1 1 FORXIGA Educational Slide Resource 732HQ12PM083 Date of preparation: October 2012

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
11
FORXIGAEducational Slide Resource
732HQ12PM083Date of preparation: October 2012
2
Introducing FORXIGA
• FORXIGA, a first-in-class SGLT2 inhibitor, removes excess glucose via an insulin-independent mechanism of action and provides:
*In patients with severe hepatic impairment, a starting dose of 5 mg is recommended. If well tolerated, the dose may be increased up to 10 mg.
1. Bailey CJ, et al. Lancet 2010;375:2223–33; 2. Bailey CJ, et al. Diabetes 2011;60(Suppl. 1):988-P; 3. Nauck MA, et al. Diabetes Care 2011;34:2015–22; 4. Nauck MA, et al. Diabetes 2011;60(Suppl. 1):Poster 40-LB; 5. FORXIGA®. Summary of product characteristics. Bristol-Myers Squibb/AstraZeneca EEIG, 2012.
• Significant and sustained HbA1c reductions1–5
• Additional benefits of weight loss1–5
and a reduction in blood pressure1,5
• Low incidence of hypoglycaemia1
• In one 10 mg tablet a day5*
“Add on for patients uncontrolled on metformin who need the additional benefit of weight loss and have normal or only mildly impaired renal function”
3
Overview
• Current challenges in Type 2 diabetes
• The role of the kidney in Type 2 diabetes
• FORXIGA (dapagliflozin)• Mechanism of action• Efficacy and safety profile• Dosing and administration
4
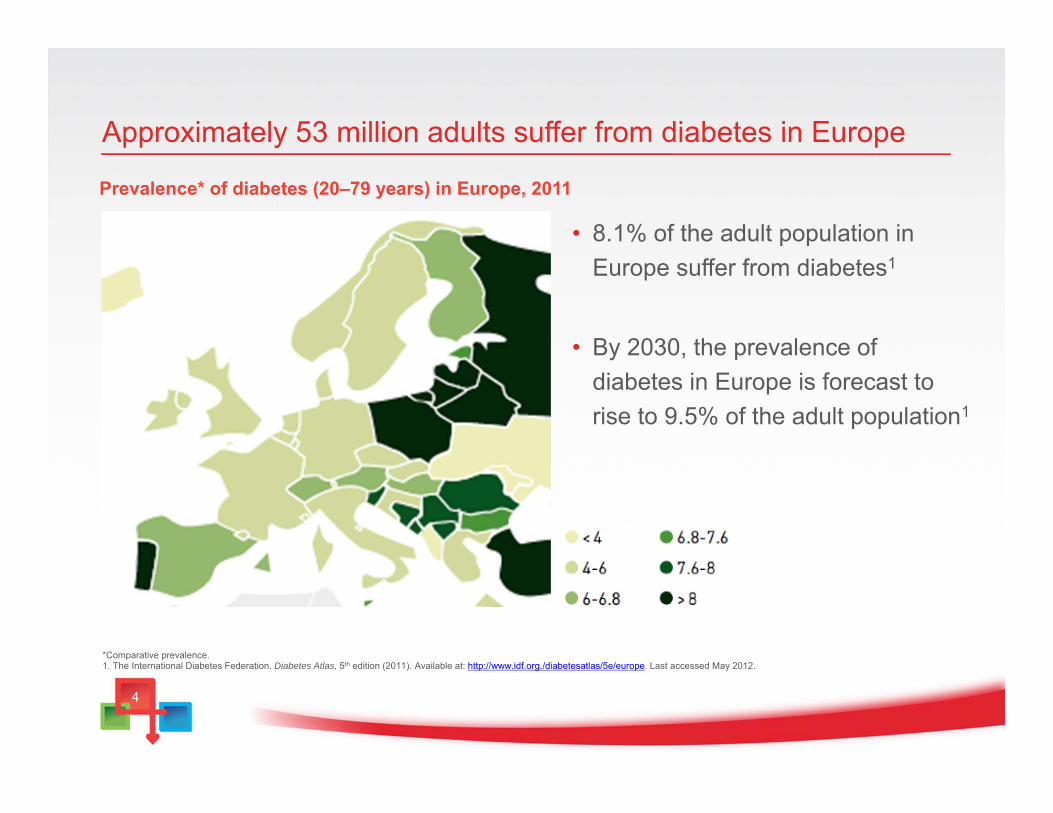
Approximately 53 million adults suffer from diabetes in Europe
Prevalence* of diabetes (20–79 years) in Europe, 2011
*Comparative prevalence.1. The International Diabetes Federation. Diabetes Atlas, 5th edition (2011). Available at: http://www.idf.org./diabetesatlas/5e/europe. Last accessed May 2012.
• 8.1% of the adult population in Europe suffer from diabetes1
• By 2030, the prevalence of diabetes in Europe is forecast to rise to 9.5% of the adult population1
5
0
20
40
60
80
100
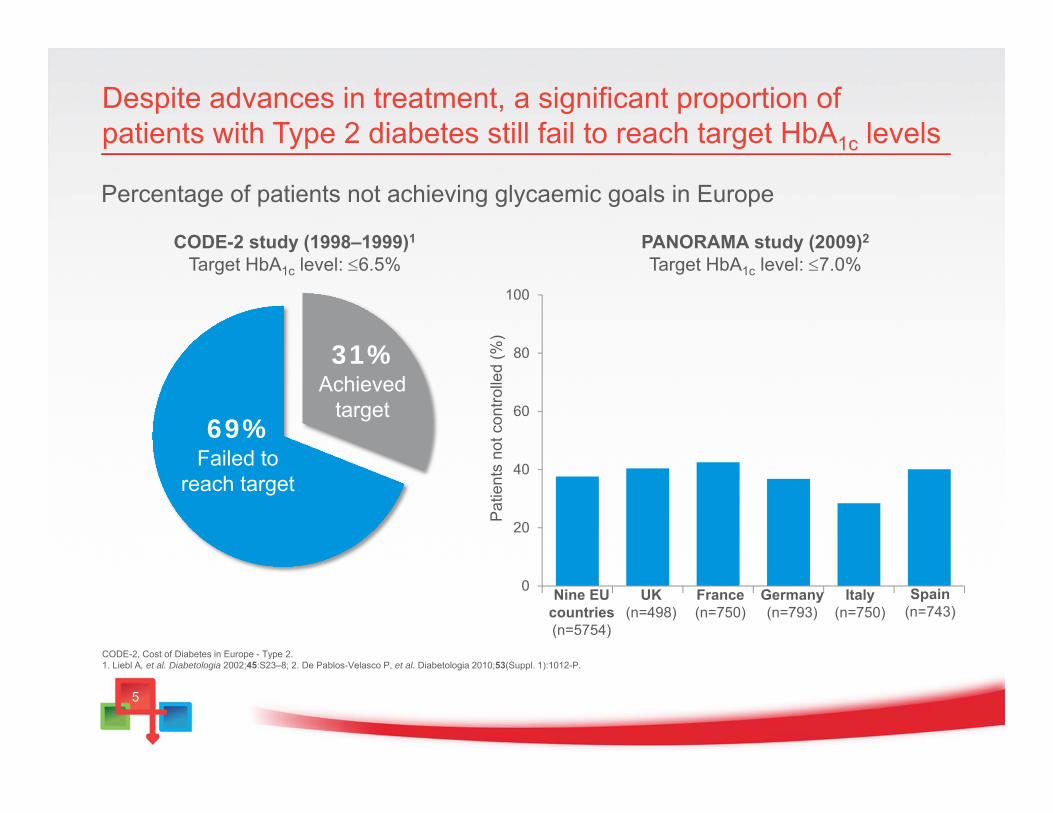
Despite advances in treatment, a significant proportion of patients with Type 2 diabetes still fail to reach target HbA1c levels
Percentage of patients not achieving glycaemic goals in Europe
CODE-2, Cost of Diabetes in Europe - Type 2. 1. Liebl A, et al. Diabetologia 2002;45:S23–8; 2. De Pablos-Velasco P, et al. Diabetologia 2010;53(Suppl. 1):1012-P.
CODE-2 study (1998–1999)1
Target HbA1c level: 6.5%
69%Failed to
reach target
31%Achieved
target
Pat
ient
s no
t con
trolle
d (%
)
UK(n=498)
France(n=750)
Germany(n=793)
Italy(n=750)
Spain(n=743)
PANORAMA study (2009)2
Target HbA1c level: 7.0%
Nine EU countries(n=5754)
6
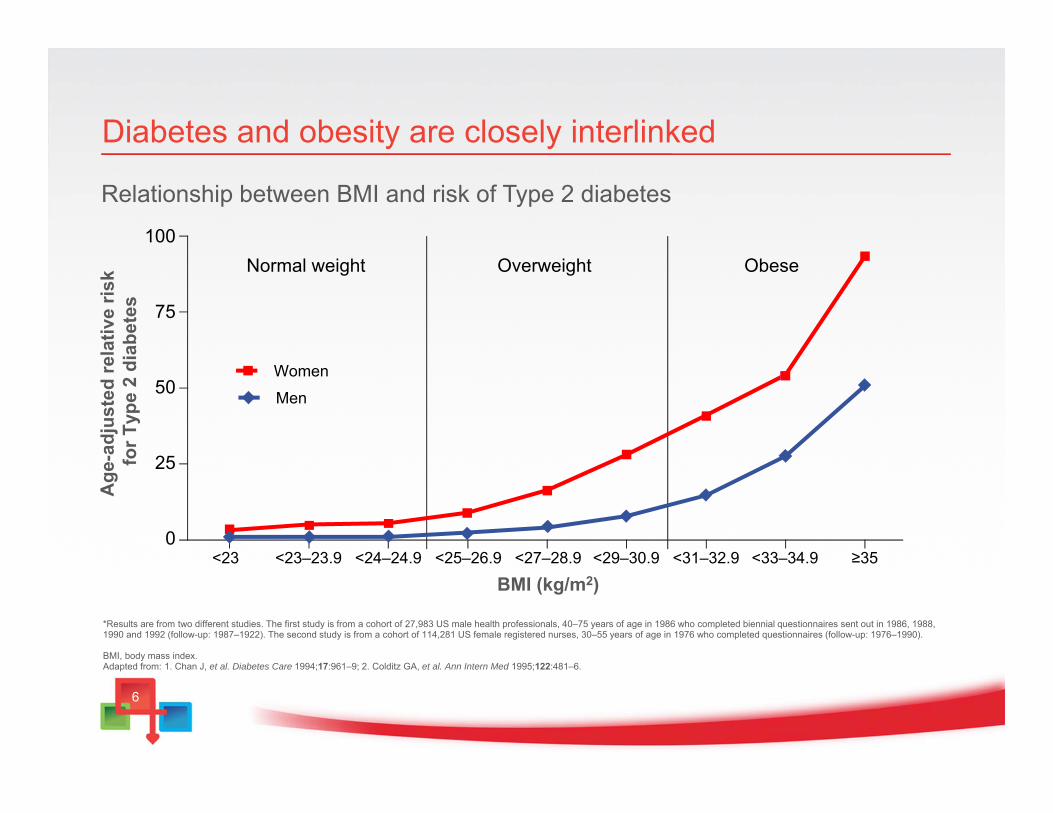
Diabetes and obesity are closely interlinked
Relationship between BMI and risk of Type 2 diabetes
*Results are from two different studies. The first study is from a cohort of 27,983 US male health professionals, 40–75 years of age in 1986 who completed biennial questionnaires sent out in 1986, 1988, 1990 and 1992 (follow-up: 1987–1922). The second study is from a cohort of 114,281 US female registered nurses, 30–55 years of age in 1976 who completed questionnaires (follow-up: 1976–1990).
BMI, body mass index.Adapted from: 1. Chan J, et al. Diabetes Care 1994;17:961–9; 2. Colditz GA, et al. Ann Intern Med 1995;122:481–6.
100
75
50
25
0<23 <23–23.9 <24–24.9 <25–26.9 <27–28.9 <29–30.9 <31–32.9 <33–34.9 ≥35
Normal weight Overweight Obese
Women
Men
Age
-adj
uste
d re
lativ
e ris
k fo
r Typ
e 2
diab
etes
BMI (kg/m2)
7
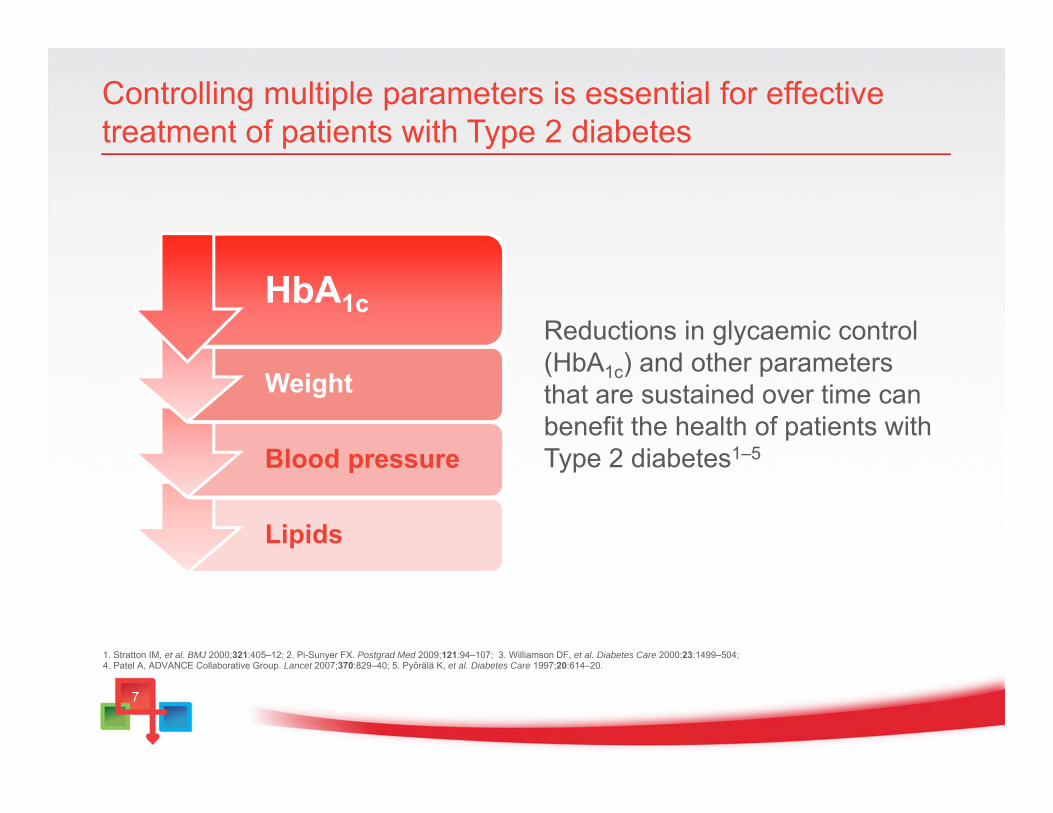
Controlling multiple parameters is essential for effective treatment of patients with Type 2 diabetes
Lipids
Blood pressure
Weight
HbA1c
1. Stratton IM, et al. BMJ 2000;321:405–12; 2. Pi-Sunyer FX. Postgrad Med 2009;121:94–107; 3. Williamson DF, et al. Diabetes Care 2000;23:1499–504; 4. Patel A, ADVANCE Collaborative Group. Lancet 2007;370:829–40; 5. Pyǒrälä K, et al. Diabetes Care 1997;20:614–20.
Reductions in glycaemic control (HbA1c) and other parameters that are sustained over time can benefit the health of patients with Type 2 diabetes1–5
8
The role of the kidney in Type 2 diabetesand SGLT2 inhibition
9
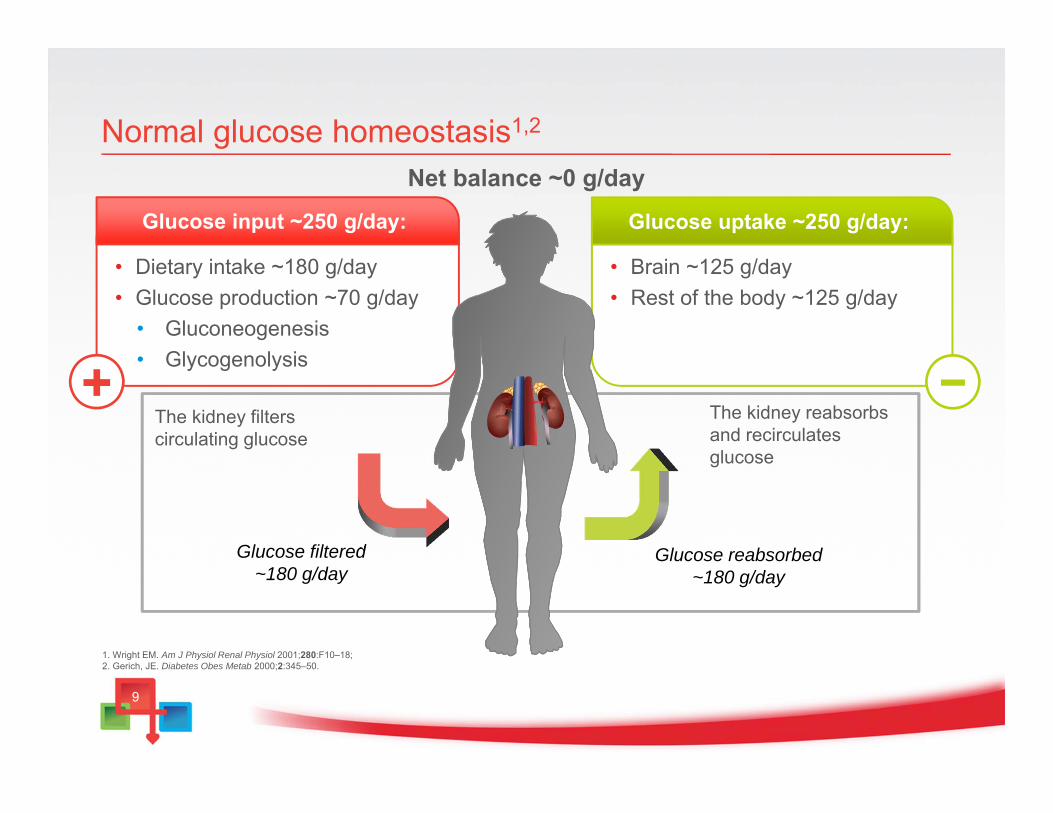
• Brain ~125 g/day• Rest of the body ~125 g/day
Glucose uptake ~250 g/day:
−
• Dietary intake ~180 g/day• Glucose production ~70 g/day
• Gluconeogenesis• Glycogenolysis
Normal glucose homeostasis1,2
+
Net balance ~0 g/day
Glucose input ~250 g/day:
The kidney filters circulating glucose
Glucose filtered~180 g/day
Glucose reabsorbed~180 g/day
The kidney reabsorbs and recirculates glucose
1. Wright EM. Am J Physiol Renal Physiol 2001;280:F10–18; 2. Gerich, JE. Diabetes Obes Metab 2000;2:345–50.
10
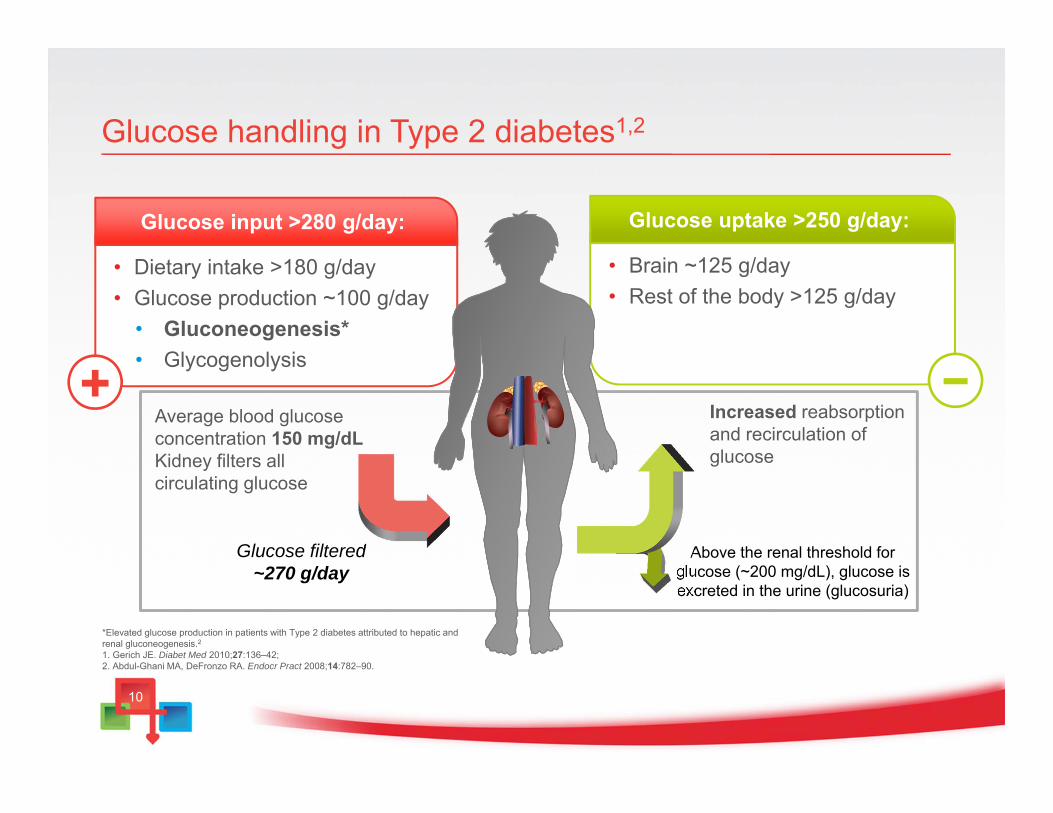
• Dietary intake >180 g/day• Glucose production ~100 g/day
• Gluconeogenesis*• Glycogenolysis
Glucose input >280 g/day:
• Brain ~125 g/day• Rest of the body >125 g/day
Glucose uptake >250 g/day:
Glucose handling in Type 2 diabetes1,2
−Increased reabsorption and recirculation of glucose
Average blood glucose concentration 150 mg/dLKidney filters allcirculating glucose
Above the renal threshold for glucose (~200 mg/dL), glucose is excreted in the urine (glucosuria)
+
Glucose filtered~270 g/day
*Elevated glucose production in patients with Type 2 diabetes attributed to hepatic and renal gluconeogenesis.21. Gerich JE. Diabet Med 2010;27:136–42; 2. Abdul-Ghani MA, DeFronzo RA. Endocr Pract 2008;14:782–90.
1111
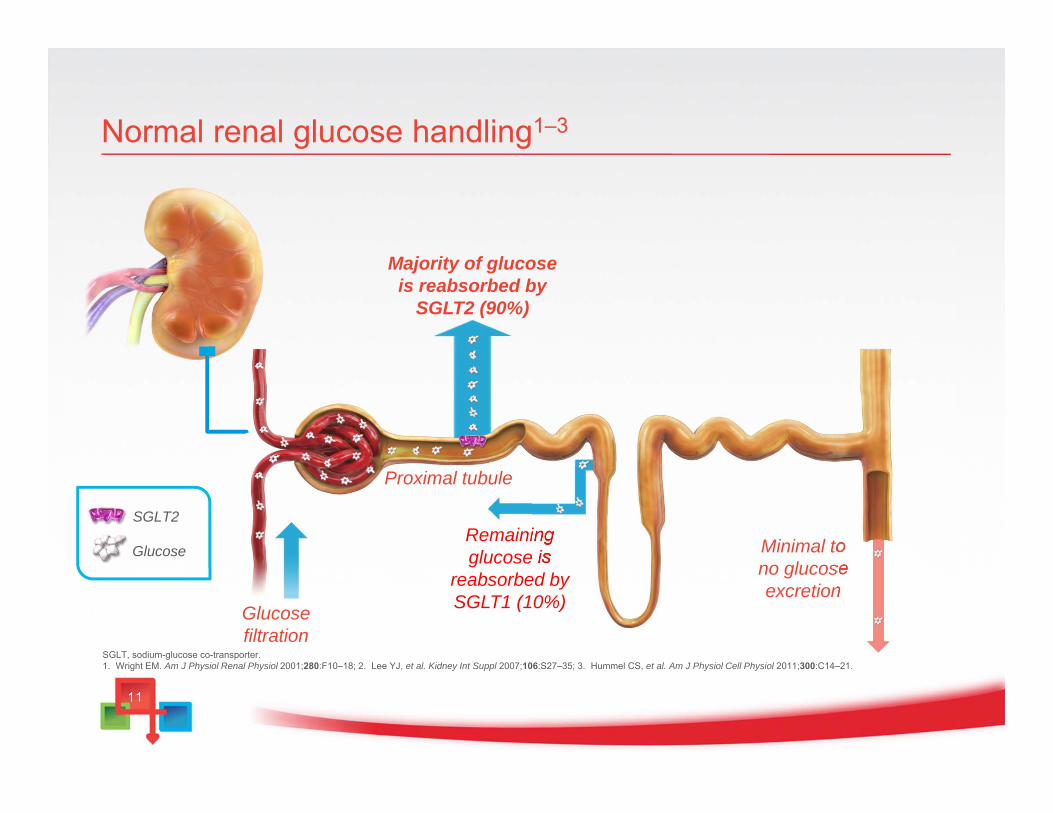
Normal renal glucose handling1–3
SGLT2
Glucose
Majority of glucose is reabsorbed by
SGLT2 (90%)
Proximal tubule
Remaining glucose is
reabsorbed by SGLT1 (10%)Glucose
filtration
Minimal to no glucose excretion
SGLT, sodium-glucose co-transporter. 1. Wright EM. Am J Physiol Renal Physiol 2001;280:F10–18; 2. Lee YJ, et al. Kidney Int Suppl 2007;106:S27–35; 3. Hummel CS, et al. Am J Physiol Cell Physiol 2011;300:C14–21.
12
1
2
3
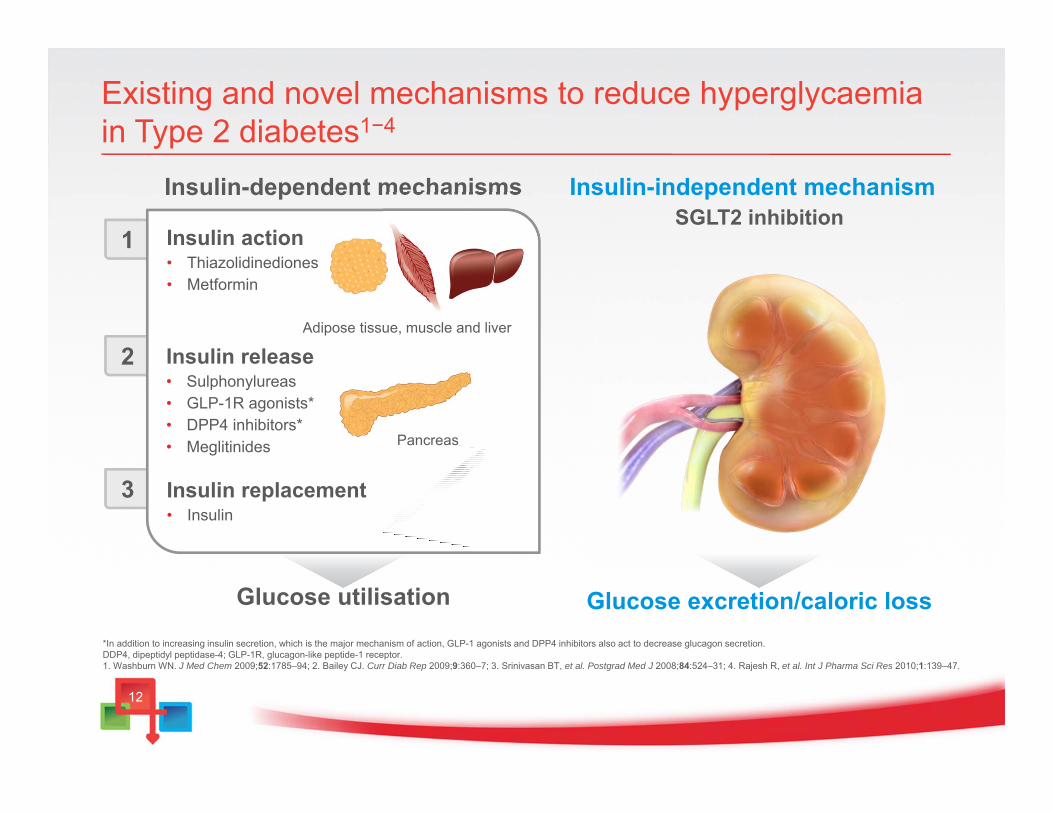
Existing and novel mechanisms to reduce hyperglycaemiain Type 2 diabetes1−4
Insulin action• Thiazolidinediones• Metformin
Insulin release• Sulphonylureas• GLP-1R agonists*• DPP4 inhibitors*• Meglitinides
Insulin replacement• Insulin
Glucose utilisation
Insulin-dependent mechanisms
Adipose tissue, muscle and liver
Glucose excretion/caloric loss
Insulin-independent mechanismSGLT2 inhibition
*In addition to increasing insulin secretion, which is the major mechanism of action, GLP-1 agonists and DPP4 inhibitors also act to decrease glucagon secretion.DDP4, dipeptidyl peptidase-4; GLP-1R, glucagon-like peptide-1 receptor. 1. Washburn WN. J Med Chem 2009;52:1785–94; 2. Bailey CJ. Curr Diab Rep 2009;9:360–7; 3. Srinivasan BT, et al. Postgrad Med J 2008;84:524–31; 4. Rajesh R, et al. Int J Pharma Sci Res 2010;1:139–47.
Pancreas
1313
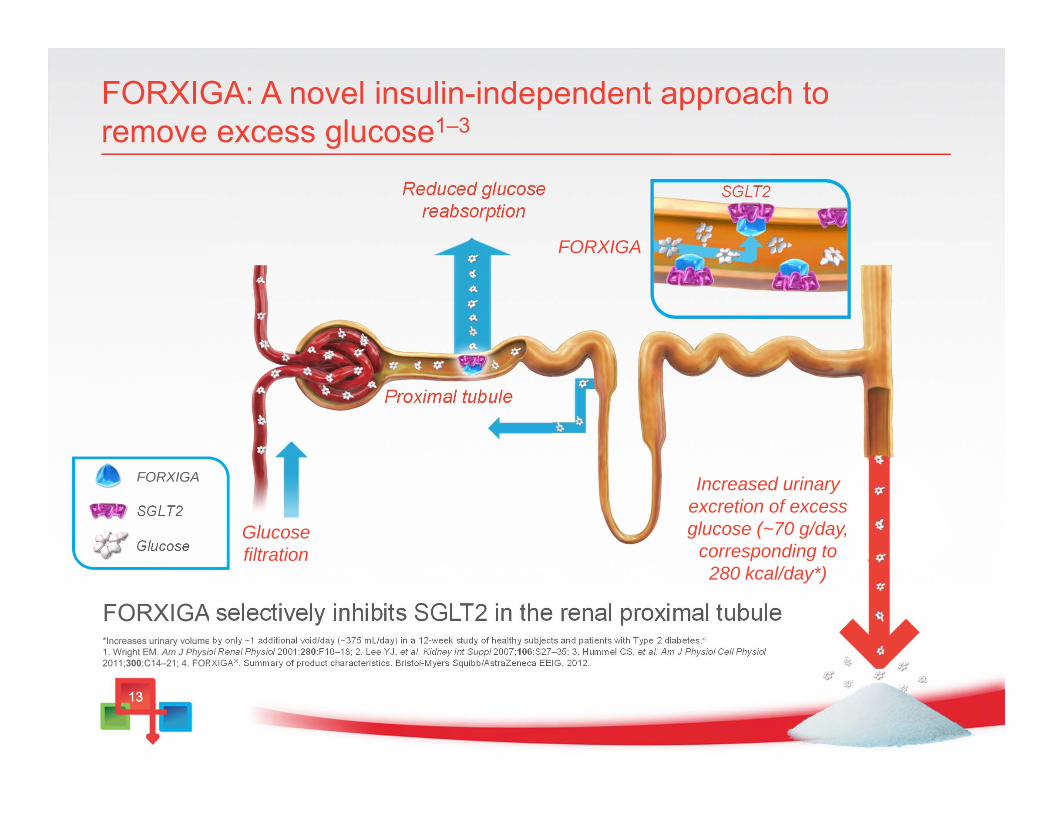
FORXIGA: A novel insulin-independent approach to remove excess glucose1–3
*Increases urinary volume by only ~1 additional void/day (~375 mL/day) in a 12-week study of healthy subjects and patients with Type 2 diabetes.41. Wright EM. Am J Physiol Renal Physiol 2001;280:F10–18; 2. Lee YJ, et al. Kidney Int Suppl 2007;106:S27–35; 3. Hummel CS, et al. Am J Physiol Cell Physiol2011;300:C14–21; 4. FORXIGA®. Summary of product characteristics. Bristol-Myers Squibb/AstraZeneca EEIG, 2012.
FORXIGA selectively inhibits SGLT2 in the renal proximal tubule
SGLT2Reduced glucose reabsorption
Increased urinary excretion of excess glucose (~70 g/day,
corresponding to 280 kcal/day*)
Proximal tubule
Glucosefiltration
SGLT2
Glucose
FORXIGA
FORXIGA
14
The benefits of FORXIGA’s unique mechanism of action
• FORXIGA’s inhibition of SGLT2 results in daily urinary excretion of excess glucose ~70 g, providing:1
• Significant HbA1c reductions2,3
• Additional benefits of weight loss and a reduction in blood pressure2
FORXIGA acts independently of insulin mechanisms2
Works regardless of β-cell function
Complements insulin-dependent
mechanisms
Low propensity for hypoglycaemia
1. List JF, et al. Diabetes Care 2009;32:650–7; 2. Bailey CJ, et al. Lancet 2010;375:2223–33; 3. Bailey CJ, et al. Diabetes 2011;60(Suppl. 1):988-P.
15
FORXIGA is indicated in adults with Type 2 diabetes to improve glycaemic control as...
• Add-on combination therapy • In combination with a monotherapy of metformin, a monotherapy of
sulphonylureas or a treatment with insulin (± oral antidiabetic drugs) when these, together with diet and exercise, do not provide adequate glycaemic control
• Monotherapy• When diet and exercise alone do not provide adequate glycaemic control
in patients for whom use of metformin is considered inappropriate due to intolerance
The use of FORXIGA with pioglitazone is not recommended. FORXIGA has not been studied in combination with DPP4 inhibitors or GLP-1 analogues. FORXIGA®. Summary of product characteristics. Bristol-Myers Squibb/AstraZeneca EEIG, 2012.
1616
FORXIGA clinical data
1717
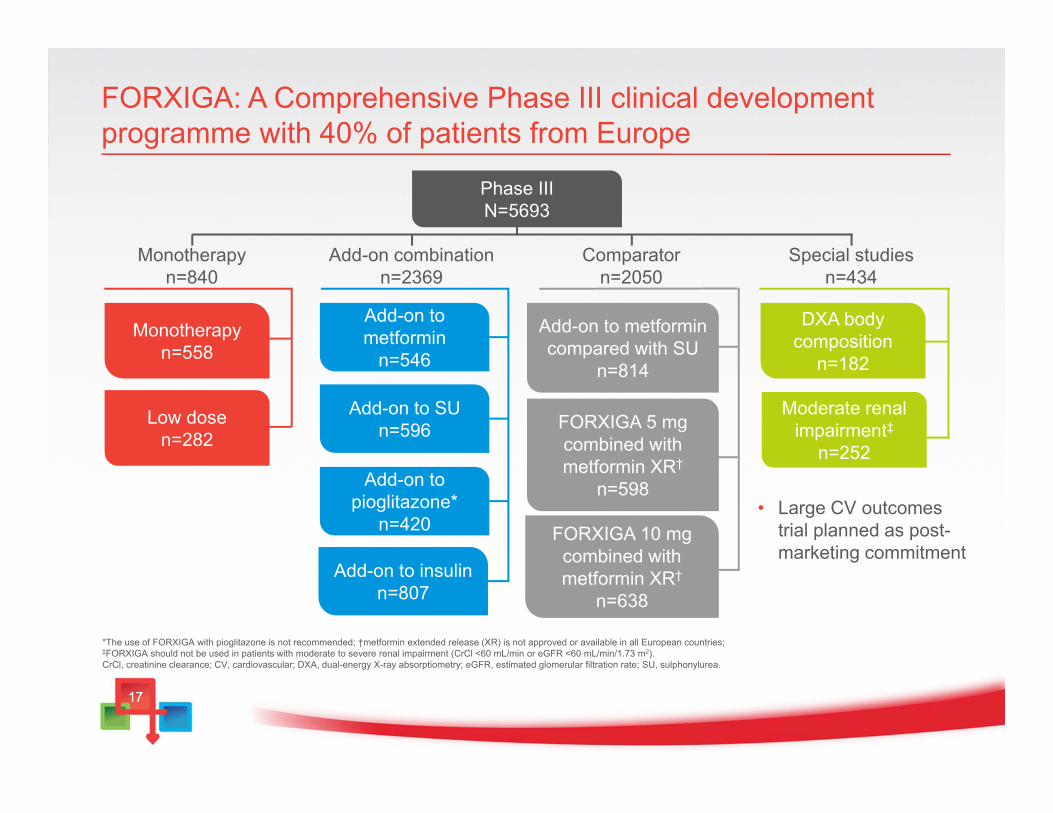
FORXIGA: A Comprehensive Phase III clinical development programme with 40% of patients from Europe
Phase IIIN=5693
Monotherapyn=840
Add-on combinationn=2369
Comparatorn=2050
Add-on to SUn=596
Add-on to metformin
n=546
Special studiesn=434
Monotherapyn=558
Low dosen=282
Add-on to pioglitazone*
n=420
Add-on to insulinn=807
Moderate renal impairment‡
n=252
DXA body composition
n=182
*The use of FORXIGA with pioglitazone is not recommended; †metformin extended release (XR) is not approved or available in all European countries; ‡FORXIGA should not be used in patients with moderate to severe renal impairment (CrCl <60 mL/min or eGFR <60 mL/min/1.73 m2).CrCl, creatinine clearance; CV, cardiovascular; DXA, dual-energy X-ray absorptiometry; eGFR, estimated glomerular filtration rate; SU, sulphonylurea.
Add-on to metformin compared with SU
n=814
FORXIGA 5 mg combined with metformin XR†
n=598
FORXIGA 10 mgcombined with metformin XR†
n=638
• Large CV outcomes trial planned as post-marketing commitment
1818
-1.0
-0.8
-0.6
-0.4
-0.2
0.0
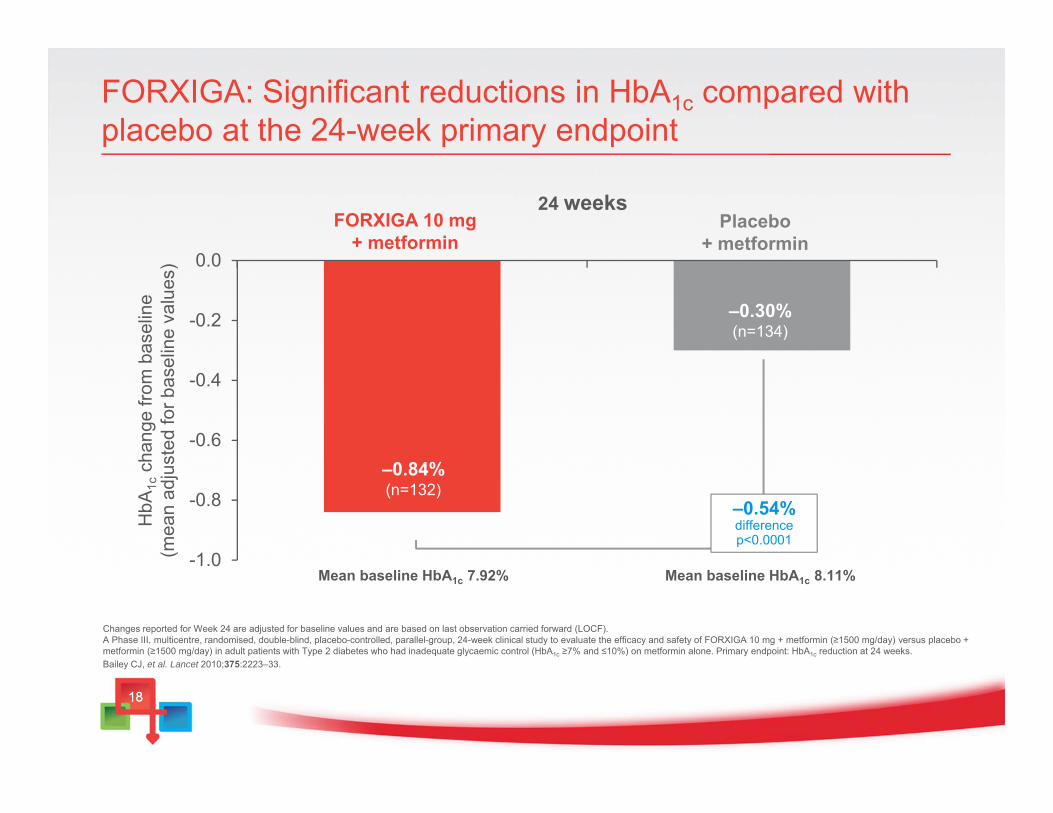
FORXIGA: Significant reductions in HbA1c compared with placebo at the 24-week primary endpoint
Changes reported for Week 24 are adjusted for baseline values and are based on last observation carried forward (LOCF). A Phase III, multicentre, randomised, double-blind, placebo-controlled, parallel-group, 24-week clinical study to evaluate the efficacy and safety of FORXIGA 10 mg + metformin (≥1500 mg/day) versus placebo + metformin (≥1500 mg/day) in adult patients with Type 2 diabetes who had inadequate glycaemic control (HbA1c ≥7% and ≤10%) on metformin alone. Primary endpoint: HbA1c reduction at 24 weeks.Bailey CJ, et al. Lancet 2010;375:2223–33.
–0.54% difference p<0.0001
HbA
1cch
ange
from
bas
elin
e(m
ean
adju
sted
for b
asel
ine
valu
es)
FORXIGA 10 mg + metformin
24 weeksPlacebo
+ metformin
–0.30%(n=134)
–0.84%(n=132)
Mean baseline HbA1c 7.92% Mean baseline HbA1c 8.11%
19
-1.0
-0.8
-0.6
-0.4
-0.2
0.0
0.2
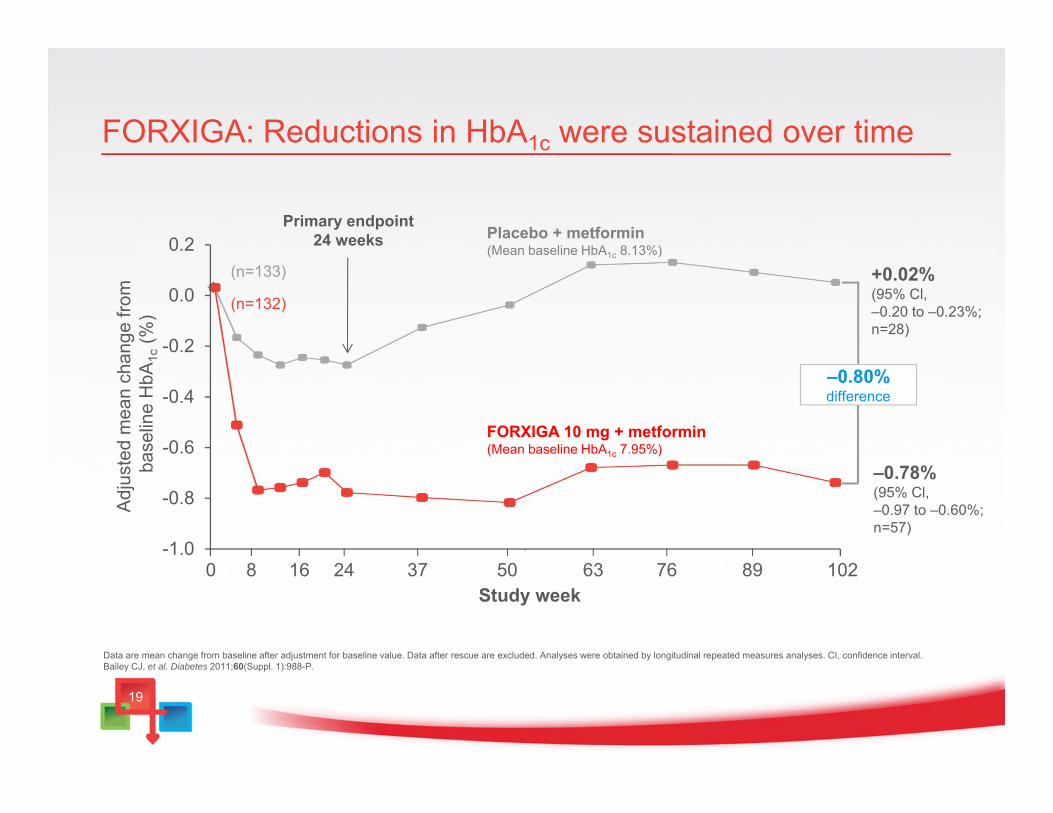
FORXIGA: Reductions in HbA1c were sustained over time
Data are mean change from baseline after adjustment for baseline value. Data after rescue are excluded. Analyses were obtained by longitudinal repeated measures analyses. CI, confidence interval. Bailey CJ, et al. Diabetes 2011;60(Suppl. 1):988-P.
Adj
uste
d m
ean
chan
ge fr
om
base
line
HbA
1c(%
)
Study week
+0.02%(95% Cl, –0.20 to –0.23%; n=28)
–0.78%(95% Cl, –0.97 to –0.60%; n=57)
FORXIGA 10 mg + metformin(Mean baseline HbA1c 7.95%)
Placebo + metformin(Mean baseline HbA1c 8.13%)
0 102
(n=133)
(n=132)
–0.80%difference
8 16 24 37 6350 76 89
Primary endpoint24 weeks
20
-4.0
-3.0
-2.0
-1.0
0.0
1.0
2.0
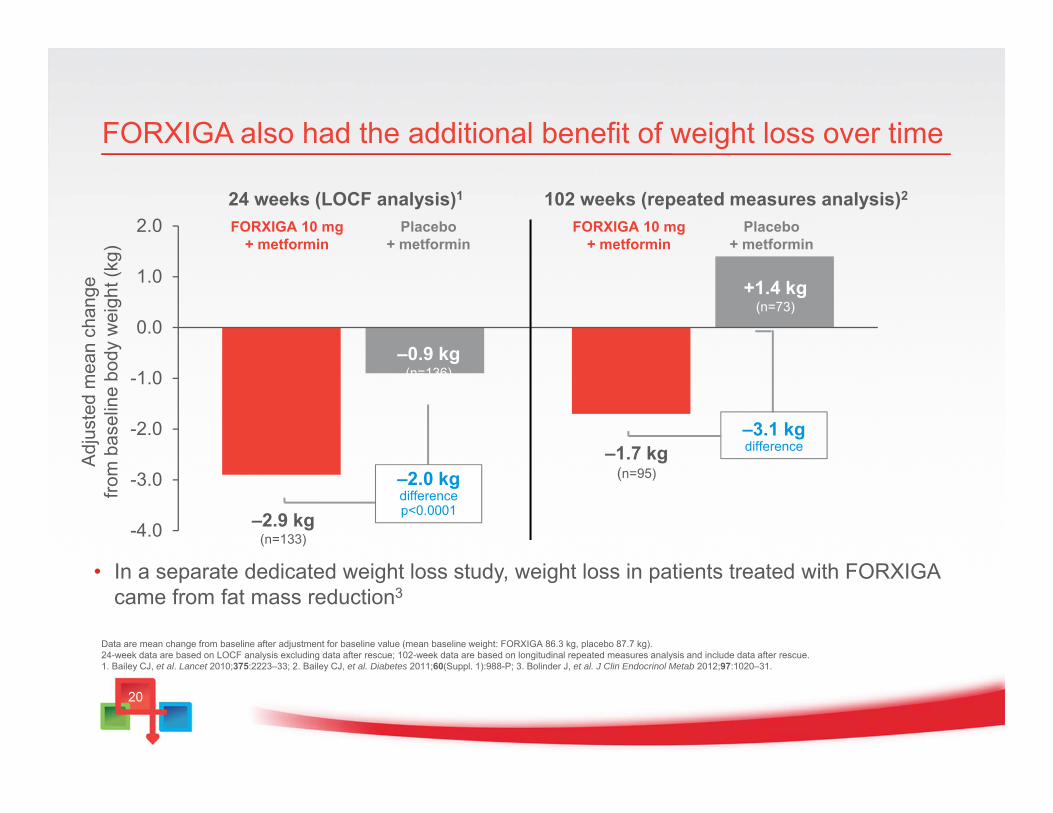
FORXIGA also had the additional benefit of weight loss over time
• In a separate dedicated weight loss study, weight loss in patients treated with FORXIGA came from fat mass reduction3
Adj
uste
d m
ean
chan
gefro
m b
asel
ine
body
wei
ght (
kg)
24 weeks (LOCF analysis)1
–1.7 kg(n=95)
–2.9 kg(n=133)
–0.9 kg(n=136)
–2.0 kg difference p<0.0001
+1.4 kg(n=73)
–3.1 kg difference
Data are mean change from baseline after adjustment for baseline value (mean baseline weight: FORXIGA 86.3 kg, placebo 87.7 kg).24-week data are based on LOCF analysis excluding data after rescue; 102-week data are based on longitudinal repeated measures analysis and include data after rescue.1. Bailey CJ, et al. Lancet 2010;375:2223–33; 2. Bailey CJ, et al. Diabetes 2011;60(Suppl. 1):988-P; 3. Bolinder J, et al. J Clin Endocrinol Metab 2012;97:1020–31.
102 weeks (repeated measures analysis)2
FORXIGA 10 mg + metformin
FORXIGA 10 mg + metformin
Placebo + metformin
Placebo + metformin
21
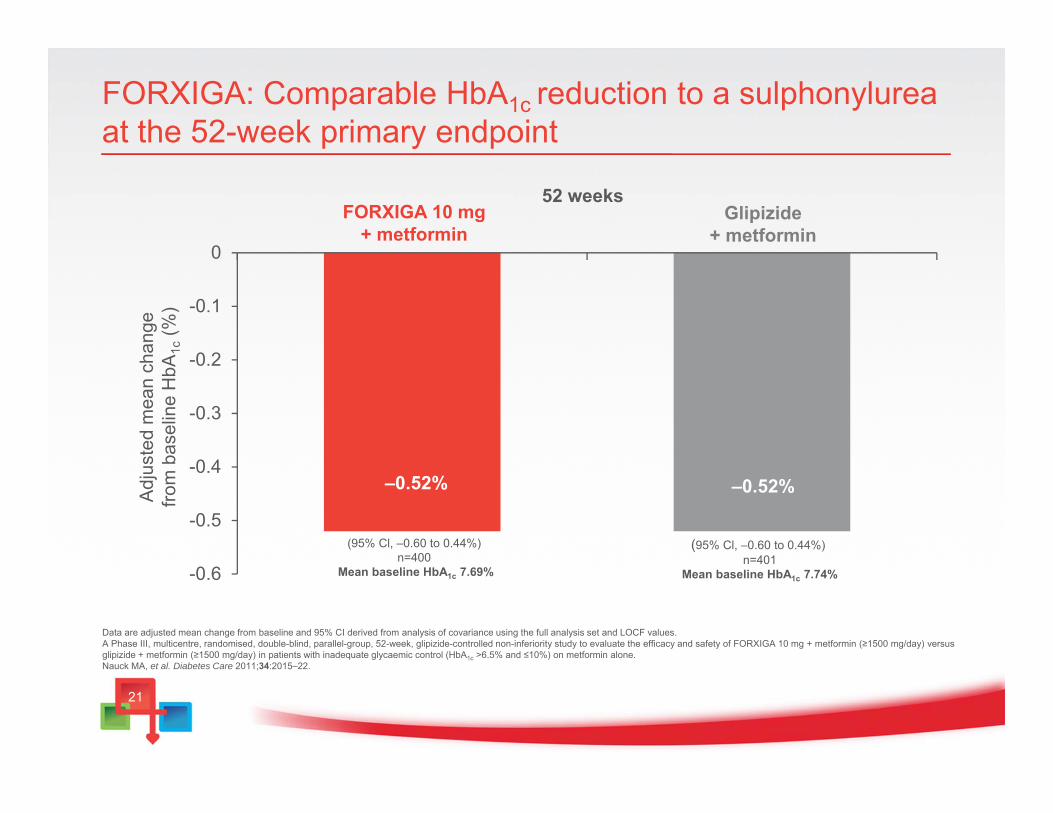
-0.6
-0.5
-0.4
-0.3
-0.2
-0.1
0
(95% Cl, –0.60 to 0.44%) n=401
Mean baseline HbA1c 7.74%
(95% Cl, –0.60 to 0.44%) n=400
Mean baseline HbA1c 7.69%
FORXIGA: Comparable HbA1c reduction to a sulphonylurea at the 52-week primary endpoint
Adj
uste
d m
ean
chan
gefro
m b
asel
ine
HbA
1c(%
)
FORXIGA 10 mg + metformin
52 weeksGlipizide
+ metformin
–0.52%
Data are adjusted mean change from baseline and 95% CI derived from analysis of covariance using the full analysis set and LOCF values. A Phase III, multicentre, randomised, double-blind, parallel-group, 52-week, glipizide-controlled non-inferiority study to evaluate the efficacy and safety of FORXIGA 10 mg + metformin (≥1500 mg/day) versus glipizide + metformin (≥1500 mg/day) in patients with inadequate glycaemic control (HbA1c >6.5% and ≤10%) on metformin alone.Nauck MA, et al. Diabetes Care 2011;34:2015–22.
–0.52%
22
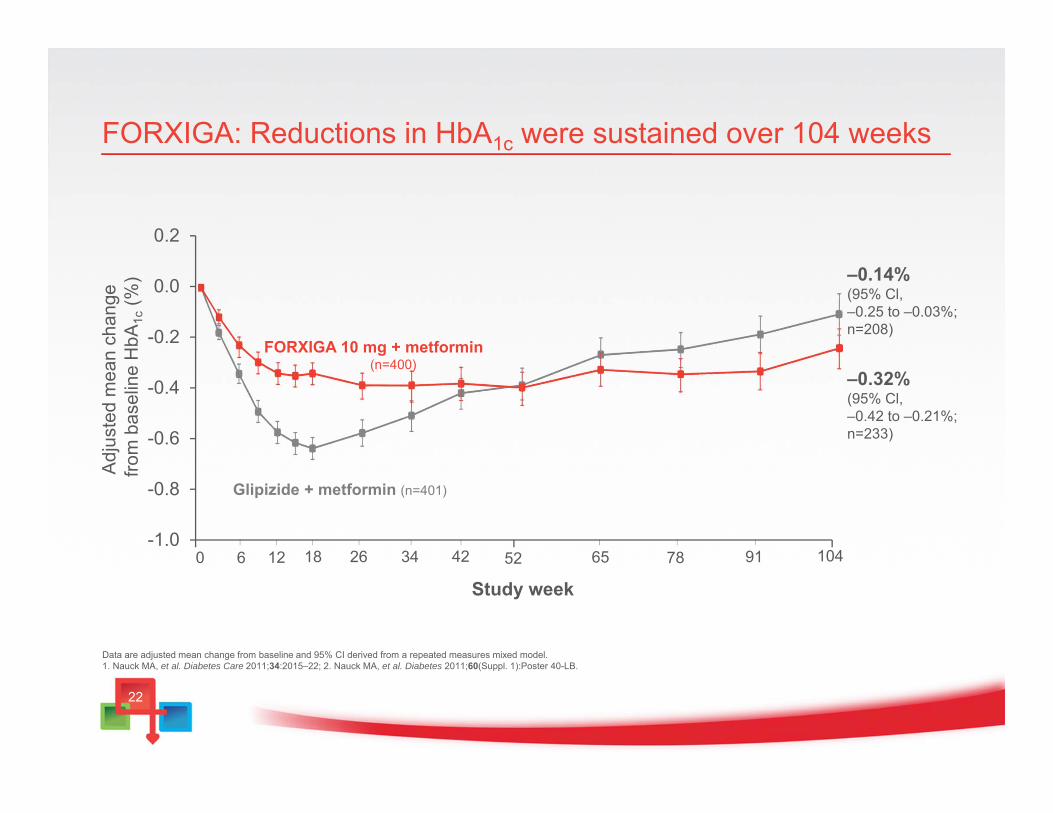
-1.0
-0.8
-0.6
-0.4
-0.2
0.0
0.2
FORXIGA 10 mg + metformin (n=400)
Glipizide + metformin (n=401)
0 10452
FORXIGA: Reductions in HbA1c were sustained over 104 weeksA
djus
ted
mea
n ch
ange
fro
m b
asel
ine
HbA
1c(%
) –0.14%(95% Cl, –0.25 to –0.03%; n=208)
–0.32%(95% Cl, –0.42 to –0.21%; n=233)
Study week6 12 18 26 34 42 65 78 91
Data are adjusted mean change from baseline and 95% CI derived from a repeated measures mixed model.1. Nauck MA, et al. Diabetes Care 2011;34:2015–22; 2. Nauck MA, et al. Diabetes 2011;60(Suppl. 1):Poster 40-LB.
23
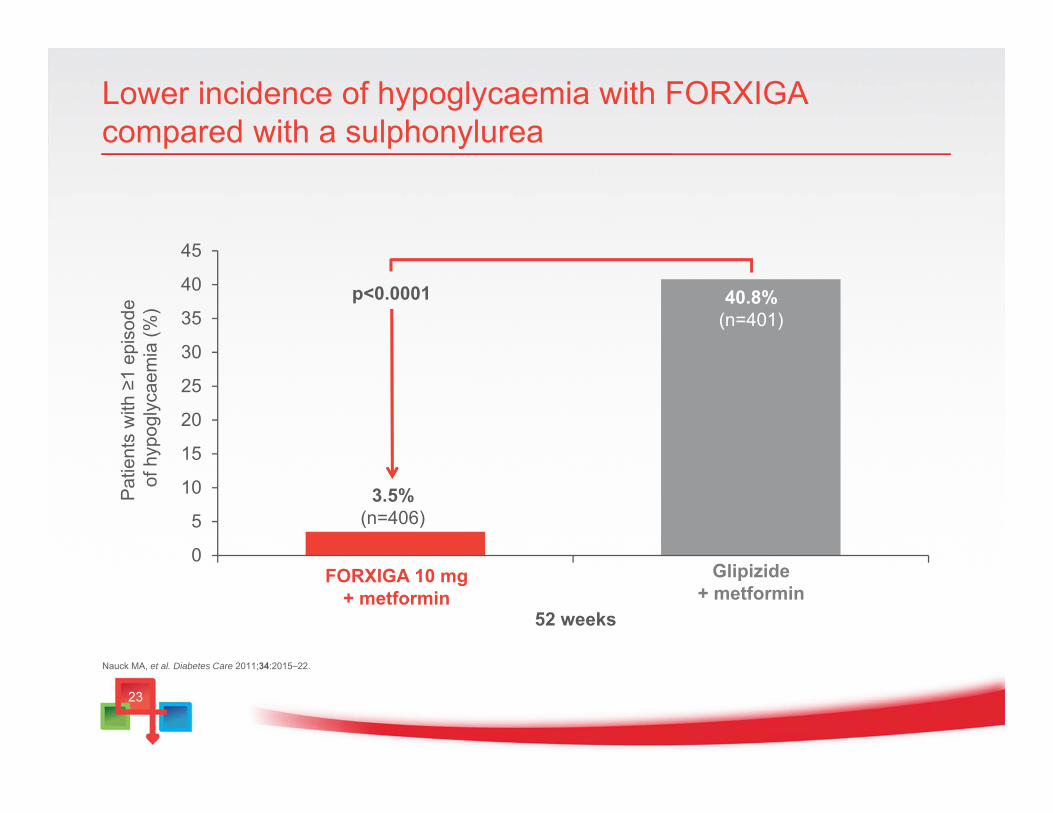
Lower incidence of hypoglycaemia with FORXIGA compared with a sulphonylurea
0
5
10
15
20
25
30
35
40
45
Pat
ient
s w
ith ≥
1 ep
isod
e of
hyp
ogly
caem
ia (%
)
52 weeks
40.8%(n=401)
3.5%(n=406)
FORXIGA 10 mg + metformin
Glipizide+ metformin
p<0.0001
Nauck MA, et al. Diabetes Care 2011;34:2015–22.
24
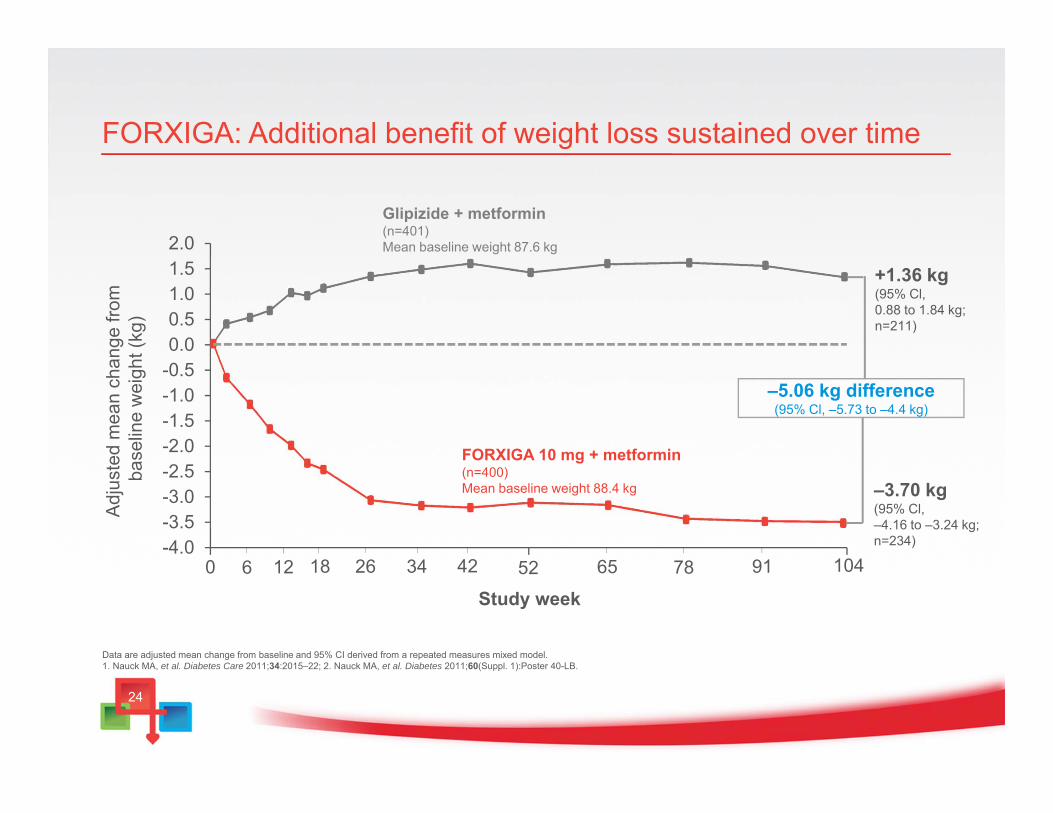
FORXIGA: Additional benefit of weight loss sustained over time
-4.0-3.5-3.0-2.5-2.0-1.5-1.0-0.50.00.51.01.52.0
FORXIGA 10 mg + metformin (n=400)Mean baseline weight 88.4 kg
Glipizide + metformin(n=401)Mean baseline weight 87.6 kg
0 10452
Adj
uste
d m
ean
chan
ge fr
om
base
line
wei
ght (
kg)
+1.36 kg(95% Cl, 0.88 to 1.84 kg; n=211)
–3.70 kg(95% Cl, –4.16 to –3.24 kg; n=234)
Study week
–5.06 kg difference(95% Cl, –5.73 to –4.4 kg)
6 12 18 26 34 42 65 78 91
Data are adjusted mean change from baseline and 95% CI derived from a repeated measures mixed model.1. Nauck MA, et al. Diabetes Care 2011;34:2015–22; 2. Nauck MA, et al. Diabetes 2011;60(Suppl. 1):Poster 40-LB.
25
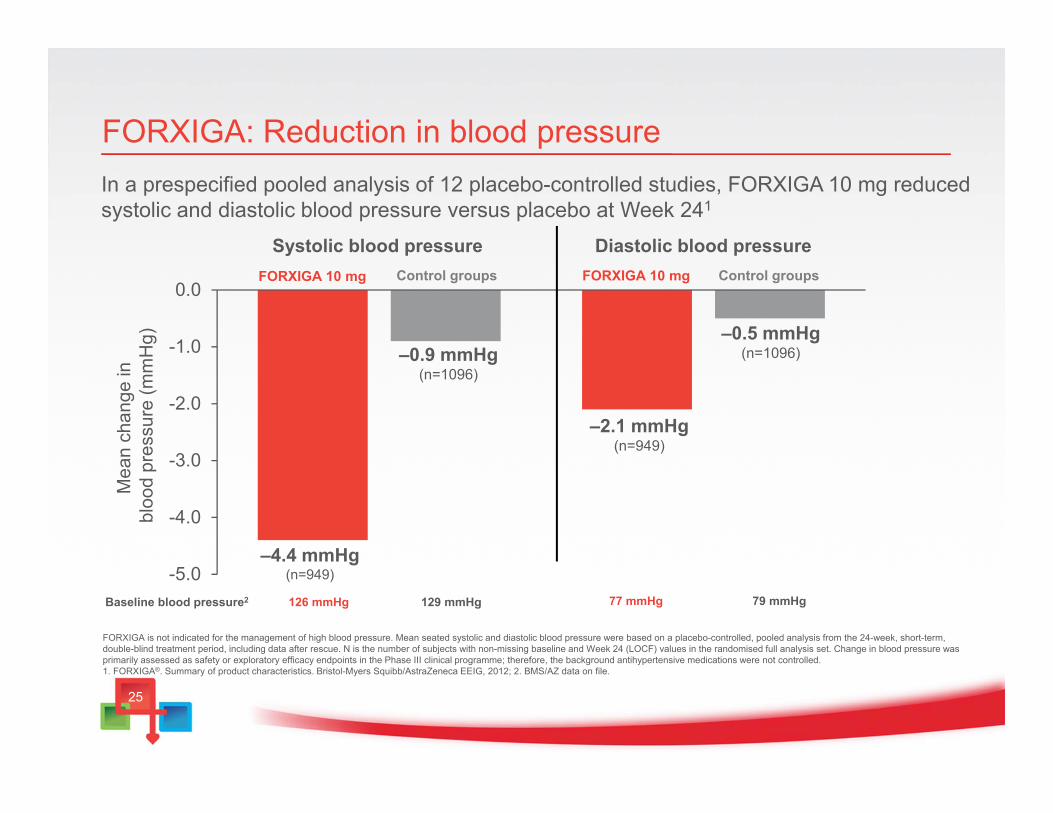
In a prespecified pooled analysis of 12 placebo-controlled studies, FORXIGA 10 mg reduced systolic and diastolic blood pressure versus placebo at Week 241
FORXIGA: Reduction in blood pressure
-5.0
-4.0
-3.0
-2.0
-1.0
0.0
Systolic blood pressure Diastolic blood pressureFORXIGA 10 mg Control groups Control groups
–4.4 mmHg(n=949)
–0.9 mmHg(n=1096)
–2.1 mmHg(n=949)
–0.5 mmHg(n=1096)
Mea
n ch
ange
in
bloo
d pr
essu
re (m
mH
g)
FORXIGA is not indicated for the management of high blood pressure. Mean seated systolic and diastolic blood pressure were based on a placebo-controlled, pooled analysis from the 24-week, short-term, double-blind treatment period, including data after rescue. N is the number of subjects with non-missing baseline and Week 24 (LOCF) values in the randomised full analysis set. Change in blood pressure was primarily assessed as safety or exploratory efficacy endpoints in the Phase III clinical programme; therefore, the background antihypertensive medications were not controlled.1. FORXIGA®. Summary of product characteristics. Bristol-Myers Squibb/AstraZeneca EEIG, 2012; 2. BMS/AZ data on file.
Baseline blood pressure2 126 mmHg 129 mmHg 77 mmHg 79 mmHg
FORXIGA 10 mg
26
Pooled safety and tolerability data
27
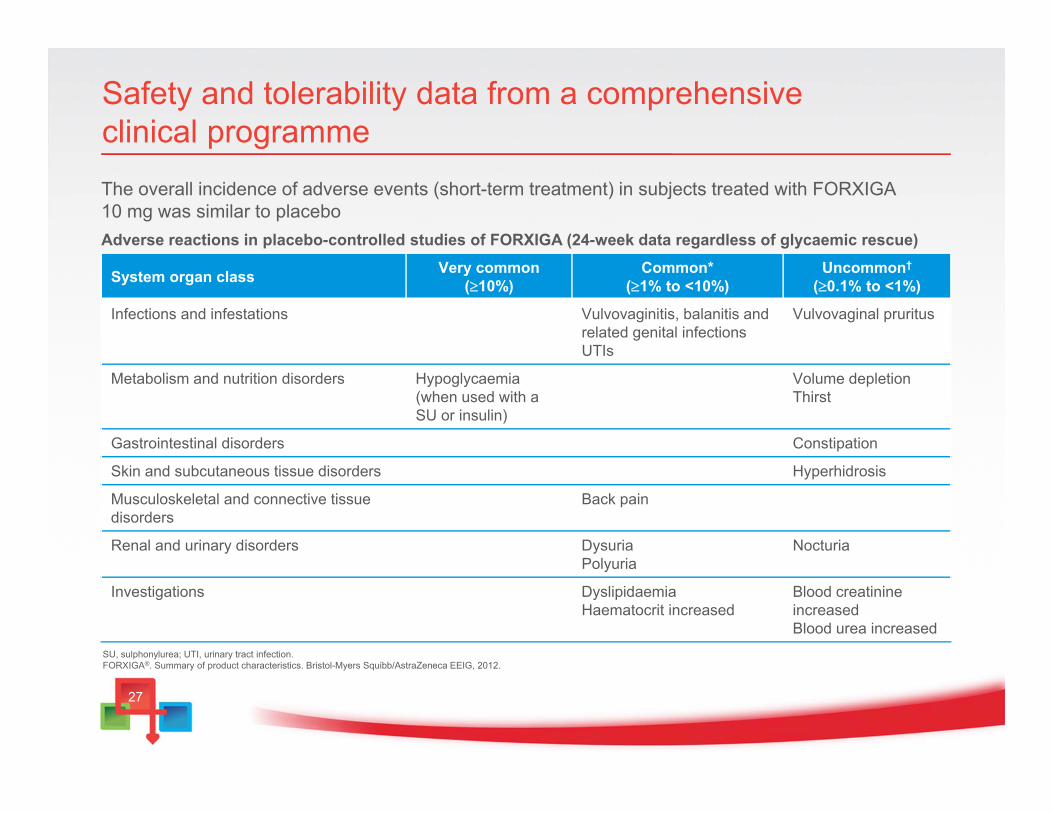
System organ class Very common(10%)
Common*(1% to <10%)
Uncommon†
(0.1% to <1%)
Infections and infestations Vulvovaginitis, balanitis and related genital infectionsUTIs
Vulvovaginal pruritus
Metabolism and nutrition disorders Hypoglycaemia (when used with a SU or insulin)
Volume depletionThirst
Gastrointestinal disorders Constipation
Skin and subcutaneous tissue disorders Hyperhidrosis
Musculoskeletal and connective tissue disorders
Back pain
Renal and urinary disorders DysuriaPolyuria
Nocturia
Investigations DyslipidaemiaHaematocrit increased
Blood creatinineincreasedBlood urea increased
Safety and tolerability data from a comprehensive clinical programme
SU, sulphonylurea; UTI, urinary tract infection.FORXIGA®. Summary of product characteristics. Bristol-Myers Squibb/AstraZeneca EEIG, 2012.
The overall incidence of adverse events (short-term treatment) in subjects treated with FORXIGA 10 mg was similar to placeboAdverse reactions in placebo-controlled studies of FORXIGA (24-week data regardless of glycaemic rescue)
28
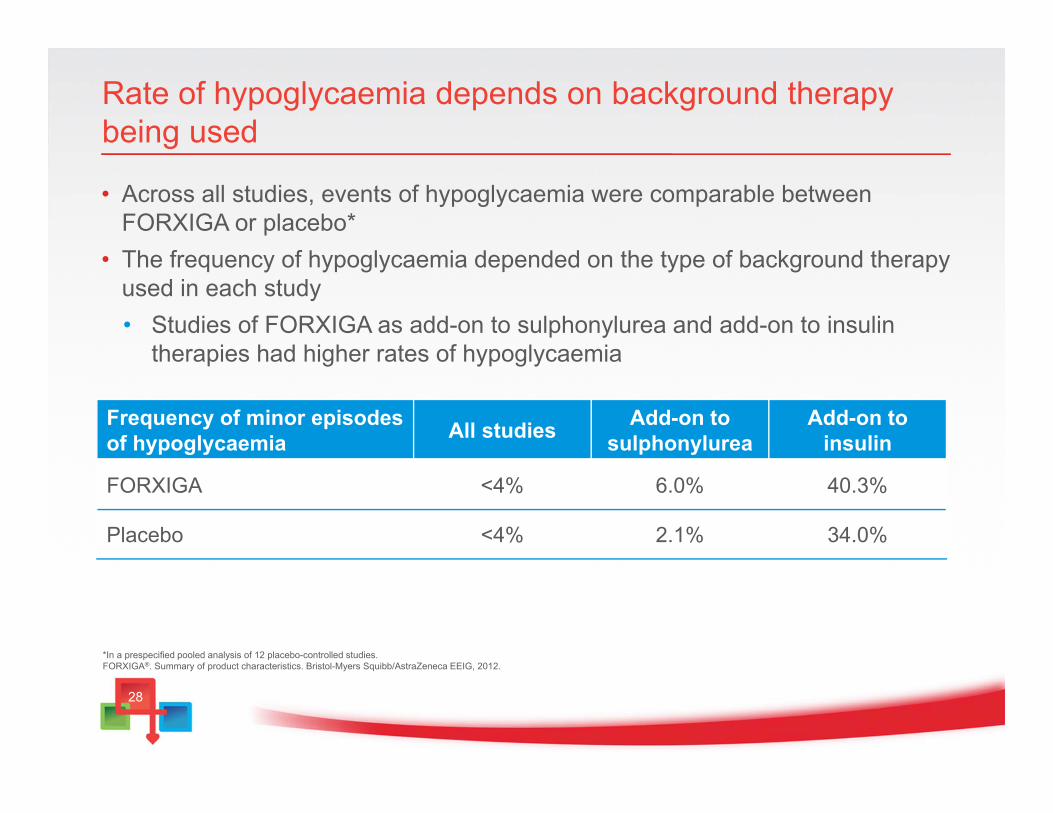
Rate of hypoglycaemia depends on background therapy being used
• Across all studies, events of hypoglycaemia were comparable between FORXIGA or placebo*
• The frequency of hypoglycaemia depended on the type of background therapy used in each study• Studies of FORXIGA as add-on to sulphonylurea and add-on to insulin
therapies had higher rates of hypoglycaemia
*In a prespecified pooled analysis of 12 placebo-controlled studies.FORXIGA®. Summary of product characteristics. Bristol-Myers Squibb/AstraZeneca EEIG, 2012.
Frequency of minor episodes of hypoglycaemia All studies Add-on to
sulphonylureaAdd-on to
insulin
FORXIGA <4% 6.0% 40.3%
Placebo <4% 2.1% 34.0%
29
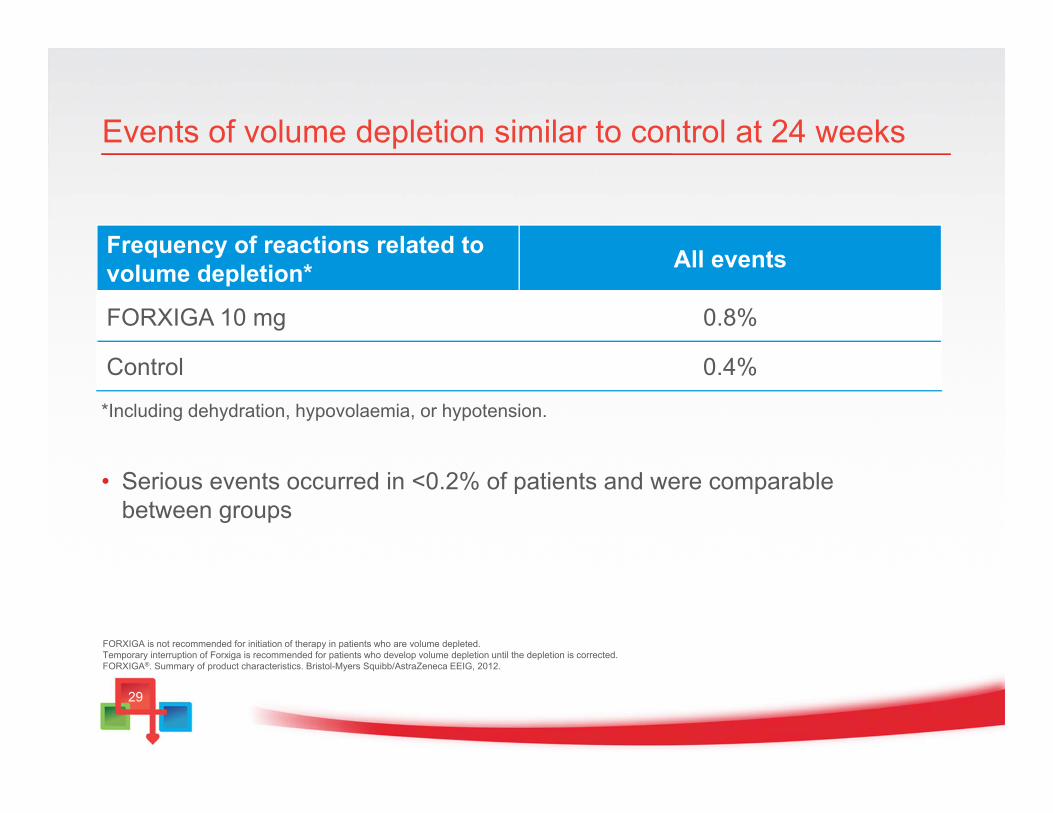
*Including dehydration, hypovolaemia, or hypotension.
• Serious events occurred in <0.2% of patients and were comparable between groups
Events of volume depletion similar to control at 24 weeks
FORXIGA is not recommended for initiation of therapy in patients who are volume depleted. Temporary interruption of Forxiga is recommended for patients who develop volume depletion until the depletion is corrected. FORXIGA®. Summary of product characteristics. Bristol-Myers Squibb/AstraZeneca EEIG, 2012.
Frequency of reactions related to volume depletion* All events
FORXIGA 10 mg 0.8%
Control 0.4%
30
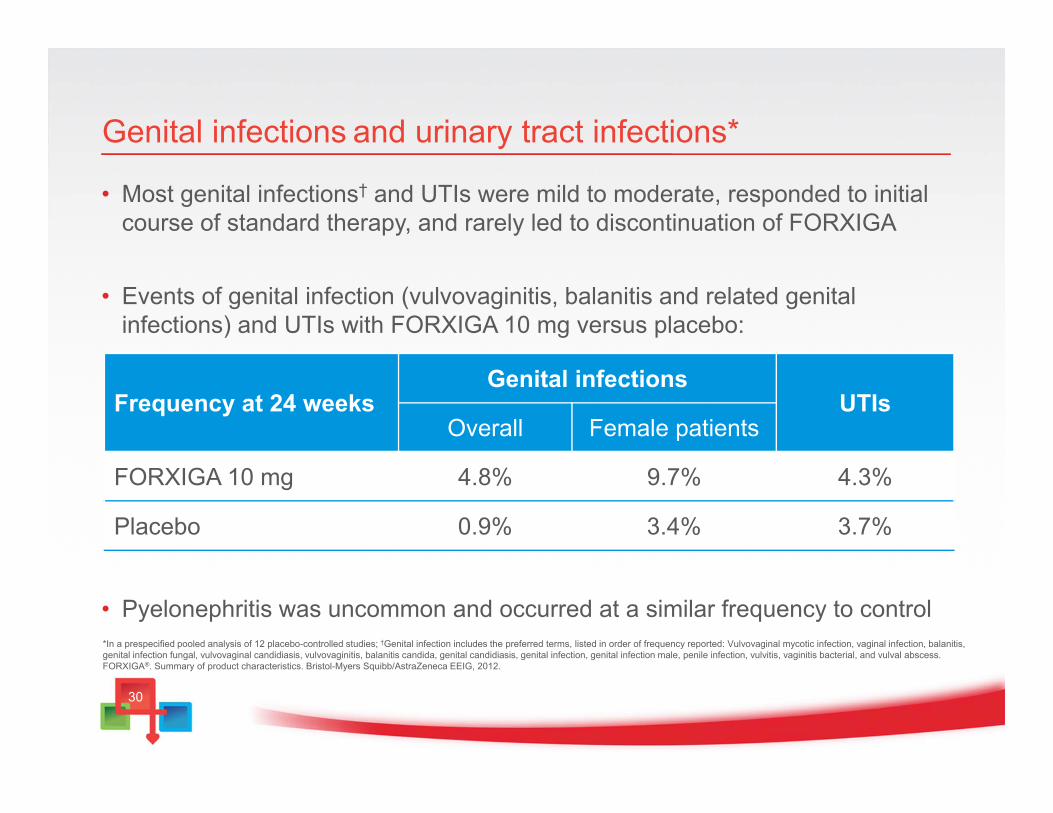
Genital infections and urinary tract infections*
• Most genital infections† and UTIs were mild to moderate, responded to initial course of standard therapy, and rarely led to discontinuation of FORXIGA
• Events of genital infection (vulvovaginitis, balanitis and related genital infections) and UTIs with FORXIGA 10 mg versus placebo:
• Pyelonephritis was uncommon and occurred at a similar frequency to control*In a prespecified pooled analysis of 12 placebo-controlled studies; †Genital infection includes the preferred terms, listed in order of frequency reported: Vulvovaginal mycotic infection, vaginal infection, balanitis, genital infection fungal, vulvovaginal candidiasis, vulvovaginitis, balanitis candida, genital candidiasis, genital infection, genital infection male, penile infection, vulvitis, vaginitis bacterial, and vulval abscess.FORXIGA®. Summary of product characteristics. Bristol-Myers Squibb/AstraZeneca EEIG, 2012.
Frequency at 24 weeksGenital infections
UTIsOverall Female patients
FORXIGA 10 mg 4.8% 9.7% 4.3%
Placebo 0.9% 3.4% 3.7%
31
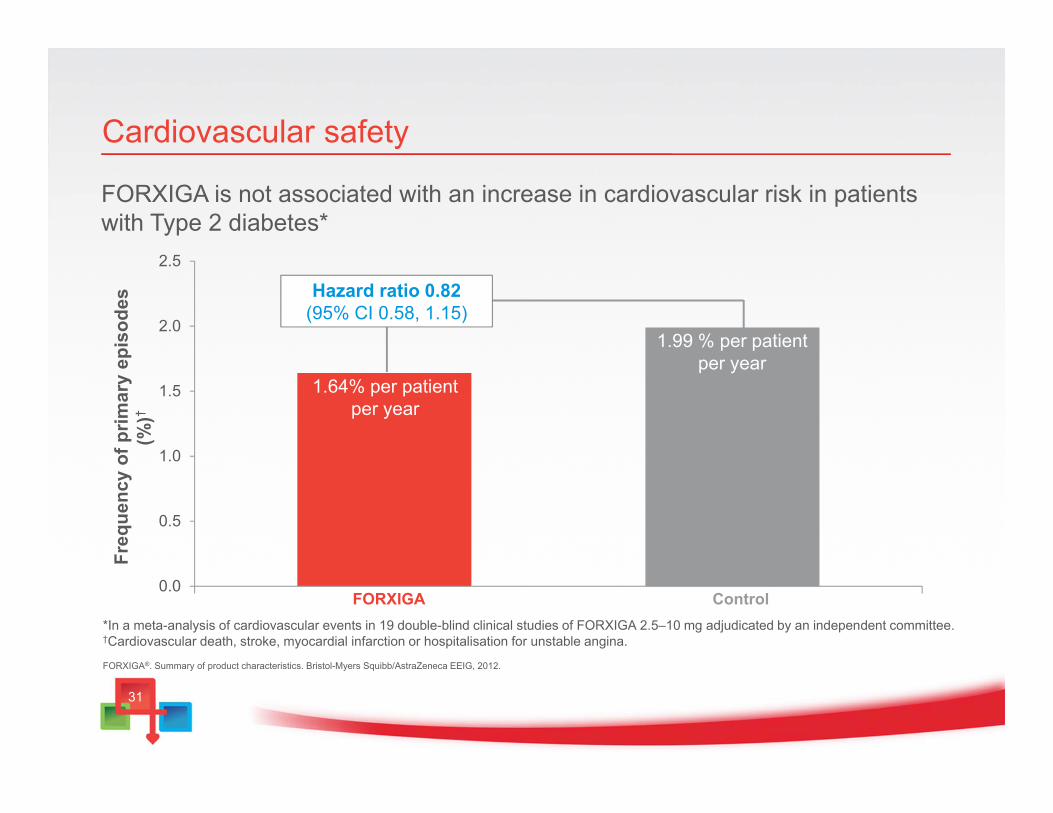
FORXIGA is not associated with an increase in cardiovascular risk in patients with Type 2 diabetes*
Cardiovascular safety
*In a meta-analysis of cardiovascular events in 19 double-blind clinical studies of FORXIGA 2.5–10 mg adjudicated by an independent committee.†Cardiovascular death, stroke, myocardial infarction or hospitalisation for unstable angina.
FORXIGA®. Summary of product characteristics. Bristol-Myers Squibb/AstraZeneca EEIG, 2012.
0.0
0.5
1.0
1.5
2.0
2.5
Freq
uenc
y of
prim
ary
epis
odes
(%
)†
FORXIGA Control
1.64% per patient per year
1.99 % per patient per year
Hazard ratio 0.82 (95% CI 0.58, 1.15)

32
Dosing and administration

33
FORXIGA: A convenient, once-daily tablet
FORXIGA®. Summary of product characteristics. Bristol-Myers Squibb/AstraZeneca EEIG, 2012.
• In patients with severe hepatic impairment, a starting dose of 5 mg is recommended. If well tolerated, the dose may be increased to 10 mg
• No known drug–drug interactions with other commonly prescribed Type 2 diabetes treatments
34
Considerations for FORXIGA dosage and administration (1)
• The efficacy of FORXIGA is dependent on renal function• FORXIGA is not recommended for use in patients with moderate to severe
renal impairment (CrCl <60 mL/min or eGFR <60 mL/min/1.73 m2)
• The monitoring of renal function is recommended as follows:• Prior to initiation of FORXIGA and at least yearly, thereafter• Prior to initiation of concomitant medicinal products that may reduce renal
function and periodically thereafter• For renal function approaching moderate renal impairment, at least 2 to 4
times per year. If renal function falls below CrCl <60 mL/min or eGFR<60 mL/min/1.73 m2, FORXIGA treatment should be discontinued
*eGFR calculated with Modification of Diet in Renal Disease Formula. FORXIGA®. Summary of product characteristics. Bristol-Myers Squibb/AstraZeneca EEIG, 2012.
35
Considerations for FORXIGA dosage and administration (2)
• FORXIGA is not recommended in:• Patients aged ≥75 years or <18 years• Patients treated concomitantly with pioglitazone• Patients receiving loop diuretics
• FORXIGA is also not recommended for initiation of therapy in patients who are volume depleted• Temporary interruption of FORXIGA is recommended for patients who
develop volume depletion until the depletion is corrected
• Caution should be exercised in patients for whom a FORXIGA-induced drop in blood pressure could pose a risk
• A lower dose of insulin or an insulin secretagogue may be required to reduce the risk of hypoglycaemia when used in combination with FORXIGA
FORXIGA®. Summary of product characteristics. Bristol-Myers Squibb/AstraZeneca EEIG, 2012.
36
FORXIGA: Considerations for patients
• As with all medicines, patients will benefit most if they understand what they are taking and the importance of lifestyle and exercise as adjuncts to successful treatment outcomes:• FORXIGA has a simple mechanism of action that means that excess
glucose is removed via the urine• FORXIGA reduces blood glucose levels and has the additional benefit of
weight loss• For the best outcomes, adherence is important as well healthy eating and
exercise
37
Summary
• FORXIGA, a first-in-class SGLT2 inhibitor, removes excess glucose via an insulin-independent mechanism of action and provides:
*In patients with severe hepatic impairment, a starting dose of 5 mg is recommended. If well tolerated, the dose may be increased up to 10 mg.
1. Bailey CJ, et al. Lancet 2010;375:2223–33; 2. Bailey CJ, et al. Diabetes 2011;60(Suppl. 1):988-P; 3. Nauck MA, et al. Diabetes Care 2011;34:2015–22; 4. Nauck MA, et al. Diabetes 2011;60(Suppl. 1):Poster 40-LB; 5. FORXIGA®. Summary of product characteristics. Bristol-Myers Squibb/AstraZeneca EEIG, 2012.
• Significant and sustained HbA1c reductions1–5
• Additional benefits of weight loss1–5
and a reduction in blood pressure1,5
• Low incidence of hypoglycaemia1
• In one 10 mg tablet a day5*
“Add on for patients uncontrolled on metforminwho need the additional benefit of weight loss and have normal or only mildly impaired renal function”
Related Documents



![POVZETEK GLAVNIH ZNAČILNOSTI ZDRAVILA 1. IME ......2020/01/08 · Zdravila Forxiga se ne sme uvesti pri bolnikih, ki imajo hitrost glomerulne filtracije [GFR] < 60 ml/min. Zdravljenje](https://static.cupdf.com/doc/110x72/60abedf8191c585f9b064500/povzetek-glavnih-znaoeilnosti-zdravila-1-ime-20200108-zdravila-forxiga.jpg)







