Overview of Co- Occurring Mental Health and Substance Use Disorders: Screening & Assessment

Overview of Co-Occurring Mental Health and Substance Use Disorders: Screening & Assessment.
Dec 30, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Overview of Co-Occurring Mental Health and Substance
Use Disorders: Screening & Assessment

Introduction:What we will cover
• Overview of the evolving field of Co-Occurring Disorders
• What is happening in the brain?
• Importance of conducting effective screening and assessment for COD
• Using motivational interviewing with this population—why and how

Co-Occurring Disorders
Co-occurring disorders • Refers to co-occurring substance use (abuse or
dependence) and mental disorders
In other words…
consumers with co-occurring disorders have:• one or more disorders relating to the use of alcohol
and/or other drugs of abuse and one or more mental disorders

Co-Occurring Disorders
Diagnosis of COD occurs when:• at least one disorder of each type can be
established independent of the other and • is not simply a cluster of symptoms resulting from
the one disorder
Clinicians knowledge of both mental health and substance abuse
is essential, but challenging to achieve
So, all of that is well and good, but…
…is dealing with drug abuse REALLY important to my job?

Prevalence of COD
• In 2006, 5.6 million adults (2.5% of persons aged 18+) met the criteria for both serious psychological distress (SPD) and substance dependence and abuse (i.e., substance use disorder, SUD)
• In 2006, 15.8 million adults (7.2% of persons aged 18+) had at least one major depressive episode (MDE) in the past year– Adults with MDE in the past year were more
likely than those without MDE to have used an illicit drug in the past year (27.7 vs. 12.9 percent)
SOURCE: 2006 National Survey on Drug Use and Health, SAMHSA.
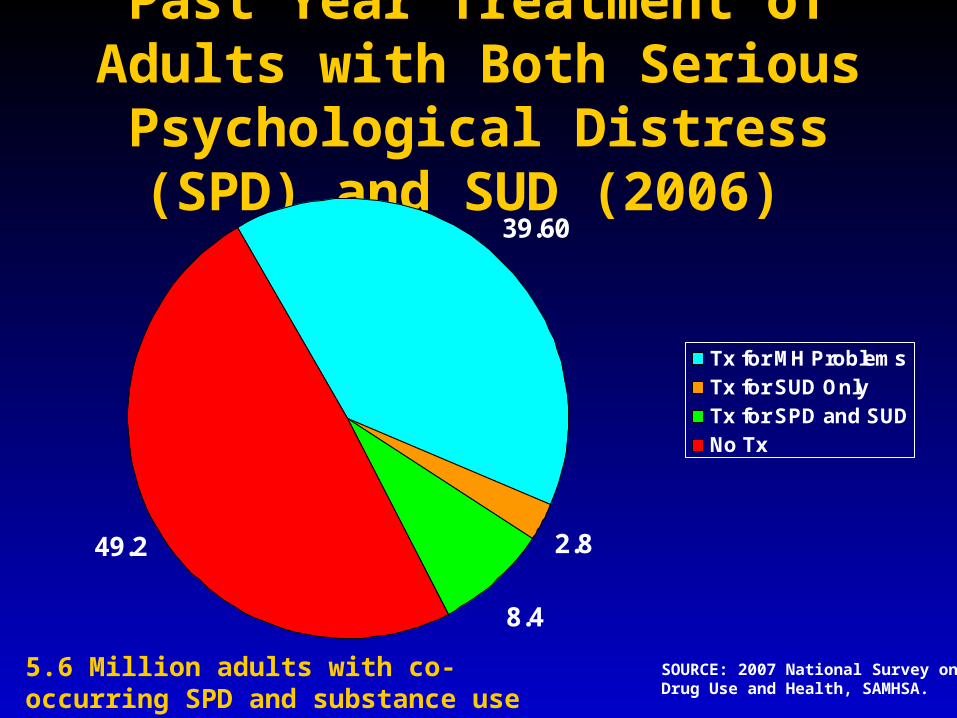
Past Year Treatment of Adults with Both Serious Psychological
Distress (SPD) and SUD (2006)
SOURCE: 2007 National Survey on Drug Use and Health, SAMHSA.
39.60
2.8
8.4
49.2
Tx for MH ProblemsTx for SUD OnlyTx for SPD and SUDNo Tx
5.6 Million adults with co-occurring SPD and substance use disorder.

Facts About Adult MDE and Alcohol Use Disorders (AUD)
• As many as 2.7 million adults had a co-occurring MDE and AUD in the past year.
• Adults who had an MDE were more than twice as likely to abuse alcohol or other drugs than persons without MDE (19.9% vs. 8.4%, respectively).
• Among adults with substance abuse or dependence, 15.6% had at least one MDE in the past year.
SOURCE: 2006 National Survey on Drug Use and Health, SAMHSA.
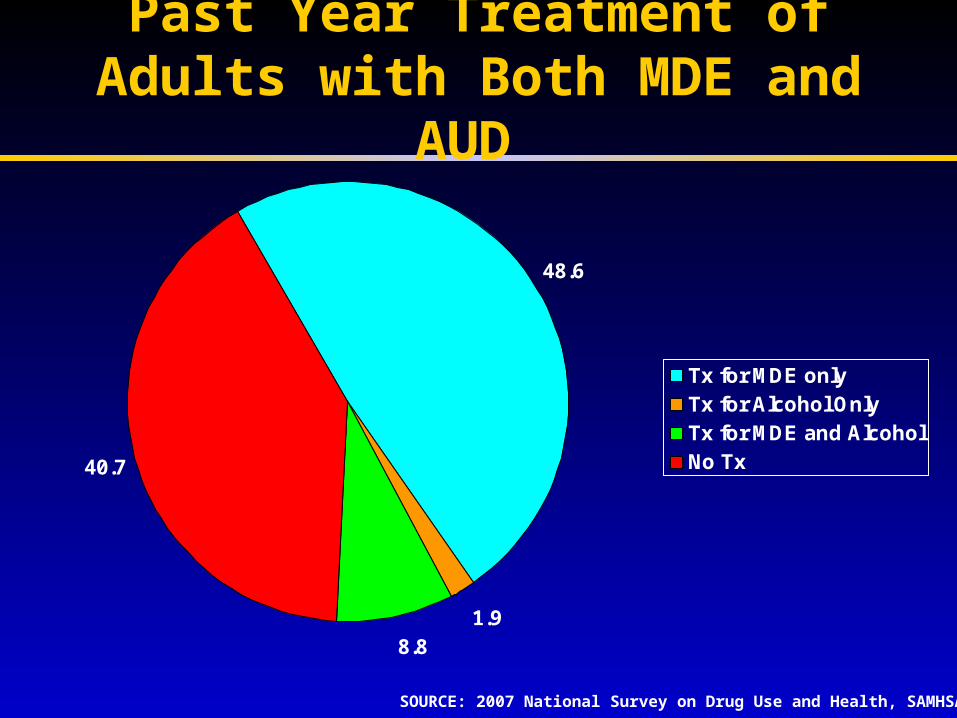
Past Year Treatment of Adults with Both MDE and AUD
SOURCE: 2007 National Survey on Drug Use and Health, SAMHSA.
48.6
1.98.8
40.7
Tx for MDE onlyTx for Alcohol OnlyTx for MDE and AlcoholNo Tx
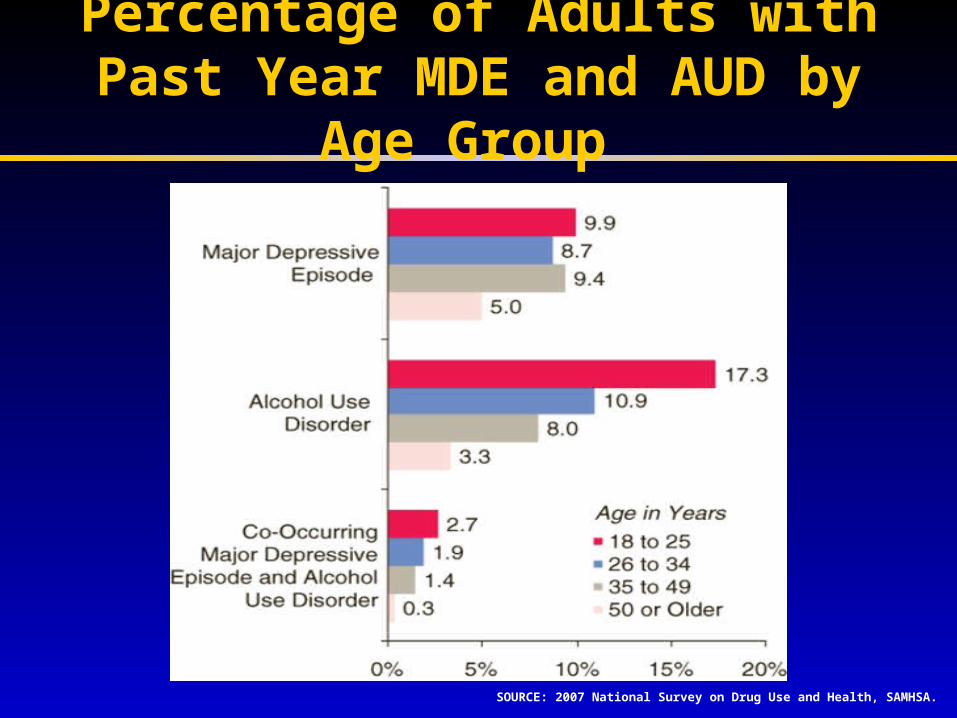
Percentage of Adults with Past Year MDE and AUD by Age Group
SOURCE: 2007 National Survey on Drug Use and Health, SAMHSA.

Prevalence and Other Data
Data now show:
• COD are common in general adult population.
• Increased prevalence of people with COD and programs for people with COD
• Rates of mental disorders increase as the number of substance use disorders increase
• If we treat the SUD, we also address mental health symptoms

So, the answer is…
We must address SUD in order to increase the
effectiveness of mental health treatment
Yes, this really IS important to your job!
Yes, this really IS important to your job!

So, How Do We Treat COD?
TIP 42
Guiding Principles and Recommendations

Six Guiding Principles (SAMHSA, TIP 42)
• Employ a recovery perspective
• Develop a phased approach to treatment
• Plan for cognitive and functional impairments
• Provide access
• Complete a full assessment
• Achieve integrated treatment
- Treatment Planning and Review
- Psychopharmacology
• Ensure continuity of care

Vision of Fully Integrated Treatment
• One program that provides treatment for both disorders
• Mental and substance use disorders are treated by the same clinicians
• The clinicians are trained in psychopathology, assessment, and treatment strategies for both disorders

Vision of Fully Integrated Treatment (continued)
• Treatment is characterized by a slow pace and a long-term perspective
• Providers offer motivational counseling
• 12-Step groups are available to those who choose to participate
• Pharmacotherapies are utilized according to consumers’ psychiatric and other medical needs
• Sensitivity to issues of trauma

Quick Exercise— Levels of Program Capacity
What challenges have you encountered in moving toward the center?
What have you done to overcome these challenges?
BeginningAddiction
Only Treatment
IntermediateAddiction
CODCapable
Fully Integrated
CODIntegrated
IntermediateMental Health
CODCapable
BeginningMental Health
OnlyTreatment
AdvancedAddiction
CODEnhanced
AdvancedMental Health
CODEnhanced

Addiction: A Brain Disease
Putting Drug Use into Context with other Mental Disorders

Onset of Mental Health Disorders
• Oppositional Defiance: 5yo
• Attention Deficit Disorder-ADHD: 1.3-2.4 yo
• Anxiety Disorders: 3.8 yo
• Conduct Disorder: 5.6 yo
• Depression: 10.1 yo
• Schizophrenia-affective disorders: mid-teens to mid-thirties

Typical Progression of Use
FAS---Substance use in-uterus
No SocialUse Experimentation Use Use Abuse Dependence-----------------------------------------------------------------------------------------------
0-2 3-5 6-8 9-10 11-12 13-14 15-16 17+Infant Child Pre- Adolescent adol
Mental Health Disorder’s onset----------------------------------

What are we talking about?
Alcoholism/Addiction Major Mental Disorders
Both heredity and environment play a roleCharacterized by chronicity and “denial”
Affects the whole familyProgresses without treatmentFeelings of shame and guilt
Inability to control behavior and emotionsOften seen as a moral issue
Leads to feelings of despair and failureBiological, psychological, social and spiritual components

Collision of Symptomology
• Differential Diagnosis is essential for accurate assessment. Is the presenting problem affected by a medical condition or substance?– Is it depression or alcohol, prescription pain killer,
heroin use?– Is it ADHD or is it methamphetamine,
cocaine use?– Is it bipolar disorder or cocaine use?– Is it schizophrenia or methamphetamine use?– Is it PTSD or polysubstance use?

A Major Reason People Take a Drug is They Like
What It Does to Their Brains
A Major Reason People Take a Drug is They Like
What It Does to Their Brains

Initially, A Person Takes A Drug Hoping to Change their Mood, Perception, or Emotional State
Initially, A Person Takes A Drug Hoping to Change their Mood, Perception, or Emotional State
Translation---Translation---
…Hoping to Change their Brain…Hoping to Change their Brain

Dopamine and the Brain

Natural Rewards Elevate Dopamine Levels
00
5050
100100
150150
200200
00 6060 120120 180180
Time (min)Time (min)
% o
f B
asal
DA
Ou
tpu
t%
of
Bas
al D
A O
utp
ut
NAc shellNAc shell
EmptyEmpty
BoxBox FeedingFeeding
Source: Di Chiara et al.Source: Di Chiara et al.
FOODFOOD
100100
150150
200200
DA
Co
nce
ntr
ati
on
(%
Bas
elin
e)D
A C
on
cen
tra
tio
n (
% B
asel
ine)
MountsMountsIntromissionsIntromissionsEjaculationsEjaculations
1515
00
55
1010
Co
pu
latio
n F
req
ue
nc
yC
op
ula
tion
Fre
qu
en
cy
SampleNumberSampleNumber
11 22 33 44 55 66 77 88 99 1010 1111 1212 1313 1414 1515 1616 1717
ScrScrScrScrBasBasFemale 1 PresentFemale 1 Present
ScrScrFemale 2 PresentFemale 2 Present
ScrScr
Source: Fiorino and PhillipsSource: Fiorino and Phillips
SEXSEX
Source: Di Chiara and ImperatoSource: Di Chiara and Imperato
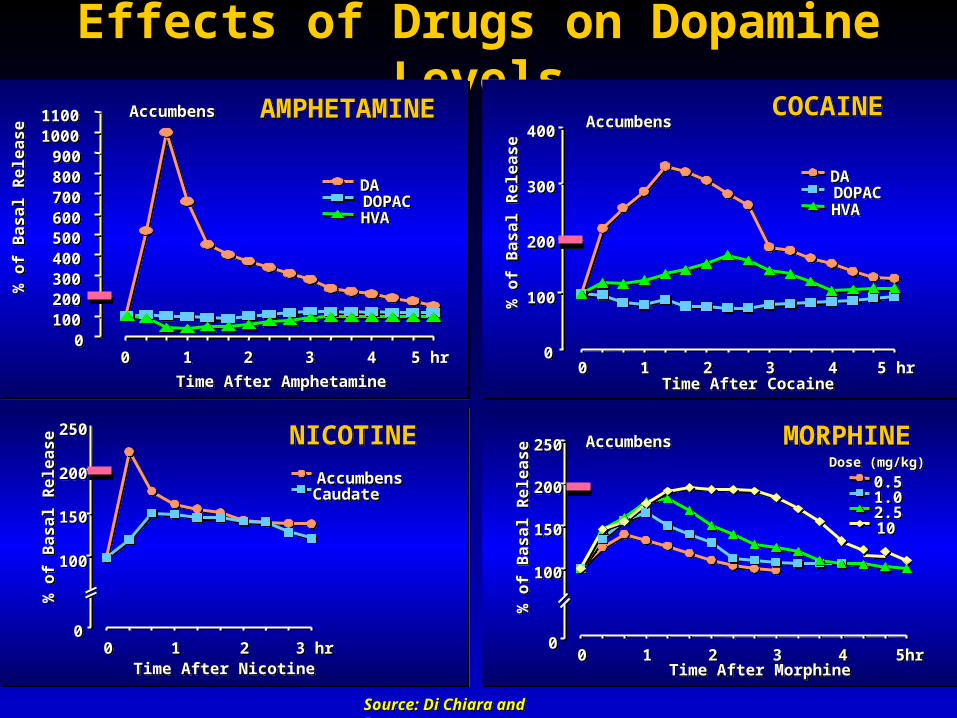
Effects of Drugs on Dopamine Levels
00100100200200300300400400500500600600700700800800900900
1000100011001100
00 11 22 33 44 5 hr5 hr
Time After AmphetamineTime After Amphetamine
% o
f B
as
al
Re
lea
se
% o
f B
as
al
Re
lea
se
DADADOPACDOPACHVAHVA
AccumbensAccumbens AMPHETAMINEAMPHETAMINE
00
100100
200200
300300
400400
00 11 22 33 44 5 hr5 hrTime After CocaineTime After Cocaine
% o
f B
as
al
Re
lea
se
% o
f B
as
al
Re
lea
se
DADADOPACDOPACHVAHVA
AccumbensAccumbensCOCAINECOCAINE
00
100100
150150
200200
250250
00 11 22 3 hr3 hrTime After NicotineTime After Nicotine
% o
f B
as
al
Re
lea
se
% o
f B
as
al
Re
lea
se
AccumbensAccumbensCaudateCaudate
NICOTINENICOTINE
00
100100
150150
200200
250250
00 11 22 33 44 5hr5hrTime After MorphineTime After Morphine
% o
f B
as
al
Re
lea
se
% o
f B
as
al
Re
lea
se
AccumbensAccumbens
0.50.51.01.02.52.51010
Dose (mg/kg)Dose (mg/kg)
MORPHINEMORPHINE

After A Person Uses Drugs For A While,
Why Can’t They Just Stop?
After A Person Uses Drugs For A While,
Why Can’t They Just Stop?
But Then…But Then…

Their Brains
have been
Re-Wired by Drug Use
Their Brains
have been
Re-Wired by Drug Use
Because…Because…

Substance Use in Action

Cognitive and
Memory Effects

Longitudinal Memory Performance
test
num
ber
corr
ect
0
5
10
15
20
25
Word Recall WordRecognition
Picture Recall PictureRecognition
controlbaseline3 mos6 mos

Control > MA
4
3
2
0
1
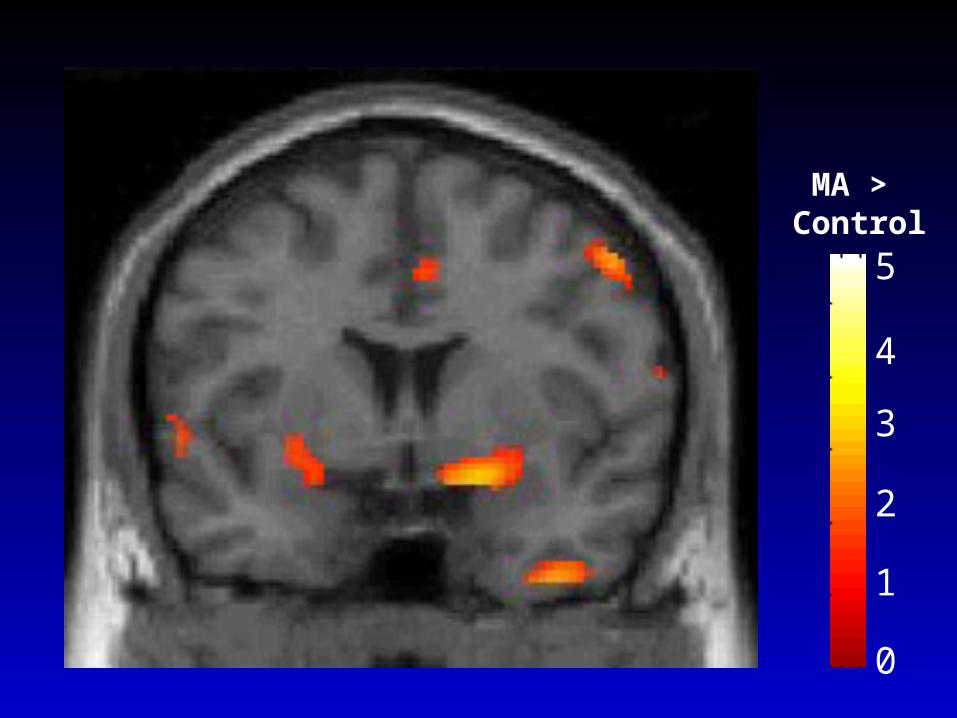
MA > Control
5
4
2
0
1
3


Addiction Is A Brain DiseaseAddiction Is A Brain DiseaseExpressed As Compulsive BehaviorExpressed As Compulsive Behavior
Both Developing and Both Developing and Recovering From It Depend onRecovering From It Depend onBehavior and Social ContextBehavior and Social Context

Screening and Assessing Consumers for COD

1. Underweight2. Unsafe sex3. High blood pressure4. Tobacco consumption5. Alcohol consumption6. Unsafe water, sanitation, &
hygiene7. Iron deficiency8. Indoor smoke from solid fuels9. High cholesterol10. Obesity
Top 10 risk factors for disease globally

Problems related to substance use
Effects of regular use include:• Specific physical and mental health problems
• Increased risk for infectious diseases
• Psychiatric symptoms
• Sleep problems
• Financial difficulties
• Legal, relationship, or work problems
• Risk of dependence
• Withdrawal symptoms when use is reduced or stopped

What is screening?
• A range of evaluation procedures and techniques to capture indicators of risk
• A preliminary assessment that indicates probability that a specific condition is present
• A single event that informs subsequent diagnosis and treatment
(Source: SAMHSA, 1994)

What is the Difference between…
Screening Assessment
What’s Going On in These Pictures?

Screening
• Conducted with large numbersof people to identify the potentialthat a problem exists
• Screening is intended to be broad scale and produce false positives
• Screening leads to more in-depth assessment and intervention for people identified with a potential problem

Benefits of screening
• Provides opportunity for education, early intervention
• Alerts provider to risks for interactions with medications or other aspects of treatment
• Offers opportunity to engage patient further• Has proved beneficial in reducing high-risk
activities for people who are not dependent
(Source: NCETA, 2004)

What can be determined through the screening and assessment process?
• The interplay between the substance use and the mental health problem
• The degree to which each disorder affects functioning (positively &/or negatively)
• The frequency, duration and quantity of use and resulting diagnosis (i.e., substance abuse or dependence)
THESE DETERMINATIONS TAKE TIME

Common Pairings of Axis I Disorders and Substances
• Depression — Alcohol, Stimulants
• Bipolar I — cannabis, stimulants
• Anxiety/panic — alcohol, benzodiazepines, cannabis
• ADHD — stimulants
• Schizophrenia/other psychosis — nicotine, cannabis

‘The Secret in the Pocket’
• Please think of one personal experience, that you have determined to keep to yourself. This can be an experience or character flaw that you are NOT proud of. YOUR SECRET.
YOU WILL NOT BE ASKED TO SHARE THIS OR SHOW THIS TO ANYONE.
Appreciating the ‘difficult to tell….’
Before we begin to ask questions, we need to:• understand and appreciate the DIFFICULT process
of sharing what is considered personal and private• understand the processes whereby individuals communicate
deeply personal information to strangers
We need to consider what might be healthy, interpersonal non-disclosure versus
unhealthy, self destructive secret-keeping
• We also need to understand how difficult it is of us to ask these questions and to hear the answers
Tasks of Mental Health Clinician:
• Our responsibility is to provide the best, most comprehensive assessment and treatment for consumers
• This requires a complete and thorough assessment
• Balance timeframes between completing necessary forms/paperwork and providing good clinical care
• Services must move at the pace set by the consumer

When do I bring up ‘the topic’?
• Ensure that sufficient rapport has been established with the consumer
• Completing paperwork and broaching specific topics may be two different events
• Using the Substance Use Screeners ensures that the topic will be raised
• Review the limits of confidentiality, especially for adolescent clients and their parents.
Assessing Risk FactorsFactors affecting risk for
involvement with substance use

Assessing Individual Risk Factors
• Favorable attitudes towards the use of substances
• Early age of onset of substance use
• Gender: Males more likely to abuse substances than females
• Genetics: Family history of substance abuse
• History of sexual/physical abuse
• Trauma/displacement

Assessing Psychological Risk Factors
• Impulsivity
• Novelty-seeking
• Childhood ADHD or conduct disorder
• Antisocial Personality Disorder
• Failure to complete high school
• Poor occupational achievement
• Low frustration tolerance
• Internalized racism/sexism/heterosexism

Assessing Sociocultural Risk Factors
• Social network
• Friends/coworkers that use
• Alcohol/drug use integrated into family culture
• Socioeconomic Status (SES)
• High crime rate/ “culture of violence”
• Degree of acculturation

Understanding the impact of age…
• It is often difficult for us to approach people who are different in age (much younger or much older)
• Not all young people act out and not all old people are depressed.
• Age often brings out our assumptions and biases– “She looks like my grandma, she couldn’t be
using drugs.”– “He’s only 10, substance abuse cannot be an
issue.”

Effecting Change through the Use of
Motivational Interviewing

How can MI be helpful for us in working with our consumers/patients?
• The successful MI therapist is able to inspire people to want to change
• Use of MI can help engage and retain consumers in treatment
• Using MI can help increase participation and involvement in treatment (thereby improving outcomes)

Where do I start?
• What you do depends on where the consumer is in the process of changing
• The first step is to be able to identify where the consumer is coming from

Stages of ChangeProchaska & DiClemente

Helping People Change
• Motivational Interviewing is the process of helping people move through the stages of change
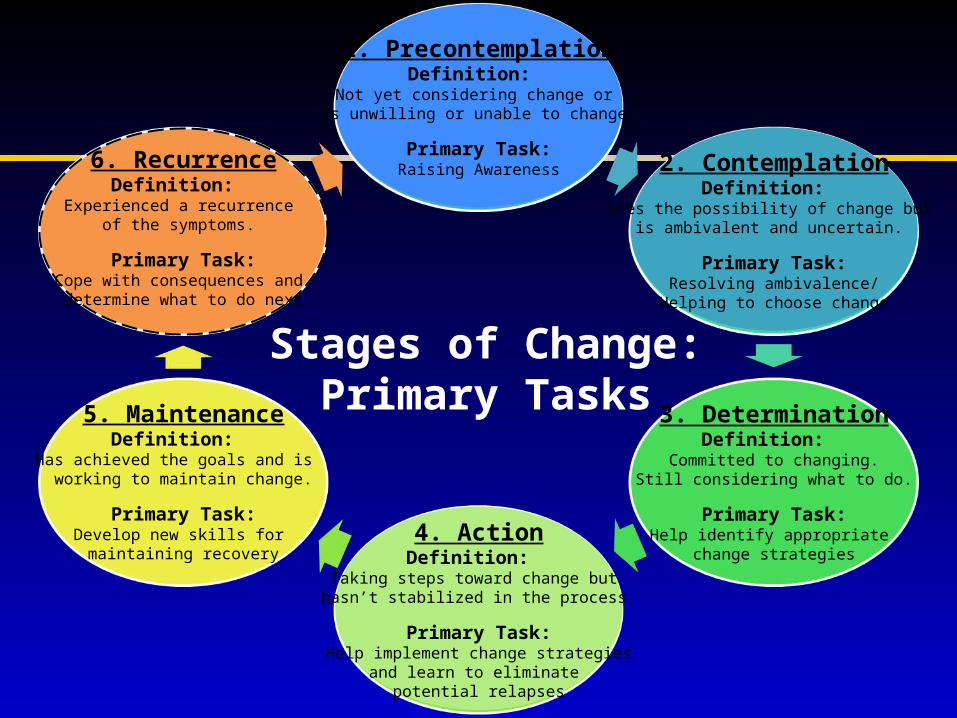
Stages of Change:Primary Tasks
1. PrecontemplationDefinition:
Not yet considering change or is unwilling or unable to change.
Primary Task:Raising Awareness 2. Contemplation
Definition: Sees the possibility of change but
is ambivalent and uncertain.
Primary Task:Resolving ambivalence/
Helping to choose change
3. DeterminationDefinition:
Committed to changing.Still considering what to do.
Primary Task:Help identify appropriate
change strategies4. ActionDefinition:
Taking steps toward change but hasn’t stabilized in the process.
Primary Task:Help implement change strategies
and learn to eliminate potential relapses
5. MaintenanceDefinition:
Has achieved the goals and is working to maintain change.
Primary Task:Develop new skills for maintaining recovery
6. RecurrenceDefinition:
Experienced a recurrence of the symptoms.
Primary Task:Cope with consequences and
determine what to do next

• Open-ended questioning
• Affirming
• Reflective listening
• Summarizing
Building Motivation OARS(the microskills)
The goal is to elicit and reinforce
self-motivational statements (Change Talk)
The goal is to elicit and reinforce
self-motivational statements (Change Talk)
Open-Ended Questions
• Solicits information in a neutral way• Helps person elaborate own view of the problem
and brainstorm possible solutions• Helps therapist avoid prejudgments• Keeps communication moving forward• Allows consumer to do most of the talking
An open-ended question is one that requires more than a yes or no response

Affirmations
• Focused on achievements of individual
• Intended to:– Support person’s persistence– Encourage continued efforts– Assist person in seeing positives– Support individual’s proven strengths

Reflective Listening Key-Concepts
• Listen to both what the person says and to what the person means
• Check out assumptions• Create an environment of empathy
(nonjudgmental)• You do not have to agree• Be aware of intonation (statement, not
question)

• Repeating – Repeating what was just said.• Rephrasing – Substituting a few words that
may slightly change the emphasis.• Paraphrasing – Major restatement of what
person said. Listener infers meaning of what was said. Can be thought of as continuing the thought.
• Reflecting Feeling - Listener reflects not just the words, but the feeling or emotion underneath what the person is saying.
Levels of Reflection

NIDA-SAMHSA Blending Initiative 69
1. Simple Reflection (repeat)
2. Amplified Reflection (rephrasing andparaphrasing)
3. Double-Sided Reflection (rephrasing,paraphrasing and reflecting feeling)
Types of Reflective Statements
Summarizing
• Summaries capture both sides of the ambivalence (“You say that ___________ but you also mentioned that ________________.”)
• They demonstrate the clinician has been listening carefully.
• Summaries also prompt clarification and further elaboration from the person.
• They prepare consumers to move forward.

DDCAT & DDCMHT
OVERVIEW

Rationale for Integrated Treatment
1. Substance use disorders are common in people with mental health disorders
2. Mental health disorders are common in people with substance use disorders
3. Co-occurring disorders lead to worse outcomes and higher costs than single disorders
4. Evidence-based models exist and can be implemented
5. Providers and consumers want a better system and services
6. Few (<10%) people get the treatments they need.


WHY DO WE NEED TO MEASURE CO-OCCURRING CAPABILITY?
1. Generic terms “integrated” or “enhanced” are “feel good” rhetoric but lack specificity.
2. Systems and providers seek guidance,objective criteria and benchmarks for providing
the best possible services.3. Patients and families should be informed aboutthe range of services, to express preferences andmake educated treatment decisions.
4. Change efforts can be focused and outcomes ofthese initiatives assessed.

IS THERE A CONCEPTUAL MODEL THAT COULD GUIDE RESEARCH AND PRACTICE FOR TREATMENT?
• The American Society of Addiction Medicine (ASAM) Patient Placement Criteria Second Edition Revised (PPC-2R) outlined the framework for a model
• The ASAM-PPC-2R is designed for addiction treatment services
• The ASAM-PPC-2R patient placement criteria have been widely adopted in public and private community addiction treatment

ASAM TAXONOMY OF DUAL DIAGNOSIS SERVICES
(ASAM, 2001)
• ADDICTION ONLY SERVICES (AOS); MENTAL HEALTH ONLY SERVICES (MHOS)
• DUAL DIAGNOSIS CAPABLE (DDC)
• DUAL DIAGNOSIS ENHANCED (DDE)

APPLYING THE FIDELITY SCALE METHODOLOGY FOR A
MORE OBJECTIVE ASSESSMENT OF DUAL DIAGNOSIS CAPABILITY
• Site visit (yields data beyond self-report)
• Multiple sources: • 1) Documents and materials• 2) Ethnographic observation
3) Interviews with staff and patients• Unit of analysis: Program
• “Triangulation” of data

DUAL DIAGNOSIS CAPABILITY IN MENTAL HEALTH TREATMENT
(DDCMHT) INDEX
• Designed by Drs. Heather Gotham, Jessica Brown & Joseph Comaty as companion to DDCAT but for use in mental health programs.
• Common metric and method: 35 items, 7 dimensions, programs categorized as Mental Health Only Services (MHOS), DDC or DDE
• More likely presentation of QIII patients in mental health system (than addiction treatment system)
• Makes comparisons between systems possible

DDCAT & DDCMHT (3.2): 7 DIMENSIONS
& CONTENT OF 35 ITEMSDimension Content of items
I Program Structure
Program mission, structure and financing, format for delivery of mental health or addiction services.
II Program Milieu
Physical, social and cultural environment for persons with psychiatric or substance use problems.
III Clinical Process: Assessment
Processes for access and entry into services, screening, assessment & diagnosis.
IV Clinical Process: Treatment
Processes for treatment including pharmacological and psychosocial evidence-based formats.
V Continuity of Care
Discharge and continuity for both substance use and psychiatric services, peer recovery supports.
VI Staffing Presence, role and integration of staff with mental health and/or addiction expertise, supervision process
VII Training Proportion of staff trained and program’s training strategy for co-occurring disorder issues.
Related Documents









![OPEN ACCESS Abuse Disorders Keywords · disorders [1]. Despite the high prevalence rates of “co-occurring” mental health and substance disorders (COD), the administration, funding](https://static.cupdf.com/doc/110x72/5edc6e63ad6a402d666715a9/open-access-abuse-disorders-keywords-disorders-1-despite-the-high-prevalence.jpg)

