CLINICAL STUDIES Over-expression of glutamine synthetase in focal nodular hyperplasia: a novel easy diagnostic tool in surgical pathology Paulette Bioulac-Sage 1,2 , Herv ´ e Laumonier 3 , Anne Rullier 1,2 , Gaelle Cubel 2 , Christophe Laurent 4 , Jessica Zucman-Rossi 5,6 and Charles Balabaud 2,7 1 Department of Pathology, Ho ˆ pital Pellegrin CHU Bordeaux, Bordeaux, France 2 Inserm U 889, Universit ´ e Victor Segalen Bordeaux 2, Bordeaux, France 3 Department of Radiology, Ho ˆ pital St Andr ´ e, CHU Bordeaux, Bordeaux, France 4 Department of Surgery, Ho ˆ pital St Andr ´ e CHU Bordeaux, Bordeaux, France 5 Inserm, U674, G ´ enomique fonctionnelle des tumeurs solides, Paris, France 6 Universit ´ e Paris 7 Denis Diderot, Institut Universitaire d’H ´ ematologie, CEPH, Paris, France 7 Department of Hepatology, Ho ˆ pital St Andr ´ e, CHU Bordeaux, Bordeaux, France Keywords focal nodular hyperplasia – glutamine synythetase – hepatocellular tumors – beta-catenin – liver pathology Correspondence Paulette Bioulac-Sage, Department of Pathology, Ho ˆ pital Pellegrin CHU Bordeaux, Bordeaux 33076, France Tel: +33 5 56 79 56 02 Fax: +33 5 56 79 60 88 e-mail: [email protected] Received 4 March 2008 Accepted 20 June 2008 DOI:10.1111/j.1478-3231.2008.01849.x Abstract Background and Aims: Glutamine synthetase (GS) is a useful marker in tumour liver pathology, including hepatocellular adenomas and nodules in cirrhosis. We investi- gated the use of GS as a marker in various clinical situations, in which FNH diagnosis had been firmly established to determine its contribution to diagnosis. Methods: Se- venty-nine cases of resected FNH, all on normal (or occasionally steatotic) livers, were retrieved from our collection. The control group was composed of hepatocellular adenomas and well-differentiated hepatocellular carcinoma. The following stains: H&E, Masson’s trichrome, Gordon-Sweet, PAS, perls and immunostains: CK7 and 19, and GS were carried out. FNH was diagnosed based on traditional pathological techniques. In case of uncertainty, particularly with hepatocellular adenoma, additional immunostainings including liver fatty acid-binding protein, serum amyloid A and b-catenin were performed. Results: Glutamine synthetase immunostaining was similar in all FNH cases. Positive GS staining of hepatocytic cytoplasms formed large areas, anastomosed in a ‘map-like’ pattern, often surrounding hepatic veins, whereas GS was not expressed in hepatocytes close to fibrotic bands containing arteries and ductules. In comparison, hepatocellular adenoma staining was completely different, even in cases of fibrotic bands due to tumour remodelling related to necrosis or haemorrhage. In hepatocellular adenomas or well-differentiated hepatocellular carcinoma presenting b- catenin mutation, GS was positive but with a completely different pattern that appeared diffuse and not ‘map-like’. Conclusion: Regardless of the FNH size or steatotic content, GS produced a similar and characteristic pattern and consequently represents a good marker for easily identifying resected FNH from other hepatocellular nodules. Focal nodular hyperplasia (FNH) has been reported in 0.6–3% of the general population (1) and is 10 times more frequently observed than hepatocellular adenomas (HCA) in referral centres (1). In about two-thirds of the cases, FNH is solitary. Most FNH are diagnosed by chance, but some cases are symptomatic. FNH is associated with vascular abnormalities including hepatic haemangiomas, which supports the concept of a vascular component in the pathogenesis of this lesion (2–6). We have recently shown (7) as hypothesized by Wanless (8) that in FNH there was a portal tract and hepatic vein injury defined by the disappearance of the portal vein, bile ducts and hepatic veins, subsequently leading to the enlarge- ment and proliferation of arteries and to venous shunts (portal and hepatic). In 70–90% of the cases depending on centres, FNH is diagnosed using imaging techniques [computed tomography scan, magnetic resonance imaging (MRI) and contrast-en- hanced sonography]. We believe that there is a role for liver biopsies in FNH, if imaging cannot firmly establish the diag- nosis. However, in some cases of FNH, the histopathological diagnosis may remain difficult, even in a resected specimen, because definitive histopathological features may be absent, inconspicuous or atypical (2). Recently, it has been shown that glutamine synthetase (GS) is a useful marker in tumour liver pathology, including HCA and nodules in cirrhosis (9, 10). We investigated whether GS could differentiate, on resected speci- mens, FNH from HCA and well-differentiated hepatocellular carcinoma (wd HCC) developed on non-cirrhotic liver, in a wide variety of clinical situations related to hepatocellular nodules. Materials and methods Cases of resected FNH, all occurring on normal (or occasionally steatotic) livers, were retrieved from our collection (Table 1). Group 1: 31 cases with a firm preoperative radiological diag- nosis, including 4 cases with additional unidentified nodule(s); group 2: 25 cases without clear radiological diagnosis (possible FNH, HCA or HCC), including seven men; group 3: 14 cases Liver International (2009) c 2009 The Authors. Journal compilation c 2009 Blackwell Publishing Ltd 459 Liver International ISSN 1478-3223

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

CL IN ICAL STUDIES
Over-expression of glutamine synthetase in focal nodular hyperplasia:a novel easydiagnostic tool in surgical pathologyPaulette Bioulac-Sage1,2, Herve Laumonier3, Anne Rullier1,2, Gaelle Cubel2, Christophe Laurent4,Jessica Zucman-Rossi5,6 and Charles Balabaud2,7
1 Department of Pathology, Hopital Pellegrin CHU Bordeaux, Bordeaux, France
2 Inserm U 889, Universite Victor Segalen Bordeaux 2, Bordeaux, France
3 Department of Radiology, Hopital St Andre, CHU Bordeaux, Bordeaux, France
4 Department of Surgery, Hopital St Andre CHU Bordeaux, Bordeaux, France
5 Inserm, U674, Genomique fonctionnelle des tumeurs solides, Paris, France
6 Universite Paris 7 Denis Diderot, Institut Universitaire d’Hematologie, CEPH, Paris, France
7 Department of Hepatology, Hopital St Andre, CHU Bordeaux, Bordeaux, France
Keywords
focal nodular hyperplasia – glutamine
synythetase – hepatocellular tumors –
beta-catenin – liver pathology
Correspondence
Paulette Bioulac-Sage, Department of
Pathology, Hopital Pellegrin CHU Bordeaux,
Bordeaux 33076, France
Tel: +33 5 56 79 56 02
Fax: +33 5 56 79 60 88
e-mail: [email protected]
Received 4 March 2008
Accepted 20 June 2008
DOI:10.1111/j.1478-3231.2008.01849.x
AbstractBackground and Aims: Glutamine synthetase (GS) is a useful marker in tumour liverpathology, including hepatocellular adenomas and nodules in cirrhosis. We investi-gated the use of GS as a marker in various clinical situations, in which FNH diagnosishad been firmly established to determine its contribution to diagnosis. Methods: Se-venty-nine cases of resected FNH, all on normal (or occasionally steatotic) livers, wereretrieved from our collection. The control group was composed of hepatocellularadenomas and well-differentiated hepatocellular carcinoma. The following stains:H&E, Masson’s trichrome, Gordon-Sweet, PAS, perls and immunostains: CK7 and 19,and GS were carried out. FNH was diagnosed based on traditional pathologicaltechniques. In case of uncertainty, particularly with hepatocellular adenoma, additionalimmunostainings including liver fatty acid-binding protein, serum amyloid A andb-catenin were performed. Results: Glutamine synthetase immunostaining was similarin all FNH cases. Positive GS staining of hepatocytic cytoplasms formed large areas,anastomosed in a ‘map-like’ pattern, often surrounding hepatic veins, whereas GS wasnot expressed in hepatocytes close to fibrotic bands containing arteries and ductules. Incomparison, hepatocellular adenoma staining was completely different, even in cases offibrotic bands due to tumour remodelling related to necrosis or haemorrhage. Inhepatocellular adenomas or well-differentiated hepatocellular carcinoma presenting b-catenin mutation, GS was positive but with a completely different pattern that appeareddiffuse and not ‘map-like’. Conclusion: Regardless of the FNH size or steatotic content,GS produced a similar and characteristic pattern and consequently represents a goodmarker for easily identifying resected FNH from other hepatocellular nodules.
Focal nodular hyperplasia (FNH) has been reported in 0.6–3%of the general population (1) and is 10 times more frequentlyobserved than hepatocellular adenomas (HCA) in referralcentres (1). In about two-thirds of the cases, FNH is solitary.Most FNH are diagnosed by chance, but some cases aresymptomatic. FNH is associated with vascular abnormalitiesincluding hepatic haemangiomas, which supports the conceptof a vascular component in the pathogenesis of this lesion(2–6). We have recently shown (7) as hypothesized by Wanless(8) that in FNH there was a portal tract and hepatic veininjury defined by the disappearance of the portal vein, bileducts and hepatic veins, subsequently leading to the enlarge-ment and proliferation of arteries and to venous shunts (portaland hepatic).
In 70–90% of the cases depending on centres, FNH isdiagnosed using imaging techniques [computed tomographyscan, magnetic resonance imaging (MRI) and contrast-en-hanced sonography]. We believe that there is a role for liverbiopsies in FNH, if imaging cannot firmly establish the diag-nosis. However, in some cases of FNH, the histopathological
diagnosis may remain difficult, even in a resected specimen,because definitive histopathological features may be absent,inconspicuous or atypical (2). Recently, it has been shown thatglutamine synthetase (GS) is a useful marker in tumour liverpathology, including HCA and nodules in cirrhosis (9, 10). Weinvestigated whether GS could differentiate, on resected speci-mens, FNH from HCA and well-differentiated hepatocellularcarcinoma (wd HCC) developed on non-cirrhotic liver, in awide variety of clinical situations related to hepatocellularnodules.
Materials and methods
Cases of resected FNH, all occurring on normal (or occasionallysteatotic) livers, were retrieved from our collection (Table 1).Group 1: 31 cases with a firm preoperative radiological diag-nosis, including 4 cases with additional unidentified nodule(s);group 2: 25 cases without clear radiological diagnosis (possibleFNH, HCA or HCC), including seven men; group 3: 14 cases
Liver International (2009)c� 2009 The Authors. Journal compilation c� 2009 Blackwell Publishing Ltd 459
Liver International ISSN 1478-3223
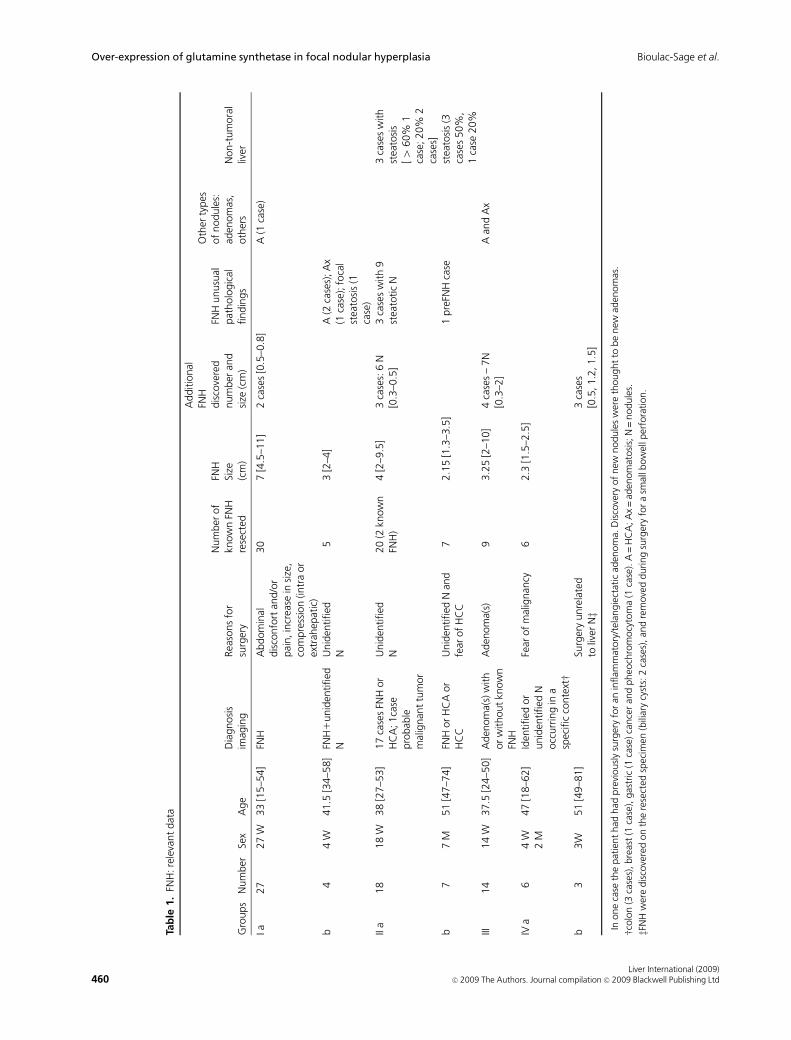
Tab
le1.
FNH
:re
leva
nt
dat
a
Gro
ups
Num
ber
Sex
Age
Dia
gnosi
sim
agin
gRea
sons
for
surg
ery
Num
ber
of
know
nFN
Hre
sect
ed
FNH
Size
(cm
)
Additio
nal
FNH
dis
cove
red
num
ber
and
size
(cm
)
FNH
unusu
alpat
holo
gic
alfindin
gs
Oth
erty
pes
of
nodule
s:ad
enom
as,
oth
ers
Non-t
um
ora
lliv
er
Ia27
27
W33
[15–5
4]
FNH
Abdom
inal
dis
confo
rtan
d/o
rpai
n,in
crea
sein
size
,co
mpre
ssio
n(in
tra
or
extr
ahep
atic
)
30
7[4
.5–1
1]
2ca
ses
[0.5
–0.8
]A
(1ca
se)
b4
4W
41.5
[34–5
8]
FNH
1unid
entified
NU
nid
entified
N5
3[2
–4]
A(2
case
s);A
x(1
case
);fo
cal
stea
tosi
s(1
case
)II
a18
18
W38
[27–5
3]
17
case
sFN
Hor
HC
A;1ca
sepro
bab
lem
alig
nan
ttu
mor
Unid
entified
N20
(2kn
ow
nFN
H)
4[2
–9.5
]3
case
s:6
N[0
.3–0
.5]
3ca
ses
with
9st
eato
tic
N3
case
sw
ith
stea
tosi
s[4
60%
1ca
se;20%
2ca
ses]
b7
7M
51
[47–7
4]
FNH
or
HC
Aor
HC
CU
nid
entified
Nan
dfe
arof
HC
C7
2.1
5[1
.3–3
.5]
1pre
FNH
case
stea
tosi
s(3
case
s50%
,1
case
20%
III14
14
W37.5
[24–5
0]
Aden
om
a(s)
with
or
without
know
nFN
H
Aden
om
a(s)�
93.2
5[2
–10]
4ca
ses
–7N
[0.3
–2]
Aan
dA
x
IVa
64
W2
M47
[18–6
2]
Iden
tified
or
unid
entified
Nocc
urr
ing
ina
spec
ific
conte
xtw
Fear
of
mal
ignan
cy6
2.3
[1.5
–2.5
]
b3
3W
51
[49–8
1]
Surg
ery
unre
late
dto
liver
Nz
3ca
ses
[0.5
,1.2
,1.5
]
� In
one
case
the
pat
ient
had
had
pre
viousl
ysu
rger
yfo
ran
inflam
mat
ory
/tel
angie
ctat
icad
enom
a.D
isco
very
of
new
nodule
sw
ere
thought
tobe
new
aden
om
as.
wcolo
n(3
case
s),bre
ast
(1ca
se),
gas
tric
(1ca
se)ca
nce
ran
dpheo
chro
mocy
tom
a(1
case
).A
=H
CA
;A
x=
aden
om
atosi
s;N
=nodule
s.
zFN
Hw
ere
dis
cove
red
on
the
rese
cted
spec
imen
(bili
ary
cyst
s:2
case
s),an
dre
move
dduring
surg
ery
for
asm
allb
ow
ellp
erfo
ration.
Liver International (2009)460 c� 2009 The Authors. Journal compilation c� 2009 Blackwell Publishing Ltd
Over-expression of glutamine synthetase in focal nodular hyperplasia Bioulac-Sage et al.
with radiological diagnosis of adenoma/adenomatosis present-ing additional FNH (known or unknown before surgery) on theresected specimen; and group 4: nine cases, including six caseswith a liver nodule removed in the context of malignancy andthree cases with nodules discovered during liver or abdominalsurgery related to solid tumours.
The control group consisted of six additional cases ofinflammatory/telangiectatic HCA with or without b-cateninmutations, three cases of HCA with mutation on b-catenin andsix cases of wd HCC (including three HCC with b-cateninmutations).
For all FNH cases, several blocks were available (from 3 to 6).The following stains: H&E, Masson’s trichrome, Gordon Sweet,
PAS, perls and immunostainings with cytokeratins (CK)7and 19, GS, and b-catenin antibodies were included. Thediagnosis of FNH was established using classic pathologicalfeatures (11).
We diagnosed HCA (including inflammatory/telangiectaticHCA) and wd HCC according to standard criteria (9, 12), usingthe same stainings as that described earlier (9). We included thefollowing additional stainings in cases of uncertainty betweenthe diagnoses of FNH and HCA, and of HCA and wd HCC:liver fatty acid-binding protein (LFABP), serum amyloid A(SAA), b-catenin and glypican 3, as published previously (9,10). b-catenin staining was systematically performed in non-FNH nodules, if immunostaining for GS was strongly positive.
(b)(a)
(c) (d)
(f)(e)
(g)
V
V
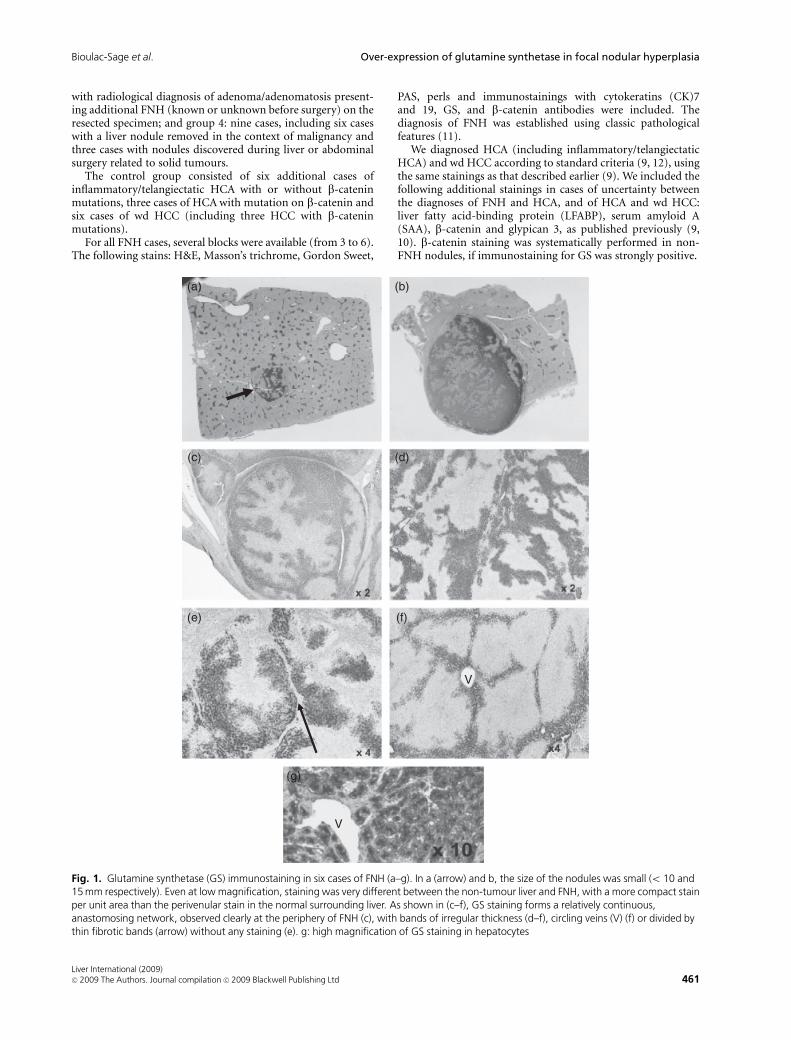
Fig. 1. Glutamine synthetase (GS) immunostaining in six cases of FNH (a–g). In a (arrow) and b, the size of the nodules was small (o 10 and15 mm respectively). Even at low magnification, staining was very different between the non-tumour liver and FNH, with a more compact stainper unit area than the perivenular stain in the normal surrounding liver. As shown in (c–f), GS staining forms a relatively continuous,anastomosing network, observed clearly at the periphery of FNH (c), with bands of irregular thickness (d–f), circling veins (V) (f) or divided bythin fibrotic bands (arrow) without any staining (e). g: high magnification of GS staining in hepatocytes
Liver International (2009)c� 2009 The Authors. Journal compilation c� 2009 Blackwell Publishing Ltd 461
Bioulac-Sage et al. Over-expression of glutamine synthetase in focal nodular hyperplasia
Results
In all FNH groups, independent of the nodule size (Table 1), GSimmunostaining was positive with similar characteristic fea-tures. GS was strongly expressed in the cytoplasm of hepato-cytes and this positive GS staining formed large hepatocyticareas, anastomosed in a ‘map-like’ pattern, often surroundinghepatic veins. GS was not expressed in hepatocytes close tofibrotic bands containing arteries and ductules. The stainingwas usually stronger at the periphery than in the centre of theFNH (Figs 1 and 2). Therefore, this pattern strikingly differsfrom GS staining observed in normal liver, where it is restrictedto 1 or 2 centrolobular plates.
In difficult FNH cases, particularly if FNH lacked character-istic features or presented some features more frequently seen inHCA such as steatosis, GS immunostaining was similar to thatdescribed above, even if sometimes more difficult to analysebecause steatosis. However, large GS-positive areas may berecognized at a distance of fibrous bands (Fig. 3).
In all FNH groups, there was no aberrant expression ofb-catenin in hepatocytes that remained membranous, as innormal hepatocytes (not shown).
Immunostainings for GS were completely different in HCAand wd HCC.
In HCA expressing wild-type b-catenin (HNF1a-mutated orinflammatory/telangiectatic HCA), peripheral hepatocytes wereeventually positive. This was also observed in a few hepatocytes
around some hepatic veins (Fig. 4), but there large areas of GSstaining were absent.
In HCA and wd HCC showing b-catenin-mutations, GS waspositive, but the distribution was diffuse and did not display the‘map-like’ pattern seen in FNH, thus appearing very differentfrom that of FNH (Fig. 5a and b). Moreover, in cases of b-catenin mutated HCA or HCC, there was also an aberrantcytoplasmic and nuclear staining with b-catenin antibody (Fig.5c). Inflammatory/telangiectatic HCA with activation ofb-catenin behaved like b-catenin HCA (not shown).
Discussion
Typical histopathological features of classic FNH include clear,well-delimited but non-encapsulated lesions composed of hepa-tocellular nodules, a central scar and radiating fibrous cords. Thefibrous regions typically contain large dystrophic arteries andductular reaction, and frequently lymphocytic infiltrate is ob-served. FNH can be diagnosed using needle liver biopsies (13, 14).
However, diagnosing FNH may be difficult if one or severalmajor signs are absent or weak (central scar, ductular reaction),if FNH is steatotic, if the nodules are small or if FNH occursunusually (i.e. in men, or in another tumoral context such asadenomatosis, primary malignant tumours,etc.), justifying theuse of several immunostains such as CK7 and 19, CD34 andmore recently immunostains used to identify HCA subtypes
(a)
(b) (c)
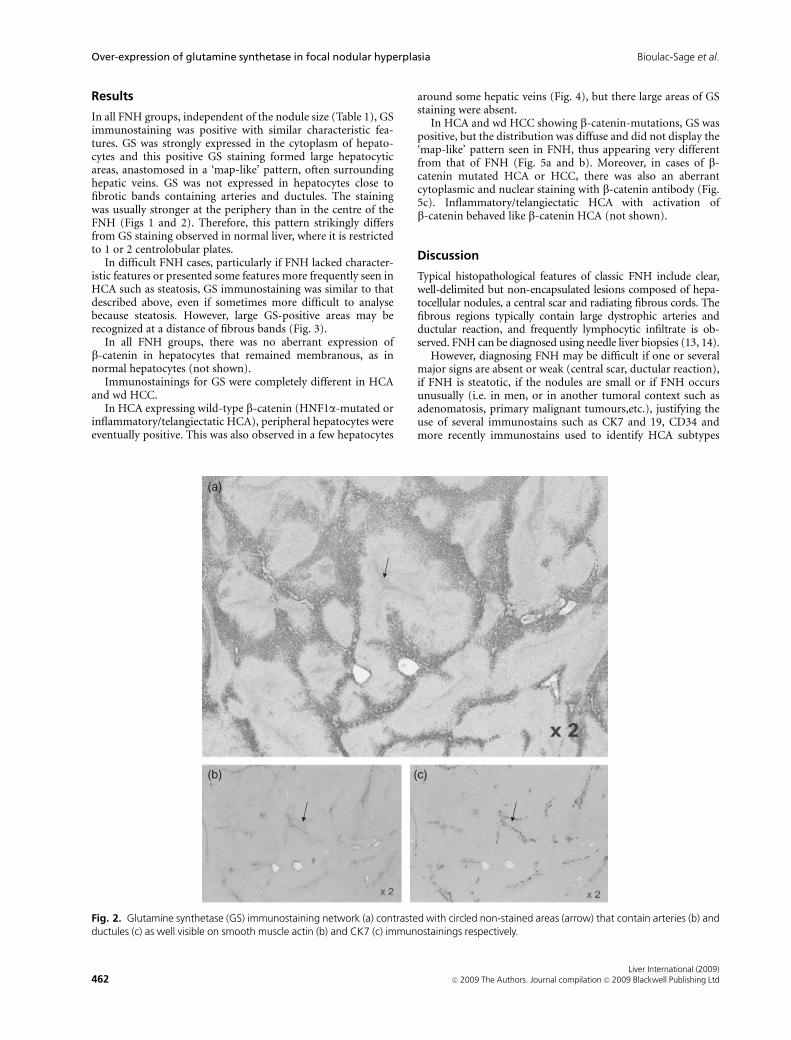
Fig. 2. Glutamine synthetase (GS) immunostaining network (a) contrasted with circled non-stained areas (arrow) that contain arteries (b) andductules (c) as well visible on smooth muscle actin (b) and CK7 (c) immunostainings respectively.
Liver International (2009)462 c� 2009 The Authors. Journal compilation c� 2009 Blackwell Publishing Ltd
Over-expression of glutamine synthetase in focal nodular hyperplasia Bioulac-Sage et al.
such as LFABP and SAA. Recently, nodules, previously termed‘telangiectatic FNH’ because they display abnormal arteriesoften associated with a ductular reaction, have been shown tobe inflammatory/telangiectatic HCA, using genotypic andphenotypic markers (9, 12, 15). In all these difficult cases, GSimmunostaining could be very useful for establishing a properdiagnosis, with no overexpression of inflammatory proteinssuch as SAA, which characterize inflammatory HCA (9).
Glutamine synthetase is one of the key enzymes in nitrogenmetabolism, catalysing the synthesis of glutamine from gluta-mate. The adult pattern of distribution of GS in the human liveris characterized by its strict pericentrolobular localization incontinuous rings of 1 or 2 plates around the central veins of thelobules (16). This pattern is highly conserved. GS is a usefulmarker in tumour liver pathology, including the diagnosis of
liver HCA and nodules in cirrhotic tissue (17, 18). As aconsequence, we tested this FNH marker in various clinicalsituations related to hepatocellular nodules.
In this study, we show that positive GS staining formed largehepatocytic areas, anastomosed in a ‘map-like’ pattern, oftensurrounding hepatic veins, whereas GS was not expressed inhepatocytes close to fibrotic bands containing arteries andductules. This staining was very useful for safe and rapididentification of FNH; this resulted in a very specific andunique staining, constant throughout the various groups stu-died, and independent of the size and the presence or absence ofmajor pathological diagnostic criteria. FNH GS staining wasdistinct from that observed in non-b-catenin HCA, inflamma-tory/telangiectatic HCA (9) as well as in b-catenin-mutatedHCA or HCC.
(a)
(b)
x 4*
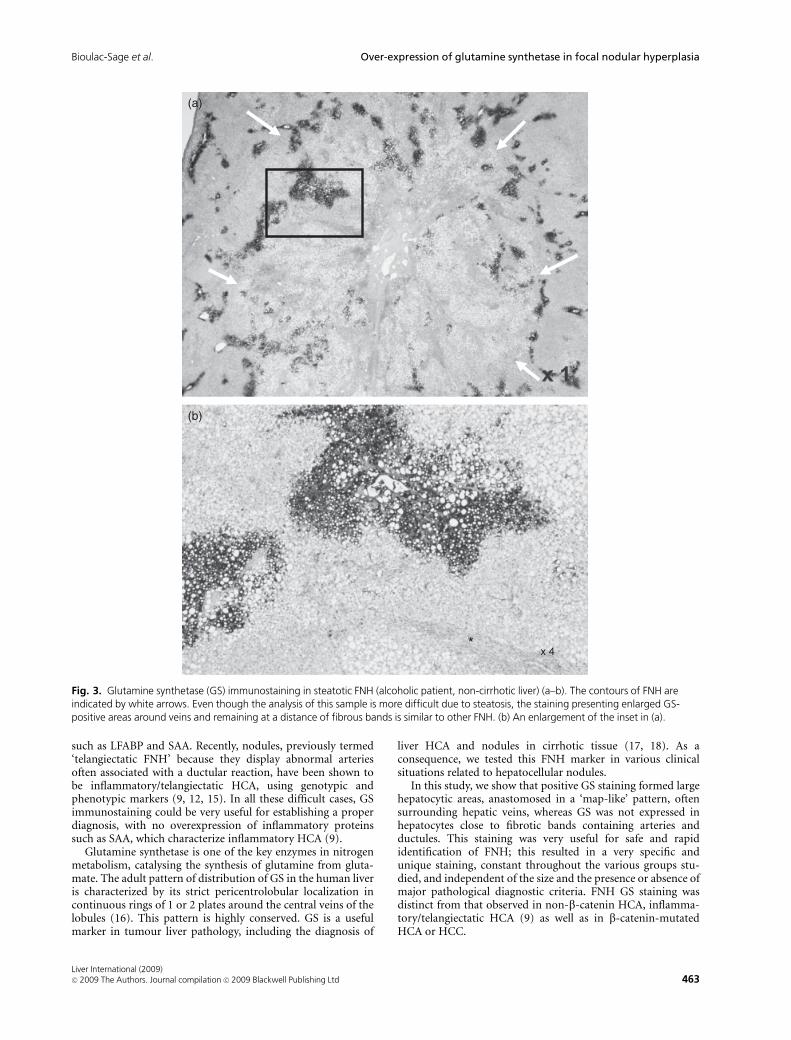
Fig. 3. Glutamine synthetase (GS) immunostaining in steatotic FNH (alcoholic patient, non-cirrhotic liver) (a–b). The contours of FNH areindicated by white arrows. Even though the analysis of this sample is more difficult due to steatosis, the staining presenting enlarged GS-positive areas around veins and remaining at a distance of fibrous bands is similar to other FNH. (b) An enlargement of the inset in (a).
Liver International (2009)c� 2009 The Authors. Journal compilation c� 2009 Blackwell Publishing Ltd 463
Bioulac-Sage et al. Over-expression of glutamine synthetase in focal nodular hyperplasia

GS was very useful for quickly solving differential diagnosesbetween HCA and FNH, particularly in the context of: (i)multiple hepatocellular tumours, such as adenomatosis ormultiple FNH, where all nodules are not always of the sameorigin (i.e. an association of adenomatosis and FNH, which isnot a rare condition); (ii) misleading steatotic FNH; and (iii)remodelled HCA with fibrotic bands.
Our overall experience with GS staining and HCA genotype/phenotype classification has resulted in the reclassification ofnodules supposed to be FNH in HCA (two cases), and in wd-HCC (one case: a small nodule in the immediate vicinity of anHCC). In addition, a small unclassified nodule was definitelyreclassified as an HCA. If this result is confirmed by othergroups and in a large series, GS staining could, in the future,have a place of choice to ascertain the diagnosis of FNH anddifferentiate from HCA in difficult cases.
We are presently testing GS on a large series of liver biopsiesto differentiate FNH from HCA and wd HCC in non-cirrhoticlivers. Preliminary data on 10 biopsies performed to differenti-ate FNH from other types of nodules showed the expected GSstaining for the diagnosis of FNH, that is to say, large areas ofGS positive hepatocytes contrasting with GS negative hepato-cytes usually in the vicinity of fibrotic bands. These biopsieswere typical of FNH based on microscopic criteria. It is, how-
ever, likely that differentiating these FNH from other noduleson biopsies will be probably more difficult from what we knowof the GS distribution in the whole specimen, due to theheterogeneous distribution of the staining, this difficulty de-pending, of course, on the biopsy length. The absence of labellingis, however, an argument for ruling out the diagnosis of FNH.
In FNH, the abnormal arteries drain indirectly into sinusoidsvia capillaries in the fibrous septa, leading to a modifiedsinusoidal endothelial cell phenotype (19). Because the fibroussepta with arteries are the location of blood inflow, they can beconsidered as ‘portal tract equivalents’. The blood compositionmay likely participate in zonal b-catenin activation. One couldtherefore hypothesize that the almost exclusive arterial inflow inFNH, without portal venous blood inflow, may cause b-cateninactivation to extend much farther towards the inflow area thanin normal liver (20).
Conclusions
In this study, we have established that GS is a good marker foreasy identification of resected FNH and for differentiating FNHfrom all other types of hepatocellular nodules developed onnormal liver.
(a) (b)
(c)
HCA
HCA
HCANTL
NTL
NTL
HCA
V
Fig. 4. Three different aspects of glutamine synthetase (GS) staining in non-mutated b-catenin adenomas (a–c). Compared with non-tumoralliver (NTL), the staining is negative in HCA (a and b), except at the border in (a). In (c), limited staining occurs at the periphery of the HCA,around the veins (V).
Liver International (2009)464 c� 2009 The Authors. Journal compilation c� 2009 Blackwell Publishing Ltd
Over-expression of glutamine synthetase in focal nodular hyperplasia Bioulac-Sage et al.
Acknowledgements
The authors wish to thank surgeons J Saric, A Sa Cunha,radiologist H Trillaud and pathologist B Le Bail, who helpedwith data collection.
References
1. Vilgrain V, Uzan F, Brancatelli G, Federle MP, Zappa M, Menu Y.
Prevalence of hepatic hemangioma in patients with focal nodular
hyperplasia: MR imaging analysis. Radiology 2003; 229: 75–9.
2. Bioulac-Sage P, Balabaud C, Wanless IR. Diagnosis of focal
nodular hyperplasia: not so easy. Am J Surg Pathol 2001; 25:
1322–13.
3. Wanless IR. Epithelioid hemangioendothelioma, multiple focal
nodular hyperplasias, and cavernous hemangiomas of the liver
[letter]. Arch Pathol Lab Med 2000; 124: 1105–7.
4. Takayama A, Wanless IR. Three-dimensional angioarchitecture of
focal nodular hyperplasia and hypothesis on the pathogenesis. Mod
Pathol 2004; 17(suppl): 313A.
5. Wanless IR, Albrecht S, Bilbao J, et al. Multiple focal nodular
hyperplasia of the liver associated with vascular malformations of
various organs and neoplasia of the brain: a new syndrome. Mod
Pathol 1989; 2: 456–62.
6. Bioulac-Sage P, Balabaud CLaennec and Elves groups et al. Patho-
logical diagnosis of liver cell adenoma and focal nodular hyperpla-
sia: Bordeaux update. J Hepatol 2007; 46: 521–7.
7. Bioulac-Sage P, Laumonier H, Cubel G, Saric J, Balabaud C. Over-
expression of glutamine synthase in focal nodular hyperplasia (part
1). Early stages in the formation support the hypothesis of a focal
hyperarterialisation with venous (portal and hepatic) and biliary
damage. Comparat Hepatol 2008; 7: 2 (online).
8. Wanless I, Sapp H, Guindy M, Olshansky D, Takayama A. The
pathogenesis of focal nodular hyperplasia/an hypothesis based on
histological review of 20 lesions including 3 occurring in early
biliary cirrhosis. Hepatology 2006; (Suppl 1): 491A.
9. Bioulac-Sage P, Rebouissou S, Thomas C, et al. Hepatocellular
adenoma subtype classification using molecular markers and im-
munohistochemistry. Hepatology 2007; 46: 740–8.
10. Di Tommaso L, Franchi G, Park YN, et al. Diagnostic value of
HSP70, glypican 3, and glutamine synthetase in hepatocellular
nodules in cirrhosis. Hepatology 2007; 45: 725–34.
11. Terminology of nodular hepatocellular lesions. International work-
ing party. Hepatology 1995; 22: 983–93.
12. Bioulac-Sage P, Rebouissou S, Sa Cunha A, et al. Clinical, morpho-
logical, and molecular features defining so-called telangiectatic
focal nodular hyperplasias of the liver. Gastroenterology 2005; 128:
1211–8.
13. Makhlouf HR, Abdul-Al HM, Goodman ZD. Diagnosis of focal
nodular hyperplasia of the liver by needle biopsy. Hum Pathol 2005;
36: 1210–6.
14. Fabre A, Audet P, Vilgrain V, et al. Histologic scoring of liver biopsy
in focal nodular hyperplasia with atypical presentation. Hepatology
2002; 35: 414–20.
15. Paradis V, Benzekri A, Dargere D, et al. Telangiectatic focal nodular
hyperplasia: a variant of hepatocellular adenoma. Gastroenterology
2004; 126: 1323–9.
16. Gebhardt R, Baldysiak-Figiel A, Krugel V, Ueberham E, Gaunitz F.
Hepatocellular expression of glutamine synthetase: an indicator of
morphogen actions as master regulators of zonation in adult liver.
Prog Histochem Cytochem 2007; 41: 201–66.
17. Racine-Samson L, Scoazec JY, D’Errico A, et al. The metabolic
organization of the adult human liver: a comparative study of
normal, fibrotic, and cirrhotic liver tissue. Hepatology 1996; 24:
104–13.
18. Gebhardt R, Reichen J. Changes in distribution and activity of
glutamine synthetase in carbon tetrachloride-induced cirrhosis in
the rat: potential role in hyperammonemia. Hepatology 1994; 20:
684–91.
19. Fukukura Y, Nakashima O, Kusaba A, Kage M Kojiro Angioarchi-
tecture and blood circulation in focal nodular hyperplasia of the
liver. J Hepatol 1998; 29: 470–5.
20. Rebouissou S, Couchy G, Libbrecht L, et al. The ß-Catenin pathway
is overexpressed in focal nodular hyperplasia but not in cirrhotic
FNH-like nodules. J Hepatol 2008; 49: 61–71.
(c)
(b)
HCA
HCC
NTL
NTL
NTL
HCA
(a)
x2
x20
x2
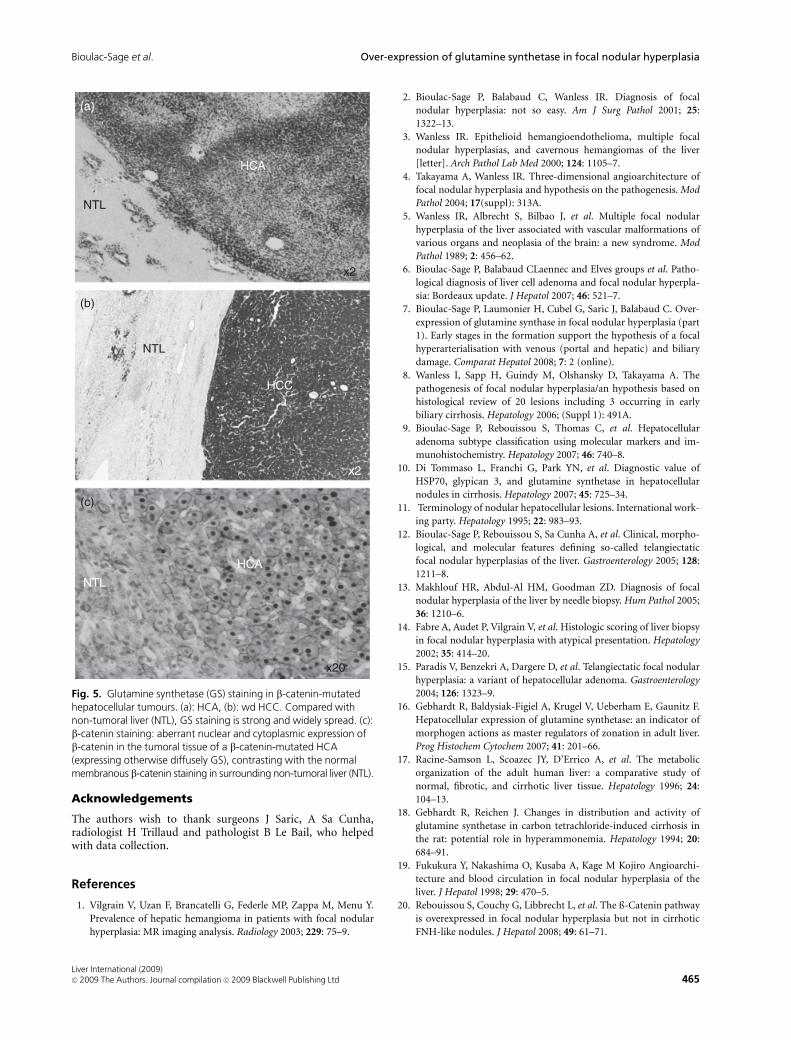
Fig. 5. Glutamine synthetase (GS) staining in b-catenin-mutatedhepatocellular tumours. (a): HCA, (b): wd HCC. Compared withnon-tumoral liver (NTL), GS staining is strong and widely spread. (c):b-catenin staining: aberrant nuclear and cytoplasmic expression ofb-catenin in the tumoral tissue of a b-catenin-mutated HCA(expressing otherwise diffusely GS), contrasting with the normalmembranous b-catenin staining in surrounding non-tumoral liver (NTL).
Liver International (2009)c� 2009 The Authors. Journal compilation c� 2009 Blackwell Publishing Ltd 465
Bioulac-Sage et al. Over-expression of glutamine synthetase in focal nodular hyperplasia
Related Documents











