidant protection The combination of the dysfunctional CFTRwith a lowered intake and absorption of dietary antioxidants producesub-optimal levels of protection from both enzymatic and non-enzymatic defense systems The former could be associated with a de-fective glutathionemetabolism and lowered intake of sulfur-containingamino acids and oligoelements such as zinc and possibly seleniumwhile fat-soluble antioxidant vitamins such as vitamin E and caroten-oids and the water-soluble vitamin C are lowered than in healthy sub-jects due to malabsorption and possibly higher consumption
The increased antioxidant demand in CF patients should be evenhigher in the presence of complications of the lung pancreas andliver Lung comorbidity is particularly important in this contextbeing associated with recurrent infections which results in the alter-nation of inflammatory exacerbates and chronic inflammation Thesesustain the flux of ROS in the airways and promote the formation ofsecond-generation byproducts by the damage of biomolecules suchas PUFA and proteins which may diffuse also at the systemic level tofurther promote adverse biological responses and toxic reactions Pan-creatic insufficiency causes malnutrition and may lead to develop en-docrine and metabolic defects associated with diabetes of CF Theseevents can be further aggravated by the concomitance of liver dys-function and a poor nutritional status Malnutrition is strongly associ-ated with poor prognosis as assessed by pulmonary function andsurvival data [138ndash140] The more aggressive nutritional interven-tions seem to produce better clinical outcomes in these patients andthe possibility of achieving higher antioxidant protection in well-nourished patients by dietary factors could be a key aspect to explainsuch a clinical advantage The assumption that food-derived compo-nentsmay help to prevent the damaging effects of oxidative stress im-proving the antioxidant defenses deserves further investigation at theclinical level This together with the investigation of appropriate
laboratory biomarkers could provide critical information to establishintervention criteria for an early nutritional management of newly di-agnosed patients [5] It is expected that a timely secondary preventionstrategy could influence the progression of CF symptoms thusaffecting with a self-feeding mechanism the same extent of malnutri-tion and oxidative stress along the life of CF patients Since severalfactors contribute to impair the nutritional status of CF patients(such as pancreatic insufficiency chronic malabsorption recurrentsinopulmonary infections and progressive lung disease chronic in-flammation increased energy expenditure suboptimal intake multi-therapy) careful monitoring of the antioxidant status should berecommended According with international guidelines fat-solublevitamin supplementation is of utmost importance in daily practice to-gether with energy intake requirements and pancreatic enzyme-replacement therapy Among these vitamin E β-carotene and ω-3FA have observed to alleviate selected biochemical signs of oxidativestress as measured for instance with well established laboratory indi-ces of lipid peroxidation and in some studies these effects werepreliminarily associated with positive clinical outcomes Notwith-standing randomizedndashcontrolled clinical trials on antioxidant supple-ments (including ω-3 FA) so far carried out in CF have failed toconclusively demonstrate significant beneficial effects on respiratorysymptoms and on the consequent impact that these have on the qual-ity of life of these patients (reviewed in [202213]) whichmay provideno support for the use of these supplements in CF An absence of effi-cacy in prevention studies on antioxidant supplements has also beenobserved in other and possibly less severe oxidative stress-relatedconditions particularly in the secondary prevention of cardiovasculardisease and some forms of cancer by vitamin E and other antioxidantssuch as vitamin C selenium and β-carotene (reviewed in [163]) Dif-ferent biases however have been identified in randomize large clini-cal trials that may account for these disappointing findings Theseinclude patient selection criteria (early interventions and primaryprevention could have more chances of success than secondaryprevention) duration and doses of the treatment use of wrong anti-oxidant formulations and administration protocols absence of verifi-cations of the biological compliance to the treatment etc The samebiases apply for the few trials carried out in CF patients Thus the ap-propriateness and efficacy of nutritional interventions with naturalfood-derived or synthetic antioxidants should be verifiedwith respectto the biological pathways of oxidative stress and clinical variablesthat are identified as end-points Profiles of blood and tissue antioxi-dants as well as of reliable surrogate markers of oxidative stresshave to be selected and determined in highly specialized laboratorieswith a well-established experience on these analyses
Well-timed (early) interventions with appropriate antioxidantformulationsprotocols need to be proposed for the next generationof trials and the development of novel CF-tailored antioxidant andanti-inflammatory agents should be promoted
As a consequence of these considerations more clinical investiga-tion is awaited to identify future successful approaches to the antiox-idant therapy as a measure to further enhance quality of life and theoverall clinical outcome of CF patients
Acknowledgments
We are indebted with the Italian Cystic Fibrosis Research Founda-tion for the support that it provided with its grant program to the re-search activity of the authors of this paper This is a scientific initiativeof the ldquoWorking Group on Inflammation in Cystic Fibrosisrdquo (BragonziA Bravo E Cabrini G Conese M Cuzzocrea S Dechecchi MC De Ales-sandri A Evangelista V Galli F Gambari R Lambiase A Lucidi VManca A Melotti P Minicucci L Motta A Pietraforte D Pompella AQuattrucci S Rizzo R Romano M Sorio C Tesse R) of the Italian Soci-ety for Cystic Fibrosis A particular thank goes to the Prof GianniMastella for the critical revision of the manuscript and for the
708 F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
stimulating research environment that he has contributed to createwithin the Italian Cystic Fibrosis Research Foundation
References
[1] BP OSullivan SD Freedman Cystic fibrosis Lancet 373 (2009) 1891ndash1904[2] P Linsdell JW Hanrahan Glutathione permeability of CFTR Am J Physiol 275
(1998) C323ndashC326[3] L Gao KJ Kim JR Yankaskas HJ Forman Abnormal glutathione transport in
cystic fibrosis airway epithelia Am J Physiol 277 (1999) L113ndashL118[4] RK Rowntree A Harris The phenotypic consequences of CFTR mutations Ann
Hum Genet 67 (2003) 471ndash485[5] EI Back C Frindt D Nohr J Frank R Ziebach M Stern M Ranke HK Biesalski
Antioxidant deficiency in cystic fibrosis when is the right time to take actionAm J Clin Nutr 80 (2004) 374ndash384
[6] LG Wood DA Fitzgerald AK Lee ML Garg Improved antioxidant and fattyacid status of patients with cystic fibrosis after antioxidant supplementation islinked to improved lung function Am J Clin Nutr 77 (2003) 150ndash159
[7] L Iuliano R Monticolo G Straface S Zullo F Galli M Boaz S Quattrucci Asso-ciation of cholesterol oxidation and abnormalities in fatty acid metabolism incystic fibrosis Am J Clin Nutr 90 (2009) 477ndash484
[8] C Libetta V Sepe P Esposito F Galli A Dal Canton Oxidative stress and inflam-mation implications in uremia and hemodialysis Clin Biochem 44 (2011)1189ndash1198
[9] G Bartosz Reactive oxygen species destroyers or messengers Biochem Phar-macol 77 (2009) 1303ndash1315
[10] T Ntimbane B Comte G Mailhot Y Berthiaume V Poitout M Prentki RRabasa-Lhoret E Levy Cystic fibrosis-related diabetes from CFTR dysfunctionto oxidative stress Clin Biochem 30 (2009) 153ndash177
[11] A van der Vliet JP Eiserich GP Marelich B Halliwell CE Cross Oxidativestress in cystic fibrosis does it occur and does it matter Adv Pharmacol 38(1997) 491ndash513
[12] AM Cantin TB White CE Cross HJ Forman RJ Sokol D Borowitz Antioxi-dants in cystic fibrosis Conclusions from the CF antioxidant workshop Bethes-da Maryland Free Radic Biol Med 42 (2007) 15ndash31
[13] LT McGrath P Mallon L Dowey B Silke E McClean M McDonnell A DevineS Copeland S Elborn Oxidative stress during acute respiratory exacerbations incystic fibrosis Thorax 54 (1999) 518ndash523
[14] E Thomson S Brennan R Senthilmohan CL Gangell AL Chapman PD SlyAJ Kettle E Balding LJ Berry JB Carlin R Carzino N de Klerk T Douglas CFoo LW Garratt GL Hall J Harrison A Kicic IA Laing KM Logie J MassieLS Mott C Murray F Parsons N Pillarisetti SR Poreddy SC RanganathanCF Robertson R Robins-Browne PJ Robinson B Skoric SM Stick ENSutanto E Williamson Identifying peroxidases and their oxidants in the earlypathology of cystic fibrosis Free Radic Biol Med 49 (2010) 1354ndash1360
[15] SP Range C Dunster AJ Knox FJ Kelly Treatment of pulmonary exacerba-tions of cystic fibrosis leads to improved antioxidant status Eur Respir J 13(1999) 560ndash564
[16] L Coppo P Ghezzi Thiol regulation of pro-inflammatory cytokines and innateimmunity protein S-thiolation as a novel molecular mechanism Biochem SocTrans 39 (2011) 1268ndash1272
[17] C Verhaeghe C Remouchamps B Hennuy A Vanderplasschen A Chariot SPTabruyn C Oury V Bours Role of IKK and ERK pathways in intrinsic inflamma-tion of cystic fibrosis airways Biochem Pharmacol 73 (2007) 1982ndash1994
[18] TL Bonfield JR Panuska MW Konstan KA Hilliard JB Hilliard H Ghnaim MBerger Inflammatory cytokines in cystic fibrosis lungs Am J Respir Crit CareMed 152 (1995) 2111ndash2118
[19] TL Noah HR Black PW Cheng RE Wood MW Leigh Nasal and bronchoal-veolar lavage fluid cytokines in early cystic fibrosis J Infect Dis 175 (1997)638ndash647
[20] MJ Welsh BW Ramsey FJ Accurso GR Cutting Cystic Fibrosis McGraw-HillNew York 2001
[21] TZ Khan JS Wagener T Bost J Martinez FJ Accurso DW Riches Early pul-monary inflammation in infants with cystic fibrosis Am J Respir Crit CareMed 151 (1995) 1075ndash1082
[22] FA Ratjen Cystic fibrosis pathogenesis and future treatment strategies RespirCare 54 (2009) 595ndash605
[23] J Jacquot O Tabary P Le Rouzic A Clement Airway epithelial cell inflamma-tory signalling in cystic fibrosis Int J Biochem Cell Biol 40 (2008)1703ndash1715
[24] CM Greene P Branagan NG McElvaney Toll-like receptors as therapeutic tar-gets in cystic fibrosis Expert Opin Ther Targets 12 (2008) 1481ndash1495
[25] M Rottner JM Freyssinet MC Martinez Mechanisms of the noxious inflam-matory cycle in cystic fibrosis Respir Res 10 (2009) 23
[26] G Cabrini V Bezzerri I Mancini E Nicolis MC Dechecchi A Tamanini ILampronti L Piccagli N Bianchi M Borgatti R Gambari Targeting transcrip-tion factor activity as a strategy to inhibit pro-inflammatory genes involved incystic fibrosis decoy oligonucleotides and low-molecular weight compoundsCurr Med Chem 17 (2010) 4392ndash4404
[27] CM Greene NG McElvaney Proteases and antiproteases in chronic neutrophiliclungdiseasemdash relevance to drug discovery Br J Pharmacol 158 (2009) 1048ndash1058
[28] AM Cantin Potential for antioxidant therapy of cystic fibrosis Curr Opin PulmMed 10 (2004) 531ndash536
[29] JF Chmiel MW Konstan Inflammation and anti-inflammatory therapies forcystic fibrosis Clin Chest Med 28 (2007) 331ndash346
[30] DP Nichols MW Konstan JF Chmiel Anti-inflammatory therapies for cys-tic fibrosis-related lung disease Clin Rev Allergy Immunol 35 (2008)135ndash153
[31] AJ Kettle T Chan I Osberg R Senthilmohan AL Chapman TJ Mocatta JSWagener Myeloperoxidase and protein oxidation in the airways of youngchildren with cystic fibrosis Am J Respir Crit Care Med 170 (2004)1317ndash1323
[32] H Fischer Mechanisms and function of DUOX in epithelia of the lung AntioxidRedox Signal 11 (2009) 2453ndash2465
[33] B Rada TL Leto Oxidative innate immune defenses by NoxDuox familyNADPH oxidases Contrib Microbiol 15 (2008) 164ndash187
[34] P Moskwa D Lorentzen KJ Excoffon J Zabner PB McCray Jr WM NauseefC Dupuy B Banfi A novel host defense system of airways is defective in cysticfibrosis Am J Respir Crit Care Med 175 (2007) 174ndash183
[35] D Lorentzen L Durairaj AA Pezzulo Y Nakano J Launspach DA Stoltz GZamba PB McCray Jr J Zabner MJ Welsh WM Nauseef B Banfi Concentra-tion of the antibacterial precursor thiocyanate in cystic fibrosis airway secre-tions Free Radic Biol Med 50 (2011) 1144ndash1150
[36] Y Xu S Szep Z Lu The antioxidant role of thiocyanate in the pathogenesis ofcystic fibrosis and other inflammation-related diseases Proc Natl Acad Sci US A 106 (2009) 20515ndash20519
[37] MP Rogan CC Taggart CM Greene PG Murphy SJ ONeill NG McElvaneyLoss of microbicidal activity and increased formation of biofilm due to decreasedlactoferrin activity in patients with cystic fibrosis J Infect Dis 190 (2004)1245ndash1253
[38] B Halliwell JM Guttridge Free Radicals in Biology and Medicine Fourth editionOxford University Press New York 2007
[39] B Rada K Lekstrom S Damian C Dupuy TL Leto The Pseudomonastoxin pyocyanin inhibits the dual oxidase-based antimicrobial system as itimposes oxidative stress on airway epithelial cells J Immunol 181 (2008)4883ndash4893
[40] C Schwarzer B Illek JH Suh SJ Remington H Fischer TE Machen Organelleredox of CF and CFTR-corrected airway epithelia Free Radic Biol Med 43(2007) 300ndash316
[41] JH Roum R Buhl NG McElvaney Z Borok RG Crystal Systemic deficiency ofglutathione in cystic fibrosis J Appl Physiol 75 (1993) 2419ndash2424
[42] VM Hudson Rethinking cystic fibrosis pathology the critical role of abnormalreduced glutathione (GSH) transport caused by CFTR mutation Free RadicBiol Med 30 (2001) 1440ndash1461
[43] PJ Barnes RA Dweik AF Gelb PG Gibson SC George H Grasemann IDPavord F Ratjen PE Silkoff DR Taylor N Zamel Exhaled nitric oxide in pul-monary diseases a comprehensive review Chest 138 (2010) 682ndash692
[44] H Grasemann E Michler M Wallot F Ratjen Decreased concentration of ex-haled nitric oxide (NO) in patients with cystic fibrosis Pediatr Pulmonol 24(1997) 173ndash177
[45] H Grasemann F Ratjen Cystic fibrosis lung disease the role of nitric oxidePediatr Pulmonol 28 (1999) 442ndash448
[46] B Gaston F Ratjen JW Vaughan NR Malhotra RG Canady AH Snyder JFHunt S Gaertig JB Goldberg Nitrogen redox balance in the cystic fibrosis air-way effects of antipseudomonal therapy Am J Respir Crit Care Med 165(2002) 387ndash390
[47] H Grasemann I Ioannidis RP Tomkiewicz H de Groot BK Rubin F RatjenNitric oxide metabolites in cystic fibrosis lung disease Arch Dis Child 78(1998) 49ndash53
[48] H Grasemann R Schwiertz S Matthiesen K Racke F Ratjen Increased argi-nase activity in cystic fibrosis airways Am J Respir Crit Care Med 172(2005) 1523ndash1528
[49] H Grasemann S Al-Saleh JA Scott D Shehnaz A Mehl R Amin M Rafii PPencharz J Belik F Ratjen Asymmetric dimethylarginine contributes to airwaynitric oxide deficiency in patients with cystic fibrosis Am J Respir Crit CareMed 183 (2011) 1363ndash1368
[50] H Grasemann F Kurtz F Ratjen Inhaled L-arginine improves exhaled nitricoxide and pulmonary function in patients with cystic fibrosis Am J RespirCrit Care Med 174 (2006) 208ndash212
[51] H Grasemann F Ratjen Emerging therapies for cystic fibrosis lung disease Ex-pert Opin Emerg Drugs 15 (2010) 653ndash659
[52] BM Morrissey K Schilling JV Weil PE Silkoff DM Rodman Nitric oxide andprotein nitration in the cystic fibrosis airway Arch Biochem Biophys 406(2002) 33ndash39
[53] R Radi Nitric oxide oxidants and protein tyrosine nitration Proc Natl AcadSci U S A 101 (2004) 4003ndash4008
[54] J Chen M Kinter S Shank C Cotton TJ Kelley AG Ziady Dysfunction of Nrf-2in CF epithelia leads to excess intracellular H2O2 and inflammatory cytokineproduction PLoS One 3 (2008) e3367
[55] F Galli M Piroddi C Annetti C Aisa E Floridi A Floridi Oxidative stress andreactive oxygen species Contrib Nephrol 149 (2005) 240ndash260
[56] DT Wright LA Cohn H Li B Fischer CM Li KB Adler Interactions of oxygenradicals with airway epithelium Environ Health Perspect 102 (Suppl 10)(1994) 85ndash90
[57] I Rahman SR Yang SK Biswas Current concepts of redox signaling in thelungs Antioxid Redox Signal 8 (2006) 681ndash689
[58] Q Li JF Engelhardt Interleukin-1beta induction of NFκB is partially regulatedby H2O2-mediated activation of NFκB-inducing kinase J Biol Chem 281(2006) 1495ndash1505
709F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
[59] E Boncoeur VS Criq E Bonvin T Roque A Henrion-Caude DC Gruenert AClement J Jacquot O Tabary Oxidative stress induces extracellular signal-regulated kinase 12 mitogen-activated protein kinase in cystic fibrosis lung ep-ithelial cells potential mechanism for excessive IL-8 expression Int J BiochemCell Biol 40 (2008) 432ndash446
[60] B Fischer J Voynow Neutrophil elastase induces MUC5AC messenger RNA ex-pression by an oxidant-dependent mechanism Chest 117 (2000) 317Sndash320S
[61] B Rada P Gardina TG Myers TL Leto Reactive oxygen species mediate in-flammatory cytokine release and EGFR-dependent mucin secretion in airwayepithelial cells exposed to Pseudomonas pyocyanin Mucosal Immunol 4(2011) 158ndash171
[62] C Schwarzer H Fischer EJ Kim KJ Barber AD Mills MJ Kurth DC GruenertJH Suh TE Machen B Illek Oxidative stress caused by pyocyanin impairs CFTRClminus transport in human bronchial epithelial cells Free Radic Biol Med 45(2008) 1653ndash1662
[63] J Hull M South P Phelan K Grimwood Surfactant composition in infants andyoung children with cystic fibrosis Am J Respir Crit Care Med 156 (1997)161ndash165
[64] KC Meyer A Sharma R Brown M Weatherly FR Moya J Lewandoski JJZimmerman Function and composition of pulmonary surfactant andsurfactant-derived fatty acid profiles are altered in young adults with cystic fi-brosis Chest 118 (2000) 164ndash174
[65] MK Pulfer RC Murphy Formation of biologically active oxysterols during ozo-nolysis of cholesterol present in lung surfactant J Biol Chem 279 (2004)26331ndash26338
[66] V Starosta E Rietschel K Paul U Baumann M Griese Oxidative changes ofbronchoalveolar proteins in cystic fibrosis Chest 129 (2006) 431ndash437
[67] V Starosta M Griese Oxidative damage to surfactant protein D in pulmonarydiseases Free Radic Res 40 (2006) 419ndash425
[68] M Griese R Essl R Schmidt E Rietschel F Ratjen M Ballmann K Paul Pulmo-nary surfactant lung function and endobronchial inflammation in cystic fibro-sis Am J Respir Crit Care Med 170 (2004) 1000ndash1005
[69] M Griese R Essl R Schmidt M Ballmann K Paul E Rietschel F Ratjen Se-quential analysis of surfactant lung function and inflammation in cystic fibrosispatients Respir Res 6 (2005) 133
[70] LG Wood DA Fitzgerald PG Gibson DM Cooper ML Garg Increased plasmafatty acid concentrations after respiratory exacerbations are associated with el-evated oxidative stress in cystic fibrosis patients Am J Clin Nutr 75 (2002)668ndash675
[71] P Montuschi SA Kharitonov G Ciabattoni M Corradi L van Rensen DM Ged-des ME Hodson PJ Barnes Exhaled 8-isoprostane as a new non-invasive bio-marker of oxidative stress in cystic fibrosis Thorax 55 (2000) 205ndash209
[72] CE Collins P Quaggiotto L Wood EV OLoughlin RL Henry ML Garg Elevat-ed plasma levels of F2 alpha isoprostane in cystic fibrosis Lipids 34 (1999)551ndash556
[73] D Hartl V Starosta K Maier I Beck-Speier C Rebhan BF Becker P Latzin RFischer F Ratjen RM Huber E Rietschel S Krauss-Etschmann M Griese In-haled glutathione decreases PGE2 and increases lymphocytes in cystic fibrosislungs Free Radic Biol Med 39 (2005) 463ndash472
[74] GL Milne H Yin JD Morrow Human biochemistry of the isoprostane pathwayJ Biol Chem 283 (2008) 15533ndash15537
[75] G Ciabattoni G Davi M Collura L Iapichino F Pardo A Ganci R Romagnoli JMaclouf C Patrono In vivo lipid peroxidation and platelet activation in cystic fi-brosis Am J Respir Crit Care Med 162 (2000) 1195ndash1201
[76] C Garenc P Julien E Levy Oxysterols in biological systems the gastrointestinaltract liver vascular wall and central nervous system Free Radic Res 44 (2011)47ndash73
[77] AM Cantin SL North RC Hubbard RG Crystal Normal alveolar epithelial lin-ing fluid contains high levels of glutathione J Appl Physiol 63 (1987) 152ndash157
[78] R Tirouvanziam CK Conrad T Bottiglieri LA Herzenberg RB Moss High-dose oral N-acetylcysteine a glutathione prodrug modulates inflammation incystic fibrosis Proc Natl Acad Sci U S A 103 (2006) 4628ndash4633
[79] LW Velsor C Kariya R Kachadourian BJ Day Mitochondrial oxidative stressin the lungs of cystic fibrosis transmembrane conductance regulator proteinmutant mice Am J Respir Cell Mol Biol 35 (2006) 579ndash586
[80] M Kelly-Aubert S Trudel J Fritsch T Nguyen-Khoa M Baudouin-Legros SMoriceau L Jeanson F Djouadi C Matar M Conti M Ollero F Brouillard AEdelman GSH monoethyl ester rescues mitochondrial defects in cystic fibrosismodels Hum Mol Genet 20 (2011) 2745ndash2759
[81] P Ghezzi Role of glutathione in immunity and inflammation in the lung Int JGen Med 4 (2011) 105ndash113
[82] N Dauletbaev K Viel R Buhl TO Wagner J Bargon Glutathione and glutathi-one peroxidase in sputum samples of adult patients with cystic fibrosis J CystFibros 3 (2004) 119ndash124
[83] CE Cross A van der Vliet CA ONeill S Louie B Halliwell Oxidants antioxi-dants and respiratory tract lining fluids Environ Health Perspect 102 (Suppl10) (1994) 185ndash191
[84] K Takeyama K Dabbagh J Jeong Shim T Dao-Pick IF Ueki JA Nadel Oxida-tive stress causes mucin synthesis via transactivation of epidermal growth factorreceptor role of neutrophils J Immunol 164 (2000) 1546ndash1552
[85] N Ballatori SM Krance S Notenboom S Shi K Tieu CL Hammond Glutathi-one dysregulation and the etiology and progression of human diseases BiolChem 390 (2009) 191ndash214
[86] SR Soltaninassab KR Sekhar MJ Meredith ML Freeman Multi-faceted regu-lation of gamma-glutamylcysteine synthetase J Cell Physiol 182 (2000)163ndash170
[87] HR Lopez-Mirabal JR Winther Redox characteristics of the eukaryotic cytosolBiochim Biophys Acta 1783 (2008) 629ndash640
[88] C Hwang AJ Sinskey HF Lodish Oxidized redox state of glutathione in the en-doplasmic reticulum Science 257 (1992) 1496ndash1502
[89] M Murphy Mitochondrial thiols in antioxidant protection and redox signallingdistinct roles for glutathionylation and other thiol modifications AntioxidRedox Signal (2011) ahead of print doi101089ars20114289
[90] BJ Day AM van Heeckeren E Min LW Velsor Role for cystic fibrosis trans-membrane conductance regulator protein in a glutathione response to bronch-opulmonary Pseudomonas infection Infect Immun 72 (2004) 2045ndash2051
[91] Y Zhang K Duan Glutathione exhibits antibacterial activity and increases tetra-cycline efficacy against Pseudomonas aeruginosa Sci China C Life Sci 52 (2009)501ndash505
[92] VM Hudson New insights into the pathogenesis of cystic fibrosis pivotal roleof glutathione system dysfunction and implications for therapy Treat RespirMed 3 (2004) 353ndash363
[93] LW Velsor A van Heeckeren BJ Day Antioxidant imbalance in the lungs ofcystic fibrosis transmembrane conductance regulator protein mutant miceAm J Physiol Lung Cell Mol Physiol 281 (2001) L31ndashL38
[94] I Kogan M Ramjeesingh C Li JF Kidd Y Wang EM Leslie SP Cole CE BearCFTR directly mediates nucleotide-regulated glutathione flux EMBO J 22(2003) 1981ndash1989
[95] NS Gould S Gauthier CT Kariya E Min J Huang DJ Brian Hypertonic salineincreases lung epithelial lining fluid glutathione and thiocyanate two protectiveCFTR-dependent thiols against oxidative injury Respir Res 11 (2010) 119
[96] VT Vasu SJ de Cruz JS Houghton KA Hayakawa BM Morrissey CE CrossJP Eiserich Evaluation of thiol-based antioxidant therapeutics in cystic fibrosissputum focus on myeloperoxidase Free Radic Res 45 (2011) 165ndash176
[97] L Roussel G Martel J Berube S Rousseau P aeruginosa drives CXCL8 synthesisvia redundant toll-like receptors and NADPH oxidase in CFTRF508 airway epi-thelial cells J Cyst Fibros 10 (2011) 107ndash113
[98] GW Lau DJ Hassett H Ran F Kong The role of pyocyanin in Pseudomonas aer-uginosa infection Trends Mol Med 10 (2004) 599ndash606
[99] R Wilson DA Sykes D Watson A Rutman GW Taylor PJ Cole Measurementof Pseudomonas aeruginosa phenazine pigments in sputum and assessment oftheir contribution to sputum sol toxicity for respiratory epithelium InfectImmun 56 (1988) 2515ndash2517
[100] M Muller Pyocyanin induces oxidative stress in human endothelial cells andmodulates the glutathione redox cycle Free Radic Biol Med 33 (2002)1527ndash1533
[101] YQ OMalley KJ Reszka BE Britigan Direct oxidation of 2prime7prime-dichlorodihy-drofluorescein by pyocyanin and other redox-active compounds independentof reactive oxygen species production Free Radic Biol Med 36 (2004)90ndash100
[102] CC Caldwell Y Chen HS Goetzmann Y Hao MT Borchers DJ Hassett LRYoung D Mavrodi L Thomashow GW Lau Pseudomonas aeruginosa exotoxinpyocyanin causes cystic fibrosis airway pathogenesis Am J Pathol 175 (2009)2473ndash2488
[103] YQ OMalley KJ Reszka DR Spitz GM Denning BE Britigan Pseudomonasaeruginosa pyocyanin directly oxidizes glutathione and decreases its levels inairway epithelial cells Am J Physiol Lung Cell Mol Physiol 287 (2004)L94ndashL103
[104] M Muller Glutathione modulates the toxicity of but is not a biologically rele-vant reductant for the Pseudomonas aeruginosa redox toxin pyocyanin FreeRadic Biol Med 50 (2011) 971ndash977
[105] R Cheluvappa R Shimmon M Dawson SN Hilmer DG Le Couteur Reactionsof Pseudomonas aeruginosa pyocyanin with reduced glutathione Acta BiochimPol 55 (2008) 571ndash580
[106] JH Widdicombe Transgenic animals may help resolve a sticky situation in cys-tic fibrosis J Clin Invest 120 (2010) 3093ndash3096
[107] X Sun H Sui JT Fisher Z Yan X Liu HJ Cho NS Joo Y Zhang W Zhou Y YiJM Kinyon DC Lei-Butters MA Griffin P Naumann M Luo J Ascher KWang T Frana JJ Wine DK Meyerholz JF Engelhardt Disease phenotype ofa ferret CFTR-knockout model of cystic fibrosis J Clin Invest 120 (2010)3149ndash3160
[108] NS Joo HJ Cho M Khansaheb JJ Wine Hyposecretion of fluid from trachealsubmucosal glands of CFTR-deficient pigs J Clin Invest 120 (2010) 3161ndash3166
[109] A Bragonzi Murine models of acute and chronic lung infection with cystic fibro-sis pathogens IJMM 300 (2010) 584ndash593
[110] AM van Heeckeren MD Schluchter Murine models of chronic Pseudomonasaeruginosa lung infection Lab Anim 36 (2002) 291ndash312
[111] A Bragonzi D Worlitzsch GB Pier P Timpert M Ulrich M Hentzer JB Ander-sen M Givskov M Conese G Doring Nonmucoid Pseudomonas aeruginosa ex-presses alginate in the lungs of patients with cystic fibrosis and in a mousemodel J Infect Dis 192 (2005) 410ndash419
[112] GS CW Bedrossian DB Singer JJ Hansen HS Rosenberg The lung in cysticfibrosis A quantitative study including prevalence of pathologic findingsamong different age groups Hum Pathol 7 (1976) 195ndash204
[113] WD HA Cash B McCullough WG Johanson Jr JA Bass A rat model of chron-ic respiratory infection with Pseudomonas aeruginosa Am Rev Respir Dis 119(1979) 453ndash459
[114] EM JR Starke C Langston CJ Baker A mouse model of chronic pulmonary in-fection with Pseudomonas aeruginosa and Pseudomonas cepacia Pediatr Res 22(1987) 698ndash702
[115] TJ AM van Heeckeren RW Walenga MW Konstan PB Davis B ErokwuMA Haxhiu TW Ferkol Effect of Pseudomonas infection on weight loss lung
710 F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
mechanics and cytokines in mice Am J Respir Crit Care Med 161 (2000)271ndash279
[116] T Aw G Wierzbicka DP Jones Oral glutathione increases tissue glutathione invivo Chem Biol Interact 80 (1991) 89ndash97
[117] F Favilli P Marraccini T Iantomasi MT Vincenzini Effect of orally adminis-tered glutathione on glutathione levels in some organs of rats role of specifictransporters Br J Nutr 78 (1997) 293ndash300
[118] C Kariya H Leitner E Min C van Heeckeren A van Heeckeren BJ Day A rolefor CFTR in the elevation of glutathione levels in the lung by oral glutathione ad-ministration Am J Physiol Lung Cell Mol Physiol 292 (2007) L1590ndashL1597
[119] K Atkuri JJ Mantovani LA Herzenberg LA Herzenberg N-Acetylcysteinemdashasafe antidote for cysteineglutathione deficiency Curr Opin Pharmacol 7(2007) 355ndash359
[120] R De Lisle E Roach K Jansson Effects of laxative and N-acetylcysteine onmucus accumulation bacterial load transit and inflammation in the cystic fi-brosis mouse small intestine Am J Physiol Gastrointest Liver Physiol 293(2007) G577ndashG584
[121] A Luciani VR Villella S Esposito N Brunetti-Pierri D Medina C Settembre MGavina L Pulze I Giardino M Pettoello-Mantovani M DApolito S Guido EMasliah B Spencer S Quaratino V Raia A Ballabio L Maiuri Defective CFTRinduces aggresome formation and lung inflammation in cystic fibrosis throughROS-mediated autophagy inhibition Nat Cell Biol 12 863ndash875
[122] M Griese J Ramakers A Krasselt V Starosta S Van Koningsbruggen R FischerF Ratjen B Mullinger RM Huber K Maier E Rietschel G Scheuch Improve-ment of alveolar glutathione and lung function but not oxidative state in cysticfibrosis Am J Respir Crit Care Med 169 (2004) 822ndash828
[123] C Bishop VM Hudson SC Hilton C Wilde A pilot study of the effect of inhaledbuffered reduced glutathione on the clinical status of patients with cystic fibro-sis Chest 127 (2005) 308ndash317
[124] WWang C Oliva G Li A Holmgren CH Lillig KL Kirk Reversible silencing of CFTRchloride channels by glutathionylation J Gen Physiol 125 (2005) 127ndash141
[125] N Dauletbaev P Fischer B Aulbach J Gross W Kusche U Thyroff-FriesingerTO Wagner J Bargon A phase II study on safety and efficacy of high-dose N-acetylcysteine in patients with cystic fibrosis Eur J Med Res 14 (2009)352ndash358
[126] R Tirouvanziam Y Gernez CK Conrad RB Moss I Schrijver CE Dunn ZADavies LA Herzenberg Profound functional and signaling changes in viable in-flammatory neutrophils homing to cystic fibrosis airways Proc Natl Acad SciU S A 105 (2008) 4335ndash4339
[127] JH Roum Z Borok NG McElvaney GJ Grimes AD Bokser R Buhl RG Crys-tal Glutathione aerosol suppresses lung epithelial surface inflammatory cell-derived oxidants in cystic fibrosis J Appl Physiol 87 (1999) 438ndash443
[128] A Visca CT Bishop SC Hilton VM Hudson Improvement in clinical markersin CF patients using a reduced glutathione regimen an uncontrolled observa-tional study J Cyst Fibros 7 (2008) 433ndash436
[129] EF Nash A Stephenson F Ratjen E Tullis Nebulized and oral thiol derivativesfor pulmonary disease in cystic fibrosis Cochrane Database Syst Rev (2009)CD007168
[130] AC foundation Drug Development Pipeline 2011[131] S Hoshida T Kuzuya N Yamashita M Nishida S Kitahara M Hori T
Kamada M Tada Gamma-glutamylcysteine ethyl ester for myocardial protec-tion in dogs during ischemia and reperfusion J Am Coll Cardiol 24 (1994)1391ndash1397
[132] J Lok W Leung S Zhao S Pallast K van Leyen S Guo X Wang A Yalcin EHLo Gamma-glutamylcysteine ethyl ester protects cerebral endothelial cells dur-ing injury and decreases bloodndashbrain barrier permeability after experimentalbrain trauma J Neurochem 118 (2011) 248ndash255
[133] Z Borok R Buhl GJ Grimes AD Bokser RC Hubbard KJ Holroyd JH RoumDB Czerski AM Cantin RG Crystal Effect of glutathione aerosol on oxidantndashantioxidant imbalance in idiopathic pulmonary fibrosis Lancet 338 (1991)215ndash216
[134] KJ Holroyd R Buhl Z Borok JH Roum AD Bokser GJ Grimes D Czerski AMCantin RG Crystal Correction of glutathione deficiency in the lower respiratorytract of HIV seropositive individuals by glutathione aerosol treatment Thorax 48(1993) 985ndash989
[135] J Hull P Vervaart K Grimwood P Phelan Pulmonary oxidative stress responsein young children with cystic fibrosis Thorax 52 (1997) 557ndash560
[136] A Corti A Paolicchi M Franzini S Dominici AF Casini A Pompella The S-thiolating activity of membrane gamma-glutamyltransferase formation ofcysteinyl-glycine mixed disulfides with cellular proteins and in the cell microen-vironment Antioxid Redox Signal 7 (2005) 911ndash918
[137] A Corti M Franzini AF Casini A Paolicchi A Pompella Vitamin C supply tobronchial epithelial cells linked to glutathione availability in elfmdasha role for se-creted gamma-glutamyltransferase J Cyst Fibros 7 (2008) 174ndash178
[138] A Munck Nutritional considerations in patients with cystic fibrosis Expert RevRespir Med 4 (2010) 47ndash56
[139] JL Matel CE Milla Nutrition in cystic fibrosis Semin Respir Crit Care Med 30(2009) 579ndash586
[140] D Salvatore R Buzzetti E Baldo MP Forneris V Lucidi D Manunza IMarinelli B Messore AS Neri V Raia ML Furnari G Mastella An overviewof international literature from cystic fibrosis registries 2 Neonatal screeningand nutritiongrowth J Cyst Fibros 9 (2010) 75ndash83
[141] KF Joosten JM Hulst Malnutrition in pediatric hospital patients current is-sues Nutrition 27 (2011) 133ndash137
[142] S Fustik T Jacovska L Spirevska S Koceva Protein-energy malnutrition as thefirst manifestation of cystic fibrosis in infancy Pediatr Int 51 (2009) 678ndash683
[143] J Himmelfarb E McMonagle Albumin is the major plasma protein target of ox-idant stress in uremia Kidney Int 60 (2001) 358ndash363
[144] P Stenvinkel JJ Carrero J Axelsson B Lindholm O Heimburger Z MassyEmerging biomarkers for evaluating cardiovascular risk in the chronic kidneydisease patient how do new pieces fit into the uremic puzzle Clin J Am SocNephrol 3 (2008) 505ndash521
[145] M Roche P Rondeau NR Singh E Tarnus E Bourdon The antioxidant proper-ties of serum albumin FEBS Lett 582 (2008) 1783ndash1787
[146] D Giustarini A Milzani I Dalle-Donne R Rossi Red blood cells as a physiolog-ical source of glutathione for extracellular fluids Blood Cells Mol Dis 40 (2008)174ndash179
[147] A Meister ME Anderson Glutathione Annu Rev Biochem 52 (1983) 711ndash760[148] B Alvarez S Carballal L Turell R Radi Formation and reactions of sulfenic acid
in human serum albumin Methods Enzymol 473 (2010) 117ndash136[149] S Carballal B Alvarez L Turell H Botti BA Freeman R Radi Sulfenic acid in
human serum albumin Amino Acids 32 (2007) 543ndash551[150] LR Barclay AM Bailey D Kong The antioxidant activity of alpha-tocopherol-
bovine serum albumin complex in micellar and liposome autoxidations J BiolChem 260 (1985) 15809ndash15814
[151] T Ishii T Ichikawa K Minoda K Kusaka S Ito Y Suzuki M Akagawa K Mochi-zuki T Goda T Nakayama Human serum albumin as an antioxidant in the ox-idation of (minus)-epigallocatechin gallate participation of reversible covalentbinding for interaction and stabilization Biosci Biotechnol Biochem 75(2011) 100ndash106
[152] F Galli S Rovidati S Benedetti U Buoncristiani C Covarelli A Floridi F Canes-trari Overexpression of erythrocyte glutathione S-transferase in uremia and di-alysis Clin Chem 45 (1999) 1781ndash1788
[153] D Borowitz RD Baker V Stallings Consensus report on nutrition for pediat-ric patients with cystic fibrosis J Pediatr Gastroenterol Nutr 35 (2002)246ndash259
[154] LJ Filer Jr SW Wright MP Manning KE Mason Absorption of alpha-tocopherol and tocopherylesters by premature and full term infants and chil-dren in health and disease Pediatrics 8 (1951) 328ndash339
[155] L Lancellotti C DOrazio G Mastella G Mazzi U Lippi Deficiency of vitamins Eand A in cystic fibrosis is independent of pancreatic function and current en-zyme and vitamin supplementation Eur J Pediatr 155 (1996) 281ndash285
[156] MN Sathe AS Patel Update in pediatrics focus on fat-soluble vitamins NutrClin Pract 25 (2010) 340ndash346
[157] MG Traber The ABCs of vitamin E and beta-carotene absorption Am J ClinNutr 80 (2004) 3ndash4
[158] TF Dolan Jr Hemolytic anemia and edema as the initial signs in infants withcystic fibrosis Consider this diagnosis even in absence of pulmonary symptomsClin Pediatr 15 (1976) 597ndash600
[159] DR James M Alfaham MC Goodchild Increased susceptibility to peroxide-induced haemolysis with normal vitamin E concentrations in cystic fibrosisClin Chim Acta 204 (1991) 279ndash290
[160] SA Peters FJ Kelly Vitamin E supplementation in cystic fibrosis J Pediatr Gas-troenterol Nutr 22 (1996) 341ndash345
[161] A Maqbool VA Stallings Update on fat-soluble vitamins in cystic fibrosis CurrOpin Pulm Med 14 (2008) 574ndash581
[162] SD Sagel MK Sontag MM Anthony P Emmett KA Papas Effect of anantioxidant-rich multivitamin supplement in cystic fibrosis J Cyst Fibros 10(2011) 31ndash36
[163] F Galli A Azzi Present trends in vitamin E research Biofactors 36 (2010)33ndash42
[164] A Hamahata P Enkhbaatar ER Kraft M Lange SW Leonard MG Traber RACox FC Schmalstieg HK Hawkins EB Whorton EM Horvath C Szabo LDTraber DN Herndon DL Traber Gamma-tocopherol nebulization by a lipidaerosolization device improves pulmonary function in sheep with burn andsmoke inhalation injury Free Radic Biol Med 45 (2008) 425ndash433
[165] JP Anais N Razzouq M Carvalho C Fernandez A Astier M Paul A AstierH Fessi AM Lorino Development of alpha-tocopherol acetate nanoparti-cles influence of preparative processes Drug Dev Ind Pharm 35 (2009)216ndash223
[166] JM Zingg Molecular and cellular activities of vitamin E analogues Mini RevMed Chem 7 (2007) 543ndash558
[167] V Viola F Pilolli M Piroddi E Pierpaoli F Orlando M Provinciali M Betti FMazzini F Galli Why tocotrienols work better insights into the in vitro anti-cancer mechanism of vitamin E Genes Nutr 7 (2011) 29ndash41
[168] F Galli F Mazzini L Bamonti L Gille S Bohmdorfer M Piroddi T Netscher FJKelly T Rosenau Tocotrienamines and tocopheramines reactions with radicalsand metal ions Bioorg Med Chem 19 (2011) 6483ndash6491
[169] A Kuhad K Chopra Attenuation of diabetic nephropathy by tocotrienol in-volvement of NFκB signaling pathway Life Sci 84 (2009) 296ndash301
[170] Q Jiang X Yin MA Lill ML Danielson H Freiser J Huang Long-chain carbox-ychromanols metabolites of vitamin E are potent inhibitors of cyclooxygenasesProc Natl Acad Sci U S A 105 (2008) 20464ndash20469
[171] ER Miller III R Pastor-Barriuso D Dalal RA Riemersma LJ Appel E GuallarMeta-analysis high-dosage vitamin E supplementation may increase all-causemortality Ann Intern Med 142 (2005) 37ndash46
[172] JN Hathcock A Azzi J Blumberg T Bray A Dickinson B Frei I Jialal CSJohnston FJ Kelly K Kraemer L Packer S Parthasarathy H Sies MG TraberVitamins E and C are safe across a broad range of intakes Am J Clin Nutr 81(2005) 736ndash745
[173] R Brigelius-Flohe F Galli Vitamin E a vitamin still awaiting the detection of itsbiological function Mol Nutr Food Res 54 (2010) 583ndash587
711F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
[174] MG Traber B Frei JS Beckman Vitamin E revisited do new data validate ben-efits for chronic disease prevention Curr Opin Lipidol 19 (2008) 30ndash38
[175] F Galli Meeting report Vitamin E Satellite Symposium (VESS) associated to theAnnual Meeting of the SFRR-Europe Rome 26 August 2009 Free Radic Res 43(2009) 1256ndash1257
[176] LJ Roberts II JA Oates MF Linton S Fazio BP Meador MD Gross Y Shyr JDMorrow The relationship between dose of vitamin E and suppression of oxida-tive stress in humans Free Radic Biol Med 43 (2007) 1388ndash1393
[177] EFSA- EFSA Scientific Opinion of the Panel on Food Additives FlavouringsProcessing Aids and Materials in Contact with Food on a request from the Com-mission on mixed tocopherols tocotrienol tocopherol and tocotrienols assources for vitamin E in EFSA- EFSA (Ed) vol 640 The EFSA Journal2008 pp 1ndash34
[178] P Rust I Eichler S Renner I Elmadfa Long-term oral beta-carotene supple-mentation in patients with cystic fibrosis mdash effects on antioxidative status andpulmonary function Ann Nutr Metab 44 (2000) 30ndash37
[179] G Lepage J Champagne N Ronco A Lamarre I Osberg RJ Sokol CC Roy Sup-plementation with carotenoids corrects increased lipid peroxidation in childrenwith cystic fibrosis Am J Clin Nutr 64 (1996) 87ndash93
[180] BM Winklhofer-Roob H Puhl G Khoschsorur MA vant Hof H EsterbauerDH Shmerling Enhanced resistance to oxidation of low density lipoproteinsand decreased lipid peroxide formation during beta-carotene supplementationin cystic fibrosis Free Radic Biol Med 18 (1995) 849ndash859
[181] RC Graham-Maar JI Schall N Stettler BS Zemel VA Stallings Elevated vita-min A intake and serum retinol in preadolescent children with cystic fibrosisAm J Clin Nutr 84 (2006) 174ndash182
[182] I Sadowska-Woda M Rachel J Pazdan E Bieszczad-Bedrejczuk K PawliszakNutritional supplement attenuates selected oxidative stress markers in pediatricpatients with cystic fibrosis Nutr Res (New York NY) 31 (2011) 509ndash518
[183] KA Papas MK Sontag C Pardee RJ Sokol SD Sagel FJ Accurso JS WagenerA pilot study on the safety and efficacy of a novel antioxidant rich formulation inpatients with cystic fibrosis J Cyst Fibros 7 (2008) 60ndash67
[184] Y Saito A Fukuhara K Nishio M Hayakawa Y Ogawa H Sakamoto K Fujii YYoshida E Niki Characterization of cellular uptake and distribution of coen-zyme Q10 and vitamin E in PC12 cells J Nutr Biochem 20 (2009) 350ndash357
[185] AA Franke CM Morrison JL Bakke LJ Custer X Li RV Cooney CoenzymeQ10 in human blood native levels and determinants of oxidation during proces-sing and storage Free Radic Biol Med 48 (2010) 1610ndash1617
[186] HN Bhagavan RK Chopra Plasma coenzyme Q10 response to oral ingestion ofcoenzyme Q10 formulations Mitochondrion 7 (2007) S78ndashS88 (Suppl)
[187] HN Bhagavan RK Chopra Coenzyme Q10 absorption tissue uptake metabo-lism and pharmacokinetics Free Radic Res 40 (2006) 445ndash453
[188] F Galli R Lee C Dunster FJ Kelly Gas chromatography mass spectrometryanalysis of carboxyethyl-hydroxychroman metabolites of alpha- and gamma-tocopherol in human plasma Free Radic Biol Med 32 (2002) 333ndash340
[189] F Galli R Lee J Atkinson A Floridi FJ Kelly Gamma-tocopherol biokineticsand transformation in humans Free Radic Res 37 (2003) 1225ndash1233
[190] TA Laguna MK Sontag I Osberg JS Wagener FJ Accurso RJ Sokol De-creased total serum coenzyme-Q10 concentrations a longitudinal study in chil-dren with cystic fibrosis J Pediatr 153 (2008) 402ndash407
[191] T Frischer JK Myung G Maurer I Eichler Z Szepfalusi G Lubec Possible dys-regulation of chaperon and metabolic proteins in cystic fibrosis bronchial tissueProteomics 6 (2006) 3381ndash3388
[192] C Andersson MM Zaman AB Jones SD Freedman Alterations in immune re-sponse and PPARLXR regulation in cystic fibrosis macrophages J Cyst Fibros 7(2008) 68ndash78
[193] SD Freedman PG Blanco MM Zaman JC Shea M Ollero IK Hopper DAWeed A Gelrud MM Regan M Laposata JG Alvarez BP OSullivan Associa-tion of cystic fibrosis with abnormalities in fatty acid metabolism N Engl JMed 350 (2004) 560ndash569
[194] S Van Biervliet G Vanbillemont JP Van Biervliet D Declercq E Robberecht AChristophe Relation between fatty acid composition and clinical status or geno-type in cystic fibrosis patients Ann Nutr Metab 51 (2007) 541ndash549
[195] SD Freedman MH Katz EM Parker M Laposata MY Urman JG AlvarezA membrane lipid imbalance plays a role in the phenotypic expression ofcystic fibrosis in cftr(minusminus) mice Proc Natl Acad Sci U S A 96 (1999)13995ndash14000
[196] S Van Biervliet S Vande Velde JP Van Biervliet E Robberecht The effect ofzinc supplements in cystic fibrosis patients Ann Nutr Metab 52 (2008)152ndash156
[197] WR Henderson Jr SJ Astley MM McCready P Kushmerick S Casey JWBecker BW Ramsey Oral absorption of omega-3 fatty acids in patients withcystic fibrosis who have pancreatic insufficiency and in healthy control subjectsJ Pediatr 124 (1994) 400ndash408
[198] I Durieu E Vericel D Guichardant H Roth JP Steghens J Drai RN JosserandE Fontaine M Lagarde G Bellon Fatty acids platelets and oxidative markersfollowing intravenous n-3 fatty acids administration in cystic fibrosis an openpilot observational study J Cyst Fibros 6 (2007) 320ndash326
[199] LG Wood DA Fitzgerald ML Garg Hypothesis vitamin E complements poly-unsaturated fatty acids in essential fatty acid deficiency in cystic fibrosis J AmColl Nutr 22 (2003) 253ndash257
[200] JD Lloyd-Still SB Johnson RT Holman Essential fatty acid status in cystic fi-brosis and the effects of safflower oil supplementation Am J Clin Nutr 34(1981) 1ndash7
[201] A Maqbool JI Schall JF Garcia-Espana BS Zemel B Strandvik VAStallings Serum linoleic acid status as a clinical indicator of essential fatty
acid status in children with cystic fibrosis J Pediatr Gastroenterol Nutr 47(2008) 635ndash644
[202] C Oliver N Jahnke Omega-3 fatty acids for cystic fibrosis Cochrane DatabaseSyst Rev (2011) CD002201
[203] B Strandvik E Gronowitz F Enlund T Martinsson J Wahlstrom Essential fattyacid deficiency in relation to genotype in patients with cystic fibrosis J Pediatr139 (2001) 650ndash655
[204] P Rise S Volpi C Colombo RF Padoan C DOrazio S Ghezzi PMelotti V BennatoC Agostoni BM Assael C Galli Whole blood fatty acid analysis with micromethodin cystic fibrosis and pulmonary disease J Cyst Fibros 9 (2010) 228ndash233
[205] H Cao K Gerhold JR Mayers MM Wiest SM Watkins GS Hotamisligil Iden-tification of a lipokine a lipid hormone linking adipose tissue to systemic me-tabolism Cell 134 (2008) 933ndash944
[206] RR Malapaka SK Khoo J Zhang JH Choi XE Zhou Y Xu Y Gong J Li ELYong MJ Chalmers L Chang JH Resau PR Griffin YE Chen HE Xu Iden-tification and mechanism of a ten carbon fatty acid as a modulating ligand ofperoxisome proliferator activated receptors J Biol Chem 287 (2012)183ndash195
[207] T Hara A Hirasawa A Ichimura I Kimura G Tsujimoto Free fatty acid recep-tors FFAR1 and GPR120 as novel therapeutic targets for metabolic disorders JPharm Sci 100 (2011) 3594ndash3601
[208] R Gupta P Rathi S Bradoo Lipase mediated upgradation of dietary fats andoils Crit Rev Food Sci Nutr 43 (2003) 635ndash644
[209] BH Jennings CC Akoh Lipase-catalyzed modification of rice bran oil to incor-porate capric acid J Agric Food Chem 48 (2000) 4439ndash4443
[210] J Hoeks M Mensink MK Hesselink K Ekroos P Schrauwen Long- andMedium-Chain Fatty Acids Induce Insulin Resistance to a Similar Extent inHumans Despite Marked Differences in Muscle Fat Accumulation J Clin Endo-crinol Metab 97 (2012) 208ndash216
[211] PJ Congden G Bruce MM Rothburn PC Clarke JM Littlewood J KelleherMS Losowsky Vitamin status in treated patients with cystic fibrosis ArchDis Child 56 (1981) 708ndash714
[212] BM Winklhofer-Roob H Ellemunter M Fruhwirth SE Schlegel-Haueter GKhoschsorur MA vant Hof DH Shmerling Plasma vitamin C concentrationsin patients with cystic fibrosis evidence of associations with lung inflammationAm J Clin Nutr 65 (1997) 1858ndash1866
[213] L Shamseer D Adams N Brown JA Johnson S Vohra Antioxidant micronutri-ents for lung disease in cystic fibrosis Cochrane Database Syst Rev (2010)CD007020
[214] C Santi S Santoro Electrophilic Selenium First edition Wiley-VCH VerlagGmbH amp Co KGaA 2012
[215] L Flohe S Toppo G Cozza F Ursini A comparison of thiol peroxidase mecha-nisms Antioxid Redox Signal 15 (2010) 763ndash780
[216] L Flohe JR Andreesen R Brigelius-Flohe M Maiorino F Ursini Selenium theelement of the moon in life on earth IUBMB Life 49 (2000) 411ndash420
[217] V Valdiglesias E Pasaro J Mendez B Laffon In vitro evaluation of seleniumgenotoxic cytotoxic and protective effects a review Arch Toxicol 84(2010) 337ndash351
[218] P Foucaud P Therond M Marchand F Brion JF Demelier J Navarro Seleniumand vitamin E in mucoviscidosis Arch Fr Pediatr 45 (1988) 383ndash386
[219] J Neve R Van Geffel M Hanocq L Molle Plasma and erythrocyte zinc copperand selenium in cystic fibrosis Acta Paediatr Scand 72 (1983) 437ndash440
[220] BM Winklhofer-Roob B Tiran PE Tuchschmid MA vant Hof DH ShmerlingEffects of pancreatic enzyme preparations on erythrocyte glutathione peroxi-dase activities and plasma selenium concentrations in cystic fibrosis FreeRadic Biol Med 25 (1998) 242ndash249
[221] JD Lloyd-Still HE Ganther Selenium and glutathione peroxidase levels in cys-tic fibrosis Pediatrics 65 (1980) 1010ndash1012
[222] D Tsavachidou TJ McDonnell S Wen X Wang F Vakar-Lopez LL Pisters CAPettaway CG Wood KA Do PF Thall C Stephens E Efstathiou R Taylor DGMenter P Troncoso SM Lippman CJ Logothetis J Kim Selenium and vitaminE cell type- and intervention-specific tissue effects in prostate cancer J NatlCancer Inst 101 (2009) 306ndash320
[223] IN Zelko TJ Mariani RJ Folz Superoxide dismutase multigene family acomparison of the CuZn-SOD (SOD1) Mn-SOD (SOD2) and EC-SOD (SOD3)gene structures evolution and expression Free Radic Biol Med 33 (2002)337ndash349
[224] RP Bowler JD Crapo Oxidative stress in airways is there a role for extracellu-lar superoxide dismutase Am J Respir Crit Care Med 166 (2002) S38ndashS43
[225] K Best K McCoy S Gemma RA Disilvestro Copper enzyme activities in cysticfibrosis before and after copper supplementation plus or minus zinc Metabo-lism 53 (2004) 37ndash41
[226] SS Percival GP Kauwell E Bowser M Wagner Altered copper status in adultmen with cystic fibrosis J Am Coll Nutr 18 (1999) 614ndash619
[227] NF Krebs JE Westcott TD Arnold BM Kluger FJ Accurso LV Miller KMHambidge Abnormalities in zinc homeostasis in young infants with cystic fibro-sis Pediatr Res 48 (2000) 256ndash261
[228] D Easley N Krebs M Jefferson L Miller J Erskine F Accurso KM HambidgeEffect of pancreatic enzymes on zinc absorption in cystic fibrosis J Pediatr Gas-troenterol Nutr 26 (1998) 136ndash139
[229] S Van Biervliet JP Van Biervliet E Robberecht Serum zinc in patients with cys-tic fibrosis at diagnosis and after one year of therapy Biol Trace Elem Res 112(2006) 205ndash211
[230] S Van Biervliet JP Van Biervliet S Vande Velde E Robberecht Serum zinc con-centrations in cystic fibrosis patients aged above 4 years a cross-sectional eval-uation Biol Trace Elem Res 119 (2007) 19ndash26
712 F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
[231] F Galli M Cristina Polidori W Stahl P Mecocci FJ Kelly Vitamin E biotransfor-mation in humans Vitam Horm 76 (2007) 263ndash280
[232] J Wiser NE Alexis Q Jiang W Wu C Robinette R Roubey DB Peden In vivogamma-tocopherol supplementation decreases systemic oxidative stress andcytokine responses of human monocytes in normal and asthmatic subjectsFree Radic Biol Med 45 (2008) 40ndash49
[233] JG Wagner Q Jiang JR Harkema B Illek DD Patel BN Ames DB PedenOzone enhancement of lower airway allergic inflammation is prevented bygamma-tocopherol Free Radic Biol Med 43 (2007) 1176ndash1188
[234] JT Harries DP Muller Absorption of different doses of fat soluble and watermiscible preparations of vitamin E in children with cystic fibrosis Arch DisChild 46 (1971) 341ndash344
[235] EI Back C Frindt E Ocenaskova D Nohr M Stern HK Biesalski Can changesin hydrophobicity increase the bioavailability of alpha-tocopherol Eur J Nutr45 (2006) 1ndash6
[236] SZ Nasr MH OLeary C Hillermeier Correction of vitamin E deficiency withfat-soluble versus water-miscible preparations of vitamin E in patients with cys-tic fibrosis J Pediatr 122 (1993) 810ndash812
[237] S Soltani-Frisk E Gronowitz H Andersson B Strandvik Water-miscibletocopherol is not superior to fat-soluble preparation for vitamin E absorptionin cystic fibrosis Acta Paediatr 90 (2001) 1112ndash1115
[238] K Papas J Kalbfleisch R Mohon Bioavailability of a novel water-soluble vi-tamin E formulation in malabsorbing patients Dig Dis Sci 52 (2007)347ndash352
[239] F Antonicelli M Parmentier EM Drost N Hirani I Rahman K Donaldson WMacNee Nacystelyn inhibits oxidant-mediated interleukin-8 expression andNF-kappaB nuclear binding in alveolar epithelial cells Free Radic Biol Med 32(2002) 492ndash502
[240] EM App D Baran I Dab A Malfroot M Coffiner F Vanderbist M King Dose-finding and 24-h monitoring for efficacy and safety of aerosolized Nacystelyn incystic fibrosis Eur Respir J 19 (2002) 294ndash302
[241] MG Traber How much vitamin E hellip Just enough Am J Clin Nutr 84 (2006)959ndash960
[242] JC McCann BN Ames Vitamin K an example of triage theory is micronu-trient inadequacy linked to diseases of aging Am J Clin Nutr 90 (2009)889ndash907
[243] M Fusaro G Crepaldi S Maggi F Galli A DAngelo L Calo S Giannini DMiozzo M Gallieni Vitamin K bone fractures and vascular calcifications inchronic kidney disease an important but poorly studied relationship J Endocri-nol Invest 34 (2010) 317ndash323
[244] JC McCann BN Ames Adaptive dysfunction of selenoproteins from the per-spective of the triage theory why modest selenium deficiency may increaserisk of diseases of aging FASEB J 25 (2011) 1793ndash1814
[245] R Apak K Guclu M Ozyurek B Bektas Oglu M Bener Cupric ion reducing an-tioxidant capacity assay for food antioxidants vitamins polyphenolics and fla-vonoids in food extracts Methods Mol Biol 477 (2008) 163ndash193
[246] F Galli Interactions of polyphenolic compounds with drug disposition and me-tabolism Curr Drug Metab 8 (2007) 830ndash838
[247] RL Prior X Wu K Schaich Standardized methods for the determination of an-tioxidant capacity and phenolics in foods and dietary supplements J Agric FoodChem 53 (2005) 4290ndash4302
[248] C Azbell S Zhang D Skinner J Fortenberry EJ Sorscher BA WoodworthHesperidin stimulates cystic fibrosis transmembrane conductance regulator-mediated chloride secretion and ciliary beat frequency in sinonasal epitheliumOtolaryngol Head Neck Surg 143 (2010) 397ndash404
[249] G Wegrzyn J Jakobkiewicz-Banecka M Gabig-Ciminska E Piotrowska M Nar-ajczyk A Kloska M Malinowska D Dziedzic I Golebiewska M Moskot AWegrzyn Genistein a natural isoflavone with a potential for treatment of ge-netic diseases Biochem Soc Trans 38 (2010) 695ndash701
[250] YC Yu H Miki Y Nakamura A Hanyuda Y Matsuzaki Y Abe M Yasui K Ta-naka TC Hwang SG Bompadre Y Sohma Curcumin and genistein additivelypotentiate G551D-CFTR J Cyst Fibros 10 (2011) 243ndash252
[251] B Illek H Fischer Flavonoids stimulate Cl conductance of human airway epithe-lium in vitro and in vivo Am J Physiol 275 (1998) L902ndashL910
[252] JL Kreindler Cystic fibrosis exploiting its genetic basis in the hunt for newtherapies Pharmacol Ther 125 (2010) 219ndash229
[253] B Illek L Zhang NC Lewis RB Moss JY Dong H Fischer Defective function ofthe cystic fibrosis-causing missense mutation G551D is recovered by genisteinAm J Physiol 277 (1999) C833ndashC839
[254] P Anandakumar S Kamaraj S Jagan G Ramakrishnan R Vinodhkumar TDevaki Capsaicin modulates pulmonary antioxidant defense system during ben-zo(a)pyrene-induced lung cancer in Swiss albinomice Phytother Res 22 (2008)529ndash533
[255] I Rahman Antioxidant therapeutic advances in COPD Ther Adv Respir Dis 2(2008) 351ndash374
[256] AW Boots H Li RP Schins R Duffin JW Heemskerk A Bast GR Haenen Thequercetin paradox Toxicol Appl Pharmacol 222 (2007) 89ndash96
[257] M Joskova S Franova V Sadlonova Acute bronchodilator effect of quercetin inexperimental allergic asthma Bratisl Lek Listy 112 (2011) 9ndash12
[258] HJ Park CM Lee ID Jung JS Lee YI Jeong JH Chang SH Chun MJ Kim IWChoi SC Ahn YK Shin SR Yeom YM Park Quercetin regulates Th1Th2 balancein a murine model of asthma Int Immunopharmacol 9 (2009) 261ndash267
[259] AP Rogerio A Kanashiro C Fontanari EV da Silva YM Lucisano-ValimEG Soares LH Faccioli Anti-inflammatory activity of quercetin and iso-quercitrin in experimental murine allergic asthma Inflamm Res 56 (2007)402ndash408
[260] M Muller Polyphenol cytotoxicity induced by the bacterial toxin pyocyaninrole of NQO1 Free Radic Biol Med 47 (2009) 84ndash91
[261] J Grassmann Terpenoids as plant antioxidants Vitam Horm 72 (2005)505ndash535
[262] P Allen Tea tree oil the science behind the antimicrobial hype Lancet 358(2001) 1245
[263] EC Dasenbrook W Checkley CA Merlo MW Konstan N Lechtzin MP BoyleAssociation between respiratory tract methicillin-resistant Staphylococcus aure-us and survival in cystic fibrosis JAMA 303 (2010) 2386ndash2392
[264] V Bezzerri M Borgatti E Nicolis I Lampronti MC Dechecchi I Mancini PRizzotti R Gambari G Cabrini Transcription factor oligodeoxynucleotides toNF-kappaB inhibit transcription of IL-8 in bronchial cells Am J Respir CellMol Biol 39 (2008) 86ndash96
[265] R Gambari M Borgatti V Bezzerri E Nicolis I Lampronti MC Dechecchi IMancini A Tamanini G Cabrini Decoy oligodeoxyribonucleotides and peptidenucleic acids-DNA chimeras targeting nuclear factor kappa-B inhibition of IL-8 gene expression in cystic fibrosis cells infected with Pseudomonas aeruginosaBiochem Pharmacol 80 (2010) 1887ndash1894
[266] M Adrian P Jeandet AC Douillet-Breuil L Tesson R Bessis Stilbene content ofmature Vitis vinifera berries in response to UV-C elicitation J Agric Food Chem48 (2000) 6103ndash6105
[267] B Paul I Masih J Deopujari C Charpentier Occurrence of resveratrol and pter-ostilbene in age-old darakchasava an ayurvedic medicine from India J Ethno-pharmacol 68 (1999) 71ndash76
[268] I Rahman Antioxidant therapies in COPD Int J Chron Obstruct Pulmon Dis 1(2006) 15ndash29
[269] M Lee S Kim OK Kwon SR Oh HK Lee K Ahn Anti-inflammatory and anti-asthmatic effects of resveratrol a polyphenolic stilbene in a mouse model ofallergic asthma Int Immunopharmacol 9 (2009) 418ndash424
[270] LG Wood PA Wark ML Garg Antioxidant and anti-inflammatory effectsof resveratrol in airway disease Antioxid Redox Signal 13 (2010)1535ndash1548
[271] KV Kiselev Perspectives for production and application of resveratrol ApplMicrobiol Biotechnol 90 (2011) 417ndash425
[272] M Shakibaei C Buhrmann A Mobasheri Resveratrol-mediated SIRT-1 interac-tions with p300 modulate receptor activator of NF-kappaB ligand (RANKL) acti-vation of NF-kappaB signaling and inhibit osteoclastogenesis in bone-derivedcells J Biol Chem 286 (2011) 11492ndash11505
[273] SF Zaidi K Ahmed T Yamamoto T Kondo K Usmanghani M Kadowaki TSugiyama Effect of resveratrol on Helicobacter pylori-induced interleukin-8 secre-tion reactive oxygen species generation and morphological changes in human gas-tric epithelial cells Biol Pharm Bull 32 (2009) 1931ndash1935
[274] JK Kundu YK Shin YJ Surh Resveratrol modulates phorbol ester-inducedpro-inflammatory signal transduction pathways in mouse skin in vivo NF-kappaB and AP-1 as prime targets Biochem Pharmacol 72 (2006)1506ndash1515
[275] NH Nam Naturally occurring NF-kappaB inhibitors Mini Rev Med Chem 6(2006) 945ndash951
[276] JM Smoliga JA Baur HA Hausenblas Resveratrol and healthmdasha comprehen-sive review of human clinical trials Mol Nutr Food Res 55 (2011) 1129ndash1141
[277] ME Juan M Maijo JM Planas Quantification of trans-resveratrol and itsmetabolites in rat plasma and tissues by HPLC J Pharm Biomed Anal 51(2010) 391ndash398
[278] JA Baur DA Sinclair Therapeutic potential of resveratrol the in vivo evidenceNat Rev 5 (2006) 493ndash506
[279] E Nicolis I Lampronti MC Dechecchi M Borgatti A Tamanini N Bianchi VBezzerri I Mancini MG Giri P Rizzotti R Gambari G Cabrini Pyrogallol anactive compound from the medicinal plant Emblica officinalis regulates expres-sion of pro-inflammatory genes in bronchial epithelial cells Int Immunophar-macol 8 (2008) 1672ndash1680
[280] E Nicolis I Lampronti MC Dechecchi M Borgatti A Tamanini V Bezzerri NBianchi M Mazzon I Mancini MG Giri P Rizzotti R Gambari G CabriniModulation of expression of IL-8 gene in bronchial epithelial cells by 5-methoxypsoralen Int Immunopharmacol 9 (2009) 1411ndash1422
[281] M Borgatti I Mancini N Bianchi A Guerrini I Lampronti D Rossi G SacchettiR Gambari Bergamot (Citrus bergamia Risso) fruit extracts and identified com-ponents alter expression of interleukin 8 gene in cystic fibrosis bronchial epithe-lial cell lines BMC Biochem 12 (2011) 15
[282] L Piccagli E Fabbri M Borgatti N Bianchi V Bezzerri I Mancini E Nicolis CMDechecchi I Lampronti G Cabrini R Gambari Virtual screening against p50NF-kappaB transcription factor for the identification of inhibitors of the NF-kappaB-DNA interaction and expression of NF-kappaB upregulated genesChemMedChem 4 (2009) 2024ndash2033
[283] L Piccagli M Borgatti E Nicolis N Bianchi I Mancini I Lampronti D VevaldiF DallAcqua G Cabrini R Gambari Virtual screening against nuclear factorkappaB (NF-kappaB) of a focus library identification of bioactive furocoumarinderivatives inhibiting NF-kappaB dependent biological functions involved incystic fibrosis Bioorg Med Chem 18 (2010) 8341ndash8349
[284] M Borgatti A Chilin L Piccagli I Lampronti N Bianchi I Mancini G Mar-zaro Da Francesco A Guiotto R Gambari Development of a novel furocou-marin derivative inhibiting NF-kappaB dependent biological functionsdesign synthesis and biological effects Eur J Med Chem 46 (2011)4870ndash4877
[285] E Georgy S Le Guellec L Vecellio E Fichant P Stordeur P Bordeau JP PerraudinFeasibility study of OSCN- and lactoferrin (Meveol) nebulization for cysticfibrosis JCyst Fibros 10 (2011) S18
713F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
[286] C Tidei M Piroddi F Galli C Santi Oxidation of thiols promoted by PhSeZnClTetrahedron Lett 53 (2012) 232ndash234
[287] L Semianrio-Vidal C van Hesuden G Mugesh ER Lazarowski Ebselen is a po-tent non-competitive inhibitor of extracellular nucleoside diphosphokinasePurinergic Signal 6 (2010) 383ndash391
[288] C ColussiMC Albertini S Coppola S Rovidati F Galli L Ghibelli H2O2-inducedblockof glycolysis as an active ADP-ribosylation reaction protecting cells from apoptosisFASEB J 14 (2000) 2266ndash2276
[289] H Xiao KL Parkin Induction of phase II enzyme activity by various seleniumcompounds Nutr Cancer 55 (2006) 210ndash223
[290] G Peluffo R Radi Biochemistry of protein tyrosine nitration in cardiovascularpathology Cardiovasc Res 75 (2007) 291ndash302
[291] B Alvarez R Radi Peroxynitrite reactivity with amino acids and proteinsAmino Acids 25 (2003) 295ndash311
[292] B Kamosinska MW Radomski M Duszyk A Radomski SF Man Nitric oxideactivates chloride currents in human lung epithelial cells Am J Physiol 272(1997) L1098ndashL1104
[293] L Chen RP Patel X Teng CA Bosworth JR Lancaster Jr S Matalon Mecha-nisms of cystic fibrosis transmembrane conductance regulator activation by S-nitrosoglutathione J Biol Chem 281 (2006) 9190ndash9199
[294] F Luchetti B CanonicoM BettiM Arcangeletti F PilolliM Piroddi L Canesi S PapaF Galli Melatonin signaling and cell protection function FASEB J 24 (2010)3603ndash3624
[295] MW Bengtsson G Jedstedt G Flemstrom Duodenal bicarbonate secretion inrats stimulation by intra-arterial and luminal guanylin and uroguanylin ActaPhysiol (Oxf) 191 (2007) 309ndash317
[296] CS Nelson JL Marino CN Allen Melatonin receptor potentiation of cyclic AMP andthe cystic fibrosis transmembrane conductance regulator ion channel J Pineal Res 26(1999) 113ndash121
[297] C de Castro-Silva VM de Bruin GM Cunha DM Nunes CAMedeiros PF de BruinMelatonin improves sleep and reduces nitrite in the exhaled breath condensate incystic fibrosismdasha randomized double-blind placebo-controlled study J Pineal Res48 (2010) 65ndash71
[298] I Hornyak E Pankotai L Kiss Z Lacza Current developments in the the-rapeutic potential of S-nitrosoglutathione an endogenous NO-donor mole-cule Curr Pharm Biotechnol (2011) Jan 11 [Epub ahead of print] - PMID21235457
[299] AH Snyder ME McPherson JF Hunt M Johnson JS Stamler B Gaston Acuteeffects of aerosolized S-nitrosoglutathione in cystic fibrosis Am J Respir CritCare Med 165 (2002) 922ndash926

707F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
A recent randomized double-blind placebo-controlled study hasexamined the effects of short term melatonin administration (3 mgfor 3 weeks) on sleep and oxidative stress markers in CF [297]According with the expected pharmacological effect of this hormonalsubstance the treatment was successful in improving sleep indicesAt the same time nitrite levels determined in exhaled breath conden-sate (EBC) were reduced to suggest a better control of NOmetabolismof CF airways (discussed above in Section 23) but these effects how-ever were not associated with a significant correction of isoprostaneas lipid peroxidation marker measured in EBC Increasing dosages ofmelatonin could be investigated for the pharmacological treatmentof oxidative stress and immune dysfunction of CF patients due tothe absence of adverse effects of this hormonal substance in humans
The S-nitrosation reaction of thiols is another interesting aspect ofNO pharmacology [53] that may find an application in the therapy oflung complications of CF This has been the case for instance of theS-nitrosothiol GSNO that has been used safely in human trials[298299] This endogenous nitrosothiol with proposed regulatory ef-fect on the CFTR of lung epithelia [292293] is well tolerated in pa-tients with CF when administered by aerosolization and mayproduce better oxygenation [299] thereby suggesting that therapyaimed at restoring endogenous GSNO levels in the CF airway maymerit further clinical evaluation Since the administered GSNO de-composes as shown by the increased levels of expired NO in CF pa-tients under treatment with this nitrosothiol [299] furtherinvestigation should be addressed to ascertain whether GSNO thera-py may merely correspond to a GSH therapy
NO dependent effects on CFTR function should be considered toevaluate mechanism of action and specificity of antioxidant therapiesthat target NO metabolism and function in the CF airways
4 Conclusions and future perspectives
The presence of clinical and biochemical symptoms of inflammationand oxidative stress implies that CF patients have a higher demand ofantioxidant protection The combination of the dysfunctional CFTRwith a lowered intake and absorption of dietary antioxidants producesub-optimal levels of protection from both enzymatic and non-enzymatic defense systems The former could be associated with a de-fective glutathionemetabolism and lowered intake of sulfur-containingamino acids and oligoelements such as zinc and possibly seleniumwhile fat-soluble antioxidant vitamins such as vitamin E and caroten-oids and the water-soluble vitamin C are lowered than in healthy sub-jects due to malabsorption and possibly higher consumption
The increased antioxidant demand in CF patients should be evenhigher in the presence of complications of the lung pancreas andliver Lung comorbidity is particularly important in this contextbeing associated with recurrent infections which results in the alter-nation of inflammatory exacerbates and chronic inflammation Thesesustain the flux of ROS in the airways and promote the formation ofsecond-generation byproducts by the damage of biomolecules suchas PUFA and proteins which may diffuse also at the systemic level tofurther promote adverse biological responses and toxic reactions Pan-creatic insufficiency causes malnutrition and may lead to develop en-docrine and metabolic defects associated with diabetes of CF Theseevents can be further aggravated by the concomitance of liver dys-function and a poor nutritional status Malnutrition is strongly associ-ated with poor prognosis as assessed by pulmonary function andsurvival data [138ndash140] The more aggressive nutritional interven-tions seem to produce better clinical outcomes in these patients andthe possibility of achieving higher antioxidant protection in well-nourished patients by dietary factors could be a key aspect to explainsuch a clinical advantage The assumption that food-derived compo-nentsmay help to prevent the damaging effects of oxidative stress im-proving the antioxidant defenses deserves further investigation at theclinical level This together with the investigation of appropriate
laboratory biomarkers could provide critical information to establishintervention criteria for an early nutritional management of newly di-agnosed patients [5] It is expected that a timely secondary preventionstrategy could influence the progression of CF symptoms thusaffecting with a self-feeding mechanism the same extent of malnutri-tion and oxidative stress along the life of CF patients Since severalfactors contribute to impair the nutritional status of CF patients(such as pancreatic insufficiency chronic malabsorption recurrentsinopulmonary infections and progressive lung disease chronic in-flammation increased energy expenditure suboptimal intake multi-therapy) careful monitoring of the antioxidant status should berecommended According with international guidelines fat-solublevitamin supplementation is of utmost importance in daily practice to-gether with energy intake requirements and pancreatic enzyme-replacement therapy Among these vitamin E β-carotene and ω-3FA have observed to alleviate selected biochemical signs of oxidativestress as measured for instance with well established laboratory indi-ces of lipid peroxidation and in some studies these effects werepreliminarily associated with positive clinical outcomes Notwith-standing randomizedndashcontrolled clinical trials on antioxidant supple-ments (including ω-3 FA) so far carried out in CF have failed toconclusively demonstrate significant beneficial effects on respiratorysymptoms and on the consequent impact that these have on the qual-ity of life of these patients (reviewed in [202213]) whichmay provideno support for the use of these supplements in CF An absence of effi-cacy in prevention studies on antioxidant supplements has also beenobserved in other and possibly less severe oxidative stress-relatedconditions particularly in the secondary prevention of cardiovasculardisease and some forms of cancer by vitamin E and other antioxidantssuch as vitamin C selenium and β-carotene (reviewed in [163]) Dif-ferent biases however have been identified in randomize large clini-cal trials that may account for these disappointing findings Theseinclude patient selection criteria (early interventions and primaryprevention could have more chances of success than secondaryprevention) duration and doses of the treatment use of wrong anti-oxidant formulations and administration protocols absence of verifi-cations of the biological compliance to the treatment etc The samebiases apply for the few trials carried out in CF patients Thus the ap-propriateness and efficacy of nutritional interventions with naturalfood-derived or synthetic antioxidants should be verifiedwith respectto the biological pathways of oxidative stress and clinical variablesthat are identified as end-points Profiles of blood and tissue antioxi-dants as well as of reliable surrogate markers of oxidative stresshave to be selected and determined in highly specialized laboratorieswith a well-established experience on these analyses
Well-timed (early) interventions with appropriate antioxidantformulationsprotocols need to be proposed for the next generationof trials and the development of novel CF-tailored antioxidant andanti-inflammatory agents should be promoted
As a consequence of these considerations more clinical investiga-tion is awaited to identify future successful approaches to the antiox-idant therapy as a measure to further enhance quality of life and theoverall clinical outcome of CF patients
Acknowledgments
We are indebted with the Italian Cystic Fibrosis Research Founda-tion for the support that it provided with its grant program to the re-search activity of the authors of this paper This is a scientific initiativeof the ldquoWorking Group on Inflammation in Cystic Fibrosisrdquo (BragonziA Bravo E Cabrini G Conese M Cuzzocrea S Dechecchi MC De Ales-sandri A Evangelista V Galli F Gambari R Lambiase A Lucidi VManca A Melotti P Minicucci L Motta A Pietraforte D Pompella AQuattrucci S Rizzo R Romano M Sorio C Tesse R) of the Italian Soci-ety for Cystic Fibrosis A particular thank goes to the Prof GianniMastella for the critical revision of the manuscript and for the
708 F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
stimulating research environment that he has contributed to createwithin the Italian Cystic Fibrosis Research Foundation
References
[1] BP OSullivan SD Freedman Cystic fibrosis Lancet 373 (2009) 1891ndash1904[2] P Linsdell JW Hanrahan Glutathione permeability of CFTR Am J Physiol 275
(1998) C323ndashC326[3] L Gao KJ Kim JR Yankaskas HJ Forman Abnormal glutathione transport in
cystic fibrosis airway epithelia Am J Physiol 277 (1999) L113ndashL118[4] RK Rowntree A Harris The phenotypic consequences of CFTR mutations Ann
Hum Genet 67 (2003) 471ndash485[5] EI Back C Frindt D Nohr J Frank R Ziebach M Stern M Ranke HK Biesalski
Antioxidant deficiency in cystic fibrosis when is the right time to take actionAm J Clin Nutr 80 (2004) 374ndash384
[6] LG Wood DA Fitzgerald AK Lee ML Garg Improved antioxidant and fattyacid status of patients with cystic fibrosis after antioxidant supplementation islinked to improved lung function Am J Clin Nutr 77 (2003) 150ndash159
[7] L Iuliano R Monticolo G Straface S Zullo F Galli M Boaz S Quattrucci Asso-ciation of cholesterol oxidation and abnormalities in fatty acid metabolism incystic fibrosis Am J Clin Nutr 90 (2009) 477ndash484
[8] C Libetta V Sepe P Esposito F Galli A Dal Canton Oxidative stress and inflam-mation implications in uremia and hemodialysis Clin Biochem 44 (2011)1189ndash1198
[9] G Bartosz Reactive oxygen species destroyers or messengers Biochem Phar-macol 77 (2009) 1303ndash1315
[10] T Ntimbane B Comte G Mailhot Y Berthiaume V Poitout M Prentki RRabasa-Lhoret E Levy Cystic fibrosis-related diabetes from CFTR dysfunctionto oxidative stress Clin Biochem 30 (2009) 153ndash177
[11] A van der Vliet JP Eiserich GP Marelich B Halliwell CE Cross Oxidativestress in cystic fibrosis does it occur and does it matter Adv Pharmacol 38(1997) 491ndash513
[12] AM Cantin TB White CE Cross HJ Forman RJ Sokol D Borowitz Antioxi-dants in cystic fibrosis Conclusions from the CF antioxidant workshop Bethes-da Maryland Free Radic Biol Med 42 (2007) 15ndash31
[13] LT McGrath P Mallon L Dowey B Silke E McClean M McDonnell A DevineS Copeland S Elborn Oxidative stress during acute respiratory exacerbations incystic fibrosis Thorax 54 (1999) 518ndash523
[14] E Thomson S Brennan R Senthilmohan CL Gangell AL Chapman PD SlyAJ Kettle E Balding LJ Berry JB Carlin R Carzino N de Klerk T Douglas CFoo LW Garratt GL Hall J Harrison A Kicic IA Laing KM Logie J MassieLS Mott C Murray F Parsons N Pillarisetti SR Poreddy SC RanganathanCF Robertson R Robins-Browne PJ Robinson B Skoric SM Stick ENSutanto E Williamson Identifying peroxidases and their oxidants in the earlypathology of cystic fibrosis Free Radic Biol Med 49 (2010) 1354ndash1360
[15] SP Range C Dunster AJ Knox FJ Kelly Treatment of pulmonary exacerba-tions of cystic fibrosis leads to improved antioxidant status Eur Respir J 13(1999) 560ndash564
[16] L Coppo P Ghezzi Thiol regulation of pro-inflammatory cytokines and innateimmunity protein S-thiolation as a novel molecular mechanism Biochem SocTrans 39 (2011) 1268ndash1272
[17] C Verhaeghe C Remouchamps B Hennuy A Vanderplasschen A Chariot SPTabruyn C Oury V Bours Role of IKK and ERK pathways in intrinsic inflamma-tion of cystic fibrosis airways Biochem Pharmacol 73 (2007) 1982ndash1994
[18] TL Bonfield JR Panuska MW Konstan KA Hilliard JB Hilliard H Ghnaim MBerger Inflammatory cytokines in cystic fibrosis lungs Am J Respir Crit CareMed 152 (1995) 2111ndash2118
[19] TL Noah HR Black PW Cheng RE Wood MW Leigh Nasal and bronchoal-veolar lavage fluid cytokines in early cystic fibrosis J Infect Dis 175 (1997)638ndash647
[20] MJ Welsh BW Ramsey FJ Accurso GR Cutting Cystic Fibrosis McGraw-HillNew York 2001
[21] TZ Khan JS Wagener T Bost J Martinez FJ Accurso DW Riches Early pul-monary inflammation in infants with cystic fibrosis Am J Respir Crit CareMed 151 (1995) 1075ndash1082
[22] FA Ratjen Cystic fibrosis pathogenesis and future treatment strategies RespirCare 54 (2009) 595ndash605
[23] J Jacquot O Tabary P Le Rouzic A Clement Airway epithelial cell inflamma-tory signalling in cystic fibrosis Int J Biochem Cell Biol 40 (2008)1703ndash1715
[24] CM Greene P Branagan NG McElvaney Toll-like receptors as therapeutic tar-gets in cystic fibrosis Expert Opin Ther Targets 12 (2008) 1481ndash1495
[25] M Rottner JM Freyssinet MC Martinez Mechanisms of the noxious inflam-matory cycle in cystic fibrosis Respir Res 10 (2009) 23
[26] G Cabrini V Bezzerri I Mancini E Nicolis MC Dechecchi A Tamanini ILampronti L Piccagli N Bianchi M Borgatti R Gambari Targeting transcrip-tion factor activity as a strategy to inhibit pro-inflammatory genes involved incystic fibrosis decoy oligonucleotides and low-molecular weight compoundsCurr Med Chem 17 (2010) 4392ndash4404
[27] CM Greene NG McElvaney Proteases and antiproteases in chronic neutrophiliclungdiseasemdash relevance to drug discovery Br J Pharmacol 158 (2009) 1048ndash1058
[28] AM Cantin Potential for antioxidant therapy of cystic fibrosis Curr Opin PulmMed 10 (2004) 531ndash536
[29] JF Chmiel MW Konstan Inflammation and anti-inflammatory therapies forcystic fibrosis Clin Chest Med 28 (2007) 331ndash346
[30] DP Nichols MW Konstan JF Chmiel Anti-inflammatory therapies for cys-tic fibrosis-related lung disease Clin Rev Allergy Immunol 35 (2008)135ndash153
[31] AJ Kettle T Chan I Osberg R Senthilmohan AL Chapman TJ Mocatta JSWagener Myeloperoxidase and protein oxidation in the airways of youngchildren with cystic fibrosis Am J Respir Crit Care Med 170 (2004)1317ndash1323
[32] H Fischer Mechanisms and function of DUOX in epithelia of the lung AntioxidRedox Signal 11 (2009) 2453ndash2465
[33] B Rada TL Leto Oxidative innate immune defenses by NoxDuox familyNADPH oxidases Contrib Microbiol 15 (2008) 164ndash187
[34] P Moskwa D Lorentzen KJ Excoffon J Zabner PB McCray Jr WM NauseefC Dupuy B Banfi A novel host defense system of airways is defective in cysticfibrosis Am J Respir Crit Care Med 175 (2007) 174ndash183
[35] D Lorentzen L Durairaj AA Pezzulo Y Nakano J Launspach DA Stoltz GZamba PB McCray Jr J Zabner MJ Welsh WM Nauseef B Banfi Concentra-tion of the antibacterial precursor thiocyanate in cystic fibrosis airway secre-tions Free Radic Biol Med 50 (2011) 1144ndash1150
[36] Y Xu S Szep Z Lu The antioxidant role of thiocyanate in the pathogenesis ofcystic fibrosis and other inflammation-related diseases Proc Natl Acad Sci US A 106 (2009) 20515ndash20519
[37] MP Rogan CC Taggart CM Greene PG Murphy SJ ONeill NG McElvaneyLoss of microbicidal activity and increased formation of biofilm due to decreasedlactoferrin activity in patients with cystic fibrosis J Infect Dis 190 (2004)1245ndash1253
[38] B Halliwell JM Guttridge Free Radicals in Biology and Medicine Fourth editionOxford University Press New York 2007
[39] B Rada K Lekstrom S Damian C Dupuy TL Leto The Pseudomonastoxin pyocyanin inhibits the dual oxidase-based antimicrobial system as itimposes oxidative stress on airway epithelial cells J Immunol 181 (2008)4883ndash4893
[40] C Schwarzer B Illek JH Suh SJ Remington H Fischer TE Machen Organelleredox of CF and CFTR-corrected airway epithelia Free Radic Biol Med 43(2007) 300ndash316
[41] JH Roum R Buhl NG McElvaney Z Borok RG Crystal Systemic deficiency ofglutathione in cystic fibrosis J Appl Physiol 75 (1993) 2419ndash2424
[42] VM Hudson Rethinking cystic fibrosis pathology the critical role of abnormalreduced glutathione (GSH) transport caused by CFTR mutation Free RadicBiol Med 30 (2001) 1440ndash1461
[43] PJ Barnes RA Dweik AF Gelb PG Gibson SC George H Grasemann IDPavord F Ratjen PE Silkoff DR Taylor N Zamel Exhaled nitric oxide in pul-monary diseases a comprehensive review Chest 138 (2010) 682ndash692
[44] H Grasemann E Michler M Wallot F Ratjen Decreased concentration of ex-haled nitric oxide (NO) in patients with cystic fibrosis Pediatr Pulmonol 24(1997) 173ndash177
[45] H Grasemann F Ratjen Cystic fibrosis lung disease the role of nitric oxidePediatr Pulmonol 28 (1999) 442ndash448
[46] B Gaston F Ratjen JW Vaughan NR Malhotra RG Canady AH Snyder JFHunt S Gaertig JB Goldberg Nitrogen redox balance in the cystic fibrosis air-way effects of antipseudomonal therapy Am J Respir Crit Care Med 165(2002) 387ndash390
[47] H Grasemann I Ioannidis RP Tomkiewicz H de Groot BK Rubin F RatjenNitric oxide metabolites in cystic fibrosis lung disease Arch Dis Child 78(1998) 49ndash53
[48] H Grasemann R Schwiertz S Matthiesen K Racke F Ratjen Increased argi-nase activity in cystic fibrosis airways Am J Respir Crit Care Med 172(2005) 1523ndash1528
[49] H Grasemann S Al-Saleh JA Scott D Shehnaz A Mehl R Amin M Rafii PPencharz J Belik F Ratjen Asymmetric dimethylarginine contributes to airwaynitric oxide deficiency in patients with cystic fibrosis Am J Respir Crit CareMed 183 (2011) 1363ndash1368
[50] H Grasemann F Kurtz F Ratjen Inhaled L-arginine improves exhaled nitricoxide and pulmonary function in patients with cystic fibrosis Am J RespirCrit Care Med 174 (2006) 208ndash212
[51] H Grasemann F Ratjen Emerging therapies for cystic fibrosis lung disease Ex-pert Opin Emerg Drugs 15 (2010) 653ndash659
[52] BM Morrissey K Schilling JV Weil PE Silkoff DM Rodman Nitric oxide andprotein nitration in the cystic fibrosis airway Arch Biochem Biophys 406(2002) 33ndash39
[53] R Radi Nitric oxide oxidants and protein tyrosine nitration Proc Natl AcadSci U S A 101 (2004) 4003ndash4008
[54] J Chen M Kinter S Shank C Cotton TJ Kelley AG Ziady Dysfunction of Nrf-2in CF epithelia leads to excess intracellular H2O2 and inflammatory cytokineproduction PLoS One 3 (2008) e3367
[55] F Galli M Piroddi C Annetti C Aisa E Floridi A Floridi Oxidative stress andreactive oxygen species Contrib Nephrol 149 (2005) 240ndash260
[56] DT Wright LA Cohn H Li B Fischer CM Li KB Adler Interactions of oxygenradicals with airway epithelium Environ Health Perspect 102 (Suppl 10)(1994) 85ndash90
[57] I Rahman SR Yang SK Biswas Current concepts of redox signaling in thelungs Antioxid Redox Signal 8 (2006) 681ndash689
[58] Q Li JF Engelhardt Interleukin-1beta induction of NFκB is partially regulatedby H2O2-mediated activation of NFκB-inducing kinase J Biol Chem 281(2006) 1495ndash1505
709F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
[59] E Boncoeur VS Criq E Bonvin T Roque A Henrion-Caude DC Gruenert AClement J Jacquot O Tabary Oxidative stress induces extracellular signal-regulated kinase 12 mitogen-activated protein kinase in cystic fibrosis lung ep-ithelial cells potential mechanism for excessive IL-8 expression Int J BiochemCell Biol 40 (2008) 432ndash446
[60] B Fischer J Voynow Neutrophil elastase induces MUC5AC messenger RNA ex-pression by an oxidant-dependent mechanism Chest 117 (2000) 317Sndash320S
[61] B Rada P Gardina TG Myers TL Leto Reactive oxygen species mediate in-flammatory cytokine release and EGFR-dependent mucin secretion in airwayepithelial cells exposed to Pseudomonas pyocyanin Mucosal Immunol 4(2011) 158ndash171
[62] C Schwarzer H Fischer EJ Kim KJ Barber AD Mills MJ Kurth DC GruenertJH Suh TE Machen B Illek Oxidative stress caused by pyocyanin impairs CFTRClminus transport in human bronchial epithelial cells Free Radic Biol Med 45(2008) 1653ndash1662
[63] J Hull M South P Phelan K Grimwood Surfactant composition in infants andyoung children with cystic fibrosis Am J Respir Crit Care Med 156 (1997)161ndash165
[64] KC Meyer A Sharma R Brown M Weatherly FR Moya J Lewandoski JJZimmerman Function and composition of pulmonary surfactant andsurfactant-derived fatty acid profiles are altered in young adults with cystic fi-brosis Chest 118 (2000) 164ndash174
[65] MK Pulfer RC Murphy Formation of biologically active oxysterols during ozo-nolysis of cholesterol present in lung surfactant J Biol Chem 279 (2004)26331ndash26338
[66] V Starosta E Rietschel K Paul U Baumann M Griese Oxidative changes ofbronchoalveolar proteins in cystic fibrosis Chest 129 (2006) 431ndash437
[67] V Starosta M Griese Oxidative damage to surfactant protein D in pulmonarydiseases Free Radic Res 40 (2006) 419ndash425
[68] M Griese R Essl R Schmidt E Rietschel F Ratjen M Ballmann K Paul Pulmo-nary surfactant lung function and endobronchial inflammation in cystic fibro-sis Am J Respir Crit Care Med 170 (2004) 1000ndash1005
[69] M Griese R Essl R Schmidt M Ballmann K Paul E Rietschel F Ratjen Se-quential analysis of surfactant lung function and inflammation in cystic fibrosispatients Respir Res 6 (2005) 133
[70] LG Wood DA Fitzgerald PG Gibson DM Cooper ML Garg Increased plasmafatty acid concentrations after respiratory exacerbations are associated with el-evated oxidative stress in cystic fibrosis patients Am J Clin Nutr 75 (2002)668ndash675
[71] P Montuschi SA Kharitonov G Ciabattoni M Corradi L van Rensen DM Ged-des ME Hodson PJ Barnes Exhaled 8-isoprostane as a new non-invasive bio-marker of oxidative stress in cystic fibrosis Thorax 55 (2000) 205ndash209
[72] CE Collins P Quaggiotto L Wood EV OLoughlin RL Henry ML Garg Elevat-ed plasma levels of F2 alpha isoprostane in cystic fibrosis Lipids 34 (1999)551ndash556
[73] D Hartl V Starosta K Maier I Beck-Speier C Rebhan BF Becker P Latzin RFischer F Ratjen RM Huber E Rietschel S Krauss-Etschmann M Griese In-haled glutathione decreases PGE2 and increases lymphocytes in cystic fibrosislungs Free Radic Biol Med 39 (2005) 463ndash472
[74] GL Milne H Yin JD Morrow Human biochemistry of the isoprostane pathwayJ Biol Chem 283 (2008) 15533ndash15537
[75] G Ciabattoni G Davi M Collura L Iapichino F Pardo A Ganci R Romagnoli JMaclouf C Patrono In vivo lipid peroxidation and platelet activation in cystic fi-brosis Am J Respir Crit Care Med 162 (2000) 1195ndash1201
[76] C Garenc P Julien E Levy Oxysterols in biological systems the gastrointestinaltract liver vascular wall and central nervous system Free Radic Res 44 (2011)47ndash73
[77] AM Cantin SL North RC Hubbard RG Crystal Normal alveolar epithelial lin-ing fluid contains high levels of glutathione J Appl Physiol 63 (1987) 152ndash157
[78] R Tirouvanziam CK Conrad T Bottiglieri LA Herzenberg RB Moss High-dose oral N-acetylcysteine a glutathione prodrug modulates inflammation incystic fibrosis Proc Natl Acad Sci U S A 103 (2006) 4628ndash4633
[79] LW Velsor C Kariya R Kachadourian BJ Day Mitochondrial oxidative stressin the lungs of cystic fibrosis transmembrane conductance regulator proteinmutant mice Am J Respir Cell Mol Biol 35 (2006) 579ndash586
[80] M Kelly-Aubert S Trudel J Fritsch T Nguyen-Khoa M Baudouin-Legros SMoriceau L Jeanson F Djouadi C Matar M Conti M Ollero F Brouillard AEdelman GSH monoethyl ester rescues mitochondrial defects in cystic fibrosismodels Hum Mol Genet 20 (2011) 2745ndash2759
[81] P Ghezzi Role of glutathione in immunity and inflammation in the lung Int JGen Med 4 (2011) 105ndash113
[82] N Dauletbaev K Viel R Buhl TO Wagner J Bargon Glutathione and glutathi-one peroxidase in sputum samples of adult patients with cystic fibrosis J CystFibros 3 (2004) 119ndash124
[83] CE Cross A van der Vliet CA ONeill S Louie B Halliwell Oxidants antioxi-dants and respiratory tract lining fluids Environ Health Perspect 102 (Suppl10) (1994) 185ndash191
[84] K Takeyama K Dabbagh J Jeong Shim T Dao-Pick IF Ueki JA Nadel Oxida-tive stress causes mucin synthesis via transactivation of epidermal growth factorreceptor role of neutrophils J Immunol 164 (2000) 1546ndash1552
[85] N Ballatori SM Krance S Notenboom S Shi K Tieu CL Hammond Glutathi-one dysregulation and the etiology and progression of human diseases BiolChem 390 (2009) 191ndash214
[86] SR Soltaninassab KR Sekhar MJ Meredith ML Freeman Multi-faceted regu-lation of gamma-glutamylcysteine synthetase J Cell Physiol 182 (2000)163ndash170
[87] HR Lopez-Mirabal JR Winther Redox characteristics of the eukaryotic cytosolBiochim Biophys Acta 1783 (2008) 629ndash640
[88] C Hwang AJ Sinskey HF Lodish Oxidized redox state of glutathione in the en-doplasmic reticulum Science 257 (1992) 1496ndash1502
[89] M Murphy Mitochondrial thiols in antioxidant protection and redox signallingdistinct roles for glutathionylation and other thiol modifications AntioxidRedox Signal (2011) ahead of print doi101089ars20114289
[90] BJ Day AM van Heeckeren E Min LW Velsor Role for cystic fibrosis trans-membrane conductance regulator protein in a glutathione response to bronch-opulmonary Pseudomonas infection Infect Immun 72 (2004) 2045ndash2051
[91] Y Zhang K Duan Glutathione exhibits antibacterial activity and increases tetra-cycline efficacy against Pseudomonas aeruginosa Sci China C Life Sci 52 (2009)501ndash505
[92] VM Hudson New insights into the pathogenesis of cystic fibrosis pivotal roleof glutathione system dysfunction and implications for therapy Treat RespirMed 3 (2004) 353ndash363
[93] LW Velsor A van Heeckeren BJ Day Antioxidant imbalance in the lungs ofcystic fibrosis transmembrane conductance regulator protein mutant miceAm J Physiol Lung Cell Mol Physiol 281 (2001) L31ndashL38
[94] I Kogan M Ramjeesingh C Li JF Kidd Y Wang EM Leslie SP Cole CE BearCFTR directly mediates nucleotide-regulated glutathione flux EMBO J 22(2003) 1981ndash1989
[95] NS Gould S Gauthier CT Kariya E Min J Huang DJ Brian Hypertonic salineincreases lung epithelial lining fluid glutathione and thiocyanate two protectiveCFTR-dependent thiols against oxidative injury Respir Res 11 (2010) 119
[96] VT Vasu SJ de Cruz JS Houghton KA Hayakawa BM Morrissey CE CrossJP Eiserich Evaluation of thiol-based antioxidant therapeutics in cystic fibrosissputum focus on myeloperoxidase Free Radic Res 45 (2011) 165ndash176
[97] L Roussel G Martel J Berube S Rousseau P aeruginosa drives CXCL8 synthesisvia redundant toll-like receptors and NADPH oxidase in CFTRF508 airway epi-thelial cells J Cyst Fibros 10 (2011) 107ndash113
[98] GW Lau DJ Hassett H Ran F Kong The role of pyocyanin in Pseudomonas aer-uginosa infection Trends Mol Med 10 (2004) 599ndash606
[99] R Wilson DA Sykes D Watson A Rutman GW Taylor PJ Cole Measurementof Pseudomonas aeruginosa phenazine pigments in sputum and assessment oftheir contribution to sputum sol toxicity for respiratory epithelium InfectImmun 56 (1988) 2515ndash2517
[100] M Muller Pyocyanin induces oxidative stress in human endothelial cells andmodulates the glutathione redox cycle Free Radic Biol Med 33 (2002)1527ndash1533
[101] YQ OMalley KJ Reszka BE Britigan Direct oxidation of 2prime7prime-dichlorodihy-drofluorescein by pyocyanin and other redox-active compounds independentof reactive oxygen species production Free Radic Biol Med 36 (2004)90ndash100
[102] CC Caldwell Y Chen HS Goetzmann Y Hao MT Borchers DJ Hassett LRYoung D Mavrodi L Thomashow GW Lau Pseudomonas aeruginosa exotoxinpyocyanin causes cystic fibrosis airway pathogenesis Am J Pathol 175 (2009)2473ndash2488
[103] YQ OMalley KJ Reszka DR Spitz GM Denning BE Britigan Pseudomonasaeruginosa pyocyanin directly oxidizes glutathione and decreases its levels inairway epithelial cells Am J Physiol Lung Cell Mol Physiol 287 (2004)L94ndashL103
[104] M Muller Glutathione modulates the toxicity of but is not a biologically rele-vant reductant for the Pseudomonas aeruginosa redox toxin pyocyanin FreeRadic Biol Med 50 (2011) 971ndash977
[105] R Cheluvappa R Shimmon M Dawson SN Hilmer DG Le Couteur Reactionsof Pseudomonas aeruginosa pyocyanin with reduced glutathione Acta BiochimPol 55 (2008) 571ndash580
[106] JH Widdicombe Transgenic animals may help resolve a sticky situation in cys-tic fibrosis J Clin Invest 120 (2010) 3093ndash3096
[107] X Sun H Sui JT Fisher Z Yan X Liu HJ Cho NS Joo Y Zhang W Zhou Y YiJM Kinyon DC Lei-Butters MA Griffin P Naumann M Luo J Ascher KWang T Frana JJ Wine DK Meyerholz JF Engelhardt Disease phenotype ofa ferret CFTR-knockout model of cystic fibrosis J Clin Invest 120 (2010)3149ndash3160
[108] NS Joo HJ Cho M Khansaheb JJ Wine Hyposecretion of fluid from trachealsubmucosal glands of CFTR-deficient pigs J Clin Invest 120 (2010) 3161ndash3166
[109] A Bragonzi Murine models of acute and chronic lung infection with cystic fibro-sis pathogens IJMM 300 (2010) 584ndash593
[110] AM van Heeckeren MD Schluchter Murine models of chronic Pseudomonasaeruginosa lung infection Lab Anim 36 (2002) 291ndash312
[111] A Bragonzi D Worlitzsch GB Pier P Timpert M Ulrich M Hentzer JB Ander-sen M Givskov M Conese G Doring Nonmucoid Pseudomonas aeruginosa ex-presses alginate in the lungs of patients with cystic fibrosis and in a mousemodel J Infect Dis 192 (2005) 410ndash419
[112] GS CW Bedrossian DB Singer JJ Hansen HS Rosenberg The lung in cysticfibrosis A quantitative study including prevalence of pathologic findingsamong different age groups Hum Pathol 7 (1976) 195ndash204
[113] WD HA Cash B McCullough WG Johanson Jr JA Bass A rat model of chron-ic respiratory infection with Pseudomonas aeruginosa Am Rev Respir Dis 119(1979) 453ndash459
[114] EM JR Starke C Langston CJ Baker A mouse model of chronic pulmonary in-fection with Pseudomonas aeruginosa and Pseudomonas cepacia Pediatr Res 22(1987) 698ndash702
[115] TJ AM van Heeckeren RW Walenga MW Konstan PB Davis B ErokwuMA Haxhiu TW Ferkol Effect of Pseudomonas infection on weight loss lung
710 F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
mechanics and cytokines in mice Am J Respir Crit Care Med 161 (2000)271ndash279
[116] T Aw G Wierzbicka DP Jones Oral glutathione increases tissue glutathione invivo Chem Biol Interact 80 (1991) 89ndash97
[117] F Favilli P Marraccini T Iantomasi MT Vincenzini Effect of orally adminis-tered glutathione on glutathione levels in some organs of rats role of specifictransporters Br J Nutr 78 (1997) 293ndash300
[118] C Kariya H Leitner E Min C van Heeckeren A van Heeckeren BJ Day A rolefor CFTR in the elevation of glutathione levels in the lung by oral glutathione ad-ministration Am J Physiol Lung Cell Mol Physiol 292 (2007) L1590ndashL1597
[119] K Atkuri JJ Mantovani LA Herzenberg LA Herzenberg N-Acetylcysteinemdashasafe antidote for cysteineglutathione deficiency Curr Opin Pharmacol 7(2007) 355ndash359
[120] R De Lisle E Roach K Jansson Effects of laxative and N-acetylcysteine onmucus accumulation bacterial load transit and inflammation in the cystic fi-brosis mouse small intestine Am J Physiol Gastrointest Liver Physiol 293(2007) G577ndashG584
[121] A Luciani VR Villella S Esposito N Brunetti-Pierri D Medina C Settembre MGavina L Pulze I Giardino M Pettoello-Mantovani M DApolito S Guido EMasliah B Spencer S Quaratino V Raia A Ballabio L Maiuri Defective CFTRinduces aggresome formation and lung inflammation in cystic fibrosis throughROS-mediated autophagy inhibition Nat Cell Biol 12 863ndash875
[122] M Griese J Ramakers A Krasselt V Starosta S Van Koningsbruggen R FischerF Ratjen B Mullinger RM Huber K Maier E Rietschel G Scheuch Improve-ment of alveolar glutathione and lung function but not oxidative state in cysticfibrosis Am J Respir Crit Care Med 169 (2004) 822ndash828
[123] C Bishop VM Hudson SC Hilton C Wilde A pilot study of the effect of inhaledbuffered reduced glutathione on the clinical status of patients with cystic fibro-sis Chest 127 (2005) 308ndash317
[124] WWang C Oliva G Li A Holmgren CH Lillig KL Kirk Reversible silencing of CFTRchloride channels by glutathionylation J Gen Physiol 125 (2005) 127ndash141
[125] N Dauletbaev P Fischer B Aulbach J Gross W Kusche U Thyroff-FriesingerTO Wagner J Bargon A phase II study on safety and efficacy of high-dose N-acetylcysteine in patients with cystic fibrosis Eur J Med Res 14 (2009)352ndash358
[126] R Tirouvanziam Y Gernez CK Conrad RB Moss I Schrijver CE Dunn ZADavies LA Herzenberg Profound functional and signaling changes in viable in-flammatory neutrophils homing to cystic fibrosis airways Proc Natl Acad SciU S A 105 (2008) 4335ndash4339
[127] JH Roum Z Borok NG McElvaney GJ Grimes AD Bokser R Buhl RG Crys-tal Glutathione aerosol suppresses lung epithelial surface inflammatory cell-derived oxidants in cystic fibrosis J Appl Physiol 87 (1999) 438ndash443
[128] A Visca CT Bishop SC Hilton VM Hudson Improvement in clinical markersin CF patients using a reduced glutathione regimen an uncontrolled observa-tional study J Cyst Fibros 7 (2008) 433ndash436
[129] EF Nash A Stephenson F Ratjen E Tullis Nebulized and oral thiol derivativesfor pulmonary disease in cystic fibrosis Cochrane Database Syst Rev (2009)CD007168
[130] AC foundation Drug Development Pipeline 2011[131] S Hoshida T Kuzuya N Yamashita M Nishida S Kitahara M Hori T
Kamada M Tada Gamma-glutamylcysteine ethyl ester for myocardial protec-tion in dogs during ischemia and reperfusion J Am Coll Cardiol 24 (1994)1391ndash1397
[132] J Lok W Leung S Zhao S Pallast K van Leyen S Guo X Wang A Yalcin EHLo Gamma-glutamylcysteine ethyl ester protects cerebral endothelial cells dur-ing injury and decreases bloodndashbrain barrier permeability after experimentalbrain trauma J Neurochem 118 (2011) 248ndash255
[133] Z Borok R Buhl GJ Grimes AD Bokser RC Hubbard KJ Holroyd JH RoumDB Czerski AM Cantin RG Crystal Effect of glutathione aerosol on oxidantndashantioxidant imbalance in idiopathic pulmonary fibrosis Lancet 338 (1991)215ndash216
[134] KJ Holroyd R Buhl Z Borok JH Roum AD Bokser GJ Grimes D Czerski AMCantin RG Crystal Correction of glutathione deficiency in the lower respiratorytract of HIV seropositive individuals by glutathione aerosol treatment Thorax 48(1993) 985ndash989
[135] J Hull P Vervaart K Grimwood P Phelan Pulmonary oxidative stress responsein young children with cystic fibrosis Thorax 52 (1997) 557ndash560
[136] A Corti A Paolicchi M Franzini S Dominici AF Casini A Pompella The S-thiolating activity of membrane gamma-glutamyltransferase formation ofcysteinyl-glycine mixed disulfides with cellular proteins and in the cell microen-vironment Antioxid Redox Signal 7 (2005) 911ndash918
[137] A Corti M Franzini AF Casini A Paolicchi A Pompella Vitamin C supply tobronchial epithelial cells linked to glutathione availability in elfmdasha role for se-creted gamma-glutamyltransferase J Cyst Fibros 7 (2008) 174ndash178
[138] A Munck Nutritional considerations in patients with cystic fibrosis Expert RevRespir Med 4 (2010) 47ndash56
[139] JL Matel CE Milla Nutrition in cystic fibrosis Semin Respir Crit Care Med 30(2009) 579ndash586
[140] D Salvatore R Buzzetti E Baldo MP Forneris V Lucidi D Manunza IMarinelli B Messore AS Neri V Raia ML Furnari G Mastella An overviewof international literature from cystic fibrosis registries 2 Neonatal screeningand nutritiongrowth J Cyst Fibros 9 (2010) 75ndash83
[141] KF Joosten JM Hulst Malnutrition in pediatric hospital patients current is-sues Nutrition 27 (2011) 133ndash137
[142] S Fustik T Jacovska L Spirevska S Koceva Protein-energy malnutrition as thefirst manifestation of cystic fibrosis in infancy Pediatr Int 51 (2009) 678ndash683
[143] J Himmelfarb E McMonagle Albumin is the major plasma protein target of ox-idant stress in uremia Kidney Int 60 (2001) 358ndash363
[144] P Stenvinkel JJ Carrero J Axelsson B Lindholm O Heimburger Z MassyEmerging biomarkers for evaluating cardiovascular risk in the chronic kidneydisease patient how do new pieces fit into the uremic puzzle Clin J Am SocNephrol 3 (2008) 505ndash521
[145] M Roche P Rondeau NR Singh E Tarnus E Bourdon The antioxidant proper-ties of serum albumin FEBS Lett 582 (2008) 1783ndash1787
[146] D Giustarini A Milzani I Dalle-Donne R Rossi Red blood cells as a physiolog-ical source of glutathione for extracellular fluids Blood Cells Mol Dis 40 (2008)174ndash179
[147] A Meister ME Anderson Glutathione Annu Rev Biochem 52 (1983) 711ndash760[148] B Alvarez S Carballal L Turell R Radi Formation and reactions of sulfenic acid
in human serum albumin Methods Enzymol 473 (2010) 117ndash136[149] S Carballal B Alvarez L Turell H Botti BA Freeman R Radi Sulfenic acid in
human serum albumin Amino Acids 32 (2007) 543ndash551[150] LR Barclay AM Bailey D Kong The antioxidant activity of alpha-tocopherol-
bovine serum albumin complex in micellar and liposome autoxidations J BiolChem 260 (1985) 15809ndash15814
[151] T Ishii T Ichikawa K Minoda K Kusaka S Ito Y Suzuki M Akagawa K Mochi-zuki T Goda T Nakayama Human serum albumin as an antioxidant in the ox-idation of (minus)-epigallocatechin gallate participation of reversible covalentbinding for interaction and stabilization Biosci Biotechnol Biochem 75(2011) 100ndash106
[152] F Galli S Rovidati S Benedetti U Buoncristiani C Covarelli A Floridi F Canes-trari Overexpression of erythrocyte glutathione S-transferase in uremia and di-alysis Clin Chem 45 (1999) 1781ndash1788
[153] D Borowitz RD Baker V Stallings Consensus report on nutrition for pediat-ric patients with cystic fibrosis J Pediatr Gastroenterol Nutr 35 (2002)246ndash259
[154] LJ Filer Jr SW Wright MP Manning KE Mason Absorption of alpha-tocopherol and tocopherylesters by premature and full term infants and chil-dren in health and disease Pediatrics 8 (1951) 328ndash339
[155] L Lancellotti C DOrazio G Mastella G Mazzi U Lippi Deficiency of vitamins Eand A in cystic fibrosis is independent of pancreatic function and current en-zyme and vitamin supplementation Eur J Pediatr 155 (1996) 281ndash285
[156] MN Sathe AS Patel Update in pediatrics focus on fat-soluble vitamins NutrClin Pract 25 (2010) 340ndash346
[157] MG Traber The ABCs of vitamin E and beta-carotene absorption Am J ClinNutr 80 (2004) 3ndash4
[158] TF Dolan Jr Hemolytic anemia and edema as the initial signs in infants withcystic fibrosis Consider this diagnosis even in absence of pulmonary symptomsClin Pediatr 15 (1976) 597ndash600
[159] DR James M Alfaham MC Goodchild Increased susceptibility to peroxide-induced haemolysis with normal vitamin E concentrations in cystic fibrosisClin Chim Acta 204 (1991) 279ndash290
[160] SA Peters FJ Kelly Vitamin E supplementation in cystic fibrosis J Pediatr Gas-troenterol Nutr 22 (1996) 341ndash345
[161] A Maqbool VA Stallings Update on fat-soluble vitamins in cystic fibrosis CurrOpin Pulm Med 14 (2008) 574ndash581
[162] SD Sagel MK Sontag MM Anthony P Emmett KA Papas Effect of anantioxidant-rich multivitamin supplement in cystic fibrosis J Cyst Fibros 10(2011) 31ndash36
[163] F Galli A Azzi Present trends in vitamin E research Biofactors 36 (2010)33ndash42
[164] A Hamahata P Enkhbaatar ER Kraft M Lange SW Leonard MG Traber RACox FC Schmalstieg HK Hawkins EB Whorton EM Horvath C Szabo LDTraber DN Herndon DL Traber Gamma-tocopherol nebulization by a lipidaerosolization device improves pulmonary function in sheep with burn andsmoke inhalation injury Free Radic Biol Med 45 (2008) 425ndash433
[165] JP Anais N Razzouq M Carvalho C Fernandez A Astier M Paul A AstierH Fessi AM Lorino Development of alpha-tocopherol acetate nanoparti-cles influence of preparative processes Drug Dev Ind Pharm 35 (2009)216ndash223
[166] JM Zingg Molecular and cellular activities of vitamin E analogues Mini RevMed Chem 7 (2007) 543ndash558
[167] V Viola F Pilolli M Piroddi E Pierpaoli F Orlando M Provinciali M Betti FMazzini F Galli Why tocotrienols work better insights into the in vitro anti-cancer mechanism of vitamin E Genes Nutr 7 (2011) 29ndash41
[168] F Galli F Mazzini L Bamonti L Gille S Bohmdorfer M Piroddi T Netscher FJKelly T Rosenau Tocotrienamines and tocopheramines reactions with radicalsand metal ions Bioorg Med Chem 19 (2011) 6483ndash6491
[169] A Kuhad K Chopra Attenuation of diabetic nephropathy by tocotrienol in-volvement of NFκB signaling pathway Life Sci 84 (2009) 296ndash301
[170] Q Jiang X Yin MA Lill ML Danielson H Freiser J Huang Long-chain carbox-ychromanols metabolites of vitamin E are potent inhibitors of cyclooxygenasesProc Natl Acad Sci U S A 105 (2008) 20464ndash20469
[171] ER Miller III R Pastor-Barriuso D Dalal RA Riemersma LJ Appel E GuallarMeta-analysis high-dosage vitamin E supplementation may increase all-causemortality Ann Intern Med 142 (2005) 37ndash46
[172] JN Hathcock A Azzi J Blumberg T Bray A Dickinson B Frei I Jialal CSJohnston FJ Kelly K Kraemer L Packer S Parthasarathy H Sies MG TraberVitamins E and C are safe across a broad range of intakes Am J Clin Nutr 81(2005) 736ndash745
[173] R Brigelius-Flohe F Galli Vitamin E a vitamin still awaiting the detection of itsbiological function Mol Nutr Food Res 54 (2010) 583ndash587
711F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
[174] MG Traber B Frei JS Beckman Vitamin E revisited do new data validate ben-efits for chronic disease prevention Curr Opin Lipidol 19 (2008) 30ndash38
[175] F Galli Meeting report Vitamin E Satellite Symposium (VESS) associated to theAnnual Meeting of the SFRR-Europe Rome 26 August 2009 Free Radic Res 43(2009) 1256ndash1257
[176] LJ Roberts II JA Oates MF Linton S Fazio BP Meador MD Gross Y Shyr JDMorrow The relationship between dose of vitamin E and suppression of oxida-tive stress in humans Free Radic Biol Med 43 (2007) 1388ndash1393
[177] EFSA- EFSA Scientific Opinion of the Panel on Food Additives FlavouringsProcessing Aids and Materials in Contact with Food on a request from the Com-mission on mixed tocopherols tocotrienol tocopherol and tocotrienols assources for vitamin E in EFSA- EFSA (Ed) vol 640 The EFSA Journal2008 pp 1ndash34
[178] P Rust I Eichler S Renner I Elmadfa Long-term oral beta-carotene supple-mentation in patients with cystic fibrosis mdash effects on antioxidative status andpulmonary function Ann Nutr Metab 44 (2000) 30ndash37
[179] G Lepage J Champagne N Ronco A Lamarre I Osberg RJ Sokol CC Roy Sup-plementation with carotenoids corrects increased lipid peroxidation in childrenwith cystic fibrosis Am J Clin Nutr 64 (1996) 87ndash93
[180] BM Winklhofer-Roob H Puhl G Khoschsorur MA vant Hof H EsterbauerDH Shmerling Enhanced resistance to oxidation of low density lipoproteinsand decreased lipid peroxide formation during beta-carotene supplementationin cystic fibrosis Free Radic Biol Med 18 (1995) 849ndash859
[181] RC Graham-Maar JI Schall N Stettler BS Zemel VA Stallings Elevated vita-min A intake and serum retinol in preadolescent children with cystic fibrosisAm J Clin Nutr 84 (2006) 174ndash182
[182] I Sadowska-Woda M Rachel J Pazdan E Bieszczad-Bedrejczuk K PawliszakNutritional supplement attenuates selected oxidative stress markers in pediatricpatients with cystic fibrosis Nutr Res (New York NY) 31 (2011) 509ndash518
[183] KA Papas MK Sontag C Pardee RJ Sokol SD Sagel FJ Accurso JS WagenerA pilot study on the safety and efficacy of a novel antioxidant rich formulation inpatients with cystic fibrosis J Cyst Fibros 7 (2008) 60ndash67
[184] Y Saito A Fukuhara K Nishio M Hayakawa Y Ogawa H Sakamoto K Fujii YYoshida E Niki Characterization of cellular uptake and distribution of coen-zyme Q10 and vitamin E in PC12 cells J Nutr Biochem 20 (2009) 350ndash357
[185] AA Franke CM Morrison JL Bakke LJ Custer X Li RV Cooney CoenzymeQ10 in human blood native levels and determinants of oxidation during proces-sing and storage Free Radic Biol Med 48 (2010) 1610ndash1617
[186] HN Bhagavan RK Chopra Plasma coenzyme Q10 response to oral ingestion ofcoenzyme Q10 formulations Mitochondrion 7 (2007) S78ndashS88 (Suppl)
[187] HN Bhagavan RK Chopra Coenzyme Q10 absorption tissue uptake metabo-lism and pharmacokinetics Free Radic Res 40 (2006) 445ndash453
[188] F Galli R Lee C Dunster FJ Kelly Gas chromatography mass spectrometryanalysis of carboxyethyl-hydroxychroman metabolites of alpha- and gamma-tocopherol in human plasma Free Radic Biol Med 32 (2002) 333ndash340
[189] F Galli R Lee J Atkinson A Floridi FJ Kelly Gamma-tocopherol biokineticsand transformation in humans Free Radic Res 37 (2003) 1225ndash1233
[190] TA Laguna MK Sontag I Osberg JS Wagener FJ Accurso RJ Sokol De-creased total serum coenzyme-Q10 concentrations a longitudinal study in chil-dren with cystic fibrosis J Pediatr 153 (2008) 402ndash407
[191] T Frischer JK Myung G Maurer I Eichler Z Szepfalusi G Lubec Possible dys-regulation of chaperon and metabolic proteins in cystic fibrosis bronchial tissueProteomics 6 (2006) 3381ndash3388
[192] C Andersson MM Zaman AB Jones SD Freedman Alterations in immune re-sponse and PPARLXR regulation in cystic fibrosis macrophages J Cyst Fibros 7(2008) 68ndash78
[193] SD Freedman PG Blanco MM Zaman JC Shea M Ollero IK Hopper DAWeed A Gelrud MM Regan M Laposata JG Alvarez BP OSullivan Associa-tion of cystic fibrosis with abnormalities in fatty acid metabolism N Engl JMed 350 (2004) 560ndash569
[194] S Van Biervliet G Vanbillemont JP Van Biervliet D Declercq E Robberecht AChristophe Relation between fatty acid composition and clinical status or geno-type in cystic fibrosis patients Ann Nutr Metab 51 (2007) 541ndash549
[195] SD Freedman MH Katz EM Parker M Laposata MY Urman JG AlvarezA membrane lipid imbalance plays a role in the phenotypic expression ofcystic fibrosis in cftr(minusminus) mice Proc Natl Acad Sci U S A 96 (1999)13995ndash14000
[196] S Van Biervliet S Vande Velde JP Van Biervliet E Robberecht The effect ofzinc supplements in cystic fibrosis patients Ann Nutr Metab 52 (2008)152ndash156
[197] WR Henderson Jr SJ Astley MM McCready P Kushmerick S Casey JWBecker BW Ramsey Oral absorption of omega-3 fatty acids in patients withcystic fibrosis who have pancreatic insufficiency and in healthy control subjectsJ Pediatr 124 (1994) 400ndash408
[198] I Durieu E Vericel D Guichardant H Roth JP Steghens J Drai RN JosserandE Fontaine M Lagarde G Bellon Fatty acids platelets and oxidative markersfollowing intravenous n-3 fatty acids administration in cystic fibrosis an openpilot observational study J Cyst Fibros 6 (2007) 320ndash326
[199] LG Wood DA Fitzgerald ML Garg Hypothesis vitamin E complements poly-unsaturated fatty acids in essential fatty acid deficiency in cystic fibrosis J AmColl Nutr 22 (2003) 253ndash257
[200] JD Lloyd-Still SB Johnson RT Holman Essential fatty acid status in cystic fi-brosis and the effects of safflower oil supplementation Am J Clin Nutr 34(1981) 1ndash7
[201] A Maqbool JI Schall JF Garcia-Espana BS Zemel B Strandvik VAStallings Serum linoleic acid status as a clinical indicator of essential fatty
acid status in children with cystic fibrosis J Pediatr Gastroenterol Nutr 47(2008) 635ndash644
[202] C Oliver N Jahnke Omega-3 fatty acids for cystic fibrosis Cochrane DatabaseSyst Rev (2011) CD002201
[203] B Strandvik E Gronowitz F Enlund T Martinsson J Wahlstrom Essential fattyacid deficiency in relation to genotype in patients with cystic fibrosis J Pediatr139 (2001) 650ndash655
[204] P Rise S Volpi C Colombo RF Padoan C DOrazio S Ghezzi PMelotti V BennatoC Agostoni BM Assael C Galli Whole blood fatty acid analysis with micromethodin cystic fibrosis and pulmonary disease J Cyst Fibros 9 (2010) 228ndash233
[205] H Cao K Gerhold JR Mayers MM Wiest SM Watkins GS Hotamisligil Iden-tification of a lipokine a lipid hormone linking adipose tissue to systemic me-tabolism Cell 134 (2008) 933ndash944
[206] RR Malapaka SK Khoo J Zhang JH Choi XE Zhou Y Xu Y Gong J Li ELYong MJ Chalmers L Chang JH Resau PR Griffin YE Chen HE Xu Iden-tification and mechanism of a ten carbon fatty acid as a modulating ligand ofperoxisome proliferator activated receptors J Biol Chem 287 (2012)183ndash195
[207] T Hara A Hirasawa A Ichimura I Kimura G Tsujimoto Free fatty acid recep-tors FFAR1 and GPR120 as novel therapeutic targets for metabolic disorders JPharm Sci 100 (2011) 3594ndash3601
[208] R Gupta P Rathi S Bradoo Lipase mediated upgradation of dietary fats andoils Crit Rev Food Sci Nutr 43 (2003) 635ndash644
[209] BH Jennings CC Akoh Lipase-catalyzed modification of rice bran oil to incor-porate capric acid J Agric Food Chem 48 (2000) 4439ndash4443
[210] J Hoeks M Mensink MK Hesselink K Ekroos P Schrauwen Long- andMedium-Chain Fatty Acids Induce Insulin Resistance to a Similar Extent inHumans Despite Marked Differences in Muscle Fat Accumulation J Clin Endo-crinol Metab 97 (2012) 208ndash216
[211] PJ Congden G Bruce MM Rothburn PC Clarke JM Littlewood J KelleherMS Losowsky Vitamin status in treated patients with cystic fibrosis ArchDis Child 56 (1981) 708ndash714
[212] BM Winklhofer-Roob H Ellemunter M Fruhwirth SE Schlegel-Haueter GKhoschsorur MA vant Hof DH Shmerling Plasma vitamin C concentrationsin patients with cystic fibrosis evidence of associations with lung inflammationAm J Clin Nutr 65 (1997) 1858ndash1866
[213] L Shamseer D Adams N Brown JA Johnson S Vohra Antioxidant micronutri-ents for lung disease in cystic fibrosis Cochrane Database Syst Rev (2010)CD007020
[214] C Santi S Santoro Electrophilic Selenium First edition Wiley-VCH VerlagGmbH amp Co KGaA 2012
[215] L Flohe S Toppo G Cozza F Ursini A comparison of thiol peroxidase mecha-nisms Antioxid Redox Signal 15 (2010) 763ndash780
[216] L Flohe JR Andreesen R Brigelius-Flohe M Maiorino F Ursini Selenium theelement of the moon in life on earth IUBMB Life 49 (2000) 411ndash420
[217] V Valdiglesias E Pasaro J Mendez B Laffon In vitro evaluation of seleniumgenotoxic cytotoxic and protective effects a review Arch Toxicol 84(2010) 337ndash351
[218] P Foucaud P Therond M Marchand F Brion JF Demelier J Navarro Seleniumand vitamin E in mucoviscidosis Arch Fr Pediatr 45 (1988) 383ndash386
[219] J Neve R Van Geffel M Hanocq L Molle Plasma and erythrocyte zinc copperand selenium in cystic fibrosis Acta Paediatr Scand 72 (1983) 437ndash440
[220] BM Winklhofer-Roob B Tiran PE Tuchschmid MA vant Hof DH ShmerlingEffects of pancreatic enzyme preparations on erythrocyte glutathione peroxi-dase activities and plasma selenium concentrations in cystic fibrosis FreeRadic Biol Med 25 (1998) 242ndash249
[221] JD Lloyd-Still HE Ganther Selenium and glutathione peroxidase levels in cys-tic fibrosis Pediatrics 65 (1980) 1010ndash1012
[222] D Tsavachidou TJ McDonnell S Wen X Wang F Vakar-Lopez LL Pisters CAPettaway CG Wood KA Do PF Thall C Stephens E Efstathiou R Taylor DGMenter P Troncoso SM Lippman CJ Logothetis J Kim Selenium and vitaminE cell type- and intervention-specific tissue effects in prostate cancer J NatlCancer Inst 101 (2009) 306ndash320
[223] IN Zelko TJ Mariani RJ Folz Superoxide dismutase multigene family acomparison of the CuZn-SOD (SOD1) Mn-SOD (SOD2) and EC-SOD (SOD3)gene structures evolution and expression Free Radic Biol Med 33 (2002)337ndash349
[224] RP Bowler JD Crapo Oxidative stress in airways is there a role for extracellu-lar superoxide dismutase Am J Respir Crit Care Med 166 (2002) S38ndashS43
[225] K Best K McCoy S Gemma RA Disilvestro Copper enzyme activities in cysticfibrosis before and after copper supplementation plus or minus zinc Metabo-lism 53 (2004) 37ndash41
[226] SS Percival GP Kauwell E Bowser M Wagner Altered copper status in adultmen with cystic fibrosis J Am Coll Nutr 18 (1999) 614ndash619
[227] NF Krebs JE Westcott TD Arnold BM Kluger FJ Accurso LV Miller KMHambidge Abnormalities in zinc homeostasis in young infants with cystic fibro-sis Pediatr Res 48 (2000) 256ndash261
[228] D Easley N Krebs M Jefferson L Miller J Erskine F Accurso KM HambidgeEffect of pancreatic enzymes on zinc absorption in cystic fibrosis J Pediatr Gas-troenterol Nutr 26 (1998) 136ndash139
[229] S Van Biervliet JP Van Biervliet E Robberecht Serum zinc in patients with cys-tic fibrosis at diagnosis and after one year of therapy Biol Trace Elem Res 112(2006) 205ndash211
[230] S Van Biervliet JP Van Biervliet S Vande Velde E Robberecht Serum zinc con-centrations in cystic fibrosis patients aged above 4 years a cross-sectional eval-uation Biol Trace Elem Res 119 (2007) 19ndash26
712 F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
[231] F Galli M Cristina Polidori W Stahl P Mecocci FJ Kelly Vitamin E biotransfor-mation in humans Vitam Horm 76 (2007) 263ndash280
[232] J Wiser NE Alexis Q Jiang W Wu C Robinette R Roubey DB Peden In vivogamma-tocopherol supplementation decreases systemic oxidative stress andcytokine responses of human monocytes in normal and asthmatic subjectsFree Radic Biol Med 45 (2008) 40ndash49
[233] JG Wagner Q Jiang JR Harkema B Illek DD Patel BN Ames DB PedenOzone enhancement of lower airway allergic inflammation is prevented bygamma-tocopherol Free Radic Biol Med 43 (2007) 1176ndash1188
[234] JT Harries DP Muller Absorption of different doses of fat soluble and watermiscible preparations of vitamin E in children with cystic fibrosis Arch DisChild 46 (1971) 341ndash344
[235] EI Back C Frindt E Ocenaskova D Nohr M Stern HK Biesalski Can changesin hydrophobicity increase the bioavailability of alpha-tocopherol Eur J Nutr45 (2006) 1ndash6
[236] SZ Nasr MH OLeary C Hillermeier Correction of vitamin E deficiency withfat-soluble versus water-miscible preparations of vitamin E in patients with cys-tic fibrosis J Pediatr 122 (1993) 810ndash812
[237] S Soltani-Frisk E Gronowitz H Andersson B Strandvik Water-miscibletocopherol is not superior to fat-soluble preparation for vitamin E absorptionin cystic fibrosis Acta Paediatr 90 (2001) 1112ndash1115
[238] K Papas J Kalbfleisch R Mohon Bioavailability of a novel water-soluble vi-tamin E formulation in malabsorbing patients Dig Dis Sci 52 (2007)347ndash352
[239] F Antonicelli M Parmentier EM Drost N Hirani I Rahman K Donaldson WMacNee Nacystelyn inhibits oxidant-mediated interleukin-8 expression andNF-kappaB nuclear binding in alveolar epithelial cells Free Radic Biol Med 32(2002) 492ndash502
[240] EM App D Baran I Dab A Malfroot M Coffiner F Vanderbist M King Dose-finding and 24-h monitoring for efficacy and safety of aerosolized Nacystelyn incystic fibrosis Eur Respir J 19 (2002) 294ndash302
[241] MG Traber How much vitamin E hellip Just enough Am J Clin Nutr 84 (2006)959ndash960
[242] JC McCann BN Ames Vitamin K an example of triage theory is micronu-trient inadequacy linked to diseases of aging Am J Clin Nutr 90 (2009)889ndash907
[243] M Fusaro G Crepaldi S Maggi F Galli A DAngelo L Calo S Giannini DMiozzo M Gallieni Vitamin K bone fractures and vascular calcifications inchronic kidney disease an important but poorly studied relationship J Endocri-nol Invest 34 (2010) 317ndash323
[244] JC McCann BN Ames Adaptive dysfunction of selenoproteins from the per-spective of the triage theory why modest selenium deficiency may increaserisk of diseases of aging FASEB J 25 (2011) 1793ndash1814
[245] R Apak K Guclu M Ozyurek B Bektas Oglu M Bener Cupric ion reducing an-tioxidant capacity assay for food antioxidants vitamins polyphenolics and fla-vonoids in food extracts Methods Mol Biol 477 (2008) 163ndash193
[246] F Galli Interactions of polyphenolic compounds with drug disposition and me-tabolism Curr Drug Metab 8 (2007) 830ndash838
[247] RL Prior X Wu K Schaich Standardized methods for the determination of an-tioxidant capacity and phenolics in foods and dietary supplements J Agric FoodChem 53 (2005) 4290ndash4302
[248] C Azbell S Zhang D Skinner J Fortenberry EJ Sorscher BA WoodworthHesperidin stimulates cystic fibrosis transmembrane conductance regulator-mediated chloride secretion and ciliary beat frequency in sinonasal epitheliumOtolaryngol Head Neck Surg 143 (2010) 397ndash404
[249] G Wegrzyn J Jakobkiewicz-Banecka M Gabig-Ciminska E Piotrowska M Nar-ajczyk A Kloska M Malinowska D Dziedzic I Golebiewska M Moskot AWegrzyn Genistein a natural isoflavone with a potential for treatment of ge-netic diseases Biochem Soc Trans 38 (2010) 695ndash701
[250] YC Yu H Miki Y Nakamura A Hanyuda Y Matsuzaki Y Abe M Yasui K Ta-naka TC Hwang SG Bompadre Y Sohma Curcumin and genistein additivelypotentiate G551D-CFTR J Cyst Fibros 10 (2011) 243ndash252
[251] B Illek H Fischer Flavonoids stimulate Cl conductance of human airway epithe-lium in vitro and in vivo Am J Physiol 275 (1998) L902ndashL910
[252] JL Kreindler Cystic fibrosis exploiting its genetic basis in the hunt for newtherapies Pharmacol Ther 125 (2010) 219ndash229
[253] B Illek L Zhang NC Lewis RB Moss JY Dong H Fischer Defective function ofthe cystic fibrosis-causing missense mutation G551D is recovered by genisteinAm J Physiol 277 (1999) C833ndashC839
[254] P Anandakumar S Kamaraj S Jagan G Ramakrishnan R Vinodhkumar TDevaki Capsaicin modulates pulmonary antioxidant defense system during ben-zo(a)pyrene-induced lung cancer in Swiss albinomice Phytother Res 22 (2008)529ndash533
[255] I Rahman Antioxidant therapeutic advances in COPD Ther Adv Respir Dis 2(2008) 351ndash374
[256] AW Boots H Li RP Schins R Duffin JW Heemskerk A Bast GR Haenen Thequercetin paradox Toxicol Appl Pharmacol 222 (2007) 89ndash96
[257] M Joskova S Franova V Sadlonova Acute bronchodilator effect of quercetin inexperimental allergic asthma Bratisl Lek Listy 112 (2011) 9ndash12
[258] HJ Park CM Lee ID Jung JS Lee YI Jeong JH Chang SH Chun MJ Kim IWChoi SC Ahn YK Shin SR Yeom YM Park Quercetin regulates Th1Th2 balancein a murine model of asthma Int Immunopharmacol 9 (2009) 261ndash267
[259] AP Rogerio A Kanashiro C Fontanari EV da Silva YM Lucisano-ValimEG Soares LH Faccioli Anti-inflammatory activity of quercetin and iso-quercitrin in experimental murine allergic asthma Inflamm Res 56 (2007)402ndash408
[260] M Muller Polyphenol cytotoxicity induced by the bacterial toxin pyocyaninrole of NQO1 Free Radic Biol Med 47 (2009) 84ndash91
[261] J Grassmann Terpenoids as plant antioxidants Vitam Horm 72 (2005)505ndash535
[262] P Allen Tea tree oil the science behind the antimicrobial hype Lancet 358(2001) 1245
[263] EC Dasenbrook W Checkley CA Merlo MW Konstan N Lechtzin MP BoyleAssociation between respiratory tract methicillin-resistant Staphylococcus aure-us and survival in cystic fibrosis JAMA 303 (2010) 2386ndash2392
[264] V Bezzerri M Borgatti E Nicolis I Lampronti MC Dechecchi I Mancini PRizzotti R Gambari G Cabrini Transcription factor oligodeoxynucleotides toNF-kappaB inhibit transcription of IL-8 in bronchial cells Am J Respir CellMol Biol 39 (2008) 86ndash96
[265] R Gambari M Borgatti V Bezzerri E Nicolis I Lampronti MC Dechecchi IMancini A Tamanini G Cabrini Decoy oligodeoxyribonucleotides and peptidenucleic acids-DNA chimeras targeting nuclear factor kappa-B inhibition of IL-8 gene expression in cystic fibrosis cells infected with Pseudomonas aeruginosaBiochem Pharmacol 80 (2010) 1887ndash1894
[266] M Adrian P Jeandet AC Douillet-Breuil L Tesson R Bessis Stilbene content ofmature Vitis vinifera berries in response to UV-C elicitation J Agric Food Chem48 (2000) 6103ndash6105
[267] B Paul I Masih J Deopujari C Charpentier Occurrence of resveratrol and pter-ostilbene in age-old darakchasava an ayurvedic medicine from India J Ethno-pharmacol 68 (1999) 71ndash76
[268] I Rahman Antioxidant therapies in COPD Int J Chron Obstruct Pulmon Dis 1(2006) 15ndash29
[269] M Lee S Kim OK Kwon SR Oh HK Lee K Ahn Anti-inflammatory and anti-asthmatic effects of resveratrol a polyphenolic stilbene in a mouse model ofallergic asthma Int Immunopharmacol 9 (2009) 418ndash424
[270] LG Wood PA Wark ML Garg Antioxidant and anti-inflammatory effectsof resveratrol in airway disease Antioxid Redox Signal 13 (2010)1535ndash1548
[271] KV Kiselev Perspectives for production and application of resveratrol ApplMicrobiol Biotechnol 90 (2011) 417ndash425
[272] M Shakibaei C Buhrmann A Mobasheri Resveratrol-mediated SIRT-1 interac-tions with p300 modulate receptor activator of NF-kappaB ligand (RANKL) acti-vation of NF-kappaB signaling and inhibit osteoclastogenesis in bone-derivedcells J Biol Chem 286 (2011) 11492ndash11505
[273] SF Zaidi K Ahmed T Yamamoto T Kondo K Usmanghani M Kadowaki TSugiyama Effect of resveratrol on Helicobacter pylori-induced interleukin-8 secre-tion reactive oxygen species generation and morphological changes in human gas-tric epithelial cells Biol Pharm Bull 32 (2009) 1931ndash1935
[274] JK Kundu YK Shin YJ Surh Resveratrol modulates phorbol ester-inducedpro-inflammatory signal transduction pathways in mouse skin in vivo NF-kappaB and AP-1 as prime targets Biochem Pharmacol 72 (2006)1506ndash1515
[275] NH Nam Naturally occurring NF-kappaB inhibitors Mini Rev Med Chem 6(2006) 945ndash951
[276] JM Smoliga JA Baur HA Hausenblas Resveratrol and healthmdasha comprehen-sive review of human clinical trials Mol Nutr Food Res 55 (2011) 1129ndash1141
[277] ME Juan M Maijo JM Planas Quantification of trans-resveratrol and itsmetabolites in rat plasma and tissues by HPLC J Pharm Biomed Anal 51(2010) 391ndash398
[278] JA Baur DA Sinclair Therapeutic potential of resveratrol the in vivo evidenceNat Rev 5 (2006) 493ndash506
[279] E Nicolis I Lampronti MC Dechecchi M Borgatti A Tamanini N Bianchi VBezzerri I Mancini MG Giri P Rizzotti R Gambari G Cabrini Pyrogallol anactive compound from the medicinal plant Emblica officinalis regulates expres-sion of pro-inflammatory genes in bronchial epithelial cells Int Immunophar-macol 8 (2008) 1672ndash1680
[280] E Nicolis I Lampronti MC Dechecchi M Borgatti A Tamanini V Bezzerri NBianchi M Mazzon I Mancini MG Giri P Rizzotti R Gambari G CabriniModulation of expression of IL-8 gene in bronchial epithelial cells by 5-methoxypsoralen Int Immunopharmacol 9 (2009) 1411ndash1422
[281] M Borgatti I Mancini N Bianchi A Guerrini I Lampronti D Rossi G SacchettiR Gambari Bergamot (Citrus bergamia Risso) fruit extracts and identified com-ponents alter expression of interleukin 8 gene in cystic fibrosis bronchial epithe-lial cell lines BMC Biochem 12 (2011) 15
[282] L Piccagli E Fabbri M Borgatti N Bianchi V Bezzerri I Mancini E Nicolis CMDechecchi I Lampronti G Cabrini R Gambari Virtual screening against p50NF-kappaB transcription factor for the identification of inhibitors of the NF-kappaB-DNA interaction and expression of NF-kappaB upregulated genesChemMedChem 4 (2009) 2024ndash2033
[283] L Piccagli M Borgatti E Nicolis N Bianchi I Mancini I Lampronti D VevaldiF DallAcqua G Cabrini R Gambari Virtual screening against nuclear factorkappaB (NF-kappaB) of a focus library identification of bioactive furocoumarinderivatives inhibiting NF-kappaB dependent biological functions involved incystic fibrosis Bioorg Med Chem 18 (2010) 8341ndash8349
[284] M Borgatti A Chilin L Piccagli I Lampronti N Bianchi I Mancini G Mar-zaro Da Francesco A Guiotto R Gambari Development of a novel furocou-marin derivative inhibiting NF-kappaB dependent biological functionsdesign synthesis and biological effects Eur J Med Chem 46 (2011)4870ndash4877
[285] E Georgy S Le Guellec L Vecellio E Fichant P Stordeur P Bordeau JP PerraudinFeasibility study of OSCN- and lactoferrin (Meveol) nebulization for cysticfibrosis JCyst Fibros 10 (2011) S18
713F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
[286] C Tidei M Piroddi F Galli C Santi Oxidation of thiols promoted by PhSeZnClTetrahedron Lett 53 (2012) 232ndash234
[287] L Semianrio-Vidal C van Hesuden G Mugesh ER Lazarowski Ebselen is a po-tent non-competitive inhibitor of extracellular nucleoside diphosphokinasePurinergic Signal 6 (2010) 383ndash391
[288] C ColussiMC Albertini S Coppola S Rovidati F Galli L Ghibelli H2O2-inducedblockof glycolysis as an active ADP-ribosylation reaction protecting cells from apoptosisFASEB J 14 (2000) 2266ndash2276
[289] H Xiao KL Parkin Induction of phase II enzyme activity by various seleniumcompounds Nutr Cancer 55 (2006) 210ndash223
[290] G Peluffo R Radi Biochemistry of protein tyrosine nitration in cardiovascularpathology Cardiovasc Res 75 (2007) 291ndash302
[291] B Alvarez R Radi Peroxynitrite reactivity with amino acids and proteinsAmino Acids 25 (2003) 295ndash311
[292] B Kamosinska MW Radomski M Duszyk A Radomski SF Man Nitric oxideactivates chloride currents in human lung epithelial cells Am J Physiol 272(1997) L1098ndashL1104
[293] L Chen RP Patel X Teng CA Bosworth JR Lancaster Jr S Matalon Mecha-nisms of cystic fibrosis transmembrane conductance regulator activation by S-nitrosoglutathione J Biol Chem 281 (2006) 9190ndash9199
[294] F Luchetti B CanonicoM BettiM Arcangeletti F PilolliM Piroddi L Canesi S PapaF Galli Melatonin signaling and cell protection function FASEB J 24 (2010)3603ndash3624
[295] MW Bengtsson G Jedstedt G Flemstrom Duodenal bicarbonate secretion inrats stimulation by intra-arterial and luminal guanylin and uroguanylin ActaPhysiol (Oxf) 191 (2007) 309ndash317
[296] CS Nelson JL Marino CN Allen Melatonin receptor potentiation of cyclic AMP andthe cystic fibrosis transmembrane conductance regulator ion channel J Pineal Res 26(1999) 113ndash121
[297] C de Castro-Silva VM de Bruin GM Cunha DM Nunes CAMedeiros PF de BruinMelatonin improves sleep and reduces nitrite in the exhaled breath condensate incystic fibrosismdasha randomized double-blind placebo-controlled study J Pineal Res48 (2010) 65ndash71
[298] I Hornyak E Pankotai L Kiss Z Lacza Current developments in the the-rapeutic potential of S-nitrosoglutathione an endogenous NO-donor mole-cule Curr Pharm Biotechnol (2011) Jan 11 [Epub ahead of print] - PMID21235457
[299] AH Snyder ME McPherson JF Hunt M Johnson JS Stamler B Gaston Acuteeffects of aerosolized S-nitrosoglutathione in cystic fibrosis Am J Respir CritCare Med 165 (2002) 922ndash926
708 F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
stimulating research environment that he has contributed to createwithin the Italian Cystic Fibrosis Research Foundation
References
[1] BP OSullivan SD Freedman Cystic fibrosis Lancet 373 (2009) 1891ndash1904[2] P Linsdell JW Hanrahan Glutathione permeability of CFTR Am J Physiol 275
(1998) C323ndashC326[3] L Gao KJ Kim JR Yankaskas HJ Forman Abnormal glutathione transport in
cystic fibrosis airway epithelia Am J Physiol 277 (1999) L113ndashL118[4] RK Rowntree A Harris The phenotypic consequences of CFTR mutations Ann
Hum Genet 67 (2003) 471ndash485[5] EI Back C Frindt D Nohr J Frank R Ziebach M Stern M Ranke HK Biesalski
Antioxidant deficiency in cystic fibrosis when is the right time to take actionAm J Clin Nutr 80 (2004) 374ndash384
[6] LG Wood DA Fitzgerald AK Lee ML Garg Improved antioxidant and fattyacid status of patients with cystic fibrosis after antioxidant supplementation islinked to improved lung function Am J Clin Nutr 77 (2003) 150ndash159
[7] L Iuliano R Monticolo G Straface S Zullo F Galli M Boaz S Quattrucci Asso-ciation of cholesterol oxidation and abnormalities in fatty acid metabolism incystic fibrosis Am J Clin Nutr 90 (2009) 477ndash484
[8] C Libetta V Sepe P Esposito F Galli A Dal Canton Oxidative stress and inflam-mation implications in uremia and hemodialysis Clin Biochem 44 (2011)1189ndash1198
[9] G Bartosz Reactive oxygen species destroyers or messengers Biochem Phar-macol 77 (2009) 1303ndash1315
[10] T Ntimbane B Comte G Mailhot Y Berthiaume V Poitout M Prentki RRabasa-Lhoret E Levy Cystic fibrosis-related diabetes from CFTR dysfunctionto oxidative stress Clin Biochem 30 (2009) 153ndash177
[11] A van der Vliet JP Eiserich GP Marelich B Halliwell CE Cross Oxidativestress in cystic fibrosis does it occur and does it matter Adv Pharmacol 38(1997) 491ndash513
[12] AM Cantin TB White CE Cross HJ Forman RJ Sokol D Borowitz Antioxi-dants in cystic fibrosis Conclusions from the CF antioxidant workshop Bethes-da Maryland Free Radic Biol Med 42 (2007) 15ndash31
[13] LT McGrath P Mallon L Dowey B Silke E McClean M McDonnell A DevineS Copeland S Elborn Oxidative stress during acute respiratory exacerbations incystic fibrosis Thorax 54 (1999) 518ndash523
[14] E Thomson S Brennan R Senthilmohan CL Gangell AL Chapman PD SlyAJ Kettle E Balding LJ Berry JB Carlin R Carzino N de Klerk T Douglas CFoo LW Garratt GL Hall J Harrison A Kicic IA Laing KM Logie J MassieLS Mott C Murray F Parsons N Pillarisetti SR Poreddy SC RanganathanCF Robertson R Robins-Browne PJ Robinson B Skoric SM Stick ENSutanto E Williamson Identifying peroxidases and their oxidants in the earlypathology of cystic fibrosis Free Radic Biol Med 49 (2010) 1354ndash1360
[15] SP Range C Dunster AJ Knox FJ Kelly Treatment of pulmonary exacerba-tions of cystic fibrosis leads to improved antioxidant status Eur Respir J 13(1999) 560ndash564
[16] L Coppo P Ghezzi Thiol regulation of pro-inflammatory cytokines and innateimmunity protein S-thiolation as a novel molecular mechanism Biochem SocTrans 39 (2011) 1268ndash1272
[17] C Verhaeghe C Remouchamps B Hennuy A Vanderplasschen A Chariot SPTabruyn C Oury V Bours Role of IKK and ERK pathways in intrinsic inflamma-tion of cystic fibrosis airways Biochem Pharmacol 73 (2007) 1982ndash1994
[18] TL Bonfield JR Panuska MW Konstan KA Hilliard JB Hilliard H Ghnaim MBerger Inflammatory cytokines in cystic fibrosis lungs Am J Respir Crit CareMed 152 (1995) 2111ndash2118
[19] TL Noah HR Black PW Cheng RE Wood MW Leigh Nasal and bronchoal-veolar lavage fluid cytokines in early cystic fibrosis J Infect Dis 175 (1997)638ndash647
[20] MJ Welsh BW Ramsey FJ Accurso GR Cutting Cystic Fibrosis McGraw-HillNew York 2001
[21] TZ Khan JS Wagener T Bost J Martinez FJ Accurso DW Riches Early pul-monary inflammation in infants with cystic fibrosis Am J Respir Crit CareMed 151 (1995) 1075ndash1082
[22] FA Ratjen Cystic fibrosis pathogenesis and future treatment strategies RespirCare 54 (2009) 595ndash605
[23] J Jacquot O Tabary P Le Rouzic A Clement Airway epithelial cell inflamma-tory signalling in cystic fibrosis Int J Biochem Cell Biol 40 (2008)1703ndash1715
[24] CM Greene P Branagan NG McElvaney Toll-like receptors as therapeutic tar-gets in cystic fibrosis Expert Opin Ther Targets 12 (2008) 1481ndash1495
[25] M Rottner JM Freyssinet MC Martinez Mechanisms of the noxious inflam-matory cycle in cystic fibrosis Respir Res 10 (2009) 23
[26] G Cabrini V Bezzerri I Mancini E Nicolis MC Dechecchi A Tamanini ILampronti L Piccagli N Bianchi M Borgatti R Gambari Targeting transcrip-tion factor activity as a strategy to inhibit pro-inflammatory genes involved incystic fibrosis decoy oligonucleotides and low-molecular weight compoundsCurr Med Chem 17 (2010) 4392ndash4404
[27] CM Greene NG McElvaney Proteases and antiproteases in chronic neutrophiliclungdiseasemdash relevance to drug discovery Br J Pharmacol 158 (2009) 1048ndash1058
[28] AM Cantin Potential for antioxidant therapy of cystic fibrosis Curr Opin PulmMed 10 (2004) 531ndash536
[29] JF Chmiel MW Konstan Inflammation and anti-inflammatory therapies forcystic fibrosis Clin Chest Med 28 (2007) 331ndash346
[30] DP Nichols MW Konstan JF Chmiel Anti-inflammatory therapies for cys-tic fibrosis-related lung disease Clin Rev Allergy Immunol 35 (2008)135ndash153
[31] AJ Kettle T Chan I Osberg R Senthilmohan AL Chapman TJ Mocatta JSWagener Myeloperoxidase and protein oxidation in the airways of youngchildren with cystic fibrosis Am J Respir Crit Care Med 170 (2004)1317ndash1323
[32] H Fischer Mechanisms and function of DUOX in epithelia of the lung AntioxidRedox Signal 11 (2009) 2453ndash2465
[33] B Rada TL Leto Oxidative innate immune defenses by NoxDuox familyNADPH oxidases Contrib Microbiol 15 (2008) 164ndash187
[34] P Moskwa D Lorentzen KJ Excoffon J Zabner PB McCray Jr WM NauseefC Dupuy B Banfi A novel host defense system of airways is defective in cysticfibrosis Am J Respir Crit Care Med 175 (2007) 174ndash183
[35] D Lorentzen L Durairaj AA Pezzulo Y Nakano J Launspach DA Stoltz GZamba PB McCray Jr J Zabner MJ Welsh WM Nauseef B Banfi Concentra-tion of the antibacterial precursor thiocyanate in cystic fibrosis airway secre-tions Free Radic Biol Med 50 (2011) 1144ndash1150
[36] Y Xu S Szep Z Lu The antioxidant role of thiocyanate in the pathogenesis ofcystic fibrosis and other inflammation-related diseases Proc Natl Acad Sci US A 106 (2009) 20515ndash20519
[37] MP Rogan CC Taggart CM Greene PG Murphy SJ ONeill NG McElvaneyLoss of microbicidal activity and increased formation of biofilm due to decreasedlactoferrin activity in patients with cystic fibrosis J Infect Dis 190 (2004)1245ndash1253
[38] B Halliwell JM Guttridge Free Radicals in Biology and Medicine Fourth editionOxford University Press New York 2007
[39] B Rada K Lekstrom S Damian C Dupuy TL Leto The Pseudomonastoxin pyocyanin inhibits the dual oxidase-based antimicrobial system as itimposes oxidative stress on airway epithelial cells J Immunol 181 (2008)4883ndash4893
[40] C Schwarzer B Illek JH Suh SJ Remington H Fischer TE Machen Organelleredox of CF and CFTR-corrected airway epithelia Free Radic Biol Med 43(2007) 300ndash316
[41] JH Roum R Buhl NG McElvaney Z Borok RG Crystal Systemic deficiency ofglutathione in cystic fibrosis J Appl Physiol 75 (1993) 2419ndash2424
[42] VM Hudson Rethinking cystic fibrosis pathology the critical role of abnormalreduced glutathione (GSH) transport caused by CFTR mutation Free RadicBiol Med 30 (2001) 1440ndash1461
[43] PJ Barnes RA Dweik AF Gelb PG Gibson SC George H Grasemann IDPavord F Ratjen PE Silkoff DR Taylor N Zamel Exhaled nitric oxide in pul-monary diseases a comprehensive review Chest 138 (2010) 682ndash692
[44] H Grasemann E Michler M Wallot F Ratjen Decreased concentration of ex-haled nitric oxide (NO) in patients with cystic fibrosis Pediatr Pulmonol 24(1997) 173ndash177
[45] H Grasemann F Ratjen Cystic fibrosis lung disease the role of nitric oxidePediatr Pulmonol 28 (1999) 442ndash448
[46] B Gaston F Ratjen JW Vaughan NR Malhotra RG Canady AH Snyder JFHunt S Gaertig JB Goldberg Nitrogen redox balance in the cystic fibrosis air-way effects of antipseudomonal therapy Am J Respir Crit Care Med 165(2002) 387ndash390
[47] H Grasemann I Ioannidis RP Tomkiewicz H de Groot BK Rubin F RatjenNitric oxide metabolites in cystic fibrosis lung disease Arch Dis Child 78(1998) 49ndash53
[48] H Grasemann R Schwiertz S Matthiesen K Racke F Ratjen Increased argi-nase activity in cystic fibrosis airways Am J Respir Crit Care Med 172(2005) 1523ndash1528
[49] H Grasemann S Al-Saleh JA Scott D Shehnaz A Mehl R Amin M Rafii PPencharz J Belik F Ratjen Asymmetric dimethylarginine contributes to airwaynitric oxide deficiency in patients with cystic fibrosis Am J Respir Crit CareMed 183 (2011) 1363ndash1368
[50] H Grasemann F Kurtz F Ratjen Inhaled L-arginine improves exhaled nitricoxide and pulmonary function in patients with cystic fibrosis Am J RespirCrit Care Med 174 (2006) 208ndash212
[51] H Grasemann F Ratjen Emerging therapies for cystic fibrosis lung disease Ex-pert Opin Emerg Drugs 15 (2010) 653ndash659
[52] BM Morrissey K Schilling JV Weil PE Silkoff DM Rodman Nitric oxide andprotein nitration in the cystic fibrosis airway Arch Biochem Biophys 406(2002) 33ndash39
[53] R Radi Nitric oxide oxidants and protein tyrosine nitration Proc Natl AcadSci U S A 101 (2004) 4003ndash4008
[54] J Chen M Kinter S Shank C Cotton TJ Kelley AG Ziady Dysfunction of Nrf-2in CF epithelia leads to excess intracellular H2O2 and inflammatory cytokineproduction PLoS One 3 (2008) e3367
[55] F Galli M Piroddi C Annetti C Aisa E Floridi A Floridi Oxidative stress andreactive oxygen species Contrib Nephrol 149 (2005) 240ndash260
[56] DT Wright LA Cohn H Li B Fischer CM Li KB Adler Interactions of oxygenradicals with airway epithelium Environ Health Perspect 102 (Suppl 10)(1994) 85ndash90
[57] I Rahman SR Yang SK Biswas Current concepts of redox signaling in thelungs Antioxid Redox Signal 8 (2006) 681ndash689
[58] Q Li JF Engelhardt Interleukin-1beta induction of NFκB is partially regulatedby H2O2-mediated activation of NFκB-inducing kinase J Biol Chem 281(2006) 1495ndash1505
709F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
[59] E Boncoeur VS Criq E Bonvin T Roque A Henrion-Caude DC Gruenert AClement J Jacquot O Tabary Oxidative stress induces extracellular signal-regulated kinase 12 mitogen-activated protein kinase in cystic fibrosis lung ep-ithelial cells potential mechanism for excessive IL-8 expression Int J BiochemCell Biol 40 (2008) 432ndash446
[60] B Fischer J Voynow Neutrophil elastase induces MUC5AC messenger RNA ex-pression by an oxidant-dependent mechanism Chest 117 (2000) 317Sndash320S
[61] B Rada P Gardina TG Myers TL Leto Reactive oxygen species mediate in-flammatory cytokine release and EGFR-dependent mucin secretion in airwayepithelial cells exposed to Pseudomonas pyocyanin Mucosal Immunol 4(2011) 158ndash171
[62] C Schwarzer H Fischer EJ Kim KJ Barber AD Mills MJ Kurth DC GruenertJH Suh TE Machen B Illek Oxidative stress caused by pyocyanin impairs CFTRClminus transport in human bronchial epithelial cells Free Radic Biol Med 45(2008) 1653ndash1662
[63] J Hull M South P Phelan K Grimwood Surfactant composition in infants andyoung children with cystic fibrosis Am J Respir Crit Care Med 156 (1997)161ndash165
[64] KC Meyer A Sharma R Brown M Weatherly FR Moya J Lewandoski JJZimmerman Function and composition of pulmonary surfactant andsurfactant-derived fatty acid profiles are altered in young adults with cystic fi-brosis Chest 118 (2000) 164ndash174
[65] MK Pulfer RC Murphy Formation of biologically active oxysterols during ozo-nolysis of cholesterol present in lung surfactant J Biol Chem 279 (2004)26331ndash26338
[66] V Starosta E Rietschel K Paul U Baumann M Griese Oxidative changes ofbronchoalveolar proteins in cystic fibrosis Chest 129 (2006) 431ndash437
[67] V Starosta M Griese Oxidative damage to surfactant protein D in pulmonarydiseases Free Radic Res 40 (2006) 419ndash425
[68] M Griese R Essl R Schmidt E Rietschel F Ratjen M Ballmann K Paul Pulmo-nary surfactant lung function and endobronchial inflammation in cystic fibro-sis Am J Respir Crit Care Med 170 (2004) 1000ndash1005
[69] M Griese R Essl R Schmidt M Ballmann K Paul E Rietschel F Ratjen Se-quential analysis of surfactant lung function and inflammation in cystic fibrosispatients Respir Res 6 (2005) 133
[70] LG Wood DA Fitzgerald PG Gibson DM Cooper ML Garg Increased plasmafatty acid concentrations after respiratory exacerbations are associated with el-evated oxidative stress in cystic fibrosis patients Am J Clin Nutr 75 (2002)668ndash675
[71] P Montuschi SA Kharitonov G Ciabattoni M Corradi L van Rensen DM Ged-des ME Hodson PJ Barnes Exhaled 8-isoprostane as a new non-invasive bio-marker of oxidative stress in cystic fibrosis Thorax 55 (2000) 205ndash209
[72] CE Collins P Quaggiotto L Wood EV OLoughlin RL Henry ML Garg Elevat-ed plasma levels of F2 alpha isoprostane in cystic fibrosis Lipids 34 (1999)551ndash556
[73] D Hartl V Starosta K Maier I Beck-Speier C Rebhan BF Becker P Latzin RFischer F Ratjen RM Huber E Rietschel S Krauss-Etschmann M Griese In-haled glutathione decreases PGE2 and increases lymphocytes in cystic fibrosislungs Free Radic Biol Med 39 (2005) 463ndash472
[74] GL Milne H Yin JD Morrow Human biochemistry of the isoprostane pathwayJ Biol Chem 283 (2008) 15533ndash15537
[75] G Ciabattoni G Davi M Collura L Iapichino F Pardo A Ganci R Romagnoli JMaclouf C Patrono In vivo lipid peroxidation and platelet activation in cystic fi-brosis Am J Respir Crit Care Med 162 (2000) 1195ndash1201
[76] C Garenc P Julien E Levy Oxysterols in biological systems the gastrointestinaltract liver vascular wall and central nervous system Free Radic Res 44 (2011)47ndash73
[77] AM Cantin SL North RC Hubbard RG Crystal Normal alveolar epithelial lin-ing fluid contains high levels of glutathione J Appl Physiol 63 (1987) 152ndash157
[78] R Tirouvanziam CK Conrad T Bottiglieri LA Herzenberg RB Moss High-dose oral N-acetylcysteine a glutathione prodrug modulates inflammation incystic fibrosis Proc Natl Acad Sci U S A 103 (2006) 4628ndash4633
[79] LW Velsor C Kariya R Kachadourian BJ Day Mitochondrial oxidative stressin the lungs of cystic fibrosis transmembrane conductance regulator proteinmutant mice Am J Respir Cell Mol Biol 35 (2006) 579ndash586
[80] M Kelly-Aubert S Trudel J Fritsch T Nguyen-Khoa M Baudouin-Legros SMoriceau L Jeanson F Djouadi C Matar M Conti M Ollero F Brouillard AEdelman GSH monoethyl ester rescues mitochondrial defects in cystic fibrosismodels Hum Mol Genet 20 (2011) 2745ndash2759
[81] P Ghezzi Role of glutathione in immunity and inflammation in the lung Int JGen Med 4 (2011) 105ndash113
[82] N Dauletbaev K Viel R Buhl TO Wagner J Bargon Glutathione and glutathi-one peroxidase in sputum samples of adult patients with cystic fibrosis J CystFibros 3 (2004) 119ndash124
[83] CE Cross A van der Vliet CA ONeill S Louie B Halliwell Oxidants antioxi-dants and respiratory tract lining fluids Environ Health Perspect 102 (Suppl10) (1994) 185ndash191
[84] K Takeyama K Dabbagh J Jeong Shim T Dao-Pick IF Ueki JA Nadel Oxida-tive stress causes mucin synthesis via transactivation of epidermal growth factorreceptor role of neutrophils J Immunol 164 (2000) 1546ndash1552
[85] N Ballatori SM Krance S Notenboom S Shi K Tieu CL Hammond Glutathi-one dysregulation and the etiology and progression of human diseases BiolChem 390 (2009) 191ndash214
[86] SR Soltaninassab KR Sekhar MJ Meredith ML Freeman Multi-faceted regu-lation of gamma-glutamylcysteine synthetase J Cell Physiol 182 (2000)163ndash170
[87] HR Lopez-Mirabal JR Winther Redox characteristics of the eukaryotic cytosolBiochim Biophys Acta 1783 (2008) 629ndash640
[88] C Hwang AJ Sinskey HF Lodish Oxidized redox state of glutathione in the en-doplasmic reticulum Science 257 (1992) 1496ndash1502
[89] M Murphy Mitochondrial thiols in antioxidant protection and redox signallingdistinct roles for glutathionylation and other thiol modifications AntioxidRedox Signal (2011) ahead of print doi101089ars20114289
[90] BJ Day AM van Heeckeren E Min LW Velsor Role for cystic fibrosis trans-membrane conductance regulator protein in a glutathione response to bronch-opulmonary Pseudomonas infection Infect Immun 72 (2004) 2045ndash2051
[91] Y Zhang K Duan Glutathione exhibits antibacterial activity and increases tetra-cycline efficacy against Pseudomonas aeruginosa Sci China C Life Sci 52 (2009)501ndash505
[92] VM Hudson New insights into the pathogenesis of cystic fibrosis pivotal roleof glutathione system dysfunction and implications for therapy Treat RespirMed 3 (2004) 353ndash363
[93] LW Velsor A van Heeckeren BJ Day Antioxidant imbalance in the lungs ofcystic fibrosis transmembrane conductance regulator protein mutant miceAm J Physiol Lung Cell Mol Physiol 281 (2001) L31ndashL38
[94] I Kogan M Ramjeesingh C Li JF Kidd Y Wang EM Leslie SP Cole CE BearCFTR directly mediates nucleotide-regulated glutathione flux EMBO J 22(2003) 1981ndash1989
[95] NS Gould S Gauthier CT Kariya E Min J Huang DJ Brian Hypertonic salineincreases lung epithelial lining fluid glutathione and thiocyanate two protectiveCFTR-dependent thiols against oxidative injury Respir Res 11 (2010) 119
[96] VT Vasu SJ de Cruz JS Houghton KA Hayakawa BM Morrissey CE CrossJP Eiserich Evaluation of thiol-based antioxidant therapeutics in cystic fibrosissputum focus on myeloperoxidase Free Radic Res 45 (2011) 165ndash176
[97] L Roussel G Martel J Berube S Rousseau P aeruginosa drives CXCL8 synthesisvia redundant toll-like receptors and NADPH oxidase in CFTRF508 airway epi-thelial cells J Cyst Fibros 10 (2011) 107ndash113
[98] GW Lau DJ Hassett H Ran F Kong The role of pyocyanin in Pseudomonas aer-uginosa infection Trends Mol Med 10 (2004) 599ndash606
[99] R Wilson DA Sykes D Watson A Rutman GW Taylor PJ Cole Measurementof Pseudomonas aeruginosa phenazine pigments in sputum and assessment oftheir contribution to sputum sol toxicity for respiratory epithelium InfectImmun 56 (1988) 2515ndash2517
[100] M Muller Pyocyanin induces oxidative stress in human endothelial cells andmodulates the glutathione redox cycle Free Radic Biol Med 33 (2002)1527ndash1533
[101] YQ OMalley KJ Reszka BE Britigan Direct oxidation of 2prime7prime-dichlorodihy-drofluorescein by pyocyanin and other redox-active compounds independentof reactive oxygen species production Free Radic Biol Med 36 (2004)90ndash100
[102] CC Caldwell Y Chen HS Goetzmann Y Hao MT Borchers DJ Hassett LRYoung D Mavrodi L Thomashow GW Lau Pseudomonas aeruginosa exotoxinpyocyanin causes cystic fibrosis airway pathogenesis Am J Pathol 175 (2009)2473ndash2488
[103] YQ OMalley KJ Reszka DR Spitz GM Denning BE Britigan Pseudomonasaeruginosa pyocyanin directly oxidizes glutathione and decreases its levels inairway epithelial cells Am J Physiol Lung Cell Mol Physiol 287 (2004)L94ndashL103
[104] M Muller Glutathione modulates the toxicity of but is not a biologically rele-vant reductant for the Pseudomonas aeruginosa redox toxin pyocyanin FreeRadic Biol Med 50 (2011) 971ndash977
[105] R Cheluvappa R Shimmon M Dawson SN Hilmer DG Le Couteur Reactionsof Pseudomonas aeruginosa pyocyanin with reduced glutathione Acta BiochimPol 55 (2008) 571ndash580
[106] JH Widdicombe Transgenic animals may help resolve a sticky situation in cys-tic fibrosis J Clin Invest 120 (2010) 3093ndash3096
[107] X Sun H Sui JT Fisher Z Yan X Liu HJ Cho NS Joo Y Zhang W Zhou Y YiJM Kinyon DC Lei-Butters MA Griffin P Naumann M Luo J Ascher KWang T Frana JJ Wine DK Meyerholz JF Engelhardt Disease phenotype ofa ferret CFTR-knockout model of cystic fibrosis J Clin Invest 120 (2010)3149ndash3160
[108] NS Joo HJ Cho M Khansaheb JJ Wine Hyposecretion of fluid from trachealsubmucosal glands of CFTR-deficient pigs J Clin Invest 120 (2010) 3161ndash3166
[109] A Bragonzi Murine models of acute and chronic lung infection with cystic fibro-sis pathogens IJMM 300 (2010) 584ndash593
[110] AM van Heeckeren MD Schluchter Murine models of chronic Pseudomonasaeruginosa lung infection Lab Anim 36 (2002) 291ndash312
[111] A Bragonzi D Worlitzsch GB Pier P Timpert M Ulrich M Hentzer JB Ander-sen M Givskov M Conese G Doring Nonmucoid Pseudomonas aeruginosa ex-presses alginate in the lungs of patients with cystic fibrosis and in a mousemodel J Infect Dis 192 (2005) 410ndash419
[112] GS CW Bedrossian DB Singer JJ Hansen HS Rosenberg The lung in cysticfibrosis A quantitative study including prevalence of pathologic findingsamong different age groups Hum Pathol 7 (1976) 195ndash204
[113] WD HA Cash B McCullough WG Johanson Jr JA Bass A rat model of chron-ic respiratory infection with Pseudomonas aeruginosa Am Rev Respir Dis 119(1979) 453ndash459
[114] EM JR Starke C Langston CJ Baker A mouse model of chronic pulmonary in-fection with Pseudomonas aeruginosa and Pseudomonas cepacia Pediatr Res 22(1987) 698ndash702
[115] TJ AM van Heeckeren RW Walenga MW Konstan PB Davis B ErokwuMA Haxhiu TW Ferkol Effect of Pseudomonas infection on weight loss lung
710 F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
mechanics and cytokines in mice Am J Respir Crit Care Med 161 (2000)271ndash279
[116] T Aw G Wierzbicka DP Jones Oral glutathione increases tissue glutathione invivo Chem Biol Interact 80 (1991) 89ndash97
[117] F Favilli P Marraccini T Iantomasi MT Vincenzini Effect of orally adminis-tered glutathione on glutathione levels in some organs of rats role of specifictransporters Br J Nutr 78 (1997) 293ndash300
[118] C Kariya H Leitner E Min C van Heeckeren A van Heeckeren BJ Day A rolefor CFTR in the elevation of glutathione levels in the lung by oral glutathione ad-ministration Am J Physiol Lung Cell Mol Physiol 292 (2007) L1590ndashL1597
[119] K Atkuri JJ Mantovani LA Herzenberg LA Herzenberg N-Acetylcysteinemdashasafe antidote for cysteineglutathione deficiency Curr Opin Pharmacol 7(2007) 355ndash359
[120] R De Lisle E Roach K Jansson Effects of laxative and N-acetylcysteine onmucus accumulation bacterial load transit and inflammation in the cystic fi-brosis mouse small intestine Am J Physiol Gastrointest Liver Physiol 293(2007) G577ndashG584
[121] A Luciani VR Villella S Esposito N Brunetti-Pierri D Medina C Settembre MGavina L Pulze I Giardino M Pettoello-Mantovani M DApolito S Guido EMasliah B Spencer S Quaratino V Raia A Ballabio L Maiuri Defective CFTRinduces aggresome formation and lung inflammation in cystic fibrosis throughROS-mediated autophagy inhibition Nat Cell Biol 12 863ndash875
[122] M Griese J Ramakers A Krasselt V Starosta S Van Koningsbruggen R FischerF Ratjen B Mullinger RM Huber K Maier E Rietschel G Scheuch Improve-ment of alveolar glutathione and lung function but not oxidative state in cysticfibrosis Am J Respir Crit Care Med 169 (2004) 822ndash828
[123] C Bishop VM Hudson SC Hilton C Wilde A pilot study of the effect of inhaledbuffered reduced glutathione on the clinical status of patients with cystic fibro-sis Chest 127 (2005) 308ndash317
[124] WWang C Oliva G Li A Holmgren CH Lillig KL Kirk Reversible silencing of CFTRchloride channels by glutathionylation J Gen Physiol 125 (2005) 127ndash141
[125] N Dauletbaev P Fischer B Aulbach J Gross W Kusche U Thyroff-FriesingerTO Wagner J Bargon A phase II study on safety and efficacy of high-dose N-acetylcysteine in patients with cystic fibrosis Eur J Med Res 14 (2009)352ndash358
[126] R Tirouvanziam Y Gernez CK Conrad RB Moss I Schrijver CE Dunn ZADavies LA Herzenberg Profound functional and signaling changes in viable in-flammatory neutrophils homing to cystic fibrosis airways Proc Natl Acad SciU S A 105 (2008) 4335ndash4339
[127] JH Roum Z Borok NG McElvaney GJ Grimes AD Bokser R Buhl RG Crys-tal Glutathione aerosol suppresses lung epithelial surface inflammatory cell-derived oxidants in cystic fibrosis J Appl Physiol 87 (1999) 438ndash443
[128] A Visca CT Bishop SC Hilton VM Hudson Improvement in clinical markersin CF patients using a reduced glutathione regimen an uncontrolled observa-tional study J Cyst Fibros 7 (2008) 433ndash436
[129] EF Nash A Stephenson F Ratjen E Tullis Nebulized and oral thiol derivativesfor pulmonary disease in cystic fibrosis Cochrane Database Syst Rev (2009)CD007168
[130] AC foundation Drug Development Pipeline 2011[131] S Hoshida T Kuzuya N Yamashita M Nishida S Kitahara M Hori T
Kamada M Tada Gamma-glutamylcysteine ethyl ester for myocardial protec-tion in dogs during ischemia and reperfusion J Am Coll Cardiol 24 (1994)1391ndash1397
[132] J Lok W Leung S Zhao S Pallast K van Leyen S Guo X Wang A Yalcin EHLo Gamma-glutamylcysteine ethyl ester protects cerebral endothelial cells dur-ing injury and decreases bloodndashbrain barrier permeability after experimentalbrain trauma J Neurochem 118 (2011) 248ndash255
[133] Z Borok R Buhl GJ Grimes AD Bokser RC Hubbard KJ Holroyd JH RoumDB Czerski AM Cantin RG Crystal Effect of glutathione aerosol on oxidantndashantioxidant imbalance in idiopathic pulmonary fibrosis Lancet 338 (1991)215ndash216
[134] KJ Holroyd R Buhl Z Borok JH Roum AD Bokser GJ Grimes D Czerski AMCantin RG Crystal Correction of glutathione deficiency in the lower respiratorytract of HIV seropositive individuals by glutathione aerosol treatment Thorax 48(1993) 985ndash989
[135] J Hull P Vervaart K Grimwood P Phelan Pulmonary oxidative stress responsein young children with cystic fibrosis Thorax 52 (1997) 557ndash560
[136] A Corti A Paolicchi M Franzini S Dominici AF Casini A Pompella The S-thiolating activity of membrane gamma-glutamyltransferase formation ofcysteinyl-glycine mixed disulfides with cellular proteins and in the cell microen-vironment Antioxid Redox Signal 7 (2005) 911ndash918
[137] A Corti M Franzini AF Casini A Paolicchi A Pompella Vitamin C supply tobronchial epithelial cells linked to glutathione availability in elfmdasha role for se-creted gamma-glutamyltransferase J Cyst Fibros 7 (2008) 174ndash178
[138] A Munck Nutritional considerations in patients with cystic fibrosis Expert RevRespir Med 4 (2010) 47ndash56
[139] JL Matel CE Milla Nutrition in cystic fibrosis Semin Respir Crit Care Med 30(2009) 579ndash586
[140] D Salvatore R Buzzetti E Baldo MP Forneris V Lucidi D Manunza IMarinelli B Messore AS Neri V Raia ML Furnari G Mastella An overviewof international literature from cystic fibrosis registries 2 Neonatal screeningand nutritiongrowth J Cyst Fibros 9 (2010) 75ndash83
[141] KF Joosten JM Hulst Malnutrition in pediatric hospital patients current is-sues Nutrition 27 (2011) 133ndash137
[142] S Fustik T Jacovska L Spirevska S Koceva Protein-energy malnutrition as thefirst manifestation of cystic fibrosis in infancy Pediatr Int 51 (2009) 678ndash683
[143] J Himmelfarb E McMonagle Albumin is the major plasma protein target of ox-idant stress in uremia Kidney Int 60 (2001) 358ndash363
[144] P Stenvinkel JJ Carrero J Axelsson B Lindholm O Heimburger Z MassyEmerging biomarkers for evaluating cardiovascular risk in the chronic kidneydisease patient how do new pieces fit into the uremic puzzle Clin J Am SocNephrol 3 (2008) 505ndash521
[145] M Roche P Rondeau NR Singh E Tarnus E Bourdon The antioxidant proper-ties of serum albumin FEBS Lett 582 (2008) 1783ndash1787
[146] D Giustarini A Milzani I Dalle-Donne R Rossi Red blood cells as a physiolog-ical source of glutathione for extracellular fluids Blood Cells Mol Dis 40 (2008)174ndash179
[147] A Meister ME Anderson Glutathione Annu Rev Biochem 52 (1983) 711ndash760[148] B Alvarez S Carballal L Turell R Radi Formation and reactions of sulfenic acid
in human serum albumin Methods Enzymol 473 (2010) 117ndash136[149] S Carballal B Alvarez L Turell H Botti BA Freeman R Radi Sulfenic acid in
human serum albumin Amino Acids 32 (2007) 543ndash551[150] LR Barclay AM Bailey D Kong The antioxidant activity of alpha-tocopherol-
bovine serum albumin complex in micellar and liposome autoxidations J BiolChem 260 (1985) 15809ndash15814
[151] T Ishii T Ichikawa K Minoda K Kusaka S Ito Y Suzuki M Akagawa K Mochi-zuki T Goda T Nakayama Human serum albumin as an antioxidant in the ox-idation of (minus)-epigallocatechin gallate participation of reversible covalentbinding for interaction and stabilization Biosci Biotechnol Biochem 75(2011) 100ndash106
[152] F Galli S Rovidati S Benedetti U Buoncristiani C Covarelli A Floridi F Canes-trari Overexpression of erythrocyte glutathione S-transferase in uremia and di-alysis Clin Chem 45 (1999) 1781ndash1788
[153] D Borowitz RD Baker V Stallings Consensus report on nutrition for pediat-ric patients with cystic fibrosis J Pediatr Gastroenterol Nutr 35 (2002)246ndash259
[154] LJ Filer Jr SW Wright MP Manning KE Mason Absorption of alpha-tocopherol and tocopherylesters by premature and full term infants and chil-dren in health and disease Pediatrics 8 (1951) 328ndash339
[155] L Lancellotti C DOrazio G Mastella G Mazzi U Lippi Deficiency of vitamins Eand A in cystic fibrosis is independent of pancreatic function and current en-zyme and vitamin supplementation Eur J Pediatr 155 (1996) 281ndash285
[156] MN Sathe AS Patel Update in pediatrics focus on fat-soluble vitamins NutrClin Pract 25 (2010) 340ndash346
[157] MG Traber The ABCs of vitamin E and beta-carotene absorption Am J ClinNutr 80 (2004) 3ndash4
[158] TF Dolan Jr Hemolytic anemia and edema as the initial signs in infants withcystic fibrosis Consider this diagnosis even in absence of pulmonary symptomsClin Pediatr 15 (1976) 597ndash600
[159] DR James M Alfaham MC Goodchild Increased susceptibility to peroxide-induced haemolysis with normal vitamin E concentrations in cystic fibrosisClin Chim Acta 204 (1991) 279ndash290
[160] SA Peters FJ Kelly Vitamin E supplementation in cystic fibrosis J Pediatr Gas-troenterol Nutr 22 (1996) 341ndash345
[161] A Maqbool VA Stallings Update on fat-soluble vitamins in cystic fibrosis CurrOpin Pulm Med 14 (2008) 574ndash581
[162] SD Sagel MK Sontag MM Anthony P Emmett KA Papas Effect of anantioxidant-rich multivitamin supplement in cystic fibrosis J Cyst Fibros 10(2011) 31ndash36
[163] F Galli A Azzi Present trends in vitamin E research Biofactors 36 (2010)33ndash42
[164] A Hamahata P Enkhbaatar ER Kraft M Lange SW Leonard MG Traber RACox FC Schmalstieg HK Hawkins EB Whorton EM Horvath C Szabo LDTraber DN Herndon DL Traber Gamma-tocopherol nebulization by a lipidaerosolization device improves pulmonary function in sheep with burn andsmoke inhalation injury Free Radic Biol Med 45 (2008) 425ndash433
[165] JP Anais N Razzouq M Carvalho C Fernandez A Astier M Paul A AstierH Fessi AM Lorino Development of alpha-tocopherol acetate nanoparti-cles influence of preparative processes Drug Dev Ind Pharm 35 (2009)216ndash223
[166] JM Zingg Molecular and cellular activities of vitamin E analogues Mini RevMed Chem 7 (2007) 543ndash558
[167] V Viola F Pilolli M Piroddi E Pierpaoli F Orlando M Provinciali M Betti FMazzini F Galli Why tocotrienols work better insights into the in vitro anti-cancer mechanism of vitamin E Genes Nutr 7 (2011) 29ndash41
[168] F Galli F Mazzini L Bamonti L Gille S Bohmdorfer M Piroddi T Netscher FJKelly T Rosenau Tocotrienamines and tocopheramines reactions with radicalsand metal ions Bioorg Med Chem 19 (2011) 6483ndash6491
[169] A Kuhad K Chopra Attenuation of diabetic nephropathy by tocotrienol in-volvement of NFκB signaling pathway Life Sci 84 (2009) 296ndash301
[170] Q Jiang X Yin MA Lill ML Danielson H Freiser J Huang Long-chain carbox-ychromanols metabolites of vitamin E are potent inhibitors of cyclooxygenasesProc Natl Acad Sci U S A 105 (2008) 20464ndash20469
[171] ER Miller III R Pastor-Barriuso D Dalal RA Riemersma LJ Appel E GuallarMeta-analysis high-dosage vitamin E supplementation may increase all-causemortality Ann Intern Med 142 (2005) 37ndash46
[172] JN Hathcock A Azzi J Blumberg T Bray A Dickinson B Frei I Jialal CSJohnston FJ Kelly K Kraemer L Packer S Parthasarathy H Sies MG TraberVitamins E and C are safe across a broad range of intakes Am J Clin Nutr 81(2005) 736ndash745
[173] R Brigelius-Flohe F Galli Vitamin E a vitamin still awaiting the detection of itsbiological function Mol Nutr Food Res 54 (2010) 583ndash587
711F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
[174] MG Traber B Frei JS Beckman Vitamin E revisited do new data validate ben-efits for chronic disease prevention Curr Opin Lipidol 19 (2008) 30ndash38
[175] F Galli Meeting report Vitamin E Satellite Symposium (VESS) associated to theAnnual Meeting of the SFRR-Europe Rome 26 August 2009 Free Radic Res 43(2009) 1256ndash1257
[176] LJ Roberts II JA Oates MF Linton S Fazio BP Meador MD Gross Y Shyr JDMorrow The relationship between dose of vitamin E and suppression of oxida-tive stress in humans Free Radic Biol Med 43 (2007) 1388ndash1393
[177] EFSA- EFSA Scientific Opinion of the Panel on Food Additives FlavouringsProcessing Aids and Materials in Contact with Food on a request from the Com-mission on mixed tocopherols tocotrienol tocopherol and tocotrienols assources for vitamin E in EFSA- EFSA (Ed) vol 640 The EFSA Journal2008 pp 1ndash34
[178] P Rust I Eichler S Renner I Elmadfa Long-term oral beta-carotene supple-mentation in patients with cystic fibrosis mdash effects on antioxidative status andpulmonary function Ann Nutr Metab 44 (2000) 30ndash37
[179] G Lepage J Champagne N Ronco A Lamarre I Osberg RJ Sokol CC Roy Sup-plementation with carotenoids corrects increased lipid peroxidation in childrenwith cystic fibrosis Am J Clin Nutr 64 (1996) 87ndash93
[180] BM Winklhofer-Roob H Puhl G Khoschsorur MA vant Hof H EsterbauerDH Shmerling Enhanced resistance to oxidation of low density lipoproteinsand decreased lipid peroxide formation during beta-carotene supplementationin cystic fibrosis Free Radic Biol Med 18 (1995) 849ndash859
[181] RC Graham-Maar JI Schall N Stettler BS Zemel VA Stallings Elevated vita-min A intake and serum retinol in preadolescent children with cystic fibrosisAm J Clin Nutr 84 (2006) 174ndash182
[182] I Sadowska-Woda M Rachel J Pazdan E Bieszczad-Bedrejczuk K PawliszakNutritional supplement attenuates selected oxidative stress markers in pediatricpatients with cystic fibrosis Nutr Res (New York NY) 31 (2011) 509ndash518
[183] KA Papas MK Sontag C Pardee RJ Sokol SD Sagel FJ Accurso JS WagenerA pilot study on the safety and efficacy of a novel antioxidant rich formulation inpatients with cystic fibrosis J Cyst Fibros 7 (2008) 60ndash67
[184] Y Saito A Fukuhara K Nishio M Hayakawa Y Ogawa H Sakamoto K Fujii YYoshida E Niki Characterization of cellular uptake and distribution of coen-zyme Q10 and vitamin E in PC12 cells J Nutr Biochem 20 (2009) 350ndash357
[185] AA Franke CM Morrison JL Bakke LJ Custer X Li RV Cooney CoenzymeQ10 in human blood native levels and determinants of oxidation during proces-sing and storage Free Radic Biol Med 48 (2010) 1610ndash1617
[186] HN Bhagavan RK Chopra Plasma coenzyme Q10 response to oral ingestion ofcoenzyme Q10 formulations Mitochondrion 7 (2007) S78ndashS88 (Suppl)
[187] HN Bhagavan RK Chopra Coenzyme Q10 absorption tissue uptake metabo-lism and pharmacokinetics Free Radic Res 40 (2006) 445ndash453
[188] F Galli R Lee C Dunster FJ Kelly Gas chromatography mass spectrometryanalysis of carboxyethyl-hydroxychroman metabolites of alpha- and gamma-tocopherol in human plasma Free Radic Biol Med 32 (2002) 333ndash340
[189] F Galli R Lee J Atkinson A Floridi FJ Kelly Gamma-tocopherol biokineticsand transformation in humans Free Radic Res 37 (2003) 1225ndash1233
[190] TA Laguna MK Sontag I Osberg JS Wagener FJ Accurso RJ Sokol De-creased total serum coenzyme-Q10 concentrations a longitudinal study in chil-dren with cystic fibrosis J Pediatr 153 (2008) 402ndash407
[191] T Frischer JK Myung G Maurer I Eichler Z Szepfalusi G Lubec Possible dys-regulation of chaperon and metabolic proteins in cystic fibrosis bronchial tissueProteomics 6 (2006) 3381ndash3388
[192] C Andersson MM Zaman AB Jones SD Freedman Alterations in immune re-sponse and PPARLXR regulation in cystic fibrosis macrophages J Cyst Fibros 7(2008) 68ndash78
[193] SD Freedman PG Blanco MM Zaman JC Shea M Ollero IK Hopper DAWeed A Gelrud MM Regan M Laposata JG Alvarez BP OSullivan Associa-tion of cystic fibrosis with abnormalities in fatty acid metabolism N Engl JMed 350 (2004) 560ndash569
[194] S Van Biervliet G Vanbillemont JP Van Biervliet D Declercq E Robberecht AChristophe Relation between fatty acid composition and clinical status or geno-type in cystic fibrosis patients Ann Nutr Metab 51 (2007) 541ndash549
[195] SD Freedman MH Katz EM Parker M Laposata MY Urman JG AlvarezA membrane lipid imbalance plays a role in the phenotypic expression ofcystic fibrosis in cftr(minusminus) mice Proc Natl Acad Sci U S A 96 (1999)13995ndash14000
[196] S Van Biervliet S Vande Velde JP Van Biervliet E Robberecht The effect ofzinc supplements in cystic fibrosis patients Ann Nutr Metab 52 (2008)152ndash156
[197] WR Henderson Jr SJ Astley MM McCready P Kushmerick S Casey JWBecker BW Ramsey Oral absorption of omega-3 fatty acids in patients withcystic fibrosis who have pancreatic insufficiency and in healthy control subjectsJ Pediatr 124 (1994) 400ndash408
[198] I Durieu E Vericel D Guichardant H Roth JP Steghens J Drai RN JosserandE Fontaine M Lagarde G Bellon Fatty acids platelets and oxidative markersfollowing intravenous n-3 fatty acids administration in cystic fibrosis an openpilot observational study J Cyst Fibros 6 (2007) 320ndash326
[199] LG Wood DA Fitzgerald ML Garg Hypothesis vitamin E complements poly-unsaturated fatty acids in essential fatty acid deficiency in cystic fibrosis J AmColl Nutr 22 (2003) 253ndash257
[200] JD Lloyd-Still SB Johnson RT Holman Essential fatty acid status in cystic fi-brosis and the effects of safflower oil supplementation Am J Clin Nutr 34(1981) 1ndash7
[201] A Maqbool JI Schall JF Garcia-Espana BS Zemel B Strandvik VAStallings Serum linoleic acid status as a clinical indicator of essential fatty
acid status in children with cystic fibrosis J Pediatr Gastroenterol Nutr 47(2008) 635ndash644
[202] C Oliver N Jahnke Omega-3 fatty acids for cystic fibrosis Cochrane DatabaseSyst Rev (2011) CD002201
[203] B Strandvik E Gronowitz F Enlund T Martinsson J Wahlstrom Essential fattyacid deficiency in relation to genotype in patients with cystic fibrosis J Pediatr139 (2001) 650ndash655
[204] P Rise S Volpi C Colombo RF Padoan C DOrazio S Ghezzi PMelotti V BennatoC Agostoni BM Assael C Galli Whole blood fatty acid analysis with micromethodin cystic fibrosis and pulmonary disease J Cyst Fibros 9 (2010) 228ndash233
[205] H Cao K Gerhold JR Mayers MM Wiest SM Watkins GS Hotamisligil Iden-tification of a lipokine a lipid hormone linking adipose tissue to systemic me-tabolism Cell 134 (2008) 933ndash944
[206] RR Malapaka SK Khoo J Zhang JH Choi XE Zhou Y Xu Y Gong J Li ELYong MJ Chalmers L Chang JH Resau PR Griffin YE Chen HE Xu Iden-tification and mechanism of a ten carbon fatty acid as a modulating ligand ofperoxisome proliferator activated receptors J Biol Chem 287 (2012)183ndash195
[207] T Hara A Hirasawa A Ichimura I Kimura G Tsujimoto Free fatty acid recep-tors FFAR1 and GPR120 as novel therapeutic targets for metabolic disorders JPharm Sci 100 (2011) 3594ndash3601
[208] R Gupta P Rathi S Bradoo Lipase mediated upgradation of dietary fats andoils Crit Rev Food Sci Nutr 43 (2003) 635ndash644
[209] BH Jennings CC Akoh Lipase-catalyzed modification of rice bran oil to incor-porate capric acid J Agric Food Chem 48 (2000) 4439ndash4443
[210] J Hoeks M Mensink MK Hesselink K Ekroos P Schrauwen Long- andMedium-Chain Fatty Acids Induce Insulin Resistance to a Similar Extent inHumans Despite Marked Differences in Muscle Fat Accumulation J Clin Endo-crinol Metab 97 (2012) 208ndash216
[211] PJ Congden G Bruce MM Rothburn PC Clarke JM Littlewood J KelleherMS Losowsky Vitamin status in treated patients with cystic fibrosis ArchDis Child 56 (1981) 708ndash714
[212] BM Winklhofer-Roob H Ellemunter M Fruhwirth SE Schlegel-Haueter GKhoschsorur MA vant Hof DH Shmerling Plasma vitamin C concentrationsin patients with cystic fibrosis evidence of associations with lung inflammationAm J Clin Nutr 65 (1997) 1858ndash1866
[213] L Shamseer D Adams N Brown JA Johnson S Vohra Antioxidant micronutri-ents for lung disease in cystic fibrosis Cochrane Database Syst Rev (2010)CD007020
[214] C Santi S Santoro Electrophilic Selenium First edition Wiley-VCH VerlagGmbH amp Co KGaA 2012
[215] L Flohe S Toppo G Cozza F Ursini A comparison of thiol peroxidase mecha-nisms Antioxid Redox Signal 15 (2010) 763ndash780
[216] L Flohe JR Andreesen R Brigelius-Flohe M Maiorino F Ursini Selenium theelement of the moon in life on earth IUBMB Life 49 (2000) 411ndash420
[217] V Valdiglesias E Pasaro J Mendez B Laffon In vitro evaluation of seleniumgenotoxic cytotoxic and protective effects a review Arch Toxicol 84(2010) 337ndash351
[218] P Foucaud P Therond M Marchand F Brion JF Demelier J Navarro Seleniumand vitamin E in mucoviscidosis Arch Fr Pediatr 45 (1988) 383ndash386
[219] J Neve R Van Geffel M Hanocq L Molle Plasma and erythrocyte zinc copperand selenium in cystic fibrosis Acta Paediatr Scand 72 (1983) 437ndash440
[220] BM Winklhofer-Roob B Tiran PE Tuchschmid MA vant Hof DH ShmerlingEffects of pancreatic enzyme preparations on erythrocyte glutathione peroxi-dase activities and plasma selenium concentrations in cystic fibrosis FreeRadic Biol Med 25 (1998) 242ndash249
[221] JD Lloyd-Still HE Ganther Selenium and glutathione peroxidase levels in cys-tic fibrosis Pediatrics 65 (1980) 1010ndash1012
[222] D Tsavachidou TJ McDonnell S Wen X Wang F Vakar-Lopez LL Pisters CAPettaway CG Wood KA Do PF Thall C Stephens E Efstathiou R Taylor DGMenter P Troncoso SM Lippman CJ Logothetis J Kim Selenium and vitaminE cell type- and intervention-specific tissue effects in prostate cancer J NatlCancer Inst 101 (2009) 306ndash320
[223] IN Zelko TJ Mariani RJ Folz Superoxide dismutase multigene family acomparison of the CuZn-SOD (SOD1) Mn-SOD (SOD2) and EC-SOD (SOD3)gene structures evolution and expression Free Radic Biol Med 33 (2002)337ndash349
[224] RP Bowler JD Crapo Oxidative stress in airways is there a role for extracellu-lar superoxide dismutase Am J Respir Crit Care Med 166 (2002) S38ndashS43
[225] K Best K McCoy S Gemma RA Disilvestro Copper enzyme activities in cysticfibrosis before and after copper supplementation plus or minus zinc Metabo-lism 53 (2004) 37ndash41
[226] SS Percival GP Kauwell E Bowser M Wagner Altered copper status in adultmen with cystic fibrosis J Am Coll Nutr 18 (1999) 614ndash619
[227] NF Krebs JE Westcott TD Arnold BM Kluger FJ Accurso LV Miller KMHambidge Abnormalities in zinc homeostasis in young infants with cystic fibro-sis Pediatr Res 48 (2000) 256ndash261
[228] D Easley N Krebs M Jefferson L Miller J Erskine F Accurso KM HambidgeEffect of pancreatic enzymes on zinc absorption in cystic fibrosis J Pediatr Gas-troenterol Nutr 26 (1998) 136ndash139
[229] S Van Biervliet JP Van Biervliet E Robberecht Serum zinc in patients with cys-tic fibrosis at diagnosis and after one year of therapy Biol Trace Elem Res 112(2006) 205ndash211
[230] S Van Biervliet JP Van Biervliet S Vande Velde E Robberecht Serum zinc con-centrations in cystic fibrosis patients aged above 4 years a cross-sectional eval-uation Biol Trace Elem Res 119 (2007) 19ndash26
712 F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
[231] F Galli M Cristina Polidori W Stahl P Mecocci FJ Kelly Vitamin E biotransfor-mation in humans Vitam Horm 76 (2007) 263ndash280
[232] J Wiser NE Alexis Q Jiang W Wu C Robinette R Roubey DB Peden In vivogamma-tocopherol supplementation decreases systemic oxidative stress andcytokine responses of human monocytes in normal and asthmatic subjectsFree Radic Biol Med 45 (2008) 40ndash49
[233] JG Wagner Q Jiang JR Harkema B Illek DD Patel BN Ames DB PedenOzone enhancement of lower airway allergic inflammation is prevented bygamma-tocopherol Free Radic Biol Med 43 (2007) 1176ndash1188
[234] JT Harries DP Muller Absorption of different doses of fat soluble and watermiscible preparations of vitamin E in children with cystic fibrosis Arch DisChild 46 (1971) 341ndash344
[235] EI Back C Frindt E Ocenaskova D Nohr M Stern HK Biesalski Can changesin hydrophobicity increase the bioavailability of alpha-tocopherol Eur J Nutr45 (2006) 1ndash6
[236] SZ Nasr MH OLeary C Hillermeier Correction of vitamin E deficiency withfat-soluble versus water-miscible preparations of vitamin E in patients with cys-tic fibrosis J Pediatr 122 (1993) 810ndash812
[237] S Soltani-Frisk E Gronowitz H Andersson B Strandvik Water-miscibletocopherol is not superior to fat-soluble preparation for vitamin E absorptionin cystic fibrosis Acta Paediatr 90 (2001) 1112ndash1115
[238] K Papas J Kalbfleisch R Mohon Bioavailability of a novel water-soluble vi-tamin E formulation in malabsorbing patients Dig Dis Sci 52 (2007)347ndash352
[239] F Antonicelli M Parmentier EM Drost N Hirani I Rahman K Donaldson WMacNee Nacystelyn inhibits oxidant-mediated interleukin-8 expression andNF-kappaB nuclear binding in alveolar epithelial cells Free Radic Biol Med 32(2002) 492ndash502
[240] EM App D Baran I Dab A Malfroot M Coffiner F Vanderbist M King Dose-finding and 24-h monitoring for efficacy and safety of aerosolized Nacystelyn incystic fibrosis Eur Respir J 19 (2002) 294ndash302
[241] MG Traber How much vitamin E hellip Just enough Am J Clin Nutr 84 (2006)959ndash960
[242] JC McCann BN Ames Vitamin K an example of triage theory is micronu-trient inadequacy linked to diseases of aging Am J Clin Nutr 90 (2009)889ndash907
[243] M Fusaro G Crepaldi S Maggi F Galli A DAngelo L Calo S Giannini DMiozzo M Gallieni Vitamin K bone fractures and vascular calcifications inchronic kidney disease an important but poorly studied relationship J Endocri-nol Invest 34 (2010) 317ndash323
[244] JC McCann BN Ames Adaptive dysfunction of selenoproteins from the per-spective of the triage theory why modest selenium deficiency may increaserisk of diseases of aging FASEB J 25 (2011) 1793ndash1814
[245] R Apak K Guclu M Ozyurek B Bektas Oglu M Bener Cupric ion reducing an-tioxidant capacity assay for food antioxidants vitamins polyphenolics and fla-vonoids in food extracts Methods Mol Biol 477 (2008) 163ndash193
[246] F Galli Interactions of polyphenolic compounds with drug disposition and me-tabolism Curr Drug Metab 8 (2007) 830ndash838
[247] RL Prior X Wu K Schaich Standardized methods for the determination of an-tioxidant capacity and phenolics in foods and dietary supplements J Agric FoodChem 53 (2005) 4290ndash4302
[248] C Azbell S Zhang D Skinner J Fortenberry EJ Sorscher BA WoodworthHesperidin stimulates cystic fibrosis transmembrane conductance regulator-mediated chloride secretion and ciliary beat frequency in sinonasal epitheliumOtolaryngol Head Neck Surg 143 (2010) 397ndash404
[249] G Wegrzyn J Jakobkiewicz-Banecka M Gabig-Ciminska E Piotrowska M Nar-ajczyk A Kloska M Malinowska D Dziedzic I Golebiewska M Moskot AWegrzyn Genistein a natural isoflavone with a potential for treatment of ge-netic diseases Biochem Soc Trans 38 (2010) 695ndash701
[250] YC Yu H Miki Y Nakamura A Hanyuda Y Matsuzaki Y Abe M Yasui K Ta-naka TC Hwang SG Bompadre Y Sohma Curcumin and genistein additivelypotentiate G551D-CFTR J Cyst Fibros 10 (2011) 243ndash252
[251] B Illek H Fischer Flavonoids stimulate Cl conductance of human airway epithe-lium in vitro and in vivo Am J Physiol 275 (1998) L902ndashL910
[252] JL Kreindler Cystic fibrosis exploiting its genetic basis in the hunt for newtherapies Pharmacol Ther 125 (2010) 219ndash229
[253] B Illek L Zhang NC Lewis RB Moss JY Dong H Fischer Defective function ofthe cystic fibrosis-causing missense mutation G551D is recovered by genisteinAm J Physiol 277 (1999) C833ndashC839
[254] P Anandakumar S Kamaraj S Jagan G Ramakrishnan R Vinodhkumar TDevaki Capsaicin modulates pulmonary antioxidant defense system during ben-zo(a)pyrene-induced lung cancer in Swiss albinomice Phytother Res 22 (2008)529ndash533
[255] I Rahman Antioxidant therapeutic advances in COPD Ther Adv Respir Dis 2(2008) 351ndash374
[256] AW Boots H Li RP Schins R Duffin JW Heemskerk A Bast GR Haenen Thequercetin paradox Toxicol Appl Pharmacol 222 (2007) 89ndash96
[257] M Joskova S Franova V Sadlonova Acute bronchodilator effect of quercetin inexperimental allergic asthma Bratisl Lek Listy 112 (2011) 9ndash12
[258] HJ Park CM Lee ID Jung JS Lee YI Jeong JH Chang SH Chun MJ Kim IWChoi SC Ahn YK Shin SR Yeom YM Park Quercetin regulates Th1Th2 balancein a murine model of asthma Int Immunopharmacol 9 (2009) 261ndash267
[259] AP Rogerio A Kanashiro C Fontanari EV da Silva YM Lucisano-ValimEG Soares LH Faccioli Anti-inflammatory activity of quercetin and iso-quercitrin in experimental murine allergic asthma Inflamm Res 56 (2007)402ndash408
[260] M Muller Polyphenol cytotoxicity induced by the bacterial toxin pyocyaninrole of NQO1 Free Radic Biol Med 47 (2009) 84ndash91
[261] J Grassmann Terpenoids as plant antioxidants Vitam Horm 72 (2005)505ndash535
[262] P Allen Tea tree oil the science behind the antimicrobial hype Lancet 358(2001) 1245
[263] EC Dasenbrook W Checkley CA Merlo MW Konstan N Lechtzin MP BoyleAssociation between respiratory tract methicillin-resistant Staphylococcus aure-us and survival in cystic fibrosis JAMA 303 (2010) 2386ndash2392
[264] V Bezzerri M Borgatti E Nicolis I Lampronti MC Dechecchi I Mancini PRizzotti R Gambari G Cabrini Transcription factor oligodeoxynucleotides toNF-kappaB inhibit transcription of IL-8 in bronchial cells Am J Respir CellMol Biol 39 (2008) 86ndash96
[265] R Gambari M Borgatti V Bezzerri E Nicolis I Lampronti MC Dechecchi IMancini A Tamanini G Cabrini Decoy oligodeoxyribonucleotides and peptidenucleic acids-DNA chimeras targeting nuclear factor kappa-B inhibition of IL-8 gene expression in cystic fibrosis cells infected with Pseudomonas aeruginosaBiochem Pharmacol 80 (2010) 1887ndash1894
[266] M Adrian P Jeandet AC Douillet-Breuil L Tesson R Bessis Stilbene content ofmature Vitis vinifera berries in response to UV-C elicitation J Agric Food Chem48 (2000) 6103ndash6105
[267] B Paul I Masih J Deopujari C Charpentier Occurrence of resveratrol and pter-ostilbene in age-old darakchasava an ayurvedic medicine from India J Ethno-pharmacol 68 (1999) 71ndash76
[268] I Rahman Antioxidant therapies in COPD Int J Chron Obstruct Pulmon Dis 1(2006) 15ndash29
[269] M Lee S Kim OK Kwon SR Oh HK Lee K Ahn Anti-inflammatory and anti-asthmatic effects of resveratrol a polyphenolic stilbene in a mouse model ofallergic asthma Int Immunopharmacol 9 (2009) 418ndash424
[270] LG Wood PA Wark ML Garg Antioxidant and anti-inflammatory effectsof resveratrol in airway disease Antioxid Redox Signal 13 (2010)1535ndash1548
[271] KV Kiselev Perspectives for production and application of resveratrol ApplMicrobiol Biotechnol 90 (2011) 417ndash425
[272] M Shakibaei C Buhrmann A Mobasheri Resveratrol-mediated SIRT-1 interac-tions with p300 modulate receptor activator of NF-kappaB ligand (RANKL) acti-vation of NF-kappaB signaling and inhibit osteoclastogenesis in bone-derivedcells J Biol Chem 286 (2011) 11492ndash11505
[273] SF Zaidi K Ahmed T Yamamoto T Kondo K Usmanghani M Kadowaki TSugiyama Effect of resveratrol on Helicobacter pylori-induced interleukin-8 secre-tion reactive oxygen species generation and morphological changes in human gas-tric epithelial cells Biol Pharm Bull 32 (2009) 1931ndash1935
[274] JK Kundu YK Shin YJ Surh Resveratrol modulates phorbol ester-inducedpro-inflammatory signal transduction pathways in mouse skin in vivo NF-kappaB and AP-1 as prime targets Biochem Pharmacol 72 (2006)1506ndash1515
[275] NH Nam Naturally occurring NF-kappaB inhibitors Mini Rev Med Chem 6(2006) 945ndash951
[276] JM Smoliga JA Baur HA Hausenblas Resveratrol and healthmdasha comprehen-sive review of human clinical trials Mol Nutr Food Res 55 (2011) 1129ndash1141
[277] ME Juan M Maijo JM Planas Quantification of trans-resveratrol and itsmetabolites in rat plasma and tissues by HPLC J Pharm Biomed Anal 51(2010) 391ndash398
[278] JA Baur DA Sinclair Therapeutic potential of resveratrol the in vivo evidenceNat Rev 5 (2006) 493ndash506
[279] E Nicolis I Lampronti MC Dechecchi M Borgatti A Tamanini N Bianchi VBezzerri I Mancini MG Giri P Rizzotti R Gambari G Cabrini Pyrogallol anactive compound from the medicinal plant Emblica officinalis regulates expres-sion of pro-inflammatory genes in bronchial epithelial cells Int Immunophar-macol 8 (2008) 1672ndash1680
[280] E Nicolis I Lampronti MC Dechecchi M Borgatti A Tamanini V Bezzerri NBianchi M Mazzon I Mancini MG Giri P Rizzotti R Gambari G CabriniModulation of expression of IL-8 gene in bronchial epithelial cells by 5-methoxypsoralen Int Immunopharmacol 9 (2009) 1411ndash1422
[281] M Borgatti I Mancini N Bianchi A Guerrini I Lampronti D Rossi G SacchettiR Gambari Bergamot (Citrus bergamia Risso) fruit extracts and identified com-ponents alter expression of interleukin 8 gene in cystic fibrosis bronchial epithe-lial cell lines BMC Biochem 12 (2011) 15
[282] L Piccagli E Fabbri M Borgatti N Bianchi V Bezzerri I Mancini E Nicolis CMDechecchi I Lampronti G Cabrini R Gambari Virtual screening against p50NF-kappaB transcription factor for the identification of inhibitors of the NF-kappaB-DNA interaction and expression of NF-kappaB upregulated genesChemMedChem 4 (2009) 2024ndash2033
[283] L Piccagli M Borgatti E Nicolis N Bianchi I Mancini I Lampronti D VevaldiF DallAcqua G Cabrini R Gambari Virtual screening against nuclear factorkappaB (NF-kappaB) of a focus library identification of bioactive furocoumarinderivatives inhibiting NF-kappaB dependent biological functions involved incystic fibrosis Bioorg Med Chem 18 (2010) 8341ndash8349
[284] M Borgatti A Chilin L Piccagli I Lampronti N Bianchi I Mancini G Mar-zaro Da Francesco A Guiotto R Gambari Development of a novel furocou-marin derivative inhibiting NF-kappaB dependent biological functionsdesign synthesis and biological effects Eur J Med Chem 46 (2011)4870ndash4877
[285] E Georgy S Le Guellec L Vecellio E Fichant P Stordeur P Bordeau JP PerraudinFeasibility study of OSCN- and lactoferrin (Meveol) nebulization for cysticfibrosis JCyst Fibros 10 (2011) S18
713F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
[286] C Tidei M Piroddi F Galli C Santi Oxidation of thiols promoted by PhSeZnClTetrahedron Lett 53 (2012) 232ndash234
[287] L Semianrio-Vidal C van Hesuden G Mugesh ER Lazarowski Ebselen is a po-tent non-competitive inhibitor of extracellular nucleoside diphosphokinasePurinergic Signal 6 (2010) 383ndash391
[288] C ColussiMC Albertini S Coppola S Rovidati F Galli L Ghibelli H2O2-inducedblockof glycolysis as an active ADP-ribosylation reaction protecting cells from apoptosisFASEB J 14 (2000) 2266ndash2276
[289] H Xiao KL Parkin Induction of phase II enzyme activity by various seleniumcompounds Nutr Cancer 55 (2006) 210ndash223
[290] G Peluffo R Radi Biochemistry of protein tyrosine nitration in cardiovascularpathology Cardiovasc Res 75 (2007) 291ndash302
[291] B Alvarez R Radi Peroxynitrite reactivity with amino acids and proteinsAmino Acids 25 (2003) 295ndash311
[292] B Kamosinska MW Radomski M Duszyk A Radomski SF Man Nitric oxideactivates chloride currents in human lung epithelial cells Am J Physiol 272(1997) L1098ndashL1104
[293] L Chen RP Patel X Teng CA Bosworth JR Lancaster Jr S Matalon Mecha-nisms of cystic fibrosis transmembrane conductance regulator activation by S-nitrosoglutathione J Biol Chem 281 (2006) 9190ndash9199
[294] F Luchetti B CanonicoM BettiM Arcangeletti F PilolliM Piroddi L Canesi S PapaF Galli Melatonin signaling and cell protection function FASEB J 24 (2010)3603ndash3624
[295] MW Bengtsson G Jedstedt G Flemstrom Duodenal bicarbonate secretion inrats stimulation by intra-arterial and luminal guanylin and uroguanylin ActaPhysiol (Oxf) 191 (2007) 309ndash317
[296] CS Nelson JL Marino CN Allen Melatonin receptor potentiation of cyclic AMP andthe cystic fibrosis transmembrane conductance regulator ion channel J Pineal Res 26(1999) 113ndash121
[297] C de Castro-Silva VM de Bruin GM Cunha DM Nunes CAMedeiros PF de BruinMelatonin improves sleep and reduces nitrite in the exhaled breath condensate incystic fibrosismdasha randomized double-blind placebo-controlled study J Pineal Res48 (2010) 65ndash71
[298] I Hornyak E Pankotai L Kiss Z Lacza Current developments in the the-rapeutic potential of S-nitrosoglutathione an endogenous NO-donor mole-cule Curr Pharm Biotechnol (2011) Jan 11 [Epub ahead of print] - PMID21235457
[299] AH Snyder ME McPherson JF Hunt M Johnson JS Stamler B Gaston Acuteeffects of aerosolized S-nitrosoglutathione in cystic fibrosis Am J Respir CritCare Med 165 (2002) 922ndash926
709F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
[59] E Boncoeur VS Criq E Bonvin T Roque A Henrion-Caude DC Gruenert AClement J Jacquot O Tabary Oxidative stress induces extracellular signal-regulated kinase 12 mitogen-activated protein kinase in cystic fibrosis lung ep-ithelial cells potential mechanism for excessive IL-8 expression Int J BiochemCell Biol 40 (2008) 432ndash446
[60] B Fischer J Voynow Neutrophil elastase induces MUC5AC messenger RNA ex-pression by an oxidant-dependent mechanism Chest 117 (2000) 317Sndash320S
[61] B Rada P Gardina TG Myers TL Leto Reactive oxygen species mediate in-flammatory cytokine release and EGFR-dependent mucin secretion in airwayepithelial cells exposed to Pseudomonas pyocyanin Mucosal Immunol 4(2011) 158ndash171
[62] C Schwarzer H Fischer EJ Kim KJ Barber AD Mills MJ Kurth DC GruenertJH Suh TE Machen B Illek Oxidative stress caused by pyocyanin impairs CFTRClminus transport in human bronchial epithelial cells Free Radic Biol Med 45(2008) 1653ndash1662
[63] J Hull M South P Phelan K Grimwood Surfactant composition in infants andyoung children with cystic fibrosis Am J Respir Crit Care Med 156 (1997)161ndash165
[64] KC Meyer A Sharma R Brown M Weatherly FR Moya J Lewandoski JJZimmerman Function and composition of pulmonary surfactant andsurfactant-derived fatty acid profiles are altered in young adults with cystic fi-brosis Chest 118 (2000) 164ndash174
[65] MK Pulfer RC Murphy Formation of biologically active oxysterols during ozo-nolysis of cholesterol present in lung surfactant J Biol Chem 279 (2004)26331ndash26338
[66] V Starosta E Rietschel K Paul U Baumann M Griese Oxidative changes ofbronchoalveolar proteins in cystic fibrosis Chest 129 (2006) 431ndash437
[67] V Starosta M Griese Oxidative damage to surfactant protein D in pulmonarydiseases Free Radic Res 40 (2006) 419ndash425
[68] M Griese R Essl R Schmidt E Rietschel F Ratjen M Ballmann K Paul Pulmo-nary surfactant lung function and endobronchial inflammation in cystic fibro-sis Am J Respir Crit Care Med 170 (2004) 1000ndash1005
[69] M Griese R Essl R Schmidt M Ballmann K Paul E Rietschel F Ratjen Se-quential analysis of surfactant lung function and inflammation in cystic fibrosispatients Respir Res 6 (2005) 133
[70] LG Wood DA Fitzgerald PG Gibson DM Cooper ML Garg Increased plasmafatty acid concentrations after respiratory exacerbations are associated with el-evated oxidative stress in cystic fibrosis patients Am J Clin Nutr 75 (2002)668ndash675
[71] P Montuschi SA Kharitonov G Ciabattoni M Corradi L van Rensen DM Ged-des ME Hodson PJ Barnes Exhaled 8-isoprostane as a new non-invasive bio-marker of oxidative stress in cystic fibrosis Thorax 55 (2000) 205ndash209
[72] CE Collins P Quaggiotto L Wood EV OLoughlin RL Henry ML Garg Elevat-ed plasma levels of F2 alpha isoprostane in cystic fibrosis Lipids 34 (1999)551ndash556
[73] D Hartl V Starosta K Maier I Beck-Speier C Rebhan BF Becker P Latzin RFischer F Ratjen RM Huber E Rietschel S Krauss-Etschmann M Griese In-haled glutathione decreases PGE2 and increases lymphocytes in cystic fibrosislungs Free Radic Biol Med 39 (2005) 463ndash472
[74] GL Milne H Yin JD Morrow Human biochemistry of the isoprostane pathwayJ Biol Chem 283 (2008) 15533ndash15537
[75] G Ciabattoni G Davi M Collura L Iapichino F Pardo A Ganci R Romagnoli JMaclouf C Patrono In vivo lipid peroxidation and platelet activation in cystic fi-brosis Am J Respir Crit Care Med 162 (2000) 1195ndash1201
[76] C Garenc P Julien E Levy Oxysterols in biological systems the gastrointestinaltract liver vascular wall and central nervous system Free Radic Res 44 (2011)47ndash73
[77] AM Cantin SL North RC Hubbard RG Crystal Normal alveolar epithelial lin-ing fluid contains high levels of glutathione J Appl Physiol 63 (1987) 152ndash157
[78] R Tirouvanziam CK Conrad T Bottiglieri LA Herzenberg RB Moss High-dose oral N-acetylcysteine a glutathione prodrug modulates inflammation incystic fibrosis Proc Natl Acad Sci U S A 103 (2006) 4628ndash4633
[79] LW Velsor C Kariya R Kachadourian BJ Day Mitochondrial oxidative stressin the lungs of cystic fibrosis transmembrane conductance regulator proteinmutant mice Am J Respir Cell Mol Biol 35 (2006) 579ndash586
[80] M Kelly-Aubert S Trudel J Fritsch T Nguyen-Khoa M Baudouin-Legros SMoriceau L Jeanson F Djouadi C Matar M Conti M Ollero F Brouillard AEdelman GSH monoethyl ester rescues mitochondrial defects in cystic fibrosismodels Hum Mol Genet 20 (2011) 2745ndash2759
[81] P Ghezzi Role of glutathione in immunity and inflammation in the lung Int JGen Med 4 (2011) 105ndash113
[82] N Dauletbaev K Viel R Buhl TO Wagner J Bargon Glutathione and glutathi-one peroxidase in sputum samples of adult patients with cystic fibrosis J CystFibros 3 (2004) 119ndash124
[83] CE Cross A van der Vliet CA ONeill S Louie B Halliwell Oxidants antioxi-dants and respiratory tract lining fluids Environ Health Perspect 102 (Suppl10) (1994) 185ndash191
[84] K Takeyama K Dabbagh J Jeong Shim T Dao-Pick IF Ueki JA Nadel Oxida-tive stress causes mucin synthesis via transactivation of epidermal growth factorreceptor role of neutrophils J Immunol 164 (2000) 1546ndash1552
[85] N Ballatori SM Krance S Notenboom S Shi K Tieu CL Hammond Glutathi-one dysregulation and the etiology and progression of human diseases BiolChem 390 (2009) 191ndash214
[86] SR Soltaninassab KR Sekhar MJ Meredith ML Freeman Multi-faceted regu-lation of gamma-glutamylcysteine synthetase J Cell Physiol 182 (2000)163ndash170
[87] HR Lopez-Mirabal JR Winther Redox characteristics of the eukaryotic cytosolBiochim Biophys Acta 1783 (2008) 629ndash640
[88] C Hwang AJ Sinskey HF Lodish Oxidized redox state of glutathione in the en-doplasmic reticulum Science 257 (1992) 1496ndash1502
[89] M Murphy Mitochondrial thiols in antioxidant protection and redox signallingdistinct roles for glutathionylation and other thiol modifications AntioxidRedox Signal (2011) ahead of print doi101089ars20114289
[90] BJ Day AM van Heeckeren E Min LW Velsor Role for cystic fibrosis trans-membrane conductance regulator protein in a glutathione response to bronch-opulmonary Pseudomonas infection Infect Immun 72 (2004) 2045ndash2051
[91] Y Zhang K Duan Glutathione exhibits antibacterial activity and increases tetra-cycline efficacy against Pseudomonas aeruginosa Sci China C Life Sci 52 (2009)501ndash505
[92] VM Hudson New insights into the pathogenesis of cystic fibrosis pivotal roleof glutathione system dysfunction and implications for therapy Treat RespirMed 3 (2004) 353ndash363
[93] LW Velsor A van Heeckeren BJ Day Antioxidant imbalance in the lungs ofcystic fibrosis transmembrane conductance regulator protein mutant miceAm J Physiol Lung Cell Mol Physiol 281 (2001) L31ndashL38
[94] I Kogan M Ramjeesingh C Li JF Kidd Y Wang EM Leslie SP Cole CE BearCFTR directly mediates nucleotide-regulated glutathione flux EMBO J 22(2003) 1981ndash1989
[95] NS Gould S Gauthier CT Kariya E Min J Huang DJ Brian Hypertonic salineincreases lung epithelial lining fluid glutathione and thiocyanate two protectiveCFTR-dependent thiols against oxidative injury Respir Res 11 (2010) 119
[96] VT Vasu SJ de Cruz JS Houghton KA Hayakawa BM Morrissey CE CrossJP Eiserich Evaluation of thiol-based antioxidant therapeutics in cystic fibrosissputum focus on myeloperoxidase Free Radic Res 45 (2011) 165ndash176
[97] L Roussel G Martel J Berube S Rousseau P aeruginosa drives CXCL8 synthesisvia redundant toll-like receptors and NADPH oxidase in CFTRF508 airway epi-thelial cells J Cyst Fibros 10 (2011) 107ndash113
[98] GW Lau DJ Hassett H Ran F Kong The role of pyocyanin in Pseudomonas aer-uginosa infection Trends Mol Med 10 (2004) 599ndash606
[99] R Wilson DA Sykes D Watson A Rutman GW Taylor PJ Cole Measurementof Pseudomonas aeruginosa phenazine pigments in sputum and assessment oftheir contribution to sputum sol toxicity for respiratory epithelium InfectImmun 56 (1988) 2515ndash2517
[100] M Muller Pyocyanin induces oxidative stress in human endothelial cells andmodulates the glutathione redox cycle Free Radic Biol Med 33 (2002)1527ndash1533
[101] YQ OMalley KJ Reszka BE Britigan Direct oxidation of 2prime7prime-dichlorodihy-drofluorescein by pyocyanin and other redox-active compounds independentof reactive oxygen species production Free Radic Biol Med 36 (2004)90ndash100
[102] CC Caldwell Y Chen HS Goetzmann Y Hao MT Borchers DJ Hassett LRYoung D Mavrodi L Thomashow GW Lau Pseudomonas aeruginosa exotoxinpyocyanin causes cystic fibrosis airway pathogenesis Am J Pathol 175 (2009)2473ndash2488
[103] YQ OMalley KJ Reszka DR Spitz GM Denning BE Britigan Pseudomonasaeruginosa pyocyanin directly oxidizes glutathione and decreases its levels inairway epithelial cells Am J Physiol Lung Cell Mol Physiol 287 (2004)L94ndashL103
[104] M Muller Glutathione modulates the toxicity of but is not a biologically rele-vant reductant for the Pseudomonas aeruginosa redox toxin pyocyanin FreeRadic Biol Med 50 (2011) 971ndash977
[105] R Cheluvappa R Shimmon M Dawson SN Hilmer DG Le Couteur Reactionsof Pseudomonas aeruginosa pyocyanin with reduced glutathione Acta BiochimPol 55 (2008) 571ndash580
[106] JH Widdicombe Transgenic animals may help resolve a sticky situation in cys-tic fibrosis J Clin Invest 120 (2010) 3093ndash3096
[107] X Sun H Sui JT Fisher Z Yan X Liu HJ Cho NS Joo Y Zhang W Zhou Y YiJM Kinyon DC Lei-Butters MA Griffin P Naumann M Luo J Ascher KWang T Frana JJ Wine DK Meyerholz JF Engelhardt Disease phenotype ofa ferret CFTR-knockout model of cystic fibrosis J Clin Invest 120 (2010)3149ndash3160
[108] NS Joo HJ Cho M Khansaheb JJ Wine Hyposecretion of fluid from trachealsubmucosal glands of CFTR-deficient pigs J Clin Invest 120 (2010) 3161ndash3166
[109] A Bragonzi Murine models of acute and chronic lung infection with cystic fibro-sis pathogens IJMM 300 (2010) 584ndash593
[110] AM van Heeckeren MD Schluchter Murine models of chronic Pseudomonasaeruginosa lung infection Lab Anim 36 (2002) 291ndash312
[111] A Bragonzi D Worlitzsch GB Pier P Timpert M Ulrich M Hentzer JB Ander-sen M Givskov M Conese G Doring Nonmucoid Pseudomonas aeruginosa ex-presses alginate in the lungs of patients with cystic fibrosis and in a mousemodel J Infect Dis 192 (2005) 410ndash419
[112] GS CW Bedrossian DB Singer JJ Hansen HS Rosenberg The lung in cysticfibrosis A quantitative study including prevalence of pathologic findingsamong different age groups Hum Pathol 7 (1976) 195ndash204
[113] WD HA Cash B McCullough WG Johanson Jr JA Bass A rat model of chron-ic respiratory infection with Pseudomonas aeruginosa Am Rev Respir Dis 119(1979) 453ndash459
[114] EM JR Starke C Langston CJ Baker A mouse model of chronic pulmonary in-fection with Pseudomonas aeruginosa and Pseudomonas cepacia Pediatr Res 22(1987) 698ndash702
[115] TJ AM van Heeckeren RW Walenga MW Konstan PB Davis B ErokwuMA Haxhiu TW Ferkol Effect of Pseudomonas infection on weight loss lung
710 F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
mechanics and cytokines in mice Am J Respir Crit Care Med 161 (2000)271ndash279
[116] T Aw G Wierzbicka DP Jones Oral glutathione increases tissue glutathione invivo Chem Biol Interact 80 (1991) 89ndash97
[117] F Favilli P Marraccini T Iantomasi MT Vincenzini Effect of orally adminis-tered glutathione on glutathione levels in some organs of rats role of specifictransporters Br J Nutr 78 (1997) 293ndash300
[118] C Kariya H Leitner E Min C van Heeckeren A van Heeckeren BJ Day A rolefor CFTR in the elevation of glutathione levels in the lung by oral glutathione ad-ministration Am J Physiol Lung Cell Mol Physiol 292 (2007) L1590ndashL1597
[119] K Atkuri JJ Mantovani LA Herzenberg LA Herzenberg N-Acetylcysteinemdashasafe antidote for cysteineglutathione deficiency Curr Opin Pharmacol 7(2007) 355ndash359
[120] R De Lisle E Roach K Jansson Effects of laxative and N-acetylcysteine onmucus accumulation bacterial load transit and inflammation in the cystic fi-brosis mouse small intestine Am J Physiol Gastrointest Liver Physiol 293(2007) G577ndashG584
[121] A Luciani VR Villella S Esposito N Brunetti-Pierri D Medina C Settembre MGavina L Pulze I Giardino M Pettoello-Mantovani M DApolito S Guido EMasliah B Spencer S Quaratino V Raia A Ballabio L Maiuri Defective CFTRinduces aggresome formation and lung inflammation in cystic fibrosis throughROS-mediated autophagy inhibition Nat Cell Biol 12 863ndash875
[122] M Griese J Ramakers A Krasselt V Starosta S Van Koningsbruggen R FischerF Ratjen B Mullinger RM Huber K Maier E Rietschel G Scheuch Improve-ment of alveolar glutathione and lung function but not oxidative state in cysticfibrosis Am J Respir Crit Care Med 169 (2004) 822ndash828
[123] C Bishop VM Hudson SC Hilton C Wilde A pilot study of the effect of inhaledbuffered reduced glutathione on the clinical status of patients with cystic fibro-sis Chest 127 (2005) 308ndash317
[124] WWang C Oliva G Li A Holmgren CH Lillig KL Kirk Reversible silencing of CFTRchloride channels by glutathionylation J Gen Physiol 125 (2005) 127ndash141
[125] N Dauletbaev P Fischer B Aulbach J Gross W Kusche U Thyroff-FriesingerTO Wagner J Bargon A phase II study on safety and efficacy of high-dose N-acetylcysteine in patients with cystic fibrosis Eur J Med Res 14 (2009)352ndash358
[126] R Tirouvanziam Y Gernez CK Conrad RB Moss I Schrijver CE Dunn ZADavies LA Herzenberg Profound functional and signaling changes in viable in-flammatory neutrophils homing to cystic fibrosis airways Proc Natl Acad SciU S A 105 (2008) 4335ndash4339
[127] JH Roum Z Borok NG McElvaney GJ Grimes AD Bokser R Buhl RG Crys-tal Glutathione aerosol suppresses lung epithelial surface inflammatory cell-derived oxidants in cystic fibrosis J Appl Physiol 87 (1999) 438ndash443
[128] A Visca CT Bishop SC Hilton VM Hudson Improvement in clinical markersin CF patients using a reduced glutathione regimen an uncontrolled observa-tional study J Cyst Fibros 7 (2008) 433ndash436
[129] EF Nash A Stephenson F Ratjen E Tullis Nebulized and oral thiol derivativesfor pulmonary disease in cystic fibrosis Cochrane Database Syst Rev (2009)CD007168
[130] AC foundation Drug Development Pipeline 2011[131] S Hoshida T Kuzuya N Yamashita M Nishida S Kitahara M Hori T
Kamada M Tada Gamma-glutamylcysteine ethyl ester for myocardial protec-tion in dogs during ischemia and reperfusion J Am Coll Cardiol 24 (1994)1391ndash1397
[132] J Lok W Leung S Zhao S Pallast K van Leyen S Guo X Wang A Yalcin EHLo Gamma-glutamylcysteine ethyl ester protects cerebral endothelial cells dur-ing injury and decreases bloodndashbrain barrier permeability after experimentalbrain trauma J Neurochem 118 (2011) 248ndash255
[133] Z Borok R Buhl GJ Grimes AD Bokser RC Hubbard KJ Holroyd JH RoumDB Czerski AM Cantin RG Crystal Effect of glutathione aerosol on oxidantndashantioxidant imbalance in idiopathic pulmonary fibrosis Lancet 338 (1991)215ndash216
[134] KJ Holroyd R Buhl Z Borok JH Roum AD Bokser GJ Grimes D Czerski AMCantin RG Crystal Correction of glutathione deficiency in the lower respiratorytract of HIV seropositive individuals by glutathione aerosol treatment Thorax 48(1993) 985ndash989
[135] J Hull P Vervaart K Grimwood P Phelan Pulmonary oxidative stress responsein young children with cystic fibrosis Thorax 52 (1997) 557ndash560
[136] A Corti A Paolicchi M Franzini S Dominici AF Casini A Pompella The S-thiolating activity of membrane gamma-glutamyltransferase formation ofcysteinyl-glycine mixed disulfides with cellular proteins and in the cell microen-vironment Antioxid Redox Signal 7 (2005) 911ndash918
[137] A Corti M Franzini AF Casini A Paolicchi A Pompella Vitamin C supply tobronchial epithelial cells linked to glutathione availability in elfmdasha role for se-creted gamma-glutamyltransferase J Cyst Fibros 7 (2008) 174ndash178
[138] A Munck Nutritional considerations in patients with cystic fibrosis Expert RevRespir Med 4 (2010) 47ndash56
[139] JL Matel CE Milla Nutrition in cystic fibrosis Semin Respir Crit Care Med 30(2009) 579ndash586
[140] D Salvatore R Buzzetti E Baldo MP Forneris V Lucidi D Manunza IMarinelli B Messore AS Neri V Raia ML Furnari G Mastella An overviewof international literature from cystic fibrosis registries 2 Neonatal screeningand nutritiongrowth J Cyst Fibros 9 (2010) 75ndash83
[141] KF Joosten JM Hulst Malnutrition in pediatric hospital patients current is-sues Nutrition 27 (2011) 133ndash137
[142] S Fustik T Jacovska L Spirevska S Koceva Protein-energy malnutrition as thefirst manifestation of cystic fibrosis in infancy Pediatr Int 51 (2009) 678ndash683
[143] J Himmelfarb E McMonagle Albumin is the major plasma protein target of ox-idant stress in uremia Kidney Int 60 (2001) 358ndash363
[144] P Stenvinkel JJ Carrero J Axelsson B Lindholm O Heimburger Z MassyEmerging biomarkers for evaluating cardiovascular risk in the chronic kidneydisease patient how do new pieces fit into the uremic puzzle Clin J Am SocNephrol 3 (2008) 505ndash521
[145] M Roche P Rondeau NR Singh E Tarnus E Bourdon The antioxidant proper-ties of serum albumin FEBS Lett 582 (2008) 1783ndash1787
[146] D Giustarini A Milzani I Dalle-Donne R Rossi Red blood cells as a physiolog-ical source of glutathione for extracellular fluids Blood Cells Mol Dis 40 (2008)174ndash179
[147] A Meister ME Anderson Glutathione Annu Rev Biochem 52 (1983) 711ndash760[148] B Alvarez S Carballal L Turell R Radi Formation and reactions of sulfenic acid
in human serum albumin Methods Enzymol 473 (2010) 117ndash136[149] S Carballal B Alvarez L Turell H Botti BA Freeman R Radi Sulfenic acid in
human serum albumin Amino Acids 32 (2007) 543ndash551[150] LR Barclay AM Bailey D Kong The antioxidant activity of alpha-tocopherol-
bovine serum albumin complex in micellar and liposome autoxidations J BiolChem 260 (1985) 15809ndash15814
[151] T Ishii T Ichikawa K Minoda K Kusaka S Ito Y Suzuki M Akagawa K Mochi-zuki T Goda T Nakayama Human serum albumin as an antioxidant in the ox-idation of (minus)-epigallocatechin gallate participation of reversible covalentbinding for interaction and stabilization Biosci Biotechnol Biochem 75(2011) 100ndash106
[152] F Galli S Rovidati S Benedetti U Buoncristiani C Covarelli A Floridi F Canes-trari Overexpression of erythrocyte glutathione S-transferase in uremia and di-alysis Clin Chem 45 (1999) 1781ndash1788
[153] D Borowitz RD Baker V Stallings Consensus report on nutrition for pediat-ric patients with cystic fibrosis J Pediatr Gastroenterol Nutr 35 (2002)246ndash259
[154] LJ Filer Jr SW Wright MP Manning KE Mason Absorption of alpha-tocopherol and tocopherylesters by premature and full term infants and chil-dren in health and disease Pediatrics 8 (1951) 328ndash339
[155] L Lancellotti C DOrazio G Mastella G Mazzi U Lippi Deficiency of vitamins Eand A in cystic fibrosis is independent of pancreatic function and current en-zyme and vitamin supplementation Eur J Pediatr 155 (1996) 281ndash285
[156] MN Sathe AS Patel Update in pediatrics focus on fat-soluble vitamins NutrClin Pract 25 (2010) 340ndash346
[157] MG Traber The ABCs of vitamin E and beta-carotene absorption Am J ClinNutr 80 (2004) 3ndash4
[158] TF Dolan Jr Hemolytic anemia and edema as the initial signs in infants withcystic fibrosis Consider this diagnosis even in absence of pulmonary symptomsClin Pediatr 15 (1976) 597ndash600
[159] DR James M Alfaham MC Goodchild Increased susceptibility to peroxide-induced haemolysis with normal vitamin E concentrations in cystic fibrosisClin Chim Acta 204 (1991) 279ndash290
[160] SA Peters FJ Kelly Vitamin E supplementation in cystic fibrosis J Pediatr Gas-troenterol Nutr 22 (1996) 341ndash345
[161] A Maqbool VA Stallings Update on fat-soluble vitamins in cystic fibrosis CurrOpin Pulm Med 14 (2008) 574ndash581
[162] SD Sagel MK Sontag MM Anthony P Emmett KA Papas Effect of anantioxidant-rich multivitamin supplement in cystic fibrosis J Cyst Fibros 10(2011) 31ndash36
[163] F Galli A Azzi Present trends in vitamin E research Biofactors 36 (2010)33ndash42
[164] A Hamahata P Enkhbaatar ER Kraft M Lange SW Leonard MG Traber RACox FC Schmalstieg HK Hawkins EB Whorton EM Horvath C Szabo LDTraber DN Herndon DL Traber Gamma-tocopherol nebulization by a lipidaerosolization device improves pulmonary function in sheep with burn andsmoke inhalation injury Free Radic Biol Med 45 (2008) 425ndash433
[165] JP Anais N Razzouq M Carvalho C Fernandez A Astier M Paul A AstierH Fessi AM Lorino Development of alpha-tocopherol acetate nanoparti-cles influence of preparative processes Drug Dev Ind Pharm 35 (2009)216ndash223
[166] JM Zingg Molecular and cellular activities of vitamin E analogues Mini RevMed Chem 7 (2007) 543ndash558
[167] V Viola F Pilolli M Piroddi E Pierpaoli F Orlando M Provinciali M Betti FMazzini F Galli Why tocotrienols work better insights into the in vitro anti-cancer mechanism of vitamin E Genes Nutr 7 (2011) 29ndash41
[168] F Galli F Mazzini L Bamonti L Gille S Bohmdorfer M Piroddi T Netscher FJKelly T Rosenau Tocotrienamines and tocopheramines reactions with radicalsand metal ions Bioorg Med Chem 19 (2011) 6483ndash6491
[169] A Kuhad K Chopra Attenuation of diabetic nephropathy by tocotrienol in-volvement of NFκB signaling pathway Life Sci 84 (2009) 296ndash301
[170] Q Jiang X Yin MA Lill ML Danielson H Freiser J Huang Long-chain carbox-ychromanols metabolites of vitamin E are potent inhibitors of cyclooxygenasesProc Natl Acad Sci U S A 105 (2008) 20464ndash20469
[171] ER Miller III R Pastor-Barriuso D Dalal RA Riemersma LJ Appel E GuallarMeta-analysis high-dosage vitamin E supplementation may increase all-causemortality Ann Intern Med 142 (2005) 37ndash46
[172] JN Hathcock A Azzi J Blumberg T Bray A Dickinson B Frei I Jialal CSJohnston FJ Kelly K Kraemer L Packer S Parthasarathy H Sies MG TraberVitamins E and C are safe across a broad range of intakes Am J Clin Nutr 81(2005) 736ndash745
[173] R Brigelius-Flohe F Galli Vitamin E a vitamin still awaiting the detection of itsbiological function Mol Nutr Food Res 54 (2010) 583ndash587
711F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
[174] MG Traber B Frei JS Beckman Vitamin E revisited do new data validate ben-efits for chronic disease prevention Curr Opin Lipidol 19 (2008) 30ndash38
[175] F Galli Meeting report Vitamin E Satellite Symposium (VESS) associated to theAnnual Meeting of the SFRR-Europe Rome 26 August 2009 Free Radic Res 43(2009) 1256ndash1257
[176] LJ Roberts II JA Oates MF Linton S Fazio BP Meador MD Gross Y Shyr JDMorrow The relationship between dose of vitamin E and suppression of oxida-tive stress in humans Free Radic Biol Med 43 (2007) 1388ndash1393
[177] EFSA- EFSA Scientific Opinion of the Panel on Food Additives FlavouringsProcessing Aids and Materials in Contact with Food on a request from the Com-mission on mixed tocopherols tocotrienol tocopherol and tocotrienols assources for vitamin E in EFSA- EFSA (Ed) vol 640 The EFSA Journal2008 pp 1ndash34
[178] P Rust I Eichler S Renner I Elmadfa Long-term oral beta-carotene supple-mentation in patients with cystic fibrosis mdash effects on antioxidative status andpulmonary function Ann Nutr Metab 44 (2000) 30ndash37
[179] G Lepage J Champagne N Ronco A Lamarre I Osberg RJ Sokol CC Roy Sup-plementation with carotenoids corrects increased lipid peroxidation in childrenwith cystic fibrosis Am J Clin Nutr 64 (1996) 87ndash93
[180] BM Winklhofer-Roob H Puhl G Khoschsorur MA vant Hof H EsterbauerDH Shmerling Enhanced resistance to oxidation of low density lipoproteinsand decreased lipid peroxide formation during beta-carotene supplementationin cystic fibrosis Free Radic Biol Med 18 (1995) 849ndash859
[181] RC Graham-Maar JI Schall N Stettler BS Zemel VA Stallings Elevated vita-min A intake and serum retinol in preadolescent children with cystic fibrosisAm J Clin Nutr 84 (2006) 174ndash182
[182] I Sadowska-Woda M Rachel J Pazdan E Bieszczad-Bedrejczuk K PawliszakNutritional supplement attenuates selected oxidative stress markers in pediatricpatients with cystic fibrosis Nutr Res (New York NY) 31 (2011) 509ndash518
[183] KA Papas MK Sontag C Pardee RJ Sokol SD Sagel FJ Accurso JS WagenerA pilot study on the safety and efficacy of a novel antioxidant rich formulation inpatients with cystic fibrosis J Cyst Fibros 7 (2008) 60ndash67
[184] Y Saito A Fukuhara K Nishio M Hayakawa Y Ogawa H Sakamoto K Fujii YYoshida E Niki Characterization of cellular uptake and distribution of coen-zyme Q10 and vitamin E in PC12 cells J Nutr Biochem 20 (2009) 350ndash357
[185] AA Franke CM Morrison JL Bakke LJ Custer X Li RV Cooney CoenzymeQ10 in human blood native levels and determinants of oxidation during proces-sing and storage Free Radic Biol Med 48 (2010) 1610ndash1617
[186] HN Bhagavan RK Chopra Plasma coenzyme Q10 response to oral ingestion ofcoenzyme Q10 formulations Mitochondrion 7 (2007) S78ndashS88 (Suppl)
[187] HN Bhagavan RK Chopra Coenzyme Q10 absorption tissue uptake metabo-lism and pharmacokinetics Free Radic Res 40 (2006) 445ndash453
[188] F Galli R Lee C Dunster FJ Kelly Gas chromatography mass spectrometryanalysis of carboxyethyl-hydroxychroman metabolites of alpha- and gamma-tocopherol in human plasma Free Radic Biol Med 32 (2002) 333ndash340
[189] F Galli R Lee J Atkinson A Floridi FJ Kelly Gamma-tocopherol biokineticsand transformation in humans Free Radic Res 37 (2003) 1225ndash1233
[190] TA Laguna MK Sontag I Osberg JS Wagener FJ Accurso RJ Sokol De-creased total serum coenzyme-Q10 concentrations a longitudinal study in chil-dren with cystic fibrosis J Pediatr 153 (2008) 402ndash407
[191] T Frischer JK Myung G Maurer I Eichler Z Szepfalusi G Lubec Possible dys-regulation of chaperon and metabolic proteins in cystic fibrosis bronchial tissueProteomics 6 (2006) 3381ndash3388
[192] C Andersson MM Zaman AB Jones SD Freedman Alterations in immune re-sponse and PPARLXR regulation in cystic fibrosis macrophages J Cyst Fibros 7(2008) 68ndash78
[193] SD Freedman PG Blanco MM Zaman JC Shea M Ollero IK Hopper DAWeed A Gelrud MM Regan M Laposata JG Alvarez BP OSullivan Associa-tion of cystic fibrosis with abnormalities in fatty acid metabolism N Engl JMed 350 (2004) 560ndash569
[194] S Van Biervliet G Vanbillemont JP Van Biervliet D Declercq E Robberecht AChristophe Relation between fatty acid composition and clinical status or geno-type in cystic fibrosis patients Ann Nutr Metab 51 (2007) 541ndash549
[195] SD Freedman MH Katz EM Parker M Laposata MY Urman JG AlvarezA membrane lipid imbalance plays a role in the phenotypic expression ofcystic fibrosis in cftr(minusminus) mice Proc Natl Acad Sci U S A 96 (1999)13995ndash14000
[196] S Van Biervliet S Vande Velde JP Van Biervliet E Robberecht The effect ofzinc supplements in cystic fibrosis patients Ann Nutr Metab 52 (2008)152ndash156
[197] WR Henderson Jr SJ Astley MM McCready P Kushmerick S Casey JWBecker BW Ramsey Oral absorption of omega-3 fatty acids in patients withcystic fibrosis who have pancreatic insufficiency and in healthy control subjectsJ Pediatr 124 (1994) 400ndash408
[198] I Durieu E Vericel D Guichardant H Roth JP Steghens J Drai RN JosserandE Fontaine M Lagarde G Bellon Fatty acids platelets and oxidative markersfollowing intravenous n-3 fatty acids administration in cystic fibrosis an openpilot observational study J Cyst Fibros 6 (2007) 320ndash326
[199] LG Wood DA Fitzgerald ML Garg Hypothesis vitamin E complements poly-unsaturated fatty acids in essential fatty acid deficiency in cystic fibrosis J AmColl Nutr 22 (2003) 253ndash257
[200] JD Lloyd-Still SB Johnson RT Holman Essential fatty acid status in cystic fi-brosis and the effects of safflower oil supplementation Am J Clin Nutr 34(1981) 1ndash7
[201] A Maqbool JI Schall JF Garcia-Espana BS Zemel B Strandvik VAStallings Serum linoleic acid status as a clinical indicator of essential fatty
acid status in children with cystic fibrosis J Pediatr Gastroenterol Nutr 47(2008) 635ndash644
[202] C Oliver N Jahnke Omega-3 fatty acids for cystic fibrosis Cochrane DatabaseSyst Rev (2011) CD002201
[203] B Strandvik E Gronowitz F Enlund T Martinsson J Wahlstrom Essential fattyacid deficiency in relation to genotype in patients with cystic fibrosis J Pediatr139 (2001) 650ndash655
[204] P Rise S Volpi C Colombo RF Padoan C DOrazio S Ghezzi PMelotti V BennatoC Agostoni BM Assael C Galli Whole blood fatty acid analysis with micromethodin cystic fibrosis and pulmonary disease J Cyst Fibros 9 (2010) 228ndash233
[205] H Cao K Gerhold JR Mayers MM Wiest SM Watkins GS Hotamisligil Iden-tification of a lipokine a lipid hormone linking adipose tissue to systemic me-tabolism Cell 134 (2008) 933ndash944
[206] RR Malapaka SK Khoo J Zhang JH Choi XE Zhou Y Xu Y Gong J Li ELYong MJ Chalmers L Chang JH Resau PR Griffin YE Chen HE Xu Iden-tification and mechanism of a ten carbon fatty acid as a modulating ligand ofperoxisome proliferator activated receptors J Biol Chem 287 (2012)183ndash195
[207] T Hara A Hirasawa A Ichimura I Kimura G Tsujimoto Free fatty acid recep-tors FFAR1 and GPR120 as novel therapeutic targets for metabolic disorders JPharm Sci 100 (2011) 3594ndash3601
[208] R Gupta P Rathi S Bradoo Lipase mediated upgradation of dietary fats andoils Crit Rev Food Sci Nutr 43 (2003) 635ndash644
[209] BH Jennings CC Akoh Lipase-catalyzed modification of rice bran oil to incor-porate capric acid J Agric Food Chem 48 (2000) 4439ndash4443
[210] J Hoeks M Mensink MK Hesselink K Ekroos P Schrauwen Long- andMedium-Chain Fatty Acids Induce Insulin Resistance to a Similar Extent inHumans Despite Marked Differences in Muscle Fat Accumulation J Clin Endo-crinol Metab 97 (2012) 208ndash216
[211] PJ Congden G Bruce MM Rothburn PC Clarke JM Littlewood J KelleherMS Losowsky Vitamin status in treated patients with cystic fibrosis ArchDis Child 56 (1981) 708ndash714
[212] BM Winklhofer-Roob H Ellemunter M Fruhwirth SE Schlegel-Haueter GKhoschsorur MA vant Hof DH Shmerling Plasma vitamin C concentrationsin patients with cystic fibrosis evidence of associations with lung inflammationAm J Clin Nutr 65 (1997) 1858ndash1866
[213] L Shamseer D Adams N Brown JA Johnson S Vohra Antioxidant micronutri-ents for lung disease in cystic fibrosis Cochrane Database Syst Rev (2010)CD007020
[214] C Santi S Santoro Electrophilic Selenium First edition Wiley-VCH VerlagGmbH amp Co KGaA 2012
[215] L Flohe S Toppo G Cozza F Ursini A comparison of thiol peroxidase mecha-nisms Antioxid Redox Signal 15 (2010) 763ndash780
[216] L Flohe JR Andreesen R Brigelius-Flohe M Maiorino F Ursini Selenium theelement of the moon in life on earth IUBMB Life 49 (2000) 411ndash420
[217] V Valdiglesias E Pasaro J Mendez B Laffon In vitro evaluation of seleniumgenotoxic cytotoxic and protective effects a review Arch Toxicol 84(2010) 337ndash351
[218] P Foucaud P Therond M Marchand F Brion JF Demelier J Navarro Seleniumand vitamin E in mucoviscidosis Arch Fr Pediatr 45 (1988) 383ndash386
[219] J Neve R Van Geffel M Hanocq L Molle Plasma and erythrocyte zinc copperand selenium in cystic fibrosis Acta Paediatr Scand 72 (1983) 437ndash440
[220] BM Winklhofer-Roob B Tiran PE Tuchschmid MA vant Hof DH ShmerlingEffects of pancreatic enzyme preparations on erythrocyte glutathione peroxi-dase activities and plasma selenium concentrations in cystic fibrosis FreeRadic Biol Med 25 (1998) 242ndash249
[221] JD Lloyd-Still HE Ganther Selenium and glutathione peroxidase levels in cys-tic fibrosis Pediatrics 65 (1980) 1010ndash1012
[222] D Tsavachidou TJ McDonnell S Wen X Wang F Vakar-Lopez LL Pisters CAPettaway CG Wood KA Do PF Thall C Stephens E Efstathiou R Taylor DGMenter P Troncoso SM Lippman CJ Logothetis J Kim Selenium and vitaminE cell type- and intervention-specific tissue effects in prostate cancer J NatlCancer Inst 101 (2009) 306ndash320
[223] IN Zelko TJ Mariani RJ Folz Superoxide dismutase multigene family acomparison of the CuZn-SOD (SOD1) Mn-SOD (SOD2) and EC-SOD (SOD3)gene structures evolution and expression Free Radic Biol Med 33 (2002)337ndash349
[224] RP Bowler JD Crapo Oxidative stress in airways is there a role for extracellu-lar superoxide dismutase Am J Respir Crit Care Med 166 (2002) S38ndashS43
[225] K Best K McCoy S Gemma RA Disilvestro Copper enzyme activities in cysticfibrosis before and after copper supplementation plus or minus zinc Metabo-lism 53 (2004) 37ndash41
[226] SS Percival GP Kauwell E Bowser M Wagner Altered copper status in adultmen with cystic fibrosis J Am Coll Nutr 18 (1999) 614ndash619
[227] NF Krebs JE Westcott TD Arnold BM Kluger FJ Accurso LV Miller KMHambidge Abnormalities in zinc homeostasis in young infants with cystic fibro-sis Pediatr Res 48 (2000) 256ndash261
[228] D Easley N Krebs M Jefferson L Miller J Erskine F Accurso KM HambidgeEffect of pancreatic enzymes on zinc absorption in cystic fibrosis J Pediatr Gas-troenterol Nutr 26 (1998) 136ndash139
[229] S Van Biervliet JP Van Biervliet E Robberecht Serum zinc in patients with cys-tic fibrosis at diagnosis and after one year of therapy Biol Trace Elem Res 112(2006) 205ndash211
[230] S Van Biervliet JP Van Biervliet S Vande Velde E Robberecht Serum zinc con-centrations in cystic fibrosis patients aged above 4 years a cross-sectional eval-uation Biol Trace Elem Res 119 (2007) 19ndash26
712 F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
[231] F Galli M Cristina Polidori W Stahl P Mecocci FJ Kelly Vitamin E biotransfor-mation in humans Vitam Horm 76 (2007) 263ndash280
[232] J Wiser NE Alexis Q Jiang W Wu C Robinette R Roubey DB Peden In vivogamma-tocopherol supplementation decreases systemic oxidative stress andcytokine responses of human monocytes in normal and asthmatic subjectsFree Radic Biol Med 45 (2008) 40ndash49
[233] JG Wagner Q Jiang JR Harkema B Illek DD Patel BN Ames DB PedenOzone enhancement of lower airway allergic inflammation is prevented bygamma-tocopherol Free Radic Biol Med 43 (2007) 1176ndash1188
[234] JT Harries DP Muller Absorption of different doses of fat soluble and watermiscible preparations of vitamin E in children with cystic fibrosis Arch DisChild 46 (1971) 341ndash344
[235] EI Back C Frindt E Ocenaskova D Nohr M Stern HK Biesalski Can changesin hydrophobicity increase the bioavailability of alpha-tocopherol Eur J Nutr45 (2006) 1ndash6
[236] SZ Nasr MH OLeary C Hillermeier Correction of vitamin E deficiency withfat-soluble versus water-miscible preparations of vitamin E in patients with cys-tic fibrosis J Pediatr 122 (1993) 810ndash812
[237] S Soltani-Frisk E Gronowitz H Andersson B Strandvik Water-miscibletocopherol is not superior to fat-soluble preparation for vitamin E absorptionin cystic fibrosis Acta Paediatr 90 (2001) 1112ndash1115
[238] K Papas J Kalbfleisch R Mohon Bioavailability of a novel water-soluble vi-tamin E formulation in malabsorbing patients Dig Dis Sci 52 (2007)347ndash352
[239] F Antonicelli M Parmentier EM Drost N Hirani I Rahman K Donaldson WMacNee Nacystelyn inhibits oxidant-mediated interleukin-8 expression andNF-kappaB nuclear binding in alveolar epithelial cells Free Radic Biol Med 32(2002) 492ndash502
[240] EM App D Baran I Dab A Malfroot M Coffiner F Vanderbist M King Dose-finding and 24-h monitoring for efficacy and safety of aerosolized Nacystelyn incystic fibrosis Eur Respir J 19 (2002) 294ndash302
[241] MG Traber How much vitamin E hellip Just enough Am J Clin Nutr 84 (2006)959ndash960
[242] JC McCann BN Ames Vitamin K an example of triage theory is micronu-trient inadequacy linked to diseases of aging Am J Clin Nutr 90 (2009)889ndash907
[243] M Fusaro G Crepaldi S Maggi F Galli A DAngelo L Calo S Giannini DMiozzo M Gallieni Vitamin K bone fractures and vascular calcifications inchronic kidney disease an important but poorly studied relationship J Endocri-nol Invest 34 (2010) 317ndash323
[244] JC McCann BN Ames Adaptive dysfunction of selenoproteins from the per-spective of the triage theory why modest selenium deficiency may increaserisk of diseases of aging FASEB J 25 (2011) 1793ndash1814
[245] R Apak K Guclu M Ozyurek B Bektas Oglu M Bener Cupric ion reducing an-tioxidant capacity assay for food antioxidants vitamins polyphenolics and fla-vonoids in food extracts Methods Mol Biol 477 (2008) 163ndash193
[246] F Galli Interactions of polyphenolic compounds with drug disposition and me-tabolism Curr Drug Metab 8 (2007) 830ndash838
[247] RL Prior X Wu K Schaich Standardized methods for the determination of an-tioxidant capacity and phenolics in foods and dietary supplements J Agric FoodChem 53 (2005) 4290ndash4302
[248] C Azbell S Zhang D Skinner J Fortenberry EJ Sorscher BA WoodworthHesperidin stimulates cystic fibrosis transmembrane conductance regulator-mediated chloride secretion and ciliary beat frequency in sinonasal epitheliumOtolaryngol Head Neck Surg 143 (2010) 397ndash404
[249] G Wegrzyn J Jakobkiewicz-Banecka M Gabig-Ciminska E Piotrowska M Nar-ajczyk A Kloska M Malinowska D Dziedzic I Golebiewska M Moskot AWegrzyn Genistein a natural isoflavone with a potential for treatment of ge-netic diseases Biochem Soc Trans 38 (2010) 695ndash701
[250] YC Yu H Miki Y Nakamura A Hanyuda Y Matsuzaki Y Abe M Yasui K Ta-naka TC Hwang SG Bompadre Y Sohma Curcumin and genistein additivelypotentiate G551D-CFTR J Cyst Fibros 10 (2011) 243ndash252
[251] B Illek H Fischer Flavonoids stimulate Cl conductance of human airway epithe-lium in vitro and in vivo Am J Physiol 275 (1998) L902ndashL910
[252] JL Kreindler Cystic fibrosis exploiting its genetic basis in the hunt for newtherapies Pharmacol Ther 125 (2010) 219ndash229
[253] B Illek L Zhang NC Lewis RB Moss JY Dong H Fischer Defective function ofthe cystic fibrosis-causing missense mutation G551D is recovered by genisteinAm J Physiol 277 (1999) C833ndashC839
[254] P Anandakumar S Kamaraj S Jagan G Ramakrishnan R Vinodhkumar TDevaki Capsaicin modulates pulmonary antioxidant defense system during ben-zo(a)pyrene-induced lung cancer in Swiss albinomice Phytother Res 22 (2008)529ndash533
[255] I Rahman Antioxidant therapeutic advances in COPD Ther Adv Respir Dis 2(2008) 351ndash374
[256] AW Boots H Li RP Schins R Duffin JW Heemskerk A Bast GR Haenen Thequercetin paradox Toxicol Appl Pharmacol 222 (2007) 89ndash96
[257] M Joskova S Franova V Sadlonova Acute bronchodilator effect of quercetin inexperimental allergic asthma Bratisl Lek Listy 112 (2011) 9ndash12
[258] HJ Park CM Lee ID Jung JS Lee YI Jeong JH Chang SH Chun MJ Kim IWChoi SC Ahn YK Shin SR Yeom YM Park Quercetin regulates Th1Th2 balancein a murine model of asthma Int Immunopharmacol 9 (2009) 261ndash267
[259] AP Rogerio A Kanashiro C Fontanari EV da Silva YM Lucisano-ValimEG Soares LH Faccioli Anti-inflammatory activity of quercetin and iso-quercitrin in experimental murine allergic asthma Inflamm Res 56 (2007)402ndash408
[260] M Muller Polyphenol cytotoxicity induced by the bacterial toxin pyocyaninrole of NQO1 Free Radic Biol Med 47 (2009) 84ndash91
[261] J Grassmann Terpenoids as plant antioxidants Vitam Horm 72 (2005)505ndash535
[262] P Allen Tea tree oil the science behind the antimicrobial hype Lancet 358(2001) 1245
[263] EC Dasenbrook W Checkley CA Merlo MW Konstan N Lechtzin MP BoyleAssociation between respiratory tract methicillin-resistant Staphylococcus aure-us and survival in cystic fibrosis JAMA 303 (2010) 2386ndash2392
[264] V Bezzerri M Borgatti E Nicolis I Lampronti MC Dechecchi I Mancini PRizzotti R Gambari G Cabrini Transcription factor oligodeoxynucleotides toNF-kappaB inhibit transcription of IL-8 in bronchial cells Am J Respir CellMol Biol 39 (2008) 86ndash96
[265] R Gambari M Borgatti V Bezzerri E Nicolis I Lampronti MC Dechecchi IMancini A Tamanini G Cabrini Decoy oligodeoxyribonucleotides and peptidenucleic acids-DNA chimeras targeting nuclear factor kappa-B inhibition of IL-8 gene expression in cystic fibrosis cells infected with Pseudomonas aeruginosaBiochem Pharmacol 80 (2010) 1887ndash1894
[266] M Adrian P Jeandet AC Douillet-Breuil L Tesson R Bessis Stilbene content ofmature Vitis vinifera berries in response to UV-C elicitation J Agric Food Chem48 (2000) 6103ndash6105
[267] B Paul I Masih J Deopujari C Charpentier Occurrence of resveratrol and pter-ostilbene in age-old darakchasava an ayurvedic medicine from India J Ethno-pharmacol 68 (1999) 71ndash76
[268] I Rahman Antioxidant therapies in COPD Int J Chron Obstruct Pulmon Dis 1(2006) 15ndash29
[269] M Lee S Kim OK Kwon SR Oh HK Lee K Ahn Anti-inflammatory and anti-asthmatic effects of resveratrol a polyphenolic stilbene in a mouse model ofallergic asthma Int Immunopharmacol 9 (2009) 418ndash424
[270] LG Wood PA Wark ML Garg Antioxidant and anti-inflammatory effectsof resveratrol in airway disease Antioxid Redox Signal 13 (2010)1535ndash1548
[271] KV Kiselev Perspectives for production and application of resveratrol ApplMicrobiol Biotechnol 90 (2011) 417ndash425
[272] M Shakibaei C Buhrmann A Mobasheri Resveratrol-mediated SIRT-1 interac-tions with p300 modulate receptor activator of NF-kappaB ligand (RANKL) acti-vation of NF-kappaB signaling and inhibit osteoclastogenesis in bone-derivedcells J Biol Chem 286 (2011) 11492ndash11505
[273] SF Zaidi K Ahmed T Yamamoto T Kondo K Usmanghani M Kadowaki TSugiyama Effect of resveratrol on Helicobacter pylori-induced interleukin-8 secre-tion reactive oxygen species generation and morphological changes in human gas-tric epithelial cells Biol Pharm Bull 32 (2009) 1931ndash1935
[274] JK Kundu YK Shin YJ Surh Resveratrol modulates phorbol ester-inducedpro-inflammatory signal transduction pathways in mouse skin in vivo NF-kappaB and AP-1 as prime targets Biochem Pharmacol 72 (2006)1506ndash1515
[275] NH Nam Naturally occurring NF-kappaB inhibitors Mini Rev Med Chem 6(2006) 945ndash951
[276] JM Smoliga JA Baur HA Hausenblas Resveratrol and healthmdasha comprehen-sive review of human clinical trials Mol Nutr Food Res 55 (2011) 1129ndash1141
[277] ME Juan M Maijo JM Planas Quantification of trans-resveratrol and itsmetabolites in rat plasma and tissues by HPLC J Pharm Biomed Anal 51(2010) 391ndash398
[278] JA Baur DA Sinclair Therapeutic potential of resveratrol the in vivo evidenceNat Rev 5 (2006) 493ndash506
[279] E Nicolis I Lampronti MC Dechecchi M Borgatti A Tamanini N Bianchi VBezzerri I Mancini MG Giri P Rizzotti R Gambari G Cabrini Pyrogallol anactive compound from the medicinal plant Emblica officinalis regulates expres-sion of pro-inflammatory genes in bronchial epithelial cells Int Immunophar-macol 8 (2008) 1672ndash1680
[280] E Nicolis I Lampronti MC Dechecchi M Borgatti A Tamanini V Bezzerri NBianchi M Mazzon I Mancini MG Giri P Rizzotti R Gambari G CabriniModulation of expression of IL-8 gene in bronchial epithelial cells by 5-methoxypsoralen Int Immunopharmacol 9 (2009) 1411ndash1422
[281] M Borgatti I Mancini N Bianchi A Guerrini I Lampronti D Rossi G SacchettiR Gambari Bergamot (Citrus bergamia Risso) fruit extracts and identified com-ponents alter expression of interleukin 8 gene in cystic fibrosis bronchial epithe-lial cell lines BMC Biochem 12 (2011) 15
[282] L Piccagli E Fabbri M Borgatti N Bianchi V Bezzerri I Mancini E Nicolis CMDechecchi I Lampronti G Cabrini R Gambari Virtual screening against p50NF-kappaB transcription factor for the identification of inhibitors of the NF-kappaB-DNA interaction and expression of NF-kappaB upregulated genesChemMedChem 4 (2009) 2024ndash2033
[283] L Piccagli M Borgatti E Nicolis N Bianchi I Mancini I Lampronti D VevaldiF DallAcqua G Cabrini R Gambari Virtual screening against nuclear factorkappaB (NF-kappaB) of a focus library identification of bioactive furocoumarinderivatives inhibiting NF-kappaB dependent biological functions involved incystic fibrosis Bioorg Med Chem 18 (2010) 8341ndash8349
[284] M Borgatti A Chilin L Piccagli I Lampronti N Bianchi I Mancini G Mar-zaro Da Francesco A Guiotto R Gambari Development of a novel furocou-marin derivative inhibiting NF-kappaB dependent biological functionsdesign synthesis and biological effects Eur J Med Chem 46 (2011)4870ndash4877
[285] E Georgy S Le Guellec L Vecellio E Fichant P Stordeur P Bordeau JP PerraudinFeasibility study of OSCN- and lactoferrin (Meveol) nebulization for cysticfibrosis JCyst Fibros 10 (2011) S18
713F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
[286] C Tidei M Piroddi F Galli C Santi Oxidation of thiols promoted by PhSeZnClTetrahedron Lett 53 (2012) 232ndash234
[287] L Semianrio-Vidal C van Hesuden G Mugesh ER Lazarowski Ebselen is a po-tent non-competitive inhibitor of extracellular nucleoside diphosphokinasePurinergic Signal 6 (2010) 383ndash391
[288] C ColussiMC Albertini S Coppola S Rovidati F Galli L Ghibelli H2O2-inducedblockof glycolysis as an active ADP-ribosylation reaction protecting cells from apoptosisFASEB J 14 (2000) 2266ndash2276
[289] H Xiao KL Parkin Induction of phase II enzyme activity by various seleniumcompounds Nutr Cancer 55 (2006) 210ndash223
[290] G Peluffo R Radi Biochemistry of protein tyrosine nitration in cardiovascularpathology Cardiovasc Res 75 (2007) 291ndash302
[291] B Alvarez R Radi Peroxynitrite reactivity with amino acids and proteinsAmino Acids 25 (2003) 295ndash311
[292] B Kamosinska MW Radomski M Duszyk A Radomski SF Man Nitric oxideactivates chloride currents in human lung epithelial cells Am J Physiol 272(1997) L1098ndashL1104
[293] L Chen RP Patel X Teng CA Bosworth JR Lancaster Jr S Matalon Mecha-nisms of cystic fibrosis transmembrane conductance regulator activation by S-nitrosoglutathione J Biol Chem 281 (2006) 9190ndash9199
[294] F Luchetti B CanonicoM BettiM Arcangeletti F PilolliM Piroddi L Canesi S PapaF Galli Melatonin signaling and cell protection function FASEB J 24 (2010)3603ndash3624
[295] MW Bengtsson G Jedstedt G Flemstrom Duodenal bicarbonate secretion inrats stimulation by intra-arterial and luminal guanylin and uroguanylin ActaPhysiol (Oxf) 191 (2007) 309ndash317
[296] CS Nelson JL Marino CN Allen Melatonin receptor potentiation of cyclic AMP andthe cystic fibrosis transmembrane conductance regulator ion channel J Pineal Res 26(1999) 113ndash121
[297] C de Castro-Silva VM de Bruin GM Cunha DM Nunes CAMedeiros PF de BruinMelatonin improves sleep and reduces nitrite in the exhaled breath condensate incystic fibrosismdasha randomized double-blind placebo-controlled study J Pineal Res48 (2010) 65ndash71
[298] I Hornyak E Pankotai L Kiss Z Lacza Current developments in the the-rapeutic potential of S-nitrosoglutathione an endogenous NO-donor mole-cule Curr Pharm Biotechnol (2011) Jan 11 [Epub ahead of print] - PMID21235457
[299] AH Snyder ME McPherson JF Hunt M Johnson JS Stamler B Gaston Acuteeffects of aerosolized S-nitrosoglutathione in cystic fibrosis Am J Respir CritCare Med 165 (2002) 922ndash926
710 F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
mechanics and cytokines in mice Am J Respir Crit Care Med 161 (2000)271ndash279
[116] T Aw G Wierzbicka DP Jones Oral glutathione increases tissue glutathione invivo Chem Biol Interact 80 (1991) 89ndash97
[117] F Favilli P Marraccini T Iantomasi MT Vincenzini Effect of orally adminis-tered glutathione on glutathione levels in some organs of rats role of specifictransporters Br J Nutr 78 (1997) 293ndash300
[118] C Kariya H Leitner E Min C van Heeckeren A van Heeckeren BJ Day A rolefor CFTR in the elevation of glutathione levels in the lung by oral glutathione ad-ministration Am J Physiol Lung Cell Mol Physiol 292 (2007) L1590ndashL1597
[119] K Atkuri JJ Mantovani LA Herzenberg LA Herzenberg N-Acetylcysteinemdashasafe antidote for cysteineglutathione deficiency Curr Opin Pharmacol 7(2007) 355ndash359
[120] R De Lisle E Roach K Jansson Effects of laxative and N-acetylcysteine onmucus accumulation bacterial load transit and inflammation in the cystic fi-brosis mouse small intestine Am J Physiol Gastrointest Liver Physiol 293(2007) G577ndashG584
[121] A Luciani VR Villella S Esposito N Brunetti-Pierri D Medina C Settembre MGavina L Pulze I Giardino M Pettoello-Mantovani M DApolito S Guido EMasliah B Spencer S Quaratino V Raia A Ballabio L Maiuri Defective CFTRinduces aggresome formation and lung inflammation in cystic fibrosis throughROS-mediated autophagy inhibition Nat Cell Biol 12 863ndash875
[122] M Griese J Ramakers A Krasselt V Starosta S Van Koningsbruggen R FischerF Ratjen B Mullinger RM Huber K Maier E Rietschel G Scheuch Improve-ment of alveolar glutathione and lung function but not oxidative state in cysticfibrosis Am J Respir Crit Care Med 169 (2004) 822ndash828
[123] C Bishop VM Hudson SC Hilton C Wilde A pilot study of the effect of inhaledbuffered reduced glutathione on the clinical status of patients with cystic fibro-sis Chest 127 (2005) 308ndash317
[124] WWang C Oliva G Li A Holmgren CH Lillig KL Kirk Reversible silencing of CFTRchloride channels by glutathionylation J Gen Physiol 125 (2005) 127ndash141
[125] N Dauletbaev P Fischer B Aulbach J Gross W Kusche U Thyroff-FriesingerTO Wagner J Bargon A phase II study on safety and efficacy of high-dose N-acetylcysteine in patients with cystic fibrosis Eur J Med Res 14 (2009)352ndash358
[126] R Tirouvanziam Y Gernez CK Conrad RB Moss I Schrijver CE Dunn ZADavies LA Herzenberg Profound functional and signaling changes in viable in-flammatory neutrophils homing to cystic fibrosis airways Proc Natl Acad SciU S A 105 (2008) 4335ndash4339
[127] JH Roum Z Borok NG McElvaney GJ Grimes AD Bokser R Buhl RG Crys-tal Glutathione aerosol suppresses lung epithelial surface inflammatory cell-derived oxidants in cystic fibrosis J Appl Physiol 87 (1999) 438ndash443
[128] A Visca CT Bishop SC Hilton VM Hudson Improvement in clinical markersin CF patients using a reduced glutathione regimen an uncontrolled observa-tional study J Cyst Fibros 7 (2008) 433ndash436
[129] EF Nash A Stephenson F Ratjen E Tullis Nebulized and oral thiol derivativesfor pulmonary disease in cystic fibrosis Cochrane Database Syst Rev (2009)CD007168
[130] AC foundation Drug Development Pipeline 2011[131] S Hoshida T Kuzuya N Yamashita M Nishida S Kitahara M Hori T
Kamada M Tada Gamma-glutamylcysteine ethyl ester for myocardial protec-tion in dogs during ischemia and reperfusion J Am Coll Cardiol 24 (1994)1391ndash1397
[132] J Lok W Leung S Zhao S Pallast K van Leyen S Guo X Wang A Yalcin EHLo Gamma-glutamylcysteine ethyl ester protects cerebral endothelial cells dur-ing injury and decreases bloodndashbrain barrier permeability after experimentalbrain trauma J Neurochem 118 (2011) 248ndash255
[133] Z Borok R Buhl GJ Grimes AD Bokser RC Hubbard KJ Holroyd JH RoumDB Czerski AM Cantin RG Crystal Effect of glutathione aerosol on oxidantndashantioxidant imbalance in idiopathic pulmonary fibrosis Lancet 338 (1991)215ndash216
[134] KJ Holroyd R Buhl Z Borok JH Roum AD Bokser GJ Grimes D Czerski AMCantin RG Crystal Correction of glutathione deficiency in the lower respiratorytract of HIV seropositive individuals by glutathione aerosol treatment Thorax 48(1993) 985ndash989
[135] J Hull P Vervaart K Grimwood P Phelan Pulmonary oxidative stress responsein young children with cystic fibrosis Thorax 52 (1997) 557ndash560
[136] A Corti A Paolicchi M Franzini S Dominici AF Casini A Pompella The S-thiolating activity of membrane gamma-glutamyltransferase formation ofcysteinyl-glycine mixed disulfides with cellular proteins and in the cell microen-vironment Antioxid Redox Signal 7 (2005) 911ndash918
[137] A Corti M Franzini AF Casini A Paolicchi A Pompella Vitamin C supply tobronchial epithelial cells linked to glutathione availability in elfmdasha role for se-creted gamma-glutamyltransferase J Cyst Fibros 7 (2008) 174ndash178
[138] A Munck Nutritional considerations in patients with cystic fibrosis Expert RevRespir Med 4 (2010) 47ndash56
[139] JL Matel CE Milla Nutrition in cystic fibrosis Semin Respir Crit Care Med 30(2009) 579ndash586
[140] D Salvatore R Buzzetti E Baldo MP Forneris V Lucidi D Manunza IMarinelli B Messore AS Neri V Raia ML Furnari G Mastella An overviewof international literature from cystic fibrosis registries 2 Neonatal screeningand nutritiongrowth J Cyst Fibros 9 (2010) 75ndash83
[141] KF Joosten JM Hulst Malnutrition in pediatric hospital patients current is-sues Nutrition 27 (2011) 133ndash137
[142] S Fustik T Jacovska L Spirevska S Koceva Protein-energy malnutrition as thefirst manifestation of cystic fibrosis in infancy Pediatr Int 51 (2009) 678ndash683
[143] J Himmelfarb E McMonagle Albumin is the major plasma protein target of ox-idant stress in uremia Kidney Int 60 (2001) 358ndash363
[144] P Stenvinkel JJ Carrero J Axelsson B Lindholm O Heimburger Z MassyEmerging biomarkers for evaluating cardiovascular risk in the chronic kidneydisease patient how do new pieces fit into the uremic puzzle Clin J Am SocNephrol 3 (2008) 505ndash521
[145] M Roche P Rondeau NR Singh E Tarnus E Bourdon The antioxidant proper-ties of serum albumin FEBS Lett 582 (2008) 1783ndash1787
[146] D Giustarini A Milzani I Dalle-Donne R Rossi Red blood cells as a physiolog-ical source of glutathione for extracellular fluids Blood Cells Mol Dis 40 (2008)174ndash179
[147] A Meister ME Anderson Glutathione Annu Rev Biochem 52 (1983) 711ndash760[148] B Alvarez S Carballal L Turell R Radi Formation and reactions of sulfenic acid
in human serum albumin Methods Enzymol 473 (2010) 117ndash136[149] S Carballal B Alvarez L Turell H Botti BA Freeman R Radi Sulfenic acid in
human serum albumin Amino Acids 32 (2007) 543ndash551[150] LR Barclay AM Bailey D Kong The antioxidant activity of alpha-tocopherol-
bovine serum albumin complex in micellar and liposome autoxidations J BiolChem 260 (1985) 15809ndash15814
[151] T Ishii T Ichikawa K Minoda K Kusaka S Ito Y Suzuki M Akagawa K Mochi-zuki T Goda T Nakayama Human serum albumin as an antioxidant in the ox-idation of (minus)-epigallocatechin gallate participation of reversible covalentbinding for interaction and stabilization Biosci Biotechnol Biochem 75(2011) 100ndash106
[152] F Galli S Rovidati S Benedetti U Buoncristiani C Covarelli A Floridi F Canes-trari Overexpression of erythrocyte glutathione S-transferase in uremia and di-alysis Clin Chem 45 (1999) 1781ndash1788
[153] D Borowitz RD Baker V Stallings Consensus report on nutrition for pediat-ric patients with cystic fibrosis J Pediatr Gastroenterol Nutr 35 (2002)246ndash259
[154] LJ Filer Jr SW Wright MP Manning KE Mason Absorption of alpha-tocopherol and tocopherylesters by premature and full term infants and chil-dren in health and disease Pediatrics 8 (1951) 328ndash339
[155] L Lancellotti C DOrazio G Mastella G Mazzi U Lippi Deficiency of vitamins Eand A in cystic fibrosis is independent of pancreatic function and current en-zyme and vitamin supplementation Eur J Pediatr 155 (1996) 281ndash285
[156] MN Sathe AS Patel Update in pediatrics focus on fat-soluble vitamins NutrClin Pract 25 (2010) 340ndash346
[157] MG Traber The ABCs of vitamin E and beta-carotene absorption Am J ClinNutr 80 (2004) 3ndash4
[158] TF Dolan Jr Hemolytic anemia and edema as the initial signs in infants withcystic fibrosis Consider this diagnosis even in absence of pulmonary symptomsClin Pediatr 15 (1976) 597ndash600
[159] DR James M Alfaham MC Goodchild Increased susceptibility to peroxide-induced haemolysis with normal vitamin E concentrations in cystic fibrosisClin Chim Acta 204 (1991) 279ndash290
[160] SA Peters FJ Kelly Vitamin E supplementation in cystic fibrosis J Pediatr Gas-troenterol Nutr 22 (1996) 341ndash345
[161] A Maqbool VA Stallings Update on fat-soluble vitamins in cystic fibrosis CurrOpin Pulm Med 14 (2008) 574ndash581
[162] SD Sagel MK Sontag MM Anthony P Emmett KA Papas Effect of anantioxidant-rich multivitamin supplement in cystic fibrosis J Cyst Fibros 10(2011) 31ndash36
[163] F Galli A Azzi Present trends in vitamin E research Biofactors 36 (2010)33ndash42
[164] A Hamahata P Enkhbaatar ER Kraft M Lange SW Leonard MG Traber RACox FC Schmalstieg HK Hawkins EB Whorton EM Horvath C Szabo LDTraber DN Herndon DL Traber Gamma-tocopherol nebulization by a lipidaerosolization device improves pulmonary function in sheep with burn andsmoke inhalation injury Free Radic Biol Med 45 (2008) 425ndash433
[165] JP Anais N Razzouq M Carvalho C Fernandez A Astier M Paul A AstierH Fessi AM Lorino Development of alpha-tocopherol acetate nanoparti-cles influence of preparative processes Drug Dev Ind Pharm 35 (2009)216ndash223
[166] JM Zingg Molecular and cellular activities of vitamin E analogues Mini RevMed Chem 7 (2007) 543ndash558
[167] V Viola F Pilolli M Piroddi E Pierpaoli F Orlando M Provinciali M Betti FMazzini F Galli Why tocotrienols work better insights into the in vitro anti-cancer mechanism of vitamin E Genes Nutr 7 (2011) 29ndash41
[168] F Galli F Mazzini L Bamonti L Gille S Bohmdorfer M Piroddi T Netscher FJKelly T Rosenau Tocotrienamines and tocopheramines reactions with radicalsand metal ions Bioorg Med Chem 19 (2011) 6483ndash6491
[169] A Kuhad K Chopra Attenuation of diabetic nephropathy by tocotrienol in-volvement of NFκB signaling pathway Life Sci 84 (2009) 296ndash301
[170] Q Jiang X Yin MA Lill ML Danielson H Freiser J Huang Long-chain carbox-ychromanols metabolites of vitamin E are potent inhibitors of cyclooxygenasesProc Natl Acad Sci U S A 105 (2008) 20464ndash20469
[171] ER Miller III R Pastor-Barriuso D Dalal RA Riemersma LJ Appel E GuallarMeta-analysis high-dosage vitamin E supplementation may increase all-causemortality Ann Intern Med 142 (2005) 37ndash46
[172] JN Hathcock A Azzi J Blumberg T Bray A Dickinson B Frei I Jialal CSJohnston FJ Kelly K Kraemer L Packer S Parthasarathy H Sies MG TraberVitamins E and C are safe across a broad range of intakes Am J Clin Nutr 81(2005) 736ndash745
[173] R Brigelius-Flohe F Galli Vitamin E a vitamin still awaiting the detection of itsbiological function Mol Nutr Food Res 54 (2010) 583ndash587
711F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
[174] MG Traber B Frei JS Beckman Vitamin E revisited do new data validate ben-efits for chronic disease prevention Curr Opin Lipidol 19 (2008) 30ndash38
[175] F Galli Meeting report Vitamin E Satellite Symposium (VESS) associated to theAnnual Meeting of the SFRR-Europe Rome 26 August 2009 Free Radic Res 43(2009) 1256ndash1257
[176] LJ Roberts II JA Oates MF Linton S Fazio BP Meador MD Gross Y Shyr JDMorrow The relationship between dose of vitamin E and suppression of oxida-tive stress in humans Free Radic Biol Med 43 (2007) 1388ndash1393
[177] EFSA- EFSA Scientific Opinion of the Panel on Food Additives FlavouringsProcessing Aids and Materials in Contact with Food on a request from the Com-mission on mixed tocopherols tocotrienol tocopherol and tocotrienols assources for vitamin E in EFSA- EFSA (Ed) vol 640 The EFSA Journal2008 pp 1ndash34
[178] P Rust I Eichler S Renner I Elmadfa Long-term oral beta-carotene supple-mentation in patients with cystic fibrosis mdash effects on antioxidative status andpulmonary function Ann Nutr Metab 44 (2000) 30ndash37
[179] G Lepage J Champagne N Ronco A Lamarre I Osberg RJ Sokol CC Roy Sup-plementation with carotenoids corrects increased lipid peroxidation in childrenwith cystic fibrosis Am J Clin Nutr 64 (1996) 87ndash93
[180] BM Winklhofer-Roob H Puhl G Khoschsorur MA vant Hof H EsterbauerDH Shmerling Enhanced resistance to oxidation of low density lipoproteinsand decreased lipid peroxide formation during beta-carotene supplementationin cystic fibrosis Free Radic Biol Med 18 (1995) 849ndash859
[181] RC Graham-Maar JI Schall N Stettler BS Zemel VA Stallings Elevated vita-min A intake and serum retinol in preadolescent children with cystic fibrosisAm J Clin Nutr 84 (2006) 174ndash182
[182] I Sadowska-Woda M Rachel J Pazdan E Bieszczad-Bedrejczuk K PawliszakNutritional supplement attenuates selected oxidative stress markers in pediatricpatients with cystic fibrosis Nutr Res (New York NY) 31 (2011) 509ndash518
[183] KA Papas MK Sontag C Pardee RJ Sokol SD Sagel FJ Accurso JS WagenerA pilot study on the safety and efficacy of a novel antioxidant rich formulation inpatients with cystic fibrosis J Cyst Fibros 7 (2008) 60ndash67
[184] Y Saito A Fukuhara K Nishio M Hayakawa Y Ogawa H Sakamoto K Fujii YYoshida E Niki Characterization of cellular uptake and distribution of coen-zyme Q10 and vitamin E in PC12 cells J Nutr Biochem 20 (2009) 350ndash357
[185] AA Franke CM Morrison JL Bakke LJ Custer X Li RV Cooney CoenzymeQ10 in human blood native levels and determinants of oxidation during proces-sing and storage Free Radic Biol Med 48 (2010) 1610ndash1617
[186] HN Bhagavan RK Chopra Plasma coenzyme Q10 response to oral ingestion ofcoenzyme Q10 formulations Mitochondrion 7 (2007) S78ndashS88 (Suppl)
[187] HN Bhagavan RK Chopra Coenzyme Q10 absorption tissue uptake metabo-lism and pharmacokinetics Free Radic Res 40 (2006) 445ndash453
[188] F Galli R Lee C Dunster FJ Kelly Gas chromatography mass spectrometryanalysis of carboxyethyl-hydroxychroman metabolites of alpha- and gamma-tocopherol in human plasma Free Radic Biol Med 32 (2002) 333ndash340
[189] F Galli R Lee J Atkinson A Floridi FJ Kelly Gamma-tocopherol biokineticsand transformation in humans Free Radic Res 37 (2003) 1225ndash1233
[190] TA Laguna MK Sontag I Osberg JS Wagener FJ Accurso RJ Sokol De-creased total serum coenzyme-Q10 concentrations a longitudinal study in chil-dren with cystic fibrosis J Pediatr 153 (2008) 402ndash407
[191] T Frischer JK Myung G Maurer I Eichler Z Szepfalusi G Lubec Possible dys-regulation of chaperon and metabolic proteins in cystic fibrosis bronchial tissueProteomics 6 (2006) 3381ndash3388
[192] C Andersson MM Zaman AB Jones SD Freedman Alterations in immune re-sponse and PPARLXR regulation in cystic fibrosis macrophages J Cyst Fibros 7(2008) 68ndash78
[193] SD Freedman PG Blanco MM Zaman JC Shea M Ollero IK Hopper DAWeed A Gelrud MM Regan M Laposata JG Alvarez BP OSullivan Associa-tion of cystic fibrosis with abnormalities in fatty acid metabolism N Engl JMed 350 (2004) 560ndash569
[194] S Van Biervliet G Vanbillemont JP Van Biervliet D Declercq E Robberecht AChristophe Relation between fatty acid composition and clinical status or geno-type in cystic fibrosis patients Ann Nutr Metab 51 (2007) 541ndash549
[195] SD Freedman MH Katz EM Parker M Laposata MY Urman JG AlvarezA membrane lipid imbalance plays a role in the phenotypic expression ofcystic fibrosis in cftr(minusminus) mice Proc Natl Acad Sci U S A 96 (1999)13995ndash14000
[196] S Van Biervliet S Vande Velde JP Van Biervliet E Robberecht The effect ofzinc supplements in cystic fibrosis patients Ann Nutr Metab 52 (2008)152ndash156
[197] WR Henderson Jr SJ Astley MM McCready P Kushmerick S Casey JWBecker BW Ramsey Oral absorption of omega-3 fatty acids in patients withcystic fibrosis who have pancreatic insufficiency and in healthy control subjectsJ Pediatr 124 (1994) 400ndash408
[198] I Durieu E Vericel D Guichardant H Roth JP Steghens J Drai RN JosserandE Fontaine M Lagarde G Bellon Fatty acids platelets and oxidative markersfollowing intravenous n-3 fatty acids administration in cystic fibrosis an openpilot observational study J Cyst Fibros 6 (2007) 320ndash326
[199] LG Wood DA Fitzgerald ML Garg Hypothesis vitamin E complements poly-unsaturated fatty acids in essential fatty acid deficiency in cystic fibrosis J AmColl Nutr 22 (2003) 253ndash257
[200] JD Lloyd-Still SB Johnson RT Holman Essential fatty acid status in cystic fi-brosis and the effects of safflower oil supplementation Am J Clin Nutr 34(1981) 1ndash7
[201] A Maqbool JI Schall JF Garcia-Espana BS Zemel B Strandvik VAStallings Serum linoleic acid status as a clinical indicator of essential fatty
acid status in children with cystic fibrosis J Pediatr Gastroenterol Nutr 47(2008) 635ndash644
[202] C Oliver N Jahnke Omega-3 fatty acids for cystic fibrosis Cochrane DatabaseSyst Rev (2011) CD002201
[203] B Strandvik E Gronowitz F Enlund T Martinsson J Wahlstrom Essential fattyacid deficiency in relation to genotype in patients with cystic fibrosis J Pediatr139 (2001) 650ndash655
[204] P Rise S Volpi C Colombo RF Padoan C DOrazio S Ghezzi PMelotti V BennatoC Agostoni BM Assael C Galli Whole blood fatty acid analysis with micromethodin cystic fibrosis and pulmonary disease J Cyst Fibros 9 (2010) 228ndash233
[205] H Cao K Gerhold JR Mayers MM Wiest SM Watkins GS Hotamisligil Iden-tification of a lipokine a lipid hormone linking adipose tissue to systemic me-tabolism Cell 134 (2008) 933ndash944
[206] RR Malapaka SK Khoo J Zhang JH Choi XE Zhou Y Xu Y Gong J Li ELYong MJ Chalmers L Chang JH Resau PR Griffin YE Chen HE Xu Iden-tification and mechanism of a ten carbon fatty acid as a modulating ligand ofperoxisome proliferator activated receptors J Biol Chem 287 (2012)183ndash195
[207] T Hara A Hirasawa A Ichimura I Kimura G Tsujimoto Free fatty acid recep-tors FFAR1 and GPR120 as novel therapeutic targets for metabolic disorders JPharm Sci 100 (2011) 3594ndash3601
[208] R Gupta P Rathi S Bradoo Lipase mediated upgradation of dietary fats andoils Crit Rev Food Sci Nutr 43 (2003) 635ndash644
[209] BH Jennings CC Akoh Lipase-catalyzed modification of rice bran oil to incor-porate capric acid J Agric Food Chem 48 (2000) 4439ndash4443
[210] J Hoeks M Mensink MK Hesselink K Ekroos P Schrauwen Long- andMedium-Chain Fatty Acids Induce Insulin Resistance to a Similar Extent inHumans Despite Marked Differences in Muscle Fat Accumulation J Clin Endo-crinol Metab 97 (2012) 208ndash216
[211] PJ Congden G Bruce MM Rothburn PC Clarke JM Littlewood J KelleherMS Losowsky Vitamin status in treated patients with cystic fibrosis ArchDis Child 56 (1981) 708ndash714
[212] BM Winklhofer-Roob H Ellemunter M Fruhwirth SE Schlegel-Haueter GKhoschsorur MA vant Hof DH Shmerling Plasma vitamin C concentrationsin patients with cystic fibrosis evidence of associations with lung inflammationAm J Clin Nutr 65 (1997) 1858ndash1866
[213] L Shamseer D Adams N Brown JA Johnson S Vohra Antioxidant micronutri-ents for lung disease in cystic fibrosis Cochrane Database Syst Rev (2010)CD007020
[214] C Santi S Santoro Electrophilic Selenium First edition Wiley-VCH VerlagGmbH amp Co KGaA 2012
[215] L Flohe S Toppo G Cozza F Ursini A comparison of thiol peroxidase mecha-nisms Antioxid Redox Signal 15 (2010) 763ndash780
[216] L Flohe JR Andreesen R Brigelius-Flohe M Maiorino F Ursini Selenium theelement of the moon in life on earth IUBMB Life 49 (2000) 411ndash420
[217] V Valdiglesias E Pasaro J Mendez B Laffon In vitro evaluation of seleniumgenotoxic cytotoxic and protective effects a review Arch Toxicol 84(2010) 337ndash351
[218] P Foucaud P Therond M Marchand F Brion JF Demelier J Navarro Seleniumand vitamin E in mucoviscidosis Arch Fr Pediatr 45 (1988) 383ndash386
[219] J Neve R Van Geffel M Hanocq L Molle Plasma and erythrocyte zinc copperand selenium in cystic fibrosis Acta Paediatr Scand 72 (1983) 437ndash440
[220] BM Winklhofer-Roob B Tiran PE Tuchschmid MA vant Hof DH ShmerlingEffects of pancreatic enzyme preparations on erythrocyte glutathione peroxi-dase activities and plasma selenium concentrations in cystic fibrosis FreeRadic Biol Med 25 (1998) 242ndash249
[221] JD Lloyd-Still HE Ganther Selenium and glutathione peroxidase levels in cys-tic fibrosis Pediatrics 65 (1980) 1010ndash1012
[222] D Tsavachidou TJ McDonnell S Wen X Wang F Vakar-Lopez LL Pisters CAPettaway CG Wood KA Do PF Thall C Stephens E Efstathiou R Taylor DGMenter P Troncoso SM Lippman CJ Logothetis J Kim Selenium and vitaminE cell type- and intervention-specific tissue effects in prostate cancer J NatlCancer Inst 101 (2009) 306ndash320
[223] IN Zelko TJ Mariani RJ Folz Superoxide dismutase multigene family acomparison of the CuZn-SOD (SOD1) Mn-SOD (SOD2) and EC-SOD (SOD3)gene structures evolution and expression Free Radic Biol Med 33 (2002)337ndash349
[224] RP Bowler JD Crapo Oxidative stress in airways is there a role for extracellu-lar superoxide dismutase Am J Respir Crit Care Med 166 (2002) S38ndashS43
[225] K Best K McCoy S Gemma RA Disilvestro Copper enzyme activities in cysticfibrosis before and after copper supplementation plus or minus zinc Metabo-lism 53 (2004) 37ndash41
[226] SS Percival GP Kauwell E Bowser M Wagner Altered copper status in adultmen with cystic fibrosis J Am Coll Nutr 18 (1999) 614ndash619
[227] NF Krebs JE Westcott TD Arnold BM Kluger FJ Accurso LV Miller KMHambidge Abnormalities in zinc homeostasis in young infants with cystic fibro-sis Pediatr Res 48 (2000) 256ndash261
[228] D Easley N Krebs M Jefferson L Miller J Erskine F Accurso KM HambidgeEffect of pancreatic enzymes on zinc absorption in cystic fibrosis J Pediatr Gas-troenterol Nutr 26 (1998) 136ndash139
[229] S Van Biervliet JP Van Biervliet E Robberecht Serum zinc in patients with cys-tic fibrosis at diagnosis and after one year of therapy Biol Trace Elem Res 112(2006) 205ndash211
[230] S Van Biervliet JP Van Biervliet S Vande Velde E Robberecht Serum zinc con-centrations in cystic fibrosis patients aged above 4 years a cross-sectional eval-uation Biol Trace Elem Res 119 (2007) 19ndash26
712 F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
[231] F Galli M Cristina Polidori W Stahl P Mecocci FJ Kelly Vitamin E biotransfor-mation in humans Vitam Horm 76 (2007) 263ndash280
[232] J Wiser NE Alexis Q Jiang W Wu C Robinette R Roubey DB Peden In vivogamma-tocopherol supplementation decreases systemic oxidative stress andcytokine responses of human monocytes in normal and asthmatic subjectsFree Radic Biol Med 45 (2008) 40ndash49
[233] JG Wagner Q Jiang JR Harkema B Illek DD Patel BN Ames DB PedenOzone enhancement of lower airway allergic inflammation is prevented bygamma-tocopherol Free Radic Biol Med 43 (2007) 1176ndash1188
[234] JT Harries DP Muller Absorption of different doses of fat soluble and watermiscible preparations of vitamin E in children with cystic fibrosis Arch DisChild 46 (1971) 341ndash344
[235] EI Back C Frindt E Ocenaskova D Nohr M Stern HK Biesalski Can changesin hydrophobicity increase the bioavailability of alpha-tocopherol Eur J Nutr45 (2006) 1ndash6
[236] SZ Nasr MH OLeary C Hillermeier Correction of vitamin E deficiency withfat-soluble versus water-miscible preparations of vitamin E in patients with cys-tic fibrosis J Pediatr 122 (1993) 810ndash812
[237] S Soltani-Frisk E Gronowitz H Andersson B Strandvik Water-miscibletocopherol is not superior to fat-soluble preparation for vitamin E absorptionin cystic fibrosis Acta Paediatr 90 (2001) 1112ndash1115
[238] K Papas J Kalbfleisch R Mohon Bioavailability of a novel water-soluble vi-tamin E formulation in malabsorbing patients Dig Dis Sci 52 (2007)347ndash352
[239] F Antonicelli M Parmentier EM Drost N Hirani I Rahman K Donaldson WMacNee Nacystelyn inhibits oxidant-mediated interleukin-8 expression andNF-kappaB nuclear binding in alveolar epithelial cells Free Radic Biol Med 32(2002) 492ndash502
[240] EM App D Baran I Dab A Malfroot M Coffiner F Vanderbist M King Dose-finding and 24-h monitoring for efficacy and safety of aerosolized Nacystelyn incystic fibrosis Eur Respir J 19 (2002) 294ndash302
[241] MG Traber How much vitamin E hellip Just enough Am J Clin Nutr 84 (2006)959ndash960
[242] JC McCann BN Ames Vitamin K an example of triage theory is micronu-trient inadequacy linked to diseases of aging Am J Clin Nutr 90 (2009)889ndash907
[243] M Fusaro G Crepaldi S Maggi F Galli A DAngelo L Calo S Giannini DMiozzo M Gallieni Vitamin K bone fractures and vascular calcifications inchronic kidney disease an important but poorly studied relationship J Endocri-nol Invest 34 (2010) 317ndash323
[244] JC McCann BN Ames Adaptive dysfunction of selenoproteins from the per-spective of the triage theory why modest selenium deficiency may increaserisk of diseases of aging FASEB J 25 (2011) 1793ndash1814
[245] R Apak K Guclu M Ozyurek B Bektas Oglu M Bener Cupric ion reducing an-tioxidant capacity assay for food antioxidants vitamins polyphenolics and fla-vonoids in food extracts Methods Mol Biol 477 (2008) 163ndash193
[246] F Galli Interactions of polyphenolic compounds with drug disposition and me-tabolism Curr Drug Metab 8 (2007) 830ndash838
[247] RL Prior X Wu K Schaich Standardized methods for the determination of an-tioxidant capacity and phenolics in foods and dietary supplements J Agric FoodChem 53 (2005) 4290ndash4302
[248] C Azbell S Zhang D Skinner J Fortenberry EJ Sorscher BA WoodworthHesperidin stimulates cystic fibrosis transmembrane conductance regulator-mediated chloride secretion and ciliary beat frequency in sinonasal epitheliumOtolaryngol Head Neck Surg 143 (2010) 397ndash404
[249] G Wegrzyn J Jakobkiewicz-Banecka M Gabig-Ciminska E Piotrowska M Nar-ajczyk A Kloska M Malinowska D Dziedzic I Golebiewska M Moskot AWegrzyn Genistein a natural isoflavone with a potential for treatment of ge-netic diseases Biochem Soc Trans 38 (2010) 695ndash701
[250] YC Yu H Miki Y Nakamura A Hanyuda Y Matsuzaki Y Abe M Yasui K Ta-naka TC Hwang SG Bompadre Y Sohma Curcumin and genistein additivelypotentiate G551D-CFTR J Cyst Fibros 10 (2011) 243ndash252
[251] B Illek H Fischer Flavonoids stimulate Cl conductance of human airway epithe-lium in vitro and in vivo Am J Physiol 275 (1998) L902ndashL910
[252] JL Kreindler Cystic fibrosis exploiting its genetic basis in the hunt for newtherapies Pharmacol Ther 125 (2010) 219ndash229
[253] B Illek L Zhang NC Lewis RB Moss JY Dong H Fischer Defective function ofthe cystic fibrosis-causing missense mutation G551D is recovered by genisteinAm J Physiol 277 (1999) C833ndashC839
[254] P Anandakumar S Kamaraj S Jagan G Ramakrishnan R Vinodhkumar TDevaki Capsaicin modulates pulmonary antioxidant defense system during ben-zo(a)pyrene-induced lung cancer in Swiss albinomice Phytother Res 22 (2008)529ndash533
[255] I Rahman Antioxidant therapeutic advances in COPD Ther Adv Respir Dis 2(2008) 351ndash374
[256] AW Boots H Li RP Schins R Duffin JW Heemskerk A Bast GR Haenen Thequercetin paradox Toxicol Appl Pharmacol 222 (2007) 89ndash96
[257] M Joskova S Franova V Sadlonova Acute bronchodilator effect of quercetin inexperimental allergic asthma Bratisl Lek Listy 112 (2011) 9ndash12
[258] HJ Park CM Lee ID Jung JS Lee YI Jeong JH Chang SH Chun MJ Kim IWChoi SC Ahn YK Shin SR Yeom YM Park Quercetin regulates Th1Th2 balancein a murine model of asthma Int Immunopharmacol 9 (2009) 261ndash267
[259] AP Rogerio A Kanashiro C Fontanari EV da Silva YM Lucisano-ValimEG Soares LH Faccioli Anti-inflammatory activity of quercetin and iso-quercitrin in experimental murine allergic asthma Inflamm Res 56 (2007)402ndash408
[260] M Muller Polyphenol cytotoxicity induced by the bacterial toxin pyocyaninrole of NQO1 Free Radic Biol Med 47 (2009) 84ndash91
[261] J Grassmann Terpenoids as plant antioxidants Vitam Horm 72 (2005)505ndash535
[262] P Allen Tea tree oil the science behind the antimicrobial hype Lancet 358(2001) 1245
[263] EC Dasenbrook W Checkley CA Merlo MW Konstan N Lechtzin MP BoyleAssociation between respiratory tract methicillin-resistant Staphylococcus aure-us and survival in cystic fibrosis JAMA 303 (2010) 2386ndash2392
[264] V Bezzerri M Borgatti E Nicolis I Lampronti MC Dechecchi I Mancini PRizzotti R Gambari G Cabrini Transcription factor oligodeoxynucleotides toNF-kappaB inhibit transcription of IL-8 in bronchial cells Am J Respir CellMol Biol 39 (2008) 86ndash96
[265] R Gambari M Borgatti V Bezzerri E Nicolis I Lampronti MC Dechecchi IMancini A Tamanini G Cabrini Decoy oligodeoxyribonucleotides and peptidenucleic acids-DNA chimeras targeting nuclear factor kappa-B inhibition of IL-8 gene expression in cystic fibrosis cells infected with Pseudomonas aeruginosaBiochem Pharmacol 80 (2010) 1887ndash1894
[266] M Adrian P Jeandet AC Douillet-Breuil L Tesson R Bessis Stilbene content ofmature Vitis vinifera berries in response to UV-C elicitation J Agric Food Chem48 (2000) 6103ndash6105
[267] B Paul I Masih J Deopujari C Charpentier Occurrence of resveratrol and pter-ostilbene in age-old darakchasava an ayurvedic medicine from India J Ethno-pharmacol 68 (1999) 71ndash76
[268] I Rahman Antioxidant therapies in COPD Int J Chron Obstruct Pulmon Dis 1(2006) 15ndash29
[269] M Lee S Kim OK Kwon SR Oh HK Lee K Ahn Anti-inflammatory and anti-asthmatic effects of resveratrol a polyphenolic stilbene in a mouse model ofallergic asthma Int Immunopharmacol 9 (2009) 418ndash424
[270] LG Wood PA Wark ML Garg Antioxidant and anti-inflammatory effectsof resveratrol in airway disease Antioxid Redox Signal 13 (2010)1535ndash1548
[271] KV Kiselev Perspectives for production and application of resveratrol ApplMicrobiol Biotechnol 90 (2011) 417ndash425
[272] M Shakibaei C Buhrmann A Mobasheri Resveratrol-mediated SIRT-1 interac-tions with p300 modulate receptor activator of NF-kappaB ligand (RANKL) acti-vation of NF-kappaB signaling and inhibit osteoclastogenesis in bone-derivedcells J Biol Chem 286 (2011) 11492ndash11505
[273] SF Zaidi K Ahmed T Yamamoto T Kondo K Usmanghani M Kadowaki TSugiyama Effect of resveratrol on Helicobacter pylori-induced interleukin-8 secre-tion reactive oxygen species generation and morphological changes in human gas-tric epithelial cells Biol Pharm Bull 32 (2009) 1931ndash1935
[274] JK Kundu YK Shin YJ Surh Resveratrol modulates phorbol ester-inducedpro-inflammatory signal transduction pathways in mouse skin in vivo NF-kappaB and AP-1 as prime targets Biochem Pharmacol 72 (2006)1506ndash1515
[275] NH Nam Naturally occurring NF-kappaB inhibitors Mini Rev Med Chem 6(2006) 945ndash951
[276] JM Smoliga JA Baur HA Hausenblas Resveratrol and healthmdasha comprehen-sive review of human clinical trials Mol Nutr Food Res 55 (2011) 1129ndash1141
[277] ME Juan M Maijo JM Planas Quantification of trans-resveratrol and itsmetabolites in rat plasma and tissues by HPLC J Pharm Biomed Anal 51(2010) 391ndash398
[278] JA Baur DA Sinclair Therapeutic potential of resveratrol the in vivo evidenceNat Rev 5 (2006) 493ndash506
[279] E Nicolis I Lampronti MC Dechecchi M Borgatti A Tamanini N Bianchi VBezzerri I Mancini MG Giri P Rizzotti R Gambari G Cabrini Pyrogallol anactive compound from the medicinal plant Emblica officinalis regulates expres-sion of pro-inflammatory genes in bronchial epithelial cells Int Immunophar-macol 8 (2008) 1672ndash1680
[280] E Nicolis I Lampronti MC Dechecchi M Borgatti A Tamanini V Bezzerri NBianchi M Mazzon I Mancini MG Giri P Rizzotti R Gambari G CabriniModulation of expression of IL-8 gene in bronchial epithelial cells by 5-methoxypsoralen Int Immunopharmacol 9 (2009) 1411ndash1422
[281] M Borgatti I Mancini N Bianchi A Guerrini I Lampronti D Rossi G SacchettiR Gambari Bergamot (Citrus bergamia Risso) fruit extracts and identified com-ponents alter expression of interleukin 8 gene in cystic fibrosis bronchial epithe-lial cell lines BMC Biochem 12 (2011) 15
[282] L Piccagli E Fabbri M Borgatti N Bianchi V Bezzerri I Mancini E Nicolis CMDechecchi I Lampronti G Cabrini R Gambari Virtual screening against p50NF-kappaB transcription factor for the identification of inhibitors of the NF-kappaB-DNA interaction and expression of NF-kappaB upregulated genesChemMedChem 4 (2009) 2024ndash2033
[283] L Piccagli M Borgatti E Nicolis N Bianchi I Mancini I Lampronti D VevaldiF DallAcqua G Cabrini R Gambari Virtual screening against nuclear factorkappaB (NF-kappaB) of a focus library identification of bioactive furocoumarinderivatives inhibiting NF-kappaB dependent biological functions involved incystic fibrosis Bioorg Med Chem 18 (2010) 8341ndash8349
[284] M Borgatti A Chilin L Piccagli I Lampronti N Bianchi I Mancini G Mar-zaro Da Francesco A Guiotto R Gambari Development of a novel furocou-marin derivative inhibiting NF-kappaB dependent biological functionsdesign synthesis and biological effects Eur J Med Chem 46 (2011)4870ndash4877
[285] E Georgy S Le Guellec L Vecellio E Fichant P Stordeur P Bordeau JP PerraudinFeasibility study of OSCN- and lactoferrin (Meveol) nebulization for cysticfibrosis JCyst Fibros 10 (2011) S18
713F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
[286] C Tidei M Piroddi F Galli C Santi Oxidation of thiols promoted by PhSeZnClTetrahedron Lett 53 (2012) 232ndash234
[287] L Semianrio-Vidal C van Hesuden G Mugesh ER Lazarowski Ebselen is a po-tent non-competitive inhibitor of extracellular nucleoside diphosphokinasePurinergic Signal 6 (2010) 383ndash391
[288] C ColussiMC Albertini S Coppola S Rovidati F Galli L Ghibelli H2O2-inducedblockof glycolysis as an active ADP-ribosylation reaction protecting cells from apoptosisFASEB J 14 (2000) 2266ndash2276
[289] H Xiao KL Parkin Induction of phase II enzyme activity by various seleniumcompounds Nutr Cancer 55 (2006) 210ndash223
[290] G Peluffo R Radi Biochemistry of protein tyrosine nitration in cardiovascularpathology Cardiovasc Res 75 (2007) 291ndash302
[291] B Alvarez R Radi Peroxynitrite reactivity with amino acids and proteinsAmino Acids 25 (2003) 295ndash311
[292] B Kamosinska MW Radomski M Duszyk A Radomski SF Man Nitric oxideactivates chloride currents in human lung epithelial cells Am J Physiol 272(1997) L1098ndashL1104
[293] L Chen RP Patel X Teng CA Bosworth JR Lancaster Jr S Matalon Mecha-nisms of cystic fibrosis transmembrane conductance regulator activation by S-nitrosoglutathione J Biol Chem 281 (2006) 9190ndash9199
[294] F Luchetti B CanonicoM BettiM Arcangeletti F PilolliM Piroddi L Canesi S PapaF Galli Melatonin signaling and cell protection function FASEB J 24 (2010)3603ndash3624
[295] MW Bengtsson G Jedstedt G Flemstrom Duodenal bicarbonate secretion inrats stimulation by intra-arterial and luminal guanylin and uroguanylin ActaPhysiol (Oxf) 191 (2007) 309ndash317
[296] CS Nelson JL Marino CN Allen Melatonin receptor potentiation of cyclic AMP andthe cystic fibrosis transmembrane conductance regulator ion channel J Pineal Res 26(1999) 113ndash121
[297] C de Castro-Silva VM de Bruin GM Cunha DM Nunes CAMedeiros PF de BruinMelatonin improves sleep and reduces nitrite in the exhaled breath condensate incystic fibrosismdasha randomized double-blind placebo-controlled study J Pineal Res48 (2010) 65ndash71
[298] I Hornyak E Pankotai L Kiss Z Lacza Current developments in the the-rapeutic potential of S-nitrosoglutathione an endogenous NO-donor mole-cule Curr Pharm Biotechnol (2011) Jan 11 [Epub ahead of print] - PMID21235457
[299] AH Snyder ME McPherson JF Hunt M Johnson JS Stamler B Gaston Acuteeffects of aerosolized S-nitrosoglutathione in cystic fibrosis Am J Respir CritCare Med 165 (2002) 922ndash926
711F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
[174] MG Traber B Frei JS Beckman Vitamin E revisited do new data validate ben-efits for chronic disease prevention Curr Opin Lipidol 19 (2008) 30ndash38
[175] F Galli Meeting report Vitamin E Satellite Symposium (VESS) associated to theAnnual Meeting of the SFRR-Europe Rome 26 August 2009 Free Radic Res 43(2009) 1256ndash1257
[176] LJ Roberts II JA Oates MF Linton S Fazio BP Meador MD Gross Y Shyr JDMorrow The relationship between dose of vitamin E and suppression of oxida-tive stress in humans Free Radic Biol Med 43 (2007) 1388ndash1393
[177] EFSA- EFSA Scientific Opinion of the Panel on Food Additives FlavouringsProcessing Aids and Materials in Contact with Food on a request from the Com-mission on mixed tocopherols tocotrienol tocopherol and tocotrienols assources for vitamin E in EFSA- EFSA (Ed) vol 640 The EFSA Journal2008 pp 1ndash34
[178] P Rust I Eichler S Renner I Elmadfa Long-term oral beta-carotene supple-mentation in patients with cystic fibrosis mdash effects on antioxidative status andpulmonary function Ann Nutr Metab 44 (2000) 30ndash37
[179] G Lepage J Champagne N Ronco A Lamarre I Osberg RJ Sokol CC Roy Sup-plementation with carotenoids corrects increased lipid peroxidation in childrenwith cystic fibrosis Am J Clin Nutr 64 (1996) 87ndash93
[180] BM Winklhofer-Roob H Puhl G Khoschsorur MA vant Hof H EsterbauerDH Shmerling Enhanced resistance to oxidation of low density lipoproteinsand decreased lipid peroxide formation during beta-carotene supplementationin cystic fibrosis Free Radic Biol Med 18 (1995) 849ndash859
[181] RC Graham-Maar JI Schall N Stettler BS Zemel VA Stallings Elevated vita-min A intake and serum retinol in preadolescent children with cystic fibrosisAm J Clin Nutr 84 (2006) 174ndash182
[182] I Sadowska-Woda M Rachel J Pazdan E Bieszczad-Bedrejczuk K PawliszakNutritional supplement attenuates selected oxidative stress markers in pediatricpatients with cystic fibrosis Nutr Res (New York NY) 31 (2011) 509ndash518
[183] KA Papas MK Sontag C Pardee RJ Sokol SD Sagel FJ Accurso JS WagenerA pilot study on the safety and efficacy of a novel antioxidant rich formulation inpatients with cystic fibrosis J Cyst Fibros 7 (2008) 60ndash67
[184] Y Saito A Fukuhara K Nishio M Hayakawa Y Ogawa H Sakamoto K Fujii YYoshida E Niki Characterization of cellular uptake and distribution of coen-zyme Q10 and vitamin E in PC12 cells J Nutr Biochem 20 (2009) 350ndash357
[185] AA Franke CM Morrison JL Bakke LJ Custer X Li RV Cooney CoenzymeQ10 in human blood native levels and determinants of oxidation during proces-sing and storage Free Radic Biol Med 48 (2010) 1610ndash1617
[186] HN Bhagavan RK Chopra Plasma coenzyme Q10 response to oral ingestion ofcoenzyme Q10 formulations Mitochondrion 7 (2007) S78ndashS88 (Suppl)
[187] HN Bhagavan RK Chopra Coenzyme Q10 absorption tissue uptake metabo-lism and pharmacokinetics Free Radic Res 40 (2006) 445ndash453
[188] F Galli R Lee C Dunster FJ Kelly Gas chromatography mass spectrometryanalysis of carboxyethyl-hydroxychroman metabolites of alpha- and gamma-tocopherol in human plasma Free Radic Biol Med 32 (2002) 333ndash340
[189] F Galli R Lee J Atkinson A Floridi FJ Kelly Gamma-tocopherol biokineticsand transformation in humans Free Radic Res 37 (2003) 1225ndash1233
[190] TA Laguna MK Sontag I Osberg JS Wagener FJ Accurso RJ Sokol De-creased total serum coenzyme-Q10 concentrations a longitudinal study in chil-dren with cystic fibrosis J Pediatr 153 (2008) 402ndash407
[191] T Frischer JK Myung G Maurer I Eichler Z Szepfalusi G Lubec Possible dys-regulation of chaperon and metabolic proteins in cystic fibrosis bronchial tissueProteomics 6 (2006) 3381ndash3388
[192] C Andersson MM Zaman AB Jones SD Freedman Alterations in immune re-sponse and PPARLXR regulation in cystic fibrosis macrophages J Cyst Fibros 7(2008) 68ndash78
[193] SD Freedman PG Blanco MM Zaman JC Shea M Ollero IK Hopper DAWeed A Gelrud MM Regan M Laposata JG Alvarez BP OSullivan Associa-tion of cystic fibrosis with abnormalities in fatty acid metabolism N Engl JMed 350 (2004) 560ndash569
[194] S Van Biervliet G Vanbillemont JP Van Biervliet D Declercq E Robberecht AChristophe Relation between fatty acid composition and clinical status or geno-type in cystic fibrosis patients Ann Nutr Metab 51 (2007) 541ndash549
[195] SD Freedman MH Katz EM Parker M Laposata MY Urman JG AlvarezA membrane lipid imbalance plays a role in the phenotypic expression ofcystic fibrosis in cftr(minusminus) mice Proc Natl Acad Sci U S A 96 (1999)13995ndash14000
[196] S Van Biervliet S Vande Velde JP Van Biervliet E Robberecht The effect ofzinc supplements in cystic fibrosis patients Ann Nutr Metab 52 (2008)152ndash156
[197] WR Henderson Jr SJ Astley MM McCready P Kushmerick S Casey JWBecker BW Ramsey Oral absorption of omega-3 fatty acids in patients withcystic fibrosis who have pancreatic insufficiency and in healthy control subjectsJ Pediatr 124 (1994) 400ndash408
[198] I Durieu E Vericel D Guichardant H Roth JP Steghens J Drai RN JosserandE Fontaine M Lagarde G Bellon Fatty acids platelets and oxidative markersfollowing intravenous n-3 fatty acids administration in cystic fibrosis an openpilot observational study J Cyst Fibros 6 (2007) 320ndash326
[199] LG Wood DA Fitzgerald ML Garg Hypothesis vitamin E complements poly-unsaturated fatty acids in essential fatty acid deficiency in cystic fibrosis J AmColl Nutr 22 (2003) 253ndash257
[200] JD Lloyd-Still SB Johnson RT Holman Essential fatty acid status in cystic fi-brosis and the effects of safflower oil supplementation Am J Clin Nutr 34(1981) 1ndash7
[201] A Maqbool JI Schall JF Garcia-Espana BS Zemel B Strandvik VAStallings Serum linoleic acid status as a clinical indicator of essential fatty
acid status in children with cystic fibrosis J Pediatr Gastroenterol Nutr 47(2008) 635ndash644
[202] C Oliver N Jahnke Omega-3 fatty acids for cystic fibrosis Cochrane DatabaseSyst Rev (2011) CD002201
[203] B Strandvik E Gronowitz F Enlund T Martinsson J Wahlstrom Essential fattyacid deficiency in relation to genotype in patients with cystic fibrosis J Pediatr139 (2001) 650ndash655
[204] P Rise S Volpi C Colombo RF Padoan C DOrazio S Ghezzi PMelotti V BennatoC Agostoni BM Assael C Galli Whole blood fatty acid analysis with micromethodin cystic fibrosis and pulmonary disease J Cyst Fibros 9 (2010) 228ndash233
[205] H Cao K Gerhold JR Mayers MM Wiest SM Watkins GS Hotamisligil Iden-tification of a lipokine a lipid hormone linking adipose tissue to systemic me-tabolism Cell 134 (2008) 933ndash944
[206] RR Malapaka SK Khoo J Zhang JH Choi XE Zhou Y Xu Y Gong J Li ELYong MJ Chalmers L Chang JH Resau PR Griffin YE Chen HE Xu Iden-tification and mechanism of a ten carbon fatty acid as a modulating ligand ofperoxisome proliferator activated receptors J Biol Chem 287 (2012)183ndash195
[207] T Hara A Hirasawa A Ichimura I Kimura G Tsujimoto Free fatty acid recep-tors FFAR1 and GPR120 as novel therapeutic targets for metabolic disorders JPharm Sci 100 (2011) 3594ndash3601
[208] R Gupta P Rathi S Bradoo Lipase mediated upgradation of dietary fats andoils Crit Rev Food Sci Nutr 43 (2003) 635ndash644
[209] BH Jennings CC Akoh Lipase-catalyzed modification of rice bran oil to incor-porate capric acid J Agric Food Chem 48 (2000) 4439ndash4443
[210] J Hoeks M Mensink MK Hesselink K Ekroos P Schrauwen Long- andMedium-Chain Fatty Acids Induce Insulin Resistance to a Similar Extent inHumans Despite Marked Differences in Muscle Fat Accumulation J Clin Endo-crinol Metab 97 (2012) 208ndash216
[211] PJ Congden G Bruce MM Rothburn PC Clarke JM Littlewood J KelleherMS Losowsky Vitamin status in treated patients with cystic fibrosis ArchDis Child 56 (1981) 708ndash714
[212] BM Winklhofer-Roob H Ellemunter M Fruhwirth SE Schlegel-Haueter GKhoschsorur MA vant Hof DH Shmerling Plasma vitamin C concentrationsin patients with cystic fibrosis evidence of associations with lung inflammationAm J Clin Nutr 65 (1997) 1858ndash1866
[213] L Shamseer D Adams N Brown JA Johnson S Vohra Antioxidant micronutri-ents for lung disease in cystic fibrosis Cochrane Database Syst Rev (2010)CD007020
[214] C Santi S Santoro Electrophilic Selenium First edition Wiley-VCH VerlagGmbH amp Co KGaA 2012
[215] L Flohe S Toppo G Cozza F Ursini A comparison of thiol peroxidase mecha-nisms Antioxid Redox Signal 15 (2010) 763ndash780
[216] L Flohe JR Andreesen R Brigelius-Flohe M Maiorino F Ursini Selenium theelement of the moon in life on earth IUBMB Life 49 (2000) 411ndash420
[217] V Valdiglesias E Pasaro J Mendez B Laffon In vitro evaluation of seleniumgenotoxic cytotoxic and protective effects a review Arch Toxicol 84(2010) 337ndash351
[218] P Foucaud P Therond M Marchand F Brion JF Demelier J Navarro Seleniumand vitamin E in mucoviscidosis Arch Fr Pediatr 45 (1988) 383ndash386
[219] J Neve R Van Geffel M Hanocq L Molle Plasma and erythrocyte zinc copperand selenium in cystic fibrosis Acta Paediatr Scand 72 (1983) 437ndash440
[220] BM Winklhofer-Roob B Tiran PE Tuchschmid MA vant Hof DH ShmerlingEffects of pancreatic enzyme preparations on erythrocyte glutathione peroxi-dase activities and plasma selenium concentrations in cystic fibrosis FreeRadic Biol Med 25 (1998) 242ndash249
[221] JD Lloyd-Still HE Ganther Selenium and glutathione peroxidase levels in cys-tic fibrosis Pediatrics 65 (1980) 1010ndash1012
[222] D Tsavachidou TJ McDonnell S Wen X Wang F Vakar-Lopez LL Pisters CAPettaway CG Wood KA Do PF Thall C Stephens E Efstathiou R Taylor DGMenter P Troncoso SM Lippman CJ Logothetis J Kim Selenium and vitaminE cell type- and intervention-specific tissue effects in prostate cancer J NatlCancer Inst 101 (2009) 306ndash320
[223] IN Zelko TJ Mariani RJ Folz Superoxide dismutase multigene family acomparison of the CuZn-SOD (SOD1) Mn-SOD (SOD2) and EC-SOD (SOD3)gene structures evolution and expression Free Radic Biol Med 33 (2002)337ndash349
[224] RP Bowler JD Crapo Oxidative stress in airways is there a role for extracellu-lar superoxide dismutase Am J Respir Crit Care Med 166 (2002) S38ndashS43
[225] K Best K McCoy S Gemma RA Disilvestro Copper enzyme activities in cysticfibrosis before and after copper supplementation plus or minus zinc Metabo-lism 53 (2004) 37ndash41
[226] SS Percival GP Kauwell E Bowser M Wagner Altered copper status in adultmen with cystic fibrosis J Am Coll Nutr 18 (1999) 614ndash619
[227] NF Krebs JE Westcott TD Arnold BM Kluger FJ Accurso LV Miller KMHambidge Abnormalities in zinc homeostasis in young infants with cystic fibro-sis Pediatr Res 48 (2000) 256ndash261
[228] D Easley N Krebs M Jefferson L Miller J Erskine F Accurso KM HambidgeEffect of pancreatic enzymes on zinc absorption in cystic fibrosis J Pediatr Gas-troenterol Nutr 26 (1998) 136ndash139
[229] S Van Biervliet JP Van Biervliet E Robberecht Serum zinc in patients with cys-tic fibrosis at diagnosis and after one year of therapy Biol Trace Elem Res 112(2006) 205ndash211
[230] S Van Biervliet JP Van Biervliet S Vande Velde E Robberecht Serum zinc con-centrations in cystic fibrosis patients aged above 4 years a cross-sectional eval-uation Biol Trace Elem Res 119 (2007) 19ndash26
712 F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
[231] F Galli M Cristina Polidori W Stahl P Mecocci FJ Kelly Vitamin E biotransfor-mation in humans Vitam Horm 76 (2007) 263ndash280
[232] J Wiser NE Alexis Q Jiang W Wu C Robinette R Roubey DB Peden In vivogamma-tocopherol supplementation decreases systemic oxidative stress andcytokine responses of human monocytes in normal and asthmatic subjectsFree Radic Biol Med 45 (2008) 40ndash49
[233] JG Wagner Q Jiang JR Harkema B Illek DD Patel BN Ames DB PedenOzone enhancement of lower airway allergic inflammation is prevented bygamma-tocopherol Free Radic Biol Med 43 (2007) 1176ndash1188
[234] JT Harries DP Muller Absorption of different doses of fat soluble and watermiscible preparations of vitamin E in children with cystic fibrosis Arch DisChild 46 (1971) 341ndash344
[235] EI Back C Frindt E Ocenaskova D Nohr M Stern HK Biesalski Can changesin hydrophobicity increase the bioavailability of alpha-tocopherol Eur J Nutr45 (2006) 1ndash6
[236] SZ Nasr MH OLeary C Hillermeier Correction of vitamin E deficiency withfat-soluble versus water-miscible preparations of vitamin E in patients with cys-tic fibrosis J Pediatr 122 (1993) 810ndash812
[237] S Soltani-Frisk E Gronowitz H Andersson B Strandvik Water-miscibletocopherol is not superior to fat-soluble preparation for vitamin E absorptionin cystic fibrosis Acta Paediatr 90 (2001) 1112ndash1115
[238] K Papas J Kalbfleisch R Mohon Bioavailability of a novel water-soluble vi-tamin E formulation in malabsorbing patients Dig Dis Sci 52 (2007)347ndash352
[239] F Antonicelli M Parmentier EM Drost N Hirani I Rahman K Donaldson WMacNee Nacystelyn inhibits oxidant-mediated interleukin-8 expression andNF-kappaB nuclear binding in alveolar epithelial cells Free Radic Biol Med 32(2002) 492ndash502
[240] EM App D Baran I Dab A Malfroot M Coffiner F Vanderbist M King Dose-finding and 24-h monitoring for efficacy and safety of aerosolized Nacystelyn incystic fibrosis Eur Respir J 19 (2002) 294ndash302
[241] MG Traber How much vitamin E hellip Just enough Am J Clin Nutr 84 (2006)959ndash960
[242] JC McCann BN Ames Vitamin K an example of triage theory is micronu-trient inadequacy linked to diseases of aging Am J Clin Nutr 90 (2009)889ndash907
[243] M Fusaro G Crepaldi S Maggi F Galli A DAngelo L Calo S Giannini DMiozzo M Gallieni Vitamin K bone fractures and vascular calcifications inchronic kidney disease an important but poorly studied relationship J Endocri-nol Invest 34 (2010) 317ndash323
[244] JC McCann BN Ames Adaptive dysfunction of selenoproteins from the per-spective of the triage theory why modest selenium deficiency may increaserisk of diseases of aging FASEB J 25 (2011) 1793ndash1814
[245] R Apak K Guclu M Ozyurek B Bektas Oglu M Bener Cupric ion reducing an-tioxidant capacity assay for food antioxidants vitamins polyphenolics and fla-vonoids in food extracts Methods Mol Biol 477 (2008) 163ndash193
[246] F Galli Interactions of polyphenolic compounds with drug disposition and me-tabolism Curr Drug Metab 8 (2007) 830ndash838
[247] RL Prior X Wu K Schaich Standardized methods for the determination of an-tioxidant capacity and phenolics in foods and dietary supplements J Agric FoodChem 53 (2005) 4290ndash4302
[248] C Azbell S Zhang D Skinner J Fortenberry EJ Sorscher BA WoodworthHesperidin stimulates cystic fibrosis transmembrane conductance regulator-mediated chloride secretion and ciliary beat frequency in sinonasal epitheliumOtolaryngol Head Neck Surg 143 (2010) 397ndash404
[249] G Wegrzyn J Jakobkiewicz-Banecka M Gabig-Ciminska E Piotrowska M Nar-ajczyk A Kloska M Malinowska D Dziedzic I Golebiewska M Moskot AWegrzyn Genistein a natural isoflavone with a potential for treatment of ge-netic diseases Biochem Soc Trans 38 (2010) 695ndash701
[250] YC Yu H Miki Y Nakamura A Hanyuda Y Matsuzaki Y Abe M Yasui K Ta-naka TC Hwang SG Bompadre Y Sohma Curcumin and genistein additivelypotentiate G551D-CFTR J Cyst Fibros 10 (2011) 243ndash252
[251] B Illek H Fischer Flavonoids stimulate Cl conductance of human airway epithe-lium in vitro and in vivo Am J Physiol 275 (1998) L902ndashL910
[252] JL Kreindler Cystic fibrosis exploiting its genetic basis in the hunt for newtherapies Pharmacol Ther 125 (2010) 219ndash229
[253] B Illek L Zhang NC Lewis RB Moss JY Dong H Fischer Defective function ofthe cystic fibrosis-causing missense mutation G551D is recovered by genisteinAm J Physiol 277 (1999) C833ndashC839
[254] P Anandakumar S Kamaraj S Jagan G Ramakrishnan R Vinodhkumar TDevaki Capsaicin modulates pulmonary antioxidant defense system during ben-zo(a)pyrene-induced lung cancer in Swiss albinomice Phytother Res 22 (2008)529ndash533
[255] I Rahman Antioxidant therapeutic advances in COPD Ther Adv Respir Dis 2(2008) 351ndash374
[256] AW Boots H Li RP Schins R Duffin JW Heemskerk A Bast GR Haenen Thequercetin paradox Toxicol Appl Pharmacol 222 (2007) 89ndash96
[257] M Joskova S Franova V Sadlonova Acute bronchodilator effect of quercetin inexperimental allergic asthma Bratisl Lek Listy 112 (2011) 9ndash12
[258] HJ Park CM Lee ID Jung JS Lee YI Jeong JH Chang SH Chun MJ Kim IWChoi SC Ahn YK Shin SR Yeom YM Park Quercetin regulates Th1Th2 balancein a murine model of asthma Int Immunopharmacol 9 (2009) 261ndash267
[259] AP Rogerio A Kanashiro C Fontanari EV da Silva YM Lucisano-ValimEG Soares LH Faccioli Anti-inflammatory activity of quercetin and iso-quercitrin in experimental murine allergic asthma Inflamm Res 56 (2007)402ndash408
[260] M Muller Polyphenol cytotoxicity induced by the bacterial toxin pyocyaninrole of NQO1 Free Radic Biol Med 47 (2009) 84ndash91
[261] J Grassmann Terpenoids as plant antioxidants Vitam Horm 72 (2005)505ndash535
[262] P Allen Tea tree oil the science behind the antimicrobial hype Lancet 358(2001) 1245
[263] EC Dasenbrook W Checkley CA Merlo MW Konstan N Lechtzin MP BoyleAssociation between respiratory tract methicillin-resistant Staphylococcus aure-us and survival in cystic fibrosis JAMA 303 (2010) 2386ndash2392
[264] V Bezzerri M Borgatti E Nicolis I Lampronti MC Dechecchi I Mancini PRizzotti R Gambari G Cabrini Transcription factor oligodeoxynucleotides toNF-kappaB inhibit transcription of IL-8 in bronchial cells Am J Respir CellMol Biol 39 (2008) 86ndash96
[265] R Gambari M Borgatti V Bezzerri E Nicolis I Lampronti MC Dechecchi IMancini A Tamanini G Cabrini Decoy oligodeoxyribonucleotides and peptidenucleic acids-DNA chimeras targeting nuclear factor kappa-B inhibition of IL-8 gene expression in cystic fibrosis cells infected with Pseudomonas aeruginosaBiochem Pharmacol 80 (2010) 1887ndash1894
[266] M Adrian P Jeandet AC Douillet-Breuil L Tesson R Bessis Stilbene content ofmature Vitis vinifera berries in response to UV-C elicitation J Agric Food Chem48 (2000) 6103ndash6105
[267] B Paul I Masih J Deopujari C Charpentier Occurrence of resveratrol and pter-ostilbene in age-old darakchasava an ayurvedic medicine from India J Ethno-pharmacol 68 (1999) 71ndash76
[268] I Rahman Antioxidant therapies in COPD Int J Chron Obstruct Pulmon Dis 1(2006) 15ndash29
[269] M Lee S Kim OK Kwon SR Oh HK Lee K Ahn Anti-inflammatory and anti-asthmatic effects of resveratrol a polyphenolic stilbene in a mouse model ofallergic asthma Int Immunopharmacol 9 (2009) 418ndash424
[270] LG Wood PA Wark ML Garg Antioxidant and anti-inflammatory effectsof resveratrol in airway disease Antioxid Redox Signal 13 (2010)1535ndash1548
[271] KV Kiselev Perspectives for production and application of resveratrol ApplMicrobiol Biotechnol 90 (2011) 417ndash425
[272] M Shakibaei C Buhrmann A Mobasheri Resveratrol-mediated SIRT-1 interac-tions with p300 modulate receptor activator of NF-kappaB ligand (RANKL) acti-vation of NF-kappaB signaling and inhibit osteoclastogenesis in bone-derivedcells J Biol Chem 286 (2011) 11492ndash11505
[273] SF Zaidi K Ahmed T Yamamoto T Kondo K Usmanghani M Kadowaki TSugiyama Effect of resveratrol on Helicobacter pylori-induced interleukin-8 secre-tion reactive oxygen species generation and morphological changes in human gas-tric epithelial cells Biol Pharm Bull 32 (2009) 1931ndash1935
[274] JK Kundu YK Shin YJ Surh Resveratrol modulates phorbol ester-inducedpro-inflammatory signal transduction pathways in mouse skin in vivo NF-kappaB and AP-1 as prime targets Biochem Pharmacol 72 (2006)1506ndash1515
[275] NH Nam Naturally occurring NF-kappaB inhibitors Mini Rev Med Chem 6(2006) 945ndash951
[276] JM Smoliga JA Baur HA Hausenblas Resveratrol and healthmdasha comprehen-sive review of human clinical trials Mol Nutr Food Res 55 (2011) 1129ndash1141
[277] ME Juan M Maijo JM Planas Quantification of trans-resveratrol and itsmetabolites in rat plasma and tissues by HPLC J Pharm Biomed Anal 51(2010) 391ndash398
[278] JA Baur DA Sinclair Therapeutic potential of resveratrol the in vivo evidenceNat Rev 5 (2006) 493ndash506
[279] E Nicolis I Lampronti MC Dechecchi M Borgatti A Tamanini N Bianchi VBezzerri I Mancini MG Giri P Rizzotti R Gambari G Cabrini Pyrogallol anactive compound from the medicinal plant Emblica officinalis regulates expres-sion of pro-inflammatory genes in bronchial epithelial cells Int Immunophar-macol 8 (2008) 1672ndash1680
[280] E Nicolis I Lampronti MC Dechecchi M Borgatti A Tamanini V Bezzerri NBianchi M Mazzon I Mancini MG Giri P Rizzotti R Gambari G CabriniModulation of expression of IL-8 gene in bronchial epithelial cells by 5-methoxypsoralen Int Immunopharmacol 9 (2009) 1411ndash1422
[281] M Borgatti I Mancini N Bianchi A Guerrini I Lampronti D Rossi G SacchettiR Gambari Bergamot (Citrus bergamia Risso) fruit extracts and identified com-ponents alter expression of interleukin 8 gene in cystic fibrosis bronchial epithe-lial cell lines BMC Biochem 12 (2011) 15
[282] L Piccagli E Fabbri M Borgatti N Bianchi V Bezzerri I Mancini E Nicolis CMDechecchi I Lampronti G Cabrini R Gambari Virtual screening against p50NF-kappaB transcription factor for the identification of inhibitors of the NF-kappaB-DNA interaction and expression of NF-kappaB upregulated genesChemMedChem 4 (2009) 2024ndash2033
[283] L Piccagli M Borgatti E Nicolis N Bianchi I Mancini I Lampronti D VevaldiF DallAcqua G Cabrini R Gambari Virtual screening against nuclear factorkappaB (NF-kappaB) of a focus library identification of bioactive furocoumarinderivatives inhibiting NF-kappaB dependent biological functions involved incystic fibrosis Bioorg Med Chem 18 (2010) 8341ndash8349
[284] M Borgatti A Chilin L Piccagli I Lampronti N Bianchi I Mancini G Mar-zaro Da Francesco A Guiotto R Gambari Development of a novel furocou-marin derivative inhibiting NF-kappaB dependent biological functionsdesign synthesis and biological effects Eur J Med Chem 46 (2011)4870ndash4877
[285] E Georgy S Le Guellec L Vecellio E Fichant P Stordeur P Bordeau JP PerraudinFeasibility study of OSCN- and lactoferrin (Meveol) nebulization for cysticfibrosis JCyst Fibros 10 (2011) S18
713F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
[286] C Tidei M Piroddi F Galli C Santi Oxidation of thiols promoted by PhSeZnClTetrahedron Lett 53 (2012) 232ndash234
[287] L Semianrio-Vidal C van Hesuden G Mugesh ER Lazarowski Ebselen is a po-tent non-competitive inhibitor of extracellular nucleoside diphosphokinasePurinergic Signal 6 (2010) 383ndash391
[288] C ColussiMC Albertini S Coppola S Rovidati F Galli L Ghibelli H2O2-inducedblockof glycolysis as an active ADP-ribosylation reaction protecting cells from apoptosisFASEB J 14 (2000) 2266ndash2276
[289] H Xiao KL Parkin Induction of phase II enzyme activity by various seleniumcompounds Nutr Cancer 55 (2006) 210ndash223
[290] G Peluffo R Radi Biochemistry of protein tyrosine nitration in cardiovascularpathology Cardiovasc Res 75 (2007) 291ndash302
[291] B Alvarez R Radi Peroxynitrite reactivity with amino acids and proteinsAmino Acids 25 (2003) 295ndash311
[292] B Kamosinska MW Radomski M Duszyk A Radomski SF Man Nitric oxideactivates chloride currents in human lung epithelial cells Am J Physiol 272(1997) L1098ndashL1104
[293] L Chen RP Patel X Teng CA Bosworth JR Lancaster Jr S Matalon Mecha-nisms of cystic fibrosis transmembrane conductance regulator activation by S-nitrosoglutathione J Biol Chem 281 (2006) 9190ndash9199
[294] F Luchetti B CanonicoM BettiM Arcangeletti F PilolliM Piroddi L Canesi S PapaF Galli Melatonin signaling and cell protection function FASEB J 24 (2010)3603ndash3624
[295] MW Bengtsson G Jedstedt G Flemstrom Duodenal bicarbonate secretion inrats stimulation by intra-arterial and luminal guanylin and uroguanylin ActaPhysiol (Oxf) 191 (2007) 309ndash317
[296] CS Nelson JL Marino CN Allen Melatonin receptor potentiation of cyclic AMP andthe cystic fibrosis transmembrane conductance regulator ion channel J Pineal Res 26(1999) 113ndash121
[297] C de Castro-Silva VM de Bruin GM Cunha DM Nunes CAMedeiros PF de BruinMelatonin improves sleep and reduces nitrite in the exhaled breath condensate incystic fibrosismdasha randomized double-blind placebo-controlled study J Pineal Res48 (2010) 65ndash71
[298] I Hornyak E Pankotai L Kiss Z Lacza Current developments in the the-rapeutic potential of S-nitrosoglutathione an endogenous NO-donor mole-cule Curr Pharm Biotechnol (2011) Jan 11 [Epub ahead of print] - PMID21235457
[299] AH Snyder ME McPherson JF Hunt M Johnson JS Stamler B Gaston Acuteeffects of aerosolized S-nitrosoglutathione in cystic fibrosis Am J Respir CritCare Med 165 (2002) 922ndash926
712 F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
[231] F Galli M Cristina Polidori W Stahl P Mecocci FJ Kelly Vitamin E biotransfor-mation in humans Vitam Horm 76 (2007) 263ndash280
[232] J Wiser NE Alexis Q Jiang W Wu C Robinette R Roubey DB Peden In vivogamma-tocopherol supplementation decreases systemic oxidative stress andcytokine responses of human monocytes in normal and asthmatic subjectsFree Radic Biol Med 45 (2008) 40ndash49
[233] JG Wagner Q Jiang JR Harkema B Illek DD Patel BN Ames DB PedenOzone enhancement of lower airway allergic inflammation is prevented bygamma-tocopherol Free Radic Biol Med 43 (2007) 1176ndash1188
[234] JT Harries DP Muller Absorption of different doses of fat soluble and watermiscible preparations of vitamin E in children with cystic fibrosis Arch DisChild 46 (1971) 341ndash344
[235] EI Back C Frindt E Ocenaskova D Nohr M Stern HK Biesalski Can changesin hydrophobicity increase the bioavailability of alpha-tocopherol Eur J Nutr45 (2006) 1ndash6
[236] SZ Nasr MH OLeary C Hillermeier Correction of vitamin E deficiency withfat-soluble versus water-miscible preparations of vitamin E in patients with cys-tic fibrosis J Pediatr 122 (1993) 810ndash812
[237] S Soltani-Frisk E Gronowitz H Andersson B Strandvik Water-miscibletocopherol is not superior to fat-soluble preparation for vitamin E absorptionin cystic fibrosis Acta Paediatr 90 (2001) 1112ndash1115
[238] K Papas J Kalbfleisch R Mohon Bioavailability of a novel water-soluble vi-tamin E formulation in malabsorbing patients Dig Dis Sci 52 (2007)347ndash352
[239] F Antonicelli M Parmentier EM Drost N Hirani I Rahman K Donaldson WMacNee Nacystelyn inhibits oxidant-mediated interleukin-8 expression andNF-kappaB nuclear binding in alveolar epithelial cells Free Radic Biol Med 32(2002) 492ndash502
[240] EM App D Baran I Dab A Malfroot M Coffiner F Vanderbist M King Dose-finding and 24-h monitoring for efficacy and safety of aerosolized Nacystelyn incystic fibrosis Eur Respir J 19 (2002) 294ndash302
[241] MG Traber How much vitamin E hellip Just enough Am J Clin Nutr 84 (2006)959ndash960
[242] JC McCann BN Ames Vitamin K an example of triage theory is micronu-trient inadequacy linked to diseases of aging Am J Clin Nutr 90 (2009)889ndash907
[243] M Fusaro G Crepaldi S Maggi F Galli A DAngelo L Calo S Giannini DMiozzo M Gallieni Vitamin K bone fractures and vascular calcifications inchronic kidney disease an important but poorly studied relationship J Endocri-nol Invest 34 (2010) 317ndash323
[244] JC McCann BN Ames Adaptive dysfunction of selenoproteins from the per-spective of the triage theory why modest selenium deficiency may increaserisk of diseases of aging FASEB J 25 (2011) 1793ndash1814
[245] R Apak K Guclu M Ozyurek B Bektas Oglu M Bener Cupric ion reducing an-tioxidant capacity assay for food antioxidants vitamins polyphenolics and fla-vonoids in food extracts Methods Mol Biol 477 (2008) 163ndash193
[246] F Galli Interactions of polyphenolic compounds with drug disposition and me-tabolism Curr Drug Metab 8 (2007) 830ndash838
[247] RL Prior X Wu K Schaich Standardized methods for the determination of an-tioxidant capacity and phenolics in foods and dietary supplements J Agric FoodChem 53 (2005) 4290ndash4302
[248] C Azbell S Zhang D Skinner J Fortenberry EJ Sorscher BA WoodworthHesperidin stimulates cystic fibrosis transmembrane conductance regulator-mediated chloride secretion and ciliary beat frequency in sinonasal epitheliumOtolaryngol Head Neck Surg 143 (2010) 397ndash404
[249] G Wegrzyn J Jakobkiewicz-Banecka M Gabig-Ciminska E Piotrowska M Nar-ajczyk A Kloska M Malinowska D Dziedzic I Golebiewska M Moskot AWegrzyn Genistein a natural isoflavone with a potential for treatment of ge-netic diseases Biochem Soc Trans 38 (2010) 695ndash701
[250] YC Yu H Miki Y Nakamura A Hanyuda Y Matsuzaki Y Abe M Yasui K Ta-naka TC Hwang SG Bompadre Y Sohma Curcumin and genistein additivelypotentiate G551D-CFTR J Cyst Fibros 10 (2011) 243ndash252
[251] B Illek H Fischer Flavonoids stimulate Cl conductance of human airway epithe-lium in vitro and in vivo Am J Physiol 275 (1998) L902ndashL910
[252] JL Kreindler Cystic fibrosis exploiting its genetic basis in the hunt for newtherapies Pharmacol Ther 125 (2010) 219ndash229
[253] B Illek L Zhang NC Lewis RB Moss JY Dong H Fischer Defective function ofthe cystic fibrosis-causing missense mutation G551D is recovered by genisteinAm J Physiol 277 (1999) C833ndashC839
[254] P Anandakumar S Kamaraj S Jagan G Ramakrishnan R Vinodhkumar TDevaki Capsaicin modulates pulmonary antioxidant defense system during ben-zo(a)pyrene-induced lung cancer in Swiss albinomice Phytother Res 22 (2008)529ndash533
[255] I Rahman Antioxidant therapeutic advances in COPD Ther Adv Respir Dis 2(2008) 351ndash374
[256] AW Boots H Li RP Schins R Duffin JW Heemskerk A Bast GR Haenen Thequercetin paradox Toxicol Appl Pharmacol 222 (2007) 89ndash96
[257] M Joskova S Franova V Sadlonova Acute bronchodilator effect of quercetin inexperimental allergic asthma Bratisl Lek Listy 112 (2011) 9ndash12
[258] HJ Park CM Lee ID Jung JS Lee YI Jeong JH Chang SH Chun MJ Kim IWChoi SC Ahn YK Shin SR Yeom YM Park Quercetin regulates Th1Th2 balancein a murine model of asthma Int Immunopharmacol 9 (2009) 261ndash267
[259] AP Rogerio A Kanashiro C Fontanari EV da Silva YM Lucisano-ValimEG Soares LH Faccioli Anti-inflammatory activity of quercetin and iso-quercitrin in experimental murine allergic asthma Inflamm Res 56 (2007)402ndash408
[260] M Muller Polyphenol cytotoxicity induced by the bacterial toxin pyocyaninrole of NQO1 Free Radic Biol Med 47 (2009) 84ndash91
[261] J Grassmann Terpenoids as plant antioxidants Vitam Horm 72 (2005)505ndash535
[262] P Allen Tea tree oil the science behind the antimicrobial hype Lancet 358(2001) 1245
[263] EC Dasenbrook W Checkley CA Merlo MW Konstan N Lechtzin MP BoyleAssociation between respiratory tract methicillin-resistant Staphylococcus aure-us and survival in cystic fibrosis JAMA 303 (2010) 2386ndash2392
[264] V Bezzerri M Borgatti E Nicolis I Lampronti MC Dechecchi I Mancini PRizzotti R Gambari G Cabrini Transcription factor oligodeoxynucleotides toNF-kappaB inhibit transcription of IL-8 in bronchial cells Am J Respir CellMol Biol 39 (2008) 86ndash96
[265] R Gambari M Borgatti V Bezzerri E Nicolis I Lampronti MC Dechecchi IMancini A Tamanini G Cabrini Decoy oligodeoxyribonucleotides and peptidenucleic acids-DNA chimeras targeting nuclear factor kappa-B inhibition of IL-8 gene expression in cystic fibrosis cells infected with Pseudomonas aeruginosaBiochem Pharmacol 80 (2010) 1887ndash1894
[266] M Adrian P Jeandet AC Douillet-Breuil L Tesson R Bessis Stilbene content ofmature Vitis vinifera berries in response to UV-C elicitation J Agric Food Chem48 (2000) 6103ndash6105
[267] B Paul I Masih J Deopujari C Charpentier Occurrence of resveratrol and pter-ostilbene in age-old darakchasava an ayurvedic medicine from India J Ethno-pharmacol 68 (1999) 71ndash76
[268] I Rahman Antioxidant therapies in COPD Int J Chron Obstruct Pulmon Dis 1(2006) 15ndash29
[269] M Lee S Kim OK Kwon SR Oh HK Lee K Ahn Anti-inflammatory and anti-asthmatic effects of resveratrol a polyphenolic stilbene in a mouse model ofallergic asthma Int Immunopharmacol 9 (2009) 418ndash424
[270] LG Wood PA Wark ML Garg Antioxidant and anti-inflammatory effectsof resveratrol in airway disease Antioxid Redox Signal 13 (2010)1535ndash1548
[271] KV Kiselev Perspectives for production and application of resveratrol ApplMicrobiol Biotechnol 90 (2011) 417ndash425
[272] M Shakibaei C Buhrmann A Mobasheri Resveratrol-mediated SIRT-1 interac-tions with p300 modulate receptor activator of NF-kappaB ligand (RANKL) acti-vation of NF-kappaB signaling and inhibit osteoclastogenesis in bone-derivedcells J Biol Chem 286 (2011) 11492ndash11505
[273] SF Zaidi K Ahmed T Yamamoto T Kondo K Usmanghani M Kadowaki TSugiyama Effect of resveratrol on Helicobacter pylori-induced interleukin-8 secre-tion reactive oxygen species generation and morphological changes in human gas-tric epithelial cells Biol Pharm Bull 32 (2009) 1931ndash1935
[274] JK Kundu YK Shin YJ Surh Resveratrol modulates phorbol ester-inducedpro-inflammatory signal transduction pathways in mouse skin in vivo NF-kappaB and AP-1 as prime targets Biochem Pharmacol 72 (2006)1506ndash1515
[275] NH Nam Naturally occurring NF-kappaB inhibitors Mini Rev Med Chem 6(2006) 945ndash951
[276] JM Smoliga JA Baur HA Hausenblas Resveratrol and healthmdasha comprehen-sive review of human clinical trials Mol Nutr Food Res 55 (2011) 1129ndash1141
[277] ME Juan M Maijo JM Planas Quantification of trans-resveratrol and itsmetabolites in rat plasma and tissues by HPLC J Pharm Biomed Anal 51(2010) 391ndash398
[278] JA Baur DA Sinclair Therapeutic potential of resveratrol the in vivo evidenceNat Rev 5 (2006) 493ndash506
[279] E Nicolis I Lampronti MC Dechecchi M Borgatti A Tamanini N Bianchi VBezzerri I Mancini MG Giri P Rizzotti R Gambari G Cabrini Pyrogallol anactive compound from the medicinal plant Emblica officinalis regulates expres-sion of pro-inflammatory genes in bronchial epithelial cells Int Immunophar-macol 8 (2008) 1672ndash1680
[280] E Nicolis I Lampronti MC Dechecchi M Borgatti A Tamanini V Bezzerri NBianchi M Mazzon I Mancini MG Giri P Rizzotti R Gambari G CabriniModulation of expression of IL-8 gene in bronchial epithelial cells by 5-methoxypsoralen Int Immunopharmacol 9 (2009) 1411ndash1422
[281] M Borgatti I Mancini N Bianchi A Guerrini I Lampronti D Rossi G SacchettiR Gambari Bergamot (Citrus bergamia Risso) fruit extracts and identified com-ponents alter expression of interleukin 8 gene in cystic fibrosis bronchial epithe-lial cell lines BMC Biochem 12 (2011) 15
[282] L Piccagli E Fabbri M Borgatti N Bianchi V Bezzerri I Mancini E Nicolis CMDechecchi I Lampronti G Cabrini R Gambari Virtual screening against p50NF-kappaB transcription factor for the identification of inhibitors of the NF-kappaB-DNA interaction and expression of NF-kappaB upregulated genesChemMedChem 4 (2009) 2024ndash2033
[283] L Piccagli M Borgatti E Nicolis N Bianchi I Mancini I Lampronti D VevaldiF DallAcqua G Cabrini R Gambari Virtual screening against nuclear factorkappaB (NF-kappaB) of a focus library identification of bioactive furocoumarinderivatives inhibiting NF-kappaB dependent biological functions involved incystic fibrosis Bioorg Med Chem 18 (2010) 8341ndash8349
[284] M Borgatti A Chilin L Piccagli I Lampronti N Bianchi I Mancini G Mar-zaro Da Francesco A Guiotto R Gambari Development of a novel furocou-marin derivative inhibiting NF-kappaB dependent biological functionsdesign synthesis and biological effects Eur J Med Chem 46 (2011)4870ndash4877
[285] E Georgy S Le Guellec L Vecellio E Fichant P Stordeur P Bordeau JP PerraudinFeasibility study of OSCN- and lactoferrin (Meveol) nebulization for cysticfibrosis JCyst Fibros 10 (2011) S18
713F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
[286] C Tidei M Piroddi F Galli C Santi Oxidation of thiols promoted by PhSeZnClTetrahedron Lett 53 (2012) 232ndash234
[287] L Semianrio-Vidal C van Hesuden G Mugesh ER Lazarowski Ebselen is a po-tent non-competitive inhibitor of extracellular nucleoside diphosphokinasePurinergic Signal 6 (2010) 383ndash391
[288] C ColussiMC Albertini S Coppola S Rovidati F Galli L Ghibelli H2O2-inducedblockof glycolysis as an active ADP-ribosylation reaction protecting cells from apoptosisFASEB J 14 (2000) 2266ndash2276
[289] H Xiao KL Parkin Induction of phase II enzyme activity by various seleniumcompounds Nutr Cancer 55 (2006) 210ndash223
[290] G Peluffo R Radi Biochemistry of protein tyrosine nitration in cardiovascularpathology Cardiovasc Res 75 (2007) 291ndash302
[291] B Alvarez R Radi Peroxynitrite reactivity with amino acids and proteinsAmino Acids 25 (2003) 295ndash311
[292] B Kamosinska MW Radomski M Duszyk A Radomski SF Man Nitric oxideactivates chloride currents in human lung epithelial cells Am J Physiol 272(1997) L1098ndashL1104
[293] L Chen RP Patel X Teng CA Bosworth JR Lancaster Jr S Matalon Mecha-nisms of cystic fibrosis transmembrane conductance regulator activation by S-nitrosoglutathione J Biol Chem 281 (2006) 9190ndash9199
[294] F Luchetti B CanonicoM BettiM Arcangeletti F PilolliM Piroddi L Canesi S PapaF Galli Melatonin signaling and cell protection function FASEB J 24 (2010)3603ndash3624
[295] MW Bengtsson G Jedstedt G Flemstrom Duodenal bicarbonate secretion inrats stimulation by intra-arterial and luminal guanylin and uroguanylin ActaPhysiol (Oxf) 191 (2007) 309ndash317
[296] CS Nelson JL Marino CN Allen Melatonin receptor potentiation of cyclic AMP andthe cystic fibrosis transmembrane conductance regulator ion channel J Pineal Res 26(1999) 113ndash121
[297] C de Castro-Silva VM de Bruin GM Cunha DM Nunes CAMedeiros PF de BruinMelatonin improves sleep and reduces nitrite in the exhaled breath condensate incystic fibrosismdasha randomized double-blind placebo-controlled study J Pineal Res48 (2010) 65ndash71
[298] I Hornyak E Pankotai L Kiss Z Lacza Current developments in the the-rapeutic potential of S-nitrosoglutathione an endogenous NO-donor mole-cule Curr Pharm Biotechnol (2011) Jan 11 [Epub ahead of print] - PMID21235457
[299] AH Snyder ME McPherson JF Hunt M Johnson JS Stamler B Gaston Acuteeffects of aerosolized S-nitrosoglutathione in cystic fibrosis Am J Respir CritCare Med 165 (2002) 922ndash926
713F Galli et al Biochimica et Biophysica Acta 1822 (2012) 690ndash713
[286] C Tidei M Piroddi F Galli C Santi Oxidation of thiols promoted by PhSeZnClTetrahedron Lett 53 (2012) 232ndash234
[287] L Semianrio-Vidal C van Hesuden G Mugesh ER Lazarowski Ebselen is a po-tent non-competitive inhibitor of extracellular nucleoside diphosphokinasePurinergic Signal 6 (2010) 383ndash391
[288] C ColussiMC Albertini S Coppola S Rovidati F Galli L Ghibelli H2O2-inducedblockof glycolysis as an active ADP-ribosylation reaction protecting cells from apoptosisFASEB J 14 (2000) 2266ndash2276
[289] H Xiao KL Parkin Induction of phase II enzyme activity by various seleniumcompounds Nutr Cancer 55 (2006) 210ndash223
[290] G Peluffo R Radi Biochemistry of protein tyrosine nitration in cardiovascularpathology Cardiovasc Res 75 (2007) 291ndash302
[291] B Alvarez R Radi Peroxynitrite reactivity with amino acids and proteinsAmino Acids 25 (2003) 295ndash311
[292] B Kamosinska MW Radomski M Duszyk A Radomski SF Man Nitric oxideactivates chloride currents in human lung epithelial cells Am J Physiol 272(1997) L1098ndashL1104
[293] L Chen RP Patel X Teng CA Bosworth JR Lancaster Jr S Matalon Mecha-nisms of cystic fibrosis transmembrane conductance regulator activation by S-nitrosoglutathione J Biol Chem 281 (2006) 9190ndash9199
[294] F Luchetti B CanonicoM BettiM Arcangeletti F PilolliM Piroddi L Canesi S PapaF Galli Melatonin signaling and cell protection function FASEB J 24 (2010)3603ndash3624
[295] MW Bengtsson G Jedstedt G Flemstrom Duodenal bicarbonate secretion inrats stimulation by intra-arterial and luminal guanylin and uroguanylin ActaPhysiol (Oxf) 191 (2007) 309ndash317
[296] CS Nelson JL Marino CN Allen Melatonin receptor potentiation of cyclic AMP andthe cystic fibrosis transmembrane conductance regulator ion channel J Pineal Res 26(1999) 113ndash121
[297] C de Castro-Silva VM de Bruin GM Cunha DM Nunes CAMedeiros PF de BruinMelatonin improves sleep and reduces nitrite in the exhaled breath condensate incystic fibrosismdasha randomized double-blind placebo-controlled study J Pineal Res48 (2010) 65ndash71
[298] I Hornyak E Pankotai L Kiss Z Lacza Current developments in the the-rapeutic potential of S-nitrosoglutathione an endogenous NO-donor mole-cule Curr Pharm Biotechnol (2011) Jan 11 [Epub ahead of print] - PMID21235457
[299] AH Snyder ME McPherson JF Hunt M Johnson JS Stamler B Gaston Acuteeffects of aerosolized S-nitrosoglutathione in cystic fibrosis Am J Respir CritCare Med 165 (2002) 922ndash926
Related Documents