Oversight and Systems Considerations to Aide in Meeting the Revised Performance Measures Nancy Albert, PhD, RN, CCNS, CCRN, NE-BC, FAHA, FCCM Senior Director Nursing Research and Innovation; CNS, Kaufman Center for Heart Failure May 2012

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Oversight and Systems Considerations to Aide in
Meeting the Revised Performance Measures
Nancy Albert, PhD, RN, CCNS, CCRN, NE-BC, FAHA, FCCM
Senior Director Nursing Research and Innovation;CNS, Kaufman Center for Heart Failure
May 2012
2
Presenter Disclosure InformationNancy Albert, PhD, RN, CCNS, CCRN, NE-BC, FAHA, FCCMOversight and Systems Considerations to Aide in Meeting the Revised Performance Measures
2
FINANCIAL DISCLOSURE:No relevant financial relationship exists

QUALITY
Review PracticeProfile Report
Select Target Performance Measure
Impact Opportunity
Create Action Plan
• Cardiologists• Nurses• Administrative Support Staff
Develop Solutions to Implementation Barriers
Evaluate and Communicate Results
to Team
Implement Improvement Action Plan
Improve Use of Evidence-Based Therapies
Performance Improvement Process
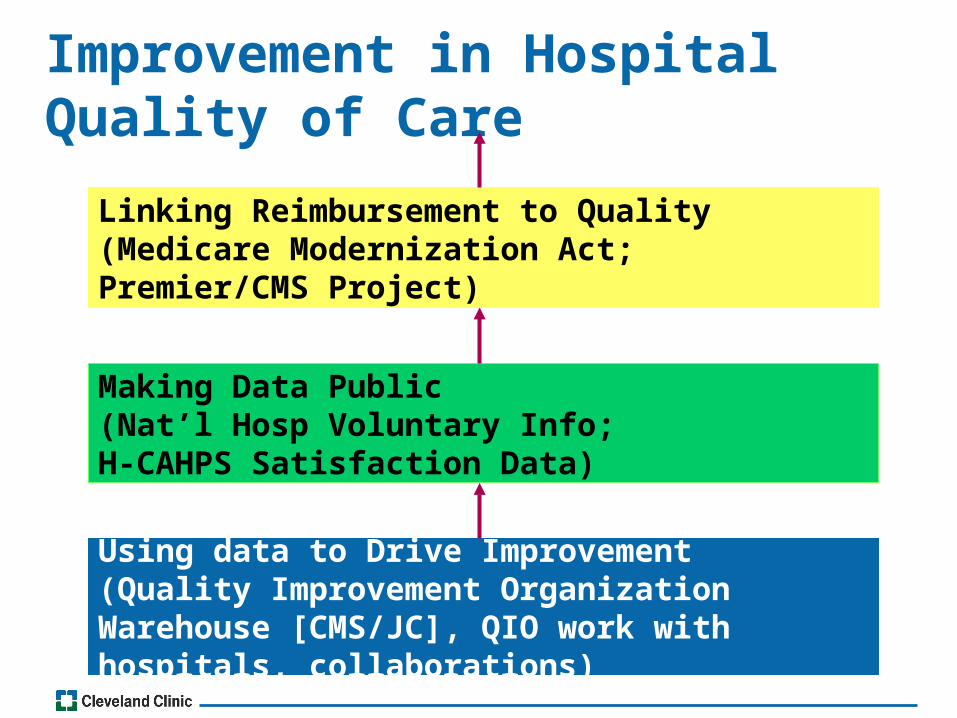
Improvement in Hospital Quality of Care
Using data to Drive Improvement(Quality Improvement Organization Warehouse [CMS/JC], QIO work with hospitals, collaborations)
Making Data Public(Nat’l Hosp Voluntary Info; H-CAHPS Satisfaction Data)
Linking Reimbursement to Quality(Medicare Modernization Act; Premier/CMS Project)
Participate in PROGRAMS to Improve Performance Measures• Usually designed to enhance quality of patient
care that promotes adoption of evidence-based, guideline-recommended therapies–Force a deeper look into actions and
practices–Requires:–Leadership–Evidence-based clinical decision support (algorithms; pocket cards, customizable order sets...)–Patient education resources
REENGINEERING QUALITY
• Reengineering:
–Starting over
–Thinking outside of the box
–Throwing out all the notions of how work was done and deciding how it can best be done now
• After identifying quality needs:
–Design how it can best be done now
–Design processes and aligning people to meet those needs
Reengineering aims at quantum gains
on the order of 30-50% or more.
QI programs stress
incremental progress,
striving for inch-by-inch gains again and again
MOVING FORWARD
• Consider how you are trying to meet the performance measure
–Have you revised electronic documentation to show conformity to a performance measure?
–Does the new “system” make a difference in quality care and patient outcomes?
• Consider who you ask to do work now
–Are nurses who are already peaked out being asked to do more?
–Do they have time to meet the request?
SYSTEMS ISSUES?
OVERSIGHT ISSUES?
Performance Measures
• Consider a “positive deviance” inquiry approach to problem solving:
• Premise: In every community there are certain individuals whose uncommon practices or behaviors enable them to find better solutions to problems than their neighbors who have access to the same resources
•What enables some members of the community (the “positive deviants”) to find better solutions to pervasive problems than their neighbors who have access to the same resources?
–Positive deviance focuses on PRACTICE (not knowledge)
–Best understood through ACTION
“It’s easier to ACT your way into a new way of THINKING, than to THINK your way into a new
way of ACTING”
Performance Measures
Using Performance Measures to ACT
• Although there are multiple, complex rationale for problems that affect practice, performance measure programs promote solutions, now/today, before all the underlying causes are addressed
• Performance measure programs utilize the 6 “Ds” of positive deviance:
1. Define the problem, its perceived causes and related current practices (situation analysis)–Define what a successful solution/outcome
would look like (described as a behavioral or status outcome)
2. Determine if there are any individuals/entities who ALREADY exhibit desired behavior or status
3. Discover uncommon practices/behaviors enabling the individuals/entities to outperform/find better solutions to the problem (than others in their “community”)
6 Ds of Positive Deviance Approach:
6 Ds of Positive Deviance Approach:
4. Design and implement activities enabling others to access and PRACTICE new behaviors (focus on “doing” rather than transfer of knowledge)
5. Discern the effectiveness of activities or project through ongoing monitoring and evaluation
6. Disseminate successful process to appropriate “other” (scaling up)

Use a ‘Phases of Innovation’ Model Inspiration Ideation Implementation
Observe & Inquire
Tell Stories
Synthesize
Brainstorm
Experiment
Execute
Spread
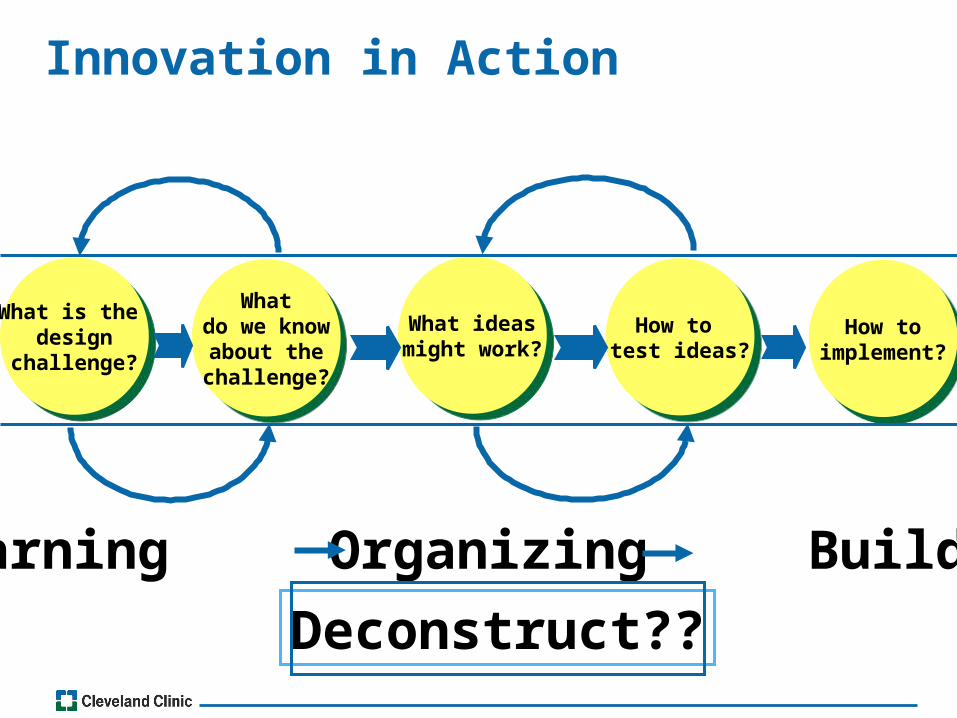
Innovation in Action
What is the design
challenge?
What is the design
challenge?
Whatdo we know
about thechallenge?
Whatdo we know
about thechallenge?
What ideasmight work?
What ideasmight work?
How to test ideas?
How to test ideas?
How toimplement?
How toimplement?
Learning Organizing Building
Deconstruct??
WHY REENGINEERING?
• Health care costs too much and achieves too little–It is inefficient
• Need for improved safety• Too much fragmented services and systems• Need better performance–Reprioritization of the healthcare provider’s
day–More time for patients
• Need to reduce tensions• Need better communication

REENGINEERING•Work is NOT a series of separate tasks to be
individually optimized
Champy J, Greenspun H. Reengineering Healthcare. FT Press; 2010

REENGINEERING
•Work is groupings of interconnected processes to be reassessed and reinvented in total
Champy J, Greenspun H. Reengineering Healthcare. FT Press; 2010
Bundling
4 Words- Keys to Reengineering
1. Fundamental: How work is performed
– Ask yourself and the team:
– Are the underlying assumptions about the design of work still valid?
–Have advances in science & technology allowed work to be carried out in new and more efficient ways?
2. Radical: Going beyond superficial changes in the way things are done
– Are old structures and operating assumptions diminishing the quality and service being delivered?
–Do you need to go back to your original roots and rethink how work should be done?
Champy J, Greenspun H. Reengineering Healthcare. FT Press; 2010
4 Words- Keys to Reengineering
1. Dramatic: NOT about marginal or incremental improvements – Not piecemeal change...need MORE– Is your efficacy threatened in a way that
only wholesale change can fix?2. Process: Group of activities– Uses 1 or more types of input to create an
output customers will value–Expanding accessibility / improving care
– Customer: patient, clinician, family or insurer paying for care
Champy J, Greenspun H. Reengineering Healthcare. FT Press; 2010
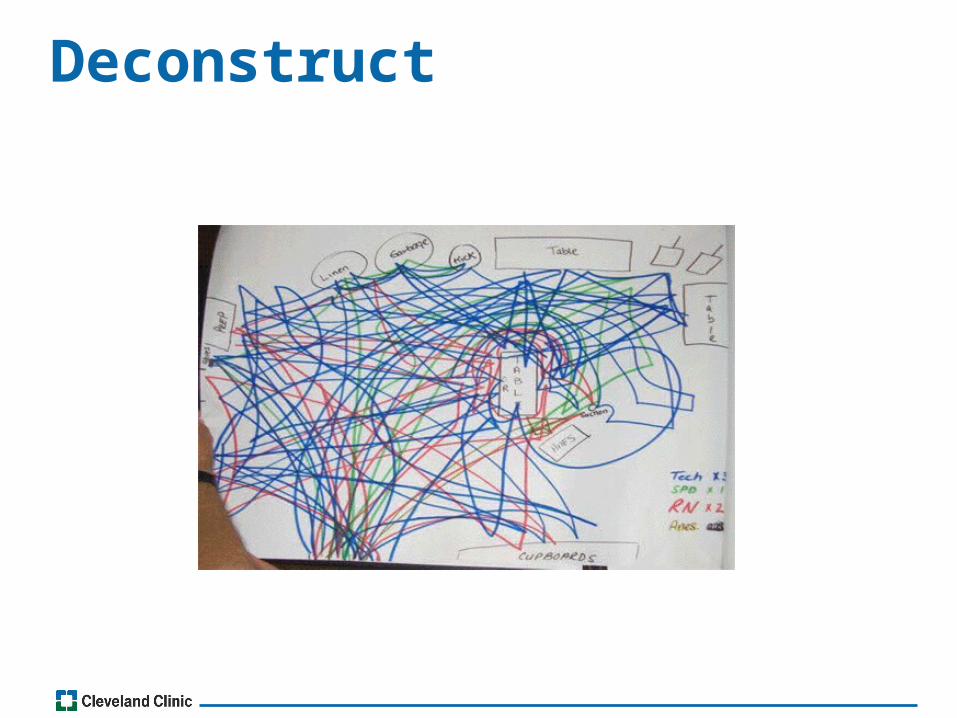
Deconstruct

•Often, we question the reliability of performance measures in specific settings–Documentation of patient education –Checking a box does not reflect delivery of quality care
REENGINEERING
1. Koelling TM, et al. Circulation 2005;111:179-185.2. Krumholz HM et al. JACC 2002;39:83-89.
• 1:1 RN-delivered comprehensive HF education during a 1-hour hospital session decreased 6-month days hospitalized or days dead1
• RN delivered, 1 hour, comprehensive hospital education + ongoing 1 year telephone-based support decreased 1-year hospital readmission rate and hospital costs2

Van der Wal MH, et al. Eur Heart J 2010;31:1486-1493
Compliance with advice on weight monitoring, low sodium diet, fluid restriction and exercise
*, P< 0.01; **P<0.05
COACH study: Death or HF Rehospitalization
COACH study: Death or HF Rehospitalization
0
20
40
60
% p
rim
ary
end
po
int
Total compliance score (0-4)
4 3 2 1 or 0
25%
38% 36%
45%*
**
*
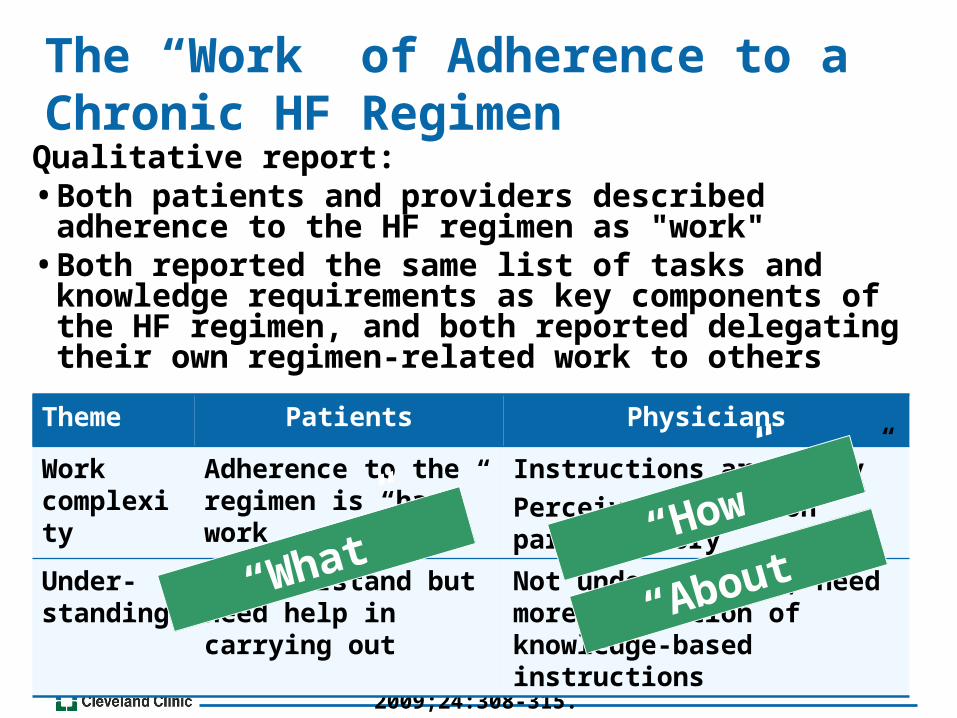
The “Work” of Adherence to a Chronic HF Regimen
Qualitative report:• Both patients and providers described adherence to the
HF regimen as "work" • Both reported the same list of tasks and knowledge
requirements as key components of the HF regimen, and both reported delegating their own regimen-related work to others
Granger BB, et al. J Cardiovasc Nurs. 2009;24:308-315.
Theme Patients Physicians
Work complexity
Adherence to the regimen is “hard” work
Instructions are “easy”
Perceive pts as non participatory
Under-standing
Do understand but need help in carrying out
Not understanding; need more repetition of knowledge-based instructions
“About”“What” “How”
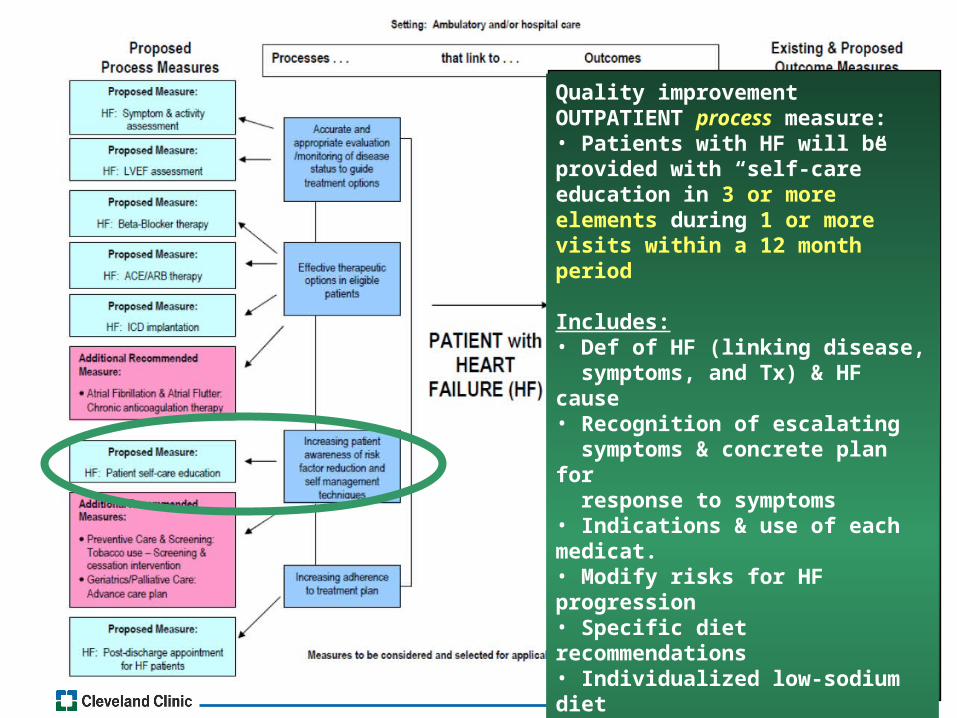
Quality improvement OUTPATIENT process measure:• Patients with HF will be provided with “self-care” education in 3 or more elements during 1 or more visits within a 12 month period
Includes:• Def of HF (linking disease, symptoms, and Tx) & HF cause• Recognition of escalating symptoms & concrete plan for response to symptoms• Indications & use of each medicat.• Modify risks for HF progression• Specific diet recommendations• Individualized low-sodium diet• Recommend for ETOH intake• Specific act./exercise recommend.• Importance of Tx adherence & behavioral strategies to promote Tx adherence• Importance of monitoring weight daily at home
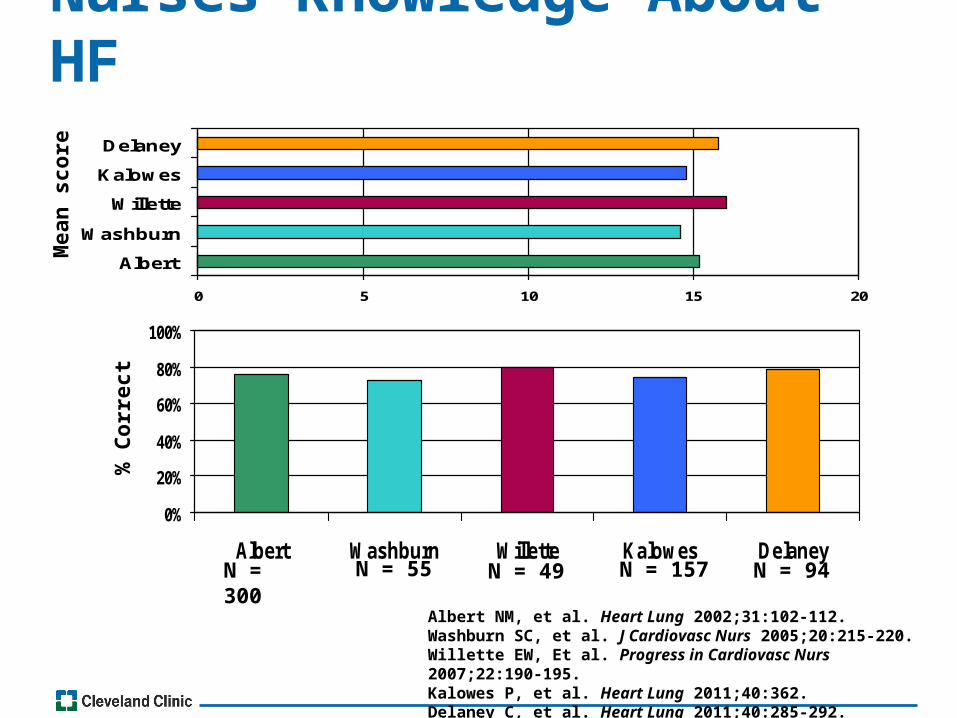
Nurses Knowledge About HF
0 5 10 15 20
Albert
Washburn
Willette
Kalowes
Delaney
0%
20%
40%
60%
80%
100%
Albert Washburn Willette Kalowes Delaney
Albert NM, et al. Heart Lung 2002;31:102-112.Washburn SC, et al. J Cardiovasc Nurs 2005;20:215-220. Willette EW, Et al. Progress in Cardiovasc Nurs 2007;22:190-195.Kalowes P, et al. Heart Lung 2011;40:362.Delaney C, et al. Heart Lung 2011;40:285-292.
N = 300 N = 55 N = 49
Mea
n s
core
% C
orr
ect
N = 157 N = 94
Nurse Education Systems Rationale:
• Based on research results:–118 nurses from 3 sites participated in
survey research on comfort and frequency in delivering HF patient education before hospital discharge–CC Main campus –2 community hospitals–CC site–Valdosta, Georgia site
–Survey created by investigators based on education themes from national guideline discharge education recommendations
Albert NM, et al. Heart & Lung 2011;40:363.
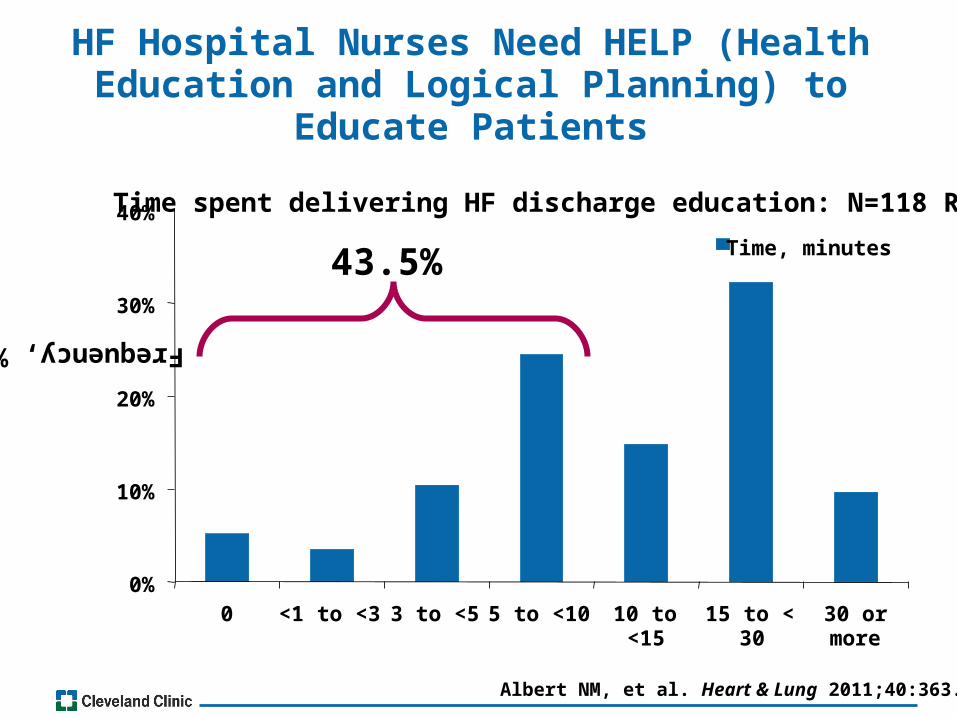
HF Hospital Nurses Need HELP (HealthEducation and Logical Planning) to
Educate Patients
Frequency, %
43.5%
Albert NM, et al. Heart & Lung 2011;40:363.
0%
10%
20%
30%
40%
0 <1 to <3 3 to <5 5 to <10 10 to<15
15 to <30
30 ormore
Time, minutes
Time spent delivering HF discharge education: N=118 RNs
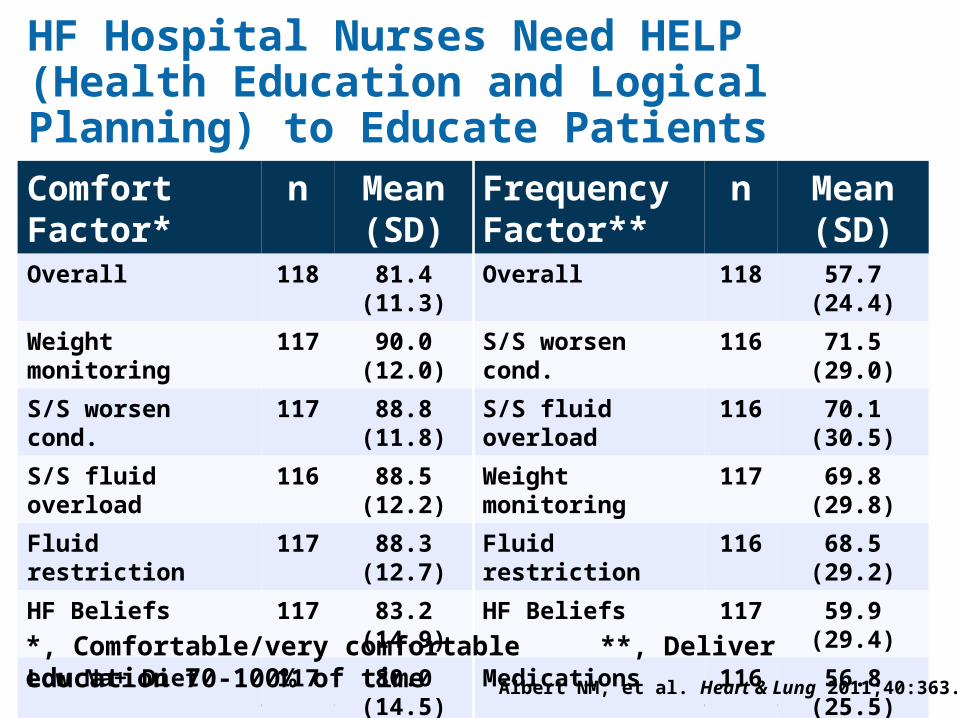
Comfort Factor*
n Mean (SD)
Frequency Factor**
n Mean (SD)
Overall 118 81.4 (11.3) Overall 118 57.7 (24.4)
Weight monitoring 117 90.0 (12.0) S/S worsen cond. 116 71.5 (29.0)
S/S worsen cond. 117 88.8 (11.8) S/S fluid overload 116 70.1 (30.5)
S/S fluid overload 116 88.5 (12.2) Weight monitoring 117 69.8 (29.8)
Fluid restriction 117 88.3 (12.7) Fluid restriction 116 68.5 (29.2)
HF Beliefs 117 83.2 (14.9) HF Beliefs 117 59.9 (29.4)
Low Na+ Diet 117 80.0 (14.5) Medications 116 56.8 (25.5)
Medications 117 78.0 (13.8) Low Na+ Diet 117 48.0 (29.2)
Activity/Exercise 117 73.0 (19.3) Activity/Exercise 117 42.7 (29.4)
Albert NM, et al. Heart & Lung 2011;40:363.
HF Hospital Nurses Need HELP (Health Education and Logical Planning) to Educate Patients
*, Comfortable/very comfortable **, Deliver education 70-100% of time
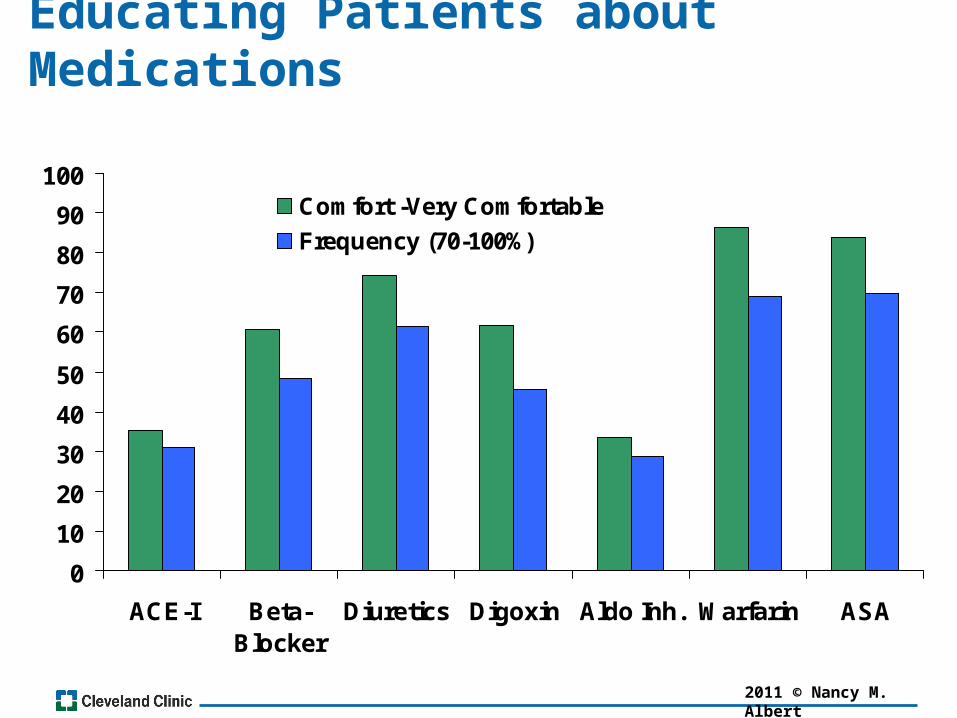
Educating Patients about Medications
0
10
20
30
40
50
60
70
80
90
100
ACE-I Beta-Blocker
Diuretics Digoxin Aldo Inh. Warfarin ASA
Comfort -Very Comfortable
Frequency (70-100%)
2011 © Nancy M. Albert
Weight Monitoring
• “If you gain 3 or more pounds in a day or 5 or more pounds in a week” call me / do something
• AHA/ACC and HFSA guidelines include weight monitoring as a component of “education”
–But, guidelines do NOT include specific wording about how to do it
Does this recommendation really work in your setting?
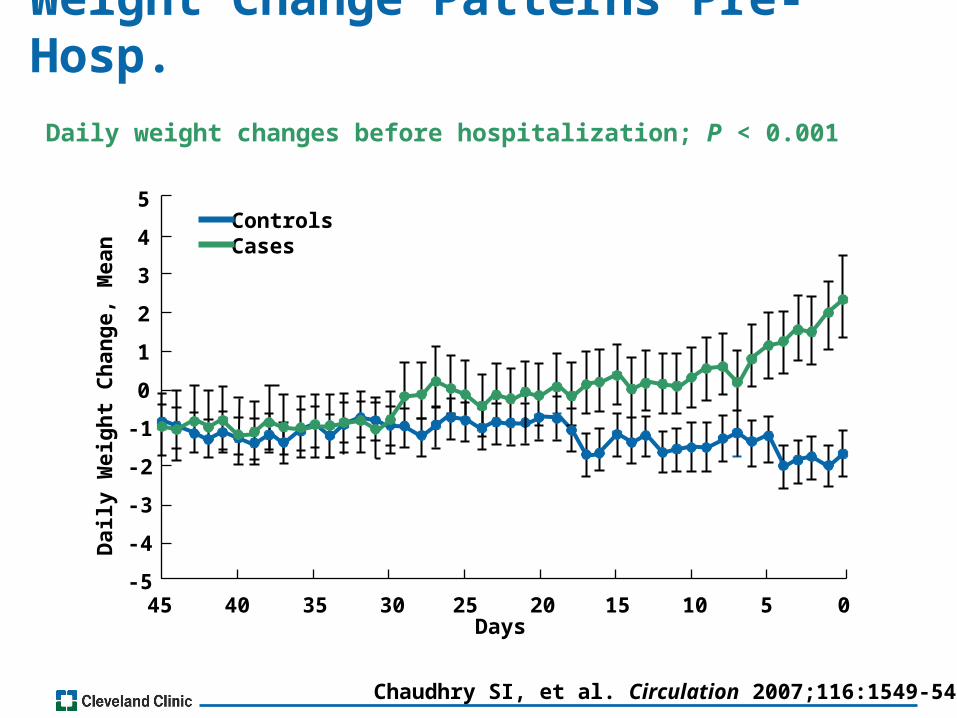
Weight Change Patterns Pre-Hosp.
Daily weight changes before hospitalization; P < 0.001
Chaudhry SI, et al. Circulation 2007;116:1549-54.
Days45 40 35 30 25 20 15 10 5 0
-5
-4
-3
-2
-1
0
1
2
3
4
5
Dai
ly W
eig
ht
Ch
ang
e, M
ean
ControlsCases
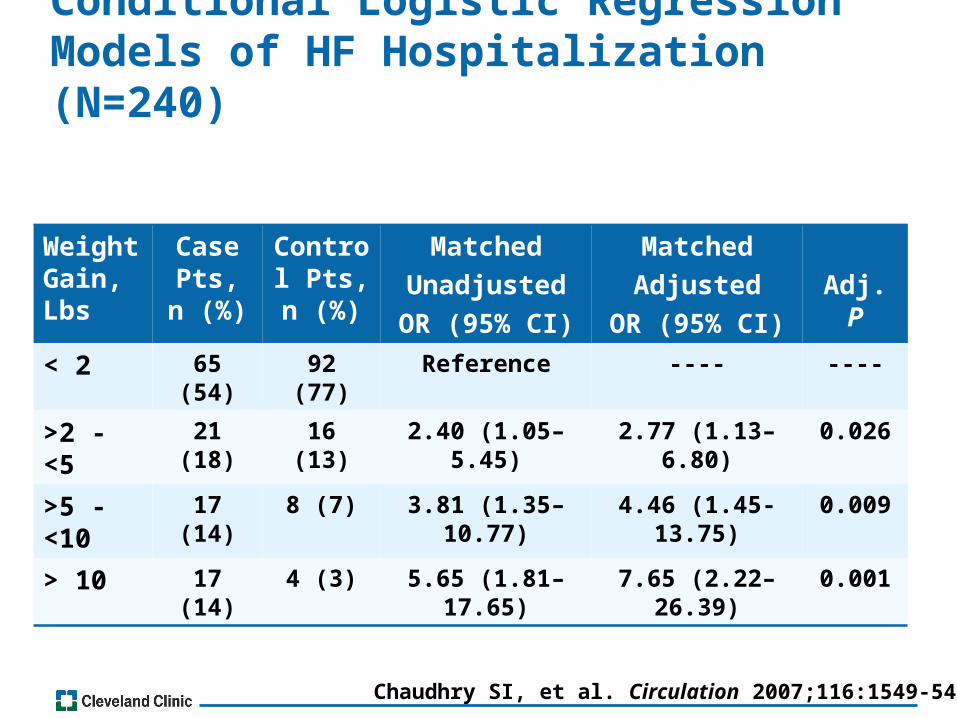
Conditional Logistic Regression Models of HF Hospitalization (N=240)
Weight Gain, Lbs
Case Pts, n
(%)
Control Pts, n
(%)
Matched
Unadjusted
OR (95% CI)
Matched
Adjusted
OR (95% CI)
Adj. P
< 2 65 (54) 92 (77) Reference ---- ----
>2 - <5 21 (18) 16 (13) 2.40 (1.05–5.45) 2.77 (1.13–6.80) 0.026
>5 - <10 17 (14) 8 (7) 3.81 (1.35–10.77) 4.46 (1.45-13.75) 0.009
> 10 17 (14) 4 (3) 5.65 (1.81–17.65) 7.65 (2.22–26.39) 0.001
Chaudhry SI, et al. Circulation 2007;116:1549-54.

Weight Monitoring
Blair JE et al. European Heart J. 2009;30:1666–1673.
HF Hospitalization
60 days 120 days 180 days
Time Post Discharge
P<0.0001(no event vs. visit prior to event groups)2.5
2
1.5
1
0.5
03169 184 401 2941 411 635 2780 411 635C
han
ge,
Bo
dy
Wei
gh
t; K
g
• 4133 Pts w HF-REF; EVEREST Trial*, Time from remote monitor to event: 32/44/56 days; time from clinic visit to event: 9/12/14 days
No eventRemote monitor before event*Clinic visit before event*
OVERSIGHT & SYSTEMS CONSIDERATIONSPatient Education in Self Care• Knowledgeable educators–Medications, Diet, Exercise
• Educators need time to educate• Select EBP daily weight reporting criteria•Medication reconciliation•Medication understanding• Across continuum: hosp. to home; hosp. to
SNF; hosp. to home care program

Reengineering - Bundled Initiatives
Focus
Changes
Patient Revised HF handbook & Quick Sheet; New focus; pages; reorgan.
Revised weight monitoring criteria
Revised Epic template to include weight expectations
Nurses 1 hour HF education; take session yearly
OPD: Document new weight protocol in Epic
Hosp: Revised HF edu. Documentation system
Team Hosp: PharmD provide pharmacy edu. & reconciliation x 2
APN assigned to SNFs; visit within 48 hrs.
CNS Care Coordinators at community hospitals
All educators: Teachback
Home care at home program w telemonitoring
Phone calls to pts 48 hrs and 10 days post discharge
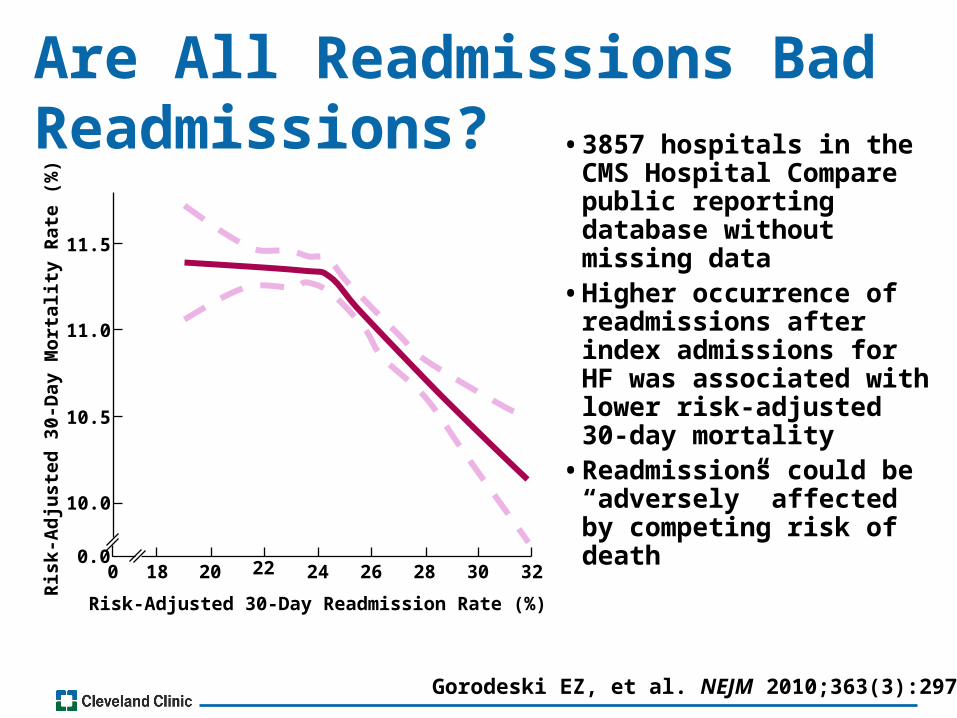
Are All Readmissions Bad Readmissions? • 3857 hospitals in the
CMS Hospital Compare public reporting database without missing data• Higher occurrence of
readmissions after index admissions for HF was associated with lower risk-adjusted 30-day mortality• Readmissions could be
“adversely” affected by competing risk of death
Gorodeski EZ, et al. NEJM 2010;363(3):297.
Risk-Adjusted 30-Day Readmission Rate (%)
0 18 20 22 24 26 28 30 320.0
10.0
10.5
11.0
11.5
Ris
k-A
dju
ste
d 3
0-D
ay M
ort
alit
y R
ate
(%
)

Related Documents











